User login
Sulfonylureas as street drugs: Hidden hypoglycemia cause
SEATTLE – .
“Physicians should be aware of this possibility and consider intentional or unintentional sulfonylurea abuse, with or without other drugs,” Amanda McKenna, MD, a first-year endocrinology fellow at the Mayo Clinic, Jacksonville, Fla., and colleagues say in a poster presented at the annual scientific & clinical congress of the American Association of Clinical Endocrinology.
The new case, seen in Florida, involves a 33-year-old man with a history of narcotic dependence and anxiety but not diabetes. At the time of presentation, the patient was unconscious and diaphoretic. The patient’s blood glucose level was 18 mg/dL. He had purchased two unmarked, light blue pills on the street which he thought were Valiums but turned out to be glyburide.
Sulfonylureas have no potential for abuse, but they physically resemble Valiums and are easier for illicit drug dealers to obtain because they’re not a controlled substance, and they can be sold for considerably more money, Dr. McKenna said in an interview.
“He thought he was getting Valium, but what he really purchased was glyburide. ... When he took it, he developed sweating and weakness. He probably thought he was having a bad trip, but it was really low blood sugar,” she said.
Similar cases go back nearly two decades
Similar cases have been reported as far back as 2004 in different parts of the United States. A 2004 article reports five cases in which people in San Francisco were “admitted to the hospital for hypoglycemia as a result of a drug purchased on the streets as a presumed benzodiazepine.”
Two more cases of “glyburide poisoning by ingestion of ‘street Valium,’ ” also from San Francisco, were reported in 2012. And in another case presented at the 2022 Endocrine Society meeting, sulfonylurea had been cut with cocaine, presumably to increase the volume.
The lead author of the 2012 article, Craig Smollin, MD, medical director of the California Poison Control System, San Francisco Division, and professor of emergency medicine at the University of California, San Francisco, told this news organization that his team has seen “a handful of cases over the years” but that “it is hard to say how common it is because hypoglycemia is common in this patient population for a variety of reasons.”
Persistent hypoglycemia led to the source
In the current case, paramedics treated the patient with D50W, and his blood glucose level increased from 18 mg/dL to 109 mg/dL. He regained consciousness but then developed recurrent hypoglycemia, and his blood glucose level dropped back to 15 mg/dL in the ED. Urine toxicology results were positive for benzodiazepines, cannabis, and cocaine.
Laboratory results showed elevations in levels of insulin (47.4 mIU/mL), C-peptide (5.4 ng/mL), and glucose (44 mg/dL). He was again treated with D50W, and his blood glucose level returned to normal over 20 hours. Once alert and oriented, he reported no personal or family history of diabetes. A 72-hour fast showed no evidence of insulinoma. A sulfonylurea screen was positive for glyburide. He was discharged home in stable condition. How many more cases have been missed?
Dr. McKenna pointed out that a typical urine toxicology screen for drugs wouldn’t detect a sulfonylurea. “The screen for hypoglycemic agents is a blood test, not a urine screen, so it’s completely different in the workup, and you really have to be thinking about that. It typically takes a while to come back,” she said.
She added that if the hypoglycemia resolves and testing isn’t conducted, the cause of the low blood sugar level might be missed. “If the hypoglycemia doesn’t persist, the [ED] physician wouldn’t consult endocrine. ... Is this happening more than we think?”
Ocreotide: A ‘unique antidote’
In their article, Dr. Smollin and colleagues describe the use of ocreotide, a long-acting somatostatin agonist that reverses the insulin-releasing effect of sulfonylureas on pancreatic beta cells, resulting in diminished insulin secretion. Unlike glucose supplementation, ocreotide doesn’t stimulate additional insulin release. It is of longer duration than glucagon, the authors say.
“The management of sulfonylurea overdose includes administration of glucose but also may include the use of octreotide, a unique antidote for sulfonylurea induced hypoglycemia,” Dr. Smollin said.
However, he also cautioned, “there is a broad differential diagnosis for hypoglycemia, and clinicians must consider many alternative diagnoses.”
Dr. McKenna and Dr. Smollin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SEATTLE – .
“Physicians should be aware of this possibility and consider intentional or unintentional sulfonylurea abuse, with or without other drugs,” Amanda McKenna, MD, a first-year endocrinology fellow at the Mayo Clinic, Jacksonville, Fla., and colleagues say in a poster presented at the annual scientific & clinical congress of the American Association of Clinical Endocrinology.
The new case, seen in Florida, involves a 33-year-old man with a history of narcotic dependence and anxiety but not diabetes. At the time of presentation, the patient was unconscious and diaphoretic. The patient’s blood glucose level was 18 mg/dL. He had purchased two unmarked, light blue pills on the street which he thought were Valiums but turned out to be glyburide.
Sulfonylureas have no potential for abuse, but they physically resemble Valiums and are easier for illicit drug dealers to obtain because they’re not a controlled substance, and they can be sold for considerably more money, Dr. McKenna said in an interview.
“He thought he was getting Valium, but what he really purchased was glyburide. ... When he took it, he developed sweating and weakness. He probably thought he was having a bad trip, but it was really low blood sugar,” she said.
Similar cases go back nearly two decades
Similar cases have been reported as far back as 2004 in different parts of the United States. A 2004 article reports five cases in which people in San Francisco were “admitted to the hospital for hypoglycemia as a result of a drug purchased on the streets as a presumed benzodiazepine.”
Two more cases of “glyburide poisoning by ingestion of ‘street Valium,’ ” also from San Francisco, were reported in 2012. And in another case presented at the 2022 Endocrine Society meeting, sulfonylurea had been cut with cocaine, presumably to increase the volume.
The lead author of the 2012 article, Craig Smollin, MD, medical director of the California Poison Control System, San Francisco Division, and professor of emergency medicine at the University of California, San Francisco, told this news organization that his team has seen “a handful of cases over the years” but that “it is hard to say how common it is because hypoglycemia is common in this patient population for a variety of reasons.”
Persistent hypoglycemia led to the source
In the current case, paramedics treated the patient with D50W, and his blood glucose level increased from 18 mg/dL to 109 mg/dL. He regained consciousness but then developed recurrent hypoglycemia, and his blood glucose level dropped back to 15 mg/dL in the ED. Urine toxicology results were positive for benzodiazepines, cannabis, and cocaine.
Laboratory results showed elevations in levels of insulin (47.4 mIU/mL), C-peptide (5.4 ng/mL), and glucose (44 mg/dL). He was again treated with D50W, and his blood glucose level returned to normal over 20 hours. Once alert and oriented, he reported no personal or family history of diabetes. A 72-hour fast showed no evidence of insulinoma. A sulfonylurea screen was positive for glyburide. He was discharged home in stable condition. How many more cases have been missed?
Dr. McKenna pointed out that a typical urine toxicology screen for drugs wouldn’t detect a sulfonylurea. “The screen for hypoglycemic agents is a blood test, not a urine screen, so it’s completely different in the workup, and you really have to be thinking about that. It typically takes a while to come back,” she said.
She added that if the hypoglycemia resolves and testing isn’t conducted, the cause of the low blood sugar level might be missed. “If the hypoglycemia doesn’t persist, the [ED] physician wouldn’t consult endocrine. ... Is this happening more than we think?”
Ocreotide: A ‘unique antidote’
In their article, Dr. Smollin and colleagues describe the use of ocreotide, a long-acting somatostatin agonist that reverses the insulin-releasing effect of sulfonylureas on pancreatic beta cells, resulting in diminished insulin secretion. Unlike glucose supplementation, ocreotide doesn’t stimulate additional insulin release. It is of longer duration than glucagon, the authors say.
“The management of sulfonylurea overdose includes administration of glucose but also may include the use of octreotide, a unique antidote for sulfonylurea induced hypoglycemia,” Dr. Smollin said.
However, he also cautioned, “there is a broad differential diagnosis for hypoglycemia, and clinicians must consider many alternative diagnoses.”
Dr. McKenna and Dr. Smollin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SEATTLE – .
“Physicians should be aware of this possibility and consider intentional or unintentional sulfonylurea abuse, with or without other drugs,” Amanda McKenna, MD, a first-year endocrinology fellow at the Mayo Clinic, Jacksonville, Fla., and colleagues say in a poster presented at the annual scientific & clinical congress of the American Association of Clinical Endocrinology.
The new case, seen in Florida, involves a 33-year-old man with a history of narcotic dependence and anxiety but not diabetes. At the time of presentation, the patient was unconscious and diaphoretic. The patient’s blood glucose level was 18 mg/dL. He had purchased two unmarked, light blue pills on the street which he thought were Valiums but turned out to be glyburide.
Sulfonylureas have no potential for abuse, but they physically resemble Valiums and are easier for illicit drug dealers to obtain because they’re not a controlled substance, and they can be sold for considerably more money, Dr. McKenna said in an interview.
“He thought he was getting Valium, but what he really purchased was glyburide. ... When he took it, he developed sweating and weakness. He probably thought he was having a bad trip, but it was really low blood sugar,” she said.
Similar cases go back nearly two decades
Similar cases have been reported as far back as 2004 in different parts of the United States. A 2004 article reports five cases in which people in San Francisco were “admitted to the hospital for hypoglycemia as a result of a drug purchased on the streets as a presumed benzodiazepine.”
Two more cases of “glyburide poisoning by ingestion of ‘street Valium,’ ” also from San Francisco, were reported in 2012. And in another case presented at the 2022 Endocrine Society meeting, sulfonylurea had been cut with cocaine, presumably to increase the volume.
The lead author of the 2012 article, Craig Smollin, MD, medical director of the California Poison Control System, San Francisco Division, and professor of emergency medicine at the University of California, San Francisco, told this news organization that his team has seen “a handful of cases over the years” but that “it is hard to say how common it is because hypoglycemia is common in this patient population for a variety of reasons.”
Persistent hypoglycemia led to the source
In the current case, paramedics treated the patient with D50W, and his blood glucose level increased from 18 mg/dL to 109 mg/dL. He regained consciousness but then developed recurrent hypoglycemia, and his blood glucose level dropped back to 15 mg/dL in the ED. Urine toxicology results were positive for benzodiazepines, cannabis, and cocaine.
Laboratory results showed elevations in levels of insulin (47.4 mIU/mL), C-peptide (5.4 ng/mL), and glucose (44 mg/dL). He was again treated with D50W, and his blood glucose level returned to normal over 20 hours. Once alert and oriented, he reported no personal or family history of diabetes. A 72-hour fast showed no evidence of insulinoma. A sulfonylurea screen was positive for glyburide. He was discharged home in stable condition. How many more cases have been missed?
Dr. McKenna pointed out that a typical urine toxicology screen for drugs wouldn’t detect a sulfonylurea. “The screen for hypoglycemic agents is a blood test, not a urine screen, so it’s completely different in the workup, and you really have to be thinking about that. It typically takes a while to come back,” she said.
She added that if the hypoglycemia resolves and testing isn’t conducted, the cause of the low blood sugar level might be missed. “If the hypoglycemia doesn’t persist, the [ED] physician wouldn’t consult endocrine. ... Is this happening more than we think?”
Ocreotide: A ‘unique antidote’
In their article, Dr. Smollin and colleagues describe the use of ocreotide, a long-acting somatostatin agonist that reverses the insulin-releasing effect of sulfonylureas on pancreatic beta cells, resulting in diminished insulin secretion. Unlike glucose supplementation, ocreotide doesn’t stimulate additional insulin release. It is of longer duration than glucagon, the authors say.
“The management of sulfonylurea overdose includes administration of glucose but also may include the use of octreotide, a unique antidote for sulfonylurea induced hypoglycemia,” Dr. Smollin said.
However, he also cautioned, “there is a broad differential diagnosis for hypoglycemia, and clinicians must consider many alternative diagnoses.”
Dr. McKenna and Dr. Smollin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT AACE 2023
Virtual care not linked with greater ED use during pandemic
Canadian family physicians’ increased use of virtual care during the first years of the pandemic was not associated with increased emergency department use among patients, a new analysis of data from Ontario suggests.
In a cross-sectional study that included almost 14,000 family physicians and almost 13 million patients in Ontario, an adjusted analysis indicated that patients with physicians who provided more than 20% of care virtually had lower rates of ED visits, compared with patients whose physicians provided the least virtual care.
“I was surprised to see that ED visit volumes in fall 2021 were below prepandemic levels,” study author Tara Kiran, MD, who practices family medicine at St. Michael’s Hospital of the University of Toronto, told this news organization.
“At that time, there was a lot in the news about how our EDs were overcrowded and an assumption that this related to higher visit volumes. But our data [suggest] there were other factors at play, including strains in staffing in the ED, hospital inpatient units, and in long-term care.” Dr. Kiran is also the Fidani chair in improvement and innovation and vice-chair of quality and innovation at the department of family and community medicine of the University of Toronto.
The study was published online in JAMA Network Open.
Embrace of telehealth
The investigators analyzed administrative data from Ontario for 13,820 family physicians (mean age, 50 years; 51.5% men) and 12,951,063 patients (mean age, 42.6 years; 51.8% women) under their care.
The family physicians had at least one primary care visit claim between Feb. 1 and Oct. 31, 2021. The researchers categorized the physicians by the percentage of total visits they delivered virtually (via telephone or video) during the study period, as follows: 0% (100% in person), greater than 0%-20%, greater than 20%-40%, greater than 40%-60%, greater than 60%-80%, greater than 80% to less than 100%, or 100%.
The percentage of virtual primary care visits peaked at 82% in the first 2 weeks of the pandemic and decreased to 49% by October 2021. ED visit rates decreased at the start of the pandemic and remained lower than in 2019 throughout the study period.
Most physicians provided between 40% and 80% of care virtually. A greater percentage of those who provided more than 80% of care virtually were aged 65 years or older, were women, and practiced in large cities.
Patient comorbidity and morbidity were similar across all categories of virtual care use. The mean number of ED visits was highest among patients whose physicians provided only in-person care (470.3 per 1,000 patients) and was lowest among those whose physicians provided greater than 0% to less than 100% of care virtually (242 per 1,000 patients).
After adjustment for patient characteristics, patients of physicians who provided more than 20% of care virtually had lower rates of ED visits, compared with patients of physicians who provided the least virtual care (for example, greater than 80% to less than 100% versus 0%-20% virtual visits in big cities; relative rate, 0.77). This pattern was consistent across all rurality of practice categories and after adjustment for 2019 ED visit rates.
The investigators observed a gradient in urban areas. Patients of physicians who provided the highest level of virtual care had the lowest ED visit rates.
Investigating virtual modalities
Some policymakers worried that inappropriate use of virtual care was leading to an increase in ED use. “Findings of this study refute this hypothesis,” the authors write. Increases in ED use seemed to coincide with decreases in COVID-19 cases, not with increases in virtual primary care visits.
Furthermore, at the population level, patients who were cared for by physicians who provided a high percentage of virtual care did not have a higher rate of ED visits, compared with those cared for by physicians who provided the lowest levels of virtual care.
During the pandemic, the switch to virtual care worked well for some of Dr. Kiran’s patients. It was more convenient, because they didn’t have to take time off work, travel to and from the clinic, find and pay for parking, or wait in the clinic before the appointment, she said.
But for others, “virtual care really didn’t work well,” she said. “This was particularly true for people who didn’t have a regular working phone, who didn’t have a private space to take calls, who weren’t fluent in English, and who were hard of hearing or had severe mental illness that resulted in paranoid thoughts.”
Clinicians also may have had different comfort levels and preferences regarding virtual visits, Dr. Kiran hypothesized. Some found it convenient and efficient, whereas others may have found it cumbersome and inefficient. “I personally find it harder to build relationships with patients when I use virtual care,” she said. “I experience more joy in work with in-person visits, but other clinicians may feel differently.”
Dr. Kiran and her colleagues are conducting a public engagement initiative called OurCare to understand public perspectives on the future of primary care. “As part of that work, we want to understand what virtual modalities are most important to the public and how the public thinks these should be integrated into primary care.”
Virtual care can support access, patient-centered care, and equity in primary care, Dr. Kiran added. “Ideally, it should be integrated into an existing relationship with a family physician and be a complement to in-person visits.”
The right dose?
In an accompanying editorial, Jesse M. Pines, MD, chief of clinical innovation at U.S. Acute Care Solutions, Canton, Ohio, writes, “There is no convincing mechanism consistent with the data for the observed outcome of lower ED use at higher telehealth use.”
Additional research is needed, he notes, to answer the “Goldilocks question” – that is, what amount of telehealth optimizes its benefits while minimizing potential problems?
“The right dose of telehealth needs to balance (1) concerns by payers and policymakers that it will increase cost and cause unintended consequences (for example, misdiagnosis or duplicative care) and (2) the desire of its proponents who want to allow clinicians to use it as they see fit, with few restrictions,” writes Dr. Pines.
“Future research would ideally use more robust research design,” he suggested. “For example, randomized trials could test different doses of telehealth, or mixed-methods studies could help elucidate how telehealth may be changing clinical management or care-seeking behavior.”
Equitable reimbursement needed
Priya Nori, MD, associate professor of infectious diseases at Montefiore Health System and associate professor at the Albert Einstein College of Medicine, both in New York, said, “I agree with their conclusions and am reassured about telehealth as a durable form of health care delivery.”
Large, population-level studies such as this one might persuade legislators to require equitable reimbursement for in-person and virtual visits “so providers have comparable incentives to provide both types of care,” she said. “Although only primary care was addressed in the study, I believe that virtual care is here to stay and can be applied to primary care, subspecialty care, and other services, like antimicrobial stewardship, infection prevention, et cetera. We need to embrace it.”
A similar study should be conducted in the United States, along with additional research “to ensure that visits done by telephone have similar outcomes as those done by video, as not all communities have adequate internet access or video conferencing technology,” said Dr. Nori.
The study was supported by ICES and grants from Ontario Health, the Canadian Institutes of Health Research, and the Health Systems Research Program of Ontario MOH. Dr. Kiran, Dr. Pines, and Dr. Nori have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Canadian family physicians’ increased use of virtual care during the first years of the pandemic was not associated with increased emergency department use among patients, a new analysis of data from Ontario suggests.
In a cross-sectional study that included almost 14,000 family physicians and almost 13 million patients in Ontario, an adjusted analysis indicated that patients with physicians who provided more than 20% of care virtually had lower rates of ED visits, compared with patients whose physicians provided the least virtual care.
“I was surprised to see that ED visit volumes in fall 2021 were below prepandemic levels,” study author Tara Kiran, MD, who practices family medicine at St. Michael’s Hospital of the University of Toronto, told this news organization.
“At that time, there was a lot in the news about how our EDs were overcrowded and an assumption that this related to higher visit volumes. But our data [suggest] there were other factors at play, including strains in staffing in the ED, hospital inpatient units, and in long-term care.” Dr. Kiran is also the Fidani chair in improvement and innovation and vice-chair of quality and innovation at the department of family and community medicine of the University of Toronto.
The study was published online in JAMA Network Open.
Embrace of telehealth
The investigators analyzed administrative data from Ontario for 13,820 family physicians (mean age, 50 years; 51.5% men) and 12,951,063 patients (mean age, 42.6 years; 51.8% women) under their care.
The family physicians had at least one primary care visit claim between Feb. 1 and Oct. 31, 2021. The researchers categorized the physicians by the percentage of total visits they delivered virtually (via telephone or video) during the study period, as follows: 0% (100% in person), greater than 0%-20%, greater than 20%-40%, greater than 40%-60%, greater than 60%-80%, greater than 80% to less than 100%, or 100%.
The percentage of virtual primary care visits peaked at 82% in the first 2 weeks of the pandemic and decreased to 49% by October 2021. ED visit rates decreased at the start of the pandemic and remained lower than in 2019 throughout the study period.
Most physicians provided between 40% and 80% of care virtually. A greater percentage of those who provided more than 80% of care virtually were aged 65 years or older, were women, and practiced in large cities.
Patient comorbidity and morbidity were similar across all categories of virtual care use. The mean number of ED visits was highest among patients whose physicians provided only in-person care (470.3 per 1,000 patients) and was lowest among those whose physicians provided greater than 0% to less than 100% of care virtually (242 per 1,000 patients).
After adjustment for patient characteristics, patients of physicians who provided more than 20% of care virtually had lower rates of ED visits, compared with patients of physicians who provided the least virtual care (for example, greater than 80% to less than 100% versus 0%-20% virtual visits in big cities; relative rate, 0.77). This pattern was consistent across all rurality of practice categories and after adjustment for 2019 ED visit rates.
The investigators observed a gradient in urban areas. Patients of physicians who provided the highest level of virtual care had the lowest ED visit rates.
Investigating virtual modalities
Some policymakers worried that inappropriate use of virtual care was leading to an increase in ED use. “Findings of this study refute this hypothesis,” the authors write. Increases in ED use seemed to coincide with decreases in COVID-19 cases, not with increases in virtual primary care visits.
Furthermore, at the population level, patients who were cared for by physicians who provided a high percentage of virtual care did not have a higher rate of ED visits, compared with those cared for by physicians who provided the lowest levels of virtual care.
During the pandemic, the switch to virtual care worked well for some of Dr. Kiran’s patients. It was more convenient, because they didn’t have to take time off work, travel to and from the clinic, find and pay for parking, or wait in the clinic before the appointment, she said.
But for others, “virtual care really didn’t work well,” she said. “This was particularly true for people who didn’t have a regular working phone, who didn’t have a private space to take calls, who weren’t fluent in English, and who were hard of hearing or had severe mental illness that resulted in paranoid thoughts.”
Clinicians also may have had different comfort levels and preferences regarding virtual visits, Dr. Kiran hypothesized. Some found it convenient and efficient, whereas others may have found it cumbersome and inefficient. “I personally find it harder to build relationships with patients when I use virtual care,” she said. “I experience more joy in work with in-person visits, but other clinicians may feel differently.”
Dr. Kiran and her colleagues are conducting a public engagement initiative called OurCare to understand public perspectives on the future of primary care. “As part of that work, we want to understand what virtual modalities are most important to the public and how the public thinks these should be integrated into primary care.”
Virtual care can support access, patient-centered care, and equity in primary care, Dr. Kiran added. “Ideally, it should be integrated into an existing relationship with a family physician and be a complement to in-person visits.”
The right dose?
In an accompanying editorial, Jesse M. Pines, MD, chief of clinical innovation at U.S. Acute Care Solutions, Canton, Ohio, writes, “There is no convincing mechanism consistent with the data for the observed outcome of lower ED use at higher telehealth use.”
Additional research is needed, he notes, to answer the “Goldilocks question” – that is, what amount of telehealth optimizes its benefits while minimizing potential problems?
“The right dose of telehealth needs to balance (1) concerns by payers and policymakers that it will increase cost and cause unintended consequences (for example, misdiagnosis or duplicative care) and (2) the desire of its proponents who want to allow clinicians to use it as they see fit, with few restrictions,” writes Dr. Pines.
“Future research would ideally use more robust research design,” he suggested. “For example, randomized trials could test different doses of telehealth, or mixed-methods studies could help elucidate how telehealth may be changing clinical management or care-seeking behavior.”
Equitable reimbursement needed
Priya Nori, MD, associate professor of infectious diseases at Montefiore Health System and associate professor at the Albert Einstein College of Medicine, both in New York, said, “I agree with their conclusions and am reassured about telehealth as a durable form of health care delivery.”
Large, population-level studies such as this one might persuade legislators to require equitable reimbursement for in-person and virtual visits “so providers have comparable incentives to provide both types of care,” she said. “Although only primary care was addressed in the study, I believe that virtual care is here to stay and can be applied to primary care, subspecialty care, and other services, like antimicrobial stewardship, infection prevention, et cetera. We need to embrace it.”
A similar study should be conducted in the United States, along with additional research “to ensure that visits done by telephone have similar outcomes as those done by video, as not all communities have adequate internet access or video conferencing technology,” said Dr. Nori.
The study was supported by ICES and grants from Ontario Health, the Canadian Institutes of Health Research, and the Health Systems Research Program of Ontario MOH. Dr. Kiran, Dr. Pines, and Dr. Nori have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Canadian family physicians’ increased use of virtual care during the first years of the pandemic was not associated with increased emergency department use among patients, a new analysis of data from Ontario suggests.
In a cross-sectional study that included almost 14,000 family physicians and almost 13 million patients in Ontario, an adjusted analysis indicated that patients with physicians who provided more than 20% of care virtually had lower rates of ED visits, compared with patients whose physicians provided the least virtual care.
“I was surprised to see that ED visit volumes in fall 2021 were below prepandemic levels,” study author Tara Kiran, MD, who practices family medicine at St. Michael’s Hospital of the University of Toronto, told this news organization.
“At that time, there was a lot in the news about how our EDs were overcrowded and an assumption that this related to higher visit volumes. But our data [suggest] there were other factors at play, including strains in staffing in the ED, hospital inpatient units, and in long-term care.” Dr. Kiran is also the Fidani chair in improvement and innovation and vice-chair of quality and innovation at the department of family and community medicine of the University of Toronto.
The study was published online in JAMA Network Open.
Embrace of telehealth
The investigators analyzed administrative data from Ontario for 13,820 family physicians (mean age, 50 years; 51.5% men) and 12,951,063 patients (mean age, 42.6 years; 51.8% women) under their care.
The family physicians had at least one primary care visit claim between Feb. 1 and Oct. 31, 2021. The researchers categorized the physicians by the percentage of total visits they delivered virtually (via telephone or video) during the study period, as follows: 0% (100% in person), greater than 0%-20%, greater than 20%-40%, greater than 40%-60%, greater than 60%-80%, greater than 80% to less than 100%, or 100%.
The percentage of virtual primary care visits peaked at 82% in the first 2 weeks of the pandemic and decreased to 49% by October 2021. ED visit rates decreased at the start of the pandemic and remained lower than in 2019 throughout the study period.
Most physicians provided between 40% and 80% of care virtually. A greater percentage of those who provided more than 80% of care virtually were aged 65 years or older, were women, and practiced in large cities.
Patient comorbidity and morbidity were similar across all categories of virtual care use. The mean number of ED visits was highest among patients whose physicians provided only in-person care (470.3 per 1,000 patients) and was lowest among those whose physicians provided greater than 0% to less than 100% of care virtually (242 per 1,000 patients).
After adjustment for patient characteristics, patients of physicians who provided more than 20% of care virtually had lower rates of ED visits, compared with patients of physicians who provided the least virtual care (for example, greater than 80% to less than 100% versus 0%-20% virtual visits in big cities; relative rate, 0.77). This pattern was consistent across all rurality of practice categories and after adjustment for 2019 ED visit rates.
The investigators observed a gradient in urban areas. Patients of physicians who provided the highest level of virtual care had the lowest ED visit rates.
Investigating virtual modalities
Some policymakers worried that inappropriate use of virtual care was leading to an increase in ED use. “Findings of this study refute this hypothesis,” the authors write. Increases in ED use seemed to coincide with decreases in COVID-19 cases, not with increases in virtual primary care visits.
Furthermore, at the population level, patients who were cared for by physicians who provided a high percentage of virtual care did not have a higher rate of ED visits, compared with those cared for by physicians who provided the lowest levels of virtual care.
During the pandemic, the switch to virtual care worked well for some of Dr. Kiran’s patients. It was more convenient, because they didn’t have to take time off work, travel to and from the clinic, find and pay for parking, or wait in the clinic before the appointment, she said.
But for others, “virtual care really didn’t work well,” she said. “This was particularly true for people who didn’t have a regular working phone, who didn’t have a private space to take calls, who weren’t fluent in English, and who were hard of hearing or had severe mental illness that resulted in paranoid thoughts.”
Clinicians also may have had different comfort levels and preferences regarding virtual visits, Dr. Kiran hypothesized. Some found it convenient and efficient, whereas others may have found it cumbersome and inefficient. “I personally find it harder to build relationships with patients when I use virtual care,” she said. “I experience more joy in work with in-person visits, but other clinicians may feel differently.”
Dr. Kiran and her colleagues are conducting a public engagement initiative called OurCare to understand public perspectives on the future of primary care. “As part of that work, we want to understand what virtual modalities are most important to the public and how the public thinks these should be integrated into primary care.”
Virtual care can support access, patient-centered care, and equity in primary care, Dr. Kiran added. “Ideally, it should be integrated into an existing relationship with a family physician and be a complement to in-person visits.”
The right dose?
In an accompanying editorial, Jesse M. Pines, MD, chief of clinical innovation at U.S. Acute Care Solutions, Canton, Ohio, writes, “There is no convincing mechanism consistent with the data for the observed outcome of lower ED use at higher telehealth use.”
Additional research is needed, he notes, to answer the “Goldilocks question” – that is, what amount of telehealth optimizes its benefits while minimizing potential problems?
“The right dose of telehealth needs to balance (1) concerns by payers and policymakers that it will increase cost and cause unintended consequences (for example, misdiagnosis or duplicative care) and (2) the desire of its proponents who want to allow clinicians to use it as they see fit, with few restrictions,” writes Dr. Pines.
“Future research would ideally use more robust research design,” he suggested. “For example, randomized trials could test different doses of telehealth, or mixed-methods studies could help elucidate how telehealth may be changing clinical management or care-seeking behavior.”
Equitable reimbursement needed
Priya Nori, MD, associate professor of infectious diseases at Montefiore Health System and associate professor at the Albert Einstein College of Medicine, both in New York, said, “I agree with their conclusions and am reassured about telehealth as a durable form of health care delivery.”
Large, population-level studies such as this one might persuade legislators to require equitable reimbursement for in-person and virtual visits “so providers have comparable incentives to provide both types of care,” she said. “Although only primary care was addressed in the study, I believe that virtual care is here to stay and can be applied to primary care, subspecialty care, and other services, like antimicrobial stewardship, infection prevention, et cetera. We need to embrace it.”
A similar study should be conducted in the United States, along with additional research “to ensure that visits done by telephone have similar outcomes as those done by video, as not all communities have adequate internet access or video conferencing technology,” said Dr. Nori.
The study was supported by ICES and grants from Ontario Health, the Canadian Institutes of Health Research, and the Health Systems Research Program of Ontario MOH. Dr. Kiran, Dr. Pines, and Dr. Nori have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Studies suggest ways to refine neonatal hernia management
WASHINGTON – Congenital diaphragmatic hernia affects many areas of pediatrics. In a trio of posters presented at the Pediatric Academic Societies annual meeting,
Initial ventilation mode shows little impact on NICU outcomes
In one study, K. Taylor Wild, MD, and colleagues investigated whether high-frequency oscillatory ventilation (HFOV) as an initial mode of ventilation in the delivery room improved gas exchange and neonatal ICU (NICU) outcomes in infants with congenital diaphragmatic hernia (CDH), compared with conventional mechanical ventilation (CMV). In 2019, HFOV became standard practice at CHOP.
The researchers reviewed data on infants with severe CDH who were born at CHOP between 2014 and 2022. Of these, 75 were placed on HFOV and 114 on CMV. The mean gestational age at birth in both groups was approximately 38 weeks, and the mean birth weight was approximately 3 kg.
Compared with CMV, use of HFOV in the delivery room was associated with significantly higher pH (7.05 vs. 7.16, P = .03) and significantly lower CO2 (85.2 vs. 64.5, P = .005). However, after adjusting for CDH severity, no significant differences appeared in length of stay and overall survival to discharge. The higher rates of extracorporeal membrane oxygenation (ECMO) use in the HFOV group, compared with the CMV group (48% vs. 29.9%), may reflect more severe disease, the researchers noted.
Prenatal brain immaturity associates with developmental delay
In a second study, Sandy Johng, MD, and colleagues found a significant association between prenatal brain immaturity in babies with CDH and developmental scores at age 12 months and older. The researchers reviewed data from a single-center patient registry for 48 infants for whom prenatal neuroimaging results were available. Based on the imaging, a fetal Total Maturation Score (fTMS) was generated and used as a measure of prenatal brain immaturity.
Results from the Bayley Scales of Infant Development-III (BSID-III) – a composite of cognitive, motor, and language scores – were available for 26 neonates at ages 12 months and under as well as at 12 months and older.
In a linear regression model, the researchers found a significant association between difference in fTMS and BSID-III composite language scores in infants 12 months and older. After adjusting for ECMO treatment, an increase in fTMS of one unit was associated with a 6.5-point increase in language scores at age 12 months and older (P < .01). No significant differences were observed between fTMS difference and language scores in infants under 12 months, or in cognitive or motor scores at any age, the researchers noted. The findings were limited by the small sample size, but the study is the first to show an association between prenatal imaging and neurodevelopmental outcomes for infants with CDH. Results suggest that the risk for neurodevelopmental impairment in this population may start in utero, the researchers concluded.
Antibiotic use stays stable
In a third study, Sabrina Flohr, MPH, and colleagues reviewed antibiotic use among infants with CDH who are at increased risk for infection. In many cases, distinguishing between infection and inherent clinical illness is challenging and may lead to unnecessarily high rates of antibiotic use, the researchers noted.
They reviewed data from 381 infants with CDH born at CHOP between January 2013 and November 2022 who were treated and survived in the NICU. Overall, 97.1% of the newborns received antibiotics for a median of 13 days. Nearly two-thirds (63.5%) received antibiotics in the first 72 hours, and 98.1% received them after 72 hours. Ampicillin and gentamicin were the antibiotics used most often in the first 72 hours (approximately 50% for both). After 72 hours, the most commonly used antibiotics were cefazolin (91.6%), vancomycin (67.7%), and cefepime (65.7%).
The results show that antibiotic use among newborns with CDH did not change significantly over time, and the choices of later antibiotics likely reflect perioperative prophylaxis and broad-spectrum treatment, the researchers noted.
Studies show larger trends
“These are three interesting studies regarding congenital diaphragmatic hernia from a center that does a high volume of repairs,” said Tim Joos, MD, a Seattle-based clinician with a combination internal medicine/pediatrics practice, in an interview.
“Each individual case can be consuming, but it is important to look for an aggregate of cases to see the larger trends in practices and outcomes,” said Dr. Joos, who was not involved in any of the studies.
The findings of the ventilation study surprised Dr. Joos. “Although high-frequency oscillatory ventilation improves initial gas exchange in the delivery room, compared with conventional mechanical ventilation, it was not associated with any larger NICU outcome,” he said. “This surprised me because my intuition would be that the HFOV would lead to less barotrauma and therefore better outcomes with the underformed lungs associated with this disorder.”
The imaging study demonstrates the need for more research on the association between CDH and neurologic outcomes, said Dr. Joos.
“Prenatal neuroimaging that shows delayed maturation with congenital diaphragmatic hernia correlates with lower language scores in early childhood, and suggests that this may be a predictor of neurologic outcome independent of the postnatal course,” he said.
Data from the antibiotics study reflect current trends, said Dr. Joos. “Antibiotics use is extremely common during the postnatal course of CDH and surgical repair,” he said. “The choice of antibiotics mirrors what we see in other neonatal conditions with regard to treatment for possible early neonatal sepsis, postsurgical prophylaxis, and later broad-spectrum empiric coverage,” he noted.
“I look forward to more studies to come out of large-volume centers like CHOP or aggregated results from many centers to help figure out best practices for this rare but very complicated and often devastating malformation,” he said.
The three posters received no outside funding. The researchers had no financial conflicts to disclose. Dr. Joos had no financial conflicts to disclose, but he serves on the Editorial Advisory Board of Pediatric News.
WASHINGTON – Congenital diaphragmatic hernia affects many areas of pediatrics. In a trio of posters presented at the Pediatric Academic Societies annual meeting,
Initial ventilation mode shows little impact on NICU outcomes
In one study, K. Taylor Wild, MD, and colleagues investigated whether high-frequency oscillatory ventilation (HFOV) as an initial mode of ventilation in the delivery room improved gas exchange and neonatal ICU (NICU) outcomes in infants with congenital diaphragmatic hernia (CDH), compared with conventional mechanical ventilation (CMV). In 2019, HFOV became standard practice at CHOP.
The researchers reviewed data on infants with severe CDH who were born at CHOP between 2014 and 2022. Of these, 75 were placed on HFOV and 114 on CMV. The mean gestational age at birth in both groups was approximately 38 weeks, and the mean birth weight was approximately 3 kg.
Compared with CMV, use of HFOV in the delivery room was associated with significantly higher pH (7.05 vs. 7.16, P = .03) and significantly lower CO2 (85.2 vs. 64.5, P = .005). However, after adjusting for CDH severity, no significant differences appeared in length of stay and overall survival to discharge. The higher rates of extracorporeal membrane oxygenation (ECMO) use in the HFOV group, compared with the CMV group (48% vs. 29.9%), may reflect more severe disease, the researchers noted.
Prenatal brain immaturity associates with developmental delay
In a second study, Sandy Johng, MD, and colleagues found a significant association between prenatal brain immaturity in babies with CDH and developmental scores at age 12 months and older. The researchers reviewed data from a single-center patient registry for 48 infants for whom prenatal neuroimaging results were available. Based on the imaging, a fetal Total Maturation Score (fTMS) was generated and used as a measure of prenatal brain immaturity.
Results from the Bayley Scales of Infant Development-III (BSID-III) – a composite of cognitive, motor, and language scores – were available for 26 neonates at ages 12 months and under as well as at 12 months and older.
In a linear regression model, the researchers found a significant association between difference in fTMS and BSID-III composite language scores in infants 12 months and older. After adjusting for ECMO treatment, an increase in fTMS of one unit was associated with a 6.5-point increase in language scores at age 12 months and older (P < .01). No significant differences were observed between fTMS difference and language scores in infants under 12 months, or in cognitive or motor scores at any age, the researchers noted. The findings were limited by the small sample size, but the study is the first to show an association between prenatal imaging and neurodevelopmental outcomes for infants with CDH. Results suggest that the risk for neurodevelopmental impairment in this population may start in utero, the researchers concluded.
Antibiotic use stays stable
In a third study, Sabrina Flohr, MPH, and colleagues reviewed antibiotic use among infants with CDH who are at increased risk for infection. In many cases, distinguishing between infection and inherent clinical illness is challenging and may lead to unnecessarily high rates of antibiotic use, the researchers noted.
They reviewed data from 381 infants with CDH born at CHOP between January 2013 and November 2022 who were treated and survived in the NICU. Overall, 97.1% of the newborns received antibiotics for a median of 13 days. Nearly two-thirds (63.5%) received antibiotics in the first 72 hours, and 98.1% received them after 72 hours. Ampicillin and gentamicin were the antibiotics used most often in the first 72 hours (approximately 50% for both). After 72 hours, the most commonly used antibiotics were cefazolin (91.6%), vancomycin (67.7%), and cefepime (65.7%).
The results show that antibiotic use among newborns with CDH did not change significantly over time, and the choices of later antibiotics likely reflect perioperative prophylaxis and broad-spectrum treatment, the researchers noted.
Studies show larger trends
“These are three interesting studies regarding congenital diaphragmatic hernia from a center that does a high volume of repairs,” said Tim Joos, MD, a Seattle-based clinician with a combination internal medicine/pediatrics practice, in an interview.
“Each individual case can be consuming, but it is important to look for an aggregate of cases to see the larger trends in practices and outcomes,” said Dr. Joos, who was not involved in any of the studies.
The findings of the ventilation study surprised Dr. Joos. “Although high-frequency oscillatory ventilation improves initial gas exchange in the delivery room, compared with conventional mechanical ventilation, it was not associated with any larger NICU outcome,” he said. “This surprised me because my intuition would be that the HFOV would lead to less barotrauma and therefore better outcomes with the underformed lungs associated with this disorder.”
The imaging study demonstrates the need for more research on the association between CDH and neurologic outcomes, said Dr. Joos.
“Prenatal neuroimaging that shows delayed maturation with congenital diaphragmatic hernia correlates with lower language scores in early childhood, and suggests that this may be a predictor of neurologic outcome independent of the postnatal course,” he said.
Data from the antibiotics study reflect current trends, said Dr. Joos. “Antibiotics use is extremely common during the postnatal course of CDH and surgical repair,” he said. “The choice of antibiotics mirrors what we see in other neonatal conditions with regard to treatment for possible early neonatal sepsis, postsurgical prophylaxis, and later broad-spectrum empiric coverage,” he noted.
“I look forward to more studies to come out of large-volume centers like CHOP or aggregated results from many centers to help figure out best practices for this rare but very complicated and often devastating malformation,” he said.
The three posters received no outside funding. The researchers had no financial conflicts to disclose. Dr. Joos had no financial conflicts to disclose, but he serves on the Editorial Advisory Board of Pediatric News.
WASHINGTON – Congenital diaphragmatic hernia affects many areas of pediatrics. In a trio of posters presented at the Pediatric Academic Societies annual meeting,
Initial ventilation mode shows little impact on NICU outcomes
In one study, K. Taylor Wild, MD, and colleagues investigated whether high-frequency oscillatory ventilation (HFOV) as an initial mode of ventilation in the delivery room improved gas exchange and neonatal ICU (NICU) outcomes in infants with congenital diaphragmatic hernia (CDH), compared with conventional mechanical ventilation (CMV). In 2019, HFOV became standard practice at CHOP.
The researchers reviewed data on infants with severe CDH who were born at CHOP between 2014 and 2022. Of these, 75 were placed on HFOV and 114 on CMV. The mean gestational age at birth in both groups was approximately 38 weeks, and the mean birth weight was approximately 3 kg.
Compared with CMV, use of HFOV in the delivery room was associated with significantly higher pH (7.05 vs. 7.16, P = .03) and significantly lower CO2 (85.2 vs. 64.5, P = .005). However, after adjusting for CDH severity, no significant differences appeared in length of stay and overall survival to discharge. The higher rates of extracorporeal membrane oxygenation (ECMO) use in the HFOV group, compared with the CMV group (48% vs. 29.9%), may reflect more severe disease, the researchers noted.
Prenatal brain immaturity associates with developmental delay
In a second study, Sandy Johng, MD, and colleagues found a significant association between prenatal brain immaturity in babies with CDH and developmental scores at age 12 months and older. The researchers reviewed data from a single-center patient registry for 48 infants for whom prenatal neuroimaging results were available. Based on the imaging, a fetal Total Maturation Score (fTMS) was generated and used as a measure of prenatal brain immaturity.
Results from the Bayley Scales of Infant Development-III (BSID-III) – a composite of cognitive, motor, and language scores – were available for 26 neonates at ages 12 months and under as well as at 12 months and older.
In a linear regression model, the researchers found a significant association between difference in fTMS and BSID-III composite language scores in infants 12 months and older. After adjusting for ECMO treatment, an increase in fTMS of one unit was associated with a 6.5-point increase in language scores at age 12 months and older (P < .01). No significant differences were observed between fTMS difference and language scores in infants under 12 months, or in cognitive or motor scores at any age, the researchers noted. The findings were limited by the small sample size, but the study is the first to show an association between prenatal imaging and neurodevelopmental outcomes for infants with CDH. Results suggest that the risk for neurodevelopmental impairment in this population may start in utero, the researchers concluded.
Antibiotic use stays stable
In a third study, Sabrina Flohr, MPH, and colleagues reviewed antibiotic use among infants with CDH who are at increased risk for infection. In many cases, distinguishing between infection and inherent clinical illness is challenging and may lead to unnecessarily high rates of antibiotic use, the researchers noted.
They reviewed data from 381 infants with CDH born at CHOP between January 2013 and November 2022 who were treated and survived in the NICU. Overall, 97.1% of the newborns received antibiotics for a median of 13 days. Nearly two-thirds (63.5%) received antibiotics in the first 72 hours, and 98.1% received them after 72 hours. Ampicillin and gentamicin were the antibiotics used most often in the first 72 hours (approximately 50% for both). After 72 hours, the most commonly used antibiotics were cefazolin (91.6%), vancomycin (67.7%), and cefepime (65.7%).
The results show that antibiotic use among newborns with CDH did not change significantly over time, and the choices of later antibiotics likely reflect perioperative prophylaxis and broad-spectrum treatment, the researchers noted.
Studies show larger trends
“These are three interesting studies regarding congenital diaphragmatic hernia from a center that does a high volume of repairs,” said Tim Joos, MD, a Seattle-based clinician with a combination internal medicine/pediatrics practice, in an interview.
“Each individual case can be consuming, but it is important to look for an aggregate of cases to see the larger trends in practices and outcomes,” said Dr. Joos, who was not involved in any of the studies.
The findings of the ventilation study surprised Dr. Joos. “Although high-frequency oscillatory ventilation improves initial gas exchange in the delivery room, compared with conventional mechanical ventilation, it was not associated with any larger NICU outcome,” he said. “This surprised me because my intuition would be that the HFOV would lead to less barotrauma and therefore better outcomes with the underformed lungs associated with this disorder.”
The imaging study demonstrates the need for more research on the association between CDH and neurologic outcomes, said Dr. Joos.
“Prenatal neuroimaging that shows delayed maturation with congenital diaphragmatic hernia correlates with lower language scores in early childhood, and suggests that this may be a predictor of neurologic outcome independent of the postnatal course,” he said.
Data from the antibiotics study reflect current trends, said Dr. Joos. “Antibiotics use is extremely common during the postnatal course of CDH and surgical repair,” he said. “The choice of antibiotics mirrors what we see in other neonatal conditions with regard to treatment for possible early neonatal sepsis, postsurgical prophylaxis, and later broad-spectrum empiric coverage,” he noted.
“I look forward to more studies to come out of large-volume centers like CHOP or aggregated results from many centers to help figure out best practices for this rare but very complicated and often devastating malformation,” he said.
The three posters received no outside funding. The researchers had no financial conflicts to disclose. Dr. Joos had no financial conflicts to disclose, but he serves on the Editorial Advisory Board of Pediatric News.
AT PAS 2023
CLL: Black patients die sooner than Whites
The findings, published in the American Journal of Hematology, hint that the racial disparity has shrunk over time, especially within the first few years of the targeted-therapy era. Still, “Black patients had a shorter median overall survival of 7 years compared to 9 years for White patients,” study coauthor Deborah Stephens, DO, of the University of Utah Huntsman Cancer Institute, said in an interview. “Clearly, more research is needed to tease out the biologic or economic barriers to achieving prolonged survival.”
As the researchers noted, CLL is far more common among White patients (5.1 cases per 100,000) than other races (Black patients: 3.2 cases per 100,000; Hispanic patients: 2.1 cases per 100,000; Asian American patients: 1.1 per 100,000). In total, non-White patients make up just 11%-13% of CLL cases in the United States.
According to Dr. Stephens, “little is known or published” about Black patients with CLL, “and it is still a mystery why fewer patients that are Black develop CLL and why this group would have shorter survival.”
Dr. Stephens and colleagues launched the new study – the largest of its kind to date – to understand disparities between White and Black patients over most of the past 20 years. The researchers especially wanted to analyze trends during the last decade, when targeted therapies revolutionized treatment of the disease.
The study authors analyzed data in the National Cancer Database for 97,804 patients diagnosed from 2004 to 2018 (90.7% White, 7.6% Black, 0.6% Asian, 1.1% other). Of patients who reported ethnicity (n = 93,555), 2.6% were Hispanic.
Black patients were more likely to have begun CLL therapy at diagnosis (35.9%) than were White patients (23.6%), a sign that Black patients had more advanced disease. Black patients also had shorter overall survival (7.0 years, 95% confidence interval [CI], 6.7–7.3 years) vs. White patients (9.1 years, 95% CI, 9.0–9.3 years, P < .001).
“This finding could be due to underlying biologic differences in the pathology of CLL, when comparing patients across racial groups,” Dr. Stephens said. “Additionally, there could be differences in access to care. Notably, there are fewer racial minorities enrolled in clinical trials, and perhaps we are not individualizing therapy for unique biologic factors seen in CLL affecting racial minorities.”
Other factors also could be at play. Black patients were more likely than were White patients to have one or more comorbidities (27.9% vs. 21.3%, P < .001), lack insurance (6.6% vs. 2.1%, P < .001) and live in lower-income neighborhoods (47.7% vs. 13.1%, P < .001).
What explains the gap in outcomes? In an interview, study lead author Victoria Vardell, MD, of the University of Utah, Salt Lake City, noted that researchers often attribute worse medical outcomes in Black patients to economic and social disparities.
“However, when we adjusted for a number of surrogate markers of health care access, including income, comorbidities, and location, among others, this disparity remained. That indicates that this may be a more complex problem in CLL in particular. Certainly, we cannot adjust for all the socioeconomic strain placed on Black Americans, including those with CLL, but there may be molecular features related to ancestry or environmental exposures that also play a role,” Dr. Vardell said.
She added that “the high cost and difficulty obtaining many novel therapies, particularly in the clinical trial setting, places significantly higher burdens on already disadvantaged populations.”
There is some good news in the new report. “Promisingly, our data suggest that the survival disparity between White and Black patients with CLL may be improving, particularly within the last 5 years, though longer follow-up is needed to confirm significance,” the researchers reported.
Alessandra Ferrajoli, MD, of M.D. Anderson Cancer Center, Houston, who has studied racial disparities in CLL, praised the study in an interview. As she noted, it examines an impressively large population.
The explanations for the disparities are still elusive, she said, although it seems clear there are multiple factors at play. “We don’t know if the disease has the same characteristics in African-Americans as in Whites,” Dr. Ferrajoli said. However, she noted, there’s “no indication that the response to treatment is different according to race.”
Moving forward, she said, the study findings “reinforce the fact that we need to pay attention to this population and be quite attentive to their characteristics.”
No study funding was reported. The authors and Dr. Ferrajoli have no disclosures.
The findings, published in the American Journal of Hematology, hint that the racial disparity has shrunk over time, especially within the first few years of the targeted-therapy era. Still, “Black patients had a shorter median overall survival of 7 years compared to 9 years for White patients,” study coauthor Deborah Stephens, DO, of the University of Utah Huntsman Cancer Institute, said in an interview. “Clearly, more research is needed to tease out the biologic or economic barriers to achieving prolonged survival.”
As the researchers noted, CLL is far more common among White patients (5.1 cases per 100,000) than other races (Black patients: 3.2 cases per 100,000; Hispanic patients: 2.1 cases per 100,000; Asian American patients: 1.1 per 100,000). In total, non-White patients make up just 11%-13% of CLL cases in the United States.
According to Dr. Stephens, “little is known or published” about Black patients with CLL, “and it is still a mystery why fewer patients that are Black develop CLL and why this group would have shorter survival.”
Dr. Stephens and colleagues launched the new study – the largest of its kind to date – to understand disparities between White and Black patients over most of the past 20 years. The researchers especially wanted to analyze trends during the last decade, when targeted therapies revolutionized treatment of the disease.
The study authors analyzed data in the National Cancer Database for 97,804 patients diagnosed from 2004 to 2018 (90.7% White, 7.6% Black, 0.6% Asian, 1.1% other). Of patients who reported ethnicity (n = 93,555), 2.6% were Hispanic.
Black patients were more likely to have begun CLL therapy at diagnosis (35.9%) than were White patients (23.6%), a sign that Black patients had more advanced disease. Black patients also had shorter overall survival (7.0 years, 95% confidence interval [CI], 6.7–7.3 years) vs. White patients (9.1 years, 95% CI, 9.0–9.3 years, P < .001).
“This finding could be due to underlying biologic differences in the pathology of CLL, when comparing patients across racial groups,” Dr. Stephens said. “Additionally, there could be differences in access to care. Notably, there are fewer racial minorities enrolled in clinical trials, and perhaps we are not individualizing therapy for unique biologic factors seen in CLL affecting racial minorities.”
Other factors also could be at play. Black patients were more likely than were White patients to have one or more comorbidities (27.9% vs. 21.3%, P < .001), lack insurance (6.6% vs. 2.1%, P < .001) and live in lower-income neighborhoods (47.7% vs. 13.1%, P < .001).
What explains the gap in outcomes? In an interview, study lead author Victoria Vardell, MD, of the University of Utah, Salt Lake City, noted that researchers often attribute worse medical outcomes in Black patients to economic and social disparities.
“However, when we adjusted for a number of surrogate markers of health care access, including income, comorbidities, and location, among others, this disparity remained. That indicates that this may be a more complex problem in CLL in particular. Certainly, we cannot adjust for all the socioeconomic strain placed on Black Americans, including those with CLL, but there may be molecular features related to ancestry or environmental exposures that also play a role,” Dr. Vardell said.
She added that “the high cost and difficulty obtaining many novel therapies, particularly in the clinical trial setting, places significantly higher burdens on already disadvantaged populations.”
There is some good news in the new report. “Promisingly, our data suggest that the survival disparity between White and Black patients with CLL may be improving, particularly within the last 5 years, though longer follow-up is needed to confirm significance,” the researchers reported.
Alessandra Ferrajoli, MD, of M.D. Anderson Cancer Center, Houston, who has studied racial disparities in CLL, praised the study in an interview. As she noted, it examines an impressively large population.
The explanations for the disparities are still elusive, she said, although it seems clear there are multiple factors at play. “We don’t know if the disease has the same characteristics in African-Americans as in Whites,” Dr. Ferrajoli said. However, she noted, there’s “no indication that the response to treatment is different according to race.”
Moving forward, she said, the study findings “reinforce the fact that we need to pay attention to this population and be quite attentive to their characteristics.”
No study funding was reported. The authors and Dr. Ferrajoli have no disclosures.
The findings, published in the American Journal of Hematology, hint that the racial disparity has shrunk over time, especially within the first few years of the targeted-therapy era. Still, “Black patients had a shorter median overall survival of 7 years compared to 9 years for White patients,” study coauthor Deborah Stephens, DO, of the University of Utah Huntsman Cancer Institute, said in an interview. “Clearly, more research is needed to tease out the biologic or economic barriers to achieving prolonged survival.”
As the researchers noted, CLL is far more common among White patients (5.1 cases per 100,000) than other races (Black patients: 3.2 cases per 100,000; Hispanic patients: 2.1 cases per 100,000; Asian American patients: 1.1 per 100,000). In total, non-White patients make up just 11%-13% of CLL cases in the United States.
According to Dr. Stephens, “little is known or published” about Black patients with CLL, “and it is still a mystery why fewer patients that are Black develop CLL and why this group would have shorter survival.”
Dr. Stephens and colleagues launched the new study – the largest of its kind to date – to understand disparities between White and Black patients over most of the past 20 years. The researchers especially wanted to analyze trends during the last decade, when targeted therapies revolutionized treatment of the disease.
The study authors analyzed data in the National Cancer Database for 97,804 patients diagnosed from 2004 to 2018 (90.7% White, 7.6% Black, 0.6% Asian, 1.1% other). Of patients who reported ethnicity (n = 93,555), 2.6% were Hispanic.
Black patients were more likely to have begun CLL therapy at diagnosis (35.9%) than were White patients (23.6%), a sign that Black patients had more advanced disease. Black patients also had shorter overall survival (7.0 years, 95% confidence interval [CI], 6.7–7.3 years) vs. White patients (9.1 years, 95% CI, 9.0–9.3 years, P < .001).
“This finding could be due to underlying biologic differences in the pathology of CLL, when comparing patients across racial groups,” Dr. Stephens said. “Additionally, there could be differences in access to care. Notably, there are fewer racial minorities enrolled in clinical trials, and perhaps we are not individualizing therapy for unique biologic factors seen in CLL affecting racial minorities.”
Other factors also could be at play. Black patients were more likely than were White patients to have one or more comorbidities (27.9% vs. 21.3%, P < .001), lack insurance (6.6% vs. 2.1%, P < .001) and live in lower-income neighborhoods (47.7% vs. 13.1%, P < .001).
What explains the gap in outcomes? In an interview, study lead author Victoria Vardell, MD, of the University of Utah, Salt Lake City, noted that researchers often attribute worse medical outcomes in Black patients to economic and social disparities.
“However, when we adjusted for a number of surrogate markers of health care access, including income, comorbidities, and location, among others, this disparity remained. That indicates that this may be a more complex problem in CLL in particular. Certainly, we cannot adjust for all the socioeconomic strain placed on Black Americans, including those with CLL, but there may be molecular features related to ancestry or environmental exposures that also play a role,” Dr. Vardell said.
She added that “the high cost and difficulty obtaining many novel therapies, particularly in the clinical trial setting, places significantly higher burdens on already disadvantaged populations.”
There is some good news in the new report. “Promisingly, our data suggest that the survival disparity between White and Black patients with CLL may be improving, particularly within the last 5 years, though longer follow-up is needed to confirm significance,” the researchers reported.
Alessandra Ferrajoli, MD, of M.D. Anderson Cancer Center, Houston, who has studied racial disparities in CLL, praised the study in an interview. As she noted, it examines an impressively large population.
The explanations for the disparities are still elusive, she said, although it seems clear there are multiple factors at play. “We don’t know if the disease has the same characteristics in African-Americans as in Whites,” Dr. Ferrajoli said. However, she noted, there’s “no indication that the response to treatment is different according to race.”
Moving forward, she said, the study findings “reinforce the fact that we need to pay attention to this population and be quite attentive to their characteristics.”
No study funding was reported. The authors and Dr. Ferrajoli have no disclosures.
FROM AMERICAN JOURNAL OF HEMATOLOGY
CRC screening rates are higher in Medicaid expansion states
CHICAGO – presented on May 6 in Chicago at the annual Digestive Disease Week®.
Researchers from the University of California, Los Angeles, reported that states with expanded Medicaid coverage had significantly higher rates of colorectal cancer (CRC) screening than states where officials refused federal support for Medicaid expansion.
Led by Megan R. McLeod, MD, an internal medicine resident at the University of California, Los Angeles, researchers compared CRC screening rates in states that did not adopt Medicaid expansion in 2021 with screening rates in states that invested Medicaid expansion into 1,284 Federally Qualified Health Centers, which are nonprofit health centers or clinics that serve medically underserved areas and populations. In this study, 76% of these centers were in states that accepted Medicaid expansion. The median colorectal cancer screening rate was 42.1% in Medicaid expansion states, compared with 36.5% in nonexpansion states
“The impact of being uninsured on CRC screening participation was profound in nonexpansion states,” said Dr. McLeod, who will be a UCLA gastroenterology fellow this year.
The study adds to a growing body of evidence that shows Medicaid expansion, which increases access to health care services to previously uninsured or underinsured patients, can improve health outcomes and may reduce racial and economic disparities.
For example, a 2019 study based on electronic health record data presented at the annual meeting of the American Society of Clinical Oncology showed that, after Medicaid expansion, racial differences in timely cancer treatment effectively disappeared. Before Medicaid expansion, Black patients were 4.8% less likely than White patients to receive timely cancer treatment, which is defined as treatment starting within 30 days of the diagnosis of an advanced or metastatic solid tumor. After Medicaid expansion, however, the difference between the racial groups dwindled to 0.8% and was no longer statistically significant.
Researchers at Weill Cornell Medical Center in New York reported in 2020 at the virtual annual meeting of the American Association for the Study of Liver Diseases that, 1 year after Medicaid expansion began on Jan. 1, 2014, the rate of liver-related mortality began to decline in 18 states with expanded coverage, whereas the rate of liver-related deaths continued to climb in 14 states that did not expand Medicaid.
The U.S. Health Resources and Services Administration funds Federally Qualified Health Centers (FQHC) that serve nearly 29 million patients throughout the country, including a large proportion whose care is covered by Medicaid. Among patients cared for in these centers, one in three have incomes below the federal poverty line, and one in five are uninsured.
Screening rates compared
Dr. McLeod and colleagues sought to determine whether Medicaid expansion would have an effect on CRC screening rates at these centers. The final analysis included 6,940,879 patients (between 50 and 74 years), of whom 1.7% were unhoused and 17.6% were uninsured.
Medicaid expansion status appeared to have a direct impact on whether screenings were even offered to patients. Centers in rural areas and those with a high proportion of uninsured patients were found to have significantly higher odds for doing fewer CRC screenings. In Medicaid expansion states, CRC screening rates were significantly lower for patients who were male, Black, Hispanic, had low income, were unhoused, or were uninsured.
In a Q&A that followed the presentation, Steven Itzkowitz, MD, director of the GI fellowship program at the Icahn School of Medicine at Mount Sinai, New York, suggested the type of CRC test patients are offered is directly related to Medicaid expansion status.
“In New York, before Cologuard (a colon and rectal cancer screening test) was covered by Medicaid, it wasn’t used very much, but once it got paid for by Medicaid, rates went up,” he said.
The study was internally supported. Dr. McLeod reported no conflicts of interest. Dr. Itzkowitz has been a consultant for Exact Sciences, the maker of Cologuard.
DDW is sponsored by the American Gastroenterological Association, the American Association for the Study of Liver Diseases, the American Society for Gastrointestinal Endoscopy, and the Society for Surgery of the Alimentary Tract.
CHICAGO – presented on May 6 in Chicago at the annual Digestive Disease Week®.
Researchers from the University of California, Los Angeles, reported that states with expanded Medicaid coverage had significantly higher rates of colorectal cancer (CRC) screening than states where officials refused federal support for Medicaid expansion.
Led by Megan R. McLeod, MD, an internal medicine resident at the University of California, Los Angeles, researchers compared CRC screening rates in states that did not adopt Medicaid expansion in 2021 with screening rates in states that invested Medicaid expansion into 1,284 Federally Qualified Health Centers, which are nonprofit health centers or clinics that serve medically underserved areas and populations. In this study, 76% of these centers were in states that accepted Medicaid expansion. The median colorectal cancer screening rate was 42.1% in Medicaid expansion states, compared with 36.5% in nonexpansion states
“The impact of being uninsured on CRC screening participation was profound in nonexpansion states,” said Dr. McLeod, who will be a UCLA gastroenterology fellow this year.
The study adds to a growing body of evidence that shows Medicaid expansion, which increases access to health care services to previously uninsured or underinsured patients, can improve health outcomes and may reduce racial and economic disparities.
For example, a 2019 study based on electronic health record data presented at the annual meeting of the American Society of Clinical Oncology showed that, after Medicaid expansion, racial differences in timely cancer treatment effectively disappeared. Before Medicaid expansion, Black patients were 4.8% less likely than White patients to receive timely cancer treatment, which is defined as treatment starting within 30 days of the diagnosis of an advanced or metastatic solid tumor. After Medicaid expansion, however, the difference between the racial groups dwindled to 0.8% and was no longer statistically significant.
Researchers at Weill Cornell Medical Center in New York reported in 2020 at the virtual annual meeting of the American Association for the Study of Liver Diseases that, 1 year after Medicaid expansion began on Jan. 1, 2014, the rate of liver-related mortality began to decline in 18 states with expanded coverage, whereas the rate of liver-related deaths continued to climb in 14 states that did not expand Medicaid.
The U.S. Health Resources and Services Administration funds Federally Qualified Health Centers (FQHC) that serve nearly 29 million patients throughout the country, including a large proportion whose care is covered by Medicaid. Among patients cared for in these centers, one in three have incomes below the federal poverty line, and one in five are uninsured.
Screening rates compared
Dr. McLeod and colleagues sought to determine whether Medicaid expansion would have an effect on CRC screening rates at these centers. The final analysis included 6,940,879 patients (between 50 and 74 years), of whom 1.7% were unhoused and 17.6% were uninsured.
Medicaid expansion status appeared to have a direct impact on whether screenings were even offered to patients. Centers in rural areas and those with a high proportion of uninsured patients were found to have significantly higher odds for doing fewer CRC screenings. In Medicaid expansion states, CRC screening rates were significantly lower for patients who were male, Black, Hispanic, had low income, were unhoused, or were uninsured.
In a Q&A that followed the presentation, Steven Itzkowitz, MD, director of the GI fellowship program at the Icahn School of Medicine at Mount Sinai, New York, suggested the type of CRC test patients are offered is directly related to Medicaid expansion status.
“In New York, before Cologuard (a colon and rectal cancer screening test) was covered by Medicaid, it wasn’t used very much, but once it got paid for by Medicaid, rates went up,” he said.
The study was internally supported. Dr. McLeod reported no conflicts of interest. Dr. Itzkowitz has been a consultant for Exact Sciences, the maker of Cologuard.
DDW is sponsored by the American Gastroenterological Association, the American Association for the Study of Liver Diseases, the American Society for Gastrointestinal Endoscopy, and the Society for Surgery of the Alimentary Tract.
CHICAGO – presented on May 6 in Chicago at the annual Digestive Disease Week®.
Researchers from the University of California, Los Angeles, reported that states with expanded Medicaid coverage had significantly higher rates of colorectal cancer (CRC) screening than states where officials refused federal support for Medicaid expansion.
Led by Megan R. McLeod, MD, an internal medicine resident at the University of California, Los Angeles, researchers compared CRC screening rates in states that did not adopt Medicaid expansion in 2021 with screening rates in states that invested Medicaid expansion into 1,284 Federally Qualified Health Centers, which are nonprofit health centers or clinics that serve medically underserved areas and populations. In this study, 76% of these centers were in states that accepted Medicaid expansion. The median colorectal cancer screening rate was 42.1% in Medicaid expansion states, compared with 36.5% in nonexpansion states
“The impact of being uninsured on CRC screening participation was profound in nonexpansion states,” said Dr. McLeod, who will be a UCLA gastroenterology fellow this year.
The study adds to a growing body of evidence that shows Medicaid expansion, which increases access to health care services to previously uninsured or underinsured patients, can improve health outcomes and may reduce racial and economic disparities.
For example, a 2019 study based on electronic health record data presented at the annual meeting of the American Society of Clinical Oncology showed that, after Medicaid expansion, racial differences in timely cancer treatment effectively disappeared. Before Medicaid expansion, Black patients were 4.8% less likely than White patients to receive timely cancer treatment, which is defined as treatment starting within 30 days of the diagnosis of an advanced or metastatic solid tumor. After Medicaid expansion, however, the difference between the racial groups dwindled to 0.8% and was no longer statistically significant.
Researchers at Weill Cornell Medical Center in New York reported in 2020 at the virtual annual meeting of the American Association for the Study of Liver Diseases that, 1 year after Medicaid expansion began on Jan. 1, 2014, the rate of liver-related mortality began to decline in 18 states with expanded coverage, whereas the rate of liver-related deaths continued to climb in 14 states that did not expand Medicaid.
The U.S. Health Resources and Services Administration funds Federally Qualified Health Centers (FQHC) that serve nearly 29 million patients throughout the country, including a large proportion whose care is covered by Medicaid. Among patients cared for in these centers, one in three have incomes below the federal poverty line, and one in five are uninsured.
Screening rates compared
Dr. McLeod and colleagues sought to determine whether Medicaid expansion would have an effect on CRC screening rates at these centers. The final analysis included 6,940,879 patients (between 50 and 74 years), of whom 1.7% were unhoused and 17.6% were uninsured.
Medicaid expansion status appeared to have a direct impact on whether screenings were even offered to patients. Centers in rural areas and those with a high proportion of uninsured patients were found to have significantly higher odds for doing fewer CRC screenings. In Medicaid expansion states, CRC screening rates were significantly lower for patients who were male, Black, Hispanic, had low income, were unhoused, or were uninsured.
In a Q&A that followed the presentation, Steven Itzkowitz, MD, director of the GI fellowship program at the Icahn School of Medicine at Mount Sinai, New York, suggested the type of CRC test patients are offered is directly related to Medicaid expansion status.
“In New York, before Cologuard (a colon and rectal cancer screening test) was covered by Medicaid, it wasn’t used very much, but once it got paid for by Medicaid, rates went up,” he said.
The study was internally supported. Dr. McLeod reported no conflicts of interest. Dr. Itzkowitz has been a consultant for Exact Sciences, the maker of Cologuard.
DDW is sponsored by the American Gastroenterological Association, the American Association for the Study of Liver Diseases, the American Society for Gastrointestinal Endoscopy, and the Society for Surgery of the Alimentary Tract.
AT DDW 2023
Familial cancer risk complex, not limited to same site
The researchers found, for instance, that children of breast cancer patients had a 27% higher risk of any discordant early-onset cancer, and patients’ siblings had a 7.6-fold higher risk of early pancreatic cancer. The analysis also indicated that children of patients’ siblings had a significantly increased risk of testicular and ovarian cancers.
“The findings suggest that the familial risk extends to discordant early-onset cancers, including ovarian, testicular, and pancreatic cancers, as well as beyond first-degree relatives,” the researchers, led by Janne M. Pitkäniemi, PhD, Finnish Cancer Registry, Institute for Statistical and Epidemiological Cancer Research, Helsinki, say. “Our findings are interesting but raise some questions about unknown [genetic] and environmental mechanisms that need to be further studied.”
Erin F. Cobain, MD, who was not involved in the research, said the findings are “not very surprising to me.”
Dr. Cobain said that at her institution, she has seen “many, many cases” of family members of early-onset breast cancer patients with discordant cancers “where we are unable to find a clear genetic cause.”
Not being able to find an identifiable cause for the clustering of early-onset cancers can be “very frustrating” for patients and their families, said Dr. Cobain, a medical oncologist at the University of Michigan Health, Ann Arbor.
The study was published online in the International Journal of Cancer.
Family members of patients with early-onset breast cancer are at elevated risk for early-onset breast cancer. However, it is “unclear whether the familial risk is limited to early-onset cancer of the same site,” the authors explained.
To investigate, the researchers studied data from the Finnish Cancer Registry and the Finnish Population System, which included 54,753 relatives from 5,562 families of females diagnosed with early-onset breast cancer, defined as probands. A proband was the first member of the family diagnosed with female breast cancer at age 40 years or younger in Finland between January 1970 and December 31, 2012. Cancers were considered familial if they occurred in a family with a previously diagnosed proband and were deemed early onset if diagnosed before age 41.
The researchers found that only 5.5% of probands’ families had a family member with a discordant early-onset cancer. The most common diagnoses were testicular cancer (0.6% of families) and cancer of the thyroid gland (also 0.6%), followed by melanoma (0.5%).
Overall, the risk of any nonbreast early-onset cancer among first-degree relatives of probands was comparable with the risk in the general population (standardized incidence ratio, 0.99; 95% confidence interval, 0.84-1.16).
However, the risk was elevated for certain family members and certain cancers.
Specifically, the children of probands had an increased risk for any discordant cancer (SIR, 1.27; 95% CI, 1.05-1.55).
The siblings of probands had an elevated risk for early-onset pancreatic cancer (SIR, 7.61) but not overall for any discordant cancer (SIR, 0.93; 95% CI, 0.68-1.25).
And siblings’ children faced an elevated risk for testicular (SIR, 1.74) and ovarian (SIR, 2.69) cancer, though not of any discordant cancer (SIR, 1.16; 95% CI, 0.97-1.37).
The researchers also found that the fathers (SIR, 0.43), mothers (SIR, 0.48), and spouses (SIR, 0.58) of probands appeared to have a decreased risk of any discordant early-onset cancer.
A potential limitation to the study was that the authors could not identify individuals with hereditary cancer syndromes or concerning gene mutations, such as BRCA carriers, because “registry data do not include comprehensive information on the gene mutation carriage status.” But the authors note that the number of BRCA carriers is likely low because of the low number of ovarian cancers observed in first-degree relatives of probands.
Dr. Cobain noted as well that the current study is potentially limited by its “very homogeneous” cohort.
But, overall, the findings indicate that familial risk is often “a much more complicated problem, mathematically and statistically,” than were there a single genetic culprit, Dr. Cobain said. One possibility is that some shared environmental exposure may be increasing the cancer risk among members of the same family.
“Genetic diversity is so vast and understanding how the interplay of multiple genes can influence an individual’s cancer risk is so much more complicated than a single BRCA1 mutation that clearly influences your breast cancer risk,” she added. However, “we’re starting to get there.”
The study was funded by the Cancer Foundation Finland and Academy of Finland. The authors and Dr. Cobain had no relevant financial relationships to declare.
A version of this article originally appeared on Medscape.com.
The researchers found, for instance, that children of breast cancer patients had a 27% higher risk of any discordant early-onset cancer, and patients’ siblings had a 7.6-fold higher risk of early pancreatic cancer. The analysis also indicated that children of patients’ siblings had a significantly increased risk of testicular and ovarian cancers.
“The findings suggest that the familial risk extends to discordant early-onset cancers, including ovarian, testicular, and pancreatic cancers, as well as beyond first-degree relatives,” the researchers, led by Janne M. Pitkäniemi, PhD, Finnish Cancer Registry, Institute for Statistical and Epidemiological Cancer Research, Helsinki, say. “Our findings are interesting but raise some questions about unknown [genetic] and environmental mechanisms that need to be further studied.”
Erin F. Cobain, MD, who was not involved in the research, said the findings are “not very surprising to me.”
Dr. Cobain said that at her institution, she has seen “many, many cases” of family members of early-onset breast cancer patients with discordant cancers “where we are unable to find a clear genetic cause.”
Not being able to find an identifiable cause for the clustering of early-onset cancers can be “very frustrating” for patients and their families, said Dr. Cobain, a medical oncologist at the University of Michigan Health, Ann Arbor.
The study was published online in the International Journal of Cancer.
Family members of patients with early-onset breast cancer are at elevated risk for early-onset breast cancer. However, it is “unclear whether the familial risk is limited to early-onset cancer of the same site,” the authors explained.
To investigate, the researchers studied data from the Finnish Cancer Registry and the Finnish Population System, which included 54,753 relatives from 5,562 families of females diagnosed with early-onset breast cancer, defined as probands. A proband was the first member of the family diagnosed with female breast cancer at age 40 years or younger in Finland between January 1970 and December 31, 2012. Cancers were considered familial if they occurred in a family with a previously diagnosed proband and were deemed early onset if diagnosed before age 41.
The researchers found that only 5.5% of probands’ families had a family member with a discordant early-onset cancer. The most common diagnoses were testicular cancer (0.6% of families) and cancer of the thyroid gland (also 0.6%), followed by melanoma (0.5%).
Overall, the risk of any nonbreast early-onset cancer among first-degree relatives of probands was comparable with the risk in the general population (standardized incidence ratio, 0.99; 95% confidence interval, 0.84-1.16).
However, the risk was elevated for certain family members and certain cancers.
Specifically, the children of probands had an increased risk for any discordant cancer (SIR, 1.27; 95% CI, 1.05-1.55).
The siblings of probands had an elevated risk for early-onset pancreatic cancer (SIR, 7.61) but not overall for any discordant cancer (SIR, 0.93; 95% CI, 0.68-1.25).
And siblings’ children faced an elevated risk for testicular (SIR, 1.74) and ovarian (SIR, 2.69) cancer, though not of any discordant cancer (SIR, 1.16; 95% CI, 0.97-1.37).
The researchers also found that the fathers (SIR, 0.43), mothers (SIR, 0.48), and spouses (SIR, 0.58) of probands appeared to have a decreased risk of any discordant early-onset cancer.
A potential limitation to the study was that the authors could not identify individuals with hereditary cancer syndromes or concerning gene mutations, such as BRCA carriers, because “registry data do not include comprehensive information on the gene mutation carriage status.” But the authors note that the number of BRCA carriers is likely low because of the low number of ovarian cancers observed in first-degree relatives of probands.
Dr. Cobain noted as well that the current study is potentially limited by its “very homogeneous” cohort.
But, overall, the findings indicate that familial risk is often “a much more complicated problem, mathematically and statistically,” than were there a single genetic culprit, Dr. Cobain said. One possibility is that some shared environmental exposure may be increasing the cancer risk among members of the same family.
“Genetic diversity is so vast and understanding how the interplay of multiple genes can influence an individual’s cancer risk is so much more complicated than a single BRCA1 mutation that clearly influences your breast cancer risk,” she added. However, “we’re starting to get there.”
The study was funded by the Cancer Foundation Finland and Academy of Finland. The authors and Dr. Cobain had no relevant financial relationships to declare.
A version of this article originally appeared on Medscape.com.
The researchers found, for instance, that children of breast cancer patients had a 27% higher risk of any discordant early-onset cancer, and patients’ siblings had a 7.6-fold higher risk of early pancreatic cancer. The analysis also indicated that children of patients’ siblings had a significantly increased risk of testicular and ovarian cancers.
“The findings suggest that the familial risk extends to discordant early-onset cancers, including ovarian, testicular, and pancreatic cancers, as well as beyond first-degree relatives,” the researchers, led by Janne M. Pitkäniemi, PhD, Finnish Cancer Registry, Institute for Statistical and Epidemiological Cancer Research, Helsinki, say. “Our findings are interesting but raise some questions about unknown [genetic] and environmental mechanisms that need to be further studied.”
Erin F. Cobain, MD, who was not involved in the research, said the findings are “not very surprising to me.”
Dr. Cobain said that at her institution, she has seen “many, many cases” of family members of early-onset breast cancer patients with discordant cancers “where we are unable to find a clear genetic cause.”
Not being able to find an identifiable cause for the clustering of early-onset cancers can be “very frustrating” for patients and their families, said Dr. Cobain, a medical oncologist at the University of Michigan Health, Ann Arbor.
The study was published online in the International Journal of Cancer.
Family members of patients with early-onset breast cancer are at elevated risk for early-onset breast cancer. However, it is “unclear whether the familial risk is limited to early-onset cancer of the same site,” the authors explained.
To investigate, the researchers studied data from the Finnish Cancer Registry and the Finnish Population System, which included 54,753 relatives from 5,562 families of females diagnosed with early-onset breast cancer, defined as probands. A proband was the first member of the family diagnosed with female breast cancer at age 40 years or younger in Finland between January 1970 and December 31, 2012. Cancers were considered familial if they occurred in a family with a previously diagnosed proband and were deemed early onset if diagnosed before age 41.
The researchers found that only 5.5% of probands’ families had a family member with a discordant early-onset cancer. The most common diagnoses were testicular cancer (0.6% of families) and cancer of the thyroid gland (also 0.6%), followed by melanoma (0.5%).
Overall, the risk of any nonbreast early-onset cancer among first-degree relatives of probands was comparable with the risk in the general population (standardized incidence ratio, 0.99; 95% confidence interval, 0.84-1.16).
However, the risk was elevated for certain family members and certain cancers.
Specifically, the children of probands had an increased risk for any discordant cancer (SIR, 1.27; 95% CI, 1.05-1.55).
The siblings of probands had an elevated risk for early-onset pancreatic cancer (SIR, 7.61) but not overall for any discordant cancer (SIR, 0.93; 95% CI, 0.68-1.25).
And siblings’ children faced an elevated risk for testicular (SIR, 1.74) and ovarian (SIR, 2.69) cancer, though not of any discordant cancer (SIR, 1.16; 95% CI, 0.97-1.37).
The researchers also found that the fathers (SIR, 0.43), mothers (SIR, 0.48), and spouses (SIR, 0.58) of probands appeared to have a decreased risk of any discordant early-onset cancer.
A potential limitation to the study was that the authors could not identify individuals with hereditary cancer syndromes or concerning gene mutations, such as BRCA carriers, because “registry data do not include comprehensive information on the gene mutation carriage status.” But the authors note that the number of BRCA carriers is likely low because of the low number of ovarian cancers observed in first-degree relatives of probands.
Dr. Cobain noted as well that the current study is potentially limited by its “very homogeneous” cohort.
But, overall, the findings indicate that familial risk is often “a much more complicated problem, mathematically and statistically,” than were there a single genetic culprit, Dr. Cobain said. One possibility is that some shared environmental exposure may be increasing the cancer risk among members of the same family.
“Genetic diversity is so vast and understanding how the interplay of multiple genes can influence an individual’s cancer risk is so much more complicated than a single BRCA1 mutation that clearly influences your breast cancer risk,” she added. However, “we’re starting to get there.”
The study was funded by the Cancer Foundation Finland and Academy of Finland. The authors and Dr. Cobain had no relevant financial relationships to declare.
A version of this article originally appeared on Medscape.com.
FROM INTERNATIONAL JOURNAL OF CANCER
Widespread prescribing of stimulants with other CNS-active meds
Investigators analyzed prescription drug claims for over 9.1 million U.S. adults over a 1-year period and found that 276,223 (3%) had used a schedule II stimulant, such as methylphenidate and amphetamines, during that time. Of these 276,223 patients, 45% combined these agents with one or more additional CNS-active drugs and almost 25% were simultaneously using two or more additional CNS-active drugs.
Close to half of the stimulant users were taking an antidepressant, while close to one-third filled prescriptions for anxiolytic/sedative/hypnotic meditations, and one-fifth received opioid prescriptions.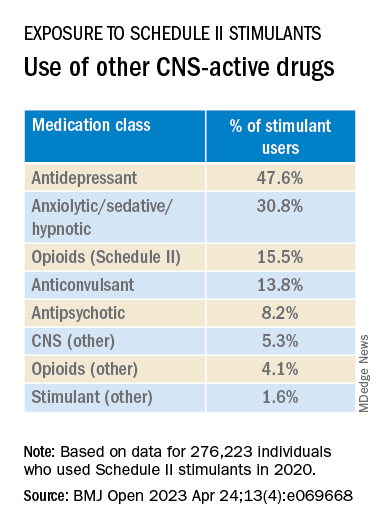
The widespread, often off-label use of these stimulants in combination therapy with antidepressants, anxiolytics, opioids, and other psychoactive drugs, “reveals new patterns of utilization beyond the approved use of stimulants as monotherapy for ADHD, but because there are so few studies of these kinds of combination therapy, both the advantages and additional risks [of this type of prescribing] remain unknown,” study investigator Thomas J. Moore, AB, faculty associate in epidemiology, Johns Hopkins Bloomberg School of Public Health and Johns Hopkins Medicine, Baltimore, told this news organization.
The study was published online in BMJ Open.
‘Dangerous’ substances
Amphetamines and methylphenidate are CNS stimulants that have been in use for almost a century. Like opioids and barbiturates, they’re considered “dangerous” and classified as schedule II Controlled Substances because of their high potential for abuse.
Over many years, these stimulants have been used for multiple purposes, including nasal congestion, narcolepsy, appetite suppression, binge eating, depression, senile behavior, lethargy, and ADHD, the researchers note.
Observational studies suggest medical use of these agents has been increasing in the United States. The investigators conducted previous research that revealed a 79% increase from 2013 to 2018 in the number of adults who self-report their use. The current study, said Mr. Moore, explores how these stimulants are being used.
For the study, data was extracted from the MarketScan 2019 and 2020 Commercial Claims and Encounters Databases, focusing on 9.1 million adults aged 19-64 years who were continuously enrolled in an included commercial benefit plan from Oct. 1, 2019 to Dec. 31, 2020.
The primary outcome consisted of an outpatient prescription claim, service date, and days’ supply for the CNS-active drugs.
The researchers defined “combination-2” therapy as 60 or more days of combination treatment with a schedule II stimulant and at least one additional CNS-active drug. “Combination-3” therapy was defined as the addition of at least two additional CNS-active drugs.
The researchers used service date and days’ supply to examine the number of stimulant and other CNS-active drugs for each of the days of 2020.
CNS-active drug classes included antidepressants, anxiolytics/sedatives/hypnotics, antipsychotics, opioids, anticonvulsants, and other CNS-active drugs.
Prescribing cascade
Of the total number of adults enrolled, 3% (n = 276,223) were taking schedule II stimulants during 2020, with a median of 8 (interquartile range, 4-11) prescriptions. These drugs provided 227 (IQR, 110-322) treatment days of exposure.
Among those taking stimulants 45.5% combined the use of at least one additional CNS-active drug for a median of 213 (IQR, 126-301) treatment days; and 24.3% used at least two additional CNS-active drugs for a median of 182 (IQR, 108-276) days.
“Clinicians should beware of the prescribing cascade. Sometimes it begins with an antidepressant that causes too much sedation, so a stimulant gets added, which leads to insomnia, so alprazolam gets added to the mix,” Mr. Moore said.
He cautioned that this “leaves a patient with multiple drugs, all with discontinuation effects of different kinds and clashing effects.”
These new findings, the investigators note, “add new public health concerns to those raised by our previous study. ... this more-detailed profile reveals several new patterns.”
Most patients become “long-term users” once treatment has started, with 75% continuing for a 1-year period.
“This underscores the possible risks of nonmedical use and dependence that have warranted the classification of these drugs as having high potential for psychological or physical dependence and their prominent appearance in toxicology drug rankings of fatal overdose cases,” they write.
They note that the data “do not indicate which intervention may have come first – a stimulant added to compensate for excess sedation from the benzodiazepine, or the alprazolam added to calm excessive CNS stimulation and/or insomnia from the stimulants or other drugs.”
Several limitations cited by the authors include the fact that, although the population encompassed 9.1 million people, it “may not represent all commercially insured adults,” and it doesn’t include people who aren’t covered by commercial insurance.
Moreover, the MarketScan dataset included up to four diagnosis codes for each outpatient and emergency department encounter; therefore, it was not possible to directly link the diagnoses to specific prescription drug claims, and thus the diagnoses were not evaluated.
“Since many providers will not accept a drug claim for a schedule II stimulant without an on-label diagnosis of ADHD,” the authors suspect that “large numbers of this diagnosis were present.”
Complex prescribing regimens
Mark Olfson, MD, MPH, professor of psychiatry, medicine, and law and professor of epidemiology, Columbia University Irving Medical Center, New York, said the report “highlights the pharmacological complexity of adults who are treated with stimulants.”

Dr. Olfson, who is a research psychiatrist at the New York State Psychiatric Institute, New York, and was not involved with the study, observed there is “evidence to support stimulants as an adjunctive therapy for treatment-resistant unipolar depression in older adults.”
However, he added, “this indication is unlikely to fully explain the high proportion of nonelderly, stimulant-treated adults who also receive antidepressants.”
These new findings “call for research to increase our understanding of the clinical contexts that motivate these complex prescribing regimens as well as their effectiveness and safety,” said Dr. Olfson.
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors. Mr. Moore declares no relevant financial relationships. Coauthor G. Caleb Alexander, MD, is past chair and a current member of the Food and Drug Administration’s Peripheral and Central Nervous System Advisory Committee; is a cofounding principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation, for whom he has served as a paid expert witness; and is a past member of OptumRx’s National P&T Committee. Dr. Olfson declares no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators analyzed prescription drug claims for over 9.1 million U.S. adults over a 1-year period and found that 276,223 (3%) had used a schedule II stimulant, such as methylphenidate and amphetamines, during that time. Of these 276,223 patients, 45% combined these agents with one or more additional CNS-active drugs and almost 25% were simultaneously using two or more additional CNS-active drugs.
Close to half of the stimulant users were taking an antidepressant, while close to one-third filled prescriptions for anxiolytic/sedative/hypnotic meditations, and one-fifth received opioid prescriptions.
The widespread, often off-label use of these stimulants in combination therapy with antidepressants, anxiolytics, opioids, and other psychoactive drugs, “reveals new patterns of utilization beyond the approved use of stimulants as monotherapy for ADHD, but because there are so few studies of these kinds of combination therapy, both the advantages and additional risks [of this type of prescribing] remain unknown,” study investigator Thomas J. Moore, AB, faculty associate in epidemiology, Johns Hopkins Bloomberg School of Public Health and Johns Hopkins Medicine, Baltimore, told this news organization.
The study was published online in BMJ Open.
‘Dangerous’ substances
Amphetamines and methylphenidate are CNS stimulants that have been in use for almost a century. Like opioids and barbiturates, they’re considered “dangerous” and classified as schedule II Controlled Substances because of their high potential for abuse.
Over many years, these stimulants have been used for multiple purposes, including nasal congestion, narcolepsy, appetite suppression, binge eating, depression, senile behavior, lethargy, and ADHD, the researchers note.
Observational studies suggest medical use of these agents has been increasing in the United States. The investigators conducted previous research that revealed a 79% increase from 2013 to 2018 in the number of adults who self-report their use. The current study, said Mr. Moore, explores how these stimulants are being used.
For the study, data was extracted from the MarketScan 2019 and 2020 Commercial Claims and Encounters Databases, focusing on 9.1 million adults aged 19-64 years who were continuously enrolled in an included commercial benefit plan from Oct. 1, 2019 to Dec. 31, 2020.
The primary outcome consisted of an outpatient prescription claim, service date, and days’ supply for the CNS-active drugs.
The researchers defined “combination-2” therapy as 60 or more days of combination treatment with a schedule II stimulant and at least one additional CNS-active drug. “Combination-3” therapy was defined as the addition of at least two additional CNS-active drugs.
The researchers used service date and days’ supply to examine the number of stimulant and other CNS-active drugs for each of the days of 2020.
CNS-active drug classes included antidepressants, anxiolytics/sedatives/hypnotics, antipsychotics, opioids, anticonvulsants, and other CNS-active drugs.
Prescribing cascade
Of the total number of adults enrolled, 3% (n = 276,223) were taking schedule II stimulants during 2020, with a median of 8 (interquartile range, 4-11) prescriptions. These drugs provided 227 (IQR, 110-322) treatment days of exposure.
Among those taking stimulants 45.5% combined the use of at least one additional CNS-active drug for a median of 213 (IQR, 126-301) treatment days; and 24.3% used at least two additional CNS-active drugs for a median of 182 (IQR, 108-276) days.
“Clinicians should beware of the prescribing cascade. Sometimes it begins with an antidepressant that causes too much sedation, so a stimulant gets added, which leads to insomnia, so alprazolam gets added to the mix,” Mr. Moore said.
He cautioned that this “leaves a patient with multiple drugs, all with discontinuation effects of different kinds and clashing effects.”
These new findings, the investigators note, “add new public health concerns to those raised by our previous study. ... this more-detailed profile reveals several new patterns.”
Most patients become “long-term users” once treatment has started, with 75% continuing for a 1-year period.
“This underscores the possible risks of nonmedical use and dependence that have warranted the classification of these drugs as having high potential for psychological or physical dependence and their prominent appearance in toxicology drug rankings of fatal overdose cases,” they write.
They note that the data “do not indicate which intervention may have come first – a stimulant added to compensate for excess sedation from the benzodiazepine, or the alprazolam added to calm excessive CNS stimulation and/or insomnia from the stimulants or other drugs.”
Several limitations cited by the authors include the fact that, although the population encompassed 9.1 million people, it “may not represent all commercially insured adults,” and it doesn’t include people who aren’t covered by commercial insurance.
Moreover, the MarketScan dataset included up to four diagnosis codes for each outpatient and emergency department encounter; therefore, it was not possible to directly link the diagnoses to specific prescription drug claims, and thus the diagnoses were not evaluated.
“Since many providers will not accept a drug claim for a schedule II stimulant without an on-label diagnosis of ADHD,” the authors suspect that “large numbers of this diagnosis were present.”
Complex prescribing regimens
Mark Olfson, MD, MPH, professor of psychiatry, medicine, and law and professor of epidemiology, Columbia University Irving Medical Center, New York, said the report “highlights the pharmacological complexity of adults who are treated with stimulants.”
Dr. Olfson, who is a research psychiatrist at the New York State Psychiatric Institute, New York, and was not involved with the study, observed there is “evidence to support stimulants as an adjunctive therapy for treatment-resistant unipolar depression in older adults.”
However, he added, “this indication is unlikely to fully explain the high proportion of nonelderly, stimulant-treated adults who also receive antidepressants.”
These new findings “call for research to increase our understanding of the clinical contexts that motivate these complex prescribing regimens as well as their effectiveness and safety,” said Dr. Olfson.
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors. Mr. Moore declares no relevant financial relationships. Coauthor G. Caleb Alexander, MD, is past chair and a current member of the Food and Drug Administration’s Peripheral and Central Nervous System Advisory Committee; is a cofounding principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation, for whom he has served as a paid expert witness; and is a past member of OptumRx’s National P&T Committee. Dr. Olfson declares no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators analyzed prescription drug claims for over 9.1 million U.S. adults over a 1-year period and found that 276,223 (3%) had used a schedule II stimulant, such as methylphenidate and amphetamines, during that time. Of these 276,223 patients, 45% combined these agents with one or more additional CNS-active drugs and almost 25% were simultaneously using two or more additional CNS-active drugs.
Close to half of the stimulant users were taking an antidepressant, while close to one-third filled prescriptions for anxiolytic/sedative/hypnotic meditations, and one-fifth received opioid prescriptions.
The widespread, often off-label use of these stimulants in combination therapy with antidepressants, anxiolytics, opioids, and other psychoactive drugs, “reveals new patterns of utilization beyond the approved use of stimulants as monotherapy for ADHD, but because there are so few studies of these kinds of combination therapy, both the advantages and additional risks [of this type of prescribing] remain unknown,” study investigator Thomas J. Moore, AB, faculty associate in epidemiology, Johns Hopkins Bloomberg School of Public Health and Johns Hopkins Medicine, Baltimore, told this news organization.
The study was published online in BMJ Open.
‘Dangerous’ substances
Amphetamines and methylphenidate are CNS stimulants that have been in use for almost a century. Like opioids and barbiturates, they’re considered “dangerous” and classified as schedule II Controlled Substances because of their high potential for abuse.
Over many years, these stimulants have been used for multiple purposes, including nasal congestion, narcolepsy, appetite suppression, binge eating, depression, senile behavior, lethargy, and ADHD, the researchers note.
Observational studies suggest medical use of these agents has been increasing in the United States. The investigators conducted previous research that revealed a 79% increase from 2013 to 2018 in the number of adults who self-report their use. The current study, said Mr. Moore, explores how these stimulants are being used.
For the study, data was extracted from the MarketScan 2019 and 2020 Commercial Claims and Encounters Databases, focusing on 9.1 million adults aged 19-64 years who were continuously enrolled in an included commercial benefit plan from Oct. 1, 2019 to Dec. 31, 2020.
The primary outcome consisted of an outpatient prescription claim, service date, and days’ supply for the CNS-active drugs.
The researchers defined “combination-2” therapy as 60 or more days of combination treatment with a schedule II stimulant and at least one additional CNS-active drug. “Combination-3” therapy was defined as the addition of at least two additional CNS-active drugs.
The researchers used service date and days’ supply to examine the number of stimulant and other CNS-active drugs for each of the days of 2020.
CNS-active drug classes included antidepressants, anxiolytics/sedatives/hypnotics, antipsychotics, opioids, anticonvulsants, and other CNS-active drugs.
Prescribing cascade
Of the total number of adults enrolled, 3% (n = 276,223) were taking schedule II stimulants during 2020, with a median of 8 (interquartile range, 4-11) prescriptions. These drugs provided 227 (IQR, 110-322) treatment days of exposure.
Among those taking stimulants 45.5% combined the use of at least one additional CNS-active drug for a median of 213 (IQR, 126-301) treatment days; and 24.3% used at least two additional CNS-active drugs for a median of 182 (IQR, 108-276) days.
“Clinicians should beware of the prescribing cascade. Sometimes it begins with an antidepressant that causes too much sedation, so a stimulant gets added, which leads to insomnia, so alprazolam gets added to the mix,” Mr. Moore said.
He cautioned that this “leaves a patient with multiple drugs, all with discontinuation effects of different kinds and clashing effects.”
These new findings, the investigators note, “add new public health concerns to those raised by our previous study. ... this more-detailed profile reveals several new patterns.”
Most patients become “long-term users” once treatment has started, with 75% continuing for a 1-year period.
“This underscores the possible risks of nonmedical use and dependence that have warranted the classification of these drugs as having high potential for psychological or physical dependence and their prominent appearance in toxicology drug rankings of fatal overdose cases,” they write.
They note that the data “do not indicate which intervention may have come first – a stimulant added to compensate for excess sedation from the benzodiazepine, or the alprazolam added to calm excessive CNS stimulation and/or insomnia from the stimulants or other drugs.”
Several limitations cited by the authors include the fact that, although the population encompassed 9.1 million people, it “may not represent all commercially insured adults,” and it doesn’t include people who aren’t covered by commercial insurance.
Moreover, the MarketScan dataset included up to four diagnosis codes for each outpatient and emergency department encounter; therefore, it was not possible to directly link the diagnoses to specific prescription drug claims, and thus the diagnoses were not evaluated.
“Since many providers will not accept a drug claim for a schedule II stimulant without an on-label diagnosis of ADHD,” the authors suspect that “large numbers of this diagnosis were present.”
Complex prescribing regimens
Mark Olfson, MD, MPH, professor of psychiatry, medicine, and law and professor of epidemiology, Columbia University Irving Medical Center, New York, said the report “highlights the pharmacological complexity of adults who are treated with stimulants.”
Dr. Olfson, who is a research psychiatrist at the New York State Psychiatric Institute, New York, and was not involved with the study, observed there is “evidence to support stimulants as an adjunctive therapy for treatment-resistant unipolar depression in older adults.”
However, he added, “this indication is unlikely to fully explain the high proportion of nonelderly, stimulant-treated adults who also receive antidepressants.”
These new findings “call for research to increase our understanding of the clinical contexts that motivate these complex prescribing regimens as well as their effectiveness and safety,” said Dr. Olfson.
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors. Mr. Moore declares no relevant financial relationships. Coauthor G. Caleb Alexander, MD, is past chair and a current member of the Food and Drug Administration’s Peripheral and Central Nervous System Advisory Committee; is a cofounding principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation, for whom he has served as a paid expert witness; and is a past member of OptumRx’s National P&T Committee. Dr. Olfson declares no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM BMJ OPEN
Asthma tied to increased risk for multiple cancers
People with asthma have an elevated risk for a variety of cancers other than lung cancer, including melanoma as well as blood, kidney, and ovarian cancers, new research suggests.
But, the authors found, treatment with an inhaled steroid may lower that risk, perhaps by keeping inflammation in check.
“Using real-world data, our study is the first to provide evidence of a positive association between asthma and cancer risk in United States patients,” Yi Guo, PhD, with the University of Florida, Gainesville, said in a news release.
The study was published online in Cancer Medicine.
The relationship between chronic inflammation and cancer remains a key area of exploration in cancer etiology. Data show that the risk for developing cancer is higher in patients with chronic inflammatory diseases, and patients with asthma have complex and chronic inflammation. However, prior studies exploring a possible link between asthma and cancer have yielded mixed results.
To investigate further, Dr. Guo and colleagues analyzed electronic health records and claims data in the OneFlorida+ clinical research network for roughly 90,000 adults with asthma and a matched cohort of about 270,000 adults without asthma.
Multivariable analysis revealed that adults with asthma were more likely to develop cancer, compared with peers without asthma (hazard ratio, 1.36), the investigators found.
Adults with asthma had an elevated cancer risk for five of the 13 cancers assessed, including melanoma (HR, 1.98), ovarian cancer (HR, 1.88), lung cancer (HR, 1.56), kidney cancer (HR, 1.48), and blood cancer (HR, 1.26).
Compared with adults without asthma, those with asthma who did not treat it with an inhaled steroid had a more pronounced overall cancer risk, compared with those who were on an inhaled steroid (HR, 1.60 vs. 1.11).
For specific cancer types, the risk was elevated for nine of 13 cancers in patients with asthma not taking an inhaled steroid: prostate (HR, 1.50), lung (HR, 1.74), colorectal (HR, 1.51), blood (HR, 1.44), melanoma (HR, 2.05), corpus uteri (HR, 1.76), kidney (HR, 1.52), ovarian (HR, 2.31), and cervical (HR, 1.46).
In contrast, in patients with asthma who did use an inhaled steroid, an elevated cancer risk was observed for only two cancers, lung cancer (HR, 1.39) and melanoma (HR, 1.92), suggesting a potential protective effect of inhaled steroid use on cancer, the researchers said.
Although prior studies have shown a protective effect of inhaled steroid use on some cancers, potentially by reducing inflammation, the “speculative nature of chronic inflammation (asthma as a common example) as a driver for pan-cancer development requires more investigation,” Dr. Guo and colleagues cautioned.
And because of the observational nature of the current study, Dr. Guo’s team stressed that these findings do not prove a causal relationship between asthma and cancer.
“More in-depth studies using real-word data are needed to further explore the causal mechanisms of asthma on cancer risk,” the researchers concluded.
Funding for the study was provided in part by grants to the researchers from the National Institutes of Health, National Cancer Institute, National Institute on Aging, and the Centers for Disease Control and Prevention. This project was supported by the Cancer Informatics Shared Resource in the University of Florida Health Cancer Center. The authors have disclosed no conflicts of interest.
A version of this article first appeared on Medscape.com.
People with asthma have an elevated risk for a variety of cancers other than lung cancer, including melanoma as well as blood, kidney, and ovarian cancers, new research suggests.
But, the authors found, treatment with an inhaled steroid may lower that risk, perhaps by keeping inflammation in check.
“Using real-world data, our study is the first to provide evidence of a positive association between asthma and cancer risk in United States patients,” Yi Guo, PhD, with the University of Florida, Gainesville, said in a news release.
The study was published online in Cancer Medicine.
The relationship between chronic inflammation and cancer remains a key area of exploration in cancer etiology. Data show that the risk for developing cancer is higher in patients with chronic inflammatory diseases, and patients with asthma have complex and chronic inflammation. However, prior studies exploring a possible link between asthma and cancer have yielded mixed results.
To investigate further, Dr. Guo and colleagues analyzed electronic health records and claims data in the OneFlorida+ clinical research network for roughly 90,000 adults with asthma and a matched cohort of about 270,000 adults without asthma.
Multivariable analysis revealed that adults with asthma were more likely to develop cancer, compared with peers without asthma (hazard ratio, 1.36), the investigators found.
Adults with asthma had an elevated cancer risk for five of the 13 cancers assessed, including melanoma (HR, 1.98), ovarian cancer (HR, 1.88), lung cancer (HR, 1.56), kidney cancer (HR, 1.48), and blood cancer (HR, 1.26).
Compared with adults without asthma, those with asthma who did not treat it with an inhaled steroid had a more pronounced overall cancer risk, compared with those who were on an inhaled steroid (HR, 1.60 vs. 1.11).
For specific cancer types, the risk was elevated for nine of 13 cancers in patients with asthma not taking an inhaled steroid: prostate (HR, 1.50), lung (HR, 1.74), colorectal (HR, 1.51), blood (HR, 1.44), melanoma (HR, 2.05), corpus uteri (HR, 1.76), kidney (HR, 1.52), ovarian (HR, 2.31), and cervical (HR, 1.46).
In contrast, in patients with asthma who did use an inhaled steroid, an elevated cancer risk was observed for only two cancers, lung cancer (HR, 1.39) and melanoma (HR, 1.92), suggesting a potential protective effect of inhaled steroid use on cancer, the researchers said.
Although prior studies have shown a protective effect of inhaled steroid use on some cancers, potentially by reducing inflammation, the “speculative nature of chronic inflammation (asthma as a common example) as a driver for pan-cancer development requires more investigation,” Dr. Guo and colleagues cautioned.
And because of the observational nature of the current study, Dr. Guo’s team stressed that these findings do not prove a causal relationship between asthma and cancer.
“More in-depth studies using real-word data are needed to further explore the causal mechanisms of asthma on cancer risk,” the researchers concluded.
Funding for the study was provided in part by grants to the researchers from the National Institutes of Health, National Cancer Institute, National Institute on Aging, and the Centers for Disease Control and Prevention. This project was supported by the Cancer Informatics Shared Resource in the University of Florida Health Cancer Center. The authors have disclosed no conflicts of interest.
A version of this article first appeared on Medscape.com.
People with asthma have an elevated risk for a variety of cancers other than lung cancer, including melanoma as well as blood, kidney, and ovarian cancers, new research suggests.
But, the authors found, treatment with an inhaled steroid may lower that risk, perhaps by keeping inflammation in check.
“Using real-world data, our study is the first to provide evidence of a positive association between asthma and cancer risk in United States patients,” Yi Guo, PhD, with the University of Florida, Gainesville, said in a news release.
The study was published online in Cancer Medicine.
The relationship between chronic inflammation and cancer remains a key area of exploration in cancer etiology. Data show that the risk for developing cancer is higher in patients with chronic inflammatory diseases, and patients with asthma have complex and chronic inflammation. However, prior studies exploring a possible link between asthma and cancer have yielded mixed results.
To investigate further, Dr. Guo and colleagues analyzed electronic health records and claims data in the OneFlorida+ clinical research network for roughly 90,000 adults with asthma and a matched cohort of about 270,000 adults without asthma.
Multivariable analysis revealed that adults with asthma were more likely to develop cancer, compared with peers without asthma (hazard ratio, 1.36), the investigators found.
Adults with asthma had an elevated cancer risk for five of the 13 cancers assessed, including melanoma (HR, 1.98), ovarian cancer (HR, 1.88), lung cancer (HR, 1.56), kidney cancer (HR, 1.48), and blood cancer (HR, 1.26).
Compared with adults without asthma, those with asthma who did not treat it with an inhaled steroid had a more pronounced overall cancer risk, compared with those who were on an inhaled steroid (HR, 1.60 vs. 1.11).
For specific cancer types, the risk was elevated for nine of 13 cancers in patients with asthma not taking an inhaled steroid: prostate (HR, 1.50), lung (HR, 1.74), colorectal (HR, 1.51), blood (HR, 1.44), melanoma (HR, 2.05), corpus uteri (HR, 1.76), kidney (HR, 1.52), ovarian (HR, 2.31), and cervical (HR, 1.46).
In contrast, in patients with asthma who did use an inhaled steroid, an elevated cancer risk was observed for only two cancers, lung cancer (HR, 1.39) and melanoma (HR, 1.92), suggesting a potential protective effect of inhaled steroid use on cancer, the researchers said.
Although prior studies have shown a protective effect of inhaled steroid use on some cancers, potentially by reducing inflammation, the “speculative nature of chronic inflammation (asthma as a common example) as a driver for pan-cancer development requires more investigation,” Dr. Guo and colleagues cautioned.
And because of the observational nature of the current study, Dr. Guo’s team stressed that these findings do not prove a causal relationship between asthma and cancer.
“More in-depth studies using real-word data are needed to further explore the causal mechanisms of asthma on cancer risk,” the researchers concluded.
Funding for the study was provided in part by grants to the researchers from the National Institutes of Health, National Cancer Institute, National Institute on Aging, and the Centers for Disease Control and Prevention. This project was supported by the Cancer Informatics Shared Resource in the University of Florida Health Cancer Center. The authors have disclosed no conflicts of interest.
A version of this article first appeared on Medscape.com.
Pausing endocrine therapy to attempt pregnancy is safe
The results provide the “strongest evidence to date on the short-term safety of this choice,” Sharon Giordano, MD, MPH, with University of Texas M.D. Anderson Cancer Center, Houston, wrote in an editorial accompanying the study.
“Physicians should now incorporate these positive data into their shared decision-making process with patients,” Dr. Giordano said.
The POSITIVE trial findings were published online in The New England Journal of Medicine.
Before the analysis, the risks associated with taking a break from endocrine therapy among young women with hormone receptor (HR)–positive breast cancer remained unclear.
In the current trial, Ann Partridge, MD, MPH, and colleagues sought prospective data on the safety associated with taking a temporary break from therapy to attempt pregnancy.
The single-group trial enrolled more than 500 premenopausal women who had received 18-30 months of endocrine therapy for mostly stage I or II HR-positive breast cancer. After a 3-month washout, the women were given 2 years to conceive, deliver, and breastfeed, if desired, before resuming treatment. Breast cancer events – the primary outcome – were defined as local, regional, or distant recurrence of invasive breast cancer or new contralateral invasive breast cancer.
The results, initially reported at San Antonio Breast Cancer Symposium (SABCS) 2022, showed that a temporary interruption of therapy to attempt pregnancy did not appear to lead to worse breast cancer outcomes.
Among 497 women who were followed for pregnancy status, 368 (74%) had at least one pregnancy, and 317 (64%) had at least one live birth.
After a median follow-up of 3.4 years, 44 women had had a breast cancer event – a result that was close to, but did not exceed, the safety threshold of 46 breast cancer events.
The 3-year incidence of breast cancer events was 8.9% (95% confidence interval [CI], 6.3-11.6) in the treatment-interruption group compared with 9.2% (95% CI, 7.6-10.8) among historical controls, which included women who would have met the entry criteria for the trial.
“These results suggest that although endocrine therapy for a period of 5-10 years substantially improves disease outcomes in patients with hormone receptor–positive early breast cancer, a temporary interruption of therapy to attempt pregnancy does not appear to have an appreciable negative short-term effect,” wrote Dr. Partridge, vice chair of medical oncology at Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston, and colleagues.
The authors cautioned, however, that the median follow-up was only 3.4 years and that 10-year follow-up data will be “critical” to confirm the safety of interruption of adjuvant endocrine therapy.
Dr. Giordano agreed, noting that “recurrences of breast cancer are reported to occur at a steady rate for up to 20 years after diagnosis among patients with hormone receptor–positive disease; the protocol-specified 10-year follow-up data will be essential to establish longer-term safety.”
The study was supported by the International Breast Cancer Study Group and by the Alliance for Clinical Trials in Oncology in North America in collaboration with the Breast International Group (BIG). Disclosures for authors and editorial writer are available at NEJM.org.
A version of this article first appeared on Medscape.com.
The results provide the “strongest evidence to date on the short-term safety of this choice,” Sharon Giordano, MD, MPH, with University of Texas M.D. Anderson Cancer Center, Houston, wrote in an editorial accompanying the study.
“Physicians should now incorporate these positive data into their shared decision-making process with patients,” Dr. Giordano said.
The POSITIVE trial findings were published online in The New England Journal of Medicine.
Before the analysis, the risks associated with taking a break from endocrine therapy among young women with hormone receptor (HR)–positive breast cancer remained unclear.
In the current trial, Ann Partridge, MD, MPH, and colleagues sought prospective data on the safety associated with taking a temporary break from therapy to attempt pregnancy.
The single-group trial enrolled more than 500 premenopausal women who had received 18-30 months of endocrine therapy for mostly stage I or II HR-positive breast cancer. After a 3-month washout, the women were given 2 years to conceive, deliver, and breastfeed, if desired, before resuming treatment. Breast cancer events – the primary outcome – were defined as local, regional, or distant recurrence of invasive breast cancer or new contralateral invasive breast cancer.
The results, initially reported at San Antonio Breast Cancer Symposium (SABCS) 2022, showed that a temporary interruption of therapy to attempt pregnancy did not appear to lead to worse breast cancer outcomes.
Among 497 women who were followed for pregnancy status, 368 (74%) had at least one pregnancy, and 317 (64%) had at least one live birth.
After a median follow-up of 3.4 years, 44 women had had a breast cancer event – a result that was close to, but did not exceed, the safety threshold of 46 breast cancer events.
The 3-year incidence of breast cancer events was 8.9% (95% confidence interval [CI], 6.3-11.6) in the treatment-interruption group compared with 9.2% (95% CI, 7.6-10.8) among historical controls, which included women who would have met the entry criteria for the trial.
“These results suggest that although endocrine therapy for a period of 5-10 years substantially improves disease outcomes in patients with hormone receptor–positive early breast cancer, a temporary interruption of therapy to attempt pregnancy does not appear to have an appreciable negative short-term effect,” wrote Dr. Partridge, vice chair of medical oncology at Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston, and colleagues.
The authors cautioned, however, that the median follow-up was only 3.4 years and that 10-year follow-up data will be “critical” to confirm the safety of interruption of adjuvant endocrine therapy.
Dr. Giordano agreed, noting that “recurrences of breast cancer are reported to occur at a steady rate for up to 20 years after diagnosis among patients with hormone receptor–positive disease; the protocol-specified 10-year follow-up data will be essential to establish longer-term safety.”
The study was supported by the International Breast Cancer Study Group and by the Alliance for Clinical Trials in Oncology in North America in collaboration with the Breast International Group (BIG). Disclosures for authors and editorial writer are available at NEJM.org.
A version of this article first appeared on Medscape.com.
The results provide the “strongest evidence to date on the short-term safety of this choice,” Sharon Giordano, MD, MPH, with University of Texas M.D. Anderson Cancer Center, Houston, wrote in an editorial accompanying the study.
“Physicians should now incorporate these positive data into their shared decision-making process with patients,” Dr. Giordano said.
The POSITIVE trial findings were published online in The New England Journal of Medicine.
Before the analysis, the risks associated with taking a break from endocrine therapy among young women with hormone receptor (HR)–positive breast cancer remained unclear.
In the current trial, Ann Partridge, MD, MPH, and colleagues sought prospective data on the safety associated with taking a temporary break from therapy to attempt pregnancy.
The single-group trial enrolled more than 500 premenopausal women who had received 18-30 months of endocrine therapy for mostly stage I or II HR-positive breast cancer. After a 3-month washout, the women were given 2 years to conceive, deliver, and breastfeed, if desired, before resuming treatment. Breast cancer events – the primary outcome – were defined as local, regional, or distant recurrence of invasive breast cancer or new contralateral invasive breast cancer.
The results, initially reported at San Antonio Breast Cancer Symposium (SABCS) 2022, showed that a temporary interruption of therapy to attempt pregnancy did not appear to lead to worse breast cancer outcomes.
Among 497 women who were followed for pregnancy status, 368 (74%) had at least one pregnancy, and 317 (64%) had at least one live birth.
After a median follow-up of 3.4 years, 44 women had had a breast cancer event – a result that was close to, but did not exceed, the safety threshold of 46 breast cancer events.
The 3-year incidence of breast cancer events was 8.9% (95% confidence interval [CI], 6.3-11.6) in the treatment-interruption group compared with 9.2% (95% CI, 7.6-10.8) among historical controls, which included women who would have met the entry criteria for the trial.
“These results suggest that although endocrine therapy for a period of 5-10 years substantially improves disease outcomes in patients with hormone receptor–positive early breast cancer, a temporary interruption of therapy to attempt pregnancy does not appear to have an appreciable negative short-term effect,” wrote Dr. Partridge, vice chair of medical oncology at Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, Boston, and colleagues.
The authors cautioned, however, that the median follow-up was only 3.4 years and that 10-year follow-up data will be “critical” to confirm the safety of interruption of adjuvant endocrine therapy.
Dr. Giordano agreed, noting that “recurrences of breast cancer are reported to occur at a steady rate for up to 20 years after diagnosis among patients with hormone receptor–positive disease; the protocol-specified 10-year follow-up data will be essential to establish longer-term safety.”
The study was supported by the International Breast Cancer Study Group and by the Alliance for Clinical Trials in Oncology in North America in collaboration with the Breast International Group (BIG). Disclosures for authors and editorial writer are available at NEJM.org.
A version of this article first appeared on Medscape.com.
FROM NEJM
New AACE type 2 diabetes algorithm individualizes care
SEATTLE – The latest American Association of Clinical Endocrinology type 2 diabetes management algorithm uses graphics to focus on individualized care while adding newly compiled information about medication access and affordability, vaccinations, and weight loss drugs.
The clinical guidance document was presented at the annual scientific & clinical congress of the American Association of Clinical Endocrinology and simultaneously published in Endocrine Practice.
Using text and colorful graphics, the document summarizes information from last year’s update and other recent AACE documents, including those addressing dyslipidemia and use of diabetes technology.
lead author Susan L. Samson, MD, PhD, chair of endocrinology, diabetes & metabolism at the Mayo Clinic Florida, Jacksonville, said in an interview.
Asked to comment, Anne L. Peters, MD, professor of clinical medicine at the University of Southern California, Los Angeles, said: “I like their simple graphics. For the Department of Health Services in Los Angeles County, we have been painstakingly trying to create our own flow diagrams. ... These will help.”
Eleven separate algorithms with text and graphics
Included are 11 visual management algorithms, with accompanying text for each one. The first lists 10 overall management principles, including “lifestyle modification underlies all therapy,” “maintain or achieve optimal weight,” “choice of therapy includes ease of use and access,” “individualize all glucose targets,” “avoid hypoglycemia,” and “comorbidities must be managed for comprehensive care.”
Three more algorithms cover the diabetes-adjacent topics of adiposity-based chronic disease, prediabetes, dyslipidemia, and hypertension.
Four separate graphics address glucose-lowering. Two are “complications-centric” and “glucose-centric” algorithms, another covers insulin initiation and titration, and a table summarizes the benefits and risks of currently available glucose-lowering medications, as well as cost.
Splitting the glucose-lowering algorithms into “complications-centric” and “glucose-centric” graphics is new, Dr. Samson said. “The complications one comes first, deliberately. You need to think about: Does my patient have a history of or high risk for cardiovascular disease, heart failure, stroke, or diabetic kidney disease? And, you want to prioritize those medications that have evidence to improve outcomes with those different diabetes complications versus a one-size-fits-all approach.”
And for patients without those complications, the glucose-centric algorithm considers obesity, hypoglycemia risk, and access/cost issues. “So, overall the diabetes medication algorithm has been split in order to emphasize that personalized approach to decision-making,” Dr. Samson explained.
Also new is a table listing the benefits and risks of weight-loss medications, and another covering immunization guidance for people with diabetes based on recommendations from the U.S. Centers for Disease Control and Prevention. “Coming out of the pandemic, we’re thinking about how can we protect our patients from infectious disease and all the comorbidities. In some cases, people with diabetes can have a much higher risk for adverse events,” Dr. Samson noted.
Regarding the weight-loss medications table, she pointed out that the task force couldn’t include the blockbuster twincretin tirzepatide because it’s not yet approved for weight loss by the U.S. Food and Drug Administration. However, it is included in the glucose-lowering drug table with weight loss listed among its benefits.
“We want this to be a living document that should be updated in a timely fashion, and so, as these new indications are approved and we see more evidence supporting their different uses, this should be updated in a really timely fashion to reflect that,” Dr. Samson said.
The end of the document includes a full page of each graphic, meant for wall posting.
Dr. Peters noted that for the most part, the AACE guidelines and algorithm align with joint guidance by the American Diabetes Association and European Association for the Study of Diabetes.
“For many years there seemed to be big differences between the AACE and ADA guidelines for the management of type 2 diabetes. Although small differences still exist ... the ADA and AACE guidelines have become quite similar,” she said.
Dr. Peters also praised the AACE algorithm for providing “a pathway for people who have issues with access and cost.”
“I am incredibly proud that in the County of Los Angeles you can get a [glucagon-like peptide-1 receptor agonist] and/or a [sodium-glucose cotransporter-2 inhibitor] even with the most restricted MediCal insurance if indications are met. But there remain many people in many places where access and cost limit options, and I am grateful that AACE includes this in their algorithms,” she said.
Dr. Samson has reported receiving research support to the Mayo Clinic from Corcept, serving on a steering committee and being a national or overall principal investigator for Chiasma and Novartis, and being a committee chair for the American Board of Internal Medicine. Dr. Peters has reported relationships with Blue Circle Health, Vertex, and Abbott Diabetes Care, receiving research grants from Abbott Diabetes Care and Insulet, and holding stock options in Teladoc and Omada Health.
A version of this article originally appeared on Medscape.com.
SEATTLE – The latest American Association of Clinical Endocrinology type 2 diabetes management algorithm uses graphics to focus on individualized care while adding newly compiled information about medication access and affordability, vaccinations, and weight loss drugs.
The clinical guidance document was presented at the annual scientific & clinical congress of the American Association of Clinical Endocrinology and simultaneously published in Endocrine Practice.
Using text and colorful graphics, the document summarizes information from last year’s update and other recent AACE documents, including those addressing dyslipidemia and use of diabetes technology.
lead author Susan L. Samson, MD, PhD, chair of endocrinology, diabetes & metabolism at the Mayo Clinic Florida, Jacksonville, said in an interview.
Asked to comment, Anne L. Peters, MD, professor of clinical medicine at the University of Southern California, Los Angeles, said: “I like their simple graphics. For the Department of Health Services in Los Angeles County, we have been painstakingly trying to create our own flow diagrams. ... These will help.”
Eleven separate algorithms with text and graphics
Included are 11 visual management algorithms, with accompanying text for each one. The first lists 10 overall management principles, including “lifestyle modification underlies all therapy,” “maintain or achieve optimal weight,” “choice of therapy includes ease of use and access,” “individualize all glucose targets,” “avoid hypoglycemia,” and “comorbidities must be managed for comprehensive care.”
Three more algorithms cover the diabetes-adjacent topics of adiposity-based chronic disease, prediabetes, dyslipidemia, and hypertension.
Four separate graphics address glucose-lowering. Two are “complications-centric” and “glucose-centric” algorithms, another covers insulin initiation and titration, and a table summarizes the benefits and risks of currently available glucose-lowering medications, as well as cost.
Splitting the glucose-lowering algorithms into “complications-centric” and “glucose-centric” graphics is new, Dr. Samson said. “The complications one comes first, deliberately. You need to think about: Does my patient have a history of or high risk for cardiovascular disease, heart failure, stroke, or diabetic kidney disease? And, you want to prioritize those medications that have evidence to improve outcomes with those different diabetes complications versus a one-size-fits-all approach.”
And for patients without those complications, the glucose-centric algorithm considers obesity, hypoglycemia risk, and access/cost issues. “So, overall the diabetes medication algorithm has been split in order to emphasize that personalized approach to decision-making,” Dr. Samson explained.
Also new is a table listing the benefits and risks of weight-loss medications, and another covering immunization guidance for people with diabetes based on recommendations from the U.S. Centers for Disease Control and Prevention. “Coming out of the pandemic, we’re thinking about how can we protect our patients from infectious disease and all the comorbidities. In some cases, people with diabetes can have a much higher risk for adverse events,” Dr. Samson noted.
Regarding the weight-loss medications table, she pointed out that the task force couldn’t include the blockbuster twincretin tirzepatide because it’s not yet approved for weight loss by the U.S. Food and Drug Administration. However, it is included in the glucose-lowering drug table with weight loss listed among its benefits.
“We want this to be a living document that should be updated in a timely fashion, and so, as these new indications are approved and we see more evidence supporting their different uses, this should be updated in a really timely fashion to reflect that,” Dr. Samson said.
The end of the document includes a full page of each graphic, meant for wall posting.
Dr. Peters noted that for the most part, the AACE guidelines and algorithm align with joint guidance by the American Diabetes Association and European Association for the Study of Diabetes.
“For many years there seemed to be big differences between the AACE and ADA guidelines for the management of type 2 diabetes. Although small differences still exist ... the ADA and AACE guidelines have become quite similar,” she said.
Dr. Peters also praised the AACE algorithm for providing “a pathway for people who have issues with access and cost.”
“I am incredibly proud that in the County of Los Angeles you can get a [glucagon-like peptide-1 receptor agonist] and/or a [sodium-glucose cotransporter-2 inhibitor] even with the most restricted MediCal insurance if indications are met. But there remain many people in many places where access and cost limit options, and I am grateful that AACE includes this in their algorithms,” she said.
Dr. Samson has reported receiving research support to the Mayo Clinic from Corcept, serving on a steering committee and being a national or overall principal investigator for Chiasma and Novartis, and being a committee chair for the American Board of Internal Medicine. Dr. Peters has reported relationships with Blue Circle Health, Vertex, and Abbott Diabetes Care, receiving research grants from Abbott Diabetes Care and Insulet, and holding stock options in Teladoc and Omada Health.
A version of this article originally appeared on Medscape.com.
SEATTLE – The latest American Association of Clinical Endocrinology type 2 diabetes management algorithm uses graphics to focus on individualized care while adding newly compiled information about medication access and affordability, vaccinations, and weight loss drugs.
The clinical guidance document was presented at the annual scientific & clinical congress of the American Association of Clinical Endocrinology and simultaneously published in Endocrine Practice.
Using text and colorful graphics, the document summarizes information from last year’s update and other recent AACE documents, including those addressing dyslipidemia and use of diabetes technology.
lead author Susan L. Samson, MD, PhD, chair of endocrinology, diabetes & metabolism at the Mayo Clinic Florida, Jacksonville, said in an interview.
Asked to comment, Anne L. Peters, MD, professor of clinical medicine at the University of Southern California, Los Angeles, said: “I like their simple graphics. For the Department of Health Services in Los Angeles County, we have been painstakingly trying to create our own flow diagrams. ... These will help.”
Eleven separate algorithms with text and graphics
Included are 11 visual management algorithms, with accompanying text for each one. The first lists 10 overall management principles, including “lifestyle modification underlies all therapy,” “maintain or achieve optimal weight,” “choice of therapy includes ease of use and access,” “individualize all glucose targets,” “avoid hypoglycemia,” and “comorbidities must be managed for comprehensive care.”
Three more algorithms cover the diabetes-adjacent topics of adiposity-based chronic disease, prediabetes, dyslipidemia, and hypertension.
Four separate graphics address glucose-lowering. Two are “complications-centric” and “glucose-centric” algorithms, another covers insulin initiation and titration, and a table summarizes the benefits and risks of currently available glucose-lowering medications, as well as cost.
Splitting the glucose-lowering algorithms into “complications-centric” and “glucose-centric” graphics is new, Dr. Samson said. “The complications one comes first, deliberately. You need to think about: Does my patient have a history of or high risk for cardiovascular disease, heart failure, stroke, or diabetic kidney disease? And, you want to prioritize those medications that have evidence to improve outcomes with those different diabetes complications versus a one-size-fits-all approach.”
And for patients without those complications, the glucose-centric algorithm considers obesity, hypoglycemia risk, and access/cost issues. “So, overall the diabetes medication algorithm has been split in order to emphasize that personalized approach to decision-making,” Dr. Samson explained.
Also new is a table listing the benefits and risks of weight-loss medications, and another covering immunization guidance for people with diabetes based on recommendations from the U.S. Centers for Disease Control and Prevention. “Coming out of the pandemic, we’re thinking about how can we protect our patients from infectious disease and all the comorbidities. In some cases, people with diabetes can have a much higher risk for adverse events,” Dr. Samson noted.
Regarding the weight-loss medications table, she pointed out that the task force couldn’t include the blockbuster twincretin tirzepatide because it’s not yet approved for weight loss by the U.S. Food and Drug Administration. However, it is included in the glucose-lowering drug table with weight loss listed among its benefits.
“We want this to be a living document that should be updated in a timely fashion, and so, as these new indications are approved and we see more evidence supporting their different uses, this should be updated in a really timely fashion to reflect that,” Dr. Samson said.
The end of the document includes a full page of each graphic, meant for wall posting.
Dr. Peters noted that for the most part, the AACE guidelines and algorithm align with joint guidance by the American Diabetes Association and European Association for the Study of Diabetes.
“For many years there seemed to be big differences between the AACE and ADA guidelines for the management of type 2 diabetes. Although small differences still exist ... the ADA and AACE guidelines have become quite similar,” she said.
Dr. Peters also praised the AACE algorithm for providing “a pathway for people who have issues with access and cost.”
“I am incredibly proud that in the County of Los Angeles you can get a [glucagon-like peptide-1 receptor agonist] and/or a [sodium-glucose cotransporter-2 inhibitor] even with the most restricted MediCal insurance if indications are met. But there remain many people in many places where access and cost limit options, and I am grateful that AACE includes this in their algorithms,” she said.
Dr. Samson has reported receiving research support to the Mayo Clinic from Corcept, serving on a steering committee and being a national or overall principal investigator for Chiasma and Novartis, and being a committee chair for the American Board of Internal Medicine. Dr. Peters has reported relationships with Blue Circle Health, Vertex, and Abbott Diabetes Care, receiving research grants from Abbott Diabetes Care and Insulet, and holding stock options in Teladoc and Omada Health.
A version of this article originally appeared on Medscape.com.
AT AACE 2023