User login
Brooklyn gastroenterologist: Good listening skills make a doctor a better teacher, person
After the 2004 Indian Ocean earthquake and tsunami, he traveled to his home country of Sri Lanka to help people who were in need and establish an orphanage. He has applied his skills as a gastroenterologist in the U.S. military and the New York City Police Department.

He was in New York during the 9-11 terrorist attacks. To this day, he treats patients with residual GI problems and precancerous changes associated with 9-11. “I’m involved in screening those people who were the first responders referred by the NYPD,” he says.
This year Dr. Iswara earned the Distinguished Clinician Award in Private Practice from the American Gastroenterological Association. “He puts his patients first in every endeavor – and every question that he asks with regards to research and education is linked to the ultimate measuring stick of improving patient care,” according to an AGA announcement of the award.
When dealing with patients and colleagues, he offers this simple pearl of advice: Listen and then listen some more.
“Once you listen more, you can find out their issues much more in depth, and you can give a satisfying answer to them and their problems. Listening is a kindness and a compassionate thing. It not only makes you become a better teacher, but a better person,” said Dr. Iswara, attending gastroenterologist at Maimonides Medical Center in New York.
In an interview, he talked more in depth about his GI beginnings, his role as a mentor, and why he always starts the day with a prayer. He also confided about the useful time management habit kept from his military days that gives him energy.
Question: What gives you joy in day-to-day practice?
Dr. Iswara: One of the main joys is my colleagues, coworkers, fellows, and my patients. The patients come No. 1. As I walk into my practice area or in the hospital, there is a sense of inner happiness in my mind to see the smiles of the patients and the greetings I get from the patients and all the coworkers. I also see smiling patients with anxiety in their face, trying to get my attention to take care of them.
After I see the patient, I change to a different mode, a kind of a professional mode to give the best to the people whom I’m caring for, who are trusting me with their lives.
One thing I do in my mind before I even start the day, I do a silent prayer to guide me, to give compassionate care and safe care. I will not harm anyone who is depending on my care.
Q: Who was your mentor?
Dr. Iswara: I was lucky enough to have been trained by Baroukh El Kodsi, MD, at Maimonides Medical Center. He recently passed away and was a legend in Brooklyn. I was his first-generation trainee, and I was able to pass on my skills to my trainees. Now so many people who are in Brooklyn; they were trained by me, so it’s kind of growth by generations.
When I finished the training with Dr. Kodsi, he hired me as an associate director of the GI department at Maimonides. I became the program director, then division chief, then I became a director of advanced endoscopy. All these gastroenterology procedures started after 1975 while I was doing the training, so I was one of the pioneers to bring all this new technology to our hospital. I’m still involved in fellowship education.
Q: Can we talk more about your accomplishments? Perhaps you can discuss your AGA award and what you received it for.
Dr. Iswara: I’m humbled and honored by this role, and I’ll be forever grateful to AGA for this prestigious honor at the late stage of my career.
I have been a continuous AGA member for the last 45 years. I probably have one of the longest durations of being an actively practicing gastroenterologist in Brooklyn. I’ve also done academic work, teaching so many young gastroenterologists, motivating several of them to become leading gastroenterologists.
Q: If you could describe a scene of your vision for the future, what it would it be in terms of how gastroenterology is practiced?
Dr. Iswara: I’d like to see the newer generation practice more of a clinical medicine than technical medicine. Sometimes when I see the young people, they sit in front of the computer more than talking and touching the patient. There has to be some sort of a balance where the newer people should be taught more bedside personal care, touching the patient, looking at the patient’s face. They are kind of under pressure to write longer notes than to examine the patient, so I think this has to change.
Q: Describe how you would spend a free Saturday afternoon.
Dr. Iswara: When I was in the military, I was told that to prevent battle fatigue you had to take a rest. I really try to take a rest almost 2 hours every day in the daytime. This rejuvenates me.
We live in New York, and I love to go to shows, especially magic shows. I love magic and illusion.
On free Saturday evenings, I also spend time with my grandchildren in the city, watching them in their baseball, soccer, swimming, and other activities. I love to spend time with them.
Lightning round
Texting or talking?
Texting
Favorite city in the U.S. besides the one you live?
Naples, Fla.
Favorite breakfast?
Pancakes
Dark Chocolate or milk chocolate?
Cadbury from England
Last movie you watched?
“To Sir, With Love”
After the 2004 Indian Ocean earthquake and tsunami, he traveled to his home country of Sri Lanka to help people who were in need and establish an orphanage. He has applied his skills as a gastroenterologist in the U.S. military and the New York City Police Department.
He was in New York during the 9-11 terrorist attacks. To this day, he treats patients with residual GI problems and precancerous changes associated with 9-11. “I’m involved in screening those people who were the first responders referred by the NYPD,” he says.
This year Dr. Iswara earned the Distinguished Clinician Award in Private Practice from the American Gastroenterological Association. “He puts his patients first in every endeavor – and every question that he asks with regards to research and education is linked to the ultimate measuring stick of improving patient care,” according to an AGA announcement of the award.
When dealing with patients and colleagues, he offers this simple pearl of advice: Listen and then listen some more.
“Once you listen more, you can find out their issues much more in depth, and you can give a satisfying answer to them and their problems. Listening is a kindness and a compassionate thing. It not only makes you become a better teacher, but a better person,” said Dr. Iswara, attending gastroenterologist at Maimonides Medical Center in New York.
In an interview, he talked more in depth about his GI beginnings, his role as a mentor, and why he always starts the day with a prayer. He also confided about the useful time management habit kept from his military days that gives him energy.
Question: What gives you joy in day-to-day practice?
Dr. Iswara: One of the main joys is my colleagues, coworkers, fellows, and my patients. The patients come No. 1. As I walk into my practice area or in the hospital, there is a sense of inner happiness in my mind to see the smiles of the patients and the greetings I get from the patients and all the coworkers. I also see smiling patients with anxiety in their face, trying to get my attention to take care of them.
After I see the patient, I change to a different mode, a kind of a professional mode to give the best to the people whom I’m caring for, who are trusting me with their lives.
One thing I do in my mind before I even start the day, I do a silent prayer to guide me, to give compassionate care and safe care. I will not harm anyone who is depending on my care.
Q: Who was your mentor?
Dr. Iswara: I was lucky enough to have been trained by Baroukh El Kodsi, MD, at Maimonides Medical Center. He recently passed away and was a legend in Brooklyn. I was his first-generation trainee, and I was able to pass on my skills to my trainees. Now so many people who are in Brooklyn; they were trained by me, so it’s kind of growth by generations.
When I finished the training with Dr. Kodsi, he hired me as an associate director of the GI department at Maimonides. I became the program director, then division chief, then I became a director of advanced endoscopy. All these gastroenterology procedures started after 1975 while I was doing the training, so I was one of the pioneers to bring all this new technology to our hospital. I’m still involved in fellowship education.
Q: Can we talk more about your accomplishments? Perhaps you can discuss your AGA award and what you received it for.
Dr. Iswara: I’m humbled and honored by this role, and I’ll be forever grateful to AGA for this prestigious honor at the late stage of my career.
I have been a continuous AGA member for the last 45 years. I probably have one of the longest durations of being an actively practicing gastroenterologist in Brooklyn. I’ve also done academic work, teaching so many young gastroenterologists, motivating several of them to become leading gastroenterologists.
Q: If you could describe a scene of your vision for the future, what it would it be in terms of how gastroenterology is practiced?
Dr. Iswara: I’d like to see the newer generation practice more of a clinical medicine than technical medicine. Sometimes when I see the young people, they sit in front of the computer more than talking and touching the patient. There has to be some sort of a balance where the newer people should be taught more bedside personal care, touching the patient, looking at the patient’s face. They are kind of under pressure to write longer notes than to examine the patient, so I think this has to change.
Q: Describe how you would spend a free Saturday afternoon.
Dr. Iswara: When I was in the military, I was told that to prevent battle fatigue you had to take a rest. I really try to take a rest almost 2 hours every day in the daytime. This rejuvenates me.
We live in New York, and I love to go to shows, especially magic shows. I love magic and illusion.
On free Saturday evenings, I also spend time with my grandchildren in the city, watching them in their baseball, soccer, swimming, and other activities. I love to spend time with them.
Lightning round
Texting or talking?
Texting
Favorite city in the U.S. besides the one you live?
Naples, Fla.
Favorite breakfast?
Pancakes
Dark Chocolate or milk chocolate?
Cadbury from England
Last movie you watched?
“To Sir, With Love”
After the 2004 Indian Ocean earthquake and tsunami, he traveled to his home country of Sri Lanka to help people who were in need and establish an orphanage. He has applied his skills as a gastroenterologist in the U.S. military and the New York City Police Department.
He was in New York during the 9-11 terrorist attacks. To this day, he treats patients with residual GI problems and precancerous changes associated with 9-11. “I’m involved in screening those people who were the first responders referred by the NYPD,” he says.
This year Dr. Iswara earned the Distinguished Clinician Award in Private Practice from the American Gastroenterological Association. “He puts his patients first in every endeavor – and every question that he asks with regards to research and education is linked to the ultimate measuring stick of improving patient care,” according to an AGA announcement of the award.
When dealing with patients and colleagues, he offers this simple pearl of advice: Listen and then listen some more.
“Once you listen more, you can find out their issues much more in depth, and you can give a satisfying answer to them and their problems. Listening is a kindness and a compassionate thing. It not only makes you become a better teacher, but a better person,” said Dr. Iswara, attending gastroenterologist at Maimonides Medical Center in New York.
In an interview, he talked more in depth about his GI beginnings, his role as a mentor, and why he always starts the day with a prayer. He also confided about the useful time management habit kept from his military days that gives him energy.
Question: What gives you joy in day-to-day practice?
Dr. Iswara: One of the main joys is my colleagues, coworkers, fellows, and my patients. The patients come No. 1. As I walk into my practice area or in the hospital, there is a sense of inner happiness in my mind to see the smiles of the patients and the greetings I get from the patients and all the coworkers. I also see smiling patients with anxiety in their face, trying to get my attention to take care of them.
After I see the patient, I change to a different mode, a kind of a professional mode to give the best to the people whom I’m caring for, who are trusting me with their lives.
One thing I do in my mind before I even start the day, I do a silent prayer to guide me, to give compassionate care and safe care. I will not harm anyone who is depending on my care.
Q: Who was your mentor?
Dr. Iswara: I was lucky enough to have been trained by Baroukh El Kodsi, MD, at Maimonides Medical Center. He recently passed away and was a legend in Brooklyn. I was his first-generation trainee, and I was able to pass on my skills to my trainees. Now so many people who are in Brooklyn; they were trained by me, so it’s kind of growth by generations.
When I finished the training with Dr. Kodsi, he hired me as an associate director of the GI department at Maimonides. I became the program director, then division chief, then I became a director of advanced endoscopy. All these gastroenterology procedures started after 1975 while I was doing the training, so I was one of the pioneers to bring all this new technology to our hospital. I’m still involved in fellowship education.
Q: Can we talk more about your accomplishments? Perhaps you can discuss your AGA award and what you received it for.
Dr. Iswara: I’m humbled and honored by this role, and I’ll be forever grateful to AGA for this prestigious honor at the late stage of my career.
I have been a continuous AGA member for the last 45 years. I probably have one of the longest durations of being an actively practicing gastroenterologist in Brooklyn. I’ve also done academic work, teaching so many young gastroenterologists, motivating several of them to become leading gastroenterologists.
Q: If you could describe a scene of your vision for the future, what it would it be in terms of how gastroenterology is practiced?
Dr. Iswara: I’d like to see the newer generation practice more of a clinical medicine than technical medicine. Sometimes when I see the young people, they sit in front of the computer more than talking and touching the patient. There has to be some sort of a balance where the newer people should be taught more bedside personal care, touching the patient, looking at the patient’s face. They are kind of under pressure to write longer notes than to examine the patient, so I think this has to change.
Q: Describe how you would spend a free Saturday afternoon.
Dr. Iswara: When I was in the military, I was told that to prevent battle fatigue you had to take a rest. I really try to take a rest almost 2 hours every day in the daytime. This rejuvenates me.
We live in New York, and I love to go to shows, especially magic shows. I love magic and illusion.
On free Saturday evenings, I also spend time with my grandchildren in the city, watching them in their baseball, soccer, swimming, and other activities. I love to spend time with them.
Lightning round
Texting or talking?
Texting
Favorite city in the U.S. besides the one you live?
Naples, Fla.
Favorite breakfast?
Pancakes
Dark Chocolate or milk chocolate?
Cadbury from England
Last movie you watched?
“To Sir, With Love”
Noninvasive Methods for the Diagnosis of Endometriosis

What is the value of considering noninvasive methods for the diagnosis of endometriosis?
Dr. Flores: There is great value in noninvasive diagnostics for endometriosis. This is because while surgical diagnosis is the “gold standard,” surgery is invasive, and waiting until a surgical diagnosis can be made further contributes to delays in diagnosis. However, more recently there has been a shift toward utilizing noninvasive approaches to the diagnosis of endometriosis, with the primary one focusing on clinically diagnosing endometriosis.
One of the first things to remember is the importance of gathering a patient history and conducting a physical exam. We've all learned this in medical school, and it comes into play even more so with a condition such as endometriosis. Endometriosis is defined as a benign gynecologic disease characterized by endometrial-like tissue outside of the uterus, but this definition does not reflect the true scope and manifestations of endometriosis. Research over the years has demonstrated that endometriosis has systemic effects—affecting regions of the brain associated with anxiety/depression, altering pain sensitization, and having inflammatory effects that can not only affect the reproductive organs but also other organ systems. As such, our questions when evaluating patients for endometriosis need to focus on these various aspects of the disease.
Endometriosis usually leads to cyclic pain. This is because just as the lining of the uterus (the endometrium) grows and sheds every month in response to hormones, endometriotic lesions—which are endometrial-like tissue outside of the uterus—also grow and shed each month. However, there is no outflow for this shed tissue and, as a result, there is an inflammatory response as well as pain. Depending on where those lesions implant, symptoms can include not only cyclic pelvic pain but also cyclic bowel/bladder pain. I’ve also had patients complain of cyclic sharp/shooting leg pain.
Many times, patients present to us after having seen several different types of providers and having been diagnosed with conditions such as irritable bowel syndrome or painful bladder syndrome. However, if you talk to patients and ask them to tell you a little bit more about this bowel or bladder pain, they will frequently endorse that their symptoms are cyclic/most severe during their menses. With respect to pelvic pain, endometriosis-related pelvic pain is usually progressive—becoming progressively more painful over the years. These symptoms are strong indicators that endometriosis is the cause. A pelvic exam is also helpful as findings of nodularity or a fixed uterus may lend further support for endometriosis; a normal exam, however, does not rule out endometriosis.
What are the primary imaging techniques used to diagnose endometriosis?
Dr. Flores: While history and physical exam are the primary components of the clinical diagnosis, imaging can also be helpful. The 2 techniques most often used are pelvic ultrasound and magnetic resonance imaging (MRI).
While transvaginal ultrasound is sensitive and specific for diagnosing endometriomas (ovarian cysts of endometriotic tissue) and may also be able to accurately identify deep-infiltrating endometriosis, it is limited in its ability to visualize peritoneal disease. MRI can improve diagnosis of endometriosis and better estimate the depth of invasion of deep-infiltrating disease, as well as confirm diagnosis of an endometrioma. While MRI is an option for peritoneal endometriosis, superficial disease is usually not detected. Lastly, computed tomography imaging of the chest can be used when thoracic endometriosis is suspected but is otherwise not routinely recommended. Imaging is also helpful in ruling in/out other potential etiologies of pelvic pain such as fibroids and adenomyosis. It is important to recognize, however, that the absence of any findings of endometriosis on imaging does not rule out the disease.
What other best practices do you implement in your day-to-day to aid in diagnosis?
Dr. Flores: Take the time to listen to your patient. Often, they’ve seen several providers before ultimately seeing a provider who can diagnosis their endometriosis without the need for surgical evaluation. We have to ask questions related to their pain and when the pain occurs, and we can’t forget to also ask about pain during intercourse, as well as non-menstrual pelvic pain. Additionally, it is important to recognize that, for patients who may have been suffering from endometriosis for several years before reaching a diagnosis, they may present with chronic pelvic pain. In this case, it is important to ask what their menstrual cycles were like before the pelvic pain became chronic, and usually patients note cyclic pelvic pain that became progressive. We also know that patients who have a first-degree relative with endometriosis are 7 times more likely to be affected by the disease, so asking about a family history of endometriosis is important.
We have to think about endometriosis as a systemic disease. Previously, endometriosis was incorrectly thought of as solely a pelvic disease, but we've been learning more and more through research that it truly is a chronic, systemic disease with multifactorial effects throughout the body. For example, we have found that endometriosis affects regions of the brain associated with anxiety and depression, as well as causing changes in metabolism. For example, a common misconception is that women with a low body mass index (BMI) were at risk for endometriosis, when in fact it's just the opposite—it is the endometriosis that is causing changes in metabolism that lead to a decreased BMI. Patients with endometriosis also frequently struggle with mood disorders; therefore, we cannot dismiss this aspect of the disease process. It is imperative that we help patients feel heard and let them know that some of the mood symptoms they are experiencing may be related to their endometriosis. Expanding our view of endometriosis as a disease that extends beyond the pelvis and thinking about the systemic effects of endometriosis is key.
We have also identified small molecules (microRNAs) that are predictive of endometriosis. They are continuing to be investigated as a noninvasive biomarker of endometriosis.
Can you talk a little more about these biomarkers?
Dr. Flores: In terms of biomarkers, this is actually some exciting work I was fortunate to be involved in with Dr. Hugh Taylor at Yale. We studied circulating molecules known as microRNAs—these are small, noncoding RNAs that can modify gene expression. In endometriosis, we've identified several that, when combined, have a high sensitivity and specificity for diagnosing endometriosis. These specific microRNAs are undergoing continued studies to ensure that they are reliable in predicting endometriosis. Hopefully they will be available soon for clinical use, as this would be of great value to help shorten the time to diagnosis of endometriosis and ultimately avoid delays in endometriosis treatment.
What is the value of considering noninvasive methods for the diagnosis of endometriosis?
Dr. Flores: There is great value in noninvasive diagnostics for endometriosis. This is because while surgical diagnosis is the “gold standard,” surgery is invasive, and waiting until a surgical diagnosis can be made further contributes to delays in diagnosis. However, more recently there has been a shift toward utilizing noninvasive approaches to the diagnosis of endometriosis, with the primary one focusing on clinically diagnosing endometriosis.
One of the first things to remember is the importance of gathering a patient history and conducting a physical exam. We've all learned this in medical school, and it comes into play even more so with a condition such as endometriosis. Endometriosis is defined as a benign gynecologic disease characterized by endometrial-like tissue outside of the uterus, but this definition does not reflect the true scope and manifestations of endometriosis. Research over the years has demonstrated that endometriosis has systemic effects—affecting regions of the brain associated with anxiety/depression, altering pain sensitization, and having inflammatory effects that can not only affect the reproductive organs but also other organ systems. As such, our questions when evaluating patients for endometriosis need to focus on these various aspects of the disease.
Endometriosis usually leads to cyclic pain. This is because just as the lining of the uterus (the endometrium) grows and sheds every month in response to hormones, endometriotic lesions—which are endometrial-like tissue outside of the uterus—also grow and shed each month. However, there is no outflow for this shed tissue and, as a result, there is an inflammatory response as well as pain. Depending on where those lesions implant, symptoms can include not only cyclic pelvic pain but also cyclic bowel/bladder pain. I’ve also had patients complain of cyclic sharp/shooting leg pain.
Many times, patients present to us after having seen several different types of providers and having been diagnosed with conditions such as irritable bowel syndrome or painful bladder syndrome. However, if you talk to patients and ask them to tell you a little bit more about this bowel or bladder pain, they will frequently endorse that their symptoms are cyclic/most severe during their menses. With respect to pelvic pain, endometriosis-related pelvic pain is usually progressive—becoming progressively more painful over the years. These symptoms are strong indicators that endometriosis is the cause. A pelvic exam is also helpful as findings of nodularity or a fixed uterus may lend further support for endometriosis; a normal exam, however, does not rule out endometriosis.
What are the primary imaging techniques used to diagnose endometriosis?
Dr. Flores: While history and physical exam are the primary components of the clinical diagnosis, imaging can also be helpful. The 2 techniques most often used are pelvic ultrasound and magnetic resonance imaging (MRI).
While transvaginal ultrasound is sensitive and specific for diagnosing endometriomas (ovarian cysts of endometriotic tissue) and may also be able to accurately identify deep-infiltrating endometriosis, it is limited in its ability to visualize peritoneal disease. MRI can improve diagnosis of endometriosis and better estimate the depth of invasion of deep-infiltrating disease, as well as confirm diagnosis of an endometrioma. While MRI is an option for peritoneal endometriosis, superficial disease is usually not detected. Lastly, computed tomography imaging of the chest can be used when thoracic endometriosis is suspected but is otherwise not routinely recommended. Imaging is also helpful in ruling in/out other potential etiologies of pelvic pain such as fibroids and adenomyosis. It is important to recognize, however, that the absence of any findings of endometriosis on imaging does not rule out the disease.
What other best practices do you implement in your day-to-day to aid in diagnosis?
Dr. Flores: Take the time to listen to your patient. Often, they’ve seen several providers before ultimately seeing a provider who can diagnosis their endometriosis without the need for surgical evaluation. We have to ask questions related to their pain and when the pain occurs, and we can’t forget to also ask about pain during intercourse, as well as non-menstrual pelvic pain. Additionally, it is important to recognize that, for patients who may have been suffering from endometriosis for several years before reaching a diagnosis, they may present with chronic pelvic pain. In this case, it is important to ask what their menstrual cycles were like before the pelvic pain became chronic, and usually patients note cyclic pelvic pain that became progressive. We also know that patients who have a first-degree relative with endometriosis are 7 times more likely to be affected by the disease, so asking about a family history of endometriosis is important.
We have to think about endometriosis as a systemic disease. Previously, endometriosis was incorrectly thought of as solely a pelvic disease, but we've been learning more and more through research that it truly is a chronic, systemic disease with multifactorial effects throughout the body. For example, we have found that endometriosis affects regions of the brain associated with anxiety and depression, as well as causing changes in metabolism. For example, a common misconception is that women with a low body mass index (BMI) were at risk for endometriosis, when in fact it's just the opposite—it is the endometriosis that is causing changes in metabolism that lead to a decreased BMI. Patients with endometriosis also frequently struggle with mood disorders; therefore, we cannot dismiss this aspect of the disease process. It is imperative that we help patients feel heard and let them know that some of the mood symptoms they are experiencing may be related to their endometriosis. Expanding our view of endometriosis as a disease that extends beyond the pelvis and thinking about the systemic effects of endometriosis is key.
We have also identified small molecules (microRNAs) that are predictive of endometriosis. They are continuing to be investigated as a noninvasive biomarker of endometriosis.
Can you talk a little more about these biomarkers?
Dr. Flores: In terms of biomarkers, this is actually some exciting work I was fortunate to be involved in with Dr. Hugh Taylor at Yale. We studied circulating molecules known as microRNAs—these are small, noncoding RNAs that can modify gene expression. In endometriosis, we've identified several that, when combined, have a high sensitivity and specificity for diagnosing endometriosis. These specific microRNAs are undergoing continued studies to ensure that they are reliable in predicting endometriosis. Hopefully they will be available soon for clinical use, as this would be of great value to help shorten the time to diagnosis of endometriosis and ultimately avoid delays in endometriosis treatment.
What is the value of considering noninvasive methods for the diagnosis of endometriosis?
Dr. Flores: There is great value in noninvasive diagnostics for endometriosis. This is because while surgical diagnosis is the “gold standard,” surgery is invasive, and waiting until a surgical diagnosis can be made further contributes to delays in diagnosis. However, more recently there has been a shift toward utilizing noninvasive approaches to the diagnosis of endometriosis, with the primary one focusing on clinically diagnosing endometriosis.
One of the first things to remember is the importance of gathering a patient history and conducting a physical exam. We've all learned this in medical school, and it comes into play even more so with a condition such as endometriosis. Endometriosis is defined as a benign gynecologic disease characterized by endometrial-like tissue outside of the uterus, but this definition does not reflect the true scope and manifestations of endometriosis. Research over the years has demonstrated that endometriosis has systemic effects—affecting regions of the brain associated with anxiety/depression, altering pain sensitization, and having inflammatory effects that can not only affect the reproductive organs but also other organ systems. As such, our questions when evaluating patients for endometriosis need to focus on these various aspects of the disease.
Endometriosis usually leads to cyclic pain. This is because just as the lining of the uterus (the endometrium) grows and sheds every month in response to hormones, endometriotic lesions—which are endometrial-like tissue outside of the uterus—also grow and shed each month. However, there is no outflow for this shed tissue and, as a result, there is an inflammatory response as well as pain. Depending on where those lesions implant, symptoms can include not only cyclic pelvic pain but also cyclic bowel/bladder pain. I’ve also had patients complain of cyclic sharp/shooting leg pain.
Many times, patients present to us after having seen several different types of providers and having been diagnosed with conditions such as irritable bowel syndrome or painful bladder syndrome. However, if you talk to patients and ask them to tell you a little bit more about this bowel or bladder pain, they will frequently endorse that their symptoms are cyclic/most severe during their menses. With respect to pelvic pain, endometriosis-related pelvic pain is usually progressive—becoming progressively more painful over the years. These symptoms are strong indicators that endometriosis is the cause. A pelvic exam is also helpful as findings of nodularity or a fixed uterus may lend further support for endometriosis; a normal exam, however, does not rule out endometriosis.
What are the primary imaging techniques used to diagnose endometriosis?
Dr. Flores: While history and physical exam are the primary components of the clinical diagnosis, imaging can also be helpful. The 2 techniques most often used are pelvic ultrasound and magnetic resonance imaging (MRI).
While transvaginal ultrasound is sensitive and specific for diagnosing endometriomas (ovarian cysts of endometriotic tissue) and may also be able to accurately identify deep-infiltrating endometriosis, it is limited in its ability to visualize peritoneal disease. MRI can improve diagnosis of endometriosis and better estimate the depth of invasion of deep-infiltrating disease, as well as confirm diagnosis of an endometrioma. While MRI is an option for peritoneal endometriosis, superficial disease is usually not detected. Lastly, computed tomography imaging of the chest can be used when thoracic endometriosis is suspected but is otherwise not routinely recommended. Imaging is also helpful in ruling in/out other potential etiologies of pelvic pain such as fibroids and adenomyosis. It is important to recognize, however, that the absence of any findings of endometriosis on imaging does not rule out the disease.
What other best practices do you implement in your day-to-day to aid in diagnosis?
Dr. Flores: Take the time to listen to your patient. Often, they’ve seen several providers before ultimately seeing a provider who can diagnosis their endometriosis without the need for surgical evaluation. We have to ask questions related to their pain and when the pain occurs, and we can’t forget to also ask about pain during intercourse, as well as non-menstrual pelvic pain. Additionally, it is important to recognize that, for patients who may have been suffering from endometriosis for several years before reaching a diagnosis, they may present with chronic pelvic pain. In this case, it is important to ask what their menstrual cycles were like before the pelvic pain became chronic, and usually patients note cyclic pelvic pain that became progressive. We also know that patients who have a first-degree relative with endometriosis are 7 times more likely to be affected by the disease, so asking about a family history of endometriosis is important.
We have to think about endometriosis as a systemic disease. Previously, endometriosis was incorrectly thought of as solely a pelvic disease, but we've been learning more and more through research that it truly is a chronic, systemic disease with multifactorial effects throughout the body. For example, we have found that endometriosis affects regions of the brain associated with anxiety and depression, as well as causing changes in metabolism. For example, a common misconception is that women with a low body mass index (BMI) were at risk for endometriosis, when in fact it's just the opposite—it is the endometriosis that is causing changes in metabolism that lead to a decreased BMI. Patients with endometriosis also frequently struggle with mood disorders; therefore, we cannot dismiss this aspect of the disease process. It is imperative that we help patients feel heard and let them know that some of the mood symptoms they are experiencing may be related to their endometriosis. Expanding our view of endometriosis as a disease that extends beyond the pelvis and thinking about the systemic effects of endometriosis is key.
We have also identified small molecules (microRNAs) that are predictive of endometriosis. They are continuing to be investigated as a noninvasive biomarker of endometriosis.
Can you talk a little more about these biomarkers?
Dr. Flores: In terms of biomarkers, this is actually some exciting work I was fortunate to be involved in with Dr. Hugh Taylor at Yale. We studied circulating molecules known as microRNAs—these are small, noncoding RNAs that can modify gene expression. In endometriosis, we've identified several that, when combined, have a high sensitivity and specificity for diagnosing endometriosis. These specific microRNAs are undergoing continued studies to ensure that they are reliable in predicting endometriosis. Hopefully they will be available soon for clinical use, as this would be of great value to help shorten the time to diagnosis of endometriosis and ultimately avoid delays in endometriosis treatment.
The AGA Research Foundation awards $2.66 million in research funding
The American Gastroenterological Association (AGA) is proud to announce the 71 recipients selected to receive research funding through its annual AGA Research Foundation Awards Program. The program serves as a catalyst for discovery and career growth among the most promising researchers in gastroenterology and hepatology.
“This year’s recipients are determined to make an impact on digestive health care through their research,” said Michael Camilleri, MD, AGAF, chair, AGA Research Foundation. “We are honored to support these talented individuals at a critical stage in their careers and research projects. We look forward to seeing their great accomplishments.”

Treatment options for digestive diseases begin with vigorous research. The AGA Research Foundation supports medical investigators as they advance our understanding of gastrointestinal and liver conditions. The AGA Research Awards Program is made possible thanks to generous donors and funders. Learn more about the AGA Research Foundation at foundation.gastro.org.
Here are this year’s award recipients:
Research Scholar Awards
AGA Research Scholar Award
Alexander Nguyen, MD, PhD, The Regent of the University of California, Los Angeles
Jeffrey W. Patterson-Fortin, MD, PhD, Dana-Farber Cancer Institute, Boston, Massachusetts
Sean Spencer, MD, PhD, Stanford Medicine, California
Ken Y. Hui, MD, PhD, Johns Hopkins University School of Medicine, Baltimore, Maryland
AGA-Gastric Cancer Foundation Ben Feinstein Memorial Research Scholar Award in Gastric Cancer
Martina Molgora, PhD, Washington University School of Medicine, St. Louis, Missouri
AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease
Brooke R. Druliner, PhD, Mayo Clinic, Rochester, Minnesota
Specialty Awards
AGA-Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer
Simon Schwörer, PhD, University of Chicago, Illinois
AGA-R. Robert & Sally Funderburg Research Award in Gastric Cancer
Bryson W. Katona, MD, PhD, University of Pennsylvania Perelman School of Medicine, Philadelphia
AGA-Amgen Fellowship-to-Faculty Transition Award
Cynthia Hsu, MD, PhD, University of California, San Diego
AGA-Bristol Myers Squibb Fellowship-to-Faculty Transition Award
Siyan Cao, MD, PhD, Washington University in St. Louis
Amit Ringel, MD, Brigham and Women’s Hospital, Boston, Massachusetts
Pilot Awards
AGA Pilot Research Award In Digestive Disease Health Disparities
Sharad Wadhwani, MD, MPH, University of California, San Francisco
AGA Pilot Research Award in Health Disparities
Enrique Soto Pérez de Celis, MD, PhD, MS, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán
AGA Pilot Research Award
Diana L. Snyder, MD, Mayo Clinic, Rochester, Minnesota
Michael Li, MD, MPH, University of California, San Francisco
Patricia Bloom, MD, University of Michigan, Ann Arbor
Edward Barnes, MD, MPH, University of North Carolina School of Medicine, Chapel Hill
AGA-Amgen Pilot Research Award In Digestive Disease Health Disparities
Laura Targownik, MD, MSHS, University of Toronto/Mount Sinai Hospital, Toronto, ON
Undergraduate Research Awards
AGA-Aman Armaan Ahmed Family Summer Undergraduate Research Award
Gwyneth Garramone, Loyola Marymount University, Los Angeles, California
Ella McLaren, University of California, San Diego
Nathan Moy, University of Southern California, Los Angeles
Hussein Elfayoumy, Johns Hopkins University, Baltimore, Maryland
Isabelle Garcia-Fischer, Tufts University, Medford, Massachusetts
Lidia Appell, University of New Mexico, Albuquerque
Katherine Burkman, Duke University, Durham, North Carolina
Alexa Boylan, Spelman College, Atlanta, Georgia
AGA-Dr. Harvey Young Education and Development Foundation’s Young Guts Scholar Program
Lucy Zhao, Massachusetts Institute of Technology Koch Institute for Integrative Cancer Research, Cambridge
Andrew Tran, Duke University, Durham, North Carolina
Sohaib Hassan, Rutgers University – Verzi Lab, New Brunswick, New Jersey
Varun Ponnusamy, University of Michigan Medical School, Ann Arbor
Daniella Montalvo, University of Miami, Coral Gables, Florida
Sara Chough, Columbia University Irving Medical Center, New York, New York
Abstract Awards
Fellow Abstract Awards
David Flores Marin, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts
Jesse Platt, MD, PhD, Massachusetts General Hospital, Boston
Devika Gandhi, MD, Loma Linda University, California
Amanda Krause, MD, University of California, San Diego
Cynthia Tsay, MD, Mphil, Johns Hopkins Hospital, Baltimore, Maryland
Suha Abushamma, MD, Cleveland Clinic Foundation, Ohio
Md Obaidul Islam, PhD, University of Miami, Coral Gables, Florida
Sakteesh Gurunathan, MD, New York University School of Medicine, New York
Aaron Yeoh, MD, Stanford Hospital & Clinics, California
Yang Xiao, PhD, Mayo Clinic, Rochester, Minnesota
Jacques Gonzales, PhD, MS, Michigan State University, East Lansing
Kai Wang, MD, PhD, Harvard T.H. Chan School of Public Health, Cambridge, Massachusetts
Hoyeol Kim, PhD, Cedars Sinai Medical Center, New York, New York
Babajide Ojo, PhD, MS, Stanford University, California
AGA Fellow Abstract of the Year Award
Stefania Tocci, PhD, MS, University of Massachusetts, Cambridge
Student Abstract Awards
Pritha Chatterjee, MS, University of California, Riverside
Ela Contreras Panta, Vanderbilt University, Nashville, Tennessee
Mihir Shah, MD, MBBS, John H. Stroger Hospital of Cook County, Chicago, Illinois
Yuhan Fu, DO, Metrohealth Medical Center, Cleveland, Ohio
Raissa Nana Sede Mbakop, MD, Piedmont Athens Regional Medical Center, Athens, Georgia
Eleazar Montalvan-Sanchez, MD, Indiana University School of Medicine, Bloomington
Sarang Gupta, MD, St. Michael’s Hospital, Toronto, Ontario
Daniel Kim, Harvard Medical School, Cambridge, Massachusetts
Hannah Hrncir, Emory University, Decatur, Georgia
Zarwa Saqib, McMaster University, Hamilton, Ontario
Ying Zhu, MD, PhD, University of Michigan, Ann Arbor
Lizeth Cifuentes, MD, University of Pittsburgh Medical Center, Pennsylvania
Sharvani Dhandibhotla, MBBS, MS, Massachusetts General Hospital, Boston
Lauren Lynch, Baylor College of Medicine, Houston, Texas
AGA Student Abstract of The Year Award
Gabrielle Waclawik, MD, MPH, University of Wisconsin, Madison
AGA Abstract Award for Health Disparities Research
Soyoun Min, PhD, Lerner Research Institute (fellow), Cleveland, Ohio
Xiaobei Zhang, PhD , David Geffen School of Medicine at University of California, Los Angeles (fellow)
Matthew Zhao, David Geffen School of Medicine at University of California, Los Angeles (student)
Hannah Fiske, MD, Brown University/Rhode Island Hospital (student), Providence
AGA-APFED Abstract Award in Eosinophilic GI Diseases
Matthew Buendia, MD, Vanderbilt University Medical Center – Monroe Carell Jr. Children’s Hospital, Nashville, Tennessee
Alexandra L. Strauss, MD, University of Pennsylvania Health System, Philadelphia
Mira Yang, Northwestern Feinberg School of Medicine, Chicago, Illinois
AGA-Moti L. & Kamla Rustgi International Travel Award
Aviv Pudipeddi, MBBS, Concord Repatriation General Hospital, Sydney, Australia
Dianqin Sun, MBBS, Mmed, Erasmus University Medical Center, Rotterdam, Netherlands
The American Gastroenterological Association (AGA) is proud to announce the 71 recipients selected to receive research funding through its annual AGA Research Foundation Awards Program. The program serves as a catalyst for discovery and career growth among the most promising researchers in gastroenterology and hepatology.
“This year’s recipients are determined to make an impact on digestive health care through their research,” said Michael Camilleri, MD, AGAF, chair, AGA Research Foundation. “We are honored to support these talented individuals at a critical stage in their careers and research projects. We look forward to seeing their great accomplishments.”
Treatment options for digestive diseases begin with vigorous research. The AGA Research Foundation supports medical investigators as they advance our understanding of gastrointestinal and liver conditions. The AGA Research Awards Program is made possible thanks to generous donors and funders. Learn more about the AGA Research Foundation at foundation.gastro.org.
Here are this year’s award recipients:
Research Scholar Awards
AGA Research Scholar Award
Alexander Nguyen, MD, PhD, The Regent of the University of California, Los Angeles
Jeffrey W. Patterson-Fortin, MD, PhD, Dana-Farber Cancer Institute, Boston, Massachusetts
Sean Spencer, MD, PhD, Stanford Medicine, California
Ken Y. Hui, MD, PhD, Johns Hopkins University School of Medicine, Baltimore, Maryland
AGA-Gastric Cancer Foundation Ben Feinstein Memorial Research Scholar Award in Gastric Cancer
Martina Molgora, PhD, Washington University School of Medicine, St. Louis, Missouri
AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease
Brooke R. Druliner, PhD, Mayo Clinic, Rochester, Minnesota
Specialty Awards
AGA-Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer
Simon Schwörer, PhD, University of Chicago, Illinois
AGA-R. Robert & Sally Funderburg Research Award in Gastric Cancer
Bryson W. Katona, MD, PhD, University of Pennsylvania Perelman School of Medicine, Philadelphia
AGA-Amgen Fellowship-to-Faculty Transition Award
Cynthia Hsu, MD, PhD, University of California, San Diego
AGA-Bristol Myers Squibb Fellowship-to-Faculty Transition Award
Siyan Cao, MD, PhD, Washington University in St. Louis
Amit Ringel, MD, Brigham and Women’s Hospital, Boston, Massachusetts
Pilot Awards
AGA Pilot Research Award In Digestive Disease Health Disparities
Sharad Wadhwani, MD, MPH, University of California, San Francisco
AGA Pilot Research Award in Health Disparities
Enrique Soto Pérez de Celis, MD, PhD, MS, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán
AGA Pilot Research Award
Diana L. Snyder, MD, Mayo Clinic, Rochester, Minnesota
Michael Li, MD, MPH, University of California, San Francisco
Patricia Bloom, MD, University of Michigan, Ann Arbor
Edward Barnes, MD, MPH, University of North Carolina School of Medicine, Chapel Hill
AGA-Amgen Pilot Research Award In Digestive Disease Health Disparities
Laura Targownik, MD, MSHS, University of Toronto/Mount Sinai Hospital, Toronto, ON
Undergraduate Research Awards
AGA-Aman Armaan Ahmed Family Summer Undergraduate Research Award
Gwyneth Garramone, Loyola Marymount University, Los Angeles, California
Ella McLaren, University of California, San Diego
Nathan Moy, University of Southern California, Los Angeles
Hussein Elfayoumy, Johns Hopkins University, Baltimore, Maryland
Isabelle Garcia-Fischer, Tufts University, Medford, Massachusetts
Lidia Appell, University of New Mexico, Albuquerque
Katherine Burkman, Duke University, Durham, North Carolina
Alexa Boylan, Spelman College, Atlanta, Georgia
AGA-Dr. Harvey Young Education and Development Foundation’s Young Guts Scholar Program
Lucy Zhao, Massachusetts Institute of Technology Koch Institute for Integrative Cancer Research, Cambridge
Andrew Tran, Duke University, Durham, North Carolina
Sohaib Hassan, Rutgers University – Verzi Lab, New Brunswick, New Jersey
Varun Ponnusamy, University of Michigan Medical School, Ann Arbor
Daniella Montalvo, University of Miami, Coral Gables, Florida
Sara Chough, Columbia University Irving Medical Center, New York, New York
Abstract Awards
Fellow Abstract Awards
David Flores Marin, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts
Jesse Platt, MD, PhD, Massachusetts General Hospital, Boston
Devika Gandhi, MD, Loma Linda University, California
Amanda Krause, MD, University of California, San Diego
Cynthia Tsay, MD, Mphil, Johns Hopkins Hospital, Baltimore, Maryland
Suha Abushamma, MD, Cleveland Clinic Foundation, Ohio
Md Obaidul Islam, PhD, University of Miami, Coral Gables, Florida
Sakteesh Gurunathan, MD, New York University School of Medicine, New York
Aaron Yeoh, MD, Stanford Hospital & Clinics, California
Yang Xiao, PhD, Mayo Clinic, Rochester, Minnesota
Jacques Gonzales, PhD, MS, Michigan State University, East Lansing
Kai Wang, MD, PhD, Harvard T.H. Chan School of Public Health, Cambridge, Massachusetts
Hoyeol Kim, PhD, Cedars Sinai Medical Center, New York, New York
Babajide Ojo, PhD, MS, Stanford University, California
AGA Fellow Abstract of the Year Award
Stefania Tocci, PhD, MS, University of Massachusetts, Cambridge
Student Abstract Awards
Pritha Chatterjee, MS, University of California, Riverside
Ela Contreras Panta, Vanderbilt University, Nashville, Tennessee
Mihir Shah, MD, MBBS, John H. Stroger Hospital of Cook County, Chicago, Illinois
Yuhan Fu, DO, Metrohealth Medical Center, Cleveland, Ohio
Raissa Nana Sede Mbakop, MD, Piedmont Athens Regional Medical Center, Athens, Georgia
Eleazar Montalvan-Sanchez, MD, Indiana University School of Medicine, Bloomington
Sarang Gupta, MD, St. Michael’s Hospital, Toronto, Ontario
Daniel Kim, Harvard Medical School, Cambridge, Massachusetts
Hannah Hrncir, Emory University, Decatur, Georgia
Zarwa Saqib, McMaster University, Hamilton, Ontario
Ying Zhu, MD, PhD, University of Michigan, Ann Arbor
Lizeth Cifuentes, MD, University of Pittsburgh Medical Center, Pennsylvania
Sharvani Dhandibhotla, MBBS, MS, Massachusetts General Hospital, Boston
Lauren Lynch, Baylor College of Medicine, Houston, Texas
AGA Student Abstract of The Year Award
Gabrielle Waclawik, MD, MPH, University of Wisconsin, Madison
AGA Abstract Award for Health Disparities Research
Soyoun Min, PhD, Lerner Research Institute (fellow), Cleveland, Ohio
Xiaobei Zhang, PhD , David Geffen School of Medicine at University of California, Los Angeles (fellow)
Matthew Zhao, David Geffen School of Medicine at University of California, Los Angeles (student)
Hannah Fiske, MD, Brown University/Rhode Island Hospital (student), Providence
AGA-APFED Abstract Award in Eosinophilic GI Diseases
Matthew Buendia, MD, Vanderbilt University Medical Center – Monroe Carell Jr. Children’s Hospital, Nashville, Tennessee
Alexandra L. Strauss, MD, University of Pennsylvania Health System, Philadelphia
Mira Yang, Northwestern Feinberg School of Medicine, Chicago, Illinois
AGA-Moti L. & Kamla Rustgi International Travel Award
Aviv Pudipeddi, MBBS, Concord Repatriation General Hospital, Sydney, Australia
Dianqin Sun, MBBS, Mmed, Erasmus University Medical Center, Rotterdam, Netherlands
The American Gastroenterological Association (AGA) is proud to announce the 71 recipients selected to receive research funding through its annual AGA Research Foundation Awards Program. The program serves as a catalyst for discovery and career growth among the most promising researchers in gastroenterology and hepatology.
“This year’s recipients are determined to make an impact on digestive health care through their research,” said Michael Camilleri, MD, AGAF, chair, AGA Research Foundation. “We are honored to support these talented individuals at a critical stage in their careers and research projects. We look forward to seeing their great accomplishments.”
Treatment options for digestive diseases begin with vigorous research. The AGA Research Foundation supports medical investigators as they advance our understanding of gastrointestinal and liver conditions. The AGA Research Awards Program is made possible thanks to generous donors and funders. Learn more about the AGA Research Foundation at foundation.gastro.org.
Here are this year’s award recipients:
Research Scholar Awards
AGA Research Scholar Award
Alexander Nguyen, MD, PhD, The Regent of the University of California, Los Angeles
Jeffrey W. Patterson-Fortin, MD, PhD, Dana-Farber Cancer Institute, Boston, Massachusetts
Sean Spencer, MD, PhD, Stanford Medicine, California
Ken Y. Hui, MD, PhD, Johns Hopkins University School of Medicine, Baltimore, Maryland
AGA-Gastric Cancer Foundation Ben Feinstein Memorial Research Scholar Award in Gastric Cancer
Martina Molgora, PhD, Washington University School of Medicine, St. Louis, Missouri
AGA-Takeda Pharmaceuticals Research Scholar Award in Inflammatory Bowel Disease
Brooke R. Druliner, PhD, Mayo Clinic, Rochester, Minnesota
Specialty Awards
AGA-Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer
Simon Schwörer, PhD, University of Chicago, Illinois
AGA-R. Robert & Sally Funderburg Research Award in Gastric Cancer
Bryson W. Katona, MD, PhD, University of Pennsylvania Perelman School of Medicine, Philadelphia
AGA-Amgen Fellowship-to-Faculty Transition Award
Cynthia Hsu, MD, PhD, University of California, San Diego
AGA-Bristol Myers Squibb Fellowship-to-Faculty Transition Award
Siyan Cao, MD, PhD, Washington University in St. Louis
Amit Ringel, MD, Brigham and Women’s Hospital, Boston, Massachusetts
Pilot Awards
AGA Pilot Research Award In Digestive Disease Health Disparities
Sharad Wadhwani, MD, MPH, University of California, San Francisco
AGA Pilot Research Award in Health Disparities
Enrique Soto Pérez de Celis, MD, PhD, MS, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán
AGA Pilot Research Award
Diana L. Snyder, MD, Mayo Clinic, Rochester, Minnesota
Michael Li, MD, MPH, University of California, San Francisco
Patricia Bloom, MD, University of Michigan, Ann Arbor
Edward Barnes, MD, MPH, University of North Carolina School of Medicine, Chapel Hill
AGA-Amgen Pilot Research Award In Digestive Disease Health Disparities
Laura Targownik, MD, MSHS, University of Toronto/Mount Sinai Hospital, Toronto, ON
Undergraduate Research Awards
AGA-Aman Armaan Ahmed Family Summer Undergraduate Research Award
Gwyneth Garramone, Loyola Marymount University, Los Angeles, California
Ella McLaren, University of California, San Diego
Nathan Moy, University of Southern California, Los Angeles
Hussein Elfayoumy, Johns Hopkins University, Baltimore, Maryland
Isabelle Garcia-Fischer, Tufts University, Medford, Massachusetts
Lidia Appell, University of New Mexico, Albuquerque
Katherine Burkman, Duke University, Durham, North Carolina
Alexa Boylan, Spelman College, Atlanta, Georgia
AGA-Dr. Harvey Young Education and Development Foundation’s Young Guts Scholar Program
Lucy Zhao, Massachusetts Institute of Technology Koch Institute for Integrative Cancer Research, Cambridge
Andrew Tran, Duke University, Durham, North Carolina
Sohaib Hassan, Rutgers University – Verzi Lab, New Brunswick, New Jersey
Varun Ponnusamy, University of Michigan Medical School, Ann Arbor
Daniella Montalvo, University of Miami, Coral Gables, Florida
Sara Chough, Columbia University Irving Medical Center, New York, New York
Abstract Awards
Fellow Abstract Awards
David Flores Marin, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts
Jesse Platt, MD, PhD, Massachusetts General Hospital, Boston
Devika Gandhi, MD, Loma Linda University, California
Amanda Krause, MD, University of California, San Diego
Cynthia Tsay, MD, Mphil, Johns Hopkins Hospital, Baltimore, Maryland
Suha Abushamma, MD, Cleveland Clinic Foundation, Ohio
Md Obaidul Islam, PhD, University of Miami, Coral Gables, Florida
Sakteesh Gurunathan, MD, New York University School of Medicine, New York
Aaron Yeoh, MD, Stanford Hospital & Clinics, California
Yang Xiao, PhD, Mayo Clinic, Rochester, Minnesota
Jacques Gonzales, PhD, MS, Michigan State University, East Lansing
Kai Wang, MD, PhD, Harvard T.H. Chan School of Public Health, Cambridge, Massachusetts
Hoyeol Kim, PhD, Cedars Sinai Medical Center, New York, New York
Babajide Ojo, PhD, MS, Stanford University, California
AGA Fellow Abstract of the Year Award
Stefania Tocci, PhD, MS, University of Massachusetts, Cambridge
Student Abstract Awards
Pritha Chatterjee, MS, University of California, Riverside
Ela Contreras Panta, Vanderbilt University, Nashville, Tennessee
Mihir Shah, MD, MBBS, John H. Stroger Hospital of Cook County, Chicago, Illinois
Yuhan Fu, DO, Metrohealth Medical Center, Cleveland, Ohio
Raissa Nana Sede Mbakop, MD, Piedmont Athens Regional Medical Center, Athens, Georgia
Eleazar Montalvan-Sanchez, MD, Indiana University School of Medicine, Bloomington
Sarang Gupta, MD, St. Michael’s Hospital, Toronto, Ontario
Daniel Kim, Harvard Medical School, Cambridge, Massachusetts
Hannah Hrncir, Emory University, Decatur, Georgia
Zarwa Saqib, McMaster University, Hamilton, Ontario
Ying Zhu, MD, PhD, University of Michigan, Ann Arbor
Lizeth Cifuentes, MD, University of Pittsburgh Medical Center, Pennsylvania
Sharvani Dhandibhotla, MBBS, MS, Massachusetts General Hospital, Boston
Lauren Lynch, Baylor College of Medicine, Houston, Texas
AGA Student Abstract of The Year Award
Gabrielle Waclawik, MD, MPH, University of Wisconsin, Madison
AGA Abstract Award for Health Disparities Research
Soyoun Min, PhD, Lerner Research Institute (fellow), Cleveland, Ohio
Xiaobei Zhang, PhD , David Geffen School of Medicine at University of California, Los Angeles (fellow)
Matthew Zhao, David Geffen School of Medicine at University of California, Los Angeles (student)
Hannah Fiske, MD, Brown University/Rhode Island Hospital (student), Providence
AGA-APFED Abstract Award in Eosinophilic GI Diseases
Matthew Buendia, MD, Vanderbilt University Medical Center – Monroe Carell Jr. Children’s Hospital, Nashville, Tennessee
Alexandra L. Strauss, MD, University of Pennsylvania Health System, Philadelphia
Mira Yang, Northwestern Feinberg School of Medicine, Chicago, Illinois
AGA-Moti L. & Kamla Rustgi International Travel Award
Aviv Pudipeddi, MBBS, Concord Repatriation General Hospital, Sydney, Australia
Dianqin Sun, MBBS, Mmed, Erasmus University Medical Center, Rotterdam, Netherlands
Membership priorities shape the AGA advocacy agenda
Here, we present key highlights from the survey findings and share opportunities for members to engage in GI advocacy.
AGA advocacy has contributed to significant recent successes that include lowering the average-risk of colorectal cancer screening age from 50 to 45 years, phasing out cost-sharing burdens associated with polypectomy at screening colonoscopy, encouraging federal support to focus on GI cancer disparities, ensuring coverage for telehealth services, expanding colonoscopy coverage after positive noninvasive colorectal cancer screening tests, and mitigating scheduled cuts in Medicare reimbursement for GI services.
Despite these important successes, the GI community faces significant challenges that include persisting GI health disparities; declines in reimbursement and increased prior authorization burdens for GI procedures and clinic visits, limited research funding to address the burden of GI disease, climate change, provider burnout, and increasing administrative burdens (such as insurance prior authorizations and step therapy policies.
The AGA sought to better understand policy priorities of the GI community by disseminating a 34-question policy priority survey to AGA members in December 2022. A total of 251 members responded to the survey with career stage and primary practice setting varying among respondents (Figure 1). The AGA vetted and selected 10 health policy issues of highest interest with 95% of survey respondents agreeing these 10 selected topics covered the top priority issues impacting gastroenterology (Figure 2).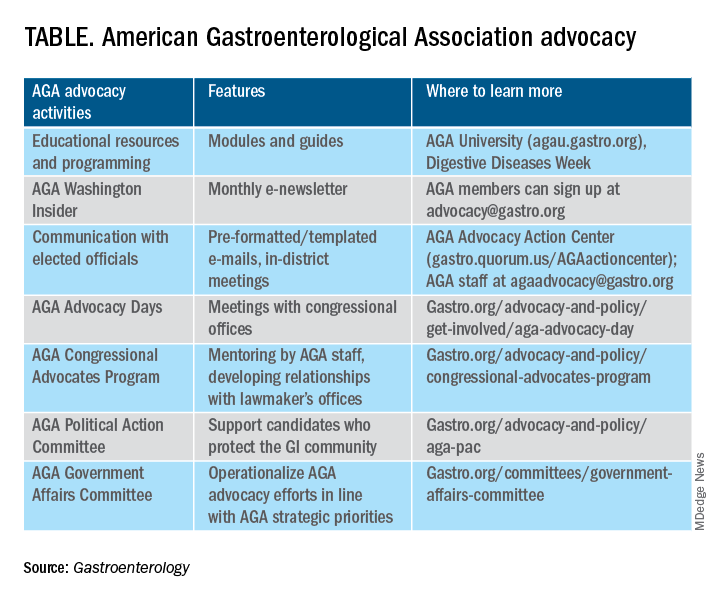
From these 10 policy issues, members were asked to identify the top 5 issues that AGA advocacy efforts should address.
The issues most frequently identified included reducing administrative burdens and patient delays in care because of increased prior authorizations (78%), ensuring fair reimbursement for GI providers (68%), reducing insurance-initiated switching of patient treatments for nonmedical reasons (58%), maintaining coverage of video and telephone evaluation and management visits (55%), and reducing delays in clinical care resulting from step therapy protocols (53%).
Other important issues included ensuring patients with pre-existing conditions have access to essential benefits and quality specialty care (43%); protecting providers from medical licensing restrictions and liability to deliver care across state lines (35%); addressing Medicare Quality Payment Program reporting requirements and lack of specialty advanced payment models (27%); increasing funding for GI health disparities (24%); and, increasing federal research funding to ensure greater opportunities for diverse early career investigators (20%).
Most problematic burdens
Survey respondents identified insurer prior authorization and step therapy burdens as especially problematic. 93% of respondents described the impact of prior authorization on their practices as “significantly burdensome” (61%) or “somewhat burdensome” (32%).
About 95% noted that prior authorization restrictions have impacted patient access to clinically appropriate treatments and patient clinical outcomes “significantly” (56%) or “somewhat” (39%) negatively. 84% described the burdens associated with prior authorization policies as having increased “significantly” (60%) or “somewhat” (24%) over the last 5 years.

Likewise, step therapy protocols were perceived by 84% of respondents as burdensome; by 88% as negatively impactful on patient access to clinically appropriate treatments; and, by 88% as negatively impactful on patient clinical outcomes.
About 84% of respondents noted increases in the frequency of nonmedical switching and dosing restrictions over the last 5 years, with 90% perceiving negative impacts on patient clinical outcomes. 73% of respondents reported increased burdens associated with compliance in the Medicare QPP over the last 5 years.
AGA’s advocacy work
About 76% of respondents were interested in learning more about the AGA’s advocacy work. We presented some of the various opportunities and resources for members to engage with and contribute to AGA advocacy efforts (see pie chart). Based on the tremendous efforts and dedication of AGA staff, some of these opportunities include educational modules on AGA University, DDW programming, the AGA Washington Insider monthly policy newsletter, preformatted communications available through the AGA Advocacy Action Center, participation in AGA Advocacy Days or the AGA Congressional Advocates Program, service on the AGA Government Affairs Committee, and/or contributing to the AGA Political Action Committee.
Overall, the survey respondents illustrate the diversity and enthusiasm of AGA membership. Importantly, 95% of AGA members responding to the survey agreed these 10 selected policy issues are inclusive of the current top priority issues of the GI community. Amidst an ever-shifting health care landscape, we – the AGA community – must remain vigilant and adaptable to best address expected and unexpected changes and challenges to our patients and colleagues. In this respect, we should encourage constructive communication and dialogue between AGA membership, leadership, other issue stakeholders, government representatives and entities, and payers.
Amit Patel, MD, is a gastroenterologist and associate professor of medicine at Duke University and the Durham Veterans Affairs Medical Center, both in Durham, N.C. He serves on the editorial review board of Gastroenterology. Rotonya McCants Carr, MD, is the Cyrus E. Rubin Chair and division head of gastroenterology at the University of Washington, Seattle. Both Dr. Patel and Dr. Carr serve on the AGA Government Affairs Committee. The contents of this article do not represent the views of the Department of Veterans Affairs.
Reference
Patel A et al. Gastroenterology. 2023 May;164[6]:847-50.
Here, we present key highlights from the survey findings and share opportunities for members to engage in GI advocacy.
AGA advocacy has contributed to significant recent successes that include lowering the average-risk of colorectal cancer screening age from 50 to 45 years, phasing out cost-sharing burdens associated with polypectomy at screening colonoscopy, encouraging federal support to focus on GI cancer disparities, ensuring coverage for telehealth services, expanding colonoscopy coverage after positive noninvasive colorectal cancer screening tests, and mitigating scheduled cuts in Medicare reimbursement for GI services.
Despite these important successes, the GI community faces significant challenges that include persisting GI health disparities; declines in reimbursement and increased prior authorization burdens for GI procedures and clinic visits, limited research funding to address the burden of GI disease, climate change, provider burnout, and increasing administrative burdens (such as insurance prior authorizations and step therapy policies.
The AGA sought to better understand policy priorities of the GI community by disseminating a 34-question policy priority survey to AGA members in December 2022. A total of 251 members responded to the survey with career stage and primary practice setting varying among respondents (Figure 1). The AGA vetted and selected 10 health policy issues of highest interest with 95% of survey respondents agreeing these 10 selected topics covered the top priority issues impacting gastroenterology (Figure 2).
From these 10 policy issues, members were asked to identify the top 5 issues that AGA advocacy efforts should address.
The issues most frequently identified included reducing administrative burdens and patient delays in care because of increased prior authorizations (78%), ensuring fair reimbursement for GI providers (68%), reducing insurance-initiated switching of patient treatments for nonmedical reasons (58%), maintaining coverage of video and telephone evaluation and management visits (55%), and reducing delays in clinical care resulting from step therapy protocols (53%).
Other important issues included ensuring patients with pre-existing conditions have access to essential benefits and quality specialty care (43%); protecting providers from medical licensing restrictions and liability to deliver care across state lines (35%); addressing Medicare Quality Payment Program reporting requirements and lack of specialty advanced payment models (27%); increasing funding for GI health disparities (24%); and, increasing federal research funding to ensure greater opportunities for diverse early career investigators (20%).
Most problematic burdens
Survey respondents identified insurer prior authorization and step therapy burdens as especially problematic. 93% of respondents described the impact of prior authorization on their practices as “significantly burdensome” (61%) or “somewhat burdensome” (32%).
About 95% noted that prior authorization restrictions have impacted patient access to clinically appropriate treatments and patient clinical outcomes “significantly” (56%) or “somewhat” (39%) negatively. 84% described the burdens associated with prior authorization policies as having increased “significantly” (60%) or “somewhat” (24%) over the last 5 years.
Likewise, step therapy protocols were perceived by 84% of respondents as burdensome; by 88% as negatively impactful on patient access to clinically appropriate treatments; and, by 88% as negatively impactful on patient clinical outcomes.
About 84% of respondents noted increases in the frequency of nonmedical switching and dosing restrictions over the last 5 years, with 90% perceiving negative impacts on patient clinical outcomes. 73% of respondents reported increased burdens associated with compliance in the Medicare QPP over the last 5 years.
AGA’s advocacy work
About 76% of respondents were interested in learning more about the AGA’s advocacy work. We presented some of the various opportunities and resources for members to engage with and contribute to AGA advocacy efforts (see pie chart). Based on the tremendous efforts and dedication of AGA staff, some of these opportunities include educational modules on AGA University, DDW programming, the AGA Washington Insider monthly policy newsletter, preformatted communications available through the AGA Advocacy Action Center, participation in AGA Advocacy Days or the AGA Congressional Advocates Program, service on the AGA Government Affairs Committee, and/or contributing to the AGA Political Action Committee.
Overall, the survey respondents illustrate the diversity and enthusiasm of AGA membership. Importantly, 95% of AGA members responding to the survey agreed these 10 selected policy issues are inclusive of the current top priority issues of the GI community. Amidst an ever-shifting health care landscape, we – the AGA community – must remain vigilant and adaptable to best address expected and unexpected changes and challenges to our patients and colleagues. In this respect, we should encourage constructive communication and dialogue between AGA membership, leadership, other issue stakeholders, government representatives and entities, and payers.
Amit Patel, MD, is a gastroenterologist and associate professor of medicine at Duke University and the Durham Veterans Affairs Medical Center, both in Durham, N.C. He serves on the editorial review board of Gastroenterology. Rotonya McCants Carr, MD, is the Cyrus E. Rubin Chair and division head of gastroenterology at the University of Washington, Seattle. Both Dr. Patel and Dr. Carr serve on the AGA Government Affairs Committee. The contents of this article do not represent the views of the Department of Veterans Affairs.
Reference
Patel A et al. Gastroenterology. 2023 May;164[6]:847-50.
Here, we present key highlights from the survey findings and share opportunities for members to engage in GI advocacy.
AGA advocacy has contributed to significant recent successes that include lowering the average-risk of colorectal cancer screening age from 50 to 45 years, phasing out cost-sharing burdens associated with polypectomy at screening colonoscopy, encouraging federal support to focus on GI cancer disparities, ensuring coverage for telehealth services, expanding colonoscopy coverage after positive noninvasive colorectal cancer screening tests, and mitigating scheduled cuts in Medicare reimbursement for GI services.
Despite these important successes, the GI community faces significant challenges that include persisting GI health disparities; declines in reimbursement and increased prior authorization burdens for GI procedures and clinic visits, limited research funding to address the burden of GI disease, climate change, provider burnout, and increasing administrative burdens (such as insurance prior authorizations and step therapy policies.
The AGA sought to better understand policy priorities of the GI community by disseminating a 34-question policy priority survey to AGA members in December 2022. A total of 251 members responded to the survey with career stage and primary practice setting varying among respondents (Figure 1). The AGA vetted and selected 10 health policy issues of highest interest with 95% of survey respondents agreeing these 10 selected topics covered the top priority issues impacting gastroenterology (Figure 2).
From these 10 policy issues, members were asked to identify the top 5 issues that AGA advocacy efforts should address.
The issues most frequently identified included reducing administrative burdens and patient delays in care because of increased prior authorizations (78%), ensuring fair reimbursement for GI providers (68%), reducing insurance-initiated switching of patient treatments for nonmedical reasons (58%), maintaining coverage of video and telephone evaluation and management visits (55%), and reducing delays in clinical care resulting from step therapy protocols (53%).
Other important issues included ensuring patients with pre-existing conditions have access to essential benefits and quality specialty care (43%); protecting providers from medical licensing restrictions and liability to deliver care across state lines (35%); addressing Medicare Quality Payment Program reporting requirements and lack of specialty advanced payment models (27%); increasing funding for GI health disparities (24%); and, increasing federal research funding to ensure greater opportunities for diverse early career investigators (20%).
Most problematic burdens
Survey respondents identified insurer prior authorization and step therapy burdens as especially problematic. 93% of respondents described the impact of prior authorization on their practices as “significantly burdensome” (61%) or “somewhat burdensome” (32%).
About 95% noted that prior authorization restrictions have impacted patient access to clinically appropriate treatments and patient clinical outcomes “significantly” (56%) or “somewhat” (39%) negatively. 84% described the burdens associated with prior authorization policies as having increased “significantly” (60%) or “somewhat” (24%) over the last 5 years.
Likewise, step therapy protocols were perceived by 84% of respondents as burdensome; by 88% as negatively impactful on patient access to clinically appropriate treatments; and, by 88% as negatively impactful on patient clinical outcomes.
About 84% of respondents noted increases in the frequency of nonmedical switching and dosing restrictions over the last 5 years, with 90% perceiving negative impacts on patient clinical outcomes. 73% of respondents reported increased burdens associated with compliance in the Medicare QPP over the last 5 years.
AGA’s advocacy work
About 76% of respondents were interested in learning more about the AGA’s advocacy work. We presented some of the various opportunities and resources for members to engage with and contribute to AGA advocacy efforts (see pie chart). Based on the tremendous efforts and dedication of AGA staff, some of these opportunities include educational modules on AGA University, DDW programming, the AGA Washington Insider monthly policy newsletter, preformatted communications available through the AGA Advocacy Action Center, participation in AGA Advocacy Days or the AGA Congressional Advocates Program, service on the AGA Government Affairs Committee, and/or contributing to the AGA Political Action Committee.
Overall, the survey respondents illustrate the diversity and enthusiasm of AGA membership. Importantly, 95% of AGA members responding to the survey agreed these 10 selected policy issues are inclusive of the current top priority issues of the GI community. Amidst an ever-shifting health care landscape, we – the AGA community – must remain vigilant and adaptable to best address expected and unexpected changes and challenges to our patients and colleagues. In this respect, we should encourage constructive communication and dialogue between AGA membership, leadership, other issue stakeholders, government representatives and entities, and payers.
Amit Patel, MD, is a gastroenterologist and associate professor of medicine at Duke University and the Durham Veterans Affairs Medical Center, both in Durham, N.C. He serves on the editorial review board of Gastroenterology. Rotonya McCants Carr, MD, is the Cyrus E. Rubin Chair and division head of gastroenterology at the University of Washington, Seattle. Both Dr. Patel and Dr. Carr serve on the AGA Government Affairs Committee. The contents of this article do not represent the views of the Department of Veterans Affairs.
Reference
Patel A et al. Gastroenterology. 2023 May;164[6]:847-50.
The power of mentorship
In a 2018 JAMA Viewpoint, Dr. Vineet Chopra, a former colleague of mine at the University of Michigan (now chair of medicine at the University of Colorado) and colleagues wrote about four archetypes of mentorship: mentor, coach, sponsor, and connector. along the way.

For me, DDW serves as an annual reminder of the power of mentorship in building and sustaining careers. Each May, trainees and early career faculty present their projects in oral or poster sessions, cheered on by their research mentors. Senior thought leaders offer career advice and guidance to more junior colleagues through structured sessions or informal conversations and facilitate introductions to new collaborators. Department chairs, division chiefs, and senior practice leaders take time to reconnect with their early mentors who believed in their potential and provided them with opportunities to take their careers to new heights. And, we see the incredible payoff of programs like AGA’s FORWARD and Future Leaders Programs in serving as springboards for career advancement and creating powerful role models and mentors for the future.
This year’s AGA presidential leadership transition served as a particularly poignant example of the power of mentorship as incoming AGA President Dr. Barbara Jung succeeded one of her early mentors, outgoing AGA President Dr. John Carethers, in this prestigious role. I hope you’ll join me in reflecting on the tremendous impact that mentors, coaches, sponsors, and connectors have had on your career, and continue to pay it forward to the next generation.
In this month’s issue, we feature several stories from DDW 2023, including summaries of the AGA presidential address and a study evaluating the impact of state Medicaid expansion on uptake of CRC screening in safety-net practices. From AGA’s flagship journals, we highlight a propensity-matched cohort study assessing the impact of pancreatic cancer surveillance of high-risk patients on important clinical outcomes and a new AGA CPU on management of extraesophageal GERD. In this month’s AGA Policy and Advocacy column, Dr. Amit Patel and Dr. Rotonya Carr review the results of a recent membership survey on policy priorities and outline the many ways you can get involved in advocacy efforts. Finally, our Member Spotlight column celebrates gastroenterologist and humanitarian Kadirawel Iswara, MD, recipient of this year’s AGA Distinguished Clinician Award in Private Practice, who is a cherished mentor to many prominent members of our field.
Megan A. Adams, M.D., J.D., MSc
Editor-in-Chief
In a 2018 JAMA Viewpoint, Dr. Vineet Chopra, a former colleague of mine at the University of Michigan (now chair of medicine at the University of Colorado) and colleagues wrote about four archetypes of mentorship: mentor, coach, sponsor, and connector. along the way.
For me, DDW serves as an annual reminder of the power of mentorship in building and sustaining careers. Each May, trainees and early career faculty present their projects in oral or poster sessions, cheered on by their research mentors. Senior thought leaders offer career advice and guidance to more junior colleagues through structured sessions or informal conversations and facilitate introductions to new collaborators. Department chairs, division chiefs, and senior practice leaders take time to reconnect with their early mentors who believed in their potential and provided them with opportunities to take their careers to new heights. And, we see the incredible payoff of programs like AGA’s FORWARD and Future Leaders Programs in serving as springboards for career advancement and creating powerful role models and mentors for the future.
This year’s AGA presidential leadership transition served as a particularly poignant example of the power of mentorship as incoming AGA President Dr. Barbara Jung succeeded one of her early mentors, outgoing AGA President Dr. John Carethers, in this prestigious role. I hope you’ll join me in reflecting on the tremendous impact that mentors, coaches, sponsors, and connectors have had on your career, and continue to pay it forward to the next generation.
In this month’s issue, we feature several stories from DDW 2023, including summaries of the AGA presidential address and a study evaluating the impact of state Medicaid expansion on uptake of CRC screening in safety-net practices. From AGA’s flagship journals, we highlight a propensity-matched cohort study assessing the impact of pancreatic cancer surveillance of high-risk patients on important clinical outcomes and a new AGA CPU on management of extraesophageal GERD. In this month’s AGA Policy and Advocacy column, Dr. Amit Patel and Dr. Rotonya Carr review the results of a recent membership survey on policy priorities and outline the many ways you can get involved in advocacy efforts. Finally, our Member Spotlight column celebrates gastroenterologist and humanitarian Kadirawel Iswara, MD, recipient of this year’s AGA Distinguished Clinician Award in Private Practice, who is a cherished mentor to many prominent members of our field.
Megan A. Adams, M.D., J.D., MSc
Editor-in-Chief
In a 2018 JAMA Viewpoint, Dr. Vineet Chopra, a former colleague of mine at the University of Michigan (now chair of medicine at the University of Colorado) and colleagues wrote about four archetypes of mentorship: mentor, coach, sponsor, and connector. along the way.
For me, DDW serves as an annual reminder of the power of mentorship in building and sustaining careers. Each May, trainees and early career faculty present their projects in oral or poster sessions, cheered on by their research mentors. Senior thought leaders offer career advice and guidance to more junior colleagues through structured sessions or informal conversations and facilitate introductions to new collaborators. Department chairs, division chiefs, and senior practice leaders take time to reconnect with their early mentors who believed in their potential and provided them with opportunities to take their careers to new heights. And, we see the incredible payoff of programs like AGA’s FORWARD and Future Leaders Programs in serving as springboards for career advancement and creating powerful role models and mentors for the future.
This year’s AGA presidential leadership transition served as a particularly poignant example of the power of mentorship as incoming AGA President Dr. Barbara Jung succeeded one of her early mentors, outgoing AGA President Dr. John Carethers, in this prestigious role. I hope you’ll join me in reflecting on the tremendous impact that mentors, coaches, sponsors, and connectors have had on your career, and continue to pay it forward to the next generation.
In this month’s issue, we feature several stories from DDW 2023, including summaries of the AGA presidential address and a study evaluating the impact of state Medicaid expansion on uptake of CRC screening in safety-net practices. From AGA’s flagship journals, we highlight a propensity-matched cohort study assessing the impact of pancreatic cancer surveillance of high-risk patients on important clinical outcomes and a new AGA CPU on management of extraesophageal GERD. In this month’s AGA Policy and Advocacy column, Dr. Amit Patel and Dr. Rotonya Carr review the results of a recent membership survey on policy priorities and outline the many ways you can get involved in advocacy efforts. Finally, our Member Spotlight column celebrates gastroenterologist and humanitarian Kadirawel Iswara, MD, recipient of this year’s AGA Distinguished Clinician Award in Private Practice, who is a cherished mentor to many prominent members of our field.
Megan A. Adams, M.D., J.D., MSc
Editor-in-Chief

Commentary: CGRP medications, COVID-19, and menopause in patients with migraine, June 2023
The field of headache medicine has changed significantly since 2018 with the advent of calcitonin gene-related peptide (CGRP)–targeted medications. Although many patients improve after their first injection, and there is even a significant portion of "super responders" who can revert to nearly zero headache days per month, the majority of patients have a moderate response. Many patients who have not had a significant decrease in the frequency and severity of migraine attacks over 12 weeks wonder whether they will eventually achieve this on a CGRP medication. Barbanti and colleagues looked specifically at the subpopulation of late responders to CGRP treatments.
This was a multicenter, prospective study lasting 24 weeks, defining the differences in responders to CGRP treatments. Participants in this study had failed three or more prior preventive medications and had high-frequency, episodic, or chronic migraine. Their response rate was determined as follows: "responder" patients had a more than 50% reduction in baseline monthly migraine days between weeks 9 and 12, and "late responder" patients achieved that reduction after 12 weeks. All three injectable CGRP monoclonal antibodies were included in this trial.
Nearly 66% of patients treated with a CGRP monoclonal antibody had a 50% or greater response at 12 weeks. Of the study participants, 34% were considered nonresponders at 12 weeks, and 55% of those nonresponders did become responders between 13 and 24 weeks. This subpopulation of late responders was noted to have higher body mass index (BMI), more frequent prior treatment failures, as well as other pain and psychiatric comorbidities. Allodynia and unilateral cranial autonomic symptoms were also noted to be significantly higher in this population.
This study helps better determine the length of a CGRP trial for prevention. Patients with more treatment failures and comorbidities should be given additional time for this class of medications to work, even beyond the initial 12 weeks.
The COVID-19 pandemic has changed the way of life for everyone, and this is especially true for people with chronic medical conditions. Hrytsenko and colleagues sought to quantify the effect that COVID-19 had on patients with a history of episodic or chronic migraine. They used a scale to determine "psycho-emotional state deterioration" in patients with migraine with and without a history of COVID-19.
The investigators included 133 participants with a prior diagnosis of migraine, either chronic or episodic. Of these, 95 had a positive polymerase chain reaction (PCR) test for COVID-19, indicating SARS-CoV-2 infection; 38 did not. The Hamilton Anxiety Rating Scale (HARS) was used to assess the severity of perceived anxiety symptoms and was used to determine psycho-emotional state. The Migraine Disability Assessment test (MIDAS) was used to determine their quality of life and degree of disability related to migraine. Patients with a history of COVID-19 had an increased usage of antimigraine medications, increased frequency of attacks, and higher HARS ratings. The average MIDAS score also increased significantly.
Many of our patients who were struggling prior to the COVID-19 pandemic unfortunately have done much worse after SARS-CoV-2 infection. A number of potential explanations exist for this, including worsening neuroinflammation in the context of COVID-19, which can specifically increase the propagation of inflammatory neurotransmitters, such as CGRP. Patients with a history of migraine respond to this with heightened frequency and severity of migraine.
There is a notable growing connection between certain neurologic conditions and vasomotor symptoms. Specifically, there appears to be an increased incidence of migraine and certain hypertensive or tachycardic conditions. Migraine is well known to be a vascular risk factor and migraine with aura even more so. Faubion and colleagues sought to quantify this in a specific menopausal population.
This was a large cross-sectional study, with an older median age compared with average migraine studies: 52.8 years. Nearly 60% of participants were postmenopausal and were recruited from a Mayo Clinic menopause registry. Participants were evaluated for a history of migraine based on The International Classification of Headache Disorders, third edition (ICHD3), criteria. They also had their symptoms measured on a menopause rating scale (the symptoms measured included hot flashes, sleep problems, physical and mental exhaustion, joint and muscular discomfort, and mood). Additional information was cross-referenced, including BMI, race, ethnicity, education, marital status, hypertension, and menopause status.
A diagnosis of migraine was associated with hypertension. There was no association between hypertension and hot flash severity, and there was a suggestion that hot flash severity and migraine history were not associated. The presence of other pain disorders also did not correlate with any other vasomotor symptoms.
This study does again link vasomotor issues with migraines. This connection remains well-founded and relevant. Antihypertensive medications have been some of the first preventive options ever offered to people with migraine. CGRP medications may actually lead to an increase in the risk for hypertension. Disconnection remains relevant and is something to discuss with patients with migraine, especially if they are at a higher risk.
The field of headache medicine has changed significantly since 2018 with the advent of calcitonin gene-related peptide (CGRP)–targeted medications. Although many patients improve after their first injection, and there is even a significant portion of "super responders" who can revert to nearly zero headache days per month, the majority of patients have a moderate response. Many patients who have not had a significant decrease in the frequency and severity of migraine attacks over 12 weeks wonder whether they will eventually achieve this on a CGRP medication. Barbanti and colleagues looked specifically at the subpopulation of late responders to CGRP treatments.
This was a multicenter, prospective study lasting 24 weeks, defining the differences in responders to CGRP treatments. Participants in this study had failed three or more prior preventive medications and had high-frequency, episodic, or chronic migraine. Their response rate was determined as follows: "responder" patients had a more than 50% reduction in baseline monthly migraine days between weeks 9 and 12, and "late responder" patients achieved that reduction after 12 weeks. All three injectable CGRP monoclonal antibodies were included in this trial.
Nearly 66% of patients treated with a CGRP monoclonal antibody had a 50% or greater response at 12 weeks. Of the study participants, 34% were considered nonresponders at 12 weeks, and 55% of those nonresponders did become responders between 13 and 24 weeks. This subpopulation of late responders was noted to have higher body mass index (BMI), more frequent prior treatment failures, as well as other pain and psychiatric comorbidities. Allodynia and unilateral cranial autonomic symptoms were also noted to be significantly higher in this population.
This study helps better determine the length of a CGRP trial for prevention. Patients with more treatment failures and comorbidities should be given additional time for this class of medications to work, even beyond the initial 12 weeks.
The COVID-19 pandemic has changed the way of life for everyone, and this is especially true for people with chronic medical conditions. Hrytsenko and colleagues sought to quantify the effect that COVID-19 had on patients with a history of episodic or chronic migraine. They used a scale to determine "psycho-emotional state deterioration" in patients with migraine with and without a history of COVID-19.
The investigators included 133 participants with a prior diagnosis of migraine, either chronic or episodic. Of these, 95 had a positive polymerase chain reaction (PCR) test for COVID-19, indicating SARS-CoV-2 infection; 38 did not. The Hamilton Anxiety Rating Scale (HARS) was used to assess the severity of perceived anxiety symptoms and was used to determine psycho-emotional state. The Migraine Disability Assessment test (MIDAS) was used to determine their quality of life and degree of disability related to migraine. Patients with a history of COVID-19 had an increased usage of antimigraine medications, increased frequency of attacks, and higher HARS ratings. The average MIDAS score also increased significantly.
Many of our patients who were struggling prior to the COVID-19 pandemic unfortunately have done much worse after SARS-CoV-2 infection. A number of potential explanations exist for this, including worsening neuroinflammation in the context of COVID-19, which can specifically increase the propagation of inflammatory neurotransmitters, such as CGRP. Patients with a history of migraine respond to this with heightened frequency and severity of migraine.
There is a notable growing connection between certain neurologic conditions and vasomotor symptoms. Specifically, there appears to be an increased incidence of migraine and certain hypertensive or tachycardic conditions. Migraine is well known to be a vascular risk factor and migraine with aura even more so. Faubion and colleagues sought to quantify this in a specific menopausal population.
This was a large cross-sectional study, with an older median age compared with average migraine studies: 52.8 years. Nearly 60% of participants were postmenopausal and were recruited from a Mayo Clinic menopause registry. Participants were evaluated for a history of migraine based on The International Classification of Headache Disorders, third edition (ICHD3), criteria. They also had their symptoms measured on a menopause rating scale (the symptoms measured included hot flashes, sleep problems, physical and mental exhaustion, joint and muscular discomfort, and mood). Additional information was cross-referenced, including BMI, race, ethnicity, education, marital status, hypertension, and menopause status.
A diagnosis of migraine was associated with hypertension. There was no association between hypertension and hot flash severity, and there was a suggestion that hot flash severity and migraine history were not associated. The presence of other pain disorders also did not correlate with any other vasomotor symptoms.
This study does again link vasomotor issues with migraines. This connection remains well-founded and relevant. Antihypertensive medications have been some of the first preventive options ever offered to people with migraine. CGRP medications may actually lead to an increase in the risk for hypertension. Disconnection remains relevant and is something to discuss with patients with migraine, especially if they are at a higher risk.
The field of headache medicine has changed significantly since 2018 with the advent of calcitonin gene-related peptide (CGRP)–targeted medications. Although many patients improve after their first injection, and there is even a significant portion of "super responders" who can revert to nearly zero headache days per month, the majority of patients have a moderate response. Many patients who have not had a significant decrease in the frequency and severity of migraine attacks over 12 weeks wonder whether they will eventually achieve this on a CGRP medication. Barbanti and colleagues looked specifically at the subpopulation of late responders to CGRP treatments.
This was a multicenter, prospective study lasting 24 weeks, defining the differences in responders to CGRP treatments. Participants in this study had failed three or more prior preventive medications and had high-frequency, episodic, or chronic migraine. Their response rate was determined as follows: "responder" patients had a more than 50% reduction in baseline monthly migraine days between weeks 9 and 12, and "late responder" patients achieved that reduction after 12 weeks. All three injectable CGRP monoclonal antibodies were included in this trial.
Nearly 66% of patients treated with a CGRP monoclonal antibody had a 50% or greater response at 12 weeks. Of the study participants, 34% were considered nonresponders at 12 weeks, and 55% of those nonresponders did become responders between 13 and 24 weeks. This subpopulation of late responders was noted to have higher body mass index (BMI), more frequent prior treatment failures, as well as other pain and psychiatric comorbidities. Allodynia and unilateral cranial autonomic symptoms were also noted to be significantly higher in this population.
This study helps better determine the length of a CGRP trial for prevention. Patients with more treatment failures and comorbidities should be given additional time for this class of medications to work, even beyond the initial 12 weeks.
The COVID-19 pandemic has changed the way of life for everyone, and this is especially true for people with chronic medical conditions. Hrytsenko and colleagues sought to quantify the effect that COVID-19 had on patients with a history of episodic or chronic migraine. They used a scale to determine "psycho-emotional state deterioration" in patients with migraine with and without a history of COVID-19.
The investigators included 133 participants with a prior diagnosis of migraine, either chronic or episodic. Of these, 95 had a positive polymerase chain reaction (PCR) test for COVID-19, indicating SARS-CoV-2 infection; 38 did not. The Hamilton Anxiety Rating Scale (HARS) was used to assess the severity of perceived anxiety symptoms and was used to determine psycho-emotional state. The Migraine Disability Assessment test (MIDAS) was used to determine their quality of life and degree of disability related to migraine. Patients with a history of COVID-19 had an increased usage of antimigraine medications, increased frequency of attacks, and higher HARS ratings. The average MIDAS score also increased significantly.
Many of our patients who were struggling prior to the COVID-19 pandemic unfortunately have done much worse after SARS-CoV-2 infection. A number of potential explanations exist for this, including worsening neuroinflammation in the context of COVID-19, which can specifically increase the propagation of inflammatory neurotransmitters, such as CGRP. Patients with a history of migraine respond to this with heightened frequency and severity of migraine.
There is a notable growing connection between certain neurologic conditions and vasomotor symptoms. Specifically, there appears to be an increased incidence of migraine and certain hypertensive or tachycardic conditions. Migraine is well known to be a vascular risk factor and migraine with aura even more so. Faubion and colleagues sought to quantify this in a specific menopausal population.
This was a large cross-sectional study, with an older median age compared with average migraine studies: 52.8 years. Nearly 60% of participants were postmenopausal and were recruited from a Mayo Clinic menopause registry. Participants were evaluated for a history of migraine based on The International Classification of Headache Disorders, third edition (ICHD3), criteria. They also had their symptoms measured on a menopause rating scale (the symptoms measured included hot flashes, sleep problems, physical and mental exhaustion, joint and muscular discomfort, and mood). Additional information was cross-referenced, including BMI, race, ethnicity, education, marital status, hypertension, and menopause status.
A diagnosis of migraine was associated with hypertension. There was no association between hypertension and hot flash severity, and there was a suggestion that hot flash severity and migraine history were not associated. The presence of other pain disorders also did not correlate with any other vasomotor symptoms.
This study does again link vasomotor issues with migraines. This connection remains well-founded and relevant. Antihypertensive medications have been some of the first preventive options ever offered to people with migraine. CGRP medications may actually lead to an increase in the risk for hypertension. Disconnection remains relevant and is something to discuss with patients with migraine, especially if they are at a higher risk.
Commentary: Evolving Treatment of CLL, June 2023
Novel therapies have transformed the management of chronic lymphocytic leukemia (CLL) over the past decade. With the advent of new options, the optimal therapy for newly diagnosed patients has become less clear. Bruton tyrosine kinase (BTK) inhibitors have led to improvement in outcomes for most patients with CLL compared with chemoimmunotherapy (CIT).1,2 Second-generation BTK inhibitors, such as acalabrutinib and zanubrutinib, are also available and appear to have an improved safety profile compared with ibrutinib. Similarly, the B-cell lymphoma 2 (BCL2) inhibitor venetoclax, in combination with obinutuzumab, is an effective option in first-line treatment that offers a time-limited approach.3 Studies combining BTK and BCL2 inhibitors are also promising in this setting.
Recently, the phase 3 GAIA-CLL13 study aimed to address the question of optimal time-limited first-line treatment for fit patients with CLL. Of note, patients with TP53 aberrations were excluded. Patients were randomly assigned to one of four treatment arms: CIT (fludarabine-cyclophosphamide-rituximab or bendamustine-rituximab), venetoclax-obinutuzumab, venetoclax-rituximab, or venetoclax-obinutuzumab-ibrutinub.
At 15 months, the rate of undetectable minimal residual disease (uMRD) was higher in the venetoclax-obinutuzumab group (86.5%; 97.5% CI 80.6-91.1) and the venetoclax-obinutuzumab-ibrutinib group (92.2%; 97.5% CI 87.3-95.7) compared with the CIT group (52.0%; 97.5% CI 44.4-59.5; P < .001 for both comparisons). The rate of uMRD for the venetoclax-rituximab group, however, was not higher than the rate in the CIT group (57.0%; 97.5%, CI 49.5-64.2; P = .32). The 3-year progression-free survival (PFS) was 90.5% in the venetoclax-obinutuzumab-ibrutinib group and 75.5% in the CIT group (hazard ratio [HR] for disease progression or death 0.32; 97.5% CI 0.19-0.54; P < .001). PFS at 3 years was also higher in the venetoclax-obinutuzumab group (87.7%; HR for disease progression or death, 0.42; 97.5% CI 0.26-0.68; P < .001), but not with venetoclax-rituximab group (80.8%; HR 0.79; 97.5% CI 0.53-1.18; P = .18). Grade 3 and grade 4 infections were more common with CIT (18.5%) and venetoclax-obinutuzumab-ibrutinib (21.2%) than with venetoclax-rituximab (10.5%) or venetoclax-obinutuzumab (13.2%).
This study confirms the role of fixed-duration venetoclax-based therapy for younger, fit patients with CLL. Interestingly, this study also suggests that rates of uMRD and PFS are superior with the use of obinutuzumab rather than with rituximab. Also of note, though the uMRD and PFS were highest with the triplet combination, it was not clearly superior to venetoclax-obinutuzumab alone and was associated with greater rates of toxicity.
Another ongoing randomized trial in first-line treatment of CLL is the FLAIR trial. This study was initially designed to compare ibrutinib-rituximab with standard CIT, though it was later modified to include an arm of ibrutinib alone and ibrutinib-venetoclax. Recently, the results of the first formal interim analysis comparing fludarabine, cyclophosphamide, and rituximab (n = 385) to ibrutinib-rituximb (n = 386), were published. This study, like the ECOG1912 study2, demonstrated improved outcomes with a BTK inhibitor over standard CIT in fit patients with CLL. After a median follow-up of 53 months, the median PFS was not reached in patients receiving ibrutinib-rituximab and was 67 months (95% CI 63 to not reached) in those receiving fludarabine, cyclophosphamide, and rituximab (HR 0.44; P < .0001). A substantial number of sudden cardiac or unexplained deaths occurred, which were more frequent in the ibrutinib-rituximab group.
Though questions regarding optimal treatment remain, there are now multiple studies to suggest an advantage of novel agents over traditional CIT. Furthermore, regardless of approach, outcomes appear favorable for patients with CLL, even among higher-risk patients.
Other studies are also evaluating alternative ways to sequence therapy. A recent phase 2 study, for example, evaluated venetoclax consolidation for patients on ibrutinib. Forty-five patients with CLL and detectable disease (≥ 0.01% minimal residual disease in bone marrow [BM]) after treatment with ibrutinib for 12 or more months who had one or more high-risk feature for disease progression were included. Patients received combined treatment with ibrutinib (previously tolerated dose) and venetoclax (escalated to 400 mg once daily) for 24 or less cycles. Venetoclax was continued until patients achieved uMRD. Patients with uMRD also had the option of discontinuing ibrutinib. Adding venetoclax to ibrutinib led to a cumulative BM uMRD rate of 73%. BM uMRD was achieved by 71% of patients after venetoclax therapy completion and by 38% and 57% of patients after 6 and 12 cycles, respectively. This trial highlights the potential use of MRD to guide treatment as well as consolidation strategies to allow for time-limited treatment.
Additional References
- Woyach JA, Ruppert AS, Heerema NA, et al. Ibrutinib regimens versus chemoimmunotherapy in older patients with untreated CLL. N Engl J Med. 2018;379:2517-2528. doi: 10.1056/NEJMoa1812836
- Shanafelt TD, Wang XV, Kay NE, et al. Ibrutinib-rituximab or chemoimmunotherapy for chronic lymphocytic leukemia. N Engl J Med. 2019;381:432-443. doi: 10.1056/NEJMoa1817073
- Fischer K, Al-Sawaf O, Bahlo J, et al. Venetoclax and obinutuzumab in patients with CLL and coexisting conditions. N Engl J Med. 2019;380:2225-2236. doi: 10.1056/NEJMoa1815281
Novel therapies have transformed the management of chronic lymphocytic leukemia (CLL) over the past decade. With the advent of new options, the optimal therapy for newly diagnosed patients has become less clear. Bruton tyrosine kinase (BTK) inhibitors have led to improvement in outcomes for most patients with CLL compared with chemoimmunotherapy (CIT).1,2 Second-generation BTK inhibitors, such as acalabrutinib and zanubrutinib, are also available and appear to have an improved safety profile compared with ibrutinib. Similarly, the B-cell lymphoma 2 (BCL2) inhibitor venetoclax, in combination with obinutuzumab, is an effective option in first-line treatment that offers a time-limited approach.3 Studies combining BTK and BCL2 inhibitors are also promising in this setting.
Recently, the phase 3 GAIA-CLL13 study aimed to address the question of optimal time-limited first-line treatment for fit patients with CLL. Of note, patients with TP53 aberrations were excluded. Patients were randomly assigned to one of four treatment arms: CIT (fludarabine-cyclophosphamide-rituximab or bendamustine-rituximab), venetoclax-obinutuzumab, venetoclax-rituximab, or venetoclax-obinutuzumab-ibrutinub.
At 15 months, the rate of undetectable minimal residual disease (uMRD) was higher in the venetoclax-obinutuzumab group (86.5%; 97.5% CI 80.6-91.1) and the venetoclax-obinutuzumab-ibrutinib group (92.2%; 97.5% CI 87.3-95.7) compared with the CIT group (52.0%; 97.5% CI 44.4-59.5; P < .001 for both comparisons). The rate of uMRD for the venetoclax-rituximab group, however, was not higher than the rate in the CIT group (57.0%; 97.5%, CI 49.5-64.2; P = .32). The 3-year progression-free survival (PFS) was 90.5% in the venetoclax-obinutuzumab-ibrutinib group and 75.5% in the CIT group (hazard ratio [HR] for disease progression or death 0.32; 97.5% CI 0.19-0.54; P < .001). PFS at 3 years was also higher in the venetoclax-obinutuzumab group (87.7%; HR for disease progression or death, 0.42; 97.5% CI 0.26-0.68; P < .001), but not with venetoclax-rituximab group (80.8%; HR 0.79; 97.5% CI 0.53-1.18; P = .18). Grade 3 and grade 4 infections were more common with CIT (18.5%) and venetoclax-obinutuzumab-ibrutinib (21.2%) than with venetoclax-rituximab (10.5%) or venetoclax-obinutuzumab (13.2%).
This study confirms the role of fixed-duration venetoclax-based therapy for younger, fit patients with CLL. Interestingly, this study also suggests that rates of uMRD and PFS are superior with the use of obinutuzumab rather than with rituximab. Also of note, though the uMRD and PFS were highest with the triplet combination, it was not clearly superior to venetoclax-obinutuzumab alone and was associated with greater rates of toxicity.
Another ongoing randomized trial in first-line treatment of CLL is the FLAIR trial. This study was initially designed to compare ibrutinib-rituximab with standard CIT, though it was later modified to include an arm of ibrutinib alone and ibrutinib-venetoclax. Recently, the results of the first formal interim analysis comparing fludarabine, cyclophosphamide, and rituximab (n = 385) to ibrutinib-rituximb (n = 386), were published. This study, like the ECOG1912 study2, demonstrated improved outcomes with a BTK inhibitor over standard CIT in fit patients with CLL. After a median follow-up of 53 months, the median PFS was not reached in patients receiving ibrutinib-rituximab and was 67 months (95% CI 63 to not reached) in those receiving fludarabine, cyclophosphamide, and rituximab (HR 0.44; P < .0001). A substantial number of sudden cardiac or unexplained deaths occurred, which were more frequent in the ibrutinib-rituximab group.
Though questions regarding optimal treatment remain, there are now multiple studies to suggest an advantage of novel agents over traditional CIT. Furthermore, regardless of approach, outcomes appear favorable for patients with CLL, even among higher-risk patients.
Other studies are also evaluating alternative ways to sequence therapy. A recent phase 2 study, for example, evaluated venetoclax consolidation for patients on ibrutinib. Forty-five patients with CLL and detectable disease (≥ 0.01% minimal residual disease in bone marrow [BM]) after treatment with ibrutinib for 12 or more months who had one or more high-risk feature for disease progression were included. Patients received combined treatment with ibrutinib (previously tolerated dose) and venetoclax (escalated to 400 mg once daily) for 24 or less cycles. Venetoclax was continued until patients achieved uMRD. Patients with uMRD also had the option of discontinuing ibrutinib. Adding venetoclax to ibrutinib led to a cumulative BM uMRD rate of 73%. BM uMRD was achieved by 71% of patients after venetoclax therapy completion and by 38% and 57% of patients after 6 and 12 cycles, respectively. This trial highlights the potential use of MRD to guide treatment as well as consolidation strategies to allow for time-limited treatment.
Additional References
- Woyach JA, Ruppert AS, Heerema NA, et al. Ibrutinib regimens versus chemoimmunotherapy in older patients with untreated CLL. N Engl J Med. 2018;379:2517-2528. doi: 10.1056/NEJMoa1812836
- Shanafelt TD, Wang XV, Kay NE, et al. Ibrutinib-rituximab or chemoimmunotherapy for chronic lymphocytic leukemia. N Engl J Med. 2019;381:432-443. doi: 10.1056/NEJMoa1817073
- Fischer K, Al-Sawaf O, Bahlo J, et al. Venetoclax and obinutuzumab in patients with CLL and coexisting conditions. N Engl J Med. 2019;380:2225-2236. doi: 10.1056/NEJMoa1815281
Novel therapies have transformed the management of chronic lymphocytic leukemia (CLL) over the past decade. With the advent of new options, the optimal therapy for newly diagnosed patients has become less clear. Bruton tyrosine kinase (BTK) inhibitors have led to improvement in outcomes for most patients with CLL compared with chemoimmunotherapy (CIT).1,2 Second-generation BTK inhibitors, such as acalabrutinib and zanubrutinib, are also available and appear to have an improved safety profile compared with ibrutinib. Similarly, the B-cell lymphoma 2 (BCL2) inhibitor venetoclax, in combination with obinutuzumab, is an effective option in first-line treatment that offers a time-limited approach.3 Studies combining BTK and BCL2 inhibitors are also promising in this setting.
Recently, the phase 3 GAIA-CLL13 study aimed to address the question of optimal time-limited first-line treatment for fit patients with CLL. Of note, patients with TP53 aberrations were excluded. Patients were randomly assigned to one of four treatment arms: CIT (fludarabine-cyclophosphamide-rituximab or bendamustine-rituximab), venetoclax-obinutuzumab, venetoclax-rituximab, or venetoclax-obinutuzumab-ibrutinub.
At 15 months, the rate of undetectable minimal residual disease (uMRD) was higher in the venetoclax-obinutuzumab group (86.5%; 97.5% CI 80.6-91.1) and the venetoclax-obinutuzumab-ibrutinib group (92.2%; 97.5% CI 87.3-95.7) compared with the CIT group (52.0%; 97.5% CI 44.4-59.5; P < .001 for both comparisons). The rate of uMRD for the venetoclax-rituximab group, however, was not higher than the rate in the CIT group (57.0%; 97.5%, CI 49.5-64.2; P = .32). The 3-year progression-free survival (PFS) was 90.5% in the venetoclax-obinutuzumab-ibrutinib group and 75.5% in the CIT group (hazard ratio [HR] for disease progression or death 0.32; 97.5% CI 0.19-0.54; P < .001). PFS at 3 years was also higher in the venetoclax-obinutuzumab group (87.7%; HR for disease progression or death, 0.42; 97.5% CI 0.26-0.68; P < .001), but not with venetoclax-rituximab group (80.8%; HR 0.79; 97.5% CI 0.53-1.18; P = .18). Grade 3 and grade 4 infections were more common with CIT (18.5%) and venetoclax-obinutuzumab-ibrutinib (21.2%) than with venetoclax-rituximab (10.5%) or venetoclax-obinutuzumab (13.2%).
This study confirms the role of fixed-duration venetoclax-based therapy for younger, fit patients with CLL. Interestingly, this study also suggests that rates of uMRD and PFS are superior with the use of obinutuzumab rather than with rituximab. Also of note, though the uMRD and PFS were highest with the triplet combination, it was not clearly superior to venetoclax-obinutuzumab alone and was associated with greater rates of toxicity.
Another ongoing randomized trial in first-line treatment of CLL is the FLAIR trial. This study was initially designed to compare ibrutinib-rituximab with standard CIT, though it was later modified to include an arm of ibrutinib alone and ibrutinib-venetoclax. Recently, the results of the first formal interim analysis comparing fludarabine, cyclophosphamide, and rituximab (n = 385) to ibrutinib-rituximb (n = 386), were published. This study, like the ECOG1912 study2, demonstrated improved outcomes with a BTK inhibitor over standard CIT in fit patients with CLL. After a median follow-up of 53 months, the median PFS was not reached in patients receiving ibrutinib-rituximab and was 67 months (95% CI 63 to not reached) in those receiving fludarabine, cyclophosphamide, and rituximab (HR 0.44; P < .0001). A substantial number of sudden cardiac or unexplained deaths occurred, which were more frequent in the ibrutinib-rituximab group.
Though questions regarding optimal treatment remain, there are now multiple studies to suggest an advantage of novel agents over traditional CIT. Furthermore, regardless of approach, outcomes appear favorable for patients with CLL, even among higher-risk patients.
Other studies are also evaluating alternative ways to sequence therapy. A recent phase 2 study, for example, evaluated venetoclax consolidation for patients on ibrutinib. Forty-five patients with CLL and detectable disease (≥ 0.01% minimal residual disease in bone marrow [BM]) after treatment with ibrutinib for 12 or more months who had one or more high-risk feature for disease progression were included. Patients received combined treatment with ibrutinib (previously tolerated dose) and venetoclax (escalated to 400 mg once daily) for 24 or less cycles. Venetoclax was continued until patients achieved uMRD. Patients with uMRD also had the option of discontinuing ibrutinib. Adding venetoclax to ibrutinib led to a cumulative BM uMRD rate of 73%. BM uMRD was achieved by 71% of patients after venetoclax therapy completion and by 38% and 57% of patients after 6 and 12 cycles, respectively. This trial highlights the potential use of MRD to guide treatment as well as consolidation strategies to allow for time-limited treatment.
Additional References
- Woyach JA, Ruppert AS, Heerema NA, et al. Ibrutinib regimens versus chemoimmunotherapy in older patients with untreated CLL. N Engl J Med. 2018;379:2517-2528. doi: 10.1056/NEJMoa1812836
- Shanafelt TD, Wang XV, Kay NE, et al. Ibrutinib-rituximab or chemoimmunotherapy for chronic lymphocytic leukemia. N Engl J Med. 2019;381:432-443. doi: 10.1056/NEJMoa1817073
- Fischer K, Al-Sawaf O, Bahlo J, et al. Venetoclax and obinutuzumab in patients with CLL and coexisting conditions. N Engl J Med. 2019;380:2225-2236. doi: 10.1056/NEJMoa1815281
Commentary: Ongoing therapy options in RA, June 2023
Several environmental risk factors are associated with the development of rheumatoid arthritis (RA), with smoking having one of the strongest associations. Exposure to airborne toxins has also been associated with development of anti–cyclic citrullinated peptide antibodies. Beidelschies and colleagues performed a cross-sectional analysis using data from the National Health and Nutrition Examination Survey to examine a potential interaction between smoking and polycyclic aromatic hydrocarbons (PAH) affecting the development of RA. Stored blood and urine samples of survey respondents were examined, and levels of PAH as well as other toxicants were measured. Of nearly 22,000 participants, about 1400 of whom reported a diagnosis of RA, toxicants were measured in about 7000. Higher levels of PAH and phthalate metabolites were more strongly associated with development of RA. Because cigarettes are a source of PAH, the authors postulated that PAH mediated the impact of smoking on development of RA, a plausible explanation given that smoking was not associated with RA after adjustment for PAH levels. However, given the cross-sectional design, causality cannot be determined.
Janus kinase (JAK) inhibitors have been found in several surveillance studies to be associated with an increased risk for cancer and cardiovascular events. Westermann and colleagues performed an observational cohort study using Danish nationwide registries to evaluate cancer risk (other than nonmelanomatous skin cancer) in patients with RA treated with tofacitinib or baricitinib. Among 875 patients treated with JAK inhibitors vs 4247 patients treated with biologic disease-modifying antirheumatic drugs (bDMARD), cancer incidence rates were similar (14.4 vs 12.9 per 1000 patient-years, respectively). Interestingly, though cancer incidence rates increased in patients > 50 and those > 65 years of age, the effect was similar between patients treated with JAK inhibitors and bDMARD. The largest difference was seen in patients up to 1 year vs > 1 year of follow-up, with hazard ratios of 1.54 vs 1.07. These findings are somewhat reassuring in light of results from the ORAL Surveillance study, suggesting increased cancer and cardiovascular risk among older patients with RA. However, as with bDMARD, increased scrutiny may be warranted among patients > 65 years, especially in the first year of treatment.
Finally, regarding withdrawal of therapy, Curtis and colleagues performed a randomized controlled study of patients with RA on combination therapy with methotrexate and etanercept and evaluated factors associated with maintenance of remission. In this study, withdrawal of methotrexate and etanercept were compared: About 250 patients whose disease was in remission, on the basis of the Simplified Disease Activity Index, were randomized in a 2:2:1 ratio to receive methotrexate monotherapy, etanercept monotherapy, or combination therapy. Prior analyses of these data have shown that continuing etanercept monotherapy showed a benefit in maintaining remission compared with continuing methotrexate monotherapy. Several baseline characteristics, including higher patient global activity at baseline and rheumatoid factor seropositivity, were associated with a lower likelihood of maintaining remission or low disease activity. Interestingly, higher serum magnesium levels seemed to negatively affect maintenance of remission, though the mechanism for this finding is not clear. In general, however, this study did not add more information to prior work in terms of shedding light on which patients may be able to stop therapy.
Several environmental risk factors are associated with the development of rheumatoid arthritis (RA), with smoking having one of the strongest associations. Exposure to airborne toxins has also been associated with development of anti–cyclic citrullinated peptide antibodies. Beidelschies and colleagues performed a cross-sectional analysis using data from the National Health and Nutrition Examination Survey to examine a potential interaction between smoking and polycyclic aromatic hydrocarbons (PAH) affecting the development of RA. Stored blood and urine samples of survey respondents were examined, and levels of PAH as well as other toxicants were measured. Of nearly 22,000 participants, about 1400 of whom reported a diagnosis of RA, toxicants were measured in about 7000. Higher levels of PAH and phthalate metabolites were more strongly associated with development of RA. Because cigarettes are a source of PAH, the authors postulated that PAH mediated the impact of smoking on development of RA, a plausible explanation given that smoking was not associated with RA after adjustment for PAH levels. However, given the cross-sectional design, causality cannot be determined.
Janus kinase (JAK) inhibitors have been found in several surveillance studies to be associated with an increased risk for cancer and cardiovascular events. Westermann and colleagues performed an observational cohort study using Danish nationwide registries to evaluate cancer risk (other than nonmelanomatous skin cancer) in patients with RA treated with tofacitinib or baricitinib. Among 875 patients treated with JAK inhibitors vs 4247 patients treated with biologic disease-modifying antirheumatic drugs (bDMARD), cancer incidence rates were similar (14.4 vs 12.9 per 1000 patient-years, respectively). Interestingly, though cancer incidence rates increased in patients > 50 and those > 65 years of age, the effect was similar between patients treated with JAK inhibitors and bDMARD. The largest difference was seen in patients up to 1 year vs > 1 year of follow-up, with hazard ratios of 1.54 vs 1.07. These findings are somewhat reassuring in light of results from the ORAL Surveillance study, suggesting increased cancer and cardiovascular risk among older patients with RA. However, as with bDMARD, increased scrutiny may be warranted among patients > 65 years, especially in the first year of treatment.
Finally, regarding withdrawal of therapy, Curtis and colleagues performed a randomized controlled study of patients with RA on combination therapy with methotrexate and etanercept and evaluated factors associated with maintenance of remission. In this study, withdrawal of methotrexate and etanercept were compared: About 250 patients whose disease was in remission, on the basis of the Simplified Disease Activity Index, were randomized in a 2:2:1 ratio to receive methotrexate monotherapy, etanercept monotherapy, or combination therapy. Prior analyses of these data have shown that continuing etanercept monotherapy showed a benefit in maintaining remission compared with continuing methotrexate monotherapy. Several baseline characteristics, including higher patient global activity at baseline and rheumatoid factor seropositivity, were associated with a lower likelihood of maintaining remission or low disease activity. Interestingly, higher serum magnesium levels seemed to negatively affect maintenance of remission, though the mechanism for this finding is not clear. In general, however, this study did not add more information to prior work in terms of shedding light on which patients may be able to stop therapy.
Several environmental risk factors are associated with the development of rheumatoid arthritis (RA), with smoking having one of the strongest associations. Exposure to airborne toxins has also been associated with development of anti–cyclic citrullinated peptide antibodies. Beidelschies and colleagues performed a cross-sectional analysis using data from the National Health and Nutrition Examination Survey to examine a potential interaction between smoking and polycyclic aromatic hydrocarbons (PAH) affecting the development of RA. Stored blood and urine samples of survey respondents were examined, and levels of PAH as well as other toxicants were measured. Of nearly 22,000 participants, about 1400 of whom reported a diagnosis of RA, toxicants were measured in about 7000. Higher levels of PAH and phthalate metabolites were more strongly associated with development of RA. Because cigarettes are a source of PAH, the authors postulated that PAH mediated the impact of smoking on development of RA, a plausible explanation given that smoking was not associated with RA after adjustment for PAH levels. However, given the cross-sectional design, causality cannot be determined.
Janus kinase (JAK) inhibitors have been found in several surveillance studies to be associated with an increased risk for cancer and cardiovascular events. Westermann and colleagues performed an observational cohort study using Danish nationwide registries to evaluate cancer risk (other than nonmelanomatous skin cancer) in patients with RA treated with tofacitinib or baricitinib. Among 875 patients treated with JAK inhibitors vs 4247 patients treated with biologic disease-modifying antirheumatic drugs (bDMARD), cancer incidence rates were similar (14.4 vs 12.9 per 1000 patient-years, respectively). Interestingly, though cancer incidence rates increased in patients > 50 and those > 65 years of age, the effect was similar between patients treated with JAK inhibitors and bDMARD. The largest difference was seen in patients up to 1 year vs > 1 year of follow-up, with hazard ratios of 1.54 vs 1.07. These findings are somewhat reassuring in light of results from the ORAL Surveillance study, suggesting increased cancer and cardiovascular risk among older patients with RA. However, as with bDMARD, increased scrutiny may be warranted among patients > 65 years, especially in the first year of treatment.
Finally, regarding withdrawal of therapy, Curtis and colleagues performed a randomized controlled study of patients with RA on combination therapy with methotrexate and etanercept and evaluated factors associated with maintenance of remission. In this study, withdrawal of methotrexate and etanercept were compared: About 250 patients whose disease was in remission, on the basis of the Simplified Disease Activity Index, were randomized in a 2:2:1 ratio to receive methotrexate monotherapy, etanercept monotherapy, or combination therapy. Prior analyses of these data have shown that continuing etanercept monotherapy showed a benefit in maintaining remission compared with continuing methotrexate monotherapy. Several baseline characteristics, including higher patient global activity at baseline and rheumatoid factor seropositivity, were associated with a lower likelihood of maintaining remission or low disease activity. Interestingly, higher serum magnesium levels seemed to negatively affect maintenance of remission, though the mechanism for this finding is not clear. In general, however, this study did not add more information to prior work in terms of shedding light on which patients may be able to stop therapy.
Survey: Family medicine earnings steady despite overall growth for physicians
according to the results of the Medscape Family Physician Compensation Report 2023.
Average compensation for the specialty, which has risen by 31% since 2015, was stagnant in 2022, showing no growth from the previous year. COVID, at least, had less of an effect on earnings, as 48% of family physicians cited pandemic-related income losses, compared with 64% in 2021, according to those who responded to Medscape’s annual survey, which was conducted from Oct. 2, 2022, to Jan. 17, 2023.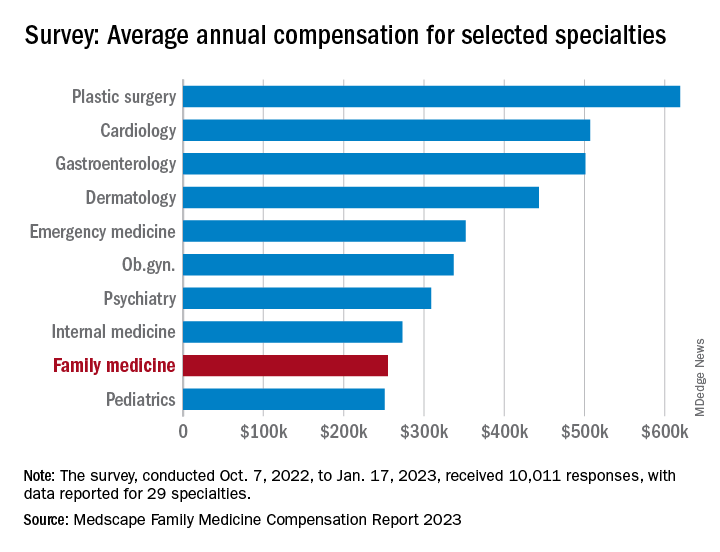
Comments from those respondents covered several areas that were already concerning physicians before the pandemic. One wrote that “decreasing Medicare reimbursement and poor payor mix destroy our income,” and another said that “patients have become rude and come with poor information from social media.” One respondent described the situation this way: “Overwhelming burnout. I had to reduce my hours to keep myself from quitting medicine completely.”
Overall physician compensation in 2022 was up by about 4% from 2021. For the 12% of the 10,011 respondents who practice family medicine, the average held at $255,000, where it had been the year before. Among the other primary care specialists, internists’ earnings were up by almost 4% and pediatricians did almost as well with a 3% increase, while ob.gyns. joined family physicians in the no-growth club, the Medscape results show.
For all physicians, average compensation in 2022 was $352,000, an increase of almost 18% since 2018. “Supply and demand is the biggest driver,” Mike Belkin, JD, of physician recruitment firm Merritt Hawkins, said in an interview. “Organizations understand it’s not getting any easier to get good candidates, and so for the most part, physicians are getting good offers.”
The lack of increase in FPs earnings among internists also included a decline of note: The disparity between mens’ and womens’ compensation dropped from 26% in 2021 to 23% in 2022. The 2022 disparity was only 16% for internists, however, even though family medicine has a considerably larger share of women (49% vs. 40%) among those surveyed, Medscape said.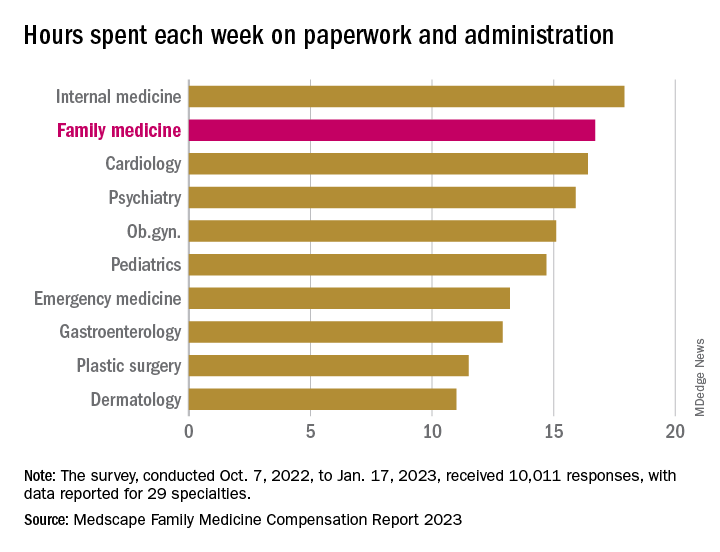
Satisfaction with their compensation, on the other hand, was higher among the family physicians (50%), compared with internists (43%). In 2022, 55% of family physicians said that they had been fairly paid.
In 2022, FP respondents reported spending an average of 16.7 hours (up from 15.6 hours in 2021) each week on paperwork and administration, just below the survey leaders, physical medicine and rehabilitation (18.5 hours) and nephrology (18.1 hours) but well above anesthesiology, lowest of the 29 specialties at 9.0 hours, and the 2022 average of 15.5 hours for all physicians, Medscape said.
When asked if they would choose medicine again, 72% of family physician respondents and 73% of all physicians said yes, with emergency medicine (65%) and dermatology (86%) representing the two extremes. A question about specialty choice showed that 66% of FPs would choose it again, putting them 28th of the 29 included specialties in their eagerness to follow the same path, above only the internists (61%), Medscape reported.
Commenters among the survey respondents were not identified by specialty, but dissatisfaction on many fronts was a definite theme:
- “Our costs go up, and our reimbursement does not.”
- “Our practice was acquired by venture capital firms; they slashed costs.”
- “My productivity bonus should have come to $45,000. Instead I was paid only $15,000. Yet cardiologists and administrators who were working from home part of the year received their full bonus.”
- “I will no longer practice cookbook mediocrity.”
according to the results of the Medscape Family Physician Compensation Report 2023.
Average compensation for the specialty, which has risen by 31% since 2015, was stagnant in 2022, showing no growth from the previous year. COVID, at least, had less of an effect on earnings, as 48% of family physicians cited pandemic-related income losses, compared with 64% in 2021, according to those who responded to Medscape’s annual survey, which was conducted from Oct. 2, 2022, to Jan. 17, 2023.
Comments from those respondents covered several areas that were already concerning physicians before the pandemic. One wrote that “decreasing Medicare reimbursement and poor payor mix destroy our income,” and another said that “patients have become rude and come with poor information from social media.” One respondent described the situation this way: “Overwhelming burnout. I had to reduce my hours to keep myself from quitting medicine completely.”
Overall physician compensation in 2022 was up by about 4% from 2021. For the 12% of the 10,011 respondents who practice family medicine, the average held at $255,000, where it had been the year before. Among the other primary care specialists, internists’ earnings were up by almost 4% and pediatricians did almost as well with a 3% increase, while ob.gyns. joined family physicians in the no-growth club, the Medscape results show.
For all physicians, average compensation in 2022 was $352,000, an increase of almost 18% since 2018. “Supply and demand is the biggest driver,” Mike Belkin, JD, of physician recruitment firm Merritt Hawkins, said in an interview. “Organizations understand it’s not getting any easier to get good candidates, and so for the most part, physicians are getting good offers.”
The lack of increase in FPs earnings among internists also included a decline of note: The disparity between mens’ and womens’ compensation dropped from 26% in 2021 to 23% in 2022. The 2022 disparity was only 16% for internists, however, even though family medicine has a considerably larger share of women (49% vs. 40%) among those surveyed, Medscape said.
Satisfaction with their compensation, on the other hand, was higher among the family physicians (50%), compared with internists (43%). In 2022, 55% of family physicians said that they had been fairly paid.
In 2022, FP respondents reported spending an average of 16.7 hours (up from 15.6 hours in 2021) each week on paperwork and administration, just below the survey leaders, physical medicine and rehabilitation (18.5 hours) and nephrology (18.1 hours) but well above anesthesiology, lowest of the 29 specialties at 9.0 hours, and the 2022 average of 15.5 hours for all physicians, Medscape said.
When asked if they would choose medicine again, 72% of family physician respondents and 73% of all physicians said yes, with emergency medicine (65%) and dermatology (86%) representing the two extremes. A question about specialty choice showed that 66% of FPs would choose it again, putting them 28th of the 29 included specialties in their eagerness to follow the same path, above only the internists (61%), Medscape reported.
Commenters among the survey respondents were not identified by specialty, but dissatisfaction on many fronts was a definite theme:
- “Our costs go up, and our reimbursement does not.”
- “Our practice was acquired by venture capital firms; they slashed costs.”
- “My productivity bonus should have come to $45,000. Instead I was paid only $15,000. Yet cardiologists and administrators who were working from home part of the year received their full bonus.”
- “I will no longer practice cookbook mediocrity.”
according to the results of the Medscape Family Physician Compensation Report 2023.
Average compensation for the specialty, which has risen by 31% since 2015, was stagnant in 2022, showing no growth from the previous year. COVID, at least, had less of an effect on earnings, as 48% of family physicians cited pandemic-related income losses, compared with 64% in 2021, according to those who responded to Medscape’s annual survey, which was conducted from Oct. 2, 2022, to Jan. 17, 2023.
Comments from those respondents covered several areas that were already concerning physicians before the pandemic. One wrote that “decreasing Medicare reimbursement and poor payor mix destroy our income,” and another said that “patients have become rude and come with poor information from social media.” One respondent described the situation this way: “Overwhelming burnout. I had to reduce my hours to keep myself from quitting medicine completely.”
Overall physician compensation in 2022 was up by about 4% from 2021. For the 12% of the 10,011 respondents who practice family medicine, the average held at $255,000, where it had been the year before. Among the other primary care specialists, internists’ earnings were up by almost 4% and pediatricians did almost as well with a 3% increase, while ob.gyns. joined family physicians in the no-growth club, the Medscape results show.
For all physicians, average compensation in 2022 was $352,000, an increase of almost 18% since 2018. “Supply and demand is the biggest driver,” Mike Belkin, JD, of physician recruitment firm Merritt Hawkins, said in an interview. “Organizations understand it’s not getting any easier to get good candidates, and so for the most part, physicians are getting good offers.”
The lack of increase in FPs earnings among internists also included a decline of note: The disparity between mens’ and womens’ compensation dropped from 26% in 2021 to 23% in 2022. The 2022 disparity was only 16% for internists, however, even though family medicine has a considerably larger share of women (49% vs. 40%) among those surveyed, Medscape said.
Satisfaction with their compensation, on the other hand, was higher among the family physicians (50%), compared with internists (43%). In 2022, 55% of family physicians said that they had been fairly paid.
In 2022, FP respondents reported spending an average of 16.7 hours (up from 15.6 hours in 2021) each week on paperwork and administration, just below the survey leaders, physical medicine and rehabilitation (18.5 hours) and nephrology (18.1 hours) but well above anesthesiology, lowest of the 29 specialties at 9.0 hours, and the 2022 average of 15.5 hours for all physicians, Medscape said.
When asked if they would choose medicine again, 72% of family physician respondents and 73% of all physicians said yes, with emergency medicine (65%) and dermatology (86%) representing the two extremes. A question about specialty choice showed that 66% of FPs would choose it again, putting them 28th of the 29 included specialties in their eagerness to follow the same path, above only the internists (61%), Medscape reported.
Commenters among the survey respondents were not identified by specialty, but dissatisfaction on many fronts was a definite theme:
- “Our costs go up, and our reimbursement does not.”
- “Our practice was acquired by venture capital firms; they slashed costs.”
- “My productivity bonus should have come to $45,000. Instead I was paid only $15,000. Yet cardiologists and administrators who were working from home part of the year received their full bonus.”
- “I will no longer practice cookbook mediocrity.”
Blood cancer patient takes on bias and ‘gaslighting’
Diagnosed with Hodgkin lymphoma in 2021, Ms. Ngon underwent port surgery to allow chemotherapy to be administered. Her right arm lost circulation and went numb, so she sought guidance from her blood cancer specialist. He dismissed her worries, saying that her tumors were pinching a nerve. She’d get better, he predicted, after more chemo.

“I knew in my body that something was wrong,” Ms. Ngon recalled. When the oncologist continued to downplay her concerns, she and a fellow communications specialist sat down together in the hospital lobby to draft an email to her physician. “We were trying to articulate the urgency in an email that expresses that I’m not being dramatic. We had to do it in a way that didn’t insult his intelligence: ‘Respectfully, you’re the doctor, but I know something is wrong.’ ”
In essence, Ms. Ngon was trying to be diplomatic and not trigger her oncologist’s defenses, while still convincing him to take action. Her approach to getting her doctor’s attention worked. He referred Ms. Ngon to a radiologist, who discovered that she had blood clots in her arm. Ms. Ngon then landed in the ICU for a week, as clinicians tried to break up the clots.
“I was the perfect person for this to happen to, because of my job and education. But it makes me sad because I understand I was in a fortunate position, with a background in communication. Most people don’t have that,” Ms. Ngon said.
This and other negative experiences during her medical saga inspired Ms. Ngon to partner with the Lymphoma Research Foundation in order to spread the word about unique challenges facing patients like her: people of color.
Ms. Ngon, who is Black, said her goal as a patient advocate is to “empower communities of color to speak up for themselves and hold oncologists responsible for listening and understanding differences across cultures.” And she wants to take a stand against the “gaslighting” of patients.
African Americans with hematologic disease like Ms. Ngon face a higher risk of poor outcomes than Whites, even as they are less likely than Whites to develop certain blood cancers. The reasons for this disparity aren’t clear, but researchers suspect they’re related to factors such as poverty, lack of insurance, genetics, and limited access to high-quality care.
Some researchers have blamed another factor: racism. A 2022 study sought to explain why Black and Hispanic patients with acute myeloid leukemia in urban areas have higher mortality rates than Whites, “despite more favorable genetics and younger age” (hazard ratio, 1.59, 95% confidence interval, 1.15-2.22 and HR, 1.25; 95% CI, 0.88-1.79). The study authors determined that “structural racism” – which they measured by examining segregation and “disadvantage” in neighborhoods where patients lived – accounted for nearly all of the disparities.
Ms. Ngon said her experiences and her awareness about poorer outcomes in medicine for African Americans – such as higher death rates for Black women during pregnancy – affect how she interacts with clinicians. “I automatically assume a barrier between me and my doctors, and it’s their responsibility to dismantle it.”
Making an connection with a physician can make a huge difference, she said. “I walked into my primary care doctor’s office and saw that she was a Latino woman. My guard went down, and I could feel her care for me as a human being. Whether that was because she was also a woman of color or not, I don’t know. But I did feel more cared for.”
However, Ms. Ngon could not find a Black oncologist to care for her in New York City, and that’s no surprise.
Ethnic and gender diversity remains an immense challenge in the hematology/oncology field. According to the American Society of Clinical Oncology, only about a third of oncologists are women, and the percentages identifying themselves as Black/African American and Hispanic are just 2.3% and 5.8%, respectively.
These numbers don’t seem likely to budge much any time soon. An analysis of medical students in U.S. oncology training programs from 2015-2020 found that just 3.8% identified themselves as Black/African American and 5.1% as Hispanic/Latino versus 52.15% as White and 31% as Asian/Pacific Islander/Native Hawaiian.
Ms. Ngon encountered challenges on other fronts during her cancer care. When she needed a wig during chemotherapy, a list of insurer-approved shops didn’t include any that catered to African Americans. Essentially, she said, she was being told that she couldn’t “purchase a wig from a place that makes you feel comfortable and from a woman who understand your needs as a Black woman. It needs to be from these specific shops that really don’t cater to my community.”
She also found it difficult to find fellow patients who shared her unique challenges. “I remember when I was diagnosed, I was looking through the support groups on Facebook, trying to find someone Black to ask about whether braiding my hair might stop it from falling out.”
Now, Ms. Ngon is in remission. And she’s happy with her oncologist, who’s White. “He listened to me, and he promised me that I would have the most boring recovery process ever, after everything I’d experienced. That explains a lot of why I felt so comfortable with him.”
She hopes to use her partnership with the Lymphoma Research Foundation to be a resource for people of color and alert them to the support that’s available for them. “I would love to let them know how to advocate for themselves as patients, how to trust their bodies, how to push back if they feel like they’re not getting the care that they deserve.”
Ms. Ngon would also like to see more support for medical students of color. “I hope to exist in a world one day where it wouldn’t be so hard to find an oncologist who looks like me in a city as large as this one,” she said.
As for oncologists, she urged them to “go the extra mile and really, really listen to what patients are saying. It’s easier said than done because there are natural biases in this world, and it’s hard to overcome those obstacles. But to not be heard and have to push every time. It was just exhausting to do that on top of trying to beat cancer.”
Diagnosed with Hodgkin lymphoma in 2021, Ms. Ngon underwent port surgery to allow chemotherapy to be administered. Her right arm lost circulation and went numb, so she sought guidance from her blood cancer specialist. He dismissed her worries, saying that her tumors were pinching a nerve. She’d get better, he predicted, after more chemo.
“I knew in my body that something was wrong,” Ms. Ngon recalled. When the oncologist continued to downplay her concerns, she and a fellow communications specialist sat down together in the hospital lobby to draft an email to her physician. “We were trying to articulate the urgency in an email that expresses that I’m not being dramatic. We had to do it in a way that didn’t insult his intelligence: ‘Respectfully, you’re the doctor, but I know something is wrong.’ ”
In essence, Ms. Ngon was trying to be diplomatic and not trigger her oncologist’s defenses, while still convincing him to take action. Her approach to getting her doctor’s attention worked. He referred Ms. Ngon to a radiologist, who discovered that she had blood clots in her arm. Ms. Ngon then landed in the ICU for a week, as clinicians tried to break up the clots.
“I was the perfect person for this to happen to, because of my job and education. But it makes me sad because I understand I was in a fortunate position, with a background in communication. Most people don’t have that,” Ms. Ngon said.
This and other negative experiences during her medical saga inspired Ms. Ngon to partner with the Lymphoma Research Foundation in order to spread the word about unique challenges facing patients like her: people of color.
Ms. Ngon, who is Black, said her goal as a patient advocate is to “empower communities of color to speak up for themselves and hold oncologists responsible for listening and understanding differences across cultures.” And she wants to take a stand against the “gaslighting” of patients.
African Americans with hematologic disease like Ms. Ngon face a higher risk of poor outcomes than Whites, even as they are less likely than Whites to develop certain blood cancers. The reasons for this disparity aren’t clear, but researchers suspect they’re related to factors such as poverty, lack of insurance, genetics, and limited access to high-quality care.
Some researchers have blamed another factor: racism. A 2022 study sought to explain why Black and Hispanic patients with acute myeloid leukemia in urban areas have higher mortality rates than Whites, “despite more favorable genetics and younger age” (hazard ratio, 1.59, 95% confidence interval, 1.15-2.22 and HR, 1.25; 95% CI, 0.88-1.79). The study authors determined that “structural racism” – which they measured by examining segregation and “disadvantage” in neighborhoods where patients lived – accounted for nearly all of the disparities.
Ms. Ngon said her experiences and her awareness about poorer outcomes in medicine for African Americans – such as higher death rates for Black women during pregnancy – affect how she interacts with clinicians. “I automatically assume a barrier between me and my doctors, and it’s their responsibility to dismantle it.”
Making an connection with a physician can make a huge difference, she said. “I walked into my primary care doctor’s office and saw that she was a Latino woman. My guard went down, and I could feel her care for me as a human being. Whether that was because she was also a woman of color or not, I don’t know. But I did feel more cared for.”
However, Ms. Ngon could not find a Black oncologist to care for her in New York City, and that’s no surprise.
Ethnic and gender diversity remains an immense challenge in the hematology/oncology field. According to the American Society of Clinical Oncology, only about a third of oncologists are women, and the percentages identifying themselves as Black/African American and Hispanic are just 2.3% and 5.8%, respectively.
These numbers don’t seem likely to budge much any time soon. An analysis of medical students in U.S. oncology training programs from 2015-2020 found that just 3.8% identified themselves as Black/African American and 5.1% as Hispanic/Latino versus 52.15% as White and 31% as Asian/Pacific Islander/Native Hawaiian.
Ms. Ngon encountered challenges on other fronts during her cancer care. When she needed a wig during chemotherapy, a list of insurer-approved shops didn’t include any that catered to African Americans. Essentially, she said, she was being told that she couldn’t “purchase a wig from a place that makes you feel comfortable and from a woman who understand your needs as a Black woman. It needs to be from these specific shops that really don’t cater to my community.”
She also found it difficult to find fellow patients who shared her unique challenges. “I remember when I was diagnosed, I was looking through the support groups on Facebook, trying to find someone Black to ask about whether braiding my hair might stop it from falling out.”
Now, Ms. Ngon is in remission. And she’s happy with her oncologist, who’s White. “He listened to me, and he promised me that I would have the most boring recovery process ever, after everything I’d experienced. That explains a lot of why I felt so comfortable with him.”
She hopes to use her partnership with the Lymphoma Research Foundation to be a resource for people of color and alert them to the support that’s available for them. “I would love to let them know how to advocate for themselves as patients, how to trust their bodies, how to push back if they feel like they’re not getting the care that they deserve.”
Ms. Ngon would also like to see more support for medical students of color. “I hope to exist in a world one day where it wouldn’t be so hard to find an oncologist who looks like me in a city as large as this one,” she said.
As for oncologists, she urged them to “go the extra mile and really, really listen to what patients are saying. It’s easier said than done because there are natural biases in this world, and it’s hard to overcome those obstacles. But to not be heard and have to push every time. It was just exhausting to do that on top of trying to beat cancer.”
Diagnosed with Hodgkin lymphoma in 2021, Ms. Ngon underwent port surgery to allow chemotherapy to be administered. Her right arm lost circulation and went numb, so she sought guidance from her blood cancer specialist. He dismissed her worries, saying that her tumors were pinching a nerve. She’d get better, he predicted, after more chemo.
“I knew in my body that something was wrong,” Ms. Ngon recalled. When the oncologist continued to downplay her concerns, she and a fellow communications specialist sat down together in the hospital lobby to draft an email to her physician. “We were trying to articulate the urgency in an email that expresses that I’m not being dramatic. We had to do it in a way that didn’t insult his intelligence: ‘Respectfully, you’re the doctor, but I know something is wrong.’ ”
In essence, Ms. Ngon was trying to be diplomatic and not trigger her oncologist’s defenses, while still convincing him to take action. Her approach to getting her doctor’s attention worked. He referred Ms. Ngon to a radiologist, who discovered that she had blood clots in her arm. Ms. Ngon then landed in the ICU for a week, as clinicians tried to break up the clots.
“I was the perfect person for this to happen to, because of my job and education. But it makes me sad because I understand I was in a fortunate position, with a background in communication. Most people don’t have that,” Ms. Ngon said.
This and other negative experiences during her medical saga inspired Ms. Ngon to partner with the Lymphoma Research Foundation in order to spread the word about unique challenges facing patients like her: people of color.
Ms. Ngon, who is Black, said her goal as a patient advocate is to “empower communities of color to speak up for themselves and hold oncologists responsible for listening and understanding differences across cultures.” And she wants to take a stand against the “gaslighting” of patients.
African Americans with hematologic disease like Ms. Ngon face a higher risk of poor outcomes than Whites, even as they are less likely than Whites to develop certain blood cancers. The reasons for this disparity aren’t clear, but researchers suspect they’re related to factors such as poverty, lack of insurance, genetics, and limited access to high-quality care.
Some researchers have blamed another factor: racism. A 2022 study sought to explain why Black and Hispanic patients with acute myeloid leukemia in urban areas have higher mortality rates than Whites, “despite more favorable genetics and younger age” (hazard ratio, 1.59, 95% confidence interval, 1.15-2.22 and HR, 1.25; 95% CI, 0.88-1.79). The study authors determined that “structural racism” – which they measured by examining segregation and “disadvantage” in neighborhoods where patients lived – accounted for nearly all of the disparities.
Ms. Ngon said her experiences and her awareness about poorer outcomes in medicine for African Americans – such as higher death rates for Black women during pregnancy – affect how she interacts with clinicians. “I automatically assume a barrier between me and my doctors, and it’s their responsibility to dismantle it.”
Making an connection with a physician can make a huge difference, she said. “I walked into my primary care doctor’s office and saw that she was a Latino woman. My guard went down, and I could feel her care for me as a human being. Whether that was because she was also a woman of color or not, I don’t know. But I did feel more cared for.”
However, Ms. Ngon could not find a Black oncologist to care for her in New York City, and that’s no surprise.
Ethnic and gender diversity remains an immense challenge in the hematology/oncology field. According to the American Society of Clinical Oncology, only about a third of oncologists are women, and the percentages identifying themselves as Black/African American and Hispanic are just 2.3% and 5.8%, respectively.
These numbers don’t seem likely to budge much any time soon. An analysis of medical students in U.S. oncology training programs from 2015-2020 found that just 3.8% identified themselves as Black/African American and 5.1% as Hispanic/Latino versus 52.15% as White and 31% as Asian/Pacific Islander/Native Hawaiian.
Ms. Ngon encountered challenges on other fronts during her cancer care. When she needed a wig during chemotherapy, a list of insurer-approved shops didn’t include any that catered to African Americans. Essentially, she said, she was being told that she couldn’t “purchase a wig from a place that makes you feel comfortable and from a woman who understand your needs as a Black woman. It needs to be from these specific shops that really don’t cater to my community.”
She also found it difficult to find fellow patients who shared her unique challenges. “I remember when I was diagnosed, I was looking through the support groups on Facebook, trying to find someone Black to ask about whether braiding my hair might stop it from falling out.”
Now, Ms. Ngon is in remission. And she’s happy with her oncologist, who’s White. “He listened to me, and he promised me that I would have the most boring recovery process ever, after everything I’d experienced. That explains a lot of why I felt so comfortable with him.”
She hopes to use her partnership with the Lymphoma Research Foundation to be a resource for people of color and alert them to the support that’s available for them. “I would love to let them know how to advocate for themselves as patients, how to trust their bodies, how to push back if they feel like they’re not getting the care that they deserve.”
Ms. Ngon would also like to see more support for medical students of color. “I hope to exist in a world one day where it wouldn’t be so hard to find an oncologist who looks like me in a city as large as this one,” she said.
As for oncologists, she urged them to “go the extra mile and really, really listen to what patients are saying. It’s easier said than done because there are natural biases in this world, and it’s hard to overcome those obstacles. But to not be heard and have to push every time. It was just exhausting to do that on top of trying to beat cancer.”