User login
Is education or screening better for type 1 diabetes?
After 100 years of insulin therapy, teplizumab, an immunotherapy for early-stage type 1 diabetes, has been approved for the first time in the United States and has been shown to delay the manifestation of clinical diabetes by 3 years on average. at the Diabetes Congress in Berlin.
Anette-Gabriele Ziegler, MD, PhD, director of the Institute for Diabetes Research in Helmholtz Munich, argued that voluntary screening for type 1 diabetes should be included in standard care. “The first immunotherapy that delays type 1 diabetes has been approved in the U.S. for early stage 2. And this early stage can only be identified through prior screening, since no symptoms have manifested by this stage,” she said. This is the only way in which as many people as possible, particularly children, will benefit from the disease-delaying therapy, she added.
Two autoantibodies
One biomarker for the early diagnosis of type 1 diabetes is evidence of at least two positive islet cell antibodies. In one study of more than 13,000 children who were observed for 20 years, the specificity of these antibodies was 100%. “Every single child with a positive autoantibody test developed type 1 diabetes later on in their life,” Dr. Ziegler said. “Based on the results of this study, the early stages of type 1 diabetes were added to multiple guidelines.”
The early stage of type 1 diabetes is divided into the following three phases, depending on autoantibody detection and the level of glucose metabolism:
- Early stage 1: Two or more islet autoantibodies and normoglycemia.
- Early stage 2: Two or more islet autoantibodies and dysglycemia.
- Early stage 3: Symptoms, hyperglycemia, insulin therapy.
The aim of the ongoing FR1DA study is to ascertain whether the general population could also be screened for type 1 diabetes using this autoantibody. “Since 2015, children of kindergarten and school age have undergone screening, and to date, more than 170,000 have been tested,” said Dr. Ziegler. “At least two autoantibodies were detected in 0.3% of those screened.”
Education and care
The families of the children in whom early-stage type 1 diabetes was diagnosed were invited to take an oral glucose tolerance test (OGTT), to undergo measurement of hemoglobin A1c, and to take part in training and monitoring. “Education and competent, ongoing care are crucial for the efficacy of the screening,” Dr. Ziegler emphasized.
The OGTT revealed that 85% of the FR1DA children were still in early stage 1, another 11% were in early stage 2, and the remaining 4% were in early stage 3.
“Unfortunately, the 4% could no longer benefit from teplizumab, since the medication is not approved for manifest diabetes,” said Dr. Ziegler. “However, the 11% could receive teplizumab immediately, and then later on, the 85%, when they developed stage 2. Therefore, further observation of the children is also important.”
The speed at which the disease progresses from early stage 1 to early stage 2 can be stratified using IA2 antibodies, the 90-minute OGTT glucose value, and the HbA1c value. With regard to progression to clinical type 1 diabetes (stage 3), it was observed that the progression risk for the FR1DA children was similar to that of international birth cohorts with increased genetic risk. “Of course, there is still no 20-year follow-up like for BABYDIAB, DIPP, and DAISY, but as of yet, the progression rate is practically identical,” said Dr. Ziegler.
Dubious benefits?
The advantages of screening for type 1 diabetes would not be limited to potential access to preventive therapies and a smooth transition to insulin therapy at the correct point in time, according to Dr. Ziegler. Participation in the FR1DA study dramatically reduced the risk of diabetic ketoacidosis (DKA). Between 2015 and 2023, the overall rate of ketoacidosis associated with the manifestation of clinical type 1 diabetes was 4.3%. In contrast, the general DKA rate in Germany has remained largely unchanged for the last 2 decades at between 20% and 25%.
In addition, the FR1DA children exhibited better beta cell function and better metabolic function at clinical diagnosis of type 1 diabetes. This finding was observed in a comparison with children with a spontaneous diabetes diagnosis from the DiMelli study. “It is important that there is a lot of data that shows how, in the long term, this is associated with a better morbidity and mortality,” said Dr. Ziegler.
Despite the impressive data from the FR1DA study, not all diabetes experts are convinced that a general screening for type 1 diabetes would be beneficial. Beate Karges, MD, PhD, of the Clinic for Pediatric and Adolescent Medicine of the Bethlehem Hospital Stolberg (Germany) and the endocrinology and diabetology department at the University Hospital Aachen (Germany), stressed, “Screening makes sense if the disease is curable in the preclinical phase or if there is a significantly better prognosis in the event of early diagnosis and treatment.”
Severe side effects
Even with an early-stage diagnosis, curing type 1 diabetes is impossible. The new anti-CD3 antibody teplizumab merely delays the manifestation of symptoms for 3 years. However, this delay has its price. The summary of product characteristics for teplizumab contains warnings of severe lymphopenia lasting many weeks, cytokine release syndrome, severe infections, and hypersensitivity reactions. Furthermore, vaccinations may not be administered during teplizumab treatment and therefore must be completed in advance.
“Preventing type 1 diabetes is still not possible, we can only delay it, and the long-term efficacy and safety of this immunotherapy are not clear,” said Dr. Karges. She added that a significant reduction in the DKA rate – as observed in the FR1DA study – may be possible even without screening. This possibility was demonstrated by a model project in Stuttgart, Germany, in which the DKA rate was significantly reduced through education alone.
Education reduces ketoacidosis
“The families were given information about the early signs of type 1 diabetes during the education investigation. Through this [education], a reduction in the ketoacidosis rate from 28% to 16% was achieved,” said Dr. Karges. It is also known from studies of familial type 1 diabetes that secondary sufferers in the family only exhibit a DKA rate of 7%. “Through education within the family and awareness campaigns, the DKA rate can be reduced by 40%-65%,” said Dr. Karges.
Dr. Karges also doubts whether starting insulin therapy earlier “at the correct point in time” elicits long-term advantages. Secondary sufferers with familial type 1 diabetes have better HbA1c values in the first few years after diagnosis. “But as they progress beyond 2, towards 10 years, the difference in HbA1c values diminishes,” said Dr. Karges.
Whether the patient has DKA at type 1 diabetes diagnosis also seems to make little difference in the long term. “There is also no difference in the HbA1c value in the 2-10 years after diagnosis,” said Dr. Karges. “Glycemic control is not permanently improved in the event that treatment is started early,” she concluded.
“Type 1 diabetes can be delayed with an immune intervention, but to do so, we must also accept possible severe side effects in an otherwise healthy child,” she said. On the other hand, type 1 diabetes can be treated well. “With pumps and continuous glucose monitoring, insulin therapy in children and adolescents has become significantly safer and more effective,” she said.
New therapeutic options
Whether voluntary screening for type 1 diabetes eventually finds its way into standard care depends on the further development of preventive medications. Dr. Ziegler stressed that future preventive therapy does not need to be limited to the anti-CD3 antibody teplizumab.
For example, strategies such as high-dose oral insulin therapy are being investigated. Verapamil, which is used to treat hypertension, is also promising, since with it, beta cells were retained in early stage 3, and it improved their function. The fusion protein abatacept fell short of statistical significance in a recently published study. For Dr. Ziegler, one thing remains true. “The therapy of type 1 diabetes is about to undergo a renaissance.”
This article was translated from the Medscape German Edition. A version of this article appeared on Medscape.com.
After 100 years of insulin therapy, teplizumab, an immunotherapy for early-stage type 1 diabetes, has been approved for the first time in the United States and has been shown to delay the manifestation of clinical diabetes by 3 years on average. at the Diabetes Congress in Berlin.
Anette-Gabriele Ziegler, MD, PhD, director of the Institute for Diabetes Research in Helmholtz Munich, argued that voluntary screening for type 1 diabetes should be included in standard care. “The first immunotherapy that delays type 1 diabetes has been approved in the U.S. for early stage 2. And this early stage can only be identified through prior screening, since no symptoms have manifested by this stage,” she said. This is the only way in which as many people as possible, particularly children, will benefit from the disease-delaying therapy, she added.
Two autoantibodies
One biomarker for the early diagnosis of type 1 diabetes is evidence of at least two positive islet cell antibodies. In one study of more than 13,000 children who were observed for 20 years, the specificity of these antibodies was 100%. “Every single child with a positive autoantibody test developed type 1 diabetes later on in their life,” Dr. Ziegler said. “Based on the results of this study, the early stages of type 1 diabetes were added to multiple guidelines.”
The early stage of type 1 diabetes is divided into the following three phases, depending on autoantibody detection and the level of glucose metabolism:
- Early stage 1: Two or more islet autoantibodies and normoglycemia.
- Early stage 2: Two or more islet autoantibodies and dysglycemia.
- Early stage 3: Symptoms, hyperglycemia, insulin therapy.
The aim of the ongoing FR1DA study is to ascertain whether the general population could also be screened for type 1 diabetes using this autoantibody. “Since 2015, children of kindergarten and school age have undergone screening, and to date, more than 170,000 have been tested,” said Dr. Ziegler. “At least two autoantibodies were detected in 0.3% of those screened.”
Education and care
The families of the children in whom early-stage type 1 diabetes was diagnosed were invited to take an oral glucose tolerance test (OGTT), to undergo measurement of hemoglobin A1c, and to take part in training and monitoring. “Education and competent, ongoing care are crucial for the efficacy of the screening,” Dr. Ziegler emphasized.
The OGTT revealed that 85% of the FR1DA children were still in early stage 1, another 11% were in early stage 2, and the remaining 4% were in early stage 3.
“Unfortunately, the 4% could no longer benefit from teplizumab, since the medication is not approved for manifest diabetes,” said Dr. Ziegler. “However, the 11% could receive teplizumab immediately, and then later on, the 85%, when they developed stage 2. Therefore, further observation of the children is also important.”
The speed at which the disease progresses from early stage 1 to early stage 2 can be stratified using IA2 antibodies, the 90-minute OGTT glucose value, and the HbA1c value. With regard to progression to clinical type 1 diabetes (stage 3), it was observed that the progression risk for the FR1DA children was similar to that of international birth cohorts with increased genetic risk. “Of course, there is still no 20-year follow-up like for BABYDIAB, DIPP, and DAISY, but as of yet, the progression rate is practically identical,” said Dr. Ziegler.
Dubious benefits?
The advantages of screening for type 1 diabetes would not be limited to potential access to preventive therapies and a smooth transition to insulin therapy at the correct point in time, according to Dr. Ziegler. Participation in the FR1DA study dramatically reduced the risk of diabetic ketoacidosis (DKA). Between 2015 and 2023, the overall rate of ketoacidosis associated with the manifestation of clinical type 1 diabetes was 4.3%. In contrast, the general DKA rate in Germany has remained largely unchanged for the last 2 decades at between 20% and 25%.
In addition, the FR1DA children exhibited better beta cell function and better metabolic function at clinical diagnosis of type 1 diabetes. This finding was observed in a comparison with children with a spontaneous diabetes diagnosis from the DiMelli study. “It is important that there is a lot of data that shows how, in the long term, this is associated with a better morbidity and mortality,” said Dr. Ziegler.
Despite the impressive data from the FR1DA study, not all diabetes experts are convinced that a general screening for type 1 diabetes would be beneficial. Beate Karges, MD, PhD, of the Clinic for Pediatric and Adolescent Medicine of the Bethlehem Hospital Stolberg (Germany) and the endocrinology and diabetology department at the University Hospital Aachen (Germany), stressed, “Screening makes sense if the disease is curable in the preclinical phase or if there is a significantly better prognosis in the event of early diagnosis and treatment.”
Severe side effects
Even with an early-stage diagnosis, curing type 1 diabetes is impossible. The new anti-CD3 antibody teplizumab merely delays the manifestation of symptoms for 3 years. However, this delay has its price. The summary of product characteristics for teplizumab contains warnings of severe lymphopenia lasting many weeks, cytokine release syndrome, severe infections, and hypersensitivity reactions. Furthermore, vaccinations may not be administered during teplizumab treatment and therefore must be completed in advance.
“Preventing type 1 diabetes is still not possible, we can only delay it, and the long-term efficacy and safety of this immunotherapy are not clear,” said Dr. Karges. She added that a significant reduction in the DKA rate – as observed in the FR1DA study – may be possible even without screening. This possibility was demonstrated by a model project in Stuttgart, Germany, in which the DKA rate was significantly reduced through education alone.
Education reduces ketoacidosis
“The families were given information about the early signs of type 1 diabetes during the education investigation. Through this [education], a reduction in the ketoacidosis rate from 28% to 16% was achieved,” said Dr. Karges. It is also known from studies of familial type 1 diabetes that secondary sufferers in the family only exhibit a DKA rate of 7%. “Through education within the family and awareness campaigns, the DKA rate can be reduced by 40%-65%,” said Dr. Karges.
Dr. Karges also doubts whether starting insulin therapy earlier “at the correct point in time” elicits long-term advantages. Secondary sufferers with familial type 1 diabetes have better HbA1c values in the first few years after diagnosis. “But as they progress beyond 2, towards 10 years, the difference in HbA1c values diminishes,” said Dr. Karges.
Whether the patient has DKA at type 1 diabetes diagnosis also seems to make little difference in the long term. “There is also no difference in the HbA1c value in the 2-10 years after diagnosis,” said Dr. Karges. “Glycemic control is not permanently improved in the event that treatment is started early,” she concluded.
“Type 1 diabetes can be delayed with an immune intervention, but to do so, we must also accept possible severe side effects in an otherwise healthy child,” she said. On the other hand, type 1 diabetes can be treated well. “With pumps and continuous glucose monitoring, insulin therapy in children and adolescents has become significantly safer and more effective,” she said.
New therapeutic options
Whether voluntary screening for type 1 diabetes eventually finds its way into standard care depends on the further development of preventive medications. Dr. Ziegler stressed that future preventive therapy does not need to be limited to the anti-CD3 antibody teplizumab.
For example, strategies such as high-dose oral insulin therapy are being investigated. Verapamil, which is used to treat hypertension, is also promising, since with it, beta cells were retained in early stage 3, and it improved their function. The fusion protein abatacept fell short of statistical significance in a recently published study. For Dr. Ziegler, one thing remains true. “The therapy of type 1 diabetes is about to undergo a renaissance.”
This article was translated from the Medscape German Edition. A version of this article appeared on Medscape.com.
After 100 years of insulin therapy, teplizumab, an immunotherapy for early-stage type 1 diabetes, has been approved for the first time in the United States and has been shown to delay the manifestation of clinical diabetes by 3 years on average. at the Diabetes Congress in Berlin.
Anette-Gabriele Ziegler, MD, PhD, director of the Institute for Diabetes Research in Helmholtz Munich, argued that voluntary screening for type 1 diabetes should be included in standard care. “The first immunotherapy that delays type 1 diabetes has been approved in the U.S. for early stage 2. And this early stage can only be identified through prior screening, since no symptoms have manifested by this stage,” she said. This is the only way in which as many people as possible, particularly children, will benefit from the disease-delaying therapy, she added.
Two autoantibodies
One biomarker for the early diagnosis of type 1 diabetes is evidence of at least two positive islet cell antibodies. In one study of more than 13,000 children who were observed for 20 years, the specificity of these antibodies was 100%. “Every single child with a positive autoantibody test developed type 1 diabetes later on in their life,” Dr. Ziegler said. “Based on the results of this study, the early stages of type 1 diabetes were added to multiple guidelines.”
The early stage of type 1 diabetes is divided into the following three phases, depending on autoantibody detection and the level of glucose metabolism:
- Early stage 1: Two or more islet autoantibodies and normoglycemia.
- Early stage 2: Two or more islet autoantibodies and dysglycemia.
- Early stage 3: Symptoms, hyperglycemia, insulin therapy.
The aim of the ongoing FR1DA study is to ascertain whether the general population could also be screened for type 1 diabetes using this autoantibody. “Since 2015, children of kindergarten and school age have undergone screening, and to date, more than 170,000 have been tested,” said Dr. Ziegler. “At least two autoantibodies were detected in 0.3% of those screened.”
Education and care
The families of the children in whom early-stage type 1 diabetes was diagnosed were invited to take an oral glucose tolerance test (OGTT), to undergo measurement of hemoglobin A1c, and to take part in training and monitoring. “Education and competent, ongoing care are crucial for the efficacy of the screening,” Dr. Ziegler emphasized.
The OGTT revealed that 85% of the FR1DA children were still in early stage 1, another 11% were in early stage 2, and the remaining 4% were in early stage 3.
“Unfortunately, the 4% could no longer benefit from teplizumab, since the medication is not approved for manifest diabetes,” said Dr. Ziegler. “However, the 11% could receive teplizumab immediately, and then later on, the 85%, when they developed stage 2. Therefore, further observation of the children is also important.”
The speed at which the disease progresses from early stage 1 to early stage 2 can be stratified using IA2 antibodies, the 90-minute OGTT glucose value, and the HbA1c value. With regard to progression to clinical type 1 diabetes (stage 3), it was observed that the progression risk for the FR1DA children was similar to that of international birth cohorts with increased genetic risk. “Of course, there is still no 20-year follow-up like for BABYDIAB, DIPP, and DAISY, but as of yet, the progression rate is practically identical,” said Dr. Ziegler.
Dubious benefits?
The advantages of screening for type 1 diabetes would not be limited to potential access to preventive therapies and a smooth transition to insulin therapy at the correct point in time, according to Dr. Ziegler. Participation in the FR1DA study dramatically reduced the risk of diabetic ketoacidosis (DKA). Between 2015 and 2023, the overall rate of ketoacidosis associated with the manifestation of clinical type 1 diabetes was 4.3%. In contrast, the general DKA rate in Germany has remained largely unchanged for the last 2 decades at between 20% and 25%.
In addition, the FR1DA children exhibited better beta cell function and better metabolic function at clinical diagnosis of type 1 diabetes. This finding was observed in a comparison with children with a spontaneous diabetes diagnosis from the DiMelli study. “It is important that there is a lot of data that shows how, in the long term, this is associated with a better morbidity and mortality,” said Dr. Ziegler.
Despite the impressive data from the FR1DA study, not all diabetes experts are convinced that a general screening for type 1 diabetes would be beneficial. Beate Karges, MD, PhD, of the Clinic for Pediatric and Adolescent Medicine of the Bethlehem Hospital Stolberg (Germany) and the endocrinology and diabetology department at the University Hospital Aachen (Germany), stressed, “Screening makes sense if the disease is curable in the preclinical phase or if there is a significantly better prognosis in the event of early diagnosis and treatment.”
Severe side effects
Even with an early-stage diagnosis, curing type 1 diabetes is impossible. The new anti-CD3 antibody teplizumab merely delays the manifestation of symptoms for 3 years. However, this delay has its price. The summary of product characteristics for teplizumab contains warnings of severe lymphopenia lasting many weeks, cytokine release syndrome, severe infections, and hypersensitivity reactions. Furthermore, vaccinations may not be administered during teplizumab treatment and therefore must be completed in advance.
“Preventing type 1 diabetes is still not possible, we can only delay it, and the long-term efficacy and safety of this immunotherapy are not clear,” said Dr. Karges. She added that a significant reduction in the DKA rate – as observed in the FR1DA study – may be possible even without screening. This possibility was demonstrated by a model project in Stuttgart, Germany, in which the DKA rate was significantly reduced through education alone.
Education reduces ketoacidosis
“The families were given information about the early signs of type 1 diabetes during the education investigation. Through this [education], a reduction in the ketoacidosis rate from 28% to 16% was achieved,” said Dr. Karges. It is also known from studies of familial type 1 diabetes that secondary sufferers in the family only exhibit a DKA rate of 7%. “Through education within the family and awareness campaigns, the DKA rate can be reduced by 40%-65%,” said Dr. Karges.
Dr. Karges also doubts whether starting insulin therapy earlier “at the correct point in time” elicits long-term advantages. Secondary sufferers with familial type 1 diabetes have better HbA1c values in the first few years after diagnosis. “But as they progress beyond 2, towards 10 years, the difference in HbA1c values diminishes,” said Dr. Karges.
Whether the patient has DKA at type 1 diabetes diagnosis also seems to make little difference in the long term. “There is also no difference in the HbA1c value in the 2-10 years after diagnosis,” said Dr. Karges. “Glycemic control is not permanently improved in the event that treatment is started early,” she concluded.
“Type 1 diabetes can be delayed with an immune intervention, but to do so, we must also accept possible severe side effects in an otherwise healthy child,” she said. On the other hand, type 1 diabetes can be treated well. “With pumps and continuous glucose monitoring, insulin therapy in children and adolescents has become significantly safer and more effective,” she said.
New therapeutic options
Whether voluntary screening for type 1 diabetes eventually finds its way into standard care depends on the further development of preventive medications. Dr. Ziegler stressed that future preventive therapy does not need to be limited to the anti-CD3 antibody teplizumab.
For example, strategies such as high-dose oral insulin therapy are being investigated. Verapamil, which is used to treat hypertension, is also promising, since with it, beta cells were retained in early stage 3, and it improved their function. The fusion protein abatacept fell short of statistical significance in a recently published study. For Dr. Ziegler, one thing remains true. “The therapy of type 1 diabetes is about to undergo a renaissance.”
This article was translated from the Medscape German Edition. A version of this article appeared on Medscape.com.
A glimmer of an answer to long COVID
Although we continue to hear a chorus of cautions from the wise folks in the public health community, most of us and our political leaders have allowed the SARS-CoV-2 pandemic to slip quietly into the dark recesses of our been-there-done-that pile. Obviously, this failure to continue learning from our mistakes is an oversight for which we will pay dearly the next time a public health crisis requiring a coordinated effort on a national and international scale raises its ugly head.
However, there is a significant portion of the population for whom the pandemic is fresh in their minds because they are experiencing the symptoms of what they have been told is long COVID. In January 2023 the Kaiser Family Foundation reported that 15% of the U.S. population feels that at some point they have experienced the symptoms of long COVID. And 6% report that they believe they currently have long COVID.

As long ago as February of 2021, Congress gave the National Institutes of Health $1.5 billion to fund a 4-year study of the prolonged health consequence of SARS-CoV-2. Sadly, 2 years into the study we aren’t too much further along in our search for answers. The Post Acute Sequelae of SARS-CoV-2 has earned an acronym, PASC, but it continues to be little more than a laundry list of vague symptoms including shortness of breath, fatigue, fever, headaches, “brain fog,” and a variety of other neurologic problems. We seem to have slipped into the same trap we find ourselves in with conditions such as chronic Lyme disease and chronic fatigue syndrome that lack workable diagnostic criteria.
However, I have just stumbled across a study in the JAMA Network Open that hints at a partial answer. Using data collected from a prospective study of nurses, investigators based at the T.H. Chan School of Public Health at Harvard found that , their chosen acronym for long COVID.
After taking into account a long list of covariants, the investigators found that women with consistently healthy sleep before and after their infection had the lowest risk of PCC when compared with women with consistently unhealthy sleep.
This finding seems to be telling us is that we shouldn’t be surprised to learn that folks who were relatively less healthy prior to contracting COVID are more likely to report feeling unhealthy after the acute phase of the illness has passed. It is unclear whether this observation is because their suboptimal health prior to the infection made them more vulnerable to its aftereffects or whether this is a return to their baseline for which we have labeled long COVID.
The results of this study are particularly important because it highlights our continued failure to acknowledge the critical role of sleep in the entire wellness picture. The broader message is of equal importance and that is when we are trying to discover what is making our patients sick, we must adhere to our traditional practice of taking a good and thorough history. When a patient asks the surgeon whether he will be able to play the violin after surgery, the prudent physician will always ask whether the patient has ever played the instrument.
As with any good study, it leaves more questions than it answers. While this study addresses the vague and neurologically based symptoms of long COVID, many of which are known symptoms associated with sleep deprivation, it doesn’t address the patients with more organically based symptoms such as those who have pulmonary or renal damage acquired during the acute phase of the illness. Many of these unfortunate individuals may have entered the pandemic with already damaged or vulnerable organ systems.
Finally, it leaves a very interesting question unanswered: Can we help the long COVID patients suffering with primarily neurologic symptoms by aggressively managing their preexisting unhealthy sleep habits? Or, has the damage already been done? I suspect and certainly hope it is the former.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Although we continue to hear a chorus of cautions from the wise folks in the public health community, most of us and our political leaders have allowed the SARS-CoV-2 pandemic to slip quietly into the dark recesses of our been-there-done-that pile. Obviously, this failure to continue learning from our mistakes is an oversight for which we will pay dearly the next time a public health crisis requiring a coordinated effort on a national and international scale raises its ugly head.
However, there is a significant portion of the population for whom the pandemic is fresh in their minds because they are experiencing the symptoms of what they have been told is long COVID. In January 2023 the Kaiser Family Foundation reported that 15% of the U.S. population feels that at some point they have experienced the symptoms of long COVID. And 6% report that they believe they currently have long COVID.
As long ago as February of 2021, Congress gave the National Institutes of Health $1.5 billion to fund a 4-year study of the prolonged health consequence of SARS-CoV-2. Sadly, 2 years into the study we aren’t too much further along in our search for answers. The Post Acute Sequelae of SARS-CoV-2 has earned an acronym, PASC, but it continues to be little more than a laundry list of vague symptoms including shortness of breath, fatigue, fever, headaches, “brain fog,” and a variety of other neurologic problems. We seem to have slipped into the same trap we find ourselves in with conditions such as chronic Lyme disease and chronic fatigue syndrome that lack workable diagnostic criteria.
However, I have just stumbled across a study in the JAMA Network Open that hints at a partial answer. Using data collected from a prospective study of nurses, investigators based at the T.H. Chan School of Public Health at Harvard found that , their chosen acronym for long COVID.
After taking into account a long list of covariants, the investigators found that women with consistently healthy sleep before and after their infection had the lowest risk of PCC when compared with women with consistently unhealthy sleep.
This finding seems to be telling us is that we shouldn’t be surprised to learn that folks who were relatively less healthy prior to contracting COVID are more likely to report feeling unhealthy after the acute phase of the illness has passed. It is unclear whether this observation is because their suboptimal health prior to the infection made them more vulnerable to its aftereffects or whether this is a return to their baseline for which we have labeled long COVID.
The results of this study are particularly important because it highlights our continued failure to acknowledge the critical role of sleep in the entire wellness picture. The broader message is of equal importance and that is when we are trying to discover what is making our patients sick, we must adhere to our traditional practice of taking a good and thorough history. When a patient asks the surgeon whether he will be able to play the violin after surgery, the prudent physician will always ask whether the patient has ever played the instrument.
As with any good study, it leaves more questions than it answers. While this study addresses the vague and neurologically based symptoms of long COVID, many of which are known symptoms associated with sleep deprivation, it doesn’t address the patients with more organically based symptoms such as those who have pulmonary or renal damage acquired during the acute phase of the illness. Many of these unfortunate individuals may have entered the pandemic with already damaged or vulnerable organ systems.
Finally, it leaves a very interesting question unanswered: Can we help the long COVID patients suffering with primarily neurologic symptoms by aggressively managing their preexisting unhealthy sleep habits? Or, has the damage already been done? I suspect and certainly hope it is the former.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Although we continue to hear a chorus of cautions from the wise folks in the public health community, most of us and our political leaders have allowed the SARS-CoV-2 pandemic to slip quietly into the dark recesses of our been-there-done-that pile. Obviously, this failure to continue learning from our mistakes is an oversight for which we will pay dearly the next time a public health crisis requiring a coordinated effort on a national and international scale raises its ugly head.
However, there is a significant portion of the population for whom the pandemic is fresh in their minds because they are experiencing the symptoms of what they have been told is long COVID. In January 2023 the Kaiser Family Foundation reported that 15% of the U.S. population feels that at some point they have experienced the symptoms of long COVID. And 6% report that they believe they currently have long COVID.
As long ago as February of 2021, Congress gave the National Institutes of Health $1.5 billion to fund a 4-year study of the prolonged health consequence of SARS-CoV-2. Sadly, 2 years into the study we aren’t too much further along in our search for answers. The Post Acute Sequelae of SARS-CoV-2 has earned an acronym, PASC, but it continues to be little more than a laundry list of vague symptoms including shortness of breath, fatigue, fever, headaches, “brain fog,” and a variety of other neurologic problems. We seem to have slipped into the same trap we find ourselves in with conditions such as chronic Lyme disease and chronic fatigue syndrome that lack workable diagnostic criteria.
However, I have just stumbled across a study in the JAMA Network Open that hints at a partial answer. Using data collected from a prospective study of nurses, investigators based at the T.H. Chan School of Public Health at Harvard found that , their chosen acronym for long COVID.
After taking into account a long list of covariants, the investigators found that women with consistently healthy sleep before and after their infection had the lowest risk of PCC when compared with women with consistently unhealthy sleep.
This finding seems to be telling us is that we shouldn’t be surprised to learn that folks who were relatively less healthy prior to contracting COVID are more likely to report feeling unhealthy after the acute phase of the illness has passed. It is unclear whether this observation is because their suboptimal health prior to the infection made them more vulnerable to its aftereffects or whether this is a return to their baseline for which we have labeled long COVID.
The results of this study are particularly important because it highlights our continued failure to acknowledge the critical role of sleep in the entire wellness picture. The broader message is of equal importance and that is when we are trying to discover what is making our patients sick, we must adhere to our traditional practice of taking a good and thorough history. When a patient asks the surgeon whether he will be able to play the violin after surgery, the prudent physician will always ask whether the patient has ever played the instrument.
As with any good study, it leaves more questions than it answers. While this study addresses the vague and neurologically based symptoms of long COVID, many of which are known symptoms associated with sleep deprivation, it doesn’t address the patients with more organically based symptoms such as those who have pulmonary or renal damage acquired during the acute phase of the illness. Many of these unfortunate individuals may have entered the pandemic with already damaged or vulnerable organ systems.
Finally, it leaves a very interesting question unanswered: Can we help the long COVID patients suffering with primarily neurologic symptoms by aggressively managing their preexisting unhealthy sleep habits? Or, has the damage already been done? I suspect and certainly hope it is the former.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
How physician-inventors create new, life-saving products
WakeMed emergency department physician and medical director, Graham Snyder, MD, has seen his fair share of deaths: an average of one or two per day. That’s part of the job. Some of the deaths were the result of risky behavior, ongoing health problems, and other natural causes.
But what he didn’t find acceptable was losing a 6-year-old girl in a backyard pool drowning at what was meant to be a celebratory birthday party and family reunion.
“There were aunts and uncles and brothers and sisters and cousins, and the pool was packed, and they’re having a great time. One of the parents looked over and saw that she was swimming around underneath but acting weird. A relative pulled her up by the arm, and she was dead,” he said. “What nobody could tell me, and what they’ll live with the rest of their life, is how long was she under water?”
So Dr. Snyder invented a solution. The catch: The goal: Improving systemic and “unsolvable” issues that harm society.
The cool part: Any MD with an idea can get in on the game.
Keeping little heads above water
Drowning is the leading cause of death in young children ages 1-4 years, and the second leading cause for children ages 5-14 years. The issue, Dr. Snyder explained, is not that rescuers couldn’t get to these children in time. “It’s that nobody knew to start looking.”
Dr. Snyder created a collar that alerts those around the swimmer that they are in trouble. The SEAL SwimSafe drowning prevention technology sets off an alarm system if a child is under water for too long. The necklace has been used to protect more than 10,000 children, including at larger swim facilities, such as the YMCA.
When Dr. Snyder first started pursuing his invention, he asked himself two key questions: “Has someone already tried this? And if they did, why did they not succeed?” These questions help counteract the potential arrogance, he says, with imagining that you are the first person to have a certain idea. And using whatever reason others didn’t succeed as your “secret sauce” helps lead to more success. He also had to consider obstacles. People might resist wearing a collar or necklace while swimming or putting one on their child, like the reluctance around wearing bicycle helmets when they gained popularity in the 1980s. He concluded that the collars would work best at larger facilities, where they were mandated.
Another obstacle was false alarms. “It was possible to trigger a false alarm, and that could really scare people,” Dr. Snyder said. He is still considering systems to prevent the collars from being stolen or from “13-year-old boys hiding them in the water drain and making everyone really scared when an alarm is going off.”
The demand is real, however, and is based on alarming data. Safe Kids has reported that 66% of natural water drownings and around half of pool drownings happened with an adult supervising. They added, however, that supervision is often lacking or insufficient, such as a parent not being within arm’s reach of a young kid. As Dr. Snyder told reporters in a 2018 story, even the most well-intentioned parents still “miss something” sometimes, and this technology is for that moment.
“This is a completely solvable problem, but not a flip-a-switch, one and done,” he said, pointing to his product as a part of a more comprehensive approach, such as in Europe, where mandated public school swimming lessons are helping to decrease drowning deaths.
The pandemic slowed progress for the SEAL SwimSafe collar, which is currently waiting on a new funder or investor to take the reins. But the concept is alive and well with competitors pursuing related ideas. Dr. Snyder is holding out hope that entrepreneurs, scientists, public health workers, researchers, and others will be interested in continuing this work.
Eliminating the stigma of incontinence
Ever had an accident before making it to the bathroom? So have two-thirds of adult women, and almost one-third of older men. Incontinence is linked to a wide variety of conditions, from pelvic-floor trauma to neurological issues to diabetes, and others. Urologist Jessica Lubahn, MD, in Portland, Ore., saw one too many patients feeling this type of shame, unaware that the condition was so common. In addition, she personally experienced childbirth-related incontinence, and helped a relative who was having incontinence after prostate cancer surgery.
“He had a great result, but he had confided in me ... it was one of the only times in his life that he’s been truly depressed,” Dr. Lubahn said. “It’s not even the amount of leakage, but the smell, the stigma is so embarrassing, that not only is it an inconvenience, but [it affects] your entire psyche.” She thought there had to be a better solution than the “demeaning” act of wearing adult diapers.
Noting the explosion of the period panty industry in the past decade, Dr. Lubahn wanted to “destigmatize” incontinence in the same way menstruation education and products have been. She created ONDR incontinence underwear, specifically meant for urine, to ease the mental and physical burden on her patients and many others.
Dr. Lubahn said a process happens when you decide to start talking about the product you want to make rather than trying to find answers on your own. “A lot of people are so afraid to talk about their ideas because they’re afraid it’s going to get stolen or scooped, or it might fail,” she said. “I just openly discussed it, kind of like cocktail party conversation – ‘Wouldn’t it be funny if you just pee into your underwear?’ ” She noticed each connection led to finding more people to help her along her journey.
Dr. Lubahn studied the apparel industry, learning that overseas manufacturers were more helpful and cost-effective. She navigated issues such as a special stitch that prevented leakage and other details. She was also intent on using eco-friendly products that offset the environmental impact of pads, liners, and diapers. She said there’s a strong entrepreneurship community that can help other physician-inventors get grants, be part of accelerator programs, and receive support.
Six years after the original idea, Dr. Lubahn’s product was released in 2020. She now sells eight types of underwear for women and men’s boxer briefs. She wears them herself daily.
Deterring carjackers, saving lives
In 2022, carjackings tripled in Chicago and Memphis. The areas have the highest rates in 30 cities that the Council on Criminal Justice analyzed in a report on pandemic crime rates. According to the report, nearly 40% of offenders used a firearm, more than a quarter of victims were injured, and only around half of the vehicles taken were recovered. In addition, vehicles are sometimes used in secondary crimes, such as drive-by shootings. William Yates, MD, former trauma surgeon, now turned hair restoration surgeon in Chicago, saw the evidence of those crimes daily.
“I was perplexed by carjacking because there wasn’t any answer, and it just kept getting worse and worse. A lot of innocent people were being affected,” he said. “I was seeing deaths – needless. If you give them any push back at all, they will shoot you.”
As a deterrent to counter this “easy crime,” he invented the Yates Device, an alarm system designed to prevent or interrupt carjacking. The driver can activate a switch located beneath the foot pedal or an app on the phone to trigger a programmed high-decibel alarm. Critically, it allows the carjacker to drive a safe distance away from the victim before it starts going off.
The alarm “turns your car into a very noisy Christmas tree on a time delay,” Dr. Yates explained. An external siren blares “stolen vehicle” repeatedly. A camera records everything in the car. Lights flash. Only the original driver can turn off the system. Later, once the car is abandoned, the police can help recover the vehicle.
In Dr. Yates’ experience, the invention process takes longer than you think. He worked through earlier iterations with strobe lights, but these could lead to bystanders getting hurt if the carjacker couldn’t see, for example. Developing the final product and applying for patents was a two-part process.
“The first is part is a pending patent phase, which secures your place in line,” he said. “After 1 year, we filed the utility patent as the final documentation that the invention is truly unique. That has been in process for a year now and the attorneys say we should receive approval soon.”
The product has initially been tested in seven cars for about 1 year. Dr. Yates is measuring how the system performs in all types of weather, including Chicago’s below-zero temperatures. The product is not available to the public for purchase yet because Dr. Yates is still seeking funding to have it mass produced, but it is currently being evaluated by Korean automakers for their car manufacturers.
“Everybody was saying ‘Let’s do something about this,’ but I didn’t see anybody doing anything yet,” Dr. Yates recalled. In the surgeon’s lounge, everybody has ideas. “You go around the room, and every doctor would have five ideas that would make them the richest doctor, but nobody takes it beyond that stage – talk. You have to synthesize that into a plan, to take action.”
Dr. Yates said that many doctors have the intellect to invent, but they aren’t in a network like entrepreneurs to bring their ideas to life.
For Dr. Yates, it takes a curious mindset to solve these daunting problems. “I’m always curious, always looking for how to improve something, to get better outcomes you have to be asking questions and just never let it go.”
A version of this article originally appeared on Medscape.com.
WakeMed emergency department physician and medical director, Graham Snyder, MD, has seen his fair share of deaths: an average of one or two per day. That’s part of the job. Some of the deaths were the result of risky behavior, ongoing health problems, and other natural causes.
But what he didn’t find acceptable was losing a 6-year-old girl in a backyard pool drowning at what was meant to be a celebratory birthday party and family reunion.
“There were aunts and uncles and brothers and sisters and cousins, and the pool was packed, and they’re having a great time. One of the parents looked over and saw that she was swimming around underneath but acting weird. A relative pulled her up by the arm, and she was dead,” he said. “What nobody could tell me, and what they’ll live with the rest of their life, is how long was she under water?”
So Dr. Snyder invented a solution. The catch: The goal: Improving systemic and “unsolvable” issues that harm society.
The cool part: Any MD with an idea can get in on the game.
Keeping little heads above water
Drowning is the leading cause of death in young children ages 1-4 years, and the second leading cause for children ages 5-14 years. The issue, Dr. Snyder explained, is not that rescuers couldn’t get to these children in time. “It’s that nobody knew to start looking.”
Dr. Snyder created a collar that alerts those around the swimmer that they are in trouble. The SEAL SwimSafe drowning prevention technology sets off an alarm system if a child is under water for too long. The necklace has been used to protect more than 10,000 children, including at larger swim facilities, such as the YMCA.
When Dr. Snyder first started pursuing his invention, he asked himself two key questions: “Has someone already tried this? And if they did, why did they not succeed?” These questions help counteract the potential arrogance, he says, with imagining that you are the first person to have a certain idea. And using whatever reason others didn’t succeed as your “secret sauce” helps lead to more success. He also had to consider obstacles. People might resist wearing a collar or necklace while swimming or putting one on their child, like the reluctance around wearing bicycle helmets when they gained popularity in the 1980s. He concluded that the collars would work best at larger facilities, where they were mandated.
Another obstacle was false alarms. “It was possible to trigger a false alarm, and that could really scare people,” Dr. Snyder said. He is still considering systems to prevent the collars from being stolen or from “13-year-old boys hiding them in the water drain and making everyone really scared when an alarm is going off.”
The demand is real, however, and is based on alarming data. Safe Kids has reported that 66% of natural water drownings and around half of pool drownings happened with an adult supervising. They added, however, that supervision is often lacking or insufficient, such as a parent not being within arm’s reach of a young kid. As Dr. Snyder told reporters in a 2018 story, even the most well-intentioned parents still “miss something” sometimes, and this technology is for that moment.
“This is a completely solvable problem, but not a flip-a-switch, one and done,” he said, pointing to his product as a part of a more comprehensive approach, such as in Europe, where mandated public school swimming lessons are helping to decrease drowning deaths.
The pandemic slowed progress for the SEAL SwimSafe collar, which is currently waiting on a new funder or investor to take the reins. But the concept is alive and well with competitors pursuing related ideas. Dr. Snyder is holding out hope that entrepreneurs, scientists, public health workers, researchers, and others will be interested in continuing this work.
Eliminating the stigma of incontinence
Ever had an accident before making it to the bathroom? So have two-thirds of adult women, and almost one-third of older men. Incontinence is linked to a wide variety of conditions, from pelvic-floor trauma to neurological issues to diabetes, and others. Urologist Jessica Lubahn, MD, in Portland, Ore., saw one too many patients feeling this type of shame, unaware that the condition was so common. In addition, she personally experienced childbirth-related incontinence, and helped a relative who was having incontinence after prostate cancer surgery.
“He had a great result, but he had confided in me ... it was one of the only times in his life that he’s been truly depressed,” Dr. Lubahn said. “It’s not even the amount of leakage, but the smell, the stigma is so embarrassing, that not only is it an inconvenience, but [it affects] your entire psyche.” She thought there had to be a better solution than the “demeaning” act of wearing adult diapers.
Noting the explosion of the period panty industry in the past decade, Dr. Lubahn wanted to “destigmatize” incontinence in the same way menstruation education and products have been. She created ONDR incontinence underwear, specifically meant for urine, to ease the mental and physical burden on her patients and many others.
Dr. Lubahn said a process happens when you decide to start talking about the product you want to make rather than trying to find answers on your own. “A lot of people are so afraid to talk about their ideas because they’re afraid it’s going to get stolen or scooped, or it might fail,” she said. “I just openly discussed it, kind of like cocktail party conversation – ‘Wouldn’t it be funny if you just pee into your underwear?’ ” She noticed each connection led to finding more people to help her along her journey.
Dr. Lubahn studied the apparel industry, learning that overseas manufacturers were more helpful and cost-effective. She navigated issues such as a special stitch that prevented leakage and other details. She was also intent on using eco-friendly products that offset the environmental impact of pads, liners, and diapers. She said there’s a strong entrepreneurship community that can help other physician-inventors get grants, be part of accelerator programs, and receive support.
Six years after the original idea, Dr. Lubahn’s product was released in 2020. She now sells eight types of underwear for women and men’s boxer briefs. She wears them herself daily.
Deterring carjackers, saving lives
In 2022, carjackings tripled in Chicago and Memphis. The areas have the highest rates in 30 cities that the Council on Criminal Justice analyzed in a report on pandemic crime rates. According to the report, nearly 40% of offenders used a firearm, more than a quarter of victims were injured, and only around half of the vehicles taken were recovered. In addition, vehicles are sometimes used in secondary crimes, such as drive-by shootings. William Yates, MD, former trauma surgeon, now turned hair restoration surgeon in Chicago, saw the evidence of those crimes daily.
“I was perplexed by carjacking because there wasn’t any answer, and it just kept getting worse and worse. A lot of innocent people were being affected,” he said. “I was seeing deaths – needless. If you give them any push back at all, they will shoot you.”
As a deterrent to counter this “easy crime,” he invented the Yates Device, an alarm system designed to prevent or interrupt carjacking. The driver can activate a switch located beneath the foot pedal or an app on the phone to trigger a programmed high-decibel alarm. Critically, it allows the carjacker to drive a safe distance away from the victim before it starts going off.
The alarm “turns your car into a very noisy Christmas tree on a time delay,” Dr. Yates explained. An external siren blares “stolen vehicle” repeatedly. A camera records everything in the car. Lights flash. Only the original driver can turn off the system. Later, once the car is abandoned, the police can help recover the vehicle.
In Dr. Yates’ experience, the invention process takes longer than you think. He worked through earlier iterations with strobe lights, but these could lead to bystanders getting hurt if the carjacker couldn’t see, for example. Developing the final product and applying for patents was a two-part process.
“The first is part is a pending patent phase, which secures your place in line,” he said. “After 1 year, we filed the utility patent as the final documentation that the invention is truly unique. That has been in process for a year now and the attorneys say we should receive approval soon.”
The product has initially been tested in seven cars for about 1 year. Dr. Yates is measuring how the system performs in all types of weather, including Chicago’s below-zero temperatures. The product is not available to the public for purchase yet because Dr. Yates is still seeking funding to have it mass produced, but it is currently being evaluated by Korean automakers for their car manufacturers.
“Everybody was saying ‘Let’s do something about this,’ but I didn’t see anybody doing anything yet,” Dr. Yates recalled. In the surgeon’s lounge, everybody has ideas. “You go around the room, and every doctor would have five ideas that would make them the richest doctor, but nobody takes it beyond that stage – talk. You have to synthesize that into a plan, to take action.”
Dr. Yates said that many doctors have the intellect to invent, but they aren’t in a network like entrepreneurs to bring their ideas to life.
For Dr. Yates, it takes a curious mindset to solve these daunting problems. “I’m always curious, always looking for how to improve something, to get better outcomes you have to be asking questions and just never let it go.”
A version of this article originally appeared on Medscape.com.
WakeMed emergency department physician and medical director, Graham Snyder, MD, has seen his fair share of deaths: an average of one or two per day. That’s part of the job. Some of the deaths were the result of risky behavior, ongoing health problems, and other natural causes.
But what he didn’t find acceptable was losing a 6-year-old girl in a backyard pool drowning at what was meant to be a celebratory birthday party and family reunion.
“There were aunts and uncles and brothers and sisters and cousins, and the pool was packed, and they’re having a great time. One of the parents looked over and saw that she was swimming around underneath but acting weird. A relative pulled her up by the arm, and she was dead,” he said. “What nobody could tell me, and what they’ll live with the rest of their life, is how long was she under water?”
So Dr. Snyder invented a solution. The catch: The goal: Improving systemic and “unsolvable” issues that harm society.
The cool part: Any MD with an idea can get in on the game.
Keeping little heads above water
Drowning is the leading cause of death in young children ages 1-4 years, and the second leading cause for children ages 5-14 years. The issue, Dr. Snyder explained, is not that rescuers couldn’t get to these children in time. “It’s that nobody knew to start looking.”
Dr. Snyder created a collar that alerts those around the swimmer that they are in trouble. The SEAL SwimSafe drowning prevention technology sets off an alarm system if a child is under water for too long. The necklace has been used to protect more than 10,000 children, including at larger swim facilities, such as the YMCA.
When Dr. Snyder first started pursuing his invention, he asked himself two key questions: “Has someone already tried this? And if they did, why did they not succeed?” These questions help counteract the potential arrogance, he says, with imagining that you are the first person to have a certain idea. And using whatever reason others didn’t succeed as your “secret sauce” helps lead to more success. He also had to consider obstacles. People might resist wearing a collar or necklace while swimming or putting one on their child, like the reluctance around wearing bicycle helmets when they gained popularity in the 1980s. He concluded that the collars would work best at larger facilities, where they were mandated.
Another obstacle was false alarms. “It was possible to trigger a false alarm, and that could really scare people,” Dr. Snyder said. He is still considering systems to prevent the collars from being stolen or from “13-year-old boys hiding them in the water drain and making everyone really scared when an alarm is going off.”
The demand is real, however, and is based on alarming data. Safe Kids has reported that 66% of natural water drownings and around half of pool drownings happened with an adult supervising. They added, however, that supervision is often lacking or insufficient, such as a parent not being within arm’s reach of a young kid. As Dr. Snyder told reporters in a 2018 story, even the most well-intentioned parents still “miss something” sometimes, and this technology is for that moment.
“This is a completely solvable problem, but not a flip-a-switch, one and done,” he said, pointing to his product as a part of a more comprehensive approach, such as in Europe, where mandated public school swimming lessons are helping to decrease drowning deaths.
The pandemic slowed progress for the SEAL SwimSafe collar, which is currently waiting on a new funder or investor to take the reins. But the concept is alive and well with competitors pursuing related ideas. Dr. Snyder is holding out hope that entrepreneurs, scientists, public health workers, researchers, and others will be interested in continuing this work.
Eliminating the stigma of incontinence
Ever had an accident before making it to the bathroom? So have two-thirds of adult women, and almost one-third of older men. Incontinence is linked to a wide variety of conditions, from pelvic-floor trauma to neurological issues to diabetes, and others. Urologist Jessica Lubahn, MD, in Portland, Ore., saw one too many patients feeling this type of shame, unaware that the condition was so common. In addition, she personally experienced childbirth-related incontinence, and helped a relative who was having incontinence after prostate cancer surgery.
“He had a great result, but he had confided in me ... it was one of the only times in his life that he’s been truly depressed,” Dr. Lubahn said. “It’s not even the amount of leakage, but the smell, the stigma is so embarrassing, that not only is it an inconvenience, but [it affects] your entire psyche.” She thought there had to be a better solution than the “demeaning” act of wearing adult diapers.
Noting the explosion of the period panty industry in the past decade, Dr. Lubahn wanted to “destigmatize” incontinence in the same way menstruation education and products have been. She created ONDR incontinence underwear, specifically meant for urine, to ease the mental and physical burden on her patients and many others.
Dr. Lubahn said a process happens when you decide to start talking about the product you want to make rather than trying to find answers on your own. “A lot of people are so afraid to talk about their ideas because they’re afraid it’s going to get stolen or scooped, or it might fail,” she said. “I just openly discussed it, kind of like cocktail party conversation – ‘Wouldn’t it be funny if you just pee into your underwear?’ ” She noticed each connection led to finding more people to help her along her journey.
Dr. Lubahn studied the apparel industry, learning that overseas manufacturers were more helpful and cost-effective. She navigated issues such as a special stitch that prevented leakage and other details. She was also intent on using eco-friendly products that offset the environmental impact of pads, liners, and diapers. She said there’s a strong entrepreneurship community that can help other physician-inventors get grants, be part of accelerator programs, and receive support.
Six years after the original idea, Dr. Lubahn’s product was released in 2020. She now sells eight types of underwear for women and men’s boxer briefs. She wears them herself daily.
Deterring carjackers, saving lives
In 2022, carjackings tripled in Chicago and Memphis. The areas have the highest rates in 30 cities that the Council on Criminal Justice analyzed in a report on pandemic crime rates. According to the report, nearly 40% of offenders used a firearm, more than a quarter of victims were injured, and only around half of the vehicles taken were recovered. In addition, vehicles are sometimes used in secondary crimes, such as drive-by shootings. William Yates, MD, former trauma surgeon, now turned hair restoration surgeon in Chicago, saw the evidence of those crimes daily.
“I was perplexed by carjacking because there wasn’t any answer, and it just kept getting worse and worse. A lot of innocent people were being affected,” he said. “I was seeing deaths – needless. If you give them any push back at all, they will shoot you.”
As a deterrent to counter this “easy crime,” he invented the Yates Device, an alarm system designed to prevent or interrupt carjacking. The driver can activate a switch located beneath the foot pedal or an app on the phone to trigger a programmed high-decibel alarm. Critically, it allows the carjacker to drive a safe distance away from the victim before it starts going off.
The alarm “turns your car into a very noisy Christmas tree on a time delay,” Dr. Yates explained. An external siren blares “stolen vehicle” repeatedly. A camera records everything in the car. Lights flash. Only the original driver can turn off the system. Later, once the car is abandoned, the police can help recover the vehicle.
In Dr. Yates’ experience, the invention process takes longer than you think. He worked through earlier iterations with strobe lights, but these could lead to bystanders getting hurt if the carjacker couldn’t see, for example. Developing the final product and applying for patents was a two-part process.
“The first is part is a pending patent phase, which secures your place in line,” he said. “After 1 year, we filed the utility patent as the final documentation that the invention is truly unique. That has been in process for a year now and the attorneys say we should receive approval soon.”
The product has initially been tested in seven cars for about 1 year. Dr. Yates is measuring how the system performs in all types of weather, including Chicago’s below-zero temperatures. The product is not available to the public for purchase yet because Dr. Yates is still seeking funding to have it mass produced, but it is currently being evaluated by Korean automakers for their car manufacturers.
“Everybody was saying ‘Let’s do something about this,’ but I didn’t see anybody doing anything yet,” Dr. Yates recalled. In the surgeon’s lounge, everybody has ideas. “You go around the room, and every doctor would have five ideas that would make them the richest doctor, but nobody takes it beyond that stage – talk. You have to synthesize that into a plan, to take action.”
Dr. Yates said that many doctors have the intellect to invent, but they aren’t in a network like entrepreneurs to bring their ideas to life.
For Dr. Yates, it takes a curious mindset to solve these daunting problems. “I’m always curious, always looking for how to improve something, to get better outcomes you have to be asking questions and just never let it go.”
A version of this article originally appeared on Medscape.com.
Cutting-edge nasal tech could usher in a new era of medicine
Noses are like caverns – twisting, turning, no two exactly the same. But if you nose past anyone’s nostrils, you’ll discover a surprisingly sprawling space.
“The size of the nasal cavity is about the same as a large handkerchief,” said Hugh Smyth, PhD, a professor of molecular pharmaceutics and drug delivery at the University of Texas at Austin.
“It’s very accessible tissue, and it has a lot of blood flow,” said Dr. Smyth. “The speed of onset can often be as fast as injections, sometimes even faster.”
It’s nothing new to get medicines via your nose. For decades, we’ve squirted various sprays into our nostrils to treat local maladies like allergies or infections. Even the ancients saw wisdom in the nasal route.
But recently, the nose has gained scientific attention as a gateway to the rest of the body – even the brain, a notoriously difficult target.
The upshot: Someday, inhaling therapies could be as routine as swallowing pills.
The nasal route is quick, needle free, and user friendly, and it often requires a smaller dose than other methods, since the drug doesn’t have to pass through the digestive tract, losing potency during digestion.
But there are challenges.
How hard can it be?
Old-school nasal sprayers, mostly unchanged since the 1800s, aren’t cut out for deep-nose delivery. “The technology is relatively limited because you’ve just got a single spray nozzle,” said Michael Hindle, PhD, a professor of pharmaceutics at Virginia Commonwealth University, Richmond.
These traditional devices (similar to perfume sprayers) don’t consistently push meds past the lower to middle sections inside the nose, called the nasal valve – if they do so at all: In a 2020 Rhinology study (doi: 10.4193/Rhin18.304) conventional nasal sprays only reached this first segment of the nose, a less-than-ideal spot to land.
Inside the nasal valve, the surface is skin-like and doesn’t absorb very well. Its narrow design slows airflow, preventing particles from moving to deeper regions, where tissue is vascular and porous like the lungs. And even if this structural roadblock is surpassed, other hurdles remain.
The nose is designed to keep stuff out. Nose hair, cilia, mucus, sneezing, coughing – all make “distributing drugs evenly across the nasal cavity difficult,” said Dr. Smyth. “The spray gets filtered out before it reaches those deeper zones,” potentially dripping out of the nostrils instead of being absorbed.
Complicating matters is how every person’s nose is different. In a 2018 study, Dr. Smyth and a research team created three dimensional–printed models of people’s nasal cavities. They varied widely. “Nasal cavities are very different in size, length, and internal geometry,” he said. “This makes it challenging to target specific areas.”
Although carefully positioning the spray nozzle can help, even something as minor as sniffing too hard (constricting the nostrils) can keep sprays from reaching the absorptive deeper regions.
Still, the benefits are enough to compel researchers to find a way in.
“This really is a drug delivery challenge we’ve been wrestling with,” said Dr. Hindle. “It’s not new formulations we hear about. It’s new devices and delivery methods trying to target the different nasal regions.”
Delivering the goods
In the late aughts, John Hoekman was a graduate student in the University of Washington’s pharmaceutics program, studying nasal drug delivery. In his experiments, he noticed that drugs distributed differently, depending on the region targeted – aiming for the upper nasal cavity led to a spike in absorption.
The results convinced Mr. Hoekman to stake his future on nasal drug delivery.
In 2008, while still in graduate school, he started his own company, now known as Impel Pharmaceuticals. In 2021, Impel released its first product: Trudhesa, a nasal spray for migraines. Although the drug itself – dihydroergotamine mesylate – was hardly novel, used for migraine relief since 1946 (Headache. 2020 Jan;60[1]:40-57), it was usually delivered through an intravenous line, often in the ED.
But with Mr. Hoekman’s POD device – short for precision olfactory delivery – the drug can be given by the patient, via the nose. This generally means faster, more reliable relief, with fewer side effects. “We were able to lower the dose and improve the overall absorption,” said Mr. Hoekman.
The POD’s nozzle is engineered to spray a soft, narrow plume. It’s gas propelled, so patients don’t have to breathe in any special way to ensure delivery. The drug can zip right through the nasal valve into the upper nasal cavity.
Another company – OptiNose – has a “bidirectional” delivery method that propels drugs, either liquid or dry powder, deep into the nose.
“You insert the nozzle into your nose, and as you blow through the mouthpiece, your soft palate closes,” said Dr. Hindle. With the throat sealed off, “the only place for the drug to go is into one nostril and out the other, coating both sides of the nasal passageways.”
The device is only available for Onzetra Xsail, a powder for migraines. But another application is on its way.
In May, OptiNose announced that the FDA is reviewing Xhance, which uses the system to direct a steroid to the sinuses. In a clinical trial, patients with chronic sinusitis who tried the drug-device combo saw a decline in congestion, facial pain, and inflammation.
Targeting the brain
Both of those migraine drugs – Trudhesa and Onzetra Xsail – are thought to penetrate the upper nasal cavity. That’s where you’ll find the olfactory zone, a sheet of neurons that connects to the olfactory bulb. Located behind the eyes, these two nerve bundles detect odors.
“The olfactory region is almost like a back door to the brain,” said Mr. Hoekman.
By bypassing the blood-brain barrier, it offers a direct pathway – the only direct pathway, actually – between an exposed area of the body and the brain. Meaning it can ferry drugs straight from the nasal cavity to the central nervous system.
Nose-to-brain treatments could be game-changing for central nervous system disorders, such as Parkinson’s disease, Alzheimer’s, or anxiety.
But reaching the olfactory zone is notoriously hard. “The vasculature in your nose is like a big freeway, and the olfactory tract is like a side alley,” explained Mr. Hoekman. “It’s very limiting in what it will allow through.” The region is also small, occupying only 3%-10% of the nasal cavity’s surface area.
Again, POD means “precision olfactory delivery.” But the device isn’t quite as laser focused on the region as its name implies. “We’re not at the stage where we’re able to exclusively deliver to one target site in the nose,” said Dr. Hindle.
While wending its way toward the olfactory zone, some of the drug will be absorbed by other regions, then circulate throughout the body.
“About 59% of the drug that we put into the upper nasal space gets absorbed into the bloodstream,” said Mr. Hoekman.
Janssen Pharmaceuticals’ Spravato – a nasal spray for drug-resistant depression – is thought to work similarly: Some goes straight to the brain via the olfactory nerves, while the rest takes a more roundabout route, passing through the blood vessels to circulate in your system.
A needle-free option
Sometimes, the bloodstream is the main target. Because the nose’s middle and upper stretches are so vascular, drugs can be rapidly absorbed.
This is especially valuable for time-sensitive conditions. “If you give something nasally, you can have peak uptake in 15-30 minutes,” said Mr. Hoekman.
Take Narcan nasal spray, which delivers a burst of naloxone to quickly reverse the effects of opioid an overdose. Or Noctiva nasal spray. Taken just half an hour before bed, it can prevent frequent nighttime urination.
There’s also a group of seizure-stopping sprays, known as “rescue treatments.” One works by temporarily loosening the space between nasal cells, allowing the seizure drug to be quickly absorbed through the vessels.
This systemic access also has potential for drugs that would otherwise have to be injected, such as biologics.
The same goes for vaccines. Mucosal tissue inside the nasal cavity offers direct access to the infection-fighting lymphatic system, making the nose a prime target for inoculation against certain viruses.
Inhaling protection against viruses
Despite the recent surge of interest, nasal vaccines faced a rocky start. After the first nasal flu vaccine hit the market in 2001, it was pulled due to potential toxicity and reports of Bell’s palsy, a type of facial paralysis.
FluMist came in 2003 and has been plagued by problems ever since. Because it contains a weakened live virus, flu-like side effects can occur. And it doesn’t always work. During the 2016-2017 flu season, FluMist protected only 3% of kids, prompting the Centers for Disease Control and Prevention to advise against the nasal route that year.
Why FluMist can be so hit-or-miss is poorly understood. But generally, the nose can pose an effectiveness challenge. “The nose is highly cycling,” said Dr. Hindle. “Anything we deposit usually gets transported out within 15-20 minutes.”
For kids – big fans of not using needles – chronically runny noses can be an issue. “You squirt it in the nose, and it will probably just come back out in their snot,” said Jay Kolls, MD, a professor of medicine and pediatrics at Tulane University, New Orleans, who is developing an intranasal pneumonia vaccine.
Even so, nasal vaccines became a hot topic among researchers after the world was shut down by a virus that invades through the nose.
“We realized that intramuscular vaccines were effective at preventing severe disease, but they weren’t that effective at preventing transmission,” said Michael Diamond, MD, PhD, an immunologist at Washington University in St. Louis.
Nasal vaccines could solve that problem by putting an immune barrier at the point of entry, denying access to the rest of the body. “You squash the infection early enough that it not only prevents disease,” said Dr. Kolls, “but potentially prevents transmission.”
And yes, a nasal COVID vaccine is on the way
In March 2020, Dr. Diamond’s team began exploring a nasal COVID vaccine. Promising results in animals prompted a vaccine development company to license the technology. The resulting nasal vaccine – the first for COVID – has been approved in India, both as a primary vaccine and a booster.
It works by stimulating an influx of IgA, a type of antibody found in the nasal passages, and production of resident memory T cells, immune cells on standby just beneath the surface tissue in the nose.
By contrast, injected vaccines generate mostly IgG antibodies, which struggle to enter the respiratory tract. Only a tiny fraction – an estimated 1% – typically reach the nose.
Nasal vaccines could also be used along with shots. The latter could prime the whole body to fight back, while a nasal spritz could pull that immune protection to the mucosal surfaces.
Nasal technology could yield more effective vaccines for infections like tuberculosis or malaria, or even safeguard against new – sometimes surprising – conditions.
In a 2021 Nature study, an intranasal vaccine derived from fentanyl was better at preventing overdose than an injected vaccine. “Through some clever chemistry, the drug [in the vaccine] isn’t fentanyl anymore,” said study author Elizabeth Norton, PhD, an assistant professor of microbiology and immunology at Tulane University. “But the immune system still has an antibody response to it.”
Novel applications like this represent the future of nasal drug delivery.
“We’re not going to innovate in asthma or COPD. We’re not going to innovate in local delivery to the nose,” said Dr. Hindle. “Innovation will only come if we look to treat new conditions.”
A version of this article originally appeared on WebMD.com.
Noses are like caverns – twisting, turning, no two exactly the same. But if you nose past anyone’s nostrils, you’ll discover a surprisingly sprawling space.
“The size of the nasal cavity is about the same as a large handkerchief,” said Hugh Smyth, PhD, a professor of molecular pharmaceutics and drug delivery at the University of Texas at Austin.
“It’s very accessible tissue, and it has a lot of blood flow,” said Dr. Smyth. “The speed of onset can often be as fast as injections, sometimes even faster.”
It’s nothing new to get medicines via your nose. For decades, we’ve squirted various sprays into our nostrils to treat local maladies like allergies or infections. Even the ancients saw wisdom in the nasal route.
But recently, the nose has gained scientific attention as a gateway to the rest of the body – even the brain, a notoriously difficult target.
The upshot: Someday, inhaling therapies could be as routine as swallowing pills.
The nasal route is quick, needle free, and user friendly, and it often requires a smaller dose than other methods, since the drug doesn’t have to pass through the digestive tract, losing potency during digestion.
But there are challenges.
How hard can it be?
Old-school nasal sprayers, mostly unchanged since the 1800s, aren’t cut out for deep-nose delivery. “The technology is relatively limited because you’ve just got a single spray nozzle,” said Michael Hindle, PhD, a professor of pharmaceutics at Virginia Commonwealth University, Richmond.
These traditional devices (similar to perfume sprayers) don’t consistently push meds past the lower to middle sections inside the nose, called the nasal valve – if they do so at all: In a 2020 Rhinology study (doi: 10.4193/Rhin18.304) conventional nasal sprays only reached this first segment of the nose, a less-than-ideal spot to land.
Inside the nasal valve, the surface is skin-like and doesn’t absorb very well. Its narrow design slows airflow, preventing particles from moving to deeper regions, where tissue is vascular and porous like the lungs. And even if this structural roadblock is surpassed, other hurdles remain.
The nose is designed to keep stuff out. Nose hair, cilia, mucus, sneezing, coughing – all make “distributing drugs evenly across the nasal cavity difficult,” said Dr. Smyth. “The spray gets filtered out before it reaches those deeper zones,” potentially dripping out of the nostrils instead of being absorbed.
Complicating matters is how every person’s nose is different. In a 2018 study, Dr. Smyth and a research team created three dimensional–printed models of people’s nasal cavities. They varied widely. “Nasal cavities are very different in size, length, and internal geometry,” he said. “This makes it challenging to target specific areas.”
Although carefully positioning the spray nozzle can help, even something as minor as sniffing too hard (constricting the nostrils) can keep sprays from reaching the absorptive deeper regions.
Still, the benefits are enough to compel researchers to find a way in.
“This really is a drug delivery challenge we’ve been wrestling with,” said Dr. Hindle. “It’s not new formulations we hear about. It’s new devices and delivery methods trying to target the different nasal regions.”
Delivering the goods
In the late aughts, John Hoekman was a graduate student in the University of Washington’s pharmaceutics program, studying nasal drug delivery. In his experiments, he noticed that drugs distributed differently, depending on the region targeted – aiming for the upper nasal cavity led to a spike in absorption.
The results convinced Mr. Hoekman to stake his future on nasal drug delivery.
In 2008, while still in graduate school, he started his own company, now known as Impel Pharmaceuticals. In 2021, Impel released its first product: Trudhesa, a nasal spray for migraines. Although the drug itself – dihydroergotamine mesylate – was hardly novel, used for migraine relief since 1946 (Headache. 2020 Jan;60[1]:40-57), it was usually delivered through an intravenous line, often in the ED.
But with Mr. Hoekman’s POD device – short for precision olfactory delivery – the drug can be given by the patient, via the nose. This generally means faster, more reliable relief, with fewer side effects. “We were able to lower the dose and improve the overall absorption,” said Mr. Hoekman.
The POD’s nozzle is engineered to spray a soft, narrow plume. It’s gas propelled, so patients don’t have to breathe in any special way to ensure delivery. The drug can zip right through the nasal valve into the upper nasal cavity.
Another company – OptiNose – has a “bidirectional” delivery method that propels drugs, either liquid or dry powder, deep into the nose.
“You insert the nozzle into your nose, and as you blow through the mouthpiece, your soft palate closes,” said Dr. Hindle. With the throat sealed off, “the only place for the drug to go is into one nostril and out the other, coating both sides of the nasal passageways.”
The device is only available for Onzetra Xsail, a powder for migraines. But another application is on its way.
In May, OptiNose announced that the FDA is reviewing Xhance, which uses the system to direct a steroid to the sinuses. In a clinical trial, patients with chronic sinusitis who tried the drug-device combo saw a decline in congestion, facial pain, and inflammation.
Targeting the brain
Both of those migraine drugs – Trudhesa and Onzetra Xsail – are thought to penetrate the upper nasal cavity. That’s where you’ll find the olfactory zone, a sheet of neurons that connects to the olfactory bulb. Located behind the eyes, these two nerve bundles detect odors.
“The olfactory region is almost like a back door to the brain,” said Mr. Hoekman.
By bypassing the blood-brain barrier, it offers a direct pathway – the only direct pathway, actually – between an exposed area of the body and the brain. Meaning it can ferry drugs straight from the nasal cavity to the central nervous system.
Nose-to-brain treatments could be game-changing for central nervous system disorders, such as Parkinson’s disease, Alzheimer’s, or anxiety.
But reaching the olfactory zone is notoriously hard. “The vasculature in your nose is like a big freeway, and the olfactory tract is like a side alley,” explained Mr. Hoekman. “It’s very limiting in what it will allow through.” The region is also small, occupying only 3%-10% of the nasal cavity’s surface area.
Again, POD means “precision olfactory delivery.” But the device isn’t quite as laser focused on the region as its name implies. “We’re not at the stage where we’re able to exclusively deliver to one target site in the nose,” said Dr. Hindle.
While wending its way toward the olfactory zone, some of the drug will be absorbed by other regions, then circulate throughout the body.
“About 59% of the drug that we put into the upper nasal space gets absorbed into the bloodstream,” said Mr. Hoekman.
Janssen Pharmaceuticals’ Spravato – a nasal spray for drug-resistant depression – is thought to work similarly: Some goes straight to the brain via the olfactory nerves, while the rest takes a more roundabout route, passing through the blood vessels to circulate in your system.
A needle-free option
Sometimes, the bloodstream is the main target. Because the nose’s middle and upper stretches are so vascular, drugs can be rapidly absorbed.
This is especially valuable for time-sensitive conditions. “If you give something nasally, you can have peak uptake in 15-30 minutes,” said Mr. Hoekman.
Take Narcan nasal spray, which delivers a burst of naloxone to quickly reverse the effects of opioid an overdose. Or Noctiva nasal spray. Taken just half an hour before bed, it can prevent frequent nighttime urination.
There’s also a group of seizure-stopping sprays, known as “rescue treatments.” One works by temporarily loosening the space between nasal cells, allowing the seizure drug to be quickly absorbed through the vessels.
This systemic access also has potential for drugs that would otherwise have to be injected, such as biologics.
The same goes for vaccines. Mucosal tissue inside the nasal cavity offers direct access to the infection-fighting lymphatic system, making the nose a prime target for inoculation against certain viruses.
Inhaling protection against viruses
Despite the recent surge of interest, nasal vaccines faced a rocky start. After the first nasal flu vaccine hit the market in 2001, it was pulled due to potential toxicity and reports of Bell’s palsy, a type of facial paralysis.
FluMist came in 2003 and has been plagued by problems ever since. Because it contains a weakened live virus, flu-like side effects can occur. And it doesn’t always work. During the 2016-2017 flu season, FluMist protected only 3% of kids, prompting the Centers for Disease Control and Prevention to advise against the nasal route that year.
Why FluMist can be so hit-or-miss is poorly understood. But generally, the nose can pose an effectiveness challenge. “The nose is highly cycling,” said Dr. Hindle. “Anything we deposit usually gets transported out within 15-20 minutes.”
For kids – big fans of not using needles – chronically runny noses can be an issue. “You squirt it in the nose, and it will probably just come back out in their snot,” said Jay Kolls, MD, a professor of medicine and pediatrics at Tulane University, New Orleans, who is developing an intranasal pneumonia vaccine.
Even so, nasal vaccines became a hot topic among researchers after the world was shut down by a virus that invades through the nose.
“We realized that intramuscular vaccines were effective at preventing severe disease, but they weren’t that effective at preventing transmission,” said Michael Diamond, MD, PhD, an immunologist at Washington University in St. Louis.
Nasal vaccines could solve that problem by putting an immune barrier at the point of entry, denying access to the rest of the body. “You squash the infection early enough that it not only prevents disease,” said Dr. Kolls, “but potentially prevents transmission.”
And yes, a nasal COVID vaccine is on the way
In March 2020, Dr. Diamond’s team began exploring a nasal COVID vaccine. Promising results in animals prompted a vaccine development company to license the technology. The resulting nasal vaccine – the first for COVID – has been approved in India, both as a primary vaccine and a booster.
It works by stimulating an influx of IgA, a type of antibody found in the nasal passages, and production of resident memory T cells, immune cells on standby just beneath the surface tissue in the nose.
By contrast, injected vaccines generate mostly IgG antibodies, which struggle to enter the respiratory tract. Only a tiny fraction – an estimated 1% – typically reach the nose.
Nasal vaccines could also be used along with shots. The latter could prime the whole body to fight back, while a nasal spritz could pull that immune protection to the mucosal surfaces.
Nasal technology could yield more effective vaccines for infections like tuberculosis or malaria, or even safeguard against new – sometimes surprising – conditions.
In a 2021 Nature study, an intranasal vaccine derived from fentanyl was better at preventing overdose than an injected vaccine. “Through some clever chemistry, the drug [in the vaccine] isn’t fentanyl anymore,” said study author Elizabeth Norton, PhD, an assistant professor of microbiology and immunology at Tulane University. “But the immune system still has an antibody response to it.”
Novel applications like this represent the future of nasal drug delivery.
“We’re not going to innovate in asthma or COPD. We’re not going to innovate in local delivery to the nose,” said Dr. Hindle. “Innovation will only come if we look to treat new conditions.”
A version of this article originally appeared on WebMD.com.
Noses are like caverns – twisting, turning, no two exactly the same. But if you nose past anyone’s nostrils, you’ll discover a surprisingly sprawling space.
“The size of the nasal cavity is about the same as a large handkerchief,” said Hugh Smyth, PhD, a professor of molecular pharmaceutics and drug delivery at the University of Texas at Austin.
“It’s very accessible tissue, and it has a lot of blood flow,” said Dr. Smyth. “The speed of onset can often be as fast as injections, sometimes even faster.”
It’s nothing new to get medicines via your nose. For decades, we’ve squirted various sprays into our nostrils to treat local maladies like allergies or infections. Even the ancients saw wisdom in the nasal route.
But recently, the nose has gained scientific attention as a gateway to the rest of the body – even the brain, a notoriously difficult target.
The upshot: Someday, inhaling therapies could be as routine as swallowing pills.
The nasal route is quick, needle free, and user friendly, and it often requires a smaller dose than other methods, since the drug doesn’t have to pass through the digestive tract, losing potency during digestion.
But there are challenges.
How hard can it be?
Old-school nasal sprayers, mostly unchanged since the 1800s, aren’t cut out for deep-nose delivery. “The technology is relatively limited because you’ve just got a single spray nozzle,” said Michael Hindle, PhD, a professor of pharmaceutics at Virginia Commonwealth University, Richmond.
These traditional devices (similar to perfume sprayers) don’t consistently push meds past the lower to middle sections inside the nose, called the nasal valve – if they do so at all: In a 2020 Rhinology study (doi: 10.4193/Rhin18.304) conventional nasal sprays only reached this first segment of the nose, a less-than-ideal spot to land.
Inside the nasal valve, the surface is skin-like and doesn’t absorb very well. Its narrow design slows airflow, preventing particles from moving to deeper regions, where tissue is vascular and porous like the lungs. And even if this structural roadblock is surpassed, other hurdles remain.
The nose is designed to keep stuff out. Nose hair, cilia, mucus, sneezing, coughing – all make “distributing drugs evenly across the nasal cavity difficult,” said Dr. Smyth. “The spray gets filtered out before it reaches those deeper zones,” potentially dripping out of the nostrils instead of being absorbed.
Complicating matters is how every person’s nose is different. In a 2018 study, Dr. Smyth and a research team created three dimensional–printed models of people’s nasal cavities. They varied widely. “Nasal cavities are very different in size, length, and internal geometry,” he said. “This makes it challenging to target specific areas.”
Although carefully positioning the spray nozzle can help, even something as minor as sniffing too hard (constricting the nostrils) can keep sprays from reaching the absorptive deeper regions.
Still, the benefits are enough to compel researchers to find a way in.
“This really is a drug delivery challenge we’ve been wrestling with,” said Dr. Hindle. “It’s not new formulations we hear about. It’s new devices and delivery methods trying to target the different nasal regions.”
Delivering the goods
In the late aughts, John Hoekman was a graduate student in the University of Washington’s pharmaceutics program, studying nasal drug delivery. In his experiments, he noticed that drugs distributed differently, depending on the region targeted – aiming for the upper nasal cavity led to a spike in absorption.
The results convinced Mr. Hoekman to stake his future on nasal drug delivery.
In 2008, while still in graduate school, he started his own company, now known as Impel Pharmaceuticals. In 2021, Impel released its first product: Trudhesa, a nasal spray for migraines. Although the drug itself – dihydroergotamine mesylate – was hardly novel, used for migraine relief since 1946 (Headache. 2020 Jan;60[1]:40-57), it was usually delivered through an intravenous line, often in the ED.
But with Mr. Hoekman’s POD device – short for precision olfactory delivery – the drug can be given by the patient, via the nose. This generally means faster, more reliable relief, with fewer side effects. “We were able to lower the dose and improve the overall absorption,” said Mr. Hoekman.
The POD’s nozzle is engineered to spray a soft, narrow plume. It’s gas propelled, so patients don’t have to breathe in any special way to ensure delivery. The drug can zip right through the nasal valve into the upper nasal cavity.
Another company – OptiNose – has a “bidirectional” delivery method that propels drugs, either liquid or dry powder, deep into the nose.
“You insert the nozzle into your nose, and as you blow through the mouthpiece, your soft palate closes,” said Dr. Hindle. With the throat sealed off, “the only place for the drug to go is into one nostril and out the other, coating both sides of the nasal passageways.”
The device is only available for Onzetra Xsail, a powder for migraines. But another application is on its way.
In May, OptiNose announced that the FDA is reviewing Xhance, which uses the system to direct a steroid to the sinuses. In a clinical trial, patients with chronic sinusitis who tried the drug-device combo saw a decline in congestion, facial pain, and inflammation.
Targeting the brain
Both of those migraine drugs – Trudhesa and Onzetra Xsail – are thought to penetrate the upper nasal cavity. That’s where you’ll find the olfactory zone, a sheet of neurons that connects to the olfactory bulb. Located behind the eyes, these two nerve bundles detect odors.
“The olfactory region is almost like a back door to the brain,” said Mr. Hoekman.
By bypassing the blood-brain barrier, it offers a direct pathway – the only direct pathway, actually – between an exposed area of the body and the brain. Meaning it can ferry drugs straight from the nasal cavity to the central nervous system.
Nose-to-brain treatments could be game-changing for central nervous system disorders, such as Parkinson’s disease, Alzheimer’s, or anxiety.
But reaching the olfactory zone is notoriously hard. “The vasculature in your nose is like a big freeway, and the olfactory tract is like a side alley,” explained Mr. Hoekman. “It’s very limiting in what it will allow through.” The region is also small, occupying only 3%-10% of the nasal cavity’s surface area.
Again, POD means “precision olfactory delivery.” But the device isn’t quite as laser focused on the region as its name implies. “We’re not at the stage where we’re able to exclusively deliver to one target site in the nose,” said Dr. Hindle.
While wending its way toward the olfactory zone, some of the drug will be absorbed by other regions, then circulate throughout the body.
“About 59% of the drug that we put into the upper nasal space gets absorbed into the bloodstream,” said Mr. Hoekman.
Janssen Pharmaceuticals’ Spravato – a nasal spray for drug-resistant depression – is thought to work similarly: Some goes straight to the brain via the olfactory nerves, while the rest takes a more roundabout route, passing through the blood vessels to circulate in your system.
A needle-free option
Sometimes, the bloodstream is the main target. Because the nose’s middle and upper stretches are so vascular, drugs can be rapidly absorbed.
This is especially valuable for time-sensitive conditions. “If you give something nasally, you can have peak uptake in 15-30 minutes,” said Mr. Hoekman.
Take Narcan nasal spray, which delivers a burst of naloxone to quickly reverse the effects of opioid an overdose. Or Noctiva nasal spray. Taken just half an hour before bed, it can prevent frequent nighttime urination.
There’s also a group of seizure-stopping sprays, known as “rescue treatments.” One works by temporarily loosening the space between nasal cells, allowing the seizure drug to be quickly absorbed through the vessels.
This systemic access also has potential for drugs that would otherwise have to be injected, such as biologics.
The same goes for vaccines. Mucosal tissue inside the nasal cavity offers direct access to the infection-fighting lymphatic system, making the nose a prime target for inoculation against certain viruses.
Inhaling protection against viruses
Despite the recent surge of interest, nasal vaccines faced a rocky start. After the first nasal flu vaccine hit the market in 2001, it was pulled due to potential toxicity and reports of Bell’s palsy, a type of facial paralysis.
FluMist came in 2003 and has been plagued by problems ever since. Because it contains a weakened live virus, flu-like side effects can occur. And it doesn’t always work. During the 2016-2017 flu season, FluMist protected only 3% of kids, prompting the Centers for Disease Control and Prevention to advise against the nasal route that year.
Why FluMist can be so hit-or-miss is poorly understood. But generally, the nose can pose an effectiveness challenge. “The nose is highly cycling,” said Dr. Hindle. “Anything we deposit usually gets transported out within 15-20 minutes.”
For kids – big fans of not using needles – chronically runny noses can be an issue. “You squirt it in the nose, and it will probably just come back out in their snot,” said Jay Kolls, MD, a professor of medicine and pediatrics at Tulane University, New Orleans, who is developing an intranasal pneumonia vaccine.
Even so, nasal vaccines became a hot topic among researchers after the world was shut down by a virus that invades through the nose.
“We realized that intramuscular vaccines were effective at preventing severe disease, but they weren’t that effective at preventing transmission,” said Michael Diamond, MD, PhD, an immunologist at Washington University in St. Louis.
Nasal vaccines could solve that problem by putting an immune barrier at the point of entry, denying access to the rest of the body. “You squash the infection early enough that it not only prevents disease,” said Dr. Kolls, “but potentially prevents transmission.”
And yes, a nasal COVID vaccine is on the way
In March 2020, Dr. Diamond’s team began exploring a nasal COVID vaccine. Promising results in animals prompted a vaccine development company to license the technology. The resulting nasal vaccine – the first for COVID – has been approved in India, both as a primary vaccine and a booster.
It works by stimulating an influx of IgA, a type of antibody found in the nasal passages, and production of resident memory T cells, immune cells on standby just beneath the surface tissue in the nose.
By contrast, injected vaccines generate mostly IgG antibodies, which struggle to enter the respiratory tract. Only a tiny fraction – an estimated 1% – typically reach the nose.
Nasal vaccines could also be used along with shots. The latter could prime the whole body to fight back, while a nasal spritz could pull that immune protection to the mucosal surfaces.
Nasal technology could yield more effective vaccines for infections like tuberculosis or malaria, or even safeguard against new – sometimes surprising – conditions.
In a 2021 Nature study, an intranasal vaccine derived from fentanyl was better at preventing overdose than an injected vaccine. “Through some clever chemistry, the drug [in the vaccine] isn’t fentanyl anymore,” said study author Elizabeth Norton, PhD, an assistant professor of microbiology and immunology at Tulane University. “But the immune system still has an antibody response to it.”
Novel applications like this represent the future of nasal drug delivery.
“We’re not going to innovate in asthma or COPD. We’re not going to innovate in local delivery to the nose,” said Dr. Hindle. “Innovation will only come if we look to treat new conditions.”
A version of this article originally appeared on WebMD.com.
Time to prescribe sauna bathing for cardiovascular health?
Is it time to start recommending regular sauna bathing to improve heart health?
While a post-workout sauna can compound the benefits of exercise, the hormetic effects of heat therapy alone can produce significant gains for microvascular and endothelial function, no workout required.
“There’s enough evidence to say that regular sauna use improves cardiovascular health,” Matthew S. Ganio, PhD, a professor of exercise science at the University of Arkansas in Fayetteville, who studies thermoregulatory responses and cardiovascular health, said.
“The more they used it, the greater the reduction in cardiovascular events like heart attack. But you don’t need to be in there more than 20-30 minutes. That’s where it seemed to have the best effect,” Dr. Ganio said, adding that studies have shown a dose-response.
A prospective cohort study published in 2015 in JAMA Internal Medicine included 20 years of data on more than 2,300 Finnish men who regularly sauna bathed. The researchers found that among participants who sat in saunas more frequently, rates of death from heart disease and stroke were lower than among those who did so less often.
Cutaneous vasodilation
The body experiences several physiologic changes when exposed to heat therapy of any kind, including sauna, hot water submerging, shortwave diathermy, and heat wrapping. Many of these changes involve elements of the cardiovascular system, said Earric Lee, PhD, an exercise physiologist and postdoctoral researcher at the University of Jyväskylä in Finland, who has studied the effects of sauna on cardiovascular health.
The mechanisms by which heat therapy improves cardiovascular fitness have not been determined, as few studies of sauna bathing have been conducted to this degree. One driver appears to be cutaneous vasodilation. To cool the body when exposed to extreme external heat, cutaneous vessels dilate and push blood to the skin, which lowers body temperature, increases heart rate, and delivers oxygen to muscles in the limbs in a way similar to aerobic exercise.
Sauna bathing has similar effects on heart rate and cardiac output. Studies have shown it can improve the circulation of blood through the body, as well as vascular endothelial function, which is closely tied to vascular tone.
“Increased cardiac output is one of the physiologic reasons sauna is good for heart health,” Dr. Ganio said.
During a sauna session, cardiac output can increase by as much as 70% in relation to elevated heart rate. And while heart rate and cardiac output rise, stroke volume remains stable. As stroke volume increases, the effort that muscle must exert increases. When heart rate rises, stroke volume often falls, which subjects the heart to less of a workout and reduces the amount of oxygen and blood circulating throughout the body.
Heat therapy also temporarily increases blood pressure, but in a way similar to exercise, which supports better long-term heart health, said Christopher Minson, PhD, the Kenneth M. and Kenda H. Singer Endowed Professor of Human Physiology at the University of Oregon in Eugene.
A small study of 19 healthy adults that was published in Complementary Therapies in Medicine in 2019 found that blood pressure and heart rate rose during a 25-minute sauna session as they might during moderate exercise, equivalent to an exercise load of about 60-100 watts. These parameters then steadily decreased for 30 minutes after the sauna. An earlier study found that in the long term, blood pressure was lower after a sauna than before a sauna.
Upregulated heat shock proteins
Both aerobic exercise and heat stress from sauna bathing increase the activity of heat shock proteins. A 2021 review published in Experimental Gerontology found that heat shock proteins become elevated in cells within 30 minutes of exposure to heat and remain elevated over time – an effect similar to exercise.
“Saunas increase heat shock proteins that break down old, dysfunctional proteins and then protect new proteins from becoming dysfunctional,” Hunter S. Waldman, PhD, an assistant professor of exercise science at the University of North Alabama in Florence, said. This effect is one way sauna bathing may quell systemic inflammation, Dr. Waldman said.
According to a 2018 review published in BioMed Research International, an abundance of heat shock proteins may increase exercise tolerance. The researchers concluded that the positive stress associated with elevated body temperature could help people be physically active for longer periods.
Added stress, especially heat-related strain, is not good for everyone, however. Dr. Waldman cautioned that heat exposure, be it through a sauna, hot tub, or other source, can be harmful for pregnant women and children and can be dangerous for people who have low blood pressure, since blood pressure often drops to rates that are lower than before taking a sauna. It also can impair semen quality for months after exposure, so people who are trying to conceive should avoid sauna bathing.
Anyone who has been diagnosed with a heart condition, including cardiac arrhythmia, coronary artery disease, and congestive heart failure, should always consult their physician prior to using sauna for the first time or before using it habitually, Dr. Lee said.
Effects compounded by exercise
Dr. Minson stressed that any type of heat therapy should be part of a lifestyle that includes mostly healthy habits overall, especially a regular exercise regime when possible.
“You have to have everything else working as well: finding time to relax, not being overly stressed, staying hydrated – all those things are critical with any exercise training and heat therapy program,” he said.
Dr. Lee said it’s easy to overhype the benefits of sauna bathing and agreed the practice should be used in tandem with other therapies, not as a replacement. So far, stacking research has shown it to be an effective extension of aerobic exercise.
A June 2023 review published in Mayo Clinic Proceedings found that while sauna bathing can produce benefits on its own, a post-workout sauna can extend the benefits of exercise. As a result, the researchers concluded, saunas likely provide the most benefit when combined with aerobic and strength training.
While some of the benefits of exercise overlap those associated with sauna bathing, “you’re going to get some benefits with exercise that you’re never going to get with sauna,” Dr. Ganio said.
For instance, strength training or aerobic exercise usually results in muscle contractions, which sauna bathing does not produce.
If a person is impaired in a way that makes exercise difficult, taking a sauna after aerobic activity can extend the cardiovascular benefits of the workout, even if muscle-building does not occur, Dr. Lee said.
“All other things considered, especially with aerobic exercise, it is very comparable, so we can look at adding sauna bathing post exercise as a way to lengthen the aerobic exercise workout,” he said. “It’s not to the same degree, but you can get many of the ranging benefits of exercising simply by going into the sauna.”
The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Is it time to start recommending regular sauna bathing to improve heart health?
While a post-workout sauna can compound the benefits of exercise, the hormetic effects of heat therapy alone can produce significant gains for microvascular and endothelial function, no workout required.
“There’s enough evidence to say that regular sauna use improves cardiovascular health,” Matthew S. Ganio, PhD, a professor of exercise science at the University of Arkansas in Fayetteville, who studies thermoregulatory responses and cardiovascular health, said.
“The more they used it, the greater the reduction in cardiovascular events like heart attack. But you don’t need to be in there more than 20-30 minutes. That’s where it seemed to have the best effect,” Dr. Ganio said, adding that studies have shown a dose-response.
A prospective cohort study published in 2015 in JAMA Internal Medicine included 20 years of data on more than 2,300 Finnish men who regularly sauna bathed. The researchers found that among participants who sat in saunas more frequently, rates of death from heart disease and stroke were lower than among those who did so less often.
Cutaneous vasodilation
The body experiences several physiologic changes when exposed to heat therapy of any kind, including sauna, hot water submerging, shortwave diathermy, and heat wrapping. Many of these changes involve elements of the cardiovascular system, said Earric Lee, PhD, an exercise physiologist and postdoctoral researcher at the University of Jyväskylä in Finland, who has studied the effects of sauna on cardiovascular health.
The mechanisms by which heat therapy improves cardiovascular fitness have not been determined, as few studies of sauna bathing have been conducted to this degree. One driver appears to be cutaneous vasodilation. To cool the body when exposed to extreme external heat, cutaneous vessels dilate and push blood to the skin, which lowers body temperature, increases heart rate, and delivers oxygen to muscles in the limbs in a way similar to aerobic exercise.
Sauna bathing has similar effects on heart rate and cardiac output. Studies have shown it can improve the circulation of blood through the body, as well as vascular endothelial function, which is closely tied to vascular tone.
“Increased cardiac output is one of the physiologic reasons sauna is good for heart health,” Dr. Ganio said.
During a sauna session, cardiac output can increase by as much as 70% in relation to elevated heart rate. And while heart rate and cardiac output rise, stroke volume remains stable. As stroke volume increases, the effort that muscle must exert increases. When heart rate rises, stroke volume often falls, which subjects the heart to less of a workout and reduces the amount of oxygen and blood circulating throughout the body.
Heat therapy also temporarily increases blood pressure, but in a way similar to exercise, which supports better long-term heart health, said Christopher Minson, PhD, the Kenneth M. and Kenda H. Singer Endowed Professor of Human Physiology at the University of Oregon in Eugene.
A small study of 19 healthy adults that was published in Complementary Therapies in Medicine in 2019 found that blood pressure and heart rate rose during a 25-minute sauna session as they might during moderate exercise, equivalent to an exercise load of about 60-100 watts. These parameters then steadily decreased for 30 minutes after the sauna. An earlier study found that in the long term, blood pressure was lower after a sauna than before a sauna.
Upregulated heat shock proteins
Both aerobic exercise and heat stress from sauna bathing increase the activity of heat shock proteins. A 2021 review published in Experimental Gerontology found that heat shock proteins become elevated in cells within 30 minutes of exposure to heat and remain elevated over time – an effect similar to exercise.
“Saunas increase heat shock proteins that break down old, dysfunctional proteins and then protect new proteins from becoming dysfunctional,” Hunter S. Waldman, PhD, an assistant professor of exercise science at the University of North Alabama in Florence, said. This effect is one way sauna bathing may quell systemic inflammation, Dr. Waldman said.
According to a 2018 review published in BioMed Research International, an abundance of heat shock proteins may increase exercise tolerance. The researchers concluded that the positive stress associated with elevated body temperature could help people be physically active for longer periods.
Added stress, especially heat-related strain, is not good for everyone, however. Dr. Waldman cautioned that heat exposure, be it through a sauna, hot tub, or other source, can be harmful for pregnant women and children and can be dangerous for people who have low blood pressure, since blood pressure often drops to rates that are lower than before taking a sauna. It also can impair semen quality for months after exposure, so people who are trying to conceive should avoid sauna bathing.
Anyone who has been diagnosed with a heart condition, including cardiac arrhythmia, coronary artery disease, and congestive heart failure, should always consult their physician prior to using sauna for the first time or before using it habitually, Dr. Lee said.
Effects compounded by exercise
Dr. Minson stressed that any type of heat therapy should be part of a lifestyle that includes mostly healthy habits overall, especially a regular exercise regime when possible.
“You have to have everything else working as well: finding time to relax, not being overly stressed, staying hydrated – all those things are critical with any exercise training and heat therapy program,” he said.
Dr. Lee said it’s easy to overhype the benefits of sauna bathing and agreed the practice should be used in tandem with other therapies, not as a replacement. So far, stacking research has shown it to be an effective extension of aerobic exercise.
A June 2023 review published in Mayo Clinic Proceedings found that while sauna bathing can produce benefits on its own, a post-workout sauna can extend the benefits of exercise. As a result, the researchers concluded, saunas likely provide the most benefit when combined with aerobic and strength training.
While some of the benefits of exercise overlap those associated with sauna bathing, “you’re going to get some benefits with exercise that you’re never going to get with sauna,” Dr. Ganio said.
For instance, strength training or aerobic exercise usually results in muscle contractions, which sauna bathing does not produce.
If a person is impaired in a way that makes exercise difficult, taking a sauna after aerobic activity can extend the cardiovascular benefits of the workout, even if muscle-building does not occur, Dr. Lee said.
“All other things considered, especially with aerobic exercise, it is very comparable, so we can look at adding sauna bathing post exercise as a way to lengthen the aerobic exercise workout,” he said. “It’s not to the same degree, but you can get many of the ranging benefits of exercising simply by going into the sauna.”
The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Is it time to start recommending regular sauna bathing to improve heart health?
While a post-workout sauna can compound the benefits of exercise, the hormetic effects of heat therapy alone can produce significant gains for microvascular and endothelial function, no workout required.
“There’s enough evidence to say that regular sauna use improves cardiovascular health,” Matthew S. Ganio, PhD, a professor of exercise science at the University of Arkansas in Fayetteville, who studies thermoregulatory responses and cardiovascular health, said.
“The more they used it, the greater the reduction in cardiovascular events like heart attack. But you don’t need to be in there more than 20-30 minutes. That’s where it seemed to have the best effect,” Dr. Ganio said, adding that studies have shown a dose-response.
A prospective cohort study published in 2015 in JAMA Internal Medicine included 20 years of data on more than 2,300 Finnish men who regularly sauna bathed. The researchers found that among participants who sat in saunas more frequently, rates of death from heart disease and stroke were lower than among those who did so less often.
Cutaneous vasodilation
The body experiences several physiologic changes when exposed to heat therapy of any kind, including sauna, hot water submerging, shortwave diathermy, and heat wrapping. Many of these changes involve elements of the cardiovascular system, said Earric Lee, PhD, an exercise physiologist and postdoctoral researcher at the University of Jyväskylä in Finland, who has studied the effects of sauna on cardiovascular health.
The mechanisms by which heat therapy improves cardiovascular fitness have not been determined, as few studies of sauna bathing have been conducted to this degree. One driver appears to be cutaneous vasodilation. To cool the body when exposed to extreme external heat, cutaneous vessels dilate and push blood to the skin, which lowers body temperature, increases heart rate, and delivers oxygen to muscles in the limbs in a way similar to aerobic exercise.
Sauna bathing has similar effects on heart rate and cardiac output. Studies have shown it can improve the circulation of blood through the body, as well as vascular endothelial function, which is closely tied to vascular tone.
“Increased cardiac output is one of the physiologic reasons sauna is good for heart health,” Dr. Ganio said.
During a sauna session, cardiac output can increase by as much as 70% in relation to elevated heart rate. And while heart rate and cardiac output rise, stroke volume remains stable. As stroke volume increases, the effort that muscle must exert increases. When heart rate rises, stroke volume often falls, which subjects the heart to less of a workout and reduces the amount of oxygen and blood circulating throughout the body.
Heat therapy also temporarily increases blood pressure, but in a way similar to exercise, which supports better long-term heart health, said Christopher Minson, PhD, the Kenneth M. and Kenda H. Singer Endowed Professor of Human Physiology at the University of Oregon in Eugene.
A small study of 19 healthy adults that was published in Complementary Therapies in Medicine in 2019 found that blood pressure and heart rate rose during a 25-minute sauna session as they might during moderate exercise, equivalent to an exercise load of about 60-100 watts. These parameters then steadily decreased for 30 minutes after the sauna. An earlier study found that in the long term, blood pressure was lower after a sauna than before a sauna.
Upregulated heat shock proteins
Both aerobic exercise and heat stress from sauna bathing increase the activity of heat shock proteins. A 2021 review published in Experimental Gerontology found that heat shock proteins become elevated in cells within 30 minutes of exposure to heat and remain elevated over time – an effect similar to exercise.
“Saunas increase heat shock proteins that break down old, dysfunctional proteins and then protect new proteins from becoming dysfunctional,” Hunter S. Waldman, PhD, an assistant professor of exercise science at the University of North Alabama in Florence, said. This effect is one way sauna bathing may quell systemic inflammation, Dr. Waldman said.
According to a 2018 review published in BioMed Research International, an abundance of heat shock proteins may increase exercise tolerance. The researchers concluded that the positive stress associated with elevated body temperature could help people be physically active for longer periods.
Added stress, especially heat-related strain, is not good for everyone, however. Dr. Waldman cautioned that heat exposure, be it through a sauna, hot tub, or other source, can be harmful for pregnant women and children and can be dangerous for people who have low blood pressure, since blood pressure often drops to rates that are lower than before taking a sauna. It also can impair semen quality for months after exposure, so people who are trying to conceive should avoid sauna bathing.
Anyone who has been diagnosed with a heart condition, including cardiac arrhythmia, coronary artery disease, and congestive heart failure, should always consult their physician prior to using sauna for the first time or before using it habitually, Dr. Lee said.
Effects compounded by exercise
Dr. Minson stressed that any type of heat therapy should be part of a lifestyle that includes mostly healthy habits overall, especially a regular exercise regime when possible.
“You have to have everything else working as well: finding time to relax, not being overly stressed, staying hydrated – all those things are critical with any exercise training and heat therapy program,” he said.
Dr. Lee said it’s easy to overhype the benefits of sauna bathing and agreed the practice should be used in tandem with other therapies, not as a replacement. So far, stacking research has shown it to be an effective extension of aerobic exercise.
A June 2023 review published in Mayo Clinic Proceedings found that while sauna bathing can produce benefits on its own, a post-workout sauna can extend the benefits of exercise. As a result, the researchers concluded, saunas likely provide the most benefit when combined with aerobic and strength training.
While some of the benefits of exercise overlap those associated with sauna bathing, “you’re going to get some benefits with exercise that you’re never going to get with sauna,” Dr. Ganio said.
For instance, strength training or aerobic exercise usually results in muscle contractions, which sauna bathing does not produce.
If a person is impaired in a way that makes exercise difficult, taking a sauna after aerobic activity can extend the cardiovascular benefits of the workout, even if muscle-building does not occur, Dr. Lee said.
“All other things considered, especially with aerobic exercise, it is very comparable, so we can look at adding sauna bathing post exercise as a way to lengthen the aerobic exercise workout,” he said. “It’s not to the same degree, but you can get many of the ranging benefits of exercising simply by going into the sauna.”
The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
West Nile virus cases rising nationwide amid mosquito season
In the past 2 weeks, new cases have been reported in Iowa and Nebraska, adding to previous 2023 reports from Arizona, Georgia, Illinois, Louisiana, Oregon, Pennsylvania, and Wyoming. A mosquito at a monitoring site near Houston tested positive last week for the potentially fatal virus, prompting local health officials to begin evening spray operations in the area where the mosquito was found, according to an announcement from Harris County Public Health.
According to the CDC, which compiles local reports, there have been 13 human cases of West Nile virus in 2023. In 2022, there were 1,126 cases, including 90 deaths.
Among this year’s 13 cases reported to the CDC so far, eight people add severe neuroinvasive disease, which means the disease spread to the nervous system. Such severe symptoms typically occur in 1 in every 150 cases of West Nile virus and can include encephalitis, which is inflammation of the brain, or meningitis, which is inflammation of the membranes that surround the brain and spinal cord. Three of the neuroinvasive cases occurred earlier this year amid an outbreak in Maricopa County, Arizona, where the disease is considered endemic, according to an April 28 report from the CDC.
The CDC says West Nile virus is the most common disease spread by mosquitoes in the continental United States. Local health officials sample mosquitoes to guide mosquito control strategies. So far this year, the CDC has received 28 reports of mosquitoes testing positive. Those mosquito testing reports came from Arizona, California, Florida, Indiana, Louisiana, and Texas.
West Nile virus is transmitted to people by the bite of an infected mosquito, but it can also be spread to humans if they handle a dead bird that is infected. The CDC says there are no medications to treat the virus in people. Most people who are infected do not feel sick, and 1 in 5 people infected develop a fever and other symptoms like headache, body ache, or a rash.
Prevention strategies are to wear insect repellent and to wear long-sleeved shirts and long pants to avoid mosquito bites.
A version of this article originally appeared on WebMD.com.
In the past 2 weeks, new cases have been reported in Iowa and Nebraska, adding to previous 2023 reports from Arizona, Georgia, Illinois, Louisiana, Oregon, Pennsylvania, and Wyoming. A mosquito at a monitoring site near Houston tested positive last week for the potentially fatal virus, prompting local health officials to begin evening spray operations in the area where the mosquito was found, according to an announcement from Harris County Public Health.
According to the CDC, which compiles local reports, there have been 13 human cases of West Nile virus in 2023. In 2022, there were 1,126 cases, including 90 deaths.
Among this year’s 13 cases reported to the CDC so far, eight people add severe neuroinvasive disease, which means the disease spread to the nervous system. Such severe symptoms typically occur in 1 in every 150 cases of West Nile virus and can include encephalitis, which is inflammation of the brain, or meningitis, which is inflammation of the membranes that surround the brain and spinal cord. Three of the neuroinvasive cases occurred earlier this year amid an outbreak in Maricopa County, Arizona, where the disease is considered endemic, according to an April 28 report from the CDC.
The CDC says West Nile virus is the most common disease spread by mosquitoes in the continental United States. Local health officials sample mosquitoes to guide mosquito control strategies. So far this year, the CDC has received 28 reports of mosquitoes testing positive. Those mosquito testing reports came from Arizona, California, Florida, Indiana, Louisiana, and Texas.
West Nile virus is transmitted to people by the bite of an infected mosquito, but it can also be spread to humans if they handle a dead bird that is infected. The CDC says there are no medications to treat the virus in people. Most people who are infected do not feel sick, and 1 in 5 people infected develop a fever and other symptoms like headache, body ache, or a rash.
Prevention strategies are to wear insect repellent and to wear long-sleeved shirts and long pants to avoid mosquito bites.
A version of this article originally appeared on WebMD.com.
In the past 2 weeks, new cases have been reported in Iowa and Nebraska, adding to previous 2023 reports from Arizona, Georgia, Illinois, Louisiana, Oregon, Pennsylvania, and Wyoming. A mosquito at a monitoring site near Houston tested positive last week for the potentially fatal virus, prompting local health officials to begin evening spray operations in the area where the mosquito was found, according to an announcement from Harris County Public Health.
According to the CDC, which compiles local reports, there have been 13 human cases of West Nile virus in 2023. In 2022, there were 1,126 cases, including 90 deaths.
Among this year’s 13 cases reported to the CDC so far, eight people add severe neuroinvasive disease, which means the disease spread to the nervous system. Such severe symptoms typically occur in 1 in every 150 cases of West Nile virus and can include encephalitis, which is inflammation of the brain, or meningitis, which is inflammation of the membranes that surround the brain and spinal cord. Three of the neuroinvasive cases occurred earlier this year amid an outbreak in Maricopa County, Arizona, where the disease is considered endemic, according to an April 28 report from the CDC.
The CDC says West Nile virus is the most common disease spread by mosquitoes in the continental United States. Local health officials sample mosquitoes to guide mosquito control strategies. So far this year, the CDC has received 28 reports of mosquitoes testing positive. Those mosquito testing reports came from Arizona, California, Florida, Indiana, Louisiana, and Texas.
West Nile virus is transmitted to people by the bite of an infected mosquito, but it can also be spread to humans if they handle a dead bird that is infected. The CDC says there are no medications to treat the virus in people. Most people who are infected do not feel sick, and 1 in 5 people infected develop a fever and other symptoms like headache, body ache, or a rash.
Prevention strategies are to wear insect repellent and to wear long-sleeved shirts and long pants to avoid mosquito bites.
A version of this article originally appeared on WebMD.com.
Raising the bar (and the OR table):Ergonomics in MIGS
Work-related musculoskeletal disorders (WMSDs) are “musculoskeletal disorders (injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs) in which the work environment and performance of work contribute significantly to the condition; and/or the condition is made worse or persists longer due to work conditions.”1 The health care industry has one of the highest rates of WMSDs, even when compared with traditional labor-intensive occupations, such as coal mining. In 2017, the health care industry reported more than a half million incidents of work-related injury and illness.2,3 In particular, surgeons are at increased risk for WMSDs, since they repetitively perform the classic tenets of poor ergonomics, including operating in static, extreme, and awkward positions and for prolonged periods of time.3
Gynecologic surgeons face unique ergonomic challenges. Operating in the pelvis requires an oblique approach that adds complexity and inhibits appropriate ergonomic positioning.4 All modalities of surgery incur their own challenges and risks to the surgeon, including minimally invasive gynecologic surgery (MIGS), which has become the standard of care for most conditions. Although MIGS has several benefits for the patient, a survey of gynecologic oncologists found that 88% of respondents reported discomfort related to MIGS.5 Several factors contribute to the development of WMSDs in surgery, including lack of ergonomic awareness, suboptimal ergonomic education and training,5,6 and ergonomically poor operating room (OR) equipment and instrument design.7 Furthermore, surgical culture does not generally prioritize ergonomics in the OR or requests for ergonomic accommodations.7,8
Within 5 years, a physician workforce shortage is projected for the United States.9 WMSDs contribute to workforce issues as they are associated with decreased productivity; time off needed for pain and treatment, including short-term disability; and possibly early retirement (as those who are older and have more work experience may be more likely to seek medical attention).10 In a 2013 study of vaginal surgeons, 14% missed work; 21% modified their work hours, work type, or amount of surgery; and 29% modified their surgical technique because of injury.10 Work-related pain also can negatively affect mental health, sleep, relationships, and quality of life.6
Recently, awareness has increased regarding WMSDs and their consequences, which has led to significant strides in the study of ergonomics among surgeons, a growing body of research on the topic, and guidance for optimizing ergonomics in the OR.
Risk factors for ergonomic strain
Several factors contribute to ergonomic strain and, subsequently, the development of WMSDs. Recognizing these factors can direct strategies for injury prevention.
Patient factors
The prevalence of obesity in the United States increased from 30.5% in 1999–2000 to 41.9% between 2017 and 2020.11 As the average patient’s body mass index (BMI) has increased, there is concern for a parallel increase in the ergonomic strain on laparoscopic surgeons.
A study of simulated laparoscopic tasks at varying model BMI levels demonstrated increased surgeon postural stress and workload at higher model BMIs (50 kg/m2) when compared with lower model BMIs (20 and 30 kg/m2).11 This result was supported in another study, which demonstrated both increased muscle activity and increased time needed to complete a surgical task with laparoscopic surgery; interestingly, when the same study measured these parameters for robotic surgery, this association was not seen.12 This suggests that a robotic rather than a laparoscopic approach may avoid some of the ergonomic strain associated with increased patient BMI.
Continue to: Surgeon factors...
Surgeon factors
Various surgeon characteristics have been shown to influence ergonomics in the OR. Surgeons with smaller hand sizes, for example, reported greater physical discomfort and demonstrated greater ergonomic workload when operating laparoscopically.13-15 In particular, those with a glove size of 6.5 or smaller have more difficulty using laparoscopic instruments, and those with a glove size smaller than 7 demonstrate a larger decline in grip strength when using laparoscopic instruments repeatedly.14,16
Surgeon height also can affect the amount of time spent in high-risk, nonergonomic positions. In a study that evaluated video recordings of surgeon posture during gynecologic laparoscopy, shorter surgeons were noted to use greater degrees of neck rotation to look at the monitor.17 Furthermore, surgeons with shorter arm lengths experienced more “extreme positions” of the nondominant shoulder and elbow.17 This trend also was seen in open and robotic surgery, where surgeons with a height of 66 cm or less reported increased pain scores after operating.18
Surgical instruments and OR setup
Surgical instrument characteristics can contribute to ergonomic strain, especially when the instruments have been designed with a one-size-fits-all mentality.8,19 In an examination of the anthropometric measurements of surgeon hand sizes and their correlation with difficulty when using a “standard” laparoscopic instrument, surgeons with smaller finger and hand spans had trouble using these instruments.19 Another study compared surgeon grip strength and ergonomic workloads after using 3 laparoscopic advanced bipolar instruments.16 Gender and hand size aside, the authors found that use of several of the laparoscopic devices led to greater decline in grip strength.16
The setup of the OR also can have a profound effect on the surgeon’s ergonomics. Monitor placement, for example, is crucial to ergonomic success. One study found that positioning the monitor directly in front of the surgeon at eye level was associated with the lowest neck muscle activity during a simulated task.20
Route of surgery
Each surgical approach has intrinsic ergonomic risks. With laparoscopy, surgeons often remain in straight head and back positions without much trunk motion, especially when compared with open surgery.21 In one study, laparoscopic surgeons spent more than 60% of a case in a static position and more than 80% of a case in a high-risk, “demanding” neck position.22
Robotic surgery, in contrast to laparoscopy, often has been cited as being more “ergonomic.” While robotic surgery has less of an effect on the neck, shoulders, arms, and legs than laparoscopy23 and often is associated with less physical discomfort than either open or laparoscopic surgery,23,24 robotic surgery still maintains its own innate ergonomic risks. Of robotic surgeons surveyed, 56.1% reported neck stiffness, finger fatigue, and eye symptoms in one study.25 In another survey study, more robotic surgeons (72%) reported physical symptoms than laparoscopic (57%) and open (49%) surgeons.26Vaginal surgery also puts surgeons at ergonomic risk. A majority of surgeons (87.2%) who completed more than 50% of their cases vaginally reported a history of WMSDs.10 Vaginal surgery places surgeons in awkward positions of the neck, shoulder, and trunk frequently and for longer durations.27
Continue to: Strategies for preventing WMSDs...
Strategies for preventing WMSDs
As factors that contribute to the development of WMSDs are identified, preventive strategies can be targeted to these individual factors. Research has focused on appropriate setup of the OR, surgeon posture, intraoperative microbreaks, and stretching both in and outside of the OR.
1. OR setup and positioning of the surgeon by MIGS route
The route of MIGS affects OR setup and surgeon posture. Ergonomic recommendations for laparoscopy, robotic surgery, and vaginal surgery are all unique to the risks posed by each particular approach.
Laparoscopic surgery. Laparoscopic monitors should face the surgeon directly, with the screen just below eye level to maintain the surgeon’s neck in a neutral position.28 The table height should be set for the tallest surgeon, and shorter surgeons should stand on steps as needed.28 The table height also should allow for the surgeon’s hands to be at elbow height, with the elbows bent at 90 degrees with the wrists straight.29 Foot pedals should be placed at the surgeons’ foot level and should be reached easily.28 Additionally, the patient’s arms should be tucked at their sides to allow surgeons a larger operative space.29 When using laparoscopic instruments, locking and ratcheting features should be used whenever possible to reduce prolonged grip or squeeze forces.28 The laparoscopic camera should be held in the palm with the wrist in a neutral position.29
Robotic surgery. Positioning and setup of the robotic console is a main focus of ergonomic recommendations. The surgeon’s chair should be brought as close to the console as possible, and the knees positioned in a 90-degree angle.30 The foot pedals should be brought toward the surgeon to maintain this angle of the knees.30 The console should be rotated toward the surgeon and then the height adjusted so that the surgeon can look through the eyepiece while sitting upright and can maintain the neck in a neutral position.28,30 The surgeon’s forehead should rest comfortably on the headrest.29 The forearms should rest on the armrest while the arms are maintained in a neutral position and the shoulders remain relaxed while the surgeon holds the robotic controls.30 It is important to utilize the armrest often to relieve stress on the arm while operating.28 Frequent use of the clutch function can keep the robotic controls in the center of the workspace.28
Vaginal surgery. Both seated and standing positions are associated with high-risk positioning of the trunk and bilateral shoulders, respectively, in vaginal surgery.31 However, surgeons who stand while operating vaginally reported more discomfort in the bilateral wrists, thighs, and lower legs than those who operated while seated.31 This suggests a potential ergonomic advantage to the seated position for vaginal surgery. Chair height should be adjusted so the surgeon can look straight ahead with the neck in a neutral position.32 Surgeons should consider using a headlamp, as this may prevent repetitive awkward movements to adjust overhead lights.32 For standing surgery, the table height should be adjusted for the tallest surgeon, and shorter surgeons or assistants should use steps as needed.3
Surgical assistants should switch sides during the course of the case to avoid excessive unilateral upper-extremity strain.32 The addition of a table-mounted vaginal retractor system may be useful in relieving physical strain for surgical assistants, but data currently are lacking to demonstrate this ergonomic benefit.33 Further studies are needed, especially since many surgeons take on the role of surgical assist in the teaching environment and subsequently report more WMSDs than their colleagues who do not work in teaching environments.10,34
2. Pain relief from individual ergonomic positioning devices
Apart from adjusting how the OR equipment is arranged or how the surgeons adjust their positioning, several devices that assist with surgeon positioning—including gel mats or insoles, exoskeletons, and “augmented reality” glasses—are being studied.
The use of gel mats or insoles in the OR has mixed evidence in the literature.35-37
Exoskeletons, external devices that support a surgeon’s posture and positioning, have been studied thus far in simulated nonsterile surgical environments. Preliminarily, it appears that use of an exoskeleton can decrease muscle activity and time spent in static positions, with a reported decrease in post-task user discomfort.38,39 More data are needed to determine if exoskeletons can be used in the sterile setting and for longer durations as may occur in actual OR cases.
Augmented reality glasses project the laparoscopic monitor image to the glasses, which frees the surgeon to place the “monitor” in a more neutral, ergonomic position. In one study, use of augmented reality glasses was associated with decreased muscle activity and a reduction in Rapid Entire Body Assessment (REBA) scores when compared with use of the conventional laparoscopic monitor.40More data are needed on these emerging technologies to determine whether adverse effects occur with prolonged use.
Continue to: 3. Implementing intraoperative microbreaks and stretching...
3. Implementing intraoperative microbreaks and stretching
The American College of Surgeons (ACS) recommends that surgeons avoid prolonged static postures during procedures.28 One strategy for preventing sustained positioning is to incorporate breaks with associated stretching routinely during surgery.28
Microbreaks. In a landmark study by Park and colleagues in 2017, 120-second long targeted stretching microbreaks (TSMBs) were completed every 20 to 40 minutes during a surgery, and results demonstrated improved postoperative surgeon pain scores without an associated increase in the length of the case.41 These surgeons reported improved pain in the neck, bilateral shoulders, bilateral hands, and lower back. Eighty-eight percent of surgeons reported either improvement or “no change” in their mental focus, and 100% reported improvement or “no change” in their physical performance after TSMBs were implemented.42 Of surveyed surgeons, 87% wanted TSMBs incorporated routinely.41,42
Stretches. Multiple resources, such as the ACS and the Mayo Clinic, for intraoperative stretches are available. The ACS recommends performing neck and shoulder stretches during intraoperative microbreaks, including a range-of-movement neck exercise, deep cervical flexor training, and standing scapular retraction.28 The ACS also demonstrates lumbrical stretches for the fingers and passive wrist extension exercises to be used intraoperatively (or between cases) (FIGURE 1).28 The Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR Stretch Instructional Video” in which the surgeon is guided through several different short stretches, including shoulder shrugging and side bends, that can be used during surgery.43
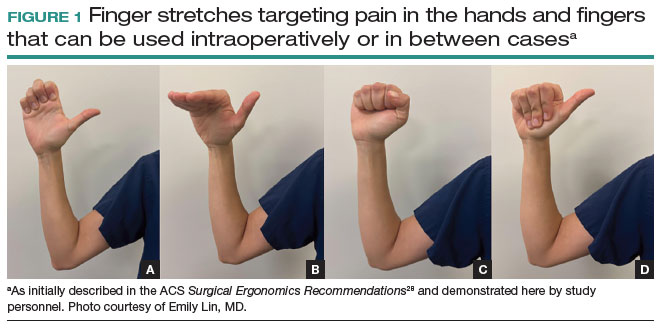
Both the ACS and the Mayo Clinic provide examples of pertinent stretch exercises for use when not in the sterile environment, between cases or after cases are complete. The ACS recommends several neck and shoulder stretches for the trapezius, levator scapulae, and pectoralis and recommends the use of a foam roller to improve thoracic mobility (FIGURE 2).28 As above, the Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR-Stretch Between Surgery Stretches Video” in which the surgeon is guided through several short stretches that are done in a seated position, including stretches for the hamstring, lower back, and arms (FIGURE 3).43
Many of the above-mentioned stretches were designed for use in the context of open, laparoscopic, or robotic surgery. For the vaginal surgeon, the intraoperative ergonomic stressors differ from those of other routes of surgery, and thus stretches tailored to the positioning during vaginal surgery are necessary. In a video recently published by the Society of Gynecologic Surgeons, several stretches are reviewed that target high-risk positions often held by the surgeon or assistant when operating vaginally.44 These stretches include cervical retraction, thoracic extension, external arm rotation, cervical side bending, and lumbar extension (FIGURE 4).44 The recommendation is to complete these exercises 2 times per day, with 8 to 10 repetitions per set.44
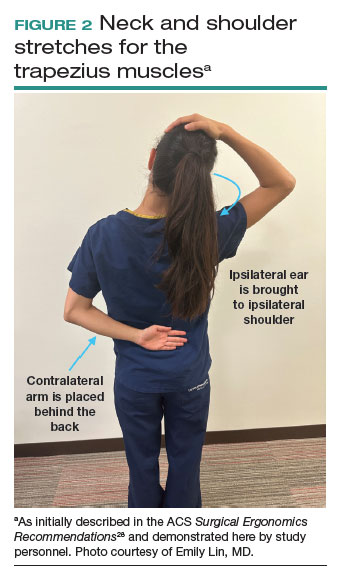
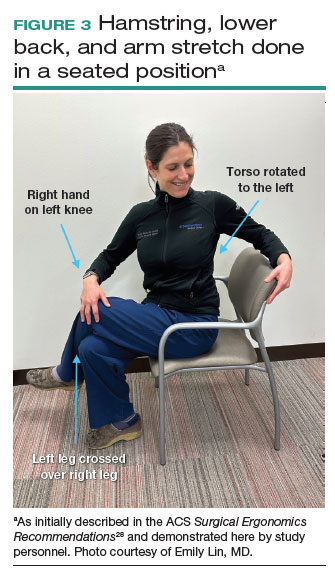
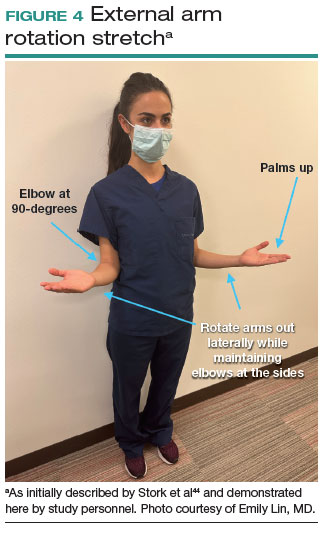
Prioritizing ergonomic awareness and training
As caregivers, it is not uncommon for us to prioritize the needs of others before those of ourselves. However, WMSDs are prevalent, and their downstream effects may cause catastrophic professional and personal losses. Cumulatively, the global impact of WMSDs is a significant issue for the health care workforce and its longevity.
To prevent WMSDs, it is imperative that surgeons are aware of the factors that contribute to injury development and the appropriate, accessible modifications for these factors. While each surgical modality confers its own ergonomic challenges, these risks can be mitigated through increased awareness of OR setup, surgeon positioning, and incorporation of microbreaks and stretching exercises during and after surgical procedures.
Formal training in surgical ergonomics is lacking across specialties, including gynecology.45 Multiple educational interventions have been proposed and studied to help fill this training gap.30,46-49When used, these interventions have been associated with increased knowledge of surgical ergonomic principles or reduction in surgeon pain scores, including trainees.50 As we become more cognizant of WMSDs, standardized resident curricula should be developed in an effort to reduce the prevalence of these potentially career-ending injuries.
In addition to education, cultivating a culture in which ergonomics is prioritized is essential. Although most surgeons report work-related pain, very few report their injuries to occupational health. For example, while 29% of gynecologic oncologists reported seeking treatment for a WMSD, only 1% had reported their injury to their employer.5 In a study of ACS members, only 19% of injuries were reported, 30% of surgeons stated that they did not know how to report an injury, and 21% felt that the resources for surgeons during and after an injury were inadequate.6
As we prioritize the health and safety of our patients, we also need to promote ergonomic awareness in the OR, respect the need for accommodations, encourage injury reporting, support surgeons who need to take time away for medical treatment, and partner with industry to develop new instruments and technology with effective ergonomic features. ●
- Workplace health glossary. Reviewed February 12, 2020. Centers for Disease Control and Prevention. Accessed May 18, 2023. https://www.cdc.gov/workplacehealthpromotion/tools-resources /glossary/glossary.html#W
- Epstein S, Sparer EH, Tran BN, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists: a systematic review and meta-analysis. JAMA Surg. 2018;153:e174947.
- Yurteri-Kaplan LA, Park AJ. Surgical ergonomics and preventing workrelated musculoskeletal disorders. Obstet Gynecol. 2023;141:455-462.
- Symer MM, Keller DS. Human factors in pelvic surgery. Eur J Surg Oncol. 2022;48:2346-2351.
- Franasiak J, Ko EM, Kidd J, et al. Physical strain and urgent need for ergonomic training among gynecologic oncologists who perform minimally invasive surgery. Gynecol Oncol. 2012;126:437-442.
- Davis WT, Fletcher SA, Guillamondegui OD. Musculoskeletal occupational injury among surgeons: effects for patients, providers, and institutions. J Surg Res. 2014;189:207-212.e6.
- Fox M. Surgeons face unique ergonomic challenges. American College of Surgeons. September 1, 2022. Accessed May 22, 2023. https://www.facs.org/for-medical-professionals/news-publications /news-and-articles/bulletin/september-2022-volume-107-issue-9 /surgeons-face-unique-ergonomic-challenges/
- Wong JMK, Carey ET, King C, et al. A call to action for ergonomic surgical devices designed for diverse surgeon end users. Obstet Gynecol. 2023;141:463-466.
- IHS Inc. The Complexities of Physician Supply and Demand: Projections from 2014 to 2025. Association of American Medical Colleges. April 5, 2016.
- Kim-Fine S, Woolley SM, Weaver AL, et al. Work-related musculoskeletal disorders among vaginal surgeons. Int Urogynecol J. 2013;24:1191-1200.
- Sers R, Forrester S, Zecca M, et al. The ergonomic impact of patient body mass index on surgeon posture during simulated laparoscopy. Appl Ergon. 2021;97:103501.
- Moss EL, Sarhanis P, Ind T, et al. Impact of obesity on surgeon ergonomics in robotic and straight-stick laparoscopic surgery. J Minim Invasive Gynecol. 2020;27:1063-1069.
- Sutton E, Irvin M, Zeigler C, et al. The ergonomics of women in surgery. Surg Endosc. 2014;28:1051-1055.
- Berguer R, Hreljac A. The relationship between hand size and difficulty using surgical instruments: a survey of 726 laparoscopic surgeons. Surg Endosc. 2004;18:508-512.
- Bellini MI, Amabile MI, Saullo P, et al. A woman’s place is in theatre, but are theatres designed with women in mind? A systematic review of ergonomics for women in surgery. J Clin Med. 2022;11:3496.
- Wong JMK, Moore KJ, Lewis P, et al. Ergonomic assessment of surgeon characteristics and laparoscopic device strain in gynecologic surgery. J Minim Invasive Gynecol. 2022;29:1357-1363.
- Aitchison LP, Cui CK, Arnold A, et al. The ergonomics of laparoscopic surgery: a quantitative study of the time and motion of laparoscopic surgeons in live surgical environments. Surg Endosc. 2016;30:5068-5076.
- Stewart C, Raoof M, Fong Y, et al. Who is hurting? A prospective study of surgeon ergonomics. Surg Endosc. 2022;36:292-299.
- Green SV, Morris DE, Naumann DN, et al. One size does not fit all: impact of hand size on ease of use of instruments for minimally invasive surgery. Surgeon. 2022;S1479-666X(22)00131-7.
- Matern U, Faist M, Kehl K, et al. Monitor position in laparoscopic surgery. Surg Endosc. 2005;19:436-440.
- Berguer R, Rab GT, Abu-Ghaida H, et al. A comparison of surgeons’ posture during laparoscopic and open surgical procedures. Surg Endosc. 1997;11:139-142.
- Athanasiadis DI, Monfared S, Asadi H, et al. An analysis of the ergonomic risk of surgical trainees and experienced surgeons during laparoscopic procedures. Surgery. 2021;169:496-501.
- Hotton J, Bogart E, Le Deley MC, et al. Ergonomic assessment of the surgeon’s physical workload during robot-assisted versus standard laparoscopy in a French multicenter randomized trial (ROBOGYN-1004 Trial). Ann Surg Oncol. 2023;30:916-923.
- Plerhoples TA, Hernandez-Boussard T, Wren SM. The aching surgeon: a survey of physical discomfort and symptoms following open, laparoscopic, and robotic surgery. J Robot Surg. 2012;6:65-72.
- Lee GI, Lee MR, Green I, et al. Surgeons’ physical discomfort and symptoms during robotic surgery: a comprehensive ergonomic survey study. Surg Endosc. 2017;31:1697-1706.
- McDonald ME, Ramirez PT, Munsell MF, et al. Physician pain and discomfort during minimally invasive gynecologic cancer surgery. Gynecol Oncol. 2014;134:243-247.
- Zhu X, Yurteri-Kaplan LA, Gutman RE, et al. Postural stress experienced by vaginal surgeons. Proc Hum Factors Ergonomics Soc Annu Meet. 2014;58:763-767.
- American College of Surgeons Division of Education and Surgical Ergonomics Committee. Surgical Ergonomics Recommendations. ACS Education. 2022.
- Cardenas-Trowers O, Kjellsson K, Hatch K. Ergonomics: making the OR a comfortable place. Int Urogynecol J. 2018;29:1065-1066.
- Hokenstad ED, Hallbeck MS, Lowndes BR, et al. Ergonomic robotic console configuration in gynecologic surgery: an interventional study. J Minim Invasive Gynecol. 2021;28:850-859.
- Singh R, Yurteri-Kaplan LA, Morrow MM, et al. Sitting versus standing makes a difference in musculoskeletal discomfort and postural load for surgeons performing vaginal surgery. Int Urogynecol J. 2019;30:231-237.
- Hullfish KL, Trowbridge ER, Bodine G. Ergonomics and gynecologic surgery: “surgeon protect thyself.” J Pelvic Med Surg. 2009;15:435-439.
- Woodburn KL, Kho RM. Vaginal surgery: don’t get bent out of shape. Am J Obstet Gynecol. 2020;223:762-763.
- Hobson DTG, Meriwether KV, Gaskins JT, et al. Learner satisfaction and experience with a high-definition telescopic camera during vaginal procedures: a randomized controlled trial. Female Pelvic Med Reconstr Surg. 2021;27:105-111.
- Speed G, Harris K, Keegel T. The effect of cushioning materials on musculoskeletal discomfort and fatigue during prolonged standing at work: a systematic review. Appl Ergon. 2018;70:300-334.
- Haramis G, Rosales JC, Palacios JM, et al. Prospective randomized evaluation of FOOT gel pads for operating room staff COMFORT during laparoscopic renal surgery. Urology. 2010;76:1405-1408.
- Voss RK, Chiang YJ, Cromwell KD, et al. Do no harm, except to ourselves? A survey of symptoms and injuries in oncologic surgeons and pilot study of an intraoperative ergonomic intervention. J Am Coll Surg. 2017;224:16-25.e1.
- Marquetand J, Gabriel J, Seibt R, et al. Ergonomics for surgeons—prototype of an external surgeon support system reduces muscular activity and fatigue. J Electromyogr Kinesiol. 2021;60:102586.
- Tetteh E, Hallbeck MS, Mirka GA. Effects of passive exoskeleton support on EMG measures of the neck, shoulder and trunk muscles while holding simulated surgical postures and performing a simulated surgical procedure. Appl Ergon. 2022;100:103646.
- Lim AK, Ryu J, Yoon HM, et al. Ergonomic effects of medical augmented reality glasses in video-assisted surgery. Surg Endosc. 2022;36:988-998.
- Park AE, Zahiri HR, Hallbeck MS, et al. Intraoperative “micro breaks” with targeted stretching enhance surgeon physical function and mental focus: a multicenter cohort study. Ann Surg. 2017;265:340-346.
- Hallbeck MS, Lowndes BR, Bingener J, et al. The impact of intraoperative microbreaks with exercises on surgeons: a multi-center cohort study. Appl Ergon. 2017;60:334-341.
- Hallbeck Human Factors Engineering Laboratories. OR Stretch Videos. Mayo Clinic, 2018. Accessed May 19, 2023. https://www.mayo .edu/research/labs/human-factors-engineering/or-stretch /or-stretch-videos
- Stork A, Bacon T, Corton M. Prevention of Work-Related Musculoskeletal Disorders in Vaginal Surgery. Video presentation at: Society of Gynecologic Surgeons’ Annual Scientific Meeting 2023, Tucson, AZ. Accessed April 3, 2023. https://sgs.eng.us/category.php?cat=2023 -video-presentations
- Aaron KA, Vaughan J, Gupta R, et al. The risk of ergonomic injury across surgical specialties. PLoS One. 2021;16:e0244868.
- Smith TG, Lowndes BR, Schmida E, et al. Course design and learning outcomes of a practical online ergonomics course for surgical residents. J Surg Educ. 2022;79:1489-1499.
- Franasiak J, Craven R, Mosaly P, et al. Feasibility and acceptance of a robotic surgery ergonomic training program. JSLS. 2014;18:e2014.00166.
- Cerier E, Hu A, Goldring A, et al. Ergonomics workshop improves musculoskeletal symptoms in general surgery residents. J Surg Res. 2022;280:567-574.
- Giagio S, Volpe G, Pillastrini P, et al. A preventive program for workrelated musculoskeletal disorders among surgeons: outcomes of a randomized controlled clinical trial. Ann Surg. 2019;270:969-975.
- Jensen MJ, Liao J, Van Gorp B, et al. Incorporating surgical ergonomics education into surgical residency curriculum. J Surg Educ. 2021;78:1209-1215.
Work-related musculoskeletal disorders (WMSDs) are “musculoskeletal disorders (injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs) in which the work environment and performance of work contribute significantly to the condition; and/or the condition is made worse or persists longer due to work conditions.”1 The health care industry has one of the highest rates of WMSDs, even when compared with traditional labor-intensive occupations, such as coal mining. In 2017, the health care industry reported more than a half million incidents of work-related injury and illness.2,3 In particular, surgeons are at increased risk for WMSDs, since they repetitively perform the classic tenets of poor ergonomics, including operating in static, extreme, and awkward positions and for prolonged periods of time.3
Gynecologic surgeons face unique ergonomic challenges. Operating in the pelvis requires an oblique approach that adds complexity and inhibits appropriate ergonomic positioning.4 All modalities of surgery incur their own challenges and risks to the surgeon, including minimally invasive gynecologic surgery (MIGS), which has become the standard of care for most conditions. Although MIGS has several benefits for the patient, a survey of gynecologic oncologists found that 88% of respondents reported discomfort related to MIGS.5 Several factors contribute to the development of WMSDs in surgery, including lack of ergonomic awareness, suboptimal ergonomic education and training,5,6 and ergonomically poor operating room (OR) equipment and instrument design.7 Furthermore, surgical culture does not generally prioritize ergonomics in the OR or requests for ergonomic accommodations.7,8
Within 5 years, a physician workforce shortage is projected for the United States.9 WMSDs contribute to workforce issues as they are associated with decreased productivity; time off needed for pain and treatment, including short-term disability; and possibly early retirement (as those who are older and have more work experience may be more likely to seek medical attention).10 In a 2013 study of vaginal surgeons, 14% missed work; 21% modified their work hours, work type, or amount of surgery; and 29% modified their surgical technique because of injury.10 Work-related pain also can negatively affect mental health, sleep, relationships, and quality of life.6
Recently, awareness has increased regarding WMSDs and their consequences, which has led to significant strides in the study of ergonomics among surgeons, a growing body of research on the topic, and guidance for optimizing ergonomics in the OR.
Risk factors for ergonomic strain
Several factors contribute to ergonomic strain and, subsequently, the development of WMSDs. Recognizing these factors can direct strategies for injury prevention.
Patient factors
The prevalence of obesity in the United States increased from 30.5% in 1999–2000 to 41.9% between 2017 and 2020.11 As the average patient’s body mass index (BMI) has increased, there is concern for a parallel increase in the ergonomic strain on laparoscopic surgeons.
A study of simulated laparoscopic tasks at varying model BMI levels demonstrated increased surgeon postural stress and workload at higher model BMIs (50 kg/m2) when compared with lower model BMIs (20 and 30 kg/m2).11 This result was supported in another study, which demonstrated both increased muscle activity and increased time needed to complete a surgical task with laparoscopic surgery; interestingly, when the same study measured these parameters for robotic surgery, this association was not seen.12 This suggests that a robotic rather than a laparoscopic approach may avoid some of the ergonomic strain associated with increased patient BMI.
Continue to: Surgeon factors...
Surgeon factors
Various surgeon characteristics have been shown to influence ergonomics in the OR. Surgeons with smaller hand sizes, for example, reported greater physical discomfort and demonstrated greater ergonomic workload when operating laparoscopically.13-15 In particular, those with a glove size of 6.5 or smaller have more difficulty using laparoscopic instruments, and those with a glove size smaller than 7 demonstrate a larger decline in grip strength when using laparoscopic instruments repeatedly.14,16
Surgeon height also can affect the amount of time spent in high-risk, nonergonomic positions. In a study that evaluated video recordings of surgeon posture during gynecologic laparoscopy, shorter surgeons were noted to use greater degrees of neck rotation to look at the monitor.17 Furthermore, surgeons with shorter arm lengths experienced more “extreme positions” of the nondominant shoulder and elbow.17 This trend also was seen in open and robotic surgery, where surgeons with a height of 66 cm or less reported increased pain scores after operating.18
Surgical instruments and OR setup
Surgical instrument characteristics can contribute to ergonomic strain, especially when the instruments have been designed with a one-size-fits-all mentality.8,19 In an examination of the anthropometric measurements of surgeon hand sizes and their correlation with difficulty when using a “standard” laparoscopic instrument, surgeons with smaller finger and hand spans had trouble using these instruments.19 Another study compared surgeon grip strength and ergonomic workloads after using 3 laparoscopic advanced bipolar instruments.16 Gender and hand size aside, the authors found that use of several of the laparoscopic devices led to greater decline in grip strength.16
The setup of the OR also can have a profound effect on the surgeon’s ergonomics. Monitor placement, for example, is crucial to ergonomic success. One study found that positioning the monitor directly in front of the surgeon at eye level was associated with the lowest neck muscle activity during a simulated task.20
Route of surgery
Each surgical approach has intrinsic ergonomic risks. With laparoscopy, surgeons often remain in straight head and back positions without much trunk motion, especially when compared with open surgery.21 In one study, laparoscopic surgeons spent more than 60% of a case in a static position and more than 80% of a case in a high-risk, “demanding” neck position.22
Robotic surgery, in contrast to laparoscopy, often has been cited as being more “ergonomic.” While robotic surgery has less of an effect on the neck, shoulders, arms, and legs than laparoscopy23 and often is associated with less physical discomfort than either open or laparoscopic surgery,23,24 robotic surgery still maintains its own innate ergonomic risks. Of robotic surgeons surveyed, 56.1% reported neck stiffness, finger fatigue, and eye symptoms in one study.25 In another survey study, more robotic surgeons (72%) reported physical symptoms than laparoscopic (57%) and open (49%) surgeons.26Vaginal surgery also puts surgeons at ergonomic risk. A majority of surgeons (87.2%) who completed more than 50% of their cases vaginally reported a history of WMSDs.10 Vaginal surgery places surgeons in awkward positions of the neck, shoulder, and trunk frequently and for longer durations.27
Continue to: Strategies for preventing WMSDs...
Strategies for preventing WMSDs
As factors that contribute to the development of WMSDs are identified, preventive strategies can be targeted to these individual factors. Research has focused on appropriate setup of the OR, surgeon posture, intraoperative microbreaks, and stretching both in and outside of the OR.
1. OR setup and positioning of the surgeon by MIGS route
The route of MIGS affects OR setup and surgeon posture. Ergonomic recommendations for laparoscopy, robotic surgery, and vaginal surgery are all unique to the risks posed by each particular approach.
Laparoscopic surgery. Laparoscopic monitors should face the surgeon directly, with the screen just below eye level to maintain the surgeon’s neck in a neutral position.28 The table height should be set for the tallest surgeon, and shorter surgeons should stand on steps as needed.28 The table height also should allow for the surgeon’s hands to be at elbow height, with the elbows bent at 90 degrees with the wrists straight.29 Foot pedals should be placed at the surgeons’ foot level and should be reached easily.28 Additionally, the patient’s arms should be tucked at their sides to allow surgeons a larger operative space.29 When using laparoscopic instruments, locking and ratcheting features should be used whenever possible to reduce prolonged grip or squeeze forces.28 The laparoscopic camera should be held in the palm with the wrist in a neutral position.29
Robotic surgery. Positioning and setup of the robotic console is a main focus of ergonomic recommendations. The surgeon’s chair should be brought as close to the console as possible, and the knees positioned in a 90-degree angle.30 The foot pedals should be brought toward the surgeon to maintain this angle of the knees.30 The console should be rotated toward the surgeon and then the height adjusted so that the surgeon can look through the eyepiece while sitting upright and can maintain the neck in a neutral position.28,30 The surgeon’s forehead should rest comfortably on the headrest.29 The forearms should rest on the armrest while the arms are maintained in a neutral position and the shoulders remain relaxed while the surgeon holds the robotic controls.30 It is important to utilize the armrest often to relieve stress on the arm while operating.28 Frequent use of the clutch function can keep the robotic controls in the center of the workspace.28
Vaginal surgery. Both seated and standing positions are associated with high-risk positioning of the trunk and bilateral shoulders, respectively, in vaginal surgery.31 However, surgeons who stand while operating vaginally reported more discomfort in the bilateral wrists, thighs, and lower legs than those who operated while seated.31 This suggests a potential ergonomic advantage to the seated position for vaginal surgery. Chair height should be adjusted so the surgeon can look straight ahead with the neck in a neutral position.32 Surgeons should consider using a headlamp, as this may prevent repetitive awkward movements to adjust overhead lights.32 For standing surgery, the table height should be adjusted for the tallest surgeon, and shorter surgeons or assistants should use steps as needed.3
Surgical assistants should switch sides during the course of the case to avoid excessive unilateral upper-extremity strain.32 The addition of a table-mounted vaginal retractor system may be useful in relieving physical strain for surgical assistants, but data currently are lacking to demonstrate this ergonomic benefit.33 Further studies are needed, especially since many surgeons take on the role of surgical assist in the teaching environment and subsequently report more WMSDs than their colleagues who do not work in teaching environments.10,34
2. Pain relief from individual ergonomic positioning devices
Apart from adjusting how the OR equipment is arranged or how the surgeons adjust their positioning, several devices that assist with surgeon positioning—including gel mats or insoles, exoskeletons, and “augmented reality” glasses—are being studied.
The use of gel mats or insoles in the OR has mixed evidence in the literature.35-37
Exoskeletons, external devices that support a surgeon’s posture and positioning, have been studied thus far in simulated nonsterile surgical environments. Preliminarily, it appears that use of an exoskeleton can decrease muscle activity and time spent in static positions, with a reported decrease in post-task user discomfort.38,39 More data are needed to determine if exoskeletons can be used in the sterile setting and for longer durations as may occur in actual OR cases.
Augmented reality glasses project the laparoscopic monitor image to the glasses, which frees the surgeon to place the “monitor” in a more neutral, ergonomic position. In one study, use of augmented reality glasses was associated with decreased muscle activity and a reduction in Rapid Entire Body Assessment (REBA) scores when compared with use of the conventional laparoscopic monitor.40More data are needed on these emerging technologies to determine whether adverse effects occur with prolonged use.
Continue to: 3. Implementing intraoperative microbreaks and stretching...
3. Implementing intraoperative microbreaks and stretching
The American College of Surgeons (ACS) recommends that surgeons avoid prolonged static postures during procedures.28 One strategy for preventing sustained positioning is to incorporate breaks with associated stretching routinely during surgery.28
Microbreaks. In a landmark study by Park and colleagues in 2017, 120-second long targeted stretching microbreaks (TSMBs) were completed every 20 to 40 minutes during a surgery, and results demonstrated improved postoperative surgeon pain scores without an associated increase in the length of the case.41 These surgeons reported improved pain in the neck, bilateral shoulders, bilateral hands, and lower back. Eighty-eight percent of surgeons reported either improvement or “no change” in their mental focus, and 100% reported improvement or “no change” in their physical performance after TSMBs were implemented.42 Of surveyed surgeons, 87% wanted TSMBs incorporated routinely.41,42
Stretches. Multiple resources, such as the ACS and the Mayo Clinic, for intraoperative stretches are available. The ACS recommends performing neck and shoulder stretches during intraoperative microbreaks, including a range-of-movement neck exercise, deep cervical flexor training, and standing scapular retraction.28 The ACS also demonstrates lumbrical stretches for the fingers and passive wrist extension exercises to be used intraoperatively (or between cases) (FIGURE 1).28 The Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR Stretch Instructional Video” in which the surgeon is guided through several different short stretches, including shoulder shrugging and side bends, that can be used during surgery.43
Both the ACS and the Mayo Clinic provide examples of pertinent stretch exercises for use when not in the sterile environment, between cases or after cases are complete. The ACS recommends several neck and shoulder stretches for the trapezius, levator scapulae, and pectoralis and recommends the use of a foam roller to improve thoracic mobility (FIGURE 2).28 As above, the Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR-Stretch Between Surgery Stretches Video” in which the surgeon is guided through several short stretches that are done in a seated position, including stretches for the hamstring, lower back, and arms (FIGURE 3).43
Many of the above-mentioned stretches were designed for use in the context of open, laparoscopic, or robotic surgery. For the vaginal surgeon, the intraoperative ergonomic stressors differ from those of other routes of surgery, and thus stretches tailored to the positioning during vaginal surgery are necessary. In a video recently published by the Society of Gynecologic Surgeons, several stretches are reviewed that target high-risk positions often held by the surgeon or assistant when operating vaginally.44 These stretches include cervical retraction, thoracic extension, external arm rotation, cervical side bending, and lumbar extension (FIGURE 4).44 The recommendation is to complete these exercises 2 times per day, with 8 to 10 repetitions per set.44
Prioritizing ergonomic awareness and training
As caregivers, it is not uncommon for us to prioritize the needs of others before those of ourselves. However, WMSDs are prevalent, and their downstream effects may cause catastrophic professional and personal losses. Cumulatively, the global impact of WMSDs is a significant issue for the health care workforce and its longevity.
To prevent WMSDs, it is imperative that surgeons are aware of the factors that contribute to injury development and the appropriate, accessible modifications for these factors. While each surgical modality confers its own ergonomic challenges, these risks can be mitigated through increased awareness of OR setup, surgeon positioning, and incorporation of microbreaks and stretching exercises during and after surgical procedures.
Formal training in surgical ergonomics is lacking across specialties, including gynecology.45 Multiple educational interventions have been proposed and studied to help fill this training gap.30,46-49When used, these interventions have been associated with increased knowledge of surgical ergonomic principles or reduction in surgeon pain scores, including trainees.50 As we become more cognizant of WMSDs, standardized resident curricula should be developed in an effort to reduce the prevalence of these potentially career-ending injuries.
In addition to education, cultivating a culture in which ergonomics is prioritized is essential. Although most surgeons report work-related pain, very few report their injuries to occupational health. For example, while 29% of gynecologic oncologists reported seeking treatment for a WMSD, only 1% had reported their injury to their employer.5 In a study of ACS members, only 19% of injuries were reported, 30% of surgeons stated that they did not know how to report an injury, and 21% felt that the resources for surgeons during and after an injury were inadequate.6
As we prioritize the health and safety of our patients, we also need to promote ergonomic awareness in the OR, respect the need for accommodations, encourage injury reporting, support surgeons who need to take time away for medical treatment, and partner with industry to develop new instruments and technology with effective ergonomic features. ●
Work-related musculoskeletal disorders (WMSDs) are “musculoskeletal disorders (injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs) in which the work environment and performance of work contribute significantly to the condition; and/or the condition is made worse or persists longer due to work conditions.”1 The health care industry has one of the highest rates of WMSDs, even when compared with traditional labor-intensive occupations, such as coal mining. In 2017, the health care industry reported more than a half million incidents of work-related injury and illness.2,3 In particular, surgeons are at increased risk for WMSDs, since they repetitively perform the classic tenets of poor ergonomics, including operating in static, extreme, and awkward positions and for prolonged periods of time.3
Gynecologic surgeons face unique ergonomic challenges. Operating in the pelvis requires an oblique approach that adds complexity and inhibits appropriate ergonomic positioning.4 All modalities of surgery incur their own challenges and risks to the surgeon, including minimally invasive gynecologic surgery (MIGS), which has become the standard of care for most conditions. Although MIGS has several benefits for the patient, a survey of gynecologic oncologists found that 88% of respondents reported discomfort related to MIGS.5 Several factors contribute to the development of WMSDs in surgery, including lack of ergonomic awareness, suboptimal ergonomic education and training,5,6 and ergonomically poor operating room (OR) equipment and instrument design.7 Furthermore, surgical culture does not generally prioritize ergonomics in the OR or requests for ergonomic accommodations.7,8
Within 5 years, a physician workforce shortage is projected for the United States.9 WMSDs contribute to workforce issues as they are associated with decreased productivity; time off needed for pain and treatment, including short-term disability; and possibly early retirement (as those who are older and have more work experience may be more likely to seek medical attention).10 In a 2013 study of vaginal surgeons, 14% missed work; 21% modified their work hours, work type, or amount of surgery; and 29% modified their surgical technique because of injury.10 Work-related pain also can negatively affect mental health, sleep, relationships, and quality of life.6
Recently, awareness has increased regarding WMSDs and their consequences, which has led to significant strides in the study of ergonomics among surgeons, a growing body of research on the topic, and guidance for optimizing ergonomics in the OR.
Risk factors for ergonomic strain
Several factors contribute to ergonomic strain and, subsequently, the development of WMSDs. Recognizing these factors can direct strategies for injury prevention.
Patient factors
The prevalence of obesity in the United States increased from 30.5% in 1999–2000 to 41.9% between 2017 and 2020.11 As the average patient’s body mass index (BMI) has increased, there is concern for a parallel increase in the ergonomic strain on laparoscopic surgeons.
A study of simulated laparoscopic tasks at varying model BMI levels demonstrated increased surgeon postural stress and workload at higher model BMIs (50 kg/m2) when compared with lower model BMIs (20 and 30 kg/m2).11 This result was supported in another study, which demonstrated both increased muscle activity and increased time needed to complete a surgical task with laparoscopic surgery; interestingly, when the same study measured these parameters for robotic surgery, this association was not seen.12 This suggests that a robotic rather than a laparoscopic approach may avoid some of the ergonomic strain associated with increased patient BMI.
Continue to: Surgeon factors...
Surgeon factors
Various surgeon characteristics have been shown to influence ergonomics in the OR. Surgeons with smaller hand sizes, for example, reported greater physical discomfort and demonstrated greater ergonomic workload when operating laparoscopically.13-15 In particular, those with a glove size of 6.5 or smaller have more difficulty using laparoscopic instruments, and those with a glove size smaller than 7 demonstrate a larger decline in grip strength when using laparoscopic instruments repeatedly.14,16
Surgeon height also can affect the amount of time spent in high-risk, nonergonomic positions. In a study that evaluated video recordings of surgeon posture during gynecologic laparoscopy, shorter surgeons were noted to use greater degrees of neck rotation to look at the monitor.17 Furthermore, surgeons with shorter arm lengths experienced more “extreme positions” of the nondominant shoulder and elbow.17 This trend also was seen in open and robotic surgery, where surgeons with a height of 66 cm or less reported increased pain scores after operating.18
Surgical instruments and OR setup
Surgical instrument characteristics can contribute to ergonomic strain, especially when the instruments have been designed with a one-size-fits-all mentality.8,19 In an examination of the anthropometric measurements of surgeon hand sizes and their correlation with difficulty when using a “standard” laparoscopic instrument, surgeons with smaller finger and hand spans had trouble using these instruments.19 Another study compared surgeon grip strength and ergonomic workloads after using 3 laparoscopic advanced bipolar instruments.16 Gender and hand size aside, the authors found that use of several of the laparoscopic devices led to greater decline in grip strength.16
The setup of the OR also can have a profound effect on the surgeon’s ergonomics. Monitor placement, for example, is crucial to ergonomic success. One study found that positioning the monitor directly in front of the surgeon at eye level was associated with the lowest neck muscle activity during a simulated task.20
Route of surgery
Each surgical approach has intrinsic ergonomic risks. With laparoscopy, surgeons often remain in straight head and back positions without much trunk motion, especially when compared with open surgery.21 In one study, laparoscopic surgeons spent more than 60% of a case in a static position and more than 80% of a case in a high-risk, “demanding” neck position.22
Robotic surgery, in contrast to laparoscopy, often has been cited as being more “ergonomic.” While robotic surgery has less of an effect on the neck, shoulders, arms, and legs than laparoscopy23 and often is associated with less physical discomfort than either open or laparoscopic surgery,23,24 robotic surgery still maintains its own innate ergonomic risks. Of robotic surgeons surveyed, 56.1% reported neck stiffness, finger fatigue, and eye symptoms in one study.25 In another survey study, more robotic surgeons (72%) reported physical symptoms than laparoscopic (57%) and open (49%) surgeons.26Vaginal surgery also puts surgeons at ergonomic risk. A majority of surgeons (87.2%) who completed more than 50% of their cases vaginally reported a history of WMSDs.10 Vaginal surgery places surgeons in awkward positions of the neck, shoulder, and trunk frequently and for longer durations.27
Continue to: Strategies for preventing WMSDs...
Strategies for preventing WMSDs
As factors that contribute to the development of WMSDs are identified, preventive strategies can be targeted to these individual factors. Research has focused on appropriate setup of the OR, surgeon posture, intraoperative microbreaks, and stretching both in and outside of the OR.
1. OR setup and positioning of the surgeon by MIGS route
The route of MIGS affects OR setup and surgeon posture. Ergonomic recommendations for laparoscopy, robotic surgery, and vaginal surgery are all unique to the risks posed by each particular approach.
Laparoscopic surgery. Laparoscopic monitors should face the surgeon directly, with the screen just below eye level to maintain the surgeon’s neck in a neutral position.28 The table height should be set for the tallest surgeon, and shorter surgeons should stand on steps as needed.28 The table height also should allow for the surgeon’s hands to be at elbow height, with the elbows bent at 90 degrees with the wrists straight.29 Foot pedals should be placed at the surgeons’ foot level and should be reached easily.28 Additionally, the patient’s arms should be tucked at their sides to allow surgeons a larger operative space.29 When using laparoscopic instruments, locking and ratcheting features should be used whenever possible to reduce prolonged grip or squeeze forces.28 The laparoscopic camera should be held in the palm with the wrist in a neutral position.29
Robotic surgery. Positioning and setup of the robotic console is a main focus of ergonomic recommendations. The surgeon’s chair should be brought as close to the console as possible, and the knees positioned in a 90-degree angle.30 The foot pedals should be brought toward the surgeon to maintain this angle of the knees.30 The console should be rotated toward the surgeon and then the height adjusted so that the surgeon can look through the eyepiece while sitting upright and can maintain the neck in a neutral position.28,30 The surgeon’s forehead should rest comfortably on the headrest.29 The forearms should rest on the armrest while the arms are maintained in a neutral position and the shoulders remain relaxed while the surgeon holds the robotic controls.30 It is important to utilize the armrest often to relieve stress on the arm while operating.28 Frequent use of the clutch function can keep the robotic controls in the center of the workspace.28
Vaginal surgery. Both seated and standing positions are associated with high-risk positioning of the trunk and bilateral shoulders, respectively, in vaginal surgery.31 However, surgeons who stand while operating vaginally reported more discomfort in the bilateral wrists, thighs, and lower legs than those who operated while seated.31 This suggests a potential ergonomic advantage to the seated position for vaginal surgery. Chair height should be adjusted so the surgeon can look straight ahead with the neck in a neutral position.32 Surgeons should consider using a headlamp, as this may prevent repetitive awkward movements to adjust overhead lights.32 For standing surgery, the table height should be adjusted for the tallest surgeon, and shorter surgeons or assistants should use steps as needed.3
Surgical assistants should switch sides during the course of the case to avoid excessive unilateral upper-extremity strain.32 The addition of a table-mounted vaginal retractor system may be useful in relieving physical strain for surgical assistants, but data currently are lacking to demonstrate this ergonomic benefit.33 Further studies are needed, especially since many surgeons take on the role of surgical assist in the teaching environment and subsequently report more WMSDs than their colleagues who do not work in teaching environments.10,34
2. Pain relief from individual ergonomic positioning devices
Apart from adjusting how the OR equipment is arranged or how the surgeons adjust their positioning, several devices that assist with surgeon positioning—including gel mats or insoles, exoskeletons, and “augmented reality” glasses—are being studied.
The use of gel mats or insoles in the OR has mixed evidence in the literature.35-37
Exoskeletons, external devices that support a surgeon’s posture and positioning, have been studied thus far in simulated nonsterile surgical environments. Preliminarily, it appears that use of an exoskeleton can decrease muscle activity and time spent in static positions, with a reported decrease in post-task user discomfort.38,39 More data are needed to determine if exoskeletons can be used in the sterile setting and for longer durations as may occur in actual OR cases.
Augmented reality glasses project the laparoscopic monitor image to the glasses, which frees the surgeon to place the “monitor” in a more neutral, ergonomic position. In one study, use of augmented reality glasses was associated with decreased muscle activity and a reduction in Rapid Entire Body Assessment (REBA) scores when compared with use of the conventional laparoscopic monitor.40More data are needed on these emerging technologies to determine whether adverse effects occur with prolonged use.
Continue to: 3. Implementing intraoperative microbreaks and stretching...
3. Implementing intraoperative microbreaks and stretching
The American College of Surgeons (ACS) recommends that surgeons avoid prolonged static postures during procedures.28 One strategy for preventing sustained positioning is to incorporate breaks with associated stretching routinely during surgery.28
Microbreaks. In a landmark study by Park and colleagues in 2017, 120-second long targeted stretching microbreaks (TSMBs) were completed every 20 to 40 minutes during a surgery, and results demonstrated improved postoperative surgeon pain scores without an associated increase in the length of the case.41 These surgeons reported improved pain in the neck, bilateral shoulders, bilateral hands, and lower back. Eighty-eight percent of surgeons reported either improvement or “no change” in their mental focus, and 100% reported improvement or “no change” in their physical performance after TSMBs were implemented.42 Of surveyed surgeons, 87% wanted TSMBs incorporated routinely.41,42
Stretches. Multiple resources, such as the ACS and the Mayo Clinic, for intraoperative stretches are available. The ACS recommends performing neck and shoulder stretches during intraoperative microbreaks, including a range-of-movement neck exercise, deep cervical flexor training, and standing scapular retraction.28 The ACS also demonstrates lumbrical stretches for the fingers and passive wrist extension exercises to be used intraoperatively (or between cases) (FIGURE 1).28 The Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR Stretch Instructional Video” in which the surgeon is guided through several different short stretches, including shoulder shrugging and side bends, that can be used during surgery.43
Both the ACS and the Mayo Clinic provide examples of pertinent stretch exercises for use when not in the sterile environment, between cases or after cases are complete. The ACS recommends several neck and shoulder stretches for the trapezius, levator scapulae, and pectoralis and recommends the use of a foam roller to improve thoracic mobility (FIGURE 2).28 As above, the Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR-Stretch Between Surgery Stretches Video” in which the surgeon is guided through several short stretches that are done in a seated position, including stretches for the hamstring, lower back, and arms (FIGURE 3).43
Many of the above-mentioned stretches were designed for use in the context of open, laparoscopic, or robotic surgery. For the vaginal surgeon, the intraoperative ergonomic stressors differ from those of other routes of surgery, and thus stretches tailored to the positioning during vaginal surgery are necessary. In a video recently published by the Society of Gynecologic Surgeons, several stretches are reviewed that target high-risk positions often held by the surgeon or assistant when operating vaginally.44 These stretches include cervical retraction, thoracic extension, external arm rotation, cervical side bending, and lumbar extension (FIGURE 4).44 The recommendation is to complete these exercises 2 times per day, with 8 to 10 repetitions per set.44
Prioritizing ergonomic awareness and training
As caregivers, it is not uncommon for us to prioritize the needs of others before those of ourselves. However, WMSDs are prevalent, and their downstream effects may cause catastrophic professional and personal losses. Cumulatively, the global impact of WMSDs is a significant issue for the health care workforce and its longevity.
To prevent WMSDs, it is imperative that surgeons are aware of the factors that contribute to injury development and the appropriate, accessible modifications for these factors. While each surgical modality confers its own ergonomic challenges, these risks can be mitigated through increased awareness of OR setup, surgeon positioning, and incorporation of microbreaks and stretching exercises during and after surgical procedures.
Formal training in surgical ergonomics is lacking across specialties, including gynecology.45 Multiple educational interventions have been proposed and studied to help fill this training gap.30,46-49When used, these interventions have been associated with increased knowledge of surgical ergonomic principles or reduction in surgeon pain scores, including trainees.50 As we become more cognizant of WMSDs, standardized resident curricula should be developed in an effort to reduce the prevalence of these potentially career-ending injuries.
In addition to education, cultivating a culture in which ergonomics is prioritized is essential. Although most surgeons report work-related pain, very few report their injuries to occupational health. For example, while 29% of gynecologic oncologists reported seeking treatment for a WMSD, only 1% had reported their injury to their employer.5 In a study of ACS members, only 19% of injuries were reported, 30% of surgeons stated that they did not know how to report an injury, and 21% felt that the resources for surgeons during and after an injury were inadequate.6
As we prioritize the health and safety of our patients, we also need to promote ergonomic awareness in the OR, respect the need for accommodations, encourage injury reporting, support surgeons who need to take time away for medical treatment, and partner with industry to develop new instruments and technology with effective ergonomic features. ●
- Workplace health glossary. Reviewed February 12, 2020. Centers for Disease Control and Prevention. Accessed May 18, 2023. https://www.cdc.gov/workplacehealthpromotion/tools-resources /glossary/glossary.html#W
- Epstein S, Sparer EH, Tran BN, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists: a systematic review and meta-analysis. JAMA Surg. 2018;153:e174947.
- Yurteri-Kaplan LA, Park AJ. Surgical ergonomics and preventing workrelated musculoskeletal disorders. Obstet Gynecol. 2023;141:455-462.
- Symer MM, Keller DS. Human factors in pelvic surgery. Eur J Surg Oncol. 2022;48:2346-2351.
- Franasiak J, Ko EM, Kidd J, et al. Physical strain and urgent need for ergonomic training among gynecologic oncologists who perform minimally invasive surgery. Gynecol Oncol. 2012;126:437-442.
- Davis WT, Fletcher SA, Guillamondegui OD. Musculoskeletal occupational injury among surgeons: effects for patients, providers, and institutions. J Surg Res. 2014;189:207-212.e6.
- Fox M. Surgeons face unique ergonomic challenges. American College of Surgeons. September 1, 2022. Accessed May 22, 2023. https://www.facs.org/for-medical-professionals/news-publications /news-and-articles/bulletin/september-2022-volume-107-issue-9 /surgeons-face-unique-ergonomic-challenges/
- Wong JMK, Carey ET, King C, et al. A call to action for ergonomic surgical devices designed for diverse surgeon end users. Obstet Gynecol. 2023;141:463-466.
- IHS Inc. The Complexities of Physician Supply and Demand: Projections from 2014 to 2025. Association of American Medical Colleges. April 5, 2016.
- Kim-Fine S, Woolley SM, Weaver AL, et al. Work-related musculoskeletal disorders among vaginal surgeons. Int Urogynecol J. 2013;24:1191-1200.
- Sers R, Forrester S, Zecca M, et al. The ergonomic impact of patient body mass index on surgeon posture during simulated laparoscopy. Appl Ergon. 2021;97:103501.
- Moss EL, Sarhanis P, Ind T, et al. Impact of obesity on surgeon ergonomics in robotic and straight-stick laparoscopic surgery. J Minim Invasive Gynecol. 2020;27:1063-1069.
- Sutton E, Irvin M, Zeigler C, et al. The ergonomics of women in surgery. Surg Endosc. 2014;28:1051-1055.
- Berguer R, Hreljac A. The relationship between hand size and difficulty using surgical instruments: a survey of 726 laparoscopic surgeons. Surg Endosc. 2004;18:508-512.
- Bellini MI, Amabile MI, Saullo P, et al. A woman’s place is in theatre, but are theatres designed with women in mind? A systematic review of ergonomics for women in surgery. J Clin Med. 2022;11:3496.
- Wong JMK, Moore KJ, Lewis P, et al. Ergonomic assessment of surgeon characteristics and laparoscopic device strain in gynecologic surgery. J Minim Invasive Gynecol. 2022;29:1357-1363.
- Aitchison LP, Cui CK, Arnold A, et al. The ergonomics of laparoscopic surgery: a quantitative study of the time and motion of laparoscopic surgeons in live surgical environments. Surg Endosc. 2016;30:5068-5076.
- Stewart C, Raoof M, Fong Y, et al. Who is hurting? A prospective study of surgeon ergonomics. Surg Endosc. 2022;36:292-299.
- Green SV, Morris DE, Naumann DN, et al. One size does not fit all: impact of hand size on ease of use of instruments for minimally invasive surgery. Surgeon. 2022;S1479-666X(22)00131-7.
- Matern U, Faist M, Kehl K, et al. Monitor position in laparoscopic surgery. Surg Endosc. 2005;19:436-440.
- Berguer R, Rab GT, Abu-Ghaida H, et al. A comparison of surgeons’ posture during laparoscopic and open surgical procedures. Surg Endosc. 1997;11:139-142.
- Athanasiadis DI, Monfared S, Asadi H, et al. An analysis of the ergonomic risk of surgical trainees and experienced surgeons during laparoscopic procedures. Surgery. 2021;169:496-501.
- Hotton J, Bogart E, Le Deley MC, et al. Ergonomic assessment of the surgeon’s physical workload during robot-assisted versus standard laparoscopy in a French multicenter randomized trial (ROBOGYN-1004 Trial). Ann Surg Oncol. 2023;30:916-923.
- Plerhoples TA, Hernandez-Boussard T, Wren SM. The aching surgeon: a survey of physical discomfort and symptoms following open, laparoscopic, and robotic surgery. J Robot Surg. 2012;6:65-72.
- Lee GI, Lee MR, Green I, et al. Surgeons’ physical discomfort and symptoms during robotic surgery: a comprehensive ergonomic survey study. Surg Endosc. 2017;31:1697-1706.
- McDonald ME, Ramirez PT, Munsell MF, et al. Physician pain and discomfort during minimally invasive gynecologic cancer surgery. Gynecol Oncol. 2014;134:243-247.
- Zhu X, Yurteri-Kaplan LA, Gutman RE, et al. Postural stress experienced by vaginal surgeons. Proc Hum Factors Ergonomics Soc Annu Meet. 2014;58:763-767.
- American College of Surgeons Division of Education and Surgical Ergonomics Committee. Surgical Ergonomics Recommendations. ACS Education. 2022.
- Cardenas-Trowers O, Kjellsson K, Hatch K. Ergonomics: making the OR a comfortable place. Int Urogynecol J. 2018;29:1065-1066.
- Hokenstad ED, Hallbeck MS, Lowndes BR, et al. Ergonomic robotic console configuration in gynecologic surgery: an interventional study. J Minim Invasive Gynecol. 2021;28:850-859.
- Singh R, Yurteri-Kaplan LA, Morrow MM, et al. Sitting versus standing makes a difference in musculoskeletal discomfort and postural load for surgeons performing vaginal surgery. Int Urogynecol J. 2019;30:231-237.
- Hullfish KL, Trowbridge ER, Bodine G. Ergonomics and gynecologic surgery: “surgeon protect thyself.” J Pelvic Med Surg. 2009;15:435-439.
- Woodburn KL, Kho RM. Vaginal surgery: don’t get bent out of shape. Am J Obstet Gynecol. 2020;223:762-763.
- Hobson DTG, Meriwether KV, Gaskins JT, et al. Learner satisfaction and experience with a high-definition telescopic camera during vaginal procedures: a randomized controlled trial. Female Pelvic Med Reconstr Surg. 2021;27:105-111.
- Speed G, Harris K, Keegel T. The effect of cushioning materials on musculoskeletal discomfort and fatigue during prolonged standing at work: a systematic review. Appl Ergon. 2018;70:300-334.
- Haramis G, Rosales JC, Palacios JM, et al. Prospective randomized evaluation of FOOT gel pads for operating room staff COMFORT during laparoscopic renal surgery. Urology. 2010;76:1405-1408.
- Voss RK, Chiang YJ, Cromwell KD, et al. Do no harm, except to ourselves? A survey of symptoms and injuries in oncologic surgeons and pilot study of an intraoperative ergonomic intervention. J Am Coll Surg. 2017;224:16-25.e1.
- Marquetand J, Gabriel J, Seibt R, et al. Ergonomics for surgeons—prototype of an external surgeon support system reduces muscular activity and fatigue. J Electromyogr Kinesiol. 2021;60:102586.
- Tetteh E, Hallbeck MS, Mirka GA. Effects of passive exoskeleton support on EMG measures of the neck, shoulder and trunk muscles while holding simulated surgical postures and performing a simulated surgical procedure. Appl Ergon. 2022;100:103646.
- Lim AK, Ryu J, Yoon HM, et al. Ergonomic effects of medical augmented reality glasses in video-assisted surgery. Surg Endosc. 2022;36:988-998.
- Park AE, Zahiri HR, Hallbeck MS, et al. Intraoperative “micro breaks” with targeted stretching enhance surgeon physical function and mental focus: a multicenter cohort study. Ann Surg. 2017;265:340-346.
- Hallbeck MS, Lowndes BR, Bingener J, et al. The impact of intraoperative microbreaks with exercises on surgeons: a multi-center cohort study. Appl Ergon. 2017;60:334-341.
- Hallbeck Human Factors Engineering Laboratories. OR Stretch Videos. Mayo Clinic, 2018. Accessed May 19, 2023. https://www.mayo .edu/research/labs/human-factors-engineering/or-stretch /or-stretch-videos
- Stork A, Bacon T, Corton M. Prevention of Work-Related Musculoskeletal Disorders in Vaginal Surgery. Video presentation at: Society of Gynecologic Surgeons’ Annual Scientific Meeting 2023, Tucson, AZ. Accessed April 3, 2023. https://sgs.eng.us/category.php?cat=2023 -video-presentations
- Aaron KA, Vaughan J, Gupta R, et al. The risk of ergonomic injury across surgical specialties. PLoS One. 2021;16:e0244868.
- Smith TG, Lowndes BR, Schmida E, et al. Course design and learning outcomes of a practical online ergonomics course for surgical residents. J Surg Educ. 2022;79:1489-1499.
- Franasiak J, Craven R, Mosaly P, et al. Feasibility and acceptance of a robotic surgery ergonomic training program. JSLS. 2014;18:e2014.00166.
- Cerier E, Hu A, Goldring A, et al. Ergonomics workshop improves musculoskeletal symptoms in general surgery residents. J Surg Res. 2022;280:567-574.
- Giagio S, Volpe G, Pillastrini P, et al. A preventive program for workrelated musculoskeletal disorders among surgeons: outcomes of a randomized controlled clinical trial. Ann Surg. 2019;270:969-975.
- Jensen MJ, Liao J, Van Gorp B, et al. Incorporating surgical ergonomics education into surgical residency curriculum. J Surg Educ. 2021;78:1209-1215.
- Workplace health glossary. Reviewed February 12, 2020. Centers for Disease Control and Prevention. Accessed May 18, 2023. https://www.cdc.gov/workplacehealthpromotion/tools-resources /glossary/glossary.html#W
- Epstein S, Sparer EH, Tran BN, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists: a systematic review and meta-analysis. JAMA Surg. 2018;153:e174947.
- Yurteri-Kaplan LA, Park AJ. Surgical ergonomics and preventing workrelated musculoskeletal disorders. Obstet Gynecol. 2023;141:455-462.
- Symer MM, Keller DS. Human factors in pelvic surgery. Eur J Surg Oncol. 2022;48:2346-2351.
- Franasiak J, Ko EM, Kidd J, et al. Physical strain and urgent need for ergonomic training among gynecologic oncologists who perform minimally invasive surgery. Gynecol Oncol. 2012;126:437-442.
- Davis WT, Fletcher SA, Guillamondegui OD. Musculoskeletal occupational injury among surgeons: effects for patients, providers, and institutions. J Surg Res. 2014;189:207-212.e6.
- Fox M. Surgeons face unique ergonomic challenges. American College of Surgeons. September 1, 2022. Accessed May 22, 2023. https://www.facs.org/for-medical-professionals/news-publications /news-and-articles/bulletin/september-2022-volume-107-issue-9 /surgeons-face-unique-ergonomic-challenges/
- Wong JMK, Carey ET, King C, et al. A call to action for ergonomic surgical devices designed for diverse surgeon end users. Obstet Gynecol. 2023;141:463-466.
- IHS Inc. The Complexities of Physician Supply and Demand: Projections from 2014 to 2025. Association of American Medical Colleges. April 5, 2016.
- Kim-Fine S, Woolley SM, Weaver AL, et al. Work-related musculoskeletal disorders among vaginal surgeons. Int Urogynecol J. 2013;24:1191-1200.
- Sers R, Forrester S, Zecca M, et al. The ergonomic impact of patient body mass index on surgeon posture during simulated laparoscopy. Appl Ergon. 2021;97:103501.
- Moss EL, Sarhanis P, Ind T, et al. Impact of obesity on surgeon ergonomics in robotic and straight-stick laparoscopic surgery. J Minim Invasive Gynecol. 2020;27:1063-1069.
- Sutton E, Irvin M, Zeigler C, et al. The ergonomics of women in surgery. Surg Endosc. 2014;28:1051-1055.
- Berguer R, Hreljac A. The relationship between hand size and difficulty using surgical instruments: a survey of 726 laparoscopic surgeons. Surg Endosc. 2004;18:508-512.
- Bellini MI, Amabile MI, Saullo P, et al. A woman’s place is in theatre, but are theatres designed with women in mind? A systematic review of ergonomics for women in surgery. J Clin Med. 2022;11:3496.
- Wong JMK, Moore KJ, Lewis P, et al. Ergonomic assessment of surgeon characteristics and laparoscopic device strain in gynecologic surgery. J Minim Invasive Gynecol. 2022;29:1357-1363.
- Aitchison LP, Cui CK, Arnold A, et al. The ergonomics of laparoscopic surgery: a quantitative study of the time and motion of laparoscopic surgeons in live surgical environments. Surg Endosc. 2016;30:5068-5076.
- Stewart C, Raoof M, Fong Y, et al. Who is hurting? A prospective study of surgeon ergonomics. Surg Endosc. 2022;36:292-299.
- Green SV, Morris DE, Naumann DN, et al. One size does not fit all: impact of hand size on ease of use of instruments for minimally invasive surgery. Surgeon. 2022;S1479-666X(22)00131-7.
- Matern U, Faist M, Kehl K, et al. Monitor position in laparoscopic surgery. Surg Endosc. 2005;19:436-440.
- Berguer R, Rab GT, Abu-Ghaida H, et al. A comparison of surgeons’ posture during laparoscopic and open surgical procedures. Surg Endosc. 1997;11:139-142.
- Athanasiadis DI, Monfared S, Asadi H, et al. An analysis of the ergonomic risk of surgical trainees and experienced surgeons during laparoscopic procedures. Surgery. 2021;169:496-501.
- Hotton J, Bogart E, Le Deley MC, et al. Ergonomic assessment of the surgeon’s physical workload during robot-assisted versus standard laparoscopy in a French multicenter randomized trial (ROBOGYN-1004 Trial). Ann Surg Oncol. 2023;30:916-923.
- Plerhoples TA, Hernandez-Boussard T, Wren SM. The aching surgeon: a survey of physical discomfort and symptoms following open, laparoscopic, and robotic surgery. J Robot Surg. 2012;6:65-72.
- Lee GI, Lee MR, Green I, et al. Surgeons’ physical discomfort and symptoms during robotic surgery: a comprehensive ergonomic survey study. Surg Endosc. 2017;31:1697-1706.
- McDonald ME, Ramirez PT, Munsell MF, et al. Physician pain and discomfort during minimally invasive gynecologic cancer surgery. Gynecol Oncol. 2014;134:243-247.
- Zhu X, Yurteri-Kaplan LA, Gutman RE, et al. Postural stress experienced by vaginal surgeons. Proc Hum Factors Ergonomics Soc Annu Meet. 2014;58:763-767.
- American College of Surgeons Division of Education and Surgical Ergonomics Committee. Surgical Ergonomics Recommendations. ACS Education. 2022.
- Cardenas-Trowers O, Kjellsson K, Hatch K. Ergonomics: making the OR a comfortable place. Int Urogynecol J. 2018;29:1065-1066.
- Hokenstad ED, Hallbeck MS, Lowndes BR, et al. Ergonomic robotic console configuration in gynecologic surgery: an interventional study. J Minim Invasive Gynecol. 2021;28:850-859.
- Singh R, Yurteri-Kaplan LA, Morrow MM, et al. Sitting versus standing makes a difference in musculoskeletal discomfort and postural load for surgeons performing vaginal surgery. Int Urogynecol J. 2019;30:231-237.
- Hullfish KL, Trowbridge ER, Bodine G. Ergonomics and gynecologic surgery: “surgeon protect thyself.” J Pelvic Med Surg. 2009;15:435-439.
- Woodburn KL, Kho RM. Vaginal surgery: don’t get bent out of shape. Am J Obstet Gynecol. 2020;223:762-763.
- Hobson DTG, Meriwether KV, Gaskins JT, et al. Learner satisfaction and experience with a high-definition telescopic camera during vaginal procedures: a randomized controlled trial. Female Pelvic Med Reconstr Surg. 2021;27:105-111.
- Speed G, Harris K, Keegel T. The effect of cushioning materials on musculoskeletal discomfort and fatigue during prolonged standing at work: a systematic review. Appl Ergon. 2018;70:300-334.
- Haramis G, Rosales JC, Palacios JM, et al. Prospective randomized evaluation of FOOT gel pads for operating room staff COMFORT during laparoscopic renal surgery. Urology. 2010;76:1405-1408.
- Voss RK, Chiang YJ, Cromwell KD, et al. Do no harm, except to ourselves? A survey of symptoms and injuries in oncologic surgeons and pilot study of an intraoperative ergonomic intervention. J Am Coll Surg. 2017;224:16-25.e1.
- Marquetand J, Gabriel J, Seibt R, et al. Ergonomics for surgeons—prototype of an external surgeon support system reduces muscular activity and fatigue. J Electromyogr Kinesiol. 2021;60:102586.
- Tetteh E, Hallbeck MS, Mirka GA. Effects of passive exoskeleton support on EMG measures of the neck, shoulder and trunk muscles while holding simulated surgical postures and performing a simulated surgical procedure. Appl Ergon. 2022;100:103646.
- Lim AK, Ryu J, Yoon HM, et al. Ergonomic effects of medical augmented reality glasses in video-assisted surgery. Surg Endosc. 2022;36:988-998.
- Park AE, Zahiri HR, Hallbeck MS, et al. Intraoperative “micro breaks” with targeted stretching enhance surgeon physical function and mental focus: a multicenter cohort study. Ann Surg. 2017;265:340-346.
- Hallbeck MS, Lowndes BR, Bingener J, et al. The impact of intraoperative microbreaks with exercises on surgeons: a multi-center cohort study. Appl Ergon. 2017;60:334-341.
- Hallbeck Human Factors Engineering Laboratories. OR Stretch Videos. Mayo Clinic, 2018. Accessed May 19, 2023. https://www.mayo .edu/research/labs/human-factors-engineering/or-stretch /or-stretch-videos
- Stork A, Bacon T, Corton M. Prevention of Work-Related Musculoskeletal Disorders in Vaginal Surgery. Video presentation at: Society of Gynecologic Surgeons’ Annual Scientific Meeting 2023, Tucson, AZ. Accessed April 3, 2023. https://sgs.eng.us/category.php?cat=2023 -video-presentations
- Aaron KA, Vaughan J, Gupta R, et al. The risk of ergonomic injury across surgical specialties. PLoS One. 2021;16:e0244868.
- Smith TG, Lowndes BR, Schmida E, et al. Course design and learning outcomes of a practical online ergonomics course for surgical residents. J Surg Educ. 2022;79:1489-1499.
- Franasiak J, Craven R, Mosaly P, et al. Feasibility and acceptance of a robotic surgery ergonomic training program. JSLS. 2014;18:e2014.00166.
- Cerier E, Hu A, Goldring A, et al. Ergonomics workshop improves musculoskeletal symptoms in general surgery residents. J Surg Res. 2022;280:567-574.
- Giagio S, Volpe G, Pillastrini P, et al. A preventive program for workrelated musculoskeletal disorders among surgeons: outcomes of a randomized controlled clinical trial. Ann Surg. 2019;270:969-975.
- Jensen MJ, Liao J, Van Gorp B, et al. Incorporating surgical ergonomics education into surgical residency curriculum. J Surg Educ. 2021;78:1209-1215.
Reducing risk for thrombosis in patients with lung cancer
CHICAGO – Having cancer is a known risk factor for thrombosis. A patient with cancer has a fourfold risk of developing venous thromboembolism (VTE).
This risk may be increased by certain cancer drugs, which seems to be the case for the combination of innovative targeted therapies lazertinib-amivantamab, as shown in patients with advanced or metastatic non–small cell lung cancer.
A study of this increased risk of VTE was presented by Nicolas Girard, MD, a respiratory medicine specialist at Curie-Montsouris Chest Center in Paris, during the annual meeting of the American Society of Clinical Oncology.
Combination therapies
Amivantamab is an EGFR and cMET bispecific antibody, and lazertinib is a third-generation EGFR tyrosine kinase inhibitor. Prescribed after osimertinib or after osimertinib plus chemotherapy, this combination of amivantamab and lazertinib has been evaluated in several cohorts of patients with EGFR-mutated advanced non–small cell lung cancer in whom targeted therapy and chemotherapy has failed.
The antitumor activity appears to be improved when both therapies are given in combination. The side effects generally are acceptable. It is these side effects, particularly the rate of VTEs, that Dr. Girard and his colleagues are interested in.
The researchers collated the data from the ongoing CHRYSALIS, CHRYSALIS-2, and LASER201 clinical trials, which assess the efficacy of these new agents as monotherapy or in combination. They initially investigated all reported thrombotic events and ruled out those that occurred during or after the 30 days before disease progression.
Increased thrombosis risk
The analysis included 560 patients who had been given amivantamab as monotherapy, 536 patients who had received amivantamab plus lazertinib in combination, and 252 who had taken lazertinib as monotherapy. The incidence of thromboembolic events was higher among patients who received amivantamab plus lazertinib in combination (21%) than in those who were given amivantamab (11%) or lazertinib (11%) as monotherapy.
The first thromboembolic event occurred an average of 84.5 days after starting treatment with amivantamab, 79 days after starting the combination therapy, and 170 days after starting treatment with lazertinib. For the amivantamab plus lazertinib combination, most VTEs developed in the first 4 months of treatment. The most common VTEs were pulmonary embolism and deep vein thrombosis.
The incidence of severe thrombotic events (grade ≥ 3), which was relatively low (amivantamab, 5%; amivantamab plus lazertinib, 6%; lazertinib, 6%) was similar regardless of the treatment, and there were no grade 5 thrombotic events among patients treated with the combination of both targeted therapies.
The significant risk factors for VTEs identified in this study were being age 60 years or older, having a score of 1 on the ECOG Performance Status Scale, and response to treatment (P < .05).
At a press conference organized by the Institut Curie before the ASCO conference, Dr. Girard said, “There has been shown to be an increased risk of blood clots with the use of this combination of targeted therapies. Preventive measures should therefore also be put forward, such as adding anticoagulant medication. This is an important study for the further development of these therapies.”
In a press release, the respiratory medicine specialist noted, “Institut Curie is particularly alert to the issue of the risk of thrombosis arising in cancer patients.” The DASTO project, dedicated to this issue and headed by the Institut Curie, “aims to cross-reference data sourced from several French cancer centers with data from the social security system to understand the risk factors, improve patient treatment, make changes to the care pathway, and prevent this unwanted occurrence from arising.”
Dr. Girard has direct links with Amgen, AstraZeneca, AbbVie, BMS, Daiichi Sankyo, Ipsen, Janssen, Roche, Lilly, Medtronic, MSD, Novartis, OSE Pharma, Pfizer, Sanofi, and Sivan.
This article was translated from the Medscape French Edition. A version of this article appeared on Medscape.com.
CHICAGO – Having cancer is a known risk factor for thrombosis. A patient with cancer has a fourfold risk of developing venous thromboembolism (VTE).
This risk may be increased by certain cancer drugs, which seems to be the case for the combination of innovative targeted therapies lazertinib-amivantamab, as shown in patients with advanced or metastatic non–small cell lung cancer.
A study of this increased risk of VTE was presented by Nicolas Girard, MD, a respiratory medicine specialist at Curie-Montsouris Chest Center in Paris, during the annual meeting of the American Society of Clinical Oncology.
Combination therapies
Amivantamab is an EGFR and cMET bispecific antibody, and lazertinib is a third-generation EGFR tyrosine kinase inhibitor. Prescribed after osimertinib or after osimertinib plus chemotherapy, this combination of amivantamab and lazertinib has been evaluated in several cohorts of patients with EGFR-mutated advanced non–small cell lung cancer in whom targeted therapy and chemotherapy has failed.
The antitumor activity appears to be improved when both therapies are given in combination. The side effects generally are acceptable. It is these side effects, particularly the rate of VTEs, that Dr. Girard and his colleagues are interested in.
The researchers collated the data from the ongoing CHRYSALIS, CHRYSALIS-2, and LASER201 clinical trials, which assess the efficacy of these new agents as monotherapy or in combination. They initially investigated all reported thrombotic events and ruled out those that occurred during or after the 30 days before disease progression.
Increased thrombosis risk
The analysis included 560 patients who had been given amivantamab as monotherapy, 536 patients who had received amivantamab plus lazertinib in combination, and 252 who had taken lazertinib as monotherapy. The incidence of thromboembolic events was higher among patients who received amivantamab plus lazertinib in combination (21%) than in those who were given amivantamab (11%) or lazertinib (11%) as monotherapy.
The first thromboembolic event occurred an average of 84.5 days after starting treatment with amivantamab, 79 days after starting the combination therapy, and 170 days after starting treatment with lazertinib. For the amivantamab plus lazertinib combination, most VTEs developed in the first 4 months of treatment. The most common VTEs were pulmonary embolism and deep vein thrombosis.
The incidence of severe thrombotic events (grade ≥ 3), which was relatively low (amivantamab, 5%; amivantamab plus lazertinib, 6%; lazertinib, 6%) was similar regardless of the treatment, and there were no grade 5 thrombotic events among patients treated with the combination of both targeted therapies.
The significant risk factors for VTEs identified in this study were being age 60 years or older, having a score of 1 on the ECOG Performance Status Scale, and response to treatment (P < .05).
At a press conference organized by the Institut Curie before the ASCO conference, Dr. Girard said, “There has been shown to be an increased risk of blood clots with the use of this combination of targeted therapies. Preventive measures should therefore also be put forward, such as adding anticoagulant medication. This is an important study for the further development of these therapies.”
In a press release, the respiratory medicine specialist noted, “Institut Curie is particularly alert to the issue of the risk of thrombosis arising in cancer patients.” The DASTO project, dedicated to this issue and headed by the Institut Curie, “aims to cross-reference data sourced from several French cancer centers with data from the social security system to understand the risk factors, improve patient treatment, make changes to the care pathway, and prevent this unwanted occurrence from arising.”
Dr. Girard has direct links with Amgen, AstraZeneca, AbbVie, BMS, Daiichi Sankyo, Ipsen, Janssen, Roche, Lilly, Medtronic, MSD, Novartis, OSE Pharma, Pfizer, Sanofi, and Sivan.
This article was translated from the Medscape French Edition. A version of this article appeared on Medscape.com.
CHICAGO – Having cancer is a known risk factor for thrombosis. A patient with cancer has a fourfold risk of developing venous thromboembolism (VTE).
This risk may be increased by certain cancer drugs, which seems to be the case for the combination of innovative targeted therapies lazertinib-amivantamab, as shown in patients with advanced or metastatic non–small cell lung cancer.
A study of this increased risk of VTE was presented by Nicolas Girard, MD, a respiratory medicine specialist at Curie-Montsouris Chest Center in Paris, during the annual meeting of the American Society of Clinical Oncology.
Combination therapies
Amivantamab is an EGFR and cMET bispecific antibody, and lazertinib is a third-generation EGFR tyrosine kinase inhibitor. Prescribed after osimertinib or after osimertinib plus chemotherapy, this combination of amivantamab and lazertinib has been evaluated in several cohorts of patients with EGFR-mutated advanced non–small cell lung cancer in whom targeted therapy and chemotherapy has failed.
The antitumor activity appears to be improved when both therapies are given in combination. The side effects generally are acceptable. It is these side effects, particularly the rate of VTEs, that Dr. Girard and his colleagues are interested in.
The researchers collated the data from the ongoing CHRYSALIS, CHRYSALIS-2, and LASER201 clinical trials, which assess the efficacy of these new agents as monotherapy or in combination. They initially investigated all reported thrombotic events and ruled out those that occurred during or after the 30 days before disease progression.
Increased thrombosis risk
The analysis included 560 patients who had been given amivantamab as monotherapy, 536 patients who had received amivantamab plus lazertinib in combination, and 252 who had taken lazertinib as monotherapy. The incidence of thromboembolic events was higher among patients who received amivantamab plus lazertinib in combination (21%) than in those who were given amivantamab (11%) or lazertinib (11%) as monotherapy.
The first thromboembolic event occurred an average of 84.5 days after starting treatment with amivantamab, 79 days after starting the combination therapy, and 170 days after starting treatment with lazertinib. For the amivantamab plus lazertinib combination, most VTEs developed in the first 4 months of treatment. The most common VTEs were pulmonary embolism and deep vein thrombosis.
The incidence of severe thrombotic events (grade ≥ 3), which was relatively low (amivantamab, 5%; amivantamab plus lazertinib, 6%; lazertinib, 6%) was similar regardless of the treatment, and there were no grade 5 thrombotic events among patients treated with the combination of both targeted therapies.
The significant risk factors for VTEs identified in this study were being age 60 years or older, having a score of 1 on the ECOG Performance Status Scale, and response to treatment (P < .05).
At a press conference organized by the Institut Curie before the ASCO conference, Dr. Girard said, “There has been shown to be an increased risk of blood clots with the use of this combination of targeted therapies. Preventive measures should therefore also be put forward, such as adding anticoagulant medication. This is an important study for the further development of these therapies.”
In a press release, the respiratory medicine specialist noted, “Institut Curie is particularly alert to the issue of the risk of thrombosis arising in cancer patients.” The DASTO project, dedicated to this issue and headed by the Institut Curie, “aims to cross-reference data sourced from several French cancer centers with data from the social security system to understand the risk factors, improve patient treatment, make changes to the care pathway, and prevent this unwanted occurrence from arising.”
Dr. Girard has direct links with Amgen, AstraZeneca, AbbVie, BMS, Daiichi Sankyo, Ipsen, Janssen, Roche, Lilly, Medtronic, MSD, Novartis, OSE Pharma, Pfizer, Sanofi, and Sivan.
This article was translated from the Medscape French Edition. A version of this article appeared on Medscape.com.
AT ASCO 2023
SGS showcases gyn surgeons’ impact on innovation, education, equity, and enterprise
The theme of the 49th Annual Scientific Meeting of the Society of Gynecologic Surgeons was Impact Factor—an allusion to scientific journal impact factor, as well as how we as gynecologic surgeons have a societal impact through our innovation, education, equity, and enterprise-level efforts. This theme and the diverse roster of speakers and presentations on contemporary and controversial issues impacting today’s gynecologic surgeons clearly resonated, breaking the prior registration record with more than 200 additional attendees than the previous year.
As always, the preconference postgraduate courses delivered relevant content that spanned the educational and surgical spectrum, including: “Innovations in training gynecologic surgeons”; “Urologic surgery for the gynecologic surgeon”; the social media workshop “Gynfluencing: Using social media to find your digital voice”; and “The sim factor: Making an impact in surgical education.” This also marked the first year of offering a specific SGS Fellows/Young Attendings’ course. The featured speaker of the SGS Equity Council was Patty Brisben, philanthropist, CEO, and founder of Pure Romance.
Dr. Beri Ridgeway, Cleveland Clinic Chief of Staff, delivered the Mark D. Walters Lecture, “Surgeon in the C-suite,” on leading approximately 5,000 physicians and the importance of surgeons and specifically ObGyns having a seat at the table. The TeLinde lecturer, Dr. Pam Moalli, Professor and Division Director for Urogynecology at the University of Pittsburgh Magee Womens Hospital, spoke on “Biomaterials for gynecologic surgeons: Toward bioinspired biomimetic devices.” The panel on the “Ergonomics of gynecologic surgery” was moderated by Dr. Amanda Fader and Dr. Kim Kho, who shared their experiences with work-related musculoskeletal injury, and featured esteemed panelists Dr. Noor Abu-Alnadi from UNC, Dr. Sue Hallbeck from Mayo Clinic, and Dr. Ladin Yurteri-Kaplan from Columbia University.
The conference also featured a new format of Ted Med Talks:
- Dr. Jason Wright, Editor-in-Chief, Obstetrics & Gynecology, and Division Director of Gynecologic Oncology at Columbia University, who spoke on “Surgical volume and outcomes for gynecologic surgery: Is more always better?”
- Dr. Kelly Wright, Division Director, Minimally Invasive Gynecologic Surgery, Cedars Sinai, on “Climate change starts at 7:15”
- Dr. Ebony Carter, Associate Editor, Equity, Obstetrics & Gynecology, and Division Director, Maternal Fetal Medicine, Washington University, on “Centering equity in reproductive health research.”
In this special section, several of these talks are presented. Additionally, Dr. Laura Homewood and her coauthors will discuss gender and racial biases in a large multi-institutional sample of more than 15,000 Press Ganey patient satisfaction surveys.
Dr. Cheryl Iglesia, SGS former president, and I hope that you will consider attending #SGS2024 in Orlando, Florida, led by Dr. Suzie As-Sanie, program chair, and Dr. Rosanne Kho, current SGS president, which promises to be another exciting meeting. ●
The theme of the 49th Annual Scientific Meeting of the Society of Gynecologic Surgeons was Impact Factor—an allusion to scientific journal impact factor, as well as how we as gynecologic surgeons have a societal impact through our innovation, education, equity, and enterprise-level efforts. This theme and the diverse roster of speakers and presentations on contemporary and controversial issues impacting today’s gynecologic surgeons clearly resonated, breaking the prior registration record with more than 200 additional attendees than the previous year.
As always, the preconference postgraduate courses delivered relevant content that spanned the educational and surgical spectrum, including: “Innovations in training gynecologic surgeons”; “Urologic surgery for the gynecologic surgeon”; the social media workshop “Gynfluencing: Using social media to find your digital voice”; and “The sim factor: Making an impact in surgical education.” This also marked the first year of offering a specific SGS Fellows/Young Attendings’ course. The featured speaker of the SGS Equity Council was Patty Brisben, philanthropist, CEO, and founder of Pure Romance.
Dr. Beri Ridgeway, Cleveland Clinic Chief of Staff, delivered the Mark D. Walters Lecture, “Surgeon in the C-suite,” on leading approximately 5,000 physicians and the importance of surgeons and specifically ObGyns having a seat at the table. The TeLinde lecturer, Dr. Pam Moalli, Professor and Division Director for Urogynecology at the University of Pittsburgh Magee Womens Hospital, spoke on “Biomaterials for gynecologic surgeons: Toward bioinspired biomimetic devices.” The panel on the “Ergonomics of gynecologic surgery” was moderated by Dr. Amanda Fader and Dr. Kim Kho, who shared their experiences with work-related musculoskeletal injury, and featured esteemed panelists Dr. Noor Abu-Alnadi from UNC, Dr. Sue Hallbeck from Mayo Clinic, and Dr. Ladin Yurteri-Kaplan from Columbia University.
The conference also featured a new format of Ted Med Talks:
- Dr. Jason Wright, Editor-in-Chief, Obstetrics & Gynecology, and Division Director of Gynecologic Oncology at Columbia University, who spoke on “Surgical volume and outcomes for gynecologic surgery: Is more always better?”
- Dr. Kelly Wright, Division Director, Minimally Invasive Gynecologic Surgery, Cedars Sinai, on “Climate change starts at 7:15”
- Dr. Ebony Carter, Associate Editor, Equity, Obstetrics & Gynecology, and Division Director, Maternal Fetal Medicine, Washington University, on “Centering equity in reproductive health research.”
In this special section, several of these talks are presented. Additionally, Dr. Laura Homewood and her coauthors will discuss gender and racial biases in a large multi-institutional sample of more than 15,000 Press Ganey patient satisfaction surveys.
Dr. Cheryl Iglesia, SGS former president, and I hope that you will consider attending #SGS2024 in Orlando, Florida, led by Dr. Suzie As-Sanie, program chair, and Dr. Rosanne Kho, current SGS president, which promises to be another exciting meeting. ●
The theme of the 49th Annual Scientific Meeting of the Society of Gynecologic Surgeons was Impact Factor—an allusion to scientific journal impact factor, as well as how we as gynecologic surgeons have a societal impact through our innovation, education, equity, and enterprise-level efforts. This theme and the diverse roster of speakers and presentations on contemporary and controversial issues impacting today’s gynecologic surgeons clearly resonated, breaking the prior registration record with more than 200 additional attendees than the previous year.
As always, the preconference postgraduate courses delivered relevant content that spanned the educational and surgical spectrum, including: “Innovations in training gynecologic surgeons”; “Urologic surgery for the gynecologic surgeon”; the social media workshop “Gynfluencing: Using social media to find your digital voice”; and “The sim factor: Making an impact in surgical education.” This also marked the first year of offering a specific SGS Fellows/Young Attendings’ course. The featured speaker of the SGS Equity Council was Patty Brisben, philanthropist, CEO, and founder of Pure Romance.
Dr. Beri Ridgeway, Cleveland Clinic Chief of Staff, delivered the Mark D. Walters Lecture, “Surgeon in the C-suite,” on leading approximately 5,000 physicians and the importance of surgeons and specifically ObGyns having a seat at the table. The TeLinde lecturer, Dr. Pam Moalli, Professor and Division Director for Urogynecology at the University of Pittsburgh Magee Womens Hospital, spoke on “Biomaterials for gynecologic surgeons: Toward bioinspired biomimetic devices.” The panel on the “Ergonomics of gynecologic surgery” was moderated by Dr. Amanda Fader and Dr. Kim Kho, who shared their experiences with work-related musculoskeletal injury, and featured esteemed panelists Dr. Noor Abu-Alnadi from UNC, Dr. Sue Hallbeck from Mayo Clinic, and Dr. Ladin Yurteri-Kaplan from Columbia University.
The conference also featured a new format of Ted Med Talks:
- Dr. Jason Wright, Editor-in-Chief, Obstetrics & Gynecology, and Division Director of Gynecologic Oncology at Columbia University, who spoke on “Surgical volume and outcomes for gynecologic surgery: Is more always better?”
- Dr. Kelly Wright, Division Director, Minimally Invasive Gynecologic Surgery, Cedars Sinai, on “Climate change starts at 7:15”
- Dr. Ebony Carter, Associate Editor, Equity, Obstetrics & Gynecology, and Division Director, Maternal Fetal Medicine, Washington University, on “Centering equity in reproductive health research.”
In this special section, several of these talks are presented. Additionally, Dr. Laura Homewood and her coauthors will discuss gender and racial biases in a large multi-institutional sample of more than 15,000 Press Ganey patient satisfaction surveys.
Dr. Cheryl Iglesia, SGS former president, and I hope that you will consider attending #SGS2024 in Orlando, Florida, led by Dr. Suzie As-Sanie, program chair, and Dr. Rosanne Kho, current SGS president, which promises to be another exciting meeting. ●
FDA OKs empagliflozin for children with type 2 diabetes
aged 10 years and older.
This approval represents only the second oral treatment option for children and adolescents with type 2 diabetes after metformin; the latter appears to be less effective for pediatric patients than for adults.
Injectable glucagonlike peptide–1 (GLP-1) agonists are also available for youth with type 2 diabetes. These include daily liraglutide (Victoza) and once-weekly extended-release exenatide (Bydureon/Bydureon BCise).
Jardiance has been approved for adults with type 2 diabetes since 2014, and Synjardy has been approved since 2015.
“Compared to adults, children with type 2 diabetes have limited treatment options, even though the disease and symptom onset generally progress more rapidly in children,” said Michelle Carey, MD, MPH.
“Today’s approvals provide much-needed additional treatment options for children with type 2 diabetes,” added Dr. Carey, associate director for therapeutic review for the division of diabetes, lipid disorders, and obesity in the FDA’s Center for Drug Evaluation and Research.
Type 2 diabetes rising exponentially in children, mainly non-Whites
Type 2 diabetes is rising exponentially in children and adolescents in the United States.
Data from the SEARCH for Diabetes in Youth study show that the incidence of type 2 diabetes among youth rose by about 5% per year between 2002 and 2015, and it continues to rise.
A more recent study found that a doubling of cases occurred during the pandemic, with youth often presenting with more severe disease. The majority of cases are among non-White racial groups.
Safety and efficacy data for empagliflozin for children came from the Diabetes Study of Linagliptin and Empagliflozin in Children and Adolescents (DINAMO) trial. That trial included 157 patients aged 10-17 years with A1c of 7% or above. Patients were randomly assigned to receive empagliflozin 10 mg or 25 mg daily, linagliptin (a DPP-4 inhibitor) 5 mg, or placebo for 26 weeks. Over 90% were also taking metformin, 40% in combination with insulin. All patients were given diet and exercise advice.
At week 26, the children treated with empagliflozin showed an average 0.2 percentage point decrease in A1c, compared with a 0.7-point increase among those taking placebo. Use of empagliflozin was also associated with lower fasting plasma glucose levels compared with placebo.
Side effects were similar to those seen in adults except for a higher risk of hypoglycemia, regardless of other glucose-lowering therapies that were being taken.
Reduction in A1c for participants treated with linagliptin was not statistically significant in comparison with placebo. There was a numerical reduction of 0.34% (P = .2935).
“Across the lifespan, we know that people living with type 2 diabetes have a high risk for many diabetes complications, so it’s important to recognize and treat diabetes early in its course,” Lori Laffel, MD, lead investigator of the DINAMO study, said in a press release from BI.
“These findings are particularly important given the need for more therapeutic options, especially oral agents, to manage type 2 diabetes in young people as, to date, metformin [has been] the only globally available oral treatment for youth,” added Dr. Laffel, chief of the pediatric, adolescent, and young adult section at the Joslin Diabetes Center and professor of pediatrics at Harvard Medical School, Boston.
A version of this article first appeared on Medscape.com.
aged 10 years and older.
This approval represents only the second oral treatment option for children and adolescents with type 2 diabetes after metformin; the latter appears to be less effective for pediatric patients than for adults.
Injectable glucagonlike peptide–1 (GLP-1) agonists are also available for youth with type 2 diabetes. These include daily liraglutide (Victoza) and once-weekly extended-release exenatide (Bydureon/Bydureon BCise).
Jardiance has been approved for adults with type 2 diabetes since 2014, and Synjardy has been approved since 2015.
“Compared to adults, children with type 2 diabetes have limited treatment options, even though the disease and symptom onset generally progress more rapidly in children,” said Michelle Carey, MD, MPH.
“Today’s approvals provide much-needed additional treatment options for children with type 2 diabetes,” added Dr. Carey, associate director for therapeutic review for the division of diabetes, lipid disorders, and obesity in the FDA’s Center for Drug Evaluation and Research.
Type 2 diabetes rising exponentially in children, mainly non-Whites
Type 2 diabetes is rising exponentially in children and adolescents in the United States.
Data from the SEARCH for Diabetes in Youth study show that the incidence of type 2 diabetes among youth rose by about 5% per year between 2002 and 2015, and it continues to rise.
A more recent study found that a doubling of cases occurred during the pandemic, with youth often presenting with more severe disease. The majority of cases are among non-White racial groups.
Safety and efficacy data for empagliflozin for children came from the Diabetes Study of Linagliptin and Empagliflozin in Children and Adolescents (DINAMO) trial. That trial included 157 patients aged 10-17 years with A1c of 7% or above. Patients were randomly assigned to receive empagliflozin 10 mg or 25 mg daily, linagliptin (a DPP-4 inhibitor) 5 mg, or placebo for 26 weeks. Over 90% were also taking metformin, 40% in combination with insulin. All patients were given diet and exercise advice.
At week 26, the children treated with empagliflozin showed an average 0.2 percentage point decrease in A1c, compared with a 0.7-point increase among those taking placebo. Use of empagliflozin was also associated with lower fasting plasma glucose levels compared with placebo.
Side effects were similar to those seen in adults except for a higher risk of hypoglycemia, regardless of other glucose-lowering therapies that were being taken.
Reduction in A1c for participants treated with linagliptin was not statistically significant in comparison with placebo. There was a numerical reduction of 0.34% (P = .2935).
“Across the lifespan, we know that people living with type 2 diabetes have a high risk for many diabetes complications, so it’s important to recognize and treat diabetes early in its course,” Lori Laffel, MD, lead investigator of the DINAMO study, said in a press release from BI.
“These findings are particularly important given the need for more therapeutic options, especially oral agents, to manage type 2 diabetes in young people as, to date, metformin [has been] the only globally available oral treatment for youth,” added Dr. Laffel, chief of the pediatric, adolescent, and young adult section at the Joslin Diabetes Center and professor of pediatrics at Harvard Medical School, Boston.
A version of this article first appeared on Medscape.com.
aged 10 years and older.
This approval represents only the second oral treatment option for children and adolescents with type 2 diabetes after metformin; the latter appears to be less effective for pediatric patients than for adults.
Injectable glucagonlike peptide–1 (GLP-1) agonists are also available for youth with type 2 diabetes. These include daily liraglutide (Victoza) and once-weekly extended-release exenatide (Bydureon/Bydureon BCise).
Jardiance has been approved for adults with type 2 diabetes since 2014, and Synjardy has been approved since 2015.
“Compared to adults, children with type 2 diabetes have limited treatment options, even though the disease and symptom onset generally progress more rapidly in children,” said Michelle Carey, MD, MPH.
“Today’s approvals provide much-needed additional treatment options for children with type 2 diabetes,” added Dr. Carey, associate director for therapeutic review for the division of diabetes, lipid disorders, and obesity in the FDA’s Center for Drug Evaluation and Research.
Type 2 diabetes rising exponentially in children, mainly non-Whites
Type 2 diabetes is rising exponentially in children and adolescents in the United States.
Data from the SEARCH for Diabetes in Youth study show that the incidence of type 2 diabetes among youth rose by about 5% per year between 2002 and 2015, and it continues to rise.
A more recent study found that a doubling of cases occurred during the pandemic, with youth often presenting with more severe disease. The majority of cases are among non-White racial groups.
Safety and efficacy data for empagliflozin for children came from the Diabetes Study of Linagliptin and Empagliflozin in Children and Adolescents (DINAMO) trial. That trial included 157 patients aged 10-17 years with A1c of 7% or above. Patients were randomly assigned to receive empagliflozin 10 mg or 25 mg daily, linagliptin (a DPP-4 inhibitor) 5 mg, or placebo for 26 weeks. Over 90% were also taking metformin, 40% in combination with insulin. All patients were given diet and exercise advice.
At week 26, the children treated with empagliflozin showed an average 0.2 percentage point decrease in A1c, compared with a 0.7-point increase among those taking placebo. Use of empagliflozin was also associated with lower fasting plasma glucose levels compared with placebo.
Side effects were similar to those seen in adults except for a higher risk of hypoglycemia, regardless of other glucose-lowering therapies that were being taken.
Reduction in A1c for participants treated with linagliptin was not statistically significant in comparison with placebo. There was a numerical reduction of 0.34% (P = .2935).
“Across the lifespan, we know that people living with type 2 diabetes have a high risk for many diabetes complications, so it’s important to recognize and treat diabetes early in its course,” Lori Laffel, MD, lead investigator of the DINAMO study, said in a press release from BI.
“These findings are particularly important given the need for more therapeutic options, especially oral agents, to manage type 2 diabetes in young people as, to date, metformin [has been] the only globally available oral treatment for youth,” added Dr. Laffel, chief of the pediatric, adolescent, and young adult section at the Joslin Diabetes Center and professor of pediatrics at Harvard Medical School, Boston.
A version of this article first appeared on Medscape.com.