User login
BEST PRACTICES IN:Treating Rosacea: Current Insights
Treating Rosacea: Current Insights
A supplement to Family Practice News. This supplement was funded by Galderma.

To view the supplement, click the image above.
•Topics
•Faculty/Faculty Disclosures
Topics
• Is it Rosacea?
• Managing Rosacea: Target Potential Triggers
• Treatment Options for Rosacea
• Newer Topical Formulations
• Surgical Therapies
• Summary
Faculty/Faculty Disclosures
Richard Odom, MD
Chair
Professor, Clinical Dermatology
University of California
San Francisco School of Medicine
San Francisco, California
Advisory committee for Johnson & Johnson.
Terry Arnold, MA, PA-C
Advanced Practice Consultants, LLC
Tulsa, Oklahoma
Speaker for Medicis; advisory board of Novartis, Warner-Chilcott; advisory board/speaker for Abbott Laboratories, Astellas, Collagenex; advisory board, speaker and consultant for Amgen, Coria Labs, Ranbaxy.
Stephen Brunton, MD
Adjunct Clinical Professor
Department of Family Medicine
University of North Carolina
Chapel Hill
Chapel Hill, North Carolina
Nothing to disclose.
Mary Knudtson, DNSc, NP
Professor, Family Medicine
Director of Family Nurse Practitioner Program
University of California, Irvine
Irvine, California
Speaker's bureau for Proctor & Gamble; consultant for sanofi aventis, Galderma.
John E. Wolf, Jr., MD, MA
Professor and Chairman
Department of Dermatology
Baylor College of Medicine
Houston, Texas
Consultant, speaker, and on the advisory board for Stiefel, PharmaDerm, Galderma, Medicis, Novartis, Warner-Chilcott, consultant for QLT and Peplin; speaker for Stiefel, sanofi-aventis (Dermik).
Copyright © 2008 Elsevier Inc.
A supplement to Family Practice News. This supplement was funded by Galderma.
To view the supplement, click the image above.
•Topics
•Faculty/Faculty Disclosures
Topics
• Is it Rosacea?
• Managing Rosacea: Target Potential Triggers
• Treatment Options for Rosacea
• Newer Topical Formulations
• Surgical Therapies
• Summary
Faculty/Faculty Disclosures
Richard Odom, MD
Chair
Professor, Clinical Dermatology
University of California
San Francisco School of Medicine
San Francisco, California
Advisory committee for Johnson & Johnson.
Terry Arnold, MA, PA-C
Advanced Practice Consultants, LLC
Tulsa, Oklahoma
Speaker for Medicis; advisory board of Novartis, Warner-Chilcott; advisory board/speaker for Abbott Laboratories, Astellas, Collagenex; advisory board, speaker and consultant for Amgen, Coria Labs, Ranbaxy.
Stephen Brunton, MD
Adjunct Clinical Professor
Department of Family Medicine
University of North Carolina
Chapel Hill
Chapel Hill, North Carolina
Nothing to disclose.
Mary Knudtson, DNSc, NP
Professor, Family Medicine
Director of Family Nurse Practitioner Program
University of California, Irvine
Irvine, California
Speaker's bureau for Proctor & Gamble; consultant for sanofi aventis, Galderma.
John E. Wolf, Jr., MD, MA
Professor and Chairman
Department of Dermatology
Baylor College of Medicine
Houston, Texas
Consultant, speaker, and on the advisory board for Stiefel, PharmaDerm, Galderma, Medicis, Novartis, Warner-Chilcott, consultant for QLT and Peplin; speaker for Stiefel, sanofi-aventis (Dermik).
Copyright © 2008 Elsevier Inc.
A supplement to Family Practice News. This supplement was funded by Galderma.
To view the supplement, click the image above.
•Topics
•Faculty/Faculty Disclosures
Topics
• Is it Rosacea?
• Managing Rosacea: Target Potential Triggers
• Treatment Options for Rosacea
• Newer Topical Formulations
• Surgical Therapies
• Summary
Faculty/Faculty Disclosures
Richard Odom, MD
Chair
Professor, Clinical Dermatology
University of California
San Francisco School of Medicine
San Francisco, California
Advisory committee for Johnson & Johnson.
Terry Arnold, MA, PA-C
Advanced Practice Consultants, LLC
Tulsa, Oklahoma
Speaker for Medicis; advisory board of Novartis, Warner-Chilcott; advisory board/speaker for Abbott Laboratories, Astellas, Collagenex; advisory board, speaker and consultant for Amgen, Coria Labs, Ranbaxy.
Stephen Brunton, MD
Adjunct Clinical Professor
Department of Family Medicine
University of North Carolina
Chapel Hill
Chapel Hill, North Carolina
Nothing to disclose.
Mary Knudtson, DNSc, NP
Professor, Family Medicine
Director of Family Nurse Practitioner Program
University of California, Irvine
Irvine, California
Speaker's bureau for Proctor & Gamble; consultant for sanofi aventis, Galderma.
John E. Wolf, Jr., MD, MA
Professor and Chairman
Department of Dermatology
Baylor College of Medicine
Houston, Texas
Consultant, speaker, and on the advisory board for Stiefel, PharmaDerm, Galderma, Medicis, Novartis, Warner-Chilcott, consultant for QLT and Peplin; speaker for Stiefel, sanofi-aventis (Dermik).
Copyright © 2008 Elsevier Inc.
Treating Rosacea: Current Insights
Treating Rosacea: Current Insights

Immediate-Release Therapy for Control of Nocturnal GERD
A supplement to Family Practice News supported by Supported by Santarus, Inc. The supplement is based on a faculty interview.

To view the supplement, click the image above.
A supplement to Family Practice News supported by Supported by Santarus, Inc. The supplement is based on a faculty interview.
To view the supplement, click the image above.
A supplement to Family Practice News supported by Supported by Santarus, Inc. The supplement is based on a faculty interview.
To view the supplement, click the image above.

Outcomes of Care by Hospitalists
The hospitalist care model as described by Drs Robert Wachter and Lee Goldman in 1996 has seen rapid growth in terms of the number of hospitalists and the number of hospitals served by hospitalists' groups in North America.16 Hospitalists were initially defined as physicians who spend a minimum of 25% to 50% of their time caring for inpatients.7 The Society of Hospital Medicine later identified hospitalists as physicians whose primary professional focus is the general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to hospital care.7, 8
Previous study results have consistently demonstrated that hospitalists may decrease overall cost and length of stay (LOS) for patients without compromising clinical outcomes.912
Like many countries around the world, tertiary hospitals in the Singapore health system grapple with the challenges of providing highly subspecialized care to patients who at the same time requires general medical care for multiple complex comorbidities. Unlike the United States, the shortage of generalists in Singapore's hospitals is partly historical, due to the fact that its health system was developed based on the British health system. Under this model of care, family doctors or general practitioners (GP) do not have a tradition of attending to their patients after they are admitted to the hospital. Care of patient is handed over to hospital specialist on admission. In the interest of improving patient care amidst increasing fragmentation of care due to subspecialization, Singapore General Hospital (SGH) developed a hospitalist care model that is adapted to the health system of Singapore.13 The hospital conducted an extensive study of the hospitalist care model which included study visits to the hospitalist programs at the Calgary Health Region in Canada and the University of California, San Francisco, CA, in the United States.14
The aim of this study was to assess the clinical outcomes of the adapted hospitalist program which uses family physicians as generalists in the hospital and compare this with the traditional model of using specialists to provide general medical care in the Singapore General Hospital. The care outcome indicators we used were hospital LOS, 30 day all‐cause readmissions, mortality, and cost of care.
Methods
Setting
SGH is the largest acute tertiary care hospital in Singapore. It has 29 clinical departments many of which are established as national referral centers. It has 1600‐beds in Singapore, serving approximately one‐fourth of its population of 4.59 million.15 It is affiliated with the Yong Loo Lin School of Medicine at the National University of Singapore (NUS) and the Duke‐NUS Graduate Medical School. Forty‐eight percent of the medical staff hold teaching appointments. It is also a major training hospital for residents, accounting for approximately 60% of the total amount of residency training in Singapore.
Intervention
In May 2006, a clinical family medicine department was established in the Singapore General Hospital with the intention of developing a local adaptation of the hospitalist care model.16 The important distinctive features of the adapted hospitalist model as compared to the model commonly found in North America include:
All attending physicians in the hospitalist teams are family physicians by training. The family medicine training program in Singapore resembles a hospital based residency program in the United States. It comprises a minimum of 2 years of structured training based in an acute hospital and 1 year in a primary care setting. The attending physicians in the hospitalist program spend a minimum of 25% of their time providing general medical care for hospitalized patients. The average time spent in inpatient care by the attending physicians was 33%(unpublished internal data). The rest of the time, they are rotated to run hospital‐based ambulatory care clinics, preoperative evaluation clinics, health assessment clinics and a home‐based intermediate care service. All the attending physicians hold teaching appointments and are involved in the teaching of medical students and residents.
Bringing family physicians into the hospital. In Singapore as it is in many health system modeled after the British system, internists work almost exclusively in the hospitals while primary care is almost exclusively provided for by family physicians who are referred to as GP. Primary physicians in Singapore do not have a tradition of managing their patients after admission to the hospital. The pace of specialization of medicine intensified after the mid‐1980s when all public hospitals in Singapore were restructured. The number of full‐time general internist dwindled dramatically and presently general medical care of patients in most hospitals in Singapore are provided for mainly by specialists.17 There had been criticism of the hospitalist care model in the United States for introducing care discontinuity between the hospital and the community.18, 19 Unlike the situation in the United States, the use of family physicians as hospitalist in Singapore is seen as a disruption of a different kind of tradition where there is a distinct divide between physicians who care for patients in the community and those who care for patients in the hospital setting.
Discharged patients with unresolved issues are followed up by the family medicine hospitalist at the ambulatory care clinics in the hospital. Patients are reviewed until they can be handed off to suitable health care providers in the community, to continue with their long term care outside the hospital. Specialist physicians of the hospital provide a similar system of follow‐up of discharged patients although they are more likely to be referred for review by different specialties according to the patients' comorbidities.
Traditionally, patients who are admitted to the Singapore General Hospital come under the care of single system specialists. Many of them are subspecialists who spend a large part of their time running specialist outpatient services and performing procedures and interventions related to their specialty. Approximately 66% of cases admitted from the emergency department to be cared for by the medical departments require specialty care and are admitted directly to the specialist departments. The rest of the patients (34%) are admitted under the category of internal medicine. The admitting physicians who work in Department of Emergency Medicine make these decisions independently. All physicians from the medical specialty departments go on a roster to provide general medical care for such patients usually with the help of specialist consultations. The reason for this form of usual care is again historically related to the fact that the Singapore health system was developed and modeled after the British system.
Patients admitted under the category of internal medicine were assigned hospital beds based on availability of beds for this category of admissions by the bed management unit of the hospital. A total of 34 beds out of 232 beds that are available for use under this category of admission are assigned to be cared for by the family medicine hospitalists in this program. The assignment is administrative and these beds are no different from other beds that accept patients admitted under the same admission category. The assignment of patients to the family medicine hospitalist or the specialist is therefore determined by the bed availability at the time of admission.
Data Source
Data of all hospitalized patients aged 18 years and above who were admitted into the Singapore General Hospital from January 1, 2008 to December 31, 2008 were collected from the hospital data warehouse at the Information Technology Department, SingHealth Group, Singapore. The collected data included demographic information such as ethnic group, gender, age, marital status, admission date, discharge date, intensive care unit (ICU) admission, disease codes under ICD‐9‐AM (International Statistical Classification of Diseases and Related Health Problems, 9th Revision, Australian Modification), and ICD‐9‐AM procedure codes. Data of patients who were readmitted to the hospital within 30‐days after the first discharge were also extracted. Available cost of care data including investigation, medication, treatment, and facility charges were also extracted based on hospital service codes. The protocol was approved by the Ethics Committee of the Singapore General Hospital with exemption from the requirement for informed consent.
Case Definition
Patients cared for by hospitalists were inpatients who were under the care of attending physicians from the Department of Family Medicine and Continuing Care using the adapted hospitalist care model. Patients cared for by nonhospitalists who were inpatients and who were cared for by all other attending specialist physicians from the other medical departments go on a roster to provide general medical care under the usual care model.
Surgical and medical conditions were determined based on the presence of ICD‐9‐AM diagnostic codes and procedure codes.20
Chronic comorbid conditions were identified by ICD‐9‐AM codes and were then studied using the Charlson Index.2123 The Charlson score was then classified into 4 previously defined grades known as the Charlson Comorbidity Index (CCI): 0 points (none), 1 to 2 points (low), 3 to 4 points (moderate), and 5 points (high).2123
Organ failure was defined by a combination of ICD‐9‐AM diagnosis and procedure codes, as outlined previously.24, 25
Statistical Analysis
Categorical variables were reported as percentages, continuous variables were reported as mean and standard deviation (SD). Hospital LOS and hospitalization cost of care were reported using geometric mean (GM) and 95% confidence interval (CI) because of their skewed distribution.
Hospital mortality rate was defined as the ratio of inpatient deaths to the total number of inpatients. Age was categorized into quintiles (18‐54, 55‐64, 65‐74, 75‐84, and >84 years) to capture the nonlinear effect of age on hospital service quality and resource utilization. Parameters were compared between patients cared for by hospitalists and nonhospitalists by chi‐square test for hospital mortality and readmission rate and by Mann‐Whitney U test for LOS and hospital cost. All hospital costs were converted to the year 2008 US dollars for presentation based on the Annual Average Rates of Exchange, Singapore (2008).26 Logistic regression was used to assess the association of hospital mortality and 30‐day all‐cause unscheduled readmission after adjusting for gender, ethnic group, ICU admission, CCI groups, number of organ failures, and the interaction among age groups, CCI groups, and numbers of organ failures. Analysis of hospital LOS and hospitalization costs were restricted to cases with values within 3 SD of the mean because of the extremely skewed nature of these data. Generalized linear model was used to assess log‐transformed LOS and cost with hospitalists care and adjusted for the above‐mentioned factors. The HosmerLemeshow chi‐square goodness‐of‐fit tests were used to exclude variables and identify clinically plausible interaction terms. Using the estimates from the regression models, we presented differences in adjusted LOS, hospitalization costs, hospital mortality, and 30‐day all‐cause unscheduled readmission between hospitalists and nonhospitalists. All P values were 2 sided. The level of statistical significance was considered to be the conventional alpha = 0.05. The data analysis was performed with SPSS 17.0 software (SPSS, Chicago, IL).
Results
A total of 3493 patients met the inclusion/exclusion criteria, in which 601 patients were under the care of hospitalists. The demographic and clinical characteristics of all patients are shown in Table 1. There were no differences in age (67.0 20.4 vs. 66.1 19.8 years, P= 0.311) and ethnic group (P= 0.253) between patients cared for by hospitalists and nonhospitalists. Patients cared for by hospitalists were less likely to be admitted to ICU (0.5% vs. 2.5%, P= 0.002) than patients cared for by nonhospitalists. There were similar CCI grades between patients cared for by hospitalists and nonhospitalists (P= 0.872). Patients cared for by hospitalists had similar numbers of organ failures as compared to patients cared for by nonhospitalists.
| Non Hospitalist, n = 2892 | Hospitalist, n = 601 | P* | |
|---|---|---|---|
| |||
| Age, year | 66.1 19.8 | 67.0 20.4 | 0.311 |
| Male sex, % | 49.2 | 44.4 | 0.033 |
| Ethnicity, % | 0.253 | ||
| Chinese | 79.2 | 76.9 | |
| Malay | 7.8 | 7.7 | |
| Indian | 9.8 | 12.5 | |
| Others | 3.3 | 3.0 | |
| ICU admission, % | 2.5 | 0.5 | 0.002 |
| Charlson Comorbidity Index, % | 0.872 | ||
| None | 43.5 | 42.3 | |
| Low | 35.5 | 36.6 | |
| Moderate | 14.0 | 14.6 | |
| High | 7.0 | 6.5 | |
| Organ failure No, % | 0.192 | ||
| 0 | 73.7 | 75.9 | |
| 1 | 21.6 | 20.5 | |
| 2 | 3.7 | 3.5 | |
| 3 | 1.0 | 0.2 | |
Unadjusted Clinical Outcomes and Resource Utilization
The in‐hospital mortality rates in patients cared for by hospitalists were similar (4.0% vs. 5.3%, P= 0.187) compared to patients cared for by nonhospitalists (Table 2). Also, there were no statistically significant differences in the 30‐day all‐cause unscheduled readmission rates between patients cared for by hospitalists and nonhospitalists (7.5% vs. 7.3%, p= 0.854). As for resource utilization, patients cared for by hospitalists had significantly shorter hospital LOS (GM, 4.6 vs. 5.7 days, P < 0.001) and lower cost (GM, $2301.0 vs. $2656.6, P= 0.001) compared with that in patients cared for by nonhospitalists (Table 2).
| Non hospitalist, n = 2892 | Hospitalist, n = 601 | Difference | P | |
|---|---|---|---|---|
| ||||
| Length of stay, day | ||||
| Un‐adjusted mean (95% CI) | 5.7 (5.4, 5.9) | 4.6 (4.2, 5.0) | 1.1 | <0.001 |
| Adjusted mean (95% CI) | 5.3 (5.3, 5.4) | 4.4 (4.3, 4.5) | 0.9 | <0.001 |
| Total hospitalization cost, $ | ||||
| Un‐adjusted mean (95% CI) | 2656.6 (2569.8, 2746.4) | 2301.0 (2125.2, 2460.1) | 335.6 | 0.001 |
| Adjusted mean (95% CI) | 2500.6 (2471.5, 2530.1) | 2250.7 (2195.9, 2306.8) | 250 | 0.003 |
| Unscheduled readmission, %* | ||||
| Un‐adjusted | 7.5 | 7.3 | 0.2 | 0.854 |
| Adjusted | 8.4 | 7.5 | 0.9 | 0.761 |
| Hospital mortality, %* | ||||
| Un‐adjusted | 5.3 | 4.0 | 1.3 | 0.187 |
| Adjusted | 5.3 | 4.2 | 1.1 | 0.307 |
Adjusted (Multivariate) Results of Hospital Clinical Outcomes and Resource Utilization
Multivariate analysis was used with adjustment for age groups, ethnic group, gender, ICU admission, numbers of organ failures, and CCI grades. Patients cared for by hospitalists, as compared with patients cared for by nonhospitalists, had a statistically significant shorter hospital LOS by 0.9 days (GM, 4.4 vs. 5.3 days, P < 0.001) and lower cost by $250 (GM, $2250.7 vs. $2500.0, P= 0.003), but similar in‐hospital mortality and 30‐day all‐cause readmission rates (both P > 0.05; Table 2). The goodness of fit of the regression model used for hospital LOS was assessed with the Hosmer‐Lemeshow test (2= 546.1, degree of freedom (df) = 3406, P= 0.160).
As for the detailed secondary cost, patients cared for by hospitalists had significantly lower treatment costs by $66 (GM, $462.9 vs. $528.1 P < 0.001) and facility costs by $127 (GM, $827.1 vs. $953.7 P < 0.001) compared with patients cared for by nonhospitalists after adjustment for age groups, ethnic group, gender, ICU admission, presence of organ failures, and CCI grades. The investigation and medication costs were comparable between the 2 groups (all P > 0.05) even after similar adjustments (Table 3).
| Non hospitalist, n = 2892 | Hospitalist, n = 601 | Difference | P | |
|---|---|---|---|---|
| ||||
| Investigation Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 828.3 (802.2, 855.3) | 772.3 (722.2, 825.8) | 24.7 | 0.196 |
| Adjusted mean (95% CI) | 776.5 (767.8, 785.2) | 759.0 (741.4, 776.9) | 17.5 | 0.673 |
| Medication Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 62.8 (58.7, 67.2) | 68.2 (59.6, 78.2) | 9.0 | 0.409 |
| Adjusted mean (95% CI) | 50.5 (49.1, 52.0) | 56.9 (53.5, 60.6) | 6.4 | 0.184 |
| Treatment Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 561.2 (542.3, 580.7) | 472.4 (442.1, 504.8) | 93.4 | <0.001 |
| Adjusted mean (95% CI) | 528.1 (522.1, 534.3) | 461.9 (450.8, 473.3) | 66.2 | <0.001 |
| Facility Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 1015.9 (978.8, 1054.4) | 847.6 (787.8, 912.0) | 178.5 | <0.001 |
| Adjusted mean (95% CI) | 953.7 (942.2, 965.4) | 827.1 (806.0, 848.9) | 126.6 | <0.001 |
| Total hospitalization cost, $ | ||||
| Un‐adjusted mean (95% CI) | 2656.6 (2569.8, 2746.4) | 2301.0 (2125.2, 2460.1) | 335.6 | 0.001 |
| Adjusted mean (95% CI) | 2500.6 (2471.5, 2530.1) | 2250.7 (2195.9, 2306.8) | 250 | 0.003 |
Discussion
We found that patients cared for by hospitalists had shorter hospital LOS (reduced by 0.9 days), and reduced cost (reduced by $250), compared with that of patients cared for by nonhospitalists. This occurred without any compromise of the clinical outcomes as measured by hospital mortality and 30‐day all‐cause unscheduled readmission. The mortality rates were 4.0%(hospitalist) and 5.3%(nonhospitalist). The difference was not statistically significant (P= 0.187). The differences in hospital LOS and cost still existed even after adjustment for age, gender, ethnic group, ICU admission, CCI, and the numbers of organ failure.
Our findings are consistent with previous reports of reduced hospital LOS and hospitalization costs in patients cared for by hospitalists in the United States.2730
Several explanations have been proposed for the favorable results. First, hospitalists' accessibility and holistic approach to the multiple problems of individual patients provide a more coordinated response to the patient's changing needs during the hospital stay. Second, studies had suggested that better coordination of care by hospitalist results in a lower use of resources and fewer specialist consultations.31 Reduced patients hospital LOS and cost may lead to an overall reduction in total revenue to the hospital, resulting in an advantage to the patients and a disadvantage to the hospital. However, this reduction in total revenue may have been partially offset by an increase in the number of patients receiving hospital care services.32 Third, fewer patients in the hospitalists group had an ICU stay and this could be another reason for an increased chance of earlier discharge from the hospital.33 The reduced LOS still existed even after adjustment for ICU admission and other factors. The total number of patients with ICU admissions was small in both groups and did not make a difference to the outcome measures used in our study. The use of ICU is significantly higher by the nonhospitalist group. It is unlikely that the difference was due to severity of illness on admission because the admitting physicians at the emergency department do not specify whether patients are to be managed by hospitalists or nonhospitalists. Assignment of the patient to the 2 groups was based only on the availability of bed at the time of admission. There is a possibility that the difference had occurred by chance due to the small number of patients requiring ICU admission. Discussion of end of life care issues and palliation as an option is known to result in lowered utilization of ICU.34 There is a possibility that hospitalists are more likely to engage the patient and family in end of life care discussions although this would require further studies to confirm. Finally, hospitalists might be more effective in navigating the complex environment of the hospital and might develop greater clinical expertise as a result of repeated experience in caring for patients in a similar setting.35 All these favorable factors were present in our adapted hospitalist care model.
While some studies of hospitalist care have shown reduced LOS without reduction of cost, our results showed significant reduction in the cost of care ($250, P= 0.001) for patient who are managed under the hospitalist program. The differences lie mainly in the cost of treatment and facilities. There were no significant differences in the cost of investigations and drugs.
There were several limitations in our study. Although hospital discharge data had numerous advantages including reliability and extensive use in various analyses in health services and health policy research,36 the dataset was administrative in nature and was not created specifically for our study. The hospital discharge data was also at risk of coding errors and omissions of important diagnoses and complications, which may affect the disease complexity estimates.37 In our study this was partly mitigated by the quality control processes instituted by the hospital and government agencies that use this data for planning and health care financing purposes. As all the data came from a single hospital, there was less risk of coding discrepancies and nonuniformity in calculating hospitalization costs. Our study was retrospective and observational in nature. Nevertheless we did use a number of statistical methods and analyses to minimize the risk of bias. Underlying differences in the patient populations of the 2 comparison groups led us to rely heavily on multivariate analysis and adjustment to minimize confounding factors. Nevertheless it is still possible that factors not included in administrative data might still exist as unmeasured confounders.28 In the period of study, we did not identify significant changes in the process of care for the patients apart from the introduction of the adapted hospitalist care model. This study was done in a single hospital. The hospital is an acute tertiary hospital. It is also a teaching hospital with affiliation to 2 medical schools (Duke‐NUS Graduate Medical School and Yong Loo Lin School of Medicine). The results might not be generalizable to other hospitals with different characteristics. Finally, this study was limited to information concerning in‐hospital deaths, and we did not have data that would have allowed us to detect differences in deaths that occurred after discharge. Similarly, we could only assess readmissions within our hospital. We do not know how frequently patients were admitted to other hospitals, a potential problem in all research of this type reported to date.30
In conclusion, our study showed that the hospitalist care model can be adapted to work in health systems outside North America with favorable outcomes. Our adapted hospitalist care model using family physicians as generalists in the hospital was associated with improvements in areas of LOS and cost reductions. There were no difference in mortality and readmissions. In health systems where hospital and primary care providers are historically divided, the deployment of family physicians as hospitalist may have the additional benefit of bridging the gap and support care continuity across the entire spectrum of care settings for patients.
Acknowledgements
The authors acknowledge Mr. Jeffrey Fong, Ms. Bessie Ang, Ms. LiSee Lou and Ms. Huicheng Tan of their contribution with the database preparation. We also thank all other staff of Family Medicine and Continuing Care and Epidemiology Unit, SGH for logistical support, and the patients who made the study possible.
- ,,,Hospitalists and the practice of inpatient medicine: results of a survey of the National Association of Inpatient Physicians.Ann Intern Med.1999;130(4 Pt 2):343–349.
- ,The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335(7):514–517.
- ,,,The status of hospital medicine groups in the United States.J Hosp Med.2006;1(2):75–80.
- ,,,. The rise of the hospitalist in California. Oakland: California Healthcare Foundation, July 2007. Available at: http://www.chcf.org/topics/hospitals/index.cfm?itemID=133365. Accessed June 2010.
- Society of Hospital Medicine. Hospital medicine specialty shows 20 percent growth 2007. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Press_Releases 2005. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=General_ Information111(8):627–632.
- ,,, et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137(11):866–874.
- ,,, et al.The positive impact of initiation of hospitalist clinician educators.J Gen Intern Med.2004;19(4):293–301.
- ,The hospitalist movement 5 years later.JAMA.2002;287(4):487–494.
- The hospitalist movement‐‐a complex adaptive response to fragmentation of care in hospitals.Ann Acad Med Singapore.2008;37(2):145–150.
- UCSF Today. Singapore Executives Learn About UCSF's Hospitalist Program. 2008. Available at: http://today.ucsf.edu/stories/singapore‐ executives‐learn‐about‐ucsfs‐hospitalist‐program/. Accessed June 2010.
- Statistics Singapore. 2007 Population (Mid‐Year Estimates). Singapore Department of Statistics,2007.
- Launch of Family Medicine Department.The College Mirror.2006;32:1–2‐.
- 1st college of physicians lecture: the role of internal medicine as a specialty in the era of subspecialisation.Ann Acad Med Singapore.2004;33(6):725–732.
- AAFP. AAFP Guidelines for Interaction in “Hospitalist” Models ‐ Communication Between the Receiving Inpatient Care Management Physician and the Referring Primary Care Physician. 2003, April Board 2009‐Reaffirmed. Available at: http://www.aafp.org/online/en/home/policy/ policies/h/hospitalists.html. Accessed June 2010.
- ,,,Continuity of care and intensive care unit use at the end of life.Arch Intern Med.2009;169(1):81–86.
- ,,,,,Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med.2001;29(7):1303–1310.
- ,,,A new method of classifying prognostic comorbidity in longitudinal studies: development and validation.J Chronic Dis.1987;40(5):373–383.
- ,,Adapting a clinical comorbidity index for use with ICD‐9‐CM administrative databases.J Clin Epidemiol.1992;45(6):613–619.
- ,,,Validation of a combined comorbidity index.J Clin Epidemiol.1994;47(11):1245–1251.
- ,,,,The effect of comorbidity and age on hospital mortality and length of stay in patients with sepsis.J Crit Care.2009.
- ,,,The epidemiology of sepsis in the United States from 1979 through 2000.N Engl J Med.2003;348(16):1546–1554.
- Inland Revenue Authority of Singapore. Annual Average Rates of Exchange 2008. Available at:http://www.iras.gov.sg/irasHome/page.aspx? id=806. Accessed June 2010.
- ,,,A comparison of two hospitalist models with traditional care in a community teaching hospital.Am J Med.2005;118(5):536–543.
- ,,,,,Outcomes of care by hospitalists, general internists, and family physicians.N Engl J Med.2007;357(25):2589–2600.
- ,Comparison of a family practice teaching service and a hospitalist model: costs, charges, length of stay, and mortality.Fam Med.2001;33(7):511–515.
- ,,Comparison of hospital costs and length of stay for community internists, hospitalists, and academicians.J Gen Intern Med.2007;22(5):662–667.
- ,,Hospital economics of the hospitalist.Health Serv Res.2003;38(3):905–918; discussion 919‐922.
- ,,, et al.Impact of a hospitalist system on length of stay and cost for children with common conditions.Pediatrics.2007;120(2):267–274.
- ,,3rd, et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med.2005;165(7):796–801‐.
- ,Admission to intensive care unit at the end‐of‐life: is it an informed decision?Palliat Med.2004;18(8):705–711.
- ,,Is volume related to outcome in health care? A systematic review and methodologic critique of the literature.Ann Intern Med.2002;137(6):511–520.
- ,,,,The Value of Hospital Discharge Databases: Final Report. NORC at the University of Chicago, The National Association of Health Data Organizations.2005. Available at: http://www.hcup‐us.ahrq.gov/reports/final_report.pdf. Accessed June 2010.
- ,,Diagnosis‐dependent misclassification of infections using administrative data variably affected incidence and mortality estimates in ICU patients.J Clin Epidemiol.2007;60(2):155–162.
The hospitalist care model as described by Drs Robert Wachter and Lee Goldman in 1996 has seen rapid growth in terms of the number of hospitalists and the number of hospitals served by hospitalists' groups in North America.16 Hospitalists were initially defined as physicians who spend a minimum of 25% to 50% of their time caring for inpatients.7 The Society of Hospital Medicine later identified hospitalists as physicians whose primary professional focus is the general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to hospital care.7, 8
Previous study results have consistently demonstrated that hospitalists may decrease overall cost and length of stay (LOS) for patients without compromising clinical outcomes.912
Like many countries around the world, tertiary hospitals in the Singapore health system grapple with the challenges of providing highly subspecialized care to patients who at the same time requires general medical care for multiple complex comorbidities. Unlike the United States, the shortage of generalists in Singapore's hospitals is partly historical, due to the fact that its health system was developed based on the British health system. Under this model of care, family doctors or general practitioners (GP) do not have a tradition of attending to their patients after they are admitted to the hospital. Care of patient is handed over to hospital specialist on admission. In the interest of improving patient care amidst increasing fragmentation of care due to subspecialization, Singapore General Hospital (SGH) developed a hospitalist care model that is adapted to the health system of Singapore.13 The hospital conducted an extensive study of the hospitalist care model which included study visits to the hospitalist programs at the Calgary Health Region in Canada and the University of California, San Francisco, CA, in the United States.14
The aim of this study was to assess the clinical outcomes of the adapted hospitalist program which uses family physicians as generalists in the hospital and compare this with the traditional model of using specialists to provide general medical care in the Singapore General Hospital. The care outcome indicators we used were hospital LOS, 30 day all‐cause readmissions, mortality, and cost of care.
Methods
Setting
SGH is the largest acute tertiary care hospital in Singapore. It has 29 clinical departments many of which are established as national referral centers. It has 1600‐beds in Singapore, serving approximately one‐fourth of its population of 4.59 million.15 It is affiliated with the Yong Loo Lin School of Medicine at the National University of Singapore (NUS) and the Duke‐NUS Graduate Medical School. Forty‐eight percent of the medical staff hold teaching appointments. It is also a major training hospital for residents, accounting for approximately 60% of the total amount of residency training in Singapore.
Intervention
In May 2006, a clinical family medicine department was established in the Singapore General Hospital with the intention of developing a local adaptation of the hospitalist care model.16 The important distinctive features of the adapted hospitalist model as compared to the model commonly found in North America include:
All attending physicians in the hospitalist teams are family physicians by training. The family medicine training program in Singapore resembles a hospital based residency program in the United States. It comprises a minimum of 2 years of structured training based in an acute hospital and 1 year in a primary care setting. The attending physicians in the hospitalist program spend a minimum of 25% of their time providing general medical care for hospitalized patients. The average time spent in inpatient care by the attending physicians was 33%(unpublished internal data). The rest of the time, they are rotated to run hospital‐based ambulatory care clinics, preoperative evaluation clinics, health assessment clinics and a home‐based intermediate care service. All the attending physicians hold teaching appointments and are involved in the teaching of medical students and residents.
Bringing family physicians into the hospital. In Singapore as it is in many health system modeled after the British system, internists work almost exclusively in the hospitals while primary care is almost exclusively provided for by family physicians who are referred to as GP. Primary physicians in Singapore do not have a tradition of managing their patients after admission to the hospital. The pace of specialization of medicine intensified after the mid‐1980s when all public hospitals in Singapore were restructured. The number of full‐time general internist dwindled dramatically and presently general medical care of patients in most hospitals in Singapore are provided for mainly by specialists.17 There had been criticism of the hospitalist care model in the United States for introducing care discontinuity between the hospital and the community.18, 19 Unlike the situation in the United States, the use of family physicians as hospitalist in Singapore is seen as a disruption of a different kind of tradition where there is a distinct divide between physicians who care for patients in the community and those who care for patients in the hospital setting.
Discharged patients with unresolved issues are followed up by the family medicine hospitalist at the ambulatory care clinics in the hospital. Patients are reviewed until they can be handed off to suitable health care providers in the community, to continue with their long term care outside the hospital. Specialist physicians of the hospital provide a similar system of follow‐up of discharged patients although they are more likely to be referred for review by different specialties according to the patients' comorbidities.
Traditionally, patients who are admitted to the Singapore General Hospital come under the care of single system specialists. Many of them are subspecialists who spend a large part of their time running specialist outpatient services and performing procedures and interventions related to their specialty. Approximately 66% of cases admitted from the emergency department to be cared for by the medical departments require specialty care and are admitted directly to the specialist departments. The rest of the patients (34%) are admitted under the category of internal medicine. The admitting physicians who work in Department of Emergency Medicine make these decisions independently. All physicians from the medical specialty departments go on a roster to provide general medical care for such patients usually with the help of specialist consultations. The reason for this form of usual care is again historically related to the fact that the Singapore health system was developed and modeled after the British system.
Patients admitted under the category of internal medicine were assigned hospital beds based on availability of beds for this category of admissions by the bed management unit of the hospital. A total of 34 beds out of 232 beds that are available for use under this category of admission are assigned to be cared for by the family medicine hospitalists in this program. The assignment is administrative and these beds are no different from other beds that accept patients admitted under the same admission category. The assignment of patients to the family medicine hospitalist or the specialist is therefore determined by the bed availability at the time of admission.
Data Source
Data of all hospitalized patients aged 18 years and above who were admitted into the Singapore General Hospital from January 1, 2008 to December 31, 2008 were collected from the hospital data warehouse at the Information Technology Department, SingHealth Group, Singapore. The collected data included demographic information such as ethnic group, gender, age, marital status, admission date, discharge date, intensive care unit (ICU) admission, disease codes under ICD‐9‐AM (International Statistical Classification of Diseases and Related Health Problems, 9th Revision, Australian Modification), and ICD‐9‐AM procedure codes. Data of patients who were readmitted to the hospital within 30‐days after the first discharge were also extracted. Available cost of care data including investigation, medication, treatment, and facility charges were also extracted based on hospital service codes. The protocol was approved by the Ethics Committee of the Singapore General Hospital with exemption from the requirement for informed consent.
Case Definition
Patients cared for by hospitalists were inpatients who were under the care of attending physicians from the Department of Family Medicine and Continuing Care using the adapted hospitalist care model. Patients cared for by nonhospitalists who were inpatients and who were cared for by all other attending specialist physicians from the other medical departments go on a roster to provide general medical care under the usual care model.
Surgical and medical conditions were determined based on the presence of ICD‐9‐AM diagnostic codes and procedure codes.20
Chronic comorbid conditions were identified by ICD‐9‐AM codes and were then studied using the Charlson Index.2123 The Charlson score was then classified into 4 previously defined grades known as the Charlson Comorbidity Index (CCI): 0 points (none), 1 to 2 points (low), 3 to 4 points (moderate), and 5 points (high).2123
Organ failure was defined by a combination of ICD‐9‐AM diagnosis and procedure codes, as outlined previously.24, 25
Statistical Analysis
Categorical variables were reported as percentages, continuous variables were reported as mean and standard deviation (SD). Hospital LOS and hospitalization cost of care were reported using geometric mean (GM) and 95% confidence interval (CI) because of their skewed distribution.
Hospital mortality rate was defined as the ratio of inpatient deaths to the total number of inpatients. Age was categorized into quintiles (18‐54, 55‐64, 65‐74, 75‐84, and >84 years) to capture the nonlinear effect of age on hospital service quality and resource utilization. Parameters were compared between patients cared for by hospitalists and nonhospitalists by chi‐square test for hospital mortality and readmission rate and by Mann‐Whitney U test for LOS and hospital cost. All hospital costs were converted to the year 2008 US dollars for presentation based on the Annual Average Rates of Exchange, Singapore (2008).26 Logistic regression was used to assess the association of hospital mortality and 30‐day all‐cause unscheduled readmission after adjusting for gender, ethnic group, ICU admission, CCI groups, number of organ failures, and the interaction among age groups, CCI groups, and numbers of organ failures. Analysis of hospital LOS and hospitalization costs were restricted to cases with values within 3 SD of the mean because of the extremely skewed nature of these data. Generalized linear model was used to assess log‐transformed LOS and cost with hospitalists care and adjusted for the above‐mentioned factors. The HosmerLemeshow chi‐square goodness‐of‐fit tests were used to exclude variables and identify clinically plausible interaction terms. Using the estimates from the regression models, we presented differences in adjusted LOS, hospitalization costs, hospital mortality, and 30‐day all‐cause unscheduled readmission between hospitalists and nonhospitalists. All P values were 2 sided. The level of statistical significance was considered to be the conventional alpha = 0.05. The data analysis was performed with SPSS 17.0 software (SPSS, Chicago, IL).
Results
A total of 3493 patients met the inclusion/exclusion criteria, in which 601 patients were under the care of hospitalists. The demographic and clinical characteristics of all patients are shown in Table 1. There were no differences in age (67.0 20.4 vs. 66.1 19.8 years, P= 0.311) and ethnic group (P= 0.253) between patients cared for by hospitalists and nonhospitalists. Patients cared for by hospitalists were less likely to be admitted to ICU (0.5% vs. 2.5%, P= 0.002) than patients cared for by nonhospitalists. There were similar CCI grades between patients cared for by hospitalists and nonhospitalists (P= 0.872). Patients cared for by hospitalists had similar numbers of organ failures as compared to patients cared for by nonhospitalists.
| Non Hospitalist, n = 2892 | Hospitalist, n = 601 | P* | |
|---|---|---|---|
| |||
| Age, year | 66.1 19.8 | 67.0 20.4 | 0.311 |
| Male sex, % | 49.2 | 44.4 | 0.033 |
| Ethnicity, % | 0.253 | ||
| Chinese | 79.2 | 76.9 | |
| Malay | 7.8 | 7.7 | |
| Indian | 9.8 | 12.5 | |
| Others | 3.3 | 3.0 | |
| ICU admission, % | 2.5 | 0.5 | 0.002 |
| Charlson Comorbidity Index, % | 0.872 | ||
| None | 43.5 | 42.3 | |
| Low | 35.5 | 36.6 | |
| Moderate | 14.0 | 14.6 | |
| High | 7.0 | 6.5 | |
| Organ failure No, % | 0.192 | ||
| 0 | 73.7 | 75.9 | |
| 1 | 21.6 | 20.5 | |
| 2 | 3.7 | 3.5 | |
| 3 | 1.0 | 0.2 | |
Unadjusted Clinical Outcomes and Resource Utilization
The in‐hospital mortality rates in patients cared for by hospitalists were similar (4.0% vs. 5.3%, P= 0.187) compared to patients cared for by nonhospitalists (Table 2). Also, there were no statistically significant differences in the 30‐day all‐cause unscheduled readmission rates between patients cared for by hospitalists and nonhospitalists (7.5% vs. 7.3%, p= 0.854). As for resource utilization, patients cared for by hospitalists had significantly shorter hospital LOS (GM, 4.6 vs. 5.7 days, P < 0.001) and lower cost (GM, $2301.0 vs. $2656.6, P= 0.001) compared with that in patients cared for by nonhospitalists (Table 2).
| Non hospitalist, n = 2892 | Hospitalist, n = 601 | Difference | P | |
|---|---|---|---|---|
| ||||
| Length of stay, day | ||||
| Un‐adjusted mean (95% CI) | 5.7 (5.4, 5.9) | 4.6 (4.2, 5.0) | 1.1 | <0.001 |
| Adjusted mean (95% CI) | 5.3 (5.3, 5.4) | 4.4 (4.3, 4.5) | 0.9 | <0.001 |
| Total hospitalization cost, $ | ||||
| Un‐adjusted mean (95% CI) | 2656.6 (2569.8, 2746.4) | 2301.0 (2125.2, 2460.1) | 335.6 | 0.001 |
| Adjusted mean (95% CI) | 2500.6 (2471.5, 2530.1) | 2250.7 (2195.9, 2306.8) | 250 | 0.003 |
| Unscheduled readmission, %* | ||||
| Un‐adjusted | 7.5 | 7.3 | 0.2 | 0.854 |
| Adjusted | 8.4 | 7.5 | 0.9 | 0.761 |
| Hospital mortality, %* | ||||
| Un‐adjusted | 5.3 | 4.0 | 1.3 | 0.187 |
| Adjusted | 5.3 | 4.2 | 1.1 | 0.307 |
Adjusted (Multivariate) Results of Hospital Clinical Outcomes and Resource Utilization
Multivariate analysis was used with adjustment for age groups, ethnic group, gender, ICU admission, numbers of organ failures, and CCI grades. Patients cared for by hospitalists, as compared with patients cared for by nonhospitalists, had a statistically significant shorter hospital LOS by 0.9 days (GM, 4.4 vs. 5.3 days, P < 0.001) and lower cost by $250 (GM, $2250.7 vs. $2500.0, P= 0.003), but similar in‐hospital mortality and 30‐day all‐cause readmission rates (both P > 0.05; Table 2). The goodness of fit of the regression model used for hospital LOS was assessed with the Hosmer‐Lemeshow test (2= 546.1, degree of freedom (df) = 3406, P= 0.160).
As for the detailed secondary cost, patients cared for by hospitalists had significantly lower treatment costs by $66 (GM, $462.9 vs. $528.1 P < 0.001) and facility costs by $127 (GM, $827.1 vs. $953.7 P < 0.001) compared with patients cared for by nonhospitalists after adjustment for age groups, ethnic group, gender, ICU admission, presence of organ failures, and CCI grades. The investigation and medication costs were comparable between the 2 groups (all P > 0.05) even after similar adjustments (Table 3).
| Non hospitalist, n = 2892 | Hospitalist, n = 601 | Difference | P | |
|---|---|---|---|---|
| ||||
| Investigation Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 828.3 (802.2, 855.3) | 772.3 (722.2, 825.8) | 24.7 | 0.196 |
| Adjusted mean (95% CI) | 776.5 (767.8, 785.2) | 759.0 (741.4, 776.9) | 17.5 | 0.673 |
| Medication Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 62.8 (58.7, 67.2) | 68.2 (59.6, 78.2) | 9.0 | 0.409 |
| Adjusted mean (95% CI) | 50.5 (49.1, 52.0) | 56.9 (53.5, 60.6) | 6.4 | 0.184 |
| Treatment Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 561.2 (542.3, 580.7) | 472.4 (442.1, 504.8) | 93.4 | <0.001 |
| Adjusted mean (95% CI) | 528.1 (522.1, 534.3) | 461.9 (450.8, 473.3) | 66.2 | <0.001 |
| Facility Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 1015.9 (978.8, 1054.4) | 847.6 (787.8, 912.0) | 178.5 | <0.001 |
| Adjusted mean (95% CI) | 953.7 (942.2, 965.4) | 827.1 (806.0, 848.9) | 126.6 | <0.001 |
| Total hospitalization cost, $ | ||||
| Un‐adjusted mean (95% CI) | 2656.6 (2569.8, 2746.4) | 2301.0 (2125.2, 2460.1) | 335.6 | 0.001 |
| Adjusted mean (95% CI) | 2500.6 (2471.5, 2530.1) | 2250.7 (2195.9, 2306.8) | 250 | 0.003 |
Discussion
We found that patients cared for by hospitalists had shorter hospital LOS (reduced by 0.9 days), and reduced cost (reduced by $250), compared with that of patients cared for by nonhospitalists. This occurred without any compromise of the clinical outcomes as measured by hospital mortality and 30‐day all‐cause unscheduled readmission. The mortality rates were 4.0%(hospitalist) and 5.3%(nonhospitalist). The difference was not statistically significant (P= 0.187). The differences in hospital LOS and cost still existed even after adjustment for age, gender, ethnic group, ICU admission, CCI, and the numbers of organ failure.
Our findings are consistent with previous reports of reduced hospital LOS and hospitalization costs in patients cared for by hospitalists in the United States.2730
Several explanations have been proposed for the favorable results. First, hospitalists' accessibility and holistic approach to the multiple problems of individual patients provide a more coordinated response to the patient's changing needs during the hospital stay. Second, studies had suggested that better coordination of care by hospitalist results in a lower use of resources and fewer specialist consultations.31 Reduced patients hospital LOS and cost may lead to an overall reduction in total revenue to the hospital, resulting in an advantage to the patients and a disadvantage to the hospital. However, this reduction in total revenue may have been partially offset by an increase in the number of patients receiving hospital care services.32 Third, fewer patients in the hospitalists group had an ICU stay and this could be another reason for an increased chance of earlier discharge from the hospital.33 The reduced LOS still existed even after adjustment for ICU admission and other factors. The total number of patients with ICU admissions was small in both groups and did not make a difference to the outcome measures used in our study. The use of ICU is significantly higher by the nonhospitalist group. It is unlikely that the difference was due to severity of illness on admission because the admitting physicians at the emergency department do not specify whether patients are to be managed by hospitalists or nonhospitalists. Assignment of the patient to the 2 groups was based only on the availability of bed at the time of admission. There is a possibility that the difference had occurred by chance due to the small number of patients requiring ICU admission. Discussion of end of life care issues and palliation as an option is known to result in lowered utilization of ICU.34 There is a possibility that hospitalists are more likely to engage the patient and family in end of life care discussions although this would require further studies to confirm. Finally, hospitalists might be more effective in navigating the complex environment of the hospital and might develop greater clinical expertise as a result of repeated experience in caring for patients in a similar setting.35 All these favorable factors were present in our adapted hospitalist care model.
While some studies of hospitalist care have shown reduced LOS without reduction of cost, our results showed significant reduction in the cost of care ($250, P= 0.001) for patient who are managed under the hospitalist program. The differences lie mainly in the cost of treatment and facilities. There were no significant differences in the cost of investigations and drugs.
There were several limitations in our study. Although hospital discharge data had numerous advantages including reliability and extensive use in various analyses in health services and health policy research,36 the dataset was administrative in nature and was not created specifically for our study. The hospital discharge data was also at risk of coding errors and omissions of important diagnoses and complications, which may affect the disease complexity estimates.37 In our study this was partly mitigated by the quality control processes instituted by the hospital and government agencies that use this data for planning and health care financing purposes. As all the data came from a single hospital, there was less risk of coding discrepancies and nonuniformity in calculating hospitalization costs. Our study was retrospective and observational in nature. Nevertheless we did use a number of statistical methods and analyses to minimize the risk of bias. Underlying differences in the patient populations of the 2 comparison groups led us to rely heavily on multivariate analysis and adjustment to minimize confounding factors. Nevertheless it is still possible that factors not included in administrative data might still exist as unmeasured confounders.28 In the period of study, we did not identify significant changes in the process of care for the patients apart from the introduction of the adapted hospitalist care model. This study was done in a single hospital. The hospital is an acute tertiary hospital. It is also a teaching hospital with affiliation to 2 medical schools (Duke‐NUS Graduate Medical School and Yong Loo Lin School of Medicine). The results might not be generalizable to other hospitals with different characteristics. Finally, this study was limited to information concerning in‐hospital deaths, and we did not have data that would have allowed us to detect differences in deaths that occurred after discharge. Similarly, we could only assess readmissions within our hospital. We do not know how frequently patients were admitted to other hospitals, a potential problem in all research of this type reported to date.30
In conclusion, our study showed that the hospitalist care model can be adapted to work in health systems outside North America with favorable outcomes. Our adapted hospitalist care model using family physicians as generalists in the hospital was associated with improvements in areas of LOS and cost reductions. There were no difference in mortality and readmissions. In health systems where hospital and primary care providers are historically divided, the deployment of family physicians as hospitalist may have the additional benefit of bridging the gap and support care continuity across the entire spectrum of care settings for patients.
Acknowledgements
The authors acknowledge Mr. Jeffrey Fong, Ms. Bessie Ang, Ms. LiSee Lou and Ms. Huicheng Tan of their contribution with the database preparation. We also thank all other staff of Family Medicine and Continuing Care and Epidemiology Unit, SGH for logistical support, and the patients who made the study possible.
The hospitalist care model as described by Drs Robert Wachter and Lee Goldman in 1996 has seen rapid growth in terms of the number of hospitalists and the number of hospitals served by hospitalists' groups in North America.16 Hospitalists were initially defined as physicians who spend a minimum of 25% to 50% of their time caring for inpatients.7 The Society of Hospital Medicine later identified hospitalists as physicians whose primary professional focus is the general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to hospital care.7, 8
Previous study results have consistently demonstrated that hospitalists may decrease overall cost and length of stay (LOS) for patients without compromising clinical outcomes.912
Like many countries around the world, tertiary hospitals in the Singapore health system grapple with the challenges of providing highly subspecialized care to patients who at the same time requires general medical care for multiple complex comorbidities. Unlike the United States, the shortage of generalists in Singapore's hospitals is partly historical, due to the fact that its health system was developed based on the British health system. Under this model of care, family doctors or general practitioners (GP) do not have a tradition of attending to their patients after they are admitted to the hospital. Care of patient is handed over to hospital specialist on admission. In the interest of improving patient care amidst increasing fragmentation of care due to subspecialization, Singapore General Hospital (SGH) developed a hospitalist care model that is adapted to the health system of Singapore.13 The hospital conducted an extensive study of the hospitalist care model which included study visits to the hospitalist programs at the Calgary Health Region in Canada and the University of California, San Francisco, CA, in the United States.14
The aim of this study was to assess the clinical outcomes of the adapted hospitalist program which uses family physicians as generalists in the hospital and compare this with the traditional model of using specialists to provide general medical care in the Singapore General Hospital. The care outcome indicators we used were hospital LOS, 30 day all‐cause readmissions, mortality, and cost of care.
Methods
Setting
SGH is the largest acute tertiary care hospital in Singapore. It has 29 clinical departments many of which are established as national referral centers. It has 1600‐beds in Singapore, serving approximately one‐fourth of its population of 4.59 million.15 It is affiliated with the Yong Loo Lin School of Medicine at the National University of Singapore (NUS) and the Duke‐NUS Graduate Medical School. Forty‐eight percent of the medical staff hold teaching appointments. It is also a major training hospital for residents, accounting for approximately 60% of the total amount of residency training in Singapore.
Intervention
In May 2006, a clinical family medicine department was established in the Singapore General Hospital with the intention of developing a local adaptation of the hospitalist care model.16 The important distinctive features of the adapted hospitalist model as compared to the model commonly found in North America include:
All attending physicians in the hospitalist teams are family physicians by training. The family medicine training program in Singapore resembles a hospital based residency program in the United States. It comprises a minimum of 2 years of structured training based in an acute hospital and 1 year in a primary care setting. The attending physicians in the hospitalist program spend a minimum of 25% of their time providing general medical care for hospitalized patients. The average time spent in inpatient care by the attending physicians was 33%(unpublished internal data). The rest of the time, they are rotated to run hospital‐based ambulatory care clinics, preoperative evaluation clinics, health assessment clinics and a home‐based intermediate care service. All the attending physicians hold teaching appointments and are involved in the teaching of medical students and residents.
Bringing family physicians into the hospital. In Singapore as it is in many health system modeled after the British system, internists work almost exclusively in the hospitals while primary care is almost exclusively provided for by family physicians who are referred to as GP. Primary physicians in Singapore do not have a tradition of managing their patients after admission to the hospital. The pace of specialization of medicine intensified after the mid‐1980s when all public hospitals in Singapore were restructured. The number of full‐time general internist dwindled dramatically and presently general medical care of patients in most hospitals in Singapore are provided for mainly by specialists.17 There had been criticism of the hospitalist care model in the United States for introducing care discontinuity between the hospital and the community.18, 19 Unlike the situation in the United States, the use of family physicians as hospitalist in Singapore is seen as a disruption of a different kind of tradition where there is a distinct divide between physicians who care for patients in the community and those who care for patients in the hospital setting.
Discharged patients with unresolved issues are followed up by the family medicine hospitalist at the ambulatory care clinics in the hospital. Patients are reviewed until they can be handed off to suitable health care providers in the community, to continue with their long term care outside the hospital. Specialist physicians of the hospital provide a similar system of follow‐up of discharged patients although they are more likely to be referred for review by different specialties according to the patients' comorbidities.
Traditionally, patients who are admitted to the Singapore General Hospital come under the care of single system specialists. Many of them are subspecialists who spend a large part of their time running specialist outpatient services and performing procedures and interventions related to their specialty. Approximately 66% of cases admitted from the emergency department to be cared for by the medical departments require specialty care and are admitted directly to the specialist departments. The rest of the patients (34%) are admitted under the category of internal medicine. The admitting physicians who work in Department of Emergency Medicine make these decisions independently. All physicians from the medical specialty departments go on a roster to provide general medical care for such patients usually with the help of specialist consultations. The reason for this form of usual care is again historically related to the fact that the Singapore health system was developed and modeled after the British system.
Patients admitted under the category of internal medicine were assigned hospital beds based on availability of beds for this category of admissions by the bed management unit of the hospital. A total of 34 beds out of 232 beds that are available for use under this category of admission are assigned to be cared for by the family medicine hospitalists in this program. The assignment is administrative and these beds are no different from other beds that accept patients admitted under the same admission category. The assignment of patients to the family medicine hospitalist or the specialist is therefore determined by the bed availability at the time of admission.
Data Source
Data of all hospitalized patients aged 18 years and above who were admitted into the Singapore General Hospital from January 1, 2008 to December 31, 2008 were collected from the hospital data warehouse at the Information Technology Department, SingHealth Group, Singapore. The collected data included demographic information such as ethnic group, gender, age, marital status, admission date, discharge date, intensive care unit (ICU) admission, disease codes under ICD‐9‐AM (International Statistical Classification of Diseases and Related Health Problems, 9th Revision, Australian Modification), and ICD‐9‐AM procedure codes. Data of patients who were readmitted to the hospital within 30‐days after the first discharge were also extracted. Available cost of care data including investigation, medication, treatment, and facility charges were also extracted based on hospital service codes. The protocol was approved by the Ethics Committee of the Singapore General Hospital with exemption from the requirement for informed consent.
Case Definition
Patients cared for by hospitalists were inpatients who were under the care of attending physicians from the Department of Family Medicine and Continuing Care using the adapted hospitalist care model. Patients cared for by nonhospitalists who were inpatients and who were cared for by all other attending specialist physicians from the other medical departments go on a roster to provide general medical care under the usual care model.
Surgical and medical conditions were determined based on the presence of ICD‐9‐AM diagnostic codes and procedure codes.20
Chronic comorbid conditions were identified by ICD‐9‐AM codes and were then studied using the Charlson Index.2123 The Charlson score was then classified into 4 previously defined grades known as the Charlson Comorbidity Index (CCI): 0 points (none), 1 to 2 points (low), 3 to 4 points (moderate), and 5 points (high).2123
Organ failure was defined by a combination of ICD‐9‐AM diagnosis and procedure codes, as outlined previously.24, 25
Statistical Analysis
Categorical variables were reported as percentages, continuous variables were reported as mean and standard deviation (SD). Hospital LOS and hospitalization cost of care were reported using geometric mean (GM) and 95% confidence interval (CI) because of their skewed distribution.
Hospital mortality rate was defined as the ratio of inpatient deaths to the total number of inpatients. Age was categorized into quintiles (18‐54, 55‐64, 65‐74, 75‐84, and >84 years) to capture the nonlinear effect of age on hospital service quality and resource utilization. Parameters were compared between patients cared for by hospitalists and nonhospitalists by chi‐square test for hospital mortality and readmission rate and by Mann‐Whitney U test for LOS and hospital cost. All hospital costs were converted to the year 2008 US dollars for presentation based on the Annual Average Rates of Exchange, Singapore (2008).26 Logistic regression was used to assess the association of hospital mortality and 30‐day all‐cause unscheduled readmission after adjusting for gender, ethnic group, ICU admission, CCI groups, number of organ failures, and the interaction among age groups, CCI groups, and numbers of organ failures. Analysis of hospital LOS and hospitalization costs were restricted to cases with values within 3 SD of the mean because of the extremely skewed nature of these data. Generalized linear model was used to assess log‐transformed LOS and cost with hospitalists care and adjusted for the above‐mentioned factors. The HosmerLemeshow chi‐square goodness‐of‐fit tests were used to exclude variables and identify clinically plausible interaction terms. Using the estimates from the regression models, we presented differences in adjusted LOS, hospitalization costs, hospital mortality, and 30‐day all‐cause unscheduled readmission between hospitalists and nonhospitalists. All P values were 2 sided. The level of statistical significance was considered to be the conventional alpha = 0.05. The data analysis was performed with SPSS 17.0 software (SPSS, Chicago, IL).
Results
A total of 3493 patients met the inclusion/exclusion criteria, in which 601 patients were under the care of hospitalists. The demographic and clinical characteristics of all patients are shown in Table 1. There were no differences in age (67.0 20.4 vs. 66.1 19.8 years, P= 0.311) and ethnic group (P= 0.253) between patients cared for by hospitalists and nonhospitalists. Patients cared for by hospitalists were less likely to be admitted to ICU (0.5% vs. 2.5%, P= 0.002) than patients cared for by nonhospitalists. There were similar CCI grades between patients cared for by hospitalists and nonhospitalists (P= 0.872). Patients cared for by hospitalists had similar numbers of organ failures as compared to patients cared for by nonhospitalists.
| Non Hospitalist, n = 2892 | Hospitalist, n = 601 | P* | |
|---|---|---|---|
| |||
| Age, year | 66.1 19.8 | 67.0 20.4 | 0.311 |
| Male sex, % | 49.2 | 44.4 | 0.033 |
| Ethnicity, % | 0.253 | ||
| Chinese | 79.2 | 76.9 | |
| Malay | 7.8 | 7.7 | |
| Indian | 9.8 | 12.5 | |
| Others | 3.3 | 3.0 | |
| ICU admission, % | 2.5 | 0.5 | 0.002 |
| Charlson Comorbidity Index, % | 0.872 | ||
| None | 43.5 | 42.3 | |
| Low | 35.5 | 36.6 | |
| Moderate | 14.0 | 14.6 | |
| High | 7.0 | 6.5 | |
| Organ failure No, % | 0.192 | ||
| 0 | 73.7 | 75.9 | |
| 1 | 21.6 | 20.5 | |
| 2 | 3.7 | 3.5 | |
| 3 | 1.0 | 0.2 | |
Unadjusted Clinical Outcomes and Resource Utilization
The in‐hospital mortality rates in patients cared for by hospitalists were similar (4.0% vs. 5.3%, P= 0.187) compared to patients cared for by nonhospitalists (Table 2). Also, there were no statistically significant differences in the 30‐day all‐cause unscheduled readmission rates between patients cared for by hospitalists and nonhospitalists (7.5% vs. 7.3%, p= 0.854). As for resource utilization, patients cared for by hospitalists had significantly shorter hospital LOS (GM, 4.6 vs. 5.7 days, P < 0.001) and lower cost (GM, $2301.0 vs. $2656.6, P= 0.001) compared with that in patients cared for by nonhospitalists (Table 2).
| Non hospitalist, n = 2892 | Hospitalist, n = 601 | Difference | P | |
|---|---|---|---|---|
| ||||
| Length of stay, day | ||||
| Un‐adjusted mean (95% CI) | 5.7 (5.4, 5.9) | 4.6 (4.2, 5.0) | 1.1 | <0.001 |
| Adjusted mean (95% CI) | 5.3 (5.3, 5.4) | 4.4 (4.3, 4.5) | 0.9 | <0.001 |
| Total hospitalization cost, $ | ||||
| Un‐adjusted mean (95% CI) | 2656.6 (2569.8, 2746.4) | 2301.0 (2125.2, 2460.1) | 335.6 | 0.001 |
| Adjusted mean (95% CI) | 2500.6 (2471.5, 2530.1) | 2250.7 (2195.9, 2306.8) | 250 | 0.003 |
| Unscheduled readmission, %* | ||||
| Un‐adjusted | 7.5 | 7.3 | 0.2 | 0.854 |
| Adjusted | 8.4 | 7.5 | 0.9 | 0.761 |
| Hospital mortality, %* | ||||
| Un‐adjusted | 5.3 | 4.0 | 1.3 | 0.187 |
| Adjusted | 5.3 | 4.2 | 1.1 | 0.307 |
Adjusted (Multivariate) Results of Hospital Clinical Outcomes and Resource Utilization
Multivariate analysis was used with adjustment for age groups, ethnic group, gender, ICU admission, numbers of organ failures, and CCI grades. Patients cared for by hospitalists, as compared with patients cared for by nonhospitalists, had a statistically significant shorter hospital LOS by 0.9 days (GM, 4.4 vs. 5.3 days, P < 0.001) and lower cost by $250 (GM, $2250.7 vs. $2500.0, P= 0.003), but similar in‐hospital mortality and 30‐day all‐cause readmission rates (both P > 0.05; Table 2). The goodness of fit of the regression model used for hospital LOS was assessed with the Hosmer‐Lemeshow test (2= 546.1, degree of freedom (df) = 3406, P= 0.160).
As for the detailed secondary cost, patients cared for by hospitalists had significantly lower treatment costs by $66 (GM, $462.9 vs. $528.1 P < 0.001) and facility costs by $127 (GM, $827.1 vs. $953.7 P < 0.001) compared with patients cared for by nonhospitalists after adjustment for age groups, ethnic group, gender, ICU admission, presence of organ failures, and CCI grades. The investigation and medication costs were comparable between the 2 groups (all P > 0.05) even after similar adjustments (Table 3).
| Non hospitalist, n = 2892 | Hospitalist, n = 601 | Difference | P | |
|---|---|---|---|---|
| ||||
| Investigation Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 828.3 (802.2, 855.3) | 772.3 (722.2, 825.8) | 24.7 | 0.196 |
| Adjusted mean (95% CI) | 776.5 (767.8, 785.2) | 759.0 (741.4, 776.9) | 17.5 | 0.673 |
| Medication Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 62.8 (58.7, 67.2) | 68.2 (59.6, 78.2) | 9.0 | 0.409 |
| Adjusted mean (95% CI) | 50.5 (49.1, 52.0) | 56.9 (53.5, 60.6) | 6.4 | 0.184 |
| Treatment Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 561.2 (542.3, 580.7) | 472.4 (442.1, 504.8) | 93.4 | <0.001 |
| Adjusted mean (95% CI) | 528.1 (522.1, 534.3) | 461.9 (450.8, 473.3) | 66.2 | <0.001 |
| Facility Cost, $ | ||||
| Un‐adjusted mean (95% CI) | 1015.9 (978.8, 1054.4) | 847.6 (787.8, 912.0) | 178.5 | <0.001 |
| Adjusted mean (95% CI) | 953.7 (942.2, 965.4) | 827.1 (806.0, 848.9) | 126.6 | <0.001 |
| Total hospitalization cost, $ | ||||
| Un‐adjusted mean (95% CI) | 2656.6 (2569.8, 2746.4) | 2301.0 (2125.2, 2460.1) | 335.6 | 0.001 |
| Adjusted mean (95% CI) | 2500.6 (2471.5, 2530.1) | 2250.7 (2195.9, 2306.8) | 250 | 0.003 |
Discussion
We found that patients cared for by hospitalists had shorter hospital LOS (reduced by 0.9 days), and reduced cost (reduced by $250), compared with that of patients cared for by nonhospitalists. This occurred without any compromise of the clinical outcomes as measured by hospital mortality and 30‐day all‐cause unscheduled readmission. The mortality rates were 4.0%(hospitalist) and 5.3%(nonhospitalist). The difference was not statistically significant (P= 0.187). The differences in hospital LOS and cost still existed even after adjustment for age, gender, ethnic group, ICU admission, CCI, and the numbers of organ failure.
Our findings are consistent with previous reports of reduced hospital LOS and hospitalization costs in patients cared for by hospitalists in the United States.2730
Several explanations have been proposed for the favorable results. First, hospitalists' accessibility and holistic approach to the multiple problems of individual patients provide a more coordinated response to the patient's changing needs during the hospital stay. Second, studies had suggested that better coordination of care by hospitalist results in a lower use of resources and fewer specialist consultations.31 Reduced patients hospital LOS and cost may lead to an overall reduction in total revenue to the hospital, resulting in an advantage to the patients and a disadvantage to the hospital. However, this reduction in total revenue may have been partially offset by an increase in the number of patients receiving hospital care services.32 Third, fewer patients in the hospitalists group had an ICU stay and this could be another reason for an increased chance of earlier discharge from the hospital.33 The reduced LOS still existed even after adjustment for ICU admission and other factors. The total number of patients with ICU admissions was small in both groups and did not make a difference to the outcome measures used in our study. The use of ICU is significantly higher by the nonhospitalist group. It is unlikely that the difference was due to severity of illness on admission because the admitting physicians at the emergency department do not specify whether patients are to be managed by hospitalists or nonhospitalists. Assignment of the patient to the 2 groups was based only on the availability of bed at the time of admission. There is a possibility that the difference had occurred by chance due to the small number of patients requiring ICU admission. Discussion of end of life care issues and palliation as an option is known to result in lowered utilization of ICU.34 There is a possibility that hospitalists are more likely to engage the patient and family in end of life care discussions although this would require further studies to confirm. Finally, hospitalists might be more effective in navigating the complex environment of the hospital and might develop greater clinical expertise as a result of repeated experience in caring for patients in a similar setting.35 All these favorable factors were present in our adapted hospitalist care model.
While some studies of hospitalist care have shown reduced LOS without reduction of cost, our results showed significant reduction in the cost of care ($250, P= 0.001) for patient who are managed under the hospitalist program. The differences lie mainly in the cost of treatment and facilities. There were no significant differences in the cost of investigations and drugs.
There were several limitations in our study. Although hospital discharge data had numerous advantages including reliability and extensive use in various analyses in health services and health policy research,36 the dataset was administrative in nature and was not created specifically for our study. The hospital discharge data was also at risk of coding errors and omissions of important diagnoses and complications, which may affect the disease complexity estimates.37 In our study this was partly mitigated by the quality control processes instituted by the hospital and government agencies that use this data for planning and health care financing purposes. As all the data came from a single hospital, there was less risk of coding discrepancies and nonuniformity in calculating hospitalization costs. Our study was retrospective and observational in nature. Nevertheless we did use a number of statistical methods and analyses to minimize the risk of bias. Underlying differences in the patient populations of the 2 comparison groups led us to rely heavily on multivariate analysis and adjustment to minimize confounding factors. Nevertheless it is still possible that factors not included in administrative data might still exist as unmeasured confounders.28 In the period of study, we did not identify significant changes in the process of care for the patients apart from the introduction of the adapted hospitalist care model. This study was done in a single hospital. The hospital is an acute tertiary hospital. It is also a teaching hospital with affiliation to 2 medical schools (Duke‐NUS Graduate Medical School and Yong Loo Lin School of Medicine). The results might not be generalizable to other hospitals with different characteristics. Finally, this study was limited to information concerning in‐hospital deaths, and we did not have data that would have allowed us to detect differences in deaths that occurred after discharge. Similarly, we could only assess readmissions within our hospital. We do not know how frequently patients were admitted to other hospitals, a potential problem in all research of this type reported to date.30
In conclusion, our study showed that the hospitalist care model can be adapted to work in health systems outside North America with favorable outcomes. Our adapted hospitalist care model using family physicians as generalists in the hospital was associated with improvements in areas of LOS and cost reductions. There were no difference in mortality and readmissions. In health systems where hospital and primary care providers are historically divided, the deployment of family physicians as hospitalist may have the additional benefit of bridging the gap and support care continuity across the entire spectrum of care settings for patients.
Acknowledgements
The authors acknowledge Mr. Jeffrey Fong, Ms. Bessie Ang, Ms. LiSee Lou and Ms. Huicheng Tan of their contribution with the database preparation. We also thank all other staff of Family Medicine and Continuing Care and Epidemiology Unit, SGH for logistical support, and the patients who made the study possible.
- ,,,Hospitalists and the practice of inpatient medicine: results of a survey of the National Association of Inpatient Physicians.Ann Intern Med.1999;130(4 Pt 2):343–349.
- ,The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335(7):514–517.
- ,,,The status of hospital medicine groups in the United States.J Hosp Med.2006;1(2):75–80.
- ,,,. The rise of the hospitalist in California. Oakland: California Healthcare Foundation, July 2007. Available at: http://www.chcf.org/topics/hospitals/index.cfm?itemID=133365. Accessed June 2010.
- Society of Hospital Medicine. Hospital medicine specialty shows 20 percent growth 2007. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Press_Releases 2005. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=General_ Information111(8):627–632.
- ,,, et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137(11):866–874.
- ,,, et al.The positive impact of initiation of hospitalist clinician educators.J Gen Intern Med.2004;19(4):293–301.
- ,The hospitalist movement 5 years later.JAMA.2002;287(4):487–494.
- The hospitalist movement‐‐a complex adaptive response to fragmentation of care in hospitals.Ann Acad Med Singapore.2008;37(2):145–150.
- UCSF Today. Singapore Executives Learn About UCSF's Hospitalist Program. 2008. Available at: http://today.ucsf.edu/stories/singapore‐ executives‐learn‐about‐ucsfs‐hospitalist‐program/. Accessed June 2010.
- Statistics Singapore. 2007 Population (Mid‐Year Estimates). Singapore Department of Statistics,2007.
- Launch of Family Medicine Department.The College Mirror.2006;32:1–2‐.
- 1st college of physicians lecture: the role of internal medicine as a specialty in the era of subspecialisation.Ann Acad Med Singapore.2004;33(6):725–732.
- AAFP. AAFP Guidelines for Interaction in “Hospitalist” Models ‐ Communication Between the Receiving Inpatient Care Management Physician and the Referring Primary Care Physician. 2003, April Board 2009‐Reaffirmed. Available at: http://www.aafp.org/online/en/home/policy/ policies/h/hospitalists.html. Accessed June 2010.
- ,,,Continuity of care and intensive care unit use at the end of life.Arch Intern Med.2009;169(1):81–86.
- ,,,,,Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med.2001;29(7):1303–1310.
- ,,,A new method of classifying prognostic comorbidity in longitudinal studies: development and validation.J Chronic Dis.1987;40(5):373–383.
- ,,Adapting a clinical comorbidity index for use with ICD‐9‐CM administrative databases.J Clin Epidemiol.1992;45(6):613–619.
- ,,,Validation of a combined comorbidity index.J Clin Epidemiol.1994;47(11):1245–1251.
- ,,,,The effect of comorbidity and age on hospital mortality and length of stay in patients with sepsis.J Crit Care.2009.
- ,,,The epidemiology of sepsis in the United States from 1979 through 2000.N Engl J Med.2003;348(16):1546–1554.
- Inland Revenue Authority of Singapore. Annual Average Rates of Exchange 2008. Available at:http://www.iras.gov.sg/irasHome/page.aspx? id=806. Accessed June 2010.
- ,,,A comparison of two hospitalist models with traditional care in a community teaching hospital.Am J Med.2005;118(5):536–543.
- ,,,,,Outcomes of care by hospitalists, general internists, and family physicians.N Engl J Med.2007;357(25):2589–2600.
- ,Comparison of a family practice teaching service and a hospitalist model: costs, charges, length of stay, and mortality.Fam Med.2001;33(7):511–515.
- ,,Comparison of hospital costs and length of stay for community internists, hospitalists, and academicians.J Gen Intern Med.2007;22(5):662–667.
- ,,Hospital economics of the hospitalist.Health Serv Res.2003;38(3):905–918; discussion 919‐922.
- ,,, et al.Impact of a hospitalist system on length of stay and cost for children with common conditions.Pediatrics.2007;120(2):267–274.
- ,,3rd, et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med.2005;165(7):796–801‐.
- ,Admission to intensive care unit at the end‐of‐life: is it an informed decision?Palliat Med.2004;18(8):705–711.
- ,,Is volume related to outcome in health care? A systematic review and methodologic critique of the literature.Ann Intern Med.2002;137(6):511–520.
- ,,,,The Value of Hospital Discharge Databases: Final Report. NORC at the University of Chicago, The National Association of Health Data Organizations.2005. Available at: http://www.hcup‐us.ahrq.gov/reports/final_report.pdf. Accessed June 2010.
- ,,Diagnosis‐dependent misclassification of infections using administrative data variably affected incidence and mortality estimates in ICU patients.J Clin Epidemiol.2007;60(2):155–162.
- ,,,Hospitalists and the practice of inpatient medicine: results of a survey of the National Association of Inpatient Physicians.Ann Intern Med.1999;130(4 Pt 2):343–349.
- ,The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335(7):514–517.
- ,,,The status of hospital medicine groups in the United States.J Hosp Med.2006;1(2):75–80.
- ,,,. The rise of the hospitalist in California. Oakland: California Healthcare Foundation, July 2007. Available at: http://www.chcf.org/topics/hospitals/index.cfm?itemID=133365. Accessed June 2010.
- Society of Hospital Medicine. Hospital medicine specialty shows 20 percent growth 2007. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Press_Releases 2005. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=General_ Information111(8):627–632.
- ,,, et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137(11):866–874.
- ,,, et al.The positive impact of initiation of hospitalist clinician educators.J Gen Intern Med.2004;19(4):293–301.
- ,The hospitalist movement 5 years later.JAMA.2002;287(4):487–494.
- The hospitalist movement‐‐a complex adaptive response to fragmentation of care in hospitals.Ann Acad Med Singapore.2008;37(2):145–150.
- UCSF Today. Singapore Executives Learn About UCSF's Hospitalist Program. 2008. Available at: http://today.ucsf.edu/stories/singapore‐ executives‐learn‐about‐ucsfs‐hospitalist‐program/. Accessed June 2010.
- Statistics Singapore. 2007 Population (Mid‐Year Estimates). Singapore Department of Statistics,2007.
- Launch of Family Medicine Department.The College Mirror.2006;32:1–2‐.
- 1st college of physicians lecture: the role of internal medicine as a specialty in the era of subspecialisation.Ann Acad Med Singapore.2004;33(6):725–732.
- AAFP. AAFP Guidelines for Interaction in “Hospitalist” Models ‐ Communication Between the Receiving Inpatient Care Management Physician and the Referring Primary Care Physician. 2003, April Board 2009‐Reaffirmed. Available at: http://www.aafp.org/online/en/home/policy/ policies/h/hospitalists.html. Accessed June 2010.
- ,,,Continuity of care and intensive care unit use at the end of life.Arch Intern Med.2009;169(1):81–86.
- ,,,,,Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med.2001;29(7):1303–1310.
- ,,,A new method of classifying prognostic comorbidity in longitudinal studies: development and validation.J Chronic Dis.1987;40(5):373–383.
- ,,Adapting a clinical comorbidity index for use with ICD‐9‐CM administrative databases.J Clin Epidemiol.1992;45(6):613–619.
- ,,,Validation of a combined comorbidity index.J Clin Epidemiol.1994;47(11):1245–1251.
- ,,,,The effect of comorbidity and age on hospital mortality and length of stay in patients with sepsis.J Crit Care.2009.
- ,,,The epidemiology of sepsis in the United States from 1979 through 2000.N Engl J Med.2003;348(16):1546–1554.
- Inland Revenue Authority of Singapore. Annual Average Rates of Exchange 2008. Available at:http://www.iras.gov.sg/irasHome/page.aspx? id=806. Accessed June 2010.
- ,,,A comparison of two hospitalist models with traditional care in a community teaching hospital.Am J Med.2005;118(5):536–543.
- ,,,,,Outcomes of care by hospitalists, general internists, and family physicians.N Engl J Med.2007;357(25):2589–2600.
- ,Comparison of a family practice teaching service and a hospitalist model: costs, charges, length of stay, and mortality.Fam Med.2001;33(7):511–515.
- ,,Comparison of hospital costs and length of stay for community internists, hospitalists, and academicians.J Gen Intern Med.2007;22(5):662–667.
- ,,Hospital economics of the hospitalist.Health Serv Res.2003;38(3):905–918; discussion 919‐922.
- ,,, et al.Impact of a hospitalist system on length of stay and cost for children with common conditions.Pediatrics.2007;120(2):267–274.
- ,,3rd, et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med.2005;165(7):796–801‐.
- ,Admission to intensive care unit at the end‐of‐life: is it an informed decision?Palliat Med.2004;18(8):705–711.
- ,,Is volume related to outcome in health care? A systematic review and methodologic critique of the literature.Ann Intern Med.2002;137(6):511–520.
- ,,,,The Value of Hospital Discharge Databases: Final Report. NORC at the University of Chicago, The National Association of Health Data Organizations.2005. Available at: http://www.hcup‐us.ahrq.gov/reports/final_report.pdf. Accessed June 2010.
- ,,Diagnosis‐dependent misclassification of infections using administrative data variably affected incidence and mortality estimates in ICU patients.J Clin Epidemiol.2007;60(2):155–162.
Copyright © 2011 Society of Hospital Medicine
Continuing Medical Education Program in
If you wish to receive credit for this activity, which beginson the next page, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Upon completion of this educational activity, participants will be better able to:
-
Identify the approximate 30‐day readmission rate of Medicare patient hospitalized initially for pneumonia.
-
Distinguish which variables were accounted and unaccounted for in the development of a pneumonia readmission model.
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to
www.blackwellpublishing.com/cme . -
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
If you wish to receive credit for this activity, which beginson the next page, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Upon completion of this educational activity, participants will be better able to:
-
Identify the approximate 30‐day readmission rate of Medicare patient hospitalized initially for pneumonia.
-
Distinguish which variables were accounted and unaccounted for in the development of a pneumonia readmission model.
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to
www.blackwellpublishing.com/cme . -
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
If you wish to receive credit for this activity, which beginson the next page, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Upon completion of this educational activity, participants will be better able to:
-
Identify the approximate 30‐day readmission rate of Medicare patient hospitalized initially for pneumonia.
-
Distinguish which variables were accounted and unaccounted for in the development of a pneumonia readmission model.
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to
www.blackwellpublishing.com/cme . -
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
SPS in Hyperkalemia
Hyperkalemia is a common and potentially life‐threatening problem encountered in many clinical settings. The incidence of hyperkalemia in hospitalized patients has been estimated to be between 1% and 10% in the United States each year.16 Medications are thought to contribute to the development of hyperkalemia in 35% to 75% of hospitalized patients.12, 9 Medications known to cause hyperkalemia include angiotensin‐converting enzyme (ACE) inhibitors, angiotensin II receptor antagonists (ARBs), potassium‐sparing diuretics, nonsteroidal anti‐inflammatory drugs (NSAIDs), potassium supplements, and antibiotics such as trimethoprim/sulfamethoxazole. Patients with hyperkalemia may develop neuromuscular symptoms such as fatigue, muscle weakness, tingling, numbness, and cramping. The most deleterious effect of hyperkalemia is cardiac toxicity, including life‐threatening arrhythmias.3, 711
Sodium polystyrene sulfonate (SPS) or Kayexalate is a cation‐exchange resin that is commonly employed to lower total body potassium in patients with mild to moderate hyperkalemia.1214 It removes potassium from the gut in exchange for sodium. SPS can be given orally or as an enema. When given orally, it is commonly administered with sorbitol to promote diarrhea. The onset of action is within 1 to 2 hours and lasts approximately 4 to 6 hours. The recommended average daily dose is 15 gm to 60 gm given as a single dose or in divided doses. An in vitro study indicated that each gram of resin binds to approximately 3.1 mEq of potassium.14 However, the majority of the exchange capacity is utilized for cations other than potassium. Therefore, the in vivo exchange capacity is thought to be no greater than 1 mEq of potassium per gram of resin.
There are conflicting data regarding the effectiveness of exchange resins.1, 13 In 1998, Guy‐Kapral et al.15 found that a 30‐gm dose of SPS failed to lower serum potassium concentration in end‐stage renal disease patients who were normokalemic. In contrast, Flinn et al.16 demonstrated effective lowering of serum potassium over a period of several days in which repeated doses of SPS were given to hyperkalemic patients. Moreover, in another study, serum potassium concentration was reduced by 1.0 mEq/L in 24 hours.17 However, this study was limited since subjects also received other potassium‐lowering agents such as insulin/glucose or sodium bicarbonate.
In 2004, Mikrut and Brockmiller‐Sell18 studied the dose response between SPS and serum potassium concentration. Their data demonstrated an average reduction in potassium concentration of approximately 1 mmol/L and 1.48 mmol/L following a 30 gm and a 60 gm dose of SPS, respectively. However, the study was small (n = 39) and only evaluated 2 dosages. In clinical practice, there is wide variability in SPS dosing. Furthermore, studies assessing the effects of different doses of SPS are lacking. Often, the dose chosen is dependent on comorbid conditions, concomitant medications and provider experience in treating hyperkalemia. The aim of our study was to examine the single‐dose effect of SPS on potassium concentration in hospitalized, hyperkalemic patients and to compare the potassium lowering effects of SPS doses commonly used.
Methods
Study Population
A retrospective cohort study involving a review of electronic medical records of inpatients receiving SPS for the treatment of hyperkalemia was conducted at the Jesse Brown Veteran Affairs Medical Center, between January 1, 2006 and December 31, 2006. Hyperkalemia was defined as a serum potassium concentration >5.1 mmol/L, as this concentration corresponded to the upper limit of normal for serum potassium at our hospital. The patient list was generated from prescription databases. Exclusion criteria included: chronic SPS use, rectal administration of SPS, multiple doses of SPS spaced less than 6 hours apart, a hemolyzed laboratory specimen, current hemodialysis, lack of a follow‐up serum potassium concentration, or other treatments started for hyperkalemia at the time of the event, specifically insulin, dextrose, albuterol, and/or furosemide. This study protocol received approval from the local Institutional Review Board and the hospital's research and development committee.
Data Collection
The Computerized Patient Record System (CPRS), the electronic medical record system used at Jesse Brown VA Medical Center (JBVAMC), was utilized to gather patient baseline demographic information consisting of age, gender, weight, and height. Data on comorbid conditions such as hypertension (HTN), diabetes mellitus (DM), chronic heart failure (CHF), chronic kidney disease (CKD), and acute renal failure (ARF) was identified from the patient's problem list in the medical record. Additionally, the authors abstracted information about concomitant hyperkalemia‐precipitating medications including ACE inhibitors, ARBs, potassium‐sparing diuretics, aldosterone antagonists, NSAIDs, potassium supplements, and antibiotics such as trimethoprim/sulfamethoxazole. Progress notes and discharge summaries were reviewed for documentation of ARF. Laboratory information including serum creatinine, blood urea nitrogen, potassium, sodium, and calcium concentrations before and after SPS administration was recorded. The date and time of laboratory draws were also collected. Data on SPS administration regarding time and date, as well as dosing information, was obtained from the medication administration records.
Outcomes
The primary outcome were the mean change in serum potassium after a single dose of SPS compared to the baseline. The data were also evaluated based on the dose of SPS that was administered, 15 gm, 30 gm, 45 gm, or 60 gm doses of SPS. Secondary outcomes were the mean change in sodium and calcium concentrations.
Statistical Analysis
In order to complete the statistical analysis for the study, continuous variables were summarized as mean standard deviation, and categorical variables were summarized as frequency counts and proportions. Group comparisons for categorical data in baseline characteristics were performed using the Fisher's exact test and the chi‐square test. The comparisons for continuous data in baseline characteristics were performed using analysis of variance (ANOVA). A paired t‐test was then used to compare changes in potassium, calcium, and sodium concentrations and again to compare the changes in potassium concentrations by different dosage groups. Subset analysis also required the paired t‐test. The differences in the change of potassium concentration between dosage groups were analyzed by ANOVA. Post hoc comparisons were performed to identify which groups were statistically different from each other. A P value less than 0.05 was considered statistically significant. The effect of dosage on primary outcome was also assessed by adjusting baseline characteristics using analysis of covariance (ANCOVA). Least square means (LSMEAN) of the primary outcome were calculated using the ANCOVA model with the SPS dosage groups as the main categorical independent variable and the baseline characteristics in Table 1 as the covariates. The LSMEAN are group means after controlling for covariates (they are the predicted group means, predicted as the population mean values of the covariates in the model). All statistical analyses were done using SAS software, version 9.1 (Cary, NC).
| All (n = 122) | 15 gm (n = 30) | 30 gm (n = 60) | 45 gm (n = 19) | 60 gm (n = 13) | P Value | |
|---|---|---|---|---|---|---|
| ||||||
| Male, n (%) | 121 (99) | 30 (100) | 60 (100) | 18 (95) | 13 (100) | 0.14 |
| Age (year) | 69.0 11.4 | 70.71 0.5 | 70.2 11.5 | 68.0 1.7 | 63.8 12.2 | 0.25 |
| Height (inch) | 69.0 3.5 | 69.2 4.6 | 68.8 3.3 | 68.2 3.0 | 70.5 1.3 | 0.31 |
| Weight (kg) | 81.4 20.7 | 77.3 15.0 | 83.1 23.3 | 82.7 21.7 | 81.6 18.1 | 0.64 |
| Hypertension, n (%) | 96 (79) | 29*(97) | 47 (78) | 12 (63) | 8 (62) | 0.01* |
| Diabetes Mellitus, n (%) | 41 (34) | 10 (33) | 21 (35) | 6 (32) | 4 (31) | 0.99 |
| Chronic kidney disease, n (%) | 46 (38) | 10 (33) | 21 (35) | 8 (42) | 7 (54) | 0.57 |
| Heart failure, n (%) | 32 (26) | 12 (40) | 13 (22) | 6 (32) | 1 (8) | 0.10 |
| Serum creatinine (mg/dL) | 2.57 2.4 | 2.09 1.5 | 2.93 3.0 | 2.37 1.2 | 2.29 2.1 | 0.41 |
| Acute renal failure, n (%) | 84 (69) | 19 (63) | 45 (75) | 12 (63) | 8 (62) | 0.55 |
| Concomitant hyperkalemia‐precipitating medications, n (%) | 60 (49) | 19 (63) | 23 (38) | 10 (53) | 8 (61) | 0.11 |
Results
Patient Characteristics
Study subjects consisted of patients who received SPS in the hospital for treatment of hyperkalemia. A total of 140 patients were identified and 122 met the inclusion criteria. Eighteen patients were excluded for current hemodialysis, receiving other treatments for hyperkalemia, and specimen hemolysis. Of those who were included in the study analysis, 30 patients received 15 gm of SPS, 60 patients received 30 gm, 19 patients received 45 gm, and 13 patients received 60 gm. Baseline characteristics of included patients are shown in Table 1. The majority of patients were male (99%) and had comorbid conditions.
At baseline, the mean serum creatinine concentration was 2.57 2.36 mg/dL. Documented acute renal dysfunction was present at the time of the hyperkalemic event in 69% of patients. Forty‐nine percent of patients were taking at least one medication that can precipitate hyperkalemia. The most common medications were ACE inhibitors (52%). All baseline characteristics were similar among the different cohorts except for HTN. There were significantly more patients with HTN in the 15 gm dosage group compared to the others. There was no effect of baseline characteristics on the primary or secondary outcomes.
Clinical Outcome
A total of 115 patients (94%) achieved normalization of potassium concentration with a single dose of SPS. The mean SPS dose given was 31.84 13.58 gm. The changes in mean electrolyte values for all patients are shown in Table 2. The mean reduction in potassium concentration was 0.99 0.51 mmol/L (P < 0.0001). The follow‐up potassium concentration was obtained on an average of 10 hours after administration of SPS. The mean reduction in calcium concentration was 0.07 0.53 mg/dL (P = 0.13). Further, the mean reduction in sodium concentration was 0.09 3.33 mg/dL (P = 0.004). Figure 1 depicts the change in serum potassium concentration in each of the SPS dosage groups. The mean change in potassium concentrations compared to baseline was statistically significant in all dosage groups. The mean reduction in potassium concentration achieved statistical significance between the 15 gm and 60 gm groups (P < 0.05) and between the 30 gm and 60 gm groups (P < 0.05) (Table 3). To adjust for the potential covariate effects in these group mean comparisons, we further calculated the LSMEAN. Table 3 presents the least square mean changes in serum potassium concentration in each of the SPS dosage groups. As shown in Table 4, the least square mean changes in potassium concentrations compared to the baseline were also statistically significant in all dosage groups. These group differences remain significant, even after the adjustment by the baseline variables.
| Electrolytes | Pre‐SPS | Post‐SPS | Mean Change | P Value |
|---|---|---|---|---|
| ||||
| K+(mmol/L) | 5.57 0.35 | 4.59 0.46 | 0.99 0.51 | <0.0001 |
| Ca2+(mg/dL) | 8.54 0.81 | 8.46 0.64 | 0.07 0.53 | 0.13 |
| Na+(mmol/L) | 136.7 4.66 | 137.6 4.65 | 0.89 3.33 | 0.004 |
| Dose (gm) | Difference Between Means | CI for Difference Between Means |
|---|---|---|
| ||
| 15‐30 | 0.13 | 0.43, 0.16 |
| 15‐45 | 0.27 | 0.66, 0.11 |
| 15‐60* | 0.64 | 1.09, 0.19 |
| 30‐45 | 0.14 | 0.48, 0.20 |
| 30‐60* | 0.50 | 0.91, 0.10 |
| 45‐60 | 0.36 | 0.82, 0.10 |
| SPS Dose | LSMEAN of Potassium Reduction | 95% Confidence Limits | |
|---|---|---|---|
| |||
| 15 gm | 0.676566 | 0.119091 | 1.234041 |
| 30 gm | 0.808860 | 0.260418 | 1.357302 |
| 45 gm | 0.951205 | 0.431039 | 1.471371 |
| 60 gm | 1.313806 | 0.718793 | 1.908818 |
Subset Analysis
To address cointervention bias, an analysis of patients who were on at least 1 medication that predisposed them to hyperkalemia such as ACE inhibitors, ARBs, potassium sparing diuretics, aldosterone antagonists, NSAIDs, potassium supplements, and antibiotics such as trimethoprim/sulfamethoxazole (n = 60) were reviewed. Of the 60 patients, 30 received SPS and had hyperkalemia‐precipitating medications adjusted and 29 patients received SPS alone. Of those who had medications adjusted, the majority of them (83%) had these medications discontinued. The mean potassium concentration before the intervention was approximately 5.6 mmol/L in both groups. The mean SPS dose given was also similar as well as the mean potassium reduction of approximately 1 mmol/L.
Discussion
In this study, we retrospectively examined inpatients who received a single dose of SPS for the treatment of hyperkalemia. In addition, we established a possible dose response relationship in the treatment of mild to moderate hyperkalemia with SPS monotherapy. Our data revealed that 94% of patients achieved normalization of serum potassium concentration with a single dose of SPS. None of the patients experienced hypokalemia as a result of SPS administration. Moreover, when compared to the work by Mikrut and Brockmiller‐Sell,18 we found a similar reduction in serum potassium associated with the 30 gm (0.95 mmol/L vs. 1 mmol/L) and 60 gm (1.40 vs. 1.48 mEq/L) doses of SPS.
As expected, patients with higher serum potassium concentrations received higher SPS doses. Our data illustrated a possible direct, dose‐response relationship between the SPS dose and the reduction in serum potassium concentration. All of the dosage groups produced a statistically significant reduction in potassium concentrations compared to baseline. Moreover, a statistically significant difference was found in the 60 gm group when compared to the 15 gm and 30 gm groups. The mean increase change in sodium of 0.89 3.33 mmol/L was found to be statistically significant (P = 0.004) but not felt to be clinically relevant. The mean change in calcium concentration of 0.07 0.53 was not statistically significant (P = 0.13).
As with any retrospective chart review, incomplete documentation limits data collection. This may have led to an underestimation of the presence of ARF or other risk factors for hyperkalemia at the time of the event. We excluded patients who received other treatment for hyperkalemia in order to truly assess the effects of SPS on potassium concentration. However, we did not account for all potential confounding variables that are likely to affect potassium concentration such as acid‐base status and glycemic control at the time of the hyperkalemic episode. Also, dietary intake of potassium was not ascertained. Absence of a control group is also a limitation of the study, as it does not allow for complete causality to be established. The sample size, although significantly larger than previous studies, was small especially in regards to the subset analysis. Results cannot be generalized to women since the sample of females was very small or to those who were excluded from the analysis by design. Finally, this study evaluated hospitalized patients and direct extrapolation of the results to outpatient settings should be done cautiously, particularly in light of nutritional considerations.
Our study demonstrates a possible dose‐response relationship in lowering potassium concentrations with SPS. The data presented in this paper can be used to develop a potential dosing guideline for the use of SPS in the clinical management of hyperkalemia in a variety of clinical settings. It provides a basis for a much needed prospective study to finalize a dosing scheme for the use of SPS. Having a dosing scheme would serve as a resource for determining what dose of SPS to give for varying degrees of hyperkalemia while being mindful that individual responses to potassium lowering effect of SPS might be variable.
Acknowledgements
The authors thank the editors and reviewers of The Journal of Hospital Medicine for their comments and suggestions. Jaclyn Ng and Kathya Valdez worked equally on manuscript as second authors.
- ,Hyperkalemia: a review.J Intensive Care Med.2005;20(5):272–290.
- Drug‐induced hyperkalemia: old culprits and new offenders.Am J Med.2000;109(4):307–314.
- ,Hyperkalemia.Am Fam Physician.2006;73(2):283–290.
- ,Indications for hospitalization of patients with hyperkalemia.Arch Intern Med.2000;160(11):1605–1611.
- Hyperkalemia: a potentially lethal clinical condition.Acta Clin Croat.2001;40(3):215–225.
- Hypokalemia and hyperkalemia.Med Clin North Am.1997;81(3):611–639.
- ,,,,Hyperkalemia in patients in hospital.BMJ.1983;286(6372):1189–1192.
- ,,,Treatment of electrolyte disorders in adult patients in the intensive care unit.Am J Health Syst Pharm.2005;62(16):1663–1682.
- ,,,Hyperkalemia revisited.Tex Heart Inst J.2006;33(1):40–47.
- Disorders of potassium homeostasis.Hypokalemia and hyperkalemia. Crit Care Clin.2002;18(2):273–288.
- ,,,Drug‐induced hyperkalemia.Medicine.1985;64(6):357–370.
- ,Therapeutic approach to hyperkalemia.Nephron.2002;92(1):33–40.
- ,Controversial issues in the treatment of hyperkalemia.Nephrol Dial Transplant.2003;18(11):2215–2218.
- Sodium polystyrene sulfonate: a cation exchange resin used in treating hyperkalemia.ANNA J.1993;20(1):93–95.
- ,,,,,Effect of single dose resin‐cathartic therapy on serum potassium concentration in patients with end‐stage renal disease.J Am Soc Nephrol.1998;9(10):1924–1930.
- ,,Treatment of the oliguric patient with a new sodium‐exchange resin and sorbitol, a preliminary report.N Engl J Med.1961;264(3):111–115.
- ,,Management of hyperkalemia with a cation exchange resin.N Engl J Med.1961;264(3):115–119.
- ,Sodium polystyrene sulfonate dosing guidelines for the treatment of adult hyperkalemia.Hosp Pharm.2004;39(8):765–771.
Hyperkalemia is a common and potentially life‐threatening problem encountered in many clinical settings. The incidence of hyperkalemia in hospitalized patients has been estimated to be between 1% and 10% in the United States each year.16 Medications are thought to contribute to the development of hyperkalemia in 35% to 75% of hospitalized patients.12, 9 Medications known to cause hyperkalemia include angiotensin‐converting enzyme (ACE) inhibitors, angiotensin II receptor antagonists (ARBs), potassium‐sparing diuretics, nonsteroidal anti‐inflammatory drugs (NSAIDs), potassium supplements, and antibiotics such as trimethoprim/sulfamethoxazole. Patients with hyperkalemia may develop neuromuscular symptoms such as fatigue, muscle weakness, tingling, numbness, and cramping. The most deleterious effect of hyperkalemia is cardiac toxicity, including life‐threatening arrhythmias.3, 711
Sodium polystyrene sulfonate (SPS) or Kayexalate is a cation‐exchange resin that is commonly employed to lower total body potassium in patients with mild to moderate hyperkalemia.1214 It removes potassium from the gut in exchange for sodium. SPS can be given orally or as an enema. When given orally, it is commonly administered with sorbitol to promote diarrhea. The onset of action is within 1 to 2 hours and lasts approximately 4 to 6 hours. The recommended average daily dose is 15 gm to 60 gm given as a single dose or in divided doses. An in vitro study indicated that each gram of resin binds to approximately 3.1 mEq of potassium.14 However, the majority of the exchange capacity is utilized for cations other than potassium. Therefore, the in vivo exchange capacity is thought to be no greater than 1 mEq of potassium per gram of resin.
There are conflicting data regarding the effectiveness of exchange resins.1, 13 In 1998, Guy‐Kapral et al.15 found that a 30‐gm dose of SPS failed to lower serum potassium concentration in end‐stage renal disease patients who were normokalemic. In contrast, Flinn et al.16 demonstrated effective lowering of serum potassium over a period of several days in which repeated doses of SPS were given to hyperkalemic patients. Moreover, in another study, serum potassium concentration was reduced by 1.0 mEq/L in 24 hours.17 However, this study was limited since subjects also received other potassium‐lowering agents such as insulin/glucose or sodium bicarbonate.
In 2004, Mikrut and Brockmiller‐Sell18 studied the dose response between SPS and serum potassium concentration. Their data demonstrated an average reduction in potassium concentration of approximately 1 mmol/L and 1.48 mmol/L following a 30 gm and a 60 gm dose of SPS, respectively. However, the study was small (n = 39) and only evaluated 2 dosages. In clinical practice, there is wide variability in SPS dosing. Furthermore, studies assessing the effects of different doses of SPS are lacking. Often, the dose chosen is dependent on comorbid conditions, concomitant medications and provider experience in treating hyperkalemia. The aim of our study was to examine the single‐dose effect of SPS on potassium concentration in hospitalized, hyperkalemic patients and to compare the potassium lowering effects of SPS doses commonly used.
Methods
Study Population
A retrospective cohort study involving a review of electronic medical records of inpatients receiving SPS for the treatment of hyperkalemia was conducted at the Jesse Brown Veteran Affairs Medical Center, between January 1, 2006 and December 31, 2006. Hyperkalemia was defined as a serum potassium concentration >5.1 mmol/L, as this concentration corresponded to the upper limit of normal for serum potassium at our hospital. The patient list was generated from prescription databases. Exclusion criteria included: chronic SPS use, rectal administration of SPS, multiple doses of SPS spaced less than 6 hours apart, a hemolyzed laboratory specimen, current hemodialysis, lack of a follow‐up serum potassium concentration, or other treatments started for hyperkalemia at the time of the event, specifically insulin, dextrose, albuterol, and/or furosemide. This study protocol received approval from the local Institutional Review Board and the hospital's research and development committee.
Data Collection
The Computerized Patient Record System (CPRS), the electronic medical record system used at Jesse Brown VA Medical Center (JBVAMC), was utilized to gather patient baseline demographic information consisting of age, gender, weight, and height. Data on comorbid conditions such as hypertension (HTN), diabetes mellitus (DM), chronic heart failure (CHF), chronic kidney disease (CKD), and acute renal failure (ARF) was identified from the patient's problem list in the medical record. Additionally, the authors abstracted information about concomitant hyperkalemia‐precipitating medications including ACE inhibitors, ARBs, potassium‐sparing diuretics, aldosterone antagonists, NSAIDs, potassium supplements, and antibiotics such as trimethoprim/sulfamethoxazole. Progress notes and discharge summaries were reviewed for documentation of ARF. Laboratory information including serum creatinine, blood urea nitrogen, potassium, sodium, and calcium concentrations before and after SPS administration was recorded. The date and time of laboratory draws were also collected. Data on SPS administration regarding time and date, as well as dosing information, was obtained from the medication administration records.
Outcomes
The primary outcome were the mean change in serum potassium after a single dose of SPS compared to the baseline. The data were also evaluated based on the dose of SPS that was administered, 15 gm, 30 gm, 45 gm, or 60 gm doses of SPS. Secondary outcomes were the mean change in sodium and calcium concentrations.
Statistical Analysis
In order to complete the statistical analysis for the study, continuous variables were summarized as mean standard deviation, and categorical variables were summarized as frequency counts and proportions. Group comparisons for categorical data in baseline characteristics were performed using the Fisher's exact test and the chi‐square test. The comparisons for continuous data in baseline characteristics were performed using analysis of variance (ANOVA). A paired t‐test was then used to compare changes in potassium, calcium, and sodium concentrations and again to compare the changes in potassium concentrations by different dosage groups. Subset analysis also required the paired t‐test. The differences in the change of potassium concentration between dosage groups were analyzed by ANOVA. Post hoc comparisons were performed to identify which groups were statistically different from each other. A P value less than 0.05 was considered statistically significant. The effect of dosage on primary outcome was also assessed by adjusting baseline characteristics using analysis of covariance (ANCOVA). Least square means (LSMEAN) of the primary outcome were calculated using the ANCOVA model with the SPS dosage groups as the main categorical independent variable and the baseline characteristics in Table 1 as the covariates. The LSMEAN are group means after controlling for covariates (they are the predicted group means, predicted as the population mean values of the covariates in the model). All statistical analyses were done using SAS software, version 9.1 (Cary, NC).
| All (n = 122) | 15 gm (n = 30) | 30 gm (n = 60) | 45 gm (n = 19) | 60 gm (n = 13) | P Value | |
|---|---|---|---|---|---|---|
| ||||||
| Male, n (%) | 121 (99) | 30 (100) | 60 (100) | 18 (95) | 13 (100) | 0.14 |
| Age (year) | 69.0 11.4 | 70.71 0.5 | 70.2 11.5 | 68.0 1.7 | 63.8 12.2 | 0.25 |
| Height (inch) | 69.0 3.5 | 69.2 4.6 | 68.8 3.3 | 68.2 3.0 | 70.5 1.3 | 0.31 |
| Weight (kg) | 81.4 20.7 | 77.3 15.0 | 83.1 23.3 | 82.7 21.7 | 81.6 18.1 | 0.64 |
| Hypertension, n (%) | 96 (79) | 29*(97) | 47 (78) | 12 (63) | 8 (62) | 0.01* |
| Diabetes Mellitus, n (%) | 41 (34) | 10 (33) | 21 (35) | 6 (32) | 4 (31) | 0.99 |
| Chronic kidney disease, n (%) | 46 (38) | 10 (33) | 21 (35) | 8 (42) | 7 (54) | 0.57 |
| Heart failure, n (%) | 32 (26) | 12 (40) | 13 (22) | 6 (32) | 1 (8) | 0.10 |
| Serum creatinine (mg/dL) | 2.57 2.4 | 2.09 1.5 | 2.93 3.0 | 2.37 1.2 | 2.29 2.1 | 0.41 |
| Acute renal failure, n (%) | 84 (69) | 19 (63) | 45 (75) | 12 (63) | 8 (62) | 0.55 |
| Concomitant hyperkalemia‐precipitating medications, n (%) | 60 (49) | 19 (63) | 23 (38) | 10 (53) | 8 (61) | 0.11 |
Results
Patient Characteristics
Study subjects consisted of patients who received SPS in the hospital for treatment of hyperkalemia. A total of 140 patients were identified and 122 met the inclusion criteria. Eighteen patients were excluded for current hemodialysis, receiving other treatments for hyperkalemia, and specimen hemolysis. Of those who were included in the study analysis, 30 patients received 15 gm of SPS, 60 patients received 30 gm, 19 patients received 45 gm, and 13 patients received 60 gm. Baseline characteristics of included patients are shown in Table 1. The majority of patients were male (99%) and had comorbid conditions.
At baseline, the mean serum creatinine concentration was 2.57 2.36 mg/dL. Documented acute renal dysfunction was present at the time of the hyperkalemic event in 69% of patients. Forty‐nine percent of patients were taking at least one medication that can precipitate hyperkalemia. The most common medications were ACE inhibitors (52%). All baseline characteristics were similar among the different cohorts except for HTN. There were significantly more patients with HTN in the 15 gm dosage group compared to the others. There was no effect of baseline characteristics on the primary or secondary outcomes.
Clinical Outcome
A total of 115 patients (94%) achieved normalization of potassium concentration with a single dose of SPS. The mean SPS dose given was 31.84 13.58 gm. The changes in mean electrolyte values for all patients are shown in Table 2. The mean reduction in potassium concentration was 0.99 0.51 mmol/L (P < 0.0001). The follow‐up potassium concentration was obtained on an average of 10 hours after administration of SPS. The mean reduction in calcium concentration was 0.07 0.53 mg/dL (P = 0.13). Further, the mean reduction in sodium concentration was 0.09 3.33 mg/dL (P = 0.004). Figure 1 depicts the change in serum potassium concentration in each of the SPS dosage groups. The mean change in potassium concentrations compared to baseline was statistically significant in all dosage groups. The mean reduction in potassium concentration achieved statistical significance between the 15 gm and 60 gm groups (P < 0.05) and between the 30 gm and 60 gm groups (P < 0.05) (Table 3). To adjust for the potential covariate effects in these group mean comparisons, we further calculated the LSMEAN. Table 3 presents the least square mean changes in serum potassium concentration in each of the SPS dosage groups. As shown in Table 4, the least square mean changes in potassium concentrations compared to the baseline were also statistically significant in all dosage groups. These group differences remain significant, even after the adjustment by the baseline variables.
| Electrolytes | Pre‐SPS | Post‐SPS | Mean Change | P Value |
|---|---|---|---|---|
| ||||
| K+(mmol/L) | 5.57 0.35 | 4.59 0.46 | 0.99 0.51 | <0.0001 |
| Ca2+(mg/dL) | 8.54 0.81 | 8.46 0.64 | 0.07 0.53 | 0.13 |
| Na+(mmol/L) | 136.7 4.66 | 137.6 4.65 | 0.89 3.33 | 0.004 |
| Dose (gm) | Difference Between Means | CI for Difference Between Means |
|---|---|---|
| ||
| 15‐30 | 0.13 | 0.43, 0.16 |
| 15‐45 | 0.27 | 0.66, 0.11 |
| 15‐60* | 0.64 | 1.09, 0.19 |
| 30‐45 | 0.14 | 0.48, 0.20 |
| 30‐60* | 0.50 | 0.91, 0.10 |
| 45‐60 | 0.36 | 0.82, 0.10 |
| SPS Dose | LSMEAN of Potassium Reduction | 95% Confidence Limits | |
|---|---|---|---|
| |||
| 15 gm | 0.676566 | 0.119091 | 1.234041 |
| 30 gm | 0.808860 | 0.260418 | 1.357302 |
| 45 gm | 0.951205 | 0.431039 | 1.471371 |
| 60 gm | 1.313806 | 0.718793 | 1.908818 |
Subset Analysis
To address cointervention bias, an analysis of patients who were on at least 1 medication that predisposed them to hyperkalemia such as ACE inhibitors, ARBs, potassium sparing diuretics, aldosterone antagonists, NSAIDs, potassium supplements, and antibiotics such as trimethoprim/sulfamethoxazole (n = 60) were reviewed. Of the 60 patients, 30 received SPS and had hyperkalemia‐precipitating medications adjusted and 29 patients received SPS alone. Of those who had medications adjusted, the majority of them (83%) had these medications discontinued. The mean potassium concentration before the intervention was approximately 5.6 mmol/L in both groups. The mean SPS dose given was also similar as well as the mean potassium reduction of approximately 1 mmol/L.
Discussion
In this study, we retrospectively examined inpatients who received a single dose of SPS for the treatment of hyperkalemia. In addition, we established a possible dose response relationship in the treatment of mild to moderate hyperkalemia with SPS monotherapy. Our data revealed that 94% of patients achieved normalization of serum potassium concentration with a single dose of SPS. None of the patients experienced hypokalemia as a result of SPS administration. Moreover, when compared to the work by Mikrut and Brockmiller‐Sell,18 we found a similar reduction in serum potassium associated with the 30 gm (0.95 mmol/L vs. 1 mmol/L) and 60 gm (1.40 vs. 1.48 mEq/L) doses of SPS.
As expected, patients with higher serum potassium concentrations received higher SPS doses. Our data illustrated a possible direct, dose‐response relationship between the SPS dose and the reduction in serum potassium concentration. All of the dosage groups produced a statistically significant reduction in potassium concentrations compared to baseline. Moreover, a statistically significant difference was found in the 60 gm group when compared to the 15 gm and 30 gm groups. The mean increase change in sodium of 0.89 3.33 mmol/L was found to be statistically significant (P = 0.004) but not felt to be clinically relevant. The mean change in calcium concentration of 0.07 0.53 was not statistically significant (P = 0.13).
As with any retrospective chart review, incomplete documentation limits data collection. This may have led to an underestimation of the presence of ARF or other risk factors for hyperkalemia at the time of the event. We excluded patients who received other treatment for hyperkalemia in order to truly assess the effects of SPS on potassium concentration. However, we did not account for all potential confounding variables that are likely to affect potassium concentration such as acid‐base status and glycemic control at the time of the hyperkalemic episode. Also, dietary intake of potassium was not ascertained. Absence of a control group is also a limitation of the study, as it does not allow for complete causality to be established. The sample size, although significantly larger than previous studies, was small especially in regards to the subset analysis. Results cannot be generalized to women since the sample of females was very small or to those who were excluded from the analysis by design. Finally, this study evaluated hospitalized patients and direct extrapolation of the results to outpatient settings should be done cautiously, particularly in light of nutritional considerations.
Our study demonstrates a possible dose‐response relationship in lowering potassium concentrations with SPS. The data presented in this paper can be used to develop a potential dosing guideline for the use of SPS in the clinical management of hyperkalemia in a variety of clinical settings. It provides a basis for a much needed prospective study to finalize a dosing scheme for the use of SPS. Having a dosing scheme would serve as a resource for determining what dose of SPS to give for varying degrees of hyperkalemia while being mindful that individual responses to potassium lowering effect of SPS might be variable.
Acknowledgements
The authors thank the editors and reviewers of The Journal of Hospital Medicine for their comments and suggestions. Jaclyn Ng and Kathya Valdez worked equally on manuscript as second authors.
Hyperkalemia is a common and potentially life‐threatening problem encountered in many clinical settings. The incidence of hyperkalemia in hospitalized patients has been estimated to be between 1% and 10% in the United States each year.16 Medications are thought to contribute to the development of hyperkalemia in 35% to 75% of hospitalized patients.12, 9 Medications known to cause hyperkalemia include angiotensin‐converting enzyme (ACE) inhibitors, angiotensin II receptor antagonists (ARBs), potassium‐sparing diuretics, nonsteroidal anti‐inflammatory drugs (NSAIDs), potassium supplements, and antibiotics such as trimethoprim/sulfamethoxazole. Patients with hyperkalemia may develop neuromuscular symptoms such as fatigue, muscle weakness, tingling, numbness, and cramping. The most deleterious effect of hyperkalemia is cardiac toxicity, including life‐threatening arrhythmias.3, 711
Sodium polystyrene sulfonate (SPS) or Kayexalate is a cation‐exchange resin that is commonly employed to lower total body potassium in patients with mild to moderate hyperkalemia.1214 It removes potassium from the gut in exchange for sodium. SPS can be given orally or as an enema. When given orally, it is commonly administered with sorbitol to promote diarrhea. The onset of action is within 1 to 2 hours and lasts approximately 4 to 6 hours. The recommended average daily dose is 15 gm to 60 gm given as a single dose or in divided doses. An in vitro study indicated that each gram of resin binds to approximately 3.1 mEq of potassium.14 However, the majority of the exchange capacity is utilized for cations other than potassium. Therefore, the in vivo exchange capacity is thought to be no greater than 1 mEq of potassium per gram of resin.
There are conflicting data regarding the effectiveness of exchange resins.1, 13 In 1998, Guy‐Kapral et al.15 found that a 30‐gm dose of SPS failed to lower serum potassium concentration in end‐stage renal disease patients who were normokalemic. In contrast, Flinn et al.16 demonstrated effective lowering of serum potassium over a period of several days in which repeated doses of SPS were given to hyperkalemic patients. Moreover, in another study, serum potassium concentration was reduced by 1.0 mEq/L in 24 hours.17 However, this study was limited since subjects also received other potassium‐lowering agents such as insulin/glucose or sodium bicarbonate.
In 2004, Mikrut and Brockmiller‐Sell18 studied the dose response between SPS and serum potassium concentration. Their data demonstrated an average reduction in potassium concentration of approximately 1 mmol/L and 1.48 mmol/L following a 30 gm and a 60 gm dose of SPS, respectively. However, the study was small (n = 39) and only evaluated 2 dosages. In clinical practice, there is wide variability in SPS dosing. Furthermore, studies assessing the effects of different doses of SPS are lacking. Often, the dose chosen is dependent on comorbid conditions, concomitant medications and provider experience in treating hyperkalemia. The aim of our study was to examine the single‐dose effect of SPS on potassium concentration in hospitalized, hyperkalemic patients and to compare the potassium lowering effects of SPS doses commonly used.
Methods
Study Population
A retrospective cohort study involving a review of electronic medical records of inpatients receiving SPS for the treatment of hyperkalemia was conducted at the Jesse Brown Veteran Affairs Medical Center, between January 1, 2006 and December 31, 2006. Hyperkalemia was defined as a serum potassium concentration >5.1 mmol/L, as this concentration corresponded to the upper limit of normal for serum potassium at our hospital. The patient list was generated from prescription databases. Exclusion criteria included: chronic SPS use, rectal administration of SPS, multiple doses of SPS spaced less than 6 hours apart, a hemolyzed laboratory specimen, current hemodialysis, lack of a follow‐up serum potassium concentration, or other treatments started for hyperkalemia at the time of the event, specifically insulin, dextrose, albuterol, and/or furosemide. This study protocol received approval from the local Institutional Review Board and the hospital's research and development committee.
Data Collection
The Computerized Patient Record System (CPRS), the electronic medical record system used at Jesse Brown VA Medical Center (JBVAMC), was utilized to gather patient baseline demographic information consisting of age, gender, weight, and height. Data on comorbid conditions such as hypertension (HTN), diabetes mellitus (DM), chronic heart failure (CHF), chronic kidney disease (CKD), and acute renal failure (ARF) was identified from the patient's problem list in the medical record. Additionally, the authors abstracted information about concomitant hyperkalemia‐precipitating medications including ACE inhibitors, ARBs, potassium‐sparing diuretics, aldosterone antagonists, NSAIDs, potassium supplements, and antibiotics such as trimethoprim/sulfamethoxazole. Progress notes and discharge summaries were reviewed for documentation of ARF. Laboratory information including serum creatinine, blood urea nitrogen, potassium, sodium, and calcium concentrations before and after SPS administration was recorded. The date and time of laboratory draws were also collected. Data on SPS administration regarding time and date, as well as dosing information, was obtained from the medication administration records.
Outcomes
The primary outcome were the mean change in serum potassium after a single dose of SPS compared to the baseline. The data were also evaluated based on the dose of SPS that was administered, 15 gm, 30 gm, 45 gm, or 60 gm doses of SPS. Secondary outcomes were the mean change in sodium and calcium concentrations.
Statistical Analysis
In order to complete the statistical analysis for the study, continuous variables were summarized as mean standard deviation, and categorical variables were summarized as frequency counts and proportions. Group comparisons for categorical data in baseline characteristics were performed using the Fisher's exact test and the chi‐square test. The comparisons for continuous data in baseline characteristics were performed using analysis of variance (ANOVA). A paired t‐test was then used to compare changes in potassium, calcium, and sodium concentrations and again to compare the changes in potassium concentrations by different dosage groups. Subset analysis also required the paired t‐test. The differences in the change of potassium concentration between dosage groups were analyzed by ANOVA. Post hoc comparisons were performed to identify which groups were statistically different from each other. A P value less than 0.05 was considered statistically significant. The effect of dosage on primary outcome was also assessed by adjusting baseline characteristics using analysis of covariance (ANCOVA). Least square means (LSMEAN) of the primary outcome were calculated using the ANCOVA model with the SPS dosage groups as the main categorical independent variable and the baseline characteristics in Table 1 as the covariates. The LSMEAN are group means after controlling for covariates (they are the predicted group means, predicted as the population mean values of the covariates in the model). All statistical analyses were done using SAS software, version 9.1 (Cary, NC).
| All (n = 122) | 15 gm (n = 30) | 30 gm (n = 60) | 45 gm (n = 19) | 60 gm (n = 13) | P Value | |
|---|---|---|---|---|---|---|
| ||||||
| Male, n (%) | 121 (99) | 30 (100) | 60 (100) | 18 (95) | 13 (100) | 0.14 |
| Age (year) | 69.0 11.4 | 70.71 0.5 | 70.2 11.5 | 68.0 1.7 | 63.8 12.2 | 0.25 |
| Height (inch) | 69.0 3.5 | 69.2 4.6 | 68.8 3.3 | 68.2 3.0 | 70.5 1.3 | 0.31 |
| Weight (kg) | 81.4 20.7 | 77.3 15.0 | 83.1 23.3 | 82.7 21.7 | 81.6 18.1 | 0.64 |
| Hypertension, n (%) | 96 (79) | 29*(97) | 47 (78) | 12 (63) | 8 (62) | 0.01* |
| Diabetes Mellitus, n (%) | 41 (34) | 10 (33) | 21 (35) | 6 (32) | 4 (31) | 0.99 |
| Chronic kidney disease, n (%) | 46 (38) | 10 (33) | 21 (35) | 8 (42) | 7 (54) | 0.57 |
| Heart failure, n (%) | 32 (26) | 12 (40) | 13 (22) | 6 (32) | 1 (8) | 0.10 |
| Serum creatinine (mg/dL) | 2.57 2.4 | 2.09 1.5 | 2.93 3.0 | 2.37 1.2 | 2.29 2.1 | 0.41 |
| Acute renal failure, n (%) | 84 (69) | 19 (63) | 45 (75) | 12 (63) | 8 (62) | 0.55 |
| Concomitant hyperkalemia‐precipitating medications, n (%) | 60 (49) | 19 (63) | 23 (38) | 10 (53) | 8 (61) | 0.11 |
Results
Patient Characteristics
Study subjects consisted of patients who received SPS in the hospital for treatment of hyperkalemia. A total of 140 patients were identified and 122 met the inclusion criteria. Eighteen patients were excluded for current hemodialysis, receiving other treatments for hyperkalemia, and specimen hemolysis. Of those who were included in the study analysis, 30 patients received 15 gm of SPS, 60 patients received 30 gm, 19 patients received 45 gm, and 13 patients received 60 gm. Baseline characteristics of included patients are shown in Table 1. The majority of patients were male (99%) and had comorbid conditions.
At baseline, the mean serum creatinine concentration was 2.57 2.36 mg/dL. Documented acute renal dysfunction was present at the time of the hyperkalemic event in 69% of patients. Forty‐nine percent of patients were taking at least one medication that can precipitate hyperkalemia. The most common medications were ACE inhibitors (52%). All baseline characteristics were similar among the different cohorts except for HTN. There were significantly more patients with HTN in the 15 gm dosage group compared to the others. There was no effect of baseline characteristics on the primary or secondary outcomes.
Clinical Outcome
A total of 115 patients (94%) achieved normalization of potassium concentration with a single dose of SPS. The mean SPS dose given was 31.84 13.58 gm. The changes in mean electrolyte values for all patients are shown in Table 2. The mean reduction in potassium concentration was 0.99 0.51 mmol/L (P < 0.0001). The follow‐up potassium concentration was obtained on an average of 10 hours after administration of SPS. The mean reduction in calcium concentration was 0.07 0.53 mg/dL (P = 0.13). Further, the mean reduction in sodium concentration was 0.09 3.33 mg/dL (P = 0.004). Figure 1 depicts the change in serum potassium concentration in each of the SPS dosage groups. The mean change in potassium concentrations compared to baseline was statistically significant in all dosage groups. The mean reduction in potassium concentration achieved statistical significance between the 15 gm and 60 gm groups (P < 0.05) and between the 30 gm and 60 gm groups (P < 0.05) (Table 3). To adjust for the potential covariate effects in these group mean comparisons, we further calculated the LSMEAN. Table 3 presents the least square mean changes in serum potassium concentration in each of the SPS dosage groups. As shown in Table 4, the least square mean changes in potassium concentrations compared to the baseline were also statistically significant in all dosage groups. These group differences remain significant, even after the adjustment by the baseline variables.
| Electrolytes | Pre‐SPS | Post‐SPS | Mean Change | P Value |
|---|---|---|---|---|
| ||||
| K+(mmol/L) | 5.57 0.35 | 4.59 0.46 | 0.99 0.51 | <0.0001 |
| Ca2+(mg/dL) | 8.54 0.81 | 8.46 0.64 | 0.07 0.53 | 0.13 |
| Na+(mmol/L) | 136.7 4.66 | 137.6 4.65 | 0.89 3.33 | 0.004 |
| Dose (gm) | Difference Between Means | CI for Difference Between Means |
|---|---|---|
| ||
| 15‐30 | 0.13 | 0.43, 0.16 |
| 15‐45 | 0.27 | 0.66, 0.11 |
| 15‐60* | 0.64 | 1.09, 0.19 |
| 30‐45 | 0.14 | 0.48, 0.20 |
| 30‐60* | 0.50 | 0.91, 0.10 |
| 45‐60 | 0.36 | 0.82, 0.10 |
| SPS Dose | LSMEAN of Potassium Reduction | 95% Confidence Limits | |
|---|---|---|---|
| |||
| 15 gm | 0.676566 | 0.119091 | 1.234041 |
| 30 gm | 0.808860 | 0.260418 | 1.357302 |
| 45 gm | 0.951205 | 0.431039 | 1.471371 |
| 60 gm | 1.313806 | 0.718793 | 1.908818 |
Subset Analysis
To address cointervention bias, an analysis of patients who were on at least 1 medication that predisposed them to hyperkalemia such as ACE inhibitors, ARBs, potassium sparing diuretics, aldosterone antagonists, NSAIDs, potassium supplements, and antibiotics such as trimethoprim/sulfamethoxazole (n = 60) were reviewed. Of the 60 patients, 30 received SPS and had hyperkalemia‐precipitating medications adjusted and 29 patients received SPS alone. Of those who had medications adjusted, the majority of them (83%) had these medications discontinued. The mean potassium concentration before the intervention was approximately 5.6 mmol/L in both groups. The mean SPS dose given was also similar as well as the mean potassium reduction of approximately 1 mmol/L.
Discussion
In this study, we retrospectively examined inpatients who received a single dose of SPS for the treatment of hyperkalemia. In addition, we established a possible dose response relationship in the treatment of mild to moderate hyperkalemia with SPS monotherapy. Our data revealed that 94% of patients achieved normalization of serum potassium concentration with a single dose of SPS. None of the patients experienced hypokalemia as a result of SPS administration. Moreover, when compared to the work by Mikrut and Brockmiller‐Sell,18 we found a similar reduction in serum potassium associated with the 30 gm (0.95 mmol/L vs. 1 mmol/L) and 60 gm (1.40 vs. 1.48 mEq/L) doses of SPS.
As expected, patients with higher serum potassium concentrations received higher SPS doses. Our data illustrated a possible direct, dose‐response relationship between the SPS dose and the reduction in serum potassium concentration. All of the dosage groups produced a statistically significant reduction in potassium concentrations compared to baseline. Moreover, a statistically significant difference was found in the 60 gm group when compared to the 15 gm and 30 gm groups. The mean increase change in sodium of 0.89 3.33 mmol/L was found to be statistically significant (P = 0.004) but not felt to be clinically relevant. The mean change in calcium concentration of 0.07 0.53 was not statistically significant (P = 0.13).
As with any retrospective chart review, incomplete documentation limits data collection. This may have led to an underestimation of the presence of ARF or other risk factors for hyperkalemia at the time of the event. We excluded patients who received other treatment for hyperkalemia in order to truly assess the effects of SPS on potassium concentration. However, we did not account for all potential confounding variables that are likely to affect potassium concentration such as acid‐base status and glycemic control at the time of the hyperkalemic episode. Also, dietary intake of potassium was not ascertained. Absence of a control group is also a limitation of the study, as it does not allow for complete causality to be established. The sample size, although significantly larger than previous studies, was small especially in regards to the subset analysis. Results cannot be generalized to women since the sample of females was very small or to those who were excluded from the analysis by design. Finally, this study evaluated hospitalized patients and direct extrapolation of the results to outpatient settings should be done cautiously, particularly in light of nutritional considerations.
Our study demonstrates a possible dose‐response relationship in lowering potassium concentrations with SPS. The data presented in this paper can be used to develop a potential dosing guideline for the use of SPS in the clinical management of hyperkalemia in a variety of clinical settings. It provides a basis for a much needed prospective study to finalize a dosing scheme for the use of SPS. Having a dosing scheme would serve as a resource for determining what dose of SPS to give for varying degrees of hyperkalemia while being mindful that individual responses to potassium lowering effect of SPS might be variable.
Acknowledgements
The authors thank the editors and reviewers of The Journal of Hospital Medicine for their comments and suggestions. Jaclyn Ng and Kathya Valdez worked equally on manuscript as second authors.
- ,Hyperkalemia: a review.J Intensive Care Med.2005;20(5):272–290.
- Drug‐induced hyperkalemia: old culprits and new offenders.Am J Med.2000;109(4):307–314.
- ,Hyperkalemia.Am Fam Physician.2006;73(2):283–290.
- ,Indications for hospitalization of patients with hyperkalemia.Arch Intern Med.2000;160(11):1605–1611.
- Hyperkalemia: a potentially lethal clinical condition.Acta Clin Croat.2001;40(3):215–225.
- Hypokalemia and hyperkalemia.Med Clin North Am.1997;81(3):611–639.
- ,,,,Hyperkalemia in patients in hospital.BMJ.1983;286(6372):1189–1192.
- ,,,Treatment of electrolyte disorders in adult patients in the intensive care unit.Am J Health Syst Pharm.2005;62(16):1663–1682.
- ,,,Hyperkalemia revisited.Tex Heart Inst J.2006;33(1):40–47.
- Disorders of potassium homeostasis.Hypokalemia and hyperkalemia. Crit Care Clin.2002;18(2):273–288.
- ,,,Drug‐induced hyperkalemia.Medicine.1985;64(6):357–370.
- ,Therapeutic approach to hyperkalemia.Nephron.2002;92(1):33–40.
- ,Controversial issues in the treatment of hyperkalemia.Nephrol Dial Transplant.2003;18(11):2215–2218.
- Sodium polystyrene sulfonate: a cation exchange resin used in treating hyperkalemia.ANNA J.1993;20(1):93–95.
- ,,,,,Effect of single dose resin‐cathartic therapy on serum potassium concentration in patients with end‐stage renal disease.J Am Soc Nephrol.1998;9(10):1924–1930.
- ,,Treatment of the oliguric patient with a new sodium‐exchange resin and sorbitol, a preliminary report.N Engl J Med.1961;264(3):111–115.
- ,,Management of hyperkalemia with a cation exchange resin.N Engl J Med.1961;264(3):115–119.
- ,Sodium polystyrene sulfonate dosing guidelines for the treatment of adult hyperkalemia.Hosp Pharm.2004;39(8):765–771.
- ,Hyperkalemia: a review.J Intensive Care Med.2005;20(5):272–290.
- Drug‐induced hyperkalemia: old culprits and new offenders.Am J Med.2000;109(4):307–314.
- ,Hyperkalemia.Am Fam Physician.2006;73(2):283–290.
- ,Indications for hospitalization of patients with hyperkalemia.Arch Intern Med.2000;160(11):1605–1611.
- Hyperkalemia: a potentially lethal clinical condition.Acta Clin Croat.2001;40(3):215–225.
- Hypokalemia and hyperkalemia.Med Clin North Am.1997;81(3):611–639.
- ,,,,Hyperkalemia in patients in hospital.BMJ.1983;286(6372):1189–1192.
- ,,,Treatment of electrolyte disorders in adult patients in the intensive care unit.Am J Health Syst Pharm.2005;62(16):1663–1682.
- ,,,Hyperkalemia revisited.Tex Heart Inst J.2006;33(1):40–47.
- Disorders of potassium homeostasis.Hypokalemia and hyperkalemia. Crit Care Clin.2002;18(2):273–288.
- ,,,Drug‐induced hyperkalemia.Medicine.1985;64(6):357–370.
- ,Therapeutic approach to hyperkalemia.Nephron.2002;92(1):33–40.
- ,Controversial issues in the treatment of hyperkalemia.Nephrol Dial Transplant.2003;18(11):2215–2218.
- Sodium polystyrene sulfonate: a cation exchange resin used in treating hyperkalemia.ANNA J.1993;20(1):93–95.
- ,,,,,Effect of single dose resin‐cathartic therapy on serum potassium concentration in patients with end‐stage renal disease.J Am Soc Nephrol.1998;9(10):1924–1930.
- ,,Treatment of the oliguric patient with a new sodium‐exchange resin and sorbitol, a preliminary report.N Engl J Med.1961;264(3):111–115.
- ,,Management of hyperkalemia with a cation exchange resin.N Engl J Med.1961;264(3):115–119.
- ,Sodium polystyrene sulfonate dosing guidelines for the treatment of adult hyperkalemia.Hosp Pharm.2004;39(8):765–771.
Copyright © 2011 Society of Hospital Medicine
Faculty Development for Hospitalists
The growth of hospitalists nationally continues at an unprecedented pace.1 In academic medical centers, the development of hospital medicine groups either as independent divisions or as part of divisions of general internal medicine (DGIM) reflects this trend. Drivers for growth in the academic setting include housestaff work hour restrictions, increased need for oversight on teaching services, development of nonhousestaff services, surgical comanagement, and greater emphasis on efficiency, quality, and safety.26 These drivers have created tremendous opportunities for hospitalists, but the rapid growth has also created challenges to achieving traditional academic success.7, 8
While hospitalists feel the traditional academic pressures to produce new knowledge and teach, the extraordinary need to expand clinical services has resulted in a young hospitalist workforce, with most lacking fellowship training. At the same time, there are few senior mentors available. Taken together, many academic hospital medicine (AHM) programs find themselves populated by large cadres of junior faculty without the support, training, and mentoring they need to succeed in a faculty career.9 For hospital medicine groups, the risk to faculty recruitment, retention, productivity, and morale is high.
In this article, we describe the development and implementation of a multifaceted Faculty Development (FD) program whose goal was to provide our faculty with clinical, educational, leadership, and scholarly skills that would promote academic output and foster work satisfaction.
Methods
Problem Identification
The University of California, San Francisco (UCSF) Medical Center operates nearly 800 beds across 2 hospitals (Parnassus and Mount Zion campuses). The UCSF Division of Hospital Medicine (DHM) provides care on the teaching service (90% of all ward months covered by a hospitalist faculty), a nonhousestaff medical service based at Mount Zion,4 a palliative care service,10 a medical consultation service, a neurosurgical comanagement service, a procedure service, and comanagement on advanced heart failure and cancer services. Like many AHM groups, ours has experienced explosive growth, more than doubling in faculty size in 3 years (50+ faculty by July 2010).
In addition, many of our new faculty joined the division directly after residency training whereas our early hospitalists were mostly former chief residents and/or fellowship‐trained. During a 2‐year period, our division lost several faculty to burnout from clinically heavy positions or because they felt their ultimate academic success was in doubt. During a 2008 divisional retreat, the single greatest need identified was to invest in the development of our first‐year faculty who were felt to be at greatest risk for burnout, dissatisfaction, and failing to integrate into the divisional mission. Based on this result, we set out to develop a program to meet this pressing need.
Needs Assessment
We formed a FD steering committee comprised of faculty from all ranks and career paths in our division (eg, educator, administrator, and investigator), with overrepresentation of recent hires to ascertain how best to meet their needs. Information from the division retreat provided the basis for the program and its priorities. The FD steering committee then outlined ideas that guided program development, which included:
New faculty should be required to meet regularly with assigned faculty mentors during their first year, and expectations for that relationship should be outlined for both parties
New faculty should be required to attend dedicated sessions that build their teaching skills
New faculty should receive a specially designed first year curriculum to provide learnings focused on high‐yield and relevant topics
New faculty should receive a set of goals, or scholarly expectations, for their first year that would foster a partnership between individual faculty and the division to meet those goals
The division should create new structures for FD that promote collaboration, sharing of personal and professional growth and challenges, and a culture of continuous learning
All of the activities that comprise our new FD program must be aligned with our stated mission: to provide the highest quality clinical care, education, system improvements, and research that benefit our patients and trainees by developing successful academic hospitalist faculty.
Program Goals and Objectives
Our DHM FD program established the goal to provide our new faculty with clinical, educational, leadership, and scholarly skills that would promote academic output and foster work satisfaction. From a broader divisional standpoint, the goal was simply to create new FD structures that fostered the division's commitment to the program. The primary objectives of the program were for new faculty to:
Increase their knowledge, skills, and attitudes about key academic hospitalist domains following participation in the program;
Demonstrate successful production of scholarly output, participation in a hospital committee, and participation in a quality or safety improvement initiative by the end of their first year;
Report high levels of satisfaction with the FD program and their first year on faculty.
Program Development Principles
We began by conducting a literature review to draw on the successes and lessons learned from existing FD programs, particularly in large departments, academic centers, and the hospitalist field.1115 We focused our program development on a set of FD principles, which included instructional improvement, organizational development, the development of professional academic skills, and the teaching of specific content.11 Furthermore, whereas many FD programs traditionally focus on mentoring or a longitudinal set of seminars, we believed a multifaceted approach could help shift our culture towards one that prioritized FD and generated a sense of community. We hoped this cultural shift would create an environment that increased faculty satisfaction with their work, with their colleagues, and in our division.
This context drove us to build programmatic activities that not only targeted new faculty, the initial focus of our planning efforts, but also the division more broadly. We wanted to adopt known strategies (eg, mentoring relationships, teaching methods for FD, and grand rounds) but also weave in new ones that targeted AHM and our Division. It was clear that successful programs used a variety of instructional methods, and often combined methods, to create active and engaged faculty. We similarly wanted to create venues for didactic and small‐group learning, but also opportunities for peer learning and facilitated discussions around important topics. Allowing new faculty to learn from each other, and having them observe more senior faculty do the same, would be an important and explicit programmatic element.
Program Description and Implementation
All new faculty meet with Divisional leadership (RMW/BAS), administrative staff (they receive an orientation binder that highlights frequently asked questions and provides service‐specific orientation documents), and the Director of FD (NLS). The latter introduces the DHM FD Program and provides the road map for their first year (Supporting Information). The checklist serves to orient, guide, and emphasize the various programmatic goals, expectations, and logistics. Discussion focuses on the activities targeted to new faculty followed by wider divisional offerings. New faculty activities include:
Coaching Program
Rather than having new faculty independently seek out an appropriate mentor, we explicitly paired each with a more senior hospitalist (eg, 3 years on faculty). We provided explicit goals and expectations for the faculty coach and used a similar road map to guide their role (Supporting Information). We chose to call them coaches rather than mentors because in the first year, we felt a new faculty member needed nuts and bolts support from a big sibling more than they needed formal academic mentoring. We placed the burden of organizing the coaching sessions on the faculty coach and provided them with periodic reminders and suggestions for topics to discuss over the course the year, including supporting the junior faculty's performance against their scholarly benchmarks. Finally, we also organized a peer mentoring session for new facultydesigned to create additional peer support and shared learnings, and establish the importance of these relationships moving forward.
Core Seminars
We created a 12‐hour curriculum to cover a broad range of relevant AHM topics (Table 1). The choice of topics was informed by our needs assessment, suggestions of the FD Steering Committee, and the new faculty themselves. The sessions included a few didactic presentations, but they were largely interactive in a workshop‐style format to allow new faculty to engage the content. For instance, a session on quality improvement asked new faculty to bring a project idea and then work through creating a project plan. We coupled three half‐day sessions with a divisional social activity and made every attempt to ensure new faculty were not distracted by clinical responsibilities (eg, not on a clinical service or coverage was provided).
|
| Core Seminars |
| Being an academic hospitalist: The nuts & bolts |
| Tools for the master clinician |
| Documentation pearls & practices: Clinical, billing, and medico‐legal issues |
| Preparing your first talk: From topic selection to power point presentation |
| Choosing a case and writing it up for a clinical vignette abstract submission |
| Searching for clinical answers: An interactive computer‐lab workshop |
| Introduction to quality improvement |
| Leadership 101: Self‐awareness, your Myers‐Briggs, and leading change |
| Project Management: An exercise in team building |
| Thinking about systems and creating a culture of safety |
| Lunch Seminars |
| Managing and updating your academic CV |
| What to do when a patient on your service dies? |
| Evaluating students & housestaffAnd giving feedback |
| Being an effective ward attending |
| Medical‐legal consultative work & being an expert witness |
| Getting involved in professional societies |
| Understanding the promotion tracks: Practical tips and career preparation |
| Getting involved in hospital committee work |
| Caring for sick family members & navigating the healthcare system as a physician |
| Retirement planning 101: Life after UCSF |
| Time management & creating scholarly work |
| Teaching medical students on the wards |
| Clinical resources: What do you use to find answers? |
Teaching Course
One of our faculty (BAS) delivered the Stanford Faculty Development Clinical Teaching program16 (a train the trainer model designed to teach faculty how to become more effective teachers) to all new faculty. The program consisted of 14 hours of highly interactive curricula, video review, and role plays. The course was offered after hours (4 PM or 5 PM) and with input from the new faculty to ensure availability and participation.
Feedback and Observation
Each new faculty received directed feedback about their teaching and supervision on the housestaff service following their first rotation. Feedback was based on housestaff evaluations and direct observation of the new faculty during patient care and teaching rounds. One of our faculty (BAS) observed each new faculty member during rounds, and met with them individually to provide feedback and generate a discussion about teaching style and improvement opportunities.
Scholarly Expectations
We developed a set of scholarly expectations for new faculty. These helped inform the coach‐new faculty meetings and our selection of content for the Core Seminars. We initially had concerns that these expectations could overwhelm new faculty, but those junior faculty (years 2‐4) on the FD steering committee urged this practice, wishing they had similar guidance in their first year.
From the divisional perspective, we also added a number of new structures.
Grand Rounds
We established a monthly continuing medical education (CME) credit‐granting DHM Grand Rounds that combined a 10‐minute Hospital Medicine Update with a 45‐minute didactic presentation. The updates were presented by new faculty in order to provide them with an opportunity to receive feedback on their teaching and presentation skills (eg, how to give a talk, make PowerPoint slides, etc.). Didactic presentations were given by senior DHM faculty as well as subspecialty colleagues or ones from other departments (eg, dermatology or neurology), disciplines (eg, risk management), or campuses.
FD Lunch Seminar Series
Our division traditionally meets each Monday over the lunch hour to talk about service or academic issues. With a growing division, we believed there was an opportunity to better organize the content of these meetings. Once monthly, we dedicated a lunch session to a Faculty Development Seminar with topics that spanned a variety of interest areas, were driven by faculty suggestions, and were focused on being facilitated discussions rather than didactics. Table 1 provides examples of these seminar topics.
| Survey Statements Reporting Level of Comfort With(% responding somewhat agree or agree) | Previous Faculty, % (n = 11) | New Faculty, % (n = 6) |
|---|---|---|
| Identifying important resources within the School of Medicine | 64 | 83 |
| Identifying important resources within the Department of Medicine | 63 | 100 |
| Identifying important resources within the Division of Hospital Medicine | 90 | 100 |
| Identifying important resources within UCSF Medical Center | 72 | 67 |
| Having a system to effectively manage my email | 64 | 67 |
| Having a system to keep my CV updated | 64 | 84 |
| Using my non‐clinical time for academic success | 54 | 67 |
| Best practices for clinical/medico‐legal documentation | 54 | 67 |
| Best practices for billing documentation | 62 | 84 |
| Being an effective supervising ward attending | 90 | 84 |
| Being an effective teacher | 90 | 84 |
| Evaluating students and housestaff performance | 90 | 83 |
| Providing feedback to students and housestaff | 90 | 100 |
| Getting involved in professional societies | 27 | 100 |
| Understanding the difference between promotion pathways | 36 | 67 |
| Getting involved in hospital committee work | 54 | 84 |
| Choosing a good case for a clinical vignette submission to a regional/national meeting | 54 | 83 |
| Creating a poster for presentation at a regional/national meeting | 36 | 84 |
| Giving a lecture to students or residents | 64 | 84 |
| Developing a PowerPoint presentation for a lecture | 45 | 100 |
| Describing my personality type and how it relates to my work | 45 | 100 |
| Understanding important aspects of being a leader | 54 | 100 |
| Explaining the basic principles of quality improvement | 45 | 84 |
| Participating and contributing to a quality improvement project | 54 | 67 |
| Explaining the basic principles of patient safety | 45 | 67 |
| Understanding the factors that contribute to medical errors | 36 | 84 |
| Creating scholarly products from my work | 27 | 50 |
| Identifying what kind of mentors I need for the future | 45 | 100 |
| Category (% completed during first year) | Previous Faculty, % (n = 11) | New Faculty, % (n = 6) |
|---|---|---|
| Medical student teaching | 90 | 100 |
| Talk for trainees | 45 | 100 |
| Hospital committee involvement | 63 | 100 |
| Participation in a quality or safety project | 33 | 67 |
| Abstract submission | 27 | 50 |
| Identified mentor for year 2 | 63 | 83 |
Quality and Safety Lunch Seminars
In addition to our FD seminars, we also used one lunch session each month to provide updates on performance measures, ongoing quality or safety improvement initiatives, or a broader quality or safety topic. Speakers were either divisional or outside experts, depending on the topic, and organized by our director for quality and safety.
Incubator Sessions
Our director of research (AA) organized a weekly works in progress meeting, to which faculty and fellows brought ideas, grant applications, early manuscript drafts, or other potential scholarship products to obtain feedback and further group mentorship.
Divisional Retreats
We began alternating annual full‐day and mini half‐day retreats as a method to bring the division together, build camaraderie, set strategic priorities, identify divisional goals, and assess needs. These helped guide the creation of additional FD opportunities as well as our overall division's strategy to achieve our academic mission. The outcomes of these retreats led to many significant initiatives and policies, such as changes in compensation models, new scheduling processes, and decisions to spend resources on areas such as quality improvement.
Program Evaluation
Our evaluation focused on measuring the FD program's impact on our new faculty. We tracked their success in completing the stated scholarly expectations and surveyed them about their satisfaction with the programmatic activities, their first year on faculty, and their preparation for year 2. Prior to implementing the program, we surveyed the previous 2 years of new faculty to provide a comparison.
Results
Seven faculty participated in the inaugural program. We compared their scholarly output and experiences (6 faculty completed the survey; 87% response rate) with that of 11 more senior faculty who completed the comparison survey. Of note, the response rate of the comparison group was 69% (5 faculty who departed from our division during the previous 2 years were not surveyed). New faculty were surveyed at the start of the academic year with the follow‐up survey completed the following June. The more senior faculty completed the survey once at the same time as the baseline survey for the new faculty. All new faculty participated in each of the Core Seminars, the Teaching Course, the required number of Coaching sessions, and the observed teaching activity. We did not track their attendance at Divisional activities such as Grand Rounds or the Lunch Seminars.
Overall, the FD programmatic offerings were rated highly by new faculty (on a scale of 1 [lowest] to 5 [highest] for a global rating of each FD activity): Core Seminars 4.83 0.41, Coaching Program 4.5 0.84, Teaching Course 4.5 0.55, Grand Rounds 4.83 0.41, and Lunch Seminars 4.5 0.84. Table 2, which compares responses to a series of end of the year statements posed to new faculty, highlights notable differences in their level of comfort with specific skills and resource awareness. Given the small sample size, statistical significance was not calculated. Table 3 illustrates similar comparisons focused on academic output, which demonstrate that new faculty gave more talks to trainees, had greater involvement in hospital committees, more actively participated in quality and safety projects, and submitted more abstracts to regional or national meetings. New faculty also responded differently to which part of the FD program was most influential with 1 suggesting the Coaching Program, 2 the Core Seminars, 2 the entire program efforts, and 1 did not specify.
Table 4 illustrates comparison responses to a series of directed statements. New faculty all reported greater degrees of satisfaction overall, measured by the above responses, compared to previous faculty.
| Categories | Previous Faculty, % (n = 11) | New Faculty, % (n = 6) |
|---|---|---|
| ||
| Success: To what degree do you feel successful as an academic hospitalist at the end of your first year? (% responding successful or very successful) | 27 | 67 |
| Prepared: To what degree do you feel prepared for academic success moving into your second year on faculty? (% responding prepared or very prepared) | 27 | 100 |
| Part of DHM: I felt like an integral part of our division after my first year on faculty (% responding somewhat agree or agree) | 45 | 84 |
| Expectations: My first year on faculty exceeded my expectations (% responding somewhat agree or agree) | 27 | 84 |
Discussion
We implemented an FD program to foster the academic development of new faculty, and to mitigate the effects of growing clinical demands and a rapid group expansion on our academic mission. The impact of the program was measured by increased work satisfaction and academic output in first year faculty, greater self‐reported comfort in a variety of skills and knowledge of resources, and an improvement in our sense of purpose behind our academic mission. Though the program is only in its second year, we believe the model is of value for other AHM groups, and perhaps even nonacademic groups, all of whom may use such an investment in their hospitalists as a method to improve recruitment, job satisfaction, and retention.
Reviewing our program's first year suggests there were at least 3 keys to our success. First, we benefited tremendously from the time spent crafting a vision for the program and relying heavily on input from the target audience of junior faculty. Moreover, we made every effort to leverage existing resources (eg, using faculty who already taught about a given topic) and time commitments (eg, reshaping our existing Monday lunch meeting). Finally, we increasingly used our FD venues to connect and build networks with colleagues outside our division and within the hospital. This was a deliberate effort to create opportunities for individual faculty to be exposed to and collaborate with nonhospitalists for academic output.
Our research has some limitations, most notably the small sample size in evaluating the program for statistical significance, and the incomplete survey return rates. However, the results were quite consistent and the nonresponses of departed faculty would tend to bias our results toward the null. We also acknowledge the possibility of other confounding factors (eg, changes in clinical compensation models) that may have played a role, although compensation changes were relatively minor during the period studied and faculty did attribute many of the benefits in job satisfaction and skill building to the FD program itself.
Hospital medicine is an unusual field in that there is low barrier to entry and exit. Providers can change jobs without having to say goodbye to a large panel of patients, and in the continued mismatch between available positions and hospitalists, alternative positions can easily and quickly be found if they are dissatisfied.17 In the academic arena, even as hospitalists are hired to fill clinical gaps, they still have to perform under more traditional academic rules in order to be promoted and receive the support and kudos of colleagues and trainees. For both these reasons, early nurturing and socialization is critical to retention and academic success. While some opportunities for FD will be offered by national organizations,18 groups also have local responsibilities to support, mentor, and develop their junior faculty. Not only is such support crucial for the junior faculty themselves, but in our young field, the mentored very quickly become the mentors. Our decision to invest in both mentees and mentors reinforced the importance of mentorship for academic success and retention while planting the seeds for continued success and growth.1923 A recent study suggested that the environment for mentoring may be as important as the mentoring itself, a finding we did not specifically measure, but would support based our anecdotal experiences.24 This orientation toward future needs and creating the right milieu is crucial because demands for continued hospitalist growth are likely to remain.
Moving into year 2 of our FD program and reflecting on the lessons learned from year 1, we've adopted the same multifaceted approach with only minor adjustments to the curriculum, greater expansion of faculty involved in teaching and coaching, and a continued focus on building a sense of community around our academic mission. For the Core Seminars, we moved away from the 3 half‐day sessions and chose to host 2‐hour sessions every other month. This allowed for the same curriculum to be delivered but was much easier to logistically orchestrate. It also had the intended effect of bringing the new faculty together more regularly. In addition, we created dedicated sessions in preparation for our national meeting to allow faculty to bring abstract submissions for review and later, posters and oral presentations for feedback. These added sessions came partly as a suggestion from new faculty in our first year program, and seemed to further energize junior faculty around converting their projects into scholarship. Finally, we continue to further develop coaching and mentoring relationships in our division, partly a result of successful new facultycoach pairings.
In conclusion, our FD program had a noted impact on our new faculty and had a meaningful impact on our division in terms of camaraderie and cohesion, a shared commitment to an academic mission, and a mechanism for recruitment and retention. We hope our practical description for development and implementation of an FD program, including our specific tools, are useful to other groups considering such an initiative.
Acknowledgements
The authors thank Katherine Li for her invaluable assistance in coordinating the DHM FD program. They are also indebted to their faculty colleagues for their time and roles in teaching and mentoring within the program. Dr. Sehgal partly developed this program as part of a project during his California Healthcare Foundation Leadership Fellowship. Dr. Sharpe delivered the teaching workshops at UCSF after completing the Stanford Faculty Development Teaching Program.
- ,,,.The status of Hospital Medicine Groups in the United States.J Hosp Med.2006;1(2):75–80.
- Accreditation Council for Graduate Medical Education: information related to the ACGME's effort to address resident duty hours and other relevant resource materials. Available at: http://www.acgme.org/acWebsite/dutyHours/dh_index.asp. Accessed August 2010.
- ,,, et al.Effects of work hour reduction on residents' lives: a systematic review.JAMA.2005;294(9):1088–1100.
- ,,,,.Non‐housestaff medicine services in academic centers: models and challenges.J Hosp Med.2008;3(3):247–255.
- ,.Surgical comanagement: a natural evolution of hospitalist practice.J Hosp Med.2008;3(5):394–397.
- ,.The expanding role of hospitalists in the United States.Swiss Med Wkly.2006;136(37–38):591–596.
- 2007–08 Hospital Medicine Survey. Society of Hospital Medicine. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Survey19(4):392–393.
- ,,, et al.Challenges and opportunities in Academic Hospital Medicine: report from the Academic Hospital Medicine Summit.J Hosp Med.2009;4(4):240–246.
- .Palliative care and hospitalists: a partnership for hope.J Hosp Med.2006;1(1):5–6.
- ,.Faculty development: principles and practices.J Vet Med Educ.2006;33(3):317–324.
- ,,, et al.A systematic review of faculty development initiatives designed to improve teaching effectiveness in medical education: BEME Guide No. 8.Med Teach.2006;28(6):497–526.
- ,.A successful approach to faculty development at an independent academic medical center.Med Teach.2008;30:e10–e14.
- ,,,.An innovative approach to supporting hospitalist physicians towards academic success.J Hosp Med.2008;3(4):314–318.
- ,,, et al.The curriculum for the Hospitalized Aging Medical Patient program: a collaborative faculty development program for hospitalists, general internists, and geriatricians.J Hosp Med.2008;3(5):384–393.
- Stanford Faculty Development Clinical Teaching Program. Available at: http://www.stanford.edu/group/SFDP. Accessed August 2010.
- ,,, et al.Trends in market demand for internal medicine 1999–2004: an analysis of physician job advertisements.J Gen Intern Med.2006;21(10):1079–1085.
- The Academic Hospitalist Academy. Available at: http://www.sgim.org/index.cfm?pageId=815. Accessed August 2010.
- ,,.Mentoring in academic medicine: a systematic review.JAMA.2006;296(9):1103–1115.
- ,,.Facilitating faculty success: outcomes and cost benefit of the UCSD National Center of Leadership in Academic Medicine.Acad Med.2004;79(10 Suppl):S9–S11.
- ,,, et al.Retention of junior faculty in academic medicine at the University of California, San Diego.Acad Med.2009;84(1):37–41.
- ,,,.Helping medical school faculty realize their dreams: an innovative, collaborative mentoring program.Acad Med.2002;77:377–384.
- ,,, et al.Physicians' perceptions of institutional and leadership factors influencing their job satisfaction at one academic medical center.Acad Med.2002;77:1235–1240.
- ,,.A systematic review of qualitative research on the meaning and characteristics of mentoring in academic medicine.J Gen Intern Med.2010;25(1);72–78.
The growth of hospitalists nationally continues at an unprecedented pace.1 In academic medical centers, the development of hospital medicine groups either as independent divisions or as part of divisions of general internal medicine (DGIM) reflects this trend. Drivers for growth in the academic setting include housestaff work hour restrictions, increased need for oversight on teaching services, development of nonhousestaff services, surgical comanagement, and greater emphasis on efficiency, quality, and safety.26 These drivers have created tremendous opportunities for hospitalists, but the rapid growth has also created challenges to achieving traditional academic success.7, 8
While hospitalists feel the traditional academic pressures to produce new knowledge and teach, the extraordinary need to expand clinical services has resulted in a young hospitalist workforce, with most lacking fellowship training. At the same time, there are few senior mentors available. Taken together, many academic hospital medicine (AHM) programs find themselves populated by large cadres of junior faculty without the support, training, and mentoring they need to succeed in a faculty career.9 For hospital medicine groups, the risk to faculty recruitment, retention, productivity, and morale is high.
In this article, we describe the development and implementation of a multifaceted Faculty Development (FD) program whose goal was to provide our faculty with clinical, educational, leadership, and scholarly skills that would promote academic output and foster work satisfaction.
Methods
Problem Identification
The University of California, San Francisco (UCSF) Medical Center operates nearly 800 beds across 2 hospitals (Parnassus and Mount Zion campuses). The UCSF Division of Hospital Medicine (DHM) provides care on the teaching service (90% of all ward months covered by a hospitalist faculty), a nonhousestaff medical service based at Mount Zion,4 a palliative care service,10 a medical consultation service, a neurosurgical comanagement service, a procedure service, and comanagement on advanced heart failure and cancer services. Like many AHM groups, ours has experienced explosive growth, more than doubling in faculty size in 3 years (50+ faculty by July 2010).
In addition, many of our new faculty joined the division directly after residency training whereas our early hospitalists were mostly former chief residents and/or fellowship‐trained. During a 2‐year period, our division lost several faculty to burnout from clinically heavy positions or because they felt their ultimate academic success was in doubt. During a 2008 divisional retreat, the single greatest need identified was to invest in the development of our first‐year faculty who were felt to be at greatest risk for burnout, dissatisfaction, and failing to integrate into the divisional mission. Based on this result, we set out to develop a program to meet this pressing need.
Needs Assessment
We formed a FD steering committee comprised of faculty from all ranks and career paths in our division (eg, educator, administrator, and investigator), with overrepresentation of recent hires to ascertain how best to meet their needs. Information from the division retreat provided the basis for the program and its priorities. The FD steering committee then outlined ideas that guided program development, which included:
New faculty should be required to meet regularly with assigned faculty mentors during their first year, and expectations for that relationship should be outlined for both parties
New faculty should be required to attend dedicated sessions that build their teaching skills
New faculty should receive a specially designed first year curriculum to provide learnings focused on high‐yield and relevant topics
New faculty should receive a set of goals, or scholarly expectations, for their first year that would foster a partnership between individual faculty and the division to meet those goals
The division should create new structures for FD that promote collaboration, sharing of personal and professional growth and challenges, and a culture of continuous learning
All of the activities that comprise our new FD program must be aligned with our stated mission: to provide the highest quality clinical care, education, system improvements, and research that benefit our patients and trainees by developing successful academic hospitalist faculty.
Program Goals and Objectives
Our DHM FD program established the goal to provide our new faculty with clinical, educational, leadership, and scholarly skills that would promote academic output and foster work satisfaction. From a broader divisional standpoint, the goal was simply to create new FD structures that fostered the division's commitment to the program. The primary objectives of the program were for new faculty to:
Increase their knowledge, skills, and attitudes about key academic hospitalist domains following participation in the program;
Demonstrate successful production of scholarly output, participation in a hospital committee, and participation in a quality or safety improvement initiative by the end of their first year;
Report high levels of satisfaction with the FD program and their first year on faculty.
Program Development Principles
We began by conducting a literature review to draw on the successes and lessons learned from existing FD programs, particularly in large departments, academic centers, and the hospitalist field.1115 We focused our program development on a set of FD principles, which included instructional improvement, organizational development, the development of professional academic skills, and the teaching of specific content.11 Furthermore, whereas many FD programs traditionally focus on mentoring or a longitudinal set of seminars, we believed a multifaceted approach could help shift our culture towards one that prioritized FD and generated a sense of community. We hoped this cultural shift would create an environment that increased faculty satisfaction with their work, with their colleagues, and in our division.
This context drove us to build programmatic activities that not only targeted new faculty, the initial focus of our planning efforts, but also the division more broadly. We wanted to adopt known strategies (eg, mentoring relationships, teaching methods for FD, and grand rounds) but also weave in new ones that targeted AHM and our Division. It was clear that successful programs used a variety of instructional methods, and often combined methods, to create active and engaged faculty. We similarly wanted to create venues for didactic and small‐group learning, but also opportunities for peer learning and facilitated discussions around important topics. Allowing new faculty to learn from each other, and having them observe more senior faculty do the same, would be an important and explicit programmatic element.
Program Description and Implementation
All new faculty meet with Divisional leadership (RMW/BAS), administrative staff (they receive an orientation binder that highlights frequently asked questions and provides service‐specific orientation documents), and the Director of FD (NLS). The latter introduces the DHM FD Program and provides the road map for their first year (Supporting Information). The checklist serves to orient, guide, and emphasize the various programmatic goals, expectations, and logistics. Discussion focuses on the activities targeted to new faculty followed by wider divisional offerings. New faculty activities include:
Coaching Program
Rather than having new faculty independently seek out an appropriate mentor, we explicitly paired each with a more senior hospitalist (eg, 3 years on faculty). We provided explicit goals and expectations for the faculty coach and used a similar road map to guide their role (Supporting Information). We chose to call them coaches rather than mentors because in the first year, we felt a new faculty member needed nuts and bolts support from a big sibling more than they needed formal academic mentoring. We placed the burden of organizing the coaching sessions on the faculty coach and provided them with periodic reminders and suggestions for topics to discuss over the course the year, including supporting the junior faculty's performance against their scholarly benchmarks. Finally, we also organized a peer mentoring session for new facultydesigned to create additional peer support and shared learnings, and establish the importance of these relationships moving forward.
Core Seminars
We created a 12‐hour curriculum to cover a broad range of relevant AHM topics (Table 1). The choice of topics was informed by our needs assessment, suggestions of the FD Steering Committee, and the new faculty themselves. The sessions included a few didactic presentations, but they were largely interactive in a workshop‐style format to allow new faculty to engage the content. For instance, a session on quality improvement asked new faculty to bring a project idea and then work through creating a project plan. We coupled three half‐day sessions with a divisional social activity and made every attempt to ensure new faculty were not distracted by clinical responsibilities (eg, not on a clinical service or coverage was provided).
|
| Core Seminars |
| Being an academic hospitalist: The nuts & bolts |
| Tools for the master clinician |
| Documentation pearls & practices: Clinical, billing, and medico‐legal issues |
| Preparing your first talk: From topic selection to power point presentation |
| Choosing a case and writing it up for a clinical vignette abstract submission |
| Searching for clinical answers: An interactive computer‐lab workshop |
| Introduction to quality improvement |
| Leadership 101: Self‐awareness, your Myers‐Briggs, and leading change |
| Project Management: An exercise in team building |
| Thinking about systems and creating a culture of safety |
| Lunch Seminars |
| Managing and updating your academic CV |
| What to do when a patient on your service dies? |
| Evaluating students & housestaffAnd giving feedback |
| Being an effective ward attending |
| Medical‐legal consultative work & being an expert witness |
| Getting involved in professional societies |
| Understanding the promotion tracks: Practical tips and career preparation |
| Getting involved in hospital committee work |
| Caring for sick family members & navigating the healthcare system as a physician |
| Retirement planning 101: Life after UCSF |
| Time management & creating scholarly work |
| Teaching medical students on the wards |
| Clinical resources: What do you use to find answers? |
Teaching Course
One of our faculty (BAS) delivered the Stanford Faculty Development Clinical Teaching program16 (a train the trainer model designed to teach faculty how to become more effective teachers) to all new faculty. The program consisted of 14 hours of highly interactive curricula, video review, and role plays. The course was offered after hours (4 PM or 5 PM) and with input from the new faculty to ensure availability and participation.
Feedback and Observation
Each new faculty received directed feedback about their teaching and supervision on the housestaff service following their first rotation. Feedback was based on housestaff evaluations and direct observation of the new faculty during patient care and teaching rounds. One of our faculty (BAS) observed each new faculty member during rounds, and met with them individually to provide feedback and generate a discussion about teaching style and improvement opportunities.
Scholarly Expectations
We developed a set of scholarly expectations for new faculty. These helped inform the coach‐new faculty meetings and our selection of content for the Core Seminars. We initially had concerns that these expectations could overwhelm new faculty, but those junior faculty (years 2‐4) on the FD steering committee urged this practice, wishing they had similar guidance in their first year.
From the divisional perspective, we also added a number of new structures.
Grand Rounds
We established a monthly continuing medical education (CME) credit‐granting DHM Grand Rounds that combined a 10‐minute Hospital Medicine Update with a 45‐minute didactic presentation. The updates were presented by new faculty in order to provide them with an opportunity to receive feedback on their teaching and presentation skills (eg, how to give a talk, make PowerPoint slides, etc.). Didactic presentations were given by senior DHM faculty as well as subspecialty colleagues or ones from other departments (eg, dermatology or neurology), disciplines (eg, risk management), or campuses.
FD Lunch Seminar Series
Our division traditionally meets each Monday over the lunch hour to talk about service or academic issues. With a growing division, we believed there was an opportunity to better organize the content of these meetings. Once monthly, we dedicated a lunch session to a Faculty Development Seminar with topics that spanned a variety of interest areas, were driven by faculty suggestions, and were focused on being facilitated discussions rather than didactics. Table 1 provides examples of these seminar topics.
| Survey Statements Reporting Level of Comfort With(% responding somewhat agree or agree) | Previous Faculty, % (n = 11) | New Faculty, % (n = 6) |
|---|---|---|
| Identifying important resources within the School of Medicine | 64 | 83 |
| Identifying important resources within the Department of Medicine | 63 | 100 |
| Identifying important resources within the Division of Hospital Medicine | 90 | 100 |
| Identifying important resources within UCSF Medical Center | 72 | 67 |
| Having a system to effectively manage my email | 64 | 67 |
| Having a system to keep my CV updated | 64 | 84 |
| Using my non‐clinical time for academic success | 54 | 67 |
| Best practices for clinical/medico‐legal documentation | 54 | 67 |
| Best practices for billing documentation | 62 | 84 |
| Being an effective supervising ward attending | 90 | 84 |
| Being an effective teacher | 90 | 84 |
| Evaluating students and housestaff performance | 90 | 83 |
| Providing feedback to students and housestaff | 90 | 100 |
| Getting involved in professional societies | 27 | 100 |
| Understanding the difference between promotion pathways | 36 | 67 |
| Getting involved in hospital committee work | 54 | 84 |
| Choosing a good case for a clinical vignette submission to a regional/national meeting | 54 | 83 |
| Creating a poster for presentation at a regional/national meeting | 36 | 84 |
| Giving a lecture to students or residents | 64 | 84 |
| Developing a PowerPoint presentation for a lecture | 45 | 100 |
| Describing my personality type and how it relates to my work | 45 | 100 |
| Understanding important aspects of being a leader | 54 | 100 |
| Explaining the basic principles of quality improvement | 45 | 84 |
| Participating and contributing to a quality improvement project | 54 | 67 |
| Explaining the basic principles of patient safety | 45 | 67 |
| Understanding the factors that contribute to medical errors | 36 | 84 |
| Creating scholarly products from my work | 27 | 50 |
| Identifying what kind of mentors I need for the future | 45 | 100 |
| Category (% completed during first year) | Previous Faculty, % (n = 11) | New Faculty, % (n = 6) |
|---|---|---|
| Medical student teaching | 90 | 100 |
| Talk for trainees | 45 | 100 |
| Hospital committee involvement | 63 | 100 |
| Participation in a quality or safety project | 33 | 67 |
| Abstract submission | 27 | 50 |
| Identified mentor for year 2 | 63 | 83 |
Quality and Safety Lunch Seminars
In addition to our FD seminars, we also used one lunch session each month to provide updates on performance measures, ongoing quality or safety improvement initiatives, or a broader quality or safety topic. Speakers were either divisional or outside experts, depending on the topic, and organized by our director for quality and safety.
Incubator Sessions
Our director of research (AA) organized a weekly works in progress meeting, to which faculty and fellows brought ideas, grant applications, early manuscript drafts, or other potential scholarship products to obtain feedback and further group mentorship.
Divisional Retreats
We began alternating annual full‐day and mini half‐day retreats as a method to bring the division together, build camaraderie, set strategic priorities, identify divisional goals, and assess needs. These helped guide the creation of additional FD opportunities as well as our overall division's strategy to achieve our academic mission. The outcomes of these retreats led to many significant initiatives and policies, such as changes in compensation models, new scheduling processes, and decisions to spend resources on areas such as quality improvement.
Program Evaluation
Our evaluation focused on measuring the FD program's impact on our new faculty. We tracked their success in completing the stated scholarly expectations and surveyed them about their satisfaction with the programmatic activities, their first year on faculty, and their preparation for year 2. Prior to implementing the program, we surveyed the previous 2 years of new faculty to provide a comparison.
Results
Seven faculty participated in the inaugural program. We compared their scholarly output and experiences (6 faculty completed the survey; 87% response rate) with that of 11 more senior faculty who completed the comparison survey. Of note, the response rate of the comparison group was 69% (5 faculty who departed from our division during the previous 2 years were not surveyed). New faculty were surveyed at the start of the academic year with the follow‐up survey completed the following June. The more senior faculty completed the survey once at the same time as the baseline survey for the new faculty. All new faculty participated in each of the Core Seminars, the Teaching Course, the required number of Coaching sessions, and the observed teaching activity. We did not track their attendance at Divisional activities such as Grand Rounds or the Lunch Seminars.
Overall, the FD programmatic offerings were rated highly by new faculty (on a scale of 1 [lowest] to 5 [highest] for a global rating of each FD activity): Core Seminars 4.83 0.41, Coaching Program 4.5 0.84, Teaching Course 4.5 0.55, Grand Rounds 4.83 0.41, and Lunch Seminars 4.5 0.84. Table 2, which compares responses to a series of end of the year statements posed to new faculty, highlights notable differences in their level of comfort with specific skills and resource awareness. Given the small sample size, statistical significance was not calculated. Table 3 illustrates similar comparisons focused on academic output, which demonstrate that new faculty gave more talks to trainees, had greater involvement in hospital committees, more actively participated in quality and safety projects, and submitted more abstracts to regional or national meetings. New faculty also responded differently to which part of the FD program was most influential with 1 suggesting the Coaching Program, 2 the Core Seminars, 2 the entire program efforts, and 1 did not specify.
Table 4 illustrates comparison responses to a series of directed statements. New faculty all reported greater degrees of satisfaction overall, measured by the above responses, compared to previous faculty.
| Categories | Previous Faculty, % (n = 11) | New Faculty, % (n = 6) |
|---|---|---|
| ||
| Success: To what degree do you feel successful as an academic hospitalist at the end of your first year? (% responding successful or very successful) | 27 | 67 |
| Prepared: To what degree do you feel prepared for academic success moving into your second year on faculty? (% responding prepared or very prepared) | 27 | 100 |
| Part of DHM: I felt like an integral part of our division after my first year on faculty (% responding somewhat agree or agree) | 45 | 84 |
| Expectations: My first year on faculty exceeded my expectations (% responding somewhat agree or agree) | 27 | 84 |
Discussion
We implemented an FD program to foster the academic development of new faculty, and to mitigate the effects of growing clinical demands and a rapid group expansion on our academic mission. The impact of the program was measured by increased work satisfaction and academic output in first year faculty, greater self‐reported comfort in a variety of skills and knowledge of resources, and an improvement in our sense of purpose behind our academic mission. Though the program is only in its second year, we believe the model is of value for other AHM groups, and perhaps even nonacademic groups, all of whom may use such an investment in their hospitalists as a method to improve recruitment, job satisfaction, and retention.
Reviewing our program's first year suggests there were at least 3 keys to our success. First, we benefited tremendously from the time spent crafting a vision for the program and relying heavily on input from the target audience of junior faculty. Moreover, we made every effort to leverage existing resources (eg, using faculty who already taught about a given topic) and time commitments (eg, reshaping our existing Monday lunch meeting). Finally, we increasingly used our FD venues to connect and build networks with colleagues outside our division and within the hospital. This was a deliberate effort to create opportunities for individual faculty to be exposed to and collaborate with nonhospitalists for academic output.
Our research has some limitations, most notably the small sample size in evaluating the program for statistical significance, and the incomplete survey return rates. However, the results were quite consistent and the nonresponses of departed faculty would tend to bias our results toward the null. We also acknowledge the possibility of other confounding factors (eg, changes in clinical compensation models) that may have played a role, although compensation changes were relatively minor during the period studied and faculty did attribute many of the benefits in job satisfaction and skill building to the FD program itself.
Hospital medicine is an unusual field in that there is low barrier to entry and exit. Providers can change jobs without having to say goodbye to a large panel of patients, and in the continued mismatch between available positions and hospitalists, alternative positions can easily and quickly be found if they are dissatisfied.17 In the academic arena, even as hospitalists are hired to fill clinical gaps, they still have to perform under more traditional academic rules in order to be promoted and receive the support and kudos of colleagues and trainees. For both these reasons, early nurturing and socialization is critical to retention and academic success. While some opportunities for FD will be offered by national organizations,18 groups also have local responsibilities to support, mentor, and develop their junior faculty. Not only is such support crucial for the junior faculty themselves, but in our young field, the mentored very quickly become the mentors. Our decision to invest in both mentees and mentors reinforced the importance of mentorship for academic success and retention while planting the seeds for continued success and growth.1923 A recent study suggested that the environment for mentoring may be as important as the mentoring itself, a finding we did not specifically measure, but would support based our anecdotal experiences.24 This orientation toward future needs and creating the right milieu is crucial because demands for continued hospitalist growth are likely to remain.
Moving into year 2 of our FD program and reflecting on the lessons learned from year 1, we've adopted the same multifaceted approach with only minor adjustments to the curriculum, greater expansion of faculty involved in teaching and coaching, and a continued focus on building a sense of community around our academic mission. For the Core Seminars, we moved away from the 3 half‐day sessions and chose to host 2‐hour sessions every other month. This allowed for the same curriculum to be delivered but was much easier to logistically orchestrate. It also had the intended effect of bringing the new faculty together more regularly. In addition, we created dedicated sessions in preparation for our national meeting to allow faculty to bring abstract submissions for review and later, posters and oral presentations for feedback. These added sessions came partly as a suggestion from new faculty in our first year program, and seemed to further energize junior faculty around converting their projects into scholarship. Finally, we continue to further develop coaching and mentoring relationships in our division, partly a result of successful new facultycoach pairings.
In conclusion, our FD program had a noted impact on our new faculty and had a meaningful impact on our division in terms of camaraderie and cohesion, a shared commitment to an academic mission, and a mechanism for recruitment and retention. We hope our practical description for development and implementation of an FD program, including our specific tools, are useful to other groups considering such an initiative.
Acknowledgements
The authors thank Katherine Li for her invaluable assistance in coordinating the DHM FD program. They are also indebted to their faculty colleagues for their time and roles in teaching and mentoring within the program. Dr. Sehgal partly developed this program as part of a project during his California Healthcare Foundation Leadership Fellowship. Dr. Sharpe delivered the teaching workshops at UCSF after completing the Stanford Faculty Development Teaching Program.
The growth of hospitalists nationally continues at an unprecedented pace.1 In academic medical centers, the development of hospital medicine groups either as independent divisions or as part of divisions of general internal medicine (DGIM) reflects this trend. Drivers for growth in the academic setting include housestaff work hour restrictions, increased need for oversight on teaching services, development of nonhousestaff services, surgical comanagement, and greater emphasis on efficiency, quality, and safety.26 These drivers have created tremendous opportunities for hospitalists, but the rapid growth has also created challenges to achieving traditional academic success.7, 8
While hospitalists feel the traditional academic pressures to produce new knowledge and teach, the extraordinary need to expand clinical services has resulted in a young hospitalist workforce, with most lacking fellowship training. At the same time, there are few senior mentors available. Taken together, many academic hospital medicine (AHM) programs find themselves populated by large cadres of junior faculty without the support, training, and mentoring they need to succeed in a faculty career.9 For hospital medicine groups, the risk to faculty recruitment, retention, productivity, and morale is high.
In this article, we describe the development and implementation of a multifaceted Faculty Development (FD) program whose goal was to provide our faculty with clinical, educational, leadership, and scholarly skills that would promote academic output and foster work satisfaction.
Methods
Problem Identification
The University of California, San Francisco (UCSF) Medical Center operates nearly 800 beds across 2 hospitals (Parnassus and Mount Zion campuses). The UCSF Division of Hospital Medicine (DHM) provides care on the teaching service (90% of all ward months covered by a hospitalist faculty), a nonhousestaff medical service based at Mount Zion,4 a palliative care service,10 a medical consultation service, a neurosurgical comanagement service, a procedure service, and comanagement on advanced heart failure and cancer services. Like many AHM groups, ours has experienced explosive growth, more than doubling in faculty size in 3 years (50+ faculty by July 2010).
In addition, many of our new faculty joined the division directly after residency training whereas our early hospitalists were mostly former chief residents and/or fellowship‐trained. During a 2‐year period, our division lost several faculty to burnout from clinically heavy positions or because they felt their ultimate academic success was in doubt. During a 2008 divisional retreat, the single greatest need identified was to invest in the development of our first‐year faculty who were felt to be at greatest risk for burnout, dissatisfaction, and failing to integrate into the divisional mission. Based on this result, we set out to develop a program to meet this pressing need.
Needs Assessment
We formed a FD steering committee comprised of faculty from all ranks and career paths in our division (eg, educator, administrator, and investigator), with overrepresentation of recent hires to ascertain how best to meet their needs. Information from the division retreat provided the basis for the program and its priorities. The FD steering committee then outlined ideas that guided program development, which included:
New faculty should be required to meet regularly with assigned faculty mentors during their first year, and expectations for that relationship should be outlined for both parties
New faculty should be required to attend dedicated sessions that build their teaching skills
New faculty should receive a specially designed first year curriculum to provide learnings focused on high‐yield and relevant topics
New faculty should receive a set of goals, or scholarly expectations, for their first year that would foster a partnership between individual faculty and the division to meet those goals
The division should create new structures for FD that promote collaboration, sharing of personal and professional growth and challenges, and a culture of continuous learning
All of the activities that comprise our new FD program must be aligned with our stated mission: to provide the highest quality clinical care, education, system improvements, and research that benefit our patients and trainees by developing successful academic hospitalist faculty.
Program Goals and Objectives
Our DHM FD program established the goal to provide our new faculty with clinical, educational, leadership, and scholarly skills that would promote academic output and foster work satisfaction. From a broader divisional standpoint, the goal was simply to create new FD structures that fostered the division's commitment to the program. The primary objectives of the program were for new faculty to:
Increase their knowledge, skills, and attitudes about key academic hospitalist domains following participation in the program;
Demonstrate successful production of scholarly output, participation in a hospital committee, and participation in a quality or safety improvement initiative by the end of their first year;
Report high levels of satisfaction with the FD program and their first year on faculty.
Program Development Principles
We began by conducting a literature review to draw on the successes and lessons learned from existing FD programs, particularly in large departments, academic centers, and the hospitalist field.1115 We focused our program development on a set of FD principles, which included instructional improvement, organizational development, the development of professional academic skills, and the teaching of specific content.11 Furthermore, whereas many FD programs traditionally focus on mentoring or a longitudinal set of seminars, we believed a multifaceted approach could help shift our culture towards one that prioritized FD and generated a sense of community. We hoped this cultural shift would create an environment that increased faculty satisfaction with their work, with their colleagues, and in our division.
This context drove us to build programmatic activities that not only targeted new faculty, the initial focus of our planning efforts, but also the division more broadly. We wanted to adopt known strategies (eg, mentoring relationships, teaching methods for FD, and grand rounds) but also weave in new ones that targeted AHM and our Division. It was clear that successful programs used a variety of instructional methods, and often combined methods, to create active and engaged faculty. We similarly wanted to create venues for didactic and small‐group learning, but also opportunities for peer learning and facilitated discussions around important topics. Allowing new faculty to learn from each other, and having them observe more senior faculty do the same, would be an important and explicit programmatic element.
Program Description and Implementation
All new faculty meet with Divisional leadership (RMW/BAS), administrative staff (they receive an orientation binder that highlights frequently asked questions and provides service‐specific orientation documents), and the Director of FD (NLS). The latter introduces the DHM FD Program and provides the road map for their first year (Supporting Information). The checklist serves to orient, guide, and emphasize the various programmatic goals, expectations, and logistics. Discussion focuses on the activities targeted to new faculty followed by wider divisional offerings. New faculty activities include:
Coaching Program
Rather than having new faculty independently seek out an appropriate mentor, we explicitly paired each with a more senior hospitalist (eg, 3 years on faculty). We provided explicit goals and expectations for the faculty coach and used a similar road map to guide their role (Supporting Information). We chose to call them coaches rather than mentors because in the first year, we felt a new faculty member needed nuts and bolts support from a big sibling more than they needed formal academic mentoring. We placed the burden of organizing the coaching sessions on the faculty coach and provided them with periodic reminders and suggestions for topics to discuss over the course the year, including supporting the junior faculty's performance against their scholarly benchmarks. Finally, we also organized a peer mentoring session for new facultydesigned to create additional peer support and shared learnings, and establish the importance of these relationships moving forward.
Core Seminars
We created a 12‐hour curriculum to cover a broad range of relevant AHM topics (Table 1). The choice of topics was informed by our needs assessment, suggestions of the FD Steering Committee, and the new faculty themselves. The sessions included a few didactic presentations, but they were largely interactive in a workshop‐style format to allow new faculty to engage the content. For instance, a session on quality improvement asked new faculty to bring a project idea and then work through creating a project plan. We coupled three half‐day sessions with a divisional social activity and made every attempt to ensure new faculty were not distracted by clinical responsibilities (eg, not on a clinical service or coverage was provided).
|
| Core Seminars |
| Being an academic hospitalist: The nuts & bolts |
| Tools for the master clinician |
| Documentation pearls & practices: Clinical, billing, and medico‐legal issues |
| Preparing your first talk: From topic selection to power point presentation |
| Choosing a case and writing it up for a clinical vignette abstract submission |
| Searching for clinical answers: An interactive computer‐lab workshop |
| Introduction to quality improvement |
| Leadership 101: Self‐awareness, your Myers‐Briggs, and leading change |
| Project Management: An exercise in team building |
| Thinking about systems and creating a culture of safety |
| Lunch Seminars |
| Managing and updating your academic CV |
| What to do when a patient on your service dies? |
| Evaluating students & housestaffAnd giving feedback |
| Being an effective ward attending |
| Medical‐legal consultative work & being an expert witness |
| Getting involved in professional societies |
| Understanding the promotion tracks: Practical tips and career preparation |
| Getting involved in hospital committee work |
| Caring for sick family members & navigating the healthcare system as a physician |
| Retirement planning 101: Life after UCSF |
| Time management & creating scholarly work |
| Teaching medical students on the wards |
| Clinical resources: What do you use to find answers? |
Teaching Course
One of our faculty (BAS) delivered the Stanford Faculty Development Clinical Teaching program16 (a train the trainer model designed to teach faculty how to become more effective teachers) to all new faculty. The program consisted of 14 hours of highly interactive curricula, video review, and role plays. The course was offered after hours (4 PM or 5 PM) and with input from the new faculty to ensure availability and participation.
Feedback and Observation
Each new faculty received directed feedback about their teaching and supervision on the housestaff service following their first rotation. Feedback was based on housestaff evaluations and direct observation of the new faculty during patient care and teaching rounds. One of our faculty (BAS) observed each new faculty member during rounds, and met with them individually to provide feedback and generate a discussion about teaching style and improvement opportunities.
Scholarly Expectations
We developed a set of scholarly expectations for new faculty. These helped inform the coach‐new faculty meetings and our selection of content for the Core Seminars. We initially had concerns that these expectations could overwhelm new faculty, but those junior faculty (years 2‐4) on the FD steering committee urged this practice, wishing they had similar guidance in their first year.
From the divisional perspective, we also added a number of new structures.
Grand Rounds
We established a monthly continuing medical education (CME) credit‐granting DHM Grand Rounds that combined a 10‐minute Hospital Medicine Update with a 45‐minute didactic presentation. The updates were presented by new faculty in order to provide them with an opportunity to receive feedback on their teaching and presentation skills (eg, how to give a talk, make PowerPoint slides, etc.). Didactic presentations were given by senior DHM faculty as well as subspecialty colleagues or ones from other departments (eg, dermatology or neurology), disciplines (eg, risk management), or campuses.
FD Lunch Seminar Series
Our division traditionally meets each Monday over the lunch hour to talk about service or academic issues. With a growing division, we believed there was an opportunity to better organize the content of these meetings. Once monthly, we dedicated a lunch session to a Faculty Development Seminar with topics that spanned a variety of interest areas, were driven by faculty suggestions, and were focused on being facilitated discussions rather than didactics. Table 1 provides examples of these seminar topics.
| Survey Statements Reporting Level of Comfort With(% responding somewhat agree or agree) | Previous Faculty, % (n = 11) | New Faculty, % (n = 6) |
|---|---|---|
| Identifying important resources within the School of Medicine | 64 | 83 |
| Identifying important resources within the Department of Medicine | 63 | 100 |
| Identifying important resources within the Division of Hospital Medicine | 90 | 100 |
| Identifying important resources within UCSF Medical Center | 72 | 67 |
| Having a system to effectively manage my email | 64 | 67 |
| Having a system to keep my CV updated | 64 | 84 |
| Using my non‐clinical time for academic success | 54 | 67 |
| Best practices for clinical/medico‐legal documentation | 54 | 67 |
| Best practices for billing documentation | 62 | 84 |
| Being an effective supervising ward attending | 90 | 84 |
| Being an effective teacher | 90 | 84 |
| Evaluating students and housestaff performance | 90 | 83 |
| Providing feedback to students and housestaff | 90 | 100 |
| Getting involved in professional societies | 27 | 100 |
| Understanding the difference between promotion pathways | 36 | 67 |
| Getting involved in hospital committee work | 54 | 84 |
| Choosing a good case for a clinical vignette submission to a regional/national meeting | 54 | 83 |
| Creating a poster for presentation at a regional/national meeting | 36 | 84 |
| Giving a lecture to students or residents | 64 | 84 |
| Developing a PowerPoint presentation for a lecture | 45 | 100 |
| Describing my personality type and how it relates to my work | 45 | 100 |
| Understanding important aspects of being a leader | 54 | 100 |
| Explaining the basic principles of quality improvement | 45 | 84 |
| Participating and contributing to a quality improvement project | 54 | 67 |
| Explaining the basic principles of patient safety | 45 | 67 |
| Understanding the factors that contribute to medical errors | 36 | 84 |
| Creating scholarly products from my work | 27 | 50 |
| Identifying what kind of mentors I need for the future | 45 | 100 |
| Category (% completed during first year) | Previous Faculty, % (n = 11) | New Faculty, % (n = 6) |
|---|---|---|
| Medical student teaching | 90 | 100 |
| Talk for trainees | 45 | 100 |
| Hospital committee involvement | 63 | 100 |
| Participation in a quality or safety project | 33 | 67 |
| Abstract submission | 27 | 50 |
| Identified mentor for year 2 | 63 | 83 |
Quality and Safety Lunch Seminars
In addition to our FD seminars, we also used one lunch session each month to provide updates on performance measures, ongoing quality or safety improvement initiatives, or a broader quality or safety topic. Speakers were either divisional or outside experts, depending on the topic, and organized by our director for quality and safety.
Incubator Sessions
Our director of research (AA) organized a weekly works in progress meeting, to which faculty and fellows brought ideas, grant applications, early manuscript drafts, or other potential scholarship products to obtain feedback and further group mentorship.
Divisional Retreats
We began alternating annual full‐day and mini half‐day retreats as a method to bring the division together, build camaraderie, set strategic priorities, identify divisional goals, and assess needs. These helped guide the creation of additional FD opportunities as well as our overall division's strategy to achieve our academic mission. The outcomes of these retreats led to many significant initiatives and policies, such as changes in compensation models, new scheduling processes, and decisions to spend resources on areas such as quality improvement.
Program Evaluation
Our evaluation focused on measuring the FD program's impact on our new faculty. We tracked their success in completing the stated scholarly expectations and surveyed them about their satisfaction with the programmatic activities, their first year on faculty, and their preparation for year 2. Prior to implementing the program, we surveyed the previous 2 years of new faculty to provide a comparison.
Results
Seven faculty participated in the inaugural program. We compared their scholarly output and experiences (6 faculty completed the survey; 87% response rate) with that of 11 more senior faculty who completed the comparison survey. Of note, the response rate of the comparison group was 69% (5 faculty who departed from our division during the previous 2 years were not surveyed). New faculty were surveyed at the start of the academic year with the follow‐up survey completed the following June. The more senior faculty completed the survey once at the same time as the baseline survey for the new faculty. All new faculty participated in each of the Core Seminars, the Teaching Course, the required number of Coaching sessions, and the observed teaching activity. We did not track their attendance at Divisional activities such as Grand Rounds or the Lunch Seminars.
Overall, the FD programmatic offerings were rated highly by new faculty (on a scale of 1 [lowest] to 5 [highest] for a global rating of each FD activity): Core Seminars 4.83 0.41, Coaching Program 4.5 0.84, Teaching Course 4.5 0.55, Grand Rounds 4.83 0.41, and Lunch Seminars 4.5 0.84. Table 2, which compares responses to a series of end of the year statements posed to new faculty, highlights notable differences in their level of comfort with specific skills and resource awareness. Given the small sample size, statistical significance was not calculated. Table 3 illustrates similar comparisons focused on academic output, which demonstrate that new faculty gave more talks to trainees, had greater involvement in hospital committees, more actively participated in quality and safety projects, and submitted more abstracts to regional or national meetings. New faculty also responded differently to which part of the FD program was most influential with 1 suggesting the Coaching Program, 2 the Core Seminars, 2 the entire program efforts, and 1 did not specify.
Table 4 illustrates comparison responses to a series of directed statements. New faculty all reported greater degrees of satisfaction overall, measured by the above responses, compared to previous faculty.
| Categories | Previous Faculty, % (n = 11) | New Faculty, % (n = 6) |
|---|---|---|
| ||
| Success: To what degree do you feel successful as an academic hospitalist at the end of your first year? (% responding successful or very successful) | 27 | 67 |
| Prepared: To what degree do you feel prepared for academic success moving into your second year on faculty? (% responding prepared or very prepared) | 27 | 100 |
| Part of DHM: I felt like an integral part of our division after my first year on faculty (% responding somewhat agree or agree) | 45 | 84 |
| Expectations: My first year on faculty exceeded my expectations (% responding somewhat agree or agree) | 27 | 84 |
Discussion
We implemented an FD program to foster the academic development of new faculty, and to mitigate the effects of growing clinical demands and a rapid group expansion on our academic mission. The impact of the program was measured by increased work satisfaction and academic output in first year faculty, greater self‐reported comfort in a variety of skills and knowledge of resources, and an improvement in our sense of purpose behind our academic mission. Though the program is only in its second year, we believe the model is of value for other AHM groups, and perhaps even nonacademic groups, all of whom may use such an investment in their hospitalists as a method to improve recruitment, job satisfaction, and retention.
Reviewing our program's first year suggests there were at least 3 keys to our success. First, we benefited tremendously from the time spent crafting a vision for the program and relying heavily on input from the target audience of junior faculty. Moreover, we made every effort to leverage existing resources (eg, using faculty who already taught about a given topic) and time commitments (eg, reshaping our existing Monday lunch meeting). Finally, we increasingly used our FD venues to connect and build networks with colleagues outside our division and within the hospital. This was a deliberate effort to create opportunities for individual faculty to be exposed to and collaborate with nonhospitalists for academic output.
Our research has some limitations, most notably the small sample size in evaluating the program for statistical significance, and the incomplete survey return rates. However, the results were quite consistent and the nonresponses of departed faculty would tend to bias our results toward the null. We also acknowledge the possibility of other confounding factors (eg, changes in clinical compensation models) that may have played a role, although compensation changes were relatively minor during the period studied and faculty did attribute many of the benefits in job satisfaction and skill building to the FD program itself.
Hospital medicine is an unusual field in that there is low barrier to entry and exit. Providers can change jobs without having to say goodbye to a large panel of patients, and in the continued mismatch between available positions and hospitalists, alternative positions can easily and quickly be found if they are dissatisfied.17 In the academic arena, even as hospitalists are hired to fill clinical gaps, they still have to perform under more traditional academic rules in order to be promoted and receive the support and kudos of colleagues and trainees. For both these reasons, early nurturing and socialization is critical to retention and academic success. While some opportunities for FD will be offered by national organizations,18 groups also have local responsibilities to support, mentor, and develop their junior faculty. Not only is such support crucial for the junior faculty themselves, but in our young field, the mentored very quickly become the mentors. Our decision to invest in both mentees and mentors reinforced the importance of mentorship for academic success and retention while planting the seeds for continued success and growth.1923 A recent study suggested that the environment for mentoring may be as important as the mentoring itself, a finding we did not specifically measure, but would support based our anecdotal experiences.24 This orientation toward future needs and creating the right milieu is crucial because demands for continued hospitalist growth are likely to remain.
Moving into year 2 of our FD program and reflecting on the lessons learned from year 1, we've adopted the same multifaceted approach with only minor adjustments to the curriculum, greater expansion of faculty involved in teaching and coaching, and a continued focus on building a sense of community around our academic mission. For the Core Seminars, we moved away from the 3 half‐day sessions and chose to host 2‐hour sessions every other month. This allowed for the same curriculum to be delivered but was much easier to logistically orchestrate. It also had the intended effect of bringing the new faculty together more regularly. In addition, we created dedicated sessions in preparation for our national meeting to allow faculty to bring abstract submissions for review and later, posters and oral presentations for feedback. These added sessions came partly as a suggestion from new faculty in our first year program, and seemed to further energize junior faculty around converting their projects into scholarship. Finally, we continue to further develop coaching and mentoring relationships in our division, partly a result of successful new facultycoach pairings.
In conclusion, our FD program had a noted impact on our new faculty and had a meaningful impact on our division in terms of camaraderie and cohesion, a shared commitment to an academic mission, and a mechanism for recruitment and retention. We hope our practical description for development and implementation of an FD program, including our specific tools, are useful to other groups considering such an initiative.
Acknowledgements
The authors thank Katherine Li for her invaluable assistance in coordinating the DHM FD program. They are also indebted to their faculty colleagues for their time and roles in teaching and mentoring within the program. Dr. Sehgal partly developed this program as part of a project during his California Healthcare Foundation Leadership Fellowship. Dr. Sharpe delivered the teaching workshops at UCSF after completing the Stanford Faculty Development Teaching Program.
- ,,,.The status of Hospital Medicine Groups in the United States.J Hosp Med.2006;1(2):75–80.
- Accreditation Council for Graduate Medical Education: information related to the ACGME's effort to address resident duty hours and other relevant resource materials. Available at: http://www.acgme.org/acWebsite/dutyHours/dh_index.asp. Accessed August 2010.
- ,,, et al.Effects of work hour reduction on residents' lives: a systematic review.JAMA.2005;294(9):1088–1100.
- ,,,,.Non‐housestaff medicine services in academic centers: models and challenges.J Hosp Med.2008;3(3):247–255.
- ,.Surgical comanagement: a natural evolution of hospitalist practice.J Hosp Med.2008;3(5):394–397.
- ,.The expanding role of hospitalists in the United States.Swiss Med Wkly.2006;136(37–38):591–596.
- 2007–08 Hospital Medicine Survey. Society of Hospital Medicine. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Survey19(4):392–393.
- ,,, et al.Challenges and opportunities in Academic Hospital Medicine: report from the Academic Hospital Medicine Summit.J Hosp Med.2009;4(4):240–246.
- .Palliative care and hospitalists: a partnership for hope.J Hosp Med.2006;1(1):5–6.
- ,.Faculty development: principles and practices.J Vet Med Educ.2006;33(3):317–324.
- ,,, et al.A systematic review of faculty development initiatives designed to improve teaching effectiveness in medical education: BEME Guide No. 8.Med Teach.2006;28(6):497–526.
- ,.A successful approach to faculty development at an independent academic medical center.Med Teach.2008;30:e10–e14.
- ,,,.An innovative approach to supporting hospitalist physicians towards academic success.J Hosp Med.2008;3(4):314–318.
- ,,, et al.The curriculum for the Hospitalized Aging Medical Patient program: a collaborative faculty development program for hospitalists, general internists, and geriatricians.J Hosp Med.2008;3(5):384–393.
- Stanford Faculty Development Clinical Teaching Program. Available at: http://www.stanford.edu/group/SFDP. Accessed August 2010.
- ,,, et al.Trends in market demand for internal medicine 1999–2004: an analysis of physician job advertisements.J Gen Intern Med.2006;21(10):1079–1085.
- The Academic Hospitalist Academy. Available at: http://www.sgim.org/index.cfm?pageId=815. Accessed August 2010.
- ,,.Mentoring in academic medicine: a systematic review.JAMA.2006;296(9):1103–1115.
- ,,.Facilitating faculty success: outcomes and cost benefit of the UCSD National Center of Leadership in Academic Medicine.Acad Med.2004;79(10 Suppl):S9–S11.
- ,,, et al.Retention of junior faculty in academic medicine at the University of California, San Diego.Acad Med.2009;84(1):37–41.
- ,,,.Helping medical school faculty realize their dreams: an innovative, collaborative mentoring program.Acad Med.2002;77:377–384.
- ,,, et al.Physicians' perceptions of institutional and leadership factors influencing their job satisfaction at one academic medical center.Acad Med.2002;77:1235–1240.
- ,,.A systematic review of qualitative research on the meaning and characteristics of mentoring in academic medicine.J Gen Intern Med.2010;25(1);72–78.
- ,,,.The status of Hospital Medicine Groups in the United States.J Hosp Med.2006;1(2):75–80.
- Accreditation Council for Graduate Medical Education: information related to the ACGME's effort to address resident duty hours and other relevant resource materials. Available at: http://www.acgme.org/acWebsite/dutyHours/dh_index.asp. Accessed August 2010.
- ,,, et al.Effects of work hour reduction on residents' lives: a systematic review.JAMA.2005;294(9):1088–1100.
- ,,,,.Non‐housestaff medicine services in academic centers: models and challenges.J Hosp Med.2008;3(3):247–255.
- ,.Surgical comanagement: a natural evolution of hospitalist practice.J Hosp Med.2008;3(5):394–397.
- ,.The expanding role of hospitalists in the United States.Swiss Med Wkly.2006;136(37–38):591–596.
- 2007–08 Hospital Medicine Survey. Society of Hospital Medicine. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Survey19(4):392–393.
- ,,, et al.Challenges and opportunities in Academic Hospital Medicine: report from the Academic Hospital Medicine Summit.J Hosp Med.2009;4(4):240–246.
- .Palliative care and hospitalists: a partnership for hope.J Hosp Med.2006;1(1):5–6.
- ,.Faculty development: principles and practices.J Vet Med Educ.2006;33(3):317–324.
- ,,, et al.A systematic review of faculty development initiatives designed to improve teaching effectiveness in medical education: BEME Guide No. 8.Med Teach.2006;28(6):497–526.
- ,.A successful approach to faculty development at an independent academic medical center.Med Teach.2008;30:e10–e14.
- ,,,.An innovative approach to supporting hospitalist physicians towards academic success.J Hosp Med.2008;3(4):314–318.
- ,,, et al.The curriculum for the Hospitalized Aging Medical Patient program: a collaborative faculty development program for hospitalists, general internists, and geriatricians.J Hosp Med.2008;3(5):384–393.
- Stanford Faculty Development Clinical Teaching Program. Available at: http://www.stanford.edu/group/SFDP. Accessed August 2010.
- ,,, et al.Trends in market demand for internal medicine 1999–2004: an analysis of physician job advertisements.J Gen Intern Med.2006;21(10):1079–1085.
- The Academic Hospitalist Academy. Available at: http://www.sgim.org/index.cfm?pageId=815. Accessed August 2010.
- ,,.Mentoring in academic medicine: a systematic review.JAMA.2006;296(9):1103–1115.
- ,,.Facilitating faculty success: outcomes and cost benefit of the UCSD National Center of Leadership in Academic Medicine.Acad Med.2004;79(10 Suppl):S9–S11.
- ,,, et al.Retention of junior faculty in academic medicine at the University of California, San Diego.Acad Med.2009;84(1):37–41.
- ,,,.Helping medical school faculty realize their dreams: an innovative, collaborative mentoring program.Acad Med.2002;77:377–384.
- ,,, et al.Physicians' perceptions of institutional and leadership factors influencing their job satisfaction at one academic medical center.Acad Med.2002;77:1235–1240.
- ,,.A systematic review of qualitative research on the meaning and characteristics of mentoring in academic medicine.J Gen Intern Med.2010;25(1);72–78.
Copyright © 2011 Society of Hospital Medicine
His Mother
Bertha Johnson is back with pneumonia again. The ED doctor on the telephone sounded both matter‐of‐fact and mildly bored when I answered her page about another admission to the hospitalist service. I hadn't met Mrs. Johnson previously, but came to know her and Douglas, her only son, well over the next few days.
The Johnsons were facing a difficult choice. Bertha was now bedbound and quadriplegic following a 40‐year battle with multiple sclerosis and gradually mounting disability. She was cognitively intact and had a solid grasp of medical realities, but was hard of hearing and quite dysarthric. Forming even short phrases and sentences took great effort. However tenuous, this ability to speak allowed her to communicate with those she loved. She had been admitted thrice in the past year with aspiration pneumonia, as she was unable to clear her secretions reliably. Repeated bronchoscopies demonstrated an inability to protect her airway. Douglas, who was also her health care proxy, favored proceeding with the tracheostomy suggested by the pulmonary team. On a prior admission, he had been distressed when his mother refused this intervention. Now she was back with the identical problem and had been given the same recommendation by her doctors. It was particularly difficult for me to discuss these sensitive issues when I had not previously met either Bertha or her son. I spoke to her primary care physician over the phone and he agreed with the need for tracheostomy. The pulmonary team had been involved in discussions about tracheostomy in all of her hospital admissions, providing continuity of care in the process. Ultimately, it was my responsibility to help Bertha and Douglas come to a decision.
After multiple discussions between the Johnsons and me, a consensus emerged to proceed with the tracheostomy. We recognized that the procedure would increase her care needs and arranged for a stay in a skilled nursing facility to provide access to round‐the‐clock suctioning. The evening prior to the tracheostomy, the floor nurse and I reviewed the procedure to ensure that Bertha was fully prepared. What followed resulted in a drastic change of plan. Bertha emphasized that she did not want to lose her only means of communication, even if the surgery would prolong her life. She admitted that she reluctantly agreed to the procedure only to please her son and doctors, because they believed it to be in her best interest. Her fear of the prospect of death from drowning in her own secretions was much less than her fear of silence and isolation that would result from her loss of speech. I shared her misgivings with Douglas, and she admitted to him that she had only agreed to the procedure for his sake. We cancelled the surgery.
Douglas later revealed that he also had been ambivalent about the procedure for sometime, as it would necessitate a nursing home stay and the loss of the caretakers who had cared for his mother so wonderfully for many years. Bertha lived alone in her own home with the help of visiting nurses and patient care assistants Douglas paid for out‐of‐pocket. Douglas lived and worked in a city over a hundred miles away, but managed to visit several times a month to facilitate his mother's care. He had supported the procedure only because the doctors had said it was the only way to avoid future pneumonias. The idea of a tracheostomy was definitively abandoned once and for all.
The Johnsons wanted Bertha to return to her home, but hospital case managers felt this would be an unsafe plan of care as she was alone for several hours a day. She was largely immobile and unable to escape if there were a fire or other emergency. Also, the caretakers were not trained to use the suction equipment, and the visiting nurses would only be available intermittently. The home care staff felt they could no longer meet her needs and declined to resume her care. Douglas became very frustrated by the delays and protracted negotiations, enough so that he threatened to sue the institution for taking over my mother's life. The threat of litigation is usually a cry for help that reflects either miscommunication or the suffering of a conflicted family.
As their hospitalist, I hoped to advocate for both the patient and Douglas while coordinating the overall care plan. I had always received consistent responses from the Johnsons, but other staff members noted that Douglas had expressed shifting views on the best site of care for his mother. At Bertha's request, I convened a meeting with her, Douglas, the social worker, case manager, visiting and staff nurses, the palliative care nurse, and floor manager. Prior to this, I met with all involved health care providers to ensure we understood each other's abilities and limitations regarding Bertha's care. As I entered the room for the family meeting, I knew it was ultimately the patient's choice whether she wanted to return home or notas long as she understood the risks involved.
During the meeting, all the team members explained the dilemmas they faced in planning for a safe disposition. Douglas's response illuminated his devotion and love for his ailing mother. He had known all along that it would be less expensive and burdensome for him for Bertha to be placed in a facility. However, he feared nursing home admission represented giving up and failing to fulfill my duty to my mother. Tears ran down the face of this otherwise well composed, immaculately dressed, articulate man in his late forties. He had assumed the responsibility for his mother's care while still a child and had carried this self‐imposed moral burden his entire life. This meeting was his first opportunity to voice explicitly to the medical team his immense love and concern for his dear mother.
I gently probed to clarify Bertha's values and goals. On a brief, prior nursing home stay, Bertha had found the experience to be scary and unfamiliar. However, as her functional abilities continued to decline, her feelings had changed. She now felt lonely and anxious at home when her caretakers were absent. She actually wanted to go to a nursing home, where there would always be company and support available! She had not told Douglas this because she knew he cared for her deeply and she didn't want to hurt his feelings; he seemed committed to caring for her the same way he had for so many years.
In short, Douglas knew it would be easier for him if his mother were in a nursing facility, but assumed she wanted to stay in her home. Oddly, Bertha was only remaining at home because she believed that was what her son wished. A few days later, Bertha was transferred to a nursing home near several relatives who would visit her regularly. Douglas was again selfless in not seeking to move her closer to him. He didn't want to uproot her more than was unavoidable.
Day‐to‐day practice reveals many examples of love and dedication, but I have never seen such blinding and unquestioning commitment as exemplified by this mother‐son duo. From them, I learned the importance of attentive and active listening. Our polite patients may only subtly hint at matters of the deepest import. If we cannot truly hear their unspoken emotions, we risk harming them and misinterpreting their words and actions. Some healthcare providers had seen Douglas as aggressive and demanding with his threat of a lawsuit, whereas Bertha had been described as unrealistic or in denial. These views distorted a much more complex reality. Time and attention to careful communication between the healthcare providers, the patient, and her son bore fruit in this case. The procedure that was really needed was the family meeting and not the tracheostomy! An undesired and invasive procedure was avoided, goals of care were clarified, quality of life maximized, a safe discharge arranged, and a new mutual understanding achieved. I was humbled, and reminded of the importance of team‐based care and the need to approach each patient and family member in a receptive, nonjudgmental, and open manner. Douglas and Bertha Johnson were linked with a profound and abiding bond that would only be severed at death.
Bertha Johnson is back with pneumonia again. The ED doctor on the telephone sounded both matter‐of‐fact and mildly bored when I answered her page about another admission to the hospitalist service. I hadn't met Mrs. Johnson previously, but came to know her and Douglas, her only son, well over the next few days.
The Johnsons were facing a difficult choice. Bertha was now bedbound and quadriplegic following a 40‐year battle with multiple sclerosis and gradually mounting disability. She was cognitively intact and had a solid grasp of medical realities, but was hard of hearing and quite dysarthric. Forming even short phrases and sentences took great effort. However tenuous, this ability to speak allowed her to communicate with those she loved. She had been admitted thrice in the past year with aspiration pneumonia, as she was unable to clear her secretions reliably. Repeated bronchoscopies demonstrated an inability to protect her airway. Douglas, who was also her health care proxy, favored proceeding with the tracheostomy suggested by the pulmonary team. On a prior admission, he had been distressed when his mother refused this intervention. Now she was back with the identical problem and had been given the same recommendation by her doctors. It was particularly difficult for me to discuss these sensitive issues when I had not previously met either Bertha or her son. I spoke to her primary care physician over the phone and he agreed with the need for tracheostomy. The pulmonary team had been involved in discussions about tracheostomy in all of her hospital admissions, providing continuity of care in the process. Ultimately, it was my responsibility to help Bertha and Douglas come to a decision.
After multiple discussions between the Johnsons and me, a consensus emerged to proceed with the tracheostomy. We recognized that the procedure would increase her care needs and arranged for a stay in a skilled nursing facility to provide access to round‐the‐clock suctioning. The evening prior to the tracheostomy, the floor nurse and I reviewed the procedure to ensure that Bertha was fully prepared. What followed resulted in a drastic change of plan. Bertha emphasized that she did not want to lose her only means of communication, even if the surgery would prolong her life. She admitted that she reluctantly agreed to the procedure only to please her son and doctors, because they believed it to be in her best interest. Her fear of the prospect of death from drowning in her own secretions was much less than her fear of silence and isolation that would result from her loss of speech. I shared her misgivings with Douglas, and she admitted to him that she had only agreed to the procedure for his sake. We cancelled the surgery.
Douglas later revealed that he also had been ambivalent about the procedure for sometime, as it would necessitate a nursing home stay and the loss of the caretakers who had cared for his mother so wonderfully for many years. Bertha lived alone in her own home with the help of visiting nurses and patient care assistants Douglas paid for out‐of‐pocket. Douglas lived and worked in a city over a hundred miles away, but managed to visit several times a month to facilitate his mother's care. He had supported the procedure only because the doctors had said it was the only way to avoid future pneumonias. The idea of a tracheostomy was definitively abandoned once and for all.
The Johnsons wanted Bertha to return to her home, but hospital case managers felt this would be an unsafe plan of care as she was alone for several hours a day. She was largely immobile and unable to escape if there were a fire or other emergency. Also, the caretakers were not trained to use the suction equipment, and the visiting nurses would only be available intermittently. The home care staff felt they could no longer meet her needs and declined to resume her care. Douglas became very frustrated by the delays and protracted negotiations, enough so that he threatened to sue the institution for taking over my mother's life. The threat of litigation is usually a cry for help that reflects either miscommunication or the suffering of a conflicted family.
As their hospitalist, I hoped to advocate for both the patient and Douglas while coordinating the overall care plan. I had always received consistent responses from the Johnsons, but other staff members noted that Douglas had expressed shifting views on the best site of care for his mother. At Bertha's request, I convened a meeting with her, Douglas, the social worker, case manager, visiting and staff nurses, the palliative care nurse, and floor manager. Prior to this, I met with all involved health care providers to ensure we understood each other's abilities and limitations regarding Bertha's care. As I entered the room for the family meeting, I knew it was ultimately the patient's choice whether she wanted to return home or notas long as she understood the risks involved.
During the meeting, all the team members explained the dilemmas they faced in planning for a safe disposition. Douglas's response illuminated his devotion and love for his ailing mother. He had known all along that it would be less expensive and burdensome for him for Bertha to be placed in a facility. However, he feared nursing home admission represented giving up and failing to fulfill my duty to my mother. Tears ran down the face of this otherwise well composed, immaculately dressed, articulate man in his late forties. He had assumed the responsibility for his mother's care while still a child and had carried this self‐imposed moral burden his entire life. This meeting was his first opportunity to voice explicitly to the medical team his immense love and concern for his dear mother.
I gently probed to clarify Bertha's values and goals. On a brief, prior nursing home stay, Bertha had found the experience to be scary and unfamiliar. However, as her functional abilities continued to decline, her feelings had changed. She now felt lonely and anxious at home when her caretakers were absent. She actually wanted to go to a nursing home, where there would always be company and support available! She had not told Douglas this because she knew he cared for her deeply and she didn't want to hurt his feelings; he seemed committed to caring for her the same way he had for so many years.
In short, Douglas knew it would be easier for him if his mother were in a nursing facility, but assumed she wanted to stay in her home. Oddly, Bertha was only remaining at home because she believed that was what her son wished. A few days later, Bertha was transferred to a nursing home near several relatives who would visit her regularly. Douglas was again selfless in not seeking to move her closer to him. He didn't want to uproot her more than was unavoidable.
Day‐to‐day practice reveals many examples of love and dedication, but I have never seen such blinding and unquestioning commitment as exemplified by this mother‐son duo. From them, I learned the importance of attentive and active listening. Our polite patients may only subtly hint at matters of the deepest import. If we cannot truly hear their unspoken emotions, we risk harming them and misinterpreting their words and actions. Some healthcare providers had seen Douglas as aggressive and demanding with his threat of a lawsuit, whereas Bertha had been described as unrealistic or in denial. These views distorted a much more complex reality. Time and attention to careful communication between the healthcare providers, the patient, and her son bore fruit in this case. The procedure that was really needed was the family meeting and not the tracheostomy! An undesired and invasive procedure was avoided, goals of care were clarified, quality of life maximized, a safe discharge arranged, and a new mutual understanding achieved. I was humbled, and reminded of the importance of team‐based care and the need to approach each patient and family member in a receptive, nonjudgmental, and open manner. Douglas and Bertha Johnson were linked with a profound and abiding bond that would only be severed at death.
Bertha Johnson is back with pneumonia again. The ED doctor on the telephone sounded both matter‐of‐fact and mildly bored when I answered her page about another admission to the hospitalist service. I hadn't met Mrs. Johnson previously, but came to know her and Douglas, her only son, well over the next few days.
The Johnsons were facing a difficult choice. Bertha was now bedbound and quadriplegic following a 40‐year battle with multiple sclerosis and gradually mounting disability. She was cognitively intact and had a solid grasp of medical realities, but was hard of hearing and quite dysarthric. Forming even short phrases and sentences took great effort. However tenuous, this ability to speak allowed her to communicate with those she loved. She had been admitted thrice in the past year with aspiration pneumonia, as she was unable to clear her secretions reliably. Repeated bronchoscopies demonstrated an inability to protect her airway. Douglas, who was also her health care proxy, favored proceeding with the tracheostomy suggested by the pulmonary team. On a prior admission, he had been distressed when his mother refused this intervention. Now she was back with the identical problem and had been given the same recommendation by her doctors. It was particularly difficult for me to discuss these sensitive issues when I had not previously met either Bertha or her son. I spoke to her primary care physician over the phone and he agreed with the need for tracheostomy. The pulmonary team had been involved in discussions about tracheostomy in all of her hospital admissions, providing continuity of care in the process. Ultimately, it was my responsibility to help Bertha and Douglas come to a decision.
After multiple discussions between the Johnsons and me, a consensus emerged to proceed with the tracheostomy. We recognized that the procedure would increase her care needs and arranged for a stay in a skilled nursing facility to provide access to round‐the‐clock suctioning. The evening prior to the tracheostomy, the floor nurse and I reviewed the procedure to ensure that Bertha was fully prepared. What followed resulted in a drastic change of plan. Bertha emphasized that she did not want to lose her only means of communication, even if the surgery would prolong her life. She admitted that she reluctantly agreed to the procedure only to please her son and doctors, because they believed it to be in her best interest. Her fear of the prospect of death from drowning in her own secretions was much less than her fear of silence and isolation that would result from her loss of speech. I shared her misgivings with Douglas, and she admitted to him that she had only agreed to the procedure for his sake. We cancelled the surgery.
Douglas later revealed that he also had been ambivalent about the procedure for sometime, as it would necessitate a nursing home stay and the loss of the caretakers who had cared for his mother so wonderfully for many years. Bertha lived alone in her own home with the help of visiting nurses and patient care assistants Douglas paid for out‐of‐pocket. Douglas lived and worked in a city over a hundred miles away, but managed to visit several times a month to facilitate his mother's care. He had supported the procedure only because the doctors had said it was the only way to avoid future pneumonias. The idea of a tracheostomy was definitively abandoned once and for all.
The Johnsons wanted Bertha to return to her home, but hospital case managers felt this would be an unsafe plan of care as she was alone for several hours a day. She was largely immobile and unable to escape if there were a fire or other emergency. Also, the caretakers were not trained to use the suction equipment, and the visiting nurses would only be available intermittently. The home care staff felt they could no longer meet her needs and declined to resume her care. Douglas became very frustrated by the delays and protracted negotiations, enough so that he threatened to sue the institution for taking over my mother's life. The threat of litigation is usually a cry for help that reflects either miscommunication or the suffering of a conflicted family.
As their hospitalist, I hoped to advocate for both the patient and Douglas while coordinating the overall care plan. I had always received consistent responses from the Johnsons, but other staff members noted that Douglas had expressed shifting views on the best site of care for his mother. At Bertha's request, I convened a meeting with her, Douglas, the social worker, case manager, visiting and staff nurses, the palliative care nurse, and floor manager. Prior to this, I met with all involved health care providers to ensure we understood each other's abilities and limitations regarding Bertha's care. As I entered the room for the family meeting, I knew it was ultimately the patient's choice whether she wanted to return home or notas long as she understood the risks involved.
During the meeting, all the team members explained the dilemmas they faced in planning for a safe disposition. Douglas's response illuminated his devotion and love for his ailing mother. He had known all along that it would be less expensive and burdensome for him for Bertha to be placed in a facility. However, he feared nursing home admission represented giving up and failing to fulfill my duty to my mother. Tears ran down the face of this otherwise well composed, immaculately dressed, articulate man in his late forties. He had assumed the responsibility for his mother's care while still a child and had carried this self‐imposed moral burden his entire life. This meeting was his first opportunity to voice explicitly to the medical team his immense love and concern for his dear mother.
I gently probed to clarify Bertha's values and goals. On a brief, prior nursing home stay, Bertha had found the experience to be scary and unfamiliar. However, as her functional abilities continued to decline, her feelings had changed. She now felt lonely and anxious at home when her caretakers were absent. She actually wanted to go to a nursing home, where there would always be company and support available! She had not told Douglas this because she knew he cared for her deeply and she didn't want to hurt his feelings; he seemed committed to caring for her the same way he had for so many years.
In short, Douglas knew it would be easier for him if his mother were in a nursing facility, but assumed she wanted to stay in her home. Oddly, Bertha was only remaining at home because she believed that was what her son wished. A few days later, Bertha was transferred to a nursing home near several relatives who would visit her regularly. Douglas was again selfless in not seeking to move her closer to him. He didn't want to uproot her more than was unavoidable.
Day‐to‐day practice reveals many examples of love and dedication, but I have never seen such blinding and unquestioning commitment as exemplified by this mother‐son duo. From them, I learned the importance of attentive and active listening. Our polite patients may only subtly hint at matters of the deepest import. If we cannot truly hear their unspoken emotions, we risk harming them and misinterpreting their words and actions. Some healthcare providers had seen Douglas as aggressive and demanding with his threat of a lawsuit, whereas Bertha had been described as unrealistic or in denial. These views distorted a much more complex reality. Time and attention to careful communication between the healthcare providers, the patient, and her son bore fruit in this case. The procedure that was really needed was the family meeting and not the tracheostomy! An undesired and invasive procedure was avoided, goals of care were clarified, quality of life maximized, a safe discharge arranged, and a new mutual understanding achieved. I was humbled, and reminded of the importance of team‐based care and the need to approach each patient and family member in a receptive, nonjudgmental, and open manner. Douglas and Bertha Johnson were linked with a profound and abiding bond that would only be severed at death.
Mapping Out Diagnosis
A 19‐year‐old Japanese man was admitted to a hospital near Kyoto, Japan, because of fever and rash. Two weeks prior to admission, he developed mild headache and low‐grade fever; a rapid test for influenza was negative. His symptoms transiently improved with acetaminophen, but 8 days prior to admission, he developed fever to 38.5C and a pruritic maculopapular rash over his back that spread to his limbs. Six days prior to admission, a chest radiograph was clear; clarithromycin was prescribed for presumed upper respiratory infection. He visited the emergency department the day before admission because of continued fever of greater than 39C, fatigue, and headache. Because there was no jolt accentuation of the headache (ie, worsening with rapid horizontal rotation), or neck pain with extreme neck flexion, he was discharged on acetaminophen. He returned the next day with worsening fatigue and was admitted. He denied chills, rigor, weight loss, photosensitivity, sore throat, neck pain, cough, dyspnea, chest pain, nausea, vomiting, diarrhea, abdominal pain, back pain, and arthralgia.
Fever and diffuse rash are often due to infection, although drugs, autoimmune processes, and cancer must be considered. The presence of headache does not focus the differential diagnosis substantially, because many of the candidate diagnoses can be accompanied by meningitis or encephalitis, or even more frequently, nonspecific headaches. In one small study, jolt‐induced aggravation of headache was shown to be a sensitive indicator of cerebrospinal fluid pleocytosis. The absence of neck stiffness and the 2‐week duration makes bacterial meningitis unlikely, but a more indolent form of aseptic meningitis may need to be evaluated with a lumbar puncture.
The 2‐week illness without rapid deterioration makes some serious causes of fever and rash, such as toxic shock syndrome, disseminated meningococcal infection, or toxic epidermal necrolysis unlikely. A viral exanthema is possible, although the 2‐week duration is longer than usual. Given his youth, however, his immunization history should be queried, and acute infection with human immunodeficiency virus (HIV) should be considered. A more indolent infection, such as subacute bacterial endocarditis, disseminated gonococcal infection, or syphilis is plausible. Among autoimmune etiologies, systemic lupus erythematosus (SLE) and Behcet's disease (which is prevalent in Japan) can involve the central nervous system and cause fever. A careful inquiry directed at prescribed, complementary, and illicit drugs is required.
The patient's past medical history was notable only for mumps at the age of 10. His medications included acetaminophen, clarithromycin, and an herbal medicine, which he had been taking for the prior several days. He reported no tobacco or illicit drug use and rarely drank alcohol. He had never been sexually active. He worked in a factory and reported occasional contact with silver. He lived with his parents; there was no family history of tuberculosis or connective tissue diseases. His father was from Kyushu (the southernmost major island in Japan) and had chronic hepatitis C. The patient denied recent animal exposure or recent travel. His childhood vaccinations were said to be up to date.
Mumps at age 10 might signal general lack of immunization, in which case childhood viral exanthema‐like measles (characterized by fever, headache, and diffuse rash) would warrant consideration. The listed medications had been started after the onset of illness and therefore are unlikely to be causal. Silver causes at least 2 skin conditionscontact dermatitis and argyriabut not the systemic illness seen here. Human T lymphotropic virus‐1 (HTLV‐1) is endemic in southern Japan, but only a minority of infected humans are afflicted with associated adult T cell leukemia/lymphoma or myelopathy. Leukemia and lymphoma are the most likely cancers to cause fever, rash, and central nervous system involvement (with T cell disorders demonstrating a particular tropism for the skin). Overall, however, the differential has not changed substantially.
On physical examination, the patient was mildly overweight and appeared acutely ill. His blood pressure was 136/78 mm Hg, pulse rate was 76 and regular, temperature was 39.2C and respiratory rate was 20 with an oxygen saturation of 98% on room air. A diffuse but nonconfluent erythematous maculopapular rash was present over his chest wall, back, medial aspects of both thighs, and around the knees. There was no jolt‐induced headache. His eyes, nose, oral cavity, and throat were all clear. The neck was supple. There were palpable lymph nodes, each about 1 cm in size, which were firm and moderately tender, in his left neck and left axilla. Lungs and heart were normal. The abdomen was soft, nontender, with normal bowel sounds and no hepatosplenomegaly. His genitalia were normal. Rectal examination revealed no masses or tenderness and a scant amount of brown stool that was negative for occult blood. Neurologic examination was unremarkable.
The multifocal lymphadenopathy does not help distinguish among the categories of disease under consideration. The diffuse maculopapular rash is similarly nonspecific, occurring more frequently with infection and drug reaction than malignancy and autoimmunity. Acute HIV, Epstein‐Barr virus (EBV), syphilis, SLE, drug exposure, or a hematologic malignancy would all be suitable explanations for fever, headache, diffuse rash, and disseminated lymphadenopathy in a previously healthy young man.
Laboratory data obtained on admission was notable for a white blood cell (WBC) count of 2100/L with 72% neutrophils, 19% lymphocytes, and 9% monocytes. Hemoglobin was 13.5 mg/dL with a mean corpuscular volume of 85 fL. Platelet count was 136,000/L. Erythrocyte sedimentation rate was 26 mm/hour. Serum chemistries revealed a sodium level of 135 mEq/L, potassium level of 3.6 mEq/L, chloride level of 100 mEq/L, blood urea nitrogen of 9.8 mg/dL, creatinine level of 1.0 mg/dL, glucose level of 101 mg/dL, calcium level of 8.8 mg/dL, albumin of 4.6 mg/dL, total protein of 8.4 mg/dL, aspartate aminotransferase of 42 IU/L (normal 35 IU/L), alanine aminotransferase of 27 IU/L, total bilirubin of 0.5 mg/dL, and lactate dehydrogenase (LDH) level of 463 IU/L (normal 260 IU/L). Chest radiography and electrocardiogram were normal.
A mild elevation in LDH is nonspecific, but without hemolysis or infarction of the kidney, lung, or muscle, it suggests a lymphoproliferative process. Leukopenia with thrombocytopenia can be seen in a number of disorders, most commonly infections including viruses (e.g., EBV, HIV, dengue), malaria, Rocky Mountain spotted fever, or ehrlichiosis/anaplasmosis. Confirmation of his lack of travel could help prioritize those considerations. An invasive bone marrow disorder cannot be excluded, although the near‐normal hemoglobin argues against it. Autoimmune cytopenias are seen in SLE. Given his age, lymphadenopathy, LDH elevation, and absence of infectious exposures, lymphoma rises to the top of the list.
Noninvasive measures should include examination of the peripheral smear, HIV testing (including HIV RNA for acute infection), EBV serologies, and tests for syphilis and SLE. Lumbar puncture (for evaluation of aseptic meningitis) and lymph node biopsy would be informative. Skin biopsy may be helpful to evaluate for aggressive T cell lymphoproliferative disorder, but this can await the results of initial testing.
The patient was given intravenous fluids and acetaminophen as needed. Blood cultures, urine culture, cytomegalovirus and EBV serologies, hepatitis B surface antigen, hepatitis C virus antibody, HIV antibody, antinuclear antibody, complement and ferritin levels, and quantiferon‐TB were ordered. The urine was normal and a urinary antigen test for Legionella was negative. Contrast‐enhanced computed tomography scan of the chest and abdomen was normal except for mild splenomegaly and an enlarged left axillary lymph node.
The ferritin may have been ordered to help evaluate for Still's disease, which is characterized by sustained fever, lymphadenopathy, and transient rash; however, the characteristic leukocytosis and arthralgias are absent. The computed tomography findings are most notable for the absence of generalized lymphadenopathy or significant hepatosplenomegaly that is seen in lymphoma, leukemia, and lymphotropic processes such as acute EBV infection. The localization of disease to the skin (where the predominant lymphocytes are of T cell origin) with relatively modest lymphadenopathy suggests a T cell lymphoma, perhaps of an indolent variety. Vertical transmission of HTLV‐1 decades ago would make adult T cell leukemia or lymphoma a major consideration.
On the third hospital day, WBC count was 1800/L with 67% neutrophils, 22% lymphocytes, and 1% atypical lymphocytes; LDH rose to 623 IU/L. He had continued fatigue and high fever while the rash gradually faded with oral antihistamines and steroid ointment. On hospital day 4, bone marrow biopsy and skin biopsy of his left thigh were performed.
The further decline in WBC and rise in LDH are modest and therefore do not significantly modify the differential diagnosis. Likewise, 1% atypical lymphocytosis is too low to pinpoint an etiology. Because unremitting fevers start to extend into their third week without a clear source of infection, the probability of malignancy and autoimmunity rise. Improvement with oral antihistamines and topical steroids frequently suggests an underlying allergic process, but the remainder of the clinical picture is not in keeping with atopy or allergy. Cutaneous lymphomas (eg, mycosis fungoides) can have waxing and waning skin manifestations, and can be temporarily or definitively treated by topical steroids. The persistence of his fatigue is of concern given the absence of anemia, cardiopulmonary involvement, or motor weakness.
Bone marrow biopsy showed normocellular marrow with no abnormal cells and some activated macrophages with hemophagocytic activity. Skin biopsy failed to show specific pathology.
His left cervical lymph nodes gradually enlarged. Ultrasound of the neck showed multiple enlarged lymph nodes (left side dominant) with dimension of 17 mm 9 mm 31 mm. Blood and urine cultures returned negative, as did HIV antibody. cytomegalovirus and EBV serologies were consistent with previous infection and the ferritin level was 578 ng/mL (normal, 39‐340 ng/mL). Toxoplasma serology and HTLV‐1 antibody were ordered.
The absence of malignant cells on bone marrow biopsy does not exclude lymphoma, but makes a myelophthisic cause of the cytopenias less likely. The macrophage hemophagocytosis reflects immune activation, which in turn is usually caused by the same viral infections, autoimmune conditions, and lymphoproliferative disorders which constitute the current differential diagnosis.
Bone marrow and skin biopsies are both subject to sampling error, and detection of cutaneous T cell lymphoma is notoriously difficult. However, taken together, the absence of cancer on 2 specimens reduces that possibility.
Sustained unilateral cervical lymphadenopathy with fever in a young Japanese man without any histologic evidence of lymphoma points to Kikuchi's disease, ie, lymphadenitis of unknown etiology associated with varying degrees of systemic manifestations. Fever is a frequent feature, we believe, but diffuse sustained rash, cytopenias, and headache are less common or are seen in severe forms of the disease. The diagnosis of Kikuchi's requires the diligent exclusion of SLE and lymphoma. Examination of the peripheral smear and a lymph node biopsy are required.
Of note, there is also a localized form of Castleman's disease, a nonmalignant lymphoproliferative disorder, that similarly is characterized by focal lymphadenopathy. In distinction to Kikuchi's, however, localized Castleman's is largely asymptomatic and responds marvelously to excision.
On hospital day 9, an excisional biopsy of his left anterior cervical lymph nodes was performed, which revealed paracortical foci with necrosis and a histiocytic cellular infiltrate consistent with subacute necrotizing lymphadenitis (Kikuchi‐Fujimoto disease). Antinuclear antibody, Toxoplasma, and HTLV‐1 antibodies returned negative.
There is no treatment for Kikuchi's. It is usually self‐limited, but steroids are sometimes given for symptomatic control.
His condition began to improve after hospital day 9 without specific treatment, including his WBC count and LDH level. He was discharged home on hospital day 15. In the outpatient clinic 1 and 3 months later, he was well and active without recurrences of any symptoms or laboratory abnormalities. His WBC count was 6600/L and LDH was 268 IU/L.
Commentary
Kikuchi‐Fujimoto disease (KFD), also called Kikuchi's disease, is a benign histiocytic necrotizing lymphadenitis described by both Kikuchi and Fujimoto in 1972.1, 2 It is rare in the United States, but seems more common in Asia, especially Japan, where at least 143 cases have been reported since 1972. The etiology has not been determined, but a viral causeincluding EBV, and human herpesvirus 6 and 8has been suggested.3 An autoimmune etiology is also implicated because of infrequent association with SLE. In general, young women are most likely to be affected. In a review of 244 cases by Kucukardali and colleagues, 77% of patients were female and the mean age was 25; 70% were younger than 30 years of age.4
The common presentation is low‐grade fever with unilateral cervical lymphadenopathy.4 Although generalized lymphadenopathy can occur, it is rare. Other common clinical manifestations include malaise, joint pain, rash, arthritis, and hepatosplenomegaly. No specific laboratory tests for diagnosis are available, but leukopenia (seen in 43% of patients), increased erythrocyte sedimentation rate (40%), and anemia (23%) may be observed.4 In this case, atypical lymphocytes were seen, and are reported in one‐third of patients.5 KFD is generally diagnosed by lymph node biopsy, which typically shows irregular paracortical areas of coagulation necrosis that can distort the nodal architecture, while different types of histiocytes are observed at the margin of necrotic areas.
Other diseases in the differential diagnosisseveral of which were considered by the discussantinclude lymphoma, tuberculosis, SLE, and even metastatic adenocarcinoma. KFD is self‐limited; symptoms typically resolve within 1 to 4 months. Patients with severe manifestations have been treated with anti‐inflammatory drugs and glucocorticosteroids. A recurrence rate of 3% to 4% has been reported.6
The clinicians taking care of this patient initially focused on ruling out those infections occasionally resulting in prolonged fever in a previously healthy young man, such as viruses from the herpes family, HIV, viral hepatitis, tuberculosis, syphilis, infective endocarditis, and intra‐abdominal abscess. Physical examination, specifically lymphadenopathy and mild splenomegaly, made Herpesviridae infections, tuberculosis, syphilis, and lymphoma difficult to exclude. Once the initial evaluation ruled out common infections, attention focused on malignancy and histiocytic necrotizing lymphadenitis, given his ethnicity and geographic location.
The discussant was similarly concerned about infection, malignancy, and noninfectious inflammatory diseases, such as SLE, as possible causes. As evidence of these treatable diseases failed to accumulate, the discussant, an American physician with teaching and clinical experience in Japan, considered endemic diseases such as Behcet's, HTLV‐1, and KFD because they fit the unfolding pattern. Given our global society, clinicians will increasingly benefit from becoming familiar with the less common diseases that afflict the various populations around the world.
Teaching Points
-
The combination of fever, lymphadenopathy, and leukopenia in young adults suggests SLE, lymphoma, and HIV. Clinicians should also consider KFD in patients from Japan and neighboring countries.
-
Lymph node biopsy is usually diagnostic of KFD, although interpretation of histopathology can be difficult and sometimes leads to confusion with SLE and lymphoma.
-
KFD typically resolves without specific treatment.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
- .Lymphadenitis showing focal reticulum cell hyperplasia with nuclear debris and phagocytes: a clinicopathological study.Acta Hematol Jpn.1972;35:379–380.
- ,,.Cervical subacute necrotizing lymphadenitis: a new clinicopathological agent.Naika.1972;20:920–927.
- ,,,.Enigmatic Kikuchi‐Fujimoto disease: a comprehensive review.Am J Clin Pathol.2004;122:141–152.
- ,,,,,.Kikuchi‐Fujimoto Disease: analysis of 244 cases.Clin Rheumatol.2007;26:50–54.
- ,,,,.Kikuchi's disease: A review and analysis of 61 cases.Otolaryngol Head Neck Surg.2003;128:650–653.
- .Histiocytic necrotizing lymphadenitis of Kikuchi and Fujimoto.Arch Pathol Lab Med.1987;11:1026–1029.
A 19‐year‐old Japanese man was admitted to a hospital near Kyoto, Japan, because of fever and rash. Two weeks prior to admission, he developed mild headache and low‐grade fever; a rapid test for influenza was negative. His symptoms transiently improved with acetaminophen, but 8 days prior to admission, he developed fever to 38.5C and a pruritic maculopapular rash over his back that spread to his limbs. Six days prior to admission, a chest radiograph was clear; clarithromycin was prescribed for presumed upper respiratory infection. He visited the emergency department the day before admission because of continued fever of greater than 39C, fatigue, and headache. Because there was no jolt accentuation of the headache (ie, worsening with rapid horizontal rotation), or neck pain with extreme neck flexion, he was discharged on acetaminophen. He returned the next day with worsening fatigue and was admitted. He denied chills, rigor, weight loss, photosensitivity, sore throat, neck pain, cough, dyspnea, chest pain, nausea, vomiting, diarrhea, abdominal pain, back pain, and arthralgia.
Fever and diffuse rash are often due to infection, although drugs, autoimmune processes, and cancer must be considered. The presence of headache does not focus the differential diagnosis substantially, because many of the candidate diagnoses can be accompanied by meningitis or encephalitis, or even more frequently, nonspecific headaches. In one small study, jolt‐induced aggravation of headache was shown to be a sensitive indicator of cerebrospinal fluid pleocytosis. The absence of neck stiffness and the 2‐week duration makes bacterial meningitis unlikely, but a more indolent form of aseptic meningitis may need to be evaluated with a lumbar puncture.
The 2‐week illness without rapid deterioration makes some serious causes of fever and rash, such as toxic shock syndrome, disseminated meningococcal infection, or toxic epidermal necrolysis unlikely. A viral exanthema is possible, although the 2‐week duration is longer than usual. Given his youth, however, his immunization history should be queried, and acute infection with human immunodeficiency virus (HIV) should be considered. A more indolent infection, such as subacute bacterial endocarditis, disseminated gonococcal infection, or syphilis is plausible. Among autoimmune etiologies, systemic lupus erythematosus (SLE) and Behcet's disease (which is prevalent in Japan) can involve the central nervous system and cause fever. A careful inquiry directed at prescribed, complementary, and illicit drugs is required.
The patient's past medical history was notable only for mumps at the age of 10. His medications included acetaminophen, clarithromycin, and an herbal medicine, which he had been taking for the prior several days. He reported no tobacco or illicit drug use and rarely drank alcohol. He had never been sexually active. He worked in a factory and reported occasional contact with silver. He lived with his parents; there was no family history of tuberculosis or connective tissue diseases. His father was from Kyushu (the southernmost major island in Japan) and had chronic hepatitis C. The patient denied recent animal exposure or recent travel. His childhood vaccinations were said to be up to date.
Mumps at age 10 might signal general lack of immunization, in which case childhood viral exanthema‐like measles (characterized by fever, headache, and diffuse rash) would warrant consideration. The listed medications had been started after the onset of illness and therefore are unlikely to be causal. Silver causes at least 2 skin conditionscontact dermatitis and argyriabut not the systemic illness seen here. Human T lymphotropic virus‐1 (HTLV‐1) is endemic in southern Japan, but only a minority of infected humans are afflicted with associated adult T cell leukemia/lymphoma or myelopathy. Leukemia and lymphoma are the most likely cancers to cause fever, rash, and central nervous system involvement (with T cell disorders demonstrating a particular tropism for the skin). Overall, however, the differential has not changed substantially.
On physical examination, the patient was mildly overweight and appeared acutely ill. His blood pressure was 136/78 mm Hg, pulse rate was 76 and regular, temperature was 39.2C and respiratory rate was 20 with an oxygen saturation of 98% on room air. A diffuse but nonconfluent erythematous maculopapular rash was present over his chest wall, back, medial aspects of both thighs, and around the knees. There was no jolt‐induced headache. His eyes, nose, oral cavity, and throat were all clear. The neck was supple. There were palpable lymph nodes, each about 1 cm in size, which were firm and moderately tender, in his left neck and left axilla. Lungs and heart were normal. The abdomen was soft, nontender, with normal bowel sounds and no hepatosplenomegaly. His genitalia were normal. Rectal examination revealed no masses or tenderness and a scant amount of brown stool that was negative for occult blood. Neurologic examination was unremarkable.
The multifocal lymphadenopathy does not help distinguish among the categories of disease under consideration. The diffuse maculopapular rash is similarly nonspecific, occurring more frequently with infection and drug reaction than malignancy and autoimmunity. Acute HIV, Epstein‐Barr virus (EBV), syphilis, SLE, drug exposure, or a hematologic malignancy would all be suitable explanations for fever, headache, diffuse rash, and disseminated lymphadenopathy in a previously healthy young man.
Laboratory data obtained on admission was notable for a white blood cell (WBC) count of 2100/L with 72% neutrophils, 19% lymphocytes, and 9% monocytes. Hemoglobin was 13.5 mg/dL with a mean corpuscular volume of 85 fL. Platelet count was 136,000/L. Erythrocyte sedimentation rate was 26 mm/hour. Serum chemistries revealed a sodium level of 135 mEq/L, potassium level of 3.6 mEq/L, chloride level of 100 mEq/L, blood urea nitrogen of 9.8 mg/dL, creatinine level of 1.0 mg/dL, glucose level of 101 mg/dL, calcium level of 8.8 mg/dL, albumin of 4.6 mg/dL, total protein of 8.4 mg/dL, aspartate aminotransferase of 42 IU/L (normal 35 IU/L), alanine aminotransferase of 27 IU/L, total bilirubin of 0.5 mg/dL, and lactate dehydrogenase (LDH) level of 463 IU/L (normal 260 IU/L). Chest radiography and electrocardiogram were normal.
A mild elevation in LDH is nonspecific, but without hemolysis or infarction of the kidney, lung, or muscle, it suggests a lymphoproliferative process. Leukopenia with thrombocytopenia can be seen in a number of disorders, most commonly infections including viruses (e.g., EBV, HIV, dengue), malaria, Rocky Mountain spotted fever, or ehrlichiosis/anaplasmosis. Confirmation of his lack of travel could help prioritize those considerations. An invasive bone marrow disorder cannot be excluded, although the near‐normal hemoglobin argues against it. Autoimmune cytopenias are seen in SLE. Given his age, lymphadenopathy, LDH elevation, and absence of infectious exposures, lymphoma rises to the top of the list.
Noninvasive measures should include examination of the peripheral smear, HIV testing (including HIV RNA for acute infection), EBV serologies, and tests for syphilis and SLE. Lumbar puncture (for evaluation of aseptic meningitis) and lymph node biopsy would be informative. Skin biopsy may be helpful to evaluate for aggressive T cell lymphoproliferative disorder, but this can await the results of initial testing.
The patient was given intravenous fluids and acetaminophen as needed. Blood cultures, urine culture, cytomegalovirus and EBV serologies, hepatitis B surface antigen, hepatitis C virus antibody, HIV antibody, antinuclear antibody, complement and ferritin levels, and quantiferon‐TB were ordered. The urine was normal and a urinary antigen test for Legionella was negative. Contrast‐enhanced computed tomography scan of the chest and abdomen was normal except for mild splenomegaly and an enlarged left axillary lymph node.
The ferritin may have been ordered to help evaluate for Still's disease, which is characterized by sustained fever, lymphadenopathy, and transient rash; however, the characteristic leukocytosis and arthralgias are absent. The computed tomography findings are most notable for the absence of generalized lymphadenopathy or significant hepatosplenomegaly that is seen in lymphoma, leukemia, and lymphotropic processes such as acute EBV infection. The localization of disease to the skin (where the predominant lymphocytes are of T cell origin) with relatively modest lymphadenopathy suggests a T cell lymphoma, perhaps of an indolent variety. Vertical transmission of HTLV‐1 decades ago would make adult T cell leukemia or lymphoma a major consideration.
On the third hospital day, WBC count was 1800/L with 67% neutrophils, 22% lymphocytes, and 1% atypical lymphocytes; LDH rose to 623 IU/L. He had continued fatigue and high fever while the rash gradually faded with oral antihistamines and steroid ointment. On hospital day 4, bone marrow biopsy and skin biopsy of his left thigh were performed.
The further decline in WBC and rise in LDH are modest and therefore do not significantly modify the differential diagnosis. Likewise, 1% atypical lymphocytosis is too low to pinpoint an etiology. Because unremitting fevers start to extend into their third week without a clear source of infection, the probability of malignancy and autoimmunity rise. Improvement with oral antihistamines and topical steroids frequently suggests an underlying allergic process, but the remainder of the clinical picture is not in keeping with atopy or allergy. Cutaneous lymphomas (eg, mycosis fungoides) can have waxing and waning skin manifestations, and can be temporarily or definitively treated by topical steroids. The persistence of his fatigue is of concern given the absence of anemia, cardiopulmonary involvement, or motor weakness.
Bone marrow biopsy showed normocellular marrow with no abnormal cells and some activated macrophages with hemophagocytic activity. Skin biopsy failed to show specific pathology.
His left cervical lymph nodes gradually enlarged. Ultrasound of the neck showed multiple enlarged lymph nodes (left side dominant) with dimension of 17 mm 9 mm 31 mm. Blood and urine cultures returned negative, as did HIV antibody. cytomegalovirus and EBV serologies were consistent with previous infection and the ferritin level was 578 ng/mL (normal, 39‐340 ng/mL). Toxoplasma serology and HTLV‐1 antibody were ordered.
The absence of malignant cells on bone marrow biopsy does not exclude lymphoma, but makes a myelophthisic cause of the cytopenias less likely. The macrophage hemophagocytosis reflects immune activation, which in turn is usually caused by the same viral infections, autoimmune conditions, and lymphoproliferative disorders which constitute the current differential diagnosis.
Bone marrow and skin biopsies are both subject to sampling error, and detection of cutaneous T cell lymphoma is notoriously difficult. However, taken together, the absence of cancer on 2 specimens reduces that possibility.
Sustained unilateral cervical lymphadenopathy with fever in a young Japanese man without any histologic evidence of lymphoma points to Kikuchi's disease, ie, lymphadenitis of unknown etiology associated with varying degrees of systemic manifestations. Fever is a frequent feature, we believe, but diffuse sustained rash, cytopenias, and headache are less common or are seen in severe forms of the disease. The diagnosis of Kikuchi's requires the diligent exclusion of SLE and lymphoma. Examination of the peripheral smear and a lymph node biopsy are required.
Of note, there is also a localized form of Castleman's disease, a nonmalignant lymphoproliferative disorder, that similarly is characterized by focal lymphadenopathy. In distinction to Kikuchi's, however, localized Castleman's is largely asymptomatic and responds marvelously to excision.
On hospital day 9, an excisional biopsy of his left anterior cervical lymph nodes was performed, which revealed paracortical foci with necrosis and a histiocytic cellular infiltrate consistent with subacute necrotizing lymphadenitis (Kikuchi‐Fujimoto disease). Antinuclear antibody, Toxoplasma, and HTLV‐1 antibodies returned negative.
There is no treatment for Kikuchi's. It is usually self‐limited, but steroids are sometimes given for symptomatic control.
His condition began to improve after hospital day 9 without specific treatment, including his WBC count and LDH level. He was discharged home on hospital day 15. In the outpatient clinic 1 and 3 months later, he was well and active without recurrences of any symptoms or laboratory abnormalities. His WBC count was 6600/L and LDH was 268 IU/L.
Commentary
Kikuchi‐Fujimoto disease (KFD), also called Kikuchi's disease, is a benign histiocytic necrotizing lymphadenitis described by both Kikuchi and Fujimoto in 1972.1, 2 It is rare in the United States, but seems more common in Asia, especially Japan, where at least 143 cases have been reported since 1972. The etiology has not been determined, but a viral causeincluding EBV, and human herpesvirus 6 and 8has been suggested.3 An autoimmune etiology is also implicated because of infrequent association with SLE. In general, young women are most likely to be affected. In a review of 244 cases by Kucukardali and colleagues, 77% of patients were female and the mean age was 25; 70% were younger than 30 years of age.4
The common presentation is low‐grade fever with unilateral cervical lymphadenopathy.4 Although generalized lymphadenopathy can occur, it is rare. Other common clinical manifestations include malaise, joint pain, rash, arthritis, and hepatosplenomegaly. No specific laboratory tests for diagnosis are available, but leukopenia (seen in 43% of patients), increased erythrocyte sedimentation rate (40%), and anemia (23%) may be observed.4 In this case, atypical lymphocytes were seen, and are reported in one‐third of patients.5 KFD is generally diagnosed by lymph node biopsy, which typically shows irregular paracortical areas of coagulation necrosis that can distort the nodal architecture, while different types of histiocytes are observed at the margin of necrotic areas.
Other diseases in the differential diagnosisseveral of which were considered by the discussantinclude lymphoma, tuberculosis, SLE, and even metastatic adenocarcinoma. KFD is self‐limited; symptoms typically resolve within 1 to 4 months. Patients with severe manifestations have been treated with anti‐inflammatory drugs and glucocorticosteroids. A recurrence rate of 3% to 4% has been reported.6
The clinicians taking care of this patient initially focused on ruling out those infections occasionally resulting in prolonged fever in a previously healthy young man, such as viruses from the herpes family, HIV, viral hepatitis, tuberculosis, syphilis, infective endocarditis, and intra‐abdominal abscess. Physical examination, specifically lymphadenopathy and mild splenomegaly, made Herpesviridae infections, tuberculosis, syphilis, and lymphoma difficult to exclude. Once the initial evaluation ruled out common infections, attention focused on malignancy and histiocytic necrotizing lymphadenitis, given his ethnicity and geographic location.
The discussant was similarly concerned about infection, malignancy, and noninfectious inflammatory diseases, such as SLE, as possible causes. As evidence of these treatable diseases failed to accumulate, the discussant, an American physician with teaching and clinical experience in Japan, considered endemic diseases such as Behcet's, HTLV‐1, and KFD because they fit the unfolding pattern. Given our global society, clinicians will increasingly benefit from becoming familiar with the less common diseases that afflict the various populations around the world.
Teaching Points
-
The combination of fever, lymphadenopathy, and leukopenia in young adults suggests SLE, lymphoma, and HIV. Clinicians should also consider KFD in patients from Japan and neighboring countries.
-
Lymph node biopsy is usually diagnostic of KFD, although interpretation of histopathology can be difficult and sometimes leads to confusion with SLE and lymphoma.
-
KFD typically resolves without specific treatment.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
A 19‐year‐old Japanese man was admitted to a hospital near Kyoto, Japan, because of fever and rash. Two weeks prior to admission, he developed mild headache and low‐grade fever; a rapid test for influenza was negative. His symptoms transiently improved with acetaminophen, but 8 days prior to admission, he developed fever to 38.5C and a pruritic maculopapular rash over his back that spread to his limbs. Six days prior to admission, a chest radiograph was clear; clarithromycin was prescribed for presumed upper respiratory infection. He visited the emergency department the day before admission because of continued fever of greater than 39C, fatigue, and headache. Because there was no jolt accentuation of the headache (ie, worsening with rapid horizontal rotation), or neck pain with extreme neck flexion, he was discharged on acetaminophen. He returned the next day with worsening fatigue and was admitted. He denied chills, rigor, weight loss, photosensitivity, sore throat, neck pain, cough, dyspnea, chest pain, nausea, vomiting, diarrhea, abdominal pain, back pain, and arthralgia.
Fever and diffuse rash are often due to infection, although drugs, autoimmune processes, and cancer must be considered. The presence of headache does not focus the differential diagnosis substantially, because many of the candidate diagnoses can be accompanied by meningitis or encephalitis, or even more frequently, nonspecific headaches. In one small study, jolt‐induced aggravation of headache was shown to be a sensitive indicator of cerebrospinal fluid pleocytosis. The absence of neck stiffness and the 2‐week duration makes bacterial meningitis unlikely, but a more indolent form of aseptic meningitis may need to be evaluated with a lumbar puncture.
The 2‐week illness without rapid deterioration makes some serious causes of fever and rash, such as toxic shock syndrome, disseminated meningococcal infection, or toxic epidermal necrolysis unlikely. A viral exanthema is possible, although the 2‐week duration is longer than usual. Given his youth, however, his immunization history should be queried, and acute infection with human immunodeficiency virus (HIV) should be considered. A more indolent infection, such as subacute bacterial endocarditis, disseminated gonococcal infection, or syphilis is plausible. Among autoimmune etiologies, systemic lupus erythematosus (SLE) and Behcet's disease (which is prevalent in Japan) can involve the central nervous system and cause fever. A careful inquiry directed at prescribed, complementary, and illicit drugs is required.
The patient's past medical history was notable only for mumps at the age of 10. His medications included acetaminophen, clarithromycin, and an herbal medicine, which he had been taking for the prior several days. He reported no tobacco or illicit drug use and rarely drank alcohol. He had never been sexually active. He worked in a factory and reported occasional contact with silver. He lived with his parents; there was no family history of tuberculosis or connective tissue diseases. His father was from Kyushu (the southernmost major island in Japan) and had chronic hepatitis C. The patient denied recent animal exposure or recent travel. His childhood vaccinations were said to be up to date.
Mumps at age 10 might signal general lack of immunization, in which case childhood viral exanthema‐like measles (characterized by fever, headache, and diffuse rash) would warrant consideration. The listed medications had been started after the onset of illness and therefore are unlikely to be causal. Silver causes at least 2 skin conditionscontact dermatitis and argyriabut not the systemic illness seen here. Human T lymphotropic virus‐1 (HTLV‐1) is endemic in southern Japan, but only a minority of infected humans are afflicted with associated adult T cell leukemia/lymphoma or myelopathy. Leukemia and lymphoma are the most likely cancers to cause fever, rash, and central nervous system involvement (with T cell disorders demonstrating a particular tropism for the skin). Overall, however, the differential has not changed substantially.
On physical examination, the patient was mildly overweight and appeared acutely ill. His blood pressure was 136/78 mm Hg, pulse rate was 76 and regular, temperature was 39.2C and respiratory rate was 20 with an oxygen saturation of 98% on room air. A diffuse but nonconfluent erythematous maculopapular rash was present over his chest wall, back, medial aspects of both thighs, and around the knees. There was no jolt‐induced headache. His eyes, nose, oral cavity, and throat were all clear. The neck was supple. There were palpable lymph nodes, each about 1 cm in size, which were firm and moderately tender, in his left neck and left axilla. Lungs and heart were normal. The abdomen was soft, nontender, with normal bowel sounds and no hepatosplenomegaly. His genitalia were normal. Rectal examination revealed no masses or tenderness and a scant amount of brown stool that was negative for occult blood. Neurologic examination was unremarkable.
The multifocal lymphadenopathy does not help distinguish among the categories of disease under consideration. The diffuse maculopapular rash is similarly nonspecific, occurring more frequently with infection and drug reaction than malignancy and autoimmunity. Acute HIV, Epstein‐Barr virus (EBV), syphilis, SLE, drug exposure, or a hematologic malignancy would all be suitable explanations for fever, headache, diffuse rash, and disseminated lymphadenopathy in a previously healthy young man.
Laboratory data obtained on admission was notable for a white blood cell (WBC) count of 2100/L with 72% neutrophils, 19% lymphocytes, and 9% monocytes. Hemoglobin was 13.5 mg/dL with a mean corpuscular volume of 85 fL. Platelet count was 136,000/L. Erythrocyte sedimentation rate was 26 mm/hour. Serum chemistries revealed a sodium level of 135 mEq/L, potassium level of 3.6 mEq/L, chloride level of 100 mEq/L, blood urea nitrogen of 9.8 mg/dL, creatinine level of 1.0 mg/dL, glucose level of 101 mg/dL, calcium level of 8.8 mg/dL, albumin of 4.6 mg/dL, total protein of 8.4 mg/dL, aspartate aminotransferase of 42 IU/L (normal 35 IU/L), alanine aminotransferase of 27 IU/L, total bilirubin of 0.5 mg/dL, and lactate dehydrogenase (LDH) level of 463 IU/L (normal 260 IU/L). Chest radiography and electrocardiogram were normal.
A mild elevation in LDH is nonspecific, but without hemolysis or infarction of the kidney, lung, or muscle, it suggests a lymphoproliferative process. Leukopenia with thrombocytopenia can be seen in a number of disorders, most commonly infections including viruses (e.g., EBV, HIV, dengue), malaria, Rocky Mountain spotted fever, or ehrlichiosis/anaplasmosis. Confirmation of his lack of travel could help prioritize those considerations. An invasive bone marrow disorder cannot be excluded, although the near‐normal hemoglobin argues against it. Autoimmune cytopenias are seen in SLE. Given his age, lymphadenopathy, LDH elevation, and absence of infectious exposures, lymphoma rises to the top of the list.
Noninvasive measures should include examination of the peripheral smear, HIV testing (including HIV RNA for acute infection), EBV serologies, and tests for syphilis and SLE. Lumbar puncture (for evaluation of aseptic meningitis) and lymph node biopsy would be informative. Skin biopsy may be helpful to evaluate for aggressive T cell lymphoproliferative disorder, but this can await the results of initial testing.
The patient was given intravenous fluids and acetaminophen as needed. Blood cultures, urine culture, cytomegalovirus and EBV serologies, hepatitis B surface antigen, hepatitis C virus antibody, HIV antibody, antinuclear antibody, complement and ferritin levels, and quantiferon‐TB were ordered. The urine was normal and a urinary antigen test for Legionella was negative. Contrast‐enhanced computed tomography scan of the chest and abdomen was normal except for mild splenomegaly and an enlarged left axillary lymph node.
The ferritin may have been ordered to help evaluate for Still's disease, which is characterized by sustained fever, lymphadenopathy, and transient rash; however, the characteristic leukocytosis and arthralgias are absent. The computed tomography findings are most notable for the absence of generalized lymphadenopathy or significant hepatosplenomegaly that is seen in lymphoma, leukemia, and lymphotropic processes such as acute EBV infection. The localization of disease to the skin (where the predominant lymphocytes are of T cell origin) with relatively modest lymphadenopathy suggests a T cell lymphoma, perhaps of an indolent variety. Vertical transmission of HTLV‐1 decades ago would make adult T cell leukemia or lymphoma a major consideration.
On the third hospital day, WBC count was 1800/L with 67% neutrophils, 22% lymphocytes, and 1% atypical lymphocytes; LDH rose to 623 IU/L. He had continued fatigue and high fever while the rash gradually faded with oral antihistamines and steroid ointment. On hospital day 4, bone marrow biopsy and skin biopsy of his left thigh were performed.
The further decline in WBC and rise in LDH are modest and therefore do not significantly modify the differential diagnosis. Likewise, 1% atypical lymphocytosis is too low to pinpoint an etiology. Because unremitting fevers start to extend into their third week without a clear source of infection, the probability of malignancy and autoimmunity rise. Improvement with oral antihistamines and topical steroids frequently suggests an underlying allergic process, but the remainder of the clinical picture is not in keeping with atopy or allergy. Cutaneous lymphomas (eg, mycosis fungoides) can have waxing and waning skin manifestations, and can be temporarily or definitively treated by topical steroids. The persistence of his fatigue is of concern given the absence of anemia, cardiopulmonary involvement, or motor weakness.
Bone marrow biopsy showed normocellular marrow with no abnormal cells and some activated macrophages with hemophagocytic activity. Skin biopsy failed to show specific pathology.
His left cervical lymph nodes gradually enlarged. Ultrasound of the neck showed multiple enlarged lymph nodes (left side dominant) with dimension of 17 mm 9 mm 31 mm. Blood and urine cultures returned negative, as did HIV antibody. cytomegalovirus and EBV serologies were consistent with previous infection and the ferritin level was 578 ng/mL (normal, 39‐340 ng/mL). Toxoplasma serology and HTLV‐1 antibody were ordered.
The absence of malignant cells on bone marrow biopsy does not exclude lymphoma, but makes a myelophthisic cause of the cytopenias less likely. The macrophage hemophagocytosis reflects immune activation, which in turn is usually caused by the same viral infections, autoimmune conditions, and lymphoproliferative disorders which constitute the current differential diagnosis.
Bone marrow and skin biopsies are both subject to sampling error, and detection of cutaneous T cell lymphoma is notoriously difficult. However, taken together, the absence of cancer on 2 specimens reduces that possibility.
Sustained unilateral cervical lymphadenopathy with fever in a young Japanese man without any histologic evidence of lymphoma points to Kikuchi's disease, ie, lymphadenitis of unknown etiology associated with varying degrees of systemic manifestations. Fever is a frequent feature, we believe, but diffuse sustained rash, cytopenias, and headache are less common or are seen in severe forms of the disease. The diagnosis of Kikuchi's requires the diligent exclusion of SLE and lymphoma. Examination of the peripheral smear and a lymph node biopsy are required.
Of note, there is also a localized form of Castleman's disease, a nonmalignant lymphoproliferative disorder, that similarly is characterized by focal lymphadenopathy. In distinction to Kikuchi's, however, localized Castleman's is largely asymptomatic and responds marvelously to excision.
On hospital day 9, an excisional biopsy of his left anterior cervical lymph nodes was performed, which revealed paracortical foci with necrosis and a histiocytic cellular infiltrate consistent with subacute necrotizing lymphadenitis (Kikuchi‐Fujimoto disease). Antinuclear antibody, Toxoplasma, and HTLV‐1 antibodies returned negative.
There is no treatment for Kikuchi's. It is usually self‐limited, but steroids are sometimes given for symptomatic control.
His condition began to improve after hospital day 9 without specific treatment, including his WBC count and LDH level. He was discharged home on hospital day 15. In the outpatient clinic 1 and 3 months later, he was well and active without recurrences of any symptoms or laboratory abnormalities. His WBC count was 6600/L and LDH was 268 IU/L.
Commentary
Kikuchi‐Fujimoto disease (KFD), also called Kikuchi's disease, is a benign histiocytic necrotizing lymphadenitis described by both Kikuchi and Fujimoto in 1972.1, 2 It is rare in the United States, but seems more common in Asia, especially Japan, where at least 143 cases have been reported since 1972. The etiology has not been determined, but a viral causeincluding EBV, and human herpesvirus 6 and 8has been suggested.3 An autoimmune etiology is also implicated because of infrequent association with SLE. In general, young women are most likely to be affected. In a review of 244 cases by Kucukardali and colleagues, 77% of patients were female and the mean age was 25; 70% were younger than 30 years of age.4
The common presentation is low‐grade fever with unilateral cervical lymphadenopathy.4 Although generalized lymphadenopathy can occur, it is rare. Other common clinical manifestations include malaise, joint pain, rash, arthritis, and hepatosplenomegaly. No specific laboratory tests for diagnosis are available, but leukopenia (seen in 43% of patients), increased erythrocyte sedimentation rate (40%), and anemia (23%) may be observed.4 In this case, atypical lymphocytes were seen, and are reported in one‐third of patients.5 KFD is generally diagnosed by lymph node biopsy, which typically shows irregular paracortical areas of coagulation necrosis that can distort the nodal architecture, while different types of histiocytes are observed at the margin of necrotic areas.
Other diseases in the differential diagnosisseveral of which were considered by the discussantinclude lymphoma, tuberculosis, SLE, and even metastatic adenocarcinoma. KFD is self‐limited; symptoms typically resolve within 1 to 4 months. Patients with severe manifestations have been treated with anti‐inflammatory drugs and glucocorticosteroids. A recurrence rate of 3% to 4% has been reported.6
The clinicians taking care of this patient initially focused on ruling out those infections occasionally resulting in prolonged fever in a previously healthy young man, such as viruses from the herpes family, HIV, viral hepatitis, tuberculosis, syphilis, infective endocarditis, and intra‐abdominal abscess. Physical examination, specifically lymphadenopathy and mild splenomegaly, made Herpesviridae infections, tuberculosis, syphilis, and lymphoma difficult to exclude. Once the initial evaluation ruled out common infections, attention focused on malignancy and histiocytic necrotizing lymphadenitis, given his ethnicity and geographic location.
The discussant was similarly concerned about infection, malignancy, and noninfectious inflammatory diseases, such as SLE, as possible causes. As evidence of these treatable diseases failed to accumulate, the discussant, an American physician with teaching and clinical experience in Japan, considered endemic diseases such as Behcet's, HTLV‐1, and KFD because they fit the unfolding pattern. Given our global society, clinicians will increasingly benefit from becoming familiar with the less common diseases that afflict the various populations around the world.
Teaching Points
-
The combination of fever, lymphadenopathy, and leukopenia in young adults suggests SLE, lymphoma, and HIV. Clinicians should also consider KFD in patients from Japan and neighboring countries.
-
Lymph node biopsy is usually diagnostic of KFD, although interpretation of histopathology can be difficult and sometimes leads to confusion with SLE and lymphoma.
-
KFD typically resolves without specific treatment.
The approach to clinical conundrums by an expert clinician is revealed through the presentation of an actual patient's case in an approach typical of a morning report. Similarly to patient care, sequential pieces of information are provided to the clinician, who is unfamiliar with the case. The focus is on the thought processes of both the clinical team caring for the patient and the discussant.
- .Lymphadenitis showing focal reticulum cell hyperplasia with nuclear debris and phagocytes: a clinicopathological study.Acta Hematol Jpn.1972;35:379–380.
- ,,.Cervical subacute necrotizing lymphadenitis: a new clinicopathological agent.Naika.1972;20:920–927.
- ,,,.Enigmatic Kikuchi‐Fujimoto disease: a comprehensive review.Am J Clin Pathol.2004;122:141–152.
- ,,,,,.Kikuchi‐Fujimoto Disease: analysis of 244 cases.Clin Rheumatol.2007;26:50–54.
- ,,,,.Kikuchi's disease: A review and analysis of 61 cases.Otolaryngol Head Neck Surg.2003;128:650–653.
- .Histiocytic necrotizing lymphadenitis of Kikuchi and Fujimoto.Arch Pathol Lab Med.1987;11:1026–1029.
- .Lymphadenitis showing focal reticulum cell hyperplasia with nuclear debris and phagocytes: a clinicopathological study.Acta Hematol Jpn.1972;35:379–380.
- ,,.Cervical subacute necrotizing lymphadenitis: a new clinicopathological agent.Naika.1972;20:920–927.
- ,,,.Enigmatic Kikuchi‐Fujimoto disease: a comprehensive review.Am J Clin Pathol.2004;122:141–152.
- ,,,,,.Kikuchi‐Fujimoto Disease: analysis of 244 cases.Clin Rheumatol.2007;26:50–54.
- ,,,,.Kikuchi's disease: A review and analysis of 61 cases.Otolaryngol Head Neck Surg.2003;128:650–653.
- .Histiocytic necrotizing lymphadenitis of Kikuchi and Fujimoto.Arch Pathol Lab Med.1987;11:1026–1029.
Physician Assistant‐Based General Medical Inpatient Care
In 2003 the Accreditation Council for Graduate Medical Education (ACGME) prescribed residency reform in the form of work hour restrictions without prescribing alternatives to resident based care.1 As a response, many academic medical centers have developed innovative models for providing inpatient care, some of which incorporate Physician Assistants (PAs).2 With further restrictions in resident work hours possible,3 teaching hospitals may increase use of these alternate models to provide inpatient care. Widespread implementation of such new and untested models could impact the care of the approximately 20 million hospitalizations that occur every year in US teaching hospitals.4
Few reports have compared the care delivered by these alternate models with the care provided by traditional resident‐based models of care.58 Roy et al.8 have provided the only recent comparison of a PA‐based model of care with a resident‐based model. They showed lower adjusted costs of inpatient care associated with PA based care but other outcomes were similar to resident‐based teams.
The objective of this study is to provide a valid and usable comparison of the outcomes of a hospitalist‐PA (H‐PA) model of inpatient care with the traditional resident‐based model. This will add to the quantity and quality of the limited research on PA‐based inpatient care, and informs the anticipated increase in the involvement of PAs in this arena.
Methods
Study Design and Setting
We conducted a retrospective cohort study at a 430‐bed urban academic medical center in the Midwestern United States.
Models of General Medical (GM) Inpatient Care at the Study Hospital During the Study Period
In November 2004, as a response to the ACGME‐mandated work hour regulations, we formed 2 Hospitalist‐PA teams (H‐PA) to supplement the 6 preexisting general medicine resident teams (RES).
The H‐PA and RES teams differed in staffing, admitting times and weekend/overnight cross coverage structure (Table 1). There were no predesigned differences between the teams in the ward location of their patients, availability of laboratory/radiology services, specialty consultation, social services/case management resources, nursing resources or documentation requirements for admission, daily care, and discharge.
| H‐PA Teams | RES Teams | |
|---|---|---|
| Attending physician | Always a hospitalist | Hospitalist, non‐hospitalist general internist or rarely a specialist |
| Attending physician role | Supervisory for some patients (about half) and sole care provider for others. | Supervisory for all patients |
| Team composition | One attending paired with 1 PA | Attending + senior resident + (2) interns + (2‐3) medical students |
| Rotation schedule | ||
| Attending | Every 2 weeks | Every 2 weeks |
| Physician assistant | Off on weekends | |
| House staff & medical students | Every month | |
| Weekend | No new admissions & hospitalist manages all patients | Accept new admissions |
| Admission times (weekdays) | 7 AM to 3 PM | Noon to 7 AM |
| Source of admissions | Emergency room, clinics, other hospitals | Emergency room, clinics, other hospitals |
| Number of admissions (weekdays) | 4‐6 patients per day per team | Noon to 5 PM: 2 teams admit a maximum of 9 patients total |
| 5 PM to 7 AM: 3 teams admit a maximum 5 patients each. | ||
| Overnight coverageroles and responsibilities | One in‐house faculty | 3 on call interns |
| Cross‐covering 2 H‐PA teams | Cross‐covering 2 teams each | |
| Performing triage | Admitting up to 5 patients each | |
| Admitting patients if necessary | ||
| Assisting residents if necessary | ||
| General medical consultation |
Admission Schedule for H‐PA or RES Teams
The admitting schedule was designed to decrease the workload of the house staff and to do so specifically during the periods of peak educational activity (morning report, attending‐led teaching rounds, and noon report). A faculty admitting medical officer (AMO) assigned patients strictly based on the time an admission was requested. Importantly, the request for admission preceded the time of actual admission recorded when the patient reached the ward. The time difference between request for admission and actual admission depended on the source of admission and the delay associated with assigning a patient room. The AMO assigned 8 to 12 new patients to the H‐PA teams every weekday between 7 AM and 3 PM and to the RES teams between noon and 7 AM the next day. There was a designed period of overlap from noon to 3 PM during which both H‐PA and RES teams could admit patients. This period allowed for flexibility in assigning patients to either type of team depending on their workload. The AMO did not use patient complexity or teaching value to assign patients.
Exceptions to Admission Schedule
Patients admitted overnight after the on call RES had reached their admission limits were assigned to H‐PA teams the next morning. In addition, recently discharged patients who were readmitted while the discharging hospitalist (H‐PA teams) or the discharging resident (RES teams) was still scheduled for inpatient duties, were assigned back to the discharging team irrespective of the admitting schedule.
The same medicine team cared for a patient from admission to discharge but on transfer to the intensive care unit (ICU), an intensivist led critical care team assumed care. On transfer out of the ICU these patients were assigned back to the original team irrespective of admitting schedulethe so called bounce back rule to promote inpatient continuity of care. But if the residents (RES teams) or the hospitalist (H‐PA teams) had changedthe bounce back rule was no longer in effect and these patients were assigned to a team according to the admission schedule.
Study Population and Study Period
We included all hospitalizations of adult patients to GM teams if both their date of admission and their date of discharge fell within the study period (January 1, 2005 to December 31, 2006). We excluded hospitalizations with admissions during the weekendwhen H‐PA teams did not admit patients; hospitalizations to GM services with transfer to nonGM service (excluding ICU) and hospitalizations involving comanagement with specialty servicesas the contribution of GM teams for these was variable; and hospitalizations of private patients.
Data Collection and Team Assignment
We collected patient data from our hospital's discharge abstract database. This database did not contain team information so to assign teams we matched the discharging attending and the day of discharge to the type of team that the discharging attending was leading that day.
We collected patient age, gender, race, insurance status, zip‐code, primary care provider, source of admission, ward type, time and day of admission, and time and day of discharge for use as independent variables. The time of admission captured in the database was the time of actual admission and not the time the admission was requested.
We grouped the principal diagnosis International Statistical Classification of Diseases and Related Health Problems, 9th edition (ICD‐9) codes into clinically relevant categories using the Clinical Classification Software.9 We created comorbidity measures using Healthcare Cost and Utilization Project Comorbidity Software, version 3.4.10
Outcome Measures
We used length of stay (LOS), charges, readmissions within 7, 14, and 30 days and inpatient mortality as our outcome measures. We calculated LOS by subtracting the discharge day and time from the admission day and time. The LOS included time spent in the ICU. We summed all charges accrued during the entire hospitalization including any stay in the ICU but did not include professional fees. We considered any repeat hospitalization to our hospital within 7, 14, and 30 days following a discharge to be a readmission except that we excluded readmissions for a planned procedure or for inpatient rehabilitation.
Statistical Analysis
Descriptive Analysis
We performed unadjusted descriptive statistics at the level of an individual hospitalization using medians and interquartile ranges for continuous data and frequencies and percentages for categorical data. We used chi‐square tests of association and KruskalWallis analysis of variance to compare H‐PA and RES teams.
Missing Data
Because we lacked data on whether a primary outpatient care provider was available for 284 (2.9%) of our study hospitalizations, we dropped them from our multivariable analyses. We used an arbitrary discharge time of noon for the 11 hospitalizations which did not have a discharge time recorded.
Multivariable Analysis
We used multivariable mixed models to risk adjust for a wide variety of variables. We included age, gender, race, insurance, presence of primary care physician, and total number of comorbidities as fixed effects in all models because of the high face validity of these variables. We then added admission source, ward, time, day of week, discharge day of week, and comorbidity measures one by one as fixed effects, including them only if significant at P < 0.01. For assessing LOS, charges, and readmissions, we added a variable identifying each patient as a random effect to account for multiple admissions for the same patient. We then added variables identifying attending physician, principal diagnostic group, and ZIP code of residence as random effects to account for clustering of hospitalizations within these categories, including them only if significant at P < 0.01. For the model assessing mortality we included variables for attending physician, principal diagnostic group, and ZIP code of residence as random effects if significant at P < 0.01. We log transformed LOS and charges because they were extremely skewed in nature. Readmissions were analyzed after excluding patients who died or were discharged alive within 7, 14, or 30 days of the end of the study period.
Sensitivity Analyses
To assess the influence of LOS outliers, we changed LOS to 6 hours if it was less than 6 hours, and 45 days if it was more than 45 daysa process called winsorizing. We consider winsorizing superior to dropping outliers because it acknowledges that outliers contribute information, but prevent them from being too influential. We chose the 6 hour cut off because we believed that was the minimum time required to admit and then discharge a patient. We chose the upper limit of 45 days on reviewing the frequency distribution for outliers. Similarly, we winsorized charges at the first and 99th percentile after reviewing the frequency distribution for outliers. We then log transformed the winsorized data before analysis.
Inpatient deaths reduce the LOS and charges associated with a hospitalization. Thus excess mortality may provide a false concession in terms of lower LOS or charges. To check if this occurred in our study we repeated the analyses after excluding inpatient deaths.
ICU stays are associated with higher LOS, charges, and mortality. In our model of care, some patients transferred to the ICU are not cared for by the original team on transfer out. Moreover, care in the ICU is not controlled by the team that discharges them. Since this might obscure differences in outcomes achieved by RES vs. H‐PA teams, we repeated these analyses after excluding hospitalizations with an ICU stay.
Since mortality can only occur during 1 hospitalization per patient, we repeated the mortality analysis using only each patient's first admission or last admission and using a randomly selected single admission for each patient.
Subgroup Analysis
To limit the effect of different physician characteristics on H‐PA and RES teams we separately analyzed the hospitalizations under the care of hospitalists who served on both H‐PA and RES teams.
To limit the effect of different admission schedules of H‐PA and RES teams we analyzed the hospitalizations with admission times between 11.00 AM and 4.00 PM. Such hospitalizations were likely to be assigned during the noon to 3 PM period when they could be assigned to either an H‐PA or RES team.
Interactions
Finally we explored interactions between the type of team and the fixed effect variables included in each model.
Statistical Software
We performed the statistical analysis using SAS software version 9.0 for UNIX (SAS Institute, Inc., Cary, NC) and R software (The R Project for Statistical Computing).
This study protocol was approved by the hospital's institutional review board.
Results
Study Population
Of the 52,391 hospitalizations to our hospital during the study period, 13,058 were admitted to general medicine. We excluded 3102 weekend admissions and 209 who met other exclusion criteria. We could not determine the team assignment for 66. Of the remaining 9681 hospitalizations, we assigned 2171 to H‐PA teams and 7510 to RES teams (Figure 1).

Descriptive Analysis
We compare patients assigned to H‐PA and RES teams in Table 2. They were similar in age, gender, race, having a primary care provider or not, and insurance status. Clinically, they had similar comorbidities and a similar distribution of common principal diagnoses. Consistent with their admitting schedule, H‐PA teams admitted and discharged more patients earlier in the day and admitted more patients earlier in the work week. Patients cared for by H‐PA teams were admitted from the Emergency Room (ER) less often and were more likely to reside on wards designated as nonmedicine by nursing specialty. Hospitalizations to H‐PA teams more often included an ICU stay.
| H‐PA (n = 2171) | RES (n = 7510) | P Value | |
|---|---|---|---|
| |||
| Age | |||
| Mean | 56.80 | 57.04 | |
| Median | 56 | 56 | 0.15 |
| Interquartile range | 43‐72 | 43‐73 | |
| Age group (years), n (%) | |||
| < 20 | 10 (0.5) | 57 (0.8) | |
| 20‐29 | 186 (8.6) | 632 (8.7) | |
| 30‐39 | 221 (10.2) | 766 (10.3) | |
| 40‐49 | 387 (17.8) | 1341 (18.1) | |
| 50‐59 | 434 (20.0) | 1492 (20.2) | 0.28 |
| 60‐69 | 325 (15.0) | 974 (12.8) | |
| 70‐79 | 271 (12.5) | 1035 (13.6) | |
| 80‐89 | 262 (12.0) | 951(12.3) | |
| 90< | 75 (3.5) | 262 (3.4) | |
| Female, n (%) | 1175 (54.1) | 4138 (55.1) | 0.42 |
| Race, n (%) | |||
| White | 1282 (59.1) | 4419 (58.9) | |
| Black | 793 (36.5) | 2754 (36.7) | 0.98 |
| Other | 96 (4.4) | 337 (4.5) | |
| Primary care provider, n (%) | 0.16 | ||
| Yes | 1537 (73.2) | 5451 (74.7) | |
| Missing: 284 | 71 (3.3) | 213 (2.8) | |
| Insurance status, n (%) | |||
| Commercial/worker's comp | 440 (20.3) | 1442 (19.2) | |
| Medicare | 1017 (46.8) | 3589 (47.8) | 0.52 |
| Medicaid/others | 714 (32.9) | 2479 (33.0) | |
| Time of admission, n (%) | |||
| 0000‐0259 | 167 (7.7) | 1068 (14.2) | |
| 0300‐0559 | 244 (11.2) | 485 (6.5) | |
| 0600‐0859 | 456 (21.0) | 270 (3.6) | |
| 0900‐1159 | 782 (36.0) | 1146 (15.3) | <0.001 |
| 1200‐1459 | 299 (13.8) | 1750 (23.3) | |
| 1500‐1759 | 155 (7.1) | 1676 (22.3) | |
| 1800‐2359 | 68 (3.1) | 1115 (14.9) | |
| Time of discharge, n (%) | |||
| 2100‐0859 | 36 (1.7) | 174 (2.3) | |
| 0900‐1159 | 275 (12.7) | 495 (6.6) | |
| 1200‐1459 | 858 (39.6) | 2608 (34.8) | <0.001 |
| 1500‐1759 | 749 (34.6) | 3122 (41.6) | |
| 1800‐2059 | 249 (11.5) | 1104 (14.7) | |
| Missing | 4 | 7 | |
| Day of week of admission, n (%) | |||
| Monday | 462 (21.3) | 1549 (20.6) | |
| Tuesday | 499 (23.0) | 1470 (19.6) | |
| Wednesday | 430 (19.8) | 1479 (19.7) | 0.001 |
| Thursday | 400 (18.4) | 1482 (19.7) | |
| Friday | 380 (17.5) | 1530 (20.4) | |
| Day of week of discharge, n (%) | |||
| Monday | 207 (9.5) | 829 (11.0) | |
| Tuesday | 268 (12.3) | 973 (13.0) | |
| Wednesday | 334 (15.4) | 1142 (15.2) | |
| Thursday | 362 (16.7) | 1297 (17.3) | 0.16 |
| Friday | 485 (22.3) | 1523 (20.3) | |
| Saturday | 330 (15.2) | 1165 (15.5) | |
| Sunday | 185 (8.5) | 581 (7.7) | |
| Admit to non‐medicine wards, n (%) | 1332 (61.4) | 2624 (34.9) | <0.001 |
| Transfer to ICU (at least once), n (%) | 299 (13.8) | 504 (6.7) | <0.001 |
| Admit from ER No (%) | 1663 (76.6) | 6063 (80.7) | <0.001 |
| 10 most frequent diagnosis (%) | Pneumonia (4.9) | Pneumonia (5.5) | |
| Congestive heart failure; nonhypertensive (4.2) | Congestive heart failure; nonhypertensive (3.9) | ||
| Sickle cell anemia (3.9) | Nonspecific chest pain (3.7) | ||
| Chronic obstructive pulmonary disease and Bronchiectasis (3.3) | Urinary tract infections(3.6) | ||
| Diabetes mellitus with complications (3.2) | Skin and subcutaneous tissue infections (3.3) | ||
| Urinary tract infections (3.2) | Sickle cell anemia (3.3) | ||
| Asthma (3.0) | Pancreatic disorders (not diabetes) (2.8) | ||
| Nonspecific chest pain (3.0) | Asthma (2.8) | ||
| Pancreatic disorders (not diabetes) (2.9) | Chronic obstructive pulmonary disease and Bronchiectasis (2.6) | ||
| Septicemia (2.2) | Diabetes mellitus with complications (2.6) | ||
| Average number of comorbidities mean (95% CI) | 0.39 (0.37‐0.42) | 0.38 (0.36‐0.39) | 0.23 |
In unadjusted comparisons of outcomes (Table 3), hospitalizations on H‐PA teams had higher lengths of stay and charges than hospitalizations on RES teams, possibly higher inpatient mortality rates but similar unadjusted readmission rates at 7, 14, and 30 days
| H‐PA (n = 2171) | RES (n = 7150) | % Difference* (CI) | P Value | |
|---|---|---|---|---|
| ||||
| LOS | Median (IQR) | Median (IQR) | ||
| Days | 3.17 (2.03‐5.30) | 2.99 (1.80‐5.08) | +8.9% (4.71‐13.29%) | <0.001 |
| Charges | ||||
| US Dollars | 9390 (6196‐16,239) | 9044 (6106‐14,805) | +5.56% (1.96‐9.28%) | 0.002 |
| Readmissions | n (%) | n (%) | Odds Ratio (CI) | |
| Within 7 days | 147 (6.96) | 571 (7.78) | 0.88 (0.73‐1.06) | 0.19 |
| Within14 days | 236 (11.34) | 924 (12.76) | 0.87 (0.75‐1.01) | 0.07 |
| Within 30 days | 383 (18.91) | 1436 (20.31) | 0.91 (0.80‐1.03) | 0.14 |
| Inpatient deaths | 39 (1.8) | 95 (1.3) | 1.36 (0.90‐2.00) | 0.06 |
Multivariable Analysis
LOS
Hospitalizations to H‐PA teams were associated with a 6.73% longer LOS (P = 0.005) (Table 4). This difference persisted when we used the winsorized data (6.45% increase, P = 0.006), excluded inpatient deaths (6.81% increase, P = 0.005), or excluded hospitalizations that involved an ICU stay (6.40%increase, P = 0.011) (Table 5).
| Overall | Subgroup: Restricted to Physicians Attending on Both H‐PA and RES Teams* | Subgroup: Restricted to Hospitalizations Between 11.00 AM and 4.00 PM | ||||
|---|---|---|---|---|---|---|
| % Difference (CI) | P Value | % Difference (CI) | P Value | % Difference (CI) | P Value | |
| ||||||
| LOS | 6.73% (1.99% to 11.70%) | 0.005 | 5.44% (0.65% to 11.91%) | 0.08 | 2.97% (4.47% to 10.98%) | 0.44 |
| Charges | 2.75% (1.30% to 6.97%) | 0.19 | 1.55% (3.76% to 7.16%) | 0.57 | 6.45% (0.62% to 14.03%) | 0.07 |
| Risk of Readmission | Adjusted OR (95%CI) | P Value | Adjusted OR (95% CI) | P Value | Adjusted OR (95% CI) | P Value |
| Within 7 days | 0.88 (0.64‐1.20) | 0.42 | 0.74 (0.40‐1.35) | 0.32 | 0.90 (0.40‐2.00) | 0.78 |
| Within14 days | 0.90 (0.69‐1.19) | 0.46 | 0.71 (0.51‐0.99) | 0.05 | 0.87 (0.36‐2.13) | 0.77 |
| Within 30 days | 0.89 (0.75‐1.06) | 0.20 | 0.75 (0.51‐1.08) | 0.12 | 0.92 (0.55‐1.54) | 0.75 |
| Inpatient mortality | 1.27 (0.82‐1.97) | 0.28 | 1.46 (0.67‐3.17) | 0.33 | 1.14 (0.47‐2.74) | 0.77 |
| Analysis With Winsorized Data | Analysis After Excluding Inpatient Deaths | Analysis After Excluding Patients With ICU Stays | ||||
|---|---|---|---|---|---|---|
| % Difference (CI) | P Value | % Difference (CI) | P Value | % Difference (CI) | P Value | |
| ||||||
| LOS | 6.45% (4.04 to 8.91%) | 0.006 | 6.81% (2.03 to 11.80%) | 0.005 | 6.40% (1.46 to 11.58%) | 0.011 |
| Charges | 2.67 (1.27 to 6.76%) | 0.187 | 2.89% (1.16 to 7.11%) | 0.164 | 0.74% (3.11 to 4.76%) | 0.710 |
Charges
Hospitalizations to H‐PA and RES teams were associated with similar charges (Table 4). The results were similar when we used winsorized data, excluded inpatient deaths or excluded hospitalizations involving an ICU stay (Table 5).
Readmissions
The risk of readmission at 7, 14, and 30 days was similar between hospitalizations to H‐PA and RES teams (Table 4).
Mortality
The risk of inpatient death was similar between all hospitalizations to H‐PA and RES teams or only hospitalizations without an ICU stay (Table 4). The results also remained the same in analyses restricted to first admissions, last admissions, or 1 randomly selected admission per patient.
Sub‐Group Analysis
On restricting the multivariable analyses to the subset of hospitalists who staffed both types of teams (Table 4), the increase in LOS associated with H‐PA care was no longer significant (5.44% higher, P = 0.081). The charges, risk of readmission at 7 and 30 days, and risk of inpatient mortality remained similar. The risk of readmission at 14 days was slightly lower following hospitalizations to H‐PA teams (odds ratio 0.71, 95% confidence interval [CI] 0.51‐0.99).
The increase in LOS associated with H‐PA care was further attenuated in analyses of the subset of admissions between 11.00 AM and 4.00 PM (2.97% higher, P = 0.444). The difference in charges approached significance (6.45% higher, P = 0.07), but risk of readmission at 7, 14, and 30 days and risk of inpatient mortality were no different (Table 4).
Interactions
On adding interaction terms between the team assignment and the fixed effect variables in each model we detected that the effect of H‐PA care on LOS (P < 0.001) and charges (P < 0.001) varied by time of admission (Figure 2a and b). Hospitalizations to H‐PA teams from 6.00 PM to 6.00 AM had greater relative increases in LOS as compared to hospitalizations to RES teams during those times. Similarly, hospitalizations during the period 3.00 PM to 3.00 AM had relatively higher charges associated with H‐PA care compared to RES care.
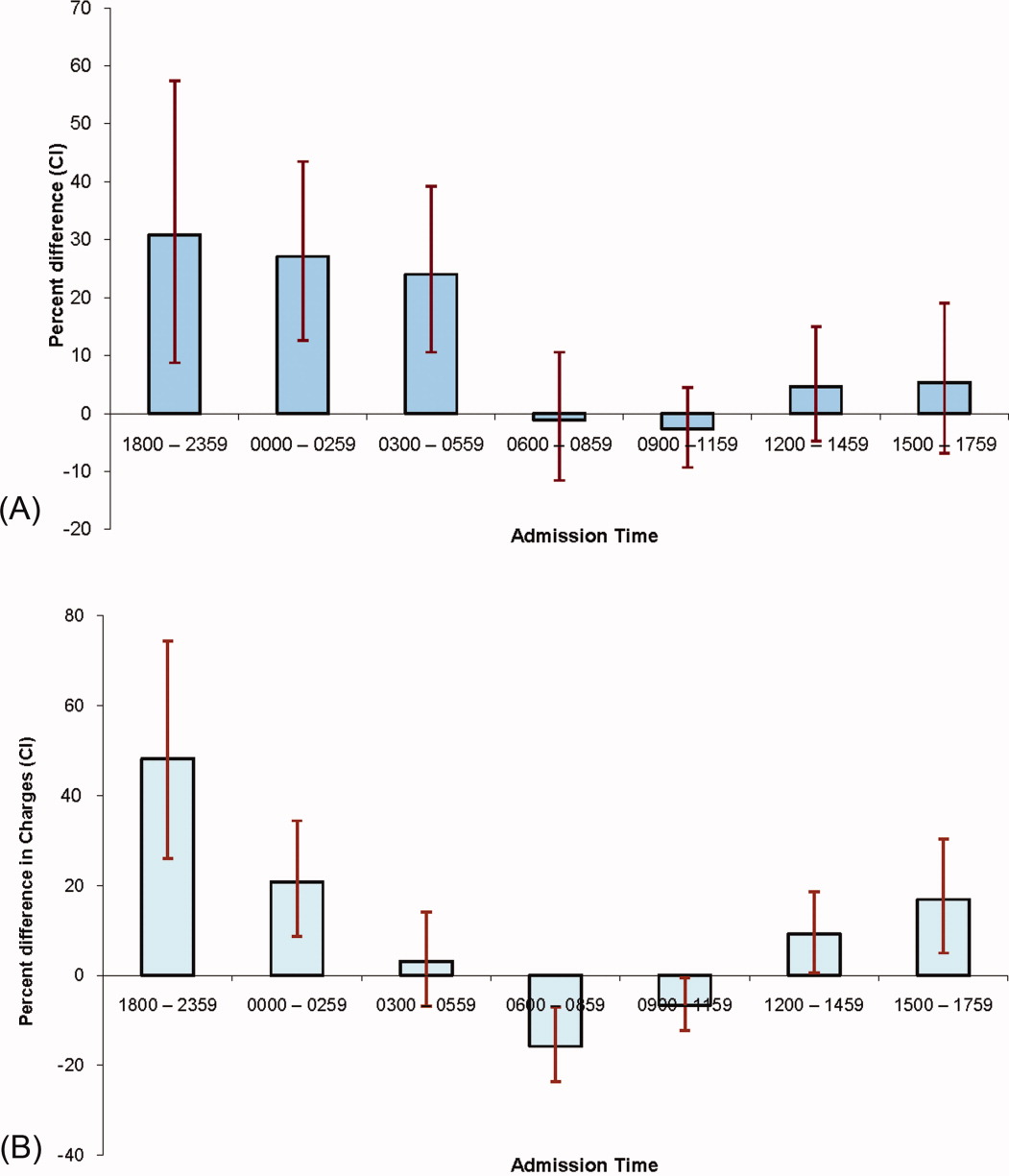
Discussion
We found that hospitalizations to our H‐PA teams had longer LOS but similar charges, readmission rates, and mortality as compared to traditional resident‐based teams. These findings were robust to multiple sensitivity and subgroup analyses but when we examined times when both types of teams could receive admissions, the difference in LOS was markedly attenuated and nonsignificant.
We note that most prior reports comparing PA‐based models of inpatient care predate the ACGME work hour regulations. In a randomized control trial (1987‐1988) Simmer et al.5 showed lower lengths of stay and charges but possibly higher risk of readmission for PA based teams as compared to resident based teams. Van Rhee et al.7 conducted a nonrandomized retrospective cohort study (1994‐1995) using administrative data which showed lower resource utilization for PA‐based inpatient care. Our results from 2005 to 2006 reflect the important changes in the organization and delivery of inpatient care since these previous investigations.
Roy et al.8 report the only previously published comparison of PA and resident based GM inpatient care after the ACGME mandated work hour regulations. They found PA‐based care was associated with lower costs, whereas we found similar charges for admissions to RES and H‐PA teams. They also found that LOS was similar for PA and resident‐based care, while we found a higher LOS for admissions to our H‐PA team. We note that although the design of Roy's study was similar to our own, patients cared for by PA‐based teams were geographically localized in their model. This may contribute to the differences in results noted between our studies.
Despite no designed differences in patients assigned to either type of team other than time of admission we noted some differences between the H‐PA and RES teams in the descriptive analysis. These differences, such as a higher proportion of hospitalizations to H‐PA teams being admitted from the ER, residing on nonmedicine wards or having an ICU stay are likely a result of our system of assigning admissions to H‐PA teams early during the workday. For example patients on H‐PA teams were more often located on nonmedicine wards as a result of later discharges and bed availability on medicine wards. The difference that deserves special comment is the much higher proportion (13.8% vs. 6.7%) of hospitalizations with an ICU stay on the H‐PA teams. Hospitalizations directly to the ICU were excluded from our study which means that the hospitalizations with an ICU stay in our study were initially admitted to either H‐PA or RES teams and then transferred to the ICU. Transfers out of the ICU usually occur early in the workday when H‐PA teams accepted patients per our admission schedule. These patients may have been preferentially assigned to H‐PA teams, if on returning from the ICU the original team's resident had changed (and the bounce back rule was not in effect). Importantly, the conclusions of our research are not altered on controlling for this difference in the teams by excluding hospitalizations with an ICU stay.
Hospitalizations to H‐PA teams were associated with higher resource utilization if they occurred later in the day or overnight (Figure 2a and b). During these times a transition of care occurred shortly after admission. For a late day admission the H‐PA teams would transfer care for overnight cross cover soon after the admission and for patients admitted overnight as overflow they would assume care of a patient from the nighttime covering physician performing the admission. On the other hand, on RES teams, interns admitting patients overnight continued to care for their patients for part of the following day (30‐hour call). Similar findings of higher resource utilization associated with transfer of care after admission in the daytime11 and nighttime12 have been previously reported. An alternative hypothesis for our findings is that the hospital maybe busier and thus less efficient during times when H‐PA teams had to admit later in the day or accept patients admitted overnight as overflow. Future research to determine the cause of this significant interaction between team assignment and time of admission on resource utilization is important as the large increases in LOS (up to 30%) and charges (up to 50%) noted, could have a potentially large impact if a higher proportion of hospitalizations were affected by this phenomenon.
Our H‐PA teams were assigned equally complex patients as our RES teams, in contrast to previous reports.8, 13 This was accomplished while improving the resident's educational experience and we have previously reported increases in our resident's board pass rates and in‐service training exam scores with that introduction of our H‐PA teams.14 We thus believe that selection of less complex patients to H‐PA teams such as ours is unnecessary and may give them a second tier status in academic settings.
Our report has limitations. It is a retrospective, nonrandomized investigation using a single institution's administrative database and has the limitations of not being able to account for unmeasured confounders, severity of illness, errors in the database, selection bias and has limited generalizability. We measured charges not actual costs,15 but we feel charges are a true reflection of relative resource use when compared between similar patients within a single institution. We also did not account for the readmissions that occur to other hospitals16 and our results do not reflect resource utilization for the healthcare system in total. For example, we could not tell if higher LOS on H‐PA teams resulted in lower readmissions for their patients in all hospitals in the region, which may reveal an overall resource savings. Additionally, we measured in‐hospital mortality and could not capture deaths related to hospital care that may occur shortly after discharge.
ACGME has proposed revised standards that may further restrict resident duty hours when they take effect in July 2011.3 This may lead to further decreases in resident‐based inpatient care. Teaching hospitals will need to continue to develop alternate models for inpatient care that do not depend on house staff. Our findings provide important evidence to inform the development of such models. Our study shows that one such model: PAs paired with hospitalists, accepting admissions early in the workday, with hospitalist coverage over the weekend and nights can care for GM inpatients as complex as those cared for by resident‐based teams without increasing readmission rates, inpatient mortality, or charges but at the cost of slightly higher LOS.
- ACGME‐Common Program Requirements for Resident Duty Hours. Available at: http://www.acgme.org/acWebsite/dutyHours/dh_ComProgrRequirmentsDutyHours0707.pdf. Accessed July 2010.
- ,,,,.Non‐housestaff medicine services in academic centers: models and challenges.J Hosp Med.2008;3(3):247–255.
- ACGME. Duty Hours: Proposed Standards for Review and comment. Available at: http://acgme‐2010standards.org/pdf/Proposed_Standards. pdf. Accessed July 22,2010.
- Agency for Health Care Policy and Research. HCUPnet: A tool for identifying, tracking, and analyzing national hospital statistics. Available at: http://hcup.ahrq.gov/HCUPnet.asp. Accessed July2010.
- ,,,,.A randomized, controlled trial of an attending staff service in general internal medicine.Med Care.1991;29(7 suppl):JS31–JS40.
- ,.Replacing an academic internal medicine residency program with a physician assistant‐‐hospitalist model: a Comparative Analysis Study.Am J Med Qual.2009;24(2):132–139.
- ,,.Resource use by physician assistant services versus teaching services.JAAPA.2002;15(1):33–42.
- ,,, et al.Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes.J Hosp Med.2008;3(5):361–368.
- AHRQ. Clinical Classifications Software (CCS) for ICD‐9‐CM. Available at: http://www.hcup‐us.ahrq.gov/toolssoftware/ccs/ccs.jsp#overview. Accessed July2010.
- AHRQ. HCUP: Comorbidity Software, Version 3.4.;Available at: http://www.hcup‐us.ahrq.gov/toolssoftware/comorbidity/comorbidity.jsp. Accessed July2010.
- ,,, et al.Effect of short call admission on length of stay and quality of care for acute decompensated heart failure.Circulation.2008;117(20):2637–2644.
- ,,,.Post‐call transfer of resident responsibility: its effect on patient care.J Gen Intern Med.1990;5(6):501–505.
- ,,,,,.The effect of nonteaching services on the distribution of inpatient cases for internal medicine residents.Acad Med.2009:84(2):220–225.
- ,,, et al.Allowing for better resident education and improving patient care: hospitalist‐physician assistant teams fill in the gaps.J Hosp Med.2007;2[S2]:1–39.
- .The distinction between cost and charges.Ann Intern Med.1982;96(1):102–109.
- ,,.Rehospitalizations among patients in the Medicare Fee‐for‐Service Program.N Engl J Med.2009;360(14):1418–1428.
In 2003 the Accreditation Council for Graduate Medical Education (ACGME) prescribed residency reform in the form of work hour restrictions without prescribing alternatives to resident based care.1 As a response, many academic medical centers have developed innovative models for providing inpatient care, some of which incorporate Physician Assistants (PAs).2 With further restrictions in resident work hours possible,3 teaching hospitals may increase use of these alternate models to provide inpatient care. Widespread implementation of such new and untested models could impact the care of the approximately 20 million hospitalizations that occur every year in US teaching hospitals.4
Few reports have compared the care delivered by these alternate models with the care provided by traditional resident‐based models of care.58 Roy et al.8 have provided the only recent comparison of a PA‐based model of care with a resident‐based model. They showed lower adjusted costs of inpatient care associated with PA based care but other outcomes were similar to resident‐based teams.
The objective of this study is to provide a valid and usable comparison of the outcomes of a hospitalist‐PA (H‐PA) model of inpatient care with the traditional resident‐based model. This will add to the quantity and quality of the limited research on PA‐based inpatient care, and informs the anticipated increase in the involvement of PAs in this arena.
Methods
Study Design and Setting
We conducted a retrospective cohort study at a 430‐bed urban academic medical center in the Midwestern United States.
Models of General Medical (GM) Inpatient Care at the Study Hospital During the Study Period
In November 2004, as a response to the ACGME‐mandated work hour regulations, we formed 2 Hospitalist‐PA teams (H‐PA) to supplement the 6 preexisting general medicine resident teams (RES).
The H‐PA and RES teams differed in staffing, admitting times and weekend/overnight cross coverage structure (Table 1). There were no predesigned differences between the teams in the ward location of their patients, availability of laboratory/radiology services, specialty consultation, social services/case management resources, nursing resources or documentation requirements for admission, daily care, and discharge.
| H‐PA Teams | RES Teams | |
|---|---|---|
| Attending physician | Always a hospitalist | Hospitalist, non‐hospitalist general internist or rarely a specialist |
| Attending physician role | Supervisory for some patients (about half) and sole care provider for others. | Supervisory for all patients |
| Team composition | One attending paired with 1 PA | Attending + senior resident + (2) interns + (2‐3) medical students |
| Rotation schedule | ||
| Attending | Every 2 weeks | Every 2 weeks |
| Physician assistant | Off on weekends | |
| House staff & medical students | Every month | |
| Weekend | No new admissions & hospitalist manages all patients | Accept new admissions |
| Admission times (weekdays) | 7 AM to 3 PM | Noon to 7 AM |
| Source of admissions | Emergency room, clinics, other hospitals | Emergency room, clinics, other hospitals |
| Number of admissions (weekdays) | 4‐6 patients per day per team | Noon to 5 PM: 2 teams admit a maximum of 9 patients total |
| 5 PM to 7 AM: 3 teams admit a maximum 5 patients each. | ||
| Overnight coverageroles and responsibilities | One in‐house faculty | 3 on call interns |
| Cross‐covering 2 H‐PA teams | Cross‐covering 2 teams each | |
| Performing triage | Admitting up to 5 patients each | |
| Admitting patients if necessary | ||
| Assisting residents if necessary | ||
| General medical consultation |
Admission Schedule for H‐PA or RES Teams
The admitting schedule was designed to decrease the workload of the house staff and to do so specifically during the periods of peak educational activity (morning report, attending‐led teaching rounds, and noon report). A faculty admitting medical officer (AMO) assigned patients strictly based on the time an admission was requested. Importantly, the request for admission preceded the time of actual admission recorded when the patient reached the ward. The time difference between request for admission and actual admission depended on the source of admission and the delay associated with assigning a patient room. The AMO assigned 8 to 12 new patients to the H‐PA teams every weekday between 7 AM and 3 PM and to the RES teams between noon and 7 AM the next day. There was a designed period of overlap from noon to 3 PM during which both H‐PA and RES teams could admit patients. This period allowed for flexibility in assigning patients to either type of team depending on their workload. The AMO did not use patient complexity or teaching value to assign patients.
Exceptions to Admission Schedule
Patients admitted overnight after the on call RES had reached their admission limits were assigned to H‐PA teams the next morning. In addition, recently discharged patients who were readmitted while the discharging hospitalist (H‐PA teams) or the discharging resident (RES teams) was still scheduled for inpatient duties, were assigned back to the discharging team irrespective of the admitting schedule.
The same medicine team cared for a patient from admission to discharge but on transfer to the intensive care unit (ICU), an intensivist led critical care team assumed care. On transfer out of the ICU these patients were assigned back to the original team irrespective of admitting schedulethe so called bounce back rule to promote inpatient continuity of care. But if the residents (RES teams) or the hospitalist (H‐PA teams) had changedthe bounce back rule was no longer in effect and these patients were assigned to a team according to the admission schedule.
Study Population and Study Period
We included all hospitalizations of adult patients to GM teams if both their date of admission and their date of discharge fell within the study period (January 1, 2005 to December 31, 2006). We excluded hospitalizations with admissions during the weekendwhen H‐PA teams did not admit patients; hospitalizations to GM services with transfer to nonGM service (excluding ICU) and hospitalizations involving comanagement with specialty servicesas the contribution of GM teams for these was variable; and hospitalizations of private patients.
Data Collection and Team Assignment
We collected patient data from our hospital's discharge abstract database. This database did not contain team information so to assign teams we matched the discharging attending and the day of discharge to the type of team that the discharging attending was leading that day.
We collected patient age, gender, race, insurance status, zip‐code, primary care provider, source of admission, ward type, time and day of admission, and time and day of discharge for use as independent variables. The time of admission captured in the database was the time of actual admission and not the time the admission was requested.
We grouped the principal diagnosis International Statistical Classification of Diseases and Related Health Problems, 9th edition (ICD‐9) codes into clinically relevant categories using the Clinical Classification Software.9 We created comorbidity measures using Healthcare Cost and Utilization Project Comorbidity Software, version 3.4.10
Outcome Measures
We used length of stay (LOS), charges, readmissions within 7, 14, and 30 days and inpatient mortality as our outcome measures. We calculated LOS by subtracting the discharge day and time from the admission day and time. The LOS included time spent in the ICU. We summed all charges accrued during the entire hospitalization including any stay in the ICU but did not include professional fees. We considered any repeat hospitalization to our hospital within 7, 14, and 30 days following a discharge to be a readmission except that we excluded readmissions for a planned procedure or for inpatient rehabilitation.
Statistical Analysis
Descriptive Analysis
We performed unadjusted descriptive statistics at the level of an individual hospitalization using medians and interquartile ranges for continuous data and frequencies and percentages for categorical data. We used chi‐square tests of association and KruskalWallis analysis of variance to compare H‐PA and RES teams.
Missing Data
Because we lacked data on whether a primary outpatient care provider was available for 284 (2.9%) of our study hospitalizations, we dropped them from our multivariable analyses. We used an arbitrary discharge time of noon for the 11 hospitalizations which did not have a discharge time recorded.
Multivariable Analysis
We used multivariable mixed models to risk adjust for a wide variety of variables. We included age, gender, race, insurance, presence of primary care physician, and total number of comorbidities as fixed effects in all models because of the high face validity of these variables. We then added admission source, ward, time, day of week, discharge day of week, and comorbidity measures one by one as fixed effects, including them only if significant at P < 0.01. For assessing LOS, charges, and readmissions, we added a variable identifying each patient as a random effect to account for multiple admissions for the same patient. We then added variables identifying attending physician, principal diagnostic group, and ZIP code of residence as random effects to account for clustering of hospitalizations within these categories, including them only if significant at P < 0.01. For the model assessing mortality we included variables for attending physician, principal diagnostic group, and ZIP code of residence as random effects if significant at P < 0.01. We log transformed LOS and charges because they were extremely skewed in nature. Readmissions were analyzed after excluding patients who died or were discharged alive within 7, 14, or 30 days of the end of the study period.
Sensitivity Analyses
To assess the influence of LOS outliers, we changed LOS to 6 hours if it was less than 6 hours, and 45 days if it was more than 45 daysa process called winsorizing. We consider winsorizing superior to dropping outliers because it acknowledges that outliers contribute information, but prevent them from being too influential. We chose the 6 hour cut off because we believed that was the minimum time required to admit and then discharge a patient. We chose the upper limit of 45 days on reviewing the frequency distribution for outliers. Similarly, we winsorized charges at the first and 99th percentile after reviewing the frequency distribution for outliers. We then log transformed the winsorized data before analysis.
Inpatient deaths reduce the LOS and charges associated with a hospitalization. Thus excess mortality may provide a false concession in terms of lower LOS or charges. To check if this occurred in our study we repeated the analyses after excluding inpatient deaths.
ICU stays are associated with higher LOS, charges, and mortality. In our model of care, some patients transferred to the ICU are not cared for by the original team on transfer out. Moreover, care in the ICU is not controlled by the team that discharges them. Since this might obscure differences in outcomes achieved by RES vs. H‐PA teams, we repeated these analyses after excluding hospitalizations with an ICU stay.
Since mortality can only occur during 1 hospitalization per patient, we repeated the mortality analysis using only each patient's first admission or last admission and using a randomly selected single admission for each patient.
Subgroup Analysis
To limit the effect of different physician characteristics on H‐PA and RES teams we separately analyzed the hospitalizations under the care of hospitalists who served on both H‐PA and RES teams.
To limit the effect of different admission schedules of H‐PA and RES teams we analyzed the hospitalizations with admission times between 11.00 AM and 4.00 PM. Such hospitalizations were likely to be assigned during the noon to 3 PM period when they could be assigned to either an H‐PA or RES team.
Interactions
Finally we explored interactions between the type of team and the fixed effect variables included in each model.
Statistical Software
We performed the statistical analysis using SAS software version 9.0 for UNIX (SAS Institute, Inc., Cary, NC) and R software (The R Project for Statistical Computing).
This study protocol was approved by the hospital's institutional review board.
Results
Study Population
Of the 52,391 hospitalizations to our hospital during the study period, 13,058 were admitted to general medicine. We excluded 3102 weekend admissions and 209 who met other exclusion criteria. We could not determine the team assignment for 66. Of the remaining 9681 hospitalizations, we assigned 2171 to H‐PA teams and 7510 to RES teams (Figure 1).
Descriptive Analysis
We compare patients assigned to H‐PA and RES teams in Table 2. They were similar in age, gender, race, having a primary care provider or not, and insurance status. Clinically, they had similar comorbidities and a similar distribution of common principal diagnoses. Consistent with their admitting schedule, H‐PA teams admitted and discharged more patients earlier in the day and admitted more patients earlier in the work week. Patients cared for by H‐PA teams were admitted from the Emergency Room (ER) less often and were more likely to reside on wards designated as nonmedicine by nursing specialty. Hospitalizations to H‐PA teams more often included an ICU stay.
| H‐PA (n = 2171) | RES (n = 7510) | P Value | |
|---|---|---|---|
| |||
| Age | |||
| Mean | 56.80 | 57.04 | |
| Median | 56 | 56 | 0.15 |
| Interquartile range | 43‐72 | 43‐73 | |
| Age group (years), n (%) | |||
| < 20 | 10 (0.5) | 57 (0.8) | |
| 20‐29 | 186 (8.6) | 632 (8.7) | |
| 30‐39 | 221 (10.2) | 766 (10.3) | |
| 40‐49 | 387 (17.8) | 1341 (18.1) | |
| 50‐59 | 434 (20.0) | 1492 (20.2) | 0.28 |
| 60‐69 | 325 (15.0) | 974 (12.8) | |
| 70‐79 | 271 (12.5) | 1035 (13.6) | |
| 80‐89 | 262 (12.0) | 951(12.3) | |
| 90< | 75 (3.5) | 262 (3.4) | |
| Female, n (%) | 1175 (54.1) | 4138 (55.1) | 0.42 |
| Race, n (%) | |||
| White | 1282 (59.1) | 4419 (58.9) | |
| Black | 793 (36.5) | 2754 (36.7) | 0.98 |
| Other | 96 (4.4) | 337 (4.5) | |
| Primary care provider, n (%) | 0.16 | ||
| Yes | 1537 (73.2) | 5451 (74.7) | |
| Missing: 284 | 71 (3.3) | 213 (2.8) | |
| Insurance status, n (%) | |||
| Commercial/worker's comp | 440 (20.3) | 1442 (19.2) | |
| Medicare | 1017 (46.8) | 3589 (47.8) | 0.52 |
| Medicaid/others | 714 (32.9) | 2479 (33.0) | |
| Time of admission, n (%) | |||
| 0000‐0259 | 167 (7.7) | 1068 (14.2) | |
| 0300‐0559 | 244 (11.2) | 485 (6.5) | |
| 0600‐0859 | 456 (21.0) | 270 (3.6) | |
| 0900‐1159 | 782 (36.0) | 1146 (15.3) | <0.001 |
| 1200‐1459 | 299 (13.8) | 1750 (23.3) | |
| 1500‐1759 | 155 (7.1) | 1676 (22.3) | |
| 1800‐2359 | 68 (3.1) | 1115 (14.9) | |
| Time of discharge, n (%) | |||
| 2100‐0859 | 36 (1.7) | 174 (2.3) | |
| 0900‐1159 | 275 (12.7) | 495 (6.6) | |
| 1200‐1459 | 858 (39.6) | 2608 (34.8) | <0.001 |
| 1500‐1759 | 749 (34.6) | 3122 (41.6) | |
| 1800‐2059 | 249 (11.5) | 1104 (14.7) | |
| Missing | 4 | 7 | |
| Day of week of admission, n (%) | |||
| Monday | 462 (21.3) | 1549 (20.6) | |
| Tuesday | 499 (23.0) | 1470 (19.6) | |
| Wednesday | 430 (19.8) | 1479 (19.7) | 0.001 |
| Thursday | 400 (18.4) | 1482 (19.7) | |
| Friday | 380 (17.5) | 1530 (20.4) | |
| Day of week of discharge, n (%) | |||
| Monday | 207 (9.5) | 829 (11.0) | |
| Tuesday | 268 (12.3) | 973 (13.0) | |
| Wednesday | 334 (15.4) | 1142 (15.2) | |
| Thursday | 362 (16.7) | 1297 (17.3) | 0.16 |
| Friday | 485 (22.3) | 1523 (20.3) | |
| Saturday | 330 (15.2) | 1165 (15.5) | |
| Sunday | 185 (8.5) | 581 (7.7) | |
| Admit to non‐medicine wards, n (%) | 1332 (61.4) | 2624 (34.9) | <0.001 |
| Transfer to ICU (at least once), n (%) | 299 (13.8) | 504 (6.7) | <0.001 |
| Admit from ER No (%) | 1663 (76.6) | 6063 (80.7) | <0.001 |
| 10 most frequent diagnosis (%) | Pneumonia (4.9) | Pneumonia (5.5) | |
| Congestive heart failure; nonhypertensive (4.2) | Congestive heart failure; nonhypertensive (3.9) | ||
| Sickle cell anemia (3.9) | Nonspecific chest pain (3.7) | ||
| Chronic obstructive pulmonary disease and Bronchiectasis (3.3) | Urinary tract infections(3.6) | ||
| Diabetes mellitus with complications (3.2) | Skin and subcutaneous tissue infections (3.3) | ||
| Urinary tract infections (3.2) | Sickle cell anemia (3.3) | ||
| Asthma (3.0) | Pancreatic disorders (not diabetes) (2.8) | ||
| Nonspecific chest pain (3.0) | Asthma (2.8) | ||
| Pancreatic disorders (not diabetes) (2.9) | Chronic obstructive pulmonary disease and Bronchiectasis (2.6) | ||
| Septicemia (2.2) | Diabetes mellitus with complications (2.6) | ||
| Average number of comorbidities mean (95% CI) | 0.39 (0.37‐0.42) | 0.38 (0.36‐0.39) | 0.23 |
In unadjusted comparisons of outcomes (Table 3), hospitalizations on H‐PA teams had higher lengths of stay and charges than hospitalizations on RES teams, possibly higher inpatient mortality rates but similar unadjusted readmission rates at 7, 14, and 30 days
| H‐PA (n = 2171) | RES (n = 7150) | % Difference* (CI) | P Value | |
|---|---|---|---|---|
| ||||
| LOS | Median (IQR) | Median (IQR) | ||
| Days | 3.17 (2.03‐5.30) | 2.99 (1.80‐5.08) | +8.9% (4.71‐13.29%) | <0.001 |
| Charges | ||||
| US Dollars | 9390 (6196‐16,239) | 9044 (6106‐14,805) | +5.56% (1.96‐9.28%) | 0.002 |
| Readmissions | n (%) | n (%) | Odds Ratio (CI) | |
| Within 7 days | 147 (6.96) | 571 (7.78) | 0.88 (0.73‐1.06) | 0.19 |
| Within14 days | 236 (11.34) | 924 (12.76) | 0.87 (0.75‐1.01) | 0.07 |
| Within 30 days | 383 (18.91) | 1436 (20.31) | 0.91 (0.80‐1.03) | 0.14 |
| Inpatient deaths | 39 (1.8) | 95 (1.3) | 1.36 (0.90‐2.00) | 0.06 |
Multivariable Analysis
LOS
Hospitalizations to H‐PA teams were associated with a 6.73% longer LOS (P = 0.005) (Table 4). This difference persisted when we used the winsorized data (6.45% increase, P = 0.006), excluded inpatient deaths (6.81% increase, P = 0.005), or excluded hospitalizations that involved an ICU stay (6.40%increase, P = 0.011) (Table 5).
| Overall | Subgroup: Restricted to Physicians Attending on Both H‐PA and RES Teams* | Subgroup: Restricted to Hospitalizations Between 11.00 AM and 4.00 PM | ||||
|---|---|---|---|---|---|---|
| % Difference (CI) | P Value | % Difference (CI) | P Value | % Difference (CI) | P Value | |
| ||||||
| LOS | 6.73% (1.99% to 11.70%) | 0.005 | 5.44% (0.65% to 11.91%) | 0.08 | 2.97% (4.47% to 10.98%) | 0.44 |
| Charges | 2.75% (1.30% to 6.97%) | 0.19 | 1.55% (3.76% to 7.16%) | 0.57 | 6.45% (0.62% to 14.03%) | 0.07 |
| Risk of Readmission | Adjusted OR (95%CI) | P Value | Adjusted OR (95% CI) | P Value | Adjusted OR (95% CI) | P Value |
| Within 7 days | 0.88 (0.64‐1.20) | 0.42 | 0.74 (0.40‐1.35) | 0.32 | 0.90 (0.40‐2.00) | 0.78 |
| Within14 days | 0.90 (0.69‐1.19) | 0.46 | 0.71 (0.51‐0.99) | 0.05 | 0.87 (0.36‐2.13) | 0.77 |
| Within 30 days | 0.89 (0.75‐1.06) | 0.20 | 0.75 (0.51‐1.08) | 0.12 | 0.92 (0.55‐1.54) | 0.75 |
| Inpatient mortality | 1.27 (0.82‐1.97) | 0.28 | 1.46 (0.67‐3.17) | 0.33 | 1.14 (0.47‐2.74) | 0.77 |
| Analysis With Winsorized Data | Analysis After Excluding Inpatient Deaths | Analysis After Excluding Patients With ICU Stays | ||||
|---|---|---|---|---|---|---|
| % Difference (CI) | P Value | % Difference (CI) | P Value | % Difference (CI) | P Value | |
| ||||||
| LOS | 6.45% (4.04 to 8.91%) | 0.006 | 6.81% (2.03 to 11.80%) | 0.005 | 6.40% (1.46 to 11.58%) | 0.011 |
| Charges | 2.67 (1.27 to 6.76%) | 0.187 | 2.89% (1.16 to 7.11%) | 0.164 | 0.74% (3.11 to 4.76%) | 0.710 |
Charges
Hospitalizations to H‐PA and RES teams were associated with similar charges (Table 4). The results were similar when we used winsorized data, excluded inpatient deaths or excluded hospitalizations involving an ICU stay (Table 5).
Readmissions
The risk of readmission at 7, 14, and 30 days was similar between hospitalizations to H‐PA and RES teams (Table 4).
Mortality
The risk of inpatient death was similar between all hospitalizations to H‐PA and RES teams or only hospitalizations without an ICU stay (Table 4). The results also remained the same in analyses restricted to first admissions, last admissions, or 1 randomly selected admission per patient.
Sub‐Group Analysis
On restricting the multivariable analyses to the subset of hospitalists who staffed both types of teams (Table 4), the increase in LOS associated with H‐PA care was no longer significant (5.44% higher, P = 0.081). The charges, risk of readmission at 7 and 30 days, and risk of inpatient mortality remained similar. The risk of readmission at 14 days was slightly lower following hospitalizations to H‐PA teams (odds ratio 0.71, 95% confidence interval [CI] 0.51‐0.99).
The increase in LOS associated with H‐PA care was further attenuated in analyses of the subset of admissions between 11.00 AM and 4.00 PM (2.97% higher, P = 0.444). The difference in charges approached significance (6.45% higher, P = 0.07), but risk of readmission at 7, 14, and 30 days and risk of inpatient mortality were no different (Table 4).
Interactions
On adding interaction terms between the team assignment and the fixed effect variables in each model we detected that the effect of H‐PA care on LOS (P < 0.001) and charges (P < 0.001) varied by time of admission (Figure 2a and b). Hospitalizations to H‐PA teams from 6.00 PM to 6.00 AM had greater relative increases in LOS as compared to hospitalizations to RES teams during those times. Similarly, hospitalizations during the period 3.00 PM to 3.00 AM had relatively higher charges associated with H‐PA care compared to RES care.
Discussion
We found that hospitalizations to our H‐PA teams had longer LOS but similar charges, readmission rates, and mortality as compared to traditional resident‐based teams. These findings were robust to multiple sensitivity and subgroup analyses but when we examined times when both types of teams could receive admissions, the difference in LOS was markedly attenuated and nonsignificant.
We note that most prior reports comparing PA‐based models of inpatient care predate the ACGME work hour regulations. In a randomized control trial (1987‐1988) Simmer et al.5 showed lower lengths of stay and charges but possibly higher risk of readmission for PA based teams as compared to resident based teams. Van Rhee et al.7 conducted a nonrandomized retrospective cohort study (1994‐1995) using administrative data which showed lower resource utilization for PA‐based inpatient care. Our results from 2005 to 2006 reflect the important changes in the organization and delivery of inpatient care since these previous investigations.
Roy et al.8 report the only previously published comparison of PA and resident based GM inpatient care after the ACGME mandated work hour regulations. They found PA‐based care was associated with lower costs, whereas we found similar charges for admissions to RES and H‐PA teams. They also found that LOS was similar for PA and resident‐based care, while we found a higher LOS for admissions to our H‐PA team. We note that although the design of Roy's study was similar to our own, patients cared for by PA‐based teams were geographically localized in their model. This may contribute to the differences in results noted between our studies.
Despite no designed differences in patients assigned to either type of team other than time of admission we noted some differences between the H‐PA and RES teams in the descriptive analysis. These differences, such as a higher proportion of hospitalizations to H‐PA teams being admitted from the ER, residing on nonmedicine wards or having an ICU stay are likely a result of our system of assigning admissions to H‐PA teams early during the workday. For example patients on H‐PA teams were more often located on nonmedicine wards as a result of later discharges and bed availability on medicine wards. The difference that deserves special comment is the much higher proportion (13.8% vs. 6.7%) of hospitalizations with an ICU stay on the H‐PA teams. Hospitalizations directly to the ICU were excluded from our study which means that the hospitalizations with an ICU stay in our study were initially admitted to either H‐PA or RES teams and then transferred to the ICU. Transfers out of the ICU usually occur early in the workday when H‐PA teams accepted patients per our admission schedule. These patients may have been preferentially assigned to H‐PA teams, if on returning from the ICU the original team's resident had changed (and the bounce back rule was not in effect). Importantly, the conclusions of our research are not altered on controlling for this difference in the teams by excluding hospitalizations with an ICU stay.
Hospitalizations to H‐PA teams were associated with higher resource utilization if they occurred later in the day or overnight (Figure 2a and b). During these times a transition of care occurred shortly after admission. For a late day admission the H‐PA teams would transfer care for overnight cross cover soon after the admission and for patients admitted overnight as overflow they would assume care of a patient from the nighttime covering physician performing the admission. On the other hand, on RES teams, interns admitting patients overnight continued to care for their patients for part of the following day (30‐hour call). Similar findings of higher resource utilization associated with transfer of care after admission in the daytime11 and nighttime12 have been previously reported. An alternative hypothesis for our findings is that the hospital maybe busier and thus less efficient during times when H‐PA teams had to admit later in the day or accept patients admitted overnight as overflow. Future research to determine the cause of this significant interaction between team assignment and time of admission on resource utilization is important as the large increases in LOS (up to 30%) and charges (up to 50%) noted, could have a potentially large impact if a higher proportion of hospitalizations were affected by this phenomenon.
Our H‐PA teams were assigned equally complex patients as our RES teams, in contrast to previous reports.8, 13 This was accomplished while improving the resident's educational experience and we have previously reported increases in our resident's board pass rates and in‐service training exam scores with that introduction of our H‐PA teams.14 We thus believe that selection of less complex patients to H‐PA teams such as ours is unnecessary and may give them a second tier status in academic settings.
Our report has limitations. It is a retrospective, nonrandomized investigation using a single institution's administrative database and has the limitations of not being able to account for unmeasured confounders, severity of illness, errors in the database, selection bias and has limited generalizability. We measured charges not actual costs,15 but we feel charges are a true reflection of relative resource use when compared between similar patients within a single institution. We also did not account for the readmissions that occur to other hospitals16 and our results do not reflect resource utilization for the healthcare system in total. For example, we could not tell if higher LOS on H‐PA teams resulted in lower readmissions for their patients in all hospitals in the region, which may reveal an overall resource savings. Additionally, we measured in‐hospital mortality and could not capture deaths related to hospital care that may occur shortly after discharge.
ACGME has proposed revised standards that may further restrict resident duty hours when they take effect in July 2011.3 This may lead to further decreases in resident‐based inpatient care. Teaching hospitals will need to continue to develop alternate models for inpatient care that do not depend on house staff. Our findings provide important evidence to inform the development of such models. Our study shows that one such model: PAs paired with hospitalists, accepting admissions early in the workday, with hospitalist coverage over the weekend and nights can care for GM inpatients as complex as those cared for by resident‐based teams without increasing readmission rates, inpatient mortality, or charges but at the cost of slightly higher LOS.
In 2003 the Accreditation Council for Graduate Medical Education (ACGME) prescribed residency reform in the form of work hour restrictions without prescribing alternatives to resident based care.1 As a response, many academic medical centers have developed innovative models for providing inpatient care, some of which incorporate Physician Assistants (PAs).2 With further restrictions in resident work hours possible,3 teaching hospitals may increase use of these alternate models to provide inpatient care. Widespread implementation of such new and untested models could impact the care of the approximately 20 million hospitalizations that occur every year in US teaching hospitals.4
Few reports have compared the care delivered by these alternate models with the care provided by traditional resident‐based models of care.58 Roy et al.8 have provided the only recent comparison of a PA‐based model of care with a resident‐based model. They showed lower adjusted costs of inpatient care associated with PA based care but other outcomes were similar to resident‐based teams.
The objective of this study is to provide a valid and usable comparison of the outcomes of a hospitalist‐PA (H‐PA) model of inpatient care with the traditional resident‐based model. This will add to the quantity and quality of the limited research on PA‐based inpatient care, and informs the anticipated increase in the involvement of PAs in this arena.
Methods
Study Design and Setting
We conducted a retrospective cohort study at a 430‐bed urban academic medical center in the Midwestern United States.
Models of General Medical (GM) Inpatient Care at the Study Hospital During the Study Period
In November 2004, as a response to the ACGME‐mandated work hour regulations, we formed 2 Hospitalist‐PA teams (H‐PA) to supplement the 6 preexisting general medicine resident teams (RES).
The H‐PA and RES teams differed in staffing, admitting times and weekend/overnight cross coverage structure (Table 1). There were no predesigned differences between the teams in the ward location of their patients, availability of laboratory/radiology services, specialty consultation, social services/case management resources, nursing resources or documentation requirements for admission, daily care, and discharge.
| H‐PA Teams | RES Teams | |
|---|---|---|
| Attending physician | Always a hospitalist | Hospitalist, non‐hospitalist general internist or rarely a specialist |
| Attending physician role | Supervisory for some patients (about half) and sole care provider for others. | Supervisory for all patients |
| Team composition | One attending paired with 1 PA | Attending + senior resident + (2) interns + (2‐3) medical students |
| Rotation schedule | ||
| Attending | Every 2 weeks | Every 2 weeks |
| Physician assistant | Off on weekends | |
| House staff & medical students | Every month | |
| Weekend | No new admissions & hospitalist manages all patients | Accept new admissions |
| Admission times (weekdays) | 7 AM to 3 PM | Noon to 7 AM |
| Source of admissions | Emergency room, clinics, other hospitals | Emergency room, clinics, other hospitals |
| Number of admissions (weekdays) | 4‐6 patients per day per team | Noon to 5 PM: 2 teams admit a maximum of 9 patients total |
| 5 PM to 7 AM: 3 teams admit a maximum 5 patients each. | ||
| Overnight coverageroles and responsibilities | One in‐house faculty | 3 on call interns |
| Cross‐covering 2 H‐PA teams | Cross‐covering 2 teams each | |
| Performing triage | Admitting up to 5 patients each | |
| Admitting patients if necessary | ||
| Assisting residents if necessary | ||
| General medical consultation |
Admission Schedule for H‐PA or RES Teams
The admitting schedule was designed to decrease the workload of the house staff and to do so specifically during the periods of peak educational activity (morning report, attending‐led teaching rounds, and noon report). A faculty admitting medical officer (AMO) assigned patients strictly based on the time an admission was requested. Importantly, the request for admission preceded the time of actual admission recorded when the patient reached the ward. The time difference between request for admission and actual admission depended on the source of admission and the delay associated with assigning a patient room. The AMO assigned 8 to 12 new patients to the H‐PA teams every weekday between 7 AM and 3 PM and to the RES teams between noon and 7 AM the next day. There was a designed period of overlap from noon to 3 PM during which both H‐PA and RES teams could admit patients. This period allowed for flexibility in assigning patients to either type of team depending on their workload. The AMO did not use patient complexity or teaching value to assign patients.
Exceptions to Admission Schedule
Patients admitted overnight after the on call RES had reached their admission limits were assigned to H‐PA teams the next morning. In addition, recently discharged patients who were readmitted while the discharging hospitalist (H‐PA teams) or the discharging resident (RES teams) was still scheduled for inpatient duties, were assigned back to the discharging team irrespective of the admitting schedule.
The same medicine team cared for a patient from admission to discharge but on transfer to the intensive care unit (ICU), an intensivist led critical care team assumed care. On transfer out of the ICU these patients were assigned back to the original team irrespective of admitting schedulethe so called bounce back rule to promote inpatient continuity of care. But if the residents (RES teams) or the hospitalist (H‐PA teams) had changedthe bounce back rule was no longer in effect and these patients were assigned to a team according to the admission schedule.
Study Population and Study Period
We included all hospitalizations of adult patients to GM teams if both their date of admission and their date of discharge fell within the study period (January 1, 2005 to December 31, 2006). We excluded hospitalizations with admissions during the weekendwhen H‐PA teams did not admit patients; hospitalizations to GM services with transfer to nonGM service (excluding ICU) and hospitalizations involving comanagement with specialty servicesas the contribution of GM teams for these was variable; and hospitalizations of private patients.
Data Collection and Team Assignment
We collected patient data from our hospital's discharge abstract database. This database did not contain team information so to assign teams we matched the discharging attending and the day of discharge to the type of team that the discharging attending was leading that day.
We collected patient age, gender, race, insurance status, zip‐code, primary care provider, source of admission, ward type, time and day of admission, and time and day of discharge for use as independent variables. The time of admission captured in the database was the time of actual admission and not the time the admission was requested.
We grouped the principal diagnosis International Statistical Classification of Diseases and Related Health Problems, 9th edition (ICD‐9) codes into clinically relevant categories using the Clinical Classification Software.9 We created comorbidity measures using Healthcare Cost and Utilization Project Comorbidity Software, version 3.4.10
Outcome Measures
We used length of stay (LOS), charges, readmissions within 7, 14, and 30 days and inpatient mortality as our outcome measures. We calculated LOS by subtracting the discharge day and time from the admission day and time. The LOS included time spent in the ICU. We summed all charges accrued during the entire hospitalization including any stay in the ICU but did not include professional fees. We considered any repeat hospitalization to our hospital within 7, 14, and 30 days following a discharge to be a readmission except that we excluded readmissions for a planned procedure or for inpatient rehabilitation.
Statistical Analysis
Descriptive Analysis
We performed unadjusted descriptive statistics at the level of an individual hospitalization using medians and interquartile ranges for continuous data and frequencies and percentages for categorical data. We used chi‐square tests of association and KruskalWallis analysis of variance to compare H‐PA and RES teams.
Missing Data
Because we lacked data on whether a primary outpatient care provider was available for 284 (2.9%) of our study hospitalizations, we dropped them from our multivariable analyses. We used an arbitrary discharge time of noon for the 11 hospitalizations which did not have a discharge time recorded.
Multivariable Analysis
We used multivariable mixed models to risk adjust for a wide variety of variables. We included age, gender, race, insurance, presence of primary care physician, and total number of comorbidities as fixed effects in all models because of the high face validity of these variables. We then added admission source, ward, time, day of week, discharge day of week, and comorbidity measures one by one as fixed effects, including them only if significant at P < 0.01. For assessing LOS, charges, and readmissions, we added a variable identifying each patient as a random effect to account for multiple admissions for the same patient. We then added variables identifying attending physician, principal diagnostic group, and ZIP code of residence as random effects to account for clustering of hospitalizations within these categories, including them only if significant at P < 0.01. For the model assessing mortality we included variables for attending physician, principal diagnostic group, and ZIP code of residence as random effects if significant at P < 0.01. We log transformed LOS and charges because they were extremely skewed in nature. Readmissions were analyzed after excluding patients who died or were discharged alive within 7, 14, or 30 days of the end of the study period.
Sensitivity Analyses
To assess the influence of LOS outliers, we changed LOS to 6 hours if it was less than 6 hours, and 45 days if it was more than 45 daysa process called winsorizing. We consider winsorizing superior to dropping outliers because it acknowledges that outliers contribute information, but prevent them from being too influential. We chose the 6 hour cut off because we believed that was the minimum time required to admit and then discharge a patient. We chose the upper limit of 45 days on reviewing the frequency distribution for outliers. Similarly, we winsorized charges at the first and 99th percentile after reviewing the frequency distribution for outliers. We then log transformed the winsorized data before analysis.
Inpatient deaths reduce the LOS and charges associated with a hospitalization. Thus excess mortality may provide a false concession in terms of lower LOS or charges. To check if this occurred in our study we repeated the analyses after excluding inpatient deaths.
ICU stays are associated with higher LOS, charges, and mortality. In our model of care, some patients transferred to the ICU are not cared for by the original team on transfer out. Moreover, care in the ICU is not controlled by the team that discharges them. Since this might obscure differences in outcomes achieved by RES vs. H‐PA teams, we repeated these analyses after excluding hospitalizations with an ICU stay.
Since mortality can only occur during 1 hospitalization per patient, we repeated the mortality analysis using only each patient's first admission or last admission and using a randomly selected single admission for each patient.
Subgroup Analysis
To limit the effect of different physician characteristics on H‐PA and RES teams we separately analyzed the hospitalizations under the care of hospitalists who served on both H‐PA and RES teams.
To limit the effect of different admission schedules of H‐PA and RES teams we analyzed the hospitalizations with admission times between 11.00 AM and 4.00 PM. Such hospitalizations were likely to be assigned during the noon to 3 PM period when they could be assigned to either an H‐PA or RES team.
Interactions
Finally we explored interactions between the type of team and the fixed effect variables included in each model.
Statistical Software
We performed the statistical analysis using SAS software version 9.0 for UNIX (SAS Institute, Inc., Cary, NC) and R software (The R Project for Statistical Computing).
This study protocol was approved by the hospital's institutional review board.
Results
Study Population
Of the 52,391 hospitalizations to our hospital during the study period, 13,058 were admitted to general medicine. We excluded 3102 weekend admissions and 209 who met other exclusion criteria. We could not determine the team assignment for 66. Of the remaining 9681 hospitalizations, we assigned 2171 to H‐PA teams and 7510 to RES teams (Figure 1).
Descriptive Analysis
We compare patients assigned to H‐PA and RES teams in Table 2. They were similar in age, gender, race, having a primary care provider or not, and insurance status. Clinically, they had similar comorbidities and a similar distribution of common principal diagnoses. Consistent with their admitting schedule, H‐PA teams admitted and discharged more patients earlier in the day and admitted more patients earlier in the work week. Patients cared for by H‐PA teams were admitted from the Emergency Room (ER) less often and were more likely to reside on wards designated as nonmedicine by nursing specialty. Hospitalizations to H‐PA teams more often included an ICU stay.
| H‐PA (n = 2171) | RES (n = 7510) | P Value | |
|---|---|---|---|
| |||
| Age | |||
| Mean | 56.80 | 57.04 | |
| Median | 56 | 56 | 0.15 |
| Interquartile range | 43‐72 | 43‐73 | |
| Age group (years), n (%) | |||
| < 20 | 10 (0.5) | 57 (0.8) | |
| 20‐29 | 186 (8.6) | 632 (8.7) | |
| 30‐39 | 221 (10.2) | 766 (10.3) | |
| 40‐49 | 387 (17.8) | 1341 (18.1) | |
| 50‐59 | 434 (20.0) | 1492 (20.2) | 0.28 |
| 60‐69 | 325 (15.0) | 974 (12.8) | |
| 70‐79 | 271 (12.5) | 1035 (13.6) | |
| 80‐89 | 262 (12.0) | 951(12.3) | |
| 90< | 75 (3.5) | 262 (3.4) | |
| Female, n (%) | 1175 (54.1) | 4138 (55.1) | 0.42 |
| Race, n (%) | |||
| White | 1282 (59.1) | 4419 (58.9) | |
| Black | 793 (36.5) | 2754 (36.7) | 0.98 |
| Other | 96 (4.4) | 337 (4.5) | |
| Primary care provider, n (%) | 0.16 | ||
| Yes | 1537 (73.2) | 5451 (74.7) | |
| Missing: 284 | 71 (3.3) | 213 (2.8) | |
| Insurance status, n (%) | |||
| Commercial/worker's comp | 440 (20.3) | 1442 (19.2) | |
| Medicare | 1017 (46.8) | 3589 (47.8) | 0.52 |
| Medicaid/others | 714 (32.9) | 2479 (33.0) | |
| Time of admission, n (%) | |||
| 0000‐0259 | 167 (7.7) | 1068 (14.2) | |
| 0300‐0559 | 244 (11.2) | 485 (6.5) | |
| 0600‐0859 | 456 (21.0) | 270 (3.6) | |
| 0900‐1159 | 782 (36.0) | 1146 (15.3) | <0.001 |
| 1200‐1459 | 299 (13.8) | 1750 (23.3) | |
| 1500‐1759 | 155 (7.1) | 1676 (22.3) | |
| 1800‐2359 | 68 (3.1) | 1115 (14.9) | |
| Time of discharge, n (%) | |||
| 2100‐0859 | 36 (1.7) | 174 (2.3) | |
| 0900‐1159 | 275 (12.7) | 495 (6.6) | |
| 1200‐1459 | 858 (39.6) | 2608 (34.8) | <0.001 |
| 1500‐1759 | 749 (34.6) | 3122 (41.6) | |
| 1800‐2059 | 249 (11.5) | 1104 (14.7) | |
| Missing | 4 | 7 | |
| Day of week of admission, n (%) | |||
| Monday | 462 (21.3) | 1549 (20.6) | |
| Tuesday | 499 (23.0) | 1470 (19.6) | |
| Wednesday | 430 (19.8) | 1479 (19.7) | 0.001 |
| Thursday | 400 (18.4) | 1482 (19.7) | |
| Friday | 380 (17.5) | 1530 (20.4) | |
| Day of week of discharge, n (%) | |||
| Monday | 207 (9.5) | 829 (11.0) | |
| Tuesday | 268 (12.3) | 973 (13.0) | |
| Wednesday | 334 (15.4) | 1142 (15.2) | |
| Thursday | 362 (16.7) | 1297 (17.3) | 0.16 |
| Friday | 485 (22.3) | 1523 (20.3) | |
| Saturday | 330 (15.2) | 1165 (15.5) | |
| Sunday | 185 (8.5) | 581 (7.7) | |
| Admit to non‐medicine wards, n (%) | 1332 (61.4) | 2624 (34.9) | <0.001 |
| Transfer to ICU (at least once), n (%) | 299 (13.8) | 504 (6.7) | <0.001 |
| Admit from ER No (%) | 1663 (76.6) | 6063 (80.7) | <0.001 |
| 10 most frequent diagnosis (%) | Pneumonia (4.9) | Pneumonia (5.5) | |
| Congestive heart failure; nonhypertensive (4.2) | Congestive heart failure; nonhypertensive (3.9) | ||
| Sickle cell anemia (3.9) | Nonspecific chest pain (3.7) | ||
| Chronic obstructive pulmonary disease and Bronchiectasis (3.3) | Urinary tract infections(3.6) | ||
| Diabetes mellitus with complications (3.2) | Skin and subcutaneous tissue infections (3.3) | ||
| Urinary tract infections (3.2) | Sickle cell anemia (3.3) | ||
| Asthma (3.0) | Pancreatic disorders (not diabetes) (2.8) | ||
| Nonspecific chest pain (3.0) | Asthma (2.8) | ||
| Pancreatic disorders (not diabetes) (2.9) | Chronic obstructive pulmonary disease and Bronchiectasis (2.6) | ||
| Septicemia (2.2) | Diabetes mellitus with complications (2.6) | ||
| Average number of comorbidities mean (95% CI) | 0.39 (0.37‐0.42) | 0.38 (0.36‐0.39) | 0.23 |
In unadjusted comparisons of outcomes (Table 3), hospitalizations on H‐PA teams had higher lengths of stay and charges than hospitalizations on RES teams, possibly higher inpatient mortality rates but similar unadjusted readmission rates at 7, 14, and 30 days
| H‐PA (n = 2171) | RES (n = 7150) | % Difference* (CI) | P Value | |
|---|---|---|---|---|
| ||||
| LOS | Median (IQR) | Median (IQR) | ||
| Days | 3.17 (2.03‐5.30) | 2.99 (1.80‐5.08) | +8.9% (4.71‐13.29%) | <0.001 |
| Charges | ||||
| US Dollars | 9390 (6196‐16,239) | 9044 (6106‐14,805) | +5.56% (1.96‐9.28%) | 0.002 |
| Readmissions | n (%) | n (%) | Odds Ratio (CI) | |
| Within 7 days | 147 (6.96) | 571 (7.78) | 0.88 (0.73‐1.06) | 0.19 |
| Within14 days | 236 (11.34) | 924 (12.76) | 0.87 (0.75‐1.01) | 0.07 |
| Within 30 days | 383 (18.91) | 1436 (20.31) | 0.91 (0.80‐1.03) | 0.14 |
| Inpatient deaths | 39 (1.8) | 95 (1.3) | 1.36 (0.90‐2.00) | 0.06 |
Multivariable Analysis
LOS
Hospitalizations to H‐PA teams were associated with a 6.73% longer LOS (P = 0.005) (Table 4). This difference persisted when we used the winsorized data (6.45% increase, P = 0.006), excluded inpatient deaths (6.81% increase, P = 0.005), or excluded hospitalizations that involved an ICU stay (6.40%increase, P = 0.011) (Table 5).
| Overall | Subgroup: Restricted to Physicians Attending on Both H‐PA and RES Teams* | Subgroup: Restricted to Hospitalizations Between 11.00 AM and 4.00 PM | ||||
|---|---|---|---|---|---|---|
| % Difference (CI) | P Value | % Difference (CI) | P Value | % Difference (CI) | P Value | |
| ||||||
| LOS | 6.73% (1.99% to 11.70%) | 0.005 | 5.44% (0.65% to 11.91%) | 0.08 | 2.97% (4.47% to 10.98%) | 0.44 |
| Charges | 2.75% (1.30% to 6.97%) | 0.19 | 1.55% (3.76% to 7.16%) | 0.57 | 6.45% (0.62% to 14.03%) | 0.07 |
| Risk of Readmission | Adjusted OR (95%CI) | P Value | Adjusted OR (95% CI) | P Value | Adjusted OR (95% CI) | P Value |
| Within 7 days | 0.88 (0.64‐1.20) | 0.42 | 0.74 (0.40‐1.35) | 0.32 | 0.90 (0.40‐2.00) | 0.78 |
| Within14 days | 0.90 (0.69‐1.19) | 0.46 | 0.71 (0.51‐0.99) | 0.05 | 0.87 (0.36‐2.13) | 0.77 |
| Within 30 days | 0.89 (0.75‐1.06) | 0.20 | 0.75 (0.51‐1.08) | 0.12 | 0.92 (0.55‐1.54) | 0.75 |
| Inpatient mortality | 1.27 (0.82‐1.97) | 0.28 | 1.46 (0.67‐3.17) | 0.33 | 1.14 (0.47‐2.74) | 0.77 |
| Analysis With Winsorized Data | Analysis After Excluding Inpatient Deaths | Analysis After Excluding Patients With ICU Stays | ||||
|---|---|---|---|---|---|---|
| % Difference (CI) | P Value | % Difference (CI) | P Value | % Difference (CI) | P Value | |
| ||||||
| LOS | 6.45% (4.04 to 8.91%) | 0.006 | 6.81% (2.03 to 11.80%) | 0.005 | 6.40% (1.46 to 11.58%) | 0.011 |
| Charges | 2.67 (1.27 to 6.76%) | 0.187 | 2.89% (1.16 to 7.11%) | 0.164 | 0.74% (3.11 to 4.76%) | 0.710 |
Charges
Hospitalizations to H‐PA and RES teams were associated with similar charges (Table 4). The results were similar when we used winsorized data, excluded inpatient deaths or excluded hospitalizations involving an ICU stay (Table 5).
Readmissions
The risk of readmission at 7, 14, and 30 days was similar between hospitalizations to H‐PA and RES teams (Table 4).
Mortality
The risk of inpatient death was similar between all hospitalizations to H‐PA and RES teams or only hospitalizations without an ICU stay (Table 4). The results also remained the same in analyses restricted to first admissions, last admissions, or 1 randomly selected admission per patient.
Sub‐Group Analysis
On restricting the multivariable analyses to the subset of hospitalists who staffed both types of teams (Table 4), the increase in LOS associated with H‐PA care was no longer significant (5.44% higher, P = 0.081). The charges, risk of readmission at 7 and 30 days, and risk of inpatient mortality remained similar. The risk of readmission at 14 days was slightly lower following hospitalizations to H‐PA teams (odds ratio 0.71, 95% confidence interval [CI] 0.51‐0.99).
The increase in LOS associated with H‐PA care was further attenuated in analyses of the subset of admissions between 11.00 AM and 4.00 PM (2.97% higher, P = 0.444). The difference in charges approached significance (6.45% higher, P = 0.07), but risk of readmission at 7, 14, and 30 days and risk of inpatient mortality were no different (Table 4).
Interactions
On adding interaction terms between the team assignment and the fixed effect variables in each model we detected that the effect of H‐PA care on LOS (P < 0.001) and charges (P < 0.001) varied by time of admission (Figure 2a and b). Hospitalizations to H‐PA teams from 6.00 PM to 6.00 AM had greater relative increases in LOS as compared to hospitalizations to RES teams during those times. Similarly, hospitalizations during the period 3.00 PM to 3.00 AM had relatively higher charges associated with H‐PA care compared to RES care.
Discussion
We found that hospitalizations to our H‐PA teams had longer LOS but similar charges, readmission rates, and mortality as compared to traditional resident‐based teams. These findings were robust to multiple sensitivity and subgroup analyses but when we examined times when both types of teams could receive admissions, the difference in LOS was markedly attenuated and nonsignificant.
We note that most prior reports comparing PA‐based models of inpatient care predate the ACGME work hour regulations. In a randomized control trial (1987‐1988) Simmer et al.5 showed lower lengths of stay and charges but possibly higher risk of readmission for PA based teams as compared to resident based teams. Van Rhee et al.7 conducted a nonrandomized retrospective cohort study (1994‐1995) using administrative data which showed lower resource utilization for PA‐based inpatient care. Our results from 2005 to 2006 reflect the important changes in the organization and delivery of inpatient care since these previous investigations.
Roy et al.8 report the only previously published comparison of PA and resident based GM inpatient care after the ACGME mandated work hour regulations. They found PA‐based care was associated with lower costs, whereas we found similar charges for admissions to RES and H‐PA teams. They also found that LOS was similar for PA and resident‐based care, while we found a higher LOS for admissions to our H‐PA team. We note that although the design of Roy's study was similar to our own, patients cared for by PA‐based teams were geographically localized in their model. This may contribute to the differences in results noted between our studies.
Despite no designed differences in patients assigned to either type of team other than time of admission we noted some differences between the H‐PA and RES teams in the descriptive analysis. These differences, such as a higher proportion of hospitalizations to H‐PA teams being admitted from the ER, residing on nonmedicine wards or having an ICU stay are likely a result of our system of assigning admissions to H‐PA teams early during the workday. For example patients on H‐PA teams were more often located on nonmedicine wards as a result of later discharges and bed availability on medicine wards. The difference that deserves special comment is the much higher proportion (13.8% vs. 6.7%) of hospitalizations with an ICU stay on the H‐PA teams. Hospitalizations directly to the ICU were excluded from our study which means that the hospitalizations with an ICU stay in our study were initially admitted to either H‐PA or RES teams and then transferred to the ICU. Transfers out of the ICU usually occur early in the workday when H‐PA teams accepted patients per our admission schedule. These patients may have been preferentially assigned to H‐PA teams, if on returning from the ICU the original team's resident had changed (and the bounce back rule was not in effect). Importantly, the conclusions of our research are not altered on controlling for this difference in the teams by excluding hospitalizations with an ICU stay.
Hospitalizations to H‐PA teams were associated with higher resource utilization if they occurred later in the day or overnight (Figure 2a and b). During these times a transition of care occurred shortly after admission. For a late day admission the H‐PA teams would transfer care for overnight cross cover soon after the admission and for patients admitted overnight as overflow they would assume care of a patient from the nighttime covering physician performing the admission. On the other hand, on RES teams, interns admitting patients overnight continued to care for their patients for part of the following day (30‐hour call). Similar findings of higher resource utilization associated with transfer of care after admission in the daytime11 and nighttime12 have been previously reported. An alternative hypothesis for our findings is that the hospital maybe busier and thus less efficient during times when H‐PA teams had to admit later in the day or accept patients admitted overnight as overflow. Future research to determine the cause of this significant interaction between team assignment and time of admission on resource utilization is important as the large increases in LOS (up to 30%) and charges (up to 50%) noted, could have a potentially large impact if a higher proportion of hospitalizations were affected by this phenomenon.
Our H‐PA teams were assigned equally complex patients as our RES teams, in contrast to previous reports.8, 13 This was accomplished while improving the resident's educational experience and we have previously reported increases in our resident's board pass rates and in‐service training exam scores with that introduction of our H‐PA teams.14 We thus believe that selection of less complex patients to H‐PA teams such as ours is unnecessary and may give them a second tier status in academic settings.
Our report has limitations. It is a retrospective, nonrandomized investigation using a single institution's administrative database and has the limitations of not being able to account for unmeasured confounders, severity of illness, errors in the database, selection bias and has limited generalizability. We measured charges not actual costs,15 but we feel charges are a true reflection of relative resource use when compared between similar patients within a single institution. We also did not account for the readmissions that occur to other hospitals16 and our results do not reflect resource utilization for the healthcare system in total. For example, we could not tell if higher LOS on H‐PA teams resulted in lower readmissions for their patients in all hospitals in the region, which may reveal an overall resource savings. Additionally, we measured in‐hospital mortality and could not capture deaths related to hospital care that may occur shortly after discharge.
ACGME has proposed revised standards that may further restrict resident duty hours when they take effect in July 2011.3 This may lead to further decreases in resident‐based inpatient care. Teaching hospitals will need to continue to develop alternate models for inpatient care that do not depend on house staff. Our findings provide important evidence to inform the development of such models. Our study shows that one such model: PAs paired with hospitalists, accepting admissions early in the workday, with hospitalist coverage over the weekend and nights can care for GM inpatients as complex as those cared for by resident‐based teams without increasing readmission rates, inpatient mortality, or charges but at the cost of slightly higher LOS.
- ACGME‐Common Program Requirements for Resident Duty Hours. Available at: http://www.acgme.org/acWebsite/dutyHours/dh_ComProgrRequirmentsDutyHours0707.pdf. Accessed July 2010.
- ,,,,.Non‐housestaff medicine services in academic centers: models and challenges.J Hosp Med.2008;3(3):247–255.
- ACGME. Duty Hours: Proposed Standards for Review and comment. Available at: http://acgme‐2010standards.org/pdf/Proposed_Standards. pdf. Accessed July 22,2010.
- Agency for Health Care Policy and Research. HCUPnet: A tool for identifying, tracking, and analyzing national hospital statistics. Available at: http://hcup.ahrq.gov/HCUPnet.asp. Accessed July2010.
- ,,,,.A randomized, controlled trial of an attending staff service in general internal medicine.Med Care.1991;29(7 suppl):JS31–JS40.
- ,.Replacing an academic internal medicine residency program with a physician assistant‐‐hospitalist model: a Comparative Analysis Study.Am J Med Qual.2009;24(2):132–139.
- ,,.Resource use by physician assistant services versus teaching services.JAAPA.2002;15(1):33–42.
- ,,, et al.Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes.J Hosp Med.2008;3(5):361–368.
- AHRQ. Clinical Classifications Software (CCS) for ICD‐9‐CM. Available at: http://www.hcup‐us.ahrq.gov/toolssoftware/ccs/ccs.jsp#overview. Accessed July2010.
- AHRQ. HCUP: Comorbidity Software, Version 3.4.;Available at: http://www.hcup‐us.ahrq.gov/toolssoftware/comorbidity/comorbidity.jsp. Accessed July2010.
- ,,, et al.Effect of short call admission on length of stay and quality of care for acute decompensated heart failure.Circulation.2008;117(20):2637–2644.
- ,,,.Post‐call transfer of resident responsibility: its effect on patient care.J Gen Intern Med.1990;5(6):501–505.
- ,,,,,.The effect of nonteaching services on the distribution of inpatient cases for internal medicine residents.Acad Med.2009:84(2):220–225.
- ,,, et al.Allowing for better resident education and improving patient care: hospitalist‐physician assistant teams fill in the gaps.J Hosp Med.2007;2[S2]:1–39.
- .The distinction between cost and charges.Ann Intern Med.1982;96(1):102–109.
- ,,.Rehospitalizations among patients in the Medicare Fee‐for‐Service Program.N Engl J Med.2009;360(14):1418–1428.
- ACGME‐Common Program Requirements for Resident Duty Hours. Available at: http://www.acgme.org/acWebsite/dutyHours/dh_ComProgrRequirmentsDutyHours0707.pdf. Accessed July 2010.
- ,,,,.Non‐housestaff medicine services in academic centers: models and challenges.J Hosp Med.2008;3(3):247–255.
- ACGME. Duty Hours: Proposed Standards for Review and comment. Available at: http://acgme‐2010standards.org/pdf/Proposed_Standards. pdf. Accessed July 22,2010.
- Agency for Health Care Policy and Research. HCUPnet: A tool for identifying, tracking, and analyzing national hospital statistics. Available at: http://hcup.ahrq.gov/HCUPnet.asp. Accessed July2010.
- ,,,,.A randomized, controlled trial of an attending staff service in general internal medicine.Med Care.1991;29(7 suppl):JS31–JS40.
- ,.Replacing an academic internal medicine residency program with a physician assistant‐‐hospitalist model: a Comparative Analysis Study.Am J Med Qual.2009;24(2):132–139.
- ,,.Resource use by physician assistant services versus teaching services.JAAPA.2002;15(1):33–42.
- ,,, et al.Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes.J Hosp Med.2008;3(5):361–368.
- AHRQ. Clinical Classifications Software (CCS) for ICD‐9‐CM. Available at: http://www.hcup‐us.ahrq.gov/toolssoftware/ccs/ccs.jsp#overview. Accessed July2010.
- AHRQ. HCUP: Comorbidity Software, Version 3.4.;Available at: http://www.hcup‐us.ahrq.gov/toolssoftware/comorbidity/comorbidity.jsp. Accessed July2010.
- ,,, et al.Effect of short call admission on length of stay and quality of care for acute decompensated heart failure.Circulation.2008;117(20):2637–2644.
- ,,,.Post‐call transfer of resident responsibility: its effect on patient care.J Gen Intern Med.1990;5(6):501–505.
- ,,,,,.The effect of nonteaching services on the distribution of inpatient cases for internal medicine residents.Acad Med.2009:84(2):220–225.
- ,,, et al.Allowing for better resident education and improving patient care: hospitalist‐physician assistant teams fill in the gaps.J Hosp Med.2007;2[S2]:1–39.
- .The distinction between cost and charges.Ann Intern Med.1982;96(1):102–109.
- ,,.Rehospitalizations among patients in the Medicare Fee‐for‐Service Program.N Engl J Med.2009;360(14):1418–1428.
Copyright © 2011 Society of Hospital Medicine
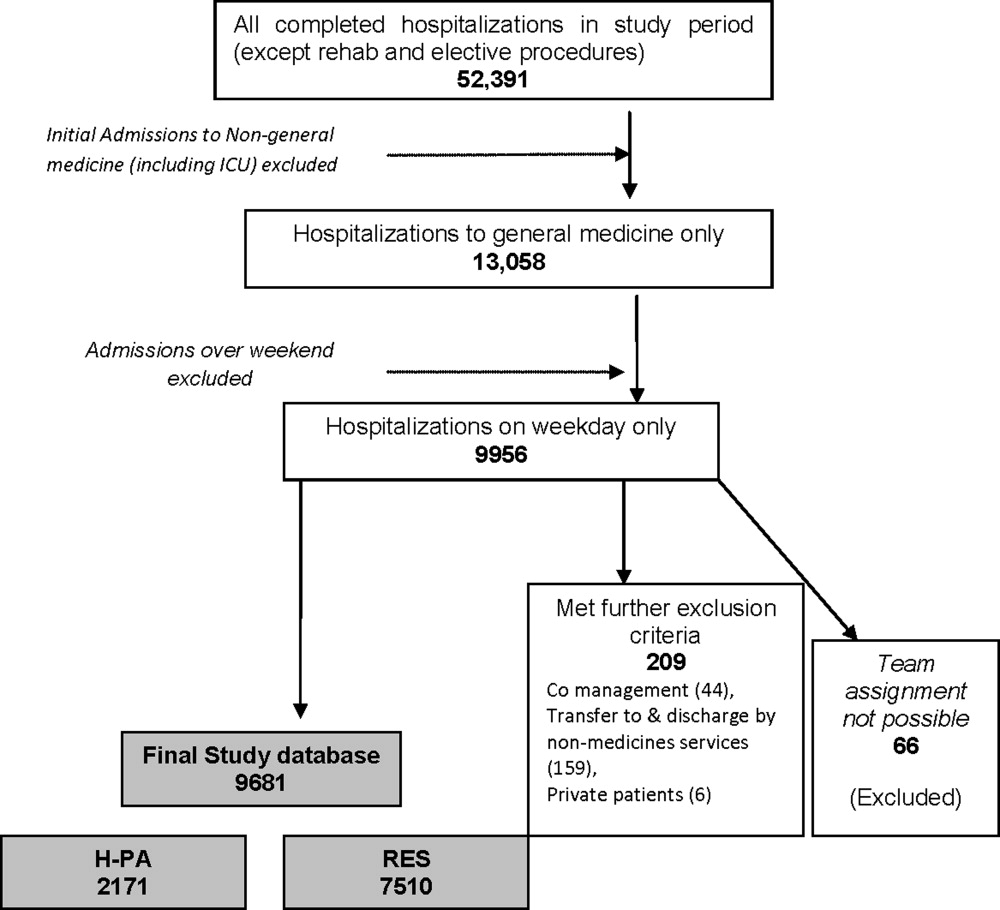
Chronic Constipation in the Elderly
A supplement to Family Practice News supported by Takeda Pharmaceuticals North America, Inc. The supplement is based on a faculty interview.

To view the supplement, click the image above.
A supplement to Family Practice News supported by Takeda Pharmaceuticals North America, Inc. The supplement is based on a faculty interview.
To view the supplement, click the image above.
A supplement to Family Practice News supported by Takeda Pharmaceuticals North America, Inc. The supplement is based on a faculty interview.
To view the supplement, click the image above.
