User login
Recognition and Management of Nighttime Reflux Symptoms
A supplement to Family Practice News supported by Santarus, Inc. The supplement is based on a faculty interview.

To view the supplement, click the image above.
A supplement to Family Practice News supported by Santarus, Inc. The supplement is based on a faculty interview.
To view the supplement, click the image above.
A supplement to Family Practice News supported by Santarus, Inc. The supplement is based on a faculty interview.
To view the supplement, click the image above.

Plastic Surgery Groups Remove Cancer-Implant Webinar After Complaints
Two plastic surgery professional organizations have removed a members-only webinar in the wake of complaints by an advocacy group that the program downplayed the risk of anaplastic large-cell lymphoma (ALCL) in women who have breast implants.
Public Citizens Health Research Group wrote to the Food and Drug Administration on Feb. 17 to urge the agency to take action against the American Society of Plastic Surgeons (ASPS) and the American Society of Aesthetic Plastic Surgery (ASAPS).
The Washington-based nonprofit said that the groups held the webinar in the wake of the FDA’s Jan. 26 announcement that there were a growing number of cases of ALCL in women with implants.
Dr. Jeffrey Shuren, director of the FDA’s Center for Devices and Radiological Health, said in a Feb. 28 letter (pdf) to Public Citizen that it had viewed the webinar and "spoke with representatives of both organizations." Dr. Shuren added that, "They informed us of their plans to remove the webinar from their Web site."
Both organizations said that they were not instructed by the FDA to take the webinar down, but that it was a voluntary decision.
In a March 2 statement, the ASAPS said that it removed the webinar "as newer information became available a week ago." That information, according to ASAPS president Felmont F. Eaves III, is "an independent, systematic review of ALCL, which will be published in an upcoming edition of Plastic and Reconstructive Surgery."
Dr. Eaves said in an interview that the Rand Corp. conducted the review and that it is his understanding that the article will be available some time in June. For the time being, the advanced copy of the article is available only to ASAPS members.
The ASPS said in a March 2 statement, "It was never our intention to downplay the risk of a very rarely occurring cancer associated with breast implants." Rather, said the Society, "We did not want to unnecessarily alarm patients when the risk of ALCL associated with breast implants is so low."
According to Public Citizen, ASPS president Phil Haeck explained in the webinar that ALCL should not be referred to as a tumor or a malignancy, but as a "condition." Dr. Haeck said, "I would recommend that you use the same terms with your patients rather than disturb them by saying this is a cancer, this is a malignancy. The best word is this is a condition," according to Public Citizen. Dr. Haeck added, "And I think you are certainly justified, with what we know now, in downplaying the malignant potential of these."
Public Citizen also objected to the webinar telling members that "surgery was curative," for ALCL.
In his response to Public Citizen, the FDA’s Dr. Shuren said, "the FDA believes the optimal treatment regimen has not been established and that additional data collection is needed to fully understand the possible relationship between ALCL and breast implants, as well as the risk factors, optimal treatment plan, and prognosis."
The FDA is asking health care providers to report confirmed cases of ALCL. The agency also notes that ASPS and others are collaborating with the agency to develop a registry tracking ALCL and implants. ASAPS said in late January that it also is supporting the registry. Details are still being worked out.
Two plastic surgery professional organizations have removed a members-only webinar in the wake of complaints by an advocacy group that the program downplayed the risk of anaplastic large-cell lymphoma (ALCL) in women who have breast implants.
Public Citizens Health Research Group wrote to the Food and Drug Administration on Feb. 17 to urge the agency to take action against the American Society of Plastic Surgeons (ASPS) and the American Society of Aesthetic Plastic Surgery (ASAPS).
The Washington-based nonprofit said that the groups held the webinar in the wake of the FDA’s Jan. 26 announcement that there were a growing number of cases of ALCL in women with implants.
Dr. Jeffrey Shuren, director of the FDA’s Center for Devices and Radiological Health, said in a Feb. 28 letter (pdf) to Public Citizen that it had viewed the webinar and "spoke with representatives of both organizations." Dr. Shuren added that, "They informed us of their plans to remove the webinar from their Web site."
Both organizations said that they were not instructed by the FDA to take the webinar down, but that it was a voluntary decision.
In a March 2 statement, the ASAPS said that it removed the webinar "as newer information became available a week ago." That information, according to ASAPS president Felmont F. Eaves III, is "an independent, systematic review of ALCL, which will be published in an upcoming edition of Plastic and Reconstructive Surgery."
Dr. Eaves said in an interview that the Rand Corp. conducted the review and that it is his understanding that the article will be available some time in June. For the time being, the advanced copy of the article is available only to ASAPS members.
The ASPS said in a March 2 statement, "It was never our intention to downplay the risk of a very rarely occurring cancer associated with breast implants." Rather, said the Society, "We did not want to unnecessarily alarm patients when the risk of ALCL associated with breast implants is so low."
According to Public Citizen, ASPS president Phil Haeck explained in the webinar that ALCL should not be referred to as a tumor or a malignancy, but as a "condition." Dr. Haeck said, "I would recommend that you use the same terms with your patients rather than disturb them by saying this is a cancer, this is a malignancy. The best word is this is a condition," according to Public Citizen. Dr. Haeck added, "And I think you are certainly justified, with what we know now, in downplaying the malignant potential of these."
Public Citizen also objected to the webinar telling members that "surgery was curative," for ALCL.
In his response to Public Citizen, the FDA’s Dr. Shuren said, "the FDA believes the optimal treatment regimen has not been established and that additional data collection is needed to fully understand the possible relationship between ALCL and breast implants, as well as the risk factors, optimal treatment plan, and prognosis."
The FDA is asking health care providers to report confirmed cases of ALCL. The agency also notes that ASPS and others are collaborating with the agency to develop a registry tracking ALCL and implants. ASAPS said in late January that it also is supporting the registry. Details are still being worked out.
Two plastic surgery professional organizations have removed a members-only webinar in the wake of complaints by an advocacy group that the program downplayed the risk of anaplastic large-cell lymphoma (ALCL) in women who have breast implants.
Public Citizens Health Research Group wrote to the Food and Drug Administration on Feb. 17 to urge the agency to take action against the American Society of Plastic Surgeons (ASPS) and the American Society of Aesthetic Plastic Surgery (ASAPS).
The Washington-based nonprofit said that the groups held the webinar in the wake of the FDA’s Jan. 26 announcement that there were a growing number of cases of ALCL in women with implants.
Dr. Jeffrey Shuren, director of the FDA’s Center for Devices and Radiological Health, said in a Feb. 28 letter (pdf) to Public Citizen that it had viewed the webinar and "spoke with representatives of both organizations." Dr. Shuren added that, "They informed us of their plans to remove the webinar from their Web site."
Both organizations said that they were not instructed by the FDA to take the webinar down, but that it was a voluntary decision.
In a March 2 statement, the ASAPS said that it removed the webinar "as newer information became available a week ago." That information, according to ASAPS president Felmont F. Eaves III, is "an independent, systematic review of ALCL, which will be published in an upcoming edition of Plastic and Reconstructive Surgery."
Dr. Eaves said in an interview that the Rand Corp. conducted the review and that it is his understanding that the article will be available some time in June. For the time being, the advanced copy of the article is available only to ASAPS members.
The ASPS said in a March 2 statement, "It was never our intention to downplay the risk of a very rarely occurring cancer associated with breast implants." Rather, said the Society, "We did not want to unnecessarily alarm patients when the risk of ALCL associated with breast implants is so low."
According to Public Citizen, ASPS president Phil Haeck explained in the webinar that ALCL should not be referred to as a tumor or a malignancy, but as a "condition." Dr. Haeck said, "I would recommend that you use the same terms with your patients rather than disturb them by saying this is a cancer, this is a malignancy. The best word is this is a condition," according to Public Citizen. Dr. Haeck added, "And I think you are certainly justified, with what we know now, in downplaying the malignant potential of these."
Public Citizen also objected to the webinar telling members that "surgery was curative," for ALCL.
In his response to Public Citizen, the FDA’s Dr. Shuren said, "the FDA believes the optimal treatment regimen has not been established and that additional data collection is needed to fully understand the possible relationship between ALCL and breast implants, as well as the risk factors, optimal treatment plan, and prognosis."
The FDA is asking health care providers to report confirmed cases of ALCL. The agency also notes that ASPS and others are collaborating with the agency to develop a registry tracking ALCL and implants. ASAPS said in late January that it also is supporting the registry. Details are still being worked out.
Triple Therapy
Dual antiplatelet therapy (DAPT) (aspirin plus a thienopyridine: clopidogrel or prasugrel) has become the standard treatment for patients with acute coronary syndromes (ACS) and after coronary stent placement (Table 1). Anticoagulant therapy with warfarin is indicated for stroke prevention in atrial fibrillation (AF), profound left ventricular dysfunction, and after mechanical heart valve replacement, as well as for treatment of deep venous thrombosis and pulmonary embolism (Table 2). It is estimated that 41% of the U.S. population over age 40 years is on some form of antiplatelet therapy,6 and 2.5 million patients, mostly elderly, are on long‐term warfarin therapy.7 More specifically, 5% of patients undergoing percutaneous coronary interventions (PCIs) also have an indication for warfarin.8 With widespread use of drug‐eluting stents (DES), the need for a longer duration of DAPT, and the increased age and complexity of hospitalized patients, the safety and challenges of triple therapy (combined DAPT and warfarin) have become more important to the practice of hospital medicine. Triple therapy may increase hospitalization rates, as the risk of major bleeding is four to five times higher than with DAPT.911 In contrast, DAPT is much less effective than warfarin alone in preventing embolic events in AF,12 and warfarin alone or in combination with aspirin (ASA) is inadequate therapy to prevent stent thrombosis. Even fewer data exist on the efficacy and safety of triple therapy in patients with mechanical valves or left ventricular dysfunction.
| Class Recommendations | Level of Evidence | |
|---|---|---|
| ||
| DAPT after PCI/stenting1 | ||
| ASA | ||
| Class I | ASA 325 mg/d after PCI for 1 mo (up to 6 mo depending on type of stent implanted) and then 7562 mg/d indefinitely | B |
| Class IIa | ASA 75‐325 mg/d indefinitely after brachytherapy unless risk of bleeding is significant | C |
| In patients at risk of bleeding, a lower dose of 75‐162 mg/d is reasonable after stent implantation | C | |
| Thienopyridine | ||
| Class I | Clopidogrel 75 mg/d after BMS for at least 1 mo and ideally up to 12 mo unless increased risk of bleeding (at least 2 wk) | B |
| Clopidogrel 75 mg/d after DES for at least 12 mo if not at high risk for bleeding | B | |
| 2009 focus update2: Clopidogrel 75 mg daily or prasugrel 10 mg daily for at least 12 mo after BMS or DES for ACS | B | |
| Class IIa | Clopidogrel 75 mg/d indefinitely after brachytherapy unless risk of bleeding is significant | C |
| Class IIb | In patients with potential for lethal or catastrophic stent thrombosis, consider platelet aggregation studies and increase clopidogrel dose to 150 mg/d if 50% inhibition of platelet aggregation is seen | C |
| Continuation of clopidogrel 75 mg/day beyond 12 mo is reasonable after DES | C | |
| 2009 focus update2: consider continuation of clopidogrel or prasugrel beyond 15 mo after DES placement | C | |
| DAPT for UA/NSTEMI without stenting3 | ||
| ASA | ||
| Class I | Continue ASA (75 to 162 mg/d) indefinitely | A |
| Clopidogrel | ||
| Class 1 | Clopidogrel (75 mg/d) for at least 1 mo (A) and ideally for up to 1 y | B |
| Dipyridamole | ||
| Class III | Dipyridamole is not recommended because it has not been shown to be effective | A |
| |
| Condition | Risk (%) |
| Atrial fibrillation (without anticoagulation)4 | |
| Low‐risk atrial fibrillation (CHADS2 score 0) | 1.9 |
| Intermediate‐risk atrial fibrillation (CHADS2 score 1) | 2.8 |
| High‐risk atrial fibrillation (CHADS2 score 2‐6) | 418 |
| Mechanical heart valve5b | |
| Mechanical heart valve (without anticoagulation) | 8.6c |
| Mechanical heart valve (treated with ASA alone) | 7.5c |
| Mechanical heart valve (treated with warfarin) | 1.8c |
| Mechanical aortic valve (treated with warfarin) | 1.1c |
| Mechanical mitral valve (treated with warfarin) | 2.7c |
Hospitalists commonly care for patients on triple therapy; certain indications are appropriate and supported from the available literature while others lack evidence. Knowledge of existing practice guidelines and of supporting research studies leads to optimal management of these complicated patients, and minimizes excessive morbidity from bleeding complications or thromboembolic events such as strokes and stent thrombosis.
In the first part of this article, we present the evidence that supports current recommendations for DAPT or warfarin in specific medical conditions. We also address controversies and unanswered questions. The second part of this review focuses on the available data and provides guidance on the optimal care of patients on triple therapy.
Dual Antiplatelet Therapy Following Acute Coronary Syndromes
Table 3 summarizes key randomized trials of DAPT versus ASA alone in several clinical scenarios. The addition of clopidogrel to ASA in patients with nonST‐elevation ACS reduced the risk of adverse ischemic outcomes in the clopidogrel in unstable angina to prevent recurrent events (CURE) trial,15 as well as in its substudy, the PCI‐CURE (patients with ACS who have undergone stenting).17 In the main CURE study, the study groups diverged within the first 30 days after randomization and the benefit of DAPT persisted throughout the 12 months of the study period. DAPT is also superior to ASA in patients with ST‐elevation myocardial infarction (MI) (CLARITYTIMI 28 and COMMIT trials).13, 14 On the basis of these findings, DAPT has become the standard of care for patients with ACS. The American College of Cardiology (ACC)/American Heart Association (AHA)3 and the European Society of Cardiology18 recommend ASA treatment indefinitely for patients with ACS whether or not they underwent PCI. Clopidogrel is recommended for at least 12 months following ACS, especially for patients who receive a coronary stent.
| Trial | Endpoints | Results |
|---|---|---|
| ||
| ST elevation MI | ||
| CLARITY‐TIMI13 | Incidence of death, infarct‐related artery occlusion, or recurrent MI | 36% reduction (95% CI 2447); P .001 |
| COMMIT14 | Incidence of death, MI, or stroke | 9% reduction (95% CI 314); P .002 |
| ACS without ST elevation | ||
| CURE15 | Incidence of death, MI, or stroke | 20% reduction (RR 0.80 [0.720.90]); P .001 |
| Bare‐metal stent placement | ||
| CREDO16 | Incidence of death, MI, or stroke | 27% reduction (95% CI 3.944.4); P .02 |
| PCI‐CURE17 | Incidence of death, MI, or urgent TVR | 30% reduction (RR 0.70 [0.500.97]); P .03 |
Despite the proven efficacy of DAPT in ACS, about 15% of patients die or experience reinfarction within 30 days of diagnosis.19 The continued risk for thrombotic events could be due to delayed onset of platelet inhibition and to patient heterogeneity in responsiveness to therapy with ASA and/or clopidogrel.20 Consequently, the optimum dose for clopidogrel and ASA following ACS is uncertain. The CURRENT‐OASIS 7 trial evaluated the efficacy and safety of high‐dose clopidogrel (600‐mg loading dose, 150 mg once daily for 7 days, followed by 75 mg/d) versus standard‐dose clopidogrel (300‐mg loading dose, followed by 75 mg/d) and ASA (75‐100 mg versus 300‐325 mg/d) in patients with ACS who were treated medically, with or without stenting.21 In the overall study population as well as in patients who did not receive stenting, there was no significant difference in the combined rate of death from cardiovascular causes, MI, and stroke between patients receiving the high‐dose and the standard‐dose clopidogrel (4.2% vs 4.4%; P = .37) and high‐dose versus low‐dose ASA (4.2% vs 4.4%; P = .47). There were no significant differences in bleeding complications between the two clopidogrel treatment arms or between the high‐dose and low‐dose ASA groups.
The ACC/AHA guidelines recommend ASA, 75‐162 mg/d indefinitely after medical therapy without stenting (class I, level of evidence: A)3 and clopidogrel 75 mg/d for at least 1 month (class IA) and optimally for 1 year (class IB). Clopidogrel monotherapy is appropriate for patients with ACS who are unable to tolerate ASA due to either hypersensitivity or recent significant gastrointestinal bleeding.
As is the case after coronary stenting, interruption of DAPT soon after ACS may subject patients to high recurrence of cardiovascular events, although few data are available to support this observation. Interruption of DAPT due to bleeding complications or surgical procedures more than 1 month after ACS may be reasonable for a patient who did not receive a stent. Clinicians should restart DAPT after the surgical procedure once the bleeding risk becomes acceptable.
Dual Antiplatelet Therapy Following Coronary Stenting
Following Bare Metal Stents
Stent thrombosis occurs in approximately 20% of patients who receive bare metal stents (BMS) without DAPT22; the risk is highest in the first 30 days after implantation. The clinical presentation of stent thrombosis is often catastrophic: MI or sudden death occurs in over 60% of cases. DAPT reduces the incidence of stent thrombosis to a clinically acceptable level.22
In the ISAR trial of 517 patients treated with BMS for MI, suboptimal angioplasty, or other high‐risk clinical and anatomic features,23 patients were randomly assigned to treatment with ASA plus ticlopidine or ASA plus anticoagulation with heparin and warfarin. The primary endpoint of cardiac death, MI, coronary bypass surgery, or repeat angioplasty occurred in 1.5% of patients assigned to DAPT and 6.2% of those assigned to anticoagulant therapy (relative risk [RR], 0.25; 95% confidence interval [CI], 0.06‐0.77). The PCI‐CURE study evaluated patients who received BMS after ACS.17 The primary endpoint was a composite of cardiovascular death, MI, or urgent target‐vessel revascularization within 30 days of PCI. Long‐term administration of clopidogrel (8 months) conferred a lower rate of cardiovascular death, MI, or any revascularization (P = .03), with no significant difference in major bleeding between the groups (P = .64). In the CREDO trial,16 investigators evaluated 2116 patients undergoing PCI at 99 North American centers. Subjects received either a 300‐mg loading dose of clopidogrel or placebo 3‐24 hours before PCI. All patients then received clopidogrel 75 mg/d through day 28. For the following 12 months, patients in the loading dose group received clopidogrel, and those in the control group received placebo. All patients received ASA throughout the study. At 1 year, loading dose plus long‐term clopidogrel therapy conferred a 27% RR reduction (3% absolute risk reduction) in the combined endpoint of death, MI, or stroke (P = .02).
Based on these trials, the ACC and AHA recommend clopidogrel (75 mg/d) for a minimum of 1 month and optimally 12 months after BMS (class 1B).2 For patients at increased risk of bleeding, the ACC/AHA recommends a minimum of 2 weeks of clopidogrel. Although lifelong therapy with ASA is recommended, the optimal dose of ASA after BMS is unknown. However, on the basis of clinical trial protocols (no randomized data), guidelines recommend ASA 162 mg‐325 mg/d for at least 1 month, followed by indefinite use at a dose of 75‐162 mg. In patients for whom there is concern about bleeding, lower doses of ASA (75‐162 mg) are acceptable for the initial period after stent implantation.
Following Drug‐Eluting Stents
Drug‐eluting stents have become the standard percutaneous treatment for patients with symptomatic coronary artery disease. In 2005, a sampling of 140 US hospitals indicated that 94% of patients treated with a stent received at least one DES.24 Compared with BMS, restenosis and the need for revascularization are significantly less frequent. In contrast, unanticipated high rates of very late (>1 year) stent thrombosis have complicated DES.25 Because of the potentially lethal consequences of stent thrombosis, several authors have questioned the long‐term safety of DES2635 and examined the role of extended DAPT in reducing this delayed complication.27, 31, 36 Although the initial pivotal randomized trials of DES mandated clopidogrel use for only 3 months after sirolimus‐eluting stent and 6 months after paclitaxel‐eluting stent,37, 38 current guidelines recommend DAPT for at least 12 months after DES placement for patients who are not at high risk of bleeding.1
Although multiple studies have confirmed the benefit of DAPT, controversy remains regarding the extended use for more than 1 year. The only randomized trial that addressed this issue was nonblinded and underpowered.39 In this study of patients from two ongoing trials, the REAL‐LATE and ZEST‐LATE, extended duration DAPT (>12 months, median duration 19.2 months), did not reduce the incidence of MI and cardiac death.39 The rate of the primary endpoint was less than 25% of that expected (underpowered), and patients had already received clopidogrel for up to 24 months before enrollment.
The results from small, nonrandomized trials regarding this issue have been contradictory. Banerjee and colleagues studied 530 consecutive patients who underwent PCI (85% received a DES), were free of cardiovascular events for 6 months after PCI, and had follow‐up available for >12 months.26 In a multivariate analysis, clopidogrel use for 1 year was associated with lower mortality (hazard ratio [HR], 0.28; 95% CI, 0.140.59); this effect was independent of traditional cardiovascular risk factors, clinical presentation, and DES use. In a study at the Duke Heart Center40 among patients with DES (n = 528) who were event‐free at 12 months, continued clopidogrel use conferred lower rates of death (0% versus 3.5%; difference, 3.5%; 95% CI, 5.9% to 1.1%; P = .004) and death or MI (0% versus 4.5%; difference, 4.5%; 95% CI, 7.1% to 1.9%; P .001) at 24 months. In the TYCOON registry,35 patients with DES receiving clopidogrel for 2 years had a rate of stent thrombosis (0.4%) that was similar to those with BMS (0.7%) but significantly lower than patients with DES and 1‐year DAPT (2.9%).
In contrast, Roy and colleagues33 found that clopidogrel cessation at 12 months did not predict stent thrombosis, and Park and colleagues32 reported that clopidogrel continuation beyond 1 year did not appear to decrease stent thrombosis or clinical events after DES implantation. Similarly, Stone et al.34 performed a landmark analysis on the basis of the prospective, double‐blind TAXUS‐II SR, TAXUS‐IV, and TAXUS‐V trials. The authors found that thienopyridine use beyond 1 year after DES may reduce stent thrombosis over the subsequent 12‐month period, but did not reduce rates of death and MI at 2 and 5 years after either DES or BMS.
Current guidelines recommend ASA 162‐325 mg/d for at least 3‐6 months, followed by treatment indefinitely at a dose of 75‐162 mg daily. Clopidogrel, on the other hand, is given at 75 mg/d for at least 12 months.
Warfarin After Acute Coronary Syndromes
Warfarin with different international normalized ratio (INR) goals alone or in combination with ASA has been evaluated after ACS. In an early trial, patients with recent (mean interval 27 days) MI were treated with warfarin alone versus placebo.41 Warfarin conferred a relative risk reduction in mortality of 24% (95% CI, 4‐44%; P = .027) at the expense of major bleeding rates of 0.6%/y. In the ASPECT trial,42 moderate to high intensity anticoagulation after MI resulted in a 53% and 40% reduction in the relative risk of reinfarction (annual incidence 2.3% versus 5.1%) and cerebrovascular events (annual incidence 0.7% versus 1.2%), respectively. In the WARIS II43 and ASPECT‐244 trials, moderate intensity warfarin (INR 2.0‐2.5) in combination with low‐dose ASA, compared with ASA alone, reduced the composite occurrence of death or nonfatal reinfarction, as well as recurrent coronary occlusion after ST‐segment elevation MI. High‐intensity warfarin therapy alone (INR 3.0‐4.0 for ASPECT, 2.8‐4.2 for WARISII) reduced ischemic vascular events compared with ASA alone. Not unexpectedly, major bleeding episodes were more common among patients receiving warfarin.
No randomized trials have compared DAPT with warfarin plus ASA for patients with ACS who did not receive stents. The ACC/AHA guidelines recommend warfarin for secondary prevention following ACS (class IIb). High‐intensity warfarin alone (INR 2.5‐3.5) or moderate intensity (INR 2.0‐2.5) with low‐dose ASA (75‐81 mg/d) may be reasonable for patients at high ischemic and low bleeding risk who are intolerant of clopidogrel (level of evidence: B). Fixed dose warfarin is not recommended by the ACC/AHA primarily on the basis of the Coumadin Aspirin Reinfarction Study (CARS) results. This study of patients following MI was discontinued prematurely because of a lack of incremental benefit of reduced‐dose ASA (80 mg/d) combined with either 1 or 3 mg of warfarin daily when compared with 160 mg/d of ASA alone.
Triple Therapy for PCI and Atrial Fibrillation
AF is the most frequent indication (70%) for long‐term therapy with warfarin in patients scheduled for stent placement.10 Clinical trials have shown that warfarin alone is superior to ASA, clopidogrel, or DAPT for prevention of stroke in patients with AF.45, 46 Although warfarin is indispensable in these settings, DAPT is similarly necessary after stent implantation. As triple therapy increases the risk of bleeding, the management of patients with AF and who have received stents remains controversial. This situation is particularly problematic among patients who have received DES and may benefit from extended DAPT. No randomized trials exist to clarify the optimal treatment in these patients; and the feasibility of such studies is questionable. Small, mostly retrospective, studies (Table 4) provide limited guidance on this issue; most studies focus on bleeding events rather than the cardiovascular efficacy of triple therapy. Because of these limitations, cardiovascular societies give IIb recommendation for either triple therapy or the combination of warfarin and clopidogrel in this setting and the level of evidence is C.1, 59, 60
| Author | Year | Type | No. | Major Bleeding, % (range) | Thrombotic Events | Comments |
|---|---|---|---|---|---|---|
| ||||||
| Studies of one group (triple therapy group) | ||||||
| Orford et al.47 | 2004 | Obs | 66 | 4.5 (0.211.2) | N/A | Bleeding occurred only with suboptimal control of INR and/or pre‐existing GI disease. |
| Porter et al.48 | 2006 | Obs | 180 | 1.6 (0.04.2) | N/A | Bleeding rates were acceptable with short‐term TT after PCI. |
| Rubboli et al.49 | 2007 | Obs | 49 | 18 (4.436.9) | N/A | Most hemorrhages occurred during TT. |
| Rogacka et al.50 | 2008 | Obs | 127 | 4.7 | N/A | One‐half of bleeding episodes were lethal and 67% occurred within the first month. |
| Studies comparing triple therapy with dual antiplatelet therapy | ||||||
| Mattichak et al.51 | 2005 | Obs | 82 | 21 vs. 3.5 (P = .028)a | Reinfarction (29% vs. 9%, P = .15) | TT did not reduce reinfarction after stenting for MI but increased rates of GI bleeding and transfusions. |
| Khurram et al.11 | 2006 | Matched cohort | 214 | 6.6 vs. 0 (P = .03) | N/A | Higher bleeding rates for TT than DAPT. INR range or ASA dosage did not influence the bleeding risk. |
| DeEugenio et al.9 | 2007 | Matched cohort | 194 | OR 5.0 (1.417.8, P = .012) | N/A | ASA dose, age, sex, BMI, DM, hypertension, and procedural anticoagulant type or use did not influence risk of major bleeding. |
| Ruiz‐Nodar et al.52 | 2008 | Obs | 426 | 14.9 vs. 9.0 (P = .19) | Mortality: OR 3.43 (1.617.54, P = .002)b MACE: OR 4.9 (2.1711.1, P .01)b | TT was associated with a nonsignificant increase in major bleeding but lower all‐cause mortality and fewer MACE. |
| Sarafoff et al.53 | 2008 | Prosp | 515 | 1.4 vs. 3.1 (P = .34). | MACCE: OR 0.76 (0.481.21, P = .25) | No difference in MACCE or bleeding at 2 y. Stent thrombosis did not differ between groups. |
| Rossini et al.54 | 2008 | Prosp | 204 | 10.8 vs. 4.9 (P = .1) | MACE: 5.8% vs. 4.9% (P = .7) | INR was targeted to the lower range (2.0‐2.5). No significant difference in bleeding rates for TT versus DAPT at 18 mo. Less bleeding for patients whose INR was within target (4.9 versus 33%, P = .00019). No significant differences in MACE between groups. |
| Uchida et al.55 | 2010 | Obs | 575 | 18 vs. 2.7 (P .001) | MACE (P = .108) | No differences in MACE rates. More bleeding for patients on TT. |
| Studies comparing triple therapy versus dual antiplatelet therapy versus wararin and single antiplatelet agent | ||||||
| Karjalainen et al.10 | 2007 | Matched cohort | 239 | OR 3.3 (1.38.6, P = .014)c | MACE: OR 1.7 (1.0‐3.0, P = 0.05)c | This study compared patients on warfarin at baseline with those not on warfarinall undergoing stenting. Patients on warfarin at baseline were treated with a variety of strategies. Baseline warfarin use increased both major bleeding and MACE at 1 y. ASA plus warfarin was inadequate to prevent stent thrombosis, and premature warfarin cessation was associated with stroke. |
| Manzano‐Fernandez et al.56 | 2008 | Obs | 104 | EB (5.8 vs. 11.3, P = .33) LB (21.6 vs. 3.8, P = .006)d | MACE: 25.5% vs. 21.0% (P = .53)d | No difference in MACE rates between TT and non‐TT (WAA or DAPT). TT conferred higher late bleeding (>48 h). |
| Gao et al.57 | 2010 | Prosp | 622 | 2.9 vs. 1.8 vs. 2.5 (P = .725)e | MACCE: 8.8% vs. 20.1% vs. 14.9% (P = .010)e | Target INR was set as 1.8‐2.5. Lower stroke and MACCE rates for TT as compared with DAPT or WAA; no difference in bleeding. |
| Studies comparing triple therapy with warfarin and single antiplatelet agent | ||||||
| Nguyen et al.58 | 2007 | Obs | 800 | 5.9 vs. 46 (P = .46) | Death: 5.1% vs. 6.5% (P = .47) Stroke: 0.7% vs. 3.4% (P = .02) MI: 3.3% vs. 4.5% (P = .49) | TT and WAA lead to similar 6‐mo bleeding, death, and MI. Fewer strokes with TT (caveat: low event rate). |
In the largest study to date, Nguyen et al.58 evaluated 800 patients who underwent stenting for ACS and were discharged on warfarin plus single antiplatelet agent or triple therapy as part of the GRACE registry. At 6 months, triple therapy conferred a significant reduction in stroke (0.7% versus 3.4%, P = .02) but not in death or MI. There were no differences in in‐hospital major bleeding events between the two groups (5.9% versus 4.6%; P = .46). Similarly, Sarafoff et al.53 reported no significant differences in the combined endpoint (death, MI, stent thrombosis or stroke) or bleeding complications among patients who received triple therapy or DAPT at 2 years of follow‐up. In contrast, Ruiz‐Nodar et al.52 showed that triple therapy, compared with DAPT, at discharge reduced the incidence of death (17.8% versus 27.8%; adjusted HR = 3.43; 95% CI, 1.617.54; P = .002) and major adverse cardiac events (26.5% versus 38.7%; adjusted HR = 4.9; 95% CI, 2.1711.1; P = .01), without a substantial increase in major bleeding events.
The value of combination antiplatelet therapy to prevent stent thrombosis in these patients is clearer in the study reported by Karjalainen et al.10 This case‐control study of 239 patients receiving warfarin at baseline who underwent PCI evaluated a primary endpoint of death, MI, target‐vessel revascularization, or stent thrombosis and a secondary endpoint of major bleeding and stroke to 12 months of follow‐up. Forty‐eight percent of patients received triple therapy, whereas 15.5% were discharged on DAPT. The remaining patients received warfarin plus a single antiplatelet agent. Stent thrombosis occurred more frequently among patients receiving warfarin plus ASA (15.2%) than among those receiving triple therapy (1.9%). As expected, stroke was more frequent in patients treated with DAPT (8.8%) than among those receiving triple therapy (2.8%). Major bleeding was similar between groups. Therapy with warfarin was an independent predictor of both major bleeding and major cardiac events at 1 year. This observation illustrates that the outcome of PCI in patients on chronic warfarin therapy is unsatisfactory irrespective of the antithrombotic combinations used, highlighting the need for better strategies to treat these patients.
Choice of Therapy and Management of Patients Eligible for Triple Therapy
Current guidelines for PCI do not provide guidance for patients with an indication for triple therapy due to a paucity of published evidence. Several ongoing prospective trials aim to address the management of these patients (AFCAS, ISAR‐TRIPLE). Pending further study, clinicians should consider the embolic risk (CHADS2 score), target INR, type of stent, bleeding risk, and duration of treatment when determining the appropriate antiplatelet/anticoagulant combinations. The CHADS2 score (Table 2) stratifies the risk for stroke among patients with AF,4 while the Outpatient Bleeding Risk Index (OBRI) allows estimation of bleeding risk.12, 61 The OBRI considers age > 65 years, prior stroke, prior gastrointestinal bleeding, and any of four comorbidities (recent MI, anemia, diabetes, or renal insufficiency) in order to stratify patients into three risk groups.61 Patients with three to four risk factors have a high risk of bleeding (23% at 3 months and 48% at 12 months) whereas patients with no risk factors have only a 3% risk of bleeding at 12 months. Unfortunately, advanced age and prior stroke appear in both OBRI and CHADS.
For patients with AF who are at high risk for embolic stroke (>3% per year), we recommend triple therapy for the shortest time possible, followed by warfarin and ASA indefinitely. In case of BMS, it is acceptable to shorten triple therapy duration to 1 month. The optimal duration of triple therapy for patients with DES is uncertain; recommended durations range from 3 months to 1 year.62 If the potential consequences of stent thrombosis are high due to a large amount of myocardium at risk, an extended period of triple therapy might be justified. For patients whose stroke risk is lower (CHADS2 score of 0‐1), the risk for bleeding likely outweighs any benefit from stroke prevention. In this instance, it is reasonable to use DAPT with ASA and clopidogrel for 1 month after BMS and 12 months after DES, followed by ASA, with or without warfarin, indefinitely. In a recently published study, patients with AF and a CHADS2 score of 1 had a yearly stroke risk of 1.25% while taking DAPT63; the risk of major bleeding for triple therapy is 6.1% per year.64
For patients who have a high bleeding risk, BMS are the preferred stent type as the duration of triple therapy might be limited to 4 weeks. To our knowledge, no randomized study has evaluated the outcome of patients with BMS compared with DES who also have an indication for warfarin. Because studies have suggested that clopidogrel is more effective than aspirin in preventing stent thrombosis and in reducing death or MI after coronary stenting,40, 65 warfarin and single antiplatelet therapy with clopidogrel might be a reasonable treatment option in patients with high bleeding risk. The WOEST study (NCT00769938), currently recruiting participants, is the first randomized study specifically designed to test this hypothesis.
Since gastrointestinal bleeding accounts for approximately 30‐40% of hemorrhagic events in patients on combined ASA and anticoagulant therapy, an expert consensus document recommended concomitant treatment with proton pump inhibitors (PPIs) to reduce this risk.66 In contrast, the 2009 Focused Updates of the ACC/AHA/SCAI Guidelines did not recommend the use of PPIs with DAPT in the setting of ACS.2 This is because of studies that show inhibition of platelet activation,67 and potential clinical harm,68 when clopidogrel is combined with certain PPIs that inhibit the CYP2C19 enzyme. However, to date there are no convincing randomized clinical trial data documenting an important clinical drug‐drug interaction. The U.S. Food and Drug Administration (FDA) advises that physicians avoid the use of clopidogrel in patients with impaired CYP2C19 function due to known genetic variation or due to concomitant use of drugs that inhibit CYP2C19 activity. More specifically, the FDA recommends avoiding the use of omeprazole and esomeprazole in patients taking clopidogrel.69
In particular, elderly patients have an increased risk of bleeding while receiving triple therapy. In a study of patients over age 65, 2.5% were hospitalized for bleeding in the first year after PCI, and the use of triple therapy was the strongest predictor of bleeding (more than threefold increase).70 One in five patients suffered death or MI at 1 year after hospitalization for bleeding.70 The basis for poor outcomes after hospitalization for bleeding in this population is multifactorial and may be due to the location of bleeding, associated hypercoagulable state, potential adverse impact of blood transfusion, withdrawal of warfarin therapy in patients with AF and PCI, and the premature discontinuation of DAPT. The use of nonsteroidal anti‐inflammatory drugs (NSAIDs) is common among the elderly and conferred a doubling of bleeding risk.70 Limiting the use of NSAID, the use of low‐dose ASA beyond 30 days after stent implantation, greater use of BMS, and maintaining INR at the lowest possible level (INR of 22.5) will reduce the risk for bleeding.57, 71
New Anticoagulants
Due to the high risk for bleeding with warfarin and the challenges inherent in INR monitoring, researchers have developed several novel anticoagulants whose advantages include fixed daily dosing and no need for monitoring. Dabigatran is a direct oral thrombin inhibitor that is already licensed in Europe and Canada for thromboprophylaxis after hip or knee surgery. It has also been studied in patients with AF. In the RE‐LY trial, patients with AF who received dabigatran 110 mg daily had rates of stroke and systemic embolism that were similar to those with warfarin, as well as lower rates of major hemorrhage.72 The randomized ReDEEM trial, reported at the AHA 2009 Scientific Sessions, was aimed at finding a dosage of dabigatran that achieves a good balance between clinical effectiveness and bleeding risk when combined with aspirin and clopidogrel after acute MI. Dosages ranging from 50 mg twice daily to 150 mg twice daily were all associated with 6‐month rates of bleeding lower than 2%. Hospitalists should view these encouraging results cautiously until the publication of ReDEEM trial results in a peer‐reviewed journal.
A variety of oral Xa antagonists are also being evaluated in patients with AF or ACS. These trials offer insight into triple therapy regimens that include ASA, clopidogrel, and an Xa antagonist. In a recent study of the oral Xa antagonist rivaroxaban, investigators stratified 3491 subjects with ACS according to whether they received concomitant ASA alone or ASA and clopidogrel.73 Subjects receiving ASA plus rivaroxaban had a modest increase in bleeding. Triple therapy, however, increased the composite bleeding rate from 3.5% in the DAPT group to approximately 6‐15% (low‐dose or high‐dose rivaroxaban, respectively). Rivaroxaban is currently under review by the FDA.
These novel agents might eventually replace warfarin for many or most indications for anticoagulation. It is imperative that future research compare the efficacy and risk of bleeding between triple therapy using these new agents and triple therapy with warfarin.
Conclusions
The management of patients on long‐term anticoagulation who require DAPT because of ACS or coronary stenting is challenging. DAPT may safely substitute for warfarin only for patients at low risk for a thromboembolic event (ie, low‐risk AF with low CHADS2 score). Clinicians should not interrupt warfarin in patients at higher risk (ie, intermediate to high‐risk AF, mechanical valves, or recent venous thromboembolism), even in the presence of DAPT. In these patients, triple therapy is the optimal approach following coronary stenting (and possibly during the initial period after ACS without stenting). As this approach confers a fivefold increase in bleeding complications compared with DAPT, careful monitoring of the INR, the addition of PPIs, and the exclusion of elderly patients who are at the highest risk for bleeding complications74 is recommended. The preferred duration of triple therapy after BMS in patients who require long‐term anticoagulation is 1 month, whereas the optimal duration after ACS or DES remains unresolved.
- ,,, et al.2007 Focused Update of the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, Writing on Behalf of the 2005 Writing Committee.Circulation2008;117:261–295.
- ,,, et al.2009 Focused Updates: ACC/AHA Guidelines for the Management of Patients With ST‐Elevation Myocardial Infarction (updating the 2004 Guideline and 2007 Focused Update) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (updating the 2005 Guideline and 2007 Focused Update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.Circulation2009;120:2271–2306.
- ,,, et al.ACC/AHA 2007 guidelines for the management of patients with unstable angina/non‐ST‐Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non‐ST‐Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine.J Am Coll Cardiol2007;50:e1–e157.
- ,,, et al.Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin.Circulation2004;110:2287–2292.
- ,,.Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses.Circulation1994;89:635–641.
- ,,,,.Aspirin use among adults aged 40 and older in the United States: results of a national survey.Am J Prev Med2007;32:403–407.
- ,,, et al.The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition).Chest2008;133:299S–339S.
- ,,, et al.Discharge antithrombotic strategies among patients with acute coronary syndrome previously on warfarin anticoagulation: physician practice in the CRUSADE registry.Am Heart J2008;155:361–368.
- ,,, et al.Risk of major bleeding with concomitant dual antiplatelet therapy after percutaneous coronary intervention in patients receiving long‐term warfarin therapy.Pharmacotherapy2007;27:691–696.
- ,,, et al.Safety and efficacy of combined antiplatelet‐warfarin therapy after coronary stenting.Eur Heart J2007;28:726–732.
- ,,, et al.Combination therapy with aspirin, clopidogrel and warfarin following coronary stenting is associated with a significant risk of bleeding.J Invasive Cardiol2006;18:162–164.
- ,,,,,.Development of a contemporary bleeding risk model for elderly warfarin recipients.Chest2006;130:1390–1396.
- ,,, et al.Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST‐segment elevation.N Engl J Med2005;352:1179–1189.
- ,,, et al.Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo‐controlled trial.Lancet2005;366:1607–1621.
- ,,,,,.Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST‐segment elevation.N Engl J Med2001;345:494–502.
- ,,, et al.Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial.JAMA2002;288:2411–2420.
- ,,, et al.Effects of pretreatment with clopidogrel and aspirin followed by long‐term therapy in patients undergoing percutaneous coronary intervention: the PCI‐CURE study.Lancet2001;358:527–533.
- ,,, et al.Guidelines for the diagnosis and treatment of non‐ST‐segment elevation acute coronary syndromes.Eur Heart J2007;28:1598–1660.
- .Burden of disease: medical and economic impact of acute coronary syndromes.Am J Manag Care2006;12:S430–S434.
- ,,,,,.Variability in platelet responsiveness to clopidogrel among 544 individuals.J Am Coll Cardiol2005;45:246–251.
- ,,, et al.Dose comparisons of clopidogrel and aspirin in acute coronary syndromes.N Engl J Med2010;363:930–942.
- ,,, et al.A clinical trial comparing three antithrombotic‐drug regimens after coronary‐artery stenting. Stent Anticoagulation Restenosis Study Investigators.N Engl J Med1998;339:1665–1671.
- ,,, et al.A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary‐artery stents.N Engl J Med1996;334:1084–1089.
- ,,.Outcomes of 6906 patients undergoing percutaneous coronary intervention in the era of drug‐eluting stents: report of the DEScover Registry.Circulation2006;114:2154–2162.
- ,,, et al.Safety and efficacy of sirolimus‐ and paclitaxel‐eluting coronary stents.N Engl J Med2007;356:998–1008.
- ,,, et al.Comparison of the impact of short (1 year) and long‐term (> or =1 year) clopidogrel use following percutaneous coronary intervention on mortality.Am J Cardiol2008;102:1159–1162.
- ,,.Stent thrombosis late after implantation of first‐generation drug‐eluting stents: a cause for concern.Circulation2007;115:1440–1455; discussion 55.
- ,,, et al.Early and late coronary stent thrombosis of sirolimus‐eluting and paclitaxel‐eluting stents in routine clinical practice: data from a large two‐institutional cohort study.Lancet2007;369:667–678.
- ,,, et al.Analysis of 14 trials comparing sirolimus‐eluting stents with bare‐metal stents.N Engl J Med2007;356:1030–1039.
- ,,,,,.Long‐term outcomes with drug‐eluting stents versus bare‐metal stents in Sweden.N Engl J Med2007;356:1009–1019.
- ,,,,,.Stent thrombosis in randomized clinical trials of drug‐eluting stents.N Engl J Med2007;356:1020–1029.
- ,,, et al.Stent thrombosis, clinical events, and influence of prolonged clopidogrel use after placement of drug‐eluting stent data from an observational cohort study of drug‐eluting versus bare‐metal stents.JACC Cardiovasc Interv2008;1:494–503.
- ,,, et al.Temporal relation between Clopidogrel cessation and stent thrombosis after drug‐eluting stent implantation.Am J Cardiol2009;103:801–805.
- ,,, et al.Effect of prolonged thienopyridine use after drug‐eluting stent implantation (from the TAXUS landmark trials data).Am J Cardiol2008;102:1017–1022.
- ,,, et al.Effectiveness of two‐year clopidogrel + aspirin in abolishing the risk of very late thrombosis after drug‐eluting stent implantation (from the TYCOON [two‐year ClOpidOgrel need] study).Am J Cardiol2009;104:1357–1361.
- ,,.Mortality in randomized controlled trials comparing drug‐eluting vs. bare metal stents in coronary artery disease: a meta‐analysis.Eur Heart J2006;27:2784–2814.
- ,,, et al.Sirolimus‐eluting stents versus standard stents in patients with stenosis in a native coronary artery.N Engl J Med2003;349:1315–1323.
- ,,, et al.A polymer‐based, paclitaxel‐eluting stent in patients with coronary artery disease.N Engl J Med2004;350:221–231.
- ,,, et al.Duration of dual antiplatelet therapy after implantation of drug‐eluting stents.N Engl J Med2010;362:1374–1382.
- ,,, et al.Clopidogrel use and long‐term clinical outcomes after drug‐eluting stent implantation.JAMA2007;297:159–168.
- ,,.The effect of warfarin on mortality and reinfarction after myocardial infarction.N Engl J Med1990;323:147–152.
- Effect of long‐term oral anticoagulant treatment on mortality and cardiovascular morbidity after myocardial infarction.Anticoagulants in the Secondary Prevention of Events in Coronary Thrombosis (ASPECT) Research Group.Lancet1994;343:499–503.
- ,,,,.Warfarin, aspirin, or both after myocardial infarction.N Engl J Med2002;347:969–974.
- ,,,,.Aspirin and coumadin after acute coronary syndromes (the ASPECT‐2 study): a randomised controlled trial.Lancet2002;360:109–113.
- ,,, et al.Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial.Lancet2006;367:1903–1912.
- ,,,.Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta‐analysis.Ann Intern Med1999;131:492–501.
- ,,, et al.Safety and efficacy of aspirin, clopidogrel, and warfarin after coronary stent placement in patients with an indication for anticoagulation.Am Heart J2004;147:463–467.
- ,,,,,.Short‐term triple therapy with aspirin, warfarin, and a thienopyridine among patients undergoing percutaneous coronary intervention.Catheter Cardiovasc Interv2006;68:56–61.
- ,,,,.Periprocedural and medium‐term antithrombotic strategies in patients with an indication for long‐term anticoagulation undergoing coronary angiography and intervention.Coron Artery Dis2007;18:193–199.
- ,,, et al.Dual antiplatelet therapy after percutaneous coronary intervention with stent implantation in patients taking chronic oral anticoagulation.JACC Cardiovasc Interv2008;1:56–61.
- ,,,,,.Evaluation of safety of warfarin in combination with antiplatelet therapy for patients treated with coronary stents for acute myocardial infarction.J Interv Cardiol2005;18:163–166.
- ,,, et al.Anticoagulant and antiplatelet therapy use in 426 patients with atrial fibrillation undergoing percutaneous coronary intervention and stent implantation implications for bleeding risk and prognosis.J Am Coll Cardiol2008;51:818–825.
- ,,, et al.Aspirin and clopidogrel with or without phenprocoumon after drug eluting coronary stent placement in patients on chronic oral anticoagulation.J Intern Med2008;264:472–480.
- ,,, et al.Long‐term outcomes in patients undergoing coronary stenting on dual oral antiplatelet treatment requiring oral anticoagulant therapy.Am J Cardiol2008;102:1618–1623.
- ,,,,.Impact of anticoagulant therapy with dual antiplatelet therapy on prognosis after treatment with drug‐eluting coronary stents.J Cardiol2010;55:362–369.
- ,,, et al.Increased major bleeding complications related to triple antithrombotic therapy usage in patients with atrial fibrillation undergoing percutaneous coronary artery stenting.Chest2008;134:559–567.
- ,,, et al.Comparison of different antithrombotic regimens for patients with atrial fibrillation undergoing drug‐eluting stent implantation.Circ J2010;74:701–708.
- ,,, et al.Combining warfarin and antiplatelet therapy after coronary stenting in the Global Registry of Acute Coronary Events: is it safe and effective to use just one antiplatelet agent?Eur Heart J2007;28:1717–1722.
- ,,, et al.2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST‐elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol2008;51:210–247.
- ,,, et al.Guidelines for percutaneous coronary interventions. The Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology.Eur Heart J2005;26:804–847.
- ,,.Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin.Am J Med1998;105:91–99.
- ,,,.Coronary stents and chronic anticoagulation.Circulation2009;119:1682–1688.
- ,,, et al.Risks and benefits of oral anticoagulation compared with clopidogrel plus aspirin in patients with atrial fibrillation according to stroke risk: the atrial fibrillation clopidogrel trial with irbesartan for prevention of vascular events (ACTIVE‐W).Stroke2008;39:1482–1486.
- ,,, et al.Early and late increased bleeding rates after angioplasty and stenting due to combined antiplatelet and anticoagulanttherapy.EuroIntervention2009;5:425–431.
- ,,, et al.Late clinical events after clopidogrel discontinuation may limit the benefit of drug‐eluting stents: an observational study of drug‐eluting versus bare‐metal stents.J Am Coll Cardiol2006;48:2584–2591.
- ,,, et al.ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents.Circulation2008;118:1894–1909.
- ,,, et al.Influence of omeprazole on the antiplatelet action of clopidogrel associated with aspirin: the randomized, double‐blind OCLA (Omeprazole CLopidogrel Aspirin) study.J Am Coll Cardiol2008;51:256–260.
- ,,, et al.Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome.JAMA2009;301:937–944.
- Follow‐Up to the January 26,2009, Early Communication about an Ongoing Safety Review of Clopidogrel Bisulfate (marketed as Plavix) and Omeprazole (marketed as Prilosec and Prilosec OTC). 11/17/2009. (Accessed at http://www.fda.gov/Drugs/DrugSafety/Postmarket DrugSafetyInformationforPatientsandProviders/DrugSafetyInformationfor HeathcareProfessionals/ucm190784.htm.)
- ,,, et al.Incidence, predictors, and prognostic implications of hospitalization for late bleeding after percutaneous coronary intervention for patients older than 65 years.Circ Cardiovasc Interv2010;3:140–147.
- ,,, et al.Antithrombotic therapy in patients treated with oral anticoagulation undergoing coronary artery stenting. An expert consensus document with focus on atrial fibrillation.Ann Med2008;40:428–436.
- ,,, et al.Dabigatran versus warfarin in patients with atrial fibrillation.N Engl J Med2009;361:1139–1151.
- ,,, et al.Rivaroxaban versus placebo in patients with acute coronary syndromes (ATLAS ACS‐TIMI 46): a randomised, double‐blind, phase II trial.Lancet2009;374:29–38.
- ,,,.Bleeding complications associated with combinations of aspirin, thienopyridine derivatives, and warfarin in elderly patients following acute myocardial infarction.Arch Intern Med2005;165:784–789.
Dual antiplatelet therapy (DAPT) (aspirin plus a thienopyridine: clopidogrel or prasugrel) has become the standard treatment for patients with acute coronary syndromes (ACS) and after coronary stent placement (Table 1). Anticoagulant therapy with warfarin is indicated for stroke prevention in atrial fibrillation (AF), profound left ventricular dysfunction, and after mechanical heart valve replacement, as well as for treatment of deep venous thrombosis and pulmonary embolism (Table 2). It is estimated that 41% of the U.S. population over age 40 years is on some form of antiplatelet therapy,6 and 2.5 million patients, mostly elderly, are on long‐term warfarin therapy.7 More specifically, 5% of patients undergoing percutaneous coronary interventions (PCIs) also have an indication for warfarin.8 With widespread use of drug‐eluting stents (DES), the need for a longer duration of DAPT, and the increased age and complexity of hospitalized patients, the safety and challenges of triple therapy (combined DAPT and warfarin) have become more important to the practice of hospital medicine. Triple therapy may increase hospitalization rates, as the risk of major bleeding is four to five times higher than with DAPT.911 In contrast, DAPT is much less effective than warfarin alone in preventing embolic events in AF,12 and warfarin alone or in combination with aspirin (ASA) is inadequate therapy to prevent stent thrombosis. Even fewer data exist on the efficacy and safety of triple therapy in patients with mechanical valves or left ventricular dysfunction.
| Class Recommendations | Level of Evidence | |
|---|---|---|
| ||
| DAPT after PCI/stenting1 | ||
| ASA | ||
| Class I | ASA 325 mg/d after PCI for 1 mo (up to 6 mo depending on type of stent implanted) and then 7562 mg/d indefinitely | B |
| Class IIa | ASA 75‐325 mg/d indefinitely after brachytherapy unless risk of bleeding is significant | C |
| In patients at risk of bleeding, a lower dose of 75‐162 mg/d is reasonable after stent implantation | C | |
| Thienopyridine | ||
| Class I | Clopidogrel 75 mg/d after BMS for at least 1 mo and ideally up to 12 mo unless increased risk of bleeding (at least 2 wk) | B |
| Clopidogrel 75 mg/d after DES for at least 12 mo if not at high risk for bleeding | B | |
| 2009 focus update2: Clopidogrel 75 mg daily or prasugrel 10 mg daily for at least 12 mo after BMS or DES for ACS | B | |
| Class IIa | Clopidogrel 75 mg/d indefinitely after brachytherapy unless risk of bleeding is significant | C |
| Class IIb | In patients with potential for lethal or catastrophic stent thrombosis, consider platelet aggregation studies and increase clopidogrel dose to 150 mg/d if 50% inhibition of platelet aggregation is seen | C |
| Continuation of clopidogrel 75 mg/day beyond 12 mo is reasonable after DES | C | |
| 2009 focus update2: consider continuation of clopidogrel or prasugrel beyond 15 mo after DES placement | C | |
| DAPT for UA/NSTEMI without stenting3 | ||
| ASA | ||
| Class I | Continue ASA (75 to 162 mg/d) indefinitely | A |
| Clopidogrel | ||
| Class 1 | Clopidogrel (75 mg/d) for at least 1 mo (A) and ideally for up to 1 y | B |
| Dipyridamole | ||
| Class III | Dipyridamole is not recommended because it has not been shown to be effective | A |
| |
| Condition | Risk (%) |
| Atrial fibrillation (without anticoagulation)4 | |
| Low‐risk atrial fibrillation (CHADS2 score 0) | 1.9 |
| Intermediate‐risk atrial fibrillation (CHADS2 score 1) | 2.8 |
| High‐risk atrial fibrillation (CHADS2 score 2‐6) | 418 |
| Mechanical heart valve5b | |
| Mechanical heart valve (without anticoagulation) | 8.6c |
| Mechanical heart valve (treated with ASA alone) | 7.5c |
| Mechanical heart valve (treated with warfarin) | 1.8c |
| Mechanical aortic valve (treated with warfarin) | 1.1c |
| Mechanical mitral valve (treated with warfarin) | 2.7c |
Hospitalists commonly care for patients on triple therapy; certain indications are appropriate and supported from the available literature while others lack evidence. Knowledge of existing practice guidelines and of supporting research studies leads to optimal management of these complicated patients, and minimizes excessive morbidity from bleeding complications or thromboembolic events such as strokes and stent thrombosis.
In the first part of this article, we present the evidence that supports current recommendations for DAPT or warfarin in specific medical conditions. We also address controversies and unanswered questions. The second part of this review focuses on the available data and provides guidance on the optimal care of patients on triple therapy.
Dual Antiplatelet Therapy Following Acute Coronary Syndromes
Table 3 summarizes key randomized trials of DAPT versus ASA alone in several clinical scenarios. The addition of clopidogrel to ASA in patients with nonST‐elevation ACS reduced the risk of adverse ischemic outcomes in the clopidogrel in unstable angina to prevent recurrent events (CURE) trial,15 as well as in its substudy, the PCI‐CURE (patients with ACS who have undergone stenting).17 In the main CURE study, the study groups diverged within the first 30 days after randomization and the benefit of DAPT persisted throughout the 12 months of the study period. DAPT is also superior to ASA in patients with ST‐elevation myocardial infarction (MI) (CLARITYTIMI 28 and COMMIT trials).13, 14 On the basis of these findings, DAPT has become the standard of care for patients with ACS. The American College of Cardiology (ACC)/American Heart Association (AHA)3 and the European Society of Cardiology18 recommend ASA treatment indefinitely for patients with ACS whether or not they underwent PCI. Clopidogrel is recommended for at least 12 months following ACS, especially for patients who receive a coronary stent.
| Trial | Endpoints | Results |
|---|---|---|
| ||
| ST elevation MI | ||
| CLARITY‐TIMI13 | Incidence of death, infarct‐related artery occlusion, or recurrent MI | 36% reduction (95% CI 2447); P .001 |
| COMMIT14 | Incidence of death, MI, or stroke | 9% reduction (95% CI 314); P .002 |
| ACS without ST elevation | ||
| CURE15 | Incidence of death, MI, or stroke | 20% reduction (RR 0.80 [0.720.90]); P .001 |
| Bare‐metal stent placement | ||
| CREDO16 | Incidence of death, MI, or stroke | 27% reduction (95% CI 3.944.4); P .02 |
| PCI‐CURE17 | Incidence of death, MI, or urgent TVR | 30% reduction (RR 0.70 [0.500.97]); P .03 |
Despite the proven efficacy of DAPT in ACS, about 15% of patients die or experience reinfarction within 30 days of diagnosis.19 The continued risk for thrombotic events could be due to delayed onset of platelet inhibition and to patient heterogeneity in responsiveness to therapy with ASA and/or clopidogrel.20 Consequently, the optimum dose for clopidogrel and ASA following ACS is uncertain. The CURRENT‐OASIS 7 trial evaluated the efficacy and safety of high‐dose clopidogrel (600‐mg loading dose, 150 mg once daily for 7 days, followed by 75 mg/d) versus standard‐dose clopidogrel (300‐mg loading dose, followed by 75 mg/d) and ASA (75‐100 mg versus 300‐325 mg/d) in patients with ACS who were treated medically, with or without stenting.21 In the overall study population as well as in patients who did not receive stenting, there was no significant difference in the combined rate of death from cardiovascular causes, MI, and stroke between patients receiving the high‐dose and the standard‐dose clopidogrel (4.2% vs 4.4%; P = .37) and high‐dose versus low‐dose ASA (4.2% vs 4.4%; P = .47). There were no significant differences in bleeding complications between the two clopidogrel treatment arms or between the high‐dose and low‐dose ASA groups.
The ACC/AHA guidelines recommend ASA, 75‐162 mg/d indefinitely after medical therapy without stenting (class I, level of evidence: A)3 and clopidogrel 75 mg/d for at least 1 month (class IA) and optimally for 1 year (class IB). Clopidogrel monotherapy is appropriate for patients with ACS who are unable to tolerate ASA due to either hypersensitivity or recent significant gastrointestinal bleeding.
As is the case after coronary stenting, interruption of DAPT soon after ACS may subject patients to high recurrence of cardiovascular events, although few data are available to support this observation. Interruption of DAPT due to bleeding complications or surgical procedures more than 1 month after ACS may be reasonable for a patient who did not receive a stent. Clinicians should restart DAPT after the surgical procedure once the bleeding risk becomes acceptable.
Dual Antiplatelet Therapy Following Coronary Stenting
Following Bare Metal Stents
Stent thrombosis occurs in approximately 20% of patients who receive bare metal stents (BMS) without DAPT22; the risk is highest in the first 30 days after implantation. The clinical presentation of stent thrombosis is often catastrophic: MI or sudden death occurs in over 60% of cases. DAPT reduces the incidence of stent thrombosis to a clinically acceptable level.22
In the ISAR trial of 517 patients treated with BMS for MI, suboptimal angioplasty, or other high‐risk clinical and anatomic features,23 patients were randomly assigned to treatment with ASA plus ticlopidine or ASA plus anticoagulation with heparin and warfarin. The primary endpoint of cardiac death, MI, coronary bypass surgery, or repeat angioplasty occurred in 1.5% of patients assigned to DAPT and 6.2% of those assigned to anticoagulant therapy (relative risk [RR], 0.25; 95% confidence interval [CI], 0.06‐0.77). The PCI‐CURE study evaluated patients who received BMS after ACS.17 The primary endpoint was a composite of cardiovascular death, MI, or urgent target‐vessel revascularization within 30 days of PCI. Long‐term administration of clopidogrel (8 months) conferred a lower rate of cardiovascular death, MI, or any revascularization (P = .03), with no significant difference in major bleeding between the groups (P = .64). In the CREDO trial,16 investigators evaluated 2116 patients undergoing PCI at 99 North American centers. Subjects received either a 300‐mg loading dose of clopidogrel or placebo 3‐24 hours before PCI. All patients then received clopidogrel 75 mg/d through day 28. For the following 12 months, patients in the loading dose group received clopidogrel, and those in the control group received placebo. All patients received ASA throughout the study. At 1 year, loading dose plus long‐term clopidogrel therapy conferred a 27% RR reduction (3% absolute risk reduction) in the combined endpoint of death, MI, or stroke (P = .02).
Based on these trials, the ACC and AHA recommend clopidogrel (75 mg/d) for a minimum of 1 month and optimally 12 months after BMS (class 1B).2 For patients at increased risk of bleeding, the ACC/AHA recommends a minimum of 2 weeks of clopidogrel. Although lifelong therapy with ASA is recommended, the optimal dose of ASA after BMS is unknown. However, on the basis of clinical trial protocols (no randomized data), guidelines recommend ASA 162 mg‐325 mg/d for at least 1 month, followed by indefinite use at a dose of 75‐162 mg. In patients for whom there is concern about bleeding, lower doses of ASA (75‐162 mg) are acceptable for the initial period after stent implantation.
Following Drug‐Eluting Stents
Drug‐eluting stents have become the standard percutaneous treatment for patients with symptomatic coronary artery disease. In 2005, a sampling of 140 US hospitals indicated that 94% of patients treated with a stent received at least one DES.24 Compared with BMS, restenosis and the need for revascularization are significantly less frequent. In contrast, unanticipated high rates of very late (>1 year) stent thrombosis have complicated DES.25 Because of the potentially lethal consequences of stent thrombosis, several authors have questioned the long‐term safety of DES2635 and examined the role of extended DAPT in reducing this delayed complication.27, 31, 36 Although the initial pivotal randomized trials of DES mandated clopidogrel use for only 3 months after sirolimus‐eluting stent and 6 months after paclitaxel‐eluting stent,37, 38 current guidelines recommend DAPT for at least 12 months after DES placement for patients who are not at high risk of bleeding.1
Although multiple studies have confirmed the benefit of DAPT, controversy remains regarding the extended use for more than 1 year. The only randomized trial that addressed this issue was nonblinded and underpowered.39 In this study of patients from two ongoing trials, the REAL‐LATE and ZEST‐LATE, extended duration DAPT (>12 months, median duration 19.2 months), did not reduce the incidence of MI and cardiac death.39 The rate of the primary endpoint was less than 25% of that expected (underpowered), and patients had already received clopidogrel for up to 24 months before enrollment.
The results from small, nonrandomized trials regarding this issue have been contradictory. Banerjee and colleagues studied 530 consecutive patients who underwent PCI (85% received a DES), were free of cardiovascular events for 6 months after PCI, and had follow‐up available for >12 months.26 In a multivariate analysis, clopidogrel use for 1 year was associated with lower mortality (hazard ratio [HR], 0.28; 95% CI, 0.140.59); this effect was independent of traditional cardiovascular risk factors, clinical presentation, and DES use. In a study at the Duke Heart Center40 among patients with DES (n = 528) who were event‐free at 12 months, continued clopidogrel use conferred lower rates of death (0% versus 3.5%; difference, 3.5%; 95% CI, 5.9% to 1.1%; P = .004) and death or MI (0% versus 4.5%; difference, 4.5%; 95% CI, 7.1% to 1.9%; P .001) at 24 months. In the TYCOON registry,35 patients with DES receiving clopidogrel for 2 years had a rate of stent thrombosis (0.4%) that was similar to those with BMS (0.7%) but significantly lower than patients with DES and 1‐year DAPT (2.9%).
In contrast, Roy and colleagues33 found that clopidogrel cessation at 12 months did not predict stent thrombosis, and Park and colleagues32 reported that clopidogrel continuation beyond 1 year did not appear to decrease stent thrombosis or clinical events after DES implantation. Similarly, Stone et al.34 performed a landmark analysis on the basis of the prospective, double‐blind TAXUS‐II SR, TAXUS‐IV, and TAXUS‐V trials. The authors found that thienopyridine use beyond 1 year after DES may reduce stent thrombosis over the subsequent 12‐month period, but did not reduce rates of death and MI at 2 and 5 years after either DES or BMS.
Current guidelines recommend ASA 162‐325 mg/d for at least 3‐6 months, followed by treatment indefinitely at a dose of 75‐162 mg daily. Clopidogrel, on the other hand, is given at 75 mg/d for at least 12 months.
Warfarin After Acute Coronary Syndromes
Warfarin with different international normalized ratio (INR) goals alone or in combination with ASA has been evaluated after ACS. In an early trial, patients with recent (mean interval 27 days) MI were treated with warfarin alone versus placebo.41 Warfarin conferred a relative risk reduction in mortality of 24% (95% CI, 4‐44%; P = .027) at the expense of major bleeding rates of 0.6%/y. In the ASPECT trial,42 moderate to high intensity anticoagulation after MI resulted in a 53% and 40% reduction in the relative risk of reinfarction (annual incidence 2.3% versus 5.1%) and cerebrovascular events (annual incidence 0.7% versus 1.2%), respectively. In the WARIS II43 and ASPECT‐244 trials, moderate intensity warfarin (INR 2.0‐2.5) in combination with low‐dose ASA, compared with ASA alone, reduced the composite occurrence of death or nonfatal reinfarction, as well as recurrent coronary occlusion after ST‐segment elevation MI. High‐intensity warfarin therapy alone (INR 3.0‐4.0 for ASPECT, 2.8‐4.2 for WARISII) reduced ischemic vascular events compared with ASA alone. Not unexpectedly, major bleeding episodes were more common among patients receiving warfarin.
No randomized trials have compared DAPT with warfarin plus ASA for patients with ACS who did not receive stents. The ACC/AHA guidelines recommend warfarin for secondary prevention following ACS (class IIb). High‐intensity warfarin alone (INR 2.5‐3.5) or moderate intensity (INR 2.0‐2.5) with low‐dose ASA (75‐81 mg/d) may be reasonable for patients at high ischemic and low bleeding risk who are intolerant of clopidogrel (level of evidence: B). Fixed dose warfarin is not recommended by the ACC/AHA primarily on the basis of the Coumadin Aspirin Reinfarction Study (CARS) results. This study of patients following MI was discontinued prematurely because of a lack of incremental benefit of reduced‐dose ASA (80 mg/d) combined with either 1 or 3 mg of warfarin daily when compared with 160 mg/d of ASA alone.
Triple Therapy for PCI and Atrial Fibrillation
AF is the most frequent indication (70%) for long‐term therapy with warfarin in patients scheduled for stent placement.10 Clinical trials have shown that warfarin alone is superior to ASA, clopidogrel, or DAPT for prevention of stroke in patients with AF.45, 46 Although warfarin is indispensable in these settings, DAPT is similarly necessary after stent implantation. As triple therapy increases the risk of bleeding, the management of patients with AF and who have received stents remains controversial. This situation is particularly problematic among patients who have received DES and may benefit from extended DAPT. No randomized trials exist to clarify the optimal treatment in these patients; and the feasibility of such studies is questionable. Small, mostly retrospective, studies (Table 4) provide limited guidance on this issue; most studies focus on bleeding events rather than the cardiovascular efficacy of triple therapy. Because of these limitations, cardiovascular societies give IIb recommendation for either triple therapy or the combination of warfarin and clopidogrel in this setting and the level of evidence is C.1, 59, 60
| Author | Year | Type | No. | Major Bleeding, % (range) | Thrombotic Events | Comments |
|---|---|---|---|---|---|---|
| ||||||
| Studies of one group (triple therapy group) | ||||||
| Orford et al.47 | 2004 | Obs | 66 | 4.5 (0.211.2) | N/A | Bleeding occurred only with suboptimal control of INR and/or pre‐existing GI disease. |
| Porter et al.48 | 2006 | Obs | 180 | 1.6 (0.04.2) | N/A | Bleeding rates were acceptable with short‐term TT after PCI. |
| Rubboli et al.49 | 2007 | Obs | 49 | 18 (4.436.9) | N/A | Most hemorrhages occurred during TT. |
| Rogacka et al.50 | 2008 | Obs | 127 | 4.7 | N/A | One‐half of bleeding episodes were lethal and 67% occurred within the first month. |
| Studies comparing triple therapy with dual antiplatelet therapy | ||||||
| Mattichak et al.51 | 2005 | Obs | 82 | 21 vs. 3.5 (P = .028)a | Reinfarction (29% vs. 9%, P = .15) | TT did not reduce reinfarction after stenting for MI but increased rates of GI bleeding and transfusions. |
| Khurram et al.11 | 2006 | Matched cohort | 214 | 6.6 vs. 0 (P = .03) | N/A | Higher bleeding rates for TT than DAPT. INR range or ASA dosage did not influence the bleeding risk. |
| DeEugenio et al.9 | 2007 | Matched cohort | 194 | OR 5.0 (1.417.8, P = .012) | N/A | ASA dose, age, sex, BMI, DM, hypertension, and procedural anticoagulant type or use did not influence risk of major bleeding. |
| Ruiz‐Nodar et al.52 | 2008 | Obs | 426 | 14.9 vs. 9.0 (P = .19) | Mortality: OR 3.43 (1.617.54, P = .002)b MACE: OR 4.9 (2.1711.1, P .01)b | TT was associated with a nonsignificant increase in major bleeding but lower all‐cause mortality and fewer MACE. |
| Sarafoff et al.53 | 2008 | Prosp | 515 | 1.4 vs. 3.1 (P = .34). | MACCE: OR 0.76 (0.481.21, P = .25) | No difference in MACCE or bleeding at 2 y. Stent thrombosis did not differ between groups. |
| Rossini et al.54 | 2008 | Prosp | 204 | 10.8 vs. 4.9 (P = .1) | MACE: 5.8% vs. 4.9% (P = .7) | INR was targeted to the lower range (2.0‐2.5). No significant difference in bleeding rates for TT versus DAPT at 18 mo. Less bleeding for patients whose INR was within target (4.9 versus 33%, P = .00019). No significant differences in MACE between groups. |
| Uchida et al.55 | 2010 | Obs | 575 | 18 vs. 2.7 (P .001) | MACE (P = .108) | No differences in MACE rates. More bleeding for patients on TT. |
| Studies comparing triple therapy versus dual antiplatelet therapy versus wararin and single antiplatelet agent | ||||||
| Karjalainen et al.10 | 2007 | Matched cohort | 239 | OR 3.3 (1.38.6, P = .014)c | MACE: OR 1.7 (1.0‐3.0, P = 0.05)c | This study compared patients on warfarin at baseline with those not on warfarinall undergoing stenting. Patients on warfarin at baseline were treated with a variety of strategies. Baseline warfarin use increased both major bleeding and MACE at 1 y. ASA plus warfarin was inadequate to prevent stent thrombosis, and premature warfarin cessation was associated with stroke. |
| Manzano‐Fernandez et al.56 | 2008 | Obs | 104 | EB (5.8 vs. 11.3, P = .33) LB (21.6 vs. 3.8, P = .006)d | MACE: 25.5% vs. 21.0% (P = .53)d | No difference in MACE rates between TT and non‐TT (WAA or DAPT). TT conferred higher late bleeding (>48 h). |
| Gao et al.57 | 2010 | Prosp | 622 | 2.9 vs. 1.8 vs. 2.5 (P = .725)e | MACCE: 8.8% vs. 20.1% vs. 14.9% (P = .010)e | Target INR was set as 1.8‐2.5. Lower stroke and MACCE rates for TT as compared with DAPT or WAA; no difference in bleeding. |
| Studies comparing triple therapy with warfarin and single antiplatelet agent | ||||||
| Nguyen et al.58 | 2007 | Obs | 800 | 5.9 vs. 46 (P = .46) | Death: 5.1% vs. 6.5% (P = .47) Stroke: 0.7% vs. 3.4% (P = .02) MI: 3.3% vs. 4.5% (P = .49) | TT and WAA lead to similar 6‐mo bleeding, death, and MI. Fewer strokes with TT (caveat: low event rate). |
In the largest study to date, Nguyen et al.58 evaluated 800 patients who underwent stenting for ACS and were discharged on warfarin plus single antiplatelet agent or triple therapy as part of the GRACE registry. At 6 months, triple therapy conferred a significant reduction in stroke (0.7% versus 3.4%, P = .02) but not in death or MI. There were no differences in in‐hospital major bleeding events between the two groups (5.9% versus 4.6%; P = .46). Similarly, Sarafoff et al.53 reported no significant differences in the combined endpoint (death, MI, stent thrombosis or stroke) or bleeding complications among patients who received triple therapy or DAPT at 2 years of follow‐up. In contrast, Ruiz‐Nodar et al.52 showed that triple therapy, compared with DAPT, at discharge reduced the incidence of death (17.8% versus 27.8%; adjusted HR = 3.43; 95% CI, 1.617.54; P = .002) and major adverse cardiac events (26.5% versus 38.7%; adjusted HR = 4.9; 95% CI, 2.1711.1; P = .01), without a substantial increase in major bleeding events.
The value of combination antiplatelet therapy to prevent stent thrombosis in these patients is clearer in the study reported by Karjalainen et al.10 This case‐control study of 239 patients receiving warfarin at baseline who underwent PCI evaluated a primary endpoint of death, MI, target‐vessel revascularization, or stent thrombosis and a secondary endpoint of major bleeding and stroke to 12 months of follow‐up. Forty‐eight percent of patients received triple therapy, whereas 15.5% were discharged on DAPT. The remaining patients received warfarin plus a single antiplatelet agent. Stent thrombosis occurred more frequently among patients receiving warfarin plus ASA (15.2%) than among those receiving triple therapy (1.9%). As expected, stroke was more frequent in patients treated with DAPT (8.8%) than among those receiving triple therapy (2.8%). Major bleeding was similar between groups. Therapy with warfarin was an independent predictor of both major bleeding and major cardiac events at 1 year. This observation illustrates that the outcome of PCI in patients on chronic warfarin therapy is unsatisfactory irrespective of the antithrombotic combinations used, highlighting the need for better strategies to treat these patients.
Choice of Therapy and Management of Patients Eligible for Triple Therapy
Current guidelines for PCI do not provide guidance for patients with an indication for triple therapy due to a paucity of published evidence. Several ongoing prospective trials aim to address the management of these patients (AFCAS, ISAR‐TRIPLE). Pending further study, clinicians should consider the embolic risk (CHADS2 score), target INR, type of stent, bleeding risk, and duration of treatment when determining the appropriate antiplatelet/anticoagulant combinations. The CHADS2 score (Table 2) stratifies the risk for stroke among patients with AF,4 while the Outpatient Bleeding Risk Index (OBRI) allows estimation of bleeding risk.12, 61 The OBRI considers age > 65 years, prior stroke, prior gastrointestinal bleeding, and any of four comorbidities (recent MI, anemia, diabetes, or renal insufficiency) in order to stratify patients into three risk groups.61 Patients with three to four risk factors have a high risk of bleeding (23% at 3 months and 48% at 12 months) whereas patients with no risk factors have only a 3% risk of bleeding at 12 months. Unfortunately, advanced age and prior stroke appear in both OBRI and CHADS.
For patients with AF who are at high risk for embolic stroke (>3% per year), we recommend triple therapy for the shortest time possible, followed by warfarin and ASA indefinitely. In case of BMS, it is acceptable to shorten triple therapy duration to 1 month. The optimal duration of triple therapy for patients with DES is uncertain; recommended durations range from 3 months to 1 year.62 If the potential consequences of stent thrombosis are high due to a large amount of myocardium at risk, an extended period of triple therapy might be justified. For patients whose stroke risk is lower (CHADS2 score of 0‐1), the risk for bleeding likely outweighs any benefit from stroke prevention. In this instance, it is reasonable to use DAPT with ASA and clopidogrel for 1 month after BMS and 12 months after DES, followed by ASA, with or without warfarin, indefinitely. In a recently published study, patients with AF and a CHADS2 score of 1 had a yearly stroke risk of 1.25% while taking DAPT63; the risk of major bleeding for triple therapy is 6.1% per year.64
For patients who have a high bleeding risk, BMS are the preferred stent type as the duration of triple therapy might be limited to 4 weeks. To our knowledge, no randomized study has evaluated the outcome of patients with BMS compared with DES who also have an indication for warfarin. Because studies have suggested that clopidogrel is more effective than aspirin in preventing stent thrombosis and in reducing death or MI after coronary stenting,40, 65 warfarin and single antiplatelet therapy with clopidogrel might be a reasonable treatment option in patients with high bleeding risk. The WOEST study (NCT00769938), currently recruiting participants, is the first randomized study specifically designed to test this hypothesis.
Since gastrointestinal bleeding accounts for approximately 30‐40% of hemorrhagic events in patients on combined ASA and anticoagulant therapy, an expert consensus document recommended concomitant treatment with proton pump inhibitors (PPIs) to reduce this risk.66 In contrast, the 2009 Focused Updates of the ACC/AHA/SCAI Guidelines did not recommend the use of PPIs with DAPT in the setting of ACS.2 This is because of studies that show inhibition of platelet activation,67 and potential clinical harm,68 when clopidogrel is combined with certain PPIs that inhibit the CYP2C19 enzyme. However, to date there are no convincing randomized clinical trial data documenting an important clinical drug‐drug interaction. The U.S. Food and Drug Administration (FDA) advises that physicians avoid the use of clopidogrel in patients with impaired CYP2C19 function due to known genetic variation or due to concomitant use of drugs that inhibit CYP2C19 activity. More specifically, the FDA recommends avoiding the use of omeprazole and esomeprazole in patients taking clopidogrel.69
In particular, elderly patients have an increased risk of bleeding while receiving triple therapy. In a study of patients over age 65, 2.5% were hospitalized for bleeding in the first year after PCI, and the use of triple therapy was the strongest predictor of bleeding (more than threefold increase).70 One in five patients suffered death or MI at 1 year after hospitalization for bleeding.70 The basis for poor outcomes after hospitalization for bleeding in this population is multifactorial and may be due to the location of bleeding, associated hypercoagulable state, potential adverse impact of blood transfusion, withdrawal of warfarin therapy in patients with AF and PCI, and the premature discontinuation of DAPT. The use of nonsteroidal anti‐inflammatory drugs (NSAIDs) is common among the elderly and conferred a doubling of bleeding risk.70 Limiting the use of NSAID, the use of low‐dose ASA beyond 30 days after stent implantation, greater use of BMS, and maintaining INR at the lowest possible level (INR of 22.5) will reduce the risk for bleeding.57, 71
New Anticoagulants
Due to the high risk for bleeding with warfarin and the challenges inherent in INR monitoring, researchers have developed several novel anticoagulants whose advantages include fixed daily dosing and no need for monitoring. Dabigatran is a direct oral thrombin inhibitor that is already licensed in Europe and Canada for thromboprophylaxis after hip or knee surgery. It has also been studied in patients with AF. In the RE‐LY trial, patients with AF who received dabigatran 110 mg daily had rates of stroke and systemic embolism that were similar to those with warfarin, as well as lower rates of major hemorrhage.72 The randomized ReDEEM trial, reported at the AHA 2009 Scientific Sessions, was aimed at finding a dosage of dabigatran that achieves a good balance between clinical effectiveness and bleeding risk when combined with aspirin and clopidogrel after acute MI. Dosages ranging from 50 mg twice daily to 150 mg twice daily were all associated with 6‐month rates of bleeding lower than 2%. Hospitalists should view these encouraging results cautiously until the publication of ReDEEM trial results in a peer‐reviewed journal.
A variety of oral Xa antagonists are also being evaluated in patients with AF or ACS. These trials offer insight into triple therapy regimens that include ASA, clopidogrel, and an Xa antagonist. In a recent study of the oral Xa antagonist rivaroxaban, investigators stratified 3491 subjects with ACS according to whether they received concomitant ASA alone or ASA and clopidogrel.73 Subjects receiving ASA plus rivaroxaban had a modest increase in bleeding. Triple therapy, however, increased the composite bleeding rate from 3.5% in the DAPT group to approximately 6‐15% (low‐dose or high‐dose rivaroxaban, respectively). Rivaroxaban is currently under review by the FDA.
These novel agents might eventually replace warfarin for many or most indications for anticoagulation. It is imperative that future research compare the efficacy and risk of bleeding between triple therapy using these new agents and triple therapy with warfarin.
Conclusions
The management of patients on long‐term anticoagulation who require DAPT because of ACS or coronary stenting is challenging. DAPT may safely substitute for warfarin only for patients at low risk for a thromboembolic event (ie, low‐risk AF with low CHADS2 score). Clinicians should not interrupt warfarin in patients at higher risk (ie, intermediate to high‐risk AF, mechanical valves, or recent venous thromboembolism), even in the presence of DAPT. In these patients, triple therapy is the optimal approach following coronary stenting (and possibly during the initial period after ACS without stenting). As this approach confers a fivefold increase in bleeding complications compared with DAPT, careful monitoring of the INR, the addition of PPIs, and the exclusion of elderly patients who are at the highest risk for bleeding complications74 is recommended. The preferred duration of triple therapy after BMS in patients who require long‐term anticoagulation is 1 month, whereas the optimal duration after ACS or DES remains unresolved.
Dual antiplatelet therapy (DAPT) (aspirin plus a thienopyridine: clopidogrel or prasugrel) has become the standard treatment for patients with acute coronary syndromes (ACS) and after coronary stent placement (Table 1). Anticoagulant therapy with warfarin is indicated for stroke prevention in atrial fibrillation (AF), profound left ventricular dysfunction, and after mechanical heart valve replacement, as well as for treatment of deep venous thrombosis and pulmonary embolism (Table 2). It is estimated that 41% of the U.S. population over age 40 years is on some form of antiplatelet therapy,6 and 2.5 million patients, mostly elderly, are on long‐term warfarin therapy.7 More specifically, 5% of patients undergoing percutaneous coronary interventions (PCIs) also have an indication for warfarin.8 With widespread use of drug‐eluting stents (DES), the need for a longer duration of DAPT, and the increased age and complexity of hospitalized patients, the safety and challenges of triple therapy (combined DAPT and warfarin) have become more important to the practice of hospital medicine. Triple therapy may increase hospitalization rates, as the risk of major bleeding is four to five times higher than with DAPT.911 In contrast, DAPT is much less effective than warfarin alone in preventing embolic events in AF,12 and warfarin alone or in combination with aspirin (ASA) is inadequate therapy to prevent stent thrombosis. Even fewer data exist on the efficacy and safety of triple therapy in patients with mechanical valves or left ventricular dysfunction.
| Class Recommendations | Level of Evidence | |
|---|---|---|
| ||
| DAPT after PCI/stenting1 | ||
| ASA | ||
| Class I | ASA 325 mg/d after PCI for 1 mo (up to 6 mo depending on type of stent implanted) and then 7562 mg/d indefinitely | B |
| Class IIa | ASA 75‐325 mg/d indefinitely after brachytherapy unless risk of bleeding is significant | C |
| In patients at risk of bleeding, a lower dose of 75‐162 mg/d is reasonable after stent implantation | C | |
| Thienopyridine | ||
| Class I | Clopidogrel 75 mg/d after BMS for at least 1 mo and ideally up to 12 mo unless increased risk of bleeding (at least 2 wk) | B |
| Clopidogrel 75 mg/d after DES for at least 12 mo if not at high risk for bleeding | B | |
| 2009 focus update2: Clopidogrel 75 mg daily or prasugrel 10 mg daily for at least 12 mo after BMS or DES for ACS | B | |
| Class IIa | Clopidogrel 75 mg/d indefinitely after brachytherapy unless risk of bleeding is significant | C |
| Class IIb | In patients with potential for lethal or catastrophic stent thrombosis, consider platelet aggregation studies and increase clopidogrel dose to 150 mg/d if 50% inhibition of platelet aggregation is seen | C |
| Continuation of clopidogrel 75 mg/day beyond 12 mo is reasonable after DES | C | |
| 2009 focus update2: consider continuation of clopidogrel or prasugrel beyond 15 mo after DES placement | C | |
| DAPT for UA/NSTEMI without stenting3 | ||
| ASA | ||
| Class I | Continue ASA (75 to 162 mg/d) indefinitely | A |
| Clopidogrel | ||
| Class 1 | Clopidogrel (75 mg/d) for at least 1 mo (A) and ideally for up to 1 y | B |
| Dipyridamole | ||
| Class III | Dipyridamole is not recommended because it has not been shown to be effective | A |
| |
| Condition | Risk (%) |
| Atrial fibrillation (without anticoagulation)4 | |
| Low‐risk atrial fibrillation (CHADS2 score 0) | 1.9 |
| Intermediate‐risk atrial fibrillation (CHADS2 score 1) | 2.8 |
| High‐risk atrial fibrillation (CHADS2 score 2‐6) | 418 |
| Mechanical heart valve5b | |
| Mechanical heart valve (without anticoagulation) | 8.6c |
| Mechanical heart valve (treated with ASA alone) | 7.5c |
| Mechanical heart valve (treated with warfarin) | 1.8c |
| Mechanical aortic valve (treated with warfarin) | 1.1c |
| Mechanical mitral valve (treated with warfarin) | 2.7c |
Hospitalists commonly care for patients on triple therapy; certain indications are appropriate and supported from the available literature while others lack evidence. Knowledge of existing practice guidelines and of supporting research studies leads to optimal management of these complicated patients, and minimizes excessive morbidity from bleeding complications or thromboembolic events such as strokes and stent thrombosis.
In the first part of this article, we present the evidence that supports current recommendations for DAPT or warfarin in specific medical conditions. We also address controversies and unanswered questions. The second part of this review focuses on the available data and provides guidance on the optimal care of patients on triple therapy.
Dual Antiplatelet Therapy Following Acute Coronary Syndromes
Table 3 summarizes key randomized trials of DAPT versus ASA alone in several clinical scenarios. The addition of clopidogrel to ASA in patients with nonST‐elevation ACS reduced the risk of adverse ischemic outcomes in the clopidogrel in unstable angina to prevent recurrent events (CURE) trial,15 as well as in its substudy, the PCI‐CURE (patients with ACS who have undergone stenting).17 In the main CURE study, the study groups diverged within the first 30 days after randomization and the benefit of DAPT persisted throughout the 12 months of the study period. DAPT is also superior to ASA in patients with ST‐elevation myocardial infarction (MI) (CLARITYTIMI 28 and COMMIT trials).13, 14 On the basis of these findings, DAPT has become the standard of care for patients with ACS. The American College of Cardiology (ACC)/American Heart Association (AHA)3 and the European Society of Cardiology18 recommend ASA treatment indefinitely for patients with ACS whether or not they underwent PCI. Clopidogrel is recommended for at least 12 months following ACS, especially for patients who receive a coronary stent.
| Trial | Endpoints | Results |
|---|---|---|
| ||
| ST elevation MI | ||
| CLARITY‐TIMI13 | Incidence of death, infarct‐related artery occlusion, or recurrent MI | 36% reduction (95% CI 2447); P .001 |
| COMMIT14 | Incidence of death, MI, or stroke | 9% reduction (95% CI 314); P .002 |
| ACS without ST elevation | ||
| CURE15 | Incidence of death, MI, or stroke | 20% reduction (RR 0.80 [0.720.90]); P .001 |
| Bare‐metal stent placement | ||
| CREDO16 | Incidence of death, MI, or stroke | 27% reduction (95% CI 3.944.4); P .02 |
| PCI‐CURE17 | Incidence of death, MI, or urgent TVR | 30% reduction (RR 0.70 [0.500.97]); P .03 |
Despite the proven efficacy of DAPT in ACS, about 15% of patients die or experience reinfarction within 30 days of diagnosis.19 The continued risk for thrombotic events could be due to delayed onset of platelet inhibition and to patient heterogeneity in responsiveness to therapy with ASA and/or clopidogrel.20 Consequently, the optimum dose for clopidogrel and ASA following ACS is uncertain. The CURRENT‐OASIS 7 trial evaluated the efficacy and safety of high‐dose clopidogrel (600‐mg loading dose, 150 mg once daily for 7 days, followed by 75 mg/d) versus standard‐dose clopidogrel (300‐mg loading dose, followed by 75 mg/d) and ASA (75‐100 mg versus 300‐325 mg/d) in patients with ACS who were treated medically, with or without stenting.21 In the overall study population as well as in patients who did not receive stenting, there was no significant difference in the combined rate of death from cardiovascular causes, MI, and stroke between patients receiving the high‐dose and the standard‐dose clopidogrel (4.2% vs 4.4%; P = .37) and high‐dose versus low‐dose ASA (4.2% vs 4.4%; P = .47). There were no significant differences in bleeding complications between the two clopidogrel treatment arms or between the high‐dose and low‐dose ASA groups.
The ACC/AHA guidelines recommend ASA, 75‐162 mg/d indefinitely after medical therapy without stenting (class I, level of evidence: A)3 and clopidogrel 75 mg/d for at least 1 month (class IA) and optimally for 1 year (class IB). Clopidogrel monotherapy is appropriate for patients with ACS who are unable to tolerate ASA due to either hypersensitivity or recent significant gastrointestinal bleeding.
As is the case after coronary stenting, interruption of DAPT soon after ACS may subject patients to high recurrence of cardiovascular events, although few data are available to support this observation. Interruption of DAPT due to bleeding complications or surgical procedures more than 1 month after ACS may be reasonable for a patient who did not receive a stent. Clinicians should restart DAPT after the surgical procedure once the bleeding risk becomes acceptable.
Dual Antiplatelet Therapy Following Coronary Stenting
Following Bare Metal Stents
Stent thrombosis occurs in approximately 20% of patients who receive bare metal stents (BMS) without DAPT22; the risk is highest in the first 30 days after implantation. The clinical presentation of stent thrombosis is often catastrophic: MI or sudden death occurs in over 60% of cases. DAPT reduces the incidence of stent thrombosis to a clinically acceptable level.22
In the ISAR trial of 517 patients treated with BMS for MI, suboptimal angioplasty, or other high‐risk clinical and anatomic features,23 patients were randomly assigned to treatment with ASA plus ticlopidine or ASA plus anticoagulation with heparin and warfarin. The primary endpoint of cardiac death, MI, coronary bypass surgery, or repeat angioplasty occurred in 1.5% of patients assigned to DAPT and 6.2% of those assigned to anticoagulant therapy (relative risk [RR], 0.25; 95% confidence interval [CI], 0.06‐0.77). The PCI‐CURE study evaluated patients who received BMS after ACS.17 The primary endpoint was a composite of cardiovascular death, MI, or urgent target‐vessel revascularization within 30 days of PCI. Long‐term administration of clopidogrel (8 months) conferred a lower rate of cardiovascular death, MI, or any revascularization (P = .03), with no significant difference in major bleeding between the groups (P = .64). In the CREDO trial,16 investigators evaluated 2116 patients undergoing PCI at 99 North American centers. Subjects received either a 300‐mg loading dose of clopidogrel or placebo 3‐24 hours before PCI. All patients then received clopidogrel 75 mg/d through day 28. For the following 12 months, patients in the loading dose group received clopidogrel, and those in the control group received placebo. All patients received ASA throughout the study. At 1 year, loading dose plus long‐term clopidogrel therapy conferred a 27% RR reduction (3% absolute risk reduction) in the combined endpoint of death, MI, or stroke (P = .02).
Based on these trials, the ACC and AHA recommend clopidogrel (75 mg/d) for a minimum of 1 month and optimally 12 months after BMS (class 1B).2 For patients at increased risk of bleeding, the ACC/AHA recommends a minimum of 2 weeks of clopidogrel. Although lifelong therapy with ASA is recommended, the optimal dose of ASA after BMS is unknown. However, on the basis of clinical trial protocols (no randomized data), guidelines recommend ASA 162 mg‐325 mg/d for at least 1 month, followed by indefinite use at a dose of 75‐162 mg. In patients for whom there is concern about bleeding, lower doses of ASA (75‐162 mg) are acceptable for the initial period after stent implantation.
Following Drug‐Eluting Stents
Drug‐eluting stents have become the standard percutaneous treatment for patients with symptomatic coronary artery disease. In 2005, a sampling of 140 US hospitals indicated that 94% of patients treated with a stent received at least one DES.24 Compared with BMS, restenosis and the need for revascularization are significantly less frequent. In contrast, unanticipated high rates of very late (>1 year) stent thrombosis have complicated DES.25 Because of the potentially lethal consequences of stent thrombosis, several authors have questioned the long‐term safety of DES2635 and examined the role of extended DAPT in reducing this delayed complication.27, 31, 36 Although the initial pivotal randomized trials of DES mandated clopidogrel use for only 3 months after sirolimus‐eluting stent and 6 months after paclitaxel‐eluting stent,37, 38 current guidelines recommend DAPT for at least 12 months after DES placement for patients who are not at high risk of bleeding.1
Although multiple studies have confirmed the benefit of DAPT, controversy remains regarding the extended use for more than 1 year. The only randomized trial that addressed this issue was nonblinded and underpowered.39 In this study of patients from two ongoing trials, the REAL‐LATE and ZEST‐LATE, extended duration DAPT (>12 months, median duration 19.2 months), did not reduce the incidence of MI and cardiac death.39 The rate of the primary endpoint was less than 25% of that expected (underpowered), and patients had already received clopidogrel for up to 24 months before enrollment.
The results from small, nonrandomized trials regarding this issue have been contradictory. Banerjee and colleagues studied 530 consecutive patients who underwent PCI (85% received a DES), were free of cardiovascular events for 6 months after PCI, and had follow‐up available for >12 months.26 In a multivariate analysis, clopidogrel use for 1 year was associated with lower mortality (hazard ratio [HR], 0.28; 95% CI, 0.140.59); this effect was independent of traditional cardiovascular risk factors, clinical presentation, and DES use. In a study at the Duke Heart Center40 among patients with DES (n = 528) who were event‐free at 12 months, continued clopidogrel use conferred lower rates of death (0% versus 3.5%; difference, 3.5%; 95% CI, 5.9% to 1.1%; P = .004) and death or MI (0% versus 4.5%; difference, 4.5%; 95% CI, 7.1% to 1.9%; P .001) at 24 months. In the TYCOON registry,35 patients with DES receiving clopidogrel for 2 years had a rate of stent thrombosis (0.4%) that was similar to those with BMS (0.7%) but significantly lower than patients with DES and 1‐year DAPT (2.9%).
In contrast, Roy and colleagues33 found that clopidogrel cessation at 12 months did not predict stent thrombosis, and Park and colleagues32 reported that clopidogrel continuation beyond 1 year did not appear to decrease stent thrombosis or clinical events after DES implantation. Similarly, Stone et al.34 performed a landmark analysis on the basis of the prospective, double‐blind TAXUS‐II SR, TAXUS‐IV, and TAXUS‐V trials. The authors found that thienopyridine use beyond 1 year after DES may reduce stent thrombosis over the subsequent 12‐month period, but did not reduce rates of death and MI at 2 and 5 years after either DES or BMS.
Current guidelines recommend ASA 162‐325 mg/d for at least 3‐6 months, followed by treatment indefinitely at a dose of 75‐162 mg daily. Clopidogrel, on the other hand, is given at 75 mg/d for at least 12 months.
Warfarin After Acute Coronary Syndromes
Warfarin with different international normalized ratio (INR) goals alone or in combination with ASA has been evaluated after ACS. In an early trial, patients with recent (mean interval 27 days) MI were treated with warfarin alone versus placebo.41 Warfarin conferred a relative risk reduction in mortality of 24% (95% CI, 4‐44%; P = .027) at the expense of major bleeding rates of 0.6%/y. In the ASPECT trial,42 moderate to high intensity anticoagulation after MI resulted in a 53% and 40% reduction in the relative risk of reinfarction (annual incidence 2.3% versus 5.1%) and cerebrovascular events (annual incidence 0.7% versus 1.2%), respectively. In the WARIS II43 and ASPECT‐244 trials, moderate intensity warfarin (INR 2.0‐2.5) in combination with low‐dose ASA, compared with ASA alone, reduced the composite occurrence of death or nonfatal reinfarction, as well as recurrent coronary occlusion after ST‐segment elevation MI. High‐intensity warfarin therapy alone (INR 3.0‐4.0 for ASPECT, 2.8‐4.2 for WARISII) reduced ischemic vascular events compared with ASA alone. Not unexpectedly, major bleeding episodes were more common among patients receiving warfarin.
No randomized trials have compared DAPT with warfarin plus ASA for patients with ACS who did not receive stents. The ACC/AHA guidelines recommend warfarin for secondary prevention following ACS (class IIb). High‐intensity warfarin alone (INR 2.5‐3.5) or moderate intensity (INR 2.0‐2.5) with low‐dose ASA (75‐81 mg/d) may be reasonable for patients at high ischemic and low bleeding risk who are intolerant of clopidogrel (level of evidence: B). Fixed dose warfarin is not recommended by the ACC/AHA primarily on the basis of the Coumadin Aspirin Reinfarction Study (CARS) results. This study of patients following MI was discontinued prematurely because of a lack of incremental benefit of reduced‐dose ASA (80 mg/d) combined with either 1 or 3 mg of warfarin daily when compared with 160 mg/d of ASA alone.
Triple Therapy for PCI and Atrial Fibrillation
AF is the most frequent indication (70%) for long‐term therapy with warfarin in patients scheduled for stent placement.10 Clinical trials have shown that warfarin alone is superior to ASA, clopidogrel, or DAPT for prevention of stroke in patients with AF.45, 46 Although warfarin is indispensable in these settings, DAPT is similarly necessary after stent implantation. As triple therapy increases the risk of bleeding, the management of patients with AF and who have received stents remains controversial. This situation is particularly problematic among patients who have received DES and may benefit from extended DAPT. No randomized trials exist to clarify the optimal treatment in these patients; and the feasibility of such studies is questionable. Small, mostly retrospective, studies (Table 4) provide limited guidance on this issue; most studies focus on bleeding events rather than the cardiovascular efficacy of triple therapy. Because of these limitations, cardiovascular societies give IIb recommendation for either triple therapy or the combination of warfarin and clopidogrel in this setting and the level of evidence is C.1, 59, 60
| Author | Year | Type | No. | Major Bleeding, % (range) | Thrombotic Events | Comments |
|---|---|---|---|---|---|---|
| ||||||
| Studies of one group (triple therapy group) | ||||||
| Orford et al.47 | 2004 | Obs | 66 | 4.5 (0.211.2) | N/A | Bleeding occurred only with suboptimal control of INR and/or pre‐existing GI disease. |
| Porter et al.48 | 2006 | Obs | 180 | 1.6 (0.04.2) | N/A | Bleeding rates were acceptable with short‐term TT after PCI. |
| Rubboli et al.49 | 2007 | Obs | 49 | 18 (4.436.9) | N/A | Most hemorrhages occurred during TT. |
| Rogacka et al.50 | 2008 | Obs | 127 | 4.7 | N/A | One‐half of bleeding episodes were lethal and 67% occurred within the first month. |
| Studies comparing triple therapy with dual antiplatelet therapy | ||||||
| Mattichak et al.51 | 2005 | Obs | 82 | 21 vs. 3.5 (P = .028)a | Reinfarction (29% vs. 9%, P = .15) | TT did not reduce reinfarction after stenting for MI but increased rates of GI bleeding and transfusions. |
| Khurram et al.11 | 2006 | Matched cohort | 214 | 6.6 vs. 0 (P = .03) | N/A | Higher bleeding rates for TT than DAPT. INR range or ASA dosage did not influence the bleeding risk. |
| DeEugenio et al.9 | 2007 | Matched cohort | 194 | OR 5.0 (1.417.8, P = .012) | N/A | ASA dose, age, sex, BMI, DM, hypertension, and procedural anticoagulant type or use did not influence risk of major bleeding. |
| Ruiz‐Nodar et al.52 | 2008 | Obs | 426 | 14.9 vs. 9.0 (P = .19) | Mortality: OR 3.43 (1.617.54, P = .002)b MACE: OR 4.9 (2.1711.1, P .01)b | TT was associated with a nonsignificant increase in major bleeding but lower all‐cause mortality and fewer MACE. |
| Sarafoff et al.53 | 2008 | Prosp | 515 | 1.4 vs. 3.1 (P = .34). | MACCE: OR 0.76 (0.481.21, P = .25) | No difference in MACCE or bleeding at 2 y. Stent thrombosis did not differ between groups. |
| Rossini et al.54 | 2008 | Prosp | 204 | 10.8 vs. 4.9 (P = .1) | MACE: 5.8% vs. 4.9% (P = .7) | INR was targeted to the lower range (2.0‐2.5). No significant difference in bleeding rates for TT versus DAPT at 18 mo. Less bleeding for patients whose INR was within target (4.9 versus 33%, P = .00019). No significant differences in MACE between groups. |
| Uchida et al.55 | 2010 | Obs | 575 | 18 vs. 2.7 (P .001) | MACE (P = .108) | No differences in MACE rates. More bleeding for patients on TT. |
| Studies comparing triple therapy versus dual antiplatelet therapy versus wararin and single antiplatelet agent | ||||||
| Karjalainen et al.10 | 2007 | Matched cohort | 239 | OR 3.3 (1.38.6, P = .014)c | MACE: OR 1.7 (1.0‐3.0, P = 0.05)c | This study compared patients on warfarin at baseline with those not on warfarinall undergoing stenting. Patients on warfarin at baseline were treated with a variety of strategies. Baseline warfarin use increased both major bleeding and MACE at 1 y. ASA plus warfarin was inadequate to prevent stent thrombosis, and premature warfarin cessation was associated with stroke. |
| Manzano‐Fernandez et al.56 | 2008 | Obs | 104 | EB (5.8 vs. 11.3, P = .33) LB (21.6 vs. 3.8, P = .006)d | MACE: 25.5% vs. 21.0% (P = .53)d | No difference in MACE rates between TT and non‐TT (WAA or DAPT). TT conferred higher late bleeding (>48 h). |
| Gao et al.57 | 2010 | Prosp | 622 | 2.9 vs. 1.8 vs. 2.5 (P = .725)e | MACCE: 8.8% vs. 20.1% vs. 14.9% (P = .010)e | Target INR was set as 1.8‐2.5. Lower stroke and MACCE rates for TT as compared with DAPT or WAA; no difference in bleeding. |
| Studies comparing triple therapy with warfarin and single antiplatelet agent | ||||||
| Nguyen et al.58 | 2007 | Obs | 800 | 5.9 vs. 46 (P = .46) | Death: 5.1% vs. 6.5% (P = .47) Stroke: 0.7% vs. 3.4% (P = .02) MI: 3.3% vs. 4.5% (P = .49) | TT and WAA lead to similar 6‐mo bleeding, death, and MI. Fewer strokes with TT (caveat: low event rate). |
In the largest study to date, Nguyen et al.58 evaluated 800 patients who underwent stenting for ACS and were discharged on warfarin plus single antiplatelet agent or triple therapy as part of the GRACE registry. At 6 months, triple therapy conferred a significant reduction in stroke (0.7% versus 3.4%, P = .02) but not in death or MI. There were no differences in in‐hospital major bleeding events between the two groups (5.9% versus 4.6%; P = .46). Similarly, Sarafoff et al.53 reported no significant differences in the combined endpoint (death, MI, stent thrombosis or stroke) or bleeding complications among patients who received triple therapy or DAPT at 2 years of follow‐up. In contrast, Ruiz‐Nodar et al.52 showed that triple therapy, compared with DAPT, at discharge reduced the incidence of death (17.8% versus 27.8%; adjusted HR = 3.43; 95% CI, 1.617.54; P = .002) and major adverse cardiac events (26.5% versus 38.7%; adjusted HR = 4.9; 95% CI, 2.1711.1; P = .01), without a substantial increase in major bleeding events.
The value of combination antiplatelet therapy to prevent stent thrombosis in these patients is clearer in the study reported by Karjalainen et al.10 This case‐control study of 239 patients receiving warfarin at baseline who underwent PCI evaluated a primary endpoint of death, MI, target‐vessel revascularization, or stent thrombosis and a secondary endpoint of major bleeding and stroke to 12 months of follow‐up. Forty‐eight percent of patients received triple therapy, whereas 15.5% were discharged on DAPT. The remaining patients received warfarin plus a single antiplatelet agent. Stent thrombosis occurred more frequently among patients receiving warfarin plus ASA (15.2%) than among those receiving triple therapy (1.9%). As expected, stroke was more frequent in patients treated with DAPT (8.8%) than among those receiving triple therapy (2.8%). Major bleeding was similar between groups. Therapy with warfarin was an independent predictor of both major bleeding and major cardiac events at 1 year. This observation illustrates that the outcome of PCI in patients on chronic warfarin therapy is unsatisfactory irrespective of the antithrombotic combinations used, highlighting the need for better strategies to treat these patients.
Choice of Therapy and Management of Patients Eligible for Triple Therapy
Current guidelines for PCI do not provide guidance for patients with an indication for triple therapy due to a paucity of published evidence. Several ongoing prospective trials aim to address the management of these patients (AFCAS, ISAR‐TRIPLE). Pending further study, clinicians should consider the embolic risk (CHADS2 score), target INR, type of stent, bleeding risk, and duration of treatment when determining the appropriate antiplatelet/anticoagulant combinations. The CHADS2 score (Table 2) stratifies the risk for stroke among patients with AF,4 while the Outpatient Bleeding Risk Index (OBRI) allows estimation of bleeding risk.12, 61 The OBRI considers age > 65 years, prior stroke, prior gastrointestinal bleeding, and any of four comorbidities (recent MI, anemia, diabetes, or renal insufficiency) in order to stratify patients into three risk groups.61 Patients with three to four risk factors have a high risk of bleeding (23% at 3 months and 48% at 12 months) whereas patients with no risk factors have only a 3% risk of bleeding at 12 months. Unfortunately, advanced age and prior stroke appear in both OBRI and CHADS.
For patients with AF who are at high risk for embolic stroke (>3% per year), we recommend triple therapy for the shortest time possible, followed by warfarin and ASA indefinitely. In case of BMS, it is acceptable to shorten triple therapy duration to 1 month. The optimal duration of triple therapy for patients with DES is uncertain; recommended durations range from 3 months to 1 year.62 If the potential consequences of stent thrombosis are high due to a large amount of myocardium at risk, an extended period of triple therapy might be justified. For patients whose stroke risk is lower (CHADS2 score of 0‐1), the risk for bleeding likely outweighs any benefit from stroke prevention. In this instance, it is reasonable to use DAPT with ASA and clopidogrel for 1 month after BMS and 12 months after DES, followed by ASA, with or without warfarin, indefinitely. In a recently published study, patients with AF and a CHADS2 score of 1 had a yearly stroke risk of 1.25% while taking DAPT63; the risk of major bleeding for triple therapy is 6.1% per year.64
For patients who have a high bleeding risk, BMS are the preferred stent type as the duration of triple therapy might be limited to 4 weeks. To our knowledge, no randomized study has evaluated the outcome of patients with BMS compared with DES who also have an indication for warfarin. Because studies have suggested that clopidogrel is more effective than aspirin in preventing stent thrombosis and in reducing death or MI after coronary stenting,40, 65 warfarin and single antiplatelet therapy with clopidogrel might be a reasonable treatment option in patients with high bleeding risk. The WOEST study (NCT00769938), currently recruiting participants, is the first randomized study specifically designed to test this hypothesis.
Since gastrointestinal bleeding accounts for approximately 30‐40% of hemorrhagic events in patients on combined ASA and anticoagulant therapy, an expert consensus document recommended concomitant treatment with proton pump inhibitors (PPIs) to reduce this risk.66 In contrast, the 2009 Focused Updates of the ACC/AHA/SCAI Guidelines did not recommend the use of PPIs with DAPT in the setting of ACS.2 This is because of studies that show inhibition of platelet activation,67 and potential clinical harm,68 when clopidogrel is combined with certain PPIs that inhibit the CYP2C19 enzyme. However, to date there are no convincing randomized clinical trial data documenting an important clinical drug‐drug interaction. The U.S. Food and Drug Administration (FDA) advises that physicians avoid the use of clopidogrel in patients with impaired CYP2C19 function due to known genetic variation or due to concomitant use of drugs that inhibit CYP2C19 activity. More specifically, the FDA recommends avoiding the use of omeprazole and esomeprazole in patients taking clopidogrel.69
In particular, elderly patients have an increased risk of bleeding while receiving triple therapy. In a study of patients over age 65, 2.5% were hospitalized for bleeding in the first year after PCI, and the use of triple therapy was the strongest predictor of bleeding (more than threefold increase).70 One in five patients suffered death or MI at 1 year after hospitalization for bleeding.70 The basis for poor outcomes after hospitalization for bleeding in this population is multifactorial and may be due to the location of bleeding, associated hypercoagulable state, potential adverse impact of blood transfusion, withdrawal of warfarin therapy in patients with AF and PCI, and the premature discontinuation of DAPT. The use of nonsteroidal anti‐inflammatory drugs (NSAIDs) is common among the elderly and conferred a doubling of bleeding risk.70 Limiting the use of NSAID, the use of low‐dose ASA beyond 30 days after stent implantation, greater use of BMS, and maintaining INR at the lowest possible level (INR of 22.5) will reduce the risk for bleeding.57, 71
New Anticoagulants
Due to the high risk for bleeding with warfarin and the challenges inherent in INR monitoring, researchers have developed several novel anticoagulants whose advantages include fixed daily dosing and no need for monitoring. Dabigatran is a direct oral thrombin inhibitor that is already licensed in Europe and Canada for thromboprophylaxis after hip or knee surgery. It has also been studied in patients with AF. In the RE‐LY trial, patients with AF who received dabigatran 110 mg daily had rates of stroke and systemic embolism that were similar to those with warfarin, as well as lower rates of major hemorrhage.72 The randomized ReDEEM trial, reported at the AHA 2009 Scientific Sessions, was aimed at finding a dosage of dabigatran that achieves a good balance between clinical effectiveness and bleeding risk when combined with aspirin and clopidogrel after acute MI. Dosages ranging from 50 mg twice daily to 150 mg twice daily were all associated with 6‐month rates of bleeding lower than 2%. Hospitalists should view these encouraging results cautiously until the publication of ReDEEM trial results in a peer‐reviewed journal.
A variety of oral Xa antagonists are also being evaluated in patients with AF or ACS. These trials offer insight into triple therapy regimens that include ASA, clopidogrel, and an Xa antagonist. In a recent study of the oral Xa antagonist rivaroxaban, investigators stratified 3491 subjects with ACS according to whether they received concomitant ASA alone or ASA and clopidogrel.73 Subjects receiving ASA plus rivaroxaban had a modest increase in bleeding. Triple therapy, however, increased the composite bleeding rate from 3.5% in the DAPT group to approximately 6‐15% (low‐dose or high‐dose rivaroxaban, respectively). Rivaroxaban is currently under review by the FDA.
These novel agents might eventually replace warfarin for many or most indications for anticoagulation. It is imperative that future research compare the efficacy and risk of bleeding between triple therapy using these new agents and triple therapy with warfarin.
Conclusions
The management of patients on long‐term anticoagulation who require DAPT because of ACS or coronary stenting is challenging. DAPT may safely substitute for warfarin only for patients at low risk for a thromboembolic event (ie, low‐risk AF with low CHADS2 score). Clinicians should not interrupt warfarin in patients at higher risk (ie, intermediate to high‐risk AF, mechanical valves, or recent venous thromboembolism), even in the presence of DAPT. In these patients, triple therapy is the optimal approach following coronary stenting (and possibly during the initial period after ACS without stenting). As this approach confers a fivefold increase in bleeding complications compared with DAPT, careful monitoring of the INR, the addition of PPIs, and the exclusion of elderly patients who are at the highest risk for bleeding complications74 is recommended. The preferred duration of triple therapy after BMS in patients who require long‐term anticoagulation is 1 month, whereas the optimal duration after ACS or DES remains unresolved.
- ,,, et al.2007 Focused Update of the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, Writing on Behalf of the 2005 Writing Committee.Circulation2008;117:261–295.
- ,,, et al.2009 Focused Updates: ACC/AHA Guidelines for the Management of Patients With ST‐Elevation Myocardial Infarction (updating the 2004 Guideline and 2007 Focused Update) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (updating the 2005 Guideline and 2007 Focused Update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.Circulation2009;120:2271–2306.
- ,,, et al.ACC/AHA 2007 guidelines for the management of patients with unstable angina/non‐ST‐Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non‐ST‐Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine.J Am Coll Cardiol2007;50:e1–e157.
- ,,, et al.Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin.Circulation2004;110:2287–2292.
- ,,.Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses.Circulation1994;89:635–641.
- ,,,,.Aspirin use among adults aged 40 and older in the United States: results of a national survey.Am J Prev Med2007;32:403–407.
- ,,, et al.The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition).Chest2008;133:299S–339S.
- ,,, et al.Discharge antithrombotic strategies among patients with acute coronary syndrome previously on warfarin anticoagulation: physician practice in the CRUSADE registry.Am Heart J2008;155:361–368.
- ,,, et al.Risk of major bleeding with concomitant dual antiplatelet therapy after percutaneous coronary intervention in patients receiving long‐term warfarin therapy.Pharmacotherapy2007;27:691–696.
- ,,, et al.Safety and efficacy of combined antiplatelet‐warfarin therapy after coronary stenting.Eur Heart J2007;28:726–732.
- ,,, et al.Combination therapy with aspirin, clopidogrel and warfarin following coronary stenting is associated with a significant risk of bleeding.J Invasive Cardiol2006;18:162–164.
- ,,,,,.Development of a contemporary bleeding risk model for elderly warfarin recipients.Chest2006;130:1390–1396.
- ,,, et al.Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST‐segment elevation.N Engl J Med2005;352:1179–1189.
- ,,, et al.Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo‐controlled trial.Lancet2005;366:1607–1621.
- ,,,,,.Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST‐segment elevation.N Engl J Med2001;345:494–502.
- ,,, et al.Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial.JAMA2002;288:2411–2420.
- ,,, et al.Effects of pretreatment with clopidogrel and aspirin followed by long‐term therapy in patients undergoing percutaneous coronary intervention: the PCI‐CURE study.Lancet2001;358:527–533.
- ,,, et al.Guidelines for the diagnosis and treatment of non‐ST‐segment elevation acute coronary syndromes.Eur Heart J2007;28:1598–1660.
- .Burden of disease: medical and economic impact of acute coronary syndromes.Am J Manag Care2006;12:S430–S434.
- ,,,,,.Variability in platelet responsiveness to clopidogrel among 544 individuals.J Am Coll Cardiol2005;45:246–251.
- ,,, et al.Dose comparisons of clopidogrel and aspirin in acute coronary syndromes.N Engl J Med2010;363:930–942.
- ,,, et al.A clinical trial comparing three antithrombotic‐drug regimens after coronary‐artery stenting. Stent Anticoagulation Restenosis Study Investigators.N Engl J Med1998;339:1665–1671.
- ,,, et al.A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary‐artery stents.N Engl J Med1996;334:1084–1089.
- ,,.Outcomes of 6906 patients undergoing percutaneous coronary intervention in the era of drug‐eluting stents: report of the DEScover Registry.Circulation2006;114:2154–2162.
- ,,, et al.Safety and efficacy of sirolimus‐ and paclitaxel‐eluting coronary stents.N Engl J Med2007;356:998–1008.
- ,,, et al.Comparison of the impact of short (1 year) and long‐term (> or =1 year) clopidogrel use following percutaneous coronary intervention on mortality.Am J Cardiol2008;102:1159–1162.
- ,,.Stent thrombosis late after implantation of first‐generation drug‐eluting stents: a cause for concern.Circulation2007;115:1440–1455; discussion 55.
- ,,, et al.Early and late coronary stent thrombosis of sirolimus‐eluting and paclitaxel‐eluting stents in routine clinical practice: data from a large two‐institutional cohort study.Lancet2007;369:667–678.
- ,,, et al.Analysis of 14 trials comparing sirolimus‐eluting stents with bare‐metal stents.N Engl J Med2007;356:1030–1039.
- ,,,,,.Long‐term outcomes with drug‐eluting stents versus bare‐metal stents in Sweden.N Engl J Med2007;356:1009–1019.
- ,,,,,.Stent thrombosis in randomized clinical trials of drug‐eluting stents.N Engl J Med2007;356:1020–1029.
- ,,, et al.Stent thrombosis, clinical events, and influence of prolonged clopidogrel use after placement of drug‐eluting stent data from an observational cohort study of drug‐eluting versus bare‐metal stents.JACC Cardiovasc Interv2008;1:494–503.
- ,,, et al.Temporal relation between Clopidogrel cessation and stent thrombosis after drug‐eluting stent implantation.Am J Cardiol2009;103:801–805.
- ,,, et al.Effect of prolonged thienopyridine use after drug‐eluting stent implantation (from the TAXUS landmark trials data).Am J Cardiol2008;102:1017–1022.
- ,,, et al.Effectiveness of two‐year clopidogrel + aspirin in abolishing the risk of very late thrombosis after drug‐eluting stent implantation (from the TYCOON [two‐year ClOpidOgrel need] study).Am J Cardiol2009;104:1357–1361.
- ,,.Mortality in randomized controlled trials comparing drug‐eluting vs. bare metal stents in coronary artery disease: a meta‐analysis.Eur Heart J2006;27:2784–2814.
- ,,, et al.Sirolimus‐eluting stents versus standard stents in patients with stenosis in a native coronary artery.N Engl J Med2003;349:1315–1323.
- ,,, et al.A polymer‐based, paclitaxel‐eluting stent in patients with coronary artery disease.N Engl J Med2004;350:221–231.
- ,,, et al.Duration of dual antiplatelet therapy after implantation of drug‐eluting stents.N Engl J Med2010;362:1374–1382.
- ,,, et al.Clopidogrel use and long‐term clinical outcomes after drug‐eluting stent implantation.JAMA2007;297:159–168.
- ,,.The effect of warfarin on mortality and reinfarction after myocardial infarction.N Engl J Med1990;323:147–152.
- Effect of long‐term oral anticoagulant treatment on mortality and cardiovascular morbidity after myocardial infarction.Anticoagulants in the Secondary Prevention of Events in Coronary Thrombosis (ASPECT) Research Group.Lancet1994;343:499–503.
- ,,,,.Warfarin, aspirin, or both after myocardial infarction.N Engl J Med2002;347:969–974.
- ,,,,.Aspirin and coumadin after acute coronary syndromes (the ASPECT‐2 study): a randomised controlled trial.Lancet2002;360:109–113.
- ,,, et al.Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial.Lancet2006;367:1903–1912.
- ,,,.Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta‐analysis.Ann Intern Med1999;131:492–501.
- ,,, et al.Safety and efficacy of aspirin, clopidogrel, and warfarin after coronary stent placement in patients with an indication for anticoagulation.Am Heart J2004;147:463–467.
- ,,,,,.Short‐term triple therapy with aspirin, warfarin, and a thienopyridine among patients undergoing percutaneous coronary intervention.Catheter Cardiovasc Interv2006;68:56–61.
- ,,,,.Periprocedural and medium‐term antithrombotic strategies in patients with an indication for long‐term anticoagulation undergoing coronary angiography and intervention.Coron Artery Dis2007;18:193–199.
- ,,, et al.Dual antiplatelet therapy after percutaneous coronary intervention with stent implantation in patients taking chronic oral anticoagulation.JACC Cardiovasc Interv2008;1:56–61.
- ,,,,,.Evaluation of safety of warfarin in combination with antiplatelet therapy for patients treated with coronary stents for acute myocardial infarction.J Interv Cardiol2005;18:163–166.
- ,,, et al.Anticoagulant and antiplatelet therapy use in 426 patients with atrial fibrillation undergoing percutaneous coronary intervention and stent implantation implications for bleeding risk and prognosis.J Am Coll Cardiol2008;51:818–825.
- ,,, et al.Aspirin and clopidogrel with or without phenprocoumon after drug eluting coronary stent placement in patients on chronic oral anticoagulation.J Intern Med2008;264:472–480.
- ,,, et al.Long‐term outcomes in patients undergoing coronary stenting on dual oral antiplatelet treatment requiring oral anticoagulant therapy.Am J Cardiol2008;102:1618–1623.
- ,,,,.Impact of anticoagulant therapy with dual antiplatelet therapy on prognosis after treatment with drug‐eluting coronary stents.J Cardiol2010;55:362–369.
- ,,, et al.Increased major bleeding complications related to triple antithrombotic therapy usage in patients with atrial fibrillation undergoing percutaneous coronary artery stenting.Chest2008;134:559–567.
- ,,, et al.Comparison of different antithrombotic regimens for patients with atrial fibrillation undergoing drug‐eluting stent implantation.Circ J2010;74:701–708.
- ,,, et al.Combining warfarin and antiplatelet therapy after coronary stenting in the Global Registry of Acute Coronary Events: is it safe and effective to use just one antiplatelet agent?Eur Heart J2007;28:1717–1722.
- ,,, et al.2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST‐elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol2008;51:210–247.
- ,,, et al.Guidelines for percutaneous coronary interventions. The Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology.Eur Heart J2005;26:804–847.
- ,,.Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin.Am J Med1998;105:91–99.
- ,,,.Coronary stents and chronic anticoagulation.Circulation2009;119:1682–1688.
- ,,, et al.Risks and benefits of oral anticoagulation compared with clopidogrel plus aspirin in patients with atrial fibrillation according to stroke risk: the atrial fibrillation clopidogrel trial with irbesartan for prevention of vascular events (ACTIVE‐W).Stroke2008;39:1482–1486.
- ,,, et al.Early and late increased bleeding rates after angioplasty and stenting due to combined antiplatelet and anticoagulanttherapy.EuroIntervention2009;5:425–431.
- ,,, et al.Late clinical events after clopidogrel discontinuation may limit the benefit of drug‐eluting stents: an observational study of drug‐eluting versus bare‐metal stents.J Am Coll Cardiol2006;48:2584–2591.
- ,,, et al.ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents.Circulation2008;118:1894–1909.
- ,,, et al.Influence of omeprazole on the antiplatelet action of clopidogrel associated with aspirin: the randomized, double‐blind OCLA (Omeprazole CLopidogrel Aspirin) study.J Am Coll Cardiol2008;51:256–260.
- ,,, et al.Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome.JAMA2009;301:937–944.
- Follow‐Up to the January 26,2009, Early Communication about an Ongoing Safety Review of Clopidogrel Bisulfate (marketed as Plavix) and Omeprazole (marketed as Prilosec and Prilosec OTC). 11/17/2009. (Accessed at http://www.fda.gov/Drugs/DrugSafety/Postmarket DrugSafetyInformationforPatientsandProviders/DrugSafetyInformationfor HeathcareProfessionals/ucm190784.htm.)
- ,,, et al.Incidence, predictors, and prognostic implications of hospitalization for late bleeding after percutaneous coronary intervention for patients older than 65 years.Circ Cardiovasc Interv2010;3:140–147.
- ,,, et al.Antithrombotic therapy in patients treated with oral anticoagulation undergoing coronary artery stenting. An expert consensus document with focus on atrial fibrillation.Ann Med2008;40:428–436.
- ,,, et al.Dabigatran versus warfarin in patients with atrial fibrillation.N Engl J Med2009;361:1139–1151.
- ,,, et al.Rivaroxaban versus placebo in patients with acute coronary syndromes (ATLAS ACS‐TIMI 46): a randomised, double‐blind, phase II trial.Lancet2009;374:29–38.
- ,,,.Bleeding complications associated with combinations of aspirin, thienopyridine derivatives, and warfarin in elderly patients following acute myocardial infarction.Arch Intern Med2005;165:784–789.
- ,,, et al.2007 Focused Update of the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, Writing on Behalf of the 2005 Writing Committee.Circulation2008;117:261–295.
- ,,, et al.2009 Focused Updates: ACC/AHA Guidelines for the Management of Patients With ST‐Elevation Myocardial Infarction (updating the 2004 Guideline and 2007 Focused Update) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (updating the 2005 Guideline and 2007 Focused Update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.Circulation2009;120:2271–2306.
- ,,, et al.ACC/AHA 2007 guidelines for the management of patients with unstable angina/non‐ST‐Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non‐ST‐Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine.J Am Coll Cardiol2007;50:e1–e157.
- ,,, et al.Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin.Circulation2004;110:2287–2292.
- ,,.Thromboembolic and bleeding complications in patients with mechanical heart valve prostheses.Circulation1994;89:635–641.
- ,,,,.Aspirin use among adults aged 40 and older in the United States: results of a national survey.Am J Prev Med2007;32:403–407.
- ,,, et al.The perioperative management of antithrombotic therapy: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition).Chest2008;133:299S–339S.
- ,,, et al.Discharge antithrombotic strategies among patients with acute coronary syndrome previously on warfarin anticoagulation: physician practice in the CRUSADE registry.Am Heart J2008;155:361–368.
- ,,, et al.Risk of major bleeding with concomitant dual antiplatelet therapy after percutaneous coronary intervention in patients receiving long‐term warfarin therapy.Pharmacotherapy2007;27:691–696.
- ,,, et al.Safety and efficacy of combined antiplatelet‐warfarin therapy after coronary stenting.Eur Heart J2007;28:726–732.
- ,,, et al.Combination therapy with aspirin, clopidogrel and warfarin following coronary stenting is associated with a significant risk of bleeding.J Invasive Cardiol2006;18:162–164.
- ,,,,,.Development of a contemporary bleeding risk model for elderly warfarin recipients.Chest2006;130:1390–1396.
- ,,, et al.Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST‐segment elevation.N Engl J Med2005;352:1179–1189.
- ,,, et al.Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo‐controlled trial.Lancet2005;366:1607–1621.
- ,,,,,.Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST‐segment elevation.N Engl J Med2001;345:494–502.
- ,,, et al.Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial.JAMA2002;288:2411–2420.
- ,,, et al.Effects of pretreatment with clopidogrel and aspirin followed by long‐term therapy in patients undergoing percutaneous coronary intervention: the PCI‐CURE study.Lancet2001;358:527–533.
- ,,, et al.Guidelines for the diagnosis and treatment of non‐ST‐segment elevation acute coronary syndromes.Eur Heart J2007;28:1598–1660.
- .Burden of disease: medical and economic impact of acute coronary syndromes.Am J Manag Care2006;12:S430–S434.
- ,,,,,.Variability in platelet responsiveness to clopidogrel among 544 individuals.J Am Coll Cardiol2005;45:246–251.
- ,,, et al.Dose comparisons of clopidogrel and aspirin in acute coronary syndromes.N Engl J Med2010;363:930–942.
- ,,, et al.A clinical trial comparing three antithrombotic‐drug regimens after coronary‐artery stenting. Stent Anticoagulation Restenosis Study Investigators.N Engl J Med1998;339:1665–1671.
- ,,, et al.A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary‐artery stents.N Engl J Med1996;334:1084–1089.
- ,,.Outcomes of 6906 patients undergoing percutaneous coronary intervention in the era of drug‐eluting stents: report of the DEScover Registry.Circulation2006;114:2154–2162.
- ,,, et al.Safety and efficacy of sirolimus‐ and paclitaxel‐eluting coronary stents.N Engl J Med2007;356:998–1008.
- ,,, et al.Comparison of the impact of short (1 year) and long‐term (> or =1 year) clopidogrel use following percutaneous coronary intervention on mortality.Am J Cardiol2008;102:1159–1162.
- ,,.Stent thrombosis late after implantation of first‐generation drug‐eluting stents: a cause for concern.Circulation2007;115:1440–1455; discussion 55.
- ,,, et al.Early and late coronary stent thrombosis of sirolimus‐eluting and paclitaxel‐eluting stents in routine clinical practice: data from a large two‐institutional cohort study.Lancet2007;369:667–678.
- ,,, et al.Analysis of 14 trials comparing sirolimus‐eluting stents with bare‐metal stents.N Engl J Med2007;356:1030–1039.
- ,,,,,.Long‐term outcomes with drug‐eluting stents versus bare‐metal stents in Sweden.N Engl J Med2007;356:1009–1019.
- ,,,,,.Stent thrombosis in randomized clinical trials of drug‐eluting stents.N Engl J Med2007;356:1020–1029.
- ,,, et al.Stent thrombosis, clinical events, and influence of prolonged clopidogrel use after placement of drug‐eluting stent data from an observational cohort study of drug‐eluting versus bare‐metal stents.JACC Cardiovasc Interv2008;1:494–503.
- ,,, et al.Temporal relation between Clopidogrel cessation and stent thrombosis after drug‐eluting stent implantation.Am J Cardiol2009;103:801–805.
- ,,, et al.Effect of prolonged thienopyridine use after drug‐eluting stent implantation (from the TAXUS landmark trials data).Am J Cardiol2008;102:1017–1022.
- ,,, et al.Effectiveness of two‐year clopidogrel + aspirin in abolishing the risk of very late thrombosis after drug‐eluting stent implantation (from the TYCOON [two‐year ClOpidOgrel need] study).Am J Cardiol2009;104:1357–1361.
- ,,.Mortality in randomized controlled trials comparing drug‐eluting vs. bare metal stents in coronary artery disease: a meta‐analysis.Eur Heart J2006;27:2784–2814.
- ,,, et al.Sirolimus‐eluting stents versus standard stents in patients with stenosis in a native coronary artery.N Engl J Med2003;349:1315–1323.
- ,,, et al.A polymer‐based, paclitaxel‐eluting stent in patients with coronary artery disease.N Engl J Med2004;350:221–231.
- ,,, et al.Duration of dual antiplatelet therapy after implantation of drug‐eluting stents.N Engl J Med2010;362:1374–1382.
- ,,, et al.Clopidogrel use and long‐term clinical outcomes after drug‐eluting stent implantation.JAMA2007;297:159–168.
- ,,.The effect of warfarin on mortality and reinfarction after myocardial infarction.N Engl J Med1990;323:147–152.
- Effect of long‐term oral anticoagulant treatment on mortality and cardiovascular morbidity after myocardial infarction.Anticoagulants in the Secondary Prevention of Events in Coronary Thrombosis (ASPECT) Research Group.Lancet1994;343:499–503.
- ,,,,.Warfarin, aspirin, or both after myocardial infarction.N Engl J Med2002;347:969–974.
- ,,,,.Aspirin and coumadin after acute coronary syndromes (the ASPECT‐2 study): a randomised controlled trial.Lancet2002;360:109–113.
- ,,, et al.Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial.Lancet2006;367:1903–1912.
- ,,,.Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta‐analysis.Ann Intern Med1999;131:492–501.
- ,,, et al.Safety and efficacy of aspirin, clopidogrel, and warfarin after coronary stent placement in patients with an indication for anticoagulation.Am Heart J2004;147:463–467.
- ,,,,,.Short‐term triple therapy with aspirin, warfarin, and a thienopyridine among patients undergoing percutaneous coronary intervention.Catheter Cardiovasc Interv2006;68:56–61.
- ,,,,.Periprocedural and medium‐term antithrombotic strategies in patients with an indication for long‐term anticoagulation undergoing coronary angiography and intervention.Coron Artery Dis2007;18:193–199.
- ,,, et al.Dual antiplatelet therapy after percutaneous coronary intervention with stent implantation in patients taking chronic oral anticoagulation.JACC Cardiovasc Interv2008;1:56–61.
- ,,,,,.Evaluation of safety of warfarin in combination with antiplatelet therapy for patients treated with coronary stents for acute myocardial infarction.J Interv Cardiol2005;18:163–166.
- ,,, et al.Anticoagulant and antiplatelet therapy use in 426 patients with atrial fibrillation undergoing percutaneous coronary intervention and stent implantation implications for bleeding risk and prognosis.J Am Coll Cardiol2008;51:818–825.
- ,,, et al.Aspirin and clopidogrel with or without phenprocoumon after drug eluting coronary stent placement in patients on chronic oral anticoagulation.J Intern Med2008;264:472–480.
- ,,, et al.Long‐term outcomes in patients undergoing coronary stenting on dual oral antiplatelet treatment requiring oral anticoagulant therapy.Am J Cardiol2008;102:1618–1623.
- ,,,,.Impact of anticoagulant therapy with dual antiplatelet therapy on prognosis after treatment with drug‐eluting coronary stents.J Cardiol2010;55:362–369.
- ,,, et al.Increased major bleeding complications related to triple antithrombotic therapy usage in patients with atrial fibrillation undergoing percutaneous coronary artery stenting.Chest2008;134:559–567.
- ,,, et al.Comparison of different antithrombotic regimens for patients with atrial fibrillation undergoing drug‐eluting stent implantation.Circ J2010;74:701–708.
- ,,, et al.Combining warfarin and antiplatelet therapy after coronary stenting in the Global Registry of Acute Coronary Events: is it safe and effective to use just one antiplatelet agent?Eur Heart J2007;28:1717–1722.
- ,,, et al.2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST‐elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol2008;51:210–247.
- ,,, et al.Guidelines for percutaneous coronary interventions. The Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology.Eur Heart J2005;26:804–847.
- ,,.Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin.Am J Med1998;105:91–99.
- ,,,.Coronary stents and chronic anticoagulation.Circulation2009;119:1682–1688.
- ,,, et al.Risks and benefits of oral anticoagulation compared with clopidogrel plus aspirin in patients with atrial fibrillation according to stroke risk: the atrial fibrillation clopidogrel trial with irbesartan for prevention of vascular events (ACTIVE‐W).Stroke2008;39:1482–1486.
- ,,, et al.Early and late increased bleeding rates after angioplasty and stenting due to combined antiplatelet and anticoagulanttherapy.EuroIntervention2009;5:425–431.
- ,,, et al.Late clinical events after clopidogrel discontinuation may limit the benefit of drug‐eluting stents: an observational study of drug‐eluting versus bare‐metal stents.J Am Coll Cardiol2006;48:2584–2591.
- ,,, et al.ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents.Circulation2008;118:1894–1909.
- ,,, et al.Influence of omeprazole on the antiplatelet action of clopidogrel associated with aspirin: the randomized, double‐blind OCLA (Omeprazole CLopidogrel Aspirin) study.J Am Coll Cardiol2008;51:256–260.
- ,,, et al.Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome.JAMA2009;301:937–944.
- Follow‐Up to the January 26,2009, Early Communication about an Ongoing Safety Review of Clopidogrel Bisulfate (marketed as Plavix) and Omeprazole (marketed as Prilosec and Prilosec OTC). 11/17/2009. (Accessed at http://www.fda.gov/Drugs/DrugSafety/Postmarket DrugSafetyInformationforPatientsandProviders/DrugSafetyInformationfor HeathcareProfessionals/ucm190784.htm.)
- ,,, et al.Incidence, predictors, and prognostic implications of hospitalization for late bleeding after percutaneous coronary intervention for patients older than 65 years.Circ Cardiovasc Interv2010;3:140–147.
- ,,, et al.Antithrombotic therapy in patients treated with oral anticoagulation undergoing coronary artery stenting. An expert consensus document with focus on atrial fibrillation.Ann Med2008;40:428–436.
- ,,, et al.Dabigatran versus warfarin in patients with atrial fibrillation.N Engl J Med2009;361:1139–1151.
- ,,, et al.Rivaroxaban versus placebo in patients with acute coronary syndromes (ATLAS ACS‐TIMI 46): a randomised, double‐blind, phase II trial.Lancet2009;374:29–38.
- ,,,.Bleeding complications associated with combinations of aspirin, thienopyridine derivatives, and warfarin in elderly patients following acute myocardial infarction.Arch Intern Med2005;165:784–789.
Treatment of Complicated Pneumonia
Community‐acquired pneumonia, the most common serious bacterial infection in childhood, may be complicated by parapneumonic effusion (ie, complicated pneumonia).1 Children with complicated pneumonia require prolonged hospitalization and frequently undergo multiple pleural fluid drainage procedures.2 Additionally, the incidence of complicated pneumonia has increased,37 making the need to define appropriate therapy even more pressing. Defining appropriate therapy is challenging for the individual physician as a result of inconsistent and insufficient evidence, and wide variation in treatment practices.2, 8
Historically, thoracotomy was performed only if initial chest tube placement did not lead to clinical improvement.9, 10 Several authors, noting the rapid resolution of symptoms in children undergoing earlier thoracotomy, advocated for the use of thoracotomy as initial therapy rather than as a procedure of last resort.114 The advent of less invasive techniques such as video‐assisted thoracoscopic surgery (VATS) has served as an additional impetus to consider surgical drainage as the initial treatment strategy.1518 Few well‐designed studies have examined the relative efficacy of these interventions.2, 1922 Published randomized trials were single center, enrolled few patients, and arrived at different conclusions.19, 21, 22 In addition, these trials did not examine other important outcomes such as requirement for additional pleural fluid drainage procedures and hospital readmission. Two large retrospective multicenter studies found modest reductions in length of stay (LOS) and substantial decreases in the requirement for additional pleural fluid drainage procedures in children undergoing initial VATS compared with initial chest tube placement.2, 20 However, Shah et al2 included relatively few patients undergoing VATS. Li et al20 combined patients undergoing initial thoracentesis, initial chest tube placement, late pleural fluid drainage (by any method), and no pleural fluid drainage into a single non‐operative management category, precluding conclusions about the relative benefits of chest tube placement compared with VATS. Neither study2, 20 examined the role of chemical fibrinolysis, a therapy which has been associated with outcomes comparable to VATS in two small randomized trials.21, 22
The objectives of this multicenter study were to describe the variation in the initial management strategy along with associated outcomes of complicated pneumonia in childhood and to determine the comparative effectiveness of different pleural fluid drainage procedures.
Methods
Data Source
The Pediatric Health Information System (PHIS), which contains resource utilization data from 40 freestanding children's hospitals, provided data for this multicenter retrospective cohort study. Participating hospitals are located in noncompeting markets of 27 states plus the District of Columbia. The PHIS database includes patient demographics, diagnoses, and procedures as well as data for all drugs, radiologic studies, laboratory tests, and supplies charged to each patient. Data are de‐identified, however encrypted medical record numbers allow for tracking individual patients across admissions. The Child Health Corporation of America (Shawnee Mission, KS) and participating hospitals jointly assure data quality and reliability as described previously.23, 24 The Children's Hospital of Philadelphia Institutional Review Board reviewed and approved this study.
Patients
Children 18 years of age receiving a pleural drainage procedure for complicated pneumonia were eligible if they were discharged from participating hospitals between January 1, 2004 and June 30, 2009. Study participants met the following criteria: 1) discharge diagnosis of pneumonia (International Classification of Diseases, 9th revision [ICD‐9] discharge diagnosis codes 480.x‐483.x, 485.x‐487.x), 2) discharge diagnosis of pleural effusion (ICD‐9 codes 510.0, 510.9, 511.0, 511.1, or 511.9), and 3) billing charge for antibiotics on the first day of hospitalization. Additionally, the primary discharge diagnosis had to be either pneumonia or pleural effusion. Patients were excluded if they did not undergo pleural fluid drainage or if their initial pleural fluid drainage procedure was thoracentesis.
Study Definitions
Pleural drainage procedures were identified using ICD‐9 procedure codes for thoracentesis (34.91), chest tube placement (34.04), VATS (34.21), and thoracotomy (34.02 or 34.09). Fibrinolysis was defined as receipt of urokinase, streptokinase, or alteplase within two days of initial chest tube placement.
Acute conditions or complications included influenza (487, 487.0, 487.1, 487.8, 488, or V04.81) and hemolytic‐uremic syndrome (283.11). Chronic comorbid conditions (CCCs) (eg, malignancy) were identified using a previously reported classification scheme.25 Billing data were used to classify receipt of mechanical ventilation and medications on the first day of hospitalization.
Measured Outcomes
The primary outcomes were hospital LOS (both overall and post‐initial procedure), requirement for additional pleural drainage procedures, total cost for index hospitalization, all‐cause readmission within 14 days after index hospital discharge, and total cost of the episode (accounting for the cost of readmissions).
Measured Exposures
The primary exposure of interest was the initial pleural fluid drainage procedure, classified as chest tube placement without fibrinolysis, chest tube placement with fibrinolysis, VATS, or thoracotomy.
Statistical Analysis
Variables were summarized using frequencies and percentages for categorical variables, and median, interquartile range (IQR), and range for continuous variables. Outcomes by initial pleural drainage procedure were compared using chi‐squared tests for categorical variables and Kruskal‐Wallis tests for continuous variables.
Multivariable analysis was performed to account for potential confounding by observed baseline variables. For dichotomous outcome variables, modeling consisted of logistic regression using generalized estimating equations to account for hospital clustering. For continuous variables, a mixed model approach was used, treating hospital as a random effect. Log transformation was applied to the right‐skewed outcome variables (LOS and cost). Cost outcomes remained skewed following log transformation, thus gamma mixed models were applied.2629 Odds ratios and 95% confidence intervals (CIs) were reported for comparison of dichotomous outcomes and the adjusted means and 95% CIs were reported for continuous outcomes after appropriate back transformation.
Additional analyses addressed the potential impact of confounding by indication inherent in any observational study. First, patients with an underlying CCC were excluded to ensure that our results would be generalizable to otherwise healthy children with community‐acquired pneumonia. Second, patients undergoing pleural drainage >2 days after hospitalization were excluded to minimize the effect of residual confounding related to differences in timing of the initial drainage procedure. Third, the analysis was repeated using a generalized propensity score as an additional method to account for confounding by indication for the initial drainage procedure.30 Propensity scores, constructed using a multivariable generalized logit model, included all variables listed in Table 1. The inverse of the propensity score was included as a weight in each multivariable model described previously. Only the primary multivariable analyses are presented as the results of the propensity score analysis were nearly identical to the primary analyses.
| Overall | Chest Tube Without Fibrinolysis | Chest Tube With Fibrinolysis | Thoracotomy | VATS | P Value | |
|---|---|---|---|---|---|---|
| ||||||
| N | 3500 | 1672 (47.8) | 623 (17.8) | 797 (22.8) | 408 (11.7) | |
| Age | ||||||
| <1 year | 335 (9.6) | 176 (10.5) | 56 (9.0) | 78 (9.8) | 25 (6.1) | |
| 1 year | 475 (13.6) | 238 (14.2) | 98 (15.7) | 92 (11.5) | 47 (11.5) | 0.003 |
| 24 years | 1230 (35.1) | 548 (32.8) | 203 (32.6) | 310 (38.9) | 169 (41.4) | |
| 59 years | 897 (25.6) | 412 (24.6) | 170 (27.3) | 199 (25.0) | 116 (28.4) | |
| 1014 years | 324 (9.3) | 167 (10.0) | 61 (9.8) | 65 (8.2) | 31 (7.6) | |
| 1518 years | 193 (5.5) | 106 (6.3) | 29 (4.6) | 40 (5.0) | 18 (4.4) | |
| >18 years | 46 (1.3) | 25 (1.5) | 6 (0.96) | 13 (1.6) | 2 (0.5) | |
| Comorbid Conditions | ||||||
| Cardiac | 69 (2.0) | 43 (2.6) | 14 (2.3) | 12 (1.5) | 0 (0.0) | 0.006 |
| Malignancy | 81 (2.3) | 31 (1.9) | 18 (2.9) | 21 (2.6) | 11 (2.7) | 0.375 |
| Neurological | 138 (3.9) | 73 (4.4) | 20 (3.2) | 34 (4.3) | 11 (2.7) | 0.313 |
| Any Other Condition | 202 (5.8) | 96 (5.7) | 40 (6.4) | 47 (5.9) | 19 (4.7) | 0.696 |
| Payer | ||||||
| Government | 1240 (35.6) | 630 (37.8) | 224 (36.0) | 259 (32.7) | 127 (31.3) | <0.001 |
| Private | 1383 (39.7) | 607 (36.4) | 283 (45.4) | 310 (39.2) | 183 (45.07) | |
| Other | 864 (24.8) | 430 (25.8) | 116 (18.6) | 222 (28.1) | 96 (23.65) | |
| Race | ||||||
| Non‐Hispanic White | 1746 (51.9) | 838 (51.6) | 358 (59.7) | 361 (47.8) | 189 (48.7) | <0.001 |
| Non‐Hispanic Black | 601 (17.9) | 318 (19.6) | 90 (15.0) | 128 (17.0) | 65 (16.8) | |
| Hispanic | 588 (17.5) | 280 (17.3) | 73 (12.2) | 155 (20.5) | 80 (20.6) | |
| Asian | 117 (3.5) | 47 (2.9) | 20 (3.3) | 37 (4.9) | 13 (3.4) | |
| Other | 314 (9.3) | 140 (8.6) | 59 (9.8) | 74 (9.8) | 41 (10.6) | |
| Male Sex | 1912 (54.6) | 923 (55.2) | 336 (53.9) | 439 (55.1) | 214 (52.5) | 0.755 |
| Radiology | ||||||
| CT, no US | 1200 (34.3) | 600 (35.9) | 184 (29.5) | 280 (35.1) | 136 (33.3) | <0.001 |
| CT and US | 221 (6.3) | 84 (5.0) | 53 (8.5) | 61 (7.7) | 23 (5.6) | |
| US, no CT | 799 (22.8) | 324 (19.4) | 178 (28.6) | 200 (25.1) | 97 (23.8) | |
| No US, no CT | 1280 (36.6) | 664 (39.7) | 208 (33.4) | 256 (32.1) | 152 (37.3) | |
| Empiric Antibiotic Regimen | ||||||
| Cephalosporins alone | 448 (12.8) | 181 (10.83) | 126 (20.2) | 73 (9.2) | 68 (16.7) | <0.001 |
| Cephalosporin and clindamycin | 797 (22.8) | 359 (21.5) | 145 (23.3) | 184 (23.1) | 109 (26.7) | |
| Other antibiotic combination | 167 (4.8) | 82 (4.9) | 30 (4.8) | 38 (4.8) | 17 (4.2) | |
| Cephalosporin and vancomycin | 2088 (59.7) | 1050 (62.8) | 322 (51.7) | 502 (63.0) | 214 (52.5) | |
| Mechanical ventilation | 494 (14.1) | 251 (15.0) | 75 (12.0) | 114 (14.3) | 54 (13.2) | 0.307 |
| Corticosteroids | 520 (14.9) | 291 (17.4) | 72 (11.6) | 114 (14.3) | 43 (10.5) | <0.001 |
| Blood product transfusionsb | 761 (21.7) | 387 (23.2) | 145 (23.3) | 161 (20.2) | 68 (16.7) | 0.018 |
| Vasoactive infusionsc | 381 (10.9) | 223 (13.3) | 63 (10.1) | 72 (9.0) | 23 (5.6) | <0.001 |
| Admission to intensive care | 1397 (39.9) | 731 (43.7) | 234 (37.6) | 296 (37.1) | 136 (33.3) | <0.001 |
| Extracorporeal membranous oxygenation | 18 (0.5) | 13 (0.8) | 2 (0.3) | 3 (0.4) | 0 (0.0) | 0.163 |
| Hemolytic‐uremic syndrome | 31 (0.9) | 15 (0.9) | 6 (1.0) | 7 (0.9) | 3 (0.7) | 0.985 |
| Influenza | 108 (3.1) | 53 (3.2) | 27 (4.3) | 23 (2.9) | 5 (1.2) | 0.044 |
| Arterial blood gas measurements | 0 (0,1) | 0 (0, 2) | 0 (0,1) | 0 (0, 1) | 0 (0, 1) | <0.001 |
| Days to first procedure | 1 (0, 3) | 1 (0, 2) | 1 (1, 3) | 1 (1, 3) | 1 (1, 3) | <0.001 |
Medical records of a randomly selected subset of subjects from 6 hospitals were reviewed to determine the accuracy of our algorithm in identifying patients with complicated pneumonia; these subjects represented 1% of the study population. For the purposes of medical record review, complicated pneumonia was defined by the following: 1) radiologically‐confirmed lung infiltrate; 2) moderate or large pleural effusion; and 3) signs and symptoms of lower respiratory tract infection. Complicated pneumonia was identified in 118 of 120 reviewed subjects for a positive predictive value of 98.3%.
All analyses were clustered by hospital. Analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC). A two‐tailed P < 0.05 was considered statistically significant.
Results
Patient Characteristics
During the study period, 9,680 subjects had complicated pneumonia. Subjects were excluded if they did not have a pleural drainage procedure (n = 5798), or if thoracentesis was the first pleural fluid drainage procedure performed (n = 382). The remaining 3500 patients were included. Demographic characteristics are summarized in Table 1. The median patient age was 4.1 years (IQR: 2.17.2 years). An underlying CCC was present in 424 (12.1%) patients. There was no association between type of drainage procedure and mechanical ventilation. However, factors associated with more severe systemic illness, such as blood product transfusion, were more common among those undergoing initial chest tube placement with or without fibrinolysis (Table 1).
Initial Pleural Fluid Drainage Procedures
The primary procedures included chest tube without fibrinolysis (47.8%); chest tube with fibrinolysis (17.8%); thoracotomy (22.8%); and VATS (11.7%) (Table 1). The proportion of patients undergoing primary chest tube placement with fibrinolysis increased over time from 14.2% in 2004 to 30.0% in 2009 (P < 0.001; chi‐squared test for trend). The initial procedure varied by hospital with the greatest proportion of patients undergoing primary chest tube placement without fibrinolysis at 28 (70.0%) hospitals, chest tube placement with fibrinolysis at 5 (12.5%) hospitals, thoracotomy at 5 (12.5%) hospitals, and VATS at 2 (5.0%) hospitals (Figure 1). The median proportion of patients undergoing primary VATS across all hospitals was 11.5% (IQR: 3.9%‐26.5%) (Figure 1). The median time to first procedure was 1 day (IQR: 03 days).
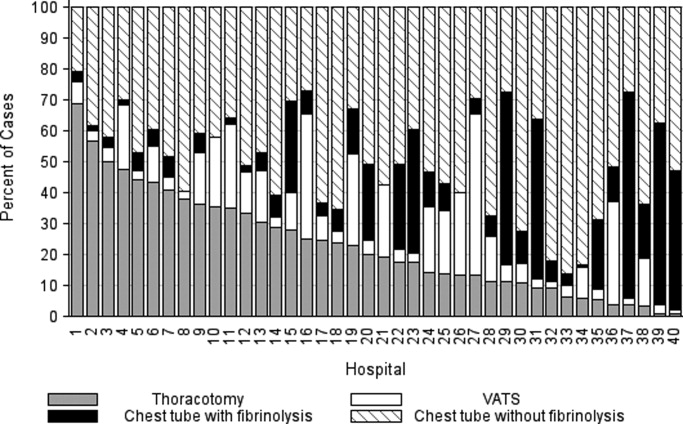
Outcome Measures
Variation in outcomes occurred across hospitals. Additional pleural drainage procedures were performed in a median of 20.9% of patients with a range of 6.8% to 44.8% (IQR: 14.5%‐25.3%) of patients across all hospitals. Median LOS was 10 days with a range of 714 days (IQR: 8.511 days) and the median LOS following the initial pleural fluid drainage procedure was 8 days with a range of 6 to 13 days (IQR: 78 days). Variation in timing of the initial pleural fluid drainage procedure explained 9.6% of the variability in LOS (Spearman rho, 0.31; P < 0.001).
Overall, 118 (3.4%) patients were readmitted within 14 days of index discharge; the median readmission rate was 3.8% with a range of 0.8% to 33.3% (IQR: 2.1%‐5.8%) across hospitals. The median total cost of the index hospitalization was $19,574 (IQR: $13,791‐$31,063). The total cost for the index hospitalization exceeded $54,215 for 10% of patients and the total cost of the episode exceeded $55,208 for 10% of patients. Unadjusted outcomes, stratified by primary pleural fluid drainage procedure, are summarized in Table 2.
| Overall | Chest Tube Without Fibrinolysis | Chest Tube With Fibrinolysis | Thoracotomy | VATS | P Valueb | |
|---|---|---|---|---|---|---|
| ||||||
| Additional Procedure | 716 (20.5) | 331 (19.8) | 144 (23.1) | 197 (24.7) | 44 (10.8) | <0.001 |
| Readmission within 14 days | 118 (3.4) | 54 (3.3) | 13 (2.1) | 32 (4.0) | 19 (4.7) | 0.096 |
| Total LOS (days) | 10 (7, 14) | 10 (7, 14) | 9 (7, 13) | 10 (7, 14) | 9 (7, 12) | <.001 |
| Post‐initial Procedure LOS (days) | 8 (5, 12) | 8 (6, 12) | 7 (5, 10) | 8 (5, 12) | 7 (5, 10) | <0.001 |
| Total Cost, Index Hospitalization ($)e | 19319 (13358, 30955) | 19951 (13576, 32018)c | 19565 (13209, 32778)d | 20352 (14351, 31343) | 17918 (13531, 25166) | 0.016 |
| Total Cost, Episode of Illness ($)e | 19831 (13927, 31749) | 20151 (13764, 32653) | 19593 (13210, 32861) | 20573 (14419, 31753) | 18344 (13835, 25462) | 0.029 |
In multivariable analysis, differences in total LOS and post‐procedure LOS were not significant (Table 3). The odds of additional drainage procedures were higher for all drainage procedures compared with initial VATS (Table 3). Patients undergoing initial chest tube placement with fibrinolysis were less likely to require readmission compared with patients undergoing initial VATS (Table 3). The total cost for the episode of illness (including the cost of readmission) was significantly less for those undergoing primary chest tube placement without fibrinolysis compared with primary VATS. The results of subanalyses excluding patients with an underlying CCC (Supporting Appendix online, Table 4) and restricting the cohort to patients undergoing pleural drainage within two days of admission (Supporting Appendix online, Table 5) were similar to the results of our primary analysis with one exception; in the latter subanalysis, children undergoing initial chest tube placement without fibrinolysis were also less likely to require readmission compared with patients undergoing initial VATS.
| Adjusted OR (95% CI)a | P Value | |
|---|---|---|
| ||
| Additional pleural drainage procedure | ||
| Chest tube without fibrinolysis | 1.82 (1.103.00) | .019 |
| Chest tube with fibrinolysis | 2.31 (1.443.72) | <0.001 |
| Thoracotomy | 2.59 (1.624.14) | <0.001 |
| VATS | Reference | |
| Readmission within 14 days | ||
| Chest tube without fibrinolysis | 0.61 (0.361.05) | .077 |
| Chest tube with fibrinolysis | 0.45 (0.230.86) | .015 |
| Thoracotomy | 0.85 (0.521.39) | .521 |
| VATS | Reference | |
| Adjusted Mean (95% CI)a | P Value | |
| Total LOS (days) | ||
| Chest tube without fibrinolysis | 8.0 (7.88.2) | .339 |
| Chest tube with fibrinolysis | 8.1 (7.98.3) | .812 |
| Thoracotomy | 8.1 (7.98.3) | .632 |
| VATS | 8.1 (7.98.3) | Ref |
| Post‐initial procedure LOS (days) | ||
| Chest tube without fibrinolysis | 7.3 (7.07.5) | .512 |
| Chest tube with fibrinolysis | 7.5 (7.27.8) | .239 |
| Thoracotomy | 7.3 (7.07.6) | .841 |
| VATS | 7.3 (7.17.6) | Reference |
| Total cost, index hospitalization ($) | ||
| Chest tube without fibrinolysis | 22928 (2200023895 | .012 |
| Chest tube with fibrinolysis | 23621 (2263124655) | .657 |
| Thoracotomy | 23386 (2241924395 | .262 |
| VATS | 23820 (2280824878) | Reference |
| Total cost, episode of illness ($) | ||
| Chest tube without fibrinolysis | 23218 (2227824199) | .004 |
| Chest tube with fibrinolysis | 23749 (2275224790) | .253 |
| Thoracotomy | 23673 (2269324696) | .131 |
| VATS | 24280 (2324425362) | Reference |
Discussion
This multicenter study is the largest to evaluate the management of children hospitalized with complicated pneumonia. We found considerable variation in initial management and outcomes across hospitals. Differences in timing of the initial drainage procedure explained only a small amount of the variability in outcomes. Children undergoing initial VATS less commonly required additional drainage procedures while children undergoing initial chest tube placement with fibrinolysis less commonly required readmission. Differences in total and post‐procedure LOS were not statistically significant. Differences in cost, while statistically significant, were of marginal relevance.
Previous studies have also shown significant variation in treatment and outcomes of children with complicated pneumonia across hospitals.2, 8 Our study provides data from additional hospitals, includes a substantially larger number of patients undergoing initial VATS, distinguishes between fibrinolysis recipients and nonrecipients, and is the first to compare outcomes between four different initial drainage strategies. The creation of national consensus guidelines might reduce variability in initial management strategies, although the variability in outcomes across hospitals in the current study could not be explained simply by differences in the type or timing of the initial drainage procedure. Thus, future studies examining hospital‐level factors may play an important role in improving quality of care for children with complicated pneumonia.
Patients with initial thoracotomy or chest tube placement with or without fibrinolysis more commonly received additional drainage procedures than patients with initial VATS. This difference remained when patients with CCCs were excluded from the analysis and when the analysis was limited to patients undergoing pleural fluid drainage within 2 days of hospitalization. Several small, randomized trials demonstrated conflicting results when comparing initial chest tube placement with fibrinolysis and VATS. St. Peter et al22 reported that 3 (17%) of 18 patients undergoing initial chest tube placement with fibrinolysis and none of the 18 patients undergoing initial VATS received additional pleural drainage procedures. Sonnappa et al21 found no differences between the two groups. Kurt et al19 did not state the proportion of patients receiving additional procedures. However, the mean number of drainage procedures was 2.25 among the 8 patients undergoing initial chest tube placement while none of the 10 patients with VATS received additional drainage.19
Thoracotomy is often perceived as a definitive procedure for treatment of complicated pneumonia. However, several possibilities exist to explain why additional procedures were performed less frequently in patients undergoing initial VATS compared with initial thoracotomy. The limited visual field in thoracotomy may lead to greater residual disease post‐operatively in those receiving thoracotomy compared with VATS.31 Additionally, thoracotomy substantially disrupts the integrity of the chest wall and is consequently associated with complications such as bleeding and air leak into the pleural cavity more often than VATS.31, 32 It is thus possible that some of the additional procedures in patients receiving initial thoracotomy were necessary for management of thoracotomy‐associated complications rather than for failure of the initial drainage procedure.
Similar to the randomized trials by Sonnappa et al21 and St. Peter et al,22 differences in the overall and post‐procedure LOS were not significant among patients undergoing initial VATS compared with initial chest tube placement with fibrinolysis. However, chest tube placement without fibrinolysis did not result in significant differences in LOS compared with initial VATS. In the only pediatric randomized trial, the 29 intrapleural urokinase recipients had a 2 day shorter LOS compared with the 29 intrapleural saline recipients.33 Several small, randomized controlled trials of adults with complicated pneumonia reported improved pleural fluid drainage among intrapleural fibrinolysis recipients compared with non‐recipients.3436 However, a large multicenter randomized trial in adults found no differences in mortality, requirement for surgical drainage, or LOS between intrapleural streptokinase and placebo recipients.37 Subsequent meta‐analyses of randomized trials in adults also demonstrated no benefit to fibrinolysis.38, 39 In the context of the increasing use of intrapleural fibrinolysis in children with complicated pneumonia, our results highlight the need for a large, multicenter randomized controlled trial to determine whether chest tube with fibrinolysis is superior to chest tube alone.
Two small randomized trials21, 22 and a decision analysis40 identified chest tube with fibrinolysis as the most economical approach to children with complicated pneumonia. However, the costs did not differ significantly between patients undergoing initial VATS or initial chest tube placement with fibrinolysis in our study. The least costly approach was initial chest tube placement without fibrinolysis. Unlike the randomized controlled trials, we considered costs associated with readmissions in determining the total costs. Shah et al41 found no difference in total charges for patients undergoing initial VATS compared with initial chest tube placement; however, patients undergoing initial VATS were concentrated in a few centers, making it difficult to determine the relative importance of procedural and hospital factors.
This multicenter observational study has several limitations. First, discharge diagnosis coding may be unreliable for specific diseases. However, our rigorous definition of complicated pneumonia, supported by the high positive predictive value as verified by medical record review, minimizes the likelihood of misclassification.
Second, unmeasured confounding or residual confounding by indication for the method of pleural drainage may occur, potentially influencing our results in two disparate ways. If patients with more severe systemic illness were too unstable for operative interventions, then our results would be biased towards worse outcomes for children undergoing initial chest tube placement. We adjusted for several variables associated with a greater systemic severity of illness, including intensive care unit admission, making this possibility less likely. We also could not account for some factors associated with more severe local disease such as the size and character of the effusion. We suspect that patients with more extensive local disease (ie, loculated effusions) would have worse outcomes than other patients, regardless of initial procedure, and that these patients would also be more likely to undergo primary surgical drainage. Thus, this study may have underestimated the benefit of initial surgical drainage (eg, VATS) compared with nonsurgical drainage (ie, chest tube placement).
Third, misclassification of the method of initial pleural drainage may have occurred. Patients transferred from another institution following chest tube placement could either be classified as not receiving pleural drainage and thus excluded from the study or classified as having initial VATS or thoracotomy if the reason for transfer was chest tube treatment failure. Additionally, we could not distinguish routine use of fibrinolysis from fibrinolysis to maintain chest tube patency. Whether such misclassification would falsely minimize or maximize differences in outcomes between the various groups remains uncertain. Fourth, because this study only included tertiary care children's hospitals, these data are not generalizable to community settings. VATS requires specialized surgical training that may be unavailable in some areas. Finally, this study demonstrates the relative efficacy of various pleural fluid drainage procedures on short‐term clinical outcomes and resource utilization. However, long‐term functional outcomes should be measured in future prospective studies.
Conclusions
In conclusion, emphasis on evidence driven treatment to optimize care has led to an increasing examination of unwarranted practice variation.42 The lack of evidence for best practice makes it difficult to define unwarranted variation in the treatment of complicated pneumonia. Our study demonstrates the large variability in practice and raises additional questions regarding the optimal drainage strategies. Published randomized trials have focused on comparisons between chest tube placement with fibrinolysis and VATS. However, our data suggest that future randomized trials should include chest tube placement without fibrinolysis as a treatment strategy. In determining the current best treatment for patients with complicated pneumonia, a clinician must weigh the impact of needing an additional procedure in approximately one‐quarter of patients undergoing initial chest tube placement (with or without fibrinolysis) with the risks of general anesthesia and readmission in patients undergoing initial VATS.
Acknowledgements
Dr. Hall had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the analysis.
- ,.Parapneumonic pleural effusion and empyema in children. Review of a 19‐year experience, 1962–1980.Clin Pediatr (Phila).1983;22:414–419.
- ,,,,.Primary early thoracoscopy and reduction in length of hospital stay and additional procedures among children with complicated pneumonia: Results of a multicenter retrospective cohort study.Arch Pediatr Adolesc Med.2008;162:675–681.
- ,.Empyema hospitalizations increased in US children despite pneumococcal conjugate vaccine.Pediatrics.2010;125:26–33.
- ,,, et al.Impact of the pneumococcal conjugate vaccine on pneumococcal parapneumonic empyema.Pediatr Infect Dis J.2006;25:250–254.
- ,,,,.Five‐fold increase in pediatric parapneumonic empyema since introduction of pneumococcal conjugate vaccine.Pediatric Infect Dis J.2008;27:1030–1032.
- ,,,.Increasing incidence of empyema complicating childhood community‐acquired pneumonia in the United States.Clin Infect Dis.2010;50:805–813.
- ,,,,.National hospitalization trends for pediatric pneumonia and associated complications.Pediatrics.2010;126:204–213.
- ,,, et al.Empyema associated with community‐acquired pneumonia: A Pediatric Investigator's Collaborative Network on Infections in Canada (PICNIC) study.BMC Infect Dis.2008;8:129.
- ,,,,.Pleural empyema in children.Ann Thorac Surg.1970;10:37–44.
- ,,.Management of streptococcal empyema.Ann Thorac Surg.1966;2:658–664.
- ,.Thoracoscopy in the management of empyema in children.J Pediatr Surg.1993;28:1128–1132.
- ,,,.Surgical treatment of parapneumonic empyema.Pediatr Pulmonol.1996;22:348–356.
- ,.The controversial role of decortication in the management of pediatric empyema.J Thorac Cardiovasc Surg.1988;96:166–170.
- ,,,,,.Postpneumonic empyema in children treated by early decortication.Eur J Pediatr Surg.1997;7:135–137.
- ,.Video‐assisted thoracoscopic surgery in the management of pediatric empyema.JSLS.1997;1:251–3.
- ,,,.Early video‐assisted thoracic surgery in the management of empyema.Pediatrics.1999;103:e63.
- ,,,,.Early definitive intervention by thoracoscopy in pediatric empyema.J Pediatr Surg.1999;34:178–180; discussion80–81.
- ,,,,.Thoracoscopy in the management of pediatric empyema.J Pediatr Surg.1995;30:1211–1215.
- ,,,,.Therapy of parapneumonic effusions in children: Video‐assisted thoracoscopic surgery versus conventional thoracostomy drainage.Pediatrics.2006;118:e547–e553.
- ,.Primary operative management for pediatric empyema: Decreases in hospital length of stay and charges in a national sample.Arch Pediatr Adolesc Med.2008;162:44–48.
- ,,, et al.Comparison of urokinase and video‐assisted thoracoscopic surgery for treatment of childhood empyema.Am J Respir Crit Care Med.2006;174:221–227.
- ,,, et al.Thoracoscopic decortication vs tube thoracostomy with fibrinolysis for empyema in children: A prospective, randomized trial.J Pediatr Surg.2009;44:106–111; discussion11.
- ,,,.Corticosteroids and mortality in children with bacterial meningitis.JAMA.2008;299:2048–2055.
- ,,,,.Intravenous immunoglobulin in children with streptococcal toxic shock syndrome.Clin Infect Dis.2009;49:1369–1376.
- ,,, et al.Deaths attributed to pediatric complex chronic conditions: National trends and implications for supportive care services.Pediatrics.2001;107:e99.
- ,.Multiple regression of cost data: Use of generalised linear models.J Health Serv Res Policy.2004;9:197–204.
- ,,,.A robustified modeling approach to analyze pediatric length of stay.Ann Epidemiol.2005;15:673–677.
- ,,.Correlates of length of stay, cost of care, and mortality among patients hospitalized for necrotizing fasciitis.Epidemiol Infect.2007;135:868–876.
- ,,,,,.Health care costs of adults treated for attention‐deficit/hyperactivity disorder who received alternative drug therapies.J Manag Care Pharm.2007;13:561–569.
- .The role of the propensity score in estimating dose‐response functions.Biometrika.2000;87:706–710.
- ,,,,.Experience with video‐assisted thoracoscopic surgery in the management of complicated pneumonia in children.J Pediatr Surg.2001;36:316–319.
- ,,, et al.VATS debridement versus thoracotomy in the treatment of loculated postpneumonia empyema.Ann Thorac Surg.1996;61:1626–1630.
- ,,,,.Randomised trial of intrapleural urokinase in the treatment of childhood empyema.Thorax.2002;57:343–347.
- ,,,,,.Intrapleural urokinase versus normal saline in the treatment of complicated parapneumonic effusions and empyema. A randomized, double‐blind study.Am J Respir Crit Care Med.1999;159:37–42.
- ,,.Randomised controlled trial of intrapleural streptokinase in community acquired pleural infection.Thorax.1997;52:416–421.
- ,,,,.Intrapleural streptokinase for empyema and complicated parapneumonic effusions.Am J Respir Crit Care Med.2004;170:49–53.
- ,,, et al.U.K. Controlled trial of intrapleural streptokinase for pleural infection.N Engl J Med.2005;352:865–874.
- ,.Intra‐pleural fibrinolytic therapy versus conservative management in the treatment of adult parapneumonic effusions and empyema.Cochrane Database Syst Rev.2008:CD002312.
- ,,,.Intrapleural fibrinolytic agents for empyema and complicated parapneumonic effusions: A meta‐analysis.Chest.2006;129:783–790.
- ,,.Cost‐effectiveness of competing strategies for the treatment of pediatric empyema.Pediatrics.2008;121:e1250–e1257.
- ,,.Costs of treating children with complicated pneumonia: A comparison of primary video‐assisted thoracoscopic surgery and chest tube placement.Pediatr Pulmonol.2010;45:71–77.
- .Unwarranted variation in pediatric medical care.Pediatr Clin North Am.2009;56:745–755.
Community‐acquired pneumonia, the most common serious bacterial infection in childhood, may be complicated by parapneumonic effusion (ie, complicated pneumonia).1 Children with complicated pneumonia require prolonged hospitalization and frequently undergo multiple pleural fluid drainage procedures.2 Additionally, the incidence of complicated pneumonia has increased,37 making the need to define appropriate therapy even more pressing. Defining appropriate therapy is challenging for the individual physician as a result of inconsistent and insufficient evidence, and wide variation in treatment practices.2, 8
Historically, thoracotomy was performed only if initial chest tube placement did not lead to clinical improvement.9, 10 Several authors, noting the rapid resolution of symptoms in children undergoing earlier thoracotomy, advocated for the use of thoracotomy as initial therapy rather than as a procedure of last resort.114 The advent of less invasive techniques such as video‐assisted thoracoscopic surgery (VATS) has served as an additional impetus to consider surgical drainage as the initial treatment strategy.1518 Few well‐designed studies have examined the relative efficacy of these interventions.2, 1922 Published randomized trials were single center, enrolled few patients, and arrived at different conclusions.19, 21, 22 In addition, these trials did not examine other important outcomes such as requirement for additional pleural fluid drainage procedures and hospital readmission. Two large retrospective multicenter studies found modest reductions in length of stay (LOS) and substantial decreases in the requirement for additional pleural fluid drainage procedures in children undergoing initial VATS compared with initial chest tube placement.2, 20 However, Shah et al2 included relatively few patients undergoing VATS. Li et al20 combined patients undergoing initial thoracentesis, initial chest tube placement, late pleural fluid drainage (by any method), and no pleural fluid drainage into a single non‐operative management category, precluding conclusions about the relative benefits of chest tube placement compared with VATS. Neither study2, 20 examined the role of chemical fibrinolysis, a therapy which has been associated with outcomes comparable to VATS in two small randomized trials.21, 22
The objectives of this multicenter study were to describe the variation in the initial management strategy along with associated outcomes of complicated pneumonia in childhood and to determine the comparative effectiveness of different pleural fluid drainage procedures.
Methods
Data Source
The Pediatric Health Information System (PHIS), which contains resource utilization data from 40 freestanding children's hospitals, provided data for this multicenter retrospective cohort study. Participating hospitals are located in noncompeting markets of 27 states plus the District of Columbia. The PHIS database includes patient demographics, diagnoses, and procedures as well as data for all drugs, radiologic studies, laboratory tests, and supplies charged to each patient. Data are de‐identified, however encrypted medical record numbers allow for tracking individual patients across admissions. The Child Health Corporation of America (Shawnee Mission, KS) and participating hospitals jointly assure data quality and reliability as described previously.23, 24 The Children's Hospital of Philadelphia Institutional Review Board reviewed and approved this study.
Patients
Children 18 years of age receiving a pleural drainage procedure for complicated pneumonia were eligible if they were discharged from participating hospitals between January 1, 2004 and June 30, 2009. Study participants met the following criteria: 1) discharge diagnosis of pneumonia (International Classification of Diseases, 9th revision [ICD‐9] discharge diagnosis codes 480.x‐483.x, 485.x‐487.x), 2) discharge diagnosis of pleural effusion (ICD‐9 codes 510.0, 510.9, 511.0, 511.1, or 511.9), and 3) billing charge for antibiotics on the first day of hospitalization. Additionally, the primary discharge diagnosis had to be either pneumonia or pleural effusion. Patients were excluded if they did not undergo pleural fluid drainage or if their initial pleural fluid drainage procedure was thoracentesis.
Study Definitions
Pleural drainage procedures were identified using ICD‐9 procedure codes for thoracentesis (34.91), chest tube placement (34.04), VATS (34.21), and thoracotomy (34.02 or 34.09). Fibrinolysis was defined as receipt of urokinase, streptokinase, or alteplase within two days of initial chest tube placement.
Acute conditions or complications included influenza (487, 487.0, 487.1, 487.8, 488, or V04.81) and hemolytic‐uremic syndrome (283.11). Chronic comorbid conditions (CCCs) (eg, malignancy) were identified using a previously reported classification scheme.25 Billing data were used to classify receipt of mechanical ventilation and medications on the first day of hospitalization.
Measured Outcomes
The primary outcomes were hospital LOS (both overall and post‐initial procedure), requirement for additional pleural drainage procedures, total cost for index hospitalization, all‐cause readmission within 14 days after index hospital discharge, and total cost of the episode (accounting for the cost of readmissions).
Measured Exposures
The primary exposure of interest was the initial pleural fluid drainage procedure, classified as chest tube placement without fibrinolysis, chest tube placement with fibrinolysis, VATS, or thoracotomy.
Statistical Analysis
Variables were summarized using frequencies and percentages for categorical variables, and median, interquartile range (IQR), and range for continuous variables. Outcomes by initial pleural drainage procedure were compared using chi‐squared tests for categorical variables and Kruskal‐Wallis tests for continuous variables.
Multivariable analysis was performed to account for potential confounding by observed baseline variables. For dichotomous outcome variables, modeling consisted of logistic regression using generalized estimating equations to account for hospital clustering. For continuous variables, a mixed model approach was used, treating hospital as a random effect. Log transformation was applied to the right‐skewed outcome variables (LOS and cost). Cost outcomes remained skewed following log transformation, thus gamma mixed models were applied.2629 Odds ratios and 95% confidence intervals (CIs) were reported for comparison of dichotomous outcomes and the adjusted means and 95% CIs were reported for continuous outcomes after appropriate back transformation.
Additional analyses addressed the potential impact of confounding by indication inherent in any observational study. First, patients with an underlying CCC were excluded to ensure that our results would be generalizable to otherwise healthy children with community‐acquired pneumonia. Second, patients undergoing pleural drainage >2 days after hospitalization were excluded to minimize the effect of residual confounding related to differences in timing of the initial drainage procedure. Third, the analysis was repeated using a generalized propensity score as an additional method to account for confounding by indication for the initial drainage procedure.30 Propensity scores, constructed using a multivariable generalized logit model, included all variables listed in Table 1. The inverse of the propensity score was included as a weight in each multivariable model described previously. Only the primary multivariable analyses are presented as the results of the propensity score analysis were nearly identical to the primary analyses.
| Overall | Chest Tube Without Fibrinolysis | Chest Tube With Fibrinolysis | Thoracotomy | VATS | P Value | |
|---|---|---|---|---|---|---|
| ||||||
| N | 3500 | 1672 (47.8) | 623 (17.8) | 797 (22.8) | 408 (11.7) | |
| Age | ||||||
| <1 year | 335 (9.6) | 176 (10.5) | 56 (9.0) | 78 (9.8) | 25 (6.1) | |
| 1 year | 475 (13.6) | 238 (14.2) | 98 (15.7) | 92 (11.5) | 47 (11.5) | 0.003 |
| 24 years | 1230 (35.1) | 548 (32.8) | 203 (32.6) | 310 (38.9) | 169 (41.4) | |
| 59 years | 897 (25.6) | 412 (24.6) | 170 (27.3) | 199 (25.0) | 116 (28.4) | |
| 1014 years | 324 (9.3) | 167 (10.0) | 61 (9.8) | 65 (8.2) | 31 (7.6) | |
| 1518 years | 193 (5.5) | 106 (6.3) | 29 (4.6) | 40 (5.0) | 18 (4.4) | |
| >18 years | 46 (1.3) | 25 (1.5) | 6 (0.96) | 13 (1.6) | 2 (0.5) | |
| Comorbid Conditions | ||||||
| Cardiac | 69 (2.0) | 43 (2.6) | 14 (2.3) | 12 (1.5) | 0 (0.0) | 0.006 |
| Malignancy | 81 (2.3) | 31 (1.9) | 18 (2.9) | 21 (2.6) | 11 (2.7) | 0.375 |
| Neurological | 138 (3.9) | 73 (4.4) | 20 (3.2) | 34 (4.3) | 11 (2.7) | 0.313 |
| Any Other Condition | 202 (5.8) | 96 (5.7) | 40 (6.4) | 47 (5.9) | 19 (4.7) | 0.696 |
| Payer | ||||||
| Government | 1240 (35.6) | 630 (37.8) | 224 (36.0) | 259 (32.7) | 127 (31.3) | <0.001 |
| Private | 1383 (39.7) | 607 (36.4) | 283 (45.4) | 310 (39.2) | 183 (45.07) | |
| Other | 864 (24.8) | 430 (25.8) | 116 (18.6) | 222 (28.1) | 96 (23.65) | |
| Race | ||||||
| Non‐Hispanic White | 1746 (51.9) | 838 (51.6) | 358 (59.7) | 361 (47.8) | 189 (48.7) | <0.001 |
| Non‐Hispanic Black | 601 (17.9) | 318 (19.6) | 90 (15.0) | 128 (17.0) | 65 (16.8) | |
| Hispanic | 588 (17.5) | 280 (17.3) | 73 (12.2) | 155 (20.5) | 80 (20.6) | |
| Asian | 117 (3.5) | 47 (2.9) | 20 (3.3) | 37 (4.9) | 13 (3.4) | |
| Other | 314 (9.3) | 140 (8.6) | 59 (9.8) | 74 (9.8) | 41 (10.6) | |
| Male Sex | 1912 (54.6) | 923 (55.2) | 336 (53.9) | 439 (55.1) | 214 (52.5) | 0.755 |
| Radiology | ||||||
| CT, no US | 1200 (34.3) | 600 (35.9) | 184 (29.5) | 280 (35.1) | 136 (33.3) | <0.001 |
| CT and US | 221 (6.3) | 84 (5.0) | 53 (8.5) | 61 (7.7) | 23 (5.6) | |
| US, no CT | 799 (22.8) | 324 (19.4) | 178 (28.6) | 200 (25.1) | 97 (23.8) | |
| No US, no CT | 1280 (36.6) | 664 (39.7) | 208 (33.4) | 256 (32.1) | 152 (37.3) | |
| Empiric Antibiotic Regimen | ||||||
| Cephalosporins alone | 448 (12.8) | 181 (10.83) | 126 (20.2) | 73 (9.2) | 68 (16.7) | <0.001 |
| Cephalosporin and clindamycin | 797 (22.8) | 359 (21.5) | 145 (23.3) | 184 (23.1) | 109 (26.7) | |
| Other antibiotic combination | 167 (4.8) | 82 (4.9) | 30 (4.8) | 38 (4.8) | 17 (4.2) | |
| Cephalosporin and vancomycin | 2088 (59.7) | 1050 (62.8) | 322 (51.7) | 502 (63.0) | 214 (52.5) | |
| Mechanical ventilation | 494 (14.1) | 251 (15.0) | 75 (12.0) | 114 (14.3) | 54 (13.2) | 0.307 |
| Corticosteroids | 520 (14.9) | 291 (17.4) | 72 (11.6) | 114 (14.3) | 43 (10.5) | <0.001 |
| Blood product transfusionsb | 761 (21.7) | 387 (23.2) | 145 (23.3) | 161 (20.2) | 68 (16.7) | 0.018 |
| Vasoactive infusionsc | 381 (10.9) | 223 (13.3) | 63 (10.1) | 72 (9.0) | 23 (5.6) | <0.001 |
| Admission to intensive care | 1397 (39.9) | 731 (43.7) | 234 (37.6) | 296 (37.1) | 136 (33.3) | <0.001 |
| Extracorporeal membranous oxygenation | 18 (0.5) | 13 (0.8) | 2 (0.3) | 3 (0.4) | 0 (0.0) | 0.163 |
| Hemolytic‐uremic syndrome | 31 (0.9) | 15 (0.9) | 6 (1.0) | 7 (0.9) | 3 (0.7) | 0.985 |
| Influenza | 108 (3.1) | 53 (3.2) | 27 (4.3) | 23 (2.9) | 5 (1.2) | 0.044 |
| Arterial blood gas measurements | 0 (0,1) | 0 (0, 2) | 0 (0,1) | 0 (0, 1) | 0 (0, 1) | <0.001 |
| Days to first procedure | 1 (0, 3) | 1 (0, 2) | 1 (1, 3) | 1 (1, 3) | 1 (1, 3) | <0.001 |
Medical records of a randomly selected subset of subjects from 6 hospitals were reviewed to determine the accuracy of our algorithm in identifying patients with complicated pneumonia; these subjects represented 1% of the study population. For the purposes of medical record review, complicated pneumonia was defined by the following: 1) radiologically‐confirmed lung infiltrate; 2) moderate or large pleural effusion; and 3) signs and symptoms of lower respiratory tract infection. Complicated pneumonia was identified in 118 of 120 reviewed subjects for a positive predictive value of 98.3%.
All analyses were clustered by hospital. Analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC). A two‐tailed P < 0.05 was considered statistically significant.
Results
Patient Characteristics
During the study period, 9,680 subjects had complicated pneumonia. Subjects were excluded if they did not have a pleural drainage procedure (n = 5798), or if thoracentesis was the first pleural fluid drainage procedure performed (n = 382). The remaining 3500 patients were included. Demographic characteristics are summarized in Table 1. The median patient age was 4.1 years (IQR: 2.17.2 years). An underlying CCC was present in 424 (12.1%) patients. There was no association between type of drainage procedure and mechanical ventilation. However, factors associated with more severe systemic illness, such as blood product transfusion, were more common among those undergoing initial chest tube placement with or without fibrinolysis (Table 1).
Initial Pleural Fluid Drainage Procedures
The primary procedures included chest tube without fibrinolysis (47.8%); chest tube with fibrinolysis (17.8%); thoracotomy (22.8%); and VATS (11.7%) (Table 1). The proportion of patients undergoing primary chest tube placement with fibrinolysis increased over time from 14.2% in 2004 to 30.0% in 2009 (P < 0.001; chi‐squared test for trend). The initial procedure varied by hospital with the greatest proportion of patients undergoing primary chest tube placement without fibrinolysis at 28 (70.0%) hospitals, chest tube placement with fibrinolysis at 5 (12.5%) hospitals, thoracotomy at 5 (12.5%) hospitals, and VATS at 2 (5.0%) hospitals (Figure 1). The median proportion of patients undergoing primary VATS across all hospitals was 11.5% (IQR: 3.9%‐26.5%) (Figure 1). The median time to first procedure was 1 day (IQR: 03 days).
Outcome Measures
Variation in outcomes occurred across hospitals. Additional pleural drainage procedures were performed in a median of 20.9% of patients with a range of 6.8% to 44.8% (IQR: 14.5%‐25.3%) of patients across all hospitals. Median LOS was 10 days with a range of 714 days (IQR: 8.511 days) and the median LOS following the initial pleural fluid drainage procedure was 8 days with a range of 6 to 13 days (IQR: 78 days). Variation in timing of the initial pleural fluid drainage procedure explained 9.6% of the variability in LOS (Spearman rho, 0.31; P < 0.001).
Overall, 118 (3.4%) patients were readmitted within 14 days of index discharge; the median readmission rate was 3.8% with a range of 0.8% to 33.3% (IQR: 2.1%‐5.8%) across hospitals. The median total cost of the index hospitalization was $19,574 (IQR: $13,791‐$31,063). The total cost for the index hospitalization exceeded $54,215 for 10% of patients and the total cost of the episode exceeded $55,208 for 10% of patients. Unadjusted outcomes, stratified by primary pleural fluid drainage procedure, are summarized in Table 2.
| Overall | Chest Tube Without Fibrinolysis | Chest Tube With Fibrinolysis | Thoracotomy | VATS | P Valueb | |
|---|---|---|---|---|---|---|
| ||||||
| Additional Procedure | 716 (20.5) | 331 (19.8) | 144 (23.1) | 197 (24.7) | 44 (10.8) | <0.001 |
| Readmission within 14 days | 118 (3.4) | 54 (3.3) | 13 (2.1) | 32 (4.0) | 19 (4.7) | 0.096 |
| Total LOS (days) | 10 (7, 14) | 10 (7, 14) | 9 (7, 13) | 10 (7, 14) | 9 (7, 12) | <.001 |
| Post‐initial Procedure LOS (days) | 8 (5, 12) | 8 (6, 12) | 7 (5, 10) | 8 (5, 12) | 7 (5, 10) | <0.001 |
| Total Cost, Index Hospitalization ($)e | 19319 (13358, 30955) | 19951 (13576, 32018)c | 19565 (13209, 32778)d | 20352 (14351, 31343) | 17918 (13531, 25166) | 0.016 |
| Total Cost, Episode of Illness ($)e | 19831 (13927, 31749) | 20151 (13764, 32653) | 19593 (13210, 32861) | 20573 (14419, 31753) | 18344 (13835, 25462) | 0.029 |
In multivariable analysis, differences in total LOS and post‐procedure LOS were not significant (Table 3). The odds of additional drainage procedures were higher for all drainage procedures compared with initial VATS (Table 3). Patients undergoing initial chest tube placement with fibrinolysis were less likely to require readmission compared with patients undergoing initial VATS (Table 3). The total cost for the episode of illness (including the cost of readmission) was significantly less for those undergoing primary chest tube placement without fibrinolysis compared with primary VATS. The results of subanalyses excluding patients with an underlying CCC (Supporting Appendix online, Table 4) and restricting the cohort to patients undergoing pleural drainage within two days of admission (Supporting Appendix online, Table 5) were similar to the results of our primary analysis with one exception; in the latter subanalysis, children undergoing initial chest tube placement without fibrinolysis were also less likely to require readmission compared with patients undergoing initial VATS.
| Adjusted OR (95% CI)a | P Value | |
|---|---|---|
| ||
| Additional pleural drainage procedure | ||
| Chest tube without fibrinolysis | 1.82 (1.103.00) | .019 |
| Chest tube with fibrinolysis | 2.31 (1.443.72) | <0.001 |
| Thoracotomy | 2.59 (1.624.14) | <0.001 |
| VATS | Reference | |
| Readmission within 14 days | ||
| Chest tube without fibrinolysis | 0.61 (0.361.05) | .077 |
| Chest tube with fibrinolysis | 0.45 (0.230.86) | .015 |
| Thoracotomy | 0.85 (0.521.39) | .521 |
| VATS | Reference | |
| Adjusted Mean (95% CI)a | P Value | |
| Total LOS (days) | ||
| Chest tube without fibrinolysis | 8.0 (7.88.2) | .339 |
| Chest tube with fibrinolysis | 8.1 (7.98.3) | .812 |
| Thoracotomy | 8.1 (7.98.3) | .632 |
| VATS | 8.1 (7.98.3) | Ref |
| Post‐initial procedure LOS (days) | ||
| Chest tube without fibrinolysis | 7.3 (7.07.5) | .512 |
| Chest tube with fibrinolysis | 7.5 (7.27.8) | .239 |
| Thoracotomy | 7.3 (7.07.6) | .841 |
| VATS | 7.3 (7.17.6) | Reference |
| Total cost, index hospitalization ($) | ||
| Chest tube without fibrinolysis | 22928 (2200023895 | .012 |
| Chest tube with fibrinolysis | 23621 (2263124655) | .657 |
| Thoracotomy | 23386 (2241924395 | .262 |
| VATS | 23820 (2280824878) | Reference |
| Total cost, episode of illness ($) | ||
| Chest tube without fibrinolysis | 23218 (2227824199) | .004 |
| Chest tube with fibrinolysis | 23749 (2275224790) | .253 |
| Thoracotomy | 23673 (2269324696) | .131 |
| VATS | 24280 (2324425362) | Reference |
Discussion
This multicenter study is the largest to evaluate the management of children hospitalized with complicated pneumonia. We found considerable variation in initial management and outcomes across hospitals. Differences in timing of the initial drainage procedure explained only a small amount of the variability in outcomes. Children undergoing initial VATS less commonly required additional drainage procedures while children undergoing initial chest tube placement with fibrinolysis less commonly required readmission. Differences in total and post‐procedure LOS were not statistically significant. Differences in cost, while statistically significant, were of marginal relevance.
Previous studies have also shown significant variation in treatment and outcomes of children with complicated pneumonia across hospitals.2, 8 Our study provides data from additional hospitals, includes a substantially larger number of patients undergoing initial VATS, distinguishes between fibrinolysis recipients and nonrecipients, and is the first to compare outcomes between four different initial drainage strategies. The creation of national consensus guidelines might reduce variability in initial management strategies, although the variability in outcomes across hospitals in the current study could not be explained simply by differences in the type or timing of the initial drainage procedure. Thus, future studies examining hospital‐level factors may play an important role in improving quality of care for children with complicated pneumonia.
Patients with initial thoracotomy or chest tube placement with or without fibrinolysis more commonly received additional drainage procedures than patients with initial VATS. This difference remained when patients with CCCs were excluded from the analysis and when the analysis was limited to patients undergoing pleural fluid drainage within 2 days of hospitalization. Several small, randomized trials demonstrated conflicting results when comparing initial chest tube placement with fibrinolysis and VATS. St. Peter et al22 reported that 3 (17%) of 18 patients undergoing initial chest tube placement with fibrinolysis and none of the 18 patients undergoing initial VATS received additional pleural drainage procedures. Sonnappa et al21 found no differences between the two groups. Kurt et al19 did not state the proportion of patients receiving additional procedures. However, the mean number of drainage procedures was 2.25 among the 8 patients undergoing initial chest tube placement while none of the 10 patients with VATS received additional drainage.19
Thoracotomy is often perceived as a definitive procedure for treatment of complicated pneumonia. However, several possibilities exist to explain why additional procedures were performed less frequently in patients undergoing initial VATS compared with initial thoracotomy. The limited visual field in thoracotomy may lead to greater residual disease post‐operatively in those receiving thoracotomy compared with VATS.31 Additionally, thoracotomy substantially disrupts the integrity of the chest wall and is consequently associated with complications such as bleeding and air leak into the pleural cavity more often than VATS.31, 32 It is thus possible that some of the additional procedures in patients receiving initial thoracotomy were necessary for management of thoracotomy‐associated complications rather than for failure of the initial drainage procedure.
Similar to the randomized trials by Sonnappa et al21 and St. Peter et al,22 differences in the overall and post‐procedure LOS were not significant among patients undergoing initial VATS compared with initial chest tube placement with fibrinolysis. However, chest tube placement without fibrinolysis did not result in significant differences in LOS compared with initial VATS. In the only pediatric randomized trial, the 29 intrapleural urokinase recipients had a 2 day shorter LOS compared with the 29 intrapleural saline recipients.33 Several small, randomized controlled trials of adults with complicated pneumonia reported improved pleural fluid drainage among intrapleural fibrinolysis recipients compared with non‐recipients.3436 However, a large multicenter randomized trial in adults found no differences in mortality, requirement for surgical drainage, or LOS between intrapleural streptokinase and placebo recipients.37 Subsequent meta‐analyses of randomized trials in adults also demonstrated no benefit to fibrinolysis.38, 39 In the context of the increasing use of intrapleural fibrinolysis in children with complicated pneumonia, our results highlight the need for a large, multicenter randomized controlled trial to determine whether chest tube with fibrinolysis is superior to chest tube alone.
Two small randomized trials21, 22 and a decision analysis40 identified chest tube with fibrinolysis as the most economical approach to children with complicated pneumonia. However, the costs did not differ significantly between patients undergoing initial VATS or initial chest tube placement with fibrinolysis in our study. The least costly approach was initial chest tube placement without fibrinolysis. Unlike the randomized controlled trials, we considered costs associated with readmissions in determining the total costs. Shah et al41 found no difference in total charges for patients undergoing initial VATS compared with initial chest tube placement; however, patients undergoing initial VATS were concentrated in a few centers, making it difficult to determine the relative importance of procedural and hospital factors.
This multicenter observational study has several limitations. First, discharge diagnosis coding may be unreliable for specific diseases. However, our rigorous definition of complicated pneumonia, supported by the high positive predictive value as verified by medical record review, minimizes the likelihood of misclassification.
Second, unmeasured confounding or residual confounding by indication for the method of pleural drainage may occur, potentially influencing our results in two disparate ways. If patients with more severe systemic illness were too unstable for operative interventions, then our results would be biased towards worse outcomes for children undergoing initial chest tube placement. We adjusted for several variables associated with a greater systemic severity of illness, including intensive care unit admission, making this possibility less likely. We also could not account for some factors associated with more severe local disease such as the size and character of the effusion. We suspect that patients with more extensive local disease (ie, loculated effusions) would have worse outcomes than other patients, regardless of initial procedure, and that these patients would also be more likely to undergo primary surgical drainage. Thus, this study may have underestimated the benefit of initial surgical drainage (eg, VATS) compared with nonsurgical drainage (ie, chest tube placement).
Third, misclassification of the method of initial pleural drainage may have occurred. Patients transferred from another institution following chest tube placement could either be classified as not receiving pleural drainage and thus excluded from the study or classified as having initial VATS or thoracotomy if the reason for transfer was chest tube treatment failure. Additionally, we could not distinguish routine use of fibrinolysis from fibrinolysis to maintain chest tube patency. Whether such misclassification would falsely minimize or maximize differences in outcomes between the various groups remains uncertain. Fourth, because this study only included tertiary care children's hospitals, these data are not generalizable to community settings. VATS requires specialized surgical training that may be unavailable in some areas. Finally, this study demonstrates the relative efficacy of various pleural fluid drainage procedures on short‐term clinical outcomes and resource utilization. However, long‐term functional outcomes should be measured in future prospective studies.
Conclusions
In conclusion, emphasis on evidence driven treatment to optimize care has led to an increasing examination of unwarranted practice variation.42 The lack of evidence for best practice makes it difficult to define unwarranted variation in the treatment of complicated pneumonia. Our study demonstrates the large variability in practice and raises additional questions regarding the optimal drainage strategies. Published randomized trials have focused on comparisons between chest tube placement with fibrinolysis and VATS. However, our data suggest that future randomized trials should include chest tube placement without fibrinolysis as a treatment strategy. In determining the current best treatment for patients with complicated pneumonia, a clinician must weigh the impact of needing an additional procedure in approximately one‐quarter of patients undergoing initial chest tube placement (with or without fibrinolysis) with the risks of general anesthesia and readmission in patients undergoing initial VATS.
Acknowledgements
Dr. Hall had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the analysis.
Community‐acquired pneumonia, the most common serious bacterial infection in childhood, may be complicated by parapneumonic effusion (ie, complicated pneumonia).1 Children with complicated pneumonia require prolonged hospitalization and frequently undergo multiple pleural fluid drainage procedures.2 Additionally, the incidence of complicated pneumonia has increased,37 making the need to define appropriate therapy even more pressing. Defining appropriate therapy is challenging for the individual physician as a result of inconsistent and insufficient evidence, and wide variation in treatment practices.2, 8
Historically, thoracotomy was performed only if initial chest tube placement did not lead to clinical improvement.9, 10 Several authors, noting the rapid resolution of symptoms in children undergoing earlier thoracotomy, advocated for the use of thoracotomy as initial therapy rather than as a procedure of last resort.114 The advent of less invasive techniques such as video‐assisted thoracoscopic surgery (VATS) has served as an additional impetus to consider surgical drainage as the initial treatment strategy.1518 Few well‐designed studies have examined the relative efficacy of these interventions.2, 1922 Published randomized trials were single center, enrolled few patients, and arrived at different conclusions.19, 21, 22 In addition, these trials did not examine other important outcomes such as requirement for additional pleural fluid drainage procedures and hospital readmission. Two large retrospective multicenter studies found modest reductions in length of stay (LOS) and substantial decreases in the requirement for additional pleural fluid drainage procedures in children undergoing initial VATS compared with initial chest tube placement.2, 20 However, Shah et al2 included relatively few patients undergoing VATS. Li et al20 combined patients undergoing initial thoracentesis, initial chest tube placement, late pleural fluid drainage (by any method), and no pleural fluid drainage into a single non‐operative management category, precluding conclusions about the relative benefits of chest tube placement compared with VATS. Neither study2, 20 examined the role of chemical fibrinolysis, a therapy which has been associated with outcomes comparable to VATS in two small randomized trials.21, 22
The objectives of this multicenter study were to describe the variation in the initial management strategy along with associated outcomes of complicated pneumonia in childhood and to determine the comparative effectiveness of different pleural fluid drainage procedures.
Methods
Data Source
The Pediatric Health Information System (PHIS), which contains resource utilization data from 40 freestanding children's hospitals, provided data for this multicenter retrospective cohort study. Participating hospitals are located in noncompeting markets of 27 states plus the District of Columbia. The PHIS database includes patient demographics, diagnoses, and procedures as well as data for all drugs, radiologic studies, laboratory tests, and supplies charged to each patient. Data are de‐identified, however encrypted medical record numbers allow for tracking individual patients across admissions. The Child Health Corporation of America (Shawnee Mission, KS) and participating hospitals jointly assure data quality and reliability as described previously.23, 24 The Children's Hospital of Philadelphia Institutional Review Board reviewed and approved this study.
Patients
Children 18 years of age receiving a pleural drainage procedure for complicated pneumonia were eligible if they were discharged from participating hospitals between January 1, 2004 and June 30, 2009. Study participants met the following criteria: 1) discharge diagnosis of pneumonia (International Classification of Diseases, 9th revision [ICD‐9] discharge diagnosis codes 480.x‐483.x, 485.x‐487.x), 2) discharge diagnosis of pleural effusion (ICD‐9 codes 510.0, 510.9, 511.0, 511.1, or 511.9), and 3) billing charge for antibiotics on the first day of hospitalization. Additionally, the primary discharge diagnosis had to be either pneumonia or pleural effusion. Patients were excluded if they did not undergo pleural fluid drainage or if their initial pleural fluid drainage procedure was thoracentesis.
Study Definitions
Pleural drainage procedures were identified using ICD‐9 procedure codes for thoracentesis (34.91), chest tube placement (34.04), VATS (34.21), and thoracotomy (34.02 or 34.09). Fibrinolysis was defined as receipt of urokinase, streptokinase, or alteplase within two days of initial chest tube placement.
Acute conditions or complications included influenza (487, 487.0, 487.1, 487.8, 488, or V04.81) and hemolytic‐uremic syndrome (283.11). Chronic comorbid conditions (CCCs) (eg, malignancy) were identified using a previously reported classification scheme.25 Billing data were used to classify receipt of mechanical ventilation and medications on the first day of hospitalization.
Measured Outcomes
The primary outcomes were hospital LOS (both overall and post‐initial procedure), requirement for additional pleural drainage procedures, total cost for index hospitalization, all‐cause readmission within 14 days after index hospital discharge, and total cost of the episode (accounting for the cost of readmissions).
Measured Exposures
The primary exposure of interest was the initial pleural fluid drainage procedure, classified as chest tube placement without fibrinolysis, chest tube placement with fibrinolysis, VATS, or thoracotomy.
Statistical Analysis
Variables were summarized using frequencies and percentages for categorical variables, and median, interquartile range (IQR), and range for continuous variables. Outcomes by initial pleural drainage procedure were compared using chi‐squared tests for categorical variables and Kruskal‐Wallis tests for continuous variables.
Multivariable analysis was performed to account for potential confounding by observed baseline variables. For dichotomous outcome variables, modeling consisted of logistic regression using generalized estimating equations to account for hospital clustering. For continuous variables, a mixed model approach was used, treating hospital as a random effect. Log transformation was applied to the right‐skewed outcome variables (LOS and cost). Cost outcomes remained skewed following log transformation, thus gamma mixed models were applied.2629 Odds ratios and 95% confidence intervals (CIs) were reported for comparison of dichotomous outcomes and the adjusted means and 95% CIs were reported for continuous outcomes after appropriate back transformation.
Additional analyses addressed the potential impact of confounding by indication inherent in any observational study. First, patients with an underlying CCC were excluded to ensure that our results would be generalizable to otherwise healthy children with community‐acquired pneumonia. Second, patients undergoing pleural drainage >2 days after hospitalization were excluded to minimize the effect of residual confounding related to differences in timing of the initial drainage procedure. Third, the analysis was repeated using a generalized propensity score as an additional method to account for confounding by indication for the initial drainage procedure.30 Propensity scores, constructed using a multivariable generalized logit model, included all variables listed in Table 1. The inverse of the propensity score was included as a weight in each multivariable model described previously. Only the primary multivariable analyses are presented as the results of the propensity score analysis were nearly identical to the primary analyses.
| Overall | Chest Tube Without Fibrinolysis | Chest Tube With Fibrinolysis | Thoracotomy | VATS | P Value | |
|---|---|---|---|---|---|---|
| ||||||
| N | 3500 | 1672 (47.8) | 623 (17.8) | 797 (22.8) | 408 (11.7) | |
| Age | ||||||
| <1 year | 335 (9.6) | 176 (10.5) | 56 (9.0) | 78 (9.8) | 25 (6.1) | |
| 1 year | 475 (13.6) | 238 (14.2) | 98 (15.7) | 92 (11.5) | 47 (11.5) | 0.003 |
| 24 years | 1230 (35.1) | 548 (32.8) | 203 (32.6) | 310 (38.9) | 169 (41.4) | |
| 59 years | 897 (25.6) | 412 (24.6) | 170 (27.3) | 199 (25.0) | 116 (28.4) | |
| 1014 years | 324 (9.3) | 167 (10.0) | 61 (9.8) | 65 (8.2) | 31 (7.6) | |
| 1518 years | 193 (5.5) | 106 (6.3) | 29 (4.6) | 40 (5.0) | 18 (4.4) | |
| >18 years | 46 (1.3) | 25 (1.5) | 6 (0.96) | 13 (1.6) | 2 (0.5) | |
| Comorbid Conditions | ||||||
| Cardiac | 69 (2.0) | 43 (2.6) | 14 (2.3) | 12 (1.5) | 0 (0.0) | 0.006 |
| Malignancy | 81 (2.3) | 31 (1.9) | 18 (2.9) | 21 (2.6) | 11 (2.7) | 0.375 |
| Neurological | 138 (3.9) | 73 (4.4) | 20 (3.2) | 34 (4.3) | 11 (2.7) | 0.313 |
| Any Other Condition | 202 (5.8) | 96 (5.7) | 40 (6.4) | 47 (5.9) | 19 (4.7) | 0.696 |
| Payer | ||||||
| Government | 1240 (35.6) | 630 (37.8) | 224 (36.0) | 259 (32.7) | 127 (31.3) | <0.001 |
| Private | 1383 (39.7) | 607 (36.4) | 283 (45.4) | 310 (39.2) | 183 (45.07) | |
| Other | 864 (24.8) | 430 (25.8) | 116 (18.6) | 222 (28.1) | 96 (23.65) | |
| Race | ||||||
| Non‐Hispanic White | 1746 (51.9) | 838 (51.6) | 358 (59.7) | 361 (47.8) | 189 (48.7) | <0.001 |
| Non‐Hispanic Black | 601 (17.9) | 318 (19.6) | 90 (15.0) | 128 (17.0) | 65 (16.8) | |
| Hispanic | 588 (17.5) | 280 (17.3) | 73 (12.2) | 155 (20.5) | 80 (20.6) | |
| Asian | 117 (3.5) | 47 (2.9) | 20 (3.3) | 37 (4.9) | 13 (3.4) | |
| Other | 314 (9.3) | 140 (8.6) | 59 (9.8) | 74 (9.8) | 41 (10.6) | |
| Male Sex | 1912 (54.6) | 923 (55.2) | 336 (53.9) | 439 (55.1) | 214 (52.5) | 0.755 |
| Radiology | ||||||
| CT, no US | 1200 (34.3) | 600 (35.9) | 184 (29.5) | 280 (35.1) | 136 (33.3) | <0.001 |
| CT and US | 221 (6.3) | 84 (5.0) | 53 (8.5) | 61 (7.7) | 23 (5.6) | |
| US, no CT | 799 (22.8) | 324 (19.4) | 178 (28.6) | 200 (25.1) | 97 (23.8) | |
| No US, no CT | 1280 (36.6) | 664 (39.7) | 208 (33.4) | 256 (32.1) | 152 (37.3) | |
| Empiric Antibiotic Regimen | ||||||
| Cephalosporins alone | 448 (12.8) | 181 (10.83) | 126 (20.2) | 73 (9.2) | 68 (16.7) | <0.001 |
| Cephalosporin and clindamycin | 797 (22.8) | 359 (21.5) | 145 (23.3) | 184 (23.1) | 109 (26.7) | |
| Other antibiotic combination | 167 (4.8) | 82 (4.9) | 30 (4.8) | 38 (4.8) | 17 (4.2) | |
| Cephalosporin and vancomycin | 2088 (59.7) | 1050 (62.8) | 322 (51.7) | 502 (63.0) | 214 (52.5) | |
| Mechanical ventilation | 494 (14.1) | 251 (15.0) | 75 (12.0) | 114 (14.3) | 54 (13.2) | 0.307 |
| Corticosteroids | 520 (14.9) | 291 (17.4) | 72 (11.6) | 114 (14.3) | 43 (10.5) | <0.001 |
| Blood product transfusionsb | 761 (21.7) | 387 (23.2) | 145 (23.3) | 161 (20.2) | 68 (16.7) | 0.018 |
| Vasoactive infusionsc | 381 (10.9) | 223 (13.3) | 63 (10.1) | 72 (9.0) | 23 (5.6) | <0.001 |
| Admission to intensive care | 1397 (39.9) | 731 (43.7) | 234 (37.6) | 296 (37.1) | 136 (33.3) | <0.001 |
| Extracorporeal membranous oxygenation | 18 (0.5) | 13 (0.8) | 2 (0.3) | 3 (0.4) | 0 (0.0) | 0.163 |
| Hemolytic‐uremic syndrome | 31 (0.9) | 15 (0.9) | 6 (1.0) | 7 (0.9) | 3 (0.7) | 0.985 |
| Influenza | 108 (3.1) | 53 (3.2) | 27 (4.3) | 23 (2.9) | 5 (1.2) | 0.044 |
| Arterial blood gas measurements | 0 (0,1) | 0 (0, 2) | 0 (0,1) | 0 (0, 1) | 0 (0, 1) | <0.001 |
| Days to first procedure | 1 (0, 3) | 1 (0, 2) | 1 (1, 3) | 1 (1, 3) | 1 (1, 3) | <0.001 |
Medical records of a randomly selected subset of subjects from 6 hospitals were reviewed to determine the accuracy of our algorithm in identifying patients with complicated pneumonia; these subjects represented 1% of the study population. For the purposes of medical record review, complicated pneumonia was defined by the following: 1) radiologically‐confirmed lung infiltrate; 2) moderate or large pleural effusion; and 3) signs and symptoms of lower respiratory tract infection. Complicated pneumonia was identified in 118 of 120 reviewed subjects for a positive predictive value of 98.3%.
All analyses were clustered by hospital. Analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC). A two‐tailed P < 0.05 was considered statistically significant.
Results
Patient Characteristics
During the study period, 9,680 subjects had complicated pneumonia. Subjects were excluded if they did not have a pleural drainage procedure (n = 5798), or if thoracentesis was the first pleural fluid drainage procedure performed (n = 382). The remaining 3500 patients were included. Demographic characteristics are summarized in Table 1. The median patient age was 4.1 years (IQR: 2.17.2 years). An underlying CCC was present in 424 (12.1%) patients. There was no association between type of drainage procedure and mechanical ventilation. However, factors associated with more severe systemic illness, such as blood product transfusion, were more common among those undergoing initial chest tube placement with or without fibrinolysis (Table 1).
Initial Pleural Fluid Drainage Procedures
The primary procedures included chest tube without fibrinolysis (47.8%); chest tube with fibrinolysis (17.8%); thoracotomy (22.8%); and VATS (11.7%) (Table 1). The proportion of patients undergoing primary chest tube placement with fibrinolysis increased over time from 14.2% in 2004 to 30.0% in 2009 (P < 0.001; chi‐squared test for trend). The initial procedure varied by hospital with the greatest proportion of patients undergoing primary chest tube placement without fibrinolysis at 28 (70.0%) hospitals, chest tube placement with fibrinolysis at 5 (12.5%) hospitals, thoracotomy at 5 (12.5%) hospitals, and VATS at 2 (5.0%) hospitals (Figure 1). The median proportion of patients undergoing primary VATS across all hospitals was 11.5% (IQR: 3.9%‐26.5%) (Figure 1). The median time to first procedure was 1 day (IQR: 03 days).
Outcome Measures
Variation in outcomes occurred across hospitals. Additional pleural drainage procedures were performed in a median of 20.9% of patients with a range of 6.8% to 44.8% (IQR: 14.5%‐25.3%) of patients across all hospitals. Median LOS was 10 days with a range of 714 days (IQR: 8.511 days) and the median LOS following the initial pleural fluid drainage procedure was 8 days with a range of 6 to 13 days (IQR: 78 days). Variation in timing of the initial pleural fluid drainage procedure explained 9.6% of the variability in LOS (Spearman rho, 0.31; P < 0.001).
Overall, 118 (3.4%) patients were readmitted within 14 days of index discharge; the median readmission rate was 3.8% with a range of 0.8% to 33.3% (IQR: 2.1%‐5.8%) across hospitals. The median total cost of the index hospitalization was $19,574 (IQR: $13,791‐$31,063). The total cost for the index hospitalization exceeded $54,215 for 10% of patients and the total cost of the episode exceeded $55,208 for 10% of patients. Unadjusted outcomes, stratified by primary pleural fluid drainage procedure, are summarized in Table 2.
| Overall | Chest Tube Without Fibrinolysis | Chest Tube With Fibrinolysis | Thoracotomy | VATS | P Valueb | |
|---|---|---|---|---|---|---|
| ||||||
| Additional Procedure | 716 (20.5) | 331 (19.8) | 144 (23.1) | 197 (24.7) | 44 (10.8) | <0.001 |
| Readmission within 14 days | 118 (3.4) | 54 (3.3) | 13 (2.1) | 32 (4.0) | 19 (4.7) | 0.096 |
| Total LOS (days) | 10 (7, 14) | 10 (7, 14) | 9 (7, 13) | 10 (7, 14) | 9 (7, 12) | <.001 |
| Post‐initial Procedure LOS (days) | 8 (5, 12) | 8 (6, 12) | 7 (5, 10) | 8 (5, 12) | 7 (5, 10) | <0.001 |
| Total Cost, Index Hospitalization ($)e | 19319 (13358, 30955) | 19951 (13576, 32018)c | 19565 (13209, 32778)d | 20352 (14351, 31343) | 17918 (13531, 25166) | 0.016 |
| Total Cost, Episode of Illness ($)e | 19831 (13927, 31749) | 20151 (13764, 32653) | 19593 (13210, 32861) | 20573 (14419, 31753) | 18344 (13835, 25462) | 0.029 |
In multivariable analysis, differences in total LOS and post‐procedure LOS were not significant (Table 3). The odds of additional drainage procedures were higher for all drainage procedures compared with initial VATS (Table 3). Patients undergoing initial chest tube placement with fibrinolysis were less likely to require readmission compared with patients undergoing initial VATS (Table 3). The total cost for the episode of illness (including the cost of readmission) was significantly less for those undergoing primary chest tube placement without fibrinolysis compared with primary VATS. The results of subanalyses excluding patients with an underlying CCC (Supporting Appendix online, Table 4) and restricting the cohort to patients undergoing pleural drainage within two days of admission (Supporting Appendix online, Table 5) were similar to the results of our primary analysis with one exception; in the latter subanalysis, children undergoing initial chest tube placement without fibrinolysis were also less likely to require readmission compared with patients undergoing initial VATS.
| Adjusted OR (95% CI)a | P Value | |
|---|---|---|
| ||
| Additional pleural drainage procedure | ||
| Chest tube without fibrinolysis | 1.82 (1.103.00) | .019 |
| Chest tube with fibrinolysis | 2.31 (1.443.72) | <0.001 |
| Thoracotomy | 2.59 (1.624.14) | <0.001 |
| VATS | Reference | |
| Readmission within 14 days | ||
| Chest tube without fibrinolysis | 0.61 (0.361.05) | .077 |
| Chest tube with fibrinolysis | 0.45 (0.230.86) | .015 |
| Thoracotomy | 0.85 (0.521.39) | .521 |
| VATS | Reference | |
| Adjusted Mean (95% CI)a | P Value | |
| Total LOS (days) | ||
| Chest tube without fibrinolysis | 8.0 (7.88.2) | .339 |
| Chest tube with fibrinolysis | 8.1 (7.98.3) | .812 |
| Thoracotomy | 8.1 (7.98.3) | .632 |
| VATS | 8.1 (7.98.3) | Ref |
| Post‐initial procedure LOS (days) | ||
| Chest tube without fibrinolysis | 7.3 (7.07.5) | .512 |
| Chest tube with fibrinolysis | 7.5 (7.27.8) | .239 |
| Thoracotomy | 7.3 (7.07.6) | .841 |
| VATS | 7.3 (7.17.6) | Reference |
| Total cost, index hospitalization ($) | ||
| Chest tube without fibrinolysis | 22928 (2200023895 | .012 |
| Chest tube with fibrinolysis | 23621 (2263124655) | .657 |
| Thoracotomy | 23386 (2241924395 | .262 |
| VATS | 23820 (2280824878) | Reference |
| Total cost, episode of illness ($) | ||
| Chest tube without fibrinolysis | 23218 (2227824199) | .004 |
| Chest tube with fibrinolysis | 23749 (2275224790) | .253 |
| Thoracotomy | 23673 (2269324696) | .131 |
| VATS | 24280 (2324425362) | Reference |
Discussion
This multicenter study is the largest to evaluate the management of children hospitalized with complicated pneumonia. We found considerable variation in initial management and outcomes across hospitals. Differences in timing of the initial drainage procedure explained only a small amount of the variability in outcomes. Children undergoing initial VATS less commonly required additional drainage procedures while children undergoing initial chest tube placement with fibrinolysis less commonly required readmission. Differences in total and post‐procedure LOS were not statistically significant. Differences in cost, while statistically significant, were of marginal relevance.
Previous studies have also shown significant variation in treatment and outcomes of children with complicated pneumonia across hospitals.2, 8 Our study provides data from additional hospitals, includes a substantially larger number of patients undergoing initial VATS, distinguishes between fibrinolysis recipients and nonrecipients, and is the first to compare outcomes between four different initial drainage strategies. The creation of national consensus guidelines might reduce variability in initial management strategies, although the variability in outcomes across hospitals in the current study could not be explained simply by differences in the type or timing of the initial drainage procedure. Thus, future studies examining hospital‐level factors may play an important role in improving quality of care for children with complicated pneumonia.
Patients with initial thoracotomy or chest tube placement with or without fibrinolysis more commonly received additional drainage procedures than patients with initial VATS. This difference remained when patients with CCCs were excluded from the analysis and when the analysis was limited to patients undergoing pleural fluid drainage within 2 days of hospitalization. Several small, randomized trials demonstrated conflicting results when comparing initial chest tube placement with fibrinolysis and VATS. St. Peter et al22 reported that 3 (17%) of 18 patients undergoing initial chest tube placement with fibrinolysis and none of the 18 patients undergoing initial VATS received additional pleural drainage procedures. Sonnappa et al21 found no differences between the two groups. Kurt et al19 did not state the proportion of patients receiving additional procedures. However, the mean number of drainage procedures was 2.25 among the 8 patients undergoing initial chest tube placement while none of the 10 patients with VATS received additional drainage.19
Thoracotomy is often perceived as a definitive procedure for treatment of complicated pneumonia. However, several possibilities exist to explain why additional procedures were performed less frequently in patients undergoing initial VATS compared with initial thoracotomy. The limited visual field in thoracotomy may lead to greater residual disease post‐operatively in those receiving thoracotomy compared with VATS.31 Additionally, thoracotomy substantially disrupts the integrity of the chest wall and is consequently associated with complications such as bleeding and air leak into the pleural cavity more often than VATS.31, 32 It is thus possible that some of the additional procedures in patients receiving initial thoracotomy were necessary for management of thoracotomy‐associated complications rather than for failure of the initial drainage procedure.
Similar to the randomized trials by Sonnappa et al21 and St. Peter et al,22 differences in the overall and post‐procedure LOS were not significant among patients undergoing initial VATS compared with initial chest tube placement with fibrinolysis. However, chest tube placement without fibrinolysis did not result in significant differences in LOS compared with initial VATS. In the only pediatric randomized trial, the 29 intrapleural urokinase recipients had a 2 day shorter LOS compared with the 29 intrapleural saline recipients.33 Several small, randomized controlled trials of adults with complicated pneumonia reported improved pleural fluid drainage among intrapleural fibrinolysis recipients compared with non‐recipients.3436 However, a large multicenter randomized trial in adults found no differences in mortality, requirement for surgical drainage, or LOS between intrapleural streptokinase and placebo recipients.37 Subsequent meta‐analyses of randomized trials in adults also demonstrated no benefit to fibrinolysis.38, 39 In the context of the increasing use of intrapleural fibrinolysis in children with complicated pneumonia, our results highlight the need for a large, multicenter randomized controlled trial to determine whether chest tube with fibrinolysis is superior to chest tube alone.
Two small randomized trials21, 22 and a decision analysis40 identified chest tube with fibrinolysis as the most economical approach to children with complicated pneumonia. However, the costs did not differ significantly between patients undergoing initial VATS or initial chest tube placement with fibrinolysis in our study. The least costly approach was initial chest tube placement without fibrinolysis. Unlike the randomized controlled trials, we considered costs associated with readmissions in determining the total costs. Shah et al41 found no difference in total charges for patients undergoing initial VATS compared with initial chest tube placement; however, patients undergoing initial VATS were concentrated in a few centers, making it difficult to determine the relative importance of procedural and hospital factors.
This multicenter observational study has several limitations. First, discharge diagnosis coding may be unreliable for specific diseases. However, our rigorous definition of complicated pneumonia, supported by the high positive predictive value as verified by medical record review, minimizes the likelihood of misclassification.
Second, unmeasured confounding or residual confounding by indication for the method of pleural drainage may occur, potentially influencing our results in two disparate ways. If patients with more severe systemic illness were too unstable for operative interventions, then our results would be biased towards worse outcomes for children undergoing initial chest tube placement. We adjusted for several variables associated with a greater systemic severity of illness, including intensive care unit admission, making this possibility less likely. We also could not account for some factors associated with more severe local disease such as the size and character of the effusion. We suspect that patients with more extensive local disease (ie, loculated effusions) would have worse outcomes than other patients, regardless of initial procedure, and that these patients would also be more likely to undergo primary surgical drainage. Thus, this study may have underestimated the benefit of initial surgical drainage (eg, VATS) compared with nonsurgical drainage (ie, chest tube placement).
Third, misclassification of the method of initial pleural drainage may have occurred. Patients transferred from another institution following chest tube placement could either be classified as not receiving pleural drainage and thus excluded from the study or classified as having initial VATS or thoracotomy if the reason for transfer was chest tube treatment failure. Additionally, we could not distinguish routine use of fibrinolysis from fibrinolysis to maintain chest tube patency. Whether such misclassification would falsely minimize or maximize differences in outcomes between the various groups remains uncertain. Fourth, because this study only included tertiary care children's hospitals, these data are not generalizable to community settings. VATS requires specialized surgical training that may be unavailable in some areas. Finally, this study demonstrates the relative efficacy of various pleural fluid drainage procedures on short‐term clinical outcomes and resource utilization. However, long‐term functional outcomes should be measured in future prospective studies.
Conclusions
In conclusion, emphasis on evidence driven treatment to optimize care has led to an increasing examination of unwarranted practice variation.42 The lack of evidence for best practice makes it difficult to define unwarranted variation in the treatment of complicated pneumonia. Our study demonstrates the large variability in practice and raises additional questions regarding the optimal drainage strategies. Published randomized trials have focused on comparisons between chest tube placement with fibrinolysis and VATS. However, our data suggest that future randomized trials should include chest tube placement without fibrinolysis as a treatment strategy. In determining the current best treatment for patients with complicated pneumonia, a clinician must weigh the impact of needing an additional procedure in approximately one‐quarter of patients undergoing initial chest tube placement (with or without fibrinolysis) with the risks of general anesthesia and readmission in patients undergoing initial VATS.
Acknowledgements
Dr. Hall had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the analysis.
- ,.Parapneumonic pleural effusion and empyema in children. Review of a 19‐year experience, 1962–1980.Clin Pediatr (Phila).1983;22:414–419.
- ,,,,.Primary early thoracoscopy and reduction in length of hospital stay and additional procedures among children with complicated pneumonia: Results of a multicenter retrospective cohort study.Arch Pediatr Adolesc Med.2008;162:675–681.
- ,.Empyema hospitalizations increased in US children despite pneumococcal conjugate vaccine.Pediatrics.2010;125:26–33.
- ,,, et al.Impact of the pneumococcal conjugate vaccine on pneumococcal parapneumonic empyema.Pediatr Infect Dis J.2006;25:250–254.
- ,,,,.Five‐fold increase in pediatric parapneumonic empyema since introduction of pneumococcal conjugate vaccine.Pediatric Infect Dis J.2008;27:1030–1032.
- ,,,.Increasing incidence of empyema complicating childhood community‐acquired pneumonia in the United States.Clin Infect Dis.2010;50:805–813.
- ,,,,.National hospitalization trends for pediatric pneumonia and associated complications.Pediatrics.2010;126:204–213.
- ,,, et al.Empyema associated with community‐acquired pneumonia: A Pediatric Investigator's Collaborative Network on Infections in Canada (PICNIC) study.BMC Infect Dis.2008;8:129.
- ,,,,.Pleural empyema in children.Ann Thorac Surg.1970;10:37–44.
- ,,.Management of streptococcal empyema.Ann Thorac Surg.1966;2:658–664.
- ,.Thoracoscopy in the management of empyema in children.J Pediatr Surg.1993;28:1128–1132.
- ,,,.Surgical treatment of parapneumonic empyema.Pediatr Pulmonol.1996;22:348–356.
- ,.The controversial role of decortication in the management of pediatric empyema.J Thorac Cardiovasc Surg.1988;96:166–170.
- ,,,,,.Postpneumonic empyema in children treated by early decortication.Eur J Pediatr Surg.1997;7:135–137.
- ,.Video‐assisted thoracoscopic surgery in the management of pediatric empyema.JSLS.1997;1:251–3.
- ,,,.Early video‐assisted thoracic surgery in the management of empyema.Pediatrics.1999;103:e63.
- ,,,,.Early definitive intervention by thoracoscopy in pediatric empyema.J Pediatr Surg.1999;34:178–180; discussion80–81.
- ,,,,.Thoracoscopy in the management of pediatric empyema.J Pediatr Surg.1995;30:1211–1215.
- ,,,,.Therapy of parapneumonic effusions in children: Video‐assisted thoracoscopic surgery versus conventional thoracostomy drainage.Pediatrics.2006;118:e547–e553.
- ,.Primary operative management for pediatric empyema: Decreases in hospital length of stay and charges in a national sample.Arch Pediatr Adolesc Med.2008;162:44–48.
- ,,, et al.Comparison of urokinase and video‐assisted thoracoscopic surgery for treatment of childhood empyema.Am J Respir Crit Care Med.2006;174:221–227.
- ,,, et al.Thoracoscopic decortication vs tube thoracostomy with fibrinolysis for empyema in children: A prospective, randomized trial.J Pediatr Surg.2009;44:106–111; discussion11.
- ,,,.Corticosteroids and mortality in children with bacterial meningitis.JAMA.2008;299:2048–2055.
- ,,,,.Intravenous immunoglobulin in children with streptococcal toxic shock syndrome.Clin Infect Dis.2009;49:1369–1376.
- ,,, et al.Deaths attributed to pediatric complex chronic conditions: National trends and implications for supportive care services.Pediatrics.2001;107:e99.
- ,.Multiple regression of cost data: Use of generalised linear models.J Health Serv Res Policy.2004;9:197–204.
- ,,,.A robustified modeling approach to analyze pediatric length of stay.Ann Epidemiol.2005;15:673–677.
- ,,.Correlates of length of stay, cost of care, and mortality among patients hospitalized for necrotizing fasciitis.Epidemiol Infect.2007;135:868–876.
- ,,,,,.Health care costs of adults treated for attention‐deficit/hyperactivity disorder who received alternative drug therapies.J Manag Care Pharm.2007;13:561–569.
- .The role of the propensity score in estimating dose‐response functions.Biometrika.2000;87:706–710.
- ,,,,.Experience with video‐assisted thoracoscopic surgery in the management of complicated pneumonia in children.J Pediatr Surg.2001;36:316–319.
- ,,, et al.VATS debridement versus thoracotomy in the treatment of loculated postpneumonia empyema.Ann Thorac Surg.1996;61:1626–1630.
- ,,,,.Randomised trial of intrapleural urokinase in the treatment of childhood empyema.Thorax.2002;57:343–347.
- ,,,,,.Intrapleural urokinase versus normal saline in the treatment of complicated parapneumonic effusions and empyema. A randomized, double‐blind study.Am J Respir Crit Care Med.1999;159:37–42.
- ,,.Randomised controlled trial of intrapleural streptokinase in community acquired pleural infection.Thorax.1997;52:416–421.
- ,,,,.Intrapleural streptokinase for empyema and complicated parapneumonic effusions.Am J Respir Crit Care Med.2004;170:49–53.
- ,,, et al.U.K. Controlled trial of intrapleural streptokinase for pleural infection.N Engl J Med.2005;352:865–874.
- ,.Intra‐pleural fibrinolytic therapy versus conservative management in the treatment of adult parapneumonic effusions and empyema.Cochrane Database Syst Rev.2008:CD002312.
- ,,,.Intrapleural fibrinolytic agents for empyema and complicated parapneumonic effusions: A meta‐analysis.Chest.2006;129:783–790.
- ,,.Cost‐effectiveness of competing strategies for the treatment of pediatric empyema.Pediatrics.2008;121:e1250–e1257.
- ,,.Costs of treating children with complicated pneumonia: A comparison of primary video‐assisted thoracoscopic surgery and chest tube placement.Pediatr Pulmonol.2010;45:71–77.
- .Unwarranted variation in pediatric medical care.Pediatr Clin North Am.2009;56:745–755.
- ,.Parapneumonic pleural effusion and empyema in children. Review of a 19‐year experience, 1962–1980.Clin Pediatr (Phila).1983;22:414–419.
- ,,,,.Primary early thoracoscopy and reduction in length of hospital stay and additional procedures among children with complicated pneumonia: Results of a multicenter retrospective cohort study.Arch Pediatr Adolesc Med.2008;162:675–681.
- ,.Empyema hospitalizations increased in US children despite pneumococcal conjugate vaccine.Pediatrics.2010;125:26–33.
- ,,, et al.Impact of the pneumococcal conjugate vaccine on pneumococcal parapneumonic empyema.Pediatr Infect Dis J.2006;25:250–254.
- ,,,,.Five‐fold increase in pediatric parapneumonic empyema since introduction of pneumococcal conjugate vaccine.Pediatric Infect Dis J.2008;27:1030–1032.
- ,,,.Increasing incidence of empyema complicating childhood community‐acquired pneumonia in the United States.Clin Infect Dis.2010;50:805–813.
- ,,,,.National hospitalization trends for pediatric pneumonia and associated complications.Pediatrics.2010;126:204–213.
- ,,, et al.Empyema associated with community‐acquired pneumonia: A Pediatric Investigator's Collaborative Network on Infections in Canada (PICNIC) study.BMC Infect Dis.2008;8:129.
- ,,,,.Pleural empyema in children.Ann Thorac Surg.1970;10:37–44.
- ,,.Management of streptococcal empyema.Ann Thorac Surg.1966;2:658–664.
- ,.Thoracoscopy in the management of empyema in children.J Pediatr Surg.1993;28:1128–1132.
- ,,,.Surgical treatment of parapneumonic empyema.Pediatr Pulmonol.1996;22:348–356.
- ,.The controversial role of decortication in the management of pediatric empyema.J Thorac Cardiovasc Surg.1988;96:166–170.
- ,,,,,.Postpneumonic empyema in children treated by early decortication.Eur J Pediatr Surg.1997;7:135–137.
- ,.Video‐assisted thoracoscopic surgery in the management of pediatric empyema.JSLS.1997;1:251–3.
- ,,,.Early video‐assisted thoracic surgery in the management of empyema.Pediatrics.1999;103:e63.
- ,,,,.Early definitive intervention by thoracoscopy in pediatric empyema.J Pediatr Surg.1999;34:178–180; discussion80–81.
- ,,,,.Thoracoscopy in the management of pediatric empyema.J Pediatr Surg.1995;30:1211–1215.
- ,,,,.Therapy of parapneumonic effusions in children: Video‐assisted thoracoscopic surgery versus conventional thoracostomy drainage.Pediatrics.2006;118:e547–e553.
- ,.Primary operative management for pediatric empyema: Decreases in hospital length of stay and charges in a national sample.Arch Pediatr Adolesc Med.2008;162:44–48.
- ,,, et al.Comparison of urokinase and video‐assisted thoracoscopic surgery for treatment of childhood empyema.Am J Respir Crit Care Med.2006;174:221–227.
- ,,, et al.Thoracoscopic decortication vs tube thoracostomy with fibrinolysis for empyema in children: A prospective, randomized trial.J Pediatr Surg.2009;44:106–111; discussion11.
- ,,,.Corticosteroids and mortality in children with bacterial meningitis.JAMA.2008;299:2048–2055.
- ,,,,.Intravenous immunoglobulin in children with streptococcal toxic shock syndrome.Clin Infect Dis.2009;49:1369–1376.
- ,,, et al.Deaths attributed to pediatric complex chronic conditions: National trends and implications for supportive care services.Pediatrics.2001;107:e99.
- ,.Multiple regression of cost data: Use of generalised linear models.J Health Serv Res Policy.2004;9:197–204.
- ,,,.A robustified modeling approach to analyze pediatric length of stay.Ann Epidemiol.2005;15:673–677.
- ,,.Correlates of length of stay, cost of care, and mortality among patients hospitalized for necrotizing fasciitis.Epidemiol Infect.2007;135:868–876.
- ,,,,,.Health care costs of adults treated for attention‐deficit/hyperactivity disorder who received alternative drug therapies.J Manag Care Pharm.2007;13:561–569.
- .The role of the propensity score in estimating dose‐response functions.Biometrika.2000;87:706–710.
- ,,,,.Experience with video‐assisted thoracoscopic surgery in the management of complicated pneumonia in children.J Pediatr Surg.2001;36:316–319.
- ,,, et al.VATS debridement versus thoracotomy in the treatment of loculated postpneumonia empyema.Ann Thorac Surg.1996;61:1626–1630.
- ,,,,.Randomised trial of intrapleural urokinase in the treatment of childhood empyema.Thorax.2002;57:343–347.
- ,,,,,.Intrapleural urokinase versus normal saline in the treatment of complicated parapneumonic effusions and empyema. A randomized, double‐blind study.Am J Respir Crit Care Med.1999;159:37–42.
- ,,.Randomised controlled trial of intrapleural streptokinase in community acquired pleural infection.Thorax.1997;52:416–421.
- ,,,,.Intrapleural streptokinase for empyema and complicated parapneumonic effusions.Am J Respir Crit Care Med.2004;170:49–53.
- ,,, et al.U.K. Controlled trial of intrapleural streptokinase for pleural infection.N Engl J Med.2005;352:865–874.
- ,.Intra‐pleural fibrinolytic therapy versus conservative management in the treatment of adult parapneumonic effusions and empyema.Cochrane Database Syst Rev.2008:CD002312.
- ,,,.Intrapleural fibrinolytic agents for empyema and complicated parapneumonic effusions: A meta‐analysis.Chest.2006;129:783–790.
- ,,.Cost‐effectiveness of competing strategies for the treatment of pediatric empyema.Pediatrics.2008;121:e1250–e1257.
- ,,.Costs of treating children with complicated pneumonia: A comparison of primary video‐assisted thoracoscopic surgery and chest tube placement.Pediatr Pulmonol.2010;45:71–77.
- .Unwarranted variation in pediatric medical care.Pediatr Clin North Am.2009;56:745–755.
Copyright © 2011 Society of Hospital Medicine
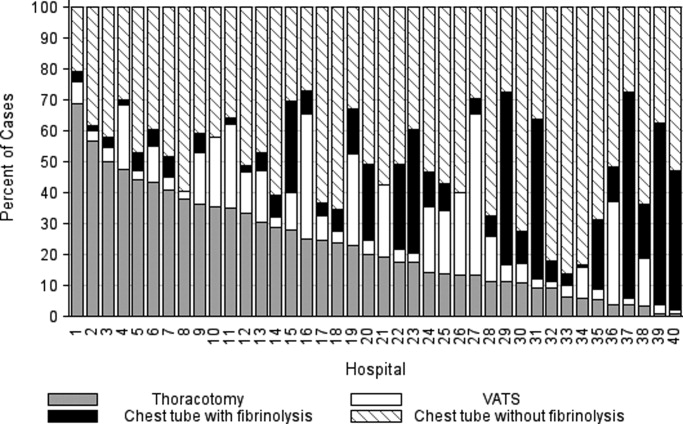
Intervention Progress
A new study of patients with ischemic stroke (JAMA. 2011;305:373-380) found that those admitted to hospitals certified as primary stroke centers had a modestly lower risk of death and serious disability.
Ying Xian, MD, PhD, of the Duke Clinical Research Institute in Durham, N.C., and colleagues compared mortality rates for 30,000 stroke patients in a New York state database, half of them admitted to certified stroke centers and the rest to nondesignated hospitals. Overall 30-day, all-cause mortality was 10.1% for the former group, 12.5% for the latter.
But this modestly lower death rate is still important, says Mark J. Alberts, MD, director of the stroke program at Northwestern University Feinberg School of Medicine in Chicago. "There aren't that many interventions we do in modern medical care that actually prevent death."
In an editorial accompanying the JAMA stroke study, Dr. Alberts portrays an emerging, multitiered system of stroke care, "with the comprehensive stroke center at the top of the pyramid, the primary stroke center in the middle, and the acute stroke-ready hospital at the base." He compares this emerging system to trauma care, which has Level 1 trauma centers at the top of its pyramid.
Not every hospital within a region might be able to pursue stroke center certification, or even become more stroke-ready, he says. But hospitals could work collaboratively to create regional stroke referral networks based on the distribution of patients and resources. Hospitalists can help promote such networks (see The Hospitalist, December 2009). "I would start by knowing your patient population, how many stroke patients present at your hospital each year," he explains.
"The overriding concept is to get stroke patients as efficiently and safely as possible to the hospital that can provide them with the most appropriate level of care," Dr. Alberts says.
More than 800 U.S. hospitals are certified as primary stroke centers by the Joint Commission. While there are not yet formal standards or requirements for an acute-stroke-ready hospital, the term suggests mobilizing resources, capabilities and expertise to receive stroke patients, stabilize them, and send them to the most appropriate facilities based on their medical needs.
A new study of patients with ischemic stroke (JAMA. 2011;305:373-380) found that those admitted to hospitals certified as primary stroke centers had a modestly lower risk of death and serious disability.
Ying Xian, MD, PhD, of the Duke Clinical Research Institute in Durham, N.C., and colleagues compared mortality rates for 30,000 stroke patients in a New York state database, half of them admitted to certified stroke centers and the rest to nondesignated hospitals. Overall 30-day, all-cause mortality was 10.1% for the former group, 12.5% for the latter.
But this modestly lower death rate is still important, says Mark J. Alberts, MD, director of the stroke program at Northwestern University Feinberg School of Medicine in Chicago. "There aren't that many interventions we do in modern medical care that actually prevent death."
In an editorial accompanying the JAMA stroke study, Dr. Alberts portrays an emerging, multitiered system of stroke care, "with the comprehensive stroke center at the top of the pyramid, the primary stroke center in the middle, and the acute stroke-ready hospital at the base." He compares this emerging system to trauma care, which has Level 1 trauma centers at the top of its pyramid.
Not every hospital within a region might be able to pursue stroke center certification, or even become more stroke-ready, he says. But hospitals could work collaboratively to create regional stroke referral networks based on the distribution of patients and resources. Hospitalists can help promote such networks (see The Hospitalist, December 2009). "I would start by knowing your patient population, how many stroke patients present at your hospital each year," he explains.
"The overriding concept is to get stroke patients as efficiently and safely as possible to the hospital that can provide them with the most appropriate level of care," Dr. Alberts says.
More than 800 U.S. hospitals are certified as primary stroke centers by the Joint Commission. While there are not yet formal standards or requirements for an acute-stroke-ready hospital, the term suggests mobilizing resources, capabilities and expertise to receive stroke patients, stabilize them, and send them to the most appropriate facilities based on their medical needs.
A new study of patients with ischemic stroke (JAMA. 2011;305:373-380) found that those admitted to hospitals certified as primary stroke centers had a modestly lower risk of death and serious disability.
Ying Xian, MD, PhD, of the Duke Clinical Research Institute in Durham, N.C., and colleagues compared mortality rates for 30,000 stroke patients in a New York state database, half of them admitted to certified stroke centers and the rest to nondesignated hospitals. Overall 30-day, all-cause mortality was 10.1% for the former group, 12.5% for the latter.
But this modestly lower death rate is still important, says Mark J. Alberts, MD, director of the stroke program at Northwestern University Feinberg School of Medicine in Chicago. "There aren't that many interventions we do in modern medical care that actually prevent death."
In an editorial accompanying the JAMA stroke study, Dr. Alberts portrays an emerging, multitiered system of stroke care, "with the comprehensive stroke center at the top of the pyramid, the primary stroke center in the middle, and the acute stroke-ready hospital at the base." He compares this emerging system to trauma care, which has Level 1 trauma centers at the top of its pyramid.
Not every hospital within a region might be able to pursue stroke center certification, or even become more stroke-ready, he says. But hospitals could work collaboratively to create regional stroke referral networks based on the distribution of patients and resources. Hospitalists can help promote such networks (see The Hospitalist, December 2009). "I would start by knowing your patient population, how many stroke patients present at your hospital each year," he explains.
"The overriding concept is to get stroke patients as efficiently and safely as possible to the hospital that can provide them with the most appropriate level of care," Dr. Alberts says.
More than 800 U.S. hospitals are certified as primary stroke centers by the Joint Commission. While there are not yet formal standards or requirements for an acute-stroke-ready hospital, the term suggests mobilizing resources, capabilities and expertise to receive stroke patients, stabilize them, and send them to the most appropriate facilities based on their medical needs.
The Facebook of Medical Records
A California hospitalist has launched a website that he envisions as an electronic health records (EHR) portal for physicians and patients alike.
MDblackbox aims to blend the interactive familiarity of such social networks as Facebook with the institutional-grade security necessary to comply with the Health Insurance Portability and Accountability Act (HIPPA), according to its inventor, Sami Bogale, MD, a hospitalist at Mills-Peninsula Medical Center in Burlingame, Calif.
"The idea is for any doctor to sign up, nationwide, and [the site] will provide uninterrupted communication" both between doctors and between physicians and patients, says Dr. Bogale, CEO of MDblackbox Inc. "The idea from the patient side is that if a patient goes out of town or goes to a new physician, they have a real copy of their medical record right there."
Dr. Bogale says he's been working on the site for the better part of three years and has spent $250,000 or so on its development. (He jokes that he doesn’t want to know how much time he’s spent on it.) He decided to launch the site this month as he saw other entrepreneurs and physicians looking to take advantage of the momentum behind EHR, buzz attributable in large part to health reform. In fact, the Centers for Medicare & Medicaid Services announced in January that registration had begun for applications to garner a piece of the $20 billion the federal government has set aside for doctors and hospitals that adopt new technologies.
Dr. Bogale continues to look for venture capitalists to back his site, which includes records management, appointment scheduling and reminder, lab orders and voice recordings that can be attached to medical files. Most services are free.
"The idea is to have a nationwide system where every doctor could pretty much have their own personal page and interact with doctors and patients," Dr. Bogale says. "I could see it really growing."
A California hospitalist has launched a website that he envisions as an electronic health records (EHR) portal for physicians and patients alike.
MDblackbox aims to blend the interactive familiarity of such social networks as Facebook with the institutional-grade security necessary to comply with the Health Insurance Portability and Accountability Act (HIPPA), according to its inventor, Sami Bogale, MD, a hospitalist at Mills-Peninsula Medical Center in Burlingame, Calif.
"The idea is for any doctor to sign up, nationwide, and [the site] will provide uninterrupted communication" both between doctors and between physicians and patients, says Dr. Bogale, CEO of MDblackbox Inc. "The idea from the patient side is that if a patient goes out of town or goes to a new physician, they have a real copy of their medical record right there."
Dr. Bogale says he's been working on the site for the better part of three years and has spent $250,000 or so on its development. (He jokes that he doesn’t want to know how much time he’s spent on it.) He decided to launch the site this month as he saw other entrepreneurs and physicians looking to take advantage of the momentum behind EHR, buzz attributable in large part to health reform. In fact, the Centers for Medicare & Medicaid Services announced in January that registration had begun for applications to garner a piece of the $20 billion the federal government has set aside for doctors and hospitals that adopt new technologies.
Dr. Bogale continues to look for venture capitalists to back his site, which includes records management, appointment scheduling and reminder, lab orders and voice recordings that can be attached to medical files. Most services are free.
"The idea is to have a nationwide system where every doctor could pretty much have their own personal page and interact with doctors and patients," Dr. Bogale says. "I could see it really growing."
A California hospitalist has launched a website that he envisions as an electronic health records (EHR) portal for physicians and patients alike.
MDblackbox aims to blend the interactive familiarity of such social networks as Facebook with the institutional-grade security necessary to comply with the Health Insurance Portability and Accountability Act (HIPPA), according to its inventor, Sami Bogale, MD, a hospitalist at Mills-Peninsula Medical Center in Burlingame, Calif.
"The idea is for any doctor to sign up, nationwide, and [the site] will provide uninterrupted communication" both between doctors and between physicians and patients, says Dr. Bogale, CEO of MDblackbox Inc. "The idea from the patient side is that if a patient goes out of town or goes to a new physician, they have a real copy of their medical record right there."
Dr. Bogale says he's been working on the site for the better part of three years and has spent $250,000 or so on its development. (He jokes that he doesn’t want to know how much time he’s spent on it.) He decided to launch the site this month as he saw other entrepreneurs and physicians looking to take advantage of the momentum behind EHR, buzz attributable in large part to health reform. In fact, the Centers for Medicare & Medicaid Services announced in January that registration had begun for applications to garner a piece of the $20 billion the federal government has set aside for doctors and hospitals that adopt new technologies.
Dr. Bogale continues to look for venture capitalists to back his site, which includes records management, appointment scheduling and reminder, lab orders and voice recordings that can be attached to medical files. Most services are free.
"The idea is to have a nationwide system where every doctor could pretty much have their own personal page and interact with doctors and patients," Dr. Bogale says. "I could see it really growing."
The Locums Litmus Test: Is Per Diem Work for You?
Family-medicine-trained hospitalist Benjamin Craig Hamilton, MD,mightrepresent the ideal locum tenens candidate. He’s single, enjoys the challenge of working in new environments, and has is licensed in six states. Currently based in Knoxville, Tenn., he values the professional and monetary rewards of per diem work.
“The beauty is that you can work three months and take three months off,” says Dr. Hamilton, one of thousands of physicians who contract to provide temporary coverage to fill staffing gaps at HM programs around the country. Dr. Hamilton works for Locum Leaders LLC, a national locums firm headquartered in Alpharetta, Ga., that focuses on hospitalists. “If you’re willing to go, you’re never without work. It’s the ultimate flexibility.”
Are You Suited?
Flexibilitytops the list of qualities locum tenens recruiters look for. “The more they [the candidates] can say ‘yes,’ the more likely that we can find a good fit for them,” says Andrea Oldendorf, physician recruiter for Nashville, Tenn.-based Cogent Healthcare. Oldendorfhandles locum tenens placements in the company’s central and western regions.
“We’re a very team-oriented company,” Oldendorf says, noting her objective is to integrate a locum physician into an HM group. “If someone comes in with a lot of limitations, such as ‘I won’t work nights’ or ‘I won’t cover ER admissions,’ that starts to narrow the pool of places where we can use them.”
Every HM program is a little different, according to Robert W. Harrington, MD, SFHM, chief medical officer at Locum Leaders LLC and chair of SHM’s Family Medicine Task Force. “Being able to work with new people, new systems, new computers, and new nursing staff is very important,” he says. Interestingly, the credentialing process provides his recruiters an avenue for gaugingcandidates’ flexibility.“There is so much paperwork, and there are certain parts of it that we can’t do. By the time they get through credentialing, we know whether they’re flexible or not.”
Temporary Work = Test Run
The monetary rewards of locums work often are cited as a major advantage. Locum physicians can gross 30% to 40% more per year (about $280,000 to $300,000) for the same number of shifts as a typical FTE hospitalist (median compensation for non-teaching hospitalists is $215,000 per year, according to the 2010 MGMA-SHM State of Hospital Medicine report). As contracted employees, locum physicians are self-employed and must report their own income and pay their own taxes; many times locum physicians need to hire an accountant.
Working locum tenens also offers a chance to sample a variety of hospital settings. “There’s a big difference between a small rural hospital and a big teaching hospital with a closed ICU,” points out Karen Belote, a physician recruiter for Locum Leaders. “[Working locums] is a great way to try some different locations and different hospitals before settling into a permanent position.”
Pitfalls and Cautions
The only pitfall Dr. Hamilton has observed is perception.“Some people have an initial gut reflex that a locums doctor is either running from something or is not of the same caliber as a permanent physician,” he says. But that notion is quickly dispelled, he says, when he or she demonstrates flexibility, competency, and eagerness to work with the team.
Dr. Hamilton has found a great fit with his current assignments and has no immediate plans to take a permanent position. “I’m learning every day,” he says. “Remember, you are the boss of your life.”
Gretchen Henkel is a freelance writer based in California.
Increase your hirability
Thinking of taking a locum tenens assignment? Consider acquiring additional procedural competencies during your third year of residency, Dr. Harrington advises.
“We are getting more and more requests for people who are comfortable with procedural skills, such as intubations, placing central lines, and vent management,” he says.
Your locum tenens agency might underwrite a procedures course, as Locum Leaders did for Dr. Hamilton. Just make sure you don’t misrepresent your abilities or your comfort level, he cautions. “Know your limits and realize that you are building your career every month,” he says.
SHM will offer a pre-course, “Medical Procedures for the Hospitalist,” at HM11 (May 9, 2011 in Grapevine, Texas), and at many of the HM regional meetings.—GH
Family-medicine-trained hospitalist Benjamin Craig Hamilton, MD,mightrepresent the ideal locum tenens candidate. He’s single, enjoys the challenge of working in new environments, and has is licensed in six states. Currently based in Knoxville, Tenn., he values the professional and monetary rewards of per diem work.
“The beauty is that you can work three months and take three months off,” says Dr. Hamilton, one of thousands of physicians who contract to provide temporary coverage to fill staffing gaps at HM programs around the country. Dr. Hamilton works for Locum Leaders LLC, a national locums firm headquartered in Alpharetta, Ga., that focuses on hospitalists. “If you’re willing to go, you’re never without work. It’s the ultimate flexibility.”
Are You Suited?
Flexibilitytops the list of qualities locum tenens recruiters look for. “The more they [the candidates] can say ‘yes,’ the more likely that we can find a good fit for them,” says Andrea Oldendorf, physician recruiter for Nashville, Tenn.-based Cogent Healthcare. Oldendorfhandles locum tenens placements in the company’s central and western regions.
“We’re a very team-oriented company,” Oldendorf says, noting her objective is to integrate a locum physician into an HM group. “If someone comes in with a lot of limitations, such as ‘I won’t work nights’ or ‘I won’t cover ER admissions,’ that starts to narrow the pool of places where we can use them.”
Every HM program is a little different, according to Robert W. Harrington, MD, SFHM, chief medical officer at Locum Leaders LLC and chair of SHM’s Family Medicine Task Force. “Being able to work with new people, new systems, new computers, and new nursing staff is very important,” he says. Interestingly, the credentialing process provides his recruiters an avenue for gaugingcandidates’ flexibility.“There is so much paperwork, and there are certain parts of it that we can’t do. By the time they get through credentialing, we know whether they’re flexible or not.”
Temporary Work = Test Run
The monetary rewards of locums work often are cited as a major advantage. Locum physicians can gross 30% to 40% more per year (about $280,000 to $300,000) for the same number of shifts as a typical FTE hospitalist (median compensation for non-teaching hospitalists is $215,000 per year, according to the 2010 MGMA-SHM State of Hospital Medicine report). As contracted employees, locum physicians are self-employed and must report their own income and pay their own taxes; many times locum physicians need to hire an accountant.
Working locum tenens also offers a chance to sample a variety of hospital settings. “There’s a big difference between a small rural hospital and a big teaching hospital with a closed ICU,” points out Karen Belote, a physician recruiter for Locum Leaders. “[Working locums] is a great way to try some different locations and different hospitals before settling into a permanent position.”
Pitfalls and Cautions
The only pitfall Dr. Hamilton has observed is perception.“Some people have an initial gut reflex that a locums doctor is either running from something or is not of the same caliber as a permanent physician,” he says. But that notion is quickly dispelled, he says, when he or she demonstrates flexibility, competency, and eagerness to work with the team.
Dr. Hamilton has found a great fit with his current assignments and has no immediate plans to take a permanent position. “I’m learning every day,” he says. “Remember, you are the boss of your life.”
Gretchen Henkel is a freelance writer based in California.
Increase your hirability
Thinking of taking a locum tenens assignment? Consider acquiring additional procedural competencies during your third year of residency, Dr. Harrington advises.
“We are getting more and more requests for people who are comfortable with procedural skills, such as intubations, placing central lines, and vent management,” he says.
Your locum tenens agency might underwrite a procedures course, as Locum Leaders did for Dr. Hamilton. Just make sure you don’t misrepresent your abilities or your comfort level, he cautions. “Know your limits and realize that you are building your career every month,” he says.
SHM will offer a pre-course, “Medical Procedures for the Hospitalist,” at HM11 (May 9, 2011 in Grapevine, Texas), and at many of the HM regional meetings.—GH
Family-medicine-trained hospitalist Benjamin Craig Hamilton, MD,mightrepresent the ideal locum tenens candidate. He’s single, enjoys the challenge of working in new environments, and has is licensed in six states. Currently based in Knoxville, Tenn., he values the professional and monetary rewards of per diem work.
“The beauty is that you can work three months and take three months off,” says Dr. Hamilton, one of thousands of physicians who contract to provide temporary coverage to fill staffing gaps at HM programs around the country. Dr. Hamilton works for Locum Leaders LLC, a national locums firm headquartered in Alpharetta, Ga., that focuses on hospitalists. “If you’re willing to go, you’re never without work. It’s the ultimate flexibility.”
Are You Suited?
Flexibilitytops the list of qualities locum tenens recruiters look for. “The more they [the candidates] can say ‘yes,’ the more likely that we can find a good fit for them,” says Andrea Oldendorf, physician recruiter for Nashville, Tenn.-based Cogent Healthcare. Oldendorfhandles locum tenens placements in the company’s central and western regions.
“We’re a very team-oriented company,” Oldendorf says, noting her objective is to integrate a locum physician into an HM group. “If someone comes in with a lot of limitations, such as ‘I won’t work nights’ or ‘I won’t cover ER admissions,’ that starts to narrow the pool of places where we can use them.”
Every HM program is a little different, according to Robert W. Harrington, MD, SFHM, chief medical officer at Locum Leaders LLC and chair of SHM’s Family Medicine Task Force. “Being able to work with new people, new systems, new computers, and new nursing staff is very important,” he says. Interestingly, the credentialing process provides his recruiters an avenue for gaugingcandidates’ flexibility.“There is so much paperwork, and there are certain parts of it that we can’t do. By the time they get through credentialing, we know whether they’re flexible or not.”
Temporary Work = Test Run
The monetary rewards of locums work often are cited as a major advantage. Locum physicians can gross 30% to 40% more per year (about $280,000 to $300,000) for the same number of shifts as a typical FTE hospitalist (median compensation for non-teaching hospitalists is $215,000 per year, according to the 2010 MGMA-SHM State of Hospital Medicine report). As contracted employees, locum physicians are self-employed and must report their own income and pay their own taxes; many times locum physicians need to hire an accountant.
Working locum tenens also offers a chance to sample a variety of hospital settings. “There’s a big difference between a small rural hospital and a big teaching hospital with a closed ICU,” points out Karen Belote, a physician recruiter for Locum Leaders. “[Working locums] is a great way to try some different locations and different hospitals before settling into a permanent position.”
Pitfalls and Cautions
The only pitfall Dr. Hamilton has observed is perception.“Some people have an initial gut reflex that a locums doctor is either running from something or is not of the same caliber as a permanent physician,” he says. But that notion is quickly dispelled, he says, when he or she demonstrates flexibility, competency, and eagerness to work with the team.
Dr. Hamilton has found a great fit with his current assignments and has no immediate plans to take a permanent position. “I’m learning every day,” he says. “Remember, you are the boss of your life.”
Gretchen Henkel is a freelance writer based in California.
Increase your hirability
Thinking of taking a locum tenens assignment? Consider acquiring additional procedural competencies during your third year of residency, Dr. Harrington advises.
“We are getting more and more requests for people who are comfortable with procedural skills, such as intubations, placing central lines, and vent management,” he says.
Your locum tenens agency might underwrite a procedures course, as Locum Leaders did for Dr. Hamilton. Just make sure you don’t misrepresent your abilities or your comfort level, he cautions. “Know your limits and realize that you are building your career every month,” he says.
SHM will offer a pre-course, “Medical Procedures for the Hospitalist,” at HM11 (May 9, 2011 in Grapevine, Texas), and at many of the HM regional meetings.—GH
Health Reform Turns 1
As America’s love-hate relationship with healthcare reform approaches its first anniversary, the law is proving just as divisive now as it was during the midterm elections. Fittingly, the Patient Protection and Affordable Care Act of 2010 (ACA), which has polarized the country, is moving forward along three separate tracks.
“Usually, at this point of the game one would only be worrying about the implementation,” says Leighton Ku, a health-policy analyst at George Washington University. “But, obviously, there’s been enough discord that the political route and the legal route are now equally important.”
Here’s a look at where the ACA stands from practical, political, and legal standpoints, along with the major players involved in the ongoing tussle.
The Battle of Public Perception
America is hopelessly divided. Despite pollsters’ best efforts to break the stalemate, the collective numbers still suggest that roughly equal numbers of respondents favor and oppose healthcare reform (with a slight advantage to opponents). It’s a trend line that has barely budged since the bill’s enactment last March.
In January, the Republican-led House of Representatives voted to repeal the entire reform act in what analysts have called a largely symbolic gesture, given that the repeal effort subsequently failed in the Democratic-controlled Senate. Even so, Ku says, the vote fulfills a Republican campaign promise and sends a strong signal to the party’s political base. “What’s driving the Republicans is that their constituencies really don’t like it,” agrees Robert J. Blendon, a professor of health policy and political analysis at the Harvard School of Public Health. “Almost all Republican congressmen who ran had on their website, ‘I will repeal this bill if elected.’ ”
But opposition doesn’t necessarily mean voters want everything repealed, a caveat also borne out by recent polling. “Where the public stands is a little more ambiguous than what the campaign rhetoric is,” Ku says. That ambiguity could present an opportunity for both parties to reframe the debate in the coming months in an effort to win over a clear majority of the public. With the economy of paramount concern, Republicans have cast healthcare reform as a “job-destroying” act that will speed the country’s descent into bankruptcy.
If the economy improves, however, opposition to the law is likely to soften. And with their “no” vote behind them, Republicans in the House will be expected to craft a coherent alternative to the legislation. “Now comes the tough part,” Ku says.
Democrats, meanwhile, have largely regrouped and are being more vocal about the law’s necessity—after a campaign season in which many conservative Democrats largely avoided talking about it, or even touted their opposition to it, and were beaten anyway.
In the absence of wholesale repeal, a few individual provisions might be stripped away. Most key elements cannot be defunded, although Republicans could cut funding streams to Health and Human Services (HHS) or the IRS to hamper implementation. Congress also could choose not to appropriate money to the estimated $106 billion worth of new spending authorizations. A sizable percentage of that pool covers popular pre-existing programs, however, which makes a “no” vote politically more risky.
A Matter of Time
The nonpartisan Congressional Budget Office has predicted that repealing the healthcare reform legislation would increase the federal deficit by $230 billion over the next decade. Even so, the law’s supporters are finding little traction among voters who have heard repeated claims by Republicans that the act itself will push the country deeper into debt (many Republicans say the CBO estimate is based on faulty numbers provided by the law’s supporters). One big reason why: The tanking economy has eroded public trust in the government. “The ratings of trust in the federal government are so low,” Blendon says, “you need a stethoscope to try to hear them.”
And then there’s the matter of time. Because the act’s biggest provisions don’t go into effect until 2014, there are no made-for-media moments—like the large numbers of previously uninsured receiving health insurance cards—to counter the dire predictions that patients will lose their doctors. Instead, the White House has tried to make the most of smaller provisions now in effect, such as one that allows children to stay on a parent’s insurance until their 26th birthday, another that lifts the lifetime caps on insurance coverage, and a third that bans insurers from dropping children with pre-existing conditions (a video explaining what the ACA does and doesn’t do, produced by the Kaiser Family Foundation, is available at http://healthreform.kff.org/The Animation.aspx).
In mid-January, on the eve of the House vote to repeal the entire act, the White House released an HHS study to bolster its contention that the law will eventually aid tens of millions, and, conversely, that any repeal would harm them (www.healthcare.gov/center/reports/preexisting.html). The study estimates that 50 million to 129 million Americans under the age of 65 have pre-existing conditions that would, theoretically, make it harder for them to buy insurance in the absence of regulations requiring coverage. But the study also reports that up to 82 million of these people already have employer-provided insurance, meaning they wouldn’t be affected either way unless they switch jobs or become unemployed.
The White House’s case has been made harder by the confluence of a poor economy, growing concern over the deficit, and the ongoing battle over whether and how to fix the Medicare reimbursement rate paid to doctors, according to Blendon. When the rate paid to doctors temporarily nosedived last June, stories about doctors refusing to see Medicare beneficiaries proliferated among alarmed seniors (Congress eventually passed another short-term patch). The memory of that lack of medical access is now being conflated with the potential side effects of the new law by the constituency most likely to vote (seniors) and most skeptical in general about healthcare reform.
Legal Limbo
More than half the states have now joined lawsuits challenging the ACA’s constitutionality. In the first of what observers expect to be a multitude of legal decisions, federal judges in two cases upheld the law, and the individual mandate requiring people to buy health insurance was ruled unconstitutional in a third.
Ultimately, most experts believe the Supreme Court will have the final say, likely before the 2012 elections. Ku says analysts already are talking about a possible 5-4 decision, with Justice Anthony Kennedy as the potential swing vote—though so far, he’s given no clear hints about which way he may be leaning. Even if the individual mandate component is struck down, Ku says, the court could uphold everything else, changing its overall impact but not the implementation of most provisions. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Key Players in the Healthcare Debate

John Boehner (R-Ohio), the new Speaker of the House, is the public face of many Republican talking points on healthcare reform and the leader in trying to maintain a unified front against the existing law.
Paul Ryan (R-Wis.), chairman of the House Budget Committee and a senior member of the Ways and Means Committee, delivered the GOP response to President Obama’s State of the Union address. He will help the party craft a coherent ACA alternative.
Many conservative “Blue Dog” Democrats either actively opposed the law or stayed silent about it—and got routed in November anyway. Most remaining Blue Dogs have since rejoined the party in highlighting the ACA’s benefits. If Republicans pass an alternative measure, it would need to attract some Democratic support to be seen as bipartisan.

Although Sen. Majority Leader Harry Reid (D-Nev.) is opposing any attempt to bring up a vote on repealing the law, Minority Leader Mitch McConnell (R-Ky.) has kept the pressure on, vowing to find a way to force a vote on repealing what he told Fox News Sunday was “the single worst piece of legislation passed in my time in the Senate.” Obama was criticized by other Democrats for not being more vocal about healthcare reform’s benefits in the leadup to the November elections. The repeal effort gives him another chance to make his case.

HHS Secretary Kathleen Sebelius likely will testify repeatedly in hearings called by the Republican leadership to scrutinize how the law is being implemented.
Supreme Court Justice Anthony Kennedy, appointed by President Reagan, is expected to be the swing vote in a closely divided court. The issue: whether an individual mandate requiring people to buy insurance is constitutional. So far, he has given little indication as to how he might rule.
—BN
As America’s love-hate relationship with healthcare reform approaches its first anniversary, the law is proving just as divisive now as it was during the midterm elections. Fittingly, the Patient Protection and Affordable Care Act of 2010 (ACA), which has polarized the country, is moving forward along three separate tracks.
“Usually, at this point of the game one would only be worrying about the implementation,” says Leighton Ku, a health-policy analyst at George Washington University. “But, obviously, there’s been enough discord that the political route and the legal route are now equally important.”
Here’s a look at where the ACA stands from practical, political, and legal standpoints, along with the major players involved in the ongoing tussle.
The Battle of Public Perception
America is hopelessly divided. Despite pollsters’ best efforts to break the stalemate, the collective numbers still suggest that roughly equal numbers of respondents favor and oppose healthcare reform (with a slight advantage to opponents). It’s a trend line that has barely budged since the bill’s enactment last March.
In January, the Republican-led House of Representatives voted to repeal the entire reform act in what analysts have called a largely symbolic gesture, given that the repeal effort subsequently failed in the Democratic-controlled Senate. Even so, Ku says, the vote fulfills a Republican campaign promise and sends a strong signal to the party’s political base. “What’s driving the Republicans is that their constituencies really don’t like it,” agrees Robert J. Blendon, a professor of health policy and political analysis at the Harvard School of Public Health. “Almost all Republican congressmen who ran had on their website, ‘I will repeal this bill if elected.’ ”
But opposition doesn’t necessarily mean voters want everything repealed, a caveat also borne out by recent polling. “Where the public stands is a little more ambiguous than what the campaign rhetoric is,” Ku says. That ambiguity could present an opportunity for both parties to reframe the debate in the coming months in an effort to win over a clear majority of the public. With the economy of paramount concern, Republicans have cast healthcare reform as a “job-destroying” act that will speed the country’s descent into bankruptcy.
If the economy improves, however, opposition to the law is likely to soften. And with their “no” vote behind them, Republicans in the House will be expected to craft a coherent alternative to the legislation. “Now comes the tough part,” Ku says.
Democrats, meanwhile, have largely regrouped and are being more vocal about the law’s necessity—after a campaign season in which many conservative Democrats largely avoided talking about it, or even touted their opposition to it, and were beaten anyway.
In the absence of wholesale repeal, a few individual provisions might be stripped away. Most key elements cannot be defunded, although Republicans could cut funding streams to Health and Human Services (HHS) or the IRS to hamper implementation. Congress also could choose not to appropriate money to the estimated $106 billion worth of new spending authorizations. A sizable percentage of that pool covers popular pre-existing programs, however, which makes a “no” vote politically more risky.
A Matter of Time
The nonpartisan Congressional Budget Office has predicted that repealing the healthcare reform legislation would increase the federal deficit by $230 billion over the next decade. Even so, the law’s supporters are finding little traction among voters who have heard repeated claims by Republicans that the act itself will push the country deeper into debt (many Republicans say the CBO estimate is based on faulty numbers provided by the law’s supporters). One big reason why: The tanking economy has eroded public trust in the government. “The ratings of trust in the federal government are so low,” Blendon says, “you need a stethoscope to try to hear them.”
And then there’s the matter of time. Because the act’s biggest provisions don’t go into effect until 2014, there are no made-for-media moments—like the large numbers of previously uninsured receiving health insurance cards—to counter the dire predictions that patients will lose their doctors. Instead, the White House has tried to make the most of smaller provisions now in effect, such as one that allows children to stay on a parent’s insurance until their 26th birthday, another that lifts the lifetime caps on insurance coverage, and a third that bans insurers from dropping children with pre-existing conditions (a video explaining what the ACA does and doesn’t do, produced by the Kaiser Family Foundation, is available at http://healthreform.kff.org/The Animation.aspx).
In mid-January, on the eve of the House vote to repeal the entire act, the White House released an HHS study to bolster its contention that the law will eventually aid tens of millions, and, conversely, that any repeal would harm them (www.healthcare.gov/center/reports/preexisting.html). The study estimates that 50 million to 129 million Americans under the age of 65 have pre-existing conditions that would, theoretically, make it harder for them to buy insurance in the absence of regulations requiring coverage. But the study also reports that up to 82 million of these people already have employer-provided insurance, meaning they wouldn’t be affected either way unless they switch jobs or become unemployed.
The White House’s case has been made harder by the confluence of a poor economy, growing concern over the deficit, and the ongoing battle over whether and how to fix the Medicare reimbursement rate paid to doctors, according to Blendon. When the rate paid to doctors temporarily nosedived last June, stories about doctors refusing to see Medicare beneficiaries proliferated among alarmed seniors (Congress eventually passed another short-term patch). The memory of that lack of medical access is now being conflated with the potential side effects of the new law by the constituency most likely to vote (seniors) and most skeptical in general about healthcare reform.
Legal Limbo
More than half the states have now joined lawsuits challenging the ACA’s constitutionality. In the first of what observers expect to be a multitude of legal decisions, federal judges in two cases upheld the law, and the individual mandate requiring people to buy health insurance was ruled unconstitutional in a third.
Ultimately, most experts believe the Supreme Court will have the final say, likely before the 2012 elections. Ku says analysts already are talking about a possible 5-4 decision, with Justice Anthony Kennedy as the potential swing vote—though so far, he’s given no clear hints about which way he may be leaning. Even if the individual mandate component is struck down, Ku says, the court could uphold everything else, changing its overall impact but not the implementation of most provisions. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Key Players in the Healthcare Debate
John Boehner (R-Ohio), the new Speaker of the House, is the public face of many Republican talking points on healthcare reform and the leader in trying to maintain a unified front against the existing law.
Paul Ryan (R-Wis.), chairman of the House Budget Committee and a senior member of the Ways and Means Committee, delivered the GOP response to President Obama’s State of the Union address. He will help the party craft a coherent ACA alternative.
Many conservative “Blue Dog” Democrats either actively opposed the law or stayed silent about it—and got routed in November anyway. Most remaining Blue Dogs have since rejoined the party in highlighting the ACA’s benefits. If Republicans pass an alternative measure, it would need to attract some Democratic support to be seen as bipartisan.
Although Sen. Majority Leader Harry Reid (D-Nev.) is opposing any attempt to bring up a vote on repealing the law, Minority Leader Mitch McConnell (R-Ky.) has kept the pressure on, vowing to find a way to force a vote on repealing what he told Fox News Sunday was “the single worst piece of legislation passed in my time in the Senate.” Obama was criticized by other Democrats for not being more vocal about healthcare reform’s benefits in the leadup to the November elections. The repeal effort gives him another chance to make his case.
HHS Secretary Kathleen Sebelius likely will testify repeatedly in hearings called by the Republican leadership to scrutinize how the law is being implemented.
Supreme Court Justice Anthony Kennedy, appointed by President Reagan, is expected to be the swing vote in a closely divided court. The issue: whether an individual mandate requiring people to buy insurance is constitutional. So far, he has given little indication as to how he might rule.
—BN
As America’s love-hate relationship with healthcare reform approaches its first anniversary, the law is proving just as divisive now as it was during the midterm elections. Fittingly, the Patient Protection and Affordable Care Act of 2010 (ACA), which has polarized the country, is moving forward along three separate tracks.
“Usually, at this point of the game one would only be worrying about the implementation,” says Leighton Ku, a health-policy analyst at George Washington University. “But, obviously, there’s been enough discord that the political route and the legal route are now equally important.”
Here’s a look at where the ACA stands from practical, political, and legal standpoints, along with the major players involved in the ongoing tussle.
The Battle of Public Perception
America is hopelessly divided. Despite pollsters’ best efforts to break the stalemate, the collective numbers still suggest that roughly equal numbers of respondents favor and oppose healthcare reform (with a slight advantage to opponents). It’s a trend line that has barely budged since the bill’s enactment last March.
In January, the Republican-led House of Representatives voted to repeal the entire reform act in what analysts have called a largely symbolic gesture, given that the repeal effort subsequently failed in the Democratic-controlled Senate. Even so, Ku says, the vote fulfills a Republican campaign promise and sends a strong signal to the party’s political base. “What’s driving the Republicans is that their constituencies really don’t like it,” agrees Robert J. Blendon, a professor of health policy and political analysis at the Harvard School of Public Health. “Almost all Republican congressmen who ran had on their website, ‘I will repeal this bill if elected.’ ”
But opposition doesn’t necessarily mean voters want everything repealed, a caveat also borne out by recent polling. “Where the public stands is a little more ambiguous than what the campaign rhetoric is,” Ku says. That ambiguity could present an opportunity for both parties to reframe the debate in the coming months in an effort to win over a clear majority of the public. With the economy of paramount concern, Republicans have cast healthcare reform as a “job-destroying” act that will speed the country’s descent into bankruptcy.
If the economy improves, however, opposition to the law is likely to soften. And with their “no” vote behind them, Republicans in the House will be expected to craft a coherent alternative to the legislation. “Now comes the tough part,” Ku says.
Democrats, meanwhile, have largely regrouped and are being more vocal about the law’s necessity—after a campaign season in which many conservative Democrats largely avoided talking about it, or even touted their opposition to it, and were beaten anyway.
In the absence of wholesale repeal, a few individual provisions might be stripped away. Most key elements cannot be defunded, although Republicans could cut funding streams to Health and Human Services (HHS) or the IRS to hamper implementation. Congress also could choose not to appropriate money to the estimated $106 billion worth of new spending authorizations. A sizable percentage of that pool covers popular pre-existing programs, however, which makes a “no” vote politically more risky.
A Matter of Time
The nonpartisan Congressional Budget Office has predicted that repealing the healthcare reform legislation would increase the federal deficit by $230 billion over the next decade. Even so, the law’s supporters are finding little traction among voters who have heard repeated claims by Republicans that the act itself will push the country deeper into debt (many Republicans say the CBO estimate is based on faulty numbers provided by the law’s supporters). One big reason why: The tanking economy has eroded public trust in the government. “The ratings of trust in the federal government are so low,” Blendon says, “you need a stethoscope to try to hear them.”
And then there’s the matter of time. Because the act’s biggest provisions don’t go into effect until 2014, there are no made-for-media moments—like the large numbers of previously uninsured receiving health insurance cards—to counter the dire predictions that patients will lose their doctors. Instead, the White House has tried to make the most of smaller provisions now in effect, such as one that allows children to stay on a parent’s insurance until their 26th birthday, another that lifts the lifetime caps on insurance coverage, and a third that bans insurers from dropping children with pre-existing conditions (a video explaining what the ACA does and doesn’t do, produced by the Kaiser Family Foundation, is available at http://healthreform.kff.org/The Animation.aspx).
In mid-January, on the eve of the House vote to repeal the entire act, the White House released an HHS study to bolster its contention that the law will eventually aid tens of millions, and, conversely, that any repeal would harm them (www.healthcare.gov/center/reports/preexisting.html). The study estimates that 50 million to 129 million Americans under the age of 65 have pre-existing conditions that would, theoretically, make it harder for them to buy insurance in the absence of regulations requiring coverage. But the study also reports that up to 82 million of these people already have employer-provided insurance, meaning they wouldn’t be affected either way unless they switch jobs or become unemployed.
The White House’s case has been made harder by the confluence of a poor economy, growing concern over the deficit, and the ongoing battle over whether and how to fix the Medicare reimbursement rate paid to doctors, according to Blendon. When the rate paid to doctors temporarily nosedived last June, stories about doctors refusing to see Medicare beneficiaries proliferated among alarmed seniors (Congress eventually passed another short-term patch). The memory of that lack of medical access is now being conflated with the potential side effects of the new law by the constituency most likely to vote (seniors) and most skeptical in general about healthcare reform.
Legal Limbo
More than half the states have now joined lawsuits challenging the ACA’s constitutionality. In the first of what observers expect to be a multitude of legal decisions, federal judges in two cases upheld the law, and the individual mandate requiring people to buy health insurance was ruled unconstitutional in a third.
Ultimately, most experts believe the Supreme Court will have the final say, likely before the 2012 elections. Ku says analysts already are talking about a possible 5-4 decision, with Justice Anthony Kennedy as the potential swing vote—though so far, he’s given no clear hints about which way he may be leaning. Even if the individual mandate component is struck down, Ku says, the court could uphold everything else, changing its overall impact but not the implementation of most provisions. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Key Players in the Healthcare Debate
John Boehner (R-Ohio), the new Speaker of the House, is the public face of many Republican talking points on healthcare reform and the leader in trying to maintain a unified front against the existing law.
Paul Ryan (R-Wis.), chairman of the House Budget Committee and a senior member of the Ways and Means Committee, delivered the GOP response to President Obama’s State of the Union address. He will help the party craft a coherent ACA alternative.
Many conservative “Blue Dog” Democrats either actively opposed the law or stayed silent about it—and got routed in November anyway. Most remaining Blue Dogs have since rejoined the party in highlighting the ACA’s benefits. If Republicans pass an alternative measure, it would need to attract some Democratic support to be seen as bipartisan.
Although Sen. Majority Leader Harry Reid (D-Nev.) is opposing any attempt to bring up a vote on repealing the law, Minority Leader Mitch McConnell (R-Ky.) has kept the pressure on, vowing to find a way to force a vote on repealing what he told Fox News Sunday was “the single worst piece of legislation passed in my time in the Senate.” Obama was criticized by other Democrats for not being more vocal about healthcare reform’s benefits in the leadup to the November elections. The repeal effort gives him another chance to make his case.
HHS Secretary Kathleen Sebelius likely will testify repeatedly in hearings called by the Republican leadership to scrutinize how the law is being implemented.
Supreme Court Justice Anthony Kennedy, appointed by President Reagan, is expected to be the swing vote in a closely divided court. The issue: whether an individual mandate requiring people to buy insurance is constitutional. So far, he has given little indication as to how he might rule.
—BN
Call of Duty
Dave Bowman, MD, doesn’t run anywhere anymore; it’s more of a fast walk. He doesn’t consider himself political, yet he does his civic duty and votes in every election. He’s not a big fan of vegetables, but he eats them to appease his wife and his conscience. Most important, Dr. Bowman doesn’t consider himself a hero. In fact, he doesn’t consider what he did that day any different from what he does every day in the hospital.
On the morning of Jan. 8, Dr. Bowman and his wife, Nancy, were thrust into the epicenter of one of the worst shooting rampages in American history. Dr. Bowman, a hospitalist, was the first physician on the scene outside the Tucson, Ariz., grocery store where a lone gunman killed six people and injured 13 others, including U.S. Representative Gabrielle Giffords (D-Ariz.).
“A hero is somebody, to me, who steps out of their element, steps up to the task that is needed, a task that is completely foreign to them, and steps up and helps people,” says Dr. Bowman, 61, executive director for IPC The Hospitalist Co.’s Tucson region. “A hero is not somebody who should be able to help in some manner and should be expected to help. … I don’t think nurses, doctors, firemen, EMTs get to be labeled as heroes. It’s what we should do, and gladly do, and in many cases took an oath to do.”
Even so, Dr. Bowman’s recollection of that frightful morning is a story laced with tragedy, courage, and hope. He remembers those who are “no longer with us.” He remembers his wife administering CPR and calling victims’ loved ones on their cellphones. And he remembers the brave men and women who not only subdued the shooter, but who worked together, selflessly, and in many cases with no medical training, to assist their injured neighbors.

“It was a pretty traumatic scene. More for others than for me; I am supposed to be the doctor and can handle all that,” he says, pausing. “But they don’t teach this course in medical school.”
Shots Ring Out, First Thought Is Help
Born and raised 100 miles south of Tucson and internal-medicine-trained at the University of Arizona, Dr. Bowman became a hospitalist in 1998 and began working with IPC in 2000. He supervises a staff of about 90 providers, including more than 50 full-time hospitalists, serving two large community hospitals, rehabilitations centers, and skilled nursing facilities in the Tucson area.
Yet he knows who the real boss is in the Bowman household. He and Nancy, an ICU nurse, had just finished a brisk walk, eaten breakfast at McDonald’s, and stopped at Safeway to pick up some vegetables on the morning of Jan. 8. “I had the oatmeal. I was so proud of myself,” Dr. Bowman says. “And, as wives will want to do, she pushes the envelope and says she wants to stop by and get some Brussels sprouts. She hadn’t had them in 20 years, and I hadn’t had them in 45 years—since my mom stunk up the house with them. So we ended up at the Safeway, because the two things that keeps a marriage together are those two words: ‘Yes, dear.’ ”
The Bowmans passed by Rep. Giffords, her staff, and about 25 people in front of the grocery store entrance. They went to the produce department and had not been in the store for more than three or four minutes before shots rang out.
“I was 150 percent sure they were gunshots,” Dr. Bowman says. “I said to my wife, ‘Let’s go, Nancy,’ and she didn’t hear me. I thought she was right behind me. But she had gone over to the Brussels sprouts and I was still in mushrooms.”
Walking to the door, Dr. Bowman saw a woman rushing in and shouting, “They shot her. They shot Congresswoman Giffords.”
“I stepped out and stood behind a pillar until no more gunshots,” he says. “They’d actually already taken down the shooter as soon as he ran out of bullets. I looked around the corner to the carnage, as you’d expect, with Congresswoman Giffords the first person I saw right at the head of the line near the front door.
“Quite frankly, I stepped over people who were no longer with us to get to her. I got her turned around and moved off to the window; she wasn’t breathing real well. I worked on her airway, cleaning her airway with the young man [Rep. Giffords’ intern, Daniel Hernandez], who then held her for the next 15 to 20 minutes until the paramedics got her ready to go to the hospital.”
From that moment, Dr. Bowman says his training and instincts took over. More important, he went into field-triage mode, “which means you can’t do anything for that one. Can’t do anything there, this one is breathing and talking, not bleeding bad, good; still breathing, good, stay right there, I will be back. You go all the way up the line from person to person, seeing who you can and can’t help.
“The problem with field triage is that you really can’t stop and do a lot, like CPR, because then the rest of the people don’t have anybody looking at them. So you just keep moving,” he explains.
He says that while it was only minutes from the first gunshot to the time police arrived and secured the scene to the time paramedics were allowed to assist with the injured, it seemed like hours. Additionally, in his haste to help, Dr. Bowman had lost track of Nancy.
“I looked back and she was not there,” he says, adding she’d been swept to the back of the grocery store. “I kept working and I looked back and she had pushed [aside] the 17-year-old sacker who was acting as a security guard. … She came outside and started doing CPR on the first person she saw. I got up the line and there was a doctor doing CPR on the young girl [Christina-Taylor Green]. He was in the parking lot when the shots rang out; he threw his wife in the car and ran up to the little girl.”
Instinct and Autopilot
In a little more than 10 seconds, the gunman had fired more than 30 rounds and killed or injured nearly 20 people.
After he’d checked on all of the wounded, Dr. Bowman says he came upon four people holding the suspected shooter down. “One of them, I didn’t know it, was one of my colleagues, Dr. Stephen Rayle,” Dr. Bowman says. “I said, ‘Hold him, and I will send the first officer over here.’ ”
From there, Dr. Bowman says, he went back up the line of injured, checking for breathing sounds and bleeding, making sure every injured person was being attended to.
“People shot in the leg were holding a hand over a chest wound on the man or woman next to them,” he says. “It was one of those chaotic scenes that you try to make some kind of order to, by deciding who you can help and who you can’t.”
When the first paramedics arrived, Dr. Bowman directed them to Rep. Giffords and the 9-year-old girl. Soon after, there were enough EMTs on scene to attend to each of the victims.
“You are just on automatic,” Dr. Bowman explains. “Actually, after I dealt with the first two victims pretty quickly, Giffords taking the most time to just get her situated, I did stop and look out in the parking lot just to see if anybody was aiming anything at us.”
The most difficult part of field triage, Dr. Bowman says, is staying calm, organized, and “not losing it emotionally.” In fact, he ushered some shell-shocked bystanders away from the scene. “Some people will step right forward and say, ‘Can I help? I know CPR.’ Other people will just stand there and scream.”
Even tougher, he says, was watching his wife try to save the life of U.S. District Judge John Roll (see “Remembering the Dead,” above). “I finally had to go to my wife, pull her off of him, and say, ‘Honey, he’s gone. I need help with this lady who has been shot in the chest laying in the street,’ ” Dr. Bowman says. “Pulling them away is pretty hard. ... It was harder for her and the bystanders, because they were the ones getting right down close with the patient, talking to them, telling patients to ‘keep looking at me.’ That is a very close bond that develops. Field triage, you just keep moving.”
Human Spirit, Cooperation, and Hope
One month after the shooting, Rep. Giffords was moving, talking, thinking, and recuperating at what her doctors at Houston’s TIRR Hermann Memorial deemed “lightning speed.” For Dr. Bowman, such news brings more than a sigh of relief.
“In truth, when I was first with her, she wasn’t responding,” he says. “She was breathing, although with a compromised airway. We got that straightened away and she had a good pulse. Daniel Hernandez, the young man with her, had some nursing training and was comfortable being with her.
“It was amazing to me, the second or third time down the line, just to look over to this guy, and he was watching for me, and he would nod and say, ‘We’re OK. She’s breathing, pulse is OK.’ I didn’t have to go back, and the third time down he said, ‘She’s moving, she’s squeezing my hand.’ ”
It was at that moment that Dr. Bowman felt the congresswoman, in spite of her severe head trauma, had a fighting chance. Others miracles were happening all around him. Each memory ceases to amaze the veteran physician.
“People who were injured holding somebody’s head in their lap because they were hit in the head and this person was hit in the chest,” he says. “It gives you hope for the human race. Those people, to me, were the heroes.”
Looking back, Dr. Bowman says, he’s played back the moment in his mind more than a few times, wondering if he did the right thing for every victim. He wonders how much he and his wife, the other doctors at the scene, and the bystanders really helped. Then, after a brief moment, he has the answer.
“It really took two weeks to really say that, when all the victims that had expired were dead at the scene, and everybody that got taken away made it and out of the hospital, it sunk in that we had made the right decisions,” he says. “Nobody died on the operating table because we didn’t pick up the gunshot wound to the back. It took two weeks to realize we did the right thing.”
Some of those answers will take many more weeks. Rep. Giffords, although she is on a positive path, still has a long road to a full recovery, and doctors are making no promises. “I don’t know how far she will make it or how long it is going to take, but there are some miracles out there,” Dr. Bowman says.
You’re a Hospitalist? You’re Ready
As a physician in the middle of a mass-casualty event, the media called upon Dr. Bowman to recount the events of the Tucson shooting. In more than a dozen interviews with local and national media, not once was Dr. Bowman referred to as a hospitalist.
“At the scene, when I kneel down, I am a doctor. Can you tell me what’s going on, can you talk to me? It goes no farther than that,” he says. “In talking with one of the interviewers, she asked, ‘What kind of doctor are you?’ I said, ‘I am an internist and a hospitalist, which is a doctor who works just in the hospital.’ They weren’t interested in that. When the cameras rolled, she said, ‘I understand you are an intern?’ I said, ‘No, I am an internist. Turn that thing off and start again.’
“That’s the level of knowledge you are dealing with, and that was a national anchorperson I was dealing with.”
It’s an all-too-common refrain for hospitalists around the country, but one Dr. Bowman and others like him have endured for years. It doesn’t bother him, and he says it shouldn’t bother others.
“Doctor or nurse was as far as it got. I can certainly understand that,” he says. “We explain what a hospitalist is every day. We’ve been doing it for 12, 13, 14 years, and people still don’t understand. It’s OK.”
What isn’t OK is hospitalist unpreparedness. In fact, Dr. Bowman says, his training as an internist and his years of HM experience played a pivotal role in managing the scene of the Tucson shooting. The first thing to do, in addition to remaining calm, is to keep your priorities straight and remember your ABCs.

“It’s airway, airway, airway,” he says. “Without an airway, people don’t live. Then you are looking for bleeding, bleeding, bleeding. Then if they are talking, not a lot of bleeding and have a pulse, that is good enough for right now. So, it’s ‘Lady, just keep pushing on the chest right there on that wound.’ … I think, if you remember your ABCs, that’s all you can do in a field triage situation.”
Although the circumstances are less stressful, hospitalists are faced with make-or-break decisions every day, Dr. Bowman says. For example, it’s 4 p.m. and the day shift physician in the ED calls and says he has six admissions he’s been working on for the past three hours. “You, based on the info given to you, have to decide, Well, who is sickest, who do I have to get to first, who is going to the ICU?” Dr. Bowman says. “You do this triage thing in your mind as you walk to the ED. If there is any corollary, it’s the fact that you, as the hospitalist, get hit with a slew of patients all at once. They don’t come in one every 15 minutes like in your office for a blood-pressure check.
“Be ready. And, by the way, you are ready,” he adds. “You take care of a stroke patient in room one, take care of a gangrenous leg in room two, a diabetic with ketoacidosis in room three. The broadness, the generality of your training, you are ready to take care of a variety of things. You’re going to be able to help. Just be ready.” TH
Jason Carris is editor of The Hospitalist.
Dave Bowman, MD, doesn’t run anywhere anymore; it’s more of a fast walk. He doesn’t consider himself political, yet he does his civic duty and votes in every election. He’s not a big fan of vegetables, but he eats them to appease his wife and his conscience. Most important, Dr. Bowman doesn’t consider himself a hero. In fact, he doesn’t consider what he did that day any different from what he does every day in the hospital.
On the morning of Jan. 8, Dr. Bowman and his wife, Nancy, were thrust into the epicenter of one of the worst shooting rampages in American history. Dr. Bowman, a hospitalist, was the first physician on the scene outside the Tucson, Ariz., grocery store where a lone gunman killed six people and injured 13 others, including U.S. Representative Gabrielle Giffords (D-Ariz.).
“A hero is somebody, to me, who steps out of their element, steps up to the task that is needed, a task that is completely foreign to them, and steps up and helps people,” says Dr. Bowman, 61, executive director for IPC The Hospitalist Co.’s Tucson region. “A hero is not somebody who should be able to help in some manner and should be expected to help. … I don’t think nurses, doctors, firemen, EMTs get to be labeled as heroes. It’s what we should do, and gladly do, and in many cases took an oath to do.”
Even so, Dr. Bowman’s recollection of that frightful morning is a story laced with tragedy, courage, and hope. He remembers those who are “no longer with us.” He remembers his wife administering CPR and calling victims’ loved ones on their cellphones. And he remembers the brave men and women who not only subdued the shooter, but who worked together, selflessly, and in many cases with no medical training, to assist their injured neighbors.
“It was a pretty traumatic scene. More for others than for me; I am supposed to be the doctor and can handle all that,” he says, pausing. “But they don’t teach this course in medical school.”
Shots Ring Out, First Thought Is Help
Born and raised 100 miles south of Tucson and internal-medicine-trained at the University of Arizona, Dr. Bowman became a hospitalist in 1998 and began working with IPC in 2000. He supervises a staff of about 90 providers, including more than 50 full-time hospitalists, serving two large community hospitals, rehabilitations centers, and skilled nursing facilities in the Tucson area.
Yet he knows who the real boss is in the Bowman household. He and Nancy, an ICU nurse, had just finished a brisk walk, eaten breakfast at McDonald’s, and stopped at Safeway to pick up some vegetables on the morning of Jan. 8. “I had the oatmeal. I was so proud of myself,” Dr. Bowman says. “And, as wives will want to do, she pushes the envelope and says she wants to stop by and get some Brussels sprouts. She hadn’t had them in 20 years, and I hadn’t had them in 45 years—since my mom stunk up the house with them. So we ended up at the Safeway, because the two things that keeps a marriage together are those two words: ‘Yes, dear.’ ”
The Bowmans passed by Rep. Giffords, her staff, and about 25 people in front of the grocery store entrance. They went to the produce department and had not been in the store for more than three or four minutes before shots rang out.
“I was 150 percent sure they were gunshots,” Dr. Bowman says. “I said to my wife, ‘Let’s go, Nancy,’ and she didn’t hear me. I thought she was right behind me. But she had gone over to the Brussels sprouts and I was still in mushrooms.”
Walking to the door, Dr. Bowman saw a woman rushing in and shouting, “They shot her. They shot Congresswoman Giffords.”
“I stepped out and stood behind a pillar until no more gunshots,” he says. “They’d actually already taken down the shooter as soon as he ran out of bullets. I looked around the corner to the carnage, as you’d expect, with Congresswoman Giffords the first person I saw right at the head of the line near the front door.
“Quite frankly, I stepped over people who were no longer with us to get to her. I got her turned around and moved off to the window; she wasn’t breathing real well. I worked on her airway, cleaning her airway with the young man [Rep. Giffords’ intern, Daniel Hernandez], who then held her for the next 15 to 20 minutes until the paramedics got her ready to go to the hospital.”
From that moment, Dr. Bowman says his training and instincts took over. More important, he went into field-triage mode, “which means you can’t do anything for that one. Can’t do anything there, this one is breathing and talking, not bleeding bad, good; still breathing, good, stay right there, I will be back. You go all the way up the line from person to person, seeing who you can and can’t help.
“The problem with field triage is that you really can’t stop and do a lot, like CPR, because then the rest of the people don’t have anybody looking at them. So you just keep moving,” he explains.
He says that while it was only minutes from the first gunshot to the time police arrived and secured the scene to the time paramedics were allowed to assist with the injured, it seemed like hours. Additionally, in his haste to help, Dr. Bowman had lost track of Nancy.
“I looked back and she was not there,” he says, adding she’d been swept to the back of the grocery store. “I kept working and I looked back and she had pushed [aside] the 17-year-old sacker who was acting as a security guard. … She came outside and started doing CPR on the first person she saw. I got up the line and there was a doctor doing CPR on the young girl [Christina-Taylor Green]. He was in the parking lot when the shots rang out; he threw his wife in the car and ran up to the little girl.”
Instinct and Autopilot
In a little more than 10 seconds, the gunman had fired more than 30 rounds and killed or injured nearly 20 people.
After he’d checked on all of the wounded, Dr. Bowman says he came upon four people holding the suspected shooter down. “One of them, I didn’t know it, was one of my colleagues, Dr. Stephen Rayle,” Dr. Bowman says. “I said, ‘Hold him, and I will send the first officer over here.’ ”
From there, Dr. Bowman says, he went back up the line of injured, checking for breathing sounds and bleeding, making sure every injured person was being attended to.
“People shot in the leg were holding a hand over a chest wound on the man or woman next to them,” he says. “It was one of those chaotic scenes that you try to make some kind of order to, by deciding who you can help and who you can’t.”
When the first paramedics arrived, Dr. Bowman directed them to Rep. Giffords and the 9-year-old girl. Soon after, there were enough EMTs on scene to attend to each of the victims.
“You are just on automatic,” Dr. Bowman explains. “Actually, after I dealt with the first two victims pretty quickly, Giffords taking the most time to just get her situated, I did stop and look out in the parking lot just to see if anybody was aiming anything at us.”
The most difficult part of field triage, Dr. Bowman says, is staying calm, organized, and “not losing it emotionally.” In fact, he ushered some shell-shocked bystanders away from the scene. “Some people will step right forward and say, ‘Can I help? I know CPR.’ Other people will just stand there and scream.”
Even tougher, he says, was watching his wife try to save the life of U.S. District Judge John Roll (see “Remembering the Dead,” above). “I finally had to go to my wife, pull her off of him, and say, ‘Honey, he’s gone. I need help with this lady who has been shot in the chest laying in the street,’ ” Dr. Bowman says. “Pulling them away is pretty hard. ... It was harder for her and the bystanders, because they were the ones getting right down close with the patient, talking to them, telling patients to ‘keep looking at me.’ That is a very close bond that develops. Field triage, you just keep moving.”
Human Spirit, Cooperation, and Hope
One month after the shooting, Rep. Giffords was moving, talking, thinking, and recuperating at what her doctors at Houston’s TIRR Hermann Memorial deemed “lightning speed.” For Dr. Bowman, such news brings more than a sigh of relief.
“In truth, when I was first with her, she wasn’t responding,” he says. “She was breathing, although with a compromised airway. We got that straightened away and she had a good pulse. Daniel Hernandez, the young man with her, had some nursing training and was comfortable being with her.
“It was amazing to me, the second or third time down the line, just to look over to this guy, and he was watching for me, and he would nod and say, ‘We’re OK. She’s breathing, pulse is OK.’ I didn’t have to go back, and the third time down he said, ‘She’s moving, she’s squeezing my hand.’ ”
It was at that moment that Dr. Bowman felt the congresswoman, in spite of her severe head trauma, had a fighting chance. Others miracles were happening all around him. Each memory ceases to amaze the veteran physician.
“People who were injured holding somebody’s head in their lap because they were hit in the head and this person was hit in the chest,” he says. “It gives you hope for the human race. Those people, to me, were the heroes.”
Looking back, Dr. Bowman says, he’s played back the moment in his mind more than a few times, wondering if he did the right thing for every victim. He wonders how much he and his wife, the other doctors at the scene, and the bystanders really helped. Then, after a brief moment, he has the answer.
“It really took two weeks to really say that, when all the victims that had expired were dead at the scene, and everybody that got taken away made it and out of the hospital, it sunk in that we had made the right decisions,” he says. “Nobody died on the operating table because we didn’t pick up the gunshot wound to the back. It took two weeks to realize we did the right thing.”
Some of those answers will take many more weeks. Rep. Giffords, although she is on a positive path, still has a long road to a full recovery, and doctors are making no promises. “I don’t know how far she will make it or how long it is going to take, but there are some miracles out there,” Dr. Bowman says.
You’re a Hospitalist? You’re Ready
As a physician in the middle of a mass-casualty event, the media called upon Dr. Bowman to recount the events of the Tucson shooting. In more than a dozen interviews with local and national media, not once was Dr. Bowman referred to as a hospitalist.
“At the scene, when I kneel down, I am a doctor. Can you tell me what’s going on, can you talk to me? It goes no farther than that,” he says. “In talking with one of the interviewers, she asked, ‘What kind of doctor are you?’ I said, ‘I am an internist and a hospitalist, which is a doctor who works just in the hospital.’ They weren’t interested in that. When the cameras rolled, she said, ‘I understand you are an intern?’ I said, ‘No, I am an internist. Turn that thing off and start again.’
“That’s the level of knowledge you are dealing with, and that was a national anchorperson I was dealing with.”
It’s an all-too-common refrain for hospitalists around the country, but one Dr. Bowman and others like him have endured for years. It doesn’t bother him, and he says it shouldn’t bother others.
“Doctor or nurse was as far as it got. I can certainly understand that,” he says. “We explain what a hospitalist is every day. We’ve been doing it for 12, 13, 14 years, and people still don’t understand. It’s OK.”
What isn’t OK is hospitalist unpreparedness. In fact, Dr. Bowman says, his training as an internist and his years of HM experience played a pivotal role in managing the scene of the Tucson shooting. The first thing to do, in addition to remaining calm, is to keep your priorities straight and remember your ABCs.
“It’s airway, airway, airway,” he says. “Without an airway, people don’t live. Then you are looking for bleeding, bleeding, bleeding. Then if they are talking, not a lot of bleeding and have a pulse, that is good enough for right now. So, it’s ‘Lady, just keep pushing on the chest right there on that wound.’ … I think, if you remember your ABCs, that’s all you can do in a field triage situation.”
Although the circumstances are less stressful, hospitalists are faced with make-or-break decisions every day, Dr. Bowman says. For example, it’s 4 p.m. and the day shift physician in the ED calls and says he has six admissions he’s been working on for the past three hours. “You, based on the info given to you, have to decide, Well, who is sickest, who do I have to get to first, who is going to the ICU?” Dr. Bowman says. “You do this triage thing in your mind as you walk to the ED. If there is any corollary, it’s the fact that you, as the hospitalist, get hit with a slew of patients all at once. They don’t come in one every 15 minutes like in your office for a blood-pressure check.
“Be ready. And, by the way, you are ready,” he adds. “You take care of a stroke patient in room one, take care of a gangrenous leg in room two, a diabetic with ketoacidosis in room three. The broadness, the generality of your training, you are ready to take care of a variety of things. You’re going to be able to help. Just be ready.” TH
Jason Carris is editor of The Hospitalist.
Dave Bowman, MD, doesn’t run anywhere anymore; it’s more of a fast walk. He doesn’t consider himself political, yet he does his civic duty and votes in every election. He’s not a big fan of vegetables, but he eats them to appease his wife and his conscience. Most important, Dr. Bowman doesn’t consider himself a hero. In fact, he doesn’t consider what he did that day any different from what he does every day in the hospital.
On the morning of Jan. 8, Dr. Bowman and his wife, Nancy, were thrust into the epicenter of one of the worst shooting rampages in American history. Dr. Bowman, a hospitalist, was the first physician on the scene outside the Tucson, Ariz., grocery store where a lone gunman killed six people and injured 13 others, including U.S. Representative Gabrielle Giffords (D-Ariz.).
“A hero is somebody, to me, who steps out of their element, steps up to the task that is needed, a task that is completely foreign to them, and steps up and helps people,” says Dr. Bowman, 61, executive director for IPC The Hospitalist Co.’s Tucson region. “A hero is not somebody who should be able to help in some manner and should be expected to help. … I don’t think nurses, doctors, firemen, EMTs get to be labeled as heroes. It’s what we should do, and gladly do, and in many cases took an oath to do.”
Even so, Dr. Bowman’s recollection of that frightful morning is a story laced with tragedy, courage, and hope. He remembers those who are “no longer with us.” He remembers his wife administering CPR and calling victims’ loved ones on their cellphones. And he remembers the brave men and women who not only subdued the shooter, but who worked together, selflessly, and in many cases with no medical training, to assist their injured neighbors.
“It was a pretty traumatic scene. More for others than for me; I am supposed to be the doctor and can handle all that,” he says, pausing. “But they don’t teach this course in medical school.”
Shots Ring Out, First Thought Is Help
Born and raised 100 miles south of Tucson and internal-medicine-trained at the University of Arizona, Dr. Bowman became a hospitalist in 1998 and began working with IPC in 2000. He supervises a staff of about 90 providers, including more than 50 full-time hospitalists, serving two large community hospitals, rehabilitations centers, and skilled nursing facilities in the Tucson area.
Yet he knows who the real boss is in the Bowman household. He and Nancy, an ICU nurse, had just finished a brisk walk, eaten breakfast at McDonald’s, and stopped at Safeway to pick up some vegetables on the morning of Jan. 8. “I had the oatmeal. I was so proud of myself,” Dr. Bowman says. “And, as wives will want to do, she pushes the envelope and says she wants to stop by and get some Brussels sprouts. She hadn’t had them in 20 years, and I hadn’t had them in 45 years—since my mom stunk up the house with them. So we ended up at the Safeway, because the two things that keeps a marriage together are those two words: ‘Yes, dear.’ ”
The Bowmans passed by Rep. Giffords, her staff, and about 25 people in front of the grocery store entrance. They went to the produce department and had not been in the store for more than three or four minutes before shots rang out.
“I was 150 percent sure they were gunshots,” Dr. Bowman says. “I said to my wife, ‘Let’s go, Nancy,’ and she didn’t hear me. I thought she was right behind me. But she had gone over to the Brussels sprouts and I was still in mushrooms.”
Walking to the door, Dr. Bowman saw a woman rushing in and shouting, “They shot her. They shot Congresswoman Giffords.”
“I stepped out and stood behind a pillar until no more gunshots,” he says. “They’d actually already taken down the shooter as soon as he ran out of bullets. I looked around the corner to the carnage, as you’d expect, with Congresswoman Giffords the first person I saw right at the head of the line near the front door.
“Quite frankly, I stepped over people who were no longer with us to get to her. I got her turned around and moved off to the window; she wasn’t breathing real well. I worked on her airway, cleaning her airway with the young man [Rep. Giffords’ intern, Daniel Hernandez], who then held her for the next 15 to 20 minutes until the paramedics got her ready to go to the hospital.”
From that moment, Dr. Bowman says his training and instincts took over. More important, he went into field-triage mode, “which means you can’t do anything for that one. Can’t do anything there, this one is breathing and talking, not bleeding bad, good; still breathing, good, stay right there, I will be back. You go all the way up the line from person to person, seeing who you can and can’t help.
“The problem with field triage is that you really can’t stop and do a lot, like CPR, because then the rest of the people don’t have anybody looking at them. So you just keep moving,” he explains.
He says that while it was only minutes from the first gunshot to the time police arrived and secured the scene to the time paramedics were allowed to assist with the injured, it seemed like hours. Additionally, in his haste to help, Dr. Bowman had lost track of Nancy.
“I looked back and she was not there,” he says, adding she’d been swept to the back of the grocery store. “I kept working and I looked back and she had pushed [aside] the 17-year-old sacker who was acting as a security guard. … She came outside and started doing CPR on the first person she saw. I got up the line and there was a doctor doing CPR on the young girl [Christina-Taylor Green]. He was in the parking lot when the shots rang out; he threw his wife in the car and ran up to the little girl.”
Instinct and Autopilot
In a little more than 10 seconds, the gunman had fired more than 30 rounds and killed or injured nearly 20 people.
After he’d checked on all of the wounded, Dr. Bowman says he came upon four people holding the suspected shooter down. “One of them, I didn’t know it, was one of my colleagues, Dr. Stephen Rayle,” Dr. Bowman says. “I said, ‘Hold him, and I will send the first officer over here.’ ”
From there, Dr. Bowman says, he went back up the line of injured, checking for breathing sounds and bleeding, making sure every injured person was being attended to.
“People shot in the leg were holding a hand over a chest wound on the man or woman next to them,” he says. “It was one of those chaotic scenes that you try to make some kind of order to, by deciding who you can help and who you can’t.”
When the first paramedics arrived, Dr. Bowman directed them to Rep. Giffords and the 9-year-old girl. Soon after, there were enough EMTs on scene to attend to each of the victims.
“You are just on automatic,” Dr. Bowman explains. “Actually, after I dealt with the first two victims pretty quickly, Giffords taking the most time to just get her situated, I did stop and look out in the parking lot just to see if anybody was aiming anything at us.”
The most difficult part of field triage, Dr. Bowman says, is staying calm, organized, and “not losing it emotionally.” In fact, he ushered some shell-shocked bystanders away from the scene. “Some people will step right forward and say, ‘Can I help? I know CPR.’ Other people will just stand there and scream.”
Even tougher, he says, was watching his wife try to save the life of U.S. District Judge John Roll (see “Remembering the Dead,” above). “I finally had to go to my wife, pull her off of him, and say, ‘Honey, he’s gone. I need help with this lady who has been shot in the chest laying in the street,’ ” Dr. Bowman says. “Pulling them away is pretty hard. ... It was harder for her and the bystanders, because they were the ones getting right down close with the patient, talking to them, telling patients to ‘keep looking at me.’ That is a very close bond that develops. Field triage, you just keep moving.”
Human Spirit, Cooperation, and Hope
One month after the shooting, Rep. Giffords was moving, talking, thinking, and recuperating at what her doctors at Houston’s TIRR Hermann Memorial deemed “lightning speed.” For Dr. Bowman, such news brings more than a sigh of relief.
“In truth, when I was first with her, she wasn’t responding,” he says. “She was breathing, although with a compromised airway. We got that straightened away and she had a good pulse. Daniel Hernandez, the young man with her, had some nursing training and was comfortable being with her.
“It was amazing to me, the second or third time down the line, just to look over to this guy, and he was watching for me, and he would nod and say, ‘We’re OK. She’s breathing, pulse is OK.’ I didn’t have to go back, and the third time down he said, ‘She’s moving, she’s squeezing my hand.’ ”
It was at that moment that Dr. Bowman felt the congresswoman, in spite of her severe head trauma, had a fighting chance. Others miracles were happening all around him. Each memory ceases to amaze the veteran physician.
“People who were injured holding somebody’s head in their lap because they were hit in the head and this person was hit in the chest,” he says. “It gives you hope for the human race. Those people, to me, were the heroes.”
Looking back, Dr. Bowman says, he’s played back the moment in his mind more than a few times, wondering if he did the right thing for every victim. He wonders how much he and his wife, the other doctors at the scene, and the bystanders really helped. Then, after a brief moment, he has the answer.
“It really took two weeks to really say that, when all the victims that had expired were dead at the scene, and everybody that got taken away made it and out of the hospital, it sunk in that we had made the right decisions,” he says. “Nobody died on the operating table because we didn’t pick up the gunshot wound to the back. It took two weeks to realize we did the right thing.”
Some of those answers will take many more weeks. Rep. Giffords, although she is on a positive path, still has a long road to a full recovery, and doctors are making no promises. “I don’t know how far she will make it or how long it is going to take, but there are some miracles out there,” Dr. Bowman says.
You’re a Hospitalist? You’re Ready
As a physician in the middle of a mass-casualty event, the media called upon Dr. Bowman to recount the events of the Tucson shooting. In more than a dozen interviews with local and national media, not once was Dr. Bowman referred to as a hospitalist.
“At the scene, when I kneel down, I am a doctor. Can you tell me what’s going on, can you talk to me? It goes no farther than that,” he says. “In talking with one of the interviewers, she asked, ‘What kind of doctor are you?’ I said, ‘I am an internist and a hospitalist, which is a doctor who works just in the hospital.’ They weren’t interested in that. When the cameras rolled, she said, ‘I understand you are an intern?’ I said, ‘No, I am an internist. Turn that thing off and start again.’
“That’s the level of knowledge you are dealing with, and that was a national anchorperson I was dealing with.”
It’s an all-too-common refrain for hospitalists around the country, but one Dr. Bowman and others like him have endured for years. It doesn’t bother him, and he says it shouldn’t bother others.
“Doctor or nurse was as far as it got. I can certainly understand that,” he says. “We explain what a hospitalist is every day. We’ve been doing it for 12, 13, 14 years, and people still don’t understand. It’s OK.”
What isn’t OK is hospitalist unpreparedness. In fact, Dr. Bowman says, his training as an internist and his years of HM experience played a pivotal role in managing the scene of the Tucson shooting. The first thing to do, in addition to remaining calm, is to keep your priorities straight and remember your ABCs.
“It’s airway, airway, airway,” he says. “Without an airway, people don’t live. Then you are looking for bleeding, bleeding, bleeding. Then if they are talking, not a lot of bleeding and have a pulse, that is good enough for right now. So, it’s ‘Lady, just keep pushing on the chest right there on that wound.’ … I think, if you remember your ABCs, that’s all you can do in a field triage situation.”
Although the circumstances are less stressful, hospitalists are faced with make-or-break decisions every day, Dr. Bowman says. For example, it’s 4 p.m. and the day shift physician in the ED calls and says he has six admissions he’s been working on for the past three hours. “You, based on the info given to you, have to decide, Well, who is sickest, who do I have to get to first, who is going to the ICU?” Dr. Bowman says. “You do this triage thing in your mind as you walk to the ED. If there is any corollary, it’s the fact that you, as the hospitalist, get hit with a slew of patients all at once. They don’t come in one every 15 minutes like in your office for a blood-pressure check.
“Be ready. And, by the way, you are ready,” he adds. “You take care of a stroke patient in room one, take care of a gangrenous leg in room two, a diabetic with ketoacidosis in room three. The broadness, the generality of your training, you are ready to take care of a variety of things. You’re going to be able to help. Just be ready.” TH
Jason Carris is editor of The Hospitalist.