User login
Identify Dyslipidemia in Children to Save Lives
With a simple blood test, you can screen and potentially improve and extend the lives of children and adolescents with dyslipidemia.
This is one of the few areas of cardiovascular medicine where your initial diagnosis will make such a significant difference into adulthood. Dyslipidemia occurs more frequently than does structural congenital disease, heart rhythm disorders, heart failure, and most other conditions pediatric cardiologists manage.

In addition, you no longer have to wonder if you should evaluate your patients for dyslipidemia. In December 2011, the National Heart, Lung, and Blood Institute published guidelines on dyslipidemia in pediatric patients. Universal screening for dyslipidemia is now expected when children are 9-11 years old, even if they have no risk factors. The American Academy of Pediatrics endorsed this guidance.
Of course, there are situations where you might want to check earlier. If you identify any risk factor – relevant family history, obesity, or diabetes – you don’t have to wait until a child is 9 years old. You can screen these children when they are as young as 2 or 3 years.
The good news is that the guidelines do not require a fasting lipid profile ("Doctors Advised to Test Cholesterol in All Children Aged 9-11 Years," Pediatric News, Nov. 15, 2011). A nonfasting lipid profile reveals relevant information (except regarding HDL cholesterol), and is therefore an appropriate initial, universal screening tool. If you get a result out of the normal range or identify any new risk factors, a follow-up fasting lipid profile is warranted.
I’m glad to see that the guideline experts do not require a fasting assay. As many pediatricians can attest, overnight fasting can be very onerous for young patients and their families – especially if the well child visit is in the afternoon.
Once dyslipidemia is diagnosed, pediatricians can effectively manage most children with this condition. However, there also is a general consensus among these experts that the most severe childhood lipid abnormalities should be managed by lipid specialists. Hypercholesterolemia with a genetic etiology is worrisome, for example, especially if it’s heterozygous familial hypercholesterolemia.
Affected children will have significant elevations of LDL cholesterol – easily over 160 mg/dL and usually over 200 mg/dL. This condition affects about 1 in 500 people in the United States. Left undiagnosed and untreated, over their lifetimes about 50% of the men and 25% of the women will experience an important event – such as peripheral arterial disease or a heart attack – by the time they are 50.
If a person unknowingly grows to adulthood with heterozygous familial hypercholesterolemia, that person might experience a heart attack with no warning at age 30 (for men) or age 40 (for women).
This is all about prevention on the part of the pediatrician. Your early identification of patients with lipid abnormalities ties into "primordial prevention." In contrast to treating adults after they’ve developed cardiovascular disease, or performing "primary prevention" to prevent disease in a patient with known risk factors, pediatricians can prevent risk factors from developing in the first place. This means screening and counseling patients before they become obese, develop prehypertension, or present with prediabetes. Primordial prevention can delay or prevent a lot of these risk factors from becoming real issues.
If you identify and treat these patients with statins, you can restore normal longevity. Researchers have shown that these agents are just as safe and effective for children as they are for adults.
Dyslipidemia screening, diagnosis, and management are clinical areas where pediatricians and cardiologists can work together and make a real difference. I can’t think of anything better for pediatricians to do.
Dr. Hardin is director of the division of pediatric cardiology, and associate professor of pediatrics, at Loyola University Health System in Maywood, Ill. He had no relevant financial disclosures.
With a simple blood test, you can screen and potentially improve and extend the lives of children and adolescents with dyslipidemia.
This is one of the few areas of cardiovascular medicine where your initial diagnosis will make such a significant difference into adulthood. Dyslipidemia occurs more frequently than does structural congenital disease, heart rhythm disorders, heart failure, and most other conditions pediatric cardiologists manage.
In addition, you no longer have to wonder if you should evaluate your patients for dyslipidemia. In December 2011, the National Heart, Lung, and Blood Institute published guidelines on dyslipidemia in pediatric patients. Universal screening for dyslipidemia is now expected when children are 9-11 years old, even if they have no risk factors. The American Academy of Pediatrics endorsed this guidance.
Of course, there are situations where you might want to check earlier. If you identify any risk factor – relevant family history, obesity, or diabetes – you don’t have to wait until a child is 9 years old. You can screen these children when they are as young as 2 or 3 years.
The good news is that the guidelines do not require a fasting lipid profile ("Doctors Advised to Test Cholesterol in All Children Aged 9-11 Years," Pediatric News, Nov. 15, 2011). A nonfasting lipid profile reveals relevant information (except regarding HDL cholesterol), and is therefore an appropriate initial, universal screening tool. If you get a result out of the normal range or identify any new risk factors, a follow-up fasting lipid profile is warranted.
I’m glad to see that the guideline experts do not require a fasting assay. As many pediatricians can attest, overnight fasting can be very onerous for young patients and their families – especially if the well child visit is in the afternoon.
Once dyslipidemia is diagnosed, pediatricians can effectively manage most children with this condition. However, there also is a general consensus among these experts that the most severe childhood lipid abnormalities should be managed by lipid specialists. Hypercholesterolemia with a genetic etiology is worrisome, for example, especially if it’s heterozygous familial hypercholesterolemia.
Affected children will have significant elevations of LDL cholesterol – easily over 160 mg/dL and usually over 200 mg/dL. This condition affects about 1 in 500 people in the United States. Left undiagnosed and untreated, over their lifetimes about 50% of the men and 25% of the women will experience an important event – such as peripheral arterial disease or a heart attack – by the time they are 50.
If a person unknowingly grows to adulthood with heterozygous familial hypercholesterolemia, that person might experience a heart attack with no warning at age 30 (for men) or age 40 (for women).
This is all about prevention on the part of the pediatrician. Your early identification of patients with lipid abnormalities ties into "primordial prevention." In contrast to treating adults after they’ve developed cardiovascular disease, or performing "primary prevention" to prevent disease in a patient with known risk factors, pediatricians can prevent risk factors from developing in the first place. This means screening and counseling patients before they become obese, develop prehypertension, or present with prediabetes. Primordial prevention can delay or prevent a lot of these risk factors from becoming real issues.
If you identify and treat these patients with statins, you can restore normal longevity. Researchers have shown that these agents are just as safe and effective for children as they are for adults.
Dyslipidemia screening, diagnosis, and management are clinical areas where pediatricians and cardiologists can work together and make a real difference. I can’t think of anything better for pediatricians to do.
Dr. Hardin is director of the division of pediatric cardiology, and associate professor of pediatrics, at Loyola University Health System in Maywood, Ill. He had no relevant financial disclosures.
With a simple blood test, you can screen and potentially improve and extend the lives of children and adolescents with dyslipidemia.
This is one of the few areas of cardiovascular medicine where your initial diagnosis will make such a significant difference into adulthood. Dyslipidemia occurs more frequently than does structural congenital disease, heart rhythm disorders, heart failure, and most other conditions pediatric cardiologists manage.
In addition, you no longer have to wonder if you should evaluate your patients for dyslipidemia. In December 2011, the National Heart, Lung, and Blood Institute published guidelines on dyslipidemia in pediatric patients. Universal screening for dyslipidemia is now expected when children are 9-11 years old, even if they have no risk factors. The American Academy of Pediatrics endorsed this guidance.
Of course, there are situations where you might want to check earlier. If you identify any risk factor – relevant family history, obesity, or diabetes – you don’t have to wait until a child is 9 years old. You can screen these children when they are as young as 2 or 3 years.
The good news is that the guidelines do not require a fasting lipid profile ("Doctors Advised to Test Cholesterol in All Children Aged 9-11 Years," Pediatric News, Nov. 15, 2011). A nonfasting lipid profile reveals relevant information (except regarding HDL cholesterol), and is therefore an appropriate initial, universal screening tool. If you get a result out of the normal range or identify any new risk factors, a follow-up fasting lipid profile is warranted.
I’m glad to see that the guideline experts do not require a fasting assay. As many pediatricians can attest, overnight fasting can be very onerous for young patients and their families – especially if the well child visit is in the afternoon.
Once dyslipidemia is diagnosed, pediatricians can effectively manage most children with this condition. However, there also is a general consensus among these experts that the most severe childhood lipid abnormalities should be managed by lipid specialists. Hypercholesterolemia with a genetic etiology is worrisome, for example, especially if it’s heterozygous familial hypercholesterolemia.
Affected children will have significant elevations of LDL cholesterol – easily over 160 mg/dL and usually over 200 mg/dL. This condition affects about 1 in 500 people in the United States. Left undiagnosed and untreated, over their lifetimes about 50% of the men and 25% of the women will experience an important event – such as peripheral arterial disease or a heart attack – by the time they are 50.
If a person unknowingly grows to adulthood with heterozygous familial hypercholesterolemia, that person might experience a heart attack with no warning at age 30 (for men) or age 40 (for women).
This is all about prevention on the part of the pediatrician. Your early identification of patients with lipid abnormalities ties into "primordial prevention." In contrast to treating adults after they’ve developed cardiovascular disease, or performing "primary prevention" to prevent disease in a patient with known risk factors, pediatricians can prevent risk factors from developing in the first place. This means screening and counseling patients before they become obese, develop prehypertension, or present with prediabetes. Primordial prevention can delay or prevent a lot of these risk factors from becoming real issues.
If you identify and treat these patients with statins, you can restore normal longevity. Researchers have shown that these agents are just as safe and effective for children as they are for adults.
Dyslipidemia screening, diagnosis, and management are clinical areas where pediatricians and cardiologists can work together and make a real difference. I can’t think of anything better for pediatricians to do.
Dr. Hardin is director of the division of pediatric cardiology, and associate professor of pediatrics, at Loyola University Health System in Maywood, Ill. He had no relevant financial disclosures.
How to Reinsert an Avulsed Permanent Tooth
STEAMBOAT SPRINGS, COLO. – Replacing a knocked-out permanent tooth is a far-less-daunting proposition than it sounds, according to Dr. Steven M. Selbst.
"This is an easy procedure that I hope every pediatrician would be comfortable in doing," he said at the meeting sponsored by the American Academy of Pediatrics.

Time is critical. A tooth reinserted within 30 minutes after being knocked out has a 90% chance of survival. After that, the success rate drops off considerably.
A common scenario is for a parent to phone the pediatrician from the scene of the mishap, perhaps a playground, the backyard trampoline, or a baseball diamond. The parent should be instructed to immerse the tooth in milk, if immediately available, while transporting the youth to the physician’s office. If milk is not at hand, water is the next best. Failing that, the adult should put the tooth under his or her own tongue, according to Dr. Selbst, professor and vice chair of pediatrics at Jefferson Medical College, Philadelphia, and an authority on emergency pediatrics.
It’s an excellent idea for every pediatrician’s office – and school nurses’ offices as well – to stock a container of the balanced salt solution known as Save-a-Tooth emergency tooth-preserving system filled with Hank’s balanced salt solution (HBSS). It’s inexpensive, available on the Internet, and extends the salvage time by several hours. As soon as the patient arrives at the office, the tooth can be placed in the HBSS while the treatment team assembles.
The tooth should always be handled by the crown, not the root. And even though the tooth may have been kicked around in the dirt, it shouldn’t be scrubbed clean; that would damage the fine root fibers that are essential to successful reattachment. Instead, the tooth can be gently irrigated with saline or tap water to clean it up.
The tooth socket is a gaping hole, often filled with a blood clot. This, too, should be gently irrigated. Wet gauze can be used to wipe away the clot.
There’s no need to anesthetize the tooth socket with a lidocaine injection.
"When the tooth got knocked out, most of the pain-carrying nerve fibers got knocked out along with it. It’s really not that painful to replace the tooth. The teenager is desperate for this procedure to be successful. He or she is going to do everything possible to help you along the way. They’ll tolerate a bit of pain or discomfort," Dr. Selbst explained.
The procedure itself is remarkably straightforward.
"You don’t need fancy equipment. You don’t need any anesthesia. You just need to have the courage to stick the tooth right back up in that big hole after you’ve cleaned it off," the pediatrician continued.
But first, make sure the tooth is correctly oriented: right side up, front facing forward.
Pretty much the only complication that can occur is if the nervous physician drops the tooth and the patient then swallows it. It’s game over at that point. For this reason, Dr. Selbst said he always has the patient sitting up to at least a 45-degree angle for the procedure rather than lying down.
The patient needs to go from the pediatrician to a dentist straight away so the tooth can be further stabilized. Have the youth bite down on a big wad of gauze to keep the loose tooth from moving around while in transit, he advised.
Dr. Selbst reported that he had no relevant financial disclosures.
STEAMBOAT SPRINGS, COLO. – Replacing a knocked-out permanent tooth is a far-less-daunting proposition than it sounds, according to Dr. Steven M. Selbst.
"This is an easy procedure that I hope every pediatrician would be comfortable in doing," he said at the meeting sponsored by the American Academy of Pediatrics.
Time is critical. A tooth reinserted within 30 minutes after being knocked out has a 90% chance of survival. After that, the success rate drops off considerably.
A common scenario is for a parent to phone the pediatrician from the scene of the mishap, perhaps a playground, the backyard trampoline, or a baseball diamond. The parent should be instructed to immerse the tooth in milk, if immediately available, while transporting the youth to the physician’s office. If milk is not at hand, water is the next best. Failing that, the adult should put the tooth under his or her own tongue, according to Dr. Selbst, professor and vice chair of pediatrics at Jefferson Medical College, Philadelphia, and an authority on emergency pediatrics.
It’s an excellent idea for every pediatrician’s office – and school nurses’ offices as well – to stock a container of the balanced salt solution known as Save-a-Tooth emergency tooth-preserving system filled with Hank’s balanced salt solution (HBSS). It’s inexpensive, available on the Internet, and extends the salvage time by several hours. As soon as the patient arrives at the office, the tooth can be placed in the HBSS while the treatment team assembles.
The tooth should always be handled by the crown, not the root. And even though the tooth may have been kicked around in the dirt, it shouldn’t be scrubbed clean; that would damage the fine root fibers that are essential to successful reattachment. Instead, the tooth can be gently irrigated with saline or tap water to clean it up.
The tooth socket is a gaping hole, often filled with a blood clot. This, too, should be gently irrigated. Wet gauze can be used to wipe away the clot.
There’s no need to anesthetize the tooth socket with a lidocaine injection.
"When the tooth got knocked out, most of the pain-carrying nerve fibers got knocked out along with it. It’s really not that painful to replace the tooth. The teenager is desperate for this procedure to be successful. He or she is going to do everything possible to help you along the way. They’ll tolerate a bit of pain or discomfort," Dr. Selbst explained.
The procedure itself is remarkably straightforward.
"You don’t need fancy equipment. You don’t need any anesthesia. You just need to have the courage to stick the tooth right back up in that big hole after you’ve cleaned it off," the pediatrician continued.
But first, make sure the tooth is correctly oriented: right side up, front facing forward.
Pretty much the only complication that can occur is if the nervous physician drops the tooth and the patient then swallows it. It’s game over at that point. For this reason, Dr. Selbst said he always has the patient sitting up to at least a 45-degree angle for the procedure rather than lying down.
The patient needs to go from the pediatrician to a dentist straight away so the tooth can be further stabilized. Have the youth bite down on a big wad of gauze to keep the loose tooth from moving around while in transit, he advised.
Dr. Selbst reported that he had no relevant financial disclosures.
STEAMBOAT SPRINGS, COLO. – Replacing a knocked-out permanent tooth is a far-less-daunting proposition than it sounds, according to Dr. Steven M. Selbst.
"This is an easy procedure that I hope every pediatrician would be comfortable in doing," he said at the meeting sponsored by the American Academy of Pediatrics.
Time is critical. A tooth reinserted within 30 minutes after being knocked out has a 90% chance of survival. After that, the success rate drops off considerably.
A common scenario is for a parent to phone the pediatrician from the scene of the mishap, perhaps a playground, the backyard trampoline, or a baseball diamond. The parent should be instructed to immerse the tooth in milk, if immediately available, while transporting the youth to the physician’s office. If milk is not at hand, water is the next best. Failing that, the adult should put the tooth under his or her own tongue, according to Dr. Selbst, professor and vice chair of pediatrics at Jefferson Medical College, Philadelphia, and an authority on emergency pediatrics.
It’s an excellent idea for every pediatrician’s office – and school nurses’ offices as well – to stock a container of the balanced salt solution known as Save-a-Tooth emergency tooth-preserving system filled with Hank’s balanced salt solution (HBSS). It’s inexpensive, available on the Internet, and extends the salvage time by several hours. As soon as the patient arrives at the office, the tooth can be placed in the HBSS while the treatment team assembles.
The tooth should always be handled by the crown, not the root. And even though the tooth may have been kicked around in the dirt, it shouldn’t be scrubbed clean; that would damage the fine root fibers that are essential to successful reattachment. Instead, the tooth can be gently irrigated with saline or tap water to clean it up.
The tooth socket is a gaping hole, often filled with a blood clot. This, too, should be gently irrigated. Wet gauze can be used to wipe away the clot.
There’s no need to anesthetize the tooth socket with a lidocaine injection.
"When the tooth got knocked out, most of the pain-carrying nerve fibers got knocked out along with it. It’s really not that painful to replace the tooth. The teenager is desperate for this procedure to be successful. He or she is going to do everything possible to help you along the way. They’ll tolerate a bit of pain or discomfort," Dr. Selbst explained.
The procedure itself is remarkably straightforward.
"You don’t need fancy equipment. You don’t need any anesthesia. You just need to have the courage to stick the tooth right back up in that big hole after you’ve cleaned it off," the pediatrician continued.
But first, make sure the tooth is correctly oriented: right side up, front facing forward.
Pretty much the only complication that can occur is if the nervous physician drops the tooth and the patient then swallows it. It’s game over at that point. For this reason, Dr. Selbst said he always has the patient sitting up to at least a 45-degree angle for the procedure rather than lying down.
The patient needs to go from the pediatrician to a dentist straight away so the tooth can be further stabilized. Have the youth bite down on a big wad of gauze to keep the loose tooth from moving around while in transit, he advised.
Dr. Selbst reported that he had no relevant financial disclosures.
EXPERT ANALYSIS FROM A MEETING ON PRACTICAL PEDIATRICS SPONSORED BY THE AMERICAN ACADEMY OF PEDIATRICS
State AGs Assess Health Reform's Individual Mandate
At a recent forum, Virginia Attorney General Ken Cuccinelli and Massachusetts Attorney General Martha Coakley offered contrasting perspectives on the constitutionality of the federal Affordable Care Act's requirement that individuals must purchase health insurance.
Reporter Alicia Ault has this video report:
At a recent forum, Virginia Attorney General Ken Cuccinelli and Massachusetts Attorney General Martha Coakley offered contrasting perspectives on the constitutionality of the federal Affordable Care Act's requirement that individuals must purchase health insurance.
Reporter Alicia Ault has this video report:
At a recent forum, Virginia Attorney General Ken Cuccinelli and Massachusetts Attorney General Martha Coakley offered contrasting perspectives on the constitutionality of the federal Affordable Care Act's requirement that individuals must purchase health insurance.
Reporter Alicia Ault has this video report:
Hospital Food Often Unhealthy
Hospitals are a place where people go to get healthy, but the same can't be said about all hospital cafeterias, according to a recent study by the Physicians Committee for Responsible Medicine (PCRM).
The study analyzed food served to patients, staff, and visitors at U.S. hospitals in all 50 states and the District of Columbia and found that some hospitals housed as many as five fast-food outlets and featured menus that were dominated by foods high in fat, cholesterol, sugar, and sodium. For hospitalists, many of whom spend 50, 70, and even 90 hours per week in the hospital, the lack of healthy eating options can be especially problematic.
"We relied on menus that were provided, and while we don't have the recipes in hand, we can tell a lot just by the fundamental ingredients," says Susan Levin, RD, PCRM's director of nutrition education and lead author of the study.
Levin says the presence of these kinds of foods in hospitals is "irresponsible," and suggests hospitals ban fast-food outlets and fill menus with low-fat, plant-based options as a way to "reverse and prevent disease."
Many hospital cafeterias around the country are doing just that. MetroWest Medical Center, just outside of Boston, has formed a "Go Green" committee that plans to group and label healthy versus nonhealthy drinks and snacks, and will reward patients and hospital staff for choosing water and other healthy options. Benioff Children's Hospital at the University of California at San Francisco (UCSF) Medical Center now offers nutritional information for entrees, and food-purchase receipts note calories and fat content.
PCRM hopes the study will encourage hospitals to lead the way in promoting healthful eating habits. "I hope that something is changing and people are thinking bigger picture and better care," Levin says.
Hospitals are a place where people go to get healthy, but the same can't be said about all hospital cafeterias, according to a recent study by the Physicians Committee for Responsible Medicine (PCRM).
The study analyzed food served to patients, staff, and visitors at U.S. hospitals in all 50 states and the District of Columbia and found that some hospitals housed as many as five fast-food outlets and featured menus that were dominated by foods high in fat, cholesterol, sugar, and sodium. For hospitalists, many of whom spend 50, 70, and even 90 hours per week in the hospital, the lack of healthy eating options can be especially problematic.
"We relied on menus that were provided, and while we don't have the recipes in hand, we can tell a lot just by the fundamental ingredients," says Susan Levin, RD, PCRM's director of nutrition education and lead author of the study.
Levin says the presence of these kinds of foods in hospitals is "irresponsible," and suggests hospitals ban fast-food outlets and fill menus with low-fat, plant-based options as a way to "reverse and prevent disease."
Many hospital cafeterias around the country are doing just that. MetroWest Medical Center, just outside of Boston, has formed a "Go Green" committee that plans to group and label healthy versus nonhealthy drinks and snacks, and will reward patients and hospital staff for choosing water and other healthy options. Benioff Children's Hospital at the University of California at San Francisco (UCSF) Medical Center now offers nutritional information for entrees, and food-purchase receipts note calories and fat content.
PCRM hopes the study will encourage hospitals to lead the way in promoting healthful eating habits. "I hope that something is changing and people are thinking bigger picture and better care," Levin says.
Hospitals are a place where people go to get healthy, but the same can't be said about all hospital cafeterias, according to a recent study by the Physicians Committee for Responsible Medicine (PCRM).
The study analyzed food served to patients, staff, and visitors at U.S. hospitals in all 50 states and the District of Columbia and found that some hospitals housed as many as five fast-food outlets and featured menus that were dominated by foods high in fat, cholesterol, sugar, and sodium. For hospitalists, many of whom spend 50, 70, and even 90 hours per week in the hospital, the lack of healthy eating options can be especially problematic.
"We relied on menus that were provided, and while we don't have the recipes in hand, we can tell a lot just by the fundamental ingredients," says Susan Levin, RD, PCRM's director of nutrition education and lead author of the study.
Levin says the presence of these kinds of foods in hospitals is "irresponsible," and suggests hospitals ban fast-food outlets and fill menus with low-fat, plant-based options as a way to "reverse and prevent disease."
Many hospital cafeterias around the country are doing just that. MetroWest Medical Center, just outside of Boston, has formed a "Go Green" committee that plans to group and label healthy versus nonhealthy drinks and snacks, and will reward patients and hospital staff for choosing water and other healthy options. Benioff Children's Hospital at the University of California at San Francisco (UCSF) Medical Center now offers nutritional information for entrees, and food-purchase receipts note calories and fat content.
PCRM hopes the study will encourage hospitals to lead the way in promoting healthful eating habits. "I hope that something is changing and people are thinking bigger picture and better care," Levin says.
Reducing Unnecessary Medical Resources as Quality Initiative
An emerging category of hospital quality initiatives, comparable to preventing medical errors and improving quality and patient safety, could be labeled “waste management” or “waste reduction.” "Waste" in this sense refers not to biohazardous substances in need of disposal, but to the overuse of medical resources—such as lab tests and pharmaceuticals—when they are not helpful to a patient's medical management.
This will be a growing focus for hospitalists, says Robert Wachter, MD, MHM, chief of the division of hospital medicine at the University of California at San Francisco (UCSF) Medical Center, and author of the HM-focused blog, Wachter's World.
"If patients are getting CAT scans they don't really need or an extra day of telemetry because we don't have criteria for who should be on telemetry, that's wasteful, it's costly, and it could be dangerous,” Dr. Wachter explained at the UCSF Management of the Hospitalized Patient meeting last October. "The data are clear that 30% of what we do in American medicine is of no value to patients—and some substantial portion of that is harmful as well. I think we as hospitalists should be identifying what these wasteful things are—and making the hard decisions to stop them."
In an academic setting such as UCSF, many of the hospitalists lead quality, safety, and "waste reduction" projects, which often use similar tools and methods but have a different focus. Dr. Wachter's colleague Niraj Sehgal, MD, MPH, the department of medicine's associate chair for quality improvement (QI) and patient safety, says that process-improvement tools such as Six Sigma and Lean methodologies can put unnecessary variation and waste under the microscope. But at UCSF, these efforts start with just looking at the data, then sharing the data with trainees and faculty.
"Clearly, attention is growing to this issue," Dr. Sehgal says. "We often talk about generating value in healthcare where value equals quality divided by cost, but we need to include the concept of appropriateness in that equation as well."
A radiology utilization awareness project at UCSF is looking at whether cost and radiation exposure information might influence the ordering of five common radiologic tests that together generate annual charges of nearly $10 million at UCSF's Moffitt-Long Medical Service. The project uses a number of educational strategies to encourage providers to think about whether the tests will change their clinical management.
"The preliminary data suggest that simply providing the cost and utilization data decreased utilization for three of the five tests evaluated," Dr. Sehgal says.
Physicians didn't necessarily ignore inefficiency and overuse in the past, he adds, but healthcare reform offers new opportunities to leverage greater cost consciousness in medical education and practice. "We're not having to convince our trainees and faculty that cost is important," he says. "They just don't always see the costs involved."
An emerging category of hospital quality initiatives, comparable to preventing medical errors and improving quality and patient safety, could be labeled “waste management” or “waste reduction.” "Waste" in this sense refers not to biohazardous substances in need of disposal, but to the overuse of medical resources—such as lab tests and pharmaceuticals—when they are not helpful to a patient's medical management.
This will be a growing focus for hospitalists, says Robert Wachter, MD, MHM, chief of the division of hospital medicine at the University of California at San Francisco (UCSF) Medical Center, and author of the HM-focused blog, Wachter's World.
"If patients are getting CAT scans they don't really need or an extra day of telemetry because we don't have criteria for who should be on telemetry, that's wasteful, it's costly, and it could be dangerous,” Dr. Wachter explained at the UCSF Management of the Hospitalized Patient meeting last October. "The data are clear that 30% of what we do in American medicine is of no value to patients—and some substantial portion of that is harmful as well. I think we as hospitalists should be identifying what these wasteful things are—and making the hard decisions to stop them."
In an academic setting such as UCSF, many of the hospitalists lead quality, safety, and "waste reduction" projects, which often use similar tools and methods but have a different focus. Dr. Wachter's colleague Niraj Sehgal, MD, MPH, the department of medicine's associate chair for quality improvement (QI) and patient safety, says that process-improvement tools such as Six Sigma and Lean methodologies can put unnecessary variation and waste under the microscope. But at UCSF, these efforts start with just looking at the data, then sharing the data with trainees and faculty.
"Clearly, attention is growing to this issue," Dr. Sehgal says. "We often talk about generating value in healthcare where value equals quality divided by cost, but we need to include the concept of appropriateness in that equation as well."
A radiology utilization awareness project at UCSF is looking at whether cost and radiation exposure information might influence the ordering of five common radiologic tests that together generate annual charges of nearly $10 million at UCSF's Moffitt-Long Medical Service. The project uses a number of educational strategies to encourage providers to think about whether the tests will change their clinical management.
"The preliminary data suggest that simply providing the cost and utilization data decreased utilization for three of the five tests evaluated," Dr. Sehgal says.
Physicians didn't necessarily ignore inefficiency and overuse in the past, he adds, but healthcare reform offers new opportunities to leverage greater cost consciousness in medical education and practice. "We're not having to convince our trainees and faculty that cost is important," he says. "They just don't always see the costs involved."
An emerging category of hospital quality initiatives, comparable to preventing medical errors and improving quality and patient safety, could be labeled “waste management” or “waste reduction.” "Waste" in this sense refers not to biohazardous substances in need of disposal, but to the overuse of medical resources—such as lab tests and pharmaceuticals—when they are not helpful to a patient's medical management.
This will be a growing focus for hospitalists, says Robert Wachter, MD, MHM, chief of the division of hospital medicine at the University of California at San Francisco (UCSF) Medical Center, and author of the HM-focused blog, Wachter's World.
"If patients are getting CAT scans they don't really need or an extra day of telemetry because we don't have criteria for who should be on telemetry, that's wasteful, it's costly, and it could be dangerous,” Dr. Wachter explained at the UCSF Management of the Hospitalized Patient meeting last October. "The data are clear that 30% of what we do in American medicine is of no value to patients—and some substantial portion of that is harmful as well. I think we as hospitalists should be identifying what these wasteful things are—and making the hard decisions to stop them."
In an academic setting such as UCSF, many of the hospitalists lead quality, safety, and "waste reduction" projects, which often use similar tools and methods but have a different focus. Dr. Wachter's colleague Niraj Sehgal, MD, MPH, the department of medicine's associate chair for quality improvement (QI) and patient safety, says that process-improvement tools such as Six Sigma and Lean methodologies can put unnecessary variation and waste under the microscope. But at UCSF, these efforts start with just looking at the data, then sharing the data with trainees and faculty.
"Clearly, attention is growing to this issue," Dr. Sehgal says. "We often talk about generating value in healthcare where value equals quality divided by cost, but we need to include the concept of appropriateness in that equation as well."
A radiology utilization awareness project at UCSF is looking at whether cost and radiation exposure information might influence the ordering of five common radiologic tests that together generate annual charges of nearly $10 million at UCSF's Moffitt-Long Medical Service. The project uses a number of educational strategies to encourage providers to think about whether the tests will change their clinical management.
"The preliminary data suggest that simply providing the cost and utilization data decreased utilization for three of the five tests evaluated," Dr. Sehgal says.
Physicians didn't necessarily ignore inefficiency and overuse in the past, he adds, but healthcare reform offers new opportunities to leverage greater cost consciousness in medical education and practice. "We're not having to convince our trainees and faculty that cost is important," he says. "They just don't always see the costs involved."
Alcohol Withdrawal Syndrome Worsens Cancer Surgery Outcomes
MIAMI BEACH – Patients with head and neck cancers who develop alcohol withdrawal syndrome perioperatively experience significantly more complications after undergoing surgery, a large database analysis indicates.
The presence of withdrawal symptoms was associated with a 25% incidence of postoperative complications, compared with 14% among patients who abused alcohol and 7% among those without alcohol abuse, Dr. Dane J. Genther said at the Triological Society’s Combined Sections Meeting. The risk for wound complications was nearly double in this population (odds ratio, 1.9).
Dr. Genther, a resident in otolaryngologyhead and neck surgery at Johns Hopkins Hospital in Baltimore, and his associates used ICD-9 codes in the Nationwide Inpatient Sample discharge database to identify more than 92,000 patients who underwent an ablative procedure for head and neck cancer in 2003-2008. The retrospective, cross-sectional study included patients with malignant oral cavity, laryngeal, hypopharyngeal, and oropharyngeal neoplasms.
In a multivariate analysis, alcohol withdrawal syndrome was significantly more likely for patients undergoing a major procedure (OR, 2.0) and was significantly associated with Medicare payer status and a need for additional health care following discharge, Dr. Genther said.
The researchers found no significant association between alcohol withdrawal syndrome and increased risk for postoperative infections or in-hospital mortality, but there was a significant increase in hospital stay and related costs associated with the syndrome.
Having a major procedure and experiencing alcohol withdrawal contributed approximately $15,000 per admission in 2011 U.S. dollars, Dr. Genther said.
The findings point to a need for alternatives to current alcohol withdrawal prevention therapies, Dr. Genther said. "Despite prophylaxis, which is our current treatment to attempt to stem the onset of alcohol withdrawal syndrome, complications do occur and they are no less severe or frequent than in the absence of prophylaxis."
Abstinence from alcohol for at least 4 weeks is another strategy proposed to minimize risk of alcohol withdrawal syndrome for any at-risk surgical patient, said Dr. Genther. However, he added, "for many cancer patients, especially those with more advanced disease, waiting a prolonged period of time to possibly gain that benefit from abstinence is not necessarily a viable option."
Another aim of the study was to assess factors contributing to alcohol abuse. Patients aged 40-64 years had the highest proportion of alcohol abuse, and this age range was a significant factor (OR, 2.37). Those who abused alcohol were more often male and more often underwent major procedures, Dr. Genther said at the meeting, which was jointly sponsored by the Triological Society and the American College of Surgeons. In addition, alcohol abuse was significantly associated with pneumonia and need for additional postdischarge health care.
Dr. Genther received a G. Slaughter Fitz-Hugh Resident Research Award for this study from the Triological Society. He reported having no financial disclosures.
MIAMI BEACH – Patients with head and neck cancers who develop alcohol withdrawal syndrome perioperatively experience significantly more complications after undergoing surgery, a large database analysis indicates.
The presence of withdrawal symptoms was associated with a 25% incidence of postoperative complications, compared with 14% among patients who abused alcohol and 7% among those without alcohol abuse, Dr. Dane J. Genther said at the Triological Society’s Combined Sections Meeting. The risk for wound complications was nearly double in this population (odds ratio, 1.9).
Dr. Genther, a resident in otolaryngologyhead and neck surgery at Johns Hopkins Hospital in Baltimore, and his associates used ICD-9 codes in the Nationwide Inpatient Sample discharge database to identify more than 92,000 patients who underwent an ablative procedure for head and neck cancer in 2003-2008. The retrospective, cross-sectional study included patients with malignant oral cavity, laryngeal, hypopharyngeal, and oropharyngeal neoplasms.
In a multivariate analysis, alcohol withdrawal syndrome was significantly more likely for patients undergoing a major procedure (OR, 2.0) and was significantly associated with Medicare payer status and a need for additional health care following discharge, Dr. Genther said.
The researchers found no significant association between alcohol withdrawal syndrome and increased risk for postoperative infections or in-hospital mortality, but there was a significant increase in hospital stay and related costs associated with the syndrome.
Having a major procedure and experiencing alcohol withdrawal contributed approximately $15,000 per admission in 2011 U.S. dollars, Dr. Genther said.
The findings point to a need for alternatives to current alcohol withdrawal prevention therapies, Dr. Genther said. "Despite prophylaxis, which is our current treatment to attempt to stem the onset of alcohol withdrawal syndrome, complications do occur and they are no less severe or frequent than in the absence of prophylaxis."
Abstinence from alcohol for at least 4 weeks is another strategy proposed to minimize risk of alcohol withdrawal syndrome for any at-risk surgical patient, said Dr. Genther. However, he added, "for many cancer patients, especially those with more advanced disease, waiting a prolonged period of time to possibly gain that benefit from abstinence is not necessarily a viable option."
Another aim of the study was to assess factors contributing to alcohol abuse. Patients aged 40-64 years had the highest proportion of alcohol abuse, and this age range was a significant factor (OR, 2.37). Those who abused alcohol were more often male and more often underwent major procedures, Dr. Genther said at the meeting, which was jointly sponsored by the Triological Society and the American College of Surgeons. In addition, alcohol abuse was significantly associated with pneumonia and need for additional postdischarge health care.
Dr. Genther received a G. Slaughter Fitz-Hugh Resident Research Award for this study from the Triological Society. He reported having no financial disclosures.
MIAMI BEACH – Patients with head and neck cancers who develop alcohol withdrawal syndrome perioperatively experience significantly more complications after undergoing surgery, a large database analysis indicates.
The presence of withdrawal symptoms was associated with a 25% incidence of postoperative complications, compared with 14% among patients who abused alcohol and 7% among those without alcohol abuse, Dr. Dane J. Genther said at the Triological Society’s Combined Sections Meeting. The risk for wound complications was nearly double in this population (odds ratio, 1.9).
Dr. Genther, a resident in otolaryngologyhead and neck surgery at Johns Hopkins Hospital in Baltimore, and his associates used ICD-9 codes in the Nationwide Inpatient Sample discharge database to identify more than 92,000 patients who underwent an ablative procedure for head and neck cancer in 2003-2008. The retrospective, cross-sectional study included patients with malignant oral cavity, laryngeal, hypopharyngeal, and oropharyngeal neoplasms.
In a multivariate analysis, alcohol withdrawal syndrome was significantly more likely for patients undergoing a major procedure (OR, 2.0) and was significantly associated with Medicare payer status and a need for additional health care following discharge, Dr. Genther said.
The researchers found no significant association between alcohol withdrawal syndrome and increased risk for postoperative infections or in-hospital mortality, but there was a significant increase in hospital stay and related costs associated with the syndrome.
Having a major procedure and experiencing alcohol withdrawal contributed approximately $15,000 per admission in 2011 U.S. dollars, Dr. Genther said.
The findings point to a need for alternatives to current alcohol withdrawal prevention therapies, Dr. Genther said. "Despite prophylaxis, which is our current treatment to attempt to stem the onset of alcohol withdrawal syndrome, complications do occur and they are no less severe or frequent than in the absence of prophylaxis."
Abstinence from alcohol for at least 4 weeks is another strategy proposed to minimize risk of alcohol withdrawal syndrome for any at-risk surgical patient, said Dr. Genther. However, he added, "for many cancer patients, especially those with more advanced disease, waiting a prolonged period of time to possibly gain that benefit from abstinence is not necessarily a viable option."
Another aim of the study was to assess factors contributing to alcohol abuse. Patients aged 40-64 years had the highest proportion of alcohol abuse, and this age range was a significant factor (OR, 2.37). Those who abused alcohol were more often male and more often underwent major procedures, Dr. Genther said at the meeting, which was jointly sponsored by the Triological Society and the American College of Surgeons. In addition, alcohol abuse was significantly associated with pneumonia and need for additional postdischarge health care.
Dr. Genther received a G. Slaughter Fitz-Hugh Resident Research Award for this study from the Triological Society. He reported having no financial disclosures.
FROM THE TRIOLOGICAL SOCIETY'S COMBINED SECTIONS MEETING
Major Finding: The presence of alcohol withdrawal symptoms was associated with a significantly higher incidence of postoperative complications, 25%, compared with 14% among patients who abused alcohol and 7% for those without alcohol abuse.
Data Source: Data were taken from a retrospective, cross-sectional study of 92,312 ablative procedures for head and neck cancer from the NIS database in 2003-2008.
Disclosures: Dr. Genther reported having no financial disclosures.
Effort of Inpatient Work
In internal medicine residency training, the most commonly used metric for measuring workload of physicians is the number of patients being followed or the number being admitted. There are data to support the importance of these census numbers. One study conducted at an academic medical center demonstrated that for patients admitted to medical services, the number of patients admitted on a call night was positively associated with mortality, even after adjustment in multivariable models.1
The problem with a census is that it is only a rough indicator of the amount of work that a given intern or resident will have. In a focus group study that our group conducted with internal medicine residents, several contributors to patient care errors were identified. Workload was identified as a major factor contributing to patient care mistakes.2 In describing workload, residents noted not only census but the complexity of the patient as contributing factors to workload.
A more comprehensive method than relying on census data has been used in anesthesia.3, 4 In 2 studies, anesthesiologists were asked to rate the effort or intensity associated with the tasks that they performed in the operating room.4, 5 In subsequent studies, this group used a trained observer to record the tasks anesthesiologists performed during a case.6, 7 Work density was calculated by multiplying the duration of each task by the previously developed task intensity score. In this way, work per unit of time can be calculated as can a cumulative workload score for a certain duration of time.
These methods provide the background for the work that we conducted in this study. The purpose of this study was to assign a task effort score to the tasks performed during periods that include admitting patients to the hospital.
METHODS
Study Site
A single 500‐bed Midwest academic institution. Residents rotate through 3 hospitals (a private community hospital, a Veterans hospital, and an academic medical center) during a typical 3‐year internal medicine residency program.
Study Design and Subjects
A cross‐sectional survey was conducted. Subjects recruited for the survey included internal medicine interns and residents, internal medicine ward attending physicians and hospitalists. Attending physicians had to have been on the wards in the past year. The survey was conducted in November, when all eligible house staff should have had at least 1 ward month. Nearly every hospitalist recruited had spent time on both teaching and nonteaching services.
Task List Compilation and Survey Development
An expert panel was convened consisting of 10 physicians representing 3 hospitals, including residents and faculty, some of which were hospitalists. During the session, the participants developed a task list and discussed the work intensity associated with some of the tasks. The task list was reviewed by the study team and organized into categories. The final list included 99 tasks divided into 6 categories: (1) direct patient care, (2) indirect patient care, (3) search for/finding things, (4) educational/academic activities, (5) personal/downtime activities, and (6) other. Table 1 gives examples of items found in each category. We used the terminology that the study participants used to describe their work (eg, they used the term eyeballing a patient to describe the process of making an initial assessment of the patient's status). This list of 99 items was formatted into a survey to allow study participants to rate each task across 3 domains: physical effort, mental effort, and psychological effort, based on previous studies in anesthesia4 (see Supporting Information). The term mental refers to cognitive effort, whereas psychological refers to emotional effort. We used the same scales with the same anchors as described in the anesthesia literature,4 but substituted the internal medicine specific tasks. Each item was rated on a 7‐point Likert‐type scale (1 = almost no stress or effort; 7 = most effort). The survey also included demographic information regarding the respondent and instructions. The instructions directed respondents to rate each item based on their average experience in performing each task. They were further instructed not to rate tasks they had never performed.
| Categories of Tasks | Examples |
|---|---|
| |
| Direct patient care | Conducting the physical examination, hand washing, putting on isolation gear |
| Indirect patient care | Writing H&P, writing orders, ordering additional labs or tests |
| Searching for/finding things | Finding a computer, finding materials for procedures, finding the patient |
| Personal/downtime activities | Eating dinner, sleep, socializing, calling family members |
| Educational/academic activities | Literature search, teaching medical students, preparing a talk |
| Other | Transporting patients, traveling from place to place, billing |
Survey Process
The potential survey participants were notified via e‐mail that they would be asked to complete the survey during a regularly scheduled meeting. The interns, residents, and faculty met during separate time slots. Data from residents and interns were obtained from teaching sessions they were required to attend (as long as their schedule permitted them to). Survey data for attending physicians were obtained from a general internal medicine meeting and a hospitalist meeting. Because of the type of meeting, subspecialists were less likely to have been included. The objectives of the study and its voluntary nature were presented to the groups, and the survey was given to all attendees at the meetings. Due to the anonymous nature of the survey, a waiver of written informed consent was granted. Time was reserved during the course of the meeting to complete the survey. Before distributing the survey, we counted the total number of people in the room so that a participation rate could be calculated. Respondents were instructed to place the survey in a designated envelope after completing it or to return a blank survey if they did not wish to complete it. There was no time limit for completion of the survey. At all of these sessions, this survey was one part of the meeting agenda.
Data Analysis
Surveys were entered into a Microsoft Excel (Redmond, WA) spreadsheet and then transferred into Stata version 8.0 (College Station, TX), which was used for analysis. Our analysis focused on (1) the description of the effort associated with individual tasks, (2) the description of the effort associated with task categories and comparisons across key categories, and (3) a comparison of effort across the task categories' physical, mental, and psychological domains.
Each task had 3 individual domain scores associated with it: physical, mental (ie, cognitive work), and psychological (ie, emotional work). A composite task effort score was calculated for each task by determining the mean of the 3 domain scores for that task.
An overall effort score was calculated for each of the 6 task categories by determining the mean of the composite task effort scores within each category. We used the composite effort score for each task to calculate the Cronbach's value for each category except other. We compared the overall category effort scores for direct versus indirect patient care using 2‐tailed paired t tests with a significance level of P < 0.05. We further evaluated differences in overall category effort scores for direct patient care between physicians of different genders and between house staff and faculty, using 2‐tailed unpaired t tests, with a significance level of P < 0.05.
Finally, we compared the physical, mental, and psychological domain scores for direct versus indirect patient care categories, using paired t tests.
Ethics
This study was approved by the Institutional Review Board at the Medical College of Wisconsin.
RESULTS
The study participation rate was 69% (59/85). The sample consisted of 31 (52%) women and 40 (68%) house staff (see Table 2). The mean age was 34 years. This participation rate represents approximately 1/3 of the internal medicine house staff and a smaller percentage of the faculty that would have been eligible.
| Demographic | Value |
|---|---|
| |
| Age, y, mean (SD) | 34 (8.8) |
| Female gender, no. (%) | 31 (52) |
| Physician description, no. (%) | |
| Intern | 7 (12) |
| Resident | 33 (56) |
| Hospitalist | 4 (7) |
| Nonhospitalist faculty | 15 (25) |
Individual Task Effort
The mean composite effort score of all 99 tasks is provided in the Supporting Information Table. Overall, the most difficult task was going to codes (in the direct patient care category), with a mean composite rating of 5.37 (standard deviation [SD] 1.5); this was also the most difficult psychological task (5.78 [SD 1.65]). The most difficult mental task was transferring an unstable patient to the intensive care unit (5.47 [SD 1.53]). The most difficult physical task was placing a central line (5.02 [SD 1.63]). The easiest task was using the Internet (in the personal/downtime activities category), with a mean composite rating of 1.41 (SD 0.74); this was also the easiest mental (1.52 [SD 1.01]), psychological (1.3 [SD 0.68]), and physical (1.42 [SD 0.76]) task.
Analysis of Task Categories
The overall and domain characteristics of each task category are given in Table 3. Categories contained between 5 and 41 tasks. The Cronbach's ranged from 0.83 for the personal/downtime activities category to 0.98 for the direct patient care category. The mean overall effort ranged from least difficult for the personal/downtime category (1.72 [SD 0.76]) to most difficult for the education category (3.61 [SD 1.06]).
| Category | No. of Items | Cronbach's | Effort Score, Mean (SD)* | |||
|---|---|---|---|---|---|---|
| Composite Effort | Physical Effort | Mental Effort | Psychological Effort | |||
| ||||||
| Direct patient care | 32 | 0.97 | 3.55 (0.91) | 3.22 (1.06) | 3.89 (0.99) | 3.52 (1.04) |
| Indirect patient care | 41 | 0.98 | 3.21 (0.92) | 2.71 (1.09) | 3.80 (1.02) | 3.20 (1.08) |
| Education | 8 | 0.92 | 3.61 (1.06) | 3.12 (1.26) | 4.27 (1.17) | 3.43 (1.30) |
| Finding things | 5 | 0.85 | 2.94 (0.91) | 3.59 (1.23) | 2.43 (1.05) | 2.79 (1.13) |
| Personal | 7 | 0.83 | 1.72 (0.76) | 1.86 (0.92) | 1.69 (0.85) | 1.63 (0.72) |
| Other | 6 | NC | NC | NC | NC | NC |
Using paired t tests, we determined that the direct patient care category was more difficult than the indirect patient care category overall (3.58 versus 3.21, P < 0.001). Direct patient care was statistically significantly more challenging than indirect patient care on the physical (3.23 vs 2.71; P < 0.001), mental (3.90 vs 3.84; P < 0.05), and psychological domains (3.57 vs 3.20; P < 0.001) as well. There were no significant differences between men and women or between house staff and faculty on the difficulty of direct patient care. We found a trend toward increased difficulty of indirect patient care for house staff versus faculty (3.36 vs 2.92; P 0.10), but no differences by gender.
DISCUSSION
In this study, we used a comprehensive list of tasks performed by internal medicine doctors while admitting patients and produced a numeric assessment of the effort associated with each. The list was generated by an expert panel and comprised 6 categories and 99 items. Residents and attending physicians then rated each task based on level of difficulty, specifically looking at the mental, psychological, and physical effort required by each.
Indirect patient care was the task category in our study that had the most tasks associated with it (41 out of 99). Direct patient care included 32 items, but 10 of these were procedures (eg, lumbar puncture), some of which are uncommonly performed. Several time‐motion studies have been performed to document the work done by residents815 and hospitalists.16, 17 Although our study did not assess the time spent on each task, the distribution of tasks across categories is consistent with these time‐motion studies, which show that the amount of time spent in direct patient care is a small fraction of the amount of time spent in the hospital,12 and that work such as interprofessional communication10 and documentation16 consume the majority of time.
This project allowed us to consider the effort required for inpatient internal medicine work on a more granular level than has been described previously. Although the difficulty of tasks associated with anesthesia and surgical work has been described,3, 4, 7, 1820 our study is a unique contribution to the internal medicine literature. Understanding the difficulty of tasks performed by inpatient physicians is an important step toward better management of workload. With concerns about burnout in hospitalists21, 22 and residents,2325 it seems wise to take the difficulty of the work they do into consideration in a more proactive manner. In addition, understanding workload may have patient safety applications. In one study of mistakes made by house staff, 51% of the survey respondents identified workload as a contributing factor.26
We assessed effort for inpatient work by generating a task list and then measuring 3 domains of each task: physical, mental, and psychological. As a result, we were able to further quantify the difficulty of work completed by physicians. Recent work from outside of medicine suggests that individuals have a finite capacity for mental workload, and when this is breached, decision‐making quality is impaired.27 This suggests that it is important to take work intensity into account when assigning work to individuals. For example, a detailed assessment of workload at the task level combined with the amount of time spent on each task would allow us to know how much effort is typically involved with admitting a new patient. This information would allow for more equal distribution of workload across admitting teams. In addition, these methods could be expanded to understand how much effort is involved in the discharge process. This could be taken into account at the beginning of a day when allocating work such as admissions and discharges between members of a team.
This methodology has the potential to be used in other ways to help quantify the effort required for the work that physicians do. Many departments are struggling to develop a system for giving credit to faculty for the time they spend on nonpatient care activities. Perhaps these methods could be used to develop effort scores associated with administrative tasks, and administrative relative value units could be calculated accordingly. Similar techniques have been used with educational relative value units.28
We know from the nursing literature that workload is related to both burnout and patient safety. Burnout is a process related to the emotional work of providing care to people.29 Our methods clearly incorporate the psychological stress of work into the workload assessment. Evaluating the amount of time spent on tasks with high psychological scores may be helpful in identifying work patterns that are more likely to produce burnout in physicians and nurses.
With respect to patient safety, higher patient‐to‐nurse ratios are associated with failure to rescue30 and nosocomial infections.31 Furthermore, researchers have demonstrated that systems issues can add substantially to nursing workload.32 Methods such as those described in our study take into account both patient‐related and systems‐related tasks, and therefore could result in more detailed workload assessments. With more detailed information about contributors to workload, better predictions about optimal staffing could be made, which would ultimately lead to fewer adverse patient events.
Our study has limitations. First, the initial task list was based on the compilation efforts from only 10 physicians. However, this group of physicians represented 3 hospitals and included both resident and attending physicians. Second, the survey data were gathered from a single institution. Although we included trainees and faculty, more participants would be needed to answer questions about how experience and setting/environmental factors affect these assessments. However, participants were instructed to reflect on their whole experience with each task, which presumably includes multiple institutions and training levels. Third, the sample size is fairly small, with more house staff than faculty (hospitalists and nonhospitalists) represented. Regardless, this study is the first attempt to define and quantify workload for internal medicine physicians using these methods. In future studies, we will expand the number of institutions and levels of experience to validate our current data. Finally, the difficulty of the tasks is clearly a subjective assessment. Although this methodology has face validity, further work needs to be done to validate these findings against other measurements of workload, such as census, or more general subjective workload assessments, such as the NASA task load index.33
In conclusion, we have described the tasks performed by inpatient physicians and the difficulty associated with them. Moreover, we have described a methodology that could be replicated at other centers for the purpose of validating our findings or quantifying workload of other types of tasks. We believe that this is the first step toward a more comprehensive understanding of the workload encountered by inpatient physicians. Because workload has implications for physician burnout and patient safety, it is essential that we fully understand the contributors to workload, including the innate difficulty of the tasks that comprise it.
Acknowledgements
The authors Alexis Visotcky, MS, and Sergey Tarima, PhD, for their assistance with statistics.
This work was presented in poster form at the Society of Hospital Medicine Annual Meeting in April 2010, the Society of General Internal Medicine Annual Meeting in May 2010, and the Society of General Internal Medicine regional meeting in September 2010.
Funding Source: The study team was supported by the following funds during this work: VA grants PPO 0925901 (Marilyn M. Schapira and Kathlyn E. Fletcher) and IIR 07201 (Marilyn M. Schapira, Siddhartha Singh, and Kathlyn E. Fletcher).
- ,,,,.House staff team workload and organization effects on patient outcomes in an academic general internal medicine inpatient service.Arch Intern Med.2007;167:47–52.
- ,,, et al.The work hour rules and contributors to patient care mistakes: A focus group study with internal medicine residentsJ Hosp Med.2008;3:228–237.
- ,,.Multiple measures of anesthesia workload during teaching and nonteaching cases.Anesth Analg.2004;98:1419–1425.
- ,,,,.Developing a technique to measure anesthesiologists' real‐time workload.Proceedings of the Human Factors and Ergonomics Society Annual Meeting.2000;44:241–244.
- ,,, et al.Quantitative description of the workload associated with airway management procedures.J Clin Anesth.2000;12:273–282.
- ,,,,,.An objective methodology for task analysis and workload assessment in anesthesia providers.Anesthesiology.1994;80:77–92.
- ,.Effects of intraoperative reading on vigilance and workload during anesthesia care in an academic medical center.Anesthesiology.2009;110:275–283.
- ,,.Resident work hours: what they are really doing.Arch Surg.2004;139:490–493; discussion, 493–494.
- ,,,,,.Analyzing the time and value of housestaff inpatient work.J Gen Intern Med.1998;13:534–540.
- ,,,.All in a day's work: an observational study to quantify how and with whom doctors on hospital wards spend their time.[see comment].Med J Aust.2008;188:506–509.
- ,,,,.How do house officers spend their nights? A time study of internal medicine house staff on call.N Engl J Med.1989;320:1673–1677.
- ,,,,.Systematic review of time studies evaluating physicians in the hospital setting.J Hosp Med.2010;5:353–359.
- ,,.Time analysis of a general medicine service: results from a random work sampling study.J Gen Intern Med.1994;9:272–277.
- ,,,.A phenomenology of scut.Ann Intern Med.1991;115:372–376.
- ,,, et al.The on‐call experience of interns in internal medicine. Medical Education Task Force of Henry Ford Hospital.Arch Intern Med.1990;150:2294–2297.
- ,,, et al.Where did the day go? A time‐motion study of hospitalists.J Hosp Med.2010;5:323–328.
- ,,.How hospitalists spend their time: insights on efficiency and safety.J Hosp Med.2006;1:88–93.
- ,,, et al.Differences in day and night shift clinical performance in anesthesiology.Hum Factors.2008;50:276–290.
- ,,,,.Assessment of the intrarater and interrater reliability of an established clinical task analysis methodology.Anesthesiology.2002;96:1129–1139.
- ,,.The effect of electronic record keeping and transesophageal echocardiography on task distribution, workload, and vigilance during cardiac anesthesia.Anesthesiology.1997;87:144–155.
- .Fight burnout while fostering experience: investing in hospitalist programs now can fight burnout later.ACP Hospitalist. July2008.
- .Hospitalist burnout: recognize it in yourself and others, and avoid or eliminate it.The Hospitalist. March2006.
- ,,,.Burnout and internal medicine resident work‐hour restrictions.Arch Intern Med.2005;165:2595–2600.
- ,,,,.The effects of work‐hour limitations on resident well‐being, patient care, and education in an internal medicine residency program.Arch Intern Med.2005;165:2601–2606.
- ,,,.Burnout and self‐reported patient care in an internal medicine residency program.Ann Intern Med.2002;136:358–367.
- ,,,.Do house officers learn from their mistakes?Qual Saf Health Care.2003;12:221–226; discussion, 227–228.
- ,,.Extraneous factors in judicial decisions.Proc Natl Acad Sci U S A.2011;108:6889–6892.
- ,.Quantifying physician teaching productivity using clinical relative value units.J Gen Intern Med.1999;14:617–621.
- .Maslach Burnout Inventory Manual.3rd ed.Palo Alto, CA:Consulting Psychology Press;1986.
- ,,,,.Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction.JAMA.2002;288:1987–1993.
- ,,,,.Patient density, nurse‐to‐patient ratio and nosocomial infection risk in a pediatric cardiac intensive care unit.Pediatr Infect Dis J.1997;16:1045–1048.
- ,.Operational failures and interruptions in hospital nursing.Health Serv Res.2006;41:643–662.
- ,.Development of NASA‐TLX (Task Load Index): results of empirical and theoretical research. In: Hancock PA, Meshkati N, eds.Human Mental Workload.Amsterdam, Netherlands:North Holland Press;1988:239–250.
In internal medicine residency training, the most commonly used metric for measuring workload of physicians is the number of patients being followed or the number being admitted. There are data to support the importance of these census numbers. One study conducted at an academic medical center demonstrated that for patients admitted to medical services, the number of patients admitted on a call night was positively associated with mortality, even after adjustment in multivariable models.1
The problem with a census is that it is only a rough indicator of the amount of work that a given intern or resident will have. In a focus group study that our group conducted with internal medicine residents, several contributors to patient care errors were identified. Workload was identified as a major factor contributing to patient care mistakes.2 In describing workload, residents noted not only census but the complexity of the patient as contributing factors to workload.
A more comprehensive method than relying on census data has been used in anesthesia.3, 4 In 2 studies, anesthesiologists were asked to rate the effort or intensity associated with the tasks that they performed in the operating room.4, 5 In subsequent studies, this group used a trained observer to record the tasks anesthesiologists performed during a case.6, 7 Work density was calculated by multiplying the duration of each task by the previously developed task intensity score. In this way, work per unit of time can be calculated as can a cumulative workload score for a certain duration of time.
These methods provide the background for the work that we conducted in this study. The purpose of this study was to assign a task effort score to the tasks performed during periods that include admitting patients to the hospital.
METHODS
Study Site
A single 500‐bed Midwest academic institution. Residents rotate through 3 hospitals (a private community hospital, a Veterans hospital, and an academic medical center) during a typical 3‐year internal medicine residency program.
Study Design and Subjects
A cross‐sectional survey was conducted. Subjects recruited for the survey included internal medicine interns and residents, internal medicine ward attending physicians and hospitalists. Attending physicians had to have been on the wards in the past year. The survey was conducted in November, when all eligible house staff should have had at least 1 ward month. Nearly every hospitalist recruited had spent time on both teaching and nonteaching services.
Task List Compilation and Survey Development
An expert panel was convened consisting of 10 physicians representing 3 hospitals, including residents and faculty, some of which were hospitalists. During the session, the participants developed a task list and discussed the work intensity associated with some of the tasks. The task list was reviewed by the study team and organized into categories. The final list included 99 tasks divided into 6 categories: (1) direct patient care, (2) indirect patient care, (3) search for/finding things, (4) educational/academic activities, (5) personal/downtime activities, and (6) other. Table 1 gives examples of items found in each category. We used the terminology that the study participants used to describe their work (eg, they used the term eyeballing a patient to describe the process of making an initial assessment of the patient's status). This list of 99 items was formatted into a survey to allow study participants to rate each task across 3 domains: physical effort, mental effort, and psychological effort, based on previous studies in anesthesia4 (see Supporting Information). The term mental refers to cognitive effort, whereas psychological refers to emotional effort. We used the same scales with the same anchors as described in the anesthesia literature,4 but substituted the internal medicine specific tasks. Each item was rated on a 7‐point Likert‐type scale (1 = almost no stress or effort; 7 = most effort). The survey also included demographic information regarding the respondent and instructions. The instructions directed respondents to rate each item based on their average experience in performing each task. They were further instructed not to rate tasks they had never performed.
| Categories of Tasks | Examples |
|---|---|
| |
| Direct patient care | Conducting the physical examination, hand washing, putting on isolation gear |
| Indirect patient care | Writing H&P, writing orders, ordering additional labs or tests |
| Searching for/finding things | Finding a computer, finding materials for procedures, finding the patient |
| Personal/downtime activities | Eating dinner, sleep, socializing, calling family members |
| Educational/academic activities | Literature search, teaching medical students, preparing a talk |
| Other | Transporting patients, traveling from place to place, billing |
Survey Process
The potential survey participants were notified via e‐mail that they would be asked to complete the survey during a regularly scheduled meeting. The interns, residents, and faculty met during separate time slots. Data from residents and interns were obtained from teaching sessions they were required to attend (as long as their schedule permitted them to). Survey data for attending physicians were obtained from a general internal medicine meeting and a hospitalist meeting. Because of the type of meeting, subspecialists were less likely to have been included. The objectives of the study and its voluntary nature were presented to the groups, and the survey was given to all attendees at the meetings. Due to the anonymous nature of the survey, a waiver of written informed consent was granted. Time was reserved during the course of the meeting to complete the survey. Before distributing the survey, we counted the total number of people in the room so that a participation rate could be calculated. Respondents were instructed to place the survey in a designated envelope after completing it or to return a blank survey if they did not wish to complete it. There was no time limit for completion of the survey. At all of these sessions, this survey was one part of the meeting agenda.
Data Analysis
Surveys were entered into a Microsoft Excel (Redmond, WA) spreadsheet and then transferred into Stata version 8.0 (College Station, TX), which was used for analysis. Our analysis focused on (1) the description of the effort associated with individual tasks, (2) the description of the effort associated with task categories and comparisons across key categories, and (3) a comparison of effort across the task categories' physical, mental, and psychological domains.
Each task had 3 individual domain scores associated with it: physical, mental (ie, cognitive work), and psychological (ie, emotional work). A composite task effort score was calculated for each task by determining the mean of the 3 domain scores for that task.
An overall effort score was calculated for each of the 6 task categories by determining the mean of the composite task effort scores within each category. We used the composite effort score for each task to calculate the Cronbach's value for each category except other. We compared the overall category effort scores for direct versus indirect patient care using 2‐tailed paired t tests with a significance level of P < 0.05. We further evaluated differences in overall category effort scores for direct patient care between physicians of different genders and between house staff and faculty, using 2‐tailed unpaired t tests, with a significance level of P < 0.05.
Finally, we compared the physical, mental, and psychological domain scores for direct versus indirect patient care categories, using paired t tests.
Ethics
This study was approved by the Institutional Review Board at the Medical College of Wisconsin.
RESULTS
The study participation rate was 69% (59/85). The sample consisted of 31 (52%) women and 40 (68%) house staff (see Table 2). The mean age was 34 years. This participation rate represents approximately 1/3 of the internal medicine house staff and a smaller percentage of the faculty that would have been eligible.
| Demographic | Value |
|---|---|
| |
| Age, y, mean (SD) | 34 (8.8) |
| Female gender, no. (%) | 31 (52) |
| Physician description, no. (%) | |
| Intern | 7 (12) |
| Resident | 33 (56) |
| Hospitalist | 4 (7) |
| Nonhospitalist faculty | 15 (25) |
Individual Task Effort
The mean composite effort score of all 99 tasks is provided in the Supporting Information Table. Overall, the most difficult task was going to codes (in the direct patient care category), with a mean composite rating of 5.37 (standard deviation [SD] 1.5); this was also the most difficult psychological task (5.78 [SD 1.65]). The most difficult mental task was transferring an unstable patient to the intensive care unit (5.47 [SD 1.53]). The most difficult physical task was placing a central line (5.02 [SD 1.63]). The easiest task was using the Internet (in the personal/downtime activities category), with a mean composite rating of 1.41 (SD 0.74); this was also the easiest mental (1.52 [SD 1.01]), psychological (1.3 [SD 0.68]), and physical (1.42 [SD 0.76]) task.
Analysis of Task Categories
The overall and domain characteristics of each task category are given in Table 3. Categories contained between 5 and 41 tasks. The Cronbach's ranged from 0.83 for the personal/downtime activities category to 0.98 for the direct patient care category. The mean overall effort ranged from least difficult for the personal/downtime category (1.72 [SD 0.76]) to most difficult for the education category (3.61 [SD 1.06]).
| Category | No. of Items | Cronbach's | Effort Score, Mean (SD)* | |||
|---|---|---|---|---|---|---|
| Composite Effort | Physical Effort | Mental Effort | Psychological Effort | |||
| ||||||
| Direct patient care | 32 | 0.97 | 3.55 (0.91) | 3.22 (1.06) | 3.89 (0.99) | 3.52 (1.04) |
| Indirect patient care | 41 | 0.98 | 3.21 (0.92) | 2.71 (1.09) | 3.80 (1.02) | 3.20 (1.08) |
| Education | 8 | 0.92 | 3.61 (1.06) | 3.12 (1.26) | 4.27 (1.17) | 3.43 (1.30) |
| Finding things | 5 | 0.85 | 2.94 (0.91) | 3.59 (1.23) | 2.43 (1.05) | 2.79 (1.13) |
| Personal | 7 | 0.83 | 1.72 (0.76) | 1.86 (0.92) | 1.69 (0.85) | 1.63 (0.72) |
| Other | 6 | NC | NC | NC | NC | NC |
Using paired t tests, we determined that the direct patient care category was more difficult than the indirect patient care category overall (3.58 versus 3.21, P < 0.001). Direct patient care was statistically significantly more challenging than indirect patient care on the physical (3.23 vs 2.71; P < 0.001), mental (3.90 vs 3.84; P < 0.05), and psychological domains (3.57 vs 3.20; P < 0.001) as well. There were no significant differences between men and women or between house staff and faculty on the difficulty of direct patient care. We found a trend toward increased difficulty of indirect patient care for house staff versus faculty (3.36 vs 2.92; P 0.10), but no differences by gender.
DISCUSSION
In this study, we used a comprehensive list of tasks performed by internal medicine doctors while admitting patients and produced a numeric assessment of the effort associated with each. The list was generated by an expert panel and comprised 6 categories and 99 items. Residents and attending physicians then rated each task based on level of difficulty, specifically looking at the mental, psychological, and physical effort required by each.
Indirect patient care was the task category in our study that had the most tasks associated with it (41 out of 99). Direct patient care included 32 items, but 10 of these were procedures (eg, lumbar puncture), some of which are uncommonly performed. Several time‐motion studies have been performed to document the work done by residents815 and hospitalists.16, 17 Although our study did not assess the time spent on each task, the distribution of tasks across categories is consistent with these time‐motion studies, which show that the amount of time spent in direct patient care is a small fraction of the amount of time spent in the hospital,12 and that work such as interprofessional communication10 and documentation16 consume the majority of time.
This project allowed us to consider the effort required for inpatient internal medicine work on a more granular level than has been described previously. Although the difficulty of tasks associated with anesthesia and surgical work has been described,3, 4, 7, 1820 our study is a unique contribution to the internal medicine literature. Understanding the difficulty of tasks performed by inpatient physicians is an important step toward better management of workload. With concerns about burnout in hospitalists21, 22 and residents,2325 it seems wise to take the difficulty of the work they do into consideration in a more proactive manner. In addition, understanding workload may have patient safety applications. In one study of mistakes made by house staff, 51% of the survey respondents identified workload as a contributing factor.26
We assessed effort for inpatient work by generating a task list and then measuring 3 domains of each task: physical, mental, and psychological. As a result, we were able to further quantify the difficulty of work completed by physicians. Recent work from outside of medicine suggests that individuals have a finite capacity for mental workload, and when this is breached, decision‐making quality is impaired.27 This suggests that it is important to take work intensity into account when assigning work to individuals. For example, a detailed assessment of workload at the task level combined with the amount of time spent on each task would allow us to know how much effort is typically involved with admitting a new patient. This information would allow for more equal distribution of workload across admitting teams. In addition, these methods could be expanded to understand how much effort is involved in the discharge process. This could be taken into account at the beginning of a day when allocating work such as admissions and discharges between members of a team.
This methodology has the potential to be used in other ways to help quantify the effort required for the work that physicians do. Many departments are struggling to develop a system for giving credit to faculty for the time they spend on nonpatient care activities. Perhaps these methods could be used to develop effort scores associated with administrative tasks, and administrative relative value units could be calculated accordingly. Similar techniques have been used with educational relative value units.28
We know from the nursing literature that workload is related to both burnout and patient safety. Burnout is a process related to the emotional work of providing care to people.29 Our methods clearly incorporate the psychological stress of work into the workload assessment. Evaluating the amount of time spent on tasks with high psychological scores may be helpful in identifying work patterns that are more likely to produce burnout in physicians and nurses.
With respect to patient safety, higher patient‐to‐nurse ratios are associated with failure to rescue30 and nosocomial infections.31 Furthermore, researchers have demonstrated that systems issues can add substantially to nursing workload.32 Methods such as those described in our study take into account both patient‐related and systems‐related tasks, and therefore could result in more detailed workload assessments. With more detailed information about contributors to workload, better predictions about optimal staffing could be made, which would ultimately lead to fewer adverse patient events.
Our study has limitations. First, the initial task list was based on the compilation efforts from only 10 physicians. However, this group of physicians represented 3 hospitals and included both resident and attending physicians. Second, the survey data were gathered from a single institution. Although we included trainees and faculty, more participants would be needed to answer questions about how experience and setting/environmental factors affect these assessments. However, participants were instructed to reflect on their whole experience with each task, which presumably includes multiple institutions and training levels. Third, the sample size is fairly small, with more house staff than faculty (hospitalists and nonhospitalists) represented. Regardless, this study is the first attempt to define and quantify workload for internal medicine physicians using these methods. In future studies, we will expand the number of institutions and levels of experience to validate our current data. Finally, the difficulty of the tasks is clearly a subjective assessment. Although this methodology has face validity, further work needs to be done to validate these findings against other measurements of workload, such as census, or more general subjective workload assessments, such as the NASA task load index.33
In conclusion, we have described the tasks performed by inpatient physicians and the difficulty associated with them. Moreover, we have described a methodology that could be replicated at other centers for the purpose of validating our findings or quantifying workload of other types of tasks. We believe that this is the first step toward a more comprehensive understanding of the workload encountered by inpatient physicians. Because workload has implications for physician burnout and patient safety, it is essential that we fully understand the contributors to workload, including the innate difficulty of the tasks that comprise it.
Acknowledgements
The authors Alexis Visotcky, MS, and Sergey Tarima, PhD, for their assistance with statistics.
This work was presented in poster form at the Society of Hospital Medicine Annual Meeting in April 2010, the Society of General Internal Medicine Annual Meeting in May 2010, and the Society of General Internal Medicine regional meeting in September 2010.
Funding Source: The study team was supported by the following funds during this work: VA grants PPO 0925901 (Marilyn M. Schapira and Kathlyn E. Fletcher) and IIR 07201 (Marilyn M. Schapira, Siddhartha Singh, and Kathlyn E. Fletcher).
In internal medicine residency training, the most commonly used metric for measuring workload of physicians is the number of patients being followed or the number being admitted. There are data to support the importance of these census numbers. One study conducted at an academic medical center demonstrated that for patients admitted to medical services, the number of patients admitted on a call night was positively associated with mortality, even after adjustment in multivariable models.1
The problem with a census is that it is only a rough indicator of the amount of work that a given intern or resident will have. In a focus group study that our group conducted with internal medicine residents, several contributors to patient care errors were identified. Workload was identified as a major factor contributing to patient care mistakes.2 In describing workload, residents noted not only census but the complexity of the patient as contributing factors to workload.
A more comprehensive method than relying on census data has been used in anesthesia.3, 4 In 2 studies, anesthesiologists were asked to rate the effort or intensity associated with the tasks that they performed in the operating room.4, 5 In subsequent studies, this group used a trained observer to record the tasks anesthesiologists performed during a case.6, 7 Work density was calculated by multiplying the duration of each task by the previously developed task intensity score. In this way, work per unit of time can be calculated as can a cumulative workload score for a certain duration of time.
These methods provide the background for the work that we conducted in this study. The purpose of this study was to assign a task effort score to the tasks performed during periods that include admitting patients to the hospital.
METHODS
Study Site
A single 500‐bed Midwest academic institution. Residents rotate through 3 hospitals (a private community hospital, a Veterans hospital, and an academic medical center) during a typical 3‐year internal medicine residency program.
Study Design and Subjects
A cross‐sectional survey was conducted. Subjects recruited for the survey included internal medicine interns and residents, internal medicine ward attending physicians and hospitalists. Attending physicians had to have been on the wards in the past year. The survey was conducted in November, when all eligible house staff should have had at least 1 ward month. Nearly every hospitalist recruited had spent time on both teaching and nonteaching services.
Task List Compilation and Survey Development
An expert panel was convened consisting of 10 physicians representing 3 hospitals, including residents and faculty, some of which were hospitalists. During the session, the participants developed a task list and discussed the work intensity associated with some of the tasks. The task list was reviewed by the study team and organized into categories. The final list included 99 tasks divided into 6 categories: (1) direct patient care, (2) indirect patient care, (3) search for/finding things, (4) educational/academic activities, (5) personal/downtime activities, and (6) other. Table 1 gives examples of items found in each category. We used the terminology that the study participants used to describe their work (eg, they used the term eyeballing a patient to describe the process of making an initial assessment of the patient's status). This list of 99 items was formatted into a survey to allow study participants to rate each task across 3 domains: physical effort, mental effort, and psychological effort, based on previous studies in anesthesia4 (see Supporting Information). The term mental refers to cognitive effort, whereas psychological refers to emotional effort. We used the same scales with the same anchors as described in the anesthesia literature,4 but substituted the internal medicine specific tasks. Each item was rated on a 7‐point Likert‐type scale (1 = almost no stress or effort; 7 = most effort). The survey also included demographic information regarding the respondent and instructions. The instructions directed respondents to rate each item based on their average experience in performing each task. They were further instructed not to rate tasks they had never performed.
| Categories of Tasks | Examples |
|---|---|
| |
| Direct patient care | Conducting the physical examination, hand washing, putting on isolation gear |
| Indirect patient care | Writing H&P, writing orders, ordering additional labs or tests |
| Searching for/finding things | Finding a computer, finding materials for procedures, finding the patient |
| Personal/downtime activities | Eating dinner, sleep, socializing, calling family members |
| Educational/academic activities | Literature search, teaching medical students, preparing a talk |
| Other | Transporting patients, traveling from place to place, billing |
Survey Process
The potential survey participants were notified via e‐mail that they would be asked to complete the survey during a regularly scheduled meeting. The interns, residents, and faculty met during separate time slots. Data from residents and interns were obtained from teaching sessions they were required to attend (as long as their schedule permitted them to). Survey data for attending physicians were obtained from a general internal medicine meeting and a hospitalist meeting. Because of the type of meeting, subspecialists were less likely to have been included. The objectives of the study and its voluntary nature were presented to the groups, and the survey was given to all attendees at the meetings. Due to the anonymous nature of the survey, a waiver of written informed consent was granted. Time was reserved during the course of the meeting to complete the survey. Before distributing the survey, we counted the total number of people in the room so that a participation rate could be calculated. Respondents were instructed to place the survey in a designated envelope after completing it or to return a blank survey if they did not wish to complete it. There was no time limit for completion of the survey. At all of these sessions, this survey was one part of the meeting agenda.
Data Analysis
Surveys were entered into a Microsoft Excel (Redmond, WA) spreadsheet and then transferred into Stata version 8.0 (College Station, TX), which was used for analysis. Our analysis focused on (1) the description of the effort associated with individual tasks, (2) the description of the effort associated with task categories and comparisons across key categories, and (3) a comparison of effort across the task categories' physical, mental, and psychological domains.
Each task had 3 individual domain scores associated with it: physical, mental (ie, cognitive work), and psychological (ie, emotional work). A composite task effort score was calculated for each task by determining the mean of the 3 domain scores for that task.
An overall effort score was calculated for each of the 6 task categories by determining the mean of the composite task effort scores within each category. We used the composite effort score for each task to calculate the Cronbach's value for each category except other. We compared the overall category effort scores for direct versus indirect patient care using 2‐tailed paired t tests with a significance level of P < 0.05. We further evaluated differences in overall category effort scores for direct patient care between physicians of different genders and between house staff and faculty, using 2‐tailed unpaired t tests, with a significance level of P < 0.05.
Finally, we compared the physical, mental, and psychological domain scores for direct versus indirect patient care categories, using paired t tests.
Ethics
This study was approved by the Institutional Review Board at the Medical College of Wisconsin.
RESULTS
The study participation rate was 69% (59/85). The sample consisted of 31 (52%) women and 40 (68%) house staff (see Table 2). The mean age was 34 years. This participation rate represents approximately 1/3 of the internal medicine house staff and a smaller percentage of the faculty that would have been eligible.
| Demographic | Value |
|---|---|
| |
| Age, y, mean (SD) | 34 (8.8) |
| Female gender, no. (%) | 31 (52) |
| Physician description, no. (%) | |
| Intern | 7 (12) |
| Resident | 33 (56) |
| Hospitalist | 4 (7) |
| Nonhospitalist faculty | 15 (25) |
Individual Task Effort
The mean composite effort score of all 99 tasks is provided in the Supporting Information Table. Overall, the most difficult task was going to codes (in the direct patient care category), with a mean composite rating of 5.37 (standard deviation [SD] 1.5); this was also the most difficult psychological task (5.78 [SD 1.65]). The most difficult mental task was transferring an unstable patient to the intensive care unit (5.47 [SD 1.53]). The most difficult physical task was placing a central line (5.02 [SD 1.63]). The easiest task was using the Internet (in the personal/downtime activities category), with a mean composite rating of 1.41 (SD 0.74); this was also the easiest mental (1.52 [SD 1.01]), psychological (1.3 [SD 0.68]), and physical (1.42 [SD 0.76]) task.
Analysis of Task Categories
The overall and domain characteristics of each task category are given in Table 3. Categories contained between 5 and 41 tasks. The Cronbach's ranged from 0.83 for the personal/downtime activities category to 0.98 for the direct patient care category. The mean overall effort ranged from least difficult for the personal/downtime category (1.72 [SD 0.76]) to most difficult for the education category (3.61 [SD 1.06]).
| Category | No. of Items | Cronbach's | Effort Score, Mean (SD)* | |||
|---|---|---|---|---|---|---|
| Composite Effort | Physical Effort | Mental Effort | Psychological Effort | |||
| ||||||
| Direct patient care | 32 | 0.97 | 3.55 (0.91) | 3.22 (1.06) | 3.89 (0.99) | 3.52 (1.04) |
| Indirect patient care | 41 | 0.98 | 3.21 (0.92) | 2.71 (1.09) | 3.80 (1.02) | 3.20 (1.08) |
| Education | 8 | 0.92 | 3.61 (1.06) | 3.12 (1.26) | 4.27 (1.17) | 3.43 (1.30) |
| Finding things | 5 | 0.85 | 2.94 (0.91) | 3.59 (1.23) | 2.43 (1.05) | 2.79 (1.13) |
| Personal | 7 | 0.83 | 1.72 (0.76) | 1.86 (0.92) | 1.69 (0.85) | 1.63 (0.72) |
| Other | 6 | NC | NC | NC | NC | NC |
Using paired t tests, we determined that the direct patient care category was more difficult than the indirect patient care category overall (3.58 versus 3.21, P < 0.001). Direct patient care was statistically significantly more challenging than indirect patient care on the physical (3.23 vs 2.71; P < 0.001), mental (3.90 vs 3.84; P < 0.05), and psychological domains (3.57 vs 3.20; P < 0.001) as well. There were no significant differences between men and women or between house staff and faculty on the difficulty of direct patient care. We found a trend toward increased difficulty of indirect patient care for house staff versus faculty (3.36 vs 2.92; P 0.10), but no differences by gender.
DISCUSSION
In this study, we used a comprehensive list of tasks performed by internal medicine doctors while admitting patients and produced a numeric assessment of the effort associated with each. The list was generated by an expert panel and comprised 6 categories and 99 items. Residents and attending physicians then rated each task based on level of difficulty, specifically looking at the mental, psychological, and physical effort required by each.
Indirect patient care was the task category in our study that had the most tasks associated with it (41 out of 99). Direct patient care included 32 items, but 10 of these were procedures (eg, lumbar puncture), some of which are uncommonly performed. Several time‐motion studies have been performed to document the work done by residents815 and hospitalists.16, 17 Although our study did not assess the time spent on each task, the distribution of tasks across categories is consistent with these time‐motion studies, which show that the amount of time spent in direct patient care is a small fraction of the amount of time spent in the hospital,12 and that work such as interprofessional communication10 and documentation16 consume the majority of time.
This project allowed us to consider the effort required for inpatient internal medicine work on a more granular level than has been described previously. Although the difficulty of tasks associated with anesthesia and surgical work has been described,3, 4, 7, 1820 our study is a unique contribution to the internal medicine literature. Understanding the difficulty of tasks performed by inpatient physicians is an important step toward better management of workload. With concerns about burnout in hospitalists21, 22 and residents,2325 it seems wise to take the difficulty of the work they do into consideration in a more proactive manner. In addition, understanding workload may have patient safety applications. In one study of mistakes made by house staff, 51% of the survey respondents identified workload as a contributing factor.26
We assessed effort for inpatient work by generating a task list and then measuring 3 domains of each task: physical, mental, and psychological. As a result, we were able to further quantify the difficulty of work completed by physicians. Recent work from outside of medicine suggests that individuals have a finite capacity for mental workload, and when this is breached, decision‐making quality is impaired.27 This suggests that it is important to take work intensity into account when assigning work to individuals. For example, a detailed assessment of workload at the task level combined with the amount of time spent on each task would allow us to know how much effort is typically involved with admitting a new patient. This information would allow for more equal distribution of workload across admitting teams. In addition, these methods could be expanded to understand how much effort is involved in the discharge process. This could be taken into account at the beginning of a day when allocating work such as admissions and discharges between members of a team.
This methodology has the potential to be used in other ways to help quantify the effort required for the work that physicians do. Many departments are struggling to develop a system for giving credit to faculty for the time they spend on nonpatient care activities. Perhaps these methods could be used to develop effort scores associated with administrative tasks, and administrative relative value units could be calculated accordingly. Similar techniques have been used with educational relative value units.28
We know from the nursing literature that workload is related to both burnout and patient safety. Burnout is a process related to the emotional work of providing care to people.29 Our methods clearly incorporate the psychological stress of work into the workload assessment. Evaluating the amount of time spent on tasks with high psychological scores may be helpful in identifying work patterns that are more likely to produce burnout in physicians and nurses.
With respect to patient safety, higher patient‐to‐nurse ratios are associated with failure to rescue30 and nosocomial infections.31 Furthermore, researchers have demonstrated that systems issues can add substantially to nursing workload.32 Methods such as those described in our study take into account both patient‐related and systems‐related tasks, and therefore could result in more detailed workload assessments. With more detailed information about contributors to workload, better predictions about optimal staffing could be made, which would ultimately lead to fewer adverse patient events.
Our study has limitations. First, the initial task list was based on the compilation efforts from only 10 physicians. However, this group of physicians represented 3 hospitals and included both resident and attending physicians. Second, the survey data were gathered from a single institution. Although we included trainees and faculty, more participants would be needed to answer questions about how experience and setting/environmental factors affect these assessments. However, participants were instructed to reflect on their whole experience with each task, which presumably includes multiple institutions and training levels. Third, the sample size is fairly small, with more house staff than faculty (hospitalists and nonhospitalists) represented. Regardless, this study is the first attempt to define and quantify workload for internal medicine physicians using these methods. In future studies, we will expand the number of institutions and levels of experience to validate our current data. Finally, the difficulty of the tasks is clearly a subjective assessment. Although this methodology has face validity, further work needs to be done to validate these findings against other measurements of workload, such as census, or more general subjective workload assessments, such as the NASA task load index.33
In conclusion, we have described the tasks performed by inpatient physicians and the difficulty associated with them. Moreover, we have described a methodology that could be replicated at other centers for the purpose of validating our findings or quantifying workload of other types of tasks. We believe that this is the first step toward a more comprehensive understanding of the workload encountered by inpatient physicians. Because workload has implications for physician burnout and patient safety, it is essential that we fully understand the contributors to workload, including the innate difficulty of the tasks that comprise it.
Acknowledgements
The authors Alexis Visotcky, MS, and Sergey Tarima, PhD, for their assistance with statistics.
This work was presented in poster form at the Society of Hospital Medicine Annual Meeting in April 2010, the Society of General Internal Medicine Annual Meeting in May 2010, and the Society of General Internal Medicine regional meeting in September 2010.
Funding Source: The study team was supported by the following funds during this work: VA grants PPO 0925901 (Marilyn M. Schapira and Kathlyn E. Fletcher) and IIR 07201 (Marilyn M. Schapira, Siddhartha Singh, and Kathlyn E. Fletcher).
- ,,,,.House staff team workload and organization effects on patient outcomes in an academic general internal medicine inpatient service.Arch Intern Med.2007;167:47–52.
- ,,, et al.The work hour rules and contributors to patient care mistakes: A focus group study with internal medicine residentsJ Hosp Med.2008;3:228–237.
- ,,.Multiple measures of anesthesia workload during teaching and nonteaching cases.Anesth Analg.2004;98:1419–1425.
- ,,,,.Developing a technique to measure anesthesiologists' real‐time workload.Proceedings of the Human Factors and Ergonomics Society Annual Meeting.2000;44:241–244.
- ,,, et al.Quantitative description of the workload associated with airway management procedures.J Clin Anesth.2000;12:273–282.
- ,,,,,.An objective methodology for task analysis and workload assessment in anesthesia providers.Anesthesiology.1994;80:77–92.
- ,.Effects of intraoperative reading on vigilance and workload during anesthesia care in an academic medical center.Anesthesiology.2009;110:275–283.
- ,,.Resident work hours: what they are really doing.Arch Surg.2004;139:490–493; discussion, 493–494.
- ,,,,,.Analyzing the time and value of housestaff inpatient work.J Gen Intern Med.1998;13:534–540.
- ,,,.All in a day's work: an observational study to quantify how and with whom doctors on hospital wards spend their time.[see comment].Med J Aust.2008;188:506–509.
- ,,,,.How do house officers spend their nights? A time study of internal medicine house staff on call.N Engl J Med.1989;320:1673–1677.
- ,,,,.Systematic review of time studies evaluating physicians in the hospital setting.J Hosp Med.2010;5:353–359.
- ,,.Time analysis of a general medicine service: results from a random work sampling study.J Gen Intern Med.1994;9:272–277.
- ,,,.A phenomenology of scut.Ann Intern Med.1991;115:372–376.
- ,,, et al.The on‐call experience of interns in internal medicine. Medical Education Task Force of Henry Ford Hospital.Arch Intern Med.1990;150:2294–2297.
- ,,, et al.Where did the day go? A time‐motion study of hospitalists.J Hosp Med.2010;5:323–328.
- ,,.How hospitalists spend their time: insights on efficiency and safety.J Hosp Med.2006;1:88–93.
- ,,, et al.Differences in day and night shift clinical performance in anesthesiology.Hum Factors.2008;50:276–290.
- ,,,,.Assessment of the intrarater and interrater reliability of an established clinical task analysis methodology.Anesthesiology.2002;96:1129–1139.
- ,,.The effect of electronic record keeping and transesophageal echocardiography on task distribution, workload, and vigilance during cardiac anesthesia.Anesthesiology.1997;87:144–155.
- .Fight burnout while fostering experience: investing in hospitalist programs now can fight burnout later.ACP Hospitalist. July2008.
- .Hospitalist burnout: recognize it in yourself and others, and avoid or eliminate it.The Hospitalist. March2006.
- ,,,.Burnout and internal medicine resident work‐hour restrictions.Arch Intern Med.2005;165:2595–2600.
- ,,,,.The effects of work‐hour limitations on resident well‐being, patient care, and education in an internal medicine residency program.Arch Intern Med.2005;165:2601–2606.
- ,,,.Burnout and self‐reported patient care in an internal medicine residency program.Ann Intern Med.2002;136:358–367.
- ,,,.Do house officers learn from their mistakes?Qual Saf Health Care.2003;12:221–226; discussion, 227–228.
- ,,.Extraneous factors in judicial decisions.Proc Natl Acad Sci U S A.2011;108:6889–6892.
- ,.Quantifying physician teaching productivity using clinical relative value units.J Gen Intern Med.1999;14:617–621.
- .Maslach Burnout Inventory Manual.3rd ed.Palo Alto, CA:Consulting Psychology Press;1986.
- ,,,,.Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction.JAMA.2002;288:1987–1993.
- ,,,,.Patient density, nurse‐to‐patient ratio and nosocomial infection risk in a pediatric cardiac intensive care unit.Pediatr Infect Dis J.1997;16:1045–1048.
- ,.Operational failures and interruptions in hospital nursing.Health Serv Res.2006;41:643–662.
- ,.Development of NASA‐TLX (Task Load Index): results of empirical and theoretical research. In: Hancock PA, Meshkati N, eds.Human Mental Workload.Amsterdam, Netherlands:North Holland Press;1988:239–250.
- ,,,,.House staff team workload and organization effects on patient outcomes in an academic general internal medicine inpatient service.Arch Intern Med.2007;167:47–52.
- ,,, et al.The work hour rules and contributors to patient care mistakes: A focus group study with internal medicine residentsJ Hosp Med.2008;3:228–237.
- ,,.Multiple measures of anesthesia workload during teaching and nonteaching cases.Anesth Analg.2004;98:1419–1425.
- ,,,,.Developing a technique to measure anesthesiologists' real‐time workload.Proceedings of the Human Factors and Ergonomics Society Annual Meeting.2000;44:241–244.
- ,,, et al.Quantitative description of the workload associated with airway management procedures.J Clin Anesth.2000;12:273–282.
- ,,,,,.An objective methodology for task analysis and workload assessment in anesthesia providers.Anesthesiology.1994;80:77–92.
- ,.Effects of intraoperative reading on vigilance and workload during anesthesia care in an academic medical center.Anesthesiology.2009;110:275–283.
- ,,.Resident work hours: what they are really doing.Arch Surg.2004;139:490–493; discussion, 493–494.
- ,,,,,.Analyzing the time and value of housestaff inpatient work.J Gen Intern Med.1998;13:534–540.
- ,,,.All in a day's work: an observational study to quantify how and with whom doctors on hospital wards spend their time.[see comment].Med J Aust.2008;188:506–509.
- ,,,,.How do house officers spend their nights? A time study of internal medicine house staff on call.N Engl J Med.1989;320:1673–1677.
- ,,,,.Systematic review of time studies evaluating physicians in the hospital setting.J Hosp Med.2010;5:353–359.
- ,,.Time analysis of a general medicine service: results from a random work sampling study.J Gen Intern Med.1994;9:272–277.
- ,,,.A phenomenology of scut.Ann Intern Med.1991;115:372–376.
- ,,, et al.The on‐call experience of interns in internal medicine. Medical Education Task Force of Henry Ford Hospital.Arch Intern Med.1990;150:2294–2297.
- ,,, et al.Where did the day go? A time‐motion study of hospitalists.J Hosp Med.2010;5:323–328.
- ,,.How hospitalists spend their time: insights on efficiency and safety.J Hosp Med.2006;1:88–93.
- ,,, et al.Differences in day and night shift clinical performance in anesthesiology.Hum Factors.2008;50:276–290.
- ,,,,.Assessment of the intrarater and interrater reliability of an established clinical task analysis methodology.Anesthesiology.2002;96:1129–1139.
- ,,.The effect of electronic record keeping and transesophageal echocardiography on task distribution, workload, and vigilance during cardiac anesthesia.Anesthesiology.1997;87:144–155.
- .Fight burnout while fostering experience: investing in hospitalist programs now can fight burnout later.ACP Hospitalist. July2008.
- .Hospitalist burnout: recognize it in yourself and others, and avoid or eliminate it.The Hospitalist. March2006.
- ,,,.Burnout and internal medicine resident work‐hour restrictions.Arch Intern Med.2005;165:2595–2600.
- ,,,,.The effects of work‐hour limitations on resident well‐being, patient care, and education in an internal medicine residency program.Arch Intern Med.2005;165:2601–2606.
- ,,,.Burnout and self‐reported patient care in an internal medicine residency program.Ann Intern Med.2002;136:358–367.
- ,,,.Do house officers learn from their mistakes?Qual Saf Health Care.2003;12:221–226; discussion, 227–228.
- ,,.Extraneous factors in judicial decisions.Proc Natl Acad Sci U S A.2011;108:6889–6892.
- ,.Quantifying physician teaching productivity using clinical relative value units.J Gen Intern Med.1999;14:617–621.
- .Maslach Burnout Inventory Manual.3rd ed.Palo Alto, CA:Consulting Psychology Press;1986.
- ,,,,.Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction.JAMA.2002;288:1987–1993.
- ,,,,.Patient density, nurse‐to‐patient ratio and nosocomial infection risk in a pediatric cardiac intensive care unit.Pediatr Infect Dis J.1997;16:1045–1048.
- ,.Operational failures and interruptions in hospital nursing.Health Serv Res.2006;41:643–662.
- ,.Development of NASA‐TLX (Task Load Index): results of empirical and theoretical research. In: Hancock PA, Meshkati N, eds.Human Mental Workload.Amsterdam, Netherlands:North Holland Press;1988:239–250.
Copyright © 2012 Society of Hospital Medicine
Physicians Often Missing Boat on Gout Therapy
SNOWMASS, COLO. – A disturbing proportion of gout cases are mismanaged by primary care physicians, and the blame falls squarely upon rheumatologists, according to one prominent gout expert.
"As rheumatologists, gout is our disease. The cause and pathophysiology are well understood, we can make the diagnosis with absolute certainty, and we’ve got great medicines. Yet today we all see people with tophi. That’s tragic. It shouldn’t exist. One of our biggest mistakes has been not being able to educate primary care physicians that having a tophus is bad, that it’s eroding cartilage and bone, and that it’s something we can prevent if we start urate-lowering therapy soon enough," Dr. Robert L. Wortmann said at the conference.
An estimated 8.3 million Americans have gout. Yet, the pharmaceutical industry says only 3.1 million of them are prescribed urate-lowering drugs. Five different studies show that a mere 40% of those on allopurinol are prescribed a dose sufficient to drive serum uric acid below 6 mg/dL, a key tenet of gout management, noted Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
Moreover, poor treatment adherence is a huge problem in gout. A study of close to 4,200 gout patients started on urate-lowering drug therapy found that 56% of them were nonadherent (Arthritis Res. Ther. 2009;11(2):R46).
"I charge you all to go back from this meeting and try to communicate with all the primary care physicians you can about the principles of managing gout. People shouldn’t suffer from this," the rheumatologist declared.
He offered these major take home points:
Don’t prescribe urate-lowering drugs for asymptomatic hyperuricemia: This practice hasn’t been shown to prevent the future development of gout, yet it exposes patients to the risk of drug toxicities.
But don’t ignore asymptomatic hyperuricemia, either: Epidemiologic studies have linked asymptomatic hyperuricemia, defined by a serum urate in excess of 6.8 mg/dL, to increased risks of hypertension, cardiovascular disease, diabetes, chronic kidney disease, and all-cause mortality. The big unanswered question is whether using medications to lower serum urate in individuals with asymptomatic hyperuricemia reduces the risk of any of these conditions. That’s the subject of ongoing large clinical trials in high-risk patients. If those studies prove positive, clinical practice will change.
While awaiting the outcome of the prevention trials, it’s worth bearing in mind that Framingham Heart Study data indicate that individuals with a serum uric acid level above 9 mg/dL have a 22% chance of developing gout within the next 5 years. The major contributors to asymptomatic hyperuricemia include obesity, metabolic syndrome, and heavy consumption of fructose-containing beverages or alcohol. Those issues should be addressed.
Losartan is the only antihypertensive agent that’s uricosuric. Fenofibrate is the sole uricosuric drug indicated for dyslipidemia. Preferential consideration could be given to the use of these drugs in hypertensive and/or hyperlipidemic patients with asymptomatic hyperuricemia.
The important thing is not which oral agent you use for treatment of acute gout, it’s to initiate therapy as early as possible, at the first hint of an attack. Colchicine, maximum-dose NSAIDs, and oral prednisone dosed at 20 mg BID until symptoms have been gone for 1 week followed by another week at 20 mg/day – they’re all effective. And since they work by different mechanisms, they can beneficially be combined in refractory patients.
The old-school colchicine dosing regimen most physicians were taught has been cast aside of late. It had a high rate of diarrhea, an inhumane side effect in gout patients hobbled by a foot too sore to walk on. The former regimen has been replaced by 1.2 mg, given in a single dose, followed by 0.6 mg 1 hour later.
"This lower dose is just as effective as the old high-dose regimen of two 0.6-mg pills given at once and then one per hour for the next 5 hours. And the lower-dose program has the same side effect profile as placebo," Dr. Wortmann said.
Get the gout patient’s serum urate below 6 mg/dL using the lowest effective dose of the urate-lowering drug you’ve selected. Physicians have traditionally started gout patients on allopurinol at the standard dose of 300 mg/day. Recently, it has been demonstrated that the risk of developing allopurinol hypersensitivity syndrome is greatly reduced by starting off at 150 mg/day, checking the urate level 2 weeks later, then increasing to 300 mg/day if the serum urate isn’t below 6 mg/dL. After 2 weeks at 300 mg/day, check the urate again, and if it still isn’t below 6 mg/dL then bump the dose to 400 mg/day. Continue testing and titrating every 2 weeks until the serum urate is less than 6 mg/dL – and preferably less than 4 mg/dL if the patient has tophi – or until the maximum approved dose of 800 mg/day is reached.
The same start-low-and-titrate strategy applies to febuxostat, with a maximum approved dose of 80 mg/day.
"We have to educate primary care physicians to check the serum urate after starting therapy, and that, if it’s not below 6 mg/dL, they need to increase the dose. And if they don’t feel comfortable with that, they need to send the patient to us," the rheumatologist said.
Fortunately, patients who have a hypersensitivity reaction to allopurinol are very unlikely to experience one with febuxostat, and vice versa.
For patients who can’t reach the target serum urate with maximum-dose therapy, take heart: Second-line agents with impressive potency are well-along in the developmental pipeline.
Many labs now list the upper limit of normal for serum urate as 8 mg/dL or 8.5 mg/dL. Ignore that. This raised ceiling is simply the result of the changing demographics among the increasingly obese U.S. population in the last several decades. The definition of asymptomatic hyperuricemia remains unchanged: a serum urate greater than 6.8 mg/dL. And the target in patients with gout is still a serum urate less than 6 mg/dL. Merely dropping a gout patient’s urate from 10 to 8 or even 6.6 mg/dL isn’t doing any favors; the disease will continue to progress if the urate is above 6 mg/dL.
All gout is tophaceous. Even if tophi aren’t apparent on clinical examination, often they are radiographically. "This is a message that has to get out," Dr. Wortmann insisted.
Proposed American College of Rheumatology gout management guidelines call for starting urate-lowering drug therapy when a patient is experiencing three attacks per year. Dr. Wortmann takes issue with that.
"I would argue that once you’ve had a third attack of gout, period, you should be treated. Maybe even sooner. We need to prevent the erosion and bony destruction that occur with tophi," he said.
One audience member complained that his gout patients with comorbid renal insufficiency and/or cardiovascular disease often get caught in a revolving door. He titrates their allopurinol to an effective dose, but when they are later admitted to the hospital because of their comorbid condition the hospitalists, nephrologists, and/or cardiologists are shocked at the allopurinol dose and either reduce it or stop it altogether. The first that the rheumatologist learns of it is when patients reappear in his office with active gout. He then resumes their allopurinol at the previous dose, and they remain well controlled until the next hospitalization, when the same thing happens.
Dr. Wortmann responded that the solution requires convincing the nonrheumatologists in one-on-one conversation that urate-lowering therapy is not a one-size-fits-all matter. They need to understand that to get rid of gout, it’s necessary to drive the serum urate to the target of less than 6 mg/dL, and it helps to reassure them that that this will be accomplished using the lowest effective dose.
He reported serving as a consultant to Savient, Takeda, URL Pharmaceuticals, Novartis, and Ardea Biosciences.
SNOWMASS, COLO. – A disturbing proportion of gout cases are mismanaged by primary care physicians, and the blame falls squarely upon rheumatologists, according to one prominent gout expert.
"As rheumatologists, gout is our disease. The cause and pathophysiology are well understood, we can make the diagnosis with absolute certainty, and we’ve got great medicines. Yet today we all see people with tophi. That’s tragic. It shouldn’t exist. One of our biggest mistakes has been not being able to educate primary care physicians that having a tophus is bad, that it’s eroding cartilage and bone, and that it’s something we can prevent if we start urate-lowering therapy soon enough," Dr. Robert L. Wortmann said at the conference.
An estimated 8.3 million Americans have gout. Yet, the pharmaceutical industry says only 3.1 million of them are prescribed urate-lowering drugs. Five different studies show that a mere 40% of those on allopurinol are prescribed a dose sufficient to drive serum uric acid below 6 mg/dL, a key tenet of gout management, noted Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
Moreover, poor treatment adherence is a huge problem in gout. A study of close to 4,200 gout patients started on urate-lowering drug therapy found that 56% of them were nonadherent (Arthritis Res. Ther. 2009;11(2):R46).
"I charge you all to go back from this meeting and try to communicate with all the primary care physicians you can about the principles of managing gout. People shouldn’t suffer from this," the rheumatologist declared.
He offered these major take home points:
Don’t prescribe urate-lowering drugs for asymptomatic hyperuricemia: This practice hasn’t been shown to prevent the future development of gout, yet it exposes patients to the risk of drug toxicities.
But don’t ignore asymptomatic hyperuricemia, either: Epidemiologic studies have linked asymptomatic hyperuricemia, defined by a serum urate in excess of 6.8 mg/dL, to increased risks of hypertension, cardiovascular disease, diabetes, chronic kidney disease, and all-cause mortality. The big unanswered question is whether using medications to lower serum urate in individuals with asymptomatic hyperuricemia reduces the risk of any of these conditions. That’s the subject of ongoing large clinical trials in high-risk patients. If those studies prove positive, clinical practice will change.
While awaiting the outcome of the prevention trials, it’s worth bearing in mind that Framingham Heart Study data indicate that individuals with a serum uric acid level above 9 mg/dL have a 22% chance of developing gout within the next 5 years. The major contributors to asymptomatic hyperuricemia include obesity, metabolic syndrome, and heavy consumption of fructose-containing beverages or alcohol. Those issues should be addressed.
Losartan is the only antihypertensive agent that’s uricosuric. Fenofibrate is the sole uricosuric drug indicated for dyslipidemia. Preferential consideration could be given to the use of these drugs in hypertensive and/or hyperlipidemic patients with asymptomatic hyperuricemia.
The important thing is not which oral agent you use for treatment of acute gout, it’s to initiate therapy as early as possible, at the first hint of an attack. Colchicine, maximum-dose NSAIDs, and oral prednisone dosed at 20 mg BID until symptoms have been gone for 1 week followed by another week at 20 mg/day – they’re all effective. And since they work by different mechanisms, they can beneficially be combined in refractory patients.
The old-school colchicine dosing regimen most physicians were taught has been cast aside of late. It had a high rate of diarrhea, an inhumane side effect in gout patients hobbled by a foot too sore to walk on. The former regimen has been replaced by 1.2 mg, given in a single dose, followed by 0.6 mg 1 hour later.
"This lower dose is just as effective as the old high-dose regimen of two 0.6-mg pills given at once and then one per hour for the next 5 hours. And the lower-dose program has the same side effect profile as placebo," Dr. Wortmann said.
Get the gout patient’s serum urate below 6 mg/dL using the lowest effective dose of the urate-lowering drug you’ve selected. Physicians have traditionally started gout patients on allopurinol at the standard dose of 300 mg/day. Recently, it has been demonstrated that the risk of developing allopurinol hypersensitivity syndrome is greatly reduced by starting off at 150 mg/day, checking the urate level 2 weeks later, then increasing to 300 mg/day if the serum urate isn’t below 6 mg/dL. After 2 weeks at 300 mg/day, check the urate again, and if it still isn’t below 6 mg/dL then bump the dose to 400 mg/day. Continue testing and titrating every 2 weeks until the serum urate is less than 6 mg/dL – and preferably less than 4 mg/dL if the patient has tophi – or until the maximum approved dose of 800 mg/day is reached.
The same start-low-and-titrate strategy applies to febuxostat, with a maximum approved dose of 80 mg/day.
"We have to educate primary care physicians to check the serum urate after starting therapy, and that, if it’s not below 6 mg/dL, they need to increase the dose. And if they don’t feel comfortable with that, they need to send the patient to us," the rheumatologist said.
Fortunately, patients who have a hypersensitivity reaction to allopurinol are very unlikely to experience one with febuxostat, and vice versa.
For patients who can’t reach the target serum urate with maximum-dose therapy, take heart: Second-line agents with impressive potency are well-along in the developmental pipeline.
Many labs now list the upper limit of normal for serum urate as 8 mg/dL or 8.5 mg/dL. Ignore that. This raised ceiling is simply the result of the changing demographics among the increasingly obese U.S. population in the last several decades. The definition of asymptomatic hyperuricemia remains unchanged: a serum urate greater than 6.8 mg/dL. And the target in patients with gout is still a serum urate less than 6 mg/dL. Merely dropping a gout patient’s urate from 10 to 8 or even 6.6 mg/dL isn’t doing any favors; the disease will continue to progress if the urate is above 6 mg/dL.
All gout is tophaceous. Even if tophi aren’t apparent on clinical examination, often they are radiographically. "This is a message that has to get out," Dr. Wortmann insisted.
Proposed American College of Rheumatology gout management guidelines call for starting urate-lowering drug therapy when a patient is experiencing three attacks per year. Dr. Wortmann takes issue with that.
"I would argue that once you’ve had a third attack of gout, period, you should be treated. Maybe even sooner. We need to prevent the erosion and bony destruction that occur with tophi," he said.
One audience member complained that his gout patients with comorbid renal insufficiency and/or cardiovascular disease often get caught in a revolving door. He titrates their allopurinol to an effective dose, but when they are later admitted to the hospital because of their comorbid condition the hospitalists, nephrologists, and/or cardiologists are shocked at the allopurinol dose and either reduce it or stop it altogether. The first that the rheumatologist learns of it is when patients reappear in his office with active gout. He then resumes their allopurinol at the previous dose, and they remain well controlled until the next hospitalization, when the same thing happens.
Dr. Wortmann responded that the solution requires convincing the nonrheumatologists in one-on-one conversation that urate-lowering therapy is not a one-size-fits-all matter. They need to understand that to get rid of gout, it’s necessary to drive the serum urate to the target of less than 6 mg/dL, and it helps to reassure them that that this will be accomplished using the lowest effective dose.
He reported serving as a consultant to Savient, Takeda, URL Pharmaceuticals, Novartis, and Ardea Biosciences.
SNOWMASS, COLO. – A disturbing proportion of gout cases are mismanaged by primary care physicians, and the blame falls squarely upon rheumatologists, according to one prominent gout expert.
"As rheumatologists, gout is our disease. The cause and pathophysiology are well understood, we can make the diagnosis with absolute certainty, and we’ve got great medicines. Yet today we all see people with tophi. That’s tragic. It shouldn’t exist. One of our biggest mistakes has been not being able to educate primary care physicians that having a tophus is bad, that it’s eroding cartilage and bone, and that it’s something we can prevent if we start urate-lowering therapy soon enough," Dr. Robert L. Wortmann said at the conference.
An estimated 8.3 million Americans have gout. Yet, the pharmaceutical industry says only 3.1 million of them are prescribed urate-lowering drugs. Five different studies show that a mere 40% of those on allopurinol are prescribed a dose sufficient to drive serum uric acid below 6 mg/dL, a key tenet of gout management, noted Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
Moreover, poor treatment adherence is a huge problem in gout. A study of close to 4,200 gout patients started on urate-lowering drug therapy found that 56% of them were nonadherent (Arthritis Res. Ther. 2009;11(2):R46).
"I charge you all to go back from this meeting and try to communicate with all the primary care physicians you can about the principles of managing gout. People shouldn’t suffer from this," the rheumatologist declared.
He offered these major take home points:
Don’t prescribe urate-lowering drugs for asymptomatic hyperuricemia: This practice hasn’t been shown to prevent the future development of gout, yet it exposes patients to the risk of drug toxicities.
But don’t ignore asymptomatic hyperuricemia, either: Epidemiologic studies have linked asymptomatic hyperuricemia, defined by a serum urate in excess of 6.8 mg/dL, to increased risks of hypertension, cardiovascular disease, diabetes, chronic kidney disease, and all-cause mortality. The big unanswered question is whether using medications to lower serum urate in individuals with asymptomatic hyperuricemia reduces the risk of any of these conditions. That’s the subject of ongoing large clinical trials in high-risk patients. If those studies prove positive, clinical practice will change.
While awaiting the outcome of the prevention trials, it’s worth bearing in mind that Framingham Heart Study data indicate that individuals with a serum uric acid level above 9 mg/dL have a 22% chance of developing gout within the next 5 years. The major contributors to asymptomatic hyperuricemia include obesity, metabolic syndrome, and heavy consumption of fructose-containing beverages or alcohol. Those issues should be addressed.
Losartan is the only antihypertensive agent that’s uricosuric. Fenofibrate is the sole uricosuric drug indicated for dyslipidemia. Preferential consideration could be given to the use of these drugs in hypertensive and/or hyperlipidemic patients with asymptomatic hyperuricemia.
The important thing is not which oral agent you use for treatment of acute gout, it’s to initiate therapy as early as possible, at the first hint of an attack. Colchicine, maximum-dose NSAIDs, and oral prednisone dosed at 20 mg BID until symptoms have been gone for 1 week followed by another week at 20 mg/day – they’re all effective. And since they work by different mechanisms, they can beneficially be combined in refractory patients.
The old-school colchicine dosing regimen most physicians were taught has been cast aside of late. It had a high rate of diarrhea, an inhumane side effect in gout patients hobbled by a foot too sore to walk on. The former regimen has been replaced by 1.2 mg, given in a single dose, followed by 0.6 mg 1 hour later.
"This lower dose is just as effective as the old high-dose regimen of two 0.6-mg pills given at once and then one per hour for the next 5 hours. And the lower-dose program has the same side effect profile as placebo," Dr. Wortmann said.
Get the gout patient’s serum urate below 6 mg/dL using the lowest effective dose of the urate-lowering drug you’ve selected. Physicians have traditionally started gout patients on allopurinol at the standard dose of 300 mg/day. Recently, it has been demonstrated that the risk of developing allopurinol hypersensitivity syndrome is greatly reduced by starting off at 150 mg/day, checking the urate level 2 weeks later, then increasing to 300 mg/day if the serum urate isn’t below 6 mg/dL. After 2 weeks at 300 mg/day, check the urate again, and if it still isn’t below 6 mg/dL then bump the dose to 400 mg/day. Continue testing and titrating every 2 weeks until the serum urate is less than 6 mg/dL – and preferably less than 4 mg/dL if the patient has tophi – or until the maximum approved dose of 800 mg/day is reached.
The same start-low-and-titrate strategy applies to febuxostat, with a maximum approved dose of 80 mg/day.
"We have to educate primary care physicians to check the serum urate after starting therapy, and that, if it’s not below 6 mg/dL, they need to increase the dose. And if they don’t feel comfortable with that, they need to send the patient to us," the rheumatologist said.
Fortunately, patients who have a hypersensitivity reaction to allopurinol are very unlikely to experience one with febuxostat, and vice versa.
For patients who can’t reach the target serum urate with maximum-dose therapy, take heart: Second-line agents with impressive potency are well-along in the developmental pipeline.
Many labs now list the upper limit of normal for serum urate as 8 mg/dL or 8.5 mg/dL. Ignore that. This raised ceiling is simply the result of the changing demographics among the increasingly obese U.S. population in the last several decades. The definition of asymptomatic hyperuricemia remains unchanged: a serum urate greater than 6.8 mg/dL. And the target in patients with gout is still a serum urate less than 6 mg/dL. Merely dropping a gout patient’s urate from 10 to 8 or even 6.6 mg/dL isn’t doing any favors; the disease will continue to progress if the urate is above 6 mg/dL.
All gout is tophaceous. Even if tophi aren’t apparent on clinical examination, often they are radiographically. "This is a message that has to get out," Dr. Wortmann insisted.
Proposed American College of Rheumatology gout management guidelines call for starting urate-lowering drug therapy when a patient is experiencing three attacks per year. Dr. Wortmann takes issue with that.
"I would argue that once you’ve had a third attack of gout, period, you should be treated. Maybe even sooner. We need to prevent the erosion and bony destruction that occur with tophi," he said.
One audience member complained that his gout patients with comorbid renal insufficiency and/or cardiovascular disease often get caught in a revolving door. He titrates their allopurinol to an effective dose, but when they are later admitted to the hospital because of their comorbid condition the hospitalists, nephrologists, and/or cardiologists are shocked at the allopurinol dose and either reduce it or stop it altogether. The first that the rheumatologist learns of it is when patients reappear in his office with active gout. He then resumes their allopurinol at the previous dose, and they remain well controlled until the next hospitalization, when the same thing happens.
Dr. Wortmann responded that the solution requires convincing the nonrheumatologists in one-on-one conversation that urate-lowering therapy is not a one-size-fits-all matter. They need to understand that to get rid of gout, it’s necessary to drive the serum urate to the target of less than 6 mg/dL, and it helps to reassure them that that this will be accomplished using the lowest effective dose.
He reported serving as a consultant to Savient, Takeda, URL Pharmaceuticals, Novartis, and Ardea Biosciences.
EXPERT ANALYSIS FROM A SYMPOSIUM SPONSORED BY THE AMERICAN COLLEGE OF RHEUMATOLOGY
Obesity Epidemic Is Skewing Face of Gout
SNOWMASS, COLO. – The epidemiology of gout has changed considerably in the past several decades, rendering treatment more challenging.
For example, today fully 21.4% of all U.S. adults are hyperuricemic as defined by a serum uric acid in excess of 6.8 mg/dL.

"When I was a fellow it was 5%. There’s a lot more uric acid in the world today," Dr. Robert L. Wortmann observed at the symposium.
Major contributing factors include metabolic syndrome, the obesity epidemic, increased consumption of high-fructose drinks and processed foods, and alcohol. Liquor has a twofold stronger urate-boosting effect than does wine, and beer’s impact is fourfold greater than wine, according to Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
"When I was in training uric acids above 9 mg/dL weren’t common; now, when I see a newly diagnosed gout patient with a uric acid level below 9, it’s exceptional. Gout patients today have uric acids of 10, 11, and 12 mg/dL as opposed to 7.5, 8, and 9 in decades past," he said.
Since 1964 the standard dose of allopurinol has been 300 mg/day. Back then, that was sufficient to reach the serum uric acid target of less than 6.0 mg/dL in about 90% of gout patients. Today, 300 mg/day gets only about 40% of patients to target, as has been shown in numerous studies.
Dr. Wortmann reported serving as a consultant to Ardea Biosciences, Novartis, Savient, Takeda, and URL Pharmaceuticals.
SNOWMASS, COLO. – The epidemiology of gout has changed considerably in the past several decades, rendering treatment more challenging.
For example, today fully 21.4% of all U.S. adults are hyperuricemic as defined by a serum uric acid in excess of 6.8 mg/dL.
"When I was a fellow it was 5%. There’s a lot more uric acid in the world today," Dr. Robert L. Wortmann observed at the symposium.
Major contributing factors include metabolic syndrome, the obesity epidemic, increased consumption of high-fructose drinks and processed foods, and alcohol. Liquor has a twofold stronger urate-boosting effect than does wine, and beer’s impact is fourfold greater than wine, according to Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
"When I was in training uric acids above 9 mg/dL weren’t common; now, when I see a newly diagnosed gout patient with a uric acid level below 9, it’s exceptional. Gout patients today have uric acids of 10, 11, and 12 mg/dL as opposed to 7.5, 8, and 9 in decades past," he said.
Since 1964 the standard dose of allopurinol has been 300 mg/day. Back then, that was sufficient to reach the serum uric acid target of less than 6.0 mg/dL in about 90% of gout patients. Today, 300 mg/day gets only about 40% of patients to target, as has been shown in numerous studies.
Dr. Wortmann reported serving as a consultant to Ardea Biosciences, Novartis, Savient, Takeda, and URL Pharmaceuticals.
SNOWMASS, COLO. – The epidemiology of gout has changed considerably in the past several decades, rendering treatment more challenging.
For example, today fully 21.4% of all U.S. adults are hyperuricemic as defined by a serum uric acid in excess of 6.8 mg/dL.
"When I was a fellow it was 5%. There’s a lot more uric acid in the world today," Dr. Robert L. Wortmann observed at the symposium.
Major contributing factors include metabolic syndrome, the obesity epidemic, increased consumption of high-fructose drinks and processed foods, and alcohol. Liquor has a twofold stronger urate-boosting effect than does wine, and beer’s impact is fourfold greater than wine, according to Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
"When I was in training uric acids above 9 mg/dL weren’t common; now, when I see a newly diagnosed gout patient with a uric acid level below 9, it’s exceptional. Gout patients today have uric acids of 10, 11, and 12 mg/dL as opposed to 7.5, 8, and 9 in decades past," he said.
Since 1964 the standard dose of allopurinol has been 300 mg/day. Back then, that was sufficient to reach the serum uric acid target of less than 6.0 mg/dL in about 90% of gout patients. Today, 300 mg/day gets only about 40% of patients to target, as has been shown in numerous studies.
Dr. Wortmann reported serving as a consultant to Ardea Biosciences, Novartis, Savient, Takeda, and URL Pharmaceuticals.
EXPERT ANALYSIS FROM A SYMPOSIUM SPONSORED BY THE AMERICAN COLLEGE OF RHEUMATOLOGY
Survey: Steady Increase in Complementary Alternative Medicine (CAM) Offerings in U.S. Hospitals
According to a survey released last fall by the Health Forum, a subsidiary of the American Hospital Association, and the Samueli Institute of Alexandria, Va., complementary and alternative medicine (CAM) services in responding hospitals increased to 42% in 2010 from 37% in 2007.
The fourth Complementary and Alternative Medicine Survey of Hospitals is a follow-up report to the 2007 survey, which The Hospitalist featured in January 2010.
Twelve percent of 5,858 hospitals answered a 42-question instrument in 2010, according to Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author. The results, Ananth says, showed that the hospitals most likely to offer CAM were urban and tended to be either medium-size (50-299 beds) or large (500+ beds) institutions.
What’s driving the increase? She believes that hospitals are simply responding to patients’ desire to have “the best that both conventional and alternative medicine can offer.”

—Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author
Sixty-five percent of hospitals responding to the survey offer CAM therapies for pain management. That figure is echoed in a 2008 National Health Statistics report (PDF) published by the Centers for Disease Control and Prevention. Back pain, neck pain, and joint pain were the three top reasons for using CAM, according to the CDC report.
“Adjacent” Treatment
Hospitalist Sanjay Reddy, MD, assistant clinical professor of medicine in the Department of Medicine at the University of California at San Francisco (UCSF), says acupuncture can be a valuable adjunct when treating patients for pain, chemotherapy-induced nausea, and insomnia. He is a trained acupuncturist and has studied complementary therapies extensively. He also is interested in exploring ways to incorporate acupuncture into the UCSF’s Osher Center for Integrative Medicine program.
David H. Gorski, MD, PhD, FACS, associate professor of surgery and director of the Breast Cancer Multidisciplinary Team at the Barbara Ann Karmanos Cancer Institute at Wayne State University School of Medicine in Detroit, strenuously objects to the incorporation of alternative therapies (often under the moniker of “integrative medicine”) in the hospital setting.
“If you accept the premise that medicine should be based in sound science and evidence, then we have an obligation not to be offering treatments that are not based in science,” he asserts. Dr. Gorski, who also blogs on such topics, finds that many of those who endorse integrative medicine have become “true believers,” and that some are mixing pseudo-science with science.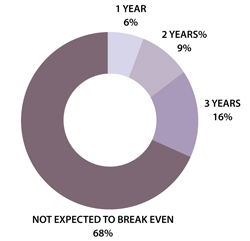
In an August 2011 post regarding the College of Physicians and Surgeons of Ontario’s draft policy on alternative treatments, Dr. Gorski wrote: “Competent adults have every right to seek out non-science-based medicine if that is what they desire. However, informed consent mandates that physicians who encounter such patients provide an honest professional assessment of such treatments based on science.”
Dr. Reddy notes that with appropriate disclosure, offering a modality such as acupuncture can be appropriate. For example, in the setting of pain relief, acupuncture offers a less sedative approach. He explains that Chinese diagnostics and treatment approaches are slightly different, so it’s difficult to study them in the context of randomized trials. (Click here to listen to more of Dr. Reddy’s discussion of appropriate indications for acupuncture.)
In the Health Forum/Samueli Institute survey, 57% of hospitals reported that their programs were not yet breaking even and only 16% said they'd be breaking even in three years (see Figure 1). In light of these results, Ananth says, hospitals undertaking complementary services should “start small and not have high expectations of breaking even for several years.”
Gretchen Henkel is a freelance writer in California.
Herbals another Matter
In the 2010 Health Forum/Samueli Institute survey, 82% of responding hospitals reported that they did not offer herbal supplements in their hospital pharmacies. Study author Sita Ananth surmises that most hospitals may be “playing it safe” by offering noninvasive therapies. Hospitalists are aware of the potentially dangerous interactions between herbal supplements and mainstream treatments, Dr. Reddy says.
A majority of the hospitals Ananth queried (67%) reported having existing policies regarding patients’ use of herbal and nutritional supplements during hospitalization. To avoid adverse events, “It’s really crucial that they are asking the right questions of their patients,” she says.—GH
According to a survey released last fall by the Health Forum, a subsidiary of the American Hospital Association, and the Samueli Institute of Alexandria, Va., complementary and alternative medicine (CAM) services in responding hospitals increased to 42% in 2010 from 37% in 2007.
The fourth Complementary and Alternative Medicine Survey of Hospitals is a follow-up report to the 2007 survey, which The Hospitalist featured in January 2010.
Twelve percent of 5,858 hospitals answered a 42-question instrument in 2010, according to Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author. The results, Ananth says, showed that the hospitals most likely to offer CAM were urban and tended to be either medium-size (50-299 beds) or large (500+ beds) institutions.
What’s driving the increase? She believes that hospitals are simply responding to patients’ desire to have “the best that both conventional and alternative medicine can offer.”
—Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author
Sixty-five percent of hospitals responding to the survey offer CAM therapies for pain management. That figure is echoed in a 2008 National Health Statistics report (PDF) published by the Centers for Disease Control and Prevention. Back pain, neck pain, and joint pain were the three top reasons for using CAM, according to the CDC report.
“Adjacent” Treatment
Hospitalist Sanjay Reddy, MD, assistant clinical professor of medicine in the Department of Medicine at the University of California at San Francisco (UCSF), says acupuncture can be a valuable adjunct when treating patients for pain, chemotherapy-induced nausea, and insomnia. He is a trained acupuncturist and has studied complementary therapies extensively. He also is interested in exploring ways to incorporate acupuncture into the UCSF’s Osher Center for Integrative Medicine program.
David H. Gorski, MD, PhD, FACS, associate professor of surgery and director of the Breast Cancer Multidisciplinary Team at the Barbara Ann Karmanos Cancer Institute at Wayne State University School of Medicine in Detroit, strenuously objects to the incorporation of alternative therapies (often under the moniker of “integrative medicine”) in the hospital setting.
“If you accept the premise that medicine should be based in sound science and evidence, then we have an obligation not to be offering treatments that are not based in science,” he asserts. Dr. Gorski, who also blogs on such topics, finds that many of those who endorse integrative medicine have become “true believers,” and that some are mixing pseudo-science with science.
In an August 2011 post regarding the College of Physicians and Surgeons of Ontario’s draft policy on alternative treatments, Dr. Gorski wrote: “Competent adults have every right to seek out non-science-based medicine if that is what they desire. However, informed consent mandates that physicians who encounter such patients provide an honest professional assessment of such treatments based on science.”
Dr. Reddy notes that with appropriate disclosure, offering a modality such as acupuncture can be appropriate. For example, in the setting of pain relief, acupuncture offers a less sedative approach. He explains that Chinese diagnostics and treatment approaches are slightly different, so it’s difficult to study them in the context of randomized trials. (Click here to listen to more of Dr. Reddy’s discussion of appropriate indications for acupuncture.)
In the Health Forum/Samueli Institute survey, 57% of hospitals reported that their programs were not yet breaking even and only 16% said they'd be breaking even in three years (see Figure 1). In light of these results, Ananth says, hospitals undertaking complementary services should “start small and not have high expectations of breaking even for several years.”
Gretchen Henkel is a freelance writer in California.
Herbals another Matter
In the 2010 Health Forum/Samueli Institute survey, 82% of responding hospitals reported that they did not offer herbal supplements in their hospital pharmacies. Study author Sita Ananth surmises that most hospitals may be “playing it safe” by offering noninvasive therapies. Hospitalists are aware of the potentially dangerous interactions between herbal supplements and mainstream treatments, Dr. Reddy says.
A majority of the hospitals Ananth queried (67%) reported having existing policies regarding patients’ use of herbal and nutritional supplements during hospitalization. To avoid adverse events, “It’s really crucial that they are asking the right questions of their patients,” she says.—GH
According to a survey released last fall by the Health Forum, a subsidiary of the American Hospital Association, and the Samueli Institute of Alexandria, Va., complementary and alternative medicine (CAM) services in responding hospitals increased to 42% in 2010 from 37% in 2007.
The fourth Complementary and Alternative Medicine Survey of Hospitals is a follow-up report to the 2007 survey, which The Hospitalist featured in January 2010.
Twelve percent of 5,858 hospitals answered a 42-question instrument in 2010, according to Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author. The results, Ananth says, showed that the hospitals most likely to offer CAM were urban and tended to be either medium-size (50-299 beds) or large (500+ beds) institutions.
What’s driving the increase? She believes that hospitals are simply responding to patients’ desire to have “the best that both conventional and alternative medicine can offer.”
—Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author
Sixty-five percent of hospitals responding to the survey offer CAM therapies for pain management. That figure is echoed in a 2008 National Health Statistics report (PDF) published by the Centers for Disease Control and Prevention. Back pain, neck pain, and joint pain were the three top reasons for using CAM, according to the CDC report.
“Adjacent” Treatment
Hospitalist Sanjay Reddy, MD, assistant clinical professor of medicine in the Department of Medicine at the University of California at San Francisco (UCSF), says acupuncture can be a valuable adjunct when treating patients for pain, chemotherapy-induced nausea, and insomnia. He is a trained acupuncturist and has studied complementary therapies extensively. He also is interested in exploring ways to incorporate acupuncture into the UCSF’s Osher Center for Integrative Medicine program.
David H. Gorski, MD, PhD, FACS, associate professor of surgery and director of the Breast Cancer Multidisciplinary Team at the Barbara Ann Karmanos Cancer Institute at Wayne State University School of Medicine in Detroit, strenuously objects to the incorporation of alternative therapies (often under the moniker of “integrative medicine”) in the hospital setting.
“If you accept the premise that medicine should be based in sound science and evidence, then we have an obligation not to be offering treatments that are not based in science,” he asserts. Dr. Gorski, who also blogs on such topics, finds that many of those who endorse integrative medicine have become “true believers,” and that some are mixing pseudo-science with science.
In an August 2011 post regarding the College of Physicians and Surgeons of Ontario’s draft policy on alternative treatments, Dr. Gorski wrote: “Competent adults have every right to seek out non-science-based medicine if that is what they desire. However, informed consent mandates that physicians who encounter such patients provide an honest professional assessment of such treatments based on science.”
Dr. Reddy notes that with appropriate disclosure, offering a modality such as acupuncture can be appropriate. For example, in the setting of pain relief, acupuncture offers a less sedative approach. He explains that Chinese diagnostics and treatment approaches are slightly different, so it’s difficult to study them in the context of randomized trials. (Click here to listen to more of Dr. Reddy’s discussion of appropriate indications for acupuncture.)
In the Health Forum/Samueli Institute survey, 57% of hospitals reported that their programs were not yet breaking even and only 16% said they'd be breaking even in three years (see Figure 1). In light of these results, Ananth says, hospitals undertaking complementary services should “start small and not have high expectations of breaking even for several years.”
Gretchen Henkel is a freelance writer in California.
Herbals another Matter
In the 2010 Health Forum/Samueli Institute survey, 82% of responding hospitals reported that they did not offer herbal supplements in their hospital pharmacies. Study author Sita Ananth surmises that most hospitals may be “playing it safe” by offering noninvasive therapies. Hospitalists are aware of the potentially dangerous interactions between herbal supplements and mainstream treatments, Dr. Reddy says.
A majority of the hospitals Ananth queried (67%) reported having existing policies regarding patients’ use of herbal and nutritional supplements during hospitalization. To avoid adverse events, “It’s really crucial that they are asking the right questions of their patients,” she says.—GH