User login
What Is the Optimal Therapy for Acute DVT?
The Case
A 55-year-old female undergoes cholecystectomy. On post-operative Day 2, she develops right-lower-extremity swelling and pain; venous ultrasound detects a proximal deep venous thrombosis (DVT). The patient denies smoking or use of hormonal medications. She has no history of venous thromboembolism (VTE), although her brother had a DVT at age 60. The hospitalist team is consulted for management of acute DVT.
Overview
VTE, including lower- and upper-extremity DVT and pulmonary embolism (PE), is one of the most common and preventable hospital diseases. DVT with PE is associated with a 10% mortality rate, and DVT with post-thrombotic syndrome can be associated with significant morbidity, including pain, edema, skin/pigment change, venous dilation, and ulcer development.1,2 Recognition of clinical symptoms and risk factors for DVT (see Table 1) in conjunction with validated clinical scoring predictors (such as the Wells Prediction Rule) and a high-sensitivity D-dimer assay can help diagnose the condition and determine the need for ultrasound.3-7
Pharmacologic Treatment
Anticoagulation should be initiated in all patients with VTE, regardless of patient symptoms. Anticoagulant options include:
- Intravenous (IV) or subcutaneous (SC) unfractionated heparin (UFH);
- SC low-molecular-weight heparins (LMWH), such as enoxaparin and dalteparin; and
- Fondaparinux (as effective as LMWH for acute treatment of VTE).8
These agents can be used while transitioning to oral vitamin K antagonists (VKA), such as warfarin.3
The 2012 American College of Chest Physicians (ACCP) guidelines on antithrombotic therapy for VTE recommend initial therapy with LMWH or fondaparinux (rather than IV or SC UFH). The guidelines suggest that LMWH once-daily dosing is favored over twice-daily dosing, based mainly on patient convenience, although this is a weak recommendation (2C) based on the overall quality of the data. The recommendation applies only if the daily dosing of the LMWH, including tinzaparin, dalteparin, and nadroparin, is equivalent to the twice-daily dosing (i.e., dalteparin may be dosed at 100 units/kg BID vs. 200 units/kg daily). Of importance, enoxaparin has not been studied at a once-daily dose (2 mg/kg), which is equivalent to the twice-daily dosing regimen (1 mg/kg twice daily). Additionally, one study suggests that once-daily dosing of enoxaparin 1.5mg/kg might be inferior to 1 mg/kg twice-daily dosing; therefore, caution must be exercised in applying this recommendation to the LMWH enoxaparin at this time.3,27,28 (updated Aug. 28, 2012)
Warfarin should be started simultaneously at a usual daily dose of 5 mg for the first two days, with subsequent doses adjusted to achieve a goal international normalized ratio (INR) of 2.0 to 3.0. Parenteral agents should be given for a minimum of five days and until the INR has been >2.0 for at least 24 hours.3
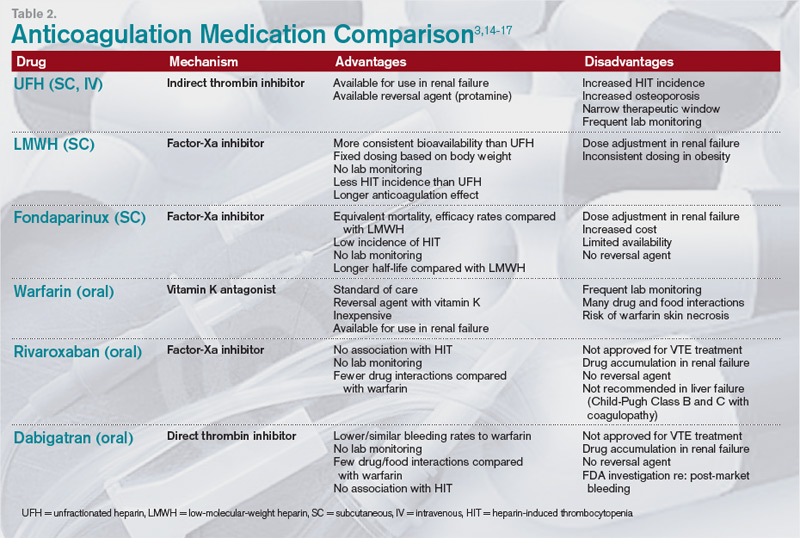
The new factor-Xa inhibitor rivaroxaban and the direct thrombin inhibitor dabigatran are promising oral alternatives to warfarin.9-11 However, neither drug is currently FDA-approved for the treatment of VTE, nor are they recommended by current guidelines (given limited data for DVT treatment and concerns of bleeding risk).3,12,13 See Table 2 (above) for comparisons of common anticoagulants.3,14-17
Duration of anticoagulation. Anticoagulant treatment of acute DVT should continue for at least three months, as shorter durations are associated with higher recurrence rates. Longer treatment may be indicated depending on the patient’s risk of recurrence.3
The ACCP guidelines estimate risk of recurrence using primary, secondary, and additional factors (see Table 3, p. 19) and recommend the following durations:
- First episode provoked: three months (proximal or distal, provoked by surgery or a nonsurgical transient risk factor);
- First episode unprovoked distal: three months (see “Considerations for isolated distal DVT,” below);
- First episode unprovoked proximal: Indefinite if low to moderate bleeding risk, three months if high bleeding risk;
- Recurrent unprovoked: Indefinite if low to moderate bleeding risk, three months if high bleeding risk; and
- With active cancer: Indefinite with LMWH due to higher risk of recurrence.3,18
These treatment duration guidelines might need to be individualized based on other factors including patient preference, ability to obtain accurate INR monitoring (for those on warfarin), treatment cost, and comorbidities.3
Considerations for isolated distal DVT. Patients with an initial episode of distal DVT, without significant symptoms or risk factors for extension (e.g. positive D-dimer, extensive clot near proximal veins, absence of a reversible provoking factor, active cancer, inpatient status, or previous VTE) might not need anticoagulation.
The DVT can be followed with serial ultrasounds for the first two weeks; anticoagulation is recommended only if the thrombus extends during that time period. The development of significant symptoms or risk factors of extension might indicate the need for anticoagulation.3
Considerations for upper-extremity DVT (UEDVT). Anticoagulation for an UEDVT is generally consistent with the above guidelines for lower-extremity DVT, with a few caveats. If an UEDVT is associated with a central venous catheter (CVC), the CVC should be removed if possible; there are no recommendations to determine whether CVC removal should be preceded by a period of anticoagulation.
A catheter-associated UEDVT requires a minimum of three months of anticoagulation; if the CVC remains in place beyond three months, anticoagulation should be continued until the catheter is removed. Unprovoked UEDVT has a lower risk of recurrence than lower-extremity DVT and three months of anticoagulation, rather than indefinite therapy, is recommended.3
Mechanical Treatment
Non-pharmacologic therapies, such as knee-high graduated compression stockings with pressure of 30 mmHg to 40 mmHg at the ankle, can help reduce the morbidity of post-thrombotic syndrome (PTS) when combined with anticoagulation. Symptomatic patients who use compression stockings as soon as feasible and for a minimum of two years can reduce their incidence of PTS by 50%.3,19,20
Thigh-length stockings are not more effective than knee-high, and while multilayer compression bandages might relieve symptoms during the first-week post-DVT, they do not reduce the one-year incidence of PTS.21,22 Early mobilization is not associated with an increased risk of PE, extension of DVT, or death; patients should ambulate as soon as physically able.23,24
Pharmacomechanical Thrombolysis
For acute DVT, ACCP guidelines recommend anticoagulation alone over pharmacomechanical thrombolysis (either systemic or catheter-directed thrombolysis and mechanical thrombus fragmentation). The rare patient with impending venous gangrene despite anticoagulation is the only clinical scenario in which thrombolysis is clearly indicated. Patients who undergo pharmacomechanical thrombolysis still need a standard course of anticoagulation.3
Role for Inferior Vena Cava Filters
The optimal role of inferior vena cava (IVC) filters remains uncertain. Only one randomized trial found that IVC filters, in conjunction with systemic anticoagulation versus systemic anticoagulation alone, were associated with short-term reductions in the incidence of PE but long-term increases in recurrent DVT, with no differences in mortality or major bleeding. However, no trials have compared anticoagulation plus IVC filter placement with IVC filter placement alone.25,26
ACCP guidelines recommend IVC filter placement only in patients with acute, proximal DVT of the lower extremity, and a contraindication to anticoagulant therapy. If the contraindication resolves, a conventional course of anticoagulation can commence. Combining an IVC filter with an anticoagulant is not recommended. The risks and benefits of retrievable filters require further investigation.3
Back to the Case
Our patient has a provoked DVT secondary to a reversible risk factor (surgery) without additional clinical risk factors. Her family history of DVT is not significant (her brother was >age 50 when it occurred). This patient should be treated with LMWH or fondaparinux with initiation of warfarin with goal INR of 2.0 to 3.0 for at least three months. She does not need an IVC filter, and she should use compression stockings to reduce the risk of PTS.
Bottom Line
In hospitalized patients, treatment of DVT should include immediate anticoagulation with LMWH, fondaparinux, or IV heparin (in patients with renal failure) with transition to warfarin and a goal INR of 2.0 to 3.0. New oral anticoagulants could prove beneficial in acute treatment of DVT but require further testing. Duration of treatment is patient-specific, but most should be anticoagulated for at least three months; some warrant indefinite therapy based on risk factors.
Dr. Sebasky is an assistant professor and Dr. DeKorte is assistant professor of medicine in the division of hospital medicine at the University of California at San Diego.
References
- Agency for Healthcare Research and Quality. Talking Points to Attract Administration Support for Venous Thromboembolism Prevention Programs. U.S. Department of Health & Human Services website. Available at: http://www.ahrq.gov/qual/vtguide/vtguideapa.htm. Accessed Feb. 4, 2012.
- Kahn SR, Shbaklo H, Lamping DL, et al. Determinants of health-related quality of life during the 2 years following deep vein thrombosis. J Thromb Haemost. 2008;6:1105-1112.
- Kearon C, Akl E, Comerota AJ, et al. Antithrombotic Therapy for VTE Disease. Antithrombotic Therapy and Prevention of Thrombosis, 9th ed.: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-e494S.
- Hirsh J, Hull RD, Raskob GE. Clinical features and diagnosis of venous thrombosis. J Am Coll Cardiol. 1986;8(6 Suppl B):114B-127B.
- Qaseem A, Snow V, Barry P, et al. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Int Med. 2007;146:454-458.
- Tapson VF, Carroll BA, Davidson BL, et al. The diagnostic approach to acute venous thromboembolism. Clinical practice guideline. American Thoracic Society. Am J Respir Crit Care Med. 1999;160:1043-1066.
- Wells PS, Owen C, Doucette S, Fergusson D, Tran H. Does this patient have deep vein thrombosis? JAMA. 2006;295:199-207.
- Büller HR, Davidson BL, Decousus H, et al. Fondaparinux or enoxaparin for the initial treatment of symptomatic deep venous thrombosis: a randomized trial. Ann Intern Med. 2004;140:867-873.
- EINSTEIN Investigators, Bauersachs R, Berkowitz SD, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363:2499-25
- Garcia, D, Libby E, Crowther M. The new oral anticoagulants. Blood. 2010;115:15-20.
- Douketis JD. Pharmacologic properties of the new oral anticoagulants: a clinician-oriented review with a focus on perioperative management. Curr Pharm Des. 2010;16:3436-3441.
- U.S. Food and Drug Administration. Pradaxa (dabigatran etexilate mesylate): Drug Safety Communication—Safety Review of Post-Market Reports of Serious Bleeding Events. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/
SafetyAlertsforHumanMedicalProducts/ucm282820.htm. Accessed March 12, 2012.
- Levi M, Erenberg E, Kamphuisen PW. Bleeding risk and reversal strategies for old and new anticoagulants and antiplatelet agents. J Thromb Haemost. 2011;9:1705.
- Erkens PM, Prins MH. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2010;8(9);CD001100.Vardi M, Zittan E, Bitterman H. Subcutaneous unfractionated heparin for the initial treatment of venous thromboembolism. Cochrane Database Syst Rev. 2009;(4):CD006771.
- Hirsh J, Levine MN. Low molecular weight heparin. Blood. 1992;79:1-17.
- Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361;2342-2352.
- Bauer KA. Long-term management of venous thromboembolism. JAMA. 2011;305:1336-1345.
- Prandoni P, Lensing AW, Prins MH, et al. Below-knee elastic compression stockings to prevent the postthrombotic syndrome: a randomized, controlled trial. Ann Intern Med. 2004;141:249-256.
- Brandjes DP, Büller HR, Heijboer H, et al. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet. 1997;349:759-762.
- Prandoni P, Noventa F, Quintavalla R, et al. Thigh-length versus below-knee compression elastic stockings for prevention of the post-thrombotic syndrome in patients with proximal-venous thrombosis: a randomized trial. Blood. 2012;119:1561-1565.
- Roumen-Klappe EM, den Heijer M, van Rossum J, et al. Multilayer compression bandaging in the acute phase of deep-vein thrombosis has no effect on the development of the post-thrombotic syndrome. J Thromb Thrombolysis. 2009;27:400-405.
- Aissaoui N, Martins E, Mouly S, Weber S, Meune C. A meta-analysis of bed rest versus early ambulation in the management of pulmonary embolism, deep venous thrombosis, or both. Int J Cardiol. 2009;137:37-41.
- Anderson CM, Overend TJ, Godwin J, Sealy C, Sunderji A. Ambulation after deep vein thrombosis: a systematic review. Physiother Can. 2009;61:133-140.
- Hann CL, Streiff MB. The role of vena caval filters in the management of venous thromboembolism. Blood Rev. 2005;19:179-202.
- Decousus H, Leizorovicz A, Page Y, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. N Engl J Med. 1998;338:409-415.
The Case
A 55-year-old female undergoes cholecystectomy. On post-operative Day 2, she develops right-lower-extremity swelling and pain; venous ultrasound detects a proximal deep venous thrombosis (DVT). The patient denies smoking or use of hormonal medications. She has no history of venous thromboembolism (VTE), although her brother had a DVT at age 60. The hospitalist team is consulted for management of acute DVT.
Overview
VTE, including lower- and upper-extremity DVT and pulmonary embolism (PE), is one of the most common and preventable hospital diseases. DVT with PE is associated with a 10% mortality rate, and DVT with post-thrombotic syndrome can be associated with significant morbidity, including pain, edema, skin/pigment change, venous dilation, and ulcer development.1,2 Recognition of clinical symptoms and risk factors for DVT (see Table 1) in conjunction with validated clinical scoring predictors (such as the Wells Prediction Rule) and a high-sensitivity D-dimer assay can help diagnose the condition and determine the need for ultrasound.3-7
Pharmacologic Treatment
Anticoagulation should be initiated in all patients with VTE, regardless of patient symptoms. Anticoagulant options include:
- Intravenous (IV) or subcutaneous (SC) unfractionated heparin (UFH);
- SC low-molecular-weight heparins (LMWH), such as enoxaparin and dalteparin; and
- Fondaparinux (as effective as LMWH for acute treatment of VTE).8
These agents can be used while transitioning to oral vitamin K antagonists (VKA), such as warfarin.3
The 2012 American College of Chest Physicians (ACCP) guidelines on antithrombotic therapy for VTE recommend initial therapy with LMWH or fondaparinux (rather than IV or SC UFH). The guidelines suggest that LMWH once-daily dosing is favored over twice-daily dosing, based mainly on patient convenience, although this is a weak recommendation (2C) based on the overall quality of the data. The recommendation applies only if the daily dosing of the LMWH, including tinzaparin, dalteparin, and nadroparin, is equivalent to the twice-daily dosing (i.e., dalteparin may be dosed at 100 units/kg BID vs. 200 units/kg daily). Of importance, enoxaparin has not been studied at a once-daily dose (2 mg/kg), which is equivalent to the twice-daily dosing regimen (1 mg/kg twice daily). Additionally, one study suggests that once-daily dosing of enoxaparin 1.5mg/kg might be inferior to 1 mg/kg twice-daily dosing; therefore, caution must be exercised in applying this recommendation to the LMWH enoxaparin at this time.3,27,28 (updated Aug. 28, 2012)
Warfarin should be started simultaneously at a usual daily dose of 5 mg for the first two days, with subsequent doses adjusted to achieve a goal international normalized ratio (INR) of 2.0 to 3.0. Parenteral agents should be given for a minimum of five days and until the INR has been >2.0 for at least 24 hours.3
The new factor-Xa inhibitor rivaroxaban and the direct thrombin inhibitor dabigatran are promising oral alternatives to warfarin.9-11 However, neither drug is currently FDA-approved for the treatment of VTE, nor are they recommended by current guidelines (given limited data for DVT treatment and concerns of bleeding risk).3,12,13 See Table 2 (above) for comparisons of common anticoagulants.3,14-17
Duration of anticoagulation. Anticoagulant treatment of acute DVT should continue for at least three months, as shorter durations are associated with higher recurrence rates. Longer treatment may be indicated depending on the patient’s risk of recurrence.3
The ACCP guidelines estimate risk of recurrence using primary, secondary, and additional factors (see Table 3, p. 19) and recommend the following durations:
- First episode provoked: three months (proximal or distal, provoked by surgery or a nonsurgical transient risk factor);
- First episode unprovoked distal: three months (see “Considerations for isolated distal DVT,” below);
- First episode unprovoked proximal: Indefinite if low to moderate bleeding risk, three months if high bleeding risk;
- Recurrent unprovoked: Indefinite if low to moderate bleeding risk, three months if high bleeding risk; and
- With active cancer: Indefinite with LMWH due to higher risk of recurrence.3,18
These treatment duration guidelines might need to be individualized based on other factors including patient preference, ability to obtain accurate INR monitoring (for those on warfarin), treatment cost, and comorbidities.3
Considerations for isolated distal DVT. Patients with an initial episode of distal DVT, without significant symptoms or risk factors for extension (e.g. positive D-dimer, extensive clot near proximal veins, absence of a reversible provoking factor, active cancer, inpatient status, or previous VTE) might not need anticoagulation.
The DVT can be followed with serial ultrasounds for the first two weeks; anticoagulation is recommended only if the thrombus extends during that time period. The development of significant symptoms or risk factors of extension might indicate the need for anticoagulation.3
Considerations for upper-extremity DVT (UEDVT). Anticoagulation for an UEDVT is generally consistent with the above guidelines for lower-extremity DVT, with a few caveats. If an UEDVT is associated with a central venous catheter (CVC), the CVC should be removed if possible; there are no recommendations to determine whether CVC removal should be preceded by a period of anticoagulation.
A catheter-associated UEDVT requires a minimum of three months of anticoagulation; if the CVC remains in place beyond three months, anticoagulation should be continued until the catheter is removed. Unprovoked UEDVT has a lower risk of recurrence than lower-extremity DVT and three months of anticoagulation, rather than indefinite therapy, is recommended.3
Mechanical Treatment
Non-pharmacologic therapies, such as knee-high graduated compression stockings with pressure of 30 mmHg to 40 mmHg at the ankle, can help reduce the morbidity of post-thrombotic syndrome (PTS) when combined with anticoagulation. Symptomatic patients who use compression stockings as soon as feasible and for a minimum of two years can reduce their incidence of PTS by 50%.3,19,20
Thigh-length stockings are not more effective than knee-high, and while multilayer compression bandages might relieve symptoms during the first-week post-DVT, they do not reduce the one-year incidence of PTS.21,22 Early mobilization is not associated with an increased risk of PE, extension of DVT, or death; patients should ambulate as soon as physically able.23,24
Pharmacomechanical Thrombolysis
For acute DVT, ACCP guidelines recommend anticoagulation alone over pharmacomechanical thrombolysis (either systemic or catheter-directed thrombolysis and mechanical thrombus fragmentation). The rare patient with impending venous gangrene despite anticoagulation is the only clinical scenario in which thrombolysis is clearly indicated. Patients who undergo pharmacomechanical thrombolysis still need a standard course of anticoagulation.3
Role for Inferior Vena Cava Filters
The optimal role of inferior vena cava (IVC) filters remains uncertain. Only one randomized trial found that IVC filters, in conjunction with systemic anticoagulation versus systemic anticoagulation alone, were associated with short-term reductions in the incidence of PE but long-term increases in recurrent DVT, with no differences in mortality or major bleeding. However, no trials have compared anticoagulation plus IVC filter placement with IVC filter placement alone.25,26
ACCP guidelines recommend IVC filter placement only in patients with acute, proximal DVT of the lower extremity, and a contraindication to anticoagulant therapy. If the contraindication resolves, a conventional course of anticoagulation can commence. Combining an IVC filter with an anticoagulant is not recommended. The risks and benefits of retrievable filters require further investigation.3
Back to the Case
Our patient has a provoked DVT secondary to a reversible risk factor (surgery) without additional clinical risk factors. Her family history of DVT is not significant (her brother was >age 50 when it occurred). This patient should be treated with LMWH or fondaparinux with initiation of warfarin with goal INR of 2.0 to 3.0 for at least three months. She does not need an IVC filter, and she should use compression stockings to reduce the risk of PTS.
Bottom Line
In hospitalized patients, treatment of DVT should include immediate anticoagulation with LMWH, fondaparinux, or IV heparin (in patients with renal failure) with transition to warfarin and a goal INR of 2.0 to 3.0. New oral anticoagulants could prove beneficial in acute treatment of DVT but require further testing. Duration of treatment is patient-specific, but most should be anticoagulated for at least three months; some warrant indefinite therapy based on risk factors.
Dr. Sebasky is an assistant professor and Dr. DeKorte is assistant professor of medicine in the division of hospital medicine at the University of California at San Diego.
References
- Agency for Healthcare Research and Quality. Talking Points to Attract Administration Support for Venous Thromboembolism Prevention Programs. U.S. Department of Health & Human Services website. Available at: http://www.ahrq.gov/qual/vtguide/vtguideapa.htm. Accessed Feb. 4, 2012.
- Kahn SR, Shbaklo H, Lamping DL, et al. Determinants of health-related quality of life during the 2 years following deep vein thrombosis. J Thromb Haemost. 2008;6:1105-1112.
- Kearon C, Akl E, Comerota AJ, et al. Antithrombotic Therapy for VTE Disease. Antithrombotic Therapy and Prevention of Thrombosis, 9th ed.: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-e494S.
- Hirsh J, Hull RD, Raskob GE. Clinical features and diagnosis of venous thrombosis. J Am Coll Cardiol. 1986;8(6 Suppl B):114B-127B.
- Qaseem A, Snow V, Barry P, et al. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Int Med. 2007;146:454-458.
- Tapson VF, Carroll BA, Davidson BL, et al. The diagnostic approach to acute venous thromboembolism. Clinical practice guideline. American Thoracic Society. Am J Respir Crit Care Med. 1999;160:1043-1066.
- Wells PS, Owen C, Doucette S, Fergusson D, Tran H. Does this patient have deep vein thrombosis? JAMA. 2006;295:199-207.
- Büller HR, Davidson BL, Decousus H, et al. Fondaparinux or enoxaparin for the initial treatment of symptomatic deep venous thrombosis: a randomized trial. Ann Intern Med. 2004;140:867-873.
- EINSTEIN Investigators, Bauersachs R, Berkowitz SD, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363:2499-25
- Garcia, D, Libby E, Crowther M. The new oral anticoagulants. Blood. 2010;115:15-20.
- Douketis JD. Pharmacologic properties of the new oral anticoagulants: a clinician-oriented review with a focus on perioperative management. Curr Pharm Des. 2010;16:3436-3441.
- U.S. Food and Drug Administration. Pradaxa (dabigatran etexilate mesylate): Drug Safety Communication—Safety Review of Post-Market Reports of Serious Bleeding Events. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/
SafetyAlertsforHumanMedicalProducts/ucm282820.htm. Accessed March 12, 2012.
- Levi M, Erenberg E, Kamphuisen PW. Bleeding risk and reversal strategies for old and new anticoagulants and antiplatelet agents. J Thromb Haemost. 2011;9:1705.
- Erkens PM, Prins MH. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2010;8(9);CD001100.Vardi M, Zittan E, Bitterman H. Subcutaneous unfractionated heparin for the initial treatment of venous thromboembolism. Cochrane Database Syst Rev. 2009;(4):CD006771.
- Hirsh J, Levine MN. Low molecular weight heparin. Blood. 1992;79:1-17.
- Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361;2342-2352.
- Bauer KA. Long-term management of venous thromboembolism. JAMA. 2011;305:1336-1345.
- Prandoni P, Lensing AW, Prins MH, et al. Below-knee elastic compression stockings to prevent the postthrombotic syndrome: a randomized, controlled trial. Ann Intern Med. 2004;141:249-256.
- Brandjes DP, Büller HR, Heijboer H, et al. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet. 1997;349:759-762.
- Prandoni P, Noventa F, Quintavalla R, et al. Thigh-length versus below-knee compression elastic stockings for prevention of the post-thrombotic syndrome in patients with proximal-venous thrombosis: a randomized trial. Blood. 2012;119:1561-1565.
- Roumen-Klappe EM, den Heijer M, van Rossum J, et al. Multilayer compression bandaging in the acute phase of deep-vein thrombosis has no effect on the development of the post-thrombotic syndrome. J Thromb Thrombolysis. 2009;27:400-405.
- Aissaoui N, Martins E, Mouly S, Weber S, Meune C. A meta-analysis of bed rest versus early ambulation in the management of pulmonary embolism, deep venous thrombosis, or both. Int J Cardiol. 2009;137:37-41.
- Anderson CM, Overend TJ, Godwin J, Sealy C, Sunderji A. Ambulation after deep vein thrombosis: a systematic review. Physiother Can. 2009;61:133-140.
- Hann CL, Streiff MB. The role of vena caval filters in the management of venous thromboembolism. Blood Rev. 2005;19:179-202.
- Decousus H, Leizorovicz A, Page Y, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. N Engl J Med. 1998;338:409-415.
The Case
A 55-year-old female undergoes cholecystectomy. On post-operative Day 2, she develops right-lower-extremity swelling and pain; venous ultrasound detects a proximal deep venous thrombosis (DVT). The patient denies smoking or use of hormonal medications. She has no history of venous thromboembolism (VTE), although her brother had a DVT at age 60. The hospitalist team is consulted for management of acute DVT.
Overview
VTE, including lower- and upper-extremity DVT and pulmonary embolism (PE), is one of the most common and preventable hospital diseases. DVT with PE is associated with a 10% mortality rate, and DVT with post-thrombotic syndrome can be associated with significant morbidity, including pain, edema, skin/pigment change, venous dilation, and ulcer development.1,2 Recognition of clinical symptoms and risk factors for DVT (see Table 1) in conjunction with validated clinical scoring predictors (such as the Wells Prediction Rule) and a high-sensitivity D-dimer assay can help diagnose the condition and determine the need for ultrasound.3-7
Pharmacologic Treatment
Anticoagulation should be initiated in all patients with VTE, regardless of patient symptoms. Anticoagulant options include:
- Intravenous (IV) or subcutaneous (SC) unfractionated heparin (UFH);
- SC low-molecular-weight heparins (LMWH), such as enoxaparin and dalteparin; and
- Fondaparinux (as effective as LMWH for acute treatment of VTE).8
These agents can be used while transitioning to oral vitamin K antagonists (VKA), such as warfarin.3
The 2012 American College of Chest Physicians (ACCP) guidelines on antithrombotic therapy for VTE recommend initial therapy with LMWH or fondaparinux (rather than IV or SC UFH). The guidelines suggest that LMWH once-daily dosing is favored over twice-daily dosing, based mainly on patient convenience, although this is a weak recommendation (2C) based on the overall quality of the data. The recommendation applies only if the daily dosing of the LMWH, including tinzaparin, dalteparin, and nadroparin, is equivalent to the twice-daily dosing (i.e., dalteparin may be dosed at 100 units/kg BID vs. 200 units/kg daily). Of importance, enoxaparin has not been studied at a once-daily dose (2 mg/kg), which is equivalent to the twice-daily dosing regimen (1 mg/kg twice daily). Additionally, one study suggests that once-daily dosing of enoxaparin 1.5mg/kg might be inferior to 1 mg/kg twice-daily dosing; therefore, caution must be exercised in applying this recommendation to the LMWH enoxaparin at this time.3,27,28 (updated Aug. 28, 2012)
Warfarin should be started simultaneously at a usual daily dose of 5 mg for the first two days, with subsequent doses adjusted to achieve a goal international normalized ratio (INR) of 2.0 to 3.0. Parenteral agents should be given for a minimum of five days and until the INR has been >2.0 for at least 24 hours.3
The new factor-Xa inhibitor rivaroxaban and the direct thrombin inhibitor dabigatran are promising oral alternatives to warfarin.9-11 However, neither drug is currently FDA-approved for the treatment of VTE, nor are they recommended by current guidelines (given limited data for DVT treatment and concerns of bleeding risk).3,12,13 See Table 2 (above) for comparisons of common anticoagulants.3,14-17
Duration of anticoagulation. Anticoagulant treatment of acute DVT should continue for at least three months, as shorter durations are associated with higher recurrence rates. Longer treatment may be indicated depending on the patient’s risk of recurrence.3
The ACCP guidelines estimate risk of recurrence using primary, secondary, and additional factors (see Table 3, p. 19) and recommend the following durations:
- First episode provoked: three months (proximal or distal, provoked by surgery or a nonsurgical transient risk factor);
- First episode unprovoked distal: three months (see “Considerations for isolated distal DVT,” below);
- First episode unprovoked proximal: Indefinite if low to moderate bleeding risk, three months if high bleeding risk;
- Recurrent unprovoked: Indefinite if low to moderate bleeding risk, three months if high bleeding risk; and
- With active cancer: Indefinite with LMWH due to higher risk of recurrence.3,18
These treatment duration guidelines might need to be individualized based on other factors including patient preference, ability to obtain accurate INR monitoring (for those on warfarin), treatment cost, and comorbidities.3
Considerations for isolated distal DVT. Patients with an initial episode of distal DVT, without significant symptoms or risk factors for extension (e.g. positive D-dimer, extensive clot near proximal veins, absence of a reversible provoking factor, active cancer, inpatient status, or previous VTE) might not need anticoagulation.
The DVT can be followed with serial ultrasounds for the first two weeks; anticoagulation is recommended only if the thrombus extends during that time period. The development of significant symptoms or risk factors of extension might indicate the need for anticoagulation.3
Considerations for upper-extremity DVT (UEDVT). Anticoagulation for an UEDVT is generally consistent with the above guidelines for lower-extremity DVT, with a few caveats. If an UEDVT is associated with a central venous catheter (CVC), the CVC should be removed if possible; there are no recommendations to determine whether CVC removal should be preceded by a period of anticoagulation.
A catheter-associated UEDVT requires a minimum of three months of anticoagulation; if the CVC remains in place beyond three months, anticoagulation should be continued until the catheter is removed. Unprovoked UEDVT has a lower risk of recurrence than lower-extremity DVT and three months of anticoagulation, rather than indefinite therapy, is recommended.3
Mechanical Treatment
Non-pharmacologic therapies, such as knee-high graduated compression stockings with pressure of 30 mmHg to 40 mmHg at the ankle, can help reduce the morbidity of post-thrombotic syndrome (PTS) when combined with anticoagulation. Symptomatic patients who use compression stockings as soon as feasible and for a minimum of two years can reduce their incidence of PTS by 50%.3,19,20
Thigh-length stockings are not more effective than knee-high, and while multilayer compression bandages might relieve symptoms during the first-week post-DVT, they do not reduce the one-year incidence of PTS.21,22 Early mobilization is not associated with an increased risk of PE, extension of DVT, or death; patients should ambulate as soon as physically able.23,24
Pharmacomechanical Thrombolysis
For acute DVT, ACCP guidelines recommend anticoagulation alone over pharmacomechanical thrombolysis (either systemic or catheter-directed thrombolysis and mechanical thrombus fragmentation). The rare patient with impending venous gangrene despite anticoagulation is the only clinical scenario in which thrombolysis is clearly indicated. Patients who undergo pharmacomechanical thrombolysis still need a standard course of anticoagulation.3
Role for Inferior Vena Cava Filters
The optimal role of inferior vena cava (IVC) filters remains uncertain. Only one randomized trial found that IVC filters, in conjunction with systemic anticoagulation versus systemic anticoagulation alone, were associated with short-term reductions in the incidence of PE but long-term increases in recurrent DVT, with no differences in mortality or major bleeding. However, no trials have compared anticoagulation plus IVC filter placement with IVC filter placement alone.25,26
ACCP guidelines recommend IVC filter placement only in patients with acute, proximal DVT of the lower extremity, and a contraindication to anticoagulant therapy. If the contraindication resolves, a conventional course of anticoagulation can commence. Combining an IVC filter with an anticoagulant is not recommended. The risks and benefits of retrievable filters require further investigation.3
Back to the Case
Our patient has a provoked DVT secondary to a reversible risk factor (surgery) without additional clinical risk factors. Her family history of DVT is not significant (her brother was >age 50 when it occurred). This patient should be treated with LMWH or fondaparinux with initiation of warfarin with goal INR of 2.0 to 3.0 for at least three months. She does not need an IVC filter, and she should use compression stockings to reduce the risk of PTS.
Bottom Line
In hospitalized patients, treatment of DVT should include immediate anticoagulation with LMWH, fondaparinux, or IV heparin (in patients with renal failure) with transition to warfarin and a goal INR of 2.0 to 3.0. New oral anticoagulants could prove beneficial in acute treatment of DVT but require further testing. Duration of treatment is patient-specific, but most should be anticoagulated for at least three months; some warrant indefinite therapy based on risk factors.
Dr. Sebasky is an assistant professor and Dr. DeKorte is assistant professor of medicine in the division of hospital medicine at the University of California at San Diego.
References
- Agency for Healthcare Research and Quality. Talking Points to Attract Administration Support for Venous Thromboembolism Prevention Programs. U.S. Department of Health & Human Services website. Available at: http://www.ahrq.gov/qual/vtguide/vtguideapa.htm. Accessed Feb. 4, 2012.
- Kahn SR, Shbaklo H, Lamping DL, et al. Determinants of health-related quality of life during the 2 years following deep vein thrombosis. J Thromb Haemost. 2008;6:1105-1112.
- Kearon C, Akl E, Comerota AJ, et al. Antithrombotic Therapy for VTE Disease. Antithrombotic Therapy and Prevention of Thrombosis, 9th ed.: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S-e494S.
- Hirsh J, Hull RD, Raskob GE. Clinical features and diagnosis of venous thrombosis. J Am Coll Cardiol. 1986;8(6 Suppl B):114B-127B.
- Qaseem A, Snow V, Barry P, et al. Current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Int Med. 2007;146:454-458.
- Tapson VF, Carroll BA, Davidson BL, et al. The diagnostic approach to acute venous thromboembolism. Clinical practice guideline. American Thoracic Society. Am J Respir Crit Care Med. 1999;160:1043-1066.
- Wells PS, Owen C, Doucette S, Fergusson D, Tran H. Does this patient have deep vein thrombosis? JAMA. 2006;295:199-207.
- Büller HR, Davidson BL, Decousus H, et al. Fondaparinux or enoxaparin for the initial treatment of symptomatic deep venous thrombosis: a randomized trial. Ann Intern Med. 2004;140:867-873.
- EINSTEIN Investigators, Bauersachs R, Berkowitz SD, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363:2499-25
- Garcia, D, Libby E, Crowther M. The new oral anticoagulants. Blood. 2010;115:15-20.
- Douketis JD. Pharmacologic properties of the new oral anticoagulants: a clinician-oriented review with a focus on perioperative management. Curr Pharm Des. 2010;16:3436-3441.
- U.S. Food and Drug Administration. Pradaxa (dabigatran etexilate mesylate): Drug Safety Communication—Safety Review of Post-Market Reports of Serious Bleeding Events. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/
SafetyAlertsforHumanMedicalProducts/ucm282820.htm. Accessed March 12, 2012.
- Levi M, Erenberg E, Kamphuisen PW. Bleeding risk and reversal strategies for old and new anticoagulants and antiplatelet agents. J Thromb Haemost. 2011;9:1705.
- Erkens PM, Prins MH. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2010;8(9);CD001100.Vardi M, Zittan E, Bitterman H. Subcutaneous unfractionated heparin for the initial treatment of venous thromboembolism. Cochrane Database Syst Rev. 2009;(4):CD006771.
- Hirsh J, Levine MN. Low molecular weight heparin. Blood. 1992;79:1-17.
- Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361;2342-2352.
- Bauer KA. Long-term management of venous thromboembolism. JAMA. 2011;305:1336-1345.
- Prandoni P, Lensing AW, Prins MH, et al. Below-knee elastic compression stockings to prevent the postthrombotic syndrome: a randomized, controlled trial. Ann Intern Med. 2004;141:249-256.
- Brandjes DP, Büller HR, Heijboer H, et al. Randomised trial of effect of compression stockings in patients with symptomatic proximal-vein thrombosis. Lancet. 1997;349:759-762.
- Prandoni P, Noventa F, Quintavalla R, et al. Thigh-length versus below-knee compression elastic stockings for prevention of the post-thrombotic syndrome in patients with proximal-venous thrombosis: a randomized trial. Blood. 2012;119:1561-1565.
- Roumen-Klappe EM, den Heijer M, van Rossum J, et al. Multilayer compression bandaging in the acute phase of deep-vein thrombosis has no effect on the development of the post-thrombotic syndrome. J Thromb Thrombolysis. 2009;27:400-405.
- Aissaoui N, Martins E, Mouly S, Weber S, Meune C. A meta-analysis of bed rest versus early ambulation in the management of pulmonary embolism, deep venous thrombosis, or both. Int J Cardiol. 2009;137:37-41.
- Anderson CM, Overend TJ, Godwin J, Sealy C, Sunderji A. Ambulation after deep vein thrombosis: a systematic review. Physiother Can. 2009;61:133-140.
- Hann CL, Streiff MB. The role of vena caval filters in the management of venous thromboembolism. Blood Rev. 2005;19:179-202.
- Decousus H, Leizorovicz A, Page Y, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. N Engl J Med. 1998;338:409-415.
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Neutral head position safe for internal jugular vein cannulation
- Thrombolysis decreases mortality in unstable patients with acute PE
- Rectal indomethacin decreases incidence of post-ERCP pancreatitis
- CHADS2-VASc and HAS-BLED as predictors in afib patients
- No readmission, mortality decreases with self-supported COPD management
- Medicare Premier P4P initiatives do not decrease mortality
- In-hospital rate of DVT/PE after hip and knee arthroplasty
- Sodium chloride prevents contrast-induced nephropathy
Neutral Head Position Is Safe for Internal Jugular Vein Cannulation
Clinical question: Is there a difference in the complication rate between neutral head position and 45-degree neck rotation during ultrasound-guided internal jugular vein cannulation?
Background: Cannulation of the internal jugular vein using ultrasound decreases the rate of major complications (carotid artery puncture, pneumothorax, and hemothorax). The relative positions of the internal jugular vein and the carotid artery change based on degree of neck rotation. The optimal position for ultrasound-guided vein puncture has not been shown.
Study design: Prospective, randomized, controlled, non-blinded study.
Setting: Tertiary neurosurgical center in Milan, Italy.
Synopsis: One thousand, three hundred thirty-two patients undergoing major neurosurgical procedures who needed central venous catheter placement were randomized to a neutral head position (NH) or a 45-degree neck rotation (HT) during ultrasound-guided internal jugular vein cannulation. Exclusion criteria were consent refusal, age <12 years, and coagulopathy. Six experienced anesthesiologists performed the procedures; blinding was not possible.
There was no difference in the rate of major complications (carotid artery puncture, pneumothorax, or hemothorax) based on head position (0.9% in NH vs. 0.6% in HT). Minor complications (multiple skin punctures, multiple vein punctures, difficulty inserting the guidewire) were similar in the two groups (13.2% in NG vs. 12.6% in HT). Neck rotation was not associated with operator-reported difficulty or vascular access time.
Limitations of the study include the inability to blind the operator. Additionally, the study involved six experienced anesthesiologists at one center who performed the procedure on patients needing an elective central line. The ability to generalize the findings to other settings, less experienced providers, and patients who need an emergency line is not certain.
Bottom line: Neutral head position is as safe as 45-degree neck rotation for elective ultrasound-guided internal jugular vein cannulation.
Citation: Lamperti M, Subert M, Cortellazzi P, et al. Is a neutral head position safer than 45-degree neck rotation during ultrasound-guided internal jugular vein cannulation? Results of a randomized controlled clinical trial. Anesth Analg. 2012;114:777-784.
Thrombolysis Decreases Mortality in Unstable Patients with Acute Pulmonary Embolism
Clinical question: Does thrombolytic therapy decrease mortality in unstable patients with acute pulmonary embolism (PE)?
Background: PE is a common problem; associated mortality is high. Despite this fact, the data supporting thrombolytic therapy in hemodynamically unstable patients are not robust, and randomized, controlled trials are unlikely to be performed.
Study design: Retrospective cohort study.
Setting: One thousand nonfederal, short-term U.S. hospitals.
Synopsis: Using data from the Nationwide Inpatient Sample database from 1999-2008, investigators found that thrombolysis decreased both all-cause and PE-specific mortality for unstable patients, defined as those either in shock or on a ventilator. Specifically for all-cause mortality, 15% of patients who received thrombolysis died vs. 47% of those who did not (RR 0.31, 95% CI 0.30-0.32). Placement of an inferior vena cava (IVC) filter further reduced mortality, to only 7.6% in patients who received both IVC filter and thrombolysis.
For PE-specific mortality, patients who received thrombolysis also had decreased rates, from 42% to 8.4% (RR 0.20; 95% CI 0.19-0.22). Across all age groups, patients who received thrombolysis had decreased all-cause and PE-specific mortality. Patients who did not receive thrombolysis had additional comorbidities.
As this study is retrospective, it might be affected by unknown confounding. In addition, it relies on coding data to identify patient stability and treatment. Despite this limitation, a randomized, controlled trial is unlikely to be performed at this stage. This study provides evidence to support use of thrombolysis in unstable patients.
Bottom line: Thrombolysis might reduce mortality in unstable patients with acute PE. In combination with IVC filters, the mortality reduction might be even greater.
Citation: Stein PD, Matta F. Thrombolytic therapy in unstable patients with acute pulmonary embolism: saves lives but underused. Am J Med. 2012;125(5):465-470.
Rectal Indomethacin Decreases Incidence of Post-ERCP Pancreatitis
Clinical question: Does rectal indomethacin reduce the incidence of pancreatitis after ERCP?
Background: Acute pancreatitis is the most common complication from endoscopic retrograde cholangiopancreatography (ERCP). No pharmacologic treatment has proven to reduce the incidence of pancreatitis. Preliminary studies, including a meta-analysis, suggest that the use of NSAIDs might reduce the incidence of post-ERCP pancreatitis.
Study design: Randomized, placebo-controlled, double-blind trial.
Setting: Multicenter trial at four university-affiliated medical centers in the U.S.
Synopsis: More than 600 patients at high risk for post-ERCP pancreatitis were randomized to receive either two 50-mg indomethacin suppositories or two identical-appearing placebo suppositories. Patients were considered at high risk for pancreatitis based on previously identified patient- and procedure-related risk factors. Most of the participants had sphincter of Oddi dysfunction (84.4% of the indomethacin group and 80.5% of the placebo group). Exclusion criteria included elevated creatinine and active peptic ulcer disease. The indomethacin or placebo suppositories were given immediately following the ERCP.
Post-ERCP pancreatitis, defined by upper abdominal pain, elevation of pancreatic enzymes, and hospitalization for at least two nights, was significantly higher in the placebo group compared with the indomethacin group (16.9% vs. 9.2%, P=0.005). Moderate or severe post-ERCP pancreatitis was significantly higher in the placebo group compared with the indomethacin group (8.8% vs. 4.4%, P=0.03).
There were no significant differences in the rates of clinically significant bleeding or acute renal failure between the two groups. The ability to generalize these findings to patients without risk factors for post-ERCP pancreatitis is not clear.
Bottom line: Rectal indomethacin decreases the rate of post-ERCP pancreatitis in patients who are at high risk for this complication.
Citation: Elmunzer BJ, Scheiman JM, Lehman GA, et al. A randomized trial of rectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med. 2012;366(15):1414-1422.
CHADS2-VASc and HAS-BLED Can Predict Thromboembolism and Bleeding Risk in Afib Patients
Clinical question: What are the risk factors for stroke/thromboembolism and bleeding from atrial fibrillation (afib), and how well do the CHADS2-VASc and HAS-BLED stroke and bleeding risk-assessment tools perform against other published stroke and bleeding risk-assessment tools (CHADS2 and HEMORR2HAGES) for patients with afib?
Background: In afib patients, the CHADS2-VASc tool might offer more comprehensive stroke assessment over the CHADS2 by identifying truly-low-risk patients with afib who might not even need antiplatelet therapy. HAS-BLED, a newer bleeding-risk-assessment tool, has been validated in previous trials and is more user-friendly than others. Use of CHADS2-VASc and HAS-BLED are recommended by the European Society of Cardiology to assess stroke and bleeding risks for patients with afib.
Study design: Prospective cohort study.
Setting: All hospitals in Sweden.
Synopsis: Investigators identified 182,678 afib patients via ICD-10 data from Sweden’s National Hospital Discharge Registry ICD-10 from 2005 to 2008. Approximately half the patients were not taking anticoagulants. Analysis assessed risk factors for stroke and bleeding and the performance of CHADS2-VASc and HAS-BLED against CHADS2 and HEMORR2HAGES stroke and bleeding risk-assessment tools.
Risk of composite thromboembolism (unspecified stroke, TIA, systemic embolism) was significantly higher in patients with increased age, peripheral arterial disease, prior myocardial infarction (MI), prior coronary artery bypass grafting (CABG), female gender, renal failure, and aspirin use, as well as hypertension, diabetes, prior thromboembolic event, or prior intracranial hemorrhage (ICH). Interestingly, a statistically increased risk was seen with aspirin use.
Conversely, history of heart failure, thyroid disease, and obesity were not associated with increased composite thromboembolic risk. The use of CHADS2-VASc was marginally better than CHADS2 in predicting stroke risk.
ICH risk was increased in patients with older age, prior ischemic stroke, prior ICH, and hypertension. Risk of composite bleeding (from ICH or other major bleeding) was significantly higher in patients with these risk factors, as well as renal failure, liver disease, anemia, dysfunctional platelets, alcohol use, and cancer. Ischemic heart disease was associated with a statistically significant lower risk of ICH, but not of composite bleeding risk.
HAS-BLED usage was as good as, and easier to use than, HEMORR2HAGES in predicting bleeding risk.
Bottom line: CHADS2-VASc might be better than CHADS2 in predicting truly-low-risk patients with nonvalvular afib; HAS-BLED is just as good as, and easier to use than, HEMORR2HAGES in predicting bleeding risk for patients with nonvalvular afib who are to receive antithrombotic therapy.
Citation: Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182,678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33(12):1500-10 [Epub 2012 Jan 13].
Supported Self-Management of COPD Does Not Decrease Readmission or Mortality Rates
Clinical question: Does supported self-management of patients with chronic obstructive pulmonary disease (COPD) decrease COPD-related hospital readmission or death?
Clinical background: Supported self-management has benefited patients with such chronic diseases as heart failure and asthma. Evidence to support such a strategy for patients with COPD is relatively lacking.
Study design: Randomized, controlled trial.
Setting: Community-based care following urban hospitalization in western Scotland.
Synopsis: From June 2007 to May 2009, and following hospitalization for COPD exacerbation, 464 patients were randomized to receive routine community-based care with or without 12 months of support and training to detect, and promptly treat, recurrent exacerbations. Independent of disease severity or demographics, investigators found no difference in combined readmission (48% vs. 47%, 95% confidence interval [CI] 0.80-1.38) or death (10% vs. 7%, 95% CI 0.71-2.61).
Based on review of appropriateness of self-management strategies used by the intervention group, unplanned exploratory subgroup analysis classified a minority of the intervention group as “successful” (42%) supported self-managers, and demonstrated decreased COPD readmissions and death (27% vs. 49%, 95% CI 0.25-0.76, P=0.003) vs. “unsuccessful” self-managers. This successful group was younger and tended to live with others. Further research to define characteristics of patients who benefit from self-management is needed.
Bottom line: Supported self-management of COPD does not reduce COPD-related readmission or death in a large population.
Citation: Bucknall CE, Miller G, Lloyd SM, et al. Glasgow supported self-management trial (GSuST) for patients with moderate to severe COPD: randomised controlled trial. BMJ. 2012;344:e1060 [Epub ahead of print].
Medicare Premier P4P Initiatives Do Not Decrease Mortality
Clinical question: Has the Medicare Premier Hospital Quality Incentive Demonstration (HQID) resulted in lower mortality?
Background: The Centers for Medicare & Medicaid Services’ (CMS) value-based purchasing program will expand to include 30-day mortality in 2013, but do pay-for-performance (P4P) initiatives result in improved mortality? Studies have demonstrated improvement in process of care but have not demonstrated mortality benefit thus far.
Study design: Cohort study.
Setting: Two hundred fifty-two hospitals participating in the Premier HQID compared with 3,363 control hospitals participating in the Hospital Compare program.
Synopsis: Researchers examined 30-day mortality for patients admitted with acute myocardial infarction, congestive heart failure, pneumonia, and for coronary artery bypass grafting (CABG) from 2003 to 2009. Results showed no difference in 30-day mortality rates over the six-year span of the program for any of the conditions studied in the Premier hospitals (participating in the voluntary pay-for-performance program) vs. non-Premier hospitals (11.82% vs. 11.74%). This held true for each condition measured individually, with a higher mortality rate for patients undergoing CABG at the Premier hospitals.
In addition, in the hospitals that underperformed initially, there was no difference with respect to rate of improvement when comparing Premier vs. non-Premier hospitals. Furthermore, mortality rate trends did not differ between those conditions that were incentivized (acute MI and CABG) compared with those that were not (congestive heart failure and pneumonia).
The authors concluded that there was “little evidence” that the Premier HQID pay-for-performance program resulted in reduced 30-day mortality.
Bottom line: Programs participating in the Medicare Premier HQID pay-for-performance program had similar 30-day mortality compared with nonparticipating programs.
Citation: Jha AK, Joynt KE, Orav EJ, Epstein AM. The long-term effect of premier pay for performance on patient outcomes. N Engl J Med. 2012;366:1606-1615.
In-Hospital Rate of DVT/PE After Hip and Knee Arthroplasty with Guideline-Recommended Prophylaxis
Clinical question: What is the rate of symptomatic DVT/PE after total or partial hip (TPHA) or knee (TPKA) arthroplasty using currently recommended prophylaxis?
Background: The rate of postoperative DVT/PE after TPHA/TPKA has dropped dramatically with use of pharmacologic prophylaxis. However, the current rate of symptomatic DVT/PE using current pharmacologic prophylaxis is not known. Such rates are needed for informed patient consent and development of patient safety benchmarks.
Study design: Systematic review.
Setting: Randomized clinical trials (RCTs) and observational studies worldwide of adult inpatients undergoing TPHA and/or TPKA from 1996 to 2011.
Synopsis: Forty-seven studies were included, of which 41 were RCTs and six were observational studies. Twenty-one studies evaluated rates after TPHA, 20 after TPKA, and six after both. More than 44,000 patients were included, with ages ranging from 58 to 74 years. The mean duration of prophylaxis was eight days, with a mean follow-up of 13 days.
In-hospital rates of symptomatic venous thromboembolism (VTE) were higher in patients undergoing TPKA than TPHA (1.09% vs. 0.53% for VTE, 0.63% vs. 0.26% for DVT, and 0.27% vs. 0.14% for PE). This is in contrast to the higher rates of VTE observed after TPHA when the post-discharge period is included. The pooled incidence of VTE was lower with use of direct inhibitors of Factors Xa or IIa when compared to low-molecular-weight heparin, although a direct efficacy comparison could not be made.
Because the majority of studies were RCTs with restrictive inclusion criteria, rates of DVT/PE in actual practice might be higher.
Bottom line: When informing patients of postoperative VTE risk, or establishing benchmarks to evaluate patient safety, one can anticipate an in-hospital VTE rate of 0.5% following TPHA and 1% following TPKA.
Citation: Januel JM, Chen G, Ruffieux C, et al. Symptomatic in-hospital deep vein thrombosis and pulmonary embolism following hip and knee arthroplasty among patients receiving recommended prophylaxis: a systematic review. JAMA. 2012;307(3):294-303.
Sodium Chloride Prevents Contrast-Induced Nephropathy
Clinical question: Is sodium chloride more effective than sodium bicarbonate for preventing contrast-induced nephropathy?
Background: Contrast-induced nephropathy can be prevented with precontrast hydration. Study authors sought to compare sodium chloride administered over 24 hours with sodium bicarbonate administered over seven hours, and with sodium bicarbonate administered orally.
Study design: Randomized, open-label, controlled trial.
Setting: Three European medical centers.
Synopsis: The study examined 258 patients with an estimated glomerular filtration rate <60mL/min/1.73m2 undergoing intravenous or intra-arterial contrast procedure. Patients with Class III or IV heart failure were excluded. The remaining patients were randomized to receive one of three regimens: sodium chloride at 1 ml/kg/hr for 12 hours prior to and 12 hours following the procedure; intravenous sodium bicarbonate for one hour prior to and six hours following the procedure; or intravenous and oral sodium bicarbonate 20 minutes prior to the procedure.
The group that received saline had a lower incidence of contrast-induced nephropathy than the bicarbonate groups (1% vs. 9% vs. 10%). The oral bicarbonate strategy was noninferior to the seven-hour intravenous bicarbonate strategy.
The authors postulated that saline should be used for high-risk patients, but that given the overall low incidence of contrast-induced nephropathy, the short-term bicarbonate strategy (intravenous followed by oral) is a viable alternative for low-risk patients.
Bottom line: Sodium chloride is more effective than sodium bicarbonate for preventing contrast-induced nephropathy, but in light of the low incidence, a short course of sodium bicarbonate is a possible convenient alternative for low-risk patients.
Citation: Klima T, Christ A, Marana I, et al. Sodium chloride vs. sodium bicarbonate for the prevention of contrast medium-induced nephropathy: a randomized controlled trial. Eur Heart J. 2012 Jan 19 [Epub ahead of print].
In This Edition
Literature At A Glance
A guide to this month’s studies
- Neutral head position safe for internal jugular vein cannulation
- Thrombolysis decreases mortality in unstable patients with acute PE
- Rectal indomethacin decreases incidence of post-ERCP pancreatitis
- CHADS2-VASc and HAS-BLED as predictors in afib patients
- No readmission, mortality decreases with self-supported COPD management
- Medicare Premier P4P initiatives do not decrease mortality
- In-hospital rate of DVT/PE after hip and knee arthroplasty
- Sodium chloride prevents contrast-induced nephropathy
Neutral Head Position Is Safe for Internal Jugular Vein Cannulation
Clinical question: Is there a difference in the complication rate between neutral head position and 45-degree neck rotation during ultrasound-guided internal jugular vein cannulation?
Background: Cannulation of the internal jugular vein using ultrasound decreases the rate of major complications (carotid artery puncture, pneumothorax, and hemothorax). The relative positions of the internal jugular vein and the carotid artery change based on degree of neck rotation. The optimal position for ultrasound-guided vein puncture has not been shown.
Study design: Prospective, randomized, controlled, non-blinded study.
Setting: Tertiary neurosurgical center in Milan, Italy.
Synopsis: One thousand, three hundred thirty-two patients undergoing major neurosurgical procedures who needed central venous catheter placement were randomized to a neutral head position (NH) or a 45-degree neck rotation (HT) during ultrasound-guided internal jugular vein cannulation. Exclusion criteria were consent refusal, age <12 years, and coagulopathy. Six experienced anesthesiologists performed the procedures; blinding was not possible.
There was no difference in the rate of major complications (carotid artery puncture, pneumothorax, or hemothorax) based on head position (0.9% in NH vs. 0.6% in HT). Minor complications (multiple skin punctures, multiple vein punctures, difficulty inserting the guidewire) were similar in the two groups (13.2% in NG vs. 12.6% in HT). Neck rotation was not associated with operator-reported difficulty or vascular access time.
Limitations of the study include the inability to blind the operator. Additionally, the study involved six experienced anesthesiologists at one center who performed the procedure on patients needing an elective central line. The ability to generalize the findings to other settings, less experienced providers, and patients who need an emergency line is not certain.
Bottom line: Neutral head position is as safe as 45-degree neck rotation for elective ultrasound-guided internal jugular vein cannulation.
Citation: Lamperti M, Subert M, Cortellazzi P, et al. Is a neutral head position safer than 45-degree neck rotation during ultrasound-guided internal jugular vein cannulation? Results of a randomized controlled clinical trial. Anesth Analg. 2012;114:777-784.
Thrombolysis Decreases Mortality in Unstable Patients with Acute Pulmonary Embolism
Clinical question: Does thrombolytic therapy decrease mortality in unstable patients with acute pulmonary embolism (PE)?
Background: PE is a common problem; associated mortality is high. Despite this fact, the data supporting thrombolytic therapy in hemodynamically unstable patients are not robust, and randomized, controlled trials are unlikely to be performed.
Study design: Retrospective cohort study.
Setting: One thousand nonfederal, short-term U.S. hospitals.
Synopsis: Using data from the Nationwide Inpatient Sample database from 1999-2008, investigators found that thrombolysis decreased both all-cause and PE-specific mortality for unstable patients, defined as those either in shock or on a ventilator. Specifically for all-cause mortality, 15% of patients who received thrombolysis died vs. 47% of those who did not (RR 0.31, 95% CI 0.30-0.32). Placement of an inferior vena cava (IVC) filter further reduced mortality, to only 7.6% in patients who received both IVC filter and thrombolysis.
For PE-specific mortality, patients who received thrombolysis also had decreased rates, from 42% to 8.4% (RR 0.20; 95% CI 0.19-0.22). Across all age groups, patients who received thrombolysis had decreased all-cause and PE-specific mortality. Patients who did not receive thrombolysis had additional comorbidities.
As this study is retrospective, it might be affected by unknown confounding. In addition, it relies on coding data to identify patient stability and treatment. Despite this limitation, a randomized, controlled trial is unlikely to be performed at this stage. This study provides evidence to support use of thrombolysis in unstable patients.
Bottom line: Thrombolysis might reduce mortality in unstable patients with acute PE. In combination with IVC filters, the mortality reduction might be even greater.
Citation: Stein PD, Matta F. Thrombolytic therapy in unstable patients with acute pulmonary embolism: saves lives but underused. Am J Med. 2012;125(5):465-470.
Rectal Indomethacin Decreases Incidence of Post-ERCP Pancreatitis
Clinical question: Does rectal indomethacin reduce the incidence of pancreatitis after ERCP?
Background: Acute pancreatitis is the most common complication from endoscopic retrograde cholangiopancreatography (ERCP). No pharmacologic treatment has proven to reduce the incidence of pancreatitis. Preliminary studies, including a meta-analysis, suggest that the use of NSAIDs might reduce the incidence of post-ERCP pancreatitis.
Study design: Randomized, placebo-controlled, double-blind trial.
Setting: Multicenter trial at four university-affiliated medical centers in the U.S.
Synopsis: More than 600 patients at high risk for post-ERCP pancreatitis were randomized to receive either two 50-mg indomethacin suppositories or two identical-appearing placebo suppositories. Patients were considered at high risk for pancreatitis based on previously identified patient- and procedure-related risk factors. Most of the participants had sphincter of Oddi dysfunction (84.4% of the indomethacin group and 80.5% of the placebo group). Exclusion criteria included elevated creatinine and active peptic ulcer disease. The indomethacin or placebo suppositories were given immediately following the ERCP.
Post-ERCP pancreatitis, defined by upper abdominal pain, elevation of pancreatic enzymes, and hospitalization for at least two nights, was significantly higher in the placebo group compared with the indomethacin group (16.9% vs. 9.2%, P=0.005). Moderate or severe post-ERCP pancreatitis was significantly higher in the placebo group compared with the indomethacin group (8.8% vs. 4.4%, P=0.03).
There were no significant differences in the rates of clinically significant bleeding or acute renal failure between the two groups. The ability to generalize these findings to patients without risk factors for post-ERCP pancreatitis is not clear.
Bottom line: Rectal indomethacin decreases the rate of post-ERCP pancreatitis in patients who are at high risk for this complication.
Citation: Elmunzer BJ, Scheiman JM, Lehman GA, et al. A randomized trial of rectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med. 2012;366(15):1414-1422.
CHADS2-VASc and HAS-BLED Can Predict Thromboembolism and Bleeding Risk in Afib Patients
Clinical question: What are the risk factors for stroke/thromboembolism and bleeding from atrial fibrillation (afib), and how well do the CHADS2-VASc and HAS-BLED stroke and bleeding risk-assessment tools perform against other published stroke and bleeding risk-assessment tools (CHADS2 and HEMORR2HAGES) for patients with afib?
Background: In afib patients, the CHADS2-VASc tool might offer more comprehensive stroke assessment over the CHADS2 by identifying truly-low-risk patients with afib who might not even need antiplatelet therapy. HAS-BLED, a newer bleeding-risk-assessment tool, has been validated in previous trials and is more user-friendly than others. Use of CHADS2-VASc and HAS-BLED are recommended by the European Society of Cardiology to assess stroke and bleeding risks for patients with afib.
Study design: Prospective cohort study.
Setting: All hospitals in Sweden.
Synopsis: Investigators identified 182,678 afib patients via ICD-10 data from Sweden’s National Hospital Discharge Registry ICD-10 from 2005 to 2008. Approximately half the patients were not taking anticoagulants. Analysis assessed risk factors for stroke and bleeding and the performance of CHADS2-VASc and HAS-BLED against CHADS2 and HEMORR2HAGES stroke and bleeding risk-assessment tools.
Risk of composite thromboembolism (unspecified stroke, TIA, systemic embolism) was significantly higher in patients with increased age, peripheral arterial disease, prior myocardial infarction (MI), prior coronary artery bypass grafting (CABG), female gender, renal failure, and aspirin use, as well as hypertension, diabetes, prior thromboembolic event, or prior intracranial hemorrhage (ICH). Interestingly, a statistically increased risk was seen with aspirin use.
Conversely, history of heart failure, thyroid disease, and obesity were not associated with increased composite thromboembolic risk. The use of CHADS2-VASc was marginally better than CHADS2 in predicting stroke risk.
ICH risk was increased in patients with older age, prior ischemic stroke, prior ICH, and hypertension. Risk of composite bleeding (from ICH or other major bleeding) was significantly higher in patients with these risk factors, as well as renal failure, liver disease, anemia, dysfunctional platelets, alcohol use, and cancer. Ischemic heart disease was associated with a statistically significant lower risk of ICH, but not of composite bleeding risk.
HAS-BLED usage was as good as, and easier to use than, HEMORR2HAGES in predicting bleeding risk.
Bottom line: CHADS2-VASc might be better than CHADS2 in predicting truly-low-risk patients with nonvalvular afib; HAS-BLED is just as good as, and easier to use than, HEMORR2HAGES in predicting bleeding risk for patients with nonvalvular afib who are to receive antithrombotic therapy.
Citation: Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182,678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33(12):1500-10 [Epub 2012 Jan 13].
Supported Self-Management of COPD Does Not Decrease Readmission or Mortality Rates
Clinical question: Does supported self-management of patients with chronic obstructive pulmonary disease (COPD) decrease COPD-related hospital readmission or death?
Clinical background: Supported self-management has benefited patients with such chronic diseases as heart failure and asthma. Evidence to support such a strategy for patients with COPD is relatively lacking.
Study design: Randomized, controlled trial.
Setting: Community-based care following urban hospitalization in western Scotland.
Synopsis: From June 2007 to May 2009, and following hospitalization for COPD exacerbation, 464 patients were randomized to receive routine community-based care with or without 12 months of support and training to detect, and promptly treat, recurrent exacerbations. Independent of disease severity or demographics, investigators found no difference in combined readmission (48% vs. 47%, 95% confidence interval [CI] 0.80-1.38) or death (10% vs. 7%, 95% CI 0.71-2.61).
Based on review of appropriateness of self-management strategies used by the intervention group, unplanned exploratory subgroup analysis classified a minority of the intervention group as “successful” (42%) supported self-managers, and demonstrated decreased COPD readmissions and death (27% vs. 49%, 95% CI 0.25-0.76, P=0.003) vs. “unsuccessful” self-managers. This successful group was younger and tended to live with others. Further research to define characteristics of patients who benefit from self-management is needed.
Bottom line: Supported self-management of COPD does not reduce COPD-related readmission or death in a large population.
Citation: Bucknall CE, Miller G, Lloyd SM, et al. Glasgow supported self-management trial (GSuST) for patients with moderate to severe COPD: randomised controlled trial. BMJ. 2012;344:e1060 [Epub ahead of print].
Medicare Premier P4P Initiatives Do Not Decrease Mortality
Clinical question: Has the Medicare Premier Hospital Quality Incentive Demonstration (HQID) resulted in lower mortality?
Background: The Centers for Medicare & Medicaid Services’ (CMS) value-based purchasing program will expand to include 30-day mortality in 2013, but do pay-for-performance (P4P) initiatives result in improved mortality? Studies have demonstrated improvement in process of care but have not demonstrated mortality benefit thus far.
Study design: Cohort study.
Setting: Two hundred fifty-two hospitals participating in the Premier HQID compared with 3,363 control hospitals participating in the Hospital Compare program.
Synopsis: Researchers examined 30-day mortality for patients admitted with acute myocardial infarction, congestive heart failure, pneumonia, and for coronary artery bypass grafting (CABG) from 2003 to 2009. Results showed no difference in 30-day mortality rates over the six-year span of the program for any of the conditions studied in the Premier hospitals (participating in the voluntary pay-for-performance program) vs. non-Premier hospitals (11.82% vs. 11.74%). This held true for each condition measured individually, with a higher mortality rate for patients undergoing CABG at the Premier hospitals.
In addition, in the hospitals that underperformed initially, there was no difference with respect to rate of improvement when comparing Premier vs. non-Premier hospitals. Furthermore, mortality rate trends did not differ between those conditions that were incentivized (acute MI and CABG) compared with those that were not (congestive heart failure and pneumonia).
The authors concluded that there was “little evidence” that the Premier HQID pay-for-performance program resulted in reduced 30-day mortality.
Bottom line: Programs participating in the Medicare Premier HQID pay-for-performance program had similar 30-day mortality compared with nonparticipating programs.
Citation: Jha AK, Joynt KE, Orav EJ, Epstein AM. The long-term effect of premier pay for performance on patient outcomes. N Engl J Med. 2012;366:1606-1615.
In-Hospital Rate of DVT/PE After Hip and Knee Arthroplasty with Guideline-Recommended Prophylaxis
Clinical question: What is the rate of symptomatic DVT/PE after total or partial hip (TPHA) or knee (TPKA) arthroplasty using currently recommended prophylaxis?
Background: The rate of postoperative DVT/PE after TPHA/TPKA has dropped dramatically with use of pharmacologic prophylaxis. However, the current rate of symptomatic DVT/PE using current pharmacologic prophylaxis is not known. Such rates are needed for informed patient consent and development of patient safety benchmarks.
Study design: Systematic review.
Setting: Randomized clinical trials (RCTs) and observational studies worldwide of adult inpatients undergoing TPHA and/or TPKA from 1996 to 2011.
Synopsis: Forty-seven studies were included, of which 41 were RCTs and six were observational studies. Twenty-one studies evaluated rates after TPHA, 20 after TPKA, and six after both. More than 44,000 patients were included, with ages ranging from 58 to 74 years. The mean duration of prophylaxis was eight days, with a mean follow-up of 13 days.
In-hospital rates of symptomatic venous thromboembolism (VTE) were higher in patients undergoing TPKA than TPHA (1.09% vs. 0.53% for VTE, 0.63% vs. 0.26% for DVT, and 0.27% vs. 0.14% for PE). This is in contrast to the higher rates of VTE observed after TPHA when the post-discharge period is included. The pooled incidence of VTE was lower with use of direct inhibitors of Factors Xa or IIa when compared to low-molecular-weight heparin, although a direct efficacy comparison could not be made.
Because the majority of studies were RCTs with restrictive inclusion criteria, rates of DVT/PE in actual practice might be higher.
Bottom line: When informing patients of postoperative VTE risk, or establishing benchmarks to evaluate patient safety, one can anticipate an in-hospital VTE rate of 0.5% following TPHA and 1% following TPKA.
Citation: Januel JM, Chen G, Ruffieux C, et al. Symptomatic in-hospital deep vein thrombosis and pulmonary embolism following hip and knee arthroplasty among patients receiving recommended prophylaxis: a systematic review. JAMA. 2012;307(3):294-303.
Sodium Chloride Prevents Contrast-Induced Nephropathy
Clinical question: Is sodium chloride more effective than sodium bicarbonate for preventing contrast-induced nephropathy?
Background: Contrast-induced nephropathy can be prevented with precontrast hydration. Study authors sought to compare sodium chloride administered over 24 hours with sodium bicarbonate administered over seven hours, and with sodium bicarbonate administered orally.
Study design: Randomized, open-label, controlled trial.
Setting: Three European medical centers.
Synopsis: The study examined 258 patients with an estimated glomerular filtration rate <60mL/min/1.73m2 undergoing intravenous or intra-arterial contrast procedure. Patients with Class III or IV heart failure were excluded. The remaining patients were randomized to receive one of three regimens: sodium chloride at 1 ml/kg/hr for 12 hours prior to and 12 hours following the procedure; intravenous sodium bicarbonate for one hour prior to and six hours following the procedure; or intravenous and oral sodium bicarbonate 20 minutes prior to the procedure.
The group that received saline had a lower incidence of contrast-induced nephropathy than the bicarbonate groups (1% vs. 9% vs. 10%). The oral bicarbonate strategy was noninferior to the seven-hour intravenous bicarbonate strategy.
The authors postulated that saline should be used for high-risk patients, but that given the overall low incidence of contrast-induced nephropathy, the short-term bicarbonate strategy (intravenous followed by oral) is a viable alternative for low-risk patients.
Bottom line: Sodium chloride is more effective than sodium bicarbonate for preventing contrast-induced nephropathy, but in light of the low incidence, a short course of sodium bicarbonate is a possible convenient alternative for low-risk patients.
Citation: Klima T, Christ A, Marana I, et al. Sodium chloride vs. sodium bicarbonate for the prevention of contrast medium-induced nephropathy: a randomized controlled trial. Eur Heart J. 2012 Jan 19 [Epub ahead of print].
In This Edition
Literature At A Glance
A guide to this month’s studies
- Neutral head position safe for internal jugular vein cannulation
- Thrombolysis decreases mortality in unstable patients with acute PE
- Rectal indomethacin decreases incidence of post-ERCP pancreatitis
- CHADS2-VASc and HAS-BLED as predictors in afib patients
- No readmission, mortality decreases with self-supported COPD management
- Medicare Premier P4P initiatives do not decrease mortality
- In-hospital rate of DVT/PE after hip and knee arthroplasty
- Sodium chloride prevents contrast-induced nephropathy
Neutral Head Position Is Safe for Internal Jugular Vein Cannulation
Clinical question: Is there a difference in the complication rate between neutral head position and 45-degree neck rotation during ultrasound-guided internal jugular vein cannulation?
Background: Cannulation of the internal jugular vein using ultrasound decreases the rate of major complications (carotid artery puncture, pneumothorax, and hemothorax). The relative positions of the internal jugular vein and the carotid artery change based on degree of neck rotation. The optimal position for ultrasound-guided vein puncture has not been shown.
Study design: Prospective, randomized, controlled, non-blinded study.
Setting: Tertiary neurosurgical center in Milan, Italy.
Synopsis: One thousand, three hundred thirty-two patients undergoing major neurosurgical procedures who needed central venous catheter placement were randomized to a neutral head position (NH) or a 45-degree neck rotation (HT) during ultrasound-guided internal jugular vein cannulation. Exclusion criteria were consent refusal, age <12 years, and coagulopathy. Six experienced anesthesiologists performed the procedures; blinding was not possible.
There was no difference in the rate of major complications (carotid artery puncture, pneumothorax, or hemothorax) based on head position (0.9% in NH vs. 0.6% in HT). Minor complications (multiple skin punctures, multiple vein punctures, difficulty inserting the guidewire) were similar in the two groups (13.2% in NG vs. 12.6% in HT). Neck rotation was not associated with operator-reported difficulty or vascular access time.
Limitations of the study include the inability to blind the operator. Additionally, the study involved six experienced anesthesiologists at one center who performed the procedure on patients needing an elective central line. The ability to generalize the findings to other settings, less experienced providers, and patients who need an emergency line is not certain.
Bottom line: Neutral head position is as safe as 45-degree neck rotation for elective ultrasound-guided internal jugular vein cannulation.
Citation: Lamperti M, Subert M, Cortellazzi P, et al. Is a neutral head position safer than 45-degree neck rotation during ultrasound-guided internal jugular vein cannulation? Results of a randomized controlled clinical trial. Anesth Analg. 2012;114:777-784.
Thrombolysis Decreases Mortality in Unstable Patients with Acute Pulmonary Embolism
Clinical question: Does thrombolytic therapy decrease mortality in unstable patients with acute pulmonary embolism (PE)?
Background: PE is a common problem; associated mortality is high. Despite this fact, the data supporting thrombolytic therapy in hemodynamically unstable patients are not robust, and randomized, controlled trials are unlikely to be performed.
Study design: Retrospective cohort study.
Setting: One thousand nonfederal, short-term U.S. hospitals.
Synopsis: Using data from the Nationwide Inpatient Sample database from 1999-2008, investigators found that thrombolysis decreased both all-cause and PE-specific mortality for unstable patients, defined as those either in shock or on a ventilator. Specifically for all-cause mortality, 15% of patients who received thrombolysis died vs. 47% of those who did not (RR 0.31, 95% CI 0.30-0.32). Placement of an inferior vena cava (IVC) filter further reduced mortality, to only 7.6% in patients who received both IVC filter and thrombolysis.
For PE-specific mortality, patients who received thrombolysis also had decreased rates, from 42% to 8.4% (RR 0.20; 95% CI 0.19-0.22). Across all age groups, patients who received thrombolysis had decreased all-cause and PE-specific mortality. Patients who did not receive thrombolysis had additional comorbidities.
As this study is retrospective, it might be affected by unknown confounding. In addition, it relies on coding data to identify patient stability and treatment. Despite this limitation, a randomized, controlled trial is unlikely to be performed at this stage. This study provides evidence to support use of thrombolysis in unstable patients.
Bottom line: Thrombolysis might reduce mortality in unstable patients with acute PE. In combination with IVC filters, the mortality reduction might be even greater.
Citation: Stein PD, Matta F. Thrombolytic therapy in unstable patients with acute pulmonary embolism: saves lives but underused. Am J Med. 2012;125(5):465-470.
Rectal Indomethacin Decreases Incidence of Post-ERCP Pancreatitis
Clinical question: Does rectal indomethacin reduce the incidence of pancreatitis after ERCP?
Background: Acute pancreatitis is the most common complication from endoscopic retrograde cholangiopancreatography (ERCP). No pharmacologic treatment has proven to reduce the incidence of pancreatitis. Preliminary studies, including a meta-analysis, suggest that the use of NSAIDs might reduce the incidence of post-ERCP pancreatitis.
Study design: Randomized, placebo-controlled, double-blind trial.
Setting: Multicenter trial at four university-affiliated medical centers in the U.S.
Synopsis: More than 600 patients at high risk for post-ERCP pancreatitis were randomized to receive either two 50-mg indomethacin suppositories or two identical-appearing placebo suppositories. Patients were considered at high risk for pancreatitis based on previously identified patient- and procedure-related risk factors. Most of the participants had sphincter of Oddi dysfunction (84.4% of the indomethacin group and 80.5% of the placebo group). Exclusion criteria included elevated creatinine and active peptic ulcer disease. The indomethacin or placebo suppositories were given immediately following the ERCP.
Post-ERCP pancreatitis, defined by upper abdominal pain, elevation of pancreatic enzymes, and hospitalization for at least two nights, was significantly higher in the placebo group compared with the indomethacin group (16.9% vs. 9.2%, P=0.005). Moderate or severe post-ERCP pancreatitis was significantly higher in the placebo group compared with the indomethacin group (8.8% vs. 4.4%, P=0.03).
There were no significant differences in the rates of clinically significant bleeding or acute renal failure between the two groups. The ability to generalize these findings to patients without risk factors for post-ERCP pancreatitis is not clear.
Bottom line: Rectal indomethacin decreases the rate of post-ERCP pancreatitis in patients who are at high risk for this complication.
Citation: Elmunzer BJ, Scheiman JM, Lehman GA, et al. A randomized trial of rectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med. 2012;366(15):1414-1422.
CHADS2-VASc and HAS-BLED Can Predict Thromboembolism and Bleeding Risk in Afib Patients
Clinical question: What are the risk factors for stroke/thromboembolism and bleeding from atrial fibrillation (afib), and how well do the CHADS2-VASc and HAS-BLED stroke and bleeding risk-assessment tools perform against other published stroke and bleeding risk-assessment tools (CHADS2 and HEMORR2HAGES) for patients with afib?
Background: In afib patients, the CHADS2-VASc tool might offer more comprehensive stroke assessment over the CHADS2 by identifying truly-low-risk patients with afib who might not even need antiplatelet therapy. HAS-BLED, a newer bleeding-risk-assessment tool, has been validated in previous trials and is more user-friendly than others. Use of CHADS2-VASc and HAS-BLED are recommended by the European Society of Cardiology to assess stroke and bleeding risks for patients with afib.
Study design: Prospective cohort study.
Setting: All hospitals in Sweden.
Synopsis: Investigators identified 182,678 afib patients via ICD-10 data from Sweden’s National Hospital Discharge Registry ICD-10 from 2005 to 2008. Approximately half the patients were not taking anticoagulants. Analysis assessed risk factors for stroke and bleeding and the performance of CHADS2-VASc and HAS-BLED against CHADS2 and HEMORR2HAGES stroke and bleeding risk-assessment tools.
Risk of composite thromboembolism (unspecified stroke, TIA, systemic embolism) was significantly higher in patients with increased age, peripheral arterial disease, prior myocardial infarction (MI), prior coronary artery bypass grafting (CABG), female gender, renal failure, and aspirin use, as well as hypertension, diabetes, prior thromboembolic event, or prior intracranial hemorrhage (ICH). Interestingly, a statistically increased risk was seen with aspirin use.
Conversely, history of heart failure, thyroid disease, and obesity were not associated with increased composite thromboembolic risk. The use of CHADS2-VASc was marginally better than CHADS2 in predicting stroke risk.
ICH risk was increased in patients with older age, prior ischemic stroke, prior ICH, and hypertension. Risk of composite bleeding (from ICH or other major bleeding) was significantly higher in patients with these risk factors, as well as renal failure, liver disease, anemia, dysfunctional platelets, alcohol use, and cancer. Ischemic heart disease was associated with a statistically significant lower risk of ICH, but not of composite bleeding risk.
HAS-BLED usage was as good as, and easier to use than, HEMORR2HAGES in predicting bleeding risk.
Bottom line: CHADS2-VASc might be better than CHADS2 in predicting truly-low-risk patients with nonvalvular afib; HAS-BLED is just as good as, and easier to use than, HEMORR2HAGES in predicting bleeding risk for patients with nonvalvular afib who are to receive antithrombotic therapy.
Citation: Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182,678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33(12):1500-10 [Epub 2012 Jan 13].
Supported Self-Management of COPD Does Not Decrease Readmission or Mortality Rates
Clinical question: Does supported self-management of patients with chronic obstructive pulmonary disease (COPD) decrease COPD-related hospital readmission or death?
Clinical background: Supported self-management has benefited patients with such chronic diseases as heart failure and asthma. Evidence to support such a strategy for patients with COPD is relatively lacking.
Study design: Randomized, controlled trial.
Setting: Community-based care following urban hospitalization in western Scotland.
Synopsis: From June 2007 to May 2009, and following hospitalization for COPD exacerbation, 464 patients were randomized to receive routine community-based care with or without 12 months of support and training to detect, and promptly treat, recurrent exacerbations. Independent of disease severity or demographics, investigators found no difference in combined readmission (48% vs. 47%, 95% confidence interval [CI] 0.80-1.38) or death (10% vs. 7%, 95% CI 0.71-2.61).
Based on review of appropriateness of self-management strategies used by the intervention group, unplanned exploratory subgroup analysis classified a minority of the intervention group as “successful” (42%) supported self-managers, and demonstrated decreased COPD readmissions and death (27% vs. 49%, 95% CI 0.25-0.76, P=0.003) vs. “unsuccessful” self-managers. This successful group was younger and tended to live with others. Further research to define characteristics of patients who benefit from self-management is needed.
Bottom line: Supported self-management of COPD does not reduce COPD-related readmission or death in a large population.
Citation: Bucknall CE, Miller G, Lloyd SM, et al. Glasgow supported self-management trial (GSuST) for patients with moderate to severe COPD: randomised controlled trial. BMJ. 2012;344:e1060 [Epub ahead of print].
Medicare Premier P4P Initiatives Do Not Decrease Mortality
Clinical question: Has the Medicare Premier Hospital Quality Incentive Demonstration (HQID) resulted in lower mortality?
Background: The Centers for Medicare & Medicaid Services’ (CMS) value-based purchasing program will expand to include 30-day mortality in 2013, but do pay-for-performance (P4P) initiatives result in improved mortality? Studies have demonstrated improvement in process of care but have not demonstrated mortality benefit thus far.
Study design: Cohort study.
Setting: Two hundred fifty-two hospitals participating in the Premier HQID compared with 3,363 control hospitals participating in the Hospital Compare program.
Synopsis: Researchers examined 30-day mortality for patients admitted with acute myocardial infarction, congestive heart failure, pneumonia, and for coronary artery bypass grafting (CABG) from 2003 to 2009. Results showed no difference in 30-day mortality rates over the six-year span of the program for any of the conditions studied in the Premier hospitals (participating in the voluntary pay-for-performance program) vs. non-Premier hospitals (11.82% vs. 11.74%). This held true for each condition measured individually, with a higher mortality rate for patients undergoing CABG at the Premier hospitals.
In addition, in the hospitals that underperformed initially, there was no difference with respect to rate of improvement when comparing Premier vs. non-Premier hospitals. Furthermore, mortality rate trends did not differ between those conditions that were incentivized (acute MI and CABG) compared with those that were not (congestive heart failure and pneumonia).
The authors concluded that there was “little evidence” that the Premier HQID pay-for-performance program resulted in reduced 30-day mortality.
Bottom line: Programs participating in the Medicare Premier HQID pay-for-performance program had similar 30-day mortality compared with nonparticipating programs.
Citation: Jha AK, Joynt KE, Orav EJ, Epstein AM. The long-term effect of premier pay for performance on patient outcomes. N Engl J Med. 2012;366:1606-1615.
In-Hospital Rate of DVT/PE After Hip and Knee Arthroplasty with Guideline-Recommended Prophylaxis
Clinical question: What is the rate of symptomatic DVT/PE after total or partial hip (TPHA) or knee (TPKA) arthroplasty using currently recommended prophylaxis?
Background: The rate of postoperative DVT/PE after TPHA/TPKA has dropped dramatically with use of pharmacologic prophylaxis. However, the current rate of symptomatic DVT/PE using current pharmacologic prophylaxis is not known. Such rates are needed for informed patient consent and development of patient safety benchmarks.
Study design: Systematic review.
Setting: Randomized clinical trials (RCTs) and observational studies worldwide of adult inpatients undergoing TPHA and/or TPKA from 1996 to 2011.
Synopsis: Forty-seven studies were included, of which 41 were RCTs and six were observational studies. Twenty-one studies evaluated rates after TPHA, 20 after TPKA, and six after both. More than 44,000 patients were included, with ages ranging from 58 to 74 years. The mean duration of prophylaxis was eight days, with a mean follow-up of 13 days.
In-hospital rates of symptomatic venous thromboembolism (VTE) were higher in patients undergoing TPKA than TPHA (1.09% vs. 0.53% for VTE, 0.63% vs. 0.26% for DVT, and 0.27% vs. 0.14% for PE). This is in contrast to the higher rates of VTE observed after TPHA when the post-discharge period is included. The pooled incidence of VTE was lower with use of direct inhibitors of Factors Xa or IIa when compared to low-molecular-weight heparin, although a direct efficacy comparison could not be made.
Because the majority of studies were RCTs with restrictive inclusion criteria, rates of DVT/PE in actual practice might be higher.
Bottom line: When informing patients of postoperative VTE risk, or establishing benchmarks to evaluate patient safety, one can anticipate an in-hospital VTE rate of 0.5% following TPHA and 1% following TPKA.
Citation: Januel JM, Chen G, Ruffieux C, et al. Symptomatic in-hospital deep vein thrombosis and pulmonary embolism following hip and knee arthroplasty among patients receiving recommended prophylaxis: a systematic review. JAMA. 2012;307(3):294-303.
Sodium Chloride Prevents Contrast-Induced Nephropathy
Clinical question: Is sodium chloride more effective than sodium bicarbonate for preventing contrast-induced nephropathy?
Background: Contrast-induced nephropathy can be prevented with precontrast hydration. Study authors sought to compare sodium chloride administered over 24 hours with sodium bicarbonate administered over seven hours, and with sodium bicarbonate administered orally.
Study design: Randomized, open-label, controlled trial.
Setting: Three European medical centers.
Synopsis: The study examined 258 patients with an estimated glomerular filtration rate <60mL/min/1.73m2 undergoing intravenous or intra-arterial contrast procedure. Patients with Class III or IV heart failure were excluded. The remaining patients were randomized to receive one of three regimens: sodium chloride at 1 ml/kg/hr for 12 hours prior to and 12 hours following the procedure; intravenous sodium bicarbonate for one hour prior to and six hours following the procedure; or intravenous and oral sodium bicarbonate 20 minutes prior to the procedure.
The group that received saline had a lower incidence of contrast-induced nephropathy than the bicarbonate groups (1% vs. 9% vs. 10%). The oral bicarbonate strategy was noninferior to the seven-hour intravenous bicarbonate strategy.
The authors postulated that saline should be used for high-risk patients, but that given the overall low incidence of contrast-induced nephropathy, the short-term bicarbonate strategy (intravenous followed by oral) is a viable alternative for low-risk patients.
Bottom line: Sodium chloride is more effective than sodium bicarbonate for preventing contrast-induced nephropathy, but in light of the low incidence, a short course of sodium bicarbonate is a possible convenient alternative for low-risk patients.
Citation: Klima T, Christ A, Marana I, et al. Sodium chloride vs. sodium bicarbonate for the prevention of contrast medium-induced nephropathy: a randomized controlled trial. Eur Heart J. 2012 Jan 19 [Epub ahead of print].
Collaboration Prevents Identification Band Errors

Clinical question: Can a quality-improvement (QI) collaborative decrease patient identification (ID) band errors?
Background: ID band errors often result in medication errors and unsafe care. Consequently, correct patient identification, through the use of at least two identifiers, has been an ongoing Joint Commission National Patient Safety Goal. Although individual sites have demonstrated improvement in accuracy of patient identification, there have not been reports of dissemination of successful practices.
Study design: Collaborative quality-improvement initiative.
Setting: Six hospitals.
Synopsis: ID band audits in 11,377 patients were performed in the learning collaborative’s six participating hospitals.
The audits were organized primarily around monthly conference calls. The hospital settings were diverse: community hospitals, hospitals within an academic medical center, and freestanding children’s hospitals. The aim of the collaborative was to reduce ID band errors by 50% within a one-year time frame across the collective sites.
Key interventions included transparent data collection and reporting; engagement of staff, families and leadership; voluntary event reporting; and auditing of failures. The mean combined ID band failure rate decreased to 4% from 22% within 13 months, representing a 77% relative reduction (P<0.001).
QI collaboratives are not designed to specifically result in generalizable knowledge, yet they might produce widespread improvement, as this effort demonstrates. The careful documentation of iterative factors implemented across sites in this initiative provides a blueprint for hospitals looking to replicate this success. Additionally, the interventions represent feasible and logical concepts within the basic constructs of improvement science methodology.
Bottom line: A QI collaborative might result in rapid and significant reductions in ID band errors.
Citation: Phillips SC, Saysana M, Worley S, Hain PD. Reduction in pediatric identification band errors: a quality collaborative. Pediatrics. 2012;129(6):e1587-e1593.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Can a quality-improvement (QI) collaborative decrease patient identification (ID) band errors?
Background: ID band errors often result in medication errors and unsafe care. Consequently, correct patient identification, through the use of at least two identifiers, has been an ongoing Joint Commission National Patient Safety Goal. Although individual sites have demonstrated improvement in accuracy of patient identification, there have not been reports of dissemination of successful practices.
Study design: Collaborative quality-improvement initiative.
Setting: Six hospitals.
Synopsis: ID band audits in 11,377 patients were performed in the learning collaborative’s six participating hospitals.
The audits were organized primarily around monthly conference calls. The hospital settings were diverse: community hospitals, hospitals within an academic medical center, and freestanding children’s hospitals. The aim of the collaborative was to reduce ID band errors by 50% within a one-year time frame across the collective sites.
Key interventions included transparent data collection and reporting; engagement of staff, families and leadership; voluntary event reporting; and auditing of failures. The mean combined ID band failure rate decreased to 4% from 22% within 13 months, representing a 77% relative reduction (P<0.001).
QI collaboratives are not designed to specifically result in generalizable knowledge, yet they might produce widespread improvement, as this effort demonstrates. The careful documentation of iterative factors implemented across sites in this initiative provides a blueprint for hospitals looking to replicate this success. Additionally, the interventions represent feasible and logical concepts within the basic constructs of improvement science methodology.
Bottom line: A QI collaborative might result in rapid and significant reductions in ID band errors.
Citation: Phillips SC, Saysana M, Worley S, Hain PD. Reduction in pediatric identification band errors: a quality collaborative. Pediatrics. 2012;129(6):e1587-e1593.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: Can a quality-improvement (QI) collaborative decrease patient identification (ID) band errors?
Background: ID band errors often result in medication errors and unsafe care. Consequently, correct patient identification, through the use of at least two identifiers, has been an ongoing Joint Commission National Patient Safety Goal. Although individual sites have demonstrated improvement in accuracy of patient identification, there have not been reports of dissemination of successful practices.
Study design: Collaborative quality-improvement initiative.
Setting: Six hospitals.
Synopsis: ID band audits in 11,377 patients were performed in the learning collaborative’s six participating hospitals.
The audits were organized primarily around monthly conference calls. The hospital settings were diverse: community hospitals, hospitals within an academic medical center, and freestanding children’s hospitals. The aim of the collaborative was to reduce ID band errors by 50% within a one-year time frame across the collective sites.
Key interventions included transparent data collection and reporting; engagement of staff, families and leadership; voluntary event reporting; and auditing of failures. The mean combined ID band failure rate decreased to 4% from 22% within 13 months, representing a 77% relative reduction (P<0.001).
QI collaboratives are not designed to specifically result in generalizable knowledge, yet they might produce widespread improvement, as this effort demonstrates. The careful documentation of iterative factors implemented across sites in this initiative provides a blueprint for hospitals looking to replicate this success. Additionally, the interventions represent feasible and logical concepts within the basic constructs of improvement science methodology.
Bottom line: A QI collaborative might result in rapid and significant reductions in ID band errors.
Citation: Phillips SC, Saysana M, Worley S, Hain PD. Reduction in pediatric identification band errors: a quality collaborative. Pediatrics. 2012;129(6):e1587-e1593.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
The Academic Hospitalist Academy Helps Researchers Get Ahead
What’s the best way to get your research noticed—and make time for more research? How can academic hospitalists get involved in patient safety and quality-improvement (QI) work? For three years, the Academic Hospitalist Academy has helped hospitalist researchers answer these and other questions they face as they develop their careers.
Now in its fourth year, the popular three-and-a-half-day course—presented by the Society of General Internal Medicine, the Association of Chiefs and Leaders of General Internal Medicine, and SHM—focuses on the unique environment, challenges, and opportunities for academic hospitalists, led by national authorities in academic hospital medicine.
Based on evaluations from the 2011 Academic Hospitalist Academy, 100% of attendees rated the meeting positively and felt the course was worth their time and money; 99% said they would recommend attending to their academic hospitalist colleagues. Check out www.academichospitalist.org testimonials to read what past attendees had to say about the academy.
What’s the best way to get your research noticed—and make time for more research? How can academic hospitalists get involved in patient safety and quality-improvement (QI) work? For three years, the Academic Hospitalist Academy has helped hospitalist researchers answer these and other questions they face as they develop their careers.
Now in its fourth year, the popular three-and-a-half-day course—presented by the Society of General Internal Medicine, the Association of Chiefs and Leaders of General Internal Medicine, and SHM—focuses on the unique environment, challenges, and opportunities for academic hospitalists, led by national authorities in academic hospital medicine.
Based on evaluations from the 2011 Academic Hospitalist Academy, 100% of attendees rated the meeting positively and felt the course was worth their time and money; 99% said they would recommend attending to their academic hospitalist colleagues. Check out www.academichospitalist.org testimonials to read what past attendees had to say about the academy.
What’s the best way to get your research noticed—and make time for more research? How can academic hospitalists get involved in patient safety and quality-improvement (QI) work? For three years, the Academic Hospitalist Academy has helped hospitalist researchers answer these and other questions they face as they develop their careers.
Now in its fourth year, the popular three-and-a-half-day course—presented by the Society of General Internal Medicine, the Association of Chiefs and Leaders of General Internal Medicine, and SHM—focuses on the unique environment, challenges, and opportunities for academic hospitalists, led by national authorities in academic hospital medicine.
Based on evaluations from the 2011 Academic Hospitalist Academy, 100% of attendees rated the meeting positively and felt the course was worth their time and money; 99% said they would recommend attending to their academic hospitalist colleagues. Check out www.academichospitalist.org testimonials to read what past attendees had to say about the academy.
Ready to Reduce Your Hospital's Readmissions?
More than 100 hospitals across the country have used Project BOOST to reduce readmissions and improve their discharge processes. You and your hospital can be next by applying for Project BOOST. The deadline for the next national cohort of Project BOOST is Sept. 1.
To improve your chances of acceptance, start soon. In addition to an online form, the application requires a letter of support from an executive sponsor from each institution.
In October, accepted Project BOOST sites will receive:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best available evidence;
- A comprehensive implementation guide that provides step-by-step instructions and project management tools, such as the “teachback” training curriculum, to help interdisciplinary teams redesign work flow and plan, implement, and evaluate the intervention;
- Longitudinal technical assistance that provides face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a “train-the-trainer” DVD and curriculum for nurses and case managers on using the teachback process, and webinars targeting the educational needs of other team members, including administrators, data analysts, physicians, nurses; and others;
- A collaboration that allows sites to communicate with and learn from each other via the BOOST listserv, BOOST community site, and quarterly all-site teleconferences and webinars; and
- Access to the BOOST data center, an online resource center that allows sites to store and benchmark data against control units and other sites and generate reports.
To start the application process, visit www.hospitalmedicine.org/boost.
Brendon Shank is SHM’s associate vice president for communications.
More than 100 hospitals across the country have used Project BOOST to reduce readmissions and improve their discharge processes. You and your hospital can be next by applying for Project BOOST. The deadline for the next national cohort of Project BOOST is Sept. 1.
To improve your chances of acceptance, start soon. In addition to an online form, the application requires a letter of support from an executive sponsor from each institution.
In October, accepted Project BOOST sites will receive:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best available evidence;
- A comprehensive implementation guide that provides step-by-step instructions and project management tools, such as the “teachback” training curriculum, to help interdisciplinary teams redesign work flow and plan, implement, and evaluate the intervention;
- Longitudinal technical assistance that provides face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a “train-the-trainer” DVD and curriculum for nurses and case managers on using the teachback process, and webinars targeting the educational needs of other team members, including administrators, data analysts, physicians, nurses; and others;
- A collaboration that allows sites to communicate with and learn from each other via the BOOST listserv, BOOST community site, and quarterly all-site teleconferences and webinars; and
- Access to the BOOST data center, an online resource center that allows sites to store and benchmark data against control units and other sites and generate reports.
To start the application process, visit www.hospitalmedicine.org/boost.
Brendon Shank is SHM’s associate vice president for communications.
More than 100 hospitals across the country have used Project BOOST to reduce readmissions and improve their discharge processes. You and your hospital can be next by applying for Project BOOST. The deadline for the next national cohort of Project BOOST is Sept. 1.
To improve your chances of acceptance, start soon. In addition to an online form, the application requires a letter of support from an executive sponsor from each institution.
In October, accepted Project BOOST sites will receive:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best available evidence;
- A comprehensive implementation guide that provides step-by-step instructions and project management tools, such as the “teachback” training curriculum, to help interdisciplinary teams redesign work flow and plan, implement, and evaluate the intervention;
- Longitudinal technical assistance that provides face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a “train-the-trainer” DVD and curriculum for nurses and case managers on using the teachback process, and webinars targeting the educational needs of other team members, including administrators, data analysts, physicians, nurses; and others;
- A collaboration that allows sites to communicate with and learn from each other via the BOOST listserv, BOOST community site, and quarterly all-site teleconferences and webinars; and
- Access to the BOOST data center, an online resource center that allows sites to store and benchmark data against control units and other sites and generate reports.
To start the application process, visit www.hospitalmedicine.org/boost.
Brendon Shank is SHM’s associate vice president for communications.
Adult Hospital Medicine Boot Camp Offers PAs, NPs Advanced Training
The Adult Hospital Medicine Boot Camp is a great way for physician assistants (PAs) and nurse practitioners (NPs) who practice as hospitalists to stay up to date on the latest in HM practice, and is the perfect opportunity to introduce new caregivers to the hospital setting.
Hosted by the American Academy of Physician Assistants (AAPA) and SHM, Adult Hospital Medicine Boot Camp will be Oct. 17-21 at the JW Marriott in New Orleans. Registration is available at www.aapa.org/bootcamp.
The specialized, education-focused “boot camp” immerses clinicians who are already practicing in HM, or who are interested in it, an intensive internal-medicine review of commonly encountered diagnoses and diseases in hospitalized adult patients. The boot camp has been approved for a maximum of 29.5 AAPA Category I CME credits.
The Adult Hospital Medicine Boot Camp is a great way for physician assistants (PAs) and nurse practitioners (NPs) who practice as hospitalists to stay up to date on the latest in HM practice, and is the perfect opportunity to introduce new caregivers to the hospital setting.
Hosted by the American Academy of Physician Assistants (AAPA) and SHM, Adult Hospital Medicine Boot Camp will be Oct. 17-21 at the JW Marriott in New Orleans. Registration is available at www.aapa.org/bootcamp.
The specialized, education-focused “boot camp” immerses clinicians who are already practicing in HM, or who are interested in it, an intensive internal-medicine review of commonly encountered diagnoses and diseases in hospitalized adult patients. The boot camp has been approved for a maximum of 29.5 AAPA Category I CME credits.
The Adult Hospital Medicine Boot Camp is a great way for physician assistants (PAs) and nurse practitioners (NPs) who practice as hospitalists to stay up to date on the latest in HM practice, and is the perfect opportunity to introduce new caregivers to the hospital setting.
Hosted by the American Academy of Physician Assistants (AAPA) and SHM, Adult Hospital Medicine Boot Camp will be Oct. 17-21 at the JW Marriott in New Orleans. Registration is available at www.aapa.org/bootcamp.
The specialized, education-focused “boot camp” immerses clinicians who are already practicing in HM, or who are interested in it, an intensive internal-medicine review of commonly encountered diagnoses and diseases in hospitalized adult patients. The boot camp has been approved for a maximum of 29.5 AAPA Category I CME credits.
Recoding: SHM’s Popular Coding Series Returns
Coding is a challenging fact of life for most hospitalists, which explains the popularity of SHM’s educational resources for helping hospitalists stay on top of best practices in coding. Due to demand from hospitalists and hospital administrators who missed the first CODE-H series, SHM will present the series again.
CODE-H, which is eligible for CME or CEU credits, gathers the country’s foremost experts in hospital coding to help HM groups capture revenue and maintain compliance through six online courses:
- Basics of E&M Coding for Hospitalists, Part 1;
- Basics of E&M Coding for Hospitalists, Part 2;
- Coding for Hospitalists’ Expanding Scope of Services;
- Staying out of Trouble;
- Integrating Physician Billing & Hospital DRG Assurance; and
- Optimizing Performance and Compliance.
In addition to being presented in a highly interactive online community, each CODE-H series subscription enables as many as 10 individuals in an HM group to participate. Course materials include extensive reference
materials, pre-tests, and post-tests. For details and registration, visit www.hospitalmedicine.org/codeh.
Coding is a challenging fact of life for most hospitalists, which explains the popularity of SHM’s educational resources for helping hospitalists stay on top of best practices in coding. Due to demand from hospitalists and hospital administrators who missed the first CODE-H series, SHM will present the series again.
CODE-H, which is eligible for CME or CEU credits, gathers the country’s foremost experts in hospital coding to help HM groups capture revenue and maintain compliance through six online courses:
- Basics of E&M Coding for Hospitalists, Part 1;
- Basics of E&M Coding for Hospitalists, Part 2;
- Coding for Hospitalists’ Expanding Scope of Services;
- Staying out of Trouble;
- Integrating Physician Billing & Hospital DRG Assurance; and
- Optimizing Performance and Compliance.
In addition to being presented in a highly interactive online community, each CODE-H series subscription enables as many as 10 individuals in an HM group to participate. Course materials include extensive reference
materials, pre-tests, and post-tests. For details and registration, visit www.hospitalmedicine.org/codeh.
Coding is a challenging fact of life for most hospitalists, which explains the popularity of SHM’s educational resources for helping hospitalists stay on top of best practices in coding. Due to demand from hospitalists and hospital administrators who missed the first CODE-H series, SHM will present the series again.
CODE-H, which is eligible for CME or CEU credits, gathers the country’s foremost experts in hospital coding to help HM groups capture revenue and maintain compliance through six online courses:
- Basics of E&M Coding for Hospitalists, Part 1;
- Basics of E&M Coding for Hospitalists, Part 2;
- Coding for Hospitalists’ Expanding Scope of Services;
- Staying out of Trouble;
- Integrating Physician Billing & Hospital DRG Assurance; and
- Optimizing Performance and Compliance.
In addition to being presented in a highly interactive online community, each CODE-H series subscription enables as many as 10 individuals in an HM group to participate. Course materials include extensive reference
materials, pre-tests, and post-tests. For details and registration, visit www.hospitalmedicine.org/codeh.
Survey Insights: Better Understand CPT Coding Intensity
Many of the practice-management-related questions we field from members here at SHM are about documentation and coding issues; members are looking for ways to benchmark their group’s coding performance against other similar groups. One helpful metric reported in the SHM/MGMA State of Hospital Medicine report is the ratio of work-RVUs to total encounters, which I refer to as “coding intensity.”
Median coding intensity for adult medicine hospitalists in the 2011 report was 1.90, up slightly from 2010 levels.
The most obvious factor that influences coding intensity is the distribution of CPT codes within specific evaluation and management code sets, such as inpatient admissions (99221-99223) or follow-up visits (99231-99233). Other considerations include the degree to which hospitalists provide high-wRVU services, such as critical care or procedures, the ratio of inpatient vs. observation patients, and the group’s average length of stay.
One interesting finding was that coding intensity varies greatly by geographic region (see Figure 1, right).
What’s going on out there in the Western states? Are those folks receiving different training than the rest of us? Or are they just mavericks, more interested in generating professional fee revenues than hospitalists elsewhere are? It’s hard to say. One big factor is that length of stay (LOS) tends to be shorter in the West than in other parts of the country. That means the typical Western hospitalist will have a larger proportion of high-wRVU value admission and discharge codes relative to their proportion of low-wRVU value subsequent visit codes.

This isn’t the whole story, though. Hospitalists in the West actually did report a significantly more aggressive code distribution for all three CPT code sets for which data were collected (inpatient admissions, subsequent visits, and discharges). And hospitalists in the South, where LOS tends to be longer, also reported the least aggressive code distributions.
Unfortunately, we don’t have a lot of clues as to why these differences exist. We don’t know, for example, whether more hospitalists in the West work in the ICU or perform more procedures compared to other parts of the country. One possibility suggested by report data is that hospitalists in Western states have the highest average proportion of their total compensation allocated to productivity incentives. Hospitalists in the East have the lowest proportion of their compensation based on productivity. So productivity-based compensation might cause hospitalists to care a lot more about doing a good job with documentation and CPT coding.
Other interesting findings include the fact that hospitalists employed by multistate hospitalist-management companies had the lowest median coding intensity, while hospitalists employed by private hospitalist-only groups had the highest coding intensity. And, perhaps not surprisingly, the small proportion of practices that did not receive any financial support had a higher average coding intensity than practices receiving financial support.
While there are no clear answers about variations in CPT coding intensity among hospitalist practices, the State of Hospital Medicine report does offer some intriguing pointers, along with a variety of useful benchmarks about hospitalist CPT coding practices. And stay tuned: The new report, due out in August, will offer even more ways of looking at coding intensity and CPT code distribution.
Leslie Flores, SHM senior advisor
Many of the practice-management-related questions we field from members here at SHM are about documentation and coding issues; members are looking for ways to benchmark their group’s coding performance against other similar groups. One helpful metric reported in the SHM/MGMA State of Hospital Medicine report is the ratio of work-RVUs to total encounters, which I refer to as “coding intensity.”
Median coding intensity for adult medicine hospitalists in the 2011 report was 1.90, up slightly from 2010 levels.
The most obvious factor that influences coding intensity is the distribution of CPT codes within specific evaluation and management code sets, such as inpatient admissions (99221-99223) or follow-up visits (99231-99233). Other considerations include the degree to which hospitalists provide high-wRVU services, such as critical care or procedures, the ratio of inpatient vs. observation patients, and the group’s average length of stay.
One interesting finding was that coding intensity varies greatly by geographic region (see Figure 1, right).
What’s going on out there in the Western states? Are those folks receiving different training than the rest of us? Or are they just mavericks, more interested in generating professional fee revenues than hospitalists elsewhere are? It’s hard to say. One big factor is that length of stay (LOS) tends to be shorter in the West than in other parts of the country. That means the typical Western hospitalist will have a larger proportion of high-wRVU value admission and discharge codes relative to their proportion of low-wRVU value subsequent visit codes.
This isn’t the whole story, though. Hospitalists in the West actually did report a significantly more aggressive code distribution for all three CPT code sets for which data were collected (inpatient admissions, subsequent visits, and discharges). And hospitalists in the South, where LOS tends to be longer, also reported the least aggressive code distributions.
Unfortunately, we don’t have a lot of clues as to why these differences exist. We don’t know, for example, whether more hospitalists in the West work in the ICU or perform more procedures compared to other parts of the country. One possibility suggested by report data is that hospitalists in Western states have the highest average proportion of their total compensation allocated to productivity incentives. Hospitalists in the East have the lowest proportion of their compensation based on productivity. So productivity-based compensation might cause hospitalists to care a lot more about doing a good job with documentation and CPT coding.
Other interesting findings include the fact that hospitalists employed by multistate hospitalist-management companies had the lowest median coding intensity, while hospitalists employed by private hospitalist-only groups had the highest coding intensity. And, perhaps not surprisingly, the small proportion of practices that did not receive any financial support had a higher average coding intensity than practices receiving financial support.
While there are no clear answers about variations in CPT coding intensity among hospitalist practices, the State of Hospital Medicine report does offer some intriguing pointers, along with a variety of useful benchmarks about hospitalist CPT coding practices. And stay tuned: The new report, due out in August, will offer even more ways of looking at coding intensity and CPT code distribution.
Leslie Flores, SHM senior advisor
Many of the practice-management-related questions we field from members here at SHM are about documentation and coding issues; members are looking for ways to benchmark their group’s coding performance against other similar groups. One helpful metric reported in the SHM/MGMA State of Hospital Medicine report is the ratio of work-RVUs to total encounters, which I refer to as “coding intensity.”
Median coding intensity for adult medicine hospitalists in the 2011 report was 1.90, up slightly from 2010 levels.
The most obvious factor that influences coding intensity is the distribution of CPT codes within specific evaluation and management code sets, such as inpatient admissions (99221-99223) or follow-up visits (99231-99233). Other considerations include the degree to which hospitalists provide high-wRVU services, such as critical care or procedures, the ratio of inpatient vs. observation patients, and the group’s average length of stay.
One interesting finding was that coding intensity varies greatly by geographic region (see Figure 1, right).
What’s going on out there in the Western states? Are those folks receiving different training than the rest of us? Or are they just mavericks, more interested in generating professional fee revenues than hospitalists elsewhere are? It’s hard to say. One big factor is that length of stay (LOS) tends to be shorter in the West than in other parts of the country. That means the typical Western hospitalist will have a larger proportion of high-wRVU value admission and discharge codes relative to their proportion of low-wRVU value subsequent visit codes.
This isn’t the whole story, though. Hospitalists in the West actually did report a significantly more aggressive code distribution for all three CPT code sets for which data were collected (inpatient admissions, subsequent visits, and discharges). And hospitalists in the South, where LOS tends to be longer, also reported the least aggressive code distributions.
Unfortunately, we don’t have a lot of clues as to why these differences exist. We don’t know, for example, whether more hospitalists in the West work in the ICU or perform more procedures compared to other parts of the country. One possibility suggested by report data is that hospitalists in Western states have the highest average proportion of their total compensation allocated to productivity incentives. Hospitalists in the East have the lowest proportion of their compensation based on productivity. So productivity-based compensation might cause hospitalists to care a lot more about doing a good job with documentation and CPT coding.
Other interesting findings include the fact that hospitalists employed by multistate hospitalist-management companies had the lowest median coding intensity, while hospitalists employed by private hospitalist-only groups had the highest coding intensity. And, perhaps not surprisingly, the small proportion of practices that did not receive any financial support had a higher average coding intensity than practices receiving financial support.
While there are no clear answers about variations in CPT coding intensity among hospitalist practices, the State of Hospital Medicine report does offer some intriguing pointers, along with a variety of useful benchmarks about hospitalist CPT coding practices. And stay tuned: The new report, due out in August, will offer even more ways of looking at coding intensity and CPT code distribution.
Leslie Flores, SHM senior advisor
Hospitalists On the Move

Casa Grande Regional Medical Center in Arizona named hospitalist Ammar Saifo, MD, its Physician of the Year. The medical center’s nursing staff praised Dr. Saifo “for his leadership, compassion, dedication, and for ‘going the extra mile’” in caring for his patients.
Bob Adams, MD, former chief hospitalist at MedWest-Harris in North Carolina, has accepted a position at Angel Medical Center in Franklin, N.C. A veteran hospitalist, he began his new position July 1.

Syed Irfan Ali, MD, a hospitalist at MaineGeneral Medical Center’s Thayer Unit in Waterville, received the 2011 NASF Humanitarian of the Year award from the Nasreen & Alam Sher Foundation. Dr. Ali earned the honor after spending several days in Pakistan providing free care to patients at Aisha Bibi Memorial Hospital (see “Hospitalist Honored for Humanitarian Work in Pakistan,” the-hospitalist.org).

J.D. Fitz, MD, FACP, has joined Sound Physicians as senior vice president of physician development. Dr. Fitz comes from MultiCare Good Samaritan Hospital, where he worked as vice president of medical affairs for five years. In his new position, Dr. Fitz will direct professional development for Sound’s more than 500 physicians.

St. Luke’s The Woodlands Hospital in The Woodlands, Texas, recently awarded Seshasree Marupudi, MD, its 2012 Physician of the Year plaque. Dr. Marupudi is a hospitalist who has been at The Woodlands Hospital since 2008. According to her colleagues, she takes an active role in patient care, as well as in communication between staff, patients, and their families.
William Lamm, MD, was named Physician of the Year by the Western Maryland Health System (WMHS) at its annual recognition gala. Dr. Lamm joined the HM program at WMHS in 2004, and he serves as a clinical instructor at the University of Maryland Medical Center’s Department of Family Medicine, where he spent his residency.

Hospital executive Greg Ohe was recently appointed president of Health Central Hospital in Orlando, Fla. Ohe had served as senior vice president of the hospital since 2004, during which time he spearheaded several of the hospital’s successful programs, including its hospitalist program.

Blal Zafar, MD, hospitalist at River Park Hospital in McMinnville, Tenn., recently was awarded the 2012 Lathem Physician Leadership Award in Hand Hygiene. The award, sponsored by Proventix Systems Inc. of Birmingham, Ala., recognizes physicians who lead by example in their dedication to excellent hand hygiene.
Casa Grande Regional Medical Center in Arizona named hospitalist Ammar Saifo, MD, its Physician of the Year. The medical center’s nursing staff praised Dr. Saifo “for his leadership, compassion, dedication, and for ‘going the extra mile’” in caring for his patients.
Bob Adams, MD, former chief hospitalist at MedWest-Harris in North Carolina, has accepted a position at Angel Medical Center in Franklin, N.C. A veteran hospitalist, he began his new position July 1.
Syed Irfan Ali, MD, a hospitalist at MaineGeneral Medical Center’s Thayer Unit in Waterville, received the 2011 NASF Humanitarian of the Year award from the Nasreen & Alam Sher Foundation. Dr. Ali earned the honor after spending several days in Pakistan providing free care to patients at Aisha Bibi Memorial Hospital (see “Hospitalist Honored for Humanitarian Work in Pakistan,” the-hospitalist.org).
J.D. Fitz, MD, FACP, has joined Sound Physicians as senior vice president of physician development. Dr. Fitz comes from MultiCare Good Samaritan Hospital, where he worked as vice president of medical affairs for five years. In his new position, Dr. Fitz will direct professional development for Sound’s more than 500 physicians.
St. Luke’s The Woodlands Hospital in The Woodlands, Texas, recently awarded Seshasree Marupudi, MD, its 2012 Physician of the Year plaque. Dr. Marupudi is a hospitalist who has been at The Woodlands Hospital since 2008. According to her colleagues, she takes an active role in patient care, as well as in communication between staff, patients, and their families.
William Lamm, MD, was named Physician of the Year by the Western Maryland Health System (WMHS) at its annual recognition gala. Dr. Lamm joined the HM program at WMHS in 2004, and he serves as a clinical instructor at the University of Maryland Medical Center’s Department of Family Medicine, where he spent his residency.
Hospital executive Greg Ohe was recently appointed president of Health Central Hospital in Orlando, Fla. Ohe had served as senior vice president of the hospital since 2004, during which time he spearheaded several of the hospital’s successful programs, including its hospitalist program.
Blal Zafar, MD, hospitalist at River Park Hospital in McMinnville, Tenn., recently was awarded the 2012 Lathem Physician Leadership Award in Hand Hygiene. The award, sponsored by Proventix Systems Inc. of Birmingham, Ala., recognizes physicians who lead by example in their dedication to excellent hand hygiene.
Casa Grande Regional Medical Center in Arizona named hospitalist Ammar Saifo, MD, its Physician of the Year. The medical center’s nursing staff praised Dr. Saifo “for his leadership, compassion, dedication, and for ‘going the extra mile’” in caring for his patients.
Bob Adams, MD, former chief hospitalist at MedWest-Harris in North Carolina, has accepted a position at Angel Medical Center in Franklin, N.C. A veteran hospitalist, he began his new position July 1.
Syed Irfan Ali, MD, a hospitalist at MaineGeneral Medical Center’s Thayer Unit in Waterville, received the 2011 NASF Humanitarian of the Year award from the Nasreen & Alam Sher Foundation. Dr. Ali earned the honor after spending several days in Pakistan providing free care to patients at Aisha Bibi Memorial Hospital (see “Hospitalist Honored for Humanitarian Work in Pakistan,” the-hospitalist.org).
J.D. Fitz, MD, FACP, has joined Sound Physicians as senior vice president of physician development. Dr. Fitz comes from MultiCare Good Samaritan Hospital, where he worked as vice president of medical affairs for five years. In his new position, Dr. Fitz will direct professional development for Sound’s more than 500 physicians.
St. Luke’s The Woodlands Hospital in The Woodlands, Texas, recently awarded Seshasree Marupudi, MD, its 2012 Physician of the Year plaque. Dr. Marupudi is a hospitalist who has been at The Woodlands Hospital since 2008. According to her colleagues, she takes an active role in patient care, as well as in communication between staff, patients, and their families.
William Lamm, MD, was named Physician of the Year by the Western Maryland Health System (WMHS) at its annual recognition gala. Dr. Lamm joined the HM program at WMHS in 2004, and he serves as a clinical instructor at the University of Maryland Medical Center’s Department of Family Medicine, where he spent his residency.
Hospital executive Greg Ohe was recently appointed president of Health Central Hospital in Orlando, Fla. Ohe had served as senior vice president of the hospital since 2004, during which time he spearheaded several of the hospital’s successful programs, including its hospitalist program.
Blal Zafar, MD, hospitalist at River Park Hospital in McMinnville, Tenn., recently was awarded the 2012 Lathem Physician Leadership Award in Hand Hygiene. The award, sponsored by Proventix Systems Inc. of Birmingham, Ala., recognizes physicians who lead by example in their dedication to excellent hand hygiene.
Established Performance Metrics Help CMS Expand Its Value-Based Purchasing Program

—Thomas B. Valuck, MD, JD, senior vice president of strategic partnerships, National Quality Forum, former CMS adviser
No longer content to be a passive purchaser of healthcare services, the Centers for Medicare & Medicaid Services (CMS) is becoming a savvier shopper, holding providers increasingly accountable for the quality and efficiency of the care they deliver. With its value-based purchasing (VPB) program for hospitals already in place, now it’s the physicians’ turn.
CMS is marching toward a value-based payment modifier program that will adjust physician reimbursement based on the relative quality and efficiency of care that physicians provide to Medicare fee-for-service patients. The program will begin January 2015 and will extend to all physicians in 2017. Like the hospital VBP program, it will be budget-neutral—meaning that payment will increase for some physicians but decrease for others.
The coming months mark a pivotal period for physicians as CMS tweaks its accountability apparatus in ways that will determine how reimbursement will rise and fall, for whom, and for what.
Menu of Metrics
In crafting the payment modifier program, CMS can tap performance metrics from several of its existing programs, including the Physician Quality Reporting System (PQRS), the soon-to-be-expanded Physician Compare website (www.medicare.gov/find-a-doctor/provider-search.aspx), and the Physician Feedback Program.
“These agendas are part of a continuum, and of equal importance, in the evolution toward physician value-based purchasing,” says Patrick J. Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee, and director of hospital medicine at St. Tammany Parish Hospital in Covington, La.
PQRS began as a voluntary “pay for reporting” system that gave physicians a modest financial bonus (currently 0.5% of allowable Medicare charges) for submitting quality data (left). The Affordable Care Act (ACA) has since authorized CMS to penalize physicians who do not participate—1.5% of allowable Medicare charges beginning in 2015, and 2% in 2016.
The Physician Compare website, launched at the end of 2010, currently contains such rudimentary information as education, gender, and whether a physician is enrolled in Medicare and satisfactorily reports data to the PQRS. But as of January, the site will begin reporting some PQRS data, as well as other metrics.
CMS’ Physician Feedback Program provides quality and cost information to physicians in an effort to encourage them to improve the care they provide and its efficiency. CMS recently combined the program with its value-based payment modifier program as it moves toward physician reimbursement that it says will reward “value rather than volume.” The program, currently being piloted in Iowa, Nebraska, Kansas, and Missouri, issues to physicians confidential quality and resource use reports (QRURs) that compare their performance to peer groups in similar specialties by tracking PQRS results, Healthcare Effectiveness Data and Information Set (HEDIS) measures, and per-capita cost data and preventable hospital admission rates for various medical conditions. CMS will roll out the program nationwide next year.
Metrics Lack Relevance
Developing performance measures that capture the most relevant activities of physicians across many different specialties with equal validity is notoriously difficult—something that CMS acknowledges.1
Assigning the right patient to the right physician (i.e. figuring out who contributed what care, in what proportion, to which patient) also is fraught with complications, especially in the inpatient care setting, where a patient is likely to see many different physicians during a hospitalization.
SHM president Shaun Frost, MD, SFHM, highlighted these challenges in a letter sent in May to acting CMS administrator Marilyn B. Tavenner in which he pointed to dramatic data deficiencies in the initial round of QRURs sent to Physician Feedback Program participants that included hospitalists in Iowa, Nebraska, Kansas and Missouri. Because hospitalists were categorized as general internal-medicine physicians in the reports, their per-capita cost of care was dramatically higher (73% higher, in one case study) than the average cost of all internal-medicine physicians. No allowance was made for distinguishing the outpatient-oriented practice of a general internist from the inherently more expensive inpatient-focused hospitalist practice.
In the case study reviewed by SHM, the hospitalist’s patients saw, on average, 28 different physicians over the course of a year, during which the hospitalist contributed to the care of many patients but did not direct the care of any one of them—facts that clearly highlight the difficulty of assigning responsibility and accountability for a patient’s care when comparing physician performance.
“Based on the measurement used in the QRUR, it seems likely that a hospitalist would be severely disadvantaged with the introduction of a value-based modifier based on the present QRUR methodology,” Dr. Frost wrote.
SHM is similarly critical of the PQRS measures, which Dr. Torcson says lack relevance to hospitalist practices. “We want to be defined as HM physicians with our own unique measures of quality and cost,” he says. “Our results will look very different from those of an internist with a primarily outpatient practice.”
Dr. Torcson notes that SHM is an active participant in providing feedback during CMS rule proposals and has offered to work with the CMS on further refining the measures. For example, SHM proposed adding additional measures related to care transitions, given their particular relevance to hospitalist practices.
Rule-Changing Reform
The disruptive innovation of CMS’ healthcare reform agenda might wind up being a game-changer that dramatically affects the contours of all provider performance reporting and incentive systems, redefining the issues of physician accountability and patient assignment.
“We’re going to need to figure out how to restructure our measurement systems to match our evolving healthcare delivery and payment systems,” says Thomas B. Valuck, MD, JD, senior vice president of strategic partnerships for the National Quality Forum and former CMS adviser to the VBP program. Healthcare quality reporting should focus more on measures that cut across care contexts and assess whether the care provided truly made a difference for patients—metrics such as health improvement, return to functional status, level of patient involvement in the management of their care, provider team coordination, and other patient needs and preferences, Dr. Valuck believes.
“We need to be focused more on measures that encourage joint responsibility and cooperation among providers, and are important to patients across hospital, post-acute, and ambulatory settings, rather than those that are compartmentalized to one setting or relevant only to specific diseases or subspecialties,” Dr. Valuck says.
Such measure sets, while still retaining some disease- and physician-specific metrics, ideally would be complementary with families of related measures at the community, state, and national levels, Dr. Valuck says. “Such a multidimensional framework can begin to tell a meaningful story about what’s happening to the patient, and how well our system is delivering the right care,” he adds.
Dr. Torcson says HM has a pioneering role to play in this evolution, and he notes that SHM has proposed that CMS harmonize measures that align hospital-based physician activities (e.g. hospital medicine, emergency medicine, anesthesia, radiology) with hospital-level performance agendas so that physicians practicing together in the hospital setting can report on measures that are relevant to both.
Christopher Guadagnino is a freelance medical writer in Philadelphia.
Reference
- Centers for Medicare & Medicaid Services. Physician Quality Reporting System Town Hall Meeting. Available at: http://www.usqualitymeasures.org/shared/content/C4M_PQRS_transcript.pdf. Accessed July 3, 2012.
—Thomas B. Valuck, MD, JD, senior vice president of strategic partnerships, National Quality Forum, former CMS adviser
No longer content to be a passive purchaser of healthcare services, the Centers for Medicare & Medicaid Services (CMS) is becoming a savvier shopper, holding providers increasingly accountable for the quality and efficiency of the care they deliver. With its value-based purchasing (VPB) program for hospitals already in place, now it’s the physicians’ turn.
CMS is marching toward a value-based payment modifier program that will adjust physician reimbursement based on the relative quality and efficiency of care that physicians provide to Medicare fee-for-service patients. The program will begin January 2015 and will extend to all physicians in 2017. Like the hospital VBP program, it will be budget-neutral—meaning that payment will increase for some physicians but decrease for others.
The coming months mark a pivotal period for physicians as CMS tweaks its accountability apparatus in ways that will determine how reimbursement will rise and fall, for whom, and for what.
Menu of Metrics
In crafting the payment modifier program, CMS can tap performance metrics from several of its existing programs, including the Physician Quality Reporting System (PQRS), the soon-to-be-expanded Physician Compare website (www.medicare.gov/find-a-doctor/provider-search.aspx), and the Physician Feedback Program.
“These agendas are part of a continuum, and of equal importance, in the evolution toward physician value-based purchasing,” says Patrick J. Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee, and director of hospital medicine at St. Tammany Parish Hospital in Covington, La.
PQRS began as a voluntary “pay for reporting” system that gave physicians a modest financial bonus (currently 0.5% of allowable Medicare charges) for submitting quality data (left). The Affordable Care Act (ACA) has since authorized CMS to penalize physicians who do not participate—1.5% of allowable Medicare charges beginning in 2015, and 2% in 2016.
The Physician Compare website, launched at the end of 2010, currently contains such rudimentary information as education, gender, and whether a physician is enrolled in Medicare and satisfactorily reports data to the PQRS. But as of January, the site will begin reporting some PQRS data, as well as other metrics.
CMS’ Physician Feedback Program provides quality and cost information to physicians in an effort to encourage them to improve the care they provide and its efficiency. CMS recently combined the program with its value-based payment modifier program as it moves toward physician reimbursement that it says will reward “value rather than volume.” The program, currently being piloted in Iowa, Nebraska, Kansas, and Missouri, issues to physicians confidential quality and resource use reports (QRURs) that compare their performance to peer groups in similar specialties by tracking PQRS results, Healthcare Effectiveness Data and Information Set (HEDIS) measures, and per-capita cost data and preventable hospital admission rates for various medical conditions. CMS will roll out the program nationwide next year.
Metrics Lack Relevance
Developing performance measures that capture the most relevant activities of physicians across many different specialties with equal validity is notoriously difficult—something that CMS acknowledges.1
Assigning the right patient to the right physician (i.e. figuring out who contributed what care, in what proportion, to which patient) also is fraught with complications, especially in the inpatient care setting, where a patient is likely to see many different physicians during a hospitalization.
SHM president Shaun Frost, MD, SFHM, highlighted these challenges in a letter sent in May to acting CMS administrator Marilyn B. Tavenner in which he pointed to dramatic data deficiencies in the initial round of QRURs sent to Physician Feedback Program participants that included hospitalists in Iowa, Nebraska, Kansas and Missouri. Because hospitalists were categorized as general internal-medicine physicians in the reports, their per-capita cost of care was dramatically higher (73% higher, in one case study) than the average cost of all internal-medicine physicians. No allowance was made for distinguishing the outpatient-oriented practice of a general internist from the inherently more expensive inpatient-focused hospitalist practice.
In the case study reviewed by SHM, the hospitalist’s patients saw, on average, 28 different physicians over the course of a year, during which the hospitalist contributed to the care of many patients but did not direct the care of any one of them—facts that clearly highlight the difficulty of assigning responsibility and accountability for a patient’s care when comparing physician performance.
“Based on the measurement used in the QRUR, it seems likely that a hospitalist would be severely disadvantaged with the introduction of a value-based modifier based on the present QRUR methodology,” Dr. Frost wrote.
SHM is similarly critical of the PQRS measures, which Dr. Torcson says lack relevance to hospitalist practices. “We want to be defined as HM physicians with our own unique measures of quality and cost,” he says. “Our results will look very different from those of an internist with a primarily outpatient practice.”
Dr. Torcson notes that SHM is an active participant in providing feedback during CMS rule proposals and has offered to work with the CMS on further refining the measures. For example, SHM proposed adding additional measures related to care transitions, given their particular relevance to hospitalist practices.
Rule-Changing Reform
The disruptive innovation of CMS’ healthcare reform agenda might wind up being a game-changer that dramatically affects the contours of all provider performance reporting and incentive systems, redefining the issues of physician accountability and patient assignment.
“We’re going to need to figure out how to restructure our measurement systems to match our evolving healthcare delivery and payment systems,” says Thomas B. Valuck, MD, JD, senior vice president of strategic partnerships for the National Quality Forum and former CMS adviser to the VBP program. Healthcare quality reporting should focus more on measures that cut across care contexts and assess whether the care provided truly made a difference for patients—metrics such as health improvement, return to functional status, level of patient involvement in the management of their care, provider team coordination, and other patient needs and preferences, Dr. Valuck believes.
“We need to be focused more on measures that encourage joint responsibility and cooperation among providers, and are important to patients across hospital, post-acute, and ambulatory settings, rather than those that are compartmentalized to one setting or relevant only to specific diseases or subspecialties,” Dr. Valuck says.
Such measure sets, while still retaining some disease- and physician-specific metrics, ideally would be complementary with families of related measures at the community, state, and national levels, Dr. Valuck says. “Such a multidimensional framework can begin to tell a meaningful story about what’s happening to the patient, and how well our system is delivering the right care,” he adds.
Dr. Torcson says HM has a pioneering role to play in this evolution, and he notes that SHM has proposed that CMS harmonize measures that align hospital-based physician activities (e.g. hospital medicine, emergency medicine, anesthesia, radiology) with hospital-level performance agendas so that physicians practicing together in the hospital setting can report on measures that are relevant to both.
Christopher Guadagnino is a freelance medical writer in Philadelphia.
Reference
- Centers for Medicare & Medicaid Services. Physician Quality Reporting System Town Hall Meeting. Available at: http://www.usqualitymeasures.org/shared/content/C4M_PQRS_transcript.pdf. Accessed July 3, 2012.
—Thomas B. Valuck, MD, JD, senior vice president of strategic partnerships, National Quality Forum, former CMS adviser
No longer content to be a passive purchaser of healthcare services, the Centers for Medicare & Medicaid Services (CMS) is becoming a savvier shopper, holding providers increasingly accountable for the quality and efficiency of the care they deliver. With its value-based purchasing (VPB) program for hospitals already in place, now it’s the physicians’ turn.
CMS is marching toward a value-based payment modifier program that will adjust physician reimbursement based on the relative quality and efficiency of care that physicians provide to Medicare fee-for-service patients. The program will begin January 2015 and will extend to all physicians in 2017. Like the hospital VBP program, it will be budget-neutral—meaning that payment will increase for some physicians but decrease for others.
The coming months mark a pivotal period for physicians as CMS tweaks its accountability apparatus in ways that will determine how reimbursement will rise and fall, for whom, and for what.
Menu of Metrics
In crafting the payment modifier program, CMS can tap performance metrics from several of its existing programs, including the Physician Quality Reporting System (PQRS), the soon-to-be-expanded Physician Compare website (www.medicare.gov/find-a-doctor/provider-search.aspx), and the Physician Feedback Program.
“These agendas are part of a continuum, and of equal importance, in the evolution toward physician value-based purchasing,” says Patrick J. Torcson, MD, MMM, FACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee, and director of hospital medicine at St. Tammany Parish Hospital in Covington, La.
PQRS began as a voluntary “pay for reporting” system that gave physicians a modest financial bonus (currently 0.5% of allowable Medicare charges) for submitting quality data (left). The Affordable Care Act (ACA) has since authorized CMS to penalize physicians who do not participate—1.5% of allowable Medicare charges beginning in 2015, and 2% in 2016.
The Physician Compare website, launched at the end of 2010, currently contains such rudimentary information as education, gender, and whether a physician is enrolled in Medicare and satisfactorily reports data to the PQRS. But as of January, the site will begin reporting some PQRS data, as well as other metrics.
CMS’ Physician Feedback Program provides quality and cost information to physicians in an effort to encourage them to improve the care they provide and its efficiency. CMS recently combined the program with its value-based payment modifier program as it moves toward physician reimbursement that it says will reward “value rather than volume.” The program, currently being piloted in Iowa, Nebraska, Kansas, and Missouri, issues to physicians confidential quality and resource use reports (QRURs) that compare their performance to peer groups in similar specialties by tracking PQRS results, Healthcare Effectiveness Data and Information Set (HEDIS) measures, and per-capita cost data and preventable hospital admission rates for various medical conditions. CMS will roll out the program nationwide next year.
Metrics Lack Relevance
Developing performance measures that capture the most relevant activities of physicians across many different specialties with equal validity is notoriously difficult—something that CMS acknowledges.1
Assigning the right patient to the right physician (i.e. figuring out who contributed what care, in what proportion, to which patient) also is fraught with complications, especially in the inpatient care setting, where a patient is likely to see many different physicians during a hospitalization.
SHM president Shaun Frost, MD, SFHM, highlighted these challenges in a letter sent in May to acting CMS administrator Marilyn B. Tavenner in which he pointed to dramatic data deficiencies in the initial round of QRURs sent to Physician Feedback Program participants that included hospitalists in Iowa, Nebraska, Kansas and Missouri. Because hospitalists were categorized as general internal-medicine physicians in the reports, their per-capita cost of care was dramatically higher (73% higher, in one case study) than the average cost of all internal-medicine physicians. No allowance was made for distinguishing the outpatient-oriented practice of a general internist from the inherently more expensive inpatient-focused hospitalist practice.
In the case study reviewed by SHM, the hospitalist’s patients saw, on average, 28 different physicians over the course of a year, during which the hospitalist contributed to the care of many patients but did not direct the care of any one of them—facts that clearly highlight the difficulty of assigning responsibility and accountability for a patient’s care when comparing physician performance.
“Based on the measurement used in the QRUR, it seems likely that a hospitalist would be severely disadvantaged with the introduction of a value-based modifier based on the present QRUR methodology,” Dr. Frost wrote.
SHM is similarly critical of the PQRS measures, which Dr. Torcson says lack relevance to hospitalist practices. “We want to be defined as HM physicians with our own unique measures of quality and cost,” he says. “Our results will look very different from those of an internist with a primarily outpatient practice.”
Dr. Torcson notes that SHM is an active participant in providing feedback during CMS rule proposals and has offered to work with the CMS on further refining the measures. For example, SHM proposed adding additional measures related to care transitions, given their particular relevance to hospitalist practices.
Rule-Changing Reform
The disruptive innovation of CMS’ healthcare reform agenda might wind up being a game-changer that dramatically affects the contours of all provider performance reporting and incentive systems, redefining the issues of physician accountability and patient assignment.
“We’re going to need to figure out how to restructure our measurement systems to match our evolving healthcare delivery and payment systems,” says Thomas B. Valuck, MD, JD, senior vice president of strategic partnerships for the National Quality Forum and former CMS adviser to the VBP program. Healthcare quality reporting should focus more on measures that cut across care contexts and assess whether the care provided truly made a difference for patients—metrics such as health improvement, return to functional status, level of patient involvement in the management of their care, provider team coordination, and other patient needs and preferences, Dr. Valuck believes.
“We need to be focused more on measures that encourage joint responsibility and cooperation among providers, and are important to patients across hospital, post-acute, and ambulatory settings, rather than those that are compartmentalized to one setting or relevant only to specific diseases or subspecialties,” Dr. Valuck says.
Such measure sets, while still retaining some disease- and physician-specific metrics, ideally would be complementary with families of related measures at the community, state, and national levels, Dr. Valuck says. “Such a multidimensional framework can begin to tell a meaningful story about what’s happening to the patient, and how well our system is delivering the right care,” he adds.
Dr. Torcson says HM has a pioneering role to play in this evolution, and he notes that SHM has proposed that CMS harmonize measures that align hospital-based physician activities (e.g. hospital medicine, emergency medicine, anesthesia, radiology) with hospital-level performance agendas so that physicians practicing together in the hospital setting can report on measures that are relevant to both.
Christopher Guadagnino is a freelance medical writer in Philadelphia.
Reference
- Centers for Medicare & Medicaid Services. Physician Quality Reporting System Town Hall Meeting. Available at: http://www.usqualitymeasures.org/shared/content/C4M_PQRS_transcript.pdf. Accessed July 3, 2012.