User login
Does mediolateral episiotomy reduce the risk of anal sphincter injury in operative vaginal delivery?
Stop performing median episiotomy!
Robert L. Barbieri, MD (Editorial, April 2012)
Episiotomy is an incision into the perineal body that is made during the second stage of labor to expedite delivery. Despite guidelines recommending restrictions on its use, episiotomy is still performed in more than 25% of vaginal deliveries in the United States. Suggested benefits include a shortened second stage of labor, the substitution of a straight surgical incision for a ragged spontaneous tear, and a reduced incidence of severe perineal injury and resultant pelvic floor dysfunction. Few data support these assertions, however.
Episiotomy is no OASIS
Absolute indications for episiotomy have yet to be established. Although there is general agreement that episiotomy may be indicated in select circumstances (such as to expedite delivery in the setting of nonreassuring fetal testing in the second stage of labor, shoulder dystocia, or at the time of operative vaginal delivery), routine use is discouraged.1,2 Besides the lack of data showing its benefit, episiotomy is associated with several potential complications, including increased blood loss, fetal injury, and localized pain. In contrast to the stated goal of reducing perineal trauma, episiotomy is associated with an increased incidence of third- or fourth-degree perineal lacerations,3,4 referred to in this study as obstetric anal sphincter injuries (OASIS).
Third- or fourth-degree tears are identified clinically at the time of vaginal delivery in 0.6% to 9% of patients.4 Studies using two-dimensional endoanal ultrasonography suggest that the true incidence of rectal injury is probably closer to 11%.5 Such injuries are associated with an increased risk of subsequent urinary or fecal incontinence (or both) and pelvic organ prolapse.
If episiotomy is indicated, how should it be performed?
There are two main types of episiotomy: median (favored in the United States) and mediolateral episiotomy. Complications—especially OASIS—are more common with median episiotomy,3,6,7 which involves a vertical midline incision from the posterior fourchette toward the rectum. Mediolateral episiotomy (favored in Europe), refers to an incision performed at a 45° angle from the posterior fourchette. OASIS is more common after median episiotomy, compared with the mediolateral approach.4,6 What is not yet clear is whether mediolateral episiotomy actually protects against OASIS.
Details of the study
de Vogel and colleagues evaluated the frequency of OASIS in women at high risk—specifically, those undergoing operative vaginal delivery; they also sought to determine whether mediolateral episiotomy is protective against OASIS. To this end, they performed a retrospective analysis of 2,861 consecutive women who delivered a singleton liveborn infant at term by vacuum, forceps, or both, from 2001–2009. Women were identified through the Netherlands Perinatal Registry, a voluntary reporting national database that includes approximately 96% of the 190,000 births that occur after 16 weeks’ gestation each year in the Netherlands. Exclusion criteria included multiple gestation, breech presentation, and use of median episiotomy.
The overall frequency of OASIS was 5.7% (162 cases among 2,861 deliveries). After logistic-regression modeling, a number of variables were significantly associated with OASIS, all of which have been identified previously: forceps delivery, occiput posterior position, primiparity, and epidural anesthesia. Women with a mediolateral episiotomy were at a significantly lower risk for OASIS, compared with women without mediolateral episiotomy (3.5% vs 15.6%, respectively; P<.001). Further analysis suggested that 8.6 mediolateral episiotomies would be needed to prevent one OASIS during vacuum extraction, whereas 5.2 procedures would be necessary to prevent one OASIS during forceps delivery. de Vogel and colleagues concluded that mediolateral episiotomy should be performed during all operative vaginal deliveries to reduce the incidence of OASIS.
Although this study included a large sample from a well-established and validated dataset (collected prospectively), it was, by design, retrospective. There was no standardization of when or how to cut the mediolateral episiotomy. However, many of these uncontrolled variables (such as cutting an episiotomy that is more median than mediolateral or cutting an episiotomy only in women who appear to be at imminent risk of sustaining a perineal laceration) would increase—not decrease—the risk of severe perineal injury. This fact suggests that the protective effect of mediolateral episiotomy may be even more dramatic than the sixfold protection reported in this study.
This study focused on women who underwent operative vaginal delivery. It remains controversial whether mediolateral episiotomy is protective in women who have a spontaneous (noninstrumental) vaginal delivery.
The study also lacks follow-up data on how many women with OASIS went on to develop fecal or urinary incontinence or pelvic organ prolapse. However, a third- or fourth-degree perineal laceration is serious enough that it can serve as an acceptable primary outcome measure even in the absence of long-term functional data.
In this study, use of median episiotomy was an exclusion, mostly likely because it is rarely performed in Europe.
While the battle over “to cut or not to cut” continues to rage, one fact is clear: median episiotomy should be abandoned. If you are going to perform episiotomy, make it mediolateral. According to this report, accoucheurs should consider cutting a mediolateral episiotomy for perineal protection each time they perform operative vaginal delivery.
ERROL R. NORWITZ, MD, PHD
After reading this article, and Dr. Barbieri’s April Editorial, we want to know if these articles have changed your practice. If you were faced with a difficult vaginal delivery, would you use a median or mediolateral episiotomy incision? Why?
We want to hear from you! Tell us what you think.
1. Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA. 2005;293(17):2141-2148.
2. Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;(1):CD000081.-
3. Helwig JT, Thorp JM, Jr, Bowes WA, Jr. Does midline episiotomy increase the risk of third- and fourth-degree lacerations in operative vaginal deliveries? Obstet Gynecol. 1993;82(2):276-279.
4. Dudding TC, Vaizey C, Kamm MA. Obstetric anal sphincter injury: incidence, risk factors, and management. Ann Surg. 2008;247(2):224-237.
5. Williams AB, Bartram CI, Halligan S, Spencer JA, Nicholls RJ, Kmiot WA. Anal sphincter damage after vaginal delivery using three-dimensional endosonography. Obstet Gynecol. 2001;97(5 Pt 1):770-775.
6. Coats PM, Chan KK, Wilkins M, Beard RJ. A comparison between midline and mediolateral episiotomies. Br J Obstet Gynaecol. 1980;87(5):408-412.
7. Kudish B, Blackwell S, McNeeley SG, et al. Operative vaginal delivery and midline episiotomy: a bad combination for the perineum. Am J Obstet Gynecol. 2006;195(3):749-754.
Stop performing median episiotomy!
Robert L. Barbieri, MD (Editorial, April 2012)
Episiotomy is an incision into the perineal body that is made during the second stage of labor to expedite delivery. Despite guidelines recommending restrictions on its use, episiotomy is still performed in more than 25% of vaginal deliveries in the United States. Suggested benefits include a shortened second stage of labor, the substitution of a straight surgical incision for a ragged spontaneous tear, and a reduced incidence of severe perineal injury and resultant pelvic floor dysfunction. Few data support these assertions, however.
Episiotomy is no OASIS
Absolute indications for episiotomy have yet to be established. Although there is general agreement that episiotomy may be indicated in select circumstances (such as to expedite delivery in the setting of nonreassuring fetal testing in the second stage of labor, shoulder dystocia, or at the time of operative vaginal delivery), routine use is discouraged.1,2 Besides the lack of data showing its benefit, episiotomy is associated with several potential complications, including increased blood loss, fetal injury, and localized pain. In contrast to the stated goal of reducing perineal trauma, episiotomy is associated with an increased incidence of third- or fourth-degree perineal lacerations,3,4 referred to in this study as obstetric anal sphincter injuries (OASIS).
Third- or fourth-degree tears are identified clinically at the time of vaginal delivery in 0.6% to 9% of patients.4 Studies using two-dimensional endoanal ultrasonography suggest that the true incidence of rectal injury is probably closer to 11%.5 Such injuries are associated with an increased risk of subsequent urinary or fecal incontinence (or both) and pelvic organ prolapse.
If episiotomy is indicated, how should it be performed?
There are two main types of episiotomy: median (favored in the United States) and mediolateral episiotomy. Complications—especially OASIS—are more common with median episiotomy,3,6,7 which involves a vertical midline incision from the posterior fourchette toward the rectum. Mediolateral episiotomy (favored in Europe), refers to an incision performed at a 45° angle from the posterior fourchette. OASIS is more common after median episiotomy, compared with the mediolateral approach.4,6 What is not yet clear is whether mediolateral episiotomy actually protects against OASIS.
Details of the study
de Vogel and colleagues evaluated the frequency of OASIS in women at high risk—specifically, those undergoing operative vaginal delivery; they also sought to determine whether mediolateral episiotomy is protective against OASIS. To this end, they performed a retrospective analysis of 2,861 consecutive women who delivered a singleton liveborn infant at term by vacuum, forceps, or both, from 2001–2009. Women were identified through the Netherlands Perinatal Registry, a voluntary reporting national database that includes approximately 96% of the 190,000 births that occur after 16 weeks’ gestation each year in the Netherlands. Exclusion criteria included multiple gestation, breech presentation, and use of median episiotomy.
The overall frequency of OASIS was 5.7% (162 cases among 2,861 deliveries). After logistic-regression modeling, a number of variables were significantly associated with OASIS, all of which have been identified previously: forceps delivery, occiput posterior position, primiparity, and epidural anesthesia. Women with a mediolateral episiotomy were at a significantly lower risk for OASIS, compared with women without mediolateral episiotomy (3.5% vs 15.6%, respectively; P<.001). Further analysis suggested that 8.6 mediolateral episiotomies would be needed to prevent one OASIS during vacuum extraction, whereas 5.2 procedures would be necessary to prevent one OASIS during forceps delivery. de Vogel and colleagues concluded that mediolateral episiotomy should be performed during all operative vaginal deliveries to reduce the incidence of OASIS.
Although this study included a large sample from a well-established and validated dataset (collected prospectively), it was, by design, retrospective. There was no standardization of when or how to cut the mediolateral episiotomy. However, many of these uncontrolled variables (such as cutting an episiotomy that is more median than mediolateral or cutting an episiotomy only in women who appear to be at imminent risk of sustaining a perineal laceration) would increase—not decrease—the risk of severe perineal injury. This fact suggests that the protective effect of mediolateral episiotomy may be even more dramatic than the sixfold protection reported in this study.
This study focused on women who underwent operative vaginal delivery. It remains controversial whether mediolateral episiotomy is protective in women who have a spontaneous (noninstrumental) vaginal delivery.
The study also lacks follow-up data on how many women with OASIS went on to develop fecal or urinary incontinence or pelvic organ prolapse. However, a third- or fourth-degree perineal laceration is serious enough that it can serve as an acceptable primary outcome measure even in the absence of long-term functional data.
In this study, use of median episiotomy was an exclusion, mostly likely because it is rarely performed in Europe.
While the battle over “to cut or not to cut” continues to rage, one fact is clear: median episiotomy should be abandoned. If you are going to perform episiotomy, make it mediolateral. According to this report, accoucheurs should consider cutting a mediolateral episiotomy for perineal protection each time they perform operative vaginal delivery.
ERROL R. NORWITZ, MD, PHD
After reading this article, and Dr. Barbieri’s April Editorial, we want to know if these articles have changed your practice. If you were faced with a difficult vaginal delivery, would you use a median or mediolateral episiotomy incision? Why?
We want to hear from you! Tell us what you think.
Stop performing median episiotomy!
Robert L. Barbieri, MD (Editorial, April 2012)
Episiotomy is an incision into the perineal body that is made during the second stage of labor to expedite delivery. Despite guidelines recommending restrictions on its use, episiotomy is still performed in more than 25% of vaginal deliveries in the United States. Suggested benefits include a shortened second stage of labor, the substitution of a straight surgical incision for a ragged spontaneous tear, and a reduced incidence of severe perineal injury and resultant pelvic floor dysfunction. Few data support these assertions, however.
Episiotomy is no OASIS
Absolute indications for episiotomy have yet to be established. Although there is general agreement that episiotomy may be indicated in select circumstances (such as to expedite delivery in the setting of nonreassuring fetal testing in the second stage of labor, shoulder dystocia, or at the time of operative vaginal delivery), routine use is discouraged.1,2 Besides the lack of data showing its benefit, episiotomy is associated with several potential complications, including increased blood loss, fetal injury, and localized pain. In contrast to the stated goal of reducing perineal trauma, episiotomy is associated with an increased incidence of third- or fourth-degree perineal lacerations,3,4 referred to in this study as obstetric anal sphincter injuries (OASIS).
Third- or fourth-degree tears are identified clinically at the time of vaginal delivery in 0.6% to 9% of patients.4 Studies using two-dimensional endoanal ultrasonography suggest that the true incidence of rectal injury is probably closer to 11%.5 Such injuries are associated with an increased risk of subsequent urinary or fecal incontinence (or both) and pelvic organ prolapse.
If episiotomy is indicated, how should it be performed?
There are two main types of episiotomy: median (favored in the United States) and mediolateral episiotomy. Complications—especially OASIS—are more common with median episiotomy,3,6,7 which involves a vertical midline incision from the posterior fourchette toward the rectum. Mediolateral episiotomy (favored in Europe), refers to an incision performed at a 45° angle from the posterior fourchette. OASIS is more common after median episiotomy, compared with the mediolateral approach.4,6 What is not yet clear is whether mediolateral episiotomy actually protects against OASIS.
Details of the study
de Vogel and colleagues evaluated the frequency of OASIS in women at high risk—specifically, those undergoing operative vaginal delivery; they also sought to determine whether mediolateral episiotomy is protective against OASIS. To this end, they performed a retrospective analysis of 2,861 consecutive women who delivered a singleton liveborn infant at term by vacuum, forceps, or both, from 2001–2009. Women were identified through the Netherlands Perinatal Registry, a voluntary reporting national database that includes approximately 96% of the 190,000 births that occur after 16 weeks’ gestation each year in the Netherlands. Exclusion criteria included multiple gestation, breech presentation, and use of median episiotomy.
The overall frequency of OASIS was 5.7% (162 cases among 2,861 deliveries). After logistic-regression modeling, a number of variables were significantly associated with OASIS, all of which have been identified previously: forceps delivery, occiput posterior position, primiparity, and epidural anesthesia. Women with a mediolateral episiotomy were at a significantly lower risk for OASIS, compared with women without mediolateral episiotomy (3.5% vs 15.6%, respectively; P<.001). Further analysis suggested that 8.6 mediolateral episiotomies would be needed to prevent one OASIS during vacuum extraction, whereas 5.2 procedures would be necessary to prevent one OASIS during forceps delivery. de Vogel and colleagues concluded that mediolateral episiotomy should be performed during all operative vaginal deliveries to reduce the incidence of OASIS.
Although this study included a large sample from a well-established and validated dataset (collected prospectively), it was, by design, retrospective. There was no standardization of when or how to cut the mediolateral episiotomy. However, many of these uncontrolled variables (such as cutting an episiotomy that is more median than mediolateral or cutting an episiotomy only in women who appear to be at imminent risk of sustaining a perineal laceration) would increase—not decrease—the risk of severe perineal injury. This fact suggests that the protective effect of mediolateral episiotomy may be even more dramatic than the sixfold protection reported in this study.
This study focused on women who underwent operative vaginal delivery. It remains controversial whether mediolateral episiotomy is protective in women who have a spontaneous (noninstrumental) vaginal delivery.
The study also lacks follow-up data on how many women with OASIS went on to develop fecal or urinary incontinence or pelvic organ prolapse. However, a third- or fourth-degree perineal laceration is serious enough that it can serve as an acceptable primary outcome measure even in the absence of long-term functional data.
In this study, use of median episiotomy was an exclusion, mostly likely because it is rarely performed in Europe.
While the battle over “to cut or not to cut” continues to rage, one fact is clear: median episiotomy should be abandoned. If you are going to perform episiotomy, make it mediolateral. According to this report, accoucheurs should consider cutting a mediolateral episiotomy for perineal protection each time they perform operative vaginal delivery.
ERROL R. NORWITZ, MD, PHD
After reading this article, and Dr. Barbieri’s April Editorial, we want to know if these articles have changed your practice. If you were faced with a difficult vaginal delivery, would you use a median or mediolateral episiotomy incision? Why?
We want to hear from you! Tell us what you think.
1. Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA. 2005;293(17):2141-2148.
2. Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;(1):CD000081.-
3. Helwig JT, Thorp JM, Jr, Bowes WA, Jr. Does midline episiotomy increase the risk of third- and fourth-degree lacerations in operative vaginal deliveries? Obstet Gynecol. 1993;82(2):276-279.
4. Dudding TC, Vaizey C, Kamm MA. Obstetric anal sphincter injury: incidence, risk factors, and management. Ann Surg. 2008;247(2):224-237.
5. Williams AB, Bartram CI, Halligan S, Spencer JA, Nicholls RJ, Kmiot WA. Anal sphincter damage after vaginal delivery using three-dimensional endosonography. Obstet Gynecol. 2001;97(5 Pt 1):770-775.
6. Coats PM, Chan KK, Wilkins M, Beard RJ. A comparison between midline and mediolateral episiotomies. Br J Obstet Gynaecol. 1980;87(5):408-412.
7. Kudish B, Blackwell S, McNeeley SG, et al. Operative vaginal delivery and midline episiotomy: a bad combination for the perineum. Am J Obstet Gynecol. 2006;195(3):749-754.
1. Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA. 2005;293(17):2141-2148.
2. Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;(1):CD000081.-
3. Helwig JT, Thorp JM, Jr, Bowes WA, Jr. Does midline episiotomy increase the risk of third- and fourth-degree lacerations in operative vaginal deliveries? Obstet Gynecol. 1993;82(2):276-279.
4. Dudding TC, Vaizey C, Kamm MA. Obstetric anal sphincter injury: incidence, risk factors, and management. Ann Surg. 2008;247(2):224-237.
5. Williams AB, Bartram CI, Halligan S, Spencer JA, Nicholls RJ, Kmiot WA. Anal sphincter damage after vaginal delivery using three-dimensional endosonography. Obstet Gynecol. 2001;97(5 Pt 1):770-775.
6. Coats PM, Chan KK, Wilkins M, Beard RJ. A comparison between midline and mediolateral episiotomies. Br J Obstet Gynaecol. 1980;87(5):408-412.
7. Kudish B, Blackwell S, McNeeley SG, et al. Operative vaginal delivery and midline episiotomy: a bad combination for the perineum. Am J Obstet Gynecol. 2006;195(3):749-754.
How to avoid major vessel injury during gynecologic laparoscopy
Update: Minimally invasive Surgery
Amy Garcia, MD (April 2012)
10 practical, evidence-based suggestions to improve your minimally invasive surgical skills now
Catherine A. Matthews, MD (April 2011)
CASE: Abdominal entry leads to life-threatening injury
A 50-year-old woman with a BMI of 25 kg/m2, a strong family history of breast and ovarian cancer, and a confirmed BRCA mutation was scheduled for prophylactic bilateral salpingo-oophorectomy via robotic laparoscopy on November 26, 2009. At the time of the procedure, the gynecologic surgeon selected a site for the camera trocar that was several centimeters above the umbilicus. After making a transverse incision, he inserted a Veress needle and insufflated the abdomen with CO2 gas until intra-abdominal pressure reached 17 mm Hg. He then thrust an 11-inch disposable trocar through the anterior abdominal wall, attached the camera to the laparoscope, confirmed proper intraperitoneal placement, and inserted two additional trocars under direct vision.
Shortly after these actions, the anesthesiologist reported that the patient’s blood pressure had dropped precipitously, along with end tidal CO2. The surgeon examined the peritoneal cavity and discovered blood in the right paracolic gutter. The anesthesiologist advised the surgeon that he could no longer detect the patient’s blood pressure; electrocardiography revealed pulseless electrical activity.
The surgical team began chest compressions, evacuated the pneumoperitoneum, and removed all trocars. Blood was noted on the camera trocar, and the device was secured by the OR staff. The surgeon performed an emergent laparotomy, making the incision within 4 minutes of the beginning of CPR. Exploration revealed a large retroperitoneal hematoma above the area of the aortic bifurcation and inferior vena cava.
General and vascular surgeons were called. The general surgeon opened the retroperitoneum and found an extreme amount of clotted and unclotted blood. The vascular surgeon described the initial injury as a 1.5-cm laceration of the distal aorta, just above the bifurcation. A cell saver was requested and recorded blood loss of 12,000 mL.
The vascular surgeon clamped the aorta proximally; he also clamped both common iliac arteries. He then repaired the lacerations on the aorta using 5-0 Prolene suture (Ethicon). The aorta was significantly narrowed, however, so the surgeon decided to replace the distal aorta, which he then resected and repaired using a 14-mm Dacron graft (DuPont).
Further inspection revealed continuing retroperitoneal bleeding. The vascular surgeon found and repaired a laceration of the inferior mesenteric vein. He also clipped multiple small veins to stop bleeding.
When a hole in the transverse colon was identified, the general surgeon—who had left the operating table—rescrubbed to repair it. He also discovered an injury to the mesentery of the transverse colon and repaired both wounds, resecting the perforated segment. The divided, stapled colon was dropped back into the abdomen because the bowel was dusky. Despite an epinephrine drip, the patient was hypotensive and coagulopathic. The abdomen was packed and covered with sterile cassette film, with towels covering the open wound.
The patient was taken to the postanesthesia care unit in guarded condition and was subsequently transferred to the ICU, where her blood pressure dropped again. She was returned to the OR, where the packs were removed and a bleeding right common iliac artery was repaired using 5-0 Prolene suture. The next day, she underwent bilateral salpingo-oophorectomy with a transverse colon colostomy.
Because of the colon injury, the vascular surgeon believed that the Dacron graft had been contaminated. On December 1, the graft was taken down, a left femoral-vein autograft was harvested, and a reconstructive conduit was created for the terminal aorta. The patient underwent three additional procedures to place mesh into the abdominal wall. When the mesh became infected, it was removed.
The patient remained in the hospital for 1 month, after which she was transferred to a long-term care facility. She suffered permanent neurologic injuries because of prolonged hypoxia and continues to require supportive care.
How could this catastrophe have been avoided?
Traumatic injury to the great retroperitoneal vessels is an emergent and life-threatening event. During gynecologic laparoscopy, it is most likely to occur during entry into the anterior abdominal wall.
Most laparoscopic procedures require entry into the anterior abdominal wall for placement of a trocar and a sleeve that serves as a portal for insertion of the endoscope. Secondary ports provide entry points for manipulative and operative tools.
The most critical entry point is primary placement of the viewing device. Secondary trocars are always inserted under direct visualization; therefore, they carry a lower risk of inflicting injury to underlying viscera and vessels.
Practice safe entry
In the early days of laparoscopy, only one method of entry existed. Over time, however, several other techniques have been devised.
The initial method—still widely utilized—is known as the closed or blind technique. The surgeon creates a pneumoperitoneum with the use of a needle that is 18 gauge to 2.5 mm in diameter; the needle is placed through a subumbilical incision. Once intraperitoneal placement is confirmed, CO2 gas is infused into the peritoneal cavity until the abdomen is tympanic to percussion (usually at pressures of 14 to 18 mm Hg).
Next, the surgeon aims the trocar toward the uterus at a 45° angle, maintaining the device in the midline. Entry is confirmed by opening the trocar’s trap-door valve and witnessing a rush of CO2 gas.
Another entry technique—the open technique—is used almost universally by general surgeons. The procedure is a type of microlaparotomy. After making the subumbilical incision, the fascia of the abdominal wall is pierced and the peritoneum is grasped and opened bluntly or sharply. Once the edges of the peritoneum are secured, a blunt trocar (Hasson trocar) is inserted. Then the trocar is removed, leaving the sleeve in place to accept the laparoscope.
Another entry variation, called direct entry, employs no pneumoperitoneum. In this approach, the surgeon grabs the anterior abdominal wall, sharply elevating it, and directly thrusts the reusable or disposable trocar into the abdominal cavity.
An extensive review of entry techniques has been published elsewhere.1
Many complications arise from entry techniques and devices
A survey of Australian gynecologists about entry techniques found that 73% of respondents used a Veress needle and pneumoperitoneum for entry and that 83% used a location other than the infraumbilical site when periumbilical adhesions were suspected. Twenty-one percent had experienced a major retroperitoneal vascular injury, but 33% lacked a plan to manage such injuries.2
In their review of entry techniques, Vilos and colleagues asserted that Veress-needle insertion should be accompanied by pneumoperitoneal pressures of 20 to 30 mm Hg rather than a predetermined volume of CO2 gas.1 They also recommended insertion in the left upper quadrant when periumbilical adhesions are suspected or when insufflation at the umbilicus fails three times.
Newer entry devices include the optical-view trocar and the radially expanding trocar. The first consists of a plastic, conically tipped instrument that is optically clear. At least hypothetically, this device permits the surgeon to view each layer of the abdominal wall as he or she thrusts the device under “direct vision” into the abdominal cavity.
The radially expanding trocar is inserted over a Veress needle into the abdominal cavity. Its initial diameter is only 3 mm; once the instrument is in place, however, a blunt plastic trocar and sleeve are pushed into the mesh-like, radially expanding tube until it reaches 11 to 12 mm in diameter. The blunt trocar is then removed, leaving the plastic sheath and mesh material in place to accept the laparoscope. One key advantage of this device is the mesh component, which resists slippage or movement as the laparoscope is moved in and out of the sheath.
Vilos and colleagues concluded that open entry was neither superior nor inferior to other entry techniques and that direct entry without pneumoperitoneum may be as safe as Veress-needle techniques and associated with a lower risk of gas embolism. They also reported that shielded trocars are not associated with fewer visceral or vascular injuries and that visual-entry trocars lack superiority, compared with other devices, for the prevention of visceral or vascular injuries.1
Other review articles about entry techniques similarly found no objective evidence that any single technique is superior.3 However, data are conflicting on the safety of the optical trocar, compared with other trocars, with some data showing marginal advantages and others demonstrating no difference.4-6
Follow a few key entry guidelines
In 1990, Yuzpe reported a mail-in survey of 800 practicing ObGyns in Canada on the topic of pneumoperitoneum and trocar injuries.7 Of the 407 physicians who responded, 16.7% reported that the pneumoperitoneum needle caused a visceral or major vessel injury, and 16.5% attributed the injury to the primary trocar. Among 109 vessel injuries, 31 were caused by the pneumoperitoneum needle, and 28 of 104 injuries were caused by the primary trocar.
To be safe, Veress needle and primary trocar entry require critical attention to the angle and direction of the thrust relative to the abdominal cavity (FIGURE, page 24). For example, if the Veress needle or the sharp tip of the trocar deviate to the right or left of the midline during entry into the abdomen, injury to the iliac vessels is a clear risk.
Most laparoscopic surgeons stand on the left-hand side of the patient and face her feet. Trocar deviation for a right-handed person tends to vector to the right, especially when a twisting motion is utilized. Correct alignment of the primary trocar is straight down the middle of the lower abdomen on a virtual or real line drawn from the center of the navel to the center of the symphysis.
An entry angle of 45° to 60° will carry the needle or trocar toward the bladder or uterus and away from the aorta and left common iliac vein. In contrast, a 90° thrust will aim the device dangerously toward the great vessels. A slightly upward and right-sided deviation from the subumbilical entry will place the needle and trocar in the direction of the inferior vena cava and right common iliac vessels. A 90° entry with deviation to the left will position the entry device at the inferior mesenteric vessels and the left common iliac vessels.
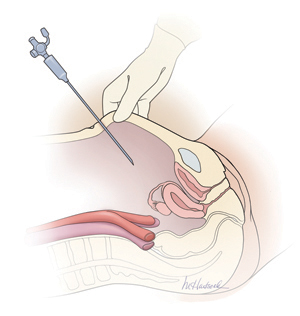
Primary abdominal entry
An entry angle of 45° to 60°, regardless of whether a needle or trocar is used, will carry the device toward the bladder or uterus and away from the aorta and left common iliac vein.In a review of access complications associated with laparoscopy, including major vascular injuries, Philips and Amaral listed variables responsible for large-vessel injury; they also documented the incidence of such injuries associated with laparoscopic cholecystectomy.8 They recommended that the patient be placed in the Trendelenburg position and that the needle or trocar be inserted at a 45° angle that stays within the midline; they also concluded that the trocar should be placed when pneumoperitoneal pressures exceed 20 mm Hg. They advised against direct insertion in patients with a history of pelvic surgery as well as in thin patients.
Place secondary trocars under direct visualization
Secondary trocars should always be placed under direct, visually controlled entry and, at least hypothetically, should never injure any great vessel. Nevertheless, secondary trocars do sometimes cause injury, most often as a result of extreme lateral entry near the inguinal ligament. The vessels at risk are the external iliac artery and vein.
Injuries are also invariably associated with adhesiolysis and anatomic problems. Precise knowledge of pelvic anatomy is not only a requisite for pelvic surgery in general but also for laparoscopic surgery, in which the operative view is less clear than it is in open procedures.
Know the risks associated with operative tools
Suturing and knot tying are not easy maneuvers during laparoscopic procedures and add significant operative time. Although they are performed more easily when robotics is utilized, few gynecologists are skilled practitioners. As a result, accessory instruments have been developed to prevent and control bleeding during laparoscopic operations. These devices include monopolar and bipolar instruments, lasers, ultrasonic tools, and stapling devices.
Avoid monopolar electrosurgery
This modality should be avoided whenever possible because the risk of injury is significantly higher than with bipolar electrosurgery. The key disadvantages of monopolar energy are high-frequency leaks; low-frequency currents; direct, indirect, and capacitative coupling; and return-electrode failures. None of these problems are common with bipolar techniques.
However, all electrosurgical devices carry a risk of thermal injury through direct tissue contact and conduction of heat to neighboring tissues and structures.
A full discussion of the physics and tissue actions of electrosurgical devices may be found elsewhere.9
CO2 is the safest laser
A variety of lasers have been used in laparoscopic surgery. The neodymium–YAG, KTP-532, and CO2 lasers have been used most frequently for gynecologic operations.
Because of its wavelength, the CO2 laser is the safest device for intra-abdominal use. Advantages include precision and control. In addition, the CO2 laser is absorbed by water very effectively. As a result, hydrodissection techniques can facilitate effective backstopping of the laser beam in strategic locations, thereby preventing injury to surrounding structures.
Laser energy is not conducted through tissue in the same way that electrosurgical energy is conducted. Therefore, the laser is ideal for vaporizing endometrial implants and cutting adhesions.
Beware of heat generated by the ultrasonic shears
This device, known more commonly as the Harmonic Scalpel (Ethicon), employs high-frequency sound waves to shear and coagulate tissue and prevent bleeding. It does not require conduction through tissues but does require contact with tissues. Because friction produces heat, these devices can become hot enough to inflict unintended burns on tissues that are inadvertently touched by the hot tip or by heat transmitted from the operative site by thermal conduction.
Stapler may inadvertently involve adjacent structures
This laparoscopic device has the advantage of not requiring or emitting energy other than the mechanical force of the operator’s hand. Disadvantages associated with the stapler center on the inadvertent inclusion of other structures within the jaws of the instrument. In addition, the staplers themselves tend to be large and somewhat unwieldy in close quarters, adding to the risk of stapling nearby viscera.
Further information on the physics and actions of lasers, ultrasonic shears, and staplers is available.10,11
Obesity may increase the risk of major vessel injury
A recent study by Baggish found obesity to be a high-risk circumstance for major vessel injury.12 In the study, 22 of 31 women who sustained injury were overweight or obese, with a BMI ranging from 26 to 30 kg/m2.
Obesity increases the risk of major vessel injury because of the greater elasticity of the anterior abdominal wall. As force secondary to the downward thrust of the trocar is placed on the abdominal wall, it is pushed inward in the direction of the posterior wall. In contrast, thin women have rigid abdominal walls with minimal elasticity, so the force of the trocar thrust does not create significant displacement.
Baggish also found that disposable trocars accounted for 90% of major vascular injuries and that use of long trocars accounted for 43% of deaths.12
Injury and death are rare but real risks
In a multicenter study in France over 9 years, investigators reviewed 29,966 diagnostic and operative laparoscopic procedures and found a mortality rate of 3.33 deaths for every 100,000 laparoscopies and an overall complication rate of 4.64 complications for every 1,000 procedures.13 They found the complication rate to be significantly correlated with the complexity of the procedure (P = .0001). One in three complications (34.1%; n = 43) occurred during set-up, and one in four (28.6%) were not identified intraoperatively.13
The risk of great vessel injury associated with laparoscopy most frequently quoted is 0.5 injury for every 1,000 procedures.14 A multicenter study reported the prevalence of this complication to be 1.05 injuries per 1,000 procedures.15
The mortality rate associated with major vessel injury has been reported in several studies to range from 8% to 17%.14-17
Two articles measured the distance from various points on the anterior abdominal wall to the great retroperitoneal vessels during laparoscopic operations; they also measured the force required for the trocar to penetrate the abdominal wall.18,19 They found significant differences in the distance from the site of primary trocar insertion to the aorta and iliac vessels, depending on the BMI of the patient. In women with a BMI below 25 kg/m2, the mean distance to the aorta was 11.21 cm. In women with a BMI of 25 to 30, it was 14.14 cm, and in women with a BMI over 30, it was 15.14 cm. They also found variations in the mean thickness of the abdominal wall, which was 3.48 cm, 3.85 cm, and 5.05 cm in women with a BMI of less than 25, 25–30, and more than 30, respectively.
As for the force required for entry, investigators found that disposable cutting trocars can traverse the anterior abdominal wall with less force and less time, compared with reusable trocars and optical viewing devices.18,19
Another study measured the thickness of the abdominal wall and the distance to the great vessels by magnetic resonance imaging or computed tomography.20 However, this study was not performed during laparoscopy with pneumoperitoneum in place.
As previously mentioned, Baggish reported on 31 cases of major-vessel injury associated with laparoscopic operations involving 49 major-vessel injuries. Twenty-eight injuries occurred as a result of entry techniques: 26 occurred during primary trocar insertion, and two were related to secondary trocar thrusts.12 Four injuries and three deaths were associated with use of an 11-inch disposable trocar.
Of the injuries associated with primary trocar insertion, 10 occurred during direct insertion and 26 after creation of pneumoperitoneum. Open laparoscopy was performed in two cases.12 The TABLE details the number of vessels injured and the sites of injury in this study.
Seven women (23%) died as a direct result of venous injury. Collateral injury to other structures was observed in 16 cases. Blood loss ranged from 1,000 mL to 7,000 mL.12
Sites of major vessel injury in one study of gynecologic laparoscopy
| Site | Number of vascular injuries |
|---|---|
| Right iliac artery | 14 |
| Right iliac vein | 12 |
| Left iliac artery | 3 |
| Left iliac vein | 9 |
| Aorta | 4 |
| Vena cava | 2 |
| Mesenteric | 2 |
| Interior epigastric* | 2 |
| Other | 1 |
| Total injuries | 49 |
| Source: Baggish12 | |
Avoid these common errors
The most common errors in gynecologic laparoscopy include:
- delayed diagnosis
- failure to act on a visible retroperitoneal hematoma
- failure to cross-match adequate supplies of blood and blood products
- failure to adequately transfuse blood and blood products
- clamping the large damaged vessel
- opening the abdomen via Pfannenstiel incision
- failure to call for a vascular surgeon in a timely manner.
When a major vascular injury occurs, a well-informed surgeon will take the following measures:
- call for a vascular surgeon immediately. (Baggish found that there was a substantial delay in getting a vascular surgeon to the operating table in four of 31 cases.12)
- open the abdomen via a midline incision
- use a sponge stick to apply direct pressure to the bleeding vessel
- obtain an emergency type and cross-match and order a minimum of 6 U of blood plus fresh frozen plasma
- obtain a baseline complete blood count, platelet count, fibrinogen level, and test for fibrin-split products
- advise the anesthesiologist to seek additional help
- call for additional OR nursing personnel
- assign one circulator to run stats and record critical data.21-33
Prevention is the best strategy
As the opening case demonstrates, major vessel injury can occur without warning and cause cascading problems that can lead to permanent disability—even death. Because most serious vessel injuries occur during entry into the anterior abdominal wall, careful attention to entry techniques and the patient’s unique circumstances (obesity, presence of adhesions) can go a long way toward averting injury. Vigilance for the possibility of injury is also important throughout the procedure. When injury does occur, it is critical to call for help as soon as possible and to have safeguards in place to manage it.
Tune in again in October 2012 for Part 2 of this series, which offers insight into gastrointestinal and urinary tract injuries during laparoscopy and offers valuable guidance on avoiding and managing related complications.
We want to hear from you! Tell us what you think.
| Dr. Baggish discusses safe abdominal entry techniques |

Michael Baggish, MD
Dr. Baggish practices Obstetrics and Gynecology at The Women’s Center at Saint Helena Hospital in Saint Helena, California. He also serves as Professor of Obstetrics and Gynecology at the University of California, San Francisco, and as Emeritus Chairman and Residency Director, Department of Obstetrics and Gynecology, Good Samaritan Hospital, Cincinnati, Ohio.
Dr. Baggish reports no financial relationships relevant to this article.
| Dr. Baggish discusses safe abdominal entry techniques |
Michael Baggish, MD
Dr. Baggish practices Obstetrics and Gynecology at The Women’s Center at Saint Helena Hospital in Saint Helena, California. He also serves as Professor of Obstetrics and Gynecology at the University of California, San Francisco, and as Emeritus Chairman and Residency Director, Department of Obstetrics and Gynecology, Good Samaritan Hospital, Cincinnati, Ohio.
Dr. Baggish reports no financial relationships relevant to this article.
| Dr. Baggish discusses safe abdominal entry techniques |
Michael Baggish, MD
Dr. Baggish practices Obstetrics and Gynecology at The Women’s Center at Saint Helena Hospital in Saint Helena, California. He also serves as Professor of Obstetrics and Gynecology at the University of California, San Francisco, and as Emeritus Chairman and Residency Director, Department of Obstetrics and Gynecology, Good Samaritan Hospital, Cincinnati, Ohio.
Dr. Baggish reports no financial relationships relevant to this article.
Update: Minimally invasive Surgery
Amy Garcia, MD (April 2012)
10 practical, evidence-based suggestions to improve your minimally invasive surgical skills now
Catherine A. Matthews, MD (April 2011)
CASE: Abdominal entry leads to life-threatening injury
A 50-year-old woman with a BMI of 25 kg/m2, a strong family history of breast and ovarian cancer, and a confirmed BRCA mutation was scheduled for prophylactic bilateral salpingo-oophorectomy via robotic laparoscopy on November 26, 2009. At the time of the procedure, the gynecologic surgeon selected a site for the camera trocar that was several centimeters above the umbilicus. After making a transverse incision, he inserted a Veress needle and insufflated the abdomen with CO2 gas until intra-abdominal pressure reached 17 mm Hg. He then thrust an 11-inch disposable trocar through the anterior abdominal wall, attached the camera to the laparoscope, confirmed proper intraperitoneal placement, and inserted two additional trocars under direct vision.
Shortly after these actions, the anesthesiologist reported that the patient’s blood pressure had dropped precipitously, along with end tidal CO2. The surgeon examined the peritoneal cavity and discovered blood in the right paracolic gutter. The anesthesiologist advised the surgeon that he could no longer detect the patient’s blood pressure; electrocardiography revealed pulseless electrical activity.
The surgical team began chest compressions, evacuated the pneumoperitoneum, and removed all trocars. Blood was noted on the camera trocar, and the device was secured by the OR staff. The surgeon performed an emergent laparotomy, making the incision within 4 minutes of the beginning of CPR. Exploration revealed a large retroperitoneal hematoma above the area of the aortic bifurcation and inferior vena cava.
General and vascular surgeons were called. The general surgeon opened the retroperitoneum and found an extreme amount of clotted and unclotted blood. The vascular surgeon described the initial injury as a 1.5-cm laceration of the distal aorta, just above the bifurcation. A cell saver was requested and recorded blood loss of 12,000 mL.
The vascular surgeon clamped the aorta proximally; he also clamped both common iliac arteries. He then repaired the lacerations on the aorta using 5-0 Prolene suture (Ethicon). The aorta was significantly narrowed, however, so the surgeon decided to replace the distal aorta, which he then resected and repaired using a 14-mm Dacron graft (DuPont).
Further inspection revealed continuing retroperitoneal bleeding. The vascular surgeon found and repaired a laceration of the inferior mesenteric vein. He also clipped multiple small veins to stop bleeding.
When a hole in the transverse colon was identified, the general surgeon—who had left the operating table—rescrubbed to repair it. He also discovered an injury to the mesentery of the transverse colon and repaired both wounds, resecting the perforated segment. The divided, stapled colon was dropped back into the abdomen because the bowel was dusky. Despite an epinephrine drip, the patient was hypotensive and coagulopathic. The abdomen was packed and covered with sterile cassette film, with towels covering the open wound.
The patient was taken to the postanesthesia care unit in guarded condition and was subsequently transferred to the ICU, where her blood pressure dropped again. She was returned to the OR, where the packs were removed and a bleeding right common iliac artery was repaired using 5-0 Prolene suture. The next day, she underwent bilateral salpingo-oophorectomy with a transverse colon colostomy.
Because of the colon injury, the vascular surgeon believed that the Dacron graft had been contaminated. On December 1, the graft was taken down, a left femoral-vein autograft was harvested, and a reconstructive conduit was created for the terminal aorta. The patient underwent three additional procedures to place mesh into the abdominal wall. When the mesh became infected, it was removed.
The patient remained in the hospital for 1 month, after which she was transferred to a long-term care facility. She suffered permanent neurologic injuries because of prolonged hypoxia and continues to require supportive care.
How could this catastrophe have been avoided?
Traumatic injury to the great retroperitoneal vessels is an emergent and life-threatening event. During gynecologic laparoscopy, it is most likely to occur during entry into the anterior abdominal wall.
Most laparoscopic procedures require entry into the anterior abdominal wall for placement of a trocar and a sleeve that serves as a portal for insertion of the endoscope. Secondary ports provide entry points for manipulative and operative tools.
The most critical entry point is primary placement of the viewing device. Secondary trocars are always inserted under direct visualization; therefore, they carry a lower risk of inflicting injury to underlying viscera and vessels.
Practice safe entry
In the early days of laparoscopy, only one method of entry existed. Over time, however, several other techniques have been devised.
The initial method—still widely utilized—is known as the closed or blind technique. The surgeon creates a pneumoperitoneum with the use of a needle that is 18 gauge to 2.5 mm in diameter; the needle is placed through a subumbilical incision. Once intraperitoneal placement is confirmed, CO2 gas is infused into the peritoneal cavity until the abdomen is tympanic to percussion (usually at pressures of 14 to 18 mm Hg).
Next, the surgeon aims the trocar toward the uterus at a 45° angle, maintaining the device in the midline. Entry is confirmed by opening the trocar’s trap-door valve and witnessing a rush of CO2 gas.
Another entry technique—the open technique—is used almost universally by general surgeons. The procedure is a type of microlaparotomy. After making the subumbilical incision, the fascia of the abdominal wall is pierced and the peritoneum is grasped and opened bluntly or sharply. Once the edges of the peritoneum are secured, a blunt trocar (Hasson trocar) is inserted. Then the trocar is removed, leaving the sleeve in place to accept the laparoscope.
Another entry variation, called direct entry, employs no pneumoperitoneum. In this approach, the surgeon grabs the anterior abdominal wall, sharply elevating it, and directly thrusts the reusable or disposable trocar into the abdominal cavity.
An extensive review of entry techniques has been published elsewhere.1
Many complications arise from entry techniques and devices
A survey of Australian gynecologists about entry techniques found that 73% of respondents used a Veress needle and pneumoperitoneum for entry and that 83% used a location other than the infraumbilical site when periumbilical adhesions were suspected. Twenty-one percent had experienced a major retroperitoneal vascular injury, but 33% lacked a plan to manage such injuries.2
In their review of entry techniques, Vilos and colleagues asserted that Veress-needle insertion should be accompanied by pneumoperitoneal pressures of 20 to 30 mm Hg rather than a predetermined volume of CO2 gas.1 They also recommended insertion in the left upper quadrant when periumbilical adhesions are suspected or when insufflation at the umbilicus fails three times.
Newer entry devices include the optical-view trocar and the radially expanding trocar. The first consists of a plastic, conically tipped instrument that is optically clear. At least hypothetically, this device permits the surgeon to view each layer of the abdominal wall as he or she thrusts the device under “direct vision” into the abdominal cavity.
The radially expanding trocar is inserted over a Veress needle into the abdominal cavity. Its initial diameter is only 3 mm; once the instrument is in place, however, a blunt plastic trocar and sleeve are pushed into the mesh-like, radially expanding tube until it reaches 11 to 12 mm in diameter. The blunt trocar is then removed, leaving the plastic sheath and mesh material in place to accept the laparoscope. One key advantage of this device is the mesh component, which resists slippage or movement as the laparoscope is moved in and out of the sheath.
Vilos and colleagues concluded that open entry was neither superior nor inferior to other entry techniques and that direct entry without pneumoperitoneum may be as safe as Veress-needle techniques and associated with a lower risk of gas embolism. They also reported that shielded trocars are not associated with fewer visceral or vascular injuries and that visual-entry trocars lack superiority, compared with other devices, for the prevention of visceral or vascular injuries.1
Other review articles about entry techniques similarly found no objective evidence that any single technique is superior.3 However, data are conflicting on the safety of the optical trocar, compared with other trocars, with some data showing marginal advantages and others demonstrating no difference.4-6
Follow a few key entry guidelines
In 1990, Yuzpe reported a mail-in survey of 800 practicing ObGyns in Canada on the topic of pneumoperitoneum and trocar injuries.7 Of the 407 physicians who responded, 16.7% reported that the pneumoperitoneum needle caused a visceral or major vessel injury, and 16.5% attributed the injury to the primary trocar. Among 109 vessel injuries, 31 were caused by the pneumoperitoneum needle, and 28 of 104 injuries were caused by the primary trocar.
To be safe, Veress needle and primary trocar entry require critical attention to the angle and direction of the thrust relative to the abdominal cavity (FIGURE, page 24). For example, if the Veress needle or the sharp tip of the trocar deviate to the right or left of the midline during entry into the abdomen, injury to the iliac vessels is a clear risk.
Most laparoscopic surgeons stand on the left-hand side of the patient and face her feet. Trocar deviation for a right-handed person tends to vector to the right, especially when a twisting motion is utilized. Correct alignment of the primary trocar is straight down the middle of the lower abdomen on a virtual or real line drawn from the center of the navel to the center of the symphysis.
An entry angle of 45° to 60° will carry the needle or trocar toward the bladder or uterus and away from the aorta and left common iliac vein. In contrast, a 90° thrust will aim the device dangerously toward the great vessels. A slightly upward and right-sided deviation from the subumbilical entry will place the needle and trocar in the direction of the inferior vena cava and right common iliac vessels. A 90° entry with deviation to the left will position the entry device at the inferior mesenteric vessels and the left common iliac vessels.
Primary abdominal entry
An entry angle of 45° to 60°, regardless of whether a needle or trocar is used, will carry the device toward the bladder or uterus and away from the aorta and left common iliac vein.In a review of access complications associated with laparoscopy, including major vascular injuries, Philips and Amaral listed variables responsible for large-vessel injury; they also documented the incidence of such injuries associated with laparoscopic cholecystectomy.8 They recommended that the patient be placed in the Trendelenburg position and that the needle or trocar be inserted at a 45° angle that stays within the midline; they also concluded that the trocar should be placed when pneumoperitoneal pressures exceed 20 mm Hg. They advised against direct insertion in patients with a history of pelvic surgery as well as in thin patients.
Place secondary trocars under direct visualization
Secondary trocars should always be placed under direct, visually controlled entry and, at least hypothetically, should never injure any great vessel. Nevertheless, secondary trocars do sometimes cause injury, most often as a result of extreme lateral entry near the inguinal ligament. The vessels at risk are the external iliac artery and vein.
Injuries are also invariably associated with adhesiolysis and anatomic problems. Precise knowledge of pelvic anatomy is not only a requisite for pelvic surgery in general but also for laparoscopic surgery, in which the operative view is less clear than it is in open procedures.
Know the risks associated with operative tools
Suturing and knot tying are not easy maneuvers during laparoscopic procedures and add significant operative time. Although they are performed more easily when robotics is utilized, few gynecologists are skilled practitioners. As a result, accessory instruments have been developed to prevent and control bleeding during laparoscopic operations. These devices include monopolar and bipolar instruments, lasers, ultrasonic tools, and stapling devices.
Avoid monopolar electrosurgery
This modality should be avoided whenever possible because the risk of injury is significantly higher than with bipolar electrosurgery. The key disadvantages of monopolar energy are high-frequency leaks; low-frequency currents; direct, indirect, and capacitative coupling; and return-electrode failures. None of these problems are common with bipolar techniques.
However, all electrosurgical devices carry a risk of thermal injury through direct tissue contact and conduction of heat to neighboring tissues and structures.
A full discussion of the physics and tissue actions of electrosurgical devices may be found elsewhere.9
CO2 is the safest laser
A variety of lasers have been used in laparoscopic surgery. The neodymium–YAG, KTP-532, and CO2 lasers have been used most frequently for gynecologic operations.
Because of its wavelength, the CO2 laser is the safest device for intra-abdominal use. Advantages include precision and control. In addition, the CO2 laser is absorbed by water very effectively. As a result, hydrodissection techniques can facilitate effective backstopping of the laser beam in strategic locations, thereby preventing injury to surrounding structures.
Laser energy is not conducted through tissue in the same way that electrosurgical energy is conducted. Therefore, the laser is ideal for vaporizing endometrial implants and cutting adhesions.
Beware of heat generated by the ultrasonic shears
This device, known more commonly as the Harmonic Scalpel (Ethicon), employs high-frequency sound waves to shear and coagulate tissue and prevent bleeding. It does not require conduction through tissues but does require contact with tissues. Because friction produces heat, these devices can become hot enough to inflict unintended burns on tissues that are inadvertently touched by the hot tip or by heat transmitted from the operative site by thermal conduction.
Stapler may inadvertently involve adjacent structures
This laparoscopic device has the advantage of not requiring or emitting energy other than the mechanical force of the operator’s hand. Disadvantages associated with the stapler center on the inadvertent inclusion of other structures within the jaws of the instrument. In addition, the staplers themselves tend to be large and somewhat unwieldy in close quarters, adding to the risk of stapling nearby viscera.
Further information on the physics and actions of lasers, ultrasonic shears, and staplers is available.10,11
Obesity may increase the risk of major vessel injury
A recent study by Baggish found obesity to be a high-risk circumstance for major vessel injury.12 In the study, 22 of 31 women who sustained injury were overweight or obese, with a BMI ranging from 26 to 30 kg/m2.
Obesity increases the risk of major vessel injury because of the greater elasticity of the anterior abdominal wall. As force secondary to the downward thrust of the trocar is placed on the abdominal wall, it is pushed inward in the direction of the posterior wall. In contrast, thin women have rigid abdominal walls with minimal elasticity, so the force of the trocar thrust does not create significant displacement.
Baggish also found that disposable trocars accounted for 90% of major vascular injuries and that use of long trocars accounted for 43% of deaths.12
Injury and death are rare but real risks
In a multicenter study in France over 9 years, investigators reviewed 29,966 diagnostic and operative laparoscopic procedures and found a mortality rate of 3.33 deaths for every 100,000 laparoscopies and an overall complication rate of 4.64 complications for every 1,000 procedures.13 They found the complication rate to be significantly correlated with the complexity of the procedure (P = .0001). One in three complications (34.1%; n = 43) occurred during set-up, and one in four (28.6%) were not identified intraoperatively.13
The risk of great vessel injury associated with laparoscopy most frequently quoted is 0.5 injury for every 1,000 procedures.14 A multicenter study reported the prevalence of this complication to be 1.05 injuries per 1,000 procedures.15
The mortality rate associated with major vessel injury has been reported in several studies to range from 8% to 17%.14-17
Two articles measured the distance from various points on the anterior abdominal wall to the great retroperitoneal vessels during laparoscopic operations; they also measured the force required for the trocar to penetrate the abdominal wall.18,19 They found significant differences in the distance from the site of primary trocar insertion to the aorta and iliac vessels, depending on the BMI of the patient. In women with a BMI below 25 kg/m2, the mean distance to the aorta was 11.21 cm. In women with a BMI of 25 to 30, it was 14.14 cm, and in women with a BMI over 30, it was 15.14 cm. They also found variations in the mean thickness of the abdominal wall, which was 3.48 cm, 3.85 cm, and 5.05 cm in women with a BMI of less than 25, 25–30, and more than 30, respectively.
As for the force required for entry, investigators found that disposable cutting trocars can traverse the anterior abdominal wall with less force and less time, compared with reusable trocars and optical viewing devices.18,19
Another study measured the thickness of the abdominal wall and the distance to the great vessels by magnetic resonance imaging or computed tomography.20 However, this study was not performed during laparoscopy with pneumoperitoneum in place.
As previously mentioned, Baggish reported on 31 cases of major-vessel injury associated with laparoscopic operations involving 49 major-vessel injuries. Twenty-eight injuries occurred as a result of entry techniques: 26 occurred during primary trocar insertion, and two were related to secondary trocar thrusts.12 Four injuries and three deaths were associated with use of an 11-inch disposable trocar.
Of the injuries associated with primary trocar insertion, 10 occurred during direct insertion and 26 after creation of pneumoperitoneum. Open laparoscopy was performed in two cases.12 The TABLE details the number of vessels injured and the sites of injury in this study.
Seven women (23%) died as a direct result of venous injury. Collateral injury to other structures was observed in 16 cases. Blood loss ranged from 1,000 mL to 7,000 mL.12
Sites of major vessel injury in one study of gynecologic laparoscopy
| Site | Number of vascular injuries |
|---|---|
| Right iliac artery | 14 |
| Right iliac vein | 12 |
| Left iliac artery | 3 |
| Left iliac vein | 9 |
| Aorta | 4 |
| Vena cava | 2 |
| Mesenteric | 2 |
| Interior epigastric* | 2 |
| Other | 1 |
| Total injuries | 49 |
| Source: Baggish12 | |
Avoid these common errors
The most common errors in gynecologic laparoscopy include:
- delayed diagnosis
- failure to act on a visible retroperitoneal hematoma
- failure to cross-match adequate supplies of blood and blood products
- failure to adequately transfuse blood and blood products
- clamping the large damaged vessel
- opening the abdomen via Pfannenstiel incision
- failure to call for a vascular surgeon in a timely manner.
When a major vascular injury occurs, a well-informed surgeon will take the following measures:
- call for a vascular surgeon immediately. (Baggish found that there was a substantial delay in getting a vascular surgeon to the operating table in four of 31 cases.12)
- open the abdomen via a midline incision
- use a sponge stick to apply direct pressure to the bleeding vessel
- obtain an emergency type and cross-match and order a minimum of 6 U of blood plus fresh frozen plasma
- obtain a baseline complete blood count, platelet count, fibrinogen level, and test for fibrin-split products
- advise the anesthesiologist to seek additional help
- call for additional OR nursing personnel
- assign one circulator to run stats and record critical data.21-33
Prevention is the best strategy
As the opening case demonstrates, major vessel injury can occur without warning and cause cascading problems that can lead to permanent disability—even death. Because most serious vessel injuries occur during entry into the anterior abdominal wall, careful attention to entry techniques and the patient’s unique circumstances (obesity, presence of adhesions) can go a long way toward averting injury. Vigilance for the possibility of injury is also important throughout the procedure. When injury does occur, it is critical to call for help as soon as possible and to have safeguards in place to manage it.
Tune in again in October 2012 for Part 2 of this series, which offers insight into gastrointestinal and urinary tract injuries during laparoscopy and offers valuable guidance on avoiding and managing related complications.
We want to hear from you! Tell us what you think.
Update: Minimally invasive Surgery
Amy Garcia, MD (April 2012)
10 practical, evidence-based suggestions to improve your minimally invasive surgical skills now
Catherine A. Matthews, MD (April 2011)
CASE: Abdominal entry leads to life-threatening injury
A 50-year-old woman with a BMI of 25 kg/m2, a strong family history of breast and ovarian cancer, and a confirmed BRCA mutation was scheduled for prophylactic bilateral salpingo-oophorectomy via robotic laparoscopy on November 26, 2009. At the time of the procedure, the gynecologic surgeon selected a site for the camera trocar that was several centimeters above the umbilicus. After making a transverse incision, he inserted a Veress needle and insufflated the abdomen with CO2 gas until intra-abdominal pressure reached 17 mm Hg. He then thrust an 11-inch disposable trocar through the anterior abdominal wall, attached the camera to the laparoscope, confirmed proper intraperitoneal placement, and inserted two additional trocars under direct vision.
Shortly after these actions, the anesthesiologist reported that the patient’s blood pressure had dropped precipitously, along with end tidal CO2. The surgeon examined the peritoneal cavity and discovered blood in the right paracolic gutter. The anesthesiologist advised the surgeon that he could no longer detect the patient’s blood pressure; electrocardiography revealed pulseless electrical activity.
The surgical team began chest compressions, evacuated the pneumoperitoneum, and removed all trocars. Blood was noted on the camera trocar, and the device was secured by the OR staff. The surgeon performed an emergent laparotomy, making the incision within 4 minutes of the beginning of CPR. Exploration revealed a large retroperitoneal hematoma above the area of the aortic bifurcation and inferior vena cava.
General and vascular surgeons were called. The general surgeon opened the retroperitoneum and found an extreme amount of clotted and unclotted blood. The vascular surgeon described the initial injury as a 1.5-cm laceration of the distal aorta, just above the bifurcation. A cell saver was requested and recorded blood loss of 12,000 mL.
The vascular surgeon clamped the aorta proximally; he also clamped both common iliac arteries. He then repaired the lacerations on the aorta using 5-0 Prolene suture (Ethicon). The aorta was significantly narrowed, however, so the surgeon decided to replace the distal aorta, which he then resected and repaired using a 14-mm Dacron graft (DuPont).
Further inspection revealed continuing retroperitoneal bleeding. The vascular surgeon found and repaired a laceration of the inferior mesenteric vein. He also clipped multiple small veins to stop bleeding.
When a hole in the transverse colon was identified, the general surgeon—who had left the operating table—rescrubbed to repair it. He also discovered an injury to the mesentery of the transverse colon and repaired both wounds, resecting the perforated segment. The divided, stapled colon was dropped back into the abdomen because the bowel was dusky. Despite an epinephrine drip, the patient was hypotensive and coagulopathic. The abdomen was packed and covered with sterile cassette film, with towels covering the open wound.
The patient was taken to the postanesthesia care unit in guarded condition and was subsequently transferred to the ICU, where her blood pressure dropped again. She was returned to the OR, where the packs were removed and a bleeding right common iliac artery was repaired using 5-0 Prolene suture. The next day, she underwent bilateral salpingo-oophorectomy with a transverse colon colostomy.
Because of the colon injury, the vascular surgeon believed that the Dacron graft had been contaminated. On December 1, the graft was taken down, a left femoral-vein autograft was harvested, and a reconstructive conduit was created for the terminal aorta. The patient underwent three additional procedures to place mesh into the abdominal wall. When the mesh became infected, it was removed.
The patient remained in the hospital for 1 month, after which she was transferred to a long-term care facility. She suffered permanent neurologic injuries because of prolonged hypoxia and continues to require supportive care.
How could this catastrophe have been avoided?
Traumatic injury to the great retroperitoneal vessels is an emergent and life-threatening event. During gynecologic laparoscopy, it is most likely to occur during entry into the anterior abdominal wall.
Most laparoscopic procedures require entry into the anterior abdominal wall for placement of a trocar and a sleeve that serves as a portal for insertion of the endoscope. Secondary ports provide entry points for manipulative and operative tools.
The most critical entry point is primary placement of the viewing device. Secondary trocars are always inserted under direct visualization; therefore, they carry a lower risk of inflicting injury to underlying viscera and vessels.
Practice safe entry
In the early days of laparoscopy, only one method of entry existed. Over time, however, several other techniques have been devised.
The initial method—still widely utilized—is known as the closed or blind technique. The surgeon creates a pneumoperitoneum with the use of a needle that is 18 gauge to 2.5 mm in diameter; the needle is placed through a subumbilical incision. Once intraperitoneal placement is confirmed, CO2 gas is infused into the peritoneal cavity until the abdomen is tympanic to percussion (usually at pressures of 14 to 18 mm Hg).
Next, the surgeon aims the trocar toward the uterus at a 45° angle, maintaining the device in the midline. Entry is confirmed by opening the trocar’s trap-door valve and witnessing a rush of CO2 gas.
Another entry technique—the open technique—is used almost universally by general surgeons. The procedure is a type of microlaparotomy. After making the subumbilical incision, the fascia of the abdominal wall is pierced and the peritoneum is grasped and opened bluntly or sharply. Once the edges of the peritoneum are secured, a blunt trocar (Hasson trocar) is inserted. Then the trocar is removed, leaving the sleeve in place to accept the laparoscope.
Another entry variation, called direct entry, employs no pneumoperitoneum. In this approach, the surgeon grabs the anterior abdominal wall, sharply elevating it, and directly thrusts the reusable or disposable trocar into the abdominal cavity.
An extensive review of entry techniques has been published elsewhere.1
Many complications arise from entry techniques and devices
A survey of Australian gynecologists about entry techniques found that 73% of respondents used a Veress needle and pneumoperitoneum for entry and that 83% used a location other than the infraumbilical site when periumbilical adhesions were suspected. Twenty-one percent had experienced a major retroperitoneal vascular injury, but 33% lacked a plan to manage such injuries.2
In their review of entry techniques, Vilos and colleagues asserted that Veress-needle insertion should be accompanied by pneumoperitoneal pressures of 20 to 30 mm Hg rather than a predetermined volume of CO2 gas.1 They also recommended insertion in the left upper quadrant when periumbilical adhesions are suspected or when insufflation at the umbilicus fails three times.
Newer entry devices include the optical-view trocar and the radially expanding trocar. The first consists of a plastic, conically tipped instrument that is optically clear. At least hypothetically, this device permits the surgeon to view each layer of the abdominal wall as he or she thrusts the device under “direct vision” into the abdominal cavity.
The radially expanding trocar is inserted over a Veress needle into the abdominal cavity. Its initial diameter is only 3 mm; once the instrument is in place, however, a blunt plastic trocar and sleeve are pushed into the mesh-like, radially expanding tube until it reaches 11 to 12 mm in diameter. The blunt trocar is then removed, leaving the plastic sheath and mesh material in place to accept the laparoscope. One key advantage of this device is the mesh component, which resists slippage or movement as the laparoscope is moved in and out of the sheath.
Vilos and colleagues concluded that open entry was neither superior nor inferior to other entry techniques and that direct entry without pneumoperitoneum may be as safe as Veress-needle techniques and associated with a lower risk of gas embolism. They also reported that shielded trocars are not associated with fewer visceral or vascular injuries and that visual-entry trocars lack superiority, compared with other devices, for the prevention of visceral or vascular injuries.1
Other review articles about entry techniques similarly found no objective evidence that any single technique is superior.3 However, data are conflicting on the safety of the optical trocar, compared with other trocars, with some data showing marginal advantages and others demonstrating no difference.4-6
Follow a few key entry guidelines
In 1990, Yuzpe reported a mail-in survey of 800 practicing ObGyns in Canada on the topic of pneumoperitoneum and trocar injuries.7 Of the 407 physicians who responded, 16.7% reported that the pneumoperitoneum needle caused a visceral or major vessel injury, and 16.5% attributed the injury to the primary trocar. Among 109 vessel injuries, 31 were caused by the pneumoperitoneum needle, and 28 of 104 injuries were caused by the primary trocar.
To be safe, Veress needle and primary trocar entry require critical attention to the angle and direction of the thrust relative to the abdominal cavity (FIGURE, page 24). For example, if the Veress needle or the sharp tip of the trocar deviate to the right or left of the midline during entry into the abdomen, injury to the iliac vessels is a clear risk.
Most laparoscopic surgeons stand on the left-hand side of the patient and face her feet. Trocar deviation for a right-handed person tends to vector to the right, especially when a twisting motion is utilized. Correct alignment of the primary trocar is straight down the middle of the lower abdomen on a virtual or real line drawn from the center of the navel to the center of the symphysis.
An entry angle of 45° to 60° will carry the needle or trocar toward the bladder or uterus and away from the aorta and left common iliac vein. In contrast, a 90° thrust will aim the device dangerously toward the great vessels. A slightly upward and right-sided deviation from the subumbilical entry will place the needle and trocar in the direction of the inferior vena cava and right common iliac vessels. A 90° entry with deviation to the left will position the entry device at the inferior mesenteric vessels and the left common iliac vessels.
Primary abdominal entry
An entry angle of 45° to 60°, regardless of whether a needle or trocar is used, will carry the device toward the bladder or uterus and away from the aorta and left common iliac vein.In a review of access complications associated with laparoscopy, including major vascular injuries, Philips and Amaral listed variables responsible for large-vessel injury; they also documented the incidence of such injuries associated with laparoscopic cholecystectomy.8 They recommended that the patient be placed in the Trendelenburg position and that the needle or trocar be inserted at a 45° angle that stays within the midline; they also concluded that the trocar should be placed when pneumoperitoneal pressures exceed 20 mm Hg. They advised against direct insertion in patients with a history of pelvic surgery as well as in thin patients.
Place secondary trocars under direct visualization
Secondary trocars should always be placed under direct, visually controlled entry and, at least hypothetically, should never injure any great vessel. Nevertheless, secondary trocars do sometimes cause injury, most often as a result of extreme lateral entry near the inguinal ligament. The vessels at risk are the external iliac artery and vein.
Injuries are also invariably associated with adhesiolysis and anatomic problems. Precise knowledge of pelvic anatomy is not only a requisite for pelvic surgery in general but also for laparoscopic surgery, in which the operative view is less clear than it is in open procedures.
Know the risks associated with operative tools
Suturing and knot tying are not easy maneuvers during laparoscopic procedures and add significant operative time. Although they are performed more easily when robotics is utilized, few gynecologists are skilled practitioners. As a result, accessory instruments have been developed to prevent and control bleeding during laparoscopic operations. These devices include monopolar and bipolar instruments, lasers, ultrasonic tools, and stapling devices.
Avoid monopolar electrosurgery
This modality should be avoided whenever possible because the risk of injury is significantly higher than with bipolar electrosurgery. The key disadvantages of monopolar energy are high-frequency leaks; low-frequency currents; direct, indirect, and capacitative coupling; and return-electrode failures. None of these problems are common with bipolar techniques.
However, all electrosurgical devices carry a risk of thermal injury through direct tissue contact and conduction of heat to neighboring tissues and structures.
A full discussion of the physics and tissue actions of electrosurgical devices may be found elsewhere.9
CO2 is the safest laser
A variety of lasers have been used in laparoscopic surgery. The neodymium–YAG, KTP-532, and CO2 lasers have been used most frequently for gynecologic operations.
Because of its wavelength, the CO2 laser is the safest device for intra-abdominal use. Advantages include precision and control. In addition, the CO2 laser is absorbed by water very effectively. As a result, hydrodissection techniques can facilitate effective backstopping of the laser beam in strategic locations, thereby preventing injury to surrounding structures.
Laser energy is not conducted through tissue in the same way that electrosurgical energy is conducted. Therefore, the laser is ideal for vaporizing endometrial implants and cutting adhesions.
Beware of heat generated by the ultrasonic shears
This device, known more commonly as the Harmonic Scalpel (Ethicon), employs high-frequency sound waves to shear and coagulate tissue and prevent bleeding. It does not require conduction through tissues but does require contact with tissues. Because friction produces heat, these devices can become hot enough to inflict unintended burns on tissues that are inadvertently touched by the hot tip or by heat transmitted from the operative site by thermal conduction.
Stapler may inadvertently involve adjacent structures
This laparoscopic device has the advantage of not requiring or emitting energy other than the mechanical force of the operator’s hand. Disadvantages associated with the stapler center on the inadvertent inclusion of other structures within the jaws of the instrument. In addition, the staplers themselves tend to be large and somewhat unwieldy in close quarters, adding to the risk of stapling nearby viscera.
Further information on the physics and actions of lasers, ultrasonic shears, and staplers is available.10,11
Obesity may increase the risk of major vessel injury
A recent study by Baggish found obesity to be a high-risk circumstance for major vessel injury.12 In the study, 22 of 31 women who sustained injury were overweight or obese, with a BMI ranging from 26 to 30 kg/m2.
Obesity increases the risk of major vessel injury because of the greater elasticity of the anterior abdominal wall. As force secondary to the downward thrust of the trocar is placed on the abdominal wall, it is pushed inward in the direction of the posterior wall. In contrast, thin women have rigid abdominal walls with minimal elasticity, so the force of the trocar thrust does not create significant displacement.
Baggish also found that disposable trocars accounted for 90% of major vascular injuries and that use of long trocars accounted for 43% of deaths.12
Injury and death are rare but real risks
In a multicenter study in France over 9 years, investigators reviewed 29,966 diagnostic and operative laparoscopic procedures and found a mortality rate of 3.33 deaths for every 100,000 laparoscopies and an overall complication rate of 4.64 complications for every 1,000 procedures.13 They found the complication rate to be significantly correlated with the complexity of the procedure (P = .0001). One in three complications (34.1%; n = 43) occurred during set-up, and one in four (28.6%) were not identified intraoperatively.13
The risk of great vessel injury associated with laparoscopy most frequently quoted is 0.5 injury for every 1,000 procedures.14 A multicenter study reported the prevalence of this complication to be 1.05 injuries per 1,000 procedures.15
The mortality rate associated with major vessel injury has been reported in several studies to range from 8% to 17%.14-17
Two articles measured the distance from various points on the anterior abdominal wall to the great retroperitoneal vessels during laparoscopic operations; they also measured the force required for the trocar to penetrate the abdominal wall.18,19 They found significant differences in the distance from the site of primary trocar insertion to the aorta and iliac vessels, depending on the BMI of the patient. In women with a BMI below 25 kg/m2, the mean distance to the aorta was 11.21 cm. In women with a BMI of 25 to 30, it was 14.14 cm, and in women with a BMI over 30, it was 15.14 cm. They also found variations in the mean thickness of the abdominal wall, which was 3.48 cm, 3.85 cm, and 5.05 cm in women with a BMI of less than 25, 25–30, and more than 30, respectively.
As for the force required for entry, investigators found that disposable cutting trocars can traverse the anterior abdominal wall with less force and less time, compared with reusable trocars and optical viewing devices.18,19
Another study measured the thickness of the abdominal wall and the distance to the great vessels by magnetic resonance imaging or computed tomography.20 However, this study was not performed during laparoscopy with pneumoperitoneum in place.
As previously mentioned, Baggish reported on 31 cases of major-vessel injury associated with laparoscopic operations involving 49 major-vessel injuries. Twenty-eight injuries occurred as a result of entry techniques: 26 occurred during primary trocar insertion, and two were related to secondary trocar thrusts.12 Four injuries and three deaths were associated with use of an 11-inch disposable trocar.
Of the injuries associated with primary trocar insertion, 10 occurred during direct insertion and 26 after creation of pneumoperitoneum. Open laparoscopy was performed in two cases.12 The TABLE details the number of vessels injured and the sites of injury in this study.
Seven women (23%) died as a direct result of venous injury. Collateral injury to other structures was observed in 16 cases. Blood loss ranged from 1,000 mL to 7,000 mL.12
Sites of major vessel injury in one study of gynecologic laparoscopy
| Site | Number of vascular injuries |
|---|---|
| Right iliac artery | 14 |
| Right iliac vein | 12 |
| Left iliac artery | 3 |
| Left iliac vein | 9 |
| Aorta | 4 |
| Vena cava | 2 |
| Mesenteric | 2 |
| Interior epigastric* | 2 |
| Other | 1 |
| Total injuries | 49 |
| Source: Baggish12 | |
Avoid these common errors
The most common errors in gynecologic laparoscopy include:
- delayed diagnosis
- failure to act on a visible retroperitoneal hematoma
- failure to cross-match adequate supplies of blood and blood products
- failure to adequately transfuse blood and blood products
- clamping the large damaged vessel
- opening the abdomen via Pfannenstiel incision
- failure to call for a vascular surgeon in a timely manner.
When a major vascular injury occurs, a well-informed surgeon will take the following measures:
- call for a vascular surgeon immediately. (Baggish found that there was a substantial delay in getting a vascular surgeon to the operating table in four of 31 cases.12)
- open the abdomen via a midline incision
- use a sponge stick to apply direct pressure to the bleeding vessel
- obtain an emergency type and cross-match and order a minimum of 6 U of blood plus fresh frozen plasma
- obtain a baseline complete blood count, platelet count, fibrinogen level, and test for fibrin-split products
- advise the anesthesiologist to seek additional help
- call for additional OR nursing personnel
- assign one circulator to run stats and record critical data.21-33
Prevention is the best strategy
As the opening case demonstrates, major vessel injury can occur without warning and cause cascading problems that can lead to permanent disability—even death. Because most serious vessel injuries occur during entry into the anterior abdominal wall, careful attention to entry techniques and the patient’s unique circumstances (obesity, presence of adhesions) can go a long way toward averting injury. Vigilance for the possibility of injury is also important throughout the procedure. When injury does occur, it is critical to call for help as soon as possible and to have safeguards in place to manage it.
Tune in again in October 2012 for Part 2 of this series, which offers insight into gastrointestinal and urinary tract injuries during laparoscopy and offers valuable guidance on avoiding and managing related complications.
We want to hear from you! Tell us what you think.
Failure to document treatment refusal proves costly . . . Enlarging uterus goes uninvestigated . . . more
When following CT guidelines isn’t enough
AN 86-YEAR-OLD MAN ON WARFARIN FAINTED AND FELL while baby-sitting his great-grandchildren. He had transient neurologic symptoms after collapsing but appeared normal by the time paramedics arrived. He was taken by private vehicle to the hospital, where an emergency department (ED) physician examined him. After tests for a myocardial infarction revealed normal enzymes, electrocardiogram, and chest radiograph, the patient was discharged home.
He returned to the hospital the following day and underwent a computed tomography (CT) scan, which showed a large cerebral hemorrhage. He died soon afterward.
PLAINTIFF’S CLAIM The patient should have had a CT scan during the first ED visit. A scan at that visit would have found the hemorrhage in time to save the patient’s life.
THE DEFENSE No discussion with family members about a blow to the head or head trauma occurred, and a CT scan wasn’t requested. The patient didn’t meet criteria for a head scan. Even if a scan had been done at the initial visit, it might not have revealed the bleed. Moreover, the patient’s age decreased the likelihood that earlier detection would have changed the outcome.
VERDICT Confidential Utah settlements. The hospital settled for a nominal sum early in the litigation process; the physician settled for a confidential amount immediately before trial.
COMMENT Even when clear guidelines for imaging exist, taking care to weigh extenuating circumstances—in this case, that the patient was on warfarin—is critical.
Failure to document treatment refusal proves costly
A 15-YEAR-OLD BOY lost consciousness at home on Halloween and needed cardiopulmonary resuscitation. When paramedics arrived on the scene, they found the boy conscious and breathing, so they left. The boy, who had a history of drug abuse, died 8 hours later of anoxic encephalopathy caused by cocaine and opiate intoxication.
PLAINTIFF’S CLAIM The paramedics were negligent in failing to evaluate the boy’s condition properly and transport him to a hospital.
THE DEFENSE The paramedics left without assessing the boy because he and his father said they didn’t want or need medical help. (The paramedics neglected to obtain signed refusal of treatment forms.)
VERDICT $5.1 million Illinois verdict.
COMMENT Here is a $5 million verdict that hinges on the completion of forms for refusal of treatment, a remarkable reminder of the importance of documentation.
Enlarging uterus goes uninvestigated
AT AN ANNUAL GYNECOLOGIC EXAMINATION, a woman’s physician noted that her uterus had enlarged since her last visit and described it as “top size” in the chart. At the patient’s next annual exam 21 months later, the uterus had grown to 14 weeks’ gestational size.
Ten months after that, when the woman returned to her physician complaining of abdominal discomfort, her uterus was larger than at the previous examination. The physician advised her to consider a hysterectomy.
About 2 months later, the patient went to the doctor again because of increasing pelvic pressure. Her uterus was 18 to 20 weeks’ gestational size. The physician ordered an ultrasound, which showed a large mass on each ovary and no fibroids or masses within the uterus. Magnetic resonance imaging confirmed the ultrasound findings.
The doctor referred the woman to an oncological gynecologist. She subsequently underwent an abdominal hysterectomy with bilateral salpingo-oophorectomy and bilateral periaortic lymph node dissection. The pathology report described ovarian cancer with an ominous prognosis.
PLAINTIFF’S CLAIM The plaintiff alleged that the physician was negligent for failing to order testing when he first noticed the abnormal size of the uterus and at the patient’s subsequent visits. Failure to do so at the first exam and subsequent visits was negligent and allowed the cancer to advance instead of allowing for surgery and cure at an early stage.
THE DEFENSE No information about the defense is available.
VERDICT $650,000 Maryland settlement.
COMMENT It’s never a good policy to ignore a changing physical exam without good documentation, including a clear discussion of medical decision making.
Third ED visit isn’t the charm
A 39-YEAR-OLD QUADRIPLEGIC MAN went to the emergency department (ED) complaining of abdominal pain. His history included involvement in a shooting when he was 16, drug abuse, homelessness, and frequent visits to the ED, where the staff knew him to be combative and ignore medical advice. The ED physician who saw the man ordered a radiograph and other testing, then released him without a conclusive diagnosis.
A month later, the man came back to the ED by ambulance, complaining of severe abdominal pain that he’d had for 4 days. Another ED physician saw him but didn’t make a diagnosis. After 4 hours, the hospital discharged the patient by ambulance to stay with family. When the family refused to accept him, the ambulance brought him back to the hospital.
With the involvement of social services, the patient was wheeled across the street to a motel. After about 5 hours, during which the motel staff said the patient was screaming in pain, the staff called an ambulance, which brought the man back to the ED covered with bloody vomit.
The same ED physician who had seen him earlier examined him, along with another ED physician. A fecal impaction was removed manually and a soap suds enema administered. The patient seemed to improve and, after about 7 hours, was released and rolled outside with a taxi voucher.
He said the hospital staff told him he was abusing the hospital’s services and the police would be called if he returned. He was taken to the house of a family member, where he was found dead 4 hours later from a ruptured duodenal ulcer.
PLAINTIFF’S CLAIM The physician who saw the patient at the first ED visit should have diagnosed peptic ulcer disease; the doctors who saw the man at the second and third visits should have diagnosed the ruptured ulcer. The hospital violated the federal Emergency Medical Treatment and Labor Act (EMTALA) by failing to stabilize the patient before discharging him.
THE DEFENSE The patient was stable and improving each time he was discharged. The hospital denied threatening to arrest the patient if he returned to the ED after the third visit.
VERDICT $1.4 million Kentucky verdict. The first trial ended in a mistrial. All defendants except the hospital settled for undisclosed amounts before a second trial, at which the hospital was found to be 15% at fault and a $1.5 million award for punitive damages was assessed against the hospital for violating EMTALA.
The hospital appealed and the matter was returned for trial after a ruling that affirmed everything except the punitive damages. At the third trial, a jury awarded $1.4 million in punitive damages.
COMMENT Most of us have a visceral reaction when faced with a drug abusing, noncompliant patient who frequently shows up at the ED. We must remember that such patients do get sick and that in this case, despite repeated visits to the ED, a tragedy occurred.
When following CT guidelines isn’t enough
AN 86-YEAR-OLD MAN ON WARFARIN FAINTED AND FELL while baby-sitting his great-grandchildren. He had transient neurologic symptoms after collapsing but appeared normal by the time paramedics arrived. He was taken by private vehicle to the hospital, where an emergency department (ED) physician examined him. After tests for a myocardial infarction revealed normal enzymes, electrocardiogram, and chest radiograph, the patient was discharged home.
He returned to the hospital the following day and underwent a computed tomography (CT) scan, which showed a large cerebral hemorrhage. He died soon afterward.
PLAINTIFF’S CLAIM The patient should have had a CT scan during the first ED visit. A scan at that visit would have found the hemorrhage in time to save the patient’s life.
THE DEFENSE No discussion with family members about a blow to the head or head trauma occurred, and a CT scan wasn’t requested. The patient didn’t meet criteria for a head scan. Even if a scan had been done at the initial visit, it might not have revealed the bleed. Moreover, the patient’s age decreased the likelihood that earlier detection would have changed the outcome.
VERDICT Confidential Utah settlements. The hospital settled for a nominal sum early in the litigation process; the physician settled for a confidential amount immediately before trial.
COMMENT Even when clear guidelines for imaging exist, taking care to weigh extenuating circumstances—in this case, that the patient was on warfarin—is critical.
Failure to document treatment refusal proves costly
A 15-YEAR-OLD BOY lost consciousness at home on Halloween and needed cardiopulmonary resuscitation. When paramedics arrived on the scene, they found the boy conscious and breathing, so they left. The boy, who had a history of drug abuse, died 8 hours later of anoxic encephalopathy caused by cocaine and opiate intoxication.
PLAINTIFF’S CLAIM The paramedics were negligent in failing to evaluate the boy’s condition properly and transport him to a hospital.
THE DEFENSE The paramedics left without assessing the boy because he and his father said they didn’t want or need medical help. (The paramedics neglected to obtain signed refusal of treatment forms.)
VERDICT $5.1 million Illinois verdict.
COMMENT Here is a $5 million verdict that hinges on the completion of forms for refusal of treatment, a remarkable reminder of the importance of documentation.
Enlarging uterus goes uninvestigated
AT AN ANNUAL GYNECOLOGIC EXAMINATION, a woman’s physician noted that her uterus had enlarged since her last visit and described it as “top size” in the chart. At the patient’s next annual exam 21 months later, the uterus had grown to 14 weeks’ gestational size.
Ten months after that, when the woman returned to her physician complaining of abdominal discomfort, her uterus was larger than at the previous examination. The physician advised her to consider a hysterectomy.
About 2 months later, the patient went to the doctor again because of increasing pelvic pressure. Her uterus was 18 to 20 weeks’ gestational size. The physician ordered an ultrasound, which showed a large mass on each ovary and no fibroids or masses within the uterus. Magnetic resonance imaging confirmed the ultrasound findings.
The doctor referred the woman to an oncological gynecologist. She subsequently underwent an abdominal hysterectomy with bilateral salpingo-oophorectomy and bilateral periaortic lymph node dissection. The pathology report described ovarian cancer with an ominous prognosis.
PLAINTIFF’S CLAIM The plaintiff alleged that the physician was negligent for failing to order testing when he first noticed the abnormal size of the uterus and at the patient’s subsequent visits. Failure to do so at the first exam and subsequent visits was negligent and allowed the cancer to advance instead of allowing for surgery and cure at an early stage.
THE DEFENSE No information about the defense is available.
VERDICT $650,000 Maryland settlement.
COMMENT It’s never a good policy to ignore a changing physical exam without good documentation, including a clear discussion of medical decision making.
Third ED visit isn’t the charm
A 39-YEAR-OLD QUADRIPLEGIC MAN went to the emergency department (ED) complaining of abdominal pain. His history included involvement in a shooting when he was 16, drug abuse, homelessness, and frequent visits to the ED, where the staff knew him to be combative and ignore medical advice. The ED physician who saw the man ordered a radiograph and other testing, then released him without a conclusive diagnosis.
A month later, the man came back to the ED by ambulance, complaining of severe abdominal pain that he’d had for 4 days. Another ED physician saw him but didn’t make a diagnosis. After 4 hours, the hospital discharged the patient by ambulance to stay with family. When the family refused to accept him, the ambulance brought him back to the hospital.
With the involvement of social services, the patient was wheeled across the street to a motel. After about 5 hours, during which the motel staff said the patient was screaming in pain, the staff called an ambulance, which brought the man back to the ED covered with bloody vomit.
The same ED physician who had seen him earlier examined him, along with another ED physician. A fecal impaction was removed manually and a soap suds enema administered. The patient seemed to improve and, after about 7 hours, was released and rolled outside with a taxi voucher.
He said the hospital staff told him he was abusing the hospital’s services and the police would be called if he returned. He was taken to the house of a family member, where he was found dead 4 hours later from a ruptured duodenal ulcer.
PLAINTIFF’S CLAIM The physician who saw the patient at the first ED visit should have diagnosed peptic ulcer disease; the doctors who saw the man at the second and third visits should have diagnosed the ruptured ulcer. The hospital violated the federal Emergency Medical Treatment and Labor Act (EMTALA) by failing to stabilize the patient before discharging him.
THE DEFENSE The patient was stable and improving each time he was discharged. The hospital denied threatening to arrest the patient if he returned to the ED after the third visit.
VERDICT $1.4 million Kentucky verdict. The first trial ended in a mistrial. All defendants except the hospital settled for undisclosed amounts before a second trial, at which the hospital was found to be 15% at fault and a $1.5 million award for punitive damages was assessed against the hospital for violating EMTALA.
The hospital appealed and the matter was returned for trial after a ruling that affirmed everything except the punitive damages. At the third trial, a jury awarded $1.4 million in punitive damages.
COMMENT Most of us have a visceral reaction when faced with a drug abusing, noncompliant patient who frequently shows up at the ED. We must remember that such patients do get sick and that in this case, despite repeated visits to the ED, a tragedy occurred.
When following CT guidelines isn’t enough
AN 86-YEAR-OLD MAN ON WARFARIN FAINTED AND FELL while baby-sitting his great-grandchildren. He had transient neurologic symptoms after collapsing but appeared normal by the time paramedics arrived. He was taken by private vehicle to the hospital, where an emergency department (ED) physician examined him. After tests for a myocardial infarction revealed normal enzymes, electrocardiogram, and chest radiograph, the patient was discharged home.
He returned to the hospital the following day and underwent a computed tomography (CT) scan, which showed a large cerebral hemorrhage. He died soon afterward.
PLAINTIFF’S CLAIM The patient should have had a CT scan during the first ED visit. A scan at that visit would have found the hemorrhage in time to save the patient’s life.
THE DEFENSE No discussion with family members about a blow to the head or head trauma occurred, and a CT scan wasn’t requested. The patient didn’t meet criteria for a head scan. Even if a scan had been done at the initial visit, it might not have revealed the bleed. Moreover, the patient’s age decreased the likelihood that earlier detection would have changed the outcome.
VERDICT Confidential Utah settlements. The hospital settled for a nominal sum early in the litigation process; the physician settled for a confidential amount immediately before trial.
COMMENT Even when clear guidelines for imaging exist, taking care to weigh extenuating circumstances—in this case, that the patient was on warfarin—is critical.
Failure to document treatment refusal proves costly
A 15-YEAR-OLD BOY lost consciousness at home on Halloween and needed cardiopulmonary resuscitation. When paramedics arrived on the scene, they found the boy conscious and breathing, so they left. The boy, who had a history of drug abuse, died 8 hours later of anoxic encephalopathy caused by cocaine and opiate intoxication.
PLAINTIFF’S CLAIM The paramedics were negligent in failing to evaluate the boy’s condition properly and transport him to a hospital.
THE DEFENSE The paramedics left without assessing the boy because he and his father said they didn’t want or need medical help. (The paramedics neglected to obtain signed refusal of treatment forms.)
VERDICT $5.1 million Illinois verdict.
COMMENT Here is a $5 million verdict that hinges on the completion of forms for refusal of treatment, a remarkable reminder of the importance of documentation.
Enlarging uterus goes uninvestigated
AT AN ANNUAL GYNECOLOGIC EXAMINATION, a woman’s physician noted that her uterus had enlarged since her last visit and described it as “top size” in the chart. At the patient’s next annual exam 21 months later, the uterus had grown to 14 weeks’ gestational size.
Ten months after that, when the woman returned to her physician complaining of abdominal discomfort, her uterus was larger than at the previous examination. The physician advised her to consider a hysterectomy.
About 2 months later, the patient went to the doctor again because of increasing pelvic pressure. Her uterus was 18 to 20 weeks’ gestational size. The physician ordered an ultrasound, which showed a large mass on each ovary and no fibroids or masses within the uterus. Magnetic resonance imaging confirmed the ultrasound findings.
The doctor referred the woman to an oncological gynecologist. She subsequently underwent an abdominal hysterectomy with bilateral salpingo-oophorectomy and bilateral periaortic lymph node dissection. The pathology report described ovarian cancer with an ominous prognosis.
PLAINTIFF’S CLAIM The plaintiff alleged that the physician was negligent for failing to order testing when he first noticed the abnormal size of the uterus and at the patient’s subsequent visits. Failure to do so at the first exam and subsequent visits was negligent and allowed the cancer to advance instead of allowing for surgery and cure at an early stage.
THE DEFENSE No information about the defense is available.
VERDICT $650,000 Maryland settlement.
COMMENT It’s never a good policy to ignore a changing physical exam without good documentation, including a clear discussion of medical decision making.
Third ED visit isn’t the charm
A 39-YEAR-OLD QUADRIPLEGIC MAN went to the emergency department (ED) complaining of abdominal pain. His history included involvement in a shooting when he was 16, drug abuse, homelessness, and frequent visits to the ED, where the staff knew him to be combative and ignore medical advice. The ED physician who saw the man ordered a radiograph and other testing, then released him without a conclusive diagnosis.
A month later, the man came back to the ED by ambulance, complaining of severe abdominal pain that he’d had for 4 days. Another ED physician saw him but didn’t make a diagnosis. After 4 hours, the hospital discharged the patient by ambulance to stay with family. When the family refused to accept him, the ambulance brought him back to the hospital.
With the involvement of social services, the patient was wheeled across the street to a motel. After about 5 hours, during which the motel staff said the patient was screaming in pain, the staff called an ambulance, which brought the man back to the ED covered with bloody vomit.
The same ED physician who had seen him earlier examined him, along with another ED physician. A fecal impaction was removed manually and a soap suds enema administered. The patient seemed to improve and, after about 7 hours, was released and rolled outside with a taxi voucher.
He said the hospital staff told him he was abusing the hospital’s services and the police would be called if he returned. He was taken to the house of a family member, where he was found dead 4 hours later from a ruptured duodenal ulcer.
PLAINTIFF’S CLAIM The physician who saw the patient at the first ED visit should have diagnosed peptic ulcer disease; the doctors who saw the man at the second and third visits should have diagnosed the ruptured ulcer. The hospital violated the federal Emergency Medical Treatment and Labor Act (EMTALA) by failing to stabilize the patient before discharging him.
THE DEFENSE The patient was stable and improving each time he was discharged. The hospital denied threatening to arrest the patient if he returned to the ED after the third visit.
VERDICT $1.4 million Kentucky verdict. The first trial ended in a mistrial. All defendants except the hospital settled for undisclosed amounts before a second trial, at which the hospital was found to be 15% at fault and a $1.5 million award for punitive damages was assessed against the hospital for violating EMTALA.
The hospital appealed and the matter was returned for trial after a ruling that affirmed everything except the punitive damages. At the third trial, a jury awarded $1.4 million in punitive damages.
COMMENT Most of us have a visceral reaction when faced with a drug abusing, noncompliant patient who frequently shows up at the ED. We must remember that such patients do get sick and that in this case, despite repeated visits to the ED, a tragedy occurred.
Injection may be the best bet for young athletes’ knee pain
Consider giving dextrose/lidocaine injections to adolescents with Osgood-Schlatter disease (OSD) that persists despite physical therapy.1
STRENGTH OF RECOMMENDATION
A: Based on one well-designed, randomized controlled trial (RCT).
Topol GA, Podesta LA, Reeves KD, et al. Hyperosmolar dextrose injection for recalcitrant Osgood-Schlatter disease. Pediatrics. 2011;128: e1121-e1128.
ILLUSTRATIVE CASE
A 13-year-old boy comes in to your office for follow-up of anterior knee pain from OSD that has not responded to 2 months of physical therapy. he is still unable to play on his recreational soccer team. What treatment can you offer to help him return to the sport he enjoys?
OSD is characterized by inflammation of the growth plate just below the knee, the result of repetitive strain on the secondary ossification center of the tibial tuberosity.2 Closure of the tibial growth plate is the definitive remedy for OSD, but the pain that some adolescents experience until that happens can be long-lasting and considerable. Nine years after diagnosis of OSD, one study found, up to 60% of patients who had received conservative treatment reported pain on kneeling and 18% had sports limitations.3
Inability to play may affect self-esteem
Adolescents whose recreational activities are limited due to OSD may experience a number of negative effects, including alienation from friends, altered peer group dynamics, and a decline in self-esteem. Surgery, which involves excision of the pain-producing ossicle with or without tuberculoplasty, relieves the pain and allows patients to return to their chosen sport in 90% to 95% of cases that have not responded to conservative treatment.4,5 For a self-limiting (although prolonged) condition like OSD, most physicians and patients would prefer to avoid surgery and opt for a more conservative approach.
Dextrose injections have been shown to be safe and effective when used for the treatment of tendon and ligamentous disorders such as Achilles tendonitis and lateral epicondylitis, although the mechanism of action is not clear.6,7 The study detailed in this PURL is the first prospective RCT of dextrose injections for the treatment of OSD.
STUDY SUMMARY: injections get adolescents back in the game
Topol et al1 sought to compare the efficacy of injections of dextrose and lidocaine with lidocaine-only injections or supervised usual care in treating OSD in young athletes. Sixty-six Argentinian boys and girls ages 9 to 17 years, all of whom had anterior knee pain and participated in kicking or jumping sports on organized teams, were considered for the study. The absence of either patellofemoral crepitus or proximal patellar tendon tenderness was a prerequisite for participation, as was reproduction of the anterior knee pain and localization of pain precisely to the tibial tuberosity during a single leg squat to confirm the OSD diagnosis.
After diagnosis, the patients completed ≥2 months of formal and gently progressive hamstring stretching, quads strengthening, and gradual reintroduction into their respective sports. Those who experienced pain during team play that persisted for ≥3 months—54 patients, all but 3 of whom were male, with a total of 65 knees requiring treatment—were included in the study. Participants were randomized to the usual care group or to one of the injection groups, which was blinded to patients, guardians, and physicians.
The injection groups received a solution of lidocaine 1%, alone or with 12.5% dextrose, at the start of the study and again at 1 and 2 months. Adequate injection was determined by complete pain relief during a single leg squat, which was also used to determine both proximal and distal points of tenderness. Both injection groups received 0.5-mL injections with a 27-gauge needle, repeated at approximately 1-cm intervals for a total of 3 to 4 midline injections. After 5 minutes, the leg squat was repeated to detect any remaining pain, and painful areas were injected until the patient could do a pain-free leg squat.
Because pain reduction may precede full healing, those in both the lidocaine-only and the dextrose-lidocaine groups received injections on all 3 occasions even if they were pain free. They were instructed to avoid running for a week after the initial treatment and then to run as tolerated. Subsequent treatments required a 3-day rest from running. Participants were able to return to their sport after the second injection and rest period.
Patients in all 3 groups received handouts explaining hamstring stretches and quadriceps strengthening exercises. The usual care group received individual instruction from a physical therapist. They were also given a video and returned at least once, both to ensure that they were performing the exercises correctly and to encourage compliance.
The primary outcome involved the Nirschl Pain Phase Scale (NPPS), a 7-point measure of sports-related symptoms and level of participation. Scores of 4 to 7 represent sports limitation resulting from pain. Scores <4 (which may involve soreness or pain but participation in the sport is unlimited) and 0 (asymptomatic participation) were the threshold goals for the study.
The groups were similar at baseline, and follow-up was 100%. At 3 months, NPPS scores improved more in dextrose-treated knees than in either the lidocaine-treated knees (3.9 vs 2.4; P=.004) or those who received usual care (3.9 vs 1.2; P=.001), and lidocaine alone was significantly better than usual care (2.4 vs 1.2; P=.024). More than 90% of participants in both injection groups achieved unlimited sports participation by 3 months. However, knees treated with dextrose were significantly more likely than lidocaine-treated knees to allow asymptomatic participation (NPPS=0), with 14 of 21 knees and 5 of 22 knees, respectively, being pain-free. After one year, more dextrose-treated knees than lidocaine-treated knees were asymptomatic with sports participation (32 of 38 vs 6 of 13; P=.024).
There were no reported adverse effects during this study and fewer than 10% of subjects required acetaminophen for postinjection pain control.
WHAT’S NEW: OSD can be safely and effectively treated
This study found dextrose injections to be safe, well tolerated, and effective in treating patients with intractable OSD symptoms. The results suggest that the duration of both the sports limitation and sports-related symptoms may be reduced with dextrose injections in adolescent athletes with recalcitrant OSD.
CAVEATS: Lack of validated measure, controls
NPPS is not an ideal measure of OSD symptoms because it has not been validated. The failure to use a validated measure of tendinopathy symptoms (eg, the Victorian Institute of Sport Assessment-Patella8) is a significant limitation of this trial. The athletes included in this study had already failed to respond to the usual treatment, which suggests that injections should be reserved for those who have tried hamstring stretching and quad-strengthening exercises.
CHALLENGES TO IMPLEMENTATION: Patient and provider comfort may be an issue
Although the injections in this study were well tolerated, there is a risk of infection, bleeding, and pain with any injection or invasive procedure. In addition, adolescents often have difficulty tolerating injections, especially repeated needlesticks like those called for in the proposed treatment. The nonviscous nature of dextrose allows 27- to 30-gauge needles to be used, which may make the injections easier for teens to tolerate. Some physicians may be hesitant to start these young patients on a new injectable therapy.
Click here to view PURL METHODOLOGY
1. Topol GA, Podesta LA, Reeves KD, et al. Hyperosmolar dextrose injection for recalcitrant Osgood-Schlatter disease. Pediatrics. 2011;128:e1121-e1128.
2. Gholve PA, Scher DM, Khakharia S, et al. Osgood-Schlatter syndrome. Curr Opin Pediatr. 2007;19:44-50.
3. Krause BL, Willimas JP, Caterall A. Natural history of OsgoodSchlatter disease. J Pediatr Orthop. 1990;10:65-68.
4. Nierenberg G, Falah M, Keren Y, et al. Surgical treatment of residual Osgood-Schlatter disease in young adults: role of the mobile osseous fragment. Orthopedics. 2011;34:176.-
5. El-Husseini TF, Abdelgawad AA. Results of surgical treatment of unresolved Osgood-Schlatter disease in adults. J Knee Surg. 2010;23:103-107.
6. Ryan M, Wong A, Taunton J. Favorable outcomes after sonographically guided intratendinous injection of hyperosmolar dextrose for chronic insertional and midportion achilles tendinosis. AJR Am J Roentgenol. 2010;194:1047-1053.
7. Scarpone M, Rabago D, Zgierska A, et al. The efficacy of prolotherapy for lateral epicondylitis: a pilot study. Clin J Sport Med. 2008;18:248-254.
8. Visentini PJ, Khan KM, Cook JL, et al. The VISA score: an index of severity of symptoms in patients with jumper’s knee (patellar tendinosis). Victorian Institute of Sport Tendon Study Group. J Sci Med Sport. 1998;1:22-28.
| Young athlete sidelined? Check to see how he’s coping Samantha O’Connell, PhD |
Mark Sakr, DO
Department of Family Medicine, University of North Carolina at Chapel Hill
Anne Mounsey, MD
Department of Family Medicine, University of North Carolina at Chapel Hill
PURLs EDITOR
John Hickner, MD, MSc
Cleveland Clinic
| Young athlete sidelined? Check to see how he’s coping Samantha O’Connell, PhD |
Mark Sakr, DO
Department of Family Medicine, University of North Carolina at Chapel Hill
Anne Mounsey, MD
Department of Family Medicine, University of North Carolina at Chapel Hill
PURLs EDITOR
John Hickner, MD, MSc
Cleveland Clinic
| Young athlete sidelined? Check to see how he’s coping Samantha O’Connell, PhD |
Mark Sakr, DO
Department of Family Medicine, University of North Carolina at Chapel Hill
Anne Mounsey, MD
Department of Family Medicine, University of North Carolina at Chapel Hill
PURLs EDITOR
John Hickner, MD, MSc
Cleveland Clinic
Consider giving dextrose/lidocaine injections to adolescents with Osgood-Schlatter disease (OSD) that persists despite physical therapy.1
STRENGTH OF RECOMMENDATION
A: Based on one well-designed, randomized controlled trial (RCT).
Topol GA, Podesta LA, Reeves KD, et al. Hyperosmolar dextrose injection for recalcitrant Osgood-Schlatter disease. Pediatrics. 2011;128: e1121-e1128.
ILLUSTRATIVE CASE
A 13-year-old boy comes in to your office for follow-up of anterior knee pain from OSD that has not responded to 2 months of physical therapy. he is still unable to play on his recreational soccer team. What treatment can you offer to help him return to the sport he enjoys?
OSD is characterized by inflammation of the growth plate just below the knee, the result of repetitive strain on the secondary ossification center of the tibial tuberosity.2 Closure of the tibial growth plate is the definitive remedy for OSD, but the pain that some adolescents experience until that happens can be long-lasting and considerable. Nine years after diagnosis of OSD, one study found, up to 60% of patients who had received conservative treatment reported pain on kneeling and 18% had sports limitations.3
Inability to play may affect self-esteem
Adolescents whose recreational activities are limited due to OSD may experience a number of negative effects, including alienation from friends, altered peer group dynamics, and a decline in self-esteem. Surgery, which involves excision of the pain-producing ossicle with or without tuberculoplasty, relieves the pain and allows patients to return to their chosen sport in 90% to 95% of cases that have not responded to conservative treatment.4,5 For a self-limiting (although prolonged) condition like OSD, most physicians and patients would prefer to avoid surgery and opt for a more conservative approach.
Dextrose injections have been shown to be safe and effective when used for the treatment of tendon and ligamentous disorders such as Achilles tendonitis and lateral epicondylitis, although the mechanism of action is not clear.6,7 The study detailed in this PURL is the first prospective RCT of dextrose injections for the treatment of OSD.
STUDY SUMMARY: injections get adolescents back in the game
Topol et al1 sought to compare the efficacy of injections of dextrose and lidocaine with lidocaine-only injections or supervised usual care in treating OSD in young athletes. Sixty-six Argentinian boys and girls ages 9 to 17 years, all of whom had anterior knee pain and participated in kicking or jumping sports on organized teams, were considered for the study. The absence of either patellofemoral crepitus or proximal patellar tendon tenderness was a prerequisite for participation, as was reproduction of the anterior knee pain and localization of pain precisely to the tibial tuberosity during a single leg squat to confirm the OSD diagnosis.
After diagnosis, the patients completed ≥2 months of formal and gently progressive hamstring stretching, quads strengthening, and gradual reintroduction into their respective sports. Those who experienced pain during team play that persisted for ≥3 months—54 patients, all but 3 of whom were male, with a total of 65 knees requiring treatment—were included in the study. Participants were randomized to the usual care group or to one of the injection groups, which was blinded to patients, guardians, and physicians.
The injection groups received a solution of lidocaine 1%, alone or with 12.5% dextrose, at the start of the study and again at 1 and 2 months. Adequate injection was determined by complete pain relief during a single leg squat, which was also used to determine both proximal and distal points of tenderness. Both injection groups received 0.5-mL injections with a 27-gauge needle, repeated at approximately 1-cm intervals for a total of 3 to 4 midline injections. After 5 minutes, the leg squat was repeated to detect any remaining pain, and painful areas were injected until the patient could do a pain-free leg squat.
Because pain reduction may precede full healing, those in both the lidocaine-only and the dextrose-lidocaine groups received injections on all 3 occasions even if they were pain free. They were instructed to avoid running for a week after the initial treatment and then to run as tolerated. Subsequent treatments required a 3-day rest from running. Participants were able to return to their sport after the second injection and rest period.
Patients in all 3 groups received handouts explaining hamstring stretches and quadriceps strengthening exercises. The usual care group received individual instruction from a physical therapist. They were also given a video and returned at least once, both to ensure that they were performing the exercises correctly and to encourage compliance.
The primary outcome involved the Nirschl Pain Phase Scale (NPPS), a 7-point measure of sports-related symptoms and level of participation. Scores of 4 to 7 represent sports limitation resulting from pain. Scores <4 (which may involve soreness or pain but participation in the sport is unlimited) and 0 (asymptomatic participation) were the threshold goals for the study.
The groups were similar at baseline, and follow-up was 100%. At 3 months, NPPS scores improved more in dextrose-treated knees than in either the lidocaine-treated knees (3.9 vs 2.4; P=.004) or those who received usual care (3.9 vs 1.2; P=.001), and lidocaine alone was significantly better than usual care (2.4 vs 1.2; P=.024). More than 90% of participants in both injection groups achieved unlimited sports participation by 3 months. However, knees treated with dextrose were significantly more likely than lidocaine-treated knees to allow asymptomatic participation (NPPS=0), with 14 of 21 knees and 5 of 22 knees, respectively, being pain-free. After one year, more dextrose-treated knees than lidocaine-treated knees were asymptomatic with sports participation (32 of 38 vs 6 of 13; P=.024).
There were no reported adverse effects during this study and fewer than 10% of subjects required acetaminophen for postinjection pain control.
WHAT’S NEW: OSD can be safely and effectively treated
This study found dextrose injections to be safe, well tolerated, and effective in treating patients with intractable OSD symptoms. The results suggest that the duration of both the sports limitation and sports-related symptoms may be reduced with dextrose injections in adolescent athletes with recalcitrant OSD.
CAVEATS: Lack of validated measure, controls
NPPS is not an ideal measure of OSD symptoms because it has not been validated. The failure to use a validated measure of tendinopathy symptoms (eg, the Victorian Institute of Sport Assessment-Patella8) is a significant limitation of this trial. The athletes included in this study had already failed to respond to the usual treatment, which suggests that injections should be reserved for those who have tried hamstring stretching and quad-strengthening exercises.
CHALLENGES TO IMPLEMENTATION: Patient and provider comfort may be an issue
Although the injections in this study were well tolerated, there is a risk of infection, bleeding, and pain with any injection or invasive procedure. In addition, adolescents often have difficulty tolerating injections, especially repeated needlesticks like those called for in the proposed treatment. The nonviscous nature of dextrose allows 27- to 30-gauge needles to be used, which may make the injections easier for teens to tolerate. Some physicians may be hesitant to start these young patients on a new injectable therapy.
Click here to view PURL METHODOLOGY
Consider giving dextrose/lidocaine injections to adolescents with Osgood-Schlatter disease (OSD) that persists despite physical therapy.1
STRENGTH OF RECOMMENDATION
A: Based on one well-designed, randomized controlled trial (RCT).
Topol GA, Podesta LA, Reeves KD, et al. Hyperosmolar dextrose injection for recalcitrant Osgood-Schlatter disease. Pediatrics. 2011;128: e1121-e1128.
ILLUSTRATIVE CASE
A 13-year-old boy comes in to your office for follow-up of anterior knee pain from OSD that has not responded to 2 months of physical therapy. he is still unable to play on his recreational soccer team. What treatment can you offer to help him return to the sport he enjoys?
OSD is characterized by inflammation of the growth plate just below the knee, the result of repetitive strain on the secondary ossification center of the tibial tuberosity.2 Closure of the tibial growth plate is the definitive remedy for OSD, but the pain that some adolescents experience until that happens can be long-lasting and considerable. Nine years after diagnosis of OSD, one study found, up to 60% of patients who had received conservative treatment reported pain on kneeling and 18% had sports limitations.3
Inability to play may affect self-esteem
Adolescents whose recreational activities are limited due to OSD may experience a number of negative effects, including alienation from friends, altered peer group dynamics, and a decline in self-esteem. Surgery, which involves excision of the pain-producing ossicle with or without tuberculoplasty, relieves the pain and allows patients to return to their chosen sport in 90% to 95% of cases that have not responded to conservative treatment.4,5 For a self-limiting (although prolonged) condition like OSD, most physicians and patients would prefer to avoid surgery and opt for a more conservative approach.
Dextrose injections have been shown to be safe and effective when used for the treatment of tendon and ligamentous disorders such as Achilles tendonitis and lateral epicondylitis, although the mechanism of action is not clear.6,7 The study detailed in this PURL is the first prospective RCT of dextrose injections for the treatment of OSD.
STUDY SUMMARY: injections get adolescents back in the game
Topol et al1 sought to compare the efficacy of injections of dextrose and lidocaine with lidocaine-only injections or supervised usual care in treating OSD in young athletes. Sixty-six Argentinian boys and girls ages 9 to 17 years, all of whom had anterior knee pain and participated in kicking or jumping sports on organized teams, were considered for the study. The absence of either patellofemoral crepitus or proximal patellar tendon tenderness was a prerequisite for participation, as was reproduction of the anterior knee pain and localization of pain precisely to the tibial tuberosity during a single leg squat to confirm the OSD diagnosis.
After diagnosis, the patients completed ≥2 months of formal and gently progressive hamstring stretching, quads strengthening, and gradual reintroduction into their respective sports. Those who experienced pain during team play that persisted for ≥3 months—54 patients, all but 3 of whom were male, with a total of 65 knees requiring treatment—were included in the study. Participants were randomized to the usual care group or to one of the injection groups, which was blinded to patients, guardians, and physicians.
The injection groups received a solution of lidocaine 1%, alone or with 12.5% dextrose, at the start of the study and again at 1 and 2 months. Adequate injection was determined by complete pain relief during a single leg squat, which was also used to determine both proximal and distal points of tenderness. Both injection groups received 0.5-mL injections with a 27-gauge needle, repeated at approximately 1-cm intervals for a total of 3 to 4 midline injections. After 5 minutes, the leg squat was repeated to detect any remaining pain, and painful areas were injected until the patient could do a pain-free leg squat.
Because pain reduction may precede full healing, those in both the lidocaine-only and the dextrose-lidocaine groups received injections on all 3 occasions even if they were pain free. They were instructed to avoid running for a week after the initial treatment and then to run as tolerated. Subsequent treatments required a 3-day rest from running. Participants were able to return to their sport after the second injection and rest period.
Patients in all 3 groups received handouts explaining hamstring stretches and quadriceps strengthening exercises. The usual care group received individual instruction from a physical therapist. They were also given a video and returned at least once, both to ensure that they were performing the exercises correctly and to encourage compliance.
The primary outcome involved the Nirschl Pain Phase Scale (NPPS), a 7-point measure of sports-related symptoms and level of participation. Scores of 4 to 7 represent sports limitation resulting from pain. Scores <4 (which may involve soreness or pain but participation in the sport is unlimited) and 0 (asymptomatic participation) were the threshold goals for the study.
The groups were similar at baseline, and follow-up was 100%. At 3 months, NPPS scores improved more in dextrose-treated knees than in either the lidocaine-treated knees (3.9 vs 2.4; P=.004) or those who received usual care (3.9 vs 1.2; P=.001), and lidocaine alone was significantly better than usual care (2.4 vs 1.2; P=.024). More than 90% of participants in both injection groups achieved unlimited sports participation by 3 months. However, knees treated with dextrose were significantly more likely than lidocaine-treated knees to allow asymptomatic participation (NPPS=0), with 14 of 21 knees and 5 of 22 knees, respectively, being pain-free. After one year, more dextrose-treated knees than lidocaine-treated knees were asymptomatic with sports participation (32 of 38 vs 6 of 13; P=.024).
There were no reported adverse effects during this study and fewer than 10% of subjects required acetaminophen for postinjection pain control.
WHAT’S NEW: OSD can be safely and effectively treated
This study found dextrose injections to be safe, well tolerated, and effective in treating patients with intractable OSD symptoms. The results suggest that the duration of both the sports limitation and sports-related symptoms may be reduced with dextrose injections in adolescent athletes with recalcitrant OSD.
CAVEATS: Lack of validated measure, controls
NPPS is not an ideal measure of OSD symptoms because it has not been validated. The failure to use a validated measure of tendinopathy symptoms (eg, the Victorian Institute of Sport Assessment-Patella8) is a significant limitation of this trial. The athletes included in this study had already failed to respond to the usual treatment, which suggests that injections should be reserved for those who have tried hamstring stretching and quad-strengthening exercises.
CHALLENGES TO IMPLEMENTATION: Patient and provider comfort may be an issue
Although the injections in this study were well tolerated, there is a risk of infection, bleeding, and pain with any injection or invasive procedure. In addition, adolescents often have difficulty tolerating injections, especially repeated needlesticks like those called for in the proposed treatment. The nonviscous nature of dextrose allows 27- to 30-gauge needles to be used, which may make the injections easier for teens to tolerate. Some physicians may be hesitant to start these young patients on a new injectable therapy.
Click here to view PURL METHODOLOGY
1. Topol GA, Podesta LA, Reeves KD, et al. Hyperosmolar dextrose injection for recalcitrant Osgood-Schlatter disease. Pediatrics. 2011;128:e1121-e1128.
2. Gholve PA, Scher DM, Khakharia S, et al. Osgood-Schlatter syndrome. Curr Opin Pediatr. 2007;19:44-50.
3. Krause BL, Willimas JP, Caterall A. Natural history of OsgoodSchlatter disease. J Pediatr Orthop. 1990;10:65-68.
4. Nierenberg G, Falah M, Keren Y, et al. Surgical treatment of residual Osgood-Schlatter disease in young adults: role of the mobile osseous fragment. Orthopedics. 2011;34:176.-
5. El-Husseini TF, Abdelgawad AA. Results of surgical treatment of unresolved Osgood-Schlatter disease in adults. J Knee Surg. 2010;23:103-107.
6. Ryan M, Wong A, Taunton J. Favorable outcomes after sonographically guided intratendinous injection of hyperosmolar dextrose for chronic insertional and midportion achilles tendinosis. AJR Am J Roentgenol. 2010;194:1047-1053.
7. Scarpone M, Rabago D, Zgierska A, et al. The efficacy of prolotherapy for lateral epicondylitis: a pilot study. Clin J Sport Med. 2008;18:248-254.
8. Visentini PJ, Khan KM, Cook JL, et al. The VISA score: an index of severity of symptoms in patients with jumper’s knee (patellar tendinosis). Victorian Institute of Sport Tendon Study Group. J Sci Med Sport. 1998;1:22-28.
1. Topol GA, Podesta LA, Reeves KD, et al. Hyperosmolar dextrose injection for recalcitrant Osgood-Schlatter disease. Pediatrics. 2011;128:e1121-e1128.
2. Gholve PA, Scher DM, Khakharia S, et al. Osgood-Schlatter syndrome. Curr Opin Pediatr. 2007;19:44-50.
3. Krause BL, Willimas JP, Caterall A. Natural history of OsgoodSchlatter disease. J Pediatr Orthop. 1990;10:65-68.
4. Nierenberg G, Falah M, Keren Y, et al. Surgical treatment of residual Osgood-Schlatter disease in young adults: role of the mobile osseous fragment. Orthopedics. 2011;34:176.-
5. El-Husseini TF, Abdelgawad AA. Results of surgical treatment of unresolved Osgood-Schlatter disease in adults. J Knee Surg. 2010;23:103-107.
6. Ryan M, Wong A, Taunton J. Favorable outcomes after sonographically guided intratendinous injection of hyperosmolar dextrose for chronic insertional and midportion achilles tendinosis. AJR Am J Roentgenol. 2010;194:1047-1053.
7. Scarpone M, Rabago D, Zgierska A, et al. The efficacy of prolotherapy for lateral epicondylitis: a pilot study. Clin J Sport Med. 2008;18:248-254.
8. Visentini PJ, Khan KM, Cook JL, et al. The VISA score: an index of severity of symptoms in patients with jumper’s knee (patellar tendinosis). Victorian Institute of Sport Tendon Study Group. J Sci Med Sport. 1998;1:22-28.
Copyright © 2012 The Family Physicians Inquiries Network. All rights reserved.
Multivitamins for healthy children: What are the true benefits?
THE BENEFITS APPEAR TO BE LIMITED. It’s doubtful that multivitamin with mineral (MVM) supplementation improves IQ in healthy, low-risk children (strength of recommendation [SOR]: B, conflicting randomized clinical trials [RCTs]).
However, MVM supplementation decreased the incidence and severity of common infectious diseases among children in peri-urban India (SOR: B, RCT).
Multivitamin (MV) use doesn’t have consistently reported harms (SOR: C, conflicting cohort studies). An association between MV use and higher rates of asthma and food allergy has been reported, but studies conflict and any such effect is small.
Evidence summary
An RCT found that MVM supplementation for one academic year didn’t improve academic achievement more than placebo in 640 children, 8 to 12 years of age, from low-income urban families.1 Scores on the Terra Nova academic achievement test of reading, math, language, science, and social sciences didn’t differ between students taking MVM supplements or placebo.
Another RCT that compared MVM supplementation with placebo among 245 children between 6 and 12 years of age found no clinically significant improvements in IQ scores overall. However, within a small subset, more children who took MVM showed a clinical increase in IQ than children who took placebo.2
Investigators randomized children to daily MVM supplementation (50% of the US recommended daily allowance) or placebo for 3 months, then measured their Wechsler IQ scores. Overall, the MVM group scored 2.5 points higher (95% confidence interval [CI], 1.85-3.15) than the placebo group (a 15-point change is clinically significant).
More children taking MVM supplements (44) than placebo (25) showed increases in nonverbal IQ scores of 15 or more points (35% compared with 21%; P<.01). The authors speculate that this result may be attributable to the fact that one in 7 schoolchildren was undernourished. A major weakness of the study was its 16% attrition rate.
Fortified milk reduced disease in young children in India
A community-based, double-blind RCT found that milk fortified with vitamins A, C, and E plus minerals reduced common illnesses over the course of a year more than unfortified milk among 633 children 1 to 3 years of age living in a peri-urban area of India.3
Children who drank fortified milk had fewer days of fever (9.1 compared with 9.7 days for placebo; P=.005), a lower incidence of diarrhea (odds ratio [OR]=0.82; 95% CI, 0.73-0.93), and a decreased rate of lower respiratory illness (OR=0.74; 95% CI, 0.57-0.97). Children 2 years and younger showed the greatest effect.
Asthma and food allergies: The data are mixed
An inception cohort study found an association between early MV use and a higher risk of asthma and food allergies.4 Investigators evaluated more than 8000 American women and their newborns over the first 3 years of life. The study population included more families with low socioeconomic status (50%), blacks (51%), and infants born before 37 weeks’ gestation (23%) than the general US population.
Exclusively formula-fed infants who took MV in the first 6 months were more likely to develop asthma (OR=1.27; 95% CI, 1.04-1.56) and food allergies (OR=1.6; 95% CI, 1.2-2.2) than formula-fed infants who didn’t take MV.
However, a birth cohort study of 2470 Swedish children that analyzed health data from parental questionnaires and compared serum immunoglobulin E (IgE) concentrations at 8 years of age found no association between MV use within the past 12 months and clinical allergic disease or specific IgE concentrations.5 Children who took MV at age 4 years or earlier had lower rates of IgE sensitization to food allergens at 8 years (OR=0.61; 95% CI, 0.39-0.97).
Recommendations
According to the American Academy of Pediatrics Committee on Nutrition,6 healthy children who are growing normally and consume a varied diet don’t need routine supplementation with vitamins and minerals. The Committee states that if parents wish to give their children supplements, a standard pediatric multivitamin generally poses no risk.
1. Perlman AI, Worobey J, O‘Sullivan Maillet J, et al. Multivitamin/mineral supplementation does not affect standardized assessment of academic performance in elementary school children. J Am Diet Assoc. 2010;110:1089-1093.
2. Schoenthaler SJ, Bier ID, Young K, et al. The effect of vitamin-mineral supplementation on the intelligence of American schoolchildren: a randomized, double-blind, placebo-controlled trial. J Altern Complement Med. 2000;6:19-29.
3. Sazawal S, Dhingra U, Dhingra P, et al. Effects of fortified milk on morbidity in young children in north India: community based, randomised, double masked, placebo controlled trial. BMJ. 2007;334:140.-
4. Milner JD, Stein DM, McCarter R, et al. Early infant multivitamin supplementation is associated with increased risk for food allergy and asthma. Pediatrics. 2004;114:27-32.
5. Marmsjö K, Rosenlund H, Kull I, et al. Use of multivitamin supplements in relation to allergic disease in 8-year-old children. Am J Clin Nutr. 2009;90:1693-1698.
6. Committee on Nutrition, American Academy of Pediatrics. Feeding the child. In: Kleinman RE, ed. Pediatric Nutrition Handbook. 6th ed. Elk Grove Village, Ill: American Academy of Pediatrics; 2009:145–174.
THE BENEFITS APPEAR TO BE LIMITED. It’s doubtful that multivitamin with mineral (MVM) supplementation improves IQ in healthy, low-risk children (strength of recommendation [SOR]: B, conflicting randomized clinical trials [RCTs]).
However, MVM supplementation decreased the incidence and severity of common infectious diseases among children in peri-urban India (SOR: B, RCT).
Multivitamin (MV) use doesn’t have consistently reported harms (SOR: C, conflicting cohort studies). An association between MV use and higher rates of asthma and food allergy has been reported, but studies conflict and any such effect is small.
Evidence summary
An RCT found that MVM supplementation for one academic year didn’t improve academic achievement more than placebo in 640 children, 8 to 12 years of age, from low-income urban families.1 Scores on the Terra Nova academic achievement test of reading, math, language, science, and social sciences didn’t differ between students taking MVM supplements or placebo.
Another RCT that compared MVM supplementation with placebo among 245 children between 6 and 12 years of age found no clinically significant improvements in IQ scores overall. However, within a small subset, more children who took MVM showed a clinical increase in IQ than children who took placebo.2
Investigators randomized children to daily MVM supplementation (50% of the US recommended daily allowance) or placebo for 3 months, then measured their Wechsler IQ scores. Overall, the MVM group scored 2.5 points higher (95% confidence interval [CI], 1.85-3.15) than the placebo group (a 15-point change is clinically significant).
More children taking MVM supplements (44) than placebo (25) showed increases in nonverbal IQ scores of 15 or more points (35% compared with 21%; P<.01). The authors speculate that this result may be attributable to the fact that one in 7 schoolchildren was undernourished. A major weakness of the study was its 16% attrition rate.
Fortified milk reduced disease in young children in India
A community-based, double-blind RCT found that milk fortified with vitamins A, C, and E plus minerals reduced common illnesses over the course of a year more than unfortified milk among 633 children 1 to 3 years of age living in a peri-urban area of India.3
Children who drank fortified milk had fewer days of fever (9.1 compared with 9.7 days for placebo; P=.005), a lower incidence of diarrhea (odds ratio [OR]=0.82; 95% CI, 0.73-0.93), and a decreased rate of lower respiratory illness (OR=0.74; 95% CI, 0.57-0.97). Children 2 years and younger showed the greatest effect.
Asthma and food allergies: The data are mixed
An inception cohort study found an association between early MV use and a higher risk of asthma and food allergies.4 Investigators evaluated more than 8000 American women and their newborns over the first 3 years of life. The study population included more families with low socioeconomic status (50%), blacks (51%), and infants born before 37 weeks’ gestation (23%) than the general US population.
Exclusively formula-fed infants who took MV in the first 6 months were more likely to develop asthma (OR=1.27; 95% CI, 1.04-1.56) and food allergies (OR=1.6; 95% CI, 1.2-2.2) than formula-fed infants who didn’t take MV.
However, a birth cohort study of 2470 Swedish children that analyzed health data from parental questionnaires and compared serum immunoglobulin E (IgE) concentrations at 8 years of age found no association between MV use within the past 12 months and clinical allergic disease or specific IgE concentrations.5 Children who took MV at age 4 years or earlier had lower rates of IgE sensitization to food allergens at 8 years (OR=0.61; 95% CI, 0.39-0.97).
Recommendations
According to the American Academy of Pediatrics Committee on Nutrition,6 healthy children who are growing normally and consume a varied diet don’t need routine supplementation with vitamins and minerals. The Committee states that if parents wish to give their children supplements, a standard pediatric multivitamin generally poses no risk.
THE BENEFITS APPEAR TO BE LIMITED. It’s doubtful that multivitamin with mineral (MVM) supplementation improves IQ in healthy, low-risk children (strength of recommendation [SOR]: B, conflicting randomized clinical trials [RCTs]).
However, MVM supplementation decreased the incidence and severity of common infectious diseases among children in peri-urban India (SOR: B, RCT).
Multivitamin (MV) use doesn’t have consistently reported harms (SOR: C, conflicting cohort studies). An association between MV use and higher rates of asthma and food allergy has been reported, but studies conflict and any such effect is small.
Evidence summary
An RCT found that MVM supplementation for one academic year didn’t improve academic achievement more than placebo in 640 children, 8 to 12 years of age, from low-income urban families.1 Scores on the Terra Nova academic achievement test of reading, math, language, science, and social sciences didn’t differ between students taking MVM supplements or placebo.
Another RCT that compared MVM supplementation with placebo among 245 children between 6 and 12 years of age found no clinically significant improvements in IQ scores overall. However, within a small subset, more children who took MVM showed a clinical increase in IQ than children who took placebo.2
Investigators randomized children to daily MVM supplementation (50% of the US recommended daily allowance) or placebo for 3 months, then measured their Wechsler IQ scores. Overall, the MVM group scored 2.5 points higher (95% confidence interval [CI], 1.85-3.15) than the placebo group (a 15-point change is clinically significant).
More children taking MVM supplements (44) than placebo (25) showed increases in nonverbal IQ scores of 15 or more points (35% compared with 21%; P<.01). The authors speculate that this result may be attributable to the fact that one in 7 schoolchildren was undernourished. A major weakness of the study was its 16% attrition rate.
Fortified milk reduced disease in young children in India
A community-based, double-blind RCT found that milk fortified with vitamins A, C, and E plus minerals reduced common illnesses over the course of a year more than unfortified milk among 633 children 1 to 3 years of age living in a peri-urban area of India.3
Children who drank fortified milk had fewer days of fever (9.1 compared with 9.7 days for placebo; P=.005), a lower incidence of diarrhea (odds ratio [OR]=0.82; 95% CI, 0.73-0.93), and a decreased rate of lower respiratory illness (OR=0.74; 95% CI, 0.57-0.97). Children 2 years and younger showed the greatest effect.
Asthma and food allergies: The data are mixed
An inception cohort study found an association between early MV use and a higher risk of asthma and food allergies.4 Investigators evaluated more than 8000 American women and their newborns over the first 3 years of life. The study population included more families with low socioeconomic status (50%), blacks (51%), and infants born before 37 weeks’ gestation (23%) than the general US population.
Exclusively formula-fed infants who took MV in the first 6 months were more likely to develop asthma (OR=1.27; 95% CI, 1.04-1.56) and food allergies (OR=1.6; 95% CI, 1.2-2.2) than formula-fed infants who didn’t take MV.
However, a birth cohort study of 2470 Swedish children that analyzed health data from parental questionnaires and compared serum immunoglobulin E (IgE) concentrations at 8 years of age found no association between MV use within the past 12 months and clinical allergic disease or specific IgE concentrations.5 Children who took MV at age 4 years or earlier had lower rates of IgE sensitization to food allergens at 8 years (OR=0.61; 95% CI, 0.39-0.97).
Recommendations
According to the American Academy of Pediatrics Committee on Nutrition,6 healthy children who are growing normally and consume a varied diet don’t need routine supplementation with vitamins and minerals. The Committee states that if parents wish to give their children supplements, a standard pediatric multivitamin generally poses no risk.
1. Perlman AI, Worobey J, O‘Sullivan Maillet J, et al. Multivitamin/mineral supplementation does not affect standardized assessment of academic performance in elementary school children. J Am Diet Assoc. 2010;110:1089-1093.
2. Schoenthaler SJ, Bier ID, Young K, et al. The effect of vitamin-mineral supplementation on the intelligence of American schoolchildren: a randomized, double-blind, placebo-controlled trial. J Altern Complement Med. 2000;6:19-29.
3. Sazawal S, Dhingra U, Dhingra P, et al. Effects of fortified milk on morbidity in young children in north India: community based, randomised, double masked, placebo controlled trial. BMJ. 2007;334:140.-
4. Milner JD, Stein DM, McCarter R, et al. Early infant multivitamin supplementation is associated with increased risk for food allergy and asthma. Pediatrics. 2004;114:27-32.
5. Marmsjö K, Rosenlund H, Kull I, et al. Use of multivitamin supplements in relation to allergic disease in 8-year-old children. Am J Clin Nutr. 2009;90:1693-1698.
6. Committee on Nutrition, American Academy of Pediatrics. Feeding the child. In: Kleinman RE, ed. Pediatric Nutrition Handbook. 6th ed. Elk Grove Village, Ill: American Academy of Pediatrics; 2009:145–174.
1. Perlman AI, Worobey J, O‘Sullivan Maillet J, et al. Multivitamin/mineral supplementation does not affect standardized assessment of academic performance in elementary school children. J Am Diet Assoc. 2010;110:1089-1093.
2. Schoenthaler SJ, Bier ID, Young K, et al. The effect of vitamin-mineral supplementation on the intelligence of American schoolchildren: a randomized, double-blind, placebo-controlled trial. J Altern Complement Med. 2000;6:19-29.
3. Sazawal S, Dhingra U, Dhingra P, et al. Effects of fortified milk on morbidity in young children in north India: community based, randomised, double masked, placebo controlled trial. BMJ. 2007;334:140.-
4. Milner JD, Stein DM, McCarter R, et al. Early infant multivitamin supplementation is associated with increased risk for food allergy and asthma. Pediatrics. 2004;114:27-32.
5. Marmsjö K, Rosenlund H, Kull I, et al. Use of multivitamin supplements in relation to allergic disease in 8-year-old children. Am J Clin Nutr. 2009;90:1693-1698.
6. Committee on Nutrition, American Academy of Pediatrics. Feeding the child. In: Kleinman RE, ed. Pediatric Nutrition Handbook. 6th ed. Elk Grove Village, Ill: American Academy of Pediatrics; 2009:145–174.
Evidence-based answers from the Family Physicians Inquiries Network
Do inhaled steroids reduce bone mineral density and increase fracture risk?
NO, except perhaps at high doses. Inhaled corticosteroids (ICS) at low to medium doses (<1500 mcg beclomethasone hydrofluoroalkane per day) for asthma and chronic obstructive pulmonary disease (COPD) don’t increase the risk of significant bone loss or fracture at 2 to 3 years follow-up (strength of recommendation [SOR]: A, systematic reviews and randomize controlled trials [RCTs]). Higher doses, however, may raise the risk of nontraumatic fracture over 1 to 4 years of follow-up (SOR: B, case control studies).
Experts recommend using the lowest effective dose to mitigate potential bone risks (SOR: C, expert consensus).
Evidence summary
A 2008 Cochrane review examined 7 RCTs comparing ICS with placebo in 1989 patients 30 to 52 years of age with mild asthma or COPD. The reviewers found no evidence of increased bone turnover, decreased bone mineral density, or increased vertebral fracture in the ICS group compared with the placebo group at 2 to 3 years’ follow-up (odds ratio [OR] for fracture=1.87; 95% confidence interval [CI], 0.5-7.0).
Steroid doses ranged from 200 to 4000 mcg beclomethasone equivalent ICS per day.1 A 100-mcg beclomethasone equivalent ICS dose is 50 mcg fluticasone, 80 mcg budesonide, or 200 mcg triamcinolone.2
A 2008 meta-analysis of 11 RCTs that examined a number of adverse effects of ICS in adult patients with COPD found 3 studies (8131 patients) that reported no significant increase in fracture risk at 36 months in the ICS group compared with the placebo group (OR=1.09; 95% CI, 0.89-1.33). Steroid doses ranged from 1000 to 2000 mcg beclomethasone equivalent ICS per day.3
Some studies suggest an association between dose and risk
A 2008 meta-analysis that included patients with COPD or asthma, average age 43 to 81 years, showed no difference in fracture risk overall at 1 to 4 years’ follow-up (OR=1.02; 95% CI, 0.96-1.08). This analysis examined 4 RCTs, 6 case-control studies, and 3 cohort studies.4
A subgroup analysis of patients taking higher-dose ICS (>1500 mcg beclomethasone equivalent ICS per day) that pooled data from case-control and cohort studies suggested an increased risk of fracture (OR=1.30; 95% CI, 1.07-1.58).4
Investigators identified a possible dose-dependent relationship in another meta-analysis of 5 case-control studies (43,783 cases, 259,936 controls).5 The meta-analysis included 4 of the studies examined in the previously discussed meta-analysis.4
The investigators found a relative risk of 1.12 (95% CI, 1.0-1.26) for nonvertebral fracture for each 1000-mcg increase in beclomethasone equivalent ICS dose per day.5 Longer follow-up time wasn’t associated with greater fracture risk.
But the relationship isn’t clear
Although some non-RCT studies discussed here show that higher doses of steroids may lead to increased fracture risk, the strength of this association isn’t clear. The authors of the Cochrane review and the meta-analyses point out that a significant number of confounding factors can put asthma and COPD patients at increased risk for fracture. They include age, smoking status, inactivity, and severity of underlying lung disease. The fact that different authors controlled differently for these factors introduced heterogeneity into the meta-analyses described here.1,3-5
Recommendations
Guidelines for the Diagnosis and Management of Asthma from the National Heart, Lung, and Blood Institute state that “most benefit is achieved with relatively low doses of ICS, whereas the risk of adverse effects increases with dose. … ICS use may be associated with a dose-dependent reduction in bone mineral content, although low or medium doses appear to have no major adverse effect. Elderly patients may be more at risk due to preexisting osteoporosis, changes in estrogen levels that affect calcium utilization, and a sedentary lifestyle.”6
1. Jones A, Fay JK, Burr M, et al. Inhaled corticosteroid effects on bone metabolism in asthma and mild chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2008;(4):CD003537.-
2. Gonelli S, Caffarelli C, Maggi S, et al. Effect of inhaled glucocorticoids and beta(2) agonists on vertebral fracture risk in COPD patients: the EOLO study. Calcif Tissue Int. 2010;87:137-143.
3. Drummond MB, Dasenbrook EC, Pitz MW, et al. Inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300:2407-2416.
4. Etminan M, Sadatsafavi M, Ganjizadeh Zavareh S, et al. Inhaled corticosteroids and the risk of fractures in older adults: a systematic review and meta-analysis. Drug Saf. 2008;31:409-414.
5. Weatherall M, James K, Clay J, et al. Dose-response relationship for risk of nonvertebral fracture with inhaled corticosteroids. Clin Exp Allergy. 2008;38:1451-1458.
6. National Heart Lung and Blood Institute. Expert Panel Report 3 (EPR3): guidelines for the diagnosis and management of asthma. Available at: www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Accessed February 25, 2012.
NO, except perhaps at high doses. Inhaled corticosteroids (ICS) at low to medium doses (<1500 mcg beclomethasone hydrofluoroalkane per day) for asthma and chronic obstructive pulmonary disease (COPD) don’t increase the risk of significant bone loss or fracture at 2 to 3 years follow-up (strength of recommendation [SOR]: A, systematic reviews and randomize controlled trials [RCTs]). Higher doses, however, may raise the risk of nontraumatic fracture over 1 to 4 years of follow-up (SOR: B, case control studies).
Experts recommend using the lowest effective dose to mitigate potential bone risks (SOR: C, expert consensus).
Evidence summary
A 2008 Cochrane review examined 7 RCTs comparing ICS with placebo in 1989 patients 30 to 52 years of age with mild asthma or COPD. The reviewers found no evidence of increased bone turnover, decreased bone mineral density, or increased vertebral fracture in the ICS group compared with the placebo group at 2 to 3 years’ follow-up (odds ratio [OR] for fracture=1.87; 95% confidence interval [CI], 0.5-7.0).
Steroid doses ranged from 200 to 4000 mcg beclomethasone equivalent ICS per day.1 A 100-mcg beclomethasone equivalent ICS dose is 50 mcg fluticasone, 80 mcg budesonide, or 200 mcg triamcinolone.2
A 2008 meta-analysis of 11 RCTs that examined a number of adverse effects of ICS in adult patients with COPD found 3 studies (8131 patients) that reported no significant increase in fracture risk at 36 months in the ICS group compared with the placebo group (OR=1.09; 95% CI, 0.89-1.33). Steroid doses ranged from 1000 to 2000 mcg beclomethasone equivalent ICS per day.3
Some studies suggest an association between dose and risk
A 2008 meta-analysis that included patients with COPD or asthma, average age 43 to 81 years, showed no difference in fracture risk overall at 1 to 4 years’ follow-up (OR=1.02; 95% CI, 0.96-1.08). This analysis examined 4 RCTs, 6 case-control studies, and 3 cohort studies.4
A subgroup analysis of patients taking higher-dose ICS (>1500 mcg beclomethasone equivalent ICS per day) that pooled data from case-control and cohort studies suggested an increased risk of fracture (OR=1.30; 95% CI, 1.07-1.58).4
Investigators identified a possible dose-dependent relationship in another meta-analysis of 5 case-control studies (43,783 cases, 259,936 controls).5 The meta-analysis included 4 of the studies examined in the previously discussed meta-analysis.4
The investigators found a relative risk of 1.12 (95% CI, 1.0-1.26) for nonvertebral fracture for each 1000-mcg increase in beclomethasone equivalent ICS dose per day.5 Longer follow-up time wasn’t associated with greater fracture risk.
But the relationship isn’t clear
Although some non-RCT studies discussed here show that higher doses of steroids may lead to increased fracture risk, the strength of this association isn’t clear. The authors of the Cochrane review and the meta-analyses point out that a significant number of confounding factors can put asthma and COPD patients at increased risk for fracture. They include age, smoking status, inactivity, and severity of underlying lung disease. The fact that different authors controlled differently for these factors introduced heterogeneity into the meta-analyses described here.1,3-5
Recommendations
Guidelines for the Diagnosis and Management of Asthma from the National Heart, Lung, and Blood Institute state that “most benefit is achieved with relatively low doses of ICS, whereas the risk of adverse effects increases with dose. … ICS use may be associated with a dose-dependent reduction in bone mineral content, although low or medium doses appear to have no major adverse effect. Elderly patients may be more at risk due to preexisting osteoporosis, changes in estrogen levels that affect calcium utilization, and a sedentary lifestyle.”6
NO, except perhaps at high doses. Inhaled corticosteroids (ICS) at low to medium doses (<1500 mcg beclomethasone hydrofluoroalkane per day) for asthma and chronic obstructive pulmonary disease (COPD) don’t increase the risk of significant bone loss or fracture at 2 to 3 years follow-up (strength of recommendation [SOR]: A, systematic reviews and randomize controlled trials [RCTs]). Higher doses, however, may raise the risk of nontraumatic fracture over 1 to 4 years of follow-up (SOR: B, case control studies).
Experts recommend using the lowest effective dose to mitigate potential bone risks (SOR: C, expert consensus).
Evidence summary
A 2008 Cochrane review examined 7 RCTs comparing ICS with placebo in 1989 patients 30 to 52 years of age with mild asthma or COPD. The reviewers found no evidence of increased bone turnover, decreased bone mineral density, or increased vertebral fracture in the ICS group compared with the placebo group at 2 to 3 years’ follow-up (odds ratio [OR] for fracture=1.87; 95% confidence interval [CI], 0.5-7.0).
Steroid doses ranged from 200 to 4000 mcg beclomethasone equivalent ICS per day.1 A 100-mcg beclomethasone equivalent ICS dose is 50 mcg fluticasone, 80 mcg budesonide, or 200 mcg triamcinolone.2
A 2008 meta-analysis of 11 RCTs that examined a number of adverse effects of ICS in adult patients with COPD found 3 studies (8131 patients) that reported no significant increase in fracture risk at 36 months in the ICS group compared with the placebo group (OR=1.09; 95% CI, 0.89-1.33). Steroid doses ranged from 1000 to 2000 mcg beclomethasone equivalent ICS per day.3
Some studies suggest an association between dose and risk
A 2008 meta-analysis that included patients with COPD or asthma, average age 43 to 81 years, showed no difference in fracture risk overall at 1 to 4 years’ follow-up (OR=1.02; 95% CI, 0.96-1.08). This analysis examined 4 RCTs, 6 case-control studies, and 3 cohort studies.4
A subgroup analysis of patients taking higher-dose ICS (>1500 mcg beclomethasone equivalent ICS per day) that pooled data from case-control and cohort studies suggested an increased risk of fracture (OR=1.30; 95% CI, 1.07-1.58).4
Investigators identified a possible dose-dependent relationship in another meta-analysis of 5 case-control studies (43,783 cases, 259,936 controls).5 The meta-analysis included 4 of the studies examined in the previously discussed meta-analysis.4
The investigators found a relative risk of 1.12 (95% CI, 1.0-1.26) for nonvertebral fracture for each 1000-mcg increase in beclomethasone equivalent ICS dose per day.5 Longer follow-up time wasn’t associated with greater fracture risk.
But the relationship isn’t clear
Although some non-RCT studies discussed here show that higher doses of steroids may lead to increased fracture risk, the strength of this association isn’t clear. The authors of the Cochrane review and the meta-analyses point out that a significant number of confounding factors can put asthma and COPD patients at increased risk for fracture. They include age, smoking status, inactivity, and severity of underlying lung disease. The fact that different authors controlled differently for these factors introduced heterogeneity into the meta-analyses described here.1,3-5
Recommendations
Guidelines for the Diagnosis and Management of Asthma from the National Heart, Lung, and Blood Institute state that “most benefit is achieved with relatively low doses of ICS, whereas the risk of adverse effects increases with dose. … ICS use may be associated with a dose-dependent reduction in bone mineral content, although low or medium doses appear to have no major adverse effect. Elderly patients may be more at risk due to preexisting osteoporosis, changes in estrogen levels that affect calcium utilization, and a sedentary lifestyle.”6
1. Jones A, Fay JK, Burr M, et al. Inhaled corticosteroid effects on bone metabolism in asthma and mild chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2008;(4):CD003537.-
2. Gonelli S, Caffarelli C, Maggi S, et al. Effect of inhaled glucocorticoids and beta(2) agonists on vertebral fracture risk in COPD patients: the EOLO study. Calcif Tissue Int. 2010;87:137-143.
3. Drummond MB, Dasenbrook EC, Pitz MW, et al. Inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300:2407-2416.
4. Etminan M, Sadatsafavi M, Ganjizadeh Zavareh S, et al. Inhaled corticosteroids and the risk of fractures in older adults: a systematic review and meta-analysis. Drug Saf. 2008;31:409-414.
5. Weatherall M, James K, Clay J, et al. Dose-response relationship for risk of nonvertebral fracture with inhaled corticosteroids. Clin Exp Allergy. 2008;38:1451-1458.
6. National Heart Lung and Blood Institute. Expert Panel Report 3 (EPR3): guidelines for the diagnosis and management of asthma. Available at: www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Accessed February 25, 2012.
1. Jones A, Fay JK, Burr M, et al. Inhaled corticosteroid effects on bone metabolism in asthma and mild chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2008;(4):CD003537.-
2. Gonelli S, Caffarelli C, Maggi S, et al. Effect of inhaled glucocorticoids and beta(2) agonists on vertebral fracture risk in COPD patients: the EOLO study. Calcif Tissue Int. 2010;87:137-143.
3. Drummond MB, Dasenbrook EC, Pitz MW, et al. Inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300:2407-2416.
4. Etminan M, Sadatsafavi M, Ganjizadeh Zavareh S, et al. Inhaled corticosteroids and the risk of fractures in older adults: a systematic review and meta-analysis. Drug Saf. 2008;31:409-414.
5. Weatherall M, James K, Clay J, et al. Dose-response relationship for risk of nonvertebral fracture with inhaled corticosteroids. Clin Exp Allergy. 2008;38:1451-1458.
6. National Heart Lung and Blood Institute. Expert Panel Report 3 (EPR3): guidelines for the diagnosis and management of asthma. Available at: www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm. Accessed February 25, 2012.
Evidence-based answers from the Family Physicians Inquiries Network
How well are we managing diabetes in long-term care?
Purpose Our objective was to compare the management of diabetes mellitus (DM) in residents of extended-care facilities with the American Diabetes Association (ADA) standards of care for ambulatory adults.
Methods We reviewed the charts of 245 residents in 14 extended-care facilities. All had a physician-documented diagnosis of type 1 or type 2 DM and had spent at least 3 of the past 12 months in the facility. We reviewed medical diagnoses, medications, laboratory reports, and consultation notes of one-year duration, then compared our findings with the ADA standards of care.
Results Of the 245 patients, 211 (86.1%) had their glucose monitored; 36.7% had a hemoglobin A1c (A1c) below 7%. Fifty-two residents (21.2%) experienced hypoglycemic events; 103 (42%) had hyperglycemic events. Of the 240 patients (98%) whose blood pressure (BP) was monitored, 107 (43.7%) met the ADA goal. Lipids were checked in 190 residents (77.6%), 89 (46.8%) of whom met the goal for low-density lipoprotein (LDL). Dilated eye examinations were provided to 133 patients (54.3%). Foot examinations were performed on 187 residents (76.3%); 170 (69.4%) had a consultation with a podiatrist.
Conclusions Our chart review demonstrates that the management of diabetes in extended-care facilities does not meet the recommended ADA standards of care for ambulatory adults. Although 36.7% of patients met the A1c goal, the A1c did not account for glucose variability. Only 46.8% of patients met the recommended LDL goal. Our results suggest the need for new standards of care for patients with diabetes residing in nursing facilities. These standards should take into account the particular needs of this patient population, specifically with regard to hypoglycemic risk, cardiovascular risk factors, and quality of life.
A surge in elderly patients with diabetes has placed a large burden on extended-care facilities. According to the Centers for Medicare and Medicaid Services, the prevalence of diabetes among nursing home residents is 33.3%.1 Between 1995 and 2004, the estimated number of long-term care residents with diabetes mellitus (DM) grew by 7.1%, from approximately 242,000 to 329,000.2 The increase adds to the challenge extended-care facilities face in attempting to provide high-quality care to patients with diabetes. No well-accepted management guidelines exist for nursing home residents with DM.3
Frail older adults with DM are more likely to suffer from cardiovascular conditions than younger patients, and are at greater risk for hypoglycemic coma and serious hyperglycemia.4,5 A high frequency of hypoglycemia, especially nocturnal hypoglycemia, has been reported among nursing home residents with diabetes.6 Intensive insulin therapy is associated with hypoglycemia and increased mortality.7 However, hyperglycemia also must be considered because it significantly impairs quality of life. Uncontrolled hyperglycemia causes osmotic diuresis, leading to polyuria, nocturia, aggravated incontinence, and disrupted sleep, as well as contributing to dehydration.4 All of these problems have serious implications for quality of life and overall health.
Although studies have identified poor glycemic control and hypertension as the major problems facing nursing home patients with DM,2,6 little research has examined how therapies targeting these problems help the elderly. Solid evidence supports the effectiveness of controlling hyperglycemia, lipid levels, and blood pressure (BP), along with aspirin therapy, in preventing microvascular disease, but does not reflect research involving older patients.8
A study of nursing homes found that health care teams did not respond to half of all significantly abnormal laboratory test results.9 Physicians who are aware of the problems associated with DM in elderly patients may hesitate to treat them because of the lack of guidelines for this patient population or concerns about adverse effects. Because of the deficiency of clinical trial data in elderly patients and the heterogenicity of the population, the American Diabetes Association (ADA) suggests that “less stringent treatment goals” may be appropriate.10
A central conflict in diabetes care for nursing home residents revolves around the need for guidelines that are both generalizable and easily individualized. Some studies support the need for individualized care, particularly with regard to A1c goals, because residents vary greatly in both disease burden and frailty.8,11 Yet individualized treatment could increase the complexity of care for nurses who must manage many patients, potentially having a negative effect on patient care.
Implementation of a treatment protocol for residents with DM is associated with a decrease in the number of hospital days for acute and chronic complications,12 but one study found that only 15% of nursing homes had such a protocol.13 Ultimately, long-term care facilities may benefit from an approach that strikes a balance between individualized care and generalized goals and does not closely mimic either acute hospital care or outpatient management of diabetes.3
In the absence of specific recommendations for extended-care residents with diabetes, our study evaluated the status of care in this population on the basis of pharmacotherapy and standards of care recommended by the ADA for ambulatory adults with DM.
Methods
Data collection
We reviewed the charts of 245 patients in 14 long-term care facilities in Ohio and West Virginia. All participating facilities signed a letter of agreement to take part in the study. The study was approved by the Ohio University Institutional Review Board.
At each facility, the director of nursing supplied a list of residents with DM. To be eligible for chart review, residents had to have a physician-documented diagnosis of type 1 or type 2 DM and have lived at the facility for at least 3 of the previous 12 months. Residents in both skilled nursing care and assisted living facilities were able to participate; short-term rehabilitation residents were not.
We performed a comprehensive review of each chart, examining the medical diagnoses, medication lists, laboratory reports, and physician and consultation notes for a one-year period. Data collection focused on diabetes-related intermediate outcomes and processes of care. Intermediate outcomes included A1c tests, lipid panels, and BP readings. Processes of care included aspirin therapy, use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers, use of statins, eye exams, foot exams, and microalbumin tests. The data collected omitted information identifying the patient, physician, or facility.
We compared the collected data with the 2011 ADA standards of care: blood glucose (fasting 80-120 mg/dL; postprandial 100-140 mg/dL), A1c (<7%), BP (<130/80 mm Hg), and lipid levels (low-density lipoprotein [LDL] <100 mg/dL; high-density lipoprotein [HDL] >40 mg/dL in men and >50 mg/dL in women; triglycerides <150 mg/dL).
Data analysis
We entered the data into an Excel database by type and key format and analyzed results using SPSS software, version 14.0 (SPSS, Chicago, IL). We used percentages and means±standard deviation to describe the data.
Results
TABLE 1 lists characteristics of the patients in the study: 24.5% were male and 75.5% were female; 9 (3.7%) were diagnosed with type 1 DM; 236 (96.3%) had type 2 DM. The mean age was 81±9 years, with a range of 44 to 103 years. Approximately 96% were Caucasian. The residents’ medical care was managed by family physicians (66.1%), internists (25.7%), geriatricians (6.9%), endocrinologists (0.8%), and other physicians (0.4%). The findings that follow are all based on a one-year period unless otherwise specified.
TABLE 1
Study population profile
| Patient characteristic | N (%) |
|---|---|
| Sex Male Female | 60 (24.5) 185 (75.5) |
| Diabetes diagnosis Type 1 Type 2 | 9 (3.7) 236 (96.3) |
| Managing physician specialty Family medicine Internal medicine Geriatrics Endocrinology Other | 162 (66.1) 63 (25.7) 17 (6.9) 2 (0.8) 1 (0.4) |
Diabetes management
Most of the residents (211 [86.1%]) underwent glucose monitoring. The proportion of residents who received specific diabetes interventions is detailed in TABLE 2.
Hypoglycemia. Fifty-two residents (24.6% of those receiving glucose monitoring and 21.2% of the total) experienced a hypoglycemic event; 103 (representing 48.8% of the monitored patients and 42% of the total) had hyperglycemic events. On average, each resident experienced 1±2 mild hypoglycemic episodes per month, with a maximum of 13 mild episodes for one resident. Severe hypoglycemia (< 50 mg/dL) occurred less often, on average 0.24±1 time per resident. One resident had 15 severe hypoglycemic events in a month. The mean low hypoglycemic episode was at a glucose level of 52±16 mg/dL.
Hyperglycemia occurred more often than hypoglycemia (8±14 times per month), with a mean high glucose level of 352±89 mg/dL. This study used a generous range for normal glucose readings (70-249 mg/dL), and 89% of blood glucose readings were within that range. Thirty-seven percent of residents had an A1c <7.0%.
Medication. Thirty-two (13.1%) patients received no oral medication or insulin, and were managed with lifestyle interventions alone. Sixty-four patients (26.1%) used only oral medications, 64 (26.1%) received only insulin, and 85 (34.7%) were treated with both. Of the patients receiving insulin, 108 (72%) were on a sliding scale regimen. Seventy-seven (51.7%) of the patients on insulin experienced hypoglycemia, vs 30 (20%) of those taking oral medication. Twenty-seven (31.8%) patients in the combined therapy group had hypoglycemic events.
TABLE 2
Interventions received by the study population
| Intervention | N (%) |
|---|---|
| Glucose monitoring | 211 (86.1) |
| Blood pressure monitoring | 240 (98.0) |
| Lipids checked | 190 (77.6) |
| Dilated eye exams | 133 (54.3) |
| Foot exams* | 187 (76.3) |
| *170 (69.4%) patients had a consultation with a podiatrist. | |
Preventive care
Foot and eye care. Dilated eye examinations were provided for 133 residents (54.3%). Most (76.3%) received foot examinations, and 69.4% were seen by a podiatrist.
Blood pressure. Of the 240 residents (98%) whose BP was monitored, 107 (43.7%) had readings lower than 125/85 mm Hg, a goal set by a team of diabetologists, endocrinologists, and geriatricians at Ohio University. One hundred residents (40.8%) were taking an angiotensin-converting enzyme inhibitor or an angiotensin II receptor blocker; 122 (49.8%) were receiving aspirin therapy. In the total population, 110 patients (44.9%) were prescribed a statin.
Lipid monitoring. Of the 190 residents (77.6%) whose lipids were monitored, only 89 (46.8%) met the LDL goal suggested by the ADA. Fifty-six (29.5%) had triglycerides <150 mg/dL.
The HDL goal recommended by the ADA is >40 mg/dL for men and >50 mg/dL for women. Three of the 24 men and 16 of the 91 women whose lipids were monitored met the HDL goal.
Discussion
Although several components of diabetes management in our study population failed to meet the ADA standards of care for ambulatory adults, some elements of care were well managed. Monthly foot exams were performed on 76.3% of patients; 69.4% were seen by a podiatrist. While the number of residents receiving foot exams had decreased by 10.7% since a previous study by our research group, the number of podiatric consults increased by 11.4%.14
Dilated eye exams were given to 54.3% of residents. More patients should be given the opportunity to have an annual eye exam. Diabetes is the leading cause of new cases of blindness among adults 20 to 74 years of age,15 and impaired vision affects patient activity levels, susceptibility to falls, and quality of life.
In addition to a good record of preventive exams, physicians were proficient in monitoring residents with diabetes with regular testing regimens. Eighty-six percent of patients underwent regular blood glucose monitoring; 84% had had their A1c tested in the past year, and 36.7% achieved the A1c goal of <7%. The average A1c reading was 6.7±1%.
While these A1c values would seem to reflect well-managed diabetes, blood glucose readings tell a different story. A comparison of A1c values and hyperglycemic events revealed a disparity between the estimated average glucose reading and the actual readings. Of the patients who underwent scheduled fingersticks, 24.6% experienced a hypoglycemic event and 48.8% had hyperglycemic events. On average, each patient had 8 hyperglycemic episodes per month. The average highest glucose reading was >350 mg/dL.
A1c is only part of the story. While A1c can be a marker of sustained hyperglycemia, it does not reflect the stability of glycemic control.16 A study by Löfgren and colleagues confirmed that elderly diabetic patients in nursing homes who have low A1c levels often suffer from hypoglycemia.6 Patients receiving insulin therapy are more likely to experience hypoglycemia.7
The mismatch between A1c and glucose readings reveals an important point about the management of diabetes in long-term care patients: A1c values do not tell the entire story about a patient’s blood glucose; thus, a physician cannot look only at A1c to assess a patient’s diabetes management. A previous study demonstrated that when physicians base treatment plans solely on A1c without consulting glucose logs or being familiar with newer treatments, adherence to evidence-based algorithms is unlikely.17
While A1c does provide information about average blood glucose levels, it does not offer perspective on hypoglycemia or glucose variability. It is vital that physicians screen the glucose log for evidence of hypo- and hyperglycemia before adjusting the patient’s treatment plan. Physicians must also keep in mind that A1c may be falsely low in elderly patients who have concomitant anemia, which lowers the value.
Controlling BP and lipids helps prevent complications. In addition to diabetes management, our study evaluated regulation of the complications of diabetes, particularly cardiovascular complications. Evidence suggests that people with DM derive the greatest mortality benefit from a treatment plan centered first on hypertension, then lipids, and finally, glycemic control.18 A renewed focus on the BP and lipid aspects of diabetes care is needed.
Our data demonstrate that, of the 240 patients who met the ADA goal of <130/80 mm Hg, only 100 (40.8%) were taking an angiotensin-converting enzyme inhibitor or an angiotensin II receptor blocker. Lowering BP to <130/80 mm Hg may provide further benefit in preventing diabetes-related macrovascular complications.8
Lipid levels are a critical gauge of cardiovascular risk. Previous studies of patients with type 2 DM have shown that treating hyperlipidemia can produce a mortality benefit within 2 to 4 years, whereas aggressive glucose management takes approximately 8 years.18
A lipid panel was performed for 77.6% of the patients in our study—an improvement over a previous study by our team in which only 33% of patients received lipid checks.14 In the current study, a mere 2.9% of patients met the ADA’s combined lipid goals (LDL <100 mg/dL; HDL >40 mg/dL in men and >50 mg/dL in women; and triglycerides<150 mg/dL). Considering the LDL goal alone, 46.8% of the 190 patients whose lipids were monitored achieved it.
One hundred ten (44.9%) of the 245 patients in our study were prescribed a statin. Various studies support the use of lipid-lowering medications to increase HDL in elderly patients with DM.8 Yet data suggest that the rate of statin use among older adults is suboptimal.19 Our study highlights the limited prescription of statins for elderly nursing home patients who need them.
The ADA lipid goals are reasonable for this patient population, especially considering the potential mortality benefit. Rather than adjust lipid and BP goals, standards of care should emphasize the importance of meeting these objectives and suggest means to achieve them, including greater use of statins.
One set of standards does not work for all patients. Our study demonstrates that the ADA standards of care for ambulatory adults with diabetes are not acceptable for long-term care residents with DM. Although stringent A1c goals are appropriate for ambulatory adults, the risk of hypoglycemic episodes among the older and frailer nursing home population is too great to adhere to such a strict approach.
We recommend new guidelines be established. Guidelines developed specifically for residents in extended care are necessary to ensure the proper care of these patients, particularly in the face of a steady increase in their number.
Study limitations. Future inquiries into this subject should take into account the weaknesses of this study. First, it was conducted solely in Ohio and West Virginia. A chart review covering more territory could explore regional differences in diabetes care provided by long-term facilities and provide more evidence of the need for a population-specific standards of care.
The study also failed to account for comorbid conditions, including dementia, and code status, and followed residents for only one year. More extensive reviews could examine the effects of therapy in this patient population and the relationship between mortality and treatment plan, spurring movement toward more uniform and effective care of patients with diabetes in the long-term care setting.
CORRESPONDENCE Jay Shubrook Jr, DO, Department of Family Medicine, Ohio University Heritage College of Osteopathic Medicine, Grosvenor Hall, Athens, OH 45701; [email protected]
1. Centers for Medicare and Medicaid Services. MDS active resident information report: third quarter 2010. Available at: https://www.cms.gov/MDSPubQIandResRep/04_activeresreport.asp?isSubmitted=res3&var=I1a&date=32. Accessed February 9, 2011.
2. Zhang X, Decker FH, Luo H, et al. Trends in the prevalence and comorbidities of diabetes mellitus in nursing home residents in the United States: 1995-2004. J Am Geriatr Soc. 2010;58:724-730.
3. Meyers RM, Reger L. Diabetes management in long-term care facilities: a practical guide. J Am Med Dir Assoc. 2009;10:589.-
4. Mayfield J, Deb P, Potter D, et al. Diabetes and long-term care. In: Diabetes in America. 2nd ed. Bethesda, MD: National Diabetes Data Group, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health; 1995:571–586.
5. Ben-Ami H, Nagachandran P, Mendelson A, et al. Drug-induced hypoglycemic coma in 102 diabetic patients. Arch Intern Med. 1999;159:281-284.
6. Löfgren UB, Rosenqvist U, Lindstrom T, et al. Diabetes control in Swedish community dwelling elderly: more often tight than poor. J Intern Med. 2004;255:96-101.
7. The Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358:2545-2559.
8. Brown AF, Mangione CM, Saliba D, et al. Guidelines for improving the care of the older person with diabetes mellitus. J Am Geriatr Soc. 2003;51:S265-S280.
9. Chalmers J, Beaven D, Sainsburg R. Are high blood sugar levels in the elderly ignored? Aust NZ J Med. 1987;17:485-490.
10. American Diabetes Association. Standards of medical care in diabetes—2011. Diabetes Care. 2011;34(suppl 1):S11-S61.
11. Meyers RM, Broton JC, Woo-Rippe KW, et al. Variability in glycosylated hemoglobin values in diabetic patients living in long-term care facilities. J Am Med Dir Assoc. 2007;8:511-514.
12. Hamman RF, Michael SL, Keefer SM, et al. Impact of policy and procedure changes on hospital days among diabetic nursing-home residents—Colorado. MMWR Morb Mortal Wkly Rep. 1984;33:621-629.
13. Feldman SM, Rosen R, DeStasio J. Status of diabetes management in the nursing home setting in 2008: a retrospective chart review and epidemiology study of diabetic nursing home residents and nursing home initiatives in diabetes management. J Am Med Dir Assoc. 2009;10:354-360.
14. Holt RM, Schwartz FL, Shubrook JH. Diabetes care in extended-care facilities: appropriate intensity of care? Diabetes Care. 2007;30:1454-1458.
15. Centers for Disease Control and Prevention. National diabetes fact sheet, 2007. Available at: http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2007.pdf. Accessed February 10, 2011.
16. Alam T, Weintraub N, Weinreb J. What is the proper use of hemoglobin A1c monitoring in the elderly? J Am Med Dir Assoc. 2006;7(3 suppl):S60-S64.
17. Alam T, Weintraub N, Weinreb J. What is the proper use of hemoglobin A1c monitoring in the elderly? J Am Med Dir Assoc. 2010;11:171-178.
18. Huang ES, Meigs JB, Singer DE. The effect of interventions to prevent cardiovascular disease in patients with type 2 diabetes mellitus. Am J Med. 2001;11:633-642.
19. Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA. 2002;288:462-467.
Purpose Our objective was to compare the management of diabetes mellitus (DM) in residents of extended-care facilities with the American Diabetes Association (ADA) standards of care for ambulatory adults.
Methods We reviewed the charts of 245 residents in 14 extended-care facilities. All had a physician-documented diagnosis of type 1 or type 2 DM and had spent at least 3 of the past 12 months in the facility. We reviewed medical diagnoses, medications, laboratory reports, and consultation notes of one-year duration, then compared our findings with the ADA standards of care.
Results Of the 245 patients, 211 (86.1%) had their glucose monitored; 36.7% had a hemoglobin A1c (A1c) below 7%. Fifty-two residents (21.2%) experienced hypoglycemic events; 103 (42%) had hyperglycemic events. Of the 240 patients (98%) whose blood pressure (BP) was monitored, 107 (43.7%) met the ADA goal. Lipids were checked in 190 residents (77.6%), 89 (46.8%) of whom met the goal for low-density lipoprotein (LDL). Dilated eye examinations were provided to 133 patients (54.3%). Foot examinations were performed on 187 residents (76.3%); 170 (69.4%) had a consultation with a podiatrist.
Conclusions Our chart review demonstrates that the management of diabetes in extended-care facilities does not meet the recommended ADA standards of care for ambulatory adults. Although 36.7% of patients met the A1c goal, the A1c did not account for glucose variability. Only 46.8% of patients met the recommended LDL goal. Our results suggest the need for new standards of care for patients with diabetes residing in nursing facilities. These standards should take into account the particular needs of this patient population, specifically with regard to hypoglycemic risk, cardiovascular risk factors, and quality of life.
A surge in elderly patients with diabetes has placed a large burden on extended-care facilities. According to the Centers for Medicare and Medicaid Services, the prevalence of diabetes among nursing home residents is 33.3%.1 Between 1995 and 2004, the estimated number of long-term care residents with diabetes mellitus (DM) grew by 7.1%, from approximately 242,000 to 329,000.2 The increase adds to the challenge extended-care facilities face in attempting to provide high-quality care to patients with diabetes. No well-accepted management guidelines exist for nursing home residents with DM.3
Frail older adults with DM are more likely to suffer from cardiovascular conditions than younger patients, and are at greater risk for hypoglycemic coma and serious hyperglycemia.4,5 A high frequency of hypoglycemia, especially nocturnal hypoglycemia, has been reported among nursing home residents with diabetes.6 Intensive insulin therapy is associated with hypoglycemia and increased mortality.7 However, hyperglycemia also must be considered because it significantly impairs quality of life. Uncontrolled hyperglycemia causes osmotic diuresis, leading to polyuria, nocturia, aggravated incontinence, and disrupted sleep, as well as contributing to dehydration.4 All of these problems have serious implications for quality of life and overall health.
Although studies have identified poor glycemic control and hypertension as the major problems facing nursing home patients with DM,2,6 little research has examined how therapies targeting these problems help the elderly. Solid evidence supports the effectiveness of controlling hyperglycemia, lipid levels, and blood pressure (BP), along with aspirin therapy, in preventing microvascular disease, but does not reflect research involving older patients.8
A study of nursing homes found that health care teams did not respond to half of all significantly abnormal laboratory test results.9 Physicians who are aware of the problems associated with DM in elderly patients may hesitate to treat them because of the lack of guidelines for this patient population or concerns about adverse effects. Because of the deficiency of clinical trial data in elderly patients and the heterogenicity of the population, the American Diabetes Association (ADA) suggests that “less stringent treatment goals” may be appropriate.10
A central conflict in diabetes care for nursing home residents revolves around the need for guidelines that are both generalizable and easily individualized. Some studies support the need for individualized care, particularly with regard to A1c goals, because residents vary greatly in both disease burden and frailty.8,11 Yet individualized treatment could increase the complexity of care for nurses who must manage many patients, potentially having a negative effect on patient care.
Implementation of a treatment protocol for residents with DM is associated with a decrease in the number of hospital days for acute and chronic complications,12 but one study found that only 15% of nursing homes had such a protocol.13 Ultimately, long-term care facilities may benefit from an approach that strikes a balance between individualized care and generalized goals and does not closely mimic either acute hospital care or outpatient management of diabetes.3
In the absence of specific recommendations for extended-care residents with diabetes, our study evaluated the status of care in this population on the basis of pharmacotherapy and standards of care recommended by the ADA for ambulatory adults with DM.
Methods
Data collection
We reviewed the charts of 245 patients in 14 long-term care facilities in Ohio and West Virginia. All participating facilities signed a letter of agreement to take part in the study. The study was approved by the Ohio University Institutional Review Board.
At each facility, the director of nursing supplied a list of residents with DM. To be eligible for chart review, residents had to have a physician-documented diagnosis of type 1 or type 2 DM and have lived at the facility for at least 3 of the previous 12 months. Residents in both skilled nursing care and assisted living facilities were able to participate; short-term rehabilitation residents were not.
We performed a comprehensive review of each chart, examining the medical diagnoses, medication lists, laboratory reports, and physician and consultation notes for a one-year period. Data collection focused on diabetes-related intermediate outcomes and processes of care. Intermediate outcomes included A1c tests, lipid panels, and BP readings. Processes of care included aspirin therapy, use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers, use of statins, eye exams, foot exams, and microalbumin tests. The data collected omitted information identifying the patient, physician, or facility.
We compared the collected data with the 2011 ADA standards of care: blood glucose (fasting 80-120 mg/dL; postprandial 100-140 mg/dL), A1c (<7%), BP (<130/80 mm Hg), and lipid levels (low-density lipoprotein [LDL] <100 mg/dL; high-density lipoprotein [HDL] >40 mg/dL in men and >50 mg/dL in women; triglycerides <150 mg/dL).
Data analysis
We entered the data into an Excel database by type and key format and analyzed results using SPSS software, version 14.0 (SPSS, Chicago, IL). We used percentages and means±standard deviation to describe the data.
Results
TABLE 1 lists characteristics of the patients in the study: 24.5% were male and 75.5% were female; 9 (3.7%) were diagnosed with type 1 DM; 236 (96.3%) had type 2 DM. The mean age was 81±9 years, with a range of 44 to 103 years. Approximately 96% were Caucasian. The residents’ medical care was managed by family physicians (66.1%), internists (25.7%), geriatricians (6.9%), endocrinologists (0.8%), and other physicians (0.4%). The findings that follow are all based on a one-year period unless otherwise specified.
TABLE 1
Study population profile
| Patient characteristic | N (%) |
|---|---|
| Sex Male Female | 60 (24.5) 185 (75.5) |
| Diabetes diagnosis Type 1 Type 2 | 9 (3.7) 236 (96.3) |
| Managing physician specialty Family medicine Internal medicine Geriatrics Endocrinology Other | 162 (66.1) 63 (25.7) 17 (6.9) 2 (0.8) 1 (0.4) |
Diabetes management
Most of the residents (211 [86.1%]) underwent glucose monitoring. The proportion of residents who received specific diabetes interventions is detailed in TABLE 2.
Hypoglycemia. Fifty-two residents (24.6% of those receiving glucose monitoring and 21.2% of the total) experienced a hypoglycemic event; 103 (representing 48.8% of the monitored patients and 42% of the total) had hyperglycemic events. On average, each resident experienced 1±2 mild hypoglycemic episodes per month, with a maximum of 13 mild episodes for one resident. Severe hypoglycemia (< 50 mg/dL) occurred less often, on average 0.24±1 time per resident. One resident had 15 severe hypoglycemic events in a month. The mean low hypoglycemic episode was at a glucose level of 52±16 mg/dL.
Hyperglycemia occurred more often than hypoglycemia (8±14 times per month), with a mean high glucose level of 352±89 mg/dL. This study used a generous range for normal glucose readings (70-249 mg/dL), and 89% of blood glucose readings were within that range. Thirty-seven percent of residents had an A1c <7.0%.
Medication. Thirty-two (13.1%) patients received no oral medication or insulin, and were managed with lifestyle interventions alone. Sixty-four patients (26.1%) used only oral medications, 64 (26.1%) received only insulin, and 85 (34.7%) were treated with both. Of the patients receiving insulin, 108 (72%) were on a sliding scale regimen. Seventy-seven (51.7%) of the patients on insulin experienced hypoglycemia, vs 30 (20%) of those taking oral medication. Twenty-seven (31.8%) patients in the combined therapy group had hypoglycemic events.
TABLE 2
Interventions received by the study population
| Intervention | N (%) |
|---|---|
| Glucose monitoring | 211 (86.1) |
| Blood pressure monitoring | 240 (98.0) |
| Lipids checked | 190 (77.6) |
| Dilated eye exams | 133 (54.3) |
| Foot exams* | 187 (76.3) |
| *170 (69.4%) patients had a consultation with a podiatrist. | |
Preventive care
Foot and eye care. Dilated eye examinations were provided for 133 residents (54.3%). Most (76.3%) received foot examinations, and 69.4% were seen by a podiatrist.
Blood pressure. Of the 240 residents (98%) whose BP was monitored, 107 (43.7%) had readings lower than 125/85 mm Hg, a goal set by a team of diabetologists, endocrinologists, and geriatricians at Ohio University. One hundred residents (40.8%) were taking an angiotensin-converting enzyme inhibitor or an angiotensin II receptor blocker; 122 (49.8%) were receiving aspirin therapy. In the total population, 110 patients (44.9%) were prescribed a statin.
Lipid monitoring. Of the 190 residents (77.6%) whose lipids were monitored, only 89 (46.8%) met the LDL goal suggested by the ADA. Fifty-six (29.5%) had triglycerides <150 mg/dL.
The HDL goal recommended by the ADA is >40 mg/dL for men and >50 mg/dL for women. Three of the 24 men and 16 of the 91 women whose lipids were monitored met the HDL goal.
Discussion
Although several components of diabetes management in our study population failed to meet the ADA standards of care for ambulatory adults, some elements of care were well managed. Monthly foot exams were performed on 76.3% of patients; 69.4% were seen by a podiatrist. While the number of residents receiving foot exams had decreased by 10.7% since a previous study by our research group, the number of podiatric consults increased by 11.4%.14
Dilated eye exams were given to 54.3% of residents. More patients should be given the opportunity to have an annual eye exam. Diabetes is the leading cause of new cases of blindness among adults 20 to 74 years of age,15 and impaired vision affects patient activity levels, susceptibility to falls, and quality of life.
In addition to a good record of preventive exams, physicians were proficient in monitoring residents with diabetes with regular testing regimens. Eighty-six percent of patients underwent regular blood glucose monitoring; 84% had had their A1c tested in the past year, and 36.7% achieved the A1c goal of <7%. The average A1c reading was 6.7±1%.
While these A1c values would seem to reflect well-managed diabetes, blood glucose readings tell a different story. A comparison of A1c values and hyperglycemic events revealed a disparity between the estimated average glucose reading and the actual readings. Of the patients who underwent scheduled fingersticks, 24.6% experienced a hypoglycemic event and 48.8% had hyperglycemic events. On average, each patient had 8 hyperglycemic episodes per month. The average highest glucose reading was >350 mg/dL.
A1c is only part of the story. While A1c can be a marker of sustained hyperglycemia, it does not reflect the stability of glycemic control.16 A study by Löfgren and colleagues confirmed that elderly diabetic patients in nursing homes who have low A1c levels often suffer from hypoglycemia.6 Patients receiving insulin therapy are more likely to experience hypoglycemia.7
The mismatch between A1c and glucose readings reveals an important point about the management of diabetes in long-term care patients: A1c values do not tell the entire story about a patient’s blood glucose; thus, a physician cannot look only at A1c to assess a patient’s diabetes management. A previous study demonstrated that when physicians base treatment plans solely on A1c without consulting glucose logs or being familiar with newer treatments, adherence to evidence-based algorithms is unlikely.17
While A1c does provide information about average blood glucose levels, it does not offer perspective on hypoglycemia or glucose variability. It is vital that physicians screen the glucose log for evidence of hypo- and hyperglycemia before adjusting the patient’s treatment plan. Physicians must also keep in mind that A1c may be falsely low in elderly patients who have concomitant anemia, which lowers the value.
Controlling BP and lipids helps prevent complications. In addition to diabetes management, our study evaluated regulation of the complications of diabetes, particularly cardiovascular complications. Evidence suggests that people with DM derive the greatest mortality benefit from a treatment plan centered first on hypertension, then lipids, and finally, glycemic control.18 A renewed focus on the BP and lipid aspects of diabetes care is needed.
Our data demonstrate that, of the 240 patients who met the ADA goal of <130/80 mm Hg, only 100 (40.8%) were taking an angiotensin-converting enzyme inhibitor or an angiotensin II receptor blocker. Lowering BP to <130/80 mm Hg may provide further benefit in preventing diabetes-related macrovascular complications.8
Lipid levels are a critical gauge of cardiovascular risk. Previous studies of patients with type 2 DM have shown that treating hyperlipidemia can produce a mortality benefit within 2 to 4 years, whereas aggressive glucose management takes approximately 8 years.18
A lipid panel was performed for 77.6% of the patients in our study—an improvement over a previous study by our team in which only 33% of patients received lipid checks.14 In the current study, a mere 2.9% of patients met the ADA’s combined lipid goals (LDL <100 mg/dL; HDL >40 mg/dL in men and >50 mg/dL in women; and triglycerides<150 mg/dL). Considering the LDL goal alone, 46.8% of the 190 patients whose lipids were monitored achieved it.
One hundred ten (44.9%) of the 245 patients in our study were prescribed a statin. Various studies support the use of lipid-lowering medications to increase HDL in elderly patients with DM.8 Yet data suggest that the rate of statin use among older adults is suboptimal.19 Our study highlights the limited prescription of statins for elderly nursing home patients who need them.
The ADA lipid goals are reasonable for this patient population, especially considering the potential mortality benefit. Rather than adjust lipid and BP goals, standards of care should emphasize the importance of meeting these objectives and suggest means to achieve them, including greater use of statins.
One set of standards does not work for all patients. Our study demonstrates that the ADA standards of care for ambulatory adults with diabetes are not acceptable for long-term care residents with DM. Although stringent A1c goals are appropriate for ambulatory adults, the risk of hypoglycemic episodes among the older and frailer nursing home population is too great to adhere to such a strict approach.
We recommend new guidelines be established. Guidelines developed specifically for residents in extended care are necessary to ensure the proper care of these patients, particularly in the face of a steady increase in their number.
Study limitations. Future inquiries into this subject should take into account the weaknesses of this study. First, it was conducted solely in Ohio and West Virginia. A chart review covering more territory could explore regional differences in diabetes care provided by long-term facilities and provide more evidence of the need for a population-specific standards of care.
The study also failed to account for comorbid conditions, including dementia, and code status, and followed residents for only one year. More extensive reviews could examine the effects of therapy in this patient population and the relationship between mortality and treatment plan, spurring movement toward more uniform and effective care of patients with diabetes in the long-term care setting.
CORRESPONDENCE Jay Shubrook Jr, DO, Department of Family Medicine, Ohio University Heritage College of Osteopathic Medicine, Grosvenor Hall, Athens, OH 45701; [email protected]
Purpose Our objective was to compare the management of diabetes mellitus (DM) in residents of extended-care facilities with the American Diabetes Association (ADA) standards of care for ambulatory adults.
Methods We reviewed the charts of 245 residents in 14 extended-care facilities. All had a physician-documented diagnosis of type 1 or type 2 DM and had spent at least 3 of the past 12 months in the facility. We reviewed medical diagnoses, medications, laboratory reports, and consultation notes of one-year duration, then compared our findings with the ADA standards of care.
Results Of the 245 patients, 211 (86.1%) had their glucose monitored; 36.7% had a hemoglobin A1c (A1c) below 7%. Fifty-two residents (21.2%) experienced hypoglycemic events; 103 (42%) had hyperglycemic events. Of the 240 patients (98%) whose blood pressure (BP) was monitored, 107 (43.7%) met the ADA goal. Lipids were checked in 190 residents (77.6%), 89 (46.8%) of whom met the goal for low-density lipoprotein (LDL). Dilated eye examinations were provided to 133 patients (54.3%). Foot examinations were performed on 187 residents (76.3%); 170 (69.4%) had a consultation with a podiatrist.
Conclusions Our chart review demonstrates that the management of diabetes in extended-care facilities does not meet the recommended ADA standards of care for ambulatory adults. Although 36.7% of patients met the A1c goal, the A1c did not account for glucose variability. Only 46.8% of patients met the recommended LDL goal. Our results suggest the need for new standards of care for patients with diabetes residing in nursing facilities. These standards should take into account the particular needs of this patient population, specifically with regard to hypoglycemic risk, cardiovascular risk factors, and quality of life.
A surge in elderly patients with diabetes has placed a large burden on extended-care facilities. According to the Centers for Medicare and Medicaid Services, the prevalence of diabetes among nursing home residents is 33.3%.1 Between 1995 and 2004, the estimated number of long-term care residents with diabetes mellitus (DM) grew by 7.1%, from approximately 242,000 to 329,000.2 The increase adds to the challenge extended-care facilities face in attempting to provide high-quality care to patients with diabetes. No well-accepted management guidelines exist for nursing home residents with DM.3
Frail older adults with DM are more likely to suffer from cardiovascular conditions than younger patients, and are at greater risk for hypoglycemic coma and serious hyperglycemia.4,5 A high frequency of hypoglycemia, especially nocturnal hypoglycemia, has been reported among nursing home residents with diabetes.6 Intensive insulin therapy is associated with hypoglycemia and increased mortality.7 However, hyperglycemia also must be considered because it significantly impairs quality of life. Uncontrolled hyperglycemia causes osmotic diuresis, leading to polyuria, nocturia, aggravated incontinence, and disrupted sleep, as well as contributing to dehydration.4 All of these problems have serious implications for quality of life and overall health.
Although studies have identified poor glycemic control and hypertension as the major problems facing nursing home patients with DM,2,6 little research has examined how therapies targeting these problems help the elderly. Solid evidence supports the effectiveness of controlling hyperglycemia, lipid levels, and blood pressure (BP), along with aspirin therapy, in preventing microvascular disease, but does not reflect research involving older patients.8
A study of nursing homes found that health care teams did not respond to half of all significantly abnormal laboratory test results.9 Physicians who are aware of the problems associated with DM in elderly patients may hesitate to treat them because of the lack of guidelines for this patient population or concerns about adverse effects. Because of the deficiency of clinical trial data in elderly patients and the heterogenicity of the population, the American Diabetes Association (ADA) suggests that “less stringent treatment goals” may be appropriate.10
A central conflict in diabetes care for nursing home residents revolves around the need for guidelines that are both generalizable and easily individualized. Some studies support the need for individualized care, particularly with regard to A1c goals, because residents vary greatly in both disease burden and frailty.8,11 Yet individualized treatment could increase the complexity of care for nurses who must manage many patients, potentially having a negative effect on patient care.
Implementation of a treatment protocol for residents with DM is associated with a decrease in the number of hospital days for acute and chronic complications,12 but one study found that only 15% of nursing homes had such a protocol.13 Ultimately, long-term care facilities may benefit from an approach that strikes a balance between individualized care and generalized goals and does not closely mimic either acute hospital care or outpatient management of diabetes.3
In the absence of specific recommendations for extended-care residents with diabetes, our study evaluated the status of care in this population on the basis of pharmacotherapy and standards of care recommended by the ADA for ambulatory adults with DM.
Methods
Data collection
We reviewed the charts of 245 patients in 14 long-term care facilities in Ohio and West Virginia. All participating facilities signed a letter of agreement to take part in the study. The study was approved by the Ohio University Institutional Review Board.
At each facility, the director of nursing supplied a list of residents with DM. To be eligible for chart review, residents had to have a physician-documented diagnosis of type 1 or type 2 DM and have lived at the facility for at least 3 of the previous 12 months. Residents in both skilled nursing care and assisted living facilities were able to participate; short-term rehabilitation residents were not.
We performed a comprehensive review of each chart, examining the medical diagnoses, medication lists, laboratory reports, and physician and consultation notes for a one-year period. Data collection focused on diabetes-related intermediate outcomes and processes of care. Intermediate outcomes included A1c tests, lipid panels, and BP readings. Processes of care included aspirin therapy, use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers, use of statins, eye exams, foot exams, and microalbumin tests. The data collected omitted information identifying the patient, physician, or facility.
We compared the collected data with the 2011 ADA standards of care: blood glucose (fasting 80-120 mg/dL; postprandial 100-140 mg/dL), A1c (<7%), BP (<130/80 mm Hg), and lipid levels (low-density lipoprotein [LDL] <100 mg/dL; high-density lipoprotein [HDL] >40 mg/dL in men and >50 mg/dL in women; triglycerides <150 mg/dL).
Data analysis
We entered the data into an Excel database by type and key format and analyzed results using SPSS software, version 14.0 (SPSS, Chicago, IL). We used percentages and means±standard deviation to describe the data.
Results
TABLE 1 lists characteristics of the patients in the study: 24.5% were male and 75.5% were female; 9 (3.7%) were diagnosed with type 1 DM; 236 (96.3%) had type 2 DM. The mean age was 81±9 years, with a range of 44 to 103 years. Approximately 96% were Caucasian. The residents’ medical care was managed by family physicians (66.1%), internists (25.7%), geriatricians (6.9%), endocrinologists (0.8%), and other physicians (0.4%). The findings that follow are all based on a one-year period unless otherwise specified.
TABLE 1
Study population profile
| Patient characteristic | N (%) |
|---|---|
| Sex Male Female | 60 (24.5) 185 (75.5) |
| Diabetes diagnosis Type 1 Type 2 | 9 (3.7) 236 (96.3) |
| Managing physician specialty Family medicine Internal medicine Geriatrics Endocrinology Other | 162 (66.1) 63 (25.7) 17 (6.9) 2 (0.8) 1 (0.4) |
Diabetes management
Most of the residents (211 [86.1%]) underwent glucose monitoring. The proportion of residents who received specific diabetes interventions is detailed in TABLE 2.
Hypoglycemia. Fifty-two residents (24.6% of those receiving glucose monitoring and 21.2% of the total) experienced a hypoglycemic event; 103 (representing 48.8% of the monitored patients and 42% of the total) had hyperglycemic events. On average, each resident experienced 1±2 mild hypoglycemic episodes per month, with a maximum of 13 mild episodes for one resident. Severe hypoglycemia (< 50 mg/dL) occurred less often, on average 0.24±1 time per resident. One resident had 15 severe hypoglycemic events in a month. The mean low hypoglycemic episode was at a glucose level of 52±16 mg/dL.
Hyperglycemia occurred more often than hypoglycemia (8±14 times per month), with a mean high glucose level of 352±89 mg/dL. This study used a generous range for normal glucose readings (70-249 mg/dL), and 89% of blood glucose readings were within that range. Thirty-seven percent of residents had an A1c <7.0%.
Medication. Thirty-two (13.1%) patients received no oral medication or insulin, and were managed with lifestyle interventions alone. Sixty-four patients (26.1%) used only oral medications, 64 (26.1%) received only insulin, and 85 (34.7%) were treated with both. Of the patients receiving insulin, 108 (72%) were on a sliding scale regimen. Seventy-seven (51.7%) of the patients on insulin experienced hypoglycemia, vs 30 (20%) of those taking oral medication. Twenty-seven (31.8%) patients in the combined therapy group had hypoglycemic events.
TABLE 2
Interventions received by the study population
| Intervention | N (%) |
|---|---|
| Glucose monitoring | 211 (86.1) |
| Blood pressure monitoring | 240 (98.0) |
| Lipids checked | 190 (77.6) |
| Dilated eye exams | 133 (54.3) |
| Foot exams* | 187 (76.3) |
| *170 (69.4%) patients had a consultation with a podiatrist. | |
Preventive care
Foot and eye care. Dilated eye examinations were provided for 133 residents (54.3%). Most (76.3%) received foot examinations, and 69.4% were seen by a podiatrist.
Blood pressure. Of the 240 residents (98%) whose BP was monitored, 107 (43.7%) had readings lower than 125/85 mm Hg, a goal set by a team of diabetologists, endocrinologists, and geriatricians at Ohio University. One hundred residents (40.8%) were taking an angiotensin-converting enzyme inhibitor or an angiotensin II receptor blocker; 122 (49.8%) were receiving aspirin therapy. In the total population, 110 patients (44.9%) were prescribed a statin.
Lipid monitoring. Of the 190 residents (77.6%) whose lipids were monitored, only 89 (46.8%) met the LDL goal suggested by the ADA. Fifty-six (29.5%) had triglycerides <150 mg/dL.
The HDL goal recommended by the ADA is >40 mg/dL for men and >50 mg/dL for women. Three of the 24 men and 16 of the 91 women whose lipids were monitored met the HDL goal.
Discussion
Although several components of diabetes management in our study population failed to meet the ADA standards of care for ambulatory adults, some elements of care were well managed. Monthly foot exams were performed on 76.3% of patients; 69.4% were seen by a podiatrist. While the number of residents receiving foot exams had decreased by 10.7% since a previous study by our research group, the number of podiatric consults increased by 11.4%.14
Dilated eye exams were given to 54.3% of residents. More patients should be given the opportunity to have an annual eye exam. Diabetes is the leading cause of new cases of blindness among adults 20 to 74 years of age,15 and impaired vision affects patient activity levels, susceptibility to falls, and quality of life.
In addition to a good record of preventive exams, physicians were proficient in monitoring residents with diabetes with regular testing regimens. Eighty-six percent of patients underwent regular blood glucose monitoring; 84% had had their A1c tested in the past year, and 36.7% achieved the A1c goal of <7%. The average A1c reading was 6.7±1%.
While these A1c values would seem to reflect well-managed diabetes, blood glucose readings tell a different story. A comparison of A1c values and hyperglycemic events revealed a disparity between the estimated average glucose reading and the actual readings. Of the patients who underwent scheduled fingersticks, 24.6% experienced a hypoglycemic event and 48.8% had hyperglycemic events. On average, each patient had 8 hyperglycemic episodes per month. The average highest glucose reading was >350 mg/dL.
A1c is only part of the story. While A1c can be a marker of sustained hyperglycemia, it does not reflect the stability of glycemic control.16 A study by Löfgren and colleagues confirmed that elderly diabetic patients in nursing homes who have low A1c levels often suffer from hypoglycemia.6 Patients receiving insulin therapy are more likely to experience hypoglycemia.7
The mismatch between A1c and glucose readings reveals an important point about the management of diabetes in long-term care patients: A1c values do not tell the entire story about a patient’s blood glucose; thus, a physician cannot look only at A1c to assess a patient’s diabetes management. A previous study demonstrated that when physicians base treatment plans solely on A1c without consulting glucose logs or being familiar with newer treatments, adherence to evidence-based algorithms is unlikely.17
While A1c does provide information about average blood glucose levels, it does not offer perspective on hypoglycemia or glucose variability. It is vital that physicians screen the glucose log for evidence of hypo- and hyperglycemia before adjusting the patient’s treatment plan. Physicians must also keep in mind that A1c may be falsely low in elderly patients who have concomitant anemia, which lowers the value.
Controlling BP and lipids helps prevent complications. In addition to diabetes management, our study evaluated regulation of the complications of diabetes, particularly cardiovascular complications. Evidence suggests that people with DM derive the greatest mortality benefit from a treatment plan centered first on hypertension, then lipids, and finally, glycemic control.18 A renewed focus on the BP and lipid aspects of diabetes care is needed.
Our data demonstrate that, of the 240 patients who met the ADA goal of <130/80 mm Hg, only 100 (40.8%) were taking an angiotensin-converting enzyme inhibitor or an angiotensin II receptor blocker. Lowering BP to <130/80 mm Hg may provide further benefit in preventing diabetes-related macrovascular complications.8
Lipid levels are a critical gauge of cardiovascular risk. Previous studies of patients with type 2 DM have shown that treating hyperlipidemia can produce a mortality benefit within 2 to 4 years, whereas aggressive glucose management takes approximately 8 years.18
A lipid panel was performed for 77.6% of the patients in our study—an improvement over a previous study by our team in which only 33% of patients received lipid checks.14 In the current study, a mere 2.9% of patients met the ADA’s combined lipid goals (LDL <100 mg/dL; HDL >40 mg/dL in men and >50 mg/dL in women; and triglycerides<150 mg/dL). Considering the LDL goal alone, 46.8% of the 190 patients whose lipids were monitored achieved it.
One hundred ten (44.9%) of the 245 patients in our study were prescribed a statin. Various studies support the use of lipid-lowering medications to increase HDL in elderly patients with DM.8 Yet data suggest that the rate of statin use among older adults is suboptimal.19 Our study highlights the limited prescription of statins for elderly nursing home patients who need them.
The ADA lipid goals are reasonable for this patient population, especially considering the potential mortality benefit. Rather than adjust lipid and BP goals, standards of care should emphasize the importance of meeting these objectives and suggest means to achieve them, including greater use of statins.
One set of standards does not work for all patients. Our study demonstrates that the ADA standards of care for ambulatory adults with diabetes are not acceptable for long-term care residents with DM. Although stringent A1c goals are appropriate for ambulatory adults, the risk of hypoglycemic episodes among the older and frailer nursing home population is too great to adhere to such a strict approach.
We recommend new guidelines be established. Guidelines developed specifically for residents in extended care are necessary to ensure the proper care of these patients, particularly in the face of a steady increase in their number.
Study limitations. Future inquiries into this subject should take into account the weaknesses of this study. First, it was conducted solely in Ohio and West Virginia. A chart review covering more territory could explore regional differences in diabetes care provided by long-term facilities and provide more evidence of the need for a population-specific standards of care.
The study also failed to account for comorbid conditions, including dementia, and code status, and followed residents for only one year. More extensive reviews could examine the effects of therapy in this patient population and the relationship between mortality and treatment plan, spurring movement toward more uniform and effective care of patients with diabetes in the long-term care setting.
CORRESPONDENCE Jay Shubrook Jr, DO, Department of Family Medicine, Ohio University Heritage College of Osteopathic Medicine, Grosvenor Hall, Athens, OH 45701; [email protected]
1. Centers for Medicare and Medicaid Services. MDS active resident information report: third quarter 2010. Available at: https://www.cms.gov/MDSPubQIandResRep/04_activeresreport.asp?isSubmitted=res3&var=I1a&date=32. Accessed February 9, 2011.
2. Zhang X, Decker FH, Luo H, et al. Trends in the prevalence and comorbidities of diabetes mellitus in nursing home residents in the United States: 1995-2004. J Am Geriatr Soc. 2010;58:724-730.
3. Meyers RM, Reger L. Diabetes management in long-term care facilities: a practical guide. J Am Med Dir Assoc. 2009;10:589.-
4. Mayfield J, Deb P, Potter D, et al. Diabetes and long-term care. In: Diabetes in America. 2nd ed. Bethesda, MD: National Diabetes Data Group, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health; 1995:571–586.
5. Ben-Ami H, Nagachandran P, Mendelson A, et al. Drug-induced hypoglycemic coma in 102 diabetic patients. Arch Intern Med. 1999;159:281-284.
6. Löfgren UB, Rosenqvist U, Lindstrom T, et al. Diabetes control in Swedish community dwelling elderly: more often tight than poor. J Intern Med. 2004;255:96-101.
7. The Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358:2545-2559.
8. Brown AF, Mangione CM, Saliba D, et al. Guidelines for improving the care of the older person with diabetes mellitus. J Am Geriatr Soc. 2003;51:S265-S280.
9. Chalmers J, Beaven D, Sainsburg R. Are high blood sugar levels in the elderly ignored? Aust NZ J Med. 1987;17:485-490.
10. American Diabetes Association. Standards of medical care in diabetes—2011. Diabetes Care. 2011;34(suppl 1):S11-S61.
11. Meyers RM, Broton JC, Woo-Rippe KW, et al. Variability in glycosylated hemoglobin values in diabetic patients living in long-term care facilities. J Am Med Dir Assoc. 2007;8:511-514.
12. Hamman RF, Michael SL, Keefer SM, et al. Impact of policy and procedure changes on hospital days among diabetic nursing-home residents—Colorado. MMWR Morb Mortal Wkly Rep. 1984;33:621-629.
13. Feldman SM, Rosen R, DeStasio J. Status of diabetes management in the nursing home setting in 2008: a retrospective chart review and epidemiology study of diabetic nursing home residents and nursing home initiatives in diabetes management. J Am Med Dir Assoc. 2009;10:354-360.
14. Holt RM, Schwartz FL, Shubrook JH. Diabetes care in extended-care facilities: appropriate intensity of care? Diabetes Care. 2007;30:1454-1458.
15. Centers for Disease Control and Prevention. National diabetes fact sheet, 2007. Available at: http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2007.pdf. Accessed February 10, 2011.
16. Alam T, Weintraub N, Weinreb J. What is the proper use of hemoglobin A1c monitoring in the elderly? J Am Med Dir Assoc. 2006;7(3 suppl):S60-S64.
17. Alam T, Weintraub N, Weinreb J. What is the proper use of hemoglobin A1c monitoring in the elderly? J Am Med Dir Assoc. 2010;11:171-178.
18. Huang ES, Meigs JB, Singer DE. The effect of interventions to prevent cardiovascular disease in patients with type 2 diabetes mellitus. Am J Med. 2001;11:633-642.
19. Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA. 2002;288:462-467.
1. Centers for Medicare and Medicaid Services. MDS active resident information report: third quarter 2010. Available at: https://www.cms.gov/MDSPubQIandResRep/04_activeresreport.asp?isSubmitted=res3&var=I1a&date=32. Accessed February 9, 2011.
2. Zhang X, Decker FH, Luo H, et al. Trends in the prevalence and comorbidities of diabetes mellitus in nursing home residents in the United States: 1995-2004. J Am Geriatr Soc. 2010;58:724-730.
3. Meyers RM, Reger L. Diabetes management in long-term care facilities: a practical guide. J Am Med Dir Assoc. 2009;10:589.-
4. Mayfield J, Deb P, Potter D, et al. Diabetes and long-term care. In: Diabetes in America. 2nd ed. Bethesda, MD: National Diabetes Data Group, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health; 1995:571–586.
5. Ben-Ami H, Nagachandran P, Mendelson A, et al. Drug-induced hypoglycemic coma in 102 diabetic patients. Arch Intern Med. 1999;159:281-284.
6. Löfgren UB, Rosenqvist U, Lindstrom T, et al. Diabetes control in Swedish community dwelling elderly: more often tight than poor. J Intern Med. 2004;255:96-101.
7. The Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358:2545-2559.
8. Brown AF, Mangione CM, Saliba D, et al. Guidelines for improving the care of the older person with diabetes mellitus. J Am Geriatr Soc. 2003;51:S265-S280.
9. Chalmers J, Beaven D, Sainsburg R. Are high blood sugar levels in the elderly ignored? Aust NZ J Med. 1987;17:485-490.
10. American Diabetes Association. Standards of medical care in diabetes—2011. Diabetes Care. 2011;34(suppl 1):S11-S61.
11. Meyers RM, Broton JC, Woo-Rippe KW, et al. Variability in glycosylated hemoglobin values in diabetic patients living in long-term care facilities. J Am Med Dir Assoc. 2007;8:511-514.
12. Hamman RF, Michael SL, Keefer SM, et al. Impact of policy and procedure changes on hospital days among diabetic nursing-home residents—Colorado. MMWR Morb Mortal Wkly Rep. 1984;33:621-629.
13. Feldman SM, Rosen R, DeStasio J. Status of diabetes management in the nursing home setting in 2008: a retrospective chart review and epidemiology study of diabetic nursing home residents and nursing home initiatives in diabetes management. J Am Med Dir Assoc. 2009;10:354-360.
14. Holt RM, Schwartz FL, Shubrook JH. Diabetes care in extended-care facilities: appropriate intensity of care? Diabetes Care. 2007;30:1454-1458.
15. Centers for Disease Control and Prevention. National diabetes fact sheet, 2007. Available at: http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2007.pdf. Accessed February 10, 2011.
16. Alam T, Weintraub N, Weinreb J. What is the proper use of hemoglobin A1c monitoring in the elderly? J Am Med Dir Assoc. 2006;7(3 suppl):S60-S64.
17. Alam T, Weintraub N, Weinreb J. What is the proper use of hemoglobin A1c monitoring in the elderly? J Am Med Dir Assoc. 2010;11:171-178.
18. Huang ES, Meigs JB, Singer DE. The effect of interventions to prevent cardiovascular disease in patients with type 2 diabetes mellitus. Am J Med. 2001;11:633-642.
19. Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA. 2002;288:462-467.
Next steps when BP won’t come down
• Review the family history of patients who do not respond to appropriate antihypertensive therapy, targeting hypertension and inherited disorders associated with high blood pressure (BP). B
• Include obstructive sleep apnea in the differential diagnosis of patients with resistant hypertension, particularly if they’re obese. B
• Include a thorough medication history in a work-up for resistant hypertension, as a number of drugs can cause or exacerbate high BP. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
What to include in the workup
Whether you’re doing an initial evaluation of a patient with high blood pressure (BP) or examining a patient with resistant hypertension, the history should focus on the duration of hypertension, previous BP levels, and comorbid conditions. It is also important to take a targeted family history, inquiring about hypertension as well as genetic disorders that increase the likelihood of secondary hypertension.
Inherited diseases associated with secondary hypertension include polycystic kidney disease, multiple endocrine neoplasia type 2 (MEN2), and von Hippel-Lindau syndrome.12,13 All are inherited in an autosomal dominant pattern. Patients with von Hippel-Lindau syndrome may present with multiple tumors, which can develop in the eyes, brain, adrenal glands, pancreas, liver, spinal cord, kidneys, or other parts of the body. Pheochromocytoma is a manifestation of both MEN2 and von Hippel-Lindau syndrome, and some specialists recommend that everyone with a family history of either condition undergo screening for pheochromocytoma.14
Table
Secondary hypertension: What you’ll see, what to test for8-11
| Secondary cause* | Signs and symptoms | Screening tests |
|---|---|---|
| Renal disease | Depends on underlying cause (eg, diabetes, polycystic kidney disease, glomerulonephritis) | Serum creatinine, urinalysis, renal ultrasound |
| Renal artery stenosis | Abdominal or flank bruits | Renal ultrasound, MRA, CT angiography |
| Primary hyperaldosteronism | Muscle cramps | PA/PRA |
| Pheochromocytoma | Paroxysms of palpitations, diaphoresis, headaches | Plasma metanephrine and normetanephrine |
| Cushing’s syndrome | Rapid weight gain, truncal obesity, abdominal striae | Measurement of 24-hour urinary free cortisol |
| OSA† | Obesity, daytime somnolence, nighttime snoring | Overnight polysomnography |
| Coarctation of the aorta‡ | Murmur of anterior and posterior thorax; claudication and weak femoral pulses | Echocardiography |
| CT, computed tomography; MRA, magnetic resonance angiography; OSA, obstructive sleep apnea; PA/PRA, plasma aldosterone-plasma renin activity. *Secondary hypertension may also be drug-induced, related to pregnancy (hypertension complicates up to 15% of pregnancies), or associated with inherited syndromes. †Highly prevalent in obese patients. ‡Higher prevalence in childhood hypertension; rarely diagnosed in adulthood. | ||
BP measurement is key
The physical examination should start with a calculation of body mass index, as well as a careful measurement of BP. The patient should be seated quietly in a chair for ≥5 minutes, with both feet on the floor and the arm being tested supported at heart level.
Unfortunately, reliability on the office BP measurement can be a confounding factor in the diagnosis of hypertension. “White coat hypertension”—in which BP is persistently elevated in the office and persistently normal in nonclinical settings—should be considered in patients who have high BP but no other signs or symptoms, and ambulatory monitoring used to rule out hypertension.15,16
Physicians also need to consider the opposite effect: Masked hypertension, characterized by normal office readings and elevated ambulatory readings, is more serious, of course, with patients at higher risk for end organ damage from unrecognized hypertension.17,18 Asking patients who self-monitor what type of BP readings they’re getting can be helpful in identifying masked hypertension. Ambulatory monitoring may be used to identify this condition, as well.
Other components in the physical workup include a fundoscopic exam; assessment of the thorax for murmurs and the abdomen for enlarged kidneys, masses, and abnormal aortic pulsation; auscultation for abdominal and carotid bruits; palpation of the thyroid gland; and palpation of the lower extremities for edema and pulses.
Include these tests in the workup
Routine tests for a patient with hypertension include:
- electrocardiogram
- blood glucose and hematocrit
- serum potassium, creatinine, and fasting lipid profiles
- urinalysis with measurement of microalbumin.
Microalbuminuria, a sensitive marker of early renal disease, is defined as a urinary albumin excretion between 30 and 300 mg/d.19 The albumin-creatinine ratio (30-300 mcg/mg), measured in spot urine specimens, is a more convenient way to detect it.20
Suspicious findings prompt further testing. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) recommends specific testing—much of it detailed below—if any aspect of the initial evaluation raises suspicion of a secondary cause or the patient has hypertension that’s of sudden onset or hard to control.21 (According to the National Heart, Lung, and Blood Institute, JNC 8 is due for release later this year.)
Kidney disease may be a consequence or a cause
The overall prevalence of hypertension in patients with renal disease is 60%,22 but varies according to the type of nephropathy. Eighty-seven percent of patients with diabetic nephropathy also have hypertension, and hypertension and diabetes are the 2 most common causes of end-stage renal disease.23,24
A combination of 2 or more drugs is usually needed to achieve the target BP of <130/80 mm Hg in patients with diabetes.21 ACE inhibitors and angiotensin receptor blockers have been found to slow the progression of diabetic nephropathy.25-27
Is renal artery stenosis to blame?
Renal artery stenosis is the most common form of secondary hypertension that’s reversible, affecting about 0.2% to 3.1% of hypertensive patients.5,6,28 The condition leads to renal ischemia, thereby stimulating the renin-angiotensin-aldosterone axis and causing secondary hyperaldosteronism.
In younger patients, especially women between 15 and 50 years of age, fibromuscular disease is the most common cause of renovascular hypertension.29,30 In older patients, atherosclerosis (which accounts for 90% of renovascular hypertension) is more likely.29,30
The choice of initial imaging tests includes duplex renal ultrasonography, magnetic resonance angiography (MRA), and spiral computed tomographic angiography. Contrast angiography is the gold standard, but it carries a risk of contrast-induced nephropathy. Duplex ultrasonography and MRA do not use iodinated contrast media, and are safe for patients with chronic kidney disease.8
Treatment. Percutaneous transluminal renal artery angioplasty is a treatment option for patients with renal artery stenosis. Angioplasty achieves higher cure rates for patients with fibromuscular dysplasia than for those with atherosclerotic renal artery stenosis.31 Most patients referred for renal artery revascularization have atherosclerosis. Because they’re generally older individuals with comorbidities, the benefits of stent revascularization for this group is controversial. Such patients require antihypertensive therapy with drugs that block the renin-angiotensin system.32
Endocrine disorders must be ruled out
Primary hyperaldosteronism is thought to be present in 0.3% to 1.4% of patients with hypertension.5,6 The prevalence varies widely from one source to another, however, and may be as high as 5% to 20% among patients with resistant hypertension.33,34
Hyperaldosteronism is related to either an aldosterone-secreting adrenal adenoma (in about 40% of cases) or bilateral adrenal hyperplasia (in the remaining 60%), and leads to increased sodium reabsorption and, typically, to a loss of potassium.35
Renin-secreting tumor, which usually arises from the juxtaglomerular cells of the kidney, is a rare cause of hyperaldosteronism. Extrarenal renin-secreting tumors have also been reported.36
What should raise your suspicion. Suspect hyperaldosteronism in patients who have both hypertension and hypokalemia, but keep in mind that not all patients with hyperaldosteronism have low serum potassium.37 Further laboratory evaluation should include a simultaneous measurement of plasma aldosterone (PA) and plasma renin activity (PRA). Patients with hyperaldosteronism will have elevated PA and suppressed PRA.
Testing considerations. It is important to ensure that the PA/PRA test is performed in the morning, with the patient in an upright position.36 He or she should be on a high sodium diet in preparation for the test, consuming 2 to 3 grams of sodium per meal for ≥2 days.37
In patients with a positive PA/PRA ratio (≥20), a 24-hour urinary aldosterone excretion test should be performed. A finding >12 to 14 mcg, along with a PRA <1.0 ng/mL per hour, confirms the diagnosis of primary hyperaldosteronism.18,37 Computed tomography or magnetic resonance imaging of the adrenal glands will distinguish between aldosterone-producing adenoma and bilateral adrenal hyperplasia.
Treatment. Laparoscopic adrenalectomy is the accepted surgical treatment of primary hyperaldosteronism.37 Patients with bilateral disease due to idiopathic hyperaldosteronism are not candidates for surgery and should be treated medically, with potassium-sparing diuretics such as spironolactone.
Cushing’s syndrome is marked by rapid weight gain
High BP may be a manifestation of Cushing’s syndrome, which affects 0.1% to 0.5% of patients with hypertension.5-7 Other signs and symptoms of Cushing’s syndrome include fatigue, weakness, hirsutism, amenorrhea, moon facies, dorsal hump, purple striae, truncal obesity, and hypokalemia. Rapid weight gain is the most common manifestation, and typically the one for which patients seek medical attention.38
The most widely used screening test for Cushing’s syndrome is a 24-hour urine collection measuring urinary-free cortisol.9 Normal urinary cortisol excretion is 20 to 100 mcg/dL in 24 hours; most patients with Cushing’s syndrome produce >250 mcg/dL in that time frame.9
Once hypercortisolism is established, determination of the cause is the next step. A serum adrenocorticotropic hormone (ACTH) level is needed to localize it. Normal (9-52 pg/mL) or elevated ACTH indicates a pituitary or ectopic source, while low levels of ACTH are an indication of an adrenal source.9,39
Treatment. Surgical resection of the tumor is often curative. For pituitary tumors (Cushing’s disease), transsphenoidal resection is the standard of care.39 For adrenal adenomas, unilateral adrenalectomy is the best option.39
Pheochromocytomas: Most are adrenal, sporadic, and benign
Pheochromocytomas—neuroendocrine, catecholamine-secreting tumors that develop from the adrenal medulla—are another cause of secondary hypertension. Catecholamines include norepinephrine and epinephrine and, rarely, dopamine secreted either intermittently or continuously. The prevalence of pheochromocytoma is 0.1% to 0.3% among patients with hypertension.5,6,28 A “rule of 10” (90:10 ratio) is often applied to pheochromocytomas because of the following:
- 90% of pheochromocytomas are located in the adrenal glands; the remaining 10% are extra-adrenal and can occur anywhere along the sympathetic chain40
- 90% are sporadic; 10% are familial41
- 90% are benign; 10% are malignant40
- 90% are found in adults; 10% affect children.42
Signs and symptoms of pheochromocytomas include palpitations, headache, dyspnea, diaphoresis, and flushing, as well as paroxysmal hypertension.40 Measurement of 24-hour urinary catecholamines and their metabolites has been the screening test of choice,43 but recent evidence suggests that measurement of plasma metanephrine and normetanephrine is a far more sensitive screen.10
Treatment. Surgical resection is the treatment of choice. Alpha blockade is started 7 to 10 days preoperatively;44,45 a beta-blocker is added only after an adequate alpha blockade has been established, as unopposed alpha stimulation could precipitate a hypertensive crisis. Laparoscopic adrenalectomy is routinely performed for small (<5 cm) pheochromocytomas.46,47
Don’t forget these (relatively) common secondary causes
Obstructive sleep apnea (OSA) is one of the most common conditions associated with resistant hypertension.48 Signs and symptoms include snoring, daytime somnolence, and obesity (body mass index ≥30 kg/m2).
OSA involves upper airway collapse during inspiration, causing intermittent hypoxemia with resultant sympathetic nervous system activation.11 The underlying mechanism of OSA-induced hypertension is strongly related to sympathetic activation.49 Overnight polysomnography is required for diagnosis.11
Continuous positive airway pressure is the treatment of choice for patients unable to lose weight.11
Pregnancy-induced hypertension is the most common medical problem encountered in pregnancy. It occurs in up to 15% of pregnancies, either during the pregnancy itself or postpartum. Postpartum hypertension may be related to preexisting chronic hypertension or to the persistence of gestational hypertension or preeclampsia, which usually occurs after 20 weeks’ gestation and is characterized by the presence of hypertension and proteinuria.50 Methyldopa and labetalol are commonly used treatments for hypertension during pregnancy.51
Drug-induced hypertension. Several drugs can cause or exacerbate hypertension, rendering it resistant to therapy. A careful review of the patient’s medication regimen is essential. Generally, drug-induced hypertension falls into 2 broad categories based on mechanism of action: volume overload and sympathetic activity.52,53
Corticosteroids can elevate BP in a dose-dependent manner, as a result of volume overload. Glycyrrhizic acid, the main ingredient in licorice, produces a state of excess mineralocorticoid, with a similar effect. Estrogen-containing oral contraceptives can cause an increased synthesis of angiotensin in the liver, resulting in greater aldosterone secretion and volume overload.
Drugs that stimulate sympathetic activity include cocaine, ephedrine, amphetamine, phenylephrine, phenylpropanolamine, caffeine, and alcohol. Nonsteroidal anti-inflammatory drugs may interfere with the action of ACE inhibitors and cause renal vasoconstriction, leading to sodium and water retention and hypertension.54
Discontinuation of the medication in question is preferable. In many cases, an agent that does not affect BP can be found to replace it.
If the patient is a child
Hypertension is uncommon in young people. However, coarctation of the aorta, a congenital narrowing associated with secondary hypertension, is typically diagnosed in childhood. In rare cases, the condition remains undetected well into adulthood.55 Clinical signs include weak femoral pulses, visible pulsations in the neck, a systolic murmur of the anterior and posterior thorax, and elevated BP in the upper extremities with low BP in the lower extremities.
Thus, once hypertension is confirmed in a young patient, BP should be measured in both arms and legs.56 Delayed or absent femoral pulses and a difference in systolic BP of ≥20 mm Hg between the arms and legs provide evidence of aortic coarctation.57 In adults, stenting is the initial treatment for this condition because of the morbidity associated with surgery.57 Stenting is an option for children with this condition, as well.58
CORRESPONDENCE Bernard M. Karnath, MD, University of Texas Medical Branch at Galveston, 301 University Boulevard, Galveston, TX 77555; [email protected]
1. Middleton K, Hing E, Xu J. National hospital ambulatory medical care survey: 2005 outpatient department summary. Adv Data. 2007;389:1-34.
2. Ong KL, Cheung BM, Man YB, et al. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999-2004. Hypertension. 2007;49:69-75.
3. Fields LE, Burt VL, Cutler JA, et al. The burden of adult hypertension in the United States 1999 to 2000: a rising tide. Hypertension. 2004;44:398-404.
4. Wang TJ, Vasan RS. Epidemiology of uncontrolled hypertension in the United States. Circulation. 2005;112:1651-1662.
5. Anderson GH, Jr, Blakeman N, Streeten DH. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J Hypertens. 1994;12:609-615.
6. Sinclair AM, Isles CG, Brown I, et al. Secondary hypertension in a blood pressure clinic. Arch Intern Med. 1987;147:1289-1293.
7. Dosh SA. The diagnosis of essential and secondary hypertension in adults. J Fam Pract. 2001;50:707-712.
8. Eardley KS, Lipkin GW. Atherosclerotic renal artery stenosis: is it worth diagnosing?J Hum Hypertens. 1999;13:217-220.
9. Boscaro M, Barzon L, Fallo F, et al. Cushing’s syndrome. Lancet. 2001;357:783-791.
10. Unger N, Pitt C, Schmidt IL. Diagnostic value of various biochemical parameters for the diagnosis of pheochromocytoma in patients with adrenal mass. Eur J Endocrinol. 2006;154:409-417.
11. Prisant LM, Dillard TA, Blanchard AR. Obstructive sleep apnea syndrome. J Clin Hypertens. 2006;8:746-750.
12. Marini F, Falchetti A, Del Monte F, et al. Multiple endocrine neoplasia type 2. Orphanet J Rare Dis. 2006;1:45.-
13. Bryant J, Farmer J, Kessler LJ, et al. Pheochromocytoma: the expanding genetic differential diagnosis. J Natl Cancer Inst. 2003;95:1196-1204.
14. Neumann HP, Berger DP, Sigmund G, et al. Pheochromocytomas, multiple endocrine neoplasia type 2, and von Hippel-Lindau disease. N Engl J Med. 1993;329:1531-1538.
15. Mancia G, Bertinieri G, Grassi G, et al. Effects of blood-pressure measurement by the doctor on patient’s blood pressure and heart rate. Lancet. 1983;2:695-698.
16. Pickering TG, James GD, Boddie C. How common is white coat hypertension? JAMA. 1988;259:225-228.
17. Kotsis V, Stabouli S, Toumanidis S, et al. Target organ damage in “white coat hypertension” and “masked hypertension”. Am J Hypertens. 2008;21:393-399.
18. Pickering TG, Davidson K, Gerin W, et al. Masked hypertension. Hypertension. 2002;40:795-796.
19. Volpe M. Microalbuminuria screening in patients with hypertension: recommendations for clinical practice. Int J Clin Pract. 2008;62:97-108.
20. Keane WF, Eknoyan G. Proteinuria, albuminuria, risk, assessment, detection, elimination (PARADE): a position paper of the National Kidney Foundation. Am J Kidney Dis. 1999;33:1004-1010.
21. Chobanian AV, Bakris GL, Black HR, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206-1252.
22. Ridao N, Luño J, García de Vinuesa S, et al. Prevalence of hypertension in renal disease. Nephrol Dial Transplant. 2001;16(suppl 1):S70-S73.
23. Foley RN, Collins AJ. End-stage renal disease in the United States: an update from the United States Renal Data System. J Am Soc Nephrol. 2007;18:2644-2648.
24. Parmar MS. Chronic renal disease. BMJ. 2002;325:85-90.
25. Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345:861-869.
26. Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.
27. Menne J, Izzo JL, Jr, Ito S, et al. Prevention of microalbuminuria in patients with type 2 diabetes and hypertension. J Hypertens. 2012;30:811-818.
28. Rossi H, Kim A, Prinz RA. Primary hyperaldosteronism in the era of laparoscopic adrenalectomy. Am Surg. 2002;68:253-256.
29. Safian RD, Textor SC. Renal artery stenosis. N Engl J Med. 2001;244:431-442.
30. Slovut DP, Olin JW. Fibromuscular dysplasia. N Engl J Med. 2004;350:1862-1871.
31. Bonelli FS, McKusick MA, Textor SC. Renal artery angioplasty: technical results and clinical outcome in 320 patients. Mayo Clin Proc. 1995;70:1041-1052.
32. Textor SC. Renovascular hypertension in 2007: where are we now? Curr Cardiol Rep. 2007;9:453-461.
33. Calhoun DA. Is there an unrecognized epidemic of primary aldosteronism? Pro. Hypertension. 2007;50:447-453.
34. Young WF, Jr. Minireview: primary aldosteronism—changing concepts in diagnosis and treatment. Endocrinology. 2003;144:2208-2213.
35. Young WF. Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf). 2007;66:607-618.
36. Pursell RN, Quinlan PM. Secondary hypertension due to a renin-producing teratoma. Am J Hypertens. 2003;16:592-595.
37. Ganguly A. Primary aldosteronism. N Engl J Med. 1998;339:1828-1834.
38. Muller M, Longo Mazzuco T, Martinie M, et al. Diagnosis of Cushing’s syndrome: a retrospective evaluation of clinical practice. Eur J Intern Med. 2006;17:334-338.
39. Norton JA, Li M, Gillary J, et al. Cushing’s syndrome. Curr Probl Surg. 2001;38:488-545.
40. Lenders JW, Eisenhofer G, Mannelli M, et al. Phaeochromocytoma. Lancet. 2005;366:665-675.
41. Bryant J, Farmer J, Kessler LJ, et al. Pheochromocytoma: the expanding genetic differential diagnosis. J Natl Cancer Inst. 2003;95:1196-1204.
42. Sullivan J, Groshong T, Tobias JD. Presenting signs and symptoms of pheochromocytoma in pediatric-aged patients. Clin Pediatr. 2005;44:715-719.
43. Young WF, Jr. Pheochromocytoma: issues in diagnosis and treatment. Compr Ther. 1997;23:319-326.
44. Kocak S, Aydintug S, Canakci N. Alpha blockade in preoperative preparation of patients with pheochromocytomas. Int Surg. 2002;87:191-194.
45. Russell WJ, Metcalfe IR, Tonkin AL, et al. The preoperative management of phaeochromocytoma. Anaesth Intensive Care. 1998;26:196-200.
46. Kalady MF, McKinlay R, Olson JA, Jr, et al. Laparoscopic adrenalectomy for pheochromocytoma. A comparison to aldosteronoma and incidentaloma. Surg Endosc. 2004;18:621-625.
47. Naya Y, Ichikawa T, Suzuki H, et al. Efficacy and safety of laparoscopic surgery for pheochromocytoma. Int J Urol. 2005;12:128-133.
48. Pedrosa RP, Drager LF, Gonzaga CC, et al. Obstructive sleep apnea: the most common secondary cause of hypertension associated with resistant hypertension. Hypertension. 2011;5:811-817.
49. Sharabi Y, Dagan Y, Grossman E. Sleep apnea as a risk factor for hypertension. Curr Opin Nephrol Hypertens. 2004;13:359-364.
50. James PR, Nelson-Piercy C. Management of hypertension before, during, and after pregnancy. Heart. 2004;90:1499-1504.
51. Solomon CG, Seely EW. Hypertension in pregnancy. Endocrinol Metab Clin North Am. 2011;40:847-863.
52. Grossman E, Messerli FH. Drug-induced hypertension: an unappreciated cause of secondary hypertension. Am J Med. 2012;125:14-22.
53. Rossi GP, Seccia TM, Maniero C, et al. Drug-related hypertension and resistance to antihypertensive treatment: a call for action. J Hypertens. 2011;29:2295-2309.
54. Grossman E, Messerli FH. Secondary hypertension: interfering substances. J Clin Hypertens. 2008;10:556-566.
55. Cicek D, Haberal C, Ozkan S, et al. A severe coarctation of aorta in a 52-year-old male: a case report. Int J Med Sci. 2010;7:340-341.
56. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(2 suppl 4th Report):S555-S576.
57. Rao PS. Coarctation of the aorta. Curr Cardiol Rep. 2005;7:425-434.
58. Rao PS. Stents in the management of aortic coarctation in young children. JACC Cardiovasc Interv. 2009;2:884-886.
• Review the family history of patients who do not respond to appropriate antihypertensive therapy, targeting hypertension and inherited disorders associated with high blood pressure (BP). B
• Include obstructive sleep apnea in the differential diagnosis of patients with resistant hypertension, particularly if they’re obese. B
• Include a thorough medication history in a work-up for resistant hypertension, as a number of drugs can cause or exacerbate high BP. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
What to include in the workup
Whether you’re doing an initial evaluation of a patient with high blood pressure (BP) or examining a patient with resistant hypertension, the history should focus on the duration of hypertension, previous BP levels, and comorbid conditions. It is also important to take a targeted family history, inquiring about hypertension as well as genetic disorders that increase the likelihood of secondary hypertension.
Inherited diseases associated with secondary hypertension include polycystic kidney disease, multiple endocrine neoplasia type 2 (MEN2), and von Hippel-Lindau syndrome.12,13 All are inherited in an autosomal dominant pattern. Patients with von Hippel-Lindau syndrome may present with multiple tumors, which can develop in the eyes, brain, adrenal glands, pancreas, liver, spinal cord, kidneys, or other parts of the body. Pheochromocytoma is a manifestation of both MEN2 and von Hippel-Lindau syndrome, and some specialists recommend that everyone with a family history of either condition undergo screening for pheochromocytoma.14
Table
Secondary hypertension: What you’ll see, what to test for8-11
| Secondary cause* | Signs and symptoms | Screening tests |
|---|---|---|
| Renal disease | Depends on underlying cause (eg, diabetes, polycystic kidney disease, glomerulonephritis) | Serum creatinine, urinalysis, renal ultrasound |
| Renal artery stenosis | Abdominal or flank bruits | Renal ultrasound, MRA, CT angiography |
| Primary hyperaldosteronism | Muscle cramps | PA/PRA |
| Pheochromocytoma | Paroxysms of palpitations, diaphoresis, headaches | Plasma metanephrine and normetanephrine |
| Cushing’s syndrome | Rapid weight gain, truncal obesity, abdominal striae | Measurement of 24-hour urinary free cortisol |
| OSA† | Obesity, daytime somnolence, nighttime snoring | Overnight polysomnography |
| Coarctation of the aorta‡ | Murmur of anterior and posterior thorax; claudication and weak femoral pulses | Echocardiography |
| CT, computed tomography; MRA, magnetic resonance angiography; OSA, obstructive sleep apnea; PA/PRA, plasma aldosterone-plasma renin activity. *Secondary hypertension may also be drug-induced, related to pregnancy (hypertension complicates up to 15% of pregnancies), or associated with inherited syndromes. †Highly prevalent in obese patients. ‡Higher prevalence in childhood hypertension; rarely diagnosed in adulthood. | ||
BP measurement is key
The physical examination should start with a calculation of body mass index, as well as a careful measurement of BP. The patient should be seated quietly in a chair for ≥5 minutes, with both feet on the floor and the arm being tested supported at heart level.
Unfortunately, reliability on the office BP measurement can be a confounding factor in the diagnosis of hypertension. “White coat hypertension”—in which BP is persistently elevated in the office and persistently normal in nonclinical settings—should be considered in patients who have high BP but no other signs or symptoms, and ambulatory monitoring used to rule out hypertension.15,16
Physicians also need to consider the opposite effect: Masked hypertension, characterized by normal office readings and elevated ambulatory readings, is more serious, of course, with patients at higher risk for end organ damage from unrecognized hypertension.17,18 Asking patients who self-monitor what type of BP readings they’re getting can be helpful in identifying masked hypertension. Ambulatory monitoring may be used to identify this condition, as well.
Other components in the physical workup include a fundoscopic exam; assessment of the thorax for murmurs and the abdomen for enlarged kidneys, masses, and abnormal aortic pulsation; auscultation for abdominal and carotid bruits; palpation of the thyroid gland; and palpation of the lower extremities for edema and pulses.
Include these tests in the workup
Routine tests for a patient with hypertension include:
- electrocardiogram
- blood glucose and hematocrit
- serum potassium, creatinine, and fasting lipid profiles
- urinalysis with measurement of microalbumin.
Microalbuminuria, a sensitive marker of early renal disease, is defined as a urinary albumin excretion between 30 and 300 mg/d.19 The albumin-creatinine ratio (30-300 mcg/mg), measured in spot urine specimens, is a more convenient way to detect it.20
Suspicious findings prompt further testing. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) recommends specific testing—much of it detailed below—if any aspect of the initial evaluation raises suspicion of a secondary cause or the patient has hypertension that’s of sudden onset or hard to control.21 (According to the National Heart, Lung, and Blood Institute, JNC 8 is due for release later this year.)
Kidney disease may be a consequence or a cause
The overall prevalence of hypertension in patients with renal disease is 60%,22 but varies according to the type of nephropathy. Eighty-seven percent of patients with diabetic nephropathy also have hypertension, and hypertension and diabetes are the 2 most common causes of end-stage renal disease.23,24
A combination of 2 or more drugs is usually needed to achieve the target BP of <130/80 mm Hg in patients with diabetes.21 ACE inhibitors and angiotensin receptor blockers have been found to slow the progression of diabetic nephropathy.25-27
Is renal artery stenosis to blame?
Renal artery stenosis is the most common form of secondary hypertension that’s reversible, affecting about 0.2% to 3.1% of hypertensive patients.5,6,28 The condition leads to renal ischemia, thereby stimulating the renin-angiotensin-aldosterone axis and causing secondary hyperaldosteronism.
In younger patients, especially women between 15 and 50 years of age, fibromuscular disease is the most common cause of renovascular hypertension.29,30 In older patients, atherosclerosis (which accounts for 90% of renovascular hypertension) is more likely.29,30
The choice of initial imaging tests includes duplex renal ultrasonography, magnetic resonance angiography (MRA), and spiral computed tomographic angiography. Contrast angiography is the gold standard, but it carries a risk of contrast-induced nephropathy. Duplex ultrasonography and MRA do not use iodinated contrast media, and are safe for patients with chronic kidney disease.8
Treatment. Percutaneous transluminal renal artery angioplasty is a treatment option for patients with renal artery stenosis. Angioplasty achieves higher cure rates for patients with fibromuscular dysplasia than for those with atherosclerotic renal artery stenosis.31 Most patients referred for renal artery revascularization have atherosclerosis. Because they’re generally older individuals with comorbidities, the benefits of stent revascularization for this group is controversial. Such patients require antihypertensive therapy with drugs that block the renin-angiotensin system.32
Endocrine disorders must be ruled out
Primary hyperaldosteronism is thought to be present in 0.3% to 1.4% of patients with hypertension.5,6 The prevalence varies widely from one source to another, however, and may be as high as 5% to 20% among patients with resistant hypertension.33,34
Hyperaldosteronism is related to either an aldosterone-secreting adrenal adenoma (in about 40% of cases) or bilateral adrenal hyperplasia (in the remaining 60%), and leads to increased sodium reabsorption and, typically, to a loss of potassium.35
Renin-secreting tumor, which usually arises from the juxtaglomerular cells of the kidney, is a rare cause of hyperaldosteronism. Extrarenal renin-secreting tumors have also been reported.36
What should raise your suspicion. Suspect hyperaldosteronism in patients who have both hypertension and hypokalemia, but keep in mind that not all patients with hyperaldosteronism have low serum potassium.37 Further laboratory evaluation should include a simultaneous measurement of plasma aldosterone (PA) and plasma renin activity (PRA). Patients with hyperaldosteronism will have elevated PA and suppressed PRA.
Testing considerations. It is important to ensure that the PA/PRA test is performed in the morning, with the patient in an upright position.36 He or she should be on a high sodium diet in preparation for the test, consuming 2 to 3 grams of sodium per meal for ≥2 days.37
In patients with a positive PA/PRA ratio (≥20), a 24-hour urinary aldosterone excretion test should be performed. A finding >12 to 14 mcg, along with a PRA <1.0 ng/mL per hour, confirms the diagnosis of primary hyperaldosteronism.18,37 Computed tomography or magnetic resonance imaging of the adrenal glands will distinguish between aldosterone-producing adenoma and bilateral adrenal hyperplasia.
Treatment. Laparoscopic adrenalectomy is the accepted surgical treatment of primary hyperaldosteronism.37 Patients with bilateral disease due to idiopathic hyperaldosteronism are not candidates for surgery and should be treated medically, with potassium-sparing diuretics such as spironolactone.
Cushing’s syndrome is marked by rapid weight gain
High BP may be a manifestation of Cushing’s syndrome, which affects 0.1% to 0.5% of patients with hypertension.5-7 Other signs and symptoms of Cushing’s syndrome include fatigue, weakness, hirsutism, amenorrhea, moon facies, dorsal hump, purple striae, truncal obesity, and hypokalemia. Rapid weight gain is the most common manifestation, and typically the one for which patients seek medical attention.38
The most widely used screening test for Cushing’s syndrome is a 24-hour urine collection measuring urinary-free cortisol.9 Normal urinary cortisol excretion is 20 to 100 mcg/dL in 24 hours; most patients with Cushing’s syndrome produce >250 mcg/dL in that time frame.9
Once hypercortisolism is established, determination of the cause is the next step. A serum adrenocorticotropic hormone (ACTH) level is needed to localize it. Normal (9-52 pg/mL) or elevated ACTH indicates a pituitary or ectopic source, while low levels of ACTH are an indication of an adrenal source.9,39
Treatment. Surgical resection of the tumor is often curative. For pituitary tumors (Cushing’s disease), transsphenoidal resection is the standard of care.39 For adrenal adenomas, unilateral adrenalectomy is the best option.39
Pheochromocytomas: Most are adrenal, sporadic, and benign
Pheochromocytomas—neuroendocrine, catecholamine-secreting tumors that develop from the adrenal medulla—are another cause of secondary hypertension. Catecholamines include norepinephrine and epinephrine and, rarely, dopamine secreted either intermittently or continuously. The prevalence of pheochromocytoma is 0.1% to 0.3% among patients with hypertension.5,6,28 A “rule of 10” (90:10 ratio) is often applied to pheochromocytomas because of the following:
- 90% of pheochromocytomas are located in the adrenal glands; the remaining 10% are extra-adrenal and can occur anywhere along the sympathetic chain40
- 90% are sporadic; 10% are familial41
- 90% are benign; 10% are malignant40
- 90% are found in adults; 10% affect children.42
Signs and symptoms of pheochromocytomas include palpitations, headache, dyspnea, diaphoresis, and flushing, as well as paroxysmal hypertension.40 Measurement of 24-hour urinary catecholamines and their metabolites has been the screening test of choice,43 but recent evidence suggests that measurement of plasma metanephrine and normetanephrine is a far more sensitive screen.10
Treatment. Surgical resection is the treatment of choice. Alpha blockade is started 7 to 10 days preoperatively;44,45 a beta-blocker is added only after an adequate alpha blockade has been established, as unopposed alpha stimulation could precipitate a hypertensive crisis. Laparoscopic adrenalectomy is routinely performed for small (<5 cm) pheochromocytomas.46,47
Don’t forget these (relatively) common secondary causes
Obstructive sleep apnea (OSA) is one of the most common conditions associated with resistant hypertension.48 Signs and symptoms include snoring, daytime somnolence, and obesity (body mass index ≥30 kg/m2).
OSA involves upper airway collapse during inspiration, causing intermittent hypoxemia with resultant sympathetic nervous system activation.11 The underlying mechanism of OSA-induced hypertension is strongly related to sympathetic activation.49 Overnight polysomnography is required for diagnosis.11
Continuous positive airway pressure is the treatment of choice for patients unable to lose weight.11
Pregnancy-induced hypertension is the most common medical problem encountered in pregnancy. It occurs in up to 15% of pregnancies, either during the pregnancy itself or postpartum. Postpartum hypertension may be related to preexisting chronic hypertension or to the persistence of gestational hypertension or preeclampsia, which usually occurs after 20 weeks’ gestation and is characterized by the presence of hypertension and proteinuria.50 Methyldopa and labetalol are commonly used treatments for hypertension during pregnancy.51
Drug-induced hypertension. Several drugs can cause or exacerbate hypertension, rendering it resistant to therapy. A careful review of the patient’s medication regimen is essential. Generally, drug-induced hypertension falls into 2 broad categories based on mechanism of action: volume overload and sympathetic activity.52,53
Corticosteroids can elevate BP in a dose-dependent manner, as a result of volume overload. Glycyrrhizic acid, the main ingredient in licorice, produces a state of excess mineralocorticoid, with a similar effect. Estrogen-containing oral contraceptives can cause an increased synthesis of angiotensin in the liver, resulting in greater aldosterone secretion and volume overload.
Drugs that stimulate sympathetic activity include cocaine, ephedrine, amphetamine, phenylephrine, phenylpropanolamine, caffeine, and alcohol. Nonsteroidal anti-inflammatory drugs may interfere with the action of ACE inhibitors and cause renal vasoconstriction, leading to sodium and water retention and hypertension.54
Discontinuation of the medication in question is preferable. In many cases, an agent that does not affect BP can be found to replace it.
If the patient is a child
Hypertension is uncommon in young people. However, coarctation of the aorta, a congenital narrowing associated with secondary hypertension, is typically diagnosed in childhood. In rare cases, the condition remains undetected well into adulthood.55 Clinical signs include weak femoral pulses, visible pulsations in the neck, a systolic murmur of the anterior and posterior thorax, and elevated BP in the upper extremities with low BP in the lower extremities.
Thus, once hypertension is confirmed in a young patient, BP should be measured in both arms and legs.56 Delayed or absent femoral pulses and a difference in systolic BP of ≥20 mm Hg between the arms and legs provide evidence of aortic coarctation.57 In adults, stenting is the initial treatment for this condition because of the morbidity associated with surgery.57 Stenting is an option for children with this condition, as well.58
CORRESPONDENCE Bernard M. Karnath, MD, University of Texas Medical Branch at Galveston, 301 University Boulevard, Galveston, TX 77555; [email protected]
• Review the family history of patients who do not respond to appropriate antihypertensive therapy, targeting hypertension and inherited disorders associated with high blood pressure (BP). B
• Include obstructive sleep apnea in the differential diagnosis of patients with resistant hypertension, particularly if they’re obese. B
• Include a thorough medication history in a work-up for resistant hypertension, as a number of drugs can cause or exacerbate high BP. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
What to include in the workup
Whether you’re doing an initial evaluation of a patient with high blood pressure (BP) or examining a patient with resistant hypertension, the history should focus on the duration of hypertension, previous BP levels, and comorbid conditions. It is also important to take a targeted family history, inquiring about hypertension as well as genetic disorders that increase the likelihood of secondary hypertension.
Inherited diseases associated with secondary hypertension include polycystic kidney disease, multiple endocrine neoplasia type 2 (MEN2), and von Hippel-Lindau syndrome.12,13 All are inherited in an autosomal dominant pattern. Patients with von Hippel-Lindau syndrome may present with multiple tumors, which can develop in the eyes, brain, adrenal glands, pancreas, liver, spinal cord, kidneys, or other parts of the body. Pheochromocytoma is a manifestation of both MEN2 and von Hippel-Lindau syndrome, and some specialists recommend that everyone with a family history of either condition undergo screening for pheochromocytoma.14
Table
Secondary hypertension: What you’ll see, what to test for8-11
| Secondary cause* | Signs and symptoms | Screening tests |
|---|---|---|
| Renal disease | Depends on underlying cause (eg, diabetes, polycystic kidney disease, glomerulonephritis) | Serum creatinine, urinalysis, renal ultrasound |
| Renal artery stenosis | Abdominal or flank bruits | Renal ultrasound, MRA, CT angiography |
| Primary hyperaldosteronism | Muscle cramps | PA/PRA |
| Pheochromocytoma | Paroxysms of palpitations, diaphoresis, headaches | Plasma metanephrine and normetanephrine |
| Cushing’s syndrome | Rapid weight gain, truncal obesity, abdominal striae | Measurement of 24-hour urinary free cortisol |
| OSA† | Obesity, daytime somnolence, nighttime snoring | Overnight polysomnography |
| Coarctation of the aorta‡ | Murmur of anterior and posterior thorax; claudication and weak femoral pulses | Echocardiography |
| CT, computed tomography; MRA, magnetic resonance angiography; OSA, obstructive sleep apnea; PA/PRA, plasma aldosterone-plasma renin activity. *Secondary hypertension may also be drug-induced, related to pregnancy (hypertension complicates up to 15% of pregnancies), or associated with inherited syndromes. †Highly prevalent in obese patients. ‡Higher prevalence in childhood hypertension; rarely diagnosed in adulthood. | ||
BP measurement is key
The physical examination should start with a calculation of body mass index, as well as a careful measurement of BP. The patient should be seated quietly in a chair for ≥5 minutes, with both feet on the floor and the arm being tested supported at heart level.
Unfortunately, reliability on the office BP measurement can be a confounding factor in the diagnosis of hypertension. “White coat hypertension”—in which BP is persistently elevated in the office and persistently normal in nonclinical settings—should be considered in patients who have high BP but no other signs or symptoms, and ambulatory monitoring used to rule out hypertension.15,16
Physicians also need to consider the opposite effect: Masked hypertension, characterized by normal office readings and elevated ambulatory readings, is more serious, of course, with patients at higher risk for end organ damage from unrecognized hypertension.17,18 Asking patients who self-monitor what type of BP readings they’re getting can be helpful in identifying masked hypertension. Ambulatory monitoring may be used to identify this condition, as well.
Other components in the physical workup include a fundoscopic exam; assessment of the thorax for murmurs and the abdomen for enlarged kidneys, masses, and abnormal aortic pulsation; auscultation for abdominal and carotid bruits; palpation of the thyroid gland; and palpation of the lower extremities for edema and pulses.
Include these tests in the workup
Routine tests for a patient with hypertension include:
- electrocardiogram
- blood glucose and hematocrit
- serum potassium, creatinine, and fasting lipid profiles
- urinalysis with measurement of microalbumin.
Microalbuminuria, a sensitive marker of early renal disease, is defined as a urinary albumin excretion between 30 and 300 mg/d.19 The albumin-creatinine ratio (30-300 mcg/mg), measured in spot urine specimens, is a more convenient way to detect it.20
Suspicious findings prompt further testing. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) recommends specific testing—much of it detailed below—if any aspect of the initial evaluation raises suspicion of a secondary cause or the patient has hypertension that’s of sudden onset or hard to control.21 (According to the National Heart, Lung, and Blood Institute, JNC 8 is due for release later this year.)
Kidney disease may be a consequence or a cause
The overall prevalence of hypertension in patients with renal disease is 60%,22 but varies according to the type of nephropathy. Eighty-seven percent of patients with diabetic nephropathy also have hypertension, and hypertension and diabetes are the 2 most common causes of end-stage renal disease.23,24
A combination of 2 or more drugs is usually needed to achieve the target BP of <130/80 mm Hg in patients with diabetes.21 ACE inhibitors and angiotensin receptor blockers have been found to slow the progression of diabetic nephropathy.25-27
Is renal artery stenosis to blame?
Renal artery stenosis is the most common form of secondary hypertension that’s reversible, affecting about 0.2% to 3.1% of hypertensive patients.5,6,28 The condition leads to renal ischemia, thereby stimulating the renin-angiotensin-aldosterone axis and causing secondary hyperaldosteronism.
In younger patients, especially women between 15 and 50 years of age, fibromuscular disease is the most common cause of renovascular hypertension.29,30 In older patients, atherosclerosis (which accounts for 90% of renovascular hypertension) is more likely.29,30
The choice of initial imaging tests includes duplex renal ultrasonography, magnetic resonance angiography (MRA), and spiral computed tomographic angiography. Contrast angiography is the gold standard, but it carries a risk of contrast-induced nephropathy. Duplex ultrasonography and MRA do not use iodinated contrast media, and are safe for patients with chronic kidney disease.8
Treatment. Percutaneous transluminal renal artery angioplasty is a treatment option for patients with renal artery stenosis. Angioplasty achieves higher cure rates for patients with fibromuscular dysplasia than for those with atherosclerotic renal artery stenosis.31 Most patients referred for renal artery revascularization have atherosclerosis. Because they’re generally older individuals with comorbidities, the benefits of stent revascularization for this group is controversial. Such patients require antihypertensive therapy with drugs that block the renin-angiotensin system.32
Endocrine disorders must be ruled out
Primary hyperaldosteronism is thought to be present in 0.3% to 1.4% of patients with hypertension.5,6 The prevalence varies widely from one source to another, however, and may be as high as 5% to 20% among patients with resistant hypertension.33,34
Hyperaldosteronism is related to either an aldosterone-secreting adrenal adenoma (in about 40% of cases) or bilateral adrenal hyperplasia (in the remaining 60%), and leads to increased sodium reabsorption and, typically, to a loss of potassium.35
Renin-secreting tumor, which usually arises from the juxtaglomerular cells of the kidney, is a rare cause of hyperaldosteronism. Extrarenal renin-secreting tumors have also been reported.36
What should raise your suspicion. Suspect hyperaldosteronism in patients who have both hypertension and hypokalemia, but keep in mind that not all patients with hyperaldosteronism have low serum potassium.37 Further laboratory evaluation should include a simultaneous measurement of plasma aldosterone (PA) and plasma renin activity (PRA). Patients with hyperaldosteronism will have elevated PA and suppressed PRA.
Testing considerations. It is important to ensure that the PA/PRA test is performed in the morning, with the patient in an upright position.36 He or she should be on a high sodium diet in preparation for the test, consuming 2 to 3 grams of sodium per meal for ≥2 days.37
In patients with a positive PA/PRA ratio (≥20), a 24-hour urinary aldosterone excretion test should be performed. A finding >12 to 14 mcg, along with a PRA <1.0 ng/mL per hour, confirms the diagnosis of primary hyperaldosteronism.18,37 Computed tomography or magnetic resonance imaging of the adrenal glands will distinguish between aldosterone-producing adenoma and bilateral adrenal hyperplasia.
Treatment. Laparoscopic adrenalectomy is the accepted surgical treatment of primary hyperaldosteronism.37 Patients with bilateral disease due to idiopathic hyperaldosteronism are not candidates for surgery and should be treated medically, with potassium-sparing diuretics such as spironolactone.
Cushing’s syndrome is marked by rapid weight gain
High BP may be a manifestation of Cushing’s syndrome, which affects 0.1% to 0.5% of patients with hypertension.5-7 Other signs and symptoms of Cushing’s syndrome include fatigue, weakness, hirsutism, amenorrhea, moon facies, dorsal hump, purple striae, truncal obesity, and hypokalemia. Rapid weight gain is the most common manifestation, and typically the one for which patients seek medical attention.38
The most widely used screening test for Cushing’s syndrome is a 24-hour urine collection measuring urinary-free cortisol.9 Normal urinary cortisol excretion is 20 to 100 mcg/dL in 24 hours; most patients with Cushing’s syndrome produce >250 mcg/dL in that time frame.9
Once hypercortisolism is established, determination of the cause is the next step. A serum adrenocorticotropic hormone (ACTH) level is needed to localize it. Normal (9-52 pg/mL) or elevated ACTH indicates a pituitary or ectopic source, while low levels of ACTH are an indication of an adrenal source.9,39
Treatment. Surgical resection of the tumor is often curative. For pituitary tumors (Cushing’s disease), transsphenoidal resection is the standard of care.39 For adrenal adenomas, unilateral adrenalectomy is the best option.39
Pheochromocytomas: Most are adrenal, sporadic, and benign
Pheochromocytomas—neuroendocrine, catecholamine-secreting tumors that develop from the adrenal medulla—are another cause of secondary hypertension. Catecholamines include norepinephrine and epinephrine and, rarely, dopamine secreted either intermittently or continuously. The prevalence of pheochromocytoma is 0.1% to 0.3% among patients with hypertension.5,6,28 A “rule of 10” (90:10 ratio) is often applied to pheochromocytomas because of the following:
- 90% of pheochromocytomas are located in the adrenal glands; the remaining 10% are extra-adrenal and can occur anywhere along the sympathetic chain40
- 90% are sporadic; 10% are familial41
- 90% are benign; 10% are malignant40
- 90% are found in adults; 10% affect children.42
Signs and symptoms of pheochromocytomas include palpitations, headache, dyspnea, diaphoresis, and flushing, as well as paroxysmal hypertension.40 Measurement of 24-hour urinary catecholamines and their metabolites has been the screening test of choice,43 but recent evidence suggests that measurement of plasma metanephrine and normetanephrine is a far more sensitive screen.10
Treatment. Surgical resection is the treatment of choice. Alpha blockade is started 7 to 10 days preoperatively;44,45 a beta-blocker is added only after an adequate alpha blockade has been established, as unopposed alpha stimulation could precipitate a hypertensive crisis. Laparoscopic adrenalectomy is routinely performed for small (<5 cm) pheochromocytomas.46,47
Don’t forget these (relatively) common secondary causes
Obstructive sleep apnea (OSA) is one of the most common conditions associated with resistant hypertension.48 Signs and symptoms include snoring, daytime somnolence, and obesity (body mass index ≥30 kg/m2).
OSA involves upper airway collapse during inspiration, causing intermittent hypoxemia with resultant sympathetic nervous system activation.11 The underlying mechanism of OSA-induced hypertension is strongly related to sympathetic activation.49 Overnight polysomnography is required for diagnosis.11
Continuous positive airway pressure is the treatment of choice for patients unable to lose weight.11
Pregnancy-induced hypertension is the most common medical problem encountered in pregnancy. It occurs in up to 15% of pregnancies, either during the pregnancy itself or postpartum. Postpartum hypertension may be related to preexisting chronic hypertension or to the persistence of gestational hypertension or preeclampsia, which usually occurs after 20 weeks’ gestation and is characterized by the presence of hypertension and proteinuria.50 Methyldopa and labetalol are commonly used treatments for hypertension during pregnancy.51
Drug-induced hypertension. Several drugs can cause or exacerbate hypertension, rendering it resistant to therapy. A careful review of the patient’s medication regimen is essential. Generally, drug-induced hypertension falls into 2 broad categories based on mechanism of action: volume overload and sympathetic activity.52,53
Corticosteroids can elevate BP in a dose-dependent manner, as a result of volume overload. Glycyrrhizic acid, the main ingredient in licorice, produces a state of excess mineralocorticoid, with a similar effect. Estrogen-containing oral contraceptives can cause an increased synthesis of angiotensin in the liver, resulting in greater aldosterone secretion and volume overload.
Drugs that stimulate sympathetic activity include cocaine, ephedrine, amphetamine, phenylephrine, phenylpropanolamine, caffeine, and alcohol. Nonsteroidal anti-inflammatory drugs may interfere with the action of ACE inhibitors and cause renal vasoconstriction, leading to sodium and water retention and hypertension.54
Discontinuation of the medication in question is preferable. In many cases, an agent that does not affect BP can be found to replace it.
If the patient is a child
Hypertension is uncommon in young people. However, coarctation of the aorta, a congenital narrowing associated with secondary hypertension, is typically diagnosed in childhood. In rare cases, the condition remains undetected well into adulthood.55 Clinical signs include weak femoral pulses, visible pulsations in the neck, a systolic murmur of the anterior and posterior thorax, and elevated BP in the upper extremities with low BP in the lower extremities.
Thus, once hypertension is confirmed in a young patient, BP should be measured in both arms and legs.56 Delayed or absent femoral pulses and a difference in systolic BP of ≥20 mm Hg between the arms and legs provide evidence of aortic coarctation.57 In adults, stenting is the initial treatment for this condition because of the morbidity associated with surgery.57 Stenting is an option for children with this condition, as well.58
CORRESPONDENCE Bernard M. Karnath, MD, University of Texas Medical Branch at Galveston, 301 University Boulevard, Galveston, TX 77555; [email protected]
1. Middleton K, Hing E, Xu J. National hospital ambulatory medical care survey: 2005 outpatient department summary. Adv Data. 2007;389:1-34.
2. Ong KL, Cheung BM, Man YB, et al. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999-2004. Hypertension. 2007;49:69-75.
3. Fields LE, Burt VL, Cutler JA, et al. The burden of adult hypertension in the United States 1999 to 2000: a rising tide. Hypertension. 2004;44:398-404.
4. Wang TJ, Vasan RS. Epidemiology of uncontrolled hypertension in the United States. Circulation. 2005;112:1651-1662.
5. Anderson GH, Jr, Blakeman N, Streeten DH. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J Hypertens. 1994;12:609-615.
6. Sinclair AM, Isles CG, Brown I, et al. Secondary hypertension in a blood pressure clinic. Arch Intern Med. 1987;147:1289-1293.
7. Dosh SA. The diagnosis of essential and secondary hypertension in adults. J Fam Pract. 2001;50:707-712.
8. Eardley KS, Lipkin GW. Atherosclerotic renal artery stenosis: is it worth diagnosing?J Hum Hypertens. 1999;13:217-220.
9. Boscaro M, Barzon L, Fallo F, et al. Cushing’s syndrome. Lancet. 2001;357:783-791.
10. Unger N, Pitt C, Schmidt IL. Diagnostic value of various biochemical parameters for the diagnosis of pheochromocytoma in patients with adrenal mass. Eur J Endocrinol. 2006;154:409-417.
11. Prisant LM, Dillard TA, Blanchard AR. Obstructive sleep apnea syndrome. J Clin Hypertens. 2006;8:746-750.
12. Marini F, Falchetti A, Del Monte F, et al. Multiple endocrine neoplasia type 2. Orphanet J Rare Dis. 2006;1:45.-
13. Bryant J, Farmer J, Kessler LJ, et al. Pheochromocytoma: the expanding genetic differential diagnosis. J Natl Cancer Inst. 2003;95:1196-1204.
14. Neumann HP, Berger DP, Sigmund G, et al. Pheochromocytomas, multiple endocrine neoplasia type 2, and von Hippel-Lindau disease. N Engl J Med. 1993;329:1531-1538.
15. Mancia G, Bertinieri G, Grassi G, et al. Effects of blood-pressure measurement by the doctor on patient’s blood pressure and heart rate. Lancet. 1983;2:695-698.
16. Pickering TG, James GD, Boddie C. How common is white coat hypertension? JAMA. 1988;259:225-228.
17. Kotsis V, Stabouli S, Toumanidis S, et al. Target organ damage in “white coat hypertension” and “masked hypertension”. Am J Hypertens. 2008;21:393-399.
18. Pickering TG, Davidson K, Gerin W, et al. Masked hypertension. Hypertension. 2002;40:795-796.
19. Volpe M. Microalbuminuria screening in patients with hypertension: recommendations for clinical practice. Int J Clin Pract. 2008;62:97-108.
20. Keane WF, Eknoyan G. Proteinuria, albuminuria, risk, assessment, detection, elimination (PARADE): a position paper of the National Kidney Foundation. Am J Kidney Dis. 1999;33:1004-1010.
21. Chobanian AV, Bakris GL, Black HR, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206-1252.
22. Ridao N, Luño J, García de Vinuesa S, et al. Prevalence of hypertension in renal disease. Nephrol Dial Transplant. 2001;16(suppl 1):S70-S73.
23. Foley RN, Collins AJ. End-stage renal disease in the United States: an update from the United States Renal Data System. J Am Soc Nephrol. 2007;18:2644-2648.
24. Parmar MS. Chronic renal disease. BMJ. 2002;325:85-90.
25. Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345:861-869.
26. Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.
27. Menne J, Izzo JL, Jr, Ito S, et al. Prevention of microalbuminuria in patients with type 2 diabetes and hypertension. J Hypertens. 2012;30:811-818.
28. Rossi H, Kim A, Prinz RA. Primary hyperaldosteronism in the era of laparoscopic adrenalectomy. Am Surg. 2002;68:253-256.
29. Safian RD, Textor SC. Renal artery stenosis. N Engl J Med. 2001;244:431-442.
30. Slovut DP, Olin JW. Fibromuscular dysplasia. N Engl J Med. 2004;350:1862-1871.
31. Bonelli FS, McKusick MA, Textor SC. Renal artery angioplasty: technical results and clinical outcome in 320 patients. Mayo Clin Proc. 1995;70:1041-1052.
32. Textor SC. Renovascular hypertension in 2007: where are we now? Curr Cardiol Rep. 2007;9:453-461.
33. Calhoun DA. Is there an unrecognized epidemic of primary aldosteronism? Pro. Hypertension. 2007;50:447-453.
34. Young WF, Jr. Minireview: primary aldosteronism—changing concepts in diagnosis and treatment. Endocrinology. 2003;144:2208-2213.
35. Young WF. Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf). 2007;66:607-618.
36. Pursell RN, Quinlan PM. Secondary hypertension due to a renin-producing teratoma. Am J Hypertens. 2003;16:592-595.
37. Ganguly A. Primary aldosteronism. N Engl J Med. 1998;339:1828-1834.
38. Muller M, Longo Mazzuco T, Martinie M, et al. Diagnosis of Cushing’s syndrome: a retrospective evaluation of clinical practice. Eur J Intern Med. 2006;17:334-338.
39. Norton JA, Li M, Gillary J, et al. Cushing’s syndrome. Curr Probl Surg. 2001;38:488-545.
40. Lenders JW, Eisenhofer G, Mannelli M, et al. Phaeochromocytoma. Lancet. 2005;366:665-675.
41. Bryant J, Farmer J, Kessler LJ, et al. Pheochromocytoma: the expanding genetic differential diagnosis. J Natl Cancer Inst. 2003;95:1196-1204.
42. Sullivan J, Groshong T, Tobias JD. Presenting signs and symptoms of pheochromocytoma in pediatric-aged patients. Clin Pediatr. 2005;44:715-719.
43. Young WF, Jr. Pheochromocytoma: issues in diagnosis and treatment. Compr Ther. 1997;23:319-326.
44. Kocak S, Aydintug S, Canakci N. Alpha blockade in preoperative preparation of patients with pheochromocytomas. Int Surg. 2002;87:191-194.
45. Russell WJ, Metcalfe IR, Tonkin AL, et al. The preoperative management of phaeochromocytoma. Anaesth Intensive Care. 1998;26:196-200.
46. Kalady MF, McKinlay R, Olson JA, Jr, et al. Laparoscopic adrenalectomy for pheochromocytoma. A comparison to aldosteronoma and incidentaloma. Surg Endosc. 2004;18:621-625.
47. Naya Y, Ichikawa T, Suzuki H, et al. Efficacy and safety of laparoscopic surgery for pheochromocytoma. Int J Urol. 2005;12:128-133.
48. Pedrosa RP, Drager LF, Gonzaga CC, et al. Obstructive sleep apnea: the most common secondary cause of hypertension associated with resistant hypertension. Hypertension. 2011;5:811-817.
49. Sharabi Y, Dagan Y, Grossman E. Sleep apnea as a risk factor for hypertension. Curr Opin Nephrol Hypertens. 2004;13:359-364.
50. James PR, Nelson-Piercy C. Management of hypertension before, during, and after pregnancy. Heart. 2004;90:1499-1504.
51. Solomon CG, Seely EW. Hypertension in pregnancy. Endocrinol Metab Clin North Am. 2011;40:847-863.
52. Grossman E, Messerli FH. Drug-induced hypertension: an unappreciated cause of secondary hypertension. Am J Med. 2012;125:14-22.
53. Rossi GP, Seccia TM, Maniero C, et al. Drug-related hypertension and resistance to antihypertensive treatment: a call for action. J Hypertens. 2011;29:2295-2309.
54. Grossman E, Messerli FH. Secondary hypertension: interfering substances. J Clin Hypertens. 2008;10:556-566.
55. Cicek D, Haberal C, Ozkan S, et al. A severe coarctation of aorta in a 52-year-old male: a case report. Int J Med Sci. 2010;7:340-341.
56. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(2 suppl 4th Report):S555-S576.
57. Rao PS. Coarctation of the aorta. Curr Cardiol Rep. 2005;7:425-434.
58. Rao PS. Stents in the management of aortic coarctation in young children. JACC Cardiovasc Interv. 2009;2:884-886.
1. Middleton K, Hing E, Xu J. National hospital ambulatory medical care survey: 2005 outpatient department summary. Adv Data. 2007;389:1-34.
2. Ong KL, Cheung BM, Man YB, et al. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999-2004. Hypertension. 2007;49:69-75.
3. Fields LE, Burt VL, Cutler JA, et al. The burden of adult hypertension in the United States 1999 to 2000: a rising tide. Hypertension. 2004;44:398-404.
4. Wang TJ, Vasan RS. Epidemiology of uncontrolled hypertension in the United States. Circulation. 2005;112:1651-1662.
5. Anderson GH, Jr, Blakeman N, Streeten DH. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J Hypertens. 1994;12:609-615.
6. Sinclair AM, Isles CG, Brown I, et al. Secondary hypertension in a blood pressure clinic. Arch Intern Med. 1987;147:1289-1293.
7. Dosh SA. The diagnosis of essential and secondary hypertension in adults. J Fam Pract. 2001;50:707-712.
8. Eardley KS, Lipkin GW. Atherosclerotic renal artery stenosis: is it worth diagnosing?J Hum Hypertens. 1999;13:217-220.
9. Boscaro M, Barzon L, Fallo F, et al. Cushing’s syndrome. Lancet. 2001;357:783-791.
10. Unger N, Pitt C, Schmidt IL. Diagnostic value of various biochemical parameters for the diagnosis of pheochromocytoma in patients with adrenal mass. Eur J Endocrinol. 2006;154:409-417.
11. Prisant LM, Dillard TA, Blanchard AR. Obstructive sleep apnea syndrome. J Clin Hypertens. 2006;8:746-750.
12. Marini F, Falchetti A, Del Monte F, et al. Multiple endocrine neoplasia type 2. Orphanet J Rare Dis. 2006;1:45.-
13. Bryant J, Farmer J, Kessler LJ, et al. Pheochromocytoma: the expanding genetic differential diagnosis. J Natl Cancer Inst. 2003;95:1196-1204.
14. Neumann HP, Berger DP, Sigmund G, et al. Pheochromocytomas, multiple endocrine neoplasia type 2, and von Hippel-Lindau disease. N Engl J Med. 1993;329:1531-1538.
15. Mancia G, Bertinieri G, Grassi G, et al. Effects of blood-pressure measurement by the doctor on patient’s blood pressure and heart rate. Lancet. 1983;2:695-698.
16. Pickering TG, James GD, Boddie C. How common is white coat hypertension? JAMA. 1988;259:225-228.
17. Kotsis V, Stabouli S, Toumanidis S, et al. Target organ damage in “white coat hypertension” and “masked hypertension”. Am J Hypertens. 2008;21:393-399.
18. Pickering TG, Davidson K, Gerin W, et al. Masked hypertension. Hypertension. 2002;40:795-796.
19. Volpe M. Microalbuminuria screening in patients with hypertension: recommendations for clinical practice. Int J Clin Pract. 2008;62:97-108.
20. Keane WF, Eknoyan G. Proteinuria, albuminuria, risk, assessment, detection, elimination (PARADE): a position paper of the National Kidney Foundation. Am J Kidney Dis. 1999;33:1004-1010.
21. Chobanian AV, Bakris GL, Black HR, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206-1252.
22. Ridao N, Luño J, García de Vinuesa S, et al. Prevalence of hypertension in renal disease. Nephrol Dial Transplant. 2001;16(suppl 1):S70-S73.
23. Foley RN, Collins AJ. End-stage renal disease in the United States: an update from the United States Renal Data System. J Am Soc Nephrol. 2007;18:2644-2648.
24. Parmar MS. Chronic renal disease. BMJ. 2002;325:85-90.
25. Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345:861-869.
26. Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851-860.
27. Menne J, Izzo JL, Jr, Ito S, et al. Prevention of microalbuminuria in patients with type 2 diabetes and hypertension. J Hypertens. 2012;30:811-818.
28. Rossi H, Kim A, Prinz RA. Primary hyperaldosteronism in the era of laparoscopic adrenalectomy. Am Surg. 2002;68:253-256.
29. Safian RD, Textor SC. Renal artery stenosis. N Engl J Med. 2001;244:431-442.
30. Slovut DP, Olin JW. Fibromuscular dysplasia. N Engl J Med. 2004;350:1862-1871.
31. Bonelli FS, McKusick MA, Textor SC. Renal artery angioplasty: technical results and clinical outcome in 320 patients. Mayo Clin Proc. 1995;70:1041-1052.
32. Textor SC. Renovascular hypertension in 2007: where are we now? Curr Cardiol Rep. 2007;9:453-461.
33. Calhoun DA. Is there an unrecognized epidemic of primary aldosteronism? Pro. Hypertension. 2007;50:447-453.
34. Young WF, Jr. Minireview: primary aldosteronism—changing concepts in diagnosis and treatment. Endocrinology. 2003;144:2208-2213.
35. Young WF. Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf). 2007;66:607-618.
36. Pursell RN, Quinlan PM. Secondary hypertension due to a renin-producing teratoma. Am J Hypertens. 2003;16:592-595.
37. Ganguly A. Primary aldosteronism. N Engl J Med. 1998;339:1828-1834.
38. Muller M, Longo Mazzuco T, Martinie M, et al. Diagnosis of Cushing’s syndrome: a retrospective evaluation of clinical practice. Eur J Intern Med. 2006;17:334-338.
39. Norton JA, Li M, Gillary J, et al. Cushing’s syndrome. Curr Probl Surg. 2001;38:488-545.
40. Lenders JW, Eisenhofer G, Mannelli M, et al. Phaeochromocytoma. Lancet. 2005;366:665-675.
41. Bryant J, Farmer J, Kessler LJ, et al. Pheochromocytoma: the expanding genetic differential diagnosis. J Natl Cancer Inst. 2003;95:1196-1204.
42. Sullivan J, Groshong T, Tobias JD. Presenting signs and symptoms of pheochromocytoma in pediatric-aged patients. Clin Pediatr. 2005;44:715-719.
43. Young WF, Jr. Pheochromocytoma: issues in diagnosis and treatment. Compr Ther. 1997;23:319-326.
44. Kocak S, Aydintug S, Canakci N. Alpha blockade in preoperative preparation of patients with pheochromocytomas. Int Surg. 2002;87:191-194.
45. Russell WJ, Metcalfe IR, Tonkin AL, et al. The preoperative management of phaeochromocytoma. Anaesth Intensive Care. 1998;26:196-200.
46. Kalady MF, McKinlay R, Olson JA, Jr, et al. Laparoscopic adrenalectomy for pheochromocytoma. A comparison to aldosteronoma and incidentaloma. Surg Endosc. 2004;18:621-625.
47. Naya Y, Ichikawa T, Suzuki H, et al. Efficacy and safety of laparoscopic surgery for pheochromocytoma. Int J Urol. 2005;12:128-133.
48. Pedrosa RP, Drager LF, Gonzaga CC, et al. Obstructive sleep apnea: the most common secondary cause of hypertension associated with resistant hypertension. Hypertension. 2011;5:811-817.
49. Sharabi Y, Dagan Y, Grossman E. Sleep apnea as a risk factor for hypertension. Curr Opin Nephrol Hypertens. 2004;13:359-364.
50. James PR, Nelson-Piercy C. Management of hypertension before, during, and after pregnancy. Heart. 2004;90:1499-1504.
51. Solomon CG, Seely EW. Hypertension in pregnancy. Endocrinol Metab Clin North Am. 2011;40:847-863.
52. Grossman E, Messerli FH. Drug-induced hypertension: an unappreciated cause of secondary hypertension. Am J Med. 2012;125:14-22.
53. Rossi GP, Seccia TM, Maniero C, et al. Drug-related hypertension and resistance to antihypertensive treatment: a call for action. J Hypertens. 2011;29:2295-2309.
54. Grossman E, Messerli FH. Secondary hypertension: interfering substances. J Clin Hypertens. 2008;10:556-566.
55. Cicek D, Haberal C, Ozkan S, et al. A severe coarctation of aorta in a 52-year-old male: a case report. Int J Med Sci. 2010;7:340-341.
56. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(2 suppl 4th Report):S555-S576.
57. Rao PS. Coarctation of the aorta. Curr Cardiol Rep. 2005;7:425-434.
58. Rao PS. Stents in the management of aortic coarctation in young children. JACC Cardiovasc Interv. 2009;2:884-886.
Biopsychosocial psychiatry
With all of the discussion about a truly comprehensive and inclusive psychiatry, it was sad to see the emptiness and one-sidedness of Dr. Nasrallah’s June editorial (“Innovative approaches to treatment-resistant depression,” From the Editor, Current Psychiatry, June 2012, p. 4-5; http://bit.ly/1GM92oV). Depression certainly is not a unified diagnosis such as measles or appendicitis. In the face of so-called treatment-resistance, the first step is to review the psychological and biologic formulation of the patient and the reasons for his or her depression. Dr. Nasrallah does not mention the need for a review of all aspects of the patient’s life. The approaches he suggests are dreary, dull, ineffective, and unchanging. It proves that patients are best cared for by psychiatrists who practice biopsychosocial psychiatry and not merely to pay lip service to it.
Arnold Robbins, MD
Private Practice
Cambridge, MA
Clinical Professor of Psychiatry
Boston University School of Medicine
Boston, MA
Dr. Nasrallah responds
I thank Dr. Robbins for his letter. As someone trained by the father of biopsychosocial psychiatry—George Engel, MD, at the University of Rochester—I agree that it is the optimal practice of psychiatry and I practice that approach with all my patients. However, I was describing innovative interventions and paradigm shifts for truly end-of-the-road refractory depression, where all psychosocial and pharmacotherapy treatments have failed and the patient is desperate, disabled, and at high risk for suicide. None of the available interventions work with such individuals and that’s why I regard the innovative breakthroughs I described in my editorial as a promise of hope, thanks to dedicated psychiatric neuroscientists. I hope psychotherapy researchers can achieve breakthroughs for these patients as well.
Henry A. Nasrallah, MD
Editor-in-Chief
Psychotherapy for GAD
I appreciated Dr. Barry’s in-depth review of current diagnostic criteria and therapy for generalized anxiety disorder (GAD) (“Generalized anxiety disorder: Helping patients overcome worry,” Current Psychiatry, May 2012, p. 40-44; http://bit.ly/1oUymyJ). However, I want to point out an error under the “Evidence-based treatments” section labeled “Psychotherapy.” Dr. Barry states that cognitive-behavioral therapy (CBT) is the preferred form of psychotherapy for GAD. In my 40 years of practice, I have found a combination of medication—preferably selective serotonin reuptake inhibitors—and psychodynamic psychotherapy is the most effective treatment for GAD and provides more enduring relief.
Jonathan Shedler, PhD, of the University of Colorado Denver School of Medicine reported on the efficacy of psychodynamic psychotherapy vs behavioral therapy.1 He compiled the results of meta-analyses of psychotherapy efficacy by 18 investigators covering 792 studies. The findings show a superior result for psychodynamic psychotherapy over behavioral therapy and the effects are more lasting.
Edward L. Parsons, MD
Private Practice
Westfield, NJ
The author responds
I appreciate Dr. Parsons’ comments and his valuable contribution to the dialogue on GAD. Dr. Parsons reemphasizes the importance of psychotherapy in this chronic condition. As demonstrated by the meta-analyses reviewed by Dr. Shedler, there is sufficient evidence in the medical literature to support either psychodynamic psychotherapy or CBT. The specific therapeutic recommendation should consider unique patient variables, such as therapist availability and expertise, the presence of co-occurring conditions or dynamics that would better align with a specific modality, and patient preference and psychological mindedness, to name a few. Regardless, psychotherapy is indicated in the treatment of GAD, and both CBT and psychodynamic psychotherapy are well-supported interventions.
Matthew J. Barry, DO
Lead Psychiatrist
Rochester Veterans Affairs Outpatient Clinic
Canandaigua Veterans Affairs Medical Center
Canandaigua, NY
Caution with prazosin
We welcome the article discussing the use of prazosin and antipsychotics for posttraumatic stress disorder (PTSD)-related nightmares (Graham RL, Leckband SG, Endow-Eyer RA. “PTSD nightmares: Prazosin and atypical antipsychotics,” Current Psychiatry, June 2012, p. 59-62; http://bit.ly/LVAlSo). The favorable outcomes associated with prazosin use combined with its low cost and general tolerability give it considerable potential. Prazosin may be particularly valuable given the unfavorable cardiometabolic risks associated with antipsychotic use, especially because evidence suggests individuals with PTSD have higher rates of cardiovascular disease.1
We believe the occurrence of adverse cardiovascular effects when starting prazosin requires further attention. As an α1-adrenergic receptor antagonist, it has been linked to orthostatic hypotension and syncope.2,3 Its cardiovascular effects may be further complicated by concomitant use of other antihypertensive medications. Therefore, we suggest a low initiation dose and gradual titration of prazosin. In individuals who initially were normotensive but then experienced hypotension following prazosin administration, we successfully used short-term sodium chloride tablets, 4 g/d. We discontinued sodium chloride after titration was completed and no postural hypotension was evident.
To minimize polypharmacy, individuals on multiple agents for hypertension may benefit from substituting prazosin for 1 of their regular anti- hypertensives. Despite the mounting evidence supporting prazosin use, it is not indicated for PTSD.
This material is the result of work supported with resources and the use of facilities of the Mental Health and Research and Development Service Lines, Atlanta Veterans Affairs Medical Center, Decatur, GA.
Arshya Vahabzadeh, MD
PGY-2, Resident Psychiatrist
Emory University School of Medicine
Erica Duncan, MD
Attending Psychiatrist
and Associate Professor
Mental Health Service Line
Atlanta Veterans Affairs Medical Center
Decatur, GA
Department of Psychiatry and Behavioral
Sciences
Emory University School of Medicine
Atlanta, GA
The authors respond
We agree with the comments by Drs. Vahabzadeh and Duncan regarding the cardiovascular adverse effects of prazosin. It is important to assess the hemodynamic status of the patient before initiating prazosin therapy, and usually, initiation is attempted only if a patient is normotensive or hypertensive because of potential orthostatic hypotension and syncope, which can occur in up to 4% of patients.1 As noted by Drs. Vahabzadeh and Duncan, prazosin often is viewed as a dual treatment for both nightmares and blood pressure in individuals who are hypertensive prior to initiation. Prazosin therapy usually is initiated at 1 mg at bedtime and titrated by 1 to 2 mg every 3 to 5 days.2 The average dose was approximately 3 mg in studies evaluating prazosin for treating PTSD-associated nightmares (dose range: 1 to 10 mg).2 Until the patient is stabilized on a prazosin dose, blood pressure should be monitored daily for inpatients. Outpatients should be educated regarding the signs and symptoms of hypotension, especially dizziness and light-headedness upon standing, along with monitoring blood pressure at his or her next clinic appointment.
Prazosin does not carry an FDA indication for PTSD. Although this is important to consider, the level of evidence in terms of treatment of nightmares also is key. Aurora et al found prazosin was the only medication with a level A rating for treating PTSD-associated nightmares, indicating it as a recommended therapy option.2 Because we do not have any medications indicated for PTSD-associated nightmares, it is crucial to practice evidence-based medicine and base therapy choices on available literature supporting the most effective and safe options.
Safety is an issue in many clinicians’ minds, especially when treating geriatric patients with PTSD because of the risk of hypotensive effects with prazosin leading to negative outcomes, such as falls. In Peskind et al’s open-label study of 9 older patients (mean age: 76) with intractable PTSD-associated nightmares treated with prazosin (mean dose: 2.3 mg; increased by 1 mg per week to a maximum dose of 4 mg), 8 patients experienced >50% reduction in nightmares after 8 weeks of treatment, and 1 patient experienced transient orthostasis when starting prazosin that resolved spontaneously with only mild decreases in blood pressure noted otherwise (<20 mm Hg decrease in systolic blood pressure upon standing).3 Although this study was small, it provides evidence that prazosin can be an effective and safe treatment option in geriatric patients and is devoid of the highly sedating side effects of some other treatment options.
Rebecca L. Graham, PharmD
Second-Year Psychiatric Pharmacy Resident
Veterans Affairs San Diego Healthcare System
(VASDHS)
Susan G. Leckband, RPh, BCPP
Clinical Psychiatric Pharmacist Specialist
VASDHS
Assistant Clinical Professor
Skaggs School of Pharmacy and
Pharmaceutical Sciences
Department of Psychiatry
University of California, San Diego
Rene A. Endow-Eyer, PharmD, BCPP
Psychiatric Clinical Pharmacy Specialist
VASDHS
Assistant Clinical Professor
Skaggs School of Pharmacy and
Pharmaceutical Sciences
Department of Psychiatry
University of California, San Diego
San Diego, CA
With all of the discussion about a truly comprehensive and inclusive psychiatry, it was sad to see the emptiness and one-sidedness of Dr. Nasrallah’s June editorial (“Innovative approaches to treatment-resistant depression,” From the Editor, Current Psychiatry, June 2012, p. 4-5; http://bit.ly/1GM92oV). Depression certainly is not a unified diagnosis such as measles or appendicitis. In the face of so-called treatment-resistance, the first step is to review the psychological and biologic formulation of the patient and the reasons for his or her depression. Dr. Nasrallah does not mention the need for a review of all aspects of the patient’s life. The approaches he suggests are dreary, dull, ineffective, and unchanging. It proves that patients are best cared for by psychiatrists who practice biopsychosocial psychiatry and not merely to pay lip service to it.
Arnold Robbins, MD
Private Practice
Cambridge, MA
Clinical Professor of Psychiatry
Boston University School of Medicine
Boston, MA
Dr. Nasrallah responds
I thank Dr. Robbins for his letter. As someone trained by the father of biopsychosocial psychiatry—George Engel, MD, at the University of Rochester—I agree that it is the optimal practice of psychiatry and I practice that approach with all my patients. However, I was describing innovative interventions and paradigm shifts for truly end-of-the-road refractory depression, where all psychosocial and pharmacotherapy treatments have failed and the patient is desperate, disabled, and at high risk for suicide. None of the available interventions work with such individuals and that’s why I regard the innovative breakthroughs I described in my editorial as a promise of hope, thanks to dedicated psychiatric neuroscientists. I hope psychotherapy researchers can achieve breakthroughs for these patients as well.
Henry A. Nasrallah, MD
Editor-in-Chief
Psychotherapy for GAD
I appreciated Dr. Barry’s in-depth review of current diagnostic criteria and therapy for generalized anxiety disorder (GAD) (“Generalized anxiety disorder: Helping patients overcome worry,” Current Psychiatry, May 2012, p. 40-44; http://bit.ly/1oUymyJ). However, I want to point out an error under the “Evidence-based treatments” section labeled “Psychotherapy.” Dr. Barry states that cognitive-behavioral therapy (CBT) is the preferred form of psychotherapy for GAD. In my 40 years of practice, I have found a combination of medication—preferably selective serotonin reuptake inhibitors—and psychodynamic psychotherapy is the most effective treatment for GAD and provides more enduring relief.
Jonathan Shedler, PhD, of the University of Colorado Denver School of Medicine reported on the efficacy of psychodynamic psychotherapy vs behavioral therapy.1 He compiled the results of meta-analyses of psychotherapy efficacy by 18 investigators covering 792 studies. The findings show a superior result for psychodynamic psychotherapy over behavioral therapy and the effects are more lasting.
Edward L. Parsons, MD
Private Practice
Westfield, NJ
The author responds
I appreciate Dr. Parsons’ comments and his valuable contribution to the dialogue on GAD. Dr. Parsons reemphasizes the importance of psychotherapy in this chronic condition. As demonstrated by the meta-analyses reviewed by Dr. Shedler, there is sufficient evidence in the medical literature to support either psychodynamic psychotherapy or CBT. The specific therapeutic recommendation should consider unique patient variables, such as therapist availability and expertise, the presence of co-occurring conditions or dynamics that would better align with a specific modality, and patient preference and psychological mindedness, to name a few. Regardless, psychotherapy is indicated in the treatment of GAD, and both CBT and psychodynamic psychotherapy are well-supported interventions.
Matthew J. Barry, DO
Lead Psychiatrist
Rochester Veterans Affairs Outpatient Clinic
Canandaigua Veterans Affairs Medical Center
Canandaigua, NY
Caution with prazosin
We welcome the article discussing the use of prazosin and antipsychotics for posttraumatic stress disorder (PTSD)-related nightmares (Graham RL, Leckband SG, Endow-Eyer RA. “PTSD nightmares: Prazosin and atypical antipsychotics,” Current Psychiatry, June 2012, p. 59-62; http://bit.ly/LVAlSo). The favorable outcomes associated with prazosin use combined with its low cost and general tolerability give it considerable potential. Prazosin may be particularly valuable given the unfavorable cardiometabolic risks associated with antipsychotic use, especially because evidence suggests individuals with PTSD have higher rates of cardiovascular disease.1
We believe the occurrence of adverse cardiovascular effects when starting prazosin requires further attention. As an α1-adrenergic receptor antagonist, it has been linked to orthostatic hypotension and syncope.2,3 Its cardiovascular effects may be further complicated by concomitant use of other antihypertensive medications. Therefore, we suggest a low initiation dose and gradual titration of prazosin. In individuals who initially were normotensive but then experienced hypotension following prazosin administration, we successfully used short-term sodium chloride tablets, 4 g/d. We discontinued sodium chloride after titration was completed and no postural hypotension was evident.
To minimize polypharmacy, individuals on multiple agents for hypertension may benefit from substituting prazosin for 1 of their regular anti- hypertensives. Despite the mounting evidence supporting prazosin use, it is not indicated for PTSD.
This material is the result of work supported with resources and the use of facilities of the Mental Health and Research and Development Service Lines, Atlanta Veterans Affairs Medical Center, Decatur, GA.
Arshya Vahabzadeh, MD
PGY-2, Resident Psychiatrist
Emory University School of Medicine
Erica Duncan, MD
Attending Psychiatrist
and Associate Professor
Mental Health Service Line
Atlanta Veterans Affairs Medical Center
Decatur, GA
Department of Psychiatry and Behavioral
Sciences
Emory University School of Medicine
Atlanta, GA
The authors respond
We agree with the comments by Drs. Vahabzadeh and Duncan regarding the cardiovascular adverse effects of prazosin. It is important to assess the hemodynamic status of the patient before initiating prazosin therapy, and usually, initiation is attempted only if a patient is normotensive or hypertensive because of potential orthostatic hypotension and syncope, which can occur in up to 4% of patients.1 As noted by Drs. Vahabzadeh and Duncan, prazosin often is viewed as a dual treatment for both nightmares and blood pressure in individuals who are hypertensive prior to initiation. Prazosin therapy usually is initiated at 1 mg at bedtime and titrated by 1 to 2 mg every 3 to 5 days.2 The average dose was approximately 3 mg in studies evaluating prazosin for treating PTSD-associated nightmares (dose range: 1 to 10 mg).2 Until the patient is stabilized on a prazosin dose, blood pressure should be monitored daily for inpatients. Outpatients should be educated regarding the signs and symptoms of hypotension, especially dizziness and light-headedness upon standing, along with monitoring blood pressure at his or her next clinic appointment.
Prazosin does not carry an FDA indication for PTSD. Although this is important to consider, the level of evidence in terms of treatment of nightmares also is key. Aurora et al found prazosin was the only medication with a level A rating for treating PTSD-associated nightmares, indicating it as a recommended therapy option.2 Because we do not have any medications indicated for PTSD-associated nightmares, it is crucial to practice evidence-based medicine and base therapy choices on available literature supporting the most effective and safe options.
Safety is an issue in many clinicians’ minds, especially when treating geriatric patients with PTSD because of the risk of hypotensive effects with prazosin leading to negative outcomes, such as falls. In Peskind et al’s open-label study of 9 older patients (mean age: 76) with intractable PTSD-associated nightmares treated with prazosin (mean dose: 2.3 mg; increased by 1 mg per week to a maximum dose of 4 mg), 8 patients experienced >50% reduction in nightmares after 8 weeks of treatment, and 1 patient experienced transient orthostasis when starting prazosin that resolved spontaneously with only mild decreases in blood pressure noted otherwise (<20 mm Hg decrease in systolic blood pressure upon standing).3 Although this study was small, it provides evidence that prazosin can be an effective and safe treatment option in geriatric patients and is devoid of the highly sedating side effects of some other treatment options.
Rebecca L. Graham, PharmD
Second-Year Psychiatric Pharmacy Resident
Veterans Affairs San Diego Healthcare System
(VASDHS)
Susan G. Leckband, RPh, BCPP
Clinical Psychiatric Pharmacist Specialist
VASDHS
Assistant Clinical Professor
Skaggs School of Pharmacy and
Pharmaceutical Sciences
Department of Psychiatry
University of California, San Diego
Rene A. Endow-Eyer, PharmD, BCPP
Psychiatric Clinical Pharmacy Specialist
VASDHS
Assistant Clinical Professor
Skaggs School of Pharmacy and
Pharmaceutical Sciences
Department of Psychiatry
University of California, San Diego
San Diego, CA
With all of the discussion about a truly comprehensive and inclusive psychiatry, it was sad to see the emptiness and one-sidedness of Dr. Nasrallah’s June editorial (“Innovative approaches to treatment-resistant depression,” From the Editor, Current Psychiatry, June 2012, p. 4-5; http://bit.ly/1GM92oV). Depression certainly is not a unified diagnosis such as measles or appendicitis. In the face of so-called treatment-resistance, the first step is to review the psychological and biologic formulation of the patient and the reasons for his or her depression. Dr. Nasrallah does not mention the need for a review of all aspects of the patient’s life. The approaches he suggests are dreary, dull, ineffective, and unchanging. It proves that patients are best cared for by psychiatrists who practice biopsychosocial psychiatry and not merely to pay lip service to it.
Arnold Robbins, MD
Private Practice
Cambridge, MA
Clinical Professor of Psychiatry
Boston University School of Medicine
Boston, MA
Dr. Nasrallah responds
I thank Dr. Robbins for his letter. As someone trained by the father of biopsychosocial psychiatry—George Engel, MD, at the University of Rochester—I agree that it is the optimal practice of psychiatry and I practice that approach with all my patients. However, I was describing innovative interventions and paradigm shifts for truly end-of-the-road refractory depression, where all psychosocial and pharmacotherapy treatments have failed and the patient is desperate, disabled, and at high risk for suicide. None of the available interventions work with such individuals and that’s why I regard the innovative breakthroughs I described in my editorial as a promise of hope, thanks to dedicated psychiatric neuroscientists. I hope psychotherapy researchers can achieve breakthroughs for these patients as well.
Henry A. Nasrallah, MD
Editor-in-Chief
Psychotherapy for GAD
I appreciated Dr. Barry’s in-depth review of current diagnostic criteria and therapy for generalized anxiety disorder (GAD) (“Generalized anxiety disorder: Helping patients overcome worry,” Current Psychiatry, May 2012, p. 40-44; http://bit.ly/1oUymyJ). However, I want to point out an error under the “Evidence-based treatments” section labeled “Psychotherapy.” Dr. Barry states that cognitive-behavioral therapy (CBT) is the preferred form of psychotherapy for GAD. In my 40 years of practice, I have found a combination of medication—preferably selective serotonin reuptake inhibitors—and psychodynamic psychotherapy is the most effective treatment for GAD and provides more enduring relief.
Jonathan Shedler, PhD, of the University of Colorado Denver School of Medicine reported on the efficacy of psychodynamic psychotherapy vs behavioral therapy.1 He compiled the results of meta-analyses of psychotherapy efficacy by 18 investigators covering 792 studies. The findings show a superior result for psychodynamic psychotherapy over behavioral therapy and the effects are more lasting.
Edward L. Parsons, MD
Private Practice
Westfield, NJ
The author responds
I appreciate Dr. Parsons’ comments and his valuable contribution to the dialogue on GAD. Dr. Parsons reemphasizes the importance of psychotherapy in this chronic condition. As demonstrated by the meta-analyses reviewed by Dr. Shedler, there is sufficient evidence in the medical literature to support either psychodynamic psychotherapy or CBT. The specific therapeutic recommendation should consider unique patient variables, such as therapist availability and expertise, the presence of co-occurring conditions or dynamics that would better align with a specific modality, and patient preference and psychological mindedness, to name a few. Regardless, psychotherapy is indicated in the treatment of GAD, and both CBT and psychodynamic psychotherapy are well-supported interventions.
Matthew J. Barry, DO
Lead Psychiatrist
Rochester Veterans Affairs Outpatient Clinic
Canandaigua Veterans Affairs Medical Center
Canandaigua, NY
Caution with prazosin
We welcome the article discussing the use of prazosin and antipsychotics for posttraumatic stress disorder (PTSD)-related nightmares (Graham RL, Leckband SG, Endow-Eyer RA. “PTSD nightmares: Prazosin and atypical antipsychotics,” Current Psychiatry, June 2012, p. 59-62; http://bit.ly/LVAlSo). The favorable outcomes associated with prazosin use combined with its low cost and general tolerability give it considerable potential. Prazosin may be particularly valuable given the unfavorable cardiometabolic risks associated with antipsychotic use, especially because evidence suggests individuals with PTSD have higher rates of cardiovascular disease.1
We believe the occurrence of adverse cardiovascular effects when starting prazosin requires further attention. As an α1-adrenergic receptor antagonist, it has been linked to orthostatic hypotension and syncope.2,3 Its cardiovascular effects may be further complicated by concomitant use of other antihypertensive medications. Therefore, we suggest a low initiation dose and gradual titration of prazosin. In individuals who initially were normotensive but then experienced hypotension following prazosin administration, we successfully used short-term sodium chloride tablets, 4 g/d. We discontinued sodium chloride after titration was completed and no postural hypotension was evident.
To minimize polypharmacy, individuals on multiple agents for hypertension may benefit from substituting prazosin for 1 of their regular anti- hypertensives. Despite the mounting evidence supporting prazosin use, it is not indicated for PTSD.
This material is the result of work supported with resources and the use of facilities of the Mental Health and Research and Development Service Lines, Atlanta Veterans Affairs Medical Center, Decatur, GA.
Arshya Vahabzadeh, MD
PGY-2, Resident Psychiatrist
Emory University School of Medicine
Erica Duncan, MD
Attending Psychiatrist
and Associate Professor
Mental Health Service Line
Atlanta Veterans Affairs Medical Center
Decatur, GA
Department of Psychiatry and Behavioral
Sciences
Emory University School of Medicine
Atlanta, GA
The authors respond
We agree with the comments by Drs. Vahabzadeh and Duncan regarding the cardiovascular adverse effects of prazosin. It is important to assess the hemodynamic status of the patient before initiating prazosin therapy, and usually, initiation is attempted only if a patient is normotensive or hypertensive because of potential orthostatic hypotension and syncope, which can occur in up to 4% of patients.1 As noted by Drs. Vahabzadeh and Duncan, prazosin often is viewed as a dual treatment for both nightmares and blood pressure in individuals who are hypertensive prior to initiation. Prazosin therapy usually is initiated at 1 mg at bedtime and titrated by 1 to 2 mg every 3 to 5 days.2 The average dose was approximately 3 mg in studies evaluating prazosin for treating PTSD-associated nightmares (dose range: 1 to 10 mg).2 Until the patient is stabilized on a prazosin dose, blood pressure should be monitored daily for inpatients. Outpatients should be educated regarding the signs and symptoms of hypotension, especially dizziness and light-headedness upon standing, along with monitoring blood pressure at his or her next clinic appointment.
Prazosin does not carry an FDA indication for PTSD. Although this is important to consider, the level of evidence in terms of treatment of nightmares also is key. Aurora et al found prazosin was the only medication with a level A rating for treating PTSD-associated nightmares, indicating it as a recommended therapy option.2 Because we do not have any medications indicated for PTSD-associated nightmares, it is crucial to practice evidence-based medicine and base therapy choices on available literature supporting the most effective and safe options.
Safety is an issue in many clinicians’ minds, especially when treating geriatric patients with PTSD because of the risk of hypotensive effects with prazosin leading to negative outcomes, such as falls. In Peskind et al’s open-label study of 9 older patients (mean age: 76) with intractable PTSD-associated nightmares treated with prazosin (mean dose: 2.3 mg; increased by 1 mg per week to a maximum dose of 4 mg), 8 patients experienced >50% reduction in nightmares after 8 weeks of treatment, and 1 patient experienced transient orthostasis when starting prazosin that resolved spontaneously with only mild decreases in blood pressure noted otherwise (<20 mm Hg decrease in systolic blood pressure upon standing).3 Although this study was small, it provides evidence that prazosin can be an effective and safe treatment option in geriatric patients and is devoid of the highly sedating side effects of some other treatment options.
Rebecca L. Graham, PharmD
Second-Year Psychiatric Pharmacy Resident
Veterans Affairs San Diego Healthcare System
(VASDHS)
Susan G. Leckband, RPh, BCPP
Clinical Psychiatric Pharmacist Specialist
VASDHS
Assistant Clinical Professor
Skaggs School of Pharmacy and
Pharmaceutical Sciences
Department of Psychiatry
University of California, San Diego
Rene A. Endow-Eyer, PharmD, BCPP
Psychiatric Clinical Pharmacy Specialist
VASDHS
Assistant Clinical Professor
Skaggs School of Pharmacy and
Pharmaceutical Sciences
Department of Psychiatry
University of California, San Diego
San Diego, CA
Recognizing and treating complicated grief
Nearly 2.5 million persons die each year in the United States.1 For the bereaved, these deaths may be among the most painful and disruptive events they will experience. In this article, we evaluate the growing body of research on complicated grief (CG)—which also has been called prolonged grief, chronic grief, traumatic grief, and pathological grief—with an emphasis on how to identify CG and distinguish it from other adaptive and maladaptive reactions to the loss of a loved one. In addition, we review empirical evidence on treating CG, including psychotherapy, pharmacotherapy, and combined treatment approaches.
The bereavement-specific syndrome we refer to as CG currently is being reviewed for possible inclusion in DSM-5 as an official diagnosis. At press time, proposals for DSM-5 included a bereavement-related adjustment disorder within the new Trauma- and Stressor-Related Disorders category, as well as a provisional diagnosis of CG entitled Persistent Complex Bereavement-Related Disorder, which, upon acceptance, would be listed in Section III.2
What is ‘normal’ grief?
Grief is highly variable across individuals and time and may range from an absence of distress to severe and persistent pain and anguish. There’s no simple definition of “normal grief.” However, as clinicians, it’s necessary to understand the range of usual reactions. We recommend 2 considerations when evaluating grief reactions.
First, be aware that grief encompasses a range of cognitions, emotions, and behaviors. It may range from a relative lack of painful thoughts and emotions to intense and disruptive sadness, loneliness, anger, guilt, intrusive thoughts, difficulty concentrating, preoccupation with loss, social withdrawal, and a sense of being overwhelmed by the loss and its consequences. In the months after a loss, bereaved individuals may look for the deceased in a crowd, speak to them, or even experience auditory or visual hallucinations of the deceased. Nonetheless, positive feelings such as relief, peace, and happiness also are common following a loss.3 Moreover, laughter and smiling when discussing a lost loved one predicts reductions in grief symptoms over time.4 Overall, grief research suggests that, far from proceeding along standard and uniform stages,5 grief is complex and comprises a broad spectrum of thoughts, feelings, and behaviors that vary within and among individuals.
Second, note that in the absence of complications, grief progresses. For those who experience elevated levels of distress, the pain and disruption of loss initially may feel overwhelming but will subside in intensity over time for most individuals.5 This is not to say that an individual will never again feel sadness or longing for the deceased; elements of grief are likely to remain. Although the trajectory of grief symptoms varies among individuals and may progress in fits and starts, over time grief becomes more intermittent, less interfering, and is balanced with a sense of interest and purpose in life.
What is CG?
As research on grief experiences has grown, there’s increasing recognition that a minority of bereaved individuals experience more extreme grief symptoms that cause substantial, persistent distress and impairment despite the passage of many months or years. Shear et al6 proposed a set of CG diagnostic criteria (Table) in which a cluster of symptoms of intense and persistent separation distress are defined as core symptoms. Similar to other psychiatric diagnoses, the symptoms must be associated with significant distress or impairment.
Table
Proposed diagnostic criteria for complicated grief
| Symptom domain | Criteria |
|---|---|
| Separation distress | The patient has ≥1 of the following 4 symptoms: 1) Persistent, intense yearning or longing for the deceased 2) Frequent feelings of intense loneliness or emptiness 3) Recurrent negative thoughts about life without the deceased or recurrent urge to join the deceased 4) Preoccupying thoughts about the deceased that impair daily functioning |
| Thoughts | The patient has ≥2 of the following 8 symptoms: 1) Rumination about circumstances of the death 2) Frequent disbelief or inability to accept the death |
| Feelings | 3) Persistent feeling of being shocked, stunned, or emotionally numb since the death 4) Recurrent feelings of anger or bitterness regarding the death 5) Difficulty trusting or caring about others since the loss 6) Experiencing pain or other somatic symptoms the deceased person had, hearing the voice of the deceased, or seeing the deceased person 7) Intense emotional reactions to memories of the deceased |
| Behaviors | 8) Excessive avoidance or excessive preoccupation with places, people, and things related to the deceased or death |
| Source: Adapted from reference 6 | |
Assessing CG symptoms
Among those with persistent elevated distress, a CG diagnosis must be considered in the context of the individual’s social and cultural environment, time since the loss, and duration of symptoms. The hallmark symptom of CG is separation distress with a focus of cognitive, behavioral, and emotional symptoms on the loss and its consequences. CG is associated with substantial distress, functional impairment, and an increased risk for suicide. See the Box for a case study.
Many individuals with CG remain undiagnosed and untreated for years despite high levels of distress and impairment and high risk for negative consequences such as suicide.7 Accordingly, there’s a need for greater CG screening. Clinically useful tools for assessing CG include a brief, 5-item dimensional screening assessment6 and the patient-rated Inventory of Complicated Grief.8
Distinguishing complicated and uncomplicated grief. Exhibiting CG symptoms in the first several months after a loss does not mean an individual has or will develop CG. Most bereaved adults report painful thoughts and emotions in the weeks and months following the loss, including distressed yearning, waves of intense grief, persistent and intrusive thoughts, images related to the death, somatic distress, and a feeling of being disconnected from others. For most individuals, the intensity of this response diminishes within 6 to 18 months after the loved one’s death.5 Although the optimal length of time to wait before establishing a diagnosis remains debatable, the earliest CG should be diagnosed is 6 months after a loss.
It’s common for grief to occasionally rise in intensity for days or weeks. This surge may occur many months or years after the loss, even in people who exhibited relatively little distress or impairment. In particular, anniversaries, holidays, or periods of stress may trigger increased grief intensity. However, these surges typically subside naturally within a short time. Accordingly, CG should be diagnosed only when symptoms persist for >1 month.
CG vs other post-loss disorders. CG, major depressive disorder (MDD), and posttraumatic stress disorder (PTSD) often are comorbid in bereaved adults. Simon et al9 found 72% of CG patients in a treatment- seeking sample reported a lifetime history of MDD and 53% reported a lifetime history of PTSD. However, CG can be distinguished from these disorders. In the same study, 25% of CG patients had no other axis I diagnosis.9 After accounting for comorbid disorders, researchers associated CG severity with work and social impairment. These findings provide clear evidence for the incremental validity of CG—ie, a CG diagnosis gives clinicians additional information that predicts impairment above and beyond other disorders. However, future research needs to further examine CG and its overlap and differentiation from MDD and PTSD.
Distinguishing CG and MDD. Intense yearning or preoccupation with the deceased is a common symptom of CG but not MDD. In addition, CG symptoms possess intentionality. For example, emotional distress such as sadness and anger are prominent features of both CG and MDD. However, in CG, these symptoms are specific to the loss or circumstances of the loss, whereas in MDD they generally are more nebulous and generalized. Similarly, CG entails proximity seeking related to the deceased, and avoidance of reminders of the deceased, whereas MDD includes a more general social withdrawal and anhedonia.
Distinguishing CG and PTSD. CG and loss-related PTSD are distinguished by the predominant emotions and focus of concern associated with each disorder. The predominant emotion in PTSD is fear, whereas in CG it is sadness and longing. In PTSD, intrusive thoughts and memories associated with the trauma generally are associated with the event itself and produce an ongoing sense of threat.10 Avoidance in PTSD is intended to reduce this threat feeling. By contrast, in CG, intrusive memories focus on the deceased or the circumstances of the death, and avoidance is aimed at preventing painful reminders of the loss or its permanence. Importantly, both syndromes may be present.
Mr. C, age 67, presents to a local emergency department (ED) with his daughter. His daughter reports that he has not been himself since his wife died in a car accident 2 years ago. He continues to live in the house he shared with his wife, despite not needing the extra space and being unable to maintain it. Although Mr. C and his daughter used to talk about her mother a great deal, she says she now tries to avoid the subject because it upsets him. More recently she became concerned when Mr. C began to tell her that his life was meaningless without his wife. He said he frequently thinks about taking his own life to end his pain and loneliness.
Mr. C tells the ED psychiatrist he feels an intense wave of grief and loneliness every morning when he realizes his wife is not with him. He often stays in bed for hours, longing for her and thinking about their time together. At times, he thinks he hears her voice downstairs but when he searches for her, she is not there. Mr. C has been unable to go through his wife’s belongings, and feels nothing should be moved in their home. He will look at her photos, yet avoids other reminders of her (eg, partaking in their favorite hobbies, going to their favorite restaurants). He feels bitter and angry about his wife’s death, and becomes agitated when describing the car accident that took her life. Mr. C feels guilty for not being with his wife when she died. He assures the psychiatrist that he loves his children, but says he feels increasingly distant from them and doesn’t understand how they can move on after their mother’s death.
Mr. C reports symptoms consistent with a diagnosis of complicated grief. Further assessment is appropriate to determine if his symptoms are severe enough to warrant treatment.
Treating CG
When is treatment indicated? For years, bereavement theorists emphasized the need to work through emotions and memories related to the deceased with particular focus on negative material. However, evidence suggests that universal application of treatment to all bereaved individuals is unhelpful. In a recent meta-analysis, Neimeyer et al11 found that the outcomes of grief therapy applied indiscriminately to all bereaved adults or all members of high-risk populations—such as parents whose child experienced a violent death—were no better than would be expected by the passage of time. In contrast, grief therapy applied only to those who develop elevated and persistent distress (eg, CG) led to greater and more enduring improvement in post-loss distress than was observed in control conditions.
These results suggest that most grieving individuals who do not meet criteria for CG (or other psychiatric disorders) will not require intervention. Those who do seek treatment for grief-related distress in the acute grief period should be assessed for bereavement-related depression, anxiety, and suicidality, and treated or referred to professional or community-based resources for support or counseling as clinically indicated.
Evidence for psychotherapy. For those who meet CG criteria, psychotherapy targeting the specific symptoms of CG is helpful. The evidence is strongest for CG treatment (CGT), a 16-session, manualized psychotherapy developed by M. Katherine Shear, MD.12 CGT is based on an attachment model and cognitive-behavioral therapy (CBT) principles, and is informed by the dual-process theory proposed by Stroebe et al.13 According to this theory, natural healing following loss comprises 2 processes:
- a loss-oriented process in which the patient comes to terms with the loss, and
- a restoration-oriented process in which the patient reinvigorates a sense of purpose and meaning in life without the deceased.
CGT focuses on both processes. To address the former, it includes clinician-guided exercises in which the patient revisits the time of the death and planned activities in which the patient reengages with people, places, or thoughts that remind him or her of the deceased. CGT aims to allow the patient to gain an increased tolerance of the distressing thoughts and emotions associated with the loss so that these thoughts can be processed and the finality of the death and its circumstances can be accepted.
The restoration process is addressed by having patients generate and discuss personal goals and aspirations for the near and distant future, as well as scheduling pleasurable and rewarding events. This is accomplished by having patients imagine what they would want for themselves if their grief was less intense and planning concrete steps to take toward these goals. The restoration-oriented process is addressed concurrent with the loss-oriented process to encourage the oscillation between processes thought to be characteristic of a natural healing process following the loss of a loved one.
Other psychotherapy approaches (eg, support groups) may have a role for some individuals, and future research may suggest alternative approaches to CGT. To date, CGT is the most targeted evidence-based psychotherapy with randomized controlled data supporting its use in CG.
Pharmacotherapy for CG. Early research suggested that antidepressants—in particular tricyclics—may effectively reduce depressive symptoms in bereavement-related depression; their effect on CG symptoms, however, may not be as strong.14 Research on pharmacologic treatment that targets CG symptoms is developing. Because of the overlap between CG, PTSD, and MDD, researchers have hypothesized that antidepressants may be effective. Two open-label studies reported that the selective serotonin reuptake inhibitor (SSRI) escitalopram may be effective for CG.15,16 Although a post-hoc comparison of paroxetine and nortriptyline17 showed significant reduction in CG and depressive symptoms with both agents, effects could not be separated from concomitant psychotherapy. Furthermore, an examination of naturalistic data on combining antidepressants with CGT suggested that antidepressants may improve outcomes for individuals receiving CGT.18 A multicenter, randomized controlled trial funded by the National Institute of Mental Health is examining the potential efficacy of citalopram, an SSRI, alone or in combination with CGT.19
The efficacy of benzodiazepines, which commonly are prescribed for bereaved individuals, has not been assessed in CG. However, recent research suggests they may not be useful for medically managing recent grief20 and that their use in the aftermath of a loss may lead to long-term dependence in geriatric patients.21
Related Resources
- Center for Anxiety and Traumatic Stress Disorders. Massachusetts General Hospital. www.bostongrief.com.
- Zisook S, Shear K. Grief and bereavement: what psychiatrists need to know. World Psychiatry. 2009;8(2):67-74.
- Bonanno G. The other side of sadness: what the new science of bereavement tells us about loss. New York, NY: Basic Books; 2009.
Drug Brand Names
- Citalopram • Celexa
- Nortriptyline • Aventyl, Pamelor
- Escitalopram • Lexapro
- Paroxetine • Paxil
Disclosures
Dr. Simon receives grant or research support from the American Cancer Society, the American Foundation for Suicide Prevention, the Department of Defense, Forest Laboratories, and the National Institute of Mental Health.
1. Kochanek KD, Xu J, Murphy SL, et al. U.S. Department of Health and Human Services. Deaths: preliminary data for 2009. http://www.cdc.gov/nchs/data/nvsr/nvsr59/nvsr59_04.pdf. Published March 16 2011. Accessed June 19, 2012.
2. American Psychiatric Association. Trauma- and stressor-related disorders. http://www.dsm5.org/ProposedRevision/Pages/TraumaandStressorRelatedDisorders.aspx. Accessed June 19 2012.
3. Bonanno GA, Kaltman S. Toward an integrative perspective on bereavement. Psychol Bull. 1999;125(6):760-776.
4. Bonanno GA, Keltner D. Facial expressions of emotion and the course of conjugal bereavement. J Abnorm Psychol. 1997;106(1):126-137.
5. Bonanno GA, Wortman CB, Lehman DR, et al. Resilience to loss and chronic grief: a prospective study from preloss to 18-months postloss. J Pers Soc Psychol. 2002;83(5):1150-1164.
6. Shear MK, Simon N, Wall M, et al. Complicated grief and related bereavement issues for DSM-5. Depress Anxiety. 2011;28(2):103-117.
7. Boelen PA, Prigerson HG. The influence of symptoms of prolonged grief disorder depression, and anxiety on quality of life among bereaved adults: a prospective study. Eur Arch Psychiatry Clin Neurosci. 2007;257(8):444-452.
8. Prigerson HG, Maciejewski PK, Reynolds CF, 3rd, et al. Inventory of Complicated Grief: a scale to measure maladaptive symptoms of loss. Psychiatry Res. 1995;59 (1-2):65-79.
9. Simon NM, Shear KM, Thompson EH, et al. The prevalence and correlates of psychiatric comorbidity in individuals with complicated grief. Compr Psychiatry. 2007;48(5):395-399.
10. Brewin CR, Holmes EA. Psychological theories of posttraumatic stress disorder. Clin Psychol Rev. 2003;23(3):339-376.
11. Neimeyer RA, Currier JM. Grief therapy: evidence of efficacy and emerging directions. Curr Dir Psychol Sci. 2009;18(6):352-356.
12. Shear K, Frank E, Houck PR, et al. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293(21):2601-2608.
13. Stroebe M, Schut H. The dual process model of coping with bereavement: rationale and description. Death Stud. 1999;23(3):197-224.
14. Reynolds CF, 3rd, Miller MD, Pasternak RE, et al. Treatment of bereavement-related major depressive episodes in later life: a controlled study of acute and continuation treatment with nortriptyline and interpersonal psychotherapy. Am J Psychiatry. 1999;156(2):202-208.
15. Simon NM, Thompson EH, Pollack MH, et al. Complicated grief: a case series using escitalopram. Am J Psychiatry. 2007;164(11):1760-1761.
16. Hensley PL, Slonimski CK, Uhlenhuth EH, et al. Escitalopram: an open-label study of bereavement-related depression and grief. J Affect Disord. 2009;113(1-2):142-149.
17. Zygmont M, Prigerson HG, Houck PR, et al. A post hoc comparison of paroxetine and nortriptyline for symptoms of traumatic grief. J Clin Psychiatry. 1998;59(5):241-245.
18. Simon NM, Shear MK, Fagiolini A, et al. Impact of concurrent naturalistic pharmacotherapy on psychotherapy of complicated grief. Psychiatry Res. 2008;159(1-2):31-36.
19. U.S. National Institutes of Health. A study of medication with or without psychotherapy for complicated grief (HEAL). http://clinicaltrials.gov/ct2/show/NCT01179568. Published June 24, 2012. Accessed June 25, 2012.
20. Warner J, Metcalfe C, King M. Evaluating the use of benzodiazepines following recent bereavement. Br J Psychiatry. 2001;178(1):36-41.
21. Cook JM, Biyanova T, Marshall R. Medicating grief with benzodiazepines: physician and patient perspectives. Arch Intern Med. 2007;167(18):2006-2007.
Nearly 2.5 million persons die each year in the United States.1 For the bereaved, these deaths may be among the most painful and disruptive events they will experience. In this article, we evaluate the growing body of research on complicated grief (CG)—which also has been called prolonged grief, chronic grief, traumatic grief, and pathological grief—with an emphasis on how to identify CG and distinguish it from other adaptive and maladaptive reactions to the loss of a loved one. In addition, we review empirical evidence on treating CG, including psychotherapy, pharmacotherapy, and combined treatment approaches.
The bereavement-specific syndrome we refer to as CG currently is being reviewed for possible inclusion in DSM-5 as an official diagnosis. At press time, proposals for DSM-5 included a bereavement-related adjustment disorder within the new Trauma- and Stressor-Related Disorders category, as well as a provisional diagnosis of CG entitled Persistent Complex Bereavement-Related Disorder, which, upon acceptance, would be listed in Section III.2
What is ‘normal’ grief?
Grief is highly variable across individuals and time and may range from an absence of distress to severe and persistent pain and anguish. There’s no simple definition of “normal grief.” However, as clinicians, it’s necessary to understand the range of usual reactions. We recommend 2 considerations when evaluating grief reactions.
First, be aware that grief encompasses a range of cognitions, emotions, and behaviors. It may range from a relative lack of painful thoughts and emotions to intense and disruptive sadness, loneliness, anger, guilt, intrusive thoughts, difficulty concentrating, preoccupation with loss, social withdrawal, and a sense of being overwhelmed by the loss and its consequences. In the months after a loss, bereaved individuals may look for the deceased in a crowd, speak to them, or even experience auditory or visual hallucinations of the deceased. Nonetheless, positive feelings such as relief, peace, and happiness also are common following a loss.3 Moreover, laughter and smiling when discussing a lost loved one predicts reductions in grief symptoms over time.4 Overall, grief research suggests that, far from proceeding along standard and uniform stages,5 grief is complex and comprises a broad spectrum of thoughts, feelings, and behaviors that vary within and among individuals.
Second, note that in the absence of complications, grief progresses. For those who experience elevated levels of distress, the pain and disruption of loss initially may feel overwhelming but will subside in intensity over time for most individuals.5 This is not to say that an individual will never again feel sadness or longing for the deceased; elements of grief are likely to remain. Although the trajectory of grief symptoms varies among individuals and may progress in fits and starts, over time grief becomes more intermittent, less interfering, and is balanced with a sense of interest and purpose in life.
What is CG?
As research on grief experiences has grown, there’s increasing recognition that a minority of bereaved individuals experience more extreme grief symptoms that cause substantial, persistent distress and impairment despite the passage of many months or years. Shear et al6 proposed a set of CG diagnostic criteria (Table) in which a cluster of symptoms of intense and persistent separation distress are defined as core symptoms. Similar to other psychiatric diagnoses, the symptoms must be associated with significant distress or impairment.
Table
Proposed diagnostic criteria for complicated grief
| Symptom domain | Criteria |
|---|---|
| Separation distress | The patient has ≥1 of the following 4 symptoms: 1) Persistent, intense yearning or longing for the deceased 2) Frequent feelings of intense loneliness or emptiness 3) Recurrent negative thoughts about life without the deceased or recurrent urge to join the deceased 4) Preoccupying thoughts about the deceased that impair daily functioning |
| Thoughts | The patient has ≥2 of the following 8 symptoms: 1) Rumination about circumstances of the death 2) Frequent disbelief or inability to accept the death |
| Feelings | 3) Persistent feeling of being shocked, stunned, or emotionally numb since the death 4) Recurrent feelings of anger or bitterness regarding the death 5) Difficulty trusting or caring about others since the loss 6) Experiencing pain or other somatic symptoms the deceased person had, hearing the voice of the deceased, or seeing the deceased person 7) Intense emotional reactions to memories of the deceased |
| Behaviors | 8) Excessive avoidance or excessive preoccupation with places, people, and things related to the deceased or death |
| Source: Adapted from reference 6 | |
Assessing CG symptoms
Among those with persistent elevated distress, a CG diagnosis must be considered in the context of the individual’s social and cultural environment, time since the loss, and duration of symptoms. The hallmark symptom of CG is separation distress with a focus of cognitive, behavioral, and emotional symptoms on the loss and its consequences. CG is associated with substantial distress, functional impairment, and an increased risk for suicide. See the Box for a case study.
Many individuals with CG remain undiagnosed and untreated for years despite high levels of distress and impairment and high risk for negative consequences such as suicide.7 Accordingly, there’s a need for greater CG screening. Clinically useful tools for assessing CG include a brief, 5-item dimensional screening assessment6 and the patient-rated Inventory of Complicated Grief.8
Distinguishing complicated and uncomplicated grief. Exhibiting CG symptoms in the first several months after a loss does not mean an individual has or will develop CG. Most bereaved adults report painful thoughts and emotions in the weeks and months following the loss, including distressed yearning, waves of intense grief, persistent and intrusive thoughts, images related to the death, somatic distress, and a feeling of being disconnected from others. For most individuals, the intensity of this response diminishes within 6 to 18 months after the loved one’s death.5 Although the optimal length of time to wait before establishing a diagnosis remains debatable, the earliest CG should be diagnosed is 6 months after a loss.
It’s common for grief to occasionally rise in intensity for days or weeks. This surge may occur many months or years after the loss, even in people who exhibited relatively little distress or impairment. In particular, anniversaries, holidays, or periods of stress may trigger increased grief intensity. However, these surges typically subside naturally within a short time. Accordingly, CG should be diagnosed only when symptoms persist for >1 month.
CG vs other post-loss disorders. CG, major depressive disorder (MDD), and posttraumatic stress disorder (PTSD) often are comorbid in bereaved adults. Simon et al9 found 72% of CG patients in a treatment- seeking sample reported a lifetime history of MDD and 53% reported a lifetime history of PTSD. However, CG can be distinguished from these disorders. In the same study, 25% of CG patients had no other axis I diagnosis.9 After accounting for comorbid disorders, researchers associated CG severity with work and social impairment. These findings provide clear evidence for the incremental validity of CG—ie, a CG diagnosis gives clinicians additional information that predicts impairment above and beyond other disorders. However, future research needs to further examine CG and its overlap and differentiation from MDD and PTSD.
Distinguishing CG and MDD. Intense yearning or preoccupation with the deceased is a common symptom of CG but not MDD. In addition, CG symptoms possess intentionality. For example, emotional distress such as sadness and anger are prominent features of both CG and MDD. However, in CG, these symptoms are specific to the loss or circumstances of the loss, whereas in MDD they generally are more nebulous and generalized. Similarly, CG entails proximity seeking related to the deceased, and avoidance of reminders of the deceased, whereas MDD includes a more general social withdrawal and anhedonia.
Distinguishing CG and PTSD. CG and loss-related PTSD are distinguished by the predominant emotions and focus of concern associated with each disorder. The predominant emotion in PTSD is fear, whereas in CG it is sadness and longing. In PTSD, intrusive thoughts and memories associated with the trauma generally are associated with the event itself and produce an ongoing sense of threat.10 Avoidance in PTSD is intended to reduce this threat feeling. By contrast, in CG, intrusive memories focus on the deceased or the circumstances of the death, and avoidance is aimed at preventing painful reminders of the loss or its permanence. Importantly, both syndromes may be present.
Mr. C, age 67, presents to a local emergency department (ED) with his daughter. His daughter reports that he has not been himself since his wife died in a car accident 2 years ago. He continues to live in the house he shared with his wife, despite not needing the extra space and being unable to maintain it. Although Mr. C and his daughter used to talk about her mother a great deal, she says she now tries to avoid the subject because it upsets him. More recently she became concerned when Mr. C began to tell her that his life was meaningless without his wife. He said he frequently thinks about taking his own life to end his pain and loneliness.
Mr. C tells the ED psychiatrist he feels an intense wave of grief and loneliness every morning when he realizes his wife is not with him. He often stays in bed for hours, longing for her and thinking about their time together. At times, he thinks he hears her voice downstairs but when he searches for her, she is not there. Mr. C has been unable to go through his wife’s belongings, and feels nothing should be moved in their home. He will look at her photos, yet avoids other reminders of her (eg, partaking in their favorite hobbies, going to their favorite restaurants). He feels bitter and angry about his wife’s death, and becomes agitated when describing the car accident that took her life. Mr. C feels guilty for not being with his wife when she died. He assures the psychiatrist that he loves his children, but says he feels increasingly distant from them and doesn’t understand how they can move on after their mother’s death.
Mr. C reports symptoms consistent with a diagnosis of complicated grief. Further assessment is appropriate to determine if his symptoms are severe enough to warrant treatment.
Treating CG
When is treatment indicated? For years, bereavement theorists emphasized the need to work through emotions and memories related to the deceased with particular focus on negative material. However, evidence suggests that universal application of treatment to all bereaved individuals is unhelpful. In a recent meta-analysis, Neimeyer et al11 found that the outcomes of grief therapy applied indiscriminately to all bereaved adults or all members of high-risk populations—such as parents whose child experienced a violent death—were no better than would be expected by the passage of time. In contrast, grief therapy applied only to those who develop elevated and persistent distress (eg, CG) led to greater and more enduring improvement in post-loss distress than was observed in control conditions.
These results suggest that most grieving individuals who do not meet criteria for CG (or other psychiatric disorders) will not require intervention. Those who do seek treatment for grief-related distress in the acute grief period should be assessed for bereavement-related depression, anxiety, and suicidality, and treated or referred to professional or community-based resources for support or counseling as clinically indicated.
Evidence for psychotherapy. For those who meet CG criteria, psychotherapy targeting the specific symptoms of CG is helpful. The evidence is strongest for CG treatment (CGT), a 16-session, manualized psychotherapy developed by M. Katherine Shear, MD.12 CGT is based on an attachment model and cognitive-behavioral therapy (CBT) principles, and is informed by the dual-process theory proposed by Stroebe et al.13 According to this theory, natural healing following loss comprises 2 processes:
- a loss-oriented process in which the patient comes to terms with the loss, and
- a restoration-oriented process in which the patient reinvigorates a sense of purpose and meaning in life without the deceased.
CGT focuses on both processes. To address the former, it includes clinician-guided exercises in which the patient revisits the time of the death and planned activities in which the patient reengages with people, places, or thoughts that remind him or her of the deceased. CGT aims to allow the patient to gain an increased tolerance of the distressing thoughts and emotions associated with the loss so that these thoughts can be processed and the finality of the death and its circumstances can be accepted.
The restoration process is addressed by having patients generate and discuss personal goals and aspirations for the near and distant future, as well as scheduling pleasurable and rewarding events. This is accomplished by having patients imagine what they would want for themselves if their grief was less intense and planning concrete steps to take toward these goals. The restoration-oriented process is addressed concurrent with the loss-oriented process to encourage the oscillation between processes thought to be characteristic of a natural healing process following the loss of a loved one.
Other psychotherapy approaches (eg, support groups) may have a role for some individuals, and future research may suggest alternative approaches to CGT. To date, CGT is the most targeted evidence-based psychotherapy with randomized controlled data supporting its use in CG.
Pharmacotherapy for CG. Early research suggested that antidepressants—in particular tricyclics—may effectively reduce depressive symptoms in bereavement-related depression; their effect on CG symptoms, however, may not be as strong.14 Research on pharmacologic treatment that targets CG symptoms is developing. Because of the overlap between CG, PTSD, and MDD, researchers have hypothesized that antidepressants may be effective. Two open-label studies reported that the selective serotonin reuptake inhibitor (SSRI) escitalopram may be effective for CG.15,16 Although a post-hoc comparison of paroxetine and nortriptyline17 showed significant reduction in CG and depressive symptoms with both agents, effects could not be separated from concomitant psychotherapy. Furthermore, an examination of naturalistic data on combining antidepressants with CGT suggested that antidepressants may improve outcomes for individuals receiving CGT.18 A multicenter, randomized controlled trial funded by the National Institute of Mental Health is examining the potential efficacy of citalopram, an SSRI, alone or in combination with CGT.19
The efficacy of benzodiazepines, which commonly are prescribed for bereaved individuals, has not been assessed in CG. However, recent research suggests they may not be useful for medically managing recent grief20 and that their use in the aftermath of a loss may lead to long-term dependence in geriatric patients.21
Related Resources
- Center for Anxiety and Traumatic Stress Disorders. Massachusetts General Hospital. www.bostongrief.com.
- Zisook S, Shear K. Grief and bereavement: what psychiatrists need to know. World Psychiatry. 2009;8(2):67-74.
- Bonanno G. The other side of sadness: what the new science of bereavement tells us about loss. New York, NY: Basic Books; 2009.
Drug Brand Names
- Citalopram • Celexa
- Nortriptyline • Aventyl, Pamelor
- Escitalopram • Lexapro
- Paroxetine • Paxil
Disclosures
Dr. Simon receives grant or research support from the American Cancer Society, the American Foundation for Suicide Prevention, the Department of Defense, Forest Laboratories, and the National Institute of Mental Health.
Nearly 2.5 million persons die each year in the United States.1 For the bereaved, these deaths may be among the most painful and disruptive events they will experience. In this article, we evaluate the growing body of research on complicated grief (CG)—which also has been called prolonged grief, chronic grief, traumatic grief, and pathological grief—with an emphasis on how to identify CG and distinguish it from other adaptive and maladaptive reactions to the loss of a loved one. In addition, we review empirical evidence on treating CG, including psychotherapy, pharmacotherapy, and combined treatment approaches.
The bereavement-specific syndrome we refer to as CG currently is being reviewed for possible inclusion in DSM-5 as an official diagnosis. At press time, proposals for DSM-5 included a bereavement-related adjustment disorder within the new Trauma- and Stressor-Related Disorders category, as well as a provisional diagnosis of CG entitled Persistent Complex Bereavement-Related Disorder, which, upon acceptance, would be listed in Section III.2
What is ‘normal’ grief?
Grief is highly variable across individuals and time and may range from an absence of distress to severe and persistent pain and anguish. There’s no simple definition of “normal grief.” However, as clinicians, it’s necessary to understand the range of usual reactions. We recommend 2 considerations when evaluating grief reactions.
First, be aware that grief encompasses a range of cognitions, emotions, and behaviors. It may range from a relative lack of painful thoughts and emotions to intense and disruptive sadness, loneliness, anger, guilt, intrusive thoughts, difficulty concentrating, preoccupation with loss, social withdrawal, and a sense of being overwhelmed by the loss and its consequences. In the months after a loss, bereaved individuals may look for the deceased in a crowd, speak to them, or even experience auditory or visual hallucinations of the deceased. Nonetheless, positive feelings such as relief, peace, and happiness also are common following a loss.3 Moreover, laughter and smiling when discussing a lost loved one predicts reductions in grief symptoms over time.4 Overall, grief research suggests that, far from proceeding along standard and uniform stages,5 grief is complex and comprises a broad spectrum of thoughts, feelings, and behaviors that vary within and among individuals.
Second, note that in the absence of complications, grief progresses. For those who experience elevated levels of distress, the pain and disruption of loss initially may feel overwhelming but will subside in intensity over time for most individuals.5 This is not to say that an individual will never again feel sadness or longing for the deceased; elements of grief are likely to remain. Although the trajectory of grief symptoms varies among individuals and may progress in fits and starts, over time grief becomes more intermittent, less interfering, and is balanced with a sense of interest and purpose in life.
What is CG?
As research on grief experiences has grown, there’s increasing recognition that a minority of bereaved individuals experience more extreme grief symptoms that cause substantial, persistent distress and impairment despite the passage of many months or years. Shear et al6 proposed a set of CG diagnostic criteria (Table) in which a cluster of symptoms of intense and persistent separation distress are defined as core symptoms. Similar to other psychiatric diagnoses, the symptoms must be associated with significant distress or impairment.
Table
Proposed diagnostic criteria for complicated grief
| Symptom domain | Criteria |
|---|---|
| Separation distress | The patient has ≥1 of the following 4 symptoms: 1) Persistent, intense yearning or longing for the deceased 2) Frequent feelings of intense loneliness or emptiness 3) Recurrent negative thoughts about life without the deceased or recurrent urge to join the deceased 4) Preoccupying thoughts about the deceased that impair daily functioning |
| Thoughts | The patient has ≥2 of the following 8 symptoms: 1) Rumination about circumstances of the death 2) Frequent disbelief or inability to accept the death |
| Feelings | 3) Persistent feeling of being shocked, stunned, or emotionally numb since the death 4) Recurrent feelings of anger or bitterness regarding the death 5) Difficulty trusting or caring about others since the loss 6) Experiencing pain or other somatic symptoms the deceased person had, hearing the voice of the deceased, or seeing the deceased person 7) Intense emotional reactions to memories of the deceased |
| Behaviors | 8) Excessive avoidance or excessive preoccupation with places, people, and things related to the deceased or death |
| Source: Adapted from reference 6 | |
Assessing CG symptoms
Among those with persistent elevated distress, a CG diagnosis must be considered in the context of the individual’s social and cultural environment, time since the loss, and duration of symptoms. The hallmark symptom of CG is separation distress with a focus of cognitive, behavioral, and emotional symptoms on the loss and its consequences. CG is associated with substantial distress, functional impairment, and an increased risk for suicide. See the Box for a case study.
Many individuals with CG remain undiagnosed and untreated for years despite high levels of distress and impairment and high risk for negative consequences such as suicide.7 Accordingly, there’s a need for greater CG screening. Clinically useful tools for assessing CG include a brief, 5-item dimensional screening assessment6 and the patient-rated Inventory of Complicated Grief.8
Distinguishing complicated and uncomplicated grief. Exhibiting CG symptoms in the first several months after a loss does not mean an individual has or will develop CG. Most bereaved adults report painful thoughts and emotions in the weeks and months following the loss, including distressed yearning, waves of intense grief, persistent and intrusive thoughts, images related to the death, somatic distress, and a feeling of being disconnected from others. For most individuals, the intensity of this response diminishes within 6 to 18 months after the loved one’s death.5 Although the optimal length of time to wait before establishing a diagnosis remains debatable, the earliest CG should be diagnosed is 6 months after a loss.
It’s common for grief to occasionally rise in intensity for days or weeks. This surge may occur many months or years after the loss, even in people who exhibited relatively little distress or impairment. In particular, anniversaries, holidays, or periods of stress may trigger increased grief intensity. However, these surges typically subside naturally within a short time. Accordingly, CG should be diagnosed only when symptoms persist for >1 month.
CG vs other post-loss disorders. CG, major depressive disorder (MDD), and posttraumatic stress disorder (PTSD) often are comorbid in bereaved adults. Simon et al9 found 72% of CG patients in a treatment- seeking sample reported a lifetime history of MDD and 53% reported a lifetime history of PTSD. However, CG can be distinguished from these disorders. In the same study, 25% of CG patients had no other axis I diagnosis.9 After accounting for comorbid disorders, researchers associated CG severity with work and social impairment. These findings provide clear evidence for the incremental validity of CG—ie, a CG diagnosis gives clinicians additional information that predicts impairment above and beyond other disorders. However, future research needs to further examine CG and its overlap and differentiation from MDD and PTSD.
Distinguishing CG and MDD. Intense yearning or preoccupation with the deceased is a common symptom of CG but not MDD. In addition, CG symptoms possess intentionality. For example, emotional distress such as sadness and anger are prominent features of both CG and MDD. However, in CG, these symptoms are specific to the loss or circumstances of the loss, whereas in MDD they generally are more nebulous and generalized. Similarly, CG entails proximity seeking related to the deceased, and avoidance of reminders of the deceased, whereas MDD includes a more general social withdrawal and anhedonia.
Distinguishing CG and PTSD. CG and loss-related PTSD are distinguished by the predominant emotions and focus of concern associated with each disorder. The predominant emotion in PTSD is fear, whereas in CG it is sadness and longing. In PTSD, intrusive thoughts and memories associated with the trauma generally are associated with the event itself and produce an ongoing sense of threat.10 Avoidance in PTSD is intended to reduce this threat feeling. By contrast, in CG, intrusive memories focus on the deceased or the circumstances of the death, and avoidance is aimed at preventing painful reminders of the loss or its permanence. Importantly, both syndromes may be present.
Mr. C, age 67, presents to a local emergency department (ED) with his daughter. His daughter reports that he has not been himself since his wife died in a car accident 2 years ago. He continues to live in the house he shared with his wife, despite not needing the extra space and being unable to maintain it. Although Mr. C and his daughter used to talk about her mother a great deal, she says she now tries to avoid the subject because it upsets him. More recently she became concerned when Mr. C began to tell her that his life was meaningless without his wife. He said he frequently thinks about taking his own life to end his pain and loneliness.
Mr. C tells the ED psychiatrist he feels an intense wave of grief and loneliness every morning when he realizes his wife is not with him. He often stays in bed for hours, longing for her and thinking about their time together. At times, he thinks he hears her voice downstairs but when he searches for her, she is not there. Mr. C has been unable to go through his wife’s belongings, and feels nothing should be moved in their home. He will look at her photos, yet avoids other reminders of her (eg, partaking in their favorite hobbies, going to their favorite restaurants). He feels bitter and angry about his wife’s death, and becomes agitated when describing the car accident that took her life. Mr. C feels guilty for not being with his wife when she died. He assures the psychiatrist that he loves his children, but says he feels increasingly distant from them and doesn’t understand how they can move on after their mother’s death.
Mr. C reports symptoms consistent with a diagnosis of complicated grief. Further assessment is appropriate to determine if his symptoms are severe enough to warrant treatment.
Treating CG
When is treatment indicated? For years, bereavement theorists emphasized the need to work through emotions and memories related to the deceased with particular focus on negative material. However, evidence suggests that universal application of treatment to all bereaved individuals is unhelpful. In a recent meta-analysis, Neimeyer et al11 found that the outcomes of grief therapy applied indiscriminately to all bereaved adults or all members of high-risk populations—such as parents whose child experienced a violent death—were no better than would be expected by the passage of time. In contrast, grief therapy applied only to those who develop elevated and persistent distress (eg, CG) led to greater and more enduring improvement in post-loss distress than was observed in control conditions.
These results suggest that most grieving individuals who do not meet criteria for CG (or other psychiatric disorders) will not require intervention. Those who do seek treatment for grief-related distress in the acute grief period should be assessed for bereavement-related depression, anxiety, and suicidality, and treated or referred to professional or community-based resources for support or counseling as clinically indicated.
Evidence for psychotherapy. For those who meet CG criteria, psychotherapy targeting the specific symptoms of CG is helpful. The evidence is strongest for CG treatment (CGT), a 16-session, manualized psychotherapy developed by M. Katherine Shear, MD.12 CGT is based on an attachment model and cognitive-behavioral therapy (CBT) principles, and is informed by the dual-process theory proposed by Stroebe et al.13 According to this theory, natural healing following loss comprises 2 processes:
- a loss-oriented process in which the patient comes to terms with the loss, and
- a restoration-oriented process in which the patient reinvigorates a sense of purpose and meaning in life without the deceased.
CGT focuses on both processes. To address the former, it includes clinician-guided exercises in which the patient revisits the time of the death and planned activities in which the patient reengages with people, places, or thoughts that remind him or her of the deceased. CGT aims to allow the patient to gain an increased tolerance of the distressing thoughts and emotions associated with the loss so that these thoughts can be processed and the finality of the death and its circumstances can be accepted.
The restoration process is addressed by having patients generate and discuss personal goals and aspirations for the near and distant future, as well as scheduling pleasurable and rewarding events. This is accomplished by having patients imagine what they would want for themselves if their grief was less intense and planning concrete steps to take toward these goals. The restoration-oriented process is addressed concurrent with the loss-oriented process to encourage the oscillation between processes thought to be characteristic of a natural healing process following the loss of a loved one.
Other psychotherapy approaches (eg, support groups) may have a role for some individuals, and future research may suggest alternative approaches to CGT. To date, CGT is the most targeted evidence-based psychotherapy with randomized controlled data supporting its use in CG.
Pharmacotherapy for CG. Early research suggested that antidepressants—in particular tricyclics—may effectively reduce depressive symptoms in bereavement-related depression; their effect on CG symptoms, however, may not be as strong.14 Research on pharmacologic treatment that targets CG symptoms is developing. Because of the overlap between CG, PTSD, and MDD, researchers have hypothesized that antidepressants may be effective. Two open-label studies reported that the selective serotonin reuptake inhibitor (SSRI) escitalopram may be effective for CG.15,16 Although a post-hoc comparison of paroxetine and nortriptyline17 showed significant reduction in CG and depressive symptoms with both agents, effects could not be separated from concomitant psychotherapy. Furthermore, an examination of naturalistic data on combining antidepressants with CGT suggested that antidepressants may improve outcomes for individuals receiving CGT.18 A multicenter, randomized controlled trial funded by the National Institute of Mental Health is examining the potential efficacy of citalopram, an SSRI, alone or in combination with CGT.19
The efficacy of benzodiazepines, which commonly are prescribed for bereaved individuals, has not been assessed in CG. However, recent research suggests they may not be useful for medically managing recent grief20 and that their use in the aftermath of a loss may lead to long-term dependence in geriatric patients.21
Related Resources
- Center for Anxiety and Traumatic Stress Disorders. Massachusetts General Hospital. www.bostongrief.com.
- Zisook S, Shear K. Grief and bereavement: what psychiatrists need to know. World Psychiatry. 2009;8(2):67-74.
- Bonanno G. The other side of sadness: what the new science of bereavement tells us about loss. New York, NY: Basic Books; 2009.
Drug Brand Names
- Citalopram • Celexa
- Nortriptyline • Aventyl, Pamelor
- Escitalopram • Lexapro
- Paroxetine • Paxil
Disclosures
Dr. Simon receives grant or research support from the American Cancer Society, the American Foundation for Suicide Prevention, the Department of Defense, Forest Laboratories, and the National Institute of Mental Health.
1. Kochanek KD, Xu J, Murphy SL, et al. U.S. Department of Health and Human Services. Deaths: preliminary data for 2009. http://www.cdc.gov/nchs/data/nvsr/nvsr59/nvsr59_04.pdf. Published March 16 2011. Accessed June 19, 2012.
2. American Psychiatric Association. Trauma- and stressor-related disorders. http://www.dsm5.org/ProposedRevision/Pages/TraumaandStressorRelatedDisorders.aspx. Accessed June 19 2012.
3. Bonanno GA, Kaltman S. Toward an integrative perspective on bereavement. Psychol Bull. 1999;125(6):760-776.
4. Bonanno GA, Keltner D. Facial expressions of emotion and the course of conjugal bereavement. J Abnorm Psychol. 1997;106(1):126-137.
5. Bonanno GA, Wortman CB, Lehman DR, et al. Resilience to loss and chronic grief: a prospective study from preloss to 18-months postloss. J Pers Soc Psychol. 2002;83(5):1150-1164.
6. Shear MK, Simon N, Wall M, et al. Complicated grief and related bereavement issues for DSM-5. Depress Anxiety. 2011;28(2):103-117.
7. Boelen PA, Prigerson HG. The influence of symptoms of prolonged grief disorder depression, and anxiety on quality of life among bereaved adults: a prospective study. Eur Arch Psychiatry Clin Neurosci. 2007;257(8):444-452.
8. Prigerson HG, Maciejewski PK, Reynolds CF, 3rd, et al. Inventory of Complicated Grief: a scale to measure maladaptive symptoms of loss. Psychiatry Res. 1995;59 (1-2):65-79.
9. Simon NM, Shear KM, Thompson EH, et al. The prevalence and correlates of psychiatric comorbidity in individuals with complicated grief. Compr Psychiatry. 2007;48(5):395-399.
10. Brewin CR, Holmes EA. Psychological theories of posttraumatic stress disorder. Clin Psychol Rev. 2003;23(3):339-376.
11. Neimeyer RA, Currier JM. Grief therapy: evidence of efficacy and emerging directions. Curr Dir Psychol Sci. 2009;18(6):352-356.
12. Shear K, Frank E, Houck PR, et al. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293(21):2601-2608.
13. Stroebe M, Schut H. The dual process model of coping with bereavement: rationale and description. Death Stud. 1999;23(3):197-224.
14. Reynolds CF, 3rd, Miller MD, Pasternak RE, et al. Treatment of bereavement-related major depressive episodes in later life: a controlled study of acute and continuation treatment with nortriptyline and interpersonal psychotherapy. Am J Psychiatry. 1999;156(2):202-208.
15. Simon NM, Thompson EH, Pollack MH, et al. Complicated grief: a case series using escitalopram. Am J Psychiatry. 2007;164(11):1760-1761.
16. Hensley PL, Slonimski CK, Uhlenhuth EH, et al. Escitalopram: an open-label study of bereavement-related depression and grief. J Affect Disord. 2009;113(1-2):142-149.
17. Zygmont M, Prigerson HG, Houck PR, et al. A post hoc comparison of paroxetine and nortriptyline for symptoms of traumatic grief. J Clin Psychiatry. 1998;59(5):241-245.
18. Simon NM, Shear MK, Fagiolini A, et al. Impact of concurrent naturalistic pharmacotherapy on psychotherapy of complicated grief. Psychiatry Res. 2008;159(1-2):31-36.
19. U.S. National Institutes of Health. A study of medication with or without psychotherapy for complicated grief (HEAL). http://clinicaltrials.gov/ct2/show/NCT01179568. Published June 24, 2012. Accessed June 25, 2012.
20. Warner J, Metcalfe C, King M. Evaluating the use of benzodiazepines following recent bereavement. Br J Psychiatry. 2001;178(1):36-41.
21. Cook JM, Biyanova T, Marshall R. Medicating grief with benzodiazepines: physician and patient perspectives. Arch Intern Med. 2007;167(18):2006-2007.
1. Kochanek KD, Xu J, Murphy SL, et al. U.S. Department of Health and Human Services. Deaths: preliminary data for 2009. http://www.cdc.gov/nchs/data/nvsr/nvsr59/nvsr59_04.pdf. Published March 16 2011. Accessed June 19, 2012.
2. American Psychiatric Association. Trauma- and stressor-related disorders. http://www.dsm5.org/ProposedRevision/Pages/TraumaandStressorRelatedDisorders.aspx. Accessed June 19 2012.
3. Bonanno GA, Kaltman S. Toward an integrative perspective on bereavement. Psychol Bull. 1999;125(6):760-776.
4. Bonanno GA, Keltner D. Facial expressions of emotion and the course of conjugal bereavement. J Abnorm Psychol. 1997;106(1):126-137.
5. Bonanno GA, Wortman CB, Lehman DR, et al. Resilience to loss and chronic grief: a prospective study from preloss to 18-months postloss. J Pers Soc Psychol. 2002;83(5):1150-1164.
6. Shear MK, Simon N, Wall M, et al. Complicated grief and related bereavement issues for DSM-5. Depress Anxiety. 2011;28(2):103-117.
7. Boelen PA, Prigerson HG. The influence of symptoms of prolonged grief disorder depression, and anxiety on quality of life among bereaved adults: a prospective study. Eur Arch Psychiatry Clin Neurosci. 2007;257(8):444-452.
8. Prigerson HG, Maciejewski PK, Reynolds CF, 3rd, et al. Inventory of Complicated Grief: a scale to measure maladaptive symptoms of loss. Psychiatry Res. 1995;59 (1-2):65-79.
9. Simon NM, Shear KM, Thompson EH, et al. The prevalence and correlates of psychiatric comorbidity in individuals with complicated grief. Compr Psychiatry. 2007;48(5):395-399.
10. Brewin CR, Holmes EA. Psychological theories of posttraumatic stress disorder. Clin Psychol Rev. 2003;23(3):339-376.
11. Neimeyer RA, Currier JM. Grief therapy: evidence of efficacy and emerging directions. Curr Dir Psychol Sci. 2009;18(6):352-356.
12. Shear K, Frank E, Houck PR, et al. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293(21):2601-2608.
13. Stroebe M, Schut H. The dual process model of coping with bereavement: rationale and description. Death Stud. 1999;23(3):197-224.
14. Reynolds CF, 3rd, Miller MD, Pasternak RE, et al. Treatment of bereavement-related major depressive episodes in later life: a controlled study of acute and continuation treatment with nortriptyline and interpersonal psychotherapy. Am J Psychiatry. 1999;156(2):202-208.
15. Simon NM, Thompson EH, Pollack MH, et al. Complicated grief: a case series using escitalopram. Am J Psychiatry. 2007;164(11):1760-1761.
16. Hensley PL, Slonimski CK, Uhlenhuth EH, et al. Escitalopram: an open-label study of bereavement-related depression and grief. J Affect Disord. 2009;113(1-2):142-149.
17. Zygmont M, Prigerson HG, Houck PR, et al. A post hoc comparison of paroxetine and nortriptyline for symptoms of traumatic grief. J Clin Psychiatry. 1998;59(5):241-245.
18. Simon NM, Shear MK, Fagiolini A, et al. Impact of concurrent naturalistic pharmacotherapy on psychotherapy of complicated grief. Psychiatry Res. 2008;159(1-2):31-36.
19. U.S. National Institutes of Health. A study of medication with or without psychotherapy for complicated grief (HEAL). http://clinicaltrials.gov/ct2/show/NCT01179568. Published June 24, 2012. Accessed June 25, 2012.
20. Warner J, Metcalfe C, King M. Evaluating the use of benzodiazepines following recent bereavement. Br J Psychiatry. 2001;178(1):36-41.
21. Cook JM, Biyanova T, Marshall R. Medicating grief with benzodiazepines: physician and patient perspectives. Arch Intern Med. 2007;167(18):2006-2007.