User login
Innovative Monitoring Technology
Treatment of hospitalized patients is becoming more and more complex as a result of rising patient age, multiple comorbidities, and more complex procedures, yet most are hospitalized in a non‐intensive care unit (non‐ICU) setting. With this rising complexity, a large proportion of hospital patients experience serious adverse events during their hospital stay, including cardiac arrest, respiratory failure, and shock, leading to unplanned admissions to the ICU, and death.1 For patients with unexpected clinical deterioration, delayed or suboptimal intervention is associated with increased morbidity and mortality.2, 3 This has prompted many hospitals to implement some form of a rapid response system (RRS) for early detection of clinical deterioration, and adequate response through rapid response teams (RRT).2, 4, 5 Still, evidence suggests that many of these systems are deficient in the detection and/or the response phase, and do not lead to the expected outcomes in terms of preventing critical events.6, 7
Researchers have established that patients frequently demonstrate clinical signs of deterioration hours before cardiac arrests or urgent transfers to ICUs.8, 9 The importance of timely interventions in many acute clinical conditions like sepsis, acute myocardial infarction, and stroke is also well established.1012 Taking these facts together with the observed shortcomings of most current rapid response systems has led experts to call for a shift of focus from the efferent limb of the RRS (the response team) to the afferent limb (the means of detecting patients at risk and obtaining help).13 A consensus conference held in 2008 emphasized the importance of accurate monitoring of vital signs for all hospitalized patients, and at the same time recommended, if practical and affordable, that all patients be monitored continuously by monitoring technology, which improves patient comfort, is easy to use, and reduces the number of false alerts.13
Technology applications that allow for continuous vital sign monitoring designed for non‐ICU settings may help hospitals achieve meaningful results by providing earlier detection of clinical deterioration, either when implemented as part of an RRS or as a stand‐alone system. To fit this description, monitors would have to be easy to use by the staff, impose little limitation on the patient, and be capable of trend analyses so that they minimize the incidence of false alerts and alert fatigue. We set out to investigate the capability of such a system to predict patient deterioration in a medical floor setting.
METHODS
Patients and Settings
We conducted a feasibility noninterventional study in two 36‐bed medicine units of two tertiary academic medical centers: Sheba Medical Center, Tel Hashomer, and Sapir Medical Center, Kfar Sababoth in Israel. The aim of the study was to define optimal cutoff values for vital signs alerts and define the accuracy of these alerts in predicting clinical deterioration. The study was approved beforehand by the independent Institutional Review Boards of both institutions.
The Earlysense system is a contactless continuous‐measurement monitor for heart rate (HR), respiration rate (RR), and bed motion. It is based on a piezoelectric sensor, sensitive to applied mechanical strain, which is placed under the patient's mattress and functions without the need for contact between patient and device. The Earlysense system was previously shown to measure accurately both HR and RR in sleep laboratory and general ICU settings.14
We chose to evaluate patients who were at increased risk for respiratory failure, which would enable us to capture more events in this study. We thus included, in the study population, patients hospitalized with an admitting diagnosis due to an acute respiratory condition including pneumonia, chronic obstructive pulmonary disease or asthma exacerbation, congestive heart failure with pulmonary edema or congestion, and patients who needed supplemental oxygen on admission. Patients were enrolled only if within the initial 24 hours of hospitalization in the study units. Dementia and inability to sign informed consent were exclusion criteria for enrollment in this study. Patients with a do not resuscitate order were not excluded from enrollment. Patient enrollment took place during the period of January to December of 2008 in Sheba Medical Center and July to November of 2008 in Sapir Medical Center. Since the study was noninterventional, and the Earlysense monitor did not produce alerts for the duration of this study, patients were still monitored by other monitoring devices, such as telemetry and pulse oximeter, as per clinical decision.
Following enrollment and informed consent, the Earlysense sensor was placed under the mattress and connected to the Earlysense bedside monitor that recorded the signals and the interpreted vital signs. The Earlysense system automatically started measuring respiratory rate, heart rate, and motion rate with no need for patient, nurse, or technician involvement, as long as the patient remained in bed. Since this was a noninterventional study, no alerts were produced from the Earlysense monitor, and floor staff was not trained to make clinical decisions based on vital sign data from the device. Patients were monitored for the full extent of their stay in the 2 medical departments. Since we had only 2 monitors at each site, in an attempt to enroll more patients, in cases where patients stayed for more than 2 weeks, a decision was made by the principal investigator whether to continue monitoring or disconnect the sensor and enroll another patient. This was based on an assessment of clinical stability and on how much longer patients were expected to stay in the unit, in an attempt to avoid a situation where a patient was utilizing 1 monitor for a very long period of time. Following patient discharge or discontinuation of the monitor, all data were downloaded to a central server for analysis. A full description of the contactless sensor and monitor was published previously.14, 15 The signal analysis determining the HR and RR from the motion waves is proprietary.
Clinical and Alert Definitions
Patients were followed for major clinical events during their hospitalization. A major clinical event was defined as any one of the following: 1) patient was transferred to an ICU (medical or cardiac); 2) patient was intubated and mechanically ventilated on the floor; or 3) patient had a cardiac arrest while in the unit.
Respiratory rate or heart rate alerts were based on vital sign readings recorded and analyzed retrospectively for this study. The Earlysense system performs signal processing in order to isolate the respiratory and the heart pulse patterns from the signal obtained by the piezoelectric sensor. Each 0.5 seconds, an updated HR reading is established based on analysis of the heart pulse pattern for the last 8 seconds, and an updated RR reading based on analysis of the last 1 minute of the respiration pattern. These specific time periods were intended to provide up‐to‐date HR and RR values, and still reduce possible false HR and RR readings caused by signal artifacts. For defining optimal cutoffs for alerts in an internal validation process, alerts were considered true‐positive if they were followed by a major clinical event within 24 hours. An alert was considered false‐positive (false alert) if no major clinical event occurred in the following 24 hours.
As a secondary outcome, we also analyzed 24‐hour trends to look for correlations with major clinical events. For trend analysis, we grouped together HR and RR readings for 6‐hour periods throughout the day in a running window fashion (data for the last 6 hours was clustered every 3 minutes). We then compared the median of the readings for each period with the corresponding period of the previous day. Post‐hoc alerts were generated when the difference (delta) between medians passed the threshold set. Only 6‐hour time windows with at least 420 valid RR or HR results were included in the analysis.
Data Analysis
In the data analysis, we excluded patients with less than 30 hours of monitoring, allowing us to evaluate the trend analysis for at least one comparable time window. We examined increasing possible cutoff values for the differences in median values that would best predict the clinical events. To find the best possible models, we performed a receiver operating characteristic (ROC) curve analysis. We looked for the optimal cutoff to yield the maximal sum of sensitivity plus specificity, and computed associated statistics (area under the curve [AUC]) and associated confidence interval; if the lower bound of interval was found to be above 0.5, the AUC was significantly different from chance. We determined a P value that tests the null hypothesis that the AUC really equals 0.5. A value below 0.05 was considered significant.
RESULTS
Of 149 patients monitored by the Earlysense system for this study, 113 had at least 30 hours of monitoring. The characteristics of these patients are presented in Table 1. Of these 113 patients, 9 had a major clinical event (8.0%), including 2 patients who were transferred to an ICU, 1 patient who was intubated and ventilated in the study unit and later had a cardiac arrest and died, and 6 more patients who developed cardiac arrest and died in the study units (overall, 10 major clinical events). Comparing patients with a major clinical event to patients without, we found no significant difference in age, gender, body mass index, or comorbidity (Charlson score), however, patients who had a clinical event stayed significantly longer than those without a clinical event (Table 1). On average, time from admission to the major clinical event was 11.6 days (range 228).
| All Patients | Patients Without a Major Clinical Event | Patients With a Major Clinical Event | P (t Test) | |
|---|---|---|---|---|
| ||||
| Patients | 113 | 104 | 9 | |
| Gender (% female) | 45.1 | 46.2 | 33.3 | 0.46 |
| Age, average SD | 69 18 | 69 18.5 | 69 16.4 | 0.99 |
| Body mass index, average (range) | 27 (1752.7) | 27.1 (1752.7) | 25.2 (17.932) | 0.41 |
| Charlson comorbidity score | 1.58 | 1.55 | 1.99 | 0.64 |
| Length of stay (days), average SD | 7.3 5.9 | 6.9 6.0 | 11.9 7.8 | 0.02 |
| Primary diagnosis | ||||
| Pneumonia | 36 | 32 | 4 | |
| CHF | 33 | 31 | 2 | |
| COPD | 17 | 16 | 1 | |
| Other respiratory* | 27 | 25 | 2 | |
Overall, this study included a total of 8628 recording hours for the 113 patients we analyzed. Using the vital signs thresholds found to provide the highest sensitivity and specificity, we recorded 898 RR alerts (average frequency of 2.4 alerts per patient‐day) and 107 HR alerts (average frequency of 0.3 alerts per patient‐day). For the entire study, we have found 63 trend alerts (46 RR and 17 HR) when using thresholds for maximal sensitivity and specificity, at a frequency of 0.2 alerts per patient‐day.
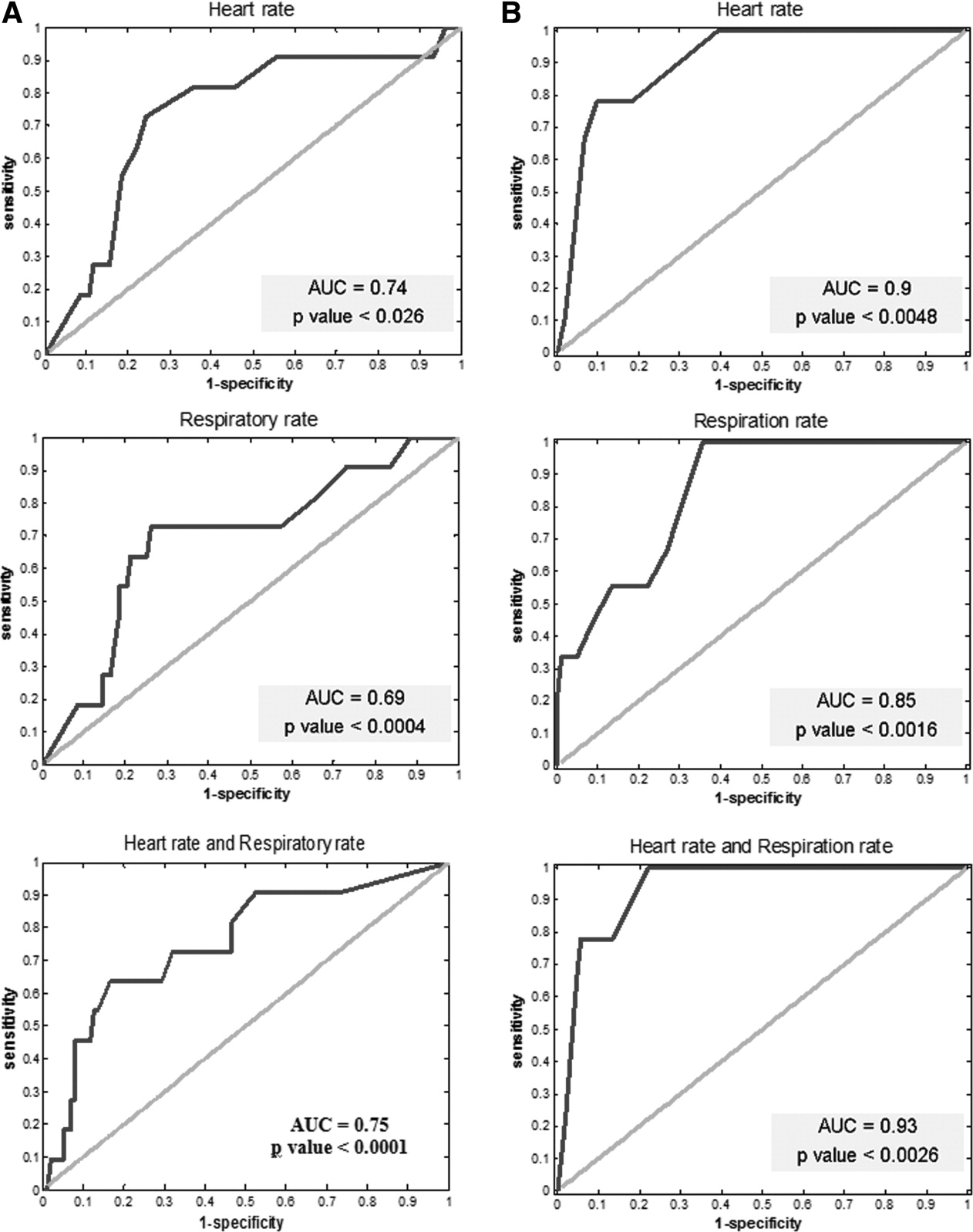
In Table 2, we summarize the sensitivity, specificity, positive predictive value, and negative predictive value of alerts in predicting a major clinical deterioration per patient for both the threshold alerts and the trend alerts. The cutoff values are those of optimal performance (maximal sensitivity plus specificity) along the ROC curves presented in Figure 1. The optimal cutoffs for the threshold alerts were HRs below 40 or above 115 beats/min, and RRs below 8 or above 40 breaths/min. For the trend alerts, when comparing between time periods, we found that a cutoff of a rise of 20 or more beats/min and 5 or more breaths/min corresponded with a maximal sensitivity and specificity, and we used these as the thresholds for the trending alerts.
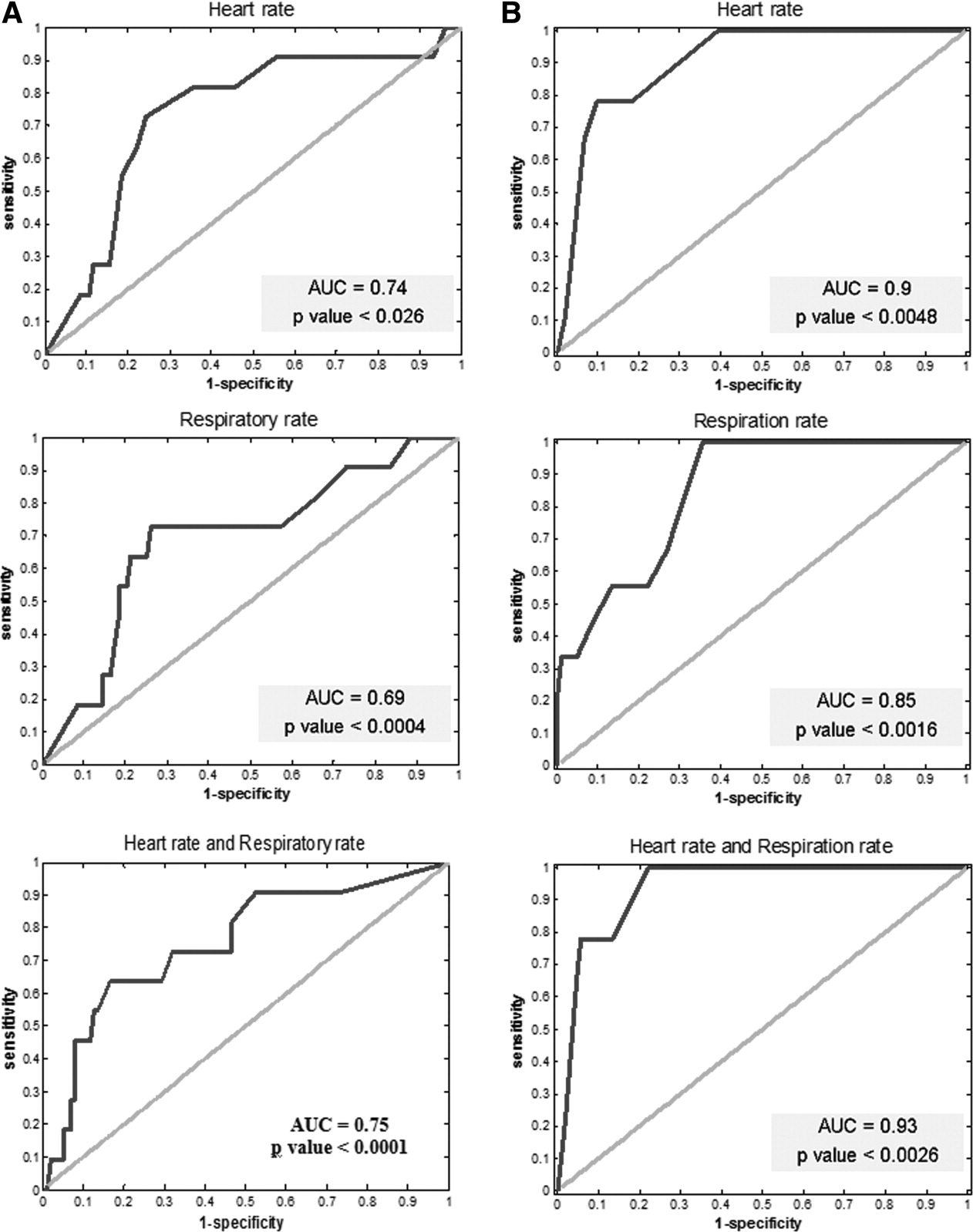
Optimal cutoffs were used when comparing time periods (20/min for HR and 5/min for RR) for maximal sum of sensitivity and specificity. Abbreviations: AUC, area under the curve.
| Sensitivity (%) | Specificity (%) | Positive Predictive Value (%) | Negative Predictive Value (%) | |
|---|---|---|---|---|
| ||||
| Threshold alerts | ||||
| HR* | 82 | 67 | 21 | 97 |
| RR | 64 | 81 | 26 | 95 |
| HR and RR | 55 | 94 | 50 | 95 |
| Trend alerts | ||||
| HR 20 | 78 | 90 | 41 | 97 |
| RR 5 | 100 | 64 | 20 | 100 |
| HR and RR | 78 | 94 | 54 | 98 |
For the determined alerts, out of the 10 clinical events, in 7 cases the alerts would have indicated the deterioration within more than 1 hour from the actual event and within 24 hours prior to the clinical event. In one case, the alert would have indicated the risk within less than 1 hour; in another case, within the 2448 hours window; and in the last case, the alerts would have done so more than 48 hours prior to the event (these last 2 cases were considered false‐negative for our post hoc analysis).
The ROC analysis for both the threshold alerts and the trend alerts for both HR and RR correlated well with the clinical events (P < 0.05 for all models) (Figure 1). When comparing the threshold alerts with the trend alerts, trend alerts had a higher AUC, suggesting that these would be more accurate in alerting for major clinical events. Specifically, the model for HR 6‐hour trend alerts demonstrated a larger AUC (0.9 and 0.85, respectively), while the combination of HR and RR had the largest AUC (0.93).
DISCUSSION
The development of monitoring systems designed for hospitalized patients on non‐ICU floors derives from the need to minimize preventable in‐hospital mortality. This study has explored one such possible solution. Through retrospective definition of optimal alert settings and internal validation within a derivation cohort, we have found the Earlysense monitor to be accurate in predicting major clinical deterioration by using both simple thresholds and a vital signs trend algorithm. We found that the post hoc determined alerts were relatively infrequent. We also found that trend alerts showed greater ability to accurately capture these deteriorations compared with simple alert thresholds, and that using a combination alert based on both HR and RR trends provided the highest accuracy and confidence for predicting clinical deterioration. These results suggest the advantages that smart alerts can bringincreasing sensitivity while lowering the alert burden and reducing the number of false alerts.
An effective and efficient patient monitoring system must be able to quickly detect acute life‐threatening events or subacute patient deterioration that will lead to a life‐threatening event; in addition, this system should have a low false‐positive rate (few false alerts). While a high sensitivity is desirable,16 this usually comes at the cost of lower specificity and higher false‐positive rates. Studies have found alerts from monitoring systems in an ICU and emergency department environment to be tremendously frequent and with an extremely high false‐positive rate.1721 Unsurprisingly, it has been reported that only about 10% of alerts are responded to by the clinical staff.22 In an attempt to improve alert relevancy and accuracy, newly designed integrated monitoring systems for ICUs use alert algorithms and trend analysis performed on data received from multiple vital signs monitors.2327 With the evident need to continuously monitor patients on hospital floors,13, 28 there is a clear gap to‐date in such experience and a need to study the implications for patients and staff as we try to optimize the monitoring tools for this environment.
As more emphasis is placed on the afferent limb of rapid response systems, we can expect to see a greater need for systems able to detect changes in clinical status that might lead to patient deterioration. The intermittent vital sign measurement performed by nurses and support staff on the floors is now regarded as inadequate by itself, because it may not be performed predictably, accurately, or completely.28 Continuous monitoring systems should complement manual intermittent vital signs monitoring and play an important role in bringing the nurse to the patient's side at the right time so that a complete assessment can be done.29, 30 There remains no substitution for a nurse evaluating the patient and making critical decisions based on his or her knowledge of the patient's condition.
While today, both electrocardiographic monitoring (telemetry) and continuous pulse oximetry provide some solution for the need for continuous monitoring on the floors, these carry disadvantages that prevent them from becoming the optimal solution. While telemetry is invaluable for higher risk cardiac patients, significant overuse of this application does occur,31 and most monitored patients gain little cardiac arrest survival benefits.32 Pulse oximetry, although regarded as one of the most important technological advancements in monitoring patients, carries important limitations that might prevent early detection of respiratory failure.33, 34 Furthermore, these 2 modalities require continuous contact of leads/sensors to the patient, a disadvantage when regarding monitoring for low/average risk patients on non‐ICU hospital floors. Related to these disadvantages, the results presented here might position the implementation of the Earlysense monitor as a preferred alternative.
This study has several important limitations. This was a retrospective noninterventional study limited to internal medicine patients. Our patients served as a derivation cohort, alert thresholds were set post hoc, and sensitivity and specificity were internally validated. It remains to be shown that the results shown here can be reproduced in a real‐time interventional study. We only included patients who were considered above average risk within medical wards, as we were hoping to capture more clinical deteriorations with a relatively small cohort. We cannot rule out that our results might be biased and may not similarly apply to all non‐ICU medical patients. Finally, the retrospective nature of this study did not allow us to assess other outcomes of appropriateness, such as staff objective assessment of alert appropriateness or change in clinical management as a result of an alert. When using these devices in the alert mode, alert thresholds may be changed by the clinical staff based on clinical judgment to further lower false alerts and alert frequency. We also did not collect information that could have allowed us to assess clinical usefulness of the alerts compared to routine clinical assessment. Documenting whether the clinical events were suspected beforehand by the clinical teams could have allowed us to assess clinical usefulness. Future interventional studies are needed to validate the Earlysense system prospectively in both medical and surgical floor settings, first using a common alert threshold alerting system and secondly using the smart trend alerts described here.
In conclusion, we found that the Earlysense monitor is able to continuously measure RR and HR, providing low alert frequency. The current study demonstrates the potential of this system to provide timely prediction of patient deterioration. Utilizing a smart trend algorithm has been shown to improve the device's accuracy and reduce associated alert burden and false‐positive alerts.
Acknowledgements
Disclosures: The study was funded by an industry grant provided by Earlysense LTD. Eyal Zimlichman, MD, MSc Ronen Rozenblum, PhD, MPH, and Jeffrey M. Rothschild, MD, MPH, have each received a research grant supported by Earlysense LTD. Martine Szyper‐Kravitz, MD, Avraham Unterman, MD, Howard Amital, MD, MHA, and Yehuda Shoenfeld, MD, report no conflicts of interest. Zvika Shinar, PhD, Tal Klap, and Shiraz Levkovich are employed by Earlysense LTD and are holding equity with the company.
- ,,,,,.Temporal trends in rates of patient harm resulting from medical care.N Engl J Med.2010;363(22):2124–2134.
- ,,, et al.Findings of the first consensus conference on medical emergency teams.Crit Care Med.2006;34(9):2463–2478.
- ,,,,.Inpatient transfers to the intensive care unit: delays are associated with increased mortality and morbidity.J Gen Intern Med.2003;18(2):77–83.
- ,,,,.Redefining in‐hospital resuscitation: the concept of the medical emergency team.Resuscitation.2001;48(2):105–110.
- Institute for Healthcare Improvement (IHI). Protecting 5 million lives from harm. Available at: www.ihi.org/ihi/programs/campaign. Accessed September 8,2011.
- ,,, et al.Introduction of the medical emergency team (MET) system: a cluster‐randomised controlled trial.Lancet.2005;365(9477):2091–2097.
- ,,,,.Rapid response teams: a systematic review and meta‐analysis.Arch Intern Med.2010;170(1):18–26.
- ,,,,,.Recognising clinical instability in hospital patients before cardiac arrest or unplanned admission to intensive care. A pilot study in a tertiary‐care hospital.Med J Aust.1999;171(1):22–25.
- ,,,,,.A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom—the ACADEMIA study.Resuscitation.2004;62(3):275–282.
- ,,, et al.Early goal‐directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med.2001;345(19):1368–1377.
- .Top ten list in myocardial infarction.Chest.2000;118(5):1477–1479.
- ,,, et al.Improvement in stroke mortality in Canada and the United States, 1990 to 2002.Circulation.2006;113(10):1335–1343.
- ,,, et al.“Identifying the hospitalised patient in crisis”—a consensus conference on the afferent limb of rapid response systems.Resuscitation.2010;81(4):375–382.
- ,,,.Contactless respiratory and heart rate monitoring: validation of an innovative tool.J Med Eng Technol.2010;35(7–8):393–398.
- ,,,,,.How is my patient doing? Evaluating hospitalized patients using continuous vital signs monitoring.Isr Med Assoc J.2009;11(6):382–394.
- ,,,,,.Medical device alarms.Biomed Tech (Berl).2011;56(2):73–83.
- ,.Poor prognosis for existing monitors in the intensive care unit.Crit Care Med.1997;25(4):614–619.
- .Crying wolf: false alarms in a pediatric intensive care unit.Crit Care Med.1994;22(6):981–985.
- ,,,,,.Intensive care unit alarms—how many do we need?Crit Care Med.2010;38(2):451–456.
- ,,,,.Alarmed: adverse events in low‐risk patients with chest pain receiving continuous electrocardiographic monitoring in the emergency department. A pilot study.Am J Emerg Med.2006;24(1):62–67.
- ,,,,,.Multicentric study of monitoring alarms in the adult intensive care unit (ICU): a descriptive analysis.Intensive Care Med.1999;25(12):1360–1366.
- .Alarms in the intensive care unit: how can the number of false alarms be reduced?Crit Care.2001;5(4):184–188.
- ,,,,,.Cardiorespiratory instability before and after implementing an integrated monitoring system.Crit Care Med.2011;39(1):65–72.
- ,,.Adaptive change detection in heart rate trend monitoring in anesthetized children.IEEE Trans Biomed Eng.2006;53(11):2211–2219.
- ,,,,,.Defining the incidence of cardiorespiratory instability in patients in step‐down units using an electronic integrated monitoring system.Arch Intern Med.2008;168(12):1300–1308.
- ,,, et al.Implementation of a real‐time computerized sepsis alert in nonintensive care unit patients.Crit Care Med.2011;39(3):469–473.
- ,,,,,.Early prediction of septic shock in hospitalized patients.J Hosp Med.2010;5(1):19–25.
- ,,.Rapid‐response teams.N Engl J Med.2011;365(2):139–146.
- ,,,.An analysis of the causes of adverse events from the Quality in Australian Health Care Study.Med J Aust.1999;170(9):411–415.
- ,.Taking your rapid response team to the next level. Society of Critical Care Medicine;2010. Available at: http://www.sccm.org/Publications/Critical_Connections/Archives/December‐2010/Pages/RapidResponseTeam.aspx. Accessed August 11,year="2011"2011.
- ,.Electrocardiographic monitoring in the hospitalized patient: a diagnostic intervention of uncertain clinical impact.Am J Emerg Med.2008;26(9):1047–1055.
- ,.Continuous electrocardiographic monitoring and cardiac arrest outcomes in 8,932 telemetry ward patients.Acad Emerg Med.2000;7(6):647–652.
- ,.The benefits and pitfalls of pulse oximetry.BMJ.1993;307(6902):457–458.
- ,.Patterns of unexpected in‐hospital deaths: a root cause analysis.Patient Saf Surg.2011;5(1):3.
Treatment of hospitalized patients is becoming more and more complex as a result of rising patient age, multiple comorbidities, and more complex procedures, yet most are hospitalized in a non‐intensive care unit (non‐ICU) setting. With this rising complexity, a large proportion of hospital patients experience serious adverse events during their hospital stay, including cardiac arrest, respiratory failure, and shock, leading to unplanned admissions to the ICU, and death.1 For patients with unexpected clinical deterioration, delayed or suboptimal intervention is associated with increased morbidity and mortality.2, 3 This has prompted many hospitals to implement some form of a rapid response system (RRS) for early detection of clinical deterioration, and adequate response through rapid response teams (RRT).2, 4, 5 Still, evidence suggests that many of these systems are deficient in the detection and/or the response phase, and do not lead to the expected outcomes in terms of preventing critical events.6, 7
Researchers have established that patients frequently demonstrate clinical signs of deterioration hours before cardiac arrests or urgent transfers to ICUs.8, 9 The importance of timely interventions in many acute clinical conditions like sepsis, acute myocardial infarction, and stroke is also well established.1012 Taking these facts together with the observed shortcomings of most current rapid response systems has led experts to call for a shift of focus from the efferent limb of the RRS (the response team) to the afferent limb (the means of detecting patients at risk and obtaining help).13 A consensus conference held in 2008 emphasized the importance of accurate monitoring of vital signs for all hospitalized patients, and at the same time recommended, if practical and affordable, that all patients be monitored continuously by monitoring technology, which improves patient comfort, is easy to use, and reduces the number of false alerts.13
Technology applications that allow for continuous vital sign monitoring designed for non‐ICU settings may help hospitals achieve meaningful results by providing earlier detection of clinical deterioration, either when implemented as part of an RRS or as a stand‐alone system. To fit this description, monitors would have to be easy to use by the staff, impose little limitation on the patient, and be capable of trend analyses so that they minimize the incidence of false alerts and alert fatigue. We set out to investigate the capability of such a system to predict patient deterioration in a medical floor setting.
METHODS
Patients and Settings
We conducted a feasibility noninterventional study in two 36‐bed medicine units of two tertiary academic medical centers: Sheba Medical Center, Tel Hashomer, and Sapir Medical Center, Kfar Sababoth in Israel. The aim of the study was to define optimal cutoff values for vital signs alerts and define the accuracy of these alerts in predicting clinical deterioration. The study was approved beforehand by the independent Institutional Review Boards of both institutions.
The Earlysense system is a contactless continuous‐measurement monitor for heart rate (HR), respiration rate (RR), and bed motion. It is based on a piezoelectric sensor, sensitive to applied mechanical strain, which is placed under the patient's mattress and functions without the need for contact between patient and device. The Earlysense system was previously shown to measure accurately both HR and RR in sleep laboratory and general ICU settings.14
We chose to evaluate patients who were at increased risk for respiratory failure, which would enable us to capture more events in this study. We thus included, in the study population, patients hospitalized with an admitting diagnosis due to an acute respiratory condition including pneumonia, chronic obstructive pulmonary disease or asthma exacerbation, congestive heart failure with pulmonary edema or congestion, and patients who needed supplemental oxygen on admission. Patients were enrolled only if within the initial 24 hours of hospitalization in the study units. Dementia and inability to sign informed consent were exclusion criteria for enrollment in this study. Patients with a do not resuscitate order were not excluded from enrollment. Patient enrollment took place during the period of January to December of 2008 in Sheba Medical Center and July to November of 2008 in Sapir Medical Center. Since the study was noninterventional, and the Earlysense monitor did not produce alerts for the duration of this study, patients were still monitored by other monitoring devices, such as telemetry and pulse oximeter, as per clinical decision.
Following enrollment and informed consent, the Earlysense sensor was placed under the mattress and connected to the Earlysense bedside monitor that recorded the signals and the interpreted vital signs. The Earlysense system automatically started measuring respiratory rate, heart rate, and motion rate with no need for patient, nurse, or technician involvement, as long as the patient remained in bed. Since this was a noninterventional study, no alerts were produced from the Earlysense monitor, and floor staff was not trained to make clinical decisions based on vital sign data from the device. Patients were monitored for the full extent of their stay in the 2 medical departments. Since we had only 2 monitors at each site, in an attempt to enroll more patients, in cases where patients stayed for more than 2 weeks, a decision was made by the principal investigator whether to continue monitoring or disconnect the sensor and enroll another patient. This was based on an assessment of clinical stability and on how much longer patients were expected to stay in the unit, in an attempt to avoid a situation where a patient was utilizing 1 monitor for a very long period of time. Following patient discharge or discontinuation of the monitor, all data were downloaded to a central server for analysis. A full description of the contactless sensor and monitor was published previously.14, 15 The signal analysis determining the HR and RR from the motion waves is proprietary.
Clinical and Alert Definitions
Patients were followed for major clinical events during their hospitalization. A major clinical event was defined as any one of the following: 1) patient was transferred to an ICU (medical or cardiac); 2) patient was intubated and mechanically ventilated on the floor; or 3) patient had a cardiac arrest while in the unit.
Respiratory rate or heart rate alerts were based on vital sign readings recorded and analyzed retrospectively for this study. The Earlysense system performs signal processing in order to isolate the respiratory and the heart pulse patterns from the signal obtained by the piezoelectric sensor. Each 0.5 seconds, an updated HR reading is established based on analysis of the heart pulse pattern for the last 8 seconds, and an updated RR reading based on analysis of the last 1 minute of the respiration pattern. These specific time periods were intended to provide up‐to‐date HR and RR values, and still reduce possible false HR and RR readings caused by signal artifacts. For defining optimal cutoffs for alerts in an internal validation process, alerts were considered true‐positive if they were followed by a major clinical event within 24 hours. An alert was considered false‐positive (false alert) if no major clinical event occurred in the following 24 hours.
As a secondary outcome, we also analyzed 24‐hour trends to look for correlations with major clinical events. For trend analysis, we grouped together HR and RR readings for 6‐hour periods throughout the day in a running window fashion (data for the last 6 hours was clustered every 3 minutes). We then compared the median of the readings for each period with the corresponding period of the previous day. Post‐hoc alerts were generated when the difference (delta) between medians passed the threshold set. Only 6‐hour time windows with at least 420 valid RR or HR results were included in the analysis.
Data Analysis
In the data analysis, we excluded patients with less than 30 hours of monitoring, allowing us to evaluate the trend analysis for at least one comparable time window. We examined increasing possible cutoff values for the differences in median values that would best predict the clinical events. To find the best possible models, we performed a receiver operating characteristic (ROC) curve analysis. We looked for the optimal cutoff to yield the maximal sum of sensitivity plus specificity, and computed associated statistics (area under the curve [AUC]) and associated confidence interval; if the lower bound of interval was found to be above 0.5, the AUC was significantly different from chance. We determined a P value that tests the null hypothesis that the AUC really equals 0.5. A value below 0.05 was considered significant.
RESULTS
Of 149 patients monitored by the Earlysense system for this study, 113 had at least 30 hours of monitoring. The characteristics of these patients are presented in Table 1. Of these 113 patients, 9 had a major clinical event (8.0%), including 2 patients who were transferred to an ICU, 1 patient who was intubated and ventilated in the study unit and later had a cardiac arrest and died, and 6 more patients who developed cardiac arrest and died in the study units (overall, 10 major clinical events). Comparing patients with a major clinical event to patients without, we found no significant difference in age, gender, body mass index, or comorbidity (Charlson score), however, patients who had a clinical event stayed significantly longer than those without a clinical event (Table 1). On average, time from admission to the major clinical event was 11.6 days (range 228).
| All Patients | Patients Without a Major Clinical Event | Patients With a Major Clinical Event | P (t Test) | |
|---|---|---|---|---|
| ||||
| Patients | 113 | 104 | 9 | |
| Gender (% female) | 45.1 | 46.2 | 33.3 | 0.46 |
| Age, average SD | 69 18 | 69 18.5 | 69 16.4 | 0.99 |
| Body mass index, average (range) | 27 (1752.7) | 27.1 (1752.7) | 25.2 (17.932) | 0.41 |
| Charlson comorbidity score | 1.58 | 1.55 | 1.99 | 0.64 |
| Length of stay (days), average SD | 7.3 5.9 | 6.9 6.0 | 11.9 7.8 | 0.02 |
| Primary diagnosis | ||||
| Pneumonia | 36 | 32 | 4 | |
| CHF | 33 | 31 | 2 | |
| COPD | 17 | 16 | 1 | |
| Other respiratory* | 27 | 25 | 2 | |
Overall, this study included a total of 8628 recording hours for the 113 patients we analyzed. Using the vital signs thresholds found to provide the highest sensitivity and specificity, we recorded 898 RR alerts (average frequency of 2.4 alerts per patient‐day) and 107 HR alerts (average frequency of 0.3 alerts per patient‐day). For the entire study, we have found 63 trend alerts (46 RR and 17 HR) when using thresholds for maximal sensitivity and specificity, at a frequency of 0.2 alerts per patient‐day.
In Table 2, we summarize the sensitivity, specificity, positive predictive value, and negative predictive value of alerts in predicting a major clinical deterioration per patient for both the threshold alerts and the trend alerts. The cutoff values are those of optimal performance (maximal sensitivity plus specificity) along the ROC curves presented in Figure 1. The optimal cutoffs for the threshold alerts were HRs below 40 or above 115 beats/min, and RRs below 8 or above 40 breaths/min. For the trend alerts, when comparing between time periods, we found that a cutoff of a rise of 20 or more beats/min and 5 or more breaths/min corresponded with a maximal sensitivity and specificity, and we used these as the thresholds for the trending alerts.
Optimal cutoffs were used when comparing time periods (20/min for HR and 5/min for RR) for maximal sum of sensitivity and specificity. Abbreviations: AUC, area under the curve.
| Sensitivity (%) | Specificity (%) | Positive Predictive Value (%) | Negative Predictive Value (%) | |
|---|---|---|---|---|
| ||||
| Threshold alerts | ||||
| HR* | 82 | 67 | 21 | 97 |
| RR | 64 | 81 | 26 | 95 |
| HR and RR | 55 | 94 | 50 | 95 |
| Trend alerts | ||||
| HR 20 | 78 | 90 | 41 | 97 |
| RR 5 | 100 | 64 | 20 | 100 |
| HR and RR | 78 | 94 | 54 | 98 |
For the determined alerts, out of the 10 clinical events, in 7 cases the alerts would have indicated the deterioration within more than 1 hour from the actual event and within 24 hours prior to the clinical event. In one case, the alert would have indicated the risk within less than 1 hour; in another case, within the 2448 hours window; and in the last case, the alerts would have done so more than 48 hours prior to the event (these last 2 cases were considered false‐negative for our post hoc analysis).
The ROC analysis for both the threshold alerts and the trend alerts for both HR and RR correlated well with the clinical events (P < 0.05 for all models) (Figure 1). When comparing the threshold alerts with the trend alerts, trend alerts had a higher AUC, suggesting that these would be more accurate in alerting for major clinical events. Specifically, the model for HR 6‐hour trend alerts demonstrated a larger AUC (0.9 and 0.85, respectively), while the combination of HR and RR had the largest AUC (0.93).
DISCUSSION
The development of monitoring systems designed for hospitalized patients on non‐ICU floors derives from the need to minimize preventable in‐hospital mortality. This study has explored one such possible solution. Through retrospective definition of optimal alert settings and internal validation within a derivation cohort, we have found the Earlysense monitor to be accurate in predicting major clinical deterioration by using both simple thresholds and a vital signs trend algorithm. We found that the post hoc determined alerts were relatively infrequent. We also found that trend alerts showed greater ability to accurately capture these deteriorations compared with simple alert thresholds, and that using a combination alert based on both HR and RR trends provided the highest accuracy and confidence for predicting clinical deterioration. These results suggest the advantages that smart alerts can bringincreasing sensitivity while lowering the alert burden and reducing the number of false alerts.
An effective and efficient patient monitoring system must be able to quickly detect acute life‐threatening events or subacute patient deterioration that will lead to a life‐threatening event; in addition, this system should have a low false‐positive rate (few false alerts). While a high sensitivity is desirable,16 this usually comes at the cost of lower specificity and higher false‐positive rates. Studies have found alerts from monitoring systems in an ICU and emergency department environment to be tremendously frequent and with an extremely high false‐positive rate.1721 Unsurprisingly, it has been reported that only about 10% of alerts are responded to by the clinical staff.22 In an attempt to improve alert relevancy and accuracy, newly designed integrated monitoring systems for ICUs use alert algorithms and trend analysis performed on data received from multiple vital signs monitors.2327 With the evident need to continuously monitor patients on hospital floors,13, 28 there is a clear gap to‐date in such experience and a need to study the implications for patients and staff as we try to optimize the monitoring tools for this environment.
As more emphasis is placed on the afferent limb of rapid response systems, we can expect to see a greater need for systems able to detect changes in clinical status that might lead to patient deterioration. The intermittent vital sign measurement performed by nurses and support staff on the floors is now regarded as inadequate by itself, because it may not be performed predictably, accurately, or completely.28 Continuous monitoring systems should complement manual intermittent vital signs monitoring and play an important role in bringing the nurse to the patient's side at the right time so that a complete assessment can be done.29, 30 There remains no substitution for a nurse evaluating the patient and making critical decisions based on his or her knowledge of the patient's condition.
While today, both electrocardiographic monitoring (telemetry) and continuous pulse oximetry provide some solution for the need for continuous monitoring on the floors, these carry disadvantages that prevent them from becoming the optimal solution. While telemetry is invaluable for higher risk cardiac patients, significant overuse of this application does occur,31 and most monitored patients gain little cardiac arrest survival benefits.32 Pulse oximetry, although regarded as one of the most important technological advancements in monitoring patients, carries important limitations that might prevent early detection of respiratory failure.33, 34 Furthermore, these 2 modalities require continuous contact of leads/sensors to the patient, a disadvantage when regarding monitoring for low/average risk patients on non‐ICU hospital floors. Related to these disadvantages, the results presented here might position the implementation of the Earlysense monitor as a preferred alternative.
This study has several important limitations. This was a retrospective noninterventional study limited to internal medicine patients. Our patients served as a derivation cohort, alert thresholds were set post hoc, and sensitivity and specificity were internally validated. It remains to be shown that the results shown here can be reproduced in a real‐time interventional study. We only included patients who were considered above average risk within medical wards, as we were hoping to capture more clinical deteriorations with a relatively small cohort. We cannot rule out that our results might be biased and may not similarly apply to all non‐ICU medical patients. Finally, the retrospective nature of this study did not allow us to assess other outcomes of appropriateness, such as staff objective assessment of alert appropriateness or change in clinical management as a result of an alert. When using these devices in the alert mode, alert thresholds may be changed by the clinical staff based on clinical judgment to further lower false alerts and alert frequency. We also did not collect information that could have allowed us to assess clinical usefulness of the alerts compared to routine clinical assessment. Documenting whether the clinical events were suspected beforehand by the clinical teams could have allowed us to assess clinical usefulness. Future interventional studies are needed to validate the Earlysense system prospectively in both medical and surgical floor settings, first using a common alert threshold alerting system and secondly using the smart trend alerts described here.
In conclusion, we found that the Earlysense monitor is able to continuously measure RR and HR, providing low alert frequency. The current study demonstrates the potential of this system to provide timely prediction of patient deterioration. Utilizing a smart trend algorithm has been shown to improve the device's accuracy and reduce associated alert burden and false‐positive alerts.
Acknowledgements
Disclosures: The study was funded by an industry grant provided by Earlysense LTD. Eyal Zimlichman, MD, MSc Ronen Rozenblum, PhD, MPH, and Jeffrey M. Rothschild, MD, MPH, have each received a research grant supported by Earlysense LTD. Martine Szyper‐Kravitz, MD, Avraham Unterman, MD, Howard Amital, MD, MHA, and Yehuda Shoenfeld, MD, report no conflicts of interest. Zvika Shinar, PhD, Tal Klap, and Shiraz Levkovich are employed by Earlysense LTD and are holding equity with the company.
Treatment of hospitalized patients is becoming more and more complex as a result of rising patient age, multiple comorbidities, and more complex procedures, yet most are hospitalized in a non‐intensive care unit (non‐ICU) setting. With this rising complexity, a large proportion of hospital patients experience serious adverse events during their hospital stay, including cardiac arrest, respiratory failure, and shock, leading to unplanned admissions to the ICU, and death.1 For patients with unexpected clinical deterioration, delayed or suboptimal intervention is associated with increased morbidity and mortality.2, 3 This has prompted many hospitals to implement some form of a rapid response system (RRS) for early detection of clinical deterioration, and adequate response through rapid response teams (RRT).2, 4, 5 Still, evidence suggests that many of these systems are deficient in the detection and/or the response phase, and do not lead to the expected outcomes in terms of preventing critical events.6, 7
Researchers have established that patients frequently demonstrate clinical signs of deterioration hours before cardiac arrests or urgent transfers to ICUs.8, 9 The importance of timely interventions in many acute clinical conditions like sepsis, acute myocardial infarction, and stroke is also well established.1012 Taking these facts together with the observed shortcomings of most current rapid response systems has led experts to call for a shift of focus from the efferent limb of the RRS (the response team) to the afferent limb (the means of detecting patients at risk and obtaining help).13 A consensus conference held in 2008 emphasized the importance of accurate monitoring of vital signs for all hospitalized patients, and at the same time recommended, if practical and affordable, that all patients be monitored continuously by monitoring technology, which improves patient comfort, is easy to use, and reduces the number of false alerts.13
Technology applications that allow for continuous vital sign monitoring designed for non‐ICU settings may help hospitals achieve meaningful results by providing earlier detection of clinical deterioration, either when implemented as part of an RRS or as a stand‐alone system. To fit this description, monitors would have to be easy to use by the staff, impose little limitation on the patient, and be capable of trend analyses so that they minimize the incidence of false alerts and alert fatigue. We set out to investigate the capability of such a system to predict patient deterioration in a medical floor setting.
METHODS
Patients and Settings
We conducted a feasibility noninterventional study in two 36‐bed medicine units of two tertiary academic medical centers: Sheba Medical Center, Tel Hashomer, and Sapir Medical Center, Kfar Sababoth in Israel. The aim of the study was to define optimal cutoff values for vital signs alerts and define the accuracy of these alerts in predicting clinical deterioration. The study was approved beforehand by the independent Institutional Review Boards of both institutions.
The Earlysense system is a contactless continuous‐measurement monitor for heart rate (HR), respiration rate (RR), and bed motion. It is based on a piezoelectric sensor, sensitive to applied mechanical strain, which is placed under the patient's mattress and functions without the need for contact between patient and device. The Earlysense system was previously shown to measure accurately both HR and RR in sleep laboratory and general ICU settings.14
We chose to evaluate patients who were at increased risk for respiratory failure, which would enable us to capture more events in this study. We thus included, in the study population, patients hospitalized with an admitting diagnosis due to an acute respiratory condition including pneumonia, chronic obstructive pulmonary disease or asthma exacerbation, congestive heart failure with pulmonary edema or congestion, and patients who needed supplemental oxygen on admission. Patients were enrolled only if within the initial 24 hours of hospitalization in the study units. Dementia and inability to sign informed consent were exclusion criteria for enrollment in this study. Patients with a do not resuscitate order were not excluded from enrollment. Patient enrollment took place during the period of January to December of 2008 in Sheba Medical Center and July to November of 2008 in Sapir Medical Center. Since the study was noninterventional, and the Earlysense monitor did not produce alerts for the duration of this study, patients were still monitored by other monitoring devices, such as telemetry and pulse oximeter, as per clinical decision.
Following enrollment and informed consent, the Earlysense sensor was placed under the mattress and connected to the Earlysense bedside monitor that recorded the signals and the interpreted vital signs. The Earlysense system automatically started measuring respiratory rate, heart rate, and motion rate with no need for patient, nurse, or technician involvement, as long as the patient remained in bed. Since this was a noninterventional study, no alerts were produced from the Earlysense monitor, and floor staff was not trained to make clinical decisions based on vital sign data from the device. Patients were monitored for the full extent of their stay in the 2 medical departments. Since we had only 2 monitors at each site, in an attempt to enroll more patients, in cases where patients stayed for more than 2 weeks, a decision was made by the principal investigator whether to continue monitoring or disconnect the sensor and enroll another patient. This was based on an assessment of clinical stability and on how much longer patients were expected to stay in the unit, in an attempt to avoid a situation where a patient was utilizing 1 monitor for a very long period of time. Following patient discharge or discontinuation of the monitor, all data were downloaded to a central server for analysis. A full description of the contactless sensor and monitor was published previously.14, 15 The signal analysis determining the HR and RR from the motion waves is proprietary.
Clinical and Alert Definitions
Patients were followed for major clinical events during their hospitalization. A major clinical event was defined as any one of the following: 1) patient was transferred to an ICU (medical or cardiac); 2) patient was intubated and mechanically ventilated on the floor; or 3) patient had a cardiac arrest while in the unit.
Respiratory rate or heart rate alerts were based on vital sign readings recorded and analyzed retrospectively for this study. The Earlysense system performs signal processing in order to isolate the respiratory and the heart pulse patterns from the signal obtained by the piezoelectric sensor. Each 0.5 seconds, an updated HR reading is established based on analysis of the heart pulse pattern for the last 8 seconds, and an updated RR reading based on analysis of the last 1 minute of the respiration pattern. These specific time periods were intended to provide up‐to‐date HR and RR values, and still reduce possible false HR and RR readings caused by signal artifacts. For defining optimal cutoffs for alerts in an internal validation process, alerts were considered true‐positive if they were followed by a major clinical event within 24 hours. An alert was considered false‐positive (false alert) if no major clinical event occurred in the following 24 hours.
As a secondary outcome, we also analyzed 24‐hour trends to look for correlations with major clinical events. For trend analysis, we grouped together HR and RR readings for 6‐hour periods throughout the day in a running window fashion (data for the last 6 hours was clustered every 3 minutes). We then compared the median of the readings for each period with the corresponding period of the previous day. Post‐hoc alerts were generated when the difference (delta) between medians passed the threshold set. Only 6‐hour time windows with at least 420 valid RR or HR results were included in the analysis.
Data Analysis
In the data analysis, we excluded patients with less than 30 hours of monitoring, allowing us to evaluate the trend analysis for at least one comparable time window. We examined increasing possible cutoff values for the differences in median values that would best predict the clinical events. To find the best possible models, we performed a receiver operating characteristic (ROC) curve analysis. We looked for the optimal cutoff to yield the maximal sum of sensitivity plus specificity, and computed associated statistics (area under the curve [AUC]) and associated confidence interval; if the lower bound of interval was found to be above 0.5, the AUC was significantly different from chance. We determined a P value that tests the null hypothesis that the AUC really equals 0.5. A value below 0.05 was considered significant.
RESULTS
Of 149 patients monitored by the Earlysense system for this study, 113 had at least 30 hours of monitoring. The characteristics of these patients are presented in Table 1. Of these 113 patients, 9 had a major clinical event (8.0%), including 2 patients who were transferred to an ICU, 1 patient who was intubated and ventilated in the study unit and later had a cardiac arrest and died, and 6 more patients who developed cardiac arrest and died in the study units (overall, 10 major clinical events). Comparing patients with a major clinical event to patients without, we found no significant difference in age, gender, body mass index, or comorbidity (Charlson score), however, patients who had a clinical event stayed significantly longer than those without a clinical event (Table 1). On average, time from admission to the major clinical event was 11.6 days (range 228).
| All Patients | Patients Without a Major Clinical Event | Patients With a Major Clinical Event | P (t Test) | |
|---|---|---|---|---|
| ||||
| Patients | 113 | 104 | 9 | |
| Gender (% female) | 45.1 | 46.2 | 33.3 | 0.46 |
| Age, average SD | 69 18 | 69 18.5 | 69 16.4 | 0.99 |
| Body mass index, average (range) | 27 (1752.7) | 27.1 (1752.7) | 25.2 (17.932) | 0.41 |
| Charlson comorbidity score | 1.58 | 1.55 | 1.99 | 0.64 |
| Length of stay (days), average SD | 7.3 5.9 | 6.9 6.0 | 11.9 7.8 | 0.02 |
| Primary diagnosis | ||||
| Pneumonia | 36 | 32 | 4 | |
| CHF | 33 | 31 | 2 | |
| COPD | 17 | 16 | 1 | |
| Other respiratory* | 27 | 25 | 2 | |
Overall, this study included a total of 8628 recording hours for the 113 patients we analyzed. Using the vital signs thresholds found to provide the highest sensitivity and specificity, we recorded 898 RR alerts (average frequency of 2.4 alerts per patient‐day) and 107 HR alerts (average frequency of 0.3 alerts per patient‐day). For the entire study, we have found 63 trend alerts (46 RR and 17 HR) when using thresholds for maximal sensitivity and specificity, at a frequency of 0.2 alerts per patient‐day.
In Table 2, we summarize the sensitivity, specificity, positive predictive value, and negative predictive value of alerts in predicting a major clinical deterioration per patient for both the threshold alerts and the trend alerts. The cutoff values are those of optimal performance (maximal sensitivity plus specificity) along the ROC curves presented in Figure 1. The optimal cutoffs for the threshold alerts were HRs below 40 or above 115 beats/min, and RRs below 8 or above 40 breaths/min. For the trend alerts, when comparing between time periods, we found that a cutoff of a rise of 20 or more beats/min and 5 or more breaths/min corresponded with a maximal sensitivity and specificity, and we used these as the thresholds for the trending alerts.
Optimal cutoffs were used when comparing time periods (20/min for HR and 5/min for RR) for maximal sum of sensitivity and specificity. Abbreviations: AUC, area under the curve.
| Sensitivity (%) | Specificity (%) | Positive Predictive Value (%) | Negative Predictive Value (%) | |
|---|---|---|---|---|
| ||||
| Threshold alerts | ||||
| HR* | 82 | 67 | 21 | 97 |
| RR | 64 | 81 | 26 | 95 |
| HR and RR | 55 | 94 | 50 | 95 |
| Trend alerts | ||||
| HR 20 | 78 | 90 | 41 | 97 |
| RR 5 | 100 | 64 | 20 | 100 |
| HR and RR | 78 | 94 | 54 | 98 |
For the determined alerts, out of the 10 clinical events, in 7 cases the alerts would have indicated the deterioration within more than 1 hour from the actual event and within 24 hours prior to the clinical event. In one case, the alert would have indicated the risk within less than 1 hour; in another case, within the 2448 hours window; and in the last case, the alerts would have done so more than 48 hours prior to the event (these last 2 cases were considered false‐negative for our post hoc analysis).
The ROC analysis for both the threshold alerts and the trend alerts for both HR and RR correlated well with the clinical events (P < 0.05 for all models) (Figure 1). When comparing the threshold alerts with the trend alerts, trend alerts had a higher AUC, suggesting that these would be more accurate in alerting for major clinical events. Specifically, the model for HR 6‐hour trend alerts demonstrated a larger AUC (0.9 and 0.85, respectively), while the combination of HR and RR had the largest AUC (0.93).
DISCUSSION
The development of monitoring systems designed for hospitalized patients on non‐ICU floors derives from the need to minimize preventable in‐hospital mortality. This study has explored one such possible solution. Through retrospective definition of optimal alert settings and internal validation within a derivation cohort, we have found the Earlysense monitor to be accurate in predicting major clinical deterioration by using both simple thresholds and a vital signs trend algorithm. We found that the post hoc determined alerts were relatively infrequent. We also found that trend alerts showed greater ability to accurately capture these deteriorations compared with simple alert thresholds, and that using a combination alert based on both HR and RR trends provided the highest accuracy and confidence for predicting clinical deterioration. These results suggest the advantages that smart alerts can bringincreasing sensitivity while lowering the alert burden and reducing the number of false alerts.
An effective and efficient patient monitoring system must be able to quickly detect acute life‐threatening events or subacute patient deterioration that will lead to a life‐threatening event; in addition, this system should have a low false‐positive rate (few false alerts). While a high sensitivity is desirable,16 this usually comes at the cost of lower specificity and higher false‐positive rates. Studies have found alerts from monitoring systems in an ICU and emergency department environment to be tremendously frequent and with an extremely high false‐positive rate.1721 Unsurprisingly, it has been reported that only about 10% of alerts are responded to by the clinical staff.22 In an attempt to improve alert relevancy and accuracy, newly designed integrated monitoring systems for ICUs use alert algorithms and trend analysis performed on data received from multiple vital signs monitors.2327 With the evident need to continuously monitor patients on hospital floors,13, 28 there is a clear gap to‐date in such experience and a need to study the implications for patients and staff as we try to optimize the monitoring tools for this environment.
As more emphasis is placed on the afferent limb of rapid response systems, we can expect to see a greater need for systems able to detect changes in clinical status that might lead to patient deterioration. The intermittent vital sign measurement performed by nurses and support staff on the floors is now regarded as inadequate by itself, because it may not be performed predictably, accurately, or completely.28 Continuous monitoring systems should complement manual intermittent vital signs monitoring and play an important role in bringing the nurse to the patient's side at the right time so that a complete assessment can be done.29, 30 There remains no substitution for a nurse evaluating the patient and making critical decisions based on his or her knowledge of the patient's condition.
While today, both electrocardiographic monitoring (telemetry) and continuous pulse oximetry provide some solution for the need for continuous monitoring on the floors, these carry disadvantages that prevent them from becoming the optimal solution. While telemetry is invaluable for higher risk cardiac patients, significant overuse of this application does occur,31 and most monitored patients gain little cardiac arrest survival benefits.32 Pulse oximetry, although regarded as one of the most important technological advancements in monitoring patients, carries important limitations that might prevent early detection of respiratory failure.33, 34 Furthermore, these 2 modalities require continuous contact of leads/sensors to the patient, a disadvantage when regarding monitoring for low/average risk patients on non‐ICU hospital floors. Related to these disadvantages, the results presented here might position the implementation of the Earlysense monitor as a preferred alternative.
This study has several important limitations. This was a retrospective noninterventional study limited to internal medicine patients. Our patients served as a derivation cohort, alert thresholds were set post hoc, and sensitivity and specificity were internally validated. It remains to be shown that the results shown here can be reproduced in a real‐time interventional study. We only included patients who were considered above average risk within medical wards, as we were hoping to capture more clinical deteriorations with a relatively small cohort. We cannot rule out that our results might be biased and may not similarly apply to all non‐ICU medical patients. Finally, the retrospective nature of this study did not allow us to assess other outcomes of appropriateness, such as staff objective assessment of alert appropriateness or change in clinical management as a result of an alert. When using these devices in the alert mode, alert thresholds may be changed by the clinical staff based on clinical judgment to further lower false alerts and alert frequency. We also did not collect information that could have allowed us to assess clinical usefulness of the alerts compared to routine clinical assessment. Documenting whether the clinical events were suspected beforehand by the clinical teams could have allowed us to assess clinical usefulness. Future interventional studies are needed to validate the Earlysense system prospectively in both medical and surgical floor settings, first using a common alert threshold alerting system and secondly using the smart trend alerts described here.
In conclusion, we found that the Earlysense monitor is able to continuously measure RR and HR, providing low alert frequency. The current study demonstrates the potential of this system to provide timely prediction of patient deterioration. Utilizing a smart trend algorithm has been shown to improve the device's accuracy and reduce associated alert burden and false‐positive alerts.
Acknowledgements
Disclosures: The study was funded by an industry grant provided by Earlysense LTD. Eyal Zimlichman, MD, MSc Ronen Rozenblum, PhD, MPH, and Jeffrey M. Rothschild, MD, MPH, have each received a research grant supported by Earlysense LTD. Martine Szyper‐Kravitz, MD, Avraham Unterman, MD, Howard Amital, MD, MHA, and Yehuda Shoenfeld, MD, report no conflicts of interest. Zvika Shinar, PhD, Tal Klap, and Shiraz Levkovich are employed by Earlysense LTD and are holding equity with the company.
- ,,,,,.Temporal trends in rates of patient harm resulting from medical care.N Engl J Med.2010;363(22):2124–2134.
- ,,, et al.Findings of the first consensus conference on medical emergency teams.Crit Care Med.2006;34(9):2463–2478.
- ,,,,.Inpatient transfers to the intensive care unit: delays are associated with increased mortality and morbidity.J Gen Intern Med.2003;18(2):77–83.
- ,,,,.Redefining in‐hospital resuscitation: the concept of the medical emergency team.Resuscitation.2001;48(2):105–110.
- Institute for Healthcare Improvement (IHI). Protecting 5 million lives from harm. Available at: www.ihi.org/ihi/programs/campaign. Accessed September 8,2011.
- ,,, et al.Introduction of the medical emergency team (MET) system: a cluster‐randomised controlled trial.Lancet.2005;365(9477):2091–2097.
- ,,,,.Rapid response teams: a systematic review and meta‐analysis.Arch Intern Med.2010;170(1):18–26.
- ,,,,,.Recognising clinical instability in hospital patients before cardiac arrest or unplanned admission to intensive care. A pilot study in a tertiary‐care hospital.Med J Aust.1999;171(1):22–25.
- ,,,,,.A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom—the ACADEMIA study.Resuscitation.2004;62(3):275–282.
- ,,, et al.Early goal‐directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med.2001;345(19):1368–1377.
- .Top ten list in myocardial infarction.Chest.2000;118(5):1477–1479.
- ,,, et al.Improvement in stroke mortality in Canada and the United States, 1990 to 2002.Circulation.2006;113(10):1335–1343.
- ,,, et al.“Identifying the hospitalised patient in crisis”—a consensus conference on the afferent limb of rapid response systems.Resuscitation.2010;81(4):375–382.
- ,,,.Contactless respiratory and heart rate monitoring: validation of an innovative tool.J Med Eng Technol.2010;35(7–8):393–398.
- ,,,,,.How is my patient doing? Evaluating hospitalized patients using continuous vital signs monitoring.Isr Med Assoc J.2009;11(6):382–394.
- ,,,,,.Medical device alarms.Biomed Tech (Berl).2011;56(2):73–83.
- ,.Poor prognosis for existing monitors in the intensive care unit.Crit Care Med.1997;25(4):614–619.
- .Crying wolf: false alarms in a pediatric intensive care unit.Crit Care Med.1994;22(6):981–985.
- ,,,,,.Intensive care unit alarms—how many do we need?Crit Care Med.2010;38(2):451–456.
- ,,,,.Alarmed: adverse events in low‐risk patients with chest pain receiving continuous electrocardiographic monitoring in the emergency department. A pilot study.Am J Emerg Med.2006;24(1):62–67.
- ,,,,,.Multicentric study of monitoring alarms in the adult intensive care unit (ICU): a descriptive analysis.Intensive Care Med.1999;25(12):1360–1366.
- .Alarms in the intensive care unit: how can the number of false alarms be reduced?Crit Care.2001;5(4):184–188.
- ,,,,,.Cardiorespiratory instability before and after implementing an integrated monitoring system.Crit Care Med.2011;39(1):65–72.
- ,,.Adaptive change detection in heart rate trend monitoring in anesthetized children.IEEE Trans Biomed Eng.2006;53(11):2211–2219.
- ,,,,,.Defining the incidence of cardiorespiratory instability in patients in step‐down units using an electronic integrated monitoring system.Arch Intern Med.2008;168(12):1300–1308.
- ,,, et al.Implementation of a real‐time computerized sepsis alert in nonintensive care unit patients.Crit Care Med.2011;39(3):469–473.
- ,,,,,.Early prediction of septic shock in hospitalized patients.J Hosp Med.2010;5(1):19–25.
- ,,.Rapid‐response teams.N Engl J Med.2011;365(2):139–146.
- ,,,.An analysis of the causes of adverse events from the Quality in Australian Health Care Study.Med J Aust.1999;170(9):411–415.
- ,.Taking your rapid response team to the next level. Society of Critical Care Medicine;2010. Available at: http://www.sccm.org/Publications/Critical_Connections/Archives/December‐2010/Pages/RapidResponseTeam.aspx. Accessed August 11,year="2011"2011.
- ,.Electrocardiographic monitoring in the hospitalized patient: a diagnostic intervention of uncertain clinical impact.Am J Emerg Med.2008;26(9):1047–1055.
- ,.Continuous electrocardiographic monitoring and cardiac arrest outcomes in 8,932 telemetry ward patients.Acad Emerg Med.2000;7(6):647–652.
- ,.The benefits and pitfalls of pulse oximetry.BMJ.1993;307(6902):457–458.
- ,.Patterns of unexpected in‐hospital deaths: a root cause analysis.Patient Saf Surg.2011;5(1):3.
- ,,,,,.Temporal trends in rates of patient harm resulting from medical care.N Engl J Med.2010;363(22):2124–2134.
- ,,, et al.Findings of the first consensus conference on medical emergency teams.Crit Care Med.2006;34(9):2463–2478.
- ,,,,.Inpatient transfers to the intensive care unit: delays are associated with increased mortality and morbidity.J Gen Intern Med.2003;18(2):77–83.
- ,,,,.Redefining in‐hospital resuscitation: the concept of the medical emergency team.Resuscitation.2001;48(2):105–110.
- Institute for Healthcare Improvement (IHI). Protecting 5 million lives from harm. Available at: www.ihi.org/ihi/programs/campaign. Accessed September 8,2011.
- ,,, et al.Introduction of the medical emergency team (MET) system: a cluster‐randomised controlled trial.Lancet.2005;365(9477):2091–2097.
- ,,,,.Rapid response teams: a systematic review and meta‐analysis.Arch Intern Med.2010;170(1):18–26.
- ,,,,,.Recognising clinical instability in hospital patients before cardiac arrest or unplanned admission to intensive care. A pilot study in a tertiary‐care hospital.Med J Aust.1999;171(1):22–25.
- ,,,,,.A comparison of antecedents to cardiac arrests, deaths and emergency intensive care admissions in Australia and New Zealand, and the United Kingdom—the ACADEMIA study.Resuscitation.2004;62(3):275–282.
- ,,, et al.Early goal‐directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med.2001;345(19):1368–1377.
- .Top ten list in myocardial infarction.Chest.2000;118(5):1477–1479.
- ,,, et al.Improvement in stroke mortality in Canada and the United States, 1990 to 2002.Circulation.2006;113(10):1335–1343.
- ,,, et al.“Identifying the hospitalised patient in crisis”—a consensus conference on the afferent limb of rapid response systems.Resuscitation.2010;81(4):375–382.
- ,,,.Contactless respiratory and heart rate monitoring: validation of an innovative tool.J Med Eng Technol.2010;35(7–8):393–398.
- ,,,,,.How is my patient doing? Evaluating hospitalized patients using continuous vital signs monitoring.Isr Med Assoc J.2009;11(6):382–394.
- ,,,,,.Medical device alarms.Biomed Tech (Berl).2011;56(2):73–83.
- ,.Poor prognosis for existing monitors in the intensive care unit.Crit Care Med.1997;25(4):614–619.
- .Crying wolf: false alarms in a pediatric intensive care unit.Crit Care Med.1994;22(6):981–985.
- ,,,,,.Intensive care unit alarms—how many do we need?Crit Care Med.2010;38(2):451–456.
- ,,,,.Alarmed: adverse events in low‐risk patients with chest pain receiving continuous electrocardiographic monitoring in the emergency department. A pilot study.Am J Emerg Med.2006;24(1):62–67.
- ,,,,,.Multicentric study of monitoring alarms in the adult intensive care unit (ICU): a descriptive analysis.Intensive Care Med.1999;25(12):1360–1366.
- .Alarms in the intensive care unit: how can the number of false alarms be reduced?Crit Care.2001;5(4):184–188.
- ,,,,,.Cardiorespiratory instability before and after implementing an integrated monitoring system.Crit Care Med.2011;39(1):65–72.
- ,,.Adaptive change detection in heart rate trend monitoring in anesthetized children.IEEE Trans Biomed Eng.2006;53(11):2211–2219.
- ,,,,,.Defining the incidence of cardiorespiratory instability in patients in step‐down units using an electronic integrated monitoring system.Arch Intern Med.2008;168(12):1300–1308.
- ,,, et al.Implementation of a real‐time computerized sepsis alert in nonintensive care unit patients.Crit Care Med.2011;39(3):469–473.
- ,,,,,.Early prediction of septic shock in hospitalized patients.J Hosp Med.2010;5(1):19–25.
- ,,.Rapid‐response teams.N Engl J Med.2011;365(2):139–146.
- ,,,.An analysis of the causes of adverse events from the Quality in Australian Health Care Study.Med J Aust.1999;170(9):411–415.
- ,.Taking your rapid response team to the next level. Society of Critical Care Medicine;2010. Available at: http://www.sccm.org/Publications/Critical_Connections/Archives/December‐2010/Pages/RapidResponseTeam.aspx. Accessed August 11,year="2011"2011.
- ,.Electrocardiographic monitoring in the hospitalized patient: a diagnostic intervention of uncertain clinical impact.Am J Emerg Med.2008;26(9):1047–1055.
- ,.Continuous electrocardiographic monitoring and cardiac arrest outcomes in 8,932 telemetry ward patients.Acad Emerg Med.2000;7(6):647–652.
- ,.The benefits and pitfalls of pulse oximetry.BMJ.1993;307(6902):457–458.
- ,.Patterns of unexpected in‐hospital deaths: a root cause analysis.Patient Saf Surg.2011;5(1):3.
Copyright © 2012 Society of Hospital Medicine
Sepsis Outcomes Across Settings
Sepsis is a major cause of death in hospitalized patients.13 It is recommended that patients with sepsis be treated with early appropriate antibiotics, as well as early goal‐directed therapy including fluid and vasopressor support according to evidence‐based guidelines.46 Following such evidence‐based protocols and process‐of‐care interventions has been shown to be associated with better patient outcomes, including decreased mortality.7, 8
Most patients with severe sepsis are cared for in intensive care units (ICUs). At times, there are no beds available in the primary ICU and patients presenting to the hospital with sepsis are cared for in other units. Patients admitted to a non‐preferred clinical inpatient setting are sometimes referred to as overflow.9 ICUs can differ significantly in staffing patterns, equipment, and training.10 It is not known if overflow sepsis patients receive similar care when admitted to non‐primary ICUs.
At our hospital, we have an active bed management system led by the hospitalist division.11 This system includes protocols to place sepsis patients in the overflow ICU if the primary ICU is full. We hypothesized that process‐of‐care interventions would be more strictly adhered to when sepsis patients were in the primary ICU rather than in the overflow unit at our institution.
METHODS
Design
This was a retrospective cohort study of all patients with sepsis admitted to either the primary medical intensive care unit (MICU) or the overflow cardiac intensive care unit (CICU) at our hospital between July 2009 and February 2010. We reviewed the admission database starting with the month of February 2010 and proceeded backwards, month by month, until we reached the target number of patients.
Setting
The study was conducted at our 320‐bed, university‐affiliated academic medical center in Baltimore, MD. The MICU and the CICU are closed units that are located adjacent to each other and have 12 beds each. They are staffed by separate pools of attending physicians trained in pulmonary/critical care medicine and cardiovascular diseases, respectively, and no attending physician attends in both units. During the study period, there were 10 unique MICU and 14 unique CICU attending physicians; while most attending physicians covered the unit for 14 days, none of the physicians were on service more than 2 of the 2‐week blocks (28 days). Each unit is additionally staffed by fellows of the respective specialties, and internal medicine residents and interns belonging to the same residency program (who rotate through both ICUs). Residents and fellows are generally assigned to these ICUs for 4 continuous weeks. The assignment of specific attendings, fellows, and residents to either ICU is performed by individual division administrators on a rotational basis based on residency, fellowship, and faculty service requirements. The teams in each ICU function independently of each other. Clinical care of patients requiring the assistance of the other specialty (pulmonary medicine or cardiology) have guidance conferred via an official consultation. Orders on patients in both ICUs are written by the residents using the same computerized order entry system (CPOE) under the supervision of their attending physicians. The nursing staff is exclusive to each ICU. The respiratory therapists spend time in both units. The nursing and respiratory therapy staff in both ICUs are similarly trained and certified, and have the same patient‐to‐nursing ratios.
Subjects
All patients admitted with a possible diagnosis of sepsis to either the MICU or CICU were identified by querying the hospital electronic triage database called etriage. This Web‐based application is used to admit patients to all the Medicine services at our hospital. We employed a wide case‐finding net using keywords that included pneumonia, sepsis, hypotension, high lactate, hypoxia, UTI (urinary tract infection)/urosepsis, SIRS (systemic inflammatory response syndrome), hypothermia, and respiratory failure. A total of 197 adult patients were identified. The charts and the electronic medical record (EMR) of these patients were then reviewed to determine the presence of a sepsis diagnosis using standard consensus criteria.12 Severe sepsis was defined by sepsis associated with organ dysfunction, hypoperfusion, or hypotension using criteria described by Bone et al.12
Fifty‐six did not meet the criteria for sepsis and were excluded from the analysis. A total of 141 patients were included in the study. This being a pilot study, we did not have any preliminary data regarding adherence to sepsis guidelines in overflow ICUs to calculate appropriate sample size. However, in 2 recent studies of dedicated ICUs (Ferrer et al13 and Castellanos‐Ortega et al14), the averaged adherence to a single measure like checking of lactate level was 27% pre‐intervention and 62% post‐intervention. With alpha level 0.05 and 80% power, one would need 31 patients in each unit to detect such differences with respect to this intervention. Although this data does not necessarily apply to overflow ICUs or for combination of processes, we used a goal of having at least 31 patients in each ICU.
The study was approved by the Johns Hopkins Institutional Review Board. The need for informed consent was waived given the retrospective nature of the study.
Data Extraction Process and Procedures
The clinical data was extracted from the EMR and patient charts using a standardized data extraction instrument, modified from a case report form (CRF) used and validated in previous studies.15, 16 The following procedures were used for the data extraction:
The data extractors included 4 physicians and 1 research assistant and were trained and tested by a single expert in data review and extraction.
Lab data was transcribed directly from the EMR. Calculation of acute physiology and chronic health evaluation (APACHE II) scores were done using the website
http://www.sfar.org/subores2/apache22.html (Socit Franaise d'Anesthsie et de Ranimation). Sepsis‐related organ failure assessment (SOFA) scores were calculated using usual criteria.17Delivery of specific treatments and interventions, including their timing, was extracted from the EMR.
The attending physicians' notes were used as the final source to assign diagnoses such as presence of acute lung injury, site of infection, and record interventions.
Data Analysis
Analyses focused primarily on assessing whether patients were treated differently between the MICU and CICU. The primary exposure variables were the process‐of‐care measures. We specifically used measurement of central venous saturation, checking of lactate level, and administration of antibiotics within 60 minutes in patients with severe sepsis as our primary process‐of‐care measures.13 Continuous variables were reported as mean standard deviation, and Student's t tests were used to compare the 2 groups. Categorical data were expressed as frequency distributions, and chi‐square tests were used to identify differences between the 2 groups. All tests were 2‐tailed with statistical significance set at 0.05. Statistical analysis was performed using SPSS version 19.0. (IBM, Armonk, NY).
To overcome data constraints, we created a dichotomous variable for each of the 3 primary processes‐of‐care (indicating receipt of process or not) and then combined them into 1 dichotomous variable indicating whether or not the patients with severe sepsis received all 3 primary processes‐of‐care. The combined variable was the key independent variable in the model.
We performed logistic regression analysis on patients with severe sepsis. The equation Logit [P(ICU Type = CICU)] = + 1Combined + 2Age describes the framework of the model, with ICU type being the dependent variable, and the combined variable of patients receiving all primary measures being the independent variable and controlled for age. Logistic regression was performed using JMP (SAS Institute, Inc, Cary, NC).
We additionally performed a secondary analysis to explore possible predictors of mortality using a logistic regression model, with the event of death as the dependent variable, and age, APACHE II scores, combined processes‐of‐care, and ICU type included as independent variables.
RESULTS
There were 100 patients admitted to the MICU and 41 patients admitted to the CICU during the study period (Table 1). The majority of the patients were admitted to the ICUs directly from the emergency department (ED) (n = 129), with a small number of patients who were transferred from the Medicine floors (n = 12).
| MICU (N =100) | CICU (N =41) | P Value | |
|---|---|---|---|
| |||
| Age in years, mean SD | 67 14.8 | 72 15.1 | 0.11 |
| Female, n (%) | 57 (57) | 27 (66) | 0.33 |
| Patients with chronic organ insufficiency, n (%) | 59 (59) | 22 (54) | 0.56 |
| Patients with severe sepsis, n (%) | 88 (88) | 21 (51) | <0.001 |
| Patients needing mechanical ventilation, n (%) | 43 (43) | 14 (34) | 0.33 |
| APACHE II score, mean SD | 25.53 9.11 | 24.37 9.53 | 0.50 |
| SOFA score on day 1, mean SD | 7.09 3.55 | 6.71 4.57 | 0.60 |
| Patients with acute lung injury on presentation, n (%) | 8 (8) | 2 (5) | 0.50 |
There were no significant differences between the 2 study groups in terms of age, sex, primary site of infection, mean APACHE II score, SOFA scores on day 1, chronic organ insufficiency, immune suppression, or need for mechanical ventilation (Table 1). The most common site of infection was lung. There were significantly more patients with severe sepsis in the MICU (88% vs 51%, P <0.001).
Sepsis Process‐of‐Care Measures
There were no significant differences in the proportion of severe sepsis patients who had central venous saturation checked (MICU: 46% vs CICU: 41%, P = 0.67), lactate level checked (95% vs 100%, P = 0.37), or received antibiotics within 60 minutes of presentation (75% vs 69%, P = 0.59) (Table 2). Multiple other processes and treatments were delivered similarly, as shown in Table 2.
| Primary Process‐of‐Care Measures (Severe Sepsis Patients) | MICU (N = 88) | CICU (N = 21) | P Value |
|---|---|---|---|
| |||
| Patients with central venous oxygen saturation checked, n (%)* | 31 (46) | 7 (41) | 0.67 |
| Patients with lactate level checked, n (%)* | 58 (95) | 16 (100) | 0.37 |
| Received antibiotics within 60 min, n (%)* | 46 (75) | 11 (69) | 0.59 |
| Patients who had all 3 above processes and treatments, n (%) | 19 (22) | 4 (19) | 0.79 |
| Received vasopressor, n (%) | 25 (28) | 8 (38) | 0.55 |
| ICU Treatments and Processes (All Sepsis Patients) | (N =100) | (N = 41) | |
| Fluid balance 24 h after admission in liters, mean SD | 1.96 2.42 | 1.42 2.63 | 0.24 |
| Patients who received stress dose steroids, n (%) | 11 (11) | 4 (10) | 0.83 |
| Patients who received Drotrecogin alfa, n (%) | 0 (0) | 0 (0) | |
| Morning glucose 24 h after admission in mg/dL, mean SD | 161 111 | 144 80 | 0.38 |
| Received DVT prophylaxis within 24 h of admission, n (%) | 74 (74) | 20 (49) | 0.004 |
| Received GI prophylaxis within 24 h of admission, n (%) | 68 (68) | 18 (44) | 0.012 |
| Received RBC transfusion within 24 h of admission, n (%) | 8 (8) | 7 (17) | 0.11 |
| Received renal replacement therapy, n (%) | 13 (13) | 3 (7) | 0.33 |
| Received a spontaneous breathing trial within 24 h of admission, n (%)* | 4 (11) | 4 (33) | 0.07 |
Logistic regression analysis examining the receipt of all 3 primary processes‐of‐care while controlling for age revealed that the odds of the being in one of the ICUs was not significantly different (P = 0.85). The secondary analysis regression models revealed that only the APACHE II score (odds ratio [OR] = 1.21; confidence interval [CI], 1.121.31) was significantly associated with higher odds of mortality. ICU‐type [MICU vs CICU] (OR = 1.85; CI, 0.428.20), age (OR = 1.01; CI, 0.971.06), and combined processes of care (OR = 0.26; CI, 0.071.01) did not have significant associations with odds of mortality.
A review of microbiologic sensitivities revealed a trend towards significance that the cultured microorganism(s) was likely to be resistant to the initial antibiotics administered in MICU vs CICU (15% vs 5%, respectively, P = 0.09).
Mechanical Ventilation Parameters
The majority of the ventilated patients were admitted to each ICU in assist control (AC) mode. There were no significant differences in categories of mean tidal volume (TV) (P = 0.3), mean plateau pressures (P = 0.12), mean fraction of inspired oxygen (FiO2) (P = 0.95), and mean positive end‐expiratory pressures (PEEP) (P = 0.98) noted across the 2 units at the time of ICU admission, and also 24 hours after ICU admission. Further comparison of measurements of tidal volumes and plateau pressures over 7 days of ICU stay revealed no significant differences in the 2 ICUs (P = 0.40 and 0.57, respectively, on day 7 of ICU admission). There was a trend towards significance in fewer patients in the MICU receiving spontaneous breathing trial within 24 hours of ICU admission (11% vs 33%, P = 0.07) (Table 2).
Patient Outcomes
There were no significant differences in ICU mortality (MICU 19% vs CICU 10%, P = 0.18), or hospital mortality (21% vs 15%, P = 0.38) across the units (Table 3). Mean ICU and hospital length of stay (LOS) and proportion of patients discharged home with unassisted breathing were similar (Table 3).
| Patient Outcomes | MICU (N = 100) | CICU (N = 41) | P Value |
|---|---|---|---|
| |||
| ICU mortality, n (%) | 19 (19) | 4 (10) | 0.18 |
| Hospital mortality, n (%) | 21 (21) | 6 (15) | 0.38 |
| Discharged home with unassisted breathing, n (%) | 33 (33) | 19 (46) | 0.14 |
| ICU length of stay in days, mean SD | 4.78 6.24 | 4.92 6.32 | 0.97 |
| Hospital length of stay in days, mean SD | 9.68 9.22 | 9.73 9.33 | 0.98 |
DISCUSSION
Since sepsis is more commonly treated in the medical ICU and some data suggests that specialty ICUs may be better at providing desired care,18, 19 we believed that patients treated in the MICU would be more likely to receive guideline‐concordant care. The study refutes our a priori hypothesis and reveals that evidence‐based processes‐of‐care associated with improved outcomes for sepsis are similarly implemented at our institution in the primary and overflow ICU. These findings are important, as ICU bed availability is a frequent problem and many hospitals overflow patients to non‐primary ICUs.9, 20
The observed equivalence in the care delivered may be a function of the relatively high number of patients with sepsis treated in the overflow unit, thereby giving the delivery teams enough experience to provide the desired care. An alternative explanation could be that the residents in CICU brought with them the experience from having previously trained in the MICU. Although, some of the care processes for sepsis patients are influenced by the CPOE (with embedded order sets and protocols), it is unlikely that CPOE can fully account for similarity in care because many processes and therapies (like use of steroids, amount of fluid delivered in first 24 hours, packed red blood cells [PRBC] transfusion, and spontaneous breathing trials) are not embedded within order sets.
The significant difference noted in the areas of deep vein thrombosis (DVT) and gastrointestinal (GI) prophylaxis within 24 hours of ICU admission was unexpected. These preventive therapies are included in initial order sets in the CPOE, which prompt physicians to order them as standard‐of‐care. With respect to DVT prophylaxis, we suspect that some of the difference might be attributable to specific contraindications to its use, which could have been more common in one of the units. There were more patients in MICU on mechanical ventilation (although not statistically significant) and with severe sepsis (statistically significant) at time of admission, which might have contributed to the difference noted in use of GI prophylaxis. It is also plausible that these differences might have disappeared if they were reassessed beyond 24 hours into the ICU admission. We cannot rule out the presence of unit‐ and physician‐level differences that contributed to this. Likewise, there was an unexpected trend towards significance, wherein more patients in CICU had spontaneous breathing trials within 24 hours of admission. This might also be explained by the higher number of patients with severe sepsis in the MICU (preempting any weaning attempts). These caveats aside, it is reassuring that, at our institution, admitting septic patients to the first available ICU bed does not adversely affect important processes‐of‐care.
One might ask whether this study's data should reassure other sites who are boarding septic patients in non‐primary ICUs. Irrespective of the number of patients studied or the degree of statistical significance of the associations, an observational study design cannot prove that boarding septic patients in non‐primary ICUs is either safe or unsafe. However, we hope that readers reflect on, and take inventory of, systems issues that may be different between unitswith an eye towards eliminating variation such that all units managing septic patients are primed to deliver guideline‐concordant care. Other hospitals that use CPOE with sepsis order sets, have protocols for sepsis care, and who train nursing and respiratory therapists to meet high standards might be pleased to see that the patients in our study received comparable, high‐quality care across the 2 units. While our data suggests that boarding patients in overflow units may be safe, these findings would need to be replicated at other sites using prospective designs to prove safety.
Length of emergency room stay prior to admission is associated with higher mortality rates.2123 At many hospitals, critical care beds are a scarce resource such that most hospitals have a policy for the triage of patients to critical care beds.24, 25 Lundberg and colleagues' study demonstrated that patients who developed septic shock on the medical wards experienced delays in receipt of intravenous fluids, inotropic agents and transfer to a critical care setting.26 Thus, rather than waiting in the ED or on the medical service for an MICU bed to become available, it may be most wise to admit a critically sick septic patient to the first available ICU bed, even to an overflow ICU. In a recent study by Sidlow and Aggarwal, 1104 patients discharged from the coronary care unit (CCU) with a non‐cardiac primary diagnosis were compared to patients admitted to the MICU in the same hospital.27 The study found no differences in patient mortality, 30‐day readmission rate, hospital LOS, ICU LOS, and safety outcomes of ventilator‐associated pneumonia and catheter‐associated bloodstream infections between ICUs. However, their study did not examine processes‐of‐care delivered between the primary ICU and the overflow unit, and did not validate the primary diagnoses of patients admitted to the ICU.
Several limitations of this study should be considered. First, this study was conducted at a single center. Second, we used a retrospective study design; however, a prospective study randomizing patients to 1 of the 2 units would likely never be possible. Third, the relatively small number of patients limited the power of the study to detect mortality differences between the units. However, this was a pilot study focused on processes of care as opposed to clinical outcomes. Fourth, it is possible that we did not capture every single patient with sepsis with our keyword search. Our use of a previously validated screening process should have limited the number of missed cases.15, 16 Fifth, although the 2 ICUs have exclusive nursing staff and attending physicians, the housestaff and respiratory therapists do rotate between the 2 ICUs and place orders in the common CPOE. The rotating housestaff may certainly represent a source for confounding, but the large numbers (>30) of evenly spread housestaff over the study period minimizes the potential for any trainee to be responsible for a large proportion of observed practice. Sixth, ICU attendings are the physicians of record and could influence the results. Because no attending physician was on service for more than 4 weeks during the study period, and patients were equally spread over this same time, concerns about clustering and biases this may have created should be minimal but cannot be ruled out. Seventh, some interventions and processes, such as antibiotic administration and measurement of lactate, may have been initiated in the ED, thereby decreasing the potential for differences between the groups. Additionally, we cannot rule out the possibility that factors other than bed availability drove the admission process (we found that the relative proportion of patients admitted to overflow ICU during hours of ambulance diversion was similar to the overflow ICU admissions during non‐ambulance diversion hours). It is possible that some selection bias by the hospitalist assigning patients to specific ICUs influenced their triage decisionsalthough all triaging doctors go through the same process of training in active bed management.11 While more patients admitted to the MICU had severe sepsis, there were no differences between groups in APACHE II or SOFA scores. However, we cannot rule out that there were other residual confounders. Finally, in a small number of cases (4/41, 10%), the CICU team consulted the MICU attending for assistance. This input had the potential to reduce disparities in care between the units.
Overflowing patients to non‐primary ICUs occurs in many hospitals. Our study demonstrates that sepsis treatment for overflow patients may be similar to that received in the primary ICU. While a large multicentered and randomized trial could determine whether significant management and outcome differences exist between primary and overflow ICUs, feasibility concerns make it unlikely that such a study will ever be conducted.
Acknowledgements
Disclosure: Dr Wright is a Miller‐Coulson Family Scholar and this work is supported by the Miller‐Coulson family through the Johns Hopkins Center for Innovative Medicine. Dr Sevransky was supported with a grant from National Institute of General Medical Sciences, NIGMS K‐23‐1399. All other authors disclose no relevant or financial conflicts of interest.
- ,,,,,.Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med.2001;29(7):1303–1310.
- ,,, et al;for the Milwaukee Initiative in Critical Care Outcomes Research (MICCOR) Group of Investigators.Nationwide trends of severe sepsis in the twenty first century (2000–2007).Chest.2011;140(5):1223–1231.
- ,,,.Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003.Crit Care Med.2007;35(5):1244–1250.
- ,,, et al.Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36(1):296–327.
- ,,, et al.Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial.JAMA.2010;303(8):739–746.
- ,,, et al.Early goal‐directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med.2001;345(19):1368–1377.
- ,,, et al.Implementation of a bundle of quality indicators for the early management of severe sepsis and septic shock is associated with decreased mortality.Crit Care Med.2007;35(4):1105–1112.
- ,,, et al.Early combination antibiotic therapy yields improved survival compared with monotherapy in septic shock: a propensity‐matched analysis.Crit Care Med.2010;38(9):1773–1785.
- .A new dimension of the PACU: the dilemma of the ICU overflow patient.J Post Anesth Nurs.1994;9(5):297–300.
- ,,, et al.Descriptive analysis of critical care units in the United States.Crit Care Med.1992;20(6):846–863.
- ,,,,,.Active bed management by hospitalists and emergency department throughput.Ann Intern Med.2008;149(11):804–811.
- ,,, et al.Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee, American College of Chest Physicians/Society of Critical Care Medicine.Chest.1992;101(6):1644–1655.
- ,,, et al.Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain.JAMA.2008;299(19):2294–2303.
- ,,, et al.Impact of the surviving sepsis campaign protocols on hospital length of stay and mortality in septic shock patients: results of a three‐year follow‐up quasi‐experimental study.Crit Care Med.2010;38(4):1036–1043.
- ,,, et al.Study protocol: the improving care of acute lung injury patients (ICAP) study.Crit Care.2006;10(1):R9.
- ,,,,,.Critical illness outcome study: an observational study of protocols and mortality in intensive care units.Open Access J Clin Trials.2011;3(September):55–65.
- ,,, et al.The SOFA (sepsis‐related organ failure assessment) score to describe organ dysfunction/failure: on behalf of the Working Group on Sepsis‐Related Problems of the European Society of Intensive Care Medicine.Intensive Care Med.1996;22(7):707–710.
- ,,,,,.Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review.JAMA.2002;288(17):2151–2162.
- ,,.Do intensivists in ICU improve outcome?Best Pract Res Clin Anaesthesiol.2005;19(1):125–135.
- .Is the postanesthesia care unit becoming an intensive care unit?J Perianesth Nurs.1999;14(2):73–77.
- ,,,,;for the DELAY‐ED Study Group.Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit.Crit Care Med.2007;35(6):1477–1483.
- ,,, et al.Association between timing of intensive care unit admission and outcomes for emergency department patients with community‐acquired pneumonia.Crit Care Med.2009;37(11):2867–2874.
- ,.Association between ambulance diversion and survival among patients with acute myocardial infarction.JAMA.2011;305(23):2440–2447.
- .Civilian triage in the intensive care unit: the ritual of the last bed.Crit Care Med.1993;21(4):598–606.
- ,,,,;for the Values Ethics and Rationing in Critical Care Task Force.Rationing critical care beds: a systematic review.Crit Care Med.2004;32(7):1588–1597.
- ,,, et al.Septic shock: an analysis of outcomes for patients with onset on hospital wards versus intensive care units.Crit Care Med.1998;26(6):1020–1024.
- ,.“The MICU is full”: one hospital's experience with an overflow triage policy.Jt Comm J Qual Patient Saf.2011;37(10):456–460.
Sepsis is a major cause of death in hospitalized patients.13 It is recommended that patients with sepsis be treated with early appropriate antibiotics, as well as early goal‐directed therapy including fluid and vasopressor support according to evidence‐based guidelines.46 Following such evidence‐based protocols and process‐of‐care interventions has been shown to be associated with better patient outcomes, including decreased mortality.7, 8
Most patients with severe sepsis are cared for in intensive care units (ICUs). At times, there are no beds available in the primary ICU and patients presenting to the hospital with sepsis are cared for in other units. Patients admitted to a non‐preferred clinical inpatient setting are sometimes referred to as overflow.9 ICUs can differ significantly in staffing patterns, equipment, and training.10 It is not known if overflow sepsis patients receive similar care when admitted to non‐primary ICUs.
At our hospital, we have an active bed management system led by the hospitalist division.11 This system includes protocols to place sepsis patients in the overflow ICU if the primary ICU is full. We hypothesized that process‐of‐care interventions would be more strictly adhered to when sepsis patients were in the primary ICU rather than in the overflow unit at our institution.
METHODS
Design
This was a retrospective cohort study of all patients with sepsis admitted to either the primary medical intensive care unit (MICU) or the overflow cardiac intensive care unit (CICU) at our hospital between July 2009 and February 2010. We reviewed the admission database starting with the month of February 2010 and proceeded backwards, month by month, until we reached the target number of patients.
Setting
The study was conducted at our 320‐bed, university‐affiliated academic medical center in Baltimore, MD. The MICU and the CICU are closed units that are located adjacent to each other and have 12 beds each. They are staffed by separate pools of attending physicians trained in pulmonary/critical care medicine and cardiovascular diseases, respectively, and no attending physician attends in both units. During the study period, there were 10 unique MICU and 14 unique CICU attending physicians; while most attending physicians covered the unit for 14 days, none of the physicians were on service more than 2 of the 2‐week blocks (28 days). Each unit is additionally staffed by fellows of the respective specialties, and internal medicine residents and interns belonging to the same residency program (who rotate through both ICUs). Residents and fellows are generally assigned to these ICUs for 4 continuous weeks. The assignment of specific attendings, fellows, and residents to either ICU is performed by individual division administrators on a rotational basis based on residency, fellowship, and faculty service requirements. The teams in each ICU function independently of each other. Clinical care of patients requiring the assistance of the other specialty (pulmonary medicine or cardiology) have guidance conferred via an official consultation. Orders on patients in both ICUs are written by the residents using the same computerized order entry system (CPOE) under the supervision of their attending physicians. The nursing staff is exclusive to each ICU. The respiratory therapists spend time in both units. The nursing and respiratory therapy staff in both ICUs are similarly trained and certified, and have the same patient‐to‐nursing ratios.
Subjects
All patients admitted with a possible diagnosis of sepsis to either the MICU or CICU were identified by querying the hospital electronic triage database called etriage. This Web‐based application is used to admit patients to all the Medicine services at our hospital. We employed a wide case‐finding net using keywords that included pneumonia, sepsis, hypotension, high lactate, hypoxia, UTI (urinary tract infection)/urosepsis, SIRS (systemic inflammatory response syndrome), hypothermia, and respiratory failure. A total of 197 adult patients were identified. The charts and the electronic medical record (EMR) of these patients were then reviewed to determine the presence of a sepsis diagnosis using standard consensus criteria.12 Severe sepsis was defined by sepsis associated with organ dysfunction, hypoperfusion, or hypotension using criteria described by Bone et al.12
Fifty‐six did not meet the criteria for sepsis and were excluded from the analysis. A total of 141 patients were included in the study. This being a pilot study, we did not have any preliminary data regarding adherence to sepsis guidelines in overflow ICUs to calculate appropriate sample size. However, in 2 recent studies of dedicated ICUs (Ferrer et al13 and Castellanos‐Ortega et al14), the averaged adherence to a single measure like checking of lactate level was 27% pre‐intervention and 62% post‐intervention. With alpha level 0.05 and 80% power, one would need 31 patients in each unit to detect such differences with respect to this intervention. Although this data does not necessarily apply to overflow ICUs or for combination of processes, we used a goal of having at least 31 patients in each ICU.
The study was approved by the Johns Hopkins Institutional Review Board. The need for informed consent was waived given the retrospective nature of the study.
Data Extraction Process and Procedures
The clinical data was extracted from the EMR and patient charts using a standardized data extraction instrument, modified from a case report form (CRF) used and validated in previous studies.15, 16 The following procedures were used for the data extraction:
The data extractors included 4 physicians and 1 research assistant and were trained and tested by a single expert in data review and extraction.
Lab data was transcribed directly from the EMR. Calculation of acute physiology and chronic health evaluation (APACHE II) scores were done using the website
http://www.sfar.org/subores2/apache22.html (Socit Franaise d'Anesthsie et de Ranimation). Sepsis‐related organ failure assessment (SOFA) scores were calculated using usual criteria.17Delivery of specific treatments and interventions, including their timing, was extracted from the EMR.
The attending physicians' notes were used as the final source to assign diagnoses such as presence of acute lung injury, site of infection, and record interventions.
Data Analysis
Analyses focused primarily on assessing whether patients were treated differently between the MICU and CICU. The primary exposure variables were the process‐of‐care measures. We specifically used measurement of central venous saturation, checking of lactate level, and administration of antibiotics within 60 minutes in patients with severe sepsis as our primary process‐of‐care measures.13 Continuous variables were reported as mean standard deviation, and Student's t tests were used to compare the 2 groups. Categorical data were expressed as frequency distributions, and chi‐square tests were used to identify differences between the 2 groups. All tests were 2‐tailed with statistical significance set at 0.05. Statistical analysis was performed using SPSS version 19.0. (IBM, Armonk, NY).
To overcome data constraints, we created a dichotomous variable for each of the 3 primary processes‐of‐care (indicating receipt of process or not) and then combined them into 1 dichotomous variable indicating whether or not the patients with severe sepsis received all 3 primary processes‐of‐care. The combined variable was the key independent variable in the model.
We performed logistic regression analysis on patients with severe sepsis. The equation Logit [P(ICU Type = CICU)] = + 1Combined + 2Age describes the framework of the model, with ICU type being the dependent variable, and the combined variable of patients receiving all primary measures being the independent variable and controlled for age. Logistic regression was performed using JMP (SAS Institute, Inc, Cary, NC).
We additionally performed a secondary analysis to explore possible predictors of mortality using a logistic regression model, with the event of death as the dependent variable, and age, APACHE II scores, combined processes‐of‐care, and ICU type included as independent variables.
RESULTS
There were 100 patients admitted to the MICU and 41 patients admitted to the CICU during the study period (Table 1). The majority of the patients were admitted to the ICUs directly from the emergency department (ED) (n = 129), with a small number of patients who were transferred from the Medicine floors (n = 12).
| MICU (N =100) | CICU (N =41) | P Value | |
|---|---|---|---|
| |||
| Age in years, mean SD | 67 14.8 | 72 15.1 | 0.11 |
| Female, n (%) | 57 (57) | 27 (66) | 0.33 |
| Patients with chronic organ insufficiency, n (%) | 59 (59) | 22 (54) | 0.56 |
| Patients with severe sepsis, n (%) | 88 (88) | 21 (51) | <0.001 |
| Patients needing mechanical ventilation, n (%) | 43 (43) | 14 (34) | 0.33 |
| APACHE II score, mean SD | 25.53 9.11 | 24.37 9.53 | 0.50 |
| SOFA score on day 1, mean SD | 7.09 3.55 | 6.71 4.57 | 0.60 |
| Patients with acute lung injury on presentation, n (%) | 8 (8) | 2 (5) | 0.50 |
There were no significant differences between the 2 study groups in terms of age, sex, primary site of infection, mean APACHE II score, SOFA scores on day 1, chronic organ insufficiency, immune suppression, or need for mechanical ventilation (Table 1). The most common site of infection was lung. There were significantly more patients with severe sepsis in the MICU (88% vs 51%, P <0.001).
Sepsis Process‐of‐Care Measures
There were no significant differences in the proportion of severe sepsis patients who had central venous saturation checked (MICU: 46% vs CICU: 41%, P = 0.67), lactate level checked (95% vs 100%, P = 0.37), or received antibiotics within 60 minutes of presentation (75% vs 69%, P = 0.59) (Table 2). Multiple other processes and treatments were delivered similarly, as shown in Table 2.
| Primary Process‐of‐Care Measures (Severe Sepsis Patients) | MICU (N = 88) | CICU (N = 21) | P Value |
|---|---|---|---|
| |||
| Patients with central venous oxygen saturation checked, n (%)* | 31 (46) | 7 (41) | 0.67 |
| Patients with lactate level checked, n (%)* | 58 (95) | 16 (100) | 0.37 |
| Received antibiotics within 60 min, n (%)* | 46 (75) | 11 (69) | 0.59 |
| Patients who had all 3 above processes and treatments, n (%) | 19 (22) | 4 (19) | 0.79 |
| Received vasopressor, n (%) | 25 (28) | 8 (38) | 0.55 |
| ICU Treatments and Processes (All Sepsis Patients) | (N =100) | (N = 41) | |
| Fluid balance 24 h after admission in liters, mean SD | 1.96 2.42 | 1.42 2.63 | 0.24 |
| Patients who received stress dose steroids, n (%) | 11 (11) | 4 (10) | 0.83 |
| Patients who received Drotrecogin alfa, n (%) | 0 (0) | 0 (0) | |
| Morning glucose 24 h after admission in mg/dL, mean SD | 161 111 | 144 80 | 0.38 |
| Received DVT prophylaxis within 24 h of admission, n (%) | 74 (74) | 20 (49) | 0.004 |
| Received GI prophylaxis within 24 h of admission, n (%) | 68 (68) | 18 (44) | 0.012 |
| Received RBC transfusion within 24 h of admission, n (%) | 8 (8) | 7 (17) | 0.11 |
| Received renal replacement therapy, n (%) | 13 (13) | 3 (7) | 0.33 |
| Received a spontaneous breathing trial within 24 h of admission, n (%)* | 4 (11) | 4 (33) | 0.07 |
Logistic regression analysis examining the receipt of all 3 primary processes‐of‐care while controlling for age revealed that the odds of the being in one of the ICUs was not significantly different (P = 0.85). The secondary analysis regression models revealed that only the APACHE II score (odds ratio [OR] = 1.21; confidence interval [CI], 1.121.31) was significantly associated with higher odds of mortality. ICU‐type [MICU vs CICU] (OR = 1.85; CI, 0.428.20), age (OR = 1.01; CI, 0.971.06), and combined processes of care (OR = 0.26; CI, 0.071.01) did not have significant associations with odds of mortality.
A review of microbiologic sensitivities revealed a trend towards significance that the cultured microorganism(s) was likely to be resistant to the initial antibiotics administered in MICU vs CICU (15% vs 5%, respectively, P = 0.09).
Mechanical Ventilation Parameters
The majority of the ventilated patients were admitted to each ICU in assist control (AC) mode. There were no significant differences in categories of mean tidal volume (TV) (P = 0.3), mean plateau pressures (P = 0.12), mean fraction of inspired oxygen (FiO2) (P = 0.95), and mean positive end‐expiratory pressures (PEEP) (P = 0.98) noted across the 2 units at the time of ICU admission, and also 24 hours after ICU admission. Further comparison of measurements of tidal volumes and plateau pressures over 7 days of ICU stay revealed no significant differences in the 2 ICUs (P = 0.40 and 0.57, respectively, on day 7 of ICU admission). There was a trend towards significance in fewer patients in the MICU receiving spontaneous breathing trial within 24 hours of ICU admission (11% vs 33%, P = 0.07) (Table 2).
Patient Outcomes
There were no significant differences in ICU mortality (MICU 19% vs CICU 10%, P = 0.18), or hospital mortality (21% vs 15%, P = 0.38) across the units (Table 3). Mean ICU and hospital length of stay (LOS) and proportion of patients discharged home with unassisted breathing were similar (Table 3).
| Patient Outcomes | MICU (N = 100) | CICU (N = 41) | P Value |
|---|---|---|---|
| |||
| ICU mortality, n (%) | 19 (19) | 4 (10) | 0.18 |
| Hospital mortality, n (%) | 21 (21) | 6 (15) | 0.38 |
| Discharged home with unassisted breathing, n (%) | 33 (33) | 19 (46) | 0.14 |
| ICU length of stay in days, mean SD | 4.78 6.24 | 4.92 6.32 | 0.97 |
| Hospital length of stay in days, mean SD | 9.68 9.22 | 9.73 9.33 | 0.98 |
DISCUSSION
Since sepsis is more commonly treated in the medical ICU and some data suggests that specialty ICUs may be better at providing desired care,18, 19 we believed that patients treated in the MICU would be more likely to receive guideline‐concordant care. The study refutes our a priori hypothesis and reveals that evidence‐based processes‐of‐care associated with improved outcomes for sepsis are similarly implemented at our institution in the primary and overflow ICU. These findings are important, as ICU bed availability is a frequent problem and many hospitals overflow patients to non‐primary ICUs.9, 20
The observed equivalence in the care delivered may be a function of the relatively high number of patients with sepsis treated in the overflow unit, thereby giving the delivery teams enough experience to provide the desired care. An alternative explanation could be that the residents in CICU brought with them the experience from having previously trained in the MICU. Although, some of the care processes for sepsis patients are influenced by the CPOE (with embedded order sets and protocols), it is unlikely that CPOE can fully account for similarity in care because many processes and therapies (like use of steroids, amount of fluid delivered in first 24 hours, packed red blood cells [PRBC] transfusion, and spontaneous breathing trials) are not embedded within order sets.
The significant difference noted in the areas of deep vein thrombosis (DVT) and gastrointestinal (GI) prophylaxis within 24 hours of ICU admission was unexpected. These preventive therapies are included in initial order sets in the CPOE, which prompt physicians to order them as standard‐of‐care. With respect to DVT prophylaxis, we suspect that some of the difference might be attributable to specific contraindications to its use, which could have been more common in one of the units. There were more patients in MICU on mechanical ventilation (although not statistically significant) and with severe sepsis (statistically significant) at time of admission, which might have contributed to the difference noted in use of GI prophylaxis. It is also plausible that these differences might have disappeared if they were reassessed beyond 24 hours into the ICU admission. We cannot rule out the presence of unit‐ and physician‐level differences that contributed to this. Likewise, there was an unexpected trend towards significance, wherein more patients in CICU had spontaneous breathing trials within 24 hours of admission. This might also be explained by the higher number of patients with severe sepsis in the MICU (preempting any weaning attempts). These caveats aside, it is reassuring that, at our institution, admitting septic patients to the first available ICU bed does not adversely affect important processes‐of‐care.
One might ask whether this study's data should reassure other sites who are boarding septic patients in non‐primary ICUs. Irrespective of the number of patients studied or the degree of statistical significance of the associations, an observational study design cannot prove that boarding septic patients in non‐primary ICUs is either safe or unsafe. However, we hope that readers reflect on, and take inventory of, systems issues that may be different between unitswith an eye towards eliminating variation such that all units managing septic patients are primed to deliver guideline‐concordant care. Other hospitals that use CPOE with sepsis order sets, have protocols for sepsis care, and who train nursing and respiratory therapists to meet high standards might be pleased to see that the patients in our study received comparable, high‐quality care across the 2 units. While our data suggests that boarding patients in overflow units may be safe, these findings would need to be replicated at other sites using prospective designs to prove safety.
Length of emergency room stay prior to admission is associated with higher mortality rates.2123 At many hospitals, critical care beds are a scarce resource such that most hospitals have a policy for the triage of patients to critical care beds.24, 25 Lundberg and colleagues' study demonstrated that patients who developed septic shock on the medical wards experienced delays in receipt of intravenous fluids, inotropic agents and transfer to a critical care setting.26 Thus, rather than waiting in the ED or on the medical service for an MICU bed to become available, it may be most wise to admit a critically sick septic patient to the first available ICU bed, even to an overflow ICU. In a recent study by Sidlow and Aggarwal, 1104 patients discharged from the coronary care unit (CCU) with a non‐cardiac primary diagnosis were compared to patients admitted to the MICU in the same hospital.27 The study found no differences in patient mortality, 30‐day readmission rate, hospital LOS, ICU LOS, and safety outcomes of ventilator‐associated pneumonia and catheter‐associated bloodstream infections between ICUs. However, their study did not examine processes‐of‐care delivered between the primary ICU and the overflow unit, and did not validate the primary diagnoses of patients admitted to the ICU.
Several limitations of this study should be considered. First, this study was conducted at a single center. Second, we used a retrospective study design; however, a prospective study randomizing patients to 1 of the 2 units would likely never be possible. Third, the relatively small number of patients limited the power of the study to detect mortality differences between the units. However, this was a pilot study focused on processes of care as opposed to clinical outcomes. Fourth, it is possible that we did not capture every single patient with sepsis with our keyword search. Our use of a previously validated screening process should have limited the number of missed cases.15, 16 Fifth, although the 2 ICUs have exclusive nursing staff and attending physicians, the housestaff and respiratory therapists do rotate between the 2 ICUs and place orders in the common CPOE. The rotating housestaff may certainly represent a source for confounding, but the large numbers (>30) of evenly spread housestaff over the study period minimizes the potential for any trainee to be responsible for a large proportion of observed practice. Sixth, ICU attendings are the physicians of record and could influence the results. Because no attending physician was on service for more than 4 weeks during the study period, and patients were equally spread over this same time, concerns about clustering and biases this may have created should be minimal but cannot be ruled out. Seventh, some interventions and processes, such as antibiotic administration and measurement of lactate, may have been initiated in the ED, thereby decreasing the potential for differences between the groups. Additionally, we cannot rule out the possibility that factors other than bed availability drove the admission process (we found that the relative proportion of patients admitted to overflow ICU during hours of ambulance diversion was similar to the overflow ICU admissions during non‐ambulance diversion hours). It is possible that some selection bias by the hospitalist assigning patients to specific ICUs influenced their triage decisionsalthough all triaging doctors go through the same process of training in active bed management.11 While more patients admitted to the MICU had severe sepsis, there were no differences between groups in APACHE II or SOFA scores. However, we cannot rule out that there were other residual confounders. Finally, in a small number of cases (4/41, 10%), the CICU team consulted the MICU attending for assistance. This input had the potential to reduce disparities in care between the units.
Overflowing patients to non‐primary ICUs occurs in many hospitals. Our study demonstrates that sepsis treatment for overflow patients may be similar to that received in the primary ICU. While a large multicentered and randomized trial could determine whether significant management and outcome differences exist between primary and overflow ICUs, feasibility concerns make it unlikely that such a study will ever be conducted.
Acknowledgements
Disclosure: Dr Wright is a Miller‐Coulson Family Scholar and this work is supported by the Miller‐Coulson family through the Johns Hopkins Center for Innovative Medicine. Dr Sevransky was supported with a grant from National Institute of General Medical Sciences, NIGMS K‐23‐1399. All other authors disclose no relevant or financial conflicts of interest.
Sepsis is a major cause of death in hospitalized patients.13 It is recommended that patients with sepsis be treated with early appropriate antibiotics, as well as early goal‐directed therapy including fluid and vasopressor support according to evidence‐based guidelines.46 Following such evidence‐based protocols and process‐of‐care interventions has been shown to be associated with better patient outcomes, including decreased mortality.7, 8
Most patients with severe sepsis are cared for in intensive care units (ICUs). At times, there are no beds available in the primary ICU and patients presenting to the hospital with sepsis are cared for in other units. Patients admitted to a non‐preferred clinical inpatient setting are sometimes referred to as overflow.9 ICUs can differ significantly in staffing patterns, equipment, and training.10 It is not known if overflow sepsis patients receive similar care when admitted to non‐primary ICUs.
At our hospital, we have an active bed management system led by the hospitalist division.11 This system includes protocols to place sepsis patients in the overflow ICU if the primary ICU is full. We hypothesized that process‐of‐care interventions would be more strictly adhered to when sepsis patients were in the primary ICU rather than in the overflow unit at our institution.
METHODS
Design
This was a retrospective cohort study of all patients with sepsis admitted to either the primary medical intensive care unit (MICU) or the overflow cardiac intensive care unit (CICU) at our hospital between July 2009 and February 2010. We reviewed the admission database starting with the month of February 2010 and proceeded backwards, month by month, until we reached the target number of patients.
Setting
The study was conducted at our 320‐bed, university‐affiliated academic medical center in Baltimore, MD. The MICU and the CICU are closed units that are located adjacent to each other and have 12 beds each. They are staffed by separate pools of attending physicians trained in pulmonary/critical care medicine and cardiovascular diseases, respectively, and no attending physician attends in both units. During the study period, there were 10 unique MICU and 14 unique CICU attending physicians; while most attending physicians covered the unit for 14 days, none of the physicians were on service more than 2 of the 2‐week blocks (28 days). Each unit is additionally staffed by fellows of the respective specialties, and internal medicine residents and interns belonging to the same residency program (who rotate through both ICUs). Residents and fellows are generally assigned to these ICUs for 4 continuous weeks. The assignment of specific attendings, fellows, and residents to either ICU is performed by individual division administrators on a rotational basis based on residency, fellowship, and faculty service requirements. The teams in each ICU function independently of each other. Clinical care of patients requiring the assistance of the other specialty (pulmonary medicine or cardiology) have guidance conferred via an official consultation. Orders on patients in both ICUs are written by the residents using the same computerized order entry system (CPOE) under the supervision of their attending physicians. The nursing staff is exclusive to each ICU. The respiratory therapists spend time in both units. The nursing and respiratory therapy staff in both ICUs are similarly trained and certified, and have the same patient‐to‐nursing ratios.
Subjects
All patients admitted with a possible diagnosis of sepsis to either the MICU or CICU were identified by querying the hospital electronic triage database called etriage. This Web‐based application is used to admit patients to all the Medicine services at our hospital. We employed a wide case‐finding net using keywords that included pneumonia, sepsis, hypotension, high lactate, hypoxia, UTI (urinary tract infection)/urosepsis, SIRS (systemic inflammatory response syndrome), hypothermia, and respiratory failure. A total of 197 adult patients were identified. The charts and the electronic medical record (EMR) of these patients were then reviewed to determine the presence of a sepsis diagnosis using standard consensus criteria.12 Severe sepsis was defined by sepsis associated with organ dysfunction, hypoperfusion, or hypotension using criteria described by Bone et al.12
Fifty‐six did not meet the criteria for sepsis and were excluded from the analysis. A total of 141 patients were included in the study. This being a pilot study, we did not have any preliminary data regarding adherence to sepsis guidelines in overflow ICUs to calculate appropriate sample size. However, in 2 recent studies of dedicated ICUs (Ferrer et al13 and Castellanos‐Ortega et al14), the averaged adherence to a single measure like checking of lactate level was 27% pre‐intervention and 62% post‐intervention. With alpha level 0.05 and 80% power, one would need 31 patients in each unit to detect such differences with respect to this intervention. Although this data does not necessarily apply to overflow ICUs or for combination of processes, we used a goal of having at least 31 patients in each ICU.
The study was approved by the Johns Hopkins Institutional Review Board. The need for informed consent was waived given the retrospective nature of the study.
Data Extraction Process and Procedures
The clinical data was extracted from the EMR and patient charts using a standardized data extraction instrument, modified from a case report form (CRF) used and validated in previous studies.15, 16 The following procedures were used for the data extraction:
The data extractors included 4 physicians and 1 research assistant and were trained and tested by a single expert in data review and extraction.
Lab data was transcribed directly from the EMR. Calculation of acute physiology and chronic health evaluation (APACHE II) scores were done using the website
http://www.sfar.org/subores2/apache22.html (Socit Franaise d'Anesthsie et de Ranimation). Sepsis‐related organ failure assessment (SOFA) scores were calculated using usual criteria.17Delivery of specific treatments and interventions, including their timing, was extracted from the EMR.
The attending physicians' notes were used as the final source to assign diagnoses such as presence of acute lung injury, site of infection, and record interventions.
Data Analysis
Analyses focused primarily on assessing whether patients were treated differently between the MICU and CICU. The primary exposure variables were the process‐of‐care measures. We specifically used measurement of central venous saturation, checking of lactate level, and administration of antibiotics within 60 minutes in patients with severe sepsis as our primary process‐of‐care measures.13 Continuous variables were reported as mean standard deviation, and Student's t tests were used to compare the 2 groups. Categorical data were expressed as frequency distributions, and chi‐square tests were used to identify differences between the 2 groups. All tests were 2‐tailed with statistical significance set at 0.05. Statistical analysis was performed using SPSS version 19.0. (IBM, Armonk, NY).
To overcome data constraints, we created a dichotomous variable for each of the 3 primary processes‐of‐care (indicating receipt of process or not) and then combined them into 1 dichotomous variable indicating whether or not the patients with severe sepsis received all 3 primary processes‐of‐care. The combined variable was the key independent variable in the model.
We performed logistic regression analysis on patients with severe sepsis. The equation Logit [P(ICU Type = CICU)] = + 1Combined + 2Age describes the framework of the model, with ICU type being the dependent variable, and the combined variable of patients receiving all primary measures being the independent variable and controlled for age. Logistic regression was performed using JMP (SAS Institute, Inc, Cary, NC).
We additionally performed a secondary analysis to explore possible predictors of mortality using a logistic regression model, with the event of death as the dependent variable, and age, APACHE II scores, combined processes‐of‐care, and ICU type included as independent variables.
RESULTS
There were 100 patients admitted to the MICU and 41 patients admitted to the CICU during the study period (Table 1). The majority of the patients were admitted to the ICUs directly from the emergency department (ED) (n = 129), with a small number of patients who were transferred from the Medicine floors (n = 12).
| MICU (N =100) | CICU (N =41) | P Value | |
|---|---|---|---|
| |||
| Age in years, mean SD | 67 14.8 | 72 15.1 | 0.11 |
| Female, n (%) | 57 (57) | 27 (66) | 0.33 |
| Patients with chronic organ insufficiency, n (%) | 59 (59) | 22 (54) | 0.56 |
| Patients with severe sepsis, n (%) | 88 (88) | 21 (51) | <0.001 |
| Patients needing mechanical ventilation, n (%) | 43 (43) | 14 (34) | 0.33 |
| APACHE II score, mean SD | 25.53 9.11 | 24.37 9.53 | 0.50 |
| SOFA score on day 1, mean SD | 7.09 3.55 | 6.71 4.57 | 0.60 |
| Patients with acute lung injury on presentation, n (%) | 8 (8) | 2 (5) | 0.50 |
There were no significant differences between the 2 study groups in terms of age, sex, primary site of infection, mean APACHE II score, SOFA scores on day 1, chronic organ insufficiency, immune suppression, or need for mechanical ventilation (Table 1). The most common site of infection was lung. There were significantly more patients with severe sepsis in the MICU (88% vs 51%, P <0.001).
Sepsis Process‐of‐Care Measures
There were no significant differences in the proportion of severe sepsis patients who had central venous saturation checked (MICU: 46% vs CICU: 41%, P = 0.67), lactate level checked (95% vs 100%, P = 0.37), or received antibiotics within 60 minutes of presentation (75% vs 69%, P = 0.59) (Table 2). Multiple other processes and treatments were delivered similarly, as shown in Table 2.
| Primary Process‐of‐Care Measures (Severe Sepsis Patients) | MICU (N = 88) | CICU (N = 21) | P Value |
|---|---|---|---|
| |||
| Patients with central venous oxygen saturation checked, n (%)* | 31 (46) | 7 (41) | 0.67 |
| Patients with lactate level checked, n (%)* | 58 (95) | 16 (100) | 0.37 |
| Received antibiotics within 60 min, n (%)* | 46 (75) | 11 (69) | 0.59 |
| Patients who had all 3 above processes and treatments, n (%) | 19 (22) | 4 (19) | 0.79 |
| Received vasopressor, n (%) | 25 (28) | 8 (38) | 0.55 |
| ICU Treatments and Processes (All Sepsis Patients) | (N =100) | (N = 41) | |
| Fluid balance 24 h after admission in liters, mean SD | 1.96 2.42 | 1.42 2.63 | 0.24 |
| Patients who received stress dose steroids, n (%) | 11 (11) | 4 (10) | 0.83 |
| Patients who received Drotrecogin alfa, n (%) | 0 (0) | 0 (0) | |
| Morning glucose 24 h after admission in mg/dL, mean SD | 161 111 | 144 80 | 0.38 |
| Received DVT prophylaxis within 24 h of admission, n (%) | 74 (74) | 20 (49) | 0.004 |
| Received GI prophylaxis within 24 h of admission, n (%) | 68 (68) | 18 (44) | 0.012 |
| Received RBC transfusion within 24 h of admission, n (%) | 8 (8) | 7 (17) | 0.11 |
| Received renal replacement therapy, n (%) | 13 (13) | 3 (7) | 0.33 |
| Received a spontaneous breathing trial within 24 h of admission, n (%)* | 4 (11) | 4 (33) | 0.07 |
Logistic regression analysis examining the receipt of all 3 primary processes‐of‐care while controlling for age revealed that the odds of the being in one of the ICUs was not significantly different (P = 0.85). The secondary analysis regression models revealed that only the APACHE II score (odds ratio [OR] = 1.21; confidence interval [CI], 1.121.31) was significantly associated with higher odds of mortality. ICU‐type [MICU vs CICU] (OR = 1.85; CI, 0.428.20), age (OR = 1.01; CI, 0.971.06), and combined processes of care (OR = 0.26; CI, 0.071.01) did not have significant associations with odds of mortality.
A review of microbiologic sensitivities revealed a trend towards significance that the cultured microorganism(s) was likely to be resistant to the initial antibiotics administered in MICU vs CICU (15% vs 5%, respectively, P = 0.09).
Mechanical Ventilation Parameters
The majority of the ventilated patients were admitted to each ICU in assist control (AC) mode. There were no significant differences in categories of mean tidal volume (TV) (P = 0.3), mean plateau pressures (P = 0.12), mean fraction of inspired oxygen (FiO2) (P = 0.95), and mean positive end‐expiratory pressures (PEEP) (P = 0.98) noted across the 2 units at the time of ICU admission, and also 24 hours after ICU admission. Further comparison of measurements of tidal volumes and plateau pressures over 7 days of ICU stay revealed no significant differences in the 2 ICUs (P = 0.40 and 0.57, respectively, on day 7 of ICU admission). There was a trend towards significance in fewer patients in the MICU receiving spontaneous breathing trial within 24 hours of ICU admission (11% vs 33%, P = 0.07) (Table 2).
Patient Outcomes
There were no significant differences in ICU mortality (MICU 19% vs CICU 10%, P = 0.18), or hospital mortality (21% vs 15%, P = 0.38) across the units (Table 3). Mean ICU and hospital length of stay (LOS) and proportion of patients discharged home with unassisted breathing were similar (Table 3).
| Patient Outcomes | MICU (N = 100) | CICU (N = 41) | P Value |
|---|---|---|---|
| |||
| ICU mortality, n (%) | 19 (19) | 4 (10) | 0.18 |
| Hospital mortality, n (%) | 21 (21) | 6 (15) | 0.38 |
| Discharged home with unassisted breathing, n (%) | 33 (33) | 19 (46) | 0.14 |
| ICU length of stay in days, mean SD | 4.78 6.24 | 4.92 6.32 | 0.97 |
| Hospital length of stay in days, mean SD | 9.68 9.22 | 9.73 9.33 | 0.98 |
DISCUSSION
Since sepsis is more commonly treated in the medical ICU and some data suggests that specialty ICUs may be better at providing desired care,18, 19 we believed that patients treated in the MICU would be more likely to receive guideline‐concordant care. The study refutes our a priori hypothesis and reveals that evidence‐based processes‐of‐care associated with improved outcomes for sepsis are similarly implemented at our institution in the primary and overflow ICU. These findings are important, as ICU bed availability is a frequent problem and many hospitals overflow patients to non‐primary ICUs.9, 20
The observed equivalence in the care delivered may be a function of the relatively high number of patients with sepsis treated in the overflow unit, thereby giving the delivery teams enough experience to provide the desired care. An alternative explanation could be that the residents in CICU brought with them the experience from having previously trained in the MICU. Although, some of the care processes for sepsis patients are influenced by the CPOE (with embedded order sets and protocols), it is unlikely that CPOE can fully account for similarity in care because many processes and therapies (like use of steroids, amount of fluid delivered in first 24 hours, packed red blood cells [PRBC] transfusion, and spontaneous breathing trials) are not embedded within order sets.
The significant difference noted in the areas of deep vein thrombosis (DVT) and gastrointestinal (GI) prophylaxis within 24 hours of ICU admission was unexpected. These preventive therapies are included in initial order sets in the CPOE, which prompt physicians to order them as standard‐of‐care. With respect to DVT prophylaxis, we suspect that some of the difference might be attributable to specific contraindications to its use, which could have been more common in one of the units. There were more patients in MICU on mechanical ventilation (although not statistically significant) and with severe sepsis (statistically significant) at time of admission, which might have contributed to the difference noted in use of GI prophylaxis. It is also plausible that these differences might have disappeared if they were reassessed beyond 24 hours into the ICU admission. We cannot rule out the presence of unit‐ and physician‐level differences that contributed to this. Likewise, there was an unexpected trend towards significance, wherein more patients in CICU had spontaneous breathing trials within 24 hours of admission. This might also be explained by the higher number of patients with severe sepsis in the MICU (preempting any weaning attempts). These caveats aside, it is reassuring that, at our institution, admitting septic patients to the first available ICU bed does not adversely affect important processes‐of‐care.
One might ask whether this study's data should reassure other sites who are boarding septic patients in non‐primary ICUs. Irrespective of the number of patients studied or the degree of statistical significance of the associations, an observational study design cannot prove that boarding septic patients in non‐primary ICUs is either safe or unsafe. However, we hope that readers reflect on, and take inventory of, systems issues that may be different between unitswith an eye towards eliminating variation such that all units managing septic patients are primed to deliver guideline‐concordant care. Other hospitals that use CPOE with sepsis order sets, have protocols for sepsis care, and who train nursing and respiratory therapists to meet high standards might be pleased to see that the patients in our study received comparable, high‐quality care across the 2 units. While our data suggests that boarding patients in overflow units may be safe, these findings would need to be replicated at other sites using prospective designs to prove safety.
Length of emergency room stay prior to admission is associated with higher mortality rates.2123 At many hospitals, critical care beds are a scarce resource such that most hospitals have a policy for the triage of patients to critical care beds.24, 25 Lundberg and colleagues' study demonstrated that patients who developed septic shock on the medical wards experienced delays in receipt of intravenous fluids, inotropic agents and transfer to a critical care setting.26 Thus, rather than waiting in the ED or on the medical service for an MICU bed to become available, it may be most wise to admit a critically sick septic patient to the first available ICU bed, even to an overflow ICU. In a recent study by Sidlow and Aggarwal, 1104 patients discharged from the coronary care unit (CCU) with a non‐cardiac primary diagnosis were compared to patients admitted to the MICU in the same hospital.27 The study found no differences in patient mortality, 30‐day readmission rate, hospital LOS, ICU LOS, and safety outcomes of ventilator‐associated pneumonia and catheter‐associated bloodstream infections between ICUs. However, their study did not examine processes‐of‐care delivered between the primary ICU and the overflow unit, and did not validate the primary diagnoses of patients admitted to the ICU.
Several limitations of this study should be considered. First, this study was conducted at a single center. Second, we used a retrospective study design; however, a prospective study randomizing patients to 1 of the 2 units would likely never be possible. Third, the relatively small number of patients limited the power of the study to detect mortality differences between the units. However, this was a pilot study focused on processes of care as opposed to clinical outcomes. Fourth, it is possible that we did not capture every single patient with sepsis with our keyword search. Our use of a previously validated screening process should have limited the number of missed cases.15, 16 Fifth, although the 2 ICUs have exclusive nursing staff and attending physicians, the housestaff and respiratory therapists do rotate between the 2 ICUs and place orders in the common CPOE. The rotating housestaff may certainly represent a source for confounding, but the large numbers (>30) of evenly spread housestaff over the study period minimizes the potential for any trainee to be responsible for a large proportion of observed practice. Sixth, ICU attendings are the physicians of record and could influence the results. Because no attending physician was on service for more than 4 weeks during the study period, and patients were equally spread over this same time, concerns about clustering and biases this may have created should be minimal but cannot be ruled out. Seventh, some interventions and processes, such as antibiotic administration and measurement of lactate, may have been initiated in the ED, thereby decreasing the potential for differences between the groups. Additionally, we cannot rule out the possibility that factors other than bed availability drove the admission process (we found that the relative proportion of patients admitted to overflow ICU during hours of ambulance diversion was similar to the overflow ICU admissions during non‐ambulance diversion hours). It is possible that some selection bias by the hospitalist assigning patients to specific ICUs influenced their triage decisionsalthough all triaging doctors go through the same process of training in active bed management.11 While more patients admitted to the MICU had severe sepsis, there were no differences between groups in APACHE II or SOFA scores. However, we cannot rule out that there were other residual confounders. Finally, in a small number of cases (4/41, 10%), the CICU team consulted the MICU attending for assistance. This input had the potential to reduce disparities in care between the units.
Overflowing patients to non‐primary ICUs occurs in many hospitals. Our study demonstrates that sepsis treatment for overflow patients may be similar to that received in the primary ICU. While a large multicentered and randomized trial could determine whether significant management and outcome differences exist between primary and overflow ICUs, feasibility concerns make it unlikely that such a study will ever be conducted.
Acknowledgements
Disclosure: Dr Wright is a Miller‐Coulson Family Scholar and this work is supported by the Miller‐Coulson family through the Johns Hopkins Center for Innovative Medicine. Dr Sevransky was supported with a grant from National Institute of General Medical Sciences, NIGMS K‐23‐1399. All other authors disclose no relevant or financial conflicts of interest.
- ,,,,,.Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med.2001;29(7):1303–1310.
- ,,, et al;for the Milwaukee Initiative in Critical Care Outcomes Research (MICCOR) Group of Investigators.Nationwide trends of severe sepsis in the twenty first century (2000–2007).Chest.2011;140(5):1223–1231.
- ,,,.Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003.Crit Care Med.2007;35(5):1244–1250.
- ,,, et al.Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36(1):296–327.
- ,,, et al.Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial.JAMA.2010;303(8):739–746.
- ,,, et al.Early goal‐directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med.2001;345(19):1368–1377.
- ,,, et al.Implementation of a bundle of quality indicators for the early management of severe sepsis and septic shock is associated with decreased mortality.Crit Care Med.2007;35(4):1105–1112.
- ,,, et al.Early combination antibiotic therapy yields improved survival compared with monotherapy in septic shock: a propensity‐matched analysis.Crit Care Med.2010;38(9):1773–1785.
- .A new dimension of the PACU: the dilemma of the ICU overflow patient.J Post Anesth Nurs.1994;9(5):297–300.
- ,,, et al.Descriptive analysis of critical care units in the United States.Crit Care Med.1992;20(6):846–863.
- ,,,,,.Active bed management by hospitalists and emergency department throughput.Ann Intern Med.2008;149(11):804–811.
- ,,, et al.Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee, American College of Chest Physicians/Society of Critical Care Medicine.Chest.1992;101(6):1644–1655.
- ,,, et al.Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain.JAMA.2008;299(19):2294–2303.
- ,,, et al.Impact of the surviving sepsis campaign protocols on hospital length of stay and mortality in septic shock patients: results of a three‐year follow‐up quasi‐experimental study.Crit Care Med.2010;38(4):1036–1043.
- ,,, et al.Study protocol: the improving care of acute lung injury patients (ICAP) study.Crit Care.2006;10(1):R9.
- ,,,,,.Critical illness outcome study: an observational study of protocols and mortality in intensive care units.Open Access J Clin Trials.2011;3(September):55–65.
- ,,, et al.The SOFA (sepsis‐related organ failure assessment) score to describe organ dysfunction/failure: on behalf of the Working Group on Sepsis‐Related Problems of the European Society of Intensive Care Medicine.Intensive Care Med.1996;22(7):707–710.
- ,,,,,.Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review.JAMA.2002;288(17):2151–2162.
- ,,.Do intensivists in ICU improve outcome?Best Pract Res Clin Anaesthesiol.2005;19(1):125–135.
- .Is the postanesthesia care unit becoming an intensive care unit?J Perianesth Nurs.1999;14(2):73–77.
- ,,,,;for the DELAY‐ED Study Group.Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit.Crit Care Med.2007;35(6):1477–1483.
- ,,, et al.Association between timing of intensive care unit admission and outcomes for emergency department patients with community‐acquired pneumonia.Crit Care Med.2009;37(11):2867–2874.
- ,.Association between ambulance diversion and survival among patients with acute myocardial infarction.JAMA.2011;305(23):2440–2447.
- .Civilian triage in the intensive care unit: the ritual of the last bed.Crit Care Med.1993;21(4):598–606.
- ,,,,;for the Values Ethics and Rationing in Critical Care Task Force.Rationing critical care beds: a systematic review.Crit Care Med.2004;32(7):1588–1597.
- ,,, et al.Septic shock: an analysis of outcomes for patients with onset on hospital wards versus intensive care units.Crit Care Med.1998;26(6):1020–1024.
- ,.“The MICU is full”: one hospital's experience with an overflow triage policy.Jt Comm J Qual Patient Saf.2011;37(10):456–460.
- ,,,,,.Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med.2001;29(7):1303–1310.
- ,,, et al;for the Milwaukee Initiative in Critical Care Outcomes Research (MICCOR) Group of Investigators.Nationwide trends of severe sepsis in the twenty first century (2000–2007).Chest.2011;140(5):1223–1231.
- ,,,.Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003.Crit Care Med.2007;35(5):1244–1250.
- ,,, et al.Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36(1):296–327.
- ,,, et al.Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial.JAMA.2010;303(8):739–746.
- ,,, et al.Early goal‐directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med.2001;345(19):1368–1377.
- ,,, et al.Implementation of a bundle of quality indicators for the early management of severe sepsis and septic shock is associated with decreased mortality.Crit Care Med.2007;35(4):1105–1112.
- ,,, et al.Early combination antibiotic therapy yields improved survival compared with monotherapy in septic shock: a propensity‐matched analysis.Crit Care Med.2010;38(9):1773–1785.
- .A new dimension of the PACU: the dilemma of the ICU overflow patient.J Post Anesth Nurs.1994;9(5):297–300.
- ,,, et al.Descriptive analysis of critical care units in the United States.Crit Care Med.1992;20(6):846–863.
- ,,,,,.Active bed management by hospitalists and emergency department throughput.Ann Intern Med.2008;149(11):804–811.
- ,,, et al.Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee, American College of Chest Physicians/Society of Critical Care Medicine.Chest.1992;101(6):1644–1655.
- ,,, et al.Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain.JAMA.2008;299(19):2294–2303.
- ,,, et al.Impact of the surviving sepsis campaign protocols on hospital length of stay and mortality in septic shock patients: results of a three‐year follow‐up quasi‐experimental study.Crit Care Med.2010;38(4):1036–1043.
- ,,, et al.Study protocol: the improving care of acute lung injury patients (ICAP) study.Crit Care.2006;10(1):R9.
- ,,,,,.Critical illness outcome study: an observational study of protocols and mortality in intensive care units.Open Access J Clin Trials.2011;3(September):55–65.
- ,,, et al.The SOFA (sepsis‐related organ failure assessment) score to describe organ dysfunction/failure: on behalf of the Working Group on Sepsis‐Related Problems of the European Society of Intensive Care Medicine.Intensive Care Med.1996;22(7):707–710.
- ,,,,,.Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review.JAMA.2002;288(17):2151–2162.
- ,,.Do intensivists in ICU improve outcome?Best Pract Res Clin Anaesthesiol.2005;19(1):125–135.
- .Is the postanesthesia care unit becoming an intensive care unit?J Perianesth Nurs.1999;14(2):73–77.
- ,,,,;for the DELAY‐ED Study Group.Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit.Crit Care Med.2007;35(6):1477–1483.
- ,,, et al.Association between timing of intensive care unit admission and outcomes for emergency department patients with community‐acquired pneumonia.Crit Care Med.2009;37(11):2867–2874.
- ,.Association between ambulance diversion and survival among patients with acute myocardial infarction.JAMA.2011;305(23):2440–2447.
- .Civilian triage in the intensive care unit: the ritual of the last bed.Crit Care Med.1993;21(4):598–606.
- ,,,,;for the Values Ethics and Rationing in Critical Care Task Force.Rationing critical care beds: a systematic review.Crit Care Med.2004;32(7):1588–1597.
- ,,, et al.Septic shock: an analysis of outcomes for patients with onset on hospital wards versus intensive care units.Crit Care Med.1998;26(6):1020–1024.
- ,.“The MICU is full”: one hospital's experience with an overflow triage policy.Jt Comm J Qual Patient Saf.2011;37(10):456–460.
Copyright © 2012 Society of Hospital Medicine
Mortality and Readmission Correlations
The Centers for Medicare & Medicaid Services (CMS) publicly reports hospital‐specific, 30‐day risk‐standardized mortality and readmission rates for Medicare fee‐for‐service patients admitted with acute myocardial infarction (AMI), heart failure (HF), and pneumonia.1 These measures are intended to reflect hospital performance on quality of care provided to patients during and after hospitalization.2, 3
Quality‐of‐care measures for a given disease are often assumed to reflect the quality of care for that particular condition. However, studies have found limited association between condition‐specific process measures and either mortality or readmission rates for those conditions.46 Mortality and readmission rates may instead reflect broader hospital‐wide or specialty‐wide structure, culture, and practice. For example, studies have previously found that hospitals differ in mortality or readmission rates according to organizational structure,7 financial structure,8 culture,9, 10 information technology,11 patient volume,1214 academic status,12 and other institution‐wide factors.12 There is now a strong policy push towards developing hospital‐wide (all‐condition) measures, beginning with readmission.15
It is not clear how much of the quality of care for a given condition is attributable to hospital‐wide influences that affect all conditions rather than disease‐specific factors. If readmission or mortality performance for a particular condition reflects, in large part, broader institutional characteristics, then improvement efforts might better be focused on hospital‐wide activities, such as team training or implementing electronic medical records. On the other hand, if the disease‐specific measures reflect quality strictly for those conditions, then improvement efforts would be better focused on disease‐specific care, such as early identification of the relevant patient population or standardizing disease‐specific care. As hospitals work to improve performance across an increasingly wide variety of conditions, it is becoming more important for hospitals to prioritize and focus their activities effectively and efficiently.
One means of determining the relative contribution of hospital versus disease factors is to explore whether outcome rates are consistent among different conditions cared for in the same hospital. If mortality (or readmission) rates across different conditions are highly correlated, it would suggest that hospital‐wide factors may play a substantive role in outcomes. Some studies have found that mortality for a particular surgical condition is a useful proxy for mortality for other surgical conditions,16, 17 while other studies have found little correlation among mortality rates for various medical conditions.18, 19 It is also possible that correlation varies according to hospital characteristics; for example, smaller or nonteaching hospitals might be more homogenous in their care than larger, less homogeneous institutions. No studies have been performed using publicly reported estimates of risk‐standardized mortality or readmission rates. In this study we use the publicly reported measures of 30‐day mortality and 30‐day readmission for AMI, HF, and pneumonia to examine whether, and to what degree, mortality rates track together within US hospitals, and separately, to what degree readmission rates track together within US hospitals.
METHODS
Data Sources
CMS calculates risk‐standardized mortality and readmission rates, and patient volume, for all acute care nonfederal hospitals with one or more eligible case of AMI, HF, and pneumonia annually based on fee‐for‐service (FFS) Medicare claims. CMS publicly releases the rates for the large subset of hospitals that participate in public reporting and have 25 or more cases for the conditions over the 3‐year period between July 2006 and June 2009. We estimated the rates for all hospitals included in the measure calculations, including those with fewer than 25 cases, using the CMS methodology and data obtained from CMS. The distribution of these rates has been previously reported.20, 21 In addition, we used the 2008 American Hospital Association (AHA) Survey to obtain data about hospital characteristics, including number of beds, hospital ownership (government, not‐for‐profit, for‐profit), teaching status (member of Council of Teaching Hospitals, other teaching hospital, nonteaching), presence of specialized cardiac capabilities (coronary artery bypass graft surgery, cardiac catheterization lab without cardiac surgery, neither), US Census Bureau core‐based statistical area (division [subarea of area with urban center >2.5 million people], metropolitan [urban center of at least 50,000 people], micropolitan [urban center of between 10,000 and 50,000 people], and rural [<10,000 people]), and safety net status22 (yes/no). Safety net status was defined as either public hospitals or private hospitals with a Medicaid caseload greater than one standard deviation above their respective state's mean private hospital Medicaid caseload using the 2007 AHA Annual Survey data.
Study Sample
This study includes 2 hospital cohorts, 1 for mortality and 1 for readmission. Hospitals were eligible for the mortality cohort if the dataset included risk‐standardized mortality rates for all 3 conditions (AMI, HF, and pneumonia). Hospitals were eligible for the readmission cohort if the dataset included risk‐standardized readmission rates for all 3 of these conditions.
Risk‐Standardized Measures
The measures include all FFS Medicare patients who are 65 years old, have been enrolled in FFS Medicare for the 12 months before the index hospitalization, are admitted with 1 of the 3 qualifying diagnoses, and do not leave the hospital against medical advice. The mortality measures include all deaths within 30 days of admission, and all deaths are attributable to the initial admitting hospital, even if the patient is then transferred to another acute care facility. Therefore, for a given hospital, transfers into the hospital are excluded from its rate, but transfers out are included. The readmission measures include all readmissions within 30 days of discharge, and all readmissions are attributable to the final discharging hospital, even if the patient was originally admitted to a different acute care facility. Therefore, for a given hospital, transfers in are included in its rate, but transfers out are excluded. For mortality measures, only 1 hospitalization for a patient in a specific year is randomly selected if the patient has multiple hospitalizations in the year. For readmission measures, admissions in which the patient died prior to discharge, and admissions within 30 days of an index admission, are not counted as index admissions.
Outcomes for all measures are all‐cause; however, for the AMI readmission measure, planned admissions for cardiac procedures are not counted as readmissions. Patients in observation status or in non‐acute care facilities are not counted as readmissions. Detailed specifications for the outcomes measures are available at the National Quality Measures Clearinghouse.23
The derivation and validation of the risk‐standardized outcome measures have been previously reported.20, 21, 2327 The measures are derived from hierarchical logistic regression models that include age, sex, clinical covariates, and a hospital‐specific random effect. The rates are calculated as the ratio of the number of predicted outcomes (obtained from a model applying the hospital‐specific effect) to the number of expected outcomes (obtained from a model applying the average effect among hospitals), multiplied by the unadjusted overall 30‐day rate.
Statistical Analysis
We examined patterns and distributions of hospital volume, risk‐standardized mortality rates, and risk‐standardized readmission rates among included hospitals. To measure the degree of association among hospitals' risk‐standardized mortality rates for AMI, HF, and pneumonia, we calculated Pearson correlation coefficients, resulting in 3 correlations for the 3 pairs of conditions (AMI and HF, AMI and pneumonia, HF and pneumonia), and tested whether they were significantly different from 0. We also conducted a factor analysis using the principal component method with a minimum eigenvalue of 1 to retain factors to determine whether there was a single common factor underlying mortality performance for the 3 conditions.28 Finally, we divided hospitals into quartiles of performance for each outcome based on the point estimate of risk‐standardized rate, and compared quartile of performance between condition pairs for each outcome. For each condition pair, we assessed the percent of hospitals in the same quartile of performance in both conditions, the percent of hospitals in either the top quartile of performance or the bottom quartile of performance for both, and the percent of hospitals in the top quartile for one and the bottom quartile for the other. We calculated the weighted kappa for agreement on quartile of performance between condition pairs for each outcome and the Spearman correlation for quartiles of performance. Then, we examined Pearson correlation coefficients in different subgroups of hospitals, including by size, ownership, teaching status, cardiac procedure capability, statistical area, and safety net status. In order to determine whether these correlations differed by hospital characteristics, we tested if the Pearson correlation coefficients were different between any 2 subgroups using the method proposed by Fisher.29 We repeated all of these analyses separately for the risk‐standardized readmission rates.
To determine whether correlations between mortality rates were significantly different than correlations between readmission rates for any given condition pair, we used the method recommended by Raghunathan et al.30 For these analyses, we included only hospitals reporting both mortality and readmission rates for the condition pairs. We used the same methods to determine whether correlations between mortality rates were significantly different than correlations between readmission rates for any given condition pair among subgroups of hospital characteristics.
All analyses and graphing were performed using the SAS statistical package version 9.2 (SAS Institute, Cary, NC). We considered a P‐value < 0.05 to be statistically significant, and all statistical tests were 2‐tailed.
RESULTS
The mortality cohort included 4559 hospitals, and the readmission cohort included 4468 hospitals. The majority of hospitals was small, nonteaching, and did not have advanced cardiac capabilities such as cardiac surgery or cardiac catheterization (Table 1).
| Description | Mortality Measures | Readmission Measures |
|---|---|---|
| Hospital N = 4559 | Hospital N = 4468 | |
| N (%)* | N (%)* | |
| ||
| No. of beds | ||
| >600 | 157 (3.4) | 156 (3.5) |
| 300600 | 628 (13.8) | 626 (14.0) |
| <300 | 3588 (78.7) | 3505 (78.5) |
| Unknown | 186 (4.08) | 181 (4.1) |
| Mean (SD) | 173.24 (189.52) | 175.23 (190.00) |
| Ownership | ||
| Not‐for‐profit | 2650 (58.1) | 2619 (58.6) |
| For‐profit | 672 (14.7) | 663 (14.8) |
| Government | 1051 (23.1) | 1005 (22.5) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Teaching status | ||
| COTH | 277 (6.1) | 276 (6.2) |
| Teaching | 505 (11.1) | 503 (11.3) |
| Nonteaching | 3591 (78.8) | 3508 (78.5) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Cardiac facility type | ||
| CABG | 1471 (32.3) | 1467 (32.8) |
| Cath lab | 578 (12.7) | 578 (12.9) |
| Neither | 2324 (51.0) | 2242 (50.2) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Core‐based statistical area | ||
| Division | 621 (13.6) | 618 (13.8) |
| Metro | 1850 (40.6) | 1835 (41.1) |
| Micro | 801 (17.6) | 788 (17.6) |
| Rural | 1101 (24.2) | 1046 (23.4) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Safety net status | ||
| No | 2995 (65.7) | 2967 (66.4) |
| Yes | 1377 (30.2) | 1319 (29.5) |
| Unknown | 187 (4.1) | 182 (4.1) |
For mortality measures, the smallest median number of cases per hospital was for AMI (48; interquartile range [IQR], 13,171), and the greatest number was for pneumonia (178; IQR, 87, 336). The same pattern held for readmission measures (AMI median 33; IQR; 9, 150; pneumonia median 191; IQR, 95, 352.5). With respect to mortality measures, AMI had the highest rate and HF the lowest rate; however, for readmission measures, HF had the highest rate and pneumonia the lowest rate (Table 2).
| Description | Mortality Measures (N = 4559) | Readmission Measures (N = 4468) | ||||
|---|---|---|---|---|---|---|
| AMI | HF | PN | AMI | HF | PN | |
| ||||||
| Total discharges | 558,653 | 1,094,960 | 1,114,706 | 546,514 | 1,314,394 | 1,152,708 |
| Hospital volume | ||||||
| Mean (SD) | 122.54 (172.52) | 240.18 (271.35) | 244.51 (220.74) | 122.32 (201.78) | 294.18 (333.2) | 257.99 (228.5) |
| Median (IQR) | 48 (13, 171) | 142 (56, 337) | 178 (87, 336) | 33 (9, 150) | 172.5 (68, 407) | 191 (95, 352.5) |
| Range min, max | 1, 1379 | 1, 2814 | 1, 2241 | 1, 1611 | 1, 3410 | 2, 2359 |
| 30‐Day risk‐standardized rate* | ||||||
| Mean (SD) | 15.7 (1.8) | 10.9 (1.6) | 11.5 (1.9) | 19.9 (1.5) | 24.8 (2.1) | 18.5 (1.7) |
| Median (IQR) | 15.7 (14.5, 16.8) | 10.8 (9.9, 11.9) | 11.3 (10.2, 12.6) | 19.9 (18.9, 20.8) | 24.7 (23.4, 26.1) | 18.4 (17.3, 19.5) |
| Range min, max | 10.3, 24.6 | 6.6, 18.2 | 6.7, 20.9 | 15.2, 26.3 | 17.3, 32.4 | 13.6, 26.7 |
Every mortality measure was significantly correlated with every other mortality measure (range of correlation coefficients, 0.270.41, P < 0.0001 for all 3 correlations). For example, the correlation between risk‐standardized mortality rates (RSMR) for HF and pneumonia was 0.41. Similarly, every readmission measure was significantly correlated with every other readmission measure (range of correlation coefficients, 0.320.47; P < 0.0001 for all 3 correlations). Overall, the lowest correlation was between risk‐standardized mortality rates for AMI and pneumonia (r = 0.27), and the highest correlation was between risk‐standardized readmission rates (RSRR) for HF and pneumonia (r = 0.47) (Table 3).
| Description | Mortality Measures | Readmission Measures | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | AMI and HF | AMI and PN | HF and PN | AMI and HF | AMI and PN | HF and PN | ||||||||
| r | P | r | P | r | P | N | r | P | r | P | r | P | ||
| ||||||||||||||
| All | 4559 | 0.30 | 0.27 | 0.41 | 4468 | 0.38 | 0.32 | 0.47 | ||||||
| Hospitals with 25 patients | 2872 | 0.33 | 0.30 | 0.44 | 2467 | 0.44 | 0.38 | 0.51 | ||||||
| No. of beds | 0.15 | 0.005 | 0.0009 | <0.0001 | <0.0001 | <0.0001 | ||||||||
| >600 | 157 | 0.38 | 0.43 | 0.51 | 156 | 0.67 | 0.50 | 0.66 | ||||||
| 300600 | 628 | 0.29 | 0.30 | 0.49 | 626 | 0.54 | 0.45 | 0.58 | ||||||
| <300 | 3588 | 0.27 | 0.23 | 0.37 | 3505 | 0.30 | 0.26 | 0.44 | ||||||
| Ownership | 0.021 | 0.05 | 0.39 | 0.0004 | 0.0004 | 0.003 | ||||||||
| Not‐for‐profit | 2650 | 0.32 | 0.28 | 0.42 | 2619 | 0.43 | 0.36 | 0.50 | ||||||
| For‐profit | 672 | 0.30 | 0.23 | 0.40 | 663 | 0.29 | 0.22 | 0.40 | ||||||
| Government | 1051 | 0.24 | 0.22 | 0.39 | 1005 | 0.32 | 0.29 | 0.45 | ||||||
| Teaching status | 0.11 | 0.08 | 0.0012 | <0.0001 | 0.0002 | 0.0003 | ||||||||
| COTH | 277 | 0.31 | 0.34 | 0.54 | 276 | 0.54 | 0.47 | 0.59 | ||||||
| Teaching | 505 | 0.22 | 0.28 | 0.43 | 503 | 0.52 | 0.42 | 0.56 | ||||||
| Nonteaching | 3591 | 0.29 | 0.24 | 0.39 | 3508 | 0.32 | 0.26 | 0.44 | ||||||
| Cardiac facility type | 0.022 | 0.006 | <0.0001 | <0.0001 | 0.0006 | 0.004 | ||||||||
| CABG | 1471 | 0.33 | 0.29 | 0.47 | 1467 | 0.48 | 0.37 | 0.52 | ||||||
| Cath lab | 578 | 0.25 | 0.26 | 0.36 | 578 | 0.32 | 0.37 | 0.47 | ||||||
| Neither | 2324 | 0.26 | 0.21 | 0.36 | 2242 | 0.28 | 0.27 | 0.44 | ||||||
| Core‐based statistical area | 0.0001 | <0.0001 | 0.002 | <0.0001 | <0.0001 | <0.0001 | ||||||||
| Division | 621 | 0.38 | 0.34 | 0.41 | 618 | 0.46 | 0.40 | 0.56 | ||||||
| Metro | 1850 | 0.26 | 0.26 | 0.42 | 1835 | 0.38 | 0.30 | 0.40 | ||||||
| Micro | 801 | 0.23 | 0.22 | 0.34 | 788 | 0.32 | 0.30 | 0.47 | ||||||
| Rural | 1101 | 0.21 | 0.13 | 0.32 | 1046 | 0.22 | 0.21 | 0.44 | ||||||
| Safety net status | 0.001 | 0.027 | 0.68 | 0.029 | 0.037 | 0.28 | ||||||||
| No | 2995 | 0.33 | 0.28 | 0.41 | 2967 | 0.40 | 0.33 | 0.48 | ||||||
| Yes | 1377 | 0.23 | 0.21 | 0.40 | 1319 | 0.34 | 0.30 | 0.45 | ||||||
Both the factor analysis for the mortality measures and the factor analysis for the readmission measures yielded only one factor with an eigenvalue >1. In each factor analysis, this single common factor kept more than half of the data based on the cumulative eigenvalue (55% for mortality measures and 60% for readmission measures). For the mortality measures, the pattern of RSMR for myocardial infarction (MI), heart failure (HF), and pneumonia (PN) in the factor was high (0.68 for MI, 0.78 for HF, and 0.76 for PN); the same was true of the RSRR in the readmission measures (0.72 for MI, 0.81 for HF, and 0.78 for PN).
For all condition pairs and both outcomes, a third or more of hospitals were in the same quartile of performance for both conditions of the pair (Table 4). Hospitals were more likely to be in the same quartile of performance if they were in the top or bottom quartile than if they were in the middle. Less than 10% of hospitals were in the top quartile for one condition in the mortality or readmission pair and in the bottom quartile for the other condition in the pair. Kappa scores for same quartile of performance between pairs of outcomes ranged from 0.16 to 0.27, and were highest for HF and pneumonia for both mortality and readmission rates.
| Condition Pair | Same Quartile (Any) (%) | Same Quartile (Q1 or Q4) (%) | Q1 in One and Q4 in Another (%) | Weighted Kappa | Spearman Correlation |
|---|---|---|---|---|---|
| |||||
| Mortality | |||||
| MI and HF | 34.8 | 20.2 | 7.9 | 0.19 | 0.25 |
| MI and PN | 32.7 | 18.8 | 8.2 | 0.16 | 0.22 |
| HF and PN | 35.9 | 21.8 | 5.0 | 0.26 | 0.36 |
| Readmission | |||||
| MI and HF | 36.6 | 21.0 | 7.5 | 0.22 | 0.28 |
| MI and PN | 34.0 | 19.6 | 8.1 | 0.19 | 0.24 |
| HF and PN | 37.1 | 22.6 | 5.4 | 0.27 | 0.37 |
In subgroup analyses, the highest mortality correlation was between HF and pneumonia in hospitals with more than 600 beds (r = 0.51, P = 0.0009), and the highest readmission correlation was between AMI and HF in hospitals with more than 600 beds (r = 0.67, P < 0.0001). Across both measures and all 3 condition pairs, correlations between conditions increased with increasing hospital bed size, presence of cardiac surgery capability, and increasing population of the hospital's Census Bureau statistical area. Furthermore, for most measures and condition pairs, correlations between conditions were highest in not‐for‐profit hospitals, hospitals belonging to the Council of Teaching Hospitals, and non‐safety net hospitals (Table 3).
For all condition pairs, the correlation between readmission rates was significantly higher than the correlation between mortality rates (P < 0.01). In subgroup analyses, readmission correlations were also significantly higher than mortality correlations for all pairs of conditions among moderate‐sized hospitals, among nonprofit hospitals, among teaching hospitals that did not belong to the Council of Teaching Hospitals, and among non‐safety net hospitals (Table 5).
| Description | AMI and HF | AMI and PN | HF and PN | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | MC | RC | P | N | MC | RC | P | N | MC | RC | P | |
| ||||||||||||
| All | 4457 | 0.31 | 0.38 | <0.0001 | 4459 | 0.27 | 0.32 | 0.007 | 4731 | 0.41 | 0.46 | 0.0004 |
| Hospitals with 25 patients | 2472 | 0.33 | 0.44 | <0.001 | 2463 | 0.31 | 0.38 | 0.01 | 4104 | 0.42 | 0.47 | 0.001 |
| No. of beds | ||||||||||||
| >600 | 156 | 0.38 | 0.67 | 0.0002 | 156 | 0.43 | 0.50 | 0.48 | 160 | 0.51 | 0.66 | 0.042 |
| 300600 | 626 | 0.29 | 0.54 | <0.0001 | 626 | 0.31 | 0.45 | 0.003 | 630 | 0.49 | 0.58 | 0.033 |
| <300 | 3494 | 0.28 | 0.30 | 0.21 | 3496 | 0.23 | 0.26 | 0.17 | 3733 | 0.37 | 0.43 | 0.003 |
| Ownership | ||||||||||||
| Not‐for‐profit | 2614 | 0.32 | 0.43 | <0.0001 | 2617 | 0.28 | 0.36 | 0.003 | 2697 | 0.42 | 0.50 | 0.0003 |
| For‐profit | 662 | 0.30 | 0.29 | 0.90 | 661 | 0.23 | 0.22 | 0.75 | 699 | 0.40 | 0.40 | 0.99 |
| Government | 1000 | 0.25 | 0.32 | 0.09 | 1000 | 0.22 | 0.29 | 0.09 | 1127 | 0.39 | 0.43 | 0.21 |
| Teaching status | ||||||||||||
| COTH | 276 | 0.31 | 0.54 | 0.001 | 277 | 0.35 | 0.46 | 0.10 | 278 | 0.54 | 0.59 | 0.41 |
| Teaching | 504 | 0.22 | 0.52 | <0.0001 | 504 | 0.28 | 0.42 | 0.012 | 508 | 0.43 | 0.56 | 0.005 |
| Nonteaching | 3496 | 0.29 | 0.32 | 0.18 | 3497 | 0.24 | 0.26 | 0.46 | 3737 | 0.39 | 0.43 | 0.016 |
| Cardiac facility type | ||||||||||||
| CABG | 1465 | 0.33 | 0.48 | <0.0001 | 1467 | 0.30 | 0.37 | 0.018 | 1483 | 0.47 | 0.51 | 0.103 |
| Cath lab | 577 | 0.25 | 0.32 | 0.18 | 577 | 0.26 | 0.37 | 0.046 | 579 | 0.36 | 0.47 | 0.022 |
| Neither | 2234 | 0.26 | 0.28 | 0.48 | 2234 | 0.21 | 0.27 | 0.037 | 2461 | 0.36 | 0.44 | 0.002 |
| Core‐based statistical area | ||||||||||||
| Division | 618 | 0.38 | 0.46 | 0.09 | 620 | 0.34 | 0.40 | 0.18 | 630 | 0.41 | 0.56 | 0.001 |
| Metro | 1833 | 0.26 | 0.38 | <0.0001 | 1832 | 0.26 | 0.30 | 0.21 | 1896 | 0.42 | 0.40 | 0.63 |
| Micro | 787 | 0.24 | 0.32 | 0.08 | 787 | 0.22 | 0.30 | 0.11 | 820 | 0.34 | 0.46 | 0.003 |
| Rural | 1038 | 0.21 | 0.22 | 0.83 | 1039 | 0.13 | 0.21 | 0.056 | 1177 | 0.32 | 0.43 | 0.002 |
| Safety net status | ||||||||||||
| No | 2961 | 0.33 | 0.40 | 0.001 | 2963 | 0.28 | 0.33 | 0.036 | 3062 | 0.41 | 0.48 | 0.001 |
| Yes | 1314 | 0.23 | 0.34 | 0.003 | 1314 | 0.22 | 0.30 | 0.015 | 1460 | 0.40 | 0.45 | 0.14 |
DISCUSSION
In this study, we found that risk‐standardized mortality rates for 3 common medical conditions were moderately correlated within institutions, as were risk‐standardized readmission rates. Readmission rates were more strongly correlated than mortality rates, and all rates tracked closest together in large, urban, and/or teaching hospitals. Very few hospitals were in the top quartile of performance for one condition and in the bottom quartile for a different condition.
Our findings are consistent with the hypothesis that 30‐day risk‐standardized mortality and 30‐day risk‐standardized readmission rates, in part, capture broad aspects of hospital quality that transcend condition‐specific activities. In this study, readmission rates tracked better together than mortality rates for every pair of conditions, suggesting that there may be a greater contribution of hospital‐wide environment, structure, and processes to readmission rates than to mortality rates. This difference is plausible because services specific to readmission, such as discharge planning, care coordination, medication reconciliation, and discharge communication with patients and outpatient clinicians, are typically hospital‐wide processes.
Our study differs from earlier studies of medical conditions in that the correlations we found were higher.18, 19 There are several possible explanations for this difference. First, during the intervening 1525 years since those studies were performed, care for these conditions has evolved substantially, such that there are now more standardized protocols available for all 3 of these diseases. Hospitals that are sufficiently organized or acculturated to systematically implement care protocols may have the infrastructure or culture to do so for all conditions, increasing correlation of performance among conditions. In addition, there are now more technologies and systems available that span care for multiple conditions, such as electronic medical records and quality committees, than were available in previous generations. Second, one of these studies utilized less robust risk‐adjustment,18 and neither used the same methodology of risk standardization. Nonetheless, it is interesting to note that Rosenthal and colleagues identified the same increase in correlation with higher volumes than we did.19 Studies investigating mortality correlations among surgical procedures, on the other hand, have generally found higher correlations than we found in these medical conditions.16, 17
Accountable care organizations will be assessed using an all‐condition readmission measure,31 several states track all‐condition readmission rates,3234 and several countries measure all‐condition mortality.35 An all‐condition measure for quality assessment first requires that there be a hospital‐wide quality signal above and beyond disease‐specific care. This study suggests that a moderate signal exists for readmission and, to a slightly lesser extent, for mortality, across 3 common conditions. There are other considerations, however, in developing all‐condition measures. There must be adequate risk adjustment for the wide variety of conditions that are included, and there must be a means of accounting for the variation in types of conditions and procedures cared for by different hospitals. Our study does not address these challenges, which have been described to be substantial for mortality measures.35
We were surprised by the finding that risk‐standardized rates correlated more strongly within larger institutions than smaller ones, because one might assume that care within smaller hospitals might be more homogenous. It may be easier, however, to detect a quality signal in hospitals with higher volumes of patients for all 3 conditions, because estimates for these hospitals are more precise. Consequently, we have greater confidence in results for larger volumes, and suspect a similar quality signal may be present but more difficult to detect statistically in smaller hospitals. Overall correlations were higher when we restricted the sample to hospitals with at least 25 cases, as is used for public reporting. It is also possible that the finding is real given that large‐volume hospitals have been demonstrated to provide better care for these conditions and are more likely to adopt systems of care that affect multiple conditions, such as electronic medical records.14, 36
The kappa scores comparing quartile of national performance for pairs of conditions were only in the fair range. There are several possible explanations for this fact: 1) outcomes for these 3 conditions are not measuring the same constructs; 2) they are all measuring the same construct, but they are unreliable in doing so; and/or 3) hospitals have similar latent quality for all 3 conditions, but the national quality of performance differs by condition, yielding variable relative performance per hospital for each condition. Based solely on our findings, we cannot distinguish which, if any, of these explanations may be true.31
Our study has several limitations. First, all 3 conditions currently publicly reported by CMS are medical diagnoses, although AMI patients may be cared for in distinct cardiology units and often undergo procedures; therefore, we cannot determine the degree to which correlations reflect hospital‐wide quality versus medicine‐wide quality. An institution may have a weak medicine department but a strong surgical department or vice versa. Second, it is possible that the correlations among conditions for readmission and among conditions for mortality are attributable to patient characteristics that are not adequately adjusted for in the risk‐adjustment model, such as socioeconomic factors, or to hospital characteristics not related to quality, such as coding practices or inter‐hospital transfer rates. For this to be true, these unmeasured characteristics would have to be consistent across different conditions within each hospital and have a consistent influence on outcomes. Third, it is possible that public reporting may have prompted disease‐specific focus on these conditions. We do not have data from non‐publicly reported conditions to test this hypothesis. Fourth, there are many small‐volume hospitals in this study; their estimates for readmission and mortality are less reliable than for large‐volume hospitals, potentially limiting our ability to detect correlations in this group of hospitals.
This study lends credence to the hypothesis that 30‐day risk‐standardized mortality and readmission rates for individual conditions may reflect aspects of hospital‐wide quality or at least medicine‐wide quality, although the correlations are not large enough to conclude that hospital‐wide factors play a dominant role, and there are other possible explanations for the correlations. Further work is warranted to better understand the causes of the correlations, and to better specify the nature of hospital factors that contribute to correlations among outcomes.
Acknowledgements
Disclosures: Dr Horwitz is supported by the National Institute on Aging (K08 AG038336) and by the American Federation of Aging Research through the Paul B. Beeson Career Development Award Program. Dr Horwitz is also a Pepper Scholar with support from the Claude D. Pepper Older Americans Independence Center at Yale University School of Medicine (P30 AG021342 NIH/NIA). Dr Krumholz is supported by grant U01 HL105270‐01 (Center for Cardiovascular Outcomes Research at Yale University) from the National Heart, Lung, and Blood Institute. Dr Krumholz chairs a cardiac scientific advisory board for UnitedHealth. Authors Drye, Krumholz, and Wang receive support from the Centers for Medicare & Medicaid Services (CMS) to develop and maintain performance measures that are used for public reporting. The analyses upon which this publication is based were performed under Contract Number HHSM‐500‐2008‐0025I Task Order T0001, entitled Measure & Instrument Development and Support (MIDS)Development and Re‐evaluation of the CMS Hospital Outcomes and Efficiency Measures, funded by the Centers for Medicare & Medicaid Services, an agency of the US Department of Health and Human Services. The Centers for Medicare & Medicaid Services reviewed and approved the use of its data for this work, and approved submission of the manuscript. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the US Government. The authors assume full responsibility for the accuracy and completeness of the ideas presented.
- US Department of Health and Human Services. Hospital Compare.2011. Available at: http://www.hospitalcompare.hhs.gov. Accessed March 5, 2011.
- ,,.Early readmissions to the department of medicine as a screening tool for monitoring quality of care problems.Medicine (Baltimore).2008;87(5):294–300.
- ,,,,.Hospital inpatient mortality. Is it a predictor of quality?N Engl J Med.1987;317(26):1674–1680.
- ,.Relationship between Medicare's hospital compare performance measures and mortality rates.JAMA.2006;296(22):2694–2702.
- ,,.Public reporting of discharge planning and rates of readmissions.N Engl J Med.2009;361(27):2637–2645.
- ,,, et al.Process of care performance measures and long‐term outcomes in patients hospitalized with heart failure.Med Care.2010;48(3):210–216.
- ,,,,,.Variations in inpatient mortality among hospitals in different system types, 1995 to 2000.Med Care.2009;47(4):466–473.
- ,,, et al.A systematic review and meta‐analysis of studies comparing mortality rates of private for‐profit and private not‐for‐profit hospitals.Can Med Assoc J.2002;166(11):1399–1406.
- ,,, et al.What distinguishes top‐performing hospitals in acute myocardial infarction mortality rates? A qualitative study.Ann Intern Med.2011;154(6):384–390.
- ,,.Perceptions of hospital safety climate and incidence of readmission.Health Serv Res.2011;46(2):596–616.
- ,,, et al.Decrease in hospital‐wide mortality rate after implementation of a commercially sold computerized physician order entry system.Pediatrics.2010;126(1):14–21.
- ,,.The condition of the literature on differences in hospital mortality.Med Care.1989;27(4):315–336.
- ,,.Threshold volumes associated with higher survival in health care: a systematic review.Med Care.2003;41(10):1129–1141.
- ,,, et al.Hospital volume and 30‐day mortality for three common medical conditions.N Engl J Med.2010;362(12):1110–1118.
- Patient Protection and Affordable Care Act Pub. L. No. 111–148, 124 Stat, §3025.2010. Available at: http://www.gpo.gov/fdsys/pkg/PLAW‐111publ148/content‐detail.html. Accessed on July 26, year="2012"2012.
- ,,.Are mortality rates for different operations related? Implications for measuring the quality of noncardiac surgery.Med Care.2006;44(8):774–778.
- ,,,.Do hospitals with low mortality rates in coronary artery bypass also perform well in valve replacement?Ann Thorac Surg.2003;76(4):1131–1137.
- ,,,,.Differences among hospitals in Medicare patient mortality.Health Serv Res.1989;24(1):1–31.
- ,,,.Variations in standardized hospital mortality rates for six common medical diagnoses: implications for profiling hospital quality.Med Care.1998;36(7):955–964.
- ,,, et al.Development, validation, and results of a measure of 30‐day readmission following hospitalization for pneumonia.J Hosp Med.2011;6(3):142–150.
- ,,, et al.An administrative claims measure suitable for profiling hospital performance on the basis of 30‐day all‐cause readmission rates among patients with heart failure.Circ Cardiovasc Qual Outcomes.2008;1:29–37.
- ,,, et al.Quality of care for acute myocardial infarction at urban safety‐net hospitals.Health Aff (Millwood).2007;26(1):238–248.
- National Quality Measures Clearinghouse.2011. Available at: http://www.qualitymeasures.ahrq.gov/. Accessed February 21,year="2011"2011.
- ,,, et al.An administrative claims model suitable for profiling hospital performance based on 30‐day mortality rates among patients with an acute myocardial infarction.Circulation.2006;113(13):1683–1692.
- ,,, et al.An administrative claims model suitable for profiling hospital performance based on 30‐day mortality rates among patients with heart failure.Circulation.2006;113(13):1693–1701.
- ,,, et al.An administrative claims model for profiling hospital 30‐day mortality rates for pneumonia patients.PLoS One.2011;6(4):e17401.
- ,,, et al.An administrative claims measure suitable for profiling hospital performance based on 30‐day all‐cause readmission rates among patients with acute myocardial infarction.Circ Cardiovasc Qual Outcomes.2011;4(2):243–252.
- .The application of electronic computers to factor analysis.Educ Psychol Meas.1960;20:141–151.
- .On the ‘probable error’ of a coefficient of correlation deduced from a small sample.Metron.1921;1:3–32.
- ,,.Comparing correlated but nonoverlapping correlations.Psychol Methods.1996;1(2):178–183.
- Centers for Medicare and Medicaid Services.Medicare Shared Savings Program: Accountable Care Organizations, Final Rule.Fed Reg.2011;76:67802–67990.
- Massachusetts Healthcare Quality and Cost Council. Potentially Preventable Readmissions.2011. Available at: http://www.mass.gov/hqcc/the‐hcqcc‐council/data‐submission‐information/potentially‐preventable‐readmissions‐ppr.html. Accessed February 29, 2012.
- Texas Medicaid. Potentially Preventable Readmission (PPR).2012. Available at: http://www.tmhp.com/Pages/Medicaid/Hospital_PPR.aspx. Accessed February 29, 2012.
- New York State. Potentially Preventable Readmissions.2011. Available at: http://www.health.ny.gov/regulations/recently_adopted/docs/2011–02‐23_potentially_preventable_readmissions.pdf. Accessed February 29, 2012.
- ,,,,.Variability in the measurement of hospital‐wide mortality rates.N Engl J Med.2010;363(26):2530–2539.
- ,,, et al.Use of electronic health records in U.S. hospitals.N Engl J Med.2009;360(16):1628–1638.
The Centers for Medicare & Medicaid Services (CMS) publicly reports hospital‐specific, 30‐day risk‐standardized mortality and readmission rates for Medicare fee‐for‐service patients admitted with acute myocardial infarction (AMI), heart failure (HF), and pneumonia.1 These measures are intended to reflect hospital performance on quality of care provided to patients during and after hospitalization.2, 3
Quality‐of‐care measures for a given disease are often assumed to reflect the quality of care for that particular condition. However, studies have found limited association between condition‐specific process measures and either mortality or readmission rates for those conditions.46 Mortality and readmission rates may instead reflect broader hospital‐wide or specialty‐wide structure, culture, and practice. For example, studies have previously found that hospitals differ in mortality or readmission rates according to organizational structure,7 financial structure,8 culture,9, 10 information technology,11 patient volume,1214 academic status,12 and other institution‐wide factors.12 There is now a strong policy push towards developing hospital‐wide (all‐condition) measures, beginning with readmission.15
It is not clear how much of the quality of care for a given condition is attributable to hospital‐wide influences that affect all conditions rather than disease‐specific factors. If readmission or mortality performance for a particular condition reflects, in large part, broader institutional characteristics, then improvement efforts might better be focused on hospital‐wide activities, such as team training or implementing electronic medical records. On the other hand, if the disease‐specific measures reflect quality strictly for those conditions, then improvement efforts would be better focused on disease‐specific care, such as early identification of the relevant patient population or standardizing disease‐specific care. As hospitals work to improve performance across an increasingly wide variety of conditions, it is becoming more important for hospitals to prioritize and focus their activities effectively and efficiently.
One means of determining the relative contribution of hospital versus disease factors is to explore whether outcome rates are consistent among different conditions cared for in the same hospital. If mortality (or readmission) rates across different conditions are highly correlated, it would suggest that hospital‐wide factors may play a substantive role in outcomes. Some studies have found that mortality for a particular surgical condition is a useful proxy for mortality for other surgical conditions,16, 17 while other studies have found little correlation among mortality rates for various medical conditions.18, 19 It is also possible that correlation varies according to hospital characteristics; for example, smaller or nonteaching hospitals might be more homogenous in their care than larger, less homogeneous institutions. No studies have been performed using publicly reported estimates of risk‐standardized mortality or readmission rates. In this study we use the publicly reported measures of 30‐day mortality and 30‐day readmission for AMI, HF, and pneumonia to examine whether, and to what degree, mortality rates track together within US hospitals, and separately, to what degree readmission rates track together within US hospitals.
METHODS
Data Sources
CMS calculates risk‐standardized mortality and readmission rates, and patient volume, for all acute care nonfederal hospitals with one or more eligible case of AMI, HF, and pneumonia annually based on fee‐for‐service (FFS) Medicare claims. CMS publicly releases the rates for the large subset of hospitals that participate in public reporting and have 25 or more cases for the conditions over the 3‐year period between July 2006 and June 2009. We estimated the rates for all hospitals included in the measure calculations, including those with fewer than 25 cases, using the CMS methodology and data obtained from CMS. The distribution of these rates has been previously reported.20, 21 In addition, we used the 2008 American Hospital Association (AHA) Survey to obtain data about hospital characteristics, including number of beds, hospital ownership (government, not‐for‐profit, for‐profit), teaching status (member of Council of Teaching Hospitals, other teaching hospital, nonteaching), presence of specialized cardiac capabilities (coronary artery bypass graft surgery, cardiac catheterization lab without cardiac surgery, neither), US Census Bureau core‐based statistical area (division [subarea of area with urban center >2.5 million people], metropolitan [urban center of at least 50,000 people], micropolitan [urban center of between 10,000 and 50,000 people], and rural [<10,000 people]), and safety net status22 (yes/no). Safety net status was defined as either public hospitals or private hospitals with a Medicaid caseload greater than one standard deviation above their respective state's mean private hospital Medicaid caseload using the 2007 AHA Annual Survey data.
Study Sample
This study includes 2 hospital cohorts, 1 for mortality and 1 for readmission. Hospitals were eligible for the mortality cohort if the dataset included risk‐standardized mortality rates for all 3 conditions (AMI, HF, and pneumonia). Hospitals were eligible for the readmission cohort if the dataset included risk‐standardized readmission rates for all 3 of these conditions.
Risk‐Standardized Measures
The measures include all FFS Medicare patients who are 65 years old, have been enrolled in FFS Medicare for the 12 months before the index hospitalization, are admitted with 1 of the 3 qualifying diagnoses, and do not leave the hospital against medical advice. The mortality measures include all deaths within 30 days of admission, and all deaths are attributable to the initial admitting hospital, even if the patient is then transferred to another acute care facility. Therefore, for a given hospital, transfers into the hospital are excluded from its rate, but transfers out are included. The readmission measures include all readmissions within 30 days of discharge, and all readmissions are attributable to the final discharging hospital, even if the patient was originally admitted to a different acute care facility. Therefore, for a given hospital, transfers in are included in its rate, but transfers out are excluded. For mortality measures, only 1 hospitalization for a patient in a specific year is randomly selected if the patient has multiple hospitalizations in the year. For readmission measures, admissions in which the patient died prior to discharge, and admissions within 30 days of an index admission, are not counted as index admissions.
Outcomes for all measures are all‐cause; however, for the AMI readmission measure, planned admissions for cardiac procedures are not counted as readmissions. Patients in observation status or in non‐acute care facilities are not counted as readmissions. Detailed specifications for the outcomes measures are available at the National Quality Measures Clearinghouse.23
The derivation and validation of the risk‐standardized outcome measures have been previously reported.20, 21, 2327 The measures are derived from hierarchical logistic regression models that include age, sex, clinical covariates, and a hospital‐specific random effect. The rates are calculated as the ratio of the number of predicted outcomes (obtained from a model applying the hospital‐specific effect) to the number of expected outcomes (obtained from a model applying the average effect among hospitals), multiplied by the unadjusted overall 30‐day rate.
Statistical Analysis
We examined patterns and distributions of hospital volume, risk‐standardized mortality rates, and risk‐standardized readmission rates among included hospitals. To measure the degree of association among hospitals' risk‐standardized mortality rates for AMI, HF, and pneumonia, we calculated Pearson correlation coefficients, resulting in 3 correlations for the 3 pairs of conditions (AMI and HF, AMI and pneumonia, HF and pneumonia), and tested whether they were significantly different from 0. We also conducted a factor analysis using the principal component method with a minimum eigenvalue of 1 to retain factors to determine whether there was a single common factor underlying mortality performance for the 3 conditions.28 Finally, we divided hospitals into quartiles of performance for each outcome based on the point estimate of risk‐standardized rate, and compared quartile of performance between condition pairs for each outcome. For each condition pair, we assessed the percent of hospitals in the same quartile of performance in both conditions, the percent of hospitals in either the top quartile of performance or the bottom quartile of performance for both, and the percent of hospitals in the top quartile for one and the bottom quartile for the other. We calculated the weighted kappa for agreement on quartile of performance between condition pairs for each outcome and the Spearman correlation for quartiles of performance. Then, we examined Pearson correlation coefficients in different subgroups of hospitals, including by size, ownership, teaching status, cardiac procedure capability, statistical area, and safety net status. In order to determine whether these correlations differed by hospital characteristics, we tested if the Pearson correlation coefficients were different between any 2 subgroups using the method proposed by Fisher.29 We repeated all of these analyses separately for the risk‐standardized readmission rates.
To determine whether correlations between mortality rates were significantly different than correlations between readmission rates for any given condition pair, we used the method recommended by Raghunathan et al.30 For these analyses, we included only hospitals reporting both mortality and readmission rates for the condition pairs. We used the same methods to determine whether correlations between mortality rates were significantly different than correlations between readmission rates for any given condition pair among subgroups of hospital characteristics.
All analyses and graphing were performed using the SAS statistical package version 9.2 (SAS Institute, Cary, NC). We considered a P‐value < 0.05 to be statistically significant, and all statistical tests were 2‐tailed.
RESULTS
The mortality cohort included 4559 hospitals, and the readmission cohort included 4468 hospitals. The majority of hospitals was small, nonteaching, and did not have advanced cardiac capabilities such as cardiac surgery or cardiac catheterization (Table 1).
| Description | Mortality Measures | Readmission Measures |
|---|---|---|
| Hospital N = 4559 | Hospital N = 4468 | |
| N (%)* | N (%)* | |
| ||
| No. of beds | ||
| >600 | 157 (3.4) | 156 (3.5) |
| 300600 | 628 (13.8) | 626 (14.0) |
| <300 | 3588 (78.7) | 3505 (78.5) |
| Unknown | 186 (4.08) | 181 (4.1) |
| Mean (SD) | 173.24 (189.52) | 175.23 (190.00) |
| Ownership | ||
| Not‐for‐profit | 2650 (58.1) | 2619 (58.6) |
| For‐profit | 672 (14.7) | 663 (14.8) |
| Government | 1051 (23.1) | 1005 (22.5) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Teaching status | ||
| COTH | 277 (6.1) | 276 (6.2) |
| Teaching | 505 (11.1) | 503 (11.3) |
| Nonteaching | 3591 (78.8) | 3508 (78.5) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Cardiac facility type | ||
| CABG | 1471 (32.3) | 1467 (32.8) |
| Cath lab | 578 (12.7) | 578 (12.9) |
| Neither | 2324 (51.0) | 2242 (50.2) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Core‐based statistical area | ||
| Division | 621 (13.6) | 618 (13.8) |
| Metro | 1850 (40.6) | 1835 (41.1) |
| Micro | 801 (17.6) | 788 (17.6) |
| Rural | 1101 (24.2) | 1046 (23.4) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Safety net status | ||
| No | 2995 (65.7) | 2967 (66.4) |
| Yes | 1377 (30.2) | 1319 (29.5) |
| Unknown | 187 (4.1) | 182 (4.1) |
For mortality measures, the smallest median number of cases per hospital was for AMI (48; interquartile range [IQR], 13,171), and the greatest number was for pneumonia (178; IQR, 87, 336). The same pattern held for readmission measures (AMI median 33; IQR; 9, 150; pneumonia median 191; IQR, 95, 352.5). With respect to mortality measures, AMI had the highest rate and HF the lowest rate; however, for readmission measures, HF had the highest rate and pneumonia the lowest rate (Table 2).
| Description | Mortality Measures (N = 4559) | Readmission Measures (N = 4468) | ||||
|---|---|---|---|---|---|---|
| AMI | HF | PN | AMI | HF | PN | |
| ||||||
| Total discharges | 558,653 | 1,094,960 | 1,114,706 | 546,514 | 1,314,394 | 1,152,708 |
| Hospital volume | ||||||
| Mean (SD) | 122.54 (172.52) | 240.18 (271.35) | 244.51 (220.74) | 122.32 (201.78) | 294.18 (333.2) | 257.99 (228.5) |
| Median (IQR) | 48 (13, 171) | 142 (56, 337) | 178 (87, 336) | 33 (9, 150) | 172.5 (68, 407) | 191 (95, 352.5) |
| Range min, max | 1, 1379 | 1, 2814 | 1, 2241 | 1, 1611 | 1, 3410 | 2, 2359 |
| 30‐Day risk‐standardized rate* | ||||||
| Mean (SD) | 15.7 (1.8) | 10.9 (1.6) | 11.5 (1.9) | 19.9 (1.5) | 24.8 (2.1) | 18.5 (1.7) |
| Median (IQR) | 15.7 (14.5, 16.8) | 10.8 (9.9, 11.9) | 11.3 (10.2, 12.6) | 19.9 (18.9, 20.8) | 24.7 (23.4, 26.1) | 18.4 (17.3, 19.5) |
| Range min, max | 10.3, 24.6 | 6.6, 18.2 | 6.7, 20.9 | 15.2, 26.3 | 17.3, 32.4 | 13.6, 26.7 |
Every mortality measure was significantly correlated with every other mortality measure (range of correlation coefficients, 0.270.41, P < 0.0001 for all 3 correlations). For example, the correlation between risk‐standardized mortality rates (RSMR) for HF and pneumonia was 0.41. Similarly, every readmission measure was significantly correlated with every other readmission measure (range of correlation coefficients, 0.320.47; P < 0.0001 for all 3 correlations). Overall, the lowest correlation was between risk‐standardized mortality rates for AMI and pneumonia (r = 0.27), and the highest correlation was between risk‐standardized readmission rates (RSRR) for HF and pneumonia (r = 0.47) (Table 3).
| Description | Mortality Measures | Readmission Measures | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | AMI and HF | AMI and PN | HF and PN | AMI and HF | AMI and PN | HF and PN | ||||||||
| r | P | r | P | r | P | N | r | P | r | P | r | P | ||
| ||||||||||||||
| All | 4559 | 0.30 | 0.27 | 0.41 | 4468 | 0.38 | 0.32 | 0.47 | ||||||
| Hospitals with 25 patients | 2872 | 0.33 | 0.30 | 0.44 | 2467 | 0.44 | 0.38 | 0.51 | ||||||
| No. of beds | 0.15 | 0.005 | 0.0009 | <0.0001 | <0.0001 | <0.0001 | ||||||||
| >600 | 157 | 0.38 | 0.43 | 0.51 | 156 | 0.67 | 0.50 | 0.66 | ||||||
| 300600 | 628 | 0.29 | 0.30 | 0.49 | 626 | 0.54 | 0.45 | 0.58 | ||||||
| <300 | 3588 | 0.27 | 0.23 | 0.37 | 3505 | 0.30 | 0.26 | 0.44 | ||||||
| Ownership | 0.021 | 0.05 | 0.39 | 0.0004 | 0.0004 | 0.003 | ||||||||
| Not‐for‐profit | 2650 | 0.32 | 0.28 | 0.42 | 2619 | 0.43 | 0.36 | 0.50 | ||||||
| For‐profit | 672 | 0.30 | 0.23 | 0.40 | 663 | 0.29 | 0.22 | 0.40 | ||||||
| Government | 1051 | 0.24 | 0.22 | 0.39 | 1005 | 0.32 | 0.29 | 0.45 | ||||||
| Teaching status | 0.11 | 0.08 | 0.0012 | <0.0001 | 0.0002 | 0.0003 | ||||||||
| COTH | 277 | 0.31 | 0.34 | 0.54 | 276 | 0.54 | 0.47 | 0.59 | ||||||
| Teaching | 505 | 0.22 | 0.28 | 0.43 | 503 | 0.52 | 0.42 | 0.56 | ||||||
| Nonteaching | 3591 | 0.29 | 0.24 | 0.39 | 3508 | 0.32 | 0.26 | 0.44 | ||||||
| Cardiac facility type | 0.022 | 0.006 | <0.0001 | <0.0001 | 0.0006 | 0.004 | ||||||||
| CABG | 1471 | 0.33 | 0.29 | 0.47 | 1467 | 0.48 | 0.37 | 0.52 | ||||||
| Cath lab | 578 | 0.25 | 0.26 | 0.36 | 578 | 0.32 | 0.37 | 0.47 | ||||||
| Neither | 2324 | 0.26 | 0.21 | 0.36 | 2242 | 0.28 | 0.27 | 0.44 | ||||||
| Core‐based statistical area | 0.0001 | <0.0001 | 0.002 | <0.0001 | <0.0001 | <0.0001 | ||||||||
| Division | 621 | 0.38 | 0.34 | 0.41 | 618 | 0.46 | 0.40 | 0.56 | ||||||
| Metro | 1850 | 0.26 | 0.26 | 0.42 | 1835 | 0.38 | 0.30 | 0.40 | ||||||
| Micro | 801 | 0.23 | 0.22 | 0.34 | 788 | 0.32 | 0.30 | 0.47 | ||||||
| Rural | 1101 | 0.21 | 0.13 | 0.32 | 1046 | 0.22 | 0.21 | 0.44 | ||||||
| Safety net status | 0.001 | 0.027 | 0.68 | 0.029 | 0.037 | 0.28 | ||||||||
| No | 2995 | 0.33 | 0.28 | 0.41 | 2967 | 0.40 | 0.33 | 0.48 | ||||||
| Yes | 1377 | 0.23 | 0.21 | 0.40 | 1319 | 0.34 | 0.30 | 0.45 | ||||||
Both the factor analysis for the mortality measures and the factor analysis for the readmission measures yielded only one factor with an eigenvalue >1. In each factor analysis, this single common factor kept more than half of the data based on the cumulative eigenvalue (55% for mortality measures and 60% for readmission measures). For the mortality measures, the pattern of RSMR for myocardial infarction (MI), heart failure (HF), and pneumonia (PN) in the factor was high (0.68 for MI, 0.78 for HF, and 0.76 for PN); the same was true of the RSRR in the readmission measures (0.72 for MI, 0.81 for HF, and 0.78 for PN).
For all condition pairs and both outcomes, a third or more of hospitals were in the same quartile of performance for both conditions of the pair (Table 4). Hospitals were more likely to be in the same quartile of performance if they were in the top or bottom quartile than if they were in the middle. Less than 10% of hospitals were in the top quartile for one condition in the mortality or readmission pair and in the bottom quartile for the other condition in the pair. Kappa scores for same quartile of performance between pairs of outcomes ranged from 0.16 to 0.27, and were highest for HF and pneumonia for both mortality and readmission rates.
| Condition Pair | Same Quartile (Any) (%) | Same Quartile (Q1 or Q4) (%) | Q1 in One and Q4 in Another (%) | Weighted Kappa | Spearman Correlation |
|---|---|---|---|---|---|
| |||||
| Mortality | |||||
| MI and HF | 34.8 | 20.2 | 7.9 | 0.19 | 0.25 |
| MI and PN | 32.7 | 18.8 | 8.2 | 0.16 | 0.22 |
| HF and PN | 35.9 | 21.8 | 5.0 | 0.26 | 0.36 |
| Readmission | |||||
| MI and HF | 36.6 | 21.0 | 7.5 | 0.22 | 0.28 |
| MI and PN | 34.0 | 19.6 | 8.1 | 0.19 | 0.24 |
| HF and PN | 37.1 | 22.6 | 5.4 | 0.27 | 0.37 |
In subgroup analyses, the highest mortality correlation was between HF and pneumonia in hospitals with more than 600 beds (r = 0.51, P = 0.0009), and the highest readmission correlation was between AMI and HF in hospitals with more than 600 beds (r = 0.67, P < 0.0001). Across both measures and all 3 condition pairs, correlations between conditions increased with increasing hospital bed size, presence of cardiac surgery capability, and increasing population of the hospital's Census Bureau statistical area. Furthermore, for most measures and condition pairs, correlations between conditions were highest in not‐for‐profit hospitals, hospitals belonging to the Council of Teaching Hospitals, and non‐safety net hospitals (Table 3).
For all condition pairs, the correlation between readmission rates was significantly higher than the correlation between mortality rates (P < 0.01). In subgroup analyses, readmission correlations were also significantly higher than mortality correlations for all pairs of conditions among moderate‐sized hospitals, among nonprofit hospitals, among teaching hospitals that did not belong to the Council of Teaching Hospitals, and among non‐safety net hospitals (Table 5).
| Description | AMI and HF | AMI and PN | HF and PN | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | MC | RC | P | N | MC | RC | P | N | MC | RC | P | |
| ||||||||||||
| All | 4457 | 0.31 | 0.38 | <0.0001 | 4459 | 0.27 | 0.32 | 0.007 | 4731 | 0.41 | 0.46 | 0.0004 |
| Hospitals with 25 patients | 2472 | 0.33 | 0.44 | <0.001 | 2463 | 0.31 | 0.38 | 0.01 | 4104 | 0.42 | 0.47 | 0.001 |
| No. of beds | ||||||||||||
| >600 | 156 | 0.38 | 0.67 | 0.0002 | 156 | 0.43 | 0.50 | 0.48 | 160 | 0.51 | 0.66 | 0.042 |
| 300600 | 626 | 0.29 | 0.54 | <0.0001 | 626 | 0.31 | 0.45 | 0.003 | 630 | 0.49 | 0.58 | 0.033 |
| <300 | 3494 | 0.28 | 0.30 | 0.21 | 3496 | 0.23 | 0.26 | 0.17 | 3733 | 0.37 | 0.43 | 0.003 |
| Ownership | ||||||||||||
| Not‐for‐profit | 2614 | 0.32 | 0.43 | <0.0001 | 2617 | 0.28 | 0.36 | 0.003 | 2697 | 0.42 | 0.50 | 0.0003 |
| For‐profit | 662 | 0.30 | 0.29 | 0.90 | 661 | 0.23 | 0.22 | 0.75 | 699 | 0.40 | 0.40 | 0.99 |
| Government | 1000 | 0.25 | 0.32 | 0.09 | 1000 | 0.22 | 0.29 | 0.09 | 1127 | 0.39 | 0.43 | 0.21 |
| Teaching status | ||||||||||||
| COTH | 276 | 0.31 | 0.54 | 0.001 | 277 | 0.35 | 0.46 | 0.10 | 278 | 0.54 | 0.59 | 0.41 |
| Teaching | 504 | 0.22 | 0.52 | <0.0001 | 504 | 0.28 | 0.42 | 0.012 | 508 | 0.43 | 0.56 | 0.005 |
| Nonteaching | 3496 | 0.29 | 0.32 | 0.18 | 3497 | 0.24 | 0.26 | 0.46 | 3737 | 0.39 | 0.43 | 0.016 |
| Cardiac facility type | ||||||||||||
| CABG | 1465 | 0.33 | 0.48 | <0.0001 | 1467 | 0.30 | 0.37 | 0.018 | 1483 | 0.47 | 0.51 | 0.103 |
| Cath lab | 577 | 0.25 | 0.32 | 0.18 | 577 | 0.26 | 0.37 | 0.046 | 579 | 0.36 | 0.47 | 0.022 |
| Neither | 2234 | 0.26 | 0.28 | 0.48 | 2234 | 0.21 | 0.27 | 0.037 | 2461 | 0.36 | 0.44 | 0.002 |
| Core‐based statistical area | ||||||||||||
| Division | 618 | 0.38 | 0.46 | 0.09 | 620 | 0.34 | 0.40 | 0.18 | 630 | 0.41 | 0.56 | 0.001 |
| Metro | 1833 | 0.26 | 0.38 | <0.0001 | 1832 | 0.26 | 0.30 | 0.21 | 1896 | 0.42 | 0.40 | 0.63 |
| Micro | 787 | 0.24 | 0.32 | 0.08 | 787 | 0.22 | 0.30 | 0.11 | 820 | 0.34 | 0.46 | 0.003 |
| Rural | 1038 | 0.21 | 0.22 | 0.83 | 1039 | 0.13 | 0.21 | 0.056 | 1177 | 0.32 | 0.43 | 0.002 |
| Safety net status | ||||||||||||
| No | 2961 | 0.33 | 0.40 | 0.001 | 2963 | 0.28 | 0.33 | 0.036 | 3062 | 0.41 | 0.48 | 0.001 |
| Yes | 1314 | 0.23 | 0.34 | 0.003 | 1314 | 0.22 | 0.30 | 0.015 | 1460 | 0.40 | 0.45 | 0.14 |
DISCUSSION
In this study, we found that risk‐standardized mortality rates for 3 common medical conditions were moderately correlated within institutions, as were risk‐standardized readmission rates. Readmission rates were more strongly correlated than mortality rates, and all rates tracked closest together in large, urban, and/or teaching hospitals. Very few hospitals were in the top quartile of performance for one condition and in the bottom quartile for a different condition.
Our findings are consistent with the hypothesis that 30‐day risk‐standardized mortality and 30‐day risk‐standardized readmission rates, in part, capture broad aspects of hospital quality that transcend condition‐specific activities. In this study, readmission rates tracked better together than mortality rates for every pair of conditions, suggesting that there may be a greater contribution of hospital‐wide environment, structure, and processes to readmission rates than to mortality rates. This difference is plausible because services specific to readmission, such as discharge planning, care coordination, medication reconciliation, and discharge communication with patients and outpatient clinicians, are typically hospital‐wide processes.
Our study differs from earlier studies of medical conditions in that the correlations we found were higher.18, 19 There are several possible explanations for this difference. First, during the intervening 1525 years since those studies were performed, care for these conditions has evolved substantially, such that there are now more standardized protocols available for all 3 of these diseases. Hospitals that are sufficiently organized or acculturated to systematically implement care protocols may have the infrastructure or culture to do so for all conditions, increasing correlation of performance among conditions. In addition, there are now more technologies and systems available that span care for multiple conditions, such as electronic medical records and quality committees, than were available in previous generations. Second, one of these studies utilized less robust risk‐adjustment,18 and neither used the same methodology of risk standardization. Nonetheless, it is interesting to note that Rosenthal and colleagues identified the same increase in correlation with higher volumes than we did.19 Studies investigating mortality correlations among surgical procedures, on the other hand, have generally found higher correlations than we found in these medical conditions.16, 17
Accountable care organizations will be assessed using an all‐condition readmission measure,31 several states track all‐condition readmission rates,3234 and several countries measure all‐condition mortality.35 An all‐condition measure for quality assessment first requires that there be a hospital‐wide quality signal above and beyond disease‐specific care. This study suggests that a moderate signal exists for readmission and, to a slightly lesser extent, for mortality, across 3 common conditions. There are other considerations, however, in developing all‐condition measures. There must be adequate risk adjustment for the wide variety of conditions that are included, and there must be a means of accounting for the variation in types of conditions and procedures cared for by different hospitals. Our study does not address these challenges, which have been described to be substantial for mortality measures.35
We were surprised by the finding that risk‐standardized rates correlated more strongly within larger institutions than smaller ones, because one might assume that care within smaller hospitals might be more homogenous. It may be easier, however, to detect a quality signal in hospitals with higher volumes of patients for all 3 conditions, because estimates for these hospitals are more precise. Consequently, we have greater confidence in results for larger volumes, and suspect a similar quality signal may be present but more difficult to detect statistically in smaller hospitals. Overall correlations were higher when we restricted the sample to hospitals with at least 25 cases, as is used for public reporting. It is also possible that the finding is real given that large‐volume hospitals have been demonstrated to provide better care for these conditions and are more likely to adopt systems of care that affect multiple conditions, such as electronic medical records.14, 36
The kappa scores comparing quartile of national performance for pairs of conditions were only in the fair range. There are several possible explanations for this fact: 1) outcomes for these 3 conditions are not measuring the same constructs; 2) they are all measuring the same construct, but they are unreliable in doing so; and/or 3) hospitals have similar latent quality for all 3 conditions, but the national quality of performance differs by condition, yielding variable relative performance per hospital for each condition. Based solely on our findings, we cannot distinguish which, if any, of these explanations may be true.31
Our study has several limitations. First, all 3 conditions currently publicly reported by CMS are medical diagnoses, although AMI patients may be cared for in distinct cardiology units and often undergo procedures; therefore, we cannot determine the degree to which correlations reflect hospital‐wide quality versus medicine‐wide quality. An institution may have a weak medicine department but a strong surgical department or vice versa. Second, it is possible that the correlations among conditions for readmission and among conditions for mortality are attributable to patient characteristics that are not adequately adjusted for in the risk‐adjustment model, such as socioeconomic factors, or to hospital characteristics not related to quality, such as coding practices or inter‐hospital transfer rates. For this to be true, these unmeasured characteristics would have to be consistent across different conditions within each hospital and have a consistent influence on outcomes. Third, it is possible that public reporting may have prompted disease‐specific focus on these conditions. We do not have data from non‐publicly reported conditions to test this hypothesis. Fourth, there are many small‐volume hospitals in this study; their estimates for readmission and mortality are less reliable than for large‐volume hospitals, potentially limiting our ability to detect correlations in this group of hospitals.
This study lends credence to the hypothesis that 30‐day risk‐standardized mortality and readmission rates for individual conditions may reflect aspects of hospital‐wide quality or at least medicine‐wide quality, although the correlations are not large enough to conclude that hospital‐wide factors play a dominant role, and there are other possible explanations for the correlations. Further work is warranted to better understand the causes of the correlations, and to better specify the nature of hospital factors that contribute to correlations among outcomes.
Acknowledgements
Disclosures: Dr Horwitz is supported by the National Institute on Aging (K08 AG038336) and by the American Federation of Aging Research through the Paul B. Beeson Career Development Award Program. Dr Horwitz is also a Pepper Scholar with support from the Claude D. Pepper Older Americans Independence Center at Yale University School of Medicine (P30 AG021342 NIH/NIA). Dr Krumholz is supported by grant U01 HL105270‐01 (Center for Cardiovascular Outcomes Research at Yale University) from the National Heart, Lung, and Blood Institute. Dr Krumholz chairs a cardiac scientific advisory board for UnitedHealth. Authors Drye, Krumholz, and Wang receive support from the Centers for Medicare & Medicaid Services (CMS) to develop and maintain performance measures that are used for public reporting. The analyses upon which this publication is based were performed under Contract Number HHSM‐500‐2008‐0025I Task Order T0001, entitled Measure & Instrument Development and Support (MIDS)Development and Re‐evaluation of the CMS Hospital Outcomes and Efficiency Measures, funded by the Centers for Medicare & Medicaid Services, an agency of the US Department of Health and Human Services. The Centers for Medicare & Medicaid Services reviewed and approved the use of its data for this work, and approved submission of the manuscript. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the US Government. The authors assume full responsibility for the accuracy and completeness of the ideas presented.
The Centers for Medicare & Medicaid Services (CMS) publicly reports hospital‐specific, 30‐day risk‐standardized mortality and readmission rates for Medicare fee‐for‐service patients admitted with acute myocardial infarction (AMI), heart failure (HF), and pneumonia.1 These measures are intended to reflect hospital performance on quality of care provided to patients during and after hospitalization.2, 3
Quality‐of‐care measures for a given disease are often assumed to reflect the quality of care for that particular condition. However, studies have found limited association between condition‐specific process measures and either mortality or readmission rates for those conditions.46 Mortality and readmission rates may instead reflect broader hospital‐wide or specialty‐wide structure, culture, and practice. For example, studies have previously found that hospitals differ in mortality or readmission rates according to organizational structure,7 financial structure,8 culture,9, 10 information technology,11 patient volume,1214 academic status,12 and other institution‐wide factors.12 There is now a strong policy push towards developing hospital‐wide (all‐condition) measures, beginning with readmission.15
It is not clear how much of the quality of care for a given condition is attributable to hospital‐wide influences that affect all conditions rather than disease‐specific factors. If readmission or mortality performance for a particular condition reflects, in large part, broader institutional characteristics, then improvement efforts might better be focused on hospital‐wide activities, such as team training or implementing electronic medical records. On the other hand, if the disease‐specific measures reflect quality strictly for those conditions, then improvement efforts would be better focused on disease‐specific care, such as early identification of the relevant patient population or standardizing disease‐specific care. As hospitals work to improve performance across an increasingly wide variety of conditions, it is becoming more important for hospitals to prioritize and focus their activities effectively and efficiently.
One means of determining the relative contribution of hospital versus disease factors is to explore whether outcome rates are consistent among different conditions cared for in the same hospital. If mortality (or readmission) rates across different conditions are highly correlated, it would suggest that hospital‐wide factors may play a substantive role in outcomes. Some studies have found that mortality for a particular surgical condition is a useful proxy for mortality for other surgical conditions,16, 17 while other studies have found little correlation among mortality rates for various medical conditions.18, 19 It is also possible that correlation varies according to hospital characteristics; for example, smaller or nonteaching hospitals might be more homogenous in their care than larger, less homogeneous institutions. No studies have been performed using publicly reported estimates of risk‐standardized mortality or readmission rates. In this study we use the publicly reported measures of 30‐day mortality and 30‐day readmission for AMI, HF, and pneumonia to examine whether, and to what degree, mortality rates track together within US hospitals, and separately, to what degree readmission rates track together within US hospitals.
METHODS
Data Sources
CMS calculates risk‐standardized mortality and readmission rates, and patient volume, for all acute care nonfederal hospitals with one or more eligible case of AMI, HF, and pneumonia annually based on fee‐for‐service (FFS) Medicare claims. CMS publicly releases the rates for the large subset of hospitals that participate in public reporting and have 25 or more cases for the conditions over the 3‐year period between July 2006 and June 2009. We estimated the rates for all hospitals included in the measure calculations, including those with fewer than 25 cases, using the CMS methodology and data obtained from CMS. The distribution of these rates has been previously reported.20, 21 In addition, we used the 2008 American Hospital Association (AHA) Survey to obtain data about hospital characteristics, including number of beds, hospital ownership (government, not‐for‐profit, for‐profit), teaching status (member of Council of Teaching Hospitals, other teaching hospital, nonteaching), presence of specialized cardiac capabilities (coronary artery bypass graft surgery, cardiac catheterization lab without cardiac surgery, neither), US Census Bureau core‐based statistical area (division [subarea of area with urban center >2.5 million people], metropolitan [urban center of at least 50,000 people], micropolitan [urban center of between 10,000 and 50,000 people], and rural [<10,000 people]), and safety net status22 (yes/no). Safety net status was defined as either public hospitals or private hospitals with a Medicaid caseload greater than one standard deviation above their respective state's mean private hospital Medicaid caseload using the 2007 AHA Annual Survey data.
Study Sample
This study includes 2 hospital cohorts, 1 for mortality and 1 for readmission. Hospitals were eligible for the mortality cohort if the dataset included risk‐standardized mortality rates for all 3 conditions (AMI, HF, and pneumonia). Hospitals were eligible for the readmission cohort if the dataset included risk‐standardized readmission rates for all 3 of these conditions.
Risk‐Standardized Measures
The measures include all FFS Medicare patients who are 65 years old, have been enrolled in FFS Medicare for the 12 months before the index hospitalization, are admitted with 1 of the 3 qualifying diagnoses, and do not leave the hospital against medical advice. The mortality measures include all deaths within 30 days of admission, and all deaths are attributable to the initial admitting hospital, even if the patient is then transferred to another acute care facility. Therefore, for a given hospital, transfers into the hospital are excluded from its rate, but transfers out are included. The readmission measures include all readmissions within 30 days of discharge, and all readmissions are attributable to the final discharging hospital, even if the patient was originally admitted to a different acute care facility. Therefore, for a given hospital, transfers in are included in its rate, but transfers out are excluded. For mortality measures, only 1 hospitalization for a patient in a specific year is randomly selected if the patient has multiple hospitalizations in the year. For readmission measures, admissions in which the patient died prior to discharge, and admissions within 30 days of an index admission, are not counted as index admissions.
Outcomes for all measures are all‐cause; however, for the AMI readmission measure, planned admissions for cardiac procedures are not counted as readmissions. Patients in observation status or in non‐acute care facilities are not counted as readmissions. Detailed specifications for the outcomes measures are available at the National Quality Measures Clearinghouse.23
The derivation and validation of the risk‐standardized outcome measures have been previously reported.20, 21, 2327 The measures are derived from hierarchical logistic regression models that include age, sex, clinical covariates, and a hospital‐specific random effect. The rates are calculated as the ratio of the number of predicted outcomes (obtained from a model applying the hospital‐specific effect) to the number of expected outcomes (obtained from a model applying the average effect among hospitals), multiplied by the unadjusted overall 30‐day rate.
Statistical Analysis
We examined patterns and distributions of hospital volume, risk‐standardized mortality rates, and risk‐standardized readmission rates among included hospitals. To measure the degree of association among hospitals' risk‐standardized mortality rates for AMI, HF, and pneumonia, we calculated Pearson correlation coefficients, resulting in 3 correlations for the 3 pairs of conditions (AMI and HF, AMI and pneumonia, HF and pneumonia), and tested whether they were significantly different from 0. We also conducted a factor analysis using the principal component method with a minimum eigenvalue of 1 to retain factors to determine whether there was a single common factor underlying mortality performance for the 3 conditions.28 Finally, we divided hospitals into quartiles of performance for each outcome based on the point estimate of risk‐standardized rate, and compared quartile of performance between condition pairs for each outcome. For each condition pair, we assessed the percent of hospitals in the same quartile of performance in both conditions, the percent of hospitals in either the top quartile of performance or the bottom quartile of performance for both, and the percent of hospitals in the top quartile for one and the bottom quartile for the other. We calculated the weighted kappa for agreement on quartile of performance between condition pairs for each outcome and the Spearman correlation for quartiles of performance. Then, we examined Pearson correlation coefficients in different subgroups of hospitals, including by size, ownership, teaching status, cardiac procedure capability, statistical area, and safety net status. In order to determine whether these correlations differed by hospital characteristics, we tested if the Pearson correlation coefficients were different between any 2 subgroups using the method proposed by Fisher.29 We repeated all of these analyses separately for the risk‐standardized readmission rates.
To determine whether correlations between mortality rates were significantly different than correlations between readmission rates for any given condition pair, we used the method recommended by Raghunathan et al.30 For these analyses, we included only hospitals reporting both mortality and readmission rates for the condition pairs. We used the same methods to determine whether correlations between mortality rates were significantly different than correlations between readmission rates for any given condition pair among subgroups of hospital characteristics.
All analyses and graphing were performed using the SAS statistical package version 9.2 (SAS Institute, Cary, NC). We considered a P‐value < 0.05 to be statistically significant, and all statistical tests were 2‐tailed.
RESULTS
The mortality cohort included 4559 hospitals, and the readmission cohort included 4468 hospitals. The majority of hospitals was small, nonteaching, and did not have advanced cardiac capabilities such as cardiac surgery or cardiac catheterization (Table 1).
| Description | Mortality Measures | Readmission Measures |
|---|---|---|
| Hospital N = 4559 | Hospital N = 4468 | |
| N (%)* | N (%)* | |
| ||
| No. of beds | ||
| >600 | 157 (3.4) | 156 (3.5) |
| 300600 | 628 (13.8) | 626 (14.0) |
| <300 | 3588 (78.7) | 3505 (78.5) |
| Unknown | 186 (4.08) | 181 (4.1) |
| Mean (SD) | 173.24 (189.52) | 175.23 (190.00) |
| Ownership | ||
| Not‐for‐profit | 2650 (58.1) | 2619 (58.6) |
| For‐profit | 672 (14.7) | 663 (14.8) |
| Government | 1051 (23.1) | 1005 (22.5) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Teaching status | ||
| COTH | 277 (6.1) | 276 (6.2) |
| Teaching | 505 (11.1) | 503 (11.3) |
| Nonteaching | 3591 (78.8) | 3508 (78.5) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Cardiac facility type | ||
| CABG | 1471 (32.3) | 1467 (32.8) |
| Cath lab | 578 (12.7) | 578 (12.9) |
| Neither | 2324 (51.0) | 2242 (50.2) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Core‐based statistical area | ||
| Division | 621 (13.6) | 618 (13.8) |
| Metro | 1850 (40.6) | 1835 (41.1) |
| Micro | 801 (17.6) | 788 (17.6) |
| Rural | 1101 (24.2) | 1046 (23.4) |
| Unknown | 186 (4.1) | 181 (4.1) |
| Safety net status | ||
| No | 2995 (65.7) | 2967 (66.4) |
| Yes | 1377 (30.2) | 1319 (29.5) |
| Unknown | 187 (4.1) | 182 (4.1) |
For mortality measures, the smallest median number of cases per hospital was for AMI (48; interquartile range [IQR], 13,171), and the greatest number was for pneumonia (178; IQR, 87, 336). The same pattern held for readmission measures (AMI median 33; IQR; 9, 150; pneumonia median 191; IQR, 95, 352.5). With respect to mortality measures, AMI had the highest rate and HF the lowest rate; however, for readmission measures, HF had the highest rate and pneumonia the lowest rate (Table 2).
| Description | Mortality Measures (N = 4559) | Readmission Measures (N = 4468) | ||||
|---|---|---|---|---|---|---|
| AMI | HF | PN | AMI | HF | PN | |
| ||||||
| Total discharges | 558,653 | 1,094,960 | 1,114,706 | 546,514 | 1,314,394 | 1,152,708 |
| Hospital volume | ||||||
| Mean (SD) | 122.54 (172.52) | 240.18 (271.35) | 244.51 (220.74) | 122.32 (201.78) | 294.18 (333.2) | 257.99 (228.5) |
| Median (IQR) | 48 (13, 171) | 142 (56, 337) | 178 (87, 336) | 33 (9, 150) | 172.5 (68, 407) | 191 (95, 352.5) |
| Range min, max | 1, 1379 | 1, 2814 | 1, 2241 | 1, 1611 | 1, 3410 | 2, 2359 |
| 30‐Day risk‐standardized rate* | ||||||
| Mean (SD) | 15.7 (1.8) | 10.9 (1.6) | 11.5 (1.9) | 19.9 (1.5) | 24.8 (2.1) | 18.5 (1.7) |
| Median (IQR) | 15.7 (14.5, 16.8) | 10.8 (9.9, 11.9) | 11.3 (10.2, 12.6) | 19.9 (18.9, 20.8) | 24.7 (23.4, 26.1) | 18.4 (17.3, 19.5) |
| Range min, max | 10.3, 24.6 | 6.6, 18.2 | 6.7, 20.9 | 15.2, 26.3 | 17.3, 32.4 | 13.6, 26.7 |
Every mortality measure was significantly correlated with every other mortality measure (range of correlation coefficients, 0.270.41, P < 0.0001 for all 3 correlations). For example, the correlation between risk‐standardized mortality rates (RSMR) for HF and pneumonia was 0.41. Similarly, every readmission measure was significantly correlated with every other readmission measure (range of correlation coefficients, 0.320.47; P < 0.0001 for all 3 correlations). Overall, the lowest correlation was between risk‐standardized mortality rates for AMI and pneumonia (r = 0.27), and the highest correlation was between risk‐standardized readmission rates (RSRR) for HF and pneumonia (r = 0.47) (Table 3).
| Description | Mortality Measures | Readmission Measures | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | AMI and HF | AMI and PN | HF and PN | AMI and HF | AMI and PN | HF and PN | ||||||||
| r | P | r | P | r | P | N | r | P | r | P | r | P | ||
| ||||||||||||||
| All | 4559 | 0.30 | 0.27 | 0.41 | 4468 | 0.38 | 0.32 | 0.47 | ||||||
| Hospitals with 25 patients | 2872 | 0.33 | 0.30 | 0.44 | 2467 | 0.44 | 0.38 | 0.51 | ||||||
| No. of beds | 0.15 | 0.005 | 0.0009 | <0.0001 | <0.0001 | <0.0001 | ||||||||
| >600 | 157 | 0.38 | 0.43 | 0.51 | 156 | 0.67 | 0.50 | 0.66 | ||||||
| 300600 | 628 | 0.29 | 0.30 | 0.49 | 626 | 0.54 | 0.45 | 0.58 | ||||||
| <300 | 3588 | 0.27 | 0.23 | 0.37 | 3505 | 0.30 | 0.26 | 0.44 | ||||||
| Ownership | 0.021 | 0.05 | 0.39 | 0.0004 | 0.0004 | 0.003 | ||||||||
| Not‐for‐profit | 2650 | 0.32 | 0.28 | 0.42 | 2619 | 0.43 | 0.36 | 0.50 | ||||||
| For‐profit | 672 | 0.30 | 0.23 | 0.40 | 663 | 0.29 | 0.22 | 0.40 | ||||||
| Government | 1051 | 0.24 | 0.22 | 0.39 | 1005 | 0.32 | 0.29 | 0.45 | ||||||
| Teaching status | 0.11 | 0.08 | 0.0012 | <0.0001 | 0.0002 | 0.0003 | ||||||||
| COTH | 277 | 0.31 | 0.34 | 0.54 | 276 | 0.54 | 0.47 | 0.59 | ||||||
| Teaching | 505 | 0.22 | 0.28 | 0.43 | 503 | 0.52 | 0.42 | 0.56 | ||||||
| Nonteaching | 3591 | 0.29 | 0.24 | 0.39 | 3508 | 0.32 | 0.26 | 0.44 | ||||||
| Cardiac facility type | 0.022 | 0.006 | <0.0001 | <0.0001 | 0.0006 | 0.004 | ||||||||
| CABG | 1471 | 0.33 | 0.29 | 0.47 | 1467 | 0.48 | 0.37 | 0.52 | ||||||
| Cath lab | 578 | 0.25 | 0.26 | 0.36 | 578 | 0.32 | 0.37 | 0.47 | ||||||
| Neither | 2324 | 0.26 | 0.21 | 0.36 | 2242 | 0.28 | 0.27 | 0.44 | ||||||
| Core‐based statistical area | 0.0001 | <0.0001 | 0.002 | <0.0001 | <0.0001 | <0.0001 | ||||||||
| Division | 621 | 0.38 | 0.34 | 0.41 | 618 | 0.46 | 0.40 | 0.56 | ||||||
| Metro | 1850 | 0.26 | 0.26 | 0.42 | 1835 | 0.38 | 0.30 | 0.40 | ||||||
| Micro | 801 | 0.23 | 0.22 | 0.34 | 788 | 0.32 | 0.30 | 0.47 | ||||||
| Rural | 1101 | 0.21 | 0.13 | 0.32 | 1046 | 0.22 | 0.21 | 0.44 | ||||||
| Safety net status | 0.001 | 0.027 | 0.68 | 0.029 | 0.037 | 0.28 | ||||||||
| No | 2995 | 0.33 | 0.28 | 0.41 | 2967 | 0.40 | 0.33 | 0.48 | ||||||
| Yes | 1377 | 0.23 | 0.21 | 0.40 | 1319 | 0.34 | 0.30 | 0.45 | ||||||
Both the factor analysis for the mortality measures and the factor analysis for the readmission measures yielded only one factor with an eigenvalue >1. In each factor analysis, this single common factor kept more than half of the data based on the cumulative eigenvalue (55% for mortality measures and 60% for readmission measures). For the mortality measures, the pattern of RSMR for myocardial infarction (MI), heart failure (HF), and pneumonia (PN) in the factor was high (0.68 for MI, 0.78 for HF, and 0.76 for PN); the same was true of the RSRR in the readmission measures (0.72 for MI, 0.81 for HF, and 0.78 for PN).
For all condition pairs and both outcomes, a third or more of hospitals were in the same quartile of performance for both conditions of the pair (Table 4). Hospitals were more likely to be in the same quartile of performance if they were in the top or bottom quartile than if they were in the middle. Less than 10% of hospitals were in the top quartile for one condition in the mortality or readmission pair and in the bottom quartile for the other condition in the pair. Kappa scores for same quartile of performance between pairs of outcomes ranged from 0.16 to 0.27, and were highest for HF and pneumonia for both mortality and readmission rates.
| Condition Pair | Same Quartile (Any) (%) | Same Quartile (Q1 or Q4) (%) | Q1 in One and Q4 in Another (%) | Weighted Kappa | Spearman Correlation |
|---|---|---|---|---|---|
| |||||
| Mortality | |||||
| MI and HF | 34.8 | 20.2 | 7.9 | 0.19 | 0.25 |
| MI and PN | 32.7 | 18.8 | 8.2 | 0.16 | 0.22 |
| HF and PN | 35.9 | 21.8 | 5.0 | 0.26 | 0.36 |
| Readmission | |||||
| MI and HF | 36.6 | 21.0 | 7.5 | 0.22 | 0.28 |
| MI and PN | 34.0 | 19.6 | 8.1 | 0.19 | 0.24 |
| HF and PN | 37.1 | 22.6 | 5.4 | 0.27 | 0.37 |
In subgroup analyses, the highest mortality correlation was between HF and pneumonia in hospitals with more than 600 beds (r = 0.51, P = 0.0009), and the highest readmission correlation was between AMI and HF in hospitals with more than 600 beds (r = 0.67, P < 0.0001). Across both measures and all 3 condition pairs, correlations between conditions increased with increasing hospital bed size, presence of cardiac surgery capability, and increasing population of the hospital's Census Bureau statistical area. Furthermore, for most measures and condition pairs, correlations between conditions were highest in not‐for‐profit hospitals, hospitals belonging to the Council of Teaching Hospitals, and non‐safety net hospitals (Table 3).
For all condition pairs, the correlation between readmission rates was significantly higher than the correlation between mortality rates (P < 0.01). In subgroup analyses, readmission correlations were also significantly higher than mortality correlations for all pairs of conditions among moderate‐sized hospitals, among nonprofit hospitals, among teaching hospitals that did not belong to the Council of Teaching Hospitals, and among non‐safety net hospitals (Table 5).
| Description | AMI and HF | AMI and PN | HF and PN | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | MC | RC | P | N | MC | RC | P | N | MC | RC | P | |
| ||||||||||||
| All | 4457 | 0.31 | 0.38 | <0.0001 | 4459 | 0.27 | 0.32 | 0.007 | 4731 | 0.41 | 0.46 | 0.0004 |
| Hospitals with 25 patients | 2472 | 0.33 | 0.44 | <0.001 | 2463 | 0.31 | 0.38 | 0.01 | 4104 | 0.42 | 0.47 | 0.001 |
| No. of beds | ||||||||||||
| >600 | 156 | 0.38 | 0.67 | 0.0002 | 156 | 0.43 | 0.50 | 0.48 | 160 | 0.51 | 0.66 | 0.042 |
| 300600 | 626 | 0.29 | 0.54 | <0.0001 | 626 | 0.31 | 0.45 | 0.003 | 630 | 0.49 | 0.58 | 0.033 |
| <300 | 3494 | 0.28 | 0.30 | 0.21 | 3496 | 0.23 | 0.26 | 0.17 | 3733 | 0.37 | 0.43 | 0.003 |
| Ownership | ||||||||||||
| Not‐for‐profit | 2614 | 0.32 | 0.43 | <0.0001 | 2617 | 0.28 | 0.36 | 0.003 | 2697 | 0.42 | 0.50 | 0.0003 |
| For‐profit | 662 | 0.30 | 0.29 | 0.90 | 661 | 0.23 | 0.22 | 0.75 | 699 | 0.40 | 0.40 | 0.99 |
| Government | 1000 | 0.25 | 0.32 | 0.09 | 1000 | 0.22 | 0.29 | 0.09 | 1127 | 0.39 | 0.43 | 0.21 |
| Teaching status | ||||||||||||
| COTH | 276 | 0.31 | 0.54 | 0.001 | 277 | 0.35 | 0.46 | 0.10 | 278 | 0.54 | 0.59 | 0.41 |
| Teaching | 504 | 0.22 | 0.52 | <0.0001 | 504 | 0.28 | 0.42 | 0.012 | 508 | 0.43 | 0.56 | 0.005 |
| Nonteaching | 3496 | 0.29 | 0.32 | 0.18 | 3497 | 0.24 | 0.26 | 0.46 | 3737 | 0.39 | 0.43 | 0.016 |
| Cardiac facility type | ||||||||||||
| CABG | 1465 | 0.33 | 0.48 | <0.0001 | 1467 | 0.30 | 0.37 | 0.018 | 1483 | 0.47 | 0.51 | 0.103 |
| Cath lab | 577 | 0.25 | 0.32 | 0.18 | 577 | 0.26 | 0.37 | 0.046 | 579 | 0.36 | 0.47 | 0.022 |
| Neither | 2234 | 0.26 | 0.28 | 0.48 | 2234 | 0.21 | 0.27 | 0.037 | 2461 | 0.36 | 0.44 | 0.002 |
| Core‐based statistical area | ||||||||||||
| Division | 618 | 0.38 | 0.46 | 0.09 | 620 | 0.34 | 0.40 | 0.18 | 630 | 0.41 | 0.56 | 0.001 |
| Metro | 1833 | 0.26 | 0.38 | <0.0001 | 1832 | 0.26 | 0.30 | 0.21 | 1896 | 0.42 | 0.40 | 0.63 |
| Micro | 787 | 0.24 | 0.32 | 0.08 | 787 | 0.22 | 0.30 | 0.11 | 820 | 0.34 | 0.46 | 0.003 |
| Rural | 1038 | 0.21 | 0.22 | 0.83 | 1039 | 0.13 | 0.21 | 0.056 | 1177 | 0.32 | 0.43 | 0.002 |
| Safety net status | ||||||||||||
| No | 2961 | 0.33 | 0.40 | 0.001 | 2963 | 0.28 | 0.33 | 0.036 | 3062 | 0.41 | 0.48 | 0.001 |
| Yes | 1314 | 0.23 | 0.34 | 0.003 | 1314 | 0.22 | 0.30 | 0.015 | 1460 | 0.40 | 0.45 | 0.14 |
DISCUSSION
In this study, we found that risk‐standardized mortality rates for 3 common medical conditions were moderately correlated within institutions, as were risk‐standardized readmission rates. Readmission rates were more strongly correlated than mortality rates, and all rates tracked closest together in large, urban, and/or teaching hospitals. Very few hospitals were in the top quartile of performance for one condition and in the bottom quartile for a different condition.
Our findings are consistent with the hypothesis that 30‐day risk‐standardized mortality and 30‐day risk‐standardized readmission rates, in part, capture broad aspects of hospital quality that transcend condition‐specific activities. In this study, readmission rates tracked better together than mortality rates for every pair of conditions, suggesting that there may be a greater contribution of hospital‐wide environment, structure, and processes to readmission rates than to mortality rates. This difference is plausible because services specific to readmission, such as discharge planning, care coordination, medication reconciliation, and discharge communication with patients and outpatient clinicians, are typically hospital‐wide processes.
Our study differs from earlier studies of medical conditions in that the correlations we found were higher.18, 19 There are several possible explanations for this difference. First, during the intervening 1525 years since those studies were performed, care for these conditions has evolved substantially, such that there are now more standardized protocols available for all 3 of these diseases. Hospitals that are sufficiently organized or acculturated to systematically implement care protocols may have the infrastructure or culture to do so for all conditions, increasing correlation of performance among conditions. In addition, there are now more technologies and systems available that span care for multiple conditions, such as electronic medical records and quality committees, than were available in previous generations. Second, one of these studies utilized less robust risk‐adjustment,18 and neither used the same methodology of risk standardization. Nonetheless, it is interesting to note that Rosenthal and colleagues identified the same increase in correlation with higher volumes than we did.19 Studies investigating mortality correlations among surgical procedures, on the other hand, have generally found higher correlations than we found in these medical conditions.16, 17
Accountable care organizations will be assessed using an all‐condition readmission measure,31 several states track all‐condition readmission rates,3234 and several countries measure all‐condition mortality.35 An all‐condition measure for quality assessment first requires that there be a hospital‐wide quality signal above and beyond disease‐specific care. This study suggests that a moderate signal exists for readmission and, to a slightly lesser extent, for mortality, across 3 common conditions. There are other considerations, however, in developing all‐condition measures. There must be adequate risk adjustment for the wide variety of conditions that are included, and there must be a means of accounting for the variation in types of conditions and procedures cared for by different hospitals. Our study does not address these challenges, which have been described to be substantial for mortality measures.35
We were surprised by the finding that risk‐standardized rates correlated more strongly within larger institutions than smaller ones, because one might assume that care within smaller hospitals might be more homogenous. It may be easier, however, to detect a quality signal in hospitals with higher volumes of patients for all 3 conditions, because estimates for these hospitals are more precise. Consequently, we have greater confidence in results for larger volumes, and suspect a similar quality signal may be present but more difficult to detect statistically in smaller hospitals. Overall correlations were higher when we restricted the sample to hospitals with at least 25 cases, as is used for public reporting. It is also possible that the finding is real given that large‐volume hospitals have been demonstrated to provide better care for these conditions and are more likely to adopt systems of care that affect multiple conditions, such as electronic medical records.14, 36
The kappa scores comparing quartile of national performance for pairs of conditions were only in the fair range. There are several possible explanations for this fact: 1) outcomes for these 3 conditions are not measuring the same constructs; 2) they are all measuring the same construct, but they are unreliable in doing so; and/or 3) hospitals have similar latent quality for all 3 conditions, but the national quality of performance differs by condition, yielding variable relative performance per hospital for each condition. Based solely on our findings, we cannot distinguish which, if any, of these explanations may be true.31
Our study has several limitations. First, all 3 conditions currently publicly reported by CMS are medical diagnoses, although AMI patients may be cared for in distinct cardiology units and often undergo procedures; therefore, we cannot determine the degree to which correlations reflect hospital‐wide quality versus medicine‐wide quality. An institution may have a weak medicine department but a strong surgical department or vice versa. Second, it is possible that the correlations among conditions for readmission and among conditions for mortality are attributable to patient characteristics that are not adequately adjusted for in the risk‐adjustment model, such as socioeconomic factors, or to hospital characteristics not related to quality, such as coding practices or inter‐hospital transfer rates. For this to be true, these unmeasured characteristics would have to be consistent across different conditions within each hospital and have a consistent influence on outcomes. Third, it is possible that public reporting may have prompted disease‐specific focus on these conditions. We do not have data from non‐publicly reported conditions to test this hypothesis. Fourth, there are many small‐volume hospitals in this study; their estimates for readmission and mortality are less reliable than for large‐volume hospitals, potentially limiting our ability to detect correlations in this group of hospitals.
This study lends credence to the hypothesis that 30‐day risk‐standardized mortality and readmission rates for individual conditions may reflect aspects of hospital‐wide quality or at least medicine‐wide quality, although the correlations are not large enough to conclude that hospital‐wide factors play a dominant role, and there are other possible explanations for the correlations. Further work is warranted to better understand the causes of the correlations, and to better specify the nature of hospital factors that contribute to correlations among outcomes.
Acknowledgements
Disclosures: Dr Horwitz is supported by the National Institute on Aging (K08 AG038336) and by the American Federation of Aging Research through the Paul B. Beeson Career Development Award Program. Dr Horwitz is also a Pepper Scholar with support from the Claude D. Pepper Older Americans Independence Center at Yale University School of Medicine (P30 AG021342 NIH/NIA). Dr Krumholz is supported by grant U01 HL105270‐01 (Center for Cardiovascular Outcomes Research at Yale University) from the National Heart, Lung, and Blood Institute. Dr Krumholz chairs a cardiac scientific advisory board for UnitedHealth. Authors Drye, Krumholz, and Wang receive support from the Centers for Medicare & Medicaid Services (CMS) to develop and maintain performance measures that are used for public reporting. The analyses upon which this publication is based were performed under Contract Number HHSM‐500‐2008‐0025I Task Order T0001, entitled Measure & Instrument Development and Support (MIDS)Development and Re‐evaluation of the CMS Hospital Outcomes and Efficiency Measures, funded by the Centers for Medicare & Medicaid Services, an agency of the US Department of Health and Human Services. The Centers for Medicare & Medicaid Services reviewed and approved the use of its data for this work, and approved submission of the manuscript. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the US Government. The authors assume full responsibility for the accuracy and completeness of the ideas presented.
- US Department of Health and Human Services. Hospital Compare.2011. Available at: http://www.hospitalcompare.hhs.gov. Accessed March 5, 2011.
- ,,.Early readmissions to the department of medicine as a screening tool for monitoring quality of care problems.Medicine (Baltimore).2008;87(5):294–300.
- ,,,,.Hospital inpatient mortality. Is it a predictor of quality?N Engl J Med.1987;317(26):1674–1680.
- ,.Relationship between Medicare's hospital compare performance measures and mortality rates.JAMA.2006;296(22):2694–2702.
- ,,.Public reporting of discharge planning and rates of readmissions.N Engl J Med.2009;361(27):2637–2645.
- ,,, et al.Process of care performance measures and long‐term outcomes in patients hospitalized with heart failure.Med Care.2010;48(3):210–216.
- ,,,,,.Variations in inpatient mortality among hospitals in different system types, 1995 to 2000.Med Care.2009;47(4):466–473.
- ,,, et al.A systematic review and meta‐analysis of studies comparing mortality rates of private for‐profit and private not‐for‐profit hospitals.Can Med Assoc J.2002;166(11):1399–1406.
- ,,, et al.What distinguishes top‐performing hospitals in acute myocardial infarction mortality rates? A qualitative study.Ann Intern Med.2011;154(6):384–390.
- ,,.Perceptions of hospital safety climate and incidence of readmission.Health Serv Res.2011;46(2):596–616.
- ,,, et al.Decrease in hospital‐wide mortality rate after implementation of a commercially sold computerized physician order entry system.Pediatrics.2010;126(1):14–21.
- ,,.The condition of the literature on differences in hospital mortality.Med Care.1989;27(4):315–336.
- ,,.Threshold volumes associated with higher survival in health care: a systematic review.Med Care.2003;41(10):1129–1141.
- ,,, et al.Hospital volume and 30‐day mortality for three common medical conditions.N Engl J Med.2010;362(12):1110–1118.
- Patient Protection and Affordable Care Act Pub. L. No. 111–148, 124 Stat, §3025.2010. Available at: http://www.gpo.gov/fdsys/pkg/PLAW‐111publ148/content‐detail.html. Accessed on July 26, year="2012"2012.
- ,,.Are mortality rates for different operations related? Implications for measuring the quality of noncardiac surgery.Med Care.2006;44(8):774–778.
- ,,,.Do hospitals with low mortality rates in coronary artery bypass also perform well in valve replacement?Ann Thorac Surg.2003;76(4):1131–1137.
- ,,,,.Differences among hospitals in Medicare patient mortality.Health Serv Res.1989;24(1):1–31.
- ,,,.Variations in standardized hospital mortality rates for six common medical diagnoses: implications for profiling hospital quality.Med Care.1998;36(7):955–964.
- ,,, et al.Development, validation, and results of a measure of 30‐day readmission following hospitalization for pneumonia.J Hosp Med.2011;6(3):142–150.
- ,,, et al.An administrative claims measure suitable for profiling hospital performance on the basis of 30‐day all‐cause readmission rates among patients with heart failure.Circ Cardiovasc Qual Outcomes.2008;1:29–37.
- ,,, et al.Quality of care for acute myocardial infarction at urban safety‐net hospitals.Health Aff (Millwood).2007;26(1):238–248.
- National Quality Measures Clearinghouse.2011. Available at: http://www.qualitymeasures.ahrq.gov/. Accessed February 21,year="2011"2011.
- ,,, et al.An administrative claims model suitable for profiling hospital performance based on 30‐day mortality rates among patients with an acute myocardial infarction.Circulation.2006;113(13):1683–1692.
- ,,, et al.An administrative claims model suitable for profiling hospital performance based on 30‐day mortality rates among patients with heart failure.Circulation.2006;113(13):1693–1701.
- ,,, et al.An administrative claims model for profiling hospital 30‐day mortality rates for pneumonia patients.PLoS One.2011;6(4):e17401.
- ,,, et al.An administrative claims measure suitable for profiling hospital performance based on 30‐day all‐cause readmission rates among patients with acute myocardial infarction.Circ Cardiovasc Qual Outcomes.2011;4(2):243–252.
- .The application of electronic computers to factor analysis.Educ Psychol Meas.1960;20:141–151.
- .On the ‘probable error’ of a coefficient of correlation deduced from a small sample.Metron.1921;1:3–32.
- ,,.Comparing correlated but nonoverlapping correlations.Psychol Methods.1996;1(2):178–183.
- Centers for Medicare and Medicaid Services.Medicare Shared Savings Program: Accountable Care Organizations, Final Rule.Fed Reg.2011;76:67802–67990.
- Massachusetts Healthcare Quality and Cost Council. Potentially Preventable Readmissions.2011. Available at: http://www.mass.gov/hqcc/the‐hcqcc‐council/data‐submission‐information/potentially‐preventable‐readmissions‐ppr.html. Accessed February 29, 2012.
- Texas Medicaid. Potentially Preventable Readmission (PPR).2012. Available at: http://www.tmhp.com/Pages/Medicaid/Hospital_PPR.aspx. Accessed February 29, 2012.
- New York State. Potentially Preventable Readmissions.2011. Available at: http://www.health.ny.gov/regulations/recently_adopted/docs/2011–02‐23_potentially_preventable_readmissions.pdf. Accessed February 29, 2012.
- ,,,,.Variability in the measurement of hospital‐wide mortality rates.N Engl J Med.2010;363(26):2530–2539.
- ,,, et al.Use of electronic health records in U.S. hospitals.N Engl J Med.2009;360(16):1628–1638.
- US Department of Health and Human Services. Hospital Compare.2011. Available at: http://www.hospitalcompare.hhs.gov. Accessed March 5, 2011.
- ,,.Early readmissions to the department of medicine as a screening tool for monitoring quality of care problems.Medicine (Baltimore).2008;87(5):294–300.
- ,,,,.Hospital inpatient mortality. Is it a predictor of quality?N Engl J Med.1987;317(26):1674–1680.
- ,.Relationship between Medicare's hospital compare performance measures and mortality rates.JAMA.2006;296(22):2694–2702.
- ,,.Public reporting of discharge planning and rates of readmissions.N Engl J Med.2009;361(27):2637–2645.
- ,,, et al.Process of care performance measures and long‐term outcomes in patients hospitalized with heart failure.Med Care.2010;48(3):210–216.
- ,,,,,.Variations in inpatient mortality among hospitals in different system types, 1995 to 2000.Med Care.2009;47(4):466–473.
- ,,, et al.A systematic review and meta‐analysis of studies comparing mortality rates of private for‐profit and private not‐for‐profit hospitals.Can Med Assoc J.2002;166(11):1399–1406.
- ,,, et al.What distinguishes top‐performing hospitals in acute myocardial infarction mortality rates? A qualitative study.Ann Intern Med.2011;154(6):384–390.
- ,,.Perceptions of hospital safety climate and incidence of readmission.Health Serv Res.2011;46(2):596–616.
- ,,, et al.Decrease in hospital‐wide mortality rate after implementation of a commercially sold computerized physician order entry system.Pediatrics.2010;126(1):14–21.
- ,,.The condition of the literature on differences in hospital mortality.Med Care.1989;27(4):315–336.
- ,,.Threshold volumes associated with higher survival in health care: a systematic review.Med Care.2003;41(10):1129–1141.
- ,,, et al.Hospital volume and 30‐day mortality for three common medical conditions.N Engl J Med.2010;362(12):1110–1118.
- Patient Protection and Affordable Care Act Pub. L. No. 111–148, 124 Stat, §3025.2010. Available at: http://www.gpo.gov/fdsys/pkg/PLAW‐111publ148/content‐detail.html. Accessed on July 26, year="2012"2012.
- ,,.Are mortality rates for different operations related? Implications for measuring the quality of noncardiac surgery.Med Care.2006;44(8):774–778.
- ,,,.Do hospitals with low mortality rates in coronary artery bypass also perform well in valve replacement?Ann Thorac Surg.2003;76(4):1131–1137.
- ,,,,.Differences among hospitals in Medicare patient mortality.Health Serv Res.1989;24(1):1–31.
- ,,,.Variations in standardized hospital mortality rates for six common medical diagnoses: implications for profiling hospital quality.Med Care.1998;36(7):955–964.
- ,,, et al.Development, validation, and results of a measure of 30‐day readmission following hospitalization for pneumonia.J Hosp Med.2011;6(3):142–150.
- ,,, et al.An administrative claims measure suitable for profiling hospital performance on the basis of 30‐day all‐cause readmission rates among patients with heart failure.Circ Cardiovasc Qual Outcomes.2008;1:29–37.
- ,,, et al.Quality of care for acute myocardial infarction at urban safety‐net hospitals.Health Aff (Millwood).2007;26(1):238–248.
- National Quality Measures Clearinghouse.2011. Available at: http://www.qualitymeasures.ahrq.gov/. Accessed February 21,year="2011"2011.
- ,,, et al.An administrative claims model suitable for profiling hospital performance based on 30‐day mortality rates among patients with an acute myocardial infarction.Circulation.2006;113(13):1683–1692.
- ,,, et al.An administrative claims model suitable for profiling hospital performance based on 30‐day mortality rates among patients with heart failure.Circulation.2006;113(13):1693–1701.
- ,,, et al.An administrative claims model for profiling hospital 30‐day mortality rates for pneumonia patients.PLoS One.2011;6(4):e17401.
- ,,, et al.An administrative claims measure suitable for profiling hospital performance based on 30‐day all‐cause readmission rates among patients with acute myocardial infarction.Circ Cardiovasc Qual Outcomes.2011;4(2):243–252.
- .The application of electronic computers to factor analysis.Educ Psychol Meas.1960;20:141–151.
- .On the ‘probable error’ of a coefficient of correlation deduced from a small sample.Metron.1921;1:3–32.
- ,,.Comparing correlated but nonoverlapping correlations.Psychol Methods.1996;1(2):178–183.
- Centers for Medicare and Medicaid Services.Medicare Shared Savings Program: Accountable Care Organizations, Final Rule.Fed Reg.2011;76:67802–67990.
- Massachusetts Healthcare Quality and Cost Council. Potentially Preventable Readmissions.2011. Available at: http://www.mass.gov/hqcc/the‐hcqcc‐council/data‐submission‐information/potentially‐preventable‐readmissions‐ppr.html. Accessed February 29, 2012.
- Texas Medicaid. Potentially Preventable Readmission (PPR).2012. Available at: http://www.tmhp.com/Pages/Medicaid/Hospital_PPR.aspx. Accessed February 29, 2012.
- New York State. Potentially Preventable Readmissions.2011. Available at: http://www.health.ny.gov/regulations/recently_adopted/docs/2011–02‐23_potentially_preventable_readmissions.pdf. Accessed February 29, 2012.
- ,,,,.Variability in the measurement of hospital‐wide mortality rates.N Engl J Med.2010;363(26):2530–2539.
- ,,, et al.Use of electronic health records in U.S. hospitals.N Engl J Med.2009;360(16):1628–1638.
Copyright © 2012 Society of Hospital Medicine
Antibiotic Decisions in the ICU
Antimicrobial use provides the selective pressure that cause bacteria to develop antimicrobial resistance.1 Currently, clones of bacteria with very limited antimicrobial sensitivity are gradually spreading around the world.2 The intensive care unit (ICU) is a focus of resistant bacteria within the hospital3 as a result of high illness severity, widespread use of invasive monitoring or therapeutic devices, frequency of bacterial infection (found in approximately 51% of patients4), and consequent extensive use of broad‐spectrum antimicrobials (in 71% of patients).4
When prescribing antimicrobials, the ICU clinician often faces a dilemma. First, the traditional symptoms and signs of infection (such as characteristic patient history, fever, increased white cell count, etc) are common in ICU patients even in the absence of infection, making distinction of infectious and noninfectious causes of patient deterioration difficult. Second, delaying antimicrobial therapy, prescribing inadequate antimicrobials, or allowing bacterial infections to go untreated, increases patient mortality,57 resulting in guideline recommendations to start broad‐spectrum antimicrobials as soon as possible in the presence of suspected severe sepsis.8 While third, and in contrast, unnecessary antimicrobial therapy increases the risk of antimicrobial‐related complications, such as Clostridium difficile colitis (with a crude mortality of up to 20%9), and potentially endangers the greater population of ICU patients by increasing the prevalence of resistant organisms. Choosing between delaying necessary antimicrobial therapy and exposing the patient to unnecessary therapy requires that 2 contrasting risks be balancedthat of untreated infection versus late antimicrobial complications.
The main aim of this study was to assess how often administration of antimicrobials for suspected infection could be justified by the presence of infection. The primary outcome measure was accuracy of antimicrobial administration, defined as the proportion of antimicrobials started for suspected infection where infection was later proven to have been present. Secondary outcome measures examined: (1) whether clinician suspicion of infection correlated with the presence of defined infection; (2) the ID specialist's accuracy for empiric antimicrobial administration; (3) whether common clinical parameters were associated with clinician certainty regarding the presence of infection; and (4) use of antimicrobials in the presence or absence of infection. These data are important in order to identify possibilities for improving antimicrobial administration.
METHODS
Setting
Data were collected on all ICU patients staying >48 hours in the 12‐bed general (mainly surgical) ICU of a 775‐bed academic tertiary referral center (the Hadassah Hebrew University Medical Center, Jerusalem, Israel) from May to August 2009. The hospital ethics committee approved the study and waived the requirement for informed consent.
Clinical antimicrobial decision‐making was at the final discretion of the ICU attending clinician. During office hours, decisions to start antimicrobials with any but first line agents (ampicillin, ampicillin/clavulanic acid, azithromycin, cefazolin, cefuroxime, ciprofloxacin, clindamycin, cloxacillin, gentamicin, and metronidazole) required authorization by the clinical ID specialist on attachment to the ICU (who performed a daily round). Out of office hours, decisions required authorization by an on‐call ID specialist (usually by phone). There was no availability of a clinical pharmacist. Microbiological studies were obtained as follows: sputum and urine cultures routinely 3 times per week, while other cultures (including blood, wound, site‐specific cultures, etc) according to clinical indications.
Antimicrobial Administration Decisions
Start and stop dates were recorded for all intravenous antimicrobials administered during the patient's ICU stay. Antimicrobial start decisions were divided into 3 groups: empirical (where antimicrobials were started for a new suspected infection), prophylaxis‐driven (antimicrobials given peri‐procedurally), and targeted therapy (antimicrobials started or changed based on receipt of culture results, or antimicrobials continued from a previous department). Although multiple antimicrobials were often started together, these were considered as a single antimicrobial start decision, if started for the same reason.
Empirical decisions represent the main focus of this study, and further data were collected for these decisions. For each empiric decision, the attending ICU clinician's name was recorded, as well as a measure of his certainty that a new infection was actually present. Certainty was determined at the time that the antimicrobials were started and was entirely subjective. The clinician was asked to categorize his certainty that an infection was present when starting empiric antimicrobials on a scale from 0 to 5: 0no infection; 1infection unlikely; 2infection possible; 3infection probable; 4infection very likely; and 5infection certain. The number of systemic inflammatory response syndrome (SIRS) criteria10 and Sequential Organ Failure Assessment (SOFA)11 score were calculated at the time each decision was made (using the last available data prior to starting antimicrobials), and for the previous 2 days (using the worst values on each calendar day). Data on demographics, admission history, comorbid conditions, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, and outcome were collected for each patient.
Antimicrobial Start Decisions and Definitions of Infection by the Study ID Specialist
Approximately 1 week after each empiric antimicrobial decision, the need for antimicrobial therapy and the presence of infection were analyzed and defined by the study ID specialist (S.B.). He was not involved in clinical decision‐making and was not acquainted with patient details. Each analysis included 2 steps: Step 1 concerning the overall requirement for antimicrobial therapy, and Step 2 regarding the presence of infection. For Step 1, data from the patient's clinical course up until the time the antimicrobial start decision was made were presented. At that point, the study ID specialist decided whether, if presented the case as a consultant, he would have recommended starting antimicrobials. For Step 2, the patient's clinical course following the antimicrobial decision point as well as laboratory, imaging, and microbiological results from the subsequent days were reviewed. The presence or absence of infection was defined by integrating all of this data, and based on the Centers for Disease Control and Prevention (CDC) surveillance criteria for the diagnosis of nosocomial infections.12 The study ID specialist used the same certainty score regarding the presence of infection as the clinicians. A certainty of a probable infection (score 3) or higher represented the cutoff to define the presence of infection. The study ID specialist's determination of the presence of infection was considered the gold standard for the presence of infection for analyses and is termed defined infection.
Accuracy of Antimicrobial Start Decisions
Accuracy was calculated for both the clinicians and the study ID specialist, and expressed as a proportion. The denominator for ICU clinician accuracy was the total number of antibiotic start decisions for suspected infection, and the numerator was the number of decisions where infection was defined by the ID specialist. For the study ID specialist, the denominator was the number of occasions when antibiotic administration was considered justified in the Step 1 analysis, and the numerator was the number of these cases where infection was defined (Figure 1). The correlation between clinician certainty and the study‐defined presence of infection was examined. The accuracy of clinical antimicrobial decisions made during the first 48 hours of ICU admission was compared to decisions made after 48 hours.
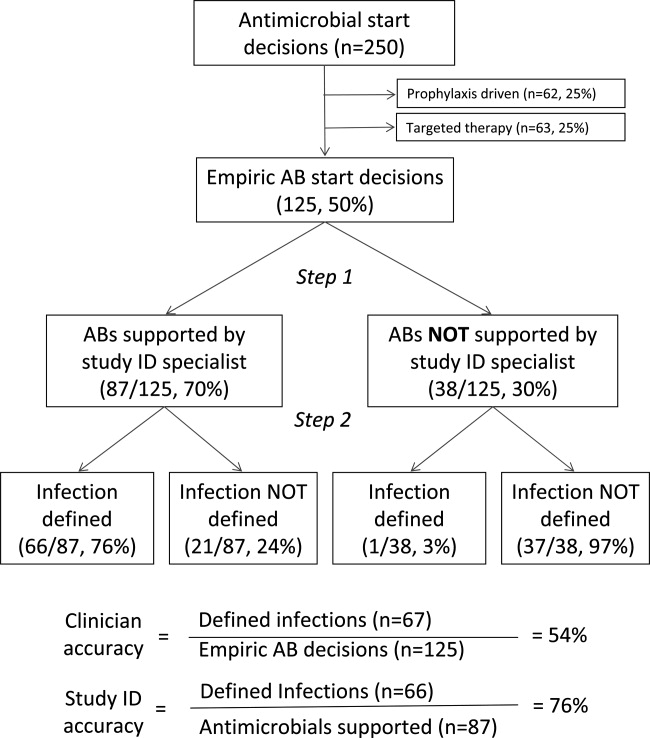
In order to assess the robustness of the study findings, the ICU clinician accuracy was examined in a sensitivity analysis. Accuracy was calculated using a lower cutoff for the study ID specialist's definition of infectionpossible infection (score 2) or above, rather than probable infection or above.
Physiological Parameters
To examine the effect of physiological variables on physician certainty, empiric antimicrobial start decisions were divided into 2 groupsa high clinician certainty group (certainty score 3) and a low certainty score (<3). Each physiological parameter comprising the SIRS and SOFA scores, the scores themselves, and changes from the previous 24 and 48 hours were compared for the 2 groups. Data used for the decision day were the last available observations prior to starting the antimicrobials. Data for the previous 2 days were the worst values present during each calendar day.
Antimicrobial Course Length
The total course given after each empirical antibiotic start decision was measured in days. The course length started with the empiric antimicrobial start decision, and ended either when antimicrobial therapy was stopped, or when a subsequent empirical start decision was made. Course length for start decisions where infection was subsequently defined was compared to decisions where infection was not defined.
Statistical Analysis
Continuous variables were compared using the Student t test, while categorical variables were compared using the chi‐square test. All P values are 2‐tailed and P < 0.05 was considered statistically significant. SAS version 8.2 (SAS Institute, Inc, Cary, NC) was used for statistical analysis.
RESULTS
Data were collected on 119 consecutive ICU patients over 4 months (Table 1). Antimicrobials were started for suspected infection in 80/119 (67%) patients, for prophylaxis in 55/119 (46%) patients, and for other reasons in 42/119 (35%) patients. More than one indication was present during the patient's ICU admission among 41/119 (34%) patients, while for 6/119 (5%) patients, no antimicrobials were prescribed at all. Among these patients, antimicrobials were administered on 250 occasions, including 125/250 (50%) occasions for suspected infection (empirical decisions), 62/250 (25%) occasions for procedural prophylaxis (prophylaxis‐driven), and on 63/250 (25%) occasions for other reasons (antimicrobial changes following receipt of culture results, or continuation of antimicrobials prescribed prior to ICU admission). Microbiological cultures were obtained from the study population on 2132 occasions, including 395 blood cultures in which significant organisms (not reflecting contamination) grew on 57/395 (14%) occasions.
| No. (%) or Mean SD | |
|---|---|
| N = 119 | |
| |
| Demographics | |
| Male gender | 66 (55) |
| Age (years) | 53 25 |
| Hospital admission prior to ICU admission | 62 (52) |
| Independent functional capacity | 99 (83) |
| Etiology for ICU admission* | |
| Surgery | 82 (69) |
| Elective | 12 (10) |
| Emergency | 70 (59) |
| Trauma | 41 (34) |
| Medical | 26 (22) |
| Comorbidities | |
| Prior antimicrobial therapy | 48 (40) |
| Severe cardiac disease | 12 (10) |
| Severe respiratory disease | 5 (4) |
| Diabetes mellitus | 22 (18) |
| Liver disease | 10 (8) |
| Dialysis | 5 (4) |
| APACHE II score | 15 8 |
| Outcome | |
| ICU length of stay (days) | 13 15 |
| Hospital length of stay (days) | 36 32 |
| ICU mortality | 16 (13) |
| Hospital mortality | 22 (18) |
Among the empiric antimicrobial start decisions, infection was defined by the study ID specialist on 67/125 (54%) occasions, representing the clinicians' diagnostic accuracy. These infections included 17 (25%) respiratory, 16 (24%) abdominal, 13 (19%) soft tissue, 11 (16%) blood stream, 6 (9%) urinary, and 4 (6%) other infections.
Three attending clinicians treated patients during the study period, and their accuracies were similar (21 infections defined/44 start decisions for suspected infection, 48%; 24/38, 63%; 22/43, 51%, for each attending; P = ns for all comparisons). Clinician accuracy was higher for empirical antimicrobial start decisions, made within 48 hours of ICU admission, compared to later decisions (35 defined infections/53 early antibiotic start decisions [66%] vs 32 defined infections/72 late antibiotic start decisions [44%]; P = 0.02).
In a sensitivity analysis, decreasing the cutoff for the study ID specialist's definition of infection from probable (and above) to possible (and above) lead to reclassification of 14/125 (11%) antimicrobial start decisions from no infection defined to infection defined. This increased physician accuracy from 67/125 (54%) to 78/125 (62%), and conversely decreased potential antimicrobial overuse from 58/125 (46%) to 47/125 (38%) decisions (P = ns).
When starting antimicrobials for suspected infection, the clinicians were asked to record their certainty in the presence of infection. Infections were defined on 6/19 (31%) occasions when the clinician certainty score was low (2) versus 61/106 (57%) when the clinician certainty score was high (3, P = 0.037; Figure 2). Correlation between the clinician certainty score and the presence of defined infection was good (r2 = 0.78).
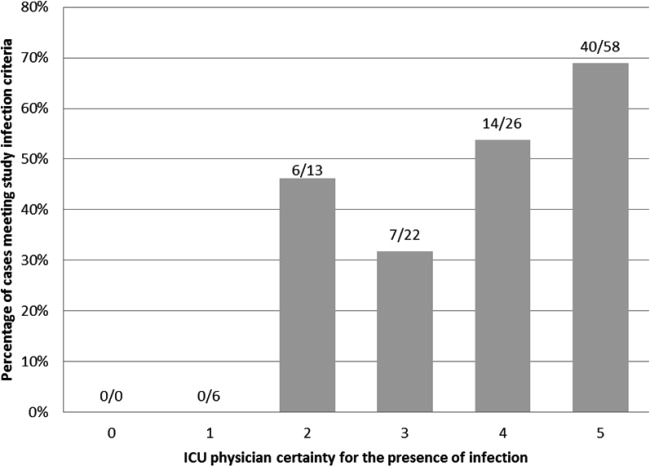
The study ID specialist agreed with the clinician's decision to start antimicrobial therapy on 87/125 (70%) occasions. Infection was subsequently defined on 66/87 (76%) occasions, representing the study ID specialist's diagnostic accuracy. The study ID specialist's accuracy was significantly higher than the clinician's (66/87 [76%] versus 67/125 [54%]; P = 0.001). Notably, there was only 1 case (3%) where empiric therapy was deemed unnecessary by the study ID specialist, and where infection was subsequently defined. In this case, the clinicians started antibiotic therapy for suspected ventilator‐associated pneumonia in a 66‐year‐old patient on the 28th day of an ICU admission for head and spinal cord trauma. The ID specialist's certainty for the presence of infection was 3probable. The patient ultimately survived and was discharged to a rehabilitation facility.
Comparing physiological data for antimicrobial start decisions with high clinician certainty (score 3) versus low certainty of infection (score 2), revealed that none of the physiological data, nor changes over time were significantly associated with clinician certainty. Further use of high doses of vasopressors (>0.1 mcg/kg/min, SOFA score 4) was present at 42/106 (40%) high certainty decisions versus 7/19 (37%) low certainty decisions (P = 0.819). This underscores the physicians' difficulty in distinguishing between infectious and inflammatory causes of deterioration (Table 2).
| Low Certainty* N = 19 | High Certainty N = 106 | ||
|---|---|---|---|
| Mean SD | Mean SD | P Value | |
| |||
| SIRS elements | |||
| Temperature (C) | 37.7 1.2 | 37.3 1.6 | 0.28 |
| WBC count ( 109/liter) | 16.7 8.1 | 15.9 10.5 | 0.72 |
| Pulse (rate/min) | 112 23 | 110 21 | 0.58 |
| Respiratory rate (rate/min) | 22 8 | 22 8 | 0.90 |
| Number of SIRS criteria (at antimicrobial start) | 3.0 0.9 | 3.2 0.9 | 0.24 |
| Change in number of SIRS criteria (24 h) | 0.1 0.9 | 0.0 0.9 | 0.68 |
| Change in number of SIRS criteria (48 h) | 0.0 0.7 | 0.3 0.9 | 0.36 |
| SOFA score elements (points) | |||
| Respiratory | 1.6 1.1 | 1.9 1.2 | 0.45 |
| Neurological | 1.8 1.7 | 2.0 1.6 | 0.50 |
| Coagulation | 0.6 1.1 | 0.6 1.1 | 0.85 |
| Hepatic | 0.6 0.8 | 0.4 0.8 | 0.37 |
| Renal | 0.7 1.1 | 0.8 1.1 | 0.51 |
| Cardiovascular | 1.5 1.9 | 1.8 1.9 | 0.47 |
| SOFA score day at antimicrobial start | 6.7 3.1 | 7.3 4.6 | 0.58 |
| SOFA score change (previous 24 h) | 1.5 3.2 | 1.0 2.9 | 0.56 |
| SOFA score change (previous 48 h) | 3.1 4.4 | 1.5 4.3 | 0.25 |
During the study period, 2541 days of antimicrobial therapy were given of which 1677 (66%), 413 (16%), and 451 (18%) were given, respectively, empirically (for suspected infection), for procedural prophylaxis, and as targeted therapy. Antimicrobial course length was 11.5 9.2 days in the presence of defined infection versus 10.7 9.1 days in the absence of defined infection (P = 0.655). Overall, 658/2541 (26%) days of therapy could potentially have been saved by reducing antimicrobial prescriptions for suspected infections which were not defined.
DISCUSSION
The use of empirical antimicrobials could be justified by the presence of defined infection on only 54% of occasions when they were administered, suggesting considerable potential overuse of these drugs. ICU‐clinician certainty for the presence of infection correlated well with the number of infections actually defined, however, infections were defined when certainty was low (Figure 2) and antimicrobials prescribed even when clinician certainty was minimal. Common clinical physiological and laboratory parameters did not seem to assist in the clinicians' decision‐making, as there were no significant differences in any of these values between empiric decisions with high or low certainty. The study ID specialist showed significantly better accuracy in antimicrobial decision‐making than the ICU clinicians. He agreed with antimicrobial administration on only 70% of occasions that clinicians started empiric therapy, and had a higher diagnostic accuracy at a cost of only 1 untreated infection.
Two main possibilities are suggested to explain the potential antimicrobial overuse. First, ICU physicians are loath to leave infections untreated and potentially cause immediate increases in mortality.8 This leads to uncertainty avoidance or risk aversive behavior that is demonstrated in our study by the inclusion of antimicrobial administration decisions made even when physicians' certainty regarding the presence of infection was low. Uncertainty avoidance has been shown to be significantly associated with antimicrobial prescribing practices,13 however, it discounts the risk of antimicrobial complications associated with unnecessary antimicrobial therapy. Second, the diagnosis of infection, and particularly nosocomial infection, in ICU patients is difficult. Symptoms cannot be elicited in obtunded ventilated ICU patients, the physical exam can be equivocal, bacterial growth in cultures (with the exception of blood cultures) often reflects colonization rather than infection, and the laboratory and imaging findings of inflammation and infection are very similar. Our data demonstrated some of these difficulties. Diagnostic accuracy was higher in infections suspected during the first 48 hours of ICU admission when compared to later, presumably as infection leading to ICU admission is associated with symptoms, signs, and an acute change in the patient's condition, factors that may be absent when a patient develops a nosocomial infection. Further, physiological parameters did not correlate with the certainty that ICU clinicians expressed in their decision, indicating the difficulty in interpreting these data. Finally, infection was defined in 30% of low certainty decisions, indicating that clinical impression alone is not a reliable tool for determining the presence of infection.
Three sets of interventions could be suggested to improve antimicrobial decision‐makingincreased use of the ID consult, improved laboratory tests for the diagnosis of infection, and a policy of de‐escalation. Use of antimicrobial stewardship (often through involvement of an ID physician) reduces antimicrobial usage and the occurrence of resistant bacteria without adverse patient outcomes.14 Indeed, our study ID consult showed more accurate antimicrobial prescribing than the ICU clinicians, although he may have been subject to the potential biases described below. All antimicrobial administration decisions taken during the study were, however, made in consultation with the clinical ID consult. The lower performance of the clinical ID consult (when compared to the study ID consult) may have resulted from difficulties in the real‐time interaction with the clinicians or from decisions taken during non‐office hours. During non‐office hours, the on‐call ICU resident presented cases to an on‐call ID specialist, neither of whom may have been familiar with all the complex case details and therefore may have preferred to err by commission than by omission.
More accurate laboratory tests, such as procalcitonin or real‐time bacterial polymerase chain reaction (PCR),15 could be beneficial as they might increase physician confidence in decision‐making. Procalcitonin has been used in a wide variety of settings1618 (including the ICU1921) to safely decrease antimicrobial starts and/or antimicrobial course length. Despite this, in a large multicenter study of procalcitonin use in ICU patients,19 compliance with the antibiotic start protocol was very low. Antibiotics were administered by the participating physicians in 73/93 (78%) cases where the procalcitonin tests indicated that antimicrobials were not required, representing protocol violations. In parallel to our study, this demonstrates the reluctance of physicians to abstain from prescribing antimicrobial therapy for suspected infection even when the likelihood of infection may be low.
A strategy of de‐escalation offers the possibility of starting broad‐spectrum antimicrobials early and, subsequently, narrowing or stopping therapy according to the clinical course and the microbiological results.22, 23 This strategy allows clinicians to start antimicrobials even when the suspicion of infection is low, but to stop them rapidly as the clinical picture clarifies. Unfortunately, the mean antimicrobial course length in this study was not influenced by the presence of infection, indicating that this strategy was not employed successfully.
The proportion of patients prescribed antimicrobials for suspected infection in our study is similar to that found in others (eg, 34% of patients in a large French survey24). The proportion of potentially unnecessary antimicrobials in other studies is also similar, ranging from 14% to 50%.2428 In the ICU, the majority of antimicrobial usage studies are microbiology‐based and examine whether bacteria cultured are resistant to the antimicrobials chosen. They have shown that inappropriate antimicrobial therapy occurs on 20%36% of occasions.6, 7, 29 The current study furthers knowledge on antimicrobials decision‐making in the ICU, by examining the actual requirement for antimicrobial therapy based on the presence of infection, ie, whether antimicrobials were needed at all.
The principal limitation of the study concerns the determination of the presence of infection. The study premise was that antimicrobials are overused, and this may have biased the study ID consult to underestimate appropriateness of antimicrobial therapy and to define fewer infections. Further, making theoretical decisions in the research office avoids the medical, ethical, and legal issues related to clinical practice, as there is no risk associated with error. This may have allowed the study ID specialist to be overly conservative in his definitions of infections. A wider team of decision‐makers to determine the presence of infection, including both ID and ICU specialists, would have lent more weight to their determinations, however, this was logistically impossible. To limit the potential bias, infections were defined as objectively as possible based on the CDC criteria.12 Further, the sensitivity analysis showed that while decreasing the study ID specialist's threshold for the definition of infection from probable and above to possible and above improved physician accuracy, over a third of antimicrobial start decisions remained unjustified by the presence of defined infection. The study was performed in only 1 center and may not reflect general ICU practice, although, as discussed above, the antibiotic decision‐making accuracy is in the same orders of magnitude as those found in other somewhat similar studies. Finally, even if unnecessary antimicrobial use was overestimated, the possibility for significant improvement in antimicrobial administration accuracy remains.
In conclusion, our data suggest that on up to 46% of occasions, empirical antimicrobials are prescribed in the absence of infection. We suggest that the potential antibiotic overuse results from difficulties in diagnosing ICU‐related infections, and from the high perceived risk of untreated infection as compared to the risks of potentially unnecessary antimicrobial therapy, representing a type of risk aversive behavior. As antimicrobial use is the primary factor promoting antibiotic resistance and may be a cause of other patient complications, efforts to improve antimicrobial‐related decision‐making should be mandatory.
- ,.Antimicrobial‐drug resistance.N Engl J Med.1996;335:1445–1453.
- ,,, et al.Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study.Lancet Infect Dis.2010;10:597–602.
- ,,, et al.Surveillance of antimicrobial use and antimicrobial resistance in United States hospitals: project ICARE phase 2. Project Intensive Care Antimicrobial Resistance Epidemiology (ICARE) hospitals.Clin Infect Dis.1999;29:245–252.
- ,,, et al.International study of the prevalence and outcomes of infection in intensive care units.JAMA.2009;302:2323–2329.
- ,,,,.Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator‐associated pneumonia.Chest.2002;122:262–268.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,, et al.Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock.Chest.2009;136:1237–1248.
- ,,, et al.Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36:296–327.
- ,,,,.Investigation of critical care unit utilization and mortality in patients infected with Clostridium difficile.J Crit Care.2010;25:282–286.
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference:definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis.Crit Care Med.1992;20:864–874.
- ,,, et al.The SOFA (Sepsis‐related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis‐Related Problems of the European Society of Intensive Care Medicine.Intensive Care Med.1996;22:707–710.
- ,,.CDC/NHSN surveillance definition of health care‐associated infection and criteria for specific types of infections in the acute care setting.Am J Infect Control.2008;36:309–332.
- ,,, et al.Are cultural dimensions relevant for explaining cross‐national differences in antibiotic use in Europe?BMC Health Serv Res.2008;8:123.
- ,,,,,.Impact of antimicrobial stewardship in critical care: a systematic review.J Antimicrob Chemother.2011;66:1223–1230.
- ,,, et al.A multicenter trial to compare blood culture with polymerase chain reaction in severe human sepsis.Intensive Care Med.2010;36:241–247.
- ,,, et al.Procalcitonin guidance of antibiotic therapy in community‐acquired pneumonia: a randomized trial.Am J Respir Crit Care Med.2006;174:84–93.
- ,,, et al.Effect of procalcitonin‐based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trial.JAMA.2009;302:1059–1066.
- ,,, et al.Antibiotic treatment of exacerbations of COPD: a randomized, controlled trial comparing procalcitonin‐guidance with standard therapy.Chest.2007;131:9–19.
- ,,, et al.Use of procalcitonin to reduce patients' exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial.Lancet.2010;375:463–474.
- ,,,,.Use of procalcitonin to shorten antibiotic treatment duration in septic patients: a randomized trial.Am J Respir Crit Care Med.2008;177:498–505.
- ,,, et al.Procalcitonin for reduced antibiotic exposure in ventilator‐associated pneumonia: a randomised study.Eur Respir J.2009;34:1364–1375.
- ,,, et al.Consensus document on controversial issues for the treatment of hospital‐associated pneumonia.Int J Infect Dis.2010;14(suppl 4):S55–S65.
- ,, et al.Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am Respir Crit Care Med.2005;171:388–416.
- ,,, et al.Strategies of initiation and streamlining of antibiotic therapy in 41 French intensive care units.Crit Care.2011;15:R17.
- ,,,.Antibiotic use at Duke University Medical Center.JAMA.1977;237:2819–2822.
- ,.A study of antimicrobial misuse in a university hospital.Am J Med Sci.1978;275:271–282.
- ,,,,.Unnecessary use of antimicrobials in hospitalized patients: current patterns of misuse with an emphasis on the antianaerobic spectrum of activity.Arch Intern Med.2003;163:972–978.
- ,,, et al.Interventions to improve antibiotic prescribing practices for hospital inpatients.Cochrane Database Syst Rev.2005;CD003543.
- ,,, et al.Patterns of antimicrobial therapy in severe nosocomial infections: empiric choices, proportion of appropriate therapy, and adaptation rates—a multicentre, observational survey in critically ill patients.Int J Antimicrob Agents.2010;35:375–381.
Antimicrobial use provides the selective pressure that cause bacteria to develop antimicrobial resistance.1 Currently, clones of bacteria with very limited antimicrobial sensitivity are gradually spreading around the world.2 The intensive care unit (ICU) is a focus of resistant bacteria within the hospital3 as a result of high illness severity, widespread use of invasive monitoring or therapeutic devices, frequency of bacterial infection (found in approximately 51% of patients4), and consequent extensive use of broad‐spectrum antimicrobials (in 71% of patients).4
When prescribing antimicrobials, the ICU clinician often faces a dilemma. First, the traditional symptoms and signs of infection (such as characteristic patient history, fever, increased white cell count, etc) are common in ICU patients even in the absence of infection, making distinction of infectious and noninfectious causes of patient deterioration difficult. Second, delaying antimicrobial therapy, prescribing inadequate antimicrobials, or allowing bacterial infections to go untreated, increases patient mortality,57 resulting in guideline recommendations to start broad‐spectrum antimicrobials as soon as possible in the presence of suspected severe sepsis.8 While third, and in contrast, unnecessary antimicrobial therapy increases the risk of antimicrobial‐related complications, such as Clostridium difficile colitis (with a crude mortality of up to 20%9), and potentially endangers the greater population of ICU patients by increasing the prevalence of resistant organisms. Choosing between delaying necessary antimicrobial therapy and exposing the patient to unnecessary therapy requires that 2 contrasting risks be balancedthat of untreated infection versus late antimicrobial complications.
The main aim of this study was to assess how often administration of antimicrobials for suspected infection could be justified by the presence of infection. The primary outcome measure was accuracy of antimicrobial administration, defined as the proportion of antimicrobials started for suspected infection where infection was later proven to have been present. Secondary outcome measures examined: (1) whether clinician suspicion of infection correlated with the presence of defined infection; (2) the ID specialist's accuracy for empiric antimicrobial administration; (3) whether common clinical parameters were associated with clinician certainty regarding the presence of infection; and (4) use of antimicrobials in the presence or absence of infection. These data are important in order to identify possibilities for improving antimicrobial administration.
METHODS
Setting
Data were collected on all ICU patients staying >48 hours in the 12‐bed general (mainly surgical) ICU of a 775‐bed academic tertiary referral center (the Hadassah Hebrew University Medical Center, Jerusalem, Israel) from May to August 2009. The hospital ethics committee approved the study and waived the requirement for informed consent.
Clinical antimicrobial decision‐making was at the final discretion of the ICU attending clinician. During office hours, decisions to start antimicrobials with any but first line agents (ampicillin, ampicillin/clavulanic acid, azithromycin, cefazolin, cefuroxime, ciprofloxacin, clindamycin, cloxacillin, gentamicin, and metronidazole) required authorization by the clinical ID specialist on attachment to the ICU (who performed a daily round). Out of office hours, decisions required authorization by an on‐call ID specialist (usually by phone). There was no availability of a clinical pharmacist. Microbiological studies were obtained as follows: sputum and urine cultures routinely 3 times per week, while other cultures (including blood, wound, site‐specific cultures, etc) according to clinical indications.
Antimicrobial Administration Decisions
Start and stop dates were recorded for all intravenous antimicrobials administered during the patient's ICU stay. Antimicrobial start decisions were divided into 3 groups: empirical (where antimicrobials were started for a new suspected infection), prophylaxis‐driven (antimicrobials given peri‐procedurally), and targeted therapy (antimicrobials started or changed based on receipt of culture results, or antimicrobials continued from a previous department). Although multiple antimicrobials were often started together, these were considered as a single antimicrobial start decision, if started for the same reason.
Empirical decisions represent the main focus of this study, and further data were collected for these decisions. For each empiric decision, the attending ICU clinician's name was recorded, as well as a measure of his certainty that a new infection was actually present. Certainty was determined at the time that the antimicrobials were started and was entirely subjective. The clinician was asked to categorize his certainty that an infection was present when starting empiric antimicrobials on a scale from 0 to 5: 0no infection; 1infection unlikely; 2infection possible; 3infection probable; 4infection very likely; and 5infection certain. The number of systemic inflammatory response syndrome (SIRS) criteria10 and Sequential Organ Failure Assessment (SOFA)11 score were calculated at the time each decision was made (using the last available data prior to starting antimicrobials), and for the previous 2 days (using the worst values on each calendar day). Data on demographics, admission history, comorbid conditions, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, and outcome were collected for each patient.
Antimicrobial Start Decisions and Definitions of Infection by the Study ID Specialist
Approximately 1 week after each empiric antimicrobial decision, the need for antimicrobial therapy and the presence of infection were analyzed and defined by the study ID specialist (S.B.). He was not involved in clinical decision‐making and was not acquainted with patient details. Each analysis included 2 steps: Step 1 concerning the overall requirement for antimicrobial therapy, and Step 2 regarding the presence of infection. For Step 1, data from the patient's clinical course up until the time the antimicrobial start decision was made were presented. At that point, the study ID specialist decided whether, if presented the case as a consultant, he would have recommended starting antimicrobials. For Step 2, the patient's clinical course following the antimicrobial decision point as well as laboratory, imaging, and microbiological results from the subsequent days were reviewed. The presence or absence of infection was defined by integrating all of this data, and based on the Centers for Disease Control and Prevention (CDC) surveillance criteria for the diagnosis of nosocomial infections.12 The study ID specialist used the same certainty score regarding the presence of infection as the clinicians. A certainty of a probable infection (score 3) or higher represented the cutoff to define the presence of infection. The study ID specialist's determination of the presence of infection was considered the gold standard for the presence of infection for analyses and is termed defined infection.
Accuracy of Antimicrobial Start Decisions
Accuracy was calculated for both the clinicians and the study ID specialist, and expressed as a proportion. The denominator for ICU clinician accuracy was the total number of antibiotic start decisions for suspected infection, and the numerator was the number of decisions where infection was defined by the ID specialist. For the study ID specialist, the denominator was the number of occasions when antibiotic administration was considered justified in the Step 1 analysis, and the numerator was the number of these cases where infection was defined (Figure 1). The correlation between clinician certainty and the study‐defined presence of infection was examined. The accuracy of clinical antimicrobial decisions made during the first 48 hours of ICU admission was compared to decisions made after 48 hours.
In order to assess the robustness of the study findings, the ICU clinician accuracy was examined in a sensitivity analysis. Accuracy was calculated using a lower cutoff for the study ID specialist's definition of infectionpossible infection (score 2) or above, rather than probable infection or above.
Physiological Parameters
To examine the effect of physiological variables on physician certainty, empiric antimicrobial start decisions were divided into 2 groupsa high clinician certainty group (certainty score 3) and a low certainty score (<3). Each physiological parameter comprising the SIRS and SOFA scores, the scores themselves, and changes from the previous 24 and 48 hours were compared for the 2 groups. Data used for the decision day were the last available observations prior to starting the antimicrobials. Data for the previous 2 days were the worst values present during each calendar day.
Antimicrobial Course Length
The total course given after each empirical antibiotic start decision was measured in days. The course length started with the empiric antimicrobial start decision, and ended either when antimicrobial therapy was stopped, or when a subsequent empirical start decision was made. Course length for start decisions where infection was subsequently defined was compared to decisions where infection was not defined.
Statistical Analysis
Continuous variables were compared using the Student t test, while categorical variables were compared using the chi‐square test. All P values are 2‐tailed and P < 0.05 was considered statistically significant. SAS version 8.2 (SAS Institute, Inc, Cary, NC) was used for statistical analysis.
RESULTS
Data were collected on 119 consecutive ICU patients over 4 months (Table 1). Antimicrobials were started for suspected infection in 80/119 (67%) patients, for prophylaxis in 55/119 (46%) patients, and for other reasons in 42/119 (35%) patients. More than one indication was present during the patient's ICU admission among 41/119 (34%) patients, while for 6/119 (5%) patients, no antimicrobials were prescribed at all. Among these patients, antimicrobials were administered on 250 occasions, including 125/250 (50%) occasions for suspected infection (empirical decisions), 62/250 (25%) occasions for procedural prophylaxis (prophylaxis‐driven), and on 63/250 (25%) occasions for other reasons (antimicrobial changes following receipt of culture results, or continuation of antimicrobials prescribed prior to ICU admission). Microbiological cultures were obtained from the study population on 2132 occasions, including 395 blood cultures in which significant organisms (not reflecting contamination) grew on 57/395 (14%) occasions.
| No. (%) or Mean SD | |
|---|---|
| N = 119 | |
| |
| Demographics | |
| Male gender | 66 (55) |
| Age (years) | 53 25 |
| Hospital admission prior to ICU admission | 62 (52) |
| Independent functional capacity | 99 (83) |
| Etiology for ICU admission* | |
| Surgery | 82 (69) |
| Elective | 12 (10) |
| Emergency | 70 (59) |
| Trauma | 41 (34) |
| Medical | 26 (22) |
| Comorbidities | |
| Prior antimicrobial therapy | 48 (40) |
| Severe cardiac disease | 12 (10) |
| Severe respiratory disease | 5 (4) |
| Diabetes mellitus | 22 (18) |
| Liver disease | 10 (8) |
| Dialysis | 5 (4) |
| APACHE II score | 15 8 |
| Outcome | |
| ICU length of stay (days) | 13 15 |
| Hospital length of stay (days) | 36 32 |
| ICU mortality | 16 (13) |
| Hospital mortality | 22 (18) |
Among the empiric antimicrobial start decisions, infection was defined by the study ID specialist on 67/125 (54%) occasions, representing the clinicians' diagnostic accuracy. These infections included 17 (25%) respiratory, 16 (24%) abdominal, 13 (19%) soft tissue, 11 (16%) blood stream, 6 (9%) urinary, and 4 (6%) other infections.
Three attending clinicians treated patients during the study period, and their accuracies were similar (21 infections defined/44 start decisions for suspected infection, 48%; 24/38, 63%; 22/43, 51%, for each attending; P = ns for all comparisons). Clinician accuracy was higher for empirical antimicrobial start decisions, made within 48 hours of ICU admission, compared to later decisions (35 defined infections/53 early antibiotic start decisions [66%] vs 32 defined infections/72 late antibiotic start decisions [44%]; P = 0.02).
In a sensitivity analysis, decreasing the cutoff for the study ID specialist's definition of infection from probable (and above) to possible (and above) lead to reclassification of 14/125 (11%) antimicrobial start decisions from no infection defined to infection defined. This increased physician accuracy from 67/125 (54%) to 78/125 (62%), and conversely decreased potential antimicrobial overuse from 58/125 (46%) to 47/125 (38%) decisions (P = ns).
When starting antimicrobials for suspected infection, the clinicians were asked to record their certainty in the presence of infection. Infections were defined on 6/19 (31%) occasions when the clinician certainty score was low (2) versus 61/106 (57%) when the clinician certainty score was high (3, P = 0.037; Figure 2). Correlation between the clinician certainty score and the presence of defined infection was good (r2 = 0.78).
The study ID specialist agreed with the clinician's decision to start antimicrobial therapy on 87/125 (70%) occasions. Infection was subsequently defined on 66/87 (76%) occasions, representing the study ID specialist's diagnostic accuracy. The study ID specialist's accuracy was significantly higher than the clinician's (66/87 [76%] versus 67/125 [54%]; P = 0.001). Notably, there was only 1 case (3%) where empiric therapy was deemed unnecessary by the study ID specialist, and where infection was subsequently defined. In this case, the clinicians started antibiotic therapy for suspected ventilator‐associated pneumonia in a 66‐year‐old patient on the 28th day of an ICU admission for head and spinal cord trauma. The ID specialist's certainty for the presence of infection was 3probable. The patient ultimately survived and was discharged to a rehabilitation facility.
Comparing physiological data for antimicrobial start decisions with high clinician certainty (score 3) versus low certainty of infection (score 2), revealed that none of the physiological data, nor changes over time were significantly associated with clinician certainty. Further use of high doses of vasopressors (>0.1 mcg/kg/min, SOFA score 4) was present at 42/106 (40%) high certainty decisions versus 7/19 (37%) low certainty decisions (P = 0.819). This underscores the physicians' difficulty in distinguishing between infectious and inflammatory causes of deterioration (Table 2).
| Low Certainty* N = 19 | High Certainty N = 106 | ||
|---|---|---|---|
| Mean SD | Mean SD | P Value | |
| |||
| SIRS elements | |||
| Temperature (C) | 37.7 1.2 | 37.3 1.6 | 0.28 |
| WBC count ( 109/liter) | 16.7 8.1 | 15.9 10.5 | 0.72 |
| Pulse (rate/min) | 112 23 | 110 21 | 0.58 |
| Respiratory rate (rate/min) | 22 8 | 22 8 | 0.90 |
| Number of SIRS criteria (at antimicrobial start) | 3.0 0.9 | 3.2 0.9 | 0.24 |
| Change in number of SIRS criteria (24 h) | 0.1 0.9 | 0.0 0.9 | 0.68 |
| Change in number of SIRS criteria (48 h) | 0.0 0.7 | 0.3 0.9 | 0.36 |
| SOFA score elements (points) | |||
| Respiratory | 1.6 1.1 | 1.9 1.2 | 0.45 |
| Neurological | 1.8 1.7 | 2.0 1.6 | 0.50 |
| Coagulation | 0.6 1.1 | 0.6 1.1 | 0.85 |
| Hepatic | 0.6 0.8 | 0.4 0.8 | 0.37 |
| Renal | 0.7 1.1 | 0.8 1.1 | 0.51 |
| Cardiovascular | 1.5 1.9 | 1.8 1.9 | 0.47 |
| SOFA score day at antimicrobial start | 6.7 3.1 | 7.3 4.6 | 0.58 |
| SOFA score change (previous 24 h) | 1.5 3.2 | 1.0 2.9 | 0.56 |
| SOFA score change (previous 48 h) | 3.1 4.4 | 1.5 4.3 | 0.25 |
During the study period, 2541 days of antimicrobial therapy were given of which 1677 (66%), 413 (16%), and 451 (18%) were given, respectively, empirically (for suspected infection), for procedural prophylaxis, and as targeted therapy. Antimicrobial course length was 11.5 9.2 days in the presence of defined infection versus 10.7 9.1 days in the absence of defined infection (P = 0.655). Overall, 658/2541 (26%) days of therapy could potentially have been saved by reducing antimicrobial prescriptions for suspected infections which were not defined.
DISCUSSION
The use of empirical antimicrobials could be justified by the presence of defined infection on only 54% of occasions when they were administered, suggesting considerable potential overuse of these drugs. ICU‐clinician certainty for the presence of infection correlated well with the number of infections actually defined, however, infections were defined when certainty was low (Figure 2) and antimicrobials prescribed even when clinician certainty was minimal. Common clinical physiological and laboratory parameters did not seem to assist in the clinicians' decision‐making, as there were no significant differences in any of these values between empiric decisions with high or low certainty. The study ID specialist showed significantly better accuracy in antimicrobial decision‐making than the ICU clinicians. He agreed with antimicrobial administration on only 70% of occasions that clinicians started empiric therapy, and had a higher diagnostic accuracy at a cost of only 1 untreated infection.
Two main possibilities are suggested to explain the potential antimicrobial overuse. First, ICU physicians are loath to leave infections untreated and potentially cause immediate increases in mortality.8 This leads to uncertainty avoidance or risk aversive behavior that is demonstrated in our study by the inclusion of antimicrobial administration decisions made even when physicians' certainty regarding the presence of infection was low. Uncertainty avoidance has been shown to be significantly associated with antimicrobial prescribing practices,13 however, it discounts the risk of antimicrobial complications associated with unnecessary antimicrobial therapy. Second, the diagnosis of infection, and particularly nosocomial infection, in ICU patients is difficult. Symptoms cannot be elicited in obtunded ventilated ICU patients, the physical exam can be equivocal, bacterial growth in cultures (with the exception of blood cultures) often reflects colonization rather than infection, and the laboratory and imaging findings of inflammation and infection are very similar. Our data demonstrated some of these difficulties. Diagnostic accuracy was higher in infections suspected during the first 48 hours of ICU admission when compared to later, presumably as infection leading to ICU admission is associated with symptoms, signs, and an acute change in the patient's condition, factors that may be absent when a patient develops a nosocomial infection. Further, physiological parameters did not correlate with the certainty that ICU clinicians expressed in their decision, indicating the difficulty in interpreting these data. Finally, infection was defined in 30% of low certainty decisions, indicating that clinical impression alone is not a reliable tool for determining the presence of infection.
Three sets of interventions could be suggested to improve antimicrobial decision‐makingincreased use of the ID consult, improved laboratory tests for the diagnosis of infection, and a policy of de‐escalation. Use of antimicrobial stewardship (often through involvement of an ID physician) reduces antimicrobial usage and the occurrence of resistant bacteria without adverse patient outcomes.14 Indeed, our study ID consult showed more accurate antimicrobial prescribing than the ICU clinicians, although he may have been subject to the potential biases described below. All antimicrobial administration decisions taken during the study were, however, made in consultation with the clinical ID consult. The lower performance of the clinical ID consult (when compared to the study ID consult) may have resulted from difficulties in the real‐time interaction with the clinicians or from decisions taken during non‐office hours. During non‐office hours, the on‐call ICU resident presented cases to an on‐call ID specialist, neither of whom may have been familiar with all the complex case details and therefore may have preferred to err by commission than by omission.
More accurate laboratory tests, such as procalcitonin or real‐time bacterial polymerase chain reaction (PCR),15 could be beneficial as they might increase physician confidence in decision‐making. Procalcitonin has been used in a wide variety of settings1618 (including the ICU1921) to safely decrease antimicrobial starts and/or antimicrobial course length. Despite this, in a large multicenter study of procalcitonin use in ICU patients,19 compliance with the antibiotic start protocol was very low. Antibiotics were administered by the participating physicians in 73/93 (78%) cases where the procalcitonin tests indicated that antimicrobials were not required, representing protocol violations. In parallel to our study, this demonstrates the reluctance of physicians to abstain from prescribing antimicrobial therapy for suspected infection even when the likelihood of infection may be low.
A strategy of de‐escalation offers the possibility of starting broad‐spectrum antimicrobials early and, subsequently, narrowing or stopping therapy according to the clinical course and the microbiological results.22, 23 This strategy allows clinicians to start antimicrobials even when the suspicion of infection is low, but to stop them rapidly as the clinical picture clarifies. Unfortunately, the mean antimicrobial course length in this study was not influenced by the presence of infection, indicating that this strategy was not employed successfully.
The proportion of patients prescribed antimicrobials for suspected infection in our study is similar to that found in others (eg, 34% of patients in a large French survey24). The proportion of potentially unnecessary antimicrobials in other studies is also similar, ranging from 14% to 50%.2428 In the ICU, the majority of antimicrobial usage studies are microbiology‐based and examine whether bacteria cultured are resistant to the antimicrobials chosen. They have shown that inappropriate antimicrobial therapy occurs on 20%36% of occasions.6, 7, 29 The current study furthers knowledge on antimicrobials decision‐making in the ICU, by examining the actual requirement for antimicrobial therapy based on the presence of infection, ie, whether antimicrobials were needed at all.
The principal limitation of the study concerns the determination of the presence of infection. The study premise was that antimicrobials are overused, and this may have biased the study ID consult to underestimate appropriateness of antimicrobial therapy and to define fewer infections. Further, making theoretical decisions in the research office avoids the medical, ethical, and legal issues related to clinical practice, as there is no risk associated with error. This may have allowed the study ID specialist to be overly conservative in his definitions of infections. A wider team of decision‐makers to determine the presence of infection, including both ID and ICU specialists, would have lent more weight to their determinations, however, this was logistically impossible. To limit the potential bias, infections were defined as objectively as possible based on the CDC criteria.12 Further, the sensitivity analysis showed that while decreasing the study ID specialist's threshold for the definition of infection from probable and above to possible and above improved physician accuracy, over a third of antimicrobial start decisions remained unjustified by the presence of defined infection. The study was performed in only 1 center and may not reflect general ICU practice, although, as discussed above, the antibiotic decision‐making accuracy is in the same orders of magnitude as those found in other somewhat similar studies. Finally, even if unnecessary antimicrobial use was overestimated, the possibility for significant improvement in antimicrobial administration accuracy remains.
In conclusion, our data suggest that on up to 46% of occasions, empirical antimicrobials are prescribed in the absence of infection. We suggest that the potential antibiotic overuse results from difficulties in diagnosing ICU‐related infections, and from the high perceived risk of untreated infection as compared to the risks of potentially unnecessary antimicrobial therapy, representing a type of risk aversive behavior. As antimicrobial use is the primary factor promoting antibiotic resistance and may be a cause of other patient complications, efforts to improve antimicrobial‐related decision‐making should be mandatory.
Antimicrobial use provides the selective pressure that cause bacteria to develop antimicrobial resistance.1 Currently, clones of bacteria with very limited antimicrobial sensitivity are gradually spreading around the world.2 The intensive care unit (ICU) is a focus of resistant bacteria within the hospital3 as a result of high illness severity, widespread use of invasive monitoring or therapeutic devices, frequency of bacterial infection (found in approximately 51% of patients4), and consequent extensive use of broad‐spectrum antimicrobials (in 71% of patients).4
When prescribing antimicrobials, the ICU clinician often faces a dilemma. First, the traditional symptoms and signs of infection (such as characteristic patient history, fever, increased white cell count, etc) are common in ICU patients even in the absence of infection, making distinction of infectious and noninfectious causes of patient deterioration difficult. Second, delaying antimicrobial therapy, prescribing inadequate antimicrobials, or allowing bacterial infections to go untreated, increases patient mortality,57 resulting in guideline recommendations to start broad‐spectrum antimicrobials as soon as possible in the presence of suspected severe sepsis.8 While third, and in contrast, unnecessary antimicrobial therapy increases the risk of antimicrobial‐related complications, such as Clostridium difficile colitis (with a crude mortality of up to 20%9), and potentially endangers the greater population of ICU patients by increasing the prevalence of resistant organisms. Choosing between delaying necessary antimicrobial therapy and exposing the patient to unnecessary therapy requires that 2 contrasting risks be balancedthat of untreated infection versus late antimicrobial complications.
The main aim of this study was to assess how often administration of antimicrobials for suspected infection could be justified by the presence of infection. The primary outcome measure was accuracy of antimicrobial administration, defined as the proportion of antimicrobials started for suspected infection where infection was later proven to have been present. Secondary outcome measures examined: (1) whether clinician suspicion of infection correlated with the presence of defined infection; (2) the ID specialist's accuracy for empiric antimicrobial administration; (3) whether common clinical parameters were associated with clinician certainty regarding the presence of infection; and (4) use of antimicrobials in the presence or absence of infection. These data are important in order to identify possibilities for improving antimicrobial administration.
METHODS
Setting
Data were collected on all ICU patients staying >48 hours in the 12‐bed general (mainly surgical) ICU of a 775‐bed academic tertiary referral center (the Hadassah Hebrew University Medical Center, Jerusalem, Israel) from May to August 2009. The hospital ethics committee approved the study and waived the requirement for informed consent.
Clinical antimicrobial decision‐making was at the final discretion of the ICU attending clinician. During office hours, decisions to start antimicrobials with any but first line agents (ampicillin, ampicillin/clavulanic acid, azithromycin, cefazolin, cefuroxime, ciprofloxacin, clindamycin, cloxacillin, gentamicin, and metronidazole) required authorization by the clinical ID specialist on attachment to the ICU (who performed a daily round). Out of office hours, decisions required authorization by an on‐call ID specialist (usually by phone). There was no availability of a clinical pharmacist. Microbiological studies were obtained as follows: sputum and urine cultures routinely 3 times per week, while other cultures (including blood, wound, site‐specific cultures, etc) according to clinical indications.
Antimicrobial Administration Decisions
Start and stop dates were recorded for all intravenous antimicrobials administered during the patient's ICU stay. Antimicrobial start decisions were divided into 3 groups: empirical (where antimicrobials were started for a new suspected infection), prophylaxis‐driven (antimicrobials given peri‐procedurally), and targeted therapy (antimicrobials started or changed based on receipt of culture results, or antimicrobials continued from a previous department). Although multiple antimicrobials were often started together, these were considered as a single antimicrobial start decision, if started for the same reason.
Empirical decisions represent the main focus of this study, and further data were collected for these decisions. For each empiric decision, the attending ICU clinician's name was recorded, as well as a measure of his certainty that a new infection was actually present. Certainty was determined at the time that the antimicrobials were started and was entirely subjective. The clinician was asked to categorize his certainty that an infection was present when starting empiric antimicrobials on a scale from 0 to 5: 0no infection; 1infection unlikely; 2infection possible; 3infection probable; 4infection very likely; and 5infection certain. The number of systemic inflammatory response syndrome (SIRS) criteria10 and Sequential Organ Failure Assessment (SOFA)11 score were calculated at the time each decision was made (using the last available data prior to starting antimicrobials), and for the previous 2 days (using the worst values on each calendar day). Data on demographics, admission history, comorbid conditions, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, and outcome were collected for each patient.
Antimicrobial Start Decisions and Definitions of Infection by the Study ID Specialist
Approximately 1 week after each empiric antimicrobial decision, the need for antimicrobial therapy and the presence of infection were analyzed and defined by the study ID specialist (S.B.). He was not involved in clinical decision‐making and was not acquainted with patient details. Each analysis included 2 steps: Step 1 concerning the overall requirement for antimicrobial therapy, and Step 2 regarding the presence of infection. For Step 1, data from the patient's clinical course up until the time the antimicrobial start decision was made were presented. At that point, the study ID specialist decided whether, if presented the case as a consultant, he would have recommended starting antimicrobials. For Step 2, the patient's clinical course following the antimicrobial decision point as well as laboratory, imaging, and microbiological results from the subsequent days were reviewed. The presence or absence of infection was defined by integrating all of this data, and based on the Centers for Disease Control and Prevention (CDC) surveillance criteria for the diagnosis of nosocomial infections.12 The study ID specialist used the same certainty score regarding the presence of infection as the clinicians. A certainty of a probable infection (score 3) or higher represented the cutoff to define the presence of infection. The study ID specialist's determination of the presence of infection was considered the gold standard for the presence of infection for analyses and is termed defined infection.
Accuracy of Antimicrobial Start Decisions
Accuracy was calculated for both the clinicians and the study ID specialist, and expressed as a proportion. The denominator for ICU clinician accuracy was the total number of antibiotic start decisions for suspected infection, and the numerator was the number of decisions where infection was defined by the ID specialist. For the study ID specialist, the denominator was the number of occasions when antibiotic administration was considered justified in the Step 1 analysis, and the numerator was the number of these cases where infection was defined (Figure 1). The correlation between clinician certainty and the study‐defined presence of infection was examined. The accuracy of clinical antimicrobial decisions made during the first 48 hours of ICU admission was compared to decisions made after 48 hours.
In order to assess the robustness of the study findings, the ICU clinician accuracy was examined in a sensitivity analysis. Accuracy was calculated using a lower cutoff for the study ID specialist's definition of infectionpossible infection (score 2) or above, rather than probable infection or above.
Physiological Parameters
To examine the effect of physiological variables on physician certainty, empiric antimicrobial start decisions were divided into 2 groupsa high clinician certainty group (certainty score 3) and a low certainty score (<3). Each physiological parameter comprising the SIRS and SOFA scores, the scores themselves, and changes from the previous 24 and 48 hours were compared for the 2 groups. Data used for the decision day were the last available observations prior to starting the antimicrobials. Data for the previous 2 days were the worst values present during each calendar day.
Antimicrobial Course Length
The total course given after each empirical antibiotic start decision was measured in days. The course length started with the empiric antimicrobial start decision, and ended either when antimicrobial therapy was stopped, or when a subsequent empirical start decision was made. Course length for start decisions where infection was subsequently defined was compared to decisions where infection was not defined.
Statistical Analysis
Continuous variables were compared using the Student t test, while categorical variables were compared using the chi‐square test. All P values are 2‐tailed and P < 0.05 was considered statistically significant. SAS version 8.2 (SAS Institute, Inc, Cary, NC) was used for statistical analysis.
RESULTS
Data were collected on 119 consecutive ICU patients over 4 months (Table 1). Antimicrobials were started for suspected infection in 80/119 (67%) patients, for prophylaxis in 55/119 (46%) patients, and for other reasons in 42/119 (35%) patients. More than one indication was present during the patient's ICU admission among 41/119 (34%) patients, while for 6/119 (5%) patients, no antimicrobials were prescribed at all. Among these patients, antimicrobials were administered on 250 occasions, including 125/250 (50%) occasions for suspected infection (empirical decisions), 62/250 (25%) occasions for procedural prophylaxis (prophylaxis‐driven), and on 63/250 (25%) occasions for other reasons (antimicrobial changes following receipt of culture results, or continuation of antimicrobials prescribed prior to ICU admission). Microbiological cultures were obtained from the study population on 2132 occasions, including 395 blood cultures in which significant organisms (not reflecting contamination) grew on 57/395 (14%) occasions.
| No. (%) or Mean SD | |
|---|---|
| N = 119 | |
| |
| Demographics | |
| Male gender | 66 (55) |
| Age (years) | 53 25 |
| Hospital admission prior to ICU admission | 62 (52) |
| Independent functional capacity | 99 (83) |
| Etiology for ICU admission* | |
| Surgery | 82 (69) |
| Elective | 12 (10) |
| Emergency | 70 (59) |
| Trauma | 41 (34) |
| Medical | 26 (22) |
| Comorbidities | |
| Prior antimicrobial therapy | 48 (40) |
| Severe cardiac disease | 12 (10) |
| Severe respiratory disease | 5 (4) |
| Diabetes mellitus | 22 (18) |
| Liver disease | 10 (8) |
| Dialysis | 5 (4) |
| APACHE II score | 15 8 |
| Outcome | |
| ICU length of stay (days) | 13 15 |
| Hospital length of stay (days) | 36 32 |
| ICU mortality | 16 (13) |
| Hospital mortality | 22 (18) |
Among the empiric antimicrobial start decisions, infection was defined by the study ID specialist on 67/125 (54%) occasions, representing the clinicians' diagnostic accuracy. These infections included 17 (25%) respiratory, 16 (24%) abdominal, 13 (19%) soft tissue, 11 (16%) blood stream, 6 (9%) urinary, and 4 (6%) other infections.
Three attending clinicians treated patients during the study period, and their accuracies were similar (21 infections defined/44 start decisions for suspected infection, 48%; 24/38, 63%; 22/43, 51%, for each attending; P = ns for all comparisons). Clinician accuracy was higher for empirical antimicrobial start decisions, made within 48 hours of ICU admission, compared to later decisions (35 defined infections/53 early antibiotic start decisions [66%] vs 32 defined infections/72 late antibiotic start decisions [44%]; P = 0.02).
In a sensitivity analysis, decreasing the cutoff for the study ID specialist's definition of infection from probable (and above) to possible (and above) lead to reclassification of 14/125 (11%) antimicrobial start decisions from no infection defined to infection defined. This increased physician accuracy from 67/125 (54%) to 78/125 (62%), and conversely decreased potential antimicrobial overuse from 58/125 (46%) to 47/125 (38%) decisions (P = ns).
When starting antimicrobials for suspected infection, the clinicians were asked to record their certainty in the presence of infection. Infections were defined on 6/19 (31%) occasions when the clinician certainty score was low (2) versus 61/106 (57%) when the clinician certainty score was high (3, P = 0.037; Figure 2). Correlation between the clinician certainty score and the presence of defined infection was good (r2 = 0.78).
The study ID specialist agreed with the clinician's decision to start antimicrobial therapy on 87/125 (70%) occasions. Infection was subsequently defined on 66/87 (76%) occasions, representing the study ID specialist's diagnostic accuracy. The study ID specialist's accuracy was significantly higher than the clinician's (66/87 [76%] versus 67/125 [54%]; P = 0.001). Notably, there was only 1 case (3%) where empiric therapy was deemed unnecessary by the study ID specialist, and where infection was subsequently defined. In this case, the clinicians started antibiotic therapy for suspected ventilator‐associated pneumonia in a 66‐year‐old patient on the 28th day of an ICU admission for head and spinal cord trauma. The ID specialist's certainty for the presence of infection was 3probable. The patient ultimately survived and was discharged to a rehabilitation facility.
Comparing physiological data for antimicrobial start decisions with high clinician certainty (score 3) versus low certainty of infection (score 2), revealed that none of the physiological data, nor changes over time were significantly associated with clinician certainty. Further use of high doses of vasopressors (>0.1 mcg/kg/min, SOFA score 4) was present at 42/106 (40%) high certainty decisions versus 7/19 (37%) low certainty decisions (P = 0.819). This underscores the physicians' difficulty in distinguishing between infectious and inflammatory causes of deterioration (Table 2).
| Low Certainty* N = 19 | High Certainty N = 106 | ||
|---|---|---|---|
| Mean SD | Mean SD | P Value | |
| |||
| SIRS elements | |||
| Temperature (C) | 37.7 1.2 | 37.3 1.6 | 0.28 |
| WBC count ( 109/liter) | 16.7 8.1 | 15.9 10.5 | 0.72 |
| Pulse (rate/min) | 112 23 | 110 21 | 0.58 |
| Respiratory rate (rate/min) | 22 8 | 22 8 | 0.90 |
| Number of SIRS criteria (at antimicrobial start) | 3.0 0.9 | 3.2 0.9 | 0.24 |
| Change in number of SIRS criteria (24 h) | 0.1 0.9 | 0.0 0.9 | 0.68 |
| Change in number of SIRS criteria (48 h) | 0.0 0.7 | 0.3 0.9 | 0.36 |
| SOFA score elements (points) | |||
| Respiratory | 1.6 1.1 | 1.9 1.2 | 0.45 |
| Neurological | 1.8 1.7 | 2.0 1.6 | 0.50 |
| Coagulation | 0.6 1.1 | 0.6 1.1 | 0.85 |
| Hepatic | 0.6 0.8 | 0.4 0.8 | 0.37 |
| Renal | 0.7 1.1 | 0.8 1.1 | 0.51 |
| Cardiovascular | 1.5 1.9 | 1.8 1.9 | 0.47 |
| SOFA score day at antimicrobial start | 6.7 3.1 | 7.3 4.6 | 0.58 |
| SOFA score change (previous 24 h) | 1.5 3.2 | 1.0 2.9 | 0.56 |
| SOFA score change (previous 48 h) | 3.1 4.4 | 1.5 4.3 | 0.25 |
During the study period, 2541 days of antimicrobial therapy were given of which 1677 (66%), 413 (16%), and 451 (18%) were given, respectively, empirically (for suspected infection), for procedural prophylaxis, and as targeted therapy. Antimicrobial course length was 11.5 9.2 days in the presence of defined infection versus 10.7 9.1 days in the absence of defined infection (P = 0.655). Overall, 658/2541 (26%) days of therapy could potentially have been saved by reducing antimicrobial prescriptions for suspected infections which were not defined.
DISCUSSION
The use of empirical antimicrobials could be justified by the presence of defined infection on only 54% of occasions when they were administered, suggesting considerable potential overuse of these drugs. ICU‐clinician certainty for the presence of infection correlated well with the number of infections actually defined, however, infections were defined when certainty was low (Figure 2) and antimicrobials prescribed even when clinician certainty was minimal. Common clinical physiological and laboratory parameters did not seem to assist in the clinicians' decision‐making, as there were no significant differences in any of these values between empiric decisions with high or low certainty. The study ID specialist showed significantly better accuracy in antimicrobial decision‐making than the ICU clinicians. He agreed with antimicrobial administration on only 70% of occasions that clinicians started empiric therapy, and had a higher diagnostic accuracy at a cost of only 1 untreated infection.
Two main possibilities are suggested to explain the potential antimicrobial overuse. First, ICU physicians are loath to leave infections untreated and potentially cause immediate increases in mortality.8 This leads to uncertainty avoidance or risk aversive behavior that is demonstrated in our study by the inclusion of antimicrobial administration decisions made even when physicians' certainty regarding the presence of infection was low. Uncertainty avoidance has been shown to be significantly associated with antimicrobial prescribing practices,13 however, it discounts the risk of antimicrobial complications associated with unnecessary antimicrobial therapy. Second, the diagnosis of infection, and particularly nosocomial infection, in ICU patients is difficult. Symptoms cannot be elicited in obtunded ventilated ICU patients, the physical exam can be equivocal, bacterial growth in cultures (with the exception of blood cultures) often reflects colonization rather than infection, and the laboratory and imaging findings of inflammation and infection are very similar. Our data demonstrated some of these difficulties. Diagnostic accuracy was higher in infections suspected during the first 48 hours of ICU admission when compared to later, presumably as infection leading to ICU admission is associated with symptoms, signs, and an acute change in the patient's condition, factors that may be absent when a patient develops a nosocomial infection. Further, physiological parameters did not correlate with the certainty that ICU clinicians expressed in their decision, indicating the difficulty in interpreting these data. Finally, infection was defined in 30% of low certainty decisions, indicating that clinical impression alone is not a reliable tool for determining the presence of infection.
Three sets of interventions could be suggested to improve antimicrobial decision‐makingincreased use of the ID consult, improved laboratory tests for the diagnosis of infection, and a policy of de‐escalation. Use of antimicrobial stewardship (often through involvement of an ID physician) reduces antimicrobial usage and the occurrence of resistant bacteria without adverse patient outcomes.14 Indeed, our study ID consult showed more accurate antimicrobial prescribing than the ICU clinicians, although he may have been subject to the potential biases described below. All antimicrobial administration decisions taken during the study were, however, made in consultation with the clinical ID consult. The lower performance of the clinical ID consult (when compared to the study ID consult) may have resulted from difficulties in the real‐time interaction with the clinicians or from decisions taken during non‐office hours. During non‐office hours, the on‐call ICU resident presented cases to an on‐call ID specialist, neither of whom may have been familiar with all the complex case details and therefore may have preferred to err by commission than by omission.
More accurate laboratory tests, such as procalcitonin or real‐time bacterial polymerase chain reaction (PCR),15 could be beneficial as they might increase physician confidence in decision‐making. Procalcitonin has been used in a wide variety of settings1618 (including the ICU1921) to safely decrease antimicrobial starts and/or antimicrobial course length. Despite this, in a large multicenter study of procalcitonin use in ICU patients,19 compliance with the antibiotic start protocol was very low. Antibiotics were administered by the participating physicians in 73/93 (78%) cases where the procalcitonin tests indicated that antimicrobials were not required, representing protocol violations. In parallel to our study, this demonstrates the reluctance of physicians to abstain from prescribing antimicrobial therapy for suspected infection even when the likelihood of infection may be low.
A strategy of de‐escalation offers the possibility of starting broad‐spectrum antimicrobials early and, subsequently, narrowing or stopping therapy according to the clinical course and the microbiological results.22, 23 This strategy allows clinicians to start antimicrobials even when the suspicion of infection is low, but to stop them rapidly as the clinical picture clarifies. Unfortunately, the mean antimicrobial course length in this study was not influenced by the presence of infection, indicating that this strategy was not employed successfully.
The proportion of patients prescribed antimicrobials for suspected infection in our study is similar to that found in others (eg, 34% of patients in a large French survey24). The proportion of potentially unnecessary antimicrobials in other studies is also similar, ranging from 14% to 50%.2428 In the ICU, the majority of antimicrobial usage studies are microbiology‐based and examine whether bacteria cultured are resistant to the antimicrobials chosen. They have shown that inappropriate antimicrobial therapy occurs on 20%36% of occasions.6, 7, 29 The current study furthers knowledge on antimicrobials decision‐making in the ICU, by examining the actual requirement for antimicrobial therapy based on the presence of infection, ie, whether antimicrobials were needed at all.
The principal limitation of the study concerns the determination of the presence of infection. The study premise was that antimicrobials are overused, and this may have biased the study ID consult to underestimate appropriateness of antimicrobial therapy and to define fewer infections. Further, making theoretical decisions in the research office avoids the medical, ethical, and legal issues related to clinical practice, as there is no risk associated with error. This may have allowed the study ID specialist to be overly conservative in his definitions of infections. A wider team of decision‐makers to determine the presence of infection, including both ID and ICU specialists, would have lent more weight to their determinations, however, this was logistically impossible. To limit the potential bias, infections were defined as objectively as possible based on the CDC criteria.12 Further, the sensitivity analysis showed that while decreasing the study ID specialist's threshold for the definition of infection from probable and above to possible and above improved physician accuracy, over a third of antimicrobial start decisions remained unjustified by the presence of defined infection. The study was performed in only 1 center and may not reflect general ICU practice, although, as discussed above, the antibiotic decision‐making accuracy is in the same orders of magnitude as those found in other somewhat similar studies. Finally, even if unnecessary antimicrobial use was overestimated, the possibility for significant improvement in antimicrobial administration accuracy remains.
In conclusion, our data suggest that on up to 46% of occasions, empirical antimicrobials are prescribed in the absence of infection. We suggest that the potential antibiotic overuse results from difficulties in diagnosing ICU‐related infections, and from the high perceived risk of untreated infection as compared to the risks of potentially unnecessary antimicrobial therapy, representing a type of risk aversive behavior. As antimicrobial use is the primary factor promoting antibiotic resistance and may be a cause of other patient complications, efforts to improve antimicrobial‐related decision‐making should be mandatory.
- ,.Antimicrobial‐drug resistance.N Engl J Med.1996;335:1445–1453.
- ,,, et al.Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study.Lancet Infect Dis.2010;10:597–602.
- ,,, et al.Surveillance of antimicrobial use and antimicrobial resistance in United States hospitals: project ICARE phase 2. Project Intensive Care Antimicrobial Resistance Epidemiology (ICARE) hospitals.Clin Infect Dis.1999;29:245–252.
- ,,, et al.International study of the prevalence and outcomes of infection in intensive care units.JAMA.2009;302:2323–2329.
- ,,,,.Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator‐associated pneumonia.Chest.2002;122:262–268.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,, et al.Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock.Chest.2009;136:1237–1248.
- ,,, et al.Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36:296–327.
- ,,,,.Investigation of critical care unit utilization and mortality in patients infected with Clostridium difficile.J Crit Care.2010;25:282–286.
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference:definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis.Crit Care Med.1992;20:864–874.
- ,,, et al.The SOFA (Sepsis‐related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis‐Related Problems of the European Society of Intensive Care Medicine.Intensive Care Med.1996;22:707–710.
- ,,.CDC/NHSN surveillance definition of health care‐associated infection and criteria for specific types of infections in the acute care setting.Am J Infect Control.2008;36:309–332.
- ,,, et al.Are cultural dimensions relevant for explaining cross‐national differences in antibiotic use in Europe?BMC Health Serv Res.2008;8:123.
- ,,,,,.Impact of antimicrobial stewardship in critical care: a systematic review.J Antimicrob Chemother.2011;66:1223–1230.
- ,,, et al.A multicenter trial to compare blood culture with polymerase chain reaction in severe human sepsis.Intensive Care Med.2010;36:241–247.
- ,,, et al.Procalcitonin guidance of antibiotic therapy in community‐acquired pneumonia: a randomized trial.Am J Respir Crit Care Med.2006;174:84–93.
- ,,, et al.Effect of procalcitonin‐based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trial.JAMA.2009;302:1059–1066.
- ,,, et al.Antibiotic treatment of exacerbations of COPD: a randomized, controlled trial comparing procalcitonin‐guidance with standard therapy.Chest.2007;131:9–19.
- ,,, et al.Use of procalcitonin to reduce patients' exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial.Lancet.2010;375:463–474.
- ,,,,.Use of procalcitonin to shorten antibiotic treatment duration in septic patients: a randomized trial.Am J Respir Crit Care Med.2008;177:498–505.
- ,,, et al.Procalcitonin for reduced antibiotic exposure in ventilator‐associated pneumonia: a randomised study.Eur Respir J.2009;34:1364–1375.
- ,,, et al.Consensus document on controversial issues for the treatment of hospital‐associated pneumonia.Int J Infect Dis.2010;14(suppl 4):S55–S65.
- ,, et al.Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am Respir Crit Care Med.2005;171:388–416.
- ,,, et al.Strategies of initiation and streamlining of antibiotic therapy in 41 French intensive care units.Crit Care.2011;15:R17.
- ,,,.Antibiotic use at Duke University Medical Center.JAMA.1977;237:2819–2822.
- ,.A study of antimicrobial misuse in a university hospital.Am J Med Sci.1978;275:271–282.
- ,,,,.Unnecessary use of antimicrobials in hospitalized patients: current patterns of misuse with an emphasis on the antianaerobic spectrum of activity.Arch Intern Med.2003;163:972–978.
- ,,, et al.Interventions to improve antibiotic prescribing practices for hospital inpatients.Cochrane Database Syst Rev.2005;CD003543.
- ,,, et al.Patterns of antimicrobial therapy in severe nosocomial infections: empiric choices, proportion of appropriate therapy, and adaptation rates—a multicentre, observational survey in critically ill patients.Int J Antimicrob Agents.2010;35:375–381.
- ,.Antimicrobial‐drug resistance.N Engl J Med.1996;335:1445–1453.
- ,,, et al.Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study.Lancet Infect Dis.2010;10:597–602.
- ,,, et al.Surveillance of antimicrobial use and antimicrobial resistance in United States hospitals: project ICARE phase 2. Project Intensive Care Antimicrobial Resistance Epidemiology (ICARE) hospitals.Clin Infect Dis.1999;29:245–252.
- ,,, et al.International study of the prevalence and outcomes of infection in intensive care units.JAMA.2009;302:2323–2329.
- ,,,,.Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator‐associated pneumonia.Chest.2002;122:262–268.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,, et al.Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock.Chest.2009;136:1237–1248.
- ,,, et al.Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36:296–327.
- ,,,,.Investigation of critical care unit utilization and mortality in patients infected with Clostridium difficile.J Crit Care.2010;25:282–286.
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference:definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis.Crit Care Med.1992;20:864–874.
- ,,, et al.The SOFA (Sepsis‐related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis‐Related Problems of the European Society of Intensive Care Medicine.Intensive Care Med.1996;22:707–710.
- ,,.CDC/NHSN surveillance definition of health care‐associated infection and criteria for specific types of infections in the acute care setting.Am J Infect Control.2008;36:309–332.
- ,,, et al.Are cultural dimensions relevant for explaining cross‐national differences in antibiotic use in Europe?BMC Health Serv Res.2008;8:123.
- ,,,,,.Impact of antimicrobial stewardship in critical care: a systematic review.J Antimicrob Chemother.2011;66:1223–1230.
- ,,, et al.A multicenter trial to compare blood culture with polymerase chain reaction in severe human sepsis.Intensive Care Med.2010;36:241–247.
- ,,, et al.Procalcitonin guidance of antibiotic therapy in community‐acquired pneumonia: a randomized trial.Am J Respir Crit Care Med.2006;174:84–93.
- ,,, et al.Effect of procalcitonin‐based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: the ProHOSP randomized controlled trial.JAMA.2009;302:1059–1066.
- ,,, et al.Antibiotic treatment of exacerbations of COPD: a randomized, controlled trial comparing procalcitonin‐guidance with standard therapy.Chest.2007;131:9–19.
- ,,, et al.Use of procalcitonin to reduce patients' exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial.Lancet.2010;375:463–474.
- ,,,,.Use of procalcitonin to shorten antibiotic treatment duration in septic patients: a randomized trial.Am J Respir Crit Care Med.2008;177:498–505.
- ,,, et al.Procalcitonin for reduced antibiotic exposure in ventilator‐associated pneumonia: a randomised study.Eur Respir J.2009;34:1364–1375.
- ,,, et al.Consensus document on controversial issues for the treatment of hospital‐associated pneumonia.Int J Infect Dis.2010;14(suppl 4):S55–S65.
- ,, et al.Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am Respir Crit Care Med.2005;171:388–416.
- ,,, et al.Strategies of initiation and streamlining of antibiotic therapy in 41 French intensive care units.Crit Care.2011;15:R17.
- ,,,.Antibiotic use at Duke University Medical Center.JAMA.1977;237:2819–2822.
- ,.A study of antimicrobial misuse in a university hospital.Am J Med Sci.1978;275:271–282.
- ,,,,.Unnecessary use of antimicrobials in hospitalized patients: current patterns of misuse with an emphasis on the antianaerobic spectrum of activity.Arch Intern Med.2003;163:972–978.
- ,,, et al.Interventions to improve antibiotic prescribing practices for hospital inpatients.Cochrane Database Syst Rev.2005;CD003543.
- ,,, et al.Patterns of antimicrobial therapy in severe nosocomial infections: empiric choices, proportion of appropriate therapy, and adaptation rates—a multicentre, observational survey in critically ill patients.Int J Antimicrob Agents.2010;35:375–381.
Copyright © 2012 Society of Hospital Medicine
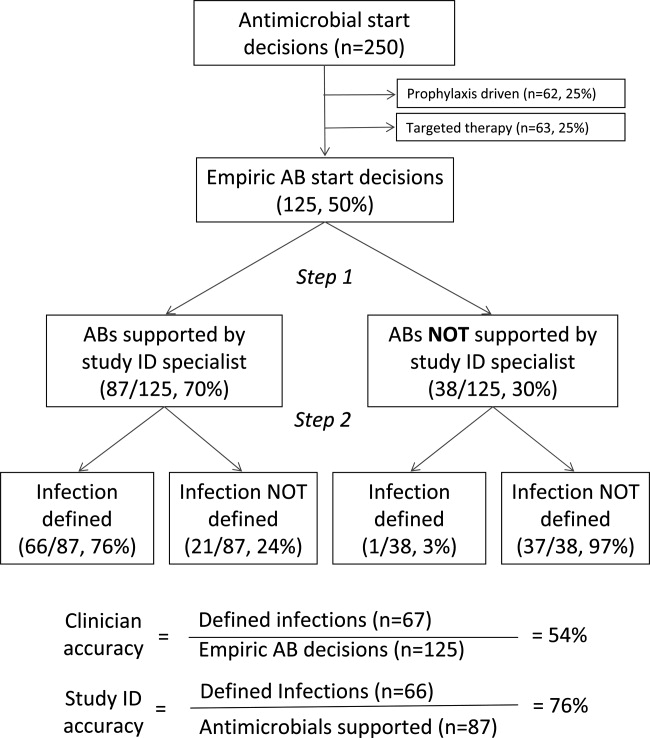
Applying Education Theory to Vascular Training
Citing a revolution in the way surgeons learn their craft, Dr. Erica L. Mitchell and Dr. Sonal Arora present an analysis of vascular training to identify key learning points and needs as residents move from novice to expert. Their report is in the August issue of the Journal of Vascular Surgery.
A shift toward competency-based training programs is now reflecting a growing emphasis on outcomes-based medical education, according to Dr. Mitchell and Dr. Arora. They discuss how pedagogy and adult learning tools can be applied to vascular training and the development of technical expertise (J Vasc Surg 2012;56:530-7).
"Surgical educators should use training and assessment methods soundly based in educational principles to develop and deliver curricula that will allow trainees to acquire the skills befitting the modern vascular surgeon," they concluded.
Find the original article by clicking here.
Citing a revolution in the way surgeons learn their craft, Dr. Erica L. Mitchell and Dr. Sonal Arora present an analysis of vascular training to identify key learning points and needs as residents move from novice to expert. Their report is in the August issue of the Journal of Vascular Surgery.
A shift toward competency-based training programs is now reflecting a growing emphasis on outcomes-based medical education, according to Dr. Mitchell and Dr. Arora. They discuss how pedagogy and adult learning tools can be applied to vascular training and the development of technical expertise (J Vasc Surg 2012;56:530-7).
"Surgical educators should use training and assessment methods soundly based in educational principles to develop and deliver curricula that will allow trainees to acquire the skills befitting the modern vascular surgeon," they concluded.
Find the original article by clicking here.
Citing a revolution in the way surgeons learn their craft, Dr. Erica L. Mitchell and Dr. Sonal Arora present an analysis of vascular training to identify key learning points and needs as residents move from novice to expert. Their report is in the August issue of the Journal of Vascular Surgery.
A shift toward competency-based training programs is now reflecting a growing emphasis on outcomes-based medical education, according to Dr. Mitchell and Dr. Arora. They discuss how pedagogy and adult learning tools can be applied to vascular training and the development of technical expertise (J Vasc Surg 2012;56:530-7).
"Surgical educators should use training and assessment methods soundly based in educational principles to develop and deliver curricula that will allow trainees to acquire the skills befitting the modern vascular surgeon," they concluded.
Find the original article by clicking here.
FROM THE JOURNAL OF VASCULAR SURGERY
Labs Find Evidence of Cancer Stem Cells
In an era of targeted cancer therapies, laboratory scientists working with mice may have found the ultimate target – a reservoir of stem cells that drive cancers to grow and metastasize.
Separate reports in the journals Science and Nature document the presence of cancer stem cells in intestinal adenomas (Science 2012 Aug. 1 [doi:10.1126/science.1224676]), squamous skin cancer, (Nature 2012 Aug. 1 [doi:10.1038/nature11344]), and glioblastoma multiforme (Nature 2012 Aug. 1 [doi:10.1038/nature11287]).
In the last study, mice with these highly lethal brain tumors were given temozolomide (Temodar), an approved treatment in humans, along with ganciclovir, an antiviral. Despite a transient therapeutic response to chemotherapy, the cancers continued to grow, driven by "a relatively quiescent subset of endogenous glioma cells, with properties similar to those proposed for cancer stem cells," the authors wrote.
Whether these reports will resolve controversy over the existence of stem cells or lead to clinically meaningful treatments remains to be seen. There is no doubt, however, that they will lead to further investigation.
In an era of targeted cancer therapies, laboratory scientists working with mice may have found the ultimate target – a reservoir of stem cells that drive cancers to grow and metastasize.
Separate reports in the journals Science and Nature document the presence of cancer stem cells in intestinal adenomas (Science 2012 Aug. 1 [doi:10.1126/science.1224676]), squamous skin cancer, (Nature 2012 Aug. 1 [doi:10.1038/nature11344]), and glioblastoma multiforme (Nature 2012 Aug. 1 [doi:10.1038/nature11287]).
In the last study, mice with these highly lethal brain tumors were given temozolomide (Temodar), an approved treatment in humans, along with ganciclovir, an antiviral. Despite a transient therapeutic response to chemotherapy, the cancers continued to grow, driven by "a relatively quiescent subset of endogenous glioma cells, with properties similar to those proposed for cancer stem cells," the authors wrote.
Whether these reports will resolve controversy over the existence of stem cells or lead to clinically meaningful treatments remains to be seen. There is no doubt, however, that they will lead to further investigation.
In an era of targeted cancer therapies, laboratory scientists working with mice may have found the ultimate target – a reservoir of stem cells that drive cancers to grow and metastasize.
Separate reports in the journals Science and Nature document the presence of cancer stem cells in intestinal adenomas (Science 2012 Aug. 1 [doi:10.1126/science.1224676]), squamous skin cancer, (Nature 2012 Aug. 1 [doi:10.1038/nature11344]), and glioblastoma multiforme (Nature 2012 Aug. 1 [doi:10.1038/nature11287]).
In the last study, mice with these highly lethal brain tumors were given temozolomide (Temodar), an approved treatment in humans, along with ganciclovir, an antiviral. Despite a transient therapeutic response to chemotherapy, the cancers continued to grow, driven by "a relatively quiescent subset of endogenous glioma cells, with properties similar to those proposed for cancer stem cells," the authors wrote.
Whether these reports will resolve controversy over the existence of stem cells or lead to clinically meaningful treatments remains to be seen. There is no doubt, however, that they will lead to further investigation.
Drug-Drug Interactions Added to Hepatitis C Drug Label
New information about interactions between boceprevir and several other drugs has been added to the prescribing information for the antiviral drug, the Food and Drug Administration announced Aug. 1.
Boceprevir (Victrelis), a protease inhibitor approved for treating hepatitis C in 2011, interacts with cyclosporine, tacrolimus (Prograf), escitalopram (Lexapro), atorvastatin (Lipitor), and pravastatin (Pravachol), according to the FDA statement.
The new information states that, when administered with boceprevir, exposure to atorvastatin increases. When the two drugs are used together, the lowest effective dose of atorvastatin should be used, not to exceed a daily dose of 40 mg, according to the FDA.
Dose adjustments of cyclosporine should be anticipated when it is given with boceprevir, and "should be guided by close monitoring of cyclosporine blood concentrations, and frequent assessments of renal function and cyclosporine-related side effects."
When administered with boceprevir, exposure of escitalopram "was slightly decreased," the statement said. Although selective serotonin reuptake inhibitors (SSRIs) such as escitalopram have a wide therapeutic index, it may be necessary to adjust the dosage when it is administered with boceprevir.
Coadministration of boceprevir with pravastatin increases exposure to pravastatin, but pravastatin can be started at the recommended dosage when coadministered with boceprevir. "Close clinical monitoring is warranted," the statement said.
Giving tacrolimus and boceprevir together "requires significant dose reduction and prolongation of the dosing interval for tacrolimus, with close monitoring of tacrolimus blood concentrations and frequent assessments of renal function and tacrolimus-related side effects," the statement said.
Boceprevir is manufactured in a capsule formulation by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., and is taken by mouth three times a day.
The drug-drug interaction data are from in vivo drug interaction trials, which the company conducted as part of its postmarketing commitments.
At a meeting in April 2011, an FDA advisory panel enthusiastically supported the approval of boceprevir for treating hepatitis C infection because of the antiviral’s efficacy but emphasized that postmarketing studies on interactions with other drugs, including antidepressants, were needed.
Serious adverse events associated with boceprevir should be reported to MedWatch or by phone at 800-332-1088.
New information about interactions between boceprevir and several other drugs has been added to the prescribing information for the antiviral drug, the Food and Drug Administration announced Aug. 1.
Boceprevir (Victrelis), a protease inhibitor approved for treating hepatitis C in 2011, interacts with cyclosporine, tacrolimus (Prograf), escitalopram (Lexapro), atorvastatin (Lipitor), and pravastatin (Pravachol), according to the FDA statement.
The new information states that, when administered with boceprevir, exposure to atorvastatin increases. When the two drugs are used together, the lowest effective dose of atorvastatin should be used, not to exceed a daily dose of 40 mg, according to the FDA.
Dose adjustments of cyclosporine should be anticipated when it is given with boceprevir, and "should be guided by close monitoring of cyclosporine blood concentrations, and frequent assessments of renal function and cyclosporine-related side effects."
When administered with boceprevir, exposure of escitalopram "was slightly decreased," the statement said. Although selective serotonin reuptake inhibitors (SSRIs) such as escitalopram have a wide therapeutic index, it may be necessary to adjust the dosage when it is administered with boceprevir.
Coadministration of boceprevir with pravastatin increases exposure to pravastatin, but pravastatin can be started at the recommended dosage when coadministered with boceprevir. "Close clinical monitoring is warranted," the statement said.
Giving tacrolimus and boceprevir together "requires significant dose reduction and prolongation of the dosing interval for tacrolimus, with close monitoring of tacrolimus blood concentrations and frequent assessments of renal function and tacrolimus-related side effects," the statement said.
Boceprevir is manufactured in a capsule formulation by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., and is taken by mouth three times a day.
The drug-drug interaction data are from in vivo drug interaction trials, which the company conducted as part of its postmarketing commitments.
At a meeting in April 2011, an FDA advisory panel enthusiastically supported the approval of boceprevir for treating hepatitis C infection because of the antiviral’s efficacy but emphasized that postmarketing studies on interactions with other drugs, including antidepressants, were needed.
Serious adverse events associated with boceprevir should be reported to MedWatch or by phone at 800-332-1088.
New information about interactions between boceprevir and several other drugs has been added to the prescribing information for the antiviral drug, the Food and Drug Administration announced Aug. 1.
Boceprevir (Victrelis), a protease inhibitor approved for treating hepatitis C in 2011, interacts with cyclosporine, tacrolimus (Prograf), escitalopram (Lexapro), atorvastatin (Lipitor), and pravastatin (Pravachol), according to the FDA statement.
The new information states that, when administered with boceprevir, exposure to atorvastatin increases. When the two drugs are used together, the lowest effective dose of atorvastatin should be used, not to exceed a daily dose of 40 mg, according to the FDA.
Dose adjustments of cyclosporine should be anticipated when it is given with boceprevir, and "should be guided by close monitoring of cyclosporine blood concentrations, and frequent assessments of renal function and cyclosporine-related side effects."
When administered with boceprevir, exposure of escitalopram "was slightly decreased," the statement said. Although selective serotonin reuptake inhibitors (SSRIs) such as escitalopram have a wide therapeutic index, it may be necessary to adjust the dosage when it is administered with boceprevir.
Coadministration of boceprevir with pravastatin increases exposure to pravastatin, but pravastatin can be started at the recommended dosage when coadministered with boceprevir. "Close clinical monitoring is warranted," the statement said.
Giving tacrolimus and boceprevir together "requires significant dose reduction and prolongation of the dosing interval for tacrolimus, with close monitoring of tacrolimus blood concentrations and frequent assessments of renal function and tacrolimus-related side effects," the statement said.
Boceprevir is manufactured in a capsule formulation by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., and is taken by mouth three times a day.
The drug-drug interaction data are from in vivo drug interaction trials, which the company conducted as part of its postmarketing commitments.
At a meeting in April 2011, an FDA advisory panel enthusiastically supported the approval of boceprevir for treating hepatitis C infection because of the antiviral’s efficacy but emphasized that postmarketing studies on interactions with other drugs, including antidepressants, were needed.
Serious adverse events associated with boceprevir should be reported to MedWatch or by phone at 800-332-1088.
Report: Pharmacist-Led Interventions Don’t Reduce Medication Errors Post-Discharge
At first blush, some hospitalists might see it as bad news that a recent report found a pharmacist-assisted medication reconciliation ("med rec") intervention did not significantly reduce clinically important medication errors after discharge. But a deeper reading of the study tells a different story, says a hospitalist who worked on the report.
"This is the latest in our growing understanding of the roles of certain interventions on transitions of care," says Jeffrey Schnipper, MD, MPH, FHM, director of clinical research and an associate physician in the general medicine division at Brigham and Women's Hospitalist Service in Boston, and co-author of the study "Effect of a Pharmacist Intervention on Clinically Important Medication Errors after Hospital Discharge." "What I don't want to have happen is for people to read this article ... and say, 'Oh, pharmacists don't make a difference.' They absolutely make a difference. This is a more nuanced issue of who do they have the biggest impact with, and 'On top of what other interventions are you doing this?'"
The researchers set out to determine whether a pharmacist-delivered intervention on patients with low health literacy (including a post-discharge telephone call) would lower adverse drug events and other clinically important medication errors. They concluded that it did not (unadjusted incidence rate ratio, 0.92 [95% CI, 0.77 to 1.10]).
Dr. Schnipper says the impact was likely muted because the patients studied had higher health-literacy levels than researchers expected. Also, because most follow-up phone calls occurred within a few days of discharge, the intervention failed to capture any events that happened in the 30 days after discharge.
He also notes that the institutions that participated in the study have already implemented multiple med-rec interventions over the past few years. Hospitals that have not focused intently on the issue could find much larger gains from implementing pharmacist-led programs.
"If you're a hospital that has not been fixated on improving medication safety and transitions of care, I think pharmacists are huge," Dr. Schnipper says. "The key, then, is to focus them on the highest-risk patients."
At first blush, some hospitalists might see it as bad news that a recent report found a pharmacist-assisted medication reconciliation ("med rec") intervention did not significantly reduce clinically important medication errors after discharge. But a deeper reading of the study tells a different story, says a hospitalist who worked on the report.
"This is the latest in our growing understanding of the roles of certain interventions on transitions of care," says Jeffrey Schnipper, MD, MPH, FHM, director of clinical research and an associate physician in the general medicine division at Brigham and Women's Hospitalist Service in Boston, and co-author of the study "Effect of a Pharmacist Intervention on Clinically Important Medication Errors after Hospital Discharge." "What I don't want to have happen is for people to read this article ... and say, 'Oh, pharmacists don't make a difference.' They absolutely make a difference. This is a more nuanced issue of who do they have the biggest impact with, and 'On top of what other interventions are you doing this?'"
The researchers set out to determine whether a pharmacist-delivered intervention on patients with low health literacy (including a post-discharge telephone call) would lower adverse drug events and other clinically important medication errors. They concluded that it did not (unadjusted incidence rate ratio, 0.92 [95% CI, 0.77 to 1.10]).
Dr. Schnipper says the impact was likely muted because the patients studied had higher health-literacy levels than researchers expected. Also, because most follow-up phone calls occurred within a few days of discharge, the intervention failed to capture any events that happened in the 30 days after discharge.
He also notes that the institutions that participated in the study have already implemented multiple med-rec interventions over the past few years. Hospitals that have not focused intently on the issue could find much larger gains from implementing pharmacist-led programs.
"If you're a hospital that has not been fixated on improving medication safety and transitions of care, I think pharmacists are huge," Dr. Schnipper says. "The key, then, is to focus them on the highest-risk patients."
At first blush, some hospitalists might see it as bad news that a recent report found a pharmacist-assisted medication reconciliation ("med rec") intervention did not significantly reduce clinically important medication errors after discharge. But a deeper reading of the study tells a different story, says a hospitalist who worked on the report.
"This is the latest in our growing understanding of the roles of certain interventions on transitions of care," says Jeffrey Schnipper, MD, MPH, FHM, director of clinical research and an associate physician in the general medicine division at Brigham and Women's Hospitalist Service in Boston, and co-author of the study "Effect of a Pharmacist Intervention on Clinically Important Medication Errors after Hospital Discharge." "What I don't want to have happen is for people to read this article ... and say, 'Oh, pharmacists don't make a difference.' They absolutely make a difference. This is a more nuanced issue of who do they have the biggest impact with, and 'On top of what other interventions are you doing this?'"
The researchers set out to determine whether a pharmacist-delivered intervention on patients with low health literacy (including a post-discharge telephone call) would lower adverse drug events and other clinically important medication errors. They concluded that it did not (unadjusted incidence rate ratio, 0.92 [95% CI, 0.77 to 1.10]).
Dr. Schnipper says the impact was likely muted because the patients studied had higher health-literacy levels than researchers expected. Also, because most follow-up phone calls occurred within a few days of discharge, the intervention failed to capture any events that happened in the 30 days after discharge.
He also notes that the institutions that participated in the study have already implemented multiple med-rec interventions over the past few years. Hospitals that have not focused intently on the issue could find much larger gains from implementing pharmacist-led programs.
"If you're a hospital that has not been fixated on improving medication safety and transitions of care, I think pharmacists are huge," Dr. Schnipper says. "The key, then, is to focus them on the highest-risk patients."
Insurers Promote Collaborative Approach to 30-Day Readmission Reductions
Although Medicare's looming financial penalties for hospitals with excessive readmissions might seem like a blunt weapon, private health plans often have the flexibility to negotiate with partnering hospitals around incentives for readmissions prevention.
"We have arrangements with private insurance companies where we put at risk future compensation, based on achieving negotiated readmissions results," says Mark Carley, vice president of managed care and network development for Centura Health, a 13-hospital system in Colorado.
Payors, including United Healthcare, have developed their own readmissions programs and reporting mechanisms, although each program’s incentives are a little different, Carley says. Target rates are negotiated based on each hospital's readmissions in the previous 12-month period and national averages. The plan can also provide helpful data on its beneficiaries and other forms of assistance, because it wants to see the hospital hit the target, he adds. "If the target has been set too high, they may be willing to renegotiate."
But the plan doesn't tell the hospital how to reach that target.
"Where the complexity comes in is how we as a system implement internal policies and procedures to improve our care coordination, discharge processes, follow-up, and communication with downstream providers," says Carley. Centura Health's approach to readmissions has included close study of past performance data in search of opportunities for improvement, fine-tuning of the discharge planning process, and follow-up phone calls to patients and providers.
"In addition, we are working with post-acute providers to provide smoother transitions in the discharge process," he says.
Although Medicare's looming financial penalties for hospitals with excessive readmissions might seem like a blunt weapon, private health plans often have the flexibility to negotiate with partnering hospitals around incentives for readmissions prevention.
"We have arrangements with private insurance companies where we put at risk future compensation, based on achieving negotiated readmissions results," says Mark Carley, vice president of managed care and network development for Centura Health, a 13-hospital system in Colorado.
Payors, including United Healthcare, have developed their own readmissions programs and reporting mechanisms, although each program’s incentives are a little different, Carley says. Target rates are negotiated based on each hospital's readmissions in the previous 12-month period and national averages. The plan can also provide helpful data on its beneficiaries and other forms of assistance, because it wants to see the hospital hit the target, he adds. "If the target has been set too high, they may be willing to renegotiate."
But the plan doesn't tell the hospital how to reach that target.
"Where the complexity comes in is how we as a system implement internal policies and procedures to improve our care coordination, discharge processes, follow-up, and communication with downstream providers," says Carley. Centura Health's approach to readmissions has included close study of past performance data in search of opportunities for improvement, fine-tuning of the discharge planning process, and follow-up phone calls to patients and providers.
"In addition, we are working with post-acute providers to provide smoother transitions in the discharge process," he says.
Although Medicare's looming financial penalties for hospitals with excessive readmissions might seem like a blunt weapon, private health plans often have the flexibility to negotiate with partnering hospitals around incentives for readmissions prevention.
"We have arrangements with private insurance companies where we put at risk future compensation, based on achieving negotiated readmissions results," says Mark Carley, vice president of managed care and network development for Centura Health, a 13-hospital system in Colorado.
Payors, including United Healthcare, have developed their own readmissions programs and reporting mechanisms, although each program’s incentives are a little different, Carley says. Target rates are negotiated based on each hospital's readmissions in the previous 12-month period and national averages. The plan can also provide helpful data on its beneficiaries and other forms of assistance, because it wants to see the hospital hit the target, he adds. "If the target has been set too high, they may be willing to renegotiate."
But the plan doesn't tell the hospital how to reach that target.
"Where the complexity comes in is how we as a system implement internal policies and procedures to improve our care coordination, discharge processes, follow-up, and communication with downstream providers," says Carley. Centura Health's approach to readmissions has included close study of past performance data in search of opportunities for improvement, fine-tuning of the discharge planning process, and follow-up phone calls to patients and providers.
"In addition, we are working with post-acute providers to provide smoother transitions in the discharge process," he says.
Transfusion Rates Vary Widely at Academic Hospitals
Wide variations in perioperative blood transfusion rates among patients undergoing major noncardiac procedures across U.S. hospitals highlight the need to further investigate evidence-based "transfusion triggers" in this population of surgical patients, according to a study published ahead of print in Annals of Surgery.
"In light of the increased risk of mortality and major complications associated with blood transfusion, the extensive variability in hospital transfusion practice in noncardiac surgery may represent an important opportunity to improve surgical outcomes," wrote Feng Qian, Ph.D., of the University of Rochester (N.Y.), and associates.
The researchers used the University HealthSystem Consortium hospital database to compare transfusion rates of allogeneic red blood cells, fresh frozen plasma, and platelets in patients undergoing elective primary total hip replacement (54,405 patients), colectomy (21,334), or pancreaticoduodenectomy (7,929) at 77 hospitals between June 2006 and September 2010. Most of the hospitals were teaching hospitals with at least 500 beds.
Transfusion rates varied widely before and after adjustment for comorbidities and other patient risk factors. Patients who were treated in hospitals with high rates of transfusions were about twice as likely to receive a blood transfusion as were patients at hospitals with average transfusion rates (Ann. Surg. 2012 July 13[doi:10.1097/SLA.0b013e31825ffc37]).
In hospitals where the transfusion rate for one procedure was high, transfusion rates also tended to be high for the other two procedures. There was some evidence indicating that a higher volume of surgical cases was associated with lower transfusion rates.
After adjusting for patient risk factors, the authors determined that transfusion rates for the different blood components among those undergoing a total hip replacement ranged from 1.3% to almost 75% (red blood cells), from 0.1% to 7.7% (fresh frozen plasma), and from 0.1% to 2% (platelets). Among colectomy patients, transfusion rates ranged from 1.9% to 47.8% (RBCs), from 1.4% to 17.7% (fresh frozen plasma), and from 1.3% to 6.2% (platelets). Among those undergoing a pancreaticoduodenectomy, the rates ranged from 3% to 78.6% (RBCs), from 1% to 47% (fresh frozen plasma), and from 1.4% to 12.6% (platelets).
The variability, the authors said, "reflects, in part, the complexity of the medical decision-making process underlying transfusion therapy." Because the data included patients from 90% of academic medical centers in the United States, the results provide "a broad and contemporary picture of transfusion practices in academic surgical centers" and "reflect transfusion practices that are being taught to the next generation of academic and private-practice clinicians during residency training," they noted.
To the best of their knowledge, the authors said, there are no large randomized studies that have compared liberal and restrictive transfusion strategies in noncardiac surgery patients, and they believe that such trials are "urgently needed to better define evidence-based transfusion triggers for patients undergoing noncardiac surgery."
The study was supported by a grant from the Agency for Healthcare and Quality Research and funding from the department of anesthesiology at the University of Rochester. No disclosures were reported by the authors.
Wide variations in perioperative blood transfusion rates among patients undergoing major noncardiac procedures across U.S. hospitals highlight the need to further investigate evidence-based "transfusion triggers" in this population of surgical patients, according to a study published ahead of print in Annals of Surgery.
"In light of the increased risk of mortality and major complications associated with blood transfusion, the extensive variability in hospital transfusion practice in noncardiac surgery may represent an important opportunity to improve surgical outcomes," wrote Feng Qian, Ph.D., of the University of Rochester (N.Y.), and associates.
The researchers used the University HealthSystem Consortium hospital database to compare transfusion rates of allogeneic red blood cells, fresh frozen plasma, and platelets in patients undergoing elective primary total hip replacement (54,405 patients), colectomy (21,334), or pancreaticoduodenectomy (7,929) at 77 hospitals between June 2006 and September 2010. Most of the hospitals were teaching hospitals with at least 500 beds.
Transfusion rates varied widely before and after adjustment for comorbidities and other patient risk factors. Patients who were treated in hospitals with high rates of transfusions were about twice as likely to receive a blood transfusion as were patients at hospitals with average transfusion rates (Ann. Surg. 2012 July 13[doi:10.1097/SLA.0b013e31825ffc37]).
In hospitals where the transfusion rate for one procedure was high, transfusion rates also tended to be high for the other two procedures. There was some evidence indicating that a higher volume of surgical cases was associated with lower transfusion rates.
After adjusting for patient risk factors, the authors determined that transfusion rates for the different blood components among those undergoing a total hip replacement ranged from 1.3% to almost 75% (red blood cells), from 0.1% to 7.7% (fresh frozen plasma), and from 0.1% to 2% (platelets). Among colectomy patients, transfusion rates ranged from 1.9% to 47.8% (RBCs), from 1.4% to 17.7% (fresh frozen plasma), and from 1.3% to 6.2% (platelets). Among those undergoing a pancreaticoduodenectomy, the rates ranged from 3% to 78.6% (RBCs), from 1% to 47% (fresh frozen plasma), and from 1.4% to 12.6% (platelets).
The variability, the authors said, "reflects, in part, the complexity of the medical decision-making process underlying transfusion therapy." Because the data included patients from 90% of academic medical centers in the United States, the results provide "a broad and contemporary picture of transfusion practices in academic surgical centers" and "reflect transfusion practices that are being taught to the next generation of academic and private-practice clinicians during residency training," they noted.
To the best of their knowledge, the authors said, there are no large randomized studies that have compared liberal and restrictive transfusion strategies in noncardiac surgery patients, and they believe that such trials are "urgently needed to better define evidence-based transfusion triggers for patients undergoing noncardiac surgery."
The study was supported by a grant from the Agency for Healthcare and Quality Research and funding from the department of anesthesiology at the University of Rochester. No disclosures were reported by the authors.
Wide variations in perioperative blood transfusion rates among patients undergoing major noncardiac procedures across U.S. hospitals highlight the need to further investigate evidence-based "transfusion triggers" in this population of surgical patients, according to a study published ahead of print in Annals of Surgery.
"In light of the increased risk of mortality and major complications associated with blood transfusion, the extensive variability in hospital transfusion practice in noncardiac surgery may represent an important opportunity to improve surgical outcomes," wrote Feng Qian, Ph.D., of the University of Rochester (N.Y.), and associates.
The researchers used the University HealthSystem Consortium hospital database to compare transfusion rates of allogeneic red blood cells, fresh frozen plasma, and platelets in patients undergoing elective primary total hip replacement (54,405 patients), colectomy (21,334), or pancreaticoduodenectomy (7,929) at 77 hospitals between June 2006 and September 2010. Most of the hospitals were teaching hospitals with at least 500 beds.
Transfusion rates varied widely before and after adjustment for comorbidities and other patient risk factors. Patients who were treated in hospitals with high rates of transfusions were about twice as likely to receive a blood transfusion as were patients at hospitals with average transfusion rates (Ann. Surg. 2012 July 13[doi:10.1097/SLA.0b013e31825ffc37]).
In hospitals where the transfusion rate for one procedure was high, transfusion rates also tended to be high for the other two procedures. There was some evidence indicating that a higher volume of surgical cases was associated with lower transfusion rates.
After adjusting for patient risk factors, the authors determined that transfusion rates for the different blood components among those undergoing a total hip replacement ranged from 1.3% to almost 75% (red blood cells), from 0.1% to 7.7% (fresh frozen plasma), and from 0.1% to 2% (platelets). Among colectomy patients, transfusion rates ranged from 1.9% to 47.8% (RBCs), from 1.4% to 17.7% (fresh frozen plasma), and from 1.3% to 6.2% (platelets). Among those undergoing a pancreaticoduodenectomy, the rates ranged from 3% to 78.6% (RBCs), from 1% to 47% (fresh frozen plasma), and from 1.4% to 12.6% (platelets).
The variability, the authors said, "reflects, in part, the complexity of the medical decision-making process underlying transfusion therapy." Because the data included patients from 90% of academic medical centers in the United States, the results provide "a broad and contemporary picture of transfusion practices in academic surgical centers" and "reflect transfusion practices that are being taught to the next generation of academic and private-practice clinicians during residency training," they noted.
To the best of their knowledge, the authors said, there are no large randomized studies that have compared liberal and restrictive transfusion strategies in noncardiac surgery patients, and they believe that such trials are "urgently needed to better define evidence-based transfusion triggers for patients undergoing noncardiac surgery."
The study was supported by a grant from the Agency for Healthcare and Quality Research and funding from the department of anesthesiology at the University of Rochester. No disclosures were reported by the authors.
FROM THE ANNALS OF SURGERY
Major Finding: Transfusion rates of red blood cells, fresh frozen plasma, and platelets among patients undergoing noncardiac procedures varied widely across different U.S. academic-affiliated hospitals.
Data Source: Data from a national database of academic medical centers were used to compare transfusions in patients undergoing one of three elective noncardiac surgical procedures at 77 academic hospitals between June 2006 and September 2010.
Disclosures: The study was supported by a grant from the Agency for Healthcare and Quality Research and funding from the department of anesthesiology at the University of Rochester (N.Y.). The authors reported no disclosures.