User login
Checklist of Safe Discharge Practices
The transition from hospital to home can expose patients to adverse events during the postdischarge period.[1, 2] Deficits in communication at hospital discharge are common,[3] and accurate information on important hospital events is often inadequately transmitted to outpatient providers, which may adversely affect patient outcomes.[4, 5, 6] Discharge bundles (multifaceted interventions including patient education, structured discharge planning, medication reconciliation, and follow‐up visits or phone calls) are strategies that provide support to patients returning home and facilitate transfer of information to primary‐care providers (PCPs).[7, 8, 9] These interventions collectively may improve patient satisfaction and possibly reduce rehospitalization.[10]
Beginning in 2012, the Centers for Medicare and Medicaid Services will be reducing payments to facilities with high rates of readmissions.[11] Thus, improving care transitions and thereby reducing avoidable readmissions are now priorities in many jurisdictions in the United States. There is a similar focus on readmission rates in the province of Ontario.[12] The Ontario Ministry of Health and Long‐Term Care convened an expert advisory panel with a mandate to provide guidance on evidence‐based practices that ensure efficient, effective, safe, and patient‐centered care transitions.[13] The objective of this study is to describe a structured panel approach to safe discharge practices, including a checklist of a recommended sequence of steps that can be followed throughout the hospital stay. This tool can aid efforts to optimize patient discharge from the hospital and improve outcomes.
METHODS
Literature Review
The research team reviewed the literature to determine the nature and format of the core information to be contained in a discharge checklist for hospitalized patients. We searched Medline (through January 2011) for relevant articles. We used combined Medical Subject Headings and keywords using patient discharge, transition, and medication reconciliation. Bibliographies of all relevant articles were reviewed to identify additional studies. In addition, we conducted a focused study of select resources, such as the systematic review examining interventions to reduce rehospitalization by Hansen and colleagues,[10] the Transitional Care Initiative for heart failure patients,[14] the Care Transitions Intervention,[15] Project RED (Re‐Engineered Hospital Discharge),[7] Project BOOST (Better Outcomes by Optimizing Safe Transitions),[16] and The King's Fund report on avoiding hospital admissions.[17] Available toolkit resources including those developed by the Commonwealth Fund in partnership with the Institute for Healthcare Improvement,[18] the World Health Organization,[19] and the Safer Healthcare Now![20] were examined in detail.
Consultation With Experts
The panel was composed of expert members from multiple disciplines and across several healthcare sectors, including PCPs, hospitalists, rehabilitation clinicians, nurses, researchers, pharmacists, academics, and hospital administrators. The aim was to create a discharge checklist to aid in transition planning based on best practices.
Checklist‐Development Process
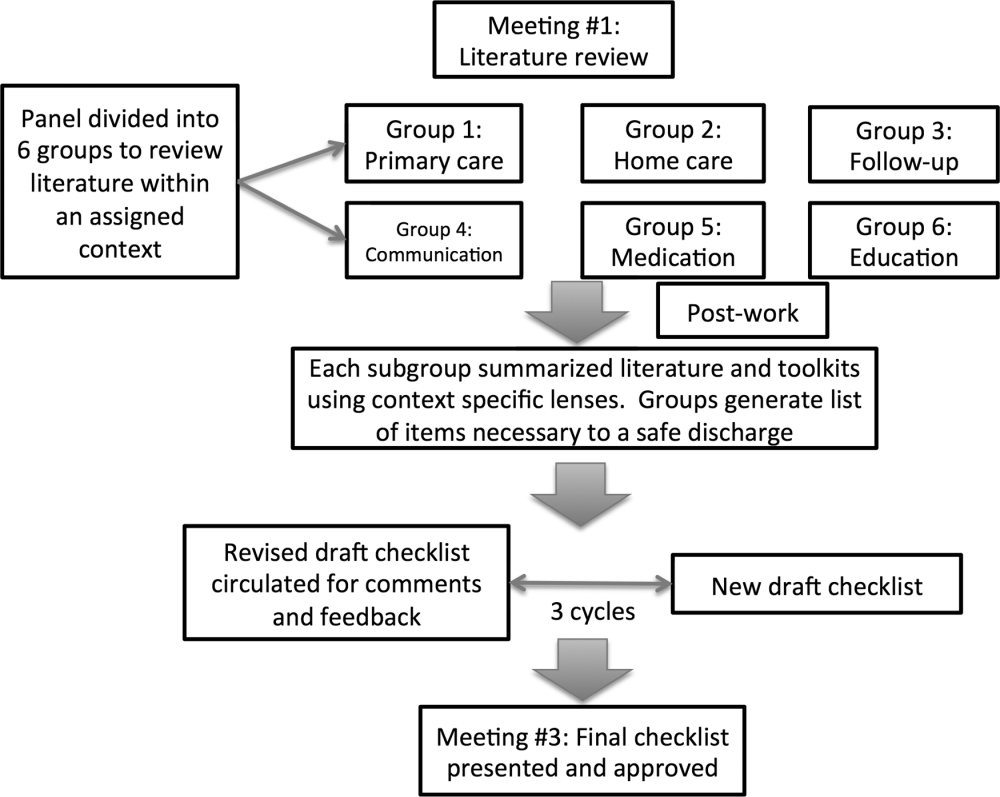
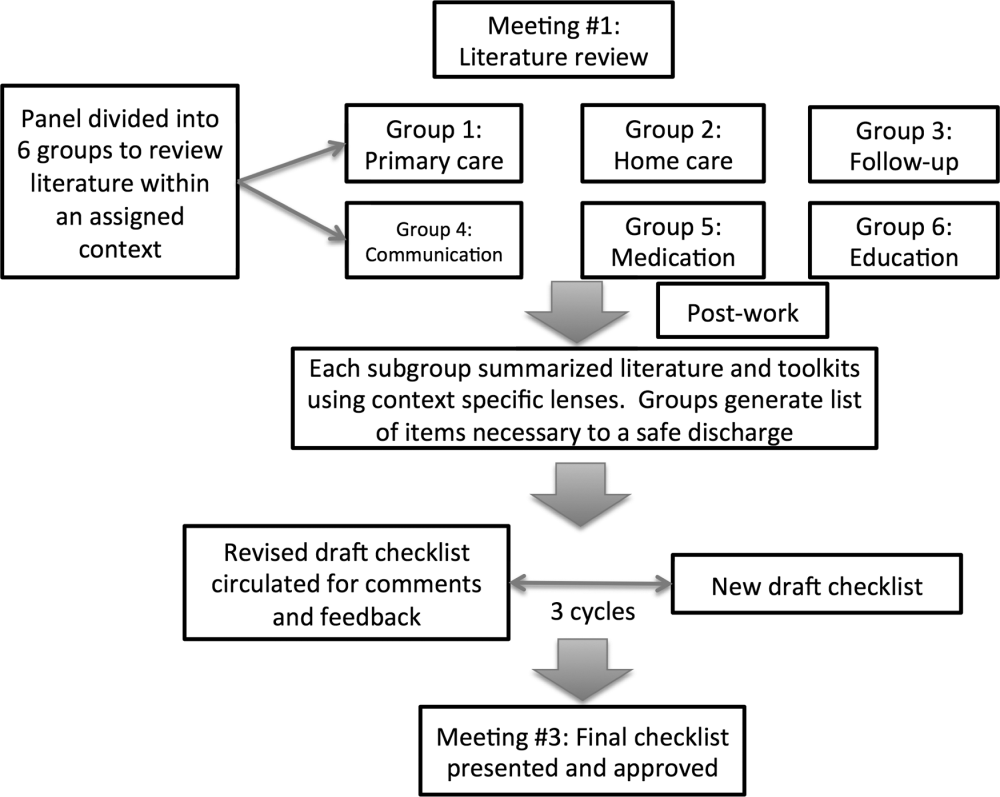
An improvement consultant (N.Z.) facilitated the process (Figure 1). The results of the literature review were circulated prior to the first meeting. The panel met 3 times in person over a period of 3 months, from January 2011 to March 2011. At the first meeting, the panel reviewed existing toolkits and evidence‐based recommendations around best discharge practices. During the meeting, panel members were assigned to 1 of 6 groups (based on specialty area) and instructed to review toolkits and literature using a context‐specific lens (primary care, home care, follow‐up plans, communication to providers and caregivers, medication, and education). The goal of this exercise was to ensure that elements necessary for a successful discharge were viewed through the perspectives of interprofessional groups involved in the care of a patient. For example, PCPs in group 1 were asked to consider an ideal discharge from the perspective of primary care. Following the meeting, each group communicated via e‐mail to generate a list of evidence‐based items necessary for a safe discharge within the context of the group's assigned lens. Every group reached consensus on items specific to its context. A preliminary draft checklist was produced based on input from all groups. The checklist was created using recommended human‐factors engineering concepts.[21] The second meeting provided the opportunity for individual comments and feedback on the draft checklist. Three cycles of checklist revision followed by comments and feedback were conducted after the meeting, through e‐mail exchange. A final meeting provided consensus of the panel on every element of the Safe Discharge Practices Checklist.
RESULTS
Evidence‐based interventions pre‐, post‐, and bridging discharge were categorized into 7 domains: (1) indication for hospitalization, (2) primary care, (3) medication safety, (4) follow‐up plans, (5) home‐care referral, (6) communication with outpatient providers, and (7) patient education (Table 1). The panel reached 100% agreement on the recommended timeline to implement elements of the discharge checklist. Given the diverse interprofessional membership of the panel, it was felt that a daily reminder of tasks to be performed would provide the best format and have the highest likelihood of engaging team members in patient care coordination. It was also felt that daily interdisciplinary (ie, bullet) rounds would serve as the most appropriate venue to utilize the checklist tool.
| Day of Admission | Subsequent Hospital Days | Discharge Day | Discharge Day +3 | |
|---|---|---|---|---|
| ||||
| 1. Hospital | ||||
| a. Assess patient to see if hospitalization is still required. | ||||
| 2. Primary care | ||||
| a. Identify and/or confirm patient has an active PCP; alert care team if no PCP and/or begin PCP search. | ||||
| b. Contact PCP and notify of patient's admission, diagnosis, and predicted discharge date. | ||||
| c. Book postdischarge PCP follow‐up appointment within 714 days of discharge (according to patient/caregiver availability and transportation needs). | ||||
| 3. Medication safety | ||||
| a. Develop BPMH and reconcile this to admission's medication orders. | ||||
| b. Teach patient how to properly use discharge medications and how these relate to the medications patient was taking prior to admission. | ||||
| c. Reconcile discharge medication order/prescription with BPMH and medications prescribed while in hospital. | ||||
| 4. Follow‐up | ||||
| a.Perform postdischarge follow‐up phone call to patient (for patients with high LACE scoresa). During call, ask: | ||||
| Has patient received new meds (if any)? | ||||
| Has patient received home care? | ||||
| Remind patient of upcoming appointments. | ||||
| If necessary, schedule patient and caregiver to come back to facility for education and training. | ||||
| b. If necessary, arrange outpatient investigations (laboratory, radiology, etc.). | ||||
| c. If necessary, book specialty‐clinic follow‐up appointment. | ||||
| 5. Home care | ||||
| a. Home‐care agency shares information, where available, about patient's existing community services. | ||||
| b. Engage home‐care agencies (eg, interdisciplinary rounds). | ||||
| c. If necessary, schedule postdischarge care. | ||||
| 6. Communication | ||||
| a. Provide patient, community pharmacy, PCP, and formal caregiver (family, LTC, home‐care agency) with copy of Discharge Summary Plan/Note and the Medication Reconciliation Form, and contact information of attending hospital physician and inpatient unit. | ||||
| 7. Patient education | ||||
| a. Clinical team performs teach‐back to patient.b | ||||
| b. Explain to patient how new medications relate to diagnosis. | ||||
| c. Thoroughly explain discharge summary to patient (use teach‐back if needed). | ||||
| d. Explain potential symptoms, what to expect while at home, and under what circumstances patient should visit ED. | ||||
The panel chose daily reminders to perform patient education around medications and clinical care for several reasons. Daily teaching provides an opportunity to assess information carried over and accurate understanding of treatment plans, as well as to review changes in care plans that may be evolving during a hospitalization. Although education starting on day 1 of admission may seem premature, we felt there was merit in addressing issues early. For example, patients admitted with heart failure can benefit from daily inpatient education around self‐monitoring, diet, and lifestyle counseling.[22]
The literature review identified communication with PCPs as an important focus to prevent adverse events when patients transition from hospital to home.[3] The expert panel agreed on admission notification, follow‐up appointment scheduling, and transfer of a high‐quality discharge summary to the patient's PCP, such as one described by Maslove and colleagues.[23] For example, summaries containing structured sections such as relevant inpatient provider contacts, diagnoses, course in hospital, results of investigations (including pending results), discharge instructions and follow‐up, and medication reconciliation have been recommended to improve communication to outpatient providers.[3] Use of validated scores such as the LACE index (a score calculated based on 4 factors: [L] length of hospital stay, [A] acuity on admission, [C] comorbidity, and [E] emergency department visits) to identify patients at high risk of readmission and targeting these individuals when arranging postdischarge follow‐up is encouraged.[24, 25] Patients with high LACE scores (10) would benefit from postdischarge follow‐up phone calls within the first 3 days of returning home. In addition, high‐risk patients may require an earlier follow‐up appointment with the PCP, and the panel supports attempts to arrange follow‐up within 7 days for at‐risk individuals. For those without a PCP, it was recommended that a search should be initiated to assist the patient in obtaining a PCP.
Medication safety is a significant source of adverse events for patients returning home from the hospital.[2, 26, 27, 28] The discharge checklist provides prompts to reconcile medications on admission and discharge, in addition to daily patient education on proper use of medications. Formal medication reconciliation programs should be tailored to the individual hospital's own resources and requirements.[29, 30]
Postdischarge care plays an important role in supporting the patient upon discharge and when part of a multifaceted discharge plan can result in decreased readmission rates and hospital utilization.[7, 9, 15, 31] The panel incorporated these elements by recommending performing postdischarge phone calls, arranging outpatient follow‐up if necessary, and coordinating home‐care services through local agencies.
To facilitate transfer of information, patients, caregivers, outpatient providers, and community pharmacies are to be provided copies of a comprehensive discharge summary, medication reconciliation, and contact information of the inpatient team under the category of Communication. Finally, as the teach‐back method is an effective tool to ensure patient understanding of their health issues, the panel recommended its use when educating patients on medication use, plan of care, and discharge instructions.[32, 33] Examples of scenarios where teach‐back would be of benefit include changes in medications with a high risk of adverse events, such as warfarin or furosemide, to ensure patients understand the dosing, frequency, and monitoring required; and self‐management skills (eg, daily weights and dietary changes) in patients with heart failure.
Finally, the panel noted that it was important to link the checklist items with relevant measures, audit, and feedback to determine associations between process and outcomes. The group avoided specific detailed recommendations to allow each institution to locally tailor appropriate process and outcome measures to assess fidelity of each component of the checklist.
DISCUSSION
A standardized, evidence‐based discharge process is critical to safe transitions for the hospitalized patient. We have used a consensus process of stakeholders to develop a Checklist of Safe Discharge Practices for Hospital Patients that details the steps of events that need to be completed for every day of a typical hospitalization. The day of discharge is often a confusing and chaotic time, with patients receiving an overwhelming volume of information on their last day in the hospital. We believe that discharge planning starts from the day of admission with daily patient education and a coordinated interdisciplinary team approach. The components of the discharge checklist should be completed throughout a patient's hospitalization to ensure a successful discharge and transmission of knowledge.
Discharge checklists have been described previously. Halasyamani and colleagues developed a checklist for elderly inpatients created through a process of literature and peer review followed by a panel discussion at the Society of Hospital Medicine Annual Meeting.[34] The resultant tool described important data elements necessary for a successful discharge and which processes were most appropriate to facilitate the transfer of information. This differs significantly from our discharge checklist, which provides specific recommendations on methods and processes to effect a safe discharge in addition to an expected timeline of when to complete each step. Kripalani et al reviewed the literature for suggested methods of promoting effective transitions of care at discharge, and their results are consistent with those summarized in our discharge checklist.[29] In contrast to both efforts, our group was multidisciplinary and had broad representation from the acute care, chronic care, home care, rehabilitation medicine, and long‐term care sectors, thereby incorporating all possible aspects of the transition process. Coordinating discharge care requires significant teamwork; our tool extends beyond a checklist of tasks to be performed, and rather serves as a platform to facilitate interprofessional collaboration. In addition, this checklist was designed to integrate discharge planning into interprofessional care rounds occurring throughout a hospital admission. As well, our paper follows an explicit and defined consensus process. Finally, our proposed tool better follows a recommended checklist format.[21]
The discharge process occurring during a patient's hospitalization is a complex, multifaceted care‐coordination plan that must begin on the first day of admission. Often, transfer of important information and medication review take place only hours before a patient leaves the hospital, a suboptimal time for patient education.[28, 35] Just as standardized treatment protocols and care plans can improve outcomes,[36] a similar approach for discharge processes may facilitate safe transition from hospital to home. Our discharge checklist prompts hospital providers to initiate steps necessary for a successful discharge while allowing for local adaptation in how each element is performed. We suggest using the checklist during daily interprofessional team rounds to ensure each task is completed, if appropriate. Institutions may consider measuring process measures such as adherence and completion of checklist, audits of discharge summaries for completion and transmission rates to PCPs (by fax or through health record departments), and documentation of patient education or medication reconciliation. Example outcome measures, if feasible, include Care Transitions Measure (CTM) scores, patient satisfaction surveys, and readmission rates.
Several limitations of this study should be considered. First, current literature on safe discharge practices is limited by low study‐design quality, with a paucity of randomized controlled trials. However, a recent systematic review found that bundled discharge interventions are likely to be most effective.[10] Individual items of the checklist may not have had an extensive evidence base; however, some of these suggested elements (eg, contact home care) have clinical face validity. Second, the heterogeneity of interventions studied pose challenges in determining generalizable best practices without considering local factors. To mitigate this, we suggest adapting the checklist to local contexts and resource availability. Third, the checklist has not been tested. The next step of this project is to pilot checklist use through small‐scale Plan‐Do‐Study‐Act (PDSA) cycles followed by large‐scale implementation. We plan to collect baseline, process, and outcome measures before and after implementation of the checklist at multiple institutions to determine utility.
Standardization of discharge practices is critical to safe transitions and preventing avoidable admissions to hospital. Our discharge checklist is an expanded tool that provides explicit guidance for each day of hospitalization and can be adapted for any hospital admission to aid interdisciplinary efforts toward a successful discharge. Future studies to evaluate the checklist in improving care‐transition processes are required to determine association with outcomes.
Disclosures
Nothing to report.
- , , , , . The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
- , , , et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143(2):121–128.
- , , , , , . Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841.
- , , , , , . “I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care. Arch Intern Med. 2004;164(20):2223–2228.
- , . Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004;141(7):533–536.
- , , , . Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004;19(6):624–631.
- , , , et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–187.
- , , , et al. A Quality improvement intervention to facilitate the transition of older adults from three hospitals back to their homes. J Am Geriatr Soc. 57(9):1540–1546.
- , , , et al. Reduction of 30‐day postdischarge hospital readmission or emergency department (ED) visit rates in high‐risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211–218.
- , , , , . Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Available at: http://cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/AcuteInpatientPPS/Readmissions‐Reduction‐Program.html.Accessed September 5, 2012.
- Ontario Ministry of Health and Long‐Term Care. The Excellent Care for All Act, 2010. Available at: http://health.gov.on.ca/en/public/programs/ecfa/default.aspx/. Accessed February 28, 2013.
- Ontario Ministry of Health and Long‐Term Care; Baker GR, ed. Enhancing the Continuum of Care: Report of the Avoidable Hospitalization Advisory Panel, November 2011. Available at: http://www.health.gov.on.ca/en/common/ministry/publications/reports/baker_2011/baker_2011.pdf. Accessed August 8, 2012.
- , , , , , . Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial [published correction appears in J Am Geriatr Soc. 2004;52(7):1228]. J Am Geriatr Soc. 2004;52(5):675–684.
- , , , . The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828.
- Society of Hospital Medicine. Project BOOST: Better Outcomes by Optimizing Safe Transitions. Available at: http://www.hospitalmedicine.org/BOOST/. Accessed October 31, 2012.
- The King's Fund; , , . Avoiding Hospital Admissions: Lessons From Evidence and Experience. Available at: http://www.kingsfund.org.uk/publications/articles/avoiding‐hospital‐admissions‐lessons‐evidence. Published October 28, 2010. Accessed September 4, 2012.
- Nielsen GA, Rutherford P, Taylor J, eds. How‐To Guide: Creating an Ideal Transition Home. Cambridge, MA: Institute for Healthcare Improvement; 2009. Available at: http://www.ihi.org or http://ah.cms‐plus.com/files/IHI_How_to_Guide_Creating_an_Ideal_Transition_Home.pdf. Accessed August 8, 2012.
- World Health Organization. Action on Patient Safety—High 5s. Available at: http://www.who.int/patientsafety/implementation/solutions/high5s/en/index.html. Accessed October 29, 2012.
- Safer Healthcare Now! Medication Reconciliation in Acute Care: Getting Started Kit. Available at: http://www.ismp‐canada.org/download/MedRec/Medrec_AC_English_GSK_V3.pdf. Accessed October 29, 2012.
- US Agency for Healthcare Research and Quality. PSNet: Patient‐safety primers, checklists. Available at: http://www.psnet.ahrq.gov/primer.aspx?primerID=14. Accessed November 1, 2012.
- , , , . Benefits of comprehensive inpatient education and discharge planning combined with outpatient support in elderly patients with congestive heart failure. Congest Heart Fail. 2005;11(6):315–321.
- , , , et al. Electronic versus dictated hospital discharge summaries: a randomized controlled trial. J Gen Intern Med. 2009;24(9):995–1001.
- , , , et al. Unplanned readmissions after hospital discharge among patients identified as being at high risk for readmission using a validated predictive algorithm. Open Med. 2011;5(2):e104–e111.
- , , , et al. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. CMAJ. 2010;182(6):551–557.
- . Will, ideas, and execution: their role in reducing adverse medication events. J Pediatr. 2005;147(6):727–728.
- , , , . Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units. Arch Intern Med. 2003;163(17):2014–2018.
- , , , et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166(5):565–571.
- , , , . Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2(5):314–323.
- , . Medication reconciliation in the hospital. Healthc Q. 2012;15:42–49.
- , , , , , . Comprehensive discharge planning for the hospitalized elderly: a randomized clinical trial. Ann Intern Med. 1994;120(12):999–1006.
- , , , et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163(1):83–90.
- , , . The effects of patient communication skills training on compliance. Arch Fam Med. 2000;9(1):57–64.
- , , , et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354–360.
- , , , , . Influence of a “discharge interview” on patient knowledge, compliance, and functional status after hospitalization. Med Care. 1983;21(8):755–767.
- , , , , . Critical pathways intervention to reduce length of hospital stay. Am J Med. 2001;110(3):175–180.
The transition from hospital to home can expose patients to adverse events during the postdischarge period.[1, 2] Deficits in communication at hospital discharge are common,[3] and accurate information on important hospital events is often inadequately transmitted to outpatient providers, which may adversely affect patient outcomes.[4, 5, 6] Discharge bundles (multifaceted interventions including patient education, structured discharge planning, medication reconciliation, and follow‐up visits or phone calls) are strategies that provide support to patients returning home and facilitate transfer of information to primary‐care providers (PCPs).[7, 8, 9] These interventions collectively may improve patient satisfaction and possibly reduce rehospitalization.[10]
Beginning in 2012, the Centers for Medicare and Medicaid Services will be reducing payments to facilities with high rates of readmissions.[11] Thus, improving care transitions and thereby reducing avoidable readmissions are now priorities in many jurisdictions in the United States. There is a similar focus on readmission rates in the province of Ontario.[12] The Ontario Ministry of Health and Long‐Term Care convened an expert advisory panel with a mandate to provide guidance on evidence‐based practices that ensure efficient, effective, safe, and patient‐centered care transitions.[13] The objective of this study is to describe a structured panel approach to safe discharge practices, including a checklist of a recommended sequence of steps that can be followed throughout the hospital stay. This tool can aid efforts to optimize patient discharge from the hospital and improve outcomes.
METHODS
Literature Review
The research team reviewed the literature to determine the nature and format of the core information to be contained in a discharge checklist for hospitalized patients. We searched Medline (through January 2011) for relevant articles. We used combined Medical Subject Headings and keywords using patient discharge, transition, and medication reconciliation. Bibliographies of all relevant articles were reviewed to identify additional studies. In addition, we conducted a focused study of select resources, such as the systematic review examining interventions to reduce rehospitalization by Hansen and colleagues,[10] the Transitional Care Initiative for heart failure patients,[14] the Care Transitions Intervention,[15] Project RED (Re‐Engineered Hospital Discharge),[7] Project BOOST (Better Outcomes by Optimizing Safe Transitions),[16] and The King's Fund report on avoiding hospital admissions.[17] Available toolkit resources including those developed by the Commonwealth Fund in partnership with the Institute for Healthcare Improvement,[18] the World Health Organization,[19] and the Safer Healthcare Now![20] were examined in detail.
Consultation With Experts
The panel was composed of expert members from multiple disciplines and across several healthcare sectors, including PCPs, hospitalists, rehabilitation clinicians, nurses, researchers, pharmacists, academics, and hospital administrators. The aim was to create a discharge checklist to aid in transition planning based on best practices.
Checklist‐Development Process
An improvement consultant (N.Z.) facilitated the process (Figure 1). The results of the literature review were circulated prior to the first meeting. The panel met 3 times in person over a period of 3 months, from January 2011 to March 2011. At the first meeting, the panel reviewed existing toolkits and evidence‐based recommendations around best discharge practices. During the meeting, panel members were assigned to 1 of 6 groups (based on specialty area) and instructed to review toolkits and literature using a context‐specific lens (primary care, home care, follow‐up plans, communication to providers and caregivers, medication, and education). The goal of this exercise was to ensure that elements necessary for a successful discharge were viewed through the perspectives of interprofessional groups involved in the care of a patient. For example, PCPs in group 1 were asked to consider an ideal discharge from the perspective of primary care. Following the meeting, each group communicated via e‐mail to generate a list of evidence‐based items necessary for a safe discharge within the context of the group's assigned lens. Every group reached consensus on items specific to its context. A preliminary draft checklist was produced based on input from all groups. The checklist was created using recommended human‐factors engineering concepts.[21] The second meeting provided the opportunity for individual comments and feedback on the draft checklist. Three cycles of checklist revision followed by comments and feedback were conducted after the meeting, through e‐mail exchange. A final meeting provided consensus of the panel on every element of the Safe Discharge Practices Checklist.
RESULTS
Evidence‐based interventions pre‐, post‐, and bridging discharge were categorized into 7 domains: (1) indication for hospitalization, (2) primary care, (3) medication safety, (4) follow‐up plans, (5) home‐care referral, (6) communication with outpatient providers, and (7) patient education (Table 1). The panel reached 100% agreement on the recommended timeline to implement elements of the discharge checklist. Given the diverse interprofessional membership of the panel, it was felt that a daily reminder of tasks to be performed would provide the best format and have the highest likelihood of engaging team members in patient care coordination. It was also felt that daily interdisciplinary (ie, bullet) rounds would serve as the most appropriate venue to utilize the checklist tool.
| Day of Admission | Subsequent Hospital Days | Discharge Day | Discharge Day +3 | |
|---|---|---|---|---|
| ||||
| 1. Hospital | ||||
| a. Assess patient to see if hospitalization is still required. | ||||
| 2. Primary care | ||||
| a. Identify and/or confirm patient has an active PCP; alert care team if no PCP and/or begin PCP search. | ||||
| b. Contact PCP and notify of patient's admission, diagnosis, and predicted discharge date. | ||||
| c. Book postdischarge PCP follow‐up appointment within 714 days of discharge (according to patient/caregiver availability and transportation needs). | ||||
| 3. Medication safety | ||||
| a. Develop BPMH and reconcile this to admission's medication orders. | ||||
| b. Teach patient how to properly use discharge medications and how these relate to the medications patient was taking prior to admission. | ||||
| c. Reconcile discharge medication order/prescription with BPMH and medications prescribed while in hospital. | ||||
| 4. Follow‐up | ||||
| a.Perform postdischarge follow‐up phone call to patient (for patients with high LACE scoresa). During call, ask: | ||||
| Has patient received new meds (if any)? | ||||
| Has patient received home care? | ||||
| Remind patient of upcoming appointments. | ||||
| If necessary, schedule patient and caregiver to come back to facility for education and training. | ||||
| b. If necessary, arrange outpatient investigations (laboratory, radiology, etc.). | ||||
| c. If necessary, book specialty‐clinic follow‐up appointment. | ||||
| 5. Home care | ||||
| a. Home‐care agency shares information, where available, about patient's existing community services. | ||||
| b. Engage home‐care agencies (eg, interdisciplinary rounds). | ||||
| c. If necessary, schedule postdischarge care. | ||||
| 6. Communication | ||||
| a. Provide patient, community pharmacy, PCP, and formal caregiver (family, LTC, home‐care agency) with copy of Discharge Summary Plan/Note and the Medication Reconciliation Form, and contact information of attending hospital physician and inpatient unit. | ||||
| 7. Patient education | ||||
| a. Clinical team performs teach‐back to patient.b | ||||
| b. Explain to patient how new medications relate to diagnosis. | ||||
| c. Thoroughly explain discharge summary to patient (use teach‐back if needed). | ||||
| d. Explain potential symptoms, what to expect while at home, and under what circumstances patient should visit ED. | ||||
The panel chose daily reminders to perform patient education around medications and clinical care for several reasons. Daily teaching provides an opportunity to assess information carried over and accurate understanding of treatment plans, as well as to review changes in care plans that may be evolving during a hospitalization. Although education starting on day 1 of admission may seem premature, we felt there was merit in addressing issues early. For example, patients admitted with heart failure can benefit from daily inpatient education around self‐monitoring, diet, and lifestyle counseling.[22]
The literature review identified communication with PCPs as an important focus to prevent adverse events when patients transition from hospital to home.[3] The expert panel agreed on admission notification, follow‐up appointment scheduling, and transfer of a high‐quality discharge summary to the patient's PCP, such as one described by Maslove and colleagues.[23] For example, summaries containing structured sections such as relevant inpatient provider contacts, diagnoses, course in hospital, results of investigations (including pending results), discharge instructions and follow‐up, and medication reconciliation have been recommended to improve communication to outpatient providers.[3] Use of validated scores such as the LACE index (a score calculated based on 4 factors: [L] length of hospital stay, [A] acuity on admission, [C] comorbidity, and [E] emergency department visits) to identify patients at high risk of readmission and targeting these individuals when arranging postdischarge follow‐up is encouraged.[24, 25] Patients with high LACE scores (10) would benefit from postdischarge follow‐up phone calls within the first 3 days of returning home. In addition, high‐risk patients may require an earlier follow‐up appointment with the PCP, and the panel supports attempts to arrange follow‐up within 7 days for at‐risk individuals. For those without a PCP, it was recommended that a search should be initiated to assist the patient in obtaining a PCP.
Medication safety is a significant source of adverse events for patients returning home from the hospital.[2, 26, 27, 28] The discharge checklist provides prompts to reconcile medications on admission and discharge, in addition to daily patient education on proper use of medications. Formal medication reconciliation programs should be tailored to the individual hospital's own resources and requirements.[29, 30]
Postdischarge care plays an important role in supporting the patient upon discharge and when part of a multifaceted discharge plan can result in decreased readmission rates and hospital utilization.[7, 9, 15, 31] The panel incorporated these elements by recommending performing postdischarge phone calls, arranging outpatient follow‐up if necessary, and coordinating home‐care services through local agencies.
To facilitate transfer of information, patients, caregivers, outpatient providers, and community pharmacies are to be provided copies of a comprehensive discharge summary, medication reconciliation, and contact information of the inpatient team under the category of Communication. Finally, as the teach‐back method is an effective tool to ensure patient understanding of their health issues, the panel recommended its use when educating patients on medication use, plan of care, and discharge instructions.[32, 33] Examples of scenarios where teach‐back would be of benefit include changes in medications with a high risk of adverse events, such as warfarin or furosemide, to ensure patients understand the dosing, frequency, and monitoring required; and self‐management skills (eg, daily weights and dietary changes) in patients with heart failure.
Finally, the panel noted that it was important to link the checklist items with relevant measures, audit, and feedback to determine associations between process and outcomes. The group avoided specific detailed recommendations to allow each institution to locally tailor appropriate process and outcome measures to assess fidelity of each component of the checklist.
DISCUSSION
A standardized, evidence‐based discharge process is critical to safe transitions for the hospitalized patient. We have used a consensus process of stakeholders to develop a Checklist of Safe Discharge Practices for Hospital Patients that details the steps of events that need to be completed for every day of a typical hospitalization. The day of discharge is often a confusing and chaotic time, with patients receiving an overwhelming volume of information on their last day in the hospital. We believe that discharge planning starts from the day of admission with daily patient education and a coordinated interdisciplinary team approach. The components of the discharge checklist should be completed throughout a patient's hospitalization to ensure a successful discharge and transmission of knowledge.
Discharge checklists have been described previously. Halasyamani and colleagues developed a checklist for elderly inpatients created through a process of literature and peer review followed by a panel discussion at the Society of Hospital Medicine Annual Meeting.[34] The resultant tool described important data elements necessary for a successful discharge and which processes were most appropriate to facilitate the transfer of information. This differs significantly from our discharge checklist, which provides specific recommendations on methods and processes to effect a safe discharge in addition to an expected timeline of when to complete each step. Kripalani et al reviewed the literature for suggested methods of promoting effective transitions of care at discharge, and their results are consistent with those summarized in our discharge checklist.[29] In contrast to both efforts, our group was multidisciplinary and had broad representation from the acute care, chronic care, home care, rehabilitation medicine, and long‐term care sectors, thereby incorporating all possible aspects of the transition process. Coordinating discharge care requires significant teamwork; our tool extends beyond a checklist of tasks to be performed, and rather serves as a platform to facilitate interprofessional collaboration. In addition, this checklist was designed to integrate discharge planning into interprofessional care rounds occurring throughout a hospital admission. As well, our paper follows an explicit and defined consensus process. Finally, our proposed tool better follows a recommended checklist format.[21]
The discharge process occurring during a patient's hospitalization is a complex, multifaceted care‐coordination plan that must begin on the first day of admission. Often, transfer of important information and medication review take place only hours before a patient leaves the hospital, a suboptimal time for patient education.[28, 35] Just as standardized treatment protocols and care plans can improve outcomes,[36] a similar approach for discharge processes may facilitate safe transition from hospital to home. Our discharge checklist prompts hospital providers to initiate steps necessary for a successful discharge while allowing for local adaptation in how each element is performed. We suggest using the checklist during daily interprofessional team rounds to ensure each task is completed, if appropriate. Institutions may consider measuring process measures such as adherence and completion of checklist, audits of discharge summaries for completion and transmission rates to PCPs (by fax or through health record departments), and documentation of patient education or medication reconciliation. Example outcome measures, if feasible, include Care Transitions Measure (CTM) scores, patient satisfaction surveys, and readmission rates.
Several limitations of this study should be considered. First, current literature on safe discharge practices is limited by low study‐design quality, with a paucity of randomized controlled trials. However, a recent systematic review found that bundled discharge interventions are likely to be most effective.[10] Individual items of the checklist may not have had an extensive evidence base; however, some of these suggested elements (eg, contact home care) have clinical face validity. Second, the heterogeneity of interventions studied pose challenges in determining generalizable best practices without considering local factors. To mitigate this, we suggest adapting the checklist to local contexts and resource availability. Third, the checklist has not been tested. The next step of this project is to pilot checklist use through small‐scale Plan‐Do‐Study‐Act (PDSA) cycles followed by large‐scale implementation. We plan to collect baseline, process, and outcome measures before and after implementation of the checklist at multiple institutions to determine utility.
Standardization of discharge practices is critical to safe transitions and preventing avoidable admissions to hospital. Our discharge checklist is an expanded tool that provides explicit guidance for each day of hospitalization and can be adapted for any hospital admission to aid interdisciplinary efforts toward a successful discharge. Future studies to evaluate the checklist in improving care‐transition processes are required to determine association with outcomes.
Disclosures
Nothing to report.
The transition from hospital to home can expose patients to adverse events during the postdischarge period.[1, 2] Deficits in communication at hospital discharge are common,[3] and accurate information on important hospital events is often inadequately transmitted to outpatient providers, which may adversely affect patient outcomes.[4, 5, 6] Discharge bundles (multifaceted interventions including patient education, structured discharge planning, medication reconciliation, and follow‐up visits or phone calls) are strategies that provide support to patients returning home and facilitate transfer of information to primary‐care providers (PCPs).[7, 8, 9] These interventions collectively may improve patient satisfaction and possibly reduce rehospitalization.[10]
Beginning in 2012, the Centers for Medicare and Medicaid Services will be reducing payments to facilities with high rates of readmissions.[11] Thus, improving care transitions and thereby reducing avoidable readmissions are now priorities in many jurisdictions in the United States. There is a similar focus on readmission rates in the province of Ontario.[12] The Ontario Ministry of Health and Long‐Term Care convened an expert advisory panel with a mandate to provide guidance on evidence‐based practices that ensure efficient, effective, safe, and patient‐centered care transitions.[13] The objective of this study is to describe a structured panel approach to safe discharge practices, including a checklist of a recommended sequence of steps that can be followed throughout the hospital stay. This tool can aid efforts to optimize patient discharge from the hospital and improve outcomes.
METHODS
Literature Review
The research team reviewed the literature to determine the nature and format of the core information to be contained in a discharge checklist for hospitalized patients. We searched Medline (through January 2011) for relevant articles. We used combined Medical Subject Headings and keywords using patient discharge, transition, and medication reconciliation. Bibliographies of all relevant articles were reviewed to identify additional studies. In addition, we conducted a focused study of select resources, such as the systematic review examining interventions to reduce rehospitalization by Hansen and colleagues,[10] the Transitional Care Initiative for heart failure patients,[14] the Care Transitions Intervention,[15] Project RED (Re‐Engineered Hospital Discharge),[7] Project BOOST (Better Outcomes by Optimizing Safe Transitions),[16] and The King's Fund report on avoiding hospital admissions.[17] Available toolkit resources including those developed by the Commonwealth Fund in partnership with the Institute for Healthcare Improvement,[18] the World Health Organization,[19] and the Safer Healthcare Now![20] were examined in detail.
Consultation With Experts
The panel was composed of expert members from multiple disciplines and across several healthcare sectors, including PCPs, hospitalists, rehabilitation clinicians, nurses, researchers, pharmacists, academics, and hospital administrators. The aim was to create a discharge checklist to aid in transition planning based on best practices.
Checklist‐Development Process
An improvement consultant (N.Z.) facilitated the process (Figure 1). The results of the literature review were circulated prior to the first meeting. The panel met 3 times in person over a period of 3 months, from January 2011 to March 2011. At the first meeting, the panel reviewed existing toolkits and evidence‐based recommendations around best discharge practices. During the meeting, panel members were assigned to 1 of 6 groups (based on specialty area) and instructed to review toolkits and literature using a context‐specific lens (primary care, home care, follow‐up plans, communication to providers and caregivers, medication, and education). The goal of this exercise was to ensure that elements necessary for a successful discharge were viewed through the perspectives of interprofessional groups involved in the care of a patient. For example, PCPs in group 1 were asked to consider an ideal discharge from the perspective of primary care. Following the meeting, each group communicated via e‐mail to generate a list of evidence‐based items necessary for a safe discharge within the context of the group's assigned lens. Every group reached consensus on items specific to its context. A preliminary draft checklist was produced based on input from all groups. The checklist was created using recommended human‐factors engineering concepts.[21] The second meeting provided the opportunity for individual comments and feedback on the draft checklist. Three cycles of checklist revision followed by comments and feedback were conducted after the meeting, through e‐mail exchange. A final meeting provided consensus of the panel on every element of the Safe Discharge Practices Checklist.
RESULTS
Evidence‐based interventions pre‐, post‐, and bridging discharge were categorized into 7 domains: (1) indication for hospitalization, (2) primary care, (3) medication safety, (4) follow‐up plans, (5) home‐care referral, (6) communication with outpatient providers, and (7) patient education (Table 1). The panel reached 100% agreement on the recommended timeline to implement elements of the discharge checklist. Given the diverse interprofessional membership of the panel, it was felt that a daily reminder of tasks to be performed would provide the best format and have the highest likelihood of engaging team members in patient care coordination. It was also felt that daily interdisciplinary (ie, bullet) rounds would serve as the most appropriate venue to utilize the checklist tool.
| Day of Admission | Subsequent Hospital Days | Discharge Day | Discharge Day +3 | |
|---|---|---|---|---|
| ||||
| 1. Hospital | ||||
| a. Assess patient to see if hospitalization is still required. | ||||
| 2. Primary care | ||||
| a. Identify and/or confirm patient has an active PCP; alert care team if no PCP and/or begin PCP search. | ||||
| b. Contact PCP and notify of patient's admission, diagnosis, and predicted discharge date. | ||||
| c. Book postdischarge PCP follow‐up appointment within 714 days of discharge (according to patient/caregiver availability and transportation needs). | ||||
| 3. Medication safety | ||||
| a. Develop BPMH and reconcile this to admission's medication orders. | ||||
| b. Teach patient how to properly use discharge medications and how these relate to the medications patient was taking prior to admission. | ||||
| c. Reconcile discharge medication order/prescription with BPMH and medications prescribed while in hospital. | ||||
| 4. Follow‐up | ||||
| a.Perform postdischarge follow‐up phone call to patient (for patients with high LACE scoresa). During call, ask: | ||||
| Has patient received new meds (if any)? | ||||
| Has patient received home care? | ||||
| Remind patient of upcoming appointments. | ||||
| If necessary, schedule patient and caregiver to come back to facility for education and training. | ||||
| b. If necessary, arrange outpatient investigations (laboratory, radiology, etc.). | ||||
| c. If necessary, book specialty‐clinic follow‐up appointment. | ||||
| 5. Home care | ||||
| a. Home‐care agency shares information, where available, about patient's existing community services. | ||||
| b. Engage home‐care agencies (eg, interdisciplinary rounds). | ||||
| c. If necessary, schedule postdischarge care. | ||||
| 6. Communication | ||||
| a. Provide patient, community pharmacy, PCP, and formal caregiver (family, LTC, home‐care agency) with copy of Discharge Summary Plan/Note and the Medication Reconciliation Form, and contact information of attending hospital physician and inpatient unit. | ||||
| 7. Patient education | ||||
| a. Clinical team performs teach‐back to patient.b | ||||
| b. Explain to patient how new medications relate to diagnosis. | ||||
| c. Thoroughly explain discharge summary to patient (use teach‐back if needed). | ||||
| d. Explain potential symptoms, what to expect while at home, and under what circumstances patient should visit ED. | ||||
The panel chose daily reminders to perform patient education around medications and clinical care for several reasons. Daily teaching provides an opportunity to assess information carried over and accurate understanding of treatment plans, as well as to review changes in care plans that may be evolving during a hospitalization. Although education starting on day 1 of admission may seem premature, we felt there was merit in addressing issues early. For example, patients admitted with heart failure can benefit from daily inpatient education around self‐monitoring, diet, and lifestyle counseling.[22]
The literature review identified communication with PCPs as an important focus to prevent adverse events when patients transition from hospital to home.[3] The expert panel agreed on admission notification, follow‐up appointment scheduling, and transfer of a high‐quality discharge summary to the patient's PCP, such as one described by Maslove and colleagues.[23] For example, summaries containing structured sections such as relevant inpatient provider contacts, diagnoses, course in hospital, results of investigations (including pending results), discharge instructions and follow‐up, and medication reconciliation have been recommended to improve communication to outpatient providers.[3] Use of validated scores such as the LACE index (a score calculated based on 4 factors: [L] length of hospital stay, [A] acuity on admission, [C] comorbidity, and [E] emergency department visits) to identify patients at high risk of readmission and targeting these individuals when arranging postdischarge follow‐up is encouraged.[24, 25] Patients with high LACE scores (10) would benefit from postdischarge follow‐up phone calls within the first 3 days of returning home. In addition, high‐risk patients may require an earlier follow‐up appointment with the PCP, and the panel supports attempts to arrange follow‐up within 7 days for at‐risk individuals. For those without a PCP, it was recommended that a search should be initiated to assist the patient in obtaining a PCP.
Medication safety is a significant source of adverse events for patients returning home from the hospital.[2, 26, 27, 28] The discharge checklist provides prompts to reconcile medications on admission and discharge, in addition to daily patient education on proper use of medications. Formal medication reconciliation programs should be tailored to the individual hospital's own resources and requirements.[29, 30]
Postdischarge care plays an important role in supporting the patient upon discharge and when part of a multifaceted discharge plan can result in decreased readmission rates and hospital utilization.[7, 9, 15, 31] The panel incorporated these elements by recommending performing postdischarge phone calls, arranging outpatient follow‐up if necessary, and coordinating home‐care services through local agencies.
To facilitate transfer of information, patients, caregivers, outpatient providers, and community pharmacies are to be provided copies of a comprehensive discharge summary, medication reconciliation, and contact information of the inpatient team under the category of Communication. Finally, as the teach‐back method is an effective tool to ensure patient understanding of their health issues, the panel recommended its use when educating patients on medication use, plan of care, and discharge instructions.[32, 33] Examples of scenarios where teach‐back would be of benefit include changes in medications with a high risk of adverse events, such as warfarin or furosemide, to ensure patients understand the dosing, frequency, and monitoring required; and self‐management skills (eg, daily weights and dietary changes) in patients with heart failure.
Finally, the panel noted that it was important to link the checklist items with relevant measures, audit, and feedback to determine associations between process and outcomes. The group avoided specific detailed recommendations to allow each institution to locally tailor appropriate process and outcome measures to assess fidelity of each component of the checklist.
DISCUSSION
A standardized, evidence‐based discharge process is critical to safe transitions for the hospitalized patient. We have used a consensus process of stakeholders to develop a Checklist of Safe Discharge Practices for Hospital Patients that details the steps of events that need to be completed for every day of a typical hospitalization. The day of discharge is often a confusing and chaotic time, with patients receiving an overwhelming volume of information on their last day in the hospital. We believe that discharge planning starts from the day of admission with daily patient education and a coordinated interdisciplinary team approach. The components of the discharge checklist should be completed throughout a patient's hospitalization to ensure a successful discharge and transmission of knowledge.
Discharge checklists have been described previously. Halasyamani and colleagues developed a checklist for elderly inpatients created through a process of literature and peer review followed by a panel discussion at the Society of Hospital Medicine Annual Meeting.[34] The resultant tool described important data elements necessary for a successful discharge and which processes were most appropriate to facilitate the transfer of information. This differs significantly from our discharge checklist, which provides specific recommendations on methods and processes to effect a safe discharge in addition to an expected timeline of when to complete each step. Kripalani et al reviewed the literature for suggested methods of promoting effective transitions of care at discharge, and their results are consistent with those summarized in our discharge checklist.[29] In contrast to both efforts, our group was multidisciplinary and had broad representation from the acute care, chronic care, home care, rehabilitation medicine, and long‐term care sectors, thereby incorporating all possible aspects of the transition process. Coordinating discharge care requires significant teamwork; our tool extends beyond a checklist of tasks to be performed, and rather serves as a platform to facilitate interprofessional collaboration. In addition, this checklist was designed to integrate discharge planning into interprofessional care rounds occurring throughout a hospital admission. As well, our paper follows an explicit and defined consensus process. Finally, our proposed tool better follows a recommended checklist format.[21]
The discharge process occurring during a patient's hospitalization is a complex, multifaceted care‐coordination plan that must begin on the first day of admission. Often, transfer of important information and medication review take place only hours before a patient leaves the hospital, a suboptimal time for patient education.[28, 35] Just as standardized treatment protocols and care plans can improve outcomes,[36] a similar approach for discharge processes may facilitate safe transition from hospital to home. Our discharge checklist prompts hospital providers to initiate steps necessary for a successful discharge while allowing for local adaptation in how each element is performed. We suggest using the checklist during daily interprofessional team rounds to ensure each task is completed, if appropriate. Institutions may consider measuring process measures such as adherence and completion of checklist, audits of discharge summaries for completion and transmission rates to PCPs (by fax or through health record departments), and documentation of patient education or medication reconciliation. Example outcome measures, if feasible, include Care Transitions Measure (CTM) scores, patient satisfaction surveys, and readmission rates.
Several limitations of this study should be considered. First, current literature on safe discharge practices is limited by low study‐design quality, with a paucity of randomized controlled trials. However, a recent systematic review found that bundled discharge interventions are likely to be most effective.[10] Individual items of the checklist may not have had an extensive evidence base; however, some of these suggested elements (eg, contact home care) have clinical face validity. Second, the heterogeneity of interventions studied pose challenges in determining generalizable best practices without considering local factors. To mitigate this, we suggest adapting the checklist to local contexts and resource availability. Third, the checklist has not been tested. The next step of this project is to pilot checklist use through small‐scale Plan‐Do‐Study‐Act (PDSA) cycles followed by large‐scale implementation. We plan to collect baseline, process, and outcome measures before and after implementation of the checklist at multiple institutions to determine utility.
Standardization of discharge practices is critical to safe transitions and preventing avoidable admissions to hospital. Our discharge checklist is an expanded tool that provides explicit guidance for each day of hospitalization and can be adapted for any hospital admission to aid interdisciplinary efforts toward a successful discharge. Future studies to evaluate the checklist in improving care‐transition processes are required to determine association with outcomes.
Disclosures
Nothing to report.
- , , , , . The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
- , , , et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143(2):121–128.
- , , , , , . Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841.
- , , , , , . “I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care. Arch Intern Med. 2004;164(20):2223–2228.
- , . Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004;141(7):533–536.
- , , , . Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004;19(6):624–631.
- , , , et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–187.
- , , , et al. A Quality improvement intervention to facilitate the transition of older adults from three hospitals back to their homes. J Am Geriatr Soc. 57(9):1540–1546.
- , , , et al. Reduction of 30‐day postdischarge hospital readmission or emergency department (ED) visit rates in high‐risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211–218.
- , , , , . Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Available at: http://cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/AcuteInpatientPPS/Readmissions‐Reduction‐Program.html.Accessed September 5, 2012.
- Ontario Ministry of Health and Long‐Term Care. The Excellent Care for All Act, 2010. Available at: http://health.gov.on.ca/en/public/programs/ecfa/default.aspx/. Accessed February 28, 2013.
- Ontario Ministry of Health and Long‐Term Care; Baker GR, ed. Enhancing the Continuum of Care: Report of the Avoidable Hospitalization Advisory Panel, November 2011. Available at: http://www.health.gov.on.ca/en/common/ministry/publications/reports/baker_2011/baker_2011.pdf. Accessed August 8, 2012.
- , , , , , . Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial [published correction appears in J Am Geriatr Soc. 2004;52(7):1228]. J Am Geriatr Soc. 2004;52(5):675–684.
- , , , . The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828.
- Society of Hospital Medicine. Project BOOST: Better Outcomes by Optimizing Safe Transitions. Available at: http://www.hospitalmedicine.org/BOOST/. Accessed October 31, 2012.
- The King's Fund; , , . Avoiding Hospital Admissions: Lessons From Evidence and Experience. Available at: http://www.kingsfund.org.uk/publications/articles/avoiding‐hospital‐admissions‐lessons‐evidence. Published October 28, 2010. Accessed September 4, 2012.
- Nielsen GA, Rutherford P, Taylor J, eds. How‐To Guide: Creating an Ideal Transition Home. Cambridge, MA: Institute for Healthcare Improvement; 2009. Available at: http://www.ihi.org or http://ah.cms‐plus.com/files/IHI_How_to_Guide_Creating_an_Ideal_Transition_Home.pdf. Accessed August 8, 2012.
- World Health Organization. Action on Patient Safety—High 5s. Available at: http://www.who.int/patientsafety/implementation/solutions/high5s/en/index.html. Accessed October 29, 2012.
- Safer Healthcare Now! Medication Reconciliation in Acute Care: Getting Started Kit. Available at: http://www.ismp‐canada.org/download/MedRec/Medrec_AC_English_GSK_V3.pdf. Accessed October 29, 2012.
- US Agency for Healthcare Research and Quality. PSNet: Patient‐safety primers, checklists. Available at: http://www.psnet.ahrq.gov/primer.aspx?primerID=14. Accessed November 1, 2012.
- , , , . Benefits of comprehensive inpatient education and discharge planning combined with outpatient support in elderly patients with congestive heart failure. Congest Heart Fail. 2005;11(6):315–321.
- , , , et al. Electronic versus dictated hospital discharge summaries: a randomized controlled trial. J Gen Intern Med. 2009;24(9):995–1001.
- , , , et al. Unplanned readmissions after hospital discharge among patients identified as being at high risk for readmission using a validated predictive algorithm. Open Med. 2011;5(2):e104–e111.
- , , , et al. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. CMAJ. 2010;182(6):551–557.
- . Will, ideas, and execution: their role in reducing adverse medication events. J Pediatr. 2005;147(6):727–728.
- , , , . Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units. Arch Intern Med. 2003;163(17):2014–2018.
- , , , et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166(5):565–571.
- , , , . Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2(5):314–323.
- , . Medication reconciliation in the hospital. Healthc Q. 2012;15:42–49.
- , , , , , . Comprehensive discharge planning for the hospitalized elderly: a randomized clinical trial. Ann Intern Med. 1994;120(12):999–1006.
- , , , et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163(1):83–90.
- , , . The effects of patient communication skills training on compliance. Arch Fam Med. 2000;9(1):57–64.
- , , , et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354–360.
- , , , , . Influence of a “discharge interview” on patient knowledge, compliance, and functional status after hospitalization. Med Care. 1983;21(8):755–767.
- , , , , . Critical pathways intervention to reduce length of hospital stay. Am J Med. 2001;110(3):175–180.
- , , , , . The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
- , , , et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143(2):121–128.
- , , , , , . Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841.
- , , , , , . “I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care. Arch Intern Med. 2004;164(20):2223–2228.
- , . Lost in transition: challenges and opportunities for improving the quality of transitional care. Ann Intern Med. 2004;141(7):533–536.
- , , , . Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004;19(6):624–631.
- , , , et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–187.
- , , , et al. A Quality improvement intervention to facilitate the transition of older adults from three hospitals back to their homes. J Am Geriatr Soc. 57(9):1540–1546.
- , , , et al. Reduction of 30‐day postdischarge hospital readmission or emergency department (ED) visit rates in high‐risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211–218.
- , , , , . Interventions to reduce 30‐day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Available at: http://cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/AcuteInpatientPPS/Readmissions‐Reduction‐Program.html.Accessed September 5, 2012.
- Ontario Ministry of Health and Long‐Term Care. The Excellent Care for All Act, 2010. Available at: http://health.gov.on.ca/en/public/programs/ecfa/default.aspx/. Accessed February 28, 2013.
- Ontario Ministry of Health and Long‐Term Care; Baker GR, ed. Enhancing the Continuum of Care: Report of the Avoidable Hospitalization Advisory Panel, November 2011. Available at: http://www.health.gov.on.ca/en/common/ministry/publications/reports/baker_2011/baker_2011.pdf. Accessed August 8, 2012.
- , , , , , . Transitional care of older adults hospitalized with heart failure: a randomized, controlled trial [published correction appears in J Am Geriatr Soc. 2004;52(7):1228]. J Am Geriatr Soc. 2004;52(5):675–684.
- , , , . The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828.
- Society of Hospital Medicine. Project BOOST: Better Outcomes by Optimizing Safe Transitions. Available at: http://www.hospitalmedicine.org/BOOST/. Accessed October 31, 2012.
- The King's Fund; , , . Avoiding Hospital Admissions: Lessons From Evidence and Experience. Available at: http://www.kingsfund.org.uk/publications/articles/avoiding‐hospital‐admissions‐lessons‐evidence. Published October 28, 2010. Accessed September 4, 2012.
- Nielsen GA, Rutherford P, Taylor J, eds. How‐To Guide: Creating an Ideal Transition Home. Cambridge, MA: Institute for Healthcare Improvement; 2009. Available at: http://www.ihi.org or http://ah.cms‐plus.com/files/IHI_How_to_Guide_Creating_an_Ideal_Transition_Home.pdf. Accessed August 8, 2012.
- World Health Organization. Action on Patient Safety—High 5s. Available at: http://www.who.int/patientsafety/implementation/solutions/high5s/en/index.html. Accessed October 29, 2012.
- Safer Healthcare Now! Medication Reconciliation in Acute Care: Getting Started Kit. Available at: http://www.ismp‐canada.org/download/MedRec/Medrec_AC_English_GSK_V3.pdf. Accessed October 29, 2012.
- US Agency for Healthcare Research and Quality. PSNet: Patient‐safety primers, checklists. Available at: http://www.psnet.ahrq.gov/primer.aspx?primerID=14. Accessed November 1, 2012.
- , , , . Benefits of comprehensive inpatient education and discharge planning combined with outpatient support in elderly patients with congestive heart failure. Congest Heart Fail. 2005;11(6):315–321.
- , , , et al. Electronic versus dictated hospital discharge summaries: a randomized controlled trial. J Gen Intern Med. 2009;24(9):995–1001.
- , , , et al. Unplanned readmissions after hospital discharge among patients identified as being at high risk for readmission using a validated predictive algorithm. Open Med. 2011;5(2):e104–e111.
- , , , et al. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. CMAJ. 2010;182(6):551–557.
- . Will, ideas, and execution: their role in reducing adverse medication events. J Pediatr. 2005;147(6):727–728.
- , , , . Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units. Arch Intern Med. 2003;163(17):2014–2018.
- , , , et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166(5):565–571.
- , , , . Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2(5):314–323.
- , . Medication reconciliation in the hospital. Healthc Q. 2012;15:42–49.
- , , , , , . Comprehensive discharge planning for the hospitalized elderly: a randomized clinical trial. Ann Intern Med. 1994;120(12):999–1006.
- , , , et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163(1):83–90.
- , , . The effects of patient communication skills training on compliance. Arch Fam Med. 2000;9(1):57–64.
- , , , et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354–360.
- , , , , . Influence of a “discharge interview” on patient knowledge, compliance, and functional status after hospitalization. Med Care. 1983;21(8):755–767.
- , , , , . Critical pathways intervention to reduce length of hospital stay. Am J Med. 2001;110(3):175–180.
Copyright © 2013 Society of Hospital Medicine
New State Law Advances Malpractice Liability Reform
A new Oregon state law that creates a process to keep frivolous medical malpractice lawsuits out of the courts is a step in the right direction, says one hospitalist.
But uncertainty remains.
Jay Ham, MD, a hospitalist at Providence Newberg Medical Center in Newberg, Ore., says many hospitalists are still learning the ins and outs of the new law, which includes a definition for adverse healthcare incidents and establishes a procedure for providers and patients to discuss those incidents outside of court. The new law also provides for a mediation process.
The lawsuit mediation bill, signed into law earlier this month by Gov. John Kitzhaber, makes discussions between health care providers and patients "confidential and inadmissible with exception." The law does not preclude patients from later filing negligence claims.
"Allowing apologies and admission of guilt in this to be inadmissible at any later civil proceedings seems a nice touch," says Dr. Ham. "Deducting any awards given in the mediation process from civil court damages, while preventing knowledge of the initial award amount, also seems fair."
But there are areas of concern, he says. While most proceedings under the process "appear protected from disclosure if a civil case does go forward," there are caveats that might discourage some physicians from using the process, such as using discussions during the private process that contradict statements made in a court case. Also, there are questions about what types of cases will qualify for discussion outside the court system.
Still, the new law brings medical malpractice liability reform a bit closer, even if it doesn't reduce liability costs, Dr. Ham says. "Changing the cost of medicine doesn't need to be the defining impetus to implement reasonable [liability] reform," Dr. Ham says.
Read SHM's position statement on medical liability reform or visit our website for more information on medical malpractice liability.
A new Oregon state law that creates a process to keep frivolous medical malpractice lawsuits out of the courts is a step in the right direction, says one hospitalist.
But uncertainty remains.
Jay Ham, MD, a hospitalist at Providence Newberg Medical Center in Newberg, Ore., says many hospitalists are still learning the ins and outs of the new law, which includes a definition for adverse healthcare incidents and establishes a procedure for providers and patients to discuss those incidents outside of court. The new law also provides for a mediation process.
The lawsuit mediation bill, signed into law earlier this month by Gov. John Kitzhaber, makes discussions between health care providers and patients "confidential and inadmissible with exception." The law does not preclude patients from later filing negligence claims.
"Allowing apologies and admission of guilt in this to be inadmissible at any later civil proceedings seems a nice touch," says Dr. Ham. "Deducting any awards given in the mediation process from civil court damages, while preventing knowledge of the initial award amount, also seems fair."
But there are areas of concern, he says. While most proceedings under the process "appear protected from disclosure if a civil case does go forward," there are caveats that might discourage some physicians from using the process, such as using discussions during the private process that contradict statements made in a court case. Also, there are questions about what types of cases will qualify for discussion outside the court system.
Still, the new law brings medical malpractice liability reform a bit closer, even if it doesn't reduce liability costs, Dr. Ham says. "Changing the cost of medicine doesn't need to be the defining impetus to implement reasonable [liability] reform," Dr. Ham says.
Read SHM's position statement on medical liability reform or visit our website for more information on medical malpractice liability.
A new Oregon state law that creates a process to keep frivolous medical malpractice lawsuits out of the courts is a step in the right direction, says one hospitalist.
But uncertainty remains.
Jay Ham, MD, a hospitalist at Providence Newberg Medical Center in Newberg, Ore., says many hospitalists are still learning the ins and outs of the new law, which includes a definition for adverse healthcare incidents and establishes a procedure for providers and patients to discuss those incidents outside of court. The new law also provides for a mediation process.
The lawsuit mediation bill, signed into law earlier this month by Gov. John Kitzhaber, makes discussions between health care providers and patients "confidential and inadmissible with exception." The law does not preclude patients from later filing negligence claims.
"Allowing apologies and admission of guilt in this to be inadmissible at any later civil proceedings seems a nice touch," says Dr. Ham. "Deducting any awards given in the mediation process from civil court damages, while preventing knowledge of the initial award amount, also seems fair."
But there are areas of concern, he says. While most proceedings under the process "appear protected from disclosure if a civil case does go forward," there are caveats that might discourage some physicians from using the process, such as using discussions during the private process that contradict statements made in a court case. Also, there are questions about what types of cases will qualify for discussion outside the court system.
Still, the new law brings medical malpractice liability reform a bit closer, even if it doesn't reduce liability costs, Dr. Ham says. "Changing the cost of medicine doesn't need to be the defining impetus to implement reasonable [liability] reform," Dr. Ham says.
Read SHM's position statement on medical liability reform or visit our website for more information on medical malpractice liability.
In the Literature: Research You Need to Know
Clinical question: Does the use of steroids and/or antivirals improve recovery in patients with newly diagnosed Bell's palsy?
Background: The American Academy of Neurology's last recommendation in 2001 stated that steroids were probably effective and antivirals possibly effective. The current review and recommendations looked at additional studies published since 2000.
Study design: Systematic review of MEDLINE and Cochrane Database of Systematic Reviews data published since June 2000.
Setting: Prospective controlled studies from Germany, Sweden, Scotland, Italy, South Korea, Japan, and Bangladesh.
Synopsis: The authors identified nine studies that fulfilled inclusion criteria. Two of these studies examined treatment with steroids alone and were judged to have the lowest risk for bias. Both studies enrolled patients within three days of symptom onset, continued treatment for 10 days, and demonstrated a significant increase in the probability of complete recovery in patients randomized to steroids (NNT 6-8). Two high-quality studies were identified that looked at the addition of antivirals to steroids. Neither study showed a statistically significant benefit.
Of note, the studies did not quantify the risk of harm from steroid use in patients with comorbidities, such as diabetes. Thus, the authors concluded that in some patients, it would be reasonable to consider limiting steroid use.
Bottom line: For patients with new-onset Bell’s palsy, steroids increase the probability of recovery of facial nerve function. Patients offered antivirals should be counseled that a benefit from antivirals has not been established and, if there is a benefit, it is modest at best.
Citation: Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Does the use of steroids and/or antivirals improve recovery in patients with newly diagnosed Bell's palsy?
Background: The American Academy of Neurology's last recommendation in 2001 stated that steroids were probably effective and antivirals possibly effective. The current review and recommendations looked at additional studies published since 2000.
Study design: Systematic review of MEDLINE and Cochrane Database of Systematic Reviews data published since June 2000.
Setting: Prospective controlled studies from Germany, Sweden, Scotland, Italy, South Korea, Japan, and Bangladesh.
Synopsis: The authors identified nine studies that fulfilled inclusion criteria. Two of these studies examined treatment with steroids alone and were judged to have the lowest risk for bias. Both studies enrolled patients within three days of symptom onset, continued treatment for 10 days, and demonstrated a significant increase in the probability of complete recovery in patients randomized to steroids (NNT 6-8). Two high-quality studies were identified that looked at the addition of antivirals to steroids. Neither study showed a statistically significant benefit.
Of note, the studies did not quantify the risk of harm from steroid use in patients with comorbidities, such as diabetes. Thus, the authors concluded that in some patients, it would be reasonable to consider limiting steroid use.
Bottom line: For patients with new-onset Bell’s palsy, steroids increase the probability of recovery of facial nerve function. Patients offered antivirals should be counseled that a benefit from antivirals has not been established and, if there is a benefit, it is modest at best.
Citation: Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Does the use of steroids and/or antivirals improve recovery in patients with newly diagnosed Bell's palsy?
Background: The American Academy of Neurology's last recommendation in 2001 stated that steroids were probably effective and antivirals possibly effective. The current review and recommendations looked at additional studies published since 2000.
Study design: Systematic review of MEDLINE and Cochrane Database of Systematic Reviews data published since June 2000.
Setting: Prospective controlled studies from Germany, Sweden, Scotland, Italy, South Korea, Japan, and Bangladesh.
Synopsis: The authors identified nine studies that fulfilled inclusion criteria. Two of these studies examined treatment with steroids alone and were judged to have the lowest risk for bias. Both studies enrolled patients within three days of symptom onset, continued treatment for 10 days, and demonstrated a significant increase in the probability of complete recovery in patients randomized to steroids (NNT 6-8). Two high-quality studies were identified that looked at the addition of antivirals to steroids. Neither study showed a statistically significant benefit.
Of note, the studies did not quantify the risk of harm from steroid use in patients with comorbidities, such as diabetes. Thus, the authors concluded that in some patients, it would be reasonable to consider limiting steroid use.
Bottom line: For patients with new-onset Bell’s palsy, steroids increase the probability of recovery of facial nerve function. Patients offered antivirals should be counseled that a benefit from antivirals has not been established and, if there is a benefit, it is modest at best.
Citation: Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213.
Visit our website for more physician reviews of recent HM-relevant literature.
Small study finds miravirsen effective in HCV-1
The microRNA inhibitor miravirsen induced a dose-dependent drop in hepatitis C virus RNA levels, according to a phase IIa clinical trial reported online March 28 in the New England Journal of Medicine.
The treatment reduced HCV RNA to undetectable levels in five patients. And there was no evidence of the virus developing resistance to miravirsen during the 18-week study, said Dr. Harry L. A. Janssen of Erasmus MC University Hospital, Rotterdam, the Netherlands, and his associates (N. Engl. J. Med. 2013 March 28 [doi:10.1056/NEJMoa1209026]).
MicroRNAs are small, endogenous RNA that are thought to regulate a wide variety of biologic processes, including cell growth and differentiation, apoptosis, and modulation of the host response to viral infection. Miravirsen inhibits microRNA-122, which is expressed at high levels in the liver "and is essential to the stability and propagation of HCV RNA," the investigators explained.
In primate studies, miravirsen induced long-lasting HCV suppression, with no evidence of viral mutations conferring resistance to the agent. In phase I human studies, no adverse events were reported in healthy volunteers who took miravirsen.
For the phase IIa study, 36 patients with treatment-naive, genotype 1chronic HCV infection were followed at seven international sites. They were randomly assigned in a double-blind fashion to receive 3-mg, 5-mg, or 7-mg/kg doses of miravirsen, or a matching placebo, injected subcutaneously in five weekly doses over 29 days.
The study patients were allowed to initiate therapy with pegylated interferon and ribavirin after completing the course of miravirsen, at the discretion of the study investigators. Twelve of the 36 patients did so.
At all three dosages, miravirsen induced declines in HCV RNA levels from baseline for the study’s 14 weeks beyond the initial 4-week treatment period.
The reduction was dose dependent: The mean maximum decrease in HCV RNA levels was 1.2 log for patients receiving 3 mg/kg, 2.9 log for those receiving 5 mg/kg, and 3.0 log for those receiving 7 mg/kg. In contrast, patients receiving placebo showed a decline of only 0.4 log.
In five patients, miravirsen decreased HCV RNA to undetectable levels. That suggests that miravirsen eventually might be appropriate as monotherapy in some patients, Dr. Janssen and his colleagues said.
However, four of those five patients showed a rebound in viral levels at the conclusion of the study, which indicates that five weekly injections were not sufficient to induce a sustained virologic response.
"It is not clear whether regimens of miravirsen of longer duration could achieve a sustained virologic response; we are currently testing the effect of a 12-week regimen," the investigators noted.
Overall, HCV RNA levels rebounded after miravirsen was discontinued in nine patients who had not begun receiving interferon plus ribavirin. That included one patient given the 3-mg dose, five patients given the 5-mg dose, and three patients given the 7-mg dose of miravirsen.
The study subjects were assessed for resistance-associated mutations in HCV RNA at week 5 and at the time of viral rebound. No such mutations were found.
"There were no dose-limiting toxic effects or treatment discontinuations because of adverse events" or laboratory abnormalities, Dr. Janssen and his associates said.
No systemic allergic reactions occurred. Five patients given miravirsen and two patients given placebo reported transient, moderately severe adverse events that may not have been related to the study drug. Those included headache, otitis, flulike symptoms, and syncope.
There was one serious adverse event: One patient fell, lost consciousness, and injured a pelvic bone 9 weeks after receiving the last 7-mg dose of miravirsen.
Lab studies showed a sustained reduction in serum alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyl transpeptidase levels with miravirsen. There were no clinically significant changes in hemoglobin levels, total white-cell counts, prothrombin time, or activated partial thromboplastin time.
A "side benefit" of the treatment was a prolonged decrease in serum total cholesterol, which was expected because inhibition of microRNA-122 is known to disrupt cholesterol homeostasis.
The findings indicate that miravirsen should be considered a potential treatment for HCV infection, the study authors said. The injections can be given as infrequently as once a month, which encourages patient compliance. And unlike protease inhibitors, miravirsen "is not a substrate for cytochrome P-450 and is therefore not expected to have significant drug-drug interactions," the researchers said.
They added that antisense therapy "may also be relevant for diseases other than chronic HCV infection," including nonalcoholic fatty liver disease. Cancer, cardiovascular diseases, and autoimmune disorders also may respond to a strategy of inhibiting microRNAs that are associated with those diseases.
Santaris Pharma funded the study. Dr. Janssen and his associates reported ties to numerous industry sources.
The findings by Janssen et al. show that "antagonizing microRNA-122, alone or in conjunction with other antiviral agents already approved or in development, could provide curative therapy for a large proportion of patients infected with all HCV strains without danger of drug resistance," said Dr. Judy Lieberman and Peter Sarnow, Ph.D.
The strategy "could also shorten the treatment time to achieve viral elimination, reduce the rate of relapse, and offer the possibility of interferon-free regimens," they noted.
Further clinical trials are needed to determine whether those possibilities are realized. Trials also are crucial to definitively establish whether inhibition of microRNA-122 in particular is safe in the long term, because microRNA-122 suppresses hepatocellular carcinoma, Dr. Lieberman and Dr. Sarnow noted.
Dr. Judy Lieberman is in the program in cellular and molecular medicine at Boston Children’s Hospital and in the department of pediatrics at Harvard Medical School, Boston. Dr. Sarnow is in the department of microbiology and immunology at Stanford (Calif.) University. Dr. Lieberman reported ties to Alnylam Pharmaceuticals. These remarks were taken from their editorial accompanying Dr. Janssen’s report (N. Engl. J. Med. 2013 March 28 [doi:10.1056/NEJMe1301348]).
The findings by Janssen et al. show that "antagonizing microRNA-122, alone or in conjunction with other antiviral agents already approved or in development, could provide curative therapy for a large proportion of patients infected with all HCV strains without danger of drug resistance," said Dr. Judy Lieberman and Peter Sarnow, Ph.D.
The strategy "could also shorten the treatment time to achieve viral elimination, reduce the rate of relapse, and offer the possibility of interferon-free regimens," they noted.
Further clinical trials are needed to determine whether those possibilities are realized. Trials also are crucial to definitively establish whether inhibition of microRNA-122 in particular is safe in the long term, because microRNA-122 suppresses hepatocellular carcinoma, Dr. Lieberman and Dr. Sarnow noted.
Dr. Judy Lieberman is in the program in cellular and molecular medicine at Boston Children’s Hospital and in the department of pediatrics at Harvard Medical School, Boston. Dr. Sarnow is in the department of microbiology and immunology at Stanford (Calif.) University. Dr. Lieberman reported ties to Alnylam Pharmaceuticals. These remarks were taken from their editorial accompanying Dr. Janssen’s report (N. Engl. J. Med. 2013 March 28 [doi:10.1056/NEJMe1301348]).
The findings by Janssen et al. show that "antagonizing microRNA-122, alone or in conjunction with other antiviral agents already approved or in development, could provide curative therapy for a large proportion of patients infected with all HCV strains without danger of drug resistance," said Dr. Judy Lieberman and Peter Sarnow, Ph.D.
The strategy "could also shorten the treatment time to achieve viral elimination, reduce the rate of relapse, and offer the possibility of interferon-free regimens," they noted.
Further clinical trials are needed to determine whether those possibilities are realized. Trials also are crucial to definitively establish whether inhibition of microRNA-122 in particular is safe in the long term, because microRNA-122 suppresses hepatocellular carcinoma, Dr. Lieberman and Dr. Sarnow noted.
Dr. Judy Lieberman is in the program in cellular and molecular medicine at Boston Children’s Hospital and in the department of pediatrics at Harvard Medical School, Boston. Dr. Sarnow is in the department of microbiology and immunology at Stanford (Calif.) University. Dr. Lieberman reported ties to Alnylam Pharmaceuticals. These remarks were taken from their editorial accompanying Dr. Janssen’s report (N. Engl. J. Med. 2013 March 28 [doi:10.1056/NEJMe1301348]).
The microRNA inhibitor miravirsen induced a dose-dependent drop in hepatitis C virus RNA levels, according to a phase IIa clinical trial reported online March 28 in the New England Journal of Medicine.
The treatment reduced HCV RNA to undetectable levels in five patients. And there was no evidence of the virus developing resistance to miravirsen during the 18-week study, said Dr. Harry L. A. Janssen of Erasmus MC University Hospital, Rotterdam, the Netherlands, and his associates (N. Engl. J. Med. 2013 March 28 [doi:10.1056/NEJMoa1209026]).
MicroRNAs are small, endogenous RNA that are thought to regulate a wide variety of biologic processes, including cell growth and differentiation, apoptosis, and modulation of the host response to viral infection. Miravirsen inhibits microRNA-122, which is expressed at high levels in the liver "and is essential to the stability and propagation of HCV RNA," the investigators explained.
In primate studies, miravirsen induced long-lasting HCV suppression, with no evidence of viral mutations conferring resistance to the agent. In phase I human studies, no adverse events were reported in healthy volunteers who took miravirsen.
For the phase IIa study, 36 patients with treatment-naive, genotype 1chronic HCV infection were followed at seven international sites. They were randomly assigned in a double-blind fashion to receive 3-mg, 5-mg, or 7-mg/kg doses of miravirsen, or a matching placebo, injected subcutaneously in five weekly doses over 29 days.
The study patients were allowed to initiate therapy with pegylated interferon and ribavirin after completing the course of miravirsen, at the discretion of the study investigators. Twelve of the 36 patients did so.
At all three dosages, miravirsen induced declines in HCV RNA levels from baseline for the study’s 14 weeks beyond the initial 4-week treatment period.
The reduction was dose dependent: The mean maximum decrease in HCV RNA levels was 1.2 log for patients receiving 3 mg/kg, 2.9 log for those receiving 5 mg/kg, and 3.0 log for those receiving 7 mg/kg. In contrast, patients receiving placebo showed a decline of only 0.4 log.
In five patients, miravirsen decreased HCV RNA to undetectable levels. That suggests that miravirsen eventually might be appropriate as monotherapy in some patients, Dr. Janssen and his colleagues said.
However, four of those five patients showed a rebound in viral levels at the conclusion of the study, which indicates that five weekly injections were not sufficient to induce a sustained virologic response.
"It is not clear whether regimens of miravirsen of longer duration could achieve a sustained virologic response; we are currently testing the effect of a 12-week regimen," the investigators noted.
Overall, HCV RNA levels rebounded after miravirsen was discontinued in nine patients who had not begun receiving interferon plus ribavirin. That included one patient given the 3-mg dose, five patients given the 5-mg dose, and three patients given the 7-mg dose of miravirsen.
The study subjects were assessed for resistance-associated mutations in HCV RNA at week 5 and at the time of viral rebound. No such mutations were found.
"There were no dose-limiting toxic effects or treatment discontinuations because of adverse events" or laboratory abnormalities, Dr. Janssen and his associates said.
No systemic allergic reactions occurred. Five patients given miravirsen and two patients given placebo reported transient, moderately severe adverse events that may not have been related to the study drug. Those included headache, otitis, flulike symptoms, and syncope.
There was one serious adverse event: One patient fell, lost consciousness, and injured a pelvic bone 9 weeks after receiving the last 7-mg dose of miravirsen.
Lab studies showed a sustained reduction in serum alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyl transpeptidase levels with miravirsen. There were no clinically significant changes in hemoglobin levels, total white-cell counts, prothrombin time, or activated partial thromboplastin time.
A "side benefit" of the treatment was a prolonged decrease in serum total cholesterol, which was expected because inhibition of microRNA-122 is known to disrupt cholesterol homeostasis.
The findings indicate that miravirsen should be considered a potential treatment for HCV infection, the study authors said. The injections can be given as infrequently as once a month, which encourages patient compliance. And unlike protease inhibitors, miravirsen "is not a substrate for cytochrome P-450 and is therefore not expected to have significant drug-drug interactions," the researchers said.
They added that antisense therapy "may also be relevant for diseases other than chronic HCV infection," including nonalcoholic fatty liver disease. Cancer, cardiovascular diseases, and autoimmune disorders also may respond to a strategy of inhibiting microRNAs that are associated with those diseases.
Santaris Pharma funded the study. Dr. Janssen and his associates reported ties to numerous industry sources.
The microRNA inhibitor miravirsen induced a dose-dependent drop in hepatitis C virus RNA levels, according to a phase IIa clinical trial reported online March 28 in the New England Journal of Medicine.
The treatment reduced HCV RNA to undetectable levels in five patients. And there was no evidence of the virus developing resistance to miravirsen during the 18-week study, said Dr. Harry L. A. Janssen of Erasmus MC University Hospital, Rotterdam, the Netherlands, and his associates (N. Engl. J. Med. 2013 March 28 [doi:10.1056/NEJMoa1209026]).
MicroRNAs are small, endogenous RNA that are thought to regulate a wide variety of biologic processes, including cell growth and differentiation, apoptosis, and modulation of the host response to viral infection. Miravirsen inhibits microRNA-122, which is expressed at high levels in the liver "and is essential to the stability and propagation of HCV RNA," the investigators explained.
In primate studies, miravirsen induced long-lasting HCV suppression, with no evidence of viral mutations conferring resistance to the agent. In phase I human studies, no adverse events were reported in healthy volunteers who took miravirsen.
For the phase IIa study, 36 patients with treatment-naive, genotype 1chronic HCV infection were followed at seven international sites. They were randomly assigned in a double-blind fashion to receive 3-mg, 5-mg, or 7-mg/kg doses of miravirsen, or a matching placebo, injected subcutaneously in five weekly doses over 29 days.
The study patients were allowed to initiate therapy with pegylated interferon and ribavirin after completing the course of miravirsen, at the discretion of the study investigators. Twelve of the 36 patients did so.
At all three dosages, miravirsen induced declines in HCV RNA levels from baseline for the study’s 14 weeks beyond the initial 4-week treatment period.
The reduction was dose dependent: The mean maximum decrease in HCV RNA levels was 1.2 log for patients receiving 3 mg/kg, 2.9 log for those receiving 5 mg/kg, and 3.0 log for those receiving 7 mg/kg. In contrast, patients receiving placebo showed a decline of only 0.4 log.
In five patients, miravirsen decreased HCV RNA to undetectable levels. That suggests that miravirsen eventually might be appropriate as monotherapy in some patients, Dr. Janssen and his colleagues said.
However, four of those five patients showed a rebound in viral levels at the conclusion of the study, which indicates that five weekly injections were not sufficient to induce a sustained virologic response.
"It is not clear whether regimens of miravirsen of longer duration could achieve a sustained virologic response; we are currently testing the effect of a 12-week regimen," the investigators noted.
Overall, HCV RNA levels rebounded after miravirsen was discontinued in nine patients who had not begun receiving interferon plus ribavirin. That included one patient given the 3-mg dose, five patients given the 5-mg dose, and three patients given the 7-mg dose of miravirsen.
The study subjects were assessed for resistance-associated mutations in HCV RNA at week 5 and at the time of viral rebound. No such mutations were found.
"There were no dose-limiting toxic effects or treatment discontinuations because of adverse events" or laboratory abnormalities, Dr. Janssen and his associates said.
No systemic allergic reactions occurred. Five patients given miravirsen and two patients given placebo reported transient, moderately severe adverse events that may not have been related to the study drug. Those included headache, otitis, flulike symptoms, and syncope.
There was one serious adverse event: One patient fell, lost consciousness, and injured a pelvic bone 9 weeks after receiving the last 7-mg dose of miravirsen.
Lab studies showed a sustained reduction in serum alanine aminotransferase, aspartate aminotransferase, and gamma-glutamyl transpeptidase levels with miravirsen. There were no clinically significant changes in hemoglobin levels, total white-cell counts, prothrombin time, or activated partial thromboplastin time.
A "side benefit" of the treatment was a prolonged decrease in serum total cholesterol, which was expected because inhibition of microRNA-122 is known to disrupt cholesterol homeostasis.
The findings indicate that miravirsen should be considered a potential treatment for HCV infection, the study authors said. The injections can be given as infrequently as once a month, which encourages patient compliance. And unlike protease inhibitors, miravirsen "is not a substrate for cytochrome P-450 and is therefore not expected to have significant drug-drug interactions," the researchers said.
They added that antisense therapy "may also be relevant for diseases other than chronic HCV infection," including nonalcoholic fatty liver disease. Cancer, cardiovascular diseases, and autoimmune disorders also may respond to a strategy of inhibiting microRNAs that are associated with those diseases.
Santaris Pharma funded the study. Dr. Janssen and his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Miravirsen cut HCV RNA levels 1.2 log at the 3-mg/kg dose, 2.9 log at the 5-mg/kg dose, and 3.0 log at the 7-mg/kg dose.
Data Source: An18-week international phase IIa clinical trial assessing the safety and activity of miravirsen in 36 patients with treatment-naive chronic HCV infection.
Disclosures: Santaris Pharma funded the study. Dr. Janssen and his associates reported ties to numerous industry sources.
Bariatric surgery advancement spurs guideline update
Weight loss surgery patients should get routine copper supplements along with other vitamins and minerals, according to newly updated bariatric surgery guidelines from the American Association of Clinical Endocrinologists, the Obesity Society, and the American Society for Metabolic and Bariatric Surgery.
The groups call for 2 mg/day to offset the potential for surgery to cause a deficiency. Although routine copper screening isn’t necessary after the procedure, copper levels should be assessed and treated as needed in patients with anemia, neutropenia, myeloneuropathy, and impaired wound healing.
The copper recommendations are new since the guidelines were last published in 2008. Other recommendations – there are 74 in all – have been revised to incorporate new advances in weight loss surgery and an improved evidence base. Changes are pointed out where they’ve been made, and the level of evidence cited for each assertion. Pre- and postoperative bariatric surgery checklists have been added as well, to help avoid errors.
"This is actually a very unique collaboration among the internists represented by the endocrinologists and the obesity people and the surgeons. We actually agreed on all these things. The main intent is to assist with clinical decision making," including selecting patients and procedures and perioperative management, said lead author Dr. Jeffrey Mechanick, president-elect of the American Association of Clinical Endocrinologists and director of metabolic support at the Mt. Sinai School of Medicine in New York.
"We scrutinized every recommendation one by one in the context of the new data. In many cases the recommendations changed," he said in an interview.
Another new recommendation is for patients to be followed by their primary care physicians and screened for cancer prior to surgery, as appropriate for age and risk. Dr. Mechanick and his colleagues have also given more attention to consent, behavioral, and psychiatric issues as well as weight loss surgery in patients with type 2 diabetes.
There’s more information on sleeve gastrectomy, as well. Considered experimental in 2008, it’s now "approved and being done more widely. There are some very nice data about its metabolic effects, independent from just the weight loss effect, effects on glycemic control, and cardiovascular risk. It was very important to devote a fair amount of time" to the procedure, he said.
The guidelines note that "sleeve gastrectomy has demonstrated benefits comparable to other bariatric procedures. ... A national risk-adjusted database positions [it] between the laparoscopic adjustable gastric band and laparoscopic Roux-en-Y gastric bypass in terms of weight loss, co-morbidity resolution, and complications."
"We [also] addressed two issues which were quite controversial, and are still rather unsettled. The first is the use of the lap band for mild obesity. The second is the use of these weight loss procedures specifically for patients with type 2 diabetes for glycemic control. Since 2008, there’ve been a lot more data" about the issues, he said, just as there’ve been more data about the need for copper supplementation.
As in 2008, the guidelines do not recommend bariatric surgery solely for glycemic control. "We still don’t have an absolute indication for ‘diabetes surgery,’ but we do recognize the existence of the salutary effects on glycemic control when these procedures are done for weight loss. It was important for the reader to be exposed to this information," Dr. Mechanick said.
Regarding surgery in the mildly obese, the guidelines note that patients with a body mass index of 30-34.9 kg/m2 with diabetes or metabolic syndrome "may also be offered a bariatric procedure, although current evidence is limited by the number of subjects studied and lack of long-term data demonstrating net benefit."
The guidelines will be published in the March/April 2013 issue of Endocrine Practice and March 2013 issue of Surgery for Obesity and Related Diseases.
Dr. Mechanick disclosed compensation from Abbott Nutrition for lectures and program development.
From preoperative evaluation through bariatric
surgery and onward through long-term postoperative health management, weight
loss surgery and the medical care associated with it is, obligatorily, a
thoroughly interdisciplinary effort. Endocrinologists and internists on the
bariatrics team spearhead lifestyle management, medical weight loss, and
long-term postoperative care and efforts to maintain durable weight loss.
Surgeons, endocrinologists, and internists work together to select patients
appropriate for bariatric surgery, to choose the weight-loss surgery best
suited to each individual patient, and to provide the proper preoperative
evaluation. Surgeons perform the appropriate bariatric operation and oversee
immediate postoperative and short-term perioperative care, and, frequently in
concert with gastroenterologists, internists, and endocrinologists, manage
complications that can result from bariatric surgery. Finally, long-term
continuity of medical care and durable maintenance of weight loss is again
directed by the endocrinologist and internist.
Thus, given that the entire bariatric care schema is
such an interdisciplinary effort, clinical practice guidelines for the
management of bariatric surgical patients must also be the product of an
analogous interdisciplinary effort. It is with this aim and in this spirit that
the American Association of Clinical Endocrinologists (AACE), The Obesity
Society (TOS), and American Society for Metabolic and Bariatric Surgery (AAMBS)
published their initial Medical Guidelines for Clinical Practice for the Perioperative
Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery
Patient in 2008. The same cooperating societies have just published their
sequel with numerous substantive additions, changes, and refinements. The
Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and
Nonsurgical Support of the Bariatric Surgery Patient – 2013 Update: Cosponsored
by American Association of Clinical Endocrinologists, The Obesity Society, and
American Society for Metabolic & Bariatric Surgery was published jointly in
the March issue of Surgery for Obesity and Related Disease, and in the
March/April issue of Endocrine Practice.
Clearly, much has changed in the bariatric landscape
in the intervening half-decade. Laparoscopic gastric band surgery has declined,
while sleeve gastrectomy has gained traction as a restrictive bariatric
operation with more robust weight loss and glycemic effects. The
increasingly recognized impact of Roux-en-Y gastric bypass surgery not only on
weight loss, but also on glycemic control and other endocrinologic endpoints
has prompted studies to determine if such benefits might also result from
restrictive-only bariatric surgeries such as sleeve gastrectomy, and initial
results appear encouraging. The arrival of more and higher-quality data with
longer-term follow up of a greater variety of endpoints has led to the ability
of these updated guidelines to provide an increasing number of more specific,
data-driven recommendations related to the broader spectrum of bariatric
surgical procedures and anatomies managed by clinicians today. They cover every
aspect of the bariatric surgical patient, from preoperative evaluation through
surgery, to postoperative management, all with more solidly outcomes-based
recommendations from over 400 references, with user-friendly and more
error-proof preoperative and postoperative care checklists, while still
arriving at such expert guidelines through interdisciplinary study and
agreement in this timely update.
John A. Martin, M.D., is associate
professor of medicine and surgery and director of endoscopy, Northwestern
University Feinberg School of Medicine, Chicago.
From preoperative evaluation through bariatric
surgery and onward through long-term postoperative health management, weight
loss surgery and the medical care associated with it is, obligatorily, a
thoroughly interdisciplinary effort. Endocrinologists and internists on the
bariatrics team spearhead lifestyle management, medical weight loss, and
long-term postoperative care and efforts to maintain durable weight loss.
Surgeons, endocrinologists, and internists work together to select patients
appropriate for bariatric surgery, to choose the weight-loss surgery best
suited to each individual patient, and to provide the proper preoperative
evaluation. Surgeons perform the appropriate bariatric operation and oversee
immediate postoperative and short-term perioperative care, and, frequently in
concert with gastroenterologists, internists, and endocrinologists, manage
complications that can result from bariatric surgery. Finally, long-term
continuity of medical care and durable maintenance of weight loss is again
directed by the endocrinologist and internist.
Thus, given that the entire bariatric care schema is
such an interdisciplinary effort, clinical practice guidelines for the
management of bariatric surgical patients must also be the product of an
analogous interdisciplinary effort. It is with this aim and in this spirit that
the American Association of Clinical Endocrinologists (AACE), The Obesity
Society (TOS), and American Society for Metabolic and Bariatric Surgery (AAMBS)
published their initial Medical Guidelines for Clinical Practice for the Perioperative
Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery
Patient in 2008. The same cooperating societies have just published their
sequel with numerous substantive additions, changes, and refinements. The
Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and
Nonsurgical Support of the Bariatric Surgery Patient – 2013 Update: Cosponsored
by American Association of Clinical Endocrinologists, The Obesity Society, and
American Society for Metabolic & Bariatric Surgery was published jointly in
the March issue of Surgery for Obesity and Related Disease, and in the
March/April issue of Endocrine Practice.
Clearly, much has changed in the bariatric landscape
in the intervening half-decade. Laparoscopic gastric band surgery has declined,
while sleeve gastrectomy has gained traction as a restrictive bariatric
operation with more robust weight loss and glycemic effects. The
increasingly recognized impact of Roux-en-Y gastric bypass surgery not only on
weight loss, but also on glycemic control and other endocrinologic endpoints
has prompted studies to determine if such benefits might also result from
restrictive-only bariatric surgeries such as sleeve gastrectomy, and initial
results appear encouraging. The arrival of more and higher-quality data with
longer-term follow up of a greater variety of endpoints has led to the ability
of these updated guidelines to provide an increasing number of more specific,
data-driven recommendations related to the broader spectrum of bariatric
surgical procedures and anatomies managed by clinicians today. They cover every
aspect of the bariatric surgical patient, from preoperative evaluation through
surgery, to postoperative management, all with more solidly outcomes-based
recommendations from over 400 references, with user-friendly and more
error-proof preoperative and postoperative care checklists, while still
arriving at such expert guidelines through interdisciplinary study and
agreement in this timely update.
John A. Martin, M.D., is associate
professor of medicine and surgery and director of endoscopy, Northwestern
University Feinberg School of Medicine, Chicago.
From preoperative evaluation through bariatric
surgery and onward through long-term postoperative health management, weight
loss surgery and the medical care associated with it is, obligatorily, a
thoroughly interdisciplinary effort. Endocrinologists and internists on the
bariatrics team spearhead lifestyle management, medical weight loss, and
long-term postoperative care and efforts to maintain durable weight loss.
Surgeons, endocrinologists, and internists work together to select patients
appropriate for bariatric surgery, to choose the weight-loss surgery best
suited to each individual patient, and to provide the proper preoperative
evaluation. Surgeons perform the appropriate bariatric operation and oversee
immediate postoperative and short-term perioperative care, and, frequently in
concert with gastroenterologists, internists, and endocrinologists, manage
complications that can result from bariatric surgery. Finally, long-term
continuity of medical care and durable maintenance of weight loss is again
directed by the endocrinologist and internist.
Thus, given that the entire bariatric care schema is
such an interdisciplinary effort, clinical practice guidelines for the
management of bariatric surgical patients must also be the product of an
analogous interdisciplinary effort. It is with this aim and in this spirit that
the American Association of Clinical Endocrinologists (AACE), The Obesity
Society (TOS), and American Society for Metabolic and Bariatric Surgery (AAMBS)
published their initial Medical Guidelines for Clinical Practice for the Perioperative
Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery
Patient in 2008. The same cooperating societies have just published their
sequel with numerous substantive additions, changes, and refinements. The
Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and
Nonsurgical Support of the Bariatric Surgery Patient – 2013 Update: Cosponsored
by American Association of Clinical Endocrinologists, The Obesity Society, and
American Society for Metabolic & Bariatric Surgery was published jointly in
the March issue of Surgery for Obesity and Related Disease, and in the
March/April issue of Endocrine Practice.
Clearly, much has changed in the bariatric landscape
in the intervening half-decade. Laparoscopic gastric band surgery has declined,
while sleeve gastrectomy has gained traction as a restrictive bariatric
operation with more robust weight loss and glycemic effects. The
increasingly recognized impact of Roux-en-Y gastric bypass surgery not only on
weight loss, but also on glycemic control and other endocrinologic endpoints
has prompted studies to determine if such benefits might also result from
restrictive-only bariatric surgeries such as sleeve gastrectomy, and initial
results appear encouraging. The arrival of more and higher-quality data with
longer-term follow up of a greater variety of endpoints has led to the ability
of these updated guidelines to provide an increasing number of more specific,
data-driven recommendations related to the broader spectrum of bariatric
surgical procedures and anatomies managed by clinicians today. They cover every
aspect of the bariatric surgical patient, from preoperative evaluation through
surgery, to postoperative management, all with more solidly outcomes-based
recommendations from over 400 references, with user-friendly and more
error-proof preoperative and postoperative care checklists, while still
arriving at such expert guidelines through interdisciplinary study and
agreement in this timely update.
John A. Martin, M.D., is associate
professor of medicine and surgery and director of endoscopy, Northwestern
University Feinberg School of Medicine, Chicago.
Weight loss surgery patients should get routine copper supplements along with other vitamins and minerals, according to newly updated bariatric surgery guidelines from the American Association of Clinical Endocrinologists, the Obesity Society, and the American Society for Metabolic and Bariatric Surgery.
The groups call for 2 mg/day to offset the potential for surgery to cause a deficiency. Although routine copper screening isn’t necessary after the procedure, copper levels should be assessed and treated as needed in patients with anemia, neutropenia, myeloneuropathy, and impaired wound healing.
The copper recommendations are new since the guidelines were last published in 2008. Other recommendations – there are 74 in all – have been revised to incorporate new advances in weight loss surgery and an improved evidence base. Changes are pointed out where they’ve been made, and the level of evidence cited for each assertion. Pre- and postoperative bariatric surgery checklists have been added as well, to help avoid errors.
"This is actually a very unique collaboration among the internists represented by the endocrinologists and the obesity people and the surgeons. We actually agreed on all these things. The main intent is to assist with clinical decision making," including selecting patients and procedures and perioperative management, said lead author Dr. Jeffrey Mechanick, president-elect of the American Association of Clinical Endocrinologists and director of metabolic support at the Mt. Sinai School of Medicine in New York.
"We scrutinized every recommendation one by one in the context of the new data. In many cases the recommendations changed," he said in an interview.
Another new recommendation is for patients to be followed by their primary care physicians and screened for cancer prior to surgery, as appropriate for age and risk. Dr. Mechanick and his colleagues have also given more attention to consent, behavioral, and psychiatric issues as well as weight loss surgery in patients with type 2 diabetes.
There’s more information on sleeve gastrectomy, as well. Considered experimental in 2008, it’s now "approved and being done more widely. There are some very nice data about its metabolic effects, independent from just the weight loss effect, effects on glycemic control, and cardiovascular risk. It was very important to devote a fair amount of time" to the procedure, he said.
The guidelines note that "sleeve gastrectomy has demonstrated benefits comparable to other bariatric procedures. ... A national risk-adjusted database positions [it] between the laparoscopic adjustable gastric band and laparoscopic Roux-en-Y gastric bypass in terms of weight loss, co-morbidity resolution, and complications."
"We [also] addressed two issues which were quite controversial, and are still rather unsettled. The first is the use of the lap band for mild obesity. The second is the use of these weight loss procedures specifically for patients with type 2 diabetes for glycemic control. Since 2008, there’ve been a lot more data" about the issues, he said, just as there’ve been more data about the need for copper supplementation.
As in 2008, the guidelines do not recommend bariatric surgery solely for glycemic control. "We still don’t have an absolute indication for ‘diabetes surgery,’ but we do recognize the existence of the salutary effects on glycemic control when these procedures are done for weight loss. It was important for the reader to be exposed to this information," Dr. Mechanick said.
Regarding surgery in the mildly obese, the guidelines note that patients with a body mass index of 30-34.9 kg/m2 with diabetes or metabolic syndrome "may also be offered a bariatric procedure, although current evidence is limited by the number of subjects studied and lack of long-term data demonstrating net benefit."
The guidelines will be published in the March/April 2013 issue of Endocrine Practice and March 2013 issue of Surgery for Obesity and Related Diseases.
Dr. Mechanick disclosed compensation from Abbott Nutrition for lectures and program development.
Weight loss surgery patients should get routine copper supplements along with other vitamins and minerals, according to newly updated bariatric surgery guidelines from the American Association of Clinical Endocrinologists, the Obesity Society, and the American Society for Metabolic and Bariatric Surgery.
The groups call for 2 mg/day to offset the potential for surgery to cause a deficiency. Although routine copper screening isn’t necessary after the procedure, copper levels should be assessed and treated as needed in patients with anemia, neutropenia, myeloneuropathy, and impaired wound healing.
The copper recommendations are new since the guidelines were last published in 2008. Other recommendations – there are 74 in all – have been revised to incorporate new advances in weight loss surgery and an improved evidence base. Changes are pointed out where they’ve been made, and the level of evidence cited for each assertion. Pre- and postoperative bariatric surgery checklists have been added as well, to help avoid errors.
"This is actually a very unique collaboration among the internists represented by the endocrinologists and the obesity people and the surgeons. We actually agreed on all these things. The main intent is to assist with clinical decision making," including selecting patients and procedures and perioperative management, said lead author Dr. Jeffrey Mechanick, president-elect of the American Association of Clinical Endocrinologists and director of metabolic support at the Mt. Sinai School of Medicine in New York.
"We scrutinized every recommendation one by one in the context of the new data. In many cases the recommendations changed," he said in an interview.
Another new recommendation is for patients to be followed by their primary care physicians and screened for cancer prior to surgery, as appropriate for age and risk. Dr. Mechanick and his colleagues have also given more attention to consent, behavioral, and psychiatric issues as well as weight loss surgery in patients with type 2 diabetes.
There’s more information on sleeve gastrectomy, as well. Considered experimental in 2008, it’s now "approved and being done more widely. There are some very nice data about its metabolic effects, independent from just the weight loss effect, effects on glycemic control, and cardiovascular risk. It was very important to devote a fair amount of time" to the procedure, he said.
The guidelines note that "sleeve gastrectomy has demonstrated benefits comparable to other bariatric procedures. ... A national risk-adjusted database positions [it] between the laparoscopic adjustable gastric band and laparoscopic Roux-en-Y gastric bypass in terms of weight loss, co-morbidity resolution, and complications."
"We [also] addressed two issues which were quite controversial, and are still rather unsettled. The first is the use of the lap band for mild obesity. The second is the use of these weight loss procedures specifically for patients with type 2 diabetes for glycemic control. Since 2008, there’ve been a lot more data" about the issues, he said, just as there’ve been more data about the need for copper supplementation.
As in 2008, the guidelines do not recommend bariatric surgery solely for glycemic control. "We still don’t have an absolute indication for ‘diabetes surgery,’ but we do recognize the existence of the salutary effects on glycemic control when these procedures are done for weight loss. It was important for the reader to be exposed to this information," Dr. Mechanick said.
Regarding surgery in the mildly obese, the guidelines note that patients with a body mass index of 30-34.9 kg/m2 with diabetes or metabolic syndrome "may also be offered a bariatric procedure, although current evidence is limited by the number of subjects studied and lack of long-term data demonstrating net benefit."
The guidelines will be published in the March/April 2013 issue of Endocrine Practice and March 2013 issue of Surgery for Obesity and Related Diseases.
Dr. Mechanick disclosed compensation from Abbott Nutrition for lectures and program development.
Veith's Viewpoint: Good doctor, good medical care: priceless
Today all we hear about is the high cost of U.S. health care, and how for our country to survive economically, it must cut doctors’ payments and spend less for health care, drugs, and medical devices. Certainly there is waste in the system and some physicians perform procedures that are unnecessary. But when one really needs good medical care and a good doctor, they are priceless.

Two recent dramatic examples in my own family made this clear to me. In one, a loved one developed a staphylococcal infection at an epidural injection site. Within 24 hours, she was desperately ill with a temperature of 104º, shaking chills, and excruciating back pain. She was expeditiously admitted to the ICU of an excellent community hospital and started on massive IV antibiotics. She underwent an urgent MRI, which revealed a paravertebral phlegmon. Blood cultures grew Staphyloccus aureus. She was seen repeatedly by her intensive care specialist and her orthopedic surgeon. When she did not improve, her orthopedic surgeon obtained a second MRI 36 hours after the first one. This, unlike the first, revealed an epidural collection, and she promptly underwent a three segment laminectomy to drain the abscess.
Although she required a second drainage procedure and careful adjustment of her IV antibiotics, she survived without any neurologic or cardiac damage. During her complicated and onerous 2½ weeks in the ICU, she was seen 2-3 times a day by both her intensivist and orthopedic surgeon, as well as by a variety of other specialists when they were needed. All made essential contributions to her recovery from this life-threatening illness. The skill and commitment of all these doctors, especially the orthopedic surgeon and the intensivist, made the difference in saving this young life. The care she received was priceless.
The second instance involved the cure of a life-threatening ventricular arrhythmia in a relatively young, productive individual. Although asymptomatic, this individual was having over 40,000 ventricular premature beats with runs of ventricular tachycardia in a 24-hour period. A highly skilled team of super-specialists in cardiac radiofrequency ablation procedures successfully eliminated the focus of these arrhythmias. However, the procedure was difficult and complicated. It took 7 hours and required both left and right heart catheterizations and crossing of the atrial septum and the aortic valve. Despite this, the individual was back at his usual work in 3 days, completely arrhythmia free. He has required no further subsequent treatment.
In both instances, the good care required by these skilled specialists and their colleagues was complicated and demanding but successful. It required enormous expertise and, more importantly, the commitment and dedication of those providing it. Sure, this care was expensive, but it was worth every penny. It was priceless, because the outcomes were life-saving and perfect. These priceless treatments restored two young, productive people to full health.
So in this rush to cut health care costs, let us remember that we in the United States have the best physicians and surgeons, the best hospitals, the best drugs, and medical devices in the world. Let us preserve these assets and not kill the goose that is laying the golden eggs of health care. Let us preserve and reward the priceless individuals and priceless care that can allow many of us in the United States to lead better, more productive lives than we otherwise would.
Dr. Veith is Professor of Surgery at New York University Medical Center and the Cleveland Clinic. He is an associate medical editor for Vascular Specialist.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or Publisher.
This months "Veith’s Viewpoint" tells two stories of patients whose lives were saved by doctors acting individually and together using the best that American medicine can offer. It brings to mind Theodore Roosevelt’s apt comment that "no one cares how much you know until they know how much you care." Nowhere did questions of work hours, EMRs, ASOs, or the subject of our "health care system" come up. Just doctors committed to patients. Over the last two decades, as the cost of heath care has made our country more insolvent and consumed more of our GDP, our so-called "system" has become increasingly fragmented. And less and less universal. What once bore at least some semblance of a system is now little more than a tattered patchwork composed of unfettered for-profit insurance companies, an under-funded Medicaid, an over-committed Medicare, a Veterans Administration system that is both vitally essential and full of redundancy, city and county hospitals that are bankrupting their communities, a workman’s compensation program that sets workers against employers, and not-for-profit hospitals that are by most important criteria no different than the for-profit ones. And the hospitals have all become "medical centers" while we doctors are "health care providers."
If all of that doesn’t make you grateful for the doctors’ professionalism and humanity that Frank Veith writes about, then I don’t know what will.
Dr. George Andros is the medical editor of Vascular Specialist.
This months "Veith’s Viewpoint" tells two stories of patients whose lives were saved by doctors acting individually and together using the best that American medicine can offer. It brings to mind Theodore Roosevelt’s apt comment that "no one cares how much you know until they know how much you care." Nowhere did questions of work hours, EMRs, ASOs, or the subject of our "health care system" come up. Just doctors committed to patients. Over the last two decades, as the cost of heath care has made our country more insolvent and consumed more of our GDP, our so-called "system" has become increasingly fragmented. And less and less universal. What once bore at least some semblance of a system is now little more than a tattered patchwork composed of unfettered for-profit insurance companies, an under-funded Medicaid, an over-committed Medicare, a Veterans Administration system that is both vitally essential and full of redundancy, city and county hospitals that are bankrupting their communities, a workman’s compensation program that sets workers against employers, and not-for-profit hospitals that are by most important criteria no different than the for-profit ones. And the hospitals have all become "medical centers" while we doctors are "health care providers."
If all of that doesn’t make you grateful for the doctors’ professionalism and humanity that Frank Veith writes about, then I don’t know what will.
Dr. George Andros is the medical editor of Vascular Specialist.
This months "Veith’s Viewpoint" tells two stories of patients whose lives were saved by doctors acting individually and together using the best that American medicine can offer. It brings to mind Theodore Roosevelt’s apt comment that "no one cares how much you know until they know how much you care." Nowhere did questions of work hours, EMRs, ASOs, or the subject of our "health care system" come up. Just doctors committed to patients. Over the last two decades, as the cost of heath care has made our country more insolvent and consumed more of our GDP, our so-called "system" has become increasingly fragmented. And less and less universal. What once bore at least some semblance of a system is now little more than a tattered patchwork composed of unfettered for-profit insurance companies, an under-funded Medicaid, an over-committed Medicare, a Veterans Administration system that is both vitally essential and full of redundancy, city and county hospitals that are bankrupting their communities, a workman’s compensation program that sets workers against employers, and not-for-profit hospitals that are by most important criteria no different than the for-profit ones. And the hospitals have all become "medical centers" while we doctors are "health care providers."
If all of that doesn’t make you grateful for the doctors’ professionalism and humanity that Frank Veith writes about, then I don’t know what will.
Dr. George Andros is the medical editor of Vascular Specialist.
Today all we hear about is the high cost of U.S. health care, and how for our country to survive economically, it must cut doctors’ payments and spend less for health care, drugs, and medical devices. Certainly there is waste in the system and some physicians perform procedures that are unnecessary. But when one really needs good medical care and a good doctor, they are priceless.
Two recent dramatic examples in my own family made this clear to me. In one, a loved one developed a staphylococcal infection at an epidural injection site. Within 24 hours, she was desperately ill with a temperature of 104º, shaking chills, and excruciating back pain. She was expeditiously admitted to the ICU of an excellent community hospital and started on massive IV antibiotics. She underwent an urgent MRI, which revealed a paravertebral phlegmon. Blood cultures grew Staphyloccus aureus. She was seen repeatedly by her intensive care specialist and her orthopedic surgeon. When she did not improve, her orthopedic surgeon obtained a second MRI 36 hours after the first one. This, unlike the first, revealed an epidural collection, and she promptly underwent a three segment laminectomy to drain the abscess.
Although she required a second drainage procedure and careful adjustment of her IV antibiotics, she survived without any neurologic or cardiac damage. During her complicated and onerous 2½ weeks in the ICU, she was seen 2-3 times a day by both her intensivist and orthopedic surgeon, as well as by a variety of other specialists when they were needed. All made essential contributions to her recovery from this life-threatening illness. The skill and commitment of all these doctors, especially the orthopedic surgeon and the intensivist, made the difference in saving this young life. The care she received was priceless.
The second instance involved the cure of a life-threatening ventricular arrhythmia in a relatively young, productive individual. Although asymptomatic, this individual was having over 40,000 ventricular premature beats with runs of ventricular tachycardia in a 24-hour period. A highly skilled team of super-specialists in cardiac radiofrequency ablation procedures successfully eliminated the focus of these arrhythmias. However, the procedure was difficult and complicated. It took 7 hours and required both left and right heart catheterizations and crossing of the atrial septum and the aortic valve. Despite this, the individual was back at his usual work in 3 days, completely arrhythmia free. He has required no further subsequent treatment.
In both instances, the good care required by these skilled specialists and their colleagues was complicated and demanding but successful. It required enormous expertise and, more importantly, the commitment and dedication of those providing it. Sure, this care was expensive, but it was worth every penny. It was priceless, because the outcomes were life-saving and perfect. These priceless treatments restored two young, productive people to full health.
So in this rush to cut health care costs, let us remember that we in the United States have the best physicians and surgeons, the best hospitals, the best drugs, and medical devices in the world. Let us preserve these assets and not kill the goose that is laying the golden eggs of health care. Let us preserve and reward the priceless individuals and priceless care that can allow many of us in the United States to lead better, more productive lives than we otherwise would.
Dr. Veith is Professor of Surgery at New York University Medical Center and the Cleveland Clinic. He is an associate medical editor for Vascular Specialist.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or Publisher.
Today all we hear about is the high cost of U.S. health care, and how for our country to survive economically, it must cut doctors’ payments and spend less for health care, drugs, and medical devices. Certainly there is waste in the system and some physicians perform procedures that are unnecessary. But when one really needs good medical care and a good doctor, they are priceless.
Two recent dramatic examples in my own family made this clear to me. In one, a loved one developed a staphylococcal infection at an epidural injection site. Within 24 hours, she was desperately ill with a temperature of 104º, shaking chills, and excruciating back pain. She was expeditiously admitted to the ICU of an excellent community hospital and started on massive IV antibiotics. She underwent an urgent MRI, which revealed a paravertebral phlegmon. Blood cultures grew Staphyloccus aureus. She was seen repeatedly by her intensive care specialist and her orthopedic surgeon. When she did not improve, her orthopedic surgeon obtained a second MRI 36 hours after the first one. This, unlike the first, revealed an epidural collection, and she promptly underwent a three segment laminectomy to drain the abscess.
Although she required a second drainage procedure and careful adjustment of her IV antibiotics, she survived without any neurologic or cardiac damage. During her complicated and onerous 2½ weeks in the ICU, she was seen 2-3 times a day by both her intensivist and orthopedic surgeon, as well as by a variety of other specialists when they were needed. All made essential contributions to her recovery from this life-threatening illness. The skill and commitment of all these doctors, especially the orthopedic surgeon and the intensivist, made the difference in saving this young life. The care she received was priceless.
The second instance involved the cure of a life-threatening ventricular arrhythmia in a relatively young, productive individual. Although asymptomatic, this individual was having over 40,000 ventricular premature beats with runs of ventricular tachycardia in a 24-hour period. A highly skilled team of super-specialists in cardiac radiofrequency ablation procedures successfully eliminated the focus of these arrhythmias. However, the procedure was difficult and complicated. It took 7 hours and required both left and right heart catheterizations and crossing of the atrial septum and the aortic valve. Despite this, the individual was back at his usual work in 3 days, completely arrhythmia free. He has required no further subsequent treatment.
In both instances, the good care required by these skilled specialists and their colleagues was complicated and demanding but successful. It required enormous expertise and, more importantly, the commitment and dedication of those providing it. Sure, this care was expensive, but it was worth every penny. It was priceless, because the outcomes were life-saving and perfect. These priceless treatments restored two young, productive people to full health.
So in this rush to cut health care costs, let us remember that we in the United States have the best physicians and surgeons, the best hospitals, the best drugs, and medical devices in the world. Let us preserve these assets and not kill the goose that is laying the golden eggs of health care. Let us preserve and reward the priceless individuals and priceless care that can allow many of us in the United States to lead better, more productive lives than we otherwise would.
Dr. Veith is Professor of Surgery at New York University Medical Center and the Cleveland Clinic. He is an associate medical editor for Vascular Specialist.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or Publisher.

New stroke guidelines stress rtPA
Expanded use of clot-busting therapy is strongly endorsed for patients with acute ischemic stroke, while mechanical thrombectomy devices garner only lukewarm support in updated acute ischemic stroke guidelines from the American Heart Association and the American Stroke Association.
The "door-to-needle time" for intravenous administration of recombinant tissue plasminogen activator (rtPA) should be within 60 minutes from hospital arrival, according to a new class I, evidence level A recommendation.
Clinicians are advised to consider a noncontrast brain CT or MRI and a series of blood tests in all patients with suspected ischemic stroke before administering rtPA, but ultimately, the guidelines state that, "The only laboratory result required in all patients before fibrinolytics therapy is initiated is a glucose determination; use of finger-stick measurement devices is acceptable"(Stroke 2013 [doi:10.1161/STR.0b013e318284056a]).
The treatment window for rtPA therapy is also extended from 3 hours to 4.5 hours after stroke onset – as recommended in the AHA/ASA 2009 update on the extended time window for administration of fibrinolytic agents (Stroke 2009;40:2945-8).
"It’s clear that time is brain," lead guideline author Dr. Edward Jauch, director of emergency medicine at the Medical University of South Carolina in Charleston, said in an interview. "We are making a much greater emphasis that patients should be evaluated as quickly as possible and get treated as quickly as possible to give them the maximum opportunity for benefit."
Dr. Jauch acknowledges that the recommendations could reignite the long-standing controversy over the use of rtPA in stroke patients, particularly in light of the Food and Drug Administration’s recent decision not to expand approval of rtPA to include treatment up to 4.5 hours, as the European Medicines Agency has done.
"The FDA makes decisions largely based on American data, and we make guidelines based on all available data," he said, noting that safety data were also obtained from Genentech, maker of the rtPA activase (Alteplase).
Two European trials – the third International Stroke Trial (Lancet 2012;379:2352-63) and a British meta-analysis (Lancet 2012;379:2364-72) – reported last year that rtPA therapy within 6 hours of symptom onset increased the proportion of people who were alive and independent on follow-up.
Dr. Patrick Lyden, director of the stroke program at Cedars-Sinai Medical Center in Los Angeles, said reducing the battery of blood tests prior to rtPA administration is particularly important and pointed out that when the FDA first approved rtPA to treat stroke on the basis of a National Institutes of Health study, it "took the research protocol and turned it into a package insert.
"It’s taken the intervening 16 years for people to do studies and realize that you don’t need to do all the things in the package insert," he said. "So the American Heart Association, for the first time, is endorsing a much more practical, a much more optimal use of tPA for stroke."
The arrival of new classes of anticoagulants has prompted the AHA/ASA to add a new recommendation that the use of intravenous or intra-arterial rtPA in patients taking direct thrombin inhibitors like dabigatran (Pradaxa) or direct factor Xa inhibitors like rivaroxaban (Xarelto) "may be harmful" and is not recommended unless specialized testing is normal, or the patient has been off the drug for more than 2 days.
"I think that’s overreaching; I don’t think the data support that," said Dr. Lyden, who was not a member of the guidelines writing committee. He added that his team has had "no safety issues whatsoever" when administering the anticoagulant argatroban in patients on rtPA.
Dr. Jauch counters that data are lacking to support the safety of rtPA in patients on the new anticoagulants. Common blood tests – such as the international normalized ratio used for warfarin – do not register the anticoagulant effects of these drugs and reversal strategies are not yet known.
"As a community, we have a ways to go to figure out the optimal way to manage stroke in patients who come in on these drugs," he said.
When mechanical thrombectomy is pursued, stent retrievers are generally preferred to coil retrievers. The guidelines acknowledge that the Merci embolus retrieval system, Penumbra System, Solitaire FR, and TREVO thrombectomy devices "can be useful" in achieving recanalization alone or in combination with fibrinolytics in carefully selected patients, but that "their ability to improve patient outcomes has not been established" and continued study in randomized trials is warranted.
While these devices can restore blood flow very quickly, part of the problem in evaluating them is that the time from when the patient develops their stroke to when they get to the catheterization lab continues to increase, Dr. Jauch said.
"One of the challenges we have is, yes, we have a great device and if you happen to have your stroke on the cath table, you’re in great luck," he said.
"But if you transfer multiple times or there’s a delay in getting the patient evaluated sufficiently, then it diminishes the chance of getting a good outcome."
If feasible, patients should be transported to the closest available certified primary care stroke center or comprehensive stroke center, which in some cases may involve air transport or hospital bypass.
An estimated 40% of Americans, however, live in remote or rural areas without direct access to a comprehensive stroke center. For these patients, the updated guidelines emphasize the use of telemedicine to extend expert stroke care and optimize the use of intravenous rtPA, said guideline coauthor Dr. Bart M. Demaerschalk, professor of neurology at Mayo Clinic in Phoenix, which serves as a hub for 12 hospitals across Arizona with limited or no neurologic support.
"Even if air transport is available, the patients generally arrive when the respective treatment window is already closed," he said. "So telemedicine often means the difference between no treatment whatsoever, which is the usual case, and treatment."
The guidelines recommend tele-radiology systems approved by the FDA or "an equivalent organization" for sites without in-house imaging expertise for prompt review of brain CT and MRI scans in patients with suspected acute stroke.
Many guidelines committee members had financial ties with drug manufacturers and device makers.
Carotid endarterectomy is the most commonly performed open arterial procedure in the US and the most effective treatment available for appropriate stroke/TIA patients. It is accepted, however, that extracranial arterial disease accounts for less than half of all stroke/TIA patients. Three stories in this month's issue dealing with stroke and TIA and their accompanying comments by our editors underscore the need for all treating doctors, including vascular surgeons, to be alert for nonextracranial causes of neuro-ischemic events, both acute and chronic. Likewise, a proper work-up should not overlook evaluation of the cervical extracranial arteries which could deny the effectiveness of CEA to those who stand to benefit from it.
Dr. George Andros is Medical Editor of Vascular Specialist.
Carotid endarterectomy is the most commonly performed open arterial procedure in the US and the most effective treatment available for appropriate stroke/TIA patients. It is accepted, however, that extracranial arterial disease accounts for less than half of all stroke/TIA patients. Three stories in this month's issue dealing with stroke and TIA and their accompanying comments by our editors underscore the need for all treating doctors, including vascular surgeons, to be alert for nonextracranial causes of neuro-ischemic events, both acute and chronic. Likewise, a proper work-up should not overlook evaluation of the cervical extracranial arteries which could deny the effectiveness of CEA to those who stand to benefit from it.
Dr. George Andros is Medical Editor of Vascular Specialist.
Carotid endarterectomy is the most commonly performed open arterial procedure in the US and the most effective treatment available for appropriate stroke/TIA patients. It is accepted, however, that extracranial arterial disease accounts for less than half of all stroke/TIA patients. Three stories in this month's issue dealing with stroke and TIA and their accompanying comments by our editors underscore the need for all treating doctors, including vascular surgeons, to be alert for nonextracranial causes of neuro-ischemic events, both acute and chronic. Likewise, a proper work-up should not overlook evaluation of the cervical extracranial arteries which could deny the effectiveness of CEA to those who stand to benefit from it.
Dr. George Andros is Medical Editor of Vascular Specialist.
Expanded use of clot-busting therapy is strongly endorsed for patients with acute ischemic stroke, while mechanical thrombectomy devices garner only lukewarm support in updated acute ischemic stroke guidelines from the American Heart Association and the American Stroke Association.
The "door-to-needle time" for intravenous administration of recombinant tissue plasminogen activator (rtPA) should be within 60 minutes from hospital arrival, according to a new class I, evidence level A recommendation.
Clinicians are advised to consider a noncontrast brain CT or MRI and a series of blood tests in all patients with suspected ischemic stroke before administering rtPA, but ultimately, the guidelines state that, "The only laboratory result required in all patients before fibrinolytics therapy is initiated is a glucose determination; use of finger-stick measurement devices is acceptable"(Stroke 2013 [doi:10.1161/STR.0b013e318284056a]).
The treatment window for rtPA therapy is also extended from 3 hours to 4.5 hours after stroke onset – as recommended in the AHA/ASA 2009 update on the extended time window for administration of fibrinolytic agents (Stroke 2009;40:2945-8).
"It’s clear that time is brain," lead guideline author Dr. Edward Jauch, director of emergency medicine at the Medical University of South Carolina in Charleston, said in an interview. "We are making a much greater emphasis that patients should be evaluated as quickly as possible and get treated as quickly as possible to give them the maximum opportunity for benefit."
Dr. Jauch acknowledges that the recommendations could reignite the long-standing controversy over the use of rtPA in stroke patients, particularly in light of the Food and Drug Administration’s recent decision not to expand approval of rtPA to include treatment up to 4.5 hours, as the European Medicines Agency has done.
"The FDA makes decisions largely based on American data, and we make guidelines based on all available data," he said, noting that safety data were also obtained from Genentech, maker of the rtPA activase (Alteplase).
Two European trials – the third International Stroke Trial (Lancet 2012;379:2352-63) and a British meta-analysis (Lancet 2012;379:2364-72) – reported last year that rtPA therapy within 6 hours of symptom onset increased the proportion of people who were alive and independent on follow-up.
Dr. Patrick Lyden, director of the stroke program at Cedars-Sinai Medical Center in Los Angeles, said reducing the battery of blood tests prior to rtPA administration is particularly important and pointed out that when the FDA first approved rtPA to treat stroke on the basis of a National Institutes of Health study, it "took the research protocol and turned it into a package insert.
"It’s taken the intervening 16 years for people to do studies and realize that you don’t need to do all the things in the package insert," he said. "So the American Heart Association, for the first time, is endorsing a much more practical, a much more optimal use of tPA for stroke."
The arrival of new classes of anticoagulants has prompted the AHA/ASA to add a new recommendation that the use of intravenous or intra-arterial rtPA in patients taking direct thrombin inhibitors like dabigatran (Pradaxa) or direct factor Xa inhibitors like rivaroxaban (Xarelto) "may be harmful" and is not recommended unless specialized testing is normal, or the patient has been off the drug for more than 2 days.
"I think that’s overreaching; I don’t think the data support that," said Dr. Lyden, who was not a member of the guidelines writing committee. He added that his team has had "no safety issues whatsoever" when administering the anticoagulant argatroban in patients on rtPA.
Dr. Jauch counters that data are lacking to support the safety of rtPA in patients on the new anticoagulants. Common blood tests – such as the international normalized ratio used for warfarin – do not register the anticoagulant effects of these drugs and reversal strategies are not yet known.
"As a community, we have a ways to go to figure out the optimal way to manage stroke in patients who come in on these drugs," he said.
When mechanical thrombectomy is pursued, stent retrievers are generally preferred to coil retrievers. The guidelines acknowledge that the Merci embolus retrieval system, Penumbra System, Solitaire FR, and TREVO thrombectomy devices "can be useful" in achieving recanalization alone or in combination with fibrinolytics in carefully selected patients, but that "their ability to improve patient outcomes has not been established" and continued study in randomized trials is warranted.
While these devices can restore blood flow very quickly, part of the problem in evaluating them is that the time from when the patient develops their stroke to when they get to the catheterization lab continues to increase, Dr. Jauch said.
"One of the challenges we have is, yes, we have a great device and if you happen to have your stroke on the cath table, you’re in great luck," he said.
"But if you transfer multiple times or there’s a delay in getting the patient evaluated sufficiently, then it diminishes the chance of getting a good outcome."
If feasible, patients should be transported to the closest available certified primary care stroke center or comprehensive stroke center, which in some cases may involve air transport or hospital bypass.
An estimated 40% of Americans, however, live in remote or rural areas without direct access to a comprehensive stroke center. For these patients, the updated guidelines emphasize the use of telemedicine to extend expert stroke care and optimize the use of intravenous rtPA, said guideline coauthor Dr. Bart M. Demaerschalk, professor of neurology at Mayo Clinic in Phoenix, which serves as a hub for 12 hospitals across Arizona with limited or no neurologic support.
"Even if air transport is available, the patients generally arrive when the respective treatment window is already closed," he said. "So telemedicine often means the difference between no treatment whatsoever, which is the usual case, and treatment."
The guidelines recommend tele-radiology systems approved by the FDA or "an equivalent organization" for sites without in-house imaging expertise for prompt review of brain CT and MRI scans in patients with suspected acute stroke.
Many guidelines committee members had financial ties with drug manufacturers and device makers.
Expanded use of clot-busting therapy is strongly endorsed for patients with acute ischemic stroke, while mechanical thrombectomy devices garner only lukewarm support in updated acute ischemic stroke guidelines from the American Heart Association and the American Stroke Association.
The "door-to-needle time" for intravenous administration of recombinant tissue plasminogen activator (rtPA) should be within 60 minutes from hospital arrival, according to a new class I, evidence level A recommendation.
Clinicians are advised to consider a noncontrast brain CT or MRI and a series of blood tests in all patients with suspected ischemic stroke before administering rtPA, but ultimately, the guidelines state that, "The only laboratory result required in all patients before fibrinolytics therapy is initiated is a glucose determination; use of finger-stick measurement devices is acceptable"(Stroke 2013 [doi:10.1161/STR.0b013e318284056a]).
The treatment window for rtPA therapy is also extended from 3 hours to 4.5 hours after stroke onset – as recommended in the AHA/ASA 2009 update on the extended time window for administration of fibrinolytic agents (Stroke 2009;40:2945-8).
"It’s clear that time is brain," lead guideline author Dr. Edward Jauch, director of emergency medicine at the Medical University of South Carolina in Charleston, said in an interview. "We are making a much greater emphasis that patients should be evaluated as quickly as possible and get treated as quickly as possible to give them the maximum opportunity for benefit."
Dr. Jauch acknowledges that the recommendations could reignite the long-standing controversy over the use of rtPA in stroke patients, particularly in light of the Food and Drug Administration’s recent decision not to expand approval of rtPA to include treatment up to 4.5 hours, as the European Medicines Agency has done.
"The FDA makes decisions largely based on American data, and we make guidelines based on all available data," he said, noting that safety data were also obtained from Genentech, maker of the rtPA activase (Alteplase).
Two European trials – the third International Stroke Trial (Lancet 2012;379:2352-63) and a British meta-analysis (Lancet 2012;379:2364-72) – reported last year that rtPA therapy within 6 hours of symptom onset increased the proportion of people who were alive and independent on follow-up.
Dr. Patrick Lyden, director of the stroke program at Cedars-Sinai Medical Center in Los Angeles, said reducing the battery of blood tests prior to rtPA administration is particularly important and pointed out that when the FDA first approved rtPA to treat stroke on the basis of a National Institutes of Health study, it "took the research protocol and turned it into a package insert.
"It’s taken the intervening 16 years for people to do studies and realize that you don’t need to do all the things in the package insert," he said. "So the American Heart Association, for the first time, is endorsing a much more practical, a much more optimal use of tPA for stroke."
The arrival of new classes of anticoagulants has prompted the AHA/ASA to add a new recommendation that the use of intravenous or intra-arterial rtPA in patients taking direct thrombin inhibitors like dabigatran (Pradaxa) or direct factor Xa inhibitors like rivaroxaban (Xarelto) "may be harmful" and is not recommended unless specialized testing is normal, or the patient has been off the drug for more than 2 days.
"I think that’s overreaching; I don’t think the data support that," said Dr. Lyden, who was not a member of the guidelines writing committee. He added that his team has had "no safety issues whatsoever" when administering the anticoagulant argatroban in patients on rtPA.
Dr. Jauch counters that data are lacking to support the safety of rtPA in patients on the new anticoagulants. Common blood tests – such as the international normalized ratio used for warfarin – do not register the anticoagulant effects of these drugs and reversal strategies are not yet known.
"As a community, we have a ways to go to figure out the optimal way to manage stroke in patients who come in on these drugs," he said.
When mechanical thrombectomy is pursued, stent retrievers are generally preferred to coil retrievers. The guidelines acknowledge that the Merci embolus retrieval system, Penumbra System, Solitaire FR, and TREVO thrombectomy devices "can be useful" in achieving recanalization alone or in combination with fibrinolytics in carefully selected patients, but that "their ability to improve patient outcomes has not been established" and continued study in randomized trials is warranted.
While these devices can restore blood flow very quickly, part of the problem in evaluating them is that the time from when the patient develops their stroke to when they get to the catheterization lab continues to increase, Dr. Jauch said.
"One of the challenges we have is, yes, we have a great device and if you happen to have your stroke on the cath table, you’re in great luck," he said.
"But if you transfer multiple times or there’s a delay in getting the patient evaluated sufficiently, then it diminishes the chance of getting a good outcome."
If feasible, patients should be transported to the closest available certified primary care stroke center or comprehensive stroke center, which in some cases may involve air transport or hospital bypass.
An estimated 40% of Americans, however, live in remote or rural areas without direct access to a comprehensive stroke center. For these patients, the updated guidelines emphasize the use of telemedicine to extend expert stroke care and optimize the use of intravenous rtPA, said guideline coauthor Dr. Bart M. Demaerschalk, professor of neurology at Mayo Clinic in Phoenix, which serves as a hub for 12 hospitals across Arizona with limited or no neurologic support.
"Even if air transport is available, the patients generally arrive when the respective treatment window is already closed," he said. "So telemedicine often means the difference between no treatment whatsoever, which is the usual case, and treatment."
The guidelines recommend tele-radiology systems approved by the FDA or "an equivalent organization" for sites without in-house imaging expertise for prompt review of brain CT and MRI scans in patients with suspected acute stroke.
Many guidelines committee members had financial ties with drug manufacturers and device makers.
Advancing treatment while respecting privacy
While reading a recent article about Richard Fee, a 25-year-old college graduate who committed suicide in 2011, I couldn’t help wondering whether things might have turned out differently had his family – particularly his parents – had more to say about his psychiatric care.
Richard’s parents reportedly had a hard time accessing appropriate care for their son and suggested that his doctors’ adherence to privacy laws might have explained their behavior. Dr. Waldo M. Ellison, the psychiatrist who conducted Richard’s initial evaluation, "explained that federal privacy laws forbade any discussion of an adult patient, even with the patient’s father," the article said ("Drowned in a Stream of Prescriptions," New York Times, Feb. 2, 2013).
The Times article discussed Richard’s struggles with attention-deficit/hyperactivity diagnoses, his dark mood and growing paranoia, and his agitated, violent behavior.
Richard’s father, Rick Fee, reportedly tried to share details about his son’s behavior with the doctor but was met with resistance. "I can’t talk to you," Mr. Fee recalled Dr. Ellison telling him. "I can’t talk with you unless your son comes with you." Later in the article, however, Mr. Fee noted that Dr. Ellison "had spoken with him about his son for 45 minutes, then they scheduled an appointment for the entire family."
The Health Insurance Portability and Accountability Act (HIPPA) sets rules for the use of health information. The intent of the federal privacy law is to give patients more control over their care, but, unfortunately, the intent is often misunderstood as restricting to whom professionals can talk. What do federal privacy laws actually say about talking with family members?
The HIPAA Privacy Rule at 45 CFR 164.510(b) specifically permits covered entities to share information that is directly relevant to the involvement of a spouse, family members, friends, or other persons identified by a patient, in the patient’s care or payment for health care.
If the patient is present, or is otherwise available prior to the disclosure, and has the capacity to make health care decisions, the covered entity may discuss this information with the family and these other persons if the patient agrees or, when given the opportunity, does not object. The covered entity also may share relevant information with the family and these other persons if it can be reasonably inferred, based on professional judgment, that the patient does not object. Under these circumstances, for example:
• A physician may instruct a patient’s roommate about proper medicine dosage when she comes to pick up her friend from the hospital.
• A physician may discuss a patient’s treatment with the patient in the presence of a friend when the patient brings the friend to a medical appointment and asks if the friend can come into the room. Even when the patient is not present because of emergency circumstances or incapacity, a covered entity may share information with the person when, in exercising professional judgment, it determines that doing so would be in the best interest of the patient. See 45 CFR 164.510(b).
In light of those allowances:
• A surgeon may, if consistent with such professional judgment, inform a patient’s spouse who accompanied her husband to the emergency room that the patient has suffered a heart attack and provide periodic updates on the patients’ progress and prognosis.
• A doctor may, if consistent with such professional judgment, discuss an incapacitated patient’s condition with a family member over the phone. In addition, the privacy rule expressly permits a covered entity to use professional judgment and experience with common practice to make reasonable inferences about the patient’s best interests in allowing another person to act on behalf of the patient to pick up a filled prescription, medical supplies, X-rays, or other similar forms of protected health information.
For example, when a person comes to a pharmacy requesting to pick up a prescription on behalf of an individual, he identifies by name, a pharmacist, based on professional judgment and experience with common practice.
What to do if a patient objects
If a family member is urgently trying to reach you, it is most likely because the person has information she deems pertinent for the safe care of your patient. You can listen to anything they say. The privacy act is about protecting patient information, so that you may not tell them details of what the patient has told you in confidence, unless there are issues of safety or the possibility of harm to self or others.
Nonemergent situations allow time for the psychiatrist to educate the patient on the benefits of family involvement. As I have written previously, the literature is quite clear: Family involvement improves the outcome of many psychiatric illnesses (Am. J. Psychiatry 2006;163:962-8). It should be part of our informed consent process that we let patients know this. For example, we might want to say something like this: "In major depression, the literature shows that patient outcome is much better if family functioning is good. Let’s schedule a family consultation, one session, to assess the family functioning." Or we might say: "With bipolar disorder, when family members are knowledgeable about the signs and symptoms of relapse, the patient has a better outcome."
Patients might fear family involvement because they think the psychiatrist will divulge secrets or because the patient fears being attacked by angry family members. The patient should be reassured that the purpose of the meeting is to promote general treatment goals, such as maintaining optimal functioning with lowest medication doses, and to work on future treatment goals as a team.
When the psychiatrist lays out a clear plan for the meeting, the patient grasps the importance of having everyone on board. This is what we should tell patients: "At the family meeting we will review your family’s concerns and your concerns. Many family members need help understanding your illness, the role of medications, and how best to manage when, for example, you miss a dose of medications or have questions about how closely they need to monitor things.
"If you all agree on what is important and what is less important, things will go more smoothly for you. The main focus is to have a plan going forward of how we should work as a team to get you the best treatment possible, maintain your health, and prevent relapses."
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. She is editor of the recently published book, "Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professions" (New York: Routledge, March 2013), and has been a member of the Association of Family Psychiatrists since 2002.
While reading a recent article about Richard Fee, a 25-year-old college graduate who committed suicide in 2011, I couldn’t help wondering whether things might have turned out differently had his family – particularly his parents – had more to say about his psychiatric care.
Richard’s parents reportedly had a hard time accessing appropriate care for their son and suggested that his doctors’ adherence to privacy laws might have explained their behavior. Dr. Waldo M. Ellison, the psychiatrist who conducted Richard’s initial evaluation, "explained that federal privacy laws forbade any discussion of an adult patient, even with the patient’s father," the article said ("Drowned in a Stream of Prescriptions," New York Times, Feb. 2, 2013).
The Times article discussed Richard’s struggles with attention-deficit/hyperactivity diagnoses, his dark mood and growing paranoia, and his agitated, violent behavior.
Richard’s father, Rick Fee, reportedly tried to share details about his son’s behavior with the doctor but was met with resistance. "I can’t talk to you," Mr. Fee recalled Dr. Ellison telling him. "I can’t talk with you unless your son comes with you." Later in the article, however, Mr. Fee noted that Dr. Ellison "had spoken with him about his son for 45 minutes, then they scheduled an appointment for the entire family."
The Health Insurance Portability and Accountability Act (HIPPA) sets rules for the use of health information. The intent of the federal privacy law is to give patients more control over their care, but, unfortunately, the intent is often misunderstood as restricting to whom professionals can talk. What do federal privacy laws actually say about talking with family members?
The HIPAA Privacy Rule at 45 CFR 164.510(b) specifically permits covered entities to share information that is directly relevant to the involvement of a spouse, family members, friends, or other persons identified by a patient, in the patient’s care or payment for health care.
If the patient is present, or is otherwise available prior to the disclosure, and has the capacity to make health care decisions, the covered entity may discuss this information with the family and these other persons if the patient agrees or, when given the opportunity, does not object. The covered entity also may share relevant information with the family and these other persons if it can be reasonably inferred, based on professional judgment, that the patient does not object. Under these circumstances, for example:
• A physician may instruct a patient’s roommate about proper medicine dosage when she comes to pick up her friend from the hospital.
• A physician may discuss a patient’s treatment with the patient in the presence of a friend when the patient brings the friend to a medical appointment and asks if the friend can come into the room. Even when the patient is not present because of emergency circumstances or incapacity, a covered entity may share information with the person when, in exercising professional judgment, it determines that doing so would be in the best interest of the patient. See 45 CFR 164.510(b).
In light of those allowances:
• A surgeon may, if consistent with such professional judgment, inform a patient’s spouse who accompanied her husband to the emergency room that the patient has suffered a heart attack and provide periodic updates on the patients’ progress and prognosis.
• A doctor may, if consistent with such professional judgment, discuss an incapacitated patient’s condition with a family member over the phone. In addition, the privacy rule expressly permits a covered entity to use professional judgment and experience with common practice to make reasonable inferences about the patient’s best interests in allowing another person to act on behalf of the patient to pick up a filled prescription, medical supplies, X-rays, or other similar forms of protected health information.
For example, when a person comes to a pharmacy requesting to pick up a prescription on behalf of an individual, he identifies by name, a pharmacist, based on professional judgment and experience with common practice.
What to do if a patient objects
If a family member is urgently trying to reach you, it is most likely because the person has information she deems pertinent for the safe care of your patient. You can listen to anything they say. The privacy act is about protecting patient information, so that you may not tell them details of what the patient has told you in confidence, unless there are issues of safety or the possibility of harm to self or others.
Nonemergent situations allow time for the psychiatrist to educate the patient on the benefits of family involvement. As I have written previously, the literature is quite clear: Family involvement improves the outcome of many psychiatric illnesses (Am. J. Psychiatry 2006;163:962-8). It should be part of our informed consent process that we let patients know this. For example, we might want to say something like this: "In major depression, the literature shows that patient outcome is much better if family functioning is good. Let’s schedule a family consultation, one session, to assess the family functioning." Or we might say: "With bipolar disorder, when family members are knowledgeable about the signs and symptoms of relapse, the patient has a better outcome."
Patients might fear family involvement because they think the psychiatrist will divulge secrets or because the patient fears being attacked by angry family members. The patient should be reassured that the purpose of the meeting is to promote general treatment goals, such as maintaining optimal functioning with lowest medication doses, and to work on future treatment goals as a team.
When the psychiatrist lays out a clear plan for the meeting, the patient grasps the importance of having everyone on board. This is what we should tell patients: "At the family meeting we will review your family’s concerns and your concerns. Many family members need help understanding your illness, the role of medications, and how best to manage when, for example, you miss a dose of medications or have questions about how closely they need to monitor things.
"If you all agree on what is important and what is less important, things will go more smoothly for you. The main focus is to have a plan going forward of how we should work as a team to get you the best treatment possible, maintain your health, and prevent relapses."
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. She is editor of the recently published book, "Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professions" (New York: Routledge, March 2013), and has been a member of the Association of Family Psychiatrists since 2002.
While reading a recent article about Richard Fee, a 25-year-old college graduate who committed suicide in 2011, I couldn’t help wondering whether things might have turned out differently had his family – particularly his parents – had more to say about his psychiatric care.
Richard’s parents reportedly had a hard time accessing appropriate care for their son and suggested that his doctors’ adherence to privacy laws might have explained their behavior. Dr. Waldo M. Ellison, the psychiatrist who conducted Richard’s initial evaluation, "explained that federal privacy laws forbade any discussion of an adult patient, even with the patient’s father," the article said ("Drowned in a Stream of Prescriptions," New York Times, Feb. 2, 2013).
The Times article discussed Richard’s struggles with attention-deficit/hyperactivity diagnoses, his dark mood and growing paranoia, and his agitated, violent behavior.
Richard’s father, Rick Fee, reportedly tried to share details about his son’s behavior with the doctor but was met with resistance. "I can’t talk to you," Mr. Fee recalled Dr. Ellison telling him. "I can’t talk with you unless your son comes with you." Later in the article, however, Mr. Fee noted that Dr. Ellison "had spoken with him about his son for 45 minutes, then they scheduled an appointment for the entire family."
The Health Insurance Portability and Accountability Act (HIPPA) sets rules for the use of health information. The intent of the federal privacy law is to give patients more control over their care, but, unfortunately, the intent is often misunderstood as restricting to whom professionals can talk. What do federal privacy laws actually say about talking with family members?
The HIPAA Privacy Rule at 45 CFR 164.510(b) specifically permits covered entities to share information that is directly relevant to the involvement of a spouse, family members, friends, or other persons identified by a patient, in the patient’s care or payment for health care.
If the patient is present, or is otherwise available prior to the disclosure, and has the capacity to make health care decisions, the covered entity may discuss this information with the family and these other persons if the patient agrees or, when given the opportunity, does not object. The covered entity also may share relevant information with the family and these other persons if it can be reasonably inferred, based on professional judgment, that the patient does not object. Under these circumstances, for example:
• A physician may instruct a patient’s roommate about proper medicine dosage when she comes to pick up her friend from the hospital.
• A physician may discuss a patient’s treatment with the patient in the presence of a friend when the patient brings the friend to a medical appointment and asks if the friend can come into the room. Even when the patient is not present because of emergency circumstances or incapacity, a covered entity may share information with the person when, in exercising professional judgment, it determines that doing so would be in the best interest of the patient. See 45 CFR 164.510(b).
In light of those allowances:
• A surgeon may, if consistent with such professional judgment, inform a patient’s spouse who accompanied her husband to the emergency room that the patient has suffered a heart attack and provide periodic updates on the patients’ progress and prognosis.
• A doctor may, if consistent with such professional judgment, discuss an incapacitated patient’s condition with a family member over the phone. In addition, the privacy rule expressly permits a covered entity to use professional judgment and experience with common practice to make reasonable inferences about the patient’s best interests in allowing another person to act on behalf of the patient to pick up a filled prescription, medical supplies, X-rays, or other similar forms of protected health information.
For example, when a person comes to a pharmacy requesting to pick up a prescription on behalf of an individual, he identifies by name, a pharmacist, based on professional judgment and experience with common practice.
What to do if a patient objects
If a family member is urgently trying to reach you, it is most likely because the person has information she deems pertinent for the safe care of your patient. You can listen to anything they say. The privacy act is about protecting patient information, so that you may not tell them details of what the patient has told you in confidence, unless there are issues of safety or the possibility of harm to self or others.
Nonemergent situations allow time for the psychiatrist to educate the patient on the benefits of family involvement. As I have written previously, the literature is quite clear: Family involvement improves the outcome of many psychiatric illnesses (Am. J. Psychiatry 2006;163:962-8). It should be part of our informed consent process that we let patients know this. For example, we might want to say something like this: "In major depression, the literature shows that patient outcome is much better if family functioning is good. Let’s schedule a family consultation, one session, to assess the family functioning." Or we might say: "With bipolar disorder, when family members are knowledgeable about the signs and symptoms of relapse, the patient has a better outcome."
Patients might fear family involvement because they think the psychiatrist will divulge secrets or because the patient fears being attacked by angry family members. The patient should be reassured that the purpose of the meeting is to promote general treatment goals, such as maintaining optimal functioning with lowest medication doses, and to work on future treatment goals as a team.
When the psychiatrist lays out a clear plan for the meeting, the patient grasps the importance of having everyone on board. This is what we should tell patients: "At the family meeting we will review your family’s concerns and your concerns. Many family members need help understanding your illness, the role of medications, and how best to manage when, for example, you miss a dose of medications or have questions about how closely they need to monitor things.
"If you all agree on what is important and what is less important, things will go more smoothly for you. The main focus is to have a plan going forward of how we should work as a team to get you the best treatment possible, maintain your health, and prevent relapses."
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. She is editor of the recently published book, "Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professions" (New York: Routledge, March 2013), and has been a member of the Association of Family Psychiatrists since 2002.

The best part of my job
One of the pleasures of a busy outpatient practice is the privilege of meeting a wide variety of people. Perhaps my imagination is limited, but I can’t think of any other profession where one gets to interact in a meaningful way with a different person every 15 minutes.
Although the work of listening to patients tell me what ails them can be mentally and emotionally exhausting, there are unquantifiable rewards of getting to know so many different people. It might be a weakness on my part, but I get attached to my patients and frequently find myself quite invested in their well-being.
It helps that I practice in a small city with many universities and only a handful of rheumatologists. I have met judges and lawyers, restaurant managers, social workers, mail carriers, firefighters, politicians, strippers, local news meteorologists, jewelry makers, religious studies professors, radio talk show hosts, biotech rising stars, artists, 90-year-old ski instructors, and professional tennis players (something called court tennis, which is different from tennis as we know it but is apparently the game from which all racquet sports evolve). The list goes on.
I’ve met people from all over the world. There are Thai, Hmong, Laotian, and Vietnamese patients. There are those from Colombia, Peru, and Brazil. There are Nigerians and South Africans and Botswanans and Liberians (one of whom used to be good friends with ousted dictator Charles Taylor). I have a number of Greek, Italian, French, British, Spanish, and Portuguese patients, but most European transplants here are from the Azores.
A recent favorite is an accountant from Eritrea. He left Eritrea in the 1970s before Eritrea was even officially a country. In talking about his country’s history, he asked me this provocative question: "What have you heard about Eritrea?" What he really meant was that the country is run by a dictator who holds a tight reign over the media, so the outside world knows nothing about the corruption, human rights abuses, and political repression that occurs there.
That question got me thinking about how insular our lives can be, and how fortunate we are to have patients who enrich us by honoring us with their stories.
I’ve heard stories as dramatic as witnessing the slaughter of one’s family at the hands of the Khmer Rouge, or as mundane as teaching a son to make "adult decisions" in his senior year of college. I’ve heard stories of love and loss, of triumph and defeat, of gratitude and grace. Each encounter is a treasure, a distillation of the repository of wisdom that these unique individuals are. The experience is at once gratifying and humbling.
So I may be tired, and I may lose a bit of myself by becoming so attached to my patients, but I can’t think of anything I would rather be doing than being a doctor.
Dr. Chan practices rheumatology in Pawtucket, R.I.
One of the pleasures of a busy outpatient practice is the privilege of meeting a wide variety of people. Perhaps my imagination is limited, but I can’t think of any other profession where one gets to interact in a meaningful way with a different person every 15 minutes.
Although the work of listening to patients tell me what ails them can be mentally and emotionally exhausting, there are unquantifiable rewards of getting to know so many different people. It might be a weakness on my part, but I get attached to my patients and frequently find myself quite invested in their well-being.
It helps that I practice in a small city with many universities and only a handful of rheumatologists. I have met judges and lawyers, restaurant managers, social workers, mail carriers, firefighters, politicians, strippers, local news meteorologists, jewelry makers, religious studies professors, radio talk show hosts, biotech rising stars, artists, 90-year-old ski instructors, and professional tennis players (something called court tennis, which is different from tennis as we know it but is apparently the game from which all racquet sports evolve). The list goes on.
I’ve met people from all over the world. There are Thai, Hmong, Laotian, and Vietnamese patients. There are those from Colombia, Peru, and Brazil. There are Nigerians and South Africans and Botswanans and Liberians (one of whom used to be good friends with ousted dictator Charles Taylor). I have a number of Greek, Italian, French, British, Spanish, and Portuguese patients, but most European transplants here are from the Azores.
A recent favorite is an accountant from Eritrea. He left Eritrea in the 1970s before Eritrea was even officially a country. In talking about his country’s history, he asked me this provocative question: "What have you heard about Eritrea?" What he really meant was that the country is run by a dictator who holds a tight reign over the media, so the outside world knows nothing about the corruption, human rights abuses, and political repression that occurs there.
That question got me thinking about how insular our lives can be, and how fortunate we are to have patients who enrich us by honoring us with their stories.
I’ve heard stories as dramatic as witnessing the slaughter of one’s family at the hands of the Khmer Rouge, or as mundane as teaching a son to make "adult decisions" in his senior year of college. I’ve heard stories of love and loss, of triumph and defeat, of gratitude and grace. Each encounter is a treasure, a distillation of the repository of wisdom that these unique individuals are. The experience is at once gratifying and humbling.
So I may be tired, and I may lose a bit of myself by becoming so attached to my patients, but I can’t think of anything I would rather be doing than being a doctor.
Dr. Chan practices rheumatology in Pawtucket, R.I.
One of the pleasures of a busy outpatient practice is the privilege of meeting a wide variety of people. Perhaps my imagination is limited, but I can’t think of any other profession where one gets to interact in a meaningful way with a different person every 15 minutes.
Although the work of listening to patients tell me what ails them can be mentally and emotionally exhausting, there are unquantifiable rewards of getting to know so many different people. It might be a weakness on my part, but I get attached to my patients and frequently find myself quite invested in their well-being.
It helps that I practice in a small city with many universities and only a handful of rheumatologists. I have met judges and lawyers, restaurant managers, social workers, mail carriers, firefighters, politicians, strippers, local news meteorologists, jewelry makers, religious studies professors, radio talk show hosts, biotech rising stars, artists, 90-year-old ski instructors, and professional tennis players (something called court tennis, which is different from tennis as we know it but is apparently the game from which all racquet sports evolve). The list goes on.
I’ve met people from all over the world. There are Thai, Hmong, Laotian, and Vietnamese patients. There are those from Colombia, Peru, and Brazil. There are Nigerians and South Africans and Botswanans and Liberians (one of whom used to be good friends with ousted dictator Charles Taylor). I have a number of Greek, Italian, French, British, Spanish, and Portuguese patients, but most European transplants here are from the Azores.
A recent favorite is an accountant from Eritrea. He left Eritrea in the 1970s before Eritrea was even officially a country. In talking about his country’s history, he asked me this provocative question: "What have you heard about Eritrea?" What he really meant was that the country is run by a dictator who holds a tight reign over the media, so the outside world knows nothing about the corruption, human rights abuses, and political repression that occurs there.
That question got me thinking about how insular our lives can be, and how fortunate we are to have patients who enrich us by honoring us with their stories.
I’ve heard stories as dramatic as witnessing the slaughter of one’s family at the hands of the Khmer Rouge, or as mundane as teaching a son to make "adult decisions" in his senior year of college. I’ve heard stories of love and loss, of triumph and defeat, of gratitude and grace. Each encounter is a treasure, a distillation of the repository of wisdom that these unique individuals are. The experience is at once gratifying and humbling.
So I may be tired, and I may lose a bit of myself by becoming so attached to my patients, but I can’t think of anything I would rather be doing than being a doctor.
Dr. Chan practices rheumatology in Pawtucket, R.I.

Being postmenopausal doubles hepatic steatosis risk
SAN FRANCISCO – Postmenopausal status is independently associated with a twofold increased risk of hepatic steatosis, the Dallas Heart Study has shown.
Among 1,018 women aged 30-65 years enrolled in the population-based study, 48% were postmenopausal. Their prevalence of hepatic steatosis as defined by greater than 5.5% hepatic fat content measured by magnetic resonance spectroscopy was 34%. In contrast, the prevalence was significantly less at 24% in the premenopausal women, Dr. Monika Sanghavi reported at the annual meeting of the American College of Cardiology.
The absolute hepatic triglyceride content in the postmenopausal cohort was 4.0%, significantly more than the 2.9% value in premenopausal women.
Of note, the prevalence of hepatic steatosis rose with greater time since the last menstrual period (LMP). The prevalence was 22% among women whose LMP was less than 2 months earlier, 31% in those whose LMP was 2-12 months earlier, and 35% in women whose LMP was more than 12 months prior, according to Dr. Sanghavi of the University of Texas Southwestern Medical Center, Dallas.
Women who were postmenopausal were, of course, substantially older on average than premenopausal women. However, they also had significantly higher average systolic blood pressure, 129 compared with 117 mm Hg; a greater prevalence of diabetes, 16% vs. 7%; a mean LDL cholesterol of 113 compared with 98 mg/dL, and an average serum triglyceride level of 107 mg/dL compared with 81 mg/dL in premenopausal women. In a multivariate analysis adjusted for these variables as well as smoking status, body mass index, and C-reactive protein level, being postmenopausal remained independently associated with a twofold increased likelihood of hepatic steatosis (odds ratio, 2.0).
Hepatic steatosis has come under increasing research scrutiny of late because it appears to be a marker of increased atherosclerotic risk. The liver abnormality is associated with the metabolic syndrome, but as the Dallas Heart Study data show, postmenopausal status confers an increased risk of hepatic steatosis through a mechanism independent of obesity, hyperlipidemia, and other conventional cardiovascular risk factors.
Dr. Sanghavi reported having no relevant financial conflicts.
SAN FRANCISCO – Postmenopausal status is independently associated with a twofold increased risk of hepatic steatosis, the Dallas Heart Study has shown.
Among 1,018 women aged 30-65 years enrolled in the population-based study, 48% were postmenopausal. Their prevalence of hepatic steatosis as defined by greater than 5.5% hepatic fat content measured by magnetic resonance spectroscopy was 34%. In contrast, the prevalence was significantly less at 24% in the premenopausal women, Dr. Monika Sanghavi reported at the annual meeting of the American College of Cardiology.
The absolute hepatic triglyceride content in the postmenopausal cohort was 4.0%, significantly more than the 2.9% value in premenopausal women.
Of note, the prevalence of hepatic steatosis rose with greater time since the last menstrual period (LMP). The prevalence was 22% among women whose LMP was less than 2 months earlier, 31% in those whose LMP was 2-12 months earlier, and 35% in women whose LMP was more than 12 months prior, according to Dr. Sanghavi of the University of Texas Southwestern Medical Center, Dallas.
Women who were postmenopausal were, of course, substantially older on average than premenopausal women. However, they also had significantly higher average systolic blood pressure, 129 compared with 117 mm Hg; a greater prevalence of diabetes, 16% vs. 7%; a mean LDL cholesterol of 113 compared with 98 mg/dL, and an average serum triglyceride level of 107 mg/dL compared with 81 mg/dL in premenopausal women. In a multivariate analysis adjusted for these variables as well as smoking status, body mass index, and C-reactive protein level, being postmenopausal remained independently associated with a twofold increased likelihood of hepatic steatosis (odds ratio, 2.0).
Hepatic steatosis has come under increasing research scrutiny of late because it appears to be a marker of increased atherosclerotic risk. The liver abnormality is associated with the metabolic syndrome, but as the Dallas Heart Study data show, postmenopausal status confers an increased risk of hepatic steatosis through a mechanism independent of obesity, hyperlipidemia, and other conventional cardiovascular risk factors.
Dr. Sanghavi reported having no relevant financial conflicts.
SAN FRANCISCO – Postmenopausal status is independently associated with a twofold increased risk of hepatic steatosis, the Dallas Heart Study has shown.
Among 1,018 women aged 30-65 years enrolled in the population-based study, 48% were postmenopausal. Their prevalence of hepatic steatosis as defined by greater than 5.5% hepatic fat content measured by magnetic resonance spectroscopy was 34%. In contrast, the prevalence was significantly less at 24% in the premenopausal women, Dr. Monika Sanghavi reported at the annual meeting of the American College of Cardiology.
The absolute hepatic triglyceride content in the postmenopausal cohort was 4.0%, significantly more than the 2.9% value in premenopausal women.
Of note, the prevalence of hepatic steatosis rose with greater time since the last menstrual period (LMP). The prevalence was 22% among women whose LMP was less than 2 months earlier, 31% in those whose LMP was 2-12 months earlier, and 35% in women whose LMP was more than 12 months prior, according to Dr. Sanghavi of the University of Texas Southwestern Medical Center, Dallas.
Women who were postmenopausal were, of course, substantially older on average than premenopausal women. However, they also had significantly higher average systolic blood pressure, 129 compared with 117 mm Hg; a greater prevalence of diabetes, 16% vs. 7%; a mean LDL cholesterol of 113 compared with 98 mg/dL, and an average serum triglyceride level of 107 mg/dL compared with 81 mg/dL in premenopausal women. In a multivariate analysis adjusted for these variables as well as smoking status, body mass index, and C-reactive protein level, being postmenopausal remained independently associated with a twofold increased likelihood of hepatic steatosis (odds ratio, 2.0).
Hepatic steatosis has come under increasing research scrutiny of late because it appears to be a marker of increased atherosclerotic risk. The liver abnormality is associated with the metabolic syndrome, but as the Dallas Heart Study data show, postmenopausal status confers an increased risk of hepatic steatosis through a mechanism independent of obesity, hyperlipidemia, and other conventional cardiovascular risk factors.
Dr. Sanghavi reported having no relevant financial conflicts.
AT ACC13
Major Finding: Postmenopausal women had a significantly greater prevalence of hepatic steatosis (34%) than did premenopausal women (24%). After multivariate adjustment, the risk of steatosis was doubled in postmenopausal women.
Data Source: The Dallas Heart Study, a multiethnic, population-based study, including 1,018 women aged 30-65.
Disclosures: The presenter reported having no relevant financial conflicts.