User login
New and Noteworthy Information—April 2013
Greater dietary fiber intake is significantly associated with a lower risk of first stroke, according to a study published online ahead of print March 28 in Stroke. Investigators searched several electronic databases for healthy participant studies published between January 1990 and May 2012 that reported fiber intake and incidence of first hemorrhagic or ischemic stroke. The group identified eight cohort studies from the United States, Europe, Australia, and Japan that met their inclusion criteria. Total dietary fiber intake was inversely associated with risk of hemorrhagic plus ischemic stroke. The researchers found evidence of heterogeneity between the studies. Soluble fiber intake of 4 g/day was not associated with stroke risk reduction, and the investigators found evidence of low heterogeneity on this point between the studies.
In women who have episodic migraine, the ratio of high molecular weight to low molecular weight ictal adiponectin (ADP) may be associated with migraine severity and predict acute treatment response, according to a study published in the March Headache. Investigators collected peripheral blood specimens from women with episodic migraine before and after acute abortive treatment with sumatriptan and naproxen sodium or placebo. In all participants, increases in the ratio of high molecular weight to low molecular weight ADP were associated with increases in pain severity. For every 0.25-μg/mL increase in low molecular weight ADP, pain severity decreased by 0.20. In treatment responders, total ADP levels were reduced at 30, 60, and 120 minutes after treatment, compared with onset.
The FDA has approved Tecfidera (dimethyl fumarate) capsules to treat adults with relapsing forms of multiple sclerosis (MS). In two clinical trials, patients with MS who took dimethyl fumarate had fewer relapses compared with people who received placebo. In one of the trials, patients who took dimethyl fumarate experienced a worsening of disability less often than patients who took a placebo. Dimethyl fumarate may decrease a person's white blood cell count, but the drug was not associated with a significant increase in infections in clinical trials. Before starting treatment, and annually thereafter, the FDA recommends that a patient's white blood cell count be assessed by a health care provider. Flushing and stomach problems were the most common adverse reactions reported. Tecfidera is manufactured by Biogen Idec (Weston, Massachusetts).
Mild cognitive impairment (MCI) at the time of Parkinson's disease diagnosis may predict a highly increased risk for early dementia, according to a study published online ahead of print March 25 in JAMA Neurology. Researchers examined data for a population-based cohort of 182 patients with incident Parkinson's disease who were monitored for three years. Significantly more patients with MCI than without MCI at baseline (27.0% versus 0.7%) progressed to dementia during follow-up. Mild cognitive impairment at the one-year visit was associated with a similar progression rate to dementia (ie, 27.8%) and reversion rate to normal cognition (ie, 19.4%). Among the 22 patients with persistent MCI at baseline and the one-year visit, 10 developed dementia and two reverted to normal cognition by the end of the study.
Higher consumption of green tea and coffee may reduce the risk of cardiovascular disease and stroke, according to a study published online ahead of print March 14 in Stroke. Investigators studied 82,369 Japanese persons between ages 45 and 74 without cardiovascular disease or cancer. Green tea and coffee consumption was assessed by a self-administered questionnaire at baseline. Compared with seldom drinking green tea, the multivariable-adjusted hazard ratios of all strokes were 0.86 and 0.80 in individuals who drank two to three and four or more cups of green tea per day, respectively. Compared with seldom drinking coffee, the multivariable-adjusted hazard ratios of all strokes were 0.89, 0.80, and 0.81 for individuals who drank coffee three to six times per week, once daily, and twice or more daily, respectively.
Updated Guidelines for the Management of Acute Cervical Spine and Spinal Cord Injuries recommend against the use of steroids, including methylprednisolone, in acute spinal cord injury in the first 24 to 48 hours after injury. The use of steroids previously was recommended for this indication with consideration of the risk–reward profile, as evaluated by the physician. In the first new treatment guidelines in a decade, which were issued by the Joint Section on Disorders of the Spine and Peripheral Nerves of the Congress of Neurological Surgeons and the American Association of Neurological Surgeons, the standard has been revised based on the lack of medical evidence supporting the benefits of these drugs in the clinical setting. The report cites strong evidence that "high-dose steroids are associated with harmful side effects, including death."
Abnormalities in cortical surface area may indicate an individual's predisposition to developing migraine, and abnormalities in cortical thickness may result from migraine-related processes, according to research published online ahead of print March 26 in Radiology. Investigators took T2-weighted and three-dimensional T1-weighted MRIs of the brain for 63 migraineurs and 18 controls. They estimated cortical thickness and cortical surface area. Compared with control subjects, patients with migraine had reduced cortical thickness and surface area in pain-processing regions. These reductions were greater in regions involved in executive functions and visual-motion processing. Cortical thickness and cortical surface area abnormalities had minimal areas of overlap. Cortical thickness and surface area abnormalities were related to aura and white matter hyperintensities, but not to disease duration and attack frequency.
Primary stroke centers are more likely to administer t-PA than noncertified hospitals, according to research published online ahead of print March 26 in the Journal of the American Heart Association. Investigators analyzed data obtained from the Nationwide Inpatient Sample between 2004 and 2009 for patients age 18 or older with a primary diagnosis of acute ischemic stroke. IV t-PA was administered to 3.1% of patients overall. The drug was given to 2.2% of patients at noncertified hospitals and to 6.7% of patients at primary stroke centers. Between 2004 and 2009, t-PA administration increased from 1.4% to 3.3% of patients at noncertified hospitals and from 6.0% to 7.6% of patients at primary stroke centers. In a multivariable model, evaluation at a primary stroke center was significantly associated with t-PA use.
Control and prevention of risk factors such as hypertension earlier in life may limit or delay neuropathologic brain changes such as Alzheimer's disease with aging, researchers reported in a study published online ahead of print March 18 in JAMA Neurology. The investigators studied 118 cognitively normal adults ages 47 to 89. Participants were classified as having hypertension if they reported a medical diagnosis of hypertension or if blood pressure exceeded 140 mm Hg systolic/90 mm Hg diastolic on seven occasions. Participants underwent Ab PET imaging with radiotracer fluorine 18–labeled florbetapir, were genotyped for apolipoprotein E, and were classified as ε4+ or ε4−. Subjects with hypertension and at least one ε4 allele had significantly more amyloid burden than those with one or no risk factors.
Physicians can discontinue chronic antipsychotic medication for many elderly adults with Alzheimer's dementia and neuropsychiatric symptoms without causing detrimental effects on their behavior, according to a review published online March 28 in the Cochrane Database of Systematic Reviews. Investigators examined data from nine randomized controlled trials that compared antipsychotic withdrawal strategies with continuation of antipsychotics in patients with dementia. Although neurologists have concerns about the potential adverse events of antipsychotics, it is not clear whether withdrawal is beneficial for patients' cognition or psychomotor status. In two studies of patients whose agitation or psychosis had previously responded well to antipsychotic treatment, discontinuation was associated with an increased risk of relapse or shorter time to relapse. Two studies suggested that patients with severe neuropsychiatric symptoms at baseline could benefit from continuing their antipsychotic medication.
Greater exposure to pathogens associated with stroke risk and atherosclerosis may correlate with poorer cognitive performance, according to research published in the March 26 Neurology. Investigators tested for various pathogens (eg, Chlamydia pneumonia and Helicobacter pylori) in 1,625 participants in the Northern Manhattan Study. The researchers assessed patients' cognitive performance at baseline and at annual follow-up visits. Higher infectious burden index was associated with worse cognition. Each standard deviation in infectious burden correlated with a 0.77-point decline in Mini-Mental State Examination (MMSE) score. Adjustment for risk factors weakened the effect, however. Infectious burden was associated with an MMSE score of 24 or lower. Infectious burden was not associated with cognitive decline over time. Past infections may contribute to cognitive impairment, said the researchers.
Smoking cessation was associated with a decreased risk of cardiovascular disease events, and subsequent weight gain did not modify this association, researchers reported in the March 13 JAMA. Investigators analyzed data collected from 1984 through 2011 in the Framingham Offspring Study. Participants' self-reported smoking status was recorded during four-year examinations. Median four-year weight gain was 2.7 kg for recent smoking quitters without diabetes, 3.6 kg for recent quitters with diabetes, and 0.9 kg for long-term quitters. After adjustment for cardiovascular risk factors, compared with smokers, recent smoking quitters had a hazard ratio for cardiovascular disease of 0.47, and long-term quitters had a hazard ratio of 0.46. The results changed minimally after further adjustment for weight change. Similar point estimates for participants with diabetes did not reach statistical significance.
Women who enter menopause prematurely after bilateral ovariectomy may have a significantly increased risk for cognitive decline and dementia, according to a study published online ahead of print March 9 in Brain. The investigators studied rats 10 weeks after they had undergone bilateral ovariectomy and found that long-term estrogen deprivation dramatically increased the hippocampal CA3 region's sensitivity to ischemic stress, which correlated with a worse cognitive outcome. Long-term ovariectomized rats had robust hyperinduction of Alzheimer's disease-related proteins in the CA3 region. Following ischemic stress, amyloid-precursor protein processing switched from nonamyloidogenic to amyloidogenic. Replacement of 17β-estradiol at the end of the estrogen-deprivation period could not prevent CA3 hypersensitivity and amyloidogenesis, but if 17β-estradiol was initiated at ovariectomy and maintained throughout the estrogen deprivation period, it completely prevented these events.
Senior Associate Editor
Greater dietary fiber intake is significantly associated with a lower risk of first stroke, according to a study published online ahead of print March 28 in Stroke. Investigators searched several electronic databases for healthy participant studies published between January 1990 and May 2012 that reported fiber intake and incidence of first hemorrhagic or ischemic stroke. The group identified eight cohort studies from the United States, Europe, Australia, and Japan that met their inclusion criteria. Total dietary fiber intake was inversely associated with risk of hemorrhagic plus ischemic stroke. The researchers found evidence of heterogeneity between the studies. Soluble fiber intake of 4 g/day was not associated with stroke risk reduction, and the investigators found evidence of low heterogeneity on this point between the studies.
In women who have episodic migraine, the ratio of high molecular weight to low molecular weight ictal adiponectin (ADP) may be associated with migraine severity and predict acute treatment response, according to a study published in the March Headache. Investigators collected peripheral blood specimens from women with episodic migraine before and after acute abortive treatment with sumatriptan and naproxen sodium or placebo. In all participants, increases in the ratio of high molecular weight to low molecular weight ADP were associated with increases in pain severity. For every 0.25-μg/mL increase in low molecular weight ADP, pain severity decreased by 0.20. In treatment responders, total ADP levels were reduced at 30, 60, and 120 minutes after treatment, compared with onset.
The FDA has approved Tecfidera (dimethyl fumarate) capsules to treat adults with relapsing forms of multiple sclerosis (MS). In two clinical trials, patients with MS who took dimethyl fumarate had fewer relapses compared with people who received placebo. In one of the trials, patients who took dimethyl fumarate experienced a worsening of disability less often than patients who took a placebo. Dimethyl fumarate may decrease a person's white blood cell count, but the drug was not associated with a significant increase in infections in clinical trials. Before starting treatment, and annually thereafter, the FDA recommends that a patient's white blood cell count be assessed by a health care provider. Flushing and stomach problems were the most common adverse reactions reported. Tecfidera is manufactured by Biogen Idec (Weston, Massachusetts).
Mild cognitive impairment (MCI) at the time of Parkinson's disease diagnosis may predict a highly increased risk for early dementia, according to a study published online ahead of print March 25 in JAMA Neurology. Researchers examined data for a population-based cohort of 182 patients with incident Parkinson's disease who were monitored for three years. Significantly more patients with MCI than without MCI at baseline (27.0% versus 0.7%) progressed to dementia during follow-up. Mild cognitive impairment at the one-year visit was associated with a similar progression rate to dementia (ie, 27.8%) and reversion rate to normal cognition (ie, 19.4%). Among the 22 patients with persistent MCI at baseline and the one-year visit, 10 developed dementia and two reverted to normal cognition by the end of the study.
Higher consumption of green tea and coffee may reduce the risk of cardiovascular disease and stroke, according to a study published online ahead of print March 14 in Stroke. Investigators studied 82,369 Japanese persons between ages 45 and 74 without cardiovascular disease or cancer. Green tea and coffee consumption was assessed by a self-administered questionnaire at baseline. Compared with seldom drinking green tea, the multivariable-adjusted hazard ratios of all strokes were 0.86 and 0.80 in individuals who drank two to three and four or more cups of green tea per day, respectively. Compared with seldom drinking coffee, the multivariable-adjusted hazard ratios of all strokes were 0.89, 0.80, and 0.81 for individuals who drank coffee three to six times per week, once daily, and twice or more daily, respectively.
Updated Guidelines for the Management of Acute Cervical Spine and Spinal Cord Injuries recommend against the use of steroids, including methylprednisolone, in acute spinal cord injury in the first 24 to 48 hours after injury. The use of steroids previously was recommended for this indication with consideration of the risk–reward profile, as evaluated by the physician. In the first new treatment guidelines in a decade, which were issued by the Joint Section on Disorders of the Spine and Peripheral Nerves of the Congress of Neurological Surgeons and the American Association of Neurological Surgeons, the standard has been revised based on the lack of medical evidence supporting the benefits of these drugs in the clinical setting. The report cites strong evidence that "high-dose steroids are associated with harmful side effects, including death."
Abnormalities in cortical surface area may indicate an individual's predisposition to developing migraine, and abnormalities in cortical thickness may result from migraine-related processes, according to research published online ahead of print March 26 in Radiology. Investigators took T2-weighted and three-dimensional T1-weighted MRIs of the brain for 63 migraineurs and 18 controls. They estimated cortical thickness and cortical surface area. Compared with control subjects, patients with migraine had reduced cortical thickness and surface area in pain-processing regions. These reductions were greater in regions involved in executive functions and visual-motion processing. Cortical thickness and cortical surface area abnormalities had minimal areas of overlap. Cortical thickness and surface area abnormalities were related to aura and white matter hyperintensities, but not to disease duration and attack frequency.
Primary stroke centers are more likely to administer t-PA than noncertified hospitals, according to research published online ahead of print March 26 in the Journal of the American Heart Association. Investigators analyzed data obtained from the Nationwide Inpatient Sample between 2004 and 2009 for patients age 18 or older with a primary diagnosis of acute ischemic stroke. IV t-PA was administered to 3.1% of patients overall. The drug was given to 2.2% of patients at noncertified hospitals and to 6.7% of patients at primary stroke centers. Between 2004 and 2009, t-PA administration increased from 1.4% to 3.3% of patients at noncertified hospitals and from 6.0% to 7.6% of patients at primary stroke centers. In a multivariable model, evaluation at a primary stroke center was significantly associated with t-PA use.
Control and prevention of risk factors such as hypertension earlier in life may limit or delay neuropathologic brain changes such as Alzheimer's disease with aging, researchers reported in a study published online ahead of print March 18 in JAMA Neurology. The investigators studied 118 cognitively normal adults ages 47 to 89. Participants were classified as having hypertension if they reported a medical diagnosis of hypertension or if blood pressure exceeded 140 mm Hg systolic/90 mm Hg diastolic on seven occasions. Participants underwent Ab PET imaging with radiotracer fluorine 18–labeled florbetapir, were genotyped for apolipoprotein E, and were classified as ε4+ or ε4−. Subjects with hypertension and at least one ε4 allele had significantly more amyloid burden than those with one or no risk factors.
Physicians can discontinue chronic antipsychotic medication for many elderly adults with Alzheimer's dementia and neuropsychiatric symptoms without causing detrimental effects on their behavior, according to a review published online March 28 in the Cochrane Database of Systematic Reviews. Investigators examined data from nine randomized controlled trials that compared antipsychotic withdrawal strategies with continuation of antipsychotics in patients with dementia. Although neurologists have concerns about the potential adverse events of antipsychotics, it is not clear whether withdrawal is beneficial for patients' cognition or psychomotor status. In two studies of patients whose agitation or psychosis had previously responded well to antipsychotic treatment, discontinuation was associated with an increased risk of relapse or shorter time to relapse. Two studies suggested that patients with severe neuropsychiatric symptoms at baseline could benefit from continuing their antipsychotic medication.
Greater exposure to pathogens associated with stroke risk and atherosclerosis may correlate with poorer cognitive performance, according to research published in the March 26 Neurology. Investigators tested for various pathogens (eg, Chlamydia pneumonia and Helicobacter pylori) in 1,625 participants in the Northern Manhattan Study. The researchers assessed patients' cognitive performance at baseline and at annual follow-up visits. Higher infectious burden index was associated with worse cognition. Each standard deviation in infectious burden correlated with a 0.77-point decline in Mini-Mental State Examination (MMSE) score. Adjustment for risk factors weakened the effect, however. Infectious burden was associated with an MMSE score of 24 or lower. Infectious burden was not associated with cognitive decline over time. Past infections may contribute to cognitive impairment, said the researchers.
Smoking cessation was associated with a decreased risk of cardiovascular disease events, and subsequent weight gain did not modify this association, researchers reported in the March 13 JAMA. Investigators analyzed data collected from 1984 through 2011 in the Framingham Offspring Study. Participants' self-reported smoking status was recorded during four-year examinations. Median four-year weight gain was 2.7 kg for recent smoking quitters without diabetes, 3.6 kg for recent quitters with diabetes, and 0.9 kg for long-term quitters. After adjustment for cardiovascular risk factors, compared with smokers, recent smoking quitters had a hazard ratio for cardiovascular disease of 0.47, and long-term quitters had a hazard ratio of 0.46. The results changed minimally after further adjustment for weight change. Similar point estimates for participants with diabetes did not reach statistical significance.
Women who enter menopause prematurely after bilateral ovariectomy may have a significantly increased risk for cognitive decline and dementia, according to a study published online ahead of print March 9 in Brain. The investigators studied rats 10 weeks after they had undergone bilateral ovariectomy and found that long-term estrogen deprivation dramatically increased the hippocampal CA3 region's sensitivity to ischemic stress, which correlated with a worse cognitive outcome. Long-term ovariectomized rats had robust hyperinduction of Alzheimer's disease-related proteins in the CA3 region. Following ischemic stress, amyloid-precursor protein processing switched from nonamyloidogenic to amyloidogenic. Replacement of 17β-estradiol at the end of the estrogen-deprivation period could not prevent CA3 hypersensitivity and amyloidogenesis, but if 17β-estradiol was initiated at ovariectomy and maintained throughout the estrogen deprivation period, it completely prevented these events.
Senior Associate Editor
Greater dietary fiber intake is significantly associated with a lower risk of first stroke, according to a study published online ahead of print March 28 in Stroke. Investigators searched several electronic databases for healthy participant studies published between January 1990 and May 2012 that reported fiber intake and incidence of first hemorrhagic or ischemic stroke. The group identified eight cohort studies from the United States, Europe, Australia, and Japan that met their inclusion criteria. Total dietary fiber intake was inversely associated with risk of hemorrhagic plus ischemic stroke. The researchers found evidence of heterogeneity between the studies. Soluble fiber intake of 4 g/day was not associated with stroke risk reduction, and the investigators found evidence of low heterogeneity on this point between the studies.
In women who have episodic migraine, the ratio of high molecular weight to low molecular weight ictal adiponectin (ADP) may be associated with migraine severity and predict acute treatment response, according to a study published in the March Headache. Investigators collected peripheral blood specimens from women with episodic migraine before and after acute abortive treatment with sumatriptan and naproxen sodium or placebo. In all participants, increases in the ratio of high molecular weight to low molecular weight ADP were associated with increases in pain severity. For every 0.25-μg/mL increase in low molecular weight ADP, pain severity decreased by 0.20. In treatment responders, total ADP levels were reduced at 30, 60, and 120 minutes after treatment, compared with onset.
The FDA has approved Tecfidera (dimethyl fumarate) capsules to treat adults with relapsing forms of multiple sclerosis (MS). In two clinical trials, patients with MS who took dimethyl fumarate had fewer relapses compared with people who received placebo. In one of the trials, patients who took dimethyl fumarate experienced a worsening of disability less often than patients who took a placebo. Dimethyl fumarate may decrease a person's white blood cell count, but the drug was not associated with a significant increase in infections in clinical trials. Before starting treatment, and annually thereafter, the FDA recommends that a patient's white blood cell count be assessed by a health care provider. Flushing and stomach problems were the most common adverse reactions reported. Tecfidera is manufactured by Biogen Idec (Weston, Massachusetts).
Mild cognitive impairment (MCI) at the time of Parkinson's disease diagnosis may predict a highly increased risk for early dementia, according to a study published online ahead of print March 25 in JAMA Neurology. Researchers examined data for a population-based cohort of 182 patients with incident Parkinson's disease who were monitored for three years. Significantly more patients with MCI than without MCI at baseline (27.0% versus 0.7%) progressed to dementia during follow-up. Mild cognitive impairment at the one-year visit was associated with a similar progression rate to dementia (ie, 27.8%) and reversion rate to normal cognition (ie, 19.4%). Among the 22 patients with persistent MCI at baseline and the one-year visit, 10 developed dementia and two reverted to normal cognition by the end of the study.
Higher consumption of green tea and coffee may reduce the risk of cardiovascular disease and stroke, according to a study published online ahead of print March 14 in Stroke. Investigators studied 82,369 Japanese persons between ages 45 and 74 without cardiovascular disease or cancer. Green tea and coffee consumption was assessed by a self-administered questionnaire at baseline. Compared with seldom drinking green tea, the multivariable-adjusted hazard ratios of all strokes were 0.86 and 0.80 in individuals who drank two to three and four or more cups of green tea per day, respectively. Compared with seldom drinking coffee, the multivariable-adjusted hazard ratios of all strokes were 0.89, 0.80, and 0.81 for individuals who drank coffee three to six times per week, once daily, and twice or more daily, respectively.
Updated Guidelines for the Management of Acute Cervical Spine and Spinal Cord Injuries recommend against the use of steroids, including methylprednisolone, in acute spinal cord injury in the first 24 to 48 hours after injury. The use of steroids previously was recommended for this indication with consideration of the risk–reward profile, as evaluated by the physician. In the first new treatment guidelines in a decade, which were issued by the Joint Section on Disorders of the Spine and Peripheral Nerves of the Congress of Neurological Surgeons and the American Association of Neurological Surgeons, the standard has been revised based on the lack of medical evidence supporting the benefits of these drugs in the clinical setting. The report cites strong evidence that "high-dose steroids are associated with harmful side effects, including death."
Abnormalities in cortical surface area may indicate an individual's predisposition to developing migraine, and abnormalities in cortical thickness may result from migraine-related processes, according to research published online ahead of print March 26 in Radiology. Investigators took T2-weighted and three-dimensional T1-weighted MRIs of the brain for 63 migraineurs and 18 controls. They estimated cortical thickness and cortical surface area. Compared with control subjects, patients with migraine had reduced cortical thickness and surface area in pain-processing regions. These reductions were greater in regions involved in executive functions and visual-motion processing. Cortical thickness and cortical surface area abnormalities had minimal areas of overlap. Cortical thickness and surface area abnormalities were related to aura and white matter hyperintensities, but not to disease duration and attack frequency.
Primary stroke centers are more likely to administer t-PA than noncertified hospitals, according to research published online ahead of print March 26 in the Journal of the American Heart Association. Investigators analyzed data obtained from the Nationwide Inpatient Sample between 2004 and 2009 for patients age 18 or older with a primary diagnosis of acute ischemic stroke. IV t-PA was administered to 3.1% of patients overall. The drug was given to 2.2% of patients at noncertified hospitals and to 6.7% of patients at primary stroke centers. Between 2004 and 2009, t-PA administration increased from 1.4% to 3.3% of patients at noncertified hospitals and from 6.0% to 7.6% of patients at primary stroke centers. In a multivariable model, evaluation at a primary stroke center was significantly associated with t-PA use.
Control and prevention of risk factors such as hypertension earlier in life may limit or delay neuropathologic brain changes such as Alzheimer's disease with aging, researchers reported in a study published online ahead of print March 18 in JAMA Neurology. The investigators studied 118 cognitively normal adults ages 47 to 89. Participants were classified as having hypertension if they reported a medical diagnosis of hypertension or if blood pressure exceeded 140 mm Hg systolic/90 mm Hg diastolic on seven occasions. Participants underwent Ab PET imaging with radiotracer fluorine 18–labeled florbetapir, were genotyped for apolipoprotein E, and were classified as ε4+ or ε4−. Subjects with hypertension and at least one ε4 allele had significantly more amyloid burden than those with one or no risk factors.
Physicians can discontinue chronic antipsychotic medication for many elderly adults with Alzheimer's dementia and neuropsychiatric symptoms without causing detrimental effects on their behavior, according to a review published online March 28 in the Cochrane Database of Systematic Reviews. Investigators examined data from nine randomized controlled trials that compared antipsychotic withdrawal strategies with continuation of antipsychotics in patients with dementia. Although neurologists have concerns about the potential adverse events of antipsychotics, it is not clear whether withdrawal is beneficial for patients' cognition or psychomotor status. In two studies of patients whose agitation or psychosis had previously responded well to antipsychotic treatment, discontinuation was associated with an increased risk of relapse or shorter time to relapse. Two studies suggested that patients with severe neuropsychiatric symptoms at baseline could benefit from continuing their antipsychotic medication.
Greater exposure to pathogens associated with stroke risk and atherosclerosis may correlate with poorer cognitive performance, according to research published in the March 26 Neurology. Investigators tested for various pathogens (eg, Chlamydia pneumonia and Helicobacter pylori) in 1,625 participants in the Northern Manhattan Study. The researchers assessed patients' cognitive performance at baseline and at annual follow-up visits. Higher infectious burden index was associated with worse cognition. Each standard deviation in infectious burden correlated with a 0.77-point decline in Mini-Mental State Examination (MMSE) score. Adjustment for risk factors weakened the effect, however. Infectious burden was associated with an MMSE score of 24 or lower. Infectious burden was not associated with cognitive decline over time. Past infections may contribute to cognitive impairment, said the researchers.
Smoking cessation was associated with a decreased risk of cardiovascular disease events, and subsequent weight gain did not modify this association, researchers reported in the March 13 JAMA. Investigators analyzed data collected from 1984 through 2011 in the Framingham Offspring Study. Participants' self-reported smoking status was recorded during four-year examinations. Median four-year weight gain was 2.7 kg for recent smoking quitters without diabetes, 3.6 kg for recent quitters with diabetes, and 0.9 kg for long-term quitters. After adjustment for cardiovascular risk factors, compared with smokers, recent smoking quitters had a hazard ratio for cardiovascular disease of 0.47, and long-term quitters had a hazard ratio of 0.46. The results changed minimally after further adjustment for weight change. Similar point estimates for participants with diabetes did not reach statistical significance.
Women who enter menopause prematurely after bilateral ovariectomy may have a significantly increased risk for cognitive decline and dementia, according to a study published online ahead of print March 9 in Brain. The investigators studied rats 10 weeks after they had undergone bilateral ovariectomy and found that long-term estrogen deprivation dramatically increased the hippocampal CA3 region's sensitivity to ischemic stress, which correlated with a worse cognitive outcome. Long-term ovariectomized rats had robust hyperinduction of Alzheimer's disease-related proteins in the CA3 region. Following ischemic stress, amyloid-precursor protein processing switched from nonamyloidogenic to amyloidogenic. Replacement of 17β-estradiol at the end of the estrogen-deprivation period could not prevent CA3 hypersensitivity and amyloidogenesis, but if 17β-estradiol was initiated at ovariectomy and maintained throughout the estrogen deprivation period, it completely prevented these events.
Senior Associate Editor
Man, 57, With Dyspnea After Chiropractic Manipulation
A 57-year-old man presented to the emergency department (ED) with a two-day history of worsening shortness of breath, light-headedness, and back pain. The patient, who had a history of ankylosing spondylitis, had been receiving weekly therapy from a chiropractor for about 10 years. One week before presenting to the ED, he had begun to undergo daily manipulations under anesthesia (MUA)—an aggressive chiropractic procedure that is administered while the patient is under monitored, procedural sedation. After the second day of treatment, the patient began to experience worsening back pain and progressive light-headedness and shortness of breath.
At a follow-up visit with his chiropractor, he was found to have decreased O2 saturation and was directed to go to the hospital for evaluation. On arrival at the ED, the patient was awake and alert. He had intact motor strength in all extremities, no sensory abnormalities, intact symmetric reflexes, and no bladder or bowel dysfunction, with a negative Babinski sign. His O2 saturation was 92% on 5 L of oxygen. An absence of breath sounds was noted on the left side.
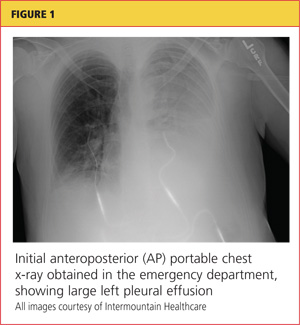
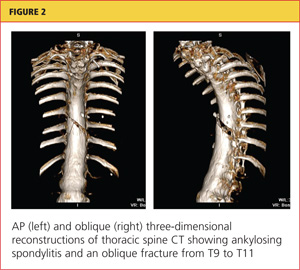
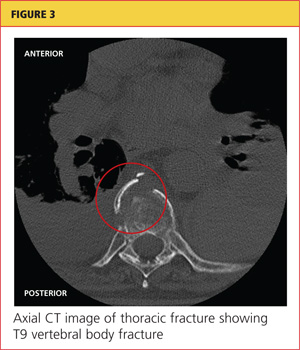
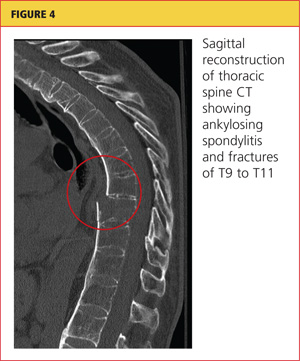
Chest x-ray (see Figure 1) was performed, which demonstrated complete opacification of the left hemithorax, consistent with a large pleural effusion or hemothorax. CT scan of the thoracic spine showed diffuse ankylosis. A complex oblique coronal and transversely oriented fracture with 7 mm of displacement was identified, beginning at the right anterior inferior lateral margin of the T8 vertebral body and extending centrally and inferiorly to the left and right into the T9 vertebral body. The fracture continued through the right T9-10 neural foramen and what was probably the right fused T9-10 facet joint. The fracture exited through the left superior and lateral margin of the T10 vertebral body and the left T10-11 neural foramen (see Figures 2, 3, and 4).
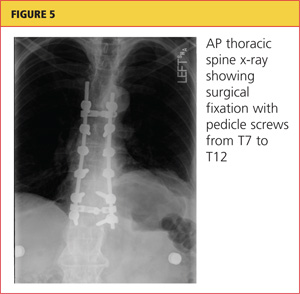
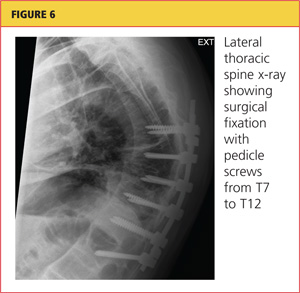
A chest tube was inserted in the ED, and 1,600 mL of old blood was immediately drained. The patient was admitted to the ICU on the trauma service. He was taken to surgery for open reduction and internal fixation of his unstable thoracic spine fracture on day 3 of hospitalization, after his pulmonary condition stabilized. Pedicle screws were placed from T7 through T12 during the spinal fusion. Good reduction of the fracture was observed following the spine surgery (see Figures 5 and 6). At the conclusion of surgery, an epidural catheter was placed in the thoracic spine to administer pain control.
After the spine portion of the procedure, the patient was repositioned and underwent video-assisted thoracoscopic surgery of the left hemithorax for evacuation of retained hemothorax. The patient tolerated the procedure well and was taken to the ICU for recovery.
On postoperative day 2, the patient complained of chest pain and experienced hypoxemia with activity. CT angiography of the chest demonstrated bilateral segmental and subsegmental pulmonary emboli. The epidural catheter was discontinued. Six hours later, a heparin drip was started, and the patient was transitioned to therapeutic enoxaparin and warfarin. When methicillin-sensitive Staphylococcus aureus (MSSA) was detected in his hemothorax fluid, he was treated with a course of nafcillin.
The patient was discharged to home on postoperative day 12. He has remained neurologically intact and has returned to his former work activities. He is not taking narcotic pain medications.
Discussion
Chiropractic care is a popular alternative health care modality in the United States. Researchers for the 2007 National Health Interview Study1 reported an annual use of chiropractic manipulation of 8.6%, while the Medical Expenditure Panel Survey2 data yielded an estimate of 12.6 million adults using chiropractic manipulation in 2006—translating to a prevalence of 5.6%. Despite the popularity of chiropractic medicine, few well-designed studies have been conducted to support its use.3,4 Because of its designation as an alternative therapy, however, chiropractic manipulation has not been subjected to rigorous efficacy and safety evaluations.5
Given the inconsistency of the evidence to support chiropractic manipulation, the practice's safety profile is a concern. The risks associated with spinal manipulation are generally described in case reports and small series. Most serious adverse events described in the literature are cerebrovascular in nature and tend to occur after cervical manipulation.6,7 Fractures after spine manipulation are exceedingly rare, and published literature on this topic consists of a few isolated case reports, with all fractures occurring in the cervical spine in patients with an underlying pathologic condition.8-10
In 2009, Gouveia et al5 reviewed the published literature regarding all adverse events resulting from chiropractic manipulation. The authors found one randomized controlled trial, two case-control studies, six prospective studies, 12 surveys, three retrospective studies, and 100 case reports. The spectrum of complications identified ranged from benign and transient, such as local discomfort, to far more serious: stroke, myelopathy, radiculopathy, subdural hematoma, spinal fluid leakage, cauda equina syndrome, herniated disc, diaphragmatic palsy, and vertebral fractures. The authors were unable to perform a true meta-analysis because of the heterogeneity of the data, but they concluded that complications associated with chiropractic procedures are "frequent."5
Manipulations Under Anesthesia
MUA is a procedure that combines chiropractic adjustments and manipulations with general anesthesia or procedural sedation.11 The theory behind this strategy is that the anesthesia or sedation reduces pain and muscle spasm that may hinder the manipulation, allowing the practitioner to more effectively break up joint adhesions and reduce segmental dysfunction than if the patient had not undergone anesthesia.11
MUA is generally indicated in patients who have not responded to a 4- to 8-week trial of traditional manipulation therapy.12 It is also considered in patients who have "painful and restricting muscular guarding [that] interferes with the performance of spinal adjustments, mobilizations, and soft tissue release techniques."13
In the chiropractic literature, between 3% and 10% of patients are estimated to be candidates for MUA.12,14 It is not completely clear, however, what diagnoses are most likely to be treated successfully with this technique. Contraindications to MUA are generally the same as those for manipulation in conscious patients. A published list of contraindications from the Committee for Manipulation under Anesthesia (2003)15 included malignancy with bony metastasis, tuberculosis of the bone, recent fracture, acute arthritis, acute gout, diabetic neuropathy, syphilitic articular lesions, excessive spinal osteoporosis, disk fragmentation, direct nerve root impingement, and evidence of cord or caudal compression by tumor, ankylosis, or other space-occupying lesions.
MUA generally begins with deep procedural sedation, managed by an anesthesiologist. Once an adequate level of sedation is achieved, the manipulations are performed. Both high- and low-velocity thrusts are used, but it is recommended that the force exerted should be much less, and the manipulations performed with more caution, than in patients who are not anesthetized.12
For the thoracic spine, the patient is manipulated in the supine position with the arms crossed over the chest. The practitioner places one hand in a fist under the spine with the other hand on the patient's crossed arms, then delivers an anterior-to-posterior thrust. This is repeated until all affected segments have been treated.11,12
Literature to support the use of MUA for various indications is largely anecdotal. The largest published series13 is of 177 patients with chronic spinal pain who each underwent three MUA sessions followed by four to six weeks of traditional manipulations. The authors found that pain, as measured by visual analog scale, was reduced by 62% in patients with cervical spine pain, and by 60% in patients with lumbar pain. No adverse events were reported in the study.
Kohlbeck and Haldeman12 reviewed the reported complications of MUA across all published literature. They found that in 17 published papers, the overall complication rate was 0.7%, mainly represented by transitory increased pain. No spinal fractures were reported.
This case demonstrates a rare but serious complication of chiropractic MUA. It is unclear exactly what mechanism of injury led to an unstable thoracic spine fracture with massive hemothorax, and the precise cause will probably never be known. The clinicians who treated the case patient find it curious that the reported rate of adverse events following this procedure is so low, but they suspect an element of reporting bias in the chiropractic literature.
Conclusion
Iatrogenic injury after chiropractic manipulation is uncommon, but it can be devastating. Few serious complications of chiropractic MUA have been reported, but the literature is lacking in well-designed research studies. Despite the dearth of clinical trials to support its safety and efficacy, use of MUA has continued in the chiropractic community. This case demonstrates that serious adverse outcomes can occur, and more rigorous studies are needed to delineate the true benefits and risks of this set of chiropractic procedures.
References
1. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;12:1-9.
2. Davis MA, Sirovich BE, Weeks WB. Utilization and expenditures on chiropractic care in the United States from 1997 to 2006. Health Serv Res. 2009;45:748-761.
3. Canadian Chiropractic Association; Canadian Federation of Chiropractic Regulatory Boards; Clinical Practice Guidelines Development Initiative; Guidelines Development Committee. Chiropractic clinical practice guideline: evidence-based treatment of adult neck pain not due to whiplash. J Can Chiropr Assoc. 2005;49:417-421.
4.
Hurwitz EL, Aker PD, Adams AH, et al. Manipulation and mobilization of the cervical spine: a systematic review of the literature. Spine (Phila Pa 1976). 1996;21:1746-1760.
5.Gouveia LO, Castanho P, Ferreira JJ. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976). 2009;34:E405-E413.
6. Di Fabio RP. Manipulation of the cervical spine: risks and benefits. Phys Ther. 1999;79:50-65.
7. Nadareishvili Z, Norris JW. Stroke from traumatic arterial dissection. Lancet. 1999;354:159-160.
8. Austin RT. Pathological vertebral fractures after spinal manipulation. Br Med J (Clin Res Ed). 1985;291:1114-1115.
9. Ea HK, Weber AJ, Yon F, Lioté F. Osteoporotic fracture of the dens revealed by cervical manipulation. Joint Bone Spine. 2004;71:246-250.
10. Schmitz A, Lutterbey G, von Engelhardt L, et al. Pathological cervical fracture after spinal manipulation in a pregnant patient. J Manipulative Physiol Ther. 2005;28:633-636.
11. Cremata E, Collins S, Clauson W, et al. Manipulation under anesthesia: a report of four cases. J Manipulative Physiol Ther. 2005;28:526-533.
12. Kohlbeck FJ, Haldeman S. Medication-assisted spinal manipulation. Spine J. 2002;2:288-302.
13. West DT, Mathews RS, Miller MR, Kent GM. Effective management of spinal pain in one hundred seventy-seven patients evaluated for manipulation under anesthesia. J Manipulative Physiol Ther. 1999;22:299-308.
14. Morey LW Jr. Osteopathic manipulation under general anesthesia. J Am Osteopath Assoc. 1973;73:116-127.
15. Tain L, Gunderson C, Cremata E, et al; Committee for Manipulation Under Anesthesia. Recommendations to the Industrial Medical Council Work Group of California for manipulation under anesthesia use for injured workers. Sacramento, CA: Industrial Medical Council; 2003.
A 57-year-old man presented to the emergency department (ED) with a two-day history of worsening shortness of breath, light-headedness, and back pain. The patient, who had a history of ankylosing spondylitis, had been receiving weekly therapy from a chiropractor for about 10 years. One week before presenting to the ED, he had begun to undergo daily manipulations under anesthesia (MUA)—an aggressive chiropractic procedure that is administered while the patient is under monitored, procedural sedation. After the second day of treatment, the patient began to experience worsening back pain and progressive light-headedness and shortness of breath.
At a follow-up visit with his chiropractor, he was found to have decreased O2 saturation and was directed to go to the hospital for evaluation. On arrival at the ED, the patient was awake and alert. He had intact motor strength in all extremities, no sensory abnormalities, intact symmetric reflexes, and no bladder or bowel dysfunction, with a negative Babinski sign. His O2 saturation was 92% on 5 L of oxygen. An absence of breath sounds was noted on the left side.
Chest x-ray (see Figure 1) was performed, which demonstrated complete opacification of the left hemithorax, consistent with a large pleural effusion or hemothorax. CT scan of the thoracic spine showed diffuse ankylosis. A complex oblique coronal and transversely oriented fracture with 7 mm of displacement was identified, beginning at the right anterior inferior lateral margin of the T8 vertebral body and extending centrally and inferiorly to the left and right into the T9 vertebral body. The fracture continued through the right T9-10 neural foramen and what was probably the right fused T9-10 facet joint. The fracture exited through the left superior and lateral margin of the T10 vertebral body and the left T10-11 neural foramen (see Figures 2, 3, and 4).
A chest tube was inserted in the ED, and 1,600 mL of old blood was immediately drained. The patient was admitted to the ICU on the trauma service. He was taken to surgery for open reduction and internal fixation of his unstable thoracic spine fracture on day 3 of hospitalization, after his pulmonary condition stabilized. Pedicle screws were placed from T7 through T12 during the spinal fusion. Good reduction of the fracture was observed following the spine surgery (see Figures 5 and 6). At the conclusion of surgery, an epidural catheter was placed in the thoracic spine to administer pain control.
After the spine portion of the procedure, the patient was repositioned and underwent video-assisted thoracoscopic surgery of the left hemithorax for evacuation of retained hemothorax. The patient tolerated the procedure well and was taken to the ICU for recovery.
On postoperative day 2, the patient complained of chest pain and experienced hypoxemia with activity. CT angiography of the chest demonstrated bilateral segmental and subsegmental pulmonary emboli. The epidural catheter was discontinued. Six hours later, a heparin drip was started, and the patient was transitioned to therapeutic enoxaparin and warfarin. When methicillin-sensitive Staphylococcus aureus (MSSA) was detected in his hemothorax fluid, he was treated with a course of nafcillin.
The patient was discharged to home on postoperative day 12. He has remained neurologically intact and has returned to his former work activities. He is not taking narcotic pain medications.
Discussion
Chiropractic care is a popular alternative health care modality in the United States. Researchers for the 2007 National Health Interview Study1 reported an annual use of chiropractic manipulation of 8.6%, while the Medical Expenditure Panel Survey2 data yielded an estimate of 12.6 million adults using chiropractic manipulation in 2006—translating to a prevalence of 5.6%. Despite the popularity of chiropractic medicine, few well-designed studies have been conducted to support its use.3,4 Because of its designation as an alternative therapy, however, chiropractic manipulation has not been subjected to rigorous efficacy and safety evaluations.5
Given the inconsistency of the evidence to support chiropractic manipulation, the practice's safety profile is a concern. The risks associated with spinal manipulation are generally described in case reports and small series. Most serious adverse events described in the literature are cerebrovascular in nature and tend to occur after cervical manipulation.6,7 Fractures after spine manipulation are exceedingly rare, and published literature on this topic consists of a few isolated case reports, with all fractures occurring in the cervical spine in patients with an underlying pathologic condition.8-10
In 2009, Gouveia et al5 reviewed the published literature regarding all adverse events resulting from chiropractic manipulation. The authors found one randomized controlled trial, two case-control studies, six prospective studies, 12 surveys, three retrospective studies, and 100 case reports. The spectrum of complications identified ranged from benign and transient, such as local discomfort, to far more serious: stroke, myelopathy, radiculopathy, subdural hematoma, spinal fluid leakage, cauda equina syndrome, herniated disc, diaphragmatic palsy, and vertebral fractures. The authors were unable to perform a true meta-analysis because of the heterogeneity of the data, but they concluded that complications associated with chiropractic procedures are "frequent."5
Manipulations Under Anesthesia
MUA is a procedure that combines chiropractic adjustments and manipulations with general anesthesia or procedural sedation.11 The theory behind this strategy is that the anesthesia or sedation reduces pain and muscle spasm that may hinder the manipulation, allowing the practitioner to more effectively break up joint adhesions and reduce segmental dysfunction than if the patient had not undergone anesthesia.11
MUA is generally indicated in patients who have not responded to a 4- to 8-week trial of traditional manipulation therapy.12 It is also considered in patients who have "painful and restricting muscular guarding [that] interferes with the performance of spinal adjustments, mobilizations, and soft tissue release techniques."13
In the chiropractic literature, between 3% and 10% of patients are estimated to be candidates for MUA.12,14 It is not completely clear, however, what diagnoses are most likely to be treated successfully with this technique. Contraindications to MUA are generally the same as those for manipulation in conscious patients. A published list of contraindications from the Committee for Manipulation under Anesthesia (2003)15 included malignancy with bony metastasis, tuberculosis of the bone, recent fracture, acute arthritis, acute gout, diabetic neuropathy, syphilitic articular lesions, excessive spinal osteoporosis, disk fragmentation, direct nerve root impingement, and evidence of cord or caudal compression by tumor, ankylosis, or other space-occupying lesions.
MUA generally begins with deep procedural sedation, managed by an anesthesiologist. Once an adequate level of sedation is achieved, the manipulations are performed. Both high- and low-velocity thrusts are used, but it is recommended that the force exerted should be much less, and the manipulations performed with more caution, than in patients who are not anesthetized.12
For the thoracic spine, the patient is manipulated in the supine position with the arms crossed over the chest. The practitioner places one hand in a fist under the spine with the other hand on the patient's crossed arms, then delivers an anterior-to-posterior thrust. This is repeated until all affected segments have been treated.11,12
Literature to support the use of MUA for various indications is largely anecdotal. The largest published series13 is of 177 patients with chronic spinal pain who each underwent three MUA sessions followed by four to six weeks of traditional manipulations. The authors found that pain, as measured by visual analog scale, was reduced by 62% in patients with cervical spine pain, and by 60% in patients with lumbar pain. No adverse events were reported in the study.
Kohlbeck and Haldeman12 reviewed the reported complications of MUA across all published literature. They found that in 17 published papers, the overall complication rate was 0.7%, mainly represented by transitory increased pain. No spinal fractures were reported.
This case demonstrates a rare but serious complication of chiropractic MUA. It is unclear exactly what mechanism of injury led to an unstable thoracic spine fracture with massive hemothorax, and the precise cause will probably never be known. The clinicians who treated the case patient find it curious that the reported rate of adverse events following this procedure is so low, but they suspect an element of reporting bias in the chiropractic literature.
Conclusion
Iatrogenic injury after chiropractic manipulation is uncommon, but it can be devastating. Few serious complications of chiropractic MUA have been reported, but the literature is lacking in well-designed research studies. Despite the dearth of clinical trials to support its safety and efficacy, use of MUA has continued in the chiropractic community. This case demonstrates that serious adverse outcomes can occur, and more rigorous studies are needed to delineate the true benefits and risks of this set of chiropractic procedures.
References
1. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;12:1-9.
2. Davis MA, Sirovich BE, Weeks WB. Utilization and expenditures on chiropractic care in the United States from 1997 to 2006. Health Serv Res. 2009;45:748-761.
3. Canadian Chiropractic Association; Canadian Federation of Chiropractic Regulatory Boards; Clinical Practice Guidelines Development Initiative; Guidelines Development Committee. Chiropractic clinical practice guideline: evidence-based treatment of adult neck pain not due to whiplash. J Can Chiropr Assoc. 2005;49:417-421.
4.
Hurwitz EL, Aker PD, Adams AH, et al. Manipulation and mobilization of the cervical spine: a systematic review of the literature. Spine (Phila Pa 1976). 1996;21:1746-1760.
5.Gouveia LO, Castanho P, Ferreira JJ. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976). 2009;34:E405-E413.
6. Di Fabio RP. Manipulation of the cervical spine: risks and benefits. Phys Ther. 1999;79:50-65.
7. Nadareishvili Z, Norris JW. Stroke from traumatic arterial dissection. Lancet. 1999;354:159-160.
8. Austin RT. Pathological vertebral fractures after spinal manipulation. Br Med J (Clin Res Ed). 1985;291:1114-1115.
9. Ea HK, Weber AJ, Yon F, Lioté F. Osteoporotic fracture of the dens revealed by cervical manipulation. Joint Bone Spine. 2004;71:246-250.
10. Schmitz A, Lutterbey G, von Engelhardt L, et al. Pathological cervical fracture after spinal manipulation in a pregnant patient. J Manipulative Physiol Ther. 2005;28:633-636.
11. Cremata E, Collins S, Clauson W, et al. Manipulation under anesthesia: a report of four cases. J Manipulative Physiol Ther. 2005;28:526-533.
12. Kohlbeck FJ, Haldeman S. Medication-assisted spinal manipulation. Spine J. 2002;2:288-302.
13. West DT, Mathews RS, Miller MR, Kent GM. Effective management of spinal pain in one hundred seventy-seven patients evaluated for manipulation under anesthesia. J Manipulative Physiol Ther. 1999;22:299-308.
14. Morey LW Jr. Osteopathic manipulation under general anesthesia. J Am Osteopath Assoc. 1973;73:116-127.
15. Tain L, Gunderson C, Cremata E, et al; Committee for Manipulation Under Anesthesia. Recommendations to the Industrial Medical Council Work Group of California for manipulation under anesthesia use for injured workers. Sacramento, CA: Industrial Medical Council; 2003.
A 57-year-old man presented to the emergency department (ED) with a two-day history of worsening shortness of breath, light-headedness, and back pain. The patient, who had a history of ankylosing spondylitis, had been receiving weekly therapy from a chiropractor for about 10 years. One week before presenting to the ED, he had begun to undergo daily manipulations under anesthesia (MUA)—an aggressive chiropractic procedure that is administered while the patient is under monitored, procedural sedation. After the second day of treatment, the patient began to experience worsening back pain and progressive light-headedness and shortness of breath.
At a follow-up visit with his chiropractor, he was found to have decreased O2 saturation and was directed to go to the hospital for evaluation. On arrival at the ED, the patient was awake and alert. He had intact motor strength in all extremities, no sensory abnormalities, intact symmetric reflexes, and no bladder or bowel dysfunction, with a negative Babinski sign. His O2 saturation was 92% on 5 L of oxygen. An absence of breath sounds was noted on the left side.
Chest x-ray (see Figure 1) was performed, which demonstrated complete opacification of the left hemithorax, consistent with a large pleural effusion or hemothorax. CT scan of the thoracic spine showed diffuse ankylosis. A complex oblique coronal and transversely oriented fracture with 7 mm of displacement was identified, beginning at the right anterior inferior lateral margin of the T8 vertebral body and extending centrally and inferiorly to the left and right into the T9 vertebral body. The fracture continued through the right T9-10 neural foramen and what was probably the right fused T9-10 facet joint. The fracture exited through the left superior and lateral margin of the T10 vertebral body and the left T10-11 neural foramen (see Figures 2, 3, and 4).
A chest tube was inserted in the ED, and 1,600 mL of old blood was immediately drained. The patient was admitted to the ICU on the trauma service. He was taken to surgery for open reduction and internal fixation of his unstable thoracic spine fracture on day 3 of hospitalization, after his pulmonary condition stabilized. Pedicle screws were placed from T7 through T12 during the spinal fusion. Good reduction of the fracture was observed following the spine surgery (see Figures 5 and 6). At the conclusion of surgery, an epidural catheter was placed in the thoracic spine to administer pain control.
After the spine portion of the procedure, the patient was repositioned and underwent video-assisted thoracoscopic surgery of the left hemithorax for evacuation of retained hemothorax. The patient tolerated the procedure well and was taken to the ICU for recovery.
On postoperative day 2, the patient complained of chest pain and experienced hypoxemia with activity. CT angiography of the chest demonstrated bilateral segmental and subsegmental pulmonary emboli. The epidural catheter was discontinued. Six hours later, a heparin drip was started, and the patient was transitioned to therapeutic enoxaparin and warfarin. When methicillin-sensitive Staphylococcus aureus (MSSA) was detected in his hemothorax fluid, he was treated with a course of nafcillin.
The patient was discharged to home on postoperative day 12. He has remained neurologically intact and has returned to his former work activities. He is not taking narcotic pain medications.
Discussion
Chiropractic care is a popular alternative health care modality in the United States. Researchers for the 2007 National Health Interview Study1 reported an annual use of chiropractic manipulation of 8.6%, while the Medical Expenditure Panel Survey2 data yielded an estimate of 12.6 million adults using chiropractic manipulation in 2006—translating to a prevalence of 5.6%. Despite the popularity of chiropractic medicine, few well-designed studies have been conducted to support its use.3,4 Because of its designation as an alternative therapy, however, chiropractic manipulation has not been subjected to rigorous efficacy and safety evaluations.5
Given the inconsistency of the evidence to support chiropractic manipulation, the practice's safety profile is a concern. The risks associated with spinal manipulation are generally described in case reports and small series. Most serious adverse events described in the literature are cerebrovascular in nature and tend to occur after cervical manipulation.6,7 Fractures after spine manipulation are exceedingly rare, and published literature on this topic consists of a few isolated case reports, with all fractures occurring in the cervical spine in patients with an underlying pathologic condition.8-10
In 2009, Gouveia et al5 reviewed the published literature regarding all adverse events resulting from chiropractic manipulation. The authors found one randomized controlled trial, two case-control studies, six prospective studies, 12 surveys, three retrospective studies, and 100 case reports. The spectrum of complications identified ranged from benign and transient, such as local discomfort, to far more serious: stroke, myelopathy, radiculopathy, subdural hematoma, spinal fluid leakage, cauda equina syndrome, herniated disc, diaphragmatic palsy, and vertebral fractures. The authors were unable to perform a true meta-analysis because of the heterogeneity of the data, but they concluded that complications associated with chiropractic procedures are "frequent."5
Manipulations Under Anesthesia
MUA is a procedure that combines chiropractic adjustments and manipulations with general anesthesia or procedural sedation.11 The theory behind this strategy is that the anesthesia or sedation reduces pain and muscle spasm that may hinder the manipulation, allowing the practitioner to more effectively break up joint adhesions and reduce segmental dysfunction than if the patient had not undergone anesthesia.11
MUA is generally indicated in patients who have not responded to a 4- to 8-week trial of traditional manipulation therapy.12 It is also considered in patients who have "painful and restricting muscular guarding [that] interferes with the performance of spinal adjustments, mobilizations, and soft tissue release techniques."13
In the chiropractic literature, between 3% and 10% of patients are estimated to be candidates for MUA.12,14 It is not completely clear, however, what diagnoses are most likely to be treated successfully with this technique. Contraindications to MUA are generally the same as those for manipulation in conscious patients. A published list of contraindications from the Committee for Manipulation under Anesthesia (2003)15 included malignancy with bony metastasis, tuberculosis of the bone, recent fracture, acute arthritis, acute gout, diabetic neuropathy, syphilitic articular lesions, excessive spinal osteoporosis, disk fragmentation, direct nerve root impingement, and evidence of cord or caudal compression by tumor, ankylosis, or other space-occupying lesions.
MUA generally begins with deep procedural sedation, managed by an anesthesiologist. Once an adequate level of sedation is achieved, the manipulations are performed. Both high- and low-velocity thrusts are used, but it is recommended that the force exerted should be much less, and the manipulations performed with more caution, than in patients who are not anesthetized.12
For the thoracic spine, the patient is manipulated in the supine position with the arms crossed over the chest. The practitioner places one hand in a fist under the spine with the other hand on the patient's crossed arms, then delivers an anterior-to-posterior thrust. This is repeated until all affected segments have been treated.11,12
Literature to support the use of MUA for various indications is largely anecdotal. The largest published series13 is of 177 patients with chronic spinal pain who each underwent three MUA sessions followed by four to six weeks of traditional manipulations. The authors found that pain, as measured by visual analog scale, was reduced by 62% in patients with cervical spine pain, and by 60% in patients with lumbar pain. No adverse events were reported in the study.
Kohlbeck and Haldeman12 reviewed the reported complications of MUA across all published literature. They found that in 17 published papers, the overall complication rate was 0.7%, mainly represented by transitory increased pain. No spinal fractures were reported.
This case demonstrates a rare but serious complication of chiropractic MUA. It is unclear exactly what mechanism of injury led to an unstable thoracic spine fracture with massive hemothorax, and the precise cause will probably never be known. The clinicians who treated the case patient find it curious that the reported rate of adverse events following this procedure is so low, but they suspect an element of reporting bias in the chiropractic literature.
Conclusion
Iatrogenic injury after chiropractic manipulation is uncommon, but it can be devastating. Few serious complications of chiropractic MUA have been reported, but the literature is lacking in well-designed research studies. Despite the dearth of clinical trials to support its safety and efficacy, use of MUA has continued in the chiropractic community. This case demonstrates that serious adverse outcomes can occur, and more rigorous studies are needed to delineate the true benefits and risks of this set of chiropractic procedures.
References
1. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;12:1-9.
2. Davis MA, Sirovich BE, Weeks WB. Utilization and expenditures on chiropractic care in the United States from 1997 to 2006. Health Serv Res. 2009;45:748-761.
3. Canadian Chiropractic Association; Canadian Federation of Chiropractic Regulatory Boards; Clinical Practice Guidelines Development Initiative; Guidelines Development Committee. Chiropractic clinical practice guideline: evidence-based treatment of adult neck pain not due to whiplash. J Can Chiropr Assoc. 2005;49:417-421.
4.
Hurwitz EL, Aker PD, Adams AH, et al. Manipulation and mobilization of the cervical spine: a systematic review of the literature. Spine (Phila Pa 1976). 1996;21:1746-1760.
5.Gouveia LO, Castanho P, Ferreira JJ. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976). 2009;34:E405-E413.
6. Di Fabio RP. Manipulation of the cervical spine: risks and benefits. Phys Ther. 1999;79:50-65.
7. Nadareishvili Z, Norris JW. Stroke from traumatic arterial dissection. Lancet. 1999;354:159-160.
8. Austin RT. Pathological vertebral fractures after spinal manipulation. Br Med J (Clin Res Ed). 1985;291:1114-1115.
9. Ea HK, Weber AJ, Yon F, Lioté F. Osteoporotic fracture of the dens revealed by cervical manipulation. Joint Bone Spine. 2004;71:246-250.
10. Schmitz A, Lutterbey G, von Engelhardt L, et al. Pathological cervical fracture after spinal manipulation in a pregnant patient. J Manipulative Physiol Ther. 2005;28:633-636.
11. Cremata E, Collins S, Clauson W, et al. Manipulation under anesthesia: a report of four cases. J Manipulative Physiol Ther. 2005;28:526-533.
12. Kohlbeck FJ, Haldeman S. Medication-assisted spinal manipulation. Spine J. 2002;2:288-302.
13. West DT, Mathews RS, Miller MR, Kent GM. Effective management of spinal pain in one hundred seventy-seven patients evaluated for manipulation under anesthesia. J Manipulative Physiol Ther. 1999;22:299-308.
14. Morey LW Jr. Osteopathic manipulation under general anesthesia. J Am Osteopath Assoc. 1973;73:116-127.
15. Tain L, Gunderson C, Cremata E, et al; Committee for Manipulation Under Anesthesia. Recommendations to the Industrial Medical Council Work Group of California for manipulation under anesthesia use for injured workers. Sacramento, CA: Industrial Medical Council; 2003.
Arthroscopic Acetabular Recession With Chondrolabral Preservation
To read the full study, click here.
To read the full study, click here.
To read the full study, click here.

Arthroscopically-Assisted Removal of Retained Loose Bodies in Acute Acetabular Fractures: A Modified Technique
Arthroscopic Acetabular Recession With Chondrolabral Preservation
Eruptive Xanthoma
Newer study shows smoking cessation aid is safe
“Counseling is a must with this smoking cessation aid,” stated a PURL published in March 2012 (J Fam Pract. 2012;61:156, 176). “Varenicline [Chantix] is associated with a small but significant harmful effect on CV outcomes.” That statement, and the PURL itself, was based on a meta-analysis published in 2011 by Singh et al.1 The meta-analysis included 14 randomized controlled trials (RCTs) that compared varenicline with placebo for the occurrence of serious cardiovascular disease (CVD) events, including myocardial infarction, coronary artery disease, arrhythmias, stroke, sudden death, and any related coronary death. RCTs that reported no CVD events were excluded.
Using a Peto odds ratio [OR] for analysis, Singh et al reported that varenicline use increased the risk of CVD events compared with placebo (OR=1.72; 95% CI, 1.09-2.71). A more recent meta-analysis by Prochaska et al,2 however, challenges the validity of the Singh meta-analysis. As members of the Family Physicians Inquiries Network, which produces the PURLs, we would like to address the questions this newer study raises about varenicline’s actual risk.
The Prochaska meta-analysis included all 14 RCTs analyzed by Singh, and used the same CVD event outcome measures. In addition, Prochaska included 8 trials in which no CVD events were reported, some of which were published after the Singh meta-analysis. And rather than use the Peto OR to estimate the risk, Prochaska calculated the absolute risk (AR). The result? The researchers found no difference in CVD events in the varenicline group compared with placebo (AR=0.27; 95% CI, -0.10 to 0.63; P=.15).
This is a good example of how inclusion criteria, subsequently published clinical trials, and the choice of statistical methods can lead to conflicting conclusions from meta-analyses on the same topic. Including studies that showed no adverse CVD events is more likely to capture the true risk than excluding them, and reporting AR is more meaningful than estimating relative risk based on the Peto OR.
Therefore, the Prochaska findings are more convincing. Given the effectiveness of varenicline and the known benefits of successful smoking cessation, it is important for clinicians to understand that the true risk of CVD adverse events attributable to varenicline is extremely low or even nonexistent.
Dionna Brown, MD
Bernard Ewigman, MD, MSPH
Chicago
1. Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
2. Prochaska JJ, Hilton JF. Risk of cardiovascular serious adverse events associated with varenicline use for tobacco cessation: systematic review and meta-analysis. BMJ. 2012;344:e2856.-
“Counseling is a must with this smoking cessation aid,” stated a PURL published in March 2012 (J Fam Pract. 2012;61:156, 176). “Varenicline [Chantix] is associated with a small but significant harmful effect on CV outcomes.” That statement, and the PURL itself, was based on a meta-analysis published in 2011 by Singh et al.1 The meta-analysis included 14 randomized controlled trials (RCTs) that compared varenicline with placebo for the occurrence of serious cardiovascular disease (CVD) events, including myocardial infarction, coronary artery disease, arrhythmias, stroke, sudden death, and any related coronary death. RCTs that reported no CVD events were excluded.
Using a Peto odds ratio [OR] for analysis, Singh et al reported that varenicline use increased the risk of CVD events compared with placebo (OR=1.72; 95% CI, 1.09-2.71). A more recent meta-analysis by Prochaska et al,2 however, challenges the validity of the Singh meta-analysis. As members of the Family Physicians Inquiries Network, which produces the PURLs, we would like to address the questions this newer study raises about varenicline’s actual risk.
The Prochaska meta-analysis included all 14 RCTs analyzed by Singh, and used the same CVD event outcome measures. In addition, Prochaska included 8 trials in which no CVD events were reported, some of which were published after the Singh meta-analysis. And rather than use the Peto OR to estimate the risk, Prochaska calculated the absolute risk (AR). The result? The researchers found no difference in CVD events in the varenicline group compared with placebo (AR=0.27; 95% CI, -0.10 to 0.63; P=.15).
This is a good example of how inclusion criteria, subsequently published clinical trials, and the choice of statistical methods can lead to conflicting conclusions from meta-analyses on the same topic. Including studies that showed no adverse CVD events is more likely to capture the true risk than excluding them, and reporting AR is more meaningful than estimating relative risk based on the Peto OR.
Therefore, the Prochaska findings are more convincing. Given the effectiveness of varenicline and the known benefits of successful smoking cessation, it is important for clinicians to understand that the true risk of CVD adverse events attributable to varenicline is extremely low or even nonexistent.
Dionna Brown, MD
Bernard Ewigman, MD, MSPH
Chicago
“Counseling is a must with this smoking cessation aid,” stated a PURL published in March 2012 (J Fam Pract. 2012;61:156, 176). “Varenicline [Chantix] is associated with a small but significant harmful effect on CV outcomes.” That statement, and the PURL itself, was based on a meta-analysis published in 2011 by Singh et al.1 The meta-analysis included 14 randomized controlled trials (RCTs) that compared varenicline with placebo for the occurrence of serious cardiovascular disease (CVD) events, including myocardial infarction, coronary artery disease, arrhythmias, stroke, sudden death, and any related coronary death. RCTs that reported no CVD events were excluded.
Using a Peto odds ratio [OR] for analysis, Singh et al reported that varenicline use increased the risk of CVD events compared with placebo (OR=1.72; 95% CI, 1.09-2.71). A more recent meta-analysis by Prochaska et al,2 however, challenges the validity of the Singh meta-analysis. As members of the Family Physicians Inquiries Network, which produces the PURLs, we would like to address the questions this newer study raises about varenicline’s actual risk.
The Prochaska meta-analysis included all 14 RCTs analyzed by Singh, and used the same CVD event outcome measures. In addition, Prochaska included 8 trials in which no CVD events were reported, some of which were published after the Singh meta-analysis. And rather than use the Peto OR to estimate the risk, Prochaska calculated the absolute risk (AR). The result? The researchers found no difference in CVD events in the varenicline group compared with placebo (AR=0.27; 95% CI, -0.10 to 0.63; P=.15).
This is a good example of how inclusion criteria, subsequently published clinical trials, and the choice of statistical methods can lead to conflicting conclusions from meta-analyses on the same topic. Including studies that showed no adverse CVD events is more likely to capture the true risk than excluding them, and reporting AR is more meaningful than estimating relative risk based on the Peto OR.
Therefore, the Prochaska findings are more convincing. Given the effectiveness of varenicline and the known benefits of successful smoking cessation, it is important for clinicians to understand that the true risk of CVD adverse events attributable to varenicline is extremely low or even nonexistent.
Dionna Brown, MD
Bernard Ewigman, MD, MSPH
Chicago
1. Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
2. Prochaska JJ, Hilton JF. Risk of cardiovascular serious adverse events associated with varenicline use for tobacco cessation: systematic review and meta-analysis. BMJ. 2012;344:e2856.-
1. Singh S, Loke YK, Spangler JG, et al. Risk of serious adverse cardiovascular events associated with varenicline: a systematic review and meta-analysis. CMAJ. 2011;183:1359-1366.
2. Prochaska JJ, Hilton JF. Risk of cardiovascular serious adverse events associated with varenicline use for tobacco cessation: systematic review and meta-analysis. BMJ. 2012;344:e2856.-
Sleepless and paranoid
CASE: Worsening insomnia
Mr. Q, age 44, presents for evaluation of altered mental status characterized by disorientation, impaired attention and concentration, paranoid delusions, and prominent auditory and visual hallucinations. His initial Folstein Mini-Mental State Examination (MMSE) score is 7 of 30, indicating severe impairment. He further describes a recent history of nausea, intermittent vomiting, and anorexia. He takes hydrocodone/acetaminophen, 5/500 mg, 4 times daily for lower back and joint pain. Additionally, he has a pacemaker, which was placed when Mr. Q was in his late 30s to treat sinus bradycardia.
Mr. Q’s fiancée describes his 6-month history of worsening sleep disturbance, noting insomnia, fractured sleep, dream enactment, and daytime fatigue. During this time, Mr. Q averaged 3 to 4 hours of sleep nightly without day-time naps. Ten days ago, he stopped sleeping completely and his cognitive function decompensated rapidly. He became increasingly paranoid, believing government agents had been dispatched to kill him. Several days before admission, Mr. Q developed auditory and visual hallucinations. He reports that he hears voices warning him of Armageddon and sees reincarnated spirits of deceased relatives. He describes his mood as “fine” and “okay” and lacks insight into his psychiatric symptoms other than his sleeplessness.
Mr. Q’s family says he has a history of transient mild depression after his older brother died from an unknown neurologic disease 3 years ago. Mr. Q did not receive pharmacotherapy or psychotherapy but his symptoms resolved. His family says that Mr. Q has been using marijuana daily for several years, but they are unaware of other substance use. They deny a family history of psychiatric illness.
On physical examination, Mr. Q appears thin, agitated, and in mild distress. He has a fever of 99.2°F. His blood pressure drops intermittently from a baseline of 120/70 mm Hg to 100/60 mm Hg, at which point he experiences transient normal sinus tachycardia. Neurologic examination reveals psychomotor agitation and diffuse myoclonic tremor.
The authors’ observations
Table 1
Differential diagnosis of insomnia
| Type of disorder | Examples |
|---|---|
| Sleep disorders | Narcolepsy, REM sleep disorder, periodic limb movement disorder, restless leg syndrome, parasomniac conditions |
| Psychiatric disorders | Mania or hypomania, psychosis, substance intoxication or withdrawal, dementia, delirium |
| Neurologic disorders | Stroke, malignancy, infection or abscess, metabolic or viral encephalopathy, seizure disorder, prion disease |
| Somatic conditions | Cardiorespiratory disease, central or obstructive sleep apnea, congestive heart failure (Cheyne-Stokes respiration), pain, nocturnal movement disorder, gastroesophageal reflux disease, nocturia |
| Other causes | Jet lag, shift work, environment, lifestyle, medication |
| REM: rapid eye movement Source: Reference 1 | |
Medications that can cause or exacerbate insomnia
| Class/category | Medication(s) |
|---|---|
| Stimulants | Bupropion, dextroamphetamine, methylphenidate |
| Decongestants | Pseudoephedrine, phenylephrine |
| Antihypertensives or antiarrythmics | α- and β-antagonists |
| Respiratory medications | Albuterol, theophylline |
| Hormones | Corticosteroids, thyroid medications |
| Anticonvulsants | Lamotrigine |
| Medications that induce rebound insomnia | Benzodiazepines, sedative-hypnotics, opioids |
| Nonprescription medications | Caffeine, alcohol, nicotine, illicit psychostimulants |
EVALUATION: Inconclusive results
Routine laboratory studies reveal mild normocytic anemia and mild hypokalemia. Liver panel, renal function, cardiac profile, brain natriuretic peptide level, folate and vitamin B12 levels, thyroid studies, and human immunodeficiency virus serology are negative or within normal limits. Urinalysis reveals the presence of ketones, indicative of Mr. Q’s recent anorexia. Chest radiography and CT imaging of the head, abdomen, and pelvis also are unremarkable. MRI is contraindicated because of Mr. Q’s implanted pacemaker. Pulse oximetry does not suggest apneic events. Mr. Q and his family refuse a lumbar puncture, which precludes cerebrospinal fluid (CSF) analysis. Electroencephalography (EEG) records normal patterns of wakefulness oscillating with transient periods of stage 1 sleep. A detailed family interview reveals that Mr. Q’s older brother had a history of epilepsy and died at age 49 following a prolonged hospitalization for recurrent seizures and similar insomnia symptoms. History from the patient’s paternal lineage is not available.
The authors’ observations
American Psychiatric Association practice guidelines3 do not support first-line use of benzodiazepines for non-alcohol withdrawal-related delirium. Benzodiazepines are ineffective for treating delirium and may exacerbate symptoms.4 Laboratory evidence confirmed Mr. Q has no history of alcohol or benzodiazepine use. Although treating the underlying cause of delirium is essential, prescribing a sedative-hypnotic medication such as zolpidem for Mr. Q’s insomnia may worsen his condition. These agents are known to impair cognition and may induce or intensify psychosis.5 Melatonin and melatonin receptor agonists, such as ramelteon, promote sleep by regulating the sleep-wake rhythm through their action on melatonin receptors in the hypothalamus.6 Recently, a randomized control trial (RCT)7 found melatonin protected against delirium in hospitalized patients age ≥65. However, no RCT has examined use of exogenous melatonin or melatonin receptor agonists to treat delirium. In Mr. Q’s case, we chose to administer haloperidol. First- and second-generation antipsychotics have shown efficacy in treating acute delirium. Although more clinical experience has accumulated using first-generation agents such as haloperidol, a 2007 Cochrane meta-analysis8 demonstrated equal benefit with second-generation antipsychotics, while noting a decreased incidence of adverse effects.
TREATMENT: Adverse effects
Mr. Q receives an IM injection of haloperidol, 5 mg, for severe agitation, followed 15 hours later by IM aripiprazole, 9.75 mg. Within hours of receiving aripiprazole, Mr. Q develops hyperkinetic perioral and tongue movements. He initially is diagnosed with acute reactionary dystonia, although closer examination reveals myoclonus consistent with his overall presentation. Additionally, his QTc interval increases by 120 ms. Subsequently, all antipsychotics are stopped. We prescribe lorazepam, 1 mg IM every 4 hours as needed, for agitation. Mr. Q receives 2 consecutive doses of lorazepam, although neither effectively reduces his agitation or promotes sleep. Mr. Q is not assessed with positron-emission tomography (PET) or polysomnography.
The authors’ observations
There was no evidence of neurologic disease on Mr. Q’s CT scan and EEG was within normal limits. Other imaging and laboratory studies did not reveal possible infection, malignancy, or cardiovascular disease. Despite its rarity, we considered the possibility of a prion disease, given Mr. Q’s unique presentation and family history. Familial fatal insomnia (FFI) is an autosomal dominant disease caused by a point mutation in the prion protein gene. Prion proteins are theorized to play a role in myelin stability. The aberrant isoform produced in FFI is structurally misfolded so that it resists degradation by proteolytic enzymes. The accumulation of irregular prion proteins in the medial thalamic nucleus results in progressive neurodegeneration. Patients with FFI present with increasingly severe insomnia, mild fever, dysautonomia, spontaneous myoclonus, cognitive dysfunction, and hallucinations.9 Generally, patients die from sudden cardiorespiratory failure or ensuing infections 9 to 24 months after symptom onset. In vivo, FFI diagnosis is suggested by a loss of sleep spindles on polysomnogram and by decreased thalamic metabolism on PET scan. Other imaging modalities and testing, including EEG and CSF analysis, lack sensitivity and/or specificity.10
OUTCOME: Improvement, discharge
On his fourth hospital day, Mr. Q’s symptoms begin to remit spontaneously. His gastrointestinal (GI) upset improves and the following night he sleeps for approximately 4 hours. As his sleep improves, his delusional thinking and hallucinations resolve. Orientation, memory, and concentration gradually improve. Before discharge, his MMSE score is 24 out of 30, indicating improved cognition. His heart rate, blood pressure, and body temperature normalize and his myoclonus improves. Mr. Q is discharged after 6 days in the hospital and returns home. He follows up with his primary care physician, denies any recurrence of sleep disturbance, and reports that his cognition and perception have returned to his baseline.
The authors’ observations
12
Table 3
DSM-IV-TR diagnostic criteria for opioid withdrawal
| A. | Either of the following:
|
| B. | ≥3 of the following, developing within minutes to several days after criterion A:
|
| C. | The symptoms of criterion B cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| D. | The symptoms are not due to a general medical condition and are not better accounted for by another mental disorder |
| Source: Reference 11 | |
- Morin CM, Benca R. Chronic insomnia. Lancet. 2012; 379(9821):1129-1141.
- Pressman MR, Orr WC, eds. Understanding sleep: the evolution and treatment of sleep disorders. Washington, DC: American Psychological Association; 1997.
- NIH State-of-the-Science Conference Statement on manifestations and management of chronic insomnia in adults. NIH Consens State Sci Statements. 2005;22(2):1-30.
- Albuterol • Proventil, Ventolin
- Aripiprazole • Abilify
- Bupropion • Wellbutrin, Zyban
- Dextroamphetamine • Dexadrine
- Haloperidol • Haldol
- Hydrocodone/Acetaminophen • Vicodin
- Lamotrigine • Lamictal
- Lorazepam • Ativan
- Methylphenidate • Methylin, Ritalin
- Phenylephrine • Neo-Synephrine
- Pseudoephedrine • Sudafed
- Ramelteon • Rozerem
- Theophylline • Elixophyllin, Slo-Phyllin
- Zolpidem • Ambien
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mai E, Buysse DJ. Insomnia: prevalence impact, pathogenesis, differential diagnosis, and evaluation. Sleep Med Clin. 2008;3(2):167-174.
2. Kennedy N, Boydell J, Kalidindi S, et al. Gender differences in incidence and age at onset of mania and bipolar disorder over a 35-year period in Camberwell, England. Am J Psychiatry. 2005;162(2):257-262.
3. Cook IA. American Psychiatric Association. Guideline watch: practice guidelines for the treatment of patients with delirium. http://psychiatryonline.org/content.aspx?bookid=28§ionid=1681952. Accessed June 20 2012.
4. Lonergan E, Luxenberg J, Areosa Sastre A, et al. Benzodiazepines for delirium. Cochrane Database Syst Rev. 2009;21(1):CD006379.-
5. Toner LC, Tsambiras BM, Catalano G, et al. Central nervous system side effects associated with zolpidem treatment. Clin Neuropharmacol. 2000;23(1):54-58.
6. Srinivasan V, Pandi-Perumal SR, Trahkt I, et al. Melatonin and melatonergic drugs on sleep: possible mechanisms of action. Int J Neurosci. 2009;119(6):821-846.
7. Al-Aama T, Brymer C, Gutmanis I, et al. Melatonin decreases delirium in elderly patients: a randomized, placebo-controlled trial. Int J Geriatr Psychiatry. 2011;26(7):687-694.
8. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;18(2):CD005594.-
9. Medori R, Tritschler HJ, LeBlanc A, et al. Fatal familial insomnia, a prion disease with a mutation codon 178 of the prion protein gene. N Engl J Med. 1992;326(7):444-449.
10. Lugaresi E, Provini F, Cortelli P. Agrypnia excitata. Sleep Med. 2011;12(suppl 2):S3-S10.
11. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
12. Jaffe JH, Strain EC. Opioid-related disorders. In: Sadock BJ Sadock VA, eds. Kaplan and Sadock’s comprehensive textbook of psychiatry. 8th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2005:1164, 1272-1274.
CASE: Worsening insomnia
Mr. Q, age 44, presents for evaluation of altered mental status characterized by disorientation, impaired attention and concentration, paranoid delusions, and prominent auditory and visual hallucinations. His initial Folstein Mini-Mental State Examination (MMSE) score is 7 of 30, indicating severe impairment. He further describes a recent history of nausea, intermittent vomiting, and anorexia. He takes hydrocodone/acetaminophen, 5/500 mg, 4 times daily for lower back and joint pain. Additionally, he has a pacemaker, which was placed when Mr. Q was in his late 30s to treat sinus bradycardia.
Mr. Q’s fiancée describes his 6-month history of worsening sleep disturbance, noting insomnia, fractured sleep, dream enactment, and daytime fatigue. During this time, Mr. Q averaged 3 to 4 hours of sleep nightly without day-time naps. Ten days ago, he stopped sleeping completely and his cognitive function decompensated rapidly. He became increasingly paranoid, believing government agents had been dispatched to kill him. Several days before admission, Mr. Q developed auditory and visual hallucinations. He reports that he hears voices warning him of Armageddon and sees reincarnated spirits of deceased relatives. He describes his mood as “fine” and “okay” and lacks insight into his psychiatric symptoms other than his sleeplessness.
Mr. Q’s family says he has a history of transient mild depression after his older brother died from an unknown neurologic disease 3 years ago. Mr. Q did not receive pharmacotherapy or psychotherapy but his symptoms resolved. His family says that Mr. Q has been using marijuana daily for several years, but they are unaware of other substance use. They deny a family history of psychiatric illness.
On physical examination, Mr. Q appears thin, agitated, and in mild distress. He has a fever of 99.2°F. His blood pressure drops intermittently from a baseline of 120/70 mm Hg to 100/60 mm Hg, at which point he experiences transient normal sinus tachycardia. Neurologic examination reveals psychomotor agitation and diffuse myoclonic tremor.
The authors’ observations
Table 1
Differential diagnosis of insomnia
| Type of disorder | Examples |
|---|---|
| Sleep disorders | Narcolepsy, REM sleep disorder, periodic limb movement disorder, restless leg syndrome, parasomniac conditions |
| Psychiatric disorders | Mania or hypomania, psychosis, substance intoxication or withdrawal, dementia, delirium |
| Neurologic disorders | Stroke, malignancy, infection or abscess, metabolic or viral encephalopathy, seizure disorder, prion disease |
| Somatic conditions | Cardiorespiratory disease, central or obstructive sleep apnea, congestive heart failure (Cheyne-Stokes respiration), pain, nocturnal movement disorder, gastroesophageal reflux disease, nocturia |
| Other causes | Jet lag, shift work, environment, lifestyle, medication |
| REM: rapid eye movement Source: Reference 1 | |
Medications that can cause or exacerbate insomnia
| Class/category | Medication(s) |
|---|---|
| Stimulants | Bupropion, dextroamphetamine, methylphenidate |
| Decongestants | Pseudoephedrine, phenylephrine |
| Antihypertensives or antiarrythmics | α- and β-antagonists |
| Respiratory medications | Albuterol, theophylline |
| Hormones | Corticosteroids, thyroid medications |
| Anticonvulsants | Lamotrigine |
| Medications that induce rebound insomnia | Benzodiazepines, sedative-hypnotics, opioids |
| Nonprescription medications | Caffeine, alcohol, nicotine, illicit psychostimulants |
EVALUATION: Inconclusive results
Routine laboratory studies reveal mild normocytic anemia and mild hypokalemia. Liver panel, renal function, cardiac profile, brain natriuretic peptide level, folate and vitamin B12 levels, thyroid studies, and human immunodeficiency virus serology are negative or within normal limits. Urinalysis reveals the presence of ketones, indicative of Mr. Q’s recent anorexia. Chest radiography and CT imaging of the head, abdomen, and pelvis also are unremarkable. MRI is contraindicated because of Mr. Q’s implanted pacemaker. Pulse oximetry does not suggest apneic events. Mr. Q and his family refuse a lumbar puncture, which precludes cerebrospinal fluid (CSF) analysis. Electroencephalography (EEG) records normal patterns of wakefulness oscillating with transient periods of stage 1 sleep. A detailed family interview reveals that Mr. Q’s older brother had a history of epilepsy and died at age 49 following a prolonged hospitalization for recurrent seizures and similar insomnia symptoms. History from the patient’s paternal lineage is not available.
The authors’ observations
American Psychiatric Association practice guidelines3 do not support first-line use of benzodiazepines for non-alcohol withdrawal-related delirium. Benzodiazepines are ineffective for treating delirium and may exacerbate symptoms.4 Laboratory evidence confirmed Mr. Q has no history of alcohol or benzodiazepine use. Although treating the underlying cause of delirium is essential, prescribing a sedative-hypnotic medication such as zolpidem for Mr. Q’s insomnia may worsen his condition. These agents are known to impair cognition and may induce or intensify psychosis.5 Melatonin and melatonin receptor agonists, such as ramelteon, promote sleep by regulating the sleep-wake rhythm through their action on melatonin receptors in the hypothalamus.6 Recently, a randomized control trial (RCT)7 found melatonin protected against delirium in hospitalized patients age ≥65. However, no RCT has examined use of exogenous melatonin or melatonin receptor agonists to treat delirium. In Mr. Q’s case, we chose to administer haloperidol. First- and second-generation antipsychotics have shown efficacy in treating acute delirium. Although more clinical experience has accumulated using first-generation agents such as haloperidol, a 2007 Cochrane meta-analysis8 demonstrated equal benefit with second-generation antipsychotics, while noting a decreased incidence of adverse effects.
TREATMENT: Adverse effects
Mr. Q receives an IM injection of haloperidol, 5 mg, for severe agitation, followed 15 hours later by IM aripiprazole, 9.75 mg. Within hours of receiving aripiprazole, Mr. Q develops hyperkinetic perioral and tongue movements. He initially is diagnosed with acute reactionary dystonia, although closer examination reveals myoclonus consistent with his overall presentation. Additionally, his QTc interval increases by 120 ms. Subsequently, all antipsychotics are stopped. We prescribe lorazepam, 1 mg IM every 4 hours as needed, for agitation. Mr. Q receives 2 consecutive doses of lorazepam, although neither effectively reduces his agitation or promotes sleep. Mr. Q is not assessed with positron-emission tomography (PET) or polysomnography.
The authors’ observations
There was no evidence of neurologic disease on Mr. Q’s CT scan and EEG was within normal limits. Other imaging and laboratory studies did not reveal possible infection, malignancy, or cardiovascular disease. Despite its rarity, we considered the possibility of a prion disease, given Mr. Q’s unique presentation and family history. Familial fatal insomnia (FFI) is an autosomal dominant disease caused by a point mutation in the prion protein gene. Prion proteins are theorized to play a role in myelin stability. The aberrant isoform produced in FFI is structurally misfolded so that it resists degradation by proteolytic enzymes. The accumulation of irregular prion proteins in the medial thalamic nucleus results in progressive neurodegeneration. Patients with FFI present with increasingly severe insomnia, mild fever, dysautonomia, spontaneous myoclonus, cognitive dysfunction, and hallucinations.9 Generally, patients die from sudden cardiorespiratory failure or ensuing infections 9 to 24 months after symptom onset. In vivo, FFI diagnosis is suggested by a loss of sleep spindles on polysomnogram and by decreased thalamic metabolism on PET scan. Other imaging modalities and testing, including EEG and CSF analysis, lack sensitivity and/or specificity.10
OUTCOME: Improvement, discharge
On his fourth hospital day, Mr. Q’s symptoms begin to remit spontaneously. His gastrointestinal (GI) upset improves and the following night he sleeps for approximately 4 hours. As his sleep improves, his delusional thinking and hallucinations resolve. Orientation, memory, and concentration gradually improve. Before discharge, his MMSE score is 24 out of 30, indicating improved cognition. His heart rate, blood pressure, and body temperature normalize and his myoclonus improves. Mr. Q is discharged after 6 days in the hospital and returns home. He follows up with his primary care physician, denies any recurrence of sleep disturbance, and reports that his cognition and perception have returned to his baseline.
The authors’ observations
12
Table 3
DSM-IV-TR diagnostic criteria for opioid withdrawal
| A. | Either of the following:
|
| B. | ≥3 of the following, developing within minutes to several days after criterion A:
|
| C. | The symptoms of criterion B cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| D. | The symptoms are not due to a general medical condition and are not better accounted for by another mental disorder |
| Source: Reference 11 | |
- Morin CM, Benca R. Chronic insomnia. Lancet. 2012; 379(9821):1129-1141.
- Pressman MR, Orr WC, eds. Understanding sleep: the evolution and treatment of sleep disorders. Washington, DC: American Psychological Association; 1997.
- NIH State-of-the-Science Conference Statement on manifestations and management of chronic insomnia in adults. NIH Consens State Sci Statements. 2005;22(2):1-30.
- Albuterol • Proventil, Ventolin
- Aripiprazole • Abilify
- Bupropion • Wellbutrin, Zyban
- Dextroamphetamine • Dexadrine
- Haloperidol • Haldol
- Hydrocodone/Acetaminophen • Vicodin
- Lamotrigine • Lamictal
- Lorazepam • Ativan
- Methylphenidate • Methylin, Ritalin
- Phenylephrine • Neo-Synephrine
- Pseudoephedrine • Sudafed
- Ramelteon • Rozerem
- Theophylline • Elixophyllin, Slo-Phyllin
- Zolpidem • Ambien
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Worsening insomnia
Mr. Q, age 44, presents for evaluation of altered mental status characterized by disorientation, impaired attention and concentration, paranoid delusions, and prominent auditory and visual hallucinations. His initial Folstein Mini-Mental State Examination (MMSE) score is 7 of 30, indicating severe impairment. He further describes a recent history of nausea, intermittent vomiting, and anorexia. He takes hydrocodone/acetaminophen, 5/500 mg, 4 times daily for lower back and joint pain. Additionally, he has a pacemaker, which was placed when Mr. Q was in his late 30s to treat sinus bradycardia.
Mr. Q’s fiancée describes his 6-month history of worsening sleep disturbance, noting insomnia, fractured sleep, dream enactment, and daytime fatigue. During this time, Mr. Q averaged 3 to 4 hours of sleep nightly without day-time naps. Ten days ago, he stopped sleeping completely and his cognitive function decompensated rapidly. He became increasingly paranoid, believing government agents had been dispatched to kill him. Several days before admission, Mr. Q developed auditory and visual hallucinations. He reports that he hears voices warning him of Armageddon and sees reincarnated spirits of deceased relatives. He describes his mood as “fine” and “okay” and lacks insight into his psychiatric symptoms other than his sleeplessness.
Mr. Q’s family says he has a history of transient mild depression after his older brother died from an unknown neurologic disease 3 years ago. Mr. Q did not receive pharmacotherapy or psychotherapy but his symptoms resolved. His family says that Mr. Q has been using marijuana daily for several years, but they are unaware of other substance use. They deny a family history of psychiatric illness.
On physical examination, Mr. Q appears thin, agitated, and in mild distress. He has a fever of 99.2°F. His blood pressure drops intermittently from a baseline of 120/70 mm Hg to 100/60 mm Hg, at which point he experiences transient normal sinus tachycardia. Neurologic examination reveals psychomotor agitation and diffuse myoclonic tremor.
The authors’ observations
Table 1
Differential diagnosis of insomnia
| Type of disorder | Examples |
|---|---|
| Sleep disorders | Narcolepsy, REM sleep disorder, periodic limb movement disorder, restless leg syndrome, parasomniac conditions |
| Psychiatric disorders | Mania or hypomania, psychosis, substance intoxication or withdrawal, dementia, delirium |
| Neurologic disorders | Stroke, malignancy, infection or abscess, metabolic or viral encephalopathy, seizure disorder, prion disease |
| Somatic conditions | Cardiorespiratory disease, central or obstructive sleep apnea, congestive heart failure (Cheyne-Stokes respiration), pain, nocturnal movement disorder, gastroesophageal reflux disease, nocturia |
| Other causes | Jet lag, shift work, environment, lifestyle, medication |
| REM: rapid eye movement Source: Reference 1 | |
Medications that can cause or exacerbate insomnia
| Class/category | Medication(s) |
|---|---|
| Stimulants | Bupropion, dextroamphetamine, methylphenidate |
| Decongestants | Pseudoephedrine, phenylephrine |
| Antihypertensives or antiarrythmics | α- and β-antagonists |
| Respiratory medications | Albuterol, theophylline |
| Hormones | Corticosteroids, thyroid medications |
| Anticonvulsants | Lamotrigine |
| Medications that induce rebound insomnia | Benzodiazepines, sedative-hypnotics, opioids |
| Nonprescription medications | Caffeine, alcohol, nicotine, illicit psychostimulants |
EVALUATION: Inconclusive results
Routine laboratory studies reveal mild normocytic anemia and mild hypokalemia. Liver panel, renal function, cardiac profile, brain natriuretic peptide level, folate and vitamin B12 levels, thyroid studies, and human immunodeficiency virus serology are negative or within normal limits. Urinalysis reveals the presence of ketones, indicative of Mr. Q’s recent anorexia. Chest radiography and CT imaging of the head, abdomen, and pelvis also are unremarkable. MRI is contraindicated because of Mr. Q’s implanted pacemaker. Pulse oximetry does not suggest apneic events. Mr. Q and his family refuse a lumbar puncture, which precludes cerebrospinal fluid (CSF) analysis. Electroencephalography (EEG) records normal patterns of wakefulness oscillating with transient periods of stage 1 sleep. A detailed family interview reveals that Mr. Q’s older brother had a history of epilepsy and died at age 49 following a prolonged hospitalization for recurrent seizures and similar insomnia symptoms. History from the patient’s paternal lineage is not available.
The authors’ observations
American Psychiatric Association practice guidelines3 do not support first-line use of benzodiazepines for non-alcohol withdrawal-related delirium. Benzodiazepines are ineffective for treating delirium and may exacerbate symptoms.4 Laboratory evidence confirmed Mr. Q has no history of alcohol or benzodiazepine use. Although treating the underlying cause of delirium is essential, prescribing a sedative-hypnotic medication such as zolpidem for Mr. Q’s insomnia may worsen his condition. These agents are known to impair cognition and may induce or intensify psychosis.5 Melatonin and melatonin receptor agonists, such as ramelteon, promote sleep by regulating the sleep-wake rhythm through their action on melatonin receptors in the hypothalamus.6 Recently, a randomized control trial (RCT)7 found melatonin protected against delirium in hospitalized patients age ≥65. However, no RCT has examined use of exogenous melatonin or melatonin receptor agonists to treat delirium. In Mr. Q’s case, we chose to administer haloperidol. First- and second-generation antipsychotics have shown efficacy in treating acute delirium. Although more clinical experience has accumulated using first-generation agents such as haloperidol, a 2007 Cochrane meta-analysis8 demonstrated equal benefit with second-generation antipsychotics, while noting a decreased incidence of adverse effects.
TREATMENT: Adverse effects
Mr. Q receives an IM injection of haloperidol, 5 mg, for severe agitation, followed 15 hours later by IM aripiprazole, 9.75 mg. Within hours of receiving aripiprazole, Mr. Q develops hyperkinetic perioral and tongue movements. He initially is diagnosed with acute reactionary dystonia, although closer examination reveals myoclonus consistent with his overall presentation. Additionally, his QTc interval increases by 120 ms. Subsequently, all antipsychotics are stopped. We prescribe lorazepam, 1 mg IM every 4 hours as needed, for agitation. Mr. Q receives 2 consecutive doses of lorazepam, although neither effectively reduces his agitation or promotes sleep. Mr. Q is not assessed with positron-emission tomography (PET) or polysomnography.
The authors’ observations
There was no evidence of neurologic disease on Mr. Q’s CT scan and EEG was within normal limits. Other imaging and laboratory studies did not reveal possible infection, malignancy, or cardiovascular disease. Despite its rarity, we considered the possibility of a prion disease, given Mr. Q’s unique presentation and family history. Familial fatal insomnia (FFI) is an autosomal dominant disease caused by a point mutation in the prion protein gene. Prion proteins are theorized to play a role in myelin stability. The aberrant isoform produced in FFI is structurally misfolded so that it resists degradation by proteolytic enzymes. The accumulation of irregular prion proteins in the medial thalamic nucleus results in progressive neurodegeneration. Patients with FFI present with increasingly severe insomnia, mild fever, dysautonomia, spontaneous myoclonus, cognitive dysfunction, and hallucinations.9 Generally, patients die from sudden cardiorespiratory failure or ensuing infections 9 to 24 months after symptom onset. In vivo, FFI diagnosis is suggested by a loss of sleep spindles on polysomnogram and by decreased thalamic metabolism on PET scan. Other imaging modalities and testing, including EEG and CSF analysis, lack sensitivity and/or specificity.10
OUTCOME: Improvement, discharge
On his fourth hospital day, Mr. Q’s symptoms begin to remit spontaneously. His gastrointestinal (GI) upset improves and the following night he sleeps for approximately 4 hours. As his sleep improves, his delusional thinking and hallucinations resolve. Orientation, memory, and concentration gradually improve. Before discharge, his MMSE score is 24 out of 30, indicating improved cognition. His heart rate, blood pressure, and body temperature normalize and his myoclonus improves. Mr. Q is discharged after 6 days in the hospital and returns home. He follows up with his primary care physician, denies any recurrence of sleep disturbance, and reports that his cognition and perception have returned to his baseline.
The authors’ observations
12
Table 3
DSM-IV-TR diagnostic criteria for opioid withdrawal
| A. | Either of the following:
|
| B. | ≥3 of the following, developing within minutes to several days after criterion A:
|
| C. | The symptoms of criterion B cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| D. | The symptoms are not due to a general medical condition and are not better accounted for by another mental disorder |
| Source: Reference 11 | |
- Morin CM, Benca R. Chronic insomnia. Lancet. 2012; 379(9821):1129-1141.
- Pressman MR, Orr WC, eds. Understanding sleep: the evolution and treatment of sleep disorders. Washington, DC: American Psychological Association; 1997.
- NIH State-of-the-Science Conference Statement on manifestations and management of chronic insomnia in adults. NIH Consens State Sci Statements. 2005;22(2):1-30.
- Albuterol • Proventil, Ventolin
- Aripiprazole • Abilify
- Bupropion • Wellbutrin, Zyban
- Dextroamphetamine • Dexadrine
- Haloperidol • Haldol
- Hydrocodone/Acetaminophen • Vicodin
- Lamotrigine • Lamictal
- Lorazepam • Ativan
- Methylphenidate • Methylin, Ritalin
- Phenylephrine • Neo-Synephrine
- Pseudoephedrine • Sudafed
- Ramelteon • Rozerem
- Theophylline • Elixophyllin, Slo-Phyllin
- Zolpidem • Ambien
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mai E, Buysse DJ. Insomnia: prevalence impact, pathogenesis, differential diagnosis, and evaluation. Sleep Med Clin. 2008;3(2):167-174.
2. Kennedy N, Boydell J, Kalidindi S, et al. Gender differences in incidence and age at onset of mania and bipolar disorder over a 35-year period in Camberwell, England. Am J Psychiatry. 2005;162(2):257-262.
3. Cook IA. American Psychiatric Association. Guideline watch: practice guidelines for the treatment of patients with delirium. http://psychiatryonline.org/content.aspx?bookid=28§ionid=1681952. Accessed June 20 2012.
4. Lonergan E, Luxenberg J, Areosa Sastre A, et al. Benzodiazepines for delirium. Cochrane Database Syst Rev. 2009;21(1):CD006379.-
5. Toner LC, Tsambiras BM, Catalano G, et al. Central nervous system side effects associated with zolpidem treatment. Clin Neuropharmacol. 2000;23(1):54-58.
6. Srinivasan V, Pandi-Perumal SR, Trahkt I, et al. Melatonin and melatonergic drugs on sleep: possible mechanisms of action. Int J Neurosci. 2009;119(6):821-846.
7. Al-Aama T, Brymer C, Gutmanis I, et al. Melatonin decreases delirium in elderly patients: a randomized, placebo-controlled trial. Int J Geriatr Psychiatry. 2011;26(7):687-694.
8. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;18(2):CD005594.-
9. Medori R, Tritschler HJ, LeBlanc A, et al. Fatal familial insomnia, a prion disease with a mutation codon 178 of the prion protein gene. N Engl J Med. 1992;326(7):444-449.
10. Lugaresi E, Provini F, Cortelli P. Agrypnia excitata. Sleep Med. 2011;12(suppl 2):S3-S10.
11. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
12. Jaffe JH, Strain EC. Opioid-related disorders. In: Sadock BJ Sadock VA, eds. Kaplan and Sadock’s comprehensive textbook of psychiatry. 8th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2005:1164, 1272-1274.
1. Mai E, Buysse DJ. Insomnia: prevalence impact, pathogenesis, differential diagnosis, and evaluation. Sleep Med Clin. 2008;3(2):167-174.
2. Kennedy N, Boydell J, Kalidindi S, et al. Gender differences in incidence and age at onset of mania and bipolar disorder over a 35-year period in Camberwell, England. Am J Psychiatry. 2005;162(2):257-262.
3. Cook IA. American Psychiatric Association. Guideline watch: practice guidelines for the treatment of patients with delirium. http://psychiatryonline.org/content.aspx?bookid=28§ionid=1681952. Accessed June 20 2012.
4. Lonergan E, Luxenberg J, Areosa Sastre A, et al. Benzodiazepines for delirium. Cochrane Database Syst Rev. 2009;21(1):CD006379.-
5. Toner LC, Tsambiras BM, Catalano G, et al. Central nervous system side effects associated with zolpidem treatment. Clin Neuropharmacol. 2000;23(1):54-58.
6. Srinivasan V, Pandi-Perumal SR, Trahkt I, et al. Melatonin and melatonergic drugs on sleep: possible mechanisms of action. Int J Neurosci. 2009;119(6):821-846.
7. Al-Aama T, Brymer C, Gutmanis I, et al. Melatonin decreases delirium in elderly patients: a randomized, placebo-controlled trial. Int J Geriatr Psychiatry. 2011;26(7):687-694.
8. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;18(2):CD005594.-
9. Medori R, Tritschler HJ, LeBlanc A, et al. Fatal familial insomnia, a prion disease with a mutation codon 178 of the prion protein gene. N Engl J Med. 1992;326(7):444-449.
10. Lugaresi E, Provini F, Cortelli P. Agrypnia excitata. Sleep Med. 2011;12(suppl 2):S3-S10.
11. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
12. Jaffe JH, Strain EC. Opioid-related disorders. In: Sadock BJ Sadock VA, eds. Kaplan and Sadock’s comprehensive textbook of psychiatry. 8th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2005:1164, 1272-1274.
Postpartum high blood pressure missed, mother suffers brain damage … and more

HOSPITALIZED TWICE FOR HYPERTENSION in the month before her child was born, a 41-year-old woman gave birth to a healthy baby by cesarean delivery. The mother was discharged 2 days later with a blood pressure (BP) of 130/90 mm Hg.
Three days later, she went to her ObGyn’s office because she was not feeling well and had extreme swelling. Her BP, taken twice by a nurse, read 170/88 mm Hg, and 168/90 mm Hg, but she was not examined by the ObGyn.
That evening, the patient had difficulty breathing and was taken to the emergency department (ED), where she was intubated. She went into cardiac arrest and suffered permanent brain damage after being without a pulse for 15 minutes. She was in a coma for 45 days. She is unable to walk without assistance, is legally blind, and her hands are so contorted that she cannot feed herself. She suffers from short-term memory loss and has difficulty speaking.
PATIENT’S CLAIM The ObGyn should have examined her when she was at the office. Her hypertension would have been properly treated and injuries avoided. She had classic signs of postpartum cardiomyopathy.
PHYSICIAN’S DEFENSE The patient had not come to the office because she was feeling ill, but to show off her baby and have her BP checked. If he had been advised of the BP readings, he would have examined her.
VERDICT A $5 million Georgia verdict was returned.
Cervical biopsy results improperly reported
A 44-YEAR-OLD WOMAN UNDERWENT a cervical biopsy in July 2007 performed by a pathologist. A few days later, the pathologist contacted the patient and reported that the biopsy revealed invasive cervical cancer that required immediate surgery. Several procedures were performed without any cancer ever being found.
A second opinion was sought, and it was determined that the cancer diagnosis was incorrect; another patient’s pathology had been reported as the patient’s.
PATIENT’S CLAIM The pathologist and hospital were negligent in reporting incorrect results of the cervical biopsy, which resulted in the patient’s physical and emotional injuries, including unnecessary surgical procedures and depression and anxiety.
DEFENDANTS’ DEFENSE The defendants did not oppose the patient’s motion for summary judgment on liability; the issue of damages was contested.
VERDICT The patient received summary judgment on liability. She then discontinued claims against the pathologist, and the matter proceeded on damages against the hospital. A $46,000 New York verdict was returned. Stipulated medical expenses were added to the verdict for a total recovery of $60,979.
Brachial plexus injury: child has significant functional disability
AT 38 6/7 WEEKS’ GESTATION, a 23-year-old woman went to the ED with contractions. She had pregestational diabetes mellitus. Her admitting glucose level was 143 mg/dL, and she had gained 25 lb during pregnancy. Her fundal height was 40 cm, and estimated fetal weight was 4000 g (8 lb 13 oz). A pelvic examination determined that she was 3 to 4 cm dilated, 100% effaced, and at minus-1 station. She was given oxytocin to aid labor. The ObGyn noted that overall fetal heart-rate tracings were reassuring, and that a pediatrician would be present for delivery due to suspected macrosomia. Shoulder dystocia occurred during delivery, but it was resolved in 40 seconds. The mother sustained a second-degree perineal laceration.
At birth, the baby’s left arm was limp. Apgar scores were 5 and 9 at 1 and 5 minutes, respectively. Her birth weight was 10 lb 2 oz. A brachial plexus injury was diagnosed, and she underwent surgery in October 2008. Despite successful nerve grafts at C5 and C6, the child has significant functional disability in the left arm.
PARENTS’ CLAIM A cesarean delivery should have been scheduled when a macrosomic fetus was suspected.
PHYSICIAN’S DEFENSE The case was settled during trial.
VERDICT A $1,475,000 Maryland settlement was reached.

DURING A MOTHER’S 38-WEEK PRENATAL VISIT, ultrasonography showed the baby was in breech position. The midwife offered two options: to schedule an external cephalic version procedure at 38 weeks or a cesarean delivery at 39 weeks. The parents agreed to schedule a cesarean delivery for 8 days later. The day before the scheduled birth, the mother awoke to find the umbilical cord between her legs. An emergency cesarean delivery was performed. The newborn required resuscitation and mechanical ventilation and suffered permanent brain damage attributed to hypoxia from umbilical cord prolapse.
PARENTS’ CLAIM The midwife’s negligence caused the baby’s injuries. Breech presentation put the pregnancy at high-risk. She did not have a physician examine the patient before scheduling a cesarean delivery and did not attempt to rotate the child back to a head-first position. She did not warn the parents about the risks of breech presentation and umbilical cord prolapse.
DEFENDANTS’ DEFENSE The choices given the parents were reasonable. Scheduling a cesarean delivery at 39 weeks was proper. A prolapsed cord is not predictable or preventable.
VERDICT A $12.6 million Pennsylvania verdict was returned against the midwife and the hospital; a confidential high/low agreement was reached.
Extensive adhesions result in bowel injury
A 58-YEAR-OLD WOMAN UNDERWENT exploratory laparotomy in May 2009. There were extensive adhesions, and the gynecologist used blind, blunt dissection to resect a large pelvic mass adhered to the sidewall. He had difficulty removing the specimen because it was too large to fit through the incision. A left salpingo-oophorectomy was also performed.
On the second postoperative day, the patient reported shortness of breath, intermittent chest pain, and had a fever of 103° F. The next day, she was unable to ambulate due to shortness of breath. CT results ruled out deep vein thrombosis or pulmonary embolism but revealed significantly decreased lung volume. She continued to experience shortness of breath and temperature spikes for 3 more days. She was discharged on the seventh postoperative day despite shortness of breath.
Two days later, she experienced severe abdominal pain and shortness of breath at home and returned to the ED by ambulance. A CT scan revealed free pelvic air, ascites, and extensive inflammatory changes, likely due to bowel perforation. She was intubated and airlifted to a regional trauma center. During exploratory surgery, the surgeon aspirated a foul-smelling fluid and identified a perforation at the rectosigmoid junction; a colostomy was created. The patient stayed in intensive care for 5 days, developed renal failure, and was transfused due to acute blood loss. She was hospitalized for 19 days. The colostomy was reversed in October 2009.
PATIENT’S CLAIM The ObGyn was negligent in injuring the bowel during surgery and in not recognizing the bowel injury and treating it in a timely manner.
PHYSICIAN’S DEFENSE The case was settled during the trial.
VERDICT A $600,000 Virginia settlement was reached.
Pregnant woman stabbed: mother and baby die
A 20-YEAR-OLD WOMAN AT 30 WEEKS’ gestation was treated in the ED for a stab wound to the shoulder. The emergency medicine (EM) physician noted internal bleeding and a possible collapsed lung on radiographs, and began efforts to have the woman transferred. One facility declined because of her pregnancy. The patient was in pain and her ability to breathe declined. An airlift was finally arranged, but she suffered cardiac arrest as the helicopter arrived. A cesarean delivery was performed, but both the mother and baby died.
ESTATE’S CLAIM The EM physician was negligent in failing to perform a thoracotomy and arrange for a more timely transfer. The physician didn’t contact a hospital that was only 8 miles away.
DEFENDANTS’ DEFENSE The federal government, which operated the facility, admitted fault.
VERDICT A $7,267,390 Mississippi verdict included $5.45 million in noneconomic damages.
What caused child’s brain damage?
DURING LABOR AND DELIVERY, electronic fetal heart-rate monitoring indicated fetal distress. Meconium-stained fluid was present. The child was born with brain damage. It is unlikely that he will walk independently, talk in full sentences, or be able to perform daily activities independently.
PARENTS’ CLAIM The fetal heart-rate monitor indicated a need for emergency cesarean delivery. The quality and quantity of meconium should have alerted the caregivers to fetal distress and caused them to perform a cesarean delivery.
DEFENDANTS’ DEFENSE Fetal heart-rate strips did not indicate a need for emergency delivery until shortly before the delivery occurred. The underlying cause of the child’s injuries was an infection that spread to the brain and was irreversible.
VERDICT A $1.71 million Massachusetts verdict was returned.
When did bladder injury occur?
AN 84-YEAR-OLD WOMAN suffered recurrent bladder cancer. She underwent a cystoscopy, and then chemotherapy. Several weeks later, she was diagnosed with a bladder perforation became septic, and died.
ESTATE’S CLAIM The bladder was lacerated during cystoscopy; she would have survived if the laceration had been treated in a timely manner.
PHYSICIAN’S DEFENSE Bladder perforation during cystoscopy is a known risk of the procedure. However, the bladder was not perforated during cystoscopy; chemotherapy may have caused the perforation.
VERDICT A Michigan defense verdict was returned.
Fetal tracings poor: Why wasn’t an internal lead used?
AT 32 WEEKS’ GESTATION, a woman’s membranes ruptured, and she was admitted. Her ObGyn planned to induce labor at 34 weeks’ gestation. She experienced contractions on the morning of the scheduled induction. Although fetal heart-rate monitoring was reassuring, the fetus was in a compound position, with the chin leading. Labor progressed rapidly to 6-cm dilation. The fetal heart rate began to show recurrent mild variable decelerations that became increasingly deeper. Although the technical quality of the external monitoring was poor, no internal lead was applied.
After 3 hours, the tracing showed severe variable decelerations. The mother was fully dilated and began to push. The tracings were of poor quality, but interpretable portions showed minimal variability and significant decelerations during contractions. The fetal baseline heart rate became tachycardic. The obstetric nurse and resident continued to note abnormalities, but there is no evidence that they called the attending ObGyn. The fetal baseline heart rate reached 190 bpm with ongoing decelerations associated with contractions. Variability remained minimal to absent. After 2 hours of pushing, meconium-stained fluid was noted. The infant was born 1 hour later. The attending ObGyn was present for the last 30 minutes of labor.
The newborn’s Apgar scores were 1, 5, and 7, at 1, 5, and 10 minutes, respectively. His arterial cord pH was significantly low. MRI of the head showed subdural and intraventricular hemorrhage and evolving, profound hypoxic ischemic injury. At 1 year of age, the child suffers from a seizure disorder, cortical blindness, and severe developmental delays.
PARENTS’ CLAIM The nurse and resident failed to respond to fetal heart-rate abnormalities and failed to insert an internal lead to obtain better quality heart-rate tracings. They did not expedite delivery when fetal distress was evident.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $4.2 million Massachusetts settlement was reached.
Hypoxic ischemic encephalopathy
DUE TO PREECLAMPSIA, a woman was admitted to the hospital 5 weeks before her due date. Her condition was monitored for 2 weeks when it was decided to induce labor with oxytocin. After 3 hours in labor, the fetal heart-rate tracing began to show significant decelerations. The baby was born at 37 weeks’ gestation with severe hypoxic ischemic encephalopathy. The child died 2 years later from severe brain damage.
PARENTS’ CLAIM The ObGyns failed to respond to signs of fetal distress by performing an emergency cesarean. The brain images would have been different if a stroke-like event had occurred.
DEFENDANTS’ DEFENSE The fetus experienced an embolic process due to a compressed umbilical cord, resulting in a stroke-like vascular event, which led to the hypoxic ischemic encephalopathy.
VERDICT A $450,000 Wisconsin settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
HOSPITALIZED TWICE FOR HYPERTENSION in the month before her child was born, a 41-year-old woman gave birth to a healthy baby by cesarean delivery. The mother was discharged 2 days later with a blood pressure (BP) of 130/90 mm Hg.
Three days later, she went to her ObGyn’s office because she was not feeling well and had extreme swelling. Her BP, taken twice by a nurse, read 170/88 mm Hg, and 168/90 mm Hg, but she was not examined by the ObGyn.
That evening, the patient had difficulty breathing and was taken to the emergency department (ED), where she was intubated. She went into cardiac arrest and suffered permanent brain damage after being without a pulse for 15 minutes. She was in a coma for 45 days. She is unable to walk without assistance, is legally blind, and her hands are so contorted that she cannot feed herself. She suffers from short-term memory loss and has difficulty speaking.
PATIENT’S CLAIM The ObGyn should have examined her when she was at the office. Her hypertension would have been properly treated and injuries avoided. She had classic signs of postpartum cardiomyopathy.
PHYSICIAN’S DEFENSE The patient had not come to the office because she was feeling ill, but to show off her baby and have her BP checked. If he had been advised of the BP readings, he would have examined her.
VERDICT A $5 million Georgia verdict was returned.
Cervical biopsy results improperly reported
A 44-YEAR-OLD WOMAN UNDERWENT a cervical biopsy in July 2007 performed by a pathologist. A few days later, the pathologist contacted the patient and reported that the biopsy revealed invasive cervical cancer that required immediate surgery. Several procedures were performed without any cancer ever being found.
A second opinion was sought, and it was determined that the cancer diagnosis was incorrect; another patient’s pathology had been reported as the patient’s.
PATIENT’S CLAIM The pathologist and hospital were negligent in reporting incorrect results of the cervical biopsy, which resulted in the patient’s physical and emotional injuries, including unnecessary surgical procedures and depression and anxiety.
DEFENDANTS’ DEFENSE The defendants did not oppose the patient’s motion for summary judgment on liability; the issue of damages was contested.
VERDICT The patient received summary judgment on liability. She then discontinued claims against the pathologist, and the matter proceeded on damages against the hospital. A $46,000 New York verdict was returned. Stipulated medical expenses were added to the verdict for a total recovery of $60,979.
Brachial plexus injury: child has significant functional disability
AT 38 6/7 WEEKS’ GESTATION, a 23-year-old woman went to the ED with contractions. She had pregestational diabetes mellitus. Her admitting glucose level was 143 mg/dL, and she had gained 25 lb during pregnancy. Her fundal height was 40 cm, and estimated fetal weight was 4000 g (8 lb 13 oz). A pelvic examination determined that she was 3 to 4 cm dilated, 100% effaced, and at minus-1 station. She was given oxytocin to aid labor. The ObGyn noted that overall fetal heart-rate tracings were reassuring, and that a pediatrician would be present for delivery due to suspected macrosomia. Shoulder dystocia occurred during delivery, but it was resolved in 40 seconds. The mother sustained a second-degree perineal laceration.
At birth, the baby’s left arm was limp. Apgar scores were 5 and 9 at 1 and 5 minutes, respectively. Her birth weight was 10 lb 2 oz. A brachial plexus injury was diagnosed, and she underwent surgery in October 2008. Despite successful nerve grafts at C5 and C6, the child has significant functional disability in the left arm.
PARENTS’ CLAIM A cesarean delivery should have been scheduled when a macrosomic fetus was suspected.
PHYSICIAN’S DEFENSE The case was settled during trial.
VERDICT A $1,475,000 Maryland settlement was reached.
DURING A MOTHER’S 38-WEEK PRENATAL VISIT, ultrasonography showed the baby was in breech position. The midwife offered two options: to schedule an external cephalic version procedure at 38 weeks or a cesarean delivery at 39 weeks. The parents agreed to schedule a cesarean delivery for 8 days later. The day before the scheduled birth, the mother awoke to find the umbilical cord between her legs. An emergency cesarean delivery was performed. The newborn required resuscitation and mechanical ventilation and suffered permanent brain damage attributed to hypoxia from umbilical cord prolapse.
PARENTS’ CLAIM The midwife’s negligence caused the baby’s injuries. Breech presentation put the pregnancy at high-risk. She did not have a physician examine the patient before scheduling a cesarean delivery and did not attempt to rotate the child back to a head-first position. She did not warn the parents about the risks of breech presentation and umbilical cord prolapse.
DEFENDANTS’ DEFENSE The choices given the parents were reasonable. Scheduling a cesarean delivery at 39 weeks was proper. A prolapsed cord is not predictable or preventable.
VERDICT A $12.6 million Pennsylvania verdict was returned against the midwife and the hospital; a confidential high/low agreement was reached.
Extensive adhesions result in bowel injury
A 58-YEAR-OLD WOMAN UNDERWENT exploratory laparotomy in May 2009. There were extensive adhesions, and the gynecologist used blind, blunt dissection to resect a large pelvic mass adhered to the sidewall. He had difficulty removing the specimen because it was too large to fit through the incision. A left salpingo-oophorectomy was also performed.
On the second postoperative day, the patient reported shortness of breath, intermittent chest pain, and had a fever of 103° F. The next day, she was unable to ambulate due to shortness of breath. CT results ruled out deep vein thrombosis or pulmonary embolism but revealed significantly decreased lung volume. She continued to experience shortness of breath and temperature spikes for 3 more days. She was discharged on the seventh postoperative day despite shortness of breath.
Two days later, she experienced severe abdominal pain and shortness of breath at home and returned to the ED by ambulance. A CT scan revealed free pelvic air, ascites, and extensive inflammatory changes, likely due to bowel perforation. She was intubated and airlifted to a regional trauma center. During exploratory surgery, the surgeon aspirated a foul-smelling fluid and identified a perforation at the rectosigmoid junction; a colostomy was created. The patient stayed in intensive care for 5 days, developed renal failure, and was transfused due to acute blood loss. She was hospitalized for 19 days. The colostomy was reversed in October 2009.
PATIENT’S CLAIM The ObGyn was negligent in injuring the bowel during surgery and in not recognizing the bowel injury and treating it in a timely manner.
PHYSICIAN’S DEFENSE The case was settled during the trial.
VERDICT A $600,000 Virginia settlement was reached.
Pregnant woman stabbed: mother and baby die
A 20-YEAR-OLD WOMAN AT 30 WEEKS’ gestation was treated in the ED for a stab wound to the shoulder. The emergency medicine (EM) physician noted internal bleeding and a possible collapsed lung on radiographs, and began efforts to have the woman transferred. One facility declined because of her pregnancy. The patient was in pain and her ability to breathe declined. An airlift was finally arranged, but she suffered cardiac arrest as the helicopter arrived. A cesarean delivery was performed, but both the mother and baby died.
ESTATE’S CLAIM The EM physician was negligent in failing to perform a thoracotomy and arrange for a more timely transfer. The physician didn’t contact a hospital that was only 8 miles away.
DEFENDANTS’ DEFENSE The federal government, which operated the facility, admitted fault.
VERDICT A $7,267,390 Mississippi verdict included $5.45 million in noneconomic damages.
What caused child’s brain damage?
DURING LABOR AND DELIVERY, electronic fetal heart-rate monitoring indicated fetal distress. Meconium-stained fluid was present. The child was born with brain damage. It is unlikely that he will walk independently, talk in full sentences, or be able to perform daily activities independently.
PARENTS’ CLAIM The fetal heart-rate monitor indicated a need for emergency cesarean delivery. The quality and quantity of meconium should have alerted the caregivers to fetal distress and caused them to perform a cesarean delivery.
DEFENDANTS’ DEFENSE Fetal heart-rate strips did not indicate a need for emergency delivery until shortly before the delivery occurred. The underlying cause of the child’s injuries was an infection that spread to the brain and was irreversible.
VERDICT A $1.71 million Massachusetts verdict was returned.
When did bladder injury occur?
AN 84-YEAR-OLD WOMAN suffered recurrent bladder cancer. She underwent a cystoscopy, and then chemotherapy. Several weeks later, she was diagnosed with a bladder perforation became septic, and died.
ESTATE’S CLAIM The bladder was lacerated during cystoscopy; she would have survived if the laceration had been treated in a timely manner.
PHYSICIAN’S DEFENSE Bladder perforation during cystoscopy is a known risk of the procedure. However, the bladder was not perforated during cystoscopy; chemotherapy may have caused the perforation.
VERDICT A Michigan defense verdict was returned.
Fetal tracings poor: Why wasn’t an internal lead used?
AT 32 WEEKS’ GESTATION, a woman’s membranes ruptured, and she was admitted. Her ObGyn planned to induce labor at 34 weeks’ gestation. She experienced contractions on the morning of the scheduled induction. Although fetal heart-rate monitoring was reassuring, the fetus was in a compound position, with the chin leading. Labor progressed rapidly to 6-cm dilation. The fetal heart rate began to show recurrent mild variable decelerations that became increasingly deeper. Although the technical quality of the external monitoring was poor, no internal lead was applied.
After 3 hours, the tracing showed severe variable decelerations. The mother was fully dilated and began to push. The tracings were of poor quality, but interpretable portions showed minimal variability and significant decelerations during contractions. The fetal baseline heart rate became tachycardic. The obstetric nurse and resident continued to note abnormalities, but there is no evidence that they called the attending ObGyn. The fetal baseline heart rate reached 190 bpm with ongoing decelerations associated with contractions. Variability remained minimal to absent. After 2 hours of pushing, meconium-stained fluid was noted. The infant was born 1 hour later. The attending ObGyn was present for the last 30 minutes of labor.
The newborn’s Apgar scores were 1, 5, and 7, at 1, 5, and 10 minutes, respectively. His arterial cord pH was significantly low. MRI of the head showed subdural and intraventricular hemorrhage and evolving, profound hypoxic ischemic injury. At 1 year of age, the child suffers from a seizure disorder, cortical blindness, and severe developmental delays.
PARENTS’ CLAIM The nurse and resident failed to respond to fetal heart-rate abnormalities and failed to insert an internal lead to obtain better quality heart-rate tracings. They did not expedite delivery when fetal distress was evident.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $4.2 million Massachusetts settlement was reached.
Hypoxic ischemic encephalopathy
DUE TO PREECLAMPSIA, a woman was admitted to the hospital 5 weeks before her due date. Her condition was monitored for 2 weeks when it was decided to induce labor with oxytocin. After 3 hours in labor, the fetal heart-rate tracing began to show significant decelerations. The baby was born at 37 weeks’ gestation with severe hypoxic ischemic encephalopathy. The child died 2 years later from severe brain damage.
PARENTS’ CLAIM The ObGyns failed to respond to signs of fetal distress by performing an emergency cesarean. The brain images would have been different if a stroke-like event had occurred.
DEFENDANTS’ DEFENSE The fetus experienced an embolic process due to a compressed umbilical cord, resulting in a stroke-like vascular event, which led to the hypoxic ischemic encephalopathy.
VERDICT A $450,000 Wisconsin settlement was reached.
HOSPITALIZED TWICE FOR HYPERTENSION in the month before her child was born, a 41-year-old woman gave birth to a healthy baby by cesarean delivery. The mother was discharged 2 days later with a blood pressure (BP) of 130/90 mm Hg.
Three days later, she went to her ObGyn’s office because she was not feeling well and had extreme swelling. Her BP, taken twice by a nurse, read 170/88 mm Hg, and 168/90 mm Hg, but she was not examined by the ObGyn.
That evening, the patient had difficulty breathing and was taken to the emergency department (ED), where she was intubated. She went into cardiac arrest and suffered permanent brain damage after being without a pulse for 15 minutes. She was in a coma for 45 days. She is unable to walk without assistance, is legally blind, and her hands are so contorted that she cannot feed herself. She suffers from short-term memory loss and has difficulty speaking.
PATIENT’S CLAIM The ObGyn should have examined her when she was at the office. Her hypertension would have been properly treated and injuries avoided. She had classic signs of postpartum cardiomyopathy.
PHYSICIAN’S DEFENSE The patient had not come to the office because she was feeling ill, but to show off her baby and have her BP checked. If he had been advised of the BP readings, he would have examined her.
VERDICT A $5 million Georgia verdict was returned.
Cervical biopsy results improperly reported
A 44-YEAR-OLD WOMAN UNDERWENT a cervical biopsy in July 2007 performed by a pathologist. A few days later, the pathologist contacted the patient and reported that the biopsy revealed invasive cervical cancer that required immediate surgery. Several procedures were performed without any cancer ever being found.
A second opinion was sought, and it was determined that the cancer diagnosis was incorrect; another patient’s pathology had been reported as the patient’s.
PATIENT’S CLAIM The pathologist and hospital were negligent in reporting incorrect results of the cervical biopsy, which resulted in the patient’s physical and emotional injuries, including unnecessary surgical procedures and depression and anxiety.
DEFENDANTS’ DEFENSE The defendants did not oppose the patient’s motion for summary judgment on liability; the issue of damages was contested.
VERDICT The patient received summary judgment on liability. She then discontinued claims against the pathologist, and the matter proceeded on damages against the hospital. A $46,000 New York verdict was returned. Stipulated medical expenses were added to the verdict for a total recovery of $60,979.
Brachial plexus injury: child has significant functional disability
AT 38 6/7 WEEKS’ GESTATION, a 23-year-old woman went to the ED with contractions. She had pregestational diabetes mellitus. Her admitting glucose level was 143 mg/dL, and she had gained 25 lb during pregnancy. Her fundal height was 40 cm, and estimated fetal weight was 4000 g (8 lb 13 oz). A pelvic examination determined that she was 3 to 4 cm dilated, 100% effaced, and at minus-1 station. She was given oxytocin to aid labor. The ObGyn noted that overall fetal heart-rate tracings were reassuring, and that a pediatrician would be present for delivery due to suspected macrosomia. Shoulder dystocia occurred during delivery, but it was resolved in 40 seconds. The mother sustained a second-degree perineal laceration.
At birth, the baby’s left arm was limp. Apgar scores were 5 and 9 at 1 and 5 minutes, respectively. Her birth weight was 10 lb 2 oz. A brachial plexus injury was diagnosed, and she underwent surgery in October 2008. Despite successful nerve grafts at C5 and C6, the child has significant functional disability in the left arm.
PARENTS’ CLAIM A cesarean delivery should have been scheduled when a macrosomic fetus was suspected.
PHYSICIAN’S DEFENSE The case was settled during trial.
VERDICT A $1,475,000 Maryland settlement was reached.
DURING A MOTHER’S 38-WEEK PRENATAL VISIT, ultrasonography showed the baby was in breech position. The midwife offered two options: to schedule an external cephalic version procedure at 38 weeks or a cesarean delivery at 39 weeks. The parents agreed to schedule a cesarean delivery for 8 days later. The day before the scheduled birth, the mother awoke to find the umbilical cord between her legs. An emergency cesarean delivery was performed. The newborn required resuscitation and mechanical ventilation and suffered permanent brain damage attributed to hypoxia from umbilical cord prolapse.
PARENTS’ CLAIM The midwife’s negligence caused the baby’s injuries. Breech presentation put the pregnancy at high-risk. She did not have a physician examine the patient before scheduling a cesarean delivery and did not attempt to rotate the child back to a head-first position. She did not warn the parents about the risks of breech presentation and umbilical cord prolapse.
DEFENDANTS’ DEFENSE The choices given the parents were reasonable. Scheduling a cesarean delivery at 39 weeks was proper. A prolapsed cord is not predictable or preventable.
VERDICT A $12.6 million Pennsylvania verdict was returned against the midwife and the hospital; a confidential high/low agreement was reached.
Extensive adhesions result in bowel injury
A 58-YEAR-OLD WOMAN UNDERWENT exploratory laparotomy in May 2009. There were extensive adhesions, and the gynecologist used blind, blunt dissection to resect a large pelvic mass adhered to the sidewall. He had difficulty removing the specimen because it was too large to fit through the incision. A left salpingo-oophorectomy was also performed.
On the second postoperative day, the patient reported shortness of breath, intermittent chest pain, and had a fever of 103° F. The next day, she was unable to ambulate due to shortness of breath. CT results ruled out deep vein thrombosis or pulmonary embolism but revealed significantly decreased lung volume. She continued to experience shortness of breath and temperature spikes for 3 more days. She was discharged on the seventh postoperative day despite shortness of breath.
Two days later, she experienced severe abdominal pain and shortness of breath at home and returned to the ED by ambulance. A CT scan revealed free pelvic air, ascites, and extensive inflammatory changes, likely due to bowel perforation. She was intubated and airlifted to a regional trauma center. During exploratory surgery, the surgeon aspirated a foul-smelling fluid and identified a perforation at the rectosigmoid junction; a colostomy was created. The patient stayed in intensive care for 5 days, developed renal failure, and was transfused due to acute blood loss. She was hospitalized for 19 days. The colostomy was reversed in October 2009.
PATIENT’S CLAIM The ObGyn was negligent in injuring the bowel during surgery and in not recognizing the bowel injury and treating it in a timely manner.
PHYSICIAN’S DEFENSE The case was settled during the trial.
VERDICT A $600,000 Virginia settlement was reached.
Pregnant woman stabbed: mother and baby die
A 20-YEAR-OLD WOMAN AT 30 WEEKS’ gestation was treated in the ED for a stab wound to the shoulder. The emergency medicine (EM) physician noted internal bleeding and a possible collapsed lung on radiographs, and began efforts to have the woman transferred. One facility declined because of her pregnancy. The patient was in pain and her ability to breathe declined. An airlift was finally arranged, but she suffered cardiac arrest as the helicopter arrived. A cesarean delivery was performed, but both the mother and baby died.
ESTATE’S CLAIM The EM physician was negligent in failing to perform a thoracotomy and arrange for a more timely transfer. The physician didn’t contact a hospital that was only 8 miles away.
DEFENDANTS’ DEFENSE The federal government, which operated the facility, admitted fault.
VERDICT A $7,267,390 Mississippi verdict included $5.45 million in noneconomic damages.
What caused child’s brain damage?
DURING LABOR AND DELIVERY, electronic fetal heart-rate monitoring indicated fetal distress. Meconium-stained fluid was present. The child was born with brain damage. It is unlikely that he will walk independently, talk in full sentences, or be able to perform daily activities independently.
PARENTS’ CLAIM The fetal heart-rate monitor indicated a need for emergency cesarean delivery. The quality and quantity of meconium should have alerted the caregivers to fetal distress and caused them to perform a cesarean delivery.
DEFENDANTS’ DEFENSE Fetal heart-rate strips did not indicate a need for emergency delivery until shortly before the delivery occurred. The underlying cause of the child’s injuries was an infection that spread to the brain and was irreversible.
VERDICT A $1.71 million Massachusetts verdict was returned.
When did bladder injury occur?
AN 84-YEAR-OLD WOMAN suffered recurrent bladder cancer. She underwent a cystoscopy, and then chemotherapy. Several weeks later, she was diagnosed with a bladder perforation became septic, and died.
ESTATE’S CLAIM The bladder was lacerated during cystoscopy; she would have survived if the laceration had been treated in a timely manner.
PHYSICIAN’S DEFENSE Bladder perforation during cystoscopy is a known risk of the procedure. However, the bladder was not perforated during cystoscopy; chemotherapy may have caused the perforation.
VERDICT A Michigan defense verdict was returned.
Fetal tracings poor: Why wasn’t an internal lead used?
AT 32 WEEKS’ GESTATION, a woman’s membranes ruptured, and she was admitted. Her ObGyn planned to induce labor at 34 weeks’ gestation. She experienced contractions on the morning of the scheduled induction. Although fetal heart-rate monitoring was reassuring, the fetus was in a compound position, with the chin leading. Labor progressed rapidly to 6-cm dilation. The fetal heart rate began to show recurrent mild variable decelerations that became increasingly deeper. Although the technical quality of the external monitoring was poor, no internal lead was applied.
After 3 hours, the tracing showed severe variable decelerations. The mother was fully dilated and began to push. The tracings were of poor quality, but interpretable portions showed minimal variability and significant decelerations during contractions. The fetal baseline heart rate became tachycardic. The obstetric nurse and resident continued to note abnormalities, but there is no evidence that they called the attending ObGyn. The fetal baseline heart rate reached 190 bpm with ongoing decelerations associated with contractions. Variability remained minimal to absent. After 2 hours of pushing, meconium-stained fluid was noted. The infant was born 1 hour later. The attending ObGyn was present for the last 30 minutes of labor.
The newborn’s Apgar scores were 1, 5, and 7, at 1, 5, and 10 minutes, respectively. His arterial cord pH was significantly low. MRI of the head showed subdural and intraventricular hemorrhage and evolving, profound hypoxic ischemic injury. At 1 year of age, the child suffers from a seizure disorder, cortical blindness, and severe developmental delays.
PARENTS’ CLAIM The nurse and resident failed to respond to fetal heart-rate abnormalities and failed to insert an internal lead to obtain better quality heart-rate tracings. They did not expedite delivery when fetal distress was evident.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $4.2 million Massachusetts settlement was reached.
Hypoxic ischemic encephalopathy
DUE TO PREECLAMPSIA, a woman was admitted to the hospital 5 weeks before her due date. Her condition was monitored for 2 weeks when it was decided to induce labor with oxytocin. After 3 hours in labor, the fetal heart-rate tracing began to show significant decelerations. The baby was born at 37 weeks’ gestation with severe hypoxic ischemic encephalopathy. The child died 2 years later from severe brain damage.
PARENTS’ CLAIM The ObGyns failed to respond to signs of fetal distress by performing an emergency cesarean. The brain images would have been different if a stroke-like event had occurred.
DEFENDANTS’ DEFENSE The fetus experienced an embolic process due to a compressed umbilical cord, resulting in a stroke-like vascular event, which led to the hypoxic ischemic encephalopathy.
VERDICT A $450,000 Wisconsin settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
STOP using synthetic mesh for routine repair of pelvic organ prolapse
Have you read these recent articles in OBG Management about the surgical use of mesh? Click here to access the list.
CASE: Stage 2 prolapse to the hymenal ring
A 54-year-old Para 3 woman presents with stage 2 prolapse to the hymenal ring. The prolapse predominantly involves the anterior vagina, with her cervix prolapsing to 2 cm within the hymenal ring. The patient is bothered by the bulge and stress urinary leakage. She does not want to use a pessary and prefers to have definitive surgical correction, including hysterectomy.
The first surgeon she consulted recommended a vaginal hysterectomy, anterior colporrhaphy, anterior synthetic mesh vaginal colpopexy, and synthetic midurethral sling. The patient was concerned about mesh placement for prolapse and the sling after seeing ads on the Internet about vaginal mesh. She presents for a second opinion about surgical alternatives.
Stop routinely offering synthetic vaginal mesh for prolapse
Advantages to the use of synthetic vaginal mesh include improved subjective and objective cure rates for prolapse (especially for the anterior compartment) and fewer repeat surgeries for recurrent prolapse. However, disadvantages include:
- mesh exposure and extrusion through the vaginal epithelium
- overall higher reoperation for mesh-related complications and de novo stress urinary incontinence.1
Synthetic vaginal mesh should be reserved for special situations. Currently, experts agree that synthetic vaginal mesh is appropriate in cases of recurrent prolapse, advanced-stage prolapse, collagen deficiency, or in cases with relative contraindications to longer endoscopic or abdominal surgery, such as medical comorbidities or adhesions.2,3 Other indications for synthetic vaginal mesh include vaginal hysteropexy procedures.
Mesh is likely not necessary in:
- primary repairs
- prolapse < POPQ (pelvic organ prolapse quantification system) stage 2
- posterior prolapse
- patients with chronic pelvic pain.
Start offering, learning, and mastering native tissue repairs
For the patient in the opening case, who has symptomatic stage 2 uterovaginal prolapse and stress urinary incontinence, surgery, including a transvaginal hysterectomy, anterior colporrhaphy, uterosacral ligament suspension, and synthetic midurethral sling, is a reasonable alternative and has a high subjective and objective cure rate—81.2% rate for anterior prolapse and 98.3% rate for apical prolapse. Better outcomes are noted with stage 2 compared with stage 3 prolapse (92.4% vs 66.8%, respectively).4
Final note
If you are offering selective transvaginal synthetic mesh for prolapse repairs:
- Undergo training specific to each device.
- Track your outcomes—including objective, subjective, quality of life, and reoperation for complications and recurrence.
- Enroll in the national pelvic floor disorders registry, which is scheduled to debut in Fall 2013.
We want to hear from you! Tell us what you think.
1. Schmid C, Maher C, Feiner B, Baessler K, Glazener C. 2012 Cochrane Review: Surgical management of pelvic organ prolapse. Int Urogynecol J. 2012;23(suppl 2).-
2. Davila GW, Baessler K, Cosson M, Cardozo L. Selection of patients in whom vaginal graft use may be appropriate. Consensus of the 2nd IUGA Grafts Roundtable: optimizing safety and appropriateness of graft use in transvaginal pelvic reconstructive surgery. Int Urogynecol J. 2012;23(suppl 1):S7-S14.
3. Committee on Gynecologic Practice. American College of Obstetricians and Gynecologists American Urogynecologic Society. Committee Opinion No. 513: Vaginal placement of synthetic mesh for pelvic organ prolapse. Obstet Gynecol. 2011;118(6):1459-1464.
4. Margulies RU, Rogers MA, Morgan DM. Outcomes of transvaginal uterosacral ligament suspension: systematic review and metaanalysis. Am J Obstet Gynecol. 2010;202(2):124-134.
EXPERT COMMENTARY

Cheryl B. Iglesia, MD
Director, Section of Female Pelvic Medicine and Reconstructive Surgery, MedStar Washington Hospital Center, and Associate Professor, Departments of Obstetrics and Gynecology and Urology, Georgetown University School of Medicine, Washington, DC. Dr. Iglesia serves on the OBG Mangement Board of Editors.
The author reports no financial relationships relevant to this article.
EXPERT COMMENTARY
Cheryl B. Iglesia, MD
Director, Section of Female Pelvic Medicine and Reconstructive Surgery, MedStar Washington Hospital Center, and Associate Professor, Departments of Obstetrics and Gynecology and Urology, Georgetown University School of Medicine, Washington, DC. Dr. Iglesia serves on the OBG Mangement Board of Editors.
The author reports no financial relationships relevant to this article.
EXPERT COMMENTARY
Cheryl B. Iglesia, MD
Director, Section of Female Pelvic Medicine and Reconstructive Surgery, MedStar Washington Hospital Center, and Associate Professor, Departments of Obstetrics and Gynecology and Urology, Georgetown University School of Medicine, Washington, DC. Dr. Iglesia serves on the OBG Mangement Board of Editors.
The author reports no financial relationships relevant to this article.
Have you read these recent articles in OBG Management about the surgical use of mesh? Click here to access the list.
CASE: Stage 2 prolapse to the hymenal ring
A 54-year-old Para 3 woman presents with stage 2 prolapse to the hymenal ring. The prolapse predominantly involves the anterior vagina, with her cervix prolapsing to 2 cm within the hymenal ring. The patient is bothered by the bulge and stress urinary leakage. She does not want to use a pessary and prefers to have definitive surgical correction, including hysterectomy.
The first surgeon she consulted recommended a vaginal hysterectomy, anterior colporrhaphy, anterior synthetic mesh vaginal colpopexy, and synthetic midurethral sling. The patient was concerned about mesh placement for prolapse and the sling after seeing ads on the Internet about vaginal mesh. She presents for a second opinion about surgical alternatives.
Stop routinely offering synthetic vaginal mesh for prolapse
Advantages to the use of synthetic vaginal mesh include improved subjective and objective cure rates for prolapse (especially for the anterior compartment) and fewer repeat surgeries for recurrent prolapse. However, disadvantages include:
- mesh exposure and extrusion through the vaginal epithelium
- overall higher reoperation for mesh-related complications and de novo stress urinary incontinence.1
Synthetic vaginal mesh should be reserved for special situations. Currently, experts agree that synthetic vaginal mesh is appropriate in cases of recurrent prolapse, advanced-stage prolapse, collagen deficiency, or in cases with relative contraindications to longer endoscopic or abdominal surgery, such as medical comorbidities or adhesions.2,3 Other indications for synthetic vaginal mesh include vaginal hysteropexy procedures.
Mesh is likely not necessary in:
- primary repairs
- prolapse < POPQ (pelvic organ prolapse quantification system) stage 2
- posterior prolapse
- patients with chronic pelvic pain.
Start offering, learning, and mastering native tissue repairs
For the patient in the opening case, who has symptomatic stage 2 uterovaginal prolapse and stress urinary incontinence, surgery, including a transvaginal hysterectomy, anterior colporrhaphy, uterosacral ligament suspension, and synthetic midurethral sling, is a reasonable alternative and has a high subjective and objective cure rate—81.2% rate for anterior prolapse and 98.3% rate for apical prolapse. Better outcomes are noted with stage 2 compared with stage 3 prolapse (92.4% vs 66.8%, respectively).4
Final note
If you are offering selective transvaginal synthetic mesh for prolapse repairs:
- Undergo training specific to each device.
- Track your outcomes—including objective, subjective, quality of life, and reoperation for complications and recurrence.
- Enroll in the national pelvic floor disorders registry, which is scheduled to debut in Fall 2013.
We want to hear from you! Tell us what you think.
Have you read these recent articles in OBG Management about the surgical use of mesh? Click here to access the list.
CASE: Stage 2 prolapse to the hymenal ring
A 54-year-old Para 3 woman presents with stage 2 prolapse to the hymenal ring. The prolapse predominantly involves the anterior vagina, with her cervix prolapsing to 2 cm within the hymenal ring. The patient is bothered by the bulge and stress urinary leakage. She does not want to use a pessary and prefers to have definitive surgical correction, including hysterectomy.
The first surgeon she consulted recommended a vaginal hysterectomy, anterior colporrhaphy, anterior synthetic mesh vaginal colpopexy, and synthetic midurethral sling. The patient was concerned about mesh placement for prolapse and the sling after seeing ads on the Internet about vaginal mesh. She presents for a second opinion about surgical alternatives.
Stop routinely offering synthetic vaginal mesh for prolapse
Advantages to the use of synthetic vaginal mesh include improved subjective and objective cure rates for prolapse (especially for the anterior compartment) and fewer repeat surgeries for recurrent prolapse. However, disadvantages include:
- mesh exposure and extrusion through the vaginal epithelium
- overall higher reoperation for mesh-related complications and de novo stress urinary incontinence.1
Synthetic vaginal mesh should be reserved for special situations. Currently, experts agree that synthetic vaginal mesh is appropriate in cases of recurrent prolapse, advanced-stage prolapse, collagen deficiency, or in cases with relative contraindications to longer endoscopic or abdominal surgery, such as medical comorbidities or adhesions.2,3 Other indications for synthetic vaginal mesh include vaginal hysteropexy procedures.
Mesh is likely not necessary in:
- primary repairs
- prolapse < POPQ (pelvic organ prolapse quantification system) stage 2
- posterior prolapse
- patients with chronic pelvic pain.
Start offering, learning, and mastering native tissue repairs
For the patient in the opening case, who has symptomatic stage 2 uterovaginal prolapse and stress urinary incontinence, surgery, including a transvaginal hysterectomy, anterior colporrhaphy, uterosacral ligament suspension, and synthetic midurethral sling, is a reasonable alternative and has a high subjective and objective cure rate—81.2% rate for anterior prolapse and 98.3% rate for apical prolapse. Better outcomes are noted with stage 2 compared with stage 3 prolapse (92.4% vs 66.8%, respectively).4
Final note
If you are offering selective transvaginal synthetic mesh for prolapse repairs:
- Undergo training specific to each device.
- Track your outcomes—including objective, subjective, quality of life, and reoperation for complications and recurrence.
- Enroll in the national pelvic floor disorders registry, which is scheduled to debut in Fall 2013.
We want to hear from you! Tell us what you think.
1. Schmid C, Maher C, Feiner B, Baessler K, Glazener C. 2012 Cochrane Review: Surgical management of pelvic organ prolapse. Int Urogynecol J. 2012;23(suppl 2).-
2. Davila GW, Baessler K, Cosson M, Cardozo L. Selection of patients in whom vaginal graft use may be appropriate. Consensus of the 2nd IUGA Grafts Roundtable: optimizing safety and appropriateness of graft use in transvaginal pelvic reconstructive surgery. Int Urogynecol J. 2012;23(suppl 1):S7-S14.
3. Committee on Gynecologic Practice. American College of Obstetricians and Gynecologists American Urogynecologic Society. Committee Opinion No. 513: Vaginal placement of synthetic mesh for pelvic organ prolapse. Obstet Gynecol. 2011;118(6):1459-1464.
4. Margulies RU, Rogers MA, Morgan DM. Outcomes of transvaginal uterosacral ligament suspension: systematic review and metaanalysis. Am J Obstet Gynecol. 2010;202(2):124-134.
1. Schmid C, Maher C, Feiner B, Baessler K, Glazener C. 2012 Cochrane Review: Surgical management of pelvic organ prolapse. Int Urogynecol J. 2012;23(suppl 2).-
2. Davila GW, Baessler K, Cosson M, Cardozo L. Selection of patients in whom vaginal graft use may be appropriate. Consensus of the 2nd IUGA Grafts Roundtable: optimizing safety and appropriateness of graft use in transvaginal pelvic reconstructive surgery. Int Urogynecol J. 2012;23(suppl 1):S7-S14.
3. Committee on Gynecologic Practice. American College of Obstetricians and Gynecologists American Urogynecologic Society. Committee Opinion No. 513: Vaginal placement of synthetic mesh for pelvic organ prolapse. Obstet Gynecol. 2011;118(6):1459-1464.
4. Margulies RU, Rogers MA, Morgan DM. Outcomes of transvaginal uterosacral ligament suspension: systematic review and metaanalysis. Am J Obstet Gynecol. 2010;202(2):124-134.