User login
New and Noteworthy Information—August 2014
Older veterans with traumatic brain injury (TBI) are 60% more likely to develop dementia later in life, compared with veterans without TBI, according to a study published online ahead of print June 25 in Neurology. The study involved 188,764 veterans ages 55 and older. At the study’s outset, each participant was free of dementia and had at least one inpatient or outpatient visit to a health care facility at baseline (2000 to 2003) and during the follow-up (2003 to 2012). A total of 1,229 veterans had a TBI diagnosis; 196 veterans with TBI (16%) developed dementia, and 18,255 (10%) of those without TBI developed dementia. On average, veterans with TBI developed dementia two years earlier than those without TBI. “If we assume that this relationship is causal, it seems likely that the same increased risk probably occurs with TBI in the civilian population as well,” said the researchers.
Higher levels of depressive symptoms, stress, and hostility are associated with a significantly increased risk of stroke or transient ischemic attack (TIA) in middle-aged and older adults, according to a study published online ahead of print July 10 in Stroke. Researchers used data from the Multi-Ethnic Study of Atherosclerosis (MESA) to determine how psychologic factors might influence the risk for chronic disease. The investigators examined data for 6,749 adults (ages 45 to 84; 53% women) as they completed questionnaires assessing chronic stress, depressive symptoms, anger, and hostility during a two-year period. Hazard ratios indicated a significantly elevated risk of stroke or TIA for the highest scoring group, compared with the lowest scoring group, for depressive symptoms (HR, 1.86), chronic stress (HR, 1.59), and hostility (HR, 2.22). No significant increased risk was associated with anger.
Patients with mild to moderate Parkinson’s disease can improve their symptoms with regular walking, according to a study published online ahead of print July 2 in Neurology. Investigators included 60 individuals who participated in a randomized trial of various exercise regimens for six months. Eighty-one percent of participants completed the study with a mean attendance of 83.3%. Subjects took additional tests to gauge their aerobic fitness, tiredness, and other factors. Brisk walking reduced tiredness by 11%, improved motor function and mood by 15%, improved attention and response control scores by 14%, and increased aerobic fitness and gait speed by 7%. With regard to motor function, participants improved by an average of 2.8 points. “The results of our study suggest that walking may provide a safe and easily accessible way of improving the symptoms of Parkinson’s disease and improve quality of life,” stated the researchers.
Mild traumatic brain injury (TBI) may result in brain damage and memory and thinking problems, according to a study published online ahead of print July 16 in Neurology. Fifty-three patients (44 with mild TBI and nine with moderate TBI) were compared with 33 participants without brain injury. Each subject underwent testing to assess his or her memory and thinking skills. Participants also had diffusion tensor imaging scans. Those with injuries had brain damage in white matter that consisted of disruption to nerve axons. Researchers also determined that scores on the verbal letter fluency task were 25% lower in individuals with injury than in individuals without injury. “We studied patients who had suffered clinically mild injuries, often from common accidents such as falling from a bicycle, or slow-speed car accidents. This finding is especially important, as 90% of all TBIs are mild to moderate,” said the researchers.
Patients with a traumatic brain injury (TBI) who received erythropoietin (EPO) or maintained a higher hemoglobin concentration through blood transfusion did not have an improved neurologic outcome at six months, according to a study published in the July 2 issue of JAMA. The randomized study included 200 patients (erythropoietin, n = 102; placebo, n = 98) with a closed head injury at neurosurgical intensive care units in two US level I trauma centers between May 2006 and August 2012. Patients were enrolled within six hours of injury and had to be unable to follow commands after initial stabilization. Overall, transfusing at higher hemoglobin concentrations was associated with a higher risk of adverse events. Researchers also observed a higher incidence of thromboembolic events for the transfusion threshold of 10 g/dL (21.8%) versus the threshold of 7 g/dL (8.1%)
Frontline Medical Communications and the National Organization for Rare Disorders (NORD) have signed a partnership agreement to develop educational programs about rare diseases for health care providers. Frontline and NORD also seek to improve awareness, recognition, and understanding of rare diseases among health care providers to accelerate diagnosis and promote optimal care for patients, facilitate the sharing of information among health care providers and rare disease medical experts, and update health care providers on new treatment options and clinical care standards. “Innovative multichannel educational programs, developed by both organizations and funded by commercial sponsors, will be distributed to more than 1.2 million health care providers using Frontline’s portfolio of 30 journal brands, corresponding websites, eNewsletters, and live events,” according to Frontline.
Upsher-Smith Laboratories (Maple Grove, Minnesota) announced that Qudexy XR (topiramate) extended-release capsules are now available in the United States. Qudexy XR, a broad-spectrum, once-daily antiepileptic drug is engineered to deliver a smooth pharmacokinetic profile. The FDA approved Qudexy XR in March 2014 as an initial monotherapy in patients 10 and older with primary generalized tonic-clonic seizures and partial-onset seizures. The drug also was approved as adjunctive therapy in patients 2 and older with primary generalized tonic-clonic seizures, partial-onset seizures, and seizures associated with Lennox-Gastaut syndrome. Overall, results from Upsher-Smith’s phase III trial showed that Qudexy XR is generally well tolerated and effective.
Transplanted brain cells producing dopamine remain viable in patients with Parkinson’s disease for several years, according to a study published June 26 in Cell Reports. The study included five patients with Parkinson’s disease who received transplants of fetal tissue-derived, dopamine-producing neurons four to 14 years earlier. Their transplanted dopamine neurons showed no signs of Parkinson’s disease–associated deterioration and appeared healthy. Researchers believe the findings provide further support for stem cells as a source for transplant-ready dopamine neurons. The investigators noted that the neuronal transplant has proven to be a durable treatment for many patients with Parkinson’s disease, with some improving for years without a need for standard medications. The study authors called the new finding “extremely encouraging,” adding that the long life of the transplanted neurons bodes well “for advancing [the technique] as a restoration therapy for Parkinson’s disease.”
Women may recover more quickly than men after a concussion, according to a study published online ahead of print May 6 in Radiology. Researchers examined the medical records and imaging results of 69 patients diagnosed with mild traumatic brain injury (TBI) between 2006 and 2013. The cohort included 47 men, 22 women, and 21 controls (10 men; median age of men, 17; median age of women, 16). Of the 47 men with TBI, 32 (68%) were injured while playing a sport, as were 10 of the 22 women (45%). Although all participants underwent the same evaluation, diffusion tensor imaging scans revealed that compared with the female patients with mild TBI, the male patients with mild TBI had significantly decreased uncinate fasciculus fractional anisotropy values. The average recovery time for all patients with concussion was 54 days. However, compared with women, who recovered in an average of 26.3 days, recovery was significantly longer for men (66.9 days).
Patients with mesial temporal lobe epilepsy who cannot be controlled with medication can now opt for a minimally invasive laser procedure performed under MRI guidance, according to a study published in the June issue of Neurosurgery. Researchers used an MRI-guided stereotactic laser amygdalohippocampotomy in 13 adult patients with epilepsy (median age, 24). During this procedure, a saline-cooled fiber-optic laser probe was targeted at the amygdalohippocampal complex. Using real-time MRI guidance, a neurosurgeon pinpointed the area of the brain responsible for seizure activity and destroyed this tissue without harming nearby brain tissue. Sixty percent of the amygdalohippocampal complex was destroyed, and the average length of the ablated area was 2.5 cm. “Such minimally invasive techniques may be more desirable to patients and result in increased use of epilepsy surgery among the large number of medically intractable epilepsy patients,” according to the investigators.
Researchers identified 10 proteins in the blood that can predict the onset of Alzheimer’s disease, according to a study published online ahead of print July 3 in Alzheimer’s & Dementia. In the international study of 1,148 individuals (220 with mild cognitive impairment [MCI], 452 elderly controls without dementia, and 476 with Alzheimer’s disease), blood samples were analyzed for 26 proteins previously associated with Alzheimer’s disease. Investigators found 16 of the 26 proteins to be strongly associated with brain shrinkage in Alzheimer’s disease or MCI. The researchers conducted a second series of tests to establish which of these proteins could predict the progression from MCI to Alzheimer’s disease. The study authors identified a combination of 10 proteins capable of predicting whether individuals with MCI would develop Alzheimer’s disease within a year with 87% accuracy. “Memory problems are common, but the challenge is identifying who is likely to develop dementia,” according to the researchers.
An international team of researchers has reviewed the diagnostic criteria for Alzheimer’s disease developed by the International Working Group (IWG) and US National Institute on Aging–Alzheimer’s Association, according to a study published in the June issue of Lancet Neurology. The team considered the strengths and weakness of the IWG criteria and proposed advances to improve the diagnostic framework. The investigators asserted that the diagnosis of Alzheimer’s disease can be simplified by requiring the presence of an appropriate clinical Alzheimer’s disease phenotype (typical or atypical) and a pathophysiologic biomarker consistent with the presence of Alzheimer’s pathology. “We propose that downstream topographic biomarkers of the disease, such as volumetric MRI and fluorodeoxyglucose PET, might better serve in the measurement and monitoring of the course of disease,” the team stated
—Kimberly D. Williams
Older veterans with traumatic brain injury (TBI) are 60% more likely to develop dementia later in life, compared with veterans without TBI, according to a study published online ahead of print June 25 in Neurology. The study involved 188,764 veterans ages 55 and older. At the study’s outset, each participant was free of dementia and had at least one inpatient or outpatient visit to a health care facility at baseline (2000 to 2003) and during the follow-up (2003 to 2012). A total of 1,229 veterans had a TBI diagnosis; 196 veterans with TBI (16%) developed dementia, and 18,255 (10%) of those without TBI developed dementia. On average, veterans with TBI developed dementia two years earlier than those without TBI. “If we assume that this relationship is causal, it seems likely that the same increased risk probably occurs with TBI in the civilian population as well,” said the researchers.
Higher levels of depressive symptoms, stress, and hostility are associated with a significantly increased risk of stroke or transient ischemic attack (TIA) in middle-aged and older adults, according to a study published online ahead of print July 10 in Stroke. Researchers used data from the Multi-Ethnic Study of Atherosclerosis (MESA) to determine how psychologic factors might influence the risk for chronic disease. The investigators examined data for 6,749 adults (ages 45 to 84; 53% women) as they completed questionnaires assessing chronic stress, depressive symptoms, anger, and hostility during a two-year period. Hazard ratios indicated a significantly elevated risk of stroke or TIA for the highest scoring group, compared with the lowest scoring group, for depressive symptoms (HR, 1.86), chronic stress (HR, 1.59), and hostility (HR, 2.22). No significant increased risk was associated with anger.
Patients with mild to moderate Parkinson’s disease can improve their symptoms with regular walking, according to a study published online ahead of print July 2 in Neurology. Investigators included 60 individuals who participated in a randomized trial of various exercise regimens for six months. Eighty-one percent of participants completed the study with a mean attendance of 83.3%. Subjects took additional tests to gauge their aerobic fitness, tiredness, and other factors. Brisk walking reduced tiredness by 11%, improved motor function and mood by 15%, improved attention and response control scores by 14%, and increased aerobic fitness and gait speed by 7%. With regard to motor function, participants improved by an average of 2.8 points. “The results of our study suggest that walking may provide a safe and easily accessible way of improving the symptoms of Parkinson’s disease and improve quality of life,” stated the researchers.
Mild traumatic brain injury (TBI) may result in brain damage and memory and thinking problems, according to a study published online ahead of print July 16 in Neurology. Fifty-three patients (44 with mild TBI and nine with moderate TBI) were compared with 33 participants without brain injury. Each subject underwent testing to assess his or her memory and thinking skills. Participants also had diffusion tensor imaging scans. Those with injuries had brain damage in white matter that consisted of disruption to nerve axons. Researchers also determined that scores on the verbal letter fluency task were 25% lower in individuals with injury than in individuals without injury. “We studied patients who had suffered clinically mild injuries, often from common accidents such as falling from a bicycle, or slow-speed car accidents. This finding is especially important, as 90% of all TBIs are mild to moderate,” said the researchers.
Patients with a traumatic brain injury (TBI) who received erythropoietin (EPO) or maintained a higher hemoglobin concentration through blood transfusion did not have an improved neurologic outcome at six months, according to a study published in the July 2 issue of JAMA. The randomized study included 200 patients (erythropoietin, n = 102; placebo, n = 98) with a closed head injury at neurosurgical intensive care units in two US level I trauma centers between May 2006 and August 2012. Patients were enrolled within six hours of injury and had to be unable to follow commands after initial stabilization. Overall, transfusing at higher hemoglobin concentrations was associated with a higher risk of adverse events. Researchers also observed a higher incidence of thromboembolic events for the transfusion threshold of 10 g/dL (21.8%) versus the threshold of 7 g/dL (8.1%)
Frontline Medical Communications and the National Organization for Rare Disorders (NORD) have signed a partnership agreement to develop educational programs about rare diseases for health care providers. Frontline and NORD also seek to improve awareness, recognition, and understanding of rare diseases among health care providers to accelerate diagnosis and promote optimal care for patients, facilitate the sharing of information among health care providers and rare disease medical experts, and update health care providers on new treatment options and clinical care standards. “Innovative multichannel educational programs, developed by both organizations and funded by commercial sponsors, will be distributed to more than 1.2 million health care providers using Frontline’s portfolio of 30 journal brands, corresponding websites, eNewsletters, and live events,” according to Frontline.
Upsher-Smith Laboratories (Maple Grove, Minnesota) announced that Qudexy XR (topiramate) extended-release capsules are now available in the United States. Qudexy XR, a broad-spectrum, once-daily antiepileptic drug is engineered to deliver a smooth pharmacokinetic profile. The FDA approved Qudexy XR in March 2014 as an initial monotherapy in patients 10 and older with primary generalized tonic-clonic seizures and partial-onset seizures. The drug also was approved as adjunctive therapy in patients 2 and older with primary generalized tonic-clonic seizures, partial-onset seizures, and seizures associated with Lennox-Gastaut syndrome. Overall, results from Upsher-Smith’s phase III trial showed that Qudexy XR is generally well tolerated and effective.
Transplanted brain cells producing dopamine remain viable in patients with Parkinson’s disease for several years, according to a study published June 26 in Cell Reports. The study included five patients with Parkinson’s disease who received transplants of fetal tissue-derived, dopamine-producing neurons four to 14 years earlier. Their transplanted dopamine neurons showed no signs of Parkinson’s disease–associated deterioration and appeared healthy. Researchers believe the findings provide further support for stem cells as a source for transplant-ready dopamine neurons. The investigators noted that the neuronal transplant has proven to be a durable treatment for many patients with Parkinson’s disease, with some improving for years without a need for standard medications. The study authors called the new finding “extremely encouraging,” adding that the long life of the transplanted neurons bodes well “for advancing [the technique] as a restoration therapy for Parkinson’s disease.”
Women may recover more quickly than men after a concussion, according to a study published online ahead of print May 6 in Radiology. Researchers examined the medical records and imaging results of 69 patients diagnosed with mild traumatic brain injury (TBI) between 2006 and 2013. The cohort included 47 men, 22 women, and 21 controls (10 men; median age of men, 17; median age of women, 16). Of the 47 men with TBI, 32 (68%) were injured while playing a sport, as were 10 of the 22 women (45%). Although all participants underwent the same evaluation, diffusion tensor imaging scans revealed that compared with the female patients with mild TBI, the male patients with mild TBI had significantly decreased uncinate fasciculus fractional anisotropy values. The average recovery time for all patients with concussion was 54 days. However, compared with women, who recovered in an average of 26.3 days, recovery was significantly longer for men (66.9 days).
Patients with mesial temporal lobe epilepsy who cannot be controlled with medication can now opt for a minimally invasive laser procedure performed under MRI guidance, according to a study published in the June issue of Neurosurgery. Researchers used an MRI-guided stereotactic laser amygdalohippocampotomy in 13 adult patients with epilepsy (median age, 24). During this procedure, a saline-cooled fiber-optic laser probe was targeted at the amygdalohippocampal complex. Using real-time MRI guidance, a neurosurgeon pinpointed the area of the brain responsible for seizure activity and destroyed this tissue without harming nearby brain tissue. Sixty percent of the amygdalohippocampal complex was destroyed, and the average length of the ablated area was 2.5 cm. “Such minimally invasive techniques may be more desirable to patients and result in increased use of epilepsy surgery among the large number of medically intractable epilepsy patients,” according to the investigators.
Researchers identified 10 proteins in the blood that can predict the onset of Alzheimer’s disease, according to a study published online ahead of print July 3 in Alzheimer’s & Dementia. In the international study of 1,148 individuals (220 with mild cognitive impairment [MCI], 452 elderly controls without dementia, and 476 with Alzheimer’s disease), blood samples were analyzed for 26 proteins previously associated with Alzheimer’s disease. Investigators found 16 of the 26 proteins to be strongly associated with brain shrinkage in Alzheimer’s disease or MCI. The researchers conducted a second series of tests to establish which of these proteins could predict the progression from MCI to Alzheimer’s disease. The study authors identified a combination of 10 proteins capable of predicting whether individuals with MCI would develop Alzheimer’s disease within a year with 87% accuracy. “Memory problems are common, but the challenge is identifying who is likely to develop dementia,” according to the researchers.
An international team of researchers has reviewed the diagnostic criteria for Alzheimer’s disease developed by the International Working Group (IWG) and US National Institute on Aging–Alzheimer’s Association, according to a study published in the June issue of Lancet Neurology. The team considered the strengths and weakness of the IWG criteria and proposed advances to improve the diagnostic framework. The investigators asserted that the diagnosis of Alzheimer’s disease can be simplified by requiring the presence of an appropriate clinical Alzheimer’s disease phenotype (typical or atypical) and a pathophysiologic biomarker consistent with the presence of Alzheimer’s pathology. “We propose that downstream topographic biomarkers of the disease, such as volumetric MRI and fluorodeoxyglucose PET, might better serve in the measurement and monitoring of the course of disease,” the team stated
—Kimberly D. Williams
Older veterans with traumatic brain injury (TBI) are 60% more likely to develop dementia later in life, compared with veterans without TBI, according to a study published online ahead of print June 25 in Neurology. The study involved 188,764 veterans ages 55 and older. At the study’s outset, each participant was free of dementia and had at least one inpatient or outpatient visit to a health care facility at baseline (2000 to 2003) and during the follow-up (2003 to 2012). A total of 1,229 veterans had a TBI diagnosis; 196 veterans with TBI (16%) developed dementia, and 18,255 (10%) of those without TBI developed dementia. On average, veterans with TBI developed dementia two years earlier than those without TBI. “If we assume that this relationship is causal, it seems likely that the same increased risk probably occurs with TBI in the civilian population as well,” said the researchers.
Higher levels of depressive symptoms, stress, and hostility are associated with a significantly increased risk of stroke or transient ischemic attack (TIA) in middle-aged and older adults, according to a study published online ahead of print July 10 in Stroke. Researchers used data from the Multi-Ethnic Study of Atherosclerosis (MESA) to determine how psychologic factors might influence the risk for chronic disease. The investigators examined data for 6,749 adults (ages 45 to 84; 53% women) as they completed questionnaires assessing chronic stress, depressive symptoms, anger, and hostility during a two-year period. Hazard ratios indicated a significantly elevated risk of stroke or TIA for the highest scoring group, compared with the lowest scoring group, for depressive symptoms (HR, 1.86), chronic stress (HR, 1.59), and hostility (HR, 2.22). No significant increased risk was associated with anger.
Patients with mild to moderate Parkinson’s disease can improve their symptoms with regular walking, according to a study published online ahead of print July 2 in Neurology. Investigators included 60 individuals who participated in a randomized trial of various exercise regimens for six months. Eighty-one percent of participants completed the study with a mean attendance of 83.3%. Subjects took additional tests to gauge their aerobic fitness, tiredness, and other factors. Brisk walking reduced tiredness by 11%, improved motor function and mood by 15%, improved attention and response control scores by 14%, and increased aerobic fitness and gait speed by 7%. With regard to motor function, participants improved by an average of 2.8 points. “The results of our study suggest that walking may provide a safe and easily accessible way of improving the symptoms of Parkinson’s disease and improve quality of life,” stated the researchers.
Mild traumatic brain injury (TBI) may result in brain damage and memory and thinking problems, according to a study published online ahead of print July 16 in Neurology. Fifty-three patients (44 with mild TBI and nine with moderate TBI) were compared with 33 participants without brain injury. Each subject underwent testing to assess his or her memory and thinking skills. Participants also had diffusion tensor imaging scans. Those with injuries had brain damage in white matter that consisted of disruption to nerve axons. Researchers also determined that scores on the verbal letter fluency task were 25% lower in individuals with injury than in individuals without injury. “We studied patients who had suffered clinically mild injuries, often from common accidents such as falling from a bicycle, or slow-speed car accidents. This finding is especially important, as 90% of all TBIs are mild to moderate,” said the researchers.
Patients with a traumatic brain injury (TBI) who received erythropoietin (EPO) or maintained a higher hemoglobin concentration through blood transfusion did not have an improved neurologic outcome at six months, according to a study published in the July 2 issue of JAMA. The randomized study included 200 patients (erythropoietin, n = 102; placebo, n = 98) with a closed head injury at neurosurgical intensive care units in two US level I trauma centers between May 2006 and August 2012. Patients were enrolled within six hours of injury and had to be unable to follow commands after initial stabilization. Overall, transfusing at higher hemoglobin concentrations was associated with a higher risk of adverse events. Researchers also observed a higher incidence of thromboembolic events for the transfusion threshold of 10 g/dL (21.8%) versus the threshold of 7 g/dL (8.1%)
Frontline Medical Communications and the National Organization for Rare Disorders (NORD) have signed a partnership agreement to develop educational programs about rare diseases for health care providers. Frontline and NORD also seek to improve awareness, recognition, and understanding of rare diseases among health care providers to accelerate diagnosis and promote optimal care for patients, facilitate the sharing of information among health care providers and rare disease medical experts, and update health care providers on new treatment options and clinical care standards. “Innovative multichannel educational programs, developed by both organizations and funded by commercial sponsors, will be distributed to more than 1.2 million health care providers using Frontline’s portfolio of 30 journal brands, corresponding websites, eNewsletters, and live events,” according to Frontline.
Upsher-Smith Laboratories (Maple Grove, Minnesota) announced that Qudexy XR (topiramate) extended-release capsules are now available in the United States. Qudexy XR, a broad-spectrum, once-daily antiepileptic drug is engineered to deliver a smooth pharmacokinetic profile. The FDA approved Qudexy XR in March 2014 as an initial monotherapy in patients 10 and older with primary generalized tonic-clonic seizures and partial-onset seizures. The drug also was approved as adjunctive therapy in patients 2 and older with primary generalized tonic-clonic seizures, partial-onset seizures, and seizures associated with Lennox-Gastaut syndrome. Overall, results from Upsher-Smith’s phase III trial showed that Qudexy XR is generally well tolerated and effective.
Transplanted brain cells producing dopamine remain viable in patients with Parkinson’s disease for several years, according to a study published June 26 in Cell Reports. The study included five patients with Parkinson’s disease who received transplants of fetal tissue-derived, dopamine-producing neurons four to 14 years earlier. Their transplanted dopamine neurons showed no signs of Parkinson’s disease–associated deterioration and appeared healthy. Researchers believe the findings provide further support for stem cells as a source for transplant-ready dopamine neurons. The investigators noted that the neuronal transplant has proven to be a durable treatment for many patients with Parkinson’s disease, with some improving for years without a need for standard medications. The study authors called the new finding “extremely encouraging,” adding that the long life of the transplanted neurons bodes well “for advancing [the technique] as a restoration therapy for Parkinson’s disease.”
Women may recover more quickly than men after a concussion, according to a study published online ahead of print May 6 in Radiology. Researchers examined the medical records and imaging results of 69 patients diagnosed with mild traumatic brain injury (TBI) between 2006 and 2013. The cohort included 47 men, 22 women, and 21 controls (10 men; median age of men, 17; median age of women, 16). Of the 47 men with TBI, 32 (68%) were injured while playing a sport, as were 10 of the 22 women (45%). Although all participants underwent the same evaluation, diffusion tensor imaging scans revealed that compared with the female patients with mild TBI, the male patients with mild TBI had significantly decreased uncinate fasciculus fractional anisotropy values. The average recovery time for all patients with concussion was 54 days. However, compared with women, who recovered in an average of 26.3 days, recovery was significantly longer for men (66.9 days).
Patients with mesial temporal lobe epilepsy who cannot be controlled with medication can now opt for a minimally invasive laser procedure performed under MRI guidance, according to a study published in the June issue of Neurosurgery. Researchers used an MRI-guided stereotactic laser amygdalohippocampotomy in 13 adult patients with epilepsy (median age, 24). During this procedure, a saline-cooled fiber-optic laser probe was targeted at the amygdalohippocampal complex. Using real-time MRI guidance, a neurosurgeon pinpointed the area of the brain responsible for seizure activity and destroyed this tissue without harming nearby brain tissue. Sixty percent of the amygdalohippocampal complex was destroyed, and the average length of the ablated area was 2.5 cm. “Such minimally invasive techniques may be more desirable to patients and result in increased use of epilepsy surgery among the large number of medically intractable epilepsy patients,” according to the investigators.
Researchers identified 10 proteins in the blood that can predict the onset of Alzheimer’s disease, according to a study published online ahead of print July 3 in Alzheimer’s & Dementia. In the international study of 1,148 individuals (220 with mild cognitive impairment [MCI], 452 elderly controls without dementia, and 476 with Alzheimer’s disease), blood samples were analyzed for 26 proteins previously associated with Alzheimer’s disease. Investigators found 16 of the 26 proteins to be strongly associated with brain shrinkage in Alzheimer’s disease or MCI. The researchers conducted a second series of tests to establish which of these proteins could predict the progression from MCI to Alzheimer’s disease. The study authors identified a combination of 10 proteins capable of predicting whether individuals with MCI would develop Alzheimer’s disease within a year with 87% accuracy. “Memory problems are common, but the challenge is identifying who is likely to develop dementia,” according to the researchers.
An international team of researchers has reviewed the diagnostic criteria for Alzheimer’s disease developed by the International Working Group (IWG) and US National Institute on Aging–Alzheimer’s Association, according to a study published in the June issue of Lancet Neurology. The team considered the strengths and weakness of the IWG criteria and proposed advances to improve the diagnostic framework. The investigators asserted that the diagnosis of Alzheimer’s disease can be simplified by requiring the presence of an appropriate clinical Alzheimer’s disease phenotype (typical or atypical) and a pathophysiologic biomarker consistent with the presence of Alzheimer’s pathology. “We propose that downstream topographic biomarkers of the disease, such as volumetric MRI and fluorodeoxyglucose PET, might better serve in the measurement and monitoring of the course of disease,” the team stated
—Kimberly D. Williams

Study reveals why HSCs falter with age

in the bone marrow
A new study helps explain how blood production declines with age and why older individuals are not suitable donors for hematopoietic stem cell (HSC) transplant.
The research also reveals a potential approach for mitigating
the negative effects of aging on the blood, which can lead to anemia,
bone marrow failure, and myeloid malignancies.
The study, conducted in mice, suggests HSCs falter with age because they lose the ability to replicate their DNA accurately and efficiently during cell division.
Emmanuelle Passegué, PhD, of the University of California San Francisco, and her colleagues reported this discovery in Nature.
The researchers analyzed old HSCs in mice and found a scarcity of protein components needed to form the mini-chromosome maintenance helicase. This molecular machine unwinds double-stranded DNA so the cell’s genetic material can be duplicated and allocated to daughter cells later in cell division.
The HSCs were stressed by the loss of this machine’s activity. As a result, they had an increased risk for DNA damage and death when forced to divide.
On the other hand, the cells tended to survive unless they were confronted with a “strong replication challenge” like transplantation.
The researchers also discovered that even after the stress associated with DNA replication, old HSCs retained molecular tags on histones, a feature often associated with DNA damage.
However, these old survivors could repair induced DNA damage as efficiently as young stem cells.
“Old stem cells are not just sitting there with damaged DNA ready to develop cancer, as it has long been postulated,” Dr Passegué said.
Of course, not all was well in the old, surviving HSCs. The molecular tags accumulated on genes needed to make ribosomes.
Dr Passegué said she will further explore the consequences of reduced protein production as part of her ongoing research. She hopes it might be possible to prevent declining stem cell populations by developing a drug to prevent the loss of the helicase components needed to unwind and replicate DNA, thereby avoiding immune system failure. ![]()
in the bone marrow
A new study helps explain how blood production declines with age and why older individuals are not suitable donors for hematopoietic stem cell (HSC) transplant.
The research also reveals a potential approach for mitigating
the negative effects of aging on the blood, which can lead to anemia,
bone marrow failure, and myeloid malignancies.
The study, conducted in mice, suggests HSCs falter with age because they lose the ability to replicate their DNA accurately and efficiently during cell division.
Emmanuelle Passegué, PhD, of the University of California San Francisco, and her colleagues reported this discovery in Nature.
The researchers analyzed old HSCs in mice and found a scarcity of protein components needed to form the mini-chromosome maintenance helicase. This molecular machine unwinds double-stranded DNA so the cell’s genetic material can be duplicated and allocated to daughter cells later in cell division.
The HSCs were stressed by the loss of this machine’s activity. As a result, they had an increased risk for DNA damage and death when forced to divide.
On the other hand, the cells tended to survive unless they were confronted with a “strong replication challenge” like transplantation.
The researchers also discovered that even after the stress associated with DNA replication, old HSCs retained molecular tags on histones, a feature often associated with DNA damage.
However, these old survivors could repair induced DNA damage as efficiently as young stem cells.
“Old stem cells are not just sitting there with damaged DNA ready to develop cancer, as it has long been postulated,” Dr Passegué said.
Of course, not all was well in the old, surviving HSCs. The molecular tags accumulated on genes needed to make ribosomes.
Dr Passegué said she will further explore the consequences of reduced protein production as part of her ongoing research. She hopes it might be possible to prevent declining stem cell populations by developing a drug to prevent the loss of the helicase components needed to unwind and replicate DNA, thereby avoiding immune system failure. ![]()
in the bone marrow
A new study helps explain how blood production declines with age and why older individuals are not suitable donors for hematopoietic stem cell (HSC) transplant.
The research also reveals a potential approach for mitigating
the negative effects of aging on the blood, which can lead to anemia,
bone marrow failure, and myeloid malignancies.
The study, conducted in mice, suggests HSCs falter with age because they lose the ability to replicate their DNA accurately and efficiently during cell division.
Emmanuelle Passegué, PhD, of the University of California San Francisco, and her colleagues reported this discovery in Nature.
The researchers analyzed old HSCs in mice and found a scarcity of protein components needed to form the mini-chromosome maintenance helicase. This molecular machine unwinds double-stranded DNA so the cell’s genetic material can be duplicated and allocated to daughter cells later in cell division.
The HSCs were stressed by the loss of this machine’s activity. As a result, they had an increased risk for DNA damage and death when forced to divide.
On the other hand, the cells tended to survive unless they were confronted with a “strong replication challenge” like transplantation.
The researchers also discovered that even after the stress associated with DNA replication, old HSCs retained molecular tags on histones, a feature often associated with DNA damage.
However, these old survivors could repair induced DNA damage as efficiently as young stem cells.
“Old stem cells are not just sitting there with damaged DNA ready to develop cancer, as it has long been postulated,” Dr Passegué said.
Of course, not all was well in the old, surviving HSCs. The molecular tags accumulated on genes needed to make ribosomes.
Dr Passegué said she will further explore the consequences of reduced protein production as part of her ongoing research. She hopes it might be possible to prevent declining stem cell populations by developing a drug to prevent the loss of the helicase components needed to unwind and replicate DNA, thereby avoiding immune system failure. ![]()
Group identifies targets for malaria vaccine

red blood cell; Credit: St Jude
Children’s Research Hospital
Scientists have uncovered a number of potential targets for a blood-stage malaria vaccine.
The team assessed how antibodies from a group of malaria-infected children responded to a library of proteins from the Plasmodium falciparum parasite.
This revealed antigens that had not previously been identified as possible vaccine targets and provided new insight into the ways antigens could be used in combination to increase protection from malaria.
“Resistance to malaria drugs is an increasing problem, so vaccines are desperately needed to battle the Plasmodium falciparum parasite before it has a chance to make people sick,” said Faith Osier, MBChB, of the Kenya Medical Research Institute in Nairobi City.
“This study presents us with a large number of new vaccine candidates that offer real hope for the future.”
Dr Osier and her colleagues described the study in Science Translational Medicine.
The researchers generated a library of correctly folded, full-length proteins from the P falciparum parasite. They then tested antibody reactivity against these proteins in a cohort of Kenyan children who were monitored for clinical episodes of malaria over 6 months.
This revealed antibodies that provide protection against clinical episodes of malaria. Some were equivalent or superior to current leading malaria vaccine candidates.
In fact, combinations consisting of 5 of the 10 top-ranked antigens (PF3D7_1136200, MSP2, RhopH3, P41, MSP11, MSP3, PF3D7_0606800, AMA1, Pf113, and MSRP1) could provide 100% protection against clinical episodes of malaria.
The researchers said these results add further weight to the theory that a successful blood-stage vaccine needs to target multiple antigens.
The team’s next step will be to generate antibodies against all of the proteins in the library and test them in different combinations to see whether combinations that appear to provide protection can directly prevent parasite invasion. ![]()
red blood cell; Credit: St Jude
Children’s Research Hospital
Scientists have uncovered a number of potential targets for a blood-stage malaria vaccine.
The team assessed how antibodies from a group of malaria-infected children responded to a library of proteins from the Plasmodium falciparum parasite.
This revealed antigens that had not previously been identified as possible vaccine targets and provided new insight into the ways antigens could be used in combination to increase protection from malaria.
“Resistance to malaria drugs is an increasing problem, so vaccines are desperately needed to battle the Plasmodium falciparum parasite before it has a chance to make people sick,” said Faith Osier, MBChB, of the Kenya Medical Research Institute in Nairobi City.
“This study presents us with a large number of new vaccine candidates that offer real hope for the future.”
Dr Osier and her colleagues described the study in Science Translational Medicine.
The researchers generated a library of correctly folded, full-length proteins from the P falciparum parasite. They then tested antibody reactivity against these proteins in a cohort of Kenyan children who were monitored for clinical episodes of malaria over 6 months.
This revealed antibodies that provide protection against clinical episodes of malaria. Some were equivalent or superior to current leading malaria vaccine candidates.
In fact, combinations consisting of 5 of the 10 top-ranked antigens (PF3D7_1136200, MSP2, RhopH3, P41, MSP11, MSP3, PF3D7_0606800, AMA1, Pf113, and MSRP1) could provide 100% protection against clinical episodes of malaria.
The researchers said these results add further weight to the theory that a successful blood-stage vaccine needs to target multiple antigens.
The team’s next step will be to generate antibodies against all of the proteins in the library and test them in different combinations to see whether combinations that appear to provide protection can directly prevent parasite invasion. ![]()
red blood cell; Credit: St Jude
Children’s Research Hospital
Scientists have uncovered a number of potential targets for a blood-stage malaria vaccine.
The team assessed how antibodies from a group of malaria-infected children responded to a library of proteins from the Plasmodium falciparum parasite.
This revealed antigens that had not previously been identified as possible vaccine targets and provided new insight into the ways antigens could be used in combination to increase protection from malaria.
“Resistance to malaria drugs is an increasing problem, so vaccines are desperately needed to battle the Plasmodium falciparum parasite before it has a chance to make people sick,” said Faith Osier, MBChB, of the Kenya Medical Research Institute in Nairobi City.
“This study presents us with a large number of new vaccine candidates that offer real hope for the future.”
Dr Osier and her colleagues described the study in Science Translational Medicine.
The researchers generated a library of correctly folded, full-length proteins from the P falciparum parasite. They then tested antibody reactivity against these proteins in a cohort of Kenyan children who were monitored for clinical episodes of malaria over 6 months.
This revealed antibodies that provide protection against clinical episodes of malaria. Some were equivalent or superior to current leading malaria vaccine candidates.
In fact, combinations consisting of 5 of the 10 top-ranked antigens (PF3D7_1136200, MSP2, RhopH3, P41, MSP11, MSP3, PF3D7_0606800, AMA1, Pf113, and MSRP1) could provide 100% protection against clinical episodes of malaria.
The researchers said these results add further weight to the theory that a successful blood-stage vaccine needs to target multiple antigens.
The team’s next step will be to generate antibodies against all of the proteins in the library and test them in different combinations to see whether combinations that appear to provide protection can directly prevent parasite invasion. ![]()
Tool aids analysis of genomic data
Credit: Christoph Bock
Computer scientists have developed a web-based tool that allows researchers to visualize and compare large amounts of genomic information from high-throughput sequencing experiments.
The group described the tool, called Epiviz, in Nature Methods.
“Prior tools limited visualization to presentation and dissemination, rather than a hybrid tool integrating interactive visualization with algorithmic analysis,” said Héctor Corrada Bravo, PhD, of the University of Maryland in College Park.
Dr Corrada Bravo and his colleagues developed Epiviz, a web-based genome browser that integrates with the widely used, open-source Bioconductor analysis software through its Epivizr Bioconductor package.
Epiviz supports many popular next-generation sequencing techniques, such as ChIP-seq, RNA-seq, and DNA methylation analyses.
The tool also implements multiple visualization methods for location-based data (such as genomic regions of interest) and feature-based data (such as gene expression).
For example, because display objects are mapped directly to data elements, Epiviz links data across different visualizations, giving users visual insights of the spatial relationships of multiple data sets. The tool is designed to allow biomedical scientists to easily incorporate their own visualizations.
In the Nature Methods paper, Dr Corrada Bravo and his colleagues describe how they used Epiviz to visualize and analyze DNA methylation and gene expression data in colon cancer.
Using Epiviz and Bioconductor, the team found consistent regions of DNA methylation changes in colon cancer samples generated by the Cancer Genome Atlas project and similar gene expression in these regions of DNA methylation changes in other cancer types.
The results were in agreement with previous experiments showing DNA methylation changes across large regions in the colon cancer genome. ![]()
Credit: Christoph Bock
Computer scientists have developed a web-based tool that allows researchers to visualize and compare large amounts of genomic information from high-throughput sequencing experiments.
The group described the tool, called Epiviz, in Nature Methods.
“Prior tools limited visualization to presentation and dissemination, rather than a hybrid tool integrating interactive visualization with algorithmic analysis,” said Héctor Corrada Bravo, PhD, of the University of Maryland in College Park.
Dr Corrada Bravo and his colleagues developed Epiviz, a web-based genome browser that integrates with the widely used, open-source Bioconductor analysis software through its Epivizr Bioconductor package.
Epiviz supports many popular next-generation sequencing techniques, such as ChIP-seq, RNA-seq, and DNA methylation analyses.
The tool also implements multiple visualization methods for location-based data (such as genomic regions of interest) and feature-based data (such as gene expression).
For example, because display objects are mapped directly to data elements, Epiviz links data across different visualizations, giving users visual insights of the spatial relationships of multiple data sets. The tool is designed to allow biomedical scientists to easily incorporate their own visualizations.
In the Nature Methods paper, Dr Corrada Bravo and his colleagues describe how they used Epiviz to visualize and analyze DNA methylation and gene expression data in colon cancer.
Using Epiviz and Bioconductor, the team found consistent regions of DNA methylation changes in colon cancer samples generated by the Cancer Genome Atlas project and similar gene expression in these regions of DNA methylation changes in other cancer types.
The results were in agreement with previous experiments showing DNA methylation changes across large regions in the colon cancer genome. ![]()
Credit: Christoph Bock
Computer scientists have developed a web-based tool that allows researchers to visualize and compare large amounts of genomic information from high-throughput sequencing experiments.
The group described the tool, called Epiviz, in Nature Methods.
“Prior tools limited visualization to presentation and dissemination, rather than a hybrid tool integrating interactive visualization with algorithmic analysis,” said Héctor Corrada Bravo, PhD, of the University of Maryland in College Park.
Dr Corrada Bravo and his colleagues developed Epiviz, a web-based genome browser that integrates with the widely used, open-source Bioconductor analysis software through its Epivizr Bioconductor package.
Epiviz supports many popular next-generation sequencing techniques, such as ChIP-seq, RNA-seq, and DNA methylation analyses.
The tool also implements multiple visualization methods for location-based data (such as genomic regions of interest) and feature-based data (such as gene expression).
For example, because display objects are mapped directly to data elements, Epiviz links data across different visualizations, giving users visual insights of the spatial relationships of multiple data sets. The tool is designed to allow biomedical scientists to easily incorporate their own visualizations.
In the Nature Methods paper, Dr Corrada Bravo and his colleagues describe how they used Epiviz to visualize and analyze DNA methylation and gene expression data in colon cancer.
Using Epiviz and Bioconductor, the team found consistent regions of DNA methylation changes in colon cancer samples generated by the Cancer Genome Atlas project and similar gene expression in these regions of DNA methylation changes in other cancer types.
The results were in agreement with previous experiments showing DNA methylation changes across large regions in the colon cancer genome. ![]()
System simplifies complex pipetting protocols

Credit: John Correa
Researchers say they’ve developed a simple system that can help scientists perform complex pipetting protocols efficiently and accurately.
The system, called iPipet, allows users to track the transfer of samples and reagents by illuminating well plates on a computer tablet.
In tests, iPipet proved more efficient than a liquid-handling robot.
The researchers have made information on iPipet available online so scientists can use the system in their own labs.
The team also described iPipet in a letter to Nature Methods.
They noted that experiments frequently rely on high-throughput methods that combine large numbers of samples with large-scale, complex pipetting designs. And pipetting errors can lead to experimental failure.
Although liquid-handling robots would seem to be a logical choice for such work, they are also extremely expensive, difficult to program, and require trained personnel. Moreover, they can be plagued by technical snafus, ranging from bent or clogged tips to an inability to capture liquids lying close to the bottoms of individual wells.
“We needed an alternative to costly robots that would allow us to execute complex pipetting protocols,” said Yaniv Erlich, PhD, of the Whitehead Institute in Cambridge, Massachusetts.
So Dr Erlich and his colleagues developed iPipet. The system illuminates individual wells of standard 96- or 384-well plates placed on top of a tablet screen, guiding users through the transfer of samples or reagents from source to destination plates according to specific designs.
Users create their own protocols in Microsoft Excel files in comma-separated format and upload them to the iPipet website, which generates a downloadable link for execution on a tablet computer. Included on the iPipet site are a variety of demos and an instructional video.
In a test of the tool against a liquid-handling robot, iPipet enabled nearly 3000 fixed-volume pipetting steps in approximately 7 hours. After significant time spent on calibration, the robot accomplished only half that number of steps in the same allotted time.
To date, one of the only challenges lab users have encountered is keeping well plates in a fixed position on the tablet screen. For that, Dr Erlich’s team provides a solution: a 3D printed plastic adaptor that users can create with a file accessible via the iPipet website.
“The entire iPipet system is open source,” Dr Erlich said. “We want to maximize the benefit for the community and allow them to further develop this new man-machine interface for biological experiments.” ![]()
Credit: John Correa
Researchers say they’ve developed a simple system that can help scientists perform complex pipetting protocols efficiently and accurately.
The system, called iPipet, allows users to track the transfer of samples and reagents by illuminating well plates on a computer tablet.
In tests, iPipet proved more efficient than a liquid-handling robot.
The researchers have made information on iPipet available online so scientists can use the system in their own labs.
The team also described iPipet in a letter to Nature Methods.
They noted that experiments frequently rely on high-throughput methods that combine large numbers of samples with large-scale, complex pipetting designs. And pipetting errors can lead to experimental failure.
Although liquid-handling robots would seem to be a logical choice for such work, they are also extremely expensive, difficult to program, and require trained personnel. Moreover, they can be plagued by technical snafus, ranging from bent or clogged tips to an inability to capture liquids lying close to the bottoms of individual wells.
“We needed an alternative to costly robots that would allow us to execute complex pipetting protocols,” said Yaniv Erlich, PhD, of the Whitehead Institute in Cambridge, Massachusetts.
So Dr Erlich and his colleagues developed iPipet. The system illuminates individual wells of standard 96- or 384-well plates placed on top of a tablet screen, guiding users through the transfer of samples or reagents from source to destination plates according to specific designs.
Users create their own protocols in Microsoft Excel files in comma-separated format and upload them to the iPipet website, which generates a downloadable link for execution on a tablet computer. Included on the iPipet site are a variety of demos and an instructional video.
In a test of the tool against a liquid-handling robot, iPipet enabled nearly 3000 fixed-volume pipetting steps in approximately 7 hours. After significant time spent on calibration, the robot accomplished only half that number of steps in the same allotted time.
To date, one of the only challenges lab users have encountered is keeping well plates in a fixed position on the tablet screen. For that, Dr Erlich’s team provides a solution: a 3D printed plastic adaptor that users can create with a file accessible via the iPipet website.
“The entire iPipet system is open source,” Dr Erlich said. “We want to maximize the benefit for the community and allow them to further develop this new man-machine interface for biological experiments.” ![]()
Credit: John Correa
Researchers say they’ve developed a simple system that can help scientists perform complex pipetting protocols efficiently and accurately.
The system, called iPipet, allows users to track the transfer of samples and reagents by illuminating well plates on a computer tablet.
In tests, iPipet proved more efficient than a liquid-handling robot.
The researchers have made information on iPipet available online so scientists can use the system in their own labs.
The team also described iPipet in a letter to Nature Methods.
They noted that experiments frequently rely on high-throughput methods that combine large numbers of samples with large-scale, complex pipetting designs. And pipetting errors can lead to experimental failure.
Although liquid-handling robots would seem to be a logical choice for such work, they are also extremely expensive, difficult to program, and require trained personnel. Moreover, they can be plagued by technical snafus, ranging from bent or clogged tips to an inability to capture liquids lying close to the bottoms of individual wells.
“We needed an alternative to costly robots that would allow us to execute complex pipetting protocols,” said Yaniv Erlich, PhD, of the Whitehead Institute in Cambridge, Massachusetts.
So Dr Erlich and his colleagues developed iPipet. The system illuminates individual wells of standard 96- or 384-well plates placed on top of a tablet screen, guiding users through the transfer of samples or reagents from source to destination plates according to specific designs.
Users create their own protocols in Microsoft Excel files in comma-separated format and upload them to the iPipet website, which generates a downloadable link for execution on a tablet computer. Included on the iPipet site are a variety of demos and an instructional video.
In a test of the tool against a liquid-handling robot, iPipet enabled nearly 3000 fixed-volume pipetting steps in approximately 7 hours. After significant time spent on calibration, the robot accomplished only half that number of steps in the same allotted time.
To date, one of the only challenges lab users have encountered is keeping well plates in a fixed position on the tablet screen. For that, Dr Erlich’s team provides a solution: a 3D printed plastic adaptor that users can create with a file accessible via the iPipet website.
“The entire iPipet system is open source,” Dr Erlich said. “We want to maximize the benefit for the community and allow them to further develop this new man-machine interface for biological experiments.” ![]()
LISTEN NOW: Highlights of the August 2014 issue of The Hospitalist newsmagazine
Highlights from The Hospitalist this month include an interview with SHM President Dr. Burke Kealey about his series of President's Desk columns. Dr. Kealey talks about how the hospital medicine movement arose and expands on the transformational nature of hospital medicine. Also in this issue, we provide a comprehensive look at medical decision making, focused on the ins and outs of turning decisions into the right codes for billing and ongoing. Dr. Christopher Moreland, a deaf teaching hospitalist at University Hospital at the University of Texas is profiled on our cover, and Team Hospitalist member Dr. Julie Fedderson tells us what drew her to the specialty. In addition, we offer a progress report of SHM’s performance assessment tool for hospital medicine groups. Our Key Clinical Question this month addresses hypontremia treatment and managment, and our In The Literature section features the latest in clinical literature.
Highlights from The Hospitalist this month include an interview with SHM President Dr. Burke Kealey about his series of President's Desk columns. Dr. Kealey talks about how the hospital medicine movement arose and expands on the transformational nature of hospital medicine. Also in this issue, we provide a comprehensive look at medical decision making, focused on the ins and outs of turning decisions into the right codes for billing and ongoing. Dr. Christopher Moreland, a deaf teaching hospitalist at University Hospital at the University of Texas is profiled on our cover, and Team Hospitalist member Dr. Julie Fedderson tells us what drew her to the specialty. In addition, we offer a progress report of SHM’s performance assessment tool for hospital medicine groups. Our Key Clinical Question this month addresses hypontremia treatment and managment, and our In The Literature section features the latest in clinical literature.
Highlights from The Hospitalist this month include an interview with SHM President Dr. Burke Kealey about his series of President's Desk columns. Dr. Kealey talks about how the hospital medicine movement arose and expands on the transformational nature of hospital medicine. Also in this issue, we provide a comprehensive look at medical decision making, focused on the ins and outs of turning decisions into the right codes for billing and ongoing. Dr. Christopher Moreland, a deaf teaching hospitalist at University Hospital at the University of Texas is profiled on our cover, and Team Hospitalist member Dr. Julie Fedderson tells us what drew her to the specialty. In addition, we offer a progress report of SHM’s performance assessment tool for hospital medicine groups. Our Key Clinical Question this month addresses hypontremia treatment and managment, and our In The Literature section features the latest in clinical literature.
Biliary pain, no gallstones—remove the gallbladder, anyway?
CASE 1 › A 28-year-old woman (G0P0) came to our office with recurrent episodes of postprandial epigastric and right upper quadrant pain. Upper and lower endoscopy, sonography, body imaging, and laboratory tests were normal. A biliary nuclear scan showed an ejection fraction (EF) of 95%; normal is >35%. We made a diagnosis of biliary dyskinesia (BD) and recommended a laparoscopic cholecystectomy. The patient underwent this procedure and her pain was relieved. She has been much improved for 2 years, although she has since been diagnosed with an autoimmune disorder.
CASE 2 › A 21-year-old woman with right upper quadrant, postprandial, colicky pain presented to the emergency department. The episode lasted approximately 30 minutes and was followed by residual soreness. This episode was one of several that had been increasing in frequency and intensity. A sonogram showed a normal gallbladder and common duct. All laboratory tests were normal. She improved and was discharged. Outpatient evaluation included body imaging and endoscopy, which were negative. A hepatobiliary (HIDA) scan revealed an EF of 90%, and the scan reproduced her symptoms.
We diagnosed BD in this patient. After reviewing the risks and benefits of cholecystectomy, the patient consented to the procedure. She has been asymptomatic for 2 years.
Family physicians often are the first to evaluate patients with recurrent biliary colic. Biliary colic without gallstones—also known as BD or acalculous cholecystitis—is a functional disorder of the gallbladder or bile duct. Approximately 8% of men and 21% of women with biliary pain do not have gallstones.1-5
BD has been successfully treated with cholecystectomy. Physicians typically have viewed cholecystectomy as being effective primarily for patients with biliary pain who have a low EF (<35%).2-4 However, recent studies and our experience with cholecystectomy in these 2 patients with high EFs suggest that EF is only one of several factors to consider when deciding whether cholecystectomy might be appropriate for a given patient.
Which patients are most likely to benefit from cholecystectomy?
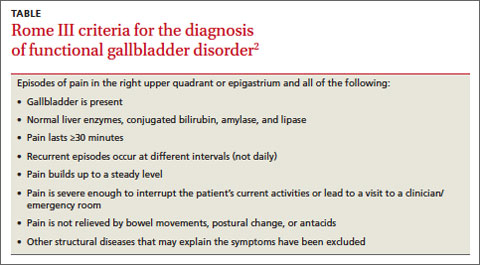
BD is a diagnosis of exclusion, considered when other upper abdominal disorders are eliminated. To receive a diagnosis of BD, patients must meet the Rome III criteria (TABLE).2
Before the advent of oral cholecystography in the 1920s, biliary disease was a clinical diagnosis confirmed by examination of the excised gallbladder.6 In 2 large studies conducted before cholecystography was in common use, researchers noted improvement in 75% to 85% of BD patients after cholecystectomy.7,8 Several years later, with the benefit, of cholecystography, Mackey9 reported similar improvement rates among patients with BD who underwent cholecystectomy.
Cholecystography has largely been replaced with HIDA scanning, which provides an objective measure of EF. Although some studies have suggested low EFs may predict which patients will benefit from cholecystectomy, others have suggested this value doesn’t tell the whole story.2,4,10,11 In some studies, patients who had biliary symptoms and a low EF (<35%) were found to be most likely to experience relief after cholecystectomy.2,4 More recently, in a chart review, DuCoin et al10 found that of 19 BD patients with an EF >35% who underwent cholecystectomy, 17 had complete symptom resolution, one had partial resolution, and one was unchanged. Only one abstract of a study of cholecystectomy for BD patients with a high EF (>80%) has been published.11 Of 28 patients who received cholecystectomy, 22 were asymptomatic after cholecystectomy and 5 others improved.11
Other tests to consider. A cholecystokinin infusion without a scan has been used to reproduce biliary colic; some physicians consider this to be diagnostic of BD and sufficient for cholecystectomy.12 Others have advocated endoscopic injection of botulinum into the sphincter of Oddi to differentiate pain arising from the sphincter of Oddi from pain in the gallbladder.5,13 If symptoms are relieved by this injection, an endoscopic biliary sphincterotomy—cutting of the biliary sphincter—is done. Cholecystectomy is reserved for patients whose pain is not relieved by botulinum. In an initial report, 25 BD patients received botulinum injections into the sphincter of Oddi; of the 11 whose pain was relieved by this injection, 10 underwent endoscopic biliary sphincterotomy, and pain resolved for all of these patients.13
Why we chose cholecystectomy for our patients
Despite a plethora of tests available to visualize and assess gallbladder and bile duct function, clinical assessment of BD by experienced physicians may be sufficient to determine which BD patients will benefit from cholecystectomy. In the cases we report on here, each patient had a high EF, but both met Rome III criteria and were experiencing clinically significant pain. Also, for both patients, a cholecystokinin infusion administered to calculate EF reproduced their pain. This clinical picture led us to recommend laparoscopic cholecystectomy, which ultimately relieved their symptoms.
CORRESPONDENCE
Mazen Iskandar, MD, The Pancreas and Biliary Center of New York, Beth Israel Medical Center, 350 East 17th Street, 16 Baird Hall, New York, NY 10010; [email protected]
1. Drossman DA, Dumitrascu DL. Rome III: new standard for functional gastrointestinal disorders. J Gastrointest Liver Dis. 2006;15:237-241.
2. Hansel SL, DiBaise JK. Functional gallbladder disorder: gallbladder dyskinesia. Gastroenterol Clin North Am. 2010;39:369-379.
3. Francis G, Baillie J. Gallbladder dyskinesia: fact or fiction? Curr Gastroenterol Rep. 2011;13:188-192.
4. Yap L, Wycherley AG, Morphett AD, et al. Acalculous biliary pain; cholecystectomy alleviates symptoms in patients with abnormal cholescintigraphy. Gastroenterology. 1991;101:786-793.
5. Behar J, Corazziari E, Guelrud M, et al. Functional gallbladder and sphincter of oddi disorders. Gastroenterology. 2006;130: 1498-1509.
6. Graham EA, Cole WH. Roentgenologic examination of the gallbladder: preliminary report of a new method utilizing the intravenous injection of tetrabromophenolphthalein. JAMA. 1924;82:613-614.
7. Blalock A. A study of eight hundred and eighty-eight cases of biliary tract disease. Johns Hopkins Hosp Bull. 1924;35:391-409.
8. Whipple AO. Surgical criteria for cholecystectomy. Bull N Y Acad Med. 1926;2:302-306.
9. Mackey WA. Cholecystitis without stone an investigation of 264 operated cases from the clinical, radiological, and pathological aspects. An attempt to determine the factors of service in estimating prognosis. Br J Surg. 1934;22:274-295.
10. DuCoin C, Faber R, Ilagan M, et al. Normokinetic biliary dyskinesia: a novel diagnosis. Surg Endosc. 2012;26:3088-3093.
11. Holes-Lewis KA, Hakim S, Rehman F, al. CCK-induced gall bladder hyperkinesia: An indication for cholecystectomy and brain-GI connectivity research. J Nucl Med. 2009;50(suppl 2):1312.
12. Carr JA, Walls J, Bryan LJ, et al. The treatment of gallbladder dyskinesia based upon symptoms: results of a 2-year, prospective, nonrandomized, concurrent cohort study. Surg Laparosc Endosc Percutan Tech. 2009;19:222-226.
13. Murray WR. Botulinum toxin-induced relaxation of the sphincter of Oddi may select patients with acalculous biliary pain who will benefit from cholecystectomy. Surg Endosc. 2011;25:813-816.
CASE 1 › A 28-year-old woman (G0P0) came to our office with recurrent episodes of postprandial epigastric and right upper quadrant pain. Upper and lower endoscopy, sonography, body imaging, and laboratory tests were normal. A biliary nuclear scan showed an ejection fraction (EF) of 95%; normal is >35%. We made a diagnosis of biliary dyskinesia (BD) and recommended a laparoscopic cholecystectomy. The patient underwent this procedure and her pain was relieved. She has been much improved for 2 years, although she has since been diagnosed with an autoimmune disorder.
CASE 2 › A 21-year-old woman with right upper quadrant, postprandial, colicky pain presented to the emergency department. The episode lasted approximately 30 minutes and was followed by residual soreness. This episode was one of several that had been increasing in frequency and intensity. A sonogram showed a normal gallbladder and common duct. All laboratory tests were normal. She improved and was discharged. Outpatient evaluation included body imaging and endoscopy, which were negative. A hepatobiliary (HIDA) scan revealed an EF of 90%, and the scan reproduced her symptoms.
We diagnosed BD in this patient. After reviewing the risks and benefits of cholecystectomy, the patient consented to the procedure. She has been asymptomatic for 2 years.
Family physicians often are the first to evaluate patients with recurrent biliary colic. Biliary colic without gallstones—also known as BD or acalculous cholecystitis—is a functional disorder of the gallbladder or bile duct. Approximately 8% of men and 21% of women with biliary pain do not have gallstones.1-5
BD has been successfully treated with cholecystectomy. Physicians typically have viewed cholecystectomy as being effective primarily for patients with biliary pain who have a low EF (<35%).2-4 However, recent studies and our experience with cholecystectomy in these 2 patients with high EFs suggest that EF is only one of several factors to consider when deciding whether cholecystectomy might be appropriate for a given patient.
Which patients are most likely to benefit from cholecystectomy?
BD is a diagnosis of exclusion, considered when other upper abdominal disorders are eliminated. To receive a diagnosis of BD, patients must meet the Rome III criteria (TABLE).2
Before the advent of oral cholecystography in the 1920s, biliary disease was a clinical diagnosis confirmed by examination of the excised gallbladder.6 In 2 large studies conducted before cholecystography was in common use, researchers noted improvement in 75% to 85% of BD patients after cholecystectomy.7,8 Several years later, with the benefit, of cholecystography, Mackey9 reported similar improvement rates among patients with BD who underwent cholecystectomy.
Cholecystography has largely been replaced with HIDA scanning, which provides an objective measure of EF. Although some studies have suggested low EFs may predict which patients will benefit from cholecystectomy, others have suggested this value doesn’t tell the whole story.2,4,10,11 In some studies, patients who had biliary symptoms and a low EF (<35%) were found to be most likely to experience relief after cholecystectomy.2,4 More recently, in a chart review, DuCoin et al10 found that of 19 BD patients with an EF >35% who underwent cholecystectomy, 17 had complete symptom resolution, one had partial resolution, and one was unchanged. Only one abstract of a study of cholecystectomy for BD patients with a high EF (>80%) has been published.11 Of 28 patients who received cholecystectomy, 22 were asymptomatic after cholecystectomy and 5 others improved.11
Other tests to consider. A cholecystokinin infusion without a scan has been used to reproduce biliary colic; some physicians consider this to be diagnostic of BD and sufficient for cholecystectomy.12 Others have advocated endoscopic injection of botulinum into the sphincter of Oddi to differentiate pain arising from the sphincter of Oddi from pain in the gallbladder.5,13 If symptoms are relieved by this injection, an endoscopic biliary sphincterotomy—cutting of the biliary sphincter—is done. Cholecystectomy is reserved for patients whose pain is not relieved by botulinum. In an initial report, 25 BD patients received botulinum injections into the sphincter of Oddi; of the 11 whose pain was relieved by this injection, 10 underwent endoscopic biliary sphincterotomy, and pain resolved for all of these patients.13
Why we chose cholecystectomy for our patients
Despite a plethora of tests available to visualize and assess gallbladder and bile duct function, clinical assessment of BD by experienced physicians may be sufficient to determine which BD patients will benefit from cholecystectomy. In the cases we report on here, each patient had a high EF, but both met Rome III criteria and were experiencing clinically significant pain. Also, for both patients, a cholecystokinin infusion administered to calculate EF reproduced their pain. This clinical picture led us to recommend laparoscopic cholecystectomy, which ultimately relieved their symptoms.
CORRESPONDENCE
Mazen Iskandar, MD, The Pancreas and Biliary Center of New York, Beth Israel Medical Center, 350 East 17th Street, 16 Baird Hall, New York, NY 10010; [email protected]
CASE 1 › A 28-year-old woman (G0P0) came to our office with recurrent episodes of postprandial epigastric and right upper quadrant pain. Upper and lower endoscopy, sonography, body imaging, and laboratory tests were normal. A biliary nuclear scan showed an ejection fraction (EF) of 95%; normal is >35%. We made a diagnosis of biliary dyskinesia (BD) and recommended a laparoscopic cholecystectomy. The patient underwent this procedure and her pain was relieved. She has been much improved for 2 years, although she has since been diagnosed with an autoimmune disorder.
CASE 2 › A 21-year-old woman with right upper quadrant, postprandial, colicky pain presented to the emergency department. The episode lasted approximately 30 minutes and was followed by residual soreness. This episode was one of several that had been increasing in frequency and intensity. A sonogram showed a normal gallbladder and common duct. All laboratory tests were normal. She improved and was discharged. Outpatient evaluation included body imaging and endoscopy, which were negative. A hepatobiliary (HIDA) scan revealed an EF of 90%, and the scan reproduced her symptoms.
We diagnosed BD in this patient. After reviewing the risks and benefits of cholecystectomy, the patient consented to the procedure. She has been asymptomatic for 2 years.
Family physicians often are the first to evaluate patients with recurrent biliary colic. Biliary colic without gallstones—also known as BD or acalculous cholecystitis—is a functional disorder of the gallbladder or bile duct. Approximately 8% of men and 21% of women with biliary pain do not have gallstones.1-5
BD has been successfully treated with cholecystectomy. Physicians typically have viewed cholecystectomy as being effective primarily for patients with biliary pain who have a low EF (<35%).2-4 However, recent studies and our experience with cholecystectomy in these 2 patients with high EFs suggest that EF is only one of several factors to consider when deciding whether cholecystectomy might be appropriate for a given patient.
Which patients are most likely to benefit from cholecystectomy?
BD is a diagnosis of exclusion, considered when other upper abdominal disorders are eliminated. To receive a diagnosis of BD, patients must meet the Rome III criteria (TABLE).2
Before the advent of oral cholecystography in the 1920s, biliary disease was a clinical diagnosis confirmed by examination of the excised gallbladder.6 In 2 large studies conducted before cholecystography was in common use, researchers noted improvement in 75% to 85% of BD patients after cholecystectomy.7,8 Several years later, with the benefit, of cholecystography, Mackey9 reported similar improvement rates among patients with BD who underwent cholecystectomy.
Cholecystography has largely been replaced with HIDA scanning, which provides an objective measure of EF. Although some studies have suggested low EFs may predict which patients will benefit from cholecystectomy, others have suggested this value doesn’t tell the whole story.2,4,10,11 In some studies, patients who had biliary symptoms and a low EF (<35%) were found to be most likely to experience relief after cholecystectomy.2,4 More recently, in a chart review, DuCoin et al10 found that of 19 BD patients with an EF >35% who underwent cholecystectomy, 17 had complete symptom resolution, one had partial resolution, and one was unchanged. Only one abstract of a study of cholecystectomy for BD patients with a high EF (>80%) has been published.11 Of 28 patients who received cholecystectomy, 22 were asymptomatic after cholecystectomy and 5 others improved.11
Other tests to consider. A cholecystokinin infusion without a scan has been used to reproduce biliary colic; some physicians consider this to be diagnostic of BD and sufficient for cholecystectomy.12 Others have advocated endoscopic injection of botulinum into the sphincter of Oddi to differentiate pain arising from the sphincter of Oddi from pain in the gallbladder.5,13 If symptoms are relieved by this injection, an endoscopic biliary sphincterotomy—cutting of the biliary sphincter—is done. Cholecystectomy is reserved for patients whose pain is not relieved by botulinum. In an initial report, 25 BD patients received botulinum injections into the sphincter of Oddi; of the 11 whose pain was relieved by this injection, 10 underwent endoscopic biliary sphincterotomy, and pain resolved for all of these patients.13
Why we chose cholecystectomy for our patients
Despite a plethora of tests available to visualize and assess gallbladder and bile duct function, clinical assessment of BD by experienced physicians may be sufficient to determine which BD patients will benefit from cholecystectomy. In the cases we report on here, each patient had a high EF, but both met Rome III criteria and were experiencing clinically significant pain. Also, for both patients, a cholecystokinin infusion administered to calculate EF reproduced their pain. This clinical picture led us to recommend laparoscopic cholecystectomy, which ultimately relieved their symptoms.
CORRESPONDENCE
Mazen Iskandar, MD, The Pancreas and Biliary Center of New York, Beth Israel Medical Center, 350 East 17th Street, 16 Baird Hall, New York, NY 10010; [email protected]
1. Drossman DA, Dumitrascu DL. Rome III: new standard for functional gastrointestinal disorders. J Gastrointest Liver Dis. 2006;15:237-241.
2. Hansel SL, DiBaise JK. Functional gallbladder disorder: gallbladder dyskinesia. Gastroenterol Clin North Am. 2010;39:369-379.
3. Francis G, Baillie J. Gallbladder dyskinesia: fact or fiction? Curr Gastroenterol Rep. 2011;13:188-192.
4. Yap L, Wycherley AG, Morphett AD, et al. Acalculous biliary pain; cholecystectomy alleviates symptoms in patients with abnormal cholescintigraphy. Gastroenterology. 1991;101:786-793.
5. Behar J, Corazziari E, Guelrud M, et al. Functional gallbladder and sphincter of oddi disorders. Gastroenterology. 2006;130: 1498-1509.
6. Graham EA, Cole WH. Roentgenologic examination of the gallbladder: preliminary report of a new method utilizing the intravenous injection of tetrabromophenolphthalein. JAMA. 1924;82:613-614.
7. Blalock A. A study of eight hundred and eighty-eight cases of biliary tract disease. Johns Hopkins Hosp Bull. 1924;35:391-409.
8. Whipple AO. Surgical criteria for cholecystectomy. Bull N Y Acad Med. 1926;2:302-306.
9. Mackey WA. Cholecystitis without stone an investigation of 264 operated cases from the clinical, radiological, and pathological aspects. An attempt to determine the factors of service in estimating prognosis. Br J Surg. 1934;22:274-295.
10. DuCoin C, Faber R, Ilagan M, et al. Normokinetic biliary dyskinesia: a novel diagnosis. Surg Endosc. 2012;26:3088-3093.
11. Holes-Lewis KA, Hakim S, Rehman F, al. CCK-induced gall bladder hyperkinesia: An indication for cholecystectomy and brain-GI connectivity research. J Nucl Med. 2009;50(suppl 2):1312.
12. Carr JA, Walls J, Bryan LJ, et al. The treatment of gallbladder dyskinesia based upon symptoms: results of a 2-year, prospective, nonrandomized, concurrent cohort study. Surg Laparosc Endosc Percutan Tech. 2009;19:222-226.
13. Murray WR. Botulinum toxin-induced relaxation of the sphincter of Oddi may select patients with acalculous biliary pain who will benefit from cholecystectomy. Surg Endosc. 2011;25:813-816.
1. Drossman DA, Dumitrascu DL. Rome III: new standard for functional gastrointestinal disorders. J Gastrointest Liver Dis. 2006;15:237-241.
2. Hansel SL, DiBaise JK. Functional gallbladder disorder: gallbladder dyskinesia. Gastroenterol Clin North Am. 2010;39:369-379.
3. Francis G, Baillie J. Gallbladder dyskinesia: fact or fiction? Curr Gastroenterol Rep. 2011;13:188-192.
4. Yap L, Wycherley AG, Morphett AD, et al. Acalculous biliary pain; cholecystectomy alleviates symptoms in patients with abnormal cholescintigraphy. Gastroenterology. 1991;101:786-793.
5. Behar J, Corazziari E, Guelrud M, et al. Functional gallbladder and sphincter of oddi disorders. Gastroenterology. 2006;130: 1498-1509.
6. Graham EA, Cole WH. Roentgenologic examination of the gallbladder: preliminary report of a new method utilizing the intravenous injection of tetrabromophenolphthalein. JAMA. 1924;82:613-614.
7. Blalock A. A study of eight hundred and eighty-eight cases of biliary tract disease. Johns Hopkins Hosp Bull. 1924;35:391-409.
8. Whipple AO. Surgical criteria for cholecystectomy. Bull N Y Acad Med. 1926;2:302-306.
9. Mackey WA. Cholecystitis without stone an investigation of 264 operated cases from the clinical, radiological, and pathological aspects. An attempt to determine the factors of service in estimating prognosis. Br J Surg. 1934;22:274-295.
10. DuCoin C, Faber R, Ilagan M, et al. Normokinetic biliary dyskinesia: a novel diagnosis. Surg Endosc. 2012;26:3088-3093.
11. Holes-Lewis KA, Hakim S, Rehman F, al. CCK-induced gall bladder hyperkinesia: An indication for cholecystectomy and brain-GI connectivity research. J Nucl Med. 2009;50(suppl 2):1312.
12. Carr JA, Walls J, Bryan LJ, et al. The treatment of gallbladder dyskinesia based upon symptoms: results of a 2-year, prospective, nonrandomized, concurrent cohort study. Surg Laparosc Endosc Percutan Tech. 2009;19:222-226.
13. Murray WR. Botulinum toxin-induced relaxation of the sphincter of Oddi may select patients with acalculous biliary pain who will benefit from cholecystectomy. Surg Endosc. 2011;25:813-816.

Failure to spot CHF leads to heart transplant
Failure to spot CHF leads to heart transplant
A 49-YEAR-OLD MAN SOUGHT TREATMENT AT AN URGENT CARE FACILITY after having shortness of breath every morning for 2 weeks. His heart rate was 119 beats/min, his blood pressure was 170/101 mm Hg, and he did not have chest pain. An electrocardiogram (EKG) was abnormal and chest x-ray showed fluid in the lung. The patient was diagnosed with pneumonia, prescribed antibiotics, and told to follow up with his physician. A follow-up chest x-ray 2 weeks later showed an enlarged heart and more fluid in the lung. A computed tomography scan indicated congestive heart failure and an EKG showed signs of a heart attack. The patient underwent a heart transplant and requires immunosuppressants.
PLAINTIFF'S CLAIM If the physician at the urgent care facility had noticed the patient’s enlarged heart, there would have been less heart damage, and the patient might have required a bypass, rather than a transplant.
THE DEFENSE No information about the defense is available.
VERDICT $1 million New Jersey verdict.
COMMENT When evaluating shortness of breath, always think lungs and heart until you have a definite diagnosis. Remember that neurological disease can present with shortness of breath, too. Consider amyotrophic lateral sclerosis, Guillain-Barré syndrome, and myasthenia gravis.
Infant suffers brain injury after delayed lab results
PARENTS BROUGHT THEIR 2-WEEK-OLD DAUGHTER TO THE EMERGENCY DEPARTMENT (ED) after she had missed several feedings and was short of breath. The ED physician ordered blood tests, but discharged the patient before receiving the results and told the parents to follow up with the infant’s pediatrician. Blood work subsequently revealed that the child had a Group B streptococcus infection, but by the time these results were communicated to the parents and treatment had begun, the infant had developed meningitis. She suffered brain injury, and was diagnosed with cerebral palsy.
PLAINTIFF'S CLAIM There was a delay in the diagnosis and treatment of the infant. Blood test results showing a bacterial infection were available the morning after discharge, but instead of notifying the parents, an additional blood culture was ordered to determine the type of bacteria present. The parents were then contacted 6 hours after the bacteria was identified as Group B streptococcus.
THE DEFENSE The defendants denied any negligence, although a nurse who cared for the infant claimed she had expressed concerns about the decision to discharge the patient.
VERDICT $7.15 million Maryland verdict.
COMMENT In newborns, the differential diagnosis for shortness of breath widens to include infection. In this case, I suspect the problem was a lack of tight follow-up, which can lead to bad outcomes—especially in newborns.
Failure to spot CHF leads to heart transplant
A 49-YEAR-OLD MAN SOUGHT TREATMENT AT AN URGENT CARE FACILITY after having shortness of breath every morning for 2 weeks. His heart rate was 119 beats/min, his blood pressure was 170/101 mm Hg, and he did not have chest pain. An electrocardiogram (EKG) was abnormal and chest x-ray showed fluid in the lung. The patient was diagnosed with pneumonia, prescribed antibiotics, and told to follow up with his physician. A follow-up chest x-ray 2 weeks later showed an enlarged heart and more fluid in the lung. A computed tomography scan indicated congestive heart failure and an EKG showed signs of a heart attack. The patient underwent a heart transplant and requires immunosuppressants.
PLAINTIFF'S CLAIM If the physician at the urgent care facility had noticed the patient’s enlarged heart, there would have been less heart damage, and the patient might have required a bypass, rather than a transplant.
THE DEFENSE No information about the defense is available.
VERDICT $1 million New Jersey verdict.
COMMENT When evaluating shortness of breath, always think lungs and heart until you have a definite diagnosis. Remember that neurological disease can present with shortness of breath, too. Consider amyotrophic lateral sclerosis, Guillain-Barré syndrome, and myasthenia gravis.
Infant suffers brain injury after delayed lab results
PARENTS BROUGHT THEIR 2-WEEK-OLD DAUGHTER TO THE EMERGENCY DEPARTMENT (ED) after she had missed several feedings and was short of breath. The ED physician ordered blood tests, but discharged the patient before receiving the results and told the parents to follow up with the infant’s pediatrician. Blood work subsequently revealed that the child had a Group B streptococcus infection, but by the time these results were communicated to the parents and treatment had begun, the infant had developed meningitis. She suffered brain injury, and was diagnosed with cerebral palsy.
PLAINTIFF'S CLAIM There was a delay in the diagnosis and treatment of the infant. Blood test results showing a bacterial infection were available the morning after discharge, but instead of notifying the parents, an additional blood culture was ordered to determine the type of bacteria present. The parents were then contacted 6 hours after the bacteria was identified as Group B streptococcus.
THE DEFENSE The defendants denied any negligence, although a nurse who cared for the infant claimed she had expressed concerns about the decision to discharge the patient.
VERDICT $7.15 million Maryland verdict.
COMMENT In newborns, the differential diagnosis for shortness of breath widens to include infection. In this case, I suspect the problem was a lack of tight follow-up, which can lead to bad outcomes—especially in newborns.
Failure to spot CHF leads to heart transplant
A 49-YEAR-OLD MAN SOUGHT TREATMENT AT AN URGENT CARE FACILITY after having shortness of breath every morning for 2 weeks. His heart rate was 119 beats/min, his blood pressure was 170/101 mm Hg, and he did not have chest pain. An electrocardiogram (EKG) was abnormal and chest x-ray showed fluid in the lung. The patient was diagnosed with pneumonia, prescribed antibiotics, and told to follow up with his physician. A follow-up chest x-ray 2 weeks later showed an enlarged heart and more fluid in the lung. A computed tomography scan indicated congestive heart failure and an EKG showed signs of a heart attack. The patient underwent a heart transplant and requires immunosuppressants.
PLAINTIFF'S CLAIM If the physician at the urgent care facility had noticed the patient’s enlarged heart, there would have been less heart damage, and the patient might have required a bypass, rather than a transplant.
THE DEFENSE No information about the defense is available.
VERDICT $1 million New Jersey verdict.
COMMENT When evaluating shortness of breath, always think lungs and heart until you have a definite diagnosis. Remember that neurological disease can present with shortness of breath, too. Consider amyotrophic lateral sclerosis, Guillain-Barré syndrome, and myasthenia gravis.
Infant suffers brain injury after delayed lab results
PARENTS BROUGHT THEIR 2-WEEK-OLD DAUGHTER TO THE EMERGENCY DEPARTMENT (ED) after she had missed several feedings and was short of breath. The ED physician ordered blood tests, but discharged the patient before receiving the results and told the parents to follow up with the infant’s pediatrician. Blood work subsequently revealed that the child had a Group B streptococcus infection, but by the time these results were communicated to the parents and treatment had begun, the infant had developed meningitis. She suffered brain injury, and was diagnosed with cerebral palsy.
PLAINTIFF'S CLAIM There was a delay in the diagnosis and treatment of the infant. Blood test results showing a bacterial infection were available the morning after discharge, but instead of notifying the parents, an additional blood culture was ordered to determine the type of bacteria present. The parents were then contacted 6 hours after the bacteria was identified as Group B streptococcus.
THE DEFENSE The defendants denied any negligence, although a nurse who cared for the infant claimed she had expressed concerns about the decision to discharge the patient.
VERDICT $7.15 million Maryland verdict.
COMMENT In newborns, the differential diagnosis for shortness of breath widens to include infection. In this case, I suspect the problem was a lack of tight follow-up, which can lead to bad outcomes—especially in newborns.
How well do physician and patient visit priorities align?
ABSTRACT
Purpose We undertook this study to explore the factors associated with differences between patients’ stated main reasons for outpatient visits and physicians’ main concerns at those same visits.
Methods This cross-sectional, mixed-methods study examined 192 outpatient visits with 4 physicians at 4 diverse primary care practices. During each visit, participating physicians elicited the patient’s main reason for the visit. Immediately after each visit, physicians documented 1) their understanding of the patient’s stated reason and 2) their main concern for the patient during that visit, and 3) assessed the extent of their alignment with the patient’s reason for visit. We assessed bivariate and multivariable associations of patient and visit characteristics with alignment, and further examined cases with unaligned physician-patient priorities to identify patterns.
Results In 69% of visits, the patient’s stated reason for the visit was completely aligned with the physician’s main concern. In 12% of visits, we observed totally unaligned priorities; 19% were only partially aligned. Uninsured or publicly-insured patients and visits with more problems addressed were less likely to be fully aligned. In many visits with unaligned priorities, patients’ stated reason for the visit was a self-limiting, symptomatic concern while physicians prioritized potentially dangerous asymptomatic conditions or ill-managed chronic conditions.
Conclusions In diverse family medicine practices, lack of alignment between physician and patient visit priorities reflects differing prioritization processes. Patients presenting with concerns unaligned with their physician’s priorities may require more time or different approaches to ensure the relevance and patient-centeredness of their care. These findings may inform the design of systems of care that promote mindful attention to patients’ priorities while addressing medically urgent or preventive services delivery.
T oday’s family physicians must balance patient’s acute concerns with chronic disease management, health promotion, and disease prevention. It’s not easy. As the content of outpatient visits expands and available time contracts,1 patients’, clinicians’, and payers’ agendas compete for attention. From a patient experience perspective, the health care encounter may seem diminished when guideline-driven agendas championing chronic disease management and preventive service delivery appear to take precedence over their personal concerns.2-4
In the matter of physician-patient alignment of visit priorities, prior research5,6 inadequately reflects current practice realities such as increased time pressure,7 greater chronic disease prevalence,8 growing expectations for preventive care,1 and increasing physician proactivity in longitudinal care.9-12 With so much to do and so little time and mounting pressure to deliver patient-centered care and patient satisfaction, it would be helpful to have a better understanding of how often and with whom physicians choose to depart from a patient’s explicitly stated reasons for a visit and instead prioritize other concerns.
We sought to examine alignment between patients’ stated main reasons for a visit as understood by the physician and the physician’s main concern during that same visit. Using a diverse sample of family physician-researchers to serve as data collectors and analysts, this study aimed to identify patient and visit characteristics associated with differing physician-patient visit priorities.
METHODS
Study design and sample
Four family physicians participating in a research fellowship undertook this cross- sectional descriptive study of a sample of their outpatient encounters. Each physician’s practice was unique: a free clinic, an inner city family practice within a teaching hospital, a geriatric home visit practice, and a suburban pediatric practice. Using the card study method pioneered by the Ambulatory Sentinel Practice Network,13,14 physicians collected observational and reflective data on a sample of 50 consecutive patients seen at his or her primary care practice. The University Hospitals Case Medical Center Institutional Review Board approved the study protocol.
Measures
Immediately following each patient visit, physicians recorded on a standardized data card the patient’s characteristics, visit characteristics, the reason for the visit provided to the office staff, the reason for visit reported by the patient at the beginning of the visit, and the physician’s own main concern for the patient during the visit. Patient characteristics included gender, age, race, type of insurance, and number of chronic conditions on the problem list. Visit characteristics included the total number of problems addressed, whether a second person (eg, family member, caregiver) was present in the exam room during the visit, and visit duration. To elicit the patient’s reason for the visit, physicians systematically asked, “How can I help you today?” If more than one problem was elicited from this prompt, the concern expressed as most important by the patient was noted.
In completing the data card, physicians also reflected on the extent to which the patient’s stated reason for the visit aligned with their own main concern for the patient during the visit, rating the relationship between their respective priorities as fully aligned, partially aligned, or totally unaligned. Visits were considered fully aligned if the patient’s reason for the visit and the physician’s concern were the same, or if the patient’s expressed concern was determined to be a symptom related to the physician’s main concern. Partial alignment occurred when the patient’s concern was shared by the physician but was not the physician’s main concern. Visit priorities were rated as totally unaligned if patient and physician concerns were different and determined not to be medically related.
Data analysis
We computed descriptive statistics and performed bivariate tests of association between physician-patient alignment of priorities and patient/visit characteristics, using chi-square statistics for categorical variables and analysis of variance (ANOVA) for continuous variables. We used logistic regression analysis to identify characteristics independently associated with either partially aligned or totally unaligned visit priorities, vs fully aligned priorities.
To better understand the unaligned cases, the study team examined all of the data cards identified as either only partially aligned or totally unaligned and categorized the nature of the disparate prioritization in each case. Study team members (PT, AW, MR, and PDG) individually reviewed and sorted the cards into similar observed patterns and wrote brief descriptions of those patterns. The group refined the preliminary descriptions of the overarching patterns and selected several cases to represent the patterns.
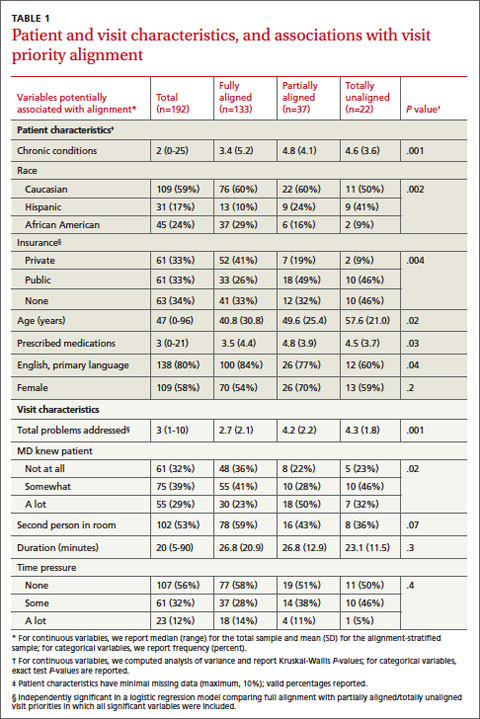
RESULTS
Quantitative findings
We collected data on 192 patients (TABLE 1). Median patient age was 47. Median number of prescription medications and chronic medical conditions were 3 and 2, respectively. Most patients (80%) primarily spoke English, 58% were female, and 59% were Caucasian. Insurance status was equally distributed among patients: 33% held private insurance, 33% had public insurance, and 34% were uninsured.
The majority of cases showed physician- patient priorities that were fully aligned (69%); only 12% were totally unaligned. TABLE 1 shows the associations between level of alignment and patient and visit characteristics. Patients whose expressed reason for their visit was less than fully aligned with their physicians’ primary concern were more likely to be older, with more chronic conditions, of Hispanic ethnicity, and either publicly insured or uninsured. Patients with some degree of unaligned concerns also tended to have greater numbers of prescribed medications and had a primary language other than English. Unaligned visit priorities were also observed more often when greater numbers of problems were addressed during the visit. Patients familiar to the physician were also more likely to express a reason for their visit that differed in some way from the primary concern of their family physician.
Multivariable logistic regression analyses showed that having more problems addressed during a visit and being publicly insured or uninsured (compared with having private insurance) were each independently associated with less than fully aligned visit priorities (indicated by § in TABLE 1).
Qualitative findings
Cases classified as partially or totally unaligned showed 2 main patterns that reflect differences in the ways that patients and physicians prioritize problems. First, when physician priorities were unaligned with the patient’s stated reason for a visit, physicians typically focused on treatable, asymptomatic conditions that could lead to long-term morbidity and mortality or, absent immediate attention, to a dangerous event. Examples include chronic disease management (eg, hypertension, diabetes, asthma) and disease prevention (eg, smoking cessation, cholesterol level monitoring, cardiac disease risk reduction). Second, in those visits that were unaligned, patients tended to show more initial concern about symptomatic problems (eg, skin rash, upper respiratory infection) that would likely resolve with minimal or no medical intervention. Most of these conditions were determined by the physician to be benign, self-limited, or not worrisome (TABLE 2).
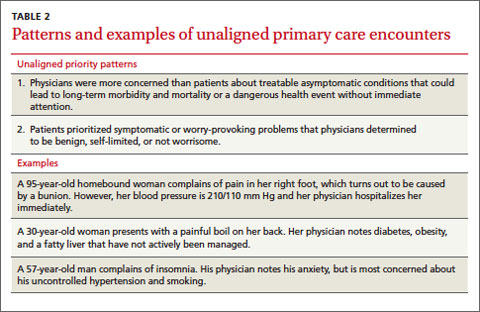
DISCUSSION
This study examined the alignment between a patient’s stated reason for a visit and the physician’s main concern. Physician-patient alignment was common, with 69% of visits showing full alignment between the patient’s reason for the visit and the physician’s main concern. While this rate is higher than that seen in prior studies,5 our method for data collection uniquely reflected how information actually is elicited and received during outpatient encounters, which likely yielded more accurate results. Also, in contrast to past approaches, our study equated patients’ symptoms to the underlying diagnosis for purposes of determining alignment.
Similar to previous studies, alignment between patient and physician concerns was less likely when the number of items addressed during the visit increased.5,6 Interestingly, physician-perceived time pressure during the visit and lack of an established patient-physician relationship were not observed to influence alignment. When time is limited, physicians may choose to prioritize the patient’s verbalized concern to avoid more complex negotiations about the agenda. In addition, during an encounter with an unfamiliar patient, prevention and chronic illness care may be deferred until the relationship becomes established.15-18
Patient insurance status was also observed to influence alignment. This finding could reflect socioeconomic or access issues among uninsured or publicly-insured patients that contribute to more complex visits.19-21 To shed further light on this finding, further research is needed that includes indicators of education or income and that separately examines Medicaid vs Medicare enrollees.
Possible study weaknesses. A potential weakness of this study is that alignment was rated by the physicians who elicited and recorded their patients’ reasons for the visit. It is possible that the central role of the physician as observer and analyst may have introduced bias and that an outside observer may have come to different conclusions about the extent to which priorities were aligned. However, by placing the physician-researcher at the center of both data collection and analysis, our study method reflects the realistic constraints of limited information on the processes of clinical discovery and sense-making that physicians regularly undertake with their patients, which we believe to be a strength of this study. While the inclusion of pediatric visits in the sample is another possible weakness, we believe that the diverse clinical settings and diverse patient populations potentially strengthen the findings. Replication with different samples of clinicians and patients is needed to assess the robustness of the findings.
Root differences in physician and patient perspectives. Collectively, these findings suggest that patients’ and physicians’ differing approaches to prioritization may limit alignment. In general, physicians tend to evaluate the full scope of the patient’s health and risk factors for future disease, while patients more often focus on symptomatically troublesome—though often self-limiting— conditions. Physicians have the knowledge and clinical experience to prioritize or deprioritize patient concerns based on an assessment of long-term risks of morbidity and mortality, yet the future-orientation of treatments and surveillance for insensible conditions (like hypertension) is less likely to align with the immediately painful or worrisome symptoms of patients. This highlights the importance of patient education on chronic disease management and disease prevention, and cooperative agenda-setting. Further work needs to be done to examine the differences in patients’ and physicians’ cognitive processes of prioritization, with the ultimate goal of providing patient-centered care through shared decision-making.
Take-home messages for all stakeholders. Amidst growing time pressures and guideline-driven protocols for care, it is important to attend to the intersecting and diverging patient, physician, and payer agendas that drive the content of the visit. Patients who are less likely to share the physician’s prioritization of their concerns—including individuals with no insurance or public insurance and those with multiple medical problems—may require more time and additional effort on the part of the physician to create a mutually acceptable agenda for the visit. Attempts at pay-for-performance should consider patients’ priorities and preferences for care, particularly when those preferences differ from the priorities of physicians or health insurance plans. A more thorough understanding of patient and physician prioritization during primary care visits could potentially guide the organization of outpatient care and inform the mindful physician’s patient-centered practice to maximize patient benefit.
CORRESPONDENCE
Susan A. Flocke, PhD, Family Medicine Research Division, Case Western Reserve University, 11000 Cedar Avenue, Suite 402, Cleveland, OH 44106; [email protected]
ACKNOWLEDGEMENTS
This study was completed as part of the culture of inquiry fellowship, supported by Academic Administrative Units in primary care Grant #D54HP05444 from the Health Resources and Services Administration, US Department of Health and Human Services. Dr. Stange’s time is supported in part by a clinical research professorship from the American Cancer Society.
1. Yarnall KS, Pollak KI, Østbye T, et al. Primary care: is there enough time for prevention? Am J Public Health. 2003;93:635-641.
2. Weyer SM, Bobiak S, Stange KC. Possible unintended consequences of a focus on performance: insights over time from the research association of practices network. Qual Manag Health Care. 2008;17:47-52.
3. Campbell SM, McDonald R, Lester H. The experience of pay for performance in English family practice: a qualitative study. Ann Fam Med. 2008;6:228-234.
4. Casalino LP. The unintended consequences of measuring quality on the quality of medical care. N Engl J Med. 1999;341:1147-1150.
5. Friedin RB, Goldman L, Cecil RR. Patient-physician concordance in problem identification in the primary care setting. Ann Intern Med. 1980;93:490-493.
6. Boland BJ, Scheitel SM, Wollan PC, et al. Patient-physician agreement on reasons for ambulatory general medical examinations. Mayo Clin Proc. 1998;73:109-117.
7. Abbo ED, Zhang Q, Zelder M, et al. The increasing number of clinical items addressed during the time of adult primary care visits. J Gen Intern Med. 2008;23:2058-2065.
8. Østbye T, Yarnall KS, Krause KM, et al. Is there time for management of patients with chronic diseases in primary care? Ann Fam Med. 2005;3:209-214.
9. Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q. 1996;74:511-544.
10. Wagner EH, Austin BT, Von Korff M. Improving outcomes in chronic illness. Manag Care Q. 1996;4:12-25.
11. Glasgow RE, Orleans CT, Wagner EH. Does the chronic care model serve also as a template for improving prevention? Milbank Q. 2001;79:579-612,iv-v.
12. Wagner EH, Bennett SM, Austin BT, et al. Finding common ground: patient-centeredness and evidence-based chronic illness care. J Altern Complement Med. 2005;11(suppl 1):S7-S15.
13. Green LA. The weekly return as a practical instrument for data collection in office based research. Fam Med. 1988;20:182-184.
14. Green LA, Reed FM, Miller RS, et al. Verification of data reported by practices for a study of spontaneous abortion. Fam Med. 1988;20:189-191.
15. Ettner SL. The relationship between continuity of care and the health behaviors of patients: Does having a usual physician make a difference? Med Care. 1999;37:547-555.
16. Parchman ML, Burge SK. The patient-physician relationship, primary care attributes, and preventive services. Fam Med. 2004;36:22-27.
17. Blewett LA, Johnson PJ, Lee B, et al. When a usual source of care and usual provider matter: adult prevention and screening services. J Gen Intern Med. 2008;23:1354-1360.
18. Flocke SA, Stange KC, Zyzanski SJ. The association of attributes of primary care with the delivery of clinical preventive services. Med Care. 1998;36(8 suppl):AS21-AS30.
19. Ayanian JZ, Weissman JS, Schneider EC, et al. Unmet health needs of uninsured adults in the United States. JAMA. 2000;284:2061-2069.
20. Fiscella K, Williams DR. Health disparities based on socioeconomic inequities: implications for urban health care. Acad Med. 2004;79:1139-1147.
21. McWilliams JM. Health consequences of uninsurance among adults in the United States: recent evidence and implications. Milbank Q. 2009;87:443-494.
ABSTRACT
Purpose We undertook this study to explore the factors associated with differences between patients’ stated main reasons for outpatient visits and physicians’ main concerns at those same visits.
Methods This cross-sectional, mixed-methods study examined 192 outpatient visits with 4 physicians at 4 diverse primary care practices. During each visit, participating physicians elicited the patient’s main reason for the visit. Immediately after each visit, physicians documented 1) their understanding of the patient’s stated reason and 2) their main concern for the patient during that visit, and 3) assessed the extent of their alignment with the patient’s reason for visit. We assessed bivariate and multivariable associations of patient and visit characteristics with alignment, and further examined cases with unaligned physician-patient priorities to identify patterns.
Results In 69% of visits, the patient’s stated reason for the visit was completely aligned with the physician’s main concern. In 12% of visits, we observed totally unaligned priorities; 19% were only partially aligned. Uninsured or publicly-insured patients and visits with more problems addressed were less likely to be fully aligned. In many visits with unaligned priorities, patients’ stated reason for the visit was a self-limiting, symptomatic concern while physicians prioritized potentially dangerous asymptomatic conditions or ill-managed chronic conditions.
Conclusions In diverse family medicine practices, lack of alignment between physician and patient visit priorities reflects differing prioritization processes. Patients presenting with concerns unaligned with their physician’s priorities may require more time or different approaches to ensure the relevance and patient-centeredness of their care. These findings may inform the design of systems of care that promote mindful attention to patients’ priorities while addressing medically urgent or preventive services delivery.
T oday’s family physicians must balance patient’s acute concerns with chronic disease management, health promotion, and disease prevention. It’s not easy. As the content of outpatient visits expands and available time contracts,1 patients’, clinicians’, and payers’ agendas compete for attention. From a patient experience perspective, the health care encounter may seem diminished when guideline-driven agendas championing chronic disease management and preventive service delivery appear to take precedence over their personal concerns.2-4
In the matter of physician-patient alignment of visit priorities, prior research5,6 inadequately reflects current practice realities such as increased time pressure,7 greater chronic disease prevalence,8 growing expectations for preventive care,1 and increasing physician proactivity in longitudinal care.9-12 With so much to do and so little time and mounting pressure to deliver patient-centered care and patient satisfaction, it would be helpful to have a better understanding of how often and with whom physicians choose to depart from a patient’s explicitly stated reasons for a visit and instead prioritize other concerns.
We sought to examine alignment between patients’ stated main reasons for a visit as understood by the physician and the physician’s main concern during that same visit. Using a diverse sample of family physician-researchers to serve as data collectors and analysts, this study aimed to identify patient and visit characteristics associated with differing physician-patient visit priorities.
METHODS
Study design and sample
Four family physicians participating in a research fellowship undertook this cross- sectional descriptive study of a sample of their outpatient encounters. Each physician’s practice was unique: a free clinic, an inner city family practice within a teaching hospital, a geriatric home visit practice, and a suburban pediatric practice. Using the card study method pioneered by the Ambulatory Sentinel Practice Network,13,14 physicians collected observational and reflective data on a sample of 50 consecutive patients seen at his or her primary care practice. The University Hospitals Case Medical Center Institutional Review Board approved the study protocol.
Measures
Immediately following each patient visit, physicians recorded on a standardized data card the patient’s characteristics, visit characteristics, the reason for the visit provided to the office staff, the reason for visit reported by the patient at the beginning of the visit, and the physician’s own main concern for the patient during the visit. Patient characteristics included gender, age, race, type of insurance, and number of chronic conditions on the problem list. Visit characteristics included the total number of problems addressed, whether a second person (eg, family member, caregiver) was present in the exam room during the visit, and visit duration. To elicit the patient’s reason for the visit, physicians systematically asked, “How can I help you today?” If more than one problem was elicited from this prompt, the concern expressed as most important by the patient was noted.
In completing the data card, physicians also reflected on the extent to which the patient’s stated reason for the visit aligned with their own main concern for the patient during the visit, rating the relationship between their respective priorities as fully aligned, partially aligned, or totally unaligned. Visits were considered fully aligned if the patient’s reason for the visit and the physician’s concern were the same, or if the patient’s expressed concern was determined to be a symptom related to the physician’s main concern. Partial alignment occurred when the patient’s concern was shared by the physician but was not the physician’s main concern. Visit priorities were rated as totally unaligned if patient and physician concerns were different and determined not to be medically related.
Data analysis
We computed descriptive statistics and performed bivariate tests of association between physician-patient alignment of priorities and patient/visit characteristics, using chi-square statistics for categorical variables and analysis of variance (ANOVA) for continuous variables. We used logistic regression analysis to identify characteristics independently associated with either partially aligned or totally unaligned visit priorities, vs fully aligned priorities.
To better understand the unaligned cases, the study team examined all of the data cards identified as either only partially aligned or totally unaligned and categorized the nature of the disparate prioritization in each case. Study team members (PT, AW, MR, and PDG) individually reviewed and sorted the cards into similar observed patterns and wrote brief descriptions of those patterns. The group refined the preliminary descriptions of the overarching patterns and selected several cases to represent the patterns.
RESULTS
Quantitative findings
We collected data on 192 patients (TABLE 1). Median patient age was 47. Median number of prescription medications and chronic medical conditions were 3 and 2, respectively. Most patients (80%) primarily spoke English, 58% were female, and 59% were Caucasian. Insurance status was equally distributed among patients: 33% held private insurance, 33% had public insurance, and 34% were uninsured.
The majority of cases showed physician- patient priorities that were fully aligned (69%); only 12% were totally unaligned. TABLE 1 shows the associations between level of alignment and patient and visit characteristics. Patients whose expressed reason for their visit was less than fully aligned with their physicians’ primary concern were more likely to be older, with more chronic conditions, of Hispanic ethnicity, and either publicly insured or uninsured. Patients with some degree of unaligned concerns also tended to have greater numbers of prescribed medications and had a primary language other than English. Unaligned visit priorities were also observed more often when greater numbers of problems were addressed during the visit. Patients familiar to the physician were also more likely to express a reason for their visit that differed in some way from the primary concern of their family physician.
Multivariable logistic regression analyses showed that having more problems addressed during a visit and being publicly insured or uninsured (compared with having private insurance) were each independently associated with less than fully aligned visit priorities (indicated by § in TABLE 1).
Qualitative findings
Cases classified as partially or totally unaligned showed 2 main patterns that reflect differences in the ways that patients and physicians prioritize problems. First, when physician priorities were unaligned with the patient’s stated reason for a visit, physicians typically focused on treatable, asymptomatic conditions that could lead to long-term morbidity and mortality or, absent immediate attention, to a dangerous event. Examples include chronic disease management (eg, hypertension, diabetes, asthma) and disease prevention (eg, smoking cessation, cholesterol level monitoring, cardiac disease risk reduction). Second, in those visits that were unaligned, patients tended to show more initial concern about symptomatic problems (eg, skin rash, upper respiratory infection) that would likely resolve with minimal or no medical intervention. Most of these conditions were determined by the physician to be benign, self-limited, or not worrisome (TABLE 2).
DISCUSSION
This study examined the alignment between a patient’s stated reason for a visit and the physician’s main concern. Physician-patient alignment was common, with 69% of visits showing full alignment between the patient’s reason for the visit and the physician’s main concern. While this rate is higher than that seen in prior studies,5 our method for data collection uniquely reflected how information actually is elicited and received during outpatient encounters, which likely yielded more accurate results. Also, in contrast to past approaches, our study equated patients’ symptoms to the underlying diagnosis for purposes of determining alignment.
Similar to previous studies, alignment between patient and physician concerns was less likely when the number of items addressed during the visit increased.5,6 Interestingly, physician-perceived time pressure during the visit and lack of an established patient-physician relationship were not observed to influence alignment. When time is limited, physicians may choose to prioritize the patient’s verbalized concern to avoid more complex negotiations about the agenda. In addition, during an encounter with an unfamiliar patient, prevention and chronic illness care may be deferred until the relationship becomes established.15-18
Patient insurance status was also observed to influence alignment. This finding could reflect socioeconomic or access issues among uninsured or publicly-insured patients that contribute to more complex visits.19-21 To shed further light on this finding, further research is needed that includes indicators of education or income and that separately examines Medicaid vs Medicare enrollees.
Possible study weaknesses. A potential weakness of this study is that alignment was rated by the physicians who elicited and recorded their patients’ reasons for the visit. It is possible that the central role of the physician as observer and analyst may have introduced bias and that an outside observer may have come to different conclusions about the extent to which priorities were aligned. However, by placing the physician-researcher at the center of both data collection and analysis, our study method reflects the realistic constraints of limited information on the processes of clinical discovery and sense-making that physicians regularly undertake with their patients, which we believe to be a strength of this study. While the inclusion of pediatric visits in the sample is another possible weakness, we believe that the diverse clinical settings and diverse patient populations potentially strengthen the findings. Replication with different samples of clinicians and patients is needed to assess the robustness of the findings.
Root differences in physician and patient perspectives. Collectively, these findings suggest that patients’ and physicians’ differing approaches to prioritization may limit alignment. In general, physicians tend to evaluate the full scope of the patient’s health and risk factors for future disease, while patients more often focus on symptomatically troublesome—though often self-limiting— conditions. Physicians have the knowledge and clinical experience to prioritize or deprioritize patient concerns based on an assessment of long-term risks of morbidity and mortality, yet the future-orientation of treatments and surveillance for insensible conditions (like hypertension) is less likely to align with the immediately painful or worrisome symptoms of patients. This highlights the importance of patient education on chronic disease management and disease prevention, and cooperative agenda-setting. Further work needs to be done to examine the differences in patients’ and physicians’ cognitive processes of prioritization, with the ultimate goal of providing patient-centered care through shared decision-making.
Take-home messages for all stakeholders. Amidst growing time pressures and guideline-driven protocols for care, it is important to attend to the intersecting and diverging patient, physician, and payer agendas that drive the content of the visit. Patients who are less likely to share the physician’s prioritization of their concerns—including individuals with no insurance or public insurance and those with multiple medical problems—may require more time and additional effort on the part of the physician to create a mutually acceptable agenda for the visit. Attempts at pay-for-performance should consider patients’ priorities and preferences for care, particularly when those preferences differ from the priorities of physicians or health insurance plans. A more thorough understanding of patient and physician prioritization during primary care visits could potentially guide the organization of outpatient care and inform the mindful physician’s patient-centered practice to maximize patient benefit.
CORRESPONDENCE
Susan A. Flocke, PhD, Family Medicine Research Division, Case Western Reserve University, 11000 Cedar Avenue, Suite 402, Cleveland, OH 44106; [email protected]
ACKNOWLEDGEMENTS
This study was completed as part of the culture of inquiry fellowship, supported by Academic Administrative Units in primary care Grant #D54HP05444 from the Health Resources and Services Administration, US Department of Health and Human Services. Dr. Stange’s time is supported in part by a clinical research professorship from the American Cancer Society.
ABSTRACT
Purpose We undertook this study to explore the factors associated with differences between patients’ stated main reasons for outpatient visits and physicians’ main concerns at those same visits.
Methods This cross-sectional, mixed-methods study examined 192 outpatient visits with 4 physicians at 4 diverse primary care practices. During each visit, participating physicians elicited the patient’s main reason for the visit. Immediately after each visit, physicians documented 1) their understanding of the patient’s stated reason and 2) their main concern for the patient during that visit, and 3) assessed the extent of their alignment with the patient’s reason for visit. We assessed bivariate and multivariable associations of patient and visit characteristics with alignment, and further examined cases with unaligned physician-patient priorities to identify patterns.
Results In 69% of visits, the patient’s stated reason for the visit was completely aligned with the physician’s main concern. In 12% of visits, we observed totally unaligned priorities; 19% were only partially aligned. Uninsured or publicly-insured patients and visits with more problems addressed were less likely to be fully aligned. In many visits with unaligned priorities, patients’ stated reason for the visit was a self-limiting, symptomatic concern while physicians prioritized potentially dangerous asymptomatic conditions or ill-managed chronic conditions.
Conclusions In diverse family medicine practices, lack of alignment between physician and patient visit priorities reflects differing prioritization processes. Patients presenting with concerns unaligned with their physician’s priorities may require more time or different approaches to ensure the relevance and patient-centeredness of their care. These findings may inform the design of systems of care that promote mindful attention to patients’ priorities while addressing medically urgent or preventive services delivery.
T oday’s family physicians must balance patient’s acute concerns with chronic disease management, health promotion, and disease prevention. It’s not easy. As the content of outpatient visits expands and available time contracts,1 patients’, clinicians’, and payers’ agendas compete for attention. From a patient experience perspective, the health care encounter may seem diminished when guideline-driven agendas championing chronic disease management and preventive service delivery appear to take precedence over their personal concerns.2-4
In the matter of physician-patient alignment of visit priorities, prior research5,6 inadequately reflects current practice realities such as increased time pressure,7 greater chronic disease prevalence,8 growing expectations for preventive care,1 and increasing physician proactivity in longitudinal care.9-12 With so much to do and so little time and mounting pressure to deliver patient-centered care and patient satisfaction, it would be helpful to have a better understanding of how often and with whom physicians choose to depart from a patient’s explicitly stated reasons for a visit and instead prioritize other concerns.
We sought to examine alignment between patients’ stated main reasons for a visit as understood by the physician and the physician’s main concern during that same visit. Using a diverse sample of family physician-researchers to serve as data collectors and analysts, this study aimed to identify patient and visit characteristics associated with differing physician-patient visit priorities.
METHODS
Study design and sample
Four family physicians participating in a research fellowship undertook this cross- sectional descriptive study of a sample of their outpatient encounters. Each physician’s practice was unique: a free clinic, an inner city family practice within a teaching hospital, a geriatric home visit practice, and a suburban pediatric practice. Using the card study method pioneered by the Ambulatory Sentinel Practice Network,13,14 physicians collected observational and reflective data on a sample of 50 consecutive patients seen at his or her primary care practice. The University Hospitals Case Medical Center Institutional Review Board approved the study protocol.
Measures
Immediately following each patient visit, physicians recorded on a standardized data card the patient’s characteristics, visit characteristics, the reason for the visit provided to the office staff, the reason for visit reported by the patient at the beginning of the visit, and the physician’s own main concern for the patient during the visit. Patient characteristics included gender, age, race, type of insurance, and number of chronic conditions on the problem list. Visit characteristics included the total number of problems addressed, whether a second person (eg, family member, caregiver) was present in the exam room during the visit, and visit duration. To elicit the patient’s reason for the visit, physicians systematically asked, “How can I help you today?” If more than one problem was elicited from this prompt, the concern expressed as most important by the patient was noted.
In completing the data card, physicians also reflected on the extent to which the patient’s stated reason for the visit aligned with their own main concern for the patient during the visit, rating the relationship between their respective priorities as fully aligned, partially aligned, or totally unaligned. Visits were considered fully aligned if the patient’s reason for the visit and the physician’s concern were the same, or if the patient’s expressed concern was determined to be a symptom related to the physician’s main concern. Partial alignment occurred when the patient’s concern was shared by the physician but was not the physician’s main concern. Visit priorities were rated as totally unaligned if patient and physician concerns were different and determined not to be medically related.
Data analysis
We computed descriptive statistics and performed bivariate tests of association between physician-patient alignment of priorities and patient/visit characteristics, using chi-square statistics for categorical variables and analysis of variance (ANOVA) for continuous variables. We used logistic regression analysis to identify characteristics independently associated with either partially aligned or totally unaligned visit priorities, vs fully aligned priorities.
To better understand the unaligned cases, the study team examined all of the data cards identified as either only partially aligned or totally unaligned and categorized the nature of the disparate prioritization in each case. Study team members (PT, AW, MR, and PDG) individually reviewed and sorted the cards into similar observed patterns and wrote brief descriptions of those patterns. The group refined the preliminary descriptions of the overarching patterns and selected several cases to represent the patterns.
RESULTS
Quantitative findings
We collected data on 192 patients (TABLE 1). Median patient age was 47. Median number of prescription medications and chronic medical conditions were 3 and 2, respectively. Most patients (80%) primarily spoke English, 58% were female, and 59% were Caucasian. Insurance status was equally distributed among patients: 33% held private insurance, 33% had public insurance, and 34% were uninsured.
The majority of cases showed physician- patient priorities that were fully aligned (69%); only 12% were totally unaligned. TABLE 1 shows the associations between level of alignment and patient and visit characteristics. Patients whose expressed reason for their visit was less than fully aligned with their physicians’ primary concern were more likely to be older, with more chronic conditions, of Hispanic ethnicity, and either publicly insured or uninsured. Patients with some degree of unaligned concerns also tended to have greater numbers of prescribed medications and had a primary language other than English. Unaligned visit priorities were also observed more often when greater numbers of problems were addressed during the visit. Patients familiar to the physician were also more likely to express a reason for their visit that differed in some way from the primary concern of their family physician.
Multivariable logistic regression analyses showed that having more problems addressed during a visit and being publicly insured or uninsured (compared with having private insurance) were each independently associated with less than fully aligned visit priorities (indicated by § in TABLE 1).
Qualitative findings
Cases classified as partially or totally unaligned showed 2 main patterns that reflect differences in the ways that patients and physicians prioritize problems. First, when physician priorities were unaligned with the patient’s stated reason for a visit, physicians typically focused on treatable, asymptomatic conditions that could lead to long-term morbidity and mortality or, absent immediate attention, to a dangerous event. Examples include chronic disease management (eg, hypertension, diabetes, asthma) and disease prevention (eg, smoking cessation, cholesterol level monitoring, cardiac disease risk reduction). Second, in those visits that were unaligned, patients tended to show more initial concern about symptomatic problems (eg, skin rash, upper respiratory infection) that would likely resolve with minimal or no medical intervention. Most of these conditions were determined by the physician to be benign, self-limited, or not worrisome (TABLE 2).
DISCUSSION
This study examined the alignment between a patient’s stated reason for a visit and the physician’s main concern. Physician-patient alignment was common, with 69% of visits showing full alignment between the patient’s reason for the visit and the physician’s main concern. While this rate is higher than that seen in prior studies,5 our method for data collection uniquely reflected how information actually is elicited and received during outpatient encounters, which likely yielded more accurate results. Also, in contrast to past approaches, our study equated patients’ symptoms to the underlying diagnosis for purposes of determining alignment.
Similar to previous studies, alignment between patient and physician concerns was less likely when the number of items addressed during the visit increased.5,6 Interestingly, physician-perceived time pressure during the visit and lack of an established patient-physician relationship were not observed to influence alignment. When time is limited, physicians may choose to prioritize the patient’s verbalized concern to avoid more complex negotiations about the agenda. In addition, during an encounter with an unfamiliar patient, prevention and chronic illness care may be deferred until the relationship becomes established.15-18
Patient insurance status was also observed to influence alignment. This finding could reflect socioeconomic or access issues among uninsured or publicly-insured patients that contribute to more complex visits.19-21 To shed further light on this finding, further research is needed that includes indicators of education or income and that separately examines Medicaid vs Medicare enrollees.
Possible study weaknesses. A potential weakness of this study is that alignment was rated by the physicians who elicited and recorded their patients’ reasons for the visit. It is possible that the central role of the physician as observer and analyst may have introduced bias and that an outside observer may have come to different conclusions about the extent to which priorities were aligned. However, by placing the physician-researcher at the center of both data collection and analysis, our study method reflects the realistic constraints of limited information on the processes of clinical discovery and sense-making that physicians regularly undertake with their patients, which we believe to be a strength of this study. While the inclusion of pediatric visits in the sample is another possible weakness, we believe that the diverse clinical settings and diverse patient populations potentially strengthen the findings. Replication with different samples of clinicians and patients is needed to assess the robustness of the findings.
Root differences in physician and patient perspectives. Collectively, these findings suggest that patients’ and physicians’ differing approaches to prioritization may limit alignment. In general, physicians tend to evaluate the full scope of the patient’s health and risk factors for future disease, while patients more often focus on symptomatically troublesome—though often self-limiting— conditions. Physicians have the knowledge and clinical experience to prioritize or deprioritize patient concerns based on an assessment of long-term risks of morbidity and mortality, yet the future-orientation of treatments and surveillance for insensible conditions (like hypertension) is less likely to align with the immediately painful or worrisome symptoms of patients. This highlights the importance of patient education on chronic disease management and disease prevention, and cooperative agenda-setting. Further work needs to be done to examine the differences in patients’ and physicians’ cognitive processes of prioritization, with the ultimate goal of providing patient-centered care through shared decision-making.
Take-home messages for all stakeholders. Amidst growing time pressures and guideline-driven protocols for care, it is important to attend to the intersecting and diverging patient, physician, and payer agendas that drive the content of the visit. Patients who are less likely to share the physician’s prioritization of their concerns—including individuals with no insurance or public insurance and those with multiple medical problems—may require more time and additional effort on the part of the physician to create a mutually acceptable agenda for the visit. Attempts at pay-for-performance should consider patients’ priorities and preferences for care, particularly when those preferences differ from the priorities of physicians or health insurance plans. A more thorough understanding of patient and physician prioritization during primary care visits could potentially guide the organization of outpatient care and inform the mindful physician’s patient-centered practice to maximize patient benefit.
CORRESPONDENCE
Susan A. Flocke, PhD, Family Medicine Research Division, Case Western Reserve University, 11000 Cedar Avenue, Suite 402, Cleveland, OH 44106; [email protected]
ACKNOWLEDGEMENTS
This study was completed as part of the culture of inquiry fellowship, supported by Academic Administrative Units in primary care Grant #D54HP05444 from the Health Resources and Services Administration, US Department of Health and Human Services. Dr. Stange’s time is supported in part by a clinical research professorship from the American Cancer Society.
1. Yarnall KS, Pollak KI, Østbye T, et al. Primary care: is there enough time for prevention? Am J Public Health. 2003;93:635-641.
2. Weyer SM, Bobiak S, Stange KC. Possible unintended consequences of a focus on performance: insights over time from the research association of practices network. Qual Manag Health Care. 2008;17:47-52.
3. Campbell SM, McDonald R, Lester H. The experience of pay for performance in English family practice: a qualitative study. Ann Fam Med. 2008;6:228-234.
4. Casalino LP. The unintended consequences of measuring quality on the quality of medical care. N Engl J Med. 1999;341:1147-1150.
5. Friedin RB, Goldman L, Cecil RR. Patient-physician concordance in problem identification in the primary care setting. Ann Intern Med. 1980;93:490-493.
6. Boland BJ, Scheitel SM, Wollan PC, et al. Patient-physician agreement on reasons for ambulatory general medical examinations. Mayo Clin Proc. 1998;73:109-117.
7. Abbo ED, Zhang Q, Zelder M, et al. The increasing number of clinical items addressed during the time of adult primary care visits. J Gen Intern Med. 2008;23:2058-2065.
8. Østbye T, Yarnall KS, Krause KM, et al. Is there time for management of patients with chronic diseases in primary care? Ann Fam Med. 2005;3:209-214.
9. Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q. 1996;74:511-544.
10. Wagner EH, Austin BT, Von Korff M. Improving outcomes in chronic illness. Manag Care Q. 1996;4:12-25.
11. Glasgow RE, Orleans CT, Wagner EH. Does the chronic care model serve also as a template for improving prevention? Milbank Q. 2001;79:579-612,iv-v.
12. Wagner EH, Bennett SM, Austin BT, et al. Finding common ground: patient-centeredness and evidence-based chronic illness care. J Altern Complement Med. 2005;11(suppl 1):S7-S15.
13. Green LA. The weekly return as a practical instrument for data collection in office based research. Fam Med. 1988;20:182-184.
14. Green LA, Reed FM, Miller RS, et al. Verification of data reported by practices for a study of spontaneous abortion. Fam Med. 1988;20:189-191.
15. Ettner SL. The relationship between continuity of care and the health behaviors of patients: Does having a usual physician make a difference? Med Care. 1999;37:547-555.
16. Parchman ML, Burge SK. The patient-physician relationship, primary care attributes, and preventive services. Fam Med. 2004;36:22-27.
17. Blewett LA, Johnson PJ, Lee B, et al. When a usual source of care and usual provider matter: adult prevention and screening services. J Gen Intern Med. 2008;23:1354-1360.
18. Flocke SA, Stange KC, Zyzanski SJ. The association of attributes of primary care with the delivery of clinical preventive services. Med Care. 1998;36(8 suppl):AS21-AS30.
19. Ayanian JZ, Weissman JS, Schneider EC, et al. Unmet health needs of uninsured adults in the United States. JAMA. 2000;284:2061-2069.
20. Fiscella K, Williams DR. Health disparities based on socioeconomic inequities: implications for urban health care. Acad Med. 2004;79:1139-1147.
21. McWilliams JM. Health consequences of uninsurance among adults in the United States: recent evidence and implications. Milbank Q. 2009;87:443-494.
1. Yarnall KS, Pollak KI, Østbye T, et al. Primary care: is there enough time for prevention? Am J Public Health. 2003;93:635-641.
2. Weyer SM, Bobiak S, Stange KC. Possible unintended consequences of a focus on performance: insights over time from the research association of practices network. Qual Manag Health Care. 2008;17:47-52.
3. Campbell SM, McDonald R, Lester H. The experience of pay for performance in English family practice: a qualitative study. Ann Fam Med. 2008;6:228-234.
4. Casalino LP. The unintended consequences of measuring quality on the quality of medical care. N Engl J Med. 1999;341:1147-1150.
5. Friedin RB, Goldman L, Cecil RR. Patient-physician concordance in problem identification in the primary care setting. Ann Intern Med. 1980;93:490-493.
6. Boland BJ, Scheitel SM, Wollan PC, et al. Patient-physician agreement on reasons for ambulatory general medical examinations. Mayo Clin Proc. 1998;73:109-117.
7. Abbo ED, Zhang Q, Zelder M, et al. The increasing number of clinical items addressed during the time of adult primary care visits. J Gen Intern Med. 2008;23:2058-2065.
8. Østbye T, Yarnall KS, Krause KM, et al. Is there time for management of patients with chronic diseases in primary care? Ann Fam Med. 2005;3:209-214.
9. Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q. 1996;74:511-544.
10. Wagner EH, Austin BT, Von Korff M. Improving outcomes in chronic illness. Manag Care Q. 1996;4:12-25.
11. Glasgow RE, Orleans CT, Wagner EH. Does the chronic care model serve also as a template for improving prevention? Milbank Q. 2001;79:579-612,iv-v.
12. Wagner EH, Bennett SM, Austin BT, et al. Finding common ground: patient-centeredness and evidence-based chronic illness care. J Altern Complement Med. 2005;11(suppl 1):S7-S15.
13. Green LA. The weekly return as a practical instrument for data collection in office based research. Fam Med. 1988;20:182-184.
14. Green LA, Reed FM, Miller RS, et al. Verification of data reported by practices for a study of spontaneous abortion. Fam Med. 1988;20:189-191.
15. Ettner SL. The relationship between continuity of care and the health behaviors of patients: Does having a usual physician make a difference? Med Care. 1999;37:547-555.
16. Parchman ML, Burge SK. The patient-physician relationship, primary care attributes, and preventive services. Fam Med. 2004;36:22-27.
17. Blewett LA, Johnson PJ, Lee B, et al. When a usual source of care and usual provider matter: adult prevention and screening services. J Gen Intern Med. 2008;23:1354-1360.
18. Flocke SA, Stange KC, Zyzanski SJ. The association of attributes of primary care with the delivery of clinical preventive services. Med Care. 1998;36(8 suppl):AS21-AS30.
19. Ayanian JZ, Weissman JS, Schneider EC, et al. Unmet health needs of uninsured adults in the United States. JAMA. 2000;284:2061-2069.
20. Fiscella K, Williams DR. Health disparities based on socioeconomic inequities: implications for urban health care. Acad Med. 2004;79:1139-1147.
21. McWilliams JM. Health consequences of uninsurance among adults in the United States: recent evidence and implications. Milbank Q. 2009;87:443-494.

What is the best nonsurgical therapy for pelvic organ prolapse?
Pelvic floor muscle training (PFMT) and pessaries are equally effective in treating symptoms of pelvic organ prolapse (POP). PFMT transiently improves patient satisfaction and reduces urinary incontinence more than pessaries do (strength of recommendation [SOR]: B, a randomized controlled trial [RCT]).
PFMT moderately improves prolapse symptoms and severity, especially following 6 months of supervised intervention (SOR: B, a systematic review of randomized trials with some methodologic flaws).
Two pessaries (ring with support and Gellhorn) reduce symptoms in as many as 60% of patients (SOR: B, a systematic review of randomized trials).
Untreated postmenopausal women with mild grades of uterine prolapse are unlikely to develop more severe prolapse; 25% to 50% improve spontaneously (SOR: C, a prospective cohort study with methodologic flaws).
EVIDENCE SUMMARY
A 2010 multicenter RCT with 445 women (mean age 49.8 years) compared PFMT, pessary use, and combined treatment.1 Investigators used the Patient Global Impression of Improvement and the stress incontinence subscale of the Pelvic Floor Distress Inventory to measure patient satisfaction and urinary incontinence symptoms.
At 3 months, equivalent numbers of women using PFMT and a pessary (49% and 40%, respectively; P=.09) reported they were “much better” or “very much better.” More women in the PFMT cohort than women using a pessary reported resolution of incontinence symptoms at 3 months (49% vs 33%; P=.006), and satisfaction with treatment (75% vs 63%; P=.02), but these differences disappeared at 12 months. Combination therapy wasn’t superior to PFMT alone.
Pelvic floor muscle training improves symptoms, especially with perseverance
A 2011 Cochrane review that compared women receiving PFMT with a control group (observed but not treated) found that PFMT moderately improved prolapse symptoms and severity, especially following 6 months of supervised intervention.2 Investigators evalu-ated 4 trials, (N=857), including 3 with fewer than 25 women per arm.
Three studies found that PFMT improved symptom severity and manometric measures. Although the authors couldn’t pool the data because of different symptom scoring instruments, typical improvements ranged from 20% to 30%. Two trials found that PFMT increased the chance of improvement in POP stage by 17% (pooled data, relative risk=.83; 95% confidence interval [CI], .71-.96). PFMT also improved urinary outcomes (approximately 30% reduction in urinary frequency and stress incontinence symptoms) in 2 of 3 trials and improved bowel symptoms in one trial (approximately 25% to 30% reduction).
Pessaries also relieve symptoms
A 2013 Cochrane Review seeking to determine the effectiveness of pessaries in POP, identified one RCT (crossover, 3 month, multicenter, United States) that compared symptom relief and change in life impact over baseline for 134 women (parous, mean age 61 years, range 30-89 years) with POP stage II or greater who were treated with ring with support or Gellhorn pessaries.3 Sixty percent of patients who completed the study (the dropout rate was 37%) reported symptom relief with both types of pessary. Outcomes were measured by multiple questionnaires and Likert scales.
Patients reported improved symptoms on both the Pelvic Organ Prolapse Distress Inventory (POPDI) and Pelvic Organ Prolapse Impact Questionnaire (POPIQ) scales (P<.05 for difference from baseline on each scale, actual scores not reported). The ring with support and Gellhorn pessaries didn’t produce different scores on either scale (POPDI, P=.99; POPIQ, P=.29).
Untreated mild prolapse postmenopause usually doesn’t progress and may regress
A cohort of 412 postmenopausal women (ages ≥50 years) with POP who were observed, but not treated, found that mild POP was unlikely to progress and sometimes improved spontaneously.4 Over a mean follow-up of 5.7 years, few women with grade 1 POP (prolapsed pelvic organs remaining within the vagina) progressed to grade 2 or 3 (probability of progression for women with cystoceles=.095, 95% CI, .07-.13; women with rectoceles=.135, 95% CI, .09-.19; and women with uterine prolapse=.019, 95% CI, .0005-.099).
Some women with grade 1 POP regressed to grade 0 (probability of regression for women with cystoceles=.235, 95% CI, .19- .28; women with rectoceles=.22, 95% CI, .16-.28; and women with uterine prolapse=.48, 95% CI, 0.34-.62). Women with grades 2 and 3 POP were less likely to regress to grade 0 (probability of regression for women with cystoceles=.093, 95% CI, .05-.14; women with rectoceles=.033, 95% CI, .011-.075; and women with uterine prolapse=0, 95% CI, 0-.37).
One flaw of this study was that the women received hormone replacement therapy, which the investigators didn’t evaluate independently. However, a 2010 Cochrane review (2 small trials, one meta-analysis) found insufficient data to determine whether hormone replacement therapy alters POP.5
RECOMMENDATIONS
The American College of Obstetricians and Gynecologists Practice Bulletin on POP recommends the following:6
- Pessaries can be fitted in most women with prolapse, regardless of prolapse stage (equivalent to grade) or site of predominant prolapse.
- Pessary use should be considered before surgical intervention in women with symptomatic prolapse.
- Women with prolapse who are asymptomatic or mildly symptomatic can be observed at regular intervals, unless new bothersome symptoms develop.
1. Richter HE, Burgio KL, Brubaker L, et al;Pelvic Floor Disorders Network. Continence pessary compared with behavioral therapy or combined therapy for stress incontinence: a randomized controlled trial. Obstet Gynecol. 2010;115:609-617.
2. Hagen S, Stark D. Conservative prevention and management of pelvic organ prolapse in women. Cochrane Database Syst Rev. 2011;12:CD003882.
3. Bugge C, Adams EJ, Gopinath D, et al. Pessaries (mechanical devices) for pelvic organ prolapse in women. Cochrane Database Syst Rev. 2013;2:CD004010.
4. Handa VL, Garrett E, Hendrix S, et al. Progression and remission of pelvic organ prolapse: a longitudinal study of menopausal women. Am J Obstet Gynecol. 2004;190:27-32.
5. Ismail SI, Bain C, Hagen S. Oestrogens for treatment or prevention of pelvic organ prolapse in postmenopausal women. Cochrane Database Syst Rev. 2010;9:CD007063.
6. ACOG Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 85: Pelvic organ prolapse. Obstet Gynecol. 2007;110:717-729.
Pelvic floor muscle training (PFMT) and pessaries are equally effective in treating symptoms of pelvic organ prolapse (POP). PFMT transiently improves patient satisfaction and reduces urinary incontinence more than pessaries do (strength of recommendation [SOR]: B, a randomized controlled trial [RCT]).
PFMT moderately improves prolapse symptoms and severity, especially following 6 months of supervised intervention (SOR: B, a systematic review of randomized trials with some methodologic flaws).
Two pessaries (ring with support and Gellhorn) reduce symptoms in as many as 60% of patients (SOR: B, a systematic review of randomized trials).
Untreated postmenopausal women with mild grades of uterine prolapse are unlikely to develop more severe prolapse; 25% to 50% improve spontaneously (SOR: C, a prospective cohort study with methodologic flaws).
EVIDENCE SUMMARY
A 2010 multicenter RCT with 445 women (mean age 49.8 years) compared PFMT, pessary use, and combined treatment.1 Investigators used the Patient Global Impression of Improvement and the stress incontinence subscale of the Pelvic Floor Distress Inventory to measure patient satisfaction and urinary incontinence symptoms.
At 3 months, equivalent numbers of women using PFMT and a pessary (49% and 40%, respectively; P=.09) reported they were “much better” or “very much better.” More women in the PFMT cohort than women using a pessary reported resolution of incontinence symptoms at 3 months (49% vs 33%; P=.006), and satisfaction with treatment (75% vs 63%; P=.02), but these differences disappeared at 12 months. Combination therapy wasn’t superior to PFMT alone.
Pelvic floor muscle training improves symptoms, especially with perseverance
A 2011 Cochrane review that compared women receiving PFMT with a control group (observed but not treated) found that PFMT moderately improved prolapse symptoms and severity, especially following 6 months of supervised intervention.2 Investigators evalu-ated 4 trials, (N=857), including 3 with fewer than 25 women per arm.
Three studies found that PFMT improved symptom severity and manometric measures. Although the authors couldn’t pool the data because of different symptom scoring instruments, typical improvements ranged from 20% to 30%. Two trials found that PFMT increased the chance of improvement in POP stage by 17% (pooled data, relative risk=.83; 95% confidence interval [CI], .71-.96). PFMT also improved urinary outcomes (approximately 30% reduction in urinary frequency and stress incontinence symptoms) in 2 of 3 trials and improved bowel symptoms in one trial (approximately 25% to 30% reduction).
Pessaries also relieve symptoms
A 2013 Cochrane Review seeking to determine the effectiveness of pessaries in POP, identified one RCT (crossover, 3 month, multicenter, United States) that compared symptom relief and change in life impact over baseline for 134 women (parous, mean age 61 years, range 30-89 years) with POP stage II or greater who were treated with ring with support or Gellhorn pessaries.3 Sixty percent of patients who completed the study (the dropout rate was 37%) reported symptom relief with both types of pessary. Outcomes were measured by multiple questionnaires and Likert scales.
Patients reported improved symptoms on both the Pelvic Organ Prolapse Distress Inventory (POPDI) and Pelvic Organ Prolapse Impact Questionnaire (POPIQ) scales (P<.05 for difference from baseline on each scale, actual scores not reported). The ring with support and Gellhorn pessaries didn’t produce different scores on either scale (POPDI, P=.99; POPIQ, P=.29).
Untreated mild prolapse postmenopause usually doesn’t progress and may regress
A cohort of 412 postmenopausal women (ages ≥50 years) with POP who were observed, but not treated, found that mild POP was unlikely to progress and sometimes improved spontaneously.4 Over a mean follow-up of 5.7 years, few women with grade 1 POP (prolapsed pelvic organs remaining within the vagina) progressed to grade 2 or 3 (probability of progression for women with cystoceles=.095, 95% CI, .07-.13; women with rectoceles=.135, 95% CI, .09-.19; and women with uterine prolapse=.019, 95% CI, .0005-.099).
Some women with grade 1 POP regressed to grade 0 (probability of regression for women with cystoceles=.235, 95% CI, .19- .28; women with rectoceles=.22, 95% CI, .16-.28; and women with uterine prolapse=.48, 95% CI, 0.34-.62). Women with grades 2 and 3 POP were less likely to regress to grade 0 (probability of regression for women with cystoceles=.093, 95% CI, .05-.14; women with rectoceles=.033, 95% CI, .011-.075; and women with uterine prolapse=0, 95% CI, 0-.37).
One flaw of this study was that the women received hormone replacement therapy, which the investigators didn’t evaluate independently. However, a 2010 Cochrane review (2 small trials, one meta-analysis) found insufficient data to determine whether hormone replacement therapy alters POP.5
RECOMMENDATIONS
The American College of Obstetricians and Gynecologists Practice Bulletin on POP recommends the following:6
- Pessaries can be fitted in most women with prolapse, regardless of prolapse stage (equivalent to grade) or site of predominant prolapse.
- Pessary use should be considered before surgical intervention in women with symptomatic prolapse.
- Women with prolapse who are asymptomatic or mildly symptomatic can be observed at regular intervals, unless new bothersome symptoms develop.
Pelvic floor muscle training (PFMT) and pessaries are equally effective in treating symptoms of pelvic organ prolapse (POP). PFMT transiently improves patient satisfaction and reduces urinary incontinence more than pessaries do (strength of recommendation [SOR]: B, a randomized controlled trial [RCT]).
PFMT moderately improves prolapse symptoms and severity, especially following 6 months of supervised intervention (SOR: B, a systematic review of randomized trials with some methodologic flaws).
Two pessaries (ring with support and Gellhorn) reduce symptoms in as many as 60% of patients (SOR: B, a systematic review of randomized trials).
Untreated postmenopausal women with mild grades of uterine prolapse are unlikely to develop more severe prolapse; 25% to 50% improve spontaneously (SOR: C, a prospective cohort study with methodologic flaws).
EVIDENCE SUMMARY
A 2010 multicenter RCT with 445 women (mean age 49.8 years) compared PFMT, pessary use, and combined treatment.1 Investigators used the Patient Global Impression of Improvement and the stress incontinence subscale of the Pelvic Floor Distress Inventory to measure patient satisfaction and urinary incontinence symptoms.
At 3 months, equivalent numbers of women using PFMT and a pessary (49% and 40%, respectively; P=.09) reported they were “much better” or “very much better.” More women in the PFMT cohort than women using a pessary reported resolution of incontinence symptoms at 3 months (49% vs 33%; P=.006), and satisfaction with treatment (75% vs 63%; P=.02), but these differences disappeared at 12 months. Combination therapy wasn’t superior to PFMT alone.
Pelvic floor muscle training improves symptoms, especially with perseverance
A 2011 Cochrane review that compared women receiving PFMT with a control group (observed but not treated) found that PFMT moderately improved prolapse symptoms and severity, especially following 6 months of supervised intervention.2 Investigators evalu-ated 4 trials, (N=857), including 3 with fewer than 25 women per arm.
Three studies found that PFMT improved symptom severity and manometric measures. Although the authors couldn’t pool the data because of different symptom scoring instruments, typical improvements ranged from 20% to 30%. Two trials found that PFMT increased the chance of improvement in POP stage by 17% (pooled data, relative risk=.83; 95% confidence interval [CI], .71-.96). PFMT also improved urinary outcomes (approximately 30% reduction in urinary frequency and stress incontinence symptoms) in 2 of 3 trials and improved bowel symptoms in one trial (approximately 25% to 30% reduction).
Pessaries also relieve symptoms
A 2013 Cochrane Review seeking to determine the effectiveness of pessaries in POP, identified one RCT (crossover, 3 month, multicenter, United States) that compared symptom relief and change in life impact over baseline for 134 women (parous, mean age 61 years, range 30-89 years) with POP stage II or greater who were treated with ring with support or Gellhorn pessaries.3 Sixty percent of patients who completed the study (the dropout rate was 37%) reported symptom relief with both types of pessary. Outcomes were measured by multiple questionnaires and Likert scales.
Patients reported improved symptoms on both the Pelvic Organ Prolapse Distress Inventory (POPDI) and Pelvic Organ Prolapse Impact Questionnaire (POPIQ) scales (P<.05 for difference from baseline on each scale, actual scores not reported). The ring with support and Gellhorn pessaries didn’t produce different scores on either scale (POPDI, P=.99; POPIQ, P=.29).
Untreated mild prolapse postmenopause usually doesn’t progress and may regress
A cohort of 412 postmenopausal women (ages ≥50 years) with POP who were observed, but not treated, found that mild POP was unlikely to progress and sometimes improved spontaneously.4 Over a mean follow-up of 5.7 years, few women with grade 1 POP (prolapsed pelvic organs remaining within the vagina) progressed to grade 2 or 3 (probability of progression for women with cystoceles=.095, 95% CI, .07-.13; women with rectoceles=.135, 95% CI, .09-.19; and women with uterine prolapse=.019, 95% CI, .0005-.099).
Some women with grade 1 POP regressed to grade 0 (probability of regression for women with cystoceles=.235, 95% CI, .19- .28; women with rectoceles=.22, 95% CI, .16-.28; and women with uterine prolapse=.48, 95% CI, 0.34-.62). Women with grades 2 and 3 POP were less likely to regress to grade 0 (probability of regression for women with cystoceles=.093, 95% CI, .05-.14; women with rectoceles=.033, 95% CI, .011-.075; and women with uterine prolapse=0, 95% CI, 0-.37).
One flaw of this study was that the women received hormone replacement therapy, which the investigators didn’t evaluate independently. However, a 2010 Cochrane review (2 small trials, one meta-analysis) found insufficient data to determine whether hormone replacement therapy alters POP.5
RECOMMENDATIONS
The American College of Obstetricians and Gynecologists Practice Bulletin on POP recommends the following:6
- Pessaries can be fitted in most women with prolapse, regardless of prolapse stage (equivalent to grade) or site of predominant prolapse.
- Pessary use should be considered before surgical intervention in women with symptomatic prolapse.
- Women with prolapse who are asymptomatic or mildly symptomatic can be observed at regular intervals, unless new bothersome symptoms develop.
1. Richter HE, Burgio KL, Brubaker L, et al;Pelvic Floor Disorders Network. Continence pessary compared with behavioral therapy or combined therapy for stress incontinence: a randomized controlled trial. Obstet Gynecol. 2010;115:609-617.
2. Hagen S, Stark D. Conservative prevention and management of pelvic organ prolapse in women. Cochrane Database Syst Rev. 2011;12:CD003882.
3. Bugge C, Adams EJ, Gopinath D, et al. Pessaries (mechanical devices) for pelvic organ prolapse in women. Cochrane Database Syst Rev. 2013;2:CD004010.
4. Handa VL, Garrett E, Hendrix S, et al. Progression and remission of pelvic organ prolapse: a longitudinal study of menopausal women. Am J Obstet Gynecol. 2004;190:27-32.
5. Ismail SI, Bain C, Hagen S. Oestrogens for treatment or prevention of pelvic organ prolapse in postmenopausal women. Cochrane Database Syst Rev. 2010;9:CD007063.
6. ACOG Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 85: Pelvic organ prolapse. Obstet Gynecol. 2007;110:717-729.
1. Richter HE, Burgio KL, Brubaker L, et al;Pelvic Floor Disorders Network. Continence pessary compared with behavioral therapy or combined therapy for stress incontinence: a randomized controlled trial. Obstet Gynecol. 2010;115:609-617.
2. Hagen S, Stark D. Conservative prevention and management of pelvic organ prolapse in women. Cochrane Database Syst Rev. 2011;12:CD003882.
3. Bugge C, Adams EJ, Gopinath D, et al. Pessaries (mechanical devices) for pelvic organ prolapse in women. Cochrane Database Syst Rev. 2013;2:CD004010.
4. Handa VL, Garrett E, Hendrix S, et al. Progression and remission of pelvic organ prolapse: a longitudinal study of menopausal women. Am J Obstet Gynecol. 2004;190:27-32.
5. Ismail SI, Bain C, Hagen S. Oestrogens for treatment or prevention of pelvic organ prolapse in postmenopausal women. Cochrane Database Syst Rev. 2010;9:CD007063.
6. ACOG Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 85: Pelvic organ prolapse. Obstet Gynecol. 2007;110:717-729.
Evidence-based answers from the Family Physicians Inquiries Network