User login
Leukemia, lymphoma cause more distress in young adults

patient and her father
Photo by Rhoda Baer
Results of 2 new studies indicate that young adults (ages 18 to 39) who have survived leukemia or lymphoma are more likely to report high distress than older survivors (age 65 and older).
Specifically, 45% of younger survivors reported moderate-to-high distress, whereas only 18% of older survivors reported similarly elevated levels.
In both groups, this distress was not affected by the amount of time since a patient received treatment. Distress was just as likely to be high in survivors who had completed treatment 4 years prior as in survivors who were 3 months out of treatment.
Whitney Jones, PhD, of the University of Colorado Denver, and her colleagues reported these findings in the Journal of Psychosocial Oncology.
In the first study, Dr Jones and her colleagues surveyed 477 cancer survivors, using a widely used measure of distress after trauma and several items from a measure of quality of life in cancer survivors.
These measures allowed the researchers to ask which factors of a cancer survivor’s life after treatment are the best predictors of persistent distress after treatment completion.
And results showed that survivors younger than 40 had the highest prevalence of distress.
Dr Jones explained the effect of age on distress using a framework called the Lifespan Perspective. Because there is an expected social, cultural, and developmental course of a person’s life, an event that is highly disruptive in one lifespan stage may be less disruptive in another.
“For younger survivors, cancer is out of context,” Dr Jones said. “When you’re under 40, you’re finishing your education, entering the workforce, starting a family, and cancer may be interpreted as disruptive and unexpected in that phase.”
“On the other hand, some of our older survivors said things like, ‘Cancer isn’t the most difficult thing I’ve experienced in life.’ And they knew friends and family members who had dealt with similar cancer experiences.”
The study also showed that people who feared recurrence were most likely to report high overall distress levels. And high financial burden due to cancer treatment predicted distress.
In the second study, the researchers used interviews with 51 leukemia and lymphoma survivors to explore the human side of these numbers and better understand the sources of distress as articulated by survivors themselves.
“For example, this was before the Affordable Care Act, and we had one survivor who talked about having only the basic college student insurance when he was diagnosed,” Dr Jones said. “After treatment, he discovered he had substantial medical debt and was uninsurable.”
“It helped to hear survivors talk about their experiences in their own words. To hear them articulate it helped us understand the real struggles behind our data.”
The interviews also helped to explain why distress lingers even years after treatment ends.
“A patient told us that, after lymphoma treatment, her doctor said that it would take 2 years to recover physically and mentally, and that almost all the gains would be in these 2 years,” Dr Jones said.
“She said something like, ‘I was really patient for 2 years, then after those 2 years passed, I didn’t feel any better and realized this is what I was going to be living with.’”
Distress detection and treatment is increasingly being seen as part of the standard of care for cancer patients and post-treatment survivors, the researchers noted.
For example, organizations like the National Comprehensive Cancer Network and the American College of Surgeons Commission on Cancer mandate distress screening and treatment in order to earn accreditation from these institutions.
“Understanding which individuals are most likely to experience elevated distress can be useful in targeting interventions to potential participants,” Dr Jones said. ![]()
patient and her father
Photo by Rhoda Baer
Results of 2 new studies indicate that young adults (ages 18 to 39) who have survived leukemia or lymphoma are more likely to report high distress than older survivors (age 65 and older).
Specifically, 45% of younger survivors reported moderate-to-high distress, whereas only 18% of older survivors reported similarly elevated levels.
In both groups, this distress was not affected by the amount of time since a patient received treatment. Distress was just as likely to be high in survivors who had completed treatment 4 years prior as in survivors who were 3 months out of treatment.
Whitney Jones, PhD, of the University of Colorado Denver, and her colleagues reported these findings in the Journal of Psychosocial Oncology.
In the first study, Dr Jones and her colleagues surveyed 477 cancer survivors, using a widely used measure of distress after trauma and several items from a measure of quality of life in cancer survivors.
These measures allowed the researchers to ask which factors of a cancer survivor’s life after treatment are the best predictors of persistent distress after treatment completion.
And results showed that survivors younger than 40 had the highest prevalence of distress.
Dr Jones explained the effect of age on distress using a framework called the Lifespan Perspective. Because there is an expected social, cultural, and developmental course of a person’s life, an event that is highly disruptive in one lifespan stage may be less disruptive in another.
“For younger survivors, cancer is out of context,” Dr Jones said. “When you’re under 40, you’re finishing your education, entering the workforce, starting a family, and cancer may be interpreted as disruptive and unexpected in that phase.”
“On the other hand, some of our older survivors said things like, ‘Cancer isn’t the most difficult thing I’ve experienced in life.’ And they knew friends and family members who had dealt with similar cancer experiences.”
The study also showed that people who feared recurrence were most likely to report high overall distress levels. And high financial burden due to cancer treatment predicted distress.
In the second study, the researchers used interviews with 51 leukemia and lymphoma survivors to explore the human side of these numbers and better understand the sources of distress as articulated by survivors themselves.
“For example, this was before the Affordable Care Act, and we had one survivor who talked about having only the basic college student insurance when he was diagnosed,” Dr Jones said. “After treatment, he discovered he had substantial medical debt and was uninsurable.”
“It helped to hear survivors talk about their experiences in their own words. To hear them articulate it helped us understand the real struggles behind our data.”
The interviews also helped to explain why distress lingers even years after treatment ends.
“A patient told us that, after lymphoma treatment, her doctor said that it would take 2 years to recover physically and mentally, and that almost all the gains would be in these 2 years,” Dr Jones said.
“She said something like, ‘I was really patient for 2 years, then after those 2 years passed, I didn’t feel any better and realized this is what I was going to be living with.’”
Distress detection and treatment is increasingly being seen as part of the standard of care for cancer patients and post-treatment survivors, the researchers noted.
For example, organizations like the National Comprehensive Cancer Network and the American College of Surgeons Commission on Cancer mandate distress screening and treatment in order to earn accreditation from these institutions.
“Understanding which individuals are most likely to experience elevated distress can be useful in targeting interventions to potential participants,” Dr Jones said. ![]()
patient and her father
Photo by Rhoda Baer
Results of 2 new studies indicate that young adults (ages 18 to 39) who have survived leukemia or lymphoma are more likely to report high distress than older survivors (age 65 and older).
Specifically, 45% of younger survivors reported moderate-to-high distress, whereas only 18% of older survivors reported similarly elevated levels.
In both groups, this distress was not affected by the amount of time since a patient received treatment. Distress was just as likely to be high in survivors who had completed treatment 4 years prior as in survivors who were 3 months out of treatment.
Whitney Jones, PhD, of the University of Colorado Denver, and her colleagues reported these findings in the Journal of Psychosocial Oncology.
In the first study, Dr Jones and her colleagues surveyed 477 cancer survivors, using a widely used measure of distress after trauma and several items from a measure of quality of life in cancer survivors.
These measures allowed the researchers to ask which factors of a cancer survivor’s life after treatment are the best predictors of persistent distress after treatment completion.
And results showed that survivors younger than 40 had the highest prevalence of distress.
Dr Jones explained the effect of age on distress using a framework called the Lifespan Perspective. Because there is an expected social, cultural, and developmental course of a person’s life, an event that is highly disruptive in one lifespan stage may be less disruptive in another.
“For younger survivors, cancer is out of context,” Dr Jones said. “When you’re under 40, you’re finishing your education, entering the workforce, starting a family, and cancer may be interpreted as disruptive and unexpected in that phase.”
“On the other hand, some of our older survivors said things like, ‘Cancer isn’t the most difficult thing I’ve experienced in life.’ And they knew friends and family members who had dealt with similar cancer experiences.”
The study also showed that people who feared recurrence were most likely to report high overall distress levels. And high financial burden due to cancer treatment predicted distress.
In the second study, the researchers used interviews with 51 leukemia and lymphoma survivors to explore the human side of these numbers and better understand the sources of distress as articulated by survivors themselves.
“For example, this was before the Affordable Care Act, and we had one survivor who talked about having only the basic college student insurance when he was diagnosed,” Dr Jones said. “After treatment, he discovered he had substantial medical debt and was uninsurable.”
“It helped to hear survivors talk about their experiences in their own words. To hear them articulate it helped us understand the real struggles behind our data.”
The interviews also helped to explain why distress lingers even years after treatment ends.
“A patient told us that, after lymphoma treatment, her doctor said that it would take 2 years to recover physically and mentally, and that almost all the gains would be in these 2 years,” Dr Jones said.
“She said something like, ‘I was really patient for 2 years, then after those 2 years passed, I didn’t feel any better and realized this is what I was going to be living with.’”
Distress detection and treatment is increasingly being seen as part of the standard of care for cancer patients and post-treatment survivors, the researchers noted.
For example, organizations like the National Comprehensive Cancer Network and the American College of Surgeons Commission on Cancer mandate distress screening and treatment in order to earn accreditation from these institutions.
“Understanding which individuals are most likely to experience elevated distress can be useful in targeting interventions to potential participants,” Dr Jones said. ![]()
Survey results support shared decision-making

Photo by Rhoda Baer
A survey of cancer patients has shown that when physicians make treatment decisions alone, patients tend to rate the quality of care lower than when physicians include patients in the decision-making process.
Researchers found this to be the case even among patients who said they preferred it when physicians made treatment decisions alone.
Kenneth L. Kehl, MD, of MD Anderson Cancer Center in Houston, Texas, and his colleagues reported these findings in JAMA Oncology.
The researchers surveyed 5315 cancer patients who reported decision roles for 10,817 treatment decisions. The team assessed the association between patients’ roles in decisions with their reports on quality of care and physician communication.
Most of the patients (58%) said they preferred shared roles in decision-making, 36% preferred patient-controlled decisions, and 6% preferred physician-controlled decisions.
The patients reported that their actual decision-making process was patient-controlled in 39% of decisions, shared in 44%, and physician-controlled in 17%. Of the treatment decisions made by patients, 42% were regarding surgery, 36% were regarding chemotherapy, and 22% were regarding radiation.
The researchers found that patients’ preferred role in decision-making was not associated with how they rated the quality of care. But when they reported that treatment decisions were controlled by physicians, the patients were less likely to rate the quality of care as excellent, as compared to shared-decision making situations.
Patients said physician care was excellent in 67.8% of cases. And 55.8% of patients gave their physicians the highest possible rating of communication.
However, patients who preferred physician-controlled decisions to shared decision-making were less likely to give top ratings to their physicians, as were patients who reported actually experiencing physician-controlled vs shared decisions.
The researchers said these results highlight the benefits of promoting shared decision-making among all patients with cancer, even those who seem to prefer less active roles in the process.
In a related commentary, Sarah T. Hawley, PhD, and Reshma Jagsi, MD, DPhil, of the University of Michigan in Ann Arbor, said they were intrigued by the fact that the association between shared decision-making and patient appraisal of care quality remained even when controlling for a patient’s preferred role in the decision-making process.
“Kehl and colleagues conclude from this finding that it is important to promote [shared decision-making], even among patients who may seek less active roles,” Drs Hawley and Jagsi wrote.
“Yet . . . prior work . . . has suggested that it is the match between patients’ preferred and actual involvement that contributes to greater satisfaction with care. These conflicting results underscore the need for further work to better quantify and link measures of [shared decision-making] to patient appraisal of care.” ![]()
Photo by Rhoda Baer
A survey of cancer patients has shown that when physicians make treatment decisions alone, patients tend to rate the quality of care lower than when physicians include patients in the decision-making process.
Researchers found this to be the case even among patients who said they preferred it when physicians made treatment decisions alone.
Kenneth L. Kehl, MD, of MD Anderson Cancer Center in Houston, Texas, and his colleagues reported these findings in JAMA Oncology.
The researchers surveyed 5315 cancer patients who reported decision roles for 10,817 treatment decisions. The team assessed the association between patients’ roles in decisions with their reports on quality of care and physician communication.
Most of the patients (58%) said they preferred shared roles in decision-making, 36% preferred patient-controlled decisions, and 6% preferred physician-controlled decisions.
The patients reported that their actual decision-making process was patient-controlled in 39% of decisions, shared in 44%, and physician-controlled in 17%. Of the treatment decisions made by patients, 42% were regarding surgery, 36% were regarding chemotherapy, and 22% were regarding radiation.
The researchers found that patients’ preferred role in decision-making was not associated with how they rated the quality of care. But when they reported that treatment decisions were controlled by physicians, the patients were less likely to rate the quality of care as excellent, as compared to shared-decision making situations.
Patients said physician care was excellent in 67.8% of cases. And 55.8% of patients gave their physicians the highest possible rating of communication.
However, patients who preferred physician-controlled decisions to shared decision-making were less likely to give top ratings to their physicians, as were patients who reported actually experiencing physician-controlled vs shared decisions.
The researchers said these results highlight the benefits of promoting shared decision-making among all patients with cancer, even those who seem to prefer less active roles in the process.
In a related commentary, Sarah T. Hawley, PhD, and Reshma Jagsi, MD, DPhil, of the University of Michigan in Ann Arbor, said they were intrigued by the fact that the association between shared decision-making and patient appraisal of care quality remained even when controlling for a patient’s preferred role in the decision-making process.
“Kehl and colleagues conclude from this finding that it is important to promote [shared decision-making], even among patients who may seek less active roles,” Drs Hawley and Jagsi wrote.
“Yet . . . prior work . . . has suggested that it is the match between patients’ preferred and actual involvement that contributes to greater satisfaction with care. These conflicting results underscore the need for further work to better quantify and link measures of [shared decision-making] to patient appraisal of care.” ![]()
Photo by Rhoda Baer
A survey of cancer patients has shown that when physicians make treatment decisions alone, patients tend to rate the quality of care lower than when physicians include patients in the decision-making process.
Researchers found this to be the case even among patients who said they preferred it when physicians made treatment decisions alone.
Kenneth L. Kehl, MD, of MD Anderson Cancer Center in Houston, Texas, and his colleagues reported these findings in JAMA Oncology.
The researchers surveyed 5315 cancer patients who reported decision roles for 10,817 treatment decisions. The team assessed the association between patients’ roles in decisions with their reports on quality of care and physician communication.
Most of the patients (58%) said they preferred shared roles in decision-making, 36% preferred patient-controlled decisions, and 6% preferred physician-controlled decisions.
The patients reported that their actual decision-making process was patient-controlled in 39% of decisions, shared in 44%, and physician-controlled in 17%. Of the treatment decisions made by patients, 42% were regarding surgery, 36% were regarding chemotherapy, and 22% were regarding radiation.
The researchers found that patients’ preferred role in decision-making was not associated with how they rated the quality of care. But when they reported that treatment decisions were controlled by physicians, the patients were less likely to rate the quality of care as excellent, as compared to shared-decision making situations.
Patients said physician care was excellent in 67.8% of cases. And 55.8% of patients gave their physicians the highest possible rating of communication.
However, patients who preferred physician-controlled decisions to shared decision-making were less likely to give top ratings to their physicians, as were patients who reported actually experiencing physician-controlled vs shared decisions.
The researchers said these results highlight the benefits of promoting shared decision-making among all patients with cancer, even those who seem to prefer less active roles in the process.
In a related commentary, Sarah T. Hawley, PhD, and Reshma Jagsi, MD, DPhil, of the University of Michigan in Ann Arbor, said they were intrigued by the fact that the association between shared decision-making and patient appraisal of care quality remained even when controlling for a patient’s preferred role in the decision-making process.
“Kehl and colleagues conclude from this finding that it is important to promote [shared decision-making], even among patients who may seek less active roles,” Drs Hawley and Jagsi wrote.
“Yet . . . prior work . . . has suggested that it is the match between patients’ preferred and actual involvement that contributes to greater satisfaction with care. These conflicting results underscore the need for further work to better quantify and link measures of [shared decision-making] to patient appraisal of care.” ![]()
Cancer patients rarely make inappropriate requests, study shows

Photo courtesy of NIH
Although it makes sense that patient requests might drive physicians to practice defensive medicine, new research suggests that may not be the case with cancer patients.
The study, conducted at outpatient oncology centers, showed that patients rarely made clinically inappropriate requests.
Only 1% of more than 5000 patient-clinician encounters resulted in a clinically inappropriate request. And physicians rarely complied with these requests.
Keerthi Gogineni, MD, of the Hospital of the University of Pennsylvania in Philadelphia, and colleagues reported these findings in JAMA Oncology.
The researchers analyzed interviews with clinicians immediately after they visited with patients to assess whether a patient had made a request, the type of request made, and the clinical appropriateness of it.
The interviews were conducted at outpatient oncology facilities at 3 Philadelphia-area hospitals between October 2013 and June 2014.
The authors evaluated 5050 patient-clinician encounters involving 3624 patients and 60 clinicians. Most of the patients were women, and the most common cancer was hematologic.
Overall, 440 (8.7%) of the encounters included a patient demand or request, such as for imaging studies, treatments, or tests. And physicians complied with 365 (83%) of them.
Of all the patient-clinician encounters, 50 (1%) included a clinically inappropriate request. Clinicians complied with 7 of them. So, in 0.14% of encounters, clinicians ordered a test or treatment based on a clinically inappropriate request.
“At least in oncology, ‘demanding patients’ seem infrequent and may not account for a significant proportion of costs,” the researchers concluded.
In a related editorial, Anthony L. Back, MD, of the Seattle Cancer Care Alliance in Washington, wrote that inappropriate patient demands appear to be “more mythical than real.”
“[W]e have to stop blaming patients for being demanding,” he wrote. “In reality, it is hardly happening. The myth of the demanding patient is more about our own responses and how lackluster communication skills can contribute to difficult situations that stick in our throats and in our memories. And when we have calmed down enough to look up, we see that what is really happening between patients and physicians these days is something quite different.”
“It is possible that what the study by Gogineni et al documents is a point in the evolution of the patient-physician relationship when both sides recognize the complexity of cancer care belies a simple fix. Perhaps this ‘negative’ study is pointing to an important truth: that we need to redirect our attention from the myths that are distracting us.” ![]()
Photo courtesy of NIH
Although it makes sense that patient requests might drive physicians to practice defensive medicine, new research suggests that may not be the case with cancer patients.
The study, conducted at outpatient oncology centers, showed that patients rarely made clinically inappropriate requests.
Only 1% of more than 5000 patient-clinician encounters resulted in a clinically inappropriate request. And physicians rarely complied with these requests.
Keerthi Gogineni, MD, of the Hospital of the University of Pennsylvania in Philadelphia, and colleagues reported these findings in JAMA Oncology.
The researchers analyzed interviews with clinicians immediately after they visited with patients to assess whether a patient had made a request, the type of request made, and the clinical appropriateness of it.
The interviews were conducted at outpatient oncology facilities at 3 Philadelphia-area hospitals between October 2013 and June 2014.
The authors evaluated 5050 patient-clinician encounters involving 3624 patients and 60 clinicians. Most of the patients were women, and the most common cancer was hematologic.
Overall, 440 (8.7%) of the encounters included a patient demand or request, such as for imaging studies, treatments, or tests. And physicians complied with 365 (83%) of them.
Of all the patient-clinician encounters, 50 (1%) included a clinically inappropriate request. Clinicians complied with 7 of them. So, in 0.14% of encounters, clinicians ordered a test or treatment based on a clinically inappropriate request.
“At least in oncology, ‘demanding patients’ seem infrequent and may not account for a significant proportion of costs,” the researchers concluded.
In a related editorial, Anthony L. Back, MD, of the Seattle Cancer Care Alliance in Washington, wrote that inappropriate patient demands appear to be “more mythical than real.”
“[W]e have to stop blaming patients for being demanding,” he wrote. “In reality, it is hardly happening. The myth of the demanding patient is more about our own responses and how lackluster communication skills can contribute to difficult situations that stick in our throats and in our memories. And when we have calmed down enough to look up, we see that what is really happening between patients and physicians these days is something quite different.”
“It is possible that what the study by Gogineni et al documents is a point in the evolution of the patient-physician relationship when both sides recognize the complexity of cancer care belies a simple fix. Perhaps this ‘negative’ study is pointing to an important truth: that we need to redirect our attention from the myths that are distracting us.” ![]()
Photo courtesy of NIH
Although it makes sense that patient requests might drive physicians to practice defensive medicine, new research suggests that may not be the case with cancer patients.
The study, conducted at outpatient oncology centers, showed that patients rarely made clinically inappropriate requests.
Only 1% of more than 5000 patient-clinician encounters resulted in a clinically inappropriate request. And physicians rarely complied with these requests.
Keerthi Gogineni, MD, of the Hospital of the University of Pennsylvania in Philadelphia, and colleagues reported these findings in JAMA Oncology.
The researchers analyzed interviews with clinicians immediately after they visited with patients to assess whether a patient had made a request, the type of request made, and the clinical appropriateness of it.
The interviews were conducted at outpatient oncology facilities at 3 Philadelphia-area hospitals between October 2013 and June 2014.
The authors evaluated 5050 patient-clinician encounters involving 3624 patients and 60 clinicians. Most of the patients were women, and the most common cancer was hematologic.
Overall, 440 (8.7%) of the encounters included a patient demand or request, such as for imaging studies, treatments, or tests. And physicians complied with 365 (83%) of them.
Of all the patient-clinician encounters, 50 (1%) included a clinically inappropriate request. Clinicians complied with 7 of them. So, in 0.14% of encounters, clinicians ordered a test or treatment based on a clinically inappropriate request.
“At least in oncology, ‘demanding patients’ seem infrequent and may not account for a significant proportion of costs,” the researchers concluded.
In a related editorial, Anthony L. Back, MD, of the Seattle Cancer Care Alliance in Washington, wrote that inappropriate patient demands appear to be “more mythical than real.”
“[W]e have to stop blaming patients for being demanding,” he wrote. “In reality, it is hardly happening. The myth of the demanding patient is more about our own responses and how lackluster communication skills can contribute to difficult situations that stick in our throats and in our memories. And when we have calmed down enough to look up, we see that what is really happening between patients and physicians these days is something quite different.”
“It is possible that what the study by Gogineni et al documents is a point in the evolution of the patient-physician relationship when both sides recognize the complexity of cancer care belies a simple fix. Perhaps this ‘negative’ study is pointing to an important truth: that we need to redirect our attention from the myths that are distracting us.” ![]()
In-flight transfusions enable better outcomes in trauma patients

Photo by Elise Amendola
In-flight red blood cell (RBC) transfusions can improve outcomes in trauma patients, according to a study published in the Journal of the American College of Surgeons.
The research showed that air-lifted trauma victims who received blood transfusions in the helicopter had higher one-day survival rates and a lower risk of shock than air-lifted patients who did not receive transfusions until they arrived at the trauma unit.
Patients who received in-flight transfusions also required fewer RBCs once they arrived at the hospital.
Joshua Brown, MD, and his colleagues at the University of Pittsburgh Medical Center (UPMC) conducted this research, evaluating the air medical evacuation strategy at UPMC, which has a network of 18 helicopter bases in Pennsylvania, Ohio, and Maryland.
The STAT MedEvac helicopter teams have been carrying blood for transfusion on their flights for about 2 decades, but this is the first study that evaluated the use of transfused blood in civilian trauma victims air-evacuated directly from the injury scene and compared them with air-evacuated trauma victims who did not receive transfused blood.
It is also the largest study to date of a civilian in-flight trauma resuscitation protocol that has been used by the military in Iraq and Afghanistan.
The researchers evaluated 240 patients who received in-flight RBC transfusions and 480 patients who were not transfused until they reached the trauma center.
Receiving an in-flight transfusion was associated with better odds of 24-hour survival (adjusted odds ratio=4.92, P=0.01), decreased odds of shock (adjusted odds ratio=0.28, P=0.03), and lower 24-hour RBC requirement (coef -3.6 RBC units, P=0.04).
Based on these data, the UPMC may modify its protocol, Dr Brown said.
“It used to be the paramedics had to give the patient 2 liters of saline before giving them blood, and we dropped that down to only 1 liter of saline,” he noted. “Now, based on this study, we’re actually looking at giving patients blood without any saline who meet the criteria of low blood pressure and elevated heart rate and are clearly in shock.”
The UPMC protocol involves giving guidelines on when to administer transfusions to the paramedics and nurses onboard flights. All the STAT MedEvac flights at the institution carry 2 units of RBCs for transfusion.
Helicopter staff can communicate with the medical command doctor at the trauma center to get the go-ahead order to give blood to patients who may not meet the guidelines for transfusion but still may benefit from receiving it.
However, there are regulatory issues that may prevent such a protocol from being adopted universally, Dr Brown noted. In Pennsylvania, paramedics who have had additional training are allowed to start a blood transfusion without a physician present, but not all states allow this.
Dr Brown also explained the logistics and challenges of storing blood away from the blood bank.
“The blood needs to be refrigerated, the helicopter base must have a freezer, and the helicopters must have coolers when they’re actually out on a mission to keep the blood at an appropriate temperature,” he said.
Meeting these requirements involves close coordination with the blood bank and having a way to return unused blood after it expires in 30 days. The University of Pittsburgh has registered all of its helicopter bases as satellite blood banks to comply with the regulations. ![]()
Photo by Elise Amendola
In-flight red blood cell (RBC) transfusions can improve outcomes in trauma patients, according to a study published in the Journal of the American College of Surgeons.
The research showed that air-lifted trauma victims who received blood transfusions in the helicopter had higher one-day survival rates and a lower risk of shock than air-lifted patients who did not receive transfusions until they arrived at the trauma unit.
Patients who received in-flight transfusions also required fewer RBCs once they arrived at the hospital.
Joshua Brown, MD, and his colleagues at the University of Pittsburgh Medical Center (UPMC) conducted this research, evaluating the air medical evacuation strategy at UPMC, which has a network of 18 helicopter bases in Pennsylvania, Ohio, and Maryland.
The STAT MedEvac helicopter teams have been carrying blood for transfusion on their flights for about 2 decades, but this is the first study that evaluated the use of transfused blood in civilian trauma victims air-evacuated directly from the injury scene and compared them with air-evacuated trauma victims who did not receive transfused blood.
It is also the largest study to date of a civilian in-flight trauma resuscitation protocol that has been used by the military in Iraq and Afghanistan.
The researchers evaluated 240 patients who received in-flight RBC transfusions and 480 patients who were not transfused until they reached the trauma center.
Receiving an in-flight transfusion was associated with better odds of 24-hour survival (adjusted odds ratio=4.92, P=0.01), decreased odds of shock (adjusted odds ratio=0.28, P=0.03), and lower 24-hour RBC requirement (coef -3.6 RBC units, P=0.04).
Based on these data, the UPMC may modify its protocol, Dr Brown said.
“It used to be the paramedics had to give the patient 2 liters of saline before giving them blood, and we dropped that down to only 1 liter of saline,” he noted. “Now, based on this study, we’re actually looking at giving patients blood without any saline who meet the criteria of low blood pressure and elevated heart rate and are clearly in shock.”
The UPMC protocol involves giving guidelines on when to administer transfusions to the paramedics and nurses onboard flights. All the STAT MedEvac flights at the institution carry 2 units of RBCs for transfusion.
Helicopter staff can communicate with the medical command doctor at the trauma center to get the go-ahead order to give blood to patients who may not meet the guidelines for transfusion but still may benefit from receiving it.
However, there are regulatory issues that may prevent such a protocol from being adopted universally, Dr Brown noted. In Pennsylvania, paramedics who have had additional training are allowed to start a blood transfusion without a physician present, but not all states allow this.
Dr Brown also explained the logistics and challenges of storing blood away from the blood bank.
“The blood needs to be refrigerated, the helicopter base must have a freezer, and the helicopters must have coolers when they’re actually out on a mission to keep the blood at an appropriate temperature,” he said.
Meeting these requirements involves close coordination with the blood bank and having a way to return unused blood after it expires in 30 days. The University of Pittsburgh has registered all of its helicopter bases as satellite blood banks to comply with the regulations. ![]()
Photo by Elise Amendola
In-flight red blood cell (RBC) transfusions can improve outcomes in trauma patients, according to a study published in the Journal of the American College of Surgeons.
The research showed that air-lifted trauma victims who received blood transfusions in the helicopter had higher one-day survival rates and a lower risk of shock than air-lifted patients who did not receive transfusions until they arrived at the trauma unit.
Patients who received in-flight transfusions also required fewer RBCs once they arrived at the hospital.
Joshua Brown, MD, and his colleagues at the University of Pittsburgh Medical Center (UPMC) conducted this research, evaluating the air medical evacuation strategy at UPMC, which has a network of 18 helicopter bases in Pennsylvania, Ohio, and Maryland.
The STAT MedEvac helicopter teams have been carrying blood for transfusion on their flights for about 2 decades, but this is the first study that evaluated the use of transfused blood in civilian trauma victims air-evacuated directly from the injury scene and compared them with air-evacuated trauma victims who did not receive transfused blood.
It is also the largest study to date of a civilian in-flight trauma resuscitation protocol that has been used by the military in Iraq and Afghanistan.
The researchers evaluated 240 patients who received in-flight RBC transfusions and 480 patients who were not transfused until they reached the trauma center.
Receiving an in-flight transfusion was associated with better odds of 24-hour survival (adjusted odds ratio=4.92, P=0.01), decreased odds of shock (adjusted odds ratio=0.28, P=0.03), and lower 24-hour RBC requirement (coef -3.6 RBC units, P=0.04).
Based on these data, the UPMC may modify its protocol, Dr Brown said.
“It used to be the paramedics had to give the patient 2 liters of saline before giving them blood, and we dropped that down to only 1 liter of saline,” he noted. “Now, based on this study, we’re actually looking at giving patients blood without any saline who meet the criteria of low blood pressure and elevated heart rate and are clearly in shock.”
The UPMC protocol involves giving guidelines on when to administer transfusions to the paramedics and nurses onboard flights. All the STAT MedEvac flights at the institution carry 2 units of RBCs for transfusion.
Helicopter staff can communicate with the medical command doctor at the trauma center to get the go-ahead order to give blood to patients who may not meet the guidelines for transfusion but still may benefit from receiving it.
However, there are regulatory issues that may prevent such a protocol from being adopted universally, Dr Brown noted. In Pennsylvania, paramedics who have had additional training are allowed to start a blood transfusion without a physician present, but not all states allow this.
Dr Brown also explained the logistics and challenges of storing blood away from the blood bank.
“The blood needs to be refrigerated, the helicopter base must have a freezer, and the helicopters must have coolers when they’re actually out on a mission to keep the blood at an appropriate temperature,” he said.
Meeting these requirements involves close coordination with the blood bank and having a way to return unused blood after it expires in 30 days. The University of Pittsburgh has registered all of its helicopter bases as satellite blood banks to comply with the regulations. ![]()
Febrile Infant CPGs
Febrile young infants are at high risk for serious bacterial infection (SBI) with reported rates of 8.5% to 12%, even higher in neonates 28 days of age.[1, 2, 3] As a result, febrile infants often undergo extensive diagnostic evaluation consisting of a combination of urine, blood, and cerebrospinal fluid (CSF) testing.[4, 5, 6] Several clinical prediction algorithms use this diagnostic testing to identify febrile infants at low risk for SBI, but they differ with respect to age range, recommended testing, antibiotic administration, and threshold for hospitalization.[4, 5, 6] Additionally, the optimal management strategy for this population has not been defined.[7] Consequently, laboratory testing, antibiotic use, and hospitalization for febrile young infants vary widely among hospitals.[8, 9, 10]
Clinical practice guidelines (CPGs) are designed to implement evidence‐based care and reduce practice variability, with the goal of improving quality of care and optimizing costs.[11] Implementation of a CPG for management of febrile young infants in the Intermountain Healthcare System was associated with greater adherence to evidence‐based care and lower costs.[12] However, when strong evidence is lacking, different interpretations of febrile infant risk classification incorporated into local CPGs may be a major driver of the across‐hospital practice variation observed in prior studies.[8, 9] Understanding sources of variability as well as determining the association of CPGs with clinicians' practice patterns can help identify quality improvement opportunities, either through national benchmarking or local efforts.
Our primary objectives were to compare (1) recommendations of pediatric emergency departmentbased institutional CPGs for febrile young infants and (2) rates of urine, blood, CSF testing, hospitalization, and ceftriaxone use at emergency department (ED) discharge based upon CPG presence and the specific CPG recommendations. Our secondary objectives were to describe the association of CPGs with healthcare costs and return visits for SBI.
METHODS
Study Design
We used the Pediatric Health Information System (PHIS) to identify febrile infants 56 days of age who presented to the ED between January 1, 2013 and December 31, 2013. We also surveyed ED providers at participating PHIS hospitals. Informed consent was obtained from survey respondents. The institutional review board at Boston Children's Hospital approved the study protocol.
Clinical Practice Guideline Survey
We sent an electronic survey to medical directors or division directors at 37 pediatric EDs to determine whether their ED utilized a CPG for the management of the febrile young infant in 2013. If no response was received after the second attempt, we queried ED fellowship directors or other ED attending physicians at nonresponding hospitals. Survey items included the presence of a febrile young infant CPG, and if present, the year of implementation, ages targeted, and CPG content. As applicable, respondents were asked to share their CPG and/or provide the specific CPG recommendations.
We collected and managed survey data using the Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Boston Children's Hospital. REDCap is a secure, Web‐based application designed to support data capture for research studies.[13]
Data Source
The PHIS database contains administrative data from 44 US children's hospitals. These hospitals, affiliated with the Children's Hospital Association, represent 85% of freestanding US children's hospitals.[14] Encrypted patient identifiers permit tracking of patients across encounters.[15] Data quality and integrity are assured jointly by the Children's Hospital Association and participating hospitals.[16] For this study, 7 hospitals were excluded due to incomplete ED data or known data‐quality issues.[17]
Patients
We identified study infants using the following International Classification of Diseases, 9th Revision (ICD‐9) admission or discharge diagnosis codes for fever as defined previously[8, 9]: 780.6, 778.4, 780.60, or 780.61. We excluded infants with a complex chronic condition[18] and those transferred from another institution, as these infants may warrant a nonstandard evaluation and/or may have incomplete data. For infants with >1 ED visit for fever during the study period, repeat visits within 3 days of an index visit were considered a revisit for the same episode of illness; visits >3 days following an index visit were considered as a new index visit.
Study Definitions
From the PHIS database, we abstracted demographic characteristics (gender, race/ethnicity), insurance status, and region where the hospital was located (using US Census categories[19]). Billing codes were used to assess whether urine, blood, and CSF testing (as defined previously[9]) were performed during the ED evaluation. To account for ED visits that spanned the midnight hour, for hospitalized patients we considered any testing or treatment occurring on the initial or second hospital day to be performed in the ED; billing code data in PHIS are based upon calendar day and do not distinguish testing performed in the ED versus inpatient setting.[8, 9] Patients billed for observation care were classified as being hospitalized.[20, 21]
We identified the presence of an SBI using ICD‐9 diagnosis codes for the following infections as described previously[9]: urinary tract infection or pyelonephritis,[22] bacteremia or sepsis, bacterial meningitis,[16] pneumonia,[23] or bacterial enteritis. To assess return visits for SBI that required inpatient management, we defined an ED revisit for an SBI as a return visit within 3 days of ED discharge[24, 25] that resulted in hospitalization with an associated ICD‐9 discharge diagnosis code for an SBI.
Hospitals charges in PHIS database were adjusted for hospital location by using the Centers for Medicare and Medicaid Services price/wage index. Costs were estimated by applying hospital‐level cost‐to‐charge ratios to charge data.[26]
Measured Exposures
The primary exposure was the presence of an ED‐based CPG for management of the febrile young infant aged 28 days and 29 to 56 days; 56 days was used as the upper age limit as all of the CPGs included infants up to this age or beyond. Six institutions utilized CPGs with different thresholds to define the age categories (eg, dichotomized at 27 or 30 days); these CPGs were classified into the aforementioned age groups to permit comparisons across standardized age groups. We classified institutions based on the presence of a CPG. To assess differences in the application of low‐risk criteria, the CPGs were further classified a priori based upon specific recommendations around laboratory testing and hospitalization, as well as ceftriaxone use for infants aged 29 to 56 days discharged from the ED. CPGs were categorized based upon whether testing, hospitalization, and ceftriaxone use were: (1) recommended for all patients, (2) recommended only if patients were classified as high risk (absence of low‐risk criteria), (3) recommended against, or (4) recommended to consider at clinician discretion.
Outcome Measures
Measured outcomes were performance of urine, blood, CSF testing, and hospitalization rate, as well as rate of ceftriaxone use for discharged infants aged 29 to 56 days, 3‐day revisits for SBI, and costs per visit, which included hospitalization costs for admitted patients.
Data Analysis
We described continuous variables using median and interquartile range or range values and categorical variables using frequencies. We compared medians using Wilcoxon rank sum and categorical variables using a [2] test. We compared rates of testing, hospitalization, ceftriaxone use, and 3‐day revisits for SBI based on the presence of a CPG, and when present, the specific CPG recommendations. Costs per visit were compared between institutions with and without CPGs and assessed separately for admitted and discharged patients. To adjust for potential confounders and clustering of patients within hospitals, we used generalized estimating equations with logistic regression to generate adjusted odd ratios (aORs) and 95% confidence intervals (CIs). Models were adjusted for geographic region, payer, race, and gender. Statistical analyses were performed by using SAS version 9.3 (SAS Institute, Cary, NC). We determined statistical significance as a 2‐tailed P value <0.05.
Febrile infants with bronchiolitis or a history of prematurity may be managed differently from full‐term febrile young infants without bronchiolitis.[6, 27] Therefore, we performed a subgroup analysis after exclusion of infants with an ICD‐9 discharge diagnosis code for bronchiolitis (466.11 and 466.19)[28] or prematurity (765).
Because our study included ED encounters in 2013, we repeated our analyses after exclusion of hospitals with CPGs implemented during the 2013 calendar year.
RESULTS
CPG by Institution
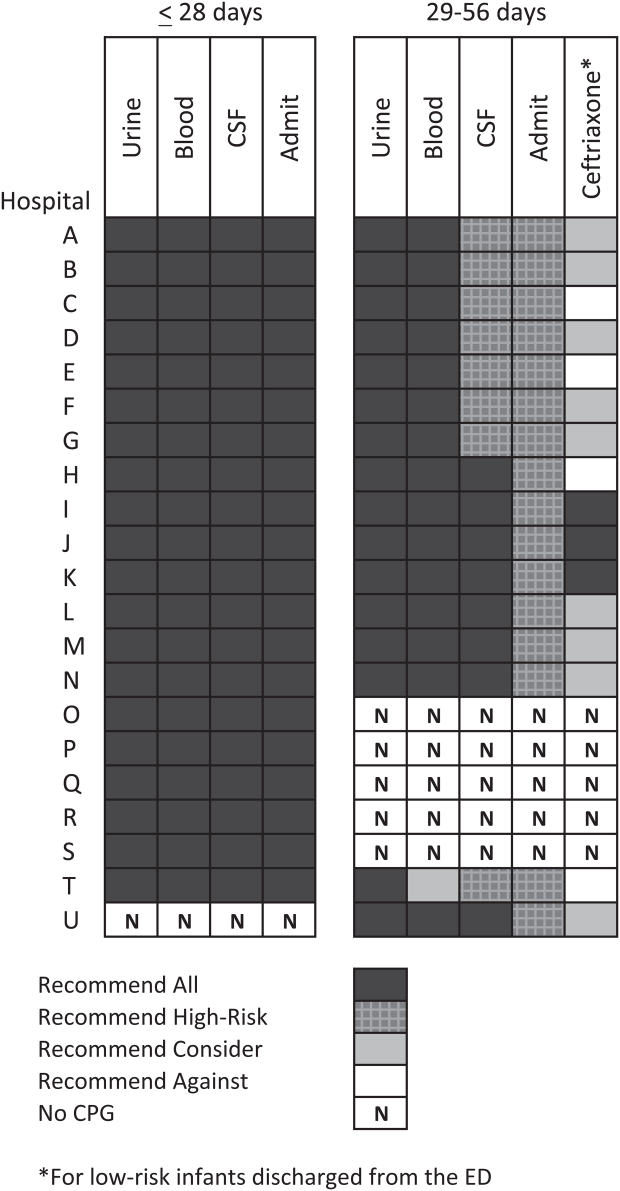
Thirty‐three (89.2%) of the 37 EDs surveyed completed the questionnaire. Overall, 21 (63.6%) of the 33 EDs had a CPG; 15 (45.5%) had a CPG for all infants 56 days of age, 5 (15.2%) had a CPG for infants 28 days only, and 1 (3.0%) had a CPG for infants 29 to 56 days but not 28 days of age (Figure 1). Seventeen EDs had an established CPG prior to 2013, and 4 hospitals implemented a CPG during the 2013 calendar year, 2 with CPGs for neonates 28 days and 2 with CPGs for both 28 days and 29 to 56 days of age. Hospitals with CPGs were more likely to be located in the Northeast and West regions of the United States and provide care to a higher proportion of non‐Hispanic white patients, as well as those with commercial insurance (Table 1).
| Characteristic | 28 Days | 2956 Days | ||||
|---|---|---|---|---|---|---|
| No CPG, n=996, N (%) | CPG, n=2,149, N (%) | P Value | No CPG, n=2,460, N (%) | CPG, n=3,772, N (%) | P Value | |
| ||||||
| Race | ||||||
| Non‐Hispanic white | 325 (32.6) | 996 (46.3) | 867 (35.2) | 1,728 (45.8) | ||
| Non‐Hispanic black | 248 (24.9) | 381 (17.7) | 593 (24.1) | 670 (17.8) | ||
| Hispanic | 243 (24.4) | 531 (24.7) | 655 (26.6) | 986 (26.1) | ||
| Asian | 28 (2.8) | 78 (3.6) | 40 (1.6) | 122 (3.2) | ||
| Other Race | 152 (15.3) | 163 (7.6) | <0.001 | 305 (12.4) | 266 (7.1) | <0.001 |
| Gender | ||||||
| Female | 435 (43.7) | 926 (43.1) | 0.76 | 1,067 (43.4) | 1,714 (45.4) | 0.22 |
| Payer | ||||||
| Commercial | 243 (24.4) | 738 (34.3) | 554 (22.5) | 1,202 (31.9) | ||
| Government | 664 (66.7) | 1,269 (59.1) | 1,798 (73.1) | 2,342 (62.1) | ||
| Other payer | 89 (8.9) | 142 (6.6) | <0.001 | 108 (4.4) | 228 (6.0) | <0.001 |
| Region | ||||||
| Northeast | 39 (3.9) | 245 (11.4) | 77 (3.1) | 572 (15.2) | ||
| South | 648 (65.1) | 915 (42.6) | 1,662 (67.6) | 1,462 (38.8) | ||
| Midwest | 271 (27.2) | 462 (21.5) | 506 (20.6) | 851 (22.6) | ||
| West | 38 (3.8) | 527 (24.5) | <0.001 | 215 (8.7) | 887 (23.5) | <0.001 |
| Serious bacterial infection | ||||||
| Overall* | 131 (13.2) | 242 (11.3) | 0.14 | 191 (7.8) | 237 (6.3) | 0.03 |
| UTI/pyelonephritis | 73 (7.3) | 153 (7.1) | 103 (4.2) | 154 (4.1) | ||
| Bacteremia/sepsis | 56 (5.6) | 91 (4.2) | 78 (3.2) | 61 (1.6) | ||
| Bacterial meningitis | 15 (1.5) | 15 (0.7) | 4 (0.2) | 14 (0.4) | ||
| Age, d, median (IQR) | 18 (11, 24) | 18 (11, 23) | 0.67 | 46 (37, 53) | 45 (37, 53) | 0.11 |
All 20 CPGs for the febrile young infant 28 days of age recommended urine, blood, CSF testing, and hospitalization for all infants (Figure 1). Of the 16 hospitals with CPGs for febrile infants aged 29 to 56 days, all recommended urine and blood testing for all patients, except for 1 CPG, which recommended consideration of blood testing but not to obtain routinely. Hospitals varied in recommendations for CSF testing among infants aged 29 to 56 days: 8 (50%) recommended CSF testing in all patients and 8 (50%) recommended CSF testing only if the patient was high risk per defined criteria (based on history, physical examination, urine, and blood testing). In all 16 CPGs, hospitalization was recommended only for high‐risk infants. For low‐risk infants aged 2956 days being discharged from the ED, 3 hospitals recommended ceftriaxone for all, 9 recommended consideration of ceftriaxone, and 4 recommended against antibiotics (Figure 1).
Study Patients
During the study period, there were 10,415 infants 56 days old with a diagnosis of fever at the 33 participating hospitals. After exclusion of 635 (6.1%) infants with a complex chronic condition and 445 (4.3%) transferred from another institution (including 42 with a complex chronic condition), 9377 infants remained in our study cohort. Approximately one‐third of the cohort was 28 days of age and two‐thirds aged 29 to 56 days. The overall SBI rate was 8.5% but varied by age (11.9% in infants 28 days and 6.9% in infants 29 to 56 days of age) (Table 1).
CPGs and Use of Diagnostic Testing, Hospitalization Rates, Ceftriaxone Use, and Revisits for SBI
For infants 28 days of age, the presence of a CPG was not associated with urine, blood, CSF testing, or hospitalization after multivariable adjustment (Table 2). Among infants aged 29 to 56 days, urine testing did not differ based on the presence of a CPG, whereas blood testing was performed less often at the 1 hospital whose CPG recommended to consider, but not routinely obtain, testing (aOR: 0.4, 95% CI: 0.3‐0.7, P=0.001). Compared to hospitals without a CPG, CSF testing was performed less often at hospitals with CPG recommendations to only obtain CSF if high risk (aOR: 0.5, 95% CI: 0.3‐0.8, P=0.002). However, the odds of hospitalization did not differ at institutions with and without a febrile infant CPG (aOR: 0.7, 95% CI: 0.5‐1.1, P=0.10). For infants aged 29 to 56 days discharged from the ED, ceftriaxone was administered more often at hospitals with CPGs that recommended ceftriaxone for all discharged patients (aOR: 4.6, 95% CI: 2.39.3, P<0.001) and less often at hospitals whose CPGs recommended against antibiotics (aOR: 0.3, 95% CI: 0.1‐0.9, P=0.03) (Table 3). Our findings were similar in the subgroup of infants without bronchiolitis or prematurity (see Supporting Tables 1 and 2 in the online version of this article). After exclusion of hospitals with a CPG implemented during the 2013 calendar year (4 hospitals excluded in the 28 days age group and 2 hospitals excluded in the 29 to 56 days age group), infants aged 29 to 56 days cared for at a hospital with a CPG experienced a lower odds of hospitalization (aOR: 0.7, 95% CI: 0.4‐0.98, P=0.04). Otherwise, our findings in both age groups did not materially differ from the main analyses.
| Testing/Hospitalization | No. of Hospitals | No. of Patients | % Received* | aOR (95% CI) | P Value |
|---|---|---|---|---|---|
| |||||
| Laboratory testing | |||||
| Urine testing | |||||
| No CPG | 13 | 996 | 75.6 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 80.7 | 1.2 (0.9‐1.7) | 0.22 |
| Blood testing | |||||
| No CPG | 13 | 996 | 76.9 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 81.8 | 1.2 (0.9‐1.7) | 0.25 |
| CSF testing‖ | |||||
| No CPG | 13 | 996 | 71.0 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 77.5 | 1.3 (1.01.7) | 0.08 |
| Disposition | |||||
| Hospitalization | |||||
| No CPG | 13 | 996 | 75.4 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 81.6 | 1.2 (0.9‐1.8) | 0.26 |
| Testing/Hospitalization | No. of Hospitals | No. of Patients | % Received* | aOR (95% CI) | P Value |
|---|---|---|---|---|---|
| |||||
| Laboratory resting | |||||
| Urine testing | |||||
| No CPG | 17 | 2,460 | 81.1 | Ref | |
| CPG: recommend for all | 16 | 3,772 | 82.1 | 0.9 (0.7‐1.4) | 0.76 |
| Blood testing | |||||
| No CPG | 17 | 2,460 | 79.4 | Ref | |
| CPG: recommend for all | 15 | 3,628 | 82.6 | 1.1 (0.7‐1.6) | 0.70 |
| CPG: recommend consider | 1 | 144 | 62.5 | 0.4 (0.3‐0.7) | 0.001 |
| CSF testing‖ | |||||
| No CPG | 17 | 2,460 | 46.3 | Ref | |
| CPG: recommend for all | 8 | 1,517 | 70.3 | 1.3 (0.9‐1.9) | 0.11 |
| CPG: recommend if high‐risk | 8 | 2,255 | 39.9 | 0.5 (0.3‐0.8) | 0.002 |
| Disposition | |||||
| Hospitalization | |||||
| No CPG | 17 | 2,460 | 47.0 | Ref | |
| CPG: recommend if high‐risk | 16 | 3,772 | 42.0 | 0.7 (0.5‐1.1) | 0.10 |
| Ceftriaxone if discharged | |||||
| No CPG | 17 | 1,304 | 11.7 | Ref | |
| CPG: recommend against | 4 | 313 | 10.9 | 0.3 (0.1‐0.9) | 0.03 |
| CPG: recommend consider | 9 | 1,567 | 14.4 | 1.5 (0.9‐2.4) | 0.09 |
| CPG: recommend for all | 3 | 306 | 64.1 | 4.6 (2.39.3) | < 0.001 |
Three‐day revisits for SBI were similarly low at hospitals with and without CPGs among infants 28 days (1.5% vs 0.8%, P=0.44) and 29 to 56 days of age (1.4% vs 1.1%, P=0.44) and did not differ after exclusion of hospitals with a CPG implemented in 2013.
CPGs and Costs
Among infants 28 days of age, costs per visit did not differ for admitted and discharged patients based on CPG presence. The presence of an ED febrile infant CPG was associated with higher costs for both admitted and discharged infants 29 to 56 days of age (Table 4). The cost analysis did not significantly differ after exclusion of hospitals with CPGs implemented in 2013.
| 28 Days, Cost, Median (IQR) | 29 to 56 Days, Cost, Median (IQR) | |||||
|---|---|---|---|---|---|---|
| No CPG | CPG | P Value | No CPG | CPG | P Value | |
| ||||||
| Admitted | $4,979 ($3,408$6,607) [n=751] | $4,715 ($3,472$6,526) [n=1,753] | 0.79 | $3,756 ($2,725$5,041) [n=1,156] | $3,923 ($3,077$5,243) [n=1,586] | <0.001 |
| Discharged | $298 ($166$510) [n=245] | $231 ($160$464) [n=396] | 0.10 | $681($398$982) [n=1,304)] | $764 ($412$1,100) [n=2,186] | <0.001 |
DISCUSSION
We described the content and association of CPGs with management of the febrile infant 56 days of age across a large sample of children's hospitals. Nearly two‐thirds of included pediatric EDs have a CPG for the management of young febrile infants. Management of febrile infants 28 days was uniform, with a majority hospitalized after urine, blood, and CSF testing regardless of the presence of a CPG. In contrast, CPGs for infants 29 to 56 days of age varied in their recommendations for CSF testing as well as ceftriaxone use for infants discharged from the ED. Consequently, we observed considerable hospital variability in CSF testing and ceftriaxone use for discharged infants, which correlates with variation in the presence and content of CPGs. Institutional CPGs may be a source of the across‐hospital variation in care of febrile young infants observed in prior study.[9]
Febrile infants 28 days of age are at particularly high risk for SBI, with a prevalence of nearly 20% or higher.[2, 3, 29] The high prevalence of SBI, combined with the inherent difficulty in distinguishing neonates with and without SBI,[2, 30] has resulted in uniform CPG recommendations to perform the full‐sepsis workup in this young age group. Similar to prior studies,[8, 9] we observed that most febrile infants 28 days undergo the full sepsis evaluation, including CSF testing, and are hospitalized regardless of the presence of a CPG.
However, given the conflicting recommendations for febrile infants 29 to 56 days of age,[4, 5, 6] the optimal management strategy is less certain.[7] The Rochester, Philadelphia, and Boston criteria, 3 published models to identify infants at low risk for SBI, primarily differ in their recommendations for CSF testing and ceftriaxone use in this age group.[4, 5, 6] Half of the CPGs recommended CSF testing for all febrile infants, and half recommended CSF testing only if the infant was high risk. Institutional guidelines that recommended selective CSF testing for febrile infants aged 29 to 56 days were associated with lower rates of CSF testing. Furthermore, ceftriaxone use varied based on CPG recommendations for low‐risk infants discharged from the ED. Therefore, the influence of febrile infant CPGs mainly relates to the limiting of CSF testing and targeted ceftriaxone use in low‐risk infants. As the rate of return visits for SBI is low across hospitals, future study should assess outcomes at hospitals with CPGs recommending selective CSF testing. Of note, infants 29 to 56 days of age were less likely to be hospitalized when cared for at a hospital with an established CPG prior to 2013 without increase in 3‐day revisits for SBI. This finding may indicate that longer duration of CPG implementation is associated with lower rates of hospitalization for low‐risk infants; this finding merits further study.
The presence of a CPG was not associated with lower costs for febrile infants in either age group. Although individual healthcare systems have achieved lower costs with CPG implementation,[12] the mere presence of a CPG is not associated with lower costs when assessed across institutions. Higher costs for admitted and discharged infants 29 to 56 days of age in the presence of a CPG likely reflects the higher rate of CSF testing at hospitals whose CPGs recommend testing for all febrile infants, as well as inpatient management strategies for hospitalized infants not captured in our study. Future investigation should include an assessment of the cost‐effectiveness of the various testing and treatment strategies employed for the febrile young infant.
Our study has several limitations. First, the validity of ICD‐9 diagnosis codes for identifying young infants with fever is not well established, and thus our study is subject to misclassification bias. To minimize missed patients, we included infants with either an ICD‐9 admission or discharge diagnosis of fever; however, utilization of diagnosis codes for patient identification may have resulted in undercapture of infants with a measured temperature of 38.0C. It is also possible that some patients who did not undergo testing were misclassified as having a fever or had temperatures below standard thresholds to prompt diagnostic testing. This is a potential reason that testing was not performed in 100% of infants, even at hospitals with CPGs that recommended testing for all patients. Additionally, some febrile infants diagnosed with SBI may not have an associated ICD‐9 diagnosis code for fever. Although the overall SBI rate observed in our study was similar to prior studies,[4, 31] the rate in neonates 28 days of age was lower than reported in recent investigations,[2, 3] which may indicate inclusion of a higher proportion of low‐risk febrile infants. With the exception of bronchiolitis, we also did not assess diagnostic testing in the presence of other identified sources of infection such as herpes simplex virus.
Second, we were unable to assess the presence or absence of a CPG at the 4 excluded EDs that did not respond to the survey or the institutions excluded for data‐quality issues. However, included and excluded hospitals did not differ in region or annual ED volume (data not shown).
Third, although we classified hospitals based upon the presence and content of CPGs, we were unable to fully evaluate adherence to the CPG at each site.
Last, though PHIS hospitals represent 85% of freestanding children's hospitals, many febrile infants are hospitalized at non‐PHIS institutions; our results may not be generalizable to care provided at nonchildren's hospitals.
CONCLUSIONS
Management of febrile neonates 28 days of age does not vary based on CPG presence. However, CPGs for the febrile infant aged 29 to 56 days vary in recommendations for CSF testing as well as ceftriaxone use for low‐risk patients, which significantly contributes to practice variation and healthcare costs across institutions.
Acknowledgements
The Febrile Young Infant Research Collaborative includes the following additional investigators who are acknowledged for their work on this study: Kao‐Ping Chua, MD, Harvard PhD Program in Health Policy, Harvard University, Cambridge, Massachusetts, and Division of Emergency Medicine, Department of Pediatrics, Boston Children's Hospital, Boston, Massachusetts; Elana A. Feldman, BA, University of Washington School of Medicine, Seattle, Washington; and Katie L. Hayes, BS, Division of Emergency Medicine, Department of Pediatrics, The Children's Hospital of Philadelphia, Philadelphia, Pennsylvania.
Disclosures
This project was funded in part by The Gerber Foundation Novice Researcher Award (Ref #18273835). Dr. Fran Balamuth received career development support from the National Institutes of Health (NHLBI K12‐HL109009). Funders were not involved in design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript. The authors have no financial relationships relevant to this article to disclose. No payment was received for the production of this article. The authors have no conflicts of interest relevant to this article to disclose.
- , , . Performance of low‐risk criteria in the evaluation of young infants with fever: review of the literature. Pediatrics. 2010;125:228–233.
- , , , , , . A week‐by‐week analysis of the low‐risk criteria for serious bacterial infection in febrile neonates. Arch Dis Child. 2009;94:287–292.
- , , , et al. Is 15 days an appropriate cut‐off age for considering serious bacterial infection in the management of febrile infants? Pediatr Infect Dis J. 2012;31:455–458.
- , , . Outpatient management without antibiotics of fever in selected infants. N Engl J Med. 1993;329:1437–1441.
- , , . Identifying febrile infants at risk for a serious bacterial infection. J Pediatr. 1993;123:489–490.
- , , , et al. Febrile infants at low risk for serious bacterial infection—an appraisal of the Rochester criteria and implications for management. Febrile Infant Collaborative Study Group. Pediatrics. 1994;94:390–396.
- American College of Emergency Physicians Clinical Policies Committee; American College of Emergency Physicians Clinical Policies Subcommittee on Pediatric Fever. Clinical policy for children younger than three years presenting to the emergency department with fever. Ann Emerg Med. 2003;42:530–545.
- , , , et al. Management of febrile neonates in US pediatric emergency departments. Pediatrics. 2014;133:187–195.
- , , , et al. Variation in care of the febrile young infant <90 days in US pediatric emergency departments. Pediatrics. 2014;134:667–677.
- , , , , . Fever survey highlights significant variations in how infants aged ≤60 days are evaluated and underline the need for guidelines. Acta Paediatr. 2014;103:379–385.
- . Evidence‐based guidelines and critical pathways for quality improvement. Pediatrics. 1999;103:225–232.
- , , , et al. Costs and infant outcomes after implementation of a care process model for febrile infants. Pediatrics. 2012;130:e16–e24.
- , , , , , . Research electronic data capture (REDCap)—a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381.
- , , , , , . Variation in occult injury screening for children with suspected abuse in selected US children's hospitals. Pediatrics. 2012;130:853–860.
- . Achieving data quality. How data from a pediatric health information system earns the trust of its users. J AHIMA. 2004;75:22–26.
- , , , . Corticosteroids and mortality in children with bacterial meningitis. JAMA. 2008;299:2048–2055.
- , , , et al. Variation in resource utilization across a national sample of pediatric emergency departments. J Pediatr. 2013;163:230–236.
- , , , , , . Deaths attributed to pediatric complex chronic conditions: national trends and implications for supportive care services. Pediatrics. 2001;107:E99.
- US Census Bureau. Geographic terms and concepts—census divisions and census regions. Available at: https://www.census.gov/geo/reference/gtc/gtc_census_divreg.html. Accessed September 10, 2014.
- , , , et al. Pediatric observation status: are we overlooking a growing population in children's hospitals? J Hosp Med. 2012;7:530–536.
- , , , et al. Differences in designations of observation care in US freestanding children's hospitals: are they virtual or real? J Hosp Med. 2012;7:287–293.
- , , , et al. Accuracy of administrative billing codes to detect urinary tract infection hospitalizations. Pediatrics. 2011;128:323–330.
- , , , et al. Identifying pediatric community‐acquired pneumonia hospitalizations: accuracy of administrative billing codes. JAMA Pediatr. 2013;167:851–858.
- , , , . Initial emergency department diagnosis and return visits: risk versus perception. Ann Emerg Med. 1998;32:569–573.
- , , , , . A national depiction of children with return visits to the emergency department within 72 hours, 2001–2007. Pediatr Emerg Care. 2012;28:606–610.
- Healthcare Cost and Utilization Project. Cost‐to‐charge ratio files. Available at: http://www.hcup‐us.ahrq.gov/db/state/costtocharge.jsp. Accessed September 11, 2014.
- , , , et al. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infections. Pediatrics. 2004;113:1728–1734.
- , , , et al. Establishing benchmarks for the hospitalized care of children with asthma, bronchiolitis, and pneumonia. Pediatrics. 2014;134:555–562.
- , , , , , . Well appearing young infants with fever without known source in the emergency department: are lumbar punctures always necessary? Eur J Emerg Med. 2010;17:167–169.
- , . Unpredictability of serious bacterial illness in febrile infants from birth to 1 month of age. Arch Pediatr Adolesc Med. 1999;153:508–511.
- , , , et al. Management and outcomes of care of fever in early infancy. JAMA. 2004;291:1203–1212.
Febrile young infants are at high risk for serious bacterial infection (SBI) with reported rates of 8.5% to 12%, even higher in neonates 28 days of age.[1, 2, 3] As a result, febrile infants often undergo extensive diagnostic evaluation consisting of a combination of urine, blood, and cerebrospinal fluid (CSF) testing.[4, 5, 6] Several clinical prediction algorithms use this diagnostic testing to identify febrile infants at low risk for SBI, but they differ with respect to age range, recommended testing, antibiotic administration, and threshold for hospitalization.[4, 5, 6] Additionally, the optimal management strategy for this population has not been defined.[7] Consequently, laboratory testing, antibiotic use, and hospitalization for febrile young infants vary widely among hospitals.[8, 9, 10]
Clinical practice guidelines (CPGs) are designed to implement evidence‐based care and reduce practice variability, with the goal of improving quality of care and optimizing costs.[11] Implementation of a CPG for management of febrile young infants in the Intermountain Healthcare System was associated with greater adherence to evidence‐based care and lower costs.[12] However, when strong evidence is lacking, different interpretations of febrile infant risk classification incorporated into local CPGs may be a major driver of the across‐hospital practice variation observed in prior studies.[8, 9] Understanding sources of variability as well as determining the association of CPGs with clinicians' practice patterns can help identify quality improvement opportunities, either through national benchmarking or local efforts.
Our primary objectives were to compare (1) recommendations of pediatric emergency departmentbased institutional CPGs for febrile young infants and (2) rates of urine, blood, CSF testing, hospitalization, and ceftriaxone use at emergency department (ED) discharge based upon CPG presence and the specific CPG recommendations. Our secondary objectives were to describe the association of CPGs with healthcare costs and return visits for SBI.
METHODS
Study Design
We used the Pediatric Health Information System (PHIS) to identify febrile infants 56 days of age who presented to the ED between January 1, 2013 and December 31, 2013. We also surveyed ED providers at participating PHIS hospitals. Informed consent was obtained from survey respondents. The institutional review board at Boston Children's Hospital approved the study protocol.
Clinical Practice Guideline Survey
We sent an electronic survey to medical directors or division directors at 37 pediatric EDs to determine whether their ED utilized a CPG for the management of the febrile young infant in 2013. If no response was received after the second attempt, we queried ED fellowship directors or other ED attending physicians at nonresponding hospitals. Survey items included the presence of a febrile young infant CPG, and if present, the year of implementation, ages targeted, and CPG content. As applicable, respondents were asked to share their CPG and/or provide the specific CPG recommendations.
We collected and managed survey data using the Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Boston Children's Hospital. REDCap is a secure, Web‐based application designed to support data capture for research studies.[13]
Data Source
The PHIS database contains administrative data from 44 US children's hospitals. These hospitals, affiliated with the Children's Hospital Association, represent 85% of freestanding US children's hospitals.[14] Encrypted patient identifiers permit tracking of patients across encounters.[15] Data quality and integrity are assured jointly by the Children's Hospital Association and participating hospitals.[16] For this study, 7 hospitals were excluded due to incomplete ED data or known data‐quality issues.[17]
Patients
We identified study infants using the following International Classification of Diseases, 9th Revision (ICD‐9) admission or discharge diagnosis codes for fever as defined previously[8, 9]: 780.6, 778.4, 780.60, or 780.61. We excluded infants with a complex chronic condition[18] and those transferred from another institution, as these infants may warrant a nonstandard evaluation and/or may have incomplete data. For infants with >1 ED visit for fever during the study period, repeat visits within 3 days of an index visit were considered a revisit for the same episode of illness; visits >3 days following an index visit were considered as a new index visit.
Study Definitions
From the PHIS database, we abstracted demographic characteristics (gender, race/ethnicity), insurance status, and region where the hospital was located (using US Census categories[19]). Billing codes were used to assess whether urine, blood, and CSF testing (as defined previously[9]) were performed during the ED evaluation. To account for ED visits that spanned the midnight hour, for hospitalized patients we considered any testing or treatment occurring on the initial or second hospital day to be performed in the ED; billing code data in PHIS are based upon calendar day and do not distinguish testing performed in the ED versus inpatient setting.[8, 9] Patients billed for observation care were classified as being hospitalized.[20, 21]
We identified the presence of an SBI using ICD‐9 diagnosis codes for the following infections as described previously[9]: urinary tract infection or pyelonephritis,[22] bacteremia or sepsis, bacterial meningitis,[16] pneumonia,[23] or bacterial enteritis. To assess return visits for SBI that required inpatient management, we defined an ED revisit for an SBI as a return visit within 3 days of ED discharge[24, 25] that resulted in hospitalization with an associated ICD‐9 discharge diagnosis code for an SBI.
Hospitals charges in PHIS database were adjusted for hospital location by using the Centers for Medicare and Medicaid Services price/wage index. Costs were estimated by applying hospital‐level cost‐to‐charge ratios to charge data.[26]
Measured Exposures
The primary exposure was the presence of an ED‐based CPG for management of the febrile young infant aged 28 days and 29 to 56 days; 56 days was used as the upper age limit as all of the CPGs included infants up to this age or beyond. Six institutions utilized CPGs with different thresholds to define the age categories (eg, dichotomized at 27 or 30 days); these CPGs were classified into the aforementioned age groups to permit comparisons across standardized age groups. We classified institutions based on the presence of a CPG. To assess differences in the application of low‐risk criteria, the CPGs were further classified a priori based upon specific recommendations around laboratory testing and hospitalization, as well as ceftriaxone use for infants aged 29 to 56 days discharged from the ED. CPGs were categorized based upon whether testing, hospitalization, and ceftriaxone use were: (1) recommended for all patients, (2) recommended only if patients were classified as high risk (absence of low‐risk criteria), (3) recommended against, or (4) recommended to consider at clinician discretion.
Outcome Measures
Measured outcomes were performance of urine, blood, CSF testing, and hospitalization rate, as well as rate of ceftriaxone use for discharged infants aged 29 to 56 days, 3‐day revisits for SBI, and costs per visit, which included hospitalization costs for admitted patients.
Data Analysis
We described continuous variables using median and interquartile range or range values and categorical variables using frequencies. We compared medians using Wilcoxon rank sum and categorical variables using a [2] test. We compared rates of testing, hospitalization, ceftriaxone use, and 3‐day revisits for SBI based on the presence of a CPG, and when present, the specific CPG recommendations. Costs per visit were compared between institutions with and without CPGs and assessed separately for admitted and discharged patients. To adjust for potential confounders and clustering of patients within hospitals, we used generalized estimating equations with logistic regression to generate adjusted odd ratios (aORs) and 95% confidence intervals (CIs). Models were adjusted for geographic region, payer, race, and gender. Statistical analyses were performed by using SAS version 9.3 (SAS Institute, Cary, NC). We determined statistical significance as a 2‐tailed P value <0.05.
Febrile infants with bronchiolitis or a history of prematurity may be managed differently from full‐term febrile young infants without bronchiolitis.[6, 27] Therefore, we performed a subgroup analysis after exclusion of infants with an ICD‐9 discharge diagnosis code for bronchiolitis (466.11 and 466.19)[28] or prematurity (765).
Because our study included ED encounters in 2013, we repeated our analyses after exclusion of hospitals with CPGs implemented during the 2013 calendar year.
RESULTS
CPG by Institution
Thirty‐three (89.2%) of the 37 EDs surveyed completed the questionnaire. Overall, 21 (63.6%) of the 33 EDs had a CPG; 15 (45.5%) had a CPG for all infants 56 days of age, 5 (15.2%) had a CPG for infants 28 days only, and 1 (3.0%) had a CPG for infants 29 to 56 days but not 28 days of age (Figure 1). Seventeen EDs had an established CPG prior to 2013, and 4 hospitals implemented a CPG during the 2013 calendar year, 2 with CPGs for neonates 28 days and 2 with CPGs for both 28 days and 29 to 56 days of age. Hospitals with CPGs were more likely to be located in the Northeast and West regions of the United States and provide care to a higher proportion of non‐Hispanic white patients, as well as those with commercial insurance (Table 1).
| Characteristic | 28 Days | 2956 Days | ||||
|---|---|---|---|---|---|---|
| No CPG, n=996, N (%) | CPG, n=2,149, N (%) | P Value | No CPG, n=2,460, N (%) | CPG, n=3,772, N (%) | P Value | |
| ||||||
| Race | ||||||
| Non‐Hispanic white | 325 (32.6) | 996 (46.3) | 867 (35.2) | 1,728 (45.8) | ||
| Non‐Hispanic black | 248 (24.9) | 381 (17.7) | 593 (24.1) | 670 (17.8) | ||
| Hispanic | 243 (24.4) | 531 (24.7) | 655 (26.6) | 986 (26.1) | ||
| Asian | 28 (2.8) | 78 (3.6) | 40 (1.6) | 122 (3.2) | ||
| Other Race | 152 (15.3) | 163 (7.6) | <0.001 | 305 (12.4) | 266 (7.1) | <0.001 |
| Gender | ||||||
| Female | 435 (43.7) | 926 (43.1) | 0.76 | 1,067 (43.4) | 1,714 (45.4) | 0.22 |
| Payer | ||||||
| Commercial | 243 (24.4) | 738 (34.3) | 554 (22.5) | 1,202 (31.9) | ||
| Government | 664 (66.7) | 1,269 (59.1) | 1,798 (73.1) | 2,342 (62.1) | ||
| Other payer | 89 (8.9) | 142 (6.6) | <0.001 | 108 (4.4) | 228 (6.0) | <0.001 |
| Region | ||||||
| Northeast | 39 (3.9) | 245 (11.4) | 77 (3.1) | 572 (15.2) | ||
| South | 648 (65.1) | 915 (42.6) | 1,662 (67.6) | 1,462 (38.8) | ||
| Midwest | 271 (27.2) | 462 (21.5) | 506 (20.6) | 851 (22.6) | ||
| West | 38 (3.8) | 527 (24.5) | <0.001 | 215 (8.7) | 887 (23.5) | <0.001 |
| Serious bacterial infection | ||||||
| Overall* | 131 (13.2) | 242 (11.3) | 0.14 | 191 (7.8) | 237 (6.3) | 0.03 |
| UTI/pyelonephritis | 73 (7.3) | 153 (7.1) | 103 (4.2) | 154 (4.1) | ||
| Bacteremia/sepsis | 56 (5.6) | 91 (4.2) | 78 (3.2) | 61 (1.6) | ||
| Bacterial meningitis | 15 (1.5) | 15 (0.7) | 4 (0.2) | 14 (0.4) | ||
| Age, d, median (IQR) | 18 (11, 24) | 18 (11, 23) | 0.67 | 46 (37, 53) | 45 (37, 53) | 0.11 |
All 20 CPGs for the febrile young infant 28 days of age recommended urine, blood, CSF testing, and hospitalization for all infants (Figure 1). Of the 16 hospitals with CPGs for febrile infants aged 29 to 56 days, all recommended urine and blood testing for all patients, except for 1 CPG, which recommended consideration of blood testing but not to obtain routinely. Hospitals varied in recommendations for CSF testing among infants aged 29 to 56 days: 8 (50%) recommended CSF testing in all patients and 8 (50%) recommended CSF testing only if the patient was high risk per defined criteria (based on history, physical examination, urine, and blood testing). In all 16 CPGs, hospitalization was recommended only for high‐risk infants. For low‐risk infants aged 2956 days being discharged from the ED, 3 hospitals recommended ceftriaxone for all, 9 recommended consideration of ceftriaxone, and 4 recommended against antibiotics (Figure 1).
Study Patients
During the study period, there were 10,415 infants 56 days old with a diagnosis of fever at the 33 participating hospitals. After exclusion of 635 (6.1%) infants with a complex chronic condition and 445 (4.3%) transferred from another institution (including 42 with a complex chronic condition), 9377 infants remained in our study cohort. Approximately one‐third of the cohort was 28 days of age and two‐thirds aged 29 to 56 days. The overall SBI rate was 8.5% but varied by age (11.9% in infants 28 days and 6.9% in infants 29 to 56 days of age) (Table 1).
CPGs and Use of Diagnostic Testing, Hospitalization Rates, Ceftriaxone Use, and Revisits for SBI
For infants 28 days of age, the presence of a CPG was not associated with urine, blood, CSF testing, or hospitalization after multivariable adjustment (Table 2). Among infants aged 29 to 56 days, urine testing did not differ based on the presence of a CPG, whereas blood testing was performed less often at the 1 hospital whose CPG recommended to consider, but not routinely obtain, testing (aOR: 0.4, 95% CI: 0.3‐0.7, P=0.001). Compared to hospitals without a CPG, CSF testing was performed less often at hospitals with CPG recommendations to only obtain CSF if high risk (aOR: 0.5, 95% CI: 0.3‐0.8, P=0.002). However, the odds of hospitalization did not differ at institutions with and without a febrile infant CPG (aOR: 0.7, 95% CI: 0.5‐1.1, P=0.10). For infants aged 29 to 56 days discharged from the ED, ceftriaxone was administered more often at hospitals with CPGs that recommended ceftriaxone for all discharged patients (aOR: 4.6, 95% CI: 2.39.3, P<0.001) and less often at hospitals whose CPGs recommended against antibiotics (aOR: 0.3, 95% CI: 0.1‐0.9, P=0.03) (Table 3). Our findings were similar in the subgroup of infants without bronchiolitis or prematurity (see Supporting Tables 1 and 2 in the online version of this article). After exclusion of hospitals with a CPG implemented during the 2013 calendar year (4 hospitals excluded in the 28 days age group and 2 hospitals excluded in the 29 to 56 days age group), infants aged 29 to 56 days cared for at a hospital with a CPG experienced a lower odds of hospitalization (aOR: 0.7, 95% CI: 0.4‐0.98, P=0.04). Otherwise, our findings in both age groups did not materially differ from the main analyses.
| Testing/Hospitalization | No. of Hospitals | No. of Patients | % Received* | aOR (95% CI) | P Value |
|---|---|---|---|---|---|
| |||||
| Laboratory testing | |||||
| Urine testing | |||||
| No CPG | 13 | 996 | 75.6 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 80.7 | 1.2 (0.9‐1.7) | 0.22 |
| Blood testing | |||||
| No CPG | 13 | 996 | 76.9 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 81.8 | 1.2 (0.9‐1.7) | 0.25 |
| CSF testing‖ | |||||
| No CPG | 13 | 996 | 71.0 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 77.5 | 1.3 (1.01.7) | 0.08 |
| Disposition | |||||
| Hospitalization | |||||
| No CPG | 13 | 996 | 75.4 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 81.6 | 1.2 (0.9‐1.8) | 0.26 |
| Testing/Hospitalization | No. of Hospitals | No. of Patients | % Received* | aOR (95% CI) | P Value |
|---|---|---|---|---|---|
| |||||
| Laboratory resting | |||||
| Urine testing | |||||
| No CPG | 17 | 2,460 | 81.1 | Ref | |
| CPG: recommend for all | 16 | 3,772 | 82.1 | 0.9 (0.7‐1.4) | 0.76 |
| Blood testing | |||||
| No CPG | 17 | 2,460 | 79.4 | Ref | |
| CPG: recommend for all | 15 | 3,628 | 82.6 | 1.1 (0.7‐1.6) | 0.70 |
| CPG: recommend consider | 1 | 144 | 62.5 | 0.4 (0.3‐0.7) | 0.001 |
| CSF testing‖ | |||||
| No CPG | 17 | 2,460 | 46.3 | Ref | |
| CPG: recommend for all | 8 | 1,517 | 70.3 | 1.3 (0.9‐1.9) | 0.11 |
| CPG: recommend if high‐risk | 8 | 2,255 | 39.9 | 0.5 (0.3‐0.8) | 0.002 |
| Disposition | |||||
| Hospitalization | |||||
| No CPG | 17 | 2,460 | 47.0 | Ref | |
| CPG: recommend if high‐risk | 16 | 3,772 | 42.0 | 0.7 (0.5‐1.1) | 0.10 |
| Ceftriaxone if discharged | |||||
| No CPG | 17 | 1,304 | 11.7 | Ref | |
| CPG: recommend against | 4 | 313 | 10.9 | 0.3 (0.1‐0.9) | 0.03 |
| CPG: recommend consider | 9 | 1,567 | 14.4 | 1.5 (0.9‐2.4) | 0.09 |
| CPG: recommend for all | 3 | 306 | 64.1 | 4.6 (2.39.3) | < 0.001 |
Three‐day revisits for SBI were similarly low at hospitals with and without CPGs among infants 28 days (1.5% vs 0.8%, P=0.44) and 29 to 56 days of age (1.4% vs 1.1%, P=0.44) and did not differ after exclusion of hospitals with a CPG implemented in 2013.
CPGs and Costs
Among infants 28 days of age, costs per visit did not differ for admitted and discharged patients based on CPG presence. The presence of an ED febrile infant CPG was associated with higher costs for both admitted and discharged infants 29 to 56 days of age (Table 4). The cost analysis did not significantly differ after exclusion of hospitals with CPGs implemented in 2013.
| 28 Days, Cost, Median (IQR) | 29 to 56 Days, Cost, Median (IQR) | |||||
|---|---|---|---|---|---|---|
| No CPG | CPG | P Value | No CPG | CPG | P Value | |
| ||||||
| Admitted | $4,979 ($3,408$6,607) [n=751] | $4,715 ($3,472$6,526) [n=1,753] | 0.79 | $3,756 ($2,725$5,041) [n=1,156] | $3,923 ($3,077$5,243) [n=1,586] | <0.001 |
| Discharged | $298 ($166$510) [n=245] | $231 ($160$464) [n=396] | 0.10 | $681($398$982) [n=1,304)] | $764 ($412$1,100) [n=2,186] | <0.001 |
DISCUSSION
We described the content and association of CPGs with management of the febrile infant 56 days of age across a large sample of children's hospitals. Nearly two‐thirds of included pediatric EDs have a CPG for the management of young febrile infants. Management of febrile infants 28 days was uniform, with a majority hospitalized after urine, blood, and CSF testing regardless of the presence of a CPG. In contrast, CPGs for infants 29 to 56 days of age varied in their recommendations for CSF testing as well as ceftriaxone use for infants discharged from the ED. Consequently, we observed considerable hospital variability in CSF testing and ceftriaxone use for discharged infants, which correlates with variation in the presence and content of CPGs. Institutional CPGs may be a source of the across‐hospital variation in care of febrile young infants observed in prior study.[9]
Febrile infants 28 days of age are at particularly high risk for SBI, with a prevalence of nearly 20% or higher.[2, 3, 29] The high prevalence of SBI, combined with the inherent difficulty in distinguishing neonates with and without SBI,[2, 30] has resulted in uniform CPG recommendations to perform the full‐sepsis workup in this young age group. Similar to prior studies,[8, 9] we observed that most febrile infants 28 days undergo the full sepsis evaluation, including CSF testing, and are hospitalized regardless of the presence of a CPG.
However, given the conflicting recommendations for febrile infants 29 to 56 days of age,[4, 5, 6] the optimal management strategy is less certain.[7] The Rochester, Philadelphia, and Boston criteria, 3 published models to identify infants at low risk for SBI, primarily differ in their recommendations for CSF testing and ceftriaxone use in this age group.[4, 5, 6] Half of the CPGs recommended CSF testing for all febrile infants, and half recommended CSF testing only if the infant was high risk. Institutional guidelines that recommended selective CSF testing for febrile infants aged 29 to 56 days were associated with lower rates of CSF testing. Furthermore, ceftriaxone use varied based on CPG recommendations for low‐risk infants discharged from the ED. Therefore, the influence of febrile infant CPGs mainly relates to the limiting of CSF testing and targeted ceftriaxone use in low‐risk infants. As the rate of return visits for SBI is low across hospitals, future study should assess outcomes at hospitals with CPGs recommending selective CSF testing. Of note, infants 29 to 56 days of age were less likely to be hospitalized when cared for at a hospital with an established CPG prior to 2013 without increase in 3‐day revisits for SBI. This finding may indicate that longer duration of CPG implementation is associated with lower rates of hospitalization for low‐risk infants; this finding merits further study.
The presence of a CPG was not associated with lower costs for febrile infants in either age group. Although individual healthcare systems have achieved lower costs with CPG implementation,[12] the mere presence of a CPG is not associated with lower costs when assessed across institutions. Higher costs for admitted and discharged infants 29 to 56 days of age in the presence of a CPG likely reflects the higher rate of CSF testing at hospitals whose CPGs recommend testing for all febrile infants, as well as inpatient management strategies for hospitalized infants not captured in our study. Future investigation should include an assessment of the cost‐effectiveness of the various testing and treatment strategies employed for the febrile young infant.
Our study has several limitations. First, the validity of ICD‐9 diagnosis codes for identifying young infants with fever is not well established, and thus our study is subject to misclassification bias. To minimize missed patients, we included infants with either an ICD‐9 admission or discharge diagnosis of fever; however, utilization of diagnosis codes for patient identification may have resulted in undercapture of infants with a measured temperature of 38.0C. It is also possible that some patients who did not undergo testing were misclassified as having a fever or had temperatures below standard thresholds to prompt diagnostic testing. This is a potential reason that testing was not performed in 100% of infants, even at hospitals with CPGs that recommended testing for all patients. Additionally, some febrile infants diagnosed with SBI may not have an associated ICD‐9 diagnosis code for fever. Although the overall SBI rate observed in our study was similar to prior studies,[4, 31] the rate in neonates 28 days of age was lower than reported in recent investigations,[2, 3] which may indicate inclusion of a higher proportion of low‐risk febrile infants. With the exception of bronchiolitis, we also did not assess diagnostic testing in the presence of other identified sources of infection such as herpes simplex virus.
Second, we were unable to assess the presence or absence of a CPG at the 4 excluded EDs that did not respond to the survey or the institutions excluded for data‐quality issues. However, included and excluded hospitals did not differ in region or annual ED volume (data not shown).
Third, although we classified hospitals based upon the presence and content of CPGs, we were unable to fully evaluate adherence to the CPG at each site.
Last, though PHIS hospitals represent 85% of freestanding children's hospitals, many febrile infants are hospitalized at non‐PHIS institutions; our results may not be generalizable to care provided at nonchildren's hospitals.
CONCLUSIONS
Management of febrile neonates 28 days of age does not vary based on CPG presence. However, CPGs for the febrile infant aged 29 to 56 days vary in recommendations for CSF testing as well as ceftriaxone use for low‐risk patients, which significantly contributes to practice variation and healthcare costs across institutions.
Acknowledgements
The Febrile Young Infant Research Collaborative includes the following additional investigators who are acknowledged for their work on this study: Kao‐Ping Chua, MD, Harvard PhD Program in Health Policy, Harvard University, Cambridge, Massachusetts, and Division of Emergency Medicine, Department of Pediatrics, Boston Children's Hospital, Boston, Massachusetts; Elana A. Feldman, BA, University of Washington School of Medicine, Seattle, Washington; and Katie L. Hayes, BS, Division of Emergency Medicine, Department of Pediatrics, The Children's Hospital of Philadelphia, Philadelphia, Pennsylvania.
Disclosures
This project was funded in part by The Gerber Foundation Novice Researcher Award (Ref #18273835). Dr. Fran Balamuth received career development support from the National Institutes of Health (NHLBI K12‐HL109009). Funders were not involved in design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript. The authors have no financial relationships relevant to this article to disclose. No payment was received for the production of this article. The authors have no conflicts of interest relevant to this article to disclose.
Febrile young infants are at high risk for serious bacterial infection (SBI) with reported rates of 8.5% to 12%, even higher in neonates 28 days of age.[1, 2, 3] As a result, febrile infants often undergo extensive diagnostic evaluation consisting of a combination of urine, blood, and cerebrospinal fluid (CSF) testing.[4, 5, 6] Several clinical prediction algorithms use this diagnostic testing to identify febrile infants at low risk for SBI, but they differ with respect to age range, recommended testing, antibiotic administration, and threshold for hospitalization.[4, 5, 6] Additionally, the optimal management strategy for this population has not been defined.[7] Consequently, laboratory testing, antibiotic use, and hospitalization for febrile young infants vary widely among hospitals.[8, 9, 10]
Clinical practice guidelines (CPGs) are designed to implement evidence‐based care and reduce practice variability, with the goal of improving quality of care and optimizing costs.[11] Implementation of a CPG for management of febrile young infants in the Intermountain Healthcare System was associated with greater adherence to evidence‐based care and lower costs.[12] However, when strong evidence is lacking, different interpretations of febrile infant risk classification incorporated into local CPGs may be a major driver of the across‐hospital practice variation observed in prior studies.[8, 9] Understanding sources of variability as well as determining the association of CPGs with clinicians' practice patterns can help identify quality improvement opportunities, either through national benchmarking or local efforts.
Our primary objectives were to compare (1) recommendations of pediatric emergency departmentbased institutional CPGs for febrile young infants and (2) rates of urine, blood, CSF testing, hospitalization, and ceftriaxone use at emergency department (ED) discharge based upon CPG presence and the specific CPG recommendations. Our secondary objectives were to describe the association of CPGs with healthcare costs and return visits for SBI.
METHODS
Study Design
We used the Pediatric Health Information System (PHIS) to identify febrile infants 56 days of age who presented to the ED between January 1, 2013 and December 31, 2013. We also surveyed ED providers at participating PHIS hospitals. Informed consent was obtained from survey respondents. The institutional review board at Boston Children's Hospital approved the study protocol.
Clinical Practice Guideline Survey
We sent an electronic survey to medical directors or division directors at 37 pediatric EDs to determine whether their ED utilized a CPG for the management of the febrile young infant in 2013. If no response was received after the second attempt, we queried ED fellowship directors or other ED attending physicians at nonresponding hospitals. Survey items included the presence of a febrile young infant CPG, and if present, the year of implementation, ages targeted, and CPG content. As applicable, respondents were asked to share their CPG and/or provide the specific CPG recommendations.
We collected and managed survey data using the Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Boston Children's Hospital. REDCap is a secure, Web‐based application designed to support data capture for research studies.[13]
Data Source
The PHIS database contains administrative data from 44 US children's hospitals. These hospitals, affiliated with the Children's Hospital Association, represent 85% of freestanding US children's hospitals.[14] Encrypted patient identifiers permit tracking of patients across encounters.[15] Data quality and integrity are assured jointly by the Children's Hospital Association and participating hospitals.[16] For this study, 7 hospitals were excluded due to incomplete ED data or known data‐quality issues.[17]
Patients
We identified study infants using the following International Classification of Diseases, 9th Revision (ICD‐9) admission or discharge diagnosis codes for fever as defined previously[8, 9]: 780.6, 778.4, 780.60, or 780.61. We excluded infants with a complex chronic condition[18] and those transferred from another institution, as these infants may warrant a nonstandard evaluation and/or may have incomplete data. For infants with >1 ED visit for fever during the study period, repeat visits within 3 days of an index visit were considered a revisit for the same episode of illness; visits >3 days following an index visit were considered as a new index visit.
Study Definitions
From the PHIS database, we abstracted demographic characteristics (gender, race/ethnicity), insurance status, and region where the hospital was located (using US Census categories[19]). Billing codes were used to assess whether urine, blood, and CSF testing (as defined previously[9]) were performed during the ED evaluation. To account for ED visits that spanned the midnight hour, for hospitalized patients we considered any testing or treatment occurring on the initial or second hospital day to be performed in the ED; billing code data in PHIS are based upon calendar day and do not distinguish testing performed in the ED versus inpatient setting.[8, 9] Patients billed for observation care were classified as being hospitalized.[20, 21]
We identified the presence of an SBI using ICD‐9 diagnosis codes for the following infections as described previously[9]: urinary tract infection or pyelonephritis,[22] bacteremia or sepsis, bacterial meningitis,[16] pneumonia,[23] or bacterial enteritis. To assess return visits for SBI that required inpatient management, we defined an ED revisit for an SBI as a return visit within 3 days of ED discharge[24, 25] that resulted in hospitalization with an associated ICD‐9 discharge diagnosis code for an SBI.
Hospitals charges in PHIS database were adjusted for hospital location by using the Centers for Medicare and Medicaid Services price/wage index. Costs were estimated by applying hospital‐level cost‐to‐charge ratios to charge data.[26]
Measured Exposures
The primary exposure was the presence of an ED‐based CPG for management of the febrile young infant aged 28 days and 29 to 56 days; 56 days was used as the upper age limit as all of the CPGs included infants up to this age or beyond. Six institutions utilized CPGs with different thresholds to define the age categories (eg, dichotomized at 27 or 30 days); these CPGs were classified into the aforementioned age groups to permit comparisons across standardized age groups. We classified institutions based on the presence of a CPG. To assess differences in the application of low‐risk criteria, the CPGs were further classified a priori based upon specific recommendations around laboratory testing and hospitalization, as well as ceftriaxone use for infants aged 29 to 56 days discharged from the ED. CPGs were categorized based upon whether testing, hospitalization, and ceftriaxone use were: (1) recommended for all patients, (2) recommended only if patients were classified as high risk (absence of low‐risk criteria), (3) recommended against, or (4) recommended to consider at clinician discretion.
Outcome Measures
Measured outcomes were performance of urine, blood, CSF testing, and hospitalization rate, as well as rate of ceftriaxone use for discharged infants aged 29 to 56 days, 3‐day revisits for SBI, and costs per visit, which included hospitalization costs for admitted patients.
Data Analysis
We described continuous variables using median and interquartile range or range values and categorical variables using frequencies. We compared medians using Wilcoxon rank sum and categorical variables using a [2] test. We compared rates of testing, hospitalization, ceftriaxone use, and 3‐day revisits for SBI based on the presence of a CPG, and when present, the specific CPG recommendations. Costs per visit were compared between institutions with and without CPGs and assessed separately for admitted and discharged patients. To adjust for potential confounders and clustering of patients within hospitals, we used generalized estimating equations with logistic regression to generate adjusted odd ratios (aORs) and 95% confidence intervals (CIs). Models were adjusted for geographic region, payer, race, and gender. Statistical analyses were performed by using SAS version 9.3 (SAS Institute, Cary, NC). We determined statistical significance as a 2‐tailed P value <0.05.
Febrile infants with bronchiolitis or a history of prematurity may be managed differently from full‐term febrile young infants without bronchiolitis.[6, 27] Therefore, we performed a subgroup analysis after exclusion of infants with an ICD‐9 discharge diagnosis code for bronchiolitis (466.11 and 466.19)[28] or prematurity (765).
Because our study included ED encounters in 2013, we repeated our analyses after exclusion of hospitals with CPGs implemented during the 2013 calendar year.
RESULTS
CPG by Institution
Thirty‐three (89.2%) of the 37 EDs surveyed completed the questionnaire. Overall, 21 (63.6%) of the 33 EDs had a CPG; 15 (45.5%) had a CPG for all infants 56 days of age, 5 (15.2%) had a CPG for infants 28 days only, and 1 (3.0%) had a CPG for infants 29 to 56 days but not 28 days of age (Figure 1). Seventeen EDs had an established CPG prior to 2013, and 4 hospitals implemented a CPG during the 2013 calendar year, 2 with CPGs for neonates 28 days and 2 with CPGs for both 28 days and 29 to 56 days of age. Hospitals with CPGs were more likely to be located in the Northeast and West regions of the United States and provide care to a higher proportion of non‐Hispanic white patients, as well as those with commercial insurance (Table 1).
| Characteristic | 28 Days | 2956 Days | ||||
|---|---|---|---|---|---|---|
| No CPG, n=996, N (%) | CPG, n=2,149, N (%) | P Value | No CPG, n=2,460, N (%) | CPG, n=3,772, N (%) | P Value | |
| ||||||
| Race | ||||||
| Non‐Hispanic white | 325 (32.6) | 996 (46.3) | 867 (35.2) | 1,728 (45.8) | ||
| Non‐Hispanic black | 248 (24.9) | 381 (17.7) | 593 (24.1) | 670 (17.8) | ||
| Hispanic | 243 (24.4) | 531 (24.7) | 655 (26.6) | 986 (26.1) | ||
| Asian | 28 (2.8) | 78 (3.6) | 40 (1.6) | 122 (3.2) | ||
| Other Race | 152 (15.3) | 163 (7.6) | <0.001 | 305 (12.4) | 266 (7.1) | <0.001 |
| Gender | ||||||
| Female | 435 (43.7) | 926 (43.1) | 0.76 | 1,067 (43.4) | 1,714 (45.4) | 0.22 |
| Payer | ||||||
| Commercial | 243 (24.4) | 738 (34.3) | 554 (22.5) | 1,202 (31.9) | ||
| Government | 664 (66.7) | 1,269 (59.1) | 1,798 (73.1) | 2,342 (62.1) | ||
| Other payer | 89 (8.9) | 142 (6.6) | <0.001 | 108 (4.4) | 228 (6.0) | <0.001 |
| Region | ||||||
| Northeast | 39 (3.9) | 245 (11.4) | 77 (3.1) | 572 (15.2) | ||
| South | 648 (65.1) | 915 (42.6) | 1,662 (67.6) | 1,462 (38.8) | ||
| Midwest | 271 (27.2) | 462 (21.5) | 506 (20.6) | 851 (22.6) | ||
| West | 38 (3.8) | 527 (24.5) | <0.001 | 215 (8.7) | 887 (23.5) | <0.001 |
| Serious bacterial infection | ||||||
| Overall* | 131 (13.2) | 242 (11.3) | 0.14 | 191 (7.8) | 237 (6.3) | 0.03 |
| UTI/pyelonephritis | 73 (7.3) | 153 (7.1) | 103 (4.2) | 154 (4.1) | ||
| Bacteremia/sepsis | 56 (5.6) | 91 (4.2) | 78 (3.2) | 61 (1.6) | ||
| Bacterial meningitis | 15 (1.5) | 15 (0.7) | 4 (0.2) | 14 (0.4) | ||
| Age, d, median (IQR) | 18 (11, 24) | 18 (11, 23) | 0.67 | 46 (37, 53) | 45 (37, 53) | 0.11 |
All 20 CPGs for the febrile young infant 28 days of age recommended urine, blood, CSF testing, and hospitalization for all infants (Figure 1). Of the 16 hospitals with CPGs for febrile infants aged 29 to 56 days, all recommended urine and blood testing for all patients, except for 1 CPG, which recommended consideration of blood testing but not to obtain routinely. Hospitals varied in recommendations for CSF testing among infants aged 29 to 56 days: 8 (50%) recommended CSF testing in all patients and 8 (50%) recommended CSF testing only if the patient was high risk per defined criteria (based on history, physical examination, urine, and blood testing). In all 16 CPGs, hospitalization was recommended only for high‐risk infants. For low‐risk infants aged 2956 days being discharged from the ED, 3 hospitals recommended ceftriaxone for all, 9 recommended consideration of ceftriaxone, and 4 recommended against antibiotics (Figure 1).
Study Patients
During the study period, there were 10,415 infants 56 days old with a diagnosis of fever at the 33 participating hospitals. After exclusion of 635 (6.1%) infants with a complex chronic condition and 445 (4.3%) transferred from another institution (including 42 with a complex chronic condition), 9377 infants remained in our study cohort. Approximately one‐third of the cohort was 28 days of age and two‐thirds aged 29 to 56 days. The overall SBI rate was 8.5% but varied by age (11.9% in infants 28 days and 6.9% in infants 29 to 56 days of age) (Table 1).
CPGs and Use of Diagnostic Testing, Hospitalization Rates, Ceftriaxone Use, and Revisits for SBI
For infants 28 days of age, the presence of a CPG was not associated with urine, blood, CSF testing, or hospitalization after multivariable adjustment (Table 2). Among infants aged 29 to 56 days, urine testing did not differ based on the presence of a CPG, whereas blood testing was performed less often at the 1 hospital whose CPG recommended to consider, but not routinely obtain, testing (aOR: 0.4, 95% CI: 0.3‐0.7, P=0.001). Compared to hospitals without a CPG, CSF testing was performed less often at hospitals with CPG recommendations to only obtain CSF if high risk (aOR: 0.5, 95% CI: 0.3‐0.8, P=0.002). However, the odds of hospitalization did not differ at institutions with and without a febrile infant CPG (aOR: 0.7, 95% CI: 0.5‐1.1, P=0.10). For infants aged 29 to 56 days discharged from the ED, ceftriaxone was administered more often at hospitals with CPGs that recommended ceftriaxone for all discharged patients (aOR: 4.6, 95% CI: 2.39.3, P<0.001) and less often at hospitals whose CPGs recommended against antibiotics (aOR: 0.3, 95% CI: 0.1‐0.9, P=0.03) (Table 3). Our findings were similar in the subgroup of infants without bronchiolitis or prematurity (see Supporting Tables 1 and 2 in the online version of this article). After exclusion of hospitals with a CPG implemented during the 2013 calendar year (4 hospitals excluded in the 28 days age group and 2 hospitals excluded in the 29 to 56 days age group), infants aged 29 to 56 days cared for at a hospital with a CPG experienced a lower odds of hospitalization (aOR: 0.7, 95% CI: 0.4‐0.98, P=0.04). Otherwise, our findings in both age groups did not materially differ from the main analyses.
| Testing/Hospitalization | No. of Hospitals | No. of Patients | % Received* | aOR (95% CI) | P Value |
|---|---|---|---|---|---|
| |||||
| Laboratory testing | |||||
| Urine testing | |||||
| No CPG | 13 | 996 | 75.6 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 80.7 | 1.2 (0.9‐1.7) | 0.22 |
| Blood testing | |||||
| No CPG | 13 | 996 | 76.9 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 81.8 | 1.2 (0.9‐1.7) | 0.25 |
| CSF testing‖ | |||||
| No CPG | 13 | 996 | 71.0 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 77.5 | 1.3 (1.01.7) | 0.08 |
| Disposition | |||||
| Hospitalization | |||||
| No CPG | 13 | 996 | 75.4 | Ref | |
| CPG: recommend for all | 20 | 2,149 | 81.6 | 1.2 (0.9‐1.8) | 0.26 |
| Testing/Hospitalization | No. of Hospitals | No. of Patients | % Received* | aOR (95% CI) | P Value |
|---|---|---|---|---|---|
| |||||
| Laboratory resting | |||||
| Urine testing | |||||
| No CPG | 17 | 2,460 | 81.1 | Ref | |
| CPG: recommend for all | 16 | 3,772 | 82.1 | 0.9 (0.7‐1.4) | 0.76 |
| Blood testing | |||||
| No CPG | 17 | 2,460 | 79.4 | Ref | |
| CPG: recommend for all | 15 | 3,628 | 82.6 | 1.1 (0.7‐1.6) | 0.70 |
| CPG: recommend consider | 1 | 144 | 62.5 | 0.4 (0.3‐0.7) | 0.001 |
| CSF testing‖ | |||||
| No CPG | 17 | 2,460 | 46.3 | Ref | |
| CPG: recommend for all | 8 | 1,517 | 70.3 | 1.3 (0.9‐1.9) | 0.11 |
| CPG: recommend if high‐risk | 8 | 2,255 | 39.9 | 0.5 (0.3‐0.8) | 0.002 |
| Disposition | |||||
| Hospitalization | |||||
| No CPG | 17 | 2,460 | 47.0 | Ref | |
| CPG: recommend if high‐risk | 16 | 3,772 | 42.0 | 0.7 (0.5‐1.1) | 0.10 |
| Ceftriaxone if discharged | |||||
| No CPG | 17 | 1,304 | 11.7 | Ref | |
| CPG: recommend against | 4 | 313 | 10.9 | 0.3 (0.1‐0.9) | 0.03 |
| CPG: recommend consider | 9 | 1,567 | 14.4 | 1.5 (0.9‐2.4) | 0.09 |
| CPG: recommend for all | 3 | 306 | 64.1 | 4.6 (2.39.3) | < 0.001 |
Three‐day revisits for SBI were similarly low at hospitals with and without CPGs among infants 28 days (1.5% vs 0.8%, P=0.44) and 29 to 56 days of age (1.4% vs 1.1%, P=0.44) and did not differ after exclusion of hospitals with a CPG implemented in 2013.
CPGs and Costs
Among infants 28 days of age, costs per visit did not differ for admitted and discharged patients based on CPG presence. The presence of an ED febrile infant CPG was associated with higher costs for both admitted and discharged infants 29 to 56 days of age (Table 4). The cost analysis did not significantly differ after exclusion of hospitals with CPGs implemented in 2013.
| 28 Days, Cost, Median (IQR) | 29 to 56 Days, Cost, Median (IQR) | |||||
|---|---|---|---|---|---|---|
| No CPG | CPG | P Value | No CPG | CPG | P Value | |
| ||||||
| Admitted | $4,979 ($3,408$6,607) [n=751] | $4,715 ($3,472$6,526) [n=1,753] | 0.79 | $3,756 ($2,725$5,041) [n=1,156] | $3,923 ($3,077$5,243) [n=1,586] | <0.001 |
| Discharged | $298 ($166$510) [n=245] | $231 ($160$464) [n=396] | 0.10 | $681($398$982) [n=1,304)] | $764 ($412$1,100) [n=2,186] | <0.001 |
DISCUSSION
We described the content and association of CPGs with management of the febrile infant 56 days of age across a large sample of children's hospitals. Nearly two‐thirds of included pediatric EDs have a CPG for the management of young febrile infants. Management of febrile infants 28 days was uniform, with a majority hospitalized after urine, blood, and CSF testing regardless of the presence of a CPG. In contrast, CPGs for infants 29 to 56 days of age varied in their recommendations for CSF testing as well as ceftriaxone use for infants discharged from the ED. Consequently, we observed considerable hospital variability in CSF testing and ceftriaxone use for discharged infants, which correlates with variation in the presence and content of CPGs. Institutional CPGs may be a source of the across‐hospital variation in care of febrile young infants observed in prior study.[9]
Febrile infants 28 days of age are at particularly high risk for SBI, with a prevalence of nearly 20% or higher.[2, 3, 29] The high prevalence of SBI, combined with the inherent difficulty in distinguishing neonates with and without SBI,[2, 30] has resulted in uniform CPG recommendations to perform the full‐sepsis workup in this young age group. Similar to prior studies,[8, 9] we observed that most febrile infants 28 days undergo the full sepsis evaluation, including CSF testing, and are hospitalized regardless of the presence of a CPG.
However, given the conflicting recommendations for febrile infants 29 to 56 days of age,[4, 5, 6] the optimal management strategy is less certain.[7] The Rochester, Philadelphia, and Boston criteria, 3 published models to identify infants at low risk for SBI, primarily differ in their recommendations for CSF testing and ceftriaxone use in this age group.[4, 5, 6] Half of the CPGs recommended CSF testing for all febrile infants, and half recommended CSF testing only if the infant was high risk. Institutional guidelines that recommended selective CSF testing for febrile infants aged 29 to 56 days were associated with lower rates of CSF testing. Furthermore, ceftriaxone use varied based on CPG recommendations for low‐risk infants discharged from the ED. Therefore, the influence of febrile infant CPGs mainly relates to the limiting of CSF testing and targeted ceftriaxone use in low‐risk infants. As the rate of return visits for SBI is low across hospitals, future study should assess outcomes at hospitals with CPGs recommending selective CSF testing. Of note, infants 29 to 56 days of age were less likely to be hospitalized when cared for at a hospital with an established CPG prior to 2013 without increase in 3‐day revisits for SBI. This finding may indicate that longer duration of CPG implementation is associated with lower rates of hospitalization for low‐risk infants; this finding merits further study.
The presence of a CPG was not associated with lower costs for febrile infants in either age group. Although individual healthcare systems have achieved lower costs with CPG implementation,[12] the mere presence of a CPG is not associated with lower costs when assessed across institutions. Higher costs for admitted and discharged infants 29 to 56 days of age in the presence of a CPG likely reflects the higher rate of CSF testing at hospitals whose CPGs recommend testing for all febrile infants, as well as inpatient management strategies for hospitalized infants not captured in our study. Future investigation should include an assessment of the cost‐effectiveness of the various testing and treatment strategies employed for the febrile young infant.
Our study has several limitations. First, the validity of ICD‐9 diagnosis codes for identifying young infants with fever is not well established, and thus our study is subject to misclassification bias. To minimize missed patients, we included infants with either an ICD‐9 admission or discharge diagnosis of fever; however, utilization of diagnosis codes for patient identification may have resulted in undercapture of infants with a measured temperature of 38.0C. It is also possible that some patients who did not undergo testing were misclassified as having a fever or had temperatures below standard thresholds to prompt diagnostic testing. This is a potential reason that testing was not performed in 100% of infants, even at hospitals with CPGs that recommended testing for all patients. Additionally, some febrile infants diagnosed with SBI may not have an associated ICD‐9 diagnosis code for fever. Although the overall SBI rate observed in our study was similar to prior studies,[4, 31] the rate in neonates 28 days of age was lower than reported in recent investigations,[2, 3] which may indicate inclusion of a higher proportion of low‐risk febrile infants. With the exception of bronchiolitis, we also did not assess diagnostic testing in the presence of other identified sources of infection such as herpes simplex virus.
Second, we were unable to assess the presence or absence of a CPG at the 4 excluded EDs that did not respond to the survey or the institutions excluded for data‐quality issues. However, included and excluded hospitals did not differ in region or annual ED volume (data not shown).
Third, although we classified hospitals based upon the presence and content of CPGs, we were unable to fully evaluate adherence to the CPG at each site.
Last, though PHIS hospitals represent 85% of freestanding children's hospitals, many febrile infants are hospitalized at non‐PHIS institutions; our results may not be generalizable to care provided at nonchildren's hospitals.
CONCLUSIONS
Management of febrile neonates 28 days of age does not vary based on CPG presence. However, CPGs for the febrile infant aged 29 to 56 days vary in recommendations for CSF testing as well as ceftriaxone use for low‐risk patients, which significantly contributes to practice variation and healthcare costs across institutions.
Acknowledgements
The Febrile Young Infant Research Collaborative includes the following additional investigators who are acknowledged for their work on this study: Kao‐Ping Chua, MD, Harvard PhD Program in Health Policy, Harvard University, Cambridge, Massachusetts, and Division of Emergency Medicine, Department of Pediatrics, Boston Children's Hospital, Boston, Massachusetts; Elana A. Feldman, BA, University of Washington School of Medicine, Seattle, Washington; and Katie L. Hayes, BS, Division of Emergency Medicine, Department of Pediatrics, The Children's Hospital of Philadelphia, Philadelphia, Pennsylvania.
Disclosures
This project was funded in part by The Gerber Foundation Novice Researcher Award (Ref #18273835). Dr. Fran Balamuth received career development support from the National Institutes of Health (NHLBI K12‐HL109009). Funders were not involved in design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript. The authors have no financial relationships relevant to this article to disclose. No payment was received for the production of this article. The authors have no conflicts of interest relevant to this article to disclose.
- , , . Performance of low‐risk criteria in the evaluation of young infants with fever: review of the literature. Pediatrics. 2010;125:228–233.
- , , , , , . A week‐by‐week analysis of the low‐risk criteria for serious bacterial infection in febrile neonates. Arch Dis Child. 2009;94:287–292.
- , , , et al. Is 15 days an appropriate cut‐off age for considering serious bacterial infection in the management of febrile infants? Pediatr Infect Dis J. 2012;31:455–458.
- , , . Outpatient management without antibiotics of fever in selected infants. N Engl J Med. 1993;329:1437–1441.
- , , . Identifying febrile infants at risk for a serious bacterial infection. J Pediatr. 1993;123:489–490.
- , , , et al. Febrile infants at low risk for serious bacterial infection—an appraisal of the Rochester criteria and implications for management. Febrile Infant Collaborative Study Group. Pediatrics. 1994;94:390–396.
- American College of Emergency Physicians Clinical Policies Committee; American College of Emergency Physicians Clinical Policies Subcommittee on Pediatric Fever. Clinical policy for children younger than three years presenting to the emergency department with fever. Ann Emerg Med. 2003;42:530–545.
- , , , et al. Management of febrile neonates in US pediatric emergency departments. Pediatrics. 2014;133:187–195.
- , , , et al. Variation in care of the febrile young infant <90 days in US pediatric emergency departments. Pediatrics. 2014;134:667–677.
- , , , , . Fever survey highlights significant variations in how infants aged ≤60 days are evaluated and underline the need for guidelines. Acta Paediatr. 2014;103:379–385.
- . Evidence‐based guidelines and critical pathways for quality improvement. Pediatrics. 1999;103:225–232.
- , , , et al. Costs and infant outcomes after implementation of a care process model for febrile infants. Pediatrics. 2012;130:e16–e24.
- , , , , , . Research electronic data capture (REDCap)—a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381.
- , , , , , . Variation in occult injury screening for children with suspected abuse in selected US children's hospitals. Pediatrics. 2012;130:853–860.
- . Achieving data quality. How data from a pediatric health information system earns the trust of its users. J AHIMA. 2004;75:22–26.
- , , , . Corticosteroids and mortality in children with bacterial meningitis. JAMA. 2008;299:2048–2055.
- , , , et al. Variation in resource utilization across a national sample of pediatric emergency departments. J Pediatr. 2013;163:230–236.
- , , , , , . Deaths attributed to pediatric complex chronic conditions: national trends and implications for supportive care services. Pediatrics. 2001;107:E99.
- US Census Bureau. Geographic terms and concepts—census divisions and census regions. Available at: https://www.census.gov/geo/reference/gtc/gtc_census_divreg.html. Accessed September 10, 2014.
- , , , et al. Pediatric observation status: are we overlooking a growing population in children's hospitals? J Hosp Med. 2012;7:530–536.
- , , , et al. Differences in designations of observation care in US freestanding children's hospitals: are they virtual or real? J Hosp Med. 2012;7:287–293.
- , , , et al. Accuracy of administrative billing codes to detect urinary tract infection hospitalizations. Pediatrics. 2011;128:323–330.
- , , , et al. Identifying pediatric community‐acquired pneumonia hospitalizations: accuracy of administrative billing codes. JAMA Pediatr. 2013;167:851–858.
- , , , . Initial emergency department diagnosis and return visits: risk versus perception. Ann Emerg Med. 1998;32:569–573.
- , , , , . A national depiction of children with return visits to the emergency department within 72 hours, 2001–2007. Pediatr Emerg Care. 2012;28:606–610.
- Healthcare Cost and Utilization Project. Cost‐to‐charge ratio files. Available at: http://www.hcup‐us.ahrq.gov/db/state/costtocharge.jsp. Accessed September 11, 2014.
- , , , et al. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infections. Pediatrics. 2004;113:1728–1734.
- , , , et al. Establishing benchmarks for the hospitalized care of children with asthma, bronchiolitis, and pneumonia. Pediatrics. 2014;134:555–562.
- , , , , , . Well appearing young infants with fever without known source in the emergency department: are lumbar punctures always necessary? Eur J Emerg Med. 2010;17:167–169.
- , . Unpredictability of serious bacterial illness in febrile infants from birth to 1 month of age. Arch Pediatr Adolesc Med. 1999;153:508–511.
- , , , et al. Management and outcomes of care of fever in early infancy. JAMA. 2004;291:1203–1212.
- , , . Performance of low‐risk criteria in the evaluation of young infants with fever: review of the literature. Pediatrics. 2010;125:228–233.
- , , , , , . A week‐by‐week analysis of the low‐risk criteria for serious bacterial infection in febrile neonates. Arch Dis Child. 2009;94:287–292.
- , , , et al. Is 15 days an appropriate cut‐off age for considering serious bacterial infection in the management of febrile infants? Pediatr Infect Dis J. 2012;31:455–458.
- , , . Outpatient management without antibiotics of fever in selected infants. N Engl J Med. 1993;329:1437–1441.
- , , . Identifying febrile infants at risk for a serious bacterial infection. J Pediatr. 1993;123:489–490.
- , , , et al. Febrile infants at low risk for serious bacterial infection—an appraisal of the Rochester criteria and implications for management. Febrile Infant Collaborative Study Group. Pediatrics. 1994;94:390–396.
- American College of Emergency Physicians Clinical Policies Committee; American College of Emergency Physicians Clinical Policies Subcommittee on Pediatric Fever. Clinical policy for children younger than three years presenting to the emergency department with fever. Ann Emerg Med. 2003;42:530–545.
- , , , et al. Management of febrile neonates in US pediatric emergency departments. Pediatrics. 2014;133:187–195.
- , , , et al. Variation in care of the febrile young infant <90 days in US pediatric emergency departments. Pediatrics. 2014;134:667–677.
- , , , , . Fever survey highlights significant variations in how infants aged ≤60 days are evaluated and underline the need for guidelines. Acta Paediatr. 2014;103:379–385.
- . Evidence‐based guidelines and critical pathways for quality improvement. Pediatrics. 1999;103:225–232.
- , , , et al. Costs and infant outcomes after implementation of a care process model for febrile infants. Pediatrics. 2012;130:e16–e24.
- , , , , , . Research electronic data capture (REDCap)—a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381.
- , , , , , . Variation in occult injury screening for children with suspected abuse in selected US children's hospitals. Pediatrics. 2012;130:853–860.
- . Achieving data quality. How data from a pediatric health information system earns the trust of its users. J AHIMA. 2004;75:22–26.
- , , , . Corticosteroids and mortality in children with bacterial meningitis. JAMA. 2008;299:2048–2055.
- , , , et al. Variation in resource utilization across a national sample of pediatric emergency departments. J Pediatr. 2013;163:230–236.
- , , , , , . Deaths attributed to pediatric complex chronic conditions: national trends and implications for supportive care services. Pediatrics. 2001;107:E99.
- US Census Bureau. Geographic terms and concepts—census divisions and census regions. Available at: https://www.census.gov/geo/reference/gtc/gtc_census_divreg.html. Accessed September 10, 2014.
- , , , et al. Pediatric observation status: are we overlooking a growing population in children's hospitals? J Hosp Med. 2012;7:530–536.
- , , , et al. Differences in designations of observation care in US freestanding children's hospitals: are they virtual or real? J Hosp Med. 2012;7:287–293.
- , , , et al. Accuracy of administrative billing codes to detect urinary tract infection hospitalizations. Pediatrics. 2011;128:323–330.
- , , , et al. Identifying pediatric community‐acquired pneumonia hospitalizations: accuracy of administrative billing codes. JAMA Pediatr. 2013;167:851–858.
- , , , . Initial emergency department diagnosis and return visits: risk versus perception. Ann Emerg Med. 1998;32:569–573.
- , , , , . A national depiction of children with return visits to the emergency department within 72 hours, 2001–2007. Pediatr Emerg Care. 2012;28:606–610.
- Healthcare Cost and Utilization Project. Cost‐to‐charge ratio files. Available at: http://www.hcup‐us.ahrq.gov/db/state/costtocharge.jsp. Accessed September 11, 2014.
- , , , et al. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infections. Pediatrics. 2004;113:1728–1734.
- , , , et al. Establishing benchmarks for the hospitalized care of children with asthma, bronchiolitis, and pneumonia. Pediatrics. 2014;134:555–562.
- , , , , , . Well appearing young infants with fever without known source in the emergency department: are lumbar punctures always necessary? Eur J Emerg Med. 2010;17:167–169.
- , . Unpredictability of serious bacterial illness in febrile infants from birth to 1 month of age. Arch Pediatr Adolesc Med. 1999;153:508–511.
- , , , et al. Management and outcomes of care of fever in early infancy. JAMA. 2004;291:1203–1212.
© 2015 Society of Hospital Medicine
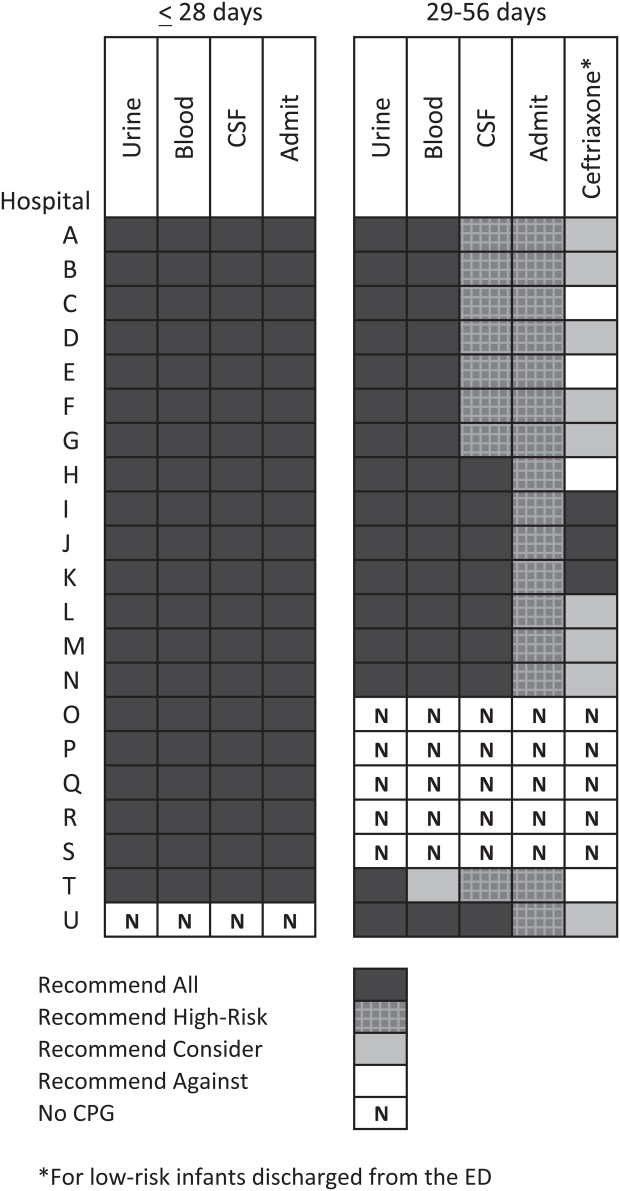
Pneumococcal Vaccination and CAP
Community‐acquired pneumonia (CAP) ranks fifth among all causes of death and is the leading infectious cause of death among persons 65 years or older (hereafter elderly) in the US.[1] Of the 1.1 million short‐stay hospital discharges for pneumonia in 2010, 55% were for elderly patients.[2] The most common cause of pneumonia in elderly patients leading to hospitalization is infection with Streptococcus pneumoniae.[1, 3, 4, 5] The 23‐valent pneumococcal polysaccharide vaccine is recommended (PPSV23) for all elderly persons and has been shown to reduce incidences of invasive pneumococcal bacteremia among immunocompetent elderly individuals.[5] However, its effect on more common manifestations of pneumococcal disease, such as pneumonia, remains controversial.[5, 6, 7, 8]
Several studies examined the association between prior PV and in‐hospital outcomes for CAP in adult patients.[9, 10, 11] Although the effect of pneumococcal vaccination (PV) on inpatient mortality was inconclusive, the studies found shortened length of stay (LOS),[9, 10] lower risk of respiratory failure and other complications,[9] faster resolution of pneumonia symptoms,[10] and fewer intensive care unit (ICU) admissions,[11] among those with prior PV. These findings suggest potential additional benefits of PV in hospitalized CAP patients.
This study examined prior PV on in‐hospital outcomes in elderly veterans hospitalized for CAP. Because PV‐vaccinated patients are also more likely to have received influenza (flu) vaccination (FV),[9, 10, 11] which could independently or additively improve CAP outcomes in hospitalized elderly patients,[12, 13, 14] we attempted to separate out the effect of FV by stratifying patients into 4 subgroups: PV alone, FV alone, both, or neither. The priori hypothesis was that PV improves in‐hospital outcomes in elderly veterans hospitalized for CAP.
METHODS
Study Cohort
This study is a retrospective cohort study of all elderly veterans admitted to any Veterans Affairs (VA) hospitals for CAP during the fiscal year 2003 (FY'03) (October 1, 2002 to September 30, 2003). Inpatient admissions for pneumonia were defined based on the principal diagnosis of nonviral pneumonia (International Classification of Diseases, 9th Revision [ICD‐9], codes 481.xx487.0x). The principal diagnosis was defined as the condition determined to be the reason for the admission.[15] To select only CAP cases, we included admissions where patients were admitted either directly or through a VA outpatient clinic. We excluded transfers from another hospital, skilled nursing facilities, intermediate care facilities, or another healthcare facility. All patients were 65 years or older on the first day of the first admission in FY'03 (index admission) and had at least 1 outpatient visit to a VA facility each year during the 5 years prior to the index admission.
Data Source
Data were drawn from Veterans Health Administration medical SAS datasets (SAS Institute Inc.,
Cary, NC). Demographic characteristics, inpatient and outpatient care utilization, and related medical diagnoses and procedure codes were extracted from national patient data extracts. Selected lab test results were drawn from the Decision Support System national extracts. This study was approved by institutional review boards at the University of Arkansas for Medical Sciences and the Central Arkansas Veterans Healthcare System.
Prior Vaccination Status
Prior PV status was determined within 5 years prior to the index admission using: ICD‐9 codes V06.6, V06.8, and V03.82, ICD‐9 procedure code 99.55, or Current Procedure Terminology (CPT) codes 90732 and 90669.[16] This 5‐year time frame was chosen for 2 reasons: (1) the Centers for Disease Control and Prevention (CDC) recommends a second dose for elderly persons if the first dose was before age 65 years and more than 5 years have passed[17]; (2) effectiveness of PV decreases over time in elderly persons, especially after 5 years since vaccination.[5, 18] Consistent with the CDC's vaccination recommendation,[18] patients with no record of prior PV were classified as not vaccinated. Prior FV status was determined in the year before the index admission using: ICD‐9 code V04.8, ICD‐9 procedure code 99.52, or CPT codes 9065590660.[16] Based on prior vaccinations, patients were classified into 4 groups: PV alone, FV alone, both, or neither.
Outcome Variables
The primary outcomes were LOS and inpatient mortality. LOS, measured in days, was the duration of a hospital stay from admission to discharge, censored at death or transfer, the occurrence of which was ascertained via the discharge type field. Inpatient mortality was defined as death from any cause that occurred before discharge or transfer. The secondary outcomes were respiratory complications and any bacteremia identified via the diagnosis field of discharge records (see Supporting Information, Appendix Table A.1, in the online version of this article for a list of ICD‐9 codes).
| PV Only, n=1,347 | FV Only, n=1,698 | Both, n=1,668 | Neither, n=2,010 | P Value* | |
|---|---|---|---|---|---|
| |||||
| Age, median (IQR) | 77 (7181) | 77 (7281) | 77 (7181) | 77 (7282) | 0.0418 |
| 6574 years | 539 (40.0%) | 619 (36.5%) | 670 (40.2%) | 733 (36.5%) | 0.0051 |
| 7584 years | 635 (47.1%) | 892 (52.5%) | 836 (50.1%) | 1058 (52.6%) | |
| 85 years | 173 (12.8%) | 187 (11.0%) | 162 (9.7%) | 219 (10.9%) | |
| Male | 1318 (97.8%) | 1657 (97.6%) | 1638 (98.2%) | 1964 (97.7%) | 0.6378 |
| Race | |||||
| White | 848 (63.0%) | 1149 (67.7%) | 1097 (65.8%) | 1272 (63.3%) | <0.0003 |
| Nonwhite | 229 (17.0%) | 214 (12.6%) | 271 (16.2%) | 289 (14.4%) | |
| Unknown | 270 (20.0%) | 335 (19.7%) | 300 (18.0%) | 449 (22.3%) | |
| Married | 726 (53.9%) | 951 (56.0%) | 930 (55.8%) | 1043 (51.9%) | 0.0419 |
| No. of non‐mental health VA outpatient visits last year, median (IQR) | 17 (1027) | 21 (1332) | 22 (1434) | 15 (926) | <0.0001 |
| CAP hospitalization last year | 87 (6.5%) | 106 (6.2%) | 100 (6.0%) | 106 (5.3%) | 0.4689 |
| Respiratory conditions in past 30 days | 149 (11.1%) | 183 (10.8%) | 173 (10.4%) | 263 (13.1%) | 0.0424 |
| Charlson Comorbidity Index, median (IQR) | 2 (14) | 3 (14) | 3 (14) | 2 (14) | <0.0001 |
| Inpatient outcomes | |||||
| LOS, d, median(IQR) | 6 (410) | 5 (39) | 5 (39) | 6 (49) | 0.0077 |
| Death | 130 (9.7%) | 119 (7.0%) | 113 (6.8%) | 166 (8.3%) | 0.0127 |
| Bacteremia | 31 (2.3%) | 56 (3.3%) | 40 (2.4%) | 68 (3.4%) | 0.1204 |
| Respiratory complications | 200 (14.8%) | 192 (11.3%) | 185 (11.1%) | 253 (12.6%) | 0.0073 |
Covariates
Covariates included patients' demographic characteristics (age, gender, race, marital status) and Charlson Comorbidity Index scores. Comorbidities were identified during the year prior to the index admission using ICD‐9 diagnoses codes based on Deyo et al. adaptation.[19] Additionally, we included prior admission for CAP within the year preceding index admission, the number of outpatient visits (excluding mental health visits; ICD‐9 codes 290.xx319.xx) within the year preceding index admission, and acute respiratory conditions experienced within 30 days preceding index admission. Development of bacteremia and respiratory complications may increase LOS, and risk of mortality and were adjusted in the regression models for these outcomes.
Race
Missing race in VA administrative data is a well‐documented problem.[20] When available, missing race was imputed using information reported during a patient's other inpatient stays available in our data as follows. We first imputed it using the most frequently reported race category. If unavailable, race was imputed by the most recently reported race category whenever available. This imputation algorithm reduced the proportion of patients with missing race information in our data to from 76% to 20%. Remaining patients with missing race information after imputation were analyzed as a separate category.
Pneumonia Severity Index Score
For patients with available lab values, we constructed an abbreviated pneumonia severity index (PSI) score adapted from Escobar et al.[21] The original PSI score developed by the Pneumonia Patient Outcomes Research Team (PORT) is a validated clinical prediction tool that permits risk stratification with regard to the likelihood of adverse outcomes in CAP patients.[22] Calculation of the PORT score requires information on patient's physical examination and radiographic findings at admission,[22] which was unavailable to us. Escobar et al. developed and validated an abbreviated form of the PORT score (PSI‐E) in CAP patients that does not incorporate physical examination and radiographic findings.[21] We calculated the PSI‐E developed by Escobar et al. with the exception that arterial pH and PaO2 test results were omitted because they were not available in the VA lab result files for the years we examined.
Data Analysis
Patients' baseline characteristics (see Covariates) were compared across the 4 vaccination groups using the Kruskal‐Wallis test for continuous variables and [2] test for categorical variables. Multiple regression analyses were used to assess the effect of prior PV and FV on inpatient outcomes during the index admission while adjusting for covariates. LOS was analyzed using a generalized linear model (GLM) with a negative binomial distribution and a logarithmic link function,[23] and incidence rate ratios (IRRs) were reported. IRRs were calculated by taking the exponential of the estimated coefficients from the GLM and are interpretable as the relative change in mean LOS associated with a 1‐unit change in a predictor variable. Risk of inpatient mortality, and development of respiratory complications or bacteremia, were analyzed using logistic regressions, and odds ratios (ORs) were reported. All regression models adjusted for covariates as described earlier. In addition, we conducted propensity score matching of PV‐vaccinated (n=2937) and unvaccinated (n=2937) patients using the GMATCH algorithm.[24] Propensity scores were estimated using a logistic regression to predict prior PV based on covariates listed earlier and prior FV status. GLM or logistic regression models were applied to the matched sample, with PV as the only predictor to generate IRRs or ORs, respectively. To account for the matched nature of the data, analyses were stratified by matched pairs.[25]
Sensitivity Analysis
Many sensitivity analyses were performed that: (1) included patients admitted from nursing homes or other inpatient facilities (n=7296); (2) excluded 0‐night admissions (n=6678); (3) varied the minimum number of VA outpatient visits to 2, 3, 4, or 5 visits each year in the previous 5 years; and (4) adjusted for the abbreviated PSI score only in patients with available information (n=3689).
Flu Season
Defining prior FV status during the previous year may have included individuals who received FV for the previous flu season (eg, a patient was admitted in December 2003, but his or her last FV was in January 2003). We conducted 2 sensitivity analyses: (1) recoded patients who were last vaccinated in the previous flu season as unvaccinated and (2) restricted to index admissions occurred during the flu season (n=5311). A flu season was defined as from September to May of the following year.
Time Since Last PV
To determine if the effectiveness of PV varies by the years elapsed since vaccination, among those with prior PV, we further classified prior PV as within 1 year (1 year), 2 years (>1 but 2 years), 3 years (>2 but 3 years), 4 years (>3 but 4 years), or 5 years (>4 but 5 years) preceding the index admission. Two‐thirds of patients received PV more than 2 years ago. We re‐estimated the regression models with indicators for the number of years since the last PV (as defined above, PV within 1 year preceding index admission as the reference group).
All analyses were conducted using SAS software (SAS Institute, Inc.). A 2‐sided P value of <0.05 was used to determine statistical significance.
RESULTS
In FY'03, 10,540 elderly VA patients had at least 1 inpatient admission for nonviral pneumonia. Among them, 3242 were excluded due to lack of VA outpatient visits in at least 1 of the 5 years prior to the index admission. Additionally, 574 patients were excluded because they were transferred from nursing homes or other inpatient facilities. The final sample consisted of 6723 elderly patients; among them, 1347(20%) had only PV, 1698(25%) had only FV, 1668 (25%) had both, and 2010 (30%) had neither prior to admission (see Supporting Information, Appendix 1, in the online version of this article) (see Supporting Information, Appendix Figure A.1, in the online version of this article).
Table 1 compares patients' baseline characteristics and inpatient outcomes across vaccination groups. Patients with prior PV and FV had the shortest LOS and were least likely to experience respiratory complications or die during the inpatient stay. They also tended to be younger, had more frequent VA nonmental health outpatient visits in the previous year, and more medical comorbidities than other groups. Although these differences were statistically significant, the actual differences were small across the groups.
Table 2 presents findings from the adjusted regression analyses. After adjusting for covariates, having prior PV alone, FV alone, or both did not significantly affect the risk of inpatient mortality, compared to patients without records of either vaccination. However, having both prior PV and FV was associated with 10% reduction in LOS (IRR: 0.90; 95% confidence interval [CI]: 0.86‐0.95; P<0.0001). PV alone were associated with an increased risk of respiratory complications (OR: 1.23; 95% CI: 1.01‐1.51; P=0.0429) and trended toward a reduced risk of bacteremia (OR: 0.67; 95% CI: 0.43‐1.03; P=0.0673). After matching on patient characteristics including prior FV status, prior PV significantly lowered the risk of developing bacteremia (OR: 0.66; 95% CI: 0.48‐0.90; P=0.0088) but was not statistically significantly associated with the other outcomes (Table 3).
| Length of Stay (Days) | Inpatient Death | |||||
|---|---|---|---|---|---|---|
| Bacteremia | Respiratory Complications | |||||
| ||||||
| Vaccination status | IRR | 95% CI | P Value | OR | 95% CI | P Value |
| PV in previous 5 Years | 1.02 | 0.97‐1.07 | 0.4561 | 1.15 | 0.89‐1.50 | 0.2901 |
| FV last year | 0.97 | 0.92‐1.02 | 0.1920 | 0.90 | 0.69‐1.17 | 0.4193 |
| Both | 0.90 | 0.86‐0.95 | <0.0001 | 0.88 | 0.67‐1.16 | 0.3646 |
| Neither | Ref | Ref | ||||
| Vaccination status | OR | 95% CI | P Value | OR | 95% CI | P Value |
| PV in previous 5 Years | 0.67 | 0.43‐1.03 | 0.0673 | 1.23 | 1.01‐1.51 | 0.0429 |
| FV last year | 0.99 | 0.69‐1.42 | 0.9536 | 0.90 | 0.74‐1.10 | 0.3085 |
| Both | 0.72 | 0.48‐1.07 | 0.1047 | 0.87 | 0.71‐1.07 | 0.1860 |
| Neither | Ref | Ref | ||||
| In‐Hospital Outcomes, Matched Sample (n=5 874) | PV vs No PV | ||
|---|---|---|---|
| IRR/OR | 95% CI | P Value | |
| |||
| Length of stay | 0.97 | 0.93‐1.01 | 0.1502 |
| Inpatient death | 1.13 | 0.94‐1.37 | 0.2027 |
| Bacteremia | 0.66 | 0.48‐0.90 | 0.0088 |
| Respiratory complications | 1.11 | 0.95‐1.30 | 0.2018 |
Findings from sensitivity analyses are included in the online appendices. Results were generally robust to various sensitivity analyses. However, in the analysis using the subset of patients with available lab information to define the PSI‐E score, having prior FV alone was also found to be associated with reduced LOS (IRR: 0.92; 95% CI: 0.86‐0.98; P<0.05). The relationship between PV and in‐patient outcomes did not vary by the time since vaccination, which is consistent with Jackson et al.[11]
DISCUSSION
Consistent with previous findings,[7, 8, 9, 10, 11] elderly VA patients hospitalized for CAP were found to have an association between prior PV and reduced risk of bacteremia. However, no associations of prior PV alone with other in‐hospital outcomes (LOS, inpatient mortality, or development of respiratory complications) were consistently found. Although, FV was not associated with a decrease in inpatient mortality in this study, having had both prior PV and FV (not necessarily given at the same time) was found to be associated with shortened LOS.
Our findings were inconsistent with 3 previous studies of prior PV on in‐hospital outcomes among adult CAP patients. Those studies found shortened LOS,[9, 10] lower risk of respiratory failure and other complications,[9] faster resolution of pneumonia symptoms,[10] and fewer ICU admissions[11] among PV‐vaccinated patients. Subanalysis of elderly patients performed in 2 of the 3 studies demonstrated a comparable survival benefit[9] or protective effect on the composite outcome of ICU admission or death[11] among elderly patients compared to nonelderly patients. However, unlike our analysis, neither study excluded patients admitted from nursing home facilities. Our database, including patients admitted from nursing homes or other inpatient facilities, estimated a slightly more favorable effect of PV alone on inpatient mortality compared to our main analysis, although the estimate remained statistically insignificant (see Supporting Information, Appendix Table A.2, in the online version of this article).
In all 3 previous studies,[9, 10, 11] an overwhelming majority of PV vaccinated patients also received FV (Mykietiuk[10]: 90.2% in PV vaccinated vs 39.9% in unvaccinated; Fisman[9]: 70% vs 2.2%; Johnstone[11]: 88% vs 9%), making it harder to distinguish the effect of having only PV from that of having both PV and FV. By defining a separate group for having both vaccinations, we found that having both PV and FV reduced LOS relative to PV alone or having had neither vaccinations. This suggests that PV alone may not be as effective in improving inpatient outcomes as shown in the previous studies, although limitations of our study prevented us from making a deterministic conclusion.
Our findings of no beneficial effects of PV alone on in‐hospital outcomes for CAP other than bacteremia in the elderly VA patients are supported by previous findings of no effect of PV on all‐cause pneumonia and all‐cause mortality,[4, 7, 8] decreasing antibody response to PV,[26, 27, 28] and decreasing vaccine effectiveness over time in the elderly patients.[5, 18] Also, in a study of patients who were previously hospitalized for CAP, PV at discharge was not associated with prevention of subsequent hospitalization for CAP or death from all causes.[29]
PV alone was found to be associated with an increased risk of respiratory complications using an unmatched sample, and this finding appears to be robust to several variations in the sample selection process (see Supporting Information, Appendix, in the online version of this article). This paradoxical finding may be a result of residual confounding despite our efforts to control for baseline differences in patients' characteristics. Using propensity matching where only those with similar observed characteristics, including comorbidity burden, were compared, the result was no longer statistically significant, although still trended in the same direction.
Up until recently, PPSV23 was the only pneumococcal vaccine recommended for all elderly individuals 65 years or older. Since September 2014, 13‐valent pneumococcal conjugate vaccine (PCV13) has also been recommended for all elderly persons in the United States. PCV13 became available in 2010 and was initially recommended only for routine use in children ages 2 to 59 months. Early evidence indicated some herd effect in adults associated with the use of PCV13 in children; however, the effect was not statistically significant in all age groups.[30] Because at the time of the study elderly patients were not vaccinated by other pneumococcal vaccines, and PCV13 was not yet in use in children, this strengthens the findings in terms of evaluating the efficacy of PPSV23, because the association was not attenuated by the herd effect of PCV13 in children or having both PPSV23 and PCV13 in the elderly population. The recent recommendation to vaccinate all elderly adults with PCV13 was based on findings from an industry‐supported placebo‐controlled trial of pneumococcal vaccine nave patients.[31] It is unknown whether PCV13 is more effective than PPSV23 in elderly adults and whether giving both would have any additional benefit in the elderly population. Future studies with population wide data on PCV13 use in elderly adults are needed.
Limitations
The major limitation for generalizing to all elderly population is that we studied elderly veterans who are almost exclusively males (98%). Previous studies have found males are at higher risk of acquiring CAP,[32] to die from CAP,[33] and to be hospitalized for CAP.[34] Vaccine effectiveness was also found to be higher in women than men.[35] These suggest that our finding may not generalize to female patients admitted for CAP.
Another important limitation is that if PV and/or FV are truly effective in reducing hospitalizations for pneumonia, then those who were hospitalized despite prior vaccinations potentially may have more severe disease and/or be less responsive to the vaccines than unvaccinated patients. If so, this potential selection bias would bias our results toward null, and may partially explain our insignificant findings of PV alone on inpatient outcomes and the low vaccination rates observed in this study.
By focusing on elderly patients admitted for CAP, our cohort is more homogeneous than many previous studies, given that PV was recommended for all elderly persons at the time of the study, and all patients in our study had CAP. Nonetheless, unmeasured selection bias may exist and could partially explain the lack of estimated beneficial effect. In particular, the PSI score could not be calculated for the whole sample due to lack of data availability. In a subsample of patients with available information to calculate the abbreviated PSI score, we continued to find no significant beneficial effect of PV on outcomes other than bacteremia.
Other limitations included the possibility that prior vaccination status may have been misclassified because of (1) the use of diagnosis and procedure codes to identify prior vaccination status and (2) the lack of linked Medicare data to obtain the complete medical service utilization history of the elderly patients with dual coverage. To address the second issue, we selected patients with at least 1 VA outpatient visit each year in the previous 5 years of the index admission, hoping to identify patients who were more likely to be VA service users. In sensitivity analyses, we further restricted our data to only patients with at least 2, 3, 4, or 5 visits per year, respectively, in the previous 5 years, and the results were generally robust to these variations (see Supporting Information, Appendix Tables A.2 and A.3, in the online version of this article). Although higher vaccination rates have been reported previously (PV: 81%89%; FV: 79%80%) for all elderly veterans in 2003,[36, 37] a lower vaccination rate may be expected among hospitalized patients for CAP, if PV and/or FV are effective in reducing hospitalizations for pneumonia as reported in previous studies.[36, 38, 39] The lower PV rate observed among hospitalized elderly patients in this study is similar to another study of hospitalized elderly patients (50% prior PV rate),[40] and is consistent with the low prior PV rates reported in other studies of CAP‐hospitalized patients, which ranges from 11% to 22%.[9, 10, 11]
Cases of CAP admissions were identified based on principal diagnosis of pneumonia. This increased precision in the identified cases but may have underidentified CAP admissions. ICD‐9 code 481.0x (influenza with pneumonia) was also used for case identification, similar to other studies[4, 9, 12, 41]; excluding this code only excluded a few and did not affect the findings. Relying exclusively on diagnosis codes to detect pneumonia may also lead to misclassification due to coding errors. The gold standard to confirm pneumonia was with x‐ray. However, such information was not available in our data.
We did not have bacteriological data to study the pneumococcal‐specific outcomes, such as pneumococcal pneumonia or pneumococcal bacteremia, which the pneumococcal vaccine is designed to protect against. Diagnosis codes for the pneumococcal‐specific outcomes have low sensitivity,[42] and will significantly underidentify those cases. This limitation will bias our result toward null, which may partially explain the insignificant findings.
CONCLUSIONS
In this study of elderly VA patients admitted for CAP, we did not find significant effects of prior PV on LOS, inpatient mortality, or respiratory complications. Although given the limitations of this study, we could not conclusively say that PV has no effect on these outcomes. Nonetheless, our findings and the findings of no significant protective effect on overall mortality and decreasing antibody response to vaccines in the elderly from other studies, does raise the question of whether the previously reported beneficial effects on in‐hospital outcomes for CAP in adults could be generalized to elderly patients. Larger electronic medical record databases with more complete information on patients' vaccination history are needed to confirm these findings. Nonetheless, given its protective effect against invasive diseases,[7, 8] the economic benefits shown,[43, 44] and relative safety, PV should still be recommended for all elderly persons, especially very old and frail nursing home residents.[45] However, significant survival benefit and improved in‐hospital outcomes for CAP as reported in previous studies may not be expected in elderly patients with prior PV, particularly if vaccination was given more than 5 years ago. This study also supports the recommendation of FV in the elderly population. Although, FV was not associated with a decrease in inpatient mortality in this study, having both PV and FV was found to be associated with shortened LOS.
Disclosures
This study was supported by the Medical Research Endowment Fund of University of Arkansas for Medical Sciences awarded to C. Li. The funding agency had no role in the study design; collection, analysis, and interpretation of data; writing of the report; or the decision to submit the article for publication. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government. All coauthors have seen and agree with the contents of the manuscript; the submission (aside from abstracts) is not under review by any other publication. All coauthors have contributed to the concept and design of the study, analysis and interpretation of data, and/or development of the manuscript. The manuscript was reviewed and revised by the coauthors to ensure that important intellectual content has been included in the final published version. C. Li is a consultant to eMaxHealth Systems on unrelated studies. The authors disclose no conflicts of interest with this study.
- , , , . Community‐acquired pneumonia in elderly patients. Aging Health. 2009;5(6):763–774.
- CDC/NCHS National Hospital Discharge Survey, 2010. Number of discharges from short‐stay hospitals, by first‐listed diagnosis and age: United States, 2010. National Center for Health Statistics. Available at: http://www.cdc.gov/nchs/data/nhds/3firstlisted/2010first3_numberage.pdf. Accessed July 14, 2014.
- , . Community‐acquired pneumonia in the elderly. Am J Geriatr Pharmacother. 2010;8(1):47–62.
- , , , et al. Effectiveness of pneumococcal polysaccharide vaccine in older adults. N Engl J Med. 2003;348:1747–1754.
- , . Pneumococcal vaccination of elderly adults: new paradigms for protection. Clin Infect Dis. 2008;47(10):1328–1338.
- , . The 23‐valent pneumococcal polysaccharide vaccine. Part 1. Efficacy of PPV in the elderly: a comparison of meta‐analysis. Eur J Epidemiol. 2004;19:353–363.
- , , , . Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst Rev. 2008;(1):CD000422.
- , , , , . Efficacy of pneumococcal vaccination in adults: a meta‐analysis. CMAJ. 2009;180(1):48–58.
- , , , , , . Prior pneumococcal vaccination is associated with reduced death, complications, and length of stay among hospitalized adults with community‐acquired pneumonia. Clin Infect Dis. 2006;42:1093–1101.
- , , , et al. Effect of prior pneumococcal vaccination on clinical outcome of hospitalized adults with community‐acquired pneumococcal pneumonia. Eur J Clin Microbiol Infect Dis. 2006;25:257–462.
- , , , . Effect of pneumococcal vaccination in hospitalized adults with community‐acquired pneumonia. Arch Intern Med. 2007;167:1938–1943.
- , , , , , . Influenza vaccination and risk of mortality among adults hospitalized with community‐acquired pneumonia. Arch Intern Med. 2007;167:53–59.
- , , , , , . Efficacy and effectiveness of influenza vaccines in elderly people: a systematic review. Lancet. 2005;366:1165–1174.
- , , , , . Effectiveness of influenza vaccine in the community‐dwelling elderly. N Engl J Med. 2007;357:1373–1381.
- VIReC Research User Guide: FY2002 VHA Medical SAS Inpatient Datasets. Hines, IL: Veterans Affairs Information Resource Center; 2003.
- Immunization Information Systems, Centers for Disease Control and Prevention. CPT codes mapped to CVX codes. Available at: http://www2a.cdc.gov/vaccines/iis/iisstandards/vaccines.asp?rpt=cpt. Accessed December 2, 2014.
- Centers for Disease Control and Prevention. Pneumococcal polysaccharide vaccine information statement. Available at: http://www.cdc.gov/vaccines/hcp/vis/vis‐statements/ppv.html. Accessed December 2, 2014.
- , , , et al. The protective efficacy of polyvalent pneumococcal polysaccharide vaccine. N Engl J Med. 1991;325:1453–1460.
- , , . Adapting a clinical comorbidity index for use with ICD‐9‐CM Administrative Databases. J Clin Epidemiol. 1992;45(6):613–619.
- , , , . Missing race/ethnicity data in Veterans Health Administration based disparities research: a systematic review. J Health Care Poor Underserved. 2006;17:128–140.
- , , , et al. Risk adjusting community‐acquired pneumonia hospital outcomes using automated databases. Am J Manag Care. 2008;14(3):158–166.
- , , , et al. A prediction rule to identify low‐risk patients with community‐acquired pneumonia. N Engl J Med. 1997;336:243–250.
- , , . A comparison of statistical modeling strategies for analyzing length of stay after CABG surgery. Health Serv Outcomes Res Methodol. 2002;3:107–133.
- , . GMATCH SAS macro. Available at: http://www.mayo.edu/research/documents/gmatchsas/DOC‐10027248. Accessed December 2, 2014.
- , , , . Analysis of Observational Health Care Data Using SAS. Cary, NC: SAS Institute; 2010.
- , , . Pneumococcal vaccination in older adults induces antibodies with low opsonic capacity and reduced antibody potency. Vaccine. 2008;26:5521–5526.
- , , . The effect of age on the response to the pneumococcal polysaccharide vaccine. BMC Infect Dis. 2010;10:60.
- , . Older adults have a low capacity to opsonize pneumococci due to low IgM antibody response to pneumococcal vaccinations. Infect Immun. 2011;79(1):314–320.
- , , , , . Impact of the pneumococcal vaccine on long‐term morbidity and mortality of adults at high risk for pneumonia. Clin Infect Dis. 2010;51(1):15–22.
- , , , , , . Effect of 13‐valent pneumococcal conjugate vaccine on admissions to hospital 2 years after its introduction in the USA: a time series analysis. Lancet Respir Med. 2014;2(5):387–394.
- American Academy of Family Physicians. ACIP recommends routine PCV13 immunization for adults 65 and older. Available at: http://www.aafp.org/news/health‐of‐the‐public/20140827pcv13vote.html. Accessed December 2, 2012.
- , , , et al. The burden of community‐acquired pneumonia in seniors: results of a population‐based study. Clin Infect Dis. 2004;39:1642–1650.
- , , , et al. Bacteremia with Streptococcus pneumoniae: sepsis and other risk factors for 30‐day mortality‐a hospital‐based cohort study. Eur J Clin Microbiol Infect Dis. 2012;13(10):2719–2725.
- , , , , . Trends in hospitalizations for pneumonia among persons aged 65 years or older in the United States, 1988–2002. JAMA. 2005;294(21):2712–2719.
- , , , et al. The effectiveness of the polysaccharide pneumococcal vaccine for the prevention of hospitalizations due to Streptococcus pneumoniae community‐acquired pneumonia in the elderly differs between the sexes: results from the Community‐Acquired Pneumonia Organization (CAPO) international cohort study. Vaccine. 2014;17:32(19):2198–2203.
- , , . Performance measures, vaccinations, and pneumonia rates among high‐risk patients in Veterans Administration health care. Am J Public Health. 2007;97(12):2167–2172.
- , , . Influenza and pneumococcal vaccination in older veterans: results from the Behavioral Risk Factor Surveillance System. J Am Geriatr Soc. 2006;54:217–223.
- , , , . The efficacy and cost effectiveness of vaccination against influenza among elderly persons living in the community. N Engl J Med. 1994;331:778–784.
- , , , . The health and economic benefits associated with pneumococcal vaccination of elderly persons with chronic lung disease. Arch Intern Med. 1999;159:2437–2442.
- , , . Pneumococcal vaccination in hospitalized elderly patients: role of the pharmacist. Pharmacotherapy. 2003;2(23):199–208.
- , , , . Accuracy of administrative data for identifying patients with pneumonia. Am J Med Qual. 2005;30:319–328.
- , , , , . International classification of diseases codes showed modest sensitivity for detecting community‐acquired pneumonia. J Clin Epidemiol. 2007;60(8):834–838.
- , , , et al. Cost‐effectiveness of pneumococcal vaccination of older people: a study in 5 western European countries. Clin Infect Dis. 2000;31:444–450.
- , , , et al. Cost‐effectiveness of pneumococcal vaccination for prevention of invasive pneumococcal disease in the elderly: an update for 10 Western European countries. Eur J Clin Microbiol Infect Dis. 2007;26(8):531–540.
- , , , et al. Efficacy of 23‐valent pneumococcal vaccine in preventing pneumonia and improving survival in nursing home residents: double blind, randomised and placebo controlled trial. BMJ. 2010;340:c1004.
Community‐acquired pneumonia (CAP) ranks fifth among all causes of death and is the leading infectious cause of death among persons 65 years or older (hereafter elderly) in the US.[1] Of the 1.1 million short‐stay hospital discharges for pneumonia in 2010, 55% were for elderly patients.[2] The most common cause of pneumonia in elderly patients leading to hospitalization is infection with Streptococcus pneumoniae.[1, 3, 4, 5] The 23‐valent pneumococcal polysaccharide vaccine is recommended (PPSV23) for all elderly persons and has been shown to reduce incidences of invasive pneumococcal bacteremia among immunocompetent elderly individuals.[5] However, its effect on more common manifestations of pneumococcal disease, such as pneumonia, remains controversial.[5, 6, 7, 8]
Several studies examined the association between prior PV and in‐hospital outcomes for CAP in adult patients.[9, 10, 11] Although the effect of pneumococcal vaccination (PV) on inpatient mortality was inconclusive, the studies found shortened length of stay (LOS),[9, 10] lower risk of respiratory failure and other complications,[9] faster resolution of pneumonia symptoms,[10] and fewer intensive care unit (ICU) admissions,[11] among those with prior PV. These findings suggest potential additional benefits of PV in hospitalized CAP patients.
This study examined prior PV on in‐hospital outcomes in elderly veterans hospitalized for CAP. Because PV‐vaccinated patients are also more likely to have received influenza (flu) vaccination (FV),[9, 10, 11] which could independently or additively improve CAP outcomes in hospitalized elderly patients,[12, 13, 14] we attempted to separate out the effect of FV by stratifying patients into 4 subgroups: PV alone, FV alone, both, or neither. The priori hypothesis was that PV improves in‐hospital outcomes in elderly veterans hospitalized for CAP.
METHODS
Study Cohort
This study is a retrospective cohort study of all elderly veterans admitted to any Veterans Affairs (VA) hospitals for CAP during the fiscal year 2003 (FY'03) (October 1, 2002 to September 30, 2003). Inpatient admissions for pneumonia were defined based on the principal diagnosis of nonviral pneumonia (International Classification of Diseases, 9th Revision [ICD‐9], codes 481.xx487.0x). The principal diagnosis was defined as the condition determined to be the reason for the admission.[15] To select only CAP cases, we included admissions where patients were admitted either directly or through a VA outpatient clinic. We excluded transfers from another hospital, skilled nursing facilities, intermediate care facilities, or another healthcare facility. All patients were 65 years or older on the first day of the first admission in FY'03 (index admission) and had at least 1 outpatient visit to a VA facility each year during the 5 years prior to the index admission.
Data Source
Data were drawn from Veterans Health Administration medical SAS datasets (SAS Institute Inc.,
Cary, NC). Demographic characteristics, inpatient and outpatient care utilization, and related medical diagnoses and procedure codes were extracted from national patient data extracts. Selected lab test results were drawn from the Decision Support System national extracts. This study was approved by institutional review boards at the University of Arkansas for Medical Sciences and the Central Arkansas Veterans Healthcare System.
Prior Vaccination Status
Prior PV status was determined within 5 years prior to the index admission using: ICD‐9 codes V06.6, V06.8, and V03.82, ICD‐9 procedure code 99.55, or Current Procedure Terminology (CPT) codes 90732 and 90669.[16] This 5‐year time frame was chosen for 2 reasons: (1) the Centers for Disease Control and Prevention (CDC) recommends a second dose for elderly persons if the first dose was before age 65 years and more than 5 years have passed[17]; (2) effectiveness of PV decreases over time in elderly persons, especially after 5 years since vaccination.[5, 18] Consistent with the CDC's vaccination recommendation,[18] patients with no record of prior PV were classified as not vaccinated. Prior FV status was determined in the year before the index admission using: ICD‐9 code V04.8, ICD‐9 procedure code 99.52, or CPT codes 9065590660.[16] Based on prior vaccinations, patients were classified into 4 groups: PV alone, FV alone, both, or neither.
Outcome Variables
The primary outcomes were LOS and inpatient mortality. LOS, measured in days, was the duration of a hospital stay from admission to discharge, censored at death or transfer, the occurrence of which was ascertained via the discharge type field. Inpatient mortality was defined as death from any cause that occurred before discharge or transfer. The secondary outcomes were respiratory complications and any bacteremia identified via the diagnosis field of discharge records (see Supporting Information, Appendix Table A.1, in the online version of this article for a list of ICD‐9 codes).
| PV Only, n=1,347 | FV Only, n=1,698 | Both, n=1,668 | Neither, n=2,010 | P Value* | |
|---|---|---|---|---|---|
| |||||
| Age, median (IQR) | 77 (7181) | 77 (7281) | 77 (7181) | 77 (7282) | 0.0418 |
| 6574 years | 539 (40.0%) | 619 (36.5%) | 670 (40.2%) | 733 (36.5%) | 0.0051 |
| 7584 years | 635 (47.1%) | 892 (52.5%) | 836 (50.1%) | 1058 (52.6%) | |
| 85 years | 173 (12.8%) | 187 (11.0%) | 162 (9.7%) | 219 (10.9%) | |
| Male | 1318 (97.8%) | 1657 (97.6%) | 1638 (98.2%) | 1964 (97.7%) | 0.6378 |
| Race | |||||
| White | 848 (63.0%) | 1149 (67.7%) | 1097 (65.8%) | 1272 (63.3%) | <0.0003 |
| Nonwhite | 229 (17.0%) | 214 (12.6%) | 271 (16.2%) | 289 (14.4%) | |
| Unknown | 270 (20.0%) | 335 (19.7%) | 300 (18.0%) | 449 (22.3%) | |
| Married | 726 (53.9%) | 951 (56.0%) | 930 (55.8%) | 1043 (51.9%) | 0.0419 |
| No. of non‐mental health VA outpatient visits last year, median (IQR) | 17 (1027) | 21 (1332) | 22 (1434) | 15 (926) | <0.0001 |
| CAP hospitalization last year | 87 (6.5%) | 106 (6.2%) | 100 (6.0%) | 106 (5.3%) | 0.4689 |
| Respiratory conditions in past 30 days | 149 (11.1%) | 183 (10.8%) | 173 (10.4%) | 263 (13.1%) | 0.0424 |
| Charlson Comorbidity Index, median (IQR) | 2 (14) | 3 (14) | 3 (14) | 2 (14) | <0.0001 |
| Inpatient outcomes | |||||
| LOS, d, median(IQR) | 6 (410) | 5 (39) | 5 (39) | 6 (49) | 0.0077 |
| Death | 130 (9.7%) | 119 (7.0%) | 113 (6.8%) | 166 (8.3%) | 0.0127 |
| Bacteremia | 31 (2.3%) | 56 (3.3%) | 40 (2.4%) | 68 (3.4%) | 0.1204 |
| Respiratory complications | 200 (14.8%) | 192 (11.3%) | 185 (11.1%) | 253 (12.6%) | 0.0073 |
Covariates
Covariates included patients' demographic characteristics (age, gender, race, marital status) and Charlson Comorbidity Index scores. Comorbidities were identified during the year prior to the index admission using ICD‐9 diagnoses codes based on Deyo et al. adaptation.[19] Additionally, we included prior admission for CAP within the year preceding index admission, the number of outpatient visits (excluding mental health visits; ICD‐9 codes 290.xx319.xx) within the year preceding index admission, and acute respiratory conditions experienced within 30 days preceding index admission. Development of bacteremia and respiratory complications may increase LOS, and risk of mortality and were adjusted in the regression models for these outcomes.
Race
Missing race in VA administrative data is a well‐documented problem.[20] When available, missing race was imputed using information reported during a patient's other inpatient stays available in our data as follows. We first imputed it using the most frequently reported race category. If unavailable, race was imputed by the most recently reported race category whenever available. This imputation algorithm reduced the proportion of patients with missing race information in our data to from 76% to 20%. Remaining patients with missing race information after imputation were analyzed as a separate category.
Pneumonia Severity Index Score
For patients with available lab values, we constructed an abbreviated pneumonia severity index (PSI) score adapted from Escobar et al.[21] The original PSI score developed by the Pneumonia Patient Outcomes Research Team (PORT) is a validated clinical prediction tool that permits risk stratification with regard to the likelihood of adverse outcomes in CAP patients.[22] Calculation of the PORT score requires information on patient's physical examination and radiographic findings at admission,[22] which was unavailable to us. Escobar et al. developed and validated an abbreviated form of the PORT score (PSI‐E) in CAP patients that does not incorporate physical examination and radiographic findings.[21] We calculated the PSI‐E developed by Escobar et al. with the exception that arterial pH and PaO2 test results were omitted because they were not available in the VA lab result files for the years we examined.
Data Analysis
Patients' baseline characteristics (see Covariates) were compared across the 4 vaccination groups using the Kruskal‐Wallis test for continuous variables and [2] test for categorical variables. Multiple regression analyses were used to assess the effect of prior PV and FV on inpatient outcomes during the index admission while adjusting for covariates. LOS was analyzed using a generalized linear model (GLM) with a negative binomial distribution and a logarithmic link function,[23] and incidence rate ratios (IRRs) were reported. IRRs were calculated by taking the exponential of the estimated coefficients from the GLM and are interpretable as the relative change in mean LOS associated with a 1‐unit change in a predictor variable. Risk of inpatient mortality, and development of respiratory complications or bacteremia, were analyzed using logistic regressions, and odds ratios (ORs) were reported. All regression models adjusted for covariates as described earlier. In addition, we conducted propensity score matching of PV‐vaccinated (n=2937) and unvaccinated (n=2937) patients using the GMATCH algorithm.[24] Propensity scores were estimated using a logistic regression to predict prior PV based on covariates listed earlier and prior FV status. GLM or logistic regression models were applied to the matched sample, with PV as the only predictor to generate IRRs or ORs, respectively. To account for the matched nature of the data, analyses were stratified by matched pairs.[25]
Sensitivity Analysis
Many sensitivity analyses were performed that: (1) included patients admitted from nursing homes or other inpatient facilities (n=7296); (2) excluded 0‐night admissions (n=6678); (3) varied the minimum number of VA outpatient visits to 2, 3, 4, or 5 visits each year in the previous 5 years; and (4) adjusted for the abbreviated PSI score only in patients with available information (n=3689).
Flu Season
Defining prior FV status during the previous year may have included individuals who received FV for the previous flu season (eg, a patient was admitted in December 2003, but his or her last FV was in January 2003). We conducted 2 sensitivity analyses: (1) recoded patients who were last vaccinated in the previous flu season as unvaccinated and (2) restricted to index admissions occurred during the flu season (n=5311). A flu season was defined as from September to May of the following year.
Time Since Last PV
To determine if the effectiveness of PV varies by the years elapsed since vaccination, among those with prior PV, we further classified prior PV as within 1 year (1 year), 2 years (>1 but 2 years), 3 years (>2 but 3 years), 4 years (>3 but 4 years), or 5 years (>4 but 5 years) preceding the index admission. Two‐thirds of patients received PV more than 2 years ago. We re‐estimated the regression models with indicators for the number of years since the last PV (as defined above, PV within 1 year preceding index admission as the reference group).
All analyses were conducted using SAS software (SAS Institute, Inc.). A 2‐sided P value of <0.05 was used to determine statistical significance.
RESULTS
In FY'03, 10,540 elderly VA patients had at least 1 inpatient admission for nonviral pneumonia. Among them, 3242 were excluded due to lack of VA outpatient visits in at least 1 of the 5 years prior to the index admission. Additionally, 574 patients were excluded because they were transferred from nursing homes or other inpatient facilities. The final sample consisted of 6723 elderly patients; among them, 1347(20%) had only PV, 1698(25%) had only FV, 1668 (25%) had both, and 2010 (30%) had neither prior to admission (see Supporting Information, Appendix 1, in the online version of this article) (see Supporting Information, Appendix Figure A.1, in the online version of this article).
Table 1 compares patients' baseline characteristics and inpatient outcomes across vaccination groups. Patients with prior PV and FV had the shortest LOS and were least likely to experience respiratory complications or die during the inpatient stay. They also tended to be younger, had more frequent VA nonmental health outpatient visits in the previous year, and more medical comorbidities than other groups. Although these differences were statistically significant, the actual differences were small across the groups.
Table 2 presents findings from the adjusted regression analyses. After adjusting for covariates, having prior PV alone, FV alone, or both did not significantly affect the risk of inpatient mortality, compared to patients without records of either vaccination. However, having both prior PV and FV was associated with 10% reduction in LOS (IRR: 0.90; 95% confidence interval [CI]: 0.86‐0.95; P<0.0001). PV alone were associated with an increased risk of respiratory complications (OR: 1.23; 95% CI: 1.01‐1.51; P=0.0429) and trended toward a reduced risk of bacteremia (OR: 0.67; 95% CI: 0.43‐1.03; P=0.0673). After matching on patient characteristics including prior FV status, prior PV significantly lowered the risk of developing bacteremia (OR: 0.66; 95% CI: 0.48‐0.90; P=0.0088) but was not statistically significantly associated with the other outcomes (Table 3).
| Length of Stay (Days) | Inpatient Death | |||||
|---|---|---|---|---|---|---|
| Bacteremia | Respiratory Complications | |||||
| ||||||
| Vaccination status | IRR | 95% CI | P Value | OR | 95% CI | P Value |
| PV in previous 5 Years | 1.02 | 0.97‐1.07 | 0.4561 | 1.15 | 0.89‐1.50 | 0.2901 |
| FV last year | 0.97 | 0.92‐1.02 | 0.1920 | 0.90 | 0.69‐1.17 | 0.4193 |
| Both | 0.90 | 0.86‐0.95 | <0.0001 | 0.88 | 0.67‐1.16 | 0.3646 |
| Neither | Ref | Ref | ||||
| Vaccination status | OR | 95% CI | P Value | OR | 95% CI | P Value |
| PV in previous 5 Years | 0.67 | 0.43‐1.03 | 0.0673 | 1.23 | 1.01‐1.51 | 0.0429 |
| FV last year | 0.99 | 0.69‐1.42 | 0.9536 | 0.90 | 0.74‐1.10 | 0.3085 |
| Both | 0.72 | 0.48‐1.07 | 0.1047 | 0.87 | 0.71‐1.07 | 0.1860 |
| Neither | Ref | Ref | ||||
| In‐Hospital Outcomes, Matched Sample (n=5 874) | PV vs No PV | ||
|---|---|---|---|
| IRR/OR | 95% CI | P Value | |
| |||
| Length of stay | 0.97 | 0.93‐1.01 | 0.1502 |
| Inpatient death | 1.13 | 0.94‐1.37 | 0.2027 |
| Bacteremia | 0.66 | 0.48‐0.90 | 0.0088 |
| Respiratory complications | 1.11 | 0.95‐1.30 | 0.2018 |
Findings from sensitivity analyses are included in the online appendices. Results were generally robust to various sensitivity analyses. However, in the analysis using the subset of patients with available lab information to define the PSI‐E score, having prior FV alone was also found to be associated with reduced LOS (IRR: 0.92; 95% CI: 0.86‐0.98; P<0.05). The relationship between PV and in‐patient outcomes did not vary by the time since vaccination, which is consistent with Jackson et al.[11]
DISCUSSION
Consistent with previous findings,[7, 8, 9, 10, 11] elderly VA patients hospitalized for CAP were found to have an association between prior PV and reduced risk of bacteremia. However, no associations of prior PV alone with other in‐hospital outcomes (LOS, inpatient mortality, or development of respiratory complications) were consistently found. Although, FV was not associated with a decrease in inpatient mortality in this study, having had both prior PV and FV (not necessarily given at the same time) was found to be associated with shortened LOS.
Our findings were inconsistent with 3 previous studies of prior PV on in‐hospital outcomes among adult CAP patients. Those studies found shortened LOS,[9, 10] lower risk of respiratory failure and other complications,[9] faster resolution of pneumonia symptoms,[10] and fewer ICU admissions[11] among PV‐vaccinated patients. Subanalysis of elderly patients performed in 2 of the 3 studies demonstrated a comparable survival benefit[9] or protective effect on the composite outcome of ICU admission or death[11] among elderly patients compared to nonelderly patients. However, unlike our analysis, neither study excluded patients admitted from nursing home facilities. Our database, including patients admitted from nursing homes or other inpatient facilities, estimated a slightly more favorable effect of PV alone on inpatient mortality compared to our main analysis, although the estimate remained statistically insignificant (see Supporting Information, Appendix Table A.2, in the online version of this article).
In all 3 previous studies,[9, 10, 11] an overwhelming majority of PV vaccinated patients also received FV (Mykietiuk[10]: 90.2% in PV vaccinated vs 39.9% in unvaccinated; Fisman[9]: 70% vs 2.2%; Johnstone[11]: 88% vs 9%), making it harder to distinguish the effect of having only PV from that of having both PV and FV. By defining a separate group for having both vaccinations, we found that having both PV and FV reduced LOS relative to PV alone or having had neither vaccinations. This suggests that PV alone may not be as effective in improving inpatient outcomes as shown in the previous studies, although limitations of our study prevented us from making a deterministic conclusion.
Our findings of no beneficial effects of PV alone on in‐hospital outcomes for CAP other than bacteremia in the elderly VA patients are supported by previous findings of no effect of PV on all‐cause pneumonia and all‐cause mortality,[4, 7, 8] decreasing antibody response to PV,[26, 27, 28] and decreasing vaccine effectiveness over time in the elderly patients.[5, 18] Also, in a study of patients who were previously hospitalized for CAP, PV at discharge was not associated with prevention of subsequent hospitalization for CAP or death from all causes.[29]
PV alone was found to be associated with an increased risk of respiratory complications using an unmatched sample, and this finding appears to be robust to several variations in the sample selection process (see Supporting Information, Appendix, in the online version of this article). This paradoxical finding may be a result of residual confounding despite our efforts to control for baseline differences in patients' characteristics. Using propensity matching where only those with similar observed characteristics, including comorbidity burden, were compared, the result was no longer statistically significant, although still trended in the same direction.
Up until recently, PPSV23 was the only pneumococcal vaccine recommended for all elderly individuals 65 years or older. Since September 2014, 13‐valent pneumococcal conjugate vaccine (PCV13) has also been recommended for all elderly persons in the United States. PCV13 became available in 2010 and was initially recommended only for routine use in children ages 2 to 59 months. Early evidence indicated some herd effect in adults associated with the use of PCV13 in children; however, the effect was not statistically significant in all age groups.[30] Because at the time of the study elderly patients were not vaccinated by other pneumococcal vaccines, and PCV13 was not yet in use in children, this strengthens the findings in terms of evaluating the efficacy of PPSV23, because the association was not attenuated by the herd effect of PCV13 in children or having both PPSV23 and PCV13 in the elderly population. The recent recommendation to vaccinate all elderly adults with PCV13 was based on findings from an industry‐supported placebo‐controlled trial of pneumococcal vaccine nave patients.[31] It is unknown whether PCV13 is more effective than PPSV23 in elderly adults and whether giving both would have any additional benefit in the elderly population. Future studies with population wide data on PCV13 use in elderly adults are needed.
Limitations
The major limitation for generalizing to all elderly population is that we studied elderly veterans who are almost exclusively males (98%). Previous studies have found males are at higher risk of acquiring CAP,[32] to die from CAP,[33] and to be hospitalized for CAP.[34] Vaccine effectiveness was also found to be higher in women than men.[35] These suggest that our finding may not generalize to female patients admitted for CAP.
Another important limitation is that if PV and/or FV are truly effective in reducing hospitalizations for pneumonia, then those who were hospitalized despite prior vaccinations potentially may have more severe disease and/or be less responsive to the vaccines than unvaccinated patients. If so, this potential selection bias would bias our results toward null, and may partially explain our insignificant findings of PV alone on inpatient outcomes and the low vaccination rates observed in this study.
By focusing on elderly patients admitted for CAP, our cohort is more homogeneous than many previous studies, given that PV was recommended for all elderly persons at the time of the study, and all patients in our study had CAP. Nonetheless, unmeasured selection bias may exist and could partially explain the lack of estimated beneficial effect. In particular, the PSI score could not be calculated for the whole sample due to lack of data availability. In a subsample of patients with available information to calculate the abbreviated PSI score, we continued to find no significant beneficial effect of PV on outcomes other than bacteremia.
Other limitations included the possibility that prior vaccination status may have been misclassified because of (1) the use of diagnosis and procedure codes to identify prior vaccination status and (2) the lack of linked Medicare data to obtain the complete medical service utilization history of the elderly patients with dual coverage. To address the second issue, we selected patients with at least 1 VA outpatient visit each year in the previous 5 years of the index admission, hoping to identify patients who were more likely to be VA service users. In sensitivity analyses, we further restricted our data to only patients with at least 2, 3, 4, or 5 visits per year, respectively, in the previous 5 years, and the results were generally robust to these variations (see Supporting Information, Appendix Tables A.2 and A.3, in the online version of this article). Although higher vaccination rates have been reported previously (PV: 81%89%; FV: 79%80%) for all elderly veterans in 2003,[36, 37] a lower vaccination rate may be expected among hospitalized patients for CAP, if PV and/or FV are effective in reducing hospitalizations for pneumonia as reported in previous studies.[36, 38, 39] The lower PV rate observed among hospitalized elderly patients in this study is similar to another study of hospitalized elderly patients (50% prior PV rate),[40] and is consistent with the low prior PV rates reported in other studies of CAP‐hospitalized patients, which ranges from 11% to 22%.[9, 10, 11]
Cases of CAP admissions were identified based on principal diagnosis of pneumonia. This increased precision in the identified cases but may have underidentified CAP admissions. ICD‐9 code 481.0x (influenza with pneumonia) was also used for case identification, similar to other studies[4, 9, 12, 41]; excluding this code only excluded a few and did not affect the findings. Relying exclusively on diagnosis codes to detect pneumonia may also lead to misclassification due to coding errors. The gold standard to confirm pneumonia was with x‐ray. However, such information was not available in our data.
We did not have bacteriological data to study the pneumococcal‐specific outcomes, such as pneumococcal pneumonia or pneumococcal bacteremia, which the pneumococcal vaccine is designed to protect against. Diagnosis codes for the pneumococcal‐specific outcomes have low sensitivity,[42] and will significantly underidentify those cases. This limitation will bias our result toward null, which may partially explain the insignificant findings.
CONCLUSIONS
In this study of elderly VA patients admitted for CAP, we did not find significant effects of prior PV on LOS, inpatient mortality, or respiratory complications. Although given the limitations of this study, we could not conclusively say that PV has no effect on these outcomes. Nonetheless, our findings and the findings of no significant protective effect on overall mortality and decreasing antibody response to vaccines in the elderly from other studies, does raise the question of whether the previously reported beneficial effects on in‐hospital outcomes for CAP in adults could be generalized to elderly patients. Larger electronic medical record databases with more complete information on patients' vaccination history are needed to confirm these findings. Nonetheless, given its protective effect against invasive diseases,[7, 8] the economic benefits shown,[43, 44] and relative safety, PV should still be recommended for all elderly persons, especially very old and frail nursing home residents.[45] However, significant survival benefit and improved in‐hospital outcomes for CAP as reported in previous studies may not be expected in elderly patients with prior PV, particularly if vaccination was given more than 5 years ago. This study also supports the recommendation of FV in the elderly population. Although, FV was not associated with a decrease in inpatient mortality in this study, having both PV and FV was found to be associated with shortened LOS.
Disclosures
This study was supported by the Medical Research Endowment Fund of University of Arkansas for Medical Sciences awarded to C. Li. The funding agency had no role in the study design; collection, analysis, and interpretation of data; writing of the report; or the decision to submit the article for publication. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government. All coauthors have seen and agree with the contents of the manuscript; the submission (aside from abstracts) is not under review by any other publication. All coauthors have contributed to the concept and design of the study, analysis and interpretation of data, and/or development of the manuscript. The manuscript was reviewed and revised by the coauthors to ensure that important intellectual content has been included in the final published version. C. Li is a consultant to eMaxHealth Systems on unrelated studies. The authors disclose no conflicts of interest with this study.
Community‐acquired pneumonia (CAP) ranks fifth among all causes of death and is the leading infectious cause of death among persons 65 years or older (hereafter elderly) in the US.[1] Of the 1.1 million short‐stay hospital discharges for pneumonia in 2010, 55% were for elderly patients.[2] The most common cause of pneumonia in elderly patients leading to hospitalization is infection with Streptococcus pneumoniae.[1, 3, 4, 5] The 23‐valent pneumococcal polysaccharide vaccine is recommended (PPSV23) for all elderly persons and has been shown to reduce incidences of invasive pneumococcal bacteremia among immunocompetent elderly individuals.[5] However, its effect on more common manifestations of pneumococcal disease, such as pneumonia, remains controversial.[5, 6, 7, 8]
Several studies examined the association between prior PV and in‐hospital outcomes for CAP in adult patients.[9, 10, 11] Although the effect of pneumococcal vaccination (PV) on inpatient mortality was inconclusive, the studies found shortened length of stay (LOS),[9, 10] lower risk of respiratory failure and other complications,[9] faster resolution of pneumonia symptoms,[10] and fewer intensive care unit (ICU) admissions,[11] among those with prior PV. These findings suggest potential additional benefits of PV in hospitalized CAP patients.
This study examined prior PV on in‐hospital outcomes in elderly veterans hospitalized for CAP. Because PV‐vaccinated patients are also more likely to have received influenza (flu) vaccination (FV),[9, 10, 11] which could independently or additively improve CAP outcomes in hospitalized elderly patients,[12, 13, 14] we attempted to separate out the effect of FV by stratifying patients into 4 subgroups: PV alone, FV alone, both, or neither. The priori hypothesis was that PV improves in‐hospital outcomes in elderly veterans hospitalized for CAP.
METHODS
Study Cohort
This study is a retrospective cohort study of all elderly veterans admitted to any Veterans Affairs (VA) hospitals for CAP during the fiscal year 2003 (FY'03) (October 1, 2002 to September 30, 2003). Inpatient admissions for pneumonia were defined based on the principal diagnosis of nonviral pneumonia (International Classification of Diseases, 9th Revision [ICD‐9], codes 481.xx487.0x). The principal diagnosis was defined as the condition determined to be the reason for the admission.[15] To select only CAP cases, we included admissions where patients were admitted either directly or through a VA outpatient clinic. We excluded transfers from another hospital, skilled nursing facilities, intermediate care facilities, or another healthcare facility. All patients were 65 years or older on the first day of the first admission in FY'03 (index admission) and had at least 1 outpatient visit to a VA facility each year during the 5 years prior to the index admission.
Data Source
Data were drawn from Veterans Health Administration medical SAS datasets (SAS Institute Inc.,
Cary, NC). Demographic characteristics, inpatient and outpatient care utilization, and related medical diagnoses and procedure codes were extracted from national patient data extracts. Selected lab test results were drawn from the Decision Support System national extracts. This study was approved by institutional review boards at the University of Arkansas for Medical Sciences and the Central Arkansas Veterans Healthcare System.
Prior Vaccination Status
Prior PV status was determined within 5 years prior to the index admission using: ICD‐9 codes V06.6, V06.8, and V03.82, ICD‐9 procedure code 99.55, or Current Procedure Terminology (CPT) codes 90732 and 90669.[16] This 5‐year time frame was chosen for 2 reasons: (1) the Centers for Disease Control and Prevention (CDC) recommends a second dose for elderly persons if the first dose was before age 65 years and more than 5 years have passed[17]; (2) effectiveness of PV decreases over time in elderly persons, especially after 5 years since vaccination.[5, 18] Consistent with the CDC's vaccination recommendation,[18] patients with no record of prior PV were classified as not vaccinated. Prior FV status was determined in the year before the index admission using: ICD‐9 code V04.8, ICD‐9 procedure code 99.52, or CPT codes 9065590660.[16] Based on prior vaccinations, patients were classified into 4 groups: PV alone, FV alone, both, or neither.
Outcome Variables
The primary outcomes were LOS and inpatient mortality. LOS, measured in days, was the duration of a hospital stay from admission to discharge, censored at death or transfer, the occurrence of which was ascertained via the discharge type field. Inpatient mortality was defined as death from any cause that occurred before discharge or transfer. The secondary outcomes were respiratory complications and any bacteremia identified via the diagnosis field of discharge records (see Supporting Information, Appendix Table A.1, in the online version of this article for a list of ICD‐9 codes).
| PV Only, n=1,347 | FV Only, n=1,698 | Both, n=1,668 | Neither, n=2,010 | P Value* | |
|---|---|---|---|---|---|
| |||||
| Age, median (IQR) | 77 (7181) | 77 (7281) | 77 (7181) | 77 (7282) | 0.0418 |
| 6574 years | 539 (40.0%) | 619 (36.5%) | 670 (40.2%) | 733 (36.5%) | 0.0051 |
| 7584 years | 635 (47.1%) | 892 (52.5%) | 836 (50.1%) | 1058 (52.6%) | |
| 85 years | 173 (12.8%) | 187 (11.0%) | 162 (9.7%) | 219 (10.9%) | |
| Male | 1318 (97.8%) | 1657 (97.6%) | 1638 (98.2%) | 1964 (97.7%) | 0.6378 |
| Race | |||||
| White | 848 (63.0%) | 1149 (67.7%) | 1097 (65.8%) | 1272 (63.3%) | <0.0003 |
| Nonwhite | 229 (17.0%) | 214 (12.6%) | 271 (16.2%) | 289 (14.4%) | |
| Unknown | 270 (20.0%) | 335 (19.7%) | 300 (18.0%) | 449 (22.3%) | |
| Married | 726 (53.9%) | 951 (56.0%) | 930 (55.8%) | 1043 (51.9%) | 0.0419 |
| No. of non‐mental health VA outpatient visits last year, median (IQR) | 17 (1027) | 21 (1332) | 22 (1434) | 15 (926) | <0.0001 |
| CAP hospitalization last year | 87 (6.5%) | 106 (6.2%) | 100 (6.0%) | 106 (5.3%) | 0.4689 |
| Respiratory conditions in past 30 days | 149 (11.1%) | 183 (10.8%) | 173 (10.4%) | 263 (13.1%) | 0.0424 |
| Charlson Comorbidity Index, median (IQR) | 2 (14) | 3 (14) | 3 (14) | 2 (14) | <0.0001 |
| Inpatient outcomes | |||||
| LOS, d, median(IQR) | 6 (410) | 5 (39) | 5 (39) | 6 (49) | 0.0077 |
| Death | 130 (9.7%) | 119 (7.0%) | 113 (6.8%) | 166 (8.3%) | 0.0127 |
| Bacteremia | 31 (2.3%) | 56 (3.3%) | 40 (2.4%) | 68 (3.4%) | 0.1204 |
| Respiratory complications | 200 (14.8%) | 192 (11.3%) | 185 (11.1%) | 253 (12.6%) | 0.0073 |
Covariates
Covariates included patients' demographic characteristics (age, gender, race, marital status) and Charlson Comorbidity Index scores. Comorbidities were identified during the year prior to the index admission using ICD‐9 diagnoses codes based on Deyo et al. adaptation.[19] Additionally, we included prior admission for CAP within the year preceding index admission, the number of outpatient visits (excluding mental health visits; ICD‐9 codes 290.xx319.xx) within the year preceding index admission, and acute respiratory conditions experienced within 30 days preceding index admission. Development of bacteremia and respiratory complications may increase LOS, and risk of mortality and were adjusted in the regression models for these outcomes.
Race
Missing race in VA administrative data is a well‐documented problem.[20] When available, missing race was imputed using information reported during a patient's other inpatient stays available in our data as follows. We first imputed it using the most frequently reported race category. If unavailable, race was imputed by the most recently reported race category whenever available. This imputation algorithm reduced the proportion of patients with missing race information in our data to from 76% to 20%. Remaining patients with missing race information after imputation were analyzed as a separate category.
Pneumonia Severity Index Score
For patients with available lab values, we constructed an abbreviated pneumonia severity index (PSI) score adapted from Escobar et al.[21] The original PSI score developed by the Pneumonia Patient Outcomes Research Team (PORT) is a validated clinical prediction tool that permits risk stratification with regard to the likelihood of adverse outcomes in CAP patients.[22] Calculation of the PORT score requires information on patient's physical examination and radiographic findings at admission,[22] which was unavailable to us. Escobar et al. developed and validated an abbreviated form of the PORT score (PSI‐E) in CAP patients that does not incorporate physical examination and radiographic findings.[21] We calculated the PSI‐E developed by Escobar et al. with the exception that arterial pH and PaO2 test results were omitted because they were not available in the VA lab result files for the years we examined.
Data Analysis
Patients' baseline characteristics (see Covariates) were compared across the 4 vaccination groups using the Kruskal‐Wallis test for continuous variables and [2] test for categorical variables. Multiple regression analyses were used to assess the effect of prior PV and FV on inpatient outcomes during the index admission while adjusting for covariates. LOS was analyzed using a generalized linear model (GLM) with a negative binomial distribution and a logarithmic link function,[23] and incidence rate ratios (IRRs) were reported. IRRs were calculated by taking the exponential of the estimated coefficients from the GLM and are interpretable as the relative change in mean LOS associated with a 1‐unit change in a predictor variable. Risk of inpatient mortality, and development of respiratory complications or bacteremia, were analyzed using logistic regressions, and odds ratios (ORs) were reported. All regression models adjusted for covariates as described earlier. In addition, we conducted propensity score matching of PV‐vaccinated (n=2937) and unvaccinated (n=2937) patients using the GMATCH algorithm.[24] Propensity scores were estimated using a logistic regression to predict prior PV based on covariates listed earlier and prior FV status. GLM or logistic regression models were applied to the matched sample, with PV as the only predictor to generate IRRs or ORs, respectively. To account for the matched nature of the data, analyses were stratified by matched pairs.[25]
Sensitivity Analysis
Many sensitivity analyses were performed that: (1) included patients admitted from nursing homes or other inpatient facilities (n=7296); (2) excluded 0‐night admissions (n=6678); (3) varied the minimum number of VA outpatient visits to 2, 3, 4, or 5 visits each year in the previous 5 years; and (4) adjusted for the abbreviated PSI score only in patients with available information (n=3689).
Flu Season
Defining prior FV status during the previous year may have included individuals who received FV for the previous flu season (eg, a patient was admitted in December 2003, but his or her last FV was in January 2003). We conducted 2 sensitivity analyses: (1) recoded patients who were last vaccinated in the previous flu season as unvaccinated and (2) restricted to index admissions occurred during the flu season (n=5311). A flu season was defined as from September to May of the following year.
Time Since Last PV
To determine if the effectiveness of PV varies by the years elapsed since vaccination, among those with prior PV, we further classified prior PV as within 1 year (1 year), 2 years (>1 but 2 years), 3 years (>2 but 3 years), 4 years (>3 but 4 years), or 5 years (>4 but 5 years) preceding the index admission. Two‐thirds of patients received PV more than 2 years ago. We re‐estimated the regression models with indicators for the number of years since the last PV (as defined above, PV within 1 year preceding index admission as the reference group).
All analyses were conducted using SAS software (SAS Institute, Inc.). A 2‐sided P value of <0.05 was used to determine statistical significance.
RESULTS
In FY'03, 10,540 elderly VA patients had at least 1 inpatient admission for nonviral pneumonia. Among them, 3242 were excluded due to lack of VA outpatient visits in at least 1 of the 5 years prior to the index admission. Additionally, 574 patients were excluded because they were transferred from nursing homes or other inpatient facilities. The final sample consisted of 6723 elderly patients; among them, 1347(20%) had only PV, 1698(25%) had only FV, 1668 (25%) had both, and 2010 (30%) had neither prior to admission (see Supporting Information, Appendix 1, in the online version of this article) (see Supporting Information, Appendix Figure A.1, in the online version of this article).
Table 1 compares patients' baseline characteristics and inpatient outcomes across vaccination groups. Patients with prior PV and FV had the shortest LOS and were least likely to experience respiratory complications or die during the inpatient stay. They also tended to be younger, had more frequent VA nonmental health outpatient visits in the previous year, and more medical comorbidities than other groups. Although these differences were statistically significant, the actual differences were small across the groups.
Table 2 presents findings from the adjusted regression analyses. After adjusting for covariates, having prior PV alone, FV alone, or both did not significantly affect the risk of inpatient mortality, compared to patients without records of either vaccination. However, having both prior PV and FV was associated with 10% reduction in LOS (IRR: 0.90; 95% confidence interval [CI]: 0.86‐0.95; P<0.0001). PV alone were associated with an increased risk of respiratory complications (OR: 1.23; 95% CI: 1.01‐1.51; P=0.0429) and trended toward a reduced risk of bacteremia (OR: 0.67; 95% CI: 0.43‐1.03; P=0.0673). After matching on patient characteristics including prior FV status, prior PV significantly lowered the risk of developing bacteremia (OR: 0.66; 95% CI: 0.48‐0.90; P=0.0088) but was not statistically significantly associated with the other outcomes (Table 3).
| Length of Stay (Days) | Inpatient Death | |||||
|---|---|---|---|---|---|---|
| Bacteremia | Respiratory Complications | |||||
| ||||||
| Vaccination status | IRR | 95% CI | P Value | OR | 95% CI | P Value |
| PV in previous 5 Years | 1.02 | 0.97‐1.07 | 0.4561 | 1.15 | 0.89‐1.50 | 0.2901 |
| FV last year | 0.97 | 0.92‐1.02 | 0.1920 | 0.90 | 0.69‐1.17 | 0.4193 |
| Both | 0.90 | 0.86‐0.95 | <0.0001 | 0.88 | 0.67‐1.16 | 0.3646 |
| Neither | Ref | Ref | ||||
| Vaccination status | OR | 95% CI | P Value | OR | 95% CI | P Value |
| PV in previous 5 Years | 0.67 | 0.43‐1.03 | 0.0673 | 1.23 | 1.01‐1.51 | 0.0429 |
| FV last year | 0.99 | 0.69‐1.42 | 0.9536 | 0.90 | 0.74‐1.10 | 0.3085 |
| Both | 0.72 | 0.48‐1.07 | 0.1047 | 0.87 | 0.71‐1.07 | 0.1860 |
| Neither | Ref | Ref | ||||
| In‐Hospital Outcomes, Matched Sample (n=5 874) | PV vs No PV | ||
|---|---|---|---|
| IRR/OR | 95% CI | P Value | |
| |||
| Length of stay | 0.97 | 0.93‐1.01 | 0.1502 |
| Inpatient death | 1.13 | 0.94‐1.37 | 0.2027 |
| Bacteremia | 0.66 | 0.48‐0.90 | 0.0088 |
| Respiratory complications | 1.11 | 0.95‐1.30 | 0.2018 |
Findings from sensitivity analyses are included in the online appendices. Results were generally robust to various sensitivity analyses. However, in the analysis using the subset of patients with available lab information to define the PSI‐E score, having prior FV alone was also found to be associated with reduced LOS (IRR: 0.92; 95% CI: 0.86‐0.98; P<0.05). The relationship between PV and in‐patient outcomes did not vary by the time since vaccination, which is consistent with Jackson et al.[11]
DISCUSSION
Consistent with previous findings,[7, 8, 9, 10, 11] elderly VA patients hospitalized for CAP were found to have an association between prior PV and reduced risk of bacteremia. However, no associations of prior PV alone with other in‐hospital outcomes (LOS, inpatient mortality, or development of respiratory complications) were consistently found. Although, FV was not associated with a decrease in inpatient mortality in this study, having had both prior PV and FV (not necessarily given at the same time) was found to be associated with shortened LOS.
Our findings were inconsistent with 3 previous studies of prior PV on in‐hospital outcomes among adult CAP patients. Those studies found shortened LOS,[9, 10] lower risk of respiratory failure and other complications,[9] faster resolution of pneumonia symptoms,[10] and fewer ICU admissions[11] among PV‐vaccinated patients. Subanalysis of elderly patients performed in 2 of the 3 studies demonstrated a comparable survival benefit[9] or protective effect on the composite outcome of ICU admission or death[11] among elderly patients compared to nonelderly patients. However, unlike our analysis, neither study excluded patients admitted from nursing home facilities. Our database, including patients admitted from nursing homes or other inpatient facilities, estimated a slightly more favorable effect of PV alone on inpatient mortality compared to our main analysis, although the estimate remained statistically insignificant (see Supporting Information, Appendix Table A.2, in the online version of this article).
In all 3 previous studies,[9, 10, 11] an overwhelming majority of PV vaccinated patients also received FV (Mykietiuk[10]: 90.2% in PV vaccinated vs 39.9% in unvaccinated; Fisman[9]: 70% vs 2.2%; Johnstone[11]: 88% vs 9%), making it harder to distinguish the effect of having only PV from that of having both PV and FV. By defining a separate group for having both vaccinations, we found that having both PV and FV reduced LOS relative to PV alone or having had neither vaccinations. This suggests that PV alone may not be as effective in improving inpatient outcomes as shown in the previous studies, although limitations of our study prevented us from making a deterministic conclusion.
Our findings of no beneficial effects of PV alone on in‐hospital outcomes for CAP other than bacteremia in the elderly VA patients are supported by previous findings of no effect of PV on all‐cause pneumonia and all‐cause mortality,[4, 7, 8] decreasing antibody response to PV,[26, 27, 28] and decreasing vaccine effectiveness over time in the elderly patients.[5, 18] Also, in a study of patients who were previously hospitalized for CAP, PV at discharge was not associated with prevention of subsequent hospitalization for CAP or death from all causes.[29]
PV alone was found to be associated with an increased risk of respiratory complications using an unmatched sample, and this finding appears to be robust to several variations in the sample selection process (see Supporting Information, Appendix, in the online version of this article). This paradoxical finding may be a result of residual confounding despite our efforts to control for baseline differences in patients' characteristics. Using propensity matching where only those with similar observed characteristics, including comorbidity burden, were compared, the result was no longer statistically significant, although still trended in the same direction.
Up until recently, PPSV23 was the only pneumococcal vaccine recommended for all elderly individuals 65 years or older. Since September 2014, 13‐valent pneumococcal conjugate vaccine (PCV13) has also been recommended for all elderly persons in the United States. PCV13 became available in 2010 and was initially recommended only for routine use in children ages 2 to 59 months. Early evidence indicated some herd effect in adults associated with the use of PCV13 in children; however, the effect was not statistically significant in all age groups.[30] Because at the time of the study elderly patients were not vaccinated by other pneumococcal vaccines, and PCV13 was not yet in use in children, this strengthens the findings in terms of evaluating the efficacy of PPSV23, because the association was not attenuated by the herd effect of PCV13 in children or having both PPSV23 and PCV13 in the elderly population. The recent recommendation to vaccinate all elderly adults with PCV13 was based on findings from an industry‐supported placebo‐controlled trial of pneumococcal vaccine nave patients.[31] It is unknown whether PCV13 is more effective than PPSV23 in elderly adults and whether giving both would have any additional benefit in the elderly population. Future studies with population wide data on PCV13 use in elderly adults are needed.
Limitations
The major limitation for generalizing to all elderly population is that we studied elderly veterans who are almost exclusively males (98%). Previous studies have found males are at higher risk of acquiring CAP,[32] to die from CAP,[33] and to be hospitalized for CAP.[34] Vaccine effectiveness was also found to be higher in women than men.[35] These suggest that our finding may not generalize to female patients admitted for CAP.
Another important limitation is that if PV and/or FV are truly effective in reducing hospitalizations for pneumonia, then those who were hospitalized despite prior vaccinations potentially may have more severe disease and/or be less responsive to the vaccines than unvaccinated patients. If so, this potential selection bias would bias our results toward null, and may partially explain our insignificant findings of PV alone on inpatient outcomes and the low vaccination rates observed in this study.
By focusing on elderly patients admitted for CAP, our cohort is more homogeneous than many previous studies, given that PV was recommended for all elderly persons at the time of the study, and all patients in our study had CAP. Nonetheless, unmeasured selection bias may exist and could partially explain the lack of estimated beneficial effect. In particular, the PSI score could not be calculated for the whole sample due to lack of data availability. In a subsample of patients with available information to calculate the abbreviated PSI score, we continued to find no significant beneficial effect of PV on outcomes other than bacteremia.
Other limitations included the possibility that prior vaccination status may have been misclassified because of (1) the use of diagnosis and procedure codes to identify prior vaccination status and (2) the lack of linked Medicare data to obtain the complete medical service utilization history of the elderly patients with dual coverage. To address the second issue, we selected patients with at least 1 VA outpatient visit each year in the previous 5 years of the index admission, hoping to identify patients who were more likely to be VA service users. In sensitivity analyses, we further restricted our data to only patients with at least 2, 3, 4, or 5 visits per year, respectively, in the previous 5 years, and the results were generally robust to these variations (see Supporting Information, Appendix Tables A.2 and A.3, in the online version of this article). Although higher vaccination rates have been reported previously (PV: 81%89%; FV: 79%80%) for all elderly veterans in 2003,[36, 37] a lower vaccination rate may be expected among hospitalized patients for CAP, if PV and/or FV are effective in reducing hospitalizations for pneumonia as reported in previous studies.[36, 38, 39] The lower PV rate observed among hospitalized elderly patients in this study is similar to another study of hospitalized elderly patients (50% prior PV rate),[40] and is consistent with the low prior PV rates reported in other studies of CAP‐hospitalized patients, which ranges from 11% to 22%.[9, 10, 11]
Cases of CAP admissions were identified based on principal diagnosis of pneumonia. This increased precision in the identified cases but may have underidentified CAP admissions. ICD‐9 code 481.0x (influenza with pneumonia) was also used for case identification, similar to other studies[4, 9, 12, 41]; excluding this code only excluded a few and did not affect the findings. Relying exclusively on diagnosis codes to detect pneumonia may also lead to misclassification due to coding errors. The gold standard to confirm pneumonia was with x‐ray. However, such information was not available in our data.
We did not have bacteriological data to study the pneumococcal‐specific outcomes, such as pneumococcal pneumonia or pneumococcal bacteremia, which the pneumococcal vaccine is designed to protect against. Diagnosis codes for the pneumococcal‐specific outcomes have low sensitivity,[42] and will significantly underidentify those cases. This limitation will bias our result toward null, which may partially explain the insignificant findings.
CONCLUSIONS
In this study of elderly VA patients admitted for CAP, we did not find significant effects of prior PV on LOS, inpatient mortality, or respiratory complications. Although given the limitations of this study, we could not conclusively say that PV has no effect on these outcomes. Nonetheless, our findings and the findings of no significant protective effect on overall mortality and decreasing antibody response to vaccines in the elderly from other studies, does raise the question of whether the previously reported beneficial effects on in‐hospital outcomes for CAP in adults could be generalized to elderly patients. Larger electronic medical record databases with more complete information on patients' vaccination history are needed to confirm these findings. Nonetheless, given its protective effect against invasive diseases,[7, 8] the economic benefits shown,[43, 44] and relative safety, PV should still be recommended for all elderly persons, especially very old and frail nursing home residents.[45] However, significant survival benefit and improved in‐hospital outcomes for CAP as reported in previous studies may not be expected in elderly patients with prior PV, particularly if vaccination was given more than 5 years ago. This study also supports the recommendation of FV in the elderly population. Although, FV was not associated with a decrease in inpatient mortality in this study, having both PV and FV was found to be associated with shortened LOS.
Disclosures
This study was supported by the Medical Research Endowment Fund of University of Arkansas for Medical Sciences awarded to C. Li. The funding agency had no role in the study design; collection, analysis, and interpretation of data; writing of the report; or the decision to submit the article for publication. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government. All coauthors have seen and agree with the contents of the manuscript; the submission (aside from abstracts) is not under review by any other publication. All coauthors have contributed to the concept and design of the study, analysis and interpretation of data, and/or development of the manuscript. The manuscript was reviewed and revised by the coauthors to ensure that important intellectual content has been included in the final published version. C. Li is a consultant to eMaxHealth Systems on unrelated studies. The authors disclose no conflicts of interest with this study.
- , , , . Community‐acquired pneumonia in elderly patients. Aging Health. 2009;5(6):763–774.
- CDC/NCHS National Hospital Discharge Survey, 2010. Number of discharges from short‐stay hospitals, by first‐listed diagnosis and age: United States, 2010. National Center for Health Statistics. Available at: http://www.cdc.gov/nchs/data/nhds/3firstlisted/2010first3_numberage.pdf. Accessed July 14, 2014.
- , . Community‐acquired pneumonia in the elderly. Am J Geriatr Pharmacother. 2010;8(1):47–62.
- , , , et al. Effectiveness of pneumococcal polysaccharide vaccine in older adults. N Engl J Med. 2003;348:1747–1754.
- , . Pneumococcal vaccination of elderly adults: new paradigms for protection. Clin Infect Dis. 2008;47(10):1328–1338.
- , . The 23‐valent pneumococcal polysaccharide vaccine. Part 1. Efficacy of PPV in the elderly: a comparison of meta‐analysis. Eur J Epidemiol. 2004;19:353–363.
- , , , . Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst Rev. 2008;(1):CD000422.
- , , , , . Efficacy of pneumococcal vaccination in adults: a meta‐analysis. CMAJ. 2009;180(1):48–58.
- , , , , , . Prior pneumococcal vaccination is associated with reduced death, complications, and length of stay among hospitalized adults with community‐acquired pneumonia. Clin Infect Dis. 2006;42:1093–1101.
- , , , et al. Effect of prior pneumococcal vaccination on clinical outcome of hospitalized adults with community‐acquired pneumococcal pneumonia. Eur J Clin Microbiol Infect Dis. 2006;25:257–462.
- , , , . Effect of pneumococcal vaccination in hospitalized adults with community‐acquired pneumonia. Arch Intern Med. 2007;167:1938–1943.
- , , , , , . Influenza vaccination and risk of mortality among adults hospitalized with community‐acquired pneumonia. Arch Intern Med. 2007;167:53–59.
- , , , , , . Efficacy and effectiveness of influenza vaccines in elderly people: a systematic review. Lancet. 2005;366:1165–1174.
- , , , , . Effectiveness of influenza vaccine in the community‐dwelling elderly. N Engl J Med. 2007;357:1373–1381.
- VIReC Research User Guide: FY2002 VHA Medical SAS Inpatient Datasets. Hines, IL: Veterans Affairs Information Resource Center; 2003.
- Immunization Information Systems, Centers for Disease Control and Prevention. CPT codes mapped to CVX codes. Available at: http://www2a.cdc.gov/vaccines/iis/iisstandards/vaccines.asp?rpt=cpt. Accessed December 2, 2014.
- Centers for Disease Control and Prevention. Pneumococcal polysaccharide vaccine information statement. Available at: http://www.cdc.gov/vaccines/hcp/vis/vis‐statements/ppv.html. Accessed December 2, 2014.
- , , , et al. The protective efficacy of polyvalent pneumococcal polysaccharide vaccine. N Engl J Med. 1991;325:1453–1460.
- , , . Adapting a clinical comorbidity index for use with ICD‐9‐CM Administrative Databases. J Clin Epidemiol. 1992;45(6):613–619.
- , , , . Missing race/ethnicity data in Veterans Health Administration based disparities research: a systematic review. J Health Care Poor Underserved. 2006;17:128–140.
- , , , et al. Risk adjusting community‐acquired pneumonia hospital outcomes using automated databases. Am J Manag Care. 2008;14(3):158–166.
- , , , et al. A prediction rule to identify low‐risk patients with community‐acquired pneumonia. N Engl J Med. 1997;336:243–250.
- , , . A comparison of statistical modeling strategies for analyzing length of stay after CABG surgery. Health Serv Outcomes Res Methodol. 2002;3:107–133.
- , . GMATCH SAS macro. Available at: http://www.mayo.edu/research/documents/gmatchsas/DOC‐10027248. Accessed December 2, 2014.
- , , , . Analysis of Observational Health Care Data Using SAS. Cary, NC: SAS Institute; 2010.
- , , . Pneumococcal vaccination in older adults induces antibodies with low opsonic capacity and reduced antibody potency. Vaccine. 2008;26:5521–5526.
- , , . The effect of age on the response to the pneumococcal polysaccharide vaccine. BMC Infect Dis. 2010;10:60.
- , . Older adults have a low capacity to opsonize pneumococci due to low IgM antibody response to pneumococcal vaccinations. Infect Immun. 2011;79(1):314–320.
- , , , , . Impact of the pneumococcal vaccine on long‐term morbidity and mortality of adults at high risk for pneumonia. Clin Infect Dis. 2010;51(1):15–22.
- , , , , , . Effect of 13‐valent pneumococcal conjugate vaccine on admissions to hospital 2 years after its introduction in the USA: a time series analysis. Lancet Respir Med. 2014;2(5):387–394.
- American Academy of Family Physicians. ACIP recommends routine PCV13 immunization for adults 65 and older. Available at: http://www.aafp.org/news/health‐of‐the‐public/20140827pcv13vote.html. Accessed December 2, 2012.
- , , , et al. The burden of community‐acquired pneumonia in seniors: results of a population‐based study. Clin Infect Dis. 2004;39:1642–1650.
- , , , et al. Bacteremia with Streptococcus pneumoniae: sepsis and other risk factors for 30‐day mortality‐a hospital‐based cohort study. Eur J Clin Microbiol Infect Dis. 2012;13(10):2719–2725.
- , , , , . Trends in hospitalizations for pneumonia among persons aged 65 years or older in the United States, 1988–2002. JAMA. 2005;294(21):2712–2719.
- , , , et al. The effectiveness of the polysaccharide pneumococcal vaccine for the prevention of hospitalizations due to Streptococcus pneumoniae community‐acquired pneumonia in the elderly differs between the sexes: results from the Community‐Acquired Pneumonia Organization (CAPO) international cohort study. Vaccine. 2014;17:32(19):2198–2203.
- , , . Performance measures, vaccinations, and pneumonia rates among high‐risk patients in Veterans Administration health care. Am J Public Health. 2007;97(12):2167–2172.
- , , . Influenza and pneumococcal vaccination in older veterans: results from the Behavioral Risk Factor Surveillance System. J Am Geriatr Soc. 2006;54:217–223.
- , , , . The efficacy and cost effectiveness of vaccination against influenza among elderly persons living in the community. N Engl J Med. 1994;331:778–784.
- , , , . The health and economic benefits associated with pneumococcal vaccination of elderly persons with chronic lung disease. Arch Intern Med. 1999;159:2437–2442.
- , , . Pneumococcal vaccination in hospitalized elderly patients: role of the pharmacist. Pharmacotherapy. 2003;2(23):199–208.
- , , , . Accuracy of administrative data for identifying patients with pneumonia. Am J Med Qual. 2005;30:319–328.
- , , , , . International classification of diseases codes showed modest sensitivity for detecting community‐acquired pneumonia. J Clin Epidemiol. 2007;60(8):834–838.
- , , , et al. Cost‐effectiveness of pneumococcal vaccination of older people: a study in 5 western European countries. Clin Infect Dis. 2000;31:444–450.
- , , , et al. Cost‐effectiveness of pneumococcal vaccination for prevention of invasive pneumococcal disease in the elderly: an update for 10 Western European countries. Eur J Clin Microbiol Infect Dis. 2007;26(8):531–540.
- , , , et al. Efficacy of 23‐valent pneumococcal vaccine in preventing pneumonia and improving survival in nursing home residents: double blind, randomised and placebo controlled trial. BMJ. 2010;340:c1004.
- , , , . Community‐acquired pneumonia in elderly patients. Aging Health. 2009;5(6):763–774.
- CDC/NCHS National Hospital Discharge Survey, 2010. Number of discharges from short‐stay hospitals, by first‐listed diagnosis and age: United States, 2010. National Center for Health Statistics. Available at: http://www.cdc.gov/nchs/data/nhds/3firstlisted/2010first3_numberage.pdf. Accessed July 14, 2014.
- , . Community‐acquired pneumonia in the elderly. Am J Geriatr Pharmacother. 2010;8(1):47–62.
- , , , et al. Effectiveness of pneumococcal polysaccharide vaccine in older adults. N Engl J Med. 2003;348:1747–1754.
- , . Pneumococcal vaccination of elderly adults: new paradigms for protection. Clin Infect Dis. 2008;47(10):1328–1338.
- , . The 23‐valent pneumococcal polysaccharide vaccine. Part 1. Efficacy of PPV in the elderly: a comparison of meta‐analysis. Eur J Epidemiol. 2004;19:353–363.
- , , , . Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst Rev. 2008;(1):CD000422.
- , , , , . Efficacy of pneumococcal vaccination in adults: a meta‐analysis. CMAJ. 2009;180(1):48–58.
- , , , , , . Prior pneumococcal vaccination is associated with reduced death, complications, and length of stay among hospitalized adults with community‐acquired pneumonia. Clin Infect Dis. 2006;42:1093–1101.
- , , , et al. Effect of prior pneumococcal vaccination on clinical outcome of hospitalized adults with community‐acquired pneumococcal pneumonia. Eur J Clin Microbiol Infect Dis. 2006;25:257–462.
- , , , . Effect of pneumococcal vaccination in hospitalized adults with community‐acquired pneumonia. Arch Intern Med. 2007;167:1938–1943.
- , , , , , . Influenza vaccination and risk of mortality among adults hospitalized with community‐acquired pneumonia. Arch Intern Med. 2007;167:53–59.
- , , , , , . Efficacy and effectiveness of influenza vaccines in elderly people: a systematic review. Lancet. 2005;366:1165–1174.
- , , , , . Effectiveness of influenza vaccine in the community‐dwelling elderly. N Engl J Med. 2007;357:1373–1381.
- VIReC Research User Guide: FY2002 VHA Medical SAS Inpatient Datasets. Hines, IL: Veterans Affairs Information Resource Center; 2003.
- Immunization Information Systems, Centers for Disease Control and Prevention. CPT codes mapped to CVX codes. Available at: http://www2a.cdc.gov/vaccines/iis/iisstandards/vaccines.asp?rpt=cpt. Accessed December 2, 2014.
- Centers for Disease Control and Prevention. Pneumococcal polysaccharide vaccine information statement. Available at: http://www.cdc.gov/vaccines/hcp/vis/vis‐statements/ppv.html. Accessed December 2, 2014.
- , , , et al. The protective efficacy of polyvalent pneumococcal polysaccharide vaccine. N Engl J Med. 1991;325:1453–1460.
- , , . Adapting a clinical comorbidity index for use with ICD‐9‐CM Administrative Databases. J Clin Epidemiol. 1992;45(6):613–619.
- , , , . Missing race/ethnicity data in Veterans Health Administration based disparities research: a systematic review. J Health Care Poor Underserved. 2006;17:128–140.
- , , , et al. Risk adjusting community‐acquired pneumonia hospital outcomes using automated databases. Am J Manag Care. 2008;14(3):158–166.
- , , , et al. A prediction rule to identify low‐risk patients with community‐acquired pneumonia. N Engl J Med. 1997;336:243–250.
- , , . A comparison of statistical modeling strategies for analyzing length of stay after CABG surgery. Health Serv Outcomes Res Methodol. 2002;3:107–133.
- , . GMATCH SAS macro. Available at: http://www.mayo.edu/research/documents/gmatchsas/DOC‐10027248. Accessed December 2, 2014.
- , , , . Analysis of Observational Health Care Data Using SAS. Cary, NC: SAS Institute; 2010.
- , , . Pneumococcal vaccination in older adults induces antibodies with low opsonic capacity and reduced antibody potency. Vaccine. 2008;26:5521–5526.
- , , . The effect of age on the response to the pneumococcal polysaccharide vaccine. BMC Infect Dis. 2010;10:60.
- , . Older adults have a low capacity to opsonize pneumococci due to low IgM antibody response to pneumococcal vaccinations. Infect Immun. 2011;79(1):314–320.
- , , , , . Impact of the pneumococcal vaccine on long‐term morbidity and mortality of adults at high risk for pneumonia. Clin Infect Dis. 2010;51(1):15–22.
- , , , , , . Effect of 13‐valent pneumococcal conjugate vaccine on admissions to hospital 2 years after its introduction in the USA: a time series analysis. Lancet Respir Med. 2014;2(5):387–394.
- American Academy of Family Physicians. ACIP recommends routine PCV13 immunization for adults 65 and older. Available at: http://www.aafp.org/news/health‐of‐the‐public/20140827pcv13vote.html. Accessed December 2, 2012.
- , , , et al. The burden of community‐acquired pneumonia in seniors: results of a population‐based study. Clin Infect Dis. 2004;39:1642–1650.
- , , , et al. Bacteremia with Streptococcus pneumoniae: sepsis and other risk factors for 30‐day mortality‐a hospital‐based cohort study. Eur J Clin Microbiol Infect Dis. 2012;13(10):2719–2725.
- , , , , . Trends in hospitalizations for pneumonia among persons aged 65 years or older in the United States, 1988–2002. JAMA. 2005;294(21):2712–2719.
- , , , et al. The effectiveness of the polysaccharide pneumococcal vaccine for the prevention of hospitalizations due to Streptococcus pneumoniae community‐acquired pneumonia in the elderly differs between the sexes: results from the Community‐Acquired Pneumonia Organization (CAPO) international cohort study. Vaccine. 2014;17:32(19):2198–2203.
- , , . Performance measures, vaccinations, and pneumonia rates among high‐risk patients in Veterans Administration health care. Am J Public Health. 2007;97(12):2167–2172.
- , , . Influenza and pneumococcal vaccination in older veterans: results from the Behavioral Risk Factor Surveillance System. J Am Geriatr Soc. 2006;54:217–223.
- , , , . The efficacy and cost effectiveness of vaccination against influenza among elderly persons living in the community. N Engl J Med. 1994;331:778–784.
- , , , . The health and economic benefits associated with pneumococcal vaccination of elderly persons with chronic lung disease. Arch Intern Med. 1999;159:2437–2442.
- , , . Pneumococcal vaccination in hospitalized elderly patients: role of the pharmacist. Pharmacotherapy. 2003;2(23):199–208.
- , , , . Accuracy of administrative data for identifying patients with pneumonia. Am J Med Qual. 2005;30:319–328.
- , , , , . International classification of diseases codes showed modest sensitivity for detecting community‐acquired pneumonia. J Clin Epidemiol. 2007;60(8):834–838.
- , , , et al. Cost‐effectiveness of pneumococcal vaccination of older people: a study in 5 western European countries. Clin Infect Dis. 2000;31:444–450.
- , , , et al. Cost‐effectiveness of pneumococcal vaccination for prevention of invasive pneumococcal disease in the elderly: an update for 10 Western European countries. Eur J Clin Microbiol Infect Dis. 2007;26(8):531–540.
- , , , et al. Efficacy of 23‐valent pneumococcal vaccine in preventing pneumonia and improving survival in nursing home residents: double blind, randomised and placebo controlled trial. BMJ. 2010;340:c1004.
© 2015 Society of Hospital Medicine
Are the implant and IUD effective beyond 3 and 5 years?
The etonogestrel contraceptive implant and the 52-mg levonorgestrel intrauterine system (LNG-IUS) remain highly effective for an additional year beyond the FDA-approved intervals of 3 and 5 years, respectively, according to a newly published prospective study.1
In the study, implant users (n = 237) contributed 229.4 women-years of follow-up, with 123 women using the implant for 4 years and 34 using it for 5 years. No pregnancies were documented—a failure rate of 0 (one-sided 97.5% confidence interval [CI], 0–1.61) per 100 women-years.
Of 263 LNG-IUS users, 197.7 women-years of follow-up found only one pregnancy—a failure rate of 0.51 (95% CI, 0.01–2.82) per 100 women-years.
Among implant users with serum etonogestrel levels assessed, the median at 3 years of use was 188.8 pg/mL (range, 63.8–802.6 pg/mL). At 4 years, the median etonogestrel level was 177.0 pg/mL (range, 67,9–470.5 pg/mL). Etonogestrel levels did not vary by body mass index at either 3 years (P = .79) or 4 years (P = .47). These serum levels indicate that the implant contains adequate hormone for ovulation suppression at the end of both 3 and 4 years of use.
Reference
1. McNicholas C, Maddipati R, Zhao Q; Swor E, Peipert JF. Use of the etonogestrel implant and levonorgestrel intrauterine device beyond the US Food and Drug Administration-approved duration. Obstet Gynecol. 2015 February 4. Published ahead of print. doi:10.1097/AOG.0000000000000690.
The etonogestrel contraceptive implant and the 52-mg levonorgestrel intrauterine system (LNG-IUS) remain highly effective for an additional year beyond the FDA-approved intervals of 3 and 5 years, respectively, according to a newly published prospective study.1
In the study, implant users (n = 237) contributed 229.4 women-years of follow-up, with 123 women using the implant for 4 years and 34 using it for 5 years. No pregnancies were documented—a failure rate of 0 (one-sided 97.5% confidence interval [CI], 0–1.61) per 100 women-years.
Of 263 LNG-IUS users, 197.7 women-years of follow-up found only one pregnancy—a failure rate of 0.51 (95% CI, 0.01–2.82) per 100 women-years.
Among implant users with serum etonogestrel levels assessed, the median at 3 years of use was 188.8 pg/mL (range, 63.8–802.6 pg/mL). At 4 years, the median etonogestrel level was 177.0 pg/mL (range, 67,9–470.5 pg/mL). Etonogestrel levels did not vary by body mass index at either 3 years (P = .79) or 4 years (P = .47). These serum levels indicate that the implant contains adequate hormone for ovulation suppression at the end of both 3 and 4 years of use.
The etonogestrel contraceptive implant and the 52-mg levonorgestrel intrauterine system (LNG-IUS) remain highly effective for an additional year beyond the FDA-approved intervals of 3 and 5 years, respectively, according to a newly published prospective study.1
In the study, implant users (n = 237) contributed 229.4 women-years of follow-up, with 123 women using the implant for 4 years and 34 using it for 5 years. No pregnancies were documented—a failure rate of 0 (one-sided 97.5% confidence interval [CI], 0–1.61) per 100 women-years.
Of 263 LNG-IUS users, 197.7 women-years of follow-up found only one pregnancy—a failure rate of 0.51 (95% CI, 0.01–2.82) per 100 women-years.
Among implant users with serum etonogestrel levels assessed, the median at 3 years of use was 188.8 pg/mL (range, 63.8–802.6 pg/mL). At 4 years, the median etonogestrel level was 177.0 pg/mL (range, 67,9–470.5 pg/mL). Etonogestrel levels did not vary by body mass index at either 3 years (P = .79) or 4 years (P = .47). These serum levels indicate that the implant contains adequate hormone for ovulation suppression at the end of both 3 and 4 years of use.
Reference
1. McNicholas C, Maddipati R, Zhao Q; Swor E, Peipert JF. Use of the etonogestrel implant and levonorgestrel intrauterine device beyond the US Food and Drug Administration-approved duration. Obstet Gynecol. 2015 February 4. Published ahead of print. doi:10.1097/AOG.0000000000000690.
Reference
1. McNicholas C, Maddipati R, Zhao Q; Swor E, Peipert JF. Use of the etonogestrel implant and levonorgestrel intrauterine device beyond the US Food and Drug Administration-approved duration. Obstet Gynecol. 2015 February 4. Published ahead of print. doi:10.1097/AOG.0000000000000690.
ECMO alone before lung transplant linked to good survival rates
SAN DIEGO – Extracorporeal membrane oxygenation with spontaneous breathing is the optimal bridging strategy for patients who have rapidly advancing pulmonary disease and are awaiting lung transplantation, based on data from over 18,000 patients who received lung transplants.
In the study, patients on extracorporeal membrane oxygenation (ECMO) alone had outcomes that were comparable to those of patients requiring no invasive support prior to transplantation, Dr. Matthew Schechter of Duke University in Durham, N.C., reported at the annual meeting of the Society of Thoracic Surgeons.
Dr. Schechter and his colleagues analyzed the United Network for Organ Sharing database for all adult patients who underwent lung transplantations between January 2000 and September 2013.
The 18,392 patients selected for study inclusion were divided into cohorts based on the type of preoperative support they received: ECMO with mechanical ventilation; ECMO only; ventilation only; and no support of any kind. Nearly 95% of the patients received no invasive preoperative support. Over 4% received mechanical ventilation alone, less than 1% received ECMO with mechanical ventilation, and about 0.5%) received ECMO only.
By using Kaplan-Meier survival analyses with log-rank testing, Dr. Schechter and his associates were able to compare survival rates for each type of preoperative support. Cox regression models were used to ascertain whether any particular type of preoperative support could definitively be associated with mortality.
At 3 years post transplantation, the survival rates of patients on ECMO alone and of those who received no preoperative support of any kind were comparable at 66% and 65%, respectively. Survival rates at 3 years after transplant were 38% in patients who received ECMO and mechanical ventilation and 52% in patients who received mechanical ventilation alone. The survival advantage in the ECMO only and no support groups was significantly better when compared to the ECMO and mechanical ventilation and the mechanical ventilation alone cohorts (P < .0001).
The findings held up after a multivariate analysis; the hazard ratio was 1.96 (95% confidence interval, 1.36-2.84) for ECMO with mechanical ventilation and 1.52 (95% CI, 1.31-1.78) for mechanical ventilation only (P < .0001 for both).
ECMO alone was not associated with any significant change in survival rate (HR = 1.07; 95% CI, 0.57-2.01; P = .843).
Patients who received just ECMO had the shortest lengths of stay after lung transplant. They also had the lowest rate of acute rejection prior to discharge, although not to an extent that was statistically significant. The incidence of new-onset dialysis was highest in patients who received ECMO with mechanical ventilation.
“ECMO alone may provide a survival advantage over other bridging strategies,” Dr. Schechter concluded. “One advantage of using ECMO only is an avoidance of the risks that come with mechanical ventilation, [which] include generalized muscle atrophy, maladapted muscle fiber remodeling in the diaphragm – which leads to a decrease in the overall durability of this muscle – as well as the induction of the pulmonary and systemic inflammatory risk responses, [all of which] have been shown to affect outcomes following lung transplantation.”
Dr. Schechter explained that patients receiving ECMO without mechanical ventilation can actively rehabilitate themselves post transplantation since nonintubated ECMO patients can participate in physical therapy.
Further study is needed to find an optimal way of assessing patients and determining exactly which ones would be best suited for ECMO with spontaneous breathing support, he said.
Dr, Schechter had no relevant financial disclosures.
SAN DIEGO – Extracorporeal membrane oxygenation with spontaneous breathing is the optimal bridging strategy for patients who have rapidly advancing pulmonary disease and are awaiting lung transplantation, based on data from over 18,000 patients who received lung transplants.
In the study, patients on extracorporeal membrane oxygenation (ECMO) alone had outcomes that were comparable to those of patients requiring no invasive support prior to transplantation, Dr. Matthew Schechter of Duke University in Durham, N.C., reported at the annual meeting of the Society of Thoracic Surgeons.
Dr. Schechter and his colleagues analyzed the United Network for Organ Sharing database for all adult patients who underwent lung transplantations between January 2000 and September 2013.
The 18,392 patients selected for study inclusion were divided into cohorts based on the type of preoperative support they received: ECMO with mechanical ventilation; ECMO only; ventilation only; and no support of any kind. Nearly 95% of the patients received no invasive preoperative support. Over 4% received mechanical ventilation alone, less than 1% received ECMO with mechanical ventilation, and about 0.5%) received ECMO only.
By using Kaplan-Meier survival analyses with log-rank testing, Dr. Schechter and his associates were able to compare survival rates for each type of preoperative support. Cox regression models were used to ascertain whether any particular type of preoperative support could definitively be associated with mortality.
At 3 years post transplantation, the survival rates of patients on ECMO alone and of those who received no preoperative support of any kind were comparable at 66% and 65%, respectively. Survival rates at 3 years after transplant were 38% in patients who received ECMO and mechanical ventilation and 52% in patients who received mechanical ventilation alone. The survival advantage in the ECMO only and no support groups was significantly better when compared to the ECMO and mechanical ventilation and the mechanical ventilation alone cohorts (P < .0001).
The findings held up after a multivariate analysis; the hazard ratio was 1.96 (95% confidence interval, 1.36-2.84) for ECMO with mechanical ventilation and 1.52 (95% CI, 1.31-1.78) for mechanical ventilation only (P < .0001 for both).
ECMO alone was not associated with any significant change in survival rate (HR = 1.07; 95% CI, 0.57-2.01; P = .843).
Patients who received just ECMO had the shortest lengths of stay after lung transplant. They also had the lowest rate of acute rejection prior to discharge, although not to an extent that was statistically significant. The incidence of new-onset dialysis was highest in patients who received ECMO with mechanical ventilation.
“ECMO alone may provide a survival advantage over other bridging strategies,” Dr. Schechter concluded. “One advantage of using ECMO only is an avoidance of the risks that come with mechanical ventilation, [which] include generalized muscle atrophy, maladapted muscle fiber remodeling in the diaphragm – which leads to a decrease in the overall durability of this muscle – as well as the induction of the pulmonary and systemic inflammatory risk responses, [all of which] have been shown to affect outcomes following lung transplantation.”
Dr. Schechter explained that patients receiving ECMO without mechanical ventilation can actively rehabilitate themselves post transplantation since nonintubated ECMO patients can participate in physical therapy.
Further study is needed to find an optimal way of assessing patients and determining exactly which ones would be best suited for ECMO with spontaneous breathing support, he said.
Dr, Schechter had no relevant financial disclosures.
SAN DIEGO – Extracorporeal membrane oxygenation with spontaneous breathing is the optimal bridging strategy for patients who have rapidly advancing pulmonary disease and are awaiting lung transplantation, based on data from over 18,000 patients who received lung transplants.
In the study, patients on extracorporeal membrane oxygenation (ECMO) alone had outcomes that were comparable to those of patients requiring no invasive support prior to transplantation, Dr. Matthew Schechter of Duke University in Durham, N.C., reported at the annual meeting of the Society of Thoracic Surgeons.
Dr. Schechter and his colleagues analyzed the United Network for Organ Sharing database for all adult patients who underwent lung transplantations between January 2000 and September 2013.
The 18,392 patients selected for study inclusion were divided into cohorts based on the type of preoperative support they received: ECMO with mechanical ventilation; ECMO only; ventilation only; and no support of any kind. Nearly 95% of the patients received no invasive preoperative support. Over 4% received mechanical ventilation alone, less than 1% received ECMO with mechanical ventilation, and about 0.5%) received ECMO only.
By using Kaplan-Meier survival analyses with log-rank testing, Dr. Schechter and his associates were able to compare survival rates for each type of preoperative support. Cox regression models were used to ascertain whether any particular type of preoperative support could definitively be associated with mortality.
At 3 years post transplantation, the survival rates of patients on ECMO alone and of those who received no preoperative support of any kind were comparable at 66% and 65%, respectively. Survival rates at 3 years after transplant were 38% in patients who received ECMO and mechanical ventilation and 52% in patients who received mechanical ventilation alone. The survival advantage in the ECMO only and no support groups was significantly better when compared to the ECMO and mechanical ventilation and the mechanical ventilation alone cohorts (P < .0001).
The findings held up after a multivariate analysis; the hazard ratio was 1.96 (95% confidence interval, 1.36-2.84) for ECMO with mechanical ventilation and 1.52 (95% CI, 1.31-1.78) for mechanical ventilation only (P < .0001 for both).
ECMO alone was not associated with any significant change in survival rate (HR = 1.07; 95% CI, 0.57-2.01; P = .843).
Patients who received just ECMO had the shortest lengths of stay after lung transplant. They also had the lowest rate of acute rejection prior to discharge, although not to an extent that was statistically significant. The incidence of new-onset dialysis was highest in patients who received ECMO with mechanical ventilation.
“ECMO alone may provide a survival advantage over other bridging strategies,” Dr. Schechter concluded. “One advantage of using ECMO only is an avoidance of the risks that come with mechanical ventilation, [which] include generalized muscle atrophy, maladapted muscle fiber remodeling in the diaphragm – which leads to a decrease in the overall durability of this muscle – as well as the induction of the pulmonary and systemic inflammatory risk responses, [all of which] have been shown to affect outcomes following lung transplantation.”
Dr. Schechter explained that patients receiving ECMO without mechanical ventilation can actively rehabilitate themselves post transplantation since nonintubated ECMO patients can participate in physical therapy.
Further study is needed to find an optimal way of assessing patients and determining exactly which ones would be best suited for ECMO with spontaneous breathing support, he said.
Dr, Schechter had no relevant financial disclosures.
FROM THE STS ANNUAL MEETING
Key clinical point: ECMO with spontaneous breathing should be considered the preferred bridging strategy for patients who have rapidly advancing pulmonary disease and are awaiting lung transplantations.
Major finding: At 3 years post transplantation, the survival rates of patients on ECMO alone and of those who received no preoperative support of any kind were comparable at 66% and 65%, respectively.
Data source: Retrospective analysis of 18,392 adult patients in the United Network for Organ Sharing database.
Disclosures: Dr. Schechter had no relevant financial disclosures.
VIDEO: Is JNC 8’s hypertension treatment threshold too high?
NASHVILLE, TENN. – Last year, the Eighth Joint National Committee revised upward its classification of hypertension in healthy adults aged 60 years and older, recommending treatment when systolic pressure hits at least 150 mm Hg, or diastolic pressure reaches at least 90 mm Hg.
But raising the treatment cut point by 10 mm Hg from the earlier JNC 7 recommendations is a bad idea, Dr. Ralph L. Sacco warned at the International Stroke Conference – very bad, in fact.
And Dr. Sacco, the Olemberg Family Chair in Neurological Disorders at the University of Miami, said he has the data to prove it.
In a video interview at the meeting, Dr. Sacco outlined the findings from a new study exploring the stroke risks of patients who might find themselves now deemed normotensive under the JNC 8 hypertension guidelines.
On Twitter @alz_gal
NASHVILLE, TENN. – Last year, the Eighth Joint National Committee revised upward its classification of hypertension in healthy adults aged 60 years and older, recommending treatment when systolic pressure hits at least 150 mm Hg, or diastolic pressure reaches at least 90 mm Hg.
But raising the treatment cut point by 10 mm Hg from the earlier JNC 7 recommendations is a bad idea, Dr. Ralph L. Sacco warned at the International Stroke Conference – very bad, in fact.
And Dr. Sacco, the Olemberg Family Chair in Neurological Disorders at the University of Miami, said he has the data to prove it.
In a video interview at the meeting, Dr. Sacco outlined the findings from a new study exploring the stroke risks of patients who might find themselves now deemed normotensive under the JNC 8 hypertension guidelines.
On Twitter @alz_gal
NASHVILLE, TENN. – Last year, the Eighth Joint National Committee revised upward its classification of hypertension in healthy adults aged 60 years and older, recommending treatment when systolic pressure hits at least 150 mm Hg, or diastolic pressure reaches at least 90 mm Hg.
But raising the treatment cut point by 10 mm Hg from the earlier JNC 7 recommendations is a bad idea, Dr. Ralph L. Sacco warned at the International Stroke Conference – very bad, in fact.
And Dr. Sacco, the Olemberg Family Chair in Neurological Disorders at the University of Miami, said he has the data to prove it.
In a video interview at the meeting, Dr. Sacco outlined the findings from a new study exploring the stroke risks of patients who might find themselves now deemed normotensive under the JNC 8 hypertension guidelines.
On Twitter @alz_gal
AT THE INTERNATIONAL STROKE CONFERENCE

Three trials cement embolectomy for acute ischemic stroke
NASHVILLE, TENN. – Treatment of selected patients with acute ischemic stroke underwent a dramatic, sudden shift with reports from three randomized, controlled trials that showed substantial added benefit and no incremental risk with the use of catheter-based embolic retrieval to open blocked intracerebral arteries when performed on top of standard thrombolytic therapy.
The three studies, each run independently and based in different countries, supported the results first reported last October and published online in December (N. Engl. J. Med. 2015;372:11-20) from the MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) study. These were the first contemporary trial results to show a jump in functional outcomes with use of a stent retriever catheter to pluck out the occluding embolus from an artery in the stroke patient’s brain to restore normal blood flow.
All three of the newly-reported studies stopped before reaching their prespecified enrollment levels because of overwhelming evidence for embolectomy’s incremental efficacy.
With four reports from prospective, randomized trials showing similar benefits and no added harm to patients, experts at the International Stroke Conference uniformly anointed catheter-based embolectomy the new standard of care for the small percentage of acute, ischemic-stroke patients who present with proximal, large-artery obstructions and also match the other strict clinical and imaging inclusion and exclusion criteria used in the studies.

“Starting now, in patients with an acute ischemic stroke due to proximal vessel occlusion, rapid endovascular treatment using a retrieval stent is the standard of care,” Dr. Mayank Goyal declared from the plenary-session podium. He is a professor of diagnostic imaging at the University of Calgary (Canada) and an investigator in two of the three trials presented at the conference, which was sponsored by the American Heart Association.
“Today the world changed. We are now in a new era, the era of highly-effective intravascular recanalization therapy,” said Dr. Jeffrey L. Saver, professor of neurology and director of the Stroke Center at the University of California, Los Angeles, and lead investigator for one of the new studies.
In three of the four studies, the researchers did not report specific numbers on how selective they were in focusing in on the ischemic stroke patients most likely to benefit from this treatment, but the one study that did, EXTEND-IA (Extending the Time for Thrombolysis in Emergency Neurological Deficits – Intra-Arterial), run at nine Australian centers and one in New Zealand, showed the extensive winnowing that occurred. Of 7,796 patients with an acute ischemic stroke who initially presented, 1,044 (13%) were eligible to receive thrombolytic therapy (alteplase in this study). And from among these 1,044 patients, a mere 70 – less than 1% of the initial group – were deemed eligible for randomization into the embolectomy trial. The top three reasons for exclusion of patients who qualified for thrombolytic treatment from the trial was an absence of a major-vessel occlusion (45% of the excluded patients), presentation outside of the times when enrollment personnel were available (22%), and poor premorbid function (16%).

But subgroup analyses in three of the four studies (EXTEND-IA with a total of 70 patients was too small for subgroup analyses) showed no subgroup of patients who failed to benefit from embolectomy, including elderly patients who in some cases were nonagenarians.
The unusual confluence of having four major trials showing remarkably consistent results meant that the stroke experts gathered at the meeting focused their attention not on whether stent retrievers should now be widely and routinely used in appropriate patients but instead on how this technology will roll out worldwide.
“From here on out we are obligated to treat patients with this technology at centers that can do this, and we are obligated to have more centers that can provide it,” said Dr. Kyra J. Becker, professor of neurology and neurological surgery and codirector of the Stroke Center at the University of Washington, Seattle. Dr. Becker had no involvement in any of the stent retriever trials. “I had been a doubter of this technology,” primarily because results reported at the International Stroke Conference a couple of years ago failed to prove the efficacy of clot retrieval in ischemic stroke patients, she noted. “Our ability to select appropriate patients and do it in a timely fashion hadn’t gotten to where it had to be until now,” Dr. Becker said in an interview.
“We only enrolled patients with blockages, we treated them quickly, and we used much better devices to open their arteries,” Dr. Saver added, explaining why the new studies succeeded when earlier studies had not.
The trial led by Dr. Saver, SWIFT-PRIME (SOLITAIRE™ FR With the Intention for Thrombectomy as Primary Endovascular Treatment for Acute Ischemic Stroke), enrolled 195 patients at 39 sites in the United States and in Europe. At 90 days after treatment, 59 patients (60%) among those treated with thrombolysis plus embolectomy had a modified Rankin Scale score of 0-2, compared with 33 patients (36%) among those treated only with thrombolysis (in this trial intravenous treatment with tissue plasminogen activator), a highly significant difference for the study’s primary endpoint.

“For every two and half patients treated, one more patient had a better disability outcome, and for every four patients treated, one more patient was independent at long-term follow-up,” Dr. Saver said. Safety measures were similar among patients in the study’s two arms.
The EXTEND-IA results showed a 90-day modified Rankin Scale score of 0-2 in 52% of the embolectomy patients, compared with 28% of those treated only with thrombolysis. The study’s co–primary endpoints were median level of reperfusion at 24 hours after treatment, 100% with embolectomy and 37% with thrombolysis only, and early neurologic recovery, defined as at least an 8-point drop from the baseline in the National Institutes of Health Stroke Scale score or a score of 0 or 1 when assessed 3 days after treatment. Patients met this second endpoint at an 80% rate with embolectomy and a 37% rate with thrombolysis only. Results of EXTEND-IA appeared in an article published online concurrently with the meeting report (N. Engl J. Med. 2015 Feb. 11 [doi:10.1056/NEJMoa1414792]).
The third, and largest, of the three studies presented at the conference, ESCAPE (Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times), enrolled 316 patients at 11 centers in Canada, 6 in the United States, 3 in South Korea, and 1 in Ireland. After 90 days, 53% of patients in the embolectomy arm had achieved a modified Rankin Scale score of 0-2, this study’s primary endpoint, compared with 29% of patients in the thrombolysis-only arm (treatment with alteplase). These results also appeared in an article published online concurrently with the conference report (N. Engl. J. Med. 2015 Feb. 11 [doi:10.1056/NEJMoa1414905]).
SWIFT PRIME was sponsored by Covidien, which markets the stent retriever used in the study. Dr. Saver and Dr. Goyal are consultants to Covidien. EXTEND-IA used stent retrievers provided by Covidien. ESCAPE received a grant from Covidien. Dr. Becker had no relevant disclosures.
On Twitter @mitchelzoler
Many U.S. centers have interventionalists who already perform endovascular treatments within intracerebral arteries, but the issue is can they do this form of embolectomy in the high-quality, highly-reliable, rapid way that it was done in these trials? Stent-retriever catheters are relatively straightforward to use by operators who are experienced doing vascular procedures in the brain, but they don’t deliver this treatment by themselves. You need a team that is focused on doing it quickly, and that will be the kind of training we’ll need to roll out this treatment broadly. We achieved it for stroke thrombolytic treatment through the Target Stroke program (JAMA 2014;311:1632-40), so we know that we can achieve this sort of goal. Delivering embolectomy requires more people and more technology than thrombolysis, but it is not rocket science; it just needs a system.

|
| Dr. Lee H. Schwamm |
Embolectomy will not replace routine thrombolysis treatment; it will piggyback on top of it. The percentage of patients with a proximal occlusion in a large artery is relatively small. The results we have seen suggest that using embolectomy plus thrombolysis has no adverse-effect downside, compared with thrombolysis alone. Once routine use of embolectomy becomes established, we can directly compare catheter treatment only against combined embolectomy and thrombolysis. My impression today is that what we’d compare is transporting stroke patients directly to a center that can perform embolectomy against taking patients to the closest center that can treat them with thrombolysis and then transporting them to the center that performs embolectomy.
The results of these three new studies plus the previously-reported results from MR CLEAN are not exactly a game changer, because many centers were already performing embolectomy but in a limited way. Now we have the data to give us confidence to do it routinely and to know which patients to select for embolectomy. Because many centers are already doing this, it will not take 5 years to diffuse the technology.
Embolectomy is already a treatment cited in the guidelines, but now it will be a level 1A recommendation.
The significance of the new reports is that they will have a dramatic impact on public health systems and in the triage of patients with stroke. It will affect how patients get triaged, and will allow us to identify which patients should go to which centers. I believe we will soon develop clinical examination tools that will allow prehospital providers to discern patients with mild strokes who can go to the nearest center that can administer thrombolysis and which patients need to go to comprehensive centers that can perform embolectomy. We now need to do what we did for thrombolysis, and help centers develop the expertise to do embolectomy as a team and to shave minutes off the delivery at every step of the process. It’s clear that it is the time from stroke onset to getting the artery open that is the key to improved patient outcomes.
If I have my way, we will launch later this year a big effort to focus on improving embolectomy delivery. Now that we know for certain that it works we need to turn the crank and make sure that as many patients as possible who qualify get this treatment.
Dr. Lee H. Schwamm is professor of neurology at Harvard Medical School, and director of acute stroke services at Massachusetts General Hospital, both in Boston. He is a consultant to Penumbra and has received research support from Genentech. He made these comments in an interview.
Many U.S. centers have interventionalists who already perform endovascular treatments within intracerebral arteries, but the issue is can they do this form of embolectomy in the high-quality, highly-reliable, rapid way that it was done in these trials? Stent-retriever catheters are relatively straightforward to use by operators who are experienced doing vascular procedures in the brain, but they don’t deliver this treatment by themselves. You need a team that is focused on doing it quickly, and that will be the kind of training we’ll need to roll out this treatment broadly. We achieved it for stroke thrombolytic treatment through the Target Stroke program (JAMA 2014;311:1632-40), so we know that we can achieve this sort of goal. Delivering embolectomy requires more people and more technology than thrombolysis, but it is not rocket science; it just needs a system.
|
|
| Dr. Lee H. Schwamm |
Embolectomy will not replace routine thrombolysis treatment; it will piggyback on top of it. The percentage of patients with a proximal occlusion in a large artery is relatively small. The results we have seen suggest that using embolectomy plus thrombolysis has no adverse-effect downside, compared with thrombolysis alone. Once routine use of embolectomy becomes established, we can directly compare catheter treatment only against combined embolectomy and thrombolysis. My impression today is that what we’d compare is transporting stroke patients directly to a center that can perform embolectomy against taking patients to the closest center that can treat them with thrombolysis and then transporting them to the center that performs embolectomy.
The results of these three new studies plus the previously-reported results from MR CLEAN are not exactly a game changer, because many centers were already performing embolectomy but in a limited way. Now we have the data to give us confidence to do it routinely and to know which patients to select for embolectomy. Because many centers are already doing this, it will not take 5 years to diffuse the technology.
Embolectomy is already a treatment cited in the guidelines, but now it will be a level 1A recommendation.
The significance of the new reports is that they will have a dramatic impact on public health systems and in the triage of patients with stroke. It will affect how patients get triaged, and will allow us to identify which patients should go to which centers. I believe we will soon develop clinical examination tools that will allow prehospital providers to discern patients with mild strokes who can go to the nearest center that can administer thrombolysis and which patients need to go to comprehensive centers that can perform embolectomy. We now need to do what we did for thrombolysis, and help centers develop the expertise to do embolectomy as a team and to shave minutes off the delivery at every step of the process. It’s clear that it is the time from stroke onset to getting the artery open that is the key to improved patient outcomes.
If I have my way, we will launch later this year a big effort to focus on improving embolectomy delivery. Now that we know for certain that it works we need to turn the crank and make sure that as many patients as possible who qualify get this treatment.
Dr. Lee H. Schwamm is professor of neurology at Harvard Medical School, and director of acute stroke services at Massachusetts General Hospital, both in Boston. He is a consultant to Penumbra and has received research support from Genentech. He made these comments in an interview.
Many U.S. centers have interventionalists who already perform endovascular treatments within intracerebral arteries, but the issue is can they do this form of embolectomy in the high-quality, highly-reliable, rapid way that it was done in these trials? Stent-retriever catheters are relatively straightforward to use by operators who are experienced doing vascular procedures in the brain, but they don’t deliver this treatment by themselves. You need a team that is focused on doing it quickly, and that will be the kind of training we’ll need to roll out this treatment broadly. We achieved it for stroke thrombolytic treatment through the Target Stroke program (JAMA 2014;311:1632-40), so we know that we can achieve this sort of goal. Delivering embolectomy requires more people and more technology than thrombolysis, but it is not rocket science; it just needs a system.
|
|
| Dr. Lee H. Schwamm |
Embolectomy will not replace routine thrombolysis treatment; it will piggyback on top of it. The percentage of patients with a proximal occlusion in a large artery is relatively small. The results we have seen suggest that using embolectomy plus thrombolysis has no adverse-effect downside, compared with thrombolysis alone. Once routine use of embolectomy becomes established, we can directly compare catheter treatment only against combined embolectomy and thrombolysis. My impression today is that what we’d compare is transporting stroke patients directly to a center that can perform embolectomy against taking patients to the closest center that can treat them with thrombolysis and then transporting them to the center that performs embolectomy.
The results of these three new studies plus the previously-reported results from MR CLEAN are not exactly a game changer, because many centers were already performing embolectomy but in a limited way. Now we have the data to give us confidence to do it routinely and to know which patients to select for embolectomy. Because many centers are already doing this, it will not take 5 years to diffuse the technology.
Embolectomy is already a treatment cited in the guidelines, but now it will be a level 1A recommendation.
The significance of the new reports is that they will have a dramatic impact on public health systems and in the triage of patients with stroke. It will affect how patients get triaged, and will allow us to identify which patients should go to which centers. I believe we will soon develop clinical examination tools that will allow prehospital providers to discern patients with mild strokes who can go to the nearest center that can administer thrombolysis and which patients need to go to comprehensive centers that can perform embolectomy. We now need to do what we did for thrombolysis, and help centers develop the expertise to do embolectomy as a team and to shave minutes off the delivery at every step of the process. It’s clear that it is the time from stroke onset to getting the artery open that is the key to improved patient outcomes.
If I have my way, we will launch later this year a big effort to focus on improving embolectomy delivery. Now that we know for certain that it works we need to turn the crank and make sure that as many patients as possible who qualify get this treatment.
Dr. Lee H. Schwamm is professor of neurology at Harvard Medical School, and director of acute stroke services at Massachusetts General Hospital, both in Boston. He is a consultant to Penumbra and has received research support from Genentech. He made these comments in an interview.
NASHVILLE, TENN. – Treatment of selected patients with acute ischemic stroke underwent a dramatic, sudden shift with reports from three randomized, controlled trials that showed substantial added benefit and no incremental risk with the use of catheter-based embolic retrieval to open blocked intracerebral arteries when performed on top of standard thrombolytic therapy.
The three studies, each run independently and based in different countries, supported the results first reported last October and published online in December (N. Engl. J. Med. 2015;372:11-20) from the MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) study. These were the first contemporary trial results to show a jump in functional outcomes with use of a stent retriever catheter to pluck out the occluding embolus from an artery in the stroke patient’s brain to restore normal blood flow.
All three of the newly-reported studies stopped before reaching their prespecified enrollment levels because of overwhelming evidence for embolectomy’s incremental efficacy.
With four reports from prospective, randomized trials showing similar benefits and no added harm to patients, experts at the International Stroke Conference uniformly anointed catheter-based embolectomy the new standard of care for the small percentage of acute, ischemic-stroke patients who present with proximal, large-artery obstructions and also match the other strict clinical and imaging inclusion and exclusion criteria used in the studies.
“Starting now, in patients with an acute ischemic stroke due to proximal vessel occlusion, rapid endovascular treatment using a retrieval stent is the standard of care,” Dr. Mayank Goyal declared from the plenary-session podium. He is a professor of diagnostic imaging at the University of Calgary (Canada) and an investigator in two of the three trials presented at the conference, which was sponsored by the American Heart Association.
“Today the world changed. We are now in a new era, the era of highly-effective intravascular recanalization therapy,” said Dr. Jeffrey L. Saver, professor of neurology and director of the Stroke Center at the University of California, Los Angeles, and lead investigator for one of the new studies.
In three of the four studies, the researchers did not report specific numbers on how selective they were in focusing in on the ischemic stroke patients most likely to benefit from this treatment, but the one study that did, EXTEND-IA (Extending the Time for Thrombolysis in Emergency Neurological Deficits – Intra-Arterial), run at nine Australian centers and one in New Zealand, showed the extensive winnowing that occurred. Of 7,796 patients with an acute ischemic stroke who initially presented, 1,044 (13%) were eligible to receive thrombolytic therapy (alteplase in this study). And from among these 1,044 patients, a mere 70 – less than 1% of the initial group – were deemed eligible for randomization into the embolectomy trial. The top three reasons for exclusion of patients who qualified for thrombolytic treatment from the trial was an absence of a major-vessel occlusion (45% of the excluded patients), presentation outside of the times when enrollment personnel were available (22%), and poor premorbid function (16%).
But subgroup analyses in three of the four studies (EXTEND-IA with a total of 70 patients was too small for subgroup analyses) showed no subgroup of patients who failed to benefit from embolectomy, including elderly patients who in some cases were nonagenarians.
The unusual confluence of having four major trials showing remarkably consistent results meant that the stroke experts gathered at the meeting focused their attention not on whether stent retrievers should now be widely and routinely used in appropriate patients but instead on how this technology will roll out worldwide.
“From here on out we are obligated to treat patients with this technology at centers that can do this, and we are obligated to have more centers that can provide it,” said Dr. Kyra J. Becker, professor of neurology and neurological surgery and codirector of the Stroke Center at the University of Washington, Seattle. Dr. Becker had no involvement in any of the stent retriever trials. “I had been a doubter of this technology,” primarily because results reported at the International Stroke Conference a couple of years ago failed to prove the efficacy of clot retrieval in ischemic stroke patients, she noted. “Our ability to select appropriate patients and do it in a timely fashion hadn’t gotten to where it had to be until now,” Dr. Becker said in an interview.
“We only enrolled patients with blockages, we treated them quickly, and we used much better devices to open their arteries,” Dr. Saver added, explaining why the new studies succeeded when earlier studies had not.
The trial led by Dr. Saver, SWIFT-PRIME (SOLITAIRE™ FR With the Intention for Thrombectomy as Primary Endovascular Treatment for Acute Ischemic Stroke), enrolled 195 patients at 39 sites in the United States and in Europe. At 90 days after treatment, 59 patients (60%) among those treated with thrombolysis plus embolectomy had a modified Rankin Scale score of 0-2, compared with 33 patients (36%) among those treated only with thrombolysis (in this trial intravenous treatment with tissue plasminogen activator), a highly significant difference for the study’s primary endpoint.
“For every two and half patients treated, one more patient had a better disability outcome, and for every four patients treated, one more patient was independent at long-term follow-up,” Dr. Saver said. Safety measures were similar among patients in the study’s two arms.
The EXTEND-IA results showed a 90-day modified Rankin Scale score of 0-2 in 52% of the embolectomy patients, compared with 28% of those treated only with thrombolysis. The study’s co–primary endpoints were median level of reperfusion at 24 hours after treatment, 100% with embolectomy and 37% with thrombolysis only, and early neurologic recovery, defined as at least an 8-point drop from the baseline in the National Institutes of Health Stroke Scale score or a score of 0 or 1 when assessed 3 days after treatment. Patients met this second endpoint at an 80% rate with embolectomy and a 37% rate with thrombolysis only. Results of EXTEND-IA appeared in an article published online concurrently with the meeting report (N. Engl J. Med. 2015 Feb. 11 [doi:10.1056/NEJMoa1414792]).
The third, and largest, of the three studies presented at the conference, ESCAPE (Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times), enrolled 316 patients at 11 centers in Canada, 6 in the United States, 3 in South Korea, and 1 in Ireland. After 90 days, 53% of patients in the embolectomy arm had achieved a modified Rankin Scale score of 0-2, this study’s primary endpoint, compared with 29% of patients in the thrombolysis-only arm (treatment with alteplase). These results also appeared in an article published online concurrently with the conference report (N. Engl. J. Med. 2015 Feb. 11 [doi:10.1056/NEJMoa1414905]).
SWIFT PRIME was sponsored by Covidien, which markets the stent retriever used in the study. Dr. Saver and Dr. Goyal are consultants to Covidien. EXTEND-IA used stent retrievers provided by Covidien. ESCAPE received a grant from Covidien. Dr. Becker had no relevant disclosures.
On Twitter @mitchelzoler
NASHVILLE, TENN. – Treatment of selected patients with acute ischemic stroke underwent a dramatic, sudden shift with reports from three randomized, controlled trials that showed substantial added benefit and no incremental risk with the use of catheter-based embolic retrieval to open blocked intracerebral arteries when performed on top of standard thrombolytic therapy.
The three studies, each run independently and based in different countries, supported the results first reported last October and published online in December (N. Engl. J. Med. 2015;372:11-20) from the MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) study. These were the first contemporary trial results to show a jump in functional outcomes with use of a stent retriever catheter to pluck out the occluding embolus from an artery in the stroke patient’s brain to restore normal blood flow.
All three of the newly-reported studies stopped before reaching their prespecified enrollment levels because of overwhelming evidence for embolectomy’s incremental efficacy.
With four reports from prospective, randomized trials showing similar benefits and no added harm to patients, experts at the International Stroke Conference uniformly anointed catheter-based embolectomy the new standard of care for the small percentage of acute, ischemic-stroke patients who present with proximal, large-artery obstructions and also match the other strict clinical and imaging inclusion and exclusion criteria used in the studies.
“Starting now, in patients with an acute ischemic stroke due to proximal vessel occlusion, rapid endovascular treatment using a retrieval stent is the standard of care,” Dr. Mayank Goyal declared from the plenary-session podium. He is a professor of diagnostic imaging at the University of Calgary (Canada) and an investigator in two of the three trials presented at the conference, which was sponsored by the American Heart Association.
“Today the world changed. We are now in a new era, the era of highly-effective intravascular recanalization therapy,” said Dr. Jeffrey L. Saver, professor of neurology and director of the Stroke Center at the University of California, Los Angeles, and lead investigator for one of the new studies.
In three of the four studies, the researchers did not report specific numbers on how selective they were in focusing in on the ischemic stroke patients most likely to benefit from this treatment, but the one study that did, EXTEND-IA (Extending the Time for Thrombolysis in Emergency Neurological Deficits – Intra-Arterial), run at nine Australian centers and one in New Zealand, showed the extensive winnowing that occurred. Of 7,796 patients with an acute ischemic stroke who initially presented, 1,044 (13%) were eligible to receive thrombolytic therapy (alteplase in this study). And from among these 1,044 patients, a mere 70 – less than 1% of the initial group – were deemed eligible for randomization into the embolectomy trial. The top three reasons for exclusion of patients who qualified for thrombolytic treatment from the trial was an absence of a major-vessel occlusion (45% of the excluded patients), presentation outside of the times when enrollment personnel were available (22%), and poor premorbid function (16%).
But subgroup analyses in three of the four studies (EXTEND-IA with a total of 70 patients was too small for subgroup analyses) showed no subgroup of patients who failed to benefit from embolectomy, including elderly patients who in some cases were nonagenarians.
The unusual confluence of having four major trials showing remarkably consistent results meant that the stroke experts gathered at the meeting focused their attention not on whether stent retrievers should now be widely and routinely used in appropriate patients but instead on how this technology will roll out worldwide.
“From here on out we are obligated to treat patients with this technology at centers that can do this, and we are obligated to have more centers that can provide it,” said Dr. Kyra J. Becker, professor of neurology and neurological surgery and codirector of the Stroke Center at the University of Washington, Seattle. Dr. Becker had no involvement in any of the stent retriever trials. “I had been a doubter of this technology,” primarily because results reported at the International Stroke Conference a couple of years ago failed to prove the efficacy of clot retrieval in ischemic stroke patients, she noted. “Our ability to select appropriate patients and do it in a timely fashion hadn’t gotten to where it had to be until now,” Dr. Becker said in an interview.
“We only enrolled patients with blockages, we treated them quickly, and we used much better devices to open their arteries,” Dr. Saver added, explaining why the new studies succeeded when earlier studies had not.
The trial led by Dr. Saver, SWIFT-PRIME (SOLITAIRE™ FR With the Intention for Thrombectomy as Primary Endovascular Treatment for Acute Ischemic Stroke), enrolled 195 patients at 39 sites in the United States and in Europe. At 90 days after treatment, 59 patients (60%) among those treated with thrombolysis plus embolectomy had a modified Rankin Scale score of 0-2, compared with 33 patients (36%) among those treated only with thrombolysis (in this trial intravenous treatment with tissue plasminogen activator), a highly significant difference for the study’s primary endpoint.
“For every two and half patients treated, one more patient had a better disability outcome, and for every four patients treated, one more patient was independent at long-term follow-up,” Dr. Saver said. Safety measures were similar among patients in the study’s two arms.
The EXTEND-IA results showed a 90-day modified Rankin Scale score of 0-2 in 52% of the embolectomy patients, compared with 28% of those treated only with thrombolysis. The study’s co–primary endpoints were median level of reperfusion at 24 hours after treatment, 100% with embolectomy and 37% with thrombolysis only, and early neurologic recovery, defined as at least an 8-point drop from the baseline in the National Institutes of Health Stroke Scale score or a score of 0 or 1 when assessed 3 days after treatment. Patients met this second endpoint at an 80% rate with embolectomy and a 37% rate with thrombolysis only. Results of EXTEND-IA appeared in an article published online concurrently with the meeting report (N. Engl J. Med. 2015 Feb. 11 [doi:10.1056/NEJMoa1414792]).
The third, and largest, of the three studies presented at the conference, ESCAPE (Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times), enrolled 316 patients at 11 centers in Canada, 6 in the United States, 3 in South Korea, and 1 in Ireland. After 90 days, 53% of patients in the embolectomy arm had achieved a modified Rankin Scale score of 0-2, this study’s primary endpoint, compared with 29% of patients in the thrombolysis-only arm (treatment with alteplase). These results also appeared in an article published online concurrently with the conference report (N. Engl. J. Med. 2015 Feb. 11 [doi:10.1056/NEJMoa1414905]).
SWIFT PRIME was sponsored by Covidien, which markets the stent retriever used in the study. Dr. Saver and Dr. Goyal are consultants to Covidien. EXTEND-IA used stent retrievers provided by Covidien. ESCAPE received a grant from Covidien. Dr. Becker had no relevant disclosures.
On Twitter @mitchelzoler
AT THE INTERNATIONAL STROKE CONFERENCE
Key clinical point: Results from three randomized, controlled trials confirmed the safety and dramatic efficacy of endovascular embolectomy for selected patients with acute, ischemic stroke.
Major finding: In SWIFT PRIME, a 90-day modified Rankin Scale score of 0-2 occurred in 60% of patients treated with thrombolysis plus embolectomy and 36% of patients treated with thrombolysis only.
Data source: SWIFT PRIME, a prospective, multicenter randomized trial that enrolled 195 patients at 39 centers in the United States and Europe.
Disclosures: SWIFT PRIME was sponsored by Covidien, which markets the stent retriever used in the study. Dr. Saver and Dr. Goyal are consultants to Covidien. EXTEND-IA used stent retrievers provided by Covidien. ESCAPE received a grant from Covidien. Dr. Becker had no relevant disclosures.
