User login
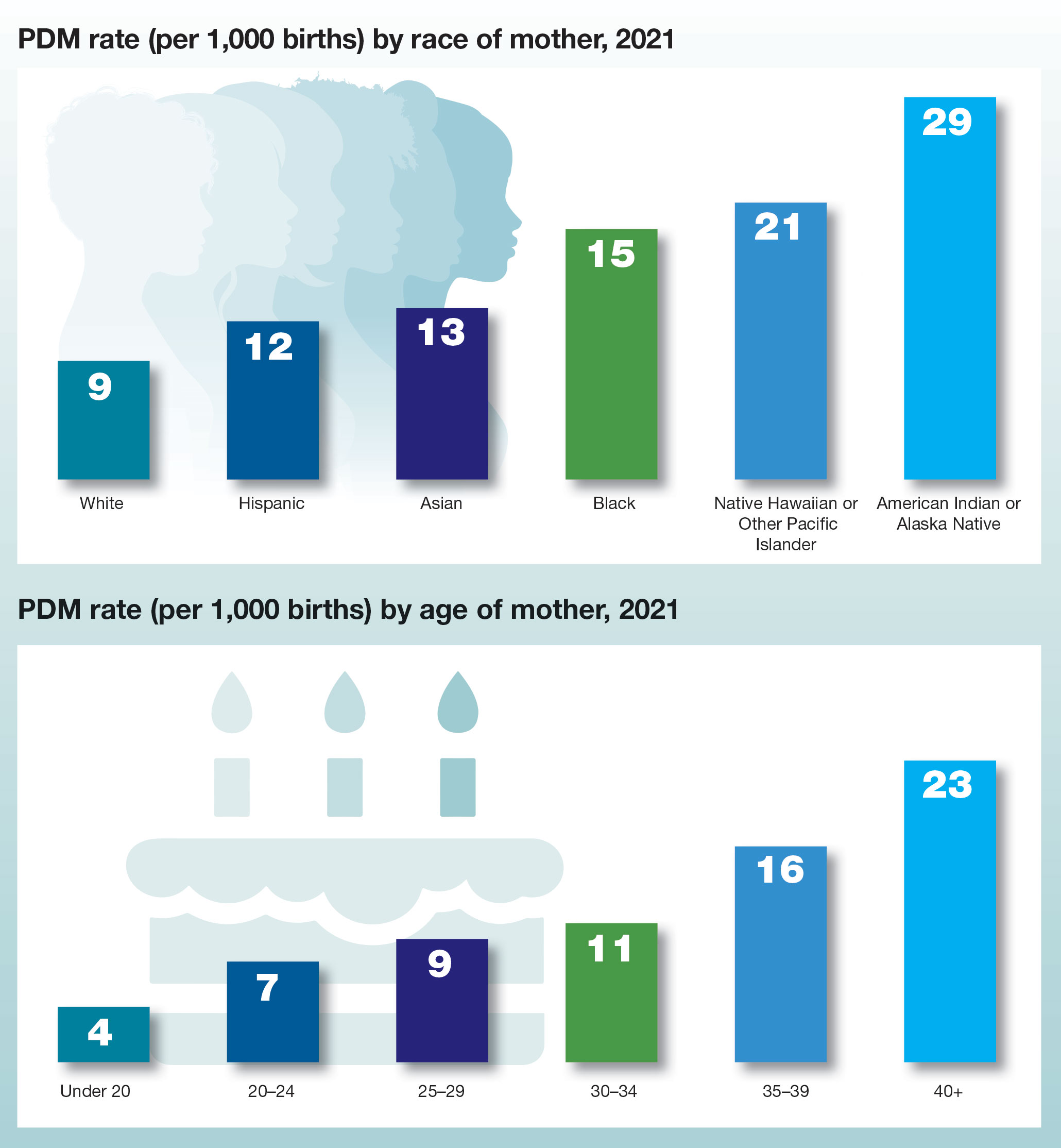
Trends in prepregnancy diabetes rates in the United States, 2016 -2021
Managing clinician burnout: Challenges and opportunities
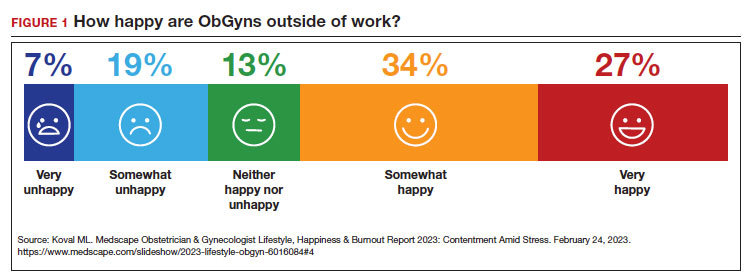
Physicians have some of the highest rates of burnout among all professions.1 Complicating matters is that clinicians (including residents)2 may avoid seeking treatment out of fear it will affect their license or privileges.3 In this article, we consider burnout in greater detail, as well as ways of successfully addressing the level of burnout in the profession (FIGURE 1), including steps individual practitioners, health care entities, and regulators should consider to reduce burnout and its harmful effects.
How burnout becomes a problem
Six general factors are commonly identified as leading to clinician career dissatisfaction and burnout:4
1. work overload
2. lack of autonomy and control
3. inadequate rewards, financial and otherwise
4. work-home schedules
5. perception of lack of fairness
6. values conflict between the clinician and employer (including a breakdown of professional community).
At the top of the list of causes of burnout is often “administrative and bureaucratic headaches.”5 More specifically, electronic health records (EHRs), including computerized order entry, is commonly cited as a major cause of burnout.6,7 According to some studies, clinicians spend as much as 49% of working time doing clerical work,8 and studies found the extension of work into home life.9
Increased measurement of performance metrics in health care services are a significant contributor to physician burnout.10 These include pressure to see more patients, perform more procedures, and respond quickly to patient requests (eg, through email).7 As we will see, medical malpractice cases, or the risk of such cases, have also played a role in burnout in some medical specialties.11 The pandemic also contributed, at least temporarily, to burnout.12,13
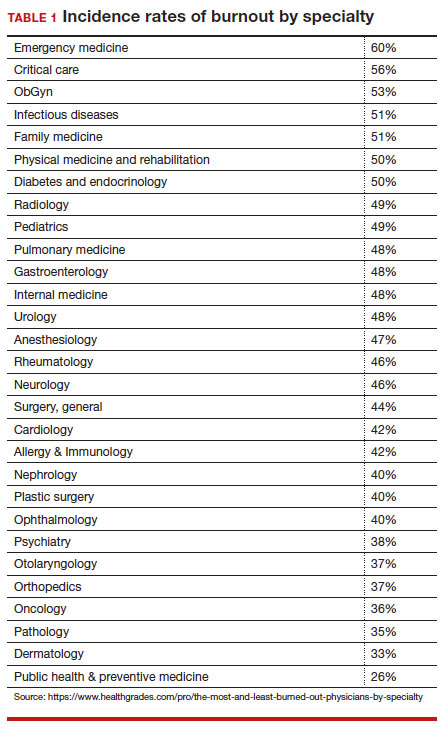
Rates of burnout among physicians are notably higher than among the general population14 or other professions.6 Although physicians have generally entered clinical practice with lower rates of burnout than the general population,15 The American College of Obstetricians and Gynecologists (ACOG) reports that 40% to 75% of ObGyns “experience some form of professional burnout.”16,17 Other source(s) cite that 53% of ObGyns report burnout (TABLE 1).
Code QD85
Burnout is a syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed. It is characterized by 3 dimensions:
- feelings of energy depletion or exhaustion
- increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job
- a sense of ineffectiveness and lack of accomplishment. Burn-out refers specifically to phenomena in the occupational context and should not be applied to describe experiences in other areas of life. Exclusions to burnout diagnosis include adjustment disorder, disorders specifically associated with stress, anxiety or fear-related disorders, and mood disorders.
Reference
1. International Classification of Diseases Eleventh Revision (ICD-11). Geneva, Switzerland: World Health Organization; 2022.
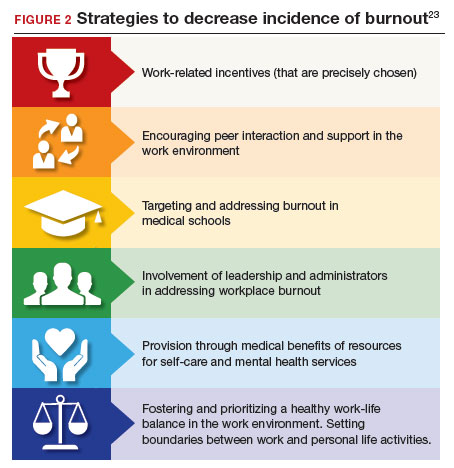
Burnout undoubtedly contributes to professionals leaving practice, leading to a significant shortage of ObGyns.18 It also raises several significant legal concerns. Despite the enormity and seriousness of the problem, there is considerable optimism and assurance that the epidemic of burnout is solvable on the individual, specialty, and profession-wide levels. ACOG and other organizations have made suggestions for physicians, the profession, and to health care institutions for reducing burnout.19 This is not to say that solutions are simple or easy for individual professionals or institutions, but they are within the reach of the profession (FIGURE 2).
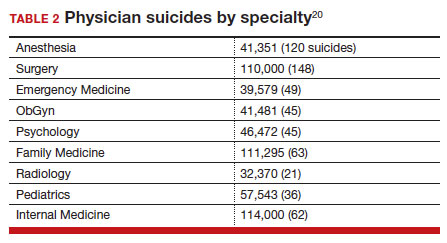
Suicide among health care professionals is one other concern (TABLE 2)20 and theoretically can stem from burnout, depression, and other psychosocial concerns.
Costs of clinician burnout
Burnout is endemic among health care providers, with numerous studies detailing the professional, emotional, and financial costs. Prior to the pandemic, one analysis of nationwide fiscal costs associated with burnout estimated an annual cost of $4.6B due to physician turnover and reduced clinical hours.21 The COVID-19 epidemic has by all accounts worsened rates of health care worker burnout, particularly for those in high patient-contact positions.22
Female clinicians appear to be differentially affected; in one recent study women reported symptoms of burnout at twice the rate of their male counterparts.23 Whether burnout rates will return to pre-pandemic levels remains an open question, but since burnout is frequently related to one’s own assessment of work-life balance, it is possible that a longer term shift in burnout rates associated with post-pandemic occupational attitudes will be observed.
Combining factors contribute to burnout
Burnout is a universal occupational hazard, but extant data suggest that physicians and other health care providers may be at higher risk. Among physicians, younger age, female gender, and front-line specialty status appear associated with higher burnout rates.24 Given that ObGyn physicians are overwhelmingly female (60% of physicians and 86% of residents),25,26 gender-related burnout factors exist alongside other specific occupational burnout risks. While gender parity has been achieved among health care providers, gender disparities persist in terms of those in leadership positions, compensation, and other factors.22
The smattering of evidence suggesting that ObGyns have higher rates of burnout than many other specialties is understandable given the unique legal challenges confronting ObGyn practice. This may be of special significance because ObGyn malpractice insurance rates are among the highest of all specialties.27 The overall shortage of ObGyns has been exacerbated by the demonstrated negative effects on training and workforce representation stemming from recent legislation that has the effect of criminalizing certain aspects of ObGyn practice;28 for instance, uncertainty regarding abortion regulations.
These negative effects are particularly heightened in states in which the law is in flux or where there are continuing efforts to substantially limit access to abortion. The efforts to increase civil and even criminal penalties related to abortion care challenge ObGyns’ professional practices, as legal rules are frequently changing. In some states, ObGyns may face additional workloads secondary to a flight of ObGyns from restrictive jurisdictions in addition to legal and professional repercussions. In a small study of 19 genetic counselors dealing with restrictive legislation in the state of Ohio,29 increased stress and burnout rates were identified as a consequence of practice uncertainties under this legislation. It is certain that other professionals working in reproductive health care are similarly affected.30
The programs provide individual resources to providers in distress, periodically survey initiatives at Stanford to assess burnout at the organizational level, and provide input designed to spur organizational change to reduce the burden of burnout. Ways that they build community and connections include:
- Live Story Rounds events (as told by Stanford Medicine physicians)
- Commensality Groups (facilitated small discussion groups built around tested evidence)
- Aim to increase sense of connection and collegiality among physicians and build comradery at work
- CME-accredited physician wellness forum, including annual doctor’s day events
Continue to: Assessment of burnout...
Assessment of burnout
Numerous scales for the assessment of burnout exist. Of these, the 22-item Maslach Burnout Inventory (MBI) is the best studied. The MBI is a well-investigated tool for assessing burnout. The MBI consists of 3 major subscales measuring overall burnout, emotional exhaustion, depersonalization, and low personal accomplishment. It exists in numerous forms. For instance, the MBI-HSS (MP), adapted for medical personnel, is available. However, the most commonly used form for assessing burnout in clinicians is the MBI-HHS (Human Services Survey); approximately 85% of all burnout studies examined in a recent meta-analysis used this survey version.31 As those authors commented, while burnout is a recognized phenomenon, a great deal of variability in study design, interpretation of subscale scores, and sample selection makes generalizations regarding burnout difficult to assess.
The MBI in various forms has been extensively used over the past 40 years to assess burnout amongst physicians and physicians in training. While not the only instrument designed to measure such factors, it is by far the most prevalent. Williamson and colleagues32 compared the MBI with several other measures of quality of life and found good correlation between the various instruments used, a finding replicated by other studies.33 Brady and colleagues compared item responses to the Stanford Professional Fulfillment Index and the Min-Z Single-item Burnout scale (a 1-item screening measure) to MBI’s Emotional Exhaustion and Depersonalization subscales. Basing their findings on a survey of more than 1,300 physicians, they found that all analyzed scales were significantly correlated with such adverse outcomes as depression, distress, or intent to leave the profession.
It is important to note that most surveys of clinician burnout were conducted prior to the pandemic. While the psychometric analyses of the MBI and other scales are likely still germane, observed rates of clinician burnout have likely increased. Thus, comparisons of pre- and post-pandemic studies should factor in an increase in the incidence and prevalence of burnout.
Management strategies
In general, there are several interventions for managing burnout34:
- individual-focused (including self-care and communications-skills workshops)
- mindfulness training
- yoga
- meditation
- organizational/structural (workload reduction, schedule realignment, teamwork training, and group-delivered stress management interventions)
- combination(s) of the above.
There is little evidence to suggest that any particular individual intervention (whether delivered in individual or group-based formats) is superior to any other in treating clinician burnout. A recent analysis of 24 studies employing mindfulness-based interventions demonstrated generally positive results for such interventions.35 Other studies have also found general support for mindfulness-based interventions, although mindfulness is often integrated with other stress-reduction techniques, such as meditation, yoga, and communication skills. Such interventions are nonspecific but generally effective.
An accumulation of evidence to date suggests that a combination of individual and organizational interventions is most effective in combatting clinician burnout. No individual intervention can be successful without addressing root causes, such as overscheduling, lack of organizational support, and the effect of restrictive legislation on practice.
Several large teaching hospitals have established programs to address physician and health care provider burnout. Notable among these is the Stanford University School of Medicine’s WellMD and WellPhD programs (https://wellmd.stanford.edu/about.html). These programs were described by Olson and colleagues36 as using a model focused on practice efficiency, organizational culture, and personal resilience to enhance physicians’ well-being. (See “Aspects of the WellMD and WellPhD programs from Stanford University.”)
A growing number of institutions have established burnout programs to support physicians experiencing work/life imbalances and other aspects of burnout.37 In general, these share common features of assessment, individual and/or group intervention, and organizational change. Fear of repercussion may be one factor preventing physicians from seeking individual treatment for burnout.38 Importantly, they emphasize the need for professional confidentiality when offering treatment to patients within organizational settings. Those authors also reported that a focus on organizational engagement may be an important factor in addressing burnout in female physicians, as they tend to report lower levels of organizational engagement.
Continue to: Legal considerations...
Legal considerations
Until recently, physician burnout “received little notice in the legal literature.”39 Although there have been burnout legal consequences in the past, the legal issues are now becoming more visible.40
Medical malpractice
A well-documented consequence of burnout is an increase in errors.14 Medical errors, of course, are at the heart of malpractice claims. Technically, malpractice is medical or professional negligence. It is the breach of a duty owed by the physician, or other provider, or organization (defendant) to the patient, which causes injury to the plaintiff/patient.41
“Medical error” is generally a meaningful deviation from the “standard of care” or accepted medical practice.42 Many medical errors do not cause injury to the patient; in those cases, the negligence does not result in liability. In instances in which the negligence causes harm, the clinician and health care facility may be subject to liability for that injury. Fortunately, however, for a variety of reasons, most harmful medical errors do not result in a medical malpractice claim or lawsuit. The absence of a good clinician-patient relationship is likely associated with an increased inclination of a patient to file a malpractice action.43Clinician burnout may, therefore, contribute to increased malpractice claims in two ways. First, burnout likely leads to increased medical errors, perhaps because burnout is associated with lower concentration, inattention, reduced cognitive vigilance, and fatigue.8,44 It may also lead to less time with patients, reduced patient empathy, and lower patient rapport, which may make injured patients more likely to file a claim or lawsuit.45 Because the relationshipbetween burnout and medical error is bidirectional, malpractice claims tend to increase burnout, which increases error. Given the time it takes to resolve most malpractice claims, the uncertainty of medical malpractice may be especially stressful for health care providers.46,47
Burnout is not a mitigating factor in malpractice. Our sympathies may go out to a professional suffering from burnout, but it does not excuse or reduce liability—it may, indeed, be an aggravating factor. Clinicians who can diagnose burnout and know its negative consequences but fail to deal with their own burnout may be demonstrating negligence if there has been harm to a patient related to the burnout.48
Institutional or corporate liability to patients
Health care institutions have obligations to avoid injury to patients. Just as poorly maintained medical equipment may harm patients, so may burned-out professionals. Therefore, institutions have some obligation to supervise and avoid the increased risks to patients posed by professionals suffering from burnout.
Respondeat superior and institutional negligence. Institutional liability may arise in two ways, the first through agency, or respondeat superior. That is, if the physician or other professional is an employee (or similar agent) of the health care institution, that institution is generally responsible for the physician’s negligence during the employment.49 Even if the physician is not an employee (for example, an independent contractor providing care or using the hospital facilities), the health care facility may be liable for the physician’s negligence.50 Liability may occur, for example, if the health care facility was aware that the physician was engaged in careless practice or was otherwise a risk to patients but the facility did not take steps to avoid those risks.51 The basis for liability is that the health care organization owes a duty to patients to take reasonable care to ensure that its facilities are not used to injure patients negligently.52 Just as it must take care that unqualified physicians are not granted privileges to practice, it also must take reasonable steps to protect patients when it is aware (through nurses or other agents) of a physician’s negligent practice.
In one case, for example, the court found liability where a staff member had “severe” burnout in a physician’s office and failed to read fetal monitoring strips. The physician was found negligent for relying on the staff member who was obviously making errors in interpretation of fetal distress.53
Continue to: Legal obligations of health care organizations to physicians and others...
Legal obligations of health care organizations to physicians and others
In addition to obligations to patients, health care organizations may have obligations to employees (and others) at risk for injury. For example, assume a patient is diagnosed with a highly contagious disease. The health care organization would be obligated to warn, and take reasonable steps to protect, the staff (employees and independent contractors) from being harmed from exposure to the disease. This principle may apply to coworkers of employees with significant burnout, thereby presenting a danger in the workplace. The liability issue is more difficult for employees experiencing job-related burnout themselves. Organizations generally compensate injured employees through no-fault workers’ compensation (an insurance-like system); for independent contractors, the liability is usually through a tort claim (negligence).54
In modern times, a focus has been on preventing those injuries, not just providing compensation after injuries have occurred. Notably, federal and state occupational health and safety laws (particularly the Occupational Safety and Health Administration [OSHA]) require most organizations (including those employing health care providers) to take steps to mitigate various kinds of worker injuries.55
Although these worker protections have commonly been applied to hospitals and other health care providers, burnout has not traditionally been a significant concern in federal or state OSHA enforcement. For example, no formal federal OSHA regulations govern work-related burnout. Regulators, including OSHA, are increasingly interested in burnout that may affect many employees. OSHA has several recommendations for reducing health care work burnout.56 The Surgeon General has expressed similar concerns.57 The federal government recently allocated $103 million from the American Rescue Plan to address burnout among health care workers.58 Also, OSHA appears to be increasing its oversight of healthcare-institution-worker injuries.55
Is burnout a “disability”?
The federal Americans with Disabilities Act (ADA) and similar state laws prohibit discrimination based on disability.59 A disability is defined as a “physical or mental impairment that substantially limits one or more major life activities” or “perceived as having such an impairment.”60 The initial issue is whether burnout is a “mental impairment.” As noted earlier, it is not officially a “medical condition.”61 To date, the United Nations has classified it as an “occupational phenomenon.”62 It may, therefore, not qualify under the ADA, even if it “interferes with a major life activity.” There is, however, some movement toward defining burnout as a mental condition. Even if defined as a disability, there would still be legal issues of how severe it must be to qualify as a disability and the proper accommodation. Apart from the legal definition of an ADA disability, as a practical matter it likely is in the best interest of health care facilities to provide accommodations that reduce burnout. A number of strategies to decrease the incidence of burnout include the role of health care systems (FIGURE 2).
In conclusion we look at several things that can be done to “treat” or reduce burnout. That effort requires the cooperation of physicians and other providers, health care facilities, training programs, licensing authorities, and professional organizations. See suggestions below.
Conclusion
There are many excellent suggestions for reducing burnout and improving patient care and practitioner satisfaction.63-65 We conclude with a summary of some of these suggestions for individual practitioners, health care organizations, the profession, and licensing. It is worth remembering, however, that it will require the efforts of each area to reduce burnout substantially.
For practitioners:
- Engage in quality coaching/therapy on mindfulness and stress management.
- Practice self-care, including exercise and relaxation techniques.
- Make work-life balance a priority.
- Take opportunities for collegial social and professional discussions.
- Prioritize (and periodically assess) your own professional satisfaction and burnout risk.
- Smile—enjoy a sense of humor (endorphins and cortisol).
For health care organizations:
- Urgently work with vendors and regulators to revise electronic health records to reduce their substantial impact on burnout.
- Reduce physicians’ time on clerical and administrative tasks (eg, by enhancing the use of quality AI, scribes, and automated notes from appointments. (This may increase the time they spend with patients.) Eliminate “pajama-time” charting.
- Provide various kinds of confidential professional counseling, therapy, and support related to burnout prevention and treatment, and avoid any penalty or stigma related to their use.
- Provide reasonable flexibility in scheduling.
- Routinely provide employees with information about burnout prevention and services.
- Appoint a wellness officer with authority to ensure the organization maximizes its prevention and treatment services.
- Constantly seek input from practitioners on how to improve the atmosphere for practice to maximize patient care and practitioner satisfaction.
- Provide ample professional and social opportunities for discussing and learning about work-life balance, resilience, intellectual stimulation, and career development.
For regulators, licensors, and professional organizations:
- Work with health care organizations and EHR vendors to substantially reduce the complexity, physician effort, and stress associated with those record systems. Streamlining should, in the future, be part of formally certifying EHR systems.
- Reduce the administrative burden on physicians by modifying complex regulations and using AI and other technology to the extent possible to obtain necessary reimbursement information.
- Eliminate unnecessary data gathering that requires practitioner time or attention.
- Licensing, educational, and certifying bodies should eliminate any questions regarding the diagnosis or treatment of mental health and focus on current (or very recent) impairments.
- Seek funding for research on burnout prevention and treatment.
Dr. H is a 58-year-old ObGyn who, after completing residency, went into solo practice. The practice grew, and Dr. H found it increasingly more challenging to cover, especially the obstetrics sector. Dr. H then merged the practice with a group of 3 other ObGyns. Their practice expanded, and began recruiting recent residency graduates. In time, the practice was bought out by the local hospital health care system. Dr. H was faced with complying with the rules and regulations of that health care system. The electronic health record (EHR) component proved challenging, as did the restrictions on staff hiring (and firing), but Dr. H did receive a paycheck each month and complied with it all. The health care system administrators had clear financial targets Dr. H was to meet each quarter, which created additional pressure. Dr. H used to love being an OB and providing excellent care for every patient, but that sense of accomplishment was being lost.
Dr. H increasingly found it difficult to focus because of mind wandering, especially in the operating room (OR). Thoughts occurred about retirement, the current challenges imposed by “the new way of practicing medicine” (more focused on financial productivity restraints and reimbursement), and EHR challenges. Then Dr. H’s attention would return to the OR case at hand. All of this resulted in considerable stress and emotional exhaustion, and sometimes a sense of being disconnected. A few times, colleagues or nurses had asked Dr. H if everything was “okay,” or if a break would help. Dr. H made more small errors than usual, but Dr. H’s self-assessment was “doing an adequate job.” Patient satisfaction scores (collected routinely by the health care system) declined over the last 9 months.
Six months ago, Dr. H finished doing a laparoscopic total hysterectomy and bilateral salpingo-oophorectomy and got into the right uterine artery. The estimated blood loss was 3,500 mL. Using minimally invasive techniques, Dr. H identified the bleeder and, with monopolar current, got everything under control. The patient went to the post-anesthesia care unit, and all appeared to be in order. Her vital signs were stable, and she was discharged home the same day.
The patient presented 1 week later with lower abdominal and right flank pain. Dr. H addressed the problem in the emergency department and admitted the patient for further evaluation and urology consultation. The right ureter was damaged and obstructed; ultimately, the urologist performed a psoas bladder hitch. The patient recovered slowly, lost several weeks of work, experienced significant pain, and had other disruptions and costs. Additional medical care related to the surgery is ongoing. A health care system committee asked Dr. H to explain the problem. Over the last 6 months, Dr. H’s frustration with practice and being tired and disconnected have increased.
Dr. H has received a letter from a law firm saying that he and the health care system are being sued for malpractice focused on an iatrogenic ureter injury. The letter names two very reputable experts who are prepared to testify that the patient’s injury resulted from clear negligence. Dr. H has told the malpractice carrier absolutely not to settle this case—it is “a sham— without merit.” The health care system has asked Dr. H to take a “burnout test.”
Legal considerations
Dr. H exhibits relatively clear signs of professional burnout. The fact that there was a bad outcome while Dr. H was experiencing burnout is not proof of negligence (or, breach of duty of care to the patient). Nor is it a defense or mitigation to any malpractice that occurred.
In the malpractice case, the plaintiff will have the burden of proving that Dr. H’s treatment was negligent in that it fell below the standard of care. Even if it was a medical error, the question is whether it was negligence. If the patient/plaintiff, using expert witnesses, can prove that Dr. H fell below the standard of care that caused injury, Dr. H may be liable for the resulting extra costs, loss of income, and pain and suffering resulting from the negligent care.
The health care system likely will also be responsible for Dr. H’s negligence, either through respondeat superior (for example, if Dr. H is an employee) or for its own negligence. The case for its negligence is that the nurses and assistants had repeatedly seen him making errors and becoming disengaged (to the extent that they asked Dr. H if “everything is okay” or if a break would help). Furthermore, Dr. H’s patient satisfaction scores have been declining for several months. The plaintiff will argue that Dr. H exhibited classic burnout symptoms with the attendant risks of medical errors. However, the health care system did not take action to protect patients or to assist Dr. H. In short, one way or another, there is some likelihood that the health care system may also be liable if patient injuries are found to have been caused by negligence.
At this point, the health care system also faces the question of how to work with Dr. H in the future. The most pressing question is whether or not to allow Dr. H to continue practicing. If, as it appears, Dr. H is dealing with burnout, the pressure of the malpractice claim could well increase the probability of other medical mistakes. The institution has asked Dr. H to take a burnout test, but it is unclear where things go if the test (as likely) demonstrates significant burnout. This is a counseling and human relations question, at least as much as a legal issue, and the institution should probably proceed in that way—which is, trying to understand and support Dr. H and determining what can be done to address the burnout. At the same time, the system must reasonably assess Dr. H’s fitness to continue practicing as the matters are resolved. Almost everyone shares the goal to provide every individual and corporate opportunity for Dr. H to deal with burnout issues and return to successful practice.
Dr. H will be represented in the malpractice case by counsel provided through the insurance carrier. However, Dr. H would be well advised to retain a trusted and knowledgeable personal attorney. For example, the instruction not to consider settlement is likely misguided, but Dr. H needs to talk with an attorney that Dr. H has chosen and trusts. In addition, the attorney can help guide Dr. H through a rational process of dealing with the health care system, putting the practice in order, and considering the options for the future.
The health care system should reconsider its processes to deal with burnout to ensure the quality of care, patient satisfaction, professional retention, and economic stability. Several burnoutresponse programs have had success in achieving these goals.
What’s the Verdict?
Dr. H received good mental health, legal, and professional advice. As a result, an out of court settlement was reached following pretrial discovery. Dr. H has continued consultation regarding burnout and has returned to productive practice.
- Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2017. Mayo Clinic Proceed. 2019;94:1681-1694.
- Smith R, Rayburn W. Burnout in obstetrician-gynecologists. Its prevalence, identification, prevention, and reversal. Obstet Gynecol Clin North Am. 2021;48:231-245. https://doi. org/10.1016/j.ogc.2021.06.003
- Patti MG, Schlottmann F, Sarr MG. The problem of burnout among surgeons. JAMA Surg. 2018;153:403-404. doi:10.1001 /jamasurg.2018.0047
- Carrau D, Janis JE. Physician burnout: solutions for individuals and organizations. Plastic and Reconstructive Surgery Global Open. 2021;91-97.
- Southwick R. The key to fixing physician burnout is the workplace not the worker. Contemporary Ob/Gyn. March 13, 2023.
- Patel RS, Bachu R, Adikey A, et al. Factors related to physician burnout and its consequences: a review. Behav Sciences. 2018;8:98.
- Melnick ER, Dyrbye LN, Sinsky CA, et al. The association between perceived electronic health record usability and professional burnout among US physicians. Mayo Clinic Proceed. 2020;95:476-487.
- Shanafelt TD, Dyrbye LN, West CP. Addressing physician burnout: the way forward. JAMA. 2017;317:901-902. doi:10.1001/jama.2017.0076
- Ommaya AK, Cipriano PF, Hoyt DB, et al. Care-centered clinical documentation in the digital environment: Solutions to alleviate burnout. National Academy of Medicine Perspectives. 2018.
- Hartzband P, Groopman J. Physician burnout, interrupted. N Engl J Med. 2020;382:2485-2487. Discussion Paper, National Academy of Medicine. Accessed July 21, 2023. https://nam .edu/care
- Ji YD, Robertson FC, Patel NA, et al. Assessment of risk factors for suicide among US health care professionals. JAMA Surg. 2020;155:713-721. centered-clinical-documentation-digital -environment-solutions-alleviate-burnout/
- Shanafelt TD, West CP, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clinic Proceed. 2022;97:2248-2258.
- Herber-Valdez C, Kupesic-Plavsic S. Satisfaction and shortfall of OB-GYN physicians and radiologists. J. Ultrasound Obstet Gynecol. 2021;15:387-392.
- Dyrbye LN, Shanafelt TD, Sinsky CA, et al. Burnout among health care professionals: a call to explore and address this underrecognized threat to safe, high-quality care. National Academy of Medicine Perspectives. Accessed July 5, 2017. https://iuhcpe.org/file_manager/1501524077-Burnout -Among-Health-Care-Professionals-A-Call-to-Explore-and -Address-This-Underrecognized-Threat.pdf
- Olson KD. Physician burnout—a leading indicator of health system performance? Mayo Clinic Proceed. 2017;92: 1608-1611.
- American College of Obstetricians and Gynecologists. Why obgyns are burning out. October 28, 2019. Accessed July 21, 2023. https://www.acog.org/news/news-articles/2019/10/why-ob -gyns-are-burning-out#:~:text=A%202017%20report%20 by%20the,exhaustion%20or%20lack%20of%20motivation
- Peckham C. National physician burnout & depression report 2018. Medscape. January 17, 2018. https://nap. nationalacademies.org/catalog/25521/taking-action -against-clinician-burnout-a-systems-approach-to -professional
- Marsa L. Labor pains: The OB-GYN shortage. AAMC News. Nov. 15, 2018. Accessed July 21, 2023. https://www.aamc.org /news-insights/labor-pains-ob-gyn-shortage
- American College of Obstetricians and Gynecologists. Coping with the stress of medical professional liability litigation. ACOG Committee Opinion. February 2005;309:453454. Accessed July 21, 2023. https://www.acog.org/clinical /clinical-guidance/committee-opinion/articles/2013/01 /coping-with-the-stress-of-medical-professional-liability -litigation
- Reith TP. Burnout in United States healthcare professionals: a narrative review. Cureus. 2018;10:e3681. doi: 10.7759 /cureus.3681
- Han S, Shanafelt TD, Sinsky CA, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med. 2019;4:784-790.
- Sullivan D, Sullivan V, Weatherspoon D, et al. Comparison of nurse burnout, before and during the COVID-19 pandemic. Nurs Clin North Am. 2022;57:79-99. doi: 10.1016 /j.cnur.2021.11.006
- Chandawarkar A, Chaparro JD. Burnout in clinicians. Curr Prob Pediatr Adolesc Health Care. 2021;51:101-104. https ://doi.org/10.1016/j.cppeds.2021.101104
- Brady KJS, Sheldrick RC, Ni P, et al. Examining the measurement equivalence of the Maslach Burnout Inventory across age, gender, and specialty groups in US physicians. J Patient-Reported Outcomes. 2021;5.
- Association of American Medical Colleges. Physician Specialty Data Report—Active Physicians by Sex and Specialty, 2021. Accessed June 19, 2023. https://www.aamc .org/data-reports/workforce/data/active-physicians-sex -specialty-2021
- Association of American Medical Colleges. Physician Specialty Data Report—ACGME Residents and Fellows by Sex and Specialty, 2021. Accessed June 19, 2023. https://www .aamc.org/data-reports/workforce/data/acgme-residents -fellows-sex-and-specialty-2021
- Painter LM, Biggans KA, Turner CT. Risk managementobstetrics and gynecology perspective. Clin Obstet Gynecol. 2023;66:331-341. DOI:10.1097/GRF.0000000000000775
- Darney BG, Boniface E, Liberty A. Assessing the effect of abortion restrictions. Obstetr Gynecol. 2023;141:233-235.
- Heuerman AC, Bessett D, Antommaria AHM, et al. Experiences of reproductive genetic counselors with abortion regulations in Ohio. J Genet Counseling. 2022;31:641-652.
- Brandi K, Gill P. Abortion restrictions threaten all reproductive health care clinicians. Am J Public Health. 2023;113:384-385.
- Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of burnout among physicians: a systematic review. JAMA. 2018;320:1131-1150. doi: 10.1001/jama.2018.1277
- Williamson K, Lank PM, Cheema N, et al. Comparing the Maslach Burnout Inventory to other well-being instruments in emergency medicine residents. J Graduate Med Education. 2018;532-536. DOI: http://dx.doi.org/10.4300 /JGME-D-18-00155.1
- Brady KJS, Sheldrick RC, Ni P, et al. Establishing crosswalks between common measures of burnout in US physicians. J Gen Intern Med. 2022;37:777-784.
- Zhang X, Song Y, Jiang T, et al. Interventions to reduce burnout of physicians and nurses: an overview of systematic reviews and meta-analyses. Medicine (Baltimore). 2020;26:e20992. DOI: 10.1097/MD.0000000000020992
- Scheepers RA, Emke H, Ronald M, et al. The impact of mindfulness-based interventions on doctors’ well-being and performance: a systematic review. Med Education. 2020;54:138-149. https://doi.org/10.1111/medu.14020
- Olson K, Marchalik D, Farley H, et al. Organizational strategies to reduce physician burnout and improve professional fulfillment. Curr Prob Pediatr Adolesc Health Care. 2019;49:12. https://doi.org/10.1016/j.cppeds.2019.100664
- Berry LL, Awdish RLA, Swensen SJ. 5 ways to restore depleted health care workers. Harvard Business Rev. February 11, 2022.
- Sullivan AB, Hersh CM, Rensel M, et al. Leadership inequity, burnout, and lower engagement of women in medicine. J Health Serv Psychol. 2023;49:33-39.
- Hoffman S. Healing the healers: legal remedies for physician burnout. Yale J Health Policy Law Ethics. 2018;18:56-113.
- Federation of State Medical Boards. Physician wellness and burnout: report and recommendations of the workgroup on physician wellness and burnout. (Policy adopted by FSMB). April 2018. Accessed July 21, 2023. https://www.fsmb.org /siteassets/advocacy/policies/policy-on-wellness-and -burnout.pdf
- Robinson C, Kettering C, Sanfilippo JS. Medical malpractice lawsuits. Clin Obstet Gynecol. 2023;66:256-260. DOI: https ://doi.org/10.1097/GRF.0000000000000777
- Gittler GJ, Goldstein EJ. The elements of medical malpractice: an overview. Clin Infect Dis. 1996;23:1152-1155.
- Bal BS. An introduction to medical malpractice in the United States. Clin Orthop Relat Res. 2009;467:339-347.
- Tawfik DS, Profit J, Morgenthaler TI, et al. Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clinic Proceed. 2018;93: 1571-1580.
- Sundholm B. Elevating physician-patient relationships in the shadow of metric mania. Drexel L Rev. 2020;12:287-330.
- Ghaith S, Campbell RL, Pollock JR, et al. Medical malpractice lawsuits involving trainees in obstetrics and gynecology in the USA. Healthcare. 2022;10:1328.
- Muller TM, Warsi S. Litigation culture causing burnout in American physicians. Trauma Mental Health Report. April 9, 2021.
- Levine AS. Legal 101: Tort law and medical malpractice for physicians. Contemp OBGYN. 2015:60;26-28, 30.
- Regan JJ, Regan WM. Medical malpractice and respondeat superior. Southern Med J. 2002;95.5:545-549. DOI 10.1097/00007611-200295050-00018
- Levin H. Hospital vicarious liability for negligence by independent contractor physicians: new rule for new times. Univ Illinois Law Rev. 2005:1291-1332.
- Darling v Charleston Hospital, 33 Ill. 2d 326, 211 N.E.2d 253 (Ill. 1965).
- Dangel R. Hospital liability for physician malpractice. Ohio State Law J. 1986;47:1077-1098.
- Reffitt v Hajjar, 892 S.W.2d 599, 605 (Ky. Ct. App. 1994).
- McMichael BJ. Malpractice. In Laws of Medicine: Core Legal Aspects for the Healthcare Professional. New York, NY: Springer International; 2022:129-150.
- Occupational Safety and Health Administration. Worker safety in hospitals: caring for our caregivers. Accessed June 8, 2023. https://www.osha.gov/hospitals
- Occupational Safety and Health Administration. Workplace stress. Accessed June 8, 2023. https://www.osha.gov /workplace-stress/understanding-the-problem
- U.S. Surgeon General’s Advisory on Building a Thriving Health Workforce. Addressing health worker burnout. Accessed July 21, 2023. https://www.hhs.gov/sites/default/files/health -worker-wellbeing-advisory.pdf
- Department of Health & Human Services. Biden-Harris administration awards $103 Million in American Rescue Plan funds to reduce burnout and promote mental health and wellness among health care workforce. January 20, 2022. Accessed July 24, 2023. https://www.hhs.gov/about /news/2022/01/20/biden-harris-administration-awards -103-million-american-rescue-plan-funds-reduce-burnout -promote-mental-health-wellness-among-health-care -workforce.html
- Rothstein LF, Irzyk J. Disabilities and the Law. 4th ed. Toronto, Canada: Thompson Reuters; 2023.
- Department of Labor. Guide to disability rights laws. February 28, 2020. Accessed July 24, 2023. https://www .ada.gov/resources/disability-rights-guide/#:~:text=An%20 individual%20with%20a%20disability%20is%20defined%20 by%20the%20ADA,as%20having%20such%20an%20 impairment
- Nadon L, De Beer LT, Morin AJS. Should burnout be conceptualized as a mental disorder? Behavioral Sci. 2022;12:82.
- World Health Organization. Burn-out an “occupational phenomenon”: International Classification of Diseases. May 28, 2019. Accessed July 21, 2023. https://www.who.int/news /item/28-05-2019-burn-out-an-occupational-phenomenon -international-classification-of-diseases
- Hoffman S. Physician burnout: why legal and regulatory systems may need to step in. The Conversation. July 9, 2019. https://theconversation.com/physician-burnout-why-legal -and-regulatory-systems-may-need-to-step-in-119705
- Jha A, Iliff A, Chaoi A, et al. A crisis in healthcare: a call to action on physician burnout. Harvard Global Health Institute. 2019. Accessed July 21, 2023. https://www.massmed.org /Publications/Research,-Studies,-and-Reports/Physician -Burnout-Report-2018/
- Arnsten AF, Shanafelt T. Physician distress and burnout: the neurobiological perspective. Mayo Clin Proceed. 2021;96:763-769.

Mr. Smith is Professor Emeritus and Dean Emeritus at California Western School of Law, San Diego, California.
Dr. Sanfilippo is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Academic Division Director, Reproductive Endocrinology and Infertility, Magee Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors.

Dr. Sammons is past CEO, National Register of Health Service Psychologists.
The authors report no financial relationships relevant to this article.
*The case presented is hypothetical. The facts are a composite of several cases.
Mr. Smith is Professor Emeritus and Dean Emeritus at California Western School of Law, San Diego, California.
Dr. Sanfilippo is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Academic Division Director, Reproductive Endocrinology and Infertility, Magee Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors.
Dr. Sammons is past CEO, National Register of Health Service Psychologists.
The authors report no financial relationships relevant to this article.
*The case presented is hypothetical. The facts are a composite of several cases.
Mr. Smith is Professor Emeritus and Dean Emeritus at California Western School of Law, San Diego, California.
Dr. Sanfilippo is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Academic Division Director, Reproductive Endocrinology and Infertility, Magee Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors.
Dr. Sammons is past CEO, National Register of Health Service Psychologists.
The authors report no financial relationships relevant to this article.
*The case presented is hypothetical. The facts are a composite of several cases.
Physicians have some of the highest rates of burnout among all professions.1 Complicating matters is that clinicians (including residents)2 may avoid seeking treatment out of fear it will affect their license or privileges.3 In this article, we consider burnout in greater detail, as well as ways of successfully addressing the level of burnout in the profession (FIGURE 1), including steps individual practitioners, health care entities, and regulators should consider to reduce burnout and its harmful effects.
How burnout becomes a problem
Six general factors are commonly identified as leading to clinician career dissatisfaction and burnout:4
1. work overload
2. lack of autonomy and control
3. inadequate rewards, financial and otherwise
4. work-home schedules
5. perception of lack of fairness
6. values conflict between the clinician and employer (including a breakdown of professional community).
At the top of the list of causes of burnout is often “administrative and bureaucratic headaches.”5 More specifically, electronic health records (EHRs), including computerized order entry, is commonly cited as a major cause of burnout.6,7 According to some studies, clinicians spend as much as 49% of working time doing clerical work,8 and studies found the extension of work into home life.9
Increased measurement of performance metrics in health care services are a significant contributor to physician burnout.10 These include pressure to see more patients, perform more procedures, and respond quickly to patient requests (eg, through email).7 As we will see, medical malpractice cases, or the risk of such cases, have also played a role in burnout in some medical specialties.11 The pandemic also contributed, at least temporarily, to burnout.12,13
Rates of burnout among physicians are notably higher than among the general population14 or other professions.6 Although physicians have generally entered clinical practice with lower rates of burnout than the general population,15 The American College of Obstetricians and Gynecologists (ACOG) reports that 40% to 75% of ObGyns “experience some form of professional burnout.”16,17 Other source(s) cite that 53% of ObGyns report burnout (TABLE 1).
Code QD85
Burnout is a syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed. It is characterized by 3 dimensions:
- feelings of energy depletion or exhaustion
- increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job
- a sense of ineffectiveness and lack of accomplishment. Burn-out refers specifically to phenomena in the occupational context and should not be applied to describe experiences in other areas of life. Exclusions to burnout diagnosis include adjustment disorder, disorders specifically associated with stress, anxiety or fear-related disorders, and mood disorders.
Reference
1. International Classification of Diseases Eleventh Revision (ICD-11). Geneva, Switzerland: World Health Organization; 2022.
Burnout undoubtedly contributes to professionals leaving practice, leading to a significant shortage of ObGyns.18 It also raises several significant legal concerns. Despite the enormity and seriousness of the problem, there is considerable optimism and assurance that the epidemic of burnout is solvable on the individual, specialty, and profession-wide levels. ACOG and other organizations have made suggestions for physicians, the profession, and to health care institutions for reducing burnout.19 This is not to say that solutions are simple or easy for individual professionals or institutions, but they are within the reach of the profession (FIGURE 2).
Suicide among health care professionals is one other concern (TABLE 2)20 and theoretically can stem from burnout, depression, and other psychosocial concerns.
Costs of clinician burnout
Burnout is endemic among health care providers, with numerous studies detailing the professional, emotional, and financial costs. Prior to the pandemic, one analysis of nationwide fiscal costs associated with burnout estimated an annual cost of $4.6B due to physician turnover and reduced clinical hours.21 The COVID-19 epidemic has by all accounts worsened rates of health care worker burnout, particularly for those in high patient-contact positions.22
Female clinicians appear to be differentially affected; in one recent study women reported symptoms of burnout at twice the rate of their male counterparts.23 Whether burnout rates will return to pre-pandemic levels remains an open question, but since burnout is frequently related to one’s own assessment of work-life balance, it is possible that a longer term shift in burnout rates associated with post-pandemic occupational attitudes will be observed.
Combining factors contribute to burnout
Burnout is a universal occupational hazard, but extant data suggest that physicians and other health care providers may be at higher risk. Among physicians, younger age, female gender, and front-line specialty status appear associated with higher burnout rates.24 Given that ObGyn physicians are overwhelmingly female (60% of physicians and 86% of residents),25,26 gender-related burnout factors exist alongside other specific occupational burnout risks. While gender parity has been achieved among health care providers, gender disparities persist in terms of those in leadership positions, compensation, and other factors.22
The smattering of evidence suggesting that ObGyns have higher rates of burnout than many other specialties is understandable given the unique legal challenges confronting ObGyn practice. This may be of special significance because ObGyn malpractice insurance rates are among the highest of all specialties.27 The overall shortage of ObGyns has been exacerbated by the demonstrated negative effects on training and workforce representation stemming from recent legislation that has the effect of criminalizing certain aspects of ObGyn practice;28 for instance, uncertainty regarding abortion regulations.
These negative effects are particularly heightened in states in which the law is in flux or where there are continuing efforts to substantially limit access to abortion. The efforts to increase civil and even criminal penalties related to abortion care challenge ObGyns’ professional practices, as legal rules are frequently changing. In some states, ObGyns may face additional workloads secondary to a flight of ObGyns from restrictive jurisdictions in addition to legal and professional repercussions. In a small study of 19 genetic counselors dealing with restrictive legislation in the state of Ohio,29 increased stress and burnout rates were identified as a consequence of practice uncertainties under this legislation. It is certain that other professionals working in reproductive health care are similarly affected.30
The programs provide individual resources to providers in distress, periodically survey initiatives at Stanford to assess burnout at the organizational level, and provide input designed to spur organizational change to reduce the burden of burnout. Ways that they build community and connections include:
- Live Story Rounds events (as told by Stanford Medicine physicians)
- Commensality Groups (facilitated small discussion groups built around tested evidence)
- Aim to increase sense of connection and collegiality among physicians and build comradery at work
- CME-accredited physician wellness forum, including annual doctor’s day events
Continue to: Assessment of burnout...
Assessment of burnout
Numerous scales for the assessment of burnout exist. Of these, the 22-item Maslach Burnout Inventory (MBI) is the best studied. The MBI is a well-investigated tool for assessing burnout. The MBI consists of 3 major subscales measuring overall burnout, emotional exhaustion, depersonalization, and low personal accomplishment. It exists in numerous forms. For instance, the MBI-HSS (MP), adapted for medical personnel, is available. However, the most commonly used form for assessing burnout in clinicians is the MBI-HHS (Human Services Survey); approximately 85% of all burnout studies examined in a recent meta-analysis used this survey version.31 As those authors commented, while burnout is a recognized phenomenon, a great deal of variability in study design, interpretation of subscale scores, and sample selection makes generalizations regarding burnout difficult to assess.
The MBI in various forms has been extensively used over the past 40 years to assess burnout amongst physicians and physicians in training. While not the only instrument designed to measure such factors, it is by far the most prevalent. Williamson and colleagues32 compared the MBI with several other measures of quality of life and found good correlation between the various instruments used, a finding replicated by other studies.33 Brady and colleagues compared item responses to the Stanford Professional Fulfillment Index and the Min-Z Single-item Burnout scale (a 1-item screening measure) to MBI’s Emotional Exhaustion and Depersonalization subscales. Basing their findings on a survey of more than 1,300 physicians, they found that all analyzed scales were significantly correlated with such adverse outcomes as depression, distress, or intent to leave the profession.
It is important to note that most surveys of clinician burnout were conducted prior to the pandemic. While the psychometric analyses of the MBI and other scales are likely still germane, observed rates of clinician burnout have likely increased. Thus, comparisons of pre- and post-pandemic studies should factor in an increase in the incidence and prevalence of burnout.
Management strategies
In general, there are several interventions for managing burnout34:
- individual-focused (including self-care and communications-skills workshops)
- mindfulness training
- yoga
- meditation
- organizational/structural (workload reduction, schedule realignment, teamwork training, and group-delivered stress management interventions)
- combination(s) of the above.
There is little evidence to suggest that any particular individual intervention (whether delivered in individual or group-based formats) is superior to any other in treating clinician burnout. A recent analysis of 24 studies employing mindfulness-based interventions demonstrated generally positive results for such interventions.35 Other studies have also found general support for mindfulness-based interventions, although mindfulness is often integrated with other stress-reduction techniques, such as meditation, yoga, and communication skills. Such interventions are nonspecific but generally effective.
An accumulation of evidence to date suggests that a combination of individual and organizational interventions is most effective in combatting clinician burnout. No individual intervention can be successful without addressing root causes, such as overscheduling, lack of organizational support, and the effect of restrictive legislation on practice.
Several large teaching hospitals have established programs to address physician and health care provider burnout. Notable among these is the Stanford University School of Medicine’s WellMD and WellPhD programs (https://wellmd.stanford.edu/about.html). These programs were described by Olson and colleagues36 as using a model focused on practice efficiency, organizational culture, and personal resilience to enhance physicians’ well-being. (See “Aspects of the WellMD and WellPhD programs from Stanford University.”)
A growing number of institutions have established burnout programs to support physicians experiencing work/life imbalances and other aspects of burnout.37 In general, these share common features of assessment, individual and/or group intervention, and organizational change. Fear of repercussion may be one factor preventing physicians from seeking individual treatment for burnout.38 Importantly, they emphasize the need for professional confidentiality when offering treatment to patients within organizational settings. Those authors also reported that a focus on organizational engagement may be an important factor in addressing burnout in female physicians, as they tend to report lower levels of organizational engagement.
Continue to: Legal considerations...
Legal considerations
Until recently, physician burnout “received little notice in the legal literature.”39 Although there have been burnout legal consequences in the past, the legal issues are now becoming more visible.40
Medical malpractice
A well-documented consequence of burnout is an increase in errors.14 Medical errors, of course, are at the heart of malpractice claims. Technically, malpractice is medical or professional negligence. It is the breach of a duty owed by the physician, or other provider, or organization (defendant) to the patient, which causes injury to the plaintiff/patient.41
“Medical error” is generally a meaningful deviation from the “standard of care” or accepted medical practice.42 Many medical errors do not cause injury to the patient; in those cases, the negligence does not result in liability. In instances in which the negligence causes harm, the clinician and health care facility may be subject to liability for that injury. Fortunately, however, for a variety of reasons, most harmful medical errors do not result in a medical malpractice claim or lawsuit. The absence of a good clinician-patient relationship is likely associated with an increased inclination of a patient to file a malpractice action.43Clinician burnout may, therefore, contribute to increased malpractice claims in two ways. First, burnout likely leads to increased medical errors, perhaps because burnout is associated with lower concentration, inattention, reduced cognitive vigilance, and fatigue.8,44 It may also lead to less time with patients, reduced patient empathy, and lower patient rapport, which may make injured patients more likely to file a claim or lawsuit.45 Because the relationshipbetween burnout and medical error is bidirectional, malpractice claims tend to increase burnout, which increases error. Given the time it takes to resolve most malpractice claims, the uncertainty of medical malpractice may be especially stressful for health care providers.46,47
Burnout is not a mitigating factor in malpractice. Our sympathies may go out to a professional suffering from burnout, but it does not excuse or reduce liability—it may, indeed, be an aggravating factor. Clinicians who can diagnose burnout and know its negative consequences but fail to deal with their own burnout may be demonstrating negligence if there has been harm to a patient related to the burnout.48
Institutional or corporate liability to patients
Health care institutions have obligations to avoid injury to patients. Just as poorly maintained medical equipment may harm patients, so may burned-out professionals. Therefore, institutions have some obligation to supervise and avoid the increased risks to patients posed by professionals suffering from burnout.
Respondeat superior and institutional negligence. Institutional liability may arise in two ways, the first through agency, or respondeat superior. That is, if the physician or other professional is an employee (or similar agent) of the health care institution, that institution is generally responsible for the physician’s negligence during the employment.49 Even if the physician is not an employee (for example, an independent contractor providing care or using the hospital facilities), the health care facility may be liable for the physician’s negligence.50 Liability may occur, for example, if the health care facility was aware that the physician was engaged in careless practice or was otherwise a risk to patients but the facility did not take steps to avoid those risks.51 The basis for liability is that the health care organization owes a duty to patients to take reasonable care to ensure that its facilities are not used to injure patients negligently.52 Just as it must take care that unqualified physicians are not granted privileges to practice, it also must take reasonable steps to protect patients when it is aware (through nurses or other agents) of a physician’s negligent practice.
In one case, for example, the court found liability where a staff member had “severe” burnout in a physician’s office and failed to read fetal monitoring strips. The physician was found negligent for relying on the staff member who was obviously making errors in interpretation of fetal distress.53
Continue to: Legal obligations of health care organizations to physicians and others...
Legal obligations of health care organizations to physicians and others
In addition to obligations to patients, health care organizations may have obligations to employees (and others) at risk for injury. For example, assume a patient is diagnosed with a highly contagious disease. The health care organization would be obligated to warn, and take reasonable steps to protect, the staff (employees and independent contractors) from being harmed from exposure to the disease. This principle may apply to coworkers of employees with significant burnout, thereby presenting a danger in the workplace. The liability issue is more difficult for employees experiencing job-related burnout themselves. Organizations generally compensate injured employees through no-fault workers’ compensation (an insurance-like system); for independent contractors, the liability is usually through a tort claim (negligence).54
In modern times, a focus has been on preventing those injuries, not just providing compensation after injuries have occurred. Notably, federal and state occupational health and safety laws (particularly the Occupational Safety and Health Administration [OSHA]) require most organizations (including those employing health care providers) to take steps to mitigate various kinds of worker injuries.55
Although these worker protections have commonly been applied to hospitals and other health care providers, burnout has not traditionally been a significant concern in federal or state OSHA enforcement. For example, no formal federal OSHA regulations govern work-related burnout. Regulators, including OSHA, are increasingly interested in burnout that may affect many employees. OSHA has several recommendations for reducing health care work burnout.56 The Surgeon General has expressed similar concerns.57 The federal government recently allocated $103 million from the American Rescue Plan to address burnout among health care workers.58 Also, OSHA appears to be increasing its oversight of healthcare-institution-worker injuries.55
Is burnout a “disability”?
The federal Americans with Disabilities Act (ADA) and similar state laws prohibit discrimination based on disability.59 A disability is defined as a “physical or mental impairment that substantially limits one or more major life activities” or “perceived as having such an impairment.”60 The initial issue is whether burnout is a “mental impairment.” As noted earlier, it is not officially a “medical condition.”61 To date, the United Nations has classified it as an “occupational phenomenon.”62 It may, therefore, not qualify under the ADA, even if it “interferes with a major life activity.” There is, however, some movement toward defining burnout as a mental condition. Even if defined as a disability, there would still be legal issues of how severe it must be to qualify as a disability and the proper accommodation. Apart from the legal definition of an ADA disability, as a practical matter it likely is in the best interest of health care facilities to provide accommodations that reduce burnout. A number of strategies to decrease the incidence of burnout include the role of health care systems (FIGURE 2).
In conclusion we look at several things that can be done to “treat” or reduce burnout. That effort requires the cooperation of physicians and other providers, health care facilities, training programs, licensing authorities, and professional organizations. See suggestions below.
Conclusion
There are many excellent suggestions for reducing burnout and improving patient care and practitioner satisfaction.63-65 We conclude with a summary of some of these suggestions for individual practitioners, health care organizations, the profession, and licensing. It is worth remembering, however, that it will require the efforts of each area to reduce burnout substantially.
For practitioners:
- Engage in quality coaching/therapy on mindfulness and stress management.
- Practice self-care, including exercise and relaxation techniques.
- Make work-life balance a priority.
- Take opportunities for collegial social and professional discussions.
- Prioritize (and periodically assess) your own professional satisfaction and burnout risk.
- Smile—enjoy a sense of humor (endorphins and cortisol).
For health care organizations:
- Urgently work with vendors and regulators to revise electronic health records to reduce their substantial impact on burnout.
- Reduce physicians’ time on clerical and administrative tasks (eg, by enhancing the use of quality AI, scribes, and automated notes from appointments. (This may increase the time they spend with patients.) Eliminate “pajama-time” charting.
- Provide various kinds of confidential professional counseling, therapy, and support related to burnout prevention and treatment, and avoid any penalty or stigma related to their use.
- Provide reasonable flexibility in scheduling.
- Routinely provide employees with information about burnout prevention and services.
- Appoint a wellness officer with authority to ensure the organization maximizes its prevention and treatment services.
- Constantly seek input from practitioners on how to improve the atmosphere for practice to maximize patient care and practitioner satisfaction.
- Provide ample professional and social opportunities for discussing and learning about work-life balance, resilience, intellectual stimulation, and career development.
For regulators, licensors, and professional organizations:
- Work with health care organizations and EHR vendors to substantially reduce the complexity, physician effort, and stress associated with those record systems. Streamlining should, in the future, be part of formally certifying EHR systems.
- Reduce the administrative burden on physicians by modifying complex regulations and using AI and other technology to the extent possible to obtain necessary reimbursement information.
- Eliminate unnecessary data gathering that requires practitioner time or attention.
- Licensing, educational, and certifying bodies should eliminate any questions regarding the diagnosis or treatment of mental health and focus on current (or very recent) impairments.
- Seek funding for research on burnout prevention and treatment.
Dr. H is a 58-year-old ObGyn who, after completing residency, went into solo practice. The practice grew, and Dr. H found it increasingly more challenging to cover, especially the obstetrics sector. Dr. H then merged the practice with a group of 3 other ObGyns. Their practice expanded, and began recruiting recent residency graduates. In time, the practice was bought out by the local hospital health care system. Dr. H was faced with complying with the rules and regulations of that health care system. The electronic health record (EHR) component proved challenging, as did the restrictions on staff hiring (and firing), but Dr. H did receive a paycheck each month and complied with it all. The health care system administrators had clear financial targets Dr. H was to meet each quarter, which created additional pressure. Dr. H used to love being an OB and providing excellent care for every patient, but that sense of accomplishment was being lost.
Dr. H increasingly found it difficult to focus because of mind wandering, especially in the operating room (OR). Thoughts occurred about retirement, the current challenges imposed by “the new way of practicing medicine” (more focused on financial productivity restraints and reimbursement), and EHR challenges. Then Dr. H’s attention would return to the OR case at hand. All of this resulted in considerable stress and emotional exhaustion, and sometimes a sense of being disconnected. A few times, colleagues or nurses had asked Dr. H if everything was “okay,” or if a break would help. Dr. H made more small errors than usual, but Dr. H’s self-assessment was “doing an adequate job.” Patient satisfaction scores (collected routinely by the health care system) declined over the last 9 months.
Six months ago, Dr. H finished doing a laparoscopic total hysterectomy and bilateral salpingo-oophorectomy and got into the right uterine artery. The estimated blood loss was 3,500 mL. Using minimally invasive techniques, Dr. H identified the bleeder and, with monopolar current, got everything under control. The patient went to the post-anesthesia care unit, and all appeared to be in order. Her vital signs were stable, and she was discharged home the same day.
The patient presented 1 week later with lower abdominal and right flank pain. Dr. H addressed the problem in the emergency department and admitted the patient for further evaluation and urology consultation. The right ureter was damaged and obstructed; ultimately, the urologist performed a psoas bladder hitch. The patient recovered slowly, lost several weeks of work, experienced significant pain, and had other disruptions and costs. Additional medical care related to the surgery is ongoing. A health care system committee asked Dr. H to explain the problem. Over the last 6 months, Dr. H’s frustration with practice and being tired and disconnected have increased.
Dr. H has received a letter from a law firm saying that he and the health care system are being sued for malpractice focused on an iatrogenic ureter injury. The letter names two very reputable experts who are prepared to testify that the patient’s injury resulted from clear negligence. Dr. H has told the malpractice carrier absolutely not to settle this case—it is “a sham— without merit.” The health care system has asked Dr. H to take a “burnout test.”
Legal considerations
Dr. H exhibits relatively clear signs of professional burnout. The fact that there was a bad outcome while Dr. H was experiencing burnout is not proof of negligence (or, breach of duty of care to the patient). Nor is it a defense or mitigation to any malpractice that occurred.
In the malpractice case, the plaintiff will have the burden of proving that Dr. H’s treatment was negligent in that it fell below the standard of care. Even if it was a medical error, the question is whether it was negligence. If the patient/plaintiff, using expert witnesses, can prove that Dr. H fell below the standard of care that caused injury, Dr. H may be liable for the resulting extra costs, loss of income, and pain and suffering resulting from the negligent care.
The health care system likely will also be responsible for Dr. H’s negligence, either through respondeat superior (for example, if Dr. H is an employee) or for its own negligence. The case for its negligence is that the nurses and assistants had repeatedly seen him making errors and becoming disengaged (to the extent that they asked Dr. H if “everything is okay” or if a break would help). Furthermore, Dr. H’s patient satisfaction scores have been declining for several months. The plaintiff will argue that Dr. H exhibited classic burnout symptoms with the attendant risks of medical errors. However, the health care system did not take action to protect patients or to assist Dr. H. In short, one way or another, there is some likelihood that the health care system may also be liable if patient injuries are found to have been caused by negligence.
At this point, the health care system also faces the question of how to work with Dr. H in the future. The most pressing question is whether or not to allow Dr. H to continue practicing. If, as it appears, Dr. H is dealing with burnout, the pressure of the malpractice claim could well increase the probability of other medical mistakes. The institution has asked Dr. H to take a burnout test, but it is unclear where things go if the test (as likely) demonstrates significant burnout. This is a counseling and human relations question, at least as much as a legal issue, and the institution should probably proceed in that way—which is, trying to understand and support Dr. H and determining what can be done to address the burnout. At the same time, the system must reasonably assess Dr. H’s fitness to continue practicing as the matters are resolved. Almost everyone shares the goal to provide every individual and corporate opportunity for Dr. H to deal with burnout issues and return to successful practice.
Dr. H will be represented in the malpractice case by counsel provided through the insurance carrier. However, Dr. H would be well advised to retain a trusted and knowledgeable personal attorney. For example, the instruction not to consider settlement is likely misguided, but Dr. H needs to talk with an attorney that Dr. H has chosen and trusts. In addition, the attorney can help guide Dr. H through a rational process of dealing with the health care system, putting the practice in order, and considering the options for the future.
The health care system should reconsider its processes to deal with burnout to ensure the quality of care, patient satisfaction, professional retention, and economic stability. Several burnoutresponse programs have had success in achieving these goals.
What’s the Verdict?
Dr. H received good mental health, legal, and professional advice. As a result, an out of court settlement was reached following pretrial discovery. Dr. H has continued consultation regarding burnout and has returned to productive practice.
Physicians have some of the highest rates of burnout among all professions.1 Complicating matters is that clinicians (including residents)2 may avoid seeking treatment out of fear it will affect their license or privileges.3 In this article, we consider burnout in greater detail, as well as ways of successfully addressing the level of burnout in the profession (FIGURE 1), including steps individual practitioners, health care entities, and regulators should consider to reduce burnout and its harmful effects.
How burnout becomes a problem
Six general factors are commonly identified as leading to clinician career dissatisfaction and burnout:4
1. work overload
2. lack of autonomy and control
3. inadequate rewards, financial and otherwise
4. work-home schedules
5. perception of lack of fairness
6. values conflict between the clinician and employer (including a breakdown of professional community).
At the top of the list of causes of burnout is often “administrative and bureaucratic headaches.”5 More specifically, electronic health records (EHRs), including computerized order entry, is commonly cited as a major cause of burnout.6,7 According to some studies, clinicians spend as much as 49% of working time doing clerical work,8 and studies found the extension of work into home life.9
Increased measurement of performance metrics in health care services are a significant contributor to physician burnout.10 These include pressure to see more patients, perform more procedures, and respond quickly to patient requests (eg, through email).7 As we will see, medical malpractice cases, or the risk of such cases, have also played a role in burnout in some medical specialties.11 The pandemic also contributed, at least temporarily, to burnout.12,13
Rates of burnout among physicians are notably higher than among the general population14 or other professions.6 Although physicians have generally entered clinical practice with lower rates of burnout than the general population,15 The American College of Obstetricians and Gynecologists (ACOG) reports that 40% to 75% of ObGyns “experience some form of professional burnout.”16,17 Other source(s) cite that 53% of ObGyns report burnout (TABLE 1).
Code QD85
Burnout is a syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed. It is characterized by 3 dimensions:
- feelings of energy depletion or exhaustion
- increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job
- a sense of ineffectiveness and lack of accomplishment. Burn-out refers specifically to phenomena in the occupational context and should not be applied to describe experiences in other areas of life. Exclusions to burnout diagnosis include adjustment disorder, disorders specifically associated with stress, anxiety or fear-related disorders, and mood disorders.
Reference
1. International Classification of Diseases Eleventh Revision (ICD-11). Geneva, Switzerland: World Health Organization; 2022.
Burnout undoubtedly contributes to professionals leaving practice, leading to a significant shortage of ObGyns.18 It also raises several significant legal concerns. Despite the enormity and seriousness of the problem, there is considerable optimism and assurance that the epidemic of burnout is solvable on the individual, specialty, and profession-wide levels. ACOG and other organizations have made suggestions for physicians, the profession, and to health care institutions for reducing burnout.19 This is not to say that solutions are simple or easy for individual professionals or institutions, but they are within the reach of the profession (FIGURE 2).
Suicide among health care professionals is one other concern (TABLE 2)20 and theoretically can stem from burnout, depression, and other psychosocial concerns.
Costs of clinician burnout
Burnout is endemic among health care providers, with numerous studies detailing the professional, emotional, and financial costs. Prior to the pandemic, one analysis of nationwide fiscal costs associated with burnout estimated an annual cost of $4.6B due to physician turnover and reduced clinical hours.21 The COVID-19 epidemic has by all accounts worsened rates of health care worker burnout, particularly for those in high patient-contact positions.22
Female clinicians appear to be differentially affected; in one recent study women reported symptoms of burnout at twice the rate of their male counterparts.23 Whether burnout rates will return to pre-pandemic levels remains an open question, but since burnout is frequently related to one’s own assessment of work-life balance, it is possible that a longer term shift in burnout rates associated with post-pandemic occupational attitudes will be observed.
Combining factors contribute to burnout
Burnout is a universal occupational hazard, but extant data suggest that physicians and other health care providers may be at higher risk. Among physicians, younger age, female gender, and front-line specialty status appear associated with higher burnout rates.24 Given that ObGyn physicians are overwhelmingly female (60% of physicians and 86% of residents),25,26 gender-related burnout factors exist alongside other specific occupational burnout risks. While gender parity has been achieved among health care providers, gender disparities persist in terms of those in leadership positions, compensation, and other factors.22
The smattering of evidence suggesting that ObGyns have higher rates of burnout than many other specialties is understandable given the unique legal challenges confronting ObGyn practice. This may be of special significance because ObGyn malpractice insurance rates are among the highest of all specialties.27 The overall shortage of ObGyns has been exacerbated by the demonstrated negative effects on training and workforce representation stemming from recent legislation that has the effect of criminalizing certain aspects of ObGyn practice;28 for instance, uncertainty regarding abortion regulations.
These negative effects are particularly heightened in states in which the law is in flux or where there are continuing efforts to substantially limit access to abortion. The efforts to increase civil and even criminal penalties related to abortion care challenge ObGyns’ professional practices, as legal rules are frequently changing. In some states, ObGyns may face additional workloads secondary to a flight of ObGyns from restrictive jurisdictions in addition to legal and professional repercussions. In a small study of 19 genetic counselors dealing with restrictive legislation in the state of Ohio,29 increased stress and burnout rates were identified as a consequence of practice uncertainties under this legislation. It is certain that other professionals working in reproductive health care are similarly affected.30
The programs provide individual resources to providers in distress, periodically survey initiatives at Stanford to assess burnout at the organizational level, and provide input designed to spur organizational change to reduce the burden of burnout. Ways that they build community and connections include:
- Live Story Rounds events (as told by Stanford Medicine physicians)
- Commensality Groups (facilitated small discussion groups built around tested evidence)
- Aim to increase sense of connection and collegiality among physicians and build comradery at work
- CME-accredited physician wellness forum, including annual doctor’s day events
Continue to: Assessment of burnout...
Assessment of burnout
Numerous scales for the assessment of burnout exist. Of these, the 22-item Maslach Burnout Inventory (MBI) is the best studied. The MBI is a well-investigated tool for assessing burnout. The MBI consists of 3 major subscales measuring overall burnout, emotional exhaustion, depersonalization, and low personal accomplishment. It exists in numerous forms. For instance, the MBI-HSS (MP), adapted for medical personnel, is available. However, the most commonly used form for assessing burnout in clinicians is the MBI-HHS (Human Services Survey); approximately 85% of all burnout studies examined in a recent meta-analysis used this survey version.31 As those authors commented, while burnout is a recognized phenomenon, a great deal of variability in study design, interpretation of subscale scores, and sample selection makes generalizations regarding burnout difficult to assess.
The MBI in various forms has been extensively used over the past 40 years to assess burnout amongst physicians and physicians in training. While not the only instrument designed to measure such factors, it is by far the most prevalent. Williamson and colleagues32 compared the MBI with several other measures of quality of life and found good correlation between the various instruments used, a finding replicated by other studies.33 Brady and colleagues compared item responses to the Stanford Professional Fulfillment Index and the Min-Z Single-item Burnout scale (a 1-item screening measure) to MBI’s Emotional Exhaustion and Depersonalization subscales. Basing their findings on a survey of more than 1,300 physicians, they found that all analyzed scales were significantly correlated with such adverse outcomes as depression, distress, or intent to leave the profession.
It is important to note that most surveys of clinician burnout were conducted prior to the pandemic. While the psychometric analyses of the MBI and other scales are likely still germane, observed rates of clinician burnout have likely increased. Thus, comparisons of pre- and post-pandemic studies should factor in an increase in the incidence and prevalence of burnout.
Management strategies
In general, there are several interventions for managing burnout34:
- individual-focused (including self-care and communications-skills workshops)
- mindfulness training
- yoga
- meditation
- organizational/structural (workload reduction, schedule realignment, teamwork training, and group-delivered stress management interventions)
- combination(s) of the above.
There is little evidence to suggest that any particular individual intervention (whether delivered in individual or group-based formats) is superior to any other in treating clinician burnout. A recent analysis of 24 studies employing mindfulness-based interventions demonstrated generally positive results for such interventions.35 Other studies have also found general support for mindfulness-based interventions, although mindfulness is often integrated with other stress-reduction techniques, such as meditation, yoga, and communication skills. Such interventions are nonspecific but generally effective.
An accumulation of evidence to date suggests that a combination of individual and organizational interventions is most effective in combatting clinician burnout. No individual intervention can be successful without addressing root causes, such as overscheduling, lack of organizational support, and the effect of restrictive legislation on practice.
Several large teaching hospitals have established programs to address physician and health care provider burnout. Notable among these is the Stanford University School of Medicine’s WellMD and WellPhD programs (https://wellmd.stanford.edu/about.html). These programs were described by Olson and colleagues36 as using a model focused on practice efficiency, organizational culture, and personal resilience to enhance physicians’ well-being. (See “Aspects of the WellMD and WellPhD programs from Stanford University.”)
A growing number of institutions have established burnout programs to support physicians experiencing work/life imbalances and other aspects of burnout.37 In general, these share common features of assessment, individual and/or group intervention, and organizational change. Fear of repercussion may be one factor preventing physicians from seeking individual treatment for burnout.38 Importantly, they emphasize the need for professional confidentiality when offering treatment to patients within organizational settings. Those authors also reported that a focus on organizational engagement may be an important factor in addressing burnout in female physicians, as they tend to report lower levels of organizational engagement.
Continue to: Legal considerations...
Legal considerations
Until recently, physician burnout “received little notice in the legal literature.”39 Although there have been burnout legal consequences in the past, the legal issues are now becoming more visible.40
Medical malpractice
A well-documented consequence of burnout is an increase in errors.14 Medical errors, of course, are at the heart of malpractice claims. Technically, malpractice is medical or professional negligence. It is the breach of a duty owed by the physician, or other provider, or organization (defendant) to the patient, which causes injury to the plaintiff/patient.41
“Medical error” is generally a meaningful deviation from the “standard of care” or accepted medical practice.42 Many medical errors do not cause injury to the patient; in those cases, the negligence does not result in liability. In instances in which the negligence causes harm, the clinician and health care facility may be subject to liability for that injury. Fortunately, however, for a variety of reasons, most harmful medical errors do not result in a medical malpractice claim or lawsuit. The absence of a good clinician-patient relationship is likely associated with an increased inclination of a patient to file a malpractice action.43Clinician burnout may, therefore, contribute to increased malpractice claims in two ways. First, burnout likely leads to increased medical errors, perhaps because burnout is associated with lower concentration, inattention, reduced cognitive vigilance, and fatigue.8,44 It may also lead to less time with patients, reduced patient empathy, and lower patient rapport, which may make injured patients more likely to file a claim or lawsuit.45 Because the relationshipbetween burnout and medical error is bidirectional, malpractice claims tend to increase burnout, which increases error. Given the time it takes to resolve most malpractice claims, the uncertainty of medical malpractice may be especially stressful for health care providers.46,47
Burnout is not a mitigating factor in malpractice. Our sympathies may go out to a professional suffering from burnout, but it does not excuse or reduce liability—it may, indeed, be an aggravating factor. Clinicians who can diagnose burnout and know its negative consequences but fail to deal with their own burnout may be demonstrating negligence if there has been harm to a patient related to the burnout.48
Institutional or corporate liability to patients
Health care institutions have obligations to avoid injury to patients. Just as poorly maintained medical equipment may harm patients, so may burned-out professionals. Therefore, institutions have some obligation to supervise and avoid the increased risks to patients posed by professionals suffering from burnout.
Respondeat superior and institutional negligence. Institutional liability may arise in two ways, the first through agency, or respondeat superior. That is, if the physician or other professional is an employee (or similar agent) of the health care institution, that institution is generally responsible for the physician’s negligence during the employment.49 Even if the physician is not an employee (for example, an independent contractor providing care or using the hospital facilities), the health care facility may be liable for the physician’s negligence.50 Liability may occur, for example, if the health care facility was aware that the physician was engaged in careless practice or was otherwise a risk to patients but the facility did not take steps to avoid those risks.51 The basis for liability is that the health care organization owes a duty to patients to take reasonable care to ensure that its facilities are not used to injure patients negligently.52 Just as it must take care that unqualified physicians are not granted privileges to practice, it also must take reasonable steps to protect patients when it is aware (through nurses or other agents) of a physician’s negligent practice.
In one case, for example, the court found liability where a staff member had “severe” burnout in a physician’s office and failed to read fetal monitoring strips. The physician was found negligent for relying on the staff member who was obviously making errors in interpretation of fetal distress.53
Continue to: Legal obligations of health care organizations to physicians and others...
Legal obligations of health care organizations to physicians and others
In addition to obligations to patients, health care organizations may have obligations to employees (and others) at risk for injury. For example, assume a patient is diagnosed with a highly contagious disease. The health care organization would be obligated to warn, and take reasonable steps to protect, the staff (employees and independent contractors) from being harmed from exposure to the disease. This principle may apply to coworkers of employees with significant burnout, thereby presenting a danger in the workplace. The liability issue is more difficult for employees experiencing job-related burnout themselves. Organizations generally compensate injured employees through no-fault workers’ compensation (an insurance-like system); for independent contractors, the liability is usually through a tort claim (negligence).54
In modern times, a focus has been on preventing those injuries, not just providing compensation after injuries have occurred. Notably, federal and state occupational health and safety laws (particularly the Occupational Safety and Health Administration [OSHA]) require most organizations (including those employing health care providers) to take steps to mitigate various kinds of worker injuries.55
Although these worker protections have commonly been applied to hospitals and other health care providers, burnout has not traditionally been a significant concern in federal or state OSHA enforcement. For example, no formal federal OSHA regulations govern work-related burnout. Regulators, including OSHA, are increasingly interested in burnout that may affect many employees. OSHA has several recommendations for reducing health care work burnout.56 The Surgeon General has expressed similar concerns.57 The federal government recently allocated $103 million from the American Rescue Plan to address burnout among health care workers.58 Also, OSHA appears to be increasing its oversight of healthcare-institution-worker injuries.55
Is burnout a “disability”?
The federal Americans with Disabilities Act (ADA) and similar state laws prohibit discrimination based on disability.59 A disability is defined as a “physical or mental impairment that substantially limits one or more major life activities” or “perceived as having such an impairment.”60 The initial issue is whether burnout is a “mental impairment.” As noted earlier, it is not officially a “medical condition.”61 To date, the United Nations has classified it as an “occupational phenomenon.”62 It may, therefore, not qualify under the ADA, even if it “interferes with a major life activity.” There is, however, some movement toward defining burnout as a mental condition. Even if defined as a disability, there would still be legal issues of how severe it must be to qualify as a disability and the proper accommodation. Apart from the legal definition of an ADA disability, as a practical matter it likely is in the best interest of health care facilities to provide accommodations that reduce burnout. A number of strategies to decrease the incidence of burnout include the role of health care systems (FIGURE 2).
In conclusion we look at several things that can be done to “treat” or reduce burnout. That effort requires the cooperation of physicians and other providers, health care facilities, training programs, licensing authorities, and professional organizations. See suggestions below.
Conclusion
There are many excellent suggestions for reducing burnout and improving patient care and practitioner satisfaction.63-65 We conclude with a summary of some of these suggestions for individual practitioners, health care organizations, the profession, and licensing. It is worth remembering, however, that it will require the efforts of each area to reduce burnout substantially.
For practitioners:
- Engage in quality coaching/therapy on mindfulness and stress management.
- Practice self-care, including exercise and relaxation techniques.
- Make work-life balance a priority.
- Take opportunities for collegial social and professional discussions.
- Prioritize (and periodically assess) your own professional satisfaction and burnout risk.
- Smile—enjoy a sense of humor (endorphins and cortisol).
For health care organizations:
- Urgently work with vendors and regulators to revise electronic health records to reduce their substantial impact on burnout.
- Reduce physicians’ time on clerical and administrative tasks (eg, by enhancing the use of quality AI, scribes, and automated notes from appointments. (This may increase the time they spend with patients.) Eliminate “pajama-time” charting.
- Provide various kinds of confidential professional counseling, therapy, and support related to burnout prevention and treatment, and avoid any penalty or stigma related to their use.
- Provide reasonable flexibility in scheduling.
- Routinely provide employees with information about burnout prevention and services.
- Appoint a wellness officer with authority to ensure the organization maximizes its prevention and treatment services.
- Constantly seek input from practitioners on how to improve the atmosphere for practice to maximize patient care and practitioner satisfaction.
- Provide ample professional and social opportunities for discussing and learning about work-life balance, resilience, intellectual stimulation, and career development.
For regulators, licensors, and professional organizations:
- Work with health care organizations and EHR vendors to substantially reduce the complexity, physician effort, and stress associated with those record systems. Streamlining should, in the future, be part of formally certifying EHR systems.
- Reduce the administrative burden on physicians by modifying complex regulations and using AI and other technology to the extent possible to obtain necessary reimbursement information.
- Eliminate unnecessary data gathering that requires practitioner time or attention.
- Licensing, educational, and certifying bodies should eliminate any questions regarding the diagnosis or treatment of mental health and focus on current (or very recent) impairments.
- Seek funding for research on burnout prevention and treatment.
Dr. H is a 58-year-old ObGyn who, after completing residency, went into solo practice. The practice grew, and Dr. H found it increasingly more challenging to cover, especially the obstetrics sector. Dr. H then merged the practice with a group of 3 other ObGyns. Their practice expanded, and began recruiting recent residency graduates. In time, the practice was bought out by the local hospital health care system. Dr. H was faced with complying with the rules and regulations of that health care system. The electronic health record (EHR) component proved challenging, as did the restrictions on staff hiring (and firing), but Dr. H did receive a paycheck each month and complied with it all. The health care system administrators had clear financial targets Dr. H was to meet each quarter, which created additional pressure. Dr. H used to love being an OB and providing excellent care for every patient, but that sense of accomplishment was being lost.
Dr. H increasingly found it difficult to focus because of mind wandering, especially in the operating room (OR). Thoughts occurred about retirement, the current challenges imposed by “the new way of practicing medicine” (more focused on financial productivity restraints and reimbursement), and EHR challenges. Then Dr. H’s attention would return to the OR case at hand. All of this resulted in considerable stress and emotional exhaustion, and sometimes a sense of being disconnected. A few times, colleagues or nurses had asked Dr. H if everything was “okay,” or if a break would help. Dr. H made more small errors than usual, but Dr. H’s self-assessment was “doing an adequate job.” Patient satisfaction scores (collected routinely by the health care system) declined over the last 9 months.
Six months ago, Dr. H finished doing a laparoscopic total hysterectomy and bilateral salpingo-oophorectomy and got into the right uterine artery. The estimated blood loss was 3,500 mL. Using minimally invasive techniques, Dr. H identified the bleeder and, with monopolar current, got everything under control. The patient went to the post-anesthesia care unit, and all appeared to be in order. Her vital signs were stable, and she was discharged home the same day.
The patient presented 1 week later with lower abdominal and right flank pain. Dr. H addressed the problem in the emergency department and admitted the patient for further evaluation and urology consultation. The right ureter was damaged and obstructed; ultimately, the urologist performed a psoas bladder hitch. The patient recovered slowly, lost several weeks of work, experienced significant pain, and had other disruptions and costs. Additional medical care related to the surgery is ongoing. A health care system committee asked Dr. H to explain the problem. Over the last 6 months, Dr. H’s frustration with practice and being tired and disconnected have increased.
Dr. H has received a letter from a law firm saying that he and the health care system are being sued for malpractice focused on an iatrogenic ureter injury. The letter names two very reputable experts who are prepared to testify that the patient’s injury resulted from clear negligence. Dr. H has told the malpractice carrier absolutely not to settle this case—it is “a sham— without merit.” The health care system has asked Dr. H to take a “burnout test.”
Legal considerations
Dr. H exhibits relatively clear signs of professional burnout. The fact that there was a bad outcome while Dr. H was experiencing burnout is not proof of negligence (or, breach of duty of care to the patient). Nor is it a defense or mitigation to any malpractice that occurred.
In the malpractice case, the plaintiff will have the burden of proving that Dr. H’s treatment was negligent in that it fell below the standard of care. Even if it was a medical error, the question is whether it was negligence. If the patient/plaintiff, using expert witnesses, can prove that Dr. H fell below the standard of care that caused injury, Dr. H may be liable for the resulting extra costs, loss of income, and pain and suffering resulting from the negligent care.
The health care system likely will also be responsible for Dr. H’s negligence, either through respondeat superior (for example, if Dr. H is an employee) or for its own negligence. The case for its negligence is that the nurses and assistants had repeatedly seen him making errors and becoming disengaged (to the extent that they asked Dr. H if “everything is okay” or if a break would help). Furthermore, Dr. H’s patient satisfaction scores have been declining for several months. The plaintiff will argue that Dr. H exhibited classic burnout symptoms with the attendant risks of medical errors. However, the health care system did not take action to protect patients or to assist Dr. H. In short, one way or another, there is some likelihood that the health care system may also be liable if patient injuries are found to have been caused by negligence.
At this point, the health care system also faces the question of how to work with Dr. H in the future. The most pressing question is whether or not to allow Dr. H to continue practicing. If, as it appears, Dr. H is dealing with burnout, the pressure of the malpractice claim could well increase the probability of other medical mistakes. The institution has asked Dr. H to take a burnout test, but it is unclear where things go if the test (as likely) demonstrates significant burnout. This is a counseling and human relations question, at least as much as a legal issue, and the institution should probably proceed in that way—which is, trying to understand and support Dr. H and determining what can be done to address the burnout. At the same time, the system must reasonably assess Dr. H’s fitness to continue practicing as the matters are resolved. Almost everyone shares the goal to provide every individual and corporate opportunity for Dr. H to deal with burnout issues and return to successful practice.
Dr. H will be represented in the malpractice case by counsel provided through the insurance carrier. However, Dr. H would be well advised to retain a trusted and knowledgeable personal attorney. For example, the instruction not to consider settlement is likely misguided, but Dr. H needs to talk with an attorney that Dr. H has chosen and trusts. In addition, the attorney can help guide Dr. H through a rational process of dealing with the health care system, putting the practice in order, and considering the options for the future.
The health care system should reconsider its processes to deal with burnout to ensure the quality of care, patient satisfaction, professional retention, and economic stability. Several burnoutresponse programs have had success in achieving these goals.
What’s the Verdict?
Dr. H received good mental health, legal, and professional advice. As a result, an out of court settlement was reached following pretrial discovery. Dr. H has continued consultation regarding burnout and has returned to productive practice.
- Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2017. Mayo Clinic Proceed. 2019;94:1681-1694.
- Smith R, Rayburn W. Burnout in obstetrician-gynecologists. Its prevalence, identification, prevention, and reversal. Obstet Gynecol Clin North Am. 2021;48:231-245. https://doi. org/10.1016/j.ogc.2021.06.003
- Patti MG, Schlottmann F, Sarr MG. The problem of burnout among surgeons. JAMA Surg. 2018;153:403-404. doi:10.1001 /jamasurg.2018.0047
- Carrau D, Janis JE. Physician burnout: solutions for individuals and organizations. Plastic and Reconstructive Surgery Global Open. 2021;91-97.
- Southwick R. The key to fixing physician burnout is the workplace not the worker. Contemporary Ob/Gyn. March 13, 2023.
- Patel RS, Bachu R, Adikey A, et al. Factors related to physician burnout and its consequences: a review. Behav Sciences. 2018;8:98.
- Melnick ER, Dyrbye LN, Sinsky CA, et al. The association between perceived electronic health record usability and professional burnout among US physicians. Mayo Clinic Proceed. 2020;95:476-487.
- Shanafelt TD, Dyrbye LN, West CP. Addressing physician burnout: the way forward. JAMA. 2017;317:901-902. doi:10.1001/jama.2017.0076
- Ommaya AK, Cipriano PF, Hoyt DB, et al. Care-centered clinical documentation in the digital environment: Solutions to alleviate burnout. National Academy of Medicine Perspectives. 2018.
- Hartzband P, Groopman J. Physician burnout, interrupted. N Engl J Med. 2020;382:2485-2487. Discussion Paper, National Academy of Medicine. Accessed July 21, 2023. https://nam .edu/care
- Ji YD, Robertson FC, Patel NA, et al. Assessment of risk factors for suicide among US health care professionals. JAMA Surg. 2020;155:713-721. centered-clinical-documentation-digital -environment-solutions-alleviate-burnout/
- Shanafelt TD, West CP, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clinic Proceed. 2022;97:2248-2258.
- Herber-Valdez C, Kupesic-Plavsic S. Satisfaction and shortfall of OB-GYN physicians and radiologists. J. Ultrasound Obstet Gynecol. 2021;15:387-392.
- Dyrbye LN, Shanafelt TD, Sinsky CA, et al. Burnout among health care professionals: a call to explore and address this underrecognized threat to safe, high-quality care. National Academy of Medicine Perspectives. Accessed July 5, 2017. https://iuhcpe.org/file_manager/1501524077-Burnout -Among-Health-Care-Professionals-A-Call-to-Explore-and -Address-This-Underrecognized-Threat.pdf
- Olson KD. Physician burnout—a leading indicator of health system performance? Mayo Clinic Proceed. 2017;92: 1608-1611.
- American College of Obstetricians and Gynecologists. Why obgyns are burning out. October 28, 2019. Accessed July 21, 2023. https://www.acog.org/news/news-articles/2019/10/why-ob -gyns-are-burning-out#:~:text=A%202017%20report%20 by%20the,exhaustion%20or%20lack%20of%20motivation
- Peckham C. National physician burnout & depression report 2018. Medscape. January 17, 2018. https://nap. nationalacademies.org/catalog/25521/taking-action -against-clinician-burnout-a-systems-approach-to -professional
- Marsa L. Labor pains: The OB-GYN shortage. AAMC News. Nov. 15, 2018. Accessed July 21, 2023. https://www.aamc.org /news-insights/labor-pains-ob-gyn-shortage
- American College of Obstetricians and Gynecologists. Coping with the stress of medical professional liability litigation. ACOG Committee Opinion. February 2005;309:453454. Accessed July 21, 2023. https://www.acog.org/clinical /clinical-guidance/committee-opinion/articles/2013/01 /coping-with-the-stress-of-medical-professional-liability -litigation
- Reith TP. Burnout in United States healthcare professionals: a narrative review. Cureus. 2018;10:e3681. doi: 10.7759 /cureus.3681
- Han S, Shanafelt TD, Sinsky CA, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med. 2019;4:784-790.
- Sullivan D, Sullivan V, Weatherspoon D, et al. Comparison of nurse burnout, before and during the COVID-19 pandemic. Nurs Clin North Am. 2022;57:79-99. doi: 10.1016 /j.cnur.2021.11.006
- Chandawarkar A, Chaparro JD. Burnout in clinicians. Curr Prob Pediatr Adolesc Health Care. 2021;51:101-104. https ://doi.org/10.1016/j.cppeds.2021.101104
- Brady KJS, Sheldrick RC, Ni P, et al. Examining the measurement equivalence of the Maslach Burnout Inventory across age, gender, and specialty groups in US physicians. J Patient-Reported Outcomes. 2021;5.
- Association of American Medical Colleges. Physician Specialty Data Report—Active Physicians by Sex and Specialty, 2021. Accessed June 19, 2023. https://www.aamc .org/data-reports/workforce/data/active-physicians-sex -specialty-2021
- Association of American Medical Colleges. Physician Specialty Data Report—ACGME Residents and Fellows by Sex and Specialty, 2021. Accessed June 19, 2023. https://www .aamc.org/data-reports/workforce/data/acgme-residents -fellows-sex-and-specialty-2021
- Painter LM, Biggans KA, Turner CT. Risk managementobstetrics and gynecology perspective. Clin Obstet Gynecol. 2023;66:331-341. DOI:10.1097/GRF.0000000000000775
- Darney BG, Boniface E, Liberty A. Assessing the effect of abortion restrictions. Obstetr Gynecol. 2023;141:233-235.
- Heuerman AC, Bessett D, Antommaria AHM, et al. Experiences of reproductive genetic counselors with abortion regulations in Ohio. J Genet Counseling. 2022;31:641-652.
- Brandi K, Gill P. Abortion restrictions threaten all reproductive health care clinicians. Am J Public Health. 2023;113:384-385.
- Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of burnout among physicians: a systematic review. JAMA. 2018;320:1131-1150. doi: 10.1001/jama.2018.1277
- Williamson K, Lank PM, Cheema N, et al. Comparing the Maslach Burnout Inventory to other well-being instruments in emergency medicine residents. J Graduate Med Education. 2018;532-536. DOI: http://dx.doi.org/10.4300 /JGME-D-18-00155.1
- Brady KJS, Sheldrick RC, Ni P, et al. Establishing crosswalks between common measures of burnout in US physicians. J Gen Intern Med. 2022;37:777-784.
- Zhang X, Song Y, Jiang T, et al. Interventions to reduce burnout of physicians and nurses: an overview of systematic reviews and meta-analyses. Medicine (Baltimore). 2020;26:e20992. DOI: 10.1097/MD.0000000000020992
- Scheepers RA, Emke H, Ronald M, et al. The impact of mindfulness-based interventions on doctors’ well-being and performance: a systematic review. Med Education. 2020;54:138-149. https://doi.org/10.1111/medu.14020
- Olson K, Marchalik D, Farley H, et al. Organizational strategies to reduce physician burnout and improve professional fulfillment. Curr Prob Pediatr Adolesc Health Care. 2019;49:12. https://doi.org/10.1016/j.cppeds.2019.100664
- Berry LL, Awdish RLA, Swensen SJ. 5 ways to restore depleted health care workers. Harvard Business Rev. February 11, 2022.
- Sullivan AB, Hersh CM, Rensel M, et al. Leadership inequity, burnout, and lower engagement of women in medicine. J Health Serv Psychol. 2023;49:33-39.
- Hoffman S. Healing the healers: legal remedies for physician burnout. Yale J Health Policy Law Ethics. 2018;18:56-113.
- Federation of State Medical Boards. Physician wellness and burnout: report and recommendations of the workgroup on physician wellness and burnout. (Policy adopted by FSMB). April 2018. Accessed July 21, 2023. https://www.fsmb.org /siteassets/advocacy/policies/policy-on-wellness-and -burnout.pdf
- Robinson C, Kettering C, Sanfilippo JS. Medical malpractice lawsuits. Clin Obstet Gynecol. 2023;66:256-260. DOI: https ://doi.org/10.1097/GRF.0000000000000777
- Gittler GJ, Goldstein EJ. The elements of medical malpractice: an overview. Clin Infect Dis. 1996;23:1152-1155.
- Bal BS. An introduction to medical malpractice in the United States. Clin Orthop Relat Res. 2009;467:339-347.
- Tawfik DS, Profit J, Morgenthaler TI, et al. Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clinic Proceed. 2018;93: 1571-1580.
- Sundholm B. Elevating physician-patient relationships in the shadow of metric mania. Drexel L Rev. 2020;12:287-330.
- Ghaith S, Campbell RL, Pollock JR, et al. Medical malpractice lawsuits involving trainees in obstetrics and gynecology in the USA. Healthcare. 2022;10:1328.
- Muller TM, Warsi S. Litigation culture causing burnout in American physicians. Trauma Mental Health Report. April 9, 2021.
- Levine AS. Legal 101: Tort law and medical malpractice for physicians. Contemp OBGYN. 2015:60;26-28, 30.
- Regan JJ, Regan WM. Medical malpractice and respondeat superior. Southern Med J. 2002;95.5:545-549. DOI 10.1097/00007611-200295050-00018
- Levin H. Hospital vicarious liability for negligence by independent contractor physicians: new rule for new times. Univ Illinois Law Rev. 2005:1291-1332.
- Darling v Charleston Hospital, 33 Ill. 2d 326, 211 N.E.2d 253 (Ill. 1965).
- Dangel R. Hospital liability for physician malpractice. Ohio State Law J. 1986;47:1077-1098.
- Reffitt v Hajjar, 892 S.W.2d 599, 605 (Ky. Ct. App. 1994).
- McMichael BJ. Malpractice. In Laws of Medicine: Core Legal Aspects for the Healthcare Professional. New York, NY: Springer International; 2022:129-150.
- Occupational Safety and Health Administration. Worker safety in hospitals: caring for our caregivers. Accessed June 8, 2023. https://www.osha.gov/hospitals
- Occupational Safety and Health Administration. Workplace stress. Accessed June 8, 2023. https://www.osha.gov /workplace-stress/understanding-the-problem
- U.S. Surgeon General’s Advisory on Building a Thriving Health Workforce. Addressing health worker burnout. Accessed July 21, 2023. https://www.hhs.gov/sites/default/files/health -worker-wellbeing-advisory.pdf
- Department of Health & Human Services. Biden-Harris administration awards $103 Million in American Rescue Plan funds to reduce burnout and promote mental health and wellness among health care workforce. January 20, 2022. Accessed July 24, 2023. https://www.hhs.gov/about /news/2022/01/20/biden-harris-administration-awards -103-million-american-rescue-plan-funds-reduce-burnout -promote-mental-health-wellness-among-health-care -workforce.html
- Rothstein LF, Irzyk J. Disabilities and the Law. 4th ed. Toronto, Canada: Thompson Reuters; 2023.
- Department of Labor. Guide to disability rights laws. February 28, 2020. Accessed July 24, 2023. https://www .ada.gov/resources/disability-rights-guide/#:~:text=An%20 individual%20with%20a%20disability%20is%20defined%20 by%20the%20ADA,as%20having%20such%20an%20 impairment
- Nadon L, De Beer LT, Morin AJS. Should burnout be conceptualized as a mental disorder? Behavioral Sci. 2022;12:82.
- World Health Organization. Burn-out an “occupational phenomenon”: International Classification of Diseases. May 28, 2019. Accessed July 21, 2023. https://www.who.int/news /item/28-05-2019-burn-out-an-occupational-phenomenon -international-classification-of-diseases
- Hoffman S. Physician burnout: why legal and regulatory systems may need to step in. The Conversation. July 9, 2019. https://theconversation.com/physician-burnout-why-legal -and-regulatory-systems-may-need-to-step-in-119705
- Jha A, Iliff A, Chaoi A, et al. A crisis in healthcare: a call to action on physician burnout. Harvard Global Health Institute. 2019. Accessed July 21, 2023. https://www.massmed.org /Publications/Research,-Studies,-and-Reports/Physician -Burnout-Report-2018/
- Arnsten AF, Shanafelt T. Physician distress and burnout: the neurobiological perspective. Mayo Clin Proceed. 2021;96:763-769.
- Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2017. Mayo Clinic Proceed. 2019;94:1681-1694.
- Smith R, Rayburn W. Burnout in obstetrician-gynecologists. Its prevalence, identification, prevention, and reversal. Obstet Gynecol Clin North Am. 2021;48:231-245. https://doi. org/10.1016/j.ogc.2021.06.003
- Patti MG, Schlottmann F, Sarr MG. The problem of burnout among surgeons. JAMA Surg. 2018;153:403-404. doi:10.1001 /jamasurg.2018.0047
- Carrau D, Janis JE. Physician burnout: solutions for individuals and organizations. Plastic and Reconstructive Surgery Global Open. 2021;91-97.
- Southwick R. The key to fixing physician burnout is the workplace not the worker. Contemporary Ob/Gyn. March 13, 2023.
- Patel RS, Bachu R, Adikey A, et al. Factors related to physician burnout and its consequences: a review. Behav Sciences. 2018;8:98.
- Melnick ER, Dyrbye LN, Sinsky CA, et al. The association between perceived electronic health record usability and professional burnout among US physicians. Mayo Clinic Proceed. 2020;95:476-487.
- Shanafelt TD, Dyrbye LN, West CP. Addressing physician burnout: the way forward. JAMA. 2017;317:901-902. doi:10.1001/jama.2017.0076
- Ommaya AK, Cipriano PF, Hoyt DB, et al. Care-centered clinical documentation in the digital environment: Solutions to alleviate burnout. National Academy of Medicine Perspectives. 2018.
- Hartzband P, Groopman J. Physician burnout, interrupted. N Engl J Med. 2020;382:2485-2487. Discussion Paper, National Academy of Medicine. Accessed July 21, 2023. https://nam .edu/care
- Ji YD, Robertson FC, Patel NA, et al. Assessment of risk factors for suicide among US health care professionals. JAMA Surg. 2020;155:713-721. centered-clinical-documentation-digital -environment-solutions-alleviate-burnout/
- Shanafelt TD, West CP, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clinic Proceed. 2022;97:2248-2258.
- Herber-Valdez C, Kupesic-Plavsic S. Satisfaction and shortfall of OB-GYN physicians and radiologists. J. Ultrasound Obstet Gynecol. 2021;15:387-392.
- Dyrbye LN, Shanafelt TD, Sinsky CA, et al. Burnout among health care professionals: a call to explore and address this underrecognized threat to safe, high-quality care. National Academy of Medicine Perspectives. Accessed July 5, 2017. https://iuhcpe.org/file_manager/1501524077-Burnout -Among-Health-Care-Professionals-A-Call-to-Explore-and -Address-This-Underrecognized-Threat.pdf
- Olson KD. Physician burnout—a leading indicator of health system performance? Mayo Clinic Proceed. 2017;92: 1608-1611.
- American College of Obstetricians and Gynecologists. Why obgyns are burning out. October 28, 2019. Accessed July 21, 2023. https://www.acog.org/news/news-articles/2019/10/why-ob -gyns-are-burning-out#:~:text=A%202017%20report%20 by%20the,exhaustion%20or%20lack%20of%20motivation
- Peckham C. National physician burnout & depression report 2018. Medscape. January 17, 2018. https://nap. nationalacademies.org/catalog/25521/taking-action -against-clinician-burnout-a-systems-approach-to -professional
- Marsa L. Labor pains: The OB-GYN shortage. AAMC News. Nov. 15, 2018. Accessed July 21, 2023. https://www.aamc.org /news-insights/labor-pains-ob-gyn-shortage
- American College of Obstetricians and Gynecologists. Coping with the stress of medical professional liability litigation. ACOG Committee Opinion. February 2005;309:453454. Accessed July 21, 2023. https://www.acog.org/clinical /clinical-guidance/committee-opinion/articles/2013/01 /coping-with-the-stress-of-medical-professional-liability -litigation
- Reith TP. Burnout in United States healthcare professionals: a narrative review. Cureus. 2018;10:e3681. doi: 10.7759 /cureus.3681
- Han S, Shanafelt TD, Sinsky CA, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med. 2019;4:784-790.
- Sullivan D, Sullivan V, Weatherspoon D, et al. Comparison of nurse burnout, before and during the COVID-19 pandemic. Nurs Clin North Am. 2022;57:79-99. doi: 10.1016 /j.cnur.2021.11.006
- Chandawarkar A, Chaparro JD. Burnout in clinicians. Curr Prob Pediatr Adolesc Health Care. 2021;51:101-104. https ://doi.org/10.1016/j.cppeds.2021.101104
- Brady KJS, Sheldrick RC, Ni P, et al. Examining the measurement equivalence of the Maslach Burnout Inventory across age, gender, and specialty groups in US physicians. J Patient-Reported Outcomes. 2021;5.
- Association of American Medical Colleges. Physician Specialty Data Report—Active Physicians by Sex and Specialty, 2021. Accessed June 19, 2023. https://www.aamc .org/data-reports/workforce/data/active-physicians-sex -specialty-2021
- Association of American Medical Colleges. Physician Specialty Data Report—ACGME Residents and Fellows by Sex and Specialty, 2021. Accessed June 19, 2023. https://www .aamc.org/data-reports/workforce/data/acgme-residents -fellows-sex-and-specialty-2021
- Painter LM, Biggans KA, Turner CT. Risk managementobstetrics and gynecology perspective. Clin Obstet Gynecol. 2023;66:331-341. DOI:10.1097/GRF.0000000000000775
- Darney BG, Boniface E, Liberty A. Assessing the effect of abortion restrictions. Obstetr Gynecol. 2023;141:233-235.
- Heuerman AC, Bessett D, Antommaria AHM, et al. Experiences of reproductive genetic counselors with abortion regulations in Ohio. J Genet Counseling. 2022;31:641-652.
- Brandi K, Gill P. Abortion restrictions threaten all reproductive health care clinicians. Am J Public Health. 2023;113:384-385.
- Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of burnout among physicians: a systematic review. JAMA. 2018;320:1131-1150. doi: 10.1001/jama.2018.1277
- Williamson K, Lank PM, Cheema N, et al. Comparing the Maslach Burnout Inventory to other well-being instruments in emergency medicine residents. J Graduate Med Education. 2018;532-536. DOI: http://dx.doi.org/10.4300 /JGME-D-18-00155.1
- Brady KJS, Sheldrick RC, Ni P, et al. Establishing crosswalks between common measures of burnout in US physicians. J Gen Intern Med. 2022;37:777-784.
- Zhang X, Song Y, Jiang T, et al. Interventions to reduce burnout of physicians and nurses: an overview of systematic reviews and meta-analyses. Medicine (Baltimore). 2020;26:e20992. DOI: 10.1097/MD.0000000000020992
- Scheepers RA, Emke H, Ronald M, et al. The impact of mindfulness-based interventions on doctors’ well-being and performance: a systematic review. Med Education. 2020;54:138-149. https://doi.org/10.1111/medu.14020
- Olson K, Marchalik D, Farley H, et al. Organizational strategies to reduce physician burnout and improve professional fulfillment. Curr Prob Pediatr Adolesc Health Care. 2019;49:12. https://doi.org/10.1016/j.cppeds.2019.100664
- Berry LL, Awdish RLA, Swensen SJ. 5 ways to restore depleted health care workers. Harvard Business Rev. February 11, 2022.
- Sullivan AB, Hersh CM, Rensel M, et al. Leadership inequity, burnout, and lower engagement of women in medicine. J Health Serv Psychol. 2023;49:33-39.
- Hoffman S. Healing the healers: legal remedies for physician burnout. Yale J Health Policy Law Ethics. 2018;18:56-113.
- Federation of State Medical Boards. Physician wellness and burnout: report and recommendations of the workgroup on physician wellness and burnout. (Policy adopted by FSMB). April 2018. Accessed July 21, 2023. https://www.fsmb.org /siteassets/advocacy/policies/policy-on-wellness-and -burnout.pdf
- Robinson C, Kettering C, Sanfilippo JS. Medical malpractice lawsuits. Clin Obstet Gynecol. 2023;66:256-260. DOI: https ://doi.org/10.1097/GRF.0000000000000777
- Gittler GJ, Goldstein EJ. The elements of medical malpractice: an overview. Clin Infect Dis. 1996;23:1152-1155.
- Bal BS. An introduction to medical malpractice in the United States. Clin Orthop Relat Res. 2009;467:339-347.
- Tawfik DS, Profit J, Morgenthaler TI, et al. Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clinic Proceed. 2018;93: 1571-1580.
- Sundholm B. Elevating physician-patient relationships in the shadow of metric mania. Drexel L Rev. 2020;12:287-330.
- Ghaith S, Campbell RL, Pollock JR, et al. Medical malpractice lawsuits involving trainees in obstetrics and gynecology in the USA. Healthcare. 2022;10:1328.
- Muller TM, Warsi S. Litigation culture causing burnout in American physicians. Trauma Mental Health Report. April 9, 2021.
- Levine AS. Legal 101: Tort law and medical malpractice for physicians. Contemp OBGYN. 2015:60;26-28, 30.
- Regan JJ, Regan WM. Medical malpractice and respondeat superior. Southern Med J. 2002;95.5:545-549. DOI 10.1097/00007611-200295050-00018
- Levin H. Hospital vicarious liability for negligence by independent contractor physicians: new rule for new times. Univ Illinois Law Rev. 2005:1291-1332.
- Darling v Charleston Hospital, 33 Ill. 2d 326, 211 N.E.2d 253 (Ill. 1965).
- Dangel R. Hospital liability for physician malpractice. Ohio State Law J. 1986;47:1077-1098.
- Reffitt v Hajjar, 892 S.W.2d 599, 605 (Ky. Ct. App. 1994).
- McMichael BJ. Malpractice. In Laws of Medicine: Core Legal Aspects for the Healthcare Professional. New York, NY: Springer International; 2022:129-150.
- Occupational Safety and Health Administration. Worker safety in hospitals: caring for our caregivers. Accessed June 8, 2023. https://www.osha.gov/hospitals
- Occupational Safety and Health Administration. Workplace stress. Accessed June 8, 2023. https://www.osha.gov /workplace-stress/understanding-the-problem
- U.S. Surgeon General’s Advisory on Building a Thriving Health Workforce. Addressing health worker burnout. Accessed July 21, 2023. https://www.hhs.gov/sites/default/files/health -worker-wellbeing-advisory.pdf
- Department of Health & Human Services. Biden-Harris administration awards $103 Million in American Rescue Plan funds to reduce burnout and promote mental health and wellness among health care workforce. January 20, 2022. Accessed July 24, 2023. https://www.hhs.gov/about /news/2022/01/20/biden-harris-administration-awards -103-million-american-rescue-plan-funds-reduce-burnout -promote-mental-health-wellness-among-health-care -workforce.html
- Rothstein LF, Irzyk J. Disabilities and the Law. 4th ed. Toronto, Canada: Thompson Reuters; 2023.
- Department of Labor. Guide to disability rights laws. February 28, 2020. Accessed July 24, 2023. https://www .ada.gov/resources/disability-rights-guide/#:~:text=An%20 individual%20with%20a%20disability%20is%20defined%20 by%20the%20ADA,as%20having%20such%20an%20 impairment
- Nadon L, De Beer LT, Morin AJS. Should burnout be conceptualized as a mental disorder? Behavioral Sci. 2022;12:82.
- World Health Organization. Burn-out an “occupational phenomenon”: International Classification of Diseases. May 28, 2019. Accessed July 21, 2023. https://www.who.int/news /item/28-05-2019-burn-out-an-occupational-phenomenon -international-classification-of-diseases
- Hoffman S. Physician burnout: why legal and regulatory systems may need to step in. The Conversation. July 9, 2019. https://theconversation.com/physician-burnout-why-legal -and-regulatory-systems-may-need-to-step-in-119705
- Jha A, Iliff A, Chaoi A, et al. A crisis in healthcare: a call to action on physician burnout. Harvard Global Health Institute. 2019. Accessed July 21, 2023. https://www.massmed.org /Publications/Research,-Studies,-and-Reports/Physician -Burnout-Report-2018/
- Arnsten AF, Shanafelt T. Physician distress and burnout: the neurobiological perspective. Mayo Clin Proceed. 2021;96:763-769.

Recurrent pregnancy loss and inherited thrombophilias: Does low molecular weight heparin improve the live birth rate?
Quenby S, Booth K, Hiller L, et al; ALIFE2 Block Writing Committee and ALIFE2 Investigators. Heparin for women with recurrent miscarriage and inherited thrombophilia (ALIFE2): an international open-label, randomised controlled trial. Lancet. 2023;402:54-61. doi:10.1016/S0140-6736(23)00693-1.
EXPERT COMMENTARY
“Follow the evidence to where it leads, even if the conclusion is uncomfortable.”
—Steven James, author
Women with RPL have endured overzealous evaluations and management despite a lack of proven efficacy. From alloimmune testing that results in paternal leukocyte immunization1 and the long-entrusted metroplasty for a septate uterus recently put under fire2 to the “hammer and nail” approach of preimplantation genetic testing for embryo aneuploid screening,3 patients have been subjected to unsubstantiated treatments.
While the evaluation of RPL has evolved, guidelines from the American Society for Reproductive Medicine (ASRM), American College of Obstetricians and Gynecologists (ACOG), and Royal College of Obstetricians and Gynaecologists (RCOG) do not recommend testing for inherited thrombophilias outside of a history for venous thromboembolism.4-6 These 3 societies support treating acquired thrombophilias that represent the antiphospholipid antibody syndrome.
Citing insufficient evidence for reducing adverse pregnancy outcomes, ACOG recommends the use of prophylactic- or intermediate-dose LMWH or unfractionated heparin (UFH) for patients with “high-risk” thrombophilias only to prevent venous thromboembolism during pregnancy and continuing postpartum.4 (High-risk thrombophilias are defined as factor V Leiden homozygosity, prothrombin gene G20210A mutation homozygosity, heterozygosity for both factor V Leiden homozygosity and prothrombin gene G20210A mutation, or an antithrombin deficiency.4)
To determine the impact of LMWH treatment versus no treatment on live birth rate, Quenby and colleagues conducted a prospective randomized controlled trial of women with RPL and inherited thrombophilias (the ALIFE2 trial). This was a follow-up to their 2010 randomized controlled trial that demonstrated no effect of LMWH with low-dose aspirin versus low-dose aspirin alone compared with placebo in women with unexplained RPL.7
 PHOTO: BETAVERSO/SHUTTERSTOCK
PHOTO: BETAVERSO/SHUTTERSTOCK
Continue to: Details of the study...
Details of the study
The ALIFE2 study took place over 8 years and involved 5 countries, including the United States, with the 2 main centers in the Netherlands and the United Kingdom. Women eligible for the study were aged 18 to 42 years, had an inherited thrombophilia (confirmed by 2 tests), experienced recurrent miscarriages (2 or more consecutive miscarriages, nonconsecutive miscarriages, or intrauterine fetal deaths, irrespective of gestational age), and were less than 7 weeks’ estimated gestational age. Study patients were randomly allocated with a positive pregnancy test to either surveillance or LMWH treatment, which was continued throughout pregnancy.
The primary outcome was live birth rate, and secondary outcomes were a history of miscarriage, ectopic pregnancy, and obstetric complications. A total of 164 women were allocated to LMWH plus standard care, and 162 women to standard care alone. LMWH was shown to be safe without major/minor bleeding or maternal heparin-induced thrombocytopenia.
The statistical calculation was by “intention to treat,” which considers all enrolled participants, including those who dropped out of the study, as opposed to a “per protocol” analysis in which only patients who completed the study were analyzed.
Results. Primary outcome data were available for 320 participants. Of the 162 women in the LMWH-treated group, 116 (72%) had live birth rates, as did 112 (71%) of 158 in the standard care group. There was no significant difference between groups (OR, 1.04; 95% CI, 0.64–1.68).
Study strengths and limitations
The outcome of the ALIFE2 study is consistent with that of a Cochrane review that found insufficient evidence for improved live birth rate in patients with RPL and inherited thrombophilias treated with LMWH versus low-dose aspirin. Of their review of the studies at low risk of bias, only 1 was placebo controlled.8
This study by Quenby and colleagues was well designed and ensured a sufficient number of enrolled participants to comply with their power analysis. However, by beginning LMWH at 7 weeks’ gestation, patients may not have received a therapeutic benefit as opposed to initiation of treatment with a positive pregnancy test. The authors did not describe when testing for thrombophilias occurred or explain the protocol and reason for repeat testing.
Study limitations included a deviation from protocol in the standard care group, which was the initiation of LMWH after 7 weeks’ gestation. In the standard care group, 30 participants received LMWH, 18 of whom started heparin treatment before 12 weeks of gestation. The other 12 participants received LMWH after 12 weeks’ gestation, and 6 of those 12 started after 28 weeks’ gestation, since they were determined to need LMWH for thromboprophylaxis according to RCOG guidelines. While this had the potential to influence outcomes, only 18 of 162 (11%) patients were involved.
The authors did not define RPL based on a clinical versus a biochemical pregnancy loss as the latter is more common and is without agreed upon criteria for testing. Additionally, a lack of patient masking to medication could play an undetermined role in affecting the outcome. ●
This elegant, and vital, randomized controlled trial provides double take-home messages: There is no value in testing for inherited thrombophilias in RPL, as they occur in a similar prevalence in the general population, and there is no significant difference in live birth rate from LMWH treatment in women with RPL and inherited thrombophilias compared with surveillance. Consequently, the increased cost of medication and testing can be averted.
MARK P. TROLICE, MD, MBA
- Wong LF, Porter TF, Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev. 2014; CD000112. doi:10.1002/14651858.CD000112
- Trolice MP. The septate uterus and metroplasty—another dogma under siege. Fertil Steril. 2021;116:693-694. doi:10.1016/j.fertnstert.2021.06.063
- Dahdouh EM, Balayla J, Garcia-Velasco JA, et al. PGT-A for recurrent pregnancy loss: evidence is growing but the issue is not resolved. Hum Reprod. 2021;36:2805-2806. doi:10.1093 /humrep/deab194
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Obstetrics. ACOG practice bulletin no. 197: inherited thrombophilias in pregnancy. Obstet Gynecol. 2018;132:e18-e34. doi:10.1097 /AOG.0000000000002703
- Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98:1103-1111. doi:10.1016/j.fertnstert.2012.06.048
- Regan L, Rai R, Saravelos S, et al; Royal College of Obstetricians and Gynaecologists. Recurrent Miscarriage Green‐top Guideline No. 17. BJOG. June 19, 2023. doi:10.1111/1471 -0528.17515
- Kaandorp SP, Goddijn M, van der Post JA, et al. Aspirin plus heparin or aspirin alone in women with recurrent miscarriage. N Engl J Med. 2010;362:1586-1596. doi:10.1056 /NEJMoa1000641
- de Jong PG, Kaandorp S, Di Nisio M, et al. Aspirin and/or heparin for women with unexplained recurrent miscarriage with or without inherited thrombophilia. Cochrane Database Syst Rev. 2014;CD004734. doi:10.1002/14651858.CD004734 .pub4
Quenby S, Booth K, Hiller L, et al; ALIFE2 Block Writing Committee and ALIFE2 Investigators. Heparin for women with recurrent miscarriage and inherited thrombophilia (ALIFE2): an international open-label, randomised controlled trial. Lancet. 2023;402:54-61. doi:10.1016/S0140-6736(23)00693-1.
EXPERT COMMENTARY
“Follow the evidence to where it leads, even if the conclusion is uncomfortable.”
—Steven James, author
Women with RPL have endured overzealous evaluations and management despite a lack of proven efficacy. From alloimmune testing that results in paternal leukocyte immunization1 and the long-entrusted metroplasty for a septate uterus recently put under fire2 to the “hammer and nail” approach of preimplantation genetic testing for embryo aneuploid screening,3 patients have been subjected to unsubstantiated treatments.
While the evaluation of RPL has evolved, guidelines from the American Society for Reproductive Medicine (ASRM), American College of Obstetricians and Gynecologists (ACOG), and Royal College of Obstetricians and Gynaecologists (RCOG) do not recommend testing for inherited thrombophilias outside of a history for venous thromboembolism.4-6 These 3 societies support treating acquired thrombophilias that represent the antiphospholipid antibody syndrome.
Citing insufficient evidence for reducing adverse pregnancy outcomes, ACOG recommends the use of prophylactic- or intermediate-dose LMWH or unfractionated heparin (UFH) for patients with “high-risk” thrombophilias only to prevent venous thromboembolism during pregnancy and continuing postpartum.4 (High-risk thrombophilias are defined as factor V Leiden homozygosity, prothrombin gene G20210A mutation homozygosity, heterozygosity for both factor V Leiden homozygosity and prothrombin gene G20210A mutation, or an antithrombin deficiency.4)
To determine the impact of LMWH treatment versus no treatment on live birth rate, Quenby and colleagues conducted a prospective randomized controlled trial of women with RPL and inherited thrombophilias (the ALIFE2 trial). This was a follow-up to their 2010 randomized controlled trial that demonstrated no effect of LMWH with low-dose aspirin versus low-dose aspirin alone compared with placebo in women with unexplained RPL.7
PHOTO: BETAVERSO/SHUTTERSTOCK
Continue to: Details of the study...
Details of the study
The ALIFE2 study took place over 8 years and involved 5 countries, including the United States, with the 2 main centers in the Netherlands and the United Kingdom. Women eligible for the study were aged 18 to 42 years, had an inherited thrombophilia (confirmed by 2 tests), experienced recurrent miscarriages (2 or more consecutive miscarriages, nonconsecutive miscarriages, or intrauterine fetal deaths, irrespective of gestational age), and were less than 7 weeks’ estimated gestational age. Study patients were randomly allocated with a positive pregnancy test to either surveillance or LMWH treatment, which was continued throughout pregnancy.
The primary outcome was live birth rate, and secondary outcomes were a history of miscarriage, ectopic pregnancy, and obstetric complications. A total of 164 women were allocated to LMWH plus standard care, and 162 women to standard care alone. LMWH was shown to be safe without major/minor bleeding or maternal heparin-induced thrombocytopenia.
The statistical calculation was by “intention to treat,” which considers all enrolled participants, including those who dropped out of the study, as opposed to a “per protocol” analysis in which only patients who completed the study were analyzed.
Results. Primary outcome data were available for 320 participants. Of the 162 women in the LMWH-treated group, 116 (72%) had live birth rates, as did 112 (71%) of 158 in the standard care group. There was no significant difference between groups (OR, 1.04; 95% CI, 0.64–1.68).
Study strengths and limitations
The outcome of the ALIFE2 study is consistent with that of a Cochrane review that found insufficient evidence for improved live birth rate in patients with RPL and inherited thrombophilias treated with LMWH versus low-dose aspirin. Of their review of the studies at low risk of bias, only 1 was placebo controlled.8
This study by Quenby and colleagues was well designed and ensured a sufficient number of enrolled participants to comply with their power analysis. However, by beginning LMWH at 7 weeks’ gestation, patients may not have received a therapeutic benefit as opposed to initiation of treatment with a positive pregnancy test. The authors did not describe when testing for thrombophilias occurred or explain the protocol and reason for repeat testing.
Study limitations included a deviation from protocol in the standard care group, which was the initiation of LMWH after 7 weeks’ gestation. In the standard care group, 30 participants received LMWH, 18 of whom started heparin treatment before 12 weeks of gestation. The other 12 participants received LMWH after 12 weeks’ gestation, and 6 of those 12 started after 28 weeks’ gestation, since they were determined to need LMWH for thromboprophylaxis according to RCOG guidelines. While this had the potential to influence outcomes, only 18 of 162 (11%) patients were involved.
The authors did not define RPL based on a clinical versus a biochemical pregnancy loss as the latter is more common and is without agreed upon criteria for testing. Additionally, a lack of patient masking to medication could play an undetermined role in affecting the outcome. ●
This elegant, and vital, randomized controlled trial provides double take-home messages: There is no value in testing for inherited thrombophilias in RPL, as they occur in a similar prevalence in the general population, and there is no significant difference in live birth rate from LMWH treatment in women with RPL and inherited thrombophilias compared with surveillance. Consequently, the increased cost of medication and testing can be averted.
MARK P. TROLICE, MD, MBA
Quenby S, Booth K, Hiller L, et al; ALIFE2 Block Writing Committee and ALIFE2 Investigators. Heparin for women with recurrent miscarriage and inherited thrombophilia (ALIFE2): an international open-label, randomised controlled trial. Lancet. 2023;402:54-61. doi:10.1016/S0140-6736(23)00693-1.
EXPERT COMMENTARY
“Follow the evidence to where it leads, even if the conclusion is uncomfortable.”
—Steven James, author
Women with RPL have endured overzealous evaluations and management despite a lack of proven efficacy. From alloimmune testing that results in paternal leukocyte immunization1 and the long-entrusted metroplasty for a septate uterus recently put under fire2 to the “hammer and nail” approach of preimplantation genetic testing for embryo aneuploid screening,3 patients have been subjected to unsubstantiated treatments.
While the evaluation of RPL has evolved, guidelines from the American Society for Reproductive Medicine (ASRM), American College of Obstetricians and Gynecologists (ACOG), and Royal College of Obstetricians and Gynaecologists (RCOG) do not recommend testing for inherited thrombophilias outside of a history for venous thromboembolism.4-6 These 3 societies support treating acquired thrombophilias that represent the antiphospholipid antibody syndrome.
Citing insufficient evidence for reducing adverse pregnancy outcomes, ACOG recommends the use of prophylactic- or intermediate-dose LMWH or unfractionated heparin (UFH) for patients with “high-risk” thrombophilias only to prevent venous thromboembolism during pregnancy and continuing postpartum.4 (High-risk thrombophilias are defined as factor V Leiden homozygosity, prothrombin gene G20210A mutation homozygosity, heterozygosity for both factor V Leiden homozygosity and prothrombin gene G20210A mutation, or an antithrombin deficiency.4)
To determine the impact of LMWH treatment versus no treatment on live birth rate, Quenby and colleagues conducted a prospective randomized controlled trial of women with RPL and inherited thrombophilias (the ALIFE2 trial). This was a follow-up to their 2010 randomized controlled trial that demonstrated no effect of LMWH with low-dose aspirin versus low-dose aspirin alone compared with placebo in women with unexplained RPL.7
PHOTO: BETAVERSO/SHUTTERSTOCK
Continue to: Details of the study...
Details of the study
The ALIFE2 study took place over 8 years and involved 5 countries, including the United States, with the 2 main centers in the Netherlands and the United Kingdom. Women eligible for the study were aged 18 to 42 years, had an inherited thrombophilia (confirmed by 2 tests), experienced recurrent miscarriages (2 or more consecutive miscarriages, nonconsecutive miscarriages, or intrauterine fetal deaths, irrespective of gestational age), and were less than 7 weeks’ estimated gestational age. Study patients were randomly allocated with a positive pregnancy test to either surveillance or LMWH treatment, which was continued throughout pregnancy.
The primary outcome was live birth rate, and secondary outcomes were a history of miscarriage, ectopic pregnancy, and obstetric complications. A total of 164 women were allocated to LMWH plus standard care, and 162 women to standard care alone. LMWH was shown to be safe without major/minor bleeding or maternal heparin-induced thrombocytopenia.
The statistical calculation was by “intention to treat,” which considers all enrolled participants, including those who dropped out of the study, as opposed to a “per protocol” analysis in which only patients who completed the study were analyzed.
Results. Primary outcome data were available for 320 participants. Of the 162 women in the LMWH-treated group, 116 (72%) had live birth rates, as did 112 (71%) of 158 in the standard care group. There was no significant difference between groups (OR, 1.04; 95% CI, 0.64–1.68).
Study strengths and limitations
The outcome of the ALIFE2 study is consistent with that of a Cochrane review that found insufficient evidence for improved live birth rate in patients with RPL and inherited thrombophilias treated with LMWH versus low-dose aspirin. Of their review of the studies at low risk of bias, only 1 was placebo controlled.8
This study by Quenby and colleagues was well designed and ensured a sufficient number of enrolled participants to comply with their power analysis. However, by beginning LMWH at 7 weeks’ gestation, patients may not have received a therapeutic benefit as opposed to initiation of treatment with a positive pregnancy test. The authors did not describe when testing for thrombophilias occurred or explain the protocol and reason for repeat testing.
Study limitations included a deviation from protocol in the standard care group, which was the initiation of LMWH after 7 weeks’ gestation. In the standard care group, 30 participants received LMWH, 18 of whom started heparin treatment before 12 weeks of gestation. The other 12 participants received LMWH after 12 weeks’ gestation, and 6 of those 12 started after 28 weeks’ gestation, since they were determined to need LMWH for thromboprophylaxis according to RCOG guidelines. While this had the potential to influence outcomes, only 18 of 162 (11%) patients were involved.
The authors did not define RPL based on a clinical versus a biochemical pregnancy loss as the latter is more common and is without agreed upon criteria for testing. Additionally, a lack of patient masking to medication could play an undetermined role in affecting the outcome. ●
This elegant, and vital, randomized controlled trial provides double take-home messages: There is no value in testing for inherited thrombophilias in RPL, as they occur in a similar prevalence in the general population, and there is no significant difference in live birth rate from LMWH treatment in women with RPL and inherited thrombophilias compared with surveillance. Consequently, the increased cost of medication and testing can be averted.
MARK P. TROLICE, MD, MBA
- Wong LF, Porter TF, Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev. 2014; CD000112. doi:10.1002/14651858.CD000112
- Trolice MP. The septate uterus and metroplasty—another dogma under siege. Fertil Steril. 2021;116:693-694. doi:10.1016/j.fertnstert.2021.06.063
- Dahdouh EM, Balayla J, Garcia-Velasco JA, et al. PGT-A for recurrent pregnancy loss: evidence is growing but the issue is not resolved. Hum Reprod. 2021;36:2805-2806. doi:10.1093 /humrep/deab194
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Obstetrics. ACOG practice bulletin no. 197: inherited thrombophilias in pregnancy. Obstet Gynecol. 2018;132:e18-e34. doi:10.1097 /AOG.0000000000002703
- Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98:1103-1111. doi:10.1016/j.fertnstert.2012.06.048
- Regan L, Rai R, Saravelos S, et al; Royal College of Obstetricians and Gynaecologists. Recurrent Miscarriage Green‐top Guideline No. 17. BJOG. June 19, 2023. doi:10.1111/1471 -0528.17515
- Kaandorp SP, Goddijn M, van der Post JA, et al. Aspirin plus heparin or aspirin alone in women with recurrent miscarriage. N Engl J Med. 2010;362:1586-1596. doi:10.1056 /NEJMoa1000641
- de Jong PG, Kaandorp S, Di Nisio M, et al. Aspirin and/or heparin for women with unexplained recurrent miscarriage with or without inherited thrombophilia. Cochrane Database Syst Rev. 2014;CD004734. doi:10.1002/14651858.CD004734 .pub4
- Wong LF, Porter TF, Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev. 2014; CD000112. doi:10.1002/14651858.CD000112
- Trolice MP. The septate uterus and metroplasty—another dogma under siege. Fertil Steril. 2021;116:693-694. doi:10.1016/j.fertnstert.2021.06.063
- Dahdouh EM, Balayla J, Garcia-Velasco JA, et al. PGT-A for recurrent pregnancy loss: evidence is growing but the issue is not resolved. Hum Reprod. 2021;36:2805-2806. doi:10.1093 /humrep/deab194
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Obstetrics. ACOG practice bulletin no. 197: inherited thrombophilias in pregnancy. Obstet Gynecol. 2018;132:e18-e34. doi:10.1097 /AOG.0000000000002703
- Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98:1103-1111. doi:10.1016/j.fertnstert.2012.06.048
- Regan L, Rai R, Saravelos S, et al; Royal College of Obstetricians and Gynaecologists. Recurrent Miscarriage Green‐top Guideline No. 17. BJOG. June 19, 2023. doi:10.1111/1471 -0528.17515
- Kaandorp SP, Goddijn M, van der Post JA, et al. Aspirin plus heparin or aspirin alone in women with recurrent miscarriage. N Engl J Med. 2010;362:1586-1596. doi:10.1056 /NEJMoa1000641
- de Jong PG, Kaandorp S, Di Nisio M, et al. Aspirin and/or heparin for women with unexplained recurrent miscarriage with or without inherited thrombophilia. Cochrane Database Syst Rev. 2014;CD004734. doi:10.1002/14651858.CD004734 .pub4

Results from halted islatravir antiretroviral trial presented
Brisbane, Australia – , according to investigators.
The nucleoside reverse transcriptase translocation inhibitor hit a roadblock in December 2021 when the U.S. Food and Drug Administration put a hold on investigational new drug applications for both the oral and implant formulations of islatravir after some patients in clinical trials showed decreases in total lymphocyte and CD4+ cell counts.
A phase 3, double-blind, randomized, controlled trial was underway at the time of once-daily islatravir (0.75 mg) in combination with 100 mg doravirine, compared with bictegravir, emtricitabine, tenofovir alafenamide (B/F/TAF) as initial therapy for HIV infection in treatment-naïve individuals. Recruitment was stopped, 83 participants short of the planned 680, but the trial could continue the full 48 weeks.
Jürgen Rockstroh, MD, professor of medicine and head of the HIV Outpatient Clinic at the University of Bonn, Germany, presented the latest results from that trial of 597 patients at the International AIDS Society conference on HIV Science.
At week 48 after starting therapy, 88.9% of participants in the islatravir and doravirine arm and 88.3% of patients in the B/F/TAF arm achieved the primary outcome of HIV-1 RNA levels below 50 copies/mL.
One patient treated with islatravir and doravirine and four patients taking B/F/TAF experienced virologic failure.
Dr. Rockstroh told the conference the patient who developed viremia with the new islatravir combination had very high viral load at baseline but showed a rapid response to treatment, which reduced his viral load down to around 1,200 copies/mL by week 4.
However, by week 24, his islatravir concentration had reduced below detectable levels, suggesting a problem with adherence. His viral load increased again, and three treatment-resistant mutations were detected.
While both arms of the study showed a significant increase in CD4+ T cell counts, Dr. Rockstroh pointed out that some individuals in the islatravir and doravirine arm had a lower absolute increase in lymphocyte counts at week 48.
Overall, the mean change in CD4+ T cell counts was 182 cells/mL in the islatravir and doravirine group, compared with 234 cells/mL in the B/F/TAF group.
More patients in the islatravir combination arm discontinued treatment due to a decrease in CD4+ T cell or total lymphocyte counts – 5.4%, compared with 2% in the B/F/TAF arm, however.
“These changes in lymphocyte counts did not lead to any difference in the amount of infection-related adverse events, which happened in both arms in relatively comparable percentages,” Dr. Rockstroh said at the conference.
New lower dose
Because of persistent concerns about the impact on CD4+ T cells and total lymphocytes, Dr. Rockstroh said another phase 3 trial is now underway using a lower 0.25 mg dose of islatravir, again combined with 100 mg doravirine, in people who are treatment-naïve and virologically suppressed.
The study also examined the impact of both treatments on weight gain and found the mean change in weight was similar between both arms – 3.45 kg gain in those on islatravir with doravirine and 3.32 kg gain in those on B/F/TAF, which was not significantly different.
There are several important reasons it is a good idea to have more treatment options available for people with HIV, Dr. Rockstroh said in an interview.
With integrase inhibitors potentially interfering with metabolic health, weight gain, hypertension, insulin resistance, and possible diabetes, “I think it’s wise that we at least have alternative strategies,” he said.
James McMahon, MD, PhD, an infectious diseases physician and head of the Infectious Diseases Clinical Research Unit at the Alfred Hospital and Monash University in Melbourne, said there is always a need for new HIV treatments, particularly ones that are more powerful.
“Whenever you get a drug that’s potent at low dose, it means you can have smaller pills, [and] you can then consider giving more of it in long-acting formulations,” Dr. McMahon said.
He pointed out that the study did not show any signal of increased infections with the lower CD4+ T cell counts in the islatravir and doravirine arm, “but that difference is enough to raise that concern that it’s not ideal, and it should be moved forward with a lower dose, which is what they’ve done.”
A version of this article first appeared on Medscape.com.
Brisbane, Australia – , according to investigators.
The nucleoside reverse transcriptase translocation inhibitor hit a roadblock in December 2021 when the U.S. Food and Drug Administration put a hold on investigational new drug applications for both the oral and implant formulations of islatravir after some patients in clinical trials showed decreases in total lymphocyte and CD4+ cell counts.
A phase 3, double-blind, randomized, controlled trial was underway at the time of once-daily islatravir (0.75 mg) in combination with 100 mg doravirine, compared with bictegravir, emtricitabine, tenofovir alafenamide (B/F/TAF) as initial therapy for HIV infection in treatment-naïve individuals. Recruitment was stopped, 83 participants short of the planned 680, but the trial could continue the full 48 weeks.
Jürgen Rockstroh, MD, professor of medicine and head of the HIV Outpatient Clinic at the University of Bonn, Germany, presented the latest results from that trial of 597 patients at the International AIDS Society conference on HIV Science.
At week 48 after starting therapy, 88.9% of participants in the islatravir and doravirine arm and 88.3% of patients in the B/F/TAF arm achieved the primary outcome of HIV-1 RNA levels below 50 copies/mL.
One patient treated with islatravir and doravirine and four patients taking B/F/TAF experienced virologic failure.
Dr. Rockstroh told the conference the patient who developed viremia with the new islatravir combination had very high viral load at baseline but showed a rapid response to treatment, which reduced his viral load down to around 1,200 copies/mL by week 4.
However, by week 24, his islatravir concentration had reduced below detectable levels, suggesting a problem with adherence. His viral load increased again, and three treatment-resistant mutations were detected.
While both arms of the study showed a significant increase in CD4+ T cell counts, Dr. Rockstroh pointed out that some individuals in the islatravir and doravirine arm had a lower absolute increase in lymphocyte counts at week 48.
Overall, the mean change in CD4+ T cell counts was 182 cells/mL in the islatravir and doravirine group, compared with 234 cells/mL in the B/F/TAF group.
More patients in the islatravir combination arm discontinued treatment due to a decrease in CD4+ T cell or total lymphocyte counts – 5.4%, compared with 2% in the B/F/TAF arm, however.
“These changes in lymphocyte counts did not lead to any difference in the amount of infection-related adverse events, which happened in both arms in relatively comparable percentages,” Dr. Rockstroh said at the conference.
New lower dose
Because of persistent concerns about the impact on CD4+ T cells and total lymphocytes, Dr. Rockstroh said another phase 3 trial is now underway using a lower 0.25 mg dose of islatravir, again combined with 100 mg doravirine, in people who are treatment-naïve and virologically suppressed.
The study also examined the impact of both treatments on weight gain and found the mean change in weight was similar between both arms – 3.45 kg gain in those on islatravir with doravirine and 3.32 kg gain in those on B/F/TAF, which was not significantly different.
There are several important reasons it is a good idea to have more treatment options available for people with HIV, Dr. Rockstroh said in an interview.
With integrase inhibitors potentially interfering with metabolic health, weight gain, hypertension, insulin resistance, and possible diabetes, “I think it’s wise that we at least have alternative strategies,” he said.
James McMahon, MD, PhD, an infectious diseases physician and head of the Infectious Diseases Clinical Research Unit at the Alfred Hospital and Monash University in Melbourne, said there is always a need for new HIV treatments, particularly ones that are more powerful.
“Whenever you get a drug that’s potent at low dose, it means you can have smaller pills, [and] you can then consider giving more of it in long-acting formulations,” Dr. McMahon said.
He pointed out that the study did not show any signal of increased infections with the lower CD4+ T cell counts in the islatravir and doravirine arm, “but that difference is enough to raise that concern that it’s not ideal, and it should be moved forward with a lower dose, which is what they’ve done.”
A version of this article first appeared on Medscape.com.
Brisbane, Australia – , according to investigators.
The nucleoside reverse transcriptase translocation inhibitor hit a roadblock in December 2021 when the U.S. Food and Drug Administration put a hold on investigational new drug applications for both the oral and implant formulations of islatravir after some patients in clinical trials showed decreases in total lymphocyte and CD4+ cell counts.
A phase 3, double-blind, randomized, controlled trial was underway at the time of once-daily islatravir (0.75 mg) in combination with 100 mg doravirine, compared with bictegravir, emtricitabine, tenofovir alafenamide (B/F/TAF) as initial therapy for HIV infection in treatment-naïve individuals. Recruitment was stopped, 83 participants short of the planned 680, but the trial could continue the full 48 weeks.
Jürgen Rockstroh, MD, professor of medicine and head of the HIV Outpatient Clinic at the University of Bonn, Germany, presented the latest results from that trial of 597 patients at the International AIDS Society conference on HIV Science.
At week 48 after starting therapy, 88.9% of participants in the islatravir and doravirine arm and 88.3% of patients in the B/F/TAF arm achieved the primary outcome of HIV-1 RNA levels below 50 copies/mL.
One patient treated with islatravir and doravirine and four patients taking B/F/TAF experienced virologic failure.
Dr. Rockstroh told the conference the patient who developed viremia with the new islatravir combination had very high viral load at baseline but showed a rapid response to treatment, which reduced his viral load down to around 1,200 copies/mL by week 4.
However, by week 24, his islatravir concentration had reduced below detectable levels, suggesting a problem with adherence. His viral load increased again, and three treatment-resistant mutations were detected.
While both arms of the study showed a significant increase in CD4+ T cell counts, Dr. Rockstroh pointed out that some individuals in the islatravir and doravirine arm had a lower absolute increase in lymphocyte counts at week 48.
Overall, the mean change in CD4+ T cell counts was 182 cells/mL in the islatravir and doravirine group, compared with 234 cells/mL in the B/F/TAF group.
More patients in the islatravir combination arm discontinued treatment due to a decrease in CD4+ T cell or total lymphocyte counts – 5.4%, compared with 2% in the B/F/TAF arm, however.
“These changes in lymphocyte counts did not lead to any difference in the amount of infection-related adverse events, which happened in both arms in relatively comparable percentages,” Dr. Rockstroh said at the conference.
New lower dose
Because of persistent concerns about the impact on CD4+ T cells and total lymphocytes, Dr. Rockstroh said another phase 3 trial is now underway using a lower 0.25 mg dose of islatravir, again combined with 100 mg doravirine, in people who are treatment-naïve and virologically suppressed.
The study also examined the impact of both treatments on weight gain and found the mean change in weight was similar between both arms – 3.45 kg gain in those on islatravir with doravirine and 3.32 kg gain in those on B/F/TAF, which was not significantly different.
There are several important reasons it is a good idea to have more treatment options available for people with HIV, Dr. Rockstroh said in an interview.
With integrase inhibitors potentially interfering with metabolic health, weight gain, hypertension, insulin resistance, and possible diabetes, “I think it’s wise that we at least have alternative strategies,” he said.
James McMahon, MD, PhD, an infectious diseases physician and head of the Infectious Diseases Clinical Research Unit at the Alfred Hospital and Monash University in Melbourne, said there is always a need for new HIV treatments, particularly ones that are more powerful.
“Whenever you get a drug that’s potent at low dose, it means you can have smaller pills, [and] you can then consider giving more of it in long-acting formulations,” Dr. McMahon said.
He pointed out that the study did not show any signal of increased infections with the lower CD4+ T cell counts in the islatravir and doravirine arm, “but that difference is enough to raise that concern that it’s not ideal, and it should be moved forward with a lower dose, which is what they’ve done.”
A version of this article first appeared on Medscape.com.
PRISm and nonspecific pattern: New insights in lung testing interpretation
The recent statement on interpretive strategies for lung testing uses the acronym PRISm for preserved ratio impaired spirometry. PRISm identifies patients with a normal forced expiratory volume in 1 second/forced vital capacity ratio but abnormal FEV1 and/or FVC (usually both). Most medical students are taught to call this a “restrictive pattern,” and every first-year pulmonary fellow orders full lung volumes when they see it. If total lung capacity (TLC) is normal, PRISm becomes the nonspecific pattern. If TLC is low, then the patient has “true” restriction, and if it’s elevated, then hyperinflation may be present.
The traditional classification scheme for basic spirometry interpretation (normal, restricted, obstructed, or mixed) is simple and conceptually clear. It turns out that many with this pattern won’t have an abnormal TLC, so the name is, in some ways, a misnomer and can be misleading. Enter PRISm, a more descriptive and inclusive term. The phrase also lends itself to a phonetic acronym that is fun to say, easy to remember, and likely to catch on with learners.
Information on occurrence and clinical behavior comes from large cohorts with basic spirometry, but without full lung volumes because PRISm no longer applies once TLC is determined. As may be expected, prevalence varies by the population studied. Estimates for general populations have been in the 7%-12% range; however, one study examining a database of patients with clinical spirometry referrals found a prevalence of 22.3%. Rates may be far higher in low- and middle-income countries. Identified risk factors include sex, tobacco use, and body mass index; the presence of PRISm is associated with respiratory symptoms and mortality. Thus, PRISm is common and it matters.
Along with PRISm, the nonspecific pattern is a new addition, if not a new concept, to the 2022 interpretative strategies statement. As with PRISm, the title is necessarily broad, though far less imaginative. Defined by reductions in FEV1 and FVC and a normal TLC, the nonspecific pattern has classically been considered a marker of early airway disease. The idea is that early, heterogeneous closure of distal segments of the bronchial tree can reduce total volume during a forced expiration before affecting the FEV1/FVC. The fact that the TLC is not a forced maneuver means there is proportionately less effect from more collapsible/susceptible smaller units. More recent data suggest that there are additional causes.
Because the nonspecific pattern requires full lung volumes, we have less population-level data than for PRISm. Estimated prevalence is approximately 9.5% in patients with complete test results. The two most common causes are obesity and airway obstruction, and the pattern is relatively stable over time. Notably, an increase in specific airway resistance or TLC minus alveolar volume difference predicts progression to frank obstruction on spirometry.
The physiologic changes that obesity inflicts on the lung have been well described. Patients with obesity breathe at lower lung volumes and are therefore susceptible to small airway closure at rest and during forced expiration. There is no doubt that the increased recognition of PRISm and the nonspecific pattern is in part related to the worldwide rise in obesity rates.
Key takeaways
In summary, PRISm and the nonspecific pattern are now part of the classification scheme we use for spirometry and full lung volumes, respectively. They should be included in interpretations given their diagnostic and predictive value. Airway disease and obesity are common causes and often coexist with either pattern. Many will not have a true, restrictive lung deficit, and a reductionist approach to interpretation is likely to lead to erroneous diagnoses. There were many important updates included in the 2022 iteration on lung testing interpretation that should not fly under the radar.
Dr. Holley is professor of medicine at Uniformed Services University in Bethesda, Md., and a pulmonary/sleep and critical care medicine physician at MedStar Washington Hospital Center in Washington. He disclosed ties with CHEST College, Metapharm, and WebMD.
A version of this article appeared on Medscape.com.
The recent statement on interpretive strategies for lung testing uses the acronym PRISm for preserved ratio impaired spirometry. PRISm identifies patients with a normal forced expiratory volume in 1 second/forced vital capacity ratio but abnormal FEV1 and/or FVC (usually both). Most medical students are taught to call this a “restrictive pattern,” and every first-year pulmonary fellow orders full lung volumes when they see it. If total lung capacity (TLC) is normal, PRISm becomes the nonspecific pattern. If TLC is low, then the patient has “true” restriction, and if it’s elevated, then hyperinflation may be present.
The traditional classification scheme for basic spirometry interpretation (normal, restricted, obstructed, or mixed) is simple and conceptually clear. It turns out that many with this pattern won’t have an abnormal TLC, so the name is, in some ways, a misnomer and can be misleading. Enter PRISm, a more descriptive and inclusive term. The phrase also lends itself to a phonetic acronym that is fun to say, easy to remember, and likely to catch on with learners.
Information on occurrence and clinical behavior comes from large cohorts with basic spirometry, but without full lung volumes because PRISm no longer applies once TLC is determined. As may be expected, prevalence varies by the population studied. Estimates for general populations have been in the 7%-12% range; however, one study examining a database of patients with clinical spirometry referrals found a prevalence of 22.3%. Rates may be far higher in low- and middle-income countries. Identified risk factors include sex, tobacco use, and body mass index; the presence of PRISm is associated with respiratory symptoms and mortality. Thus, PRISm is common and it matters.
Along with PRISm, the nonspecific pattern is a new addition, if not a new concept, to the 2022 interpretative strategies statement. As with PRISm, the title is necessarily broad, though far less imaginative. Defined by reductions in FEV1 and FVC and a normal TLC, the nonspecific pattern has classically been considered a marker of early airway disease. The idea is that early, heterogeneous closure of distal segments of the bronchial tree can reduce total volume during a forced expiration before affecting the FEV1/FVC. The fact that the TLC is not a forced maneuver means there is proportionately less effect from more collapsible/susceptible smaller units. More recent data suggest that there are additional causes.
Because the nonspecific pattern requires full lung volumes, we have less population-level data than for PRISm. Estimated prevalence is approximately 9.5% in patients with complete test results. The two most common causes are obesity and airway obstruction, and the pattern is relatively stable over time. Notably, an increase in specific airway resistance or TLC minus alveolar volume difference predicts progression to frank obstruction on spirometry.
The physiologic changes that obesity inflicts on the lung have been well described. Patients with obesity breathe at lower lung volumes and are therefore susceptible to small airway closure at rest and during forced expiration. There is no doubt that the increased recognition of PRISm and the nonspecific pattern is in part related to the worldwide rise in obesity rates.
Key takeaways
In summary, PRISm and the nonspecific pattern are now part of the classification scheme we use for spirometry and full lung volumes, respectively. They should be included in interpretations given their diagnostic and predictive value. Airway disease and obesity are common causes and often coexist with either pattern. Many will not have a true, restrictive lung deficit, and a reductionist approach to interpretation is likely to lead to erroneous diagnoses. There were many important updates included in the 2022 iteration on lung testing interpretation that should not fly under the radar.
Dr. Holley is professor of medicine at Uniformed Services University in Bethesda, Md., and a pulmonary/sleep and critical care medicine physician at MedStar Washington Hospital Center in Washington. He disclosed ties with CHEST College, Metapharm, and WebMD.
A version of this article appeared on Medscape.com.
The recent statement on interpretive strategies for lung testing uses the acronym PRISm for preserved ratio impaired spirometry. PRISm identifies patients with a normal forced expiratory volume in 1 second/forced vital capacity ratio but abnormal FEV1 and/or FVC (usually both). Most medical students are taught to call this a “restrictive pattern,” and every first-year pulmonary fellow orders full lung volumes when they see it. If total lung capacity (TLC) is normal, PRISm becomes the nonspecific pattern. If TLC is low, then the patient has “true” restriction, and if it’s elevated, then hyperinflation may be present.
The traditional classification scheme for basic spirometry interpretation (normal, restricted, obstructed, or mixed) is simple and conceptually clear. It turns out that many with this pattern won’t have an abnormal TLC, so the name is, in some ways, a misnomer and can be misleading. Enter PRISm, a more descriptive and inclusive term. The phrase also lends itself to a phonetic acronym that is fun to say, easy to remember, and likely to catch on with learners.
Information on occurrence and clinical behavior comes from large cohorts with basic spirometry, but without full lung volumes because PRISm no longer applies once TLC is determined. As may be expected, prevalence varies by the population studied. Estimates for general populations have been in the 7%-12% range; however, one study examining a database of patients with clinical spirometry referrals found a prevalence of 22.3%. Rates may be far higher in low- and middle-income countries. Identified risk factors include sex, tobacco use, and body mass index; the presence of PRISm is associated with respiratory symptoms and mortality. Thus, PRISm is common and it matters.
Along with PRISm, the nonspecific pattern is a new addition, if not a new concept, to the 2022 interpretative strategies statement. As with PRISm, the title is necessarily broad, though far less imaginative. Defined by reductions in FEV1 and FVC and a normal TLC, the nonspecific pattern has classically been considered a marker of early airway disease. The idea is that early, heterogeneous closure of distal segments of the bronchial tree can reduce total volume during a forced expiration before affecting the FEV1/FVC. The fact that the TLC is not a forced maneuver means there is proportionately less effect from more collapsible/susceptible smaller units. More recent data suggest that there are additional causes.
Because the nonspecific pattern requires full lung volumes, we have less population-level data than for PRISm. Estimated prevalence is approximately 9.5% in patients with complete test results. The two most common causes are obesity and airway obstruction, and the pattern is relatively stable over time. Notably, an increase in specific airway resistance or TLC minus alveolar volume difference predicts progression to frank obstruction on spirometry.
The physiologic changes that obesity inflicts on the lung have been well described. Patients with obesity breathe at lower lung volumes and are therefore susceptible to small airway closure at rest and during forced expiration. There is no doubt that the increased recognition of PRISm and the nonspecific pattern is in part related to the worldwide rise in obesity rates.
Key takeaways
In summary, PRISm and the nonspecific pattern are now part of the classification scheme we use for spirometry and full lung volumes, respectively. They should be included in interpretations given their diagnostic and predictive value. Airway disease and obesity are common causes and often coexist with either pattern. Many will not have a true, restrictive lung deficit, and a reductionist approach to interpretation is likely to lead to erroneous diagnoses. There were many important updates included in the 2022 iteration on lung testing interpretation that should not fly under the radar.
Dr. Holley is professor of medicine at Uniformed Services University in Bethesda, Md., and a pulmonary/sleep and critical care medicine physician at MedStar Washington Hospital Center in Washington. He disclosed ties with CHEST College, Metapharm, and WebMD.
A version of this article appeared on Medscape.com.
New AHA/ACC performance, quality metrics for coronary revascularization

“Performance measures are helpful to accelerate translation of scientific evidence into clinical practice and are intended to provide practitioners and institutions with tools to measure the quality of care provided and identify opportunities for improvement,” writing group chair Gregory J. Dehmer, MD, Carilion Clinic Cardiology, Roanoke, Va., said in an interview.
Performance measures are “evidence-based, have exceptions and exclusions supported by evidence, and should be actionable,” Dr. Dehmer added. They typically target meaningful gaps in the quality of care and are based on Class 1 clinical practice guidelines.
The 44-page document was published online in the Journal of the American College of Cardiology.
Topics addressed in the 15 performance measures include the following:
- The importance of using coronary physiological measurements rather than visual assessment of an intermediate severity lesion.
- Dual antiplatelet therapy (DAPT) with percutaneous coronary intervention (PCI), as a “cornerstone” of therapy for prevention of thrombotic complications and reduction of ischemic events.
- Antiplatelets and anticoagulation after PCI, which provide “an important outcome benefit” and represent “an existing gap in care,” especially in patients with atrial fibrillation (AF).
- P2Y12 inhibitors with fibrinolytic therapy to reduce recurrent ischemia and avoid increased risk of bleeding relative to aspirin.
Other performance measures address aspirin in patients undergoing coronary artery bypass grafting (CABG), lipid management, glycemic control during and after CABG, use of internal mammary artery for CABG, arterial access for PCI, noninfarct artery revascularization in ST-segment elevation myocardial infarction (STEMI), noninfarct artery PCI in STEMI with shock, management of ventricular arrhythmias, and referral to cardiac rehabilitation from inpatient and outpatient settings.
“The measures are structured in a typical format with the goal to seek a higher performance score, ideally nearing 100%,” Dr. Dehmer said.
The document also includes five quality measures. These measures are “important but are not based on Class 1 clinical practice guidelines or are lacking in other important characteristics (e.g., questions of feasibility, validity),” the writing group notes.
“If additional evidence supports the importance of the proposed quality measures, they may be changed to performance measures in the future,” they point out.
The quality measures emphasize shared decision-making and informed consent; periprocedural hydration in cardiovascular angiography; smoking cessation after revascularization; risk assessment before CABG; and reduction of AF after CABG.
The document also includes two structural measures. One focuses on preprocedural assessment and fostering collaborative efforts among cardiovascular specialists, and the other encourages registry participation to measure performance.
Areas for future research
The writing group notes that the field of coronary artery revascularization “continues to evolve rapidly.”
They say areas for further research include determining the optimal role and timing for revascularization in cardiogenic shock, research on conduits and techniques for CABG, the use of mechanical support for high-risk PCI, defining the role of drug-coated balloons, and the optimal duration of antiplatelet therapy after PCI and in the setting of AF.
New devices for PCI continue to enter the marketplace, and research is needed to better define their safety and effectiveness in real-world populations, they add.
Chronic total occlusions are another area in need of additional research.
“Whereas many chronic total occlusions were once thought too difficult to treat, newer techniques for the recanalization of these vessels are being developed, but more research is needed to determine the role of chronic total occlusion therapies on long-term outcomes such as death, heart failure events, and optimal case selection,” the writing group points out.
They also note that several studies have shown that an initial strategy of guideline-directed medical therapy alone, compared with guideline-directed medical therapy plus revascularization, in selected patients with chronic coronary disease has similar effects on cardiovascular outcomes such as death, MI, heart failure, and hospitalization for unstable angina.
More investigation is needed to compare the long-term effects of these two therapies and identify subgroups of stable patients that may have a mortality benefit from early revascularization as well as the effects of these two therapeutic strategies on symptoms and quality of life.
More research is also needed to identify gender-based differences in responses to available therapies.
The document was developed in collaboration with the American Association for Thoracic Surgery and the Society for Cardiovascular Angiography and Interventions.
It has been endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation, American Society for Preventive Cardiology, American Society of Health-System Pharmacists, Association of Black Cardiologists, Heart Failure Society of America, Heart Rhythm Society, International Society for Heart and Lung Transplantation, Outpatient Endovascular and Interventional Society, and the Preventive Cardiovascular Nurses Association.
This research had no commercial funding. Dr. Dehmer has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
“Performance measures are helpful to accelerate translation of scientific evidence into clinical practice and are intended to provide practitioners and institutions with tools to measure the quality of care provided and identify opportunities for improvement,” writing group chair Gregory J. Dehmer, MD, Carilion Clinic Cardiology, Roanoke, Va., said in an interview.
Performance measures are “evidence-based, have exceptions and exclusions supported by evidence, and should be actionable,” Dr. Dehmer added. They typically target meaningful gaps in the quality of care and are based on Class 1 clinical practice guidelines.
The 44-page document was published online in the Journal of the American College of Cardiology.
Topics addressed in the 15 performance measures include the following:
- The importance of using coronary physiological measurements rather than visual assessment of an intermediate severity lesion.
- Dual antiplatelet therapy (DAPT) with percutaneous coronary intervention (PCI), as a “cornerstone” of therapy for prevention of thrombotic complications and reduction of ischemic events.
- Antiplatelets and anticoagulation after PCI, which provide “an important outcome benefit” and represent “an existing gap in care,” especially in patients with atrial fibrillation (AF).
- P2Y12 inhibitors with fibrinolytic therapy to reduce recurrent ischemia and avoid increased risk of bleeding relative to aspirin.
Other performance measures address aspirin in patients undergoing coronary artery bypass grafting (CABG), lipid management, glycemic control during and after CABG, use of internal mammary artery for CABG, arterial access for PCI, noninfarct artery revascularization in ST-segment elevation myocardial infarction (STEMI), noninfarct artery PCI in STEMI with shock, management of ventricular arrhythmias, and referral to cardiac rehabilitation from inpatient and outpatient settings.
“The measures are structured in a typical format with the goal to seek a higher performance score, ideally nearing 100%,” Dr. Dehmer said.
The document also includes five quality measures. These measures are “important but are not based on Class 1 clinical practice guidelines or are lacking in other important characteristics (e.g., questions of feasibility, validity),” the writing group notes.
“If additional evidence supports the importance of the proposed quality measures, they may be changed to performance measures in the future,” they point out.
The quality measures emphasize shared decision-making and informed consent; periprocedural hydration in cardiovascular angiography; smoking cessation after revascularization; risk assessment before CABG; and reduction of AF after CABG.
The document also includes two structural measures. One focuses on preprocedural assessment and fostering collaborative efforts among cardiovascular specialists, and the other encourages registry participation to measure performance.
Areas for future research
The writing group notes that the field of coronary artery revascularization “continues to evolve rapidly.”
They say areas for further research include determining the optimal role and timing for revascularization in cardiogenic shock, research on conduits and techniques for CABG, the use of mechanical support for high-risk PCI, defining the role of drug-coated balloons, and the optimal duration of antiplatelet therapy after PCI and in the setting of AF.
New devices for PCI continue to enter the marketplace, and research is needed to better define their safety and effectiveness in real-world populations, they add.
Chronic total occlusions are another area in need of additional research.
“Whereas many chronic total occlusions were once thought too difficult to treat, newer techniques for the recanalization of these vessels are being developed, but more research is needed to determine the role of chronic total occlusion therapies on long-term outcomes such as death, heart failure events, and optimal case selection,” the writing group points out.
They also note that several studies have shown that an initial strategy of guideline-directed medical therapy alone, compared with guideline-directed medical therapy plus revascularization, in selected patients with chronic coronary disease has similar effects on cardiovascular outcomes such as death, MI, heart failure, and hospitalization for unstable angina.
More investigation is needed to compare the long-term effects of these two therapies and identify subgroups of stable patients that may have a mortality benefit from early revascularization as well as the effects of these two therapeutic strategies on symptoms and quality of life.
More research is also needed to identify gender-based differences in responses to available therapies.
The document was developed in collaboration with the American Association for Thoracic Surgery and the Society for Cardiovascular Angiography and Interventions.
It has been endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation, American Society for Preventive Cardiology, American Society of Health-System Pharmacists, Association of Black Cardiologists, Heart Failure Society of America, Heart Rhythm Society, International Society for Heart and Lung Transplantation, Outpatient Endovascular and Interventional Society, and the Preventive Cardiovascular Nurses Association.
This research had no commercial funding. Dr. Dehmer has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
“Performance measures are helpful to accelerate translation of scientific evidence into clinical practice and are intended to provide practitioners and institutions with tools to measure the quality of care provided and identify opportunities for improvement,” writing group chair Gregory J. Dehmer, MD, Carilion Clinic Cardiology, Roanoke, Va., said in an interview.
Performance measures are “evidence-based, have exceptions and exclusions supported by evidence, and should be actionable,” Dr. Dehmer added. They typically target meaningful gaps in the quality of care and are based on Class 1 clinical practice guidelines.
The 44-page document was published online in the Journal of the American College of Cardiology.
Topics addressed in the 15 performance measures include the following:
- The importance of using coronary physiological measurements rather than visual assessment of an intermediate severity lesion.
- Dual antiplatelet therapy (DAPT) with percutaneous coronary intervention (PCI), as a “cornerstone” of therapy for prevention of thrombotic complications and reduction of ischemic events.
- Antiplatelets and anticoagulation after PCI, which provide “an important outcome benefit” and represent “an existing gap in care,” especially in patients with atrial fibrillation (AF).
- P2Y12 inhibitors with fibrinolytic therapy to reduce recurrent ischemia and avoid increased risk of bleeding relative to aspirin.
Other performance measures address aspirin in patients undergoing coronary artery bypass grafting (CABG), lipid management, glycemic control during and after CABG, use of internal mammary artery for CABG, arterial access for PCI, noninfarct artery revascularization in ST-segment elevation myocardial infarction (STEMI), noninfarct artery PCI in STEMI with shock, management of ventricular arrhythmias, and referral to cardiac rehabilitation from inpatient and outpatient settings.
“The measures are structured in a typical format with the goal to seek a higher performance score, ideally nearing 100%,” Dr. Dehmer said.
The document also includes five quality measures. These measures are “important but are not based on Class 1 clinical practice guidelines or are lacking in other important characteristics (e.g., questions of feasibility, validity),” the writing group notes.
“If additional evidence supports the importance of the proposed quality measures, they may be changed to performance measures in the future,” they point out.
The quality measures emphasize shared decision-making and informed consent; periprocedural hydration in cardiovascular angiography; smoking cessation after revascularization; risk assessment before CABG; and reduction of AF after CABG.
The document also includes two structural measures. One focuses on preprocedural assessment and fostering collaborative efforts among cardiovascular specialists, and the other encourages registry participation to measure performance.
Areas for future research
The writing group notes that the field of coronary artery revascularization “continues to evolve rapidly.”
They say areas for further research include determining the optimal role and timing for revascularization in cardiogenic shock, research on conduits and techniques for CABG, the use of mechanical support for high-risk PCI, defining the role of drug-coated balloons, and the optimal duration of antiplatelet therapy after PCI and in the setting of AF.
New devices for PCI continue to enter the marketplace, and research is needed to better define their safety and effectiveness in real-world populations, they add.
Chronic total occlusions are another area in need of additional research.
“Whereas many chronic total occlusions were once thought too difficult to treat, newer techniques for the recanalization of these vessels are being developed, but more research is needed to determine the role of chronic total occlusion therapies on long-term outcomes such as death, heart failure events, and optimal case selection,” the writing group points out.
They also note that several studies have shown that an initial strategy of guideline-directed medical therapy alone, compared with guideline-directed medical therapy plus revascularization, in selected patients with chronic coronary disease has similar effects on cardiovascular outcomes such as death, MI, heart failure, and hospitalization for unstable angina.
More investigation is needed to compare the long-term effects of these two therapies and identify subgroups of stable patients that may have a mortality benefit from early revascularization as well as the effects of these two therapeutic strategies on symptoms and quality of life.
More research is also needed to identify gender-based differences in responses to available therapies.
The document was developed in collaboration with the American Association for Thoracic Surgery and the Society for Cardiovascular Angiography and Interventions.
It has been endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation, American Society for Preventive Cardiology, American Society of Health-System Pharmacists, Association of Black Cardiologists, Heart Failure Society of America, Heart Rhythm Society, International Society for Heart and Lung Transplantation, Outpatient Endovascular and Interventional Society, and the Preventive Cardiovascular Nurses Association.
This research had no commercial funding. Dr. Dehmer has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Obesity cardiomyopathy tied to sudden cardiac death
a new case-control study suggests.
Researchers who analyzed hearts taken at autopsy from people who had died from sudden cardiac death found that a number of the hearts obtained from obese decedents were heavier than those from normal-weight decedents and that the hazard ratio of unexplained cardiomegaly in this cohort was 5.3, compared with normal-weight individuals.
“Even when we ruled out any conditions that could potentially cause enlargement of the heart, including hypertension, heart valve problems, diabetes, and other cardiovascular risk factors, the association with obesity cardiomyopathy, or OCM, and sudden cardiac death remained,” lead author Joseph Westaby, PhD, from the Cardiac Risk in the Young (CRY) Cardiovascular Pathology Laboratories at St George’s University of London, said in an interview.
The study was published online in JACC: Advances.
Intrigued by this finding, Dr. Westaby and associates sought to characterize the clinical and pathological features of OCM associated with sudden cardiac death by comparing this population to two control groups: sudden cardiac death patients who were either obese or of normal weight, and had morphologically normal hearts.
Their group is uniquely positioned to do such research, Dr. Westaby explained.
“Here at St George’s University of London, we have a specialized cardiovascular pathology service. ... All hearts obtained at autopsy from individuals who have died from sudden cardiac death, or who were suspected to have had a cardiovascular cause of death, anywhere in the U.K., are referred to the CRY Centre for further analysis,” he said.
Patients were divided into two groups according to body mass index: an obesity group (BMI > 30 kg/m2) and a normal-weight group (BMI, 18.5-24.9).
An increased heart weight above 550 g in men and 450 g in women in the absence of coronary artery disease, hypertension, diabetes, or valvular disease was classified as unexplained cardiomegaly, and individuals with obesity and cardiomegaly were defined as obesity cardiomyopathy.
Age- and sex-matched controls with obesity (n = 106) were selected based on a BMI greater than 30, with a morphologically normal heart weighing less than 550 g in men and than 450 g in women.
Age- and sex-matched normal weight controls (n = 106) were selected based on a BMI of 18.5-24.9 and a morphologically normal heart weighing less than 550 g in men and less than 450 g in women.
The researchers identified 53 OCM cases from a cohort of more than 4,500 sudden cardiac death cases that had BMI measurements. In normal-weight patients, there were 14 cases of unexplained cardiomegaly.
The mean age at death of individuals with OCM was 42 years (range, 30-54 years). Most of the deaths occurred in men (n = 34; 64%), who also died younger than women (40 ± 13 years vs. 45 ± 10 years; P = .036).
The average heart weight in OCM patients was 598 ± 93 g. Risk of sudden cardiac death increased when BMI reached 35.
Compared with matched controls, there were increases in right and left ventricular wall thickness (all P < .05) in OCM cases. Right ventricular epicardial fat was increased in OCM cases, compared with normal-weight controls only.
Left ventricular fibrosis was identified in seven (13%) OCM cases.
Role of genetics to be explored
“This study highlights the need for further investigation into these individuals because, at the moment, we can’t be sure that the only contributing factor to this is the obesity,” said Dr. Westaby.
In the works are plans to see if there may be an underlying genetic predisposition in obese individuals that may have contributed to the development of an enlarged heart. The group also plans to study the families of the deceased individuals to determine if they are at risk of developing cardiomegaly, he said.
“This paper makes an important contribution to the literature that raises many important questions for future research,” Timothy P. Fitzgibbons, MD, PhD, from the University of Massachusetts, Worcester, wrote in an accompanying editorial.
Being able to access so many autopsy samples gives the current study considerable heft, Dr. Fitzgibbons said in an interview.
“A lot has been made of the obesity paradox and the perhaps benign nature of obesity but this paper suggests the opposite, that it is a very serious problem and can, in fact, in and of itself, cause heart abnormalities that could cause sudden death,” he noted.
The fact that only 13% of OCM cases had fibrosis on histology suggests that fibrosis was not the main cause of sudden cardiac death, he said.
“Often we will do MRIs to look for areas of fibrosis within the heart because those areas make patients prone to re-entry arrhythmias, in particular, ventricular tachycardia. But the authors suggest that the enlarged myocytes may themselves be predisposing to arrhythmias, rather than fibrosis,” Dr. Fitzgibbons said.
The study was supported by Cardiac Risk in the Young. Dr. Westaby and Dr. Fitzgibbons have reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
a new case-control study suggests.
Researchers who analyzed hearts taken at autopsy from people who had died from sudden cardiac death found that a number of the hearts obtained from obese decedents were heavier than those from normal-weight decedents and that the hazard ratio of unexplained cardiomegaly in this cohort was 5.3, compared with normal-weight individuals.
“Even when we ruled out any conditions that could potentially cause enlargement of the heart, including hypertension, heart valve problems, diabetes, and other cardiovascular risk factors, the association with obesity cardiomyopathy, or OCM, and sudden cardiac death remained,” lead author Joseph Westaby, PhD, from the Cardiac Risk in the Young (CRY) Cardiovascular Pathology Laboratories at St George’s University of London, said in an interview.
The study was published online in JACC: Advances.
Intrigued by this finding, Dr. Westaby and associates sought to characterize the clinical and pathological features of OCM associated with sudden cardiac death by comparing this population to two control groups: sudden cardiac death patients who were either obese or of normal weight, and had morphologically normal hearts.
Their group is uniquely positioned to do such research, Dr. Westaby explained.
“Here at St George’s University of London, we have a specialized cardiovascular pathology service. ... All hearts obtained at autopsy from individuals who have died from sudden cardiac death, or who were suspected to have had a cardiovascular cause of death, anywhere in the U.K., are referred to the CRY Centre for further analysis,” he said.
Patients were divided into two groups according to body mass index: an obesity group (BMI > 30 kg/m2) and a normal-weight group (BMI, 18.5-24.9).
An increased heart weight above 550 g in men and 450 g in women in the absence of coronary artery disease, hypertension, diabetes, or valvular disease was classified as unexplained cardiomegaly, and individuals with obesity and cardiomegaly were defined as obesity cardiomyopathy.
Age- and sex-matched controls with obesity (n = 106) were selected based on a BMI greater than 30, with a morphologically normal heart weighing less than 550 g in men and than 450 g in women.
Age- and sex-matched normal weight controls (n = 106) were selected based on a BMI of 18.5-24.9 and a morphologically normal heart weighing less than 550 g in men and less than 450 g in women.
The researchers identified 53 OCM cases from a cohort of more than 4,500 sudden cardiac death cases that had BMI measurements. In normal-weight patients, there were 14 cases of unexplained cardiomegaly.
The mean age at death of individuals with OCM was 42 years (range, 30-54 years). Most of the deaths occurred in men (n = 34; 64%), who also died younger than women (40 ± 13 years vs. 45 ± 10 years; P = .036).
The average heart weight in OCM patients was 598 ± 93 g. Risk of sudden cardiac death increased when BMI reached 35.
Compared with matched controls, there were increases in right and left ventricular wall thickness (all P < .05) in OCM cases. Right ventricular epicardial fat was increased in OCM cases, compared with normal-weight controls only.
Left ventricular fibrosis was identified in seven (13%) OCM cases.
Role of genetics to be explored
“This study highlights the need for further investigation into these individuals because, at the moment, we can’t be sure that the only contributing factor to this is the obesity,” said Dr. Westaby.
In the works are plans to see if there may be an underlying genetic predisposition in obese individuals that may have contributed to the development of an enlarged heart. The group also plans to study the families of the deceased individuals to determine if they are at risk of developing cardiomegaly, he said.
“This paper makes an important contribution to the literature that raises many important questions for future research,” Timothy P. Fitzgibbons, MD, PhD, from the University of Massachusetts, Worcester, wrote in an accompanying editorial.
Being able to access so many autopsy samples gives the current study considerable heft, Dr. Fitzgibbons said in an interview.
“A lot has been made of the obesity paradox and the perhaps benign nature of obesity but this paper suggests the opposite, that it is a very serious problem and can, in fact, in and of itself, cause heart abnormalities that could cause sudden death,” he noted.
The fact that only 13% of OCM cases had fibrosis on histology suggests that fibrosis was not the main cause of sudden cardiac death, he said.
“Often we will do MRIs to look for areas of fibrosis within the heart because those areas make patients prone to re-entry arrhythmias, in particular, ventricular tachycardia. But the authors suggest that the enlarged myocytes may themselves be predisposing to arrhythmias, rather than fibrosis,” Dr. Fitzgibbons said.
The study was supported by Cardiac Risk in the Young. Dr. Westaby and Dr. Fitzgibbons have reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
a new case-control study suggests.
Researchers who analyzed hearts taken at autopsy from people who had died from sudden cardiac death found that a number of the hearts obtained from obese decedents were heavier than those from normal-weight decedents and that the hazard ratio of unexplained cardiomegaly in this cohort was 5.3, compared with normal-weight individuals.
“Even when we ruled out any conditions that could potentially cause enlargement of the heart, including hypertension, heart valve problems, diabetes, and other cardiovascular risk factors, the association with obesity cardiomyopathy, or OCM, and sudden cardiac death remained,” lead author Joseph Westaby, PhD, from the Cardiac Risk in the Young (CRY) Cardiovascular Pathology Laboratories at St George’s University of London, said in an interview.
The study was published online in JACC: Advances.
Intrigued by this finding, Dr. Westaby and associates sought to characterize the clinical and pathological features of OCM associated with sudden cardiac death by comparing this population to two control groups: sudden cardiac death patients who were either obese or of normal weight, and had morphologically normal hearts.
Their group is uniquely positioned to do such research, Dr. Westaby explained.
“Here at St George’s University of London, we have a specialized cardiovascular pathology service. ... All hearts obtained at autopsy from individuals who have died from sudden cardiac death, or who were suspected to have had a cardiovascular cause of death, anywhere in the U.K., are referred to the CRY Centre for further analysis,” he said.
Patients were divided into two groups according to body mass index: an obesity group (BMI > 30 kg/m2) and a normal-weight group (BMI, 18.5-24.9).
An increased heart weight above 550 g in men and 450 g in women in the absence of coronary artery disease, hypertension, diabetes, or valvular disease was classified as unexplained cardiomegaly, and individuals with obesity and cardiomegaly were defined as obesity cardiomyopathy.
Age- and sex-matched controls with obesity (n = 106) were selected based on a BMI greater than 30, with a morphologically normal heart weighing less than 550 g in men and than 450 g in women.
Age- and sex-matched normal weight controls (n = 106) were selected based on a BMI of 18.5-24.9 and a morphologically normal heart weighing less than 550 g in men and less than 450 g in women.
The researchers identified 53 OCM cases from a cohort of more than 4,500 sudden cardiac death cases that had BMI measurements. In normal-weight patients, there were 14 cases of unexplained cardiomegaly.
The mean age at death of individuals with OCM was 42 years (range, 30-54 years). Most of the deaths occurred in men (n = 34; 64%), who also died younger than women (40 ± 13 years vs. 45 ± 10 years; P = .036).
The average heart weight in OCM patients was 598 ± 93 g. Risk of sudden cardiac death increased when BMI reached 35.
Compared with matched controls, there were increases in right and left ventricular wall thickness (all P < .05) in OCM cases. Right ventricular epicardial fat was increased in OCM cases, compared with normal-weight controls only.
Left ventricular fibrosis was identified in seven (13%) OCM cases.
Role of genetics to be explored
“This study highlights the need for further investigation into these individuals because, at the moment, we can’t be sure that the only contributing factor to this is the obesity,” said Dr. Westaby.
In the works are plans to see if there may be an underlying genetic predisposition in obese individuals that may have contributed to the development of an enlarged heart. The group also plans to study the families of the deceased individuals to determine if they are at risk of developing cardiomegaly, he said.
“This paper makes an important contribution to the literature that raises many important questions for future research,” Timothy P. Fitzgibbons, MD, PhD, from the University of Massachusetts, Worcester, wrote in an accompanying editorial.
Being able to access so many autopsy samples gives the current study considerable heft, Dr. Fitzgibbons said in an interview.
“A lot has been made of the obesity paradox and the perhaps benign nature of obesity but this paper suggests the opposite, that it is a very serious problem and can, in fact, in and of itself, cause heart abnormalities that could cause sudden death,” he noted.
The fact that only 13% of OCM cases had fibrosis on histology suggests that fibrosis was not the main cause of sudden cardiac death, he said.
“Often we will do MRIs to look for areas of fibrosis within the heart because those areas make patients prone to re-entry arrhythmias, in particular, ventricular tachycardia. But the authors suggest that the enlarged myocytes may themselves be predisposing to arrhythmias, rather than fibrosis,” Dr. Fitzgibbons said.
The study was supported by Cardiac Risk in the Young. Dr. Westaby and Dr. Fitzgibbons have reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM JACC: ADVANCES
LAAO tied to fewer post-fall bleeds than DOACs in AF
Left atrial appendage occlusion (LAAO) is associated with fewer injuries and less bleeding from falls than anticoagulant medications in patients with atrial fibrillation (AF) and a previous stroke, a new cohort study suggests.
Investigators prospectively followed more than 1,250 patients with AF and a previous ischemic stroke. Approximately half underwent LAAO, while the other half were treated with direct oral anticoagulants (DOACs). Patients were followed for close to 2 years.
Slightly more than 20% of patients fell during that period in each group, and , who were not taking anticoagulants. The risk for a major bleed, including an intracranial bleed, was 70% lower in the LAAO group.
LAAO has previously been considered for people at risk of bleeding events – for example, those with gastrointestinal (GI) bleeds, bruising, or intracranial bleeding – but had not yet been studied in those at risk for falls, coauthor Moussa Mansour, MD, professor of medicine, Harvard Medical School, and director of the Atrial Fibrillation Program at Massachusetts General Hospital, Boston, said in an interview.
This is the first study to focus on LAAO specifically for those at risk for falling and demonstrated that the LAAO has utility in this population as well, which is important because the U.S. population is an aging population, and at advanced ages, “people’s balance becomes unsteady and they are at high risk of falling,” he said.
The findings were published online as a research letter in the Journal of the American College of Cardiology.
Multidisciplinary collaboration
“More than one in five of our neurology patients with AF fall – many with devastating consequences – making stroke prevention extremely challenging,” senior author MingMing Ning, MD, MMsc, associate professor of neurology, Harvard Medical School, and director of the Cardio-Neurology and the Clinical Proteomics Research Center at Massachusetts General Hospital, Boston, said in an interview.
“There is a dire need to tailor treatment to keep our patients safe while preventing future strokes,” she said.
Anticoagulants are effective in stroke prevention in these patients but are associated with a higher risk for major bleeding, especially after a fall.
The current prospective observational study recruited 1,266 stroke patients who were treated either with LAAO or DOACs (n = 570 and 696, respectively). Patients were followed for a median of 1.8 years (IQR: 0.9-3.0).
During the follow-up period, 22.6% of LAAO-treated patients and 22.7% of DOAC-treated patients sustained a fall (mean age 78.9 years, 57.4% male and 79.1 years, 52.5% male respectively).
Fall severity, evaluated via the Injury Severity Score, was less in the LAAO vs. the DOAC group, with ISS scores of 1 (IQR 1-4) vs. 4 (IQR 1.75-9).
LAAO was associated with significantly reduced severity of fall-related injuries (OR, –1.09, 95% confidence interval [CI], –1.52 to –0.66; P < .001) – a finding that remained statistically significant after adjustment for confounders such as age, sex, and comorbidities contributing to fall risk, such as hypertension, hyperlipidemia, and diabetes.
The incidence of major trauma (defined as ISS >15) was lower in the LAAO group, compared to the DOAC group (0.8% vs. 6.3%, respectively, P = .026), and LAAO-treated patients had a shorter length of hospital stay, with fewer LAAO patients compared with DOAC patients staying in the hospital for more than 3 days (17% vs. 29.1%, respectively, P = .018).
The risk for major post-fall bleeding was lower in the LAAO vs. the DOAC group (4.7% vs. 15.2%, AOR, 0.29; 95% CI, 0.11-0.73; P = .009) – a finding that included intracranial bleeding (3.1% vs. 9.5%; AOR, 0.29; 95% CI, 0.09-0.90; P = .033).
“Many people are living to advanced ages, where their balance becomes unsteady, and in addition, we have an increase in the prevalence of AF because people are living longer and it’s a disease of the elderly, because we have more hypertension, and we also have more tools to diagnose AF. It’s almost a ‘perfect storm’ situation, and we need effective interventions in this population,” said Dr. Mansour.
Before the study, people at risk for falling were not being considered for LAAO; but now, “we believe they should be considered,” he added. “And although people in the current study had all experienced an ischemic stroke, any patient at risk of a fall will potentially benefit.”
Beyond demonstrating the role of LAAO in reducing the risk of post-fall bleeding injuries, the study – which was conducted by specialists in neurology and cardiology among other fields – highlights the importance of multidisciplinary collaboration, which is “key” for effective stroke prevention, Dr. Ning said.
She emphasized that “we need to learn from our patients and tailor treatment to their needs. A patient’s risk of falling, lifestyle, and medication adherence are all important for individualizing care and improving quality of life.”
Better option
Commenting for this article, Andrea Natale, MD, executive medical director, Texas Cardiac Arrhythmia Institute at St. David’s Medical Center, Austin, said the authors “should be commended for this prospective study on real-world patients that has yielded highly meaningful data from a clinical standpoint.”
Dr. Natale, who was not involved with the study, said it has “several strong points,” such as a fairly large sample size, exclusive population with a history of AF-related stroke, long follow-up duration, evaluation of fall incidents by blinded experts, and severity of fall assessed by a validated questionnaire.
“This is the first study that directly compared the outcomes of traumatic fall in patients receiving LAAO vs. DOAC,” he said. “Given that history of fall is an independent predictor of bleeding and death, the study findings by Deng et al. offer the hope for a safer life with the LAAO option in the aging, fall-prone AF population.”
The take-home message is that, in patients with history of stroke, LAAO “is a better option, in terms of significantly reduced injury severity and shortened hospital length of stay after traumatic falls,” Dr. Natale said.
This study was supported in part by research grants from Boston Scientific, the Leducq Foundation, and the National Institutes of Health. The authors reported no relevant financial relationships. Dr. Natale is a consultant for Abbott, Baylis, Biosense Webster, Biotronik, Boston Scientific, and Medtronic.
A version of this article appeared on Medscape.com.
Left atrial appendage occlusion (LAAO) is associated with fewer injuries and less bleeding from falls than anticoagulant medications in patients with atrial fibrillation (AF) and a previous stroke, a new cohort study suggests.
Investigators prospectively followed more than 1,250 patients with AF and a previous ischemic stroke. Approximately half underwent LAAO, while the other half were treated with direct oral anticoagulants (DOACs). Patients were followed for close to 2 years.
Slightly more than 20% of patients fell during that period in each group, and , who were not taking anticoagulants. The risk for a major bleed, including an intracranial bleed, was 70% lower in the LAAO group.
LAAO has previously been considered for people at risk of bleeding events – for example, those with gastrointestinal (GI) bleeds, bruising, or intracranial bleeding – but had not yet been studied in those at risk for falls, coauthor Moussa Mansour, MD, professor of medicine, Harvard Medical School, and director of the Atrial Fibrillation Program at Massachusetts General Hospital, Boston, said in an interview.
This is the first study to focus on LAAO specifically for those at risk for falling and demonstrated that the LAAO has utility in this population as well, which is important because the U.S. population is an aging population, and at advanced ages, “people’s balance becomes unsteady and they are at high risk of falling,” he said.
The findings were published online as a research letter in the Journal of the American College of Cardiology.
Multidisciplinary collaboration
“More than one in five of our neurology patients with AF fall – many with devastating consequences – making stroke prevention extremely challenging,” senior author MingMing Ning, MD, MMsc, associate professor of neurology, Harvard Medical School, and director of the Cardio-Neurology and the Clinical Proteomics Research Center at Massachusetts General Hospital, Boston, said in an interview.
“There is a dire need to tailor treatment to keep our patients safe while preventing future strokes,” she said.
Anticoagulants are effective in stroke prevention in these patients but are associated with a higher risk for major bleeding, especially after a fall.
The current prospective observational study recruited 1,266 stroke patients who were treated either with LAAO or DOACs (n = 570 and 696, respectively). Patients were followed for a median of 1.8 years (IQR: 0.9-3.0).
During the follow-up period, 22.6% of LAAO-treated patients and 22.7% of DOAC-treated patients sustained a fall (mean age 78.9 years, 57.4% male and 79.1 years, 52.5% male respectively).
Fall severity, evaluated via the Injury Severity Score, was less in the LAAO vs. the DOAC group, with ISS scores of 1 (IQR 1-4) vs. 4 (IQR 1.75-9).
LAAO was associated with significantly reduced severity of fall-related injuries (OR, –1.09, 95% confidence interval [CI], –1.52 to –0.66; P < .001) – a finding that remained statistically significant after adjustment for confounders such as age, sex, and comorbidities contributing to fall risk, such as hypertension, hyperlipidemia, and diabetes.
The incidence of major trauma (defined as ISS >15) was lower in the LAAO group, compared to the DOAC group (0.8% vs. 6.3%, respectively, P = .026), and LAAO-treated patients had a shorter length of hospital stay, with fewer LAAO patients compared with DOAC patients staying in the hospital for more than 3 days (17% vs. 29.1%, respectively, P = .018).
The risk for major post-fall bleeding was lower in the LAAO vs. the DOAC group (4.7% vs. 15.2%, AOR, 0.29; 95% CI, 0.11-0.73; P = .009) – a finding that included intracranial bleeding (3.1% vs. 9.5%; AOR, 0.29; 95% CI, 0.09-0.90; P = .033).
“Many people are living to advanced ages, where their balance becomes unsteady, and in addition, we have an increase in the prevalence of AF because people are living longer and it’s a disease of the elderly, because we have more hypertension, and we also have more tools to diagnose AF. It’s almost a ‘perfect storm’ situation, and we need effective interventions in this population,” said Dr. Mansour.
Before the study, people at risk for falling were not being considered for LAAO; but now, “we believe they should be considered,” he added. “And although people in the current study had all experienced an ischemic stroke, any patient at risk of a fall will potentially benefit.”
Beyond demonstrating the role of LAAO in reducing the risk of post-fall bleeding injuries, the study – which was conducted by specialists in neurology and cardiology among other fields – highlights the importance of multidisciplinary collaboration, which is “key” for effective stroke prevention, Dr. Ning said.
She emphasized that “we need to learn from our patients and tailor treatment to their needs. A patient’s risk of falling, lifestyle, and medication adherence are all important for individualizing care and improving quality of life.”
Better option
Commenting for this article, Andrea Natale, MD, executive medical director, Texas Cardiac Arrhythmia Institute at St. David’s Medical Center, Austin, said the authors “should be commended for this prospective study on real-world patients that has yielded highly meaningful data from a clinical standpoint.”
Dr. Natale, who was not involved with the study, said it has “several strong points,” such as a fairly large sample size, exclusive population with a history of AF-related stroke, long follow-up duration, evaluation of fall incidents by blinded experts, and severity of fall assessed by a validated questionnaire.
“This is the first study that directly compared the outcomes of traumatic fall in patients receiving LAAO vs. DOAC,” he said. “Given that history of fall is an independent predictor of bleeding and death, the study findings by Deng et al. offer the hope for a safer life with the LAAO option in the aging, fall-prone AF population.”
The take-home message is that, in patients with history of stroke, LAAO “is a better option, in terms of significantly reduced injury severity and shortened hospital length of stay after traumatic falls,” Dr. Natale said.
This study was supported in part by research grants from Boston Scientific, the Leducq Foundation, and the National Institutes of Health. The authors reported no relevant financial relationships. Dr. Natale is a consultant for Abbott, Baylis, Biosense Webster, Biotronik, Boston Scientific, and Medtronic.
A version of this article appeared on Medscape.com.
Left atrial appendage occlusion (LAAO) is associated with fewer injuries and less bleeding from falls than anticoagulant medications in patients with atrial fibrillation (AF) and a previous stroke, a new cohort study suggests.
Investigators prospectively followed more than 1,250 patients with AF and a previous ischemic stroke. Approximately half underwent LAAO, while the other half were treated with direct oral anticoagulants (DOACs). Patients were followed for close to 2 years.
Slightly more than 20% of patients fell during that period in each group, and , who were not taking anticoagulants. The risk for a major bleed, including an intracranial bleed, was 70% lower in the LAAO group.
LAAO has previously been considered for people at risk of bleeding events – for example, those with gastrointestinal (GI) bleeds, bruising, or intracranial bleeding – but had not yet been studied in those at risk for falls, coauthor Moussa Mansour, MD, professor of medicine, Harvard Medical School, and director of the Atrial Fibrillation Program at Massachusetts General Hospital, Boston, said in an interview.
This is the first study to focus on LAAO specifically for those at risk for falling and demonstrated that the LAAO has utility in this population as well, which is important because the U.S. population is an aging population, and at advanced ages, “people’s balance becomes unsteady and they are at high risk of falling,” he said.
The findings were published online as a research letter in the Journal of the American College of Cardiology.
Multidisciplinary collaboration
“More than one in five of our neurology patients with AF fall – many with devastating consequences – making stroke prevention extremely challenging,” senior author MingMing Ning, MD, MMsc, associate professor of neurology, Harvard Medical School, and director of the Cardio-Neurology and the Clinical Proteomics Research Center at Massachusetts General Hospital, Boston, said in an interview.
“There is a dire need to tailor treatment to keep our patients safe while preventing future strokes,” she said.
Anticoagulants are effective in stroke prevention in these patients but are associated with a higher risk for major bleeding, especially after a fall.
The current prospective observational study recruited 1,266 stroke patients who were treated either with LAAO or DOACs (n = 570 and 696, respectively). Patients were followed for a median of 1.8 years (IQR: 0.9-3.0).
During the follow-up period, 22.6% of LAAO-treated patients and 22.7% of DOAC-treated patients sustained a fall (mean age 78.9 years, 57.4% male and 79.1 years, 52.5% male respectively).
Fall severity, evaluated via the Injury Severity Score, was less in the LAAO vs. the DOAC group, with ISS scores of 1 (IQR 1-4) vs. 4 (IQR 1.75-9).
LAAO was associated with significantly reduced severity of fall-related injuries (OR, –1.09, 95% confidence interval [CI], –1.52 to –0.66; P < .001) – a finding that remained statistically significant after adjustment for confounders such as age, sex, and comorbidities contributing to fall risk, such as hypertension, hyperlipidemia, and diabetes.
The incidence of major trauma (defined as ISS >15) was lower in the LAAO group, compared to the DOAC group (0.8% vs. 6.3%, respectively, P = .026), and LAAO-treated patients had a shorter length of hospital stay, with fewer LAAO patients compared with DOAC patients staying in the hospital for more than 3 days (17% vs. 29.1%, respectively, P = .018).
The risk for major post-fall bleeding was lower in the LAAO vs. the DOAC group (4.7% vs. 15.2%, AOR, 0.29; 95% CI, 0.11-0.73; P = .009) – a finding that included intracranial bleeding (3.1% vs. 9.5%; AOR, 0.29; 95% CI, 0.09-0.90; P = .033).
“Many people are living to advanced ages, where their balance becomes unsteady, and in addition, we have an increase in the prevalence of AF because people are living longer and it’s a disease of the elderly, because we have more hypertension, and we also have more tools to diagnose AF. It’s almost a ‘perfect storm’ situation, and we need effective interventions in this population,” said Dr. Mansour.
Before the study, people at risk for falling were not being considered for LAAO; but now, “we believe they should be considered,” he added. “And although people in the current study had all experienced an ischemic stroke, any patient at risk of a fall will potentially benefit.”
Beyond demonstrating the role of LAAO in reducing the risk of post-fall bleeding injuries, the study – which was conducted by specialists in neurology and cardiology among other fields – highlights the importance of multidisciplinary collaboration, which is “key” for effective stroke prevention, Dr. Ning said.
She emphasized that “we need to learn from our patients and tailor treatment to their needs. A patient’s risk of falling, lifestyle, and medication adherence are all important for individualizing care and improving quality of life.”
Better option
Commenting for this article, Andrea Natale, MD, executive medical director, Texas Cardiac Arrhythmia Institute at St. David’s Medical Center, Austin, said the authors “should be commended for this prospective study on real-world patients that has yielded highly meaningful data from a clinical standpoint.”
Dr. Natale, who was not involved with the study, said it has “several strong points,” such as a fairly large sample size, exclusive population with a history of AF-related stroke, long follow-up duration, evaluation of fall incidents by blinded experts, and severity of fall assessed by a validated questionnaire.
“This is the first study that directly compared the outcomes of traumatic fall in patients receiving LAAO vs. DOAC,” he said. “Given that history of fall is an independent predictor of bleeding and death, the study findings by Deng et al. offer the hope for a safer life with the LAAO option in the aging, fall-prone AF population.”
The take-home message is that, in patients with history of stroke, LAAO “is a better option, in terms of significantly reduced injury severity and shortened hospital length of stay after traumatic falls,” Dr. Natale said.
This study was supported in part by research grants from Boston Scientific, the Leducq Foundation, and the National Institutes of Health. The authors reported no relevant financial relationships. Dr. Natale is a consultant for Abbott, Baylis, Biosense Webster, Biotronik, Boston Scientific, and Medtronic.
A version of this article appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Studies link GLP-1 agonists to progression of diabetic retinopathy
SEATTLE – A family of blockbuster drugs for managing blood glucose – and now for promoting weight loss – has been linked to exacerbation of macular disease that frequently accompanies diabetes, new data show.
Two studies presented at the annual meeting of the American Society of Retina Specialists (ASRS) have found that
Clinicians should be aware of these effects of GLP-1 inhibitors to ensure appropriate monitoring of patients for the possibility that retinopathy may accelerate, according to Ehsan Rahimy, MD, an adjunct clinical professor at Stanford (Calif.) University, and colleagues.
Dr. Rahimy presented results of a retrospective study of retinopathy progression in patients taking either GLP-1 agonists or sodium-glucose transporter-2 (SGLT-2) inhibitors, also known as gliflozins. “When we looked at the conversion to proliferative disease, you can see it was statistically higher in the GLP-1 group at all time points,” he said.
GLP-1 agonists can promote considerable weight loss in patients with and without diabetes. Moreover, the finding that gliflozins improve cardiovascular and renal function in patients with type 2 diabetes has accelerated the use of these agents for blood glucose control.
Using a repository of data from more than 13,500 people taking either of the two kinds of medication, the researchers looked for conversion of diabetic eye disease to proliferative diabetic retinopathy (PDR) or DME. Secondary outcomes were the need for intravitreal injections, panretinal photocoagulation (PRP), or pars plana vitrectomy (PPV).
Propensity score matching for age, sex, race, ethnicity, and baseline hemoglobin A1c resulted in the inclusion of 5,446 participants in each treatment group. After matching, the mean age of participants in either group was 64 years, and the mean A1c was 8.5%. Slightly more than half the participants were insulin-dependent.
Patients taking GLP-1 inhibitors had higher rates of conversion to PDR than those taking gliflozins at 3 years (6% vs. 4%; P < .01), the researchers found. Nearly 25% of those taking a GLP-1 agonist had progressed to DME after 3 years, compared with 18% of those taking a gliflozin.
People in the group taking GLP-1 inhibitors also had a greater need for interventions than those on a gliflozin; 8% vs. roughly 6%, respectively, required intravitreal injections, Dr. Rahimy reported. Similar trends were noted for need for PRP and PPV, he added, although the absolute numbers of patients were small.
Albiglutide the key culprit?
In other research reported at the meeting, a meta-analysis of data collected in 93 randomized clinical trials of the seven currently available GLP-1 agonists found only albiglutide was associated with diabetic retinopathy to a statistically significant degree. Compared with placebo, albiglutide more than doubled the risk for early-stage diabetic retinopathy (relative risk 2.18; 95% confidence interval, 1.01-4.67; P = .05).
Other GLP-1 agonists evaluated in the meta-analysis included semaglutide, tirzepatide, dulaglutide, exenatide, liraglutide, and lixisenatide. These findings were reported in a poster presented at the meeting by Ishani Kapoor, MD candidate, Drexel University, Philadelphia.
“The strength of these effects depends on the specific GLP-1 receptor agonist used, patient-specific clinical characteristics, and demographics,” Ms. Kapoor and coauthors reported. “Further studies are needed to clarify the patient populations that would benefit from GLP-1 receptor agonists and those at risk for [the] development of additional ocular damage.”
What causes progression?
Whether worsening of retinopathy stems from rapid weight loss and acute reductions in concentrations of blood glucose or is a direct effect of GLP-1 agonists on the eye is unclear.
“That rapid reduction is thought to play some role,” Dr. Rahimy said. “But if you actually look out there in the basic science literature, it’s suggested that there are direct effects of these medications on the retina too. That being said, it’s suggested that they may be protective to the retina. And I think that’s where we’ve gotten a lot of mixed signals in our community between what we’ve seen on the basic science side vs. what we’re seeing on the real-world side.”
The study was independently funded. Dr. Rahimy reports consultancies or speakerships with AbbVie, Allergan, Apellis, Carl Zeiss, Genentech, and Google, and research support from Regeneron. Ms. Kapoor reports no relevant financial relationships.
A version of this article appeared on Medscape.com.
SEATTLE – A family of blockbuster drugs for managing blood glucose – and now for promoting weight loss – has been linked to exacerbation of macular disease that frequently accompanies diabetes, new data show.
Two studies presented at the annual meeting of the American Society of Retina Specialists (ASRS) have found that
Clinicians should be aware of these effects of GLP-1 inhibitors to ensure appropriate monitoring of patients for the possibility that retinopathy may accelerate, according to Ehsan Rahimy, MD, an adjunct clinical professor at Stanford (Calif.) University, and colleagues.
Dr. Rahimy presented results of a retrospective study of retinopathy progression in patients taking either GLP-1 agonists or sodium-glucose transporter-2 (SGLT-2) inhibitors, also known as gliflozins. “When we looked at the conversion to proliferative disease, you can see it was statistically higher in the GLP-1 group at all time points,” he said.
GLP-1 agonists can promote considerable weight loss in patients with and without diabetes. Moreover, the finding that gliflozins improve cardiovascular and renal function in patients with type 2 diabetes has accelerated the use of these agents for blood glucose control.
Using a repository of data from more than 13,500 people taking either of the two kinds of medication, the researchers looked for conversion of diabetic eye disease to proliferative diabetic retinopathy (PDR) or DME. Secondary outcomes were the need for intravitreal injections, panretinal photocoagulation (PRP), or pars plana vitrectomy (PPV).
Propensity score matching for age, sex, race, ethnicity, and baseline hemoglobin A1c resulted in the inclusion of 5,446 participants in each treatment group. After matching, the mean age of participants in either group was 64 years, and the mean A1c was 8.5%. Slightly more than half the participants were insulin-dependent.
Patients taking GLP-1 inhibitors had higher rates of conversion to PDR than those taking gliflozins at 3 years (6% vs. 4%; P < .01), the researchers found. Nearly 25% of those taking a GLP-1 agonist had progressed to DME after 3 years, compared with 18% of those taking a gliflozin.
People in the group taking GLP-1 inhibitors also had a greater need for interventions than those on a gliflozin; 8% vs. roughly 6%, respectively, required intravitreal injections, Dr. Rahimy reported. Similar trends were noted for need for PRP and PPV, he added, although the absolute numbers of patients were small.
Albiglutide the key culprit?
In other research reported at the meeting, a meta-analysis of data collected in 93 randomized clinical trials of the seven currently available GLP-1 agonists found only albiglutide was associated with diabetic retinopathy to a statistically significant degree. Compared with placebo, albiglutide more than doubled the risk for early-stage diabetic retinopathy (relative risk 2.18; 95% confidence interval, 1.01-4.67; P = .05).
Other GLP-1 agonists evaluated in the meta-analysis included semaglutide, tirzepatide, dulaglutide, exenatide, liraglutide, and lixisenatide. These findings were reported in a poster presented at the meeting by Ishani Kapoor, MD candidate, Drexel University, Philadelphia.
“The strength of these effects depends on the specific GLP-1 receptor agonist used, patient-specific clinical characteristics, and demographics,” Ms. Kapoor and coauthors reported. “Further studies are needed to clarify the patient populations that would benefit from GLP-1 receptor agonists and those at risk for [the] development of additional ocular damage.”
What causes progression?
Whether worsening of retinopathy stems from rapid weight loss and acute reductions in concentrations of blood glucose or is a direct effect of GLP-1 agonists on the eye is unclear.
“That rapid reduction is thought to play some role,” Dr. Rahimy said. “But if you actually look out there in the basic science literature, it’s suggested that there are direct effects of these medications on the retina too. That being said, it’s suggested that they may be protective to the retina. And I think that’s where we’ve gotten a lot of mixed signals in our community between what we’ve seen on the basic science side vs. what we’re seeing on the real-world side.”
The study was independently funded. Dr. Rahimy reports consultancies or speakerships with AbbVie, Allergan, Apellis, Carl Zeiss, Genentech, and Google, and research support from Regeneron. Ms. Kapoor reports no relevant financial relationships.
A version of this article appeared on Medscape.com.
SEATTLE – A family of blockbuster drugs for managing blood glucose – and now for promoting weight loss – has been linked to exacerbation of macular disease that frequently accompanies diabetes, new data show.
Two studies presented at the annual meeting of the American Society of Retina Specialists (ASRS) have found that
Clinicians should be aware of these effects of GLP-1 inhibitors to ensure appropriate monitoring of patients for the possibility that retinopathy may accelerate, according to Ehsan Rahimy, MD, an adjunct clinical professor at Stanford (Calif.) University, and colleagues.
Dr. Rahimy presented results of a retrospective study of retinopathy progression in patients taking either GLP-1 agonists or sodium-glucose transporter-2 (SGLT-2) inhibitors, also known as gliflozins. “When we looked at the conversion to proliferative disease, you can see it was statistically higher in the GLP-1 group at all time points,” he said.
GLP-1 agonists can promote considerable weight loss in patients with and without diabetes. Moreover, the finding that gliflozins improve cardiovascular and renal function in patients with type 2 diabetes has accelerated the use of these agents for blood glucose control.
Using a repository of data from more than 13,500 people taking either of the two kinds of medication, the researchers looked for conversion of diabetic eye disease to proliferative diabetic retinopathy (PDR) or DME. Secondary outcomes were the need for intravitreal injections, panretinal photocoagulation (PRP), or pars plana vitrectomy (PPV).
Propensity score matching for age, sex, race, ethnicity, and baseline hemoglobin A1c resulted in the inclusion of 5,446 participants in each treatment group. After matching, the mean age of participants in either group was 64 years, and the mean A1c was 8.5%. Slightly more than half the participants were insulin-dependent.
Patients taking GLP-1 inhibitors had higher rates of conversion to PDR than those taking gliflozins at 3 years (6% vs. 4%; P < .01), the researchers found. Nearly 25% of those taking a GLP-1 agonist had progressed to DME after 3 years, compared with 18% of those taking a gliflozin.
People in the group taking GLP-1 inhibitors also had a greater need for interventions than those on a gliflozin; 8% vs. roughly 6%, respectively, required intravitreal injections, Dr. Rahimy reported. Similar trends were noted for need for PRP and PPV, he added, although the absolute numbers of patients were small.
Albiglutide the key culprit?
In other research reported at the meeting, a meta-analysis of data collected in 93 randomized clinical trials of the seven currently available GLP-1 agonists found only albiglutide was associated with diabetic retinopathy to a statistically significant degree. Compared with placebo, albiglutide more than doubled the risk for early-stage diabetic retinopathy (relative risk 2.18; 95% confidence interval, 1.01-4.67; P = .05).
Other GLP-1 agonists evaluated in the meta-analysis included semaglutide, tirzepatide, dulaglutide, exenatide, liraglutide, and lixisenatide. These findings were reported in a poster presented at the meeting by Ishani Kapoor, MD candidate, Drexel University, Philadelphia.
“The strength of these effects depends on the specific GLP-1 receptor agonist used, patient-specific clinical characteristics, and demographics,” Ms. Kapoor and coauthors reported. “Further studies are needed to clarify the patient populations that would benefit from GLP-1 receptor agonists and those at risk for [the] development of additional ocular damage.”
What causes progression?
Whether worsening of retinopathy stems from rapid weight loss and acute reductions in concentrations of blood glucose or is a direct effect of GLP-1 agonists on the eye is unclear.
“That rapid reduction is thought to play some role,” Dr. Rahimy said. “But if you actually look out there in the basic science literature, it’s suggested that there are direct effects of these medications on the retina too. That being said, it’s suggested that they may be protective to the retina. And I think that’s where we’ve gotten a lot of mixed signals in our community between what we’ve seen on the basic science side vs. what we’re seeing on the real-world side.”
The study was independently funded. Dr. Rahimy reports consultancies or speakerships with AbbVie, Allergan, Apellis, Carl Zeiss, Genentech, and Google, and research support from Regeneron. Ms. Kapoor reports no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM ASRS 2023
Clinicians debate the usefulness of NAFLD name change
Some clinicians say it’s “confusing” and “ridiculous” to change the name and diagnostic criteria of an established liver disease, while others bemoan the seemingly political reasons why it happened. Yet recently, 236 panelists from 56 countries decided that the terms nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH) rely on “exclusionary confounder terms and the use of potentially stigmatizing language.”
In a report published in Hepatology, the panelists, members of the NAFLD Nomenclature Consensus Group, determined that steatotic liver disease (SLD) would be used as an “overarching term to encompass the various etiologies of steatosis.”
Metabolic dysfunction–associated steatotic liver disease (MASLD) was chosen to replace NAFLD, and the definition was changed to include at least one of five cardiometabolic risk factors.
Metabolic dysfunction–associated steatohepatitis (MASH) replaces NASH.
Those with no metabolic parameters and no known cause will be diagnosed with cryptogenic SLD.
A new category, MetALD, now describes those with MASLD who drink more alcohol per week – 140-350 g for men and 210-420 g for women.
The changes did not sit well with this news organization’s readers from diverse specialties, including family practice, critical care, and gastroenterology.
In its report, the consensus group wrote that 74% of respondents to its rounds of surveys felt the current nomenclature “was sufficiently flawed to consider a name change.”
The terms “nonalcoholic” and “fatty” were felt to be stigmatizing by 61% and 66% of respondents, respectively, according to the group, a multi-stakeholder effort under the auspices of the American Association for Study of Liver Disease and the European Association for Study of the Liver, in collaboration with the Asociación Latinoamericana para el Estudio del Hígado.
Consensus was defined a priori as a supermajority (67%) vote.
“The new nomenclature and diagnostic criteria are widely supported, nonstigmatizing, and can improve awareness and patient identification,” the group concluded.
“No way” sums up many of the almost 60 reader comments received on this news organization’s story covering the change. Readers must share medical credentials to publicly comment on stories.
‘Confusing’ and ‘ridiculous’
A number of readers questioned how the changes will help practice.
“Once again, the specialists and other experts are changing the nomenclature to make the subject even more confusing for us primary care practitioners,” an HIV/AIDS physician wrote. “They obviously have no idea what [primary care practitioners] have to put up with day in and day out. All such revisions do is increase the cynicism and anger so many [primary care practitioners] have.”
Similarly, an internist said, “These new terms are going to confuse both doctors and patients. When you give a patient a diagnosis like this, they will not understand it, and will not be able to act as they should to correct it.”
“ ‘Fatty liver’ is a jargon-free diagnosis, easy to understand and easy for patients to know what they need to do,” the internist continued. “You think patients are gonna be educated when you tell them they have a ‘metabolic disease’? 100% they will not know what you’re talking about.”
Yet another wondered, “If SLD is the ‘umbrella’ term, why (are) MetALD and ALD not MetASLD and ASLD, respectively? Furthermore, efforts to ‘destigmatize’ terminology will inadvertently condemn cryptogenic SLD (CSLD) as the new ‘closet alcoholic.’ “
“Perhaps a subclassification, CSLD-HDIRDD (CSLD–Honest, Doc, I Really Don’t Drink),” the reader added.
“Everything about this is ridiculous,” a family physician wrote. “How long will it be until the experts change obesity to ‘gravitationally challenged’ as a diagnosis!”
“I was thinking of ‘circumferentially challenged,’” a reader in Canada chimed in. “But that would be ‘body shaming’ would it not?”
This reader continued, asking, “What about returning to the old practice of using Latin names patients don’t understand so there is no ‘shame’ attached to them? Or what about this revolutionary idea: To just say it as it is – fat?”
Acceding to ‘wokeness’
A sizable number of readers felt the name changes were motivated by a “woke” awareness.
“The effect of this new ‘woke’ clarity is ridiculous and simply not worth it! Can we justify the cost of this? Patients will have to learn all over again how to discuss their condition,” said one reader.
The reader continued, saying, “The Internet and social media freely use the term ‘fat’ – and despite not wanting to offend – there seems to be universal agreement that FAT, in certain conditions or places, is unhealthy and undesirable.
“Why is the medical community so afraid to tell it like it is? I might hurt your feelings, but I could save your life,” concluded the reader.
Defending change
One commentator, a hepatologist in France, defended the changes and responded to some of complaints.
“Maybe people who comment here should read the article, reflect, and understand the reasons why the old nomenclature and definition were scientifically inaccurate and needed to be changed,” the commentator wrote.
“It was an exclusionary, negative definition not recognizing the root of the disease (adipose tissue dysfunction with insulin resistance – instead defining it by what it is not ...) and not allowing the recognition of a large segment of the population [that] accumulates metabolic risk factors and moderate alcohol consumption. These patients were left out of all studies. Those were the main reasons for change and not the stigma part – with the word ‘fatty’ only being an issue in English-speaking countries, not elsewhere,” the commentator continued.
“Calls for change have been voiced for 20 years and a first comprehensive attempt (called MAFLD) was introduced 3 years ago (J Hepatol. 2020;73:202-9). Please, a little bit of respect and restraint in the comments recognizing the research efforts and publications for those that contributed to the field over the past 25 years ...” the hepatologist wrote.
The reader added, “Clinicians and researchers were dissatisfied for a long time, but it took years to gather overwhelming evidence demonstrating what causes the disease and then to kickstart a process under the auspices of several multinational scientific societies and come up with something consensually agreed upon by a large number of clinician researchers.
“Now you can tell your patient that he has metabolic liver disease instead of telling him that the problem at the root of his disease is that he is not drinking alcohol (nonalcoholic steatohepatitis). So, again, it is not so much about changing a name but about redefining diagnostic criteria and a nosological framework,” the reader wrote.
Other readers responded to the defender:
“This nomenclature issue has been churned for 20+ years? Well, the mountain has labored heavily, and given birth to a mouse,” one said.
“Still, how is this going to help in the clinical management? The whole gamut of conditions are evaluated and treated as a whole, not in isolation,” a general practitioner in India said. “If someone has a risk factor or not, continuous follow-up is required as a whole, whether it’s nonalcoholic or alcoholic, or whatever term is coined up.”
Finally, a family physician said, “It just rolls off the tongue, doesn’t it? But I have to admit, it’s the one place where ‘persons’ from 56 countries can get together and agree on something. Not even politicians can do that! Me, I’m sticking with NAFLD.”
A version of this article first appeared on Medscape.com.
Some clinicians say it’s “confusing” and “ridiculous” to change the name and diagnostic criteria of an established liver disease, while others bemoan the seemingly political reasons why it happened. Yet recently, 236 panelists from 56 countries decided that the terms nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH) rely on “exclusionary confounder terms and the use of potentially stigmatizing language.”
In a report published in Hepatology, the panelists, members of the NAFLD Nomenclature Consensus Group, determined that steatotic liver disease (SLD) would be used as an “overarching term to encompass the various etiologies of steatosis.”
Metabolic dysfunction–associated steatotic liver disease (MASLD) was chosen to replace NAFLD, and the definition was changed to include at least one of five cardiometabolic risk factors.
Metabolic dysfunction–associated steatohepatitis (MASH) replaces NASH.
Those with no metabolic parameters and no known cause will be diagnosed with cryptogenic SLD.
A new category, MetALD, now describes those with MASLD who drink more alcohol per week – 140-350 g for men and 210-420 g for women.
The changes did not sit well with this news organization’s readers from diverse specialties, including family practice, critical care, and gastroenterology.
In its report, the consensus group wrote that 74% of respondents to its rounds of surveys felt the current nomenclature “was sufficiently flawed to consider a name change.”
The terms “nonalcoholic” and “fatty” were felt to be stigmatizing by 61% and 66% of respondents, respectively, according to the group, a multi-stakeholder effort under the auspices of the American Association for Study of Liver Disease and the European Association for Study of the Liver, in collaboration with the Asociación Latinoamericana para el Estudio del Hígado.
Consensus was defined a priori as a supermajority (67%) vote.
“The new nomenclature and diagnostic criteria are widely supported, nonstigmatizing, and can improve awareness and patient identification,” the group concluded.
“No way” sums up many of the almost 60 reader comments received on this news organization’s story covering the change. Readers must share medical credentials to publicly comment on stories.
‘Confusing’ and ‘ridiculous’
A number of readers questioned how the changes will help practice.
“Once again, the specialists and other experts are changing the nomenclature to make the subject even more confusing for us primary care practitioners,” an HIV/AIDS physician wrote. “They obviously have no idea what [primary care practitioners] have to put up with day in and day out. All such revisions do is increase the cynicism and anger so many [primary care practitioners] have.”
Similarly, an internist said, “These new terms are going to confuse both doctors and patients. When you give a patient a diagnosis like this, they will not understand it, and will not be able to act as they should to correct it.”
“ ‘Fatty liver’ is a jargon-free diagnosis, easy to understand and easy for patients to know what they need to do,” the internist continued. “You think patients are gonna be educated when you tell them they have a ‘metabolic disease’? 100% they will not know what you’re talking about.”
Yet another wondered, “If SLD is the ‘umbrella’ term, why (are) MetALD and ALD not MetASLD and ASLD, respectively? Furthermore, efforts to ‘destigmatize’ terminology will inadvertently condemn cryptogenic SLD (CSLD) as the new ‘closet alcoholic.’ “
“Perhaps a subclassification, CSLD-HDIRDD (CSLD–Honest, Doc, I Really Don’t Drink),” the reader added.
“Everything about this is ridiculous,” a family physician wrote. “How long will it be until the experts change obesity to ‘gravitationally challenged’ as a diagnosis!”
“I was thinking of ‘circumferentially challenged,’” a reader in Canada chimed in. “But that would be ‘body shaming’ would it not?”
This reader continued, asking, “What about returning to the old practice of using Latin names patients don’t understand so there is no ‘shame’ attached to them? Or what about this revolutionary idea: To just say it as it is – fat?”
Acceding to ‘wokeness’
A sizable number of readers felt the name changes were motivated by a “woke” awareness.
“The effect of this new ‘woke’ clarity is ridiculous and simply not worth it! Can we justify the cost of this? Patients will have to learn all over again how to discuss their condition,” said one reader.
The reader continued, saying, “The Internet and social media freely use the term ‘fat’ – and despite not wanting to offend – there seems to be universal agreement that FAT, in certain conditions or places, is unhealthy and undesirable.
“Why is the medical community so afraid to tell it like it is? I might hurt your feelings, but I could save your life,” concluded the reader.
Defending change
One commentator, a hepatologist in France, defended the changes and responded to some of complaints.
“Maybe people who comment here should read the article, reflect, and understand the reasons why the old nomenclature and definition were scientifically inaccurate and needed to be changed,” the commentator wrote.
“It was an exclusionary, negative definition not recognizing the root of the disease (adipose tissue dysfunction with insulin resistance – instead defining it by what it is not ...) and not allowing the recognition of a large segment of the population [that] accumulates metabolic risk factors and moderate alcohol consumption. These patients were left out of all studies. Those were the main reasons for change and not the stigma part – with the word ‘fatty’ only being an issue in English-speaking countries, not elsewhere,” the commentator continued.
“Calls for change have been voiced for 20 years and a first comprehensive attempt (called MAFLD) was introduced 3 years ago (J Hepatol. 2020;73:202-9). Please, a little bit of respect and restraint in the comments recognizing the research efforts and publications for those that contributed to the field over the past 25 years ...” the hepatologist wrote.
The reader added, “Clinicians and researchers were dissatisfied for a long time, but it took years to gather overwhelming evidence demonstrating what causes the disease and then to kickstart a process under the auspices of several multinational scientific societies and come up with something consensually agreed upon by a large number of clinician researchers.
“Now you can tell your patient that he has metabolic liver disease instead of telling him that the problem at the root of his disease is that he is not drinking alcohol (nonalcoholic steatohepatitis). So, again, it is not so much about changing a name but about redefining diagnostic criteria and a nosological framework,” the reader wrote.
Other readers responded to the defender:
“This nomenclature issue has been churned for 20+ years? Well, the mountain has labored heavily, and given birth to a mouse,” one said.
“Still, how is this going to help in the clinical management? The whole gamut of conditions are evaluated and treated as a whole, not in isolation,” a general practitioner in India said. “If someone has a risk factor or not, continuous follow-up is required as a whole, whether it’s nonalcoholic or alcoholic, or whatever term is coined up.”
Finally, a family physician said, “It just rolls off the tongue, doesn’t it? But I have to admit, it’s the one place where ‘persons’ from 56 countries can get together and agree on something. Not even politicians can do that! Me, I’m sticking with NAFLD.”
A version of this article first appeared on Medscape.com.
Some clinicians say it’s “confusing” and “ridiculous” to change the name and diagnostic criteria of an established liver disease, while others bemoan the seemingly political reasons why it happened. Yet recently, 236 panelists from 56 countries decided that the terms nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH) rely on “exclusionary confounder terms and the use of potentially stigmatizing language.”
In a report published in Hepatology, the panelists, members of the NAFLD Nomenclature Consensus Group, determined that steatotic liver disease (SLD) would be used as an “overarching term to encompass the various etiologies of steatosis.”
Metabolic dysfunction–associated steatotic liver disease (MASLD) was chosen to replace NAFLD, and the definition was changed to include at least one of five cardiometabolic risk factors.
Metabolic dysfunction–associated steatohepatitis (MASH) replaces NASH.
Those with no metabolic parameters and no known cause will be diagnosed with cryptogenic SLD.
A new category, MetALD, now describes those with MASLD who drink more alcohol per week – 140-350 g for men and 210-420 g for women.
The changes did not sit well with this news organization’s readers from diverse specialties, including family practice, critical care, and gastroenterology.
In its report, the consensus group wrote that 74% of respondents to its rounds of surveys felt the current nomenclature “was sufficiently flawed to consider a name change.”
The terms “nonalcoholic” and “fatty” were felt to be stigmatizing by 61% and 66% of respondents, respectively, according to the group, a multi-stakeholder effort under the auspices of the American Association for Study of Liver Disease and the European Association for Study of the Liver, in collaboration with the Asociación Latinoamericana para el Estudio del Hígado.
Consensus was defined a priori as a supermajority (67%) vote.
“The new nomenclature and diagnostic criteria are widely supported, nonstigmatizing, and can improve awareness and patient identification,” the group concluded.
“No way” sums up many of the almost 60 reader comments received on this news organization’s story covering the change. Readers must share medical credentials to publicly comment on stories.
‘Confusing’ and ‘ridiculous’
A number of readers questioned how the changes will help practice.
“Once again, the specialists and other experts are changing the nomenclature to make the subject even more confusing for us primary care practitioners,” an HIV/AIDS physician wrote. “They obviously have no idea what [primary care practitioners] have to put up with day in and day out. All such revisions do is increase the cynicism and anger so many [primary care practitioners] have.”
Similarly, an internist said, “These new terms are going to confuse both doctors and patients. When you give a patient a diagnosis like this, they will not understand it, and will not be able to act as they should to correct it.”
“ ‘Fatty liver’ is a jargon-free diagnosis, easy to understand and easy for patients to know what they need to do,” the internist continued. “You think patients are gonna be educated when you tell them they have a ‘metabolic disease’? 100% they will not know what you’re talking about.”
Yet another wondered, “If SLD is the ‘umbrella’ term, why (are) MetALD and ALD not MetASLD and ASLD, respectively? Furthermore, efforts to ‘destigmatize’ terminology will inadvertently condemn cryptogenic SLD (CSLD) as the new ‘closet alcoholic.’ “
“Perhaps a subclassification, CSLD-HDIRDD (CSLD–Honest, Doc, I Really Don’t Drink),” the reader added.
“Everything about this is ridiculous,” a family physician wrote. “How long will it be until the experts change obesity to ‘gravitationally challenged’ as a diagnosis!”
“I was thinking of ‘circumferentially challenged,’” a reader in Canada chimed in. “But that would be ‘body shaming’ would it not?”
This reader continued, asking, “What about returning to the old practice of using Latin names patients don’t understand so there is no ‘shame’ attached to them? Or what about this revolutionary idea: To just say it as it is – fat?”
Acceding to ‘wokeness’
A sizable number of readers felt the name changes were motivated by a “woke” awareness.
“The effect of this new ‘woke’ clarity is ridiculous and simply not worth it! Can we justify the cost of this? Patients will have to learn all over again how to discuss their condition,” said one reader.
The reader continued, saying, “The Internet and social media freely use the term ‘fat’ – and despite not wanting to offend – there seems to be universal agreement that FAT, in certain conditions or places, is unhealthy and undesirable.
“Why is the medical community so afraid to tell it like it is? I might hurt your feelings, but I could save your life,” concluded the reader.
Defending change
One commentator, a hepatologist in France, defended the changes and responded to some of complaints.
“Maybe people who comment here should read the article, reflect, and understand the reasons why the old nomenclature and definition were scientifically inaccurate and needed to be changed,” the commentator wrote.
“It was an exclusionary, negative definition not recognizing the root of the disease (adipose tissue dysfunction with insulin resistance – instead defining it by what it is not ...) and not allowing the recognition of a large segment of the population [that] accumulates metabolic risk factors and moderate alcohol consumption. These patients were left out of all studies. Those were the main reasons for change and not the stigma part – with the word ‘fatty’ only being an issue in English-speaking countries, not elsewhere,” the commentator continued.
“Calls for change have been voiced for 20 years and a first comprehensive attempt (called MAFLD) was introduced 3 years ago (J Hepatol. 2020;73:202-9). Please, a little bit of respect and restraint in the comments recognizing the research efforts and publications for those that contributed to the field over the past 25 years ...” the hepatologist wrote.
The reader added, “Clinicians and researchers were dissatisfied for a long time, but it took years to gather overwhelming evidence demonstrating what causes the disease and then to kickstart a process under the auspices of several multinational scientific societies and come up with something consensually agreed upon by a large number of clinician researchers.
“Now you can tell your patient that he has metabolic liver disease instead of telling him that the problem at the root of his disease is that he is not drinking alcohol (nonalcoholic steatohepatitis). So, again, it is not so much about changing a name but about redefining diagnostic criteria and a nosological framework,” the reader wrote.
Other readers responded to the defender:
“This nomenclature issue has been churned for 20+ years? Well, the mountain has labored heavily, and given birth to a mouse,” one said.
“Still, how is this going to help in the clinical management? The whole gamut of conditions are evaluated and treated as a whole, not in isolation,” a general practitioner in India said. “If someone has a risk factor or not, continuous follow-up is required as a whole, whether it’s nonalcoholic or alcoholic, or whatever term is coined up.”
Finally, a family physician said, “It just rolls off the tongue, doesn’t it? But I have to admit, it’s the one place where ‘persons’ from 56 countries can get together and agree on something. Not even politicians can do that! Me, I’m sticking with NAFLD.”
A version of this article first appeared on Medscape.com.