HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
HM15 presenters: Verity Schaye, Michael Janjigian, Frank Volpicelli, Susan Hunt.
Performing a physical exam is the standard of care for evaluating patients. It has been shown to have higher diagnostic utility than many technology based tests. The physical exam is the Gold Standard for dermatological and mental status assessment for which technological tests are not readily available. The tradition “laying on of hands” has important benefits for the physician patient relationship.
The teaching of physical exam skills is increasingly problematic. Barriers include attending time, comfort and skill level as well as challenges of patient comfort and potential isolation issues.
The Peyton Model provides a better means of teaching physical exam skills than the traditional “See one, do one, teach one” model. The Peyton Model has four steps:
Demonstration. The teacher performs the exam at normal speed without commentary.
Deconstruction. The teacher performs the exam while describing the steps.
Comprehension. The teacher performs the exam while the learner describes the steps.
Performance. The learner performs the exam while also describing the steps.
This approach can be abbreviated for more advanced learners with the middle two steps being combined to a discussion between the teacher and learner to highlight any differences or changes in technique. TH
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
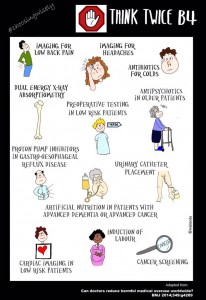
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
Question: Choose the single best answer to complete the statement, “A class-action lawsuit ...”
A. Is a legal cause of action for a wrongful act perpetrated by a class of wrongdoers.
B. Requires prior certification by a judge before it can go forward.
C. Is appropriate where the claims of a few injured victims can be joined together against a common wrongdoer.
D. Fulfills twin criteria of numerosity and commonality.
E. Can only be filed where there are substantial monetary damages at issue.
Answer: B. A class-action lawsuit describes a legal cause of action where a representative plaintiff(s), known as the lead plaintiff, asserts claims on behalf of a large class of similarly injured members, who then give up their rights to pursue an individual lawsuit. Class-action suits are distinguished from the usual lawsuit, which characteristically affects only one or a few plaintiffs.
Dr. Siang Yong Tan
Four prerequisites govern an action before it can be deemed a class action: numerosity, commonality, typicality, and adequacy. These are words of art, with specific definitions.
Numerosity denotes a large class membership, usually exceeding 30-40, and sometimes numbering in the thousands, such that the usual joining together of a few injured plaintiffs is not practical. Commonality speaks to common questions of fact and law, typicality requires the claim(s) of the representative plaintiff to match that of the class members, and adequacy demands that the representation of the class members be adequate.
These rules, as well as other important technicalities governing class action, are enumerated in the Federal Rules of Civil Procedure under Rule 23.12Wal-Mart Stores, Inc. v. Dukes et al., where Wal-Mart was alleged to have violated Title VII of the Civil Rights Act of 1964 by having disparate wages and promotion reflecting gender discrimination.3 The plaintiffs sought an injunction against the alleged practice, as well as monetary damages. An earlier ruling of the U.S. Court of Appeals for the Ninth Circuit gave the green light to this sprawling nationwide class action.
It had started out with Betty Dukes and five other women employees, but grew to more than 1.5 million female Wal-Mart employees. However, on appeal, the U.S. Supreme Court reversed, holding that the certification of the plaintiff class was not consistent with Rule 23(a), as the prerequisite of commonality was not fulfilled. The Supreme Court also disallowed the claim for monetary relief, as it was not incidental or secondary to the injunction sought.
Class-action suits are commonly encountered in mass torts, where a product or accident causes injury to numerous individuals. Other situations include environmental pollution, securities fraud, and improper employment practices.
A favorite target is in the health care industry, where manufacturers of drugs and medical devices face allegations that defective products have been allowed to enter the market, causing harm to end users.
An example is the silicon breast implant litigation of the 1990s. The Food and Drug Administration had placed breast implants in the category of medical products and learned that the Dow Corning Corporation, which manufactured the silicon implants, had withheld safety information. The FDA severely restricted the use of these implants, which predictably led to widespread litigation with billions of dollars of judgment awards and settlements.45 and the FDA subsequently required the revision of the package insert of Lipitor and other statins to warn of this association. In 2013, a large Canadian study confirmed the increased incidence of new-onset diabetes in patients taking atorvastatin (hazard ratio, 1.22) or simvastatin.6
However, the outcome of the trial may turn on whether the clear health benefit of lowering serum cholesterol outweighs any purported safety concern.
A fast-growing trend is the filing of class-action suits against nursing homes for providing inadequate care. This is not unexpected, because large numbers of nursing home residents have a common concern over any breach of safety, hygiene, or other statutorily mandated standards of nursing home care. This important topic will be taken up in a subsequent column.
4. Snyder JW. Silicon breast implants. Can emerging medical, legal and scientific concepts be reconciled? J. Leg. Med. 1997;18:133-220.
5. Sattar N, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet 2010;375:735-42.
6. Carter AC, et al. Risk of incident diabetes among patients treated with statins: population based study. BMJ 2013;346:f2610.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: Choose the single best answer to complete the statement, “A class-action lawsuit ...”
A. Is a legal cause of action for a wrongful act perpetrated by a class of wrongdoers.
B. Requires prior certification by a judge before it can go forward.
C. Is appropriate where the claims of a few injured victims can be joined together against a common wrongdoer.
D. Fulfills twin criteria of numerosity and commonality.
E. Can only be filed where there are substantial monetary damages at issue.
Answer: B. A class-action lawsuit describes a legal cause of action where a representative plaintiff(s), known as the lead plaintiff, asserts claims on behalf of a large class of similarly injured members, who then give up their rights to pursue an individual lawsuit. Class-action suits are distinguished from the usual lawsuit, which characteristically affects only one or a few plaintiffs.
Dr. Siang Yong Tan
Four prerequisites govern an action before it can be deemed a class action: numerosity, commonality, typicality, and adequacy. These are words of art, with specific definitions.
Numerosity denotes a large class membership, usually exceeding 30-40, and sometimes numbering in the thousands, such that the usual joining together of a few injured plaintiffs is not practical. Commonality speaks to common questions of fact and law, typicality requires the claim(s) of the representative plaintiff to match that of the class members, and adequacy demands that the representation of the class members be adequate.
These rules, as well as other important technicalities governing class action, are enumerated in the Federal Rules of Civil Procedure under Rule 23.12Wal-Mart Stores, Inc. v. Dukes et al., where Wal-Mart was alleged to have violated Title VII of the Civil Rights Act of 1964 by having disparate wages and promotion reflecting gender discrimination.3 The plaintiffs sought an injunction against the alleged practice, as well as monetary damages. An earlier ruling of the U.S. Court of Appeals for the Ninth Circuit gave the green light to this sprawling nationwide class action.
It had started out with Betty Dukes and five other women employees, but grew to more than 1.5 million female Wal-Mart employees. However, on appeal, the U.S. Supreme Court reversed, holding that the certification of the plaintiff class was not consistent with Rule 23(a), as the prerequisite of commonality was not fulfilled. The Supreme Court also disallowed the claim for monetary relief, as it was not incidental or secondary to the injunction sought.
Class-action suits are commonly encountered in mass torts, where a product or accident causes injury to numerous individuals. Other situations include environmental pollution, securities fraud, and improper employment practices.
A favorite target is in the health care industry, where manufacturers of drugs and medical devices face allegations that defective products have been allowed to enter the market, causing harm to end users.
An example is the silicon breast implant litigation of the 1990s. The Food and Drug Administration had placed breast implants in the category of medical products and learned that the Dow Corning Corporation, which manufactured the silicon implants, had withheld safety information. The FDA severely restricted the use of these implants, which predictably led to widespread litigation with billions of dollars of judgment awards and settlements.45 and the FDA subsequently required the revision of the package insert of Lipitor and other statins to warn of this association. In 2013, a large Canadian study confirmed the increased incidence of new-onset diabetes in patients taking atorvastatin (hazard ratio, 1.22) or simvastatin.6
However, the outcome of the trial may turn on whether the clear health benefit of lowering serum cholesterol outweighs any purported safety concern.
A fast-growing trend is the filing of class-action suits against nursing homes for providing inadequate care. This is not unexpected, because large numbers of nursing home residents have a common concern over any breach of safety, hygiene, or other statutorily mandated standards of nursing home care. This important topic will be taken up in a subsequent column.
4. Snyder JW. Silicon breast implants. Can emerging medical, legal and scientific concepts be reconciled? J. Leg. Med. 1997;18:133-220.
5. Sattar N, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet 2010;375:735-42.
6. Carter AC, et al. Risk of incident diabetes among patients treated with statins: population based study. BMJ 2013;346:f2610.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Question: Choose the single best answer to complete the statement, “A class-action lawsuit ...”
A. Is a legal cause of action for a wrongful act perpetrated by a class of wrongdoers.
B. Requires prior certification by a judge before it can go forward.
C. Is appropriate where the claims of a few injured victims can be joined together against a common wrongdoer.
D. Fulfills twin criteria of numerosity and commonality.
E. Can only be filed where there are substantial monetary damages at issue.
Answer: B. A class-action lawsuit describes a legal cause of action where a representative plaintiff(s), known as the lead plaintiff, asserts claims on behalf of a large class of similarly injured members, who then give up their rights to pursue an individual lawsuit. Class-action suits are distinguished from the usual lawsuit, which characteristically affects only one or a few plaintiffs.
Dr. Siang Yong Tan
Four prerequisites govern an action before it can be deemed a class action: numerosity, commonality, typicality, and adequacy. These are words of art, with specific definitions.
Numerosity denotes a large class membership, usually exceeding 30-40, and sometimes numbering in the thousands, such that the usual joining together of a few injured plaintiffs is not practical. Commonality speaks to common questions of fact and law, typicality requires the claim(s) of the representative plaintiff to match that of the class members, and adequacy demands that the representation of the class members be adequate.
These rules, as well as other important technicalities governing class action, are enumerated in the Federal Rules of Civil Procedure under Rule 23.12Wal-Mart Stores, Inc. v. Dukes et al., where Wal-Mart was alleged to have violated Title VII of the Civil Rights Act of 1964 by having disparate wages and promotion reflecting gender discrimination.3 The plaintiffs sought an injunction against the alleged practice, as well as monetary damages. An earlier ruling of the U.S. Court of Appeals for the Ninth Circuit gave the green light to this sprawling nationwide class action.
It had started out with Betty Dukes and five other women employees, but grew to more than 1.5 million female Wal-Mart employees. However, on appeal, the U.S. Supreme Court reversed, holding that the certification of the plaintiff class was not consistent with Rule 23(a), as the prerequisite of commonality was not fulfilled. The Supreme Court also disallowed the claim for monetary relief, as it was not incidental or secondary to the injunction sought.
Class-action suits are commonly encountered in mass torts, where a product or accident causes injury to numerous individuals. Other situations include environmental pollution, securities fraud, and improper employment practices.
A favorite target is in the health care industry, where manufacturers of drugs and medical devices face allegations that defective products have been allowed to enter the market, causing harm to end users.
An example is the silicon breast implant litigation of the 1990s. The Food and Drug Administration had placed breast implants in the category of medical products and learned that the Dow Corning Corporation, which manufactured the silicon implants, had withheld safety information. The FDA severely restricted the use of these implants, which predictably led to widespread litigation with billions of dollars of judgment awards and settlements.45 and the FDA subsequently required the revision of the package insert of Lipitor and other statins to warn of this association. In 2013, a large Canadian study confirmed the increased incidence of new-onset diabetes in patients taking atorvastatin (hazard ratio, 1.22) or simvastatin.6
However, the outcome of the trial may turn on whether the clear health benefit of lowering serum cholesterol outweighs any purported safety concern.
A fast-growing trend is the filing of class-action suits against nursing homes for providing inadequate care. This is not unexpected, because large numbers of nursing home residents have a common concern over any breach of safety, hygiene, or other statutorily mandated standards of nursing home care. This important topic will be taken up in a subsequent column.
4. Snyder JW. Silicon breast implants. Can emerging medical, legal and scientific concepts be reconciled? J. Leg. Med. 1997;18:133-220.
5. Sattar N, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet 2010;375:735-42.
6. Carter AC, et al. Risk of incident diabetes among patients treated with statins: population based study. BMJ 2013;346:f2610.
Dr. Tan is emeritus professor of medicine and former adjunct professor of law at the University of Hawaii, and currently directs the St. Francis International Center for Healthcare Ethics in Honolulu. This article is meant to be educational and does not constitute medical, ethical, or legal advice. Some of the articles in this series are adapted from the author’s 2006 book, “Medical Malpractice: Understanding the Law, Managing the Risk,” and his 2012 Halsbury treatise, “Medical Negligence and Professional Misconduct.” For additional information, readers may contact the author at [email protected].
Consider prescribing oral naltrexone (50 mg/d) for patients with alcohol use disorder who wish to maintain abstinence after a brief period of detoxification.1
Strength of recommendation
A: Based on a meta-analysis of 95 randomized controlled trials.
Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311:1889-1900.
Illustrative case
Your patient, a 42-year-old man with alcohol use disorder (AUD), detoxifies from alcohol during a recent hospitalization. He doesn’t want to resume drinking, but reports frequent cravings. Are there any medications you can prescribe to help prevent relapse?
Excessive alcohol consumption is responsible for 1 of every 10 deaths among US adults ages 20 to 64 years.2 Twenty percent to 36% of patients seen in a primary care office have AUD.3 Up to 70% of people who quit with psychosocial support alone will relapse.3
The US Preventive Services Task Force gives a grade B recommendation to screening all adults for AUD, indicating that physicians should provide this service.4 For patients with AUD who wish to abstain but struggle with cravings and relapse, the National Institute on Alcohol Abuse and Alcoholism (NIAAA) recommends considering medication as an adjunct to brief behavioral counseling.5
STUDY SUMMARY: Evidence shows naltrexone can prevent a return to drinking
In a meta-analysis, Jonas et al1 reviewed 123 studies (N=22,803) of pharmacotherapy for AUD. After excluding 28 studies (7 were the only study of a given drug, one was a prospective cohort, and 20 had insufficient data), 95 randomized control trials were included in the analysis. Twenty-two were placebo-controlled for acamprosate (1000-3000 mg/d), 44 for naltrexone (50 mg/d oral, 100 mg/d oral, or injectable) and 4 compared the 2 drugs. Additional studies evaluated disulfiram as well as 23 other off-label medications such as valproic acid and topiramate.
Two investigators independently reviewed the studies, checking for completeness and accuracy. Studies were also analyzed for bias using predefined criteria; those with high or unclear risk of bias were excluded from the main analysis but included in the sensitivity analysis. Funnel plots showed no evidence of publication bias.
Participants were primarily recruited as inpatients and in most studies the mean age was in the 40s. Most patients were diagnosed with alcohol dependence based on criteria in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV-TR); this diagnosis translates to likely moderate to severe AUD in DSM-5. Prior to starting medications, participants underwent detoxification or achieved at least 3 days of sobriety. Most studies included psychosocial intervention in addition to medication, but the types of interventions varied. The duration of the trials ranged from 12 to 52 weeks.
Researchers analyzed 5 drinking outcomes—return to any drinking, return to heavy drinking (defined as ≥4 drinks/d for women and ≥5 drinks/d for men), number of drinking days, number of heavy drinking days, and drinks per drinking day. They also evaluated health outcomes (accidents, injuries, quality of life, function, and mortality) and adverse effects.
Acamprosate and oral naltrexone (50 mg/d) significantly decreased return to any drinking, with a number needed to treat (NNT) of 12 (95% confidence interval [CI], 8-26) for acamprosate and 20 (95% CI, 11-500) for naltrexone. Oral naltrexone (50 mg/d) also decreased return to heavy drinking (NNT=12; 95% CI, 8-26), while acamprosate did not. Neither medication showed a decrease in heavy drinking days. In a post hoc subgroup analysis of acamprosate for return to any drinking, the drug appeared to be more effective in studies with a higher risk of bias and less effective in studies with a lower risk of bias; the 2 studies with the lowest risk of bias found no significant effect.
Disulfiram had no effect on any of the drinking outcomes analyzed.
Of the off-label medications, topiramate showed a decrease in drinking days (weighted mean difference [WMD]=-6.5%; 95% CI, -12.0% to -1.0%), heavy drinking days (WMD=-9.0%; 95% CI, -15.3% to -2.7%), and drinks per drinking day (WMD=-1.0; 95% CI, -1.6 to -0.48).
Oral naltrexone 50 mg/d significantly decreased the number of patients who resumed drinking after detoxification.
There were no significant differences in health outcomes for any of the medications. Adverse events were greater in treatment groups than placebo groups. Acamprosate was associated with increased risk of diarrhea (number needed to harm [NNH]=11; 95% CI, 6-34), vomiting (NNH=42; 95% CI, 24-143), and anxiety (NNH=7; 95% CI, 5-11). Naltrexone was associated with increased risk of nausea (NNH=9; 95% CI, 7-14), vomiting (NNH=24; 95% CI, 17-44), and dizziness (NNH 16; 95% CI, 12-28).
WHAT'S NEW: Consider prescribing naltrexone to prevent relapse
While previous studies suggested that pharmacotherapy could help patients with AUD remain abstinent, this methodologically rigorous meta-analysis compared the efficacy of several commonly used medications and found clear evidence favoring oral naltrexone. Prescribe oral naltrexone 50 mg/d to help patients with moderate to severe AUD avoid returning to any drinking or heavy drinking after alcohol detoxification. Acamprosate may also decrease return to drinking, although the evidence is not as strong (the studies with low bias showed no effect).
CAVEATS: Medication should be used with psychosocial treatments
Pharmacotherapy for AUD should be reserved for patients who want to quit drinking and used in conjunction with psychosocial intervention.3 Only one of the studies analyzed by Jonas et al1 was conducted in primary care. That said, many of the psychosocial interventions—such as regular follow-up visits to encourage adherence and monitor for adverse effects, in conjunction with attendance at Alcoholics Anonymous meetings—could be done in primary care settings.
Comorbidities may limit therapy options. Naltrexone is contraindicated in acute hepatitis and liver failure, and in combination with opioids.5 Acamprosate is contraindicated in renal disease.5
CHALLENGES TO IMPLEMENTATION: Cost, adherence may be factors for some patients
Perhaps the greatest hurdle in pharmacotherapy for AUD in primary care is a lack of familiarity with these medications. For physicians who are comfortable with prescribing these medications, implementation may be hindered by a lack of available psychosocial resources for successful abstinence.
Medications for alcohol use disorder should be reserved for patients who want to quit drinking, and should be combined with psychosocial interventions.
Additionally, the medications are expensive. The branded version of naltrexone 50 mg costs approximately $118 for a 30-day supply,6 and the branded version of acamprosate costs approximately $284 for a 30-day supply.7
As is the case with any chronic medical condition, medication adherence is a challenge. Naltrexone is taken once daily, while acamprosate is taken 3 times a day. The risk of relapse is high until 6 to 12 months of sobriety and then wanes over several years.5 The NIAAA recommends treatment for a minimum of 3 months.5
ACKNOWLEDGEMENT The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311:1889-1900.
2. Centers for Disease Control and Prevention. Fact sheets - Alcohol use and your health. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/alcohol/fact-sheets/alcohol-use.htm. Updated November 7, 2014. Accessed January 6, 2015.
5. US Department of Health and Human Services; National Institutes of Health; National Institute on Alcohol Abuse and Alcoholism. Excerpt from Helping Patients Who Drink Too Much: A Clinician’s Guide. National Institute on Alcohol Abuse and Alcoholism Web site. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/PrescribingMeds.pdf. Updated October 2008. Accessed January 6, 2015.
6. Drugs.com. Revia prices, coupons and patient assistance programs. Drugs.com Web site. Available at: http://www.drugs.com/price-guide/revia. Accessed February 18, 2015.
7. Drugs.com. Campral prices, coupons and patient assistance programs. Drugs.com Web site. Available at: http://www.drugs.com/price-guide/campral. Accessed February 18, 2015.
Sydney Hendry, MD; Anne Mounsey, MD; naltrexone; AUD; alcohol use disorder; naltrexone; National Institute on Alcohol Abuse and Alcoholism; NIAAA; acamprosate; addiction
Consider prescribing oral naltrexone (50 mg/d) for patients with alcohol use disorder who wish to maintain abstinence after a brief period of detoxification.1
Strength of recommendation
A: Based on a meta-analysis of 95 randomized controlled trials.
Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311:1889-1900.
Illustrative case
Your patient, a 42-year-old man with alcohol use disorder (AUD), detoxifies from alcohol during a recent hospitalization. He doesn’t want to resume drinking, but reports frequent cravings. Are there any medications you can prescribe to help prevent relapse?
Excessive alcohol consumption is responsible for 1 of every 10 deaths among US adults ages 20 to 64 years.2 Twenty percent to 36% of patients seen in a primary care office have AUD.3 Up to 70% of people who quit with psychosocial support alone will relapse.3
The US Preventive Services Task Force gives a grade B recommendation to screening all adults for AUD, indicating that physicians should provide this service.4 For patients with AUD who wish to abstain but struggle with cravings and relapse, the National Institute on Alcohol Abuse and Alcoholism (NIAAA) recommends considering medication as an adjunct to brief behavioral counseling.5
STUDY SUMMARY: Evidence shows naltrexone can prevent a return to drinking
In a meta-analysis, Jonas et al1 reviewed 123 studies (N=22,803) of pharmacotherapy for AUD. After excluding 28 studies (7 were the only study of a given drug, one was a prospective cohort, and 20 had insufficient data), 95 randomized control trials were included in the analysis. Twenty-two were placebo-controlled for acamprosate (1000-3000 mg/d), 44 for naltrexone (50 mg/d oral, 100 mg/d oral, or injectable) and 4 compared the 2 drugs. Additional studies evaluated disulfiram as well as 23 other off-label medications such as valproic acid and topiramate.
Two investigators independently reviewed the studies, checking for completeness and accuracy. Studies were also analyzed for bias using predefined criteria; those with high or unclear risk of bias were excluded from the main analysis but included in the sensitivity analysis. Funnel plots showed no evidence of publication bias.
Participants were primarily recruited as inpatients and in most studies the mean age was in the 40s. Most patients were diagnosed with alcohol dependence based on criteria in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV-TR); this diagnosis translates to likely moderate to severe AUD in DSM-5. Prior to starting medications, participants underwent detoxification or achieved at least 3 days of sobriety. Most studies included psychosocial intervention in addition to medication, but the types of interventions varied. The duration of the trials ranged from 12 to 52 weeks.
Researchers analyzed 5 drinking outcomes—return to any drinking, return to heavy drinking (defined as ≥4 drinks/d for women and ≥5 drinks/d for men), number of drinking days, number of heavy drinking days, and drinks per drinking day. They also evaluated health outcomes (accidents, injuries, quality of life, function, and mortality) and adverse effects.
Acamprosate and oral naltrexone (50 mg/d) significantly decreased return to any drinking, with a number needed to treat (NNT) of 12 (95% confidence interval [CI], 8-26) for acamprosate and 20 (95% CI, 11-500) for naltrexone. Oral naltrexone (50 mg/d) also decreased return to heavy drinking (NNT=12; 95% CI, 8-26), while acamprosate did not. Neither medication showed a decrease in heavy drinking days. In a post hoc subgroup analysis of acamprosate for return to any drinking, the drug appeared to be more effective in studies with a higher risk of bias and less effective in studies with a lower risk of bias; the 2 studies with the lowest risk of bias found no significant effect.
Disulfiram had no effect on any of the drinking outcomes analyzed.
Of the off-label medications, topiramate showed a decrease in drinking days (weighted mean difference [WMD]=-6.5%; 95% CI, -12.0% to -1.0%), heavy drinking days (WMD=-9.0%; 95% CI, -15.3% to -2.7%), and drinks per drinking day (WMD=-1.0; 95% CI, -1.6 to -0.48).
Oral naltrexone 50 mg/d significantly decreased the number of patients who resumed drinking after detoxification.
There were no significant differences in health outcomes for any of the medications. Adverse events were greater in treatment groups than placebo groups. Acamprosate was associated with increased risk of diarrhea (number needed to harm [NNH]=11; 95% CI, 6-34), vomiting (NNH=42; 95% CI, 24-143), and anxiety (NNH=7; 95% CI, 5-11). Naltrexone was associated with increased risk of nausea (NNH=9; 95% CI, 7-14), vomiting (NNH=24; 95% CI, 17-44), and dizziness (NNH 16; 95% CI, 12-28).
WHAT'S NEW: Consider prescribing naltrexone to prevent relapse
While previous studies suggested that pharmacotherapy could help patients with AUD remain abstinent, this methodologically rigorous meta-analysis compared the efficacy of several commonly used medications and found clear evidence favoring oral naltrexone. Prescribe oral naltrexone 50 mg/d to help patients with moderate to severe AUD avoid returning to any drinking or heavy drinking after alcohol detoxification. Acamprosate may also decrease return to drinking, although the evidence is not as strong (the studies with low bias showed no effect).
CAVEATS: Medication should be used with psychosocial treatments
Pharmacotherapy for AUD should be reserved for patients who want to quit drinking and used in conjunction with psychosocial intervention.3 Only one of the studies analyzed by Jonas et al1 was conducted in primary care. That said, many of the psychosocial interventions—such as regular follow-up visits to encourage adherence and monitor for adverse effects, in conjunction with attendance at Alcoholics Anonymous meetings—could be done in primary care settings.
Comorbidities may limit therapy options. Naltrexone is contraindicated in acute hepatitis and liver failure, and in combination with opioids.5 Acamprosate is contraindicated in renal disease.5
CHALLENGES TO IMPLEMENTATION: Cost, adherence may be factors for some patients
Perhaps the greatest hurdle in pharmacotherapy for AUD in primary care is a lack of familiarity with these medications. For physicians who are comfortable with prescribing these medications, implementation may be hindered by a lack of available psychosocial resources for successful abstinence.
Medications for alcohol use disorder should be reserved for patients who want to quit drinking, and should be combined with psychosocial interventions.
Additionally, the medications are expensive. The branded version of naltrexone 50 mg costs approximately $118 for a 30-day supply,6 and the branded version of acamprosate costs approximately $284 for a 30-day supply.7
As is the case with any chronic medical condition, medication adherence is a challenge. Naltrexone is taken once daily, while acamprosate is taken 3 times a day. The risk of relapse is high until 6 to 12 months of sobriety and then wanes over several years.5 The NIAAA recommends treatment for a minimum of 3 months.5
ACKNOWLEDGEMENT The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
PRACTICE CHANGER
Consider prescribing oral naltrexone (50 mg/d) for patients with alcohol use disorder who wish to maintain abstinence after a brief period of detoxification.1
Strength of recommendation
A: Based on a meta-analysis of 95 randomized controlled trials.
Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311:1889-1900.
Illustrative case
Your patient, a 42-year-old man with alcohol use disorder (AUD), detoxifies from alcohol during a recent hospitalization. He doesn’t want to resume drinking, but reports frequent cravings. Are there any medications you can prescribe to help prevent relapse?
Excessive alcohol consumption is responsible for 1 of every 10 deaths among US adults ages 20 to 64 years.2 Twenty percent to 36% of patients seen in a primary care office have AUD.3 Up to 70% of people who quit with psychosocial support alone will relapse.3
The US Preventive Services Task Force gives a grade B recommendation to screening all adults for AUD, indicating that physicians should provide this service.4 For patients with AUD who wish to abstain but struggle with cravings and relapse, the National Institute on Alcohol Abuse and Alcoholism (NIAAA) recommends considering medication as an adjunct to brief behavioral counseling.5
STUDY SUMMARY: Evidence shows naltrexone can prevent a return to drinking
In a meta-analysis, Jonas et al1 reviewed 123 studies (N=22,803) of pharmacotherapy for AUD. After excluding 28 studies (7 were the only study of a given drug, one was a prospective cohort, and 20 had insufficient data), 95 randomized control trials were included in the analysis. Twenty-two were placebo-controlled for acamprosate (1000-3000 mg/d), 44 for naltrexone (50 mg/d oral, 100 mg/d oral, or injectable) and 4 compared the 2 drugs. Additional studies evaluated disulfiram as well as 23 other off-label medications such as valproic acid and topiramate.
Two investigators independently reviewed the studies, checking for completeness and accuracy. Studies were also analyzed for bias using predefined criteria; those with high or unclear risk of bias were excluded from the main analysis but included in the sensitivity analysis. Funnel plots showed no evidence of publication bias.
Participants were primarily recruited as inpatients and in most studies the mean age was in the 40s. Most patients were diagnosed with alcohol dependence based on criteria in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV-TR); this diagnosis translates to likely moderate to severe AUD in DSM-5. Prior to starting medications, participants underwent detoxification or achieved at least 3 days of sobriety. Most studies included psychosocial intervention in addition to medication, but the types of interventions varied. The duration of the trials ranged from 12 to 52 weeks.
Researchers analyzed 5 drinking outcomes—return to any drinking, return to heavy drinking (defined as ≥4 drinks/d for women and ≥5 drinks/d for men), number of drinking days, number of heavy drinking days, and drinks per drinking day. They also evaluated health outcomes (accidents, injuries, quality of life, function, and mortality) and adverse effects.
Acamprosate and oral naltrexone (50 mg/d) significantly decreased return to any drinking, with a number needed to treat (NNT) of 12 (95% confidence interval [CI], 8-26) for acamprosate and 20 (95% CI, 11-500) for naltrexone. Oral naltrexone (50 mg/d) also decreased return to heavy drinking (NNT=12; 95% CI, 8-26), while acamprosate did not. Neither medication showed a decrease in heavy drinking days. In a post hoc subgroup analysis of acamprosate for return to any drinking, the drug appeared to be more effective in studies with a higher risk of bias and less effective in studies with a lower risk of bias; the 2 studies with the lowest risk of bias found no significant effect.
Disulfiram had no effect on any of the drinking outcomes analyzed.
Of the off-label medications, topiramate showed a decrease in drinking days (weighted mean difference [WMD]=-6.5%; 95% CI, -12.0% to -1.0%), heavy drinking days (WMD=-9.0%; 95% CI, -15.3% to -2.7%), and drinks per drinking day (WMD=-1.0; 95% CI, -1.6 to -0.48).
Oral naltrexone 50 mg/d significantly decreased the number of patients who resumed drinking after detoxification.
There were no significant differences in health outcomes for any of the medications. Adverse events were greater in treatment groups than placebo groups. Acamprosate was associated with increased risk of diarrhea (number needed to harm [NNH]=11; 95% CI, 6-34), vomiting (NNH=42; 95% CI, 24-143), and anxiety (NNH=7; 95% CI, 5-11). Naltrexone was associated with increased risk of nausea (NNH=9; 95% CI, 7-14), vomiting (NNH=24; 95% CI, 17-44), and dizziness (NNH 16; 95% CI, 12-28).
WHAT'S NEW: Consider prescribing naltrexone to prevent relapse
While previous studies suggested that pharmacotherapy could help patients with AUD remain abstinent, this methodologically rigorous meta-analysis compared the efficacy of several commonly used medications and found clear evidence favoring oral naltrexone. Prescribe oral naltrexone 50 mg/d to help patients with moderate to severe AUD avoid returning to any drinking or heavy drinking after alcohol detoxification. Acamprosate may also decrease return to drinking, although the evidence is not as strong (the studies with low bias showed no effect).
CAVEATS: Medication should be used with psychosocial treatments
Pharmacotherapy for AUD should be reserved for patients who want to quit drinking and used in conjunction with psychosocial intervention.3 Only one of the studies analyzed by Jonas et al1 was conducted in primary care. That said, many of the psychosocial interventions—such as regular follow-up visits to encourage adherence and monitor for adverse effects, in conjunction with attendance at Alcoholics Anonymous meetings—could be done in primary care settings.
Comorbidities may limit therapy options. Naltrexone is contraindicated in acute hepatitis and liver failure, and in combination with opioids.5 Acamprosate is contraindicated in renal disease.5
CHALLENGES TO IMPLEMENTATION: Cost, adherence may be factors for some patients
Perhaps the greatest hurdle in pharmacotherapy for AUD in primary care is a lack of familiarity with these medications. For physicians who are comfortable with prescribing these medications, implementation may be hindered by a lack of available psychosocial resources for successful abstinence.
Medications for alcohol use disorder should be reserved for patients who want to quit drinking, and should be combined with psychosocial interventions.
Additionally, the medications are expensive. The branded version of naltrexone 50 mg costs approximately $118 for a 30-day supply,6 and the branded version of acamprosate costs approximately $284 for a 30-day supply.7
As is the case with any chronic medical condition, medication adherence is a challenge. Naltrexone is taken once daily, while acamprosate is taken 3 times a day. The risk of relapse is high until 6 to 12 months of sobriety and then wanes over several years.5 The NIAAA recommends treatment for a minimum of 3 months.5
ACKNOWLEDGEMENT The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
References
1. Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311:1889-1900.
2. Centers for Disease Control and Prevention. Fact sheets - Alcohol use and your health. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/alcohol/fact-sheets/alcohol-use.htm. Updated November 7, 2014. Accessed January 6, 2015.
5. US Department of Health and Human Services; National Institutes of Health; National Institute on Alcohol Abuse and Alcoholism. Excerpt from Helping Patients Who Drink Too Much: A Clinician’s Guide. National Institute on Alcohol Abuse and Alcoholism Web site. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/PrescribingMeds.pdf. Updated October 2008. Accessed January 6, 2015.
6. Drugs.com. Revia prices, coupons and patient assistance programs. Drugs.com Web site. Available at: http://www.drugs.com/price-guide/revia. Accessed February 18, 2015.
7. Drugs.com. Campral prices, coupons and patient assistance programs. Drugs.com Web site. Available at: http://www.drugs.com/price-guide/campral. Accessed February 18, 2015.
References
1. Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311:1889-1900.
2. Centers for Disease Control and Prevention. Fact sheets - Alcohol use and your health. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/alcohol/fact-sheets/alcohol-use.htm. Updated November 7, 2014. Accessed January 6, 2015.
5. US Department of Health and Human Services; National Institutes of Health; National Institute on Alcohol Abuse and Alcoholism. Excerpt from Helping Patients Who Drink Too Much: A Clinician’s Guide. National Institute on Alcohol Abuse and Alcoholism Web site. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/PrescribingMeds.pdf. Updated October 2008. Accessed January 6, 2015.
6. Drugs.com. Revia prices, coupons and patient assistance programs. Drugs.com Web site. Available at: http://www.drugs.com/price-guide/revia. Accessed February 18, 2015.
7. Drugs.com. Campral prices, coupons and patient assistance programs. Drugs.com Web site. Available at: http://www.drugs.com/price-guide/campral. Accessed February 18, 2015.
Consider these medications to help patients stay sober
Display Headline
Consider these medications to help patients stay sober
Legacy Keywords
Sydney Hendry, MD; Anne Mounsey, MD; naltrexone; AUD; alcohol use disorder; naltrexone; National Institute on Alcohol Abuse and Alcoholism; NIAAA; acamprosate; addiction
Legacy Keywords
Sydney Hendry, MD; Anne Mounsey, MD; naltrexone; AUD; alcohol use disorder; naltrexone; National Institute on Alcohol Abuse and Alcoholism; NIAAA; acamprosate; addiction
Failure to recognize impending MI has tragic consequences
A 55-YEAR-OLD WOMAN WENT TO HER MEDICAL CLINIC because she had heartburn and bilateral arm pain with numbness and tingling in her forearms. She said she’d had intermittent arm pain over the previous 7 to 10 days. A physician’s assistant diagnosed gastroesophageal reflux disease, gave the patient an antacid medication, and instructed her to return in 2 to 3 weeks. The patient came back to the clinic 10 days later with increased heartburn and continued arm pain with tingling. Because no clinicians were available to see her at that time, a prescription for ranitidine was called in and the patient was sent home. That evening, the patient died of a myocardial infarction (MI).
PLAINTIFF’S CLAIM There were specific, objective signs of an impending MI that were not recognized.
The patient should have been seen by a medical provider on the day of her death or referred to an emergency department.
THE DEFENSE No information about the defense is available.
VERDICT $275,000 California settlement.
COMMENTThere was clearly an opportunity to make the correct diagnosis for this woman, especially when she returned a second time. The one lesson I have learned from reviewing malpractice cases for 15 years is that if a patient returns unimproved, you must up the ante with the evaluation. Start all over again and think through the entire history very carefully; you are likely to find a clue to the correct diagnosis.
Pulmonary embolism mistaken for respiratory infection
A 40-YEAR-OLD MAN SOUGHT TREATMENT FOR SYMPTOMS OF A COLD. He also complained of shortness of breath, dizziness, and pain in his left calf. His family physician (FP) treated him for a respiratory infection. Three days later, the patient returned to the office with continued shortness of breath. The FP scheduled a cardiac work-up. Two days before the work-up, the patient died from a pulmonary embolism (PE).
PLAINTIFF'S CLAIM No information about the plaintiff’s claim is available.
If a patient returns unimproved, start the evaluation over again and think through the entire history; you’ll likely find a clue to the correct diagnosis.
THE DEFENSE No information about the defense is available.
VERDICT $1.1 million Virginia settlement.
COMMENTPE has clearly unseated syphilis as “The Great Masquerader.” We cannot tell from this short synopsis how significant the patient’s calf pain was and whether or not there were any physical findings of deep vein thrombosis. However, when the patient returned 3 days later with increasing shortness of breath, PE should have been toward the top of the differential diagnosis.
Back spasms—or something far more serious?
A 47-YEAR-OLD WOMAN WENT TO THE EMERGENCY DEPARTMENT (ED) seeking treatment for severe back and abdominal pain. The patient had previously undergone gastric bypass surgery. The ED physician diagnosed back spasms, but admitted her to the hospital for observation. The next day, the patient died from a bowel obstruction.
PLAINTIFF'S CLAIM The ED physician failed to order testing and consult with a specialist to diagnose bowel obstruction, which is a known complication of gastric bypass surgery.
THE DEFENSE No information about the defense is available.
VERDICT $2.4 million Illinois verdict.
COMMENTBowel obstruction with back pain only? And dead the next day from bowel obstruction? I can only presume the history was inadequate, which led to a failure to do an abdominal exam.
Failure to recognize impending MI has tragic consequences
A 55-YEAR-OLD WOMAN WENT TO HER MEDICAL CLINIC because she had heartburn and bilateral arm pain with numbness and tingling in her forearms. She said she’d had intermittent arm pain over the previous 7 to 10 days. A physician’s assistant diagnosed gastroesophageal reflux disease, gave the patient an antacid medication, and instructed her to return in 2 to 3 weeks. The patient came back to the clinic 10 days later with increased heartburn and continued arm pain with tingling. Because no clinicians were available to see her at that time, a prescription for ranitidine was called in and the patient was sent home. That evening, the patient died of a myocardial infarction (MI).
PLAINTIFF’S CLAIM There were specific, objective signs of an impending MI that were not recognized.
The patient should have been seen by a medical provider on the day of her death or referred to an emergency department.
THE DEFENSE No information about the defense is available.
VERDICT $275,000 California settlement.
COMMENTThere was clearly an opportunity to make the correct diagnosis for this woman, especially when she returned a second time. The one lesson I have learned from reviewing malpractice cases for 15 years is that if a patient returns unimproved, you must up the ante with the evaluation. Start all over again and think through the entire history very carefully; you are likely to find a clue to the correct diagnosis.
Pulmonary embolism mistaken for respiratory infection
A 40-YEAR-OLD MAN SOUGHT TREATMENT FOR SYMPTOMS OF A COLD. He also complained of shortness of breath, dizziness, and pain in his left calf. His family physician (FP) treated him for a respiratory infection. Three days later, the patient returned to the office with continued shortness of breath. The FP scheduled a cardiac work-up. Two days before the work-up, the patient died from a pulmonary embolism (PE).
PLAINTIFF'S CLAIM No information about the plaintiff’s claim is available.
If a patient returns unimproved, start the evaluation over again and think through the entire history; you’ll likely find a clue to the correct diagnosis.
THE DEFENSE No information about the defense is available.
VERDICT $1.1 million Virginia settlement.
COMMENTPE has clearly unseated syphilis as “The Great Masquerader.” We cannot tell from this short synopsis how significant the patient’s calf pain was and whether or not there were any physical findings of deep vein thrombosis. However, when the patient returned 3 days later with increasing shortness of breath, PE should have been toward the top of the differential diagnosis.
Back spasms—or something far more serious?
A 47-YEAR-OLD WOMAN WENT TO THE EMERGENCY DEPARTMENT (ED) seeking treatment for severe back and abdominal pain. The patient had previously undergone gastric bypass surgery. The ED physician diagnosed back spasms, but admitted her to the hospital for observation. The next day, the patient died from a bowel obstruction.
PLAINTIFF'S CLAIM The ED physician failed to order testing and consult with a specialist to diagnose bowel obstruction, which is a known complication of gastric bypass surgery.
THE DEFENSE No information about the defense is available.
VERDICT $2.4 million Illinois verdict.
COMMENTBowel obstruction with back pain only? And dead the next day from bowel obstruction? I can only presume the history was inadequate, which led to a failure to do an abdominal exam.
Failure to recognize impending MI has tragic consequences
A 55-YEAR-OLD WOMAN WENT TO HER MEDICAL CLINIC because she had heartburn and bilateral arm pain with numbness and tingling in her forearms. She said she’d had intermittent arm pain over the previous 7 to 10 days. A physician’s assistant diagnosed gastroesophageal reflux disease, gave the patient an antacid medication, and instructed her to return in 2 to 3 weeks. The patient came back to the clinic 10 days later with increased heartburn and continued arm pain with tingling. Because no clinicians were available to see her at that time, a prescription for ranitidine was called in and the patient was sent home. That evening, the patient died of a myocardial infarction (MI).
PLAINTIFF’S CLAIM There were specific, objective signs of an impending MI that were not recognized.
The patient should have been seen by a medical provider on the day of her death or referred to an emergency department.
THE DEFENSE No information about the defense is available.
VERDICT $275,000 California settlement.
COMMENTThere was clearly an opportunity to make the correct diagnosis for this woman, especially when she returned a second time. The one lesson I have learned from reviewing malpractice cases for 15 years is that if a patient returns unimproved, you must up the ante with the evaluation. Start all over again and think through the entire history very carefully; you are likely to find a clue to the correct diagnosis.
Pulmonary embolism mistaken for respiratory infection
A 40-YEAR-OLD MAN SOUGHT TREATMENT FOR SYMPTOMS OF A COLD. He also complained of shortness of breath, dizziness, and pain in his left calf. His family physician (FP) treated him for a respiratory infection. Three days later, the patient returned to the office with continued shortness of breath. The FP scheduled a cardiac work-up. Two days before the work-up, the patient died from a pulmonary embolism (PE).
PLAINTIFF'S CLAIM No information about the plaintiff’s claim is available.
If a patient returns unimproved, start the evaluation over again and think through the entire history; you’ll likely find a clue to the correct diagnosis.
THE DEFENSE No information about the defense is available.
VERDICT $1.1 million Virginia settlement.
COMMENTPE has clearly unseated syphilis as “The Great Masquerader.” We cannot tell from this short synopsis how significant the patient’s calf pain was and whether or not there were any physical findings of deep vein thrombosis. However, when the patient returned 3 days later with increasing shortness of breath, PE should have been toward the top of the differential diagnosis.
Back spasms—or something far more serious?
A 47-YEAR-OLD WOMAN WENT TO THE EMERGENCY DEPARTMENT (ED) seeking treatment for severe back and abdominal pain. The patient had previously undergone gastric bypass surgery. The ED physician diagnosed back spasms, but admitted her to the hospital for observation. The next day, the patient died from a bowel obstruction.
PLAINTIFF'S CLAIM The ED physician failed to order testing and consult with a specialist to diagnose bowel obstruction, which is a known complication of gastric bypass surgery.
THE DEFENSE No information about the defense is available.
VERDICT $2.4 million Illinois verdict.
COMMENTBowel obstruction with back pain only? And dead the next day from bowel obstruction? I can only presume the history was inadequate, which led to a failure to do an abdominal exam.
SAN FRANCISCO – What role does nanotechnology play in photoprotection? How is the current regulatory climate helping and hurting innovation and product development? What are the real and perceived safety issues? These and other questions were addressed in a roundtable discussion hosted by the Nanodermatology Society at the annual meeting of the American Academy of Dermatology. Participants included dermatology practitioners and researchers, along with representatives of industry and the media.
“We have good data on a lot of the filters that are out there,” emphasized Dr. Adnan Nasir, president of the Nanodermatology Society and moderator of the roundtable.
Given the epidemic of skin cancer in the United States, “I hope that we can target our message as a public health message” and increase the confidence of physicians in discussing photoprotection and the confidence of patients in their doctors’ opinions on this important topic, Dr. Nasir said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN FRANCISCO – What role does nanotechnology play in photoprotection? How is the current regulatory climate helping and hurting innovation and product development? What are the real and perceived safety issues? These and other questions were addressed in a roundtable discussion hosted by the Nanodermatology Society at the annual meeting of the American Academy of Dermatology. Participants included dermatology practitioners and researchers, along with representatives of industry and the media.
“We have good data on a lot of the filters that are out there,” emphasized Dr. Adnan Nasir, president of the Nanodermatology Society and moderator of the roundtable.
Given the epidemic of skin cancer in the United States, “I hope that we can target our message as a public health message” and increase the confidence of physicians in discussing photoprotection and the confidence of patients in their doctors’ opinions on this important topic, Dr. Nasir said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN FRANCISCO – What role does nanotechnology play in photoprotection? How is the current regulatory climate helping and hurting innovation and product development? What are the real and perceived safety issues? These and other questions were addressed in a roundtable discussion hosted by the Nanodermatology Society at the annual meeting of the American Academy of Dermatology. Participants included dermatology practitioners and researchers, along with representatives of industry and the media.
“We have good data on a lot of the filters that are out there,” emphasized Dr. Adnan Nasir, president of the Nanodermatology Society and moderator of the roundtable.
Given the epidemic of skin cancer in the United States, “I hope that we can target our message as a public health message” and increase the confidence of physicians in discussing photoprotection and the confidence of patients in their doctors’ opinions on this important topic, Dr. Nasir said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
A 21-year-old college student was referred to us by the counseling center at our university for a psychiatric evaluation after 11 psychotherapy sessions over 3 months had failed to reduce her feelings of anxiety and panic.
During our evaluation, the patient described feeling “not quite right” for many months. She had been experiencing mental fogginess, fatigue, and worsening concentration/ memory. Her anxiety, which had been gradually increasing, was the result of being unsure about her gait. She first noticed this while walking down some bleachers; she felt dizzy, was afraid of falling, and couldn’t walk down without assistance. All episodes of “panic” occurred in situations where she experienced disequilibrium, unsteady gait, and fear of falling. She grew fearful of driving or going anywhere without assistance.
The patient had celiac disease that was well controlled with a gluten-free diet. She had no personal or family psychiatric history and no history of substance abuse.
THE DIAGNOSIS
Physical exam and lab studies, including a complete blood count, comprehensive metabolic panel, and thyrotropin and folate levels, were normal. Her homocysteine level was 11.8 μmol/L (reference range, 5.4-11.9 μmol/L) and vitamin B12 level was 292 pg/mL (reference range, 200-1100 pg/mL). Her lab report included a note that read, “Although the reference range for vitamin B12 is 200 to 1100 pg/mL, it has been reported that between 5% and 10% of patients with values between 200 and 400 pg/mL may experience neuropsychiatric and hematologic abnormalities due to occult B12 deficiency; <1% of patients with values >400 pg/mL will have symptoms.”
Based on this vitamin B12 level, the patient’s symptoms, and her borderline high homocysteine level, we diagnosed vitamin B12 deficiency.
DISCUSSION
There are no recommendations by the US Preventive Services Task Force or any other major US medical society for routine vitamin B12 screening.1 In Canada, the Medical Services Commission of the British Columbia Ministry of Health recommends B12 screening for patients who present with macrocytic anemia or unexplained neurologic symptoms (eg, paresthesia, numbness, poor motor coordination, memory lapses, or cognitive or personality changes).2
Vitamin B12 deficiency can be caused by numerous conditions, including those that cause malabsorption (such as gastric bypass). It can also be caused by diseases such as human immunodeficiency virus infection or Crohn’s disease, long-term adherence to a vegetarian or vegan diet, or by any other lack of dietary intake.1 The condition can cause hematologic-related signs and symptoms such as megaloblastic anemia, fatigue, and syncope. It also can have neurologic manifestations, including paresthesia, weakness, motor disturbances (including gait abnormalities), vision loss, and a wide range of cognitive and behavioral changes.1 Anemia is uncommon because since 1998, the US Food and Drug Administration has required fortification of all enriched grain and cereal products with folic acid; thus, vitamin B12 deficiency may proceed without anemia revealing its presence.1
A controversial topic. Vitamin B12 deficiency is a complicated and controversial subject. Specifically, there is uncertainty about the clinical importance of lower serum levels of vitamin B12 (200-400 pg/mL), their impact on well-being, and the need for treatment. In addition to measuring a patient’s serum B12 level, testing a second biomarker (such as homocysteine or methylmalonic acid) can be helpful in establishing a diagnosis of B12 deficiency.1 Levels of each of these are elevated in patients with B12 deficiency.1
Some evidence suggests B12 supplementation may improve symptoms of depression and anxiety.
Although vitamin B12 deficiency has been well studied in older patients,3 little has been published about the condition in young adults. National Health and Nutrition Examination Survey (NHANES) data from 2000 to 2004 shows that almost 40% of people ages 19 to 30 years have a B12 level <400 pg/mL.1 How many of these individuals are at risk of complications of B12 deficiency is unknown.
B12 supplementation is inexpensive and has no significant adverse effects.1 It can be administered orally, parenterally (intramuscularly or subcutaneously), or intranasally.1 A common oral regimen is 1 mg/d; parental regimens vary widely, but might include a 1-mg injection once a week for 8 weeks, then once a month for life.1
Some evidence suggests B12 supplementation may improve symptoms of depression and anxiety. A Pakistani study randomized 73 patients with depression and “low normal” B12 levels (190-300 pg/mL) to an antidepressant only (equivalent to imipramine 100-250 mg/d or fluoxetine 20-40 mg/d) or an antidepressant plus parenteral B12 (1000 mcg once a week).4 At 3 months follow-up, 100% of the treatment group showed at least a 20% reduction in their Hamilton Depression Rating Scale (HAM-D) score, compared to 69% in the control arm (P<.001).4
A Swedish study analyzed the effects of several B vitamins, including 0.5 mg/d of B12 vs placebo on mood in 65 celiac patients on a gluten-free diet who had borderline/low normal B12 levels (>191 pg/mL).5 Patients who scored low on a measure of psychological well-being at the beginning of the study and who received B12 experienced significant improvements in anxiety and depressed mood compared to those who received placebo.
Our patient
Because neurologic and psychiatric symptoms require assured compliance and urgent treatment, our patient received vitamin B12 parenterally as cyanocobalamin 1 mg/mL. She was given this dosage intramuscularly once a day for 5 days, then once a week for 4 weeks. She will continue to receive it once a month indefinitely.
The patient was advised that if she wished to switch to oral therapy, she could do so after several months of parenteral treatment, as long as she had close follow-up with frequent B12 measurements to assure that she was absorbing oral therapy. Her anxiety and mood symptoms resolved within one month, and her disequilibrium was almost entirely resolved within 3 months of treatment.
THE TAKEAWAY
Although more common in older patients, vitamin B12 deficiency can also affect younger patients. “Low normal” B12 levels (200-400 pg/mL) may affect psychological well-being.
Consider testing serum B12 and a second biomarker—such as homocysteine or methylmalonic acid, if indicated—in patients who present with depressed mood, anxiety, cognitive symptoms, and/or fatigue. Vitamin B12 supplementation can be administered orally and has no major adverse effects.
References
1. Centers for Disease Control and Prevention. Why vitamin B12 deficiency should be on your radar screen. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/ncbddd/b12/. Accessed February 26, 2015.
2. Guidelines and Protocols Advisory Committee, Medical Services Commission, British Columbia Ministry of Health. Cobalamin (vitamin B12) Deficiency - Investigation & Management. British Columbia Ministry of Health Web site. Available at: http://www.bcguidelines.ca/guideline_cobalamin.html. Accessed March 13, 2015.
3. Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence of cobalamin deficiency in elderly outpatients. J Am Geriatr Soc. 1992;40:1197-1204.
4. Syed EU, Wasay M, Awan S. Vitamin B12 supplementation in treating major depressive disorder: a randomized controlled trial. Open Neurol J. 2013;7:44-48
5. Hallert C, Svensson M, Tholstrup J, et al. Clinical trial: B vitamins improve health in patients with coeliac disease living on a gluten-free diet. Ailment Pharmacol Ther. 2009;29:811-816.
A 21-year-old college student was referred to us by the counseling center at our university for a psychiatric evaluation after 11 psychotherapy sessions over 3 months had failed to reduce her feelings of anxiety and panic.
During our evaluation, the patient described feeling “not quite right” for many months. She had been experiencing mental fogginess, fatigue, and worsening concentration/ memory. Her anxiety, which had been gradually increasing, was the result of being unsure about her gait. She first noticed this while walking down some bleachers; she felt dizzy, was afraid of falling, and couldn’t walk down without assistance. All episodes of “panic” occurred in situations where she experienced disequilibrium, unsteady gait, and fear of falling. She grew fearful of driving or going anywhere without assistance.
The patient had celiac disease that was well controlled with a gluten-free diet. She had no personal or family psychiatric history and no history of substance abuse.
THE DIAGNOSIS
Physical exam and lab studies, including a complete blood count, comprehensive metabolic panel, and thyrotropin and folate levels, were normal. Her homocysteine level was 11.8 μmol/L (reference range, 5.4-11.9 μmol/L) and vitamin B12 level was 292 pg/mL (reference range, 200-1100 pg/mL). Her lab report included a note that read, “Although the reference range for vitamin B12 is 200 to 1100 pg/mL, it has been reported that between 5% and 10% of patients with values between 200 and 400 pg/mL may experience neuropsychiatric and hematologic abnormalities due to occult B12 deficiency; <1% of patients with values >400 pg/mL will have symptoms.”
Based on this vitamin B12 level, the patient’s symptoms, and her borderline high homocysteine level, we diagnosed vitamin B12 deficiency.
DISCUSSION
There are no recommendations by the US Preventive Services Task Force or any other major US medical society for routine vitamin B12 screening.1 In Canada, the Medical Services Commission of the British Columbia Ministry of Health recommends B12 screening for patients who present with macrocytic anemia or unexplained neurologic symptoms (eg, paresthesia, numbness, poor motor coordination, memory lapses, or cognitive or personality changes).2
Vitamin B12 deficiency can be caused by numerous conditions, including those that cause malabsorption (such as gastric bypass). It can also be caused by diseases such as human immunodeficiency virus infection or Crohn’s disease, long-term adherence to a vegetarian or vegan diet, or by any other lack of dietary intake.1 The condition can cause hematologic-related signs and symptoms such as megaloblastic anemia, fatigue, and syncope. It also can have neurologic manifestations, including paresthesia, weakness, motor disturbances (including gait abnormalities), vision loss, and a wide range of cognitive and behavioral changes.1 Anemia is uncommon because since 1998, the US Food and Drug Administration has required fortification of all enriched grain and cereal products with folic acid; thus, vitamin B12 deficiency may proceed without anemia revealing its presence.1
A controversial topic. Vitamin B12 deficiency is a complicated and controversial subject. Specifically, there is uncertainty about the clinical importance of lower serum levels of vitamin B12 (200-400 pg/mL), their impact on well-being, and the need for treatment. In addition to measuring a patient’s serum B12 level, testing a second biomarker (such as homocysteine or methylmalonic acid) can be helpful in establishing a diagnosis of B12 deficiency.1 Levels of each of these are elevated in patients with B12 deficiency.1
Some evidence suggests B12 supplementation may improve symptoms of depression and anxiety.
Although vitamin B12 deficiency has been well studied in older patients,3 little has been published about the condition in young adults. National Health and Nutrition Examination Survey (NHANES) data from 2000 to 2004 shows that almost 40% of people ages 19 to 30 years have a B12 level <400 pg/mL.1 How many of these individuals are at risk of complications of B12 deficiency is unknown.
B12 supplementation is inexpensive and has no significant adverse effects.1 It can be administered orally, parenterally (intramuscularly or subcutaneously), or intranasally.1 A common oral regimen is 1 mg/d; parental regimens vary widely, but might include a 1-mg injection once a week for 8 weeks, then once a month for life.1
Some evidence suggests B12 supplementation may improve symptoms of depression and anxiety. A Pakistani study randomized 73 patients with depression and “low normal” B12 levels (190-300 pg/mL) to an antidepressant only (equivalent to imipramine 100-250 mg/d or fluoxetine 20-40 mg/d) or an antidepressant plus parenteral B12 (1000 mcg once a week).4 At 3 months follow-up, 100% of the treatment group showed at least a 20% reduction in their Hamilton Depression Rating Scale (HAM-D) score, compared to 69% in the control arm (P<.001).4
A Swedish study analyzed the effects of several B vitamins, including 0.5 mg/d of B12 vs placebo on mood in 65 celiac patients on a gluten-free diet who had borderline/low normal B12 levels (>191 pg/mL).5 Patients who scored low on a measure of psychological well-being at the beginning of the study and who received B12 experienced significant improvements in anxiety and depressed mood compared to those who received placebo.
Our patient
Because neurologic and psychiatric symptoms require assured compliance and urgent treatment, our patient received vitamin B12 parenterally as cyanocobalamin 1 mg/mL. She was given this dosage intramuscularly once a day for 5 days, then once a week for 4 weeks. She will continue to receive it once a month indefinitely.
The patient was advised that if she wished to switch to oral therapy, she could do so after several months of parenteral treatment, as long as she had close follow-up with frequent B12 measurements to assure that she was absorbing oral therapy. Her anxiety and mood symptoms resolved within one month, and her disequilibrium was almost entirely resolved within 3 months of treatment.
THE TAKEAWAY
Although more common in older patients, vitamin B12 deficiency can also affect younger patients. “Low normal” B12 levels (200-400 pg/mL) may affect psychological well-being.
Consider testing serum B12 and a second biomarker—such as homocysteine or methylmalonic acid, if indicated—in patients who present with depressed mood, anxiety, cognitive symptoms, and/or fatigue. Vitamin B12 supplementation can be administered orally and has no major adverse effects.
THE CASE
A 21-year-old college student was referred to us by the counseling center at our university for a psychiatric evaluation after 11 psychotherapy sessions over 3 months had failed to reduce her feelings of anxiety and panic.
During our evaluation, the patient described feeling “not quite right” for many months. She had been experiencing mental fogginess, fatigue, and worsening concentration/ memory. Her anxiety, which had been gradually increasing, was the result of being unsure about her gait. She first noticed this while walking down some bleachers; she felt dizzy, was afraid of falling, and couldn’t walk down without assistance. All episodes of “panic” occurred in situations where she experienced disequilibrium, unsteady gait, and fear of falling. She grew fearful of driving or going anywhere without assistance.
The patient had celiac disease that was well controlled with a gluten-free diet. She had no personal or family psychiatric history and no history of substance abuse.
THE DIAGNOSIS
Physical exam and lab studies, including a complete blood count, comprehensive metabolic panel, and thyrotropin and folate levels, were normal. Her homocysteine level was 11.8 μmol/L (reference range, 5.4-11.9 μmol/L) and vitamin B12 level was 292 pg/mL (reference range, 200-1100 pg/mL). Her lab report included a note that read, “Although the reference range for vitamin B12 is 200 to 1100 pg/mL, it has been reported that between 5% and 10% of patients with values between 200 and 400 pg/mL may experience neuropsychiatric and hematologic abnormalities due to occult B12 deficiency; <1% of patients with values >400 pg/mL will have symptoms.”
Based on this vitamin B12 level, the patient’s symptoms, and her borderline high homocysteine level, we diagnosed vitamin B12 deficiency.
DISCUSSION
There are no recommendations by the US Preventive Services Task Force or any other major US medical society for routine vitamin B12 screening.1 In Canada, the Medical Services Commission of the British Columbia Ministry of Health recommends B12 screening for patients who present with macrocytic anemia or unexplained neurologic symptoms (eg, paresthesia, numbness, poor motor coordination, memory lapses, or cognitive or personality changes).2
Vitamin B12 deficiency can be caused by numerous conditions, including those that cause malabsorption (such as gastric bypass). It can also be caused by diseases such as human immunodeficiency virus infection or Crohn’s disease, long-term adherence to a vegetarian or vegan diet, or by any other lack of dietary intake.1 The condition can cause hematologic-related signs and symptoms such as megaloblastic anemia, fatigue, and syncope. It also can have neurologic manifestations, including paresthesia, weakness, motor disturbances (including gait abnormalities), vision loss, and a wide range of cognitive and behavioral changes.1 Anemia is uncommon because since 1998, the US Food and Drug Administration has required fortification of all enriched grain and cereal products with folic acid; thus, vitamin B12 deficiency may proceed without anemia revealing its presence.1
A controversial topic. Vitamin B12 deficiency is a complicated and controversial subject. Specifically, there is uncertainty about the clinical importance of lower serum levels of vitamin B12 (200-400 pg/mL), their impact on well-being, and the need for treatment. In addition to measuring a patient’s serum B12 level, testing a second biomarker (such as homocysteine or methylmalonic acid) can be helpful in establishing a diagnosis of B12 deficiency.1 Levels of each of these are elevated in patients with B12 deficiency.1
Some evidence suggests B12 supplementation may improve symptoms of depression and anxiety.
Although vitamin B12 deficiency has been well studied in older patients,3 little has been published about the condition in young adults. National Health and Nutrition Examination Survey (NHANES) data from 2000 to 2004 shows that almost 40% of people ages 19 to 30 years have a B12 level <400 pg/mL.1 How many of these individuals are at risk of complications of B12 deficiency is unknown.
B12 supplementation is inexpensive and has no significant adverse effects.1 It can be administered orally, parenterally (intramuscularly or subcutaneously), or intranasally.1 A common oral regimen is 1 mg/d; parental regimens vary widely, but might include a 1-mg injection once a week for 8 weeks, then once a month for life.1
Some evidence suggests B12 supplementation may improve symptoms of depression and anxiety. A Pakistani study randomized 73 patients with depression and “low normal” B12 levels (190-300 pg/mL) to an antidepressant only (equivalent to imipramine 100-250 mg/d or fluoxetine 20-40 mg/d) or an antidepressant plus parenteral B12 (1000 mcg once a week).4 At 3 months follow-up, 100% of the treatment group showed at least a 20% reduction in their Hamilton Depression Rating Scale (HAM-D) score, compared to 69% in the control arm (P<.001).4
A Swedish study analyzed the effects of several B vitamins, including 0.5 mg/d of B12 vs placebo on mood in 65 celiac patients on a gluten-free diet who had borderline/low normal B12 levels (>191 pg/mL).5 Patients who scored low on a measure of psychological well-being at the beginning of the study and who received B12 experienced significant improvements in anxiety and depressed mood compared to those who received placebo.
Our patient
Because neurologic and psychiatric symptoms require assured compliance and urgent treatment, our patient received vitamin B12 parenterally as cyanocobalamin 1 mg/mL. She was given this dosage intramuscularly once a day for 5 days, then once a week for 4 weeks. She will continue to receive it once a month indefinitely.
The patient was advised that if she wished to switch to oral therapy, she could do so after several months of parenteral treatment, as long as she had close follow-up with frequent B12 measurements to assure that she was absorbing oral therapy. Her anxiety and mood symptoms resolved within one month, and her disequilibrium was almost entirely resolved within 3 months of treatment.
THE TAKEAWAY
Although more common in older patients, vitamin B12 deficiency can also affect younger patients. “Low normal” B12 levels (200-400 pg/mL) may affect psychological well-being.
Consider testing serum B12 and a second biomarker—such as homocysteine or methylmalonic acid, if indicated—in patients who present with depressed mood, anxiety, cognitive symptoms, and/or fatigue. Vitamin B12 supplementation can be administered orally and has no major adverse effects.
References
1. Centers for Disease Control and Prevention. Why vitamin B12 deficiency should be on your radar screen. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/ncbddd/b12/. Accessed February 26, 2015.
2. Guidelines and Protocols Advisory Committee, Medical Services Commission, British Columbia Ministry of Health. Cobalamin (vitamin B12) Deficiency - Investigation & Management. British Columbia Ministry of Health Web site. Available at: http://www.bcguidelines.ca/guideline_cobalamin.html. Accessed March 13, 2015.
3. Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence of cobalamin deficiency in elderly outpatients. J Am Geriatr Soc. 1992;40:1197-1204.
4. Syed EU, Wasay M, Awan S. Vitamin B12 supplementation in treating major depressive disorder: a randomized controlled trial. Open Neurol J. 2013;7:44-48
5. Hallert C, Svensson M, Tholstrup J, et al. Clinical trial: B vitamins improve health in patients with coeliac disease living on a gluten-free diet. Ailment Pharmacol Ther. 2009;29:811-816.
References
1. Centers for Disease Control and Prevention. Why vitamin B12 deficiency should be on your radar screen. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/ncbddd/b12/. Accessed February 26, 2015.
2. Guidelines and Protocols Advisory Committee, Medical Services Commission, British Columbia Ministry of Health. Cobalamin (vitamin B12) Deficiency - Investigation & Management. British Columbia Ministry of Health Web site. Available at: http://www.bcguidelines.ca/guideline_cobalamin.html. Accessed March 13, 2015.
3. Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence of cobalamin deficiency in elderly outpatients. J Am Geriatr Soc. 1992;40:1197-1204.
4. Syed EU, Wasay M, Awan S. Vitamin B12 supplementation in treating major depressive disorder: a randomized controlled trial. Open Neurol J. 2013;7:44-48
5. Hallert C, Svensson M, Tholstrup J, et al. Clinical trial: B vitamins improve health in patients with coeliac disease living on a gluten-free diet. Ailment Pharmacol Ther. 2009;29:811-816.
Yes. Statin therapy produces a small increase in the incidence of diabetes: one additional case per 255 patients taking statins over 4 years (strength of recommendation [SOR]: A, meta-analysis). Intensive statin therapy, compared with moderate therapy, produces an additional 2 cases of diabetes per 1000 patient years (SOR: B, meta-analysis with significant heterogeneity among trials).
EVIDENCE SUMMARY
A meta-analysis of 13 randomized, placebo or standard of care-controlled statin trials (113,148 patients, 81% without diabetes at enrollment, mean ages 55-76 years) found that statin therapy increased the incidence of diabetes by 9% over 4 years (odds ratio [OR]=1.09; 95% confidence interval [CI], 1.02-1.17), or one additional case per 255 patients.1 The increased risk was similar for lipophilic (pravastatin, rosuvastatin) and hydrophilic (atorvastatin, simvastatin, lovastatin) statins, although the analysis wasn’t adjusted for doses used.
In a meta-regression analysis, baseline body mass index or percentage change in low-density lipoprotein cholesterol didn’t appear to confer additional risk. The risk of diabetes with statins was generally higher in studies with older patients (data given graphically).
Higher statin doses mean higher risk
A meta-analysis of 5 placebo and standard-of-care randomized controlled trials (39,612 patients, 83% without diabetes at enrollment, mean age 58-64 years) found that the risk of diabetes was higher with higher-dose statins.2 Therapy with atorvastatin 80 mg or simvastatin 40 to 80 mg was defined as intensive. Treatment with simvastatin 20 to 40 mg, atorvastatin 10 mg, or pravastatin 40 mg was defined as moderate.
At a mean follow-up of 4.9 years, intensive statin therapy was associated with a higher risk of developing diabetes than moderate therapy (OR=1.12; 95% CI, 1.04-1.22) with 2 additional cases of diabetes per 1000 patient-years in the intensive therapy group. The authors noted significant heterogeneity between trials with regard to major cardiovascular events.
Similar results were found in a subsequent population-based cohort study of 471,250 nondiabetic patients older than 66 years who were newly prescribed a statin.3 The study authors used the incidence of new diabetes in patients taking pravastatin as the baseline, since it had been associated with reduced rates of diabetes in a large cardiovascular prevention trial.4 Without adjusting for dose, patients were at significantly higher risk of diabetes if prescribed atorvastatin (hazard ratio [HR]=1.22; 95% CI, 1.15-1.29), rosuvastatin (HR=1.18; 95% CI, 1.10-1.26), or simvastatin (HR=1.10; 95% CI, 1.04-1.17) compared with pravastatin. The risk with fluvastatin and lovastatin was similar to pravastatin.
A subanalysis that compared moderate- and high-dose statin therapy with low-dose therapy (atorvastatin <20 mg, rosuvastatin <10 mg, simvastatin <80 mg, or any dose of fluvastatin, lovastatin, or pravastatin) found a 22% increased risk of diabetes (HR=1.22; 95% CI, 1.19-1.26) for moderate-dose therapy (atorvastatin 20-79 mg, rosuvastatin 10-39 mg, or simvastatin >80 mg) and a 30% increased risk (HR=1.3; 95% CI, 1.2-1.4) for high-dose therapy (atorvastatin ≥80 mg or rosuvastatin ≥40 mg).
A cohort trial also shows increased diabetes risk
A smaller subsequent cohort trial based on data from Taiwan National Health Insurance records compared 8412 nondiabetic adult patients (mean age 63 years) taking statins with 33,648 age- and risk-matched controls not taking statins over a mean duration of 7.2 years.5 Statin use was associated with a 15% higher risk of developing diabetes (HR=1.15; 95% CI, 1.08-1.22).
RECOMMENDATIONS
The 2013 American College of Cardiology/American Heart Association guidelines for lipid-lowering therapy recommend that patients taking statins be screened for diabetes according to current screening recommendations.6 The guidelines advise encouraging patients who develop diabetes while on statin therapy to adhere to a heart-healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce the risk of cardiovascular events.
References
1. Sattar N, Preiss D, Murray HM, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet. 2010;375:735-742.
2. Preiss D, Seshasai SR, Welsh P, et al. Risk of incident diabetes with intensive-dose compared with moderatedose statin therapy: a meta-analysis. JAMA. 2011;305:2556-2564.
3. Carter AA, Gomes T, Camacho X, et al. Risk of incident diabetes among patients treated with statins: population-based study. BMJ. 2013;346:f2610.
4. Freeman DJ, Morrie J, Sattar N, et al. Pravastatin and the development of diabetes mellitus: evidence for a protective treatment effect in the West of Scotland Coronary Prevention Study. Circulation. 2001;103:357-362.
5. Wang KL, Liu CJ, Chao TF, et al. Statins, risk of diabetes and implications on outcomes in the general population. J Am Coll Cardiol. 2012;60:1231-1238.
6. Stone NJ, Robinson JG, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S1-S45.
Kristin Parker, DO; Karen Dohr, PharmD; Jon O. Neher, MD; Gary Kelsberg, MD; Leilani St. Anna, MLIS, AHIP; diabetes; statins; American College of Cardiology/American Heart Association
Yes. Statin therapy produces a small increase in the incidence of diabetes: one additional case per 255 patients taking statins over 4 years (strength of recommendation [SOR]: A, meta-analysis). Intensive statin therapy, compared with moderate therapy, produces an additional 2 cases of diabetes per 1000 patient years (SOR: B, meta-analysis with significant heterogeneity among trials).
EVIDENCE SUMMARY
A meta-analysis of 13 randomized, placebo or standard of care-controlled statin trials (113,148 patients, 81% without diabetes at enrollment, mean ages 55-76 years) found that statin therapy increased the incidence of diabetes by 9% over 4 years (odds ratio [OR]=1.09; 95% confidence interval [CI], 1.02-1.17), or one additional case per 255 patients.1 The increased risk was similar for lipophilic (pravastatin, rosuvastatin) and hydrophilic (atorvastatin, simvastatin, lovastatin) statins, although the analysis wasn’t adjusted for doses used.
In a meta-regression analysis, baseline body mass index or percentage change in low-density lipoprotein cholesterol didn’t appear to confer additional risk. The risk of diabetes with statins was generally higher in studies with older patients (data given graphically).
Higher statin doses mean higher risk
A meta-analysis of 5 placebo and standard-of-care randomized controlled trials (39,612 patients, 83% without diabetes at enrollment, mean age 58-64 years) found that the risk of diabetes was higher with higher-dose statins.2 Therapy with atorvastatin 80 mg or simvastatin 40 to 80 mg was defined as intensive. Treatment with simvastatin 20 to 40 mg, atorvastatin 10 mg, or pravastatin 40 mg was defined as moderate.
At a mean follow-up of 4.9 years, intensive statin therapy was associated with a higher risk of developing diabetes than moderate therapy (OR=1.12; 95% CI, 1.04-1.22) with 2 additional cases of diabetes per 1000 patient-years in the intensive therapy group. The authors noted significant heterogeneity between trials with regard to major cardiovascular events.
Similar results were found in a subsequent population-based cohort study of 471,250 nondiabetic patients older than 66 years who were newly prescribed a statin.3 The study authors used the incidence of new diabetes in patients taking pravastatin as the baseline, since it had been associated with reduced rates of diabetes in a large cardiovascular prevention trial.4 Without adjusting for dose, patients were at significantly higher risk of diabetes if prescribed atorvastatin (hazard ratio [HR]=1.22; 95% CI, 1.15-1.29), rosuvastatin (HR=1.18; 95% CI, 1.10-1.26), or simvastatin (HR=1.10; 95% CI, 1.04-1.17) compared with pravastatin. The risk with fluvastatin and lovastatin was similar to pravastatin.
A subanalysis that compared moderate- and high-dose statin therapy with low-dose therapy (atorvastatin <20 mg, rosuvastatin <10 mg, simvastatin <80 mg, or any dose of fluvastatin, lovastatin, or pravastatin) found a 22% increased risk of diabetes (HR=1.22; 95% CI, 1.19-1.26) for moderate-dose therapy (atorvastatin 20-79 mg, rosuvastatin 10-39 mg, or simvastatin >80 mg) and a 30% increased risk (HR=1.3; 95% CI, 1.2-1.4) for high-dose therapy (atorvastatin ≥80 mg or rosuvastatin ≥40 mg).
A cohort trial also shows increased diabetes risk
A smaller subsequent cohort trial based on data from Taiwan National Health Insurance records compared 8412 nondiabetic adult patients (mean age 63 years) taking statins with 33,648 age- and risk-matched controls not taking statins over a mean duration of 7.2 years.5 Statin use was associated with a 15% higher risk of developing diabetes (HR=1.15; 95% CI, 1.08-1.22).
RECOMMENDATIONS
The 2013 American College of Cardiology/American Heart Association guidelines for lipid-lowering therapy recommend that patients taking statins be screened for diabetes according to current screening recommendations.6 The guidelines advise encouraging patients who develop diabetes while on statin therapy to adhere to a heart-healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce the risk of cardiovascular events.
EVIDENCE-BASED ANSWER:
Yes. Statin therapy produces a small increase in the incidence of diabetes: one additional case per 255 patients taking statins over 4 years (strength of recommendation [SOR]: A, meta-analysis). Intensive statin therapy, compared with moderate therapy, produces an additional 2 cases of diabetes per 1000 patient years (SOR: B, meta-analysis with significant heterogeneity among trials).
EVIDENCE SUMMARY
A meta-analysis of 13 randomized, placebo or standard of care-controlled statin trials (113,148 patients, 81% without diabetes at enrollment, mean ages 55-76 years) found that statin therapy increased the incidence of diabetes by 9% over 4 years (odds ratio [OR]=1.09; 95% confidence interval [CI], 1.02-1.17), or one additional case per 255 patients.1 The increased risk was similar for lipophilic (pravastatin, rosuvastatin) and hydrophilic (atorvastatin, simvastatin, lovastatin) statins, although the analysis wasn’t adjusted for doses used.
In a meta-regression analysis, baseline body mass index or percentage change in low-density lipoprotein cholesterol didn’t appear to confer additional risk. The risk of diabetes with statins was generally higher in studies with older patients (data given graphically).
Higher statin doses mean higher risk
A meta-analysis of 5 placebo and standard-of-care randomized controlled trials (39,612 patients, 83% without diabetes at enrollment, mean age 58-64 years) found that the risk of diabetes was higher with higher-dose statins.2 Therapy with atorvastatin 80 mg or simvastatin 40 to 80 mg was defined as intensive. Treatment with simvastatin 20 to 40 mg, atorvastatin 10 mg, or pravastatin 40 mg was defined as moderate.
At a mean follow-up of 4.9 years, intensive statin therapy was associated with a higher risk of developing diabetes than moderate therapy (OR=1.12; 95% CI, 1.04-1.22) with 2 additional cases of diabetes per 1000 patient-years in the intensive therapy group. The authors noted significant heterogeneity between trials with regard to major cardiovascular events.
Similar results were found in a subsequent population-based cohort study of 471,250 nondiabetic patients older than 66 years who were newly prescribed a statin.3 The study authors used the incidence of new diabetes in patients taking pravastatin as the baseline, since it had been associated with reduced rates of diabetes in a large cardiovascular prevention trial.4 Without adjusting for dose, patients were at significantly higher risk of diabetes if prescribed atorvastatin (hazard ratio [HR]=1.22; 95% CI, 1.15-1.29), rosuvastatin (HR=1.18; 95% CI, 1.10-1.26), or simvastatin (HR=1.10; 95% CI, 1.04-1.17) compared with pravastatin. The risk with fluvastatin and lovastatin was similar to pravastatin.
A subanalysis that compared moderate- and high-dose statin therapy with low-dose therapy (atorvastatin <20 mg, rosuvastatin <10 mg, simvastatin <80 mg, or any dose of fluvastatin, lovastatin, or pravastatin) found a 22% increased risk of diabetes (HR=1.22; 95% CI, 1.19-1.26) for moderate-dose therapy (atorvastatin 20-79 mg, rosuvastatin 10-39 mg, or simvastatin >80 mg) and a 30% increased risk (HR=1.3; 95% CI, 1.2-1.4) for high-dose therapy (atorvastatin ≥80 mg or rosuvastatin ≥40 mg).
A cohort trial also shows increased diabetes risk
A smaller subsequent cohort trial based on data from Taiwan National Health Insurance records compared 8412 nondiabetic adult patients (mean age 63 years) taking statins with 33,648 age- and risk-matched controls not taking statins over a mean duration of 7.2 years.5 Statin use was associated with a 15% higher risk of developing diabetes (HR=1.15; 95% CI, 1.08-1.22).
RECOMMENDATIONS
The 2013 American College of Cardiology/American Heart Association guidelines for lipid-lowering therapy recommend that patients taking statins be screened for diabetes according to current screening recommendations.6 The guidelines advise encouraging patients who develop diabetes while on statin therapy to adhere to a heart-healthy dietary pattern, engage in physical activity, achieve and maintain a healthy body weight, cease tobacco use, and continue statin therapy to reduce the risk of cardiovascular events.
References
1. Sattar N, Preiss D, Murray HM, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet. 2010;375:735-742.
2. Preiss D, Seshasai SR, Welsh P, et al. Risk of incident diabetes with intensive-dose compared with moderatedose statin therapy: a meta-analysis. JAMA. 2011;305:2556-2564.
3. Carter AA, Gomes T, Camacho X, et al. Risk of incident diabetes among patients treated with statins: population-based study. BMJ. 2013;346:f2610.
4. Freeman DJ, Morrie J, Sattar N, et al. Pravastatin and the development of diabetes mellitus: evidence for a protective treatment effect in the West of Scotland Coronary Prevention Study. Circulation. 2001;103:357-362.
5. Wang KL, Liu CJ, Chao TF, et al. Statins, risk of diabetes and implications on outcomes in the general population. J Am Coll Cardiol. 2012;60:1231-1238.
6. Stone NJ, Robinson JG, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S1-S45.
References
1. Sattar N, Preiss D, Murray HM, et al. Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. Lancet. 2010;375:735-742.
2. Preiss D, Seshasai SR, Welsh P, et al. Risk of incident diabetes with intensive-dose compared with moderatedose statin therapy: a meta-analysis. JAMA. 2011;305:2556-2564.
3. Carter AA, Gomes T, Camacho X, et al. Risk of incident diabetes among patients treated with statins: population-based study. BMJ. 2013;346:f2610.
4. Freeman DJ, Morrie J, Sattar N, et al. Pravastatin and the development of diabetes mellitus: evidence for a protective treatment effect in the West of Scotland Coronary Prevention Study. Circulation. 2001;103:357-362.
5. Wang KL, Liu CJ, Chao TF, et al. Statins, risk of diabetes and implications on outcomes in the general population. J Am Coll Cardiol. 2012;60:1231-1238.
6. Stone NJ, Robinson JG, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S1-S45.
Do statins increase the risk of developing diabetes?
Display Headline
Do statins increase the risk of developing diabetes?
Legacy Keywords
Kristin Parker, DO; Karen Dohr, PharmD; Jon O. Neher, MD; Gary Kelsberg, MD; Leilani St. Anna, MLIS, AHIP; diabetes; statins; American College of Cardiology/American Heart Association
Legacy Keywords
Kristin Parker, DO; Karen Dohr, PharmD; Jon O. Neher, MD; Gary Kelsberg, MD; Leilani St. Anna, MLIS, AHIP; diabetes; statins; American College of Cardiology/American Heart Association