User login
Upper-limb deep vein thrombosis in Paget-Schroetter syndrome
A 43-year-old man with no medical history presented with pain and swelling in his left arm for 2 weeks. He was a regular weight lifter, and his exercise routine included repetitive hyperextension and hyperabduction of his arms while lifting heavy weights.
He had no history of recent trauma or venous cannulation of the left arm. His family history was negative for thrombophilic disorders. Physical examination revealed a swollen and erythematous left arm and visible venous collaterals at the neck, shoulder, and chest. There was no evidence of arterial insufficiency.
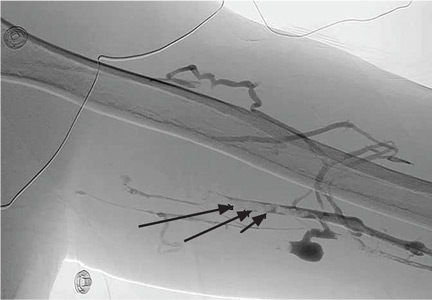
Duplex ultrasonography confirmed thrombosis of the left brachial, axillary, and subclavian veins. Further evaluation with computed tomography showed no intrathoracic mass but revealed several subsegmental pulmonary thrombi in the right lung. A screen for thrombophilia was negative. Venography confirmed complete thrombotic occlusion of the subclavian, axillary, and brachial veins (Figure 1).
Catheter-directed thrombolysis with tissue plasminogen activator resulted in complete resolution of the thrombosis, but venography after 3 days of thrombolysis showed 50% residual stenosis of the left subclavian vein where it passes under the first rib (Figure 2). The redness and swelling had markedly improved 2 days after thrombolytic therapy. He was discharged home on rivaroxaban 20 mg daily.
Follow-up venography 2 months later (Figure 3), with the patient performing hyperabduction of the arms, showed a patent subclavian vein with no thrombosis, but dynamic compression and occlusion of the subclavian vein where it passes the first rib. Magnetic resonance imaging (MRI) of the neck showed no cervical (ie, extra) rib and no soft-tissue abnormalities of the scalene triangle.
Following this, the patient underwent resection of the left first rib for decompression of the venous thoracic outlet, which resulted in resolution of his symptoms. He remained asymptomatic at 6-month follow-up.
PAGET-SCHROETTER SYNDROME
Paget-Schroetter syndrome, also referred to as effort-induced or effort thrombosis, is thrombosis of the axillary or subclavian vein associated with strenuous and repetitive activity of the arms. Anatomic abnormalities at the thoracic outlet—cervical rib, congenital bands, hypertrophy of scalene tendons, abnormal insertion of the costoclavicular ligament—and repetitive trauma to the endothelium of the subclavian vein are key factors in its initiation and progression.
The condition is seen primarily in young people who participate in strenuous activities such as rowing, weight lifting, and baseball pitching. It is estimated to be the cause of 40% of cases of primary upper-extremity deep vein thrombosis in the absence of an obvious risk factor or trigger such as a central venous catheter, pacemaker, port, or occult malignancy.1
A provocative test such as the Adson test or hyperabduction test during MRI or venography helps confirm thoracic outlet obstruction by demonstrating dynamic obstruction.2
TREATMENT CONSIDERATIONS
There are no universal guidelines for the treatment of Paget-Schroetter syndrome. However, the available data3–5 suggest a multimodal approach that involves early catheter-directed thrombolysis and subsequent surgical decompression of the thoracic outlet. This can restore venous patency and reduce the risk of long-term complications such as rethrombosis and postthrombotic syndrome.3–5
Surgical treatment includes resection of the first rib and division of the scalene muscles and the costoclavicular ligament. MRI with provocative testing helps guide the surgical approach. Anticoagulation therapy alone—ie, without thrombolysis and surgical decompression—is inadequate as it leads to recurrence of thrombosis and residual symptoms.6
Paget-Schroetter syndrome should not be managed the same as lower-extremity deep vein thrombosis because the cause and the exacerbating factors are different.
Unanswered questions
Because we have no data from randomized controlled trials, questions about management remain. What should be the duration of anticoagulation, especially in the absence of coexisting thrombophilia? Is thrombophilia screening useful? What is the optimal timing for starting thrombolytic therapy?
A careful history and heightened suspicion are required to make this diagnosis. If undiagnosed, it carries a risk of significant long-term morbidity and death. Dynamic obstruction during venography, in addition to MRI, can help identify an anatomic obstruction.
- Bernardi E, Pesavento R, Prandoni P. Upper extremity deep venous thrombosis. Semin Thromb Hemost 2006; 32:729–736.
- Demirbag D, Unlu E, Ozdemir F, et al. The relationship between magnetic resonance imaging findings and postural maneuver and physical examination tests in patients with thoracic outlet syndrome: results of a double-blind, controlled study. Arch Phys Med Rehabil 2007; 88:844–851.
- Alla VM, Natarajan N, Kaushik M, Warrier R, Nair CK. Paget-Schroetter syndrome: review of pathogenesis and treatment of effort thrombosis. West J Emerg Med 2010; 11:358–362.
- Molina JE, Hunter DW, Dietz CA. Paget-Schroetter syndrome treated with thrombolytics and immediate surgery. J Vasc Surg 2007; 45:328–334.
- Thompson RW. Comprehensive management of subclavian vein effort thrombosis. Semin Intervent Radiol 2012; 29:44–51.
- AbuRahma AF, Robinson PA. Effort subclavian vein thrombosis: evolution of management. J Endovasc Ther 2000; 7:302–308.
A 43-year-old man with no medical history presented with pain and swelling in his left arm for 2 weeks. He was a regular weight lifter, and his exercise routine included repetitive hyperextension and hyperabduction of his arms while lifting heavy weights.
He had no history of recent trauma or venous cannulation of the left arm. His family history was negative for thrombophilic disorders. Physical examination revealed a swollen and erythematous left arm and visible venous collaterals at the neck, shoulder, and chest. There was no evidence of arterial insufficiency.
Duplex ultrasonography confirmed thrombosis of the left brachial, axillary, and subclavian veins. Further evaluation with computed tomography showed no intrathoracic mass but revealed several subsegmental pulmonary thrombi in the right lung. A screen for thrombophilia was negative. Venography confirmed complete thrombotic occlusion of the subclavian, axillary, and brachial veins (Figure 1).
Catheter-directed thrombolysis with tissue plasminogen activator resulted in complete resolution of the thrombosis, but venography after 3 days of thrombolysis showed 50% residual stenosis of the left subclavian vein where it passes under the first rib (Figure 2). The redness and swelling had markedly improved 2 days after thrombolytic therapy. He was discharged home on rivaroxaban 20 mg daily.
Follow-up venography 2 months later (Figure 3), with the patient performing hyperabduction of the arms, showed a patent subclavian vein with no thrombosis, but dynamic compression and occlusion of the subclavian vein where it passes the first rib. Magnetic resonance imaging (MRI) of the neck showed no cervical (ie, extra) rib and no soft-tissue abnormalities of the scalene triangle.
Following this, the patient underwent resection of the left first rib for decompression of the venous thoracic outlet, which resulted in resolution of his symptoms. He remained asymptomatic at 6-month follow-up.
PAGET-SCHROETTER SYNDROME
Paget-Schroetter syndrome, also referred to as effort-induced or effort thrombosis, is thrombosis of the axillary or subclavian vein associated with strenuous and repetitive activity of the arms. Anatomic abnormalities at the thoracic outlet—cervical rib, congenital bands, hypertrophy of scalene tendons, abnormal insertion of the costoclavicular ligament—and repetitive trauma to the endothelium of the subclavian vein are key factors in its initiation and progression.
The condition is seen primarily in young people who participate in strenuous activities such as rowing, weight lifting, and baseball pitching. It is estimated to be the cause of 40% of cases of primary upper-extremity deep vein thrombosis in the absence of an obvious risk factor or trigger such as a central venous catheter, pacemaker, port, or occult malignancy.1
A provocative test such as the Adson test or hyperabduction test during MRI or venography helps confirm thoracic outlet obstruction by demonstrating dynamic obstruction.2
TREATMENT CONSIDERATIONS
There are no universal guidelines for the treatment of Paget-Schroetter syndrome. However, the available data3–5 suggest a multimodal approach that involves early catheter-directed thrombolysis and subsequent surgical decompression of the thoracic outlet. This can restore venous patency and reduce the risk of long-term complications such as rethrombosis and postthrombotic syndrome.3–5
Surgical treatment includes resection of the first rib and division of the scalene muscles and the costoclavicular ligament. MRI with provocative testing helps guide the surgical approach. Anticoagulation therapy alone—ie, without thrombolysis and surgical decompression—is inadequate as it leads to recurrence of thrombosis and residual symptoms.6
Paget-Schroetter syndrome should not be managed the same as lower-extremity deep vein thrombosis because the cause and the exacerbating factors are different.
Unanswered questions
Because we have no data from randomized controlled trials, questions about management remain. What should be the duration of anticoagulation, especially in the absence of coexisting thrombophilia? Is thrombophilia screening useful? What is the optimal timing for starting thrombolytic therapy?
A careful history and heightened suspicion are required to make this diagnosis. If undiagnosed, it carries a risk of significant long-term morbidity and death. Dynamic obstruction during venography, in addition to MRI, can help identify an anatomic obstruction.
A 43-year-old man with no medical history presented with pain and swelling in his left arm for 2 weeks. He was a regular weight lifter, and his exercise routine included repetitive hyperextension and hyperabduction of his arms while lifting heavy weights.
He had no history of recent trauma or venous cannulation of the left arm. His family history was negative for thrombophilic disorders. Physical examination revealed a swollen and erythematous left arm and visible venous collaterals at the neck, shoulder, and chest. There was no evidence of arterial insufficiency.
Duplex ultrasonography confirmed thrombosis of the left brachial, axillary, and subclavian veins. Further evaluation with computed tomography showed no intrathoracic mass but revealed several subsegmental pulmonary thrombi in the right lung. A screen for thrombophilia was negative. Venography confirmed complete thrombotic occlusion of the subclavian, axillary, and brachial veins (Figure 1).
Catheter-directed thrombolysis with tissue plasminogen activator resulted in complete resolution of the thrombosis, but venography after 3 days of thrombolysis showed 50% residual stenosis of the left subclavian vein where it passes under the first rib (Figure 2). The redness and swelling had markedly improved 2 days after thrombolytic therapy. He was discharged home on rivaroxaban 20 mg daily.
Follow-up venography 2 months later (Figure 3), with the patient performing hyperabduction of the arms, showed a patent subclavian vein with no thrombosis, but dynamic compression and occlusion of the subclavian vein where it passes the first rib. Magnetic resonance imaging (MRI) of the neck showed no cervical (ie, extra) rib and no soft-tissue abnormalities of the scalene triangle.
Following this, the patient underwent resection of the left first rib for decompression of the venous thoracic outlet, which resulted in resolution of his symptoms. He remained asymptomatic at 6-month follow-up.
PAGET-SCHROETTER SYNDROME
Paget-Schroetter syndrome, also referred to as effort-induced or effort thrombosis, is thrombosis of the axillary or subclavian vein associated with strenuous and repetitive activity of the arms. Anatomic abnormalities at the thoracic outlet—cervical rib, congenital bands, hypertrophy of scalene tendons, abnormal insertion of the costoclavicular ligament—and repetitive trauma to the endothelium of the subclavian vein are key factors in its initiation and progression.
The condition is seen primarily in young people who participate in strenuous activities such as rowing, weight lifting, and baseball pitching. It is estimated to be the cause of 40% of cases of primary upper-extremity deep vein thrombosis in the absence of an obvious risk factor or trigger such as a central venous catheter, pacemaker, port, or occult malignancy.1
A provocative test such as the Adson test or hyperabduction test during MRI or venography helps confirm thoracic outlet obstruction by demonstrating dynamic obstruction.2
TREATMENT CONSIDERATIONS
There are no universal guidelines for the treatment of Paget-Schroetter syndrome. However, the available data3–5 suggest a multimodal approach that involves early catheter-directed thrombolysis and subsequent surgical decompression of the thoracic outlet. This can restore venous patency and reduce the risk of long-term complications such as rethrombosis and postthrombotic syndrome.3–5
Surgical treatment includes resection of the first rib and division of the scalene muscles and the costoclavicular ligament. MRI with provocative testing helps guide the surgical approach. Anticoagulation therapy alone—ie, without thrombolysis and surgical decompression—is inadequate as it leads to recurrence of thrombosis and residual symptoms.6
Paget-Schroetter syndrome should not be managed the same as lower-extremity deep vein thrombosis because the cause and the exacerbating factors are different.
Unanswered questions
Because we have no data from randomized controlled trials, questions about management remain. What should be the duration of anticoagulation, especially in the absence of coexisting thrombophilia? Is thrombophilia screening useful? What is the optimal timing for starting thrombolytic therapy?
A careful history and heightened suspicion are required to make this diagnosis. If undiagnosed, it carries a risk of significant long-term morbidity and death. Dynamic obstruction during venography, in addition to MRI, can help identify an anatomic obstruction.
- Bernardi E, Pesavento R, Prandoni P. Upper extremity deep venous thrombosis. Semin Thromb Hemost 2006; 32:729–736.
- Demirbag D, Unlu E, Ozdemir F, et al. The relationship between magnetic resonance imaging findings and postural maneuver and physical examination tests in patients with thoracic outlet syndrome: results of a double-blind, controlled study. Arch Phys Med Rehabil 2007; 88:844–851.
- Alla VM, Natarajan N, Kaushik M, Warrier R, Nair CK. Paget-Schroetter syndrome: review of pathogenesis and treatment of effort thrombosis. West J Emerg Med 2010; 11:358–362.
- Molina JE, Hunter DW, Dietz CA. Paget-Schroetter syndrome treated with thrombolytics and immediate surgery. J Vasc Surg 2007; 45:328–334.
- Thompson RW. Comprehensive management of subclavian vein effort thrombosis. Semin Intervent Radiol 2012; 29:44–51.
- AbuRahma AF, Robinson PA. Effort subclavian vein thrombosis: evolution of management. J Endovasc Ther 2000; 7:302–308.
- Bernardi E, Pesavento R, Prandoni P. Upper extremity deep venous thrombosis. Semin Thromb Hemost 2006; 32:729–736.
- Demirbag D, Unlu E, Ozdemir F, et al. The relationship between magnetic resonance imaging findings and postural maneuver and physical examination tests in patients with thoracic outlet syndrome: results of a double-blind, controlled study. Arch Phys Med Rehabil 2007; 88:844–851.
- Alla VM, Natarajan N, Kaushik M, Warrier R, Nair CK. Paget-Schroetter syndrome: review of pathogenesis and treatment of effort thrombosis. West J Emerg Med 2010; 11:358–362.
- Molina JE, Hunter DW, Dietz CA. Paget-Schroetter syndrome treated with thrombolytics and immediate surgery. J Vasc Surg 2007; 45:328–334.
- Thompson RW. Comprehensive management of subclavian vein effort thrombosis. Semin Intervent Radiol 2012; 29:44–51.
- AbuRahma AF, Robinson PA. Effort subclavian vein thrombosis: evolution of management. J Endovasc Ther 2000; 7:302–308.
What can we offer patients with mild cognitive impairment?
We can promote healthy nutrition, physical activity, socialization, and mental activity. These interventions help stabilize and even improve cognition, as well as enhance quality of life and mood, delay institutionalization, and reduce disruptive behaviors. However, no medication is approved by the US Food and Drug Administration for treating mild cognitive impairment (MCI).
WHAT IS MILD COGNITIVE IMPAIRMENT?
MCI is a dynamic stage between normal aging and dementia. It is diagnosed in patients with an objective cognitive deficit but preserved function.
Population-based studies have found a wide range of rates of MCI incidence (21.5–71.3 per 1,000 person-years) and prevalence (3%–42%).1 The risk of progression from MCI to dementia ranges from 5% to 25% per year and is highest with MCI that involves memory loss (amnestic MCI).2,3
MCI can be regarded as a syndrome that is often associated with Alzheimer pathology and that has variable outcomes. In MCI due to Alzheimer disease, the primary complaint is short-term memory loss.4 Patients who have multiple impaired cognitive domains with prominent deficits in attention and executive function and relatively unimpaired short-term memory (nonamnestic MCI) are more likely to have vascular or Lewy body pathologies.5 Although distinctions between amnestic and nonamnestic MCI can be useful for counseling patients, both subtypes have similar proportions of “pure” Alzheimer disease pathology, vascular infarcts, and other pathologies at autopsy.5,6
GENERAL MANAGEMENT—IMPROVE OVERALL HEALTH
Primary management of MCI should focus on improving lifestyle factors and treating comorbid conditions that can affect cognition (eg, depression, nutritional deficiencies).
An important goal of management is to preserve working memory, ie, the ability to maintain and manipulate information while ignoring distractions. Preservation of working memory but not short-term memory is associated with slower functional decline in MCI and early Alzheimer disease.7 Lifestyle factors including sleep, stress, and exercise affect working memory performance and, thus, functional ability.
Minimizing the risk of traumatic brain injury by reducing the risk of falling is also important. Although the role of alcohol consumption as it relates to cognition is controversial, physicians may counsel older adults with MCI to reduce their alcohol consumption even if they are consuming no more than one standard drink in a 24-hour period, in order to reduce the risk of falls and their sequelae.
Optimally controlling blood pressure, lipids, and blood sugar can reduce cardiovascular risk and may slow progression of MCI to dementia.2
Smoking should be stopped and polypharmacy avoided, with particular emphasis on eliminating medications included in the Beers criteria.8
A HEALTHY DIET MAY HELP
Although evidence supporting the benefits of various diets for MCI remains scarce with mixed results, a healthy diet may favorably affect cognition. A 2009 systematic review found that observational studies showed that long-chain omega-3 fatty acids had a positive influence on cognition, but results from clinical trials were equivocal.9 Studies investigating the impact on cognition of the Mediterranean diet—rich in vegetables, fruits, whole grains, lean protein, and olive oil—remain mixed (possibly because of dietary and cognitive measurement variations between studies) but suggest that it promotes slower cognitive decline.10
PHYSICAL ACTIVITY HAS MULTIPLE BENEFITS
Physical activity has many health benefits in the elderly: it reduces muscle loss, increases functional capacity, and decreases the risk of falls.11 Several randomized controlled trials have explored the relationship between physical activity and cognition in patients with varying degrees of cognitive impairment. Although the optimal type and duration of exercise needed to achieve a specific benefit remains unclear, physical activity has been found to be helpful in more studies than not.12 Baker et al13 found that 45 to 60 minutes of high-intensity aerobic activity 4 days a week for 6 months improved executive function.
MAINTAIN SOCIAL ACTIVITIES
Social engagement—which can include a range of activities from conversation to structured group activities—is important for maintaining cognitive function.
A prospective cohort study14 that followed participants for 1 to 3 years after MCI diagnosis found that those who progressed from mild to severe cognitive impairment were less likely to attend a place of worship, work, or volunteer.
A longitudinal study of 89 elderly people without known dementia evaluated measures of socialization, global cognitive function, and Alzheimer disease pathology seen on brain autopsy. Lower cognitive function was associated with more disease pathology, but social network size modified this relationship: cognitive function was less impaired than expected for those with a large social network, even for those with a high burden of brain pathology.15
ENCOURAGE BRAIN EXERCISE
Activities can include “cognitive hobbies” such as playing board games, reading, playing a musical instrument, and doing crossword puzzles. Specific cognitive training strategies (eg, mnemonics, calligraphy therapy, computer-based interventions) have shown benefits, although it is unclear if some interventions are more effective than others.12
MULTIMODAL STRATEGIES
There are no data supporting strategies that combine multiple interventions compared with a single intervention on cognitive outcome. However, most single interventions likely contain socialization as an unstated intervention. For example, group settings for a cognitive or physical activity may include interactions with an instructor and interactions with other participants. It is thus difficult to identify truly unimodal interventions.
An example of a multimodal approach for cognitive impairment is tai chi. Physical activity in tai chi is used for coordinated movements and balance; attention, visual imagery, and memory provide cognitive stimulation; and it is frequently performed in a group setting or with an instructor. A 1-year trial in 389 MCI patients found that those who practiced tai chi had lower clinical dementia rating scale scores than the control group who participated in stretching and toning exercises.16
Table 1 summarizes recommendations for patients with MCI. In addition, referral to a geriatrician should be considered for assistance with evaluation and management, particularly if the patient lacks a capable caregiver or if the caregiver is under stress.
- Ward A, Arrighi HM, Michels S, Cedarbaum JM. Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimers Dement 2012; 8:14–21.
- Mariani E, Monastero R, Mecocci P. Mild cognitive impairment: a systematic review. J Alzheimers Dis 2007; 12:23–35.
- Jean L, Bergeron ME, Thivierge S, Simard M. Cognitive intervention programs for individuals with mild cognitive impairment: systematic review of the literature. Am J Geriatr Psychiatry 2010; 18:281–296.
- Petersen RC, Parisi JE, Dickson DW, et al. Neuropathologic features of amnestic mild cognitive impairment. Arch Neurol 2006; 63:665–672.
- Schneider JA, Arvanitakis Z, Leurgans SE, Bennett DA. The neuropathology of probable Alzheimer disease and mild cognitive impairment. Ann Neurol 2009; 66:200–208.
- Ferman TJ, Smith GE, Kantarci K, et al. Nonamnestic mild cognitive impairment progresses to dementia with Lewy bodies. Neurology 2013; 81:2032–2038.
- Pillai JA, Bonner-Jackson A, Walker E, Mourany L, Cummings JL. Higher working memory predicts slower functional decline in autopsy-confirmed Alzheimer’s disease. Dement Geriatr Cogn Disord 2014; 38:224–233.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012; 60:616–631.
- Fotuhi M, Mohassel P, Yaffe K. Fish consumption, long-chain omega-3 fatty acids and risk of cognitive decline or Alzheimer disease: a complex association. Nat Clin Pract Neurol 2009; 5:140–152.
- Kuczmarski MF, Allegro D, Stave E. The association of healthful diets and cognitive function: a review. J Nutr Gerontol Geriatr 2014; 33:69–90.
- Heyn P, Abreu BC, Ottenbacher KJ. The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Arch Phys Med Rehabil 2004; 85:1694–1704.
- Horr T, Messinger-Rapport B, Pillai JA. Systematic review of strengths and limitations of randomized controlled trials for non-pharmacological interventions in mild cognitive impairment: focus on Alzheimer’s disease. J Nutr Health Aging 2015; 19:141–153.
- Baker LD, Frank LL, Foster-Schubert K, et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol 2010; 67:71-79.
- Hughes TF, Flatt JD, Fu B, Chang CC, Ganguli M. Engagement in social activities and progression from mild to severe cognitive impairment: the MYHAT study. Int Psychogeriatr 2013; 25:587–595.
- Bennett DA, Schneider JA, Tang Y, Arnold SE, Wilson RS. The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: a longitudinal cohort study. Lancet Neurol 2006; 5:406–412.
- Lam LC, Chau RC, Wong BM, et al. A 1-year randomized controlled trial comparing mind body exercise (tai chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc 2012; 13:568.e15–568.e20.
We can promote healthy nutrition, physical activity, socialization, and mental activity. These interventions help stabilize and even improve cognition, as well as enhance quality of life and mood, delay institutionalization, and reduce disruptive behaviors. However, no medication is approved by the US Food and Drug Administration for treating mild cognitive impairment (MCI).
WHAT IS MILD COGNITIVE IMPAIRMENT?
MCI is a dynamic stage between normal aging and dementia. It is diagnosed in patients with an objective cognitive deficit but preserved function.
Population-based studies have found a wide range of rates of MCI incidence (21.5–71.3 per 1,000 person-years) and prevalence (3%–42%).1 The risk of progression from MCI to dementia ranges from 5% to 25% per year and is highest with MCI that involves memory loss (amnestic MCI).2,3
MCI can be regarded as a syndrome that is often associated with Alzheimer pathology and that has variable outcomes. In MCI due to Alzheimer disease, the primary complaint is short-term memory loss.4 Patients who have multiple impaired cognitive domains with prominent deficits in attention and executive function and relatively unimpaired short-term memory (nonamnestic MCI) are more likely to have vascular or Lewy body pathologies.5 Although distinctions between amnestic and nonamnestic MCI can be useful for counseling patients, both subtypes have similar proportions of “pure” Alzheimer disease pathology, vascular infarcts, and other pathologies at autopsy.5,6
GENERAL MANAGEMENT—IMPROVE OVERALL HEALTH
Primary management of MCI should focus on improving lifestyle factors and treating comorbid conditions that can affect cognition (eg, depression, nutritional deficiencies).
An important goal of management is to preserve working memory, ie, the ability to maintain and manipulate information while ignoring distractions. Preservation of working memory but not short-term memory is associated with slower functional decline in MCI and early Alzheimer disease.7 Lifestyle factors including sleep, stress, and exercise affect working memory performance and, thus, functional ability.
Minimizing the risk of traumatic brain injury by reducing the risk of falling is also important. Although the role of alcohol consumption as it relates to cognition is controversial, physicians may counsel older adults with MCI to reduce their alcohol consumption even if they are consuming no more than one standard drink in a 24-hour period, in order to reduce the risk of falls and their sequelae.
Optimally controlling blood pressure, lipids, and blood sugar can reduce cardiovascular risk and may slow progression of MCI to dementia.2
Smoking should be stopped and polypharmacy avoided, with particular emphasis on eliminating medications included in the Beers criteria.8
A HEALTHY DIET MAY HELP
Although evidence supporting the benefits of various diets for MCI remains scarce with mixed results, a healthy diet may favorably affect cognition. A 2009 systematic review found that observational studies showed that long-chain omega-3 fatty acids had a positive influence on cognition, but results from clinical trials were equivocal.9 Studies investigating the impact on cognition of the Mediterranean diet—rich in vegetables, fruits, whole grains, lean protein, and olive oil—remain mixed (possibly because of dietary and cognitive measurement variations between studies) but suggest that it promotes slower cognitive decline.10
PHYSICAL ACTIVITY HAS MULTIPLE BENEFITS
Physical activity has many health benefits in the elderly: it reduces muscle loss, increases functional capacity, and decreases the risk of falls.11 Several randomized controlled trials have explored the relationship between physical activity and cognition in patients with varying degrees of cognitive impairment. Although the optimal type and duration of exercise needed to achieve a specific benefit remains unclear, physical activity has been found to be helpful in more studies than not.12 Baker et al13 found that 45 to 60 minutes of high-intensity aerobic activity 4 days a week for 6 months improved executive function.
MAINTAIN SOCIAL ACTIVITIES
Social engagement—which can include a range of activities from conversation to structured group activities—is important for maintaining cognitive function.
A prospective cohort study14 that followed participants for 1 to 3 years after MCI diagnosis found that those who progressed from mild to severe cognitive impairment were less likely to attend a place of worship, work, or volunteer.
A longitudinal study of 89 elderly people without known dementia evaluated measures of socialization, global cognitive function, and Alzheimer disease pathology seen on brain autopsy. Lower cognitive function was associated with more disease pathology, but social network size modified this relationship: cognitive function was less impaired than expected for those with a large social network, even for those with a high burden of brain pathology.15
ENCOURAGE BRAIN EXERCISE
Activities can include “cognitive hobbies” such as playing board games, reading, playing a musical instrument, and doing crossword puzzles. Specific cognitive training strategies (eg, mnemonics, calligraphy therapy, computer-based interventions) have shown benefits, although it is unclear if some interventions are more effective than others.12
MULTIMODAL STRATEGIES
There are no data supporting strategies that combine multiple interventions compared with a single intervention on cognitive outcome. However, most single interventions likely contain socialization as an unstated intervention. For example, group settings for a cognitive or physical activity may include interactions with an instructor and interactions with other participants. It is thus difficult to identify truly unimodal interventions.
An example of a multimodal approach for cognitive impairment is tai chi. Physical activity in tai chi is used for coordinated movements and balance; attention, visual imagery, and memory provide cognitive stimulation; and it is frequently performed in a group setting or with an instructor. A 1-year trial in 389 MCI patients found that those who practiced tai chi had lower clinical dementia rating scale scores than the control group who participated in stretching and toning exercises.16
Table 1 summarizes recommendations for patients with MCI. In addition, referral to a geriatrician should be considered for assistance with evaluation and management, particularly if the patient lacks a capable caregiver or if the caregiver is under stress.
We can promote healthy nutrition, physical activity, socialization, and mental activity. These interventions help stabilize and even improve cognition, as well as enhance quality of life and mood, delay institutionalization, and reduce disruptive behaviors. However, no medication is approved by the US Food and Drug Administration for treating mild cognitive impairment (MCI).
WHAT IS MILD COGNITIVE IMPAIRMENT?
MCI is a dynamic stage between normal aging and dementia. It is diagnosed in patients with an objective cognitive deficit but preserved function.
Population-based studies have found a wide range of rates of MCI incidence (21.5–71.3 per 1,000 person-years) and prevalence (3%–42%).1 The risk of progression from MCI to dementia ranges from 5% to 25% per year and is highest with MCI that involves memory loss (amnestic MCI).2,3
MCI can be regarded as a syndrome that is often associated with Alzheimer pathology and that has variable outcomes. In MCI due to Alzheimer disease, the primary complaint is short-term memory loss.4 Patients who have multiple impaired cognitive domains with prominent deficits in attention and executive function and relatively unimpaired short-term memory (nonamnestic MCI) are more likely to have vascular or Lewy body pathologies.5 Although distinctions between amnestic and nonamnestic MCI can be useful for counseling patients, both subtypes have similar proportions of “pure” Alzheimer disease pathology, vascular infarcts, and other pathologies at autopsy.5,6
GENERAL MANAGEMENT—IMPROVE OVERALL HEALTH
Primary management of MCI should focus on improving lifestyle factors and treating comorbid conditions that can affect cognition (eg, depression, nutritional deficiencies).
An important goal of management is to preserve working memory, ie, the ability to maintain and manipulate information while ignoring distractions. Preservation of working memory but not short-term memory is associated with slower functional decline in MCI and early Alzheimer disease.7 Lifestyle factors including sleep, stress, and exercise affect working memory performance and, thus, functional ability.
Minimizing the risk of traumatic brain injury by reducing the risk of falling is also important. Although the role of alcohol consumption as it relates to cognition is controversial, physicians may counsel older adults with MCI to reduce their alcohol consumption even if they are consuming no more than one standard drink in a 24-hour period, in order to reduce the risk of falls and their sequelae.
Optimally controlling blood pressure, lipids, and blood sugar can reduce cardiovascular risk and may slow progression of MCI to dementia.2
Smoking should be stopped and polypharmacy avoided, with particular emphasis on eliminating medications included in the Beers criteria.8
A HEALTHY DIET MAY HELP
Although evidence supporting the benefits of various diets for MCI remains scarce with mixed results, a healthy diet may favorably affect cognition. A 2009 systematic review found that observational studies showed that long-chain omega-3 fatty acids had a positive influence on cognition, but results from clinical trials were equivocal.9 Studies investigating the impact on cognition of the Mediterranean diet—rich in vegetables, fruits, whole grains, lean protein, and olive oil—remain mixed (possibly because of dietary and cognitive measurement variations between studies) but suggest that it promotes slower cognitive decline.10
PHYSICAL ACTIVITY HAS MULTIPLE BENEFITS
Physical activity has many health benefits in the elderly: it reduces muscle loss, increases functional capacity, and decreases the risk of falls.11 Several randomized controlled trials have explored the relationship between physical activity and cognition in patients with varying degrees of cognitive impairment. Although the optimal type and duration of exercise needed to achieve a specific benefit remains unclear, physical activity has been found to be helpful in more studies than not.12 Baker et al13 found that 45 to 60 minutes of high-intensity aerobic activity 4 days a week for 6 months improved executive function.
MAINTAIN SOCIAL ACTIVITIES
Social engagement—which can include a range of activities from conversation to structured group activities—is important for maintaining cognitive function.
A prospective cohort study14 that followed participants for 1 to 3 years after MCI diagnosis found that those who progressed from mild to severe cognitive impairment were less likely to attend a place of worship, work, or volunteer.
A longitudinal study of 89 elderly people without known dementia evaluated measures of socialization, global cognitive function, and Alzheimer disease pathology seen on brain autopsy. Lower cognitive function was associated with more disease pathology, but social network size modified this relationship: cognitive function was less impaired than expected for those with a large social network, even for those with a high burden of brain pathology.15
ENCOURAGE BRAIN EXERCISE
Activities can include “cognitive hobbies” such as playing board games, reading, playing a musical instrument, and doing crossword puzzles. Specific cognitive training strategies (eg, mnemonics, calligraphy therapy, computer-based interventions) have shown benefits, although it is unclear if some interventions are more effective than others.12
MULTIMODAL STRATEGIES
There are no data supporting strategies that combine multiple interventions compared with a single intervention on cognitive outcome. However, most single interventions likely contain socialization as an unstated intervention. For example, group settings for a cognitive or physical activity may include interactions with an instructor and interactions with other participants. It is thus difficult to identify truly unimodal interventions.
An example of a multimodal approach for cognitive impairment is tai chi. Physical activity in tai chi is used for coordinated movements and balance; attention, visual imagery, and memory provide cognitive stimulation; and it is frequently performed in a group setting or with an instructor. A 1-year trial in 389 MCI patients found that those who practiced tai chi had lower clinical dementia rating scale scores than the control group who participated in stretching and toning exercises.16
Table 1 summarizes recommendations for patients with MCI. In addition, referral to a geriatrician should be considered for assistance with evaluation and management, particularly if the patient lacks a capable caregiver or if the caregiver is under stress.
- Ward A, Arrighi HM, Michels S, Cedarbaum JM. Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimers Dement 2012; 8:14–21.
- Mariani E, Monastero R, Mecocci P. Mild cognitive impairment: a systematic review. J Alzheimers Dis 2007; 12:23–35.
- Jean L, Bergeron ME, Thivierge S, Simard M. Cognitive intervention programs for individuals with mild cognitive impairment: systematic review of the literature. Am J Geriatr Psychiatry 2010; 18:281–296.
- Petersen RC, Parisi JE, Dickson DW, et al. Neuropathologic features of amnestic mild cognitive impairment. Arch Neurol 2006; 63:665–672.
- Schneider JA, Arvanitakis Z, Leurgans SE, Bennett DA. The neuropathology of probable Alzheimer disease and mild cognitive impairment. Ann Neurol 2009; 66:200–208.
- Ferman TJ, Smith GE, Kantarci K, et al. Nonamnestic mild cognitive impairment progresses to dementia with Lewy bodies. Neurology 2013; 81:2032–2038.
- Pillai JA, Bonner-Jackson A, Walker E, Mourany L, Cummings JL. Higher working memory predicts slower functional decline in autopsy-confirmed Alzheimer’s disease. Dement Geriatr Cogn Disord 2014; 38:224–233.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012; 60:616–631.
- Fotuhi M, Mohassel P, Yaffe K. Fish consumption, long-chain omega-3 fatty acids and risk of cognitive decline or Alzheimer disease: a complex association. Nat Clin Pract Neurol 2009; 5:140–152.
- Kuczmarski MF, Allegro D, Stave E. The association of healthful diets and cognitive function: a review. J Nutr Gerontol Geriatr 2014; 33:69–90.
- Heyn P, Abreu BC, Ottenbacher KJ. The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Arch Phys Med Rehabil 2004; 85:1694–1704.
- Horr T, Messinger-Rapport B, Pillai JA. Systematic review of strengths and limitations of randomized controlled trials for non-pharmacological interventions in mild cognitive impairment: focus on Alzheimer’s disease. J Nutr Health Aging 2015; 19:141–153.
- Baker LD, Frank LL, Foster-Schubert K, et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol 2010; 67:71-79.
- Hughes TF, Flatt JD, Fu B, Chang CC, Ganguli M. Engagement in social activities and progression from mild to severe cognitive impairment: the MYHAT study. Int Psychogeriatr 2013; 25:587–595.
- Bennett DA, Schneider JA, Tang Y, Arnold SE, Wilson RS. The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: a longitudinal cohort study. Lancet Neurol 2006; 5:406–412.
- Lam LC, Chau RC, Wong BM, et al. A 1-year randomized controlled trial comparing mind body exercise (tai chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc 2012; 13:568.e15–568.e20.
- Ward A, Arrighi HM, Michels S, Cedarbaum JM. Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimers Dement 2012; 8:14–21.
- Mariani E, Monastero R, Mecocci P. Mild cognitive impairment: a systematic review. J Alzheimers Dis 2007; 12:23–35.
- Jean L, Bergeron ME, Thivierge S, Simard M. Cognitive intervention programs for individuals with mild cognitive impairment: systematic review of the literature. Am J Geriatr Psychiatry 2010; 18:281–296.
- Petersen RC, Parisi JE, Dickson DW, et al. Neuropathologic features of amnestic mild cognitive impairment. Arch Neurol 2006; 63:665–672.
- Schneider JA, Arvanitakis Z, Leurgans SE, Bennett DA. The neuropathology of probable Alzheimer disease and mild cognitive impairment. Ann Neurol 2009; 66:200–208.
- Ferman TJ, Smith GE, Kantarci K, et al. Nonamnestic mild cognitive impairment progresses to dementia with Lewy bodies. Neurology 2013; 81:2032–2038.
- Pillai JA, Bonner-Jackson A, Walker E, Mourany L, Cummings JL. Higher working memory predicts slower functional decline in autopsy-confirmed Alzheimer’s disease. Dement Geriatr Cogn Disord 2014; 38:224–233.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012; 60:616–631.
- Fotuhi M, Mohassel P, Yaffe K. Fish consumption, long-chain omega-3 fatty acids and risk of cognitive decline or Alzheimer disease: a complex association. Nat Clin Pract Neurol 2009; 5:140–152.
- Kuczmarski MF, Allegro D, Stave E. The association of healthful diets and cognitive function: a review. J Nutr Gerontol Geriatr 2014; 33:69–90.
- Heyn P, Abreu BC, Ottenbacher KJ. The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Arch Phys Med Rehabil 2004; 85:1694–1704.
- Horr T, Messinger-Rapport B, Pillai JA. Systematic review of strengths and limitations of randomized controlled trials for non-pharmacological interventions in mild cognitive impairment: focus on Alzheimer’s disease. J Nutr Health Aging 2015; 19:141–153.
- Baker LD, Frank LL, Foster-Schubert K, et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol 2010; 67:71-79.
- Hughes TF, Flatt JD, Fu B, Chang CC, Ganguli M. Engagement in social activities and progression from mild to severe cognitive impairment: the MYHAT study. Int Psychogeriatr 2013; 25:587–595.
- Bennett DA, Schneider JA, Tang Y, Arnold SE, Wilson RS. The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: a longitudinal cohort study. Lancet Neurol 2006; 5:406–412.
- Lam LC, Chau RC, Wong BM, et al. A 1-year randomized controlled trial comparing mind body exercise (tai chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc 2012; 13:568.e15–568.e20.

Lady Windermere syndrome: Mycobacterium of sophistication
A 75-year-old woman was referred to our pulmonary clinic with a 4-year history of intermittent episodes of persistent cough, occasionally productive of sputum, and mild exertional dyspnea. She had been treated with azithromycin for presumed community-acquired pneumonia, and her symptoms had initially improved. Subsequently, she experienced discrete, recurrent episodes of “bronchitis,” with productive cough and mild exertional dyspnea. Testing for latent tuberculosis had been negative. She reported a 10-pack-year smoking history in the remote past.
Her medical history included asthma, atrial fibrillation, gastroesophageal reflux disorder, hyperlipidemia, osteopenia, hypothyroidism, and allergic rhinitis. Her current medications were metoprolol, propafenone, and warfarin.
ABNORMALITIES ON PREVIOUS IMAGING
Computed tomography (CT) in April 2010 had revealed scattered linear, nodular, and “tree-in-bud” opacities involving the bilateral apices and the upper, middle, and lower lobes of the right lung, suggestive of bronchiolitis. Mild bronchiectasis had also been noted (Figure 1). Chest radiography had demonstrated signs of bronchiectasis and several scattered nodules (Figure 2). These abnormalities were still present on another CT scan in May 2013.
The patient had not undergone bronchoscopy before she was referred to our clinic.
WORKUP AT OUR CLINIC
On examination, the patient was lean, with a body mass index of 20.53 kg/m2. She appeared calm, well-groomed, and well-dressed, and had a very polite manner. When she coughed, she tried to suppress it, as if she were self-conscious about it. Her heart rhythm was irregularly irregular with a normal rate.
Expectorated sputum samples were obtained. Stains for acid-fast bacilli were negative, but three cultures were positive for acid-fast bacilli consistent with Mycobacterium avium-intracellulare. Serologic studies were negative for fungal infection and immunoglobulin deficiency.
Based on her symptoms and on the findings of imaging studies and sputum culture, we arrived at the diagnosis of nontuberculous mycobacterial lung infection, specifically, Lady Windermere syndrome.
NONTUBERCULOUS MYOCOBACTERIAL LUNG INFECTION
The diagnosis of nontuberculous mycobacterial lung infection is based on respiratory symptoms, findings on imaging (eg, nodular or cavitary opacities on radiography, or multifocal bronchiectasis and multiple small nodules on CT), and a positive culture for nontuberculous mycobacterial infection in more than two specimens of expectorated sputum or in more than one specimen from bronchoalveolar lavage. Lung biopsy with tissue culture is another way to confirm the diagnosis.
LADY WINDERMERE SYNDROME
Lady Windermere syndrome was described more than 20 years ago.1 The name derives from the lead character in Oscar Wilde’s play Lady Windermere’s Fan, which satirizes the strict morals and polite manners typical of the Victorian era in Great Britain.2
The patient with Lady Windermere syndrome is typically a thin, lean, well-mannered elderly woman who voluntarily suppresses her cough out of politeness. Suppression of the cough is thought to predispose to lung infection by allowing secretions to collect in the airways, especially in the right middle lobe, which has the longest and narrowest of the lobar bronchi.3,4
Symptoms of Lady Windermere syndrome include cough, sputum production, and fatigue similar to that of acute or chronic bronchitis. Dyspnea, fever, and hemoptysis are less common.5 The differential diagnosis for these symptoms is broad and includes asthma, chronic obstructive pulmonary disease, gastroesophageal reflux disease, pneumonia, bronchiectasis, cystic fibrosis, interstitial lung disease, postnasal drip, lung cancer, and heart failure.
A prospective cohort study by Kim et al6 yielded descriptions of typical patients with Lady Windermere syndrome. Patients were tall and lean, tended to have scoliosis, and more commonly had pectus excavatum or mitral valve prolapse; 95% were women, 91% were white, and the average age was 60. The morphologic features are thought to contribute to impaired clearance of airway secretions by altered mechanics during coughing.
HALLMARKS ON IMAGING
Kim et al6 reported that the most common findings on lung imaging in nontuberculous mycobacterial infection were bronchiectasis involving the right middle lobe (90%), nodules involving the right lower lobe (73%) and right middle lobe (71%), and, less commonly, a cavitary infiltrate involving the right upper lobe (17%) or right middle lobe (10%).
Key findings on imaging in Lady Windermere syndrome include opacities and “cylindrical bronchiectasis” predominantly involving the right middle lobe or lingula.5 Bronchiolar inflammation in response to nontuberculous mycobacterial infection may cause a nodular appearance, often progressing to a tree-in-bud appearance on CT.
Other diagnostic considerations for tree-in-bud appearance on CT include fungal, viral, or other bacterial infection, aspiration pneumonitis, inhalation of a foreign substance, cystic fibrosis, rheumatoid arthritis, SjÖgren syndrome, bronchiolitis obliterans, and neoplastic disease.
CURRENT TREATMENT OPTIONS
Treatment of nontuberculous mycobacterial lung infection, including Lady Windermere syndrome, is not necessary in every case, given the variability in clinical symptoms and in disease progression. Patients with progressive symptoms or radiographic changes should be considered candidates for treatment.
Management is directed at the underlying infection. M avium-intracellulare is ubiquitous in the environment, including in soil and water, and it has been reported as the most common pathogen in nontuberculous mycobacterial lung infection.7
Nodular-bronchiectatic nontuberculous mycobacterial lung disease typically progresses more slowly than fibrocavitary disease. For patients with nodular-bronchiectatic disease, follow-up over months or years may be needed before clinical or radiographic changes become apparent.
When treatment is indicated for nodular-bronchiectatic nontuberculous mycobacterial lung infection, it should include a macrolide antibiotic, ethambutol, and rifampin.7,8 Monotherapy with a macrolide is not recommended because of the risk of macrolide resistance. Addition of an aminoglycoside may be considered when treating fibrocavitary disease or widespread nodular bronchiectatic disease.
Management of bronchiectasis, when present, includes chest physiotherapy, pulmonary hygiene therapy, and awareness of the predisposition for nonmycobacterial lung infection. The decision to prescribe antimicrobials should take into consideration the risks and benefits for each patient.
Because treatment involves multidrug regimens, drug interactions and adverse effects need to be considered and monitored, especially in elderly patients, who may already be taking multiple medications. Treatment should be continued until a patient has negative sputum cultures for acid-fast bacilli while on therapy, for 1 year.
- Reich JM, Johnson RE. Mycobacterium avium complex pulmonary disease presenting as an isolated lingular or middle lobe pattern. The Lady Windermere syndrome. Chest 1992; 101:1605–1609.
- Kasthoori JJ, Liam CK, Wastie ML. Lady Windermere syndrome: an inappropriate eponym for an increasingly important condition. Singapore Med J 2008; 49:e47–e49.
- Dhillon SS, Watanakunakorn C. Lady Windermere syndrome: middle lobe bronchiectasis and mycobacterium avium complex infection due to voluntary cough suppression. Clin Infect Dis 2000; 30:572–575.
- Reich JM. Pathogenesis of Lady Windermere syndrome. Scand J Infect Dis 2012; 44:1–2.
- Glassroth J. Pulmonary disease due to nontuberculous mycobacteria. Chest 2008; 133:243–251.
- Kim RD, Greenberg DE, Ehrmantraut ME, et al. Pulmonary nontuberculous mycobacterial disease: prospective study of a distinct preexisting syndrome. Am J Respir Crit Care Med 2008; 178:1066–1074.
- Griffith DE, Aksamit T, Brown-Elliott BA, et al; ATS Mycobacterial Diseases Subcommittee; American Thoracic Society; Infectious Disease Society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007; 175:367–416.
- Mason RJ, Broaddus VC, Martin T, et al, editors. Murray and Nadel’s Textbook of Respiratory Medicine. 5th ed. Philadelphia, PA: Saunders; 2010.
A 75-year-old woman was referred to our pulmonary clinic with a 4-year history of intermittent episodes of persistent cough, occasionally productive of sputum, and mild exertional dyspnea. She had been treated with azithromycin for presumed community-acquired pneumonia, and her symptoms had initially improved. Subsequently, she experienced discrete, recurrent episodes of “bronchitis,” with productive cough and mild exertional dyspnea. Testing for latent tuberculosis had been negative. She reported a 10-pack-year smoking history in the remote past.
Her medical history included asthma, atrial fibrillation, gastroesophageal reflux disorder, hyperlipidemia, osteopenia, hypothyroidism, and allergic rhinitis. Her current medications were metoprolol, propafenone, and warfarin.
ABNORMALITIES ON PREVIOUS IMAGING
Computed tomography (CT) in April 2010 had revealed scattered linear, nodular, and “tree-in-bud” opacities involving the bilateral apices and the upper, middle, and lower lobes of the right lung, suggestive of bronchiolitis. Mild bronchiectasis had also been noted (Figure 1). Chest radiography had demonstrated signs of bronchiectasis and several scattered nodules (Figure 2). These abnormalities were still present on another CT scan in May 2013.
The patient had not undergone bronchoscopy before she was referred to our clinic.
WORKUP AT OUR CLINIC
On examination, the patient was lean, with a body mass index of 20.53 kg/m2. She appeared calm, well-groomed, and well-dressed, and had a very polite manner. When she coughed, she tried to suppress it, as if she were self-conscious about it. Her heart rhythm was irregularly irregular with a normal rate.
Expectorated sputum samples were obtained. Stains for acid-fast bacilli were negative, but three cultures were positive for acid-fast bacilli consistent with Mycobacterium avium-intracellulare. Serologic studies were negative for fungal infection and immunoglobulin deficiency.
Based on her symptoms and on the findings of imaging studies and sputum culture, we arrived at the diagnosis of nontuberculous mycobacterial lung infection, specifically, Lady Windermere syndrome.
NONTUBERCULOUS MYOCOBACTERIAL LUNG INFECTION
The diagnosis of nontuberculous mycobacterial lung infection is based on respiratory symptoms, findings on imaging (eg, nodular or cavitary opacities on radiography, or multifocal bronchiectasis and multiple small nodules on CT), and a positive culture for nontuberculous mycobacterial infection in more than two specimens of expectorated sputum or in more than one specimen from bronchoalveolar lavage. Lung biopsy with tissue culture is another way to confirm the diagnosis.
LADY WINDERMERE SYNDROME
Lady Windermere syndrome was described more than 20 years ago.1 The name derives from the lead character in Oscar Wilde’s play Lady Windermere’s Fan, which satirizes the strict morals and polite manners typical of the Victorian era in Great Britain.2
The patient with Lady Windermere syndrome is typically a thin, lean, well-mannered elderly woman who voluntarily suppresses her cough out of politeness. Suppression of the cough is thought to predispose to lung infection by allowing secretions to collect in the airways, especially in the right middle lobe, which has the longest and narrowest of the lobar bronchi.3,4
Symptoms of Lady Windermere syndrome include cough, sputum production, and fatigue similar to that of acute or chronic bronchitis. Dyspnea, fever, and hemoptysis are less common.5 The differential diagnosis for these symptoms is broad and includes asthma, chronic obstructive pulmonary disease, gastroesophageal reflux disease, pneumonia, bronchiectasis, cystic fibrosis, interstitial lung disease, postnasal drip, lung cancer, and heart failure.
A prospective cohort study by Kim et al6 yielded descriptions of typical patients with Lady Windermere syndrome. Patients were tall and lean, tended to have scoliosis, and more commonly had pectus excavatum or mitral valve prolapse; 95% were women, 91% were white, and the average age was 60. The morphologic features are thought to contribute to impaired clearance of airway secretions by altered mechanics during coughing.
HALLMARKS ON IMAGING
Kim et al6 reported that the most common findings on lung imaging in nontuberculous mycobacterial infection were bronchiectasis involving the right middle lobe (90%), nodules involving the right lower lobe (73%) and right middle lobe (71%), and, less commonly, a cavitary infiltrate involving the right upper lobe (17%) or right middle lobe (10%).
Key findings on imaging in Lady Windermere syndrome include opacities and “cylindrical bronchiectasis” predominantly involving the right middle lobe or lingula.5 Bronchiolar inflammation in response to nontuberculous mycobacterial infection may cause a nodular appearance, often progressing to a tree-in-bud appearance on CT.
Other diagnostic considerations for tree-in-bud appearance on CT include fungal, viral, or other bacterial infection, aspiration pneumonitis, inhalation of a foreign substance, cystic fibrosis, rheumatoid arthritis, SjÖgren syndrome, bronchiolitis obliterans, and neoplastic disease.
CURRENT TREATMENT OPTIONS
Treatment of nontuberculous mycobacterial lung infection, including Lady Windermere syndrome, is not necessary in every case, given the variability in clinical symptoms and in disease progression. Patients with progressive symptoms or radiographic changes should be considered candidates for treatment.
Management is directed at the underlying infection. M avium-intracellulare is ubiquitous in the environment, including in soil and water, and it has been reported as the most common pathogen in nontuberculous mycobacterial lung infection.7
Nodular-bronchiectatic nontuberculous mycobacterial lung disease typically progresses more slowly than fibrocavitary disease. For patients with nodular-bronchiectatic disease, follow-up over months or years may be needed before clinical or radiographic changes become apparent.
When treatment is indicated for nodular-bronchiectatic nontuberculous mycobacterial lung infection, it should include a macrolide antibiotic, ethambutol, and rifampin.7,8 Monotherapy with a macrolide is not recommended because of the risk of macrolide resistance. Addition of an aminoglycoside may be considered when treating fibrocavitary disease or widespread nodular bronchiectatic disease.
Management of bronchiectasis, when present, includes chest physiotherapy, pulmonary hygiene therapy, and awareness of the predisposition for nonmycobacterial lung infection. The decision to prescribe antimicrobials should take into consideration the risks and benefits for each patient.
Because treatment involves multidrug regimens, drug interactions and adverse effects need to be considered and monitored, especially in elderly patients, who may already be taking multiple medications. Treatment should be continued until a patient has negative sputum cultures for acid-fast bacilli while on therapy, for 1 year.
A 75-year-old woman was referred to our pulmonary clinic with a 4-year history of intermittent episodes of persistent cough, occasionally productive of sputum, and mild exertional dyspnea. She had been treated with azithromycin for presumed community-acquired pneumonia, and her symptoms had initially improved. Subsequently, she experienced discrete, recurrent episodes of “bronchitis,” with productive cough and mild exertional dyspnea. Testing for latent tuberculosis had been negative. She reported a 10-pack-year smoking history in the remote past.
Her medical history included asthma, atrial fibrillation, gastroesophageal reflux disorder, hyperlipidemia, osteopenia, hypothyroidism, and allergic rhinitis. Her current medications were metoprolol, propafenone, and warfarin.
ABNORMALITIES ON PREVIOUS IMAGING
Computed tomography (CT) in April 2010 had revealed scattered linear, nodular, and “tree-in-bud” opacities involving the bilateral apices and the upper, middle, and lower lobes of the right lung, suggestive of bronchiolitis. Mild bronchiectasis had also been noted (Figure 1). Chest radiography had demonstrated signs of bronchiectasis and several scattered nodules (Figure 2). These abnormalities were still present on another CT scan in May 2013.
The patient had not undergone bronchoscopy before she was referred to our clinic.
WORKUP AT OUR CLINIC
On examination, the patient was lean, with a body mass index of 20.53 kg/m2. She appeared calm, well-groomed, and well-dressed, and had a very polite manner. When she coughed, she tried to suppress it, as if she were self-conscious about it. Her heart rhythm was irregularly irregular with a normal rate.
Expectorated sputum samples were obtained. Stains for acid-fast bacilli were negative, but three cultures were positive for acid-fast bacilli consistent with Mycobacterium avium-intracellulare. Serologic studies were negative for fungal infection and immunoglobulin deficiency.
Based on her symptoms and on the findings of imaging studies and sputum culture, we arrived at the diagnosis of nontuberculous mycobacterial lung infection, specifically, Lady Windermere syndrome.
NONTUBERCULOUS MYOCOBACTERIAL LUNG INFECTION
The diagnosis of nontuberculous mycobacterial lung infection is based on respiratory symptoms, findings on imaging (eg, nodular or cavitary opacities on radiography, or multifocal bronchiectasis and multiple small nodules on CT), and a positive culture for nontuberculous mycobacterial infection in more than two specimens of expectorated sputum or in more than one specimen from bronchoalveolar lavage. Lung biopsy with tissue culture is another way to confirm the diagnosis.
LADY WINDERMERE SYNDROME
Lady Windermere syndrome was described more than 20 years ago.1 The name derives from the lead character in Oscar Wilde’s play Lady Windermere’s Fan, which satirizes the strict morals and polite manners typical of the Victorian era in Great Britain.2
The patient with Lady Windermere syndrome is typically a thin, lean, well-mannered elderly woman who voluntarily suppresses her cough out of politeness. Suppression of the cough is thought to predispose to lung infection by allowing secretions to collect in the airways, especially in the right middle lobe, which has the longest and narrowest of the lobar bronchi.3,4
Symptoms of Lady Windermere syndrome include cough, sputum production, and fatigue similar to that of acute or chronic bronchitis. Dyspnea, fever, and hemoptysis are less common.5 The differential diagnosis for these symptoms is broad and includes asthma, chronic obstructive pulmonary disease, gastroesophageal reflux disease, pneumonia, bronchiectasis, cystic fibrosis, interstitial lung disease, postnasal drip, lung cancer, and heart failure.
A prospective cohort study by Kim et al6 yielded descriptions of typical patients with Lady Windermere syndrome. Patients were tall and lean, tended to have scoliosis, and more commonly had pectus excavatum or mitral valve prolapse; 95% were women, 91% were white, and the average age was 60. The morphologic features are thought to contribute to impaired clearance of airway secretions by altered mechanics during coughing.
HALLMARKS ON IMAGING
Kim et al6 reported that the most common findings on lung imaging in nontuberculous mycobacterial infection were bronchiectasis involving the right middle lobe (90%), nodules involving the right lower lobe (73%) and right middle lobe (71%), and, less commonly, a cavitary infiltrate involving the right upper lobe (17%) or right middle lobe (10%).
Key findings on imaging in Lady Windermere syndrome include opacities and “cylindrical bronchiectasis” predominantly involving the right middle lobe or lingula.5 Bronchiolar inflammation in response to nontuberculous mycobacterial infection may cause a nodular appearance, often progressing to a tree-in-bud appearance on CT.
Other diagnostic considerations for tree-in-bud appearance on CT include fungal, viral, or other bacterial infection, aspiration pneumonitis, inhalation of a foreign substance, cystic fibrosis, rheumatoid arthritis, SjÖgren syndrome, bronchiolitis obliterans, and neoplastic disease.
CURRENT TREATMENT OPTIONS
Treatment of nontuberculous mycobacterial lung infection, including Lady Windermere syndrome, is not necessary in every case, given the variability in clinical symptoms and in disease progression. Patients with progressive symptoms or radiographic changes should be considered candidates for treatment.
Management is directed at the underlying infection. M avium-intracellulare is ubiquitous in the environment, including in soil and water, and it has been reported as the most common pathogen in nontuberculous mycobacterial lung infection.7
Nodular-bronchiectatic nontuberculous mycobacterial lung disease typically progresses more slowly than fibrocavitary disease. For patients with nodular-bronchiectatic disease, follow-up over months or years may be needed before clinical or radiographic changes become apparent.
When treatment is indicated for nodular-bronchiectatic nontuberculous mycobacterial lung infection, it should include a macrolide antibiotic, ethambutol, and rifampin.7,8 Monotherapy with a macrolide is not recommended because of the risk of macrolide resistance. Addition of an aminoglycoside may be considered when treating fibrocavitary disease or widespread nodular bronchiectatic disease.
Management of bronchiectasis, when present, includes chest physiotherapy, pulmonary hygiene therapy, and awareness of the predisposition for nonmycobacterial lung infection. The decision to prescribe antimicrobials should take into consideration the risks and benefits for each patient.
Because treatment involves multidrug regimens, drug interactions and adverse effects need to be considered and monitored, especially in elderly patients, who may already be taking multiple medications. Treatment should be continued until a patient has negative sputum cultures for acid-fast bacilli while on therapy, for 1 year.
- Reich JM, Johnson RE. Mycobacterium avium complex pulmonary disease presenting as an isolated lingular or middle lobe pattern. The Lady Windermere syndrome. Chest 1992; 101:1605–1609.
- Kasthoori JJ, Liam CK, Wastie ML. Lady Windermere syndrome: an inappropriate eponym for an increasingly important condition. Singapore Med J 2008; 49:e47–e49.
- Dhillon SS, Watanakunakorn C. Lady Windermere syndrome: middle lobe bronchiectasis and mycobacterium avium complex infection due to voluntary cough suppression. Clin Infect Dis 2000; 30:572–575.
- Reich JM. Pathogenesis of Lady Windermere syndrome. Scand J Infect Dis 2012; 44:1–2.
- Glassroth J. Pulmonary disease due to nontuberculous mycobacteria. Chest 2008; 133:243–251.
- Kim RD, Greenberg DE, Ehrmantraut ME, et al. Pulmonary nontuberculous mycobacterial disease: prospective study of a distinct preexisting syndrome. Am J Respir Crit Care Med 2008; 178:1066–1074.
- Griffith DE, Aksamit T, Brown-Elliott BA, et al; ATS Mycobacterial Diseases Subcommittee; American Thoracic Society; Infectious Disease Society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007; 175:367–416.
- Mason RJ, Broaddus VC, Martin T, et al, editors. Murray and Nadel’s Textbook of Respiratory Medicine. 5th ed. Philadelphia, PA: Saunders; 2010.
- Reich JM, Johnson RE. Mycobacterium avium complex pulmonary disease presenting as an isolated lingular or middle lobe pattern. The Lady Windermere syndrome. Chest 1992; 101:1605–1609.
- Kasthoori JJ, Liam CK, Wastie ML. Lady Windermere syndrome: an inappropriate eponym for an increasingly important condition. Singapore Med J 2008; 49:e47–e49.
- Dhillon SS, Watanakunakorn C. Lady Windermere syndrome: middle lobe bronchiectasis and mycobacterium avium complex infection due to voluntary cough suppression. Clin Infect Dis 2000; 30:572–575.
- Reich JM. Pathogenesis of Lady Windermere syndrome. Scand J Infect Dis 2012; 44:1–2.
- Glassroth J. Pulmonary disease due to nontuberculous mycobacteria. Chest 2008; 133:243–251.
- Kim RD, Greenberg DE, Ehrmantraut ME, et al. Pulmonary nontuberculous mycobacterial disease: prospective study of a distinct preexisting syndrome. Am J Respir Crit Care Med 2008; 178:1066–1074.
- Griffith DE, Aksamit T, Brown-Elliott BA, et al; ATS Mycobacterial Diseases Subcommittee; American Thoracic Society; Infectious Disease Society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007; 175:367–416.
- Mason RJ, Broaddus VC, Martin T, et al, editors. Murray and Nadel’s Textbook of Respiratory Medicine. 5th ed. Philadelphia, PA: Saunders; 2010.

Reflux redux

Symptoms compatible with gastroesophageal reflux disease (GERD) are incredibly prevalent. The typical ones are common, and the atypical ones are so often attributed to GERD that they too are extremely common. It seems that few patients in my clinic are not taking a proton pump inhibitor (PPI).
Drs. Alzubaidi and Gabbard, in their review of GERD in this issue, note that up to 40% of people experience symptoms of GERD at least once monthly. Since these symptoms can be intermittent, diagnosis poses a problem when the diagnostic algorithm includes a trial of a PPI. It is sometimes unclear whether PPI therapy relieved the symptoms or whether the symptoms abated for other reasons. I suspect that many patients remain on PPI therapy longer than needed (and often longer than initially intended) because of a false sense of improvement and continued need. When patients are diagnosed on clinical grounds, we need to intermittently reassess the continued need for PPI therapy. The authors discuss and place in reasonable perspective a few of the potential complications of chronic PPI use, but not the effects on absorption of iron, calcium, and micronutrients, or PPI-associated gastric polyposis. These can be clinically significant in some patients.
I believe that some atypical symptoms such as cough and hoarseness are overly attributed to GERD, so that PPI therapy is started, continued, and escalated due to premature closure of the diagnosis. I believe that the diagnosis should be reassessed at least once with observed withdrawal of PPI therapy in patients who did not have a firm physiologic diagnosis. Asking the patient to keep a symptom diary may help.
Lack of a significant response to PPI therapy should cast doubt on the diagnosis of GERD and warrant exploration for an alternative cause of the symptoms (eg, eosinophilic esophagitis, bile reflux, sinus disease, dysmotility). The possibility that the patient was not given an optimal trial of a PPI must also be considered: eg, the dose may have been inadequate, the timing of administration may have been suboptimal (not preprandial), or the patient may have been taking over-the-counter NSAIDs.
GERD is so prevalent in the general population that we must train ourselves to consider the possibility that, even if totally relieved by PPI therapy, the symptoms might be associated with aggravating comorbid conditions such as obstructive sleep apnea, Raynaud phenomenon, drugs that can decrease the tone of the lower esophageal sphincter, or even scleroderma.
Finally, in patients who have had a less-than-total response to full-dose PPI therapy and have had other diagnoses excluded, we shouldn’t forget the value of adding appropriately timed histamine 2 receptor antagonist therapy (and asking the patient about use of medications that can exacerbate symptoms).
Even the diseases we deal with every day sometimes warrant a second look.
Symptoms compatible with gastroesophageal reflux disease (GERD) are incredibly prevalent. The typical ones are common, and the atypical ones are so often attributed to GERD that they too are extremely common. It seems that few patients in my clinic are not taking a proton pump inhibitor (PPI).
Drs. Alzubaidi and Gabbard, in their review of GERD in this issue, note that up to 40% of people experience symptoms of GERD at least once monthly. Since these symptoms can be intermittent, diagnosis poses a problem when the diagnostic algorithm includes a trial of a PPI. It is sometimes unclear whether PPI therapy relieved the symptoms or whether the symptoms abated for other reasons. I suspect that many patients remain on PPI therapy longer than needed (and often longer than initially intended) because of a false sense of improvement and continued need. When patients are diagnosed on clinical grounds, we need to intermittently reassess the continued need for PPI therapy. The authors discuss and place in reasonable perspective a few of the potential complications of chronic PPI use, but not the effects on absorption of iron, calcium, and micronutrients, or PPI-associated gastric polyposis. These can be clinically significant in some patients.
I believe that some atypical symptoms such as cough and hoarseness are overly attributed to GERD, so that PPI therapy is started, continued, and escalated due to premature closure of the diagnosis. I believe that the diagnosis should be reassessed at least once with observed withdrawal of PPI therapy in patients who did not have a firm physiologic diagnosis. Asking the patient to keep a symptom diary may help.
Lack of a significant response to PPI therapy should cast doubt on the diagnosis of GERD and warrant exploration for an alternative cause of the symptoms (eg, eosinophilic esophagitis, bile reflux, sinus disease, dysmotility). The possibility that the patient was not given an optimal trial of a PPI must also be considered: eg, the dose may have been inadequate, the timing of administration may have been suboptimal (not preprandial), or the patient may have been taking over-the-counter NSAIDs.
GERD is so prevalent in the general population that we must train ourselves to consider the possibility that, even if totally relieved by PPI therapy, the symptoms might be associated with aggravating comorbid conditions such as obstructive sleep apnea, Raynaud phenomenon, drugs that can decrease the tone of the lower esophageal sphincter, or even scleroderma.
Finally, in patients who have had a less-than-total response to full-dose PPI therapy and have had other diagnoses excluded, we shouldn’t forget the value of adding appropriately timed histamine 2 receptor antagonist therapy (and asking the patient about use of medications that can exacerbate symptoms).
Even the diseases we deal with every day sometimes warrant a second look.
Symptoms compatible with gastroesophageal reflux disease (GERD) are incredibly prevalent. The typical ones are common, and the atypical ones are so often attributed to GERD that they too are extremely common. It seems that few patients in my clinic are not taking a proton pump inhibitor (PPI).
Drs. Alzubaidi and Gabbard, in their review of GERD in this issue, note that up to 40% of people experience symptoms of GERD at least once monthly. Since these symptoms can be intermittent, diagnosis poses a problem when the diagnostic algorithm includes a trial of a PPI. It is sometimes unclear whether PPI therapy relieved the symptoms or whether the symptoms abated for other reasons. I suspect that many patients remain on PPI therapy longer than needed (and often longer than initially intended) because of a false sense of improvement and continued need. When patients are diagnosed on clinical grounds, we need to intermittently reassess the continued need for PPI therapy. The authors discuss and place in reasonable perspective a few of the potential complications of chronic PPI use, but not the effects on absorption of iron, calcium, and micronutrients, or PPI-associated gastric polyposis. These can be clinically significant in some patients.
I believe that some atypical symptoms such as cough and hoarseness are overly attributed to GERD, so that PPI therapy is started, continued, and escalated due to premature closure of the diagnosis. I believe that the diagnosis should be reassessed at least once with observed withdrawal of PPI therapy in patients who did not have a firm physiologic diagnosis. Asking the patient to keep a symptom diary may help.
Lack of a significant response to PPI therapy should cast doubt on the diagnosis of GERD and warrant exploration for an alternative cause of the symptoms (eg, eosinophilic esophagitis, bile reflux, sinus disease, dysmotility). The possibility that the patient was not given an optimal trial of a PPI must also be considered: eg, the dose may have been inadequate, the timing of administration may have been suboptimal (not preprandial), or the patient may have been taking over-the-counter NSAIDs.
GERD is so prevalent in the general population that we must train ourselves to consider the possibility that, even if totally relieved by PPI therapy, the symptoms might be associated with aggravating comorbid conditions such as obstructive sleep apnea, Raynaud phenomenon, drugs that can decrease the tone of the lower esophageal sphincter, or even scleroderma.
Finally, in patients who have had a less-than-total response to full-dose PPI therapy and have had other diagnoses excluded, we shouldn’t forget the value of adding appropriately timed histamine 2 receptor antagonist therapy (and asking the patient about use of medications that can exacerbate symptoms).
Even the diseases we deal with every day sometimes warrant a second look.
GERD: Diagnosing and treating the burn
Gastroesophageal reflux disease (GERD) is a chronic and common medical problem, with up to 40% of the population experiencing its symptoms at least once per month.1 The condition develops when the reflux of stomach contents causes troublesome symptoms or complications.2
GERD symptoms can range from heartburn and regurgitation to cough and hoarseness. While many patients’ symptoms respond to medical treatment, the diagnosis and treatment in those whose symptoms do not respond to a proton pump inhibitor (PPI) may be challenging.
This article reviews the diagnosis and treatment options for GERD.
SYMPTOMS: TYPICAL, ATYPICAL, AND ALARM
Symptoms of GERD (Table 1) can be classified as typical (heartburn and regurgitation) or atypical (cough, asthma, hoarseness, chronic laryngitis, throat-clearing, chest pain, dyspepsia, and nausea). Atypical symptoms are more likely to be due to GERD if patients also have typical symptoms and if the symptoms respond to a trial of a PPI.3
Alarm symptoms. Keep in mind that extraesophageal presentations may be multifactorial, and it may be difficult to establish that reflux, even if present, is actually the cause. While chest pain may be due to GERD, it is important to rule out cardiac chest pain before considering GERD as a cause. Similarly, dysphagia along with typical or atypical symptoms warrants investigation for potential complications such as underlying motility disorder, esophageal stricture, esophageal ring, or malignancy.4 Other alarm symptoms include odynophagia, bleeding, weight loss, and anemia.
DIAGNOSING GERD: RESPONSE TO A PPI IS DIAGNOSTIC
Patients with typical symptoms that respond to PPI therapy need no further evaluation for a diagnosis of GERD to be made.5 On the other hand, further testing should be undertaken in patients with typical symptoms that do not respond to PPI therapy, in patients presenting with atypical symptoms, and in patients in whom antireflux surgery is being considered. Figure 1 shows our proposed algorithm.
Try a PPI for 6–8 weeks
Relief of heartburn and regurgitation after a 6- to 8-week course of a PPI strongly suggests GERD.6 However, a negative trial of a PPI does not rule out GERD, as this approach has been found to have a sensitivity of 78% and specificity of 54%.6
Despite this limitation, a trial of PPI therapy should be offered to patients presenting with typical symptoms and no alarm features. This approach has been found to be more cost-effective than proceeding directly to diagnostic testing.7
Endoscopy
Endoscopic findings in GERD can include erosive esophagitis, peptic stricture, and Barrett esophagus. Esophageal erosions are a highly specific sign of GERD; the Los Angeles classification system, a standardized scale for grading the severity of erosive esophagitis (from A to D, with D the most severe) provides an objective way to assess severity.8 However, most patients with heartburn and regurgitation do not have erosive disease, thus limiting the sensitivity of upper endoscopy as an initial diagnostic test in patients with suspected GERD.9
We recommend endoscopy for patients who present with alarm symptoms, patients with noncardiac chest pain, PPI nonresponders, and patients with chronic GERD symptoms and multiple risk factors for Barrett esophagus besides GERD, such as older age, male sex, white race, overweight, and smoking.10
Ambulatory pH and impedance monitoring
Ambulatory pH monitoring is the gold standard test for pathologic acid exposure in the esophagus. pH testing is indicated in PPI nonresponders, patients presenting with atypical symptoms, and before antireflux surgery.
In general, pH testing should be performed after the patient has been off PPI therapy for at least 7 days, as the test is highly unlikely to be abnormal while a patient is on a PPI.11 It is done either with a transnasal catheter for 24 hours, or with a wireless capsule (Bravo pH System, Given Imaging Ltd, Duluth, GA), which collects 48 to 96 hours of data. Studies of the wireless system have shown that its sensitivity increases 12% to 25% when it is performed for 48 hours compared with 24 hours.12,13
The pH test can be combined with impedance testing to evaluate for nonacid reflux.14 However, the clinical significance of nonacid reflux remains controversial, and for this reason the Esophageal Diagnostic Advisory Panel recommends that the decision to perform antireflux surgery should not be based on abnormal impedance testing.15
During pH and impedance testing, special software can calculate how closely the patient’s symptoms correlate with esophageal acid exposure. The symptom index (SI) and symptom association probability (SAP) are the symptom measurements most commonly used in practice. The SI measures the overall strength of the relationship, and an SI greater than 50% is considered positive.16 The SAP determines whether this relationship could have occurred by chance, and an SAP greater than 95% is statistically significant.17 In patients with normal levels of esophageal acid exposure, an elevated SI or SAP may indicate a component of esophageal hypersensitivity in symptom generation.
At our institution, we generally perform pH-only transnasal or wireless testing off PPI therapy to establish that the patient has pathologic acid exposure in the distal esophagus. Combined pH-impedance testing is typically reserved for patients with atypical symptoms unresponsive to PPI therapy and abnormal results on previous pH testing, which allows for correlation of nonacid reflux and symptoms.
Other tests
Esophageal manometry and barium esophagography have limited value in the primary diagnosis of GERD. However, they should be considered to rule out achalasia and other esophageal motility disorders in patients whose symptoms do not respond to PPIs. For this reason, esophageal manometry should be performed before considering antireflux surgery.
MANAGING GERD
Table 2 summarizes the various treatments for GERD.
Lifestyle modifications
Lifestyle modifications are the first-line therapy for GERD. Modifications that have been studied include weight loss, head-of-bed elevation, and avoidance of tobacco, alcohol, and late-night meals. Another modification that has been suggested is avoiding foods that can aggravate reflux symptoms—eg, caffeine, coffee, chocolate, spicy foods, highly acidic foods (oranges, tomatoes), and fatty foods. Of these, only weight loss and head-of-bed elevation have been proven effective.18
Three randomized controlled trials demonstrated that GERD symptoms and esophageal pH values improved with head-of-bed elevation using blocks or incline foam wedges.19–21 Several cohort studies demonstrated reduction in GERD symptoms with weight loss.22,23 Recently, a prospective cohort study also found that smoking cessation significantly improved GERD symptoms in patients with normal body mass index and severe symptoms.24
Antacids
Several antacids (eg, sodium bicarbonate, calcium carbonate, magnesium hydroxide, aluminum hydroxide) are available over the counter.
Antacids were thought to control heartburn symptoms by increasing the pH of gastric contents that might subsequently reflux into the esophagus. However, well-controlled studies have shown that they relieve heartburn by neutralizing acid in the esophagus, with no significant effect on gastric pH.25,26
Antacids provide rapid but short-lived relief from an existing episode of heartburn. Because they do not significantly raise the gastric pH, they do not prevent subsequent reflux episodes from repeatedly exposing the esophagus to gastric acid and causing heartburn. Additionally, antacids have not been shown to contribute to healing of erosive esophagitis.27 Hence, they may not be optimal for treating frequent reflux heartburn.
Sodium alginate
Gastric acid pockets are unbuffered pools of acid that float on top of ingested food.28 They develop as a result of poor mixing of newly secreted acid and food in the proximal stomach, which remains relatively quiescent after a meal compared with the distal stomach.29 In GERD, proximal extension of the acid pocket above the diaphragm increases the risk of acid reflux.30 The acid pocket is therefore an important source of postprandial acid in GERD and, as such, represents a unique therapeutic target.
Emerging evidence suggests that alginates may act directly on the acid pocket. Alginates are natural polysaccharide polymers that, on contact with gastric acid, precipitate within minutes into a low-density viscous gel of near-neutral pH. The change in pH triggers the sodium bicarbonate in the formulation to release carbon dioxide that becomes trapped in the alginate gel, causing it to float to the top of the gastric contents like a raft.31
A randomized controlled trial demonstrated that sodium alginate was as effective as omeprazole in relieving symptoms in patients with nonerosive reflux disease.32 Alginate has also been shown to provide more postprandial reflux relief than antacids.33
Histamine-2 receptor antagonists
Histamine-2 receptor antagonists act more swiftly and increase postprandial gastric pH more rapidly than PPIs, thus making them a good option for prophylaxis against postprandial GERD.34 Taking these drugs at bedtime may help in patients with objective nighttime reflux despite optimal PPI use. However, tachyphylaxis may occur as early as 1 week after starting combination therapy.35
Proton pump inhibitors
There are currently seven available PPIs, including four that can be obtained over the counter (omeprazole, lansoprazole, esomeprazole, and omeprazole-sodium bicarbonate) and three available only by prescription (rabeprazole, pantoprazole, and dexlansoprazole). Studies have shown than a standard 6- to 8-week course of a PPI provides complete symptom relief in 70% to 80% of patients with erosive reflux disease and in 60% of patients with nonerosive reflux disease.36,37 Clinically, PPIs all appear to be similar in their symptom relief.38
Most PPIs should be taken 30 to 60 minutes before meals. Exceptions are omeprazole-sodium bicarbonate and dexlansoprazole, which can be taken without regard to meals. At our institution, we usually start PPIs in a once-daily standard dose for 6 to 8 weeks and consider increasing to twice-daily dosing if symptoms do not respond completely. Patients with mild intermittent GERD symptoms may benefit from “on-demand” use of PPIs. This approach is best suited for patients with nonerosive reflux disease without evidence of Barrett esophagus on endoscopy.
Safety and adverse effects of PPIs
PPIs are generally safe but can cause adverse effects (Table 3).
Osteoporosis. In 2010, the US Food and Drug Administration issued warnings regarding the potential for wrist, hip, and spine fractures in PPI users.26 Most recent evidence suggests that PPIs may be associated with a small increase in risk of hip fractures in patients already at high risk.39,40 However, the 2013 American College of Gastroenterology (ACG) guidelines say that patients with known osteoporosis can remain on PPI therapy, and concern for hip fractures and osteoporosis should not affect the decision to use PPIs long-term except in patients with other risk factors for hip fracture.41
Community-acquired pneumonia. An increased risk of community-acquired pneumonia cannot be clearly documented in association with PPI therapy. Multiple studies, including randomized controlled trials, investigated this potential correlation. However, evidence suggests that short-term but not long-term PPI use may be associated with an overall increased risk of community-acquired pneumonia.42,43 Current guidelines suggest that in patients who need a PPI, the drug should not be withheld on the basis of a potential risk of community-acquired pneumonia.41
Clostridium difficile infection. In theory, PPIs may increase the risk of C difficile infection by increasing the ability of the spore to convert to the vegetative form and to survive intraluminally. In fact, studies and meta-analyses have suggested that PPIs do increase the risk of development and recurrence of C difficile infection.44,45 Therefore, PPIs should be used with care in patients who are at risk.41
Interaction with clopidogrel. The antiplatelet activity of clopidogrel requires activation by CYP2C19, the same pathway required for metabolism of some PPIs. Concern was raised about decreased antiplatelet activity of clopidogrel in the presence of PPIs. This was extensively studied, and there now appears to be no increased risk of adverse cardiovascular events in patients on PPIs, based on data from well-controlled randomized trials.46,47 A consensus panel of the American College of Cardiology Foundation, the American Heart Association, and the ACG said that PPIs may be used for appropriate indications in patients taking clopidogrel.47
Hypomagnesemia. By an unknown molecular mechanism, PPIs are thought to reduce intestinal magnesium absorption, leading to hypomagnesemia. A meta-analysis published in 2011 showed that PPI-induced hypomagnesemia is a drug-class effect and occurred after a median of 5.5 years of PPI use. Stopping the PPI resulted in magnesium recovery in 4 days, and rechallenge led to recurrence within 4 days.48
Hence, to avoid putting patients on long-term PPI therapy at risk, clinicians should anticipate this problem. Our practice is to check the magnesium level before starting a patient on long-term PPI therapy, and then to repeat the measurement every 1 to 2 years.
Baclofen
Transient lower esophageal sphincter relaxation has been shown to be a cause of reflux in healthy people and in patients with GERD.49
Baclofen, a muscle relaxant with selective gamma-aminobutyric acid receptor class B agonist properties, reduces transient lower esophageal sphincter relaxation in humans.50 In a well-designed, double-blind, randomized controlled trial, baclofen was associated with a significant decrease in upright reflux on 24-hour pH monitoring and significant improvement in belching and overall reflux symptoms.51 However, baclofen is not approved by the US Food and Drug Administration for the treatment of GERD, and its use may be limited by side effects such as somnolence and dizziness.
Antireflux surgery
Antireflux surgery is a reasonable option for selected patients with chronic GERD. The main types of surgery are laparoscopic fundoplication and, for obese patients, gastric bypass. Reasons to consider antireflux surgery include desire to stop PPI therapy, esophagitis not healed by PPIs, symptomatic hiatal hernia, and refractory reflux documented by pH testing.41
In general, surgical therapy may be considered in patients who respond to PPIs, but patients who do not respond to PPIs are less likely to respond to antireflux surgery.15 Other patients less likely to respond are those with symptoms of dyspepsia, such as nausea, vomiting, and epigastric pain.41
Common adverse effects of antireflux surgery include gas-bloat syndrome (up to 85% of patients), dysphagia (10% to 50% of patients), diarrhea (18% to 33% of patients), and recurrent heartburn (10% to 62% of patients).52
Endoscopic and minimally invasive antireflux procedures include endoscopic plication of the lower esophageal sphincter, radiofrequency augmentation of the lower esophageal sphincter, and sphincter augmentation by a string of titanium beads. While some have shown promise, they are not recommended by the most recent ACG guidelines, given lack of long-term data.41
REFRACTORY GERD
There is no consensus on the definition of refractory GERD. However, for the sake of simplicity, we can define it as persistence of suspected GERD symptoms despite treatment with a PPI. This may vary from a partial response to PPI therapy to a complete absence of response.
It is extremely important to rule out non-GERD causes of the ongoing symptoms, such as achalasia, gastroparesis, eosinophilic esophagitis, rumination, and aerophagia. PPI nonresponders are more likely to be obese, poorly compliant, and have extraesophageal symptoms.53–56 As previously discussed, PPIs should be taken 30 to 60 minutes before meals. For patients whose symptoms fail to respond to standard-dose daily PPI therapy, switching to another PPI or doubling the dose is common, although data to support this practice are limited. Of note, omeprazole-sodium bicarbonate has been shown to provide more symptom relief in nocturnal GERD.57 Additionally, adding a nighttime histamine-2 receptor antagonist may also help in patients with objective nighttime reflux.41
After noncompliance and suboptimal PPI dosing have been ruled out, PPI nonresponders with typical symptoms should undergo upper endoscopy and subsequent pH monitoring. Normal esophageal acid exposure on pH testing suggests functional heartburn or functional dyspepsia. Negative pH testing in a patient with atypical symptoms suggests a non-GERD cause of symptoms, and referral to an otolaryngologist, pulmonologist, or allergist is often warranted.
While antireflux surgery can be considered for patients with nonacid reflux on impedance testing, it should again be noted that GERD in patients with no response to PPIs is less likely to respond to antireflux surgery.15
TAKE-HOME POINTS
- GERD is a common medical condition, affecting up to 40% of US adults at least once monthly.
- GERD can result in a wide variety of symptoms, including typical heartburn and regurgitation as well as atypical symptoms such as cough.
- On the other hand, keep in mind that multiple non-GERD causes of heartburn and regurgitation may exist.
- Testing for GERD includes endoscopy and pH testing as well as functional testing such as esophageal manometry.
- While in most patients GERD will respond to lifestyle changes and antisecretory therapy such as a PPI, careful attention must be given to patients with symptoms refractory to PPI therapy.
- For a subset of patients, antireflux surgery may be a reasonable option, but care must be taken to exclude patients with a lower likelihood of responding to surgery.
- Locke GR 3rd, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ 3rd. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology 1997; 112:1448–1456.
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R; Globale Konsensusgrupp. [The Montreal definition and classification of gastroesophageal reflux disease: a global, evidence-based consensus paper]. Z Gastroenterol 2007; 45:1125–1240. In German.
- Gerson LB, Kahrilas PJ, Fass R. Insights into gastroesophageal reflux disease-associated dyspeptic symptoms. Clin Gastroenterol Hepatol 2011; 9:824–833.
- Vakil NB, Traxler B, Levine D. Dysphagia in patients with erosive esophagitis: prevalence, severity, and response to proton pump inhibitor treatment. Clin Gastroenterol Hepatol 2004; 2:665–668.
- Kahrilas PJ, Shaheen NJ, aezi MF, et al; American Gastroenterological Association. American Gastroenterological Association Medical Position Statement on the management of gastroesophageal reflux disease. Gastroenterology 2008; 135:1383–1391 e1–5.
- Numans ME, Lau J, de Wit NJ, Bonis PA. Short-term treatment with proton-pump inhibitors as a test for gastroesophageal reflux disease: a meta-analysis of diagnostic test characteristics. Ann Intern Med 2004; 140:518–527.
- Fass R. Empirical trials in treatment of gastroesophageal reflux disease. Dig Dis 2000; 18:20–26.
- Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut 1999; 45:172–180.
- Johansson KE, Ask P, Boeryd B, Fransson SG, Tibbling L. Oesophagitis, signs of reflux, and gastric acid secretion in patients with symptoms of gastro-oesophageal reflux disease. Scand J Gastroenterol 1986; 21:837–847.
- Becher A, Dent J. Systematic review: ageing and gastro-oesophageal reflux disease symptoms, oesophageal function and reflux oesophagitis. Aliment Pharmacol Ther 2011; 33:442–454.
- Charbel S, Khandwala F, Vaezi MF. The role of esophageal pH monitoring in symptomatic patients on PPI therapy. Am J Gastroenterol 2005; 100:283–289.
- Pandolfino JE, Richter JE, Ours T, Guardino JM, Chapman J, Kahrilas PJ. Ambulatory esophageal pH monitoring using a wireless system. Am J Gastroenterol 2003; 98:740–749.
- Prakash C, Clouse RE. Value of extended recording time with wireless pH monitoring in evaluating gastroesophageal reflux disease. Clin Gastroenterol Hepatol 2005; 3:329–334.
- Hirano I, Richter JE; Practice Parameters Committee of the American College of Gastroenterology. ACG practice guidelines: esophageal reflux testing. Am J Gastroenterol 2007; 102:668–685.
- Jobe BA, Richter JE, Hoppo T, et al. Preoperative diagnostic workup before antireflux surgery: an evidence and experience-based consensus of the Esophageal Diagnostic Advisory Panel. J Am Coll Surg 2013; 217:586–597.
- Singh S, Richter JE, Bradley LA, Haile JM. The symptom index. Differential usefulness in suspected acid-related complaints of heartburn and chest pain. Dig Dis Sci 1993; 38:1402–1408.
- Weusten BL, Roelofs JM, Akkermans LM, Van Berge-Henegouwen GP, Smout AJ. The symptom-association probability: an improved method for symptom analysis of 24-hour esophageal pH data. Gastroenterology 1994; 107:1741–1745.
- Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidence-based approach. Arch Intern Med 2006; 166:965–971.
- Hamilton JW, Boisen RJ, Yamamoto DT, Wagner JL, Reichelderfer M. Sleeping on a wedge diminishes exposure of the esophagus to refluxed acid. Dig Dis Sci 1988; 33:518–522.
- Pollmann H, Zillessen E, Pohl J, et al. [Effect of elevated head position in bed in therapy of gastroesophageal reflux]. Z Gastroenterol 1996; 34(suppl 2):93–99. In German.
- Stanciu C, Bennett JR. Effects of posture on gastro-oesophageal reflux. Digestion 1977; 15:104–109.
- Fraser-Moodie CA, Norton B, Gornall C, Magnago S, Weale AR, Holmes GK. Weight loss has an independent beneficial effect on symptoms of gastro-oesophageal reflux in patients who are overweight. Scand J Gastroenterol 1999; 34:337–340.
- Mathus-Vliegen LM, Tytgat GN. Twenty-four-hour pH measurements in morbid obesity: effects of massive overweight, weight loss and gastric distension. Eur J Gastroenterol Hepatol 1996; 8:635–640.
- Ness-Jensen E, Lindam A, Lagergren J, Hveem K. Tobacco smoking cessation and improved gastroesophageal reflux: a prospective population-based cohort study: the HUNT study. Am J Gastroenterol 2014; 109:171–177.
- Collings KL, Rodriguez-Stanley S, Proskin HM, Robinson M, Miner PB Jr. Clinical effectiveness of a new antacid chewing gum on heartburn and oesophageal pH control. Aliment Pharmacol Ther 2002; 16:2029–2035.
- Decktor DL, Robinson M, Maton PN, Lanza FL, Gottlieb S. Effects of aluminum/magnesium hydroxide and calcium carbonate on esophageal and gastric pH in subjects with heartburn. Am J Ther 1995; 2:546–552.
- Pettit M. Treatment of gastroesophageal reflux disease. Pharm World Sci 2005; 27:432–435.
- Fletcher J, Wirz A, Young J, Vallance R, McColl KE. Unbuffered highly acidic gastric juice exists at the gastroesophageal junction after a meal. Gastroenterology 2001; 121:775–783.
- Sauter M, Curcic J, Menne D, et al. Measuring the interaction of meal and gastric secretion: a combined quantitative magnetic resonance imaging and pharmacokinetic modeling approach. Neurogastroenterol Motil 2012; 24:632–638, e272–e273.
- Beaumont H, Bennink RJ, de Jong J, Boeckxstaens GE. The position of the acid pocket as a major risk factor for acidic reflux in healthy subjects and patients with GORD. Gut 2010; 59:441–451.
- Tytgat GN, Simoneau G. Clinical and laboratory studies of the antacid and raft-forming properties of Rennie alginate suspension. Aliment Pharmacol Ther 2006; 23:759–765.
- Chiu CT, Hsu CM, Wang CC, et al. Randomised clinical trial: sodium alginate oral suspension is non-inferior to omeprazole in the treatment of patients with non-erosive gastroesophageal disease. Aliment Pharmacol Ther 2013; 38:1054–1064.
- Rohof WO, Bennink RJ, Smout AJ, Thomas E, Boeckxstaens GE. An alginate-antacid formulation localizes to the acid pocket to reduce acid reflux in patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol 2013; 11:1585–1591.
- Khoury RM, Katz PO, Castell DO. Post-prandial ranitidine is superior to post-prandial omeprazole in control of gastric acidity in healthy volunteers. Aliment Pharmacol Ther 1999; 13:1211–1214.
- Fackler WK, Ours TM, Vaezi MF, Richter JE. Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology 2002; 122:625–632.
- Robinson M, Sahba B, Avner D, Jhala N, Greski-Rose PA, Jennings DE. A comparison of lansoprazole and ranitidine in the treatment of erosive oesophagitis. Multicentre Investigational Group. Aliment Pharmacol Ther 1995; 9:25–31.
- Vantrappen G, Rutgeerts L, Schurmans P, Coenegrachts JL. Omeprazole (40 mg) is superior to ranitidine in short-term treatment of ulcerative reflux esophagitis. Dig Dis Sci 1988; 33:523–529.
- Gralnek IM, Dulai GS, Fennerty MB, Spiegel BM. Esomeprazole versus other proton pump inhibitors in erosive esophagitis: a meta-analysis of randomized clinical trials. Clin Gastroenterol Hepatol 2006; 4:1452–1458.
- Targownik LE, Lix LM, Leung S, Leslie WD. Proton-pump inhibitor use is not associated with osteoporosis or accelerated bone mineral density loss. Gastroenterology 2010; 138:896–904.
- Corley DA, Kubo A, Zhao W, Quesenberry C. Proton pump inhibitors and histamine-2 receptor antagonists are associated with hip fractures among at-risk patients. Gastroenterology 2010; 139:93–101.
- Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 2013; 108:308–328.
- Giuliano C, Wilhelm SM, Kale-Pradhan PB. Are proton pump inhibitors associated with the development of community-acquired pneumonia? A meta-analysis. Expert Rev Clin Pharmacol 2012; 5:337–344.
- Hermos JA, Young MM, Fonda JR, Gagnon DR, Fiore LD, Lawler EV. Risk of community-acquired pneumonia in veteran patients to whom proton pump inhibitors were dispensed. Clin Infect Dis 2012; 54:33–42.
- Linsky A, Gupta K, Lawler EV, Fonda JR, Hermos JA. Proton pump inhibitors and risk for recurrent Clostridium difficile infection. Arch Intern Med 2010; 170:772–778.
- Bavishi C, Dupont HL. Systematic review: the use of proton pump inhibitors and increased susceptibility to enteric infection. Aliment Pharmacol Ther 2011; 34:1269–1281.
- Bhatt DL, Cryer BL, Contant CF, et al; COGENT Investigators. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med 2010; 363:1909–1917.
- O’Donoghue ML, Braunwald E, Antman EM, et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomised trials. Lancet 2009; 374:989–997.
- Hess MW, Hoenderop JG, Bindels RJ, Drenth JP. Systematic review: hypomagnesaemia induced by proton pump inhibition. Aliment Pharmacol Ther 2012; 36:405–413.
- Mittal RK, McCallum RW. Characteristics and frequency of transient relaxations of the lower esophageal sphincter in patients with reflux esophagitis. Gastroenterology 1988; 95:593–599.
- Lidums I, Lehmann A, Checklin H, Dent J, Holloway RH. Control of transient lower esophageal sphincter relaxations and reflux by the GABA(B) agonist baclofen in normal subjects. Gastroenterology 2000; 118:7–13.
- Cossentino MJ, Mann K, Armbruster SP, Lake JM, Maydonovitch C, Wong RK. Randomised clinical trial: the effect of baclofen in patients with gastro-oesophageal reflux—a randomised prospective study. Aliment Pharmacol Ther 2012; 35:1036–1044.
- Richter JE. Gastroesophageal reflux disease treatment: side effects and complications of fundoplication. Clin Gastroenterol Hepatol 2013; 11:465–471.
- Dickman R, Boaz M, Aizic S, Beniashvili Z, Fass R, Niv Y. Comparison of clinical characteristics of patients with gastroesophageal reflux disease who failed proton pump inhibitor therapy versus those who fully responded. J Neurogastroenterol Motil 2011; 17:387–394.
- Chan WW, Chiou E, Obstein KL, Tignor AS, Whitlock TL. The efficacy of proton pump inhibitors for the treatment of asthma in adults: a meta-analysis. Arch Intern Med 2011; 171:620–629.
- Chang AB, Lasserson TJ, Gaffney J, Connor FL, Garske LA. Gastro-oesophageal reflux treatment for prolonged non-specific cough in children and adults. Cochrane Database Syst Rev 2011; 1:CD004823.
- Qadeer MA, Phillips CO, Lopez AR, et al. Proton pump inhibitor therapy for suspected GERD-related chronic laryngitis: a meta-analysis of randomized controlled trials. Am J Gastroenterol 2006; 101:2646–2654.
- Gerson LB, Mitra S, Bleker WF, Yeung P. Control of intra-oesophageal pH in patients with Barrett's oesophagus on omeprazole-sodium bicarbonate therapy. Aliment Pharmacol Ther 2012; 35:803–809.
Gastroesophageal reflux disease (GERD) is a chronic and common medical problem, with up to 40% of the population experiencing its symptoms at least once per month.1 The condition develops when the reflux of stomach contents causes troublesome symptoms or complications.2
GERD symptoms can range from heartburn and regurgitation to cough and hoarseness. While many patients’ symptoms respond to medical treatment, the diagnosis and treatment in those whose symptoms do not respond to a proton pump inhibitor (PPI) may be challenging.
This article reviews the diagnosis and treatment options for GERD.
SYMPTOMS: TYPICAL, ATYPICAL, AND ALARM
Symptoms of GERD (Table 1) can be classified as typical (heartburn and regurgitation) or atypical (cough, asthma, hoarseness, chronic laryngitis, throat-clearing, chest pain, dyspepsia, and nausea). Atypical symptoms are more likely to be due to GERD if patients also have typical symptoms and if the symptoms respond to a trial of a PPI.3
Alarm symptoms. Keep in mind that extraesophageal presentations may be multifactorial, and it may be difficult to establish that reflux, even if present, is actually the cause. While chest pain may be due to GERD, it is important to rule out cardiac chest pain before considering GERD as a cause. Similarly, dysphagia along with typical or atypical symptoms warrants investigation for potential complications such as underlying motility disorder, esophageal stricture, esophageal ring, or malignancy.4 Other alarm symptoms include odynophagia, bleeding, weight loss, and anemia.
DIAGNOSING GERD: RESPONSE TO A PPI IS DIAGNOSTIC
Patients with typical symptoms that respond to PPI therapy need no further evaluation for a diagnosis of GERD to be made.5 On the other hand, further testing should be undertaken in patients with typical symptoms that do not respond to PPI therapy, in patients presenting with atypical symptoms, and in patients in whom antireflux surgery is being considered. Figure 1 shows our proposed algorithm.
Try a PPI for 6–8 weeks
Relief of heartburn and regurgitation after a 6- to 8-week course of a PPI strongly suggests GERD.6 However, a negative trial of a PPI does not rule out GERD, as this approach has been found to have a sensitivity of 78% and specificity of 54%.6
Despite this limitation, a trial of PPI therapy should be offered to patients presenting with typical symptoms and no alarm features. This approach has been found to be more cost-effective than proceeding directly to diagnostic testing.7
Endoscopy
Endoscopic findings in GERD can include erosive esophagitis, peptic stricture, and Barrett esophagus. Esophageal erosions are a highly specific sign of GERD; the Los Angeles classification system, a standardized scale for grading the severity of erosive esophagitis (from A to D, with D the most severe) provides an objective way to assess severity.8 However, most patients with heartburn and regurgitation do not have erosive disease, thus limiting the sensitivity of upper endoscopy as an initial diagnostic test in patients with suspected GERD.9
We recommend endoscopy for patients who present with alarm symptoms, patients with noncardiac chest pain, PPI nonresponders, and patients with chronic GERD symptoms and multiple risk factors for Barrett esophagus besides GERD, such as older age, male sex, white race, overweight, and smoking.10
Ambulatory pH and impedance monitoring
Ambulatory pH monitoring is the gold standard test for pathologic acid exposure in the esophagus. pH testing is indicated in PPI nonresponders, patients presenting with atypical symptoms, and before antireflux surgery.
In general, pH testing should be performed after the patient has been off PPI therapy for at least 7 days, as the test is highly unlikely to be abnormal while a patient is on a PPI.11 It is done either with a transnasal catheter for 24 hours, or with a wireless capsule (Bravo pH System, Given Imaging Ltd, Duluth, GA), which collects 48 to 96 hours of data. Studies of the wireless system have shown that its sensitivity increases 12% to 25% when it is performed for 48 hours compared with 24 hours.12,13
The pH test can be combined with impedance testing to evaluate for nonacid reflux.14 However, the clinical significance of nonacid reflux remains controversial, and for this reason the Esophageal Diagnostic Advisory Panel recommends that the decision to perform antireflux surgery should not be based on abnormal impedance testing.15
During pH and impedance testing, special software can calculate how closely the patient’s symptoms correlate with esophageal acid exposure. The symptom index (SI) and symptom association probability (SAP) are the symptom measurements most commonly used in practice. The SI measures the overall strength of the relationship, and an SI greater than 50% is considered positive.16 The SAP determines whether this relationship could have occurred by chance, and an SAP greater than 95% is statistically significant.17 In patients with normal levels of esophageal acid exposure, an elevated SI or SAP may indicate a component of esophageal hypersensitivity in symptom generation.
At our institution, we generally perform pH-only transnasal or wireless testing off PPI therapy to establish that the patient has pathologic acid exposure in the distal esophagus. Combined pH-impedance testing is typically reserved for patients with atypical symptoms unresponsive to PPI therapy and abnormal results on previous pH testing, which allows for correlation of nonacid reflux and symptoms.
Other tests
Esophageal manometry and barium esophagography have limited value in the primary diagnosis of GERD. However, they should be considered to rule out achalasia and other esophageal motility disorders in patients whose symptoms do not respond to PPIs. For this reason, esophageal manometry should be performed before considering antireflux surgery.
MANAGING GERD
Table 2 summarizes the various treatments for GERD.
Lifestyle modifications
Lifestyle modifications are the first-line therapy for GERD. Modifications that have been studied include weight loss, head-of-bed elevation, and avoidance of tobacco, alcohol, and late-night meals. Another modification that has been suggested is avoiding foods that can aggravate reflux symptoms—eg, caffeine, coffee, chocolate, spicy foods, highly acidic foods (oranges, tomatoes), and fatty foods. Of these, only weight loss and head-of-bed elevation have been proven effective.18
Three randomized controlled trials demonstrated that GERD symptoms and esophageal pH values improved with head-of-bed elevation using blocks or incline foam wedges.19–21 Several cohort studies demonstrated reduction in GERD symptoms with weight loss.22,23 Recently, a prospective cohort study also found that smoking cessation significantly improved GERD symptoms in patients with normal body mass index and severe symptoms.24
Antacids
Several antacids (eg, sodium bicarbonate, calcium carbonate, magnesium hydroxide, aluminum hydroxide) are available over the counter.
Antacids were thought to control heartburn symptoms by increasing the pH of gastric contents that might subsequently reflux into the esophagus. However, well-controlled studies have shown that they relieve heartburn by neutralizing acid in the esophagus, with no significant effect on gastric pH.25,26
Antacids provide rapid but short-lived relief from an existing episode of heartburn. Because they do not significantly raise the gastric pH, they do not prevent subsequent reflux episodes from repeatedly exposing the esophagus to gastric acid and causing heartburn. Additionally, antacids have not been shown to contribute to healing of erosive esophagitis.27 Hence, they may not be optimal for treating frequent reflux heartburn.
Sodium alginate
Gastric acid pockets are unbuffered pools of acid that float on top of ingested food.28 They develop as a result of poor mixing of newly secreted acid and food in the proximal stomach, which remains relatively quiescent after a meal compared with the distal stomach.29 In GERD, proximal extension of the acid pocket above the diaphragm increases the risk of acid reflux.30 The acid pocket is therefore an important source of postprandial acid in GERD and, as such, represents a unique therapeutic target.
Emerging evidence suggests that alginates may act directly on the acid pocket. Alginates are natural polysaccharide polymers that, on contact with gastric acid, precipitate within minutes into a low-density viscous gel of near-neutral pH. The change in pH triggers the sodium bicarbonate in the formulation to release carbon dioxide that becomes trapped in the alginate gel, causing it to float to the top of the gastric contents like a raft.31
A randomized controlled trial demonstrated that sodium alginate was as effective as omeprazole in relieving symptoms in patients with nonerosive reflux disease.32 Alginate has also been shown to provide more postprandial reflux relief than antacids.33
Histamine-2 receptor antagonists
Histamine-2 receptor antagonists act more swiftly and increase postprandial gastric pH more rapidly than PPIs, thus making them a good option for prophylaxis against postprandial GERD.34 Taking these drugs at bedtime may help in patients with objective nighttime reflux despite optimal PPI use. However, tachyphylaxis may occur as early as 1 week after starting combination therapy.35
Proton pump inhibitors
There are currently seven available PPIs, including four that can be obtained over the counter (omeprazole, lansoprazole, esomeprazole, and omeprazole-sodium bicarbonate) and three available only by prescription (rabeprazole, pantoprazole, and dexlansoprazole). Studies have shown than a standard 6- to 8-week course of a PPI provides complete symptom relief in 70% to 80% of patients with erosive reflux disease and in 60% of patients with nonerosive reflux disease.36,37 Clinically, PPIs all appear to be similar in their symptom relief.38
Most PPIs should be taken 30 to 60 minutes before meals. Exceptions are omeprazole-sodium bicarbonate and dexlansoprazole, which can be taken without regard to meals. At our institution, we usually start PPIs in a once-daily standard dose for 6 to 8 weeks and consider increasing to twice-daily dosing if symptoms do not respond completely. Patients with mild intermittent GERD symptoms may benefit from “on-demand” use of PPIs. This approach is best suited for patients with nonerosive reflux disease without evidence of Barrett esophagus on endoscopy.
Safety and adverse effects of PPIs
PPIs are generally safe but can cause adverse effects (Table 3).
Osteoporosis. In 2010, the US Food and Drug Administration issued warnings regarding the potential for wrist, hip, and spine fractures in PPI users.26 Most recent evidence suggests that PPIs may be associated with a small increase in risk of hip fractures in patients already at high risk.39,40 However, the 2013 American College of Gastroenterology (ACG) guidelines say that patients with known osteoporosis can remain on PPI therapy, and concern for hip fractures and osteoporosis should not affect the decision to use PPIs long-term except in patients with other risk factors for hip fracture.41
Community-acquired pneumonia. An increased risk of community-acquired pneumonia cannot be clearly documented in association with PPI therapy. Multiple studies, including randomized controlled trials, investigated this potential correlation. However, evidence suggests that short-term but not long-term PPI use may be associated with an overall increased risk of community-acquired pneumonia.42,43 Current guidelines suggest that in patients who need a PPI, the drug should not be withheld on the basis of a potential risk of community-acquired pneumonia.41
Clostridium difficile infection. In theory, PPIs may increase the risk of C difficile infection by increasing the ability of the spore to convert to the vegetative form and to survive intraluminally. In fact, studies and meta-analyses have suggested that PPIs do increase the risk of development and recurrence of C difficile infection.44,45 Therefore, PPIs should be used with care in patients who are at risk.41
Interaction with clopidogrel. The antiplatelet activity of clopidogrel requires activation by CYP2C19, the same pathway required for metabolism of some PPIs. Concern was raised about decreased antiplatelet activity of clopidogrel in the presence of PPIs. This was extensively studied, and there now appears to be no increased risk of adverse cardiovascular events in patients on PPIs, based on data from well-controlled randomized trials.46,47 A consensus panel of the American College of Cardiology Foundation, the American Heart Association, and the ACG said that PPIs may be used for appropriate indications in patients taking clopidogrel.47
Hypomagnesemia. By an unknown molecular mechanism, PPIs are thought to reduce intestinal magnesium absorption, leading to hypomagnesemia. A meta-analysis published in 2011 showed that PPI-induced hypomagnesemia is a drug-class effect and occurred after a median of 5.5 years of PPI use. Stopping the PPI resulted in magnesium recovery in 4 days, and rechallenge led to recurrence within 4 days.48
Hence, to avoid putting patients on long-term PPI therapy at risk, clinicians should anticipate this problem. Our practice is to check the magnesium level before starting a patient on long-term PPI therapy, and then to repeat the measurement every 1 to 2 years.
Baclofen
Transient lower esophageal sphincter relaxation has been shown to be a cause of reflux in healthy people and in patients with GERD.49
Baclofen, a muscle relaxant with selective gamma-aminobutyric acid receptor class B agonist properties, reduces transient lower esophageal sphincter relaxation in humans.50 In a well-designed, double-blind, randomized controlled trial, baclofen was associated with a significant decrease in upright reflux on 24-hour pH monitoring and significant improvement in belching and overall reflux symptoms.51 However, baclofen is not approved by the US Food and Drug Administration for the treatment of GERD, and its use may be limited by side effects such as somnolence and dizziness.
Antireflux surgery
Antireflux surgery is a reasonable option for selected patients with chronic GERD. The main types of surgery are laparoscopic fundoplication and, for obese patients, gastric bypass. Reasons to consider antireflux surgery include desire to stop PPI therapy, esophagitis not healed by PPIs, symptomatic hiatal hernia, and refractory reflux documented by pH testing.41
In general, surgical therapy may be considered in patients who respond to PPIs, but patients who do not respond to PPIs are less likely to respond to antireflux surgery.15 Other patients less likely to respond are those with symptoms of dyspepsia, such as nausea, vomiting, and epigastric pain.41
Common adverse effects of antireflux surgery include gas-bloat syndrome (up to 85% of patients), dysphagia (10% to 50% of patients), diarrhea (18% to 33% of patients), and recurrent heartburn (10% to 62% of patients).52
Endoscopic and minimally invasive antireflux procedures include endoscopic plication of the lower esophageal sphincter, radiofrequency augmentation of the lower esophageal sphincter, and sphincter augmentation by a string of titanium beads. While some have shown promise, they are not recommended by the most recent ACG guidelines, given lack of long-term data.41
REFRACTORY GERD
There is no consensus on the definition of refractory GERD. However, for the sake of simplicity, we can define it as persistence of suspected GERD symptoms despite treatment with a PPI. This may vary from a partial response to PPI therapy to a complete absence of response.
It is extremely important to rule out non-GERD causes of the ongoing symptoms, such as achalasia, gastroparesis, eosinophilic esophagitis, rumination, and aerophagia. PPI nonresponders are more likely to be obese, poorly compliant, and have extraesophageal symptoms.53–56 As previously discussed, PPIs should be taken 30 to 60 minutes before meals. For patients whose symptoms fail to respond to standard-dose daily PPI therapy, switching to another PPI or doubling the dose is common, although data to support this practice are limited. Of note, omeprazole-sodium bicarbonate has been shown to provide more symptom relief in nocturnal GERD.57 Additionally, adding a nighttime histamine-2 receptor antagonist may also help in patients with objective nighttime reflux.41
After noncompliance and suboptimal PPI dosing have been ruled out, PPI nonresponders with typical symptoms should undergo upper endoscopy and subsequent pH monitoring. Normal esophageal acid exposure on pH testing suggests functional heartburn or functional dyspepsia. Negative pH testing in a patient with atypical symptoms suggests a non-GERD cause of symptoms, and referral to an otolaryngologist, pulmonologist, or allergist is often warranted.
While antireflux surgery can be considered for patients with nonacid reflux on impedance testing, it should again be noted that GERD in patients with no response to PPIs is less likely to respond to antireflux surgery.15
TAKE-HOME POINTS
- GERD is a common medical condition, affecting up to 40% of US adults at least once monthly.
- GERD can result in a wide variety of symptoms, including typical heartburn and regurgitation as well as atypical symptoms such as cough.
- On the other hand, keep in mind that multiple non-GERD causes of heartburn and regurgitation may exist.
- Testing for GERD includes endoscopy and pH testing as well as functional testing such as esophageal manometry.
- While in most patients GERD will respond to lifestyle changes and antisecretory therapy such as a PPI, careful attention must be given to patients with symptoms refractory to PPI therapy.
- For a subset of patients, antireflux surgery may be a reasonable option, but care must be taken to exclude patients with a lower likelihood of responding to surgery.
Gastroesophageal reflux disease (GERD) is a chronic and common medical problem, with up to 40% of the population experiencing its symptoms at least once per month.1 The condition develops when the reflux of stomach contents causes troublesome symptoms or complications.2
GERD symptoms can range from heartburn and regurgitation to cough and hoarseness. While many patients’ symptoms respond to medical treatment, the diagnosis and treatment in those whose symptoms do not respond to a proton pump inhibitor (PPI) may be challenging.
This article reviews the diagnosis and treatment options for GERD.
SYMPTOMS: TYPICAL, ATYPICAL, AND ALARM
Symptoms of GERD (Table 1) can be classified as typical (heartburn and regurgitation) or atypical (cough, asthma, hoarseness, chronic laryngitis, throat-clearing, chest pain, dyspepsia, and nausea). Atypical symptoms are more likely to be due to GERD if patients also have typical symptoms and if the symptoms respond to a trial of a PPI.3
Alarm symptoms. Keep in mind that extraesophageal presentations may be multifactorial, and it may be difficult to establish that reflux, even if present, is actually the cause. While chest pain may be due to GERD, it is important to rule out cardiac chest pain before considering GERD as a cause. Similarly, dysphagia along with typical or atypical symptoms warrants investigation for potential complications such as underlying motility disorder, esophageal stricture, esophageal ring, or malignancy.4 Other alarm symptoms include odynophagia, bleeding, weight loss, and anemia.
DIAGNOSING GERD: RESPONSE TO A PPI IS DIAGNOSTIC
Patients with typical symptoms that respond to PPI therapy need no further evaluation for a diagnosis of GERD to be made.5 On the other hand, further testing should be undertaken in patients with typical symptoms that do not respond to PPI therapy, in patients presenting with atypical symptoms, and in patients in whom antireflux surgery is being considered. Figure 1 shows our proposed algorithm.
Try a PPI for 6–8 weeks
Relief of heartburn and regurgitation after a 6- to 8-week course of a PPI strongly suggests GERD.6 However, a negative trial of a PPI does not rule out GERD, as this approach has been found to have a sensitivity of 78% and specificity of 54%.6
Despite this limitation, a trial of PPI therapy should be offered to patients presenting with typical symptoms and no alarm features. This approach has been found to be more cost-effective than proceeding directly to diagnostic testing.7
Endoscopy
Endoscopic findings in GERD can include erosive esophagitis, peptic stricture, and Barrett esophagus. Esophageal erosions are a highly specific sign of GERD; the Los Angeles classification system, a standardized scale for grading the severity of erosive esophagitis (from A to D, with D the most severe) provides an objective way to assess severity.8 However, most patients with heartburn and regurgitation do not have erosive disease, thus limiting the sensitivity of upper endoscopy as an initial diagnostic test in patients with suspected GERD.9
We recommend endoscopy for patients who present with alarm symptoms, patients with noncardiac chest pain, PPI nonresponders, and patients with chronic GERD symptoms and multiple risk factors for Barrett esophagus besides GERD, such as older age, male sex, white race, overweight, and smoking.10
Ambulatory pH and impedance monitoring
Ambulatory pH monitoring is the gold standard test for pathologic acid exposure in the esophagus. pH testing is indicated in PPI nonresponders, patients presenting with atypical symptoms, and before antireflux surgery.
In general, pH testing should be performed after the patient has been off PPI therapy for at least 7 days, as the test is highly unlikely to be abnormal while a patient is on a PPI.11 It is done either with a transnasal catheter for 24 hours, or with a wireless capsule (Bravo pH System, Given Imaging Ltd, Duluth, GA), which collects 48 to 96 hours of data. Studies of the wireless system have shown that its sensitivity increases 12% to 25% when it is performed for 48 hours compared with 24 hours.12,13
The pH test can be combined with impedance testing to evaluate for nonacid reflux.14 However, the clinical significance of nonacid reflux remains controversial, and for this reason the Esophageal Diagnostic Advisory Panel recommends that the decision to perform antireflux surgery should not be based on abnormal impedance testing.15
During pH and impedance testing, special software can calculate how closely the patient’s symptoms correlate with esophageal acid exposure. The symptom index (SI) and symptom association probability (SAP) are the symptom measurements most commonly used in practice. The SI measures the overall strength of the relationship, and an SI greater than 50% is considered positive.16 The SAP determines whether this relationship could have occurred by chance, and an SAP greater than 95% is statistically significant.17 In patients with normal levels of esophageal acid exposure, an elevated SI or SAP may indicate a component of esophageal hypersensitivity in symptom generation.
At our institution, we generally perform pH-only transnasal or wireless testing off PPI therapy to establish that the patient has pathologic acid exposure in the distal esophagus. Combined pH-impedance testing is typically reserved for patients with atypical symptoms unresponsive to PPI therapy and abnormal results on previous pH testing, which allows for correlation of nonacid reflux and symptoms.
Other tests
Esophageal manometry and barium esophagography have limited value in the primary diagnosis of GERD. However, they should be considered to rule out achalasia and other esophageal motility disorders in patients whose symptoms do not respond to PPIs. For this reason, esophageal manometry should be performed before considering antireflux surgery.
MANAGING GERD
Table 2 summarizes the various treatments for GERD.
Lifestyle modifications
Lifestyle modifications are the first-line therapy for GERD. Modifications that have been studied include weight loss, head-of-bed elevation, and avoidance of tobacco, alcohol, and late-night meals. Another modification that has been suggested is avoiding foods that can aggravate reflux symptoms—eg, caffeine, coffee, chocolate, spicy foods, highly acidic foods (oranges, tomatoes), and fatty foods. Of these, only weight loss and head-of-bed elevation have been proven effective.18
Three randomized controlled trials demonstrated that GERD symptoms and esophageal pH values improved with head-of-bed elevation using blocks or incline foam wedges.19–21 Several cohort studies demonstrated reduction in GERD symptoms with weight loss.22,23 Recently, a prospective cohort study also found that smoking cessation significantly improved GERD symptoms in patients with normal body mass index and severe symptoms.24
Antacids
Several antacids (eg, sodium bicarbonate, calcium carbonate, magnesium hydroxide, aluminum hydroxide) are available over the counter.
Antacids were thought to control heartburn symptoms by increasing the pH of gastric contents that might subsequently reflux into the esophagus. However, well-controlled studies have shown that they relieve heartburn by neutralizing acid in the esophagus, with no significant effect on gastric pH.25,26
Antacids provide rapid but short-lived relief from an existing episode of heartburn. Because they do not significantly raise the gastric pH, they do not prevent subsequent reflux episodes from repeatedly exposing the esophagus to gastric acid and causing heartburn. Additionally, antacids have not been shown to contribute to healing of erosive esophagitis.27 Hence, they may not be optimal for treating frequent reflux heartburn.
Sodium alginate
Gastric acid pockets are unbuffered pools of acid that float on top of ingested food.28 They develop as a result of poor mixing of newly secreted acid and food in the proximal stomach, which remains relatively quiescent after a meal compared with the distal stomach.29 In GERD, proximal extension of the acid pocket above the diaphragm increases the risk of acid reflux.30 The acid pocket is therefore an important source of postprandial acid in GERD and, as such, represents a unique therapeutic target.
Emerging evidence suggests that alginates may act directly on the acid pocket. Alginates are natural polysaccharide polymers that, on contact with gastric acid, precipitate within minutes into a low-density viscous gel of near-neutral pH. The change in pH triggers the sodium bicarbonate in the formulation to release carbon dioxide that becomes trapped in the alginate gel, causing it to float to the top of the gastric contents like a raft.31
A randomized controlled trial demonstrated that sodium alginate was as effective as omeprazole in relieving symptoms in patients with nonerosive reflux disease.32 Alginate has also been shown to provide more postprandial reflux relief than antacids.33
Histamine-2 receptor antagonists
Histamine-2 receptor antagonists act more swiftly and increase postprandial gastric pH more rapidly than PPIs, thus making them a good option for prophylaxis against postprandial GERD.34 Taking these drugs at bedtime may help in patients with objective nighttime reflux despite optimal PPI use. However, tachyphylaxis may occur as early as 1 week after starting combination therapy.35
Proton pump inhibitors
There are currently seven available PPIs, including four that can be obtained over the counter (omeprazole, lansoprazole, esomeprazole, and omeprazole-sodium bicarbonate) and three available only by prescription (rabeprazole, pantoprazole, and dexlansoprazole). Studies have shown than a standard 6- to 8-week course of a PPI provides complete symptom relief in 70% to 80% of patients with erosive reflux disease and in 60% of patients with nonerosive reflux disease.36,37 Clinically, PPIs all appear to be similar in their symptom relief.38
Most PPIs should be taken 30 to 60 minutes before meals. Exceptions are omeprazole-sodium bicarbonate and dexlansoprazole, which can be taken without regard to meals. At our institution, we usually start PPIs in a once-daily standard dose for 6 to 8 weeks and consider increasing to twice-daily dosing if symptoms do not respond completely. Patients with mild intermittent GERD symptoms may benefit from “on-demand” use of PPIs. This approach is best suited for patients with nonerosive reflux disease without evidence of Barrett esophagus on endoscopy.
Safety and adverse effects of PPIs
PPIs are generally safe but can cause adverse effects (Table 3).
Osteoporosis. In 2010, the US Food and Drug Administration issued warnings regarding the potential for wrist, hip, and spine fractures in PPI users.26 Most recent evidence suggests that PPIs may be associated with a small increase in risk of hip fractures in patients already at high risk.39,40 However, the 2013 American College of Gastroenterology (ACG) guidelines say that patients with known osteoporosis can remain on PPI therapy, and concern for hip fractures and osteoporosis should not affect the decision to use PPIs long-term except in patients with other risk factors for hip fracture.41
Community-acquired pneumonia. An increased risk of community-acquired pneumonia cannot be clearly documented in association with PPI therapy. Multiple studies, including randomized controlled trials, investigated this potential correlation. However, evidence suggests that short-term but not long-term PPI use may be associated with an overall increased risk of community-acquired pneumonia.42,43 Current guidelines suggest that in patients who need a PPI, the drug should not be withheld on the basis of a potential risk of community-acquired pneumonia.41
Clostridium difficile infection. In theory, PPIs may increase the risk of C difficile infection by increasing the ability of the spore to convert to the vegetative form and to survive intraluminally. In fact, studies and meta-analyses have suggested that PPIs do increase the risk of development and recurrence of C difficile infection.44,45 Therefore, PPIs should be used with care in patients who are at risk.41
Interaction with clopidogrel. The antiplatelet activity of clopidogrel requires activation by CYP2C19, the same pathway required for metabolism of some PPIs. Concern was raised about decreased antiplatelet activity of clopidogrel in the presence of PPIs. This was extensively studied, and there now appears to be no increased risk of adverse cardiovascular events in patients on PPIs, based on data from well-controlled randomized trials.46,47 A consensus panel of the American College of Cardiology Foundation, the American Heart Association, and the ACG said that PPIs may be used for appropriate indications in patients taking clopidogrel.47
Hypomagnesemia. By an unknown molecular mechanism, PPIs are thought to reduce intestinal magnesium absorption, leading to hypomagnesemia. A meta-analysis published in 2011 showed that PPI-induced hypomagnesemia is a drug-class effect and occurred after a median of 5.5 years of PPI use. Stopping the PPI resulted in magnesium recovery in 4 days, and rechallenge led to recurrence within 4 days.48
Hence, to avoid putting patients on long-term PPI therapy at risk, clinicians should anticipate this problem. Our practice is to check the magnesium level before starting a patient on long-term PPI therapy, and then to repeat the measurement every 1 to 2 years.
Baclofen
Transient lower esophageal sphincter relaxation has been shown to be a cause of reflux in healthy people and in patients with GERD.49
Baclofen, a muscle relaxant with selective gamma-aminobutyric acid receptor class B agonist properties, reduces transient lower esophageal sphincter relaxation in humans.50 In a well-designed, double-blind, randomized controlled trial, baclofen was associated with a significant decrease in upright reflux on 24-hour pH monitoring and significant improvement in belching and overall reflux symptoms.51 However, baclofen is not approved by the US Food and Drug Administration for the treatment of GERD, and its use may be limited by side effects such as somnolence and dizziness.
Antireflux surgery
Antireflux surgery is a reasonable option for selected patients with chronic GERD. The main types of surgery are laparoscopic fundoplication and, for obese patients, gastric bypass. Reasons to consider antireflux surgery include desire to stop PPI therapy, esophagitis not healed by PPIs, symptomatic hiatal hernia, and refractory reflux documented by pH testing.41
In general, surgical therapy may be considered in patients who respond to PPIs, but patients who do not respond to PPIs are less likely to respond to antireflux surgery.15 Other patients less likely to respond are those with symptoms of dyspepsia, such as nausea, vomiting, and epigastric pain.41
Common adverse effects of antireflux surgery include gas-bloat syndrome (up to 85% of patients), dysphagia (10% to 50% of patients), diarrhea (18% to 33% of patients), and recurrent heartburn (10% to 62% of patients).52
Endoscopic and minimally invasive antireflux procedures include endoscopic plication of the lower esophageal sphincter, radiofrequency augmentation of the lower esophageal sphincter, and sphincter augmentation by a string of titanium beads. While some have shown promise, they are not recommended by the most recent ACG guidelines, given lack of long-term data.41
REFRACTORY GERD
There is no consensus on the definition of refractory GERD. However, for the sake of simplicity, we can define it as persistence of suspected GERD symptoms despite treatment with a PPI. This may vary from a partial response to PPI therapy to a complete absence of response.
It is extremely important to rule out non-GERD causes of the ongoing symptoms, such as achalasia, gastroparesis, eosinophilic esophagitis, rumination, and aerophagia. PPI nonresponders are more likely to be obese, poorly compliant, and have extraesophageal symptoms.53–56 As previously discussed, PPIs should be taken 30 to 60 minutes before meals. For patients whose symptoms fail to respond to standard-dose daily PPI therapy, switching to another PPI or doubling the dose is common, although data to support this practice are limited. Of note, omeprazole-sodium bicarbonate has been shown to provide more symptom relief in nocturnal GERD.57 Additionally, adding a nighttime histamine-2 receptor antagonist may also help in patients with objective nighttime reflux.41
After noncompliance and suboptimal PPI dosing have been ruled out, PPI nonresponders with typical symptoms should undergo upper endoscopy and subsequent pH monitoring. Normal esophageal acid exposure on pH testing suggests functional heartburn or functional dyspepsia. Negative pH testing in a patient with atypical symptoms suggests a non-GERD cause of symptoms, and referral to an otolaryngologist, pulmonologist, or allergist is often warranted.
While antireflux surgery can be considered for patients with nonacid reflux on impedance testing, it should again be noted that GERD in patients with no response to PPIs is less likely to respond to antireflux surgery.15
TAKE-HOME POINTS
- GERD is a common medical condition, affecting up to 40% of US adults at least once monthly.
- GERD can result in a wide variety of symptoms, including typical heartburn and regurgitation as well as atypical symptoms such as cough.
- On the other hand, keep in mind that multiple non-GERD causes of heartburn and regurgitation may exist.
- Testing for GERD includes endoscopy and pH testing as well as functional testing such as esophageal manometry.
- While in most patients GERD will respond to lifestyle changes and antisecretory therapy such as a PPI, careful attention must be given to patients with symptoms refractory to PPI therapy.
- For a subset of patients, antireflux surgery may be a reasonable option, but care must be taken to exclude patients with a lower likelihood of responding to surgery.
- Locke GR 3rd, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ 3rd. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology 1997; 112:1448–1456.
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R; Globale Konsensusgrupp. [The Montreal definition and classification of gastroesophageal reflux disease: a global, evidence-based consensus paper]. Z Gastroenterol 2007; 45:1125–1240. In German.
- Gerson LB, Kahrilas PJ, Fass R. Insights into gastroesophageal reflux disease-associated dyspeptic symptoms. Clin Gastroenterol Hepatol 2011; 9:824–833.
- Vakil NB, Traxler B, Levine D. Dysphagia in patients with erosive esophagitis: prevalence, severity, and response to proton pump inhibitor treatment. Clin Gastroenterol Hepatol 2004; 2:665–668.
- Kahrilas PJ, Shaheen NJ, aezi MF, et al; American Gastroenterological Association. American Gastroenterological Association Medical Position Statement on the management of gastroesophageal reflux disease. Gastroenterology 2008; 135:1383–1391 e1–5.
- Numans ME, Lau J, de Wit NJ, Bonis PA. Short-term treatment with proton-pump inhibitors as a test for gastroesophageal reflux disease: a meta-analysis of diagnostic test characteristics. Ann Intern Med 2004; 140:518–527.
- Fass R. Empirical trials in treatment of gastroesophageal reflux disease. Dig Dis 2000; 18:20–26.
- Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut 1999; 45:172–180.
- Johansson KE, Ask P, Boeryd B, Fransson SG, Tibbling L. Oesophagitis, signs of reflux, and gastric acid secretion in patients with symptoms of gastro-oesophageal reflux disease. Scand J Gastroenterol 1986; 21:837–847.
- Becher A, Dent J. Systematic review: ageing and gastro-oesophageal reflux disease symptoms, oesophageal function and reflux oesophagitis. Aliment Pharmacol Ther 2011; 33:442–454.
- Charbel S, Khandwala F, Vaezi MF. The role of esophageal pH monitoring in symptomatic patients on PPI therapy. Am J Gastroenterol 2005; 100:283–289.
- Pandolfino JE, Richter JE, Ours T, Guardino JM, Chapman J, Kahrilas PJ. Ambulatory esophageal pH monitoring using a wireless system. Am J Gastroenterol 2003; 98:740–749.
- Prakash C, Clouse RE. Value of extended recording time with wireless pH monitoring in evaluating gastroesophageal reflux disease. Clin Gastroenterol Hepatol 2005; 3:329–334.
- Hirano I, Richter JE; Practice Parameters Committee of the American College of Gastroenterology. ACG practice guidelines: esophageal reflux testing. Am J Gastroenterol 2007; 102:668–685.
- Jobe BA, Richter JE, Hoppo T, et al. Preoperative diagnostic workup before antireflux surgery: an evidence and experience-based consensus of the Esophageal Diagnostic Advisory Panel. J Am Coll Surg 2013; 217:586–597.
- Singh S, Richter JE, Bradley LA, Haile JM. The symptom index. Differential usefulness in suspected acid-related complaints of heartburn and chest pain. Dig Dis Sci 1993; 38:1402–1408.
- Weusten BL, Roelofs JM, Akkermans LM, Van Berge-Henegouwen GP, Smout AJ. The symptom-association probability: an improved method for symptom analysis of 24-hour esophageal pH data. Gastroenterology 1994; 107:1741–1745.
- Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidence-based approach. Arch Intern Med 2006; 166:965–971.
- Hamilton JW, Boisen RJ, Yamamoto DT, Wagner JL, Reichelderfer M. Sleeping on a wedge diminishes exposure of the esophagus to refluxed acid. Dig Dis Sci 1988; 33:518–522.
- Pollmann H, Zillessen E, Pohl J, et al. [Effect of elevated head position in bed in therapy of gastroesophageal reflux]. Z Gastroenterol 1996; 34(suppl 2):93–99. In German.
- Stanciu C, Bennett JR. Effects of posture on gastro-oesophageal reflux. Digestion 1977; 15:104–109.
- Fraser-Moodie CA, Norton B, Gornall C, Magnago S, Weale AR, Holmes GK. Weight loss has an independent beneficial effect on symptoms of gastro-oesophageal reflux in patients who are overweight. Scand J Gastroenterol 1999; 34:337–340.
- Mathus-Vliegen LM, Tytgat GN. Twenty-four-hour pH measurements in morbid obesity: effects of massive overweight, weight loss and gastric distension. Eur J Gastroenterol Hepatol 1996; 8:635–640.
- Ness-Jensen E, Lindam A, Lagergren J, Hveem K. Tobacco smoking cessation and improved gastroesophageal reflux: a prospective population-based cohort study: the HUNT study. Am J Gastroenterol 2014; 109:171–177.
- Collings KL, Rodriguez-Stanley S, Proskin HM, Robinson M, Miner PB Jr. Clinical effectiveness of a new antacid chewing gum on heartburn and oesophageal pH control. Aliment Pharmacol Ther 2002; 16:2029–2035.
- Decktor DL, Robinson M, Maton PN, Lanza FL, Gottlieb S. Effects of aluminum/magnesium hydroxide and calcium carbonate on esophageal and gastric pH in subjects with heartburn. Am J Ther 1995; 2:546–552.
- Pettit M. Treatment of gastroesophageal reflux disease. Pharm World Sci 2005; 27:432–435.
- Fletcher J, Wirz A, Young J, Vallance R, McColl KE. Unbuffered highly acidic gastric juice exists at the gastroesophageal junction after a meal. Gastroenterology 2001; 121:775–783.
- Sauter M, Curcic J, Menne D, et al. Measuring the interaction of meal and gastric secretion: a combined quantitative magnetic resonance imaging and pharmacokinetic modeling approach. Neurogastroenterol Motil 2012; 24:632–638, e272–e273.
- Beaumont H, Bennink RJ, de Jong J, Boeckxstaens GE. The position of the acid pocket as a major risk factor for acidic reflux in healthy subjects and patients with GORD. Gut 2010; 59:441–451.
- Tytgat GN, Simoneau G. Clinical and laboratory studies of the antacid and raft-forming properties of Rennie alginate suspension. Aliment Pharmacol Ther 2006; 23:759–765.
- Chiu CT, Hsu CM, Wang CC, et al. Randomised clinical trial: sodium alginate oral suspension is non-inferior to omeprazole in the treatment of patients with non-erosive gastroesophageal disease. Aliment Pharmacol Ther 2013; 38:1054–1064.
- Rohof WO, Bennink RJ, Smout AJ, Thomas E, Boeckxstaens GE. An alginate-antacid formulation localizes to the acid pocket to reduce acid reflux in patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol 2013; 11:1585–1591.
- Khoury RM, Katz PO, Castell DO. Post-prandial ranitidine is superior to post-prandial omeprazole in control of gastric acidity in healthy volunteers. Aliment Pharmacol Ther 1999; 13:1211–1214.
- Fackler WK, Ours TM, Vaezi MF, Richter JE. Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology 2002; 122:625–632.
- Robinson M, Sahba B, Avner D, Jhala N, Greski-Rose PA, Jennings DE. A comparison of lansoprazole and ranitidine in the treatment of erosive oesophagitis. Multicentre Investigational Group. Aliment Pharmacol Ther 1995; 9:25–31.
- Vantrappen G, Rutgeerts L, Schurmans P, Coenegrachts JL. Omeprazole (40 mg) is superior to ranitidine in short-term treatment of ulcerative reflux esophagitis. Dig Dis Sci 1988; 33:523–529.
- Gralnek IM, Dulai GS, Fennerty MB, Spiegel BM. Esomeprazole versus other proton pump inhibitors in erosive esophagitis: a meta-analysis of randomized clinical trials. Clin Gastroenterol Hepatol 2006; 4:1452–1458.
- Targownik LE, Lix LM, Leung S, Leslie WD. Proton-pump inhibitor use is not associated with osteoporosis or accelerated bone mineral density loss. Gastroenterology 2010; 138:896–904.
- Corley DA, Kubo A, Zhao W, Quesenberry C. Proton pump inhibitors and histamine-2 receptor antagonists are associated with hip fractures among at-risk patients. Gastroenterology 2010; 139:93–101.
- Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 2013; 108:308–328.
- Giuliano C, Wilhelm SM, Kale-Pradhan PB. Are proton pump inhibitors associated with the development of community-acquired pneumonia? A meta-analysis. Expert Rev Clin Pharmacol 2012; 5:337–344.
- Hermos JA, Young MM, Fonda JR, Gagnon DR, Fiore LD, Lawler EV. Risk of community-acquired pneumonia in veteran patients to whom proton pump inhibitors were dispensed. Clin Infect Dis 2012; 54:33–42.
- Linsky A, Gupta K, Lawler EV, Fonda JR, Hermos JA. Proton pump inhibitors and risk for recurrent Clostridium difficile infection. Arch Intern Med 2010; 170:772–778.
- Bavishi C, Dupont HL. Systematic review: the use of proton pump inhibitors and increased susceptibility to enteric infection. Aliment Pharmacol Ther 2011; 34:1269–1281.
- Bhatt DL, Cryer BL, Contant CF, et al; COGENT Investigators. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med 2010; 363:1909–1917.
- O’Donoghue ML, Braunwald E, Antman EM, et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomised trials. Lancet 2009; 374:989–997.
- Hess MW, Hoenderop JG, Bindels RJ, Drenth JP. Systematic review: hypomagnesaemia induced by proton pump inhibition. Aliment Pharmacol Ther 2012; 36:405–413.
- Mittal RK, McCallum RW. Characteristics and frequency of transient relaxations of the lower esophageal sphincter in patients with reflux esophagitis. Gastroenterology 1988; 95:593–599.
- Lidums I, Lehmann A, Checklin H, Dent J, Holloway RH. Control of transient lower esophageal sphincter relaxations and reflux by the GABA(B) agonist baclofen in normal subjects. Gastroenterology 2000; 118:7–13.
- Cossentino MJ, Mann K, Armbruster SP, Lake JM, Maydonovitch C, Wong RK. Randomised clinical trial: the effect of baclofen in patients with gastro-oesophageal reflux—a randomised prospective study. Aliment Pharmacol Ther 2012; 35:1036–1044.
- Richter JE. Gastroesophageal reflux disease treatment: side effects and complications of fundoplication. Clin Gastroenterol Hepatol 2013; 11:465–471.
- Dickman R, Boaz M, Aizic S, Beniashvili Z, Fass R, Niv Y. Comparison of clinical characteristics of patients with gastroesophageal reflux disease who failed proton pump inhibitor therapy versus those who fully responded. J Neurogastroenterol Motil 2011; 17:387–394.
- Chan WW, Chiou E, Obstein KL, Tignor AS, Whitlock TL. The efficacy of proton pump inhibitors for the treatment of asthma in adults: a meta-analysis. Arch Intern Med 2011; 171:620–629.
- Chang AB, Lasserson TJ, Gaffney J, Connor FL, Garske LA. Gastro-oesophageal reflux treatment for prolonged non-specific cough in children and adults. Cochrane Database Syst Rev 2011; 1:CD004823.
- Qadeer MA, Phillips CO, Lopez AR, et al. Proton pump inhibitor therapy for suspected GERD-related chronic laryngitis: a meta-analysis of randomized controlled trials. Am J Gastroenterol 2006; 101:2646–2654.
- Gerson LB, Mitra S, Bleker WF, Yeung P. Control of intra-oesophageal pH in patients with Barrett's oesophagus on omeprazole-sodium bicarbonate therapy. Aliment Pharmacol Ther 2012; 35:803–809.
- Locke GR 3rd, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ 3rd. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology 1997; 112:1448–1456.
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R; Globale Konsensusgrupp. [The Montreal definition and classification of gastroesophageal reflux disease: a global, evidence-based consensus paper]. Z Gastroenterol 2007; 45:1125–1240. In German.
- Gerson LB, Kahrilas PJ, Fass R. Insights into gastroesophageal reflux disease-associated dyspeptic symptoms. Clin Gastroenterol Hepatol 2011; 9:824–833.
- Vakil NB, Traxler B, Levine D. Dysphagia in patients with erosive esophagitis: prevalence, severity, and response to proton pump inhibitor treatment. Clin Gastroenterol Hepatol 2004; 2:665–668.
- Kahrilas PJ, Shaheen NJ, aezi MF, et al; American Gastroenterological Association. American Gastroenterological Association Medical Position Statement on the management of gastroesophageal reflux disease. Gastroenterology 2008; 135:1383–1391 e1–5.
- Numans ME, Lau J, de Wit NJ, Bonis PA. Short-term treatment with proton-pump inhibitors as a test for gastroesophageal reflux disease: a meta-analysis of diagnostic test characteristics. Ann Intern Med 2004; 140:518–527.
- Fass R. Empirical trials in treatment of gastroesophageal reflux disease. Dig Dis 2000; 18:20–26.
- Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut 1999; 45:172–180.
- Johansson KE, Ask P, Boeryd B, Fransson SG, Tibbling L. Oesophagitis, signs of reflux, and gastric acid secretion in patients with symptoms of gastro-oesophageal reflux disease. Scand J Gastroenterol 1986; 21:837–847.
- Becher A, Dent J. Systematic review: ageing and gastro-oesophageal reflux disease symptoms, oesophageal function and reflux oesophagitis. Aliment Pharmacol Ther 2011; 33:442–454.
- Charbel S, Khandwala F, Vaezi MF. The role of esophageal pH monitoring in symptomatic patients on PPI therapy. Am J Gastroenterol 2005; 100:283–289.
- Pandolfino JE, Richter JE, Ours T, Guardino JM, Chapman J, Kahrilas PJ. Ambulatory esophageal pH monitoring using a wireless system. Am J Gastroenterol 2003; 98:740–749.
- Prakash C, Clouse RE. Value of extended recording time with wireless pH monitoring in evaluating gastroesophageal reflux disease. Clin Gastroenterol Hepatol 2005; 3:329–334.
- Hirano I, Richter JE; Practice Parameters Committee of the American College of Gastroenterology. ACG practice guidelines: esophageal reflux testing. Am J Gastroenterol 2007; 102:668–685.
- Jobe BA, Richter JE, Hoppo T, et al. Preoperative diagnostic workup before antireflux surgery: an evidence and experience-based consensus of the Esophageal Diagnostic Advisory Panel. J Am Coll Surg 2013; 217:586–597.
- Singh S, Richter JE, Bradley LA, Haile JM. The symptom index. Differential usefulness in suspected acid-related complaints of heartburn and chest pain. Dig Dis Sci 1993; 38:1402–1408.
- Weusten BL, Roelofs JM, Akkermans LM, Van Berge-Henegouwen GP, Smout AJ. The symptom-association probability: an improved method for symptom analysis of 24-hour esophageal pH data. Gastroenterology 1994; 107:1741–1745.
- Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidence-based approach. Arch Intern Med 2006; 166:965–971.
- Hamilton JW, Boisen RJ, Yamamoto DT, Wagner JL, Reichelderfer M. Sleeping on a wedge diminishes exposure of the esophagus to refluxed acid. Dig Dis Sci 1988; 33:518–522.
- Pollmann H, Zillessen E, Pohl J, et al. [Effect of elevated head position in bed in therapy of gastroesophageal reflux]. Z Gastroenterol 1996; 34(suppl 2):93–99. In German.
- Stanciu C, Bennett JR. Effects of posture on gastro-oesophageal reflux. Digestion 1977; 15:104–109.
- Fraser-Moodie CA, Norton B, Gornall C, Magnago S, Weale AR, Holmes GK. Weight loss has an independent beneficial effect on symptoms of gastro-oesophageal reflux in patients who are overweight. Scand J Gastroenterol 1999; 34:337–340.
- Mathus-Vliegen LM, Tytgat GN. Twenty-four-hour pH measurements in morbid obesity: effects of massive overweight, weight loss and gastric distension. Eur J Gastroenterol Hepatol 1996; 8:635–640.
- Ness-Jensen E, Lindam A, Lagergren J, Hveem K. Tobacco smoking cessation and improved gastroesophageal reflux: a prospective population-based cohort study: the HUNT study. Am J Gastroenterol 2014; 109:171–177.
- Collings KL, Rodriguez-Stanley S, Proskin HM, Robinson M, Miner PB Jr. Clinical effectiveness of a new antacid chewing gum on heartburn and oesophageal pH control. Aliment Pharmacol Ther 2002; 16:2029–2035.
- Decktor DL, Robinson M, Maton PN, Lanza FL, Gottlieb S. Effects of aluminum/magnesium hydroxide and calcium carbonate on esophageal and gastric pH in subjects with heartburn. Am J Ther 1995; 2:546–552.
- Pettit M. Treatment of gastroesophageal reflux disease. Pharm World Sci 2005; 27:432–435.
- Fletcher J, Wirz A, Young J, Vallance R, McColl KE. Unbuffered highly acidic gastric juice exists at the gastroesophageal junction after a meal. Gastroenterology 2001; 121:775–783.
- Sauter M, Curcic J, Menne D, et al. Measuring the interaction of meal and gastric secretion: a combined quantitative magnetic resonance imaging and pharmacokinetic modeling approach. Neurogastroenterol Motil 2012; 24:632–638, e272–e273.
- Beaumont H, Bennink RJ, de Jong J, Boeckxstaens GE. The position of the acid pocket as a major risk factor for acidic reflux in healthy subjects and patients with GORD. Gut 2010; 59:441–451.
- Tytgat GN, Simoneau G. Clinical and laboratory studies of the antacid and raft-forming properties of Rennie alginate suspension. Aliment Pharmacol Ther 2006; 23:759–765.
- Chiu CT, Hsu CM, Wang CC, et al. Randomised clinical trial: sodium alginate oral suspension is non-inferior to omeprazole in the treatment of patients with non-erosive gastroesophageal disease. Aliment Pharmacol Ther 2013; 38:1054–1064.
- Rohof WO, Bennink RJ, Smout AJ, Thomas E, Boeckxstaens GE. An alginate-antacid formulation localizes to the acid pocket to reduce acid reflux in patients with gastroesophageal reflux disease. Clin Gastroenterol Hepatol 2013; 11:1585–1591.
- Khoury RM, Katz PO, Castell DO. Post-prandial ranitidine is superior to post-prandial omeprazole in control of gastric acidity in healthy volunteers. Aliment Pharmacol Ther 1999; 13:1211–1214.
- Fackler WK, Ours TM, Vaezi MF, Richter JE. Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology 2002; 122:625–632.
- Robinson M, Sahba B, Avner D, Jhala N, Greski-Rose PA, Jennings DE. A comparison of lansoprazole and ranitidine in the treatment of erosive oesophagitis. Multicentre Investigational Group. Aliment Pharmacol Ther 1995; 9:25–31.
- Vantrappen G, Rutgeerts L, Schurmans P, Coenegrachts JL. Omeprazole (40 mg) is superior to ranitidine in short-term treatment of ulcerative reflux esophagitis. Dig Dis Sci 1988; 33:523–529.
- Gralnek IM, Dulai GS, Fennerty MB, Spiegel BM. Esomeprazole versus other proton pump inhibitors in erosive esophagitis: a meta-analysis of randomized clinical trials. Clin Gastroenterol Hepatol 2006; 4:1452–1458.
- Targownik LE, Lix LM, Leung S, Leslie WD. Proton-pump inhibitor use is not associated with osteoporosis or accelerated bone mineral density loss. Gastroenterology 2010; 138:896–904.
- Corley DA, Kubo A, Zhao W, Quesenberry C. Proton pump inhibitors and histamine-2 receptor antagonists are associated with hip fractures among at-risk patients. Gastroenterology 2010; 139:93–101.
- Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 2013; 108:308–328.
- Giuliano C, Wilhelm SM, Kale-Pradhan PB. Are proton pump inhibitors associated with the development of community-acquired pneumonia? A meta-analysis. Expert Rev Clin Pharmacol 2012; 5:337–344.
- Hermos JA, Young MM, Fonda JR, Gagnon DR, Fiore LD, Lawler EV. Risk of community-acquired pneumonia in veteran patients to whom proton pump inhibitors were dispensed. Clin Infect Dis 2012; 54:33–42.
- Linsky A, Gupta K, Lawler EV, Fonda JR, Hermos JA. Proton pump inhibitors and risk for recurrent Clostridium difficile infection. Arch Intern Med 2010; 170:772–778.
- Bavishi C, Dupont HL. Systematic review: the use of proton pump inhibitors and increased susceptibility to enteric infection. Aliment Pharmacol Ther 2011; 34:1269–1281.
- Bhatt DL, Cryer BL, Contant CF, et al; COGENT Investigators. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med 2010; 363:1909–1917.
- O’Donoghue ML, Braunwald E, Antman EM, et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomised trials. Lancet 2009; 374:989–997.
- Hess MW, Hoenderop JG, Bindels RJ, Drenth JP. Systematic review: hypomagnesaemia induced by proton pump inhibition. Aliment Pharmacol Ther 2012; 36:405–413.
- Mittal RK, McCallum RW. Characteristics and frequency of transient relaxations of the lower esophageal sphincter in patients with reflux esophagitis. Gastroenterology 1988; 95:593–599.
- Lidums I, Lehmann A, Checklin H, Dent J, Holloway RH. Control of transient lower esophageal sphincter relaxations and reflux by the GABA(B) agonist baclofen in normal subjects. Gastroenterology 2000; 118:7–13.
- Cossentino MJ, Mann K, Armbruster SP, Lake JM, Maydonovitch C, Wong RK. Randomised clinical trial: the effect of baclofen in patients with gastro-oesophageal reflux—a randomised prospective study. Aliment Pharmacol Ther 2012; 35:1036–1044.
- Richter JE. Gastroesophageal reflux disease treatment: side effects and complications of fundoplication. Clin Gastroenterol Hepatol 2013; 11:465–471.
- Dickman R, Boaz M, Aizic S, Beniashvili Z, Fass R, Niv Y. Comparison of clinical characteristics of patients with gastroesophageal reflux disease who failed proton pump inhibitor therapy versus those who fully responded. J Neurogastroenterol Motil 2011; 17:387–394.
- Chan WW, Chiou E, Obstein KL, Tignor AS, Whitlock TL. The efficacy of proton pump inhibitors for the treatment of asthma in adults: a meta-analysis. Arch Intern Med 2011; 171:620–629.
- Chang AB, Lasserson TJ, Gaffney J, Connor FL, Garske LA. Gastro-oesophageal reflux treatment for prolonged non-specific cough in children and adults. Cochrane Database Syst Rev 2011; 1:CD004823.
- Qadeer MA, Phillips CO, Lopez AR, et al. Proton pump inhibitor therapy for suspected GERD-related chronic laryngitis: a meta-analysis of randomized controlled trials. Am J Gastroenterol 2006; 101:2646–2654.
- Gerson LB, Mitra S, Bleker WF, Yeung P. Control of intra-oesophageal pH in patients with Barrett's oesophagus on omeprazole-sodium bicarbonate therapy. Aliment Pharmacol Ther 2012; 35:803–809.
KEY POINTS
- GERD symptoms may be typical (eg, heartburn, regurgitation) or atypical (eg, cough, chest pain, hoarseness).
- In patients with typical symptoms, a 6- to 8-week trial of a PPI is a reasonable and cost-effective approach to diagnosing GERD.
- Endoscopy is indicated for patients who have alarm symptoms such as dysphagia, weight loss, and bleeding; it is unnecessary in patients who have typical GERD symptoms.
- Ambulatory pH monitoring should be used in patients whose symptoms do not respond to a PPI and those in whom antireflux surgery is being considered.
- Weight loss and head-of-bed elevation are the only lifestyle interventions that have been proven effective for GERD.
- While risks of PPI use are rare, they should be discussed with patients on long-term therapy.
- Symptoms that do not respond to a PPI are less likely to improve with antireflux surgery.
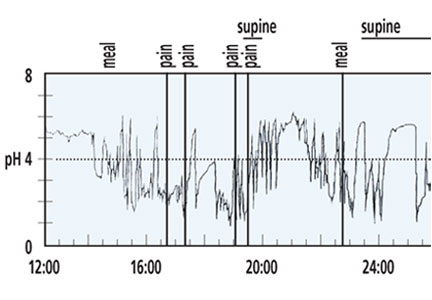
Vaginal hysterectomy with basic instrumentation
In the United States, gynecologic surgeons remove approximately one uterus every minute of the year.1 That rate translates to more than 525,000 hysterectomies annually in this country alone. Yet, despite the widespread availability of information on the benefits of a vaginal approach to hysterectomy, the great majority of these operations—close to 50%—are still performed via an open abdominal approach.2
As I pointed out last month in my “Update on Vaginal Hysterectomy,” the vaginal approach not only is more cosmetically pleasing than laparoscopic and robot-assisted hysterectomy (not to mention open abdominal surgery) but also has a lower complication rate.3
As I also noted, one reason for the low rate of vaginal hysterectomy may be the assumption, on the part of many gynecologic surgeons, that the techniques and tools they learned to use during training are still the only options available today. That assumption is wrong.
In this article, I describe the technique for vaginal hysterectomy using basic instru mentation. This article is based on a master class in vaginal hysterectomy produced by the AAGL and co-sponsored by the Am erican College of Obstetricians and Gynecologists and the Society of Gynecologic Surgeons. This master class offers continuing medical education credits and is avail able at http://www.aagl.org/vaghystwebinar.
For a look at innovative tools for this procedure, see my “Update on Vaginal Hysterectomy” in the September 2015 issue of this journal at obgmanagement.com.
Vaginal hysterectomy has few contraindications
Many commonly cited contraindications to the vaginal approach are not, in fact, absolute contraindications. An open or laparoscopic approach is preferred when the patient has a known cancer, of course, and when deep infiltrating endometriosis is present at the rectovaginal septum. However, previous pelvic surgery, nulliparity, an enlarged uterus, or lack of a prior vaginal delivery need not exclude the vaginal approach. Nor does a narrow introitus necessarily mandate a laparoscopic or open abdominal approach. In fact, in this article, I describe my basic technique in a patient (a cadaver) with a very narrow pubic arch, and I offer strategies for gaining some needed mobility and avoiding complications (TABLES 1 and 2).
Next month, in the November issue of OBG Management, John B. Gebhart, MD, will describe his vaginal technique for right salpingectomy with ovarian preservation, as well as his technique for right salpingo-oophorectomy.
Proper patient positioning is key
You can simplify the operation by positioning the patient so that her buttocks are over the edge of the table fairly far—at least 1 inch beyond the edge of the table for optimal exposure and greater access. If the patient is thin, it then becomes important to pad the sacrum because, when she is positioned that far off the table, all her weight comes to rest on the sacrum. In overweight patients, this is not an issue, but for thin patients, I place a bit of egg crate or gel beneath the sacrum.
For the procedure, I prefer to place my instruments on a tray that is kept on my lap. This arrangement frees the scrub technician from having to hand tools over my shoulder—and it saves time. I use a narrow, covered Mayo stand, and I place a stepstool beneath my feet to keep my knees at right angles so that things don’t slip during the operation.
Surgical technique
Choose an appropriate retractor
In a woman with a narrow introitus, I find that a posterior weighted speculum takes up too much space. Once I place a clamp on the cervix with that speculum in place, I don’t have much room to work. However, if I substitute a small Deaver retractor, which is narrower, I gain more workspace.
Inject the uterosacral ligaments
Grasp the cervix using a Jacobs vulsellum tenaculum. Use of a single tenaculum allows for much more movement than the use of instruments placed anteriorly and posteriorly. The Jacobs tenaculum obtains a better purchase on the tissue than a single tooth and is considerably less likely to tear through the tissue.
Before beginning the hysterectomy, locate the uterosacral ligaments and inject each one at its junction with the cervix, aspirating slightly before infiltrating the ligament with 0.25% to 0.50% bupivacaine with epinephrine, with dilute vasopressin mixed in. (I place 1 unit in 20 mL of the local solution.) Injection of this solution achieves 2 goals:
- improved intraoperative hemostasis
- postoperative pain relief.
Use a short needle with a needle extender attached to a control syringe rather than a spinal needle for greater control.
Enter the posterior peritoneal cavity
Before entering the peritoneal cavity, create a right angle with the Jacobs tenaculum and Deaver retractor in relation to the surgical field (FIGURE 1). This right angle is difficult to achieve when you are using a weighted speculum in a tight vagina. Once you have a right angle, tent the vaginal tissue in the midline (FIGURE 2).
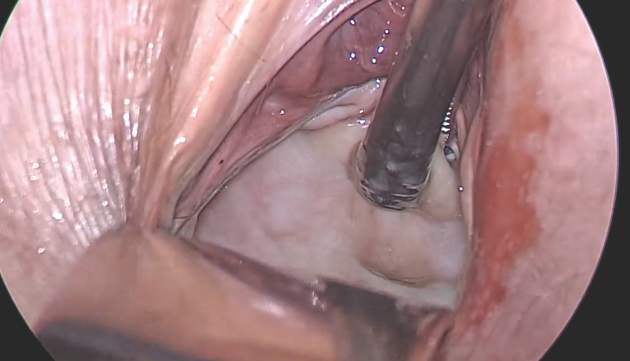
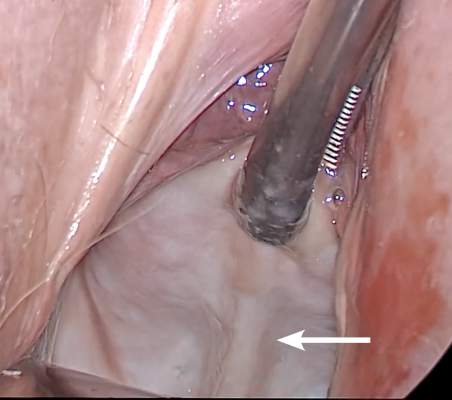
In a nulliparous patient or a woman with a tight pelvis, you may discover that the peritoneum is pulled up between the uterosacral ligaments. One common pitfall arises when the surgeon, having dissected the vaginal epithelium, continues cutting into the vaginal epithelium instead of reaching into the peritoneal cavity. Palpate the tissue to ensure that there is no bowel in the way and stay at right angles while confidently grasping the peritoneum with a toothed forceps.
I like to use a bit of electrosurgery to incise the vaginal wall. I don’t begin at the cervix but incise more distally into the vaginal epithelium approximately 2 cm from the cervicovaginal junction. This strategy prevents dissection into the cervix and/or rectovaginal septum rather than the posterior
cul-de-sac (FIGURE 3).
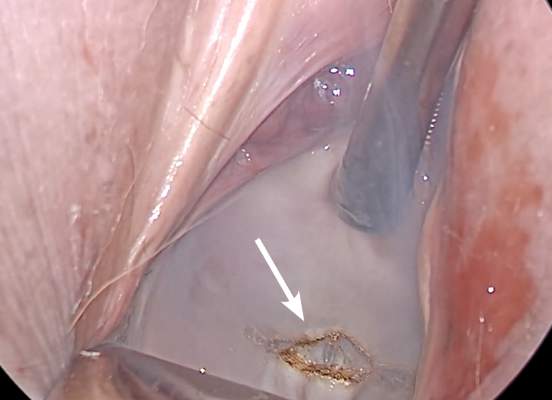
Once the incision is made, it is possible to feel the posterior peritoneum. And as you tent the peritoneum, you can then very confidently extend the incision and enter the cavity posteriorly.
In a patient with significant adhesions such as this one, I feel around posteriorly to determine exactly where I am. One tactic I use is to release the tenaculum and regrasp the cervix with it. This allows for improved visualization and movement of the cervix as the procedure progresses. Depending on the case, it may be necessary to insert a sponge to hold bowel out of the way.
Avoid the bladder
Move the Deaver retractor to the anterior position, switch the Jacobs clamp to the anterior cervix, and pull straight down. Now that you have incised the vaginal epithelium posteriorly, the length of the cervix should be apparent to you, and you can easily determine the location of the bladder reflection.
Keep in mind that, in a postmenopausal patient, there will be fewer vaginal rugae to guide you. Place the Jacobs tenaculum as close to the midline as possible so that you can confidently grab the tissue without fear of grabbing the bladder. If you tilt the Jacobs clamp, you can feel the edge of the bladder reflection. Remember that postmenopausal patients with prolapse (or, occasionally, obese patients with cervical elongation but little actual descensus) may have altered anatomy.
You can create a bit more space in which to dissect by injecting the bupivacaine/ epinephrine solution into the vaginal epithelium. This technique also ensures that the vaginal epithelial incisions won’t bleed.
Now, tilt the Jacobs tenaculum downward and push the junction of the cervix with the bladder reflection toward you so that you have a good sense of how deeply to incise.
Once you’ve made the incision, reclamp the Jacobs tenaculum so that it holds all of that tissue, and repeat the maneuver, tilting the clamp downward and pushing the junction toward you. In this way, you create traction and countertraction, sweeping the tissue out of your way.
Always use sharp dissection. When adhesions are present, surgeons often get into trouble using blunt dissection and may inadvertently enter the bladder if they use a sponge-covered digit for dissection, because adhesions can be much denser than normal tissue. In such cases, the bladder tears open rather than the adhesions being swept away.
Consider this: You don’t need to enter the peritoneal cavity anteriorly in order to continue working on the procedure. You can safely protect the bladder throughout the case, until the very end, if necessary, in patients who have undergone multiple previous surgeries or cesarean deliveries.
Rather than enter the anterior peritoneum, I dissect as much of the vaginal epithelium as possible and place a second Deaver retractor posteriorly.
I massage the uterosacral ligament for about 10 seconds to lengthen it and create more descensus, then place a Ballantine Heaney clamp on the ligament.
Next, I cut the pedicle and suture it, maintaining a clamp on the uterosacral ligament suture so that I can use it later for repair of the vaginal cuff.
I recommend a vessel-sealing device to secure the major blood supply, but I do suture the uterosacral and round ligaments for attachment to the apex at the conclusion of the hysterectomy. I suggest that you place straight clamps to hold the uterosacral ligament sutures and curved clamps on the round ligament ties to help you keep track of what you’re doing.
I generally prefer to use a smaller vessel-sealing device, such as the LigaSure Max (Covidien), because it allows me to take very small bites of tissue. It is also less expensive because it uses a disposable electrode within a reusable Heaney-type clamp.
Many people have argued that we need to teach surgeons to suture vaginally and, for that reason, should avoid vessel sealing. My response: Why wouldn’t we want to use the very best technology available? Randomized trials have demonstrated a 50% reduction in pain relief postoperatively when we use vessel sealing.4 Less foreign material is left in the pelvis, lowering the risk of infection. And it really doesn’t matter which vessel-sealing technology you use, as long as you’re familiar with the specifics of the system you choose. Another advantage: There is no need to pass needles back and forth.
Take small bites of tissue
Because this patient has a very small uterus, a small bite of tissue will get you close to where you want to be. When you take a bite with the vessel sealer, try to protect the vaginal epithelium and vulva from the steam that is emitted. The clamp itself does not heat up, but the steam that is released from the tissue is 100° C, so place a finger between the clamp and the sidewall for protection. It is preferable to burn your own finger than to burn the patient.
Because you haven’t entered the peritoneal cavity anteriorly, it is important to ensure that you don’t take too big of a bite with the vessel sealer. Rather, stay where you know you’ve done your dissection, where things are safe.
One cardinal principle of surgery is that you shouldn’t operate where you can’t feel or see. One of the common errors in vaginal surgery is that surgeons start dissecting higher than they can see. It’s easy to get into trouble when you start pushing tissue or dissecting tissue that you can’t visualize.
At this point, the anterior Deaver retractor is not essential, so I remove it. If you don’t need it, don’t use it. I try to avoid metal when I can.
If I were using suture rather than vessel sealing, I would place a Heaney clamp on the uterosacral ligament and cut. Using a clamp-cut-tie technique, I would pull on the pedicle and cut just beyond the tip of the clamp to ensure that the suture will be secure (FIGURE 4). This approach would not be appropriate during use of a vessel sealer. In that case, you would want to cut to but not beyond the tip of the clamp.
One of the skills helpful in suturing is learning to move your elbow and wrist to achieve the proper angle. Determine where you want the suture to exit the tissue, and then angle your elbow and wrist so that the suture comes out where you want it. It’s easy to lose track of the needle tip, especially when you’re working in a limited space under the pubic symphysis, so use your shoulder, elbow, and wrist to control
suture placement.

Protect the anterior epithelium
Because you have not yet entered the peritoneal cavity anteriorly, it is important to protect the anterior epithelium and bladder. Reinsert a narrow Deaver retractor anteriorly, remove the Jacobs clamp, and replace the clamp laterally so that the cervix can be pulled off to the side (FIGURE 5).

One nice thing about some vessel sealers is that the surgeon can twist them in any direction. It isn’t necessary to move your hand; you simply move the device itself.
Once you have taken at least the descending branch of the uterine artery, remove the posterior retractor and pull downward on the Jacobs tenaculum. You should have reached just about to the level of the uterine fundus, with the anatomy well visualized (FIGURE 6). Next, open the anterior peritoneum.
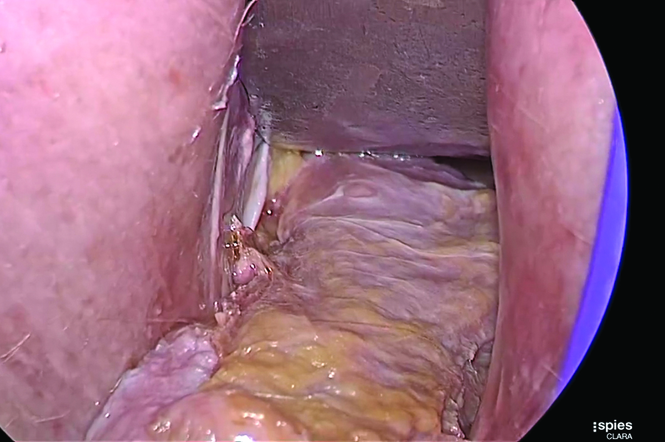
Pay attention to the surgical field
Now that you have entered the peritoneum anteriorly as well as posteriorly, identify the broad ligament, keeping in mind that the ureter is retroperitoneal, not intraperitoneal. If you were to place a clamp from the posterior leaf of the broad ligament across to the anterior leaf of the broad ligament, you would be grasping all the vessels but not the ureter. In fact, the anterior Deaver retractor is lifting both ureters up and out of the way. If you pull the cervix off to the opposite side, you create an additional couple of centimeters—a safe space for the vessel sealer
(FIGURE 7).
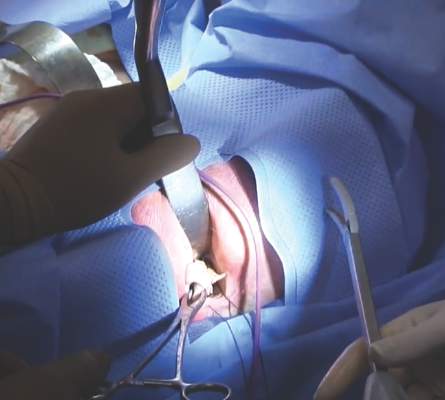
In placing the vessel sealer, there is no need to move out laterally, as there is no need for space to place suture. Instead, hug the uterus. At this point, the main concern is the risk of damaging any small bowel behind the uterine fundus that might be coming down into the surgical field, obscured from vision. And because there may be steam emitted at the tip of the vessel-sealing clamp, keep a finger back there to protect anything that might be in the field.
Last steps
Before taking the last bite of tissue on the right-hand side, place the round ligament in a Heaney clamp. Now that the round and utero-ovarian ligaments have been skeletonized, you can grasp the pedicle in a clamp. If the pedicle is especially thick, it may be beneficial to close the clamp, leave it on for a few seconds, and then reapply it. In that way, you obtain a better purchase.
Next, free the rest of the tissue with a vessel sealer, or cut it. I prefer to use a vessel sealer, and I again protect the adjacent tissue with my fingers anteriorly and posteriorly.
With the clamp remaining on the round ligament and utero-ovarian ligament
(FIGURE 8), which will be sutured, push the uterine tissue out of the way, back into the pelvis, to make room for suturing.

Because a postmenopausal vulva may be cut by the suture, it’s important to take pains not to abrade that tissue. Once you have finished suturing the round/utero-ovarian pedicle, leave the needle on the suture so that you can reconnect the round ligament to the anterior pubocervical ring to reconstruct the vaginal apex. For safekeeping, clamp the needle out of the way and tuck it beneath the drape.
Switching to the other side, use a Lahey clamp to flip the uterus, then clamp the pedicle and use the vessel sealer to separate it, again protecting the tissue beneath and ahead of the clamp. Sometimes, with an especially thick pedicle, the vessel sealer will signal that the tissue hasn’t been completely sealed. In that case, get another purchase of the pedicle, protect the adjacent tissue, and seal again.
Once the uterus has been removed completely, suture the utero-ovarian and round ligament on this side.
One tip to aid in the placement of suture is to move your clamped tissue in such a way as to prevent inadvertent suturing of other tissue (FIGURE 9).

An additional strategy for pain relief at this point is to infiltrate the round ligaments with local anesthetic. We know that we’re working with higher-level fibers—T10 to T12—through the round ligaments. By infiltrating them with anesthetic, you achieve denser pain relief for post- operative management.
Uterine reduction strategies facilitate vaginal removal of tissue
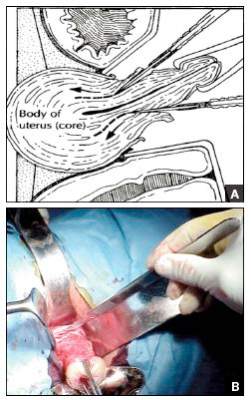
When the uterus is too large to remove intact through the vagina, there are a number of techniques for coring, wedging, and morcellating the tissue. As always, a complete knowledge of anatomy is essential, as well as an understanding that fibroids can frequently distort the uterus, twisting it to the left or right. It is important to anticipate such distortion to avoid the inadvertent destruction of anatomic landmarks or damage to the adnexae.
One straight-forward strategy is to debulk the uterus using a knife to core it, removing the central portion. In cases in which you need to keep the entire endometrial cavity intact, you can core the central portion of the uterus while grasping the cervix so that you can remove the endometrium intact for the pathologist (FIGURE).
For this strategy it is important to protect the vaginal sidewalls with metal. You can use another retractor to do that, pulling down on the cervix and beginning the morcellation. I generally prefer to use a short knife handle only because I want to be sure I’m not tempted to cut any higher than I can see.
For more on coring and wedging techniques, see the introductory video for the ACOG/SGS/AAGL master class on vaginal hysterectomy at http://www.aagl.org/vaghystwebinar.
Close the vaginal cuff
The reconstruction of the vaginal cuff is a critical component of any hysterectomy. My approach is to reattach the uterosacral ligaments to the posterior cuff and the round ligaments to the anterior cuff, thereby re- creating an intact pubocervical ring. It is not necessary to include the peritoneum in the cuff closure. In fact, kinking of the ureters is more likely when the peritoneum is closed.
Attach one uterosacral ligament, then place a running, full-thickness stitch across the posterior cuff, and attach the uterosacral ligament on the opposite side. Use the needle you left attached to the round ligament to bring the right pedicle to the anterior cuff at 10 o’clock (be sure you grasp the full thickness of the vaginal epithelium without compromising the bladder). Attach the left round-ligament pedicle at the 2 o’clock position. Then close the cuff side to side down to the uterosacral ligaments. This completely reconstructs the pubocervical ring and provides excellent support at the apex.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Brigham and Women’s Hospital. Minimally Invasive Gynecologic Surgery: Hysterectomy Options. http://www .brighamandwomens.org/Departments_and_Services/obgyn /services/mininvgynsurg/mininvoptions/hysterectomy.aspx. Published October 3, 2014. Accessed September 2, 2015.
- American Congress of Obstetricians and Gynecologists. 2011 Women’s Health Stats & Facts. Washington, DC: ACOG; 2011. http://www.acog.org/~/media/NewsRoom/MediaKit.pdf. Accessed August 6, 2015.
- American College of Obstetricians and Gynecologists. Committee Opinion No. 444: Choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2009; 114(5):1156–1158.
- Silva-Filho AL, Rodrigues AM, Vale de Castro Monteiro M, et al. Randomized study of bipolar vessel sealing system versus conventional suture ligature for vaginal hysterectomy. Eur J Obstet Gynecol Reprod Biol. 2009;146(2):200–203.
Barbara S. Levy, MD

Dr. Levy is Vice President for Health Policy at the American Congress of Obstetricians and Gynecologists in Washington, DC, and a past president of AAGL.
The author reports no financial relationships relevant to this article.
Barbara S. Levy, MD
Dr. Levy is Vice President for Health Policy at the American Congress of Obstetricians and Gynecologists in Washington, DC, and a past president of AAGL.
The author reports no financial relationships relevant to this article.
Barbara S. Levy, MD
Dr. Levy is Vice President for Health Policy at the American Congress of Obstetricians and Gynecologists in Washington, DC, and a past president of AAGL.
The author reports no financial relationships relevant to this article.
In the United States, gynecologic surgeons remove approximately one uterus every minute of the year.1 That rate translates to more than 525,000 hysterectomies annually in this country alone. Yet, despite the widespread availability of information on the benefits of a vaginal approach to hysterectomy, the great majority of these operations—close to 50%—are still performed via an open abdominal approach.2
As I pointed out last month in my “Update on Vaginal Hysterectomy,” the vaginal approach not only is more cosmetically pleasing than laparoscopic and robot-assisted hysterectomy (not to mention open abdominal surgery) but also has a lower complication rate.3
As I also noted, one reason for the low rate of vaginal hysterectomy may be the assumption, on the part of many gynecologic surgeons, that the techniques and tools they learned to use during training are still the only options available today. That assumption is wrong.
In this article, I describe the technique for vaginal hysterectomy using basic instru mentation. This article is based on a master class in vaginal hysterectomy produced by the AAGL and co-sponsored by the Am erican College of Obstetricians and Gynecologists and the Society of Gynecologic Surgeons. This master class offers continuing medical education credits and is avail able at http://www.aagl.org/vaghystwebinar.
For a look at innovative tools for this procedure, see my “Update on Vaginal Hysterectomy” in the September 2015 issue of this journal at obgmanagement.com.
Vaginal hysterectomy has few contraindications
Many commonly cited contraindications to the vaginal approach are not, in fact, absolute contraindications. An open or laparoscopic approach is preferred when the patient has a known cancer, of course, and when deep infiltrating endometriosis is present at the rectovaginal septum. However, previous pelvic surgery, nulliparity, an enlarged uterus, or lack of a prior vaginal delivery need not exclude the vaginal approach. Nor does a narrow introitus necessarily mandate a laparoscopic or open abdominal approach. In fact, in this article, I describe my basic technique in a patient (a cadaver) with a very narrow pubic arch, and I offer strategies for gaining some needed mobility and avoiding complications (TABLES 1 and 2).
Next month, in the November issue of OBG Management, John B. Gebhart, MD, will describe his vaginal technique for right salpingectomy with ovarian preservation, as well as his technique for right salpingo-oophorectomy.
Proper patient positioning is key
You can simplify the operation by positioning the patient so that her buttocks are over the edge of the table fairly far—at least 1 inch beyond the edge of the table for optimal exposure and greater access. If the patient is thin, it then becomes important to pad the sacrum because, when she is positioned that far off the table, all her weight comes to rest on the sacrum. In overweight patients, this is not an issue, but for thin patients, I place a bit of egg crate or gel beneath the sacrum.
For the procedure, I prefer to place my instruments on a tray that is kept on my lap. This arrangement frees the scrub technician from having to hand tools over my shoulder—and it saves time. I use a narrow, covered Mayo stand, and I place a stepstool beneath my feet to keep my knees at right angles so that things don’t slip during the operation.
Surgical technique
Choose an appropriate retractor
In a woman with a narrow introitus, I find that a posterior weighted speculum takes up too much space. Once I place a clamp on the cervix with that speculum in place, I don’t have much room to work. However, if I substitute a small Deaver retractor, which is narrower, I gain more workspace.
Inject the uterosacral ligaments
Grasp the cervix using a Jacobs vulsellum tenaculum. Use of a single tenaculum allows for much more movement than the use of instruments placed anteriorly and posteriorly. The Jacobs tenaculum obtains a better purchase on the tissue than a single tooth and is considerably less likely to tear through the tissue.
Before beginning the hysterectomy, locate the uterosacral ligaments and inject each one at its junction with the cervix, aspirating slightly before infiltrating the ligament with 0.25% to 0.50% bupivacaine with epinephrine, with dilute vasopressin mixed in. (I place 1 unit in 20 mL of the local solution.) Injection of this solution achieves 2 goals:
- improved intraoperative hemostasis
- postoperative pain relief.
Use a short needle with a needle extender attached to a control syringe rather than a spinal needle for greater control.
Enter the posterior peritoneal cavity
Before entering the peritoneal cavity, create a right angle with the Jacobs tenaculum and Deaver retractor in relation to the surgical field (FIGURE 1). This right angle is difficult to achieve when you are using a weighted speculum in a tight vagina. Once you have a right angle, tent the vaginal tissue in the midline (FIGURE 2).
In a nulliparous patient or a woman with a tight pelvis, you may discover that the peritoneum is pulled up between the uterosacral ligaments. One common pitfall arises when the surgeon, having dissected the vaginal epithelium, continues cutting into the vaginal epithelium instead of reaching into the peritoneal cavity. Palpate the tissue to ensure that there is no bowel in the way and stay at right angles while confidently grasping the peritoneum with a toothed forceps.
I like to use a bit of electrosurgery to incise the vaginal wall. I don’t begin at the cervix but incise more distally into the vaginal epithelium approximately 2 cm from the cervicovaginal junction. This strategy prevents dissection into the cervix and/or rectovaginal septum rather than the posterior
cul-de-sac (FIGURE 3).
Once the incision is made, it is possible to feel the posterior peritoneum. And as you tent the peritoneum, you can then very confidently extend the incision and enter the cavity posteriorly.
In a patient with significant adhesions such as this one, I feel around posteriorly to determine exactly where I am. One tactic I use is to release the tenaculum and regrasp the cervix with it. This allows for improved visualization and movement of the cervix as the procedure progresses. Depending on the case, it may be necessary to insert a sponge to hold bowel out of the way.
Avoid the bladder
Move the Deaver retractor to the anterior position, switch the Jacobs clamp to the anterior cervix, and pull straight down. Now that you have incised the vaginal epithelium posteriorly, the length of the cervix should be apparent to you, and you can easily determine the location of the bladder reflection.
Keep in mind that, in a postmenopausal patient, there will be fewer vaginal rugae to guide you. Place the Jacobs tenaculum as close to the midline as possible so that you can confidently grab the tissue without fear of grabbing the bladder. If you tilt the Jacobs clamp, you can feel the edge of the bladder reflection. Remember that postmenopausal patients with prolapse (or, occasionally, obese patients with cervical elongation but little actual descensus) may have altered anatomy.
You can create a bit more space in which to dissect by injecting the bupivacaine/ epinephrine solution into the vaginal epithelium. This technique also ensures that the vaginal epithelial incisions won’t bleed.
Now, tilt the Jacobs tenaculum downward and push the junction of the cervix with the bladder reflection toward you so that you have a good sense of how deeply to incise.
Once you’ve made the incision, reclamp the Jacobs tenaculum so that it holds all of that tissue, and repeat the maneuver, tilting the clamp downward and pushing the junction toward you. In this way, you create traction and countertraction, sweeping the tissue out of your way.
Always use sharp dissection. When adhesions are present, surgeons often get into trouble using blunt dissection and may inadvertently enter the bladder if they use a sponge-covered digit for dissection, because adhesions can be much denser than normal tissue. In such cases, the bladder tears open rather than the adhesions being swept away.
Consider this: You don’t need to enter the peritoneal cavity anteriorly in order to continue working on the procedure. You can safely protect the bladder throughout the case, until the very end, if necessary, in patients who have undergone multiple previous surgeries or cesarean deliveries.
Rather than enter the anterior peritoneum, I dissect as much of the vaginal epithelium as possible and place a second Deaver retractor posteriorly.
I massage the uterosacral ligament for about 10 seconds to lengthen it and create more descensus, then place a Ballantine Heaney clamp on the ligament.
Next, I cut the pedicle and suture it, maintaining a clamp on the uterosacral ligament suture so that I can use it later for repair of the vaginal cuff.
I recommend a vessel-sealing device to secure the major blood supply, but I do suture the uterosacral and round ligaments for attachment to the apex at the conclusion of the hysterectomy. I suggest that you place straight clamps to hold the uterosacral ligament sutures and curved clamps on the round ligament ties to help you keep track of what you’re doing.
I generally prefer to use a smaller vessel-sealing device, such as the LigaSure Max (Covidien), because it allows me to take very small bites of tissue. It is also less expensive because it uses a disposable electrode within a reusable Heaney-type clamp.
Many people have argued that we need to teach surgeons to suture vaginally and, for that reason, should avoid vessel sealing. My response: Why wouldn’t we want to use the very best technology available? Randomized trials have demonstrated a 50% reduction in pain relief postoperatively when we use vessel sealing.4 Less foreign material is left in the pelvis, lowering the risk of infection. And it really doesn’t matter which vessel-sealing technology you use, as long as you’re familiar with the specifics of the system you choose. Another advantage: There is no need to pass needles back and forth.
Take small bites of tissue
Because this patient has a very small uterus, a small bite of tissue will get you close to where you want to be. When you take a bite with the vessel sealer, try to protect the vaginal epithelium and vulva from the steam that is emitted. The clamp itself does not heat up, but the steam that is released from the tissue is 100° C, so place a finger between the clamp and the sidewall for protection. It is preferable to burn your own finger than to burn the patient.
Because you haven’t entered the peritoneal cavity anteriorly, it is important to ensure that you don’t take too big of a bite with the vessel sealer. Rather, stay where you know you’ve done your dissection, where things are safe.
One cardinal principle of surgery is that you shouldn’t operate where you can’t feel or see. One of the common errors in vaginal surgery is that surgeons start dissecting higher than they can see. It’s easy to get into trouble when you start pushing tissue or dissecting tissue that you can’t visualize.
At this point, the anterior Deaver retractor is not essential, so I remove it. If you don’t need it, don’t use it. I try to avoid metal when I can.
If I were using suture rather than vessel sealing, I would place a Heaney clamp on the uterosacral ligament and cut. Using a clamp-cut-tie technique, I would pull on the pedicle and cut just beyond the tip of the clamp to ensure that the suture will be secure (FIGURE 4). This approach would not be appropriate during use of a vessel sealer. In that case, you would want to cut to but not beyond the tip of the clamp.
One of the skills helpful in suturing is learning to move your elbow and wrist to achieve the proper angle. Determine where you want the suture to exit the tissue, and then angle your elbow and wrist so that the suture comes out where you want it. It’s easy to lose track of the needle tip, especially when you’re working in a limited space under the pubic symphysis, so use your shoulder, elbow, and wrist to control
suture placement.
Protect the anterior epithelium
Because you have not yet entered the peritoneal cavity anteriorly, it is important to protect the anterior epithelium and bladder. Reinsert a narrow Deaver retractor anteriorly, remove the Jacobs clamp, and replace the clamp laterally so that the cervix can be pulled off to the side (FIGURE 5).
One nice thing about some vessel sealers is that the surgeon can twist them in any direction. It isn’t necessary to move your hand; you simply move the device itself.
Once you have taken at least the descending branch of the uterine artery, remove the posterior retractor and pull downward on the Jacobs tenaculum. You should have reached just about to the level of the uterine fundus, with the anatomy well visualized (FIGURE 6). Next, open the anterior peritoneum.
Pay attention to the surgical field
Now that you have entered the peritoneum anteriorly as well as posteriorly, identify the broad ligament, keeping in mind that the ureter is retroperitoneal, not intraperitoneal. If you were to place a clamp from the posterior leaf of the broad ligament across to the anterior leaf of the broad ligament, you would be grasping all the vessels but not the ureter. In fact, the anterior Deaver retractor is lifting both ureters up and out of the way. If you pull the cervix off to the opposite side, you create an additional couple of centimeters—a safe space for the vessel sealer
(FIGURE 7).
In placing the vessel sealer, there is no need to move out laterally, as there is no need for space to place suture. Instead, hug the uterus. At this point, the main concern is the risk of damaging any small bowel behind the uterine fundus that might be coming down into the surgical field, obscured from vision. And because there may be steam emitted at the tip of the vessel-sealing clamp, keep a finger back there to protect anything that might be in the field.
Last steps
Before taking the last bite of tissue on the right-hand side, place the round ligament in a Heaney clamp. Now that the round and utero-ovarian ligaments have been skeletonized, you can grasp the pedicle in a clamp. If the pedicle is especially thick, it may be beneficial to close the clamp, leave it on for a few seconds, and then reapply it. In that way, you obtain a better purchase.
Next, free the rest of the tissue with a vessel sealer, or cut it. I prefer to use a vessel sealer, and I again protect the adjacent tissue with my fingers anteriorly and posteriorly.
With the clamp remaining on the round ligament and utero-ovarian ligament
(FIGURE 8), which will be sutured, push the uterine tissue out of the way, back into the pelvis, to make room for suturing.
Because a postmenopausal vulva may be cut by the suture, it’s important to take pains not to abrade that tissue. Once you have finished suturing the round/utero-ovarian pedicle, leave the needle on the suture so that you can reconnect the round ligament to the anterior pubocervical ring to reconstruct the vaginal apex. For safekeeping, clamp the needle out of the way and tuck it beneath the drape.
Switching to the other side, use a Lahey clamp to flip the uterus, then clamp the pedicle and use the vessel sealer to separate it, again protecting the tissue beneath and ahead of the clamp. Sometimes, with an especially thick pedicle, the vessel sealer will signal that the tissue hasn’t been completely sealed. In that case, get another purchase of the pedicle, protect the adjacent tissue, and seal again.
Once the uterus has been removed completely, suture the utero-ovarian and round ligament on this side.
One tip to aid in the placement of suture is to move your clamped tissue in such a way as to prevent inadvertent suturing of other tissue (FIGURE 9).
An additional strategy for pain relief at this point is to infiltrate the round ligaments with local anesthetic. We know that we’re working with higher-level fibers—T10 to T12—through the round ligaments. By infiltrating them with anesthetic, you achieve denser pain relief for post- operative management.
Uterine reduction strategies facilitate vaginal removal of tissue
When the uterus is too large to remove intact through the vagina, there are a number of techniques for coring, wedging, and morcellating the tissue. As always, a complete knowledge of anatomy is essential, as well as an understanding that fibroids can frequently distort the uterus, twisting it to the left or right. It is important to anticipate such distortion to avoid the inadvertent destruction of anatomic landmarks or damage to the adnexae.
One straight-forward strategy is to debulk the uterus using a knife to core it, removing the central portion. In cases in which you need to keep the entire endometrial cavity intact, you can core the central portion of the uterus while grasping the cervix so that you can remove the endometrium intact for the pathologist (FIGURE).
For this strategy it is important to protect the vaginal sidewalls with metal. You can use another retractor to do that, pulling down on the cervix and beginning the morcellation. I generally prefer to use a short knife handle only because I want to be sure I’m not tempted to cut any higher than I can see.
For more on coring and wedging techniques, see the introductory video for the ACOG/SGS/AAGL master class on vaginal hysterectomy at http://www.aagl.org/vaghystwebinar.
Close the vaginal cuff
The reconstruction of the vaginal cuff is a critical component of any hysterectomy. My approach is to reattach the uterosacral ligaments to the posterior cuff and the round ligaments to the anterior cuff, thereby re- creating an intact pubocervical ring. It is not necessary to include the peritoneum in the cuff closure. In fact, kinking of the ureters is more likely when the peritoneum is closed.
Attach one uterosacral ligament, then place a running, full-thickness stitch across the posterior cuff, and attach the uterosacral ligament on the opposite side. Use the needle you left attached to the round ligament to bring the right pedicle to the anterior cuff at 10 o’clock (be sure you grasp the full thickness of the vaginal epithelium without compromising the bladder). Attach the left round-ligament pedicle at the 2 o’clock position. Then close the cuff side to side down to the uterosacral ligaments. This completely reconstructs the pubocervical ring and provides excellent support at the apex.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In the United States, gynecologic surgeons remove approximately one uterus every minute of the year.1 That rate translates to more than 525,000 hysterectomies annually in this country alone. Yet, despite the widespread availability of information on the benefits of a vaginal approach to hysterectomy, the great majority of these operations—close to 50%—are still performed via an open abdominal approach.2
As I pointed out last month in my “Update on Vaginal Hysterectomy,” the vaginal approach not only is more cosmetically pleasing than laparoscopic and robot-assisted hysterectomy (not to mention open abdominal surgery) but also has a lower complication rate.3
As I also noted, one reason for the low rate of vaginal hysterectomy may be the assumption, on the part of many gynecologic surgeons, that the techniques and tools they learned to use during training are still the only options available today. That assumption is wrong.
In this article, I describe the technique for vaginal hysterectomy using basic instru mentation. This article is based on a master class in vaginal hysterectomy produced by the AAGL and co-sponsored by the Am erican College of Obstetricians and Gynecologists and the Society of Gynecologic Surgeons. This master class offers continuing medical education credits and is avail able at http://www.aagl.org/vaghystwebinar.
For a look at innovative tools for this procedure, see my “Update on Vaginal Hysterectomy” in the September 2015 issue of this journal at obgmanagement.com.
Vaginal hysterectomy has few contraindications
Many commonly cited contraindications to the vaginal approach are not, in fact, absolute contraindications. An open or laparoscopic approach is preferred when the patient has a known cancer, of course, and when deep infiltrating endometriosis is present at the rectovaginal septum. However, previous pelvic surgery, nulliparity, an enlarged uterus, or lack of a prior vaginal delivery need not exclude the vaginal approach. Nor does a narrow introitus necessarily mandate a laparoscopic or open abdominal approach. In fact, in this article, I describe my basic technique in a patient (a cadaver) with a very narrow pubic arch, and I offer strategies for gaining some needed mobility and avoiding complications (TABLES 1 and 2).
Next month, in the November issue of OBG Management, John B. Gebhart, MD, will describe his vaginal technique for right salpingectomy with ovarian preservation, as well as his technique for right salpingo-oophorectomy.
Proper patient positioning is key
You can simplify the operation by positioning the patient so that her buttocks are over the edge of the table fairly far—at least 1 inch beyond the edge of the table for optimal exposure and greater access. If the patient is thin, it then becomes important to pad the sacrum because, when she is positioned that far off the table, all her weight comes to rest on the sacrum. In overweight patients, this is not an issue, but for thin patients, I place a bit of egg crate or gel beneath the sacrum.
For the procedure, I prefer to place my instruments on a tray that is kept on my lap. This arrangement frees the scrub technician from having to hand tools over my shoulder—and it saves time. I use a narrow, covered Mayo stand, and I place a stepstool beneath my feet to keep my knees at right angles so that things don’t slip during the operation.
Surgical technique
Choose an appropriate retractor
In a woman with a narrow introitus, I find that a posterior weighted speculum takes up too much space. Once I place a clamp on the cervix with that speculum in place, I don’t have much room to work. However, if I substitute a small Deaver retractor, which is narrower, I gain more workspace.
Inject the uterosacral ligaments
Grasp the cervix using a Jacobs vulsellum tenaculum. Use of a single tenaculum allows for much more movement than the use of instruments placed anteriorly and posteriorly. The Jacobs tenaculum obtains a better purchase on the tissue than a single tooth and is considerably less likely to tear through the tissue.
Before beginning the hysterectomy, locate the uterosacral ligaments and inject each one at its junction with the cervix, aspirating slightly before infiltrating the ligament with 0.25% to 0.50% bupivacaine with epinephrine, with dilute vasopressin mixed in. (I place 1 unit in 20 mL of the local solution.) Injection of this solution achieves 2 goals:
- improved intraoperative hemostasis
- postoperative pain relief.
Use a short needle with a needle extender attached to a control syringe rather than a spinal needle for greater control.
Enter the posterior peritoneal cavity
Before entering the peritoneal cavity, create a right angle with the Jacobs tenaculum and Deaver retractor in relation to the surgical field (FIGURE 1). This right angle is difficult to achieve when you are using a weighted speculum in a tight vagina. Once you have a right angle, tent the vaginal tissue in the midline (FIGURE 2).
In a nulliparous patient or a woman with a tight pelvis, you may discover that the peritoneum is pulled up between the uterosacral ligaments. One common pitfall arises when the surgeon, having dissected the vaginal epithelium, continues cutting into the vaginal epithelium instead of reaching into the peritoneal cavity. Palpate the tissue to ensure that there is no bowel in the way and stay at right angles while confidently grasping the peritoneum with a toothed forceps.
I like to use a bit of electrosurgery to incise the vaginal wall. I don’t begin at the cervix but incise more distally into the vaginal epithelium approximately 2 cm from the cervicovaginal junction. This strategy prevents dissection into the cervix and/or rectovaginal septum rather than the posterior
cul-de-sac (FIGURE 3).
Once the incision is made, it is possible to feel the posterior peritoneum. And as you tent the peritoneum, you can then very confidently extend the incision and enter the cavity posteriorly.
In a patient with significant adhesions such as this one, I feel around posteriorly to determine exactly where I am. One tactic I use is to release the tenaculum and regrasp the cervix with it. This allows for improved visualization and movement of the cervix as the procedure progresses. Depending on the case, it may be necessary to insert a sponge to hold bowel out of the way.
Avoid the bladder
Move the Deaver retractor to the anterior position, switch the Jacobs clamp to the anterior cervix, and pull straight down. Now that you have incised the vaginal epithelium posteriorly, the length of the cervix should be apparent to you, and you can easily determine the location of the bladder reflection.
Keep in mind that, in a postmenopausal patient, there will be fewer vaginal rugae to guide you. Place the Jacobs tenaculum as close to the midline as possible so that you can confidently grab the tissue without fear of grabbing the bladder. If you tilt the Jacobs clamp, you can feel the edge of the bladder reflection. Remember that postmenopausal patients with prolapse (or, occasionally, obese patients with cervical elongation but little actual descensus) may have altered anatomy.
You can create a bit more space in which to dissect by injecting the bupivacaine/ epinephrine solution into the vaginal epithelium. This technique also ensures that the vaginal epithelial incisions won’t bleed.
Now, tilt the Jacobs tenaculum downward and push the junction of the cervix with the bladder reflection toward you so that you have a good sense of how deeply to incise.
Once you’ve made the incision, reclamp the Jacobs tenaculum so that it holds all of that tissue, and repeat the maneuver, tilting the clamp downward and pushing the junction toward you. In this way, you create traction and countertraction, sweeping the tissue out of your way.
Always use sharp dissection. When adhesions are present, surgeons often get into trouble using blunt dissection and may inadvertently enter the bladder if they use a sponge-covered digit for dissection, because adhesions can be much denser than normal tissue. In such cases, the bladder tears open rather than the adhesions being swept away.
Consider this: You don’t need to enter the peritoneal cavity anteriorly in order to continue working on the procedure. You can safely protect the bladder throughout the case, until the very end, if necessary, in patients who have undergone multiple previous surgeries or cesarean deliveries.
Rather than enter the anterior peritoneum, I dissect as much of the vaginal epithelium as possible and place a second Deaver retractor posteriorly.
I massage the uterosacral ligament for about 10 seconds to lengthen it and create more descensus, then place a Ballantine Heaney clamp on the ligament.
Next, I cut the pedicle and suture it, maintaining a clamp on the uterosacral ligament suture so that I can use it later for repair of the vaginal cuff.
I recommend a vessel-sealing device to secure the major blood supply, but I do suture the uterosacral and round ligaments for attachment to the apex at the conclusion of the hysterectomy. I suggest that you place straight clamps to hold the uterosacral ligament sutures and curved clamps on the round ligament ties to help you keep track of what you’re doing.
I generally prefer to use a smaller vessel-sealing device, such as the LigaSure Max (Covidien), because it allows me to take very small bites of tissue. It is also less expensive because it uses a disposable electrode within a reusable Heaney-type clamp.
Many people have argued that we need to teach surgeons to suture vaginally and, for that reason, should avoid vessel sealing. My response: Why wouldn’t we want to use the very best technology available? Randomized trials have demonstrated a 50% reduction in pain relief postoperatively when we use vessel sealing.4 Less foreign material is left in the pelvis, lowering the risk of infection. And it really doesn’t matter which vessel-sealing technology you use, as long as you’re familiar with the specifics of the system you choose. Another advantage: There is no need to pass needles back and forth.
Take small bites of tissue
Because this patient has a very small uterus, a small bite of tissue will get you close to where you want to be. When you take a bite with the vessel sealer, try to protect the vaginal epithelium and vulva from the steam that is emitted. The clamp itself does not heat up, but the steam that is released from the tissue is 100° C, so place a finger between the clamp and the sidewall for protection. It is preferable to burn your own finger than to burn the patient.
Because you haven’t entered the peritoneal cavity anteriorly, it is important to ensure that you don’t take too big of a bite with the vessel sealer. Rather, stay where you know you’ve done your dissection, where things are safe.
One cardinal principle of surgery is that you shouldn’t operate where you can’t feel or see. One of the common errors in vaginal surgery is that surgeons start dissecting higher than they can see. It’s easy to get into trouble when you start pushing tissue or dissecting tissue that you can’t visualize.
At this point, the anterior Deaver retractor is not essential, so I remove it. If you don’t need it, don’t use it. I try to avoid metal when I can.
If I were using suture rather than vessel sealing, I would place a Heaney clamp on the uterosacral ligament and cut. Using a clamp-cut-tie technique, I would pull on the pedicle and cut just beyond the tip of the clamp to ensure that the suture will be secure (FIGURE 4). This approach would not be appropriate during use of a vessel sealer. In that case, you would want to cut to but not beyond the tip of the clamp.
One of the skills helpful in suturing is learning to move your elbow and wrist to achieve the proper angle. Determine where you want the suture to exit the tissue, and then angle your elbow and wrist so that the suture comes out where you want it. It’s easy to lose track of the needle tip, especially when you’re working in a limited space under the pubic symphysis, so use your shoulder, elbow, and wrist to control
suture placement.
Protect the anterior epithelium
Because you have not yet entered the peritoneal cavity anteriorly, it is important to protect the anterior epithelium and bladder. Reinsert a narrow Deaver retractor anteriorly, remove the Jacobs clamp, and replace the clamp laterally so that the cervix can be pulled off to the side (FIGURE 5).
One nice thing about some vessel sealers is that the surgeon can twist them in any direction. It isn’t necessary to move your hand; you simply move the device itself.
Once you have taken at least the descending branch of the uterine artery, remove the posterior retractor and pull downward on the Jacobs tenaculum. You should have reached just about to the level of the uterine fundus, with the anatomy well visualized (FIGURE 6). Next, open the anterior peritoneum.
Pay attention to the surgical field
Now that you have entered the peritoneum anteriorly as well as posteriorly, identify the broad ligament, keeping in mind that the ureter is retroperitoneal, not intraperitoneal. If you were to place a clamp from the posterior leaf of the broad ligament across to the anterior leaf of the broad ligament, you would be grasping all the vessels but not the ureter. In fact, the anterior Deaver retractor is lifting both ureters up and out of the way. If you pull the cervix off to the opposite side, you create an additional couple of centimeters—a safe space for the vessel sealer
(FIGURE 7).
In placing the vessel sealer, there is no need to move out laterally, as there is no need for space to place suture. Instead, hug the uterus. At this point, the main concern is the risk of damaging any small bowel behind the uterine fundus that might be coming down into the surgical field, obscured from vision. And because there may be steam emitted at the tip of the vessel-sealing clamp, keep a finger back there to protect anything that might be in the field.
Last steps
Before taking the last bite of tissue on the right-hand side, place the round ligament in a Heaney clamp. Now that the round and utero-ovarian ligaments have been skeletonized, you can grasp the pedicle in a clamp. If the pedicle is especially thick, it may be beneficial to close the clamp, leave it on for a few seconds, and then reapply it. In that way, you obtain a better purchase.
Next, free the rest of the tissue with a vessel sealer, or cut it. I prefer to use a vessel sealer, and I again protect the adjacent tissue with my fingers anteriorly and posteriorly.
With the clamp remaining on the round ligament and utero-ovarian ligament
(FIGURE 8), which will be sutured, push the uterine tissue out of the way, back into the pelvis, to make room for suturing.
Because a postmenopausal vulva may be cut by the suture, it’s important to take pains not to abrade that tissue. Once you have finished suturing the round/utero-ovarian pedicle, leave the needle on the suture so that you can reconnect the round ligament to the anterior pubocervical ring to reconstruct the vaginal apex. For safekeeping, clamp the needle out of the way and tuck it beneath the drape.
Switching to the other side, use a Lahey clamp to flip the uterus, then clamp the pedicle and use the vessel sealer to separate it, again protecting the tissue beneath and ahead of the clamp. Sometimes, with an especially thick pedicle, the vessel sealer will signal that the tissue hasn’t been completely sealed. In that case, get another purchase of the pedicle, protect the adjacent tissue, and seal again.
Once the uterus has been removed completely, suture the utero-ovarian and round ligament on this side.
One tip to aid in the placement of suture is to move your clamped tissue in such a way as to prevent inadvertent suturing of other tissue (FIGURE 9).
An additional strategy for pain relief at this point is to infiltrate the round ligaments with local anesthetic. We know that we’re working with higher-level fibers—T10 to T12—through the round ligaments. By infiltrating them with anesthetic, you achieve denser pain relief for post- operative management.
Uterine reduction strategies facilitate vaginal removal of tissue
When the uterus is too large to remove intact through the vagina, there are a number of techniques for coring, wedging, and morcellating the tissue. As always, a complete knowledge of anatomy is essential, as well as an understanding that fibroids can frequently distort the uterus, twisting it to the left or right. It is important to anticipate such distortion to avoid the inadvertent destruction of anatomic landmarks or damage to the adnexae.
One straight-forward strategy is to debulk the uterus using a knife to core it, removing the central portion. In cases in which you need to keep the entire endometrial cavity intact, you can core the central portion of the uterus while grasping the cervix so that you can remove the endometrium intact for the pathologist (FIGURE).
For this strategy it is important to protect the vaginal sidewalls with metal. You can use another retractor to do that, pulling down on the cervix and beginning the morcellation. I generally prefer to use a short knife handle only because I want to be sure I’m not tempted to cut any higher than I can see.
For more on coring and wedging techniques, see the introductory video for the ACOG/SGS/AAGL master class on vaginal hysterectomy at http://www.aagl.org/vaghystwebinar.
Close the vaginal cuff
The reconstruction of the vaginal cuff is a critical component of any hysterectomy. My approach is to reattach the uterosacral ligaments to the posterior cuff and the round ligaments to the anterior cuff, thereby re- creating an intact pubocervical ring. It is not necessary to include the peritoneum in the cuff closure. In fact, kinking of the ureters is more likely when the peritoneum is closed.
Attach one uterosacral ligament, then place a running, full-thickness stitch across the posterior cuff, and attach the uterosacral ligament on the opposite side. Use the needle you left attached to the round ligament to bring the right pedicle to the anterior cuff at 10 o’clock (be sure you grasp the full thickness of the vaginal epithelium without compromising the bladder). Attach the left round-ligament pedicle at the 2 o’clock position. Then close the cuff side to side down to the uterosacral ligaments. This completely reconstructs the pubocervical ring and provides excellent support at the apex.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Brigham and Women’s Hospital. Minimally Invasive Gynecologic Surgery: Hysterectomy Options. http://www .brighamandwomens.org/Departments_and_Services/obgyn /services/mininvgynsurg/mininvoptions/hysterectomy.aspx. Published October 3, 2014. Accessed September 2, 2015.
- American Congress of Obstetricians and Gynecologists. 2011 Women’s Health Stats & Facts. Washington, DC: ACOG; 2011. http://www.acog.org/~/media/NewsRoom/MediaKit.pdf. Accessed August 6, 2015.
- American College of Obstetricians and Gynecologists. Committee Opinion No. 444: Choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2009; 114(5):1156–1158.
- Silva-Filho AL, Rodrigues AM, Vale de Castro Monteiro M, et al. Randomized study of bipolar vessel sealing system versus conventional suture ligature for vaginal hysterectomy. Eur J Obstet Gynecol Reprod Biol. 2009;146(2):200–203.
- Brigham and Women’s Hospital. Minimally Invasive Gynecologic Surgery: Hysterectomy Options. http://www .brighamandwomens.org/Departments_and_Services/obgyn /services/mininvgynsurg/mininvoptions/hysterectomy.aspx. Published October 3, 2014. Accessed September 2, 2015.
- American Congress of Obstetricians and Gynecologists. 2011 Women’s Health Stats & Facts. Washington, DC: ACOG; 2011. http://www.acog.org/~/media/NewsRoom/MediaKit.pdf. Accessed August 6, 2015.
- American College of Obstetricians and Gynecologists. Committee Opinion No. 444: Choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2009; 114(5):1156–1158.
- Silva-Filho AL, Rodrigues AM, Vale de Castro Monteiro M, et al. Randomized study of bipolar vessel sealing system versus conventional suture ligature for vaginal hysterectomy. Eur J Obstet Gynecol Reprod Biol. 2009;146(2):200–203.
In this Article
- 5 solutions to difficult vaginal access
- The need to take small bites of tissue
- Uterine reduction strategies
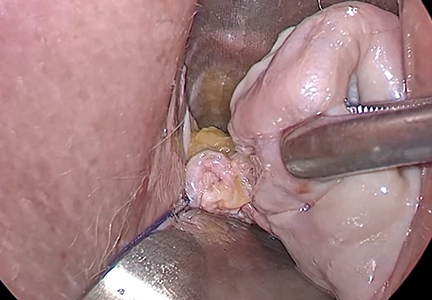
Does hormone therapy reduce mortality in recently menopausal women?
Clinicians work to maximize the quality of life and longevity of every patient. For women with moderate to severe menopausal symptoms, oral estrogen therapy can improve quality of life, but at the cost of significant adverse effects. The Women’s Health Initiative (WHI) reported that for postmenopausal women with a uterus, conjugated estrogen plus medroxyprogesterone acetate (CEE+MPA) hormone therapy (HT) versus placebo significantly increased the risk of cardiovascular events (relative risk [RR], 1.13), breast cancer (RR, 1.24), stroke (RR, 1.37), deep vein thrombosis (RR, 1.87), and pulmonary embolism (RR, 1.98).1 In postmeno pausal women without a uterus, CEE HT did not increase the risk of breast cancer (RR, 0.79), compared with placebo, but it did significantly in crease the risk of cardiovascular events (RR, 1.11), stroke (RR, 1.35), deep vein thrombosis (RR, 1.48), and pulmonary embolism (RR, 1.35).1
Clinicians prescribing estrogen must individualize therapy according to its benefits and risks. An important issue that has received insufficient at tention is, “What is the effect of HT on mortality in recently menopausal women?” Here, I examine this issue.
HT reduces mortality in recently menopausal women
Pooling the results of the WHI CEE+MPA and CEE-only trials reveals that there were 70 deaths in the HT-treated groups and 98 deaths in the placebo groups among women aged 50 to 59 years.1 With 4,706 and 4,259 women alive at the conclusion of the study in the HT and placebo groups, respectively, the women in the placebo group had significantly more deaths than the women in the HT-treated groups (Fisher exact test, P = .0194, χ2 test with Yates correction, P = .0226).
Using pooled data from the WHI, the RR of death in the HT versus placebo group was estimated at 0.70 (95% confidence interval [CI], 0.51−0.96), representing approximately 5 fewer deaths per 1,000 women per 5 years of therapy.2 In women aged 60 to 69 years and 70 to 79 years there were no significant differences in death rates between the HT- and placebo-treated women.
My interpretation of these results is that HT likely is associated with a reduced risk of death in recently menopausal women, but not in women distant from menopause onset.
Cochrane review of HT and mortality
Consistent with the WHI findings, authors of a recent Cochrane meta-analysis of 19 randomized trials including 40,410 menopausal women reported that HT significantly increased the risk of stroke (RR, 1.24; 95% CI, 1.10−1.41), venous thromboembolism (RR, 1.92; 95% CI, 1.36−2.69), and pulmonary emboli (RR, 1.81; 95% CI, 1.32−2.48).3 However, among women treated with oral HT within 10 years after the start of menopause, there was a reduced risk of coronary heart disease (RR, 0.52; 95% CI, 0.29−0.96). Using data from 5 clinical trials, the Cochrane meta-analysis researchers reported that, compared with placebo, HT reduced mortality (RR, 0.70; 95% CI, 0.52−0.95).3
Results of the Cochrane meta-analysis are consistent with those of a previous meta-analysis of 19 randomized trials involving 16,000 women. In this analysis, investigators found a reduced risk of death in recently menopausal women treated with hormone therapy (RR, 0.73; 95% CI, 0.52−0.96).4
Early menopause, HT, and mortality
Authors of multiple large epidemiologic studies have reported that early menopause is associated with an increased risk of death if HT is not initiated.5−7 For example, results of a study of women in Olmsted County, Minnesota, conducted from 1950 to 1987, indicated that, for women younger than age 45 years who underwent bilateral oophorectomy, the risk of death was increased among those who did not initiate HT, compared with women who did not undergo oophorectomy (hazard ratio [HR], 1.84; 95% CI, 1.27−2.68; P = .001).7
By contrast, women younger than 45 years who underwent bilateral oophorectomy and initiated estrogen therapy did not have an increased risk of death compared with women who did not undergo oophorectomy (HR, 0.65; 95% CI, 0.30−1.41; P = .28).7 An excess number of cardiovascular events appeared to account for the increased mortality among women with early surgical menopause who did not initiate HT.
The “timing hypothesis” proposes that the initiation of HT soon after the onset of menopause is associated with beneficial cardiovascular effects, but initiation more than 10 years after the onset of menopause is not associated with beneficial cardiovascular effects. The timing hypothesis is supported by the finding that, in recently menopausal women, HT is associated with reduced carotid intima-media thickness (CIMT), compared with placebo.8 Greater CIMT thickness is associated with an increased risk of cardiovascular events.
In my experience, few primary care clinicians are aware of these data. Often, these clinicians over-emphasize the risks and withhold HT in this vulnerable group of women.
HT: Minimizing the risks of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer
Results of multiple studies have shown that certain HT regimens increase the risk of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer. Is it possible to prescribe HT in a way that reduces these risks?
Results of observational studies indicate that, compared with oral estrogen therapy, transdermal HT is associated with a lower risk of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer (TABLE).9−15
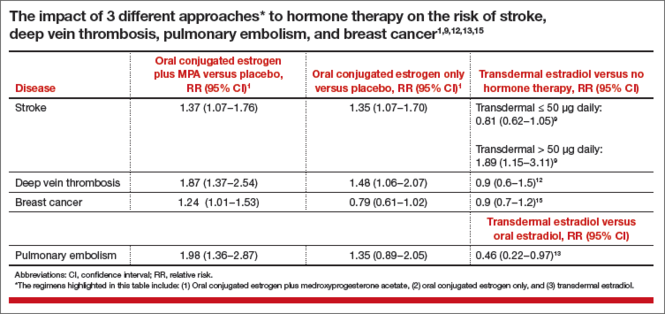
Reducing the risk of stroke caused by HT is an important goal. In a study of 15,710 women who had stroke and 59,958 control women aged 50 to 79 years, transdermal estradiol at a dose of 50 µg or less daily was not associated with an increased risk of stroke, compared with HT nonuse (rate ratio, 0.81; 95% CI, 0.62−1.05).9 Compared with HT nonuse, the use of oral estrogen (rate ratio, 1.28; 95% CI, 1.15−1.42) or transdermal estradiol 50 µg or greater daily (rate ratio, 1.89; 95% CI, 1.15−3.11) was associated with an increased risk of stroke.9
Reducing the risks of deep venous thromboembolism (VTE) and pulmonary embolism caused by HT is an important goal. In a meta-analysis of the risk of VTE with HT, compared with nonusers, oral estrogen therapy was associated with a significantly increased risk of VTE (odds ratio [OR], 2.5; 95% CI, 1.9−3.4). Compared with nonuse, transdermal estrogen therapy was not associated with an increased risk of VTE (OR, 1.2; 95% CI, 0.9−1.7).11 In a study comparing oral versus transdermal estradiol, transdermal estradiol was associated with a reduced risk of pulmonary embolism (0.46 [95% CI, 0.22−0.97]).13
Reducing the risk of breast cancer caused by HT is an important goal. Results of one study showed that the combination of oral estrogen plus synthetic progestin was associated with an increased risk of breast cancer, compared with nonuse (RR, 1.5; 95% CI, 1.1−1.9). By contrast, the combination of transdermal estradiol plus micronized progesterone was not associated with an increased risk of breast cancer, compared with nonuse (RR, 0.9; 95% CI, 0.7−1.2).15
The bottom line
In recently menopausal women with moderate to severe hot flashes, HT improves quality of life and appears to decrease mortality. However, HT with oral estrogen plus synthetic progestin is associated with an increased risk of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer. Compared with oral estrogen, transdermal estradiol treatment is associated with a lower risk of stroke, deep vein thrombosis, and pulmonary embolism. Compared with oral estrogen plus a synthetic progestin, transdermal estradiol plus micronized progesterone is associated with a lower risk of breast cancer. The benefits of HT are likely maximized by initiating therapy in the perimenopause transition or early in the postmenopause, and the risks are minimized by using transdermal estradiol.16−18
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended post-stopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353−1368.
- Santen RJ, Allred DC, Ardoin SP, et al. J Clin Endocrinol Metab. 2010;95(suppl 1):S1−S66.
- Boardman HM, Hartley L, Eisinga A, et al. Hormone therapy for preventing cardiovascular disease in postmenopausal women. Cochrane Database Syst Rev. 2015;3:CD002229.
- Salpeter SR, Cheng J, Thabane L, Buckley NS, Salpeter EE. Bayesian meta-analysis of hormone therapy and mortality in younger post-menopausal women. Am J Med. 2009;122(11):1016−1022.
- Gordon T, Kannel WB, Hjortland MC, McNamara PM. Menopause and coronary heart disease: The Framingham Study. Ann Intern Med. 1978;89(2):157−161.
- Stampfer MJ, Colditz GA, Willet WC, et al. Postmenopausal estrogen therapy and cardiovascular disease. Ten-year follow-up from the Nurses Health Study. N Engl J Med. 1991;325(11):756−762.
- Rivera CM, Grossardt BR, Rhodes DJ, et al. Increased cardiovascular mortality after early bilateral oophorectomy. Menopause. 2009;16(1):15−23.
- Hodis HN, Mack WJ, Shoupe D, et al. Testing the menopausal hormone therapy timing hypothesis: the early versus late intervention trial with estradiol [abstract 13283]. American Heart Association Meeting 2014. Circulation. 2014;130:A13283.
- Renoux C, Dell’Aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519
- Renoux C, Dell’Aniello S, Suissa S. Hormone replacement therapy and the risk of venous thromboembolism: a population-based study. J Thromb Haemost. 2010;8(5):979−986.
- Canonico M, Plu-Bureau G, Lowe GD, Scarabin PY. Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: systematic review and meta-analysis. BMJ. 2008;336(7655):1227−1231.
- Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol. 2010;30(2):340−345.
- Laliberte F, Dea K, Duh MS, Kahler KH, Rolli M, Lefebvre P. Does the route of administration for estrogen hormone therapy impact the risk of venous thromboembolism? Estradiol transdermal system versus oral estrogen-only hormone therapy. Menopause. 2011;18(10):1052−1059.
- Sweetland S, Beral V, Balkwill A, et al. Venous thromboembolism risk in relation to different types of postmenopausal hormone therapy in a large prospective study. J Thromb Haemost. 2012;10(11):2277−2286.
- Fournier A, Berrino F, Riboli E, Avenel V, Clavel-Chapelon F. Breast cancer risk in relation to different types of hormone replacement therapy in the E3N-EPIC cohort. Int J Cancer. 2005;114(3):448−454.
- L’Hermite M. HRT optimization, using transdermal estradiol plus micronized progesterone, a safer HRT. Climacteric. 2013;16(suppl 1):44−53.
- Simon JA. What’s new in hormone replacement therapy: focus on transdermal estradiol and micronized progesterone. Climacteric. 2012;15(suppl 1):3−10.
- Mueck AO. Postmenopausal hormone replacement therapy and cardiovascular disease: the value of transdermal estradiol and micronized progesterone. Climacteric. 2012;15(suppl 1): 11−17.
Robert L. Barbieri, MD

Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Dr. Barbieri is Editor in Chief, OBG Management; Chair, Obstetrics and Gynecology, at Brigham and Women’s Hospital, Boston, Massachusetts; and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology at Harvard Medical School, Boston.
Dr. Barbieri reports no financial relationships relevant to this article.
Clinicians work to maximize the quality of life and longevity of every patient. For women with moderate to severe menopausal symptoms, oral estrogen therapy can improve quality of life, but at the cost of significant adverse effects. The Women’s Health Initiative (WHI) reported that for postmenopausal women with a uterus, conjugated estrogen plus medroxyprogesterone acetate (CEE+MPA) hormone therapy (HT) versus placebo significantly increased the risk of cardiovascular events (relative risk [RR], 1.13), breast cancer (RR, 1.24), stroke (RR, 1.37), deep vein thrombosis (RR, 1.87), and pulmonary embolism (RR, 1.98).1 In postmeno pausal women without a uterus, CEE HT did not increase the risk of breast cancer (RR, 0.79), compared with placebo, but it did significantly in crease the risk of cardiovascular events (RR, 1.11), stroke (RR, 1.35), deep vein thrombosis (RR, 1.48), and pulmonary embolism (RR, 1.35).1
Clinicians prescribing estrogen must individualize therapy according to its benefits and risks. An important issue that has received insufficient at tention is, “What is the effect of HT on mortality in recently menopausal women?” Here, I examine this issue.
HT reduces mortality in recently menopausal women
Pooling the results of the WHI CEE+MPA and CEE-only trials reveals that there were 70 deaths in the HT-treated groups and 98 deaths in the placebo groups among women aged 50 to 59 years.1 With 4,706 and 4,259 women alive at the conclusion of the study in the HT and placebo groups, respectively, the women in the placebo group had significantly more deaths than the women in the HT-treated groups (Fisher exact test, P = .0194, χ2 test with Yates correction, P = .0226).
Using pooled data from the WHI, the RR of death in the HT versus placebo group was estimated at 0.70 (95% confidence interval [CI], 0.51−0.96), representing approximately 5 fewer deaths per 1,000 women per 5 years of therapy.2 In women aged 60 to 69 years and 70 to 79 years there were no significant differences in death rates between the HT- and placebo-treated women.
My interpretation of these results is that HT likely is associated with a reduced risk of death in recently menopausal women, but not in women distant from menopause onset.
Cochrane review of HT and mortality
Consistent with the WHI findings, authors of a recent Cochrane meta-analysis of 19 randomized trials including 40,410 menopausal women reported that HT significantly increased the risk of stroke (RR, 1.24; 95% CI, 1.10−1.41), venous thromboembolism (RR, 1.92; 95% CI, 1.36−2.69), and pulmonary emboli (RR, 1.81; 95% CI, 1.32−2.48).3 However, among women treated with oral HT within 10 years after the start of menopause, there was a reduced risk of coronary heart disease (RR, 0.52; 95% CI, 0.29−0.96). Using data from 5 clinical trials, the Cochrane meta-analysis researchers reported that, compared with placebo, HT reduced mortality (RR, 0.70; 95% CI, 0.52−0.95).3
Results of the Cochrane meta-analysis are consistent with those of a previous meta-analysis of 19 randomized trials involving 16,000 women. In this analysis, investigators found a reduced risk of death in recently menopausal women treated with hormone therapy (RR, 0.73; 95% CI, 0.52−0.96).4
Early menopause, HT, and mortality
Authors of multiple large epidemiologic studies have reported that early menopause is associated with an increased risk of death if HT is not initiated.5−7 For example, results of a study of women in Olmsted County, Minnesota, conducted from 1950 to 1987, indicated that, for women younger than age 45 years who underwent bilateral oophorectomy, the risk of death was increased among those who did not initiate HT, compared with women who did not undergo oophorectomy (hazard ratio [HR], 1.84; 95% CI, 1.27−2.68; P = .001).7
By contrast, women younger than 45 years who underwent bilateral oophorectomy and initiated estrogen therapy did not have an increased risk of death compared with women who did not undergo oophorectomy (HR, 0.65; 95% CI, 0.30−1.41; P = .28).7 An excess number of cardiovascular events appeared to account for the increased mortality among women with early surgical menopause who did not initiate HT.
The “timing hypothesis” proposes that the initiation of HT soon after the onset of menopause is associated with beneficial cardiovascular effects, but initiation more than 10 years after the onset of menopause is not associated with beneficial cardiovascular effects. The timing hypothesis is supported by the finding that, in recently menopausal women, HT is associated with reduced carotid intima-media thickness (CIMT), compared with placebo.8 Greater CIMT thickness is associated with an increased risk of cardiovascular events.
In my experience, few primary care clinicians are aware of these data. Often, these clinicians over-emphasize the risks and withhold HT in this vulnerable group of women.
HT: Minimizing the risks of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer
Results of multiple studies have shown that certain HT regimens increase the risk of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer. Is it possible to prescribe HT in a way that reduces these risks?
Results of observational studies indicate that, compared with oral estrogen therapy, transdermal HT is associated with a lower risk of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer (TABLE).9−15
Reducing the risk of stroke caused by HT is an important goal. In a study of 15,710 women who had stroke and 59,958 control women aged 50 to 79 years, transdermal estradiol at a dose of 50 µg or less daily was not associated with an increased risk of stroke, compared with HT nonuse (rate ratio, 0.81; 95% CI, 0.62−1.05).9 Compared with HT nonuse, the use of oral estrogen (rate ratio, 1.28; 95% CI, 1.15−1.42) or transdermal estradiol 50 µg or greater daily (rate ratio, 1.89; 95% CI, 1.15−3.11) was associated with an increased risk of stroke.9
Reducing the risks of deep venous thromboembolism (VTE) and pulmonary embolism caused by HT is an important goal. In a meta-analysis of the risk of VTE with HT, compared with nonusers, oral estrogen therapy was associated with a significantly increased risk of VTE (odds ratio [OR], 2.5; 95% CI, 1.9−3.4). Compared with nonuse, transdermal estrogen therapy was not associated with an increased risk of VTE (OR, 1.2; 95% CI, 0.9−1.7).11 In a study comparing oral versus transdermal estradiol, transdermal estradiol was associated with a reduced risk of pulmonary embolism (0.46 [95% CI, 0.22−0.97]).13
Reducing the risk of breast cancer caused by HT is an important goal. Results of one study showed that the combination of oral estrogen plus synthetic progestin was associated with an increased risk of breast cancer, compared with nonuse (RR, 1.5; 95% CI, 1.1−1.9). By contrast, the combination of transdermal estradiol plus micronized progesterone was not associated with an increased risk of breast cancer, compared with nonuse (RR, 0.9; 95% CI, 0.7−1.2).15
The bottom line
In recently menopausal women with moderate to severe hot flashes, HT improves quality of life and appears to decrease mortality. However, HT with oral estrogen plus synthetic progestin is associated with an increased risk of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer. Compared with oral estrogen, transdermal estradiol treatment is associated with a lower risk of stroke, deep vein thrombosis, and pulmonary embolism. Compared with oral estrogen plus a synthetic progestin, transdermal estradiol plus micronized progesterone is associated with a lower risk of breast cancer. The benefits of HT are likely maximized by initiating therapy in the perimenopause transition or early in the postmenopause, and the risks are minimized by using transdermal estradiol.16−18
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Clinicians work to maximize the quality of life and longevity of every patient. For women with moderate to severe menopausal symptoms, oral estrogen therapy can improve quality of life, but at the cost of significant adverse effects. The Women’s Health Initiative (WHI) reported that for postmenopausal women with a uterus, conjugated estrogen plus medroxyprogesterone acetate (CEE+MPA) hormone therapy (HT) versus placebo significantly increased the risk of cardiovascular events (relative risk [RR], 1.13), breast cancer (RR, 1.24), stroke (RR, 1.37), deep vein thrombosis (RR, 1.87), and pulmonary embolism (RR, 1.98).1 In postmeno pausal women without a uterus, CEE HT did not increase the risk of breast cancer (RR, 0.79), compared with placebo, but it did significantly in crease the risk of cardiovascular events (RR, 1.11), stroke (RR, 1.35), deep vein thrombosis (RR, 1.48), and pulmonary embolism (RR, 1.35).1
Clinicians prescribing estrogen must individualize therapy according to its benefits and risks. An important issue that has received insufficient at tention is, “What is the effect of HT on mortality in recently menopausal women?” Here, I examine this issue.
HT reduces mortality in recently menopausal women
Pooling the results of the WHI CEE+MPA and CEE-only trials reveals that there were 70 deaths in the HT-treated groups and 98 deaths in the placebo groups among women aged 50 to 59 years.1 With 4,706 and 4,259 women alive at the conclusion of the study in the HT and placebo groups, respectively, the women in the placebo group had significantly more deaths than the women in the HT-treated groups (Fisher exact test, P = .0194, χ2 test with Yates correction, P = .0226).
Using pooled data from the WHI, the RR of death in the HT versus placebo group was estimated at 0.70 (95% confidence interval [CI], 0.51−0.96), representing approximately 5 fewer deaths per 1,000 women per 5 years of therapy.2 In women aged 60 to 69 years and 70 to 79 years there were no significant differences in death rates between the HT- and placebo-treated women.
My interpretation of these results is that HT likely is associated with a reduced risk of death in recently menopausal women, but not in women distant from menopause onset.
Cochrane review of HT and mortality
Consistent with the WHI findings, authors of a recent Cochrane meta-analysis of 19 randomized trials including 40,410 menopausal women reported that HT significantly increased the risk of stroke (RR, 1.24; 95% CI, 1.10−1.41), venous thromboembolism (RR, 1.92; 95% CI, 1.36−2.69), and pulmonary emboli (RR, 1.81; 95% CI, 1.32−2.48).3 However, among women treated with oral HT within 10 years after the start of menopause, there was a reduced risk of coronary heart disease (RR, 0.52; 95% CI, 0.29−0.96). Using data from 5 clinical trials, the Cochrane meta-analysis researchers reported that, compared with placebo, HT reduced mortality (RR, 0.70; 95% CI, 0.52−0.95).3
Results of the Cochrane meta-analysis are consistent with those of a previous meta-analysis of 19 randomized trials involving 16,000 women. In this analysis, investigators found a reduced risk of death in recently menopausal women treated with hormone therapy (RR, 0.73; 95% CI, 0.52−0.96).4
Early menopause, HT, and mortality
Authors of multiple large epidemiologic studies have reported that early menopause is associated with an increased risk of death if HT is not initiated.5−7 For example, results of a study of women in Olmsted County, Minnesota, conducted from 1950 to 1987, indicated that, for women younger than age 45 years who underwent bilateral oophorectomy, the risk of death was increased among those who did not initiate HT, compared with women who did not undergo oophorectomy (hazard ratio [HR], 1.84; 95% CI, 1.27−2.68; P = .001).7
By contrast, women younger than 45 years who underwent bilateral oophorectomy and initiated estrogen therapy did not have an increased risk of death compared with women who did not undergo oophorectomy (HR, 0.65; 95% CI, 0.30−1.41; P = .28).7 An excess number of cardiovascular events appeared to account for the increased mortality among women with early surgical menopause who did not initiate HT.
The “timing hypothesis” proposes that the initiation of HT soon after the onset of menopause is associated with beneficial cardiovascular effects, but initiation more than 10 years after the onset of menopause is not associated with beneficial cardiovascular effects. The timing hypothesis is supported by the finding that, in recently menopausal women, HT is associated with reduced carotid intima-media thickness (CIMT), compared with placebo.8 Greater CIMT thickness is associated with an increased risk of cardiovascular events.
In my experience, few primary care clinicians are aware of these data. Often, these clinicians over-emphasize the risks and withhold HT in this vulnerable group of women.
HT: Minimizing the risks of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer
Results of multiple studies have shown that certain HT regimens increase the risk of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer. Is it possible to prescribe HT in a way that reduces these risks?
Results of observational studies indicate that, compared with oral estrogen therapy, transdermal HT is associated with a lower risk of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer (TABLE).9−15
Reducing the risk of stroke caused by HT is an important goal. In a study of 15,710 women who had stroke and 59,958 control women aged 50 to 79 years, transdermal estradiol at a dose of 50 µg or less daily was not associated with an increased risk of stroke, compared with HT nonuse (rate ratio, 0.81; 95% CI, 0.62−1.05).9 Compared with HT nonuse, the use of oral estrogen (rate ratio, 1.28; 95% CI, 1.15−1.42) or transdermal estradiol 50 µg or greater daily (rate ratio, 1.89; 95% CI, 1.15−3.11) was associated with an increased risk of stroke.9
Reducing the risks of deep venous thromboembolism (VTE) and pulmonary embolism caused by HT is an important goal. In a meta-analysis of the risk of VTE with HT, compared with nonusers, oral estrogen therapy was associated with a significantly increased risk of VTE (odds ratio [OR], 2.5; 95% CI, 1.9−3.4). Compared with nonuse, transdermal estrogen therapy was not associated with an increased risk of VTE (OR, 1.2; 95% CI, 0.9−1.7).11 In a study comparing oral versus transdermal estradiol, transdermal estradiol was associated with a reduced risk of pulmonary embolism (0.46 [95% CI, 0.22−0.97]).13
Reducing the risk of breast cancer caused by HT is an important goal. Results of one study showed that the combination of oral estrogen plus synthetic progestin was associated with an increased risk of breast cancer, compared with nonuse (RR, 1.5; 95% CI, 1.1−1.9). By contrast, the combination of transdermal estradiol plus micronized progesterone was not associated with an increased risk of breast cancer, compared with nonuse (RR, 0.9; 95% CI, 0.7−1.2).15
The bottom line
In recently menopausal women with moderate to severe hot flashes, HT improves quality of life and appears to decrease mortality. However, HT with oral estrogen plus synthetic progestin is associated with an increased risk of stroke, deep vein thrombosis, pulmonary embolism, and breast cancer. Compared with oral estrogen, transdermal estradiol treatment is associated with a lower risk of stroke, deep vein thrombosis, and pulmonary embolism. Compared with oral estrogen plus a synthetic progestin, transdermal estradiol plus micronized progesterone is associated with a lower risk of breast cancer. The benefits of HT are likely maximized by initiating therapy in the perimenopause transition or early in the postmenopause, and the risks are minimized by using transdermal estradiol.16−18
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended post-stopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353−1368.
- Santen RJ, Allred DC, Ardoin SP, et al. J Clin Endocrinol Metab. 2010;95(suppl 1):S1−S66.
- Boardman HM, Hartley L, Eisinga A, et al. Hormone therapy for preventing cardiovascular disease in postmenopausal women. Cochrane Database Syst Rev. 2015;3:CD002229.
- Salpeter SR, Cheng J, Thabane L, Buckley NS, Salpeter EE. Bayesian meta-analysis of hormone therapy and mortality in younger post-menopausal women. Am J Med. 2009;122(11):1016−1022.
- Gordon T, Kannel WB, Hjortland MC, McNamara PM. Menopause and coronary heart disease: The Framingham Study. Ann Intern Med. 1978;89(2):157−161.
- Stampfer MJ, Colditz GA, Willet WC, et al. Postmenopausal estrogen therapy and cardiovascular disease. Ten-year follow-up from the Nurses Health Study. N Engl J Med. 1991;325(11):756−762.
- Rivera CM, Grossardt BR, Rhodes DJ, et al. Increased cardiovascular mortality after early bilateral oophorectomy. Menopause. 2009;16(1):15−23.
- Hodis HN, Mack WJ, Shoupe D, et al. Testing the menopausal hormone therapy timing hypothesis: the early versus late intervention trial with estradiol [abstract 13283]. American Heart Association Meeting 2014. Circulation. 2014;130:A13283.
- Renoux C, Dell’Aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519
- Renoux C, Dell’Aniello S, Suissa S. Hormone replacement therapy and the risk of venous thromboembolism: a population-based study. J Thromb Haemost. 2010;8(5):979−986.
- Canonico M, Plu-Bureau G, Lowe GD, Scarabin PY. Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: systematic review and meta-analysis. BMJ. 2008;336(7655):1227−1231.
- Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol. 2010;30(2):340−345.
- Laliberte F, Dea K, Duh MS, Kahler KH, Rolli M, Lefebvre P. Does the route of administration for estrogen hormone therapy impact the risk of venous thromboembolism? Estradiol transdermal system versus oral estrogen-only hormone therapy. Menopause. 2011;18(10):1052−1059.
- Sweetland S, Beral V, Balkwill A, et al. Venous thromboembolism risk in relation to different types of postmenopausal hormone therapy in a large prospective study. J Thromb Haemost. 2012;10(11):2277−2286.
- Fournier A, Berrino F, Riboli E, Avenel V, Clavel-Chapelon F. Breast cancer risk in relation to different types of hormone replacement therapy in the E3N-EPIC cohort. Int J Cancer. 2005;114(3):448−454.
- L’Hermite M. HRT optimization, using transdermal estradiol plus micronized progesterone, a safer HRT. Climacteric. 2013;16(suppl 1):44−53.
- Simon JA. What’s new in hormone replacement therapy: focus on transdermal estradiol and micronized progesterone. Climacteric. 2012;15(suppl 1):3−10.
- Mueck AO. Postmenopausal hormone replacement therapy and cardiovascular disease: the value of transdermal estradiol and micronized progesterone. Climacteric. 2012;15(suppl 1): 11−17.
- Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended post-stopping phases of the Women’s Health Initiative randomized trials. JAMA. 2013;310(13):1353−1368.
- Santen RJ, Allred DC, Ardoin SP, et al. J Clin Endocrinol Metab. 2010;95(suppl 1):S1−S66.
- Boardman HM, Hartley L, Eisinga A, et al. Hormone therapy for preventing cardiovascular disease in postmenopausal women. Cochrane Database Syst Rev. 2015;3:CD002229.
- Salpeter SR, Cheng J, Thabane L, Buckley NS, Salpeter EE. Bayesian meta-analysis of hormone therapy and mortality in younger post-menopausal women. Am J Med. 2009;122(11):1016−1022.
- Gordon T, Kannel WB, Hjortland MC, McNamara PM. Menopause and coronary heart disease: The Framingham Study. Ann Intern Med. 1978;89(2):157−161.
- Stampfer MJ, Colditz GA, Willet WC, et al. Postmenopausal estrogen therapy and cardiovascular disease. Ten-year follow-up from the Nurses Health Study. N Engl J Med. 1991;325(11):756−762.
- Rivera CM, Grossardt BR, Rhodes DJ, et al. Increased cardiovascular mortality after early bilateral oophorectomy. Menopause. 2009;16(1):15−23.
- Hodis HN, Mack WJ, Shoupe D, et al. Testing the menopausal hormone therapy timing hypothesis: the early versus late intervention trial with estradiol [abstract 13283]. American Heart Association Meeting 2014. Circulation. 2014;130:A13283.
- Renoux C, Dell’Aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519
- Renoux C, Dell’Aniello S, Suissa S. Hormone replacement therapy and the risk of venous thromboembolism: a population-based study. J Thromb Haemost. 2010;8(5):979−986.
- Canonico M, Plu-Bureau G, Lowe GD, Scarabin PY. Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: systematic review and meta-analysis. BMJ. 2008;336(7655):1227−1231.
- Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol. 2010;30(2):340−345.
- Laliberte F, Dea K, Duh MS, Kahler KH, Rolli M, Lefebvre P. Does the route of administration for estrogen hormone therapy impact the risk of venous thromboembolism? Estradiol transdermal system versus oral estrogen-only hormone therapy. Menopause. 2011;18(10):1052−1059.
- Sweetland S, Beral V, Balkwill A, et al. Venous thromboembolism risk in relation to different types of postmenopausal hormone therapy in a large prospective study. J Thromb Haemost. 2012;10(11):2277−2286.
- Fournier A, Berrino F, Riboli E, Avenel V, Clavel-Chapelon F. Breast cancer risk in relation to different types of hormone replacement therapy in the E3N-EPIC cohort. Int J Cancer. 2005;114(3):448−454.
- L’Hermite M. HRT optimization, using transdermal estradiol plus micronized progesterone, a safer HRT. Climacteric. 2013;16(suppl 1):44−53.
- Simon JA. What’s new in hormone replacement therapy: focus on transdermal estradiol and micronized progesterone. Climacteric. 2012;15(suppl 1):3−10.
- Mueck AO. Postmenopausal hormone replacement therapy and cardiovascular disease: the value of transdermal estradiol and micronized progesterone. Climacteric. 2012;15(suppl 1): 11−17.

Innovations in patient safety for women's health: Minimally invasive gynecologic surgery
Click here to download the PDF.
Every surgeon knows that, if you operate, complications will follow. Surgeons are perfectionists and strive to reduce complications through years of diligent personal training and continuous quality improvement. Surgeons hate complications, especially those that might be preventable (such as retained foreign bodies, wrong site surgery, and medication errors).
In this special issue of OBG Management, world-renowned experts focus on topical issues in safety in minimally invasive gynecologic surgery (MIGS). In a roundtable, Drs. Neal Lonky, John Gebhart, Rosanne Kho, and Malcolm Munro discuss important issues in MIGS, including the need to prioritize the vaginal and laparoscopic routes of hysterectomy and the role of single-port surgery. In a concise yet detailed discussion of safety issues related to radiofrequency and ultrasound energy devices, Dr. Munro alerts us to the dangers of heat injury and direct and capacitative coupling. Drs. Andrew Sokol and Katelyn Smithling provide guidance on preventing apical prolapse of the vagina following hysterectomy. And Dr. Antonio Gargiulo explores the rapidly expanding role of simulation training with computer-assisted (robotic) surgical simulators and predicts that, instead of learning surgery on patients, future trainees will gain skills in a simulation environment.
We thank the master surgeons who participated in this special issue for providing guidance and helping us to reduce complications. Our patients are the beneficiaries of the wisdom provided herein.
>>Robert L. Barbieri, MD
Editor in Chief, OBG Management
To view the video, "McCall" culdoplasty technique by Mickey Karram, MD, that accompanies the article by Sokol et al in this supplement, click here.
Click here to download the PDF.
Every surgeon knows that, if you operate, complications will follow. Surgeons are perfectionists and strive to reduce complications through years of diligent personal training and continuous quality improvement. Surgeons hate complications, especially those that might be preventable (such as retained foreign bodies, wrong site surgery, and medication errors).
In this special issue of OBG Management, world-renowned experts focus on topical issues in safety in minimally invasive gynecologic surgery (MIGS). In a roundtable, Drs. Neal Lonky, John Gebhart, Rosanne Kho, and Malcolm Munro discuss important issues in MIGS, including the need to prioritize the vaginal and laparoscopic routes of hysterectomy and the role of single-port surgery. In a concise yet detailed discussion of safety issues related to radiofrequency and ultrasound energy devices, Dr. Munro alerts us to the dangers of heat injury and direct and capacitative coupling. Drs. Andrew Sokol and Katelyn Smithling provide guidance on preventing apical prolapse of the vagina following hysterectomy. And Dr. Antonio Gargiulo explores the rapidly expanding role of simulation training with computer-assisted (robotic) surgical simulators and predicts that, instead of learning surgery on patients, future trainees will gain skills in a simulation environment.
We thank the master surgeons who participated in this special issue for providing guidance and helping us to reduce complications. Our patients are the beneficiaries of the wisdom provided herein.
>>Robert L. Barbieri, MD
Editor in Chief, OBG Management
To view the video, "McCall" culdoplasty technique by Mickey Karram, MD, that accompanies the article by Sokol et al in this supplement, click here.
Click here to download the PDF.
Every surgeon knows that, if you operate, complications will follow. Surgeons are perfectionists and strive to reduce complications through years of diligent personal training and continuous quality improvement. Surgeons hate complications, especially those that might be preventable (such as retained foreign bodies, wrong site surgery, and medication errors).
In this special issue of OBG Management, world-renowned experts focus on topical issues in safety in minimally invasive gynecologic surgery (MIGS). In a roundtable, Drs. Neal Lonky, John Gebhart, Rosanne Kho, and Malcolm Munro discuss important issues in MIGS, including the need to prioritize the vaginal and laparoscopic routes of hysterectomy and the role of single-port surgery. In a concise yet detailed discussion of safety issues related to radiofrequency and ultrasound energy devices, Dr. Munro alerts us to the dangers of heat injury and direct and capacitative coupling. Drs. Andrew Sokol and Katelyn Smithling provide guidance on preventing apical prolapse of the vagina following hysterectomy. And Dr. Antonio Gargiulo explores the rapidly expanding role of simulation training with computer-assisted (robotic) surgical simulators and predicts that, instead of learning surgery on patients, future trainees will gain skills in a simulation environment.
We thank the master surgeons who participated in this special issue for providing guidance and helping us to reduce complications. Our patients are the beneficiaries of the wisdom provided herein.
>>Robert L. Barbieri, MD
Editor in Chief, OBG Management
To view the video, "McCall" culdoplasty technique by Mickey Karram, MD, that accompanies the article by Sokol et al in this supplement, click here.
CLL: No symptoms, no treatment still appropriate
CHICAGO – Despite exciting new advances in the understanding of chronic lymphocytic leukemia, particularly with respect to prognostic features that predict risk for relapse, a watch-and-wait approach remains appropriate for asymptomatic disease pending outcomes data for newer approaches, according to Dr. John G. Gribben.
“When the disease is diagnosed, if it is asymptomatic, the correct approach – of course – is to continue to watch and wait,” Dr. Gribben of Barts Cancer Institute, Queen Mary University of London, said at the American Society of Hematology Meeting on Hematologic Malignancies.

Numerous clinical trials have demonstrated no advantage of early treatment vs. watch and wait, he said, adding that all of the trials published to date have used treatment of all-comers, and have used chlorambucil (CLB) as the treatment.
“There has been a whole variety of more modern trials that have used select prognostic features to identify subgroups of people who are at higher risk of relapse, who then go on to receive earlier treatment with either FCR [fludarabine, cyclophosphamide, rituximab], or more recently, ibrutinib,” he said.
These treatments are interesting, and the trials have demonstrated that prognostic features can identify patients who will progress more rapidly, but none have reported, he explained.
“In the absence of any published trial, I continue to ‘watch and wait’ patients, and there are no high-risk features which will make me alter that approach. Even the highest-risk features of complex karyotype and p53 abnormalities are not indications to treat patients until they become symptomatic,” he said.
It is striking how white counts vary widely in both asymptomatic and symptomatic patients, he noted.
“I don’t personally have any particular white count which is the number at which I’ll treat a patient. I don’t treat white counts, I treat patients,” he said.
When patients become symptomatic, the treatment of choice is now immunochemotherapies, irrespective of performance status, he said.
“Within the past year we have seen approval of obinutuzumab and ofatumumab for treatment of previously untreated CLL, as well as ibrutinib and idelalisib plus rituximab for treatment of both previously untreated CLL and those with 17p deletions for relapsed/refractory disease, as well as for up-front treatment,” he said, adding that these new agents greatly increase the available options for treating CLL.
Dr. Gribben said he considers these questions when it comes to treating CLL:
• Does the patient require treatment, or is watching and waiting appropriate?
• What is the goal of therapy? This is determined through conversation with the patient and the patient’s family regarding the side-effect profile they are willing to tolerate vs. the potential longer duration of response.
• What comorbidities are present to determine “fitness” for specific immunochemotherapy? Specifically, is the patient fit for an FCR-type approach, or is an alternative more appropriate?
• Is there a 17p deletion or P53 mutation that would make chemotherapy a less attractive option, and use of novel agents a more attractive option?
His approach, based on the answers to these questions, is as follows:
• In Rai stage 0-II patients with inactive disease, fitness and 17p deletion or p53 mutation status is irrelevant; no therapy is given.
• For active disease or Rai III-IV disease, a “go-go” patient, (or patient in good physical condition) is treated based on the presence or absence of 17p deletion or p53 mutation status. Those without 17p deletions or p53 mutations can be treated with FCR (his preference), or fludarabine-rituximab (FR). Bendamustine-rituximab (BR) is also an attractive option in certain cases, he said.
• For patients with active disease or Rai stage III-IV disease who do have a 17p deletion, his treatment of choice is either ibrutinib or idelalisib plus rituximab, depending on the patient.
• In “slow-go” patients (those with poorer physical condition) treatment is again based on mutational analysis. Those without mutation receive either FR, BR, or CLB plus obinutuzumab. These are very good options, and represent a spectrum to choose from based on the patient’s core abilities and ability to withstand particular types of treatments, he said.
“If they do have a 17p deletion, these patients are just as eligible for ibrutinib or idelalisib plus rituximab as the younger patients,” he noted.
His choices are based largely on the findings from the CLL8 trial (Lancet 2010 Oct;376[9747]:1164-74) which demonstrated an overall survival advantage with chemoimmunotherapy for front-line therapy vs. chemotherapy alone (hazard ratio, 0.68).
Over time, the advantage has become even more pronounced, according to follow-up data.
Starting with something “gentle” and saving the best treatment for later in the event of relapse was recently considered a reasonable approach, but in the wake of the CLL8 findings, this is no longer an acceptable plan, Dr. Gribben said.
“That’s why for my choice, FCR remains the treatment of choice for those patients who are fit enough to tolerate this type of approach,” he said.
In those with 17p deletions or P53 mutations, the CLL8 trial showed poor outcomes with FCR.
“This is a group of patients whom I believe chemoimmunotherapy would no longer be the treatment of choice,” he said, adding that newer findings suggest outcomes in these patients are better with novel agents.
He also noted that patients with 11q abnormalities, which were previously associated with a poor prognosis, were found in CLL8 to respond well to chemoimmunotherapy when used front line.
While there are special considerations in the elderly, and different strategies in relapsed and refractory disease, the future of CLL treatment is promising. The benefit of adding rituximab to combination chemotherapy is well established, the benefit of novel agents is also now established, and the future likely involves combining targeted therapies with each other and with immunochemotherapies, and combining targeted therapies across different pathways.
“And of course the hope is that we’re going to use the biology of the disease to decide what specific therapy is ideal for that patient. Better understanding of biology and genetics is facilitating rational development of new treatments,” he said, adding that whenever possible, patients should be treated within clinical trials.
Dr. Gribben has received research funding from the NIH, Cancer Research UK, MRC, and Wellcome Trust. He has received honoraria from Roche/Genentech, Celgene, Janssen, Pharmacyclics, Gilead, Mundipharma, Infinity, TG Therapeutics, and Ascerta, and he has a patent or receives royalties from Celgene. He also has been the principal investigator on a clinical trial for Roche, Takeda, Pharmacyclics, Gilead, and Infinity.
CHICAGO – Despite exciting new advances in the understanding of chronic lymphocytic leukemia, particularly with respect to prognostic features that predict risk for relapse, a watch-and-wait approach remains appropriate for asymptomatic disease pending outcomes data for newer approaches, according to Dr. John G. Gribben.
“When the disease is diagnosed, if it is asymptomatic, the correct approach – of course – is to continue to watch and wait,” Dr. Gribben of Barts Cancer Institute, Queen Mary University of London, said at the American Society of Hematology Meeting on Hematologic Malignancies.
Numerous clinical trials have demonstrated no advantage of early treatment vs. watch and wait, he said, adding that all of the trials published to date have used treatment of all-comers, and have used chlorambucil (CLB) as the treatment.
“There has been a whole variety of more modern trials that have used select prognostic features to identify subgroups of people who are at higher risk of relapse, who then go on to receive earlier treatment with either FCR [fludarabine, cyclophosphamide, rituximab], or more recently, ibrutinib,” he said.
These treatments are interesting, and the trials have demonstrated that prognostic features can identify patients who will progress more rapidly, but none have reported, he explained.
“In the absence of any published trial, I continue to ‘watch and wait’ patients, and there are no high-risk features which will make me alter that approach. Even the highest-risk features of complex karyotype and p53 abnormalities are not indications to treat patients until they become symptomatic,” he said.
It is striking how white counts vary widely in both asymptomatic and symptomatic patients, he noted.
“I don’t personally have any particular white count which is the number at which I’ll treat a patient. I don’t treat white counts, I treat patients,” he said.
When patients become symptomatic, the treatment of choice is now immunochemotherapies, irrespective of performance status, he said.
“Within the past year we have seen approval of obinutuzumab and ofatumumab for treatment of previously untreated CLL, as well as ibrutinib and idelalisib plus rituximab for treatment of both previously untreated CLL and those with 17p deletions for relapsed/refractory disease, as well as for up-front treatment,” he said, adding that these new agents greatly increase the available options for treating CLL.
Dr. Gribben said he considers these questions when it comes to treating CLL:
• Does the patient require treatment, or is watching and waiting appropriate?
• What is the goal of therapy? This is determined through conversation with the patient and the patient’s family regarding the side-effect profile they are willing to tolerate vs. the potential longer duration of response.
• What comorbidities are present to determine “fitness” for specific immunochemotherapy? Specifically, is the patient fit for an FCR-type approach, or is an alternative more appropriate?
• Is there a 17p deletion or P53 mutation that would make chemotherapy a less attractive option, and use of novel agents a more attractive option?
His approach, based on the answers to these questions, is as follows:
• In Rai stage 0-II patients with inactive disease, fitness and 17p deletion or p53 mutation status is irrelevant; no therapy is given.
• For active disease or Rai III-IV disease, a “go-go” patient, (or patient in good physical condition) is treated based on the presence or absence of 17p deletion or p53 mutation status. Those without 17p deletions or p53 mutations can be treated with FCR (his preference), or fludarabine-rituximab (FR). Bendamustine-rituximab (BR) is also an attractive option in certain cases, he said.
• For patients with active disease or Rai stage III-IV disease who do have a 17p deletion, his treatment of choice is either ibrutinib or idelalisib plus rituximab, depending on the patient.
• In “slow-go” patients (those with poorer physical condition) treatment is again based on mutational analysis. Those without mutation receive either FR, BR, or CLB plus obinutuzumab. These are very good options, and represent a spectrum to choose from based on the patient’s core abilities and ability to withstand particular types of treatments, he said.
“If they do have a 17p deletion, these patients are just as eligible for ibrutinib or idelalisib plus rituximab as the younger patients,” he noted.
His choices are based largely on the findings from the CLL8 trial (Lancet 2010 Oct;376[9747]:1164-74) which demonstrated an overall survival advantage with chemoimmunotherapy for front-line therapy vs. chemotherapy alone (hazard ratio, 0.68).
Over time, the advantage has become even more pronounced, according to follow-up data.
Starting with something “gentle” and saving the best treatment for later in the event of relapse was recently considered a reasonable approach, but in the wake of the CLL8 findings, this is no longer an acceptable plan, Dr. Gribben said.
“That’s why for my choice, FCR remains the treatment of choice for those patients who are fit enough to tolerate this type of approach,” he said.
In those with 17p deletions or P53 mutations, the CLL8 trial showed poor outcomes with FCR.
“This is a group of patients whom I believe chemoimmunotherapy would no longer be the treatment of choice,” he said, adding that newer findings suggest outcomes in these patients are better with novel agents.
He also noted that patients with 11q abnormalities, which were previously associated with a poor prognosis, were found in CLL8 to respond well to chemoimmunotherapy when used front line.
While there are special considerations in the elderly, and different strategies in relapsed and refractory disease, the future of CLL treatment is promising. The benefit of adding rituximab to combination chemotherapy is well established, the benefit of novel agents is also now established, and the future likely involves combining targeted therapies with each other and with immunochemotherapies, and combining targeted therapies across different pathways.
“And of course the hope is that we’re going to use the biology of the disease to decide what specific therapy is ideal for that patient. Better understanding of biology and genetics is facilitating rational development of new treatments,” he said, adding that whenever possible, patients should be treated within clinical trials.
Dr. Gribben has received research funding from the NIH, Cancer Research UK, MRC, and Wellcome Trust. He has received honoraria from Roche/Genentech, Celgene, Janssen, Pharmacyclics, Gilead, Mundipharma, Infinity, TG Therapeutics, and Ascerta, and he has a patent or receives royalties from Celgene. He also has been the principal investigator on a clinical trial for Roche, Takeda, Pharmacyclics, Gilead, and Infinity.
CHICAGO – Despite exciting new advances in the understanding of chronic lymphocytic leukemia, particularly with respect to prognostic features that predict risk for relapse, a watch-and-wait approach remains appropriate for asymptomatic disease pending outcomes data for newer approaches, according to Dr. John G. Gribben.
“When the disease is diagnosed, if it is asymptomatic, the correct approach – of course – is to continue to watch and wait,” Dr. Gribben of Barts Cancer Institute, Queen Mary University of London, said at the American Society of Hematology Meeting on Hematologic Malignancies.
Numerous clinical trials have demonstrated no advantage of early treatment vs. watch and wait, he said, adding that all of the trials published to date have used treatment of all-comers, and have used chlorambucil (CLB) as the treatment.
“There has been a whole variety of more modern trials that have used select prognostic features to identify subgroups of people who are at higher risk of relapse, who then go on to receive earlier treatment with either FCR [fludarabine, cyclophosphamide, rituximab], or more recently, ibrutinib,” he said.
These treatments are interesting, and the trials have demonstrated that prognostic features can identify patients who will progress more rapidly, but none have reported, he explained.
“In the absence of any published trial, I continue to ‘watch and wait’ patients, and there are no high-risk features which will make me alter that approach. Even the highest-risk features of complex karyotype and p53 abnormalities are not indications to treat patients until they become symptomatic,” he said.
It is striking how white counts vary widely in both asymptomatic and symptomatic patients, he noted.
“I don’t personally have any particular white count which is the number at which I’ll treat a patient. I don’t treat white counts, I treat patients,” he said.
When patients become symptomatic, the treatment of choice is now immunochemotherapies, irrespective of performance status, he said.
“Within the past year we have seen approval of obinutuzumab and ofatumumab for treatment of previously untreated CLL, as well as ibrutinib and idelalisib plus rituximab for treatment of both previously untreated CLL and those with 17p deletions for relapsed/refractory disease, as well as for up-front treatment,” he said, adding that these new agents greatly increase the available options for treating CLL.
Dr. Gribben said he considers these questions when it comes to treating CLL:
• Does the patient require treatment, or is watching and waiting appropriate?
• What is the goal of therapy? This is determined through conversation with the patient and the patient’s family regarding the side-effect profile they are willing to tolerate vs. the potential longer duration of response.
• What comorbidities are present to determine “fitness” for specific immunochemotherapy? Specifically, is the patient fit for an FCR-type approach, or is an alternative more appropriate?
• Is there a 17p deletion or P53 mutation that would make chemotherapy a less attractive option, and use of novel agents a more attractive option?
His approach, based on the answers to these questions, is as follows:
• In Rai stage 0-II patients with inactive disease, fitness and 17p deletion or p53 mutation status is irrelevant; no therapy is given.
• For active disease or Rai III-IV disease, a “go-go” patient, (or patient in good physical condition) is treated based on the presence or absence of 17p deletion or p53 mutation status. Those without 17p deletions or p53 mutations can be treated with FCR (his preference), or fludarabine-rituximab (FR). Bendamustine-rituximab (BR) is also an attractive option in certain cases, he said.
• For patients with active disease or Rai stage III-IV disease who do have a 17p deletion, his treatment of choice is either ibrutinib or idelalisib plus rituximab, depending on the patient.
• In “slow-go” patients (those with poorer physical condition) treatment is again based on mutational analysis. Those without mutation receive either FR, BR, or CLB plus obinutuzumab. These are very good options, and represent a spectrum to choose from based on the patient’s core abilities and ability to withstand particular types of treatments, he said.
“If they do have a 17p deletion, these patients are just as eligible for ibrutinib or idelalisib plus rituximab as the younger patients,” he noted.
His choices are based largely on the findings from the CLL8 trial (Lancet 2010 Oct;376[9747]:1164-74) which demonstrated an overall survival advantage with chemoimmunotherapy for front-line therapy vs. chemotherapy alone (hazard ratio, 0.68).
Over time, the advantage has become even more pronounced, according to follow-up data.
Starting with something “gentle” and saving the best treatment for later in the event of relapse was recently considered a reasonable approach, but in the wake of the CLL8 findings, this is no longer an acceptable plan, Dr. Gribben said.
“That’s why for my choice, FCR remains the treatment of choice for those patients who are fit enough to tolerate this type of approach,” he said.
In those with 17p deletions or P53 mutations, the CLL8 trial showed poor outcomes with FCR.
“This is a group of patients whom I believe chemoimmunotherapy would no longer be the treatment of choice,” he said, adding that newer findings suggest outcomes in these patients are better with novel agents.
He also noted that patients with 11q abnormalities, which were previously associated with a poor prognosis, were found in CLL8 to respond well to chemoimmunotherapy when used front line.
While there are special considerations in the elderly, and different strategies in relapsed and refractory disease, the future of CLL treatment is promising. The benefit of adding rituximab to combination chemotherapy is well established, the benefit of novel agents is also now established, and the future likely involves combining targeted therapies with each other and with immunochemotherapies, and combining targeted therapies across different pathways.
“And of course the hope is that we’re going to use the biology of the disease to decide what specific therapy is ideal for that patient. Better understanding of biology and genetics is facilitating rational development of new treatments,” he said, adding that whenever possible, patients should be treated within clinical trials.
Dr. Gribben has received research funding from the NIH, Cancer Research UK, MRC, and Wellcome Trust. He has received honoraria from Roche/Genentech, Celgene, Janssen, Pharmacyclics, Gilead, Mundipharma, Infinity, TG Therapeutics, and Ascerta, and he has a patent or receives royalties from Celgene. He also has been the principal investigator on a clinical trial for Roche, Takeda, Pharmacyclics, Gilead, and Infinity.
EXPERT ANALYSIS FROM MHM 2015

Metabolic monitoring of antipsychotic meds
Introduction
The use of antipsychotic medications has become more common in children and adolescents over the past 2 decades (Arch Gen Psychiatry. 2012 Dec;69[12]:1247-56). Whether or not one agrees that the trend in prescribing these agents is problematic (and I do), often the prescription and monitoring of antipsychotic medication falls to the primary care clinician who may have concerns about how to manage them. Here, we present a case to illustrate just such an issue.
Case summary
James is a 17-year-old young man with a diagnosis of bipolar disorder made earlier this year after an inpatient day at a local hospital. James had a history of attention-deficit/hyperactivity disorder (ADHD) growing up, but also had a strong family history of bipolar disorder. He began having increasing difficulty during the summer after his junior year, and then had a clear manic episode with elation and grandiosity that necessitated the hospitalization. During the relatively short stay on the psychiatric unit, he was placed on lithium carbonate and risperidone to treat the mania, which did respond. Although it was recommended that he follow up with a child and adolescent psychiatrist, through a series of happenstances he missed two appointments for an intake. He is now only able to get a new intake that is 4 months off.

You have continued to prescribe for him, waiting for what always seemed to be an imminent appointment. But now he comes to the office for a follow-up visit that can no longer wait. His mood symptoms are actually doing quite well. However, you have always known James to have a relatively thin build in the 25th percentile for weight and the 75th percentile for height. Now (is it possible?) 6 months after starting the risperidone and lithium, he returns to the office in the 50th percentile for weight and remains in the 75th percentile for height. There is nothing else noted to be concerning on physical or mental status examination, but you wonder what should be done for monitoring of his weight, should you be doing it, and whether there are other metabolic parameters that you should be measuring?
Case discussion
Regardless of your stance on pediatric bipolar disorder and the treatments for it, James has been placed on medications that need to be monitored. While it appears that James will, eventually, have a prescriber who can monitor his medication for side effects, it is incumbent on all of his providers to make sure that monitoring is occurring. Recent studies have demonstrated that guidelines for monitoring of antipsychotic use are not consistently being adhered to. For example, Rettew et al. (Pediatrics. 2015 Apr;135[4]:658-65) recently reported that metabolic monitoring that included laboratory tests was reported in only 57.2% of cases where an antipsychotic was prescribed.
Children and adolescents placed on these agents should be monitored in a number of ways. First, height and weight should be taken at baseline and at follow-up visits – at least every 6 months. The American Academy of Child and Adolescent Psychiatry practice parameters state that “consideration of weight management interventions and increased regularity of blood glucose and lipid levels should be implemented if [atypical antipsychotic agent]–induced weight gain exceeds 90th percentile body mass index (BMI) for age, or a change of five BMI units in those youths who were obese at the beginning of treatment.” Fasting blood sugar, fasting triglyceride, and cholesterol panels should be done at baseline and at approximately 6-month intervals. Screening for dystonic movements with an Abnormal Involuntary Movement Scale (AIMS) should be done at 6-month intervals. In the case of risperidone, if there are any questions about gynecomastia, galactorrhea, and/or sexual dysfunction, a prolactin level should be considered. Certain other antipsychotics require specific monitoring (for example, ECG for prolonged QT interval for ziprasidone, CBC for clozapine, and an eye exam for quetiapine).
The most important kinds of monitoring are for dose and efficacy. While the antipsychotic medications may have a role, they are not a panacea and do carry longer-term risks of metabolic problems and obesity, among others. If it is possible to provide interventions to reduce the dose or duration of use, that is preferable. If not, it’s best to work with the psychiatrist (if available) to determine who will perform the monitoring and how often it will be done to stave off metabolic problems as early as possible.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at [email protected].
Introduction
The use of antipsychotic medications has become more common in children and adolescents over the past 2 decades (Arch Gen Psychiatry. 2012 Dec;69[12]:1247-56). Whether or not one agrees that the trend in prescribing these agents is problematic (and I do), often the prescription and monitoring of antipsychotic medication falls to the primary care clinician who may have concerns about how to manage them. Here, we present a case to illustrate just such an issue.
Case summary
James is a 17-year-old young man with a diagnosis of bipolar disorder made earlier this year after an inpatient day at a local hospital. James had a history of attention-deficit/hyperactivity disorder (ADHD) growing up, but also had a strong family history of bipolar disorder. He began having increasing difficulty during the summer after his junior year, and then had a clear manic episode with elation and grandiosity that necessitated the hospitalization. During the relatively short stay on the psychiatric unit, he was placed on lithium carbonate and risperidone to treat the mania, which did respond. Although it was recommended that he follow up with a child and adolescent psychiatrist, through a series of happenstances he missed two appointments for an intake. He is now only able to get a new intake that is 4 months off.
You have continued to prescribe for him, waiting for what always seemed to be an imminent appointment. But now he comes to the office for a follow-up visit that can no longer wait. His mood symptoms are actually doing quite well. However, you have always known James to have a relatively thin build in the 25th percentile for weight and the 75th percentile for height. Now (is it possible?) 6 months after starting the risperidone and lithium, he returns to the office in the 50th percentile for weight and remains in the 75th percentile for height. There is nothing else noted to be concerning on physical or mental status examination, but you wonder what should be done for monitoring of his weight, should you be doing it, and whether there are other metabolic parameters that you should be measuring?
Case discussion
Regardless of your stance on pediatric bipolar disorder and the treatments for it, James has been placed on medications that need to be monitored. While it appears that James will, eventually, have a prescriber who can monitor his medication for side effects, it is incumbent on all of his providers to make sure that monitoring is occurring. Recent studies have demonstrated that guidelines for monitoring of antipsychotic use are not consistently being adhered to. For example, Rettew et al. (Pediatrics. 2015 Apr;135[4]:658-65) recently reported that metabolic monitoring that included laboratory tests was reported in only 57.2% of cases where an antipsychotic was prescribed.
Children and adolescents placed on these agents should be monitored in a number of ways. First, height and weight should be taken at baseline and at follow-up visits – at least every 6 months. The American Academy of Child and Adolescent Psychiatry practice parameters state that “consideration of weight management interventions and increased regularity of blood glucose and lipid levels should be implemented if [atypical antipsychotic agent]–induced weight gain exceeds 90th percentile body mass index (BMI) for age, or a change of five BMI units in those youths who were obese at the beginning of treatment.” Fasting blood sugar, fasting triglyceride, and cholesterol panels should be done at baseline and at approximately 6-month intervals. Screening for dystonic movements with an Abnormal Involuntary Movement Scale (AIMS) should be done at 6-month intervals. In the case of risperidone, if there are any questions about gynecomastia, galactorrhea, and/or sexual dysfunction, a prolactin level should be considered. Certain other antipsychotics require specific monitoring (for example, ECG for prolonged QT interval for ziprasidone, CBC for clozapine, and an eye exam for quetiapine).
The most important kinds of monitoring are for dose and efficacy. While the antipsychotic medications may have a role, they are not a panacea and do carry longer-term risks of metabolic problems and obesity, among others. If it is possible to provide interventions to reduce the dose or duration of use, that is preferable. If not, it’s best to work with the psychiatrist (if available) to determine who will perform the monitoring and how often it will be done to stave off metabolic problems as early as possible.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at [email protected].
Introduction
The use of antipsychotic medications has become more common in children and adolescents over the past 2 decades (Arch Gen Psychiatry. 2012 Dec;69[12]:1247-56). Whether or not one agrees that the trend in prescribing these agents is problematic (and I do), often the prescription and monitoring of antipsychotic medication falls to the primary care clinician who may have concerns about how to manage them. Here, we present a case to illustrate just such an issue.
Case summary
James is a 17-year-old young man with a diagnosis of bipolar disorder made earlier this year after an inpatient day at a local hospital. James had a history of attention-deficit/hyperactivity disorder (ADHD) growing up, but also had a strong family history of bipolar disorder. He began having increasing difficulty during the summer after his junior year, and then had a clear manic episode with elation and grandiosity that necessitated the hospitalization. During the relatively short stay on the psychiatric unit, he was placed on lithium carbonate and risperidone to treat the mania, which did respond. Although it was recommended that he follow up with a child and adolescent psychiatrist, through a series of happenstances he missed two appointments for an intake. He is now only able to get a new intake that is 4 months off.
You have continued to prescribe for him, waiting for what always seemed to be an imminent appointment. But now he comes to the office for a follow-up visit that can no longer wait. His mood symptoms are actually doing quite well. However, you have always known James to have a relatively thin build in the 25th percentile for weight and the 75th percentile for height. Now (is it possible?) 6 months after starting the risperidone and lithium, he returns to the office in the 50th percentile for weight and remains in the 75th percentile for height. There is nothing else noted to be concerning on physical or mental status examination, but you wonder what should be done for monitoring of his weight, should you be doing it, and whether there are other metabolic parameters that you should be measuring?
Case discussion
Regardless of your stance on pediatric bipolar disorder and the treatments for it, James has been placed on medications that need to be monitored. While it appears that James will, eventually, have a prescriber who can monitor his medication for side effects, it is incumbent on all of his providers to make sure that monitoring is occurring. Recent studies have demonstrated that guidelines for monitoring of antipsychotic use are not consistently being adhered to. For example, Rettew et al. (Pediatrics. 2015 Apr;135[4]:658-65) recently reported that metabolic monitoring that included laboratory tests was reported in only 57.2% of cases where an antipsychotic was prescribed.
Children and adolescents placed on these agents should be monitored in a number of ways. First, height and weight should be taken at baseline and at follow-up visits – at least every 6 months. The American Academy of Child and Adolescent Psychiatry practice parameters state that “consideration of weight management interventions and increased regularity of blood glucose and lipid levels should be implemented if [atypical antipsychotic agent]–induced weight gain exceeds 90th percentile body mass index (BMI) for age, or a change of five BMI units in those youths who were obese at the beginning of treatment.” Fasting blood sugar, fasting triglyceride, and cholesterol panels should be done at baseline and at approximately 6-month intervals. Screening for dystonic movements with an Abnormal Involuntary Movement Scale (AIMS) should be done at 6-month intervals. In the case of risperidone, if there are any questions about gynecomastia, galactorrhea, and/or sexual dysfunction, a prolactin level should be considered. Certain other antipsychotics require specific monitoring (for example, ECG for prolonged QT interval for ziprasidone, CBC for clozapine, and an eye exam for quetiapine).
The most important kinds of monitoring are for dose and efficacy. While the antipsychotic medications may have a role, they are not a panacea and do carry longer-term risks of metabolic problems and obesity, among others. If it is possible to provide interventions to reduce the dose or duration of use, that is preferable. If not, it’s best to work with the psychiatrist (if available) to determine who will perform the monitoring and how often it will be done to stave off metabolic problems as early as possible.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at [email protected].
