User login
Findings may help advance treatment of malaria

infecting a red blood cell
Image courtesy of St. Jude
Children’s Research Hospital
Researchers have found that a screening model can classify antimalarial drugs and reveal drug targets for Plasmodium falciparum, according to a paper published in Scientific Reports.
The team performed chemogenomic profiling of P falciparum for the first time.
They used a collection of malaria parasite mutants that each had altered metabolism linked to a defect in a single P falciparum gene.
They then screened 53 drugs and compounds against 71 of these P falciparum piggyBac single-insertion mutant parasites.
Computational analysis of the response patterns linked the different antimalarial drug candidates and metabolic inhibitors to the specific gene defect.
This revealed new insights into the drugs’ mechanism of action and uncovered 6 new genes that were involved in P falciparum’s response to artemisinin but were associated with increased susceptibility to the drugs tested.
“That represents 6 new targets potentially as effective as artemisinin for killing the malaria parasite,” said study author Dennis Kyle, PhD, of the University of South Florida in Tampa.
“There is definitely a sense of urgency for discovering new antimalarial drugs that may replace artemisinin, or work better with artemisinin, to prevent or delay drug resistance.”
P falciparum, which is becoming increasingly resistant to artemisinin, causes three-quarters of all malaria cases in Africa and 95% of malaria deaths worldwide. ![]()
infecting a red blood cell
Image courtesy of St. Jude
Children’s Research Hospital
Researchers have found that a screening model can classify antimalarial drugs and reveal drug targets for Plasmodium falciparum, according to a paper published in Scientific Reports.
The team performed chemogenomic profiling of P falciparum for the first time.
They used a collection of malaria parasite mutants that each had altered metabolism linked to a defect in a single P falciparum gene.
They then screened 53 drugs and compounds against 71 of these P falciparum piggyBac single-insertion mutant parasites.
Computational analysis of the response patterns linked the different antimalarial drug candidates and metabolic inhibitors to the specific gene defect.
This revealed new insights into the drugs’ mechanism of action and uncovered 6 new genes that were involved in P falciparum’s response to artemisinin but were associated with increased susceptibility to the drugs tested.
“That represents 6 new targets potentially as effective as artemisinin for killing the malaria parasite,” said study author Dennis Kyle, PhD, of the University of South Florida in Tampa.
“There is definitely a sense of urgency for discovering new antimalarial drugs that may replace artemisinin, or work better with artemisinin, to prevent or delay drug resistance.”
P falciparum, which is becoming increasingly resistant to artemisinin, causes three-quarters of all malaria cases in Africa and 95% of malaria deaths worldwide. ![]()
infecting a red blood cell
Image courtesy of St. Jude
Children’s Research Hospital
Researchers have found that a screening model can classify antimalarial drugs and reveal drug targets for Plasmodium falciparum, according to a paper published in Scientific Reports.
The team performed chemogenomic profiling of P falciparum for the first time.
They used a collection of malaria parasite mutants that each had altered metabolism linked to a defect in a single P falciparum gene.
They then screened 53 drugs and compounds against 71 of these P falciparum piggyBac single-insertion mutant parasites.
Computational analysis of the response patterns linked the different antimalarial drug candidates and metabolic inhibitors to the specific gene defect.
This revealed new insights into the drugs’ mechanism of action and uncovered 6 new genes that were involved in P falciparum’s response to artemisinin but were associated with increased susceptibility to the drugs tested.
“That represents 6 new targets potentially as effective as artemisinin for killing the malaria parasite,” said study author Dennis Kyle, PhD, of the University of South Florida in Tampa.
“There is definitely a sense of urgency for discovering new antimalarial drugs that may replace artemisinin, or work better with artemisinin, to prevent or delay drug resistance.”
P falciparum, which is becoming increasingly resistant to artemisinin, causes three-quarters of all malaria cases in Africa and 95% of malaria deaths worldwide. ![]()
Managing Patients With Alopecia
What does the patient need to know at the first visit?
When I communicate with alopecia patients at the first visit, I make sure they know that I’m there to help them—that I won’t minimize their concerns and that I understand how important their condition is to them. Alopecia can be frustrating for both the patient and the physician, and there often is a confounding background of psychosocial stress and/or a history of physicians who have dismissed the patient’s concerns about his or her hair loss as trivial. Establishing an effective doctor-patient relationship is key in treating alopecia. Physicians sometimes may be left feeling like the patient wants to keep them in the room until his or her hair regrows, but in reality you simply need to reassure the patient that you are comfortable with the evaluation and treatment of alopecia and that several steps will be required but you will get started today.
How do you use punch biopsies to determine the best treatment options?
My most important tips regarding alopecia diagnosis relate to scalp biopsies, which usually are required in distinguishing chronic cutaneous lupus erythematosus from other scarring alopecias. First, an absorbable gelatin compressed sponge is your best friend. A small strip inserted into the punch biopsy wound results in prompt hemostasis without the need for sutures, and the resulting scar often looks as good or better than that produced by suturing. Next, don’t biopsy the active advancing borders of an alopecia patch, as the findings usually are nonspecific. Instead, biopsy a well-established portion that has been present for at least 4 to 6 months but is still active. In inconclusive cases, a biopsy of a scarred area stained with Verhoeff elastic stain can demonstrate characteristic patterns of elastic tissue loss and often establish a diagnosis. It is important to distinguish chronic cutaneous lupus erythematosus from other forms of scarring alopecia, as it is more likely to respond to antimalarials.
What are your go-to treatments? Are your recommendations anecdotal or evidence based?
There isn’t an extensive arsenal of evidence-based therapy for refractory scarring alopecia, but that doesn’t mean we don’t have effective therapies; it simply means that our treatments are based on experience without accompanying randomized controlled trials. We need to produce more evidence, but patients with severe disease still need to be treated in the meantime. It’s important to remember that therapeutic complacency can result in permanent irreversible scarring. The presence of easily extractable anagen hairs is a sign of active disease. This simple test is helpful to monitor therapeutic progress.
Topical and intralesional corticosteroids can be extremely useful and often are underused. In general, the risk of scarring and atrophy from untreated disease is much greater than that from the corticosteroid. On the scalp, atrophy often presents as erythema, which should not be confused with erythema related to active disease. Dermoscopy is useful to demonstrate that the redness represents dermal atrophy with prominence of the subpapillary plexus of vessels.
When systemic therapy is required, antimalarials, retinoids, dapsone, thalidomide, sulfasalazine, mycophenolate mofetil, and methotrexate have all been used successfully in the setting of cutaneous lupus erythematosus, while topical tazarotene and topical calcineurin inhibitors are generally disappointing.
For the treatment of lichen planopilaris, intralesional corticosteroids, oral retinoids, and excimer laser can be effective. In contrast, antimalarials usually are not effective in preventing disease progression. The peroxisome proliferator-activated receptor-γ agonist pioglitazone can be effective, but reported results vary widely. In my experience, mycophenolate mofetil is generally reliable in patients with refractory disease. Dutasteride can be effective as a first-line therapy in the setting of frontal fibrosing alopecia, although some of the noted improvement may relate to the nonscarring portion of the disease in patients with a background of pattern alopecia.
How do you keep patients compliant with treatment?
Again, the key to treatment compliance is to establish an effective doctor-patient relationship. Whenever possible, begin with adequately potent therapy to give patients an early response. Don’t hesitate to use prednisone initially for inflammatory scarring alopecia. Patients need to see signs of progress in order to stay compliant with treatment, and long trials of ineffective therapies destroy trust. Adequate doses of intralesional or oral corticosteroids often are appropriate to ensure an early response with subsequent transition to steroid-sparing agents.
What do you do if they refuse treatment?
Try to find out why—often it’s simply fear of side effects. Patient education is key, and it can help tremendously to share with them the number of patients you have treated safely with the medication in question and assure them that you know how to monitor for the important side effects.
What resources do you recommend to patients for more information?
It is helpful to keep a handy list of patient advocacy Web sites. Well-established support groups such as the National Alopecia Areata Foundation (https://www.naaf.org) and the Cicatricial Alopecia Research Foundation (http://www.carfintl.org) provide excellent information for patients and help to support research to improve outcomes for these difficult disorders.
What does the patient need to know at the first visit?
When I communicate with alopecia patients at the first visit, I make sure they know that I’m there to help them—that I won’t minimize their concerns and that I understand how important their condition is to them. Alopecia can be frustrating for both the patient and the physician, and there often is a confounding background of psychosocial stress and/or a history of physicians who have dismissed the patient’s concerns about his or her hair loss as trivial. Establishing an effective doctor-patient relationship is key in treating alopecia. Physicians sometimes may be left feeling like the patient wants to keep them in the room until his or her hair regrows, but in reality you simply need to reassure the patient that you are comfortable with the evaluation and treatment of alopecia and that several steps will be required but you will get started today.
How do you use punch biopsies to determine the best treatment options?
My most important tips regarding alopecia diagnosis relate to scalp biopsies, which usually are required in distinguishing chronic cutaneous lupus erythematosus from other scarring alopecias. First, an absorbable gelatin compressed sponge is your best friend. A small strip inserted into the punch biopsy wound results in prompt hemostasis without the need for sutures, and the resulting scar often looks as good or better than that produced by suturing. Next, don’t biopsy the active advancing borders of an alopecia patch, as the findings usually are nonspecific. Instead, biopsy a well-established portion that has been present for at least 4 to 6 months but is still active. In inconclusive cases, a biopsy of a scarred area stained with Verhoeff elastic stain can demonstrate characteristic patterns of elastic tissue loss and often establish a diagnosis. It is important to distinguish chronic cutaneous lupus erythematosus from other forms of scarring alopecia, as it is more likely to respond to antimalarials.
What are your go-to treatments? Are your recommendations anecdotal or evidence based?
There isn’t an extensive arsenal of evidence-based therapy for refractory scarring alopecia, but that doesn’t mean we don’t have effective therapies; it simply means that our treatments are based on experience without accompanying randomized controlled trials. We need to produce more evidence, but patients with severe disease still need to be treated in the meantime. It’s important to remember that therapeutic complacency can result in permanent irreversible scarring. The presence of easily extractable anagen hairs is a sign of active disease. This simple test is helpful to monitor therapeutic progress.
Topical and intralesional corticosteroids can be extremely useful and often are underused. In general, the risk of scarring and atrophy from untreated disease is much greater than that from the corticosteroid. On the scalp, atrophy often presents as erythema, which should not be confused with erythema related to active disease. Dermoscopy is useful to demonstrate that the redness represents dermal atrophy with prominence of the subpapillary plexus of vessels.
When systemic therapy is required, antimalarials, retinoids, dapsone, thalidomide, sulfasalazine, mycophenolate mofetil, and methotrexate have all been used successfully in the setting of cutaneous lupus erythematosus, while topical tazarotene and topical calcineurin inhibitors are generally disappointing.
For the treatment of lichen planopilaris, intralesional corticosteroids, oral retinoids, and excimer laser can be effective. In contrast, antimalarials usually are not effective in preventing disease progression. The peroxisome proliferator-activated receptor-γ agonist pioglitazone can be effective, but reported results vary widely. In my experience, mycophenolate mofetil is generally reliable in patients with refractory disease. Dutasteride can be effective as a first-line therapy in the setting of frontal fibrosing alopecia, although some of the noted improvement may relate to the nonscarring portion of the disease in patients with a background of pattern alopecia.
How do you keep patients compliant with treatment?
Again, the key to treatment compliance is to establish an effective doctor-patient relationship. Whenever possible, begin with adequately potent therapy to give patients an early response. Don’t hesitate to use prednisone initially for inflammatory scarring alopecia. Patients need to see signs of progress in order to stay compliant with treatment, and long trials of ineffective therapies destroy trust. Adequate doses of intralesional or oral corticosteroids often are appropriate to ensure an early response with subsequent transition to steroid-sparing agents.
What do you do if they refuse treatment?
Try to find out why—often it’s simply fear of side effects. Patient education is key, and it can help tremendously to share with them the number of patients you have treated safely with the medication in question and assure them that you know how to monitor for the important side effects.
What resources do you recommend to patients for more information?
It is helpful to keep a handy list of patient advocacy Web sites. Well-established support groups such as the National Alopecia Areata Foundation (https://www.naaf.org) and the Cicatricial Alopecia Research Foundation (http://www.carfintl.org) provide excellent information for patients and help to support research to improve outcomes for these difficult disorders.
What does the patient need to know at the first visit?
When I communicate with alopecia patients at the first visit, I make sure they know that I’m there to help them—that I won’t minimize their concerns and that I understand how important their condition is to them. Alopecia can be frustrating for both the patient and the physician, and there often is a confounding background of psychosocial stress and/or a history of physicians who have dismissed the patient’s concerns about his or her hair loss as trivial. Establishing an effective doctor-patient relationship is key in treating alopecia. Physicians sometimes may be left feeling like the patient wants to keep them in the room until his or her hair regrows, but in reality you simply need to reassure the patient that you are comfortable with the evaluation and treatment of alopecia and that several steps will be required but you will get started today.
How do you use punch biopsies to determine the best treatment options?
My most important tips regarding alopecia diagnosis relate to scalp biopsies, which usually are required in distinguishing chronic cutaneous lupus erythematosus from other scarring alopecias. First, an absorbable gelatin compressed sponge is your best friend. A small strip inserted into the punch biopsy wound results in prompt hemostasis without the need for sutures, and the resulting scar often looks as good or better than that produced by suturing. Next, don’t biopsy the active advancing borders of an alopecia patch, as the findings usually are nonspecific. Instead, biopsy a well-established portion that has been present for at least 4 to 6 months but is still active. In inconclusive cases, a biopsy of a scarred area stained with Verhoeff elastic stain can demonstrate characteristic patterns of elastic tissue loss and often establish a diagnosis. It is important to distinguish chronic cutaneous lupus erythematosus from other forms of scarring alopecia, as it is more likely to respond to antimalarials.
What are your go-to treatments? Are your recommendations anecdotal or evidence based?
There isn’t an extensive arsenal of evidence-based therapy for refractory scarring alopecia, but that doesn’t mean we don’t have effective therapies; it simply means that our treatments are based on experience without accompanying randomized controlled trials. We need to produce more evidence, but patients with severe disease still need to be treated in the meantime. It’s important to remember that therapeutic complacency can result in permanent irreversible scarring. The presence of easily extractable anagen hairs is a sign of active disease. This simple test is helpful to monitor therapeutic progress.
Topical and intralesional corticosteroids can be extremely useful and often are underused. In general, the risk of scarring and atrophy from untreated disease is much greater than that from the corticosteroid. On the scalp, atrophy often presents as erythema, which should not be confused with erythema related to active disease. Dermoscopy is useful to demonstrate that the redness represents dermal atrophy with prominence of the subpapillary plexus of vessels.
When systemic therapy is required, antimalarials, retinoids, dapsone, thalidomide, sulfasalazine, mycophenolate mofetil, and methotrexate have all been used successfully in the setting of cutaneous lupus erythematosus, while topical tazarotene and topical calcineurin inhibitors are generally disappointing.
For the treatment of lichen planopilaris, intralesional corticosteroids, oral retinoids, and excimer laser can be effective. In contrast, antimalarials usually are not effective in preventing disease progression. The peroxisome proliferator-activated receptor-γ agonist pioglitazone can be effective, but reported results vary widely. In my experience, mycophenolate mofetil is generally reliable in patients with refractory disease. Dutasteride can be effective as a first-line therapy in the setting of frontal fibrosing alopecia, although some of the noted improvement may relate to the nonscarring portion of the disease in patients with a background of pattern alopecia.
How do you keep patients compliant with treatment?
Again, the key to treatment compliance is to establish an effective doctor-patient relationship. Whenever possible, begin with adequately potent therapy to give patients an early response. Don’t hesitate to use prednisone initially for inflammatory scarring alopecia. Patients need to see signs of progress in order to stay compliant with treatment, and long trials of ineffective therapies destroy trust. Adequate doses of intralesional or oral corticosteroids often are appropriate to ensure an early response with subsequent transition to steroid-sparing agents.
What do you do if they refuse treatment?
Try to find out why—often it’s simply fear of side effects. Patient education is key, and it can help tremendously to share with them the number of patients you have treated safely with the medication in question and assure them that you know how to monitor for the important side effects.
What resources do you recommend to patients for more information?
It is helpful to keep a handy list of patient advocacy Web sites. Well-established support groups such as the National Alopecia Areata Foundation (https://www.naaf.org) and the Cicatricial Alopecia Research Foundation (http://www.carfintl.org) provide excellent information for patients and help to support research to improve outcomes for these difficult disorders.

AAGL 2015: Conference social highlights
Tune in daily for social media coverage of AAGL 2015 from OBG Management and ObGyn News. Share your thoughts with us, and we may highlight them below. Thank you for your social contributions!

|
Tune in daily for social media coverage of AAGL 2015 from OBG Management and ObGyn News. Share your thoughts with us, and we may highlight them below. Thank you for your social contributions!
|
|
Tune in daily for social media coverage of AAGL 2015 from OBG Management and ObGyn News. Share your thoughts with us, and we may highlight them below. Thank you for your social contributions!
|
|

Iron deficiency may explain persistent hypothyroidism symptoms
LAKE BUENA VISTA, FLA. – Between 30% and 50% of hypothyroid patients with persistent symptoms despite adequate levothyroxine therapy may have covert iron deficiency, findings from a small study suggest.
The findings cast “a dark shadow of doubt on the validity of the studies on the effect of T3 therapy in these patients,” Dr. Esa Soppi reported in a poster at the International Thyroid Congress.

Study subjects were women with a history of overt hypothyroidism who had persistent symptoms after appropriate and ongoing treatment with L-T4. L-T4 dosing was adjusted as necessary to achieve a thyroid-stimulating hormone concentration of 1-2 mU/L, and diabetes, B12-vitamin deficiency, celiac disease, hypercalcemia, and vitamin D deficiency were ruled out as causes for the persistent symptoms.
Further, none of the patients had anemia, and red cell indices were within the reference range.
Five of the women had serum ferritin of less than 15 mcg/L, and two of those had serum iron, transferrin, or soluble transferrin receptor concentration or transferrin saturation out of range, suggesting iron deficiency. The remaining 20 women had a serum ferritin concentration between 15 mcg/L and 60 mcg/L, Dr. Soppi of Eira Hospital, Helsinki, noted at the meeting held by the American Thyroid Association, Asia-Oceania Thyroid Association , European Thyroid Association, and Latin American Thyroid Society.
Four of the five women with serum ferritin less than 15 mcg/L, and 14 of the 20 with less than 15-60 mcg/L became symptom free when treated with oral iron substitution therapy for 6-12 months, Dr. Soppi said.
“All patients were advised to take their thyroxine dose at the fasting state in the morning and start breakfast 30 minutes later. The interval between the iron and thyroxine was at least 4 hours. The response was observed at a serum ferritin concentration approaching 70-100 mcg/L,” Dr. Soppi wrote, noting that in one patient – a 28-year-old woman with type 1 diabetes and hypothyroidism – all symptoms of fatigue, failure to thrive, and lethargy experienced before the start of the iron therapy disappeared after about 4 months of oral iron therapy at a dose of 100 mg twice daily.
However, another patient – an 18-year-old woman with hypothyroidism after total thyroidectomy performed because of a suspected thyroid malignancy – was found to have no malignancy; disabling tiredness, and failure to thrive emerged after the thyroidectomy and persisted despite iron therapy given at 100 mg twice daily.
“Iron deficiency is as common as hypothyroidism and its symptoms resemble those of hypothyroidism. However, the diagnosis of iron deficiency without anemia is extremely challenging since all indicators of iron status may be ‘normal.’ A clinical suspicion is key to diagnosis of covert iron deficiency,” Dr. Soppi wrote, noting that the serum ferritin concentration may be helpful, and restoration of ferritin above 100 mcg/L seems to ameliorate symptoms in about two-thirds of patients, and that it is not currently known why some iron-deficient patients fail to respond to restoration of their functional iron stores.
LAKE BUENA VISTA, FLA. – Between 30% and 50% of hypothyroid patients with persistent symptoms despite adequate levothyroxine therapy may have covert iron deficiency, findings from a small study suggest.
The findings cast “a dark shadow of doubt on the validity of the studies on the effect of T3 therapy in these patients,” Dr. Esa Soppi reported in a poster at the International Thyroid Congress.
Study subjects were women with a history of overt hypothyroidism who had persistent symptoms after appropriate and ongoing treatment with L-T4. L-T4 dosing was adjusted as necessary to achieve a thyroid-stimulating hormone concentration of 1-2 mU/L, and diabetes, B12-vitamin deficiency, celiac disease, hypercalcemia, and vitamin D deficiency were ruled out as causes for the persistent symptoms.
Further, none of the patients had anemia, and red cell indices were within the reference range.
Five of the women had serum ferritin of less than 15 mcg/L, and two of those had serum iron, transferrin, or soluble transferrin receptor concentration or transferrin saturation out of range, suggesting iron deficiency. The remaining 20 women had a serum ferritin concentration between 15 mcg/L and 60 mcg/L, Dr. Soppi of Eira Hospital, Helsinki, noted at the meeting held by the American Thyroid Association, Asia-Oceania Thyroid Association , European Thyroid Association, and Latin American Thyroid Society.
Four of the five women with serum ferritin less than 15 mcg/L, and 14 of the 20 with less than 15-60 mcg/L became symptom free when treated with oral iron substitution therapy for 6-12 months, Dr. Soppi said.
“All patients were advised to take their thyroxine dose at the fasting state in the morning and start breakfast 30 minutes later. The interval between the iron and thyroxine was at least 4 hours. The response was observed at a serum ferritin concentration approaching 70-100 mcg/L,” Dr. Soppi wrote, noting that in one patient – a 28-year-old woman with type 1 diabetes and hypothyroidism – all symptoms of fatigue, failure to thrive, and lethargy experienced before the start of the iron therapy disappeared after about 4 months of oral iron therapy at a dose of 100 mg twice daily.
However, another patient – an 18-year-old woman with hypothyroidism after total thyroidectomy performed because of a suspected thyroid malignancy – was found to have no malignancy; disabling tiredness, and failure to thrive emerged after the thyroidectomy and persisted despite iron therapy given at 100 mg twice daily.
“Iron deficiency is as common as hypothyroidism and its symptoms resemble those of hypothyroidism. However, the diagnosis of iron deficiency without anemia is extremely challenging since all indicators of iron status may be ‘normal.’ A clinical suspicion is key to diagnosis of covert iron deficiency,” Dr. Soppi wrote, noting that the serum ferritin concentration may be helpful, and restoration of ferritin above 100 mcg/L seems to ameliorate symptoms in about two-thirds of patients, and that it is not currently known why some iron-deficient patients fail to respond to restoration of their functional iron stores.
LAKE BUENA VISTA, FLA. – Between 30% and 50% of hypothyroid patients with persistent symptoms despite adequate levothyroxine therapy may have covert iron deficiency, findings from a small study suggest.
The findings cast “a dark shadow of doubt on the validity of the studies on the effect of T3 therapy in these patients,” Dr. Esa Soppi reported in a poster at the International Thyroid Congress.
Study subjects were women with a history of overt hypothyroidism who had persistent symptoms after appropriate and ongoing treatment with L-T4. L-T4 dosing was adjusted as necessary to achieve a thyroid-stimulating hormone concentration of 1-2 mU/L, and diabetes, B12-vitamin deficiency, celiac disease, hypercalcemia, and vitamin D deficiency were ruled out as causes for the persistent symptoms.
Further, none of the patients had anemia, and red cell indices were within the reference range.
Five of the women had serum ferritin of less than 15 mcg/L, and two of those had serum iron, transferrin, or soluble transferrin receptor concentration or transferrin saturation out of range, suggesting iron deficiency. The remaining 20 women had a serum ferritin concentration between 15 mcg/L and 60 mcg/L, Dr. Soppi of Eira Hospital, Helsinki, noted at the meeting held by the American Thyroid Association, Asia-Oceania Thyroid Association , European Thyroid Association, and Latin American Thyroid Society.
Four of the five women with serum ferritin less than 15 mcg/L, and 14 of the 20 with less than 15-60 mcg/L became symptom free when treated with oral iron substitution therapy for 6-12 months, Dr. Soppi said.
“All patients were advised to take their thyroxine dose at the fasting state in the morning and start breakfast 30 minutes later. The interval between the iron and thyroxine was at least 4 hours. The response was observed at a serum ferritin concentration approaching 70-100 mcg/L,” Dr. Soppi wrote, noting that in one patient – a 28-year-old woman with type 1 diabetes and hypothyroidism – all symptoms of fatigue, failure to thrive, and lethargy experienced before the start of the iron therapy disappeared after about 4 months of oral iron therapy at a dose of 100 mg twice daily.
However, another patient – an 18-year-old woman with hypothyroidism after total thyroidectomy performed because of a suspected thyroid malignancy – was found to have no malignancy; disabling tiredness, and failure to thrive emerged after the thyroidectomy and persisted despite iron therapy given at 100 mg twice daily.
“Iron deficiency is as common as hypothyroidism and its symptoms resemble those of hypothyroidism. However, the diagnosis of iron deficiency without anemia is extremely challenging since all indicators of iron status may be ‘normal.’ A clinical suspicion is key to diagnosis of covert iron deficiency,” Dr. Soppi wrote, noting that the serum ferritin concentration may be helpful, and restoration of ferritin above 100 mcg/L seems to ameliorate symptoms in about two-thirds of patients, and that it is not currently known why some iron-deficient patients fail to respond to restoration of their functional iron stores.
AT THE INTERNATIONAL THYROID CONGRESS
Key clinical point: Between 30% and 50% of hypothyroid patients with persistent symptoms despite adequate levothyroxine therapy may have covert iron deficiency, findings from a small study suggest.
Major finding: Four of five women with serum ferritin less than 15 mcg/L, and 14 of 20 with less than 15-60 mcg/L became symptom free when treated with oral iron substitution therapy for 6-12 months.
Data source: A prospective study of 25 women.
Disclosures: Dr. Soppi reported having no disclosures.

ACS: Watchful waiting for some rectal cancers almost ready for ‘prime time’
CHICAGO – Watchful waiting with careful surveillance may become an option for the majority of locally advanced rectal cancer patients who have a complete clinical response to neoadjuvant therapy, according to a review of 442 rectal cancer patients at Memorial Sloan Kettering Cancer Center in New York.
Seventy-three of those patients had a complete clinical response to neoadjuvant therapy and opted for watchful waiting instead of surgery after weighing the risks and benefits – including about a 25% chance of local recurrence – with their doctors.

At 4 years’ follow-up, 54 (74%) remained cancer free. Nineteen patients had local tumor recurrence, generally within 13 months. Two of those patients had successful local excisions, and the remaining 17 had salvage total mesorectal excisions (TME).
There were no statistically significant differences in 4-year disease-specific and overall survival among the 73 patients and 72 other patients who opted for TME after neoadjuvant chemotherapy and were found to have had pathologic complete responses.
“In our cohort, watch and wait was safe. It’s an effective treatment strategy achieving a high rate of rectal preservation in tumors that respond to neoadjuvant therapy. I don’t think the rectum needs to come out in everybody,” said investigator Dr. J. Joshua Smith, a surgical oncologist at Sloan Kettering.
Several studies have reported similar results similar to the Sloan Kettering study, but other investigations have been retrospective, so optimal patient selection, assessment of response, surveillance protocols, and other matters remain uncertain. Sloan Kettering and about 20 other cancer centers in United States – all members of the Rectal Cancer Consortium – recently launched a randomized clinical trial to get a better handle on those issues.
Locally advanced rectal cancer patients will be randomized to either chemoradiation for 5.5 weeks followed by folinic acid, fluorouracil, and oxaliplatin (FOLFOX) or capecitabine and oxaliplatin (CapeOX) over about 16 weeks, or FOLFOX/CapeOX first and chemoradiation second. Those who have a significant clinical response will then undergo watchful waiting; those who do not will have TME.
About 50 patients have enrolled in the phase II trial so far; the investigators are looking for more than 200.
“I think ‘prime time for watchful waiting’ is around the corner, but not yet here. It must be preceded by a prospective trial.” Meanwhile, “how we define complete clinical response is important” when considering watchful waiting, Dr. Smith said at the annual clinical congress of the American College of Surgeons..
At Sloan Kettering, where watchful waiting has become more popular in recent years, complete clinical response means no tumor or lymph nodes on imaging, and, on digital rectal exam (DRE) and proctoscopy, normal flat mucosa, smooth induration, no mass, no nodules, no ulcerations, and no luminal narrowing; a pale scar and telangiectasias are okay.
In the first year, surveillance includes DRE and endoscopy every 3 months and imaging every 6 months. In the second year, DRE and endoscopy come every 4 months, and imaging again every 6 months. From years 3 to 5, DRE and endoscopy are done every 6 months, and imaging every 6-12 months. After 5 years, surveillance is by yearly DRE and endoscopy.
When discussing the option with patients, they need to know – besides the risk of recurrence – that watchful waiting is currently not standard medical management; surveillance must be frequent; they are at risk for a more extensive salvage TME than they might have had otherwise; and the approach might compromise the chance of a cure, Dr. Smith said.
Dr. Smith said he has no relevant disclosures.
CHICAGO – Watchful waiting with careful surveillance may become an option for the majority of locally advanced rectal cancer patients who have a complete clinical response to neoadjuvant therapy, according to a review of 442 rectal cancer patients at Memorial Sloan Kettering Cancer Center in New York.
Seventy-three of those patients had a complete clinical response to neoadjuvant therapy and opted for watchful waiting instead of surgery after weighing the risks and benefits – including about a 25% chance of local recurrence – with their doctors.
At 4 years’ follow-up, 54 (74%) remained cancer free. Nineteen patients had local tumor recurrence, generally within 13 months. Two of those patients had successful local excisions, and the remaining 17 had salvage total mesorectal excisions (TME).
There were no statistically significant differences in 4-year disease-specific and overall survival among the 73 patients and 72 other patients who opted for TME after neoadjuvant chemotherapy and were found to have had pathologic complete responses.
“In our cohort, watch and wait was safe. It’s an effective treatment strategy achieving a high rate of rectal preservation in tumors that respond to neoadjuvant therapy. I don’t think the rectum needs to come out in everybody,” said investigator Dr. J. Joshua Smith, a surgical oncologist at Sloan Kettering.
Several studies have reported similar results similar to the Sloan Kettering study, but other investigations have been retrospective, so optimal patient selection, assessment of response, surveillance protocols, and other matters remain uncertain. Sloan Kettering and about 20 other cancer centers in United States – all members of the Rectal Cancer Consortium – recently launched a randomized clinical trial to get a better handle on those issues.
Locally advanced rectal cancer patients will be randomized to either chemoradiation for 5.5 weeks followed by folinic acid, fluorouracil, and oxaliplatin (FOLFOX) or capecitabine and oxaliplatin (CapeOX) over about 16 weeks, or FOLFOX/CapeOX first and chemoradiation second. Those who have a significant clinical response will then undergo watchful waiting; those who do not will have TME.
About 50 patients have enrolled in the phase II trial so far; the investigators are looking for more than 200.
“I think ‘prime time for watchful waiting’ is around the corner, but not yet here. It must be preceded by a prospective trial.” Meanwhile, “how we define complete clinical response is important” when considering watchful waiting, Dr. Smith said at the annual clinical congress of the American College of Surgeons..
At Sloan Kettering, where watchful waiting has become more popular in recent years, complete clinical response means no tumor or lymph nodes on imaging, and, on digital rectal exam (DRE) and proctoscopy, normal flat mucosa, smooth induration, no mass, no nodules, no ulcerations, and no luminal narrowing; a pale scar and telangiectasias are okay.
In the first year, surveillance includes DRE and endoscopy every 3 months and imaging every 6 months. In the second year, DRE and endoscopy come every 4 months, and imaging again every 6 months. From years 3 to 5, DRE and endoscopy are done every 6 months, and imaging every 6-12 months. After 5 years, surveillance is by yearly DRE and endoscopy.
When discussing the option with patients, they need to know – besides the risk of recurrence – that watchful waiting is currently not standard medical management; surveillance must be frequent; they are at risk for a more extensive salvage TME than they might have had otherwise; and the approach might compromise the chance of a cure, Dr. Smith said.
Dr. Smith said he has no relevant disclosures.
CHICAGO – Watchful waiting with careful surveillance may become an option for the majority of locally advanced rectal cancer patients who have a complete clinical response to neoadjuvant therapy, according to a review of 442 rectal cancer patients at Memorial Sloan Kettering Cancer Center in New York.
Seventy-three of those patients had a complete clinical response to neoadjuvant therapy and opted for watchful waiting instead of surgery after weighing the risks and benefits – including about a 25% chance of local recurrence – with their doctors.
At 4 years’ follow-up, 54 (74%) remained cancer free. Nineteen patients had local tumor recurrence, generally within 13 months. Two of those patients had successful local excisions, and the remaining 17 had salvage total mesorectal excisions (TME).
There were no statistically significant differences in 4-year disease-specific and overall survival among the 73 patients and 72 other patients who opted for TME after neoadjuvant chemotherapy and were found to have had pathologic complete responses.
“In our cohort, watch and wait was safe. It’s an effective treatment strategy achieving a high rate of rectal preservation in tumors that respond to neoadjuvant therapy. I don’t think the rectum needs to come out in everybody,” said investigator Dr. J. Joshua Smith, a surgical oncologist at Sloan Kettering.
Several studies have reported similar results similar to the Sloan Kettering study, but other investigations have been retrospective, so optimal patient selection, assessment of response, surveillance protocols, and other matters remain uncertain. Sloan Kettering and about 20 other cancer centers in United States – all members of the Rectal Cancer Consortium – recently launched a randomized clinical trial to get a better handle on those issues.
Locally advanced rectal cancer patients will be randomized to either chemoradiation for 5.5 weeks followed by folinic acid, fluorouracil, and oxaliplatin (FOLFOX) or capecitabine and oxaliplatin (CapeOX) over about 16 weeks, or FOLFOX/CapeOX first and chemoradiation second. Those who have a significant clinical response will then undergo watchful waiting; those who do not will have TME.
About 50 patients have enrolled in the phase II trial so far; the investigators are looking for more than 200.
“I think ‘prime time for watchful waiting’ is around the corner, but not yet here. It must be preceded by a prospective trial.” Meanwhile, “how we define complete clinical response is important” when considering watchful waiting, Dr. Smith said at the annual clinical congress of the American College of Surgeons..
At Sloan Kettering, where watchful waiting has become more popular in recent years, complete clinical response means no tumor or lymph nodes on imaging, and, on digital rectal exam (DRE) and proctoscopy, normal flat mucosa, smooth induration, no mass, no nodules, no ulcerations, and no luminal narrowing; a pale scar and telangiectasias are okay.
In the first year, surveillance includes DRE and endoscopy every 3 months and imaging every 6 months. In the second year, DRE and endoscopy come every 4 months, and imaging again every 6 months. From years 3 to 5, DRE and endoscopy are done every 6 months, and imaging every 6-12 months. After 5 years, surveillance is by yearly DRE and endoscopy.
When discussing the option with patients, they need to know – besides the risk of recurrence – that watchful waiting is currently not standard medical management; surveillance must be frequent; they are at risk for a more extensive salvage TME than they might have had otherwise; and the approach might compromise the chance of a cure, Dr. Smith said.
Dr. Smith said he has no relevant disclosures.
AT THE ACS CLINICAL CONGRESS
Key clinical point: Organ preservation seems to be a valid option when locally advanced rectal cancers respond completely to neoadjuvant therapy.
Major finding: Almost three-quarters of 73 patients who opted for watchful waiting after complete clinical responses to neodjuvant therapy remained cancer free at 4 years.
Data source: Review of 442 patients at Memorial Sloan Kettering Cancer Center.
Disclosures: The presenting investigator has no relevant financial disclosures.

Status Report From the American Acne & Rosacea Society on Medical Management of Acne in Adult Women, Part 2: Topical Therapies
It seems intuitive that clinicians in dermatology would automatically recognize the importance of proper selection and integration of skin care products and techniques in the management of acne vulgaris (AV). However, an understanding of the fundamental importance of skin care in AV management and the scientific basis for maintaining epidermal barrier (EpB) function and repair cannot be assumed. In fact, there is limited scientific information about EpB dysfunction and AV or the adjunctive benefits of specific skin care products. However, some data have emerged that can be successfully applied by clinicians.1-9
In part 2 of this series, emphasis is placed on skin care and topical therapies for the treatment of AV in adult women. In addition to the plethora of cleanser and moisturizer formulations that exist in the marketplace, there are many over-the-counter (OTC) products marketed to treat AV that contain benzoyl peroxide (BP) and salicylic acid. Importantly, women tend to be selective about what they use to cleanse and moisturize their skin, and use of OTC products to treat AV is common among adult women.10,11
A thorough discussion of EpB impairment, related inflammatory cascades, and potential relevance to AV are beyond the scope of this article. In short, appropriate skin care products can reduce the inflammation and sensitivity associated with increased transepidermal water loss and reduced stratum corneum hydration and can mitigate EpB impairments induced by certain acne medications or vehicles.1,12 Available data support the adjunctive benefit of proper skin care in the management of AV by mitigating cutaneous irritation and potentially contributing to a reduction in AV lesions.2-4,7,13 Use of a formulation that also provides broad-spectrum photoprotection also is helpful.3,4
Another challenge is the myriad of cosmeceuticals that are heavily marketed to adult women with AV.13,14 Unfortunately, the scientific evidence supporting these products for treatment of AV is limited, resulting in the clinician’s inability to make specific recommendations. The core message is to incorporate skin care products that can reduce EpB impairment and mitigate cutaneous irritation associated with some AV therapies.1-4,7-9,12
OTC Topical Therapies
The marketplace is replete with several OTC products for treatment of AV, most of which contain BP and salicylic acid.15,16 There is a lack of efficacy data for OTC products for AV, including cleansers and topical medications, although some may be beneficial for milder cases. A variety of formulations are available to choose from, usually without the advice of a clinician. Additionally, heavy marketing is directed at adult women with AV, which may promote the use of therapies that may not be optimal for their respective AV severity or may cause facial skin irritation. Self-treatment may also cause delay in seeking dermatologic care, increasing the risk of persistent or permanent sequelae. Delay in adequate treatment is a major risk factor for the development of acne scars.17
Prescription Topical Therapies
Despite the high prevalence of AV in adult women, there is a paucity of studies evaluating topical therapies for AV in this subset.18-24 Reports in the literature on AV in adult women have focused on systemic hormonal agents (eg, oral contraceptives, spironolactone); however, more recent reports have addressed the use of topical therapies in this subpopulation.11,25-30 Published data on topical formulations are predominantly post hoc analyses from pivotal randomized controlled trials (RCTs) that included adolescents and adults of both genders with facial AV located above the jawline and predominantly moderate in severity.11,26,28,30 Participants in all of these studies presented with non-nodular, mixed inflammatory, and comedonal facial AV above the jawline, with inclusion criteria that required a minimum of 20 comedonal lesions and 20 papulopustular lesions at baseline. An important differentiating factor among these various post hoc analyses evaluating adult women versus adolescent girls with AV are the ages used to separate adults from adolescents. A dividing line of 18 years and older was used in some reports (eg, adapalene gel 0.3%, dapsone gel 5%), while other reports used 25 years and older to separate adolescent girls from adult women (ie, clindamycin phosphate [CP] 1.2%– BP 3.75% gel, adapalene 0.1%–BP 2.5% gel).11,26,28,30
Importantly, these studies included adult women with AV who presented with mixed comedonal and inflammatory AV (mixed pattern AV) similar to adolescents. None of the studies included women with a U-shaped AV pattern or lower facial AV characterized by deep inflammatory lesions that are often tender and few in number. Unfortunately, there is a lack of data evaluating topical therapies for these patterns of AV in adult women, including AV below the jawline and on the trunk. Although mixed pattern AV has been reported to affect 75% to 90% of adult women with AV, epidemiologic data quantifying the clinical AV patterns affecting adult women are limited.11,22,29,31,32 More well-designed studies are needed.
The treatment of AV in adult women may incorporate any of the topical therapies used to treat AV in adolescents, especially as studies encompass both the adolescent and adult age ranges. This is especially true with mixed pattern AV, which is the predominant presentation in participants enrolled in clinical trials with topical therapies, especially of moderate severity.
Herein we provide a summary of the topical therapies that have been evaluated by post hoc analyses of data from pivotal studies in adult women with AV.
Adapalene Gel 0.3%
Adapalene exhibits retinoid activity with efficacy in reducing inflammatory and comedonal AV lesions shown with both 0.1% and 0.3% concentrations.33-35 Post hoc analyses of 2 pivotal RCTs of patients with facial AV showed that adapalene gel 0.3% once daily (n=74; mean age, 27.2 years) was superior to vehicle once daily (n=43; mean age, 25.2 years) in both mean and median percentage reductions of comedonal, inflammatory, and total lesions in women 18 years and older who were treated for 12 weeks; the difference in mean percentage lesion reduction from vehicle for total AV lesions was statistically significant at 12 weeks (P=.045).26 Adapalene gel 0.3% produced a favorable skin tolerability profile similar to adapalene gel 0.1%, with the most common adverse reactions being discomfort and dryness.
Advantages of topical retinoid therapy in adult women with facial AV are reduction in postinflammatory hyperpigmentation and therapeutic modulation of chronic photodamage (eg, fine lines, rough texture, dyschromia).29,36,37 Disadvantages include signs and symptoms of cutaneous irritation, although this tends to occur less frequently on facial skin with adapalene gel 0.3% as compared to other topical retinoids that exhibit comparable efficacy.33-37 Topical retinoid therapy on the anterior neck and upper chest should be used cautiously, as these anatomic sites appear to be more prone to cutaneous irritation.
Dapsone Gel 5%
Dapsone is a sulfone antimicrobial and anti-inflammatory agent that has been shown to be effective, safe, and well tolerated in the treatment of AV in a topical 5% formulation.38,39 A post hoc analysis of pivotal 12-week trial data suggested that dapsone gel 5% twice daily produced greater AV reductions in females compared to males; no gender differences were noted in adverse effects, which were low in frequency.39 A separate subgroup analysis compared outcomes among adult women (≥18 years of age; n=434) and adolescent girls (12–17 years of age; n=347) treated with dapsone gel 5%.11 The proportion with no or minimal acne based on the Global Acne Assessment Score at week 12 was greater in adult women (53.5%) versus adolescent girls (45.3%, P=.022), with significantly greater percentage reductions in both noninflammatory (P<.0001) and total lesion counts (P=.0008) observed in the adult group. Percentage reductions in inflammatory lesions were similar in both groups. No major safety or tolerability issues or new safety signals were noted. Advantages of dapsone gel 5% are highly favorable tolerability and the perception of decreased oily skin in some participants.38,39
Clindamycin Phosphate 1.2%–Benzoyl Peroxide 3.75% Gel
The combination formulation of CP 1.2%– BP 3.75% gel applied once daily has been shown to be effective, well tolerated, and safe for the treatment of facial AV, with a gender analysis noting an apparent greater efficacy in females.40,41 A post hoc analysis from the 12-week pivotal study data in adult women aged 25 years and older showed a mean percentage change from baseline in inflammatory and noninflammatory lesion counts and the percentage of participants who achieved a 2-grade improvement by global assessment to be 68.7%, 60.4%, and 52.7% in actively treated participants (n=29), respectively, which was significantly superior to vehicle applied once daily (n=43; P=.019, P=.020, and P=.074, respectively).42 No relevant differences in tolerability were noted among treatment groups, and no participants discontinued therapy due to adverse events. Advantages of CP 1.2%–BP 3.75% gel are highly favorable skin tolerability and the perception of decreased oily skin in some participants.41-43
Adapalene 0.1%–Benzoyl Peroxide 2.5% Gel
A meta-analysis of pooled data from 3 RCTs evaluated use of adapalene 0.1%–BP 2.5% gel applied once daily in adult women aged 25 years and older with facial AV (n=130) versus vehicle gel applied once daily (n=124).30 The percentage of participants who achieved investigator global assessment ratings of clear or almost clear was 39.2% in actively treated participants versus 18.5% with vehicle (P<.001), and median percentage lesion reduction was approximately 30% greater in those treated with adapalene 0.1%–BP 2.5% gel versus vehicle gel. Tolerability and safety were favorable.
Other Agents
Topical azelaic acid (20% cream formulation, 15% gel formulation) has been suggested as a treatment option for adult women with AV, including patients with darker skin who are more prone to persistent hyperpigmentation.29
Conclusion
Proper skin care is an important component in the management of AV in adult women. Data for topical therapies in this subpopulation are limited; however, post hoc analyses provide some information regarding their efficacy in treating mixed pattern AV. More well-designed studies are needed to better evaluate the use of topical agents in adult women with AV. Although most topical AV therapies appear to be safe for use during pregnancy when properly used and limited to facial application, their use in women of childbearing potential and during pregnancy warrants individual consideration; topical retinoids are best avoided during pregnancy, especially tazarotene, which is rated category X.44 In part 3 of this series, oral therapies used to treat AV in adult women will be discussed.
1. Thiboutot D, Del Rosso JQ. Acne vulgaris and the epidermal barrier: is acne vulgaris associated with inherent epidermal abnormalities that cause impairment of barrier functions? do any topical acne therapies alter the structural and/or functional integrity of the epidermal barrier? J Clin Aesthet Dermatol. 2013;6:18-24.
2. Subramanyan K. Role of mild cleansing in the management of patient skin. Dermatol Ther. 2004;17(suppl 1):26-34.
3. Del Rosso JQ, Gold M, Rueda MJ, et al. Efficacy, safety, and subject satisfaction of a specified skin care regimen to cleanse, medicate, moisturize, and protect the skin of patients under treatment for acne vulgaris. J Clin Aesthet Dermatol. 2015;8:22-30.
4. Del Rosso JQ, Brandt S. The role of skin care as an integral component in the management of acne vulgaris: part 2: tolerability and performance of a designated skin care regimen using a foam wash and moisturizer SPF 30 in patients with acne vulgaris undergoing active treatment. J Clin Aesthet Dermatol. 2013;6:28-36.
5. Draelos ZD. Facial cosmetics for acne patients. Cosmetics in Dermatology. 2nd ed. New York, NY: Churchill Livingstone Inc; 1995:22-23.
6. Leyden JJ, Del Rosso JQ, Baum EW. The use of isotretinoin in the treatment of acne vulgaris: clinical considerations and future directions. J Clin Aesthet Dermatol. 2014;7(suppl 2):S3-S21.
7. Hayashi N, Kawashima M. Study of the usefulness of moisturizers on adherence of acne patients treated with adapalene. J Dermatol. 2014;41:592-597.
8. Isoda K, Seki T, Inoue Y, et al. Efficacy of the combined use of a facial cleanser and moisturizers for the care of mild acne patients with sensitive skin. J Dermatol. 2015;42:181-188.
9. Hensley D, Meckfessel MH. Tolerability of a skin care regimen formulated for acne-prone skin in children. Pediatr Dermatol. 2015;32:501-505.
10. Tanghetti EA, Kawata AK, Daniels SR, et al. Understanding the burden of adult female acne. J Clin Aesthet Dermatol. 2014;7:22-30.
11. Del Rosso JQ, Kircik L, Gallagher CJ. Comparative efficacy and tolerability of dapsone 5% gel in adult versus adolescent females with acne vulgaris. J Clin Aesthet Dermatol. 2015;8:31-37.
12. Del Rosso JQ, Levin J. The clinical relevance of maintaining the functional integrity of the stratum corneum in both healthy and disease-affected skin. J Clin Aesthet Dermatol. 2011;4:22-42.
13. Levin J, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? J Clin Aesthet Dermatol. 2010;3:22-41.
14. Draelos ZD. Acne. In: Draelos ZD, ed. Cosmeceuticals. 2nd ed. Philadelphia, PA: Saunders-Elsevier; 2009:175-180.
15. Kircik LH, Gwazdauskas J, Butners V, et al. Evaluation of the efficacy, tolerability, and safety of an over-the-counter acne regimen containing benzoyl peroxide and salicylic acid in subjects with acne. J Drugs Dermatol. 2013;12:259-264.
16. Decker A, Graber EM. Over-the-counter acne treatments: a review. J Clin Aesthet Dermatol. 2012;5:32-40.
17. Layton AM, Henderson C, Cunliffe WJ. A clinical evaluation of acne scarring and its incidence. Clin Exp Dermatol. 1994;19:303-308.
18. Perkins AC, Maglione J, Hillebrand GG, et al. Acne vulgaris in women: prevalence across the life span. J Womens Health. 2012;21:223-230.
19. Poli F, Dreno B, Verschoore M. An epidemiological study of acne in female adults: results of a survey conducted in France. J Eur Acad Dermatol Venereol. 2001;15:541-545.
20. Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56-59.
21. Capitanio B, Sinagra JL, Bordignon V, et al. Underestimated clinical features of postadolescent acne. J Am Acad Dermatol. 2010;63:782-788.
22. Holzmann R, Shakery K. Postadolescent acne in females. Skin Pharmacol Physiol. 2014;27(suppl 1):3-8.
23. Williams C, Layton AM. Persistent acne in women: implications for the patient and for therapy. Am J Clin Dermatol. 2006;7:281-290.
24. Rendon MI, Rodriguez DA, Kawata AK, et al. Acne treatment patterns, expectations, and satisfaction among adult females of different races/ethnicities. Clin Cosmet Investig Dermatol. 2015;8:231-238.
25. Villasenor J, Berson DS, Kroshinsky D. Treatment guidelines in adult women. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:198-207.
26. Berson D, Alexis A. Adapalene 0.3% for the treatment of acne in women. J Clin Aesthet Dermatol. 2013;6:32-35.
27. Del Rosso JQ. Topical therapy for acne in women: is there a role for clindamycin phosphate–benzoyl peroxide gel? Cutis. 2014;94:177-182.
28. Zeichner JA. The efficacy and tolerability of a fixed combination (1.2%) and benzoyl peroxide (3.75%) aqueous gel in adult females with facial acne vulgaris. J Clin Aesthet Dermatol. 2015;8:21-25.
29. Fisk WA, Lev-Tov HA, Sivamani RK. Epidemiology and management of acne in adult women. Curr Derm Rep. 2014;3:29-39.
30. Stein-Gold L. Adapalene 0.1%-benzoyl peroxide 2.5% gel in adult female acne. Poster presented at: Winter Clinical Dermatology Conference; January 16–21, 2015; Maui, Hawaii.
31. Dréno B, Thiboutot D, Layton AM, et al. Large-scale international study enhances understanding of an emerging acne population: adult females. J Euro Acad Dermatol Venereol. 2015;29:1096-1106.
32. Dréno B, Layton AM, Zouboulis CC, et al. Adult female acne: a new paradigm. J Euro Acad Dermatol Venereol. 2013;27:1063-1070.
33. Shalita A, Weiss JS, Chalker DK, et al. A comparison of the efficacy and safety of adapalene gel 0.1% and tretinoin gel 0.025% in the treatment of acne vulgaris: a multicenter trial. J Am Acad Dermatol. 1996;34:482-485.
34. Pariser DM, Thiboutot DM, Clark SD, et al. The efficacy and safety of adapalene gel 0.3% in the treatment of acne vulgaris: a randomized, multicenter, investigator-blinded, controlled comparison study versus adapalene gel 0.1% and vehicle. Cutis. 2005;76:145-151.
35. Thiboutot D, Pariser DM, Egan N, et al. Adapalene gel 0.3% for the treatment of acne vulgaris: a multicenter, randomized, double-blind, controlled, phase III trial. J Am Acad Dermatol. 2006;54:242-250.
36. Tanghetti E, Dhawan S, Green L, et al. Randomized comparison of the safety and efficacy of tazarotene 0.1% cream and adapalene 0.3% gel in the treatment of patients with at least moderate facial acne vulgaris. J Drugs Dermatol. 2010;9:549-558.
37. Hui AM, Shalita AR. Topical retinoids. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:86-94.
38. Draelos Z, Carter E, Maloney JM, et al. Two randomized studies demonstrate the efficacy and safety of dapsone gel 5% for the treatment of acne vulgaris. J Am Acad Dermatol. 2007;56:439.e1-439.e10.
39. Tanghetti E, Harper JC, Oefelein MG. The efficacy and tolerability of dapsone 5% gel in female vs male patients with facial acne vulgaris: gender as a clinically relevant outcome variable. J Drugs Dermatol. 2012;11:1417-1421.
40. Pariser DM, Rich P, Cook-Bolden FE, et al. An aqueous gel fixed combination of clindamycin phosphate 1.2% and benzoyl peroxide 3.75% for the once-daily treatment of moderate to severe acne vulgaris. J Drugs Dermatol. 2014;13:1083-1089.
41. Harper JC. The efficacy and tolerability of a fixed combination clindamycin (1.2%) and benzoyl peroxide (3.75%) aqueous gel in patients with facial acne vulgaris: gender as a clinically relevant outcome variable. J Drugs Dermatol. 2015;14:381-384.
42. Zeichner JA. The efficacy and tolerability of a fixed combination clindamycin (1.2%) and benzoyl peroxide (3.75%) aqueous gel in adult female patients with facial acne vulgaris. J Clin Aesthet Dermatol. 2015;8:21-25.
43. Coley MK, Berson DS, Callendar VD. Overview of treatment principles for skin of color. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:70-85.
44. Ebede TL, Berson DS. Acne in pregnancy. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:177-181.
It seems intuitive that clinicians in dermatology would automatically recognize the importance of proper selection and integration of skin care products and techniques in the management of acne vulgaris (AV). However, an understanding of the fundamental importance of skin care in AV management and the scientific basis for maintaining epidermal barrier (EpB) function and repair cannot be assumed. In fact, there is limited scientific information about EpB dysfunction and AV or the adjunctive benefits of specific skin care products. However, some data have emerged that can be successfully applied by clinicians.1-9
In part 2 of this series, emphasis is placed on skin care and topical therapies for the treatment of AV in adult women. In addition to the plethora of cleanser and moisturizer formulations that exist in the marketplace, there are many over-the-counter (OTC) products marketed to treat AV that contain benzoyl peroxide (BP) and salicylic acid. Importantly, women tend to be selective about what they use to cleanse and moisturize their skin, and use of OTC products to treat AV is common among adult women.10,11
A thorough discussion of EpB impairment, related inflammatory cascades, and potential relevance to AV are beyond the scope of this article. In short, appropriate skin care products can reduce the inflammation and sensitivity associated with increased transepidermal water loss and reduced stratum corneum hydration and can mitigate EpB impairments induced by certain acne medications or vehicles.1,12 Available data support the adjunctive benefit of proper skin care in the management of AV by mitigating cutaneous irritation and potentially contributing to a reduction in AV lesions.2-4,7,13 Use of a formulation that also provides broad-spectrum photoprotection also is helpful.3,4
Another challenge is the myriad of cosmeceuticals that are heavily marketed to adult women with AV.13,14 Unfortunately, the scientific evidence supporting these products for treatment of AV is limited, resulting in the clinician’s inability to make specific recommendations. The core message is to incorporate skin care products that can reduce EpB impairment and mitigate cutaneous irritation associated with some AV therapies.1-4,7-9,12
OTC Topical Therapies
The marketplace is replete with several OTC products for treatment of AV, most of which contain BP and salicylic acid.15,16 There is a lack of efficacy data for OTC products for AV, including cleansers and topical medications, although some may be beneficial for milder cases. A variety of formulations are available to choose from, usually without the advice of a clinician. Additionally, heavy marketing is directed at adult women with AV, which may promote the use of therapies that may not be optimal for their respective AV severity or may cause facial skin irritation. Self-treatment may also cause delay in seeking dermatologic care, increasing the risk of persistent or permanent sequelae. Delay in adequate treatment is a major risk factor for the development of acne scars.17
Prescription Topical Therapies
Despite the high prevalence of AV in adult women, there is a paucity of studies evaluating topical therapies for AV in this subset.18-24 Reports in the literature on AV in adult women have focused on systemic hormonal agents (eg, oral contraceptives, spironolactone); however, more recent reports have addressed the use of topical therapies in this subpopulation.11,25-30 Published data on topical formulations are predominantly post hoc analyses from pivotal randomized controlled trials (RCTs) that included adolescents and adults of both genders with facial AV located above the jawline and predominantly moderate in severity.11,26,28,30 Participants in all of these studies presented with non-nodular, mixed inflammatory, and comedonal facial AV above the jawline, with inclusion criteria that required a minimum of 20 comedonal lesions and 20 papulopustular lesions at baseline. An important differentiating factor among these various post hoc analyses evaluating adult women versus adolescent girls with AV are the ages used to separate adults from adolescents. A dividing line of 18 years and older was used in some reports (eg, adapalene gel 0.3%, dapsone gel 5%), while other reports used 25 years and older to separate adolescent girls from adult women (ie, clindamycin phosphate [CP] 1.2%– BP 3.75% gel, adapalene 0.1%–BP 2.5% gel).11,26,28,30
Importantly, these studies included adult women with AV who presented with mixed comedonal and inflammatory AV (mixed pattern AV) similar to adolescents. None of the studies included women with a U-shaped AV pattern or lower facial AV characterized by deep inflammatory lesions that are often tender and few in number. Unfortunately, there is a lack of data evaluating topical therapies for these patterns of AV in adult women, including AV below the jawline and on the trunk. Although mixed pattern AV has been reported to affect 75% to 90% of adult women with AV, epidemiologic data quantifying the clinical AV patterns affecting adult women are limited.11,22,29,31,32 More well-designed studies are needed.
The treatment of AV in adult women may incorporate any of the topical therapies used to treat AV in adolescents, especially as studies encompass both the adolescent and adult age ranges. This is especially true with mixed pattern AV, which is the predominant presentation in participants enrolled in clinical trials with topical therapies, especially of moderate severity.
Herein we provide a summary of the topical therapies that have been evaluated by post hoc analyses of data from pivotal studies in adult women with AV.
Adapalene Gel 0.3%
Adapalene exhibits retinoid activity with efficacy in reducing inflammatory and comedonal AV lesions shown with both 0.1% and 0.3% concentrations.33-35 Post hoc analyses of 2 pivotal RCTs of patients with facial AV showed that adapalene gel 0.3% once daily (n=74; mean age, 27.2 years) was superior to vehicle once daily (n=43; mean age, 25.2 years) in both mean and median percentage reductions of comedonal, inflammatory, and total lesions in women 18 years and older who were treated for 12 weeks; the difference in mean percentage lesion reduction from vehicle for total AV lesions was statistically significant at 12 weeks (P=.045).26 Adapalene gel 0.3% produced a favorable skin tolerability profile similar to adapalene gel 0.1%, with the most common adverse reactions being discomfort and dryness.
Advantages of topical retinoid therapy in adult women with facial AV are reduction in postinflammatory hyperpigmentation and therapeutic modulation of chronic photodamage (eg, fine lines, rough texture, dyschromia).29,36,37 Disadvantages include signs and symptoms of cutaneous irritation, although this tends to occur less frequently on facial skin with adapalene gel 0.3% as compared to other topical retinoids that exhibit comparable efficacy.33-37 Topical retinoid therapy on the anterior neck and upper chest should be used cautiously, as these anatomic sites appear to be more prone to cutaneous irritation.
Dapsone Gel 5%
Dapsone is a sulfone antimicrobial and anti-inflammatory agent that has been shown to be effective, safe, and well tolerated in the treatment of AV in a topical 5% formulation.38,39 A post hoc analysis of pivotal 12-week trial data suggested that dapsone gel 5% twice daily produced greater AV reductions in females compared to males; no gender differences were noted in adverse effects, which were low in frequency.39 A separate subgroup analysis compared outcomes among adult women (≥18 years of age; n=434) and adolescent girls (12–17 years of age; n=347) treated with dapsone gel 5%.11 The proportion with no or minimal acne based on the Global Acne Assessment Score at week 12 was greater in adult women (53.5%) versus adolescent girls (45.3%, P=.022), with significantly greater percentage reductions in both noninflammatory (P<.0001) and total lesion counts (P=.0008) observed in the adult group. Percentage reductions in inflammatory lesions were similar in both groups. No major safety or tolerability issues or new safety signals were noted. Advantages of dapsone gel 5% are highly favorable tolerability and the perception of decreased oily skin in some participants.38,39
Clindamycin Phosphate 1.2%–Benzoyl Peroxide 3.75% Gel
The combination formulation of CP 1.2%– BP 3.75% gel applied once daily has been shown to be effective, well tolerated, and safe for the treatment of facial AV, with a gender analysis noting an apparent greater efficacy in females.40,41 A post hoc analysis from the 12-week pivotal study data in adult women aged 25 years and older showed a mean percentage change from baseline in inflammatory and noninflammatory lesion counts and the percentage of participants who achieved a 2-grade improvement by global assessment to be 68.7%, 60.4%, and 52.7% in actively treated participants (n=29), respectively, which was significantly superior to vehicle applied once daily (n=43; P=.019, P=.020, and P=.074, respectively).42 No relevant differences in tolerability were noted among treatment groups, and no participants discontinued therapy due to adverse events. Advantages of CP 1.2%–BP 3.75% gel are highly favorable skin tolerability and the perception of decreased oily skin in some participants.41-43
Adapalene 0.1%–Benzoyl Peroxide 2.5% Gel
A meta-analysis of pooled data from 3 RCTs evaluated use of adapalene 0.1%–BP 2.5% gel applied once daily in adult women aged 25 years and older with facial AV (n=130) versus vehicle gel applied once daily (n=124).30 The percentage of participants who achieved investigator global assessment ratings of clear or almost clear was 39.2% in actively treated participants versus 18.5% with vehicle (P<.001), and median percentage lesion reduction was approximately 30% greater in those treated with adapalene 0.1%–BP 2.5% gel versus vehicle gel. Tolerability and safety were favorable.
Other Agents
Topical azelaic acid (20% cream formulation, 15% gel formulation) has been suggested as a treatment option for adult women with AV, including patients with darker skin who are more prone to persistent hyperpigmentation.29
Conclusion
Proper skin care is an important component in the management of AV in adult women. Data for topical therapies in this subpopulation are limited; however, post hoc analyses provide some information regarding their efficacy in treating mixed pattern AV. More well-designed studies are needed to better evaluate the use of topical agents in adult women with AV. Although most topical AV therapies appear to be safe for use during pregnancy when properly used and limited to facial application, their use in women of childbearing potential and during pregnancy warrants individual consideration; topical retinoids are best avoided during pregnancy, especially tazarotene, which is rated category X.44 In part 3 of this series, oral therapies used to treat AV in adult women will be discussed.
It seems intuitive that clinicians in dermatology would automatically recognize the importance of proper selection and integration of skin care products and techniques in the management of acne vulgaris (AV). However, an understanding of the fundamental importance of skin care in AV management and the scientific basis for maintaining epidermal barrier (EpB) function and repair cannot be assumed. In fact, there is limited scientific information about EpB dysfunction and AV or the adjunctive benefits of specific skin care products. However, some data have emerged that can be successfully applied by clinicians.1-9
In part 2 of this series, emphasis is placed on skin care and topical therapies for the treatment of AV in adult women. In addition to the plethora of cleanser and moisturizer formulations that exist in the marketplace, there are many over-the-counter (OTC) products marketed to treat AV that contain benzoyl peroxide (BP) and salicylic acid. Importantly, women tend to be selective about what they use to cleanse and moisturize their skin, and use of OTC products to treat AV is common among adult women.10,11
A thorough discussion of EpB impairment, related inflammatory cascades, and potential relevance to AV are beyond the scope of this article. In short, appropriate skin care products can reduce the inflammation and sensitivity associated with increased transepidermal water loss and reduced stratum corneum hydration and can mitigate EpB impairments induced by certain acne medications or vehicles.1,12 Available data support the adjunctive benefit of proper skin care in the management of AV by mitigating cutaneous irritation and potentially contributing to a reduction in AV lesions.2-4,7,13 Use of a formulation that also provides broad-spectrum photoprotection also is helpful.3,4
Another challenge is the myriad of cosmeceuticals that are heavily marketed to adult women with AV.13,14 Unfortunately, the scientific evidence supporting these products for treatment of AV is limited, resulting in the clinician’s inability to make specific recommendations. The core message is to incorporate skin care products that can reduce EpB impairment and mitigate cutaneous irritation associated with some AV therapies.1-4,7-9,12
OTC Topical Therapies
The marketplace is replete with several OTC products for treatment of AV, most of which contain BP and salicylic acid.15,16 There is a lack of efficacy data for OTC products for AV, including cleansers and topical medications, although some may be beneficial for milder cases. A variety of formulations are available to choose from, usually without the advice of a clinician. Additionally, heavy marketing is directed at adult women with AV, which may promote the use of therapies that may not be optimal for their respective AV severity or may cause facial skin irritation. Self-treatment may also cause delay in seeking dermatologic care, increasing the risk of persistent or permanent sequelae. Delay in adequate treatment is a major risk factor for the development of acne scars.17
Prescription Topical Therapies
Despite the high prevalence of AV in adult women, there is a paucity of studies evaluating topical therapies for AV in this subset.18-24 Reports in the literature on AV in adult women have focused on systemic hormonal agents (eg, oral contraceptives, spironolactone); however, more recent reports have addressed the use of topical therapies in this subpopulation.11,25-30 Published data on topical formulations are predominantly post hoc analyses from pivotal randomized controlled trials (RCTs) that included adolescents and adults of both genders with facial AV located above the jawline and predominantly moderate in severity.11,26,28,30 Participants in all of these studies presented with non-nodular, mixed inflammatory, and comedonal facial AV above the jawline, with inclusion criteria that required a minimum of 20 comedonal lesions and 20 papulopustular lesions at baseline. An important differentiating factor among these various post hoc analyses evaluating adult women versus adolescent girls with AV are the ages used to separate adults from adolescents. A dividing line of 18 years and older was used in some reports (eg, adapalene gel 0.3%, dapsone gel 5%), while other reports used 25 years and older to separate adolescent girls from adult women (ie, clindamycin phosphate [CP] 1.2%– BP 3.75% gel, adapalene 0.1%–BP 2.5% gel).11,26,28,30
Importantly, these studies included adult women with AV who presented with mixed comedonal and inflammatory AV (mixed pattern AV) similar to adolescents. None of the studies included women with a U-shaped AV pattern or lower facial AV characterized by deep inflammatory lesions that are often tender and few in number. Unfortunately, there is a lack of data evaluating topical therapies for these patterns of AV in adult women, including AV below the jawline and on the trunk. Although mixed pattern AV has been reported to affect 75% to 90% of adult women with AV, epidemiologic data quantifying the clinical AV patterns affecting adult women are limited.11,22,29,31,32 More well-designed studies are needed.
The treatment of AV in adult women may incorporate any of the topical therapies used to treat AV in adolescents, especially as studies encompass both the adolescent and adult age ranges. This is especially true with mixed pattern AV, which is the predominant presentation in participants enrolled in clinical trials with topical therapies, especially of moderate severity.
Herein we provide a summary of the topical therapies that have been evaluated by post hoc analyses of data from pivotal studies in adult women with AV.
Adapalene Gel 0.3%
Adapalene exhibits retinoid activity with efficacy in reducing inflammatory and comedonal AV lesions shown with both 0.1% and 0.3% concentrations.33-35 Post hoc analyses of 2 pivotal RCTs of patients with facial AV showed that adapalene gel 0.3% once daily (n=74; mean age, 27.2 years) was superior to vehicle once daily (n=43; mean age, 25.2 years) in both mean and median percentage reductions of comedonal, inflammatory, and total lesions in women 18 years and older who were treated for 12 weeks; the difference in mean percentage lesion reduction from vehicle for total AV lesions was statistically significant at 12 weeks (P=.045).26 Adapalene gel 0.3% produced a favorable skin tolerability profile similar to adapalene gel 0.1%, with the most common adverse reactions being discomfort and dryness.
Advantages of topical retinoid therapy in adult women with facial AV are reduction in postinflammatory hyperpigmentation and therapeutic modulation of chronic photodamage (eg, fine lines, rough texture, dyschromia).29,36,37 Disadvantages include signs and symptoms of cutaneous irritation, although this tends to occur less frequently on facial skin with adapalene gel 0.3% as compared to other topical retinoids that exhibit comparable efficacy.33-37 Topical retinoid therapy on the anterior neck and upper chest should be used cautiously, as these anatomic sites appear to be more prone to cutaneous irritation.
Dapsone Gel 5%
Dapsone is a sulfone antimicrobial and anti-inflammatory agent that has been shown to be effective, safe, and well tolerated in the treatment of AV in a topical 5% formulation.38,39 A post hoc analysis of pivotal 12-week trial data suggested that dapsone gel 5% twice daily produced greater AV reductions in females compared to males; no gender differences were noted in adverse effects, which were low in frequency.39 A separate subgroup analysis compared outcomes among adult women (≥18 years of age; n=434) and adolescent girls (12–17 years of age; n=347) treated with dapsone gel 5%.11 The proportion with no or minimal acne based on the Global Acne Assessment Score at week 12 was greater in adult women (53.5%) versus adolescent girls (45.3%, P=.022), with significantly greater percentage reductions in both noninflammatory (P<.0001) and total lesion counts (P=.0008) observed in the adult group. Percentage reductions in inflammatory lesions were similar in both groups. No major safety or tolerability issues or new safety signals were noted. Advantages of dapsone gel 5% are highly favorable tolerability and the perception of decreased oily skin in some participants.38,39
Clindamycin Phosphate 1.2%–Benzoyl Peroxide 3.75% Gel
The combination formulation of CP 1.2%– BP 3.75% gel applied once daily has been shown to be effective, well tolerated, and safe for the treatment of facial AV, with a gender analysis noting an apparent greater efficacy in females.40,41 A post hoc analysis from the 12-week pivotal study data in adult women aged 25 years and older showed a mean percentage change from baseline in inflammatory and noninflammatory lesion counts and the percentage of participants who achieved a 2-grade improvement by global assessment to be 68.7%, 60.4%, and 52.7% in actively treated participants (n=29), respectively, which was significantly superior to vehicle applied once daily (n=43; P=.019, P=.020, and P=.074, respectively).42 No relevant differences in tolerability were noted among treatment groups, and no participants discontinued therapy due to adverse events. Advantages of CP 1.2%–BP 3.75% gel are highly favorable skin tolerability and the perception of decreased oily skin in some participants.41-43
Adapalene 0.1%–Benzoyl Peroxide 2.5% Gel
A meta-analysis of pooled data from 3 RCTs evaluated use of adapalene 0.1%–BP 2.5% gel applied once daily in adult women aged 25 years and older with facial AV (n=130) versus vehicle gel applied once daily (n=124).30 The percentage of participants who achieved investigator global assessment ratings of clear or almost clear was 39.2% in actively treated participants versus 18.5% with vehicle (P<.001), and median percentage lesion reduction was approximately 30% greater in those treated with adapalene 0.1%–BP 2.5% gel versus vehicle gel. Tolerability and safety were favorable.
Other Agents
Topical azelaic acid (20% cream formulation, 15% gel formulation) has been suggested as a treatment option for adult women with AV, including patients with darker skin who are more prone to persistent hyperpigmentation.29
Conclusion
Proper skin care is an important component in the management of AV in adult women. Data for topical therapies in this subpopulation are limited; however, post hoc analyses provide some information regarding their efficacy in treating mixed pattern AV. More well-designed studies are needed to better evaluate the use of topical agents in adult women with AV. Although most topical AV therapies appear to be safe for use during pregnancy when properly used and limited to facial application, their use in women of childbearing potential and during pregnancy warrants individual consideration; topical retinoids are best avoided during pregnancy, especially tazarotene, which is rated category X.44 In part 3 of this series, oral therapies used to treat AV in adult women will be discussed.
1. Thiboutot D, Del Rosso JQ. Acne vulgaris and the epidermal barrier: is acne vulgaris associated with inherent epidermal abnormalities that cause impairment of barrier functions? do any topical acne therapies alter the structural and/or functional integrity of the epidermal barrier? J Clin Aesthet Dermatol. 2013;6:18-24.
2. Subramanyan K. Role of mild cleansing in the management of patient skin. Dermatol Ther. 2004;17(suppl 1):26-34.
3. Del Rosso JQ, Gold M, Rueda MJ, et al. Efficacy, safety, and subject satisfaction of a specified skin care regimen to cleanse, medicate, moisturize, and protect the skin of patients under treatment for acne vulgaris. J Clin Aesthet Dermatol. 2015;8:22-30.
4. Del Rosso JQ, Brandt S. The role of skin care as an integral component in the management of acne vulgaris: part 2: tolerability and performance of a designated skin care regimen using a foam wash and moisturizer SPF 30 in patients with acne vulgaris undergoing active treatment. J Clin Aesthet Dermatol. 2013;6:28-36.
5. Draelos ZD. Facial cosmetics for acne patients. Cosmetics in Dermatology. 2nd ed. New York, NY: Churchill Livingstone Inc; 1995:22-23.
6. Leyden JJ, Del Rosso JQ, Baum EW. The use of isotretinoin in the treatment of acne vulgaris: clinical considerations and future directions. J Clin Aesthet Dermatol. 2014;7(suppl 2):S3-S21.
7. Hayashi N, Kawashima M. Study of the usefulness of moisturizers on adherence of acne patients treated with adapalene. J Dermatol. 2014;41:592-597.
8. Isoda K, Seki T, Inoue Y, et al. Efficacy of the combined use of a facial cleanser and moisturizers for the care of mild acne patients with sensitive skin. J Dermatol. 2015;42:181-188.
9. Hensley D, Meckfessel MH. Tolerability of a skin care regimen formulated for acne-prone skin in children. Pediatr Dermatol. 2015;32:501-505.
10. Tanghetti EA, Kawata AK, Daniels SR, et al. Understanding the burden of adult female acne. J Clin Aesthet Dermatol. 2014;7:22-30.
11. Del Rosso JQ, Kircik L, Gallagher CJ. Comparative efficacy and tolerability of dapsone 5% gel in adult versus adolescent females with acne vulgaris. J Clin Aesthet Dermatol. 2015;8:31-37.
12. Del Rosso JQ, Levin J. The clinical relevance of maintaining the functional integrity of the stratum corneum in both healthy and disease-affected skin. J Clin Aesthet Dermatol. 2011;4:22-42.
13. Levin J, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? J Clin Aesthet Dermatol. 2010;3:22-41.
14. Draelos ZD. Acne. In: Draelos ZD, ed. Cosmeceuticals. 2nd ed. Philadelphia, PA: Saunders-Elsevier; 2009:175-180.
15. Kircik LH, Gwazdauskas J, Butners V, et al. Evaluation of the efficacy, tolerability, and safety of an over-the-counter acne regimen containing benzoyl peroxide and salicylic acid in subjects with acne. J Drugs Dermatol. 2013;12:259-264.
16. Decker A, Graber EM. Over-the-counter acne treatments: a review. J Clin Aesthet Dermatol. 2012;5:32-40.
17. Layton AM, Henderson C, Cunliffe WJ. A clinical evaluation of acne scarring and its incidence. Clin Exp Dermatol. 1994;19:303-308.
18. Perkins AC, Maglione J, Hillebrand GG, et al. Acne vulgaris in women: prevalence across the life span. J Womens Health. 2012;21:223-230.
19. Poli F, Dreno B, Verschoore M. An epidemiological study of acne in female adults: results of a survey conducted in France. J Eur Acad Dermatol Venereol. 2001;15:541-545.
20. Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56-59.
21. Capitanio B, Sinagra JL, Bordignon V, et al. Underestimated clinical features of postadolescent acne. J Am Acad Dermatol. 2010;63:782-788.
22. Holzmann R, Shakery K. Postadolescent acne in females. Skin Pharmacol Physiol. 2014;27(suppl 1):3-8.
23. Williams C, Layton AM. Persistent acne in women: implications for the patient and for therapy. Am J Clin Dermatol. 2006;7:281-290.
24. Rendon MI, Rodriguez DA, Kawata AK, et al. Acne treatment patterns, expectations, and satisfaction among adult females of different races/ethnicities. Clin Cosmet Investig Dermatol. 2015;8:231-238.
25. Villasenor J, Berson DS, Kroshinsky D. Treatment guidelines in adult women. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:198-207.
26. Berson D, Alexis A. Adapalene 0.3% for the treatment of acne in women. J Clin Aesthet Dermatol. 2013;6:32-35.
27. Del Rosso JQ. Topical therapy for acne in women: is there a role for clindamycin phosphate–benzoyl peroxide gel? Cutis. 2014;94:177-182.
28. Zeichner JA. The efficacy and tolerability of a fixed combination (1.2%) and benzoyl peroxide (3.75%) aqueous gel in adult females with facial acne vulgaris. J Clin Aesthet Dermatol. 2015;8:21-25.
29. Fisk WA, Lev-Tov HA, Sivamani RK. Epidemiology and management of acne in adult women. Curr Derm Rep. 2014;3:29-39.
30. Stein-Gold L. Adapalene 0.1%-benzoyl peroxide 2.5% gel in adult female acne. Poster presented at: Winter Clinical Dermatology Conference; January 16–21, 2015; Maui, Hawaii.
31. Dréno B, Thiboutot D, Layton AM, et al. Large-scale international study enhances understanding of an emerging acne population: adult females. J Euro Acad Dermatol Venereol. 2015;29:1096-1106.
32. Dréno B, Layton AM, Zouboulis CC, et al. Adult female acne: a new paradigm. J Euro Acad Dermatol Venereol. 2013;27:1063-1070.
33. Shalita A, Weiss JS, Chalker DK, et al. A comparison of the efficacy and safety of adapalene gel 0.1% and tretinoin gel 0.025% in the treatment of acne vulgaris: a multicenter trial. J Am Acad Dermatol. 1996;34:482-485.
34. Pariser DM, Thiboutot DM, Clark SD, et al. The efficacy and safety of adapalene gel 0.3% in the treatment of acne vulgaris: a randomized, multicenter, investigator-blinded, controlled comparison study versus adapalene gel 0.1% and vehicle. Cutis. 2005;76:145-151.
35. Thiboutot D, Pariser DM, Egan N, et al. Adapalene gel 0.3% for the treatment of acne vulgaris: a multicenter, randomized, double-blind, controlled, phase III trial. J Am Acad Dermatol. 2006;54:242-250.
36. Tanghetti E, Dhawan S, Green L, et al. Randomized comparison of the safety and efficacy of tazarotene 0.1% cream and adapalene 0.3% gel in the treatment of patients with at least moderate facial acne vulgaris. J Drugs Dermatol. 2010;9:549-558.
37. Hui AM, Shalita AR. Topical retinoids. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:86-94.
38. Draelos Z, Carter E, Maloney JM, et al. Two randomized studies demonstrate the efficacy and safety of dapsone gel 5% for the treatment of acne vulgaris. J Am Acad Dermatol. 2007;56:439.e1-439.e10.
39. Tanghetti E, Harper JC, Oefelein MG. The efficacy and tolerability of dapsone 5% gel in female vs male patients with facial acne vulgaris: gender as a clinically relevant outcome variable. J Drugs Dermatol. 2012;11:1417-1421.
40. Pariser DM, Rich P, Cook-Bolden FE, et al. An aqueous gel fixed combination of clindamycin phosphate 1.2% and benzoyl peroxide 3.75% for the once-daily treatment of moderate to severe acne vulgaris. J Drugs Dermatol. 2014;13:1083-1089.
41. Harper JC. The efficacy and tolerability of a fixed combination clindamycin (1.2%) and benzoyl peroxide (3.75%) aqueous gel in patients with facial acne vulgaris: gender as a clinically relevant outcome variable. J Drugs Dermatol. 2015;14:381-384.
42. Zeichner JA. The efficacy and tolerability of a fixed combination clindamycin (1.2%) and benzoyl peroxide (3.75%) aqueous gel in adult female patients with facial acne vulgaris. J Clin Aesthet Dermatol. 2015;8:21-25.
43. Coley MK, Berson DS, Callendar VD. Overview of treatment principles for skin of color. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:70-85.
44. Ebede TL, Berson DS. Acne in pregnancy. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:177-181.
1. Thiboutot D, Del Rosso JQ. Acne vulgaris and the epidermal barrier: is acne vulgaris associated with inherent epidermal abnormalities that cause impairment of barrier functions? do any topical acne therapies alter the structural and/or functional integrity of the epidermal barrier? J Clin Aesthet Dermatol. 2013;6:18-24.
2. Subramanyan K. Role of mild cleansing in the management of patient skin. Dermatol Ther. 2004;17(suppl 1):26-34.
3. Del Rosso JQ, Gold M, Rueda MJ, et al. Efficacy, safety, and subject satisfaction of a specified skin care regimen to cleanse, medicate, moisturize, and protect the skin of patients under treatment for acne vulgaris. J Clin Aesthet Dermatol. 2015;8:22-30.
4. Del Rosso JQ, Brandt S. The role of skin care as an integral component in the management of acne vulgaris: part 2: tolerability and performance of a designated skin care regimen using a foam wash and moisturizer SPF 30 in patients with acne vulgaris undergoing active treatment. J Clin Aesthet Dermatol. 2013;6:28-36.
5. Draelos ZD. Facial cosmetics for acne patients. Cosmetics in Dermatology. 2nd ed. New York, NY: Churchill Livingstone Inc; 1995:22-23.
6. Leyden JJ, Del Rosso JQ, Baum EW. The use of isotretinoin in the treatment of acne vulgaris: clinical considerations and future directions. J Clin Aesthet Dermatol. 2014;7(suppl 2):S3-S21.
7. Hayashi N, Kawashima M. Study of the usefulness of moisturizers on adherence of acne patients treated with adapalene. J Dermatol. 2014;41:592-597.
8. Isoda K, Seki T, Inoue Y, et al. Efficacy of the combined use of a facial cleanser and moisturizers for the care of mild acne patients with sensitive skin. J Dermatol. 2015;42:181-188.
9. Hensley D, Meckfessel MH. Tolerability of a skin care regimen formulated for acne-prone skin in children. Pediatr Dermatol. 2015;32:501-505.
10. Tanghetti EA, Kawata AK, Daniels SR, et al. Understanding the burden of adult female acne. J Clin Aesthet Dermatol. 2014;7:22-30.
11. Del Rosso JQ, Kircik L, Gallagher CJ. Comparative efficacy and tolerability of dapsone 5% gel in adult versus adolescent females with acne vulgaris. J Clin Aesthet Dermatol. 2015;8:31-37.
12. Del Rosso JQ, Levin J. The clinical relevance of maintaining the functional integrity of the stratum corneum in both healthy and disease-affected skin. J Clin Aesthet Dermatol. 2011;4:22-42.
13. Levin J, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? J Clin Aesthet Dermatol. 2010;3:22-41.
14. Draelos ZD. Acne. In: Draelos ZD, ed. Cosmeceuticals. 2nd ed. Philadelphia, PA: Saunders-Elsevier; 2009:175-180.
15. Kircik LH, Gwazdauskas J, Butners V, et al. Evaluation of the efficacy, tolerability, and safety of an over-the-counter acne regimen containing benzoyl peroxide and salicylic acid in subjects with acne. J Drugs Dermatol. 2013;12:259-264.
16. Decker A, Graber EM. Over-the-counter acne treatments: a review. J Clin Aesthet Dermatol. 2012;5:32-40.
17. Layton AM, Henderson C, Cunliffe WJ. A clinical evaluation of acne scarring and its incidence. Clin Exp Dermatol. 1994;19:303-308.
18. Perkins AC, Maglione J, Hillebrand GG, et al. Acne vulgaris in women: prevalence across the life span. J Womens Health. 2012;21:223-230.
19. Poli F, Dreno B, Verschoore M. An epidemiological study of acne in female adults: results of a survey conducted in France. J Eur Acad Dermatol Venereol. 2001;15:541-545.
20. Collier CN, Harper JC, Cafardi JA, et al. The prevalence of acne in adults 20 years and older. J Am Acad Dermatol. 2008;58:56-59.
21. Capitanio B, Sinagra JL, Bordignon V, et al. Underestimated clinical features of postadolescent acne. J Am Acad Dermatol. 2010;63:782-788.
22. Holzmann R, Shakery K. Postadolescent acne in females. Skin Pharmacol Physiol. 2014;27(suppl 1):3-8.
23. Williams C, Layton AM. Persistent acne in women: implications for the patient and for therapy. Am J Clin Dermatol. 2006;7:281-290.
24. Rendon MI, Rodriguez DA, Kawata AK, et al. Acne treatment patterns, expectations, and satisfaction among adult females of different races/ethnicities. Clin Cosmet Investig Dermatol. 2015;8:231-238.
25. Villasenor J, Berson DS, Kroshinsky D. Treatment guidelines in adult women. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:198-207.
26. Berson D, Alexis A. Adapalene 0.3% for the treatment of acne in women. J Clin Aesthet Dermatol. 2013;6:32-35.
27. Del Rosso JQ. Topical therapy for acne in women: is there a role for clindamycin phosphate–benzoyl peroxide gel? Cutis. 2014;94:177-182.
28. Zeichner JA. The efficacy and tolerability of a fixed combination (1.2%) and benzoyl peroxide (3.75%) aqueous gel in adult females with facial acne vulgaris. J Clin Aesthet Dermatol. 2015;8:21-25.
29. Fisk WA, Lev-Tov HA, Sivamani RK. Epidemiology and management of acne in adult women. Curr Derm Rep. 2014;3:29-39.
30. Stein-Gold L. Adapalene 0.1%-benzoyl peroxide 2.5% gel in adult female acne. Poster presented at: Winter Clinical Dermatology Conference; January 16–21, 2015; Maui, Hawaii.
31. Dréno B, Thiboutot D, Layton AM, et al. Large-scale international study enhances understanding of an emerging acne population: adult females. J Euro Acad Dermatol Venereol. 2015;29:1096-1106.
32. Dréno B, Layton AM, Zouboulis CC, et al. Adult female acne: a new paradigm. J Euro Acad Dermatol Venereol. 2013;27:1063-1070.
33. Shalita A, Weiss JS, Chalker DK, et al. A comparison of the efficacy and safety of adapalene gel 0.1% and tretinoin gel 0.025% in the treatment of acne vulgaris: a multicenter trial. J Am Acad Dermatol. 1996;34:482-485.
34. Pariser DM, Thiboutot DM, Clark SD, et al. The efficacy and safety of adapalene gel 0.3% in the treatment of acne vulgaris: a randomized, multicenter, investigator-blinded, controlled comparison study versus adapalene gel 0.1% and vehicle. Cutis. 2005;76:145-151.
35. Thiboutot D, Pariser DM, Egan N, et al. Adapalene gel 0.3% for the treatment of acne vulgaris: a multicenter, randomized, double-blind, controlled, phase III trial. J Am Acad Dermatol. 2006;54:242-250.
36. Tanghetti E, Dhawan S, Green L, et al. Randomized comparison of the safety and efficacy of tazarotene 0.1% cream and adapalene 0.3% gel in the treatment of patients with at least moderate facial acne vulgaris. J Drugs Dermatol. 2010;9:549-558.
37. Hui AM, Shalita AR. Topical retinoids. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:86-94.
38. Draelos Z, Carter E, Maloney JM, et al. Two randomized studies demonstrate the efficacy and safety of dapsone gel 5% for the treatment of acne vulgaris. J Am Acad Dermatol. 2007;56:439.e1-439.e10.
39. Tanghetti E, Harper JC, Oefelein MG. The efficacy and tolerability of dapsone 5% gel in female vs male patients with facial acne vulgaris: gender as a clinically relevant outcome variable. J Drugs Dermatol. 2012;11:1417-1421.
40. Pariser DM, Rich P, Cook-Bolden FE, et al. An aqueous gel fixed combination of clindamycin phosphate 1.2% and benzoyl peroxide 3.75% for the once-daily treatment of moderate to severe acne vulgaris. J Drugs Dermatol. 2014;13:1083-1089.
41. Harper JC. The efficacy and tolerability of a fixed combination clindamycin (1.2%) and benzoyl peroxide (3.75%) aqueous gel in patients with facial acne vulgaris: gender as a clinically relevant outcome variable. J Drugs Dermatol. 2015;14:381-384.
42. Zeichner JA. The efficacy and tolerability of a fixed combination clindamycin (1.2%) and benzoyl peroxide (3.75%) aqueous gel in adult female patients with facial acne vulgaris. J Clin Aesthet Dermatol. 2015;8:21-25.
43. Coley MK, Berson DS, Callendar VD. Overview of treatment principles for skin of color. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:70-85.
44. Ebede TL, Berson DS. Acne in pregnancy. In: Shalita AR, Del Rosso JQ, Webster GF, eds. Acne Vulgaris. London, United Kingdom: Informa Healthcare; 2011:177-181.
Practice Points
- Data from randomized controlled clinical trials (RCTs) of topical agents used for the treatment of acne in adult women has been gleaned through subanalyses of larger pivotal studies with adapalene gel 0.3%, dapsone gel 5%, clindamycin phosphate 1.2%–benzoyl peroxide 3.75% gel, and adapalene 0.1%–benzoyl peroxide 2.5% gel.
- Efficacy and tolerability/safety results from RCTs of these topical agents evaluated outcomes for the clinical pattern of mixed inflammatory, comedonal, and non-nodular acne located on the face above the jawline margin.
- More data are needed on the treatment of acne in adult women with topical agents, systemic agents, and combination regimens, including results for the full spectrum of clinical presentations.

A Novel Cream Formulation Containing Nicotinamide 4%, Arbutin 3%, Bisabolol 1%, and Retinaldehyde 0.05% for Treatment of Epidermal Melasma
Epidermal melasma is a common hyperpigmentation disorder that can be challenging to treat. The pathogenesis of melasma is not fully understood but has been associated with increased melanin and melanocyte activity.1,2 Melasma is characterized by jagged, light- to dark-brown patches on areas of the skin most often exposed to the sun—primarily the cheeks, forehead, upper lip, nose, and chin.3 Although it can affect both sexes and all races, melasma is more common in Fitzpatrick skin types II to IV and frequently is seen in Asian or Hispanic women residing in geographic locations with high levels of sun exposure (eg, tropical areas).2 Melasma presents more frequently in adult women of childbearing age, especially during pregnancy, but also can begin postmenopause. Onset may occur as early as menarche but typically is observed between the ages of 30 and 55 years.3,4 Only 10% of melasma cases are known to occur in males4 and are influenced by such factors as ethnicity, hormones, and level of sun exposure.2
Topical therapies for melasma attempt to inhibit melanocytic activation at each level of melanin formation until the deposited pigment is removed; however, results may vary greatly, as melasma often recurs due to the migration of new melanocytes from hair follicles to the skin’s surface, leading to new development of hyperpigmentation. The current standard of treatment for melasma involves the use of hydroquinone and other bleaching agents, but long-term use of these treatments has been associated with concerns regarding unstable preparations (which may lose their therapeutic properties) and adverse effects (eg, ochronosis, depigmentation).5 Cosmetic agents that recently have been evaluated for melasma treatment include nicotinamide (a form of vitamin B3), which inhibits the transfer of melanosomes from melanocytes to keratinocytes; arbutin, which inhibits melanin synthesis by inhibiting tyrosinase activity6; bisabolol, which prevents anti-inflammatory activity7; and retinaldehyde (RAL), a precursor of retinoic acid (RA) that has powerful bleaching action and low levels of cutaneous irritability.8
This prospective, single-arm, open-label study, evaluated the efficacy and safety of a novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05% in the treatment of epidermal melasma.
Study Product Ingredients and Background
Nicotinamide
Nicotinamide is a water-soluble amide of nicotinic acid (niacin) and one of the 2 principal forms of vitamin B3. It is a component of the coenzymes nicotinamide adenine dinucleotide and nicotinamide adenine dinucleotide phosphate. Nicotinamide essentially acts as an antioxidant, with most of its effects exerted through poly(adenosine diphosphate–ribose) polymerase inhibition. Interest has increased in the role of nicotinamide in the prevention and treatment of several skin diseases, such as acne and UV radiation–induced deleterious molecular and immunological events. Nicotinamide also has gained consideration as a potential agent in sunscreen preparations due to its possible skin-lightening effects, stimulation of DNA repair, suppression of UV photocarcinogenesis, and other antiaging effects.9
Arbutin
Arbutin is a molecule that has proven effective in treating melasma.10 Its pigment-lightening ingredients include botanicals that are structurally similar to hydroquinone. Arbutin is obtained from the leaves of the bearberry plant but also is found in lesser quantities in cranberry and blueberry leaves. A naturally occurring gluconopyranoside, arbutin reduces tyrosinase activity without affecting messenger RNA expression.11 Arbutin also inhibits melanosome maturation, is nontoxic to melanocytes, and is used in Japan in a variety of pigment-lightening preparations at 3% concentrations.12
Bisabolol
Bisabolol is a natural monocyclic sesquiterpene alcohol found in the oils of chamomile and other plants. Bisabolol often is included in cosmetics due to its favorable anti-inflammatory and depigmentation properties. Its downregulation of inducible nitric oxide synthase and cyclooxygenase-2 suggests that it may have anti-inflammatory effects.7
Retinaldehyde
Retinaldehyde is an RA precursor that forms as an intermediate metabolite in the transformation of retinol to RA in human keratinocytes. Topical RAL is well tolerated by human skin, and several of its biologic effects are identical to those of RA. Using the tails of C57BL/6 mouse models, RAL 0.05% has been found to have significantly more potent depigmenting effects than RA 0.05% (P<.001 vs P<.01, respectively) when compared to vehicle.13
Although combination therapy with RAL and arbutin could potentially cause skin irritation, the addition of bisabolol to the combination cream used in this study is believed to have conferred anti-inflammatory properties because it inhibits the release of histamine and relieves irritation.
Methods
This single-center, single-arm, prospective, open-label study evaluated the efficacy and safety of a novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05% in treating epidermal melasma. Clinical evaluation included assessment of Melasma Area and Severity Index (MASI) score, photographic analysis, and in vivo reflectance confocal microscopy (RCM) analysis.
The study population included women aged 18 to 50 years with Fitzpatrick skin types I through V who had clinically diagnosed epidermal melasma on the face. Eligibility requirements included confirmation of epidermal pigmentation on Wood lamp examination and RCM analysis and a MASI score of less than 10.5. A total of 35 participants were enrolled in the study (intention to treat [ITT] population). Thirty-three participants were included in the analysis of treatment effectiveness (ITTe population), as 2 were excluded due to lack of follow-up postbaseline. Four participants were prematurely withdrawn from the study—3 due to loss to follow-up and 1 due to treatment discontinuation following an adverse event (AE). The last observation carried forward method was used to input missing data from these 4 participants excluding repeated measure analysis that used the generalized estimated equation method.
At baseline, a 25-g tube of the study cream containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05% was distributed to all participants for once-daily application to the entire face for 30 days. Participants were instructed to apply the product in the evening after using a gentle cleanser, which also was to be used in the morning to remove the product residue. Additionally, participants were given a sunscreen with a sun protection factor of 30 to apply daily on the entire face in the morning, after lunch, and midafternoon. During the 30-day treatment period, treatment interruption of up to 5 consecutive days or 10 nonconsecutive days in total was permitted. At day 30, participants received another 30-day supply of the study product and sunscreen to be applied according to the same regimen for an additional 30-day treatment period.
Clinical Evaluation
At baseline, demographic data and medical history was recorded for all participants and dermatologic and physical examination was performed documenting weight, height, blood pressure, heart rate, and baseline MASI score. Following Wood lamp examination, participants’ faces were photographed and catalogued using medical imaging software that allowed for measurement of the total melasma surface area (Figure 1A). The photographs also were cross-polarized for further analysis of the pigmentation (Figure 1B).
| 
| |
Figure 1. Clinical (A) and cross-polarized (B) photographs of a patient before treatment with the novel compound containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05%. | ||
A questionnaire evaluating treatment satisfaction was administered to participants (ITTe population [n=33]) at baseline and days 30 and 60. Questionnaire items pertained to skin blemishes, signs of facial aging, overall appearance, texture, oiliness, brightness, and hydration. Participants were instructed to rate their satisfaction for each item on a scale of 1 to 10 (1=bad, 10=excellent). For investigator analysis, scores of 1 to 4 were classified as “dissatisfied,” scores of 5 to 6 were classified as “satisfied,” and scores of 7 to 10 were classified as “completely satisfied.” A questionnaire evaluating product appreciation was administered at day 60 to participants who completed the study (n=29). Questionnaire items asked participants to rate the study cream’s ease of application, consistency, smell, absorption, and overall satisfaction using ratings of “bad,” “regular,” “good,” “very good,” or “excellent.”
Treatment efficacy in all participants was assessed by the investigators at days 30 and 60. Investigators evaluated reductions in pigmentation and total melasma surface area using ratings of “none,” “regular,” “good,” “very good,” or “excellent.” Local tolerance also was evaluated at both time points, and AEs were recorded and analyzed with respect to their duration, intensity, frequency, and severity.
Targeted hyperpigmented skin was selected for in vivo RCM analysis. At each time point, a sequence of block images was acquired at 4 levels of skin: (1) superficial dermis, (2) suprabasal layer/ dermoepidermal junction, (3) spinous layer, and (4) superficial granular layer. Blind evaluation of these images to assess the reduction in melanin quantity was conducted by a dermatopathologist at baseline and days 30 and 60. Melanin quantity present in each layer was graded according to 4 categories (0%–25%, 25.1%–50%, 50.1%–75%, 75.1%–100%). The mean value was used for statistical evaluation.
Results
Efficacy evaluation
The primary efficacy variable was the mean reduction in MASI score from baseline to the end of treatment (day 60), which was 2.25 ± 1.87 (P<.0001). The reduction in mean MASI score was significant from baseline to day 30 (P<.0001) and from day 30 to day 60 (P<.0001). The least root-mean-square error estimates of MASI score variation at days 30 and 60 were 1.40 and 2.25, respectively.
The mean total melasma surface area (as measured in analysis of clinical photographs using medical imaging software) was significantly reduced from 1398.5 mm2 at baseline to 1116.9 mm2 at day 30 (P<.0001) and 923.4 at day 60 (P<.0001). From baseline to end of treatment, the overall reduction in mean total melasma surface area was 475.1 mm2 (P<.0001)(Figure 2). Clinical and cross-polarized photographs taken at day 60 demonstrated a visible reduction in melasma surface area (Figure 3), which was confirmed using medical imaging software.
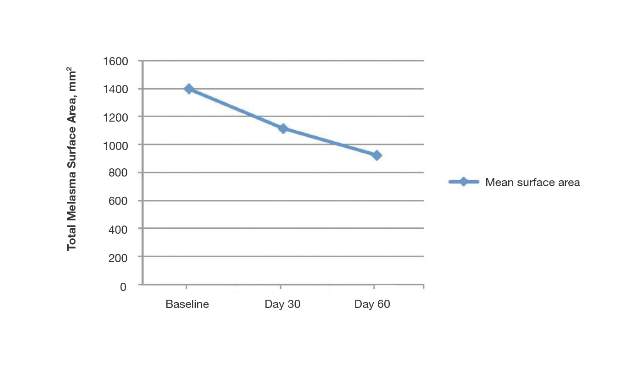

| 
| |
Figure 3. Clinical (A) and cross-polarized (B) photographs of a patient after 60 days of treatment with the novel compound containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05%. | ||
In vivo RCM analyses at each time point showed reduction in pigmentation in the 4 levels of the skin that were evaluated, but the results were not statistically significant.
Participant satisfaction
There was strong statistical evidence of patient satisfaction with the treatment results at the end of the study period (P<.0001). At baseline, 75.8% (25/33) of participants were dissatisfied with the appearance of their skin as compared with 15.2% (5/33) at day 60. Additionally, 18.1% (6/33) and 6.1% (2/33) of the participants were satisfied and completely satisfied at baseline compared with 33.3% (11/33) and 51.5% (17/33) at day 60, respectively. Participant satisfaction with signs of facial aging also increased over the study period (P=.0104). At baseline, 60.6% (20/33) were dissatisfied, 12.1% (4/33) were satisfied, and 27.3% (9/33) were completely satisfied; at the end of treatment, 30.3% (10/33) were dissatisfied, 36.4% (12/33) were satisfied, and 33.3% (11/33) were completely satisfied with the improvement in signs of facial aging.
Increased patient satisfaction with facial skin texture at baseline compared to day 60 also was statistically significant (P=.0157). At baseline, 39.4% (13/33) of the participants were dissatisfied, 30.3% (10/33) were satisfied, and 30.3% (10/33) were completely satisfied with facial texture; at day 60, 15.1% (5/33) were dissatisfied, 30.3% (10/33) were satisfied, and 54.6% (18/33) were completely satisfied. Significant improvement from baseline to day 60 also was observed in participant assessment of skin oiliness (P=.0210), brightness (P=.0003), overall appearance (P<.0001), and hydration (P<.0001).
Product appreciation
At day 60, 89.7% (26/29) of the participants who completed the study rated the product’s ease of application as being at least “good,” with more than half of participants (55.2% [16/29]) rating it as “very good” or “excellent.” Overall satisfaction with the product was rated as “very good” or “excellent” by 48.3% (14/29) of the participants. Similar results were observed in participant assessments of consistency, smell, and absorption (Figure 4).

Safety evaluation
A total of 52 AEs were observed in 23 (69.7%) participants, which were recorded by participants in diary entries throughout treatment and evaluated by investigators at each time point. Among these AEs, 48 (92.3%) were considered possibly, probably, or conditionally related to treatment by the investigators based on clinical observation. The most common presumed treatment-related AE was a burning sensation on the skin, reported by 30.3% (10/33) of the participants at day 30 and 13.8% (4/29) at day 60. Of the reported AEs related to treatment, 91.7% (44/48) were of mild intensity and 93.8% (45/48) required no treatment or other action. There were no reported serious AEs related to the investigational product. Blood pressure, heart rate, and weight remained stable among all participants throughout the study.
The intensity of the AEs was described as “light” in 91.7% (44/48) of cases and “moderate” in 8.3% (4/48) of cases. The frequency of AEs was classified as “unique,” “intermittent,” or “continuous” in 45.8% (22/48), 39.6% (19/48), and14.6% (7/48) of cases, respectively. Of the 48 AEs, 3 (6.3%) occurred in 1 participant, necessitating interruption of treatment, application of the topical corticosteroid cream mometasone, and removal from the study.
Comment
Following treatment with the study cream containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05%, the mean reduction in MASI score (P<.0001) and the mean reduction in total melasma surface area from baseline to end of treatment were statistically significant (P<.0001). The study product was associated with strong statistical evidence of patient satisfaction (P<.0001) regarding improvement in facial skin texture, skin oiliness, brightness, overall appearance, and hydration. Participants also responded favorably to the product and considered it safe and effective. In vivo RCM analysis demonstrated a reduction in the amount of melanin in 4 levels of the skin (superficial dermis, suprabasal layer/dermoepidermal junction, spinous layer, superficial granular layer) following treatment with the study cream; however, over the course of the 60-day treatment period, it did not reveal statistically significant reductions. This finding likely is due to the large ranges used to classify the amount of melanin present in each layer of the skin. These limitations suggest that scales used in future in vivo RCM analyses of melasma should be narrower.
Epidermal melasma is one of the most difficult dermatologic diseases to treat and control. Maintenance of clear, undamaged skin remains a treatment target for all dermatologists. This novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05% has proven to be an effective, safe, and tolerable treatment option for patients with epidermal melasma.
1. Grimes PE, Yamada N, Bhawan J. Light microscopic, immunohistochemical, and ultrastructural alterations in patients with melasma. Am J Dermatopathol. 2005;27:96-101.
2. Kang WH, Yoon KH, Lee ES, et al. Melasma: histopathological characteristics in 56 Korean patients. Br J Dermatol. 2002;146:228-237.
3. Cestari T, Arellano I, Hexsel D, et al. Melasma in Latin America: options the therapy and treatment algorithm. JEADV. 2009;23:760-772.
4. Miot LDB, Miot HA, Silva MG, et al. Fisiopatologia do Melasma. An Bras Dermatol. 2009;84:623-635.
5. Draelos Z. Skin lightening preparations and the hydroquinone controversy. Dermatol Ther. 2007;20:308-313.
6. Parvez S, Kang M, Chung HS, et al. Survey and mechanism of skin depigmenting and lightening agents. Phytoter Res. 2006;20:921-934.
7. Kim S, Jung E, Kim JH, et al. Inhibitory effects of (-)-α-bisabolol on LPS-induced inflammatory response in RAW264.7 macrophages. Food Chem Toxicol. 2011;49:2580-2585.
8. Ortonne JP. Retinoid therapy of pigmentary disorders. Dermatol Ther. 2006;19:280-288.
9. Namazi MR. Nicotinamide-containing sunscreens for use in Australasian countries and cancer-provoking conditions. Med Hypotheses. 2003;60:544-545.
10. Ertam I, Mutlu B, Unal I, et al. Efficiency of ellagic acid and arbutin in melasma: a randomized, prospective, open-label study. J Dermatol. 2008;35:570-574.
11. Hori I, Nihei K, Kubo I. Structural criteria for depigmenting mechanism of arbutin. Phytother Res. 2004;18:475-469.
12. Ethnic skin and pigmentation. In: Draelos ZD. Cosmetics and Dermatologic Problems and Solutions. 3rd ed. Boca Raton, FL: CRC Press; 2011:52-55.
13. Kasraee B, Tran C, Sorg O, et al. The depigmenting effect of RALGA in C57BL/6 mice. Dermatology. 2005;210(suppl 1):30-34.
Epidermal melasma is a common hyperpigmentation disorder that can be challenging to treat. The pathogenesis of melasma is not fully understood but has been associated with increased melanin and melanocyte activity.1,2 Melasma is characterized by jagged, light- to dark-brown patches on areas of the skin most often exposed to the sun—primarily the cheeks, forehead, upper lip, nose, and chin.3 Although it can affect both sexes and all races, melasma is more common in Fitzpatrick skin types II to IV and frequently is seen in Asian or Hispanic women residing in geographic locations with high levels of sun exposure (eg, tropical areas).2 Melasma presents more frequently in adult women of childbearing age, especially during pregnancy, but also can begin postmenopause. Onset may occur as early as menarche but typically is observed between the ages of 30 and 55 years.3,4 Only 10% of melasma cases are known to occur in males4 and are influenced by such factors as ethnicity, hormones, and level of sun exposure.2
Topical therapies for melasma attempt to inhibit melanocytic activation at each level of melanin formation until the deposited pigment is removed; however, results may vary greatly, as melasma often recurs due to the migration of new melanocytes from hair follicles to the skin’s surface, leading to new development of hyperpigmentation. The current standard of treatment for melasma involves the use of hydroquinone and other bleaching agents, but long-term use of these treatments has been associated with concerns regarding unstable preparations (which may lose their therapeutic properties) and adverse effects (eg, ochronosis, depigmentation).5 Cosmetic agents that recently have been evaluated for melasma treatment include nicotinamide (a form of vitamin B3), which inhibits the transfer of melanosomes from melanocytes to keratinocytes; arbutin, which inhibits melanin synthesis by inhibiting tyrosinase activity6; bisabolol, which prevents anti-inflammatory activity7; and retinaldehyde (RAL), a precursor of retinoic acid (RA) that has powerful bleaching action and low levels of cutaneous irritability.8
This prospective, single-arm, open-label study, evaluated the efficacy and safety of a novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05% in the treatment of epidermal melasma.
Study Product Ingredients and Background
Nicotinamide
Nicotinamide is a water-soluble amide of nicotinic acid (niacin) and one of the 2 principal forms of vitamin B3. It is a component of the coenzymes nicotinamide adenine dinucleotide and nicotinamide adenine dinucleotide phosphate. Nicotinamide essentially acts as an antioxidant, with most of its effects exerted through poly(adenosine diphosphate–ribose) polymerase inhibition. Interest has increased in the role of nicotinamide in the prevention and treatment of several skin diseases, such as acne and UV radiation–induced deleterious molecular and immunological events. Nicotinamide also has gained consideration as a potential agent in sunscreen preparations due to its possible skin-lightening effects, stimulation of DNA repair, suppression of UV photocarcinogenesis, and other antiaging effects.9
Arbutin
Arbutin is a molecule that has proven effective in treating melasma.10 Its pigment-lightening ingredients include botanicals that are structurally similar to hydroquinone. Arbutin is obtained from the leaves of the bearberry plant but also is found in lesser quantities in cranberry and blueberry leaves. A naturally occurring gluconopyranoside, arbutin reduces tyrosinase activity without affecting messenger RNA expression.11 Arbutin also inhibits melanosome maturation, is nontoxic to melanocytes, and is used in Japan in a variety of pigment-lightening preparations at 3% concentrations.12
Bisabolol
Bisabolol is a natural monocyclic sesquiterpene alcohol found in the oils of chamomile and other plants. Bisabolol often is included in cosmetics due to its favorable anti-inflammatory and depigmentation properties. Its downregulation of inducible nitric oxide synthase and cyclooxygenase-2 suggests that it may have anti-inflammatory effects.7
Retinaldehyde
Retinaldehyde is an RA precursor that forms as an intermediate metabolite in the transformation of retinol to RA in human keratinocytes. Topical RAL is well tolerated by human skin, and several of its biologic effects are identical to those of RA. Using the tails of C57BL/6 mouse models, RAL 0.05% has been found to have significantly more potent depigmenting effects than RA 0.05% (P<.001 vs P<.01, respectively) when compared to vehicle.13
Although combination therapy with RAL and arbutin could potentially cause skin irritation, the addition of bisabolol to the combination cream used in this study is believed to have conferred anti-inflammatory properties because it inhibits the release of histamine and relieves irritation.
Methods
This single-center, single-arm, prospective, open-label study evaluated the efficacy and safety of a novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05% in treating epidermal melasma. Clinical evaluation included assessment of Melasma Area and Severity Index (MASI) score, photographic analysis, and in vivo reflectance confocal microscopy (RCM) analysis.
The study population included women aged 18 to 50 years with Fitzpatrick skin types I through V who had clinically diagnosed epidermal melasma on the face. Eligibility requirements included confirmation of epidermal pigmentation on Wood lamp examination and RCM analysis and a MASI score of less than 10.5. A total of 35 participants were enrolled in the study (intention to treat [ITT] population). Thirty-three participants were included in the analysis of treatment effectiveness (ITTe population), as 2 were excluded due to lack of follow-up postbaseline. Four participants were prematurely withdrawn from the study—3 due to loss to follow-up and 1 due to treatment discontinuation following an adverse event (AE). The last observation carried forward method was used to input missing data from these 4 participants excluding repeated measure analysis that used the generalized estimated equation method.
At baseline, a 25-g tube of the study cream containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05% was distributed to all participants for once-daily application to the entire face for 30 days. Participants were instructed to apply the product in the evening after using a gentle cleanser, which also was to be used in the morning to remove the product residue. Additionally, participants were given a sunscreen with a sun protection factor of 30 to apply daily on the entire face in the morning, after lunch, and midafternoon. During the 30-day treatment period, treatment interruption of up to 5 consecutive days or 10 nonconsecutive days in total was permitted. At day 30, participants received another 30-day supply of the study product and sunscreen to be applied according to the same regimen for an additional 30-day treatment period.
Clinical Evaluation
At baseline, demographic data and medical history was recorded for all participants and dermatologic and physical examination was performed documenting weight, height, blood pressure, heart rate, and baseline MASI score. Following Wood lamp examination, participants’ faces were photographed and catalogued using medical imaging software that allowed for measurement of the total melasma surface area (Figure 1A). The photographs also were cross-polarized for further analysis of the pigmentation (Figure 1B).
|
|
| |
Figure 1. Clinical (A) and cross-polarized (B) photographs of a patient before treatment with the novel compound containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05%. | ||
A questionnaire evaluating treatment satisfaction was administered to participants (ITTe population [n=33]) at baseline and days 30 and 60. Questionnaire items pertained to skin blemishes, signs of facial aging, overall appearance, texture, oiliness, brightness, and hydration. Participants were instructed to rate their satisfaction for each item on a scale of 1 to 10 (1=bad, 10=excellent). For investigator analysis, scores of 1 to 4 were classified as “dissatisfied,” scores of 5 to 6 were classified as “satisfied,” and scores of 7 to 10 were classified as “completely satisfied.” A questionnaire evaluating product appreciation was administered at day 60 to participants who completed the study (n=29). Questionnaire items asked participants to rate the study cream’s ease of application, consistency, smell, absorption, and overall satisfaction using ratings of “bad,” “regular,” “good,” “very good,” or “excellent.”
Treatment efficacy in all participants was assessed by the investigators at days 30 and 60. Investigators evaluated reductions in pigmentation and total melasma surface area using ratings of “none,” “regular,” “good,” “very good,” or “excellent.” Local tolerance also was evaluated at both time points, and AEs were recorded and analyzed with respect to their duration, intensity, frequency, and severity.
Targeted hyperpigmented skin was selected for in vivo RCM analysis. At each time point, a sequence of block images was acquired at 4 levels of skin: (1) superficial dermis, (2) suprabasal layer/ dermoepidermal junction, (3) spinous layer, and (4) superficial granular layer. Blind evaluation of these images to assess the reduction in melanin quantity was conducted by a dermatopathologist at baseline and days 30 and 60. Melanin quantity present in each layer was graded according to 4 categories (0%–25%, 25.1%–50%, 50.1%–75%, 75.1%–100%). The mean value was used for statistical evaluation.
Results
Efficacy evaluation
The primary efficacy variable was the mean reduction in MASI score from baseline to the end of treatment (day 60), which was 2.25 ± 1.87 (P<.0001). The reduction in mean MASI score was significant from baseline to day 30 (P<.0001) and from day 30 to day 60 (P<.0001). The least root-mean-square error estimates of MASI score variation at days 30 and 60 were 1.40 and 2.25, respectively.
The mean total melasma surface area (as measured in analysis of clinical photographs using medical imaging software) was significantly reduced from 1398.5 mm2 at baseline to 1116.9 mm2 at day 30 (P<.0001) and 923.4 at day 60 (P<.0001). From baseline to end of treatment, the overall reduction in mean total melasma surface area was 475.1 mm2 (P<.0001)(Figure 2). Clinical and cross-polarized photographs taken at day 60 demonstrated a visible reduction in melasma surface area (Figure 3), which was confirmed using medical imaging software.
|
|
| |
Figure 3. Clinical (A) and cross-polarized (B) photographs of a patient after 60 days of treatment with the novel compound containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05%. | ||
In vivo RCM analyses at each time point showed reduction in pigmentation in the 4 levels of the skin that were evaluated, but the results were not statistically significant.
Participant satisfaction
There was strong statistical evidence of patient satisfaction with the treatment results at the end of the study period (P<.0001). At baseline, 75.8% (25/33) of participants were dissatisfied with the appearance of their skin as compared with 15.2% (5/33) at day 60. Additionally, 18.1% (6/33) and 6.1% (2/33) of the participants were satisfied and completely satisfied at baseline compared with 33.3% (11/33) and 51.5% (17/33) at day 60, respectively. Participant satisfaction with signs of facial aging also increased over the study period (P=.0104). At baseline, 60.6% (20/33) were dissatisfied, 12.1% (4/33) were satisfied, and 27.3% (9/33) were completely satisfied; at the end of treatment, 30.3% (10/33) were dissatisfied, 36.4% (12/33) were satisfied, and 33.3% (11/33) were completely satisfied with the improvement in signs of facial aging.
Increased patient satisfaction with facial skin texture at baseline compared to day 60 also was statistically significant (P=.0157). At baseline, 39.4% (13/33) of the participants were dissatisfied, 30.3% (10/33) were satisfied, and 30.3% (10/33) were completely satisfied with facial texture; at day 60, 15.1% (5/33) were dissatisfied, 30.3% (10/33) were satisfied, and 54.6% (18/33) were completely satisfied. Significant improvement from baseline to day 60 also was observed in participant assessment of skin oiliness (P=.0210), brightness (P=.0003), overall appearance (P<.0001), and hydration (P<.0001).
Product appreciation
At day 60, 89.7% (26/29) of the participants who completed the study rated the product’s ease of application as being at least “good,” with more than half of participants (55.2% [16/29]) rating it as “very good” or “excellent.” Overall satisfaction with the product was rated as “very good” or “excellent” by 48.3% (14/29) of the participants. Similar results were observed in participant assessments of consistency, smell, and absorption (Figure 4).
Safety evaluation
A total of 52 AEs were observed in 23 (69.7%) participants, which were recorded by participants in diary entries throughout treatment and evaluated by investigators at each time point. Among these AEs, 48 (92.3%) were considered possibly, probably, or conditionally related to treatment by the investigators based on clinical observation. The most common presumed treatment-related AE was a burning sensation on the skin, reported by 30.3% (10/33) of the participants at day 30 and 13.8% (4/29) at day 60. Of the reported AEs related to treatment, 91.7% (44/48) were of mild intensity and 93.8% (45/48) required no treatment or other action. There were no reported serious AEs related to the investigational product. Blood pressure, heart rate, and weight remained stable among all participants throughout the study.
The intensity of the AEs was described as “light” in 91.7% (44/48) of cases and “moderate” in 8.3% (4/48) of cases. The frequency of AEs was classified as “unique,” “intermittent,” or “continuous” in 45.8% (22/48), 39.6% (19/48), and14.6% (7/48) of cases, respectively. Of the 48 AEs, 3 (6.3%) occurred in 1 participant, necessitating interruption of treatment, application of the topical corticosteroid cream mometasone, and removal from the study.
Comment
Following treatment with the study cream containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05%, the mean reduction in MASI score (P<.0001) and the mean reduction in total melasma surface area from baseline to end of treatment were statistically significant (P<.0001). The study product was associated with strong statistical evidence of patient satisfaction (P<.0001) regarding improvement in facial skin texture, skin oiliness, brightness, overall appearance, and hydration. Participants also responded favorably to the product and considered it safe and effective. In vivo RCM analysis demonstrated a reduction in the amount of melanin in 4 levels of the skin (superficial dermis, suprabasal layer/dermoepidermal junction, spinous layer, superficial granular layer) following treatment with the study cream; however, over the course of the 60-day treatment period, it did not reveal statistically significant reductions. This finding likely is due to the large ranges used to classify the amount of melanin present in each layer of the skin. These limitations suggest that scales used in future in vivo RCM analyses of melasma should be narrower.
Epidermal melasma is one of the most difficult dermatologic diseases to treat and control. Maintenance of clear, undamaged skin remains a treatment target for all dermatologists. This novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05% has proven to be an effective, safe, and tolerable treatment option for patients with epidermal melasma.
Epidermal melasma is a common hyperpigmentation disorder that can be challenging to treat. The pathogenesis of melasma is not fully understood but has been associated with increased melanin and melanocyte activity.1,2 Melasma is characterized by jagged, light- to dark-brown patches on areas of the skin most often exposed to the sun—primarily the cheeks, forehead, upper lip, nose, and chin.3 Although it can affect both sexes and all races, melasma is more common in Fitzpatrick skin types II to IV and frequently is seen in Asian or Hispanic women residing in geographic locations with high levels of sun exposure (eg, tropical areas).2 Melasma presents more frequently in adult women of childbearing age, especially during pregnancy, but also can begin postmenopause. Onset may occur as early as menarche but typically is observed between the ages of 30 and 55 years.3,4 Only 10% of melasma cases are known to occur in males4 and are influenced by such factors as ethnicity, hormones, and level of sun exposure.2
Topical therapies for melasma attempt to inhibit melanocytic activation at each level of melanin formation until the deposited pigment is removed; however, results may vary greatly, as melasma often recurs due to the migration of new melanocytes from hair follicles to the skin’s surface, leading to new development of hyperpigmentation. The current standard of treatment for melasma involves the use of hydroquinone and other bleaching agents, but long-term use of these treatments has been associated with concerns regarding unstable preparations (which may lose their therapeutic properties) and adverse effects (eg, ochronosis, depigmentation).5 Cosmetic agents that recently have been evaluated for melasma treatment include nicotinamide (a form of vitamin B3), which inhibits the transfer of melanosomes from melanocytes to keratinocytes; arbutin, which inhibits melanin synthesis by inhibiting tyrosinase activity6; bisabolol, which prevents anti-inflammatory activity7; and retinaldehyde (RAL), a precursor of retinoic acid (RA) that has powerful bleaching action and low levels of cutaneous irritability.8
This prospective, single-arm, open-label study, evaluated the efficacy and safety of a novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05% in the treatment of epidermal melasma.
Study Product Ingredients and Background
Nicotinamide
Nicotinamide is a water-soluble amide of nicotinic acid (niacin) and one of the 2 principal forms of vitamin B3. It is a component of the coenzymes nicotinamide adenine dinucleotide and nicotinamide adenine dinucleotide phosphate. Nicotinamide essentially acts as an antioxidant, with most of its effects exerted through poly(adenosine diphosphate–ribose) polymerase inhibition. Interest has increased in the role of nicotinamide in the prevention and treatment of several skin diseases, such as acne and UV radiation–induced deleterious molecular and immunological events. Nicotinamide also has gained consideration as a potential agent in sunscreen preparations due to its possible skin-lightening effects, stimulation of DNA repair, suppression of UV photocarcinogenesis, and other antiaging effects.9
Arbutin
Arbutin is a molecule that has proven effective in treating melasma.10 Its pigment-lightening ingredients include botanicals that are structurally similar to hydroquinone. Arbutin is obtained from the leaves of the bearberry plant but also is found in lesser quantities in cranberry and blueberry leaves. A naturally occurring gluconopyranoside, arbutin reduces tyrosinase activity without affecting messenger RNA expression.11 Arbutin also inhibits melanosome maturation, is nontoxic to melanocytes, and is used in Japan in a variety of pigment-lightening preparations at 3% concentrations.12
Bisabolol
Bisabolol is a natural monocyclic sesquiterpene alcohol found in the oils of chamomile and other plants. Bisabolol often is included in cosmetics due to its favorable anti-inflammatory and depigmentation properties. Its downregulation of inducible nitric oxide synthase and cyclooxygenase-2 suggests that it may have anti-inflammatory effects.7
Retinaldehyde
Retinaldehyde is an RA precursor that forms as an intermediate metabolite in the transformation of retinol to RA in human keratinocytes. Topical RAL is well tolerated by human skin, and several of its biologic effects are identical to those of RA. Using the tails of C57BL/6 mouse models, RAL 0.05% has been found to have significantly more potent depigmenting effects than RA 0.05% (P<.001 vs P<.01, respectively) when compared to vehicle.13
Although combination therapy with RAL and arbutin could potentially cause skin irritation, the addition of bisabolol to the combination cream used in this study is believed to have conferred anti-inflammatory properties because it inhibits the release of histamine and relieves irritation.
Methods
This single-center, single-arm, prospective, open-label study evaluated the efficacy and safety of a novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05% in treating epidermal melasma. Clinical evaluation included assessment of Melasma Area and Severity Index (MASI) score, photographic analysis, and in vivo reflectance confocal microscopy (RCM) analysis.
The study population included women aged 18 to 50 years with Fitzpatrick skin types I through V who had clinically diagnosed epidermal melasma on the face. Eligibility requirements included confirmation of epidermal pigmentation on Wood lamp examination and RCM analysis and a MASI score of less than 10.5. A total of 35 participants were enrolled in the study (intention to treat [ITT] population). Thirty-three participants were included in the analysis of treatment effectiveness (ITTe population), as 2 were excluded due to lack of follow-up postbaseline. Four participants were prematurely withdrawn from the study—3 due to loss to follow-up and 1 due to treatment discontinuation following an adverse event (AE). The last observation carried forward method was used to input missing data from these 4 participants excluding repeated measure analysis that used the generalized estimated equation method.
At baseline, a 25-g tube of the study cream containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05% was distributed to all participants for once-daily application to the entire face for 30 days. Participants were instructed to apply the product in the evening after using a gentle cleanser, which also was to be used in the morning to remove the product residue. Additionally, participants were given a sunscreen with a sun protection factor of 30 to apply daily on the entire face in the morning, after lunch, and midafternoon. During the 30-day treatment period, treatment interruption of up to 5 consecutive days or 10 nonconsecutive days in total was permitted. At day 30, participants received another 30-day supply of the study product and sunscreen to be applied according to the same regimen for an additional 30-day treatment period.
Clinical Evaluation
At baseline, demographic data and medical history was recorded for all participants and dermatologic and physical examination was performed documenting weight, height, blood pressure, heart rate, and baseline MASI score. Following Wood lamp examination, participants’ faces were photographed and catalogued using medical imaging software that allowed for measurement of the total melasma surface area (Figure 1A). The photographs also were cross-polarized for further analysis of the pigmentation (Figure 1B).
|
|
| |
Figure 1. Clinical (A) and cross-polarized (B) photographs of a patient before treatment with the novel compound containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05%. | ||
A questionnaire evaluating treatment satisfaction was administered to participants (ITTe population [n=33]) at baseline and days 30 and 60. Questionnaire items pertained to skin blemishes, signs of facial aging, overall appearance, texture, oiliness, brightness, and hydration. Participants were instructed to rate their satisfaction for each item on a scale of 1 to 10 (1=bad, 10=excellent). For investigator analysis, scores of 1 to 4 were classified as “dissatisfied,” scores of 5 to 6 were classified as “satisfied,” and scores of 7 to 10 were classified as “completely satisfied.” A questionnaire evaluating product appreciation was administered at day 60 to participants who completed the study (n=29). Questionnaire items asked participants to rate the study cream’s ease of application, consistency, smell, absorption, and overall satisfaction using ratings of “bad,” “regular,” “good,” “very good,” or “excellent.”
Treatment efficacy in all participants was assessed by the investigators at days 30 and 60. Investigators evaluated reductions in pigmentation and total melasma surface area using ratings of “none,” “regular,” “good,” “very good,” or “excellent.” Local tolerance also was evaluated at both time points, and AEs were recorded and analyzed with respect to their duration, intensity, frequency, and severity.
Targeted hyperpigmented skin was selected for in vivo RCM analysis. At each time point, a sequence of block images was acquired at 4 levels of skin: (1) superficial dermis, (2) suprabasal layer/ dermoepidermal junction, (3) spinous layer, and (4) superficial granular layer. Blind evaluation of these images to assess the reduction in melanin quantity was conducted by a dermatopathologist at baseline and days 30 and 60. Melanin quantity present in each layer was graded according to 4 categories (0%–25%, 25.1%–50%, 50.1%–75%, 75.1%–100%). The mean value was used for statistical evaluation.
Results
Efficacy evaluation
The primary efficacy variable was the mean reduction in MASI score from baseline to the end of treatment (day 60), which was 2.25 ± 1.87 (P<.0001). The reduction in mean MASI score was significant from baseline to day 30 (P<.0001) and from day 30 to day 60 (P<.0001). The least root-mean-square error estimates of MASI score variation at days 30 and 60 were 1.40 and 2.25, respectively.
The mean total melasma surface area (as measured in analysis of clinical photographs using medical imaging software) was significantly reduced from 1398.5 mm2 at baseline to 1116.9 mm2 at day 30 (P<.0001) and 923.4 at day 60 (P<.0001). From baseline to end of treatment, the overall reduction in mean total melasma surface area was 475.1 mm2 (P<.0001)(Figure 2). Clinical and cross-polarized photographs taken at day 60 demonstrated a visible reduction in melasma surface area (Figure 3), which was confirmed using medical imaging software.
|
|
| |
Figure 3. Clinical (A) and cross-polarized (B) photographs of a patient after 60 days of treatment with the novel compound containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05%. | ||
In vivo RCM analyses at each time point showed reduction in pigmentation in the 4 levels of the skin that were evaluated, but the results were not statistically significant.
Participant satisfaction
There was strong statistical evidence of patient satisfaction with the treatment results at the end of the study period (P<.0001). At baseline, 75.8% (25/33) of participants were dissatisfied with the appearance of their skin as compared with 15.2% (5/33) at day 60. Additionally, 18.1% (6/33) and 6.1% (2/33) of the participants were satisfied and completely satisfied at baseline compared with 33.3% (11/33) and 51.5% (17/33) at day 60, respectively. Participant satisfaction with signs of facial aging also increased over the study period (P=.0104). At baseline, 60.6% (20/33) were dissatisfied, 12.1% (4/33) were satisfied, and 27.3% (9/33) were completely satisfied; at the end of treatment, 30.3% (10/33) were dissatisfied, 36.4% (12/33) were satisfied, and 33.3% (11/33) were completely satisfied with the improvement in signs of facial aging.
Increased patient satisfaction with facial skin texture at baseline compared to day 60 also was statistically significant (P=.0157). At baseline, 39.4% (13/33) of the participants were dissatisfied, 30.3% (10/33) were satisfied, and 30.3% (10/33) were completely satisfied with facial texture; at day 60, 15.1% (5/33) were dissatisfied, 30.3% (10/33) were satisfied, and 54.6% (18/33) were completely satisfied. Significant improvement from baseline to day 60 also was observed in participant assessment of skin oiliness (P=.0210), brightness (P=.0003), overall appearance (P<.0001), and hydration (P<.0001).
Product appreciation
At day 60, 89.7% (26/29) of the participants who completed the study rated the product’s ease of application as being at least “good,” with more than half of participants (55.2% [16/29]) rating it as “very good” or “excellent.” Overall satisfaction with the product was rated as “very good” or “excellent” by 48.3% (14/29) of the participants. Similar results were observed in participant assessments of consistency, smell, and absorption (Figure 4).
Safety evaluation
A total of 52 AEs were observed in 23 (69.7%) participants, which were recorded by participants in diary entries throughout treatment and evaluated by investigators at each time point. Among these AEs, 48 (92.3%) were considered possibly, probably, or conditionally related to treatment by the investigators based on clinical observation. The most common presumed treatment-related AE was a burning sensation on the skin, reported by 30.3% (10/33) of the participants at day 30 and 13.8% (4/29) at day 60. Of the reported AEs related to treatment, 91.7% (44/48) were of mild intensity and 93.8% (45/48) required no treatment or other action. There were no reported serious AEs related to the investigational product. Blood pressure, heart rate, and weight remained stable among all participants throughout the study.
The intensity of the AEs was described as “light” in 91.7% (44/48) of cases and “moderate” in 8.3% (4/48) of cases. The frequency of AEs was classified as “unique,” “intermittent,” or “continuous” in 45.8% (22/48), 39.6% (19/48), and14.6% (7/48) of cases, respectively. Of the 48 AEs, 3 (6.3%) occurred in 1 participant, necessitating interruption of treatment, application of the topical corticosteroid cream mometasone, and removal from the study.
Comment
Following treatment with the study cream containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05%, the mean reduction in MASI score (P<.0001) and the mean reduction in total melasma surface area from baseline to end of treatment were statistically significant (P<.0001). The study product was associated with strong statistical evidence of patient satisfaction (P<.0001) regarding improvement in facial skin texture, skin oiliness, brightness, overall appearance, and hydration. Participants also responded favorably to the product and considered it safe and effective. In vivo RCM analysis demonstrated a reduction in the amount of melanin in 4 levels of the skin (superficial dermis, suprabasal layer/dermoepidermal junction, spinous layer, superficial granular layer) following treatment with the study cream; however, over the course of the 60-day treatment period, it did not reveal statistically significant reductions. This finding likely is due to the large ranges used to classify the amount of melanin present in each layer of the skin. These limitations suggest that scales used in future in vivo RCM analyses of melasma should be narrower.
Epidermal melasma is one of the most difficult dermatologic diseases to treat and control. Maintenance of clear, undamaged skin remains a treatment target for all dermatologists. This novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and RAL 0.05% has proven to be an effective, safe, and tolerable treatment option for patients with epidermal melasma.
1. Grimes PE, Yamada N, Bhawan J. Light microscopic, immunohistochemical, and ultrastructural alterations in patients with melasma. Am J Dermatopathol. 2005;27:96-101.
2. Kang WH, Yoon KH, Lee ES, et al. Melasma: histopathological characteristics in 56 Korean patients. Br J Dermatol. 2002;146:228-237.
3. Cestari T, Arellano I, Hexsel D, et al. Melasma in Latin America: options the therapy and treatment algorithm. JEADV. 2009;23:760-772.
4. Miot LDB, Miot HA, Silva MG, et al. Fisiopatologia do Melasma. An Bras Dermatol. 2009;84:623-635.
5. Draelos Z. Skin lightening preparations and the hydroquinone controversy. Dermatol Ther. 2007;20:308-313.
6. Parvez S, Kang M, Chung HS, et al. Survey and mechanism of skin depigmenting and lightening agents. Phytoter Res. 2006;20:921-934.
7. Kim S, Jung E, Kim JH, et al. Inhibitory effects of (-)-α-bisabolol on LPS-induced inflammatory response in RAW264.7 macrophages. Food Chem Toxicol. 2011;49:2580-2585.
8. Ortonne JP. Retinoid therapy of pigmentary disorders. Dermatol Ther. 2006;19:280-288.
9. Namazi MR. Nicotinamide-containing sunscreens for use in Australasian countries and cancer-provoking conditions. Med Hypotheses. 2003;60:544-545.
10. Ertam I, Mutlu B, Unal I, et al. Efficiency of ellagic acid and arbutin in melasma: a randomized, prospective, open-label study. J Dermatol. 2008;35:570-574.
11. Hori I, Nihei K, Kubo I. Structural criteria for depigmenting mechanism of arbutin. Phytother Res. 2004;18:475-469.
12. Ethnic skin and pigmentation. In: Draelos ZD. Cosmetics and Dermatologic Problems and Solutions. 3rd ed. Boca Raton, FL: CRC Press; 2011:52-55.
13. Kasraee B, Tran C, Sorg O, et al. The depigmenting effect of RALGA in C57BL/6 mice. Dermatology. 2005;210(suppl 1):30-34.
1. Grimes PE, Yamada N, Bhawan J. Light microscopic, immunohistochemical, and ultrastructural alterations in patients with melasma. Am J Dermatopathol. 2005;27:96-101.
2. Kang WH, Yoon KH, Lee ES, et al. Melasma: histopathological characteristics in 56 Korean patients. Br J Dermatol. 2002;146:228-237.
3. Cestari T, Arellano I, Hexsel D, et al. Melasma in Latin America: options the therapy and treatment algorithm. JEADV. 2009;23:760-772.
4. Miot LDB, Miot HA, Silva MG, et al. Fisiopatologia do Melasma. An Bras Dermatol. 2009;84:623-635.
5. Draelos Z. Skin lightening preparations and the hydroquinone controversy. Dermatol Ther. 2007;20:308-313.
6. Parvez S, Kang M, Chung HS, et al. Survey and mechanism of skin depigmenting and lightening agents. Phytoter Res. 2006;20:921-934.
7. Kim S, Jung E, Kim JH, et al. Inhibitory effects of (-)-α-bisabolol on LPS-induced inflammatory response in RAW264.7 macrophages. Food Chem Toxicol. 2011;49:2580-2585.
8. Ortonne JP. Retinoid therapy of pigmentary disorders. Dermatol Ther. 2006;19:280-288.
9. Namazi MR. Nicotinamide-containing sunscreens for use in Australasian countries and cancer-provoking conditions. Med Hypotheses. 2003;60:544-545.
10. Ertam I, Mutlu B, Unal I, et al. Efficiency of ellagic acid and arbutin in melasma: a randomized, prospective, open-label study. J Dermatol. 2008;35:570-574.
11. Hori I, Nihei K, Kubo I. Structural criteria for depigmenting mechanism of arbutin. Phytother Res. 2004;18:475-469.
12. Ethnic skin and pigmentation. In: Draelos ZD. Cosmetics and Dermatologic Problems and Solutions. 3rd ed. Boca Raton, FL: CRC Press; 2011:52-55.
13. Kasraee B, Tran C, Sorg O, et al. The depigmenting effect of RALGA in C57BL/6 mice. Dermatology. 2005;210(suppl 1):30-34.
Practice Points
- Epidermal melasma is a common hyperpigmentation disorder characterized by the appearance of abnormal melanin deposits in different layers of the skin.
- Melasma can be difficult to treat and often recurs due to the migration of new melanocytes from hair follicles to the skin’s surface.
- A novel cream formulation containing nicotinamide 4%, arbutin 3%, bisabolol 1%, and retinaldehyde 0.05% offers a safe and effective option for treatment of epidermal melasma.

Coding for Biopsies, Shave Removals, and Excisions
In dermatology, samples of skin and subcutaneous tissue are routinely removed to establish a diagnosis, treat symptomatic lesions, or remove potential tumors. The Current Procedural Terminology (CPT) codes used in billing for these procedures typically are generic, but it is important to differentiate between 3 degrees of tissue removal—biopsy, shave removal, and excision—when billing for these services since different codes may be appropriate in each of these circumstances.
Biopsy
Specifically, biopsy (CPT codes 11100/11101) is described as an “independent…procedure to obtain tissue for pathologic examination.”1 The method of biopsy is not specified by CPT and can include any of the following, as long as the primary purpose of the procedure is to remove tissue for analysis: removal by scissors, shaving with a blade or specialized instrument to any level including the subcutaneous fat, extraction using a punch, and excision down to the subcutaneous fat with a scalpel. The feature that differentiates biopsy from shave removal or excision is not depth or extent of tissue mobilization but the intent “to remove a portion of skin, suspect lesion, or entire lesion so that it can be examined histologically.”2 The underlying assumption is that neither definitive clinical nor histologic diagnosis exists prior to biopsy, the purpose of which is to help establish the identity of the lesion.
If the tissue within a large, single lesion is sampled at several separate locations at the same visit, then only a single unit of a single biopsy code (eg, either 11100, 11101, or some site-specific code) should be reported.In contrast, if a number of discrete lesions in the same approximate anatomic area were sampled for diagnoses, each sample taken from separate lesions would constitute a distinct biopsy and would be billed as a separate unit of service.
Shave Removals and Excisions
Shave removal of skin lesions (CPT codes 11300–11313) includes the removal of tangential or saucerized skin lesions to a level no deeper than the base of the dermis. The CPT provides no detailed guidance regarding differentiation of codes for shave removal versus biopsy when a specimen is submitted for histopathologic examination other than the definition of biopsy that was discussed previously. If the tissue is removed specifically for establishing diagnosis, then by definition the procedure should be coded as a biopsy. On the other hand, shave removal implies the intent to completely remove a lesion that already has a presumptive clinical or histologic diagnosis or is being removed for some purpose other than diagnosis (eg, symptomatic relief).
Shave removals are, however, clearly different than excisions (CPT codes 11400–11646), which must proceed through the entire dermis to the subcutis. Additionally, skin lesion excisions include margins, as the intent of an excision procedure is to remove the entire lesion along with a margin of normal skin around it.2
Specialized Biopsy and Excision Codes
While most biopsies, shave removals, and excisions are performed using generic codes, there are specialized circumstances when more specific codes may be preferable. For instance, there are site-specific skin biopsy codes for the nail unit (11755), vermilion and mucosal lip (40490), penis (54100), vulva (56605), and external ear (69100) that take into account the additional complexity of biopsy at these anatomic locations. There also is a site-specific code for eyelid biopsy (67810), which was redefined in 2013 as an “incisional biopsy of eyelid skin including lid margin.”1 Therefore, biopsies of eyelid skin that do not remove the eyelid margin must be coded as 11100/11101, or if the entire cutaneous lesion was removed, can be reclassified as shave removals, which would be coded in the 11310 to 11313 range.
Specialized excision codes include those of the soft tissue. Soft tissue excision codes typically used by dermatologists are not numbered consecutively, are site-specific, and are typically used for resection of benign tumors confined to the subcutaneous tissue below the skin but above the deep fascia. Cysts of all types, including epidermoid and pilar cysts, are specifically excluded from this code set regardless of how large or complex they may be, as they protrude into the dermis or above and are not exclusively in the subcutis. However, lipomas meet the definition for soft-tissue excision, and therefore site-specific soft tissue excision codes can be used in lieu of traditional skin excision codes. The soft-tissue excision codes are distributed throughout the CPT manual, with distinct codes for the abdominal wall (22902, 22903); leg or ankle (27618, 27632); back or flank (21930, 21931); external auditory canal (69145); upper arm or elbow (24075, 24071); face or scalp (21011, 21012); hand or finger (26115, 26111); foot or toe (28043, 28039); forearm or wrist (25075, 25071); hip or pelvis (27047, 27043); thigh or knee (27327, 27337); neck or anterior thorax (21555, 21552); and shoulder (23075, 23071). In general, there are 2 codes for each area—one for smaller and one for larger excisions—but they frequently are out of order (ie, the code associated with a higher numerical value may correspond with the smaller excision). Care should be taken in selecting the correct code. The specific size cutoffs for the various soft tissue excision code sets are different, so it is important to be familiar with the particular CPT descriptions for each.
Final Thoughts
In summary, biopsies, shave removals, and excisions are different procedures and therefore should be coded differently. Although the distinction between biopsies and shave removals is ill defined, remember that biopsies are intended to establish a diagnosis and shave removals are intended to remove the entire lesion. By definition, excisions must include margins and proceed through the dermis to the subcutis. In particular circumstances, site-specific biopsy codes may be appropriate and can be used to code for lipoma excisions.
1. Current Procedural Terminology 2015, Professional Edition. Chicago, Illinois: American Medical Association; 2014.
2. American Medical Association. Biopsy. CPT Assistant. Chicago, IL: American Medical Association: October 2004:4.
In dermatology, samples of skin and subcutaneous tissue are routinely removed to establish a diagnosis, treat symptomatic lesions, or remove potential tumors. The Current Procedural Terminology (CPT) codes used in billing for these procedures typically are generic, but it is important to differentiate between 3 degrees of tissue removal—biopsy, shave removal, and excision—when billing for these services since different codes may be appropriate in each of these circumstances.
Biopsy
Specifically, biopsy (CPT codes 11100/11101) is described as an “independent…procedure to obtain tissue for pathologic examination.”1 The method of biopsy is not specified by CPT and can include any of the following, as long as the primary purpose of the procedure is to remove tissue for analysis: removal by scissors, shaving with a blade or specialized instrument to any level including the subcutaneous fat, extraction using a punch, and excision down to the subcutaneous fat with a scalpel. The feature that differentiates biopsy from shave removal or excision is not depth or extent of tissue mobilization but the intent “to remove a portion of skin, suspect lesion, or entire lesion so that it can be examined histologically.”2 The underlying assumption is that neither definitive clinical nor histologic diagnosis exists prior to biopsy, the purpose of which is to help establish the identity of the lesion.
If the tissue within a large, single lesion is sampled at several separate locations at the same visit, then only a single unit of a single biopsy code (eg, either 11100, 11101, or some site-specific code) should be reported.In contrast, if a number of discrete lesions in the same approximate anatomic area were sampled for diagnoses, each sample taken from separate lesions would constitute a distinct biopsy and would be billed as a separate unit of service.
Shave Removals and Excisions
Shave removal of skin lesions (CPT codes 11300–11313) includes the removal of tangential or saucerized skin lesions to a level no deeper than the base of the dermis. The CPT provides no detailed guidance regarding differentiation of codes for shave removal versus biopsy when a specimen is submitted for histopathologic examination other than the definition of biopsy that was discussed previously. If the tissue is removed specifically for establishing diagnosis, then by definition the procedure should be coded as a biopsy. On the other hand, shave removal implies the intent to completely remove a lesion that already has a presumptive clinical or histologic diagnosis or is being removed for some purpose other than diagnosis (eg, symptomatic relief).
Shave removals are, however, clearly different than excisions (CPT codes 11400–11646), which must proceed through the entire dermis to the subcutis. Additionally, skin lesion excisions include margins, as the intent of an excision procedure is to remove the entire lesion along with a margin of normal skin around it.2
Specialized Biopsy and Excision Codes
While most biopsies, shave removals, and excisions are performed using generic codes, there are specialized circumstances when more specific codes may be preferable. For instance, there are site-specific skin biopsy codes for the nail unit (11755), vermilion and mucosal lip (40490), penis (54100), vulva (56605), and external ear (69100) that take into account the additional complexity of biopsy at these anatomic locations. There also is a site-specific code for eyelid biopsy (67810), which was redefined in 2013 as an “incisional biopsy of eyelid skin including lid margin.”1 Therefore, biopsies of eyelid skin that do not remove the eyelid margin must be coded as 11100/11101, or if the entire cutaneous lesion was removed, can be reclassified as shave removals, which would be coded in the 11310 to 11313 range.
Specialized excision codes include those of the soft tissue. Soft tissue excision codes typically used by dermatologists are not numbered consecutively, are site-specific, and are typically used for resection of benign tumors confined to the subcutaneous tissue below the skin but above the deep fascia. Cysts of all types, including epidermoid and pilar cysts, are specifically excluded from this code set regardless of how large or complex they may be, as they protrude into the dermis or above and are not exclusively in the subcutis. However, lipomas meet the definition for soft-tissue excision, and therefore site-specific soft tissue excision codes can be used in lieu of traditional skin excision codes. The soft-tissue excision codes are distributed throughout the CPT manual, with distinct codes for the abdominal wall (22902, 22903); leg or ankle (27618, 27632); back or flank (21930, 21931); external auditory canal (69145); upper arm or elbow (24075, 24071); face or scalp (21011, 21012); hand or finger (26115, 26111); foot or toe (28043, 28039); forearm or wrist (25075, 25071); hip or pelvis (27047, 27043); thigh or knee (27327, 27337); neck or anterior thorax (21555, 21552); and shoulder (23075, 23071). In general, there are 2 codes for each area—one for smaller and one for larger excisions—but they frequently are out of order (ie, the code associated with a higher numerical value may correspond with the smaller excision). Care should be taken in selecting the correct code. The specific size cutoffs for the various soft tissue excision code sets are different, so it is important to be familiar with the particular CPT descriptions for each.
Final Thoughts
In summary, biopsies, shave removals, and excisions are different procedures and therefore should be coded differently. Although the distinction between biopsies and shave removals is ill defined, remember that biopsies are intended to establish a diagnosis and shave removals are intended to remove the entire lesion. By definition, excisions must include margins and proceed through the dermis to the subcutis. In particular circumstances, site-specific biopsy codes may be appropriate and can be used to code for lipoma excisions.
In dermatology, samples of skin and subcutaneous tissue are routinely removed to establish a diagnosis, treat symptomatic lesions, or remove potential tumors. The Current Procedural Terminology (CPT) codes used in billing for these procedures typically are generic, but it is important to differentiate between 3 degrees of tissue removal—biopsy, shave removal, and excision—when billing for these services since different codes may be appropriate in each of these circumstances.
Biopsy
Specifically, biopsy (CPT codes 11100/11101) is described as an “independent…procedure to obtain tissue for pathologic examination.”1 The method of biopsy is not specified by CPT and can include any of the following, as long as the primary purpose of the procedure is to remove tissue for analysis: removal by scissors, shaving with a blade or specialized instrument to any level including the subcutaneous fat, extraction using a punch, and excision down to the subcutaneous fat with a scalpel. The feature that differentiates biopsy from shave removal or excision is not depth or extent of tissue mobilization but the intent “to remove a portion of skin, suspect lesion, or entire lesion so that it can be examined histologically.”2 The underlying assumption is that neither definitive clinical nor histologic diagnosis exists prior to biopsy, the purpose of which is to help establish the identity of the lesion.
If the tissue within a large, single lesion is sampled at several separate locations at the same visit, then only a single unit of a single biopsy code (eg, either 11100, 11101, or some site-specific code) should be reported.In contrast, if a number of discrete lesions in the same approximate anatomic area were sampled for diagnoses, each sample taken from separate lesions would constitute a distinct biopsy and would be billed as a separate unit of service.
Shave Removals and Excisions
Shave removal of skin lesions (CPT codes 11300–11313) includes the removal of tangential or saucerized skin lesions to a level no deeper than the base of the dermis. The CPT provides no detailed guidance regarding differentiation of codes for shave removal versus biopsy when a specimen is submitted for histopathologic examination other than the definition of biopsy that was discussed previously. If the tissue is removed specifically for establishing diagnosis, then by definition the procedure should be coded as a biopsy. On the other hand, shave removal implies the intent to completely remove a lesion that already has a presumptive clinical or histologic diagnosis or is being removed for some purpose other than diagnosis (eg, symptomatic relief).
Shave removals are, however, clearly different than excisions (CPT codes 11400–11646), which must proceed through the entire dermis to the subcutis. Additionally, skin lesion excisions include margins, as the intent of an excision procedure is to remove the entire lesion along with a margin of normal skin around it.2
Specialized Biopsy and Excision Codes
While most biopsies, shave removals, and excisions are performed using generic codes, there are specialized circumstances when more specific codes may be preferable. For instance, there are site-specific skin biopsy codes for the nail unit (11755), vermilion and mucosal lip (40490), penis (54100), vulva (56605), and external ear (69100) that take into account the additional complexity of biopsy at these anatomic locations. There also is a site-specific code for eyelid biopsy (67810), which was redefined in 2013 as an “incisional biopsy of eyelid skin including lid margin.”1 Therefore, biopsies of eyelid skin that do not remove the eyelid margin must be coded as 11100/11101, or if the entire cutaneous lesion was removed, can be reclassified as shave removals, which would be coded in the 11310 to 11313 range.
Specialized excision codes include those of the soft tissue. Soft tissue excision codes typically used by dermatologists are not numbered consecutively, are site-specific, and are typically used for resection of benign tumors confined to the subcutaneous tissue below the skin but above the deep fascia. Cysts of all types, including epidermoid and pilar cysts, are specifically excluded from this code set regardless of how large or complex they may be, as they protrude into the dermis or above and are not exclusively in the subcutis. However, lipomas meet the definition for soft-tissue excision, and therefore site-specific soft tissue excision codes can be used in lieu of traditional skin excision codes. The soft-tissue excision codes are distributed throughout the CPT manual, with distinct codes for the abdominal wall (22902, 22903); leg or ankle (27618, 27632); back or flank (21930, 21931); external auditory canal (69145); upper arm or elbow (24075, 24071); face or scalp (21011, 21012); hand or finger (26115, 26111); foot or toe (28043, 28039); forearm or wrist (25075, 25071); hip or pelvis (27047, 27043); thigh or knee (27327, 27337); neck or anterior thorax (21555, 21552); and shoulder (23075, 23071). In general, there are 2 codes for each area—one for smaller and one for larger excisions—but they frequently are out of order (ie, the code associated with a higher numerical value may correspond with the smaller excision). Care should be taken in selecting the correct code. The specific size cutoffs for the various soft tissue excision code sets are different, so it is important to be familiar with the particular CPT descriptions for each.
Final Thoughts
In summary, biopsies, shave removals, and excisions are different procedures and therefore should be coded differently. Although the distinction between biopsies and shave removals is ill defined, remember that biopsies are intended to establish a diagnosis and shave removals are intended to remove the entire lesion. By definition, excisions must include margins and proceed through the dermis to the subcutis. In particular circumstances, site-specific biopsy codes may be appropriate and can be used to code for lipoma excisions.
1. Current Procedural Terminology 2015, Professional Edition. Chicago, Illinois: American Medical Association; 2014.
2. American Medical Association. Biopsy. CPT Assistant. Chicago, IL: American Medical Association: October 2004:4.
1. Current Procedural Terminology 2015, Professional Edition. Chicago, Illinois: American Medical Association; 2014.
2. American Medical Association. Biopsy. CPT Assistant. Chicago, IL: American Medical Association: October 2004:4.
Practice Points
- Biopsies are coded when there is an independent procedure to remove skin for histologic analysis to help establish a definitive histologic diagnosis.
- Coding for shave removals and excisions requires the intent to remove the entire lesion.
- Unlike shave removals, excisions can be coded only if the lesion is removed to the level of the subcutaneous fat.
- When available, site-specific biopsy or soft tissue excision codes may better describe a procedure than standard biopsy or excision codes.

Outpatient Care Costly for Hospitals
NEW YORK - Outpatient care may cost more when hospitals own the medical practices or employ the physicians, a U.S. study suggests.
Hospital employment of doctors and ownership of physician practices has grown over the past decade as health care providers seek to curb expenses with economies of scale and deliver better-coordinated treatment to patients.
Research reported in an article online October 19 in JAMA Internal Medicine examined how the rise of tighter financial integration between doctors and hospitals affected costs for people enrolled in private health insurance plans from 2008 to 2012.
In communities with the sharpest increase in financial integration between doctors and hospitals over the study period, average annual outpatient costs for each person with private health insurance increased by $75, while the amount of outpatient services they used was little changed.
"We document an increase in spending driven by prices, without any change in utilization," lead author Hannah Neprash, a health policy researcher at Harvard University in Boston, said by email.
"Some price increases may be acceptable - particularly if they are accompanied with improved quality of care," Neprash added. This study, however, didn't look at changes in quality associated with physician-hospital integration, she said.
Using Medicare claims data for 240 metropolitan areas nationwide, the researchers identified physicians who were either directly employed by hospitals or who worked for practices owned by hospitals.
Overall, the proportion of physicians with close financial ties to hospitals rose from 18% in 2008 to 21.3% in 2012.
Next, the researchers analyzed spending and prices for nearly 7.4 million non-elderly adults in these regions with two common types of private health insurance coverage: preferred-provider organizations (PPO) or point-of-service (POS) plans. These types of insurance may tie patients' out-of-pocket fees to the prices doctors charge.
The cost increase seen with greater financial integration of doctors and hospitals was confined to outpatient spending, bringing the average outpatient cost per enrollee in the PPO and POS plans in 2012 to about $2,400.
The average cost of $872 for inpatient treatments, however, was unaffected by financial ties between doctors and hospitals, the study found.
One shortcoming of the study is that the researchers didn't assess quality of care, the authors acknowledge. Better quality outpatient care might justify higher prices, they note.
Newer payment arrangements, however, are starting to hold providers more accountable for both inpatient and outpatient spending and for outcomes, senior study author Dr. J. Michael McWilliams of Harvard Medical School and Brigham and Women's Hospital in Boston, said by email.
Over time, this means "physician-hospital integration could conceivably offer some distinct efficiencies in terms of higher quality of care at a lower cost," Dr. McWilliams said.
Still, price hikes for people with private insurance - often provided to U.S. workers by their employers - are probably going to lead to higher out-of-pocket costs for patients, noted Dr. James Reschovsky and Dr. Eugene Rich of Mathematica Policy Research in Washington, D.C., in an accompanying editorial.
"The higher prices in hospital outpatient departments are passed on to employers in the form of higher premiums, and ultimately to workers in the form of less generous health benefits, higher premium cost sharing, or lower wages," Dr. Reschovsky said by email. "Certainly patients with co-insurance would pay more out-of-pocket when the price of service is higher."
The Robert Wood Johnson Foundation supported this research. One coauthor reported being formerly employed by Truven Health Analytics.
NEW YORK - Outpatient care may cost more when hospitals own the medical practices or employ the physicians, a U.S. study suggests.
Hospital employment of doctors and ownership of physician practices has grown over the past decade as health care providers seek to curb expenses with economies of scale and deliver better-coordinated treatment to patients.
Research reported in an article online October 19 in JAMA Internal Medicine examined how the rise of tighter financial integration between doctors and hospitals affected costs for people enrolled in private health insurance plans from 2008 to 2012.
In communities with the sharpest increase in financial integration between doctors and hospitals over the study period, average annual outpatient costs for each person with private health insurance increased by $75, while the amount of outpatient services they used was little changed.
"We document an increase in spending driven by prices, without any change in utilization," lead author Hannah Neprash, a health policy researcher at Harvard University in Boston, said by email.
"Some price increases may be acceptable - particularly if they are accompanied with improved quality of care," Neprash added. This study, however, didn't look at changes in quality associated with physician-hospital integration, she said.
Using Medicare claims data for 240 metropolitan areas nationwide, the researchers identified physicians who were either directly employed by hospitals or who worked for practices owned by hospitals.
Overall, the proportion of physicians with close financial ties to hospitals rose from 18% in 2008 to 21.3% in 2012.
Next, the researchers analyzed spending and prices for nearly 7.4 million non-elderly adults in these regions with two common types of private health insurance coverage: preferred-provider organizations (PPO) or point-of-service (POS) plans. These types of insurance may tie patients' out-of-pocket fees to the prices doctors charge.
The cost increase seen with greater financial integration of doctors and hospitals was confined to outpatient spending, bringing the average outpatient cost per enrollee in the PPO and POS plans in 2012 to about $2,400.
The average cost of $872 for inpatient treatments, however, was unaffected by financial ties between doctors and hospitals, the study found.
One shortcoming of the study is that the researchers didn't assess quality of care, the authors acknowledge. Better quality outpatient care might justify higher prices, they note.
Newer payment arrangements, however, are starting to hold providers more accountable for both inpatient and outpatient spending and for outcomes, senior study author Dr. J. Michael McWilliams of Harvard Medical School and Brigham and Women's Hospital in Boston, said by email.
Over time, this means "physician-hospital integration could conceivably offer some distinct efficiencies in terms of higher quality of care at a lower cost," Dr. McWilliams said.
Still, price hikes for people with private insurance - often provided to U.S. workers by their employers - are probably going to lead to higher out-of-pocket costs for patients, noted Dr. James Reschovsky and Dr. Eugene Rich of Mathematica Policy Research in Washington, D.C., in an accompanying editorial.
"The higher prices in hospital outpatient departments are passed on to employers in the form of higher premiums, and ultimately to workers in the form of less generous health benefits, higher premium cost sharing, or lower wages," Dr. Reschovsky said by email. "Certainly patients with co-insurance would pay more out-of-pocket when the price of service is higher."
The Robert Wood Johnson Foundation supported this research. One coauthor reported being formerly employed by Truven Health Analytics.
NEW YORK - Outpatient care may cost more when hospitals own the medical practices or employ the physicians, a U.S. study suggests.
Hospital employment of doctors and ownership of physician practices has grown over the past decade as health care providers seek to curb expenses with economies of scale and deliver better-coordinated treatment to patients.
Research reported in an article online October 19 in JAMA Internal Medicine examined how the rise of tighter financial integration between doctors and hospitals affected costs for people enrolled in private health insurance plans from 2008 to 2012.
In communities with the sharpest increase in financial integration between doctors and hospitals over the study period, average annual outpatient costs for each person with private health insurance increased by $75, while the amount of outpatient services they used was little changed.
"We document an increase in spending driven by prices, without any change in utilization," lead author Hannah Neprash, a health policy researcher at Harvard University in Boston, said by email.
"Some price increases may be acceptable - particularly if they are accompanied with improved quality of care," Neprash added. This study, however, didn't look at changes in quality associated with physician-hospital integration, she said.
Using Medicare claims data for 240 metropolitan areas nationwide, the researchers identified physicians who were either directly employed by hospitals or who worked for practices owned by hospitals.
Overall, the proportion of physicians with close financial ties to hospitals rose from 18% in 2008 to 21.3% in 2012.
Next, the researchers analyzed spending and prices for nearly 7.4 million non-elderly adults in these regions with two common types of private health insurance coverage: preferred-provider organizations (PPO) or point-of-service (POS) plans. These types of insurance may tie patients' out-of-pocket fees to the prices doctors charge.
The cost increase seen with greater financial integration of doctors and hospitals was confined to outpatient spending, bringing the average outpatient cost per enrollee in the PPO and POS plans in 2012 to about $2,400.
The average cost of $872 for inpatient treatments, however, was unaffected by financial ties between doctors and hospitals, the study found.
One shortcoming of the study is that the researchers didn't assess quality of care, the authors acknowledge. Better quality outpatient care might justify higher prices, they note.
Newer payment arrangements, however, are starting to hold providers more accountable for both inpatient and outpatient spending and for outcomes, senior study author Dr. J. Michael McWilliams of Harvard Medical School and Brigham and Women's Hospital in Boston, said by email.
Over time, this means "physician-hospital integration could conceivably offer some distinct efficiencies in terms of higher quality of care at a lower cost," Dr. McWilliams said.
Still, price hikes for people with private insurance - often provided to U.S. workers by their employers - are probably going to lead to higher out-of-pocket costs for patients, noted Dr. James Reschovsky and Dr. Eugene Rich of Mathematica Policy Research in Washington, D.C., in an accompanying editorial.
"The higher prices in hospital outpatient departments are passed on to employers in the form of higher premiums, and ultimately to workers in the form of less generous health benefits, higher premium cost sharing, or lower wages," Dr. Reschovsky said by email. "Certainly patients with co-insurance would pay more out-of-pocket when the price of service is higher."
The Robert Wood Johnson Foundation supported this research. One coauthor reported being formerly employed by Truven Health Analytics.
Suicide rate high in patients with head and neck cancer
Patients with head and neck cancer had a threefold higher risk of suicide, compared with the general population, with higher rates among male patients and those with later-stage disease, according to an analysis of SEER data.
Patients with cancers of the hypopharynx had the highest rates (standardized mortality ratio, compared with the general population, 13.91), followed by cancer of the larynx (5.48) and cancer of the oral cavity and oropharynx (5.23).
“Routine screening for suicide risk may not be needed in every patient,” said David Kam, a medical student at Rutgers New Jersey Medical School, Newark, and his colleagues, “but we have identified a certain subset of patients often seen by otolaryngologists as being at increased risk (those who are older, male, with cancers of the hypopharynx, or with history of radiation therapy)” (JAMA Otolaryngol Head Neck Surg. 2015 Nov 12. doi: 10.1001/jamaoto.2015.2480).
Patients who underwent radiation therapy without surgery had about twice the suicide risk as those who underwent surgery alone (5.12 vs. 2.57). The researchers noted a potential selection bias among those treated with radiation alone, as patients with unresectable disease or significant comorbidities may undergo radiation instead of surgery.
Radiation therapy is integral to treating many head and neck cancers but is associated with a lower quality of life because of related morbidity. Despite improvements in quality of life measures associated with intensity-modulated radiation therapy (IMRT), the analysis showed no improvement in suicide rates after 2005, when IMRT was widely commercially available and a large fraction of patients would presumably have received the newer treatment.
An analysis of SEER (Surveillance, Epidemiology, and End Results) data from 1973 to 2011 showed 857 suicides among 350,413 individuals with head and neck cancer. Among all patients, the greatest increase in suicide rates occurred in the first 5 years after diagnosis.
Because of the significantly increased suicide risk among patients with head and neck cancers, research on survival outcomes should expand to include the psychological toll that the cancer, treatments, and resulting morbidity have on patients, the researchers said.
Patients with head and neck cancer had a threefold higher risk of suicide, compared with the general population, with higher rates among male patients and those with later-stage disease, according to an analysis of SEER data.
Patients with cancers of the hypopharynx had the highest rates (standardized mortality ratio, compared with the general population, 13.91), followed by cancer of the larynx (5.48) and cancer of the oral cavity and oropharynx (5.23).
“Routine screening for suicide risk may not be needed in every patient,” said David Kam, a medical student at Rutgers New Jersey Medical School, Newark, and his colleagues, “but we have identified a certain subset of patients often seen by otolaryngologists as being at increased risk (those who are older, male, with cancers of the hypopharynx, or with history of radiation therapy)” (JAMA Otolaryngol Head Neck Surg. 2015 Nov 12. doi: 10.1001/jamaoto.2015.2480).
Patients who underwent radiation therapy without surgery had about twice the suicide risk as those who underwent surgery alone (5.12 vs. 2.57). The researchers noted a potential selection bias among those treated with radiation alone, as patients with unresectable disease or significant comorbidities may undergo radiation instead of surgery.
Radiation therapy is integral to treating many head and neck cancers but is associated with a lower quality of life because of related morbidity. Despite improvements in quality of life measures associated with intensity-modulated radiation therapy (IMRT), the analysis showed no improvement in suicide rates after 2005, when IMRT was widely commercially available and a large fraction of patients would presumably have received the newer treatment.
An analysis of SEER (Surveillance, Epidemiology, and End Results) data from 1973 to 2011 showed 857 suicides among 350,413 individuals with head and neck cancer. Among all patients, the greatest increase in suicide rates occurred in the first 5 years after diagnosis.
Because of the significantly increased suicide risk among patients with head and neck cancers, research on survival outcomes should expand to include the psychological toll that the cancer, treatments, and resulting morbidity have on patients, the researchers said.
Patients with head and neck cancer had a threefold higher risk of suicide, compared with the general population, with higher rates among male patients and those with later-stage disease, according to an analysis of SEER data.
Patients with cancers of the hypopharynx had the highest rates (standardized mortality ratio, compared with the general population, 13.91), followed by cancer of the larynx (5.48) and cancer of the oral cavity and oropharynx (5.23).
“Routine screening for suicide risk may not be needed in every patient,” said David Kam, a medical student at Rutgers New Jersey Medical School, Newark, and his colleagues, “but we have identified a certain subset of patients often seen by otolaryngologists as being at increased risk (those who are older, male, with cancers of the hypopharynx, or with history of radiation therapy)” (JAMA Otolaryngol Head Neck Surg. 2015 Nov 12. doi: 10.1001/jamaoto.2015.2480).
Patients who underwent radiation therapy without surgery had about twice the suicide risk as those who underwent surgery alone (5.12 vs. 2.57). The researchers noted a potential selection bias among those treated with radiation alone, as patients with unresectable disease or significant comorbidities may undergo radiation instead of surgery.
Radiation therapy is integral to treating many head and neck cancers but is associated with a lower quality of life because of related morbidity. Despite improvements in quality of life measures associated with intensity-modulated radiation therapy (IMRT), the analysis showed no improvement in suicide rates after 2005, when IMRT was widely commercially available and a large fraction of patients would presumably have received the newer treatment.
An analysis of SEER (Surveillance, Epidemiology, and End Results) data from 1973 to 2011 showed 857 suicides among 350,413 individuals with head and neck cancer. Among all patients, the greatest increase in suicide rates occurred in the first 5 years after diagnosis.
Because of the significantly increased suicide risk among patients with head and neck cancers, research on survival outcomes should expand to include the psychological toll that the cancer, treatments, and resulting morbidity have on patients, the researchers said.
Key clinical point: Patients with head and neck cancer have a significantly higher suicide rate than the general population.
Major finding: The standardized suicide ratio for patients with head and neck cancer, compared with the general population, was 3.21.
Data source: An analysis of SEER data from 1973 to 2011 showed 857 suicides among 350,413 individuals with head and neck cancer.
Disclosures: David Kam and his coauthors reported having no relevant financial disclosures.