User login
CAR exhibits activity in resistant B-cell malignancies

Photo courtesy of ASH
ORLANDO, FL—Allogeneic chimeric antigen receptor (CAR) T cells directed against CD19 can have “significant” activity against resistant B-cell malignancies, even when given without prior chemotherapy, according to a presentation at the 2015 ASH Annual Meeting.
Nine of 20 patients responded to treatment with the CAR T cells, despite having failed prior allogeneic transplant. The best responses were observed in patients with acute lymphoblastic leukemia (ALL) and chronic lymphocytic leukemia (CLL).
“Malignancies that were resistant to allogeneic transplants and standard donor lymphocyte infusions regressed after infusions of allogeneic anti-CD19 CAR T cells,” said James N. Kochenderfer, MD, of the National Cancer Institute in Bethesda, Maryland.
“Allogeneic anti-CD19 CAR T cells seem to be particularly effective against ALL and CLL, suggesting a possible antigenic stimulation that may be more pronounced in these malignancies.”
Adverse events associated with these CAR T cells included severe but reversible cytokine release syndrome, mild aphasia, and muscle damage. There were no cases of acute graft-vs-host disease (GVHD).
Dr Kochenderfer presented these results at ASH as abstract 99.
For this phase 1 study, researchers tested a CAR T-cell therapy that was originally developed by Dr Kochenderfer and his colleagues. The therapy is now known as KTE-C19 and is under development by Kite Pharmaceuticals. However, the company did not sponsor this trial.
The study was open to patients with any CD19+ B-cell malignancy that persisted after allogeneic transplant.
All patients except those with ALL were required to have received at least one standard donor lymphocyte infusion. In addition, patients were only eligible if they had minimal or no GVHD and were not receiving any systemic immunosuppressive drugs.
The trial included 20 patients—5 each with ALL, CLL, mantle cell lymphoma (MCL), and diffuse large B-cell lymphoma (DLBCL).
All patients received a single infusion of CAR T cells derived from their original transplant donor. Production of these cells took 8 days. The highest dose of CAR T cells given was 107 cells/kg.
Four of the ALL patients obtained a minimal-residual disease-negative complete response (CR), but 2 of these patients subsequently relapsed. Of the other 2 patients, 1 remains in CR at 18 months of follow-up, and the other went on to receive a second allogeneic transplant. That patient remains in CR today.
Among the CLL patients, 1 achieved a CR, and 1 achieved a partial response (PR). One patient had stable disease (SD), and the other 2 progressed. Both the CR and the PR are ongoing at 36 and 18 months of follow-up, respectively.
One MCL patient achieved a CR, 1 had a PR, and 3 had SD. The CR is ongoing at 31 months. One DLBCL patient achieved a CR, 3 had SD, and 1 progressed.
Dr Kochenderfer noted that response was associated with higher blood CAR T-cell levels. There was a significant difference in CAR T-cell levels between responders and nonresponders (P=0.001).
In addition, the presence of blood B-cell levels before CAR T-cell infusion was associated with higher blood CAR T-cell levels. Patients with normal or high B lymphocytes had higher levels of CAR T cells in their blood (P=0.04).
Patients with high tumor burdens developed severe cytokine-release syndrome with fever, tachycardia, and hypotension. The ALL patients were particularly susceptible to cytokine-release syndrome.
Dr Kochenderfer said neurologic toxicity was rare and mild. There was 1 case of mild aphasia.
There were 2 patients with elevations in CPK, indicating muscle damage. Those patients also reported muscle pain, and 1 patient reported weakness.
“This is one of the first reports, I think, of muscle damage in CAR T-cell patients,” Dr Kochenderfer said.
None of the patients developed acute GVHD after CAR T-cell therapy. One patient had continued worsening of pre-existing chronic GVHD after treatment, and 1 patient developed mild chronic eye GVHD more than a year after CAR T-cell infusion.
Dr Kochenderfer said additional details from this trial will be published in an upcoming issue of the Journal of Clinical Oncology. ![]()
Photo courtesy of ASH
ORLANDO, FL—Allogeneic chimeric antigen receptor (CAR) T cells directed against CD19 can have “significant” activity against resistant B-cell malignancies, even when given without prior chemotherapy, according to a presentation at the 2015 ASH Annual Meeting.
Nine of 20 patients responded to treatment with the CAR T cells, despite having failed prior allogeneic transplant. The best responses were observed in patients with acute lymphoblastic leukemia (ALL) and chronic lymphocytic leukemia (CLL).
“Malignancies that were resistant to allogeneic transplants and standard donor lymphocyte infusions regressed after infusions of allogeneic anti-CD19 CAR T cells,” said James N. Kochenderfer, MD, of the National Cancer Institute in Bethesda, Maryland.
“Allogeneic anti-CD19 CAR T cells seem to be particularly effective against ALL and CLL, suggesting a possible antigenic stimulation that may be more pronounced in these malignancies.”
Adverse events associated with these CAR T cells included severe but reversible cytokine release syndrome, mild aphasia, and muscle damage. There were no cases of acute graft-vs-host disease (GVHD).
Dr Kochenderfer presented these results at ASH as abstract 99.
For this phase 1 study, researchers tested a CAR T-cell therapy that was originally developed by Dr Kochenderfer and his colleagues. The therapy is now known as KTE-C19 and is under development by Kite Pharmaceuticals. However, the company did not sponsor this trial.
The study was open to patients with any CD19+ B-cell malignancy that persisted after allogeneic transplant.
All patients except those with ALL were required to have received at least one standard donor lymphocyte infusion. In addition, patients were only eligible if they had minimal or no GVHD and were not receiving any systemic immunosuppressive drugs.
The trial included 20 patients—5 each with ALL, CLL, mantle cell lymphoma (MCL), and diffuse large B-cell lymphoma (DLBCL).
All patients received a single infusion of CAR T cells derived from their original transplant donor. Production of these cells took 8 days. The highest dose of CAR T cells given was 107 cells/kg.
Four of the ALL patients obtained a minimal-residual disease-negative complete response (CR), but 2 of these patients subsequently relapsed. Of the other 2 patients, 1 remains in CR at 18 months of follow-up, and the other went on to receive a second allogeneic transplant. That patient remains in CR today.
Among the CLL patients, 1 achieved a CR, and 1 achieved a partial response (PR). One patient had stable disease (SD), and the other 2 progressed. Both the CR and the PR are ongoing at 36 and 18 months of follow-up, respectively.
One MCL patient achieved a CR, 1 had a PR, and 3 had SD. The CR is ongoing at 31 months. One DLBCL patient achieved a CR, 3 had SD, and 1 progressed.
Dr Kochenderfer noted that response was associated with higher blood CAR T-cell levels. There was a significant difference in CAR T-cell levels between responders and nonresponders (P=0.001).
In addition, the presence of blood B-cell levels before CAR T-cell infusion was associated with higher blood CAR T-cell levels. Patients with normal or high B lymphocytes had higher levels of CAR T cells in their blood (P=0.04).
Patients with high tumor burdens developed severe cytokine-release syndrome with fever, tachycardia, and hypotension. The ALL patients were particularly susceptible to cytokine-release syndrome.
Dr Kochenderfer said neurologic toxicity was rare and mild. There was 1 case of mild aphasia.
There were 2 patients with elevations in CPK, indicating muscle damage. Those patients also reported muscle pain, and 1 patient reported weakness.
“This is one of the first reports, I think, of muscle damage in CAR T-cell patients,” Dr Kochenderfer said.
None of the patients developed acute GVHD after CAR T-cell therapy. One patient had continued worsening of pre-existing chronic GVHD after treatment, and 1 patient developed mild chronic eye GVHD more than a year after CAR T-cell infusion.
Dr Kochenderfer said additional details from this trial will be published in an upcoming issue of the Journal of Clinical Oncology. ![]()
Photo courtesy of ASH
ORLANDO, FL—Allogeneic chimeric antigen receptor (CAR) T cells directed against CD19 can have “significant” activity against resistant B-cell malignancies, even when given without prior chemotherapy, according to a presentation at the 2015 ASH Annual Meeting.
Nine of 20 patients responded to treatment with the CAR T cells, despite having failed prior allogeneic transplant. The best responses were observed in patients with acute lymphoblastic leukemia (ALL) and chronic lymphocytic leukemia (CLL).
“Malignancies that were resistant to allogeneic transplants and standard donor lymphocyte infusions regressed after infusions of allogeneic anti-CD19 CAR T cells,” said James N. Kochenderfer, MD, of the National Cancer Institute in Bethesda, Maryland.
“Allogeneic anti-CD19 CAR T cells seem to be particularly effective against ALL and CLL, suggesting a possible antigenic stimulation that may be more pronounced in these malignancies.”
Adverse events associated with these CAR T cells included severe but reversible cytokine release syndrome, mild aphasia, and muscle damage. There were no cases of acute graft-vs-host disease (GVHD).
Dr Kochenderfer presented these results at ASH as abstract 99.
For this phase 1 study, researchers tested a CAR T-cell therapy that was originally developed by Dr Kochenderfer and his colleagues. The therapy is now known as KTE-C19 and is under development by Kite Pharmaceuticals. However, the company did not sponsor this trial.
The study was open to patients with any CD19+ B-cell malignancy that persisted after allogeneic transplant.
All patients except those with ALL were required to have received at least one standard donor lymphocyte infusion. In addition, patients were only eligible if they had minimal or no GVHD and were not receiving any systemic immunosuppressive drugs.
The trial included 20 patients—5 each with ALL, CLL, mantle cell lymphoma (MCL), and diffuse large B-cell lymphoma (DLBCL).
All patients received a single infusion of CAR T cells derived from their original transplant donor. Production of these cells took 8 days. The highest dose of CAR T cells given was 107 cells/kg.
Four of the ALL patients obtained a minimal-residual disease-negative complete response (CR), but 2 of these patients subsequently relapsed. Of the other 2 patients, 1 remains in CR at 18 months of follow-up, and the other went on to receive a second allogeneic transplant. That patient remains in CR today.
Among the CLL patients, 1 achieved a CR, and 1 achieved a partial response (PR). One patient had stable disease (SD), and the other 2 progressed. Both the CR and the PR are ongoing at 36 and 18 months of follow-up, respectively.
One MCL patient achieved a CR, 1 had a PR, and 3 had SD. The CR is ongoing at 31 months. One DLBCL patient achieved a CR, 3 had SD, and 1 progressed.
Dr Kochenderfer noted that response was associated with higher blood CAR T-cell levels. There was a significant difference in CAR T-cell levels between responders and nonresponders (P=0.001).
In addition, the presence of blood B-cell levels before CAR T-cell infusion was associated with higher blood CAR T-cell levels. Patients with normal or high B lymphocytes had higher levels of CAR T cells in their blood (P=0.04).
Patients with high tumor burdens developed severe cytokine-release syndrome with fever, tachycardia, and hypotension. The ALL patients were particularly susceptible to cytokine-release syndrome.
Dr Kochenderfer said neurologic toxicity was rare and mild. There was 1 case of mild aphasia.
There were 2 patients with elevations in CPK, indicating muscle damage. Those patients also reported muscle pain, and 1 patient reported weakness.
“This is one of the first reports, I think, of muscle damage in CAR T-cell patients,” Dr Kochenderfer said.
None of the patients developed acute GVHD after CAR T-cell therapy. One patient had continued worsening of pre-existing chronic GVHD after treatment, and 1 patient developed mild chronic eye GVHD more than a year after CAR T-cell infusion.
Dr Kochenderfer said additional details from this trial will be published in an upcoming issue of the Journal of Clinical Oncology. ![]()
Mixing warfarin, sulfonylurea may cause serious events

A retrospective study published in The BMJ suggests the possibility of a significant drug interaction between warfarin and the sulfonylureas glipizide and glimepiride.
Taking either of these diabetes drugs in conjunction with warfarin was linked to increased hospitalizations for falls, altered mental state, and insulin shock among patients 65 and older.
Hospital admissions or emergency room visits were nearly 22% higher for patients who were taking warfarin with glipizide or glimepiride, compared to patients taking the diabetes drugs alone.
Clinical references warn doctors of a potential interaction between these drugs, but evidence of it has been thin, according to lead study author John Romley, PhD, of the University of Southern California (USC) in Los Angeles.
He and his colleagues said that, in their study, evidence of the drug-to-drug interaction was clear.
When taken with glipizide or glimepiride, warfarin can intensify their effects and send blood sugar levels crashing. Patients experiencing hypoglycemia may seem drunk, lightheaded, and confused, and are at risk of falling.
“The take-home message is simply that an interaction can occur that has clinical significance, so providers need to be aware in order to prevent a low blood sugar issue from occurring,” said Anne Peters, MD, also of USC.
“Sometimes this means having the patient monitor their blood sugar levels more often. There are many ways to deal with the issue if one is forewarned.”
Pharmacists don’t need to change patient instructions, added Bradley Williams, PharmD, of USC.
“What it does require is for pharmacists and other clinicians to be more vigilant when a sulfonylurea is added to a regimen that includes warfarin, as well as when a patient who is taking both has a change in their medical status,” Dr Williams said.
“I think additional research into the potential interactions between medications for diabetes and warfarin, as well as other drugs that affect blood clotting, is warranted because of the potential consequences of excessive bleeding.”
For the current study, the researchers analyzed a random sample of 465,918 Medicare beneficiaries with diabetes who filled a prescription for glipizide or glimepiride between 2006 and 2011. About 15% of these patients (n=71,895) also filled a prescription for warfarin.
The researchers found that hospital admissions or emergency department visits for hypoglycemia were more common with concurrent warfarin and glipizide/glimepiride use than with glipizide/glimepiride use alone. The adjusted odds ratio (AOR) was 1.22.
The risk of hypoglycemia associated with concurrent use was higher among patients taking warfarin for the first time, as well as in patients ages 65 to 74.
Concurrent use of warfarin and glipizide/glimepiride was also associated with hospital admission or emergency department visits for fall-related fractures (AOR=1.47) and altered consciousness/mental status (AOR=1.22).
The researchers said these findings may not be generalizable beyond the elderly Medicare population.
They also noted that their findings could be confounded by some unmeasured characteristics in patients that may be connected to warfarin use or a risk for hypoglycemia. Another limitation of this study is that the researchers did not measure drug use directly. ![]()
A retrospective study published in The BMJ suggests the possibility of a significant drug interaction between warfarin and the sulfonylureas glipizide and glimepiride.
Taking either of these diabetes drugs in conjunction with warfarin was linked to increased hospitalizations for falls, altered mental state, and insulin shock among patients 65 and older.
Hospital admissions or emergency room visits were nearly 22% higher for patients who were taking warfarin with glipizide or glimepiride, compared to patients taking the diabetes drugs alone.
Clinical references warn doctors of a potential interaction between these drugs, but evidence of it has been thin, according to lead study author John Romley, PhD, of the University of Southern California (USC) in Los Angeles.
He and his colleagues said that, in their study, evidence of the drug-to-drug interaction was clear.
When taken with glipizide or glimepiride, warfarin can intensify their effects and send blood sugar levels crashing. Patients experiencing hypoglycemia may seem drunk, lightheaded, and confused, and are at risk of falling.
“The take-home message is simply that an interaction can occur that has clinical significance, so providers need to be aware in order to prevent a low blood sugar issue from occurring,” said Anne Peters, MD, also of USC.
“Sometimes this means having the patient monitor their blood sugar levels more often. There are many ways to deal with the issue if one is forewarned.”
Pharmacists don’t need to change patient instructions, added Bradley Williams, PharmD, of USC.
“What it does require is for pharmacists and other clinicians to be more vigilant when a sulfonylurea is added to a regimen that includes warfarin, as well as when a patient who is taking both has a change in their medical status,” Dr Williams said.
“I think additional research into the potential interactions between medications for diabetes and warfarin, as well as other drugs that affect blood clotting, is warranted because of the potential consequences of excessive bleeding.”
For the current study, the researchers analyzed a random sample of 465,918 Medicare beneficiaries with diabetes who filled a prescription for glipizide or glimepiride between 2006 and 2011. About 15% of these patients (n=71,895) also filled a prescription for warfarin.
The researchers found that hospital admissions or emergency department visits for hypoglycemia were more common with concurrent warfarin and glipizide/glimepiride use than with glipizide/glimepiride use alone. The adjusted odds ratio (AOR) was 1.22.
The risk of hypoglycemia associated with concurrent use was higher among patients taking warfarin for the first time, as well as in patients ages 65 to 74.
Concurrent use of warfarin and glipizide/glimepiride was also associated with hospital admission or emergency department visits for fall-related fractures (AOR=1.47) and altered consciousness/mental status (AOR=1.22).
The researchers said these findings may not be generalizable beyond the elderly Medicare population.
They also noted that their findings could be confounded by some unmeasured characteristics in patients that may be connected to warfarin use or a risk for hypoglycemia. Another limitation of this study is that the researchers did not measure drug use directly. ![]()
A retrospective study published in The BMJ suggests the possibility of a significant drug interaction between warfarin and the sulfonylureas glipizide and glimepiride.
Taking either of these diabetes drugs in conjunction with warfarin was linked to increased hospitalizations for falls, altered mental state, and insulin shock among patients 65 and older.
Hospital admissions or emergency room visits were nearly 22% higher for patients who were taking warfarin with glipizide or glimepiride, compared to patients taking the diabetes drugs alone.
Clinical references warn doctors of a potential interaction between these drugs, but evidence of it has been thin, according to lead study author John Romley, PhD, of the University of Southern California (USC) in Los Angeles.
He and his colleagues said that, in their study, evidence of the drug-to-drug interaction was clear.
When taken with glipizide or glimepiride, warfarin can intensify their effects and send blood sugar levels crashing. Patients experiencing hypoglycemia may seem drunk, lightheaded, and confused, and are at risk of falling.
“The take-home message is simply that an interaction can occur that has clinical significance, so providers need to be aware in order to prevent a low blood sugar issue from occurring,” said Anne Peters, MD, also of USC.
“Sometimes this means having the patient monitor their blood sugar levels more often. There are many ways to deal with the issue if one is forewarned.”
Pharmacists don’t need to change patient instructions, added Bradley Williams, PharmD, of USC.
“What it does require is for pharmacists and other clinicians to be more vigilant when a sulfonylurea is added to a regimen that includes warfarin, as well as when a patient who is taking both has a change in their medical status,” Dr Williams said.
“I think additional research into the potential interactions between medications for diabetes and warfarin, as well as other drugs that affect blood clotting, is warranted because of the potential consequences of excessive bleeding.”
For the current study, the researchers analyzed a random sample of 465,918 Medicare beneficiaries with diabetes who filled a prescription for glipizide or glimepiride between 2006 and 2011. About 15% of these patients (n=71,895) also filled a prescription for warfarin.
The researchers found that hospital admissions or emergency department visits for hypoglycemia were more common with concurrent warfarin and glipizide/glimepiride use than with glipizide/glimepiride use alone. The adjusted odds ratio (AOR) was 1.22.
The risk of hypoglycemia associated with concurrent use was higher among patients taking warfarin for the first time, as well as in patients ages 65 to 74.
Concurrent use of warfarin and glipizide/glimepiride was also associated with hospital admission or emergency department visits for fall-related fractures (AOR=1.47) and altered consciousness/mental status (AOR=1.22).
The researchers said these findings may not be generalizable beyond the elderly Medicare population.
They also noted that their findings could be confounded by some unmeasured characteristics in patients that may be connected to warfarin use or a risk for hypoglycemia. Another limitation of this study is that the researchers did not measure drug use directly. ![]()
FDA approves recombinant product for VWD
The US Food and Drug Administration (FDA) has approved a recombinant von Willebrand factor product, Vonvendi (formerly BAX 111), for use in adults with von Willebrand disease (VWD).
Vonvendi is the first FDA-approved recombinant von Willebrand factor.
It is now approved for the on-demand treatment and control of bleeding episodes in VWD patients 18 years of age and older.
Vonvendi is expected to be broadly available in the US in late 2016.
Compared to other marketed von Willebrand factor concentrates, Vonvendi contains a more consistent concentration of ultra-large-molecular-weight multimers. And the product is developed using a plasma- and albumin-free manufacturing method.
Vonvendi is the first von Willebrand factor concentrate in the US that contains only trace amounts of factor VIII (FVIII), offering the flexibility to administer FVIII only when needed.
The FDA’s approval of Vonvendi was based on results from a phase 3 trial recently published in Blood. The study included 49 patients with WWD who received Vonvendi with and without recombinant FVIII.
All participants reported successful treatment of bleeding episodes. Most (96.9%) treated bleeds (n=192 bleeds in 22 patients) achieved an “excellent” efficacy rating.
Most bleeds (81.8%) were resolved with a single infusion of Vonvendi, and the treatment had a mean half-life of 21.9 hours.
There were 8 adverse events considered related to Vonvendi, but only 2 of these were serious. One patient experienced 2 simultaneous serious adverse events—chest discomfort and increased heart rate—but these were resolved.
There were no thrombotic events in this trial, no treatment-related binding or neutralizing antibodies against von Willebrand factor, and no neutralizing antibodies against FVIII.
Vonvendi is manufactured by Baxalta Incorporated. Baxalta said it is building a robust clinical development program to optimize patient access to Vonvendi worldwide. A series of clinical programs are planned to evaluate its use for prophylaxis, surgical, and pediatric indications.
Baxalta expects to file for regulatory approvals in Europe in 2017 and in other markets around the world.
For more details on Vonvendi, see the product information. ![]()
The US Food and Drug Administration (FDA) has approved a recombinant von Willebrand factor product, Vonvendi (formerly BAX 111), for use in adults with von Willebrand disease (VWD).
Vonvendi is the first FDA-approved recombinant von Willebrand factor.
It is now approved for the on-demand treatment and control of bleeding episodes in VWD patients 18 years of age and older.
Vonvendi is expected to be broadly available in the US in late 2016.
Compared to other marketed von Willebrand factor concentrates, Vonvendi contains a more consistent concentration of ultra-large-molecular-weight multimers. And the product is developed using a plasma- and albumin-free manufacturing method.
Vonvendi is the first von Willebrand factor concentrate in the US that contains only trace amounts of factor VIII (FVIII), offering the flexibility to administer FVIII only when needed.
The FDA’s approval of Vonvendi was based on results from a phase 3 trial recently published in Blood. The study included 49 patients with WWD who received Vonvendi with and without recombinant FVIII.
All participants reported successful treatment of bleeding episodes. Most (96.9%) treated bleeds (n=192 bleeds in 22 patients) achieved an “excellent” efficacy rating.
Most bleeds (81.8%) were resolved with a single infusion of Vonvendi, and the treatment had a mean half-life of 21.9 hours.
There were 8 adverse events considered related to Vonvendi, but only 2 of these were serious. One patient experienced 2 simultaneous serious adverse events—chest discomfort and increased heart rate—but these were resolved.
There were no thrombotic events in this trial, no treatment-related binding or neutralizing antibodies against von Willebrand factor, and no neutralizing antibodies against FVIII.
Vonvendi is manufactured by Baxalta Incorporated. Baxalta said it is building a robust clinical development program to optimize patient access to Vonvendi worldwide. A series of clinical programs are planned to evaluate its use for prophylaxis, surgical, and pediatric indications.
Baxalta expects to file for regulatory approvals in Europe in 2017 and in other markets around the world.
For more details on Vonvendi, see the product information. ![]()
The US Food and Drug Administration (FDA) has approved a recombinant von Willebrand factor product, Vonvendi (formerly BAX 111), for use in adults with von Willebrand disease (VWD).
Vonvendi is the first FDA-approved recombinant von Willebrand factor.
It is now approved for the on-demand treatment and control of bleeding episodes in VWD patients 18 years of age and older.
Vonvendi is expected to be broadly available in the US in late 2016.
Compared to other marketed von Willebrand factor concentrates, Vonvendi contains a more consistent concentration of ultra-large-molecular-weight multimers. And the product is developed using a plasma- and albumin-free manufacturing method.
Vonvendi is the first von Willebrand factor concentrate in the US that contains only trace amounts of factor VIII (FVIII), offering the flexibility to administer FVIII only when needed.
The FDA’s approval of Vonvendi was based on results from a phase 3 trial recently published in Blood. The study included 49 patients with WWD who received Vonvendi with and without recombinant FVIII.
All participants reported successful treatment of bleeding episodes. Most (96.9%) treated bleeds (n=192 bleeds in 22 patients) achieved an “excellent” efficacy rating.
Most bleeds (81.8%) were resolved with a single infusion of Vonvendi, and the treatment had a mean half-life of 21.9 hours.
There were 8 adverse events considered related to Vonvendi, but only 2 of these were serious. One patient experienced 2 simultaneous serious adverse events—chest discomfort and increased heart rate—but these were resolved.
There were no thrombotic events in this trial, no treatment-related binding or neutralizing antibodies against von Willebrand factor, and no neutralizing antibodies against FVIII.
Vonvendi is manufactured by Baxalta Incorporated. Baxalta said it is building a robust clinical development program to optimize patient access to Vonvendi worldwide. A series of clinical programs are planned to evaluate its use for prophylaxis, surgical, and pediatric indications.
Baxalta expects to file for regulatory approvals in Europe in 2017 and in other markets around the world.
For more details on Vonvendi, see the product information. ![]()
Antiplatelet agent proves ineffective in SCD

Photo courtesy of St. Jude
Children’s Research Hospital
Treatment with the antiplatelet agent prasugrel does not significantly reduce the rate of pain crises or severe lung complications in children with sickle cell disease (SCD), according to one of the largest and most geographically diverse international trials on SCD to date.
The DOVE trial was a double blind, randomized, placebo-controlled phase 3 study conducted at 51 sites across 13 nations in the Americas, Europe, the Middle East, Asia, and Africa.
“Although we were disappointed that prasugrel does not appear to ease the suffering of children with sickle cell disease, the fact that this study incorporated patients in the wide range of countries where the disease occurs is hugely significant,” said Carolyn Hoppe, MD, of UCSF Benioff Children’s Hospital Oakland in California.
“The logistical challenges that we addressed in designing and implementing the study can serve as a model for future research.”
The results of the study were published in NEJM. The research was sponsored by Daiichi Sankyo Company, Ltd. and Eli Lilly and Company.
The goal of the DOVE trial was to determine whether prasugrel could significantly reduce the rate of vaso-occlusive crises (VOCs)—defined as pain crises or acute chest syndrome—in children with SCD.
The trial enrolled 341 patients. About half of them (n=170) received daily oral prasugrel for between 9 and 24 months at individualized, blinded doses intended to maintain a selected target range of platelet activity. The remaining patients received a placebo.
All patients were monitored for VOCs prompting medical visits and for any increased risk of bleeding due to reduced platelet activity. In addition, patients 4 years old and older kept a daily electronic pain diary to aid in the reporting of painful events between visits.
At the end of the study period, there was no significant difference between the treatment arms in the overall rate of VOCs. The rate was 2.3 episodes per person-year in the prasugrel arm and 2.8 episodes per person-year in the placebo arm (P=0.12).
Similarly, prasugrel did not have a significant effect on the trial’s secondary outcome measures—VOC-related hospitalization rate, duration of hospitalization, time between VOCs, incidence of ischemic attack or ischemic stroke, transfusion rate, rate of pain, intensity of pain, use of analgesics, or missed school due to SCD-related pain.
The data did reveal a trend toward reduced VOC rates among patients ages 12 to 18 (P=0.06) and among patients who were not taking hydroxyurea (P=0.06). However, these trends were not statistically significant and require further research to determine their validity.
The investigators noted no adverse events related to prasugrel.
“Even though prasugrel did not achieve significant results, the findings should not detract from the fact that this team successfully completed a rigorous, sophisticated trial in a disease where the barriers to conducting large-scale international, patient-focused research are quite high,” said Matthew M. Heeney, MD, of the Dana–Farber/Boston Children’s Cancer and Blood Disorders Center in Massachusetts.
To conduct the study successfully on such a broad geographical scale, the investigators had to address several obstacles, such as varying standards of care, local technological resources, and infrastructure challenges, such as a lack of reliable electrical power. ![]()
Photo courtesy of St. Jude
Children’s Research Hospital
Treatment with the antiplatelet agent prasugrel does not significantly reduce the rate of pain crises or severe lung complications in children with sickle cell disease (SCD), according to one of the largest and most geographically diverse international trials on SCD to date.
The DOVE trial was a double blind, randomized, placebo-controlled phase 3 study conducted at 51 sites across 13 nations in the Americas, Europe, the Middle East, Asia, and Africa.
“Although we were disappointed that prasugrel does not appear to ease the suffering of children with sickle cell disease, the fact that this study incorporated patients in the wide range of countries where the disease occurs is hugely significant,” said Carolyn Hoppe, MD, of UCSF Benioff Children’s Hospital Oakland in California.
“The logistical challenges that we addressed in designing and implementing the study can serve as a model for future research.”
The results of the study were published in NEJM. The research was sponsored by Daiichi Sankyo Company, Ltd. and Eli Lilly and Company.
The goal of the DOVE trial was to determine whether prasugrel could significantly reduce the rate of vaso-occlusive crises (VOCs)—defined as pain crises or acute chest syndrome—in children with SCD.
The trial enrolled 341 patients. About half of them (n=170) received daily oral prasugrel for between 9 and 24 months at individualized, blinded doses intended to maintain a selected target range of platelet activity. The remaining patients received a placebo.
All patients were monitored for VOCs prompting medical visits and for any increased risk of bleeding due to reduced platelet activity. In addition, patients 4 years old and older kept a daily electronic pain diary to aid in the reporting of painful events between visits.
At the end of the study period, there was no significant difference between the treatment arms in the overall rate of VOCs. The rate was 2.3 episodes per person-year in the prasugrel arm and 2.8 episodes per person-year in the placebo arm (P=0.12).
Similarly, prasugrel did not have a significant effect on the trial’s secondary outcome measures—VOC-related hospitalization rate, duration of hospitalization, time between VOCs, incidence of ischemic attack or ischemic stroke, transfusion rate, rate of pain, intensity of pain, use of analgesics, or missed school due to SCD-related pain.
The data did reveal a trend toward reduced VOC rates among patients ages 12 to 18 (P=0.06) and among patients who were not taking hydroxyurea (P=0.06). However, these trends were not statistically significant and require further research to determine their validity.
The investigators noted no adverse events related to prasugrel.
“Even though prasugrel did not achieve significant results, the findings should not detract from the fact that this team successfully completed a rigorous, sophisticated trial in a disease where the barriers to conducting large-scale international, patient-focused research are quite high,” said Matthew M. Heeney, MD, of the Dana–Farber/Boston Children’s Cancer and Blood Disorders Center in Massachusetts.
To conduct the study successfully on such a broad geographical scale, the investigators had to address several obstacles, such as varying standards of care, local technological resources, and infrastructure challenges, such as a lack of reliable electrical power. ![]()
Photo courtesy of St. Jude
Children’s Research Hospital
Treatment with the antiplatelet agent prasugrel does not significantly reduce the rate of pain crises or severe lung complications in children with sickle cell disease (SCD), according to one of the largest and most geographically diverse international trials on SCD to date.
The DOVE trial was a double blind, randomized, placebo-controlled phase 3 study conducted at 51 sites across 13 nations in the Americas, Europe, the Middle East, Asia, and Africa.
“Although we were disappointed that prasugrel does not appear to ease the suffering of children with sickle cell disease, the fact that this study incorporated patients in the wide range of countries where the disease occurs is hugely significant,” said Carolyn Hoppe, MD, of UCSF Benioff Children’s Hospital Oakland in California.
“The logistical challenges that we addressed in designing and implementing the study can serve as a model for future research.”
The results of the study were published in NEJM. The research was sponsored by Daiichi Sankyo Company, Ltd. and Eli Lilly and Company.
The goal of the DOVE trial was to determine whether prasugrel could significantly reduce the rate of vaso-occlusive crises (VOCs)—defined as pain crises or acute chest syndrome—in children with SCD.
The trial enrolled 341 patients. About half of them (n=170) received daily oral prasugrel for between 9 and 24 months at individualized, blinded doses intended to maintain a selected target range of platelet activity. The remaining patients received a placebo.
All patients were monitored for VOCs prompting medical visits and for any increased risk of bleeding due to reduced platelet activity. In addition, patients 4 years old and older kept a daily electronic pain diary to aid in the reporting of painful events between visits.
At the end of the study period, there was no significant difference between the treatment arms in the overall rate of VOCs. The rate was 2.3 episodes per person-year in the prasugrel arm and 2.8 episodes per person-year in the placebo arm (P=0.12).
Similarly, prasugrel did not have a significant effect on the trial’s secondary outcome measures—VOC-related hospitalization rate, duration of hospitalization, time between VOCs, incidence of ischemic attack or ischemic stroke, transfusion rate, rate of pain, intensity of pain, use of analgesics, or missed school due to SCD-related pain.
The data did reveal a trend toward reduced VOC rates among patients ages 12 to 18 (P=0.06) and among patients who were not taking hydroxyurea (P=0.06). However, these trends were not statistically significant and require further research to determine their validity.
The investigators noted no adverse events related to prasugrel.
“Even though prasugrel did not achieve significant results, the findings should not detract from the fact that this team successfully completed a rigorous, sophisticated trial in a disease where the barriers to conducting large-scale international, patient-focused research are quite high,” said Matthew M. Heeney, MD, of the Dana–Farber/Boston Children’s Cancer and Blood Disorders Center in Massachusetts.
To conduct the study successfully on such a broad geographical scale, the investigators had to address several obstacles, such as varying standards of care, local technological resources, and infrastructure challenges, such as a lack of reliable electrical power. ![]()
A Practical Approach to Weight Loss Maintenance and a Possible Role for Primary Care
Study Overview
Objective. To determine whether in-person visits for primary care patients resulted in improved weight loss maintenance relative to monthly mailings, with both groups receiving access to portion-controlled meals.
Design. Randomized clinical trial.
Setting and participants. This study took place within 2 university-affiliated primary care clinics in Colorado. For the first phase of the study, investigators enrolled 104 obese adult patients (18–79 years; BMI 30–49.9 kg/m2) who had been diagnosed with at least one of the following: type 2 diabetes, sleep apnea, hypertension, or hyperlipidemia. Patients who had independently lost weight prior to trial entry (> 5% in 6 months), were on weight-gain–promoting medications such as steroids, or had previously undergone bariatric surgery were excluded. The trial started with a 6-month run-in phase where active weight loss was promoted using a high-intensity behavioral intervention based on the Diabetes Prevention Program as well as access to subsidized portion-controlled foods (Nutrisystem). At the end of the 6-month run-in, the remaining participants (n = 84, 79.3%) were then randomized, stratified by gender and whether or not they achieved 5% weight loss, into the 2 main study arms.
Intervention. The experimental study arm (n = 41, “intensified maintenance”) relied on monthly in-person visits and monthly phone calls to prevent weight regain (thus, these participants had twice monthly contact during maintenance). Both visit types in this arm were conducted by a graduate-level research assistant and included some structured educational content as well as problem-solving around diet and lifestyle issues. In contrast, the control arm (n = 43, “standard maintenance”) relied just on monthly mailings (or emails) of educational and support materials to promote weight loss maintenance. Participants in both groups had the opportunity to purchase subsidized portion-controlled foods/meals from Nutrisystem in order to facilitate continued adherence to the caloric restriction required for weight loss maintenance.
Main outcome measures. The primary outcome for this trial was change in weight, measured in kgs, during the 12-month maintenance period. Other biometric outcomes included changes in blood pressure, serum glucose, lipid levels, and the inflammatory marker hs-CRP. Patient-reported outcomes included changes in medication use. The investigators used intention-to-treat analysis, with mixed linear models adjusted for age and gender. No imputation techniques for missing data are reported, although complete follow-up data was obtained on 94% of patients.
Results. Participants in the standard and intensified weight maintenance arms of the trial were similar with respect to measured baseline characteristics. The average age of participants was 56 years, and three-quarters (75%) were female. The majority in both groups were white (77% in standard arm; 88% in intense), and over half had either a college or advanced degree (58.1% in standard arm, 51.2% in intense). Approximately one- third had diabetes (32.6% in standard arm, 34.1% in intense) and over half had hypertension (67.4% in standard arm, 63.4% in intense). Of the 84 participants who were randomized in the weight maintenance phase of the study, 79 completed the 12-month follow up (94%; no difference in attrition between groups).
After 12 months of maintenance, participants in the intensified maintenance arm regained just 1.6 (± 1.3) kg of lost weight, while those in the standard arm regained 5.0 (± 0.8) kg, a statistically significant difference (P = 0.01). The investigators also examined the subgroup of participants who, after the 6-month run-in, had lost at least 5% of their initial body weight. For these individuals, almost three-quarters in the intensified maintenance arm (71.9%) maintained that > 5% loss by 18 months, compared to 51.7% in the standard group. This difference between groups was not statistically significant. There was a significant difference between groups for change in hs-CRP over the 12-month maintenance period, with the intensive group’s hs-CRP ending up an average of 1.46 mg/L lower than that of the standard group (P = 0.03). Although there was a similar trend favoring the intensive intervention for other biometric measures (change in waist circumference, glucose, blood pressure, and lipids were all more favorable in this arm), the between-group differences for these measures did not reach statistical significance. No significant differences between groups were observed with respect to changes in medication use over the 12-month maintenance intervention.
Conclusion. After 5 months of active weight loss, twice-monthly contact (using one in-person and one phone visit) plus portion-controlled foods during a 12-month weight maintenance phase resulted in significantly less weight regain than monthly mail or email-based counseling plus portion-controlled foods.
Commentary
Behavioral weight loss interventions, which typically require high-intensity in-person counseling over several months to a year, may be difficult to accomplish in the average primary care practice [1]. On the other hand, it may be the case that primary care practices are well-suited to assist patients who have already lost weight, as they enter weight-loss maintenance. While numerous studies have shown that patients who adhere to calorie-restricted diets (almost regardless of diet composition) are able to achieve clinically significant weight loss, less is known about effective methods of preventing weight regain. Several large trials have suggested that, as is the case with behavioral weight loss interventions, maintenance interventions are also more successful if they include regular contact, at least some of which is face-to-face [2,3]. These visits, along with other practices such as self-weighing and food diaries, may help patients maintain the energy balance necessary to stay at their new, lower body weight. There remains a gap, however, in terms of knowing whether the maintenance interventions from large randomized trials can be translated into the sometimes messy real world of clinical practice, where clinicians and patients are typically overburdened and busy.
The current study by Tsai et al does address some aspects of this important question. By recruiting “real-world” chronically ill patients from a primary care practice to participate in the trial, the results of this study may be more likely to generalize to the patient populations seen by practicing clinicians than the typically healthier, younger, community-recruited volunteers in large trials. Additionally, although the interventions in this study were not delivered by the primary care practice per se, they were low enough in intensity that they could theoretically be translated into most clinical practice settings, assuming reimbursement is not an issue. Monthly in-person visits certainly could be done by a physician (as under current CMS reimbursement guidelines), but would not have to be (the visits in this study were done by a graduate student with no formal training in behavioral interventions), and telephone visits could easily be done by clinical support staff. Even with this low level of visit intensity, patients had significantly less weight regain than those who were receiving monthly email or postal mail support (which, realistically, would still require some work on the part of primary care practices). Furthermore, there were suggestions of numerous parallel cardiometabolic benefits that might have been statistically significant with a larger sample size. This study benefited from several strengths in addition to its highly practical point of view. It was a randomized trial with a strong control group and long follow-up duration (18 months total). It used a run-in period for weight loss so that all who entered maintenance were doing so based on exposure to the same weight loss intervention. Happily, though, the investigators did not require successful weight loss (> 5%) for entry into the maintenance phase, which likely further contributed to the generalizability of their results. Another area where the run-in likely helped was with retention of subjects—94% of those randomized for maintenance contributed complete data at the end of the 12-month study period.
As acknowledged by the authors, this study also has some important limitations. As with most weight loss/diet interventions, the participants in this study were mostly female, and mostly non-Hispanic white, and thus a substantially less diverse population than is represented by patients with obesity in the US. Furthermore, although some aspects of the patient population did promote generalizability (recruitment from primary care, chronic illness burden), these patients were fairly highly educated, which may have impacted their adherence and results.
The use of subsidized portion-controlled meals in this study, while evidence-based, may have clouded the results somewhat. Perhaps the effect of both interventions would have been less pronounced had patients not been provided with subsidies to access these foods. In their discussion, the investigators acknowledge that the study lacked a comparison group with no access to portion-controlled foods and that, in a post-hoc analysis, greater use of these foods corresponded with better weight loss and weight loss maintenance among all participants.
Finally, although it was beyond the scope of this study, this trial does not provide any information about how weight loss medications in either the weight loss or maintenance phases might impact these types of interventions. Now that the FDA has approved a number of such medications for long-term use, it would be very helpful to have more information about how medications might be integrated into these types of strategies, for interested patients, as physicians could clearly play an integral role in the pharmacologic management of weight, alongside effective behavioral interventions.
Applications for Clinical Practice
Low-to-moderate intensity in-person and telephone-based visits during weight maintenance may help to protect against weight regain, and could realistically be an option for many primary care practices and their patients. However, aside from Medicare patients, for whom monthly primary care–based weight maintenance visits are now covered, physicians would need to understand how to code and bill such visits appropriately in order to avoid having patients face unexpected charges.
—Kristina Lewis, MD, MPH
1. Tsai AG, Wadden TA. Treatment of obesity in primary care practice in the United States: a systematic review. J Gen Intern Med 2009;24:1073–9.
2. Wing RR, Tate DF, Gorin AA, et al. A self-regulation program for maintenance of weight loss. N Engl J Med 2006;355:1563–71.
3. Svetkey LP, Stevens VJ, Brantley PJ, et al. Comparison of strategies for sustaining weight loss: the weight loss maintenance randomized controlled trial. JAMA 2008;299:1139–48.
Study Overview
Objective. To determine whether in-person visits for primary care patients resulted in improved weight loss maintenance relative to monthly mailings, with both groups receiving access to portion-controlled meals.
Design. Randomized clinical trial.
Setting and participants. This study took place within 2 university-affiliated primary care clinics in Colorado. For the first phase of the study, investigators enrolled 104 obese adult patients (18–79 years; BMI 30–49.9 kg/m2) who had been diagnosed with at least one of the following: type 2 diabetes, sleep apnea, hypertension, or hyperlipidemia. Patients who had independently lost weight prior to trial entry (> 5% in 6 months), were on weight-gain–promoting medications such as steroids, or had previously undergone bariatric surgery were excluded. The trial started with a 6-month run-in phase where active weight loss was promoted using a high-intensity behavioral intervention based on the Diabetes Prevention Program as well as access to subsidized portion-controlled foods (Nutrisystem). At the end of the 6-month run-in, the remaining participants (n = 84, 79.3%) were then randomized, stratified by gender and whether or not they achieved 5% weight loss, into the 2 main study arms.
Intervention. The experimental study arm (n = 41, “intensified maintenance”) relied on monthly in-person visits and monthly phone calls to prevent weight regain (thus, these participants had twice monthly contact during maintenance). Both visit types in this arm were conducted by a graduate-level research assistant and included some structured educational content as well as problem-solving around diet and lifestyle issues. In contrast, the control arm (n = 43, “standard maintenance”) relied just on monthly mailings (or emails) of educational and support materials to promote weight loss maintenance. Participants in both groups had the opportunity to purchase subsidized portion-controlled foods/meals from Nutrisystem in order to facilitate continued adherence to the caloric restriction required for weight loss maintenance.
Main outcome measures. The primary outcome for this trial was change in weight, measured in kgs, during the 12-month maintenance period. Other biometric outcomes included changes in blood pressure, serum glucose, lipid levels, and the inflammatory marker hs-CRP. Patient-reported outcomes included changes in medication use. The investigators used intention-to-treat analysis, with mixed linear models adjusted for age and gender. No imputation techniques for missing data are reported, although complete follow-up data was obtained on 94% of patients.
Results. Participants in the standard and intensified weight maintenance arms of the trial were similar with respect to measured baseline characteristics. The average age of participants was 56 years, and three-quarters (75%) were female. The majority in both groups were white (77% in standard arm; 88% in intense), and over half had either a college or advanced degree (58.1% in standard arm, 51.2% in intense). Approximately one- third had diabetes (32.6% in standard arm, 34.1% in intense) and over half had hypertension (67.4% in standard arm, 63.4% in intense). Of the 84 participants who were randomized in the weight maintenance phase of the study, 79 completed the 12-month follow up (94%; no difference in attrition between groups).
After 12 months of maintenance, participants in the intensified maintenance arm regained just 1.6 (± 1.3) kg of lost weight, while those in the standard arm regained 5.0 (± 0.8) kg, a statistically significant difference (P = 0.01). The investigators also examined the subgroup of participants who, after the 6-month run-in, had lost at least 5% of their initial body weight. For these individuals, almost three-quarters in the intensified maintenance arm (71.9%) maintained that > 5% loss by 18 months, compared to 51.7% in the standard group. This difference between groups was not statistically significant. There was a significant difference between groups for change in hs-CRP over the 12-month maintenance period, with the intensive group’s hs-CRP ending up an average of 1.46 mg/L lower than that of the standard group (P = 0.03). Although there was a similar trend favoring the intensive intervention for other biometric measures (change in waist circumference, glucose, blood pressure, and lipids were all more favorable in this arm), the between-group differences for these measures did not reach statistical significance. No significant differences between groups were observed with respect to changes in medication use over the 12-month maintenance intervention.
Conclusion. After 5 months of active weight loss, twice-monthly contact (using one in-person and one phone visit) plus portion-controlled foods during a 12-month weight maintenance phase resulted in significantly less weight regain than monthly mail or email-based counseling plus portion-controlled foods.
Commentary
Behavioral weight loss interventions, which typically require high-intensity in-person counseling over several months to a year, may be difficult to accomplish in the average primary care practice [1]. On the other hand, it may be the case that primary care practices are well-suited to assist patients who have already lost weight, as they enter weight-loss maintenance. While numerous studies have shown that patients who adhere to calorie-restricted diets (almost regardless of diet composition) are able to achieve clinically significant weight loss, less is known about effective methods of preventing weight regain. Several large trials have suggested that, as is the case with behavioral weight loss interventions, maintenance interventions are also more successful if they include regular contact, at least some of which is face-to-face [2,3]. These visits, along with other practices such as self-weighing and food diaries, may help patients maintain the energy balance necessary to stay at their new, lower body weight. There remains a gap, however, in terms of knowing whether the maintenance interventions from large randomized trials can be translated into the sometimes messy real world of clinical practice, where clinicians and patients are typically overburdened and busy.
The current study by Tsai et al does address some aspects of this important question. By recruiting “real-world” chronically ill patients from a primary care practice to participate in the trial, the results of this study may be more likely to generalize to the patient populations seen by practicing clinicians than the typically healthier, younger, community-recruited volunteers in large trials. Additionally, although the interventions in this study were not delivered by the primary care practice per se, they were low enough in intensity that they could theoretically be translated into most clinical practice settings, assuming reimbursement is not an issue. Monthly in-person visits certainly could be done by a physician (as under current CMS reimbursement guidelines), but would not have to be (the visits in this study were done by a graduate student with no formal training in behavioral interventions), and telephone visits could easily be done by clinical support staff. Even with this low level of visit intensity, patients had significantly less weight regain than those who were receiving monthly email or postal mail support (which, realistically, would still require some work on the part of primary care practices). Furthermore, there were suggestions of numerous parallel cardiometabolic benefits that might have been statistically significant with a larger sample size. This study benefited from several strengths in addition to its highly practical point of view. It was a randomized trial with a strong control group and long follow-up duration (18 months total). It used a run-in period for weight loss so that all who entered maintenance were doing so based on exposure to the same weight loss intervention. Happily, though, the investigators did not require successful weight loss (> 5%) for entry into the maintenance phase, which likely further contributed to the generalizability of their results. Another area where the run-in likely helped was with retention of subjects—94% of those randomized for maintenance contributed complete data at the end of the 12-month study period.
As acknowledged by the authors, this study also has some important limitations. As with most weight loss/diet interventions, the participants in this study were mostly female, and mostly non-Hispanic white, and thus a substantially less diverse population than is represented by patients with obesity in the US. Furthermore, although some aspects of the patient population did promote generalizability (recruitment from primary care, chronic illness burden), these patients were fairly highly educated, which may have impacted their adherence and results.
The use of subsidized portion-controlled meals in this study, while evidence-based, may have clouded the results somewhat. Perhaps the effect of both interventions would have been less pronounced had patients not been provided with subsidies to access these foods. In their discussion, the investigators acknowledge that the study lacked a comparison group with no access to portion-controlled foods and that, in a post-hoc analysis, greater use of these foods corresponded with better weight loss and weight loss maintenance among all participants.
Finally, although it was beyond the scope of this study, this trial does not provide any information about how weight loss medications in either the weight loss or maintenance phases might impact these types of interventions. Now that the FDA has approved a number of such medications for long-term use, it would be very helpful to have more information about how medications might be integrated into these types of strategies, for interested patients, as physicians could clearly play an integral role in the pharmacologic management of weight, alongside effective behavioral interventions.
Applications for Clinical Practice
Low-to-moderate intensity in-person and telephone-based visits during weight maintenance may help to protect against weight regain, and could realistically be an option for many primary care practices and their patients. However, aside from Medicare patients, for whom monthly primary care–based weight maintenance visits are now covered, physicians would need to understand how to code and bill such visits appropriately in order to avoid having patients face unexpected charges.
—Kristina Lewis, MD, MPH
Study Overview
Objective. To determine whether in-person visits for primary care patients resulted in improved weight loss maintenance relative to monthly mailings, with both groups receiving access to portion-controlled meals.
Design. Randomized clinical trial.
Setting and participants. This study took place within 2 university-affiliated primary care clinics in Colorado. For the first phase of the study, investigators enrolled 104 obese adult patients (18–79 years; BMI 30–49.9 kg/m2) who had been diagnosed with at least one of the following: type 2 diabetes, sleep apnea, hypertension, or hyperlipidemia. Patients who had independently lost weight prior to trial entry (> 5% in 6 months), were on weight-gain–promoting medications such as steroids, or had previously undergone bariatric surgery were excluded. The trial started with a 6-month run-in phase where active weight loss was promoted using a high-intensity behavioral intervention based on the Diabetes Prevention Program as well as access to subsidized portion-controlled foods (Nutrisystem). At the end of the 6-month run-in, the remaining participants (n = 84, 79.3%) were then randomized, stratified by gender and whether or not they achieved 5% weight loss, into the 2 main study arms.
Intervention. The experimental study arm (n = 41, “intensified maintenance”) relied on monthly in-person visits and monthly phone calls to prevent weight regain (thus, these participants had twice monthly contact during maintenance). Both visit types in this arm were conducted by a graduate-level research assistant and included some structured educational content as well as problem-solving around diet and lifestyle issues. In contrast, the control arm (n = 43, “standard maintenance”) relied just on monthly mailings (or emails) of educational and support materials to promote weight loss maintenance. Participants in both groups had the opportunity to purchase subsidized portion-controlled foods/meals from Nutrisystem in order to facilitate continued adherence to the caloric restriction required for weight loss maintenance.
Main outcome measures. The primary outcome for this trial was change in weight, measured in kgs, during the 12-month maintenance period. Other biometric outcomes included changes in blood pressure, serum glucose, lipid levels, and the inflammatory marker hs-CRP. Patient-reported outcomes included changes in medication use. The investigators used intention-to-treat analysis, with mixed linear models adjusted for age and gender. No imputation techniques for missing data are reported, although complete follow-up data was obtained on 94% of patients.
Results. Participants in the standard and intensified weight maintenance arms of the trial were similar with respect to measured baseline characteristics. The average age of participants was 56 years, and three-quarters (75%) were female. The majority in both groups were white (77% in standard arm; 88% in intense), and over half had either a college or advanced degree (58.1% in standard arm, 51.2% in intense). Approximately one- third had diabetes (32.6% in standard arm, 34.1% in intense) and over half had hypertension (67.4% in standard arm, 63.4% in intense). Of the 84 participants who were randomized in the weight maintenance phase of the study, 79 completed the 12-month follow up (94%; no difference in attrition between groups).
After 12 months of maintenance, participants in the intensified maintenance arm regained just 1.6 (± 1.3) kg of lost weight, while those in the standard arm regained 5.0 (± 0.8) kg, a statistically significant difference (P = 0.01). The investigators also examined the subgroup of participants who, after the 6-month run-in, had lost at least 5% of their initial body weight. For these individuals, almost three-quarters in the intensified maintenance arm (71.9%) maintained that > 5% loss by 18 months, compared to 51.7% in the standard group. This difference between groups was not statistically significant. There was a significant difference between groups for change in hs-CRP over the 12-month maintenance period, with the intensive group’s hs-CRP ending up an average of 1.46 mg/L lower than that of the standard group (P = 0.03). Although there was a similar trend favoring the intensive intervention for other biometric measures (change in waist circumference, glucose, blood pressure, and lipids were all more favorable in this arm), the between-group differences for these measures did not reach statistical significance. No significant differences between groups were observed with respect to changes in medication use over the 12-month maintenance intervention.
Conclusion. After 5 months of active weight loss, twice-monthly contact (using one in-person and one phone visit) plus portion-controlled foods during a 12-month weight maintenance phase resulted in significantly less weight regain than monthly mail or email-based counseling plus portion-controlled foods.
Commentary
Behavioral weight loss interventions, which typically require high-intensity in-person counseling over several months to a year, may be difficult to accomplish in the average primary care practice [1]. On the other hand, it may be the case that primary care practices are well-suited to assist patients who have already lost weight, as they enter weight-loss maintenance. While numerous studies have shown that patients who adhere to calorie-restricted diets (almost regardless of diet composition) are able to achieve clinically significant weight loss, less is known about effective methods of preventing weight regain. Several large trials have suggested that, as is the case with behavioral weight loss interventions, maintenance interventions are also more successful if they include regular contact, at least some of which is face-to-face [2,3]. These visits, along with other practices such as self-weighing and food diaries, may help patients maintain the energy balance necessary to stay at their new, lower body weight. There remains a gap, however, in terms of knowing whether the maintenance interventions from large randomized trials can be translated into the sometimes messy real world of clinical practice, where clinicians and patients are typically overburdened and busy.
The current study by Tsai et al does address some aspects of this important question. By recruiting “real-world” chronically ill patients from a primary care practice to participate in the trial, the results of this study may be more likely to generalize to the patient populations seen by practicing clinicians than the typically healthier, younger, community-recruited volunteers in large trials. Additionally, although the interventions in this study were not delivered by the primary care practice per se, they were low enough in intensity that they could theoretically be translated into most clinical practice settings, assuming reimbursement is not an issue. Monthly in-person visits certainly could be done by a physician (as under current CMS reimbursement guidelines), but would not have to be (the visits in this study were done by a graduate student with no formal training in behavioral interventions), and telephone visits could easily be done by clinical support staff. Even with this low level of visit intensity, patients had significantly less weight regain than those who were receiving monthly email or postal mail support (which, realistically, would still require some work on the part of primary care practices). Furthermore, there were suggestions of numerous parallel cardiometabolic benefits that might have been statistically significant with a larger sample size. This study benefited from several strengths in addition to its highly practical point of view. It was a randomized trial with a strong control group and long follow-up duration (18 months total). It used a run-in period for weight loss so that all who entered maintenance were doing so based on exposure to the same weight loss intervention. Happily, though, the investigators did not require successful weight loss (> 5%) for entry into the maintenance phase, which likely further contributed to the generalizability of their results. Another area where the run-in likely helped was with retention of subjects—94% of those randomized for maintenance contributed complete data at the end of the 12-month study period.
As acknowledged by the authors, this study also has some important limitations. As with most weight loss/diet interventions, the participants in this study were mostly female, and mostly non-Hispanic white, and thus a substantially less diverse population than is represented by patients with obesity in the US. Furthermore, although some aspects of the patient population did promote generalizability (recruitment from primary care, chronic illness burden), these patients were fairly highly educated, which may have impacted their adherence and results.
The use of subsidized portion-controlled meals in this study, while evidence-based, may have clouded the results somewhat. Perhaps the effect of both interventions would have been less pronounced had patients not been provided with subsidies to access these foods. In their discussion, the investigators acknowledge that the study lacked a comparison group with no access to portion-controlled foods and that, in a post-hoc analysis, greater use of these foods corresponded with better weight loss and weight loss maintenance among all participants.
Finally, although it was beyond the scope of this study, this trial does not provide any information about how weight loss medications in either the weight loss or maintenance phases might impact these types of interventions. Now that the FDA has approved a number of such medications for long-term use, it would be very helpful to have more information about how medications might be integrated into these types of strategies, for interested patients, as physicians could clearly play an integral role in the pharmacologic management of weight, alongside effective behavioral interventions.
Applications for Clinical Practice
Low-to-moderate intensity in-person and telephone-based visits during weight maintenance may help to protect against weight regain, and could realistically be an option for many primary care practices and their patients. However, aside from Medicare patients, for whom monthly primary care–based weight maintenance visits are now covered, physicians would need to understand how to code and bill such visits appropriately in order to avoid having patients face unexpected charges.
—Kristina Lewis, MD, MPH
1. Tsai AG, Wadden TA. Treatment of obesity in primary care practice in the United States: a systematic review. J Gen Intern Med 2009;24:1073–9.
2. Wing RR, Tate DF, Gorin AA, et al. A self-regulation program for maintenance of weight loss. N Engl J Med 2006;355:1563–71.
3. Svetkey LP, Stevens VJ, Brantley PJ, et al. Comparison of strategies for sustaining weight loss: the weight loss maintenance randomized controlled trial. JAMA 2008;299:1139–48.
1. Tsai AG, Wadden TA. Treatment of obesity in primary care practice in the United States: a systematic review. J Gen Intern Med 2009;24:1073–9.
2. Wing RR, Tate DF, Gorin AA, et al. A self-regulation program for maintenance of weight loss. N Engl J Med 2006;355:1563–71.
3. Svetkey LP, Stevens VJ, Brantley PJ, et al. Comparison of strategies for sustaining weight loss: the weight loss maintenance randomized controlled trial. JAMA 2008;299:1139–48.
Enhancing the Communication Skills of Critical Care Nurses: Focus on Prognosis and Goals of Care Discussions
From the University of California Irvine Health/Chao Family Comprehensive Cancer Center Orange, CA (Ms. Boyle) and the University of California San Francisco Medical Center, San Francisco, CA (Dr. Anderson).
Abstract
- Objective: To describe components of a unique interactive workshop focusing on the enhancement of critical care nurses’ communication skills within the realm of prognosis and goals of care discussions with family members and physicians.
- Methods: A series of one-day workshops were offered to critical care nurses practicing in the 5 University of California hospital settings. After workshop attendance, nurse participants were followed by workshop facilitators in their units to ensure new communication skills were being integrated into practice and to problem solve if barriers were met.
- Results: Improvement in nurses’ self-confidence in engaging in these discussions was seen. This confidence was sustained months following workshop participation.
- Conclusion: The combination of critical care nurse workshop participation that involved skill enhancement through role-playing, in combination with clinical follow-up with attendees, resulted in positive affirmation of nurse communication skills specific to prognosis and goals of care discussions with family members and physicians.
There is increasing evidence that in the absence of quality communication between professional caregivers and those they care for, negative outcomes may prevail, such as reduced patient/family satisfaction, lower health status awareness, and a decreased sense of being cared about and cared for [1–5]. Communication skill competency is a critical corollary of nursing practice. In the intensive care unit (ICU) setting, patients and families have cited skilled communication as a core element of high-quality care [3,6]. Proficiency in this realm enhances nurses’ understanding of the patient and family’s encounter with health care and provides a vehicle to gather information, inform, teach, and offer emotional support. Additionally, it identifies values, goals, health care preferences, worries and concerns, and facilitates the nurses’ coordination of care [7]. Despite this skill’s importance, however, it is generally not taught in basic education and until recently has been overlooked as a key competency [8,9].
Skilled communication in palliative and end-of-life care is pivotal for discussing prognosis and care planning. In the acute care setting this is particularly relevant as the majority of Americans die in hospitals versus their preferred site of home [10]. Additionally, 1 in 5 Americans die during or shortly after receiving care in an ICU [11]. Hence, while the ICU is a setting in which intensive effort to save lives is employed, it is also a setting where death frequently occurs. The complexity and highly emotive nature of critical care often results in family needs for information and support not being met [12]. A number of reasons for this occurrence have been proposed. In this paper, we will delineate barriers to critical care nurses’ involvement in prognosis and goals of care discussions, identify why nurse involvement in this communication is needed, describe a unique workshop exemplar with a sample role play that characterizes the workshop, and offer recommendations for colleagues interested in replicating similar education offerings.
Barriers to Communication
In the ICU, the sheer number of professionals families interact with may cause confusion. In particular, numerous medical consultants commonly offer opposing opinions. Additionally, each specialist may provide information that focuses on their area of expertise such that the “big picture” is not relayed to the patient and family. Emotional discomfort on the part of the health professional around discussions of poor prognosis, goals of care, and code status may prompt limiting discussion time with patients and families and even the avoidance of interpersonal exchanges [13–15]. Health professionals have also reported concern that end-of-life discussions will increase patient distress [16]. Among health care professionals, the subject of mortality may prompt personal anxiety, trigger unresolved grief, or fear that they will “become emotional” in front of the patient/family [7]. Lack of knowledge about cultural and religious norms has been cited as a barrier, as has time constraints [17,18]. Most frequently, inadequate or absent communication skill training is noted as a significant barrier [19,20]. Many ICU nurses also report feeling marginalized due their exclusion from goals of care and decision-making discussions with patients and families they know well [21,22].
Nurses As Key Palliative Care Communicators
Education efforts that foster communication proficiency during serious illness have traditionally focused on training physicians. Recently, nursing has become a focus of communication skill enhancement in recognition of nurses’ intense and protracted interactions with patients and families in the acute care setting. Nurses are the ‘constant’ in the patient and family’s journey through the fragmented health care system [21,23]. They often have the best knowledge of, and strongest relationship with, the family and often have had extensive discussions with them about their loved one’s status [24]. Nurses are aware of the patients’ symptom experiences and are privy to valuable information about the concerns and priorities of patients and families [12]. Additionally, having the most continuous presence, nurses have seen and heard interactions with clinicians from numerous disciplines. Nurses are the most visible, constant resource for patient and family education, information and support, and thus they perceive one of their most important roles to be that of advocate for the patient and family [20,21].
Communication Training Programs for Critical Care Nurses
Education is critical to enhance communication skills within palliative care [7,15,17,20,21,24]. The preferred teaching style within this realm is role play, where skills can be practiced and the affective component of engaging in sensitive discussions can be addressed [25–27]. Role play also demonstrates firsthand the importance of nonverbal communication (eg, body language, proximity, use of gestures, tone of voice) [7,20] and facilitates nurses’ gaining a sense of comfort with wordless communication [18].
Communication skills training programs have been designed to provide bedside critical care nurses with the tools they need to be active participants in discussions of prognosis, goals of care, and palliative care with families and physicians [27,28]. These programs have demonstrated improvement in nurses’ confidence to engage in key palliative care-related discussions. Essential elements of these programs include (1) delineation of the role of the bedside nurse in palliative care communication; (2) presentation and learner-centered practice of communication skills using role play; and (3) a reflection session focused on self-care and sustainability.
Across the 5 academic University of California medical centers (San Francisco, Davis, Los Angeles, Irvine, and San Diego), a communication training program based on this work has been implemented [29]. The one-day workshop, entitled IMPACT-ICU (Integrating Multidisciplinary Palliative Care into the ICU), has taught a total of 527 critical care nurses across the 5 centers. In addition to classroom training, the IMPACT-ICU program also includes proactive specialty palliative nursing support for bedside nurses by facilitating the availability of palliative care advanced practice nurses and nurse educators resources. This support helps nurses to apply the skills learned in the workshop in their practice. During rounds at the bedside, the nurse resources coach the bedside staff on the “how” and “when” of addressing palliative care needs. Education and support on a range of topics are offered, including clarifying goals and interventions provided by palliative care teams, the specifics of how to provide family emotional support and delivery of understandable information, the assessment and management of symptoms distress, and the nurses’ role in organizing and participating in family meetings. Case-specific consultations are also offered that address how to interface with resistant medical staff. The importance of nurse documentation of these varied exchanges is also emphasized.
IMPACT-ICU Workshop
A maximum of 15 nurses participate in each 8-hour workshop. The session begins with introductions and small group discussions about what the participants perceive to be the greatest barriers to goals of care discussions and fostering patient/family decision-making in the ICU. Participants are also asked to reflect on what they want to learn as a result of their workshop attendance.
A short didactic session then reviews the definition of palliative care and its core components, addresses the nurses’ role in communication within palliative care, a social worker’s perspective of what it is like to be a family member in the ICU, and the outline of the day. This includes delineation of expectations for involvement within the role plays and the various roles to be enacted. An emphasis is placed on the workshop being a safe place to explore and trial skills with the support of colleagues, and that practice is the optimum way to integrate communication expertise into the nurses’ skill set.
The “4 Cs” serves as the instructional basis for nurse communication skill enhancement [27]. This model outlines 4 key nursing roles in optimizing communication within palliative care:
Convening: Making sure multidisciplinary patient/family/clinician communication occurs.
Checking: Identifying the patient and family needs for information; ensuring that patients and families clearly receive desired information; ensuring that clinicians understand patient and family perspectives.
Caring: Naming emotions and responding to feeling.
Continuing: Following up after discussions to clarify and reinforce information and provide support.
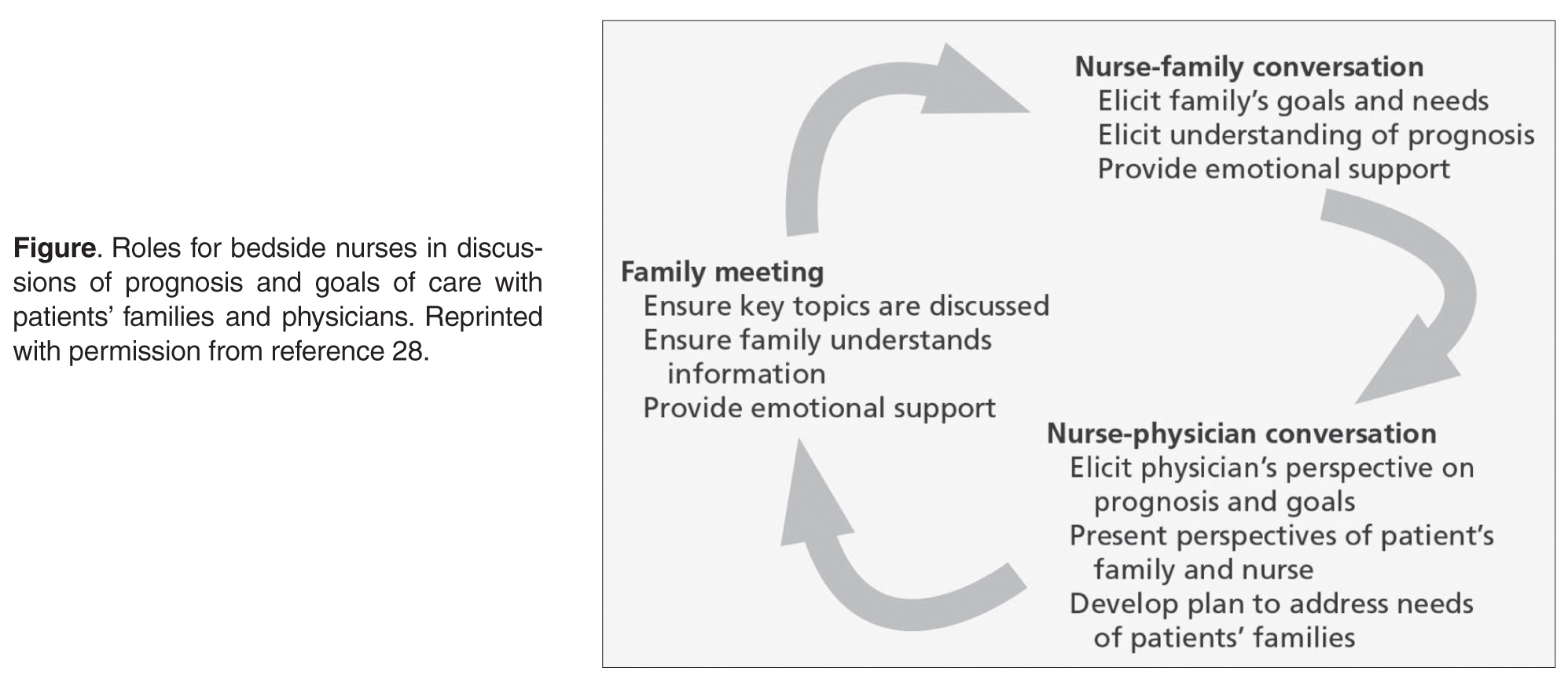
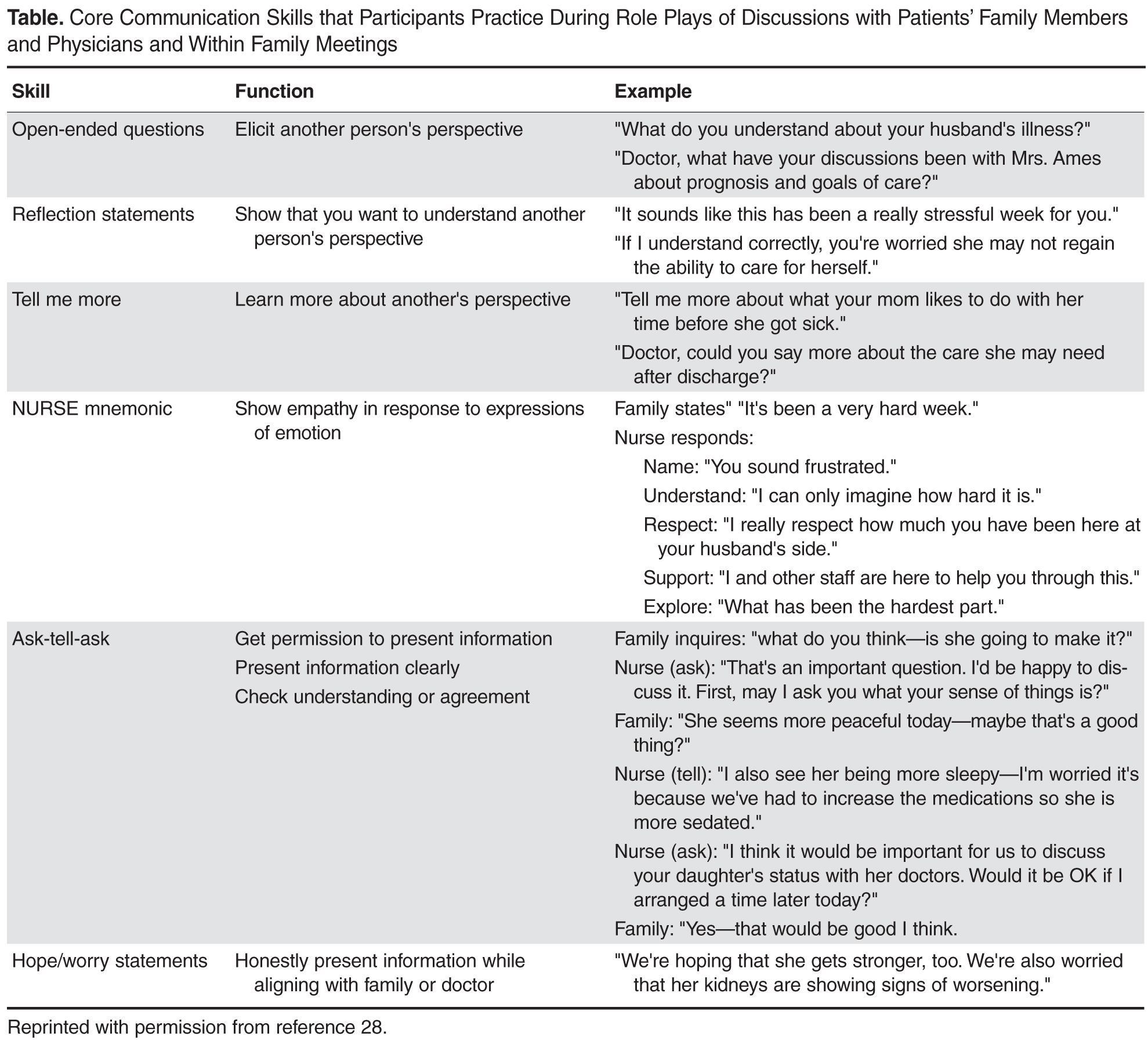
Sample Role Play
Facilitator: So our first role play is focused on eliciting patient and family perspectives and needs. I need a learner and someone to play the role of the family member.
Learner: I’ll give it a try.
Facilitator: Lisa, you’re going to do great. Who wants to play the family member?
Workshop Participant: I’ll do it.
Facilitator: So Mary (who has agreed to play the role of the wife), why don’t you read us the scenario. (She reads it out loud to the group).
Facilitator: Lisa, as the nurse, I want you to look at your guide and tell me what your goal is for this conversation with Mrs. Ames and then which skill you want to practice.
Learner: I think I want to try eliciting the patient and family’s needs for information and I’ll try “Tell Me More” statements.
Facilitator: Alright. So remember Lisa, if you feel the conversation isn’t going well, you can call a “time out.” I can do this as well if I feel you need to start over. I’ll also call a time out when I feel you have met your goal. Sound OK? Mary, do you have any questions playing the part of Mrs. Ames?
Wife Role: Well, how hard should I make this for her? Should I be one of those “difficult” family members?
Facilitator: Our goal here is not to “stump” you or make it particularly difficult. We want you to try out these skills and get a sense of your “comfort zone.” So let’s start with some basic communication skills, OK?
Wife Role: Alright.
Facilitator: Why don’t we set the stage, such that Lisa, you are Mr. Ames’ nurse assessing him at the start of your shift, when Mrs. Ames enters. This is the first time you have taken care of him. The night nurse has told you that he has been requiring increasing ventilator support and his renal function is declining. Per Mrs. Ames’ request, the night nurse called her to let her know how he was doing and Mrs. Ames told her she would be in shortly.
Wife Role: (nervously enters the room and grasps her husband’s hand and looks at the nurse). How’s he doing? Is he better? The night nurse called me and I was so worried I rushed over here.
Learner: (Turns to Mrs. Ames and extends her hand). Are you Mrs. Ames? I’m Lisa and I am going to be taking care of Mr. Ames today. Let me just finish my assessment and how about we talk then? Will that be OK? It will be just a few minutes.
Wife Role: Alright, I’ll be in the waiting area but please come get me as soon as you can.
Learner: I will. (Nurse then shortly comes into the waiting area and asks Mrs. Ames to come back into the ICU where she invites her to sit just outside Mr. Ames’ room). Mrs. Ames, how are you doing? This must be so stressful for you, having your husband in the ICU.
Wife Role: It’s awful. He’s never been in the hospital before this and look at him, all hooked up to machines. I’m so worried. He seems to be getting worse instead of better.
Learner: What’s your understanding of what is going on?
Wife Role: I really don’t know. One doctor comes in and says one thing and then another comes in and tells me the opposite. I’m so confused I don’t know what to think.
Learner: Would having a better idea of his condition from the doctors who are treating him help you have a better understanding?
Wife Role: Oh, yes, but they always seem in such a hurry.
Learner: What exactly would you like to know?
Wife: Well, I want to know when he can get off that breathing machine because we have been planning to go to our son’s house for Thanksgiving.
Facilitator: Time out. Lisa, did you meet your conversation goal?
Learner: Um, I’m not sure, I guess so.
Facilitator: (Turns to Observers). What do you think, did she meet her goal?
Observer: Yes, she determined Mrs. Ames’ need for more information and she asked her what she wanted to know exactly.
Facilitator: What else did we see Lisa do to enhance communication with Mrs. Ames?
Observer: Well, when Mrs. Ames rushed into the room and asked her for information, Lisa didn’t just jump in and spout out values for the ventilator and his output. She took the time to introduce herself and de-escalate Mrs. Ames’ anxiety and she followed up on her promise to come get her in the waiting room as soon as she could.
Facilitator: Why do you think was important?
Observer: It helps establish trust.
Facilitator: Did Lisa use the skill she wanted to try out?
Observer: Yes.
Facilitator: How do you know? What did you hear her say?
Observer: She said, “What’s your understanding of what is going on with Mr. Ames?”
Facilitator: Absolutely. Great job, Lisa. And who wants to take a guess at how long Lisa’s exchange with Mrs. Ames took?
Observer: Less than two minutes?
Facilitator: That’s right. So just as you consider how long it takes, and how proficient you are, in starting an IV or inserting a Foley catheter, when you have a goal in mind and have practiced the skills to do it well, any skill can be mastered.
Feedback
Participants in the workshops uniformly report an enhanced sense of self-confidence in their palliative care communication skills as a result of their participation [29]. Key to the success of the workshop is the ongoing contact by the workshop facilitators with participants. Rounding is routinely planned such that each participant is visited weekly by a workshop facilitator in their clinical area to determine if the bedside nurse has practiced the new skills and if so, how the interaction transpired. Positive feedback is given for attempts to engage in new behaviors and participants are reminded that with any new skill, repetitive trials are necessary to foster success.
Lessons Learned and Next Steps
One of our major lessons learned was recognizing that it was difficult for many critical care nurses to practice the new communication skills. Nurses are trained to fix problems and perform medico-technical tasks; “listening” has not always been recognized as real work [18]. We needed to reinforce that skills like eliciting another’s perspective or making reflection statements are equally important to those associated with behavioral/technical proficiency.
While our program has been successful, we recognize that the next step in fostering ideal palliative care communication is to provide education within an interdisciplinary context. We recommend that colleagues interested in replicating this or a similar education intervention, survey nurse participants prior to and following workshop participation to measure attitudes, self confidence and perceived barriers over time [30]. We hope to translate our positive experience into a program that engages multiple professionals in the enhancement of optimum palliative care communication proficiency.
Corresponding author: Deborah A. Boyle MSN, RN, AOCNS, Department of Nursing Quality, Research and Education, University of California, Irvine Health, 101 The City Drive, Bldg 22A, Room 3104, Orange, CA 92868.
1. Leung JM, Udris EM, Uman J, et al. The effect of end-of-life discussions on perceived quality of care and health status among patients with COPD. Chest 2012;142:128–33.
2. Osborn TR, Curtis JR, Nielsen EL, et al. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control and ICU atmosphere. Chest 2012;142:1185–92.
3. Nelson JE, Puntillo K, Pronovost PJ, et al. In their own words: patients and families define high-quality palliative care in the ICU. Crit Care Med 2010;38:808–18.
4. Nels W, Gabrijel S, Kiss S, et al. Communication skill training significantly improves lung cancer patients understanding. J Palliat Care Med 2014;4:182.
5. Van Vliet LM, Epstein AS. Current state of the art and science of patient-clinician communication in progressive disease: patients’ need to know and feel known. J Clin Oncol 2014;32:3474-8.
6. Troug RD, Campbell ML, Curtis JR, et al. Recommendations for end of life care in the intensive care unit: a consensus statement by the American College of Critical Care Medicine. Crit Care Med 2008;36:953–63.
7. Dahlin CM, Wittenberg E. Communication in palliative care. In: Ferrell BR, Coyle N, Paice J, editors. Oxford textbook of palliative nursing. 4th ed. Oxford: Oxford University Press; 2014:81–109.
8. Baer L, Weinstein E. Improving oncology nurses’ communication skills for difficult conversations. Clin J Oncol Nurs 2013;17:E45–E51.
9. Treece PD. Communication in the intensive care unit about end of life care. AACN Adv Crit Care 2007;18:406–14.
10. Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end of life care at the last place of care. JAMA 2004;291:88–92.
11. Angus DC, Barnato AE, Linde-Zwirble WT, et al. Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med 2004;32:638–43.
12. Hamric AB, Blackhall LJ. Nurse-physician perspectives on the care of dying patients in intensive care units: collaboration, moral distress, and ethical climate. Crit Care Med 2007;35:422–9.
13. Back AL, Trinidad SB, Hopley EK, Edwards KA. Reframing the goals of care conversation: “We’re in a different place.” J Palliat Med 2014;17:1010–24.
14. Aslakson RA, Wyskiel R, Thornton I, et al. Nurse perceived barriers to effective communication regarding prognosis and optimal end of life care for surgical ICU patients: a qualitative exploration. J Palliat Med 2012;15:910–5.
15. Erickson J. Bedside nurse involvement in end of life decision-making. Dimens Crit Care Nurs 2013;32:65–8.
16. Bernacki RE, Block SD for the American College of Physicians High Value Care Task Force. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med 2014;174:1994–2003.
17. You JJ, Downar J, Fowler RA, et al. Barriers to goals of care discussion with ‘seriously’ ill hospitalized patients and their families: a multicenter survey of clinicians. JAMA Intern Med 2015;175:549–56.
18. Strang S, Henoch I, Danielson E, et al. Communication about existential issues with patients close to death: nurses’ reflections on content, process, and meaning. Psychooncology 2014;23:562–8.
19. Slatore CG, Hensen L, Gauzine L, et al. Communication by nurses in the intensive care unit: qualitative analysis of domains in patient-centered care. Am J Crit Care 2012;21:410–8.
20. Wittenberg-Lyles E, Goldsmith J, Platt CS. Palliative care communication. Sem Oncol Nurs 2014;30:280–6.
21. Fox MY. Improving communication with patients and families in the ICU: palliative care strategies for intensive care unit nurses. J Hospice Palliat Nurs 2014;16:93–8.
22. Beckstrand RL, Callister LC, Kirchhoff KT. Providing a ‘good death’: critical care nurses’ suggestions for improving end of life care. Am J Crit Care 2006;15:38–45.
23. Peereboom K, Coyle N. Facilitating goals of care discus.sions for patients with life-limiting disease: communication strategies for nurses. J Hospice Palliat Nurs 2012; 14:251–8.
24. Nelson JE, Cortez TB, Curtis JR, et al. Integrating palliative care in the ICU: the nurse in the leading role. J Hospice Palliat Nurs 2011;13:89–94.
25. Jors K, Seibel K, Bardenheuer H, et al. Education in end of life care: what do experienced professionals find important? J Cancer Educ 2015 March 15.
26. Roze des Ordons AL, Sharma N, Heyland DK, et al. Strategies for effective goals of care discussions and decision-making: perspective from a multi-centre survey of Canadian hospital-based health care providers. BMC Palliat Care 2015;14:38.
27. Krimshtein NS, Luhrs CA, Puntillo KA, et al. Training nurses for interdisciplinary communication with families in the ICU. J Palliat Med 2011;14:1325–32.
28. Milic MM, Puntillo K, Turner K, et al. Communicating with patients’ families and physicians about prognosis and goals of care. Am J Crit Care 2015;24:e56–e64.
29. Anderson W, Puntillo K, Barbour S, et al. The IMPACT-ICU Project: expanding palliative care nursing across University of California Centers ICUs to advance palliative care. Center to Advance Palliative Care (CAPC) national seminar. Nov 7–9, 2013. Dallas, TX.
30. Anderson WG, Puntillo K, Boyle D, et al. ICU bedside nurses’ involvement in palliative care communication: a multicenter survey. J Pain Symptom Manage. In press.
From the University of California Irvine Health/Chao Family Comprehensive Cancer Center Orange, CA (Ms. Boyle) and the University of California San Francisco Medical Center, San Francisco, CA (Dr. Anderson).
Abstract
- Objective: To describe components of a unique interactive workshop focusing on the enhancement of critical care nurses’ communication skills within the realm of prognosis and goals of care discussions with family members and physicians.
- Methods: A series of one-day workshops were offered to critical care nurses practicing in the 5 University of California hospital settings. After workshop attendance, nurse participants were followed by workshop facilitators in their units to ensure new communication skills were being integrated into practice and to problem solve if barriers were met.
- Results: Improvement in nurses’ self-confidence in engaging in these discussions was seen. This confidence was sustained months following workshop participation.
- Conclusion: The combination of critical care nurse workshop participation that involved skill enhancement through role-playing, in combination with clinical follow-up with attendees, resulted in positive affirmation of nurse communication skills specific to prognosis and goals of care discussions with family members and physicians.
There is increasing evidence that in the absence of quality communication between professional caregivers and those they care for, negative outcomes may prevail, such as reduced patient/family satisfaction, lower health status awareness, and a decreased sense of being cared about and cared for [1–5]. Communication skill competency is a critical corollary of nursing practice. In the intensive care unit (ICU) setting, patients and families have cited skilled communication as a core element of high-quality care [3,6]. Proficiency in this realm enhances nurses’ understanding of the patient and family’s encounter with health care and provides a vehicle to gather information, inform, teach, and offer emotional support. Additionally, it identifies values, goals, health care preferences, worries and concerns, and facilitates the nurses’ coordination of care [7]. Despite this skill’s importance, however, it is generally not taught in basic education and until recently has been overlooked as a key competency [8,9].
Skilled communication in palliative and end-of-life care is pivotal for discussing prognosis and care planning. In the acute care setting this is particularly relevant as the majority of Americans die in hospitals versus their preferred site of home [10]. Additionally, 1 in 5 Americans die during or shortly after receiving care in an ICU [11]. Hence, while the ICU is a setting in which intensive effort to save lives is employed, it is also a setting where death frequently occurs. The complexity and highly emotive nature of critical care often results in family needs for information and support not being met [12]. A number of reasons for this occurrence have been proposed. In this paper, we will delineate barriers to critical care nurses’ involvement in prognosis and goals of care discussions, identify why nurse involvement in this communication is needed, describe a unique workshop exemplar with a sample role play that characterizes the workshop, and offer recommendations for colleagues interested in replicating similar education offerings.
Barriers to Communication
In the ICU, the sheer number of professionals families interact with may cause confusion. In particular, numerous medical consultants commonly offer opposing opinions. Additionally, each specialist may provide information that focuses on their area of expertise such that the “big picture” is not relayed to the patient and family. Emotional discomfort on the part of the health professional around discussions of poor prognosis, goals of care, and code status may prompt limiting discussion time with patients and families and even the avoidance of interpersonal exchanges [13–15]. Health professionals have also reported concern that end-of-life discussions will increase patient distress [16]. Among health care professionals, the subject of mortality may prompt personal anxiety, trigger unresolved grief, or fear that they will “become emotional” in front of the patient/family [7]. Lack of knowledge about cultural and religious norms has been cited as a barrier, as has time constraints [17,18]. Most frequently, inadequate or absent communication skill training is noted as a significant barrier [19,20]. Many ICU nurses also report feeling marginalized due their exclusion from goals of care and decision-making discussions with patients and families they know well [21,22].
Nurses As Key Palliative Care Communicators
Education efforts that foster communication proficiency during serious illness have traditionally focused on training physicians. Recently, nursing has become a focus of communication skill enhancement in recognition of nurses’ intense and protracted interactions with patients and families in the acute care setting. Nurses are the ‘constant’ in the patient and family’s journey through the fragmented health care system [21,23]. They often have the best knowledge of, and strongest relationship with, the family and often have had extensive discussions with them about their loved one’s status [24]. Nurses are aware of the patients’ symptom experiences and are privy to valuable information about the concerns and priorities of patients and families [12]. Additionally, having the most continuous presence, nurses have seen and heard interactions with clinicians from numerous disciplines. Nurses are the most visible, constant resource for patient and family education, information and support, and thus they perceive one of their most important roles to be that of advocate for the patient and family [20,21].
Communication Training Programs for Critical Care Nurses
Education is critical to enhance communication skills within palliative care [7,15,17,20,21,24]. The preferred teaching style within this realm is role play, where skills can be practiced and the affective component of engaging in sensitive discussions can be addressed [25–27]. Role play also demonstrates firsthand the importance of nonverbal communication (eg, body language, proximity, use of gestures, tone of voice) [7,20] and facilitates nurses’ gaining a sense of comfort with wordless communication [18].
Communication skills training programs have been designed to provide bedside critical care nurses with the tools they need to be active participants in discussions of prognosis, goals of care, and palliative care with families and physicians [27,28]. These programs have demonstrated improvement in nurses’ confidence to engage in key palliative care-related discussions. Essential elements of these programs include (1) delineation of the role of the bedside nurse in palliative care communication; (2) presentation and learner-centered practice of communication skills using role play; and (3) a reflection session focused on self-care and sustainability.
Across the 5 academic University of California medical centers (San Francisco, Davis, Los Angeles, Irvine, and San Diego), a communication training program based on this work has been implemented [29]. The one-day workshop, entitled IMPACT-ICU (Integrating Multidisciplinary Palliative Care into the ICU), has taught a total of 527 critical care nurses across the 5 centers. In addition to classroom training, the IMPACT-ICU program also includes proactive specialty palliative nursing support for bedside nurses by facilitating the availability of palliative care advanced practice nurses and nurse educators resources. This support helps nurses to apply the skills learned in the workshop in their practice. During rounds at the bedside, the nurse resources coach the bedside staff on the “how” and “when” of addressing palliative care needs. Education and support on a range of topics are offered, including clarifying goals and interventions provided by palliative care teams, the specifics of how to provide family emotional support and delivery of understandable information, the assessment and management of symptoms distress, and the nurses’ role in organizing and participating in family meetings. Case-specific consultations are also offered that address how to interface with resistant medical staff. The importance of nurse documentation of these varied exchanges is also emphasized.
IMPACT-ICU Workshop
A maximum of 15 nurses participate in each 8-hour workshop. The session begins with introductions and small group discussions about what the participants perceive to be the greatest barriers to goals of care discussions and fostering patient/family decision-making in the ICU. Participants are also asked to reflect on what they want to learn as a result of their workshop attendance.
A short didactic session then reviews the definition of palliative care and its core components, addresses the nurses’ role in communication within palliative care, a social worker’s perspective of what it is like to be a family member in the ICU, and the outline of the day. This includes delineation of expectations for involvement within the role plays and the various roles to be enacted. An emphasis is placed on the workshop being a safe place to explore and trial skills with the support of colleagues, and that practice is the optimum way to integrate communication expertise into the nurses’ skill set.
The “4 Cs” serves as the instructional basis for nurse communication skill enhancement [27]. This model outlines 4 key nursing roles in optimizing communication within palliative care:
Convening: Making sure multidisciplinary patient/family/clinician communication occurs.
Checking: Identifying the patient and family needs for information; ensuring that patients and families clearly receive desired information; ensuring that clinicians understand patient and family perspectives.
Caring: Naming emotions and responding to feeling.
Continuing: Following up after discussions to clarify and reinforce information and provide support.
Sample Role Play
Facilitator: So our first role play is focused on eliciting patient and family perspectives and needs. I need a learner and someone to play the role of the family member.
Learner: I’ll give it a try.
Facilitator: Lisa, you’re going to do great. Who wants to play the family member?
Workshop Participant: I’ll do it.
Facilitator: So Mary (who has agreed to play the role of the wife), why don’t you read us the scenario. (She reads it out loud to the group).
Facilitator: Lisa, as the nurse, I want you to look at your guide and tell me what your goal is for this conversation with Mrs. Ames and then which skill you want to practice.
Learner: I think I want to try eliciting the patient and family’s needs for information and I’ll try “Tell Me More” statements.
Facilitator: Alright. So remember Lisa, if you feel the conversation isn’t going well, you can call a “time out.” I can do this as well if I feel you need to start over. I’ll also call a time out when I feel you have met your goal. Sound OK? Mary, do you have any questions playing the part of Mrs. Ames?
Wife Role: Well, how hard should I make this for her? Should I be one of those “difficult” family members?
Facilitator: Our goal here is not to “stump” you or make it particularly difficult. We want you to try out these skills and get a sense of your “comfort zone.” So let’s start with some basic communication skills, OK?
Wife Role: Alright.
Facilitator: Why don’t we set the stage, such that Lisa, you are Mr. Ames’ nurse assessing him at the start of your shift, when Mrs. Ames enters. This is the first time you have taken care of him. The night nurse has told you that he has been requiring increasing ventilator support and his renal function is declining. Per Mrs. Ames’ request, the night nurse called her to let her know how he was doing and Mrs. Ames told her she would be in shortly.
Wife Role: (nervously enters the room and grasps her husband’s hand and looks at the nurse). How’s he doing? Is he better? The night nurse called me and I was so worried I rushed over here.
Learner: (Turns to Mrs. Ames and extends her hand). Are you Mrs. Ames? I’m Lisa and I am going to be taking care of Mr. Ames today. Let me just finish my assessment and how about we talk then? Will that be OK? It will be just a few minutes.
Wife Role: Alright, I’ll be in the waiting area but please come get me as soon as you can.
Learner: I will. (Nurse then shortly comes into the waiting area and asks Mrs. Ames to come back into the ICU where she invites her to sit just outside Mr. Ames’ room). Mrs. Ames, how are you doing? This must be so stressful for you, having your husband in the ICU.
Wife Role: It’s awful. He’s never been in the hospital before this and look at him, all hooked up to machines. I’m so worried. He seems to be getting worse instead of better.
Learner: What’s your understanding of what is going on?
Wife Role: I really don’t know. One doctor comes in and says one thing and then another comes in and tells me the opposite. I’m so confused I don’t know what to think.
Learner: Would having a better idea of his condition from the doctors who are treating him help you have a better understanding?
Wife Role: Oh, yes, but they always seem in such a hurry.
Learner: What exactly would you like to know?
Wife: Well, I want to know when he can get off that breathing machine because we have been planning to go to our son’s house for Thanksgiving.
Facilitator: Time out. Lisa, did you meet your conversation goal?
Learner: Um, I’m not sure, I guess so.
Facilitator: (Turns to Observers). What do you think, did she meet her goal?
Observer: Yes, she determined Mrs. Ames’ need for more information and she asked her what she wanted to know exactly.
Facilitator: What else did we see Lisa do to enhance communication with Mrs. Ames?
Observer: Well, when Mrs. Ames rushed into the room and asked her for information, Lisa didn’t just jump in and spout out values for the ventilator and his output. She took the time to introduce herself and de-escalate Mrs. Ames’ anxiety and she followed up on her promise to come get her in the waiting room as soon as she could.
Facilitator: Why do you think was important?
Observer: It helps establish trust.
Facilitator: Did Lisa use the skill she wanted to try out?
Observer: Yes.
Facilitator: How do you know? What did you hear her say?
Observer: She said, “What’s your understanding of what is going on with Mr. Ames?”
Facilitator: Absolutely. Great job, Lisa. And who wants to take a guess at how long Lisa’s exchange with Mrs. Ames took?
Observer: Less than two minutes?
Facilitator: That’s right. So just as you consider how long it takes, and how proficient you are, in starting an IV or inserting a Foley catheter, when you have a goal in mind and have practiced the skills to do it well, any skill can be mastered.
Feedback
Participants in the workshops uniformly report an enhanced sense of self-confidence in their palliative care communication skills as a result of their participation [29]. Key to the success of the workshop is the ongoing contact by the workshop facilitators with participants. Rounding is routinely planned such that each participant is visited weekly by a workshop facilitator in their clinical area to determine if the bedside nurse has practiced the new skills and if so, how the interaction transpired. Positive feedback is given for attempts to engage in new behaviors and participants are reminded that with any new skill, repetitive trials are necessary to foster success.
Lessons Learned and Next Steps
One of our major lessons learned was recognizing that it was difficult for many critical care nurses to practice the new communication skills. Nurses are trained to fix problems and perform medico-technical tasks; “listening” has not always been recognized as real work [18]. We needed to reinforce that skills like eliciting another’s perspective or making reflection statements are equally important to those associated with behavioral/technical proficiency.
While our program has been successful, we recognize that the next step in fostering ideal palliative care communication is to provide education within an interdisciplinary context. We recommend that colleagues interested in replicating this or a similar education intervention, survey nurse participants prior to and following workshop participation to measure attitudes, self confidence and perceived barriers over time [30]. We hope to translate our positive experience into a program that engages multiple professionals in the enhancement of optimum palliative care communication proficiency.
Corresponding author: Deborah A. Boyle MSN, RN, AOCNS, Department of Nursing Quality, Research and Education, University of California, Irvine Health, 101 The City Drive, Bldg 22A, Room 3104, Orange, CA 92868.
From the University of California Irvine Health/Chao Family Comprehensive Cancer Center Orange, CA (Ms. Boyle) and the University of California San Francisco Medical Center, San Francisco, CA (Dr. Anderson).
Abstract
- Objective: To describe components of a unique interactive workshop focusing on the enhancement of critical care nurses’ communication skills within the realm of prognosis and goals of care discussions with family members and physicians.
- Methods: A series of one-day workshops were offered to critical care nurses practicing in the 5 University of California hospital settings. After workshop attendance, nurse participants were followed by workshop facilitators in their units to ensure new communication skills were being integrated into practice and to problem solve if barriers were met.
- Results: Improvement in nurses’ self-confidence in engaging in these discussions was seen. This confidence was sustained months following workshop participation.
- Conclusion: The combination of critical care nurse workshop participation that involved skill enhancement through role-playing, in combination with clinical follow-up with attendees, resulted in positive affirmation of nurse communication skills specific to prognosis and goals of care discussions with family members and physicians.
There is increasing evidence that in the absence of quality communication between professional caregivers and those they care for, negative outcomes may prevail, such as reduced patient/family satisfaction, lower health status awareness, and a decreased sense of being cared about and cared for [1–5]. Communication skill competency is a critical corollary of nursing practice. In the intensive care unit (ICU) setting, patients and families have cited skilled communication as a core element of high-quality care [3,6]. Proficiency in this realm enhances nurses’ understanding of the patient and family’s encounter with health care and provides a vehicle to gather information, inform, teach, and offer emotional support. Additionally, it identifies values, goals, health care preferences, worries and concerns, and facilitates the nurses’ coordination of care [7]. Despite this skill’s importance, however, it is generally not taught in basic education and until recently has been overlooked as a key competency [8,9].
Skilled communication in palliative and end-of-life care is pivotal for discussing prognosis and care planning. In the acute care setting this is particularly relevant as the majority of Americans die in hospitals versus their preferred site of home [10]. Additionally, 1 in 5 Americans die during or shortly after receiving care in an ICU [11]. Hence, while the ICU is a setting in which intensive effort to save lives is employed, it is also a setting where death frequently occurs. The complexity and highly emotive nature of critical care often results in family needs for information and support not being met [12]. A number of reasons for this occurrence have been proposed. In this paper, we will delineate barriers to critical care nurses’ involvement in prognosis and goals of care discussions, identify why nurse involvement in this communication is needed, describe a unique workshop exemplar with a sample role play that characterizes the workshop, and offer recommendations for colleagues interested in replicating similar education offerings.
Barriers to Communication
In the ICU, the sheer number of professionals families interact with may cause confusion. In particular, numerous medical consultants commonly offer opposing opinions. Additionally, each specialist may provide information that focuses on their area of expertise such that the “big picture” is not relayed to the patient and family. Emotional discomfort on the part of the health professional around discussions of poor prognosis, goals of care, and code status may prompt limiting discussion time with patients and families and even the avoidance of interpersonal exchanges [13–15]. Health professionals have also reported concern that end-of-life discussions will increase patient distress [16]. Among health care professionals, the subject of mortality may prompt personal anxiety, trigger unresolved grief, or fear that they will “become emotional” in front of the patient/family [7]. Lack of knowledge about cultural and religious norms has been cited as a barrier, as has time constraints [17,18]. Most frequently, inadequate or absent communication skill training is noted as a significant barrier [19,20]. Many ICU nurses also report feeling marginalized due their exclusion from goals of care and decision-making discussions with patients and families they know well [21,22].
Nurses As Key Palliative Care Communicators
Education efforts that foster communication proficiency during serious illness have traditionally focused on training physicians. Recently, nursing has become a focus of communication skill enhancement in recognition of nurses’ intense and protracted interactions with patients and families in the acute care setting. Nurses are the ‘constant’ in the patient and family’s journey through the fragmented health care system [21,23]. They often have the best knowledge of, and strongest relationship with, the family and often have had extensive discussions with them about their loved one’s status [24]. Nurses are aware of the patients’ symptom experiences and are privy to valuable information about the concerns and priorities of patients and families [12]. Additionally, having the most continuous presence, nurses have seen and heard interactions with clinicians from numerous disciplines. Nurses are the most visible, constant resource for patient and family education, information and support, and thus they perceive one of their most important roles to be that of advocate for the patient and family [20,21].
Communication Training Programs for Critical Care Nurses
Education is critical to enhance communication skills within palliative care [7,15,17,20,21,24]. The preferred teaching style within this realm is role play, where skills can be practiced and the affective component of engaging in sensitive discussions can be addressed [25–27]. Role play also demonstrates firsthand the importance of nonverbal communication (eg, body language, proximity, use of gestures, tone of voice) [7,20] and facilitates nurses’ gaining a sense of comfort with wordless communication [18].
Communication skills training programs have been designed to provide bedside critical care nurses with the tools they need to be active participants in discussions of prognosis, goals of care, and palliative care with families and physicians [27,28]. These programs have demonstrated improvement in nurses’ confidence to engage in key palliative care-related discussions. Essential elements of these programs include (1) delineation of the role of the bedside nurse in palliative care communication; (2) presentation and learner-centered practice of communication skills using role play; and (3) a reflection session focused on self-care and sustainability.
Across the 5 academic University of California medical centers (San Francisco, Davis, Los Angeles, Irvine, and San Diego), a communication training program based on this work has been implemented [29]. The one-day workshop, entitled IMPACT-ICU (Integrating Multidisciplinary Palliative Care into the ICU), has taught a total of 527 critical care nurses across the 5 centers. In addition to classroom training, the IMPACT-ICU program also includes proactive specialty palliative nursing support for bedside nurses by facilitating the availability of palliative care advanced practice nurses and nurse educators resources. This support helps nurses to apply the skills learned in the workshop in their practice. During rounds at the bedside, the nurse resources coach the bedside staff on the “how” and “when” of addressing palliative care needs. Education and support on a range of topics are offered, including clarifying goals and interventions provided by palliative care teams, the specifics of how to provide family emotional support and delivery of understandable information, the assessment and management of symptoms distress, and the nurses’ role in organizing and participating in family meetings. Case-specific consultations are also offered that address how to interface with resistant medical staff. The importance of nurse documentation of these varied exchanges is also emphasized.
IMPACT-ICU Workshop
A maximum of 15 nurses participate in each 8-hour workshop. The session begins with introductions and small group discussions about what the participants perceive to be the greatest barriers to goals of care discussions and fostering patient/family decision-making in the ICU. Participants are also asked to reflect on what they want to learn as a result of their workshop attendance.
A short didactic session then reviews the definition of palliative care and its core components, addresses the nurses’ role in communication within palliative care, a social worker’s perspective of what it is like to be a family member in the ICU, and the outline of the day. This includes delineation of expectations for involvement within the role plays and the various roles to be enacted. An emphasis is placed on the workshop being a safe place to explore and trial skills with the support of colleagues, and that practice is the optimum way to integrate communication expertise into the nurses’ skill set.
The “4 Cs” serves as the instructional basis for nurse communication skill enhancement [27]. This model outlines 4 key nursing roles in optimizing communication within palliative care:
Convening: Making sure multidisciplinary patient/family/clinician communication occurs.
Checking: Identifying the patient and family needs for information; ensuring that patients and families clearly receive desired information; ensuring that clinicians understand patient and family perspectives.
Caring: Naming emotions and responding to feeling.
Continuing: Following up after discussions to clarify and reinforce information and provide support.
Sample Role Play
Facilitator: So our first role play is focused on eliciting patient and family perspectives and needs. I need a learner and someone to play the role of the family member.
Learner: I’ll give it a try.
Facilitator: Lisa, you’re going to do great. Who wants to play the family member?
Workshop Participant: I’ll do it.
Facilitator: So Mary (who has agreed to play the role of the wife), why don’t you read us the scenario. (She reads it out loud to the group).
Facilitator: Lisa, as the nurse, I want you to look at your guide and tell me what your goal is for this conversation with Mrs. Ames and then which skill you want to practice.
Learner: I think I want to try eliciting the patient and family’s needs for information and I’ll try “Tell Me More” statements.
Facilitator: Alright. So remember Lisa, if you feel the conversation isn’t going well, you can call a “time out.” I can do this as well if I feel you need to start over. I’ll also call a time out when I feel you have met your goal. Sound OK? Mary, do you have any questions playing the part of Mrs. Ames?
Wife Role: Well, how hard should I make this for her? Should I be one of those “difficult” family members?
Facilitator: Our goal here is not to “stump” you or make it particularly difficult. We want you to try out these skills and get a sense of your “comfort zone.” So let’s start with some basic communication skills, OK?
Wife Role: Alright.
Facilitator: Why don’t we set the stage, such that Lisa, you are Mr. Ames’ nurse assessing him at the start of your shift, when Mrs. Ames enters. This is the first time you have taken care of him. The night nurse has told you that he has been requiring increasing ventilator support and his renal function is declining. Per Mrs. Ames’ request, the night nurse called her to let her know how he was doing and Mrs. Ames told her she would be in shortly.
Wife Role: (nervously enters the room and grasps her husband’s hand and looks at the nurse). How’s he doing? Is he better? The night nurse called me and I was so worried I rushed over here.
Learner: (Turns to Mrs. Ames and extends her hand). Are you Mrs. Ames? I’m Lisa and I am going to be taking care of Mr. Ames today. Let me just finish my assessment and how about we talk then? Will that be OK? It will be just a few minutes.
Wife Role: Alright, I’ll be in the waiting area but please come get me as soon as you can.
Learner: I will. (Nurse then shortly comes into the waiting area and asks Mrs. Ames to come back into the ICU where she invites her to sit just outside Mr. Ames’ room). Mrs. Ames, how are you doing? This must be so stressful for you, having your husband in the ICU.
Wife Role: It’s awful. He’s never been in the hospital before this and look at him, all hooked up to machines. I’m so worried. He seems to be getting worse instead of better.
Learner: What’s your understanding of what is going on?
Wife Role: I really don’t know. One doctor comes in and says one thing and then another comes in and tells me the opposite. I’m so confused I don’t know what to think.
Learner: Would having a better idea of his condition from the doctors who are treating him help you have a better understanding?
Wife Role: Oh, yes, but they always seem in such a hurry.
Learner: What exactly would you like to know?
Wife: Well, I want to know when he can get off that breathing machine because we have been planning to go to our son’s house for Thanksgiving.
Facilitator: Time out. Lisa, did you meet your conversation goal?
Learner: Um, I’m not sure, I guess so.
Facilitator: (Turns to Observers). What do you think, did she meet her goal?
Observer: Yes, she determined Mrs. Ames’ need for more information and she asked her what she wanted to know exactly.
Facilitator: What else did we see Lisa do to enhance communication with Mrs. Ames?
Observer: Well, when Mrs. Ames rushed into the room and asked her for information, Lisa didn’t just jump in and spout out values for the ventilator and his output. She took the time to introduce herself and de-escalate Mrs. Ames’ anxiety and she followed up on her promise to come get her in the waiting room as soon as she could.
Facilitator: Why do you think was important?
Observer: It helps establish trust.
Facilitator: Did Lisa use the skill she wanted to try out?
Observer: Yes.
Facilitator: How do you know? What did you hear her say?
Observer: She said, “What’s your understanding of what is going on with Mr. Ames?”
Facilitator: Absolutely. Great job, Lisa. And who wants to take a guess at how long Lisa’s exchange with Mrs. Ames took?
Observer: Less than two minutes?
Facilitator: That’s right. So just as you consider how long it takes, and how proficient you are, in starting an IV or inserting a Foley catheter, when you have a goal in mind and have practiced the skills to do it well, any skill can be mastered.
Feedback
Participants in the workshops uniformly report an enhanced sense of self-confidence in their palliative care communication skills as a result of their participation [29]. Key to the success of the workshop is the ongoing contact by the workshop facilitators with participants. Rounding is routinely planned such that each participant is visited weekly by a workshop facilitator in their clinical area to determine if the bedside nurse has practiced the new skills and if so, how the interaction transpired. Positive feedback is given for attempts to engage in new behaviors and participants are reminded that with any new skill, repetitive trials are necessary to foster success.
Lessons Learned and Next Steps
One of our major lessons learned was recognizing that it was difficult for many critical care nurses to practice the new communication skills. Nurses are trained to fix problems and perform medico-technical tasks; “listening” has not always been recognized as real work [18]. We needed to reinforce that skills like eliciting another’s perspective or making reflection statements are equally important to those associated with behavioral/technical proficiency.
While our program has been successful, we recognize that the next step in fostering ideal palliative care communication is to provide education within an interdisciplinary context. We recommend that colleagues interested in replicating this or a similar education intervention, survey nurse participants prior to and following workshop participation to measure attitudes, self confidence and perceived barriers over time [30]. We hope to translate our positive experience into a program that engages multiple professionals in the enhancement of optimum palliative care communication proficiency.
Corresponding author: Deborah A. Boyle MSN, RN, AOCNS, Department of Nursing Quality, Research and Education, University of California, Irvine Health, 101 The City Drive, Bldg 22A, Room 3104, Orange, CA 92868.
1. Leung JM, Udris EM, Uman J, et al. The effect of end-of-life discussions on perceived quality of care and health status among patients with COPD. Chest 2012;142:128–33.
2. Osborn TR, Curtis JR, Nielsen EL, et al. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control and ICU atmosphere. Chest 2012;142:1185–92.
3. Nelson JE, Puntillo K, Pronovost PJ, et al. In their own words: patients and families define high-quality palliative care in the ICU. Crit Care Med 2010;38:808–18.
4. Nels W, Gabrijel S, Kiss S, et al. Communication skill training significantly improves lung cancer patients understanding. J Palliat Care Med 2014;4:182.
5. Van Vliet LM, Epstein AS. Current state of the art and science of patient-clinician communication in progressive disease: patients’ need to know and feel known. J Clin Oncol 2014;32:3474-8.
6. Troug RD, Campbell ML, Curtis JR, et al. Recommendations for end of life care in the intensive care unit: a consensus statement by the American College of Critical Care Medicine. Crit Care Med 2008;36:953–63.
7. Dahlin CM, Wittenberg E. Communication in palliative care. In: Ferrell BR, Coyle N, Paice J, editors. Oxford textbook of palliative nursing. 4th ed. Oxford: Oxford University Press; 2014:81–109.
8. Baer L, Weinstein E. Improving oncology nurses’ communication skills for difficult conversations. Clin J Oncol Nurs 2013;17:E45–E51.
9. Treece PD. Communication in the intensive care unit about end of life care. AACN Adv Crit Care 2007;18:406–14.
10. Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end of life care at the last place of care. JAMA 2004;291:88–92.
11. Angus DC, Barnato AE, Linde-Zwirble WT, et al. Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med 2004;32:638–43.
12. Hamric AB, Blackhall LJ. Nurse-physician perspectives on the care of dying patients in intensive care units: collaboration, moral distress, and ethical climate. Crit Care Med 2007;35:422–9.
13. Back AL, Trinidad SB, Hopley EK, Edwards KA. Reframing the goals of care conversation: “We’re in a different place.” J Palliat Med 2014;17:1010–24.
14. Aslakson RA, Wyskiel R, Thornton I, et al. Nurse perceived barriers to effective communication regarding prognosis and optimal end of life care for surgical ICU patients: a qualitative exploration. J Palliat Med 2012;15:910–5.
15. Erickson J. Bedside nurse involvement in end of life decision-making. Dimens Crit Care Nurs 2013;32:65–8.
16. Bernacki RE, Block SD for the American College of Physicians High Value Care Task Force. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med 2014;174:1994–2003.
17. You JJ, Downar J, Fowler RA, et al. Barriers to goals of care discussion with ‘seriously’ ill hospitalized patients and their families: a multicenter survey of clinicians. JAMA Intern Med 2015;175:549–56.
18. Strang S, Henoch I, Danielson E, et al. Communication about existential issues with patients close to death: nurses’ reflections on content, process, and meaning. Psychooncology 2014;23:562–8.
19. Slatore CG, Hensen L, Gauzine L, et al. Communication by nurses in the intensive care unit: qualitative analysis of domains in patient-centered care. Am J Crit Care 2012;21:410–8.
20. Wittenberg-Lyles E, Goldsmith J, Platt CS. Palliative care communication. Sem Oncol Nurs 2014;30:280–6.
21. Fox MY. Improving communication with patients and families in the ICU: palliative care strategies for intensive care unit nurses. J Hospice Palliat Nurs 2014;16:93–8.
22. Beckstrand RL, Callister LC, Kirchhoff KT. Providing a ‘good death’: critical care nurses’ suggestions for improving end of life care. Am J Crit Care 2006;15:38–45.
23. Peereboom K, Coyle N. Facilitating goals of care discus.sions for patients with life-limiting disease: communication strategies for nurses. J Hospice Palliat Nurs 2012; 14:251–8.
24. Nelson JE, Cortez TB, Curtis JR, et al. Integrating palliative care in the ICU: the nurse in the leading role. J Hospice Palliat Nurs 2011;13:89–94.
25. Jors K, Seibel K, Bardenheuer H, et al. Education in end of life care: what do experienced professionals find important? J Cancer Educ 2015 March 15.
26. Roze des Ordons AL, Sharma N, Heyland DK, et al. Strategies for effective goals of care discussions and decision-making: perspective from a multi-centre survey of Canadian hospital-based health care providers. BMC Palliat Care 2015;14:38.
27. Krimshtein NS, Luhrs CA, Puntillo KA, et al. Training nurses for interdisciplinary communication with families in the ICU. J Palliat Med 2011;14:1325–32.
28. Milic MM, Puntillo K, Turner K, et al. Communicating with patients’ families and physicians about prognosis and goals of care. Am J Crit Care 2015;24:e56–e64.
29. Anderson W, Puntillo K, Barbour S, et al. The IMPACT-ICU Project: expanding palliative care nursing across University of California Centers ICUs to advance palliative care. Center to Advance Palliative Care (CAPC) national seminar. Nov 7–9, 2013. Dallas, TX.
30. Anderson WG, Puntillo K, Boyle D, et al. ICU bedside nurses’ involvement in palliative care communication: a multicenter survey. J Pain Symptom Manage. In press.
1. Leung JM, Udris EM, Uman J, et al. The effect of end-of-life discussions on perceived quality of care and health status among patients with COPD. Chest 2012;142:128–33.
2. Osborn TR, Curtis JR, Nielsen EL, et al. Identifying elements of ICU care that families report as important but unsatisfactory: decision-making, control and ICU atmosphere. Chest 2012;142:1185–92.
3. Nelson JE, Puntillo K, Pronovost PJ, et al. In their own words: patients and families define high-quality palliative care in the ICU. Crit Care Med 2010;38:808–18.
4. Nels W, Gabrijel S, Kiss S, et al. Communication skill training significantly improves lung cancer patients understanding. J Palliat Care Med 2014;4:182.
5. Van Vliet LM, Epstein AS. Current state of the art and science of patient-clinician communication in progressive disease: patients’ need to know and feel known. J Clin Oncol 2014;32:3474-8.
6. Troug RD, Campbell ML, Curtis JR, et al. Recommendations for end of life care in the intensive care unit: a consensus statement by the American College of Critical Care Medicine. Crit Care Med 2008;36:953–63.
7. Dahlin CM, Wittenberg E. Communication in palliative care. In: Ferrell BR, Coyle N, Paice J, editors. Oxford textbook of palliative nursing. 4th ed. Oxford: Oxford University Press; 2014:81–109.
8. Baer L, Weinstein E. Improving oncology nurses’ communication skills for difficult conversations. Clin J Oncol Nurs 2013;17:E45–E51.
9. Treece PD. Communication in the intensive care unit about end of life care. AACN Adv Crit Care 2007;18:406–14.
10. Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end of life care at the last place of care. JAMA 2004;291:88–92.
11. Angus DC, Barnato AE, Linde-Zwirble WT, et al. Robert Wood Johnson Foundation ICU End-of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med 2004;32:638–43.
12. Hamric AB, Blackhall LJ. Nurse-physician perspectives on the care of dying patients in intensive care units: collaboration, moral distress, and ethical climate. Crit Care Med 2007;35:422–9.
13. Back AL, Trinidad SB, Hopley EK, Edwards KA. Reframing the goals of care conversation: “We’re in a different place.” J Palliat Med 2014;17:1010–24.
14. Aslakson RA, Wyskiel R, Thornton I, et al. Nurse perceived barriers to effective communication regarding prognosis and optimal end of life care for surgical ICU patients: a qualitative exploration. J Palliat Med 2012;15:910–5.
15. Erickson J. Bedside nurse involvement in end of life decision-making. Dimens Crit Care Nurs 2013;32:65–8.
16. Bernacki RE, Block SD for the American College of Physicians High Value Care Task Force. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med 2014;174:1994–2003.
17. You JJ, Downar J, Fowler RA, et al. Barriers to goals of care discussion with ‘seriously’ ill hospitalized patients and their families: a multicenter survey of clinicians. JAMA Intern Med 2015;175:549–56.
18. Strang S, Henoch I, Danielson E, et al. Communication about existential issues with patients close to death: nurses’ reflections on content, process, and meaning. Psychooncology 2014;23:562–8.
19. Slatore CG, Hensen L, Gauzine L, et al. Communication by nurses in the intensive care unit: qualitative analysis of domains in patient-centered care. Am J Crit Care 2012;21:410–8.
20. Wittenberg-Lyles E, Goldsmith J, Platt CS. Palliative care communication. Sem Oncol Nurs 2014;30:280–6.
21. Fox MY. Improving communication with patients and families in the ICU: palliative care strategies for intensive care unit nurses. J Hospice Palliat Nurs 2014;16:93–8.
22. Beckstrand RL, Callister LC, Kirchhoff KT. Providing a ‘good death’: critical care nurses’ suggestions for improving end of life care. Am J Crit Care 2006;15:38–45.
23. Peereboom K, Coyle N. Facilitating goals of care discus.sions for patients with life-limiting disease: communication strategies for nurses. J Hospice Palliat Nurs 2012; 14:251–8.
24. Nelson JE, Cortez TB, Curtis JR, et al. Integrating palliative care in the ICU: the nurse in the leading role. J Hospice Palliat Nurs 2011;13:89–94.
25. Jors K, Seibel K, Bardenheuer H, et al. Education in end of life care: what do experienced professionals find important? J Cancer Educ 2015 March 15.
26. Roze des Ordons AL, Sharma N, Heyland DK, et al. Strategies for effective goals of care discussions and decision-making: perspective from a multi-centre survey of Canadian hospital-based health care providers. BMC Palliat Care 2015;14:38.
27. Krimshtein NS, Luhrs CA, Puntillo KA, et al. Training nurses for interdisciplinary communication with families in the ICU. J Palliat Med 2011;14:1325–32.
28. Milic MM, Puntillo K, Turner K, et al. Communicating with patients’ families and physicians about prognosis and goals of care. Am J Crit Care 2015;24:e56–e64.
29. Anderson W, Puntillo K, Barbour S, et al. The IMPACT-ICU Project: expanding palliative care nursing across University of California Centers ICUs to advance palliative care. Center to Advance Palliative Care (CAPC) national seminar. Nov 7–9, 2013. Dallas, TX.
30. Anderson WG, Puntillo K, Boyle D, et al. ICU bedside nurses’ involvement in palliative care communication: a multicenter survey. J Pain Symptom Manage. In press.
Evaluation and Management of Pancreatic Cystic Lesions
From the Department of Medicine, Stanford University School of Medicine, Stanford, CA.
Abstract
- Objective: To review the diagnosis and management of pancreatic cystic lesions.
- Methods: Narrative review of the literature.
- Results: Pancreatic cystic lesions are clinically relevant as some are precursor lesions to pancreatic adenocarcinoma. Mucinous cystic neoplasms and intraductal papillary mucinous neoplasms are 2 commonly encountered pre-cancerous pancreatic cysts. Many cysts are identified incidentally due to frequent use of high-resolution CT and MRI imaging technology. Proposed diagnostic and management algorithms exist to guide clinical practice but are limited by a lack of evidence and discordance among various guidelines. New cyst fluid biomarkers are under development to diagnose cyst types and risk of cancer.
- Conclusion: Pancreatic cysts are increasingly encountered in clinical practice and represent a growing problem. Diagnostic and management algorithms are available to assist practice but are limited by the available evidence. A multidisciplinary approach is recommended.
In the United States there were an estimated 46,420 new cases of pancreatic cancer in 2014 [1]. Of all major cancers, pancreatic cancer had the lowest 5-year survival rate at 6% [1]. Of the 3 known precursor lesions to pancreas adenocarcinoma, 2 are pancreatic cysts [2]. Correctly identifying those with cancer, those with cancer potential (premalignant), and those that are benign (harboring no malignant potential) can be difficult.
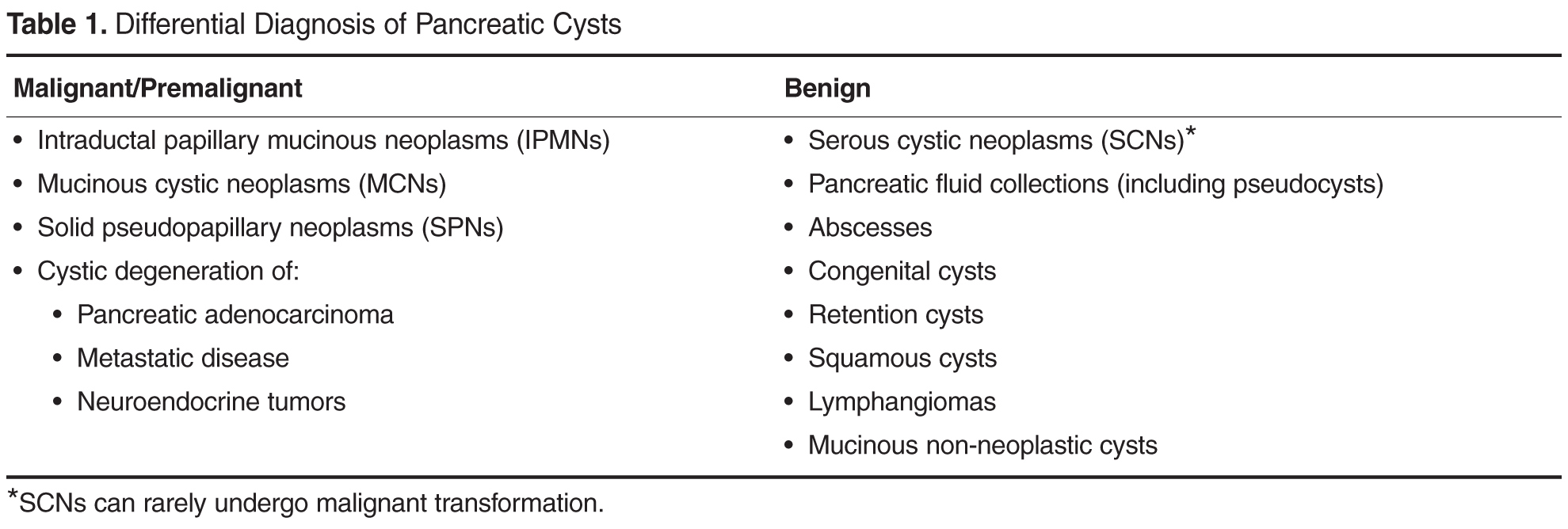
Case 1
A 57-year-old male had a 1.5-cm pancreatic cyst located in the head that was found on computed tomography (CT) imaging for suspected renal colic. He had no history or complaints suspicious for pancreatic disease. A CT pancreas protocol scan was obtained, which demonstrated a simple appearing cyst with no mural nodules. The pancreatic and biliary ducts were normal. His laboratory evaluations including liver function testing and lipase were normal.
• What is the approach to incidentally discovered pancreatic cysts?
While many pancreatic cysts are first discovered by cross sectional imaging (CT or MRI), the diagnostic accuracy of defining cyst type and the presence of malignancy is imperfect. The area under the curve (AUC) for differentiating malignant from benign pancreatic cysts ranges from 0.64 to 0.82 for CT and 0.73 to 0.91 for MRI, and no difference between the 2 were observed [12,13]. Several guidelines are currently available to offer guidance on management [6,14,15,16,17]. Much of the current evidence includes retrospective case series with no randomized control trials. The guidelines, therefore, mostly represent consensus-based expert extrapolation of available data.

The American Gastroenterological Association (AGA) recently produced guidelines in 2015 [14]. In comparison to the international consensus guidelines, there are a few key differences, which have now become a point of vigorous debate and disagreement among pancreatologists and confusion among general gastroenterologists and surgeons in the community. Where the international consensus guidelines have stricter criteria to define the appropriateness of surgery, the AGA guidelines are more liberal. AGA defined cysts appropriate for surgery as having 2 out of 3 of the following features: (1) cyst size ≥ 3 cm, (2) presence of a solid component in the cyst, and (3) dilation of the main pancreatic duct. Those having 1 out of 3 criteria were defined as needing further investigation with EUS [14]. These criteria are more relaxed and will likely lead to more surgical resections.
Another difference involves surveillance recommendations. The international consensus guidelines do not define a period when surveillance can be safely stopped. The AGA guidelines define 5 years as the period where if there is no significant change in the cyst from surveillance MRIs performed every 1 to 2 years, then surveillance can be stopped [14]. As the natural history of these cysts remain substantially uncertain, with evidence that malignant transformation occurs after 5 years, this particular recommendation by the AGA remains highly controversial [18,19]. Other differences between these 2 guidelines are summarized in Table 2 [6,14].
Until the surveillance recommendations by the AGA are validated with further studies, we generally follow the 2012 international consensus guidelines. We generally prefer MRI for initial and surveillance evaluations of pancreatic cysts. Besides the lack of radiation exposure, some studies show MRI to have better inter-reader variability [20], better resolution to show cyst communication with the main pancreatic duct [21], and better characterization of peripheral pancreatic cysts [22]. At our center, when a solid mass is suspected, a CT pancreas protocol is preferred in lieu of an MRI by our surgical team.
Case 1 Continued
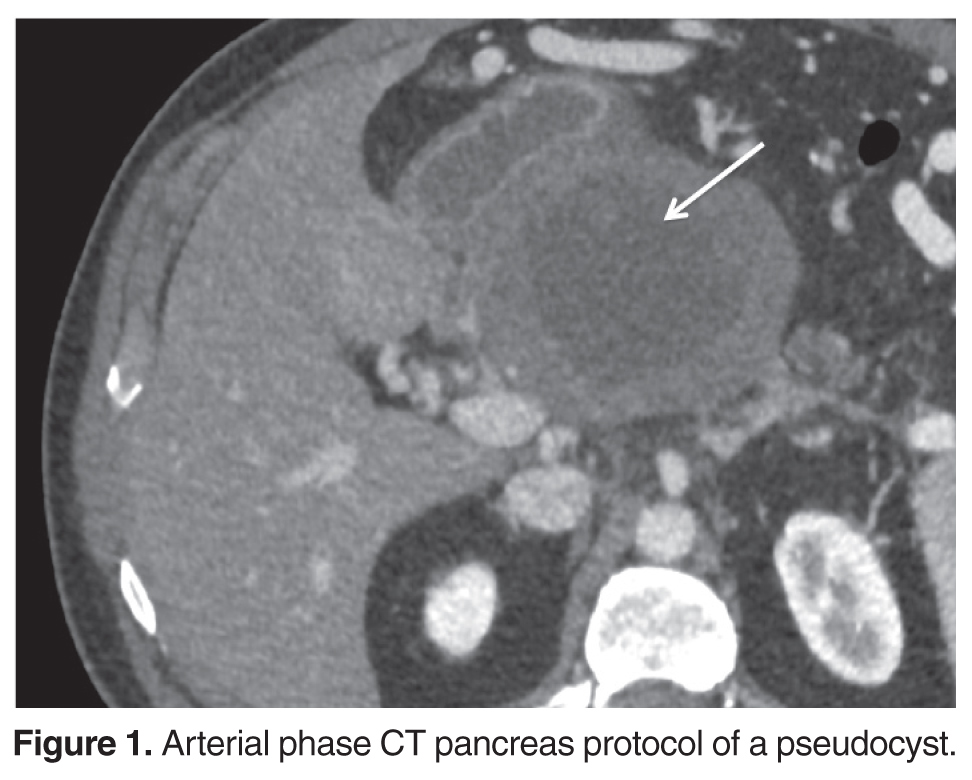
Despite the reassuring CEA and cytology results, a high concern for a malignant cystic lesion remained based on cyst size, main pancreatic duct dilation, and atrophy noted in the distal pancreas. The patient underwent surgical resection including subtotal pancreatectomy, splenectomy, subtotal gastrectomy, and superior mesenteric and portal vein resection with reconstruction. Pathology revealed the cyst to be a benign pseudocyst.
This case reflects some of the critical challenges in current management of pancreatic cysts. By history, this patient had no suspicion for pancreatitis, making a pseudocyst less likely in a differential diagnosis. When the patient presented 7 years later, again with no reported history of pancreatitis, there was clinical concern for a branch duct IPMN. Although the cyst fluid CEA and cytology were reassuring, the patient met surgical criteria by the 2006 international consensus criteria and the more recent AGA guidelines. Interestingly, the narrowed 2012 international consensus guidelines for surgical resection would have recommended observation. This case highlights the need for better diagnostic tests.
• What is the epidemiology of pancreatic fluid collections and how do they present?
Pancreatic fluid collections are not true cysts as they lack an epithelial cell lining. They often occur in the context of either acute or chronic pancreatitis, and are considered benign or nonmucinous cysts [7,8]. Duct disruption occurs causing pancreatic fluid accumulation, initially defined as an acute peri-pancreatic fluid collection, or an acute necrotic collection if necrosis is present. Over about 4 weeks a more defined cyst wall forms and the cyst is now classified as either a pseudocyst or walled-off pancreatic necrosis [23]. In one review, the median age at presentation was 49 with a male:female ratio of 2:1. Only 52% of fluid collections were discovered following an acute attack of pancreatitis [24]. The risk factors for pancreatic fluid collections are similar to the risk factors for pancreatitis, with the most common being alcohol use and gallstones [24]. Potential symptoms include abdominal pain, weight loss, gastrointestinal bleeding from pseudoaneurysms, obstructive symptoms, sepsis from super infection, and obstructive jaundice [8,24,25,26,27].
• How are pancreatic fluid collections diagnosed and managed?
Clinical suspicion for pancreatic fluid collections should increase if a cyst is diagnosed in the context of acute or chronic pancreatitis [28]. However, other types of cysts can cause ductal obstruction and pancreatitis, so further investigation may be needed, including review of prior imaging if available. The presence of internal debris, the presence of imaging findings of acute or chronic pancreatitis, and fluid extension beyond the pancreas and taking the shape of the retroperitoneum are often characteristics found in pancreatic fluid collections [29,28,30]. If needed, FNA with assay of amylase may be helpful. An amylase value of 5680 IU/L or greater was 84% sensitive and 64% specific (AUC 0.69) for pseudocysts in one study [31].
Management of pancreatic fluid collections is largely based on surgical series. Drainage procedures for pancreatic fluid collections are often undertaken for intractable symptoms or concerns of infection [8,24,25,26]. Asymptomatic pseudocysts can be safely followed. Specific techniques used for pancreatic fluid collection management vary by institutional expertise. Endoscopic drainage can be done by transpapillary stenting if main duct communication is present, or transgastric/transduodenal stenting if the cyst wall is mature and accessible by these approaches [32]. If necrosis is present this can be debrided endoscopically [33]. Laparoscopic surgical options are preferred to open approaches, and can be performed in 1 procedure where endoscopic approaches may require multiple procedures. The most common approach is to drain the cyst by creating a cyst-gastrostomy, or when not feasible a cyst-duodenostomy or cyst-jejunostomy [26,34]. Percutaneous drainage is less commonly performed and used for unstable patients as it can lead to cutaneous fistulas [34]. The best technique for intervention should be decided in the context of a multidisciplinary team. The option for conservative management should be considered as well because about 60% of those managed conservatively will have resolution in 1 year [35].
Case 2
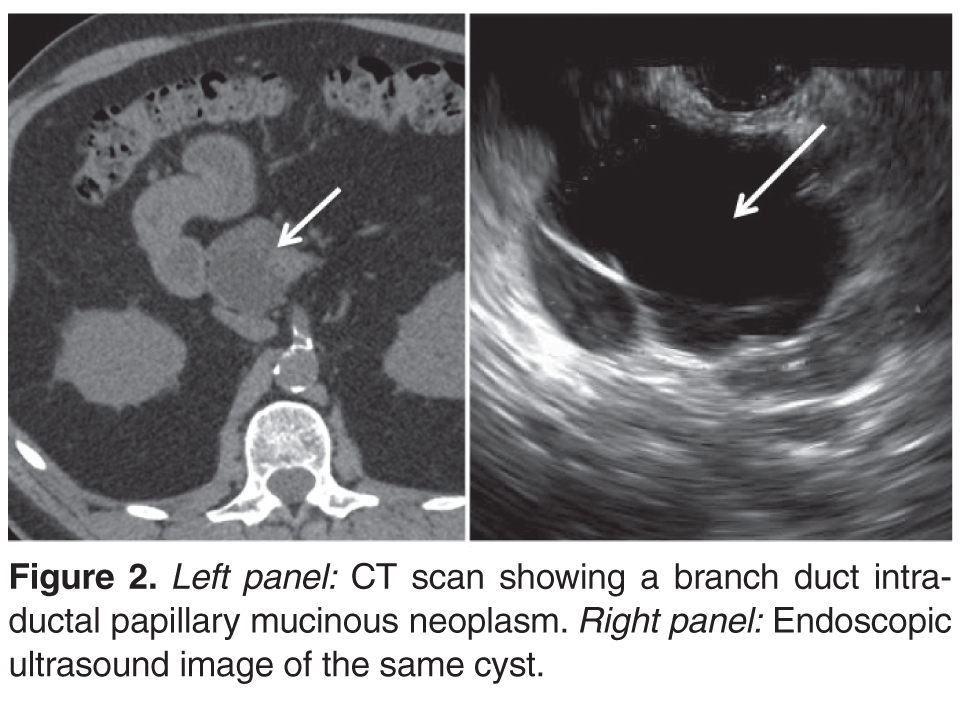
• What is the role of endoscopic ultrasound with FNA in the diagnosis of pancreatic cysts?
While more invasive than CT or MRI, EUS provides detailed imaging to characterize relevant clinical features and allows fine needle aspiration of the cyst fluid and tissue of intra-cystic masses (Table 2) [6,14]. While MRI imaging resolution is continuing to improve [22,36,37], EUS is generally considered superior [38] for diagnosing high-risk lesions. A limitation of EUS, however, is significant inter-observer variability when compared with MRI [37,39,40].
EUS enables FNA of the cyst, which offers unique oppor-tunities for diagnosis. Cyst fluid cytology unfortunately has limited diagnostic yield, with a recent meta-analysis showing sensitivity 63%, specificity 88%, and AUC of 0.89 in differentiating mucinous from nonmucinous cysts [41]. The low sensitivity is likely because cyst fluid is paucicellular. Techniques that include targeting the cyst wall are under investigation and may improve the diagnostic yield of cytological analysis [42]. Tumor markers such as CEA have been widely used in the cyst fluid, with a value > 192 ng/mL having 63% sensitivity and 88% specificity (AUC of 0.79) for mucinous pancreatic cysts [43]. Other cyst fluid markers have been or are being developed including mutated KRAS DNA [44], mutated GNAS DNA [45,46], micro RNA [47,48], glucose [49], proteomic analysis [50], and multiple other molecules [51]. At this time, many of these markers are under investigation.
Case 2 Continued
An endoscopic ultrasound was performed and showed normal main pancreatic and common bile ducts. No intra-cystic mural nodules were observed. FNA was performed. Cytology showed “paucicellular fluid” and the cyst fluid CEA was 319 ng/mL. Having met the original consensus criteria for surgical resection [17] based on size, the presence of mural nodules, and due to suspicion for a mucinous cyst based on the CEA level, the patient underwent a Whipple procedure. The final pathology was a branch-duct IPMN with moderate dysplasia.
• What interventions exist for treating pancreatic cysts?
Surgery is the mainstay of treatment for pancreatic cysts. The most common surgical procedure for worrisome cysts in the head of the pancreas is a pancreatoduodenectomy (Whipple procedure). For cysts in the distal pancreas, a laparoscopic distal pancreatectomy can be performed [52,53]. Middle pancreatectomy, total pancreatectomy, and enucleation are less commonly performed and remain under investigation. The most common complications after surgery are surgical site and nonsurgical site infection, bleeding, pancreatic fistula, and delayed gastric emptying [52,53]. Overall complication rate for pancreatic cyst surgery is 27% to 39%, and perioperative mortality is 0.5% to 4% at high-volume centers [52,53].
An area of active investigation involves EUS-directed chemical cyst ablation. Prior studies using ethanol intra-cystic injection alone showed cyst resolution in 33% of patients [54]. A combination of ethanol and paclitaxel showed cyst resolution in 62% of patients [55]. Though these techniques offer a less invasive alternative to surgery, the complete eradication of dysplastic cystic epithelium remains uncertain and long-term efficacy is unclear. Thus, these techniques should only be considered in the context of a clinical trial or perhaps in patients who are not surgical candidates [56].
Case 3

• What is the epidemiology of IPMNs and how do they present?
IPMNs are mucin-producing lesions (mucinous cysts) of the exocrine pancreas involving either the main or branch ducts that have the potential to develop into pancreatic adenocarcinoma [57]. The mean age at presentation for both branch duct IPMNs (BD-IPMNs) and main duct IPMNs (MD-IPMNs) is around 65 years [58,59]. In the United States, the male to female prevalence ratio is equal, though there is some geographic variation among different countries [58]. Risk factors for IPMN formation include diabetes, chronic pancreatitis, and a family history of pancreatic adenocarcinoma [60]. Presentation is often asymptomatic but may present with pancreatitis, abdominal pain, weight loss, jaundice, and pancreatic exocrine insufficiency [61]. They tend to occur in the pancreatic head [29]. IPMNs involve either the main pancreatic duct or branch duct or both [62], but this is not always visible by imaging [21]. MRI with MRCP is considered superior to CT in characterizing these lesions, specifically in identifying a connection with the pancreatic ducts [21].
• How are IPMNs diagnosed and managed?
MD-IPMNs harbor a higher risk of malignancy than BD-IPMNs. In one series, 64% of MD-IPMN resected specimens contained cancer [63]. Because of the high cancer risk, all guidelines recommend surgical resection for appropriate patients [6,14,15,16,17]. BD-IPMNs have a lower risk of cancer at diagnosis, present in 19.5% of resected specimens in one study [63]. As a surgical series, this may overstate the true prevalence, which is supported by another study. A cohort of 103 suspected BD-IPMNs patients were observed and those with high-risk features were resected. The overall rate of cancer at 5 years was 2.6%, and only 1 of 103 patients developed non-resectable disease [64]. For these reasons, suspected BD-IPMNs can often be safely monitored if they do not harbor any high risk stigmata as defined by the international consensus criteria (Table 2)[6]. Otherwise, suspected BD-IPMNs are managed in a similar manner to other pancreatic cysts (Table 2) [6,14].
Prognosis after resection is more favorable for IPMNs than for pancreatic adenocarcinoma, possibly due to earlier stage of detection. The 5-year survival for BD-IPMN is 90% after resection, and 47% for MD-IPMN after resection [62]. Survival rates for IPMNs with invasive adenocarcinoma are lower with a combined overall survival 24% to 42% at 5 years. Survival rates are similar to the survival rate for non-cystic pancreatic adenocarcinoma when controlling for size, invasiveness, and lymph node metastasis [65,66].
Guidelines for surveillance after resection have even fewer applicable studies. The 5-year postoperative recurrence rate is 0 to 20% for IPMNs [6]. The revised international consensus guidelines recommends surveillance 6 months after resection with CT or MRI for all IPMNs, but with no recommendation given on how long to continue surveillance [6]. For patients with invasive disease, the same follow up is recommended as for standard invasive adenocarcinoma [6]. The AGA recommends yearly MRI only for only patients with high-grade dysplasia or invasive disease, with consideration for lifelong surveillance [14].
Case 4
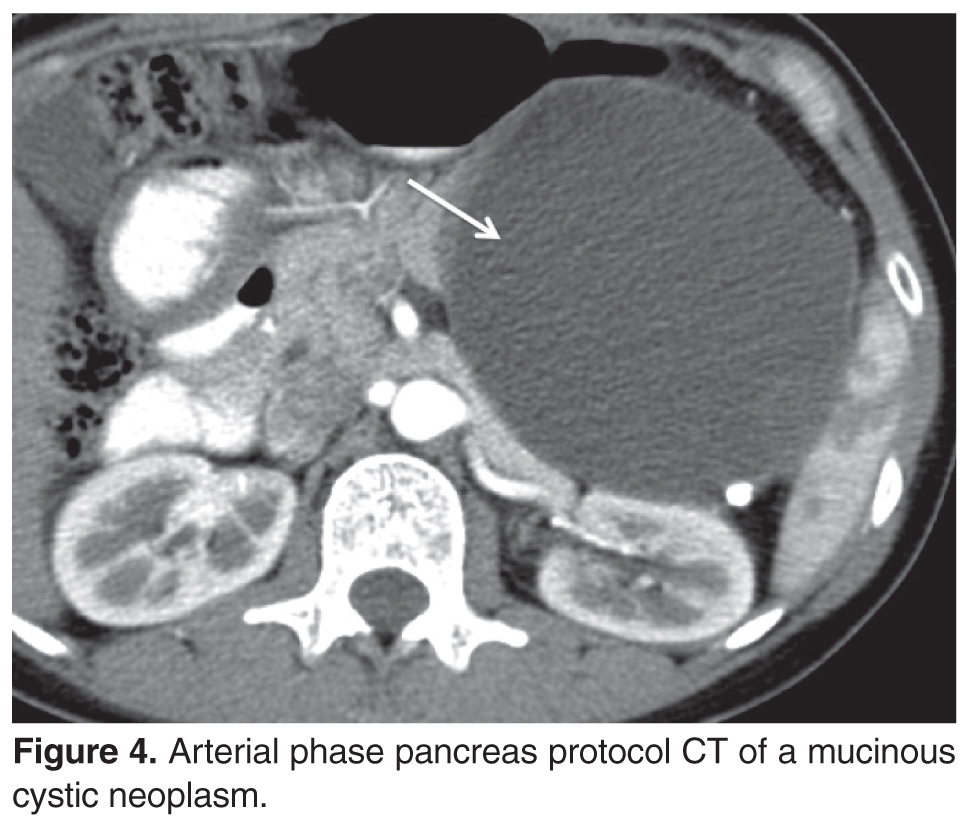
• What is the epidemiology of MCNs and how do they present?
MCNs are mucin-producing lesions (mucinous cysts) of the exocrine pancreas histologically defined by the presence of ovarian stroma [67]. They have the potential to develop into pancreatic adenocarcinoma. Unlike IPMNs, MCNs occur almost exclusively in women, and patients are generally younger. In one series, 99.7% of MCNs occurred in females, with a mean age of 47 [67]. Presenting symptoms, as with other cysts, are often vague. These include abdominal pain, fatigue, weight loss, pancreatitis, and a palpable mass. Only 25% of patients are asymptomatic [68].
• How are MCNs diagnosed and managed?
Approximately 95% of MCNs are located in the body or tail of the pancreas [67]. These lesions do not communicate with the pancreatic ducts unlike IPMNs, though they may still cause ductal obstruction and dilation [29]. They are often one large unilocular cyst with a thick cyst wall, but in 20% of cases they can have multiple septations [29]. Peripheral eggshell calcification on CT is present in roughly 25% of cases, which is sometimes helpful in differentiating these lesions from serous cystic neoplasms, which often have central calcification [69].
When diagnosed, MCNs are surgically removed [6,14]. A recent surgical series found that the rate of high-grade dysplasia in resected specimens was 5.5%, and the risk of invasive disease was 4.4% [70]. This data suggests that a more conservative approach of observation rather than immediate resection may be reasonable for some patients [70]. The prognosis is very good after MCN resection, with a 5-year survival of 97% to 100% for all comers [68,70]. However, invasive MCNs have a lower 5-year survival rate ranging from 15% to 75% [70,71]. Per the AGA guidelines, patients with invasive disease or dysplasia should undergo yearly surveillance with MRI [14]. This recommendation is based on a potential field defect described with IPMNs. However, the international consensus guidelines only recommends surveillance if invasive disease is present [6,68,71,72].
Case 5
A 59-year-old male presents for evaluation of sudden onset abdominal pain and an 8-pound weight loss over the past few months. Seven years ago a pancreatic cyst was diagnosed and has since been observed by serial imaging. His lipase was 400 U/L (normal < 82) with normal liver function tests. A CT scan of the abdomen and pelvis showed peri-pancreatic stranding consistent with pancreatitis and a large complex cyst in the head of the pancreas.

• What is the epidemiology of SCNs and how do they present?
SCNs are benign non–mucin-producing cystic lesions that are characterized by a glycogen-rich epithelium on histology [73]. Of patients with SCNs, 74% are female, with a median age 58 [10]. When diagnosed, most patients are usually asymptomatic (61%), but 27% present with abdominal pain. Other symptoms include jaundice, pancreatitis, nausea, and presence of a palpable abdominal mass. SCNs are more common in patients with von Hippel-Lindau syndrome [74].
• How are SCNs diagnosed and managed?
These cysts have fairly even distribution when discovered in the pancreas [53]. About 74% of lesions have smaller micro-cystic components [75]. About 20% of lesions have a characteristic honeycomb appearance, which is highly suggestive of an SCN [76]. About 30% of patients have a characteristic central stellate scar on CT which is also highly suggestive of an SCN [76]. Unlike mucinous neoplasms, peripheral calcification is usually not seen [69].
Malignancy associated with these cysts is very rare, with the largest cohort study reporting a rate of 0.1% [10]. The diagnosis can commonly be made by its unique imaging appearance [10]. Diagnostic biomarkers that may identify such cysts with more certainty are under active investigation [77]. Resection is reasonable and often performed for SCNs when they cause debilitating symptoms including refractory abdominal pain or pancreatitis. When resected and confirmed by pathology, no surveillance is required [14,78].
Conclusion
Pancreatic cysts are common incidental findings in clinical practice today. Many cause anxiety due to their association with pancreas cancer, but most are indolent and safe to observe. Even those cysts with malignant potential grow slowly and immediate surgery is often unnecessary. Several guidelines have been developed, and while there are similarities between them, there are enough critical differences unfortunately to cause some confusion among practitioners today. Further robust research is needed to help address and reconcile these differences. In the meantime, a multidisciplinary approach is highly recommended at dedicated centers of excellence for pancreatic diseases.
Corresponding author: Walter G. Park, MD, MS, 300 Pasteur Drive, MC: 5187, Stanford, CA 94305, [email protected].
Funding/support: Dr. Park is funded by an American College of Gastroenterology Junior Faculty Development Award and is a subcontinent for the National Cancer Institute's Early Detection Research Network.
Financial disclosures: None.
Author contributions: conception and design, TZ, WGP; analysis and interpretation of data, WGP; drafting of article, TZ, WGP; critical revision of the article, TZ, WGP.
1. DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin 2014;64:252–71.
2. Hruban RH, Maitra A, Kern SE, Goggins M. Precursors to pancreatic cancer. Gastroenterol Clin North Am 2007;36:831–49.
3. Laffan TA, Horton KM, Klein AP, et al. Prevalence of unsuspected pancreatic cysts on MDCT. Am J Roentgenol 2008;191:802–7.
4. Lee KS, Sekhar A, Rofsky NM, Pedrosa I. Prevalence of incidental pancreatic cysts in the adult population on MR imaging. Am J Gastroenterol 2010;105:2079–84.
5. Volkan Adsay N. Cystic lesions of the pancreas. Mod Pathol 20(1 Suppl):S71–93.
6. Tanaka M, Fernández-del Castillo C, Adsay V, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012;12:183–97.
7. Galanis C, Zamani A, Cameron J, et al. Resected serous cystic neoplasms of the pancreas: a review of 158 patients with recommendations for treatment. J Gastrointest Surg 2007;11:820–6.
8. Vitas G, Sarr M. Selected management of pancreatic pseudocysts: operative versus expectant management. Surgery 1992;111:123–30.
9. Jani N, Bani Hani M, Schulick RD, et al. Diagnosis and management of cystic lesions of the pancreas. Diagn Ther Endosc 2011;2011:478913.
10. Jais B, Rebours V, Malleo G, et al. Serous cystic neoplasm of the pancreas: a multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas). Gut 2015 Jun 4.
11. Kim YS, Cho JH. Rare nonneoplastic cysts of pancreas. Clin Endosc 2015;48:31–8.
12. Visser BC, Yeh BM, Qayyum A, et al. Characterization of cystic pancreatic masses: relative accuracy of CT and MRI. Am J Roentgenol 2007;189:648–56.
13. Lee H-J, Kim M-J, Choi J-Y, et al. Relative accuracy of CT and MRI in the differentiation of benign from malignant pancreatic cystic lesions. Clin Radiol 2011;66:315–21.
14. Scheiman JM, Hwang JH, Moayyedi P. American Gastroenterological Association technical review on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology 2015;148:824–48.
15. Berland LL, Silverman SG, Gore RM, et al. Managing incidental findings on abdominal CT: white paper of the ACR Incidental Findings Committee. J Am Coll Radiol 2010;7:754–73.
16. Khalid A, Brugge W. ACG practice guidelines for the diagnosis and management of neoplastic pancreatic cysts. Am J Gastroenterol 2007;102:2339–49.
17. Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatol Off J Int Assoc Pancreatol IAP Al 2006;6(1-2).
18. Ahn D-W, Lee SH, Kim J, et al. Long-term outcome of cystic lesions in the pancreas: a retrospective cohort study. Gut Liver 2012;6:493–500.
19. Khannoussi W, Vullierme MP, Rebours V, et al. The long term risk of malignancy in patients with branch duct intraductal papillary mucinous neoplasms of the pancreas. Pancreatol Off J Int Assoc Pancreatol IAP Al 2012;12:198–202.
20. Grieser C, Heine G, Stelter L, et al. Morphological analysis and differentiation of benign cystic neoplasms of the pancreas using computed tomography and magnetic resonance imaging. Fortschr Röntgenstr 2013;185:219–27.
21. Waters J, Schmidt CM, Pinchot J, et al. CT vs MRCP: optimal classification of IPMN type and extent. J Gastrointest Surg 2008;12:101–9.
22. Duconseil P, Turrini O, Ewald J, et al. “Peripheric” pancreatic cysts: performance of CT scan, MRI and endoscopy according to final pathological examination. HPB 2015;17:485–9.
23. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102–11.
24. Sanfey H, Aguilar M, Jones R. Pseudocysts of the pancreas, a review of 97 cases. Am Surg 1994;60:661–8.
25. Cheruvu CVN, Clarke MG, Prentice M, Eyre-Brook IA. Conservative treatment as an option in the management of pancreatic pseudocyst. Ann R Coll Surg Engl 2003;85:313–6.
26. Usatoff V, Brancatisano R, Williamson RCN. Operative treatment of pseudocysts in patients with chronic pancreatitis. Br J Surg 2000;87:1494–9.
27. Marshall G, Howell DA, Hansen BL, et al. Multidisciplinary approach to pseudoaneurysms complicating pancreatic pseudocysts: Impact of pretreatment diagnosis. Arch Surg 1996;131:278–83.
28. Sahani DV, Kadavigere R, Saokar A, et al. Cystic pancreatic lesions: a simple imaging-based classification system for guiding management. RadioGraphics 2005;25:1471–84.
29. Tirkes T, Aisen A, Cramer H, et al. Cystic neoplasms of the pancreas; findings on magnetic resonance imaging with pathological, surgical, and clinical correlation. Abdom Imaging 2014;39:1088–101.
30. Macari M, Finn ME, Bennett GL, et al. Differentiating Pancreatic cystic neoplasms from pancreatic pseudocysts at MR Imaging: value of perceived internal debris. Radiology 2009;251:77–84.
31. Park WG, Mascarenhas R, Palaez-Luna M, et al. Diagnostic performance of cyst fluid carcinoembryonic antigen and amylase in histologically confirmed pancreatic cysts. Pancreas 2011;40:42–5.
32. Braden B, Dietrich CF. Endoscopic ultrasonography-guided endoscopic treatment of pancreatic pseudocysts and walled-off necrosis: New technical developments. World J Gastroenterol WJG 2014;20:16191–6.
33. van Brunschot S, Fockens P, Bakker O, et al. Endoscopic transluminal necrosectomy in necrotising pancreatitis: a systematic review. Surg Endosc 2014;28:1425–38.
34. Pan G, Wan MH, Xie K-L, et al. Classification and management of pancreatic pseudocysts. Medicine (Baltimore). 2015;94:e960.
35. Yeo CJ, Bastidas JA, Lynch-Nyhan A, et al. The natural history of pancreatic pseudocysts documented by computed tomography. Surg Gynecol Obstet 1990;170:411–7.
36. Chebib I, Yaeger K, Mino-Kenudson M, Pitman MB. The role of cytopathology and cyst fluid analysis in the preoperative diagnosis and management of pancreatic cysts >3 cm. Cancer Cytopathol 2014;122:804–9.
37. Kim JH, Eun HW, Park H-J, et al. Diagnostic performance of MRI and EUS in the differentiation of benign from malignant pancreatic cyst and cyst communication with the main duct. Eur J Radiol 2012;81:2927–35.
38. Khashab MA, Kim K, Lennon AM, et al. Should we do EUS/FNA on patients with pancreatic cysts? the incremental diagnostic yield of EUS over CT/MRI for prediction of cystic neoplasms. Pancreas 2013;42:717–21.
39. de Jong K, Verlaan T, Dijkgraaf MG, et al. Interobserver agreement for endosonography in the diagnosis of pancreatic cysts. Endoscopy 2011;43:579–84.
40. Harinck F, Konings ICAW, Kluijt I, Poley JW, van Hooft JE, van Dullemen HM, et al. A multicentre comparative prospective blinded analysis of EUS and MRI for screening of pancreatic cancer in high-risk individuals. Gut 2015 May 18.
41. Thosani N, Thosani S, Qiao W, et al. Role of EUS-FNA based cytology in diagnosis of mucinous pancreatic cystic lesions: a systematic review and meta-analysis. Dig Dis Sci 2010;55:2756–66.
42. Hong S-KS, Loren DE, Rogart JN, et al. Targeted cyst wall puncture and aspiration during EUS-FNA increases the diagnostic yield of premalignant and malignant pancreatic cysts. Gastrointest Endosc 2012;75:775–82.
43. Thornton G, McPhail M, Nayagam S, et al. Endoscopic ultrasound guided fine needle aspiration for the diagnosis of pancreatic cystic neoplasms: a meta-analysis. Pancreatology 2013;13:48–57.
44. Khalid A, Zahid M, Finkelstein SD, et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: a report of the PANDA study. Gastrointest Endosc 2009;May;69:1095–102.
45. Wu J, Matthaei H, Maitra A, et al. Recurrent GNAS mutations define an unexpected pathway for pancreatic cyst development. Sci Transl Med 2011;3:92ra66.
46. Springer S, Wang Y, Molin MD, et al. A Combination of molecular markers and clinical features improve the classification of pancreatic cysts. Gastroenterology 2015 Aug 4.
47. Ryu JK, Matthaei H, dal Molin M, et al. Elevated microRNA miR-21 Levels in Pancreatic cyst fluid are predictive of mucinous precursor lesions of ductal adenocarcinoma. Pancreatology 2011;11:343–50.
48. Matthaei H, Wylie D, Lloyd MB, et al. miRNA Biomarkers in cyst fluid augment the diagnosis and management of pancreatic cysts. Clin Cancer Res 2012;18 :4713–24.
49. Zikos T, Pham K, Bowen R, et al. Cyst fluid glucose is rapidly feasible and accurate in diagnosing mucinous pancreatic cysts. Am J Gastroenterol 2015;110:909–14.
50. Corcos O, Couvelard A, Dargère D, et al. Proteomic assessment of markers for malignancy in the mucus of intraductal papillary mucinous neoplasms of the pancreas. Pancreas 2012;41:169–74.
51. Thiruvengadam N, Park W. Systematic review of pancreatic cyst fluid biomarkers: the path forward. Clin Transl Gastroenterol 2015;11:e88.
52. Plichta JK, Brosius JA, Pappas SG, et al. The changing spectrum of surgically treated cystic neoplasms of the pancreas. HPB Surg 2015;2015:791704.
53. Valsangkar NP, Morales-Oyarvide V, Thayer SP, et al. 851 resected cystic tumors of the pancreas: A 33-year experience at the Massachusetts General Hospital. Surgery 2012;152:S4–12.
54. DeWitt J, McGreevy K, Schmidt CM, Brugge WR. EUS-guided ethanol versus saline solution lavage for pancreatic cysts: a randomized, double-blind study. Gastrointest Endosc 2009;70:710–23.
55. Oh H-C, Seo DW, Song TJ, et al. Endoscopic ultrasonography-guided ethanol lavage with paclitaxel injection treats patients with pancreatic cysts. Gastroenterology 2011;140:172–9.
56. Gavini H, Lee JH. Endoscopic ultrasound-guided endotherapy. J Clin Gastroenterol 2015;49:185–93.
57. Grutzmann R, Niedergethmann M, Pilarsky C, et al. Intraductal papillary mucinous tumors of the pancreas: biology, diagnosis, and treatment. Ooncologist 2010;15:1294–309.
58. Ingkakul T, Warshaw AL, Fernández-Del Castillo C. Epidemiology of intraductal papillary mucinous neoplasms of the pancreas: sex differences between 3 geographic regions. Pancreas 2011;40:779–80.
59. Brugge WR, Lauwers GY, Sahani D, et al. Cystic neoplasms of the pancreas. N Engl J Med 2004;351:1218–26.
60. Capurso G, Boccia S, Salvia R, et al. Risk factors for intraductal papillary mucinous neoplasm (IPMN) of the pancreas: a multicentre case-control study. Am J Gastroenterol 2013n;108:1003–9.
61. Lubezky N, Ben-Haim M, Nakache R, et al. Clinical presentation can predict disease course in patients with intraductal papillary mucinous neoplasm of the pancreas. World J Surg 2010;34:126–32.
62. Kobari M, Egawa S, Shibuya K, et al. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg Chic Ill 1960. 1999;134:1131–6.
63. Serikawa M, Sasaki T, Fujimoto Y, et al. Management of intraductal papillary-mucinous neoplasm of the pancreas: treatment strategy based on morphologic classification. J Clin Gastroenterol 2006;40:856–62.
64. Sawai Y, Yamao K, Bhatia V, et al. Development of pancreatic cancers during long-term follow-up of side-branch intraductal papillary mucinous neoplasms. Endoscopy 2010;42:1077–84.
65. Poultsides GA, Reddy S, Cameron JL, et al. Histopathologic basis for the favorable survival after resection of intraductal papillary mucinous neoplasm-associated invasive adenocarcinoma of the pancreas. Ann Surg 201 Mar;251:470–6.
66. Worni M, Akushevich I, Gloor B, et al. Adjuvant radiotherapy in the treatment of invasive intraductal papillary mucinous neoplasm of the pancreas: an analysis of the surveillance, epidemiology, and end results registry. Ann Surg Oncol 2012;19:1316–23.
67. Goh BKP, Tan Y-M, Chung Y-FA, et al. A review of mucinous cystic neoplasms of the pancreas defined by ovarian-type stroma: clinicopathological features of 344 patients. World J Surg 2006;30:2236–45.
68. Crippa S, Salvia R, Warshaw AL, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: lessons from 163 resected patients. Ann Surg 2008;247:571–9.
69. Curry CA, Eng J, Horton KM, et al. CT of primary cystic pancreatic neoplasms: can CT be used for patient triage and treatment? AJR Am J Roentgenol 2000;175:99–103.
70. Park JW, Jang J-Y, Kang MJ, et al. Mucinous cystic neoplasm of the pancreas: Is surgical resection recommended for all surgically fit patients? Pancreatology 2014;14:131–6.
71. Sakorafas GH, Smyrniotis V, Reid-Lombardo KM, Sarr MG. Primary pancreatic cystic neoplasms revisited: Part II. Mucinous cystic neoplasms. Surg Oncol 2011;20:e93–101.
72. Sarr MG, Carpenter HA, Prabhakar LP, et al. Clinical and pathologic correlation of 84 mucinous cystic neoplasms of the pancreas: can one reliably differentiate benign from malignant (or premalignant) neoplasms? Ann Surg 2000;231:205–12.
73. Reid MD, Choi H, Balci S, et al. Serous cystic neoplasms of the pancreas: Clinicopathologic and molecular characteristics. Pancreat Neoplasms 2014;31:475–83.
74. Charlesworth M, Verbeke CS, Falk GA, et al. Pancreatic lesions in von Hippel-Lindau disease? A systematic review and meta-synthesis of the literature. J Gastrointest Surg Off J Soc Surg Aliment Tract 2012;16:1422–8.
75. Kimura W, Moriya T, Hirai I, et al. Multicenter study of serous cystic neoplasm of the Japan pancreas society. Pancreas 2012;41):380–7.
76. Sarr MG, Murr M, Smyrk TC, et al. Primary cystic neoplasms of the pancreas. Neoplastic disorders of emerging importance-current state-of-the-art and unanswered questions. J Gastrointest Surg Off J Soc Surg Aliment Tract 2003;7:417–28.
77. Yip-Schneider MT, Wu H, Dumas RP, et al. Vascular endothelial growth factor, a novel and highly accurate pancreatic fluid biomarker for serous pancreatic cysts. J Am Coll Surg 2014;218:608–17.
78. Del Chiaro M, Verbeke C, Salvia R, et al. European experts consensus statement on cystic tumours of the pancreas. Dig Liver Dis 2013;45:703–11.
From the Department of Medicine, Stanford University School of Medicine, Stanford, CA.
Abstract
- Objective: To review the diagnosis and management of pancreatic cystic lesions.
- Methods: Narrative review of the literature.
- Results: Pancreatic cystic lesions are clinically relevant as some are precursor lesions to pancreatic adenocarcinoma. Mucinous cystic neoplasms and intraductal papillary mucinous neoplasms are 2 commonly encountered pre-cancerous pancreatic cysts. Many cysts are identified incidentally due to frequent use of high-resolution CT and MRI imaging technology. Proposed diagnostic and management algorithms exist to guide clinical practice but are limited by a lack of evidence and discordance among various guidelines. New cyst fluid biomarkers are under development to diagnose cyst types and risk of cancer.
- Conclusion: Pancreatic cysts are increasingly encountered in clinical practice and represent a growing problem. Diagnostic and management algorithms are available to assist practice but are limited by the available evidence. A multidisciplinary approach is recommended.
In the United States there were an estimated 46,420 new cases of pancreatic cancer in 2014 [1]. Of all major cancers, pancreatic cancer had the lowest 5-year survival rate at 6% [1]. Of the 3 known precursor lesions to pancreas adenocarcinoma, 2 are pancreatic cysts [2]. Correctly identifying those with cancer, those with cancer potential (premalignant), and those that are benign (harboring no malignant potential) can be difficult.
Case 1
A 57-year-old male had a 1.5-cm pancreatic cyst located in the head that was found on computed tomography (CT) imaging for suspected renal colic. He had no history or complaints suspicious for pancreatic disease. A CT pancreas protocol scan was obtained, which demonstrated a simple appearing cyst with no mural nodules. The pancreatic and biliary ducts were normal. His laboratory evaluations including liver function testing and lipase were normal.
• What is the approach to incidentally discovered pancreatic cysts?
While many pancreatic cysts are first discovered by cross sectional imaging (CT or MRI), the diagnostic accuracy of defining cyst type and the presence of malignancy is imperfect. The area under the curve (AUC) for differentiating malignant from benign pancreatic cysts ranges from 0.64 to 0.82 for CT and 0.73 to 0.91 for MRI, and no difference between the 2 were observed [12,13]. Several guidelines are currently available to offer guidance on management [6,14,15,16,17]. Much of the current evidence includes retrospective case series with no randomized control trials. The guidelines, therefore, mostly represent consensus-based expert extrapolation of available data.
The American Gastroenterological Association (AGA) recently produced guidelines in 2015 [14]. In comparison to the international consensus guidelines, there are a few key differences, which have now become a point of vigorous debate and disagreement among pancreatologists and confusion among general gastroenterologists and surgeons in the community. Where the international consensus guidelines have stricter criteria to define the appropriateness of surgery, the AGA guidelines are more liberal. AGA defined cysts appropriate for surgery as having 2 out of 3 of the following features: (1) cyst size ≥ 3 cm, (2) presence of a solid component in the cyst, and (3) dilation of the main pancreatic duct. Those having 1 out of 3 criteria were defined as needing further investigation with EUS [14]. These criteria are more relaxed and will likely lead to more surgical resections.
Another difference involves surveillance recommendations. The international consensus guidelines do not define a period when surveillance can be safely stopped. The AGA guidelines define 5 years as the period where if there is no significant change in the cyst from surveillance MRIs performed every 1 to 2 years, then surveillance can be stopped [14]. As the natural history of these cysts remain substantially uncertain, with evidence that malignant transformation occurs after 5 years, this particular recommendation by the AGA remains highly controversial [18,19]. Other differences between these 2 guidelines are summarized in Table 2 [6,14].
Until the surveillance recommendations by the AGA are validated with further studies, we generally follow the 2012 international consensus guidelines. We generally prefer MRI for initial and surveillance evaluations of pancreatic cysts. Besides the lack of radiation exposure, some studies show MRI to have better inter-reader variability [20], better resolution to show cyst communication with the main pancreatic duct [21], and better characterization of peripheral pancreatic cysts [22]. At our center, when a solid mass is suspected, a CT pancreas protocol is preferred in lieu of an MRI by our surgical team.
Case 1 Continued
Despite the reassuring CEA and cytology results, a high concern for a malignant cystic lesion remained based on cyst size, main pancreatic duct dilation, and atrophy noted in the distal pancreas. The patient underwent surgical resection including subtotal pancreatectomy, splenectomy, subtotal gastrectomy, and superior mesenteric and portal vein resection with reconstruction. Pathology revealed the cyst to be a benign pseudocyst.
This case reflects some of the critical challenges in current management of pancreatic cysts. By history, this patient had no suspicion for pancreatitis, making a pseudocyst less likely in a differential diagnosis. When the patient presented 7 years later, again with no reported history of pancreatitis, there was clinical concern for a branch duct IPMN. Although the cyst fluid CEA and cytology were reassuring, the patient met surgical criteria by the 2006 international consensus criteria and the more recent AGA guidelines. Interestingly, the narrowed 2012 international consensus guidelines for surgical resection would have recommended observation. This case highlights the need for better diagnostic tests.
• What is the epidemiology of pancreatic fluid collections and how do they present?
Pancreatic fluid collections are not true cysts as they lack an epithelial cell lining. They often occur in the context of either acute or chronic pancreatitis, and are considered benign or nonmucinous cysts [7,8]. Duct disruption occurs causing pancreatic fluid accumulation, initially defined as an acute peri-pancreatic fluid collection, or an acute necrotic collection if necrosis is present. Over about 4 weeks a more defined cyst wall forms and the cyst is now classified as either a pseudocyst or walled-off pancreatic necrosis [23]. In one review, the median age at presentation was 49 with a male:female ratio of 2:1. Only 52% of fluid collections were discovered following an acute attack of pancreatitis [24]. The risk factors for pancreatic fluid collections are similar to the risk factors for pancreatitis, with the most common being alcohol use and gallstones [24]. Potential symptoms include abdominal pain, weight loss, gastrointestinal bleeding from pseudoaneurysms, obstructive symptoms, sepsis from super infection, and obstructive jaundice [8,24,25,26,27].
• How are pancreatic fluid collections diagnosed and managed?
Clinical suspicion for pancreatic fluid collections should increase if a cyst is diagnosed in the context of acute or chronic pancreatitis [28]. However, other types of cysts can cause ductal obstruction and pancreatitis, so further investigation may be needed, including review of prior imaging if available. The presence of internal debris, the presence of imaging findings of acute or chronic pancreatitis, and fluid extension beyond the pancreas and taking the shape of the retroperitoneum are often characteristics found in pancreatic fluid collections [29,28,30]. If needed, FNA with assay of amylase may be helpful. An amylase value of 5680 IU/L or greater was 84% sensitive and 64% specific (AUC 0.69) for pseudocysts in one study [31].
Management of pancreatic fluid collections is largely based on surgical series. Drainage procedures for pancreatic fluid collections are often undertaken for intractable symptoms or concerns of infection [8,24,25,26]. Asymptomatic pseudocysts can be safely followed. Specific techniques used for pancreatic fluid collection management vary by institutional expertise. Endoscopic drainage can be done by transpapillary stenting if main duct communication is present, or transgastric/transduodenal stenting if the cyst wall is mature and accessible by these approaches [32]. If necrosis is present this can be debrided endoscopically [33]. Laparoscopic surgical options are preferred to open approaches, and can be performed in 1 procedure where endoscopic approaches may require multiple procedures. The most common approach is to drain the cyst by creating a cyst-gastrostomy, or when not feasible a cyst-duodenostomy or cyst-jejunostomy [26,34]. Percutaneous drainage is less commonly performed and used for unstable patients as it can lead to cutaneous fistulas [34]. The best technique for intervention should be decided in the context of a multidisciplinary team. The option for conservative management should be considered as well because about 60% of those managed conservatively will have resolution in 1 year [35].
Case 2
• What is the role of endoscopic ultrasound with FNA in the diagnosis of pancreatic cysts?
While more invasive than CT or MRI, EUS provides detailed imaging to characterize relevant clinical features and allows fine needle aspiration of the cyst fluid and tissue of intra-cystic masses (Table 2) [6,14]. While MRI imaging resolution is continuing to improve [22,36,37], EUS is generally considered superior [38] for diagnosing high-risk lesions. A limitation of EUS, however, is significant inter-observer variability when compared with MRI [37,39,40].
EUS enables FNA of the cyst, which offers unique oppor-tunities for diagnosis. Cyst fluid cytology unfortunately has limited diagnostic yield, with a recent meta-analysis showing sensitivity 63%, specificity 88%, and AUC of 0.89 in differentiating mucinous from nonmucinous cysts [41]. The low sensitivity is likely because cyst fluid is paucicellular. Techniques that include targeting the cyst wall are under investigation and may improve the diagnostic yield of cytological analysis [42]. Tumor markers such as CEA have been widely used in the cyst fluid, with a value > 192 ng/mL having 63% sensitivity and 88% specificity (AUC of 0.79) for mucinous pancreatic cysts [43]. Other cyst fluid markers have been or are being developed including mutated KRAS DNA [44], mutated GNAS DNA [45,46], micro RNA [47,48], glucose [49], proteomic analysis [50], and multiple other molecules [51]. At this time, many of these markers are under investigation.
Case 2 Continued
An endoscopic ultrasound was performed and showed normal main pancreatic and common bile ducts. No intra-cystic mural nodules were observed. FNA was performed. Cytology showed “paucicellular fluid” and the cyst fluid CEA was 319 ng/mL. Having met the original consensus criteria for surgical resection [17] based on size, the presence of mural nodules, and due to suspicion for a mucinous cyst based on the CEA level, the patient underwent a Whipple procedure. The final pathology was a branch-duct IPMN with moderate dysplasia.
• What interventions exist for treating pancreatic cysts?
Surgery is the mainstay of treatment for pancreatic cysts. The most common surgical procedure for worrisome cysts in the head of the pancreas is a pancreatoduodenectomy (Whipple procedure). For cysts in the distal pancreas, a laparoscopic distal pancreatectomy can be performed [52,53]. Middle pancreatectomy, total pancreatectomy, and enucleation are less commonly performed and remain under investigation. The most common complications after surgery are surgical site and nonsurgical site infection, bleeding, pancreatic fistula, and delayed gastric emptying [52,53]. Overall complication rate for pancreatic cyst surgery is 27% to 39%, and perioperative mortality is 0.5% to 4% at high-volume centers [52,53].
An area of active investigation involves EUS-directed chemical cyst ablation. Prior studies using ethanol intra-cystic injection alone showed cyst resolution in 33% of patients [54]. A combination of ethanol and paclitaxel showed cyst resolution in 62% of patients [55]. Though these techniques offer a less invasive alternative to surgery, the complete eradication of dysplastic cystic epithelium remains uncertain and long-term efficacy is unclear. Thus, these techniques should only be considered in the context of a clinical trial or perhaps in patients who are not surgical candidates [56].
Case 3
• What is the epidemiology of IPMNs and how do they present?
IPMNs are mucin-producing lesions (mucinous cysts) of the exocrine pancreas involving either the main or branch ducts that have the potential to develop into pancreatic adenocarcinoma [57]. The mean age at presentation for both branch duct IPMNs (BD-IPMNs) and main duct IPMNs (MD-IPMNs) is around 65 years [58,59]. In the United States, the male to female prevalence ratio is equal, though there is some geographic variation among different countries [58]. Risk factors for IPMN formation include diabetes, chronic pancreatitis, and a family history of pancreatic adenocarcinoma [60]. Presentation is often asymptomatic but may present with pancreatitis, abdominal pain, weight loss, jaundice, and pancreatic exocrine insufficiency [61]. They tend to occur in the pancreatic head [29]. IPMNs involve either the main pancreatic duct or branch duct or both [62], but this is not always visible by imaging [21]. MRI with MRCP is considered superior to CT in characterizing these lesions, specifically in identifying a connection with the pancreatic ducts [21].
• How are IPMNs diagnosed and managed?
MD-IPMNs harbor a higher risk of malignancy than BD-IPMNs. In one series, 64% of MD-IPMN resected specimens contained cancer [63]. Because of the high cancer risk, all guidelines recommend surgical resection for appropriate patients [6,14,15,16,17]. BD-IPMNs have a lower risk of cancer at diagnosis, present in 19.5% of resected specimens in one study [63]. As a surgical series, this may overstate the true prevalence, which is supported by another study. A cohort of 103 suspected BD-IPMNs patients were observed and those with high-risk features were resected. The overall rate of cancer at 5 years was 2.6%, and only 1 of 103 patients developed non-resectable disease [64]. For these reasons, suspected BD-IPMNs can often be safely monitored if they do not harbor any high risk stigmata as defined by the international consensus criteria (Table 2)[6]. Otherwise, suspected BD-IPMNs are managed in a similar manner to other pancreatic cysts (Table 2) [6,14].
Prognosis after resection is more favorable for IPMNs than for pancreatic adenocarcinoma, possibly due to earlier stage of detection. The 5-year survival for BD-IPMN is 90% after resection, and 47% for MD-IPMN after resection [62]. Survival rates for IPMNs with invasive adenocarcinoma are lower with a combined overall survival 24% to 42% at 5 years. Survival rates are similar to the survival rate for non-cystic pancreatic adenocarcinoma when controlling for size, invasiveness, and lymph node metastasis [65,66].
Guidelines for surveillance after resection have even fewer applicable studies. The 5-year postoperative recurrence rate is 0 to 20% for IPMNs [6]. The revised international consensus guidelines recommends surveillance 6 months after resection with CT or MRI for all IPMNs, but with no recommendation given on how long to continue surveillance [6]. For patients with invasive disease, the same follow up is recommended as for standard invasive adenocarcinoma [6]. The AGA recommends yearly MRI only for only patients with high-grade dysplasia or invasive disease, with consideration for lifelong surveillance [14].
Case 4
• What is the epidemiology of MCNs and how do they present?
MCNs are mucin-producing lesions (mucinous cysts) of the exocrine pancreas histologically defined by the presence of ovarian stroma [67]. They have the potential to develop into pancreatic adenocarcinoma. Unlike IPMNs, MCNs occur almost exclusively in women, and patients are generally younger. In one series, 99.7% of MCNs occurred in females, with a mean age of 47 [67]. Presenting symptoms, as with other cysts, are often vague. These include abdominal pain, fatigue, weight loss, pancreatitis, and a palpable mass. Only 25% of patients are asymptomatic [68].
• How are MCNs diagnosed and managed?
Approximately 95% of MCNs are located in the body or tail of the pancreas [67]. These lesions do not communicate with the pancreatic ducts unlike IPMNs, though they may still cause ductal obstruction and dilation [29]. They are often one large unilocular cyst with a thick cyst wall, but in 20% of cases they can have multiple septations [29]. Peripheral eggshell calcification on CT is present in roughly 25% of cases, which is sometimes helpful in differentiating these lesions from serous cystic neoplasms, which often have central calcification [69].
When diagnosed, MCNs are surgically removed [6,14]. A recent surgical series found that the rate of high-grade dysplasia in resected specimens was 5.5%, and the risk of invasive disease was 4.4% [70]. This data suggests that a more conservative approach of observation rather than immediate resection may be reasonable for some patients [70]. The prognosis is very good after MCN resection, with a 5-year survival of 97% to 100% for all comers [68,70]. However, invasive MCNs have a lower 5-year survival rate ranging from 15% to 75% [70,71]. Per the AGA guidelines, patients with invasive disease or dysplasia should undergo yearly surveillance with MRI [14]. This recommendation is based on a potential field defect described with IPMNs. However, the international consensus guidelines only recommends surveillance if invasive disease is present [6,68,71,72].
Case 5
A 59-year-old male presents for evaluation of sudden onset abdominal pain and an 8-pound weight loss over the past few months. Seven years ago a pancreatic cyst was diagnosed and has since been observed by serial imaging. His lipase was 400 U/L (normal < 82) with normal liver function tests. A CT scan of the abdomen and pelvis showed peri-pancreatic stranding consistent with pancreatitis and a large complex cyst in the head of the pancreas.
• What is the epidemiology of SCNs and how do they present?
SCNs are benign non–mucin-producing cystic lesions that are characterized by a glycogen-rich epithelium on histology [73]. Of patients with SCNs, 74% are female, with a median age 58 [10]. When diagnosed, most patients are usually asymptomatic (61%), but 27% present with abdominal pain. Other symptoms include jaundice, pancreatitis, nausea, and presence of a palpable abdominal mass. SCNs are more common in patients with von Hippel-Lindau syndrome [74].
• How are SCNs diagnosed and managed?
These cysts have fairly even distribution when discovered in the pancreas [53]. About 74% of lesions have smaller micro-cystic components [75]. About 20% of lesions have a characteristic honeycomb appearance, which is highly suggestive of an SCN [76]. About 30% of patients have a characteristic central stellate scar on CT which is also highly suggestive of an SCN [76]. Unlike mucinous neoplasms, peripheral calcification is usually not seen [69].
Malignancy associated with these cysts is very rare, with the largest cohort study reporting a rate of 0.1% [10]. The diagnosis can commonly be made by its unique imaging appearance [10]. Diagnostic biomarkers that may identify such cysts with more certainty are under active investigation [77]. Resection is reasonable and often performed for SCNs when they cause debilitating symptoms including refractory abdominal pain or pancreatitis. When resected and confirmed by pathology, no surveillance is required [14,78].
Conclusion
Pancreatic cysts are common incidental findings in clinical practice today. Many cause anxiety due to their association with pancreas cancer, but most are indolent and safe to observe. Even those cysts with malignant potential grow slowly and immediate surgery is often unnecessary. Several guidelines have been developed, and while there are similarities between them, there are enough critical differences unfortunately to cause some confusion among practitioners today. Further robust research is needed to help address and reconcile these differences. In the meantime, a multidisciplinary approach is highly recommended at dedicated centers of excellence for pancreatic diseases.
Corresponding author: Walter G. Park, MD, MS, 300 Pasteur Drive, MC: 5187, Stanford, CA 94305, [email protected].
Funding/support: Dr. Park is funded by an American College of Gastroenterology Junior Faculty Development Award and is a subcontinent for the National Cancer Institute's Early Detection Research Network.
Financial disclosures: None.
Author contributions: conception and design, TZ, WGP; analysis and interpretation of data, WGP; drafting of article, TZ, WGP; critical revision of the article, TZ, WGP.
From the Department of Medicine, Stanford University School of Medicine, Stanford, CA.
Abstract
- Objective: To review the diagnosis and management of pancreatic cystic lesions.
- Methods: Narrative review of the literature.
- Results: Pancreatic cystic lesions are clinically relevant as some are precursor lesions to pancreatic adenocarcinoma. Mucinous cystic neoplasms and intraductal papillary mucinous neoplasms are 2 commonly encountered pre-cancerous pancreatic cysts. Many cysts are identified incidentally due to frequent use of high-resolution CT and MRI imaging technology. Proposed diagnostic and management algorithms exist to guide clinical practice but are limited by a lack of evidence and discordance among various guidelines. New cyst fluid biomarkers are under development to diagnose cyst types and risk of cancer.
- Conclusion: Pancreatic cysts are increasingly encountered in clinical practice and represent a growing problem. Diagnostic and management algorithms are available to assist practice but are limited by the available evidence. A multidisciplinary approach is recommended.
In the United States there were an estimated 46,420 new cases of pancreatic cancer in 2014 [1]. Of all major cancers, pancreatic cancer had the lowest 5-year survival rate at 6% [1]. Of the 3 known precursor lesions to pancreas adenocarcinoma, 2 are pancreatic cysts [2]. Correctly identifying those with cancer, those with cancer potential (premalignant), and those that are benign (harboring no malignant potential) can be difficult.
Case 1
A 57-year-old male had a 1.5-cm pancreatic cyst located in the head that was found on computed tomography (CT) imaging for suspected renal colic. He had no history or complaints suspicious for pancreatic disease. A CT pancreas protocol scan was obtained, which demonstrated a simple appearing cyst with no mural nodules. The pancreatic and biliary ducts were normal. His laboratory evaluations including liver function testing and lipase were normal.
• What is the approach to incidentally discovered pancreatic cysts?
While many pancreatic cysts are first discovered by cross sectional imaging (CT or MRI), the diagnostic accuracy of defining cyst type and the presence of malignancy is imperfect. The area under the curve (AUC) for differentiating malignant from benign pancreatic cysts ranges from 0.64 to 0.82 for CT and 0.73 to 0.91 for MRI, and no difference between the 2 were observed [12,13]. Several guidelines are currently available to offer guidance on management [6,14,15,16,17]. Much of the current evidence includes retrospective case series with no randomized control trials. The guidelines, therefore, mostly represent consensus-based expert extrapolation of available data.
The American Gastroenterological Association (AGA) recently produced guidelines in 2015 [14]. In comparison to the international consensus guidelines, there are a few key differences, which have now become a point of vigorous debate and disagreement among pancreatologists and confusion among general gastroenterologists and surgeons in the community. Where the international consensus guidelines have stricter criteria to define the appropriateness of surgery, the AGA guidelines are more liberal. AGA defined cysts appropriate for surgery as having 2 out of 3 of the following features: (1) cyst size ≥ 3 cm, (2) presence of a solid component in the cyst, and (3) dilation of the main pancreatic duct. Those having 1 out of 3 criteria were defined as needing further investigation with EUS [14]. These criteria are more relaxed and will likely lead to more surgical resections.
Another difference involves surveillance recommendations. The international consensus guidelines do not define a period when surveillance can be safely stopped. The AGA guidelines define 5 years as the period where if there is no significant change in the cyst from surveillance MRIs performed every 1 to 2 years, then surveillance can be stopped [14]. As the natural history of these cysts remain substantially uncertain, with evidence that malignant transformation occurs after 5 years, this particular recommendation by the AGA remains highly controversial [18,19]. Other differences between these 2 guidelines are summarized in Table 2 [6,14].
Until the surveillance recommendations by the AGA are validated with further studies, we generally follow the 2012 international consensus guidelines. We generally prefer MRI for initial and surveillance evaluations of pancreatic cysts. Besides the lack of radiation exposure, some studies show MRI to have better inter-reader variability [20], better resolution to show cyst communication with the main pancreatic duct [21], and better characterization of peripheral pancreatic cysts [22]. At our center, when a solid mass is suspected, a CT pancreas protocol is preferred in lieu of an MRI by our surgical team.
Case 1 Continued
Despite the reassuring CEA and cytology results, a high concern for a malignant cystic lesion remained based on cyst size, main pancreatic duct dilation, and atrophy noted in the distal pancreas. The patient underwent surgical resection including subtotal pancreatectomy, splenectomy, subtotal gastrectomy, and superior mesenteric and portal vein resection with reconstruction. Pathology revealed the cyst to be a benign pseudocyst.
This case reflects some of the critical challenges in current management of pancreatic cysts. By history, this patient had no suspicion for pancreatitis, making a pseudocyst less likely in a differential diagnosis. When the patient presented 7 years later, again with no reported history of pancreatitis, there was clinical concern for a branch duct IPMN. Although the cyst fluid CEA and cytology were reassuring, the patient met surgical criteria by the 2006 international consensus criteria and the more recent AGA guidelines. Interestingly, the narrowed 2012 international consensus guidelines for surgical resection would have recommended observation. This case highlights the need for better diagnostic tests.
• What is the epidemiology of pancreatic fluid collections and how do they present?
Pancreatic fluid collections are not true cysts as they lack an epithelial cell lining. They often occur in the context of either acute or chronic pancreatitis, and are considered benign or nonmucinous cysts [7,8]. Duct disruption occurs causing pancreatic fluid accumulation, initially defined as an acute peri-pancreatic fluid collection, or an acute necrotic collection if necrosis is present. Over about 4 weeks a more defined cyst wall forms and the cyst is now classified as either a pseudocyst or walled-off pancreatic necrosis [23]. In one review, the median age at presentation was 49 with a male:female ratio of 2:1. Only 52% of fluid collections were discovered following an acute attack of pancreatitis [24]. The risk factors for pancreatic fluid collections are similar to the risk factors for pancreatitis, with the most common being alcohol use and gallstones [24]. Potential symptoms include abdominal pain, weight loss, gastrointestinal bleeding from pseudoaneurysms, obstructive symptoms, sepsis from super infection, and obstructive jaundice [8,24,25,26,27].
• How are pancreatic fluid collections diagnosed and managed?
Clinical suspicion for pancreatic fluid collections should increase if a cyst is diagnosed in the context of acute or chronic pancreatitis [28]. However, other types of cysts can cause ductal obstruction and pancreatitis, so further investigation may be needed, including review of prior imaging if available. The presence of internal debris, the presence of imaging findings of acute or chronic pancreatitis, and fluid extension beyond the pancreas and taking the shape of the retroperitoneum are often characteristics found in pancreatic fluid collections [29,28,30]. If needed, FNA with assay of amylase may be helpful. An amylase value of 5680 IU/L or greater was 84% sensitive and 64% specific (AUC 0.69) for pseudocysts in one study [31].
Management of pancreatic fluid collections is largely based on surgical series. Drainage procedures for pancreatic fluid collections are often undertaken for intractable symptoms or concerns of infection [8,24,25,26]. Asymptomatic pseudocysts can be safely followed. Specific techniques used for pancreatic fluid collection management vary by institutional expertise. Endoscopic drainage can be done by transpapillary stenting if main duct communication is present, or transgastric/transduodenal stenting if the cyst wall is mature and accessible by these approaches [32]. If necrosis is present this can be debrided endoscopically [33]. Laparoscopic surgical options are preferred to open approaches, and can be performed in 1 procedure where endoscopic approaches may require multiple procedures. The most common approach is to drain the cyst by creating a cyst-gastrostomy, or when not feasible a cyst-duodenostomy or cyst-jejunostomy [26,34]. Percutaneous drainage is less commonly performed and used for unstable patients as it can lead to cutaneous fistulas [34]. The best technique for intervention should be decided in the context of a multidisciplinary team. The option for conservative management should be considered as well because about 60% of those managed conservatively will have resolution in 1 year [35].
Case 2
• What is the role of endoscopic ultrasound with FNA in the diagnosis of pancreatic cysts?
While more invasive than CT or MRI, EUS provides detailed imaging to characterize relevant clinical features and allows fine needle aspiration of the cyst fluid and tissue of intra-cystic masses (Table 2) [6,14]. While MRI imaging resolution is continuing to improve [22,36,37], EUS is generally considered superior [38] for diagnosing high-risk lesions. A limitation of EUS, however, is significant inter-observer variability when compared with MRI [37,39,40].
EUS enables FNA of the cyst, which offers unique oppor-tunities for diagnosis. Cyst fluid cytology unfortunately has limited diagnostic yield, with a recent meta-analysis showing sensitivity 63%, specificity 88%, and AUC of 0.89 in differentiating mucinous from nonmucinous cysts [41]. The low sensitivity is likely because cyst fluid is paucicellular. Techniques that include targeting the cyst wall are under investigation and may improve the diagnostic yield of cytological analysis [42]. Tumor markers such as CEA have been widely used in the cyst fluid, with a value > 192 ng/mL having 63% sensitivity and 88% specificity (AUC of 0.79) for mucinous pancreatic cysts [43]. Other cyst fluid markers have been or are being developed including mutated KRAS DNA [44], mutated GNAS DNA [45,46], micro RNA [47,48], glucose [49], proteomic analysis [50], and multiple other molecules [51]. At this time, many of these markers are under investigation.
Case 2 Continued
An endoscopic ultrasound was performed and showed normal main pancreatic and common bile ducts. No intra-cystic mural nodules were observed. FNA was performed. Cytology showed “paucicellular fluid” and the cyst fluid CEA was 319 ng/mL. Having met the original consensus criteria for surgical resection [17] based on size, the presence of mural nodules, and due to suspicion for a mucinous cyst based on the CEA level, the patient underwent a Whipple procedure. The final pathology was a branch-duct IPMN with moderate dysplasia.
• What interventions exist for treating pancreatic cysts?
Surgery is the mainstay of treatment for pancreatic cysts. The most common surgical procedure for worrisome cysts in the head of the pancreas is a pancreatoduodenectomy (Whipple procedure). For cysts in the distal pancreas, a laparoscopic distal pancreatectomy can be performed [52,53]. Middle pancreatectomy, total pancreatectomy, and enucleation are less commonly performed and remain under investigation. The most common complications after surgery are surgical site and nonsurgical site infection, bleeding, pancreatic fistula, and delayed gastric emptying [52,53]. Overall complication rate for pancreatic cyst surgery is 27% to 39%, and perioperative mortality is 0.5% to 4% at high-volume centers [52,53].
An area of active investigation involves EUS-directed chemical cyst ablation. Prior studies using ethanol intra-cystic injection alone showed cyst resolution in 33% of patients [54]. A combination of ethanol and paclitaxel showed cyst resolution in 62% of patients [55]. Though these techniques offer a less invasive alternative to surgery, the complete eradication of dysplastic cystic epithelium remains uncertain and long-term efficacy is unclear. Thus, these techniques should only be considered in the context of a clinical trial or perhaps in patients who are not surgical candidates [56].
Case 3
• What is the epidemiology of IPMNs and how do they present?
IPMNs are mucin-producing lesions (mucinous cysts) of the exocrine pancreas involving either the main or branch ducts that have the potential to develop into pancreatic adenocarcinoma [57]. The mean age at presentation for both branch duct IPMNs (BD-IPMNs) and main duct IPMNs (MD-IPMNs) is around 65 years [58,59]. In the United States, the male to female prevalence ratio is equal, though there is some geographic variation among different countries [58]. Risk factors for IPMN formation include diabetes, chronic pancreatitis, and a family history of pancreatic adenocarcinoma [60]. Presentation is often asymptomatic but may present with pancreatitis, abdominal pain, weight loss, jaundice, and pancreatic exocrine insufficiency [61]. They tend to occur in the pancreatic head [29]. IPMNs involve either the main pancreatic duct or branch duct or both [62], but this is not always visible by imaging [21]. MRI with MRCP is considered superior to CT in characterizing these lesions, specifically in identifying a connection with the pancreatic ducts [21].
• How are IPMNs diagnosed and managed?
MD-IPMNs harbor a higher risk of malignancy than BD-IPMNs. In one series, 64% of MD-IPMN resected specimens contained cancer [63]. Because of the high cancer risk, all guidelines recommend surgical resection for appropriate patients [6,14,15,16,17]. BD-IPMNs have a lower risk of cancer at diagnosis, present in 19.5% of resected specimens in one study [63]. As a surgical series, this may overstate the true prevalence, which is supported by another study. A cohort of 103 suspected BD-IPMNs patients were observed and those with high-risk features were resected. The overall rate of cancer at 5 years was 2.6%, and only 1 of 103 patients developed non-resectable disease [64]. For these reasons, suspected BD-IPMNs can often be safely monitored if they do not harbor any high risk stigmata as defined by the international consensus criteria (Table 2)[6]. Otherwise, suspected BD-IPMNs are managed in a similar manner to other pancreatic cysts (Table 2) [6,14].
Prognosis after resection is more favorable for IPMNs than for pancreatic adenocarcinoma, possibly due to earlier stage of detection. The 5-year survival for BD-IPMN is 90% after resection, and 47% for MD-IPMN after resection [62]. Survival rates for IPMNs with invasive adenocarcinoma are lower with a combined overall survival 24% to 42% at 5 years. Survival rates are similar to the survival rate for non-cystic pancreatic adenocarcinoma when controlling for size, invasiveness, and lymph node metastasis [65,66].
Guidelines for surveillance after resection have even fewer applicable studies. The 5-year postoperative recurrence rate is 0 to 20% for IPMNs [6]. The revised international consensus guidelines recommends surveillance 6 months after resection with CT or MRI for all IPMNs, but with no recommendation given on how long to continue surveillance [6]. For patients with invasive disease, the same follow up is recommended as for standard invasive adenocarcinoma [6]. The AGA recommends yearly MRI only for only patients with high-grade dysplasia or invasive disease, with consideration for lifelong surveillance [14].
Case 4
• What is the epidemiology of MCNs and how do they present?
MCNs are mucin-producing lesions (mucinous cysts) of the exocrine pancreas histologically defined by the presence of ovarian stroma [67]. They have the potential to develop into pancreatic adenocarcinoma. Unlike IPMNs, MCNs occur almost exclusively in women, and patients are generally younger. In one series, 99.7% of MCNs occurred in females, with a mean age of 47 [67]. Presenting symptoms, as with other cysts, are often vague. These include abdominal pain, fatigue, weight loss, pancreatitis, and a palpable mass. Only 25% of patients are asymptomatic [68].
• How are MCNs diagnosed and managed?
Approximately 95% of MCNs are located in the body or tail of the pancreas [67]. These lesions do not communicate with the pancreatic ducts unlike IPMNs, though they may still cause ductal obstruction and dilation [29]. They are often one large unilocular cyst with a thick cyst wall, but in 20% of cases they can have multiple septations [29]. Peripheral eggshell calcification on CT is present in roughly 25% of cases, which is sometimes helpful in differentiating these lesions from serous cystic neoplasms, which often have central calcification [69].
When diagnosed, MCNs are surgically removed [6,14]. A recent surgical series found that the rate of high-grade dysplasia in resected specimens was 5.5%, and the risk of invasive disease was 4.4% [70]. This data suggests that a more conservative approach of observation rather than immediate resection may be reasonable for some patients [70]. The prognosis is very good after MCN resection, with a 5-year survival of 97% to 100% for all comers [68,70]. However, invasive MCNs have a lower 5-year survival rate ranging from 15% to 75% [70,71]. Per the AGA guidelines, patients with invasive disease or dysplasia should undergo yearly surveillance with MRI [14]. This recommendation is based on a potential field defect described with IPMNs. However, the international consensus guidelines only recommends surveillance if invasive disease is present [6,68,71,72].
Case 5
A 59-year-old male presents for evaluation of sudden onset abdominal pain and an 8-pound weight loss over the past few months. Seven years ago a pancreatic cyst was diagnosed and has since been observed by serial imaging. His lipase was 400 U/L (normal < 82) with normal liver function tests. A CT scan of the abdomen and pelvis showed peri-pancreatic stranding consistent with pancreatitis and a large complex cyst in the head of the pancreas.
• What is the epidemiology of SCNs and how do they present?
SCNs are benign non–mucin-producing cystic lesions that are characterized by a glycogen-rich epithelium on histology [73]. Of patients with SCNs, 74% are female, with a median age 58 [10]. When diagnosed, most patients are usually asymptomatic (61%), but 27% present with abdominal pain. Other symptoms include jaundice, pancreatitis, nausea, and presence of a palpable abdominal mass. SCNs are more common in patients with von Hippel-Lindau syndrome [74].
• How are SCNs diagnosed and managed?
These cysts have fairly even distribution when discovered in the pancreas [53]. About 74% of lesions have smaller micro-cystic components [75]. About 20% of lesions have a characteristic honeycomb appearance, which is highly suggestive of an SCN [76]. About 30% of patients have a characteristic central stellate scar on CT which is also highly suggestive of an SCN [76]. Unlike mucinous neoplasms, peripheral calcification is usually not seen [69].
Malignancy associated with these cysts is very rare, with the largest cohort study reporting a rate of 0.1% [10]. The diagnosis can commonly be made by its unique imaging appearance [10]. Diagnostic biomarkers that may identify such cysts with more certainty are under active investigation [77]. Resection is reasonable and often performed for SCNs when they cause debilitating symptoms including refractory abdominal pain or pancreatitis. When resected and confirmed by pathology, no surveillance is required [14,78].
Conclusion
Pancreatic cysts are common incidental findings in clinical practice today. Many cause anxiety due to their association with pancreas cancer, but most are indolent and safe to observe. Even those cysts with malignant potential grow slowly and immediate surgery is often unnecessary. Several guidelines have been developed, and while there are similarities between them, there are enough critical differences unfortunately to cause some confusion among practitioners today. Further robust research is needed to help address and reconcile these differences. In the meantime, a multidisciplinary approach is highly recommended at dedicated centers of excellence for pancreatic diseases.
Corresponding author: Walter G. Park, MD, MS, 300 Pasteur Drive, MC: 5187, Stanford, CA 94305, [email protected].
Funding/support: Dr. Park is funded by an American College of Gastroenterology Junior Faculty Development Award and is a subcontinent for the National Cancer Institute's Early Detection Research Network.
Financial disclosures: None.
Author contributions: conception and design, TZ, WGP; analysis and interpretation of data, WGP; drafting of article, TZ, WGP; critical revision of the article, TZ, WGP.
1. DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin 2014;64:252–71.
2. Hruban RH, Maitra A, Kern SE, Goggins M. Precursors to pancreatic cancer. Gastroenterol Clin North Am 2007;36:831–49.
3. Laffan TA, Horton KM, Klein AP, et al. Prevalence of unsuspected pancreatic cysts on MDCT. Am J Roentgenol 2008;191:802–7.
4. Lee KS, Sekhar A, Rofsky NM, Pedrosa I. Prevalence of incidental pancreatic cysts in the adult population on MR imaging. Am J Gastroenterol 2010;105:2079–84.
5. Volkan Adsay N. Cystic lesions of the pancreas. Mod Pathol 20(1 Suppl):S71–93.
6. Tanaka M, Fernández-del Castillo C, Adsay V, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012;12:183–97.
7. Galanis C, Zamani A, Cameron J, et al. Resected serous cystic neoplasms of the pancreas: a review of 158 patients with recommendations for treatment. J Gastrointest Surg 2007;11:820–6.
8. Vitas G, Sarr M. Selected management of pancreatic pseudocysts: operative versus expectant management. Surgery 1992;111:123–30.
9. Jani N, Bani Hani M, Schulick RD, et al. Diagnosis and management of cystic lesions of the pancreas. Diagn Ther Endosc 2011;2011:478913.
10. Jais B, Rebours V, Malleo G, et al. Serous cystic neoplasm of the pancreas: a multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas). Gut 2015 Jun 4.
11. Kim YS, Cho JH. Rare nonneoplastic cysts of pancreas. Clin Endosc 2015;48:31–8.
12. Visser BC, Yeh BM, Qayyum A, et al. Characterization of cystic pancreatic masses: relative accuracy of CT and MRI. Am J Roentgenol 2007;189:648–56.
13. Lee H-J, Kim M-J, Choi J-Y, et al. Relative accuracy of CT and MRI in the differentiation of benign from malignant pancreatic cystic lesions. Clin Radiol 2011;66:315–21.
14. Scheiman JM, Hwang JH, Moayyedi P. American Gastroenterological Association technical review on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology 2015;148:824–48.
15. Berland LL, Silverman SG, Gore RM, et al. Managing incidental findings on abdominal CT: white paper of the ACR Incidental Findings Committee. J Am Coll Radiol 2010;7:754–73.
16. Khalid A, Brugge W. ACG practice guidelines for the diagnosis and management of neoplastic pancreatic cysts. Am J Gastroenterol 2007;102:2339–49.
17. Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatol Off J Int Assoc Pancreatol IAP Al 2006;6(1-2).
18. Ahn D-W, Lee SH, Kim J, et al. Long-term outcome of cystic lesions in the pancreas: a retrospective cohort study. Gut Liver 2012;6:493–500.
19. Khannoussi W, Vullierme MP, Rebours V, et al. The long term risk of malignancy in patients with branch duct intraductal papillary mucinous neoplasms of the pancreas. Pancreatol Off J Int Assoc Pancreatol IAP Al 2012;12:198–202.
20. Grieser C, Heine G, Stelter L, et al. Morphological analysis and differentiation of benign cystic neoplasms of the pancreas using computed tomography and magnetic resonance imaging. Fortschr Röntgenstr 2013;185:219–27.
21. Waters J, Schmidt CM, Pinchot J, et al. CT vs MRCP: optimal classification of IPMN type and extent. J Gastrointest Surg 2008;12:101–9.
22. Duconseil P, Turrini O, Ewald J, et al. “Peripheric” pancreatic cysts: performance of CT scan, MRI and endoscopy according to final pathological examination. HPB 2015;17:485–9.
23. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102–11.
24. Sanfey H, Aguilar M, Jones R. Pseudocysts of the pancreas, a review of 97 cases. Am Surg 1994;60:661–8.
25. Cheruvu CVN, Clarke MG, Prentice M, Eyre-Brook IA. Conservative treatment as an option in the management of pancreatic pseudocyst. Ann R Coll Surg Engl 2003;85:313–6.
26. Usatoff V, Brancatisano R, Williamson RCN. Operative treatment of pseudocysts in patients with chronic pancreatitis. Br J Surg 2000;87:1494–9.
27. Marshall G, Howell DA, Hansen BL, et al. Multidisciplinary approach to pseudoaneurysms complicating pancreatic pseudocysts: Impact of pretreatment diagnosis. Arch Surg 1996;131:278–83.
28. Sahani DV, Kadavigere R, Saokar A, et al. Cystic pancreatic lesions: a simple imaging-based classification system for guiding management. RadioGraphics 2005;25:1471–84.
29. Tirkes T, Aisen A, Cramer H, et al. Cystic neoplasms of the pancreas; findings on magnetic resonance imaging with pathological, surgical, and clinical correlation. Abdom Imaging 2014;39:1088–101.
30. Macari M, Finn ME, Bennett GL, et al. Differentiating Pancreatic cystic neoplasms from pancreatic pseudocysts at MR Imaging: value of perceived internal debris. Radiology 2009;251:77–84.
31. Park WG, Mascarenhas R, Palaez-Luna M, et al. Diagnostic performance of cyst fluid carcinoembryonic antigen and amylase in histologically confirmed pancreatic cysts. Pancreas 2011;40:42–5.
32. Braden B, Dietrich CF. Endoscopic ultrasonography-guided endoscopic treatment of pancreatic pseudocysts and walled-off necrosis: New technical developments. World J Gastroenterol WJG 2014;20:16191–6.
33. van Brunschot S, Fockens P, Bakker O, et al. Endoscopic transluminal necrosectomy in necrotising pancreatitis: a systematic review. Surg Endosc 2014;28:1425–38.
34. Pan G, Wan MH, Xie K-L, et al. Classification and management of pancreatic pseudocysts. Medicine (Baltimore). 2015;94:e960.
35. Yeo CJ, Bastidas JA, Lynch-Nyhan A, et al. The natural history of pancreatic pseudocysts documented by computed tomography. Surg Gynecol Obstet 1990;170:411–7.
36. Chebib I, Yaeger K, Mino-Kenudson M, Pitman MB. The role of cytopathology and cyst fluid analysis in the preoperative diagnosis and management of pancreatic cysts >3 cm. Cancer Cytopathol 2014;122:804–9.
37. Kim JH, Eun HW, Park H-J, et al. Diagnostic performance of MRI and EUS in the differentiation of benign from malignant pancreatic cyst and cyst communication with the main duct. Eur J Radiol 2012;81:2927–35.
38. Khashab MA, Kim K, Lennon AM, et al. Should we do EUS/FNA on patients with pancreatic cysts? the incremental diagnostic yield of EUS over CT/MRI for prediction of cystic neoplasms. Pancreas 2013;42:717–21.
39. de Jong K, Verlaan T, Dijkgraaf MG, et al. Interobserver agreement for endosonography in the diagnosis of pancreatic cysts. Endoscopy 2011;43:579–84.
40. Harinck F, Konings ICAW, Kluijt I, Poley JW, van Hooft JE, van Dullemen HM, et al. A multicentre comparative prospective blinded analysis of EUS and MRI for screening of pancreatic cancer in high-risk individuals. Gut 2015 May 18.
41. Thosani N, Thosani S, Qiao W, et al. Role of EUS-FNA based cytology in diagnosis of mucinous pancreatic cystic lesions: a systematic review and meta-analysis. Dig Dis Sci 2010;55:2756–66.
42. Hong S-KS, Loren DE, Rogart JN, et al. Targeted cyst wall puncture and aspiration during EUS-FNA increases the diagnostic yield of premalignant and malignant pancreatic cysts. Gastrointest Endosc 2012;75:775–82.
43. Thornton G, McPhail M, Nayagam S, et al. Endoscopic ultrasound guided fine needle aspiration for the diagnosis of pancreatic cystic neoplasms: a meta-analysis. Pancreatology 2013;13:48–57.
44. Khalid A, Zahid M, Finkelstein SD, et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: a report of the PANDA study. Gastrointest Endosc 2009;May;69:1095–102.
45. Wu J, Matthaei H, Maitra A, et al. Recurrent GNAS mutations define an unexpected pathway for pancreatic cyst development. Sci Transl Med 2011;3:92ra66.
46. Springer S, Wang Y, Molin MD, et al. A Combination of molecular markers and clinical features improve the classification of pancreatic cysts. Gastroenterology 2015 Aug 4.
47. Ryu JK, Matthaei H, dal Molin M, et al. Elevated microRNA miR-21 Levels in Pancreatic cyst fluid are predictive of mucinous precursor lesions of ductal adenocarcinoma. Pancreatology 2011;11:343–50.
48. Matthaei H, Wylie D, Lloyd MB, et al. miRNA Biomarkers in cyst fluid augment the diagnosis and management of pancreatic cysts. Clin Cancer Res 2012;18 :4713–24.
49. Zikos T, Pham K, Bowen R, et al. Cyst fluid glucose is rapidly feasible and accurate in diagnosing mucinous pancreatic cysts. Am J Gastroenterol 2015;110:909–14.
50. Corcos O, Couvelard A, Dargère D, et al. Proteomic assessment of markers for malignancy in the mucus of intraductal papillary mucinous neoplasms of the pancreas. Pancreas 2012;41:169–74.
51. Thiruvengadam N, Park W. Systematic review of pancreatic cyst fluid biomarkers: the path forward. Clin Transl Gastroenterol 2015;11:e88.
52. Plichta JK, Brosius JA, Pappas SG, et al. The changing spectrum of surgically treated cystic neoplasms of the pancreas. HPB Surg 2015;2015:791704.
53. Valsangkar NP, Morales-Oyarvide V, Thayer SP, et al. 851 resected cystic tumors of the pancreas: A 33-year experience at the Massachusetts General Hospital. Surgery 2012;152:S4–12.
54. DeWitt J, McGreevy K, Schmidt CM, Brugge WR. EUS-guided ethanol versus saline solution lavage for pancreatic cysts: a randomized, double-blind study. Gastrointest Endosc 2009;70:710–23.
55. Oh H-C, Seo DW, Song TJ, et al. Endoscopic ultrasonography-guided ethanol lavage with paclitaxel injection treats patients with pancreatic cysts. Gastroenterology 2011;140:172–9.
56. Gavini H, Lee JH. Endoscopic ultrasound-guided endotherapy. J Clin Gastroenterol 2015;49:185–93.
57. Grutzmann R, Niedergethmann M, Pilarsky C, et al. Intraductal papillary mucinous tumors of the pancreas: biology, diagnosis, and treatment. Ooncologist 2010;15:1294–309.
58. Ingkakul T, Warshaw AL, Fernández-Del Castillo C. Epidemiology of intraductal papillary mucinous neoplasms of the pancreas: sex differences between 3 geographic regions. Pancreas 2011;40:779–80.
59. Brugge WR, Lauwers GY, Sahani D, et al. Cystic neoplasms of the pancreas. N Engl J Med 2004;351:1218–26.
60. Capurso G, Boccia S, Salvia R, et al. Risk factors for intraductal papillary mucinous neoplasm (IPMN) of the pancreas: a multicentre case-control study. Am J Gastroenterol 2013n;108:1003–9.
61. Lubezky N, Ben-Haim M, Nakache R, et al. Clinical presentation can predict disease course in patients with intraductal papillary mucinous neoplasm of the pancreas. World J Surg 2010;34:126–32.
62. Kobari M, Egawa S, Shibuya K, et al. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg Chic Ill 1960. 1999;134:1131–6.
63. Serikawa M, Sasaki T, Fujimoto Y, et al. Management of intraductal papillary-mucinous neoplasm of the pancreas: treatment strategy based on morphologic classification. J Clin Gastroenterol 2006;40:856–62.
64. Sawai Y, Yamao K, Bhatia V, et al. Development of pancreatic cancers during long-term follow-up of side-branch intraductal papillary mucinous neoplasms. Endoscopy 2010;42:1077–84.
65. Poultsides GA, Reddy S, Cameron JL, et al. Histopathologic basis for the favorable survival after resection of intraductal papillary mucinous neoplasm-associated invasive adenocarcinoma of the pancreas. Ann Surg 201 Mar;251:470–6.
66. Worni M, Akushevich I, Gloor B, et al. Adjuvant radiotherapy in the treatment of invasive intraductal papillary mucinous neoplasm of the pancreas: an analysis of the surveillance, epidemiology, and end results registry. Ann Surg Oncol 2012;19:1316–23.
67. Goh BKP, Tan Y-M, Chung Y-FA, et al. A review of mucinous cystic neoplasms of the pancreas defined by ovarian-type stroma: clinicopathological features of 344 patients. World J Surg 2006;30:2236–45.
68. Crippa S, Salvia R, Warshaw AL, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: lessons from 163 resected patients. Ann Surg 2008;247:571–9.
69. Curry CA, Eng J, Horton KM, et al. CT of primary cystic pancreatic neoplasms: can CT be used for patient triage and treatment? AJR Am J Roentgenol 2000;175:99–103.
70. Park JW, Jang J-Y, Kang MJ, et al. Mucinous cystic neoplasm of the pancreas: Is surgical resection recommended for all surgically fit patients? Pancreatology 2014;14:131–6.
71. Sakorafas GH, Smyrniotis V, Reid-Lombardo KM, Sarr MG. Primary pancreatic cystic neoplasms revisited: Part II. Mucinous cystic neoplasms. Surg Oncol 2011;20:e93–101.
72. Sarr MG, Carpenter HA, Prabhakar LP, et al. Clinical and pathologic correlation of 84 mucinous cystic neoplasms of the pancreas: can one reliably differentiate benign from malignant (or premalignant) neoplasms? Ann Surg 2000;231:205–12.
73. Reid MD, Choi H, Balci S, et al. Serous cystic neoplasms of the pancreas: Clinicopathologic and molecular characteristics. Pancreat Neoplasms 2014;31:475–83.
74. Charlesworth M, Verbeke CS, Falk GA, et al. Pancreatic lesions in von Hippel-Lindau disease? A systematic review and meta-synthesis of the literature. J Gastrointest Surg Off J Soc Surg Aliment Tract 2012;16:1422–8.
75. Kimura W, Moriya T, Hirai I, et al. Multicenter study of serous cystic neoplasm of the Japan pancreas society. Pancreas 2012;41):380–7.
76. Sarr MG, Murr M, Smyrk TC, et al. Primary cystic neoplasms of the pancreas. Neoplastic disorders of emerging importance-current state-of-the-art and unanswered questions. J Gastrointest Surg Off J Soc Surg Aliment Tract 2003;7:417–28.
77. Yip-Schneider MT, Wu H, Dumas RP, et al. Vascular endothelial growth factor, a novel and highly accurate pancreatic fluid biomarker for serous pancreatic cysts. J Am Coll Surg 2014;218:608–17.
78. Del Chiaro M, Verbeke C, Salvia R, et al. European experts consensus statement on cystic tumours of the pancreas. Dig Liver Dis 2013;45:703–11.
1. DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin 2014;64:252–71.
2. Hruban RH, Maitra A, Kern SE, Goggins M. Precursors to pancreatic cancer. Gastroenterol Clin North Am 2007;36:831–49.
3. Laffan TA, Horton KM, Klein AP, et al. Prevalence of unsuspected pancreatic cysts on MDCT. Am J Roentgenol 2008;191:802–7.
4. Lee KS, Sekhar A, Rofsky NM, Pedrosa I. Prevalence of incidental pancreatic cysts in the adult population on MR imaging. Am J Gastroenterol 2010;105:2079–84.
5. Volkan Adsay N. Cystic lesions of the pancreas. Mod Pathol 20(1 Suppl):S71–93.
6. Tanaka M, Fernández-del Castillo C, Adsay V, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012;12:183–97.
7. Galanis C, Zamani A, Cameron J, et al. Resected serous cystic neoplasms of the pancreas: a review of 158 patients with recommendations for treatment. J Gastrointest Surg 2007;11:820–6.
8. Vitas G, Sarr M. Selected management of pancreatic pseudocysts: operative versus expectant management. Surgery 1992;111:123–30.
9. Jani N, Bani Hani M, Schulick RD, et al. Diagnosis and management of cystic lesions of the pancreas. Diagn Ther Endosc 2011;2011:478913.
10. Jais B, Rebours V, Malleo G, et al. Serous cystic neoplasm of the pancreas: a multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas). Gut 2015 Jun 4.
11. Kim YS, Cho JH. Rare nonneoplastic cysts of pancreas. Clin Endosc 2015;48:31–8.
12. Visser BC, Yeh BM, Qayyum A, et al. Characterization of cystic pancreatic masses: relative accuracy of CT and MRI. Am J Roentgenol 2007;189:648–56.
13. Lee H-J, Kim M-J, Choi J-Y, et al. Relative accuracy of CT and MRI in the differentiation of benign from malignant pancreatic cystic lesions. Clin Radiol 2011;66:315–21.
14. Scheiman JM, Hwang JH, Moayyedi P. American Gastroenterological Association technical review on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology 2015;148:824–48.
15. Berland LL, Silverman SG, Gore RM, et al. Managing incidental findings on abdominal CT: white paper of the ACR Incidental Findings Committee. J Am Coll Radiol 2010;7:754–73.
16. Khalid A, Brugge W. ACG practice guidelines for the diagnosis and management of neoplastic pancreatic cysts. Am J Gastroenterol 2007;102:2339–49.
17. Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatol Off J Int Assoc Pancreatol IAP Al 2006;6(1-2).
18. Ahn D-W, Lee SH, Kim J, et al. Long-term outcome of cystic lesions in the pancreas: a retrospective cohort study. Gut Liver 2012;6:493–500.
19. Khannoussi W, Vullierme MP, Rebours V, et al. The long term risk of malignancy in patients with branch duct intraductal papillary mucinous neoplasms of the pancreas. Pancreatol Off J Int Assoc Pancreatol IAP Al 2012;12:198–202.
20. Grieser C, Heine G, Stelter L, et al. Morphological analysis and differentiation of benign cystic neoplasms of the pancreas using computed tomography and magnetic resonance imaging. Fortschr Röntgenstr 2013;185:219–27.
21. Waters J, Schmidt CM, Pinchot J, et al. CT vs MRCP: optimal classification of IPMN type and extent. J Gastrointest Surg 2008;12:101–9.
22. Duconseil P, Turrini O, Ewald J, et al. “Peripheric” pancreatic cysts: performance of CT scan, MRI and endoscopy according to final pathological examination. HPB 2015;17:485–9.
23. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102–11.
24. Sanfey H, Aguilar M, Jones R. Pseudocysts of the pancreas, a review of 97 cases. Am Surg 1994;60:661–8.
25. Cheruvu CVN, Clarke MG, Prentice M, Eyre-Brook IA. Conservative treatment as an option in the management of pancreatic pseudocyst. Ann R Coll Surg Engl 2003;85:313–6.
26. Usatoff V, Brancatisano R, Williamson RCN. Operative treatment of pseudocysts in patients with chronic pancreatitis. Br J Surg 2000;87:1494–9.
27. Marshall G, Howell DA, Hansen BL, et al. Multidisciplinary approach to pseudoaneurysms complicating pancreatic pseudocysts: Impact of pretreatment diagnosis. Arch Surg 1996;131:278–83.
28. Sahani DV, Kadavigere R, Saokar A, et al. Cystic pancreatic lesions: a simple imaging-based classification system for guiding management. RadioGraphics 2005;25:1471–84.
29. Tirkes T, Aisen A, Cramer H, et al. Cystic neoplasms of the pancreas; findings on magnetic resonance imaging with pathological, surgical, and clinical correlation. Abdom Imaging 2014;39:1088–101.
30. Macari M, Finn ME, Bennett GL, et al. Differentiating Pancreatic cystic neoplasms from pancreatic pseudocysts at MR Imaging: value of perceived internal debris. Radiology 2009;251:77–84.
31. Park WG, Mascarenhas R, Palaez-Luna M, et al. Diagnostic performance of cyst fluid carcinoembryonic antigen and amylase in histologically confirmed pancreatic cysts. Pancreas 2011;40:42–5.
32. Braden B, Dietrich CF. Endoscopic ultrasonography-guided endoscopic treatment of pancreatic pseudocysts and walled-off necrosis: New technical developments. World J Gastroenterol WJG 2014;20:16191–6.
33. van Brunschot S, Fockens P, Bakker O, et al. Endoscopic transluminal necrosectomy in necrotising pancreatitis: a systematic review. Surg Endosc 2014;28:1425–38.
34. Pan G, Wan MH, Xie K-L, et al. Classification and management of pancreatic pseudocysts. Medicine (Baltimore). 2015;94:e960.
35. Yeo CJ, Bastidas JA, Lynch-Nyhan A, et al. The natural history of pancreatic pseudocysts documented by computed tomography. Surg Gynecol Obstet 1990;170:411–7.
36. Chebib I, Yaeger K, Mino-Kenudson M, Pitman MB. The role of cytopathology and cyst fluid analysis in the preoperative diagnosis and management of pancreatic cysts >3 cm. Cancer Cytopathol 2014;122:804–9.
37. Kim JH, Eun HW, Park H-J, et al. Diagnostic performance of MRI and EUS in the differentiation of benign from malignant pancreatic cyst and cyst communication with the main duct. Eur J Radiol 2012;81:2927–35.
38. Khashab MA, Kim K, Lennon AM, et al. Should we do EUS/FNA on patients with pancreatic cysts? the incremental diagnostic yield of EUS over CT/MRI for prediction of cystic neoplasms. Pancreas 2013;42:717–21.
39. de Jong K, Verlaan T, Dijkgraaf MG, et al. Interobserver agreement for endosonography in the diagnosis of pancreatic cysts. Endoscopy 2011;43:579–84.
40. Harinck F, Konings ICAW, Kluijt I, Poley JW, van Hooft JE, van Dullemen HM, et al. A multicentre comparative prospective blinded analysis of EUS and MRI for screening of pancreatic cancer in high-risk individuals. Gut 2015 May 18.
41. Thosani N, Thosani S, Qiao W, et al. Role of EUS-FNA based cytology in diagnosis of mucinous pancreatic cystic lesions: a systematic review and meta-analysis. Dig Dis Sci 2010;55:2756–66.
42. Hong S-KS, Loren DE, Rogart JN, et al. Targeted cyst wall puncture and aspiration during EUS-FNA increases the diagnostic yield of premalignant and malignant pancreatic cysts. Gastrointest Endosc 2012;75:775–82.
43. Thornton G, McPhail M, Nayagam S, et al. Endoscopic ultrasound guided fine needle aspiration for the diagnosis of pancreatic cystic neoplasms: a meta-analysis. Pancreatology 2013;13:48–57.
44. Khalid A, Zahid M, Finkelstein SD, et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: a report of the PANDA study. Gastrointest Endosc 2009;May;69:1095–102.
45. Wu J, Matthaei H, Maitra A, et al. Recurrent GNAS mutations define an unexpected pathway for pancreatic cyst development. Sci Transl Med 2011;3:92ra66.
46. Springer S, Wang Y, Molin MD, et al. A Combination of molecular markers and clinical features improve the classification of pancreatic cysts. Gastroenterology 2015 Aug 4.
47. Ryu JK, Matthaei H, dal Molin M, et al. Elevated microRNA miR-21 Levels in Pancreatic cyst fluid are predictive of mucinous precursor lesions of ductal adenocarcinoma. Pancreatology 2011;11:343–50.
48. Matthaei H, Wylie D, Lloyd MB, et al. miRNA Biomarkers in cyst fluid augment the diagnosis and management of pancreatic cysts. Clin Cancer Res 2012;18 :4713–24.
49. Zikos T, Pham K, Bowen R, et al. Cyst fluid glucose is rapidly feasible and accurate in diagnosing mucinous pancreatic cysts. Am J Gastroenterol 2015;110:909–14.
50. Corcos O, Couvelard A, Dargère D, et al. Proteomic assessment of markers for malignancy in the mucus of intraductal papillary mucinous neoplasms of the pancreas. Pancreas 2012;41:169–74.
51. Thiruvengadam N, Park W. Systematic review of pancreatic cyst fluid biomarkers: the path forward. Clin Transl Gastroenterol 2015;11:e88.
52. Plichta JK, Brosius JA, Pappas SG, et al. The changing spectrum of surgically treated cystic neoplasms of the pancreas. HPB Surg 2015;2015:791704.
53. Valsangkar NP, Morales-Oyarvide V, Thayer SP, et al. 851 resected cystic tumors of the pancreas: A 33-year experience at the Massachusetts General Hospital. Surgery 2012;152:S4–12.
54. DeWitt J, McGreevy K, Schmidt CM, Brugge WR. EUS-guided ethanol versus saline solution lavage for pancreatic cysts: a randomized, double-blind study. Gastrointest Endosc 2009;70:710–23.
55. Oh H-C, Seo DW, Song TJ, et al. Endoscopic ultrasonography-guided ethanol lavage with paclitaxel injection treats patients with pancreatic cysts. Gastroenterology 2011;140:172–9.
56. Gavini H, Lee JH. Endoscopic ultrasound-guided endotherapy. J Clin Gastroenterol 2015;49:185–93.
57. Grutzmann R, Niedergethmann M, Pilarsky C, et al. Intraductal papillary mucinous tumors of the pancreas: biology, diagnosis, and treatment. Ooncologist 2010;15:1294–309.
58. Ingkakul T, Warshaw AL, Fernández-Del Castillo C. Epidemiology of intraductal papillary mucinous neoplasms of the pancreas: sex differences between 3 geographic regions. Pancreas 2011;40:779–80.
59. Brugge WR, Lauwers GY, Sahani D, et al. Cystic neoplasms of the pancreas. N Engl J Med 2004;351:1218–26.
60. Capurso G, Boccia S, Salvia R, et al. Risk factors for intraductal papillary mucinous neoplasm (IPMN) of the pancreas: a multicentre case-control study. Am J Gastroenterol 2013n;108:1003–9.
61. Lubezky N, Ben-Haim M, Nakache R, et al. Clinical presentation can predict disease course in patients with intraductal papillary mucinous neoplasm of the pancreas. World J Surg 2010;34:126–32.
62. Kobari M, Egawa S, Shibuya K, et al. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg Chic Ill 1960. 1999;134:1131–6.
63. Serikawa M, Sasaki T, Fujimoto Y, et al. Management of intraductal papillary-mucinous neoplasm of the pancreas: treatment strategy based on morphologic classification. J Clin Gastroenterol 2006;40:856–62.
64. Sawai Y, Yamao K, Bhatia V, et al. Development of pancreatic cancers during long-term follow-up of side-branch intraductal papillary mucinous neoplasms. Endoscopy 2010;42:1077–84.
65. Poultsides GA, Reddy S, Cameron JL, et al. Histopathologic basis for the favorable survival after resection of intraductal papillary mucinous neoplasm-associated invasive adenocarcinoma of the pancreas. Ann Surg 201 Mar;251:470–6.
66. Worni M, Akushevich I, Gloor B, et al. Adjuvant radiotherapy in the treatment of invasive intraductal papillary mucinous neoplasm of the pancreas: an analysis of the surveillance, epidemiology, and end results registry. Ann Surg Oncol 2012;19:1316–23.
67. Goh BKP, Tan Y-M, Chung Y-FA, et al. A review of mucinous cystic neoplasms of the pancreas defined by ovarian-type stroma: clinicopathological features of 344 patients. World J Surg 2006;30:2236–45.
68. Crippa S, Salvia R, Warshaw AL, et al. Mucinous cystic neoplasm of the pancreas is not an aggressive entity: lessons from 163 resected patients. Ann Surg 2008;247:571–9.
69. Curry CA, Eng J, Horton KM, et al. CT of primary cystic pancreatic neoplasms: can CT be used for patient triage and treatment? AJR Am J Roentgenol 2000;175:99–103.
70. Park JW, Jang J-Y, Kang MJ, et al. Mucinous cystic neoplasm of the pancreas: Is surgical resection recommended for all surgically fit patients? Pancreatology 2014;14:131–6.
71. Sakorafas GH, Smyrniotis V, Reid-Lombardo KM, Sarr MG. Primary pancreatic cystic neoplasms revisited: Part II. Mucinous cystic neoplasms. Surg Oncol 2011;20:e93–101.
72. Sarr MG, Carpenter HA, Prabhakar LP, et al. Clinical and pathologic correlation of 84 mucinous cystic neoplasms of the pancreas: can one reliably differentiate benign from malignant (or premalignant) neoplasms? Ann Surg 2000;231:205–12.
73. Reid MD, Choi H, Balci S, et al. Serous cystic neoplasms of the pancreas: Clinicopathologic and molecular characteristics. Pancreat Neoplasms 2014;31:475–83.
74. Charlesworth M, Verbeke CS, Falk GA, et al. Pancreatic lesions in von Hippel-Lindau disease? A systematic review and meta-synthesis of the literature. J Gastrointest Surg Off J Soc Surg Aliment Tract 2012;16:1422–8.
75. Kimura W, Moriya T, Hirai I, et al. Multicenter study of serous cystic neoplasm of the Japan pancreas society. Pancreas 2012;41):380–7.
76. Sarr MG, Murr M, Smyrk TC, et al. Primary cystic neoplasms of the pancreas. Neoplastic disorders of emerging importance-current state-of-the-art and unanswered questions. J Gastrointest Surg Off J Soc Surg Aliment Tract 2003;7:417–28.
77. Yip-Schneider MT, Wu H, Dumas RP, et al. Vascular endothelial growth factor, a novel and highly accurate pancreatic fluid biomarker for serous pancreatic cysts. J Am Coll Surg 2014;218:608–17.
78. Del Chiaro M, Verbeke C, Salvia R, et al. European experts consensus statement on cystic tumours of the pancreas. Dig Liver Dis 2013;45:703–11.
46 experts pen open letter to the FDA on uterine power morcellation
As gynecologists are well aware, in November 2014, the FDA issued a safety communication, warning “against the use of laparoscopic power morcellators in the majority of women undergoing myomectomy or hysterectomy for treatment of fibroids.” Now, a group of 46 experts in gynecologic surgery, including Dr. Eva Chalas, question the FDA’s decision and provide their own clinical recommendations for FDA consideration.
In this interview with Dr. Chalas, she discusses:
|
Reference
- US Food and Drug Administration. Updated: Laparoscopic Uterine Power Morcellation in Hysterectomy and Myomectomy: FDA Safety Communication. November 24, 2014. http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm424443.htm. Accessed November 19, 2015.
As gynecologists are well aware, in November 2014, the FDA issued a safety communication, warning “against the use of laparoscopic power morcellators in the majority of women undergoing myomectomy or hysterectomy for treatment of fibroids.” Now, a group of 46 experts in gynecologic surgery, including Dr. Eva Chalas, question the FDA’s decision and provide their own clinical recommendations for FDA consideration.
In this interview with Dr. Chalas, she discusses:
|
As gynecologists are well aware, in November 2014, the FDA issued a safety communication, warning “against the use of laparoscopic power morcellators in the majority of women undergoing myomectomy or hysterectomy for treatment of fibroids.” Now, a group of 46 experts in gynecologic surgery, including Dr. Eva Chalas, question the FDA’s decision and provide their own clinical recommendations for FDA consideration.
In this interview with Dr. Chalas, she discusses:
|
Reference
- US Food and Drug Administration. Updated: Laparoscopic Uterine Power Morcellation in Hysterectomy and Myomectomy: FDA Safety Communication. November 24, 2014. http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm424443.htm. Accessed November 19, 2015.
Reference
- US Food and Drug Administration. Updated: Laparoscopic Uterine Power Morcellation in Hysterectomy and Myomectomy: FDA Safety Communication. November 24, 2014. http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm424443.htm. Accessed November 19, 2015.
Selecting a Direct Oral Anticoagulant for the Geriatric Patient with Nonvalvular Atrial Fibrillation
From the Ernest Mario School of Pharmacy, Rutgers University, Piscataway, NJ.
Abstract
- Objective: To provide a clinical summary of the available data evaluating the use of direct oral anticoagulants (DOACs) in geriatric patients with nonvalvular atrial fibrillation.
- Methods: MEDLINE, Web of Science, and Google Scholar were used to identify pertinent systematic reviews, randomized controlled trials, observational studies, and pharmacokinetic studies evaluating use of DOACs in the geriatric population.
- Results: A total of 8 systemic reviews, 5 randomized controlled trials, 2 observational trials, and 5 pharmacokinetic studies of relevance were identified for inclusion in this review. The landscape of anticoagulation has dramatically changed over the past 5 years beginning with the development and marketing of an oral direct thrombin inhibitor and followed by 3 oral direct factor Xa inhibitors. Despite significant advances in this oral anticoagulation arena, many questions remain as to the best therapeutic approach in the geriatric population as the literature is lacking. This population has a higher risk of stroke; however, due to the increased risk of bleeding clinicians may often defer anticoagulant therapy due to the fear of hemorrhagic complications. Clinicians must consider the risk-benefit ratio and the associated outcomes in geriatric patients compared to other patient populations.
- Conclusions: Interpreting the available literature and understanding the benefits and limitations of the DOACs is critical when selecting the most appropriate pharmacologic strategy in geriatric patients.
Anticoagulants are among the top 5 drug classes associated with patient harm in the US [1] and are commonly reported as contributing to hospitalizations [2]. In just one quarter in 2012 alone, warfarin, dabigatran, and rivaroxaban accounted for 1734 of 50,289 adverse events reported to the Food and Drug Administration (FDA), including 233 deaths [3]. Appropriate use of anticoagulant agents and consideration of individual patient risk factors are essential to mitigate the occurrence of adverse consequences, especially in the geriatric population. This population is more likely to have risk factors for adverse drug events, for example, polypharmacy, age-related changes in pharmacokinetics and pharmacodynamics, and diminished organ function (ie, renal and hepatic) [4,5]. Another important consideration is the lack of consensus on the definition of a “geriatric” or “elderly” patient. Although many consider a chronological age of > 65 years as the defining variable for a geriatric individual, this definition does not account for overall health status [6,7]. Clinicians should consider this shortcoming when evaluating the quality of geriatric studies. For example, a study claiming to evaluate the pharmacokinetics of a drug in a geriatric population enrolling healthy subjects aged > 65 years may result in data that do not translate to clinical practice.
Compounding the concern for iatrogenic events is the frequency of anticoagulant use in the geriatric population, as several indications are found more commonly in this age-group. Stroke prevention in nonvalvular atrial fibrillation (AF), the most common arrhythmia in the elderly, is a common indication for long-term anticoagulation [8]. The prevalence of AF increases with age and is usually higher in men than in women [9,10]. AF is generally uncommon before 60 years of age, but the prevalence increases noticeably thereafter, affecting approximately 10% of the overall population by 80 years of age [11]. The median age of patients who have AF is 75 years with approximately 70% of patients between 65 and 85 years of age [8,12]. Currently in the United States, an estimated 2.3 million people are diagnosed with AF [8]. In 2020, the AF population is predicted to increase to 7.5 million individuals with an expected prevalence of 13.5% among individuals ≥ 75 years of age, and 18.2% for those ≥ 85 years of age [13]. These data underscore the importance of considering the influence of age on the balance between efficacy and safety of anticoagulant therapy.
Direct oral anticoagulants (DOACs) represent the first alternatives to warfarin in over 6 decades. Currently available products in US include apixaban, dabigatran, edoxaban, and rivaroxaban. DOACs possess many of the characteristics of an ideal anticoagulant, including predictable pharmacokinetics, a wider therapeutic window compared to warfarin, minimal drug interactions, a fixed dose, and no need for routine evaluation of coagulation parameters. The safety and efficacy of the DOACs for stroke prevention in nonvalvular AF have been substantiated in several landmark clinical trials [14–16]. Yet there are several important questions that need to be addressed, such as management of excessive anticoagulation, clinical outcome data with renally adjusted doses (an exclusion criterion in many landmark studies was a creatinine clearance of < 25–30 mL/min), whether monitoring of coagulation parameters could enhance efficacy and safety, and optimal dosing strategies in geriatric patients. This review provides clinicians a summary of data from landmark studies, post-marketing surveillance, and pharmacokinetic evaluations to support DOAC selection in the geriatric population.
Evaluating Bleeding Risk

These tools have been extensively evaluated with warfarin therapy, but their performance in predicting DOAC-related bleeding has not been definitively established. Nonetheless, until tools evaluated specifically for DOACs are developed, it is reasonable to use these for risk-prediction in combination with clinical judgment. As an example, the European Society of Cardiology guideline on the use of non–vitamin K antagonist (VKA) anticoagulants in patients with nonvalvular AF suggests that the HAS-BLED score may be used to identify risk factors for bleeding and correct those that are modifiable [20]. The HAS-BLED score is validated for VKA and non-VKA anticoagulants (early-generation oral direct thrombin inhibitor ximelgatran) [21] and is the only bleeding risk score predictive for intracranial hemorrhage [19]. In a 2013 “real world” comparison, HAS-BLED was easier to use and had better predictive accuracy that ATRIA [22].
One of the major challenges in geriatric patients is that those at highest risk for bleeding are those who would have the greatest benefit from anticoagulation [23]. The prediction scores can help clinicians balance the risk-benefit ratio for anticoagulation on a case by case basis. Although the scoring systems take into consideration several factors, including medical conditions that have been shown to significantly increase bleeding risk, including hypertension, cerebrovascular disease, ischemic stroke, serious heart disease, diabetes, renal insufficiency, alcoholism and liver disease, not all are included in every scoring scheme [23]. These conditions are more common among elderly patients, and this should be taken into account when estimating the risk-benefit ratio of oral anticoagulation [15]. Patients’ preferences should also be taken into account. It is essential for clinicians to clearly discuss treatment options with patients as data suggest that clinician and patient perceptions of anticoagulation are often mismatched [24–26].
Performance of TSOACS in Landmark Studies

Some specific differences in outcomes seen in landmark studies that may facilitate selection among the DOACs include the risk of major bleeding, risk of gastrointestinal bleeding, risk of acute coronary syndrome, exclusion of valvular heart disease, and noninferiority versus superiority as the primary endpoint when compared to warfarin.
Major Bleeding


Gastrointestinal Bleeding
Among all of the DOACs, gastrointestinal (GI) bleeding was significantly greater with dabigatran, edoxaban, and rivaroxaban when compared to warfarin (HR, 1.49; 95% CI, 1.21–1.84; HR, 1.23; 95% CI, 1.02–1.50; and HR, 1.61; 95% CI, 1.30–1.99, respectively; P < 0.05 for all) [14–16] in landmark studies. Based on these data, clinicians may consider the selection of apixaban in patients with a previous history of GI pathology. GI bleeding may be more common in elderly patients due to the potential for preexisting GI pathology and high local concentrations of drug [29]. Clemens and colleagues suggested an “anticoagulation GI stress test” may predict GI malignancy [33]. They found that patients on DOACs that presented with a GI bleed were more likely to present with a GI malignancy. As such, it is reasonable to screen patients with a fecal occult blood test within the first month after initiating TSOAC treatment and then annually.
Acute Coronary Syndrome
A higher rate of myocardial infarction was observed with dabigatran 150 mg versus warfarin (0.74% vs 0.53% per year; P = 0.048) in the RE-LY study [16]. Whether the increase in myocardial infarction was due to dabigatran as a causative agent or warfarin’s ability to reduce the risk of myocardial infarction to a larger extent compared with dabigatran is unknown. Nonetheless, it may be prudent to use an alternative therapy in patients with a history of acute coronary syndrome.
Valvular Heart Disease
The risk of stroke and systemic embolism is higher in patients with valvular heart disease [34]. Patients with moderate to severe mitral stenosis or mechanical prosthetic heart valves were excluded from the DOAC landmark studies. Dabigatran was evaluated for prevention of stroke and systemic embolism in patients with valvular heart disease in the RE-ALIGN study [35,36]. Patients were randomized to warfarin titrated to a target INR of 2 to 3 or 2.5 to 3.5 on the basis of thromboembolic risk or dabigatran 150 mg, 220 mg, or 300 mg twice daily adjusted to a targeted trough of ≥ 50 ng/mL. The trial was terminated early due to a worse primary outcome (composite of stroke, systemic embolism, myocardial infarction, and death) with dabigatran versus warfarin (HR, 3.37, 95% CI, 0.76–14.95; P = 0.11). In addition, bleeding rates (any bleeding) was significantly greater with dabigatran (27%) versus warfarin (12%) (P = 0.01). Based on these data and the lack of data with the other TSOACs, warfarin remains the standard of care for valvular heart disease [37]. In patients with a previous bioprosthetic valve with AF, patients with mitral insufficiency, or aortic stensosis, TSOACs may be considered [37].
Landmark Study Efficacy Endpoints
The primary endpoint in each of the landmark studies was a composite of stroke (ischemic or hemorrhagic) and systemic embolism. For the primary endpoint only dabigatran 150 mg twice daily and apixaban 5 mg twice daily were found to be superior to warfarin for the prevention of stroke or systemic embolism in nonvalvular AF (HR, 0.66; 95% CI, 0.53–0.82; P < 0.001 and HR, 0.66; 95% CI, 0.66–0.95; P = 0.01, respectively). Both edoxaban (60 mg and 30 mg daily) and rivaroxaban were noninferior to warfarin for the primary endpoint. In terms of ischemic stroke, only dabigatran 150 mg twice daily was superior to warfarin for the reduction in ischemic stroke in patients with nonvalvular AF (HR, 0.76; 95% CI, 0.60–0.98; P = 0.03) [19]. All of the DOACs demonstrated a reduction in hemorrhagic stroke.
TSOAC Use in Elderly Patitents
Pharmacokinetic Evaluations
Several pharmacokinetic studies have evaluated the influence of age on DOAC disposition. In a study evaluating the influence of age on apixaban disposition, the area under the concentration-time curve to infinity was 32% higher in the elderly (aged 65 years or older) compared to the younger subjects (< age 40 years) [38]. These data provide the rationale for dosage adjustment in individuals aged 80 years or older with either low body mass (weight less than or equal to 60 kg) or renal impairment (serum creatinine 1.5 mg/dL or higher). In a pharmacokinetic study evaluating dabigatran in patients > 65 years of age, the time to steady state ranged from 2 to 3 days, correlating to a half-life of 12 to 14 hours, and peak concentrations (256 ng/mL females, 255 ng/mL males) were reached after a median of 3 hours (range, 2.0–4.0 hours) [39]. These data suggest a 1.7- to twofold increase in bioavailability. The area under the curve of rivaroxaban was significantly higher in subjects > 75 years versus subjects 18-45 years, while total and renal clearance were decreased [40].However, the time to maximum factor Xa inhibition and Cmax were not influenced by age.
Clinical Evaluations
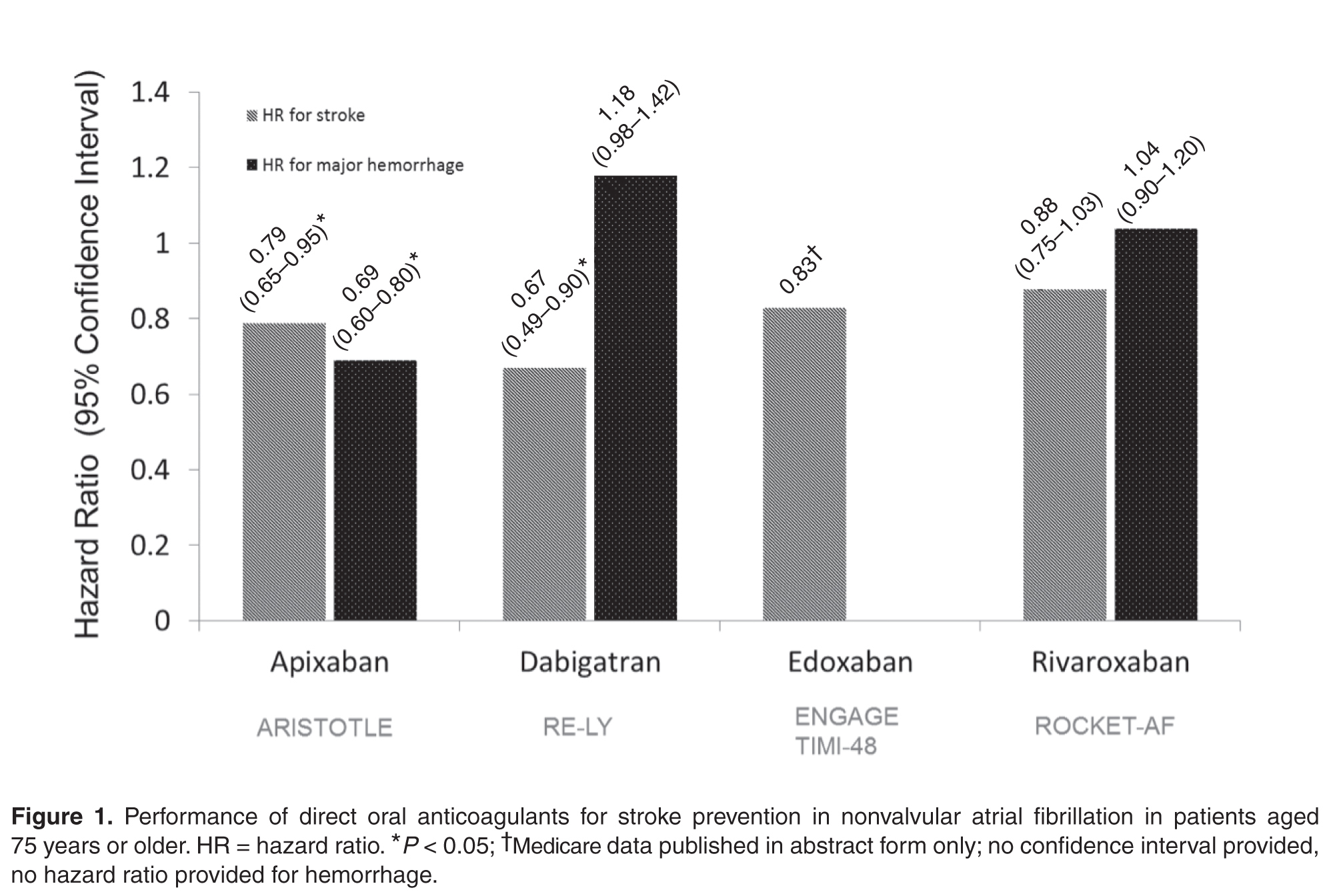
Dabigatran
In a post-hoc analysis of the RE-LY trial, Eikelboom and colleagues found that patients 75 years of age and older treated with dabigatran 150 mg twice daily had a greater incidence of GI bleeding irrespective of renal function compared with those on warfarin (1.85%/year vs. 1.25%/year; P < 0.001) [29]. A higher risk in major bleeding also was seen in dabigatran patients (5.10% versus 4.37%; P = 0.07). As a result, the 2012 Beer’s Criteria lists dabigatran as a potentially inappropriate medication. An analysis was conducted of 134,414 elderly Medicare patients (defined as age > 65 years) with 37,587 person-years of follow-up who were treated with dabigatran or warfarin [44]. Approximately 60% of patients included in the analysis were over age 75 years. Dabigatran was associated with a significant reduction in ischemic stroke: HR 0.80 (CI 0.67–0.96); intracranial hemorrhage: HR 0.34 (CI 0.26–0.46); and death: HR 0.86 (CI 0.77–0.96) when compared with warfarin. As in the Eikelboom study, major gastrointestinal bleeding was significantly increased with dabigatran (HR, 1.28 [95% CI, 1.14–1.44]).
Rivaroxaban
For rivaroxaban, a subgroup analysis of patients ≥ 75 years in the ROCKET-AF trial reported similar rates of major bleeding (HR, 1.11; 95% CI, 0.92–1.34) with rivaroxaban compared with warfarin [31]. Clinically relevant non-major bleeding was significantly higher for patients aged ≥ 75 years compared with patients aged < 75 years (P = 0.01).
Apixaban
Halvorsen and colleagues found that age did not influence the benefits of apixaban in terms of efficacy and safety [47]. In the cohort of patients aged 75 years or older, major bleeding was significantly reduced compared to warfarin (HR, 0.64; 95% CI, 0.52–0.79). The safety benefits persisted even in the setting of age greater than 75 years and renal impairment. A significant reduction in major bleeding (HR, 0.35; 95% CI, 0.14–0.86) was seen in elderly patients with a CrCl; ≤ 30 mL/min (n = 221) treated with apixaban versus warfarin. Similarly, in elderly patients with a CrCl 30 to 50 mL/min (n = 1898) a significant reduction in major bleeding was reported (HR, 0.53; 95% CI, 0.37–0.76). These data are consistent with a meta-regression analysis that found a linear relationship between the relative risk of major bleeding and the magnitude of renal excretion for the DOACs (r2=0.66, P = 0.03) [48]. In this analysis, apixaban had the most favorable outcomes in terms of major bleeding compared to the other DOACs and also has the least dependence on renal function for clearance. In a pooled analysis of data from landmark trials, Ng and colleagues found that in elderly patients (defined as age > 75 years) with nonvalvular AF, only apixaban was associated with a significant reduction in both stroke and major hemorrhage (Figure 1) [49,50].
Edoxaban
Kato and colleagues performed a subgroup analysis of patients aged 75 years or older enrolled in the ENGAGE TIMI 48 study [50]. Currently the results are only published in abstract form. Regardless of treatment, the risk of major bleeding and stroke significantly increased with age (P < 0.001). An absolute risk reduction in major bleeding was reported with both 60 mg and 30 mg of edoxaban versus warfarin (4.0%/year and 2.2%/year versus 4.8%/year, respectively; no P value provided).
Therapeuti Drug Monitoring
Collectively, the data on assessment of the anticoagulant activity of DOACs using coagulation assays is evolving. These tests include but are not limited to prothrombin time (PT), activated partial thromboplastin time (aPTT), thrombin clotting time (TT), dilute TT, activated clotting time (ACT), anti factor Xa, and ecarin clotting time (ECT) assays. Although routine monitoring is not desirable, the ability to assess degree of anticoagulation in select patient populations may prove beneficial. Future studies are essential to confirm whether assessing DOAC activity using coagulation assays in vulnerable populations such as the elderly improves clinical outcomes. Several reviews on this subject matter have been published [51–55]. The reader is encouraged to review these data as there are significant limitations to currently available assays and incorrect interpretation may lead to suboptimal treatment decisions.
Renal and Hepatic Dysfunction
Depending on the specific agents, DOACs renal clearance varies from 27% to 80% [56–59]. Clinical trials often use the Cockcroft-Gault formula (CG) based on actual body weight to estimate renal function. Landmark trials evaluating the DOACs differed in their strategy for estimation of renal function using CG. For example, RE-LY and ROCKET-AF used actual body weight for the estimation of renal function, while ARISTOTLE did not specify which body weight to use. Estimation of renal function or glomerular filtration rate (GFR) by CG is frequently in discordance with actual renal function in the elderly [60]. MDRD (modification of diet in renal disease) and Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) are also common estimations that provide an estimate of GFR. In a cross-sectional study, comparing the CG, MDRD, and EPI formulas in a clinical setting, data from potential kidney donors and adult patients who underwent a GFR measurement revealed that MDRD has the smallest mean bias. The influence of age was the absolute bias for estimation of renal function for all formulas. CG is additionally influenced by body weight and body mass index. When compared to CG, MDRD actually reported more accurate predictor of GFR in adults < 70 years old [61]. However, package inserts recommend dose adjustments based on estimation of CrCl using CG formula. This poses a problem in adjusting DOAC doses in elderly patients who are subject to overestimation of renal function with this antiquated equation. Among elderly patients with renal impairment, discordance between estimated and actual renal function was higher for dabigatran and rivaroxaban than for apixaban dosages [61].

Renal excretion of unchanged dabigatran is the predominant pathway for elimination (~80%) [58]. The FDA-approved dosing strategy in the US for dabigatran is 150 mg twice daily in patients with a CrCl ≥ 30 mL/min, 75 mg twice daily in patients with severe renal impairment (CrCl 15–30 mL/min), and is contraindicated in patients with a CrCl < 15 mL/min [58]. By comparison, the Canadian and the European Medicines Agency have listed patients with a CrCl < 30 mL/min (severe renal impairment) as a contraindication for use. The US-approved dosage for severe renal impairment was derived during the approval phase of dabigatran using a simulation pharmacokinetic model [62,63]. The dosage was estimated by pharmacokinetic simulation to provide similar Cmax and Cmin concentrations compared to the 150 mg twice-daily dosage in moderate renal impairment. Compared to patients with CrCl ≥ 80 mL/min, there was a 1.29- and a 1.47-fold increase in dabigatran trough plasma concentration in the CrCl 50–80 mL/min patients and the CrCl 30–50 mL/min patients, respectively. There have been many postmarketing reports of hemorrhage with dabigatran [36,84,85]. Although reporting bias is likely due to the novelty of the agent, clinicians may take key clinical pearls away from these reports. Patients often had risk factors, including low body weight, renal impairment, and polypharmacy with interacting drugs (eg, amiodarone). These risk factors are also important with the other DOACs.
A subgroup analysis of ROCKET-AF evaluating rivaroxaban 15 mg daily in patients with a CrCl of 30–49 mL/min did not identify any differences in endpoints with the exception of fatal bleeding, which occurred less often with rivaroxaban (0.28%/yr vs. 0.74%/yr; P = 0.047) [64].
Monitoring of renal function is essential to mitigate the risk of drug accumulation. Clinicians should consider obtaining a baseline renal assessment with annual reassessments in patients with normal (CrCl ≥ 80 mL/min) or mild (CrCl 50–79 mL/min) renal impairment, and 2 to 3 times per year in patients with moderate (CrCl 30–49 mL/min) renal impairment [65]. A summary of renal dose adjustments for DOAC therapy may be found in Table 5 [56–59].
In addition to renal function, hepatic impairment can also affect the metabolism of anticoagulants. Severe hepatic impairment can lead to prolonged PT. Therefore, patients who have liver dysfunction and are treated with anticoagulation have increased risk of hemorrhagic events. Large pivotal trials on the key indications of dabigatran, apixaban, and rivaroxaban excluded patients with significant signs of hepatic impairment. Table 5 provides dosing recommendations for the different DOACs in the setting of hepatic impairment [56–59].
Polypharmacy And The Potential For Adverse Consequences
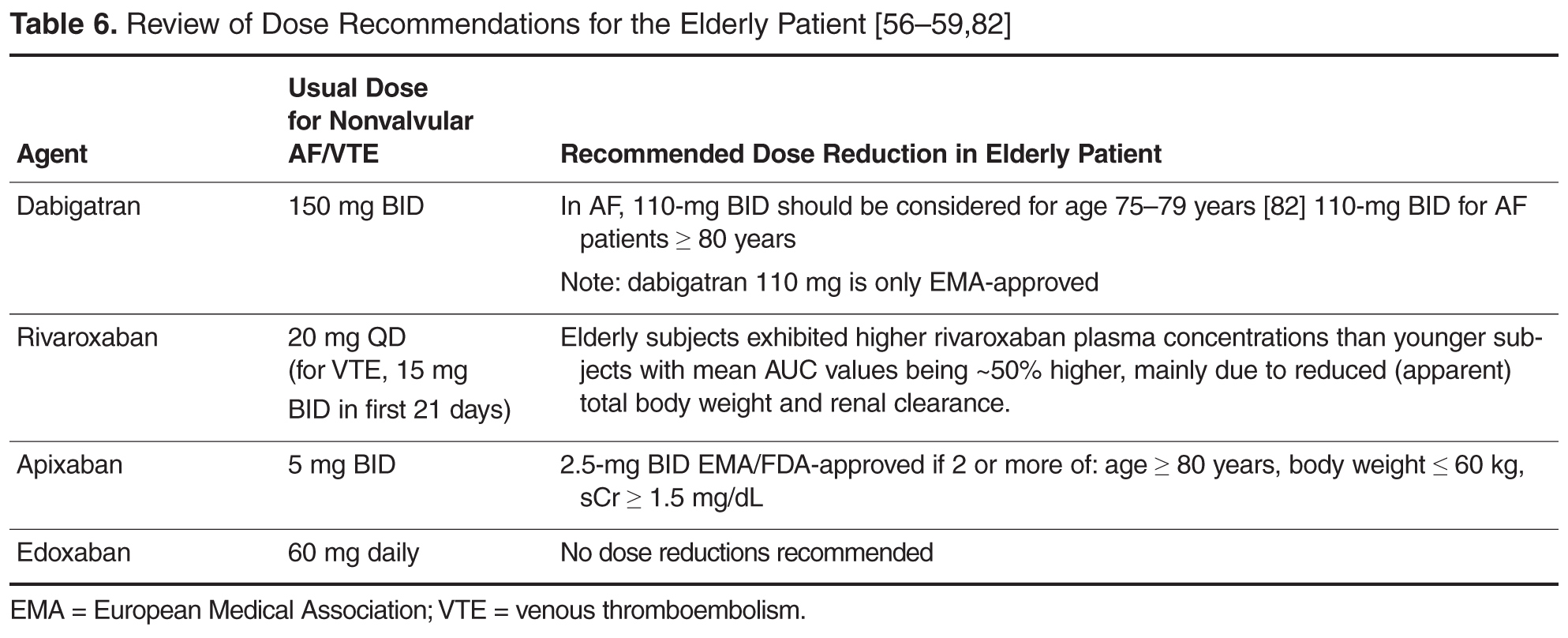

Costs And Cost-Effectiveness of DOACS
With the high burden of AF and the aging population, analysis of cost and value is an important consideration [76]. There are limited publications comparing the cost-effectiveness between the anticoagulation options. However, numerous cost-effectiveness studies have evaluated the individual DOACs [71–79]. Overall, the studies suggest that the DOACs are a cost-effective alternative to warfarin in the general and elderly populations. One analysis reported that dabigatran may not be cost-effective in patients with a low CHADS2 score (≤ 2) [71].
Harrington et al [80] compared the cost-effectiveness of dabigatran, rivaroxaban, and apixaban versus warfarin. This cost-effectiveness study used published clinical trial data to build a decision model, and results indicated that for patients ≥ 70 years of age with an increased risk for stroke, normal renal function, and no previous contraindications to anticoagulant therapy, apixaban 5 mg, dabigatran 150 mg, and rivaroxaban 20 mg were cost-effective substitutes for warfarin for the prevention of stroke in nonvalvular AF [80]. Apixaban was the preferred anticoagulant for their hypothetical cohort of 70-year-old patients with nonvalvular AF, as it was most likely to be the cost-effective treatment option at all willing-to-pay thresholds > $40,000 per quality-adjusted life-year gained [76,81].
Prescription costs may vary depending on payor and level of insurance. If a patient does not have prescription insurance, the annual price of generic warfarin is roughly $200 to $360, depending on dosage. Approximate annual costs for the DOACs are greater than 20 times the cost of warfarin (apixaban $4500, dabigatran $4500, and rivaroxaban $4800) [82]. However, most patients on these medications are over 65 years old and have prescription coverage through Medicare Part D. Of note, patients may have more of a burden if or when they reach the “donut hole” coverage gap. Currently, once patients spend $2960 (for 2015) and $3310 (for 2016) on covered drugs they will fall into the donut hole unless they qualify for additional assistance. At this point Medicare Part D will reimburse 45% of the cost of the newer anticoagulants since generics are currently unavailable. As a result, individual affordability may become an issue. Further complicating the scenario is the inability to apply coupon and rebate cards in the setting of government-funded prescription coverage. Clinicians should discuss these issues with their patients to help select the most valuable therapy.
Conclusions And Recommendations

Corresponding author: Luigi Brunetti, PharmD, MPH, Rutgers University, 160 Frelinghuysen Rd, Piscataway, NJ 08854, [email protected].
1. Fanikos J, Stapinski C, Koo S, et al. Medication errors associated with anticoagulant therapy in the hospital. Am J Cardiol 2004;94:532–5.
2. Budnitz DS, Lovegrove MC, Shehab N, Richards CL. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med2011;365:2002–12.
3. Institute for Safe Medication Practices. QuarterWatch. 9 January 2013. Available at http://www.ismp.org/quarterwatch/pdfs/2012Q2.pdf.
4. Hajjar ER, Hanlon JT, Artz MB, Let al. Adverse drug reaction risk factors in older outpatients. Am J Geriatr Pharmacother 2003;1:82–9.
5. Gurwitz JH, Field TS, Harrold LR, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA 2003;289:1107–16.
6. Singh S. Defining ‘elderly’ in clinical practice guidelines for pharmacotherapy. Pharm Pract 2014;12:489.
7. Singh S, Bajorek B. Pharmacotherapy in the aging patient: The impact of age per se (a review). Ageing Res Rev 2015 Jul 28. pii: S1568-1637(15)30008-8.
8. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the anticoagulation and risk factors in atrial fibrillation (ATRIA) Study. JAMA 2001;285:2370–5.
9. Lip GY, Brechin CM, Lane DA. The global burden of atrial fibrillation and stroke: a systematic review of the epidemiology of atrial fibrillation in regions outside North America and Europe Chest 2012;142:1489–98.
10. Camm AJ, Lip GY, De Caterina R, et al. 2012 Focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation-developed with the special contribution of the European Heart Rhythm Association Europace 2012;14:1385–413.
11. Kannel WB, Benjamin EJ. Status of the epidemiology of atrial fibrillation. Med Clin North Am 2008;92:17–40.
12. Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a global burden 2010 study. Circulation 2014;129:837-47.
13. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114:119–25.
14. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139–51.
15. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365:883–91.
16. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365:981–92.
17. Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORR2HAGES, ATRIA, and HAS-BLED Bleeding Risk–Prediction Scores in Patients With Atrial Fibrillation Undergoing Anticoagulation: The AMADEUS (Evaluating the Use of SR34006 Compared to Warfarin or Acenocoumarol in Patients With Atrial Fibrillation) Study. J Am Coll Cardiol 2012;60:861–7.
18. Fang MC, Go AS, Chang Y, et al. A new risk scheme to predict warfarin-associated hemorrhage: the ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) study. J Am Coll Cardiol 2011;58:395–401.
19. Pisters R, Lane DA, Nieuwlaat R, et al. A novel user-friendly score (has-bled) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010;138:1093–100.
20. Heidbuchel H, Verhamme P, Alings M, et al. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace 2015;17:1467–507.
21. Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am Coll Cardiol 2011;57:173–80.
22. Roldán V, Marín F, Fernández H, et al. Predictive value of the HAS-BLED and ATRIA bleeding scores for the risk of serious bleeding in a "real-world" population with atrial fibrillation receiving anticoagulant therapy. Chest 2013;43:179–84.
23. Robert-Ebadi H, Le Gal G, Righini M. Use of anticoagulants in elderly patients: practical recommendations. Clin Interv Aging 2009;4:165–77.
24. Barcellona D, Contu P, Sorano GG, et al. The management of oral anticoagulant therapy: the patient's point of view. Thromb Haemost 2000;83:49–53.
25. Lancaster TR, Singer DE, Sheehan MA, et al. The impact of long-term warfarin therapy on quality of life. Evidence from a randomized trial. Boston Area Anticoagulation Trial for Atrial Fibrillation Investigators. Arch Intern Med 1991;151:1944–9.
26. Devereaux PJ, Anderson DR, Gardner MJ, et al. Differences between perspectives of physicians and patients on anticoagulation in patients with atrial fibrillation: observational study. BMJ 2001;323:1218–22.
27. Giugliano RP, Ruff CT, Braunwald E, Murphy SA. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2013;369:2093–104.
28. Barco S, Cheung YW, Eikelboom JW, Coppens M. New oral anticoagulants in elderly patients. Best Pract Res Clin Haematol 2013;26:215–24
29. Eikelboom JW, Wallentin L, Connolly SJ, et al. Risk of bleeding with 2 doses of dabigatran compared with warfarin in older and younger patients with atrial fibrillation: an analysis of the randomized evaluation of long-term anticoagulant therapy (RE-LY) trial. Circulation 2011;123:2363–72.
30. Coppens M, Eikelboom JW, Ezekowitz M, et al. Dabigatran versus warfarin in very elderly patients with atrial fibrillation: results from the RE-LY trial. Abstract. Circulation 2012;126:A15l537.
31. Halperin JL, Wojdyla D, Piccini JP, et al. Efficacy and safety of rivaroxaban compared with warfarin among elderly patients with nonvalvular atrial fibrillation in the ROCKET-AF trial. Abstract. Stroke 2012;43:A148.
32. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 2014;383:955–62
33. Clemens A, Strack A, Noack H, et al. Anticoagulant-related gastrointestinal bleeding—could this facilitate early detection of benign or malignant gastrointestinal lesions? Ann Med 2014;46:672–8.
34. Petty GW, Khandheria BK, Whisnant JP, et al. Predictors of cerebrovascular events and death among patients with valvular heart disease: A population-based study. Stroke 2000;31:2628–35.
35. Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med 2013;369:1206–14.
36. Schomburg JL, Medina EM, Lahti MT, Bianco RW. Dabigatran versus warfarin after mechanical mitral valve replacement in the swine model. J Invest Surg 2012;25:150–5.
37. Douketis J, Bell AD, Eikelboom J, Liew A. Approach to the new oral anticoagulants in family practice: part 2: addressing frequently asked questions. Can Fam Physician 2014;60:997–1001.
38. Frost CE, Nepal S, Barrett YC, LaCreta F. Effects of age and gender on the singledose pharmacokinetics (PK) and pharmacodynamics (PD) of apixaban. Abstract. J Thromb Haemost 2009;7(Suppl 2):PP-MO-407..
39. Stangier J, Stahle H, Rathgen K et al. Pharmacokinetics and pharmacodynamics of the direct oral thrombin inhibitor dabigatran in healthy elderly subjects. Clin Pharmacokinet 2008;47:47–59.
40. Kubitza D, Becka M, Mueck W. The effect of extreme age, and gender on the pharmacology and tolerability of rivaroxaban, an oral direct factor Xa inhibitor. Blood 2006;108: Abstract 905.
41. Siegal DM, Crowther MA. Acute management of bleeding in patients on novel oral anticoagulants. Eur Heart J 2013;34:489–98.
42. Evans A, Kalra L. Are the results of randomized controlled trials on anticoagulation in patients with atrial fibrillation generalizable to clinical practice? Arch Intern Med 2001;161:1443–7.
43. Harper P, Young L, Merriman E. Bleeding risk with dabigatran in the frail elderly. N Engl J Med 2012;366:864–6.
44. Graham DJ, Reichman ME, Wernecke M, et al. Cardiovascular, bleeding, and mortality risks in elderly Medicare patients treated with dabigatran or warfarin for nonvalvular atrial fibrillation. Circulation 2015;131:157–64.
45. Avgil-Tsadok M, Jackevicius CA, Essebag V, et al. Dabigatran use in elderly patients with atrial fibrillation. Thromb Haemost 2015;115(1).
46. Uchino K, Hernandez AV. Dabigatran association with higher risk of acute coronary events: meta-analysis of noninferiority randomized controlled trials. Arch Intern Med 2012;172:397–402.
47. Halvorsen S, Atar D, Yang H, et al. Efficacy and safety of apixaban compared with warfarin according to age for stroke prevention in atrial fibrillation: observations from the ARISTOTLE trial. Eur Heart J 2014;35:1864–72.
48. Lega JC, Bertoletti L, Gremillet C, et al. Consistency of safety profile of new oral anticoagulants in patients with renal failure. J Thromb Haemost 2014;12:337–43.
49. Ng KH, Hart RG, Eikelboom JW. Anticoagulation in patients aged ≥ 75 years with atrial fibrillation: role of novel oral anticoagulants. Cardiol Ther 2013;2:135–49.
50. Kato ET, Guigliano RP, Ruff CT, et al. Efficacy and safety of edoxaban for the management of elderly patients with atrial fibrillation: Engage-AF TIMI 48. Circulation 2014;130:A16612.
51. Tripodi A. The laboratory and the new oral anticoagulants. Clin Chem 2013;59:353–62.
52. Tripodi A, Di Iorio G, Lippi G, et al. Position paper on laboratory testing for patients taking new oral anticoagulants. Consensus document of FCSA, SIMeL, SIBioC and CISMEL. Clin Chem Lab Med 2012;50:2137-40.
53. Heidbuchel H, Verhamme P, Alings M, et al. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Europace 2013;15:625–51.
54. Chin PK, Wright DF, Patterson DM, et al. A proposal for dose-adjustment of dabigatran etexilate in atrial fibrillation guided by thrombin time. Br J Clin Pharmacol 2014;78:599–609.
55. Miyares MA, Davis K. Newer oral anticoagulants: a review of laboratory monitoring options and reversal agents in the hemorrhagic patient. Am J Health Syst Pharm 2012;69:1473–84.
56. Xarelto [package insert]. Titusville, NJ. Janssen Pharmaceuticals. September 2014.
57. Eliquis [package insert]. Princeton, NJ: Bristol-Meyers Squibb. June 2015.
58. Pradaxa [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals. October 2010.
59. Savaysa [package insert]. Parsippany, NJ: Daiichi Sankyo. September 2015.
60. Michels WM, Grootendorst DC, Verduijn M, et al. Performance of the Cockcroft-Gault, MDRD, and new CKDEPI formulas in relation to GFR, age, and body size. Clin J Am Soc Nephrol 2010;5: 1003–9.
61. Poulsen BK, Grove EL, Husted SE. New oral anticoagulants: a review of the literature with particular emphasis on patients with impaired renal function. Drugs 2012;72:1739–53.
62. Hariharan S, Madabushi R. Clinical pharmacology basis of deriving dosing recommendations for dabigatran in patients with severe renal impairment. J Clin Pharmacol 2012;52:119S–25S.
63. Lehr T, Haertter S, Liesenfeld KH, et al. Dabigatran etexilate in atrial fibrillation patients with severe renal impairment: dose identification using pharmacokinetic modeling and simulation. J Clin Pharmacol 2012;52:1373–8.
64. Fox KAA, Piccini JP, Wojdyla D, et al. Prevention of stroke and systemic embolism with rivaroxaban compared with warfarin in patients with non-valvular atrial fibrillation and moderate renal impairment. Eur Heart J 2011;32:2387–94.
65. Pengo V, Crippa L, Falanga A et al. Questions and answers on the use of dabigatran and perspectives on the use of other new oral anticoagulants in patients with atrial fibrillation. A consensus document of the Italian Federation of Thrombosis Centers (FCSA). Thromb Haemost 2011;106:868–76.
66. Atkin PA, Veitch PC, Veitch EM, Ogle SJ. The epidemiology of serious adverse drug reactions among the elderly. Drugs Aging 1999;14:141–52.
67. Qato DM, Alexander GC, Conti RM, et al. Use of prescription and over-the-counter medications and dietary supplements among older adults in the United States. JAMA 2008;300:2867–78.
68. Skov J, Bladbjerg EM, Sidelmann J, et al. Plenty of pills: polypharmacy prevails in patients of a Danish anticoagulant clinic. Eur J Clin Pharmacol 2011;67:1169–74.
69. Ukena C, Bohm M, Schirmer SH. Hot topics in cardiology: data from IABP-SHOCK II, TRILOGY-ACS, WOEST, ALTIDUDE, FAME II and more. Clin Res Cardiol 2012;101):861–74.
70. Dewilde, Willem JM, Oirbans T, et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomised, controlled trial. Lancet;381:1107–15.
71. Shah SV, Gage BF. Cost-effectiveness of dabigatran for stroke prophylaxis in atrial fibrillation. Circulation 2011;123:
2562–70.
72. Sorensen SV, Kansal AR, Connolly S, et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation: a Canadian payer perspective. Thromb Haemost 2011;105:908–19.
73. Adcock AK, Lee-Iannotti JK, Aguilar MI, et al. Is dabigatran cost effective compared with warfarin for stroke prevention in atrial fibrillation?: a critically appraised topic. Neurologist 2012;18:102–7.
74. Kamel H, Johnston SC, Easton JD, Kim AS. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in patients with atrial fibrillation and prior stroke or transient ischemic attack. Stroke 2012;43:881–3.
75. Langkilde LK, Bergholdt AM, Overgaard M. Cost-effectiveness of dabigatran etexilate for stroke prevention in non-valvular atrial fibrillation. J Med Econ 2012;15:695-703.
76. Kansal AR, Sorensen SV, Gani R, et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in UK patients with atrial fibrillation. Heart 2012; 98:573–8.
77. Freeman JV, Zhu RP, Owens DK, et al. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in atrial fibrillation. Ann Intern Med 2011;154:1–11.
78. Pink J, Lane S, Pirmohamed M, Hughes DA. Dabigatran etexilate versus warfarin in management of non-valvular atrial fibrillation in UK context: quantitative benefit-harm and economic analyses. BMJ 2011;343:d6333.
79. Ali A, Bailey C, Abdelhafiz AH. Stroke prophylaxis with warfarin or dabigatran for patients with non-valvular atrial fibrillation-cost analysis. Age Ageing 2012;41:681–4.
80. Harrington AR, Armstrong EP, Nolan PE Jr, Malone DC. Cost effectiveness of apixaban, dabigatran, rivaroxaban, and warfarin for stroke prevention in atrial fibrillation. Stroke 2013;44:1676–81.
81. Amin A, Lingohr-Smith M, Bruno A, et al. Economic evaluations of medical cost differences: use of targeted-specific oral anticoagulants vs. warfarin among patients with nonvalvular atrial fibrillation and venous thromboembolism in the US. J Hematol Thrombo Dis 2015;3:209.
82. Lexicomp, Lexi-Drugs. Hudson, OH: Lexi-Comp.
83. U.S. Food and Drug Administration, Center for Drug Evaluation and Research. Apixaban NDA 202155/S-002 approval letter. Jan 30 2014. Available at http://www.accessdata.fda.gov/drugsatfda_docs/appletter/2014/202155Orig1s002ltr.pdf
84. Hinojar R, Jimenez-Natcher JJ, Fernandez-Golfin C, Zamorano JL. New oral anticoagulants: a practical guide for physicians. Eur Heart J Cardiovasc Pharmacother 2015;1:134-45.
85. Connolly SJ, Eikelboom J, Joyner C, et al. Apixaban in patiets with atrial fibrillation. N Engl J Med 2011;364;806–17.
From the Ernest Mario School of Pharmacy, Rutgers University, Piscataway, NJ.
Abstract
- Objective: To provide a clinical summary of the available data evaluating the use of direct oral anticoagulants (DOACs) in geriatric patients with nonvalvular atrial fibrillation.
- Methods: MEDLINE, Web of Science, and Google Scholar were used to identify pertinent systematic reviews, randomized controlled trials, observational studies, and pharmacokinetic studies evaluating use of DOACs in the geriatric population.
- Results: A total of 8 systemic reviews, 5 randomized controlled trials, 2 observational trials, and 5 pharmacokinetic studies of relevance were identified for inclusion in this review. The landscape of anticoagulation has dramatically changed over the past 5 years beginning with the development and marketing of an oral direct thrombin inhibitor and followed by 3 oral direct factor Xa inhibitors. Despite significant advances in this oral anticoagulation arena, many questions remain as to the best therapeutic approach in the geriatric population as the literature is lacking. This population has a higher risk of stroke; however, due to the increased risk of bleeding clinicians may often defer anticoagulant therapy due to the fear of hemorrhagic complications. Clinicians must consider the risk-benefit ratio and the associated outcomes in geriatric patients compared to other patient populations.
- Conclusions: Interpreting the available literature and understanding the benefits and limitations of the DOACs is critical when selecting the most appropriate pharmacologic strategy in geriatric patients.
Anticoagulants are among the top 5 drug classes associated with patient harm in the US [1] and are commonly reported as contributing to hospitalizations [2]. In just one quarter in 2012 alone, warfarin, dabigatran, and rivaroxaban accounted for 1734 of 50,289 adverse events reported to the Food and Drug Administration (FDA), including 233 deaths [3]. Appropriate use of anticoagulant agents and consideration of individual patient risk factors are essential to mitigate the occurrence of adverse consequences, especially in the geriatric population. This population is more likely to have risk factors for adverse drug events, for example, polypharmacy, age-related changes in pharmacokinetics and pharmacodynamics, and diminished organ function (ie, renal and hepatic) [4,5]. Another important consideration is the lack of consensus on the definition of a “geriatric” or “elderly” patient. Although many consider a chronological age of > 65 years as the defining variable for a geriatric individual, this definition does not account for overall health status [6,7]. Clinicians should consider this shortcoming when evaluating the quality of geriatric studies. For example, a study claiming to evaluate the pharmacokinetics of a drug in a geriatric population enrolling healthy subjects aged > 65 years may result in data that do not translate to clinical practice.
Compounding the concern for iatrogenic events is the frequency of anticoagulant use in the geriatric population, as several indications are found more commonly in this age-group. Stroke prevention in nonvalvular atrial fibrillation (AF), the most common arrhythmia in the elderly, is a common indication for long-term anticoagulation [8]. The prevalence of AF increases with age and is usually higher in men than in women [9,10]. AF is generally uncommon before 60 years of age, but the prevalence increases noticeably thereafter, affecting approximately 10% of the overall population by 80 years of age [11]. The median age of patients who have AF is 75 years with approximately 70% of patients between 65 and 85 years of age [8,12]. Currently in the United States, an estimated 2.3 million people are diagnosed with AF [8]. In 2020, the AF population is predicted to increase to 7.5 million individuals with an expected prevalence of 13.5% among individuals ≥ 75 years of age, and 18.2% for those ≥ 85 years of age [13]. These data underscore the importance of considering the influence of age on the balance between efficacy and safety of anticoagulant therapy.
Direct oral anticoagulants (DOACs) represent the first alternatives to warfarin in over 6 decades. Currently available products in US include apixaban, dabigatran, edoxaban, and rivaroxaban. DOACs possess many of the characteristics of an ideal anticoagulant, including predictable pharmacokinetics, a wider therapeutic window compared to warfarin, minimal drug interactions, a fixed dose, and no need for routine evaluation of coagulation parameters. The safety and efficacy of the DOACs for stroke prevention in nonvalvular AF have been substantiated in several landmark clinical trials [14–16]. Yet there are several important questions that need to be addressed, such as management of excessive anticoagulation, clinical outcome data with renally adjusted doses (an exclusion criterion in many landmark studies was a creatinine clearance of < 25–30 mL/min), whether monitoring of coagulation parameters could enhance efficacy and safety, and optimal dosing strategies in geriatric patients. This review provides clinicians a summary of data from landmark studies, post-marketing surveillance, and pharmacokinetic evaluations to support DOAC selection in the geriatric population.
Evaluating Bleeding Risk
These tools have been extensively evaluated with warfarin therapy, but their performance in predicting DOAC-related bleeding has not been definitively established. Nonetheless, until tools evaluated specifically for DOACs are developed, it is reasonable to use these for risk-prediction in combination with clinical judgment. As an example, the European Society of Cardiology guideline on the use of non–vitamin K antagonist (VKA) anticoagulants in patients with nonvalvular AF suggests that the HAS-BLED score may be used to identify risk factors for bleeding and correct those that are modifiable [20]. The HAS-BLED score is validated for VKA and non-VKA anticoagulants (early-generation oral direct thrombin inhibitor ximelgatran) [21] and is the only bleeding risk score predictive for intracranial hemorrhage [19]. In a 2013 “real world” comparison, HAS-BLED was easier to use and had better predictive accuracy that ATRIA [22].
One of the major challenges in geriatric patients is that those at highest risk for bleeding are those who would have the greatest benefit from anticoagulation [23]. The prediction scores can help clinicians balance the risk-benefit ratio for anticoagulation on a case by case basis. Although the scoring systems take into consideration several factors, including medical conditions that have been shown to significantly increase bleeding risk, including hypertension, cerebrovascular disease, ischemic stroke, serious heart disease, diabetes, renal insufficiency, alcoholism and liver disease, not all are included in every scoring scheme [23]. These conditions are more common among elderly patients, and this should be taken into account when estimating the risk-benefit ratio of oral anticoagulation [15]. Patients’ preferences should also be taken into account. It is essential for clinicians to clearly discuss treatment options with patients as data suggest that clinician and patient perceptions of anticoagulation are often mismatched [24–26].
Performance of TSOACS in Landmark Studies
Some specific differences in outcomes seen in landmark studies that may facilitate selection among the DOACs include the risk of major bleeding, risk of gastrointestinal bleeding, risk of acute coronary syndrome, exclusion of valvular heart disease, and noninferiority versus superiority as the primary endpoint when compared to warfarin.
Major Bleeding
Gastrointestinal Bleeding
Among all of the DOACs, gastrointestinal (GI) bleeding was significantly greater with dabigatran, edoxaban, and rivaroxaban when compared to warfarin (HR, 1.49; 95% CI, 1.21–1.84; HR, 1.23; 95% CI, 1.02–1.50; and HR, 1.61; 95% CI, 1.30–1.99, respectively; P < 0.05 for all) [14–16] in landmark studies. Based on these data, clinicians may consider the selection of apixaban in patients with a previous history of GI pathology. GI bleeding may be more common in elderly patients due to the potential for preexisting GI pathology and high local concentrations of drug [29]. Clemens and colleagues suggested an “anticoagulation GI stress test” may predict GI malignancy [33]. They found that patients on DOACs that presented with a GI bleed were more likely to present with a GI malignancy. As such, it is reasonable to screen patients with a fecal occult blood test within the first month after initiating TSOAC treatment and then annually.
Acute Coronary Syndrome
A higher rate of myocardial infarction was observed with dabigatran 150 mg versus warfarin (0.74% vs 0.53% per year; P = 0.048) in the RE-LY study [16]. Whether the increase in myocardial infarction was due to dabigatran as a causative agent or warfarin’s ability to reduce the risk of myocardial infarction to a larger extent compared with dabigatran is unknown. Nonetheless, it may be prudent to use an alternative therapy in patients with a history of acute coronary syndrome.
Valvular Heart Disease
The risk of stroke and systemic embolism is higher in patients with valvular heart disease [34]. Patients with moderate to severe mitral stenosis or mechanical prosthetic heart valves were excluded from the DOAC landmark studies. Dabigatran was evaluated for prevention of stroke and systemic embolism in patients with valvular heart disease in the RE-ALIGN study [35,36]. Patients were randomized to warfarin titrated to a target INR of 2 to 3 or 2.5 to 3.5 on the basis of thromboembolic risk or dabigatran 150 mg, 220 mg, or 300 mg twice daily adjusted to a targeted trough of ≥ 50 ng/mL. The trial was terminated early due to a worse primary outcome (composite of stroke, systemic embolism, myocardial infarction, and death) with dabigatran versus warfarin (HR, 3.37, 95% CI, 0.76–14.95; P = 0.11). In addition, bleeding rates (any bleeding) was significantly greater with dabigatran (27%) versus warfarin (12%) (P = 0.01). Based on these data and the lack of data with the other TSOACs, warfarin remains the standard of care for valvular heart disease [37]. In patients with a previous bioprosthetic valve with AF, patients with mitral insufficiency, or aortic stensosis, TSOACs may be considered [37].
Landmark Study Efficacy Endpoints
The primary endpoint in each of the landmark studies was a composite of stroke (ischemic or hemorrhagic) and systemic embolism. For the primary endpoint only dabigatran 150 mg twice daily and apixaban 5 mg twice daily were found to be superior to warfarin for the prevention of stroke or systemic embolism in nonvalvular AF (HR, 0.66; 95% CI, 0.53–0.82; P < 0.001 and HR, 0.66; 95% CI, 0.66–0.95; P = 0.01, respectively). Both edoxaban (60 mg and 30 mg daily) and rivaroxaban were noninferior to warfarin for the primary endpoint. In terms of ischemic stroke, only dabigatran 150 mg twice daily was superior to warfarin for the reduction in ischemic stroke in patients with nonvalvular AF (HR, 0.76; 95% CI, 0.60–0.98; P = 0.03) [19]. All of the DOACs demonstrated a reduction in hemorrhagic stroke.
TSOAC Use in Elderly Patitents
Pharmacokinetic Evaluations
Several pharmacokinetic studies have evaluated the influence of age on DOAC disposition. In a study evaluating the influence of age on apixaban disposition, the area under the concentration-time curve to infinity was 32% higher in the elderly (aged 65 years or older) compared to the younger subjects (< age 40 years) [38]. These data provide the rationale for dosage adjustment in individuals aged 80 years or older with either low body mass (weight less than or equal to 60 kg) or renal impairment (serum creatinine 1.5 mg/dL or higher). In a pharmacokinetic study evaluating dabigatran in patients > 65 years of age, the time to steady state ranged from 2 to 3 days, correlating to a half-life of 12 to 14 hours, and peak concentrations (256 ng/mL females, 255 ng/mL males) were reached after a median of 3 hours (range, 2.0–4.0 hours) [39]. These data suggest a 1.7- to twofold increase in bioavailability. The area under the curve of rivaroxaban was significantly higher in subjects > 75 years versus subjects 18-45 years, while total and renal clearance were decreased [40].However, the time to maximum factor Xa inhibition and Cmax were not influenced by age.
Clinical Evaluations
Dabigatran
In a post-hoc analysis of the RE-LY trial, Eikelboom and colleagues found that patients 75 years of age and older treated with dabigatran 150 mg twice daily had a greater incidence of GI bleeding irrespective of renal function compared with those on warfarin (1.85%/year vs. 1.25%/year; P < 0.001) [29]. A higher risk in major bleeding also was seen in dabigatran patients (5.10% versus 4.37%; P = 0.07). As a result, the 2012 Beer’s Criteria lists dabigatran as a potentially inappropriate medication. An analysis was conducted of 134,414 elderly Medicare patients (defined as age > 65 years) with 37,587 person-years of follow-up who were treated with dabigatran or warfarin [44]. Approximately 60% of patients included in the analysis were over age 75 years. Dabigatran was associated with a significant reduction in ischemic stroke: HR 0.80 (CI 0.67–0.96); intracranial hemorrhage: HR 0.34 (CI 0.26–0.46); and death: HR 0.86 (CI 0.77–0.96) when compared with warfarin. As in the Eikelboom study, major gastrointestinal bleeding was significantly increased with dabigatran (HR, 1.28 [95% CI, 1.14–1.44]).
Rivaroxaban
For rivaroxaban, a subgroup analysis of patients ≥ 75 years in the ROCKET-AF trial reported similar rates of major bleeding (HR, 1.11; 95% CI, 0.92–1.34) with rivaroxaban compared with warfarin [31]. Clinically relevant non-major bleeding was significantly higher for patients aged ≥ 75 years compared with patients aged < 75 years (P = 0.01).
Apixaban
Halvorsen and colleagues found that age did not influence the benefits of apixaban in terms of efficacy and safety [47]. In the cohort of patients aged 75 years or older, major bleeding was significantly reduced compared to warfarin (HR, 0.64; 95% CI, 0.52–0.79). The safety benefits persisted even in the setting of age greater than 75 years and renal impairment. A significant reduction in major bleeding (HR, 0.35; 95% CI, 0.14–0.86) was seen in elderly patients with a CrCl; ≤ 30 mL/min (n = 221) treated with apixaban versus warfarin. Similarly, in elderly patients with a CrCl 30 to 50 mL/min (n = 1898) a significant reduction in major bleeding was reported (HR, 0.53; 95% CI, 0.37–0.76). These data are consistent with a meta-regression analysis that found a linear relationship between the relative risk of major bleeding and the magnitude of renal excretion for the DOACs (r2=0.66, P = 0.03) [48]. In this analysis, apixaban had the most favorable outcomes in terms of major bleeding compared to the other DOACs and also has the least dependence on renal function for clearance. In a pooled analysis of data from landmark trials, Ng and colleagues found that in elderly patients (defined as age > 75 years) with nonvalvular AF, only apixaban was associated with a significant reduction in both stroke and major hemorrhage (Figure 1) [49,50].
Edoxaban
Kato and colleagues performed a subgroup analysis of patients aged 75 years or older enrolled in the ENGAGE TIMI 48 study [50]. Currently the results are only published in abstract form. Regardless of treatment, the risk of major bleeding and stroke significantly increased with age (P < 0.001). An absolute risk reduction in major bleeding was reported with both 60 mg and 30 mg of edoxaban versus warfarin (4.0%/year and 2.2%/year versus 4.8%/year, respectively; no P value provided).
Therapeuti Drug Monitoring
Collectively, the data on assessment of the anticoagulant activity of DOACs using coagulation assays is evolving. These tests include but are not limited to prothrombin time (PT), activated partial thromboplastin time (aPTT), thrombin clotting time (TT), dilute TT, activated clotting time (ACT), anti factor Xa, and ecarin clotting time (ECT) assays. Although routine monitoring is not desirable, the ability to assess degree of anticoagulation in select patient populations may prove beneficial. Future studies are essential to confirm whether assessing DOAC activity using coagulation assays in vulnerable populations such as the elderly improves clinical outcomes. Several reviews on this subject matter have been published [51–55]. The reader is encouraged to review these data as there are significant limitations to currently available assays and incorrect interpretation may lead to suboptimal treatment decisions.
Renal and Hepatic Dysfunction
Depending on the specific agents, DOACs renal clearance varies from 27% to 80% [56–59]. Clinical trials often use the Cockcroft-Gault formula (CG) based on actual body weight to estimate renal function. Landmark trials evaluating the DOACs differed in their strategy for estimation of renal function using CG. For example, RE-LY and ROCKET-AF used actual body weight for the estimation of renal function, while ARISTOTLE did not specify which body weight to use. Estimation of renal function or glomerular filtration rate (GFR) by CG is frequently in discordance with actual renal function in the elderly [60]. MDRD (modification of diet in renal disease) and Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) are also common estimations that provide an estimate of GFR. In a cross-sectional study, comparing the CG, MDRD, and EPI formulas in a clinical setting, data from potential kidney donors and adult patients who underwent a GFR measurement revealed that MDRD has the smallest mean bias. The influence of age was the absolute bias for estimation of renal function for all formulas. CG is additionally influenced by body weight and body mass index. When compared to CG, MDRD actually reported more accurate predictor of GFR in adults < 70 years old [61]. However, package inserts recommend dose adjustments based on estimation of CrCl using CG formula. This poses a problem in adjusting DOAC doses in elderly patients who are subject to overestimation of renal function with this antiquated equation. Among elderly patients with renal impairment, discordance between estimated and actual renal function was higher for dabigatran and rivaroxaban than for apixaban dosages [61].
Renal excretion of unchanged dabigatran is the predominant pathway for elimination (~80%) [58]. The FDA-approved dosing strategy in the US for dabigatran is 150 mg twice daily in patients with a CrCl ≥ 30 mL/min, 75 mg twice daily in patients with severe renal impairment (CrCl 15–30 mL/min), and is contraindicated in patients with a CrCl < 15 mL/min [58]. By comparison, the Canadian and the European Medicines Agency have listed patients with a CrCl < 30 mL/min (severe renal impairment) as a contraindication for use. The US-approved dosage for severe renal impairment was derived during the approval phase of dabigatran using a simulation pharmacokinetic model [62,63]. The dosage was estimated by pharmacokinetic simulation to provide similar Cmax and Cmin concentrations compared to the 150 mg twice-daily dosage in moderate renal impairment. Compared to patients with CrCl ≥ 80 mL/min, there was a 1.29- and a 1.47-fold increase in dabigatran trough plasma concentration in the CrCl 50–80 mL/min patients and the CrCl 30–50 mL/min patients, respectively. There have been many postmarketing reports of hemorrhage with dabigatran [36,84,85]. Although reporting bias is likely due to the novelty of the agent, clinicians may take key clinical pearls away from these reports. Patients often had risk factors, including low body weight, renal impairment, and polypharmacy with interacting drugs (eg, amiodarone). These risk factors are also important with the other DOACs.
A subgroup analysis of ROCKET-AF evaluating rivaroxaban 15 mg daily in patients with a CrCl of 30–49 mL/min did not identify any differences in endpoints with the exception of fatal bleeding, which occurred less often with rivaroxaban (0.28%/yr vs. 0.74%/yr; P = 0.047) [64].
Monitoring of renal function is essential to mitigate the risk of drug accumulation. Clinicians should consider obtaining a baseline renal assessment with annual reassessments in patients with normal (CrCl ≥ 80 mL/min) or mild (CrCl 50–79 mL/min) renal impairment, and 2 to 3 times per year in patients with moderate (CrCl 30–49 mL/min) renal impairment [65]. A summary of renal dose adjustments for DOAC therapy may be found in Table 5 [56–59].
In addition to renal function, hepatic impairment can also affect the metabolism of anticoagulants. Severe hepatic impairment can lead to prolonged PT. Therefore, patients who have liver dysfunction and are treated with anticoagulation have increased risk of hemorrhagic events. Large pivotal trials on the key indications of dabigatran, apixaban, and rivaroxaban excluded patients with significant signs of hepatic impairment. Table 5 provides dosing recommendations for the different DOACs in the setting of hepatic impairment [56–59].
Polypharmacy And The Potential For Adverse Consequences
Costs And Cost-Effectiveness of DOACS
With the high burden of AF and the aging population, analysis of cost and value is an important consideration [76]. There are limited publications comparing the cost-effectiveness between the anticoagulation options. However, numerous cost-effectiveness studies have evaluated the individual DOACs [71–79]. Overall, the studies suggest that the DOACs are a cost-effective alternative to warfarin in the general and elderly populations. One analysis reported that dabigatran may not be cost-effective in patients with a low CHADS2 score (≤ 2) [71].
Harrington et al [80] compared the cost-effectiveness of dabigatran, rivaroxaban, and apixaban versus warfarin. This cost-effectiveness study used published clinical trial data to build a decision model, and results indicated that for patients ≥ 70 years of age with an increased risk for stroke, normal renal function, and no previous contraindications to anticoagulant therapy, apixaban 5 mg, dabigatran 150 mg, and rivaroxaban 20 mg were cost-effective substitutes for warfarin for the prevention of stroke in nonvalvular AF [80]. Apixaban was the preferred anticoagulant for their hypothetical cohort of 70-year-old patients with nonvalvular AF, as it was most likely to be the cost-effective treatment option at all willing-to-pay thresholds > $40,000 per quality-adjusted life-year gained [76,81].
Prescription costs may vary depending on payor and level of insurance. If a patient does not have prescription insurance, the annual price of generic warfarin is roughly $200 to $360, depending on dosage. Approximate annual costs for the DOACs are greater than 20 times the cost of warfarin (apixaban $4500, dabigatran $4500, and rivaroxaban $4800) [82]. However, most patients on these medications are over 65 years old and have prescription coverage through Medicare Part D. Of note, patients may have more of a burden if or when they reach the “donut hole” coverage gap. Currently, once patients spend $2960 (for 2015) and $3310 (for 2016) on covered drugs they will fall into the donut hole unless they qualify for additional assistance. At this point Medicare Part D will reimburse 45% of the cost of the newer anticoagulants since generics are currently unavailable. As a result, individual affordability may become an issue. Further complicating the scenario is the inability to apply coupon and rebate cards in the setting of government-funded prescription coverage. Clinicians should discuss these issues with their patients to help select the most valuable therapy.
Conclusions And Recommendations
Corresponding author: Luigi Brunetti, PharmD, MPH, Rutgers University, 160 Frelinghuysen Rd, Piscataway, NJ 08854, [email protected].
From the Ernest Mario School of Pharmacy, Rutgers University, Piscataway, NJ.
Abstract
- Objective: To provide a clinical summary of the available data evaluating the use of direct oral anticoagulants (DOACs) in geriatric patients with nonvalvular atrial fibrillation.
- Methods: MEDLINE, Web of Science, and Google Scholar were used to identify pertinent systematic reviews, randomized controlled trials, observational studies, and pharmacokinetic studies evaluating use of DOACs in the geriatric population.
- Results: A total of 8 systemic reviews, 5 randomized controlled trials, 2 observational trials, and 5 pharmacokinetic studies of relevance were identified for inclusion in this review. The landscape of anticoagulation has dramatically changed over the past 5 years beginning with the development and marketing of an oral direct thrombin inhibitor and followed by 3 oral direct factor Xa inhibitors. Despite significant advances in this oral anticoagulation arena, many questions remain as to the best therapeutic approach in the geriatric population as the literature is lacking. This population has a higher risk of stroke; however, due to the increased risk of bleeding clinicians may often defer anticoagulant therapy due to the fear of hemorrhagic complications. Clinicians must consider the risk-benefit ratio and the associated outcomes in geriatric patients compared to other patient populations.
- Conclusions: Interpreting the available literature and understanding the benefits and limitations of the DOACs is critical when selecting the most appropriate pharmacologic strategy in geriatric patients.
Anticoagulants are among the top 5 drug classes associated with patient harm in the US [1] and are commonly reported as contributing to hospitalizations [2]. In just one quarter in 2012 alone, warfarin, dabigatran, and rivaroxaban accounted for 1734 of 50,289 adverse events reported to the Food and Drug Administration (FDA), including 233 deaths [3]. Appropriate use of anticoagulant agents and consideration of individual patient risk factors are essential to mitigate the occurrence of adverse consequences, especially in the geriatric population. This population is more likely to have risk factors for adverse drug events, for example, polypharmacy, age-related changes in pharmacokinetics and pharmacodynamics, and diminished organ function (ie, renal and hepatic) [4,5]. Another important consideration is the lack of consensus on the definition of a “geriatric” or “elderly” patient. Although many consider a chronological age of > 65 years as the defining variable for a geriatric individual, this definition does not account for overall health status [6,7]. Clinicians should consider this shortcoming when evaluating the quality of geriatric studies. For example, a study claiming to evaluate the pharmacokinetics of a drug in a geriatric population enrolling healthy subjects aged > 65 years may result in data that do not translate to clinical practice.
Compounding the concern for iatrogenic events is the frequency of anticoagulant use in the geriatric population, as several indications are found more commonly in this age-group. Stroke prevention in nonvalvular atrial fibrillation (AF), the most common arrhythmia in the elderly, is a common indication for long-term anticoagulation [8]. The prevalence of AF increases with age and is usually higher in men than in women [9,10]. AF is generally uncommon before 60 years of age, but the prevalence increases noticeably thereafter, affecting approximately 10% of the overall population by 80 years of age [11]. The median age of patients who have AF is 75 years with approximately 70% of patients between 65 and 85 years of age [8,12]. Currently in the United States, an estimated 2.3 million people are diagnosed with AF [8]. In 2020, the AF population is predicted to increase to 7.5 million individuals with an expected prevalence of 13.5% among individuals ≥ 75 years of age, and 18.2% for those ≥ 85 years of age [13]. These data underscore the importance of considering the influence of age on the balance between efficacy and safety of anticoagulant therapy.
Direct oral anticoagulants (DOACs) represent the first alternatives to warfarin in over 6 decades. Currently available products in US include apixaban, dabigatran, edoxaban, and rivaroxaban. DOACs possess many of the characteristics of an ideal anticoagulant, including predictable pharmacokinetics, a wider therapeutic window compared to warfarin, minimal drug interactions, a fixed dose, and no need for routine evaluation of coagulation parameters. The safety and efficacy of the DOACs for stroke prevention in nonvalvular AF have been substantiated in several landmark clinical trials [14–16]. Yet there are several important questions that need to be addressed, such as management of excessive anticoagulation, clinical outcome data with renally adjusted doses (an exclusion criterion in many landmark studies was a creatinine clearance of < 25–30 mL/min), whether monitoring of coagulation parameters could enhance efficacy and safety, and optimal dosing strategies in geriatric patients. This review provides clinicians a summary of data from landmark studies, post-marketing surveillance, and pharmacokinetic evaluations to support DOAC selection in the geriatric population.
Evaluating Bleeding Risk
These tools have been extensively evaluated with warfarin therapy, but their performance in predicting DOAC-related bleeding has not been definitively established. Nonetheless, until tools evaluated specifically for DOACs are developed, it is reasonable to use these for risk-prediction in combination with clinical judgment. As an example, the European Society of Cardiology guideline on the use of non–vitamin K antagonist (VKA) anticoagulants in patients with nonvalvular AF suggests that the HAS-BLED score may be used to identify risk factors for bleeding and correct those that are modifiable [20]. The HAS-BLED score is validated for VKA and non-VKA anticoagulants (early-generation oral direct thrombin inhibitor ximelgatran) [21] and is the only bleeding risk score predictive for intracranial hemorrhage [19]. In a 2013 “real world” comparison, HAS-BLED was easier to use and had better predictive accuracy that ATRIA [22].
One of the major challenges in geriatric patients is that those at highest risk for bleeding are those who would have the greatest benefit from anticoagulation [23]. The prediction scores can help clinicians balance the risk-benefit ratio for anticoagulation on a case by case basis. Although the scoring systems take into consideration several factors, including medical conditions that have been shown to significantly increase bleeding risk, including hypertension, cerebrovascular disease, ischemic stroke, serious heart disease, diabetes, renal insufficiency, alcoholism and liver disease, not all are included in every scoring scheme [23]. These conditions are more common among elderly patients, and this should be taken into account when estimating the risk-benefit ratio of oral anticoagulation [15]. Patients’ preferences should also be taken into account. It is essential for clinicians to clearly discuss treatment options with patients as data suggest that clinician and patient perceptions of anticoagulation are often mismatched [24–26].
Performance of TSOACS in Landmark Studies
Some specific differences in outcomes seen in landmark studies that may facilitate selection among the DOACs include the risk of major bleeding, risk of gastrointestinal bleeding, risk of acute coronary syndrome, exclusion of valvular heart disease, and noninferiority versus superiority as the primary endpoint when compared to warfarin.
Major Bleeding
Gastrointestinal Bleeding
Among all of the DOACs, gastrointestinal (GI) bleeding was significantly greater with dabigatran, edoxaban, and rivaroxaban when compared to warfarin (HR, 1.49; 95% CI, 1.21–1.84; HR, 1.23; 95% CI, 1.02–1.50; and HR, 1.61; 95% CI, 1.30–1.99, respectively; P < 0.05 for all) [14–16] in landmark studies. Based on these data, clinicians may consider the selection of apixaban in patients with a previous history of GI pathology. GI bleeding may be more common in elderly patients due to the potential for preexisting GI pathology and high local concentrations of drug [29]. Clemens and colleagues suggested an “anticoagulation GI stress test” may predict GI malignancy [33]. They found that patients on DOACs that presented with a GI bleed were more likely to present with a GI malignancy. As such, it is reasonable to screen patients with a fecal occult blood test within the first month after initiating TSOAC treatment and then annually.
Acute Coronary Syndrome
A higher rate of myocardial infarction was observed with dabigatran 150 mg versus warfarin (0.74% vs 0.53% per year; P = 0.048) in the RE-LY study [16]. Whether the increase in myocardial infarction was due to dabigatran as a causative agent or warfarin’s ability to reduce the risk of myocardial infarction to a larger extent compared with dabigatran is unknown. Nonetheless, it may be prudent to use an alternative therapy in patients with a history of acute coronary syndrome.
Valvular Heart Disease
The risk of stroke and systemic embolism is higher in patients with valvular heart disease [34]. Patients with moderate to severe mitral stenosis or mechanical prosthetic heart valves were excluded from the DOAC landmark studies. Dabigatran was evaluated for prevention of stroke and systemic embolism in patients with valvular heart disease in the RE-ALIGN study [35,36]. Patients were randomized to warfarin titrated to a target INR of 2 to 3 or 2.5 to 3.5 on the basis of thromboembolic risk or dabigatran 150 mg, 220 mg, or 300 mg twice daily adjusted to a targeted trough of ≥ 50 ng/mL. The trial was terminated early due to a worse primary outcome (composite of stroke, systemic embolism, myocardial infarction, and death) with dabigatran versus warfarin (HR, 3.37, 95% CI, 0.76–14.95; P = 0.11). In addition, bleeding rates (any bleeding) was significantly greater with dabigatran (27%) versus warfarin (12%) (P = 0.01). Based on these data and the lack of data with the other TSOACs, warfarin remains the standard of care for valvular heart disease [37]. In patients with a previous bioprosthetic valve with AF, patients with mitral insufficiency, or aortic stensosis, TSOACs may be considered [37].
Landmark Study Efficacy Endpoints
The primary endpoint in each of the landmark studies was a composite of stroke (ischemic or hemorrhagic) and systemic embolism. For the primary endpoint only dabigatran 150 mg twice daily and apixaban 5 mg twice daily were found to be superior to warfarin for the prevention of stroke or systemic embolism in nonvalvular AF (HR, 0.66; 95% CI, 0.53–0.82; P < 0.001 and HR, 0.66; 95% CI, 0.66–0.95; P = 0.01, respectively). Both edoxaban (60 mg and 30 mg daily) and rivaroxaban were noninferior to warfarin for the primary endpoint. In terms of ischemic stroke, only dabigatran 150 mg twice daily was superior to warfarin for the reduction in ischemic stroke in patients with nonvalvular AF (HR, 0.76; 95% CI, 0.60–0.98; P = 0.03) [19]. All of the DOACs demonstrated a reduction in hemorrhagic stroke.
TSOAC Use in Elderly Patitents
Pharmacokinetic Evaluations
Several pharmacokinetic studies have evaluated the influence of age on DOAC disposition. In a study evaluating the influence of age on apixaban disposition, the area under the concentration-time curve to infinity was 32% higher in the elderly (aged 65 years or older) compared to the younger subjects (< age 40 years) [38]. These data provide the rationale for dosage adjustment in individuals aged 80 years or older with either low body mass (weight less than or equal to 60 kg) or renal impairment (serum creatinine 1.5 mg/dL or higher). In a pharmacokinetic study evaluating dabigatran in patients > 65 years of age, the time to steady state ranged from 2 to 3 days, correlating to a half-life of 12 to 14 hours, and peak concentrations (256 ng/mL females, 255 ng/mL males) were reached after a median of 3 hours (range, 2.0–4.0 hours) [39]. These data suggest a 1.7- to twofold increase in bioavailability. The area under the curve of rivaroxaban was significantly higher in subjects > 75 years versus subjects 18-45 years, while total and renal clearance were decreased [40].However, the time to maximum factor Xa inhibition and Cmax were not influenced by age.
Clinical Evaluations
Dabigatran
In a post-hoc analysis of the RE-LY trial, Eikelboom and colleagues found that patients 75 years of age and older treated with dabigatran 150 mg twice daily had a greater incidence of GI bleeding irrespective of renal function compared with those on warfarin (1.85%/year vs. 1.25%/year; P < 0.001) [29]. A higher risk in major bleeding also was seen in dabigatran patients (5.10% versus 4.37%; P = 0.07). As a result, the 2012 Beer’s Criteria lists dabigatran as a potentially inappropriate medication. An analysis was conducted of 134,414 elderly Medicare patients (defined as age > 65 years) with 37,587 person-years of follow-up who were treated with dabigatran or warfarin [44]. Approximately 60% of patients included in the analysis were over age 75 years. Dabigatran was associated with a significant reduction in ischemic stroke: HR 0.80 (CI 0.67–0.96); intracranial hemorrhage: HR 0.34 (CI 0.26–0.46); and death: HR 0.86 (CI 0.77–0.96) when compared with warfarin. As in the Eikelboom study, major gastrointestinal bleeding was significantly increased with dabigatran (HR, 1.28 [95% CI, 1.14–1.44]).
Rivaroxaban
For rivaroxaban, a subgroup analysis of patients ≥ 75 years in the ROCKET-AF trial reported similar rates of major bleeding (HR, 1.11; 95% CI, 0.92–1.34) with rivaroxaban compared with warfarin [31]. Clinically relevant non-major bleeding was significantly higher for patients aged ≥ 75 years compared with patients aged < 75 years (P = 0.01).
Apixaban
Halvorsen and colleagues found that age did not influence the benefits of apixaban in terms of efficacy and safety [47]. In the cohort of patients aged 75 years or older, major bleeding was significantly reduced compared to warfarin (HR, 0.64; 95% CI, 0.52–0.79). The safety benefits persisted even in the setting of age greater than 75 years and renal impairment. A significant reduction in major bleeding (HR, 0.35; 95% CI, 0.14–0.86) was seen in elderly patients with a CrCl; ≤ 30 mL/min (n = 221) treated with apixaban versus warfarin. Similarly, in elderly patients with a CrCl 30 to 50 mL/min (n = 1898) a significant reduction in major bleeding was reported (HR, 0.53; 95% CI, 0.37–0.76). These data are consistent with a meta-regression analysis that found a linear relationship between the relative risk of major bleeding and the magnitude of renal excretion for the DOACs (r2=0.66, P = 0.03) [48]. In this analysis, apixaban had the most favorable outcomes in terms of major bleeding compared to the other DOACs and also has the least dependence on renal function for clearance. In a pooled analysis of data from landmark trials, Ng and colleagues found that in elderly patients (defined as age > 75 years) with nonvalvular AF, only apixaban was associated with a significant reduction in both stroke and major hemorrhage (Figure 1) [49,50].
Edoxaban
Kato and colleagues performed a subgroup analysis of patients aged 75 years or older enrolled in the ENGAGE TIMI 48 study [50]. Currently the results are only published in abstract form. Regardless of treatment, the risk of major bleeding and stroke significantly increased with age (P < 0.001). An absolute risk reduction in major bleeding was reported with both 60 mg and 30 mg of edoxaban versus warfarin (4.0%/year and 2.2%/year versus 4.8%/year, respectively; no P value provided).
Therapeuti Drug Monitoring
Collectively, the data on assessment of the anticoagulant activity of DOACs using coagulation assays is evolving. These tests include but are not limited to prothrombin time (PT), activated partial thromboplastin time (aPTT), thrombin clotting time (TT), dilute TT, activated clotting time (ACT), anti factor Xa, and ecarin clotting time (ECT) assays. Although routine monitoring is not desirable, the ability to assess degree of anticoagulation in select patient populations may prove beneficial. Future studies are essential to confirm whether assessing DOAC activity using coagulation assays in vulnerable populations such as the elderly improves clinical outcomes. Several reviews on this subject matter have been published [51–55]. The reader is encouraged to review these data as there are significant limitations to currently available assays and incorrect interpretation may lead to suboptimal treatment decisions.
Renal and Hepatic Dysfunction
Depending on the specific agents, DOACs renal clearance varies from 27% to 80% [56–59]. Clinical trials often use the Cockcroft-Gault formula (CG) based on actual body weight to estimate renal function. Landmark trials evaluating the DOACs differed in their strategy for estimation of renal function using CG. For example, RE-LY and ROCKET-AF used actual body weight for the estimation of renal function, while ARISTOTLE did not specify which body weight to use. Estimation of renal function or glomerular filtration rate (GFR) by CG is frequently in discordance with actual renal function in the elderly [60]. MDRD (modification of diet in renal disease) and Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) are also common estimations that provide an estimate of GFR. In a cross-sectional study, comparing the CG, MDRD, and EPI formulas in a clinical setting, data from potential kidney donors and adult patients who underwent a GFR measurement revealed that MDRD has the smallest mean bias. The influence of age was the absolute bias for estimation of renal function for all formulas. CG is additionally influenced by body weight and body mass index. When compared to CG, MDRD actually reported more accurate predictor of GFR in adults < 70 years old [61]. However, package inserts recommend dose adjustments based on estimation of CrCl using CG formula. This poses a problem in adjusting DOAC doses in elderly patients who are subject to overestimation of renal function with this antiquated equation. Among elderly patients with renal impairment, discordance between estimated and actual renal function was higher for dabigatran and rivaroxaban than for apixaban dosages [61].
Renal excretion of unchanged dabigatran is the predominant pathway for elimination (~80%) [58]. The FDA-approved dosing strategy in the US for dabigatran is 150 mg twice daily in patients with a CrCl ≥ 30 mL/min, 75 mg twice daily in patients with severe renal impairment (CrCl 15–30 mL/min), and is contraindicated in patients with a CrCl < 15 mL/min [58]. By comparison, the Canadian and the European Medicines Agency have listed patients with a CrCl < 30 mL/min (severe renal impairment) as a contraindication for use. The US-approved dosage for severe renal impairment was derived during the approval phase of dabigatran using a simulation pharmacokinetic model [62,63]. The dosage was estimated by pharmacokinetic simulation to provide similar Cmax and Cmin concentrations compared to the 150 mg twice-daily dosage in moderate renal impairment. Compared to patients with CrCl ≥ 80 mL/min, there was a 1.29- and a 1.47-fold increase in dabigatran trough plasma concentration in the CrCl 50–80 mL/min patients and the CrCl 30–50 mL/min patients, respectively. There have been many postmarketing reports of hemorrhage with dabigatran [36,84,85]. Although reporting bias is likely due to the novelty of the agent, clinicians may take key clinical pearls away from these reports. Patients often had risk factors, including low body weight, renal impairment, and polypharmacy with interacting drugs (eg, amiodarone). These risk factors are also important with the other DOACs.
A subgroup analysis of ROCKET-AF evaluating rivaroxaban 15 mg daily in patients with a CrCl of 30–49 mL/min did not identify any differences in endpoints with the exception of fatal bleeding, which occurred less often with rivaroxaban (0.28%/yr vs. 0.74%/yr; P = 0.047) [64].
Monitoring of renal function is essential to mitigate the risk of drug accumulation. Clinicians should consider obtaining a baseline renal assessment with annual reassessments in patients with normal (CrCl ≥ 80 mL/min) or mild (CrCl 50–79 mL/min) renal impairment, and 2 to 3 times per year in patients with moderate (CrCl 30–49 mL/min) renal impairment [65]. A summary of renal dose adjustments for DOAC therapy may be found in Table 5 [56–59].
In addition to renal function, hepatic impairment can also affect the metabolism of anticoagulants. Severe hepatic impairment can lead to prolonged PT. Therefore, patients who have liver dysfunction and are treated with anticoagulation have increased risk of hemorrhagic events. Large pivotal trials on the key indications of dabigatran, apixaban, and rivaroxaban excluded patients with significant signs of hepatic impairment. Table 5 provides dosing recommendations for the different DOACs in the setting of hepatic impairment [56–59].
Polypharmacy And The Potential For Adverse Consequences
Costs And Cost-Effectiveness of DOACS
With the high burden of AF and the aging population, analysis of cost and value is an important consideration [76]. There are limited publications comparing the cost-effectiveness between the anticoagulation options. However, numerous cost-effectiveness studies have evaluated the individual DOACs [71–79]. Overall, the studies suggest that the DOACs are a cost-effective alternative to warfarin in the general and elderly populations. One analysis reported that dabigatran may not be cost-effective in patients with a low CHADS2 score (≤ 2) [71].
Harrington et al [80] compared the cost-effectiveness of dabigatran, rivaroxaban, and apixaban versus warfarin. This cost-effectiveness study used published clinical trial data to build a decision model, and results indicated that for patients ≥ 70 years of age with an increased risk for stroke, normal renal function, and no previous contraindications to anticoagulant therapy, apixaban 5 mg, dabigatran 150 mg, and rivaroxaban 20 mg were cost-effective substitutes for warfarin for the prevention of stroke in nonvalvular AF [80]. Apixaban was the preferred anticoagulant for their hypothetical cohort of 70-year-old patients with nonvalvular AF, as it was most likely to be the cost-effective treatment option at all willing-to-pay thresholds > $40,000 per quality-adjusted life-year gained [76,81].
Prescription costs may vary depending on payor and level of insurance. If a patient does not have prescription insurance, the annual price of generic warfarin is roughly $200 to $360, depending on dosage. Approximate annual costs for the DOACs are greater than 20 times the cost of warfarin (apixaban $4500, dabigatran $4500, and rivaroxaban $4800) [82]. However, most patients on these medications are over 65 years old and have prescription coverage through Medicare Part D. Of note, patients may have more of a burden if or when they reach the “donut hole” coverage gap. Currently, once patients spend $2960 (for 2015) and $3310 (for 2016) on covered drugs they will fall into the donut hole unless they qualify for additional assistance. At this point Medicare Part D will reimburse 45% of the cost of the newer anticoagulants since generics are currently unavailable. As a result, individual affordability may become an issue. Further complicating the scenario is the inability to apply coupon and rebate cards in the setting of government-funded prescription coverage. Clinicians should discuss these issues with their patients to help select the most valuable therapy.
Conclusions And Recommendations
Corresponding author: Luigi Brunetti, PharmD, MPH, Rutgers University, 160 Frelinghuysen Rd, Piscataway, NJ 08854, [email protected].
1. Fanikos J, Stapinski C, Koo S, et al. Medication errors associated with anticoagulant therapy in the hospital. Am J Cardiol 2004;94:532–5.
2. Budnitz DS, Lovegrove MC, Shehab N, Richards CL. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med2011;365:2002–12.
3. Institute for Safe Medication Practices. QuarterWatch. 9 January 2013. Available at http://www.ismp.org/quarterwatch/pdfs/2012Q2.pdf.
4. Hajjar ER, Hanlon JT, Artz MB, Let al. Adverse drug reaction risk factors in older outpatients. Am J Geriatr Pharmacother 2003;1:82–9.
5. Gurwitz JH, Field TS, Harrold LR, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA 2003;289:1107–16.
6. Singh S. Defining ‘elderly’ in clinical practice guidelines for pharmacotherapy. Pharm Pract 2014;12:489.
7. Singh S, Bajorek B. Pharmacotherapy in the aging patient: The impact of age per se (a review). Ageing Res Rev 2015 Jul 28. pii: S1568-1637(15)30008-8.
8. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the anticoagulation and risk factors in atrial fibrillation (ATRIA) Study. JAMA 2001;285:2370–5.
9. Lip GY, Brechin CM, Lane DA. The global burden of atrial fibrillation and stroke: a systematic review of the epidemiology of atrial fibrillation in regions outside North America and Europe Chest 2012;142:1489–98.
10. Camm AJ, Lip GY, De Caterina R, et al. 2012 Focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation-developed with the special contribution of the European Heart Rhythm Association Europace 2012;14:1385–413.
11. Kannel WB, Benjamin EJ. Status of the epidemiology of atrial fibrillation. Med Clin North Am 2008;92:17–40.
12. Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a global burden 2010 study. Circulation 2014;129:837-47.
13. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114:119–25.
14. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139–51.
15. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365:883–91.
16. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365:981–92.
17. Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORR2HAGES, ATRIA, and HAS-BLED Bleeding Risk–Prediction Scores in Patients With Atrial Fibrillation Undergoing Anticoagulation: The AMADEUS (Evaluating the Use of SR34006 Compared to Warfarin or Acenocoumarol in Patients With Atrial Fibrillation) Study. J Am Coll Cardiol 2012;60:861–7.
18. Fang MC, Go AS, Chang Y, et al. A new risk scheme to predict warfarin-associated hemorrhage: the ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) study. J Am Coll Cardiol 2011;58:395–401.
19. Pisters R, Lane DA, Nieuwlaat R, et al. A novel user-friendly score (has-bled) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010;138:1093–100.
20. Heidbuchel H, Verhamme P, Alings M, et al. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace 2015;17:1467–507.
21. Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am Coll Cardiol 2011;57:173–80.
22. Roldán V, Marín F, Fernández H, et al. Predictive value of the HAS-BLED and ATRIA bleeding scores for the risk of serious bleeding in a "real-world" population with atrial fibrillation receiving anticoagulant therapy. Chest 2013;43:179–84.
23. Robert-Ebadi H, Le Gal G, Righini M. Use of anticoagulants in elderly patients: practical recommendations. Clin Interv Aging 2009;4:165–77.
24. Barcellona D, Contu P, Sorano GG, et al. The management of oral anticoagulant therapy: the patient's point of view. Thromb Haemost 2000;83:49–53.
25. Lancaster TR, Singer DE, Sheehan MA, et al. The impact of long-term warfarin therapy on quality of life. Evidence from a randomized trial. Boston Area Anticoagulation Trial for Atrial Fibrillation Investigators. Arch Intern Med 1991;151:1944–9.
26. Devereaux PJ, Anderson DR, Gardner MJ, et al. Differences between perspectives of physicians and patients on anticoagulation in patients with atrial fibrillation: observational study. BMJ 2001;323:1218–22.
27. Giugliano RP, Ruff CT, Braunwald E, Murphy SA. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2013;369:2093–104.
28. Barco S, Cheung YW, Eikelboom JW, Coppens M. New oral anticoagulants in elderly patients. Best Pract Res Clin Haematol 2013;26:215–24
29. Eikelboom JW, Wallentin L, Connolly SJ, et al. Risk of bleeding with 2 doses of dabigatran compared with warfarin in older and younger patients with atrial fibrillation: an analysis of the randomized evaluation of long-term anticoagulant therapy (RE-LY) trial. Circulation 2011;123:2363–72.
30. Coppens M, Eikelboom JW, Ezekowitz M, et al. Dabigatran versus warfarin in very elderly patients with atrial fibrillation: results from the RE-LY trial. Abstract. Circulation 2012;126:A15l537.
31. Halperin JL, Wojdyla D, Piccini JP, et al. Efficacy and safety of rivaroxaban compared with warfarin among elderly patients with nonvalvular atrial fibrillation in the ROCKET-AF trial. Abstract. Stroke 2012;43:A148.
32. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 2014;383:955–62
33. Clemens A, Strack A, Noack H, et al. Anticoagulant-related gastrointestinal bleeding—could this facilitate early detection of benign or malignant gastrointestinal lesions? Ann Med 2014;46:672–8.
34. Petty GW, Khandheria BK, Whisnant JP, et al. Predictors of cerebrovascular events and death among patients with valvular heart disease: A population-based study. Stroke 2000;31:2628–35.
35. Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med 2013;369:1206–14.
36. Schomburg JL, Medina EM, Lahti MT, Bianco RW. Dabigatran versus warfarin after mechanical mitral valve replacement in the swine model. J Invest Surg 2012;25:150–5.
37. Douketis J, Bell AD, Eikelboom J, Liew A. Approach to the new oral anticoagulants in family practice: part 2: addressing frequently asked questions. Can Fam Physician 2014;60:997–1001.
38. Frost CE, Nepal S, Barrett YC, LaCreta F. Effects of age and gender on the singledose pharmacokinetics (PK) and pharmacodynamics (PD) of apixaban. Abstract. J Thromb Haemost 2009;7(Suppl 2):PP-MO-407..
39. Stangier J, Stahle H, Rathgen K et al. Pharmacokinetics and pharmacodynamics of the direct oral thrombin inhibitor dabigatran in healthy elderly subjects. Clin Pharmacokinet 2008;47:47–59.
40. Kubitza D, Becka M, Mueck W. The effect of extreme age, and gender on the pharmacology and tolerability of rivaroxaban, an oral direct factor Xa inhibitor. Blood 2006;108: Abstract 905.
41. Siegal DM, Crowther MA. Acute management of bleeding in patients on novel oral anticoagulants. Eur Heart J 2013;34:489–98.
42. Evans A, Kalra L. Are the results of randomized controlled trials on anticoagulation in patients with atrial fibrillation generalizable to clinical practice? Arch Intern Med 2001;161:1443–7.
43. Harper P, Young L, Merriman E. Bleeding risk with dabigatran in the frail elderly. N Engl J Med 2012;366:864–6.
44. Graham DJ, Reichman ME, Wernecke M, et al. Cardiovascular, bleeding, and mortality risks in elderly Medicare patients treated with dabigatran or warfarin for nonvalvular atrial fibrillation. Circulation 2015;131:157–64.
45. Avgil-Tsadok M, Jackevicius CA, Essebag V, et al. Dabigatran use in elderly patients with atrial fibrillation. Thromb Haemost 2015;115(1).
46. Uchino K, Hernandez AV. Dabigatran association with higher risk of acute coronary events: meta-analysis of noninferiority randomized controlled trials. Arch Intern Med 2012;172:397–402.
47. Halvorsen S, Atar D, Yang H, et al. Efficacy and safety of apixaban compared with warfarin according to age for stroke prevention in atrial fibrillation: observations from the ARISTOTLE trial. Eur Heart J 2014;35:1864–72.
48. Lega JC, Bertoletti L, Gremillet C, et al. Consistency of safety profile of new oral anticoagulants in patients with renal failure. J Thromb Haemost 2014;12:337–43.
49. Ng KH, Hart RG, Eikelboom JW. Anticoagulation in patients aged ≥ 75 years with atrial fibrillation: role of novel oral anticoagulants. Cardiol Ther 2013;2:135–49.
50. Kato ET, Guigliano RP, Ruff CT, et al. Efficacy and safety of edoxaban for the management of elderly patients with atrial fibrillation: Engage-AF TIMI 48. Circulation 2014;130:A16612.
51. Tripodi A. The laboratory and the new oral anticoagulants. Clin Chem 2013;59:353–62.
52. Tripodi A, Di Iorio G, Lippi G, et al. Position paper on laboratory testing for patients taking new oral anticoagulants. Consensus document of FCSA, SIMeL, SIBioC and CISMEL. Clin Chem Lab Med 2012;50:2137-40.
53. Heidbuchel H, Verhamme P, Alings M, et al. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Europace 2013;15:625–51.
54. Chin PK, Wright DF, Patterson DM, et al. A proposal for dose-adjustment of dabigatran etexilate in atrial fibrillation guided by thrombin time. Br J Clin Pharmacol 2014;78:599–609.
55. Miyares MA, Davis K. Newer oral anticoagulants: a review of laboratory monitoring options and reversal agents in the hemorrhagic patient. Am J Health Syst Pharm 2012;69:1473–84.
56. Xarelto [package insert]. Titusville, NJ. Janssen Pharmaceuticals. September 2014.
57. Eliquis [package insert]. Princeton, NJ: Bristol-Meyers Squibb. June 2015.
58. Pradaxa [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals. October 2010.
59. Savaysa [package insert]. Parsippany, NJ: Daiichi Sankyo. September 2015.
60. Michels WM, Grootendorst DC, Verduijn M, et al. Performance of the Cockcroft-Gault, MDRD, and new CKDEPI formulas in relation to GFR, age, and body size. Clin J Am Soc Nephrol 2010;5: 1003–9.
61. Poulsen BK, Grove EL, Husted SE. New oral anticoagulants: a review of the literature with particular emphasis on patients with impaired renal function. Drugs 2012;72:1739–53.
62. Hariharan S, Madabushi R. Clinical pharmacology basis of deriving dosing recommendations for dabigatran in patients with severe renal impairment. J Clin Pharmacol 2012;52:119S–25S.
63. Lehr T, Haertter S, Liesenfeld KH, et al. Dabigatran etexilate in atrial fibrillation patients with severe renal impairment: dose identification using pharmacokinetic modeling and simulation. J Clin Pharmacol 2012;52:1373–8.
64. Fox KAA, Piccini JP, Wojdyla D, et al. Prevention of stroke and systemic embolism with rivaroxaban compared with warfarin in patients with non-valvular atrial fibrillation and moderate renal impairment. Eur Heart J 2011;32:2387–94.
65. Pengo V, Crippa L, Falanga A et al. Questions and answers on the use of dabigatran and perspectives on the use of other new oral anticoagulants in patients with atrial fibrillation. A consensus document of the Italian Federation of Thrombosis Centers (FCSA). Thromb Haemost 2011;106:868–76.
66. Atkin PA, Veitch PC, Veitch EM, Ogle SJ. The epidemiology of serious adverse drug reactions among the elderly. Drugs Aging 1999;14:141–52.
67. Qato DM, Alexander GC, Conti RM, et al. Use of prescription and over-the-counter medications and dietary supplements among older adults in the United States. JAMA 2008;300:2867–78.
68. Skov J, Bladbjerg EM, Sidelmann J, et al. Plenty of pills: polypharmacy prevails in patients of a Danish anticoagulant clinic. Eur J Clin Pharmacol 2011;67:1169–74.
69. Ukena C, Bohm M, Schirmer SH. Hot topics in cardiology: data from IABP-SHOCK II, TRILOGY-ACS, WOEST, ALTIDUDE, FAME II and more. Clin Res Cardiol 2012;101):861–74.
70. Dewilde, Willem JM, Oirbans T, et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomised, controlled trial. Lancet;381:1107–15.
71. Shah SV, Gage BF. Cost-effectiveness of dabigatran for stroke prophylaxis in atrial fibrillation. Circulation 2011;123:
2562–70.
72. Sorensen SV, Kansal AR, Connolly S, et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation: a Canadian payer perspective. Thromb Haemost 2011;105:908–19.
73. Adcock AK, Lee-Iannotti JK, Aguilar MI, et al. Is dabigatran cost effective compared with warfarin for stroke prevention in atrial fibrillation?: a critically appraised topic. Neurologist 2012;18:102–7.
74. Kamel H, Johnston SC, Easton JD, Kim AS. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in patients with atrial fibrillation and prior stroke or transient ischemic attack. Stroke 2012;43:881–3.
75. Langkilde LK, Bergholdt AM, Overgaard M. Cost-effectiveness of dabigatran etexilate for stroke prevention in non-valvular atrial fibrillation. J Med Econ 2012;15:695-703.
76. Kansal AR, Sorensen SV, Gani R, et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in UK patients with atrial fibrillation. Heart 2012; 98:573–8.
77. Freeman JV, Zhu RP, Owens DK, et al. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in atrial fibrillation. Ann Intern Med 2011;154:1–11.
78. Pink J, Lane S, Pirmohamed M, Hughes DA. Dabigatran etexilate versus warfarin in management of non-valvular atrial fibrillation in UK context: quantitative benefit-harm and economic analyses. BMJ 2011;343:d6333.
79. Ali A, Bailey C, Abdelhafiz AH. Stroke prophylaxis with warfarin or dabigatran for patients with non-valvular atrial fibrillation-cost analysis. Age Ageing 2012;41:681–4.
80. Harrington AR, Armstrong EP, Nolan PE Jr, Malone DC. Cost effectiveness of apixaban, dabigatran, rivaroxaban, and warfarin for stroke prevention in atrial fibrillation. Stroke 2013;44:1676–81.
81. Amin A, Lingohr-Smith M, Bruno A, et al. Economic evaluations of medical cost differences: use of targeted-specific oral anticoagulants vs. warfarin among patients with nonvalvular atrial fibrillation and venous thromboembolism in the US. J Hematol Thrombo Dis 2015;3:209.
82. Lexicomp, Lexi-Drugs. Hudson, OH: Lexi-Comp.
83. U.S. Food and Drug Administration, Center for Drug Evaluation and Research. Apixaban NDA 202155/S-002 approval letter. Jan 30 2014. Available at http://www.accessdata.fda.gov/drugsatfda_docs/appletter/2014/202155Orig1s002ltr.pdf
84. Hinojar R, Jimenez-Natcher JJ, Fernandez-Golfin C, Zamorano JL. New oral anticoagulants: a practical guide for physicians. Eur Heart J Cardiovasc Pharmacother 2015;1:134-45.
85. Connolly SJ, Eikelboom J, Joyner C, et al. Apixaban in patiets with atrial fibrillation. N Engl J Med 2011;364;806–17.
1. Fanikos J, Stapinski C, Koo S, et al. Medication errors associated with anticoagulant therapy in the hospital. Am J Cardiol 2004;94:532–5.
2. Budnitz DS, Lovegrove MC, Shehab N, Richards CL. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med2011;365:2002–12.
3. Institute for Safe Medication Practices. QuarterWatch. 9 January 2013. Available at http://www.ismp.org/quarterwatch/pdfs/2012Q2.pdf.
4. Hajjar ER, Hanlon JT, Artz MB, Let al. Adverse drug reaction risk factors in older outpatients. Am J Geriatr Pharmacother 2003;1:82–9.
5. Gurwitz JH, Field TS, Harrold LR, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA 2003;289:1107–16.
6. Singh S. Defining ‘elderly’ in clinical practice guidelines for pharmacotherapy. Pharm Pract 2014;12:489.
7. Singh S, Bajorek B. Pharmacotherapy in the aging patient: The impact of age per se (a review). Ageing Res Rev 2015 Jul 28. pii: S1568-1637(15)30008-8.
8. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the anticoagulation and risk factors in atrial fibrillation (ATRIA) Study. JAMA 2001;285:2370–5.
9. Lip GY, Brechin CM, Lane DA. The global burden of atrial fibrillation and stroke: a systematic review of the epidemiology of atrial fibrillation in regions outside North America and Europe Chest 2012;142:1489–98.
10. Camm AJ, Lip GY, De Caterina R, et al. 2012 Focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation-developed with the special contribution of the European Heart Rhythm Association Europace 2012;14:1385–413.
11. Kannel WB, Benjamin EJ. Status of the epidemiology of atrial fibrillation. Med Clin North Am 2008;92:17–40.
12. Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a global burden 2010 study. Circulation 2014;129:837-47.
13. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114:119–25.
14. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139–51.
15. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365:883–91.
16. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011;365:981–92.
17. Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORR2HAGES, ATRIA, and HAS-BLED Bleeding Risk–Prediction Scores in Patients With Atrial Fibrillation Undergoing Anticoagulation: The AMADEUS (Evaluating the Use of SR34006 Compared to Warfarin or Acenocoumarol in Patients With Atrial Fibrillation) Study. J Am Coll Cardiol 2012;60:861–7.
18. Fang MC, Go AS, Chang Y, et al. A new risk scheme to predict warfarin-associated hemorrhage: the ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) study. J Am Coll Cardiol 2011;58:395–401.
19. Pisters R, Lane DA, Nieuwlaat R, et al. A novel user-friendly score (has-bled) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010;138:1093–100.
20. Heidbuchel H, Verhamme P, Alings M, et al. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace 2015;17:1467–507.
21. Lip GY, Frison L, Halperin JL, Lane DA. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am Coll Cardiol 2011;57:173–80.
22. Roldán V, Marín F, Fernández H, et al. Predictive value of the HAS-BLED and ATRIA bleeding scores for the risk of serious bleeding in a "real-world" population with atrial fibrillation receiving anticoagulant therapy. Chest 2013;43:179–84.
23. Robert-Ebadi H, Le Gal G, Righini M. Use of anticoagulants in elderly patients: practical recommendations. Clin Interv Aging 2009;4:165–77.
24. Barcellona D, Contu P, Sorano GG, et al. The management of oral anticoagulant therapy: the patient's point of view. Thromb Haemost 2000;83:49–53.
25. Lancaster TR, Singer DE, Sheehan MA, et al. The impact of long-term warfarin therapy on quality of life. Evidence from a randomized trial. Boston Area Anticoagulation Trial for Atrial Fibrillation Investigators. Arch Intern Med 1991;151:1944–9.
26. Devereaux PJ, Anderson DR, Gardner MJ, et al. Differences between perspectives of physicians and patients on anticoagulation in patients with atrial fibrillation: observational study. BMJ 2001;323:1218–22.
27. Giugliano RP, Ruff CT, Braunwald E, Murphy SA. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2013;369:2093–104.
28. Barco S, Cheung YW, Eikelboom JW, Coppens M. New oral anticoagulants in elderly patients. Best Pract Res Clin Haematol 2013;26:215–24
29. Eikelboom JW, Wallentin L, Connolly SJ, et al. Risk of bleeding with 2 doses of dabigatran compared with warfarin in older and younger patients with atrial fibrillation: an analysis of the randomized evaluation of long-term anticoagulant therapy (RE-LY) trial. Circulation 2011;123:2363–72.
30. Coppens M, Eikelboom JW, Ezekowitz M, et al. Dabigatran versus warfarin in very elderly patients with atrial fibrillation: results from the RE-LY trial. Abstract. Circulation 2012;126:A15l537.
31. Halperin JL, Wojdyla D, Piccini JP, et al. Efficacy and safety of rivaroxaban compared with warfarin among elderly patients with nonvalvular atrial fibrillation in the ROCKET-AF trial. Abstract. Stroke 2012;43:A148.
32. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 2014;383:955–62
33. Clemens A, Strack A, Noack H, et al. Anticoagulant-related gastrointestinal bleeding—could this facilitate early detection of benign or malignant gastrointestinal lesions? Ann Med 2014;46:672–8.
34. Petty GW, Khandheria BK, Whisnant JP, et al. Predictors of cerebrovascular events and death among patients with valvular heart disease: A population-based study. Stroke 2000;31:2628–35.
35. Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med 2013;369:1206–14.
36. Schomburg JL, Medina EM, Lahti MT, Bianco RW. Dabigatran versus warfarin after mechanical mitral valve replacement in the swine model. J Invest Surg 2012;25:150–5.
37. Douketis J, Bell AD, Eikelboom J, Liew A. Approach to the new oral anticoagulants in family practice: part 2: addressing frequently asked questions. Can Fam Physician 2014;60:997–1001.
38. Frost CE, Nepal S, Barrett YC, LaCreta F. Effects of age and gender on the singledose pharmacokinetics (PK) and pharmacodynamics (PD) of apixaban. Abstract. J Thromb Haemost 2009;7(Suppl 2):PP-MO-407..
39. Stangier J, Stahle H, Rathgen K et al. Pharmacokinetics and pharmacodynamics of the direct oral thrombin inhibitor dabigatran in healthy elderly subjects. Clin Pharmacokinet 2008;47:47–59.
40. Kubitza D, Becka M, Mueck W. The effect of extreme age, and gender on the pharmacology and tolerability of rivaroxaban, an oral direct factor Xa inhibitor. Blood 2006;108: Abstract 905.
41. Siegal DM, Crowther MA. Acute management of bleeding in patients on novel oral anticoagulants. Eur Heart J 2013;34:489–98.
42. Evans A, Kalra L. Are the results of randomized controlled trials on anticoagulation in patients with atrial fibrillation generalizable to clinical practice? Arch Intern Med 2001;161:1443–7.
43. Harper P, Young L, Merriman E. Bleeding risk with dabigatran in the frail elderly. N Engl J Med 2012;366:864–6.
44. Graham DJ, Reichman ME, Wernecke M, et al. Cardiovascular, bleeding, and mortality risks in elderly Medicare patients treated with dabigatran or warfarin for nonvalvular atrial fibrillation. Circulation 2015;131:157–64.
45. Avgil-Tsadok M, Jackevicius CA, Essebag V, et al. Dabigatran use in elderly patients with atrial fibrillation. Thromb Haemost 2015;115(1).
46. Uchino K, Hernandez AV. Dabigatran association with higher risk of acute coronary events: meta-analysis of noninferiority randomized controlled trials. Arch Intern Med 2012;172:397–402.
47. Halvorsen S, Atar D, Yang H, et al. Efficacy and safety of apixaban compared with warfarin according to age for stroke prevention in atrial fibrillation: observations from the ARISTOTLE trial. Eur Heart J 2014;35:1864–72.
48. Lega JC, Bertoletti L, Gremillet C, et al. Consistency of safety profile of new oral anticoagulants in patients with renal failure. J Thromb Haemost 2014;12:337–43.
49. Ng KH, Hart RG, Eikelboom JW. Anticoagulation in patients aged ≥ 75 years with atrial fibrillation: role of novel oral anticoagulants. Cardiol Ther 2013;2:135–49.
50. Kato ET, Guigliano RP, Ruff CT, et al. Efficacy and safety of edoxaban for the management of elderly patients with atrial fibrillation: Engage-AF TIMI 48. Circulation 2014;130:A16612.
51. Tripodi A. The laboratory and the new oral anticoagulants. Clin Chem 2013;59:353–62.
52. Tripodi A, Di Iorio G, Lippi G, et al. Position paper on laboratory testing for patients taking new oral anticoagulants. Consensus document of FCSA, SIMeL, SIBioC and CISMEL. Clin Chem Lab Med 2012;50:2137-40.
53. Heidbuchel H, Verhamme P, Alings M, et al. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Europace 2013;15:625–51.
54. Chin PK, Wright DF, Patterson DM, et al. A proposal for dose-adjustment of dabigatran etexilate in atrial fibrillation guided by thrombin time. Br J Clin Pharmacol 2014;78:599–609.
55. Miyares MA, Davis K. Newer oral anticoagulants: a review of laboratory monitoring options and reversal agents in the hemorrhagic patient. Am J Health Syst Pharm 2012;69:1473–84.
56. Xarelto [package insert]. Titusville, NJ. Janssen Pharmaceuticals. September 2014.
57. Eliquis [package insert]. Princeton, NJ: Bristol-Meyers Squibb. June 2015.
58. Pradaxa [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals. October 2010.
59. Savaysa [package insert]. Parsippany, NJ: Daiichi Sankyo. September 2015.
60. Michels WM, Grootendorst DC, Verduijn M, et al. Performance of the Cockcroft-Gault, MDRD, and new CKDEPI formulas in relation to GFR, age, and body size. Clin J Am Soc Nephrol 2010;5: 1003–9.
61. Poulsen BK, Grove EL, Husted SE. New oral anticoagulants: a review of the literature with particular emphasis on patients with impaired renal function. Drugs 2012;72:1739–53.
62. Hariharan S, Madabushi R. Clinical pharmacology basis of deriving dosing recommendations for dabigatran in patients with severe renal impairment. J Clin Pharmacol 2012;52:119S–25S.
63. Lehr T, Haertter S, Liesenfeld KH, et al. Dabigatran etexilate in atrial fibrillation patients with severe renal impairment: dose identification using pharmacokinetic modeling and simulation. J Clin Pharmacol 2012;52:1373–8.
64. Fox KAA, Piccini JP, Wojdyla D, et al. Prevention of stroke and systemic embolism with rivaroxaban compared with warfarin in patients with non-valvular atrial fibrillation and moderate renal impairment. Eur Heart J 2011;32:2387–94.
65. Pengo V, Crippa L, Falanga A et al. Questions and answers on the use of dabigatran and perspectives on the use of other new oral anticoagulants in patients with atrial fibrillation. A consensus document of the Italian Federation of Thrombosis Centers (FCSA). Thromb Haemost 2011;106:868–76.
66. Atkin PA, Veitch PC, Veitch EM, Ogle SJ. The epidemiology of serious adverse drug reactions among the elderly. Drugs Aging 1999;14:141–52.
67. Qato DM, Alexander GC, Conti RM, et al. Use of prescription and over-the-counter medications and dietary supplements among older adults in the United States. JAMA 2008;300:2867–78.
68. Skov J, Bladbjerg EM, Sidelmann J, et al. Plenty of pills: polypharmacy prevails in patients of a Danish anticoagulant clinic. Eur J Clin Pharmacol 2011;67:1169–74.
69. Ukena C, Bohm M, Schirmer SH. Hot topics in cardiology: data from IABP-SHOCK II, TRILOGY-ACS, WOEST, ALTIDUDE, FAME II and more. Clin Res Cardiol 2012;101):861–74.
70. Dewilde, Willem JM, Oirbans T, et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: an open-label, randomised, controlled trial. Lancet;381:1107–15.
71. Shah SV, Gage BF. Cost-effectiveness of dabigatran for stroke prophylaxis in atrial fibrillation. Circulation 2011;123:
2562–70.
72. Sorensen SV, Kansal AR, Connolly S, et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation: a Canadian payer perspective. Thromb Haemost 2011;105:908–19.
73. Adcock AK, Lee-Iannotti JK, Aguilar MI, et al. Is dabigatran cost effective compared with warfarin for stroke prevention in atrial fibrillation?: a critically appraised topic. Neurologist 2012;18:102–7.
74. Kamel H, Johnston SC, Easton JD, Kim AS. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in patients with atrial fibrillation and prior stroke or transient ischemic attack. Stroke 2012;43:881–3.
75. Langkilde LK, Bergholdt AM, Overgaard M. Cost-effectiveness of dabigatran etexilate for stroke prevention in non-valvular atrial fibrillation. J Med Econ 2012;15:695-703.
76. Kansal AR, Sorensen SV, Gani R, et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in UK patients with atrial fibrillation. Heart 2012; 98:573–8.
77. Freeman JV, Zhu RP, Owens DK, et al. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in atrial fibrillation. Ann Intern Med 2011;154:1–11.
78. Pink J, Lane S, Pirmohamed M, Hughes DA. Dabigatran etexilate versus warfarin in management of non-valvular atrial fibrillation in UK context: quantitative benefit-harm and economic analyses. BMJ 2011;343:d6333.
79. Ali A, Bailey C, Abdelhafiz AH. Stroke prophylaxis with warfarin or dabigatran for patients with non-valvular atrial fibrillation-cost analysis. Age Ageing 2012;41:681–4.
80. Harrington AR, Armstrong EP, Nolan PE Jr, Malone DC. Cost effectiveness of apixaban, dabigatran, rivaroxaban, and warfarin for stroke prevention in atrial fibrillation. Stroke 2013;44:1676–81.
81. Amin A, Lingohr-Smith M, Bruno A, et al. Economic evaluations of medical cost differences: use of targeted-specific oral anticoagulants vs. warfarin among patients with nonvalvular atrial fibrillation and venous thromboembolism in the US. J Hematol Thrombo Dis 2015;3:209.
82. Lexicomp, Lexi-Drugs. Hudson, OH: Lexi-Comp.
83. U.S. Food and Drug Administration, Center for Drug Evaluation and Research. Apixaban NDA 202155/S-002 approval letter. Jan 30 2014. Available at http://www.accessdata.fda.gov/drugsatfda_docs/appletter/2014/202155Orig1s002ltr.pdf
84. Hinojar R, Jimenez-Natcher JJ, Fernandez-Golfin C, Zamorano JL. New oral anticoagulants: a practical guide for physicians. Eur Heart J Cardiovasc Pharmacother 2015;1:134-45.
85. Connolly SJ, Eikelboom J, Joyner C, et al. Apixaban in patiets with atrial fibrillation. N Engl J Med 2011;364;806–17.
More Than Skin Deep
1. About a year ago, this 40-year-old man developed scaling on the distal one-third of his thumbnail. The condition began to worsen, leaving most of his thumb covered by thick adherent white scales on a pinkish base with sharply defined margins. The adjacent thumbnail has focal areas of pitting in the nail plate, as well as yellowish discoloration on the distal edge.

Diagnosis: The most likely diagnosis is psoriasis, which can manifest with localized involvement.
For more information, see “Thumb: Scaling with Pitted Nail Plate.” Clin Rev. 2013 March;23(3):11.
For the next photograph, proceed to the next page >>
2. A 10-year-old girl has had patches of dry skin appearing and disappearing on her arms, legs, and neck for years. Recently manifested on her extensor forearm is an annular, distinctly salmon-pink plaque with a tenacious white scale. Scaly areas are observed in both postauricular sulci; several tiny pits are seen on her fingernails.

Diagnosis: It would be difficult to imagine a more clear-cut case of psoriasis, not only manifesting with a classic plaque on the extensor forearm but also with corroboratory stigmata behind the ears and classic fingernail pits.
It’s helpful to know that psoriasis affects almost 3% of the white population in the United States, meaning that you will see it with considerable frequency. It would also help if you knew the diagnosis can be corroborated by identification of other, lesser known features.
For more information, see “Girl, 10, Asks Tough Questions About Skin Problem.” Clin Rev. 2015;25(8):W2.
For the next photograph, proceed to the next page >>
3. A 62-year-old woman complained bitterly of itching on the soles of both feet. Both insteps are covered with discrete, confluent papules and tiny pustules on an erythematous and hyperpigmented (brown), sharply demarcated, and highly symmetrical base. No such lesions appear elsewhere.

Diagnosis: Palmoplantar pustulosis is the term most often used to describe a fairly common form of psoriasis typified by this case. Many patients are genetically predisposed to psoriasis, but they may require a trigger to set it off, such as strep infection or occasionally, medication. Notable among the latter are the b-blockers and lithium. Stress is often involved as well.
The bilateral symmetrical involvement of both insteps is highly suggestive of this diagnosis, which often also affects either peripheral or central palms. A secondary form of neurodermatitis (itch–scratch–itch cycle) can follow, complicating the picture and perpetuating the problem.
For more information, see “Pruritic Rash on Both Soles.” Clin Rev. 2012 Jan;22(1).
For the next photograph, proceed to the next page >>
4. The patient presented with fiery red, burned looking skin covering ≥90% of the skin surface and shedding in large "sheets" instead of smaller scales. He was monitored for fever, systemic symptoms, and multiorgan dysfunction.

Photo courtesy of Peter A. Lio, MD, and Alisa McQueen, MD
Diagnosis: This patient was given a diagnosis of erythrodermic psoriasis. This form of psoriasis can be life-threatening.
For more information, see “Derm emergencies— detecting early signs of trouble.” J Fam Pract. 2012 February;61(2):71-78.
For the next photograph, proceed to the next page >>
5. This 18-year-old patient had multiple, erythematous papules and plaques with a fine scale over her face, neck, trunk, and lower legs. She noted that the eruption had developed after a sore throat 2 weeks earlier and that it was itchy.

Photos courtesy of David A. Boyd, MD
Diagnosis: Guttate psoriasis was diagnosed in this patient based on her history and physical exam, a throat culture that was positive for group A beta-hemolytic streptococci, and blood work that showed an elevated antistreptolysin O titer. Further confirmation was obtained via punch biopsy.
Guttate psoriasis is a fairly uncommon form of psoriasis, affecting approximately 2% of patients with psoriasis.1 It is characterized by the abrupt onset of pruritic, salmon-pink 1- to 10-mm droplike lesions with fine scale that may spread to the face, but spare the palms and soles. It’s uncommon for this sub-type of psoriasis to involve the nails.
Guttate psoriasis affects individuals younger than 30; there appears to be no gender predilection.2 The rash usually appears 2 to 3 weeks after an upper respiratory group A beta-hemolytic streptococci infection. Although less common, there have also been reports of guttate psoriasis associated with perianal streptococcal disease.2
1. Habif TP. Clinical Dermatology. 4th ed. St. Louis, Mo: Mosby; 2004;209-239
2. Honig PJ. Guttate psoriasis associated with perianal streptococcal disease. J Pediatr. 1988;113:1037-1039.
For more information, see “Teen with a diffuse erythematous, pruritic eruption.” J Fam Pract. 2011 January;60(1):37-39.
1. About a year ago, this 40-year-old man developed scaling on the distal one-third of his thumbnail. The condition began to worsen, leaving most of his thumb covered by thick adherent white scales on a pinkish base with sharply defined margins. The adjacent thumbnail has focal areas of pitting in the nail plate, as well as yellowish discoloration on the distal edge.
Diagnosis: The most likely diagnosis is psoriasis, which can manifest with localized involvement.
For more information, see “Thumb: Scaling with Pitted Nail Plate.” Clin Rev. 2013 March;23(3):11.
For the next photograph, proceed to the next page >>
2. A 10-year-old girl has had patches of dry skin appearing and disappearing on her arms, legs, and neck for years. Recently manifested on her extensor forearm is an annular, distinctly salmon-pink plaque with a tenacious white scale. Scaly areas are observed in both postauricular sulci; several tiny pits are seen on her fingernails.
Diagnosis: It would be difficult to imagine a more clear-cut case of psoriasis, not only manifesting with a classic plaque on the extensor forearm but also with corroboratory stigmata behind the ears and classic fingernail pits.
It’s helpful to know that psoriasis affects almost 3% of the white population in the United States, meaning that you will see it with considerable frequency. It would also help if you knew the diagnosis can be corroborated by identification of other, lesser known features.
For more information, see “Girl, 10, Asks Tough Questions About Skin Problem.” Clin Rev. 2015;25(8):W2.
For the next photograph, proceed to the next page >>
3. A 62-year-old woman complained bitterly of itching on the soles of both feet. Both insteps are covered with discrete, confluent papules and tiny pustules on an erythematous and hyperpigmented (brown), sharply demarcated, and highly symmetrical base. No such lesions appear elsewhere.
Diagnosis: Palmoplantar pustulosis is the term most often used to describe a fairly common form of psoriasis typified by this case. Many patients are genetically predisposed to psoriasis, but they may require a trigger to set it off, such as strep infection or occasionally, medication. Notable among the latter are the b-blockers and lithium. Stress is often involved as well.
The bilateral symmetrical involvement of both insteps is highly suggestive of this diagnosis, which often also affects either peripheral or central palms. A secondary form of neurodermatitis (itch–scratch–itch cycle) can follow, complicating the picture and perpetuating the problem.
For more information, see “Pruritic Rash on Both Soles.” Clin Rev. 2012 Jan;22(1).
For the next photograph, proceed to the next page >>
4. The patient presented with fiery red, burned looking skin covering ≥90% of the skin surface and shedding in large "sheets" instead of smaller scales. He was monitored for fever, systemic symptoms, and multiorgan dysfunction.
Photo courtesy of Peter A. Lio, MD, and Alisa McQueen, MD
Diagnosis: This patient was given a diagnosis of erythrodermic psoriasis. This form of psoriasis can be life-threatening.
For more information, see “Derm emergencies— detecting early signs of trouble.” J Fam Pract. 2012 February;61(2):71-78.
For the next photograph, proceed to the next page >>
5. This 18-year-old patient had multiple, erythematous papules and plaques with a fine scale over her face, neck, trunk, and lower legs. She noted that the eruption had developed after a sore throat 2 weeks earlier and that it was itchy.
Photos courtesy of David A. Boyd, MD
Diagnosis: Guttate psoriasis was diagnosed in this patient based on her history and physical exam, a throat culture that was positive for group A beta-hemolytic streptococci, and blood work that showed an elevated antistreptolysin O titer. Further confirmation was obtained via punch biopsy.
Guttate psoriasis is a fairly uncommon form of psoriasis, affecting approximately 2% of patients with psoriasis.1 It is characterized by the abrupt onset of pruritic, salmon-pink 1- to 10-mm droplike lesions with fine scale that may spread to the face, but spare the palms and soles. It’s uncommon for this sub-type of psoriasis to involve the nails.
Guttate psoriasis affects individuals younger than 30; there appears to be no gender predilection.2 The rash usually appears 2 to 3 weeks after an upper respiratory group A beta-hemolytic streptococci infection. Although less common, there have also been reports of guttate psoriasis associated with perianal streptococcal disease.2
1. Habif TP. Clinical Dermatology. 4th ed. St. Louis, Mo: Mosby; 2004;209-239
2. Honig PJ. Guttate psoriasis associated with perianal streptococcal disease. J Pediatr. 1988;113:1037-1039.
For more information, see “Teen with a diffuse erythematous, pruritic eruption.” J Fam Pract. 2011 January;60(1):37-39.
1. About a year ago, this 40-year-old man developed scaling on the distal one-third of his thumbnail. The condition began to worsen, leaving most of his thumb covered by thick adherent white scales on a pinkish base with sharply defined margins. The adjacent thumbnail has focal areas of pitting in the nail plate, as well as yellowish discoloration on the distal edge.
Diagnosis: The most likely diagnosis is psoriasis, which can manifest with localized involvement.
For more information, see “Thumb: Scaling with Pitted Nail Plate.” Clin Rev. 2013 March;23(3):11.
For the next photograph, proceed to the next page >>
2. A 10-year-old girl has had patches of dry skin appearing and disappearing on her arms, legs, and neck for years. Recently manifested on her extensor forearm is an annular, distinctly salmon-pink plaque with a tenacious white scale. Scaly areas are observed in both postauricular sulci; several tiny pits are seen on her fingernails.
Diagnosis: It would be difficult to imagine a more clear-cut case of psoriasis, not only manifesting with a classic plaque on the extensor forearm but also with corroboratory stigmata behind the ears and classic fingernail pits.
It’s helpful to know that psoriasis affects almost 3% of the white population in the United States, meaning that you will see it with considerable frequency. It would also help if you knew the diagnosis can be corroborated by identification of other, lesser known features.
For more information, see “Girl, 10, Asks Tough Questions About Skin Problem.” Clin Rev. 2015;25(8):W2.
For the next photograph, proceed to the next page >>
3. A 62-year-old woman complained bitterly of itching on the soles of both feet. Both insteps are covered with discrete, confluent papules and tiny pustules on an erythematous and hyperpigmented (brown), sharply demarcated, and highly symmetrical base. No such lesions appear elsewhere.
Diagnosis: Palmoplantar pustulosis is the term most often used to describe a fairly common form of psoriasis typified by this case. Many patients are genetically predisposed to psoriasis, but they may require a trigger to set it off, such as strep infection or occasionally, medication. Notable among the latter are the b-blockers and lithium. Stress is often involved as well.
The bilateral symmetrical involvement of both insteps is highly suggestive of this diagnosis, which often also affects either peripheral or central palms. A secondary form of neurodermatitis (itch–scratch–itch cycle) can follow, complicating the picture and perpetuating the problem.
For more information, see “Pruritic Rash on Both Soles.” Clin Rev. 2012 Jan;22(1).
For the next photograph, proceed to the next page >>
4. The patient presented with fiery red, burned looking skin covering ≥90% of the skin surface and shedding in large "sheets" instead of smaller scales. He was monitored for fever, systemic symptoms, and multiorgan dysfunction.
Photo courtesy of Peter A. Lio, MD, and Alisa McQueen, MD
Diagnosis: This patient was given a diagnosis of erythrodermic psoriasis. This form of psoriasis can be life-threatening.
For more information, see “Derm emergencies— detecting early signs of trouble.” J Fam Pract. 2012 February;61(2):71-78.
For the next photograph, proceed to the next page >>
5. This 18-year-old patient had multiple, erythematous papules and plaques with a fine scale over her face, neck, trunk, and lower legs. She noted that the eruption had developed after a sore throat 2 weeks earlier and that it was itchy.
Photos courtesy of David A. Boyd, MD
Diagnosis: Guttate psoriasis was diagnosed in this patient based on her history and physical exam, a throat culture that was positive for group A beta-hemolytic streptococci, and blood work that showed an elevated antistreptolysin O titer. Further confirmation was obtained via punch biopsy.
Guttate psoriasis is a fairly uncommon form of psoriasis, affecting approximately 2% of patients with psoriasis.1 It is characterized by the abrupt onset of pruritic, salmon-pink 1- to 10-mm droplike lesions with fine scale that may spread to the face, but spare the palms and soles. It’s uncommon for this sub-type of psoriasis to involve the nails.
Guttate psoriasis affects individuals younger than 30; there appears to be no gender predilection.2 The rash usually appears 2 to 3 weeks after an upper respiratory group A beta-hemolytic streptococci infection. Although less common, there have also been reports of guttate psoriasis associated with perianal streptococcal disease.2
1. Habif TP. Clinical Dermatology. 4th ed. St. Louis, Mo: Mosby; 2004;209-239
2. Honig PJ. Guttate psoriasis associated with perianal streptococcal disease. J Pediatr. 1988;113:1037-1039.
For more information, see “Teen with a diffuse erythematous, pruritic eruption.” J Fam Pract. 2011 January;60(1):37-39.