User login
New COVID strain may evade vaccines, alarming health officials
The strain is called BA.2.86 and is of particular concern because of its more than 30 mutations, which means it may behave very differently than previous versions of the virus. That number of mutations is on par with the difference between variants so serious that they were formally named, such as between Delta and Omicron, the CDC explained in the risk assessment issued Aug. 23.
Worldwide, health agencies are issuing a flurry of updates on BA.2.86. The strain only recently landed on the World Health Organization’s radar when it was named a “variant under monitoring” on Aug. 17. The CDC announced the same day that it had been detected in the United States.
Among the characteristics the CDC monitors for are how contagious a strain is, how well it responds to treatment, and how severely it affects people.
“BA.2.86 may be more capable of causing infection in people who have previously had COVID-19 or who have received COVID-19 vaccines,” the CDC risk assessment stated.
The agency is evaluating how well the forthcoming updated vaccine, due out in September, performs against BA.2.86.
A new forecast also released this week by the CDC predicts hospitalizations due to the virus will continue their upward trend through at least mid-September. Currently, about 1,800 people are hospitalized daily with COVID-19. The new prediction shows that number has a small potential to drop as low as 1,100 daily, but it could also increase by as many as 7,500 per day. The most likely scenario lands somewhere in the middle of that range, with daily hospital admissions of between 2,000 and 4,000 people by Sept. 18.
The CDC said there is “no evidence” that BA.2.86 is causing more severe illness but said that could change as more information becomes available. Health experts typically gauge severity by the rate of COVID hospitalizations.
The journal Nature reported that many scientists see similarities between the emergence of BA.2.86 and that of Omicron, which rapidly spread around the world in late 2021.
“There’s a little bit of déjà vu all over again,” University of Michigan virologist Adam Lauring, MD, PhD, whose lab detected one of the first U.S. cases of BA.2.86, told Nature.
Dr. Lauring, as well as the CDC and the WHO, all caution that more data is needed to truly understand the threat posed by BA.2.86.
“There’s good reason to think it won’t be like the Omicron wave, but it’s early days,” Dr. Lauring said.
A version of this article first appeared on Medscape.com.
The strain is called BA.2.86 and is of particular concern because of its more than 30 mutations, which means it may behave very differently than previous versions of the virus. That number of mutations is on par with the difference between variants so serious that they were formally named, such as between Delta and Omicron, the CDC explained in the risk assessment issued Aug. 23.
Worldwide, health agencies are issuing a flurry of updates on BA.2.86. The strain only recently landed on the World Health Organization’s radar when it was named a “variant under monitoring” on Aug. 17. The CDC announced the same day that it had been detected in the United States.
Among the characteristics the CDC monitors for are how contagious a strain is, how well it responds to treatment, and how severely it affects people.
“BA.2.86 may be more capable of causing infection in people who have previously had COVID-19 or who have received COVID-19 vaccines,” the CDC risk assessment stated.
The agency is evaluating how well the forthcoming updated vaccine, due out in September, performs against BA.2.86.
A new forecast also released this week by the CDC predicts hospitalizations due to the virus will continue their upward trend through at least mid-September. Currently, about 1,800 people are hospitalized daily with COVID-19. The new prediction shows that number has a small potential to drop as low as 1,100 daily, but it could also increase by as many as 7,500 per day. The most likely scenario lands somewhere in the middle of that range, with daily hospital admissions of between 2,000 and 4,000 people by Sept. 18.
The CDC said there is “no evidence” that BA.2.86 is causing more severe illness but said that could change as more information becomes available. Health experts typically gauge severity by the rate of COVID hospitalizations.
The journal Nature reported that many scientists see similarities between the emergence of BA.2.86 and that of Omicron, which rapidly spread around the world in late 2021.
“There’s a little bit of déjà vu all over again,” University of Michigan virologist Adam Lauring, MD, PhD, whose lab detected one of the first U.S. cases of BA.2.86, told Nature.
Dr. Lauring, as well as the CDC and the WHO, all caution that more data is needed to truly understand the threat posed by BA.2.86.
“There’s good reason to think it won’t be like the Omicron wave, but it’s early days,” Dr. Lauring said.
A version of this article first appeared on Medscape.com.
The strain is called BA.2.86 and is of particular concern because of its more than 30 mutations, which means it may behave very differently than previous versions of the virus. That number of mutations is on par with the difference between variants so serious that they were formally named, such as between Delta and Omicron, the CDC explained in the risk assessment issued Aug. 23.
Worldwide, health agencies are issuing a flurry of updates on BA.2.86. The strain only recently landed on the World Health Organization’s radar when it was named a “variant under monitoring” on Aug. 17. The CDC announced the same day that it had been detected in the United States.
Among the characteristics the CDC monitors for are how contagious a strain is, how well it responds to treatment, and how severely it affects people.
“BA.2.86 may be more capable of causing infection in people who have previously had COVID-19 or who have received COVID-19 vaccines,” the CDC risk assessment stated.
The agency is evaluating how well the forthcoming updated vaccine, due out in September, performs against BA.2.86.
A new forecast also released this week by the CDC predicts hospitalizations due to the virus will continue their upward trend through at least mid-September. Currently, about 1,800 people are hospitalized daily with COVID-19. The new prediction shows that number has a small potential to drop as low as 1,100 daily, but it could also increase by as many as 7,500 per day. The most likely scenario lands somewhere in the middle of that range, with daily hospital admissions of between 2,000 and 4,000 people by Sept. 18.
The CDC said there is “no evidence” that BA.2.86 is causing more severe illness but said that could change as more information becomes available. Health experts typically gauge severity by the rate of COVID hospitalizations.
The journal Nature reported that many scientists see similarities between the emergence of BA.2.86 and that of Omicron, which rapidly spread around the world in late 2021.
“There’s a little bit of déjà vu all over again,” University of Michigan virologist Adam Lauring, MD, PhD, whose lab detected one of the first U.S. cases of BA.2.86, told Nature.
Dr. Lauring, as well as the CDC and the WHO, all caution that more data is needed to truly understand the threat posed by BA.2.86.
“There’s good reason to think it won’t be like the Omicron wave, but it’s early days,” Dr. Lauring said.
A version of this article first appeared on Medscape.com.
Breast cancer: Hope in sight for improved tamoxifen therapy?
A team at Lyon’s Cancer Research Center (CRCL) has revealed the role of an enzyme, PRMT5, in the response to tamoxifen, a drug used to prevent relapse in premenopausal women with breast cancer.
Muriel Le Romancer, MD, director of research at France’s Institute of Health and Medical Research, explained the issues involved in this discovery in an interview. She jointly led this research along with Olivier Trédan, MD, PhD, oncologist at Lyon’s Léon Bérard Clinic. The research concluded with the publication of a study in EMBO Molecular Medicine. The researchers both head up the CRCL’s hormone resistance, methylation, and breast cancer team.
Although the enzyme’s involvement in the mode of action of tamoxifen has been observed in close to 900 patients with breast cancer, these results need to be validated in other at-risk patient cohorts before the biomarker can be considered for routine use, said Dr. Le Romancer. She estimated that 2 more years of research are needed.
Can you tell us which cases involve the use of tamoxifen and what its mode of action is?
Dr. Le Romancer: Tamoxifen is a hormone therapy used to reduce the risk of breast cancer relapse. It is prescribed to premenopausal women with hormone-sensitive cancer, which equates to roughly 25% of women with breast cancer: 15,000 women each year. The drug, which is taken every day via oral administration, is an estrogen antagonist. By binding to these receptors, it blocks estrogen from mediating its biological effect in the breasts. Aromatase inhibitors are the preferred choice in postmenopausal women, as they have been shown to be more effective. These also have an antiestrogenic effect, but by inhibiting estrogen production.
Tamoxifen therapy is prescribed for a minimum period of 5 years. Despite this, 25% of women treated with tamoxifen relapse. Tamoxifen resistance is unique in that it occurs very late on, generally 10-15 years after starting treatment. This means that it’s really important for us to identify predictive markers of the response to hormone therapy to adapt treatment as best we can. For the moment, the only criteria used to prescribe tamoxifen are patient age and the presence of estrogen receptors within the tumor.
Exactly how would treatment be improved if a decisive predictive marker of response to tamoxifen could be identified?
Dr. Le Romancer: Currently, when a patient’s breast cancer relapses after several years of treatment with tamoxifen, we don’t know if the relapse is linked to tamoxifen resistance or not. This makes it difficult to choose the right treatment to manage such relapses, which remain complicated to treat. Lots of patients die because of metastases.
By predicting the response to tamoxifen using a marker, we will be able to either use another hormone therapy to prevent the relapse or prescribe tamoxifen alongside a molecule that stops resistance from developing. We hope that this will significantly reduce the rate of relapse.
You put forward PRMT5 as a potential predictive marker of response to tamoxifen. What makes you think it could be used in this way?
Dr. Le Romancer: Our research has allowed us to demonstrate that PRMT5, when present in the nuclei of tumor cells, is involved in the mechanisms of action of tamoxifen. Remember that estrogen receptors are located in cell nuclei. For tamoxifen to exert its antitumoral action, PRMT5, an enzyme, needs to enter the nucleus to modify the estrogen receptor. It’s this modification that allows tamoxifen to inhibit tumor growth. The proliferative effect induced by the estrogens is also blocked.
The results of our study showed that high nuclear expression of PRMT5, specifically in the nuclei of breast cancer cells, is associated with a prolonged survival of tamoxifen-treated patients. Until now, we thought this enzyme had an oncogenic role when present in the cytoplasm. It turns out that it also has the opposite effect when acting within the nucleus, at least in this patient cohort: women with hormone-sensitive breast cancer treated with tamoxifen.
What are the next steps in your research before we can begin to think about its use in clinical practice?
Dr. Le Romancer: Our next research will focus on understanding the circumstances surrounding PRMT5 entering and leaving the nucleus. We have also shown that in some patients, tamoxifen causes PRMT5 to enter the cell nucleus. This translocation is only seen in women who respond to tamoxifen, not in those who are resistant to treatment with the drug. All that remains is for us to work out how tamoxifen facilitates this translocation.
Once the elements promoting this translocation have been identified, we will be able to propose a treatment aimed at forcing the enzyme to enter the nucleus and stay there. Eventually, the idea is to combine treatment with antiestrogens with a medicinal product that promotes localization of PRMT5 in the nucleus to guarantee response to tamoxifen. It will be a few years of research before we can apply our findings to clinical practice.
Could we use this biomarker as is just to identify tamoxifen resistance?
Dr. Le Romancer: In the short term, yes, we could use this biomarker to better guide treatment choices at time of diagnosis. We have demonstrated the role of PRMT5 in response to tamoxifen by studying two cohorts of 900 patients with breast cancer receiving treatment at the Léon Bérard Center, Lyon. Before moving on to routine testing, we need to replicate these results in other cohorts, especially in high-risk patients with, for example, greater cell proliferation or those who experience relapse.
The use of this biomarker is based on histological examination of cancer tissue. Single antibody tissue staining targeting PRMT5 reveals the localization of the enzyme in the cells and provides a score evaluating its presence in the nucleus. Using this score, it would be possible to determine the level of response to tamoxifen and decide whether the treatment should be used. This biomarker is the first of its kind undergoing validation as part of the examination of resistance to hormone therapy. We should be able to confirm the findings within the next 2 years.
If clinical tests using this biomarker predict tamoxifen resistance, what alternative treatments are available to these patients?
Dr. Le Romancer: We could give them an aromatase inhibitor or one of the new estrogen antagonists that are currently in development. In a phase 3 study, fulvestrant (Faslodex), for example, demonstrated a significant benefit in treating women with hormone-sensitive advanced breast cancer when administered via injection. The same goes for oral treatment, elacestrant (Orserdu), which has recently been approved by the Food and Drug Administration. These treatments are usually deemed second line after tamoxifen, but they could certainly be used as first-line therapy in resistant patients.
The results obtained from research into novel estrogen antagonists are certainly encouraging. Can tamoxifen retain its prominent position while still ensuring its efficacy?
Dr. Le Romancer: Keeping in mind the current trend for personalized medicine, we should keep as many treatment options open as possible. When a patient relapses, there need to be other treatments available to them. Tamoxifen has been ousted in favor of aromatase inhibitors for postmenopausal women, but it’s still the gold standard for premenopausal women and has been for over 20 years. Despite having been replaced by a novel estrogen antagonist, it will still have a prominent place in the therapeutic arsenal of premenopausal women with breast cancer.
With the development of PRMT5 as a predictive biomarker, we could even see tamoxifen being proposed as first-line therapy for postmenopausal women in whom high levels of PRMT5 are found in the nuclei of their cancer cells. By predicting their response, we could achieve greater efficacy of tamoxifen, compared with aromatase inhibitors. For now, this remains a hypothesis and must be verified in further clinical studies.
This article was translated from the Medscape French Edition. A version appeared on Medscape.com.
A team at Lyon’s Cancer Research Center (CRCL) has revealed the role of an enzyme, PRMT5, in the response to tamoxifen, a drug used to prevent relapse in premenopausal women with breast cancer.
Muriel Le Romancer, MD, director of research at France’s Institute of Health and Medical Research, explained the issues involved in this discovery in an interview. She jointly led this research along with Olivier Trédan, MD, PhD, oncologist at Lyon’s Léon Bérard Clinic. The research concluded with the publication of a study in EMBO Molecular Medicine. The researchers both head up the CRCL’s hormone resistance, methylation, and breast cancer team.
Although the enzyme’s involvement in the mode of action of tamoxifen has been observed in close to 900 patients with breast cancer, these results need to be validated in other at-risk patient cohorts before the biomarker can be considered for routine use, said Dr. Le Romancer. She estimated that 2 more years of research are needed.
Can you tell us which cases involve the use of tamoxifen and what its mode of action is?
Dr. Le Romancer: Tamoxifen is a hormone therapy used to reduce the risk of breast cancer relapse. It is prescribed to premenopausal women with hormone-sensitive cancer, which equates to roughly 25% of women with breast cancer: 15,000 women each year. The drug, which is taken every day via oral administration, is an estrogen antagonist. By binding to these receptors, it blocks estrogen from mediating its biological effect in the breasts. Aromatase inhibitors are the preferred choice in postmenopausal women, as they have been shown to be more effective. These also have an antiestrogenic effect, but by inhibiting estrogen production.
Tamoxifen therapy is prescribed for a minimum period of 5 years. Despite this, 25% of women treated with tamoxifen relapse. Tamoxifen resistance is unique in that it occurs very late on, generally 10-15 years after starting treatment. This means that it’s really important for us to identify predictive markers of the response to hormone therapy to adapt treatment as best we can. For the moment, the only criteria used to prescribe tamoxifen are patient age and the presence of estrogen receptors within the tumor.
Exactly how would treatment be improved if a decisive predictive marker of response to tamoxifen could be identified?
Dr. Le Romancer: Currently, when a patient’s breast cancer relapses after several years of treatment with tamoxifen, we don’t know if the relapse is linked to tamoxifen resistance or not. This makes it difficult to choose the right treatment to manage such relapses, which remain complicated to treat. Lots of patients die because of metastases.
By predicting the response to tamoxifen using a marker, we will be able to either use another hormone therapy to prevent the relapse or prescribe tamoxifen alongside a molecule that stops resistance from developing. We hope that this will significantly reduce the rate of relapse.
You put forward PRMT5 as a potential predictive marker of response to tamoxifen. What makes you think it could be used in this way?
Dr. Le Romancer: Our research has allowed us to demonstrate that PRMT5, when present in the nuclei of tumor cells, is involved in the mechanisms of action of tamoxifen. Remember that estrogen receptors are located in cell nuclei. For tamoxifen to exert its antitumoral action, PRMT5, an enzyme, needs to enter the nucleus to modify the estrogen receptor. It’s this modification that allows tamoxifen to inhibit tumor growth. The proliferative effect induced by the estrogens is also blocked.
The results of our study showed that high nuclear expression of PRMT5, specifically in the nuclei of breast cancer cells, is associated with a prolonged survival of tamoxifen-treated patients. Until now, we thought this enzyme had an oncogenic role when present in the cytoplasm. It turns out that it also has the opposite effect when acting within the nucleus, at least in this patient cohort: women with hormone-sensitive breast cancer treated with tamoxifen.
What are the next steps in your research before we can begin to think about its use in clinical practice?
Dr. Le Romancer: Our next research will focus on understanding the circumstances surrounding PRMT5 entering and leaving the nucleus. We have also shown that in some patients, tamoxifen causes PRMT5 to enter the cell nucleus. This translocation is only seen in women who respond to tamoxifen, not in those who are resistant to treatment with the drug. All that remains is for us to work out how tamoxifen facilitates this translocation.
Once the elements promoting this translocation have been identified, we will be able to propose a treatment aimed at forcing the enzyme to enter the nucleus and stay there. Eventually, the idea is to combine treatment with antiestrogens with a medicinal product that promotes localization of PRMT5 in the nucleus to guarantee response to tamoxifen. It will be a few years of research before we can apply our findings to clinical practice.
Could we use this biomarker as is just to identify tamoxifen resistance?
Dr. Le Romancer: In the short term, yes, we could use this biomarker to better guide treatment choices at time of diagnosis. We have demonstrated the role of PRMT5 in response to tamoxifen by studying two cohorts of 900 patients with breast cancer receiving treatment at the Léon Bérard Center, Lyon. Before moving on to routine testing, we need to replicate these results in other cohorts, especially in high-risk patients with, for example, greater cell proliferation or those who experience relapse.
The use of this biomarker is based on histological examination of cancer tissue. Single antibody tissue staining targeting PRMT5 reveals the localization of the enzyme in the cells and provides a score evaluating its presence in the nucleus. Using this score, it would be possible to determine the level of response to tamoxifen and decide whether the treatment should be used. This biomarker is the first of its kind undergoing validation as part of the examination of resistance to hormone therapy. We should be able to confirm the findings within the next 2 years.
If clinical tests using this biomarker predict tamoxifen resistance, what alternative treatments are available to these patients?
Dr. Le Romancer: We could give them an aromatase inhibitor or one of the new estrogen antagonists that are currently in development. In a phase 3 study, fulvestrant (Faslodex), for example, demonstrated a significant benefit in treating women with hormone-sensitive advanced breast cancer when administered via injection. The same goes for oral treatment, elacestrant (Orserdu), which has recently been approved by the Food and Drug Administration. These treatments are usually deemed second line after tamoxifen, but they could certainly be used as first-line therapy in resistant patients.
The results obtained from research into novel estrogen antagonists are certainly encouraging. Can tamoxifen retain its prominent position while still ensuring its efficacy?
Dr. Le Romancer: Keeping in mind the current trend for personalized medicine, we should keep as many treatment options open as possible. When a patient relapses, there need to be other treatments available to them. Tamoxifen has been ousted in favor of aromatase inhibitors for postmenopausal women, but it’s still the gold standard for premenopausal women and has been for over 20 years. Despite having been replaced by a novel estrogen antagonist, it will still have a prominent place in the therapeutic arsenal of premenopausal women with breast cancer.
With the development of PRMT5 as a predictive biomarker, we could even see tamoxifen being proposed as first-line therapy for postmenopausal women in whom high levels of PRMT5 are found in the nuclei of their cancer cells. By predicting their response, we could achieve greater efficacy of tamoxifen, compared with aromatase inhibitors. For now, this remains a hypothesis and must be verified in further clinical studies.
This article was translated from the Medscape French Edition. A version appeared on Medscape.com.
A team at Lyon’s Cancer Research Center (CRCL) has revealed the role of an enzyme, PRMT5, in the response to tamoxifen, a drug used to prevent relapse in premenopausal women with breast cancer.
Muriel Le Romancer, MD, director of research at France’s Institute of Health and Medical Research, explained the issues involved in this discovery in an interview. She jointly led this research along with Olivier Trédan, MD, PhD, oncologist at Lyon’s Léon Bérard Clinic. The research concluded with the publication of a study in EMBO Molecular Medicine. The researchers both head up the CRCL’s hormone resistance, methylation, and breast cancer team.
Although the enzyme’s involvement in the mode of action of tamoxifen has been observed in close to 900 patients with breast cancer, these results need to be validated in other at-risk patient cohorts before the biomarker can be considered for routine use, said Dr. Le Romancer. She estimated that 2 more years of research are needed.
Can you tell us which cases involve the use of tamoxifen and what its mode of action is?
Dr. Le Romancer: Tamoxifen is a hormone therapy used to reduce the risk of breast cancer relapse. It is prescribed to premenopausal women with hormone-sensitive cancer, which equates to roughly 25% of women with breast cancer: 15,000 women each year. The drug, which is taken every day via oral administration, is an estrogen antagonist. By binding to these receptors, it blocks estrogen from mediating its biological effect in the breasts. Aromatase inhibitors are the preferred choice in postmenopausal women, as they have been shown to be more effective. These also have an antiestrogenic effect, but by inhibiting estrogen production.
Tamoxifen therapy is prescribed for a minimum period of 5 years. Despite this, 25% of women treated with tamoxifen relapse. Tamoxifen resistance is unique in that it occurs very late on, generally 10-15 years after starting treatment. This means that it’s really important for us to identify predictive markers of the response to hormone therapy to adapt treatment as best we can. For the moment, the only criteria used to prescribe tamoxifen are patient age and the presence of estrogen receptors within the tumor.
Exactly how would treatment be improved if a decisive predictive marker of response to tamoxifen could be identified?
Dr. Le Romancer: Currently, when a patient’s breast cancer relapses after several years of treatment with tamoxifen, we don’t know if the relapse is linked to tamoxifen resistance or not. This makes it difficult to choose the right treatment to manage such relapses, which remain complicated to treat. Lots of patients die because of metastases.
By predicting the response to tamoxifen using a marker, we will be able to either use another hormone therapy to prevent the relapse or prescribe tamoxifen alongside a molecule that stops resistance from developing. We hope that this will significantly reduce the rate of relapse.
You put forward PRMT5 as a potential predictive marker of response to tamoxifen. What makes you think it could be used in this way?
Dr. Le Romancer: Our research has allowed us to demonstrate that PRMT5, when present in the nuclei of tumor cells, is involved in the mechanisms of action of tamoxifen. Remember that estrogen receptors are located in cell nuclei. For tamoxifen to exert its antitumoral action, PRMT5, an enzyme, needs to enter the nucleus to modify the estrogen receptor. It’s this modification that allows tamoxifen to inhibit tumor growth. The proliferative effect induced by the estrogens is also blocked.
The results of our study showed that high nuclear expression of PRMT5, specifically in the nuclei of breast cancer cells, is associated with a prolonged survival of tamoxifen-treated patients. Until now, we thought this enzyme had an oncogenic role when present in the cytoplasm. It turns out that it also has the opposite effect when acting within the nucleus, at least in this patient cohort: women with hormone-sensitive breast cancer treated with tamoxifen.
What are the next steps in your research before we can begin to think about its use in clinical practice?
Dr. Le Romancer: Our next research will focus on understanding the circumstances surrounding PRMT5 entering and leaving the nucleus. We have also shown that in some patients, tamoxifen causes PRMT5 to enter the cell nucleus. This translocation is only seen in women who respond to tamoxifen, not in those who are resistant to treatment with the drug. All that remains is for us to work out how tamoxifen facilitates this translocation.
Once the elements promoting this translocation have been identified, we will be able to propose a treatment aimed at forcing the enzyme to enter the nucleus and stay there. Eventually, the idea is to combine treatment with antiestrogens with a medicinal product that promotes localization of PRMT5 in the nucleus to guarantee response to tamoxifen. It will be a few years of research before we can apply our findings to clinical practice.
Could we use this biomarker as is just to identify tamoxifen resistance?
Dr. Le Romancer: In the short term, yes, we could use this biomarker to better guide treatment choices at time of diagnosis. We have demonstrated the role of PRMT5 in response to tamoxifen by studying two cohorts of 900 patients with breast cancer receiving treatment at the Léon Bérard Center, Lyon. Before moving on to routine testing, we need to replicate these results in other cohorts, especially in high-risk patients with, for example, greater cell proliferation or those who experience relapse.
The use of this biomarker is based on histological examination of cancer tissue. Single antibody tissue staining targeting PRMT5 reveals the localization of the enzyme in the cells and provides a score evaluating its presence in the nucleus. Using this score, it would be possible to determine the level of response to tamoxifen and decide whether the treatment should be used. This biomarker is the first of its kind undergoing validation as part of the examination of resistance to hormone therapy. We should be able to confirm the findings within the next 2 years.
If clinical tests using this biomarker predict tamoxifen resistance, what alternative treatments are available to these patients?
Dr. Le Romancer: We could give them an aromatase inhibitor or one of the new estrogen antagonists that are currently in development. In a phase 3 study, fulvestrant (Faslodex), for example, demonstrated a significant benefit in treating women with hormone-sensitive advanced breast cancer when administered via injection. The same goes for oral treatment, elacestrant (Orserdu), which has recently been approved by the Food and Drug Administration. These treatments are usually deemed second line after tamoxifen, but they could certainly be used as first-line therapy in resistant patients.
The results obtained from research into novel estrogen antagonists are certainly encouraging. Can tamoxifen retain its prominent position while still ensuring its efficacy?
Dr. Le Romancer: Keeping in mind the current trend for personalized medicine, we should keep as many treatment options open as possible. When a patient relapses, there need to be other treatments available to them. Tamoxifen has been ousted in favor of aromatase inhibitors for postmenopausal women, but it’s still the gold standard for premenopausal women and has been for over 20 years. Despite having been replaced by a novel estrogen antagonist, it will still have a prominent place in the therapeutic arsenal of premenopausal women with breast cancer.
With the development of PRMT5 as a predictive biomarker, we could even see tamoxifen being proposed as first-line therapy for postmenopausal women in whom high levels of PRMT5 are found in the nuclei of their cancer cells. By predicting their response, we could achieve greater efficacy of tamoxifen, compared with aromatase inhibitors. For now, this remains a hypothesis and must be verified in further clinical studies.
This article was translated from the Medscape French Edition. A version appeared on Medscape.com.
Poor sleep and chronic pain prove pesky bedfellows
Early in his career as a pain researcher, Daniel Whibley, PhD, was struck by an article that drew parallels between methods of torture and the experiences of patients with insomnia and chronic pain.
The author of that article, Nicole Tang, DPhil, observed that two methods used by torturers – pain infliction and sleep deprivation – harm people in ways that also are experienced by many patients with pain and sleep conditions.
Patients are “essentially living in this perpetually undesirable, at best, situation where both of these features are playing out in their lives,” said Dr. Whibley, a research assistant professor of physical medicine and rehabilitation at the University of Michigan, Ann Arbor.
The problems create a “kind of vicious circle,” he said. Pain disrupts sleep. Insufficient sleep worsens pain.
Studies have established important relationships between the conditions, but investigators are still trying to clarify the mechanisms that connect them and the best ways to intervene to improve patient outcomes.
To that end, Dr. Whibley has developed an intervention known as Move & Snooze to benefit patients with pain associated with osteoarthritis.
The program includes remote exercise coaching and an automated 6-week course of digital cognitive-behavioral therapy for insomnia (CBT-I).
He and his colleagues have tested the intervention in a feasibility study and are in the process of securing grant funding to test it in a large, nationwide trial.
Losing sleep for science
Michael Smith, PhD, is examining the sleep-pain connection from a different angle.
Dr. Smith, the director of the Behavioral Medicine Research Laboratory at Johns Hopkins University, Baltimore, is recruiting healthy adults to endure restless nights and painful stimuli.
His team is conducting a study known as Sleep-MOR that aims to reveal how different types of sleep disturbances influence pain and a person’s response to opioids.
Nearly three dozen participants have completed the study so far, Dr. Smith said, out of what he hopes will be 200 in all.
Participants are randomly assigned to sleep normally or to undergo an experimental condition that is designed to mimic the sleep disturbances of insomnia or obstructive sleep apnea (OSA).
In a “forced awakening” group, participants are awakened for 20-minute intervals every hour and for a full hour-long window during the night. In this condition, they could sleep for about four hours in all. Forced awakening is intended to represent insomnia
A “sleep fragmentation” group is meant to represent patients with OSA. About 30 times per hour, tones and tactile buzzers rouse sleeping participants without fully waking them up. Although the experiment involves brief arousals such as those experienced by patients with OSA, it does not capture another important feature of sleep apnea – the cessation of breathing, Dr. Smith noted.
The next day, researchers perform pain testing and brain imaging and see how opioid receptors respond to pain medication.
“Some of the forms of sleep loss that we are studying may actually alter the efficacy of the binding of those receptors, and that might then require you to have higher doses of an opioid to get the same effect,” Dr. Smith said. “That’s our hypothesis.”
If that bears out, disturbed sleep may play a role in the development of opioid use disorder and have implications for patients who receive opioids after surgery, he said.
In the lab, researchers examine pain thresholds using techniques such as thermal pain testing, in which a thermode attached to a participant’s arm heats up. The temperature “slowly goes up and the patient just says: ‘Ouch,’ when it first hurts. Then we have their pain threshold,” Dr. Smith said.
A bidirectional relationship
Epidemiologic studies have found that, if you follow women who do not have pain, those with complaints about sleep are more than twice as likely to develop fibromyalgia.
Dr. Smith’s group and others have shown that if you deprive a healthy person of sleep, they become more sensitive to pain.
Inflammation could be one possible reason for this effect. In one study, participants who experienced forced awakening experienced less slow-wave sleep, which was tied to more inflammation in the morning. Increased inflammation was linked to greater pain sensitivity.
“We are starting to piece together some of the pathways. That’s just one,” Dr. Smith said.
A recent study by researchers at Harvard University and elsewhere investigated how sleep disturbances affected three pain pathways. In that study, the results varied by sex. The data indicate that optimal treatment approaches might differ for men and women, the researchers said.
Waking up to the problem
Sleep problems can be neglected in medical school and in the clinic. “People just have other things to focus on that they clearly know what they can do about it,” Dr. Smith said.
But clinicians should not hesitate to screen for conditions such as insomnia or OSA and refer patients to a specialist. If a patient has had pain for 6 months and treatments are not working, the chance that they have a treatable sleep disorder “is very high, above 50%,” Dr. Smith said. Many could have more than one sleep disorder, he added.
Continuous positive airway pressure for OSA and CBT for insomnia can improve sleep. Dr. Smith said he expects these measures will improve overall pain management as well.
If treating a sleep disorder fails to help with pain, however, it may still help prevent other sleep-related problems, such as depression, poor glucose control, and heart disease. It also could improve patients’ ability to function day to day, he said.
Evidence on whether treating sleep problems reduces pain has so far been mixed.
“We’ve done some studies showing that if you have CBT-I and you have knee arthritis, improvements in the amount of time you spend awake at night translate into improvements in pain at 6 months. There is a signal there, but it’s not as strong as we would like,” he said. “It may be that it takes longer than anyone would like” to have an effect.
A structured intervention such as CBT-I is likely more beneficial than education about sleep hygiene alone in resolving sleep disturbances, Dr. Whibley said. CBT-I includes active components such as sleep restriction therapy and stimulus control therapy and is recommended by the American Academy of Sleep Medicine as the first-line treatment for chronic insomnia (J Clin Sleep Med. 2008 Oct 15;4[5]:487-504).
Patients should consider the role that sleep may play in their chronic pain condition, he said.
“An increasing number of researchers and clinicians are becoming more interested in this as a foundational pillar of health, alongside activity and diet,” Dr. Whibley said. “Sleep is recognized as just as important but doesn’t seem to get the airtime.”
Clinicians, he added, should regularly assess their patients’ sleep and know where to refer those whom they feel would benefit from more advanced management: “They [should] know that they have at least got it on their radar to check as one of the important pillars of health that you should be able to control.”
Sleep trials seeking pain patients
Researchers around the United States are conducting dozens of studies related to sleep and pain. The following trials are recruiting participants, according to ClinicalTrials.gov.
Sleep and Pain Interventions in Women With Fibromyalgia (SPIN-II). Investigators at the University of Missouri–Columbia are examining two cognitive-behavioral treatments for women with fibromyalgia and insomnia. “This trial will yield important information about the roles of sleep, arousal, and brain structure and function in the development and maintenance of chronic pain in women with fibromyalgia,” the researchers say.
Prospective Randomized Trial of CPAP for SDB in Patients Who Use Opioids (PRESTO). At the University of California, San Diego, researchers are investigating whether patients with chronic pain who use opioids and have sleep-disordered breathing may benefit from treatment with continuous positive airway pressure. They plan to assess the intervention’s effects on sleep quality, pain, and quality of life. They also will see which patients are least likely to benefit from this treatment approach.
Latent Aging Mechanisms in Pain and Sleep (LAMPS). Researchers at the University of Florida are studying the effects of oral gamma-aminobutyric acid in older adults with chronic pain and sleep difficulties.
Sleep and Pain in Sickle Cell Disease. At Johns Hopkins University, investigators are evaluating how behavioral sleep interventions influence pain and brain function in patients with sickle cell disease.
Pain in Long COVID-19: The Role of Sleep. Researchers at Beth Israel Deaconess Medical Center are conducting an observational study of patients with long COVID who have pain and sleep disturbances. The study aims “to understand the role of sleep in the development and persistence of pain symptoms in long COVID.”
Intervention for Sleep and Pain in Youth: A Randomized Controlled Trial (I-SPY-RCT). Adolescents with migraine are being recruited by a team at Seattle Children’s Hospital for a randomized controlled trial. The study will examine the effects of CBT-I as well as the combined effect of CBT-I and pain interventions on reducing insomnia symptoms and headache-related disability in this population.
A version of this article appeared on Medscape.com.
Early in his career as a pain researcher, Daniel Whibley, PhD, was struck by an article that drew parallels between methods of torture and the experiences of patients with insomnia and chronic pain.
The author of that article, Nicole Tang, DPhil, observed that two methods used by torturers – pain infliction and sleep deprivation – harm people in ways that also are experienced by many patients with pain and sleep conditions.
Patients are “essentially living in this perpetually undesirable, at best, situation where both of these features are playing out in their lives,” said Dr. Whibley, a research assistant professor of physical medicine and rehabilitation at the University of Michigan, Ann Arbor.
The problems create a “kind of vicious circle,” he said. Pain disrupts sleep. Insufficient sleep worsens pain.
Studies have established important relationships between the conditions, but investigators are still trying to clarify the mechanisms that connect them and the best ways to intervene to improve patient outcomes.
To that end, Dr. Whibley has developed an intervention known as Move & Snooze to benefit patients with pain associated with osteoarthritis.
The program includes remote exercise coaching and an automated 6-week course of digital cognitive-behavioral therapy for insomnia (CBT-I).
He and his colleagues have tested the intervention in a feasibility study and are in the process of securing grant funding to test it in a large, nationwide trial.
Losing sleep for science
Michael Smith, PhD, is examining the sleep-pain connection from a different angle.
Dr. Smith, the director of the Behavioral Medicine Research Laboratory at Johns Hopkins University, Baltimore, is recruiting healthy adults to endure restless nights and painful stimuli.
His team is conducting a study known as Sleep-MOR that aims to reveal how different types of sleep disturbances influence pain and a person’s response to opioids.
Nearly three dozen participants have completed the study so far, Dr. Smith said, out of what he hopes will be 200 in all.
Participants are randomly assigned to sleep normally or to undergo an experimental condition that is designed to mimic the sleep disturbances of insomnia or obstructive sleep apnea (OSA).
In a “forced awakening” group, participants are awakened for 20-minute intervals every hour and for a full hour-long window during the night. In this condition, they could sleep for about four hours in all. Forced awakening is intended to represent insomnia
A “sleep fragmentation” group is meant to represent patients with OSA. About 30 times per hour, tones and tactile buzzers rouse sleeping participants without fully waking them up. Although the experiment involves brief arousals such as those experienced by patients with OSA, it does not capture another important feature of sleep apnea – the cessation of breathing, Dr. Smith noted.
The next day, researchers perform pain testing and brain imaging and see how opioid receptors respond to pain medication.
“Some of the forms of sleep loss that we are studying may actually alter the efficacy of the binding of those receptors, and that might then require you to have higher doses of an opioid to get the same effect,” Dr. Smith said. “That’s our hypothesis.”
If that bears out, disturbed sleep may play a role in the development of opioid use disorder and have implications for patients who receive opioids after surgery, he said.
In the lab, researchers examine pain thresholds using techniques such as thermal pain testing, in which a thermode attached to a participant’s arm heats up. The temperature “slowly goes up and the patient just says: ‘Ouch,’ when it first hurts. Then we have their pain threshold,” Dr. Smith said.
A bidirectional relationship
Epidemiologic studies have found that, if you follow women who do not have pain, those with complaints about sleep are more than twice as likely to develop fibromyalgia.
Dr. Smith’s group and others have shown that if you deprive a healthy person of sleep, they become more sensitive to pain.
Inflammation could be one possible reason for this effect. In one study, participants who experienced forced awakening experienced less slow-wave sleep, which was tied to more inflammation in the morning. Increased inflammation was linked to greater pain sensitivity.
“We are starting to piece together some of the pathways. That’s just one,” Dr. Smith said.
A recent study by researchers at Harvard University and elsewhere investigated how sleep disturbances affected three pain pathways. In that study, the results varied by sex. The data indicate that optimal treatment approaches might differ for men and women, the researchers said.
Waking up to the problem
Sleep problems can be neglected in medical school and in the clinic. “People just have other things to focus on that they clearly know what they can do about it,” Dr. Smith said.
But clinicians should not hesitate to screen for conditions such as insomnia or OSA and refer patients to a specialist. If a patient has had pain for 6 months and treatments are not working, the chance that they have a treatable sleep disorder “is very high, above 50%,” Dr. Smith said. Many could have more than one sleep disorder, he added.
Continuous positive airway pressure for OSA and CBT for insomnia can improve sleep. Dr. Smith said he expects these measures will improve overall pain management as well.
If treating a sleep disorder fails to help with pain, however, it may still help prevent other sleep-related problems, such as depression, poor glucose control, and heart disease. It also could improve patients’ ability to function day to day, he said.
Evidence on whether treating sleep problems reduces pain has so far been mixed.
“We’ve done some studies showing that if you have CBT-I and you have knee arthritis, improvements in the amount of time you spend awake at night translate into improvements in pain at 6 months. There is a signal there, but it’s not as strong as we would like,” he said. “It may be that it takes longer than anyone would like” to have an effect.
A structured intervention such as CBT-I is likely more beneficial than education about sleep hygiene alone in resolving sleep disturbances, Dr. Whibley said. CBT-I includes active components such as sleep restriction therapy and stimulus control therapy and is recommended by the American Academy of Sleep Medicine as the first-line treatment for chronic insomnia (J Clin Sleep Med. 2008 Oct 15;4[5]:487-504).
Patients should consider the role that sleep may play in their chronic pain condition, he said.
“An increasing number of researchers and clinicians are becoming more interested in this as a foundational pillar of health, alongside activity and diet,” Dr. Whibley said. “Sleep is recognized as just as important but doesn’t seem to get the airtime.”
Clinicians, he added, should regularly assess their patients’ sleep and know where to refer those whom they feel would benefit from more advanced management: “They [should] know that they have at least got it on their radar to check as one of the important pillars of health that you should be able to control.”
Sleep trials seeking pain patients
Researchers around the United States are conducting dozens of studies related to sleep and pain. The following trials are recruiting participants, according to ClinicalTrials.gov.
Sleep and Pain Interventions in Women With Fibromyalgia (SPIN-II). Investigators at the University of Missouri–Columbia are examining two cognitive-behavioral treatments for women with fibromyalgia and insomnia. “This trial will yield important information about the roles of sleep, arousal, and brain structure and function in the development and maintenance of chronic pain in women with fibromyalgia,” the researchers say.
Prospective Randomized Trial of CPAP for SDB in Patients Who Use Opioids (PRESTO). At the University of California, San Diego, researchers are investigating whether patients with chronic pain who use opioids and have sleep-disordered breathing may benefit from treatment with continuous positive airway pressure. They plan to assess the intervention’s effects on sleep quality, pain, and quality of life. They also will see which patients are least likely to benefit from this treatment approach.
Latent Aging Mechanisms in Pain and Sleep (LAMPS). Researchers at the University of Florida are studying the effects of oral gamma-aminobutyric acid in older adults with chronic pain and sleep difficulties.
Sleep and Pain in Sickle Cell Disease. At Johns Hopkins University, investigators are evaluating how behavioral sleep interventions influence pain and brain function in patients with sickle cell disease.
Pain in Long COVID-19: The Role of Sleep. Researchers at Beth Israel Deaconess Medical Center are conducting an observational study of patients with long COVID who have pain and sleep disturbances. The study aims “to understand the role of sleep in the development and persistence of pain symptoms in long COVID.”
Intervention for Sleep and Pain in Youth: A Randomized Controlled Trial (I-SPY-RCT). Adolescents with migraine are being recruited by a team at Seattle Children’s Hospital for a randomized controlled trial. The study will examine the effects of CBT-I as well as the combined effect of CBT-I and pain interventions on reducing insomnia symptoms and headache-related disability in this population.
A version of this article appeared on Medscape.com.
Early in his career as a pain researcher, Daniel Whibley, PhD, was struck by an article that drew parallels between methods of torture and the experiences of patients with insomnia and chronic pain.
The author of that article, Nicole Tang, DPhil, observed that two methods used by torturers – pain infliction and sleep deprivation – harm people in ways that also are experienced by many patients with pain and sleep conditions.
Patients are “essentially living in this perpetually undesirable, at best, situation where both of these features are playing out in their lives,” said Dr. Whibley, a research assistant professor of physical medicine and rehabilitation at the University of Michigan, Ann Arbor.
The problems create a “kind of vicious circle,” he said. Pain disrupts sleep. Insufficient sleep worsens pain.
Studies have established important relationships between the conditions, but investigators are still trying to clarify the mechanisms that connect them and the best ways to intervene to improve patient outcomes.
To that end, Dr. Whibley has developed an intervention known as Move & Snooze to benefit patients with pain associated with osteoarthritis.
The program includes remote exercise coaching and an automated 6-week course of digital cognitive-behavioral therapy for insomnia (CBT-I).
He and his colleagues have tested the intervention in a feasibility study and are in the process of securing grant funding to test it in a large, nationwide trial.
Losing sleep for science
Michael Smith, PhD, is examining the sleep-pain connection from a different angle.
Dr. Smith, the director of the Behavioral Medicine Research Laboratory at Johns Hopkins University, Baltimore, is recruiting healthy adults to endure restless nights and painful stimuli.
His team is conducting a study known as Sleep-MOR that aims to reveal how different types of sleep disturbances influence pain and a person’s response to opioids.
Nearly three dozen participants have completed the study so far, Dr. Smith said, out of what he hopes will be 200 in all.
Participants are randomly assigned to sleep normally or to undergo an experimental condition that is designed to mimic the sleep disturbances of insomnia or obstructive sleep apnea (OSA).
In a “forced awakening” group, participants are awakened for 20-minute intervals every hour and for a full hour-long window during the night. In this condition, they could sleep for about four hours in all. Forced awakening is intended to represent insomnia
A “sleep fragmentation” group is meant to represent patients with OSA. About 30 times per hour, tones and tactile buzzers rouse sleeping participants without fully waking them up. Although the experiment involves brief arousals such as those experienced by patients with OSA, it does not capture another important feature of sleep apnea – the cessation of breathing, Dr. Smith noted.
The next day, researchers perform pain testing and brain imaging and see how opioid receptors respond to pain medication.
“Some of the forms of sleep loss that we are studying may actually alter the efficacy of the binding of those receptors, and that might then require you to have higher doses of an opioid to get the same effect,” Dr. Smith said. “That’s our hypothesis.”
If that bears out, disturbed sleep may play a role in the development of opioid use disorder and have implications for patients who receive opioids after surgery, he said.
In the lab, researchers examine pain thresholds using techniques such as thermal pain testing, in which a thermode attached to a participant’s arm heats up. The temperature “slowly goes up and the patient just says: ‘Ouch,’ when it first hurts. Then we have their pain threshold,” Dr. Smith said.
A bidirectional relationship
Epidemiologic studies have found that, if you follow women who do not have pain, those with complaints about sleep are more than twice as likely to develop fibromyalgia.
Dr. Smith’s group and others have shown that if you deprive a healthy person of sleep, they become more sensitive to pain.
Inflammation could be one possible reason for this effect. In one study, participants who experienced forced awakening experienced less slow-wave sleep, which was tied to more inflammation in the morning. Increased inflammation was linked to greater pain sensitivity.
“We are starting to piece together some of the pathways. That’s just one,” Dr. Smith said.
A recent study by researchers at Harvard University and elsewhere investigated how sleep disturbances affected three pain pathways. In that study, the results varied by sex. The data indicate that optimal treatment approaches might differ for men and women, the researchers said.
Waking up to the problem
Sleep problems can be neglected in medical school and in the clinic. “People just have other things to focus on that they clearly know what they can do about it,” Dr. Smith said.
But clinicians should not hesitate to screen for conditions such as insomnia or OSA and refer patients to a specialist. If a patient has had pain for 6 months and treatments are not working, the chance that they have a treatable sleep disorder “is very high, above 50%,” Dr. Smith said. Many could have more than one sleep disorder, he added.
Continuous positive airway pressure for OSA and CBT for insomnia can improve sleep. Dr. Smith said he expects these measures will improve overall pain management as well.
If treating a sleep disorder fails to help with pain, however, it may still help prevent other sleep-related problems, such as depression, poor glucose control, and heart disease. It also could improve patients’ ability to function day to day, he said.
Evidence on whether treating sleep problems reduces pain has so far been mixed.
“We’ve done some studies showing that if you have CBT-I and you have knee arthritis, improvements in the amount of time you spend awake at night translate into improvements in pain at 6 months. There is a signal there, but it’s not as strong as we would like,” he said. “It may be that it takes longer than anyone would like” to have an effect.
A structured intervention such as CBT-I is likely more beneficial than education about sleep hygiene alone in resolving sleep disturbances, Dr. Whibley said. CBT-I includes active components such as sleep restriction therapy and stimulus control therapy and is recommended by the American Academy of Sleep Medicine as the first-line treatment for chronic insomnia (J Clin Sleep Med. 2008 Oct 15;4[5]:487-504).
Patients should consider the role that sleep may play in their chronic pain condition, he said.
“An increasing number of researchers and clinicians are becoming more interested in this as a foundational pillar of health, alongside activity and diet,” Dr. Whibley said. “Sleep is recognized as just as important but doesn’t seem to get the airtime.”
Clinicians, he added, should regularly assess their patients’ sleep and know where to refer those whom they feel would benefit from more advanced management: “They [should] know that they have at least got it on their radar to check as one of the important pillars of health that you should be able to control.”
Sleep trials seeking pain patients
Researchers around the United States are conducting dozens of studies related to sleep and pain. The following trials are recruiting participants, according to ClinicalTrials.gov.
Sleep and Pain Interventions in Women With Fibromyalgia (SPIN-II). Investigators at the University of Missouri–Columbia are examining two cognitive-behavioral treatments for women with fibromyalgia and insomnia. “This trial will yield important information about the roles of sleep, arousal, and brain structure and function in the development and maintenance of chronic pain in women with fibromyalgia,” the researchers say.
Prospective Randomized Trial of CPAP for SDB in Patients Who Use Opioids (PRESTO). At the University of California, San Diego, researchers are investigating whether patients with chronic pain who use opioids and have sleep-disordered breathing may benefit from treatment with continuous positive airway pressure. They plan to assess the intervention’s effects on sleep quality, pain, and quality of life. They also will see which patients are least likely to benefit from this treatment approach.
Latent Aging Mechanisms in Pain and Sleep (LAMPS). Researchers at the University of Florida are studying the effects of oral gamma-aminobutyric acid in older adults with chronic pain and sleep difficulties.
Sleep and Pain in Sickle Cell Disease. At Johns Hopkins University, investigators are evaluating how behavioral sleep interventions influence pain and brain function in patients with sickle cell disease.
Pain in Long COVID-19: The Role of Sleep. Researchers at Beth Israel Deaconess Medical Center are conducting an observational study of patients with long COVID who have pain and sleep disturbances. The study aims “to understand the role of sleep in the development and persistence of pain symptoms in long COVID.”
Intervention for Sleep and Pain in Youth: A Randomized Controlled Trial (I-SPY-RCT). Adolescents with migraine are being recruited by a team at Seattle Children’s Hospital for a randomized controlled trial. The study will examine the effects of CBT-I as well as the combined effect of CBT-I and pain interventions on reducing insomnia symptoms and headache-related disability in this population.
A version of this article appeared on Medscape.com.
COVID vax: Primary care back at forefront of care delivery
With COVID-19 hospitalizations up by 22% and deaths up by 8% as of Aug. 12, primary care clinicians are readying to distribute the new COVID-19 booster that is expected to arrive in September.
David Cutler, MD, is hoping to vaccinate as many of his patients who want the shots. He and other primary care clinicians are finally back in the business of prevention after being sidelined during the pandemic.
Most primary care clinicians weren’t provided with the vaccine through the height of the pandemic, when federal officials instead focused their efforts on vaccine distribution through hospital systems and retail pharmacies. The consequence, primary care clinicians say, is that they have no records for patients who need the vaccine; they cannot send patients reminders; and they have no idea if an at-risk patient is ready for a booster.
“The role of primary care is educating people about COVID-19, testing for COVID-19 and other infections, providing access to vaccines and treatment, and sustaining our health care system to provide care, fight disease, and save lives,” said Dr. Cutler, a family physician at Providence Saint John’s Health Center in Santa Monica, Calif.
A study published in Health Affairs confirmed that primary care practices were not included in the federal vaccine strategy. The researchers found that by the end of 2021, 43.1% of 2,000 primary care practices had no records of COVID-19 vaccinations for patients. More than 90% had records for historically routine immunizations, such as influenza and shingles.
“I do believe if PCPs had earlier access to the vaccine, we could have done a better job vaccinating more people,” said Ann Greiner, MCP, president and chief executive officer of the Primary Care Collaborative, a nonprofit organization. “We need to make sure they’re back in that seat, providing the lion’s share of those vaccines.”
The roadblocks to vaccines
More than 20,000 primary care clinicians applied to distribute vaccines to patients as of April 2021, according to the Centers for Disease Control and Prevention. A quarter of those received the shots. Fewer than 5% of all vaccine doses were provided to primary care offices during that early stage of rollout.
Natasha Beauvais, MD, MPH, a family physician at Northern Virginia Family Practice in Alexandria, Va., said trying to vaccinate patients back then was a herculean task.
“We were desperate to get the vaccine, like many practices,” Dr. Beauvais said.
It was only by chance – through one of the physician’s work connections – that they got in touch with the city’s health department to request a supply of immunizations.
The requirements for becoming a vaccine provider were stringent: Dr. Beauvais had to show that her practice could appropriately refrigerate or freeze doses at much colder temperatures than most immunizations, monitor the storage unit at all times, and accurately record and schedule every dose. What’s more, most primary care practices lacked the bandwidth to conduct mass vaccinations like larger medical systems.
Robert L. Phillips Jr., MD, MSPH, founding executive director at the American Board of Family Medicine Foundation, said that the decision to sideline primary care practices, along with a poor records system, left clinicians struggling to leverage relationships with patients to boost rates of vaccination.
“Primary care is where most people have trusted health relationships, and it should be more than a footnote in the nation’s epidemic response plans,” said Dr. Phillips, a corresponding author of the Health Affairs study.
The exclusion of primary care has deep roots: These clinicians were mentioned as a footnote in the CDC’s 2017 Pandemic Influenza Plan, according to Dr. Phillips.
“There’s no one in the federal government who wakes up in the morning thinking of primary care,” Dr. Phillips said. “It’s not the only reason the numbers were down, but a big reason.”
Other countries, including Australia, utilized the specialty for vaccine distribution. A 2022 article in Australian Health Review noted that the success of Australia’s COVID-19 vaccine rollout came down to the involvement of primary care.
Dr. Cutler said his clinic also did as much as they could during the early pandemic – from keeping their urgent care clinic open to providing COVID-19 antibody testing and infusions. His practice was able to start vaccinating patients in March 2021, and by that summer, the office had provided the immunization to 4,000 patients. Dr. Cutler was also able to address any health problems these patients reported during their vaccination visit.
“A vaccine is not just a vaccine: It’s an opportunity to have a conversation between a primary care physician and a patient about other health issues, and it encultures people to get important preventive care,” Ms. Greiner said.
The Health Affairs study was supported by the CDC.
A version of this article first appeared on Medscape.com.
With COVID-19 hospitalizations up by 22% and deaths up by 8% as of Aug. 12, primary care clinicians are readying to distribute the new COVID-19 booster that is expected to arrive in September.
David Cutler, MD, is hoping to vaccinate as many of his patients who want the shots. He and other primary care clinicians are finally back in the business of prevention after being sidelined during the pandemic.
Most primary care clinicians weren’t provided with the vaccine through the height of the pandemic, when federal officials instead focused their efforts on vaccine distribution through hospital systems and retail pharmacies. The consequence, primary care clinicians say, is that they have no records for patients who need the vaccine; they cannot send patients reminders; and they have no idea if an at-risk patient is ready for a booster.
“The role of primary care is educating people about COVID-19, testing for COVID-19 and other infections, providing access to vaccines and treatment, and sustaining our health care system to provide care, fight disease, and save lives,” said Dr. Cutler, a family physician at Providence Saint John’s Health Center in Santa Monica, Calif.
A study published in Health Affairs confirmed that primary care practices were not included in the federal vaccine strategy. The researchers found that by the end of 2021, 43.1% of 2,000 primary care practices had no records of COVID-19 vaccinations for patients. More than 90% had records for historically routine immunizations, such as influenza and shingles.
“I do believe if PCPs had earlier access to the vaccine, we could have done a better job vaccinating more people,” said Ann Greiner, MCP, president and chief executive officer of the Primary Care Collaborative, a nonprofit organization. “We need to make sure they’re back in that seat, providing the lion’s share of those vaccines.”
The roadblocks to vaccines
More than 20,000 primary care clinicians applied to distribute vaccines to patients as of April 2021, according to the Centers for Disease Control and Prevention. A quarter of those received the shots. Fewer than 5% of all vaccine doses were provided to primary care offices during that early stage of rollout.
Natasha Beauvais, MD, MPH, a family physician at Northern Virginia Family Practice in Alexandria, Va., said trying to vaccinate patients back then was a herculean task.
“We were desperate to get the vaccine, like many practices,” Dr. Beauvais said.
It was only by chance – through one of the physician’s work connections – that they got in touch with the city’s health department to request a supply of immunizations.
The requirements for becoming a vaccine provider were stringent: Dr. Beauvais had to show that her practice could appropriately refrigerate or freeze doses at much colder temperatures than most immunizations, monitor the storage unit at all times, and accurately record and schedule every dose. What’s more, most primary care practices lacked the bandwidth to conduct mass vaccinations like larger medical systems.
Robert L. Phillips Jr., MD, MSPH, founding executive director at the American Board of Family Medicine Foundation, said that the decision to sideline primary care practices, along with a poor records system, left clinicians struggling to leverage relationships with patients to boost rates of vaccination.
“Primary care is where most people have trusted health relationships, and it should be more than a footnote in the nation’s epidemic response plans,” said Dr. Phillips, a corresponding author of the Health Affairs study.
The exclusion of primary care has deep roots: These clinicians were mentioned as a footnote in the CDC’s 2017 Pandemic Influenza Plan, according to Dr. Phillips.
“There’s no one in the federal government who wakes up in the morning thinking of primary care,” Dr. Phillips said. “It’s not the only reason the numbers were down, but a big reason.”
Other countries, including Australia, utilized the specialty for vaccine distribution. A 2022 article in Australian Health Review noted that the success of Australia’s COVID-19 vaccine rollout came down to the involvement of primary care.
Dr. Cutler said his clinic also did as much as they could during the early pandemic – from keeping their urgent care clinic open to providing COVID-19 antibody testing and infusions. His practice was able to start vaccinating patients in March 2021, and by that summer, the office had provided the immunization to 4,000 patients. Dr. Cutler was also able to address any health problems these patients reported during their vaccination visit.
“A vaccine is not just a vaccine: It’s an opportunity to have a conversation between a primary care physician and a patient about other health issues, and it encultures people to get important preventive care,” Ms. Greiner said.
The Health Affairs study was supported by the CDC.
A version of this article first appeared on Medscape.com.
With COVID-19 hospitalizations up by 22% and deaths up by 8% as of Aug. 12, primary care clinicians are readying to distribute the new COVID-19 booster that is expected to arrive in September.
David Cutler, MD, is hoping to vaccinate as many of his patients who want the shots. He and other primary care clinicians are finally back in the business of prevention after being sidelined during the pandemic.
Most primary care clinicians weren’t provided with the vaccine through the height of the pandemic, when federal officials instead focused their efforts on vaccine distribution through hospital systems and retail pharmacies. The consequence, primary care clinicians say, is that they have no records for patients who need the vaccine; they cannot send patients reminders; and they have no idea if an at-risk patient is ready for a booster.
“The role of primary care is educating people about COVID-19, testing for COVID-19 and other infections, providing access to vaccines and treatment, and sustaining our health care system to provide care, fight disease, and save lives,” said Dr. Cutler, a family physician at Providence Saint John’s Health Center in Santa Monica, Calif.
A study published in Health Affairs confirmed that primary care practices were not included in the federal vaccine strategy. The researchers found that by the end of 2021, 43.1% of 2,000 primary care practices had no records of COVID-19 vaccinations for patients. More than 90% had records for historically routine immunizations, such as influenza and shingles.
“I do believe if PCPs had earlier access to the vaccine, we could have done a better job vaccinating more people,” said Ann Greiner, MCP, president and chief executive officer of the Primary Care Collaborative, a nonprofit organization. “We need to make sure they’re back in that seat, providing the lion’s share of those vaccines.”
The roadblocks to vaccines
More than 20,000 primary care clinicians applied to distribute vaccines to patients as of April 2021, according to the Centers for Disease Control and Prevention. A quarter of those received the shots. Fewer than 5% of all vaccine doses were provided to primary care offices during that early stage of rollout.
Natasha Beauvais, MD, MPH, a family physician at Northern Virginia Family Practice in Alexandria, Va., said trying to vaccinate patients back then was a herculean task.
“We were desperate to get the vaccine, like many practices,” Dr. Beauvais said.
It was only by chance – through one of the physician’s work connections – that they got in touch with the city’s health department to request a supply of immunizations.
The requirements for becoming a vaccine provider were stringent: Dr. Beauvais had to show that her practice could appropriately refrigerate or freeze doses at much colder temperatures than most immunizations, monitor the storage unit at all times, and accurately record and schedule every dose. What’s more, most primary care practices lacked the bandwidth to conduct mass vaccinations like larger medical systems.
Robert L. Phillips Jr., MD, MSPH, founding executive director at the American Board of Family Medicine Foundation, said that the decision to sideline primary care practices, along with a poor records system, left clinicians struggling to leverage relationships with patients to boost rates of vaccination.
“Primary care is where most people have trusted health relationships, and it should be more than a footnote in the nation’s epidemic response plans,” said Dr. Phillips, a corresponding author of the Health Affairs study.
The exclusion of primary care has deep roots: These clinicians were mentioned as a footnote in the CDC’s 2017 Pandemic Influenza Plan, according to Dr. Phillips.
“There’s no one in the federal government who wakes up in the morning thinking of primary care,” Dr. Phillips said. “It’s not the only reason the numbers were down, but a big reason.”
Other countries, including Australia, utilized the specialty for vaccine distribution. A 2022 article in Australian Health Review noted that the success of Australia’s COVID-19 vaccine rollout came down to the involvement of primary care.
Dr. Cutler said his clinic also did as much as they could during the early pandemic – from keeping their urgent care clinic open to providing COVID-19 antibody testing and infusions. His practice was able to start vaccinating patients in March 2021, and by that summer, the office had provided the immunization to 4,000 patients. Dr. Cutler was also able to address any health problems these patients reported during their vaccination visit.
“A vaccine is not just a vaccine: It’s an opportunity to have a conversation between a primary care physician and a patient about other health issues, and it encultures people to get important preventive care,” Ms. Greiner said.
The Health Affairs study was supported by the CDC.
A version of this article first appeared on Medscape.com.
Atopic dermatitis may be a risk factor for GBS colonization in pregnancy
suggest.
“The rate of GBS colonization among pregnant females with a history of AD has not been previously reported, but AD could be a risk factor for maternal carriage of GBS,” corresponding author David J. Margolis, MD, PhD, of the department of dermatology at the University of Pennsylvania, Philadelphia, and colleagues wrote in the study, which was published as a letter to the editor online in the Journal of Investigative Dermatology. “GBS reporting in a large administrative database represents a unique opportunity to conduct a population-based evaluation of GBS carriage with AD. Understanding this association could expand our understanding of microbial changes associated with AD,” they noted.
To determine if an association between GBS and AD in pregnant women exists, the researchers performed a cross-sectional study using a random sample from an Optum administrative database of pregnant women who had vaginal deliveries between May of 2007 and September 2021. The primary outcome of interest was the presence of GBS based on American College of Obstetricians and Gynecologists–recommended codes for GBS during 36 0/7 to 37 6/7 weeks of pregnancy. They used descriptive statistics to summarize categorical and continuous variables as proportions and means, and logistic regression to examine the association between AD and GBS status.
The cohort included 566,467 pregnant women with an average age of 38.8 years. Of these, 2.9% had a diagnosis of AD or a history of AD, and 24.9% had diagnoses of asthma, seasonal allergies, or both. Women with AD had an increased odds ratio of asthma (OR, 2.55), seasonal allergies (OR, 3.39), or both (OR, 5.35), compared with those without AD.
GBS was reported in 20.6% of the cohort. The median time of follow-up for those with and without GBS was 494 days and 468 days, respectively (P = .134). Among the women with AD, 24.1% had GBS, compared with 20.51% of the women without AD (P <.0001), which translated into an OR of 1.23 (95% confidence interval, 1.18-1.27).
Among the women with GBS, the OR of asthma was 1.08 (95% CI, 1.06-1.10) and was 1.07 (95% CI, 1.05-1.09) among those with seasonal allergies. When adjusted for potential confounders, these findings did not change substantively.
“It is not apparent why pregnant females with AD are more likely to specifically carry GBS,” the authors wrote. “However, several studies have shown that individuals with AD are more likely to carry [Staphylococcus] aureus and that individuals with AD might be deficient in host defenses against S. aureus and other pathogens,” they added.
“Individuals with AD frequently receive antibiotics as part of their AD treatment and this might alter their resident microbiome. Carriage rates may be enhanced by the inhibition of an important barrier protein called filaggrin (FLG) and FLG loss of function genetic variation is known to decrease barrier proteins thought to inhibit the colonization of S. aureus and other pathogens,” the researchers wrote.
They acknowledged certain limitations of their study, including its reliance on an administrative database that does not contain information on past disease.
Asked to comment on the results, Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, who was not involved with the study, characterized AD as “the poster child for cutaneous dysbiosis – an altered petri dish, so to speak, [that] facilitates survival of the few, leading to decreased microbial diversity that can both enable potential pathogen invasion and immune dysregulation.”
Though it’s not surprising that pregnant AD patients have dysbiosis, the focus on GBS, “which can be a bad actor in the perinatal period, is an interesting connection,” he said. “Will this change practices? Pregnant women should be screened for GBS regardless, but maybe more attention or counseling can be offered to AD patients about the importance of screening. Would decolonization regimens be employed early in pregnancy? This study can’t answer that but certainly raises good questions.”
Dr. Margolis disclosed that he is or recently has been a consultant for Pfizer, Leo, and Sanofi with respect to studies of atopic dermatitis and served on an advisory board for the National Eczema Association. Another author disclosed receiving grants from companies related to work with AD; other authors had no disclosures. Dr. Friedman reported having no relevant disclosures.
suggest.
“The rate of GBS colonization among pregnant females with a history of AD has not been previously reported, but AD could be a risk factor for maternal carriage of GBS,” corresponding author David J. Margolis, MD, PhD, of the department of dermatology at the University of Pennsylvania, Philadelphia, and colleagues wrote in the study, which was published as a letter to the editor online in the Journal of Investigative Dermatology. “GBS reporting in a large administrative database represents a unique opportunity to conduct a population-based evaluation of GBS carriage with AD. Understanding this association could expand our understanding of microbial changes associated with AD,” they noted.
To determine if an association between GBS and AD in pregnant women exists, the researchers performed a cross-sectional study using a random sample from an Optum administrative database of pregnant women who had vaginal deliveries between May of 2007 and September 2021. The primary outcome of interest was the presence of GBS based on American College of Obstetricians and Gynecologists–recommended codes for GBS during 36 0/7 to 37 6/7 weeks of pregnancy. They used descriptive statistics to summarize categorical and continuous variables as proportions and means, and logistic regression to examine the association between AD and GBS status.
The cohort included 566,467 pregnant women with an average age of 38.8 years. Of these, 2.9% had a diagnosis of AD or a history of AD, and 24.9% had diagnoses of asthma, seasonal allergies, or both. Women with AD had an increased odds ratio of asthma (OR, 2.55), seasonal allergies (OR, 3.39), or both (OR, 5.35), compared with those without AD.
GBS was reported in 20.6% of the cohort. The median time of follow-up for those with and without GBS was 494 days and 468 days, respectively (P = .134). Among the women with AD, 24.1% had GBS, compared with 20.51% of the women without AD (P <.0001), which translated into an OR of 1.23 (95% confidence interval, 1.18-1.27).
Among the women with GBS, the OR of asthma was 1.08 (95% CI, 1.06-1.10) and was 1.07 (95% CI, 1.05-1.09) among those with seasonal allergies. When adjusted for potential confounders, these findings did not change substantively.
“It is not apparent why pregnant females with AD are more likely to specifically carry GBS,” the authors wrote. “However, several studies have shown that individuals with AD are more likely to carry [Staphylococcus] aureus and that individuals with AD might be deficient in host defenses against S. aureus and other pathogens,” they added.
“Individuals with AD frequently receive antibiotics as part of their AD treatment and this might alter their resident microbiome. Carriage rates may be enhanced by the inhibition of an important barrier protein called filaggrin (FLG) and FLG loss of function genetic variation is known to decrease barrier proteins thought to inhibit the colonization of S. aureus and other pathogens,” the researchers wrote.
They acknowledged certain limitations of their study, including its reliance on an administrative database that does not contain information on past disease.
Asked to comment on the results, Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, who was not involved with the study, characterized AD as “the poster child for cutaneous dysbiosis – an altered petri dish, so to speak, [that] facilitates survival of the few, leading to decreased microbial diversity that can both enable potential pathogen invasion and immune dysregulation.”
Though it’s not surprising that pregnant AD patients have dysbiosis, the focus on GBS, “which can be a bad actor in the perinatal period, is an interesting connection,” he said. “Will this change practices? Pregnant women should be screened for GBS regardless, but maybe more attention or counseling can be offered to AD patients about the importance of screening. Would decolonization regimens be employed early in pregnancy? This study can’t answer that but certainly raises good questions.”
Dr. Margolis disclosed that he is or recently has been a consultant for Pfizer, Leo, and Sanofi with respect to studies of atopic dermatitis and served on an advisory board for the National Eczema Association. Another author disclosed receiving grants from companies related to work with AD; other authors had no disclosures. Dr. Friedman reported having no relevant disclosures.
suggest.
“The rate of GBS colonization among pregnant females with a history of AD has not been previously reported, but AD could be a risk factor for maternal carriage of GBS,” corresponding author David J. Margolis, MD, PhD, of the department of dermatology at the University of Pennsylvania, Philadelphia, and colleagues wrote in the study, which was published as a letter to the editor online in the Journal of Investigative Dermatology. “GBS reporting in a large administrative database represents a unique opportunity to conduct a population-based evaluation of GBS carriage with AD. Understanding this association could expand our understanding of microbial changes associated with AD,” they noted.
To determine if an association between GBS and AD in pregnant women exists, the researchers performed a cross-sectional study using a random sample from an Optum administrative database of pregnant women who had vaginal deliveries between May of 2007 and September 2021. The primary outcome of interest was the presence of GBS based on American College of Obstetricians and Gynecologists–recommended codes for GBS during 36 0/7 to 37 6/7 weeks of pregnancy. They used descriptive statistics to summarize categorical and continuous variables as proportions and means, and logistic regression to examine the association between AD and GBS status.
The cohort included 566,467 pregnant women with an average age of 38.8 years. Of these, 2.9% had a diagnosis of AD or a history of AD, and 24.9% had diagnoses of asthma, seasonal allergies, or both. Women with AD had an increased odds ratio of asthma (OR, 2.55), seasonal allergies (OR, 3.39), or both (OR, 5.35), compared with those without AD.
GBS was reported in 20.6% of the cohort. The median time of follow-up for those with and without GBS was 494 days and 468 days, respectively (P = .134). Among the women with AD, 24.1% had GBS, compared with 20.51% of the women without AD (P <.0001), which translated into an OR of 1.23 (95% confidence interval, 1.18-1.27).
Among the women with GBS, the OR of asthma was 1.08 (95% CI, 1.06-1.10) and was 1.07 (95% CI, 1.05-1.09) among those with seasonal allergies. When adjusted for potential confounders, these findings did not change substantively.
“It is not apparent why pregnant females with AD are more likely to specifically carry GBS,” the authors wrote. “However, several studies have shown that individuals with AD are more likely to carry [Staphylococcus] aureus and that individuals with AD might be deficient in host defenses against S. aureus and other pathogens,” they added.
“Individuals with AD frequently receive antibiotics as part of their AD treatment and this might alter their resident microbiome. Carriage rates may be enhanced by the inhibition of an important barrier protein called filaggrin (FLG) and FLG loss of function genetic variation is known to decrease barrier proteins thought to inhibit the colonization of S. aureus and other pathogens,” the researchers wrote.
They acknowledged certain limitations of their study, including its reliance on an administrative database that does not contain information on past disease.
Asked to comment on the results, Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington, who was not involved with the study, characterized AD as “the poster child for cutaneous dysbiosis – an altered petri dish, so to speak, [that] facilitates survival of the few, leading to decreased microbial diversity that can both enable potential pathogen invasion and immune dysregulation.”
Though it’s not surprising that pregnant AD patients have dysbiosis, the focus on GBS, “which can be a bad actor in the perinatal period, is an interesting connection,” he said. “Will this change practices? Pregnant women should be screened for GBS regardless, but maybe more attention or counseling can be offered to AD patients about the importance of screening. Would decolonization regimens be employed early in pregnancy? This study can’t answer that but certainly raises good questions.”
Dr. Margolis disclosed that he is or recently has been a consultant for Pfizer, Leo, and Sanofi with respect to studies of atopic dermatitis and served on an advisory board for the National Eczema Association. Another author disclosed receiving grants from companies related to work with AD; other authors had no disclosures. Dr. Friedman reported having no relevant disclosures.
FROM THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
What’s New in Diffuse Large B-cell Lymphoma?
Diffuse large B-cell lymphoma (DLBCL) is the most diagnosed non-Hodgkin lymphoma (NHL), accounting for up to one-third of cases. For many decades, R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) has been the standard first-line treatment approach for eligible patients in the first-line setting, resulting in long-term remissions in about two-thirds of patients. However, as our understanding of the biologic heterogeneity of this disease has advanced with the ability to perform more sophisticated molecular testing at diagnosis, researchers have been able to identify high-risk patient subtypes with suboptimal outcomes. While survival outcomes among low-risk patient subgroups are favorable with first-line immunochemotherapy, the majority of high-risk patients will experience relapse and often succumb to their disease.
Given the poor outcomes among patients with relapsed or refractory (R/R) DLBCL, there has been a massive research effort over the last decade to improve survival in this setting. Many experts agree that the approval of chimeric antigen receptor (CAR) T-cell therapy was the first major victory in this uphill battle. First approved in October of 2017, axicabtagene ciloleucel was the first of the 3 currently available commercial CAR T-cell therapy constructs to be approved in the third-line setting for DLBCL. Compared to historical controls, CAR T-cell therapy is associated with significant improvement in patient survival with complete response (CR) rates of 40%-50% compared to <20% with standard salvage immunochemotherapy.
Following approval in the third-line setting, these agents were quickly expedited to second-line therapy with pivotal trials demonstrating superiority with CAR T-cell therapy in the second line compared to salvage immunochemotherapy followed by autologous stem cell transplant. In 2022 the ZUMA-7 study reported a 24-month event-free survival (EFS) of 41% with axicabtagene ciloleucel compared to 16% with standard of care, and the TRANSFORM study documented a median EFS not yet reached with lisocabtagene ciloleucel compared to 2.3 months with standard of care. Despite these drastic improvements in patient outcomes, more than half of patients will still fail CAR T-cell therapy and require further systemic therapy.
Thankfully, this year has seen even more advancement in the treatment landscape of R/R DLBCL with two new commercially approved agents in yet another novel therapeutic category: bispecific antibodies. The following is a description of the newest data leading to the latest approvals by the US Food and Drug Administration.
Bispecific antibodies (BsAbs) are an off-the-shelf product that activate endogenous immune cells by cotargeting both tumor antigens as well as host T cells or natural killer cells. Several different experimental agents with varying constructs are under active observation in a wide variety of both hematologic and solid malignancies. Specifically within the realm of B-cell NHL, however, this class of agents is extremely promising and possibly represents the next significant milestone in the treatment of lymphoma.
The toxicity profile of these agents has been reliably predictable in most early phase clinical studies and is related predominantly to T-cell overactivation. The most commonly reported adverse events consist of cytokine release syndrome (CRS) as well as neutropenia, anemia, and hypophosphatemia. While neurologic toxicity has been reported, the incidence is low, and the mechanism is thought to be different than that reported with CAR T-cell therapy given that BsAbs are not likely to cross the blood–brain barrier.
Epcoritamab is a subcutaneously administered bispecific antibody that targets CD3 and CD20 in a 1:1 ratio and activates T cells to destroy CD20-expressing malignant cells. The recent EPCORE NHL-1 clinical trial investigated epcoritamab monotherapy in R/R mature B-cell lymphomas. This agent is administered with a step-up dosing strategy seen consistently across the BsAb drug class. Patients receive a first priming dose of 0.16 mg on cycle 1 day 1, followed by an intermediate dose of 0.8 mg on cycle 1 day 8, followed by the first full dose of 48 mg on cycle 1 day 15. Subsequent doses are administered once weekly for cycles 1-3 followed by every 2 weeks for cycles 4-9, and every 4 weeks starting with cycle 10.
The study enrolled 157 patients globally with median age of 64 and 3 median prior lines of antilymphoma therapy. Nearly 40% of patients had received at least 4 prior lines of therapy, and 83% of patients were refractory to last systemic therapy. Thirty-nine percent of patients had received prior CAR T-cell therapy; 75% of these patients developed progressive disease within 6 months of CAR T-cell therapy.
Among patients treated in the study, the results were as follows:
CR rate 39% with an overall response rate (ORR) of 63%
Duration of response 12 months; duration of objective response not reached in patients with CR
Duration of CR 12 months
Median PFS 4.4 months; median OS not reached
Time to CR of 2.7 months
Toxicity profile was notable for the following:
Any grade CRS in 50%, grade ≥3 in 2.5%
Most CRS occurs with first full dose on cycle 1 day 15 with median time to onset of 20 hours and median time to resolution of 48 hours
Any grade neutropenia in 22%, grade ≥3 in 15%, febrile neutropenia in 2.5%
Any grade anemia in 18%, grade ≥3 in 10%
Injection site reaction, any grade, in 20%
Any grade neurotoxicity in 6%, grade ≥3 in 1 patient (0.6%)
Epcoritamab was granted accelerated approval on May 19, 2023, for use in patients with R/R DLBCL who have received at least 2 prior lines of systemic therapy.
Glofitamab is the more recently approved BsAb for DLBCL. This agent is distinguished by its 2:1 binding configuration that confers bivalency for the CD20 binding site. Glofitamab is delivered intravenously and requires pretreatment with obinutuzumab 1000 mg 7 days before the first dose. With a similar step-up dosing strategy, patients receive a priming dose of 2.5mg on cycle 1 day 8, an intermediate dose of 10mg on cycle 1 day 15, and a first full dose of 30mg on cycle 2 day 1. Subsequent treatments are administered every 21 days for up to 12 cycles.
The open-label phase 1-2 clinical trial of glofitamab monotherapy enrolled 155 patients with a median age of 66 and 3 median prior lines of therapy. Thirty-three percent of patients had received prior CAR T-cell therapy, and 86% were refractory to last line of therapy with 30% refractory to CAR T-cell therapy.
Results were as follows:
CR rate of 39%, ORR 52%
Median duration of CR not reached, median duration of objective response 18.4 months
Median PFS 4.9 months, median OS not reached
Toxicity profile demonstrated the following:
Any grade CRS 66%, grade ≥ 2 in 18%
Median time to onset 13.5 hours from cycle 1 day 8, median duration 30.5 hours
Any grade neutropenia in 38%, grade ≥ 3 in 27%
Grade ≥ 2 neurologic event in 15%
Glofitamab received accelerated approval from the FDA on June 15, 2023, with an identical indication to epcoritamab.
The introduction of BsAbs in DLBCL has highlighted some important issues. Will BsAbs supplant CAR T-cell therapy in DLBCL? Experts can be found on both sides of this debate. BsAbs circumvent the logistics surrounding the production of CAR T-cell therapy products and can, for the large part, be administered in the outpatient setting. However, CAR T-cell therapy has significantly longer follow-up times, which speaks to the curative potential of these agents even in the third-line setting. BsAbs, some may argue, seem to carry a more favorable toxicity profile with the CRS mitigation strategies. However, we still have much to learn about the downstream side effects with prolonged T-cell activation and the potential for T-cell exhaustion.
Finally, with the continued development of new agents in this arena, the art of sequencing therapies will become ever more important. What is the efficacy of CAR T-cell therapy after BsAb exposure? Can BsAbs be used as bridging therapy to a curative option with CAR T-cell therapy? With longer-term follow-up in several years, will we see late relapses after CR with BsAbs? Ongoing clinical trials investigating combination strategies and CAR T-cell therapy consolidation with BsAbs will hopefully eventually clarify some of these questions.
Diffuse large B-cell lymphoma (DLBCL) is the most diagnosed non-Hodgkin lymphoma (NHL), accounting for up to one-third of cases. For many decades, R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) has been the standard first-line treatment approach for eligible patients in the first-line setting, resulting in long-term remissions in about two-thirds of patients. However, as our understanding of the biologic heterogeneity of this disease has advanced with the ability to perform more sophisticated molecular testing at diagnosis, researchers have been able to identify high-risk patient subtypes with suboptimal outcomes. While survival outcomes among low-risk patient subgroups are favorable with first-line immunochemotherapy, the majority of high-risk patients will experience relapse and often succumb to their disease.
Given the poor outcomes among patients with relapsed or refractory (R/R) DLBCL, there has been a massive research effort over the last decade to improve survival in this setting. Many experts agree that the approval of chimeric antigen receptor (CAR) T-cell therapy was the first major victory in this uphill battle. First approved in October of 2017, axicabtagene ciloleucel was the first of the 3 currently available commercial CAR T-cell therapy constructs to be approved in the third-line setting for DLBCL. Compared to historical controls, CAR T-cell therapy is associated with significant improvement in patient survival with complete response (CR) rates of 40%-50% compared to <20% with standard salvage immunochemotherapy.
Following approval in the third-line setting, these agents were quickly expedited to second-line therapy with pivotal trials demonstrating superiority with CAR T-cell therapy in the second line compared to salvage immunochemotherapy followed by autologous stem cell transplant. In 2022 the ZUMA-7 study reported a 24-month event-free survival (EFS) of 41% with axicabtagene ciloleucel compared to 16% with standard of care, and the TRANSFORM study documented a median EFS not yet reached with lisocabtagene ciloleucel compared to 2.3 months with standard of care. Despite these drastic improvements in patient outcomes, more than half of patients will still fail CAR T-cell therapy and require further systemic therapy.
Thankfully, this year has seen even more advancement in the treatment landscape of R/R DLBCL with two new commercially approved agents in yet another novel therapeutic category: bispecific antibodies. The following is a description of the newest data leading to the latest approvals by the US Food and Drug Administration.
Bispecific antibodies (BsAbs) are an off-the-shelf product that activate endogenous immune cells by cotargeting both tumor antigens as well as host T cells or natural killer cells. Several different experimental agents with varying constructs are under active observation in a wide variety of both hematologic and solid malignancies. Specifically within the realm of B-cell NHL, however, this class of agents is extremely promising and possibly represents the next significant milestone in the treatment of lymphoma.
The toxicity profile of these agents has been reliably predictable in most early phase clinical studies and is related predominantly to T-cell overactivation. The most commonly reported adverse events consist of cytokine release syndrome (CRS) as well as neutropenia, anemia, and hypophosphatemia. While neurologic toxicity has been reported, the incidence is low, and the mechanism is thought to be different than that reported with CAR T-cell therapy given that BsAbs are not likely to cross the blood–brain barrier.
Epcoritamab is a subcutaneously administered bispecific antibody that targets CD3 and CD20 in a 1:1 ratio and activates T cells to destroy CD20-expressing malignant cells. The recent EPCORE NHL-1 clinical trial investigated epcoritamab monotherapy in R/R mature B-cell lymphomas. This agent is administered with a step-up dosing strategy seen consistently across the BsAb drug class. Patients receive a first priming dose of 0.16 mg on cycle 1 day 1, followed by an intermediate dose of 0.8 mg on cycle 1 day 8, followed by the first full dose of 48 mg on cycle 1 day 15. Subsequent doses are administered once weekly for cycles 1-3 followed by every 2 weeks for cycles 4-9, and every 4 weeks starting with cycle 10.
The study enrolled 157 patients globally with median age of 64 and 3 median prior lines of antilymphoma therapy. Nearly 40% of patients had received at least 4 prior lines of therapy, and 83% of patients were refractory to last systemic therapy. Thirty-nine percent of patients had received prior CAR T-cell therapy; 75% of these patients developed progressive disease within 6 months of CAR T-cell therapy.
Among patients treated in the study, the results were as follows:
CR rate 39% with an overall response rate (ORR) of 63%
Duration of response 12 months; duration of objective response not reached in patients with CR
Duration of CR 12 months
Median PFS 4.4 months; median OS not reached
Time to CR of 2.7 months
Toxicity profile was notable for the following:
Any grade CRS in 50%, grade ≥3 in 2.5%
Most CRS occurs with first full dose on cycle 1 day 15 with median time to onset of 20 hours and median time to resolution of 48 hours
Any grade neutropenia in 22%, grade ≥3 in 15%, febrile neutropenia in 2.5%
Any grade anemia in 18%, grade ≥3 in 10%
Injection site reaction, any grade, in 20%
Any grade neurotoxicity in 6%, grade ≥3 in 1 patient (0.6%)
Epcoritamab was granted accelerated approval on May 19, 2023, for use in patients with R/R DLBCL who have received at least 2 prior lines of systemic therapy.
Glofitamab is the more recently approved BsAb for DLBCL. This agent is distinguished by its 2:1 binding configuration that confers bivalency for the CD20 binding site. Glofitamab is delivered intravenously and requires pretreatment with obinutuzumab 1000 mg 7 days before the first dose. With a similar step-up dosing strategy, patients receive a priming dose of 2.5mg on cycle 1 day 8, an intermediate dose of 10mg on cycle 1 day 15, and a first full dose of 30mg on cycle 2 day 1. Subsequent treatments are administered every 21 days for up to 12 cycles.
The open-label phase 1-2 clinical trial of glofitamab monotherapy enrolled 155 patients with a median age of 66 and 3 median prior lines of therapy. Thirty-three percent of patients had received prior CAR T-cell therapy, and 86% were refractory to last line of therapy with 30% refractory to CAR T-cell therapy.
Results were as follows:
CR rate of 39%, ORR 52%
Median duration of CR not reached, median duration of objective response 18.4 months
Median PFS 4.9 months, median OS not reached
Toxicity profile demonstrated the following:
Any grade CRS 66%, grade ≥ 2 in 18%
Median time to onset 13.5 hours from cycle 1 day 8, median duration 30.5 hours
Any grade neutropenia in 38%, grade ≥ 3 in 27%
Grade ≥ 2 neurologic event in 15%
Glofitamab received accelerated approval from the FDA on June 15, 2023, with an identical indication to epcoritamab.
The introduction of BsAbs in DLBCL has highlighted some important issues. Will BsAbs supplant CAR T-cell therapy in DLBCL? Experts can be found on both sides of this debate. BsAbs circumvent the logistics surrounding the production of CAR T-cell therapy products and can, for the large part, be administered in the outpatient setting. However, CAR T-cell therapy has significantly longer follow-up times, which speaks to the curative potential of these agents even in the third-line setting. BsAbs, some may argue, seem to carry a more favorable toxicity profile with the CRS mitigation strategies. However, we still have much to learn about the downstream side effects with prolonged T-cell activation and the potential for T-cell exhaustion.
Finally, with the continued development of new agents in this arena, the art of sequencing therapies will become ever more important. What is the efficacy of CAR T-cell therapy after BsAb exposure? Can BsAbs be used as bridging therapy to a curative option with CAR T-cell therapy? With longer-term follow-up in several years, will we see late relapses after CR with BsAbs? Ongoing clinical trials investigating combination strategies and CAR T-cell therapy consolidation with BsAbs will hopefully eventually clarify some of these questions.
Diffuse large B-cell lymphoma (DLBCL) is the most diagnosed non-Hodgkin lymphoma (NHL), accounting for up to one-third of cases. For many decades, R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) has been the standard first-line treatment approach for eligible patients in the first-line setting, resulting in long-term remissions in about two-thirds of patients. However, as our understanding of the biologic heterogeneity of this disease has advanced with the ability to perform more sophisticated molecular testing at diagnosis, researchers have been able to identify high-risk patient subtypes with suboptimal outcomes. While survival outcomes among low-risk patient subgroups are favorable with first-line immunochemotherapy, the majority of high-risk patients will experience relapse and often succumb to their disease.
Given the poor outcomes among patients with relapsed or refractory (R/R) DLBCL, there has been a massive research effort over the last decade to improve survival in this setting. Many experts agree that the approval of chimeric antigen receptor (CAR) T-cell therapy was the first major victory in this uphill battle. First approved in October of 2017, axicabtagene ciloleucel was the first of the 3 currently available commercial CAR T-cell therapy constructs to be approved in the third-line setting for DLBCL. Compared to historical controls, CAR T-cell therapy is associated with significant improvement in patient survival with complete response (CR) rates of 40%-50% compared to <20% with standard salvage immunochemotherapy.
Following approval in the third-line setting, these agents were quickly expedited to second-line therapy with pivotal trials demonstrating superiority with CAR T-cell therapy in the second line compared to salvage immunochemotherapy followed by autologous stem cell transplant. In 2022 the ZUMA-7 study reported a 24-month event-free survival (EFS) of 41% with axicabtagene ciloleucel compared to 16% with standard of care, and the TRANSFORM study documented a median EFS not yet reached with lisocabtagene ciloleucel compared to 2.3 months with standard of care. Despite these drastic improvements in patient outcomes, more than half of patients will still fail CAR T-cell therapy and require further systemic therapy.
Thankfully, this year has seen even more advancement in the treatment landscape of R/R DLBCL with two new commercially approved agents in yet another novel therapeutic category: bispecific antibodies. The following is a description of the newest data leading to the latest approvals by the US Food and Drug Administration.
Bispecific antibodies (BsAbs) are an off-the-shelf product that activate endogenous immune cells by cotargeting both tumor antigens as well as host T cells or natural killer cells. Several different experimental agents with varying constructs are under active observation in a wide variety of both hematologic and solid malignancies. Specifically within the realm of B-cell NHL, however, this class of agents is extremely promising and possibly represents the next significant milestone in the treatment of lymphoma.
The toxicity profile of these agents has been reliably predictable in most early phase clinical studies and is related predominantly to T-cell overactivation. The most commonly reported adverse events consist of cytokine release syndrome (CRS) as well as neutropenia, anemia, and hypophosphatemia. While neurologic toxicity has been reported, the incidence is low, and the mechanism is thought to be different than that reported with CAR T-cell therapy given that BsAbs are not likely to cross the blood–brain barrier.
Epcoritamab is a subcutaneously administered bispecific antibody that targets CD3 and CD20 in a 1:1 ratio and activates T cells to destroy CD20-expressing malignant cells. The recent EPCORE NHL-1 clinical trial investigated epcoritamab monotherapy in R/R mature B-cell lymphomas. This agent is administered with a step-up dosing strategy seen consistently across the BsAb drug class. Patients receive a first priming dose of 0.16 mg on cycle 1 day 1, followed by an intermediate dose of 0.8 mg on cycle 1 day 8, followed by the first full dose of 48 mg on cycle 1 day 15. Subsequent doses are administered once weekly for cycles 1-3 followed by every 2 weeks for cycles 4-9, and every 4 weeks starting with cycle 10.
The study enrolled 157 patients globally with median age of 64 and 3 median prior lines of antilymphoma therapy. Nearly 40% of patients had received at least 4 prior lines of therapy, and 83% of patients were refractory to last systemic therapy. Thirty-nine percent of patients had received prior CAR T-cell therapy; 75% of these patients developed progressive disease within 6 months of CAR T-cell therapy.
Among patients treated in the study, the results were as follows:
CR rate 39% with an overall response rate (ORR) of 63%
Duration of response 12 months; duration of objective response not reached in patients with CR
Duration of CR 12 months
Median PFS 4.4 months; median OS not reached
Time to CR of 2.7 months
Toxicity profile was notable for the following:
Any grade CRS in 50%, grade ≥3 in 2.5%
Most CRS occurs with first full dose on cycle 1 day 15 with median time to onset of 20 hours and median time to resolution of 48 hours
Any grade neutropenia in 22%, grade ≥3 in 15%, febrile neutropenia in 2.5%
Any grade anemia in 18%, grade ≥3 in 10%
Injection site reaction, any grade, in 20%
Any grade neurotoxicity in 6%, grade ≥3 in 1 patient (0.6%)
Epcoritamab was granted accelerated approval on May 19, 2023, for use in patients with R/R DLBCL who have received at least 2 prior lines of systemic therapy.
Glofitamab is the more recently approved BsAb for DLBCL. This agent is distinguished by its 2:1 binding configuration that confers bivalency for the CD20 binding site. Glofitamab is delivered intravenously and requires pretreatment with obinutuzumab 1000 mg 7 days before the first dose. With a similar step-up dosing strategy, patients receive a priming dose of 2.5mg on cycle 1 day 8, an intermediate dose of 10mg on cycle 1 day 15, and a first full dose of 30mg on cycle 2 day 1. Subsequent treatments are administered every 21 days for up to 12 cycles.
The open-label phase 1-2 clinical trial of glofitamab monotherapy enrolled 155 patients with a median age of 66 and 3 median prior lines of therapy. Thirty-three percent of patients had received prior CAR T-cell therapy, and 86% were refractory to last line of therapy with 30% refractory to CAR T-cell therapy.
Results were as follows:
CR rate of 39%, ORR 52%
Median duration of CR not reached, median duration of objective response 18.4 months
Median PFS 4.9 months, median OS not reached
Toxicity profile demonstrated the following:
Any grade CRS 66%, grade ≥ 2 in 18%
Median time to onset 13.5 hours from cycle 1 day 8, median duration 30.5 hours
Any grade neutropenia in 38%, grade ≥ 3 in 27%
Grade ≥ 2 neurologic event in 15%
Glofitamab received accelerated approval from the FDA on June 15, 2023, with an identical indication to epcoritamab.
The introduction of BsAbs in DLBCL has highlighted some important issues. Will BsAbs supplant CAR T-cell therapy in DLBCL? Experts can be found on both sides of this debate. BsAbs circumvent the logistics surrounding the production of CAR T-cell therapy products and can, for the large part, be administered in the outpatient setting. However, CAR T-cell therapy has significantly longer follow-up times, which speaks to the curative potential of these agents even in the third-line setting. BsAbs, some may argue, seem to carry a more favorable toxicity profile with the CRS mitigation strategies. However, we still have much to learn about the downstream side effects with prolonged T-cell activation and the potential for T-cell exhaustion.
Finally, with the continued development of new agents in this arena, the art of sequencing therapies will become ever more important. What is the efficacy of CAR T-cell therapy after BsAb exposure? Can BsAbs be used as bridging therapy to a curative option with CAR T-cell therapy? With longer-term follow-up in several years, will we see late relapses after CR with BsAbs? Ongoing clinical trials investigating combination strategies and CAR T-cell therapy consolidation with BsAbs will hopefully eventually clarify some of these questions.
Post-SCT, better survival in children with healthy gut diversity
“To the best of our knowledge, we present the first evidence of an association between pretransplantation lower gut microbiota diversity and poorer outcome in children undergoing allo-HSCT,” the authors report, in research published in the journal Blood. “Our findings underscore the importance of pre-transplant gut microbiota diversity and compositional structure in influencing allo-HSCT-related clinical outcomes in the pediatric setting.”
While allogeneic hematopoietic stem cell transplantation (allo-HSCT) can be potentially curative of hematologic malignancies, the stem cell transplantation process can wreak havoc on gut microbiota, because of factors including the conditioning regimen, antibiotic exposure, and dietary changes.
Specifically, the process can cause a substantial decrease in necessary alpha diversity and a potential expansion of possibly pathogenic bacteria.
While poor gut microbiota diversity has been linked to higher mortality in adult patients receiving allo-HSCT, research on the effects in pediatric patients is lacking.
“The gut microbiota of children differs from adults’ one, and this accounts for the need for specific pediatric studies on the gut microbiota-to–allo-HSCT relationship,” the authors write.
For the multicenter study, first author Riccardo Masetti, MD, PhD, of the department of pediatric oncology and hematology at the University of Bologna, Italy, and colleagues analyzed the gut microbiota diversity of 90 pediatric allo-HSCT recipients at four centers in Italy and one in Poland, stratifying the patients into groups of higher and lower diversity pretransplantation and again at the time of neutrophil engraftment.
Overall, gut microbiota diversity significantly declined from before allo-HSCT to afterward, at the time of neutrophil engraftment (P < .0001), with lower diversity observed in patients 3 years of age or younger.
With a median follow-up of 52 months, compared with the lower diversity group, those with higher diversity prior to transplantation had a significantly higher probability of overall survival (hazard ratio, 0.26; P = .011), after adjustment for age, graft source, donor type, intensity of conditioning regimen, center, and type of disease, with estimated overall survival at 52 months after allo-HSCT of 88.9% for the higher diversity group and 62.7% for the lower diversity group.
The cumulative incidence of grade II-IV acute GvHD was significantly lower for the higher diversity group versus lower diversity (20.0 versus 44.4, respectively; P = .017), as were the incidence rates of grade III-IV acute GvHD (2.2 versus 20.0; P = .007).
There were, however, no significant differences between the low and high diversity gut microbiota groups in relapse-free survival (P = .091).
The higher diversity group notably had higher relative abundances of potentially health-related bacterial families, including Ruminococcaceae and Oscillospiraceae, while the lower diversity group showed an overabundance of Enterococcaceae and Enterobacteriaceae.
Of note, the results differ from those observed in adults, among whom gut microbiota diversity before as well as after transplantation has been significantly associated with transplant outcomes, whereas with children, the association was limited to diversity prior to transplant.
In general, children have significantly lower diversity of gut microbiota than adults, with varying functional properties, and microbiota that is more easily modified by environmental factors, with larger changes occurring upon exposure to external stressors, the authors explain.
“Considering these different ecological properties compared to adults, we hypothesize that allo-HSCT–induced dysbiosis in the pediatric setting may imply loss of age-related gut microbiota signatures, including alpha diversity, with high interpatient variability,” they say.
Characteristics that were associated with higher or lower gut microbiota diversity prior to allo-HSCT included the treating center, suggesting that the geographical region may affect the diversity and the type of antibiotic exposure prior to the transplant.
Limitations included that “we didn’t assess other pretransplant characteristics such as the type of chemotherapy received, or the lifestyle, and this should be addressed in future studies on larger cohorts,” Dr. Masetti said in an interview.
While lengthy delays in screening of samples are barriers in the use of the gut microbiome as a tool in clinical practice, he noted that clinicians can take key measures to improve the microbiota.
“[Preventive measures] include the avoidance of unnecessary antibiotic treatment, which has a detrimental effect on the microbiota,” he said. “Moreover, some dietary changes may promote microbiota health.”
In addition, key measures can be taken during the allo-HSCT to preserve the microbiota, he added.
“In our center, we use enteral nutrition with a nasogastric tube rather than parenteral nutrition, which helps the microbiota to recover faster,” Dr. Masetti explained. “Moreover, other interventional measures such as fecal microbiota transplantation or the use of probiotics are under testing.”
“In particular, our data emphasize the importance of an overall healthy network, rather than the abundance of specific families or genera, in preventing complications and unfavorable outcomes.”
Commenting on the study, Robert Jenq, MD, an assistant professor in the departments of genomic medicine and stem cell transplantation and cellular therapy at the University of Texas M.D. Anderson Cancer Center, Houston, noted that with the growing evidence of the effects of poor gut microbiota diversity on clinical outcomes, multiple early-phase clinical trials are being conducted to test various strategies to prevent or treat gut injury.
“I’m not aware of any one approach that has shown enough promise to warrant being tested in multicenter studies yet, but it’s still a bit early,” Dr. Jenq said.“In the meantime, discontinuing or de-escalating antibiotics when medically safe, and encouraging patients to eat as much as they’re able to is a reasonable recommendation.”
Dr. Jenq added that, with most of the data on the issue being retrospective, a causative role has not been established, and “the finding of an association between the gut microbiota composition and survival, while interesting and provocative, does not provide evidence that intervening on the gut microbiota will lead to a clinical benefit.”
“I’m hopeful that randomized clinical trials will eventually demonstrate that we can protect or restore the gut microbiota, and this will lead to substantial clinical benefits, but this remains to be seen,” he said.
The authors had no disclosures to report. Dr. Jenq is an advisor for Seres Therapeutics, Prolacta Biosciences, and MaaT Pharma.
“To the best of our knowledge, we present the first evidence of an association between pretransplantation lower gut microbiota diversity and poorer outcome in children undergoing allo-HSCT,” the authors report, in research published in the journal Blood. “Our findings underscore the importance of pre-transplant gut microbiota diversity and compositional structure in influencing allo-HSCT-related clinical outcomes in the pediatric setting.”
While allogeneic hematopoietic stem cell transplantation (allo-HSCT) can be potentially curative of hematologic malignancies, the stem cell transplantation process can wreak havoc on gut microbiota, because of factors including the conditioning regimen, antibiotic exposure, and dietary changes.
Specifically, the process can cause a substantial decrease in necessary alpha diversity and a potential expansion of possibly pathogenic bacteria.
While poor gut microbiota diversity has been linked to higher mortality in adult patients receiving allo-HSCT, research on the effects in pediatric patients is lacking.
“The gut microbiota of children differs from adults’ one, and this accounts for the need for specific pediatric studies on the gut microbiota-to–allo-HSCT relationship,” the authors write.
For the multicenter study, first author Riccardo Masetti, MD, PhD, of the department of pediatric oncology and hematology at the University of Bologna, Italy, and colleagues analyzed the gut microbiota diversity of 90 pediatric allo-HSCT recipients at four centers in Italy and one in Poland, stratifying the patients into groups of higher and lower diversity pretransplantation and again at the time of neutrophil engraftment.
Overall, gut microbiota diversity significantly declined from before allo-HSCT to afterward, at the time of neutrophil engraftment (P < .0001), with lower diversity observed in patients 3 years of age or younger.
With a median follow-up of 52 months, compared with the lower diversity group, those with higher diversity prior to transplantation had a significantly higher probability of overall survival (hazard ratio, 0.26; P = .011), after adjustment for age, graft source, donor type, intensity of conditioning regimen, center, and type of disease, with estimated overall survival at 52 months after allo-HSCT of 88.9% for the higher diversity group and 62.7% for the lower diversity group.
The cumulative incidence of grade II-IV acute GvHD was significantly lower for the higher diversity group versus lower diversity (20.0 versus 44.4, respectively; P = .017), as were the incidence rates of grade III-IV acute GvHD (2.2 versus 20.0; P = .007).
There were, however, no significant differences between the low and high diversity gut microbiota groups in relapse-free survival (P = .091).
The higher diversity group notably had higher relative abundances of potentially health-related bacterial families, including Ruminococcaceae and Oscillospiraceae, while the lower diversity group showed an overabundance of Enterococcaceae and Enterobacteriaceae.
Of note, the results differ from those observed in adults, among whom gut microbiota diversity before as well as after transplantation has been significantly associated with transplant outcomes, whereas with children, the association was limited to diversity prior to transplant.
In general, children have significantly lower diversity of gut microbiota than adults, with varying functional properties, and microbiota that is more easily modified by environmental factors, with larger changes occurring upon exposure to external stressors, the authors explain.
“Considering these different ecological properties compared to adults, we hypothesize that allo-HSCT–induced dysbiosis in the pediatric setting may imply loss of age-related gut microbiota signatures, including alpha diversity, with high interpatient variability,” they say.
Characteristics that were associated with higher or lower gut microbiota diversity prior to allo-HSCT included the treating center, suggesting that the geographical region may affect the diversity and the type of antibiotic exposure prior to the transplant.
Limitations included that “we didn’t assess other pretransplant characteristics such as the type of chemotherapy received, or the lifestyle, and this should be addressed in future studies on larger cohorts,” Dr. Masetti said in an interview.
While lengthy delays in screening of samples are barriers in the use of the gut microbiome as a tool in clinical practice, he noted that clinicians can take key measures to improve the microbiota.
“[Preventive measures] include the avoidance of unnecessary antibiotic treatment, which has a detrimental effect on the microbiota,” he said. “Moreover, some dietary changes may promote microbiota health.”
In addition, key measures can be taken during the allo-HSCT to preserve the microbiota, he added.
“In our center, we use enteral nutrition with a nasogastric tube rather than parenteral nutrition, which helps the microbiota to recover faster,” Dr. Masetti explained. “Moreover, other interventional measures such as fecal microbiota transplantation or the use of probiotics are under testing.”
“In particular, our data emphasize the importance of an overall healthy network, rather than the abundance of specific families or genera, in preventing complications and unfavorable outcomes.”
Commenting on the study, Robert Jenq, MD, an assistant professor in the departments of genomic medicine and stem cell transplantation and cellular therapy at the University of Texas M.D. Anderson Cancer Center, Houston, noted that with the growing evidence of the effects of poor gut microbiota diversity on clinical outcomes, multiple early-phase clinical trials are being conducted to test various strategies to prevent or treat gut injury.
“I’m not aware of any one approach that has shown enough promise to warrant being tested in multicenter studies yet, but it’s still a bit early,” Dr. Jenq said.“In the meantime, discontinuing or de-escalating antibiotics when medically safe, and encouraging patients to eat as much as they’re able to is a reasonable recommendation.”
Dr. Jenq added that, with most of the data on the issue being retrospective, a causative role has not been established, and “the finding of an association between the gut microbiota composition and survival, while interesting and provocative, does not provide evidence that intervening on the gut microbiota will lead to a clinical benefit.”
“I’m hopeful that randomized clinical trials will eventually demonstrate that we can protect or restore the gut microbiota, and this will lead to substantial clinical benefits, but this remains to be seen,” he said.
The authors had no disclosures to report. Dr. Jenq is an advisor for Seres Therapeutics, Prolacta Biosciences, and MaaT Pharma.
“To the best of our knowledge, we present the first evidence of an association between pretransplantation lower gut microbiota diversity and poorer outcome in children undergoing allo-HSCT,” the authors report, in research published in the journal Blood. “Our findings underscore the importance of pre-transplant gut microbiota diversity and compositional structure in influencing allo-HSCT-related clinical outcomes in the pediatric setting.”
While allogeneic hematopoietic stem cell transplantation (allo-HSCT) can be potentially curative of hematologic malignancies, the stem cell transplantation process can wreak havoc on gut microbiota, because of factors including the conditioning regimen, antibiotic exposure, and dietary changes.
Specifically, the process can cause a substantial decrease in necessary alpha diversity and a potential expansion of possibly pathogenic bacteria.
While poor gut microbiota diversity has been linked to higher mortality in adult patients receiving allo-HSCT, research on the effects in pediatric patients is lacking.
“The gut microbiota of children differs from adults’ one, and this accounts for the need for specific pediatric studies on the gut microbiota-to–allo-HSCT relationship,” the authors write.
For the multicenter study, first author Riccardo Masetti, MD, PhD, of the department of pediatric oncology and hematology at the University of Bologna, Italy, and colleagues analyzed the gut microbiota diversity of 90 pediatric allo-HSCT recipients at four centers in Italy and one in Poland, stratifying the patients into groups of higher and lower diversity pretransplantation and again at the time of neutrophil engraftment.
Overall, gut microbiota diversity significantly declined from before allo-HSCT to afterward, at the time of neutrophil engraftment (P < .0001), with lower diversity observed in patients 3 years of age or younger.
With a median follow-up of 52 months, compared with the lower diversity group, those with higher diversity prior to transplantation had a significantly higher probability of overall survival (hazard ratio, 0.26; P = .011), after adjustment for age, graft source, donor type, intensity of conditioning regimen, center, and type of disease, with estimated overall survival at 52 months after allo-HSCT of 88.9% for the higher diversity group and 62.7% for the lower diversity group.
The cumulative incidence of grade II-IV acute GvHD was significantly lower for the higher diversity group versus lower diversity (20.0 versus 44.4, respectively; P = .017), as were the incidence rates of grade III-IV acute GvHD (2.2 versus 20.0; P = .007).
There were, however, no significant differences between the low and high diversity gut microbiota groups in relapse-free survival (P = .091).
The higher diversity group notably had higher relative abundances of potentially health-related bacterial families, including Ruminococcaceae and Oscillospiraceae, while the lower diversity group showed an overabundance of Enterococcaceae and Enterobacteriaceae.
Of note, the results differ from those observed in adults, among whom gut microbiota diversity before as well as after transplantation has been significantly associated with transplant outcomes, whereas with children, the association was limited to diversity prior to transplant.
In general, children have significantly lower diversity of gut microbiota than adults, with varying functional properties, and microbiota that is more easily modified by environmental factors, with larger changes occurring upon exposure to external stressors, the authors explain.
“Considering these different ecological properties compared to adults, we hypothesize that allo-HSCT–induced dysbiosis in the pediatric setting may imply loss of age-related gut microbiota signatures, including alpha diversity, with high interpatient variability,” they say.
Characteristics that were associated with higher or lower gut microbiota diversity prior to allo-HSCT included the treating center, suggesting that the geographical region may affect the diversity and the type of antibiotic exposure prior to the transplant.
Limitations included that “we didn’t assess other pretransplant characteristics such as the type of chemotherapy received, or the lifestyle, and this should be addressed in future studies on larger cohorts,” Dr. Masetti said in an interview.
While lengthy delays in screening of samples are barriers in the use of the gut microbiome as a tool in clinical practice, he noted that clinicians can take key measures to improve the microbiota.
“[Preventive measures] include the avoidance of unnecessary antibiotic treatment, which has a detrimental effect on the microbiota,” he said. “Moreover, some dietary changes may promote microbiota health.”
In addition, key measures can be taken during the allo-HSCT to preserve the microbiota, he added.
“In our center, we use enteral nutrition with a nasogastric tube rather than parenteral nutrition, which helps the microbiota to recover faster,” Dr. Masetti explained. “Moreover, other interventional measures such as fecal microbiota transplantation or the use of probiotics are under testing.”
“In particular, our data emphasize the importance of an overall healthy network, rather than the abundance of specific families or genera, in preventing complications and unfavorable outcomes.”
Commenting on the study, Robert Jenq, MD, an assistant professor in the departments of genomic medicine and stem cell transplantation and cellular therapy at the University of Texas M.D. Anderson Cancer Center, Houston, noted that with the growing evidence of the effects of poor gut microbiota diversity on clinical outcomes, multiple early-phase clinical trials are being conducted to test various strategies to prevent or treat gut injury.
“I’m not aware of any one approach that has shown enough promise to warrant being tested in multicenter studies yet, but it’s still a bit early,” Dr. Jenq said.“In the meantime, discontinuing or de-escalating antibiotics when medically safe, and encouraging patients to eat as much as they’re able to is a reasonable recommendation.”
Dr. Jenq added that, with most of the data on the issue being retrospective, a causative role has not been established, and “the finding of an association between the gut microbiota composition and survival, while interesting and provocative, does not provide evidence that intervening on the gut microbiota will lead to a clinical benefit.”
“I’m hopeful that randomized clinical trials will eventually demonstrate that we can protect or restore the gut microbiota, and this will lead to substantial clinical benefits, but this remains to be seen,” he said.
The authors had no disclosures to report. Dr. Jenq is an advisor for Seres Therapeutics, Prolacta Biosciences, and MaaT Pharma.
FROM BLOOD
New recommendation expands antiretroviral guidance for HIV
.
“With these new options we could potentially extend pre-exposure prophylaxis (PrEP) to a wider population,” says James Stevermer, MD, a member of the task force and a professor of family and community medicine at the University of Missouri–Columbia.
The guidance, published in JAMA, updates the group’s previous recommendation from 2019 to take into account the new options that have become available since the U.S. Food and Drug Administration approvals that included a long-acting injectable form.
In the original report, daily oral tenofovir disoproxil fumarate with emtricitabine was the only approved medication available and the task force recommended it. Since then, two new regimens have been approved: daily oral tenofovir alafenamide with emtricitabine and the long-acting injectable cabotegravir.
The task force is backing all three options and is recommending that clinicians use whichever formulation is most appropriate for their patients at risk for HIV infection.
Task force in primary and preventive care
The USPSTF is a volunteer group of experts in primary and preventive care who make recommendations on the best preventative interventions clinicians should take on everything from cancer screening, to preventive aspirin use, to behavioral counseling. The group is convened and supported by the Agency for Healthcare Research and Quality.
Recommendations from this group are particularly helpful for clinicians who may not see HIV as their area of expertise, says Carolyn Chu, MD, chief medical officer of the American Academy of HIV Medicine. “Hopefully, this will catch the eye of people who are not tracking all of the HIV updates,” she says.
A person’s risk for infection is mostly based on their behavior, Dr. Stevermer says. Those who use injectable drugs, particularly if they share needles, those who use condoms inconsistently and do not know their partner’s HIV status, and those who have recently had bacterial sexually transmitted infections like gonorrhea and syphilis are all at higher risk.
The efficacy of each of the three options is close enough to equal that it doesn’t usually matter which is prescribed, according to the task force. However, daily oral tenofovir alafenamide with emtricitabine is not approved for use by people engaging in receptive vaginal sex. For most people, the best medication option is the one they are most likely able to integrate into their routine. Cabotegravir, for example, which requires injections every 2 months, is an easier method for some people, particularly those who don’t think they could successfully take a daily pill.
Reducing risk
“The evidence is very clear that being able to adhere to taking the medication daily was very closely associated with the effectiveness of PrEP,” Dr. Stevermer says. “So, everything that we can do to make sure that the person who wants to prevent HIV is getting their PrEP as it is supposed to be taken makes it that much more effective.”
Expanding access to antiretrovirals among at-risk groups is an important part of the Ending the HIV Epidemic in the United States initiative that aims to reduce new HIV cases by 90% by 2030.
But an editorial published alongside the recommendation in JAMA notes that uptake of PrEP has been disproportionately low among populations most heavily affected by HIV.
In 2021, 78% of White people expected to benefit from PrEP received it, compared with just 11% of Black people and 21% of Hispanic people, despite both of those populations having a higher incidence of HIV than Whites. PrEP use is also substantially lower among cisgender and transgender women, youth, and people who inject drugs.
“We have an intervention that can markedly reduce people’s risk of getting HIV and so we want to make sure we get this out to all those populations at increased risk,” Dr. Stevermer says.
Having multiple options when it comes to PrEP is a big part of expanding access to the treatment for underserved groups, Dr. Chu says. “Even though oral tenofovir disoproxil fumarate with emtricitabine has been out for a while, we know it’s not getting to everyone, and there may be clinical circumstances that means it’s not the right option,” she says. “Making sure we are supporting choices so people can make the decision for themselves is important.”
But doctors also need to be willing to have an open conversation with their patients and bring up the topic of PrEP in a way that doesn’t feel judgmental or stigmatizing, Dr. Chu says.
It is also important not to make assumptions about who would want to talk about medication, she adds. “How can we change the narrative around PrEP?” she asks. “The evidence is there, these medications are effective and safe; weave PrEP into your preventive care portfolio to at least start the conversation.”
A version of this article appeared on Medscape.com.
.
“With these new options we could potentially extend pre-exposure prophylaxis (PrEP) to a wider population,” says James Stevermer, MD, a member of the task force and a professor of family and community medicine at the University of Missouri–Columbia.
The guidance, published in JAMA, updates the group’s previous recommendation from 2019 to take into account the new options that have become available since the U.S. Food and Drug Administration approvals that included a long-acting injectable form.
In the original report, daily oral tenofovir disoproxil fumarate with emtricitabine was the only approved medication available and the task force recommended it. Since then, two new regimens have been approved: daily oral tenofovir alafenamide with emtricitabine and the long-acting injectable cabotegravir.
The task force is backing all three options and is recommending that clinicians use whichever formulation is most appropriate for their patients at risk for HIV infection.
Task force in primary and preventive care
The USPSTF is a volunteer group of experts in primary and preventive care who make recommendations on the best preventative interventions clinicians should take on everything from cancer screening, to preventive aspirin use, to behavioral counseling. The group is convened and supported by the Agency for Healthcare Research and Quality.
Recommendations from this group are particularly helpful for clinicians who may not see HIV as their area of expertise, says Carolyn Chu, MD, chief medical officer of the American Academy of HIV Medicine. “Hopefully, this will catch the eye of people who are not tracking all of the HIV updates,” she says.
A person’s risk for infection is mostly based on their behavior, Dr. Stevermer says. Those who use injectable drugs, particularly if they share needles, those who use condoms inconsistently and do not know their partner’s HIV status, and those who have recently had bacterial sexually transmitted infections like gonorrhea and syphilis are all at higher risk.
The efficacy of each of the three options is close enough to equal that it doesn’t usually matter which is prescribed, according to the task force. However, daily oral tenofovir alafenamide with emtricitabine is not approved for use by people engaging in receptive vaginal sex. For most people, the best medication option is the one they are most likely able to integrate into their routine. Cabotegravir, for example, which requires injections every 2 months, is an easier method for some people, particularly those who don’t think they could successfully take a daily pill.
Reducing risk
“The evidence is very clear that being able to adhere to taking the medication daily was very closely associated with the effectiveness of PrEP,” Dr. Stevermer says. “So, everything that we can do to make sure that the person who wants to prevent HIV is getting their PrEP as it is supposed to be taken makes it that much more effective.”
Expanding access to antiretrovirals among at-risk groups is an important part of the Ending the HIV Epidemic in the United States initiative that aims to reduce new HIV cases by 90% by 2030.
But an editorial published alongside the recommendation in JAMA notes that uptake of PrEP has been disproportionately low among populations most heavily affected by HIV.
In 2021, 78% of White people expected to benefit from PrEP received it, compared with just 11% of Black people and 21% of Hispanic people, despite both of those populations having a higher incidence of HIV than Whites. PrEP use is also substantially lower among cisgender and transgender women, youth, and people who inject drugs.
“We have an intervention that can markedly reduce people’s risk of getting HIV and so we want to make sure we get this out to all those populations at increased risk,” Dr. Stevermer says.
Having multiple options when it comes to PrEP is a big part of expanding access to the treatment for underserved groups, Dr. Chu says. “Even though oral tenofovir disoproxil fumarate with emtricitabine has been out for a while, we know it’s not getting to everyone, and there may be clinical circumstances that means it’s not the right option,” she says. “Making sure we are supporting choices so people can make the decision for themselves is important.”
But doctors also need to be willing to have an open conversation with their patients and bring up the topic of PrEP in a way that doesn’t feel judgmental or stigmatizing, Dr. Chu says.
It is also important not to make assumptions about who would want to talk about medication, she adds. “How can we change the narrative around PrEP?” she asks. “The evidence is there, these medications are effective and safe; weave PrEP into your preventive care portfolio to at least start the conversation.”
A version of this article appeared on Medscape.com.
.
“With these new options we could potentially extend pre-exposure prophylaxis (PrEP) to a wider population,” says James Stevermer, MD, a member of the task force and a professor of family and community medicine at the University of Missouri–Columbia.
The guidance, published in JAMA, updates the group’s previous recommendation from 2019 to take into account the new options that have become available since the U.S. Food and Drug Administration approvals that included a long-acting injectable form.
In the original report, daily oral tenofovir disoproxil fumarate with emtricitabine was the only approved medication available and the task force recommended it. Since then, two new regimens have been approved: daily oral tenofovir alafenamide with emtricitabine and the long-acting injectable cabotegravir.
The task force is backing all three options and is recommending that clinicians use whichever formulation is most appropriate for their patients at risk for HIV infection.
Task force in primary and preventive care
The USPSTF is a volunteer group of experts in primary and preventive care who make recommendations on the best preventative interventions clinicians should take on everything from cancer screening, to preventive aspirin use, to behavioral counseling. The group is convened and supported by the Agency for Healthcare Research and Quality.
Recommendations from this group are particularly helpful for clinicians who may not see HIV as their area of expertise, says Carolyn Chu, MD, chief medical officer of the American Academy of HIV Medicine. “Hopefully, this will catch the eye of people who are not tracking all of the HIV updates,” she says.
A person’s risk for infection is mostly based on their behavior, Dr. Stevermer says. Those who use injectable drugs, particularly if they share needles, those who use condoms inconsistently and do not know their partner’s HIV status, and those who have recently had bacterial sexually transmitted infections like gonorrhea and syphilis are all at higher risk.
The efficacy of each of the three options is close enough to equal that it doesn’t usually matter which is prescribed, according to the task force. However, daily oral tenofovir alafenamide with emtricitabine is not approved for use by people engaging in receptive vaginal sex. For most people, the best medication option is the one they are most likely able to integrate into their routine. Cabotegravir, for example, which requires injections every 2 months, is an easier method for some people, particularly those who don’t think they could successfully take a daily pill.
Reducing risk
“The evidence is very clear that being able to adhere to taking the medication daily was very closely associated with the effectiveness of PrEP,” Dr. Stevermer says. “So, everything that we can do to make sure that the person who wants to prevent HIV is getting their PrEP as it is supposed to be taken makes it that much more effective.”
Expanding access to antiretrovirals among at-risk groups is an important part of the Ending the HIV Epidemic in the United States initiative that aims to reduce new HIV cases by 90% by 2030.
But an editorial published alongside the recommendation in JAMA notes that uptake of PrEP has been disproportionately low among populations most heavily affected by HIV.
In 2021, 78% of White people expected to benefit from PrEP received it, compared with just 11% of Black people and 21% of Hispanic people, despite both of those populations having a higher incidence of HIV than Whites. PrEP use is also substantially lower among cisgender and transgender women, youth, and people who inject drugs.
“We have an intervention that can markedly reduce people’s risk of getting HIV and so we want to make sure we get this out to all those populations at increased risk,” Dr. Stevermer says.
Having multiple options when it comes to PrEP is a big part of expanding access to the treatment for underserved groups, Dr. Chu says. “Even though oral tenofovir disoproxil fumarate with emtricitabine has been out for a while, we know it’s not getting to everyone, and there may be clinical circumstances that means it’s not the right option,” she says. “Making sure we are supporting choices so people can make the decision for themselves is important.”
But doctors also need to be willing to have an open conversation with their patients and bring up the topic of PrEP in a way that doesn’t feel judgmental or stigmatizing, Dr. Chu says.
It is also important not to make assumptions about who would want to talk about medication, she adds. “How can we change the narrative around PrEP?” she asks. “The evidence is there, these medications are effective and safe; weave PrEP into your preventive care portfolio to at least start the conversation.”
A version of this article appeared on Medscape.com.
Mohs found to confer survival benefit in localized Merkel cell carcinoma
results from a national retrospective cohort study suggest.
The study found that, in patients with pathologically confirmed, localized T1/T2 MCC, “treatment with MMS was associated with an approximately 40% reduction in hazard of death compared with WLE,” reported John A. Carucci, MD, PhD, and colleagues in the department of dermatology at NYU Langone Health, New York. The results provide “preliminary data suggesting that treatment of localized, early-stage MCC with MMS may result in the most optimal patient survival outcomes for this aggressive form of skin cancer,” they added. The study was published online in JAMA Dermatology.
“Although data for keratinocytic nonmelanoma skin cancers have been definitive in demonstrating the advantage of peripheral and deep en face margin assessment over conventional WLE or NME [narrow-margin excision], the data for MCC, likely because of the disease’s rarity and limitations of available data sets, have been mixed,” they wrote.
Results from national studies published in the Journal of the National Cancer Institute and the Journal of the American Academy of Dermatology found no difference in survival among patients with localized MCC treated with WLE versus MMS. “However, these studies did not have confirmed pathologic node status, a substantial limitation considering that clinically node-negative cases of localized MCC have sentinel lymph node positivity rates ranging from 25% to 40%,” the authors noted.
To evaluate the association of the surgical excision modality and patient survival for pathologically confirmed localized T1/T2 MCC, Dr. Carucci and coauthors examined a cohort of 2,313 patients from the National Cancer Database with T1/T2 MCC diagnosed between Jan. 1, 2004, and Dec. 31, 2018, with pathologically confirmed, negative regional lymph nodes and treated with surgery. Their mean age was 71 years and 57.9% were male. Of the 2,313 patients, 1,452 underwent WLE, 104 underwent MMS, and 757 underwent NME.
The unadjusted analysis revealed that, compared with WLE, excision with MMS had the best unadjusted mean survival rates: 87.4% versus 86.1%, respectively, at 3 years, 84.5% versus 76.9% at 5 years, and 81.8% versus 60.9% at 10 years. Patients treated with NME had similar mean survival rates as those treated with WLE: 84.8% at 3 years, 78.3% at 5 years, and 60.8% at 10 years.
Multivariable survival analysis demonstrated that treatment with MMS was associated with significantly improved survival, compared with WLE (hazard ratio, 0.59; 95% CI, 0.36-0.97; P = .04).
“These data suggest that MMS may provide a survival benefit in the treatment of localized MCC, although further prospective work studying this issue is required,” the authors concluded. “Future directions may also focus on elucidating the benefit of adjuvant radiotherapy in localized cases treated with MMS.”
They acknowledged certain limitations of the study, including the fewer numbers of patients receiving MMS surgery, lack of randomization, and potential for selection bias.
In an interview, Travis W. Blalock, MD, director of dermatologic surgery, Mohs micrographic surgery, and cutaneous oncology at Emory University, Atlanta, who was asked to comment on the study, said that the field of MCC “has undergone rapid and robust transformation over the past 20 years. These changes encompass advancements in diagnosing the condition, identifying linked viruses, and developing systemic treatments.”
The study findings “imply that comprehensive assessment of histologic margins might offer advantages beyond minimizing scars, minimizing functional impact, and reducing the likelihood of local recurrence,” he said.
“It’s beyond doubt,” he added, that the study “furnishes us with yet another set of real-world insights that will undoubtedly influence patient outcomes. These insights serve to bring clarity to the ways in which we can deliver precisely targeted surgical treatment with durable outcomes for localized MCC.”
Patricia M. Richey, MD, director of Mohs surgery at Boston University, who was also asked to comment on the study, added that, because of the nature of the National Cancer Database, “the authors of this study were unfortunately unable to report disease-specific survival or immunosuppression status. That being said, the preliminary data presented are convincing and should result in us further exploring this topic, as well as readdressing and questioning related issues such as whether or not adjuvant radiotherapy is truly beneficial in cases with histologic clearance via Mohs.”
Dr. Carucci reported receiving grant funding from Regeneron for investigator-initiated basic research. No other author disclosures were reported. Neither Dr. Blalock nor Dr. Richey had relevant disclosures.
results from a national retrospective cohort study suggest.
The study found that, in patients with pathologically confirmed, localized T1/T2 MCC, “treatment with MMS was associated with an approximately 40% reduction in hazard of death compared with WLE,” reported John A. Carucci, MD, PhD, and colleagues in the department of dermatology at NYU Langone Health, New York. The results provide “preliminary data suggesting that treatment of localized, early-stage MCC with MMS may result in the most optimal patient survival outcomes for this aggressive form of skin cancer,” they added. The study was published online in JAMA Dermatology.
“Although data for keratinocytic nonmelanoma skin cancers have been definitive in demonstrating the advantage of peripheral and deep en face margin assessment over conventional WLE or NME [narrow-margin excision], the data for MCC, likely because of the disease’s rarity and limitations of available data sets, have been mixed,” they wrote.
Results from national studies published in the Journal of the National Cancer Institute and the Journal of the American Academy of Dermatology found no difference in survival among patients with localized MCC treated with WLE versus MMS. “However, these studies did not have confirmed pathologic node status, a substantial limitation considering that clinically node-negative cases of localized MCC have sentinel lymph node positivity rates ranging from 25% to 40%,” the authors noted.
To evaluate the association of the surgical excision modality and patient survival for pathologically confirmed localized T1/T2 MCC, Dr. Carucci and coauthors examined a cohort of 2,313 patients from the National Cancer Database with T1/T2 MCC diagnosed between Jan. 1, 2004, and Dec. 31, 2018, with pathologically confirmed, negative regional lymph nodes and treated with surgery. Their mean age was 71 years and 57.9% were male. Of the 2,313 patients, 1,452 underwent WLE, 104 underwent MMS, and 757 underwent NME.
The unadjusted analysis revealed that, compared with WLE, excision with MMS had the best unadjusted mean survival rates: 87.4% versus 86.1%, respectively, at 3 years, 84.5% versus 76.9% at 5 years, and 81.8% versus 60.9% at 10 years. Patients treated with NME had similar mean survival rates as those treated with WLE: 84.8% at 3 years, 78.3% at 5 years, and 60.8% at 10 years.
Multivariable survival analysis demonstrated that treatment with MMS was associated with significantly improved survival, compared with WLE (hazard ratio, 0.59; 95% CI, 0.36-0.97; P = .04).
“These data suggest that MMS may provide a survival benefit in the treatment of localized MCC, although further prospective work studying this issue is required,” the authors concluded. “Future directions may also focus on elucidating the benefit of adjuvant radiotherapy in localized cases treated with MMS.”
They acknowledged certain limitations of the study, including the fewer numbers of patients receiving MMS surgery, lack of randomization, and potential for selection bias.
In an interview, Travis W. Blalock, MD, director of dermatologic surgery, Mohs micrographic surgery, and cutaneous oncology at Emory University, Atlanta, who was asked to comment on the study, said that the field of MCC “has undergone rapid and robust transformation over the past 20 years. These changes encompass advancements in diagnosing the condition, identifying linked viruses, and developing systemic treatments.”
The study findings “imply that comprehensive assessment of histologic margins might offer advantages beyond minimizing scars, minimizing functional impact, and reducing the likelihood of local recurrence,” he said.
“It’s beyond doubt,” he added, that the study “furnishes us with yet another set of real-world insights that will undoubtedly influence patient outcomes. These insights serve to bring clarity to the ways in which we can deliver precisely targeted surgical treatment with durable outcomes for localized MCC.”
Patricia M. Richey, MD, director of Mohs surgery at Boston University, who was also asked to comment on the study, added that, because of the nature of the National Cancer Database, “the authors of this study were unfortunately unable to report disease-specific survival or immunosuppression status. That being said, the preliminary data presented are convincing and should result in us further exploring this topic, as well as readdressing and questioning related issues such as whether or not adjuvant radiotherapy is truly beneficial in cases with histologic clearance via Mohs.”
Dr. Carucci reported receiving grant funding from Regeneron for investigator-initiated basic research. No other author disclosures were reported. Neither Dr. Blalock nor Dr. Richey had relevant disclosures.
results from a national retrospective cohort study suggest.
The study found that, in patients with pathologically confirmed, localized T1/T2 MCC, “treatment with MMS was associated with an approximately 40% reduction in hazard of death compared with WLE,” reported John A. Carucci, MD, PhD, and colleagues in the department of dermatology at NYU Langone Health, New York. The results provide “preliminary data suggesting that treatment of localized, early-stage MCC with MMS may result in the most optimal patient survival outcomes for this aggressive form of skin cancer,” they added. The study was published online in JAMA Dermatology.
“Although data for keratinocytic nonmelanoma skin cancers have been definitive in demonstrating the advantage of peripheral and deep en face margin assessment over conventional WLE or NME [narrow-margin excision], the data for MCC, likely because of the disease’s rarity and limitations of available data sets, have been mixed,” they wrote.
Results from national studies published in the Journal of the National Cancer Institute and the Journal of the American Academy of Dermatology found no difference in survival among patients with localized MCC treated with WLE versus MMS. “However, these studies did not have confirmed pathologic node status, a substantial limitation considering that clinically node-negative cases of localized MCC have sentinel lymph node positivity rates ranging from 25% to 40%,” the authors noted.
To evaluate the association of the surgical excision modality and patient survival for pathologically confirmed localized T1/T2 MCC, Dr. Carucci and coauthors examined a cohort of 2,313 patients from the National Cancer Database with T1/T2 MCC diagnosed between Jan. 1, 2004, and Dec. 31, 2018, with pathologically confirmed, negative regional lymph nodes and treated with surgery. Their mean age was 71 years and 57.9% were male. Of the 2,313 patients, 1,452 underwent WLE, 104 underwent MMS, and 757 underwent NME.
The unadjusted analysis revealed that, compared with WLE, excision with MMS had the best unadjusted mean survival rates: 87.4% versus 86.1%, respectively, at 3 years, 84.5% versus 76.9% at 5 years, and 81.8% versus 60.9% at 10 years. Patients treated with NME had similar mean survival rates as those treated with WLE: 84.8% at 3 years, 78.3% at 5 years, and 60.8% at 10 years.
Multivariable survival analysis demonstrated that treatment with MMS was associated with significantly improved survival, compared with WLE (hazard ratio, 0.59; 95% CI, 0.36-0.97; P = .04).
“These data suggest that MMS may provide a survival benefit in the treatment of localized MCC, although further prospective work studying this issue is required,” the authors concluded. “Future directions may also focus on elucidating the benefit of adjuvant radiotherapy in localized cases treated with MMS.”
They acknowledged certain limitations of the study, including the fewer numbers of patients receiving MMS surgery, lack of randomization, and potential for selection bias.
In an interview, Travis W. Blalock, MD, director of dermatologic surgery, Mohs micrographic surgery, and cutaneous oncology at Emory University, Atlanta, who was asked to comment on the study, said that the field of MCC “has undergone rapid and robust transformation over the past 20 years. These changes encompass advancements in diagnosing the condition, identifying linked viruses, and developing systemic treatments.”
The study findings “imply that comprehensive assessment of histologic margins might offer advantages beyond minimizing scars, minimizing functional impact, and reducing the likelihood of local recurrence,” he said.
“It’s beyond doubt,” he added, that the study “furnishes us with yet another set of real-world insights that will undoubtedly influence patient outcomes. These insights serve to bring clarity to the ways in which we can deliver precisely targeted surgical treatment with durable outcomes for localized MCC.”
Patricia M. Richey, MD, director of Mohs surgery at Boston University, who was also asked to comment on the study, added that, because of the nature of the National Cancer Database, “the authors of this study were unfortunately unable to report disease-specific survival or immunosuppression status. That being said, the preliminary data presented are convincing and should result in us further exploring this topic, as well as readdressing and questioning related issues such as whether or not adjuvant radiotherapy is truly beneficial in cases with histologic clearance via Mohs.”
Dr. Carucci reported receiving grant funding from Regeneron for investigator-initiated basic research. No other author disclosures were reported. Neither Dr. Blalock nor Dr. Richey had relevant disclosures.
FROM JAMA DERMATOLOGY
Human frailty is a cash cow
Doctor, if you are caring for patients with diabetes, I sure hope you know more about it than I do. The longer I live, it seems, the less I understand.
In a free society, people can do what they want, and that’s great except when it isn’t. That’s why societies develop ethics and even public laws if ethics are not strong enough to protect us from ourselves and others.
Sugar, sugar
When I was growing up in small-town Alabama during the Depression and World War II, we called it sugar diabetes. Eat too much sugar, you got fat; your blood sugar went up, and you spilled sugar into your urine. Diabetes was fairly rare, and so was obesity. Doctors treated it by limiting the intake of sugar (and various sweet foods), along with attempting weight loss. If that didn’t do the trick, insulin injections.
From then until now, note these trends.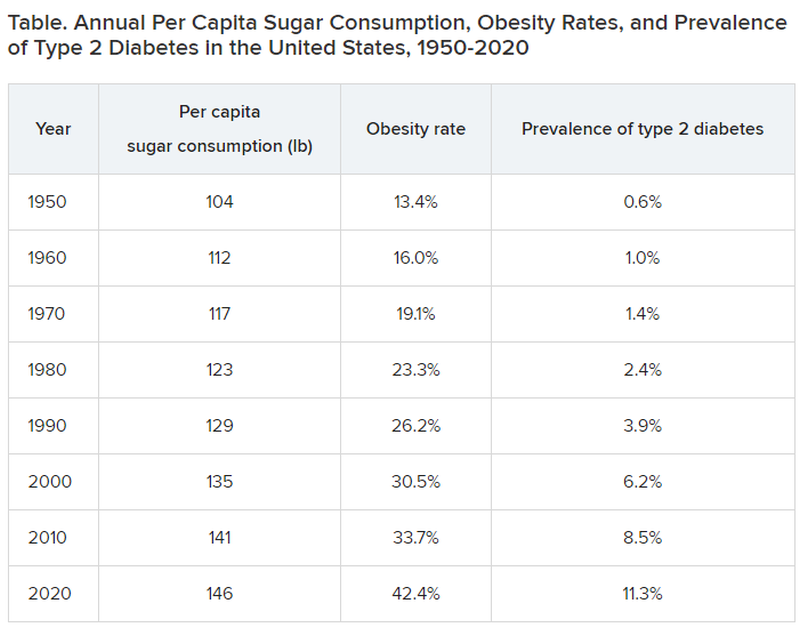
Type 2 diabetes was diagnosed even more infrequently before 1950:
- 1920: 0.2% of the population
- 1930: 0.3% of the population
- 1940: 0.4% of the population
In 2020, although 11.3% of the population was diagnosed with type 2 diabetes, the unknown undiagnosed proportion could be much higher.
Notice a correlation between sugar consumption and prevalence of diabetes? Of course, correlation is not causation, but at the same time, it sure as hell is not negation. Such concordance can be considered hypothesis generating. It may not be true causation, but it’s a good bet when 89% of people with diabetes have overweight or obesity.
What did the entire medical, public health, government, agriculture, nursing, food manufacturing, marketing, advertising, restaurant, and education constituencies do about this as it was happening? They observed, documented, gave lip service, and wrung their hands in public a bit. I do not believe that this is an organized active conspiracy; it would take too many players cooperating over too long a period of time. But it certainly may be a passive conspiracy, and primary care physicians and their patients are trapped.
The proper daily practice of medicine consists of one patient, one physician, one moment, and one decision. Let it be a shared decision, informed by the best evidence and taking cost into consideration. That encounter represents an opportunity, a responsibility, and a conundrum.
Individual health is subsumed under the collective health of the public. As such, a patient’s health is out of the control of both physician and patient; instead, patients are the beneficiaries or victims of the “marketplace.” Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.
Rethinking diabetes
Consider diabetes as one of many examples. What a terrific deal for capitalism. then it discovers (invents) long-term, very expensive, compelling treatments to slim us down, with no end in sight, and still without ever understanding the true nature of diabetes.
Gary Taubes’s great new book, “Rethinking Diabetes: What Science Reveals About Diet, Insulin, and Successful Treatments,” is being published by Alfred A. Knopf in early 2024.
It is 404 pages of (dense) text, with 401 numbered references and footnotes, a bibliography of 790 references, alphabetically arranged for easy cross-checking, and a 25-page index.
Remember Mr. Taubes’s earlier definitive historical treatises: “Good Calories, Bad Calories” (2007), “Why We Get Fat” (2010), “The Case Against Sugar” (2016), and “The Case for Keto” (2020)?
This new book is more like “Good Calories, Bad Calories”: long, dense, detailed, definitive, and of great historical reference value, including original research information from other countries in other languages. The author told me that the many early research reference sources were available only in German and that his use of generative artificial intelligence as an assistant researcher was of great value.
Nonphysician author Mr. Taubes uses his deep understanding of science and history to inform his long-honed talents of impartial investigative journalism as he attempts to understand and then explain why after all these years, the medical scientific community still does not have a sound consensus about the essence of diabetes, diet, insulin, and proper prevention and treatment at a level that is actually effective – amazing and so sad.
To signal these evolved and evolving conflicts, the book includes the following chapters:
- “Rise of the Carbohydrate-Rich and Very-Low-Carbohydrate Diets”
- “The Fear of Fat and High-Fat Diets”
- “Insulin and The End of Carbohydrate Restriction and Low Blood Sugar”
Yes, it is difficult. Imagine the bookend segments: “The Nature of Medical Knowledge” and “The Conflicts of Evidence-Based Medicine.” There is also a detailed discussion of good versus bad science spanning three long chapters.
If all that reads like a greatly confused mess to you then you’re beginning to understand. If you are a fan of an unbiased explication of the evolution of understanding the ins and outs of scientific history in richly documented detail, this is a book for you. It’s not a quick nor easy read. And don’t expect to discover whether the newest wonder drugs for weight loss and control of diabetes will be the long-term solution for people with obesity and diabetes worldwide.
Obesity and overweight are major risk factors for type 2 diabetes. About 90% of patients with diabetes have either overweight or obesity. Thus, the complications of these two conditions, which largely overlap, include atherosclerotic cardiovascular disease; myocardial infarction; stroke; hypertension; metabolic syndrome; lower-extremity gangrene; chronic kidney disease; retinopathy; glaucoma; cataracts; disabling osteoarthritis; breast, endometrial, colon, and other cancers; fatty liver; sleep apnea; and peripheral neuropathy. These diseases create a major lucrative business for a wide swathe of medical and surgical specialties, plus hospital, clinic, device, pharmaceutical, and food industries.
In summary, we’ve just been through 40 years of failure to recognize the sugar-elephant in the room and intervene with serious preventive efforts. Forty years of fleshing out both the populace and the American medical-industrial complex (AMIC). Talk about a sweet spot. The only successful long-term treatment of obesity (and with it, diabetes) is prevention. Don’t emphasize losing weight. Focus on preventing excessive weight gain, right now, for the population, beginning with yourselves. Otherwise, we continue openly to perpetuate a terrific deal for the AMIC, a travesty for everyone else. Time for some industrial grade penance and a course correction.
Meanwhile, here we are living out Big Pharma’s dream of a big populace, produced by the agriculture and food industries, enjoyed by capitalism after failures of education, medicine, and public health: a seemingly endless supply of people living with big complications who are ready for big (expensive, new) medications to fix the world’s big health problems.
Dr. Lundberg is editor in chief, Cancer Commons. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Doctor, if you are caring for patients with diabetes, I sure hope you know more about it than I do. The longer I live, it seems, the less I understand.
In a free society, people can do what they want, and that’s great except when it isn’t. That’s why societies develop ethics and even public laws if ethics are not strong enough to protect us from ourselves and others.
Sugar, sugar
When I was growing up in small-town Alabama during the Depression and World War II, we called it sugar diabetes. Eat too much sugar, you got fat; your blood sugar went up, and you spilled sugar into your urine. Diabetes was fairly rare, and so was obesity. Doctors treated it by limiting the intake of sugar (and various sweet foods), along with attempting weight loss. If that didn’t do the trick, insulin injections.
From then until now, note these trends.
Type 2 diabetes was diagnosed even more infrequently before 1950:
- 1920: 0.2% of the population
- 1930: 0.3% of the population
- 1940: 0.4% of the population
In 2020, although 11.3% of the population was diagnosed with type 2 diabetes, the unknown undiagnosed proportion could be much higher.
Notice a correlation between sugar consumption and prevalence of diabetes? Of course, correlation is not causation, but at the same time, it sure as hell is not negation. Such concordance can be considered hypothesis generating. It may not be true causation, but it’s a good bet when 89% of people with diabetes have overweight or obesity.
What did the entire medical, public health, government, agriculture, nursing, food manufacturing, marketing, advertising, restaurant, and education constituencies do about this as it was happening? They observed, documented, gave lip service, and wrung their hands in public a bit. I do not believe that this is an organized active conspiracy; it would take too many players cooperating over too long a period of time. But it certainly may be a passive conspiracy, and primary care physicians and their patients are trapped.
The proper daily practice of medicine consists of one patient, one physician, one moment, and one decision. Let it be a shared decision, informed by the best evidence and taking cost into consideration. That encounter represents an opportunity, a responsibility, and a conundrum.
Individual health is subsumed under the collective health of the public. As such, a patient’s health is out of the control of both physician and patient; instead, patients are the beneficiaries or victims of the “marketplace.” Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.
Rethinking diabetes
Consider diabetes as one of many examples. What a terrific deal for capitalism. then it discovers (invents) long-term, very expensive, compelling treatments to slim us down, with no end in sight, and still without ever understanding the true nature of diabetes.
Gary Taubes’s great new book, “Rethinking Diabetes: What Science Reveals About Diet, Insulin, and Successful Treatments,” is being published by Alfred A. Knopf in early 2024.
It is 404 pages of (dense) text, with 401 numbered references and footnotes, a bibliography of 790 references, alphabetically arranged for easy cross-checking, and a 25-page index.
Remember Mr. Taubes’s earlier definitive historical treatises: “Good Calories, Bad Calories” (2007), “Why We Get Fat” (2010), “The Case Against Sugar” (2016), and “The Case for Keto” (2020)?
This new book is more like “Good Calories, Bad Calories”: long, dense, detailed, definitive, and of great historical reference value, including original research information from other countries in other languages. The author told me that the many early research reference sources were available only in German and that his use of generative artificial intelligence as an assistant researcher was of great value.
Nonphysician author Mr. Taubes uses his deep understanding of science and history to inform his long-honed talents of impartial investigative journalism as he attempts to understand and then explain why after all these years, the medical scientific community still does not have a sound consensus about the essence of diabetes, diet, insulin, and proper prevention and treatment at a level that is actually effective – amazing and so sad.
To signal these evolved and evolving conflicts, the book includes the following chapters:
- “Rise of the Carbohydrate-Rich and Very-Low-Carbohydrate Diets”
- “The Fear of Fat and High-Fat Diets”
- “Insulin and The End of Carbohydrate Restriction and Low Blood Sugar”
Yes, it is difficult. Imagine the bookend segments: “The Nature of Medical Knowledge” and “The Conflicts of Evidence-Based Medicine.” There is also a detailed discussion of good versus bad science spanning three long chapters.
If all that reads like a greatly confused mess to you then you’re beginning to understand. If you are a fan of an unbiased explication of the evolution of understanding the ins and outs of scientific history in richly documented detail, this is a book for you. It’s not a quick nor easy read. And don’t expect to discover whether the newest wonder drugs for weight loss and control of diabetes will be the long-term solution for people with obesity and diabetes worldwide.
Obesity and overweight are major risk factors for type 2 diabetes. About 90% of patients with diabetes have either overweight or obesity. Thus, the complications of these two conditions, which largely overlap, include atherosclerotic cardiovascular disease; myocardial infarction; stroke; hypertension; metabolic syndrome; lower-extremity gangrene; chronic kidney disease; retinopathy; glaucoma; cataracts; disabling osteoarthritis; breast, endometrial, colon, and other cancers; fatty liver; sleep apnea; and peripheral neuropathy. These diseases create a major lucrative business for a wide swathe of medical and surgical specialties, plus hospital, clinic, device, pharmaceutical, and food industries.
In summary, we’ve just been through 40 years of failure to recognize the sugar-elephant in the room and intervene with serious preventive efforts. Forty years of fleshing out both the populace and the American medical-industrial complex (AMIC). Talk about a sweet spot. The only successful long-term treatment of obesity (and with it, diabetes) is prevention. Don’t emphasize losing weight. Focus on preventing excessive weight gain, right now, for the population, beginning with yourselves. Otherwise, we continue openly to perpetuate a terrific deal for the AMIC, a travesty for everyone else. Time for some industrial grade penance and a course correction.
Meanwhile, here we are living out Big Pharma’s dream of a big populace, produced by the agriculture and food industries, enjoyed by capitalism after failures of education, medicine, and public health: a seemingly endless supply of people living with big complications who are ready for big (expensive, new) medications to fix the world’s big health problems.
Dr. Lundberg is editor in chief, Cancer Commons. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Doctor, if you are caring for patients with diabetes, I sure hope you know more about it than I do. The longer I live, it seems, the less I understand.
In a free society, people can do what they want, and that’s great except when it isn’t. That’s why societies develop ethics and even public laws if ethics are not strong enough to protect us from ourselves and others.
Sugar, sugar
When I was growing up in small-town Alabama during the Depression and World War II, we called it sugar diabetes. Eat too much sugar, you got fat; your blood sugar went up, and you spilled sugar into your urine. Diabetes was fairly rare, and so was obesity. Doctors treated it by limiting the intake of sugar (and various sweet foods), along with attempting weight loss. If that didn’t do the trick, insulin injections.
From then until now, note these trends.
Type 2 diabetes was diagnosed even more infrequently before 1950:
- 1920: 0.2% of the population
- 1930: 0.3% of the population
- 1940: 0.4% of the population
In 2020, although 11.3% of the population was diagnosed with type 2 diabetes, the unknown undiagnosed proportion could be much higher.
Notice a correlation between sugar consumption and prevalence of diabetes? Of course, correlation is not causation, but at the same time, it sure as hell is not negation. Such concordance can be considered hypothesis generating. It may not be true causation, but it’s a good bet when 89% of people with diabetes have overweight or obesity.
What did the entire medical, public health, government, agriculture, nursing, food manufacturing, marketing, advertising, restaurant, and education constituencies do about this as it was happening? They observed, documented, gave lip service, and wrung their hands in public a bit. I do not believe that this is an organized active conspiracy; it would take too many players cooperating over too long a period of time. But it certainly may be a passive conspiracy, and primary care physicians and their patients are trapped.
The proper daily practice of medicine consists of one patient, one physician, one moment, and one decision. Let it be a shared decision, informed by the best evidence and taking cost into consideration. That encounter represents an opportunity, a responsibility, and a conundrum.
Individual health is subsumed under the collective health of the public. As such, a patient’s health is out of the control of both physician and patient; instead, patients are the beneficiaries or victims of the “marketplace.” Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.
Rethinking diabetes
Consider diabetes as one of many examples. What a terrific deal for capitalism. then it discovers (invents) long-term, very expensive, compelling treatments to slim us down, with no end in sight, and still without ever understanding the true nature of diabetes.
Gary Taubes’s great new book, “Rethinking Diabetes: What Science Reveals About Diet, Insulin, and Successful Treatments,” is being published by Alfred A. Knopf in early 2024.
It is 404 pages of (dense) text, with 401 numbered references and footnotes, a bibliography of 790 references, alphabetically arranged for easy cross-checking, and a 25-page index.
Remember Mr. Taubes’s earlier definitive historical treatises: “Good Calories, Bad Calories” (2007), “Why We Get Fat” (2010), “The Case Against Sugar” (2016), and “The Case for Keto” (2020)?
This new book is more like “Good Calories, Bad Calories”: long, dense, detailed, definitive, and of great historical reference value, including original research information from other countries in other languages. The author told me that the many early research reference sources were available only in German and that his use of generative artificial intelligence as an assistant researcher was of great value.
Nonphysician author Mr. Taubes uses his deep understanding of science and history to inform his long-honed talents of impartial investigative journalism as he attempts to understand and then explain why after all these years, the medical scientific community still does not have a sound consensus about the essence of diabetes, diet, insulin, and proper prevention and treatment at a level that is actually effective – amazing and so sad.
To signal these evolved and evolving conflicts, the book includes the following chapters:
- “Rise of the Carbohydrate-Rich and Very-Low-Carbohydrate Diets”
- “The Fear of Fat and High-Fat Diets”
- “Insulin and The End of Carbohydrate Restriction and Low Blood Sugar”
Yes, it is difficult. Imagine the bookend segments: “The Nature of Medical Knowledge” and “The Conflicts of Evidence-Based Medicine.” There is also a detailed discussion of good versus bad science spanning three long chapters.
If all that reads like a greatly confused mess to you then you’re beginning to understand. If you are a fan of an unbiased explication of the evolution of understanding the ins and outs of scientific history in richly documented detail, this is a book for you. It’s not a quick nor easy read. And don’t expect to discover whether the newest wonder drugs for weight loss and control of diabetes will be the long-term solution for people with obesity and diabetes worldwide.
Obesity and overweight are major risk factors for type 2 diabetes. About 90% of patients with diabetes have either overweight or obesity. Thus, the complications of these two conditions, which largely overlap, include atherosclerotic cardiovascular disease; myocardial infarction; stroke; hypertension; metabolic syndrome; lower-extremity gangrene; chronic kidney disease; retinopathy; glaucoma; cataracts; disabling osteoarthritis; breast, endometrial, colon, and other cancers; fatty liver; sleep apnea; and peripheral neuropathy. These diseases create a major lucrative business for a wide swathe of medical and surgical specialties, plus hospital, clinic, device, pharmaceutical, and food industries.
In summary, we’ve just been through 40 years of failure to recognize the sugar-elephant in the room and intervene with serious preventive efforts. Forty years of fleshing out both the populace and the American medical-industrial complex (AMIC). Talk about a sweet spot. The only successful long-term treatment of obesity (and with it, diabetes) is prevention. Don’t emphasize losing weight. Focus on preventing excessive weight gain, right now, for the population, beginning with yourselves. Otherwise, we continue openly to perpetuate a terrific deal for the AMIC, a travesty for everyone else. Time for some industrial grade penance and a course correction.
Meanwhile, here we are living out Big Pharma’s dream of a big populace, produced by the agriculture and food industries, enjoyed by capitalism after failures of education, medicine, and public health: a seemingly endless supply of people living with big complications who are ready for big (expensive, new) medications to fix the world’s big health problems.
Dr. Lundberg is editor in chief, Cancer Commons. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.