User login
Growing Subcutaneous Mass on the Thigh
The Diagnosis: Eccrine Angiomatous Hamartoma
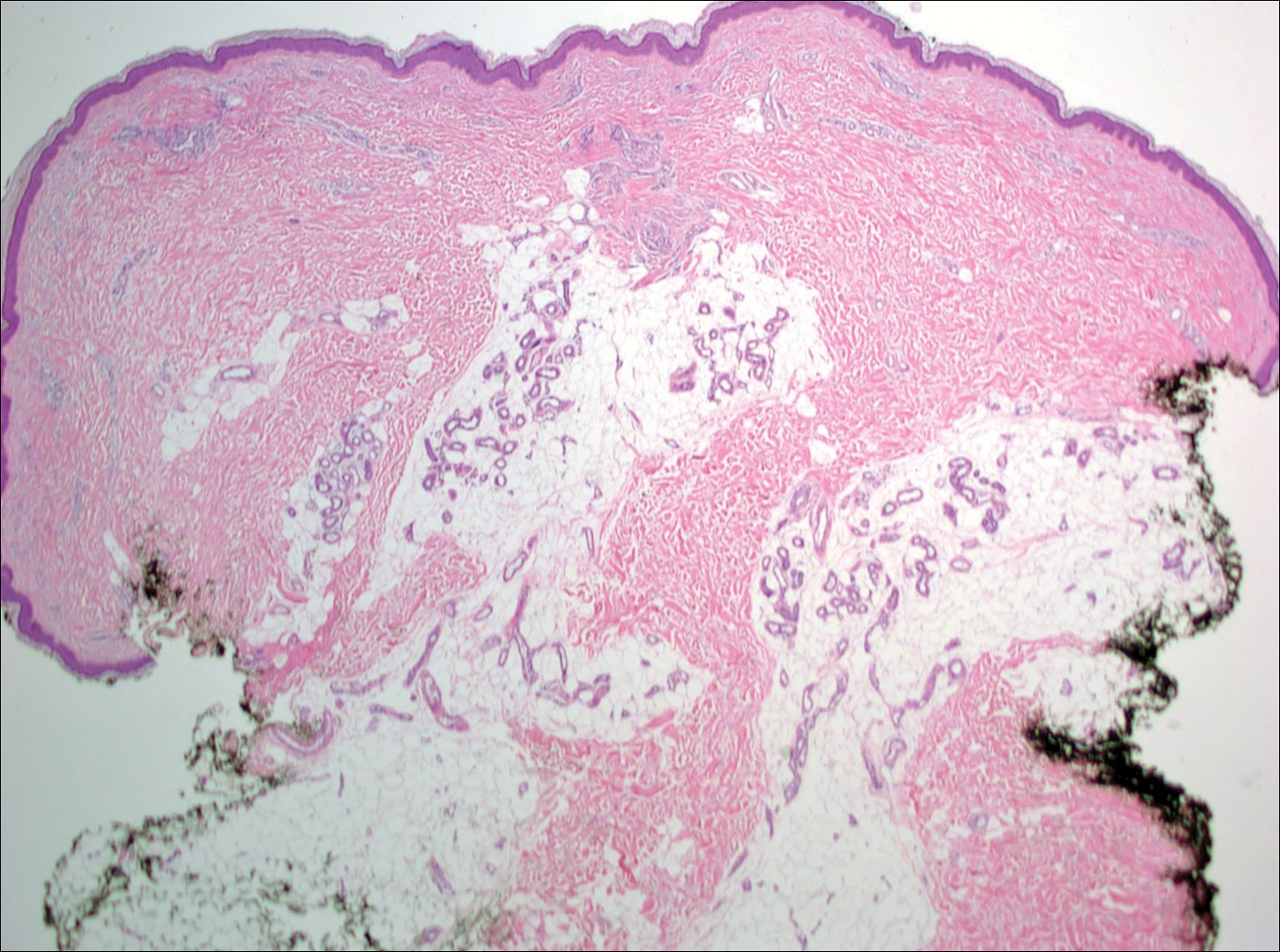
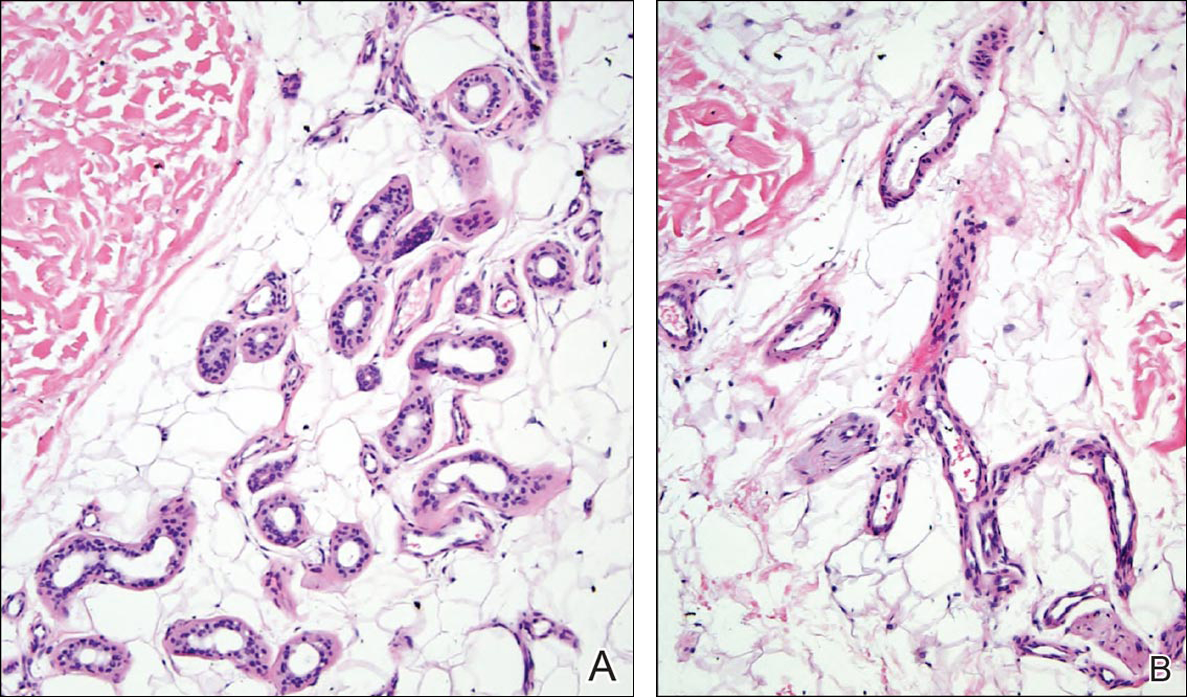
Given the progression of symptoms 3 months prior to presentation, an excisional biopsy was performed (Figure 1). Hematoxylin and eosin staining showed prominent eccrine sweat glands and vessels surrounded by superficially located adipose tissue in the mid and deep dermis (Figure 2).
Eccrine angiomatous hamartoma (EAH) is an uncommon benign tumor typically located on the arms and legs or trunk. It is usually solitary, though cases with multiple lesions have been reported.1,2 Most cases are diagnosed in childhood as either congenital or acquired lesions. However, EAHs can develop in adulthood and have been described in patients up to 70 years of age.3 The median age of diagnosis is 10 years,2 indicating that EAH is primarily a pediatric tumor. There is no gender predilection.
Approximately 35% to 66% of patients report pain, pruritus, or hyperhidrosis associated with EAHs, though this incidence may be overrepresented because patients tend to present when the lesions become symptomatic.2-5 The pain is attributed to nerve fibers infiltrating the tumor. Hypertrichosis also has been described and is thought to be due to hair follicles within the hamartoma.
Histologically, EAHs are characterized by normal-appearing eccrine glands mingled with venules and capillaries. Additional variable pathologic findings include lipomatous, pilar, lymphatic, or mucinous features.2 Other vascular anomalies such as hemangiomas or arteriovenous malformations occasionally have been described in association with EAH. The vessels stain for ulex europaeus 1 and factor VIII. Eccrine glands stain for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and cytokeratin CAM 5.2. In light of a publication proposing that EAH is a lymphatic proliferation,6 a D2-40 stain was performed on the specimen and was negative.
Eccrine angiomatous hamartoma has been reported to grow mainly during childhood, puberty, or pregnancy, presumably due to hormonal influences.7 There are few reports of EAH enlarging in middle-aged adults, and even fewer without pain during the growth phase. It is unclear what triggered the growth in our otherwise healthy postmenopausal patient.
Eccrine angiomatous hamartoma does not have malignant potential and thus treatment is optional and based on relief of symptoms. Simple excision of the EAH usually is curative, but recurrences can occur.4 Botulinum toxin also has been used to treat hyperhidrosis in tumors that are too large for resection. Treatment with lasers such as the pulsed dye laser and Nd:YAG laser has not been successful.8 A case of spontaneous regression has been reported.1
Liposuction was considered in our patient given the substantial adipose tissue on biopsy. The patient ultimately declined treatment. This case highlights that EAH can present in adulthood and should be considered in the differential diagnosis of an enlarging but otherwise asymptomatic vascular tumor.
- Tay YK, Sim CS. Eccrine angiomatous hamartoma associated with spontaneous regression. Pediatr Dermatol. 2006;23:516-517.
- Pelle MT, Pride HB, Tyler WB. Eccrine angiomatous hamartoma. J Am Acad Dermatol. 2002;47:429-435.
- Shin J, Jang YH, Kim SC, et al. Eccrine angiomatous hamartoma: a review of ten cases [published online May 10, 2013]. Ann Dermatol. 2013;25:208-212.
- Lin YT, Chen CM, Yang CH, et al. Eccrine angiomatous hamartoma: a retrospective study of 15 cases. Chang Gung Med J. 2012;35:167-177.
- Nakatsui TC, Schloss E, Krol A, et al. Eccrine angiomatous hamartoma: report of a case and literature review. J Am Acad Dermatol. 1999;41:109-111.
- Wang L, Wang S, Gao T, et al. Eccrine angiomatous hamartoma is a lymphatic proliferation. Eur J Dermatol. 2013;23:614-617.
- Kikusawa A, Oka M, Taguchi K, et al. Eccrine angiomatous hamartoma with sudden enlargement and pain in an adolescent girl after menarche [published online October 1, 2011]. Dermatoendocrinol. 2011;3:266-268.
- Barco D, Baselga E, Alegre M, et al. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 2009;145:241-243.
The Diagnosis: Eccrine Angiomatous Hamartoma
Given the progression of symptoms 3 months prior to presentation, an excisional biopsy was performed (Figure 1). Hematoxylin and eosin staining showed prominent eccrine sweat glands and vessels surrounded by superficially located adipose tissue in the mid and deep dermis (Figure 2).
Eccrine angiomatous hamartoma (EAH) is an uncommon benign tumor typically located on the arms and legs or trunk. It is usually solitary, though cases with multiple lesions have been reported.1,2 Most cases are diagnosed in childhood as either congenital or acquired lesions. However, EAHs can develop in adulthood and have been described in patients up to 70 years of age.3 The median age of diagnosis is 10 years,2 indicating that EAH is primarily a pediatric tumor. There is no gender predilection.
Approximately 35% to 66% of patients report pain, pruritus, or hyperhidrosis associated with EAHs, though this incidence may be overrepresented because patients tend to present when the lesions become symptomatic.2-5 The pain is attributed to nerve fibers infiltrating the tumor. Hypertrichosis also has been described and is thought to be due to hair follicles within the hamartoma.
Histologically, EAHs are characterized by normal-appearing eccrine glands mingled with venules and capillaries. Additional variable pathologic findings include lipomatous, pilar, lymphatic, or mucinous features.2 Other vascular anomalies such as hemangiomas or arteriovenous malformations occasionally have been described in association with EAH. The vessels stain for ulex europaeus 1 and factor VIII. Eccrine glands stain for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and cytokeratin CAM 5.2. In light of a publication proposing that EAH is a lymphatic proliferation,6 a D2-40 stain was performed on the specimen and was negative.
Eccrine angiomatous hamartoma has been reported to grow mainly during childhood, puberty, or pregnancy, presumably due to hormonal influences.7 There are few reports of EAH enlarging in middle-aged adults, and even fewer without pain during the growth phase. It is unclear what triggered the growth in our otherwise healthy postmenopausal patient.
Eccrine angiomatous hamartoma does not have malignant potential and thus treatment is optional and based on relief of symptoms. Simple excision of the EAH usually is curative, but recurrences can occur.4 Botulinum toxin also has been used to treat hyperhidrosis in tumors that are too large for resection. Treatment with lasers such as the pulsed dye laser and Nd:YAG laser has not been successful.8 A case of spontaneous regression has been reported.1
Liposuction was considered in our patient given the substantial adipose tissue on biopsy. The patient ultimately declined treatment. This case highlights that EAH can present in adulthood and should be considered in the differential diagnosis of an enlarging but otherwise asymptomatic vascular tumor.
The Diagnosis: Eccrine Angiomatous Hamartoma
Given the progression of symptoms 3 months prior to presentation, an excisional biopsy was performed (Figure 1). Hematoxylin and eosin staining showed prominent eccrine sweat glands and vessels surrounded by superficially located adipose tissue in the mid and deep dermis (Figure 2).
Eccrine angiomatous hamartoma (EAH) is an uncommon benign tumor typically located on the arms and legs or trunk. It is usually solitary, though cases with multiple lesions have been reported.1,2 Most cases are diagnosed in childhood as either congenital or acquired lesions. However, EAHs can develop in adulthood and have been described in patients up to 70 years of age.3 The median age of diagnosis is 10 years,2 indicating that EAH is primarily a pediatric tumor. There is no gender predilection.
Approximately 35% to 66% of patients report pain, pruritus, or hyperhidrosis associated with EAHs, though this incidence may be overrepresented because patients tend to present when the lesions become symptomatic.2-5 The pain is attributed to nerve fibers infiltrating the tumor. Hypertrichosis also has been described and is thought to be due to hair follicles within the hamartoma.
Histologically, EAHs are characterized by normal-appearing eccrine glands mingled with venules and capillaries. Additional variable pathologic findings include lipomatous, pilar, lymphatic, or mucinous features.2 Other vascular anomalies such as hemangiomas or arteriovenous malformations occasionally have been described in association with EAH. The vessels stain for ulex europaeus 1 and factor VIII. Eccrine glands stain for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and cytokeratin CAM 5.2. In light of a publication proposing that EAH is a lymphatic proliferation,6 a D2-40 stain was performed on the specimen and was negative.
Eccrine angiomatous hamartoma has been reported to grow mainly during childhood, puberty, or pregnancy, presumably due to hormonal influences.7 There are few reports of EAH enlarging in middle-aged adults, and even fewer without pain during the growth phase. It is unclear what triggered the growth in our otherwise healthy postmenopausal patient.
Eccrine angiomatous hamartoma does not have malignant potential and thus treatment is optional and based on relief of symptoms. Simple excision of the EAH usually is curative, but recurrences can occur.4 Botulinum toxin also has been used to treat hyperhidrosis in tumors that are too large for resection. Treatment with lasers such as the pulsed dye laser and Nd:YAG laser has not been successful.8 A case of spontaneous regression has been reported.1
Liposuction was considered in our patient given the substantial adipose tissue on biopsy. The patient ultimately declined treatment. This case highlights that EAH can present in adulthood and should be considered in the differential diagnosis of an enlarging but otherwise asymptomatic vascular tumor.
- Tay YK, Sim CS. Eccrine angiomatous hamartoma associated with spontaneous regression. Pediatr Dermatol. 2006;23:516-517.
- Pelle MT, Pride HB, Tyler WB. Eccrine angiomatous hamartoma. J Am Acad Dermatol. 2002;47:429-435.
- Shin J, Jang YH, Kim SC, et al. Eccrine angiomatous hamartoma: a review of ten cases [published online May 10, 2013]. Ann Dermatol. 2013;25:208-212.
- Lin YT, Chen CM, Yang CH, et al. Eccrine angiomatous hamartoma: a retrospective study of 15 cases. Chang Gung Med J. 2012;35:167-177.
- Nakatsui TC, Schloss E, Krol A, et al. Eccrine angiomatous hamartoma: report of a case and literature review. J Am Acad Dermatol. 1999;41:109-111.
- Wang L, Wang S, Gao T, et al. Eccrine angiomatous hamartoma is a lymphatic proliferation. Eur J Dermatol. 2013;23:614-617.
- Kikusawa A, Oka M, Taguchi K, et al. Eccrine angiomatous hamartoma with sudden enlargement and pain in an adolescent girl after menarche [published online October 1, 2011]. Dermatoendocrinol. 2011;3:266-268.
- Barco D, Baselga E, Alegre M, et al. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 2009;145:241-243.
- Tay YK, Sim CS. Eccrine angiomatous hamartoma associated with spontaneous regression. Pediatr Dermatol. 2006;23:516-517.
- Pelle MT, Pride HB, Tyler WB. Eccrine angiomatous hamartoma. J Am Acad Dermatol. 2002;47:429-435.
- Shin J, Jang YH, Kim SC, et al. Eccrine angiomatous hamartoma: a review of ten cases [published online May 10, 2013]. Ann Dermatol. 2013;25:208-212.
- Lin YT, Chen CM, Yang CH, et al. Eccrine angiomatous hamartoma: a retrospective study of 15 cases. Chang Gung Med J. 2012;35:167-177.
- Nakatsui TC, Schloss E, Krol A, et al. Eccrine angiomatous hamartoma: report of a case and literature review. J Am Acad Dermatol. 1999;41:109-111.
- Wang L, Wang S, Gao T, et al. Eccrine angiomatous hamartoma is a lymphatic proliferation. Eur J Dermatol. 2013;23:614-617.
- Kikusawa A, Oka M, Taguchi K, et al. Eccrine angiomatous hamartoma with sudden enlargement and pain in an adolescent girl after menarche [published online October 1, 2011]. Dermatoendocrinol. 2011;3:266-268.
- Barco D, Baselga E, Alegre M, et al. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 2009;145:241-243.
Histologic examination of anastomotic stapler doughnuts may not yield clinical benefit
LOS ANGELES – A multicenter of patients who had low anterior resection with stapled anastomosis for rectal cancer found no clinical or economic benefit in routinely sending anastomotic doughnuts for histopathological evaluation.
“Several small studies outside the United States have found no benefit in histologic examination of anastomotic stapler doughnuts,” lead study author Dr. Jeremy Sugrue said at the annual meeting of the American Society of Colon and Rectal Surgeons. “We wanted to see if this held true in our population.”

Dr. Sugrue, of the division of colon and rectal surgery in the department of surgery at the University of Illinois at Chicago, and his associates performed a retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions. The primary outcome was pathologic findings in the doughnuts and their impact on patient management. Secondary outcomes included tumor characteristics that may influence how often a surgeon may send a doughnut to pathology, along with approximate cost.
The mean age of the 486 patients was 60 years, 55% were male, and the mean gross distal margin of the primary tumor specimen was 2.9 cm. “The majority of tumors were located in the middle rectum, and the rest were evenly distributed between the lower rectum, upper rectum, and rectosigmoid regions,” said Dr. Sugrue, who is a general surgery resident. About half of the patients received neoadjuvant radiation or chemotherapy.
Benign findings were found in 33 patients. Among these, 16 had inflammatory changes, including 12 who had nonspecific changes, 3 who had changes from radiation, and 1 had inflammatory bowel disease changes. In addition, 13 patients with benign findings had polyps in their doughnuts (10 hyperplastic and 3 adenomatous), while 4 patients had miscellaneous changes including two cases of vessel micro calcification, one case of diverticuli, and one case of melanosis coli.
Among the 412 patients with malignant findings, 410 (99.5%) had no cancer in the doughnuts and no cancer at the distal resection margin in the primary tumor specimens. “In the two patients where we found cancer in the doughnuts, these patients also had a positive distal margin,” Dr. Sugrue said. “We did not find any patients with a positive distal margin and a negative doughnut. Likewise, we did not find any patients with a negative distal margin or an unexpectedly positive doughnut.”
The researchers also found that patients with low rectal tumors were significantly more likely to have their doughnut sent to pathology, compared with those with rectosigmoid tumors. “However, when we looked at distal margin comparing patients who had doughnuts reported on pathology with those who did not, there was no statistically significant difference,” Dr. Sugrue said. After averaging pathology professional fees and technical fees across all three institutions, he and his associates determined that doughnuts add $643 in cost when processed by pathology as a unique specimen.
Limitations of the study, he said, include its retrospective design, “which inherently introduces selection bias, and we did not perform a precise cost-benefit analysis.”
Dr. Sugrue reported having no financial disclosures.
LOS ANGELES – A multicenter of patients who had low anterior resection with stapled anastomosis for rectal cancer found no clinical or economic benefit in routinely sending anastomotic doughnuts for histopathological evaluation.
“Several small studies outside the United States have found no benefit in histologic examination of anastomotic stapler doughnuts,” lead study author Dr. Jeremy Sugrue said at the annual meeting of the American Society of Colon and Rectal Surgeons. “We wanted to see if this held true in our population.”
Dr. Sugrue, of the division of colon and rectal surgery in the department of surgery at the University of Illinois at Chicago, and his associates performed a retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions. The primary outcome was pathologic findings in the doughnuts and their impact on patient management. Secondary outcomes included tumor characteristics that may influence how often a surgeon may send a doughnut to pathology, along with approximate cost.
The mean age of the 486 patients was 60 years, 55% were male, and the mean gross distal margin of the primary tumor specimen was 2.9 cm. “The majority of tumors were located in the middle rectum, and the rest were evenly distributed between the lower rectum, upper rectum, and rectosigmoid regions,” said Dr. Sugrue, who is a general surgery resident. About half of the patients received neoadjuvant radiation or chemotherapy.
Benign findings were found in 33 patients. Among these, 16 had inflammatory changes, including 12 who had nonspecific changes, 3 who had changes from radiation, and 1 had inflammatory bowel disease changes. In addition, 13 patients with benign findings had polyps in their doughnuts (10 hyperplastic and 3 adenomatous), while 4 patients had miscellaneous changes including two cases of vessel micro calcification, one case of diverticuli, and one case of melanosis coli.
Among the 412 patients with malignant findings, 410 (99.5%) had no cancer in the doughnuts and no cancer at the distal resection margin in the primary tumor specimens. “In the two patients where we found cancer in the doughnuts, these patients also had a positive distal margin,” Dr. Sugrue said. “We did not find any patients with a positive distal margin and a negative doughnut. Likewise, we did not find any patients with a negative distal margin or an unexpectedly positive doughnut.”
The researchers also found that patients with low rectal tumors were significantly more likely to have their doughnut sent to pathology, compared with those with rectosigmoid tumors. “However, when we looked at distal margin comparing patients who had doughnuts reported on pathology with those who did not, there was no statistically significant difference,” Dr. Sugrue said. After averaging pathology professional fees and technical fees across all three institutions, he and his associates determined that doughnuts add $643 in cost when processed by pathology as a unique specimen.
Limitations of the study, he said, include its retrospective design, “which inherently introduces selection bias, and we did not perform a precise cost-benefit analysis.”
Dr. Sugrue reported having no financial disclosures.
LOS ANGELES – A multicenter of patients who had low anterior resection with stapled anastomosis for rectal cancer found no clinical or economic benefit in routinely sending anastomotic doughnuts for histopathological evaluation.
“Several small studies outside the United States have found no benefit in histologic examination of anastomotic stapler doughnuts,” lead study author Dr. Jeremy Sugrue said at the annual meeting of the American Society of Colon and Rectal Surgeons. “We wanted to see if this held true in our population.”
Dr. Sugrue, of the division of colon and rectal surgery in the department of surgery at the University of Illinois at Chicago, and his associates performed a retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions. The primary outcome was pathologic findings in the doughnuts and their impact on patient management. Secondary outcomes included tumor characteristics that may influence how often a surgeon may send a doughnut to pathology, along with approximate cost.
The mean age of the 486 patients was 60 years, 55% were male, and the mean gross distal margin of the primary tumor specimen was 2.9 cm. “The majority of tumors were located in the middle rectum, and the rest were evenly distributed between the lower rectum, upper rectum, and rectosigmoid regions,” said Dr. Sugrue, who is a general surgery resident. About half of the patients received neoadjuvant radiation or chemotherapy.
Benign findings were found in 33 patients. Among these, 16 had inflammatory changes, including 12 who had nonspecific changes, 3 who had changes from radiation, and 1 had inflammatory bowel disease changes. In addition, 13 patients with benign findings had polyps in their doughnuts (10 hyperplastic and 3 adenomatous), while 4 patients had miscellaneous changes including two cases of vessel micro calcification, one case of diverticuli, and one case of melanosis coli.
Among the 412 patients with malignant findings, 410 (99.5%) had no cancer in the doughnuts and no cancer at the distal resection margin in the primary tumor specimens. “In the two patients where we found cancer in the doughnuts, these patients also had a positive distal margin,” Dr. Sugrue said. “We did not find any patients with a positive distal margin and a negative doughnut. Likewise, we did not find any patients with a negative distal margin or an unexpectedly positive doughnut.”
The researchers also found that patients with low rectal tumors were significantly more likely to have their doughnut sent to pathology, compared with those with rectosigmoid tumors. “However, when we looked at distal margin comparing patients who had doughnuts reported on pathology with those who did not, there was no statistically significant difference,” Dr. Sugrue said. After averaging pathology professional fees and technical fees across all three institutions, he and his associates determined that doughnuts add $643 in cost when processed by pathology as a unique specimen.
Limitations of the study, he said, include its retrospective design, “which inherently introduces selection bias, and we did not perform a precise cost-benefit analysis.”
Dr. Sugrue reported having no financial disclosures.
AT THE ASCRS ANNUAL MEETING
Key clinical point: The routine histologic examination of anastomotic doughnuts at lower anterior resection for rectal cancer has no clinical benefit.
Major finding: Of the 412 patients with anastomotic doughnuts included in their pathology reports, only 2 had cancer cells in their doughnuts and both of these patients also had a positive distal margin in their primary tumor specimen.
Data source: A retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions.
Disclosures: Dr. Sugrue reported having no financial disclosures.

VIDEO: Experts discuss progress in schizophrenia treatment
ATLANTA – Over the last 20 years, there have been many signs of progress in treating schizophrenia, two experts said at the annual meeting of the American Psychiatric Association.
In this video, Dr. Henry A. Nasrallah and Dr. Michael Y. Hwang review the latest research in everything from genetic profiles predisposed to schizophrenia to their relationship with addiction, as well as the interplay between schizophrenia. They also discuss medical and psychiatric comorbidities – particularly obsessive-compulsive disorder. “We did a study where we looked at the onset of schizophrenia vs. the onset of OCD,” Dr. Nasrallah said. “We found that OCD symptoms precede the onset of psychosis by about a year.”
In addition, Dr. Nasrallah and Dr. Hwang discuss the impact of heterogeneity in schizophrenia not only when it comes to identifying appropriate interventions but also to conducting clinical trials.
Dr. Nasrallah is the Sydney W. Souers Professor and chair of the department of neurology and psychiatry at Saint Louis University. He has multiple disclosures, including Alkermes, Boehringer Ingelheim, Lundbeck, Otsuka, Sunovion, and others. Dr. Hwang, a staff physician at the East Orange (N.J.) Veterans Administration Medical Center, did not have any relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
ATLANTA – Over the last 20 years, there have been many signs of progress in treating schizophrenia, two experts said at the annual meeting of the American Psychiatric Association.
In this video, Dr. Henry A. Nasrallah and Dr. Michael Y. Hwang review the latest research in everything from genetic profiles predisposed to schizophrenia to their relationship with addiction, as well as the interplay between schizophrenia. They also discuss medical and psychiatric comorbidities – particularly obsessive-compulsive disorder. “We did a study where we looked at the onset of schizophrenia vs. the onset of OCD,” Dr. Nasrallah said. “We found that OCD symptoms precede the onset of psychosis by about a year.”
In addition, Dr. Nasrallah and Dr. Hwang discuss the impact of heterogeneity in schizophrenia not only when it comes to identifying appropriate interventions but also to conducting clinical trials.
Dr. Nasrallah is the Sydney W. Souers Professor and chair of the department of neurology and psychiatry at Saint Louis University. He has multiple disclosures, including Alkermes, Boehringer Ingelheim, Lundbeck, Otsuka, Sunovion, and others. Dr. Hwang, a staff physician at the East Orange (N.J.) Veterans Administration Medical Center, did not have any relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
ATLANTA – Over the last 20 years, there have been many signs of progress in treating schizophrenia, two experts said at the annual meeting of the American Psychiatric Association.
In this video, Dr. Henry A. Nasrallah and Dr. Michael Y. Hwang review the latest research in everything from genetic profiles predisposed to schizophrenia to their relationship with addiction, as well as the interplay between schizophrenia. They also discuss medical and psychiatric comorbidities – particularly obsessive-compulsive disorder. “We did a study where we looked at the onset of schizophrenia vs. the onset of OCD,” Dr. Nasrallah said. “We found that OCD symptoms precede the onset of psychosis by about a year.”
In addition, Dr. Nasrallah and Dr. Hwang discuss the impact of heterogeneity in schizophrenia not only when it comes to identifying appropriate interventions but also to conducting clinical trials.
Dr. Nasrallah is the Sydney W. Souers Professor and chair of the department of neurology and psychiatry at Saint Louis University. He has multiple disclosures, including Alkermes, Boehringer Ingelheim, Lundbeck, Otsuka, Sunovion, and others. Dr. Hwang, a staff physician at the East Orange (N.J.) Veterans Administration Medical Center, did not have any relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM THE APA ANNUAL MEETING

VIDEO: Identifying patients who will benefit from pulmonary metastasectomy
BALTIMORE – New research from Memorial Sloan Kettering Cancer Center in New York could help surgeons better determine which patients with soft tissue sarcoma may benefit most from pulmonary metastasectomy.
The results of the research, presented at the annual meeting of the American Association for Thoracic Surgery, suggest that preoperative factors such as primary tumor histology and size, number of metastases, time from initial resection of the primary, absence of extrapulmonary disease, and thoracoscopic resection are associated with improved survival in STS patients.
Dr. Garrett L. Walsh, professor of surgery at the University of Texas MD Anderson Cancer Center, Houston, and a discussant on the paper at the meeting, said the study was important because it showed the power of a prospective surgical database, retrospectively viewed in this particular case. He said that the Sloan Kettering research was likely “as good as it’s going to get,” given that a randomized controlled trial is unlikely ever to occur with STS patients.
“Trying to select the patients we think are going to do well with surgery has always been one of the challenging aspects of thoracic surgery,” Dr. Walsh said in a video interview. “This paper may help with better selection of patients from that large cohort who are referred to us for pulmonary metastasectomy.”
Dr. Walsh reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – New research from Memorial Sloan Kettering Cancer Center in New York could help surgeons better determine which patients with soft tissue sarcoma may benefit most from pulmonary metastasectomy.
The results of the research, presented at the annual meeting of the American Association for Thoracic Surgery, suggest that preoperative factors such as primary tumor histology and size, number of metastases, time from initial resection of the primary, absence of extrapulmonary disease, and thoracoscopic resection are associated with improved survival in STS patients.
Dr. Garrett L. Walsh, professor of surgery at the University of Texas MD Anderson Cancer Center, Houston, and a discussant on the paper at the meeting, said the study was important because it showed the power of a prospective surgical database, retrospectively viewed in this particular case. He said that the Sloan Kettering research was likely “as good as it’s going to get,” given that a randomized controlled trial is unlikely ever to occur with STS patients.
“Trying to select the patients we think are going to do well with surgery has always been one of the challenging aspects of thoracic surgery,” Dr. Walsh said in a video interview. “This paper may help with better selection of patients from that large cohort who are referred to us for pulmonary metastasectomy.”
Dr. Walsh reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – New research from Memorial Sloan Kettering Cancer Center in New York could help surgeons better determine which patients with soft tissue sarcoma may benefit most from pulmonary metastasectomy.
The results of the research, presented at the annual meeting of the American Association for Thoracic Surgery, suggest that preoperative factors such as primary tumor histology and size, number of metastases, time from initial resection of the primary, absence of extrapulmonary disease, and thoracoscopic resection are associated with improved survival in STS patients.
Dr. Garrett L. Walsh, professor of surgery at the University of Texas MD Anderson Cancer Center, Houston, and a discussant on the paper at the meeting, said the study was important because it showed the power of a prospective surgical database, retrospectively viewed in this particular case. He said that the Sloan Kettering research was likely “as good as it’s going to get,” given that a randomized controlled trial is unlikely ever to occur with STS patients.
“Trying to select the patients we think are going to do well with surgery has always been one of the challenging aspects of thoracic surgery,” Dr. Walsh said in a video interview. “This paper may help with better selection of patients from that large cohort who are referred to us for pulmonary metastasectomy.”
Dr. Walsh reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
AT THE AATS ANNUAL MEETING

Novel drug shows preclinical success in pancreatic cancer
SAN DIEGO – The experimental drug Metavert was effective in a mouse model of aggressive pancreatic cancer, and phase I trials in humans are expected to begin in early 2017.
“Metavert significantly slows tumor growth with less toxicity in preclinical trials. The drug prevents metastasis and reduces resistance to chemotherapy. Hopefully the drug will be a good partner with other drugs,” said presenting author Mouad Edderkaoui, Ph.D., of Cedars-Sinai, Los Angeles. “We hope this drug will improve the outcome of treatment of pancreatic cancer, knowing that the drugs now available are not effective and outcome is dismal. The last drug approved for pancreatic cancer – nab-paclitaxel – extended survival by only 7 weeks.”

Dr. Edderkaoui and Dr. Stephen Pandol, director, basic and translational pancreas research, gastroenterology, at Cedars-Sinai, are cofounders of Avenzoar Pharmaceuticals, the developer of Metavert.
Metavert is a small molecular dual inhibitor that targets two procancer pathways. Preclinical results show strong prevention of pancreatic cancer growth and metastasis with no significant toxicity, according to Dr. Edderkaoui, who explained that the novel agent has two linked moieties that target the glycogen synthase kinase–3 (GSK-3) beta and histone deacetylase (HDAC).
GSK-3 beta, which is highly expressed in pancreatic cancer, stimulates proliferation and resistance to apoptosis in cancer cells. HDAC inhibits epithelial cells. In combination, the two should simultaneously affect proliferation and metastasis.
The investigators studied pancreatic cell lines and KPC mice – an animal model of aggressive pancreatic cancer that carries KRAS and p53 mutations. Metavert reduced the survival of cancer cell lines but not of normal cells.
“The [combination] drug was more potent in cell lines than the two inhibitors separately,” he said. In dose-dependent fashion, Metavert inhibited GSK-3 beta and HDAC, decreased markers of epithelial to mesenchymal transition, and decreased migration of pancreatic cancer cells.
Further, Metavert sensitized pancreatic cancer cells to chemotherapy with gemcitabine and to radiation.
In KPC mice with advanced pancreatic cancer, treatment with Metavert increased survival by about 50%. At 6 months, all control mice had died, while 42% of Metavert-treated mice were still alive.
Tumor shrinkage was observed in Metavert-treated mice. Micrometastasis was seen in 29% of controls and in none of the Metavert-treated mice.
Fibrosis was not significantly affected by treatment, and the level of M2 macrophages significantly declined in treated mice.
SAN DIEGO – The experimental drug Metavert was effective in a mouse model of aggressive pancreatic cancer, and phase I trials in humans are expected to begin in early 2017.
“Metavert significantly slows tumor growth with less toxicity in preclinical trials. The drug prevents metastasis and reduces resistance to chemotherapy. Hopefully the drug will be a good partner with other drugs,” said presenting author Mouad Edderkaoui, Ph.D., of Cedars-Sinai, Los Angeles. “We hope this drug will improve the outcome of treatment of pancreatic cancer, knowing that the drugs now available are not effective and outcome is dismal. The last drug approved for pancreatic cancer – nab-paclitaxel – extended survival by only 7 weeks.”
Dr. Edderkaoui and Dr. Stephen Pandol, director, basic and translational pancreas research, gastroenterology, at Cedars-Sinai, are cofounders of Avenzoar Pharmaceuticals, the developer of Metavert.
Metavert is a small molecular dual inhibitor that targets two procancer pathways. Preclinical results show strong prevention of pancreatic cancer growth and metastasis with no significant toxicity, according to Dr. Edderkaoui, who explained that the novel agent has two linked moieties that target the glycogen synthase kinase–3 (GSK-3) beta and histone deacetylase (HDAC).
GSK-3 beta, which is highly expressed in pancreatic cancer, stimulates proliferation and resistance to apoptosis in cancer cells. HDAC inhibits epithelial cells. In combination, the two should simultaneously affect proliferation and metastasis.
The investigators studied pancreatic cell lines and KPC mice – an animal model of aggressive pancreatic cancer that carries KRAS and p53 mutations. Metavert reduced the survival of cancer cell lines but not of normal cells.
“The [combination] drug was more potent in cell lines than the two inhibitors separately,” he said. In dose-dependent fashion, Metavert inhibited GSK-3 beta and HDAC, decreased markers of epithelial to mesenchymal transition, and decreased migration of pancreatic cancer cells.
Further, Metavert sensitized pancreatic cancer cells to chemotherapy with gemcitabine and to radiation.
In KPC mice with advanced pancreatic cancer, treatment with Metavert increased survival by about 50%. At 6 months, all control mice had died, while 42% of Metavert-treated mice were still alive.
Tumor shrinkage was observed in Metavert-treated mice. Micrometastasis was seen in 29% of controls and in none of the Metavert-treated mice.
Fibrosis was not significantly affected by treatment, and the level of M2 macrophages significantly declined in treated mice.
SAN DIEGO – The experimental drug Metavert was effective in a mouse model of aggressive pancreatic cancer, and phase I trials in humans are expected to begin in early 2017.
“Metavert significantly slows tumor growth with less toxicity in preclinical trials. The drug prevents metastasis and reduces resistance to chemotherapy. Hopefully the drug will be a good partner with other drugs,” said presenting author Mouad Edderkaoui, Ph.D., of Cedars-Sinai, Los Angeles. “We hope this drug will improve the outcome of treatment of pancreatic cancer, knowing that the drugs now available are not effective and outcome is dismal. The last drug approved for pancreatic cancer – nab-paclitaxel – extended survival by only 7 weeks.”
Dr. Edderkaoui and Dr. Stephen Pandol, director, basic and translational pancreas research, gastroenterology, at Cedars-Sinai, are cofounders of Avenzoar Pharmaceuticals, the developer of Metavert.
Metavert is a small molecular dual inhibitor that targets two procancer pathways. Preclinical results show strong prevention of pancreatic cancer growth and metastasis with no significant toxicity, according to Dr. Edderkaoui, who explained that the novel agent has two linked moieties that target the glycogen synthase kinase–3 (GSK-3) beta and histone deacetylase (HDAC).
GSK-3 beta, which is highly expressed in pancreatic cancer, stimulates proliferation and resistance to apoptosis in cancer cells. HDAC inhibits epithelial cells. In combination, the two should simultaneously affect proliferation and metastasis.
The investigators studied pancreatic cell lines and KPC mice – an animal model of aggressive pancreatic cancer that carries KRAS and p53 mutations. Metavert reduced the survival of cancer cell lines but not of normal cells.
“The [combination] drug was more potent in cell lines than the two inhibitors separately,” he said. In dose-dependent fashion, Metavert inhibited GSK-3 beta and HDAC, decreased markers of epithelial to mesenchymal transition, and decreased migration of pancreatic cancer cells.
Further, Metavert sensitized pancreatic cancer cells to chemotherapy with gemcitabine and to radiation.
In KPC mice with advanced pancreatic cancer, treatment with Metavert increased survival by about 50%. At 6 months, all control mice had died, while 42% of Metavert-treated mice were still alive.
Tumor shrinkage was observed in Metavert-treated mice. Micrometastasis was seen in 29% of controls and in none of the Metavert-treated mice.
Fibrosis was not significantly affected by treatment, and the level of M2 macrophages significantly declined in treated mice.
AT DDW® 2016
Key clinical point: A novel compound appears to have potential in the treatment of pancreatic cancer.
Major finding: In experimental animal models of pancreatic cancer, Metavert improved survival by 50% and prevented micrometastasis.
Data source: Cell lines and a mouse model of pancreatic cancer.
Disclosures: Metavert was developed with financial support from the Hirshberg Foundation, NIH/VA Awards, and the Cedars-Sinai Intellectual Property office.

VIDEO: Two good options for mitral valve repair
BALTIMORE – Degenerative mitral regurgitation due to anterior or bileaflet prolapse can be treated with excellent results by both the traditional double orifice edge-to-edge repair or the implantation of artificial chordae, combined with ring annuloplasty, according to a study presented at the annual meeting of the American Association for Thoracic Surgery.
Researchers at San Raffaele University Hospital in Milan undertook a long-term comparison between the two methods of degenerative MR repair and found no differences in outcomes in cases of bileaflet prolapse, whereas in isolated anterior leaflet prolapse, the double orifice repair actually appeared to be more effective.
Mitral valve repair is a very well-accepted modality to fix posterior leaflet prolapse, according to Dr. Marc Ruel, chief of cardiac surgery at the University of Ottawa Heart Institute and a discussant on the paper at the meeting. But anterior mitral leaflet prolapse is a much more challenging operation, he said, and surgeons are looking for a “foolproof” way to address it.
“The double orifice repair, for most surgeons, is a much simpler procedure than doing artificial chordae, so this is good news,” Dr. Ruel said. “It shows that a fairly reproducible way of repairing the mitral valve seems to work as well, and likely better in some lesions, than the more complex way of addressing it.”
Dr. Ruel, who discusses the study in this video interview, reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – Degenerative mitral regurgitation due to anterior or bileaflet prolapse can be treated with excellent results by both the traditional double orifice edge-to-edge repair or the implantation of artificial chordae, combined with ring annuloplasty, according to a study presented at the annual meeting of the American Association for Thoracic Surgery.
Researchers at San Raffaele University Hospital in Milan undertook a long-term comparison between the two methods of degenerative MR repair and found no differences in outcomes in cases of bileaflet prolapse, whereas in isolated anterior leaflet prolapse, the double orifice repair actually appeared to be more effective.
Mitral valve repair is a very well-accepted modality to fix posterior leaflet prolapse, according to Dr. Marc Ruel, chief of cardiac surgery at the University of Ottawa Heart Institute and a discussant on the paper at the meeting. But anterior mitral leaflet prolapse is a much more challenging operation, he said, and surgeons are looking for a “foolproof” way to address it.
“The double orifice repair, for most surgeons, is a much simpler procedure than doing artificial chordae, so this is good news,” Dr. Ruel said. “It shows that a fairly reproducible way of repairing the mitral valve seems to work as well, and likely better in some lesions, than the more complex way of addressing it.”
Dr. Ruel, who discusses the study in this video interview, reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – Degenerative mitral regurgitation due to anterior or bileaflet prolapse can be treated with excellent results by both the traditional double orifice edge-to-edge repair or the implantation of artificial chordae, combined with ring annuloplasty, according to a study presented at the annual meeting of the American Association for Thoracic Surgery.
Researchers at San Raffaele University Hospital in Milan undertook a long-term comparison between the two methods of degenerative MR repair and found no differences in outcomes in cases of bileaflet prolapse, whereas in isolated anterior leaflet prolapse, the double orifice repair actually appeared to be more effective.
Mitral valve repair is a very well-accepted modality to fix posterior leaflet prolapse, according to Dr. Marc Ruel, chief of cardiac surgery at the University of Ottawa Heart Institute and a discussant on the paper at the meeting. But anterior mitral leaflet prolapse is a much more challenging operation, he said, and surgeons are looking for a “foolproof” way to address it.
“The double orifice repair, for most surgeons, is a much simpler procedure than doing artificial chordae, so this is good news,” Dr. Ruel said. “It shows that a fairly reproducible way of repairing the mitral valve seems to work as well, and likely better in some lesions, than the more complex way of addressing it.”
Dr. Ruel, who discusses the study in this video interview, reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
AT THE AATS ANNUAL MEETING

Putting an end to ENDS
Recent legislation to ban the sale of e-cigarettes to persons younger than 18 years of age, and to prevent distribution of free samples and placement in vending machines where teens may be present, was a major win for the fight for the health and well-being of our adolescents.1
The electronic nicotine delivery system, or ENDS, was developed as an alternative to smoking cigarettes, reducing the intake of harmful fumes that lead to lung cancer. It was a great idea for those wishing to decrease or completely stop smoking. Its sleek design and flavor assortment made it very appealing, not only to adults, but to teenagers as well.
The history of e-cigs goes back to the 1960s when first developed, but because smoking was so socially acceptable the idea did not take hold. It wasn’t until 2003 when they started to become popular. Initially, e-cigs were met with resistance from the Food and Drug Administration, which stated that they were dangerous. But as the need for an alternative to smoking increased and preventable deaths continued to rise, there was more pressure to make them available. In 2013, sales started to skyrocket, but no restrictions for sale or product information was required. This made them readily available to teens and heralded the start of a whole new crisis. The Centers for Disease Control and Prevention reported that between 2011 and 2014, e-cig use rose from 0.6% to 5.3% among middle schoolers and from 1.5% to 16% among high school students.2

Because the marketing for e-cigs suggests they carry a reduced risk for cancer and are a healthier alternative to cigarettes, the perception is that they are not harmful. But research shows the contrary. Nicotine exposure of any level to the developing brain has been found to have negative effects, particularly in the prefrontal cortex where altered synapses have been identified.3 Symptoms of nicotine dependence at lower doses of nicotine is evident in adolescents. Long-term effects in adolescents are reported in working memory, attention, and predilection to major depressive disorder, panic disorder, academic problems, and addiction to other substances.3
The American Academy of Pediatrics 2015 statement on e-cigarettes stated increasing use by teens “threatens 5 decades of public health gains in successfully deglamorizing, restricting, and decreasing the use of tobacco products” and called for an FDA ban on the products.4 Although the FDA recently did place new restrictions, it will take several years for them to go fully into effect. A recent incident where a toddler ingested the liquid nicotine from an e-cig and died also brought to light other dangers of nicotine.5 These nicotine solutions come in colors and a variety of flavors, which makes them even more desirable to toddlers.Just one confirmed death has been reported from e-cig solution ingestion, but there has been a significant jump in calls to poison control centers associated with the liquids. Nicotine from these solutions also can be absorbed through the skin.

More than 3 million middle and high school students were current users of e-cigarettes in 2015,1 and e-cigs were the most commonly used tobacco product among middle and high school students that year.2 Early introduction of ENDS causes a combination of early dependence and addiction with long-term impairment of cognitive skills, promoting an even more grim future for the health of our teens. Education and awareness is imperative to slow the current trends and prevent an even worse crisis than the one ENDS was created to improve.
References
1. http://www.fda.gov/TobaccoProducts/Labeling/ProductsIngredientsComponents/ucm456610.htm
2. MMWR Morb Mortal Wkly Rep. 2016 Apr 15;65(14):361-7.
3. Cold Spring Harbor Perspectives in Medicine. 2012;2(12):10.1101/cshperspect.a012120 a012120.
4. Pediatrics. 2015 Nov.10.1542/peds.2015-3222.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at [email protected].
Recent legislation to ban the sale of e-cigarettes to persons younger than 18 years of age, and to prevent distribution of free samples and placement in vending machines where teens may be present, was a major win for the fight for the health and well-being of our adolescents.1
The electronic nicotine delivery system, or ENDS, was developed as an alternative to smoking cigarettes, reducing the intake of harmful fumes that lead to lung cancer. It was a great idea for those wishing to decrease or completely stop smoking. Its sleek design and flavor assortment made it very appealing, not only to adults, but to teenagers as well.
The history of e-cigs goes back to the 1960s when first developed, but because smoking was so socially acceptable the idea did not take hold. It wasn’t until 2003 when they started to become popular. Initially, e-cigs were met with resistance from the Food and Drug Administration, which stated that they were dangerous. But as the need for an alternative to smoking increased and preventable deaths continued to rise, there was more pressure to make them available. In 2013, sales started to skyrocket, but no restrictions for sale or product information was required. This made them readily available to teens and heralded the start of a whole new crisis. The Centers for Disease Control and Prevention reported that between 2011 and 2014, e-cig use rose from 0.6% to 5.3% among middle schoolers and from 1.5% to 16% among high school students.2
Because the marketing for e-cigs suggests they carry a reduced risk for cancer and are a healthier alternative to cigarettes, the perception is that they are not harmful. But research shows the contrary. Nicotine exposure of any level to the developing brain has been found to have negative effects, particularly in the prefrontal cortex where altered synapses have been identified.3 Symptoms of nicotine dependence at lower doses of nicotine is evident in adolescents. Long-term effects in adolescents are reported in working memory, attention, and predilection to major depressive disorder, panic disorder, academic problems, and addiction to other substances.3
The American Academy of Pediatrics 2015 statement on e-cigarettes stated increasing use by teens “threatens 5 decades of public health gains in successfully deglamorizing, restricting, and decreasing the use of tobacco products” and called for an FDA ban on the products.4 Although the FDA recently did place new restrictions, it will take several years for them to go fully into effect. A recent incident where a toddler ingested the liquid nicotine from an e-cig and died also brought to light other dangers of nicotine.5 These nicotine solutions come in colors and a variety of flavors, which makes them even more desirable to toddlers.Just one confirmed death has been reported from e-cig solution ingestion, but there has been a significant jump in calls to poison control centers associated with the liquids. Nicotine from these solutions also can be absorbed through the skin.
More than 3 million middle and high school students were current users of e-cigarettes in 2015,1 and e-cigs were the most commonly used tobacco product among middle and high school students that year.2 Early introduction of ENDS causes a combination of early dependence and addiction with long-term impairment of cognitive skills, promoting an even more grim future for the health of our teens. Education and awareness is imperative to slow the current trends and prevent an even worse crisis than the one ENDS was created to improve.
References
1. http://www.fda.gov/TobaccoProducts/Labeling/ProductsIngredientsComponents/ucm456610.htm
2. MMWR Morb Mortal Wkly Rep. 2016 Apr 15;65(14):361-7.
3. Cold Spring Harbor Perspectives in Medicine. 2012;2(12):10.1101/cshperspect.a012120 a012120.
4. Pediatrics. 2015 Nov.10.1542/peds.2015-3222.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at [email protected].
Recent legislation to ban the sale of e-cigarettes to persons younger than 18 years of age, and to prevent distribution of free samples and placement in vending machines where teens may be present, was a major win for the fight for the health and well-being of our adolescents.1
The electronic nicotine delivery system, or ENDS, was developed as an alternative to smoking cigarettes, reducing the intake of harmful fumes that lead to lung cancer. It was a great idea for those wishing to decrease or completely stop smoking. Its sleek design and flavor assortment made it very appealing, not only to adults, but to teenagers as well.
The history of e-cigs goes back to the 1960s when first developed, but because smoking was so socially acceptable the idea did not take hold. It wasn’t until 2003 when they started to become popular. Initially, e-cigs were met with resistance from the Food and Drug Administration, which stated that they were dangerous. But as the need for an alternative to smoking increased and preventable deaths continued to rise, there was more pressure to make them available. In 2013, sales started to skyrocket, but no restrictions for sale or product information was required. This made them readily available to teens and heralded the start of a whole new crisis. The Centers for Disease Control and Prevention reported that between 2011 and 2014, e-cig use rose from 0.6% to 5.3% among middle schoolers and from 1.5% to 16% among high school students.2
Because the marketing for e-cigs suggests they carry a reduced risk for cancer and are a healthier alternative to cigarettes, the perception is that they are not harmful. But research shows the contrary. Nicotine exposure of any level to the developing brain has been found to have negative effects, particularly in the prefrontal cortex where altered synapses have been identified.3 Symptoms of nicotine dependence at lower doses of nicotine is evident in adolescents. Long-term effects in adolescents are reported in working memory, attention, and predilection to major depressive disorder, panic disorder, academic problems, and addiction to other substances.3
The American Academy of Pediatrics 2015 statement on e-cigarettes stated increasing use by teens “threatens 5 decades of public health gains in successfully deglamorizing, restricting, and decreasing the use of tobacco products” and called for an FDA ban on the products.4 Although the FDA recently did place new restrictions, it will take several years for them to go fully into effect. A recent incident where a toddler ingested the liquid nicotine from an e-cig and died also brought to light other dangers of nicotine.5 These nicotine solutions come in colors and a variety of flavors, which makes them even more desirable to toddlers.Just one confirmed death has been reported from e-cig solution ingestion, but there has been a significant jump in calls to poison control centers associated with the liquids. Nicotine from these solutions also can be absorbed through the skin.
More than 3 million middle and high school students were current users of e-cigarettes in 2015,1 and e-cigs were the most commonly used tobacco product among middle and high school students that year.2 Early introduction of ENDS causes a combination of early dependence and addiction with long-term impairment of cognitive skills, promoting an even more grim future for the health of our teens. Education and awareness is imperative to slow the current trends and prevent an even worse crisis than the one ENDS was created to improve.
References
1. http://www.fda.gov/TobaccoProducts/Labeling/ProductsIngredientsComponents/ucm456610.htm
2. MMWR Morb Mortal Wkly Rep. 2016 Apr 15;65(14):361-7.
3. Cold Spring Harbor Perspectives in Medicine. 2012;2(12):10.1101/cshperspect.a012120 a012120.
4. Pediatrics. 2015 Nov.10.1542/peds.2015-3222.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at [email protected].

Pregnancy alters pharmacodynamics of infliximab, adalimumab in women with IBD
SAN DIEGO – Blood levels of infliximab rose during pregnancy, while adalimumab levels remained stable, even after researchers accounted for changes in albumin, body mass index, and C-reactive protein levels, according to a novel single-center study of 25 women with inflammatory bowel disease (IBD).
Furthermore, blood levels of both anti–tumor necrosis factor agents varied considerably among patients, reported Dr. Cynthia Seow, a gastroenterologist at the University of Calgary (Alta.). “We should consider therapeutic drug monitoring during the prepregnancy period in order to optimize the dose during pregnancy,” she said. “Therapeutic drug monitoring may also be considered for pregnant women receiving infliximab in the second trimester to guide third-trimester dosing.

Active IBD during pregnancy increases the risk of relapse and preterm birth, Dr. Seow noted at the annual Digestive Diseases Week. Thus, infliximab and adalimumab are used to keep IBD in check during pregnancy, even though they cross the placenta and reach higher levels in the cord blood and newborn (Clin Gastroenterol Hepatol. 2013 March;11[3]:286-92) than in the mother. “However, it is not known how pregnancy itself influences the pharmacokinetics of anti-TNF agents, or the implications of this on prescribed dosing,” said Dr. Seow.
Therefore, she and her colleagues analyzed blood samples from 25 women receiving stable maintenance anti-TNF therapy for IBD, who attended a median of three prenatal visits at the University of Calgary IBD Pregnancy Clinic. Fifteen women received infliximab during 15 pregnancies, and 10 women received adalimumab during 11 pregnancies. Infliximab levels were drawn at trough times, while adalimumab levels were usually drawn 3 days before the next injection. Blood samples were tested only after delivery, and anti-TNF doses were not adjusted during pregnancy.
The infliximab group included eight women with Crohn’s disease and seven women with ulcerative colitis, and the adalimumab group included nine women with Crohn’s disease and one with ulcerative colitis, said Dr. Seow. The treatment groups were similar in terms of age at diagnosis and pregnancy, time on anti-TNF agents, and average gestational age at delivery, which was 39.2 weeks (range, 38.1-40.2 weeks) for the infliximab group and 38.4 weeks (range, 37.2-39.6 weeks) for the adalimumab patients.
Median infliximab concentrations rose from 8.5 mcg/mL in the first trimester to a peak of 21 mcg/mL during the middle of the third trimester (P = .04), and then dropped to nearly preconception levels after delivery, Dr. Seow reported. “This change persisted irrespective of disease phenotype,” she added. Albumin levels correlated inversely with infliximab levels. In contrast, median adalimumab levels ranged between 8.6 and 12.2 mcg/mL during pregnancy, dropped to 6.8 mcg/mL after birth, and were unrelated to albumin levels.
Body mass index and C-reactive protein levels did not affect blood levels of either drug, and the researchers found no differences in pharmacokinetics in subgroups of patients who had only two blood draws, subtherapeutic drug levels, or consistently absent drug levels, Dr. Seow said. Three patients had detectable antibodies during pregnancy, all of whom had a stable clinical course, she said. “The antibody levels appeared to decrease as the pregnancy progressed, and then appeared to increase again after delivery.” A third of infliximab patients and nearly half of adalimumab patients were receiving combination treatments for IBD, and their anti-TNF blood levels resembled those of patients on monotherapy, she also noted.
The researchers did not test cord blood or blood sample from the newborns, but based on past evidence, fetal anti-TNF exposure has implications for current live vaccination recommendations in infants, Dr. Seow emphasized. “The long-term consequences of anti-TNF exposure remain unknown,” she concluded.
Dr. Seow disclosed ties with Janssen, AbbVie, Takeda, Shire, and Actavis.
SAN DIEGO – Blood levels of infliximab rose during pregnancy, while adalimumab levels remained stable, even after researchers accounted for changes in albumin, body mass index, and C-reactive protein levels, according to a novel single-center study of 25 women with inflammatory bowel disease (IBD).
Furthermore, blood levels of both anti–tumor necrosis factor agents varied considerably among patients, reported Dr. Cynthia Seow, a gastroenterologist at the University of Calgary (Alta.). “We should consider therapeutic drug monitoring during the prepregnancy period in order to optimize the dose during pregnancy,” she said. “Therapeutic drug monitoring may also be considered for pregnant women receiving infliximab in the second trimester to guide third-trimester dosing.
Active IBD during pregnancy increases the risk of relapse and preterm birth, Dr. Seow noted at the annual Digestive Diseases Week. Thus, infliximab and adalimumab are used to keep IBD in check during pregnancy, even though they cross the placenta and reach higher levels in the cord blood and newborn (Clin Gastroenterol Hepatol. 2013 March;11[3]:286-92) than in the mother. “However, it is not known how pregnancy itself influences the pharmacokinetics of anti-TNF agents, or the implications of this on prescribed dosing,” said Dr. Seow.
Therefore, she and her colleagues analyzed blood samples from 25 women receiving stable maintenance anti-TNF therapy for IBD, who attended a median of three prenatal visits at the University of Calgary IBD Pregnancy Clinic. Fifteen women received infliximab during 15 pregnancies, and 10 women received adalimumab during 11 pregnancies. Infliximab levels were drawn at trough times, while adalimumab levels were usually drawn 3 days before the next injection. Blood samples were tested only after delivery, and anti-TNF doses were not adjusted during pregnancy.
The infliximab group included eight women with Crohn’s disease and seven women with ulcerative colitis, and the adalimumab group included nine women with Crohn’s disease and one with ulcerative colitis, said Dr. Seow. The treatment groups were similar in terms of age at diagnosis and pregnancy, time on anti-TNF agents, and average gestational age at delivery, which was 39.2 weeks (range, 38.1-40.2 weeks) for the infliximab group and 38.4 weeks (range, 37.2-39.6 weeks) for the adalimumab patients.
Median infliximab concentrations rose from 8.5 mcg/mL in the first trimester to a peak of 21 mcg/mL during the middle of the third trimester (P = .04), and then dropped to nearly preconception levels after delivery, Dr. Seow reported. “This change persisted irrespective of disease phenotype,” she added. Albumin levels correlated inversely with infliximab levels. In contrast, median adalimumab levels ranged between 8.6 and 12.2 mcg/mL during pregnancy, dropped to 6.8 mcg/mL after birth, and were unrelated to albumin levels.
Body mass index and C-reactive protein levels did not affect blood levels of either drug, and the researchers found no differences in pharmacokinetics in subgroups of patients who had only two blood draws, subtherapeutic drug levels, or consistently absent drug levels, Dr. Seow said. Three patients had detectable antibodies during pregnancy, all of whom had a stable clinical course, she said. “The antibody levels appeared to decrease as the pregnancy progressed, and then appeared to increase again after delivery.” A third of infliximab patients and nearly half of adalimumab patients were receiving combination treatments for IBD, and their anti-TNF blood levels resembled those of patients on monotherapy, she also noted.
The researchers did not test cord blood or blood sample from the newborns, but based on past evidence, fetal anti-TNF exposure has implications for current live vaccination recommendations in infants, Dr. Seow emphasized. “The long-term consequences of anti-TNF exposure remain unknown,” she concluded.
Dr. Seow disclosed ties with Janssen, AbbVie, Takeda, Shire, and Actavis.
SAN DIEGO – Blood levels of infliximab rose during pregnancy, while adalimumab levels remained stable, even after researchers accounted for changes in albumin, body mass index, and C-reactive protein levels, according to a novel single-center study of 25 women with inflammatory bowel disease (IBD).
Furthermore, blood levels of both anti–tumor necrosis factor agents varied considerably among patients, reported Dr. Cynthia Seow, a gastroenterologist at the University of Calgary (Alta.). “We should consider therapeutic drug monitoring during the prepregnancy period in order to optimize the dose during pregnancy,” she said. “Therapeutic drug monitoring may also be considered for pregnant women receiving infliximab in the second trimester to guide third-trimester dosing.
Active IBD during pregnancy increases the risk of relapse and preterm birth, Dr. Seow noted at the annual Digestive Diseases Week. Thus, infliximab and adalimumab are used to keep IBD in check during pregnancy, even though they cross the placenta and reach higher levels in the cord blood and newborn (Clin Gastroenterol Hepatol. 2013 March;11[3]:286-92) than in the mother. “However, it is not known how pregnancy itself influences the pharmacokinetics of anti-TNF agents, or the implications of this on prescribed dosing,” said Dr. Seow.
Therefore, she and her colleagues analyzed blood samples from 25 women receiving stable maintenance anti-TNF therapy for IBD, who attended a median of three prenatal visits at the University of Calgary IBD Pregnancy Clinic. Fifteen women received infliximab during 15 pregnancies, and 10 women received adalimumab during 11 pregnancies. Infliximab levels were drawn at trough times, while adalimumab levels were usually drawn 3 days before the next injection. Blood samples were tested only after delivery, and anti-TNF doses were not adjusted during pregnancy.
The infliximab group included eight women with Crohn’s disease and seven women with ulcerative colitis, and the adalimumab group included nine women with Crohn’s disease and one with ulcerative colitis, said Dr. Seow. The treatment groups were similar in terms of age at diagnosis and pregnancy, time on anti-TNF agents, and average gestational age at delivery, which was 39.2 weeks (range, 38.1-40.2 weeks) for the infliximab group and 38.4 weeks (range, 37.2-39.6 weeks) for the adalimumab patients.
Median infliximab concentrations rose from 8.5 mcg/mL in the first trimester to a peak of 21 mcg/mL during the middle of the third trimester (P = .04), and then dropped to nearly preconception levels after delivery, Dr. Seow reported. “This change persisted irrespective of disease phenotype,” she added. Albumin levels correlated inversely with infliximab levels. In contrast, median adalimumab levels ranged between 8.6 and 12.2 mcg/mL during pregnancy, dropped to 6.8 mcg/mL after birth, and were unrelated to albumin levels.
Body mass index and C-reactive protein levels did not affect blood levels of either drug, and the researchers found no differences in pharmacokinetics in subgroups of patients who had only two blood draws, subtherapeutic drug levels, or consistently absent drug levels, Dr. Seow said. Three patients had detectable antibodies during pregnancy, all of whom had a stable clinical course, she said. “The antibody levels appeared to decrease as the pregnancy progressed, and then appeared to increase again after delivery.” A third of infliximab patients and nearly half of adalimumab patients were receiving combination treatments for IBD, and their anti-TNF blood levels resembled those of patients on monotherapy, she also noted.
The researchers did not test cord blood or blood sample from the newborns, but based on past evidence, fetal anti-TNF exposure has implications for current live vaccination recommendations in infants, Dr. Seow emphasized. “The long-term consequences of anti-TNF exposure remain unknown,” she concluded.
Dr. Seow disclosed ties with Janssen, AbbVie, Takeda, Shire, and Actavis.
AT DDW® 2016
Key clinical point: Blood levels of infliximab rose during pregnancy, while adalimumab levels remained stable, even after researchers accounted for changes in albumin, body mass index, and C-reactive protein levels.
Major finding: Median infliximab concentrations rose from 8.5 mcg/mL in the first trimester to a peak of 21 mcg/mL during the middle of the third trimester (P = .04). Median adalimumab levels ranged between 8.6 and 12.2 mcg/mL during pregnancy.
Data source: A prospective study of 25 pregnant women with ulcerative colitis or Crohn’s disease.
Disclosures: Dr. Seow disclosed ties with Janssen, AbbVie, Takeda, Shire, and Actavis.

NPY signaling pathway might induce noneosinophilic asthma
The neuropeptide Y (NPY) gene appears to play an essential role in airway reactivity and may be a target for treating noneosinophilic asthma.
Higher expression of the NPY signaling molecule was seen in mice lacking Foxp1 and Foxp4 transcription factors. NPY induced noneosinophilic airway hyperreactivity by activating smooth muscle myosin light-chain phosphorylation, researchers reported in the Journal of Clinical Investigation.
Deleting the NPY gene in mice reduced airway hyperreactivity almost to normal levels, while incubating human lung tissue with recombinant NPY triggered bronchoconstriction, said Dr. Shanru Li and his associates at the University of Pennsylvania in Philadelphia. Future treatments for noneosinophilic asthma might target paracrine signaling from the airway epithelium to underlying smooth muscle.
The researchers also used transcriptome analysis to identify 10 genes that were significantly upregulated in the knockout mice and acted on airway smooth muscle cells to trigger airway hyperresponsiveness (AHR) in a paracrine manner. Among these, NPY was expressed at the highest levels, and deleting this gene in the Foxp1/Foxp4 knockout mice caused AHR to fall almost to normal levels. Incubating recombinant NPY with human and mouse lung tissue triggered marked bronchoconstriction in response to a methacholine challenge. Furthermore, phosphorylation of myosin light chain (pMLC), “a critical signaling event required for airway smooth muscle contraction,” increased with the methacholine challenge, but rose even more with concurrent exposure to NPY.
“Foxp1 and Foxp4 double mutants represent a model for noneosinophilic asthma, which remains poorly understood,” the researchers concluded. “The studies are among the first, to our knowledge, to mechanistically link a critical transcription pathway in airway epithelium that activates a paracrine response to the promotion of AHR in the absence of a Th2-induced eosinophilic inflammatory response.”
Most asthma therapies do not improve nonimmune asthma, which accounts for about half of asthma cases overall. While NPY gene variants have been linked to asthma, the specific molecular pathway was unknown, the researchers said. They found that Foxp1/4 knockout mice had greater airway smooth muscle contraction than control mice, especially after exposure to airway irritants. Notably, they did not find increased levels of the eosinophilic marker IL-13 or the neutrophilic inflammatory markers IL-17, IL-6, or keratinocyte-derived chemokine (KC) in airway epithelium from the knockout mice. “We did observe a modest increase in the numbers of neutrophils, but not macrophages, eosinophils, or lymphocytes in the bronchoalveolar lavage fluid in the Foxp1/4 knockout mutants,” they added (J Clin Invest. 2016 Apr. doi: 10.1172/JCI81389).
The National Institutes of Health funded the studies. The investigators had no disclosures.
The neuropeptide Y (NPY) gene appears to play an essential role in airway reactivity and may be a target for treating noneosinophilic asthma.
Higher expression of the NPY signaling molecule was seen in mice lacking Foxp1 and Foxp4 transcription factors. NPY induced noneosinophilic airway hyperreactivity by activating smooth muscle myosin light-chain phosphorylation, researchers reported in the Journal of Clinical Investigation.
Deleting the NPY gene in mice reduced airway hyperreactivity almost to normal levels, while incubating human lung tissue with recombinant NPY triggered bronchoconstriction, said Dr. Shanru Li and his associates at the University of Pennsylvania in Philadelphia. Future treatments for noneosinophilic asthma might target paracrine signaling from the airway epithelium to underlying smooth muscle.
The researchers also used transcriptome analysis to identify 10 genes that were significantly upregulated in the knockout mice and acted on airway smooth muscle cells to trigger airway hyperresponsiveness (AHR) in a paracrine manner. Among these, NPY was expressed at the highest levels, and deleting this gene in the Foxp1/Foxp4 knockout mice caused AHR to fall almost to normal levels. Incubating recombinant NPY with human and mouse lung tissue triggered marked bronchoconstriction in response to a methacholine challenge. Furthermore, phosphorylation of myosin light chain (pMLC), “a critical signaling event required for airway smooth muscle contraction,” increased with the methacholine challenge, but rose even more with concurrent exposure to NPY.
“Foxp1 and Foxp4 double mutants represent a model for noneosinophilic asthma, which remains poorly understood,” the researchers concluded. “The studies are among the first, to our knowledge, to mechanistically link a critical transcription pathway in airway epithelium that activates a paracrine response to the promotion of AHR in the absence of a Th2-induced eosinophilic inflammatory response.”
Most asthma therapies do not improve nonimmune asthma, which accounts for about half of asthma cases overall. While NPY gene variants have been linked to asthma, the specific molecular pathway was unknown, the researchers said. They found that Foxp1/4 knockout mice had greater airway smooth muscle contraction than control mice, especially after exposure to airway irritants. Notably, they did not find increased levels of the eosinophilic marker IL-13 or the neutrophilic inflammatory markers IL-17, IL-6, or keratinocyte-derived chemokine (KC) in airway epithelium from the knockout mice. “We did observe a modest increase in the numbers of neutrophils, but not macrophages, eosinophils, or lymphocytes in the bronchoalveolar lavage fluid in the Foxp1/4 knockout mutants,” they added (J Clin Invest. 2016 Apr. doi: 10.1172/JCI81389).
The National Institutes of Health funded the studies. The investigators had no disclosures.
The neuropeptide Y (NPY) gene appears to play an essential role in airway reactivity and may be a target for treating noneosinophilic asthma.
Higher expression of the NPY signaling molecule was seen in mice lacking Foxp1 and Foxp4 transcription factors. NPY induced noneosinophilic airway hyperreactivity by activating smooth muscle myosin light-chain phosphorylation, researchers reported in the Journal of Clinical Investigation.
Deleting the NPY gene in mice reduced airway hyperreactivity almost to normal levels, while incubating human lung tissue with recombinant NPY triggered bronchoconstriction, said Dr. Shanru Li and his associates at the University of Pennsylvania in Philadelphia. Future treatments for noneosinophilic asthma might target paracrine signaling from the airway epithelium to underlying smooth muscle.
The researchers also used transcriptome analysis to identify 10 genes that were significantly upregulated in the knockout mice and acted on airway smooth muscle cells to trigger airway hyperresponsiveness (AHR) in a paracrine manner. Among these, NPY was expressed at the highest levels, and deleting this gene in the Foxp1/Foxp4 knockout mice caused AHR to fall almost to normal levels. Incubating recombinant NPY with human and mouse lung tissue triggered marked bronchoconstriction in response to a methacholine challenge. Furthermore, phosphorylation of myosin light chain (pMLC), “a critical signaling event required for airway smooth muscle contraction,” increased with the methacholine challenge, but rose even more with concurrent exposure to NPY.
“Foxp1 and Foxp4 double mutants represent a model for noneosinophilic asthma, which remains poorly understood,” the researchers concluded. “The studies are among the first, to our knowledge, to mechanistically link a critical transcription pathway in airway epithelium that activates a paracrine response to the promotion of AHR in the absence of a Th2-induced eosinophilic inflammatory response.”
Most asthma therapies do not improve nonimmune asthma, which accounts for about half of asthma cases overall. While NPY gene variants have been linked to asthma, the specific molecular pathway was unknown, the researchers said. They found that Foxp1/4 knockout mice had greater airway smooth muscle contraction than control mice, especially after exposure to airway irritants. Notably, they did not find increased levels of the eosinophilic marker IL-13 or the neutrophilic inflammatory markers IL-17, IL-6, or keratinocyte-derived chemokine (KC) in airway epithelium from the knockout mice. “We did observe a modest increase in the numbers of neutrophils, but not macrophages, eosinophils, or lymphocytes in the bronchoalveolar lavage fluid in the Foxp1/4 knockout mutants,” they added (J Clin Invest. 2016 Apr. doi: 10.1172/JCI81389).
The National Institutes of Health funded the studies. The investigators had no disclosures.
FROM THE JOURNAL OF CLINICAL INVESTIGATION
Key clinical point: Loss of Foxp1 and Foxp4 expression is associated with overexpression of the NPY signaling molecule, which induced a phenotype resembling noneosinophilic asthma.
Major finding: Compared with control mice, Foxp1/Foxp4 knockout mice had substantially higher NPY levels and airway hyperresponsiveness in response to airway irritants.
Data source: Laboratory studies of Foxp1/Foxp4 knockout mice, control mice, and mouse and human lung tissue.
Disclosures: The National Institutes of Health funded the studies. The investigators had no disclosures.
Colorectal cancer threatens younger people
The rate of colorectal cancer diagnosis has risen in younger patients, with later-stage tumors predominant, according to findings from a study based on the large National Cancer Database.
Over a 10-year period, the number of colorectal cancer (CRC) cases increased by 11.4% among patients younger than 50 years, which translates to an average increase of 1.28% per year, or 136 new cases each year. By contrast, the number of newly diagnosed CRC cases in those over 50 years of age, dropped by 2.5% over the same period, according to data presented in a teleconference in advance of the annual Digestive Disease Week.
More advanced cancers were diagnosed in the younger group: stage 3, in 30.6% of patients under 50 years of age vs. 25.1% in those over that age; stage 4, in 25.6% vs. 18.2%, respectively.
“Last year, colorectal cancer was the second leading cause of cancer deaths in the U.S., second only to lung cancer. The health care system has done a great deal to heighten patient awareness and increase screenings, but these efforts have focused on people over the age of 50. Our findings show that more efforts need to be aimed at younger people, a group not normally considered at risk,” said lead author Dr. Elie Sutton. “Further, it is very concerning that within younger patients, a higher percentage were diagnosed at later stages.”
The study was based on more than 1 million CRC cases in the National Cancer Database from 2004 to 2013. Factors examined included a comparison of variables between younger-onset and older-onset CRC, such as stage at diagnosis, length of inpatient hospital stay, demographics, and 30-day and 90-day mortality.
In patients for whom data on metastatic disease were available, liver metastasis was reported in 19.4% of younger-onset patients vs. 13.8% of older-onset patients (P less than .001).
As would be expected, hospital stays were shorter for younger-onset patients, who are typically more resilient than older patients. A hospital stay of 5 days or less was recorded for 56.6% of younger-onset patients vs. 43.3% of older-onset patients (P = .001).
Short-term mortality was better for younger patients. Thirty-day mortality was 0.6% for younger-onset patients vs. 3.5% for older-onset patients (P less than .001). Ninety-day mortality was reported in 1.6% vs. 6.4%, respectively (P less than .001), and 8.5% of younger-onset patients had no insurance vs. 2.8% of older-onset patients (P less than .001).
These data are not a surprise, Dr. Sutton commented, in light of the fact that another study showed a similar trend about 5 years ago. “This means we have not adequately addressed risk of CRC in young patients under the age of 50,” he said. “Health care providers should be more vigilant and encourage screening in younger patients,” he emphasized.
Future studies will look at the trends in CRC over time. “We will continue to analyze the National Cancer Database. These insights may be helpful when revisiting colorectal cancer screening guidelines,” Dr. Sutton stated.
Dr. Sutton had no relevant financial disclosures.
The rate of colorectal cancer diagnosis has risen in younger patients, with later-stage tumors predominant, according to findings from a study based on the large National Cancer Database.
Over a 10-year period, the number of colorectal cancer (CRC) cases increased by 11.4% among patients younger than 50 years, which translates to an average increase of 1.28% per year, or 136 new cases each year. By contrast, the number of newly diagnosed CRC cases in those over 50 years of age, dropped by 2.5% over the same period, according to data presented in a teleconference in advance of the annual Digestive Disease Week.
More advanced cancers were diagnosed in the younger group: stage 3, in 30.6% of patients under 50 years of age vs. 25.1% in those over that age; stage 4, in 25.6% vs. 18.2%, respectively.
“Last year, colorectal cancer was the second leading cause of cancer deaths in the U.S., second only to lung cancer. The health care system has done a great deal to heighten patient awareness and increase screenings, but these efforts have focused on people over the age of 50. Our findings show that more efforts need to be aimed at younger people, a group not normally considered at risk,” said lead author Dr. Elie Sutton. “Further, it is very concerning that within younger patients, a higher percentage were diagnosed at later stages.”
The study was based on more than 1 million CRC cases in the National Cancer Database from 2004 to 2013. Factors examined included a comparison of variables between younger-onset and older-onset CRC, such as stage at diagnosis, length of inpatient hospital stay, demographics, and 30-day and 90-day mortality.
In patients for whom data on metastatic disease were available, liver metastasis was reported in 19.4% of younger-onset patients vs. 13.8% of older-onset patients (P less than .001).
As would be expected, hospital stays were shorter for younger-onset patients, who are typically more resilient than older patients. A hospital stay of 5 days or less was recorded for 56.6% of younger-onset patients vs. 43.3% of older-onset patients (P = .001).
Short-term mortality was better for younger patients. Thirty-day mortality was 0.6% for younger-onset patients vs. 3.5% for older-onset patients (P less than .001). Ninety-day mortality was reported in 1.6% vs. 6.4%, respectively (P less than .001), and 8.5% of younger-onset patients had no insurance vs. 2.8% of older-onset patients (P less than .001).
These data are not a surprise, Dr. Sutton commented, in light of the fact that another study showed a similar trend about 5 years ago. “This means we have not adequately addressed risk of CRC in young patients under the age of 50,” he said. “Health care providers should be more vigilant and encourage screening in younger patients,” he emphasized.
Future studies will look at the trends in CRC over time. “We will continue to analyze the National Cancer Database. These insights may be helpful when revisiting colorectal cancer screening guidelines,” Dr. Sutton stated.
Dr. Sutton had no relevant financial disclosures.
The rate of colorectal cancer diagnosis has risen in younger patients, with later-stage tumors predominant, according to findings from a study based on the large National Cancer Database.
Over a 10-year period, the number of colorectal cancer (CRC) cases increased by 11.4% among patients younger than 50 years, which translates to an average increase of 1.28% per year, or 136 new cases each year. By contrast, the number of newly diagnosed CRC cases in those over 50 years of age, dropped by 2.5% over the same period, according to data presented in a teleconference in advance of the annual Digestive Disease Week.
More advanced cancers were diagnosed in the younger group: stage 3, in 30.6% of patients under 50 years of age vs. 25.1% in those over that age; stage 4, in 25.6% vs. 18.2%, respectively.
“Last year, colorectal cancer was the second leading cause of cancer deaths in the U.S., second only to lung cancer. The health care system has done a great deal to heighten patient awareness and increase screenings, but these efforts have focused on people over the age of 50. Our findings show that more efforts need to be aimed at younger people, a group not normally considered at risk,” said lead author Dr. Elie Sutton. “Further, it is very concerning that within younger patients, a higher percentage were diagnosed at later stages.”
The study was based on more than 1 million CRC cases in the National Cancer Database from 2004 to 2013. Factors examined included a comparison of variables between younger-onset and older-onset CRC, such as stage at diagnosis, length of inpatient hospital stay, demographics, and 30-day and 90-day mortality.
In patients for whom data on metastatic disease were available, liver metastasis was reported in 19.4% of younger-onset patients vs. 13.8% of older-onset patients (P less than .001).
As would be expected, hospital stays were shorter for younger-onset patients, who are typically more resilient than older patients. A hospital stay of 5 days or less was recorded for 56.6% of younger-onset patients vs. 43.3% of older-onset patients (P = .001).
Short-term mortality was better for younger patients. Thirty-day mortality was 0.6% for younger-onset patients vs. 3.5% for older-onset patients (P less than .001). Ninety-day mortality was reported in 1.6% vs. 6.4%, respectively (P less than .001), and 8.5% of younger-onset patients had no insurance vs. 2.8% of older-onset patients (P less than .001).
These data are not a surprise, Dr. Sutton commented, in light of the fact that another study showed a similar trend about 5 years ago. “This means we have not adequately addressed risk of CRC in young patients under the age of 50,” he said. “Health care providers should be more vigilant and encourage screening in younger patients,” he emphasized.
Future studies will look at the trends in CRC over time. “We will continue to analyze the National Cancer Database. These insights may be helpful when revisiting colorectal cancer screening guidelines,” Dr. Sutton stated.
Dr. Sutton had no relevant financial disclosures.
FROM DDW® 2016
Key clinical point: The incidence of colorectal cancer is declining overall in the United States, but is increasing in people under age 50.
Major finding: Over a period of a decade, the number of young-onset cases of colorectal cancer increased by 11.4%, while the number of cases in patients over age 50 fell by 2.5%.
Data source: A retrospective study of more than 1 million colorectal cancer cases in the National Cancer Database from 2004 to 2013.
Disclosures: Dr. Sutton had no relevant financial disclosures