User login
Lesions on lower abdomen

At first, the FP considered the diagnosis of seborrheic keratosis, as the lesions were verrucous and pigmented. But after asking to see the patient’s genital area, the FP made the diagnosis of condyloma acuminata.
This is a good example of how seeing the whole picture beyond what the patient shows you can lead to a more accurate diagnosis. Verrucous lesions on the penis are usually condyloma acuminata, but it is important to know that condyloma can spread up the abdomen and onto the upper thighs, as was seen in this case. The lesions can also be hyperpigmented in people of color. If any doubts remain, a shave biopsy of one of the abdominal lesions would prove the diagnosis of condyloma by demonstrating human papillomavirus (HPV) changes histologically.
In this case, the FP discussed the risk of other sexually transmitted infections with the patient. Syphilis and human immunodeficiency virus tests were ordered, and both turned out to be negative.
The patient chose cryotherapy as a treatment option and the lesions were frozen with liquid nitrogen using a standard cryo-gun and a 1 mm halo, creating an appropriate freeze ball for each lesion. The patient tolerated the procedure well and was willing to have a second freeze thaw cycle for a more rapid treatment response. The FP suggested a follow-up visit in 3 to 4 weeks for a second round of cryotherapy. The patient indicated that he would be willing to try topical imiquimod after the next visit if the cryotherapy didn’t fully work.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ, Usatine R. Genital warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:759-765.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
At first, the FP considered the diagnosis of seborrheic keratosis, as the lesions were verrucous and pigmented. But after asking to see the patient’s genital area, the FP made the diagnosis of condyloma acuminata.
This is a good example of how seeing the whole picture beyond what the patient shows you can lead to a more accurate diagnosis. Verrucous lesions on the penis are usually condyloma acuminata, but it is important to know that condyloma can spread up the abdomen and onto the upper thighs, as was seen in this case. The lesions can also be hyperpigmented in people of color. If any doubts remain, a shave biopsy of one of the abdominal lesions would prove the diagnosis of condyloma by demonstrating human papillomavirus (HPV) changes histologically.
In this case, the FP discussed the risk of other sexually transmitted infections with the patient. Syphilis and human immunodeficiency virus tests were ordered, and both turned out to be negative.
The patient chose cryotherapy as a treatment option and the lesions were frozen with liquid nitrogen using a standard cryo-gun and a 1 mm halo, creating an appropriate freeze ball for each lesion. The patient tolerated the procedure well and was willing to have a second freeze thaw cycle for a more rapid treatment response. The FP suggested a follow-up visit in 3 to 4 weeks for a second round of cryotherapy. The patient indicated that he would be willing to try topical imiquimod after the next visit if the cryotherapy didn’t fully work.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ, Usatine R. Genital warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:759-765.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
At first, the FP considered the diagnosis of seborrheic keratosis, as the lesions were verrucous and pigmented. But after asking to see the patient’s genital area, the FP made the diagnosis of condyloma acuminata.
This is a good example of how seeing the whole picture beyond what the patient shows you can lead to a more accurate diagnosis. Verrucous lesions on the penis are usually condyloma acuminata, but it is important to know that condyloma can spread up the abdomen and onto the upper thighs, as was seen in this case. The lesions can also be hyperpigmented in people of color. If any doubts remain, a shave biopsy of one of the abdominal lesions would prove the diagnosis of condyloma by demonstrating human papillomavirus (HPV) changes histologically.
In this case, the FP discussed the risk of other sexually transmitted infections with the patient. Syphilis and human immunodeficiency virus tests were ordered, and both turned out to be negative.
The patient chose cryotherapy as a treatment option and the lesions were frozen with liquid nitrogen using a standard cryo-gun and a 1 mm halo, creating an appropriate freeze ball for each lesion. The patient tolerated the procedure well and was willing to have a second freeze thaw cycle for a more rapid treatment response. The FP suggested a follow-up visit in 3 to 4 weeks for a second round of cryotherapy. The patient indicated that he would be willing to try topical imiquimod after the next visit if the cryotherapy didn’t fully work.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Mayeaux EJ, Usatine R. Genital warts. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:759-765.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

Study identifies distinct OA fatigue trajectories
A new study has identified three distinct trajectories of fatigue levels in patients with early symptomatic osteoarthritis (OA) in the knee and hip, report Jadran Botterman, MSc, and coauthors from the department of psychology, health, and technology at the University of Twente (the Netherlands).
Six years of data were collected from the CHECK (Cohort Hip and Cohort Knee) participants and then separated into distinct trajectories using growth mixture modeling. Three distinct fatigue trajectories were found: low fatigue, low to high fatigue, and high fatigue.
The authors found a significant association between trajectory and patient characteristics. Women, patients with comorbid disease, and patients using medications were more likely to have a high fatigue trajectory, Dr. Botterman and his colleagues reported.
“Identification of these trajectories with differing patient characteristics may warrant tailored psychosocial interventions for patients with elevated levels of fatigue,” the authors concluded.
Read the full article in the Journal of Rheumatology.
A new study has identified three distinct trajectories of fatigue levels in patients with early symptomatic osteoarthritis (OA) in the knee and hip, report Jadran Botterman, MSc, and coauthors from the department of psychology, health, and technology at the University of Twente (the Netherlands).
Six years of data were collected from the CHECK (Cohort Hip and Cohort Knee) participants and then separated into distinct trajectories using growth mixture modeling. Three distinct fatigue trajectories were found: low fatigue, low to high fatigue, and high fatigue.
The authors found a significant association between trajectory and patient characteristics. Women, patients with comorbid disease, and patients using medications were more likely to have a high fatigue trajectory, Dr. Botterman and his colleagues reported.
“Identification of these trajectories with differing patient characteristics may warrant tailored psychosocial interventions for patients with elevated levels of fatigue,” the authors concluded.
Read the full article in the Journal of Rheumatology.
A new study has identified three distinct trajectories of fatigue levels in patients with early symptomatic osteoarthritis (OA) in the knee and hip, report Jadran Botterman, MSc, and coauthors from the department of psychology, health, and technology at the University of Twente (the Netherlands).
Six years of data were collected from the CHECK (Cohort Hip and Cohort Knee) participants and then separated into distinct trajectories using growth mixture modeling. Three distinct fatigue trajectories were found: low fatigue, low to high fatigue, and high fatigue.
The authors found a significant association between trajectory and patient characteristics. Women, patients with comorbid disease, and patients using medications were more likely to have a high fatigue trajectory, Dr. Botterman and his colleagues reported.
“Identification of these trajectories with differing patient characteristics may warrant tailored psychosocial interventions for patients with elevated levels of fatigue,” the authors concluded.
Read the full article in the Journal of Rheumatology.
FROM THE JOURNAL OF RHEUMATOLOGY
Three-drug regimen boosts progression-free survival in patients with relapsed CLL and adverse prognostic features
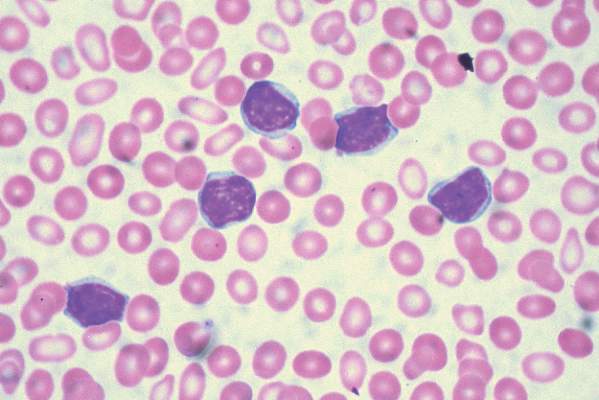
Progression-free survival was improved for poor prognosis patients with relapsed chronic lymphocytic leukemia when idelalisib was added to bendamustine and rituximab, based on the results of a randomized, double-blind, placebo-controlled phase III study.
The findings support the three-drug approach as an important treatment option for patients with relapsed CLL and adverse prognostic features, but the regimen also was associated with more grade 3 or greater adverse events, primarily neutropenia and opportunistic infections, that led to more study drug discontinuation, Jacqueline Claudia Barrientos, M.D., and her colleagues reported at the annual meeting of the American Society of Clinical Oncology.
The overall response rates were 68% in the three-drug group and 45% in the two-drug plus placebo group.
For the study, 416 patients were stratified based on whether they had 17p deletions or TP53 mutations, their IGHV mutation status, and whether they had refractory or relapsed disease. The 207 patients who received idelalisib, bendamustine, and rituximab had consistently better progression-free survival than the 209 patients who received placebo, bendamustine, and rituximab. The median progression-free survival was 23 months in the group that received idelalisib and 11 months in the group that received placebo, with an overall hazard ratio of 0.33 at a median follow-up of 12 months.
For those with 17p deletions or TP53 mutations, the median progression-free survival was 11 months with the three-drug regimen and 8 months for the two-drug plus placebo regimen. For those with neither of these abnormalities, progression-free survival was more than 24 months for patients given the three active drugs and 11 months for patients given two drugs plus placebo.
For those with the 11q deletion, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and 9 months with placebo, bendamustine, and rituximab, said Dr. Barrientos of Hofstra University, Hempstead, N.Y.
For those with IGHV mutations, the median progression-free survival has not been reached in the idelalisib, bendamustine, and rituximab group and was 11 months in the placebo, bendamustine, and rituximab group.
Among patients with tumor burdens exceeding 5 cm, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and about 10 months with placebo, bendamustine, and rituximab.
Grade 3 or greater adverse events affected 97% of patients given the three active drugs and 76% of patients given bendamustine and rituximab plus placebo. Adverse events resulted in drug dose reductions in 11% of those given the three active drugs and in 6% of those given bendamustine and rituximab plus placebo. The study drug was discontinued in 26% of those in the idelalisib, bendamustine, and rituximab group and in 13% of the placebo, bendamustine, and rituximab group. Death occurred in 10% of the study patients given idelalisib, bendamustine, and rituximab and in 7% of the patients given placebo, bendamustine, and rituximab.
To be eligible for the study (NCT01569295), patients needed to have previously treated recurrent CLL, have measurable lymphadenopathy, require therapy for CLL, and have experienced CLL progression for less than 36 months since the completion of their last prior therapy.
The treatment regimen consisted of 6 cycles every 28 days of bendamustine (70 mg/m2 on day 1 and day 2 of each cycle), rituximab (375 mg/m2 in cycle 1 and 500 mg/m2 in cycles 2-6), and idelalisib (150 mg twice daily) or placebo. Idelalisib or placebo was continued until an independent review committee confirmed disease progression, death, intolerable toxicity, or withdrawal of consent.
The study was sponsored by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Barrientos receives research funding from Gilead Sciences and Abbvie, and serves as a consultant or adviser to Celgene, Genentech, and Pharmacyclics.
On Twitter @maryjodales
Progression-free survival was improved for poor prognosis patients with relapsed chronic lymphocytic leukemia when idelalisib was added to bendamustine and rituximab, based on the results of a randomized, double-blind, placebo-controlled phase III study.
The findings support the three-drug approach as an important treatment option for patients with relapsed CLL and adverse prognostic features, but the regimen also was associated with more grade 3 or greater adverse events, primarily neutropenia and opportunistic infections, that led to more study drug discontinuation, Jacqueline Claudia Barrientos, M.D., and her colleagues reported at the annual meeting of the American Society of Clinical Oncology.
The overall response rates were 68% in the three-drug group and 45% in the two-drug plus placebo group.
For the study, 416 patients were stratified based on whether they had 17p deletions or TP53 mutations, their IGHV mutation status, and whether they had refractory or relapsed disease. The 207 patients who received idelalisib, bendamustine, and rituximab had consistently better progression-free survival than the 209 patients who received placebo, bendamustine, and rituximab. The median progression-free survival was 23 months in the group that received idelalisib and 11 months in the group that received placebo, with an overall hazard ratio of 0.33 at a median follow-up of 12 months.
For those with 17p deletions or TP53 mutations, the median progression-free survival was 11 months with the three-drug regimen and 8 months for the two-drug plus placebo regimen. For those with neither of these abnormalities, progression-free survival was more than 24 months for patients given the three active drugs and 11 months for patients given two drugs plus placebo.
For those with the 11q deletion, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and 9 months with placebo, bendamustine, and rituximab, said Dr. Barrientos of Hofstra University, Hempstead, N.Y.
For those with IGHV mutations, the median progression-free survival has not been reached in the idelalisib, bendamustine, and rituximab group and was 11 months in the placebo, bendamustine, and rituximab group.
Among patients with tumor burdens exceeding 5 cm, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and about 10 months with placebo, bendamustine, and rituximab.
Grade 3 or greater adverse events affected 97% of patients given the three active drugs and 76% of patients given bendamustine and rituximab plus placebo. Adverse events resulted in drug dose reductions in 11% of those given the three active drugs and in 6% of those given bendamustine and rituximab plus placebo. The study drug was discontinued in 26% of those in the idelalisib, bendamustine, and rituximab group and in 13% of the placebo, bendamustine, and rituximab group. Death occurred in 10% of the study patients given idelalisib, bendamustine, and rituximab and in 7% of the patients given placebo, bendamustine, and rituximab.
To be eligible for the study (NCT01569295), patients needed to have previously treated recurrent CLL, have measurable lymphadenopathy, require therapy for CLL, and have experienced CLL progression for less than 36 months since the completion of their last prior therapy.
The treatment regimen consisted of 6 cycles every 28 days of bendamustine (70 mg/m2 on day 1 and day 2 of each cycle), rituximab (375 mg/m2 in cycle 1 and 500 mg/m2 in cycles 2-6), and idelalisib (150 mg twice daily) or placebo. Idelalisib or placebo was continued until an independent review committee confirmed disease progression, death, intolerable toxicity, or withdrawal of consent.
The study was sponsored by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Barrientos receives research funding from Gilead Sciences and Abbvie, and serves as a consultant or adviser to Celgene, Genentech, and Pharmacyclics.
On Twitter @maryjodales
Progression-free survival was improved for poor prognosis patients with relapsed chronic lymphocytic leukemia when idelalisib was added to bendamustine and rituximab, based on the results of a randomized, double-blind, placebo-controlled phase III study.
The findings support the three-drug approach as an important treatment option for patients with relapsed CLL and adverse prognostic features, but the regimen also was associated with more grade 3 or greater adverse events, primarily neutropenia and opportunistic infections, that led to more study drug discontinuation, Jacqueline Claudia Barrientos, M.D., and her colleagues reported at the annual meeting of the American Society of Clinical Oncology.
The overall response rates were 68% in the three-drug group and 45% in the two-drug plus placebo group.
For the study, 416 patients were stratified based on whether they had 17p deletions or TP53 mutations, their IGHV mutation status, and whether they had refractory or relapsed disease. The 207 patients who received idelalisib, bendamustine, and rituximab had consistently better progression-free survival than the 209 patients who received placebo, bendamustine, and rituximab. The median progression-free survival was 23 months in the group that received idelalisib and 11 months in the group that received placebo, with an overall hazard ratio of 0.33 at a median follow-up of 12 months.
For those with 17p deletions or TP53 mutations, the median progression-free survival was 11 months with the three-drug regimen and 8 months for the two-drug plus placebo regimen. For those with neither of these abnormalities, progression-free survival was more than 24 months for patients given the three active drugs and 11 months for patients given two drugs plus placebo.
For those with the 11q deletion, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and 9 months with placebo, bendamustine, and rituximab, said Dr. Barrientos of Hofstra University, Hempstead, N.Y.
For those with IGHV mutations, the median progression-free survival has not been reached in the idelalisib, bendamustine, and rituximab group and was 11 months in the placebo, bendamustine, and rituximab group.
Among patients with tumor burdens exceeding 5 cm, median progression-free survival was 23 months with idelalisib, bendamustine, and rituximab and about 10 months with placebo, bendamustine, and rituximab.
Grade 3 or greater adverse events affected 97% of patients given the three active drugs and 76% of patients given bendamustine and rituximab plus placebo. Adverse events resulted in drug dose reductions in 11% of those given the three active drugs and in 6% of those given bendamustine and rituximab plus placebo. The study drug was discontinued in 26% of those in the idelalisib, bendamustine, and rituximab group and in 13% of the placebo, bendamustine, and rituximab group. Death occurred in 10% of the study patients given idelalisib, bendamustine, and rituximab and in 7% of the patients given placebo, bendamustine, and rituximab.
To be eligible for the study (NCT01569295), patients needed to have previously treated recurrent CLL, have measurable lymphadenopathy, require therapy for CLL, and have experienced CLL progression for less than 36 months since the completion of their last prior therapy.
The treatment regimen consisted of 6 cycles every 28 days of bendamustine (70 mg/m2 on day 1 and day 2 of each cycle), rituximab (375 mg/m2 in cycle 1 and 500 mg/m2 in cycles 2-6), and idelalisib (150 mg twice daily) or placebo. Idelalisib or placebo was continued until an independent review committee confirmed disease progression, death, intolerable toxicity, or withdrawal of consent.
The study was sponsored by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Barrientos receives research funding from Gilead Sciences and Abbvie, and serves as a consultant or adviser to Celgene, Genentech, and Pharmacyclics.
On Twitter @maryjodales
FROM 2016 ASCO ANNUAL MEETING
Key clinical point: Progression-free survival was improved for poor prognosis patients with relapsed chronic lymphocytic leukemia when idelalisib was added to bendamustine, and rituximab.
Major finding: The median progression-free survival was 23 months in the group that received idelalisib and 11 months in the group that received placebo, with an overall hazard ratio of 0.33 at a median follow-up of 12 months.
Data source: A randomized, double-blind, placebo-controlled phase III study of 416 patients stratified on the basis of 17p deletions or TP53 mutations, IGHV mutation status, and whether they had refractory or relapsed disease.
Disclosures: The study was sponsored by Gilead Sciences, the maker of idelalisib (Zydelig). Dr. Barrientos receives research funding from Gilead Sciences and Abbvie, and serves as a consultant or adviser to Celgene, Genentech, and Pharmacyclics.
Triple Therapy Helped Type 1 Patients Improve Glycemia
NEW ORLEANS – The addition of dapagliflozin to insulin and liraglutide in patients with type 1 diabetes resulted in a significant improvement in glycemia, results from a single-center randomized trial showed.
“Because liraglutide suppresses glucagon and lowers free fatty acids while SGLT-2 inhibitors increase glucagon and risk of diabetic ketoacidosis, it’s possible that the combination of the two agents may neutralize the diabetic ketoacidosis risk,” Paresh Dandona, MD, said at the annual scientific sessions of the American Diabetes Association.

In a recent study Dr. Dandona, chief of endocrinology at the University of Buffalo (N.Y.), and his associates showed that the addition of liraglutide to insulin significantly improved glycemic control in patients with type 1 diabetes (Diabetes Care 2016 Jun; 39[6]:1027-35). The purpose of the current study was to investigate whether the addition of dapagliflozin, a sodium-glucose cotransporter–2 inhibitor, to the combination of insulin and liraglutide would further improve glycemic control.
A total of 30 type 1 diabetes patients on insulin and liraglutide therapy for a minimum of 6 months were randomized to receive either dapagliflozin 10 mg or placebo daily for 12 weeks. Dapagliflozin was initiated at 5 mg daily for 1 week and increased to 10 mg daily thereafter. All patients had type 1 diabetes for at least 1 year, were on insulin therapy, had no detectable C-peptide in plasma, and were on 1.8 mg of liraglutide for 7 months. These patients were evaluated every week for the first and last 2 weeks and then every 2 weeks for 12 weeks. Blood and 24-hour urine samples were collected before and after intervention.
At baseline, the mean age of patients was 54 years and both groups were similar in terms of mean hemoglobin A1c, glucose levels, and insulin dosages. After 12 weeks, the mean HbA1c did not change in the placebo group, but it dropped significantly in the triple-therapy group, by .66% (P less than .01). In addition, the average weekly glucose concentration fell in the triple-therapy group by 13 mg/dL (P = .35) and there was a reduction in standard deviations of glycemic excursions. The triple-therapy group also experienced a small reduction in the total insulin dose, compared with the placebo group (–3.5 vs. –.4 units, respectively; P = .29)
Dr. Dandona went on to note that the episodes of hypoglycemia did not increase after triple therapy but body weight fell by 1.9 kg after 12 weeks, while there was no real change in the placebo arm. Two patients had to withdraw from the study because they developed diabetic ketoacidosis within a day after increasing the dose of dapagliflozin to 10 mg. “One of these patients had euglycemic DKA with blood glucose concentrations of less than 160 mg/dL, while the other had marked hyperglycemia with unchanged insulin dose at 26 units,” Dr. Dandona said. “This patient had experienced a marked reduction in insulin dose during the time she was on liraglutide prior to starting on dapagliflozin.”
Dr. Dandona disclosed that he has received research support from AstraZeneca and Novo Nordisk.
NEW ORLEANS – The addition of dapagliflozin to insulin and liraglutide in patients with type 1 diabetes resulted in a significant improvement in glycemia, results from a single-center randomized trial showed.
“Because liraglutide suppresses glucagon and lowers free fatty acids while SGLT-2 inhibitors increase glucagon and risk of diabetic ketoacidosis, it’s possible that the combination of the two agents may neutralize the diabetic ketoacidosis risk,” Paresh Dandona, MD, said at the annual scientific sessions of the American Diabetes Association.
In a recent study Dr. Dandona, chief of endocrinology at the University of Buffalo (N.Y.), and his associates showed that the addition of liraglutide to insulin significantly improved glycemic control in patients with type 1 diabetes (Diabetes Care 2016 Jun; 39[6]:1027-35). The purpose of the current study was to investigate whether the addition of dapagliflozin, a sodium-glucose cotransporter–2 inhibitor, to the combination of insulin and liraglutide would further improve glycemic control.
A total of 30 type 1 diabetes patients on insulin and liraglutide therapy for a minimum of 6 months were randomized to receive either dapagliflozin 10 mg or placebo daily for 12 weeks. Dapagliflozin was initiated at 5 mg daily for 1 week and increased to 10 mg daily thereafter. All patients had type 1 diabetes for at least 1 year, were on insulin therapy, had no detectable C-peptide in plasma, and were on 1.8 mg of liraglutide for 7 months. These patients were evaluated every week for the first and last 2 weeks and then every 2 weeks for 12 weeks. Blood and 24-hour urine samples were collected before and after intervention.
At baseline, the mean age of patients was 54 years and both groups were similar in terms of mean hemoglobin A1c, glucose levels, and insulin dosages. After 12 weeks, the mean HbA1c did not change in the placebo group, but it dropped significantly in the triple-therapy group, by .66% (P less than .01). In addition, the average weekly glucose concentration fell in the triple-therapy group by 13 mg/dL (P = .35) and there was a reduction in standard deviations of glycemic excursions. The triple-therapy group also experienced a small reduction in the total insulin dose, compared with the placebo group (–3.5 vs. –.4 units, respectively; P = .29)
Dr. Dandona went on to note that the episodes of hypoglycemia did not increase after triple therapy but body weight fell by 1.9 kg after 12 weeks, while there was no real change in the placebo arm. Two patients had to withdraw from the study because they developed diabetic ketoacidosis within a day after increasing the dose of dapagliflozin to 10 mg. “One of these patients had euglycemic DKA with blood glucose concentrations of less than 160 mg/dL, while the other had marked hyperglycemia with unchanged insulin dose at 26 units,” Dr. Dandona said. “This patient had experienced a marked reduction in insulin dose during the time she was on liraglutide prior to starting on dapagliflozin.”
Dr. Dandona disclosed that he has received research support from AstraZeneca and Novo Nordisk.
NEW ORLEANS – The addition of dapagliflozin to insulin and liraglutide in patients with type 1 diabetes resulted in a significant improvement in glycemia, results from a single-center randomized trial showed.
“Because liraglutide suppresses glucagon and lowers free fatty acids while SGLT-2 inhibitors increase glucagon and risk of diabetic ketoacidosis, it’s possible that the combination of the two agents may neutralize the diabetic ketoacidosis risk,” Paresh Dandona, MD, said at the annual scientific sessions of the American Diabetes Association.
In a recent study Dr. Dandona, chief of endocrinology at the University of Buffalo (N.Y.), and his associates showed that the addition of liraglutide to insulin significantly improved glycemic control in patients with type 1 diabetes (Diabetes Care 2016 Jun; 39[6]:1027-35). The purpose of the current study was to investigate whether the addition of dapagliflozin, a sodium-glucose cotransporter–2 inhibitor, to the combination of insulin and liraglutide would further improve glycemic control.
A total of 30 type 1 diabetes patients on insulin and liraglutide therapy for a minimum of 6 months were randomized to receive either dapagliflozin 10 mg or placebo daily for 12 weeks. Dapagliflozin was initiated at 5 mg daily for 1 week and increased to 10 mg daily thereafter. All patients had type 1 diabetes for at least 1 year, were on insulin therapy, had no detectable C-peptide in plasma, and were on 1.8 mg of liraglutide for 7 months. These patients were evaluated every week for the first and last 2 weeks and then every 2 weeks for 12 weeks. Blood and 24-hour urine samples were collected before and after intervention.
At baseline, the mean age of patients was 54 years and both groups were similar in terms of mean hemoglobin A1c, glucose levels, and insulin dosages. After 12 weeks, the mean HbA1c did not change in the placebo group, but it dropped significantly in the triple-therapy group, by .66% (P less than .01). In addition, the average weekly glucose concentration fell in the triple-therapy group by 13 mg/dL (P = .35) and there was a reduction in standard deviations of glycemic excursions. The triple-therapy group also experienced a small reduction in the total insulin dose, compared with the placebo group (–3.5 vs. –.4 units, respectively; P = .29)
Dr. Dandona went on to note that the episodes of hypoglycemia did not increase after triple therapy but body weight fell by 1.9 kg after 12 weeks, while there was no real change in the placebo arm. Two patients had to withdraw from the study because they developed diabetic ketoacidosis within a day after increasing the dose of dapagliflozin to 10 mg. “One of these patients had euglycemic DKA with blood glucose concentrations of less than 160 mg/dL, while the other had marked hyperglycemia with unchanged insulin dose at 26 units,” Dr. Dandona said. “This patient had experienced a marked reduction in insulin dose during the time she was on liraglutide prior to starting on dapagliflozin.”
Dr. Dandona disclosed that he has received research support from AstraZeneca and Novo Nordisk.
AT THE ADA ANNUAL SCIENTIFIC SESSIONS

Triple therapy helped type 1 patients improve glycemia
NEW ORLEANS – The addition of dapagliflozin to insulin and liraglutide in patients with type 1 diabetes resulted in a significant improvement in glycemia, results from a single-center randomized trial showed.
“Because liraglutide suppresses glucagon and lowers free fatty acids while SGLT-2 inhibitors increase glucagon and risk of diabetic ketoacidosis, it’s possible that the combination of the two agents may neutralize the diabetic ketoacidosis risk,” Paresh Dandona, MD, said at the annual scientific sessions of the American Diabetes Association.

In a recent study Dr. Dandona, chief of endocrinology at the University of Buffalo (N.Y.), and his associates showed that the addition of liraglutide to insulin significantly improved glycemic control in patients with type 1 diabetes (Diabetes Care 2016 Jun; 39[6]:1027-35). The purpose of the current study was to investigate whether the addition of dapagliflozin, a sodium-glucose cotransporter–2 inhibitor, to the combination of insulin and liraglutide would further improve glycemic control.
A total of 30 type 1 diabetes patients on insulin and liraglutide therapy for a minimum of 6 months were randomized to receive either dapagliflozin 10 mg or placebo daily for 12 weeks. Dapagliflozin was initiated at 5 mg daily for 1 week and increased to 10 mg daily thereafter. All patients had type 1 diabetes for at least 1 year, were on insulin therapy, had no detectable C-peptide in plasma, and were on 1.8 mg of liraglutide for 7 months. These patients were evaluated every week for the first and last 2 weeks and then every 2 weeks for 12 weeks. Blood and 24-hour urine samples were collected before and after intervention.
At baseline, the mean age of patients was 54 years and both groups were similar in terms of mean hemoglobin A1c, glucose levels, and insulin dosages. After 12 weeks, the mean HbA1c did not change in the placebo group, but it dropped significantly in the triple-therapy group, by .66% (P less than .01). In addition, the average weekly glucose concentration fell in the triple-therapy group by 13 mg/dL (P = .35) and there was a reduction in standard deviations of glycemic excursions. The triple-therapy group also experienced a small reduction in the total insulin dose, compared with the placebo group (–3.5 vs. –.4 units, respectively; P = .29)
Dr. Dandona went on to note that the episodes of hypoglycemia did not increase after triple therapy but body weight fell by 1.9 kg after 12 weeks, while there was no real change in the placebo arm. Two patients had to withdraw from the study because they developed diabetic ketoacidosis within a day after increasing the dose of dapagliflozin to 10 mg. “One of these patients had euglycemic DKA with blood glucose concentrations of less than 160 mg/dL, while the other had marked hyperglycemia with unchanged insulin dose at 26 units,” Dr. Dandona said. “This patient had experienced a marked reduction in insulin dose during the time she was on liraglutide prior to starting on dapagliflozin.”
Dr. Dandona disclosed that he has received research support from AstraZeneca and Novo Nordisk.
NEW ORLEANS – The addition of dapagliflozin to insulin and liraglutide in patients with type 1 diabetes resulted in a significant improvement in glycemia, results from a single-center randomized trial showed.
“Because liraglutide suppresses glucagon and lowers free fatty acids while SGLT-2 inhibitors increase glucagon and risk of diabetic ketoacidosis, it’s possible that the combination of the two agents may neutralize the diabetic ketoacidosis risk,” Paresh Dandona, MD, said at the annual scientific sessions of the American Diabetes Association.
In a recent study Dr. Dandona, chief of endocrinology at the University of Buffalo (N.Y.), and his associates showed that the addition of liraglutide to insulin significantly improved glycemic control in patients with type 1 diabetes (Diabetes Care 2016 Jun; 39[6]:1027-35). The purpose of the current study was to investigate whether the addition of dapagliflozin, a sodium-glucose cotransporter–2 inhibitor, to the combination of insulin and liraglutide would further improve glycemic control.
A total of 30 type 1 diabetes patients on insulin and liraglutide therapy for a minimum of 6 months were randomized to receive either dapagliflozin 10 mg or placebo daily for 12 weeks. Dapagliflozin was initiated at 5 mg daily for 1 week and increased to 10 mg daily thereafter. All patients had type 1 diabetes for at least 1 year, were on insulin therapy, had no detectable C-peptide in plasma, and were on 1.8 mg of liraglutide for 7 months. These patients were evaluated every week for the first and last 2 weeks and then every 2 weeks for 12 weeks. Blood and 24-hour urine samples were collected before and after intervention.
At baseline, the mean age of patients was 54 years and both groups were similar in terms of mean hemoglobin A1c, glucose levels, and insulin dosages. After 12 weeks, the mean HbA1c did not change in the placebo group, but it dropped significantly in the triple-therapy group, by .66% (P less than .01). In addition, the average weekly glucose concentration fell in the triple-therapy group by 13 mg/dL (P = .35) and there was a reduction in standard deviations of glycemic excursions. The triple-therapy group also experienced a small reduction in the total insulin dose, compared with the placebo group (–3.5 vs. –.4 units, respectively; P = .29)
Dr. Dandona went on to note that the episodes of hypoglycemia did not increase after triple therapy but body weight fell by 1.9 kg after 12 weeks, while there was no real change in the placebo arm. Two patients had to withdraw from the study because they developed diabetic ketoacidosis within a day after increasing the dose of dapagliflozin to 10 mg. “One of these patients had euglycemic DKA with blood glucose concentrations of less than 160 mg/dL, while the other had marked hyperglycemia with unchanged insulin dose at 26 units,” Dr. Dandona said. “This patient had experienced a marked reduction in insulin dose during the time she was on liraglutide prior to starting on dapagliflozin.”
Dr. Dandona disclosed that he has received research support from AstraZeneca and Novo Nordisk.
NEW ORLEANS – The addition of dapagliflozin to insulin and liraglutide in patients with type 1 diabetes resulted in a significant improvement in glycemia, results from a single-center randomized trial showed.
“Because liraglutide suppresses glucagon and lowers free fatty acids while SGLT-2 inhibitors increase glucagon and risk of diabetic ketoacidosis, it’s possible that the combination of the two agents may neutralize the diabetic ketoacidosis risk,” Paresh Dandona, MD, said at the annual scientific sessions of the American Diabetes Association.
In a recent study Dr. Dandona, chief of endocrinology at the University of Buffalo (N.Y.), and his associates showed that the addition of liraglutide to insulin significantly improved glycemic control in patients with type 1 diabetes (Diabetes Care 2016 Jun; 39[6]:1027-35). The purpose of the current study was to investigate whether the addition of dapagliflozin, a sodium-glucose cotransporter–2 inhibitor, to the combination of insulin and liraglutide would further improve glycemic control.
A total of 30 type 1 diabetes patients on insulin and liraglutide therapy for a minimum of 6 months were randomized to receive either dapagliflozin 10 mg or placebo daily for 12 weeks. Dapagliflozin was initiated at 5 mg daily for 1 week and increased to 10 mg daily thereafter. All patients had type 1 diabetes for at least 1 year, were on insulin therapy, had no detectable C-peptide in plasma, and were on 1.8 mg of liraglutide for 7 months. These patients were evaluated every week for the first and last 2 weeks and then every 2 weeks for 12 weeks. Blood and 24-hour urine samples were collected before and after intervention.
At baseline, the mean age of patients was 54 years and both groups were similar in terms of mean hemoglobin A1c, glucose levels, and insulin dosages. After 12 weeks, the mean HbA1c did not change in the placebo group, but it dropped significantly in the triple-therapy group, by .66% (P less than .01). In addition, the average weekly glucose concentration fell in the triple-therapy group by 13 mg/dL (P = .35) and there was a reduction in standard deviations of glycemic excursions. The triple-therapy group also experienced a small reduction in the total insulin dose, compared with the placebo group (–3.5 vs. –.4 units, respectively; P = .29)
Dr. Dandona went on to note that the episodes of hypoglycemia did not increase after triple therapy but body weight fell by 1.9 kg after 12 weeks, while there was no real change in the placebo arm. Two patients had to withdraw from the study because they developed diabetic ketoacidosis within a day after increasing the dose of dapagliflozin to 10 mg. “One of these patients had euglycemic DKA with blood glucose concentrations of less than 160 mg/dL, while the other had marked hyperglycemia with unchanged insulin dose at 26 units,” Dr. Dandona said. “This patient had experienced a marked reduction in insulin dose during the time she was on liraglutide prior to starting on dapagliflozin.”
Dr. Dandona disclosed that he has received research support from AstraZeneca and Novo Nordisk.
AT THE ADA ANNUAL SCIENTIFIC SESSIONS
Key clinical point: Adding dapagliflozin to insulin and liraglutide in patients with type 1 diabetes led to a significant improvement in glycemia.
Major finding: After 12 weeks, the mean HbA1c did not change in the placebo group, but it dropped in the triple-therapy group by 0.66% (P less than .01).
Data source: A single-center study in which 30 type 1 diabetes patients on insulin and liraglutide therapy for a minimum of 6 months were randomized to receive either dapagliflozin 10 mg or placebo daily for 12 weeks.
Disclosures: Dr. Dandona disclosed that he has received research support from AstraZeneca and Novo Nordisk.

New antibiotics targeting MDR pathogens are expensive, but not impressive
The U.S. Food and Drug Administration has approved a number of new antibiotics targeting multidrug-resistant bacteria in the past 5 years, but the new drugs have not led to a substantial improvement in patient outcomes when compared with existing antibiotics, according to a recent analysis in the Annals of Internal Medicine.
The eight new antibiotics approved by the FDA between January 2010 and December 2015 were ceftaroline, fidaxomicin, bedaquiline, dalbavancin, tedizolid, oritavancin, ceftolozane/tazobactam, and ceftazidime/avibactam. Of those eight drugs, only three showed in vitro activity against the so-called ESKAPE pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumonia, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species). Only one drug, fidaxomicin, demonstrated in vitro activity against an urgent-threat pathogen from the Centers for Disease Control and Prevention, Clostridium difficile. Bedaquiline was the only new antibiotic specifically indicated for a disease from a multidrug-resistant pathogen, although the investigators said most of the drugs demonstrated in vitro activity against gram-positive drug-resistant pathogens.

Importantly, the authors noted that in vitro activity does not necessarily reflect benefits on actual patient clinical outcomes, as exemplified by such drugs as tigecycline and doripenem.
The researchers found what they called “important deficiencies in the clinical trials leading to approval of these new antibiotic products.” Most pivotal trial designs were primarily noninferiority trials, and the antibiotics were not studied to evaluate whether they have substantial benefits in efficacy over what is currently available, they noted. Additionally, none of the trials evaluated direct patient outcomes as primary end points, and some drugs did not have confirmatory evidence from a second independent trial or did not have any confirmatory trials.
Researchers also examined the prices of a single dose of the new antibiotics. The prices ranged from $1,195 to $4,183 (4-14 days of ceftolozane/tazobactam for acute pyelonephritis and intra-abdominal infections) to $69,702 (24 weeks of bedaquiline) – quite a premium for antibiotics showing unclear evidence of additional benefit.
“As antibiotic innovation continues to move forward, greater attention needs to be paid to incentives for developing high-quality new products with demonstrated superiority to existing products on outcomes in patients with multidrug-resistant disease, replacing the current focus on quantity and presumed future benefits,” researchers concluded.
Read the full study in the Annals of Internal Medicine (doi: 10.7326/M16-0291).
The U.S. Food and Drug Administration has approved a number of new antibiotics targeting multidrug-resistant bacteria in the past 5 years, but the new drugs have not led to a substantial improvement in patient outcomes when compared with existing antibiotics, according to a recent analysis in the Annals of Internal Medicine.
The eight new antibiotics approved by the FDA between January 2010 and December 2015 were ceftaroline, fidaxomicin, bedaquiline, dalbavancin, tedizolid, oritavancin, ceftolozane/tazobactam, and ceftazidime/avibactam. Of those eight drugs, only three showed in vitro activity against the so-called ESKAPE pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumonia, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species). Only one drug, fidaxomicin, demonstrated in vitro activity against an urgent-threat pathogen from the Centers for Disease Control and Prevention, Clostridium difficile. Bedaquiline was the only new antibiotic specifically indicated for a disease from a multidrug-resistant pathogen, although the investigators said most of the drugs demonstrated in vitro activity against gram-positive drug-resistant pathogens.
Importantly, the authors noted that in vitro activity does not necessarily reflect benefits on actual patient clinical outcomes, as exemplified by such drugs as tigecycline and doripenem.
The researchers found what they called “important deficiencies in the clinical trials leading to approval of these new antibiotic products.” Most pivotal trial designs were primarily noninferiority trials, and the antibiotics were not studied to evaluate whether they have substantial benefits in efficacy over what is currently available, they noted. Additionally, none of the trials evaluated direct patient outcomes as primary end points, and some drugs did not have confirmatory evidence from a second independent trial or did not have any confirmatory trials.
Researchers also examined the prices of a single dose of the new antibiotics. The prices ranged from $1,195 to $4,183 (4-14 days of ceftolozane/tazobactam for acute pyelonephritis and intra-abdominal infections) to $69,702 (24 weeks of bedaquiline) – quite a premium for antibiotics showing unclear evidence of additional benefit.
“As antibiotic innovation continues to move forward, greater attention needs to be paid to incentives for developing high-quality new products with demonstrated superiority to existing products on outcomes in patients with multidrug-resistant disease, replacing the current focus on quantity and presumed future benefits,” researchers concluded.
Read the full study in the Annals of Internal Medicine (doi: 10.7326/M16-0291).
The U.S. Food and Drug Administration has approved a number of new antibiotics targeting multidrug-resistant bacteria in the past 5 years, but the new drugs have not led to a substantial improvement in patient outcomes when compared with existing antibiotics, according to a recent analysis in the Annals of Internal Medicine.
The eight new antibiotics approved by the FDA between January 2010 and December 2015 were ceftaroline, fidaxomicin, bedaquiline, dalbavancin, tedizolid, oritavancin, ceftolozane/tazobactam, and ceftazidime/avibactam. Of those eight drugs, only three showed in vitro activity against the so-called ESKAPE pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumonia, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species). Only one drug, fidaxomicin, demonstrated in vitro activity against an urgent-threat pathogen from the Centers for Disease Control and Prevention, Clostridium difficile. Bedaquiline was the only new antibiotic specifically indicated for a disease from a multidrug-resistant pathogen, although the investigators said most of the drugs demonstrated in vitro activity against gram-positive drug-resistant pathogens.
Importantly, the authors noted that in vitro activity does not necessarily reflect benefits on actual patient clinical outcomes, as exemplified by such drugs as tigecycline and doripenem.
The researchers found what they called “important deficiencies in the clinical trials leading to approval of these new antibiotic products.” Most pivotal trial designs were primarily noninferiority trials, and the antibiotics were not studied to evaluate whether they have substantial benefits in efficacy over what is currently available, they noted. Additionally, none of the trials evaluated direct patient outcomes as primary end points, and some drugs did not have confirmatory evidence from a second independent trial or did not have any confirmatory trials.
Researchers also examined the prices of a single dose of the new antibiotics. The prices ranged from $1,195 to $4,183 (4-14 days of ceftolozane/tazobactam for acute pyelonephritis and intra-abdominal infections) to $69,702 (24 weeks of bedaquiline) – quite a premium for antibiotics showing unclear evidence of additional benefit.
“As antibiotic innovation continues to move forward, greater attention needs to be paid to incentives for developing high-quality new products with demonstrated superiority to existing products on outcomes in patients with multidrug-resistant disease, replacing the current focus on quantity and presumed future benefits,” researchers concluded.
Read the full study in the Annals of Internal Medicine (doi: 10.7326/M16-0291).
FROM ANNALS OF INTERNAL MEDICINE

Study links adipocytes and myeloma progression

A study published in Cancer Letters suggests that adipocytes contribute to the growth and progression of multiple myeloma (MM).
Researchers co-cultured MM cells with adipocytes derived from patients defined as normal weight, overweight, obese, or super obese.
This revealed a positive correlation between adipocytes and indicators of MM progression, which was most pronounced in cells from obese and super obese individuals.
“Once a person with cancer is out of the normal weight category, their BMI [body mass index] is contributing to multiple myeloma growth and progression,” said study author Katie DeCicco-Skinner, PhD, of American University in Washington, DC.
For this study, Dr DeCicco-Skinner and her colleagues obtained human adipose-derived stem cells from 29 patients who underwent liposuction and were defined as normal weight (BMI = 20–25 kg/m2), overweight (25–30 kg/m2), obese (30–35 kg/m2), or super obese (35–40 kg/m2).
Once the cells matured into adipocytes, they were co-cultured with the MM cell lines RPMI-8226 and NCI-H929.
The researchers found that adipocytes from overweight, obese, and super obese patients had increased levels of proteins linked to cancer, including PPAR-gamma, cytochrome C, interleukin-6, and leptin.
In addition, adipocyte-conditioned media from obese and super obese patients significantly increased MM cell adhesion.
And conditioned media from overweight, obese, and super obese patients increased angiogenic potential and expression of matrix metalloproteinase-2.
“We know multiple myeloma cells will anchor into bone marrow, and fat cells in the bone marrow will support the growth and spread of the cancer,” Dr DeCicco-Skinner said.
“In our study, as BMI increased, we started seeing an increase in the ability of multiple myeloma cells to adhere, which causes the cancer to better anchor. With angiogenesis, cancer cells cannot exist without their own blood supply. We also found the amount of blood vessels that developed was directly proportional to a patient’s BMI.”
Dr DeCicco-Skinner and her colleagues had assumed that cancer proliferation would benefit from a higher-than-normal BMI because of the epidemiological link between obesity and cancer. But the relationship between MM and the BMI of obese and super obese patients was drastic.
“We found that fat cells from obese or morbidly obese patients secreted a high amount of inflammatory proteins, which contributed to tumor progression,” Dr DeCicco-Skinner said.
These findings suggest a new approach for MM treatment, according to the researchers. They say physicians may want to consider tailoring drugs based on a patient’s BMI because a drug may not be as effective in obese or super obese patients.
“A patient may need to receive drugs to block inflammatory or other obesity-specific proteins, in addition to standard anticancer drugs they receive,” Dr DeCicco-Skinner said.
“Obesity increasingly plays a role in cancer cases, as the numbers of those who are obese rise. Improving our understanding of how fat cells and cancer cells communicate with each other, and how the communication changes during obesity, is critical.” ![]()
A study published in Cancer Letters suggests that adipocytes contribute to the growth and progression of multiple myeloma (MM).
Researchers co-cultured MM cells with adipocytes derived from patients defined as normal weight, overweight, obese, or super obese.
This revealed a positive correlation between adipocytes and indicators of MM progression, which was most pronounced in cells from obese and super obese individuals.
“Once a person with cancer is out of the normal weight category, their BMI [body mass index] is contributing to multiple myeloma growth and progression,” said study author Katie DeCicco-Skinner, PhD, of American University in Washington, DC.
For this study, Dr DeCicco-Skinner and her colleagues obtained human adipose-derived stem cells from 29 patients who underwent liposuction and were defined as normal weight (BMI = 20–25 kg/m2), overweight (25–30 kg/m2), obese (30–35 kg/m2), or super obese (35–40 kg/m2).
Once the cells matured into adipocytes, they were co-cultured with the MM cell lines RPMI-8226 and NCI-H929.
The researchers found that adipocytes from overweight, obese, and super obese patients had increased levels of proteins linked to cancer, including PPAR-gamma, cytochrome C, interleukin-6, and leptin.
In addition, adipocyte-conditioned media from obese and super obese patients significantly increased MM cell adhesion.
And conditioned media from overweight, obese, and super obese patients increased angiogenic potential and expression of matrix metalloproteinase-2.
“We know multiple myeloma cells will anchor into bone marrow, and fat cells in the bone marrow will support the growth and spread of the cancer,” Dr DeCicco-Skinner said.
“In our study, as BMI increased, we started seeing an increase in the ability of multiple myeloma cells to adhere, which causes the cancer to better anchor. With angiogenesis, cancer cells cannot exist without their own blood supply. We also found the amount of blood vessels that developed was directly proportional to a patient’s BMI.”
Dr DeCicco-Skinner and her colleagues had assumed that cancer proliferation would benefit from a higher-than-normal BMI because of the epidemiological link between obesity and cancer. But the relationship between MM and the BMI of obese and super obese patients was drastic.
“We found that fat cells from obese or morbidly obese patients secreted a high amount of inflammatory proteins, which contributed to tumor progression,” Dr DeCicco-Skinner said.
These findings suggest a new approach for MM treatment, according to the researchers. They say physicians may want to consider tailoring drugs based on a patient’s BMI because a drug may not be as effective in obese or super obese patients.
“A patient may need to receive drugs to block inflammatory or other obesity-specific proteins, in addition to standard anticancer drugs they receive,” Dr DeCicco-Skinner said.
“Obesity increasingly plays a role in cancer cases, as the numbers of those who are obese rise. Improving our understanding of how fat cells and cancer cells communicate with each other, and how the communication changes during obesity, is critical.” ![]()
A study published in Cancer Letters suggests that adipocytes contribute to the growth and progression of multiple myeloma (MM).
Researchers co-cultured MM cells with adipocytes derived from patients defined as normal weight, overweight, obese, or super obese.
This revealed a positive correlation between adipocytes and indicators of MM progression, which was most pronounced in cells from obese and super obese individuals.
“Once a person with cancer is out of the normal weight category, their BMI [body mass index] is contributing to multiple myeloma growth and progression,” said study author Katie DeCicco-Skinner, PhD, of American University in Washington, DC.
For this study, Dr DeCicco-Skinner and her colleagues obtained human adipose-derived stem cells from 29 patients who underwent liposuction and were defined as normal weight (BMI = 20–25 kg/m2), overweight (25–30 kg/m2), obese (30–35 kg/m2), or super obese (35–40 kg/m2).
Once the cells matured into adipocytes, they were co-cultured with the MM cell lines RPMI-8226 and NCI-H929.
The researchers found that adipocytes from overweight, obese, and super obese patients had increased levels of proteins linked to cancer, including PPAR-gamma, cytochrome C, interleukin-6, and leptin.
In addition, adipocyte-conditioned media from obese and super obese patients significantly increased MM cell adhesion.
And conditioned media from overweight, obese, and super obese patients increased angiogenic potential and expression of matrix metalloproteinase-2.
“We know multiple myeloma cells will anchor into bone marrow, and fat cells in the bone marrow will support the growth and spread of the cancer,” Dr DeCicco-Skinner said.
“In our study, as BMI increased, we started seeing an increase in the ability of multiple myeloma cells to adhere, which causes the cancer to better anchor. With angiogenesis, cancer cells cannot exist without their own blood supply. We also found the amount of blood vessels that developed was directly proportional to a patient’s BMI.”
Dr DeCicco-Skinner and her colleagues had assumed that cancer proliferation would benefit from a higher-than-normal BMI because of the epidemiological link between obesity and cancer. But the relationship between MM and the BMI of obese and super obese patients was drastic.
“We found that fat cells from obese or morbidly obese patients secreted a high amount of inflammatory proteins, which contributed to tumor progression,” Dr DeCicco-Skinner said.
These findings suggest a new approach for MM treatment, according to the researchers. They say physicians may want to consider tailoring drugs based on a patient’s BMI because a drug may not be as effective in obese or super obese patients.
“A patient may need to receive drugs to block inflammatory or other obesity-specific proteins, in addition to standard anticancer drugs they receive,” Dr DeCicco-Skinner said.
“Obesity increasingly plays a role in cancer cases, as the numbers of those who are obese rise. Improving our understanding of how fat cells and cancer cells communicate with each other, and how the communication changes during obesity, is critical.” ![]()
INR monitoring systems to be pulled from market

The Alere INRatio® and INRatio®2 PT/INR Monitoring Systems are being withdrawn from the US market because they may provide inaccurate international normalized ratio (INR) results.
These handheld blood coagulation systems, which consist of a small monitor and disposable test strips, are used to monitor patients taking warfarin.
The manufacturer of these systems, Alere Inc., said it is working with the US Food and Drug Administration (FDA) to determine the most appropriate timing for product discontinuation.
The company also said it will provide guidance on transitioning patients using the INRatio systems to an alternate solution to allow them to continue anticoagulation monitoring in the least disruptive manner possible.
Background on the withdrawal
In December 2014, Alere initiated a voluntary correction to inform users of the INRatio® and INRatio®2 PT/INR Monitoring Systems that patients with certain medical conditions should not be tested with the systems.
The company found that, in certain cases, the systems provided an INR result that was clinically significantly lower than a result obtained using a reference INR system (laboratory method).
In fact, there has been speculation that this issue may have affected the results of the ROCKET AF trial, a comparison of rivaroxaban and warfarin in which INRs were measured with the INRatio systems.
The FDA is currently investigating this possibility, although the European Medicines Agency has said the study’s overall results were not affected by the issue.
After Alere reported the issue with the INRatio systems to the FDA, the company began conducting its own investigation.
Over the past 2 years, Alere invested in the research and development of software enhancements to address the potential of the INRatio systems to deliver results that differ from laboratory INR measurement.
Alere said it is confident the software enhancements it developed and submitted to the FDA at the end of 2015 effectively address this issue.
However, the FDA said the company’s studies do not adequately demonstrate the effectiveness of the software modification. The agency therefore advised Alere to submit a proposed plan to voluntarily remove the INRatio systems from the market.
The company decided to follow this recommendation and plans to provide a timeline to discontinue the product line. Alere said it will provide further information on patient transition to patients and healthcare providers.
For more information regarding this product discontinuation, visit http://www.inr-care.com. ![]()
The Alere INRatio® and INRatio®2 PT/INR Monitoring Systems are being withdrawn from the US market because they may provide inaccurate international normalized ratio (INR) results.
These handheld blood coagulation systems, which consist of a small monitor and disposable test strips, are used to monitor patients taking warfarin.
The manufacturer of these systems, Alere Inc., said it is working with the US Food and Drug Administration (FDA) to determine the most appropriate timing for product discontinuation.
The company also said it will provide guidance on transitioning patients using the INRatio systems to an alternate solution to allow them to continue anticoagulation monitoring in the least disruptive manner possible.
Background on the withdrawal
In December 2014, Alere initiated a voluntary correction to inform users of the INRatio® and INRatio®2 PT/INR Monitoring Systems that patients with certain medical conditions should not be tested with the systems.
The company found that, in certain cases, the systems provided an INR result that was clinically significantly lower than a result obtained using a reference INR system (laboratory method).
In fact, there has been speculation that this issue may have affected the results of the ROCKET AF trial, a comparison of rivaroxaban and warfarin in which INRs were measured with the INRatio systems.
The FDA is currently investigating this possibility, although the European Medicines Agency has said the study’s overall results were not affected by the issue.
After Alere reported the issue with the INRatio systems to the FDA, the company began conducting its own investigation.
Over the past 2 years, Alere invested in the research and development of software enhancements to address the potential of the INRatio systems to deliver results that differ from laboratory INR measurement.
Alere said it is confident the software enhancements it developed and submitted to the FDA at the end of 2015 effectively address this issue.
However, the FDA said the company’s studies do not adequately demonstrate the effectiveness of the software modification. The agency therefore advised Alere to submit a proposed plan to voluntarily remove the INRatio systems from the market.
The company decided to follow this recommendation and plans to provide a timeline to discontinue the product line. Alere said it will provide further information on patient transition to patients and healthcare providers.
For more information regarding this product discontinuation, visit http://www.inr-care.com. ![]()
The Alere INRatio® and INRatio®2 PT/INR Monitoring Systems are being withdrawn from the US market because they may provide inaccurate international normalized ratio (INR) results.
These handheld blood coagulation systems, which consist of a small monitor and disposable test strips, are used to monitor patients taking warfarin.
The manufacturer of these systems, Alere Inc., said it is working with the US Food and Drug Administration (FDA) to determine the most appropriate timing for product discontinuation.
The company also said it will provide guidance on transitioning patients using the INRatio systems to an alternate solution to allow them to continue anticoagulation monitoring in the least disruptive manner possible.
Background on the withdrawal
In December 2014, Alere initiated a voluntary correction to inform users of the INRatio® and INRatio®2 PT/INR Monitoring Systems that patients with certain medical conditions should not be tested with the systems.
The company found that, in certain cases, the systems provided an INR result that was clinically significantly lower than a result obtained using a reference INR system (laboratory method).
In fact, there has been speculation that this issue may have affected the results of the ROCKET AF trial, a comparison of rivaroxaban and warfarin in which INRs were measured with the INRatio systems.
The FDA is currently investigating this possibility, although the European Medicines Agency has said the study’s overall results were not affected by the issue.
After Alere reported the issue with the INRatio systems to the FDA, the company began conducting its own investigation.
Over the past 2 years, Alere invested in the research and development of software enhancements to address the potential of the INRatio systems to deliver results that differ from laboratory INR measurement.
Alere said it is confident the software enhancements it developed and submitted to the FDA at the end of 2015 effectively address this issue.
However, the FDA said the company’s studies do not adequately demonstrate the effectiveness of the software modification. The agency therefore advised Alere to submit a proposed plan to voluntarily remove the INRatio systems from the market.
The company decided to follow this recommendation and plans to provide a timeline to discontinue the product line. Alere said it will provide further information on patient transition to patients and healthcare providers.
For more information regarding this product discontinuation, visit http://www.inr-care.com. ![]()
COMP recommends orphan status for drug to treat PNH

The European Medicines Agency’s Committee for Orphan Medicinal Products (COMP) has issued a positive opinion recommending orphan designation for Coversin for the treatment of paroxysmal nocturnal hemoglobinuria (PNH).
Coversin is a second-generation complement inhibitor that acts on complement component-C5, preventing release of C5a and formation of C5b-9 (also known as the membrane attack complex).
Coversin is a recombinant small protein (16,740 Da) derived from a native protein found in the saliva of the Ornithodoros moubata tick.
The drug is being developed by Akari Therapeutics.
In vitro experiments have shown that Coversin inhibits red blood cell lysis in PNH, and the drug can achieve full complement inhibition in the blood of PNH patients who are resistant to the drug eculizumab.
In a phase 1a trial of healthy volunteers, Coversin completely inhibited complement C5 activity within 12 hours of administration.
Akari Therapeutics is currently conducting a phase 1b study of Coversin in healthy volunteers and is administering the drug to a patient with eculizumab-resistant PNH. Thus far, Coversin has prevented hemolytic episodes and improved disease symptoms in this patient. And the only drug-related adverse event has been occasional local and transient irritation at the injection site.
Coversin is also being studied in atypical hemolytic uremic syndrome and Guillain Barré syndrome.
About orphan designation
The COMP adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision.
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat a life-threatening or chronically debilitating condition affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity in the European Union if the drug receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure. ![]()
The European Medicines Agency’s Committee for Orphan Medicinal Products (COMP) has issued a positive opinion recommending orphan designation for Coversin for the treatment of paroxysmal nocturnal hemoglobinuria (PNH).
Coversin is a second-generation complement inhibitor that acts on complement component-C5, preventing release of C5a and formation of C5b-9 (also known as the membrane attack complex).
Coversin is a recombinant small protein (16,740 Da) derived from a native protein found in the saliva of the Ornithodoros moubata tick.
The drug is being developed by Akari Therapeutics.
In vitro experiments have shown that Coversin inhibits red blood cell lysis in PNH, and the drug can achieve full complement inhibition in the blood of PNH patients who are resistant to the drug eculizumab.
In a phase 1a trial of healthy volunteers, Coversin completely inhibited complement C5 activity within 12 hours of administration.
Akari Therapeutics is currently conducting a phase 1b study of Coversin in healthy volunteers and is administering the drug to a patient with eculizumab-resistant PNH. Thus far, Coversin has prevented hemolytic episodes and improved disease symptoms in this patient. And the only drug-related adverse event has been occasional local and transient irritation at the injection site.
Coversin is also being studied in atypical hemolytic uremic syndrome and Guillain Barré syndrome.
About orphan designation
The COMP adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision.
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat a life-threatening or chronically debilitating condition affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity in the European Union if the drug receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure. ![]()
The European Medicines Agency’s Committee for Orphan Medicinal Products (COMP) has issued a positive opinion recommending orphan designation for Coversin for the treatment of paroxysmal nocturnal hemoglobinuria (PNH).
Coversin is a second-generation complement inhibitor that acts on complement component-C5, preventing release of C5a and formation of C5b-9 (also known as the membrane attack complex).
Coversin is a recombinant small protein (16,740 Da) derived from a native protein found in the saliva of the Ornithodoros moubata tick.
The drug is being developed by Akari Therapeutics.
In vitro experiments have shown that Coversin inhibits red blood cell lysis in PNH, and the drug can achieve full complement inhibition in the blood of PNH patients who are resistant to the drug eculizumab.
In a phase 1a trial of healthy volunteers, Coversin completely inhibited complement C5 activity within 12 hours of administration.
Akari Therapeutics is currently conducting a phase 1b study of Coversin in healthy volunteers and is administering the drug to a patient with eculizumab-resistant PNH. Thus far, Coversin has prevented hemolytic episodes and improved disease symptoms in this patient. And the only drug-related adverse event has been occasional local and transient irritation at the injection site.
Coversin is also being studied in atypical hemolytic uremic syndrome and Guillain Barré syndrome.
About orphan designation
The COMP adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision.
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat a life-threatening or chronically debilitating condition affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity in the European Union if the drug receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure. ![]()
Drug could be disease-modifying for SCD, team says

Image by Graham Beards
Researchers say the small molecule GBT440 could be a disease-modifying agent for patients with sickle cell disease (SCD).
Preclinical data showed that GBT440 can reduce sickling, extend the circulating half-life of red blood cells (RBCs), and decrease excessive erythropoiesis in SCD.
GBT440 binds specifically to hemoglobin and is designed to inhibit sickle hemoglobin (HbS) polymer formation.
“One promising strategy for preventing red blood cell sickling and subsequently modifying sickle cell disease over the long term involves inhibiting polymerization of HbS in red blood cells,” said David R. Archer, PhD, of Emory University School of Medicine in Atlanta, Georgia.
“This can be achieved by increasing the proportion of oxygenated HbS in those cells. We believe our preclinical results provide strong evidence that GBT440 inhibits HbS polymerization and red blood cell sickling, which is important because it addresses the underlying pathophysiology of sickle cell disease and has the potential to change its devastating clinical course.”
Dr Archer and his colleagues reported these results in the British Journal of Haematology. The research was supported by Global Blood Therapeutics, Inc., the company developing GBT440.
The researchers reported that, in vitro, GBT440 dose-dependently increased the affinity of HbS for oxygen, delayed polymerization of HbS, and reduced the number of sickled RBCs in whole blood from SCD patients.
In an animal model of SCD, GBT440 inhibited RBC sickling, prolonged the half-life of RBCs, and reduced reticulocyte counts.
The researchers said the drug also exhibited favorable pharmacokinetic properties in various animal species, suggesting the potential for once-daily oral dosing in SCD patients.
“Our preclinical work has developed a foundation of evidence that GBT440 is a potent inhibitor of the polymerization of HbS,” said Ted W. Love, MD, chief executive officer of Global Blood Therapeutics, Inc.
“We continue to build on these data with our ongoing phase 1/2 study, which has shown that GBT440 was well-tolerated over 90 days of dosing and that all SCD patients who received multiple doses of GBT440 exhibited improvements in one or more clinical markers of hemolysis and anemia. Our next step is to initiate a pivotal trial in adults with SCD later this year.” ![]()
Image by Graham Beards
Researchers say the small molecule GBT440 could be a disease-modifying agent for patients with sickle cell disease (SCD).
Preclinical data showed that GBT440 can reduce sickling, extend the circulating half-life of red blood cells (RBCs), and decrease excessive erythropoiesis in SCD.
GBT440 binds specifically to hemoglobin and is designed to inhibit sickle hemoglobin (HbS) polymer formation.
“One promising strategy for preventing red blood cell sickling and subsequently modifying sickle cell disease over the long term involves inhibiting polymerization of HbS in red blood cells,” said David R. Archer, PhD, of Emory University School of Medicine in Atlanta, Georgia.
“This can be achieved by increasing the proportion of oxygenated HbS in those cells. We believe our preclinical results provide strong evidence that GBT440 inhibits HbS polymerization and red blood cell sickling, which is important because it addresses the underlying pathophysiology of sickle cell disease and has the potential to change its devastating clinical course.”
Dr Archer and his colleagues reported these results in the British Journal of Haematology. The research was supported by Global Blood Therapeutics, Inc., the company developing GBT440.
The researchers reported that, in vitro, GBT440 dose-dependently increased the affinity of HbS for oxygen, delayed polymerization of HbS, and reduced the number of sickled RBCs in whole blood from SCD patients.
In an animal model of SCD, GBT440 inhibited RBC sickling, prolonged the half-life of RBCs, and reduced reticulocyte counts.
The researchers said the drug also exhibited favorable pharmacokinetic properties in various animal species, suggesting the potential for once-daily oral dosing in SCD patients.
“Our preclinical work has developed a foundation of evidence that GBT440 is a potent inhibitor of the polymerization of HbS,” said Ted W. Love, MD, chief executive officer of Global Blood Therapeutics, Inc.
“We continue to build on these data with our ongoing phase 1/2 study, which has shown that GBT440 was well-tolerated over 90 days of dosing and that all SCD patients who received multiple doses of GBT440 exhibited improvements in one or more clinical markers of hemolysis and anemia. Our next step is to initiate a pivotal trial in adults with SCD later this year.” ![]()
Image by Graham Beards
Researchers say the small molecule GBT440 could be a disease-modifying agent for patients with sickle cell disease (SCD).
Preclinical data showed that GBT440 can reduce sickling, extend the circulating half-life of red blood cells (RBCs), and decrease excessive erythropoiesis in SCD.
GBT440 binds specifically to hemoglobin and is designed to inhibit sickle hemoglobin (HbS) polymer formation.
“One promising strategy for preventing red blood cell sickling and subsequently modifying sickle cell disease over the long term involves inhibiting polymerization of HbS in red blood cells,” said David R. Archer, PhD, of Emory University School of Medicine in Atlanta, Georgia.
“This can be achieved by increasing the proportion of oxygenated HbS in those cells. We believe our preclinical results provide strong evidence that GBT440 inhibits HbS polymerization and red blood cell sickling, which is important because it addresses the underlying pathophysiology of sickle cell disease and has the potential to change its devastating clinical course.”
Dr Archer and his colleagues reported these results in the British Journal of Haematology. The research was supported by Global Blood Therapeutics, Inc., the company developing GBT440.
The researchers reported that, in vitro, GBT440 dose-dependently increased the affinity of HbS for oxygen, delayed polymerization of HbS, and reduced the number of sickled RBCs in whole blood from SCD patients.
In an animal model of SCD, GBT440 inhibited RBC sickling, prolonged the half-life of RBCs, and reduced reticulocyte counts.
The researchers said the drug also exhibited favorable pharmacokinetic properties in various animal species, suggesting the potential for once-daily oral dosing in SCD patients.
“Our preclinical work has developed a foundation of evidence that GBT440 is a potent inhibitor of the polymerization of HbS,” said Ted W. Love, MD, chief executive officer of Global Blood Therapeutics, Inc.
“We continue to build on these data with our ongoing phase 1/2 study, which has shown that GBT440 was well-tolerated over 90 days of dosing and that all SCD patients who received multiple doses of GBT440 exhibited improvements in one or more clinical markers of hemolysis and anemia. Our next step is to initiate a pivotal trial in adults with SCD later this year.” ![]()