User login
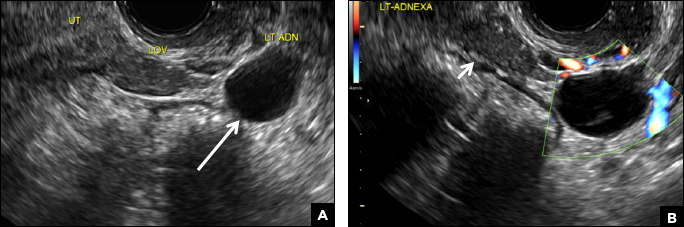
32-year-old woman with pelvic pain and irregular menstrual periods
(A) Paratubal cyst CORRECT
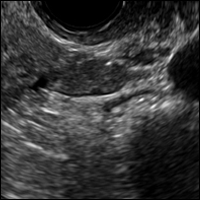
Paratubal, or paraovarian, cysts typically are round or oval avascular hypoechoic cysts (long arrow) separate from the adjacent ovary (short arrow). Since they are congenital remnants of the Wolffian duct, they arise from the mesosalpinx, specifically the broad ligament or fallopian tube.1,2 They usually are seen in close proximity to but separate from the ovary without distorting the ovary’s architecture.1,2
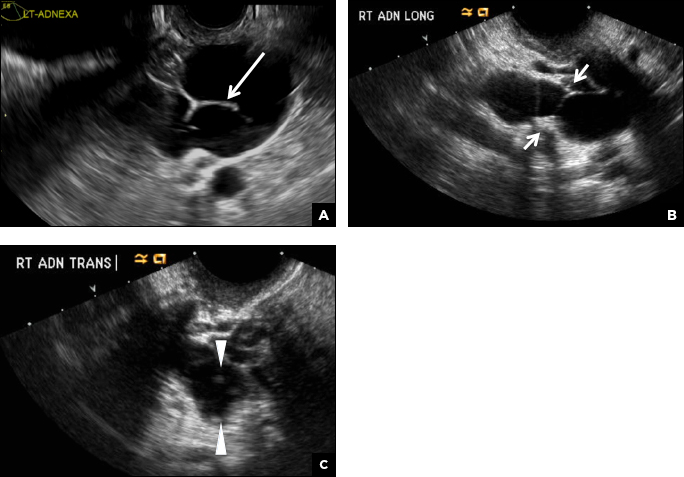
B) Hydrosalpinx INCORRECT
A hydrosalpinx appears as an elongated C- or S-shaped, thin-walled tubular serpiginous cystic lesion separate from the ovary. It often has incomplete septations that are infolding of the tube on itself (long arrow).3 Other findings include diametrically opposed indentations (short arrows) of the wall (Waist sign) and short linear mucosal or submucosal folds (arrowhead) that when viewed in cross section appear similar to the spokes of a cogwheel (Cogwheel sign).1–3 Prior tubal infection or gynecologic surgery represent risk factors for hydrosalpinx.
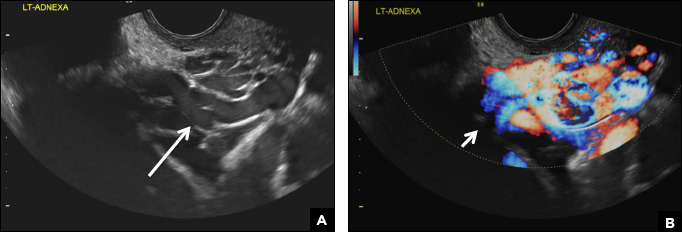
C) Peritoneal inclusion cyst INCORRECT
A peritoneal inclusion cyst appears as an anechoic cystic mass that conforms passively to the shape of the peritoneal cavity/pelvic sidewall (long arrow) and may contain entrapped ovaries (short arrow) within or along the periphery of the fluid collection.1,2 Septations within it are likely from peritoneal adhesions (arrowhead) and may show vascularity.2 Prior (often multiple) gynecologic surgeries represent a risk factor for peritoneal inclusion cysts.

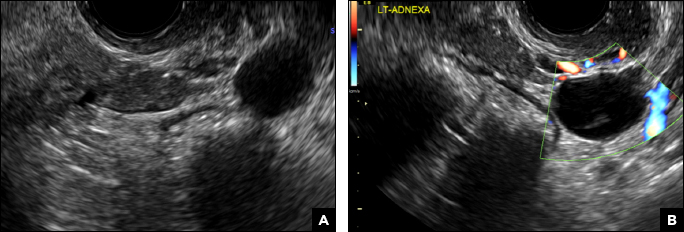
D) Dilated pelvic veins INCORRECT
Dilated pelvic veins appear on sonography as a cluster of elongated and tubular cystic lesions in the adnexa along the broad ligament and demonstrate low level echoes due to sluggish flow (long arrow) and visible red blood cell rouleaux formation. This can be confirmed on color Doppler images (short arrow) and help differentiate it from hydrosalpinx.
- Laing FC, Allison SF. US of the ovary and adnexa: to worry or not to worry? Radiographics. 2012:32(6):1621−1639.
- Moyle PL, Kataoka MY, Nakai A, Takahata A, Reinhold C, Sala E. Nonovarian cystic lesions of the pelvis. Radiographics. 2010;30(4):921−938.
- Rezvani M, Shaaban AM. Fallopian tube disease in the nonpregnant patient. Radiographics. 2011;31(2):527−548.

Dr. Kanmaniraja is Assistant Professor and Chief, Division of Abdominal Imaging, Department of Radiology, University of Florida College of Medicine–Jacksonville.

Dr. Kaunitz is University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He is Medical Director and Director of Menopause and Gynecologic Ultrasound Services at UF Women’s Health Specialists–Emerson. He also serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this quiz.
Dr. Kanmaniraja is Assistant Professor and Chief, Division of Abdominal Imaging, Department of Radiology, University of Florida College of Medicine–Jacksonville.
Dr. Kaunitz is University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He is Medical Director and Director of Menopause and Gynecologic Ultrasound Services at UF Women’s Health Specialists–Emerson. He also serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this quiz.
Dr. Kanmaniraja is Assistant Professor and Chief, Division of Abdominal Imaging, Department of Radiology, University of Florida College of Medicine–Jacksonville.
Dr. Kaunitz is University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He is Medical Director and Director of Menopause and Gynecologic Ultrasound Services at UF Women’s Health Specialists–Emerson. He also serves on the OBG Management Board of Editors.
The authors report no financial relationships relevant to this quiz.
(A) Paratubal cyst CORRECT
Paratubal, or paraovarian, cysts typically are round or oval avascular hypoechoic cysts (long arrow) separate from the adjacent ovary (short arrow). Since they are congenital remnants of the Wolffian duct, they arise from the mesosalpinx, specifically the broad ligament or fallopian tube.1,2 They usually are seen in close proximity to but separate from the ovary without distorting the ovary’s architecture.1,2
B) Hydrosalpinx INCORRECT
A hydrosalpinx appears as an elongated C- or S-shaped, thin-walled tubular serpiginous cystic lesion separate from the ovary. It often has incomplete septations that are infolding of the tube on itself (long arrow).3 Other findings include diametrically opposed indentations (short arrows) of the wall (Waist sign) and short linear mucosal or submucosal folds (arrowhead) that when viewed in cross section appear similar to the spokes of a cogwheel (Cogwheel sign).1–3 Prior tubal infection or gynecologic surgery represent risk factors for hydrosalpinx.
C) Peritoneal inclusion cyst INCORRECT
A peritoneal inclusion cyst appears as an anechoic cystic mass that conforms passively to the shape of the peritoneal cavity/pelvic sidewall (long arrow) and may contain entrapped ovaries (short arrow) within or along the periphery of the fluid collection.1,2 Septations within it are likely from peritoneal adhesions (arrowhead) and may show vascularity.2 Prior (often multiple) gynecologic surgeries represent a risk factor for peritoneal inclusion cysts.
D) Dilated pelvic veins INCORRECT
Dilated pelvic veins appear on sonography as a cluster of elongated and tubular cystic lesions in the adnexa along the broad ligament and demonstrate low level echoes due to sluggish flow (long arrow) and visible red blood cell rouleaux formation. This can be confirmed on color Doppler images (short arrow) and help differentiate it from hydrosalpinx.
(A) Paratubal cyst CORRECT
Paratubal, or paraovarian, cysts typically are round or oval avascular hypoechoic cysts (long arrow) separate from the adjacent ovary (short arrow). Since they are congenital remnants of the Wolffian duct, they arise from the mesosalpinx, specifically the broad ligament or fallopian tube.1,2 They usually are seen in close proximity to but separate from the ovary without distorting the ovary’s architecture.1,2
B) Hydrosalpinx INCORRECT
A hydrosalpinx appears as an elongated C- or S-shaped, thin-walled tubular serpiginous cystic lesion separate from the ovary. It often has incomplete septations that are infolding of the tube on itself (long arrow).3 Other findings include diametrically opposed indentations (short arrows) of the wall (Waist sign) and short linear mucosal or submucosal folds (arrowhead) that when viewed in cross section appear similar to the spokes of a cogwheel (Cogwheel sign).1–3 Prior tubal infection or gynecologic surgery represent risk factors for hydrosalpinx.
C) Peritoneal inclusion cyst INCORRECT
A peritoneal inclusion cyst appears as an anechoic cystic mass that conforms passively to the shape of the peritoneal cavity/pelvic sidewall (long arrow) and may contain entrapped ovaries (short arrow) within or along the periphery of the fluid collection.1,2 Septations within it are likely from peritoneal adhesions (arrowhead) and may show vascularity.2 Prior (often multiple) gynecologic surgeries represent a risk factor for peritoneal inclusion cysts.
D) Dilated pelvic veins INCORRECT
Dilated pelvic veins appear on sonography as a cluster of elongated and tubular cystic lesions in the adnexa along the broad ligament and demonstrate low level echoes due to sluggish flow (long arrow) and visible red blood cell rouleaux formation. This can be confirmed on color Doppler images (short arrow) and help differentiate it from hydrosalpinx.
- Laing FC, Allison SF. US of the ovary and adnexa: to worry or not to worry? Radiographics. 2012:32(6):1621−1639.
- Moyle PL, Kataoka MY, Nakai A, Takahata A, Reinhold C, Sala E. Nonovarian cystic lesions of the pelvis. Radiographics. 2010;30(4):921−938.
- Rezvani M, Shaaban AM. Fallopian tube disease in the nonpregnant patient. Radiographics. 2011;31(2):527−548.
- Laing FC, Allison SF. US of the ovary and adnexa: to worry or not to worry? Radiographics. 2012:32(6):1621−1639.
- Moyle PL, Kataoka MY, Nakai A, Takahata A, Reinhold C, Sala E. Nonovarian cystic lesions of the pelvis. Radiographics. 2010;30(4):921−938.
- Rezvani M, Shaaban AM. Fallopian tube disease in the nonpregnant patient. Radiographics. 2011;31(2):527−548.
A 32-year-old women presents to her gynecologist’s office reporting pelvic pain and irregular menstrual periods. Results of a urine pregnancy test are negative. Pelvic ultrasonography is performed, with gray scale ( A ) and color Doppler ( B ) images of the left adnexa obtained. Figures shown above.
VIDEO: Clot aspiration equals retrieval for ischemic stroke
HOUSTON – Intracerebral clot aspiration was as safe and effective as stent retriever thrombectomy for restoring cerebral blood flow in a French multicenter, randomized trial with 381 acute ischemic stroke patients.
This study is the “first direct comparison of aspiration versus stent retrieval” as the initial strategy for clot removal in acute ischemic stroke, and it “opens the door to add a new tool” for clot removal, Bertrand Lapergue, MD, said at the International Stroke Conference sponsored by the American Heart Association.

The new results “are the first to show that aspiration first is as good as a stent retriever, but we need to also see the results from COMPASS,” a U.S. multicenter trial that is in the process of making the same comparison, commented Ricardo A. Hanel, MD, a vascular neurosurgeon at Baptist Health in Jacksonville, Fla. The COMPASS Trial: a Direct Aspiration First Pass Technique has now enrolled about two-thirds of its target patient number, and until the study is complete the role of direct aspiration for clot removal in stroke remains investigational for U.S. practice, said Dr. Hanel, a COMPASS investigator.
The aspiration catheter tested in ASTER is marketed by Penumbra and has already received Food and Drug Administration approval for revascularization of ischemic stroke patients. U.S. use of aspiration for treating acute ischemic stroke, however, has remained limited because there is no clear evidence of the method’s efficacy. Dr. Hanel said that he occasionally uses aspiration as an adjunct to clot removal with a stent retriever.

ASTER’s primary endpoint was the percentage of patients who achieved thrombolysis in cerebral infarction (TICI) 2b or 3 flow at the end of treatment, which occurred in 85% of patients treated with aspiration first and in 83% of those treated by clot removal first, a difference that was not statistically significant, Dr. Lapergue reported. The rate of patients who achieved either TICI 2b or 3 flow after the initial strategy only was 63% with aspiration and 68% with clot removal, also a nonsignificant difference. The two strategies also showed no significant difference for any measured safety parameter. The results showed a trend toward more vasospasm with clot removal – a 6% rate, versus 3% with clot aspiration – but this did not reach statistical significance.
Results from additional analyses of the clinical outcomes of patients in the trial and of cost efficacy will be reported later in 2017, Dr. Lapergue said.
ASTER received an unrestricted research grant from Penumbra, a company that markets clot removal aspiration catheters. Dr. Lapergue had no personal disclosures. Dr. Hanel has been a consultant to and received grant support from Medtronic. He has received research grants from MicroVention and has an ownership interest in InNeuroCo.
[email protected]
On Twitter @mitchelzoler
ASTER is an important trial. It shows for the first time that an aspiration device is probably as safe and reasonable for opening an acute occlusion in a large cerebral artery as is a stent retriever.
ASTER, however, was done entirely in a French population, making it uncertain whether the results are applicable to other populations. For example, U.S. acute ischemic stroke patients, especially African Americans and Hispanics, generally have more intracerebral atherostenotic disease than do patients from European countries, while French patients tend to have more embolic disease. Will aspiration be as effective in U.S. patients with atherostenotic blockages? I would love to see this study repeated in a U.S. population of ischemic stroke patients, and that is now happening in the COMPASS trial. It would be helpful to know if there are selected U.S. patients who might be better treated using either aspiration or a stent retriever first.
Although aspiration catheters have already received Food and Drug Administration approval for clot removal in acute ischemic stroke patients, many U.S. interventionalists have moved to deploying stent retrievers based on the very positive results reported with these devices about 2 years ago. For the moment, stent retrievers remain the most prominent devices to open large vessel occlusions.
Ralph L. Sacco, MD, is professor and chairman of neurology at the University of Miami. He had no relevant disclosures. He made these comments in a video interview and during a press conference.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ASTER is an important trial. It shows for the first time that an aspiration device is probably as safe and reasonable for opening an acute occlusion in a large cerebral artery as is a stent retriever.
ASTER, however, was done entirely in a French population, making it uncertain whether the results are applicable to other populations. For example, U.S. acute ischemic stroke patients, especially African Americans and Hispanics, generally have more intracerebral atherostenotic disease than do patients from European countries, while French patients tend to have more embolic disease. Will aspiration be as effective in U.S. patients with atherostenotic blockages? I would love to see this study repeated in a U.S. population of ischemic stroke patients, and that is now happening in the COMPASS trial. It would be helpful to know if there are selected U.S. patients who might be better treated using either aspiration or a stent retriever first.
Although aspiration catheters have already received Food and Drug Administration approval for clot removal in acute ischemic stroke patients, many U.S. interventionalists have moved to deploying stent retrievers based on the very positive results reported with these devices about 2 years ago. For the moment, stent retrievers remain the most prominent devices to open large vessel occlusions.
Ralph L. Sacco, MD, is professor and chairman of neurology at the University of Miami. He had no relevant disclosures. He made these comments in a video interview and during a press conference.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ASTER is an important trial. It shows for the first time that an aspiration device is probably as safe and reasonable for opening an acute occlusion in a large cerebral artery as is a stent retriever.
ASTER, however, was done entirely in a French population, making it uncertain whether the results are applicable to other populations. For example, U.S. acute ischemic stroke patients, especially African Americans and Hispanics, generally have more intracerebral atherostenotic disease than do patients from European countries, while French patients tend to have more embolic disease. Will aspiration be as effective in U.S. patients with atherostenotic blockages? I would love to see this study repeated in a U.S. population of ischemic stroke patients, and that is now happening in the COMPASS trial. It would be helpful to know if there are selected U.S. patients who might be better treated using either aspiration or a stent retriever first.
Although aspiration catheters have already received Food and Drug Administration approval for clot removal in acute ischemic stroke patients, many U.S. interventionalists have moved to deploying stent retrievers based on the very positive results reported with these devices about 2 years ago. For the moment, stent retrievers remain the most prominent devices to open large vessel occlusions.
Ralph L. Sacco, MD, is professor and chairman of neurology at the University of Miami. He had no relevant disclosures. He made these comments in a video interview and during a press conference.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
HOUSTON – Intracerebral clot aspiration was as safe and effective as stent retriever thrombectomy for restoring cerebral blood flow in a French multicenter, randomized trial with 381 acute ischemic stroke patients.
This study is the “first direct comparison of aspiration versus stent retrieval” as the initial strategy for clot removal in acute ischemic stroke, and it “opens the door to add a new tool” for clot removal, Bertrand Lapergue, MD, said at the International Stroke Conference sponsored by the American Heart Association.
The new results “are the first to show that aspiration first is as good as a stent retriever, but we need to also see the results from COMPASS,” a U.S. multicenter trial that is in the process of making the same comparison, commented Ricardo A. Hanel, MD, a vascular neurosurgeon at Baptist Health in Jacksonville, Fla. The COMPASS Trial: a Direct Aspiration First Pass Technique has now enrolled about two-thirds of its target patient number, and until the study is complete the role of direct aspiration for clot removal in stroke remains investigational for U.S. practice, said Dr. Hanel, a COMPASS investigator.
The aspiration catheter tested in ASTER is marketed by Penumbra and has already received Food and Drug Administration approval for revascularization of ischemic stroke patients. U.S. use of aspiration for treating acute ischemic stroke, however, has remained limited because there is no clear evidence of the method’s efficacy. Dr. Hanel said that he occasionally uses aspiration as an adjunct to clot removal with a stent retriever.
ASTER’s primary endpoint was the percentage of patients who achieved thrombolysis in cerebral infarction (TICI) 2b or 3 flow at the end of treatment, which occurred in 85% of patients treated with aspiration first and in 83% of those treated by clot removal first, a difference that was not statistically significant, Dr. Lapergue reported. The rate of patients who achieved either TICI 2b or 3 flow after the initial strategy only was 63% with aspiration and 68% with clot removal, also a nonsignificant difference. The two strategies also showed no significant difference for any measured safety parameter. The results showed a trend toward more vasospasm with clot removal – a 6% rate, versus 3% with clot aspiration – but this did not reach statistical significance.
Results from additional analyses of the clinical outcomes of patients in the trial and of cost efficacy will be reported later in 2017, Dr. Lapergue said.
ASTER received an unrestricted research grant from Penumbra, a company that markets clot removal aspiration catheters. Dr. Lapergue had no personal disclosures. Dr. Hanel has been a consultant to and received grant support from Medtronic. He has received research grants from MicroVention and has an ownership interest in InNeuroCo.
[email protected]
On Twitter @mitchelzoler
HOUSTON – Intracerebral clot aspiration was as safe and effective as stent retriever thrombectomy for restoring cerebral blood flow in a French multicenter, randomized trial with 381 acute ischemic stroke patients.
This study is the “first direct comparison of aspiration versus stent retrieval” as the initial strategy for clot removal in acute ischemic stroke, and it “opens the door to add a new tool” for clot removal, Bertrand Lapergue, MD, said at the International Stroke Conference sponsored by the American Heart Association.
The new results “are the first to show that aspiration first is as good as a stent retriever, but we need to also see the results from COMPASS,” a U.S. multicenter trial that is in the process of making the same comparison, commented Ricardo A. Hanel, MD, a vascular neurosurgeon at Baptist Health in Jacksonville, Fla. The COMPASS Trial: a Direct Aspiration First Pass Technique has now enrolled about two-thirds of its target patient number, and until the study is complete the role of direct aspiration for clot removal in stroke remains investigational for U.S. practice, said Dr. Hanel, a COMPASS investigator.
The aspiration catheter tested in ASTER is marketed by Penumbra and has already received Food and Drug Administration approval for revascularization of ischemic stroke patients. U.S. use of aspiration for treating acute ischemic stroke, however, has remained limited because there is no clear evidence of the method’s efficacy. Dr. Hanel said that he occasionally uses aspiration as an adjunct to clot removal with a stent retriever.
ASTER’s primary endpoint was the percentage of patients who achieved thrombolysis in cerebral infarction (TICI) 2b or 3 flow at the end of treatment, which occurred in 85% of patients treated with aspiration first and in 83% of those treated by clot removal first, a difference that was not statistically significant, Dr. Lapergue reported. The rate of patients who achieved either TICI 2b or 3 flow after the initial strategy only was 63% with aspiration and 68% with clot removal, also a nonsignificant difference. The two strategies also showed no significant difference for any measured safety parameter. The results showed a trend toward more vasospasm with clot removal – a 6% rate, versus 3% with clot aspiration – but this did not reach statistical significance.
Results from additional analyses of the clinical outcomes of patients in the trial and of cost efficacy will be reported later in 2017, Dr. Lapergue said.
ASTER received an unrestricted research grant from Penumbra, a company that markets clot removal aspiration catheters. Dr. Lapergue had no personal disclosures. Dr. Hanel has been a consultant to and received grant support from Medtronic. He has received research grants from MicroVention and has an ownership interest in InNeuroCo.
[email protected]
On Twitter @mitchelzoler
AT THE INTERNATIONAL STROKE CONFERENCE
Key clinical point:
Major finding: Recanalization occurred in 85% of patients treated with aspiration first and 83% treated with clot removal first.
Data source: ASTER, a multicenter, randomized French trial with 381 patients.
Disclosures: ASTER received an unrestricted research grant from Penumbra, a company that markets clot removal aspiration catheters. Dr. Lapergue had no personal disclosures. Dr. Hanel has been a consultant to and received grant support from Medtronic. He has received research grants from MicroVention and has an ownership interest in InNeuroCo.
Low-volume PEG linked to hypokalemia in at-risk patients
FROM GASTROINTESTINAL ENDOSCOPY
Bowel preparation with low-volume polyethylene glycol led to hypokalemia in nearly 25% of high-risk patients who were normokalemic at baseline, according to a first-in-kind large single-center prospective study.
“Hypokalemia is frequently encountered after low-volume PEG bowel cleansing in high-risk patients,” wrote Ankie Reumkens, MD, and her associates at Maastricht University Medical Center, Maastricht, the Netherlands. The report was published online in Gastrointestinal Endoscopy. “Additional large-scale studies are needed on the prevalence of hypokalemia in nonselected populations undergoing bowel cleansing and on the occurrence of potentially very serious side effects in order to decide on screening of high-risk groups in daily clinical practice.”
Good bowel preparation is crucial to colonoscopy. Bowel preparation with both sodium phosphate and high-volume polyethylene glycol (PEG) has caused hypokalemia, but whether this is true of low-volume PEG is unclear, the investigators said. Recently, at their institution, two colonoscopy patients developed severe hypokalemia and died of ventricular arrhythmias after receiving low-volume PEG. These deaths spurred the researchers to prospectively study 1,822 colonoscopy patients who underwent bowel preparation with low-volume PEG in 2014 and who were considered at high risk of hypokalemia by their gastroenterologists or because of hospitalization or diuretic use.
The researchers measured serum potassium levels of all patients before bowel cleansing. After bowel testing, they retested a subgroup of 301 patients who were normokalemic (3.5-5 mmol/L) at baseline (Gastrointest Endosc. 2017 Feb 7. doi: 10.1016/j.gie.2017.01.040).
In all, 77 patients (4%) were hypokalemic before bowel cleansing, the researchers said. Fully one-third were hospitalized, and hospitalization remained a significant risk factor for baseline hypokalemia even after the researchers controlled for diuretic use, age, sex, and reason for colonoscopy (odds ratio, 2.5; 95% confidence interval, 1.5 to 4.2; P less than .001).
Follow-up testing showed that 71 patients (24%) who were normokalemic at baseline became hypokalemic (serum potassium less than 3.5 mmol/L) after bowel preparation with low-volume PEG. Only diuretic use remained significantly associated with this outcome after researchers accounted for age, sex, reason for colonoscopy, and hospitalization status (odds ratio, 2.3; 95% confidence interval, 1.3 to 4.0; P = .004).
This study included preselected groups of diuretic users and hospitalized patients, making it difficult to assess specific and detailed risk factors for hypokalemia, the researchers said. “Despite this limitation, our study clearly shows that hypokalemia may develop in a substantial percentage of patients after the ingestion of low-volume PEG,” they emphasized. But they recommended population-based studies to determine the true prevalence of hypokalemia after colonoscopy, examine risk factors for this outcome, and consider whether it makes sense to screen subgroups at risk.
The protocol at their hospital is to measure serum potassium before bowel cleansing in hospitalized patients and those on diuretics, they noted. Hypokalemic patients then receive oral potassium if their potassium level was 2.5-3.0 mmol/L, and intravenous potassium if their level was below 2.5 mmol/L.
The investigators reported having no funding sources and no competing interests.
FROM GASTROINTESTINAL ENDOSCOPY
Bowel preparation with low-volume polyethylene glycol led to hypokalemia in nearly 25% of high-risk patients who were normokalemic at baseline, according to a first-in-kind large single-center prospective study.
“Hypokalemia is frequently encountered after low-volume PEG bowel cleansing in high-risk patients,” wrote Ankie Reumkens, MD, and her associates at Maastricht University Medical Center, Maastricht, the Netherlands. The report was published online in Gastrointestinal Endoscopy. “Additional large-scale studies are needed on the prevalence of hypokalemia in nonselected populations undergoing bowel cleansing and on the occurrence of potentially very serious side effects in order to decide on screening of high-risk groups in daily clinical practice.”
Good bowel preparation is crucial to colonoscopy. Bowel preparation with both sodium phosphate and high-volume polyethylene glycol (PEG) has caused hypokalemia, but whether this is true of low-volume PEG is unclear, the investigators said. Recently, at their institution, two colonoscopy patients developed severe hypokalemia and died of ventricular arrhythmias after receiving low-volume PEG. These deaths spurred the researchers to prospectively study 1,822 colonoscopy patients who underwent bowel preparation with low-volume PEG in 2014 and who were considered at high risk of hypokalemia by their gastroenterologists or because of hospitalization or diuretic use.
The researchers measured serum potassium levels of all patients before bowel cleansing. After bowel testing, they retested a subgroup of 301 patients who were normokalemic (3.5-5 mmol/L) at baseline (Gastrointest Endosc. 2017 Feb 7. doi: 10.1016/j.gie.2017.01.040).
In all, 77 patients (4%) were hypokalemic before bowel cleansing, the researchers said. Fully one-third were hospitalized, and hospitalization remained a significant risk factor for baseline hypokalemia even after the researchers controlled for diuretic use, age, sex, and reason for colonoscopy (odds ratio, 2.5; 95% confidence interval, 1.5 to 4.2; P less than .001).
Follow-up testing showed that 71 patients (24%) who were normokalemic at baseline became hypokalemic (serum potassium less than 3.5 mmol/L) after bowel preparation with low-volume PEG. Only diuretic use remained significantly associated with this outcome after researchers accounted for age, sex, reason for colonoscopy, and hospitalization status (odds ratio, 2.3; 95% confidence interval, 1.3 to 4.0; P = .004).
This study included preselected groups of diuretic users and hospitalized patients, making it difficult to assess specific and detailed risk factors for hypokalemia, the researchers said. “Despite this limitation, our study clearly shows that hypokalemia may develop in a substantial percentage of patients after the ingestion of low-volume PEG,” they emphasized. But they recommended population-based studies to determine the true prevalence of hypokalemia after colonoscopy, examine risk factors for this outcome, and consider whether it makes sense to screen subgroups at risk.
The protocol at their hospital is to measure serum potassium before bowel cleansing in hospitalized patients and those on diuretics, they noted. Hypokalemic patients then receive oral potassium if their potassium level was 2.5-3.0 mmol/L, and intravenous potassium if their level was below 2.5 mmol/L.
The investigators reported having no funding sources and no competing interests.
FROM GASTROINTESTINAL ENDOSCOPY
Bowel preparation with low-volume polyethylene glycol led to hypokalemia in nearly 25% of high-risk patients who were normokalemic at baseline, according to a first-in-kind large single-center prospective study.
“Hypokalemia is frequently encountered after low-volume PEG bowel cleansing in high-risk patients,” wrote Ankie Reumkens, MD, and her associates at Maastricht University Medical Center, Maastricht, the Netherlands. The report was published online in Gastrointestinal Endoscopy. “Additional large-scale studies are needed on the prevalence of hypokalemia in nonselected populations undergoing bowel cleansing and on the occurrence of potentially very serious side effects in order to decide on screening of high-risk groups in daily clinical practice.”
Good bowel preparation is crucial to colonoscopy. Bowel preparation with both sodium phosphate and high-volume polyethylene glycol (PEG) has caused hypokalemia, but whether this is true of low-volume PEG is unclear, the investigators said. Recently, at their institution, two colonoscopy patients developed severe hypokalemia and died of ventricular arrhythmias after receiving low-volume PEG. These deaths spurred the researchers to prospectively study 1,822 colonoscopy patients who underwent bowel preparation with low-volume PEG in 2014 and who were considered at high risk of hypokalemia by their gastroenterologists or because of hospitalization or diuretic use.
The researchers measured serum potassium levels of all patients before bowel cleansing. After bowel testing, they retested a subgroup of 301 patients who were normokalemic (3.5-5 mmol/L) at baseline (Gastrointest Endosc. 2017 Feb 7. doi: 10.1016/j.gie.2017.01.040).
In all, 77 patients (4%) were hypokalemic before bowel cleansing, the researchers said. Fully one-third were hospitalized, and hospitalization remained a significant risk factor for baseline hypokalemia even after the researchers controlled for diuretic use, age, sex, and reason for colonoscopy (odds ratio, 2.5; 95% confidence interval, 1.5 to 4.2; P less than .001).
Follow-up testing showed that 71 patients (24%) who were normokalemic at baseline became hypokalemic (serum potassium less than 3.5 mmol/L) after bowel preparation with low-volume PEG. Only diuretic use remained significantly associated with this outcome after researchers accounted for age, sex, reason for colonoscopy, and hospitalization status (odds ratio, 2.3; 95% confidence interval, 1.3 to 4.0; P = .004).
This study included preselected groups of diuretic users and hospitalized patients, making it difficult to assess specific and detailed risk factors for hypokalemia, the researchers said. “Despite this limitation, our study clearly shows that hypokalemia may develop in a substantial percentage of patients after the ingestion of low-volume PEG,” they emphasized. But they recommended population-based studies to determine the true prevalence of hypokalemia after colonoscopy, examine risk factors for this outcome, and consider whether it makes sense to screen subgroups at risk.
The protocol at their hospital is to measure serum potassium before bowel cleansing in hospitalized patients and those on diuretics, they noted. Hypokalemic patients then receive oral potassium if their potassium level was 2.5-3.0 mmol/L, and intravenous potassium if their level was below 2.5 mmol/L.
The investigators reported having no funding sources and no competing interests.
Key clinical point. Bowel preparation with low-volume polyethylene glycol (PEG) led to hypokalemia in at-risk patients.
Major finding: In all, 24% of patients who were normokalemic before bowel cleansing developed hypokalemia afterward. Diuretic use was a significant risk factor for hypokalemia (odds ratio, 2.3; P = .004).
Data source: A prospective study of 1,822 colonoscopy patients considered at high risk of hypokalemia.
Disclosures: The investigators reported having no funding sources and no competing interests.
Unrestricted DAA access halved Dutch HCV incidence in HIV
SEATTLE – New hepatitis C infections among HIV-positive men who have sex with men (MSM) were halved in the Netherlands by unrestricted access to direct-acting antivirals (DAAs), primarily ledipasvir/sofosbuvir tablets (Harvoni), according to Dutch investigators.
Since 2015, DAAs have been available to all newly acquired hepatitis C virus (HCV) patients without restriction. Due to the high cost of the drugs, payers in the United States and some other Western countries limit access to only patients with severe liver disease.*
The Dutch government, however, requires insurers to cover them, and has negotiated price discounts with makers. “The price that is paid is secret,” but it’s less than the standard cost of, for instance, €45,000 for a 3-month course of [ledipasvir/sofosbuvir] in the Netherlands, said senior investigator Bart Rijnders, MD, an infectious diseases assistant professor at Erasmus University Medical Center, Rotterdam.

The study compared the incidence of acute HCV (aHCV) in HIV-positive MSM in 2014, before unrestricted access to DAAs, to the incidence of aHCV in 2016, after limits were lifted. The investigators used data from 18 HIV treatment centers spread across the Netherlands, capturing about 80% of Dutch MSM being treated for HIV.
In 2014, there were 93 aHCV infections diagnosed among the men, translating to an incidence of 11.2 cases per 1,000 person-years of follow-up (95% CI, 9.1-13.7 cases). In 2016, there were 49 aHCV cases, an incidence of 5.5 cases per 1,000 person-years (95% CI, 4.1–7.2, P less than .001). At the same time, there was a substantial increase in new syphilis cases, indicating that the 51% reduction in aHCV over 2 years was not due to changes in behavior.
Meanwhile, “within 14 months after these drugs became available to all, 75% of the HIV-positive MSM in the Netherlands were cured of their infection,” Dr. Rijnders said at the Conference on Retroviruses & Opportunistic Infections in partnership with the International Antiviral Society.
Ledipasvir/sofosbuvir was the DAA used by about 90% of the men.
In short, unrestricted access to DAAs wiped out the infection so that men were no longer passing it to other men. The results are “an example of what is possible if you search for HCV and treat it as soon as you find it. You cure patients and prevent new infections. In the long run, you may save money,” he said, especially as more DAA options come on the market and prices fall.
Almost all the subjects were seen in their HIV clinic at least twice a year. An uptick in liver enzymes triggered HCV testing. The investigators checked positive results against patients’ own stored blood samples to distinguish new from chronic infections.
The study wasn’t funded, but Dr. Rijnders is a paid researcher for Merck’s DAA option, elbasvir/grazoprevir (Zepatier).
*This story was updated on February 24, 2017.
This is the first proof that early treatment of acute HCV could be a form of prevention. By removing the fibrosis requirement and restrictions forbidding treatment of people who are actively engaged in high-risk behaviors, they are reducing new infections.

We are far behind in the United States; 90% of states have restrictions that don’t allow uniform uptake of hepatitis C treatment and many forbid treatment for people who are actively using drugs. Having restrictions on people that don’t have enough liver disease is like telling a person with HIV they can’t be treated because their CD4 count isn’t below 200.
David Thomas, MD, is professor of medicine and director of the division of infectious diseases at Johns Hopkins University, Baltimore. He wasn’t involved with the work.
This is the first proof that early treatment of acute HCV could be a form of prevention. By removing the fibrosis requirement and restrictions forbidding treatment of people who are actively engaged in high-risk behaviors, they are reducing new infections.
We are far behind in the United States; 90% of states have restrictions that don’t allow uniform uptake of hepatitis C treatment and many forbid treatment for people who are actively using drugs. Having restrictions on people that don’t have enough liver disease is like telling a person with HIV they can’t be treated because their CD4 count isn’t below 200.
David Thomas, MD, is professor of medicine and director of the division of infectious diseases at Johns Hopkins University, Baltimore. He wasn’t involved with the work.
This is the first proof that early treatment of acute HCV could be a form of prevention. By removing the fibrosis requirement and restrictions forbidding treatment of people who are actively engaged in high-risk behaviors, they are reducing new infections.
We are far behind in the United States; 90% of states have restrictions that don’t allow uniform uptake of hepatitis C treatment and many forbid treatment for people who are actively using drugs. Having restrictions on people that don’t have enough liver disease is like telling a person with HIV they can’t be treated because their CD4 count isn’t below 200.
David Thomas, MD, is professor of medicine and director of the division of infectious diseases at Johns Hopkins University, Baltimore. He wasn’t involved with the work.
SEATTLE – New hepatitis C infections among HIV-positive men who have sex with men (MSM) were halved in the Netherlands by unrestricted access to direct-acting antivirals (DAAs), primarily ledipasvir/sofosbuvir tablets (Harvoni), according to Dutch investigators.
Since 2015, DAAs have been available to all newly acquired hepatitis C virus (HCV) patients without restriction. Due to the high cost of the drugs, payers in the United States and some other Western countries limit access to only patients with severe liver disease.*
The Dutch government, however, requires insurers to cover them, and has negotiated price discounts with makers. “The price that is paid is secret,” but it’s less than the standard cost of, for instance, €45,000 for a 3-month course of [ledipasvir/sofosbuvir] in the Netherlands, said senior investigator Bart Rijnders, MD, an infectious diseases assistant professor at Erasmus University Medical Center, Rotterdam.
The study compared the incidence of acute HCV (aHCV) in HIV-positive MSM in 2014, before unrestricted access to DAAs, to the incidence of aHCV in 2016, after limits were lifted. The investigators used data from 18 HIV treatment centers spread across the Netherlands, capturing about 80% of Dutch MSM being treated for HIV.
In 2014, there were 93 aHCV infections diagnosed among the men, translating to an incidence of 11.2 cases per 1,000 person-years of follow-up (95% CI, 9.1-13.7 cases). In 2016, there were 49 aHCV cases, an incidence of 5.5 cases per 1,000 person-years (95% CI, 4.1–7.2, P less than .001). At the same time, there was a substantial increase in new syphilis cases, indicating that the 51% reduction in aHCV over 2 years was not due to changes in behavior.
Meanwhile, “within 14 months after these drugs became available to all, 75% of the HIV-positive MSM in the Netherlands were cured of their infection,” Dr. Rijnders said at the Conference on Retroviruses & Opportunistic Infections in partnership with the International Antiviral Society.
Ledipasvir/sofosbuvir was the DAA used by about 90% of the men.
In short, unrestricted access to DAAs wiped out the infection so that men were no longer passing it to other men. The results are “an example of what is possible if you search for HCV and treat it as soon as you find it. You cure patients and prevent new infections. In the long run, you may save money,” he said, especially as more DAA options come on the market and prices fall.
Almost all the subjects were seen in their HIV clinic at least twice a year. An uptick in liver enzymes triggered HCV testing. The investigators checked positive results against patients’ own stored blood samples to distinguish new from chronic infections.
The study wasn’t funded, but Dr. Rijnders is a paid researcher for Merck’s DAA option, elbasvir/grazoprevir (Zepatier).
*This story was updated on February 24, 2017.
SEATTLE – New hepatitis C infections among HIV-positive men who have sex with men (MSM) were halved in the Netherlands by unrestricted access to direct-acting antivirals (DAAs), primarily ledipasvir/sofosbuvir tablets (Harvoni), according to Dutch investigators.
Since 2015, DAAs have been available to all newly acquired hepatitis C virus (HCV) patients without restriction. Due to the high cost of the drugs, payers in the United States and some other Western countries limit access to only patients with severe liver disease.*
The Dutch government, however, requires insurers to cover them, and has negotiated price discounts with makers. “The price that is paid is secret,” but it’s less than the standard cost of, for instance, €45,000 for a 3-month course of [ledipasvir/sofosbuvir] in the Netherlands, said senior investigator Bart Rijnders, MD, an infectious diseases assistant professor at Erasmus University Medical Center, Rotterdam.
The study compared the incidence of acute HCV (aHCV) in HIV-positive MSM in 2014, before unrestricted access to DAAs, to the incidence of aHCV in 2016, after limits were lifted. The investigators used data from 18 HIV treatment centers spread across the Netherlands, capturing about 80% of Dutch MSM being treated for HIV.
In 2014, there were 93 aHCV infections diagnosed among the men, translating to an incidence of 11.2 cases per 1,000 person-years of follow-up (95% CI, 9.1-13.7 cases). In 2016, there were 49 aHCV cases, an incidence of 5.5 cases per 1,000 person-years (95% CI, 4.1–7.2, P less than .001). At the same time, there was a substantial increase in new syphilis cases, indicating that the 51% reduction in aHCV over 2 years was not due to changes in behavior.
Meanwhile, “within 14 months after these drugs became available to all, 75% of the HIV-positive MSM in the Netherlands were cured of their infection,” Dr. Rijnders said at the Conference on Retroviruses & Opportunistic Infections in partnership with the International Antiviral Society.
Ledipasvir/sofosbuvir was the DAA used by about 90% of the men.
In short, unrestricted access to DAAs wiped out the infection so that men were no longer passing it to other men. The results are “an example of what is possible if you search for HCV and treat it as soon as you find it. You cure patients and prevent new infections. In the long run, you may save money,” he said, especially as more DAA options come on the market and prices fall.
Almost all the subjects were seen in their HIV clinic at least twice a year. An uptick in liver enzymes triggered HCV testing. The investigators checked positive results against patients’ own stored blood samples to distinguish new from chronic infections.
The study wasn’t funded, but Dr. Rijnders is a paid researcher for Merck’s DAA option, elbasvir/grazoprevir (Zepatier).
*This story was updated on February 24, 2017.
AT CROI
Key clinical point:
Major finding: In 2014, there were 93 acute HCV infections diagnosed among HIV-positive men who have sex with men, translating to an incidence of 11.2 cases per 1,000 person-years of follow-up (95% CI, 9.1-13.7 cases). In 2016, there were 49 cases, an incidence of 5.5 cases per 1,000 person years (95% CI, 4.1–7.2, P less than .001).
Data source: HIV treatment centers in the Netherlands
Disclosures: The study wasn’t funded, but the senior investigator is a paid researcher for Merck’s DAA option, elbasvir/grazoprevir (Zepatier).
Sarcoidosis doubles hospitalized infection risk
Persons with sarcoidosis were found to have double the risk of hospitalization, compared with age-matched controls in a population-based cohort study that also linked glucocorticoid use with an increased risk of hospitalization in this group.
Using data from the Rochester Epidemiology Project record-linkage system, Patompong Ungprasert, MD, an assistant professor of medicine at the Mayo Clinic in Rochester, Minn., and his colleagues identified 345 incident cases of sarcoidosis recorded between 1976 and 2013, confirmed by individual medical records (Ann Am Thorac Soc. 2017 Feb 8. doi: 10.1513/AnnalsATS.201610-750OC). Using random selection, each patient was age- and sex-matched with sarcoidosis-free controls taken from the same database. Medical records across the study were examined for community-acquired infections requiring hospitalization that occurred after the index date or the date of diagnosis.

Dr. Ungprasert and his coinvestigators found that those with sarcoidosis had double the risk of all forms of specific hospitalized infection when compared with controls – a 2.00 hazard ratio (95% confidence interval, 1.41-2.84). The results were similar when adjusted for infection risk factors: 2.13 HR (95% CI, 1.35-3.34).
The risk of hospitalized infection in the sarcoidosis arm was higher than in controls regardless of disease stage: an HR of 1.70 (95% CI, 1.12-2.58, P = .013) in those with Stage I; an HR of 2.00 (95% CI, 1.22-3.29, P = .006) among those with stage II; and an HR of 2.63 (95% CI, 1.58-4.39, P less than .001) in those with Stage III and Stage IV disease.
Biopsies taken in 251 cases resulted in 229 positive results for noncaseating granuloma, and just over half of patients had stage I disease. Stage II disease was found in 29%, Stage III in 15%, and Stage IV in 2%.
Patients in the sarcoidosis group who had not been exposed to immunosuppressive treatment had significantly higher risk of hospitalization with an HR of 1.73 (95% CI, 1.16-2.60; P = .008) when compared with controls. The risk was even higher in study patients who had received immunosuppressive therapy: an HR of 2.41 (95% CI, 1.60-3.64; P less than .001), when compared with controls. Less than half of all sarcoidosis patients required immunosuppressive therapy at any point during follow-up: about 37% by year 30 after original diagnosis. Oral glucocorticoids were the most commonly prescribed medication, used in 113 cases.
A baseline diffusing capacity of the lung for carbon monoxide was associated with an overall increased risk of hospitalized infection, with an HR of 1.15 per decrease of 10% predicted in diffusing capacity of the lung for carbon monoxide (95% CI, 1.01-1.32). A baseline forced vital capacity was associated with an increased hospitalized pneumonia risk with an HR of 1.15 per decrease of 10% predicted in forced vital capacity (95% CI, 1.01-1.32).
Although the use of immunosuppressive agents was not significantly associated with the risk of hospitalized infection (HR, 1.43; 95% CI, 0.94-2.19), current use of oral glucocorticoids, whether alone or as adjunct to immunosuppressive therapy, significantly predicted risk of infection in patients with sarcoidosis, with an HR of 3.03 (95% CI, 1.33-6.90) for oral glucocorticoids up to 10 mg per day, and an HR of 4.48 (95% CI, 1.33-6.90) in patients taking oral glucocorticoids at more than 10 mg per day, when compared with controls.
In an interview, Dr. Ungprasert said the results were not surprising, but provided the following takeaways from this study for physicians caring for patients with sarcoidosis.
“These patients are at an increased risk of serious infection and should seek medical attention as soon as possible when they develop symptoms of infection, such as fever or chills,” he said in an interview. “Keeping current with vaccinations is also important for them.”
Dr. Ungprasert also said the study serves as a reminder to use oral glucocorticoids judiciously. “When considering their use, the physician should keep in mind that a large number of patients with sarcoidosis will have a spontaneous resolution of the disease.”
There were no relevant disclosures. The study was funded in part by the National Institute on Aging.
[email protected]
On Twitter @whitneymcknight
Persons with sarcoidosis were found to have double the risk of hospitalization, compared with age-matched controls in a population-based cohort study that also linked glucocorticoid use with an increased risk of hospitalization in this group.
Using data from the Rochester Epidemiology Project record-linkage system, Patompong Ungprasert, MD, an assistant professor of medicine at the Mayo Clinic in Rochester, Minn., and his colleagues identified 345 incident cases of sarcoidosis recorded between 1976 and 2013, confirmed by individual medical records (Ann Am Thorac Soc. 2017 Feb 8. doi: 10.1513/AnnalsATS.201610-750OC). Using random selection, each patient was age- and sex-matched with sarcoidosis-free controls taken from the same database. Medical records across the study were examined for community-acquired infections requiring hospitalization that occurred after the index date or the date of diagnosis.
Dr. Ungprasert and his coinvestigators found that those with sarcoidosis had double the risk of all forms of specific hospitalized infection when compared with controls – a 2.00 hazard ratio (95% confidence interval, 1.41-2.84). The results were similar when adjusted for infection risk factors: 2.13 HR (95% CI, 1.35-3.34).
The risk of hospitalized infection in the sarcoidosis arm was higher than in controls regardless of disease stage: an HR of 1.70 (95% CI, 1.12-2.58, P = .013) in those with Stage I; an HR of 2.00 (95% CI, 1.22-3.29, P = .006) among those with stage II; and an HR of 2.63 (95% CI, 1.58-4.39, P less than .001) in those with Stage III and Stage IV disease.
Biopsies taken in 251 cases resulted in 229 positive results for noncaseating granuloma, and just over half of patients had stage I disease. Stage II disease was found in 29%, Stage III in 15%, and Stage IV in 2%.
Patients in the sarcoidosis group who had not been exposed to immunosuppressive treatment had significantly higher risk of hospitalization with an HR of 1.73 (95% CI, 1.16-2.60; P = .008) when compared with controls. The risk was even higher in study patients who had received immunosuppressive therapy: an HR of 2.41 (95% CI, 1.60-3.64; P less than .001), when compared with controls. Less than half of all sarcoidosis patients required immunosuppressive therapy at any point during follow-up: about 37% by year 30 after original diagnosis. Oral glucocorticoids were the most commonly prescribed medication, used in 113 cases.
A baseline diffusing capacity of the lung for carbon monoxide was associated with an overall increased risk of hospitalized infection, with an HR of 1.15 per decrease of 10% predicted in diffusing capacity of the lung for carbon monoxide (95% CI, 1.01-1.32). A baseline forced vital capacity was associated with an increased hospitalized pneumonia risk with an HR of 1.15 per decrease of 10% predicted in forced vital capacity (95% CI, 1.01-1.32).
Although the use of immunosuppressive agents was not significantly associated with the risk of hospitalized infection (HR, 1.43; 95% CI, 0.94-2.19), current use of oral glucocorticoids, whether alone or as adjunct to immunosuppressive therapy, significantly predicted risk of infection in patients with sarcoidosis, with an HR of 3.03 (95% CI, 1.33-6.90) for oral glucocorticoids up to 10 mg per day, and an HR of 4.48 (95% CI, 1.33-6.90) in patients taking oral glucocorticoids at more than 10 mg per day, when compared with controls.
In an interview, Dr. Ungprasert said the results were not surprising, but provided the following takeaways from this study for physicians caring for patients with sarcoidosis.
“These patients are at an increased risk of serious infection and should seek medical attention as soon as possible when they develop symptoms of infection, such as fever or chills,” he said in an interview. “Keeping current with vaccinations is also important for them.”
Dr. Ungprasert also said the study serves as a reminder to use oral glucocorticoids judiciously. “When considering their use, the physician should keep in mind that a large number of patients with sarcoidosis will have a spontaneous resolution of the disease.”
There were no relevant disclosures. The study was funded in part by the National Institute on Aging.
[email protected]
On Twitter @whitneymcknight
Persons with sarcoidosis were found to have double the risk of hospitalization, compared with age-matched controls in a population-based cohort study that also linked glucocorticoid use with an increased risk of hospitalization in this group.
Using data from the Rochester Epidemiology Project record-linkage system, Patompong Ungprasert, MD, an assistant professor of medicine at the Mayo Clinic in Rochester, Minn., and his colleagues identified 345 incident cases of sarcoidosis recorded between 1976 and 2013, confirmed by individual medical records (Ann Am Thorac Soc. 2017 Feb 8. doi: 10.1513/AnnalsATS.201610-750OC). Using random selection, each patient was age- and sex-matched with sarcoidosis-free controls taken from the same database. Medical records across the study were examined for community-acquired infections requiring hospitalization that occurred after the index date or the date of diagnosis.
Dr. Ungprasert and his coinvestigators found that those with sarcoidosis had double the risk of all forms of specific hospitalized infection when compared with controls – a 2.00 hazard ratio (95% confidence interval, 1.41-2.84). The results were similar when adjusted for infection risk factors: 2.13 HR (95% CI, 1.35-3.34).
The risk of hospitalized infection in the sarcoidosis arm was higher than in controls regardless of disease stage: an HR of 1.70 (95% CI, 1.12-2.58, P = .013) in those with Stage I; an HR of 2.00 (95% CI, 1.22-3.29, P = .006) among those with stage II; and an HR of 2.63 (95% CI, 1.58-4.39, P less than .001) in those with Stage III and Stage IV disease.
Biopsies taken in 251 cases resulted in 229 positive results for noncaseating granuloma, and just over half of patients had stage I disease. Stage II disease was found in 29%, Stage III in 15%, and Stage IV in 2%.
Patients in the sarcoidosis group who had not been exposed to immunosuppressive treatment had significantly higher risk of hospitalization with an HR of 1.73 (95% CI, 1.16-2.60; P = .008) when compared with controls. The risk was even higher in study patients who had received immunosuppressive therapy: an HR of 2.41 (95% CI, 1.60-3.64; P less than .001), when compared with controls. Less than half of all sarcoidosis patients required immunosuppressive therapy at any point during follow-up: about 37% by year 30 after original diagnosis. Oral glucocorticoids were the most commonly prescribed medication, used in 113 cases.
A baseline diffusing capacity of the lung for carbon monoxide was associated with an overall increased risk of hospitalized infection, with an HR of 1.15 per decrease of 10% predicted in diffusing capacity of the lung for carbon monoxide (95% CI, 1.01-1.32). A baseline forced vital capacity was associated with an increased hospitalized pneumonia risk with an HR of 1.15 per decrease of 10% predicted in forced vital capacity (95% CI, 1.01-1.32).
Although the use of immunosuppressive agents was not significantly associated with the risk of hospitalized infection (HR, 1.43; 95% CI, 0.94-2.19), current use of oral glucocorticoids, whether alone or as adjunct to immunosuppressive therapy, significantly predicted risk of infection in patients with sarcoidosis, with an HR of 3.03 (95% CI, 1.33-6.90) for oral glucocorticoids up to 10 mg per day, and an HR of 4.48 (95% CI, 1.33-6.90) in patients taking oral glucocorticoids at more than 10 mg per day, when compared with controls.
In an interview, Dr. Ungprasert said the results were not surprising, but provided the following takeaways from this study for physicians caring for patients with sarcoidosis.
“These patients are at an increased risk of serious infection and should seek medical attention as soon as possible when they develop symptoms of infection, such as fever or chills,” he said in an interview. “Keeping current with vaccinations is also important for them.”
Dr. Ungprasert also said the study serves as a reminder to use oral glucocorticoids judiciously. “When considering their use, the physician should keep in mind that a large number of patients with sarcoidosis will have a spontaneous resolution of the disease.”
There were no relevant disclosures. The study was funded in part by the National Institute on Aging.
[email protected]
On Twitter @whitneymcknight
FROM ANNALS OF THE AMERICAN THORACIC SOCIETY
Key clinical point:
Major finding: 345 patients with sarcoidosis had a hazard ratio of 2.00 (95% CI, 1.41-2.84) for hospitalized infection, compared with controls.
Data source: Olmsted County, Minn. epidemiology records from 1976 to 2013.
Disclosures: There were no relevant disclosures. The study was funded in part by the National Institute on Aging.
New significantly mutated genes detected in prostate cancer
A new large study has identified 78 significantly mutated genes (SMGs) and has enlarged the genetic landscape of prostate cancer. In addition, 37 genes that were not previously reported as SMGs in prostate cancer and 23 that were not previously identified as recurrently altered in cancer, were identified.
“Through aggregation and uniform genomic analysis, we refined the map of somatic mutations in prostate cancer and identified cancer genes and pathways not previously associated with this disease,” said lead author Dr. Joshua Armenia, of the Memorial Sloan Kettering Cancer Center, New York.
“Our findings may inform patient stratification and translational investigation,” Dr. Armenia said in a press briefing held in 2017 genitourinary cancers symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
The mutational landscapes of primary and metastatic prostate cancer have been robustly analyzed in multiple whole exome sequencing (WES) studies.
But prostate cancer is a very heterogenous disease, explained Dr. Armenia. Aggregation and uniform genomic analysis of larger cohorts can reveal significantly mutated genes and pathways in the “long tail” (1%-5% of cases).
The power to detect genes is significantly proportional to the number of samples used, and the size of the cohort. “Our knowledge of prostate cancer genes is incomplete,” said Dr. Armenia.
He and his colleagues hypothesized that an aggregate, uniform analysis of all data generated to date would enable discovery of new significantly mutated genes and pathways not previously associated with prostate cancer and shed more light onto the genetic differences between primary and metastatic prostate cancer.
They analyzed 918 tumors, with a total of 583 primary tumors and 335 metastasis, with a mutational significance analysis that uses statistical and biological approaches to determine which genes and pathways are recurrently altered.
This approach led to the identification of 78 SMGs, and 37 of the genes are novel prostate cancer genes implicated in other tumor types; SPEN, SETD2, ARID1A, CUL3 ARID2, SMARCAD1, U2AF1.
“These genes have never been implicated in prostate cancer but are found in other tumor types,” said Dr. Armenia. “We stratified them by pathway, and we found 21% of the tumors show mutations in epigenetic regulators and chromatin remodelers.”
The investigators found that 14% of these tumors show alterations in the ubiquitin pathway in prostate cancer. The novel mutations in CUL3 (M299R hotspot) are mutually exclusive with SPOP mutations.
“Unexpectedly, we also found alterations in splicing pathway alterations in prostate cancer,” Dr. Armenia noted.
There were 38 altered tumors (4% of the 918 total) that had alterations in genes such as U2AF1 (0.5%) and SF3B1 (1%), GEMINS (0.8%), TCERG1 (1.3%), and PRPFB (1.3%).
The researchers found another “interesting” gene, SPEN, which is a novel prostate cancer gene. It is a hormone regulator gene that has been described in breast cancer, where it is associated with tamoxifen resistance. Truncating mutations were found in SPEN, which is a hormone inducible transcriptional repressor, in 2.8% of samples which is a rate similar to the frequency observed in breast tumors. SPEN in prostate cancer may have a similar role to the one it has in breast cancer.
“We performed enrichment analysis of genomic alterations in metastatic tumors to be able to identify markers of advanced disease,” he explained. “And what we found that TP53, AR, PTEN, FOXA1, APC, and BRCA2 alterations are enriched in metastatic samples.”
Alterations in epigenetic regulators (KMT2C, KMT2D) are significantly enriched in metastatic tumors while SPOP mutations and FOXP1/RYBP deletions are enriched in primary tumors.
Dr. Armenia and colleagues also identified a subclass of epigenetically mutated prostate cancer, representing 21% of prostate cancers and insignificantly enriched tumors lacking an ETS fusion.
“We discovered novel pathways in prostate cancer including SW1/SNF and splicing, as well as novel prostate cancer genes that include CUL3 and SPEN, and a set of genomic markers enriched in advanced disease,” he concluded.
A new large study has identified 78 significantly mutated genes (SMGs) and has enlarged the genetic landscape of prostate cancer. In addition, 37 genes that were not previously reported as SMGs in prostate cancer and 23 that were not previously identified as recurrently altered in cancer, were identified.
“Through aggregation and uniform genomic analysis, we refined the map of somatic mutations in prostate cancer and identified cancer genes and pathways not previously associated with this disease,” said lead author Dr. Joshua Armenia, of the Memorial Sloan Kettering Cancer Center, New York.
“Our findings may inform patient stratification and translational investigation,” Dr. Armenia said in a press briefing held in 2017 genitourinary cancers symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
The mutational landscapes of primary and metastatic prostate cancer have been robustly analyzed in multiple whole exome sequencing (WES) studies.
But prostate cancer is a very heterogenous disease, explained Dr. Armenia. Aggregation and uniform genomic analysis of larger cohorts can reveal significantly mutated genes and pathways in the “long tail” (1%-5% of cases).
The power to detect genes is significantly proportional to the number of samples used, and the size of the cohort. “Our knowledge of prostate cancer genes is incomplete,” said Dr. Armenia.
He and his colleagues hypothesized that an aggregate, uniform analysis of all data generated to date would enable discovery of new significantly mutated genes and pathways not previously associated with prostate cancer and shed more light onto the genetic differences between primary and metastatic prostate cancer.
They analyzed 918 tumors, with a total of 583 primary tumors and 335 metastasis, with a mutational significance analysis that uses statistical and biological approaches to determine which genes and pathways are recurrently altered.
This approach led to the identification of 78 SMGs, and 37 of the genes are novel prostate cancer genes implicated in other tumor types; SPEN, SETD2, ARID1A, CUL3 ARID2, SMARCAD1, U2AF1.
“These genes have never been implicated in prostate cancer but are found in other tumor types,” said Dr. Armenia. “We stratified them by pathway, and we found 21% of the tumors show mutations in epigenetic regulators and chromatin remodelers.”
The investigators found that 14% of these tumors show alterations in the ubiquitin pathway in prostate cancer. The novel mutations in CUL3 (M299R hotspot) are mutually exclusive with SPOP mutations.
“Unexpectedly, we also found alterations in splicing pathway alterations in prostate cancer,” Dr. Armenia noted.
There were 38 altered tumors (4% of the 918 total) that had alterations in genes such as U2AF1 (0.5%) and SF3B1 (1%), GEMINS (0.8%), TCERG1 (1.3%), and PRPFB (1.3%).
The researchers found another “interesting” gene, SPEN, which is a novel prostate cancer gene. It is a hormone regulator gene that has been described in breast cancer, where it is associated with tamoxifen resistance. Truncating mutations were found in SPEN, which is a hormone inducible transcriptional repressor, in 2.8% of samples which is a rate similar to the frequency observed in breast tumors. SPEN in prostate cancer may have a similar role to the one it has in breast cancer.
“We performed enrichment analysis of genomic alterations in metastatic tumors to be able to identify markers of advanced disease,” he explained. “And what we found that TP53, AR, PTEN, FOXA1, APC, and BRCA2 alterations are enriched in metastatic samples.”
Alterations in epigenetic regulators (KMT2C, KMT2D) are significantly enriched in metastatic tumors while SPOP mutations and FOXP1/RYBP deletions are enriched in primary tumors.
Dr. Armenia and colleagues also identified a subclass of epigenetically mutated prostate cancer, representing 21% of prostate cancers and insignificantly enriched tumors lacking an ETS fusion.
“We discovered novel pathways in prostate cancer including SW1/SNF and splicing, as well as novel prostate cancer genes that include CUL3 and SPEN, and a set of genomic markers enriched in advanced disease,” he concluded.
A new large study has identified 78 significantly mutated genes (SMGs) and has enlarged the genetic landscape of prostate cancer. In addition, 37 genes that were not previously reported as SMGs in prostate cancer and 23 that were not previously identified as recurrently altered in cancer, were identified.
“Through aggregation and uniform genomic analysis, we refined the map of somatic mutations in prostate cancer and identified cancer genes and pathways not previously associated with this disease,” said lead author Dr. Joshua Armenia, of the Memorial Sloan Kettering Cancer Center, New York.
“Our findings may inform patient stratification and translational investigation,” Dr. Armenia said in a press briefing held in 2017 genitourinary cancers symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
The mutational landscapes of primary and metastatic prostate cancer have been robustly analyzed in multiple whole exome sequencing (WES) studies.
But prostate cancer is a very heterogenous disease, explained Dr. Armenia. Aggregation and uniform genomic analysis of larger cohorts can reveal significantly mutated genes and pathways in the “long tail” (1%-5% of cases).
The power to detect genes is significantly proportional to the number of samples used, and the size of the cohort. “Our knowledge of prostate cancer genes is incomplete,” said Dr. Armenia.
He and his colleagues hypothesized that an aggregate, uniform analysis of all data generated to date would enable discovery of new significantly mutated genes and pathways not previously associated with prostate cancer and shed more light onto the genetic differences between primary and metastatic prostate cancer.
They analyzed 918 tumors, with a total of 583 primary tumors and 335 metastasis, with a mutational significance analysis that uses statistical and biological approaches to determine which genes and pathways are recurrently altered.
This approach led to the identification of 78 SMGs, and 37 of the genes are novel prostate cancer genes implicated in other tumor types; SPEN, SETD2, ARID1A, CUL3 ARID2, SMARCAD1, U2AF1.
“These genes have never been implicated in prostate cancer but are found in other tumor types,” said Dr. Armenia. “We stratified them by pathway, and we found 21% of the tumors show mutations in epigenetic regulators and chromatin remodelers.”
The investigators found that 14% of these tumors show alterations in the ubiquitin pathway in prostate cancer. The novel mutations in CUL3 (M299R hotspot) are mutually exclusive with SPOP mutations.
“Unexpectedly, we also found alterations in splicing pathway alterations in prostate cancer,” Dr. Armenia noted.
There were 38 altered tumors (4% of the 918 total) that had alterations in genes such as U2AF1 (0.5%) and SF3B1 (1%), GEMINS (0.8%), TCERG1 (1.3%), and PRPFB (1.3%).
The researchers found another “interesting” gene, SPEN, which is a novel prostate cancer gene. It is a hormone regulator gene that has been described in breast cancer, where it is associated with tamoxifen resistance. Truncating mutations were found in SPEN, which is a hormone inducible transcriptional repressor, in 2.8% of samples which is a rate similar to the frequency observed in breast tumors. SPEN in prostate cancer may have a similar role to the one it has in breast cancer.
“We performed enrichment analysis of genomic alterations in metastatic tumors to be able to identify markers of advanced disease,” he explained. “And what we found that TP53, AR, PTEN, FOXA1, APC, and BRCA2 alterations are enriched in metastatic samples.”
Alterations in epigenetic regulators (KMT2C, KMT2D) are significantly enriched in metastatic tumors while SPOP mutations and FOXP1/RYBP deletions are enriched in primary tumors.
Dr. Armenia and colleagues also identified a subclass of epigenetically mutated prostate cancer, representing 21% of prostate cancers and insignificantly enriched tumors lacking an ETS fusion.
“We discovered novel pathways in prostate cancer including SW1/SNF and splicing, as well as novel prostate cancer genes that include CUL3 and SPEN, and a set of genomic markers enriched in advanced disease,” he concluded.
Key clinical point: New findings on prostate cancer genetics may help inform patient stratification and translational research.
Major finding: A total of 78 significantly mutated genes were identified in prostate cancer along with 37 genes that were not previously reported as significantly mutated.
Data source: An experimental study that analyzed 918 tumors obtained from prostate cancer patients.
Disclosures: The study does not list a funding source. Dr. Armenia has no disclosures but several coauthors report relationships with industry.
Management of Proximal Biceps Pathology in Overhead Athletes: What Is the Role of Biceps Tenodesis?
Take Home Points
- Outcomes after SLAP repair remain guarded.
- Physical examination is key in determining proper management of biceps pathology.
- When performing SLAP repair, knotless technology may prevent future cartilage or rotator cuff injury.
- Revision of SLAP repair is best handled with biceps tenodesis.
- Subpectoral biceps tenodesis avoids residual groove pain.
In recent decades, the long head of the biceps (LHB) tendon has been recognized as a pain generator in the shoulder of throwing athletes. The LHB muscle and its role in glenohumeral kinematics remains largely in question. The LHB tendon varies in size but most commonly is 5 mm to 6mm in diameter and about 9 cm in length, inserting on the superior labrum and supraglenoid tubercle after traveling through the bicipital groove.1 The many conditions that can develop along the course of the biceps tendon include overall biceps tendonitis, biceps tendon subluxation or instability, and injuries to the superior anterior to posterior area of the labrum.
These injuries can occur in young overhead athletes as well as manual laborers and older overhead recreational athletes. Pitching is the most common activity that leads to proximal biceps tendon disorders. The 6 phases of the pitch are linked in a kinetic chain that generates energy that is then translated to high velocity. The amount of force that is exerted on the shoulder during pitching and especially after ball release is impressive, and the athlete’s shoulder changes in many ways as it adapts to the motion.2-5 The late-cocking and deceleration phases are most commonly associated with proximal biceps pathology and the “peel-back” phenomenon. Other common activities that lead to biceps tendon issues in a young population are volleyball, baseball, tennis, softball, swimming, and cricket. Shoulder arthroscopies performed in older patients show degenerative biceps and labrum tears, which should be treated appropriately but perhaps different from how they are treated in overhead athletes.6-8 Further, many professional athletes have asymptomatic superior labrum anterior-posterior (SLAP) tears.9
Mechanism of Injury
Overhead throwing is commonly thought to be the mechanism by which lesions are created in the biceps–labrum complex (BLC). Pitching in particular generates incredible force and torque within the shoulder. In professional pitchers, the resulting throwing speed creates forces regularly in excess of 1000 N.3 These forces effect internal compensatory changes and internal derangement of the BLC. These changes often involve internal rotation deficits and alterations in the rotator cuff, which may contribute to glenohumeral instability and altered joint kinematics.10
Repetitive overhead activity is largely considered the mechanism of injury in this population, though more specific mechanisms have been described, including the peel-back mechanism11 and the posterior superior glenoid impingement. There is little evidence that preventive programs have any effect on decreasing the incidence of SLAP tears in overhead athletes.
Preoperative Evaluation
Preoperative evaluation is arguably the most important step in treating a patient with persistent or recurrent symptoms consistent with a SLAP tear. Evaluation includes thorough history, physical examination, and review of any prior injuries or surgical procedures. The physical examination should focus on maneuvers that define where the problem is occurring. Although SLAP tears are most common in this population, disorders of the biceps tendon within the groove, including inflammation and instability, should be ruled out with physical examination and advanced imaging. Palpation for groove tenderness, impingement-type complaints, internal rotation loss, and SLAP provocative testing are crucial in the diagnosis.12,13 The cause of symptoms may be multifactorial and include the often encountered concomitant pathology of rotator cuff tears, internal impingement, and instability.
Standard radiographs (Grashey anteroposterior, scapular/lateral, axillary lateral) and magnetic resonance imaging (MRI) with or without arthrography can be helpful in identifying and characterizing most SLAP tears as well as failed SLAP tear repairs. However, MRI is often positive for SLAP tears in asymptomatic patients, and diagnosing SLAP tears with MRI is often a challenge.14 MRI can help in determining concomitant pathology, including rotator cuff injury and cysts causing nerve compression. Correlation with clinical examination and patient history is most crucial. Conservative treatment (rest, activity modification, use of oral anti-inflammatory medications) typically is attempted and coordinated with respect to the athlete’s season of play.15,16
Classification
In overhead throwing athletes, SLAP tears typically are associated with anterior shoulder pain. Associated shoulder instability and significant glenohumeral dysfunction are not uncommon in athletes with lesions of the BLC. In 1985, Andrews and colleagues17 were the first to describe SLAP tears in overhead athletes (73 patients). Later, Snyder and colleagues18,19 further classified these lesions into 4 types based on tear stability and location, and they coined the acronym SLAP (Figure 1). 
Type I lesions typically are described as fraying at the inner margin of the labrum and are common in throwers, even asymptomatic throwers. Type II lesions, separations of the biceps and labrum from the superior glenoid (≥5 mm of excursion), are the most commonly occurring and treated variant in throwing athletes.20-22 Intraoperative evaluation for a peel-back lesion (placing the arm in abduction with external rotation), rather than for a sulcus of 1 mm to 2 mm, may confirm a type II SLAP tear.20,23,24 It is often important to consider the direction of tear propagation as well. Type III lesions include those with an intact BLC (but with a bucket-handle tear of the superior labral complex and an intact biceps tendon), whereas type IV lesions involve additional extension of the tear into the biceps tendon.18,19The classification systems are well defined. Nevertheless, management of SLAP lesions remains controversial.
Options for Surgical Treatment
SLAP Tear Repair—Outcomes
The incidence of SLAP tear repairs has increased dramatically in recent years.6,25 There are various SLAP tear repair methods, but the most common consists of repairing the labrum and biceps anchor. Management of type II SLAP lesions remains controversial. Several prospective studies have found overall improvement after SLAP tear repair.26-31 Other series have reported less encouraging outcomes, including dissatisfaction with persistent pain and inability to return to throwing.28,32 A 2010 systematic review found that the percentage of patients who returned to their preinjury level of play was only 64%, and outcomes for overhead throwing athletes were even worse—only 22% to 60% of these patients returned to their previous level.33 The right surgery for SLAP tears in this population continues to be an area of uncertainty for many surgeons.
Failed SLAP tear repairs (poor outcomes) have become common in overhead throwing athletes. The reasons for these failed repairs are unclear, but several possible explanations have been offered. One is that labral repair may result in permanent alterations in pitching biomechanics, which may lead to an inability to regain velocity and command.3 Another is that the athlete’s shoulder may remain unstable even after repair.10Hardware complications are a significant concern in this high-level population. Suture anchor pullout or iatrogenic cartilage damage may occur during instrumentation or as a result of suture anchor reactive changes. In addition, there are several reports of glenoid osteochondrolysis (Figure 2) caused by prominent hardware or prominent knots.34-39 

Stiffness after SLAP tear repair is a significant problem, with most patients taking up to 6 months to regain full motion.26,48 Overtensioning of the labrum and the glenohumeral ligaments may be the cause, and the solution may be to place anchors posterior (vs anterior) to the biceps insertion. In a large prospective military study, mean forward flexion and external rotation were reduced at final follow-up.31 These outcomes are less acceptable to overhead throwing athletes, who rely on motion for high-end throwing activities.
Primary Biceps Tenodesis—Outcomes
A 2015 database study found a 1.7-fold increase in biceps tenodesis over the preceding 5 years.49 However, relatively few procedures included in the study were performed in patients age younger than 30 years. For many older non-overhead throwers with type II tears, SLAP tear repair has become less popular as a treatment option.32 There is a dearth of knowledge about the outcomes of subpectoral biceps tenodesis as a primary treatment for biceps tendonitis and an associated SLAP tear. Although type I tears historically have been treated with débridement, débridement is seldom used for concomitant biceps tendonitis. It should be coupled with careful clinical examination.
In recent years, biceps tenodesis has been proposed as an alternative to repair for SLAP tears, particularly in older patients.24,44 For obvious reasons, however, there has been some trepidation about performing biceps tenodesis in throwing athletes. Some authors have proposed biceps tenodesis as primary treatment for isolated SLAP tears. Boileau and colleagues44 compared the outcomes of treatment of isolated type II SLAP lesions in 25 consecutive patients. For 10 patients, repair involved suture anchors; for the other 15, arthroscopic biceps tenodesis was performed with an absorbable interference screw. Six of the 10 suture anchor patients were disappointed with their outcome (persistent pain or inability to return to sport), whereas 14 of the 15 biceps tenodesis patients were satisfied. The authors concluded that arthroscopic biceps tenodesis is an effective alternative to repair for type II SLAP lesions, though their study was not isolated to overhead athletes (tenodesis group mean age, 52 years).
In a 2014 series of cases, Ek and colleagues50 reported good outcomes of SLAP tear repair and biceps tenodesis. Again, though, tenodesis was used in older patients, and repair in younger, more active patients, with no high-level athletes in either group. There was no difference in return to sport between groups. In a study of patients who underwent primary biceps tenodesis, Gupta and colleagues51 found 80% excellent outcomes (improved shoulder outcome scores) in select SLAP tear patients, including 8 athletes, 88% of whom were overhead athletes. Gottschalk and colleagues52 reported on differences in prospectively collected outcome data (age, sex, SLAP lesion type II or IV) for primary biceps tenodesis in a series of 33 patients. Twenty-six of the 29 patients who completed follow-up returned to their previous level of activity. These studies suggest that primary biceps tenodesis may be an alternative with lower failure rates in the treatment of SLAP tears in middle-aged patients, and in overhead athletes, though additional specific studies are needed to focus on overhead athletes on a larger scale.
Revision SLAP Tear Repair Versus Biceps Tenodesis
Failed arthroscopic SLAP tear repairs, which are increasingly common, present a unique treatment challenge. In a 2013 prospective cohort series, Gupta and colleagues46 found excellent clinical outcomes of subpectoral biceps tenodesis for failed type II SLAP tears. The authors reported a postoperative SANE (Single Assessment Numeric Evaluation) score of 70.4%, an SST (Simple Shoulder Test) score of 9.33, and an ASES (American Shoulder and Elbow Surgeons) score of 77.96, along with reasonable health-related quality-of-life scores. Werner and colleagues53 evaluated 2-year outcomes of biceps tenodesis performed after SLAP tear repair in 24 patients and found a return to almost normal range of motion as well as good clinical outcome scores. Significantly worse outcomes were found for patients with open worker’s compensation claims.
McCormick and colleagues26 prospectively evaluated the efficacy of biceps tenodesis for failed type II SLAP tear repair in 46 patients. Improvement was noted across all outcome assessments during follow-up (mean, 3.6 years). From these findings, we might conclude that biceps tenodesis is a more predictable option for failed SLAP tear repair, and that it has a relatively low complication rate. However, most investigators have used a heterogeneous patient population, as opposed to overhead athletes specifically. To our knowledge, no one has evaluated the specific population of overhead throwers with failed SLAP tear repairs. In addition, no one has conducted randomized controlled trials comparing débridement, biceps tenodesis, and repair for failed SLAP tear repairs.
Postoperative Considerations
When overhead athletes and their surgeons are considering surgical options, they must take rehabilitation and return to play into account. Many surgeons think the possible marginal clinical benefit of SLAP tear repair may not be worth the protracted rehabilitation. In most practices, rehabilitation after biceps tenodesis is less involved. Discussing the advantages and disadvantages of these 2 procedures can be helpful in decision making.
Dein and colleagues54 reported the case of a middle-aged pitcher who sustained a fracture after biceps tenodesis with an interference screw. Cases like this are concerning. Surgeons should consider altering the rehabilitation regimen when planning postoperative care in cases of biceps tenodesis in throwers. Other reported complications of open tenodesis are deep infection, thrombosis, postoperative stiffness, and nerve injury.55-58
Consequences for Overhead Throwers
The unknown role of the BLC leaves surgeons wary when considering biceps tenodesis for elite athletes. Some have postulated that removing the intra-articular portion of the LHB may cause microinstability and alter joint kinematics.10,59-61 Others have suggested the biceps is desynchronized from the other musculature and is not functionally important.62 Disruption of one portion of the superior labrum may result in instability on the opposite side of the glenoid.10,61 Biomechanical studies, both cadaveric and in vivo, have tried to create proper loads to the LHB and evaluate the kinematics of the shoulder before and after biceps tenodesis and SLAP tear repair.59,60 Using a cadaveric model, Strauss and colleagues63 found that type II SLAP lesions resulted in increased glenohumeral translation compared with baseline. Biceps tenodesis did not restore normal translation, but this did not negatively affect stability in the presence of a SLAP lesion. The consensus is that the role of the biceps is controversial at best.
Several studies have used electromyography (EMG) to evaluate LHB functioning. In 2014, Chalmers and colleagues59 used surface EMG and motion analysis to evaluate 18 pitchers: 6 underwent SLAP tear repair, 5 underwent biceps tenodesis, and 7 were uninjured controls. There were no significant differences in the activity of the LHB muscle, the short head of the biceps muscle, the deltoid, the infraspinatus, or the latissimus among the 3 groups. Motion analysis showed that the normal pattern of muscular activation within the LHB muscle was more closely restored by biceps tenodesis than by SLAP tear repair. In addition, thoracic rotation patterns were significantly more altered in the SLAP tear repair patients than in the uninjured controls. As the authors noted, given the low frequency with which biceps tenodesis is performed in overhead athletes, it is unlikely that larger scale studies will be conducted without a multicenter effort.
Recommendations and Our Preferred Technique
Which surgical option is best for treating symptomatic SLAP lesions in overhead athletes remains unclear. Many athletes struggle to return to high-level play after SLAP tear repair. Whether the same is true after biceps tenodesis is yet to be determined because of the low frequency with which biceps tenodesis is performed in high-level overhead athletes. The options for fixation, technique, and fixation location are equally broad. In this section, we outline our general line of thinking for cases of proximal biceps pathology.
In each case, we perform glenohumeral arthroscopy to evaluate the BLC and identify any other pathology. For overhead athletes who are younger than 30 years and lack bicipital groove pain or signs of gross tendinopathy, we favor arthroscopic SLAP tear repair. Repair is usually performed through an anterior working portal for suture passage and a Wilmington portal for anchor placement. We use knotless technology to achieve stable fixation and stay posterior to the biceps anchor insertion.
For the prevention of any potential pain from the bicipital groove in carefully selected patients—recreational overhead athletes and patients who want a less involved surgical recovery—we favor open subpectoral biceps tenodesis rather than arthroscopic tenodesis. The outcomes of biceps tenodesis are consistent, according to the literature.47,57,64 Moreover, the open approach is favored for the incidence of postoperative stiffness in the arthroscopic population.65 Tendons can be fixed with multiple procedures, including soft-tissue tenodesis, interference screw fixation, and surface anchors. We favor using a tenodesis screw in the subpectoral location, as outlined by Mazzocca and colleagues.64Our algorithm for SLAP lesions is evolving with our understanding of this complex disease process. For young overhead throwers with type II SLAP lesions, we favor arthroscopic SLAP tear repair with knotless technology. For older recreational overhead athletes, we favor biceps tenodesis in the subpectoral region after diagnostic arthroscopy plus biceps tenotomy with or without additional SLAP tear fixation, depending on the stability of the biceps anchor (Figures 4A, 4B). 
Conclusion
Overhead athletes who present with symptomatic SLAP lesions often provide a treatment dilemma. Although SLAP tear repair historically has been standard treatment, biceps tenodesis represents a consistent surgical option with low complication rates and low revision rates. It is likely that, as additional data on glenohumeral kinematics and outcomes in young athletes become available, improved decision-making algorithms will follow.
Am J Orthop. 2017;46(1):E71-E78. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Elser F, Braun S, Dewing CB, Giphart JE, Millett PJ. Anatomy, function, injuries, and treatment of the long head of the biceps brachii tendon. Arthroscopy. 2011;27(4):581-592.
2. Fedoriw WW, Ramkumar P, McCulloch PC, Lintner DM. Return to play after treatment of superior labral tears in professional baseball players. Am J Sports Med. 2014;42(5):1155-1160.
3. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23(2):233-239.
4. Aydin N, Sirin E, Arya A. Superior labrum anterior to posterior lesions of the shoulder: diagnosis and arthroscopic management. World J Orthop. 2014;5(3):344-350.
5. Barber A, Field LD, Ryu R. Biceps tendon and superior labrum injuries: decision-marking. J Bone Joint Surg Am. 2007;89(8):1844-1855.
6. Onyekwelu I, Khatib O, Zuckerman JD, Rokito AS, Kwon YW. The rising incidence of arthroscopic superior labrum anterior and posterior (SLAP) repairs. J Shoulder Elbow Surg. 2012;21(6):728-731.
7. Patterson BM, Creighton RA, Spang JT, Roberson JR, Kamath GV. Surgical trends in the treatment of superior labrum anterior and posterior lesions of the shoulder: analysis of data from the American Board of Orthopaedic Surgery Certification Examination Database. Am J Sports Med. 2014;42(8):1904-1910.
8. Walton DM, Sadi J. Identifying SLAP lesions: a meta-analysis of clinical tests and exercise in clinical reasoning. Phys Ther Sport. 2008;9(4):167-176.
9. Lesniak BP, Baraga MG, Jose J, Smith MK, Cunningham S, Kaplan LD. Glenohumeral findings on magnetic resonance imaging correlate with innings pitched in asymptomatic pitchers. Am J Sports Med. 2013;41(9):2022-2027.
10. Mihata T, McGarry MH, Tibone JE, Fitzpatrick MJ, Kinoshita M, Lee TQ. Biomechanical assessment of type II superior labral anterior-posterior (SLAP) lesions associated with anterior shoulder capsular laxity as seen in throwers: a cadaveric study. Am J Sports Med. 2008;36(8):1604-1610.
11. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part II: evaluation and treatment of SLAP lesions in throwers. Arthroscopy. 2003;19(5):531-539.
12. Meserve BB, Cleland JA, Boucher TR. A meta-analysis examining clinical test utility for assessing superior labral anterior posterior lesions. Am J Sports Med. 2009;37(11):2252-2258.
13. Pandya NK, Colton A, Webner D, Sennett B, Huffman GR. Physical examination and magnetic resonance imaging in the diagnosis of superior labrum anterior-posterior lesions of the shoulder: a sensitivity analysis. Arthroscopy. 2008;24(3):311-317.
14. Amin MF, Youssef AO. The diagnostic value of magnetic resonance arthrography of the shoulder in detection and grading of SLAP lesions: comparison with arthroscopic findings. Eur J Radiol. 2012;81(9):2343-2347.
15. Cook C, Beaty S, Kissenberth MJ, Siffri P, Pill SG, Hawkins RJ. Diagnostic accuracy of five orthopedic clinical tests for diagnosis of superior labrum anterior posterior (SLAP) lesions. J Shoulder Elbow Surg. 2012;21(1):13-22.
16. Edwards SL, Lee JA, Bell JE, et al. Nonoperative treatment of superior labrum anterior posterior tears: improvements in pain, function, and quality of life. Am J Sports Med. 2010;38(7):1456-1461.
17. Andrews JR, Carson WG Jr, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985;13(5):337-341.
18. Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990;6(4):274-279.
19. Snyder SJ, Banas MP, Karzel RP. An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg. 1995;4(4):243-248.
20. Morgan CD, Burkhart SS, Palmeri M, Gillespie M. Type II SLAP lesions: three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy. 1998;14(6):553-565.
21. Weber SC, Martin DF, Seiler JG 3rd, Harrast JJ. Superior labrum anterior and posterior lesions of the shoulder: incidence rates, complications, and outcomes as reported by American Board of Orthopedic Surgery. Part II candidates. Am J Sports Med. 2012;40(7):1538-1543.
22. Keener JD, Brophy RH. Superior labral tears of the shoulder: pathogenesis, evaluation, and treatment. J Am Acad Orthop Surg. 2009;17(10):627-637.
23. Chen CH, Hsu KY, Chen WJ, Shih CH. Incidence and severity of biceps long head tendon lesion in patients with complete rotator cuff tears. J Trauma. 2005;58(6):1189-1193.
24. Nho SJ, Strauss EJ, Lenart BA, et al. Long head of the biceps tendinopathy: diagnosis and management. J Am Acad Orthop Surg. 2010;18(11):645-656.
25. Zhang AL, Kreulen C, Ngo SS, Hame SL, Wang JC, Gamradt SC. Demographic trends in arthroscopic SLAP repair in the United States. Am J Sports Med. 2012;40(5):1144-1147.
26. McCormick F, Bhatia S, Chalmers P, Gupta A, Verma N, Romeo AA. The management of type II superior labral anterior to posterior injuries. Orthop Clin North Am. 2014;45(1):121-128.
27. Brockmeier SF, Voos JE, Williams RJ 3rd, Altchek DW, Cordasco FA, Allen AA; Hospital for Special Surgery Sports Medicine and Shoulder Service. Outcomes after arthroscopic repair of type-II SLAP lesions. J Bone Joint Surg Am. 2009;91(7):1595-1603.
28. Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009;37(5):929-936.
29. Denard PJ, Lädermann A, Burkhart SS. Long-term outcome after arthroscopic repair of type II SLAP lesions: results according to age and workers’ compensation status. Arthroscopy. 2012;28(4):451-457.
30. Friel NA, Karas V, Slabaugh MA, Cole BJ. Outcomes of type II superior labrum, anterior to posterior (SLAP) repair: prospective evaluation at a minimum two-year follow-up. J Shoulder Elbow Surg. 2010;19(6):859-867.
31. Provencher MT, McCormick F, Dewing C, McIntire S, Solomon D. A prospective analysis of 179 type 2 superior labrum anterior and posterior repairs: outcomes and factors associated with success and failure. Am J Sports Med. 2013;41(4):880-886.
32. Gupta AK, Chalmers PN, Klosterman EL, et al. Subpectoral biceps tenodesis for bicipital tendonitis with SLAP tear. Orthopedics. 2015;38(1):e48-e53.
33. Gorantla K, Gill C, Wright RW. The outcome of type II SLAP repair: a systematic review. Arthroscopy. 2010;26(4):537-545.
34. Katz LM, Hsu S, Miller SL, et al. Poor outcomes after SLAP repair: descriptive analysis and prognosis. Arthroscopy. 2009;25(8):849-855.
35. Park MJ, Hsu JE, Harper C, Sennett BJ, Huffman GR. Poly-L/D-lactic acid anchors are associated with reoperation and failure of SLAP repairs. Arthroscopy. 2011;27(10):1335-1340.
36. Sassmannshausen G, Sukay M, Mair SD. Broken or dislodged poly-L-lactic acid bioabsorbable tacks in patients after SLAP lesion surgery. Arthroscopy. 2006;22(6):615-619.
37. Uggen C, Wei A, Glousman RE, et al. Biomechanical comparison of knotless anchor repair versus simple suture repair for type II SLAP lesions. Arthroscopy. 2009;25(10):1085-1092.
38. Weber SC. Surgical management of the failed SLAP repair. Sports Med Arthrosc. 2010;18(3):162-166.
39. Wilkerson JP, Zvijac JE, Uribe JW, Schürhoff MR, Green JB. Failure of polymerized lactic acid tacks in shoulder surgery. J Shoulder Elbow Surg. 2003;12(2):117-121.
40. Weber S. Surgical management of the failed SLAP lesion. Arthroscopy. 2008;24(suppl):e8-e9.
41. Schrøder CP, Skare O, Gjengedal E, Uppheim G, Reikerås O, Brox JI. Long-term results after SLAP repair: a 5-year follow-up study of 107 patients with comparison of patients aged over and under 40 years. Arthroscopy. 2012;28(11):1601-1607.
42. Mazzocca AD, Cote MP, Arciero CL, Romeo AA, Arciero RA. Clinical outcomes after subpectoral biceps tenodesis with an interference screw. Am J Sports Med. 2008;36(10):1922-1929.
43. Mazzocca AD, McCarthy MB, Ledgard FA, et al. Histomorphologic changes of the long head of the biceps tendon in common shoulder pathologies. Arthroscopy. 2013;29(6):972-981.
44. Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009;37(5):929-936.
45. Boileau P, Krishnan SG, Coste JS, Walch G. Arthroscopic biceps tenodesis: a new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002;18(9):1002-1012.
46. Gupta AK, Bruce B, Klosterman EL, McCormick F, Harris J, Romeo AA. Subpectoral biceps tenodesis for failed type II SLAP repair. Orthopedics. 2013;36(6):e723-e728.
47. Provencher MT, LeClere LE, Romeo AA. Subpectoral biceps tenodesis. Sports Med Arthrosc. 2008;16(3):170-176.
48. McCarty LP 3rd, Buss DD, Datta MW, Freehill MQ, Giveans MR. Complications observed following labral or rotator cuff repair with use of poly-L-lactic acid implants. J Bone Joint Surg Am. 2013;95(6):507-511.
49. Werner BC, Brockmeier SF, Gwathmey FW. Trends in long head biceps tenodesis. Am J Sports Med. 2015;43(3):570-578.
50. Ek ET, Shi LL, Tompson JD, Freehill MT, Warner JJ. Surgical treatment of isolated type II superior labrum anterior-posterior (SLAP) lesions: repair versus biceps tenodesis. J Shoulder Elbow Surg. 2014;23(7):1059-1065.
51. Gupta AK, Chalmers PN, Klosterman EL, et al. Subpectoral biceps tenodesis for bicipital tendonitis with SLAP tear. Orthopedics. 2015;38(1):e48-e53.
52. Gottschalk MB, Karas SG, Ghattas TN, Burdette R. Subpectoral biceps tenodesis for the treatment of type II and IV superior labral anterior and posterior lesions. Am J Sports Med. 2014;42(9):2128-2135.
53. Werner BC, Pehlivan HC, Hart JM, et al. Biceps tenodesis is a viable option for salvage of failed SLAP repair. J Shoulder Elbow Surg. 2014;23(8):e179-e184.
54. Dein EJ, Huri G, Gordon JC, McFarland EG. A humerus fracture in a baseball pitcher after biceps tenodesis [published correction appears in Am J Sports Med. 2014;42(6):NP39]. Am J Sports Med. 2014;42(4):877-879.
55. Nho SJ, Reiff SN, Verma NN, Slabaugh MA, Mazzocca AD, Romeo AA. Complications associated with subpectoral biceps tenodesis: low rates of incidence following surgery. J Shoulder Elbow Surg. 2010;19(5):764-768.
56. Osbahr DC, Diamond AB, Speer KP. The cosmetic appearance of the biceps muscle after long-head tenotomy versus tenodesis. Arthroscopy. 2002;18(5):483-487.
57. Romeo AA, Mazzocca AD, Tauro JC. Arthroscopic biceps tenodesis. Arthroscopy. 2004;20(2):206-213.
58. Ma H, Van Heest A, Glisson C, Patel S. Musculocutaneous nerve entrapment: an unusual complication after biceps tenodesis. Am J Sports Med. 2009;37(12):2467-2469.
59. Chalmers PN, Trombley R, Cip J, et al. Postoperative restoration of upper extremity motion and neuromuscular control during the overhand pitch: evaluation of tenodesis and repair for superior labral anterior-posterior tears. Am J Sports Med. 2014;42(12):2825-2836.
60. Giphart JE, Elser F, Dewing CB, Torry MR, Millett PJ. The long head of the biceps tendon has minimal effect on in vivo glenohumeral kinematics: a biplane fluoroscopy study. Am J Sports Med. 2012;40(1):202-212.
61. Grossman MG, Tibone JE, McGarry MH, Schneider DJ, Veneziani S, Lee TQ. A cadaveric model of the throwing shoulder: a possible etiology of superior labrum anterior-to-posterior lesions. J Bone Joint Surg Am. 2005;87(4):824-831.
62. Hawkes DH, Alizadehkhaiyat O, Fisher AC, Kemp GJ, Roebuck MM, Frostick SP. Normal shoulder muscular activation and co-ordination during a shoulder elevation task based on activities of daily living: an electromyographic study. J Orthop Res. 2012;30(1):53-60.
63. Strauss EJ, Salata MJ, Sershon RA, et al. Role of the superior labrum after biceps tenodesis in glenohumeral stability. J Shoulder Elbow Surg. 2014;23(4):485-491.
64. Mazzocca AD, Bicos J, Santangelo S, Romeo AA, Arciero RA. The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis. Arthroscopy. 2005;21(11):1296-1306.
65. Werner BC, Pehlivan HC, Hart JM, et al. Increased incidence of postoperative stiffness after arthroscopic compared with open biceps tenodesis. Arthroscopy. 2014;30(9):1075-1084.
66. Denard PJ, Dai X, Hanypsiak BT, Burkhart SS. Anatomy of the biceps tendon: implications for restoring physiological length–tension relation during biceps tenodesis with interference screw fixation. Arthroscopy. 2012;28(10):1352-1358.
67. Mazzocca AD, Rios CG, Romeo AA, Arciero RA. Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy. 2005;21(7):896.
Take Home Points
- Outcomes after SLAP repair remain guarded.
- Physical examination is key in determining proper management of biceps pathology.
- When performing SLAP repair, knotless technology may prevent future cartilage or rotator cuff injury.
- Revision of SLAP repair is best handled with biceps tenodesis.
- Subpectoral biceps tenodesis avoids residual groove pain.
In recent decades, the long head of the biceps (LHB) tendon has been recognized as a pain generator in the shoulder of throwing athletes. The LHB muscle and its role in glenohumeral kinematics remains largely in question. The LHB tendon varies in size but most commonly is 5 mm to 6mm in diameter and about 9 cm in length, inserting on the superior labrum and supraglenoid tubercle after traveling through the bicipital groove.1 The many conditions that can develop along the course of the biceps tendon include overall biceps tendonitis, biceps tendon subluxation or instability, and injuries to the superior anterior to posterior area of the labrum.
These injuries can occur in young overhead athletes as well as manual laborers and older overhead recreational athletes. Pitching is the most common activity that leads to proximal biceps tendon disorders. The 6 phases of the pitch are linked in a kinetic chain that generates energy that is then translated to high velocity. The amount of force that is exerted on the shoulder during pitching and especially after ball release is impressive, and the athlete’s shoulder changes in many ways as it adapts to the motion.2-5 The late-cocking and deceleration phases are most commonly associated with proximal biceps pathology and the “peel-back” phenomenon. Other common activities that lead to biceps tendon issues in a young population are volleyball, baseball, tennis, softball, swimming, and cricket. Shoulder arthroscopies performed in older patients show degenerative biceps and labrum tears, which should be treated appropriately but perhaps different from how they are treated in overhead athletes.6-8 Further, many professional athletes have asymptomatic superior labrum anterior-posterior (SLAP) tears.9
Mechanism of Injury
Overhead throwing is commonly thought to be the mechanism by which lesions are created in the biceps–labrum complex (BLC). Pitching in particular generates incredible force and torque within the shoulder. In professional pitchers, the resulting throwing speed creates forces regularly in excess of 1000 N.3 These forces effect internal compensatory changes and internal derangement of the BLC. These changes often involve internal rotation deficits and alterations in the rotator cuff, which may contribute to glenohumeral instability and altered joint kinematics.10
Repetitive overhead activity is largely considered the mechanism of injury in this population, though more specific mechanisms have been described, including the peel-back mechanism11 and the posterior superior glenoid impingement. There is little evidence that preventive programs have any effect on decreasing the incidence of SLAP tears in overhead athletes.
Preoperative Evaluation
Preoperative evaluation is arguably the most important step in treating a patient with persistent or recurrent symptoms consistent with a SLAP tear. Evaluation includes thorough history, physical examination, and review of any prior injuries or surgical procedures. The physical examination should focus on maneuvers that define where the problem is occurring. Although SLAP tears are most common in this population, disorders of the biceps tendon within the groove, including inflammation and instability, should be ruled out with physical examination and advanced imaging. Palpation for groove tenderness, impingement-type complaints, internal rotation loss, and SLAP provocative testing are crucial in the diagnosis.12,13 The cause of symptoms may be multifactorial and include the often encountered concomitant pathology of rotator cuff tears, internal impingement, and instability.
Standard radiographs (Grashey anteroposterior, scapular/lateral, axillary lateral) and magnetic resonance imaging (MRI) with or without arthrography can be helpful in identifying and characterizing most SLAP tears as well as failed SLAP tear repairs. However, MRI is often positive for SLAP tears in asymptomatic patients, and diagnosing SLAP tears with MRI is often a challenge.14 MRI can help in determining concomitant pathology, including rotator cuff injury and cysts causing nerve compression. Correlation with clinical examination and patient history is most crucial. Conservative treatment (rest, activity modification, use of oral anti-inflammatory medications) typically is attempted and coordinated with respect to the athlete’s season of play.15,16
Classification
In overhead throwing athletes, SLAP tears typically are associated with anterior shoulder pain. Associated shoulder instability and significant glenohumeral dysfunction are not uncommon in athletes with lesions of the BLC. In 1985, Andrews and colleagues17 were the first to describe SLAP tears in overhead athletes (73 patients). Later, Snyder and colleagues18,19 further classified these lesions into 4 types based on tear stability and location, and they coined the acronym SLAP (Figure 1).
Type I lesions typically are described as fraying at the inner margin of the labrum and are common in throwers, even asymptomatic throwers. Type II lesions, separations of the biceps and labrum from the superior glenoid (≥5 mm of excursion), are the most commonly occurring and treated variant in throwing athletes.20-22 Intraoperative evaluation for a peel-back lesion (placing the arm in abduction with external rotation), rather than for a sulcus of 1 mm to 2 mm, may confirm a type II SLAP tear.20,23,24 It is often important to consider the direction of tear propagation as well. Type III lesions include those with an intact BLC (but with a bucket-handle tear of the superior labral complex and an intact biceps tendon), whereas type IV lesions involve additional extension of the tear into the biceps tendon.18,19The classification systems are well defined. Nevertheless, management of SLAP lesions remains controversial.
Options for Surgical Treatment
SLAP Tear Repair—Outcomes
The incidence of SLAP tear repairs has increased dramatically in recent years.6,25 There are various SLAP tear repair methods, but the most common consists of repairing the labrum and biceps anchor. Management of type II SLAP lesions remains controversial. Several prospective studies have found overall improvement after SLAP tear repair.26-31 Other series have reported less encouraging outcomes, including dissatisfaction with persistent pain and inability to return to throwing.28,32 A 2010 systematic review found that the percentage of patients who returned to their preinjury level of play was only 64%, and outcomes for overhead throwing athletes were even worse—only 22% to 60% of these patients returned to their previous level.33 The right surgery for SLAP tears in this population continues to be an area of uncertainty for many surgeons.
Failed SLAP tear repairs (poor outcomes) have become common in overhead throwing athletes. The reasons for these failed repairs are unclear, but several possible explanations have been offered. One is that labral repair may result in permanent alterations in pitching biomechanics, which may lead to an inability to regain velocity and command.3 Another is that the athlete’s shoulder may remain unstable even after repair.10Hardware complications are a significant concern in this high-level population. Suture anchor pullout or iatrogenic cartilage damage may occur during instrumentation or as a result of suture anchor reactive changes. In addition, there are several reports of glenoid osteochondrolysis (Figure 2) caused by prominent hardware or prominent knots.34-39
Stiffness after SLAP tear repair is a significant problem, with most patients taking up to 6 months to regain full motion.26,48 Overtensioning of the labrum and the glenohumeral ligaments may be the cause, and the solution may be to place anchors posterior (vs anterior) to the biceps insertion. In a large prospective military study, mean forward flexion and external rotation were reduced at final follow-up.31 These outcomes are less acceptable to overhead throwing athletes, who rely on motion for high-end throwing activities.
Primary Biceps Tenodesis—Outcomes
A 2015 database study found a 1.7-fold increase in biceps tenodesis over the preceding 5 years.49 However, relatively few procedures included in the study were performed in patients age younger than 30 years. For many older non-overhead throwers with type II tears, SLAP tear repair has become less popular as a treatment option.32 There is a dearth of knowledge about the outcomes of subpectoral biceps tenodesis as a primary treatment for biceps tendonitis and an associated SLAP tear. Although type I tears historically have been treated with débridement, débridement is seldom used for concomitant biceps tendonitis. It should be coupled with careful clinical examination.
In recent years, biceps tenodesis has been proposed as an alternative to repair for SLAP tears, particularly in older patients.24,44 For obvious reasons, however, there has been some trepidation about performing biceps tenodesis in throwing athletes. Some authors have proposed biceps tenodesis as primary treatment for isolated SLAP tears. Boileau and colleagues44 compared the outcomes of treatment of isolated type II SLAP lesions in 25 consecutive patients. For 10 patients, repair involved suture anchors; for the other 15, arthroscopic biceps tenodesis was performed with an absorbable interference screw. Six of the 10 suture anchor patients were disappointed with their outcome (persistent pain or inability to return to sport), whereas 14 of the 15 biceps tenodesis patients were satisfied. The authors concluded that arthroscopic biceps tenodesis is an effective alternative to repair for type II SLAP lesions, though their study was not isolated to overhead athletes (tenodesis group mean age, 52 years).
In a 2014 series of cases, Ek and colleagues50 reported good outcomes of SLAP tear repair and biceps tenodesis. Again, though, tenodesis was used in older patients, and repair in younger, more active patients, with no high-level athletes in either group. There was no difference in return to sport between groups. In a study of patients who underwent primary biceps tenodesis, Gupta and colleagues51 found 80% excellent outcomes (improved shoulder outcome scores) in select SLAP tear patients, including 8 athletes, 88% of whom were overhead athletes. Gottschalk and colleagues52 reported on differences in prospectively collected outcome data (age, sex, SLAP lesion type II or IV) for primary biceps tenodesis in a series of 33 patients. Twenty-six of the 29 patients who completed follow-up returned to their previous level of activity. These studies suggest that primary biceps tenodesis may be an alternative with lower failure rates in the treatment of SLAP tears in middle-aged patients, and in overhead athletes, though additional specific studies are needed to focus on overhead athletes on a larger scale.
Revision SLAP Tear Repair Versus Biceps Tenodesis
Failed arthroscopic SLAP tear repairs, which are increasingly common, present a unique treatment challenge. In a 2013 prospective cohort series, Gupta and colleagues46 found excellent clinical outcomes of subpectoral biceps tenodesis for failed type II SLAP tears. The authors reported a postoperative SANE (Single Assessment Numeric Evaluation) score of 70.4%, an SST (Simple Shoulder Test) score of 9.33, and an ASES (American Shoulder and Elbow Surgeons) score of 77.96, along with reasonable health-related quality-of-life scores. Werner and colleagues53 evaluated 2-year outcomes of biceps tenodesis performed after SLAP tear repair in 24 patients and found a return to almost normal range of motion as well as good clinical outcome scores. Significantly worse outcomes were found for patients with open worker’s compensation claims.
McCormick and colleagues26 prospectively evaluated the efficacy of biceps tenodesis for failed type II SLAP tear repair in 46 patients. Improvement was noted across all outcome assessments during follow-up (mean, 3.6 years). From these findings, we might conclude that biceps tenodesis is a more predictable option for failed SLAP tear repair, and that it has a relatively low complication rate. However, most investigators have used a heterogeneous patient population, as opposed to overhead athletes specifically. To our knowledge, no one has evaluated the specific population of overhead throwers with failed SLAP tear repairs. In addition, no one has conducted randomized controlled trials comparing débridement, biceps tenodesis, and repair for failed SLAP tear repairs.
Postoperative Considerations
When overhead athletes and their surgeons are considering surgical options, they must take rehabilitation and return to play into account. Many surgeons think the possible marginal clinical benefit of SLAP tear repair may not be worth the protracted rehabilitation. In most practices, rehabilitation after biceps tenodesis is less involved. Discussing the advantages and disadvantages of these 2 procedures can be helpful in decision making.
Dein and colleagues54 reported the case of a middle-aged pitcher who sustained a fracture after biceps tenodesis with an interference screw. Cases like this are concerning. Surgeons should consider altering the rehabilitation regimen when planning postoperative care in cases of biceps tenodesis in throwers. Other reported complications of open tenodesis are deep infection, thrombosis, postoperative stiffness, and nerve injury.55-58
Consequences for Overhead Throwers
The unknown role of the BLC leaves surgeons wary when considering biceps tenodesis for elite athletes. Some have postulated that removing the intra-articular portion of the LHB may cause microinstability and alter joint kinematics.10,59-61 Others have suggested the biceps is desynchronized from the other musculature and is not functionally important.62 Disruption of one portion of the superior labrum may result in instability on the opposite side of the glenoid.10,61 Biomechanical studies, both cadaveric and in vivo, have tried to create proper loads to the LHB and evaluate the kinematics of the shoulder before and after biceps tenodesis and SLAP tear repair.59,60 Using a cadaveric model, Strauss and colleagues63 found that type II SLAP lesions resulted in increased glenohumeral translation compared with baseline. Biceps tenodesis did not restore normal translation, but this did not negatively affect stability in the presence of a SLAP lesion. The consensus is that the role of the biceps is controversial at best.
Several studies have used electromyography (EMG) to evaluate LHB functioning. In 2014, Chalmers and colleagues59 used surface EMG and motion analysis to evaluate 18 pitchers: 6 underwent SLAP tear repair, 5 underwent biceps tenodesis, and 7 were uninjured controls. There were no significant differences in the activity of the LHB muscle, the short head of the biceps muscle, the deltoid, the infraspinatus, or the latissimus among the 3 groups. Motion analysis showed that the normal pattern of muscular activation within the LHB muscle was more closely restored by biceps tenodesis than by SLAP tear repair. In addition, thoracic rotation patterns were significantly more altered in the SLAP tear repair patients than in the uninjured controls. As the authors noted, given the low frequency with which biceps tenodesis is performed in overhead athletes, it is unlikely that larger scale studies will be conducted without a multicenter effort.
Recommendations and Our Preferred Technique
Which surgical option is best for treating symptomatic SLAP lesions in overhead athletes remains unclear. Many athletes struggle to return to high-level play after SLAP tear repair. Whether the same is true after biceps tenodesis is yet to be determined because of the low frequency with which biceps tenodesis is performed in high-level overhead athletes. The options for fixation, technique, and fixation location are equally broad. In this section, we outline our general line of thinking for cases of proximal biceps pathology.
In each case, we perform glenohumeral arthroscopy to evaluate the BLC and identify any other pathology. For overhead athletes who are younger than 30 years and lack bicipital groove pain or signs of gross tendinopathy, we favor arthroscopic SLAP tear repair. Repair is usually performed through an anterior working portal for suture passage and a Wilmington portal for anchor placement. We use knotless technology to achieve stable fixation and stay posterior to the biceps anchor insertion.
For the prevention of any potential pain from the bicipital groove in carefully selected patients—recreational overhead athletes and patients who want a less involved surgical recovery—we favor open subpectoral biceps tenodesis rather than arthroscopic tenodesis. The outcomes of biceps tenodesis are consistent, according to the literature.47,57,64 Moreover, the open approach is favored for the incidence of postoperative stiffness in the arthroscopic population.65 Tendons can be fixed with multiple procedures, including soft-tissue tenodesis, interference screw fixation, and surface anchors. We favor using a tenodesis screw in the subpectoral location, as outlined by Mazzocca and colleagues.64Our algorithm for SLAP lesions is evolving with our understanding of this complex disease process. For young overhead throwers with type II SLAP lesions, we favor arthroscopic SLAP tear repair with knotless technology. For older recreational overhead athletes, we favor biceps tenodesis in the subpectoral region after diagnostic arthroscopy plus biceps tenotomy with or without additional SLAP tear fixation, depending on the stability of the biceps anchor (Figures 4A, 4B).
Conclusion
Overhead athletes who present with symptomatic SLAP lesions often provide a treatment dilemma. Although SLAP tear repair historically has been standard treatment, biceps tenodesis represents a consistent surgical option with low complication rates and low revision rates. It is likely that, as additional data on glenohumeral kinematics and outcomes in young athletes become available, improved decision-making algorithms will follow.
Am J Orthop. 2017;46(1):E71-E78. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
Take Home Points
- Outcomes after SLAP repair remain guarded.
- Physical examination is key in determining proper management of biceps pathology.
- When performing SLAP repair, knotless technology may prevent future cartilage or rotator cuff injury.
- Revision of SLAP repair is best handled with biceps tenodesis.
- Subpectoral biceps tenodesis avoids residual groove pain.
In recent decades, the long head of the biceps (LHB) tendon has been recognized as a pain generator in the shoulder of throwing athletes. The LHB muscle and its role in glenohumeral kinematics remains largely in question. The LHB tendon varies in size but most commonly is 5 mm to 6mm in diameter and about 9 cm in length, inserting on the superior labrum and supraglenoid tubercle after traveling through the bicipital groove.1 The many conditions that can develop along the course of the biceps tendon include overall biceps tendonitis, biceps tendon subluxation or instability, and injuries to the superior anterior to posterior area of the labrum.
These injuries can occur in young overhead athletes as well as manual laborers and older overhead recreational athletes. Pitching is the most common activity that leads to proximal biceps tendon disorders. The 6 phases of the pitch are linked in a kinetic chain that generates energy that is then translated to high velocity. The amount of force that is exerted on the shoulder during pitching and especially after ball release is impressive, and the athlete’s shoulder changes in many ways as it adapts to the motion.2-5 The late-cocking and deceleration phases are most commonly associated with proximal biceps pathology and the “peel-back” phenomenon. Other common activities that lead to biceps tendon issues in a young population are volleyball, baseball, tennis, softball, swimming, and cricket. Shoulder arthroscopies performed in older patients show degenerative biceps and labrum tears, which should be treated appropriately but perhaps different from how they are treated in overhead athletes.6-8 Further, many professional athletes have asymptomatic superior labrum anterior-posterior (SLAP) tears.9
Mechanism of Injury
Overhead throwing is commonly thought to be the mechanism by which lesions are created in the biceps–labrum complex (BLC). Pitching in particular generates incredible force and torque within the shoulder. In professional pitchers, the resulting throwing speed creates forces regularly in excess of 1000 N.3 These forces effect internal compensatory changes and internal derangement of the BLC. These changes often involve internal rotation deficits and alterations in the rotator cuff, which may contribute to glenohumeral instability and altered joint kinematics.10
Repetitive overhead activity is largely considered the mechanism of injury in this population, though more specific mechanisms have been described, including the peel-back mechanism11 and the posterior superior glenoid impingement. There is little evidence that preventive programs have any effect on decreasing the incidence of SLAP tears in overhead athletes.
Preoperative Evaluation
Preoperative evaluation is arguably the most important step in treating a patient with persistent or recurrent symptoms consistent with a SLAP tear. Evaluation includes thorough history, physical examination, and review of any prior injuries or surgical procedures. The physical examination should focus on maneuvers that define where the problem is occurring. Although SLAP tears are most common in this population, disorders of the biceps tendon within the groove, including inflammation and instability, should be ruled out with physical examination and advanced imaging. Palpation for groove tenderness, impingement-type complaints, internal rotation loss, and SLAP provocative testing are crucial in the diagnosis.12,13 The cause of symptoms may be multifactorial and include the often encountered concomitant pathology of rotator cuff tears, internal impingement, and instability.
Standard radiographs (Grashey anteroposterior, scapular/lateral, axillary lateral) and magnetic resonance imaging (MRI) with or without arthrography can be helpful in identifying and characterizing most SLAP tears as well as failed SLAP tear repairs. However, MRI is often positive for SLAP tears in asymptomatic patients, and diagnosing SLAP tears with MRI is often a challenge.14 MRI can help in determining concomitant pathology, including rotator cuff injury and cysts causing nerve compression. Correlation with clinical examination and patient history is most crucial. Conservative treatment (rest, activity modification, use of oral anti-inflammatory medications) typically is attempted and coordinated with respect to the athlete’s season of play.15,16
Classification
In overhead throwing athletes, SLAP tears typically are associated with anterior shoulder pain. Associated shoulder instability and significant glenohumeral dysfunction are not uncommon in athletes with lesions of the BLC. In 1985, Andrews and colleagues17 were the first to describe SLAP tears in overhead athletes (73 patients). Later, Snyder and colleagues18,19 further classified these lesions into 4 types based on tear stability and location, and they coined the acronym SLAP (Figure 1).
Type I lesions typically are described as fraying at the inner margin of the labrum and are common in throwers, even asymptomatic throwers. Type II lesions, separations of the biceps and labrum from the superior glenoid (≥5 mm of excursion), are the most commonly occurring and treated variant in throwing athletes.20-22 Intraoperative evaluation for a peel-back lesion (placing the arm in abduction with external rotation), rather than for a sulcus of 1 mm to 2 mm, may confirm a type II SLAP tear.20,23,24 It is often important to consider the direction of tear propagation as well. Type III lesions include those with an intact BLC (but with a bucket-handle tear of the superior labral complex and an intact biceps tendon), whereas type IV lesions involve additional extension of the tear into the biceps tendon.18,19The classification systems are well defined. Nevertheless, management of SLAP lesions remains controversial.
Options for Surgical Treatment
SLAP Tear Repair—Outcomes
The incidence of SLAP tear repairs has increased dramatically in recent years.6,25 There are various SLAP tear repair methods, but the most common consists of repairing the labrum and biceps anchor. Management of type II SLAP lesions remains controversial. Several prospective studies have found overall improvement after SLAP tear repair.26-31 Other series have reported less encouraging outcomes, including dissatisfaction with persistent pain and inability to return to throwing.28,32 A 2010 systematic review found that the percentage of patients who returned to their preinjury level of play was only 64%, and outcomes for overhead throwing athletes were even worse—only 22% to 60% of these patients returned to their previous level.33 The right surgery for SLAP tears in this population continues to be an area of uncertainty for many surgeons.
Failed SLAP tear repairs (poor outcomes) have become common in overhead throwing athletes. The reasons for these failed repairs are unclear, but several possible explanations have been offered. One is that labral repair may result in permanent alterations in pitching biomechanics, which may lead to an inability to regain velocity and command.3 Another is that the athlete’s shoulder may remain unstable even after repair.10Hardware complications are a significant concern in this high-level population. Suture anchor pullout or iatrogenic cartilage damage may occur during instrumentation or as a result of suture anchor reactive changes. In addition, there are several reports of glenoid osteochondrolysis (Figure 2) caused by prominent hardware or prominent knots.34-39
Stiffness after SLAP tear repair is a significant problem, with most patients taking up to 6 months to regain full motion.26,48 Overtensioning of the labrum and the glenohumeral ligaments may be the cause, and the solution may be to place anchors posterior (vs anterior) to the biceps insertion. In a large prospective military study, mean forward flexion and external rotation were reduced at final follow-up.31 These outcomes are less acceptable to overhead throwing athletes, who rely on motion for high-end throwing activities.
Primary Biceps Tenodesis—Outcomes
A 2015 database study found a 1.7-fold increase in biceps tenodesis over the preceding 5 years.49 However, relatively few procedures included in the study were performed in patients age younger than 30 years. For many older non-overhead throwers with type II tears, SLAP tear repair has become less popular as a treatment option.32 There is a dearth of knowledge about the outcomes of subpectoral biceps tenodesis as a primary treatment for biceps tendonitis and an associated SLAP tear. Although type I tears historically have been treated with débridement, débridement is seldom used for concomitant biceps tendonitis. It should be coupled with careful clinical examination.
In recent years, biceps tenodesis has been proposed as an alternative to repair for SLAP tears, particularly in older patients.24,44 For obvious reasons, however, there has been some trepidation about performing biceps tenodesis in throwing athletes. Some authors have proposed biceps tenodesis as primary treatment for isolated SLAP tears. Boileau and colleagues44 compared the outcomes of treatment of isolated type II SLAP lesions in 25 consecutive patients. For 10 patients, repair involved suture anchors; for the other 15, arthroscopic biceps tenodesis was performed with an absorbable interference screw. Six of the 10 suture anchor patients were disappointed with their outcome (persistent pain or inability to return to sport), whereas 14 of the 15 biceps tenodesis patients were satisfied. The authors concluded that arthroscopic biceps tenodesis is an effective alternative to repair for type II SLAP lesions, though their study was not isolated to overhead athletes (tenodesis group mean age, 52 years).
In a 2014 series of cases, Ek and colleagues50 reported good outcomes of SLAP tear repair and biceps tenodesis. Again, though, tenodesis was used in older patients, and repair in younger, more active patients, with no high-level athletes in either group. There was no difference in return to sport between groups. In a study of patients who underwent primary biceps tenodesis, Gupta and colleagues51 found 80% excellent outcomes (improved shoulder outcome scores) in select SLAP tear patients, including 8 athletes, 88% of whom were overhead athletes. Gottschalk and colleagues52 reported on differences in prospectively collected outcome data (age, sex, SLAP lesion type II or IV) for primary biceps tenodesis in a series of 33 patients. Twenty-six of the 29 patients who completed follow-up returned to their previous level of activity. These studies suggest that primary biceps tenodesis may be an alternative with lower failure rates in the treatment of SLAP tears in middle-aged patients, and in overhead athletes, though additional specific studies are needed to focus on overhead athletes on a larger scale.
Revision SLAP Tear Repair Versus Biceps Tenodesis
Failed arthroscopic SLAP tear repairs, which are increasingly common, present a unique treatment challenge. In a 2013 prospective cohort series, Gupta and colleagues46 found excellent clinical outcomes of subpectoral biceps tenodesis for failed type II SLAP tears. The authors reported a postoperative SANE (Single Assessment Numeric Evaluation) score of 70.4%, an SST (Simple Shoulder Test) score of 9.33, and an ASES (American Shoulder and Elbow Surgeons) score of 77.96, along with reasonable health-related quality-of-life scores. Werner and colleagues53 evaluated 2-year outcomes of biceps tenodesis performed after SLAP tear repair in 24 patients and found a return to almost normal range of motion as well as good clinical outcome scores. Significantly worse outcomes were found for patients with open worker’s compensation claims.
McCormick and colleagues26 prospectively evaluated the efficacy of biceps tenodesis for failed type II SLAP tear repair in 46 patients. Improvement was noted across all outcome assessments during follow-up (mean, 3.6 years). From these findings, we might conclude that biceps tenodesis is a more predictable option for failed SLAP tear repair, and that it has a relatively low complication rate. However, most investigators have used a heterogeneous patient population, as opposed to overhead athletes specifically. To our knowledge, no one has evaluated the specific population of overhead throwers with failed SLAP tear repairs. In addition, no one has conducted randomized controlled trials comparing débridement, biceps tenodesis, and repair for failed SLAP tear repairs.
Postoperative Considerations
When overhead athletes and their surgeons are considering surgical options, they must take rehabilitation and return to play into account. Many surgeons think the possible marginal clinical benefit of SLAP tear repair may not be worth the protracted rehabilitation. In most practices, rehabilitation after biceps tenodesis is less involved. Discussing the advantages and disadvantages of these 2 procedures can be helpful in decision making.
Dein and colleagues54 reported the case of a middle-aged pitcher who sustained a fracture after biceps tenodesis with an interference screw. Cases like this are concerning. Surgeons should consider altering the rehabilitation regimen when planning postoperative care in cases of biceps tenodesis in throwers. Other reported complications of open tenodesis are deep infection, thrombosis, postoperative stiffness, and nerve injury.55-58
Consequences for Overhead Throwers
The unknown role of the BLC leaves surgeons wary when considering biceps tenodesis for elite athletes. Some have postulated that removing the intra-articular portion of the LHB may cause microinstability and alter joint kinematics.10,59-61 Others have suggested the biceps is desynchronized from the other musculature and is not functionally important.62 Disruption of one portion of the superior labrum may result in instability on the opposite side of the glenoid.10,61 Biomechanical studies, both cadaveric and in vivo, have tried to create proper loads to the LHB and evaluate the kinematics of the shoulder before and after biceps tenodesis and SLAP tear repair.59,60 Using a cadaveric model, Strauss and colleagues63 found that type II SLAP lesions resulted in increased glenohumeral translation compared with baseline. Biceps tenodesis did not restore normal translation, but this did not negatively affect stability in the presence of a SLAP lesion. The consensus is that the role of the biceps is controversial at best.
Several studies have used electromyography (EMG) to evaluate LHB functioning. In 2014, Chalmers and colleagues59 used surface EMG and motion analysis to evaluate 18 pitchers: 6 underwent SLAP tear repair, 5 underwent biceps tenodesis, and 7 were uninjured controls. There were no significant differences in the activity of the LHB muscle, the short head of the biceps muscle, the deltoid, the infraspinatus, or the latissimus among the 3 groups. Motion analysis showed that the normal pattern of muscular activation within the LHB muscle was more closely restored by biceps tenodesis than by SLAP tear repair. In addition, thoracic rotation patterns were significantly more altered in the SLAP tear repair patients than in the uninjured controls. As the authors noted, given the low frequency with which biceps tenodesis is performed in overhead athletes, it is unlikely that larger scale studies will be conducted without a multicenter effort.
Recommendations and Our Preferred Technique
Which surgical option is best for treating symptomatic SLAP lesions in overhead athletes remains unclear. Many athletes struggle to return to high-level play after SLAP tear repair. Whether the same is true after biceps tenodesis is yet to be determined because of the low frequency with which biceps tenodesis is performed in high-level overhead athletes. The options for fixation, technique, and fixation location are equally broad. In this section, we outline our general line of thinking for cases of proximal biceps pathology.
In each case, we perform glenohumeral arthroscopy to evaluate the BLC and identify any other pathology. For overhead athletes who are younger than 30 years and lack bicipital groove pain or signs of gross tendinopathy, we favor arthroscopic SLAP tear repair. Repair is usually performed through an anterior working portal for suture passage and a Wilmington portal for anchor placement. We use knotless technology to achieve stable fixation and stay posterior to the biceps anchor insertion.
For the prevention of any potential pain from the bicipital groove in carefully selected patients—recreational overhead athletes and patients who want a less involved surgical recovery—we favor open subpectoral biceps tenodesis rather than arthroscopic tenodesis. The outcomes of biceps tenodesis are consistent, according to the literature.47,57,64 Moreover, the open approach is favored for the incidence of postoperative stiffness in the arthroscopic population.65 Tendons can be fixed with multiple procedures, including soft-tissue tenodesis, interference screw fixation, and surface anchors. We favor using a tenodesis screw in the subpectoral location, as outlined by Mazzocca and colleagues.64Our algorithm for SLAP lesions is evolving with our understanding of this complex disease process. For young overhead throwers with type II SLAP lesions, we favor arthroscopic SLAP tear repair with knotless technology. For older recreational overhead athletes, we favor biceps tenodesis in the subpectoral region after diagnostic arthroscopy plus biceps tenotomy with or without additional SLAP tear fixation, depending on the stability of the biceps anchor (Figures 4A, 4B).
Conclusion
Overhead athletes who present with symptomatic SLAP lesions often provide a treatment dilemma. Although SLAP tear repair historically has been standard treatment, biceps tenodesis represents a consistent surgical option with low complication rates and low revision rates. It is likely that, as additional data on glenohumeral kinematics and outcomes in young athletes become available, improved decision-making algorithms will follow.
Am J Orthop. 2017;46(1):E71-E78. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Elser F, Braun S, Dewing CB, Giphart JE, Millett PJ. Anatomy, function, injuries, and treatment of the long head of the biceps brachii tendon. Arthroscopy. 2011;27(4):581-592.
2. Fedoriw WW, Ramkumar P, McCulloch PC, Lintner DM. Return to play after treatment of superior labral tears in professional baseball players. Am J Sports Med. 2014;42(5):1155-1160.
3. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23(2):233-239.
4. Aydin N, Sirin E, Arya A. Superior labrum anterior to posterior lesions of the shoulder: diagnosis and arthroscopic management. World J Orthop. 2014;5(3):344-350.
5. Barber A, Field LD, Ryu R. Biceps tendon and superior labrum injuries: decision-marking. J Bone Joint Surg Am. 2007;89(8):1844-1855.
6. Onyekwelu I, Khatib O, Zuckerman JD, Rokito AS, Kwon YW. The rising incidence of arthroscopic superior labrum anterior and posterior (SLAP) repairs. J Shoulder Elbow Surg. 2012;21(6):728-731.
7. Patterson BM, Creighton RA, Spang JT, Roberson JR, Kamath GV. Surgical trends in the treatment of superior labrum anterior and posterior lesions of the shoulder: analysis of data from the American Board of Orthopaedic Surgery Certification Examination Database. Am J Sports Med. 2014;42(8):1904-1910.
8. Walton DM, Sadi J. Identifying SLAP lesions: a meta-analysis of clinical tests and exercise in clinical reasoning. Phys Ther Sport. 2008;9(4):167-176.
9. Lesniak BP, Baraga MG, Jose J, Smith MK, Cunningham S, Kaplan LD. Glenohumeral findings on magnetic resonance imaging correlate with innings pitched in asymptomatic pitchers. Am J Sports Med. 2013;41(9):2022-2027.
10. Mihata T, McGarry MH, Tibone JE, Fitzpatrick MJ, Kinoshita M, Lee TQ. Biomechanical assessment of type II superior labral anterior-posterior (SLAP) lesions associated with anterior shoulder capsular laxity as seen in throwers: a cadaveric study. Am J Sports Med. 2008;36(8):1604-1610.
11. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part II: evaluation and treatment of SLAP lesions in throwers. Arthroscopy. 2003;19(5):531-539.
12. Meserve BB, Cleland JA, Boucher TR. A meta-analysis examining clinical test utility for assessing superior labral anterior posterior lesions. Am J Sports Med. 2009;37(11):2252-2258.
13. Pandya NK, Colton A, Webner D, Sennett B, Huffman GR. Physical examination and magnetic resonance imaging in the diagnosis of superior labrum anterior-posterior lesions of the shoulder: a sensitivity analysis. Arthroscopy. 2008;24(3):311-317.
14. Amin MF, Youssef AO. The diagnostic value of magnetic resonance arthrography of the shoulder in detection and grading of SLAP lesions: comparison with arthroscopic findings. Eur J Radiol. 2012;81(9):2343-2347.
15. Cook C, Beaty S, Kissenberth MJ, Siffri P, Pill SG, Hawkins RJ. Diagnostic accuracy of five orthopedic clinical tests for diagnosis of superior labrum anterior posterior (SLAP) lesions. J Shoulder Elbow Surg. 2012;21(1):13-22.
16. Edwards SL, Lee JA, Bell JE, et al. Nonoperative treatment of superior labrum anterior posterior tears: improvements in pain, function, and quality of life. Am J Sports Med. 2010;38(7):1456-1461.
17. Andrews JR, Carson WG Jr, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985;13(5):337-341.
18. Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990;6(4):274-279.
19. Snyder SJ, Banas MP, Karzel RP. An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg. 1995;4(4):243-248.
20. Morgan CD, Burkhart SS, Palmeri M, Gillespie M. Type II SLAP lesions: three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy. 1998;14(6):553-565.
21. Weber SC, Martin DF, Seiler JG 3rd, Harrast JJ. Superior labrum anterior and posterior lesions of the shoulder: incidence rates, complications, and outcomes as reported by American Board of Orthopedic Surgery. Part II candidates. Am J Sports Med. 2012;40(7):1538-1543.
22. Keener JD, Brophy RH. Superior labral tears of the shoulder: pathogenesis, evaluation, and treatment. J Am Acad Orthop Surg. 2009;17(10):627-637.
23. Chen CH, Hsu KY, Chen WJ, Shih CH. Incidence and severity of biceps long head tendon lesion in patients with complete rotator cuff tears. J Trauma. 2005;58(6):1189-1193.
24. Nho SJ, Strauss EJ, Lenart BA, et al. Long head of the biceps tendinopathy: diagnosis and management. J Am Acad Orthop Surg. 2010;18(11):645-656.
25. Zhang AL, Kreulen C, Ngo SS, Hame SL, Wang JC, Gamradt SC. Demographic trends in arthroscopic SLAP repair in the United States. Am J Sports Med. 2012;40(5):1144-1147.
26. McCormick F, Bhatia S, Chalmers P, Gupta A, Verma N, Romeo AA. The management of type II superior labral anterior to posterior injuries. Orthop Clin North Am. 2014;45(1):121-128.
27. Brockmeier SF, Voos JE, Williams RJ 3rd, Altchek DW, Cordasco FA, Allen AA; Hospital for Special Surgery Sports Medicine and Shoulder Service. Outcomes after arthroscopic repair of type-II SLAP lesions. J Bone Joint Surg Am. 2009;91(7):1595-1603.
28. Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009;37(5):929-936.
29. Denard PJ, Lädermann A, Burkhart SS. Long-term outcome after arthroscopic repair of type II SLAP lesions: results according to age and workers’ compensation status. Arthroscopy. 2012;28(4):451-457.
30. Friel NA, Karas V, Slabaugh MA, Cole BJ. Outcomes of type II superior labrum, anterior to posterior (SLAP) repair: prospective evaluation at a minimum two-year follow-up. J Shoulder Elbow Surg. 2010;19(6):859-867.
31. Provencher MT, McCormick F, Dewing C, McIntire S, Solomon D. A prospective analysis of 179 type 2 superior labrum anterior and posterior repairs: outcomes and factors associated with success and failure. Am J Sports Med. 2013;41(4):880-886.
32. Gupta AK, Chalmers PN, Klosterman EL, et al. Subpectoral biceps tenodesis for bicipital tendonitis with SLAP tear. Orthopedics. 2015;38(1):e48-e53.
33. Gorantla K, Gill C, Wright RW. The outcome of type II SLAP repair: a systematic review. Arthroscopy. 2010;26(4):537-545.
34. Katz LM, Hsu S, Miller SL, et al. Poor outcomes after SLAP repair: descriptive analysis and prognosis. Arthroscopy. 2009;25(8):849-855.
35. Park MJ, Hsu JE, Harper C, Sennett BJ, Huffman GR. Poly-L/D-lactic acid anchors are associated with reoperation and failure of SLAP repairs. Arthroscopy. 2011;27(10):1335-1340.
36. Sassmannshausen G, Sukay M, Mair SD. Broken or dislodged poly-L-lactic acid bioabsorbable tacks in patients after SLAP lesion surgery. Arthroscopy. 2006;22(6):615-619.
37. Uggen C, Wei A, Glousman RE, et al. Biomechanical comparison of knotless anchor repair versus simple suture repair for type II SLAP lesions. Arthroscopy. 2009;25(10):1085-1092.
38. Weber SC. Surgical management of the failed SLAP repair. Sports Med Arthrosc. 2010;18(3):162-166.
39. Wilkerson JP, Zvijac JE, Uribe JW, Schürhoff MR, Green JB. Failure of polymerized lactic acid tacks in shoulder surgery. J Shoulder Elbow Surg. 2003;12(2):117-121.
40. Weber S. Surgical management of the failed SLAP lesion. Arthroscopy. 2008;24(suppl):e8-e9.
41. Schrøder CP, Skare O, Gjengedal E, Uppheim G, Reikerås O, Brox JI. Long-term results after SLAP repair: a 5-year follow-up study of 107 patients with comparison of patients aged over and under 40 years. Arthroscopy. 2012;28(11):1601-1607.
42. Mazzocca AD, Cote MP, Arciero CL, Romeo AA, Arciero RA. Clinical outcomes after subpectoral biceps tenodesis with an interference screw. Am J Sports Med. 2008;36(10):1922-1929.
43. Mazzocca AD, McCarthy MB, Ledgard FA, et al. Histomorphologic changes of the long head of the biceps tendon in common shoulder pathologies. Arthroscopy. 2013;29(6):972-981.
44. Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009;37(5):929-936.
45. Boileau P, Krishnan SG, Coste JS, Walch G. Arthroscopic biceps tenodesis: a new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002;18(9):1002-1012.
46. Gupta AK, Bruce B, Klosterman EL, McCormick F, Harris J, Romeo AA. Subpectoral biceps tenodesis for failed type II SLAP repair. Orthopedics. 2013;36(6):e723-e728.
47. Provencher MT, LeClere LE, Romeo AA. Subpectoral biceps tenodesis. Sports Med Arthrosc. 2008;16(3):170-176.
48. McCarty LP 3rd, Buss DD, Datta MW, Freehill MQ, Giveans MR. Complications observed following labral or rotator cuff repair with use of poly-L-lactic acid implants. J Bone Joint Surg Am. 2013;95(6):507-511.
49. Werner BC, Brockmeier SF, Gwathmey FW. Trends in long head biceps tenodesis. Am J Sports Med. 2015;43(3):570-578.
50. Ek ET, Shi LL, Tompson JD, Freehill MT, Warner JJ. Surgical treatment of isolated type II superior labrum anterior-posterior (SLAP) lesions: repair versus biceps tenodesis. J Shoulder Elbow Surg. 2014;23(7):1059-1065.
51. Gupta AK, Chalmers PN, Klosterman EL, et al. Subpectoral biceps tenodesis for bicipital tendonitis with SLAP tear. Orthopedics. 2015;38(1):e48-e53.
52. Gottschalk MB, Karas SG, Ghattas TN, Burdette R. Subpectoral biceps tenodesis for the treatment of type II and IV superior labral anterior and posterior lesions. Am J Sports Med. 2014;42(9):2128-2135.
53. Werner BC, Pehlivan HC, Hart JM, et al. Biceps tenodesis is a viable option for salvage of failed SLAP repair. J Shoulder Elbow Surg. 2014;23(8):e179-e184.
54. Dein EJ, Huri G, Gordon JC, McFarland EG. A humerus fracture in a baseball pitcher after biceps tenodesis [published correction appears in Am J Sports Med. 2014;42(6):NP39]. Am J Sports Med. 2014;42(4):877-879.
55. Nho SJ, Reiff SN, Verma NN, Slabaugh MA, Mazzocca AD, Romeo AA. Complications associated with subpectoral biceps tenodesis: low rates of incidence following surgery. J Shoulder Elbow Surg. 2010;19(5):764-768.
56. Osbahr DC, Diamond AB, Speer KP. The cosmetic appearance of the biceps muscle after long-head tenotomy versus tenodesis. Arthroscopy. 2002;18(5):483-487.
57. Romeo AA, Mazzocca AD, Tauro JC. Arthroscopic biceps tenodesis. Arthroscopy. 2004;20(2):206-213.
58. Ma H, Van Heest A, Glisson C, Patel S. Musculocutaneous nerve entrapment: an unusual complication after biceps tenodesis. Am J Sports Med. 2009;37(12):2467-2469.
59. Chalmers PN, Trombley R, Cip J, et al. Postoperative restoration of upper extremity motion and neuromuscular control during the overhand pitch: evaluation of tenodesis and repair for superior labral anterior-posterior tears. Am J Sports Med. 2014;42(12):2825-2836.
60. Giphart JE, Elser F, Dewing CB, Torry MR, Millett PJ. The long head of the biceps tendon has minimal effect on in vivo glenohumeral kinematics: a biplane fluoroscopy study. Am J Sports Med. 2012;40(1):202-212.
61. Grossman MG, Tibone JE, McGarry MH, Schneider DJ, Veneziani S, Lee TQ. A cadaveric model of the throwing shoulder: a possible etiology of superior labrum anterior-to-posterior lesions. J Bone Joint Surg Am. 2005;87(4):824-831.
62. Hawkes DH, Alizadehkhaiyat O, Fisher AC, Kemp GJ, Roebuck MM, Frostick SP. Normal shoulder muscular activation and co-ordination during a shoulder elevation task based on activities of daily living: an electromyographic study. J Orthop Res. 2012;30(1):53-60.
63. Strauss EJ, Salata MJ, Sershon RA, et al. Role of the superior labrum after biceps tenodesis in glenohumeral stability. J Shoulder Elbow Surg. 2014;23(4):485-491.
64. Mazzocca AD, Bicos J, Santangelo S, Romeo AA, Arciero RA. The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis. Arthroscopy. 2005;21(11):1296-1306.
65. Werner BC, Pehlivan HC, Hart JM, et al. Increased incidence of postoperative stiffness after arthroscopic compared with open biceps tenodesis. Arthroscopy. 2014;30(9):1075-1084.
66. Denard PJ, Dai X, Hanypsiak BT, Burkhart SS. Anatomy of the biceps tendon: implications for restoring physiological length–tension relation during biceps tenodesis with interference screw fixation. Arthroscopy. 2012;28(10):1352-1358.
67. Mazzocca AD, Rios CG, Romeo AA, Arciero RA. Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy. 2005;21(7):896.
1. Elser F, Braun S, Dewing CB, Giphart JE, Millett PJ. Anatomy, function, injuries, and treatment of the long head of the biceps brachii tendon. Arthroscopy. 2011;27(4):581-592.
2. Fedoriw WW, Ramkumar P, McCulloch PC, Lintner DM. Return to play after treatment of superior labral tears in professional baseball players. Am J Sports Med. 2014;42(5):1155-1160.
3. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23(2):233-239.
4. Aydin N, Sirin E, Arya A. Superior labrum anterior to posterior lesions of the shoulder: diagnosis and arthroscopic management. World J Orthop. 2014;5(3):344-350.
5. Barber A, Field LD, Ryu R. Biceps tendon and superior labrum injuries: decision-marking. J Bone Joint Surg Am. 2007;89(8):1844-1855.
6. Onyekwelu I, Khatib O, Zuckerman JD, Rokito AS, Kwon YW. The rising incidence of arthroscopic superior labrum anterior and posterior (SLAP) repairs. J Shoulder Elbow Surg. 2012;21(6):728-731.
7. Patterson BM, Creighton RA, Spang JT, Roberson JR, Kamath GV. Surgical trends in the treatment of superior labrum anterior and posterior lesions of the shoulder: analysis of data from the American Board of Orthopaedic Surgery Certification Examination Database. Am J Sports Med. 2014;42(8):1904-1910.
8. Walton DM, Sadi J. Identifying SLAP lesions: a meta-analysis of clinical tests and exercise in clinical reasoning. Phys Ther Sport. 2008;9(4):167-176.
9. Lesniak BP, Baraga MG, Jose J, Smith MK, Cunningham S, Kaplan LD. Glenohumeral findings on magnetic resonance imaging correlate with innings pitched in asymptomatic pitchers. Am J Sports Med. 2013;41(9):2022-2027.
10. Mihata T, McGarry MH, Tibone JE, Fitzpatrick MJ, Kinoshita M, Lee TQ. Biomechanical assessment of type II superior labral anterior-posterior (SLAP) lesions associated with anterior shoulder capsular laxity as seen in throwers: a cadaveric study. Am J Sports Med. 2008;36(8):1604-1610.
11. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part II: evaluation and treatment of SLAP lesions in throwers. Arthroscopy. 2003;19(5):531-539.
12. Meserve BB, Cleland JA, Boucher TR. A meta-analysis examining clinical test utility for assessing superior labral anterior posterior lesions. Am J Sports Med. 2009;37(11):2252-2258.
13. Pandya NK, Colton A, Webner D, Sennett B, Huffman GR. Physical examination and magnetic resonance imaging in the diagnosis of superior labrum anterior-posterior lesions of the shoulder: a sensitivity analysis. Arthroscopy. 2008;24(3):311-317.
14. Amin MF, Youssef AO. The diagnostic value of magnetic resonance arthrography of the shoulder in detection and grading of SLAP lesions: comparison with arthroscopic findings. Eur J Radiol. 2012;81(9):2343-2347.
15. Cook C, Beaty S, Kissenberth MJ, Siffri P, Pill SG, Hawkins RJ. Diagnostic accuracy of five orthopedic clinical tests for diagnosis of superior labrum anterior posterior (SLAP) lesions. J Shoulder Elbow Surg. 2012;21(1):13-22.
16. Edwards SL, Lee JA, Bell JE, et al. Nonoperative treatment of superior labrum anterior posterior tears: improvements in pain, function, and quality of life. Am J Sports Med. 2010;38(7):1456-1461.
17. Andrews JR, Carson WG Jr, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985;13(5):337-341.
18. Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990;6(4):274-279.
19. Snyder SJ, Banas MP, Karzel RP. An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg. 1995;4(4):243-248.
20. Morgan CD, Burkhart SS, Palmeri M, Gillespie M. Type II SLAP lesions: three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy. 1998;14(6):553-565.
21. Weber SC, Martin DF, Seiler JG 3rd, Harrast JJ. Superior labrum anterior and posterior lesions of the shoulder: incidence rates, complications, and outcomes as reported by American Board of Orthopedic Surgery. Part II candidates. Am J Sports Med. 2012;40(7):1538-1543.
22. Keener JD, Brophy RH. Superior labral tears of the shoulder: pathogenesis, evaluation, and treatment. J Am Acad Orthop Surg. 2009;17(10):627-637.
23. Chen CH, Hsu KY, Chen WJ, Shih CH. Incidence and severity of biceps long head tendon lesion in patients with complete rotator cuff tears. J Trauma. 2005;58(6):1189-1193.
24. Nho SJ, Strauss EJ, Lenart BA, et al. Long head of the biceps tendinopathy: diagnosis and management. J Am Acad Orthop Surg. 2010;18(11):645-656.
25. Zhang AL, Kreulen C, Ngo SS, Hame SL, Wang JC, Gamradt SC. Demographic trends in arthroscopic SLAP repair in the United States. Am J Sports Med. 2012;40(5):1144-1147.
26. McCormick F, Bhatia S, Chalmers P, Gupta A, Verma N, Romeo AA. The management of type II superior labral anterior to posterior injuries. Orthop Clin North Am. 2014;45(1):121-128.
27. Brockmeier SF, Voos JE, Williams RJ 3rd, Altchek DW, Cordasco FA, Allen AA; Hospital for Special Surgery Sports Medicine and Shoulder Service. Outcomes after arthroscopic repair of type-II SLAP lesions. J Bone Joint Surg Am. 2009;91(7):1595-1603.
28. Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009;37(5):929-936.
29. Denard PJ, Lädermann A, Burkhart SS. Long-term outcome after arthroscopic repair of type II SLAP lesions: results according to age and workers’ compensation status. Arthroscopy. 2012;28(4):451-457.
30. Friel NA, Karas V, Slabaugh MA, Cole BJ. Outcomes of type II superior labrum, anterior to posterior (SLAP) repair: prospective evaluation at a minimum two-year follow-up. J Shoulder Elbow Surg. 2010;19(6):859-867.
31. Provencher MT, McCormick F, Dewing C, McIntire S, Solomon D. A prospective analysis of 179 type 2 superior labrum anterior and posterior repairs: outcomes and factors associated with success and failure. Am J Sports Med. 2013;41(4):880-886.
32. Gupta AK, Chalmers PN, Klosterman EL, et al. Subpectoral biceps tenodesis for bicipital tendonitis with SLAP tear. Orthopedics. 2015;38(1):e48-e53.
33. Gorantla K, Gill C, Wright RW. The outcome of type II SLAP repair: a systematic review. Arthroscopy. 2010;26(4):537-545.
34. Katz LM, Hsu S, Miller SL, et al. Poor outcomes after SLAP repair: descriptive analysis and prognosis. Arthroscopy. 2009;25(8):849-855.
35. Park MJ, Hsu JE, Harper C, Sennett BJ, Huffman GR. Poly-L/D-lactic acid anchors are associated with reoperation and failure of SLAP repairs. Arthroscopy. 2011;27(10):1335-1340.
36. Sassmannshausen G, Sukay M, Mair SD. Broken or dislodged poly-L-lactic acid bioabsorbable tacks in patients after SLAP lesion surgery. Arthroscopy. 2006;22(6):615-619.
37. Uggen C, Wei A, Glousman RE, et al. Biomechanical comparison of knotless anchor repair versus simple suture repair for type II SLAP lesions. Arthroscopy. 2009;25(10):1085-1092.
38. Weber SC. Surgical management of the failed SLAP repair. Sports Med Arthrosc. 2010;18(3):162-166.
39. Wilkerson JP, Zvijac JE, Uribe JW, Schürhoff MR, Green JB. Failure of polymerized lactic acid tacks in shoulder surgery. J Shoulder Elbow Surg. 2003;12(2):117-121.
40. Weber S. Surgical management of the failed SLAP lesion. Arthroscopy. 2008;24(suppl):e8-e9.
41. Schrøder CP, Skare O, Gjengedal E, Uppheim G, Reikerås O, Brox JI. Long-term results after SLAP repair: a 5-year follow-up study of 107 patients with comparison of patients aged over and under 40 years. Arthroscopy. 2012;28(11):1601-1607.
42. Mazzocca AD, Cote MP, Arciero CL, Romeo AA, Arciero RA. Clinical outcomes after subpectoral biceps tenodesis with an interference screw. Am J Sports Med. 2008;36(10):1922-1929.
43. Mazzocca AD, McCarthy MB, Ledgard FA, et al. Histomorphologic changes of the long head of the biceps tendon in common shoulder pathologies. Arthroscopy. 2013;29(6):972-981.
44. Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009;37(5):929-936.
45. Boileau P, Krishnan SG, Coste JS, Walch G. Arthroscopic biceps tenodesis: a new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002;18(9):1002-1012.
46. Gupta AK, Bruce B, Klosterman EL, McCormick F, Harris J, Romeo AA. Subpectoral biceps tenodesis for failed type II SLAP repair. Orthopedics. 2013;36(6):e723-e728.
47. Provencher MT, LeClere LE, Romeo AA. Subpectoral biceps tenodesis. Sports Med Arthrosc. 2008;16(3):170-176.
48. McCarty LP 3rd, Buss DD, Datta MW, Freehill MQ, Giveans MR. Complications observed following labral or rotator cuff repair with use of poly-L-lactic acid implants. J Bone Joint Surg Am. 2013;95(6):507-511.
49. Werner BC, Brockmeier SF, Gwathmey FW. Trends in long head biceps tenodesis. Am J Sports Med. 2015;43(3):570-578.
50. Ek ET, Shi LL, Tompson JD, Freehill MT, Warner JJ. Surgical treatment of isolated type II superior labrum anterior-posterior (SLAP) lesions: repair versus biceps tenodesis. J Shoulder Elbow Surg. 2014;23(7):1059-1065.
51. Gupta AK, Chalmers PN, Klosterman EL, et al. Subpectoral biceps tenodesis for bicipital tendonitis with SLAP tear. Orthopedics. 2015;38(1):e48-e53.
52. Gottschalk MB, Karas SG, Ghattas TN, Burdette R. Subpectoral biceps tenodesis for the treatment of type II and IV superior labral anterior and posterior lesions. Am J Sports Med. 2014;42(9):2128-2135.
53. Werner BC, Pehlivan HC, Hart JM, et al. Biceps tenodesis is a viable option for salvage of failed SLAP repair. J Shoulder Elbow Surg. 2014;23(8):e179-e184.
54. Dein EJ, Huri G, Gordon JC, McFarland EG. A humerus fracture in a baseball pitcher after biceps tenodesis [published correction appears in Am J Sports Med. 2014;42(6):NP39]. Am J Sports Med. 2014;42(4):877-879.
55. Nho SJ, Reiff SN, Verma NN, Slabaugh MA, Mazzocca AD, Romeo AA. Complications associated with subpectoral biceps tenodesis: low rates of incidence following surgery. J Shoulder Elbow Surg. 2010;19(5):764-768.
56. Osbahr DC, Diamond AB, Speer KP. The cosmetic appearance of the biceps muscle after long-head tenotomy versus tenodesis. Arthroscopy. 2002;18(5):483-487.
57. Romeo AA, Mazzocca AD, Tauro JC. Arthroscopic biceps tenodesis. Arthroscopy. 2004;20(2):206-213.
58. Ma H, Van Heest A, Glisson C, Patel S. Musculocutaneous nerve entrapment: an unusual complication after biceps tenodesis. Am J Sports Med. 2009;37(12):2467-2469.
59. Chalmers PN, Trombley R, Cip J, et al. Postoperative restoration of upper extremity motion and neuromuscular control during the overhand pitch: evaluation of tenodesis and repair for superior labral anterior-posterior tears. Am J Sports Med. 2014;42(12):2825-2836.
60. Giphart JE, Elser F, Dewing CB, Torry MR, Millett PJ. The long head of the biceps tendon has minimal effect on in vivo glenohumeral kinematics: a biplane fluoroscopy study. Am J Sports Med. 2012;40(1):202-212.
61. Grossman MG, Tibone JE, McGarry MH, Schneider DJ, Veneziani S, Lee TQ. A cadaveric model of the throwing shoulder: a possible etiology of superior labrum anterior-to-posterior lesions. J Bone Joint Surg Am. 2005;87(4):824-831.
62. Hawkes DH, Alizadehkhaiyat O, Fisher AC, Kemp GJ, Roebuck MM, Frostick SP. Normal shoulder muscular activation and co-ordination during a shoulder elevation task based on activities of daily living: an electromyographic study. J Orthop Res. 2012;30(1):53-60.
63. Strauss EJ, Salata MJ, Sershon RA, et al. Role of the superior labrum after biceps tenodesis in glenohumeral stability. J Shoulder Elbow Surg. 2014;23(4):485-491.
64. Mazzocca AD, Bicos J, Santangelo S, Romeo AA, Arciero RA. The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis. Arthroscopy. 2005;21(11):1296-1306.
65. Werner BC, Pehlivan HC, Hart JM, et al. Increased incidence of postoperative stiffness after arthroscopic compared with open biceps tenodesis. Arthroscopy. 2014;30(9):1075-1084.
66. Denard PJ, Dai X, Hanypsiak BT, Burkhart SS. Anatomy of the biceps tendon: implications for restoring physiological length–tension relation during biceps tenodesis with interference screw fixation. Arthroscopy. 2012;28(10):1352-1358.
67. Mazzocca AD, Rios CG, Romeo AA, Arciero RA. Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy. 2005;21(7):896.
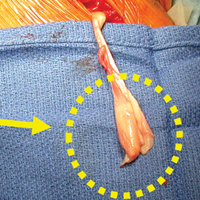
Make the Diagnosis - January 2017
Pemphigus vulgaris

Pemphigus vulgaris is the most common type of pemphigus. The average age of onset of 40-60 years. Clinically, patients may present with mucosal blisters and/or erosions. The most common site of mucosal lesions is the oral cavity, where the disease often manifests. Autoantibodies are produced against desmoglein 3 or both desmoglein 1 and desmoglein 3 in pemphigus vulgaris. Blistering is commonly induced with mechanical pressure at th edge of a blister or on normal skin, which is known as the Nikolsky sign. Pemphigus vulgaris has two uncommon clinical variants, pemphigus vegetans and pemphigus herpetiformis. Lack of prompt treatment of pemphigus vulgaris leads to epitope spreading and increased difficulty in management. Treatment with systemic glucocorticoids is the current standard of care to achieve control of the disease, and nonsteroidal immunomodulatory agents such as azathioprine, mycophenolate mofetil, and dapsone can be used in conjunction to help reduce adverse effects associated with long-term glucocorticoid therapy.
Pemphigus foliaceus results from autoantibodies against desmoglein 1. Patients usually present with small, scattered superficial cutaneous blisters that transition into scaly, crusted erosions. The scalp, neck, and trunk are the most common sites of presentation, with sparing of the mucous membranes. Like pemphigus vulgaris, the Nikolsky sign is frequently present in patients with pemphigus foliaceus. However, pemphigus foliaceus is readily distinguished from pemphigus vulgaris by its lack of mucous membrane involvement. The mainstays of treatment of pemphigus foliaceus are similar to those of pemphigus vulgaris, with systemic glucocorticoids and nonsteroidal adjuvant therapies playing a major role in controlling disease.
IgA pemphigus may occur at any age and is characterized by vesicles that progress into pustules commonly present on the trunk and proximal extremities. Erythematous plaques are frequently present alongside the vesicles and pustules. Like pemphigus foliaceus, IgA pemphigus usually spares the mucous membranes. The lesions may be pruritic but can also be asymptomatic. All other types of pemphigus are caused by IgG autoantibodies; however, IgA pemphigus results from IgA autoantibodies against target keratinocyte antigens. Several reports have shown dapsone to be a successful first-line adjuvant therapy for the treatment of IgA pemphigus.
Paraneoplastic pemphigus affects both genders and can occur at any age. It is most commonly the result of a malignancy. It is not clear which autoantibodies are actually responsible for the pathogenicity of most cases of paraneoplastic pemphigus. Clinically, it presents as a combination of severe erosive stomatitis, polymorphous cutaneous lesions, and possible pulmonary involvement. Severe, painful, and erosive mucositis is ubiquitous to the disease, and oral erosions are the most common initial presentation of paraneoplastic pemphigus, with a characteristic involvement of the tongue. Skin lesions commonly manifest after the onset of mucosal lesions. Cutaneous involvement is highly varied from patient to patient, with lesions resembling bullae, inflammatory violaceous papules, targetoid lesions, and desquamation. Management consists of treatment of the underlying neoplasm and control of the disease itself using a variety of agents including immunosuppressants and rituximab.
The patient’s biopsy came back consistent with pemphigus vulgaris. He was started on topical steroid gel for the mucosal lesions, topical steroid cream for the cutaneous lesions, and oral prednisone.
This case and photo were submitted by Natasha Cowan, University of California, San Diego, and Brooke Resh Sateesh, MD, San Diego Family Dermatology.
Donna Bilu Martin, MD, is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
Pemphigus vulgaris
Pemphigus vulgaris is the most common type of pemphigus. The average age of onset of 40-60 years. Clinically, patients may present with mucosal blisters and/or erosions. The most common site of mucosal lesions is the oral cavity, where the disease often manifests. Autoantibodies are produced against desmoglein 3 or both desmoglein 1 and desmoglein 3 in pemphigus vulgaris. Blistering is commonly induced with mechanical pressure at th edge of a blister or on normal skin, which is known as the Nikolsky sign. Pemphigus vulgaris has two uncommon clinical variants, pemphigus vegetans and pemphigus herpetiformis. Lack of prompt treatment of pemphigus vulgaris leads to epitope spreading and increased difficulty in management. Treatment with systemic glucocorticoids is the current standard of care to achieve control of the disease, and nonsteroidal immunomodulatory agents such as azathioprine, mycophenolate mofetil, and dapsone can be used in conjunction to help reduce adverse effects associated with long-term glucocorticoid therapy.
Pemphigus foliaceus results from autoantibodies against desmoglein 1. Patients usually present with small, scattered superficial cutaneous blisters that transition into scaly, crusted erosions. The scalp, neck, and trunk are the most common sites of presentation, with sparing of the mucous membranes. Like pemphigus vulgaris, the Nikolsky sign is frequently present in patients with pemphigus foliaceus. However, pemphigus foliaceus is readily distinguished from pemphigus vulgaris by its lack of mucous membrane involvement. The mainstays of treatment of pemphigus foliaceus are similar to those of pemphigus vulgaris, with systemic glucocorticoids and nonsteroidal adjuvant therapies playing a major role in controlling disease.
IgA pemphigus may occur at any age and is characterized by vesicles that progress into pustules commonly present on the trunk and proximal extremities. Erythematous plaques are frequently present alongside the vesicles and pustules. Like pemphigus foliaceus, IgA pemphigus usually spares the mucous membranes. The lesions may be pruritic but can also be asymptomatic. All other types of pemphigus are caused by IgG autoantibodies; however, IgA pemphigus results from IgA autoantibodies against target keratinocyte antigens. Several reports have shown dapsone to be a successful first-line adjuvant therapy for the treatment of IgA pemphigus.
Paraneoplastic pemphigus affects both genders and can occur at any age. It is most commonly the result of a malignancy. It is not clear which autoantibodies are actually responsible for the pathogenicity of most cases of paraneoplastic pemphigus. Clinically, it presents as a combination of severe erosive stomatitis, polymorphous cutaneous lesions, and possible pulmonary involvement. Severe, painful, and erosive mucositis is ubiquitous to the disease, and oral erosions are the most common initial presentation of paraneoplastic pemphigus, with a characteristic involvement of the tongue. Skin lesions commonly manifest after the onset of mucosal lesions. Cutaneous involvement is highly varied from patient to patient, with lesions resembling bullae, inflammatory violaceous papules, targetoid lesions, and desquamation. Management consists of treatment of the underlying neoplasm and control of the disease itself using a variety of agents including immunosuppressants and rituximab.
The patient’s biopsy came back consistent with pemphigus vulgaris. He was started on topical steroid gel for the mucosal lesions, topical steroid cream for the cutaneous lesions, and oral prednisone.
This case and photo were submitted by Natasha Cowan, University of California, San Diego, and Brooke Resh Sateesh, MD, San Diego Family Dermatology.
Donna Bilu Martin, MD, is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
Pemphigus vulgaris
Pemphigus vulgaris is the most common type of pemphigus. The average age of onset of 40-60 years. Clinically, patients may present with mucosal blisters and/or erosions. The most common site of mucosal lesions is the oral cavity, where the disease often manifests. Autoantibodies are produced against desmoglein 3 or both desmoglein 1 and desmoglein 3 in pemphigus vulgaris. Blistering is commonly induced with mechanical pressure at th edge of a blister or on normal skin, which is known as the Nikolsky sign. Pemphigus vulgaris has two uncommon clinical variants, pemphigus vegetans and pemphigus herpetiformis. Lack of prompt treatment of pemphigus vulgaris leads to epitope spreading and increased difficulty in management. Treatment with systemic glucocorticoids is the current standard of care to achieve control of the disease, and nonsteroidal immunomodulatory agents such as azathioprine, mycophenolate mofetil, and dapsone can be used in conjunction to help reduce adverse effects associated with long-term glucocorticoid therapy.
Pemphigus foliaceus results from autoantibodies against desmoglein 1. Patients usually present with small, scattered superficial cutaneous blisters that transition into scaly, crusted erosions. The scalp, neck, and trunk are the most common sites of presentation, with sparing of the mucous membranes. Like pemphigus vulgaris, the Nikolsky sign is frequently present in patients with pemphigus foliaceus. However, pemphigus foliaceus is readily distinguished from pemphigus vulgaris by its lack of mucous membrane involvement. The mainstays of treatment of pemphigus foliaceus are similar to those of pemphigus vulgaris, with systemic glucocorticoids and nonsteroidal adjuvant therapies playing a major role in controlling disease.
IgA pemphigus may occur at any age and is characterized by vesicles that progress into pustules commonly present on the trunk and proximal extremities. Erythematous plaques are frequently present alongside the vesicles and pustules. Like pemphigus foliaceus, IgA pemphigus usually spares the mucous membranes. The lesions may be pruritic but can also be asymptomatic. All other types of pemphigus are caused by IgG autoantibodies; however, IgA pemphigus results from IgA autoantibodies against target keratinocyte antigens. Several reports have shown dapsone to be a successful first-line adjuvant therapy for the treatment of IgA pemphigus.
Paraneoplastic pemphigus affects both genders and can occur at any age. It is most commonly the result of a malignancy. It is not clear which autoantibodies are actually responsible for the pathogenicity of most cases of paraneoplastic pemphigus. Clinically, it presents as a combination of severe erosive stomatitis, polymorphous cutaneous lesions, and possible pulmonary involvement. Severe, painful, and erosive mucositis is ubiquitous to the disease, and oral erosions are the most common initial presentation of paraneoplastic pemphigus, with a characteristic involvement of the tongue. Skin lesions commonly manifest after the onset of mucosal lesions. Cutaneous involvement is highly varied from patient to patient, with lesions resembling bullae, inflammatory violaceous papules, targetoid lesions, and desquamation. Management consists of treatment of the underlying neoplasm and control of the disease itself using a variety of agents including immunosuppressants and rituximab.
The patient’s biopsy came back consistent with pemphigus vulgaris. He was started on topical steroid gel for the mucosal lesions, topical steroid cream for the cutaneous lesions, and oral prednisone.
This case and photo were submitted by Natasha Cowan, University of California, San Diego, and Brooke Resh Sateesh, MD, San Diego Family Dermatology.
Donna Bilu Martin, MD, is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
A 50 year old Hispanic male presented with a two day history of blisters on his lips, extremities, and upper body. He complained of soreness on his lips. Bullae were flaccid and some had crusting.
Term ultrasound shown unreliable for diagnosing macrosomia
LAS VEGAS – Fetal macrosomia can be challenging to detect by ultrasound performed just before delivery, which had 41% sensitivity and 58% positive predictive value in a prospective study of more than 2,300 pregnancies.
The results also showed that fetal macrosomia (defined as birth weight of more than 4,000 grams) is significantly linked with increased rates of prolonged labor, delivery by either operative vaginal or cesarean approaches, and postpartum hemorrhage, Daniel M. Galvin, MD, said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.

Because all clinicians involved with these deliveries were blinded to the prenatal ultrasound results, the findings suggest that prolonged labor, postpartum hemorrhage, and need for either operative vaginal delivery or cesarean delivery are all outcomes driven by macrosomia itself rather than by clinical actions taken because of an expectation of macrosomia, said Dr. Galvin, an ob.gyn. with Perinatal Ireland, a Dublin-based consortium of eight Irish fetal medicine centers that is examining ways to improve delivery outcomes.
The study used “a pure population of pregnancies with unsuspected fetal macrosomia,” he explained.
Dr. Galvin and his colleagues used data collected in GENESIS, a prospective study run by the Perinatal Ireland multicenter consortium with the primary goal of determining whether late-pregnancy fetal head circumference can predict labor dystocia and intrapartum cesarean delivery. They examined two secondary outcomes: the reliability of ultrasound to estimate fetal size, and the consequences of fetal macrosomia when it is not recognized until delivery is already underway.
The study enrolled 2,336 nulliparous women with singleton pregnancies that ranged from the start of 39 weeks’ gestational age through the end of 40 weeks. The women underwent a standard ultrasound examination to assess fetal biometrics. The study excluded pregnancies with an estimated fetal size greater than 5,000 g. Mothers carrying a fetus estimated to be less than 4,000 g constituted 88% of the study group, with 12% carrying pregnancies with an estimated fetal weight greater than 4,000 g.
The ultrasound examination worked reasonably well for ruling out macrosomia, with an 89% rate of correctly identifying fetuses with a birth weight of less than 4,000 g. Near-term ultrasound was less useful for a positive identification of macrosomia; it flagged 58% of the fetuses born heavier than 4,000 g.
Analysis of delivery mode showed that infants born weighing more than 4,000 g had a statistically significant 56% reduced rate of spontaneous vaginal deliveries compared with smaller neonates, a 63% greater rate of cesarean deliveries, and a 49% greater rate of operative vaginal deliveries, compared with small babies, Dr. Galvin reported. All three between-group differences were statistically significant.
The analysis also showed that compared with the smaller babies, the larger neonates were twice as likely to be born during prolonged labor of more than 12 hours. Delivery of larger neonates was also twice as likely to trigger postpartum hemorrhage. But deliveries of larger babies had no significant link with increased rates of neonatal intensive care admissions, anal sphincter injuries, shoulder dystocias or birth injuries, compared with deliveries of smaller babies.
Dr. Galvin reported having no financial disclosures.
[email protected]
On Twitter @mitchelzoler
LAS VEGAS – Fetal macrosomia can be challenging to detect by ultrasound performed just before delivery, which had 41% sensitivity and 58% positive predictive value in a prospective study of more than 2,300 pregnancies.
The results also showed that fetal macrosomia (defined as birth weight of more than 4,000 grams) is significantly linked with increased rates of prolonged labor, delivery by either operative vaginal or cesarean approaches, and postpartum hemorrhage, Daniel M. Galvin, MD, said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Because all clinicians involved with these deliveries were blinded to the prenatal ultrasound results, the findings suggest that prolonged labor, postpartum hemorrhage, and need for either operative vaginal delivery or cesarean delivery are all outcomes driven by macrosomia itself rather than by clinical actions taken because of an expectation of macrosomia, said Dr. Galvin, an ob.gyn. with Perinatal Ireland, a Dublin-based consortium of eight Irish fetal medicine centers that is examining ways to improve delivery outcomes.
The study used “a pure population of pregnancies with unsuspected fetal macrosomia,” he explained.
Dr. Galvin and his colleagues used data collected in GENESIS, a prospective study run by the Perinatal Ireland multicenter consortium with the primary goal of determining whether late-pregnancy fetal head circumference can predict labor dystocia and intrapartum cesarean delivery. They examined two secondary outcomes: the reliability of ultrasound to estimate fetal size, and the consequences of fetal macrosomia when it is not recognized until delivery is already underway.
The study enrolled 2,336 nulliparous women with singleton pregnancies that ranged from the start of 39 weeks’ gestational age through the end of 40 weeks. The women underwent a standard ultrasound examination to assess fetal biometrics. The study excluded pregnancies with an estimated fetal size greater than 5,000 g. Mothers carrying a fetus estimated to be less than 4,000 g constituted 88% of the study group, with 12% carrying pregnancies with an estimated fetal weight greater than 4,000 g.
The ultrasound examination worked reasonably well for ruling out macrosomia, with an 89% rate of correctly identifying fetuses with a birth weight of less than 4,000 g. Near-term ultrasound was less useful for a positive identification of macrosomia; it flagged 58% of the fetuses born heavier than 4,000 g.
Analysis of delivery mode showed that infants born weighing more than 4,000 g had a statistically significant 56% reduced rate of spontaneous vaginal deliveries compared with smaller neonates, a 63% greater rate of cesarean deliveries, and a 49% greater rate of operative vaginal deliveries, compared with small babies, Dr. Galvin reported. All three between-group differences were statistically significant.
The analysis also showed that compared with the smaller babies, the larger neonates were twice as likely to be born during prolonged labor of more than 12 hours. Delivery of larger neonates was also twice as likely to trigger postpartum hemorrhage. But deliveries of larger babies had no significant link with increased rates of neonatal intensive care admissions, anal sphincter injuries, shoulder dystocias or birth injuries, compared with deliveries of smaller babies.
Dr. Galvin reported having no financial disclosures.
[email protected]
On Twitter @mitchelzoler
LAS VEGAS – Fetal macrosomia can be challenging to detect by ultrasound performed just before delivery, which had 41% sensitivity and 58% positive predictive value in a prospective study of more than 2,300 pregnancies.
The results also showed that fetal macrosomia (defined as birth weight of more than 4,000 grams) is significantly linked with increased rates of prolonged labor, delivery by either operative vaginal or cesarean approaches, and postpartum hemorrhage, Daniel M. Galvin, MD, said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Because all clinicians involved with these deliveries were blinded to the prenatal ultrasound results, the findings suggest that prolonged labor, postpartum hemorrhage, and need for either operative vaginal delivery or cesarean delivery are all outcomes driven by macrosomia itself rather than by clinical actions taken because of an expectation of macrosomia, said Dr. Galvin, an ob.gyn. with Perinatal Ireland, a Dublin-based consortium of eight Irish fetal medicine centers that is examining ways to improve delivery outcomes.
The study used “a pure population of pregnancies with unsuspected fetal macrosomia,” he explained.
Dr. Galvin and his colleagues used data collected in GENESIS, a prospective study run by the Perinatal Ireland multicenter consortium with the primary goal of determining whether late-pregnancy fetal head circumference can predict labor dystocia and intrapartum cesarean delivery. They examined two secondary outcomes: the reliability of ultrasound to estimate fetal size, and the consequences of fetal macrosomia when it is not recognized until delivery is already underway.
The study enrolled 2,336 nulliparous women with singleton pregnancies that ranged from the start of 39 weeks’ gestational age through the end of 40 weeks. The women underwent a standard ultrasound examination to assess fetal biometrics. The study excluded pregnancies with an estimated fetal size greater than 5,000 g. Mothers carrying a fetus estimated to be less than 4,000 g constituted 88% of the study group, with 12% carrying pregnancies with an estimated fetal weight greater than 4,000 g.
The ultrasound examination worked reasonably well for ruling out macrosomia, with an 89% rate of correctly identifying fetuses with a birth weight of less than 4,000 g. Near-term ultrasound was less useful for a positive identification of macrosomia; it flagged 58% of the fetuses born heavier than 4,000 g.
Analysis of delivery mode showed that infants born weighing more than 4,000 g had a statistically significant 56% reduced rate of spontaneous vaginal deliveries compared with smaller neonates, a 63% greater rate of cesarean deliveries, and a 49% greater rate of operative vaginal deliveries, compared with small babies, Dr. Galvin reported. All three between-group differences were statistically significant.
The analysis also showed that compared with the smaller babies, the larger neonates were twice as likely to be born during prolonged labor of more than 12 hours. Delivery of larger neonates was also twice as likely to trigger postpartum hemorrhage. But deliveries of larger babies had no significant link with increased rates of neonatal intensive care admissions, anal sphincter injuries, shoulder dystocias or birth injuries, compared with deliveries of smaller babies.
Dr. Galvin reported having no financial disclosures.
[email protected]
On Twitter @mitchelzoler
AT THE PREGNANCY MEETING
Key clinical point:
Major finding: Near-term ultrasound identified 58% of fetuses born weighing more than 4,000 g.
Data source: Prospective, multicenter study of 2,336 singleton pregnancies.
Disclosures: Dr. Galvin reported having no financial disclosures.
When the iPad is on the other foot
Sometimes patients take a few notes when I talk, but Niles was different. As I started to spout words of wisdom about his granuloma annulare, he whipped out a tablet and started to type.
“How do you spell that again?” he wanted to know.
I spelled it out, and Niles tapped away. I launched into my usual explanation – how the cause is unknown, how it is roundish but not a fungus, how it usually has no systemic significance, and so on. At each point, looking down at the keyboard, he stopped me.

“Wait, you say it isn’t fungal?”
“No ...”
Typing. “And you don’t know the cause?”
“No, the medical term for that is ‘idiopathic’ ...”
“Wait, how do you spell that?”
I regretted using the word. “I-D-I-O-P-A-T-H-I-C.”
More typing. “Wait, hold on. OK, got it. And what did you say you want to treat it with?”
“A cream. Betamethasone dipropionate.”
“Hold on! How do you spell that?”
I spelled it out, along with “augmented” and “0.05%.”
The interview continued a bit longer. As we concluded, Niles thanked me for seeing him. At no time did he raise his eyes from the tablet, even as he was putting it back into its case. He acted the same way my staff does when I walk into the lunchroom. There I see three or four people sitting around a table with a sandwich or salad in front of them, staring at their smartphones. The same way groups of people do nowadays, everywhere. (A couple of years ago, I took some of my grandchildren out on a rowboat on the Charles River on a sunny summer afternoon. There we saw two young women, oars across their laps, examining their phones.)

When my student and I left the room, I took him aside.
“Did you see anything unusual about how that visit went?” I asked.
When he looked blank, I explained: “The patient didn’t look me in the eye once.”
Yes, come to think of it, the student had noticed that.
“Not very satisfying, was it?” I asked. “It’s hard to talk to somebody who isn’t looking at you. It’s even a little insulting, don’t you think?” He agreed.
“When you’re out in practice in a few years,” I said, “the person in the exam room looking at the computer and not making eye contact is likely to be you. Think about how it felt to watch me talking at the top of the patient’s head, and then imagine how your patients are likely to feel when they’re talking to the top of your head. Unless of course your laptop has a screen that blocks your head altogether.
“I just bring a clipboard with sheets of paper on it into the exam room,” I said. “The way things are working out, I think I’ll be able to make it to the end of my career without being forced to use an electronic device.
“You have your whole career ahead of you, though,” I told him. “I guess you’ll figure out how to make communication work.”
He will too, no doubt. He’ll have to. As the Romans used to say, times change, and we change with them.
No need to spell this out for the younger generation, literally or otherwise.
Just a short addendum from the world of artificial intelligence, as applied to voice recognition software:
Last week I saw Chad, who had seen my colleague a year earlier and come back for a skin check. She had described Chad’s occupation:
“The patient is a flight attendant for Diflucan Airlines.”
Check them out. Their restrooms are so clean you can go barefoot.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
Sometimes patients take a few notes when I talk, but Niles was different. As I started to spout words of wisdom about his granuloma annulare, he whipped out a tablet and started to type.
“How do you spell that again?” he wanted to know.
I spelled it out, and Niles tapped away. I launched into my usual explanation – how the cause is unknown, how it is roundish but not a fungus, how it usually has no systemic significance, and so on. At each point, looking down at the keyboard, he stopped me.
“Wait, you say it isn’t fungal?”
“No ...”
Typing. “And you don’t know the cause?”
“No, the medical term for that is ‘idiopathic’ ...”
“Wait, how do you spell that?”
I regretted using the word. “I-D-I-O-P-A-T-H-I-C.”
More typing. “Wait, hold on. OK, got it. And what did you say you want to treat it with?”
“A cream. Betamethasone dipropionate.”
“Hold on! How do you spell that?”
I spelled it out, along with “augmented” and “0.05%.”
The interview continued a bit longer. As we concluded, Niles thanked me for seeing him. At no time did he raise his eyes from the tablet, even as he was putting it back into its case. He acted the same way my staff does when I walk into the lunchroom. There I see three or four people sitting around a table with a sandwich or salad in front of them, staring at their smartphones. The same way groups of people do nowadays, everywhere. (A couple of years ago, I took some of my grandchildren out on a rowboat on the Charles River on a sunny summer afternoon. There we saw two young women, oars across their laps, examining their phones.)
When my student and I left the room, I took him aside.
“Did you see anything unusual about how that visit went?” I asked.
When he looked blank, I explained: “The patient didn’t look me in the eye once.”
Yes, come to think of it, the student had noticed that.
“Not very satisfying, was it?” I asked. “It’s hard to talk to somebody who isn’t looking at you. It’s even a little insulting, don’t you think?” He agreed.
“When you’re out in practice in a few years,” I said, “the person in the exam room looking at the computer and not making eye contact is likely to be you. Think about how it felt to watch me talking at the top of the patient’s head, and then imagine how your patients are likely to feel when they’re talking to the top of your head. Unless of course your laptop has a screen that blocks your head altogether.
“I just bring a clipboard with sheets of paper on it into the exam room,” I said. “The way things are working out, I think I’ll be able to make it to the end of my career without being forced to use an electronic device.
“You have your whole career ahead of you, though,” I told him. “I guess you’ll figure out how to make communication work.”
He will too, no doubt. He’ll have to. As the Romans used to say, times change, and we change with them.
No need to spell this out for the younger generation, literally or otherwise.
Just a short addendum from the world of artificial intelligence, as applied to voice recognition software:
Last week I saw Chad, who had seen my colleague a year earlier and come back for a skin check. She had described Chad’s occupation:
“The patient is a flight attendant for Diflucan Airlines.”
Check them out. Their restrooms are so clean you can go barefoot.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].
Sometimes patients take a few notes when I talk, but Niles was different. As I started to spout words of wisdom about his granuloma annulare, he whipped out a tablet and started to type.
“How do you spell that again?” he wanted to know.
I spelled it out, and Niles tapped away. I launched into my usual explanation – how the cause is unknown, how it is roundish but not a fungus, how it usually has no systemic significance, and so on. At each point, looking down at the keyboard, he stopped me.
“Wait, you say it isn’t fungal?”
“No ...”
Typing. “And you don’t know the cause?”
“No, the medical term for that is ‘idiopathic’ ...”
“Wait, how do you spell that?”
I regretted using the word. “I-D-I-O-P-A-T-H-I-C.”
More typing. “Wait, hold on. OK, got it. And what did you say you want to treat it with?”
“A cream. Betamethasone dipropionate.”
“Hold on! How do you spell that?”
I spelled it out, along with “augmented” and “0.05%.”
The interview continued a bit longer. As we concluded, Niles thanked me for seeing him. At no time did he raise his eyes from the tablet, even as he was putting it back into its case. He acted the same way my staff does when I walk into the lunchroom. There I see three or four people sitting around a table with a sandwich or salad in front of them, staring at their smartphones. The same way groups of people do nowadays, everywhere. (A couple of years ago, I took some of my grandchildren out on a rowboat on the Charles River on a sunny summer afternoon. There we saw two young women, oars across their laps, examining their phones.)
When my student and I left the room, I took him aside.
“Did you see anything unusual about how that visit went?” I asked.
When he looked blank, I explained: “The patient didn’t look me in the eye once.”
Yes, come to think of it, the student had noticed that.
“Not very satisfying, was it?” I asked. “It’s hard to talk to somebody who isn’t looking at you. It’s even a little insulting, don’t you think?” He agreed.
“When you’re out in practice in a few years,” I said, “the person in the exam room looking at the computer and not making eye contact is likely to be you. Think about how it felt to watch me talking at the top of the patient’s head, and then imagine how your patients are likely to feel when they’re talking to the top of your head. Unless of course your laptop has a screen that blocks your head altogether.
“I just bring a clipboard with sheets of paper on it into the exam room,” I said. “The way things are working out, I think I’ll be able to make it to the end of my career without being forced to use an electronic device.
“You have your whole career ahead of you, though,” I told him. “I guess you’ll figure out how to make communication work.”
He will too, no doubt. He’ll have to. As the Romans used to say, times change, and we change with them.
No need to spell this out for the younger generation, literally or otherwise.
Just a short addendum from the world of artificial intelligence, as applied to voice recognition software:
Last week I saw Chad, who had seen my colleague a year earlier and come back for a skin check. She had described Chad’s occupation:
“The patient is a flight attendant for Diflucan Airlines.”
Check them out. Their restrooms are so clean you can go barefoot.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His new book “Act Like a Doctor, Think Like a Patient” is now available at amazon.com and barnesandnoble.com. This is his second book. Write to him at [email protected].