User login
Military Brats: Members of a Lost Tribe
Some of you who are reading this column likely are military brats from one branch or another. Many of us felt the call to give back by either joining the military, PHS, or working in organizations like the VA, treating former service members. That certainly was a huge motivation for me to become a VA physician. I always felt more welcomed, even felt at home, at the VA or at a military hospital than I did at any civilian health care facility. And many of my colleagues feel the same way. Other brats have never interacted much with the military except for their being raised by family members in the armed forces; yet this designation is still a part of their identity,
The percentage of adults > 50 years old who have an immediate family member who served in the military is 77%; the percentage of those aged 30 to 49 years is 57%; and aged < 30 years, only 33%.1 Almost 5% of adult Americans are military brats. This demographic trend brings with it an increasing chance that current and former service members may feel socially isolated and that many health care professionals will struggle to relate to, and appreciate, their unique cultural background.
Authors always should acknowledge any material conflict of interest, and as a double Army brat, I am far from objective on this subject. I was born and raised on an army base. My father was a career military physician, and my mother, albeit briefly, was an army nurse. Some of my earliest memories are of being with my father and driving around Fort Sam Houston when everyone and everything stopped upon hearing the sound of a bugle (at the time, it was still a real bugle). My father and I would get out of the car. He would salute, and I would stand as still as a small active child can while we turned toward the flag being lowered over the base.
In reading about army brats, this memory seems to be a common one. Many individuals have commented on how this repeated experience from their youth instilled in them a sense of respect for our flag and country and an appreciation of order and discipline that stayed with them long after they became adults.
Obviously, while those of us claiming this identity use it positively as a phrase of winsome nostalgia and civic pride, in everyday language a brat is a pejorative reference. The online magazine Military Brat Life, defines the term as “someone, who, as a child, grows up in a family where one or more parents are ‘career’ military, and where the children move from base to base, experiencing life in several different places and possibly different countries.”2 The phrase denotes an individual whose parents at some point served full-time in the military, no duration is specified or whether the parents had to be active duty, reserve or National Guard members. The prefix for the label comes from the military branch in which the parents primarily served, though like hyphenated names some younger generations will introduce themselves as a Navy-Air Force brat. Other sites suggest that it doesn’t refer to a spoiled child at all but actually is yet another of the acronyms that proliferate in military environments. Although after I read these possible theories, many seemed retrospective attempts to jettison the negative connotations.
I learned that like others sharing similar formative experiences, military brats are considered a subculture or a third culture, in some of the literature. There is a dearth of scholarly data about the phenomenology and social psychology of adults who spent some of their formative years under the auspices of military culture. As in any foray into cultural competence, avoiding stereotypes is crucial. However, research has shown that the experience of growing up in the military is one that bestows resilience and risk.3 It is also an important piece of a patient’s narrative that health care professionals in and out of the federal system should consider to provide patient-centered care.
A childhood in a military environment is often romanticized as shaping an adult who is worldly, cosmopolitan, resilient, and tolerant. Although these are adaptive traits that children of military personnel develop, there also is a far darker side emerging in the research.4 We are all too aware of the epidemic of suicide, opioid use, and posttraumatic stress disorder that has developed in the wake of our country’s latest and lasting conflicts. The reverberations of these mental health problems are felt by the children who lived through them or who lost loved ones to war or suicide. The DoD has begun recognizing this collateral damage and is developing innovative programs to help children and adolescents.
We need to do more though, not just in this arena when the wounds occur, but also later when those wounded come to nurse practitioners and psychologists, social workers, and physicians. Our growing number of community partners through Choice and other programs also need to be aware of the potential mental health impacts of being a military brat or family member.
In the introduction to one of the best books written on the subject, Military Brats: Legacies of Childhood Inside the Fortress, author Pat Conroy wrote, “I thought I was singular in all this, one of a kind.... I discovered that I speak in the multitongued, deep-throated voice of my tribe. It’s a language I was not even aware I spoke... a secret family I did not know I had.... Military brats, my lost tribe, spent their entire youth in service to this country, and no one even knew we were there.”5
1. Pew Research Center. The military-civilian gap: fewer family connections. http://www.pewsocialtrends.org/2011/11/23/the-military-civilian-gap-fewer-family-connections. Published November 23, 2011. Accessed July 12, 2017.
2. Baker V. What is a military brat? http://militarybratlife.com/what-is-a-military-brat. Published January 22, 2015. Accessed July 13, 2017.
3. Park N. Military children and families: strengths and challenges in war and peace. Am Psychol. 2011;66(1):65-72.
4. McGuire AC, Kanesarajah J, Runge CE, Ireland R, Waller M, Dobson AJ. Effect of multiple deployments on military families: a cross-sectional study of health and well-being of partners and children. Mill Med. 2016;181(4):319-327.
5. Wertsch ME. Military Brats: Legacies of Childhood Inside the Fortress. St. Louis, MO: Brightwell Publishing; 2011.
Some of you who are reading this column likely are military brats from one branch or another. Many of us felt the call to give back by either joining the military, PHS, or working in organizations like the VA, treating former service members. That certainly was a huge motivation for me to become a VA physician. I always felt more welcomed, even felt at home, at the VA or at a military hospital than I did at any civilian health care facility. And many of my colleagues feel the same way. Other brats have never interacted much with the military except for their being raised by family members in the armed forces; yet this designation is still a part of their identity,
The percentage of adults > 50 years old who have an immediate family member who served in the military is 77%; the percentage of those aged 30 to 49 years is 57%; and aged < 30 years, only 33%.1 Almost 5% of adult Americans are military brats. This demographic trend brings with it an increasing chance that current and former service members may feel socially isolated and that many health care professionals will struggle to relate to, and appreciate, their unique cultural background.
Authors always should acknowledge any material conflict of interest, and as a double Army brat, I am far from objective on this subject. I was born and raised on an army base. My father was a career military physician, and my mother, albeit briefly, was an army nurse. Some of my earliest memories are of being with my father and driving around Fort Sam Houston when everyone and everything stopped upon hearing the sound of a bugle (at the time, it was still a real bugle). My father and I would get out of the car. He would salute, and I would stand as still as a small active child can while we turned toward the flag being lowered over the base.
In reading about army brats, this memory seems to be a common one. Many individuals have commented on how this repeated experience from their youth instilled in them a sense of respect for our flag and country and an appreciation of order and discipline that stayed with them long after they became adults.
Obviously, while those of us claiming this identity use it positively as a phrase of winsome nostalgia and civic pride, in everyday language a brat is a pejorative reference. The online magazine Military Brat Life, defines the term as “someone, who, as a child, grows up in a family where one or more parents are ‘career’ military, and where the children move from base to base, experiencing life in several different places and possibly different countries.”2 The phrase denotes an individual whose parents at some point served full-time in the military, no duration is specified or whether the parents had to be active duty, reserve or National Guard members. The prefix for the label comes from the military branch in which the parents primarily served, though like hyphenated names some younger generations will introduce themselves as a Navy-Air Force brat. Other sites suggest that it doesn’t refer to a spoiled child at all but actually is yet another of the acronyms that proliferate in military environments. Although after I read these possible theories, many seemed retrospective attempts to jettison the negative connotations.
I learned that like others sharing similar formative experiences, military brats are considered a subculture or a third culture, in some of the literature. There is a dearth of scholarly data about the phenomenology and social psychology of adults who spent some of their formative years under the auspices of military culture. As in any foray into cultural competence, avoiding stereotypes is crucial. However, research has shown that the experience of growing up in the military is one that bestows resilience and risk.3 It is also an important piece of a patient’s narrative that health care professionals in and out of the federal system should consider to provide patient-centered care.
A childhood in a military environment is often romanticized as shaping an adult who is worldly, cosmopolitan, resilient, and tolerant. Although these are adaptive traits that children of military personnel develop, there also is a far darker side emerging in the research.4 We are all too aware of the epidemic of suicide, opioid use, and posttraumatic stress disorder that has developed in the wake of our country’s latest and lasting conflicts. The reverberations of these mental health problems are felt by the children who lived through them or who lost loved ones to war or suicide. The DoD has begun recognizing this collateral damage and is developing innovative programs to help children and adolescents.
We need to do more though, not just in this arena when the wounds occur, but also later when those wounded come to nurse practitioners and psychologists, social workers, and physicians. Our growing number of community partners through Choice and other programs also need to be aware of the potential mental health impacts of being a military brat or family member.
In the introduction to one of the best books written on the subject, Military Brats: Legacies of Childhood Inside the Fortress, author Pat Conroy wrote, “I thought I was singular in all this, one of a kind.... I discovered that I speak in the multitongued, deep-throated voice of my tribe. It’s a language I was not even aware I spoke... a secret family I did not know I had.... Military brats, my lost tribe, spent their entire youth in service to this country, and no one even knew we were there.”5
Some of you who are reading this column likely are military brats from one branch or another. Many of us felt the call to give back by either joining the military, PHS, or working in organizations like the VA, treating former service members. That certainly was a huge motivation for me to become a VA physician. I always felt more welcomed, even felt at home, at the VA or at a military hospital than I did at any civilian health care facility. And many of my colleagues feel the same way. Other brats have never interacted much with the military except for their being raised by family members in the armed forces; yet this designation is still a part of their identity,
The percentage of adults > 50 years old who have an immediate family member who served in the military is 77%; the percentage of those aged 30 to 49 years is 57%; and aged < 30 years, only 33%.1 Almost 5% of adult Americans are military brats. This demographic trend brings with it an increasing chance that current and former service members may feel socially isolated and that many health care professionals will struggle to relate to, and appreciate, their unique cultural background.
Authors always should acknowledge any material conflict of interest, and as a double Army brat, I am far from objective on this subject. I was born and raised on an army base. My father was a career military physician, and my mother, albeit briefly, was an army nurse. Some of my earliest memories are of being with my father and driving around Fort Sam Houston when everyone and everything stopped upon hearing the sound of a bugle (at the time, it was still a real bugle). My father and I would get out of the car. He would salute, and I would stand as still as a small active child can while we turned toward the flag being lowered over the base.
In reading about army brats, this memory seems to be a common one. Many individuals have commented on how this repeated experience from their youth instilled in them a sense of respect for our flag and country and an appreciation of order and discipline that stayed with them long after they became adults.
Obviously, while those of us claiming this identity use it positively as a phrase of winsome nostalgia and civic pride, in everyday language a brat is a pejorative reference. The online magazine Military Brat Life, defines the term as “someone, who, as a child, grows up in a family where one or more parents are ‘career’ military, and where the children move from base to base, experiencing life in several different places and possibly different countries.”2 The phrase denotes an individual whose parents at some point served full-time in the military, no duration is specified or whether the parents had to be active duty, reserve or National Guard members. The prefix for the label comes from the military branch in which the parents primarily served, though like hyphenated names some younger generations will introduce themselves as a Navy-Air Force brat. Other sites suggest that it doesn’t refer to a spoiled child at all but actually is yet another of the acronyms that proliferate in military environments. Although after I read these possible theories, many seemed retrospective attempts to jettison the negative connotations.
I learned that like others sharing similar formative experiences, military brats are considered a subculture or a third culture, in some of the literature. There is a dearth of scholarly data about the phenomenology and social psychology of adults who spent some of their formative years under the auspices of military culture. As in any foray into cultural competence, avoiding stereotypes is crucial. However, research has shown that the experience of growing up in the military is one that bestows resilience and risk.3 It is also an important piece of a patient’s narrative that health care professionals in and out of the federal system should consider to provide patient-centered care.
A childhood in a military environment is often romanticized as shaping an adult who is worldly, cosmopolitan, resilient, and tolerant. Although these are adaptive traits that children of military personnel develop, there also is a far darker side emerging in the research.4 We are all too aware of the epidemic of suicide, opioid use, and posttraumatic stress disorder that has developed in the wake of our country’s latest and lasting conflicts. The reverberations of these mental health problems are felt by the children who lived through them or who lost loved ones to war or suicide. The DoD has begun recognizing this collateral damage and is developing innovative programs to help children and adolescents.
We need to do more though, not just in this arena when the wounds occur, but also later when those wounded come to nurse practitioners and psychologists, social workers, and physicians. Our growing number of community partners through Choice and other programs also need to be aware of the potential mental health impacts of being a military brat or family member.
In the introduction to one of the best books written on the subject, Military Brats: Legacies of Childhood Inside the Fortress, author Pat Conroy wrote, “I thought I was singular in all this, one of a kind.... I discovered that I speak in the multitongued, deep-throated voice of my tribe. It’s a language I was not even aware I spoke... a secret family I did not know I had.... Military brats, my lost tribe, spent their entire youth in service to this country, and no one even knew we were there.”5
1. Pew Research Center. The military-civilian gap: fewer family connections. http://www.pewsocialtrends.org/2011/11/23/the-military-civilian-gap-fewer-family-connections. Published November 23, 2011. Accessed July 12, 2017.
2. Baker V. What is a military brat? http://militarybratlife.com/what-is-a-military-brat. Published January 22, 2015. Accessed July 13, 2017.
3. Park N. Military children and families: strengths and challenges in war and peace. Am Psychol. 2011;66(1):65-72.
4. McGuire AC, Kanesarajah J, Runge CE, Ireland R, Waller M, Dobson AJ. Effect of multiple deployments on military families: a cross-sectional study of health and well-being of partners and children. Mill Med. 2016;181(4):319-327.
5. Wertsch ME. Military Brats: Legacies of Childhood Inside the Fortress. St. Louis, MO: Brightwell Publishing; 2011.
1. Pew Research Center. The military-civilian gap: fewer family connections. http://www.pewsocialtrends.org/2011/11/23/the-military-civilian-gap-fewer-family-connections. Published November 23, 2011. Accessed July 12, 2017.
2. Baker V. What is a military brat? http://militarybratlife.com/what-is-a-military-brat. Published January 22, 2015. Accessed July 13, 2017.
3. Park N. Military children and families: strengths and challenges in war and peace. Am Psychol. 2011;66(1):65-72.
4. McGuire AC, Kanesarajah J, Runge CE, Ireland R, Waller M, Dobson AJ. Effect of multiple deployments on military families: a cross-sectional study of health and well-being of partners and children. Mill Med. 2016;181(4):319-327.
5. Wertsch ME. Military Brats: Legacies of Childhood Inside the Fortress. St. Louis, MO: Brightwell Publishing; 2011.

Studies support early use of genetic tests in early childhood disorders
Results from two new studies suggest that genetic testing early in the diagnostic pathway may allow for earlier and more precise diagnoses in early-life epilepsies and a range of other childhood-onset disorders, and potentially limit costs associated with a long diagnostic course.
Both papers, published online July 31 in JAMA Pediatrics, showed the diagnostic yield of genetic testing approaches, including whole-exome sequencing (WES), to be high.
The results also argue for the incorporation of genetic testing into the first diagnostic assessments; not limiting it to severe presentations only; and for broad testing methods to be employed in lieu of narrower ones.

Of these patients, just under half (n = 327) underwent various forms of genetic testing at the discretion of the treating physician, including karyotyping, microarrays, epilepsy gene panels, WES, mitochondrial panels, and other tests. Pathogenic variants were discovered in 132 children, or 40% of those receiving genetic testing (JAMA Pediatr. 2017 July 31. doi: 10.1001/jamapediatrics.2017.1743).
Of all the genetic testing methods employed in the study, diagnostic yields were significantly greater for epilepsy gene panels (29.2%) and WES (27.8%), compared with chromosome microarray (7.9%).
The results, the investigators said, provide “added impetus to move the diagnosis of the specific cause to the point of initial presentation ... it is time to provide greater emphasis on and support for thorough genetic evaluations, particularly sequencing-based evaluations, for children with newly presenting epilepsies in the first few years of life.”
In addition to aiding management decisions, early genetic testing “ends the diagnostic odyssey during which parents and physicians spend untold amounts of time searching for an explanation for a child’s epilepsy and reduces associated costs,” Dr. Berg and her colleagues concluded.
In a separate study led by Tiong Yang Tan, MBBS, PhD, of Victorian Clinical Genetics Services in Melbourne, Australia, and his colleagues, singleton WES was used in 44 children recruited at outpatient clinics of a Melbourne hospital system (JAMA Pediatr. 2017 July 31. doi: 10.1001/jamapediatrics.2017.1755).
Children in the study were aged 2-18 years (with mean age at presentation 28 months) and had a wide variety of suspected genetic disorders, including skeletal, skin, neurometabolic, and intellectual disorders. Some of these had features overlapping several conditions. The children in the cohort had not received prior genetic testing before undergoing WES.
The molecular test resulted in a diagnosis in 52% (n = 23) of the children, including unexpected diagnoses in eight of these. Clinical management was altered as result of sequencing findings in six children.
“Although phenotyping is critical, 35% of children had a diagnosis caused by a gene outside the initially prioritized gene list. This finding not only possibly reflects lack of clinical recognition but also underscores the utility of WES in achieving a diagnosis even when the a priori hypothesis is imprecise,” Dr. Tan and his associates wrote in their analysis.
Dr. Tan and his colleagues conducted a cost analysis that found WES performed at initial tertiary presentation resulted in a cost savings of U.S. $6,838 per additional diagnosis (95% confidence interval, U.S. $3,263-$11,678), compared with the standard diagnostic pathway. The figures reflect costs in an Australian care setting.
The children in the study had a mean diagnostic odyssey of 6 years, including a mean of 19 tests and four clinical genetics and four non–genetics specialist consultations. A quarter of them had undergone at least one diagnostic procedure under general anesthesia.
“The diagnostic odyssey of children suspected of having monogenic disorders is protracted and painful and may not provide a precise diagnosis,” Dr. Tan and his colleagues wrote in their analysis. “This paradigm has markedly shifted with the advent of WES.”
WES is best targeted to children “with genetically heterogeneous disorders or features overlapping several conditions,” the investigators concluded. “Our findings suggest that these children are best served by early recognition by their pediatrician and expedited referral to clinical genetics with WES applied after chromosomal microarray but before an extensive diagnostic process.”
Dr. Tan and his colleagues’ study was funded by the Melbourne Genomics Health Alliance and state and national governments in Australia. None of the authors declared conflicts of interest. Dr. Berg and her colleagues’ study was funded by the Pediatric Epilepsy Research Foundation, and none of its authors disclosed commercial conflicts of interest.
The studies by Tan et al. and Berg et al. demonstrate the dramatic effect of the diagnostic yield of different genetic testing approaches on cost-effectiveness and the potential design of testing strategies in children with suspected monogenic conditions. Both studies emphasize the effect of the results of genetic testing. Whereas Tan et al. showed that, in 26% of cases, the result enabled a specific modification of patient care, Berg et al. also demonstrated that there is no basis for identifying optimal, targeted treatments, when testing is not performed and genetic diagnoses are not made.
However, in the absence of targeted treatments, a genetic diagnosis is of high value for the patients, their families, and treating physicians. A clear diagnosis may not only be of prognostic value but also put an end to a possibly stressful and demanding diagnostic odyssey. It may enable patient care that is explicitly focused on the individual needs of the patient. A clear diagnosis usually also allows a better assessment of the risks of recurrence in the family and possibly enables prenatal testing in relatives. Finally, it enables research and a better scientific understanding of the underlying pathophysiology, which may ideally lead to the identification of novel therapeutic prospects. Seven years ago, an international consensus statement endorsed the replacement of classic cytogenetic karyotype analysis by chromosomal microarrays as a first-tier diagnostic test in individuals with developmental disabilities or congenital anomalies. The studies add to the growing evidence that this consensus may already be outdated, as high-throughput sequencing techniques may achieve even higher diagnostic yields and, thus, are capable to become the new first-tier diagnostic test in congenital and early-onset disorders.
Johannes R. Lemke, MD, is with the Institute of Human Genetics at the University of Leipzig (Germany) Hospitals and Clinics. He reports no conflicts of interest associated with his editorial, which accompanied the JAMA Pediatrics reports (JAMA Pediatr. 2017 July 31. doi: 10.1001/jamapediatrics.2017.1743).
The studies by Tan et al. and Berg et al. demonstrate the dramatic effect of the diagnostic yield of different genetic testing approaches on cost-effectiveness and the potential design of testing strategies in children with suspected monogenic conditions. Both studies emphasize the effect of the results of genetic testing. Whereas Tan et al. showed that, in 26% of cases, the result enabled a specific modification of patient care, Berg et al. also demonstrated that there is no basis for identifying optimal, targeted treatments, when testing is not performed and genetic diagnoses are not made.
However, in the absence of targeted treatments, a genetic diagnosis is of high value for the patients, their families, and treating physicians. A clear diagnosis may not only be of prognostic value but also put an end to a possibly stressful and demanding diagnostic odyssey. It may enable patient care that is explicitly focused on the individual needs of the patient. A clear diagnosis usually also allows a better assessment of the risks of recurrence in the family and possibly enables prenatal testing in relatives. Finally, it enables research and a better scientific understanding of the underlying pathophysiology, which may ideally lead to the identification of novel therapeutic prospects. Seven years ago, an international consensus statement endorsed the replacement of classic cytogenetic karyotype analysis by chromosomal microarrays as a first-tier diagnostic test in individuals with developmental disabilities or congenital anomalies. The studies add to the growing evidence that this consensus may already be outdated, as high-throughput sequencing techniques may achieve even higher diagnostic yields and, thus, are capable to become the new first-tier diagnostic test in congenital and early-onset disorders.
Johannes R. Lemke, MD, is with the Institute of Human Genetics at the University of Leipzig (Germany) Hospitals and Clinics. He reports no conflicts of interest associated with his editorial, which accompanied the JAMA Pediatrics reports (JAMA Pediatr. 2017 July 31. doi: 10.1001/jamapediatrics.2017.1743).
The studies by Tan et al. and Berg et al. demonstrate the dramatic effect of the diagnostic yield of different genetic testing approaches on cost-effectiveness and the potential design of testing strategies in children with suspected monogenic conditions. Both studies emphasize the effect of the results of genetic testing. Whereas Tan et al. showed that, in 26% of cases, the result enabled a specific modification of patient care, Berg et al. also demonstrated that there is no basis for identifying optimal, targeted treatments, when testing is not performed and genetic diagnoses are not made.
However, in the absence of targeted treatments, a genetic diagnosis is of high value for the patients, their families, and treating physicians. A clear diagnosis may not only be of prognostic value but also put an end to a possibly stressful and demanding diagnostic odyssey. It may enable patient care that is explicitly focused on the individual needs of the patient. A clear diagnosis usually also allows a better assessment of the risks of recurrence in the family and possibly enables prenatal testing in relatives. Finally, it enables research and a better scientific understanding of the underlying pathophysiology, which may ideally lead to the identification of novel therapeutic prospects. Seven years ago, an international consensus statement endorsed the replacement of classic cytogenetic karyotype analysis by chromosomal microarrays as a first-tier diagnostic test in individuals with developmental disabilities or congenital anomalies. The studies add to the growing evidence that this consensus may already be outdated, as high-throughput sequencing techniques may achieve even higher diagnostic yields and, thus, are capable to become the new first-tier diagnostic test in congenital and early-onset disorders.
Johannes R. Lemke, MD, is with the Institute of Human Genetics at the University of Leipzig (Germany) Hospitals and Clinics. He reports no conflicts of interest associated with his editorial, which accompanied the JAMA Pediatrics reports (JAMA Pediatr. 2017 July 31. doi: 10.1001/jamapediatrics.2017.1743).
Results from two new studies suggest that genetic testing early in the diagnostic pathway may allow for earlier and more precise diagnoses in early-life epilepsies and a range of other childhood-onset disorders, and potentially limit costs associated with a long diagnostic course.
Both papers, published online July 31 in JAMA Pediatrics, showed the diagnostic yield of genetic testing approaches, including whole-exome sequencing (WES), to be high.
The results also argue for the incorporation of genetic testing into the first diagnostic assessments; not limiting it to severe presentations only; and for broad testing methods to be employed in lieu of narrower ones.
Of these patients, just under half (n = 327) underwent various forms of genetic testing at the discretion of the treating physician, including karyotyping, microarrays, epilepsy gene panels, WES, mitochondrial panels, and other tests. Pathogenic variants were discovered in 132 children, or 40% of those receiving genetic testing (JAMA Pediatr. 2017 July 31. doi: 10.1001/jamapediatrics.2017.1743).
Of all the genetic testing methods employed in the study, diagnostic yields were significantly greater for epilepsy gene panels (29.2%) and WES (27.8%), compared with chromosome microarray (7.9%).
The results, the investigators said, provide “added impetus to move the diagnosis of the specific cause to the point of initial presentation ... it is time to provide greater emphasis on and support for thorough genetic evaluations, particularly sequencing-based evaluations, for children with newly presenting epilepsies in the first few years of life.”
In addition to aiding management decisions, early genetic testing “ends the diagnostic odyssey during which parents and physicians spend untold amounts of time searching for an explanation for a child’s epilepsy and reduces associated costs,” Dr. Berg and her colleagues concluded.
In a separate study led by Tiong Yang Tan, MBBS, PhD, of Victorian Clinical Genetics Services in Melbourne, Australia, and his colleagues, singleton WES was used in 44 children recruited at outpatient clinics of a Melbourne hospital system (JAMA Pediatr. 2017 July 31. doi: 10.1001/jamapediatrics.2017.1755).
Children in the study were aged 2-18 years (with mean age at presentation 28 months) and had a wide variety of suspected genetic disorders, including skeletal, skin, neurometabolic, and intellectual disorders. Some of these had features overlapping several conditions. The children in the cohort had not received prior genetic testing before undergoing WES.
The molecular test resulted in a diagnosis in 52% (n = 23) of the children, including unexpected diagnoses in eight of these. Clinical management was altered as result of sequencing findings in six children.
“Although phenotyping is critical, 35% of children had a diagnosis caused by a gene outside the initially prioritized gene list. This finding not only possibly reflects lack of clinical recognition but also underscores the utility of WES in achieving a diagnosis even when the a priori hypothesis is imprecise,” Dr. Tan and his associates wrote in their analysis.
Dr. Tan and his colleagues conducted a cost analysis that found WES performed at initial tertiary presentation resulted in a cost savings of U.S. $6,838 per additional diagnosis (95% confidence interval, U.S. $3,263-$11,678), compared with the standard diagnostic pathway. The figures reflect costs in an Australian care setting.
The children in the study had a mean diagnostic odyssey of 6 years, including a mean of 19 tests and four clinical genetics and four non–genetics specialist consultations. A quarter of them had undergone at least one diagnostic procedure under general anesthesia.
“The diagnostic odyssey of children suspected of having monogenic disorders is protracted and painful and may not provide a precise diagnosis,” Dr. Tan and his colleagues wrote in their analysis. “This paradigm has markedly shifted with the advent of WES.”
WES is best targeted to children “with genetically heterogeneous disorders or features overlapping several conditions,” the investigators concluded. “Our findings suggest that these children are best served by early recognition by their pediatrician and expedited referral to clinical genetics with WES applied after chromosomal microarray but before an extensive diagnostic process.”
Dr. Tan and his colleagues’ study was funded by the Melbourne Genomics Health Alliance and state and national governments in Australia. None of the authors declared conflicts of interest. Dr. Berg and her colleagues’ study was funded by the Pediatric Epilepsy Research Foundation, and none of its authors disclosed commercial conflicts of interest.
Results from two new studies suggest that genetic testing early in the diagnostic pathway may allow for earlier and more precise diagnoses in early-life epilepsies and a range of other childhood-onset disorders, and potentially limit costs associated with a long diagnostic course.
Both papers, published online July 31 in JAMA Pediatrics, showed the diagnostic yield of genetic testing approaches, including whole-exome sequencing (WES), to be high.
The results also argue for the incorporation of genetic testing into the first diagnostic assessments; not limiting it to severe presentations only; and for broad testing methods to be employed in lieu of narrower ones.
Of these patients, just under half (n = 327) underwent various forms of genetic testing at the discretion of the treating physician, including karyotyping, microarrays, epilepsy gene panels, WES, mitochondrial panels, and other tests. Pathogenic variants were discovered in 132 children, or 40% of those receiving genetic testing (JAMA Pediatr. 2017 July 31. doi: 10.1001/jamapediatrics.2017.1743).
Of all the genetic testing methods employed in the study, diagnostic yields were significantly greater for epilepsy gene panels (29.2%) and WES (27.8%), compared with chromosome microarray (7.9%).
The results, the investigators said, provide “added impetus to move the diagnosis of the specific cause to the point of initial presentation ... it is time to provide greater emphasis on and support for thorough genetic evaluations, particularly sequencing-based evaluations, for children with newly presenting epilepsies in the first few years of life.”
In addition to aiding management decisions, early genetic testing “ends the diagnostic odyssey during which parents and physicians spend untold amounts of time searching for an explanation for a child’s epilepsy and reduces associated costs,” Dr. Berg and her colleagues concluded.
In a separate study led by Tiong Yang Tan, MBBS, PhD, of Victorian Clinical Genetics Services in Melbourne, Australia, and his colleagues, singleton WES was used in 44 children recruited at outpatient clinics of a Melbourne hospital system (JAMA Pediatr. 2017 July 31. doi: 10.1001/jamapediatrics.2017.1755).
Children in the study were aged 2-18 years (with mean age at presentation 28 months) and had a wide variety of suspected genetic disorders, including skeletal, skin, neurometabolic, and intellectual disorders. Some of these had features overlapping several conditions. The children in the cohort had not received prior genetic testing before undergoing WES.
The molecular test resulted in a diagnosis in 52% (n = 23) of the children, including unexpected diagnoses in eight of these. Clinical management was altered as result of sequencing findings in six children.
“Although phenotyping is critical, 35% of children had a diagnosis caused by a gene outside the initially prioritized gene list. This finding not only possibly reflects lack of clinical recognition but also underscores the utility of WES in achieving a diagnosis even when the a priori hypothesis is imprecise,” Dr. Tan and his associates wrote in their analysis.
Dr. Tan and his colleagues conducted a cost analysis that found WES performed at initial tertiary presentation resulted in a cost savings of U.S. $6,838 per additional diagnosis (95% confidence interval, U.S. $3,263-$11,678), compared with the standard diagnostic pathway. The figures reflect costs in an Australian care setting.
The children in the study had a mean diagnostic odyssey of 6 years, including a mean of 19 tests and four clinical genetics and four non–genetics specialist consultations. A quarter of them had undergone at least one diagnostic procedure under general anesthesia.
“The diagnostic odyssey of children suspected of having monogenic disorders is protracted and painful and may not provide a precise diagnosis,” Dr. Tan and his colleagues wrote in their analysis. “This paradigm has markedly shifted with the advent of WES.”
WES is best targeted to children “with genetically heterogeneous disorders or features overlapping several conditions,” the investigators concluded. “Our findings suggest that these children are best served by early recognition by their pediatrician and expedited referral to clinical genetics with WES applied after chromosomal microarray but before an extensive diagnostic process.”
Dr. Tan and his colleagues’ study was funded by the Melbourne Genomics Health Alliance and state and national governments in Australia. None of the authors declared conflicts of interest. Dr. Berg and her colleagues’ study was funded by the Pediatric Epilepsy Research Foundation, and none of its authors disclosed commercial conflicts of interest.
FROM JAMA PEDIATRICS
Which Acute Myeloid Leukemia Patients are Good Immunotherapy Candidates?
Some patients with acute myeloid leukemia (AML) may have trouble with immunotherapy following chemotherapy. Researchers from the National Heart, Lung and Blood Institute may have found a reason why.
Related: Novel Treatment Shows Promise for Acute Lymphoblastic Leukemia
The researchers wanted to perform a “deep assessment” of the state of the adaptive immune system in AML patients in remission after chemotherapy. They used these patients’ response to seasonal influenza vaccination as a surrogate for the robustness of the immune system. The researchers say their approach was unique in that they established a comprehensive picture of the adaptive “immunome” by simultaneously examining the genetic, phenotypic, and functional consequences of chemotherapy.
Their assessment revealed a “dramatic impact” in the B-cell compartment, which appeared slower to recover than the T-cell compartment. Of 10 patients in the study, only 2 generated protective titers in response to vaccination. Most had abnormal frequencies of transitional and memory B-cells. The researchers say the inability of AML patients to produce protective antibody titers in response to influenza vaccination is likely due to multiple B-cell abnormalities.
Related: Six Open Clinical Trials That Are Expanding Our Understanding of Immunotherapies
The researchers “strikingly” found similar patterns of immune dysfunction across all the patients in the study. When they ranked patients based on time elapsed since chemotherapy, the degree of dysfunction was shown to be less in patients who had the most time elapsed form their chemotherapy treatment.
The researchers conclude the “consistent finding” of a reduction of memory B-cells in all the AML patients suggests that humoral immunity reconstitution is “a very long process.” They add that a better understanding of the changes in adaptive immune cell subsets after chemotherapy will be useful in designing immunotherapies that can work with existing immune capacity.
Source:
Goswami M, Prince G, Biancotto A, et al. J Transl Med. 2017;15:155.
doi: 10.1186/s12967-017-1252-2
Some patients with acute myeloid leukemia (AML) may have trouble with immunotherapy following chemotherapy. Researchers from the National Heart, Lung and Blood Institute may have found a reason why.
Related: Novel Treatment Shows Promise for Acute Lymphoblastic Leukemia
The researchers wanted to perform a “deep assessment” of the state of the adaptive immune system in AML patients in remission after chemotherapy. They used these patients’ response to seasonal influenza vaccination as a surrogate for the robustness of the immune system. The researchers say their approach was unique in that they established a comprehensive picture of the adaptive “immunome” by simultaneously examining the genetic, phenotypic, and functional consequences of chemotherapy.
Their assessment revealed a “dramatic impact” in the B-cell compartment, which appeared slower to recover than the T-cell compartment. Of 10 patients in the study, only 2 generated protective titers in response to vaccination. Most had abnormal frequencies of transitional and memory B-cells. The researchers say the inability of AML patients to produce protective antibody titers in response to influenza vaccination is likely due to multiple B-cell abnormalities.
Related: Six Open Clinical Trials That Are Expanding Our Understanding of Immunotherapies
The researchers “strikingly” found similar patterns of immune dysfunction across all the patients in the study. When they ranked patients based on time elapsed since chemotherapy, the degree of dysfunction was shown to be less in patients who had the most time elapsed form their chemotherapy treatment.
The researchers conclude the “consistent finding” of a reduction of memory B-cells in all the AML patients suggests that humoral immunity reconstitution is “a very long process.” They add that a better understanding of the changes in adaptive immune cell subsets after chemotherapy will be useful in designing immunotherapies that can work with existing immune capacity.
Source:
Goswami M, Prince G, Biancotto A, et al. J Transl Med. 2017;15:155.
doi: 10.1186/s12967-017-1252-2
Some patients with acute myeloid leukemia (AML) may have trouble with immunotherapy following chemotherapy. Researchers from the National Heart, Lung and Blood Institute may have found a reason why.
Related: Novel Treatment Shows Promise for Acute Lymphoblastic Leukemia
The researchers wanted to perform a “deep assessment” of the state of the adaptive immune system in AML patients in remission after chemotherapy. They used these patients’ response to seasonal influenza vaccination as a surrogate for the robustness of the immune system. The researchers say their approach was unique in that they established a comprehensive picture of the adaptive “immunome” by simultaneously examining the genetic, phenotypic, and functional consequences of chemotherapy.
Their assessment revealed a “dramatic impact” in the B-cell compartment, which appeared slower to recover than the T-cell compartment. Of 10 patients in the study, only 2 generated protective titers in response to vaccination. Most had abnormal frequencies of transitional and memory B-cells. The researchers say the inability of AML patients to produce protective antibody titers in response to influenza vaccination is likely due to multiple B-cell abnormalities.
Related: Six Open Clinical Trials That Are Expanding Our Understanding of Immunotherapies
The researchers “strikingly” found similar patterns of immune dysfunction across all the patients in the study. When they ranked patients based on time elapsed since chemotherapy, the degree of dysfunction was shown to be less in patients who had the most time elapsed form their chemotherapy treatment.
The researchers conclude the “consistent finding” of a reduction of memory B-cells in all the AML patients suggests that humoral immunity reconstitution is “a very long process.” They add that a better understanding of the changes in adaptive immune cell subsets after chemotherapy will be useful in designing immunotherapies that can work with existing immune capacity.
Source:
Goswami M, Prince G, Biancotto A, et al. J Transl Med. 2017;15:155.
doi: 10.1186/s12967-017-1252-2
August 2017 Digital Edition
Click here to access the August 2017 Digital Edition.
Table of Contents
- Collaboration of the NIH and PHS Commissioned Corps in the International Ebola Clinical Research Response
- Parkinsonism and Vitamin C Deficiency
- Right Paraduodenal Hernia
- Military Brats: Members of a Lost Tribe
- Practitioner Cognitive Reframing: Working More Effectively in Addictions
- The Role of Methicillin-Resistant Staphylococcus aureus Polymerase Chain Reaction Nasal Swabs in Clinical Decision Making
- Improving Veteran Engagement With Mental Health Care
Click here to access the August 2017 Digital Edition.
Table of Contents
- Collaboration of the NIH and PHS Commissioned Corps in the International Ebola Clinical Research Response
- Parkinsonism and Vitamin C Deficiency
- Right Paraduodenal Hernia
- Military Brats: Members of a Lost Tribe
- Practitioner Cognitive Reframing: Working More Effectively in Addictions
- The Role of Methicillin-Resistant Staphylococcus aureus Polymerase Chain Reaction Nasal Swabs in Clinical Decision Making
- Improving Veteran Engagement With Mental Health Care
Click here to access the August 2017 Digital Edition.
Table of Contents
- Collaboration of the NIH and PHS Commissioned Corps in the International Ebola Clinical Research Response
- Parkinsonism and Vitamin C Deficiency
- Right Paraduodenal Hernia
- Military Brats: Members of a Lost Tribe
- Practitioner Cognitive Reframing: Working More Effectively in Addictions
- The Role of Methicillin-Resistant Staphylococcus aureus Polymerase Chain Reaction Nasal Swabs in Clinical Decision Making
- Improving Veteran Engagement With Mental Health Care
Post-Treatment Follow-Up by Oncologic Specialists as a Relevant Component of Cancer Survivorship for Veteran Patients Living in Rural Area
Purpose: To present a lesson learned from a pilot project aiming to improve post-radiotherapy (RT) followup (FU) care for Veterans living in rural area within our VISN, thereby questioning if FU care as dictated by oncologic specialists would be beneficial in a rural Veteran’s cancer survivorship.
Methods: A team of radiation oncology (RO) specialists was assembled to include clinical providers and medical physicists. A 2-pronged approach was employed: 1 by inperson visit at selected rural community-based outpatient clinic (rCBOC), the other via telehealth link. Target population included rural Veterans who had received RT at either a VA or Non-VA Care Center (NVCC) facility. On-site visits were done by RO specialists at each rCBOC. Patient satisfaction was evaluated via feedback survey. Mileage and time saved were calculated for each Veteran who might otherwise travel to see a VA RO specialist.
Results: In a span of 14 months, 9 separate rCBOC visits were made for 3 sites and a total of 49 Veteran visits. Excellent patient satisfaction was obtained, and the average mileage and time saved per Veteran visit was 217.2 miles and 201 min (off-traffic peak), respectively. However, 4 of 5 NVCC treatment plans encountered contained physics quality assurance (QA) data not considered to have met professional standards. Dedicated telehealth equipment was acquired and connections validated. Challenges faced included: soliciting timely assistance of administrative leadership, identifying patients to be seen and accessing their records, and obtaining clinical privilege and EHR access at rCBOCs.
Implications: Access to post-treatment cancer care for rural Veterans can be improved with in-person visits by VA oncologic specialists at corresponding rCBOCs. Barriers due to distance and time can be reduced significantly, with excellent patient satisfaction outcome. The efficacy of telehealth link requires further clinical testing. Furthermore, the inadvertent finding of physics QA deficiencies at NVCC sites raised plausible concern for overall quality of RT care, reflecting the probable need for future oversight by VA specialists. By reaching out to rural Veterans proactively, VA oncologic specialists can enhance their post-treatment cancer care, thereby improving their cancer survivorship.
Purpose: To present a lesson learned from a pilot project aiming to improve post-radiotherapy (RT) followup (FU) care for Veterans living in rural area within our VISN, thereby questioning if FU care as dictated by oncologic specialists would be beneficial in a rural Veteran’s cancer survivorship.
Methods: A team of radiation oncology (RO) specialists was assembled to include clinical providers and medical physicists. A 2-pronged approach was employed: 1 by inperson visit at selected rural community-based outpatient clinic (rCBOC), the other via telehealth link. Target population included rural Veterans who had received RT at either a VA or Non-VA Care Center (NVCC) facility. On-site visits were done by RO specialists at each rCBOC. Patient satisfaction was evaluated via feedback survey. Mileage and time saved were calculated for each Veteran who might otherwise travel to see a VA RO specialist.
Results: In a span of 14 months, 9 separate rCBOC visits were made for 3 sites and a total of 49 Veteran visits. Excellent patient satisfaction was obtained, and the average mileage and time saved per Veteran visit was 217.2 miles and 201 min (off-traffic peak), respectively. However, 4 of 5 NVCC treatment plans encountered contained physics quality assurance (QA) data not considered to have met professional standards. Dedicated telehealth equipment was acquired and connections validated. Challenges faced included: soliciting timely assistance of administrative leadership, identifying patients to be seen and accessing their records, and obtaining clinical privilege and EHR access at rCBOCs.
Implications: Access to post-treatment cancer care for rural Veterans can be improved with in-person visits by VA oncologic specialists at corresponding rCBOCs. Barriers due to distance and time can be reduced significantly, with excellent patient satisfaction outcome. The efficacy of telehealth link requires further clinical testing. Furthermore, the inadvertent finding of physics QA deficiencies at NVCC sites raised plausible concern for overall quality of RT care, reflecting the probable need for future oversight by VA specialists. By reaching out to rural Veterans proactively, VA oncologic specialists can enhance their post-treatment cancer care, thereby improving their cancer survivorship.
Purpose: To present a lesson learned from a pilot project aiming to improve post-radiotherapy (RT) followup (FU) care for Veterans living in rural area within our VISN, thereby questioning if FU care as dictated by oncologic specialists would be beneficial in a rural Veteran’s cancer survivorship.
Methods: A team of radiation oncology (RO) specialists was assembled to include clinical providers and medical physicists. A 2-pronged approach was employed: 1 by inperson visit at selected rural community-based outpatient clinic (rCBOC), the other via telehealth link. Target population included rural Veterans who had received RT at either a VA or Non-VA Care Center (NVCC) facility. On-site visits were done by RO specialists at each rCBOC. Patient satisfaction was evaluated via feedback survey. Mileage and time saved were calculated for each Veteran who might otherwise travel to see a VA RO specialist.
Results: In a span of 14 months, 9 separate rCBOC visits were made for 3 sites and a total of 49 Veteran visits. Excellent patient satisfaction was obtained, and the average mileage and time saved per Veteran visit was 217.2 miles and 201 min (off-traffic peak), respectively. However, 4 of 5 NVCC treatment plans encountered contained physics quality assurance (QA) data not considered to have met professional standards. Dedicated telehealth equipment was acquired and connections validated. Challenges faced included: soliciting timely assistance of administrative leadership, identifying patients to be seen and accessing their records, and obtaining clinical privilege and EHR access at rCBOCs.
Implications: Access to post-treatment cancer care for rural Veterans can be improved with in-person visits by VA oncologic specialists at corresponding rCBOCs. Barriers due to distance and time can be reduced significantly, with excellent patient satisfaction outcome. The efficacy of telehealth link requires further clinical testing. Furthermore, the inadvertent finding of physics QA deficiencies at NVCC sites raised plausible concern for overall quality of RT care, reflecting the probable need for future oversight by VA specialists. By reaching out to rural Veterans proactively, VA oncologic specialists can enhance their post-treatment cancer care, thereby improving their cancer survivorship.
Update on the VA Precision Oncology Program
Purpose: To inform VA stakeholders of the availability of precision oncology (PO) services for Veterans with advanced cancer.
Background: PO offers the promise of effective, low-toxicity targeted therapies tailored to individual tumor genomics but is unequally available within VHA. A systemwide PO program (POP), including patients in rural areas, launched in July 2016.
Methods: Patients tested with multigene next generation sequencing (NGS) tumor testing through 2 contracted vendors were identified from POP records and cancer characteristics were extracted from POP and medical records. Drug use data were obtained from the VA Corporate Data Warehouse. NGS testing results, and annotations were extracted from POP records.
Results: 1,442 tumor samples were sent for NGS testing as of 5/21/17 from 61 facilities. Rural patient testing (35%) was similar to VHA rurality (33%) and more than twice the US rate (14%). Most common diagnoses: lung (688: adeno 482, squamous 134), unknown (114), colorectal (103), skin (96), prostate (76), and H&N (66). Sample test requests increased rapidly after national implementation in July 2016 (23 samples/month prior to implementation to mean 126 samples/month 3 months later) as did the number of participating facilities (10/quarter to 39/month). Sequencing success rate increased from 68% to 71% over the same interval, while mean turn around time remained similar at 19.7 and 19.1 days, respectively. To date, 26 patients received a recommended drug outside a clinical trial, some more than 9 months after NGS. 5 additional patients had received an NGS-recommended drug prior to testing. NGS results are available for a cohort of 344 patients including: lung 200 (adeno 138, squamous 51), skin 28, LN 20, liver 19, GI 16. 979 variants were found most commonly in TP53, KRAS, STK11, APC, PIK3CA, and CDKN2A. 228 patients (66%) had actionable results (on-label drug 24, off-label drug 165, clinical trial 213). A PO consultation service (available by IFC) and a liquid biopsy are now available nationally.
Conclusions: Implementation of tumor NGS testing in VHA has been successful. Further program expansion, addition of hematological malignancies, deployment of informatics tools and efforts to expand access to appropriate drugs are ongoing.
Purpose: To inform VA stakeholders of the availability of precision oncology (PO) services for Veterans with advanced cancer.
Background: PO offers the promise of effective, low-toxicity targeted therapies tailored to individual tumor genomics but is unequally available within VHA. A systemwide PO program (POP), including patients in rural areas, launched in July 2016.
Methods: Patients tested with multigene next generation sequencing (NGS) tumor testing through 2 contracted vendors were identified from POP records and cancer characteristics were extracted from POP and medical records. Drug use data were obtained from the VA Corporate Data Warehouse. NGS testing results, and annotations were extracted from POP records.
Results: 1,442 tumor samples were sent for NGS testing as of 5/21/17 from 61 facilities. Rural patient testing (35%) was similar to VHA rurality (33%) and more than twice the US rate (14%). Most common diagnoses: lung (688: adeno 482, squamous 134), unknown (114), colorectal (103), skin (96), prostate (76), and H&N (66). Sample test requests increased rapidly after national implementation in July 2016 (23 samples/month prior to implementation to mean 126 samples/month 3 months later) as did the number of participating facilities (10/quarter to 39/month). Sequencing success rate increased from 68% to 71% over the same interval, while mean turn around time remained similar at 19.7 and 19.1 days, respectively. To date, 26 patients received a recommended drug outside a clinical trial, some more than 9 months after NGS. 5 additional patients had received an NGS-recommended drug prior to testing. NGS results are available for a cohort of 344 patients including: lung 200 (adeno 138, squamous 51), skin 28, LN 20, liver 19, GI 16. 979 variants were found most commonly in TP53, KRAS, STK11, APC, PIK3CA, and CDKN2A. 228 patients (66%) had actionable results (on-label drug 24, off-label drug 165, clinical trial 213). A PO consultation service (available by IFC) and a liquid biopsy are now available nationally.
Conclusions: Implementation of tumor NGS testing in VHA has been successful. Further program expansion, addition of hematological malignancies, deployment of informatics tools and efforts to expand access to appropriate drugs are ongoing.
Purpose: To inform VA stakeholders of the availability of precision oncology (PO) services for Veterans with advanced cancer.
Background: PO offers the promise of effective, low-toxicity targeted therapies tailored to individual tumor genomics but is unequally available within VHA. A systemwide PO program (POP), including patients in rural areas, launched in July 2016.
Methods: Patients tested with multigene next generation sequencing (NGS) tumor testing through 2 contracted vendors were identified from POP records and cancer characteristics were extracted from POP and medical records. Drug use data were obtained from the VA Corporate Data Warehouse. NGS testing results, and annotations were extracted from POP records.
Results: 1,442 tumor samples were sent for NGS testing as of 5/21/17 from 61 facilities. Rural patient testing (35%) was similar to VHA rurality (33%) and more than twice the US rate (14%). Most common diagnoses: lung (688: adeno 482, squamous 134), unknown (114), colorectal (103), skin (96), prostate (76), and H&N (66). Sample test requests increased rapidly after national implementation in July 2016 (23 samples/month prior to implementation to mean 126 samples/month 3 months later) as did the number of participating facilities (10/quarter to 39/month). Sequencing success rate increased from 68% to 71% over the same interval, while mean turn around time remained similar at 19.7 and 19.1 days, respectively. To date, 26 patients received a recommended drug outside a clinical trial, some more than 9 months after NGS. 5 additional patients had received an NGS-recommended drug prior to testing. NGS results are available for a cohort of 344 patients including: lung 200 (adeno 138, squamous 51), skin 28, LN 20, liver 19, GI 16. 979 variants were found most commonly in TP53, KRAS, STK11, APC, PIK3CA, and CDKN2A. 228 patients (66%) had actionable results (on-label drug 24, off-label drug 165, clinical trial 213). A PO consultation service (available by IFC) and a liquid biopsy are now available nationally.
Conclusions: Implementation of tumor NGS testing in VHA has been successful. Further program expansion, addition of hematological malignancies, deployment of informatics tools and efforts to expand access to appropriate drugs are ongoing.
DDSEP® 8 Quick quiz - August 2017 Question 2
Q2: Answer: D
The history of weight loss, intermittent diarrhea, and bloating are suspicious for celiac disease. While lactose intolerance can explain the pain, diarrhea, and bloating, there does not appear to be any correlation with the ingestion of particular foods, nor should there be any weight loss. While inflammatory bowel disease is certainly a possible explanation for his symptoms, it would be premature to jump to upper and lower endoscopy as initial evaluations.
Tissue transglutaminase antibodies are a sensitive and specific screening test for celiac disease, with published sensitivities and specificities greater than 95%. Obtaining a total serum IgA level at the time of screening is recommended to exclude IgA deficiency, which may result in a false-negative test.
Reference
1. Husby S., Koletzko S., Korponay-Szabo I.R., et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54:136-60.
2. Olen O., Gudjonsdottir A., Browaldh L., et al. Antibodies against deamindated gliadin peptides and tissue transglutaminase for diagnosis of pediatric celiac disease. J Pediatr Gastroenterol Nutr. 2012;55:695-700.
Q2: Answer: D
The history of weight loss, intermittent diarrhea, and bloating are suspicious for celiac disease. While lactose intolerance can explain the pain, diarrhea, and bloating, there does not appear to be any correlation with the ingestion of particular foods, nor should there be any weight loss. While inflammatory bowel disease is certainly a possible explanation for his symptoms, it would be premature to jump to upper and lower endoscopy as initial evaluations.
Tissue transglutaminase antibodies are a sensitive and specific screening test for celiac disease, with published sensitivities and specificities greater than 95%. Obtaining a total serum IgA level at the time of screening is recommended to exclude IgA deficiency, which may result in a false-negative test.
Reference
1. Husby S., Koletzko S., Korponay-Szabo I.R., et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54:136-60.
2. Olen O., Gudjonsdottir A., Browaldh L., et al. Antibodies against deamindated gliadin peptides and tissue transglutaminase for diagnosis of pediatric celiac disease. J Pediatr Gastroenterol Nutr. 2012;55:695-700.
Q2: Answer: D
The history of weight loss, intermittent diarrhea, and bloating are suspicious for celiac disease. While lactose intolerance can explain the pain, diarrhea, and bloating, there does not appear to be any correlation with the ingestion of particular foods, nor should there be any weight loss. While inflammatory bowel disease is certainly a possible explanation for his symptoms, it would be premature to jump to upper and lower endoscopy as initial evaluations.
Tissue transglutaminase antibodies are a sensitive and specific screening test for celiac disease, with published sensitivities and specificities greater than 95%. Obtaining a total serum IgA level at the time of screening is recommended to exclude IgA deficiency, which may result in a false-negative test.
Reference
1. Husby S., Koletzko S., Korponay-Szabo I.R., et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54:136-60.
2. Olen O., Gudjonsdottir A., Browaldh L., et al. Antibodies against deamindated gliadin peptides and tissue transglutaminase for diagnosis of pediatric celiac disease. J Pediatr Gastroenterol Nutr. 2012;55:695-700.
A 10-year-old boy is referred after he was noted to have lost weight over the past year during a routine physical exam. He denies trying to lose weight. He has occasional abdominal pain and intermittent watery nonbloody diarrhea, which do not seem associated with particular foods. He also complains of feeling bloated and his mother reports that “his belly always looks swollen.” He has had no other symptoms of illness. On physical exam, he is slender and has a mildly distended and tympanitic abdomen.
Opioid abuse and overdose: Keep your patients safe
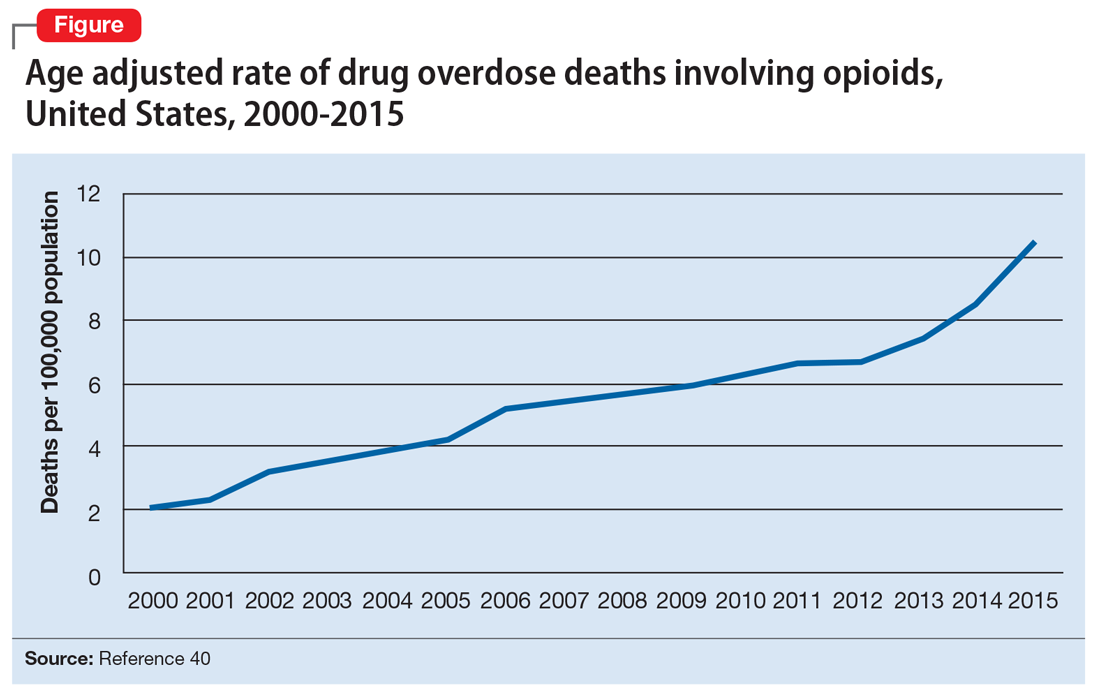
Opioid abuse and overdose are large and growing problems, and in recent years the numbers have been staggering. Overdose deaths related to opioids increased from 28,647 in 2014 to 33,091 in 2015 (Figure).1 More than 2 million individuals in the United States had opioid use disorder in 2015,2 and approximately 80% of them received no treatment,3 even though effective treatment could reduce the scope of abuse.4,5
Although psychiatrists typically are not the primary prescribers of opioid medications, they often treat psychiatric disorders in patients with chronic pain who take prescription opioids. A recent study found that, despite representing only 16% of the adult population, adults with mental health disorders receive more than one-half of all opioid prescriptions distributed each year in the United States.6 Therefore, psychiatrists must be aware of risk assessment strategies for patients receiving opioids.
In this article, we provide recommendations for managing individuals with opioid use disorder, including:
- how to identify risk factors for opioid use disorder and use screening tools
- how to evaluate a patient with suspected opioid use disorder and make the diagnosis
- how to treat a patient with opioid use disorder, including a review of approved pharmaceutical agents.
Risk factors for opioid abuse and overdose
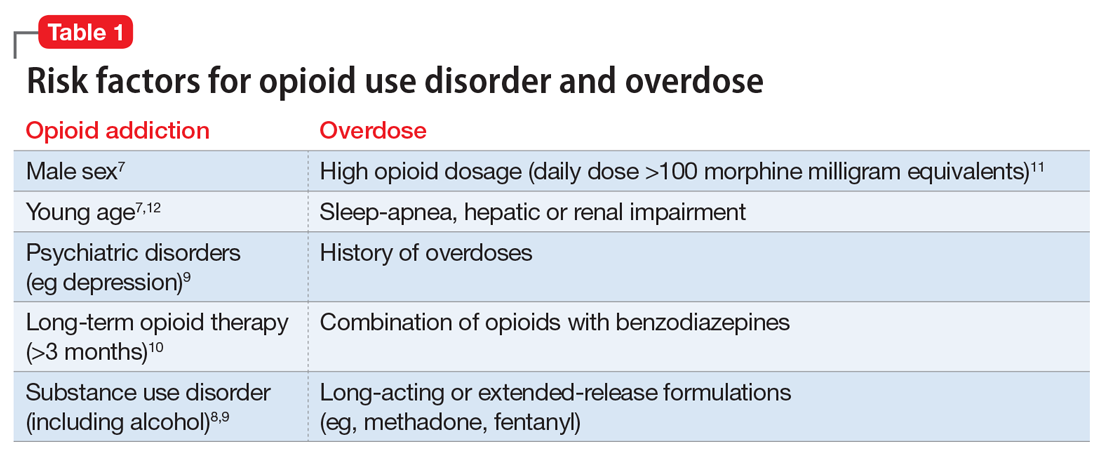
Patients with a history of mental health and/or substance use disorders or at least 3 months of prescribed opioid treatment are at risk for opioid abuse. Those taking a high daily dose of opioids or who have a history of overdose are at risk for overdose from opioid abuse (Table 1).7-12 Standardized tools, such as the Opioid Risk Tool, can be used to screen to assess risk for opioid abuse among individuals prescribed opioids for treatment of chronic pain.12 However, clinicians must be aware that even patients without characteristic risk factors can become dependent on opioids and/or be at risk for an accidental or intentional overdose. For example, opioid therapy following surgical procedures, even in patients who do not have a history of opioid use, increases risk of developing opioid use disorder.13
Evaluation and diagnosis
DSM-5 criteria define 3 degrees of opioid use disorder, depending on how many of the following traits a patient exhibits (mild, 2 to 3; moderate, 4 to 5; and severe, ≥6 )14:
- taking more than the initially intended quantities of opioids or for a longer period of time than intended
- continuous attempts to reduce or otherwise manage opioid use or desires to do so
- a great deal of time using, recovering from, or acquiring opioids
- reports of strong cravings to use opioids
- failing to meet personal objectives at home, work, or school
- continued opioid use even though it causes recurrent social problems
- reduction or elimination of activities the patient once considered important due to opioid use
- opioid use in situations where it is physically dangerous
- continued opioid use despite persistent psychological or physiologic problems despite knowing that continued use is causing or worsening those problems
- tolerance to opioids (not consequential for the diagnosis if the patient is taking opioids under appropriate medical supervision)
- withdrawal or use of opioids (or related substances) to prevent withdrawal (not consequential for the diagnosis if the patient is taking opioids under appropriate medical supervision).
Clinicians should be vigilant for symptoms of opioid use or withdrawal, such as needle marks and weight loss, during the interview (Table 2). High-risk populations that require regular screening include individuals with a history of opioid use disorder, patients taking chronic pain medication, and psychiatric patients.15 During the interview, clinicians should take an nonjudgmental approach and avoid “shame and blame.”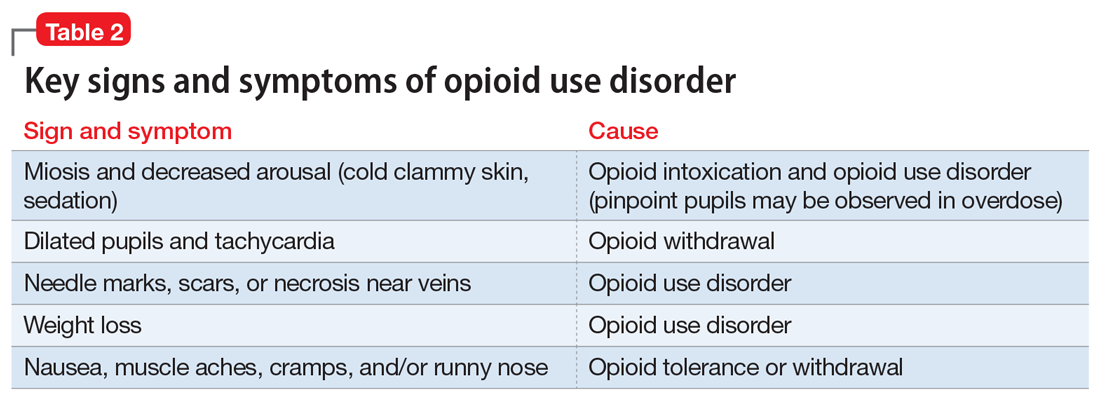
Patients often will withhold information about drug use for various reasons.16 Therefore, collateral information from the patient’s family, close friends, or a referral source is important.
Standardized scales. Various standardized scales can be used to evaluate patients for opioid withdrawal and risk for substance use disorder. Scales for assessing opioid withdrawal include:
- Clinical Opiate Withdrawal Scale
- Subjective Opiate Withdrawal Scale.
Substance use disorder screening tools include:
- Drug Abuse Screen Test-10
- Alcohol Use Disorders Identification Test
- National Institute on Drug Abuse (NIDA) Drug Screening Tool.17
Examination findings. A brief physical examination is necessary to document key findings (Table 2). Patients should undergo a urine drug screen; gas chromatography/mass spectroscopy can confirm positive results. During the examination, clinicians should look for signs and symptoms of co-occurring substance use (eg, benzodiazepines, marijuana, alcohol, cocaine) or mental disorders (mood, anxiety, attention-deficit).18-21 Because nonprescription opioid use is associated with increased risk of suicide attempts and ideation,22 a suicide risk assessment is necessary.
Managing opioid use disorder
Detoxification is a 3-tiered approach that requires judicious prescription of medication, psychosocial support, and supervision to relieve opioid withdrawal symptoms. In both inpatient and outpatient settings, medications used for opioid detoxification include buprenorphine, clonidine, and methadone administered in doses tapered over 5 to 7 days. Appropriate detoxification increases treatment retention for continuing care.23,24
Buprenorphine or buprenorphine/naloxone is the first-line option for outpatient and inpatient detoxification. Short-term detoxification schedules include starting doses between 4 and 16 mg/d, tapered over 5 to 7 days. Compared with methadone, buprenorphine has a lower risk of overdose25 and abuse potential and can be given in an office-based setting. Clonidine, 0.3 to 1.2 mg/d in divided doses, is an alternative to buprenorphine and can be used in inpatient settings.26
Clonidine is not as effective as buprenorphine for detoxification, but it may be used when buprenorphine is contraindicated. Clonidine may require adjuvant symptomatic treatment for insomnia (eg, trazodone, 100 mg at bedtime), anxiety (eg, hydroxyzine, 25 mg, twice a day), or diarrhea (loperamide, 2 mg/d). If a patient needs more structure and monitoring, he (she) should be referred for inpatient detoxification or to a methadone program.27
Medication-assisted therapies
Detoxification alone often is not sufficient treatment. Medication-assisted therapy (MAT) is typically recommended by federal guidelines provided by the Substance Abuse and Mental Health Administration (SAMHSA) for patients with opioid use disorders.3 Patients can be directly transitioned from currently abused opioids to MAT on an outpatient basis. FDA-approved medications for MAT for opioid use disorder include buprenorphine, naltrexone (oral and long-acting injectable), and methadone (Table 3). Choice of MAT depends on several factors, including cost, patient preference, and availability of methadone programs and buprenorphine providers.28

MAT should include psychosocial support29-33 and active monitoring with urine drug screens. Maintenance therapy with medications is usually long-term and has been shown to have better outcomes than detoxification alone or short-term treatment.34 Relapse during MAT should not be cause to discontinue treatment; instead, the patient should be referred to a higher level of care.
Some patients require individualized treatment approaches. For example, the SAMHSA has developed specific treatment improvement protocols to tailor treatments to address specific needs of adolescents.32 The American Academy of Pediatrics recommends MAT with buprenorphine in adolescents with opioid use disorder.33 Although methadone has been approved for pregnant, opioid-dependent patients, recent data indicate buprenorphine is as effective with lower intensity of neonatal abstinence syndrome.34
Buprenorphine. This long-acting (half-life of 24 to 42 hours) opioid partial agonist is approved for treating opioid use disorder in office-based settings according to the Drug Abuse Treatment Act of 2000. Buprenorphine is administered in doses of 8 to 16 mg/d in film or tablet form (sublingual or buccal) and is available in various formulations (Table 4). It is well tolerated; constipation and unpleasant taste are the most common adverse effects. Physicians are required to have a federal waiver to obtain the Drug Enforcement Administration license to prescribe buprenorphine for opioid use disorder in an office setting.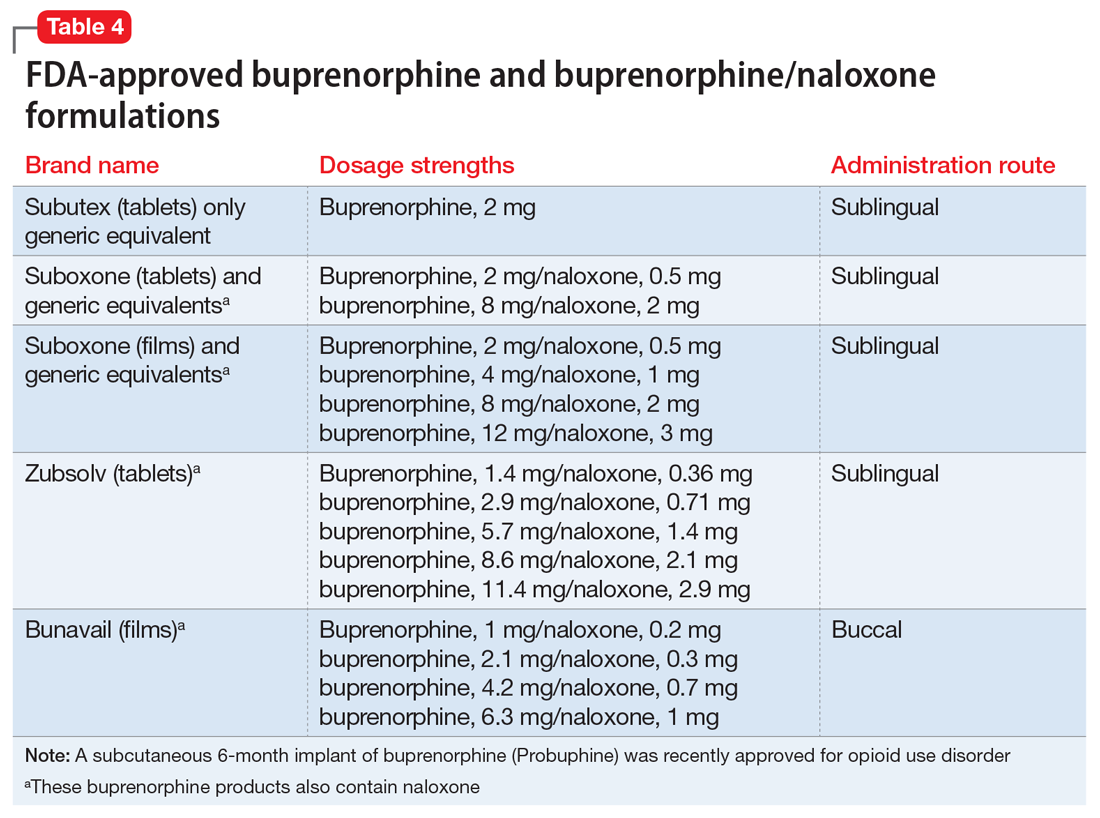
Buprenorphine reduces or eliminates cravings and withdrawal symptoms and helps improve outcomes of abstinence from opioids and retention in treatment.31 Formulations of naloxone combined with buprenorphine reduce the risk of abuse via injection.35 Buprenorphine is safe; however, overdoses can occur when it is combined with benzodiazepines and/or other opiates.
Methadone. This long-acting (half-life 8 to 59 hours), full opioid agonist is approved to treat opioid addiction in federal- and state-regulated opioid treatment programs, also known as methadone maintenance programs. These programs are highly structured and include intensive counseling, monitoring, and dispensing to reduce relapse. Methadone is administered orally either via powder, liquid concentrate, tablet, or solution of diskette. Typically, methadone is dispensed daily in doses of 60 to 100 mg, although higher doses are sometimes necessary. Patients who meet certain criteria for stability may be allowed to take home supplies of methadone.
Methadone has a “black-box” warning for overdose, QT prolongation, and risk for respiratory depression when used in combination with benzodiazepines. Because of its long and unpredictable half-life and tissue accumulation, methadone carries a high overdose risk, particularly with rapidly titrated doses during therapy initiation.35 However, most overdose deaths have occurred with methadone prescribed for pain management. When prescribed and monitored in an opioid treatment program, methadone has shown a high safety profile with respect to overdoses.36
Injectable and oral naltrexone. Used for prevention of relapse to opioid dependence, naltrexone is a pure opioid antagonist that is available as an oral or IM form. Naltrexone has high affinity for the opioid receptors and in therapeutic doses provides an effective blockade for heroin or opioids. Compliance with oral naltrexone has been poor, leading to development of an IM form of naltrexone that can be administered as a single 380-mg dose once every 4 weeks for 6 months or sometimes longer. Naltrexone is also approved for alcohol dependence.
To avoid precipitated withdrawal, patients should be detoxified from opioids for 7 to 10 days before they begin naltrexone, which has no potential for abuse. Common adverse effects include fatigue, nausea, headache, and, for the IM formulation, injection site reactions. There is a “black-box” warning for liver toxicity; therefore, baseline and periodic liver function tests are necessary.
A NIDA review reported poor compliance with oral naltrexone compared with methadone.35 However, naltrexone has been shown to be effective in highly motivated patients (eg, impaired physicians) and the criminal justice population and for preventing relapse following taper from buprenorphine or methadone.37,38
Treatment for opioid overdose
Naloxone is a highly effective treatment to reverse opioid overdose that is delivered via IM or IV injection or by nasal application. Naloxone has no abuse potential. In doses of 0.4 to 2 mg, naloxone reverses overdose within 2 minutes and is effective for 30 to 90 minutes.39 One should call 911 as soon as possible after naloxone is administered. In several states, naloxone is available without a prescription for patients and family members to combat opioid overdoses. The CDC recommends offering naloxone to patients who have risk factors for opioid overdose.40
1. Centers for Disease Control and Prevention. Opioid data analysis. http://www.cdc.gov/drugoverdose/data/analysis.html. Updated February 9, 2017. Accessed June 27, 2017.
2. Substance Abuse and Mental Health Services Administration. Results from the 2015 National Survey on Drug Use and Health: detailed tables. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015.pdf.
3. Substance Abuse and Mental Health Services Administration. Medication-assisted treatment of opioid use disorder pocket guide. https://store.samhsa.gov/shin/content//SMA16-4892PG/SMA16-4892PG.pdf. Accessed June 29, 2017.
4. Mutlu C, Demirci AC, Yalcin O, et al. One-year follow-up of heroin-dependent adolescents treated with buprenorphine/naloxone for the first time in a substance treatment unit. J Subst Abuse Treat. 2016;67:1-8.
5. Sharma B, Bruner A, Barnett G, et al. Opioid use disorders. Child Adolesc Psychiatr Clin N Am. 2016;25(3):473-487.
6. Davis MA, Lin LA, Liu H, Sites BD. Prescription Opioid Use among Adults with mental health disorders in the United States. J Am Board Fam Med. 2017;30:42-47.
7. Icahn School of Medicine at Mount Sinai. Substance use: prescription drugs. http://www.mountsinai.org/patient-care/health-library/diseases-and-conditions/opioid-abuse#risk. Accessed June 27, 2017.
8. Boscarino JA, Rukstalis M, Hoffman SN, et al. Risk factors for drug dependence among out-patients on opioid therapy in a large US health-care system. Addiction. 2010;105(10):1776-1782.
9. Edlund M, Steffick D, Hudson T, et al. Risk factors for clinically recognized opioid abuse and dependence among veterans using opioids for chronic non-cancer pain. Pain. 2007;129(3):355-362.
10. Compton WM, Volkow ND. Major increases in opioid analgesic abuse in the United States: concerns and strategies. Drug Alcohol Depend. 2006;81(2):103-107.
11. Bohnert AS, Valenstein M, Bair M, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011;305(13):1315-1321.
12. Webster LR, Webster RM. Predicting aberrant behaviors in opioid-treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005;6(6):432.
13. Sun EC, Darnall BD, Baker LC, et al. Incidence of and risk factors for chronic opioid use among opioid-naive patients in the postoperative period. JAMA Intern Med. 2016;176(9):1286-1293.
14. Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013.
15. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Internal Med. 2010;152(11):712-720.
16. Substance Abuse and Mental Health Services Administration. Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction: a treatment improvement protocol: TIP 40. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2004.
17. NIDA drug screening tool: clinician’s screening tool for drug use in general medical settings. National Institutes of Health. https://www.drugabuse.gov/nmassist. Accessed June 27, 2017.
18. Fareed A, Eilender P, Haber M, et al. Comorbid posttraumatic stress disorder and opiate addiction: a literature review. J Addict Dis. 2013;32(2):168-179.
19. Rosen D, Smith ML, Reynolds CF 3rd. The prevalence of mental and physical health disorders among older methadone patients. Am J Geriatr Psychiatry. 2008;16(6):488-497.
20. Goldner EM, Lusted A, Roerecke M, et al. Prevalence of Axis-1 psychiatric (with focus on depression and anxiety) disorder and symptomatology among non-medical prescription opioid users in substance use treatment: systematic review and meta-analyses. Addict Behav. 2014;39(3):520-531.
21. Barry DT, Cutter CJ, Beitel M, et al. Psychiatric disorders among patients seeking treatment for co-occurring chronic pain and opioid use disorder. J Clin Psychiatry. 2016;77(10):1413-1419.
22. Kuramoto SJ, Chilcoat HD, Ko J, et al. Suicidal ideation and suicide attempt across stages of nonmedical prescription opioid use and presence of prescription opioid disorders among U.S. adults. J Stud Alcohol Drugs. 2012;73(2):178-184.
23. Mattick RP, Breen C, Kimber J, et al. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;(2):CD002207. doi: 10.1002/14651858.CD002207.pub4.
24. Evans E, Li L, Min J, et al. Mortality among individuals accessing pharmacological treatment for opioid dependence in California, 2006-10. Addiction. 2015;110(6):996-1005.
25. Marteu D, McDonald R, Patel K. The relative risk of fatal poisoning by methadone or buprenorphine within the wider population of England and Wales. BMJ Open. 2015;5(5):e007629. doi: 10.1136/bmjopen-2015-007629.
26. Jasinski DR, Johnson RE, Kocher TR. Clonidine in morphine withdrawal. Differential effects on signs and symptoms. Arch Gen Psychiatry. 1985;42(11):1063-1066.
27. Whelan PJ, Remski K. Buprenorphine vs methadone treatment: a review of evidence in both developed and developing worlds. J Neurosci Rural Pract. 2012;3(1):45-50.
28. Schuckit MA. Treatment of opioid-use disorders. N Engl J Med. 2016;375(4):357-368.
29. Dutra L, Stathopoulou G, Basden SL, et al. A meta-analytic review of psychosocial interventions for substance use disorders. Am J Psychiatry. 2008;165(2):179-187.
30. Brown HL, Britton KA, Mahaffey D, et al. Methadone maintenance in pregnancy: a reappraisal. Am J Obstet Gynecol. 1998;179(2):459-463.
31. Center for Substance Abuse Treatment. Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Treatment Improvement Protocol (TIP) 43.
32. Zimlich R. AAP recommends on medication assisted therapy for adolescent opioid addiction. Contemporary Pediatrics. http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/news/aap-recommends-medication-assisted-therapy-adolescent-opioid-addiction. Published September 15, 2016. Accessed June 29, 2017.
33. Patkar A, Lee J, Burgess D. Opioid use disorder. BMJ Publishing Group. http://bestpractice.bmj.com/best-practice/monograph/200.html. Published 2015. Accessed July 6, 2017.
34. Alho H, Sinclair D, Vuori E, et al. Abuse liability of buprenorphine-naloxone tablets in untreated IV drug users. Drug Alcohol Depend. 2007;88(1):75-78.
35. Centers for Disease Control and Prevention (CDC). Vital signs: risk for overdose from methadone used for pain relief - United States, 1999-2010. MMWR Morb Mortal Wkly Rep. 2012;61(26):493-497.
36. Soyka M. New developments in the management of opioid dependence: focus on sublingual buprenorphine-naloxone. Subst Abuse Rehabil. 2015;6:1-14.
37. Lee JD, Friedmann PD, Kinlock TW, et al. Extended-Release Naltrexone to Prevent Opioid Relapse in Criminal Justice Offenders N Engl J Med. 2016;374(13):1232-1242.
38. Vo HT, Robbins E, Westwood M, et al. Relapse prevention medications in community treatment for young adults with opioid addiction. Subst Abus. 2016;37(3):392-397.
39. McDonald R, Campbell ND, Strang J. Twenty years of take-home naloxone for the prevention of overdose deaths from heroin and other opioids-conception and maturation. Drug Alcohol Depend. 2017;178:176-187.
40. Centers for Disease Control and Prevention. Overdose prevention. https://www.cdc.gov/drugoverdose/opioids/odprevention.html. Updated February 9, 2017. Accessed July 6, 2017.
Opioid abuse and overdose are large and growing problems, and in recent years the numbers have been staggering. Overdose deaths related to opioids increased from 28,647 in 2014 to 33,091 in 2015 (Figure).1 More than 2 million individuals in the United States had opioid use disorder in 2015,2 and approximately 80% of them received no treatment,3 even though effective treatment could reduce the scope of abuse.4,5
Although psychiatrists typically are not the primary prescribers of opioid medications, they often treat psychiatric disorders in patients with chronic pain who take prescription opioids. A recent study found that, despite representing only 16% of the adult population, adults with mental health disorders receive more than one-half of all opioid prescriptions distributed each year in the United States.6 Therefore, psychiatrists must be aware of risk assessment strategies for patients receiving opioids.
In this article, we provide recommendations for managing individuals with opioid use disorder, including:
- how to identify risk factors for opioid use disorder and use screening tools
- how to evaluate a patient with suspected opioid use disorder and make the diagnosis
- how to treat a patient with opioid use disorder, including a review of approved pharmaceutical agents.
Risk factors for opioid abuse and overdose
Patients with a history of mental health and/or substance use disorders or at least 3 months of prescribed opioid treatment are at risk for opioid abuse. Those taking a high daily dose of opioids or who have a history of overdose are at risk for overdose from opioid abuse (Table 1).7-12 Standardized tools, such as the Opioid Risk Tool, can be used to screen to assess risk for opioid abuse among individuals prescribed opioids for treatment of chronic pain.12 However, clinicians must be aware that even patients without characteristic risk factors can become dependent on opioids and/or be at risk for an accidental or intentional overdose. For example, opioid therapy following surgical procedures, even in patients who do not have a history of opioid use, increases risk of developing opioid use disorder.13
Evaluation and diagnosis
DSM-5 criteria define 3 degrees of opioid use disorder, depending on how many of the following traits a patient exhibits (mild, 2 to 3; moderate, 4 to 5; and severe, ≥6 )14:
- taking more than the initially intended quantities of opioids or for a longer period of time than intended
- continuous attempts to reduce or otherwise manage opioid use or desires to do so
- a great deal of time using, recovering from, or acquiring opioids
- reports of strong cravings to use opioids
- failing to meet personal objectives at home, work, or school
- continued opioid use even though it causes recurrent social problems
- reduction or elimination of activities the patient once considered important due to opioid use
- opioid use in situations where it is physically dangerous
- continued opioid use despite persistent psychological or physiologic problems despite knowing that continued use is causing or worsening those problems
- tolerance to opioids (not consequential for the diagnosis if the patient is taking opioids under appropriate medical supervision)
- withdrawal or use of opioids (or related substances) to prevent withdrawal (not consequential for the diagnosis if the patient is taking opioids under appropriate medical supervision).
Clinicians should be vigilant for symptoms of opioid use or withdrawal, such as needle marks and weight loss, during the interview (Table 2). High-risk populations that require regular screening include individuals with a history of opioid use disorder, patients taking chronic pain medication, and psychiatric patients.15 During the interview, clinicians should take an nonjudgmental approach and avoid “shame and blame.”
Patients often will withhold information about drug use for various reasons.16 Therefore, collateral information from the patient’s family, close friends, or a referral source is important.
Standardized scales. Various standardized scales can be used to evaluate patients for opioid withdrawal and risk for substance use disorder. Scales for assessing opioid withdrawal include:
- Clinical Opiate Withdrawal Scale
- Subjective Opiate Withdrawal Scale.
Substance use disorder screening tools include:
- Drug Abuse Screen Test-10
- Alcohol Use Disorders Identification Test
- National Institute on Drug Abuse (NIDA) Drug Screening Tool.17
Examination findings. A brief physical examination is necessary to document key findings (Table 2). Patients should undergo a urine drug screen; gas chromatography/mass spectroscopy can confirm positive results. During the examination, clinicians should look for signs and symptoms of co-occurring substance use (eg, benzodiazepines, marijuana, alcohol, cocaine) or mental disorders (mood, anxiety, attention-deficit).18-21 Because nonprescription opioid use is associated with increased risk of suicide attempts and ideation,22 a suicide risk assessment is necessary.
Managing opioid use disorder
Detoxification is a 3-tiered approach that requires judicious prescription of medication, psychosocial support, and supervision to relieve opioid withdrawal symptoms. In both inpatient and outpatient settings, medications used for opioid detoxification include buprenorphine, clonidine, and methadone administered in doses tapered over 5 to 7 days. Appropriate detoxification increases treatment retention for continuing care.23,24
Buprenorphine or buprenorphine/naloxone is the first-line option for outpatient and inpatient detoxification. Short-term detoxification schedules include starting doses between 4 and 16 mg/d, tapered over 5 to 7 days. Compared with methadone, buprenorphine has a lower risk of overdose25 and abuse potential and can be given in an office-based setting. Clonidine, 0.3 to 1.2 mg/d in divided doses, is an alternative to buprenorphine and can be used in inpatient settings.26
Clonidine is not as effective as buprenorphine for detoxification, but it may be used when buprenorphine is contraindicated. Clonidine may require adjuvant symptomatic treatment for insomnia (eg, trazodone, 100 mg at bedtime), anxiety (eg, hydroxyzine, 25 mg, twice a day), or diarrhea (loperamide, 2 mg/d). If a patient needs more structure and monitoring, he (she) should be referred for inpatient detoxification or to a methadone program.27
Medication-assisted therapies
Detoxification alone often is not sufficient treatment. Medication-assisted therapy (MAT) is typically recommended by federal guidelines provided by the Substance Abuse and Mental Health Administration (SAMHSA) for patients with opioid use disorders.3 Patients can be directly transitioned from currently abused opioids to MAT on an outpatient basis. FDA-approved medications for MAT for opioid use disorder include buprenorphine, naltrexone (oral and long-acting injectable), and methadone (Table 3). Choice of MAT depends on several factors, including cost, patient preference, and availability of methadone programs and buprenorphine providers.28
MAT should include psychosocial support29-33 and active monitoring with urine drug screens. Maintenance therapy with medications is usually long-term and has been shown to have better outcomes than detoxification alone or short-term treatment.34 Relapse during MAT should not be cause to discontinue treatment; instead, the patient should be referred to a higher level of care.
Some patients require individualized treatment approaches. For example, the SAMHSA has developed specific treatment improvement protocols to tailor treatments to address specific needs of adolescents.32 The American Academy of Pediatrics recommends MAT with buprenorphine in adolescents with opioid use disorder.33 Although methadone has been approved for pregnant, opioid-dependent patients, recent data indicate buprenorphine is as effective with lower intensity of neonatal abstinence syndrome.34
Buprenorphine. This long-acting (half-life of 24 to 42 hours) opioid partial agonist is approved for treating opioid use disorder in office-based settings according to the Drug Abuse Treatment Act of 2000. Buprenorphine is administered in doses of 8 to 16 mg/d in film or tablet form (sublingual or buccal) and is available in various formulations (Table 4). It is well tolerated; constipation and unpleasant taste are the most common adverse effects. Physicians are required to have a federal waiver to obtain the Drug Enforcement Administration license to prescribe buprenorphine for opioid use disorder in an office setting.
Buprenorphine reduces or eliminates cravings and withdrawal symptoms and helps improve outcomes of abstinence from opioids and retention in treatment.31 Formulations of naloxone combined with buprenorphine reduce the risk of abuse via injection.35 Buprenorphine is safe; however, overdoses can occur when it is combined with benzodiazepines and/or other opiates.
Methadone. This long-acting (half-life 8 to 59 hours), full opioid agonist is approved to treat opioid addiction in federal- and state-regulated opioid treatment programs, also known as methadone maintenance programs. These programs are highly structured and include intensive counseling, monitoring, and dispensing to reduce relapse. Methadone is administered orally either via powder, liquid concentrate, tablet, or solution of diskette. Typically, methadone is dispensed daily in doses of 60 to 100 mg, although higher doses are sometimes necessary. Patients who meet certain criteria for stability may be allowed to take home supplies of methadone.
Methadone has a “black-box” warning for overdose, QT prolongation, and risk for respiratory depression when used in combination with benzodiazepines. Because of its long and unpredictable half-life and tissue accumulation, methadone carries a high overdose risk, particularly with rapidly titrated doses during therapy initiation.35 However, most overdose deaths have occurred with methadone prescribed for pain management. When prescribed and monitored in an opioid treatment program, methadone has shown a high safety profile with respect to overdoses.36
Injectable and oral naltrexone. Used for prevention of relapse to opioid dependence, naltrexone is a pure opioid antagonist that is available as an oral or IM form. Naltrexone has high affinity for the opioid receptors and in therapeutic doses provides an effective blockade for heroin or opioids. Compliance with oral naltrexone has been poor, leading to development of an IM form of naltrexone that can be administered as a single 380-mg dose once every 4 weeks for 6 months or sometimes longer. Naltrexone is also approved for alcohol dependence.
To avoid precipitated withdrawal, patients should be detoxified from opioids for 7 to 10 days before they begin naltrexone, which has no potential for abuse. Common adverse effects include fatigue, nausea, headache, and, for the IM formulation, injection site reactions. There is a “black-box” warning for liver toxicity; therefore, baseline and periodic liver function tests are necessary.
A NIDA review reported poor compliance with oral naltrexone compared with methadone.35 However, naltrexone has been shown to be effective in highly motivated patients (eg, impaired physicians) and the criminal justice population and for preventing relapse following taper from buprenorphine or methadone.37,38
Treatment for opioid overdose
Naloxone is a highly effective treatment to reverse opioid overdose that is delivered via IM or IV injection or by nasal application. Naloxone has no abuse potential. In doses of 0.4 to 2 mg, naloxone reverses overdose within 2 minutes and is effective for 30 to 90 minutes.39 One should call 911 as soon as possible after naloxone is administered. In several states, naloxone is available without a prescription for patients and family members to combat opioid overdoses. The CDC recommends offering naloxone to patients who have risk factors for opioid overdose.40
Opioid abuse and overdose are large and growing problems, and in recent years the numbers have been staggering. Overdose deaths related to opioids increased from 28,647 in 2014 to 33,091 in 2015 (Figure).1 More than 2 million individuals in the United States had opioid use disorder in 2015,2 and approximately 80% of them received no treatment,3 even though effective treatment could reduce the scope of abuse.4,5
Although psychiatrists typically are not the primary prescribers of opioid medications, they often treat psychiatric disorders in patients with chronic pain who take prescription opioids. A recent study found that, despite representing only 16% of the adult population, adults with mental health disorders receive more than one-half of all opioid prescriptions distributed each year in the United States.6 Therefore, psychiatrists must be aware of risk assessment strategies for patients receiving opioids.
In this article, we provide recommendations for managing individuals with opioid use disorder, including:
- how to identify risk factors for opioid use disorder and use screening tools
- how to evaluate a patient with suspected opioid use disorder and make the diagnosis
- how to treat a patient with opioid use disorder, including a review of approved pharmaceutical agents.
Risk factors for opioid abuse and overdose
Patients with a history of mental health and/or substance use disorders or at least 3 months of prescribed opioid treatment are at risk for opioid abuse. Those taking a high daily dose of opioids or who have a history of overdose are at risk for overdose from opioid abuse (Table 1).7-12 Standardized tools, such as the Opioid Risk Tool, can be used to screen to assess risk for opioid abuse among individuals prescribed opioids for treatment of chronic pain.12 However, clinicians must be aware that even patients without characteristic risk factors can become dependent on opioids and/or be at risk for an accidental or intentional overdose. For example, opioid therapy following surgical procedures, even in patients who do not have a history of opioid use, increases risk of developing opioid use disorder.13
Evaluation and diagnosis
DSM-5 criteria define 3 degrees of opioid use disorder, depending on how many of the following traits a patient exhibits (mild, 2 to 3; moderate, 4 to 5; and severe, ≥6 )14:
- taking more than the initially intended quantities of opioids or for a longer period of time than intended
- continuous attempts to reduce or otherwise manage opioid use or desires to do so
- a great deal of time using, recovering from, or acquiring opioids
- reports of strong cravings to use opioids
- failing to meet personal objectives at home, work, or school
- continued opioid use even though it causes recurrent social problems
- reduction or elimination of activities the patient once considered important due to opioid use
- opioid use in situations where it is physically dangerous
- continued opioid use despite persistent psychological or physiologic problems despite knowing that continued use is causing or worsening those problems
- tolerance to opioids (not consequential for the diagnosis if the patient is taking opioids under appropriate medical supervision)
- withdrawal or use of opioids (or related substances) to prevent withdrawal (not consequential for the diagnosis if the patient is taking opioids under appropriate medical supervision).
Clinicians should be vigilant for symptoms of opioid use or withdrawal, such as needle marks and weight loss, during the interview (Table 2). High-risk populations that require regular screening include individuals with a history of opioid use disorder, patients taking chronic pain medication, and psychiatric patients.15 During the interview, clinicians should take an nonjudgmental approach and avoid “shame and blame.”
Patients often will withhold information about drug use for various reasons.16 Therefore, collateral information from the patient’s family, close friends, or a referral source is important.
Standardized scales. Various standardized scales can be used to evaluate patients for opioid withdrawal and risk for substance use disorder. Scales for assessing opioid withdrawal include:
- Clinical Opiate Withdrawal Scale
- Subjective Opiate Withdrawal Scale.
Substance use disorder screening tools include:
- Drug Abuse Screen Test-10
- Alcohol Use Disorders Identification Test
- National Institute on Drug Abuse (NIDA) Drug Screening Tool.17
Examination findings. A brief physical examination is necessary to document key findings (Table 2). Patients should undergo a urine drug screen; gas chromatography/mass spectroscopy can confirm positive results. During the examination, clinicians should look for signs and symptoms of co-occurring substance use (eg, benzodiazepines, marijuana, alcohol, cocaine) or mental disorders (mood, anxiety, attention-deficit).18-21 Because nonprescription opioid use is associated with increased risk of suicide attempts and ideation,22 a suicide risk assessment is necessary.
Managing opioid use disorder
Detoxification is a 3-tiered approach that requires judicious prescription of medication, psychosocial support, and supervision to relieve opioid withdrawal symptoms. In both inpatient and outpatient settings, medications used for opioid detoxification include buprenorphine, clonidine, and methadone administered in doses tapered over 5 to 7 days. Appropriate detoxification increases treatment retention for continuing care.23,24
Buprenorphine or buprenorphine/naloxone is the first-line option for outpatient and inpatient detoxification. Short-term detoxification schedules include starting doses between 4 and 16 mg/d, tapered over 5 to 7 days. Compared with methadone, buprenorphine has a lower risk of overdose25 and abuse potential and can be given in an office-based setting. Clonidine, 0.3 to 1.2 mg/d in divided doses, is an alternative to buprenorphine and can be used in inpatient settings.26
Clonidine is not as effective as buprenorphine for detoxification, but it may be used when buprenorphine is contraindicated. Clonidine may require adjuvant symptomatic treatment for insomnia (eg, trazodone, 100 mg at bedtime), anxiety (eg, hydroxyzine, 25 mg, twice a day), or diarrhea (loperamide, 2 mg/d). If a patient needs more structure and monitoring, he (she) should be referred for inpatient detoxification or to a methadone program.27
Medication-assisted therapies
Detoxification alone often is not sufficient treatment. Medication-assisted therapy (MAT) is typically recommended by federal guidelines provided by the Substance Abuse and Mental Health Administration (SAMHSA) for patients with opioid use disorders.3 Patients can be directly transitioned from currently abused opioids to MAT on an outpatient basis. FDA-approved medications for MAT for opioid use disorder include buprenorphine, naltrexone (oral and long-acting injectable), and methadone (Table 3). Choice of MAT depends on several factors, including cost, patient preference, and availability of methadone programs and buprenorphine providers.28
MAT should include psychosocial support29-33 and active monitoring with urine drug screens. Maintenance therapy with medications is usually long-term and has been shown to have better outcomes than detoxification alone or short-term treatment.34 Relapse during MAT should not be cause to discontinue treatment; instead, the patient should be referred to a higher level of care.
Some patients require individualized treatment approaches. For example, the SAMHSA has developed specific treatment improvement protocols to tailor treatments to address specific needs of adolescents.32 The American Academy of Pediatrics recommends MAT with buprenorphine in adolescents with opioid use disorder.33 Although methadone has been approved for pregnant, opioid-dependent patients, recent data indicate buprenorphine is as effective with lower intensity of neonatal abstinence syndrome.34
Buprenorphine. This long-acting (half-life of 24 to 42 hours) opioid partial agonist is approved for treating opioid use disorder in office-based settings according to the Drug Abuse Treatment Act of 2000. Buprenorphine is administered in doses of 8 to 16 mg/d in film or tablet form (sublingual or buccal) and is available in various formulations (Table 4). It is well tolerated; constipation and unpleasant taste are the most common adverse effects. Physicians are required to have a federal waiver to obtain the Drug Enforcement Administration license to prescribe buprenorphine for opioid use disorder in an office setting.
Buprenorphine reduces or eliminates cravings and withdrawal symptoms and helps improve outcomes of abstinence from opioids and retention in treatment.31 Formulations of naloxone combined with buprenorphine reduce the risk of abuse via injection.35 Buprenorphine is safe; however, overdoses can occur when it is combined with benzodiazepines and/or other opiates.
Methadone. This long-acting (half-life 8 to 59 hours), full opioid agonist is approved to treat opioid addiction in federal- and state-regulated opioid treatment programs, also known as methadone maintenance programs. These programs are highly structured and include intensive counseling, monitoring, and dispensing to reduce relapse. Methadone is administered orally either via powder, liquid concentrate, tablet, or solution of diskette. Typically, methadone is dispensed daily in doses of 60 to 100 mg, although higher doses are sometimes necessary. Patients who meet certain criteria for stability may be allowed to take home supplies of methadone.
Methadone has a “black-box” warning for overdose, QT prolongation, and risk for respiratory depression when used in combination with benzodiazepines. Because of its long and unpredictable half-life and tissue accumulation, methadone carries a high overdose risk, particularly with rapidly titrated doses during therapy initiation.35 However, most overdose deaths have occurred with methadone prescribed for pain management. When prescribed and monitored in an opioid treatment program, methadone has shown a high safety profile with respect to overdoses.36
Injectable and oral naltrexone. Used for prevention of relapse to opioid dependence, naltrexone is a pure opioid antagonist that is available as an oral or IM form. Naltrexone has high affinity for the opioid receptors and in therapeutic doses provides an effective blockade for heroin or opioids. Compliance with oral naltrexone has been poor, leading to development of an IM form of naltrexone that can be administered as a single 380-mg dose once every 4 weeks for 6 months or sometimes longer. Naltrexone is also approved for alcohol dependence.
To avoid precipitated withdrawal, patients should be detoxified from opioids for 7 to 10 days before they begin naltrexone, which has no potential for abuse. Common adverse effects include fatigue, nausea, headache, and, for the IM formulation, injection site reactions. There is a “black-box” warning for liver toxicity; therefore, baseline and periodic liver function tests are necessary.
A NIDA review reported poor compliance with oral naltrexone compared with methadone.35 However, naltrexone has been shown to be effective in highly motivated patients (eg, impaired physicians) and the criminal justice population and for preventing relapse following taper from buprenorphine or methadone.37,38
Treatment for opioid overdose
Naloxone is a highly effective treatment to reverse opioid overdose that is delivered via IM or IV injection or by nasal application. Naloxone has no abuse potential. In doses of 0.4 to 2 mg, naloxone reverses overdose within 2 minutes and is effective for 30 to 90 minutes.39 One should call 911 as soon as possible after naloxone is administered. In several states, naloxone is available without a prescription for patients and family members to combat opioid overdoses. The CDC recommends offering naloxone to patients who have risk factors for opioid overdose.40
1. Centers for Disease Control and Prevention. Opioid data analysis. http://www.cdc.gov/drugoverdose/data/analysis.html. Updated February 9, 2017. Accessed June 27, 2017.
2. Substance Abuse and Mental Health Services Administration. Results from the 2015 National Survey on Drug Use and Health: detailed tables. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015.pdf.
3. Substance Abuse and Mental Health Services Administration. Medication-assisted treatment of opioid use disorder pocket guide. https://store.samhsa.gov/shin/content//SMA16-4892PG/SMA16-4892PG.pdf. Accessed June 29, 2017.
4. Mutlu C, Demirci AC, Yalcin O, et al. One-year follow-up of heroin-dependent adolescents treated with buprenorphine/naloxone for the first time in a substance treatment unit. J Subst Abuse Treat. 2016;67:1-8.
5. Sharma B, Bruner A, Barnett G, et al. Opioid use disorders. Child Adolesc Psychiatr Clin N Am. 2016;25(3):473-487.
6. Davis MA, Lin LA, Liu H, Sites BD. Prescription Opioid Use among Adults with mental health disorders in the United States. J Am Board Fam Med. 2017;30:42-47.
7. Icahn School of Medicine at Mount Sinai. Substance use: prescription drugs. http://www.mountsinai.org/patient-care/health-library/diseases-and-conditions/opioid-abuse#risk. Accessed June 27, 2017.
8. Boscarino JA, Rukstalis M, Hoffman SN, et al. Risk factors for drug dependence among out-patients on opioid therapy in a large US health-care system. Addiction. 2010;105(10):1776-1782.
9. Edlund M, Steffick D, Hudson T, et al. Risk factors for clinically recognized opioid abuse and dependence among veterans using opioids for chronic non-cancer pain. Pain. 2007;129(3):355-362.
10. Compton WM, Volkow ND. Major increases in opioid analgesic abuse in the United States: concerns and strategies. Drug Alcohol Depend. 2006;81(2):103-107.
11. Bohnert AS, Valenstein M, Bair M, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011;305(13):1315-1321.
12. Webster LR, Webster RM. Predicting aberrant behaviors in opioid-treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005;6(6):432.
13. Sun EC, Darnall BD, Baker LC, et al. Incidence of and risk factors for chronic opioid use among opioid-naive patients in the postoperative period. JAMA Intern Med. 2016;176(9):1286-1293.
14. Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013.
15. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Internal Med. 2010;152(11):712-720.
16. Substance Abuse and Mental Health Services Administration. Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction: a treatment improvement protocol: TIP 40. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2004.
17. NIDA drug screening tool: clinician’s screening tool for drug use in general medical settings. National Institutes of Health. https://www.drugabuse.gov/nmassist. Accessed June 27, 2017.
18. Fareed A, Eilender P, Haber M, et al. Comorbid posttraumatic stress disorder and opiate addiction: a literature review. J Addict Dis. 2013;32(2):168-179.
19. Rosen D, Smith ML, Reynolds CF 3rd. The prevalence of mental and physical health disorders among older methadone patients. Am J Geriatr Psychiatry. 2008;16(6):488-497.
20. Goldner EM, Lusted A, Roerecke M, et al. Prevalence of Axis-1 psychiatric (with focus on depression and anxiety) disorder and symptomatology among non-medical prescription opioid users in substance use treatment: systematic review and meta-analyses. Addict Behav. 2014;39(3):520-531.
21. Barry DT, Cutter CJ, Beitel M, et al. Psychiatric disorders among patients seeking treatment for co-occurring chronic pain and opioid use disorder. J Clin Psychiatry. 2016;77(10):1413-1419.
22. Kuramoto SJ, Chilcoat HD, Ko J, et al. Suicidal ideation and suicide attempt across stages of nonmedical prescription opioid use and presence of prescription opioid disorders among U.S. adults. J Stud Alcohol Drugs. 2012;73(2):178-184.
23. Mattick RP, Breen C, Kimber J, et al. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;(2):CD002207. doi: 10.1002/14651858.CD002207.pub4.
24. Evans E, Li L, Min J, et al. Mortality among individuals accessing pharmacological treatment for opioid dependence in California, 2006-10. Addiction. 2015;110(6):996-1005.
25. Marteu D, McDonald R, Patel K. The relative risk of fatal poisoning by methadone or buprenorphine within the wider population of England and Wales. BMJ Open. 2015;5(5):e007629. doi: 10.1136/bmjopen-2015-007629.
26. Jasinski DR, Johnson RE, Kocher TR. Clonidine in morphine withdrawal. Differential effects on signs and symptoms. Arch Gen Psychiatry. 1985;42(11):1063-1066.
27. Whelan PJ, Remski K. Buprenorphine vs methadone treatment: a review of evidence in both developed and developing worlds. J Neurosci Rural Pract. 2012;3(1):45-50.
28. Schuckit MA. Treatment of opioid-use disorders. N Engl J Med. 2016;375(4):357-368.
29. Dutra L, Stathopoulou G, Basden SL, et al. A meta-analytic review of psychosocial interventions for substance use disorders. Am J Psychiatry. 2008;165(2):179-187.
30. Brown HL, Britton KA, Mahaffey D, et al. Methadone maintenance in pregnancy: a reappraisal. Am J Obstet Gynecol. 1998;179(2):459-463.
31. Center for Substance Abuse Treatment. Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Treatment Improvement Protocol (TIP) 43.
32. Zimlich R. AAP recommends on medication assisted therapy for adolescent opioid addiction. Contemporary Pediatrics. http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/news/aap-recommends-medication-assisted-therapy-adolescent-opioid-addiction. Published September 15, 2016. Accessed June 29, 2017.
33. Patkar A, Lee J, Burgess D. Opioid use disorder. BMJ Publishing Group. http://bestpractice.bmj.com/best-practice/monograph/200.html. Published 2015. Accessed July 6, 2017.
34. Alho H, Sinclair D, Vuori E, et al. Abuse liability of buprenorphine-naloxone tablets in untreated IV drug users. Drug Alcohol Depend. 2007;88(1):75-78.
35. Centers for Disease Control and Prevention (CDC). Vital signs: risk for overdose from methadone used for pain relief - United States, 1999-2010. MMWR Morb Mortal Wkly Rep. 2012;61(26):493-497.
36. Soyka M. New developments in the management of opioid dependence: focus on sublingual buprenorphine-naloxone. Subst Abuse Rehabil. 2015;6:1-14.
37. Lee JD, Friedmann PD, Kinlock TW, et al. Extended-Release Naltrexone to Prevent Opioid Relapse in Criminal Justice Offenders N Engl J Med. 2016;374(13):1232-1242.
38. Vo HT, Robbins E, Westwood M, et al. Relapse prevention medications in community treatment for young adults with opioid addiction. Subst Abus. 2016;37(3):392-397.
39. McDonald R, Campbell ND, Strang J. Twenty years of take-home naloxone for the prevention of overdose deaths from heroin and other opioids-conception and maturation. Drug Alcohol Depend. 2017;178:176-187.
40. Centers for Disease Control and Prevention. Overdose prevention. https://www.cdc.gov/drugoverdose/opioids/odprevention.html. Updated February 9, 2017. Accessed July 6, 2017.
1. Centers for Disease Control and Prevention. Opioid data analysis. http://www.cdc.gov/drugoverdose/data/analysis.html. Updated February 9, 2017. Accessed June 27, 2017.
2. Substance Abuse and Mental Health Services Administration. Results from the 2015 National Survey on Drug Use and Health: detailed tables. https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015.pdf.
3. Substance Abuse and Mental Health Services Administration. Medication-assisted treatment of opioid use disorder pocket guide. https://store.samhsa.gov/shin/content//SMA16-4892PG/SMA16-4892PG.pdf. Accessed June 29, 2017.
4. Mutlu C, Demirci AC, Yalcin O, et al. One-year follow-up of heroin-dependent adolescents treated with buprenorphine/naloxone for the first time in a substance treatment unit. J Subst Abuse Treat. 2016;67:1-8.
5. Sharma B, Bruner A, Barnett G, et al. Opioid use disorders. Child Adolesc Psychiatr Clin N Am. 2016;25(3):473-487.
6. Davis MA, Lin LA, Liu H, Sites BD. Prescription Opioid Use among Adults with mental health disorders in the United States. J Am Board Fam Med. 2017;30:42-47.
7. Icahn School of Medicine at Mount Sinai. Substance use: prescription drugs. http://www.mountsinai.org/patient-care/health-library/diseases-and-conditions/opioid-abuse#risk. Accessed June 27, 2017.
8. Boscarino JA, Rukstalis M, Hoffman SN, et al. Risk factors for drug dependence among out-patients on opioid therapy in a large US health-care system. Addiction. 2010;105(10):1776-1782.
9. Edlund M, Steffick D, Hudson T, et al. Risk factors for clinically recognized opioid abuse and dependence among veterans using opioids for chronic non-cancer pain. Pain. 2007;129(3):355-362.
10. Compton WM, Volkow ND. Major increases in opioid analgesic abuse in the United States: concerns and strategies. Drug Alcohol Depend. 2006;81(2):103-107.
11. Bohnert AS, Valenstein M, Bair M, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011;305(13):1315-1321.
12. Webster LR, Webster RM. Predicting aberrant behaviors in opioid-treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005;6(6):432.
13. Sun EC, Darnall BD, Baker LC, et al. Incidence of and risk factors for chronic opioid use among opioid-naive patients in the postoperative period. JAMA Intern Med. 2016;176(9):1286-1293.
14. Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013.
15. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Internal Med. 2010;152(11):712-720.
16. Substance Abuse and Mental Health Services Administration. Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction: a treatment improvement protocol: TIP 40. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2004.
17. NIDA drug screening tool: clinician’s screening tool for drug use in general medical settings. National Institutes of Health. https://www.drugabuse.gov/nmassist. Accessed June 27, 2017.
18. Fareed A, Eilender P, Haber M, et al. Comorbid posttraumatic stress disorder and opiate addiction: a literature review. J Addict Dis. 2013;32(2):168-179.
19. Rosen D, Smith ML, Reynolds CF 3rd. The prevalence of mental and physical health disorders among older methadone patients. Am J Geriatr Psychiatry. 2008;16(6):488-497.
20. Goldner EM, Lusted A, Roerecke M, et al. Prevalence of Axis-1 psychiatric (with focus on depression and anxiety) disorder and symptomatology among non-medical prescription opioid users in substance use treatment: systematic review and meta-analyses. Addict Behav. 2014;39(3):520-531.
21. Barry DT, Cutter CJ, Beitel M, et al. Psychiatric disorders among patients seeking treatment for co-occurring chronic pain and opioid use disorder. J Clin Psychiatry. 2016;77(10):1413-1419.
22. Kuramoto SJ, Chilcoat HD, Ko J, et al. Suicidal ideation and suicide attempt across stages of nonmedical prescription opioid use and presence of prescription opioid disorders among U.S. adults. J Stud Alcohol Drugs. 2012;73(2):178-184.
23. Mattick RP, Breen C, Kimber J, et al. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;(2):CD002207. doi: 10.1002/14651858.CD002207.pub4.
24. Evans E, Li L, Min J, et al. Mortality among individuals accessing pharmacological treatment for opioid dependence in California, 2006-10. Addiction. 2015;110(6):996-1005.
25. Marteu D, McDonald R, Patel K. The relative risk of fatal poisoning by methadone or buprenorphine within the wider population of England and Wales. BMJ Open. 2015;5(5):e007629. doi: 10.1136/bmjopen-2015-007629.
26. Jasinski DR, Johnson RE, Kocher TR. Clonidine in morphine withdrawal. Differential effects on signs and symptoms. Arch Gen Psychiatry. 1985;42(11):1063-1066.
27. Whelan PJ, Remski K. Buprenorphine vs methadone treatment: a review of evidence in both developed and developing worlds. J Neurosci Rural Pract. 2012;3(1):45-50.
28. Schuckit MA. Treatment of opioid-use disorders. N Engl J Med. 2016;375(4):357-368.
29. Dutra L, Stathopoulou G, Basden SL, et al. A meta-analytic review of psychosocial interventions for substance use disorders. Am J Psychiatry. 2008;165(2):179-187.
30. Brown HL, Britton KA, Mahaffey D, et al. Methadone maintenance in pregnancy: a reappraisal. Am J Obstet Gynecol. 1998;179(2):459-463.
31. Center for Substance Abuse Treatment. Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Treatment Improvement Protocol (TIP) 43.
32. Zimlich R. AAP recommends on medication assisted therapy for adolescent opioid addiction. Contemporary Pediatrics. http://contemporarypediatrics.modernmedicine.com/contemporary-pediatrics/news/aap-recommends-medication-assisted-therapy-adolescent-opioid-addiction. Published September 15, 2016. Accessed June 29, 2017.
33. Patkar A, Lee J, Burgess D. Opioid use disorder. BMJ Publishing Group. http://bestpractice.bmj.com/best-practice/monograph/200.html. Published 2015. Accessed July 6, 2017.
34. Alho H, Sinclair D, Vuori E, et al. Abuse liability of buprenorphine-naloxone tablets in untreated IV drug users. Drug Alcohol Depend. 2007;88(1):75-78.
35. Centers for Disease Control and Prevention (CDC). Vital signs: risk for overdose from methadone used for pain relief - United States, 1999-2010. MMWR Morb Mortal Wkly Rep. 2012;61(26):493-497.
36. Soyka M. New developments in the management of opioid dependence: focus on sublingual buprenorphine-naloxone. Subst Abuse Rehabil. 2015;6:1-14.
37. Lee JD, Friedmann PD, Kinlock TW, et al. Extended-Release Naltrexone to Prevent Opioid Relapse in Criminal Justice Offenders N Engl J Med. 2016;374(13):1232-1242.
38. Vo HT, Robbins E, Westwood M, et al. Relapse prevention medications in community treatment for young adults with opioid addiction. Subst Abus. 2016;37(3):392-397.
39. McDonald R, Campbell ND, Strang J. Twenty years of take-home naloxone for the prevention of overdose deaths from heroin and other opioids-conception and maturation. Drug Alcohol Depend. 2017;178:176-187.
40. Centers for Disease Control and Prevention. Overdose prevention. https://www.cdc.gov/drugoverdose/opioids/odprevention.html. Updated February 9, 2017. Accessed July 6, 2017.

