User login
The full scope of GI advances
What distinguished this year’s course offering was the overall approach and philosophy to utilize educational processes and educational theory resulting in an educational program that adhered to the AGA’s commitment to high-quality, evidence-based, and theory-driven programming.
As a first step in planning the course, we performed a needs assessment. By identifying what learners need to know, we endeavored to develop the ideal course. Our course directors, supported by the AGA staff, reviewed past course evaluations, and in particular, the comments related to suggestions for future programs. We also reviewed and discussed with experts the emerging trend topics and need-to-know areas in GI and hepatology. In doing so, an outline of topics was created, which was subsequently approved by AGA Institute’s Education and Training Committee.

Objectives
At the completion of this course the attendee will be able to:
1. Identify new strategies in the evaluation and management of GI and hepatobiliary problems
2. Recognize medical, surgical, and technological advances in the field of GI and hepatology
3. Apply new strategies for evaluation, therapeutic options, and technology to the optimal care of patients
It is challenging to craft large audience educational experiences so that they also address adult learning principles. We know that adult learners benefit from experiences that are relevant, are problem-centered (rather than content oriented), promote active learning, and provide feedback to the learner. We therefore requested that each session begin with a brief case. Having clinical examples helps learners frame the disease process, and can help demonstrate the importance of learning the material. Finally, all participants were given the opportunity to review each session, and the course in its entirety, to help us improve future programming.
Lunch sessions promoted active learning with the opportunity for interaction, and we also included case-based breakout sessions. Not only was CME accreditation provided, but Maintenance of Certification (MOC) credit was also available.
This educational offering provided a setting to hear from leaders in GI and hepatology, and for learners to gain new insights to take home and apply to the care of patients. The sections that follow provide brief summaries of the sessions from the course written by the moderators.
Please visit http://pgcourse.gastro.org/home to access the content from DDW.
Dr. Rose is a professor of medicine, the Senior Associate Dean for Education, University of Connecticut School of Medicine, Farmington, and the 2017 AGA Postgraduate Course Director. This is a summary provided by the moderator of one of the AGA Postgraduate Courses held at DDW 2017.
What distinguished this year’s course offering was the overall approach and philosophy to utilize educational processes and educational theory resulting in an educational program that adhered to the AGA’s commitment to high-quality, evidence-based, and theory-driven programming.
As a first step in planning the course, we performed a needs assessment. By identifying what learners need to know, we endeavored to develop the ideal course. Our course directors, supported by the AGA staff, reviewed past course evaluations, and in particular, the comments related to suggestions for future programs. We also reviewed and discussed with experts the emerging trend topics and need-to-know areas in GI and hepatology. In doing so, an outline of topics was created, which was subsequently approved by AGA Institute’s Education and Training Committee.
Objectives
At the completion of this course the attendee will be able to:
1. Identify new strategies in the evaluation and management of GI and hepatobiliary problems
2. Recognize medical, surgical, and technological advances in the field of GI and hepatology
3. Apply new strategies for evaluation, therapeutic options, and technology to the optimal care of patients
It is challenging to craft large audience educational experiences so that they also address adult learning principles. We know that adult learners benefit from experiences that are relevant, are problem-centered (rather than content oriented), promote active learning, and provide feedback to the learner. We therefore requested that each session begin with a brief case. Having clinical examples helps learners frame the disease process, and can help demonstrate the importance of learning the material. Finally, all participants were given the opportunity to review each session, and the course in its entirety, to help us improve future programming.
Lunch sessions promoted active learning with the opportunity for interaction, and we also included case-based breakout sessions. Not only was CME accreditation provided, but Maintenance of Certification (MOC) credit was also available.
This educational offering provided a setting to hear from leaders in GI and hepatology, and for learners to gain new insights to take home and apply to the care of patients. The sections that follow provide brief summaries of the sessions from the course written by the moderators.
Please visit http://pgcourse.gastro.org/home to access the content from DDW.
Dr. Rose is a professor of medicine, the Senior Associate Dean for Education, University of Connecticut School of Medicine, Farmington, and the 2017 AGA Postgraduate Course Director. This is a summary provided by the moderator of one of the AGA Postgraduate Courses held at DDW 2017.
What distinguished this year’s course offering was the overall approach and philosophy to utilize educational processes and educational theory resulting in an educational program that adhered to the AGA’s commitment to high-quality, evidence-based, and theory-driven programming.
As a first step in planning the course, we performed a needs assessment. By identifying what learners need to know, we endeavored to develop the ideal course. Our course directors, supported by the AGA staff, reviewed past course evaluations, and in particular, the comments related to suggestions for future programs. We also reviewed and discussed with experts the emerging trend topics and need-to-know areas in GI and hepatology. In doing so, an outline of topics was created, which was subsequently approved by AGA Institute’s Education and Training Committee.
Objectives
At the completion of this course the attendee will be able to:
1. Identify new strategies in the evaluation and management of GI and hepatobiliary problems
2. Recognize medical, surgical, and technological advances in the field of GI and hepatology
3. Apply new strategies for evaluation, therapeutic options, and technology to the optimal care of patients
It is challenging to craft large audience educational experiences so that they also address adult learning principles. We know that adult learners benefit from experiences that are relevant, are problem-centered (rather than content oriented), promote active learning, and provide feedback to the learner. We therefore requested that each session begin with a brief case. Having clinical examples helps learners frame the disease process, and can help demonstrate the importance of learning the material. Finally, all participants were given the opportunity to review each session, and the course in its entirety, to help us improve future programming.
Lunch sessions promoted active learning with the opportunity for interaction, and we also included case-based breakout sessions. Not only was CME accreditation provided, but Maintenance of Certification (MOC) credit was also available.
This educational offering provided a setting to hear from leaders in GI and hepatology, and for learners to gain new insights to take home and apply to the care of patients. The sections that follow provide brief summaries of the sessions from the course written by the moderators.
Please visit http://pgcourse.gastro.org/home to access the content from DDW.
Dr. Rose is a professor of medicine, the Senior Associate Dean for Education, University of Connecticut School of Medicine, Farmington, and the 2017 AGA Postgraduate Course Director. This is a summary provided by the moderator of one of the AGA Postgraduate Courses held at DDW 2017.
Amyloid PET May Influence Care of Patients With Cognitive Problems
LONDON—Amyloid PET imaging may change the care plan for a large proportion of patients with mild cognitive impairment (MCI) or dementia, according to interim results presented at the 2017 Alzheimer’s Association International Conference. The most common change following PET imaging may involve pharmaceutical treatment. The study could influence the reimbursement of PET imaging for appropriately selected patients.
Amyloid PET imaging detects amyloid plaques in the brains of living people. The technique can clarify the diagnosis of patients with cognitive impairment of uncertain cause. In a 2013 National Coverage Decision, the Centers for Medicare and Medicaid Services stated that they would not reimburse clinicians for amyloid PET imaging because “the evidence is insufficient to conclude that the use of PET amyloid-beta imaging is reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of … Medicare beneficiaries with dementia or neurodegenerative disease.”
Examining Care Plans Before and After Imaging
Gil D. Rabinovici, MD, Professor of Neurology at the University of California, San Francisco, and colleagues initiated the Imaging Dementia Evidence for Amyloid Scanning (IDEAS) study with the goals of assessing the effect of amyloid PET on the patient care plan at three months, and assessing the scan’s effect on health outcomes at one year. More than 1,100 participating clinicians across the United States plan to enroll 18,500 Medicare beneficiaries with MCI or dementia of uncertain etiology.

In the study, referring clinicians document their care plans for their patients before the patients undergo amyloid imaging. After patients undergo imaging, the clinicians receive the results and make recommendations accordingly. Patients return for a follow-up visit 90 days later. Finally, the clinicians record what management changes have been implemented.
Dr. Rabinovici reported the results of a prespecified interim analysis of the first 3,979 patients enrolled in the study. The analysis was intended to determine the feasibility of detecting a 30% change in the patient management plan. The composite end point includes changes in the use of medications specifically indicated for Alzheimer’s disease, changes in other neurologic medications, and finally, counseling about safety and future planning.
Most Patients’ Care Plans Changed
Approximately 64% of participants had MCI, and about 36% had dementia. The population’s mean age was 75. Approximately 51% of patients were women. In 76% of participants, the suspected cause of cognitive impairment was Alzheimer’s disease. PET scans were positive for 54.3% of patients with MCI and 70.5% of patients with dementia.
The care plan changed for 67.6% of participants, and the percentage change was similar between patients with MCI (67.8%) and those with dementia (65.9%). The most common change was in the use of Alzheimer’s-disease-specific medications (about 48% in the MCI and dementia groups), followed by the use of other neurologic medications (36.0% for the MCI group and 32.2% for the dementia group) and counseling (23.9% in the MCI group and 15.9% in the dementia group). “Each patient might have had changes in two, or even all three, of these components, and this would be counted as only one change in the composite for that patient,” said Dr. Rabinovici.
PET led to a more precise diagnosis and treatment plan for participants, he added. Among patients with a positive amyloid PET scan, the rate of Alzheimer’s disease diagnosis increased from 78.5% to 95.2%. In patients with a negative scan, the rate of Alzheimer’s diagnosis decreased from 73.0% to 14.5%. “Many patients would have otherwise been diagnosed with Alzheimer’s disease, and yet there was no biologic evidence of amyloid plaques in the brain,” said Dr. Rabinovici.
These changes in diagnosis led to appropriate treatment. For patients with a positive scan, the use of Alzheimer’s-disease-specific drugs increased from 50.9% to 83.8%. For patients with a negative scan, the use of these drugs decreased from 39.1% to 30.8%.
“The pivotal trials for cholinesterase inhibitors and memantine in Alzheimer’s disease did not require a biomarker, so we do not really know that only amyloid-positive patients benefit,” said Dr. Rabinovici. “Also, patients with Lewy body dementia have been shown to benefit from cholinesterase inhibitors, and [they] can be negative on amyloid PET.”
Imaging May Dispel Uncertainty
“These are partial results reflecting one-third of the sample,” said Dr. Rabinovici. Recruitment is ongoing and may be complete by early 2018. After enrollment is complete, a year of follow-up will be required to determine whether amyloid PET improves participants’ outcomes. The researchers may finish the study earlier than they had anticipated, and final results pertaining to changes in management may be available in one year.
“One thing that this study is not capturing is the meaning of diagnosis,” said Dr. Rabinovici. “Patients want to know what is going on in their brain. They want to understand what the cause of cognitive impairment is…. A lot of times, the uncertainty is worse than the certainty, even when the information is bad news.”
—Erik Greb
Suggested Reading
Jack CR Jr, Barrio JR, Kepe V. Cerebral amyloid PET imaging in Alzheimer’s disease. Acta Neuropathol. 2013; 126(5):643-657.
Johnson KA, Minoshima S, Bohnen NI, et al. Appropriate use criteria for amyloid PET: a report of the Amyloid Imaging Task Force, the Society of Nuclear Medicine and Molecular Imaging, and the Alzheimer’s Association. Alzheimers Dement. 2013;9(1):e-1-16.
Vandenberghe R, Adamczuk K, Van Laere K. The interest of amyloid PET imaging in the diagnosis of Alzheimer’s disease. Curr Opin Neurol. 2013;26(6):646-655.
LONDON—Amyloid PET imaging may change the care plan for a large proportion of patients with mild cognitive impairment (MCI) or dementia, according to interim results presented at the 2017 Alzheimer’s Association International Conference. The most common change following PET imaging may involve pharmaceutical treatment. The study could influence the reimbursement of PET imaging for appropriately selected patients.
Amyloid PET imaging detects amyloid plaques in the brains of living people. The technique can clarify the diagnosis of patients with cognitive impairment of uncertain cause. In a 2013 National Coverage Decision, the Centers for Medicare and Medicaid Services stated that they would not reimburse clinicians for amyloid PET imaging because “the evidence is insufficient to conclude that the use of PET amyloid-beta imaging is reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of … Medicare beneficiaries with dementia or neurodegenerative disease.”
Examining Care Plans Before and After Imaging
Gil D. Rabinovici, MD, Professor of Neurology at the University of California, San Francisco, and colleagues initiated the Imaging Dementia Evidence for Amyloid Scanning (IDEAS) study with the goals of assessing the effect of amyloid PET on the patient care plan at three months, and assessing the scan’s effect on health outcomes at one year. More than 1,100 participating clinicians across the United States plan to enroll 18,500 Medicare beneficiaries with MCI or dementia of uncertain etiology.
In the study, referring clinicians document their care plans for their patients before the patients undergo amyloid imaging. After patients undergo imaging, the clinicians receive the results and make recommendations accordingly. Patients return for a follow-up visit 90 days later. Finally, the clinicians record what management changes have been implemented.
Dr. Rabinovici reported the results of a prespecified interim analysis of the first 3,979 patients enrolled in the study. The analysis was intended to determine the feasibility of detecting a 30% change in the patient management plan. The composite end point includes changes in the use of medications specifically indicated for Alzheimer’s disease, changes in other neurologic medications, and finally, counseling about safety and future planning.
Most Patients’ Care Plans Changed
Approximately 64% of participants had MCI, and about 36% had dementia. The population’s mean age was 75. Approximately 51% of patients were women. In 76% of participants, the suspected cause of cognitive impairment was Alzheimer’s disease. PET scans were positive for 54.3% of patients with MCI and 70.5% of patients with dementia.
The care plan changed for 67.6% of participants, and the percentage change was similar between patients with MCI (67.8%) and those with dementia (65.9%). The most common change was in the use of Alzheimer’s-disease-specific medications (about 48% in the MCI and dementia groups), followed by the use of other neurologic medications (36.0% for the MCI group and 32.2% for the dementia group) and counseling (23.9% in the MCI group and 15.9% in the dementia group). “Each patient might have had changes in two, or even all three, of these components, and this would be counted as only one change in the composite for that patient,” said Dr. Rabinovici.
PET led to a more precise diagnosis and treatment plan for participants, he added. Among patients with a positive amyloid PET scan, the rate of Alzheimer’s disease diagnosis increased from 78.5% to 95.2%. In patients with a negative scan, the rate of Alzheimer’s diagnosis decreased from 73.0% to 14.5%. “Many patients would have otherwise been diagnosed with Alzheimer’s disease, and yet there was no biologic evidence of amyloid plaques in the brain,” said Dr. Rabinovici.
These changes in diagnosis led to appropriate treatment. For patients with a positive scan, the use of Alzheimer’s-disease-specific drugs increased from 50.9% to 83.8%. For patients with a negative scan, the use of these drugs decreased from 39.1% to 30.8%.
“The pivotal trials for cholinesterase inhibitors and memantine in Alzheimer’s disease did not require a biomarker, so we do not really know that only amyloid-positive patients benefit,” said Dr. Rabinovici. “Also, patients with Lewy body dementia have been shown to benefit from cholinesterase inhibitors, and [they] can be negative on amyloid PET.”
Imaging May Dispel Uncertainty
“These are partial results reflecting one-third of the sample,” said Dr. Rabinovici. Recruitment is ongoing and may be complete by early 2018. After enrollment is complete, a year of follow-up will be required to determine whether amyloid PET improves participants’ outcomes. The researchers may finish the study earlier than they had anticipated, and final results pertaining to changes in management may be available in one year.
“One thing that this study is not capturing is the meaning of diagnosis,” said Dr. Rabinovici. “Patients want to know what is going on in their brain. They want to understand what the cause of cognitive impairment is…. A lot of times, the uncertainty is worse than the certainty, even when the information is bad news.”
—Erik Greb
Suggested Reading
Jack CR Jr, Barrio JR, Kepe V. Cerebral amyloid PET imaging in Alzheimer’s disease. Acta Neuropathol. 2013; 126(5):643-657.
Johnson KA, Minoshima S, Bohnen NI, et al. Appropriate use criteria for amyloid PET: a report of the Amyloid Imaging Task Force, the Society of Nuclear Medicine and Molecular Imaging, and the Alzheimer’s Association. Alzheimers Dement. 2013;9(1):e-1-16.
Vandenberghe R, Adamczuk K, Van Laere K. The interest of amyloid PET imaging in the diagnosis of Alzheimer’s disease. Curr Opin Neurol. 2013;26(6):646-655.
LONDON—Amyloid PET imaging may change the care plan for a large proportion of patients with mild cognitive impairment (MCI) or dementia, according to interim results presented at the 2017 Alzheimer’s Association International Conference. The most common change following PET imaging may involve pharmaceutical treatment. The study could influence the reimbursement of PET imaging for appropriately selected patients.
Amyloid PET imaging detects amyloid plaques in the brains of living people. The technique can clarify the diagnosis of patients with cognitive impairment of uncertain cause. In a 2013 National Coverage Decision, the Centers for Medicare and Medicaid Services stated that they would not reimburse clinicians for amyloid PET imaging because “the evidence is insufficient to conclude that the use of PET amyloid-beta imaging is reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of … Medicare beneficiaries with dementia or neurodegenerative disease.”
Examining Care Plans Before and After Imaging
Gil D. Rabinovici, MD, Professor of Neurology at the University of California, San Francisco, and colleagues initiated the Imaging Dementia Evidence for Amyloid Scanning (IDEAS) study with the goals of assessing the effect of amyloid PET on the patient care plan at three months, and assessing the scan’s effect on health outcomes at one year. More than 1,100 participating clinicians across the United States plan to enroll 18,500 Medicare beneficiaries with MCI or dementia of uncertain etiology.
In the study, referring clinicians document their care plans for their patients before the patients undergo amyloid imaging. After patients undergo imaging, the clinicians receive the results and make recommendations accordingly. Patients return for a follow-up visit 90 days later. Finally, the clinicians record what management changes have been implemented.
Dr. Rabinovici reported the results of a prespecified interim analysis of the first 3,979 patients enrolled in the study. The analysis was intended to determine the feasibility of detecting a 30% change in the patient management plan. The composite end point includes changes in the use of medications specifically indicated for Alzheimer’s disease, changes in other neurologic medications, and finally, counseling about safety and future planning.
Most Patients’ Care Plans Changed
Approximately 64% of participants had MCI, and about 36% had dementia. The population’s mean age was 75. Approximately 51% of patients were women. In 76% of participants, the suspected cause of cognitive impairment was Alzheimer’s disease. PET scans were positive for 54.3% of patients with MCI and 70.5% of patients with dementia.
The care plan changed for 67.6% of participants, and the percentage change was similar between patients with MCI (67.8%) and those with dementia (65.9%). The most common change was in the use of Alzheimer’s-disease-specific medications (about 48% in the MCI and dementia groups), followed by the use of other neurologic medications (36.0% for the MCI group and 32.2% for the dementia group) and counseling (23.9% in the MCI group and 15.9% in the dementia group). “Each patient might have had changes in two, or even all three, of these components, and this would be counted as only one change in the composite for that patient,” said Dr. Rabinovici.
PET led to a more precise diagnosis and treatment plan for participants, he added. Among patients with a positive amyloid PET scan, the rate of Alzheimer’s disease diagnosis increased from 78.5% to 95.2%. In patients with a negative scan, the rate of Alzheimer’s diagnosis decreased from 73.0% to 14.5%. “Many patients would have otherwise been diagnosed with Alzheimer’s disease, and yet there was no biologic evidence of amyloid plaques in the brain,” said Dr. Rabinovici.
These changes in diagnosis led to appropriate treatment. For patients with a positive scan, the use of Alzheimer’s-disease-specific drugs increased from 50.9% to 83.8%. For patients with a negative scan, the use of these drugs decreased from 39.1% to 30.8%.
“The pivotal trials for cholinesterase inhibitors and memantine in Alzheimer’s disease did not require a biomarker, so we do not really know that only amyloid-positive patients benefit,” said Dr. Rabinovici. “Also, patients with Lewy body dementia have been shown to benefit from cholinesterase inhibitors, and [they] can be negative on amyloid PET.”
Imaging May Dispel Uncertainty
“These are partial results reflecting one-third of the sample,” said Dr. Rabinovici. Recruitment is ongoing and may be complete by early 2018. After enrollment is complete, a year of follow-up will be required to determine whether amyloid PET improves participants’ outcomes. The researchers may finish the study earlier than they had anticipated, and final results pertaining to changes in management may be available in one year.
“One thing that this study is not capturing is the meaning of diagnosis,” said Dr. Rabinovici. “Patients want to know what is going on in their brain. They want to understand what the cause of cognitive impairment is…. A lot of times, the uncertainty is worse than the certainty, even when the information is bad news.”
—Erik Greb
Suggested Reading
Jack CR Jr, Barrio JR, Kepe V. Cerebral amyloid PET imaging in Alzheimer’s disease. Acta Neuropathol. 2013; 126(5):643-657.
Johnson KA, Minoshima S, Bohnen NI, et al. Appropriate use criteria for amyloid PET: a report of the Amyloid Imaging Task Force, the Society of Nuclear Medicine and Molecular Imaging, and the Alzheimer’s Association. Alzheimers Dement. 2013;9(1):e-1-16.
Vandenberghe R, Adamczuk K, Van Laere K. The interest of amyloid PET imaging in the diagnosis of Alzheimer’s disease. Curr Opin Neurol. 2013;26(6):646-655.
Intraoperative ketamine makes no dent in postop delirium or pain
Postoperative delirium remains a problem without an effective solution, wrote Michael S. Avidan, MBBCh, FCASA, of Washington University, Saint Louis, and his colleagues (Lancet 2017;390[10091]:267-75).
Recent guidelines published by the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council include ketamine as a recommended component of multimodal pain therapy for several commonly performed surgeries. “Before recommending widespread administration of an intraoperative bolus of subanaesthetic ketamine, demonstrating that ketamine decreases either delirium or pain, or both, without incurring adverse effects in a large, pragmatic trial was warranted,” the researchers said.
In the PODCAST (Prevention of Delirium and Complications Associated With Surgical Treatments) trial, the researchers randomized 672 patients over the age of 60 undergoing major open surgery under general anesthesia (such as open cardiac or noncardiac surgery, urological surgery, gynecologic surgery, or intra-abdominal surgery) to 0.5 mg/kg ketamine (227), 1.0 mg/kg ketamine (223), or placebo (222). The ketamine or placebo was given after anesthesia and before surgical incision.
Overall, no difference in the incidence of delirium occurred between patients in the combined ketamine groups (19.5%) and the placebo group (19.8%), and there was no significant difference in delirium across all three treatment groups.
No differences in pain based on visual analog scale scores were observed across the three groups, and overall adverse event rates were similar as well: approximately 40.8% in the 1.0-mg ketamine group, 39.6% in the 0.5-mg ketamine group, and 36.9% in the placebo group.
The study findings were limited by several factors, including a study population potentially too small to show an effect of ketamine on delirium, and a lack of data on other variables that might contribute to delirium and pain, the researchers noted. However, the results suggest that “despite present evidence and guidelines, the administration of a subanaesthetic ketamine dose during surgery is not useful for preventing postoperative delirium (primary outcome) or reducing postoperative pain and minimising opioid consumption (related secondary outcomes),” and appears to increase postoperative hallucinations and nightmares to an extent that might be prohibitive, they said.
The National Institutes of Health and Cancer Center Support funded the study. The researchers had no financial conflicts to disclose.
Postoperative delirium remains a problem without an effective solution, wrote Michael S. Avidan, MBBCh, FCASA, of Washington University, Saint Louis, and his colleagues (Lancet 2017;390[10091]:267-75).
Recent guidelines published by the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council include ketamine as a recommended component of multimodal pain therapy for several commonly performed surgeries. “Before recommending widespread administration of an intraoperative bolus of subanaesthetic ketamine, demonstrating that ketamine decreases either delirium or pain, or both, without incurring adverse effects in a large, pragmatic trial was warranted,” the researchers said.
In the PODCAST (Prevention of Delirium and Complications Associated With Surgical Treatments) trial, the researchers randomized 672 patients over the age of 60 undergoing major open surgery under general anesthesia (such as open cardiac or noncardiac surgery, urological surgery, gynecologic surgery, or intra-abdominal surgery) to 0.5 mg/kg ketamine (227), 1.0 mg/kg ketamine (223), or placebo (222). The ketamine or placebo was given after anesthesia and before surgical incision.
Overall, no difference in the incidence of delirium occurred between patients in the combined ketamine groups (19.5%) and the placebo group (19.8%), and there was no significant difference in delirium across all three treatment groups.
No differences in pain based on visual analog scale scores were observed across the three groups, and overall adverse event rates were similar as well: approximately 40.8% in the 1.0-mg ketamine group, 39.6% in the 0.5-mg ketamine group, and 36.9% in the placebo group.
The study findings were limited by several factors, including a study population potentially too small to show an effect of ketamine on delirium, and a lack of data on other variables that might contribute to delirium and pain, the researchers noted. However, the results suggest that “despite present evidence and guidelines, the administration of a subanaesthetic ketamine dose during surgery is not useful for preventing postoperative delirium (primary outcome) or reducing postoperative pain and minimising opioid consumption (related secondary outcomes),” and appears to increase postoperative hallucinations and nightmares to an extent that might be prohibitive, they said.
The National Institutes of Health and Cancer Center Support funded the study. The researchers had no financial conflicts to disclose.
Postoperative delirium remains a problem without an effective solution, wrote Michael S. Avidan, MBBCh, FCASA, of Washington University, Saint Louis, and his colleagues (Lancet 2017;390[10091]:267-75).
Recent guidelines published by the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council include ketamine as a recommended component of multimodal pain therapy for several commonly performed surgeries. “Before recommending widespread administration of an intraoperative bolus of subanaesthetic ketamine, demonstrating that ketamine decreases either delirium or pain, or both, without incurring adverse effects in a large, pragmatic trial was warranted,” the researchers said.
In the PODCAST (Prevention of Delirium and Complications Associated With Surgical Treatments) trial, the researchers randomized 672 patients over the age of 60 undergoing major open surgery under general anesthesia (such as open cardiac or noncardiac surgery, urological surgery, gynecologic surgery, or intra-abdominal surgery) to 0.5 mg/kg ketamine (227), 1.0 mg/kg ketamine (223), or placebo (222). The ketamine or placebo was given after anesthesia and before surgical incision.
Overall, no difference in the incidence of delirium occurred between patients in the combined ketamine groups (19.5%) and the placebo group (19.8%), and there was no significant difference in delirium across all three treatment groups.
No differences in pain based on visual analog scale scores were observed across the three groups, and overall adverse event rates were similar as well: approximately 40.8% in the 1.0-mg ketamine group, 39.6% in the 0.5-mg ketamine group, and 36.9% in the placebo group.
The study findings were limited by several factors, including a study population potentially too small to show an effect of ketamine on delirium, and a lack of data on other variables that might contribute to delirium and pain, the researchers noted. However, the results suggest that “despite present evidence and guidelines, the administration of a subanaesthetic ketamine dose during surgery is not useful for preventing postoperative delirium (primary outcome) or reducing postoperative pain and minimising opioid consumption (related secondary outcomes),” and appears to increase postoperative hallucinations and nightmares to an extent that might be prohibitive, they said.
The National Institutes of Health and Cancer Center Support funded the study. The researchers had no financial conflicts to disclose.
FROM THE LANCET
Key clinical point: Ketamine failed to reduce postoperative delirium in older adults.
Major finding: No difference was observed in the incidence of postoperative delirium between patients given ketamine before surgical incision and patients on placebo.
Data source: The Prevention of Delirium and Complications Associated With Surgical Treatments study, a randomized, multicenter trial of 672 adults older than 60 years.
Disclosures: The National Institutes of Health and Cancer Center Support funded the study. The researchers had no financial conflicts to disclose.
Mental health courts: Is recidivism what counts?
In 2004, the federal government authorized $50 million for state initiatives to coordinate crime control efforts between the criminal justice and mental health systems. Some of that money was dedicated toward expansion of state mental health courts in an attempt to reduce the number of people with serious mental illness in jails and prisons.
Unlike traditional criminal courts, a mental health court is a nonadversarial problem-solving program that brings together all the stakeholders involved in a defendant’s criminal case and mental health care. A criminal defendant who agrees to participate in mental health court must participate in regular status hearings during which a judge reviews the defendant’s adherence to a court-imposed treatment plan and monitors his progress while on probation. The judge considers input from the prosecutor and the defense attorney, and also from the court’s social worker or case manager. A defendant who agrees to mental health court involvement is often placed on probation rather than sentenced to incarceration and is usually incarcerated for a shorter time pending trial.

Although mental health courts have been in existence for 20 years, data about program efficacy have been mixed. Outcome studies have been hampered by lack of truly blind subject assignment, inadequate controls, and selection bias because many mental health courts exclude defendants charged with serious violent crimes or sex offenses. Also, mental health courts are voluntary programs with significant dropout rates. Nevertheless, proponents of mental health courts believe that they prevent crime, reduce violent offending, and serve to stabilize people with serious mental illness in the community.
In a study published recently in Psychiatric Services (2017 Aug 15. doi: 10.1176/appi.ps.201700107), researchers from North Carolina University, Raleigh, addressed the effect of mental health court involvement on criminal recidivism. Lowder et al. looked at 17 outcome studies of mental health court participants published between 2004 and 2015. These studies included 16,129 participants followed for a minimum of 1 year.
Most of the included studies defined recidivism as a new arrest. For the purpose of the meta-analysis, researchers also included any incarceration, conviction, or new charge. Each study also included a comparison group of defendants processed through usual criminal procedures. Included studies generally looked at reoffending in the year after entry into the program or in the year following exit from the program.
The meta-analysis found a small but significant reduction in criminal recidivism, although the degree of this effect varied considerably between studies, and the effect disappeared completely when only moderate and high-quality studies were considered.
These results should not surprise anyone. Crime is a complex human behavior mediated by more than just psychiatric issues. Poverty, stressful life events, and substance abuse all play a role. And as an outcome variable, an arrest is not a sensitive measure because many crimes go unreported. Defendants with lower rates of reoffending may simply have more forgiving victims; for people with mental illness, that victim is often a family member.
Fortunately, crime prevention is not the sole justification for mental health programs. There are also the intangible social benefits that aren’t measured in these studies – benefits like improved quality of life, restored relationships, and the ability to participate more fully in all the joys that life has to offer. For people with serious mental illness who graduate from mental health court, that’s the outcome that counts.
Dr. Hanson is a forensic psychiatrist and coauthor of “Committed: The Battle over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). The opinions expressed are those of the author only and do not represent those of any of Dr. Hanson’s employers or consultees, including the Maryland Department of Health and Mental Hygiene and the Maryland Division of Correction.
In 2004, the federal government authorized $50 million for state initiatives to coordinate crime control efforts between the criminal justice and mental health systems. Some of that money was dedicated toward expansion of state mental health courts in an attempt to reduce the number of people with serious mental illness in jails and prisons.
Unlike traditional criminal courts, a mental health court is a nonadversarial problem-solving program that brings together all the stakeholders involved in a defendant’s criminal case and mental health care. A criminal defendant who agrees to participate in mental health court must participate in regular status hearings during which a judge reviews the defendant’s adherence to a court-imposed treatment plan and monitors his progress while on probation. The judge considers input from the prosecutor and the defense attorney, and also from the court’s social worker or case manager. A defendant who agrees to mental health court involvement is often placed on probation rather than sentenced to incarceration and is usually incarcerated for a shorter time pending trial.
Although mental health courts have been in existence for 20 years, data about program efficacy have been mixed. Outcome studies have been hampered by lack of truly blind subject assignment, inadequate controls, and selection bias because many mental health courts exclude defendants charged with serious violent crimes or sex offenses. Also, mental health courts are voluntary programs with significant dropout rates. Nevertheless, proponents of mental health courts believe that they prevent crime, reduce violent offending, and serve to stabilize people with serious mental illness in the community.
In a study published recently in Psychiatric Services (2017 Aug 15. doi: 10.1176/appi.ps.201700107), researchers from North Carolina University, Raleigh, addressed the effect of mental health court involvement on criminal recidivism. Lowder et al. looked at 17 outcome studies of mental health court participants published between 2004 and 2015. These studies included 16,129 participants followed for a minimum of 1 year.
Most of the included studies defined recidivism as a new arrest. For the purpose of the meta-analysis, researchers also included any incarceration, conviction, or new charge. Each study also included a comparison group of defendants processed through usual criminal procedures. Included studies generally looked at reoffending in the year after entry into the program or in the year following exit from the program.
The meta-analysis found a small but significant reduction in criminal recidivism, although the degree of this effect varied considerably between studies, and the effect disappeared completely when only moderate and high-quality studies were considered.
These results should not surprise anyone. Crime is a complex human behavior mediated by more than just psychiatric issues. Poverty, stressful life events, and substance abuse all play a role. And as an outcome variable, an arrest is not a sensitive measure because many crimes go unreported. Defendants with lower rates of reoffending may simply have more forgiving victims; for people with mental illness, that victim is often a family member.
Fortunately, crime prevention is not the sole justification for mental health programs. There are also the intangible social benefits that aren’t measured in these studies – benefits like improved quality of life, restored relationships, and the ability to participate more fully in all the joys that life has to offer. For people with serious mental illness who graduate from mental health court, that’s the outcome that counts.
Dr. Hanson is a forensic psychiatrist and coauthor of “Committed: The Battle over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). The opinions expressed are those of the author only and do not represent those of any of Dr. Hanson’s employers or consultees, including the Maryland Department of Health and Mental Hygiene and the Maryland Division of Correction.
In 2004, the federal government authorized $50 million for state initiatives to coordinate crime control efforts between the criminal justice and mental health systems. Some of that money was dedicated toward expansion of state mental health courts in an attempt to reduce the number of people with serious mental illness in jails and prisons.
Unlike traditional criminal courts, a mental health court is a nonadversarial problem-solving program that brings together all the stakeholders involved in a defendant’s criminal case and mental health care. A criminal defendant who agrees to participate in mental health court must participate in regular status hearings during which a judge reviews the defendant’s adherence to a court-imposed treatment plan and monitors his progress while on probation. The judge considers input from the prosecutor and the defense attorney, and also from the court’s social worker or case manager. A defendant who agrees to mental health court involvement is often placed on probation rather than sentenced to incarceration and is usually incarcerated for a shorter time pending trial.
Although mental health courts have been in existence for 20 years, data about program efficacy have been mixed. Outcome studies have been hampered by lack of truly blind subject assignment, inadequate controls, and selection bias because many mental health courts exclude defendants charged with serious violent crimes or sex offenses. Also, mental health courts are voluntary programs with significant dropout rates. Nevertheless, proponents of mental health courts believe that they prevent crime, reduce violent offending, and serve to stabilize people with serious mental illness in the community.
In a study published recently in Psychiatric Services (2017 Aug 15. doi: 10.1176/appi.ps.201700107), researchers from North Carolina University, Raleigh, addressed the effect of mental health court involvement on criminal recidivism. Lowder et al. looked at 17 outcome studies of mental health court participants published between 2004 and 2015. These studies included 16,129 participants followed for a minimum of 1 year.
Most of the included studies defined recidivism as a new arrest. For the purpose of the meta-analysis, researchers also included any incarceration, conviction, or new charge. Each study also included a comparison group of defendants processed through usual criminal procedures. Included studies generally looked at reoffending in the year after entry into the program or in the year following exit from the program.
The meta-analysis found a small but significant reduction in criminal recidivism, although the degree of this effect varied considerably between studies, and the effect disappeared completely when only moderate and high-quality studies were considered.
These results should not surprise anyone. Crime is a complex human behavior mediated by more than just psychiatric issues. Poverty, stressful life events, and substance abuse all play a role. And as an outcome variable, an arrest is not a sensitive measure because many crimes go unreported. Defendants with lower rates of reoffending may simply have more forgiving victims; for people with mental illness, that victim is often a family member.
Fortunately, crime prevention is not the sole justification for mental health programs. There are also the intangible social benefits that aren’t measured in these studies – benefits like improved quality of life, restored relationships, and the ability to participate more fully in all the joys that life has to offer. For people with serious mental illness who graduate from mental health court, that’s the outcome that counts.
Dr. Hanson is a forensic psychiatrist and coauthor of “Committed: The Battle over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016). The opinions expressed are those of the author only and do not represent those of any of Dr. Hanson’s employers or consultees, including the Maryland Department of Health and Mental Hygiene and the Maryland Division of Correction.
Safety issues not that unusual in medical offices
More than a quarter of medical offices report that they are contacted by pharmacies on a daily or weekly basis to clarify or correct prescriptions, according to the Agency for Healthcare Research and Quality.
That safety issue – reported by 27% of outpatient medical offices – was the most common among those included in the Medical Office Survey on Patient Safety Culture from November 2013 to November 2015, the AHRQ said in its annual National Healthcare Quality and Disparities Report. Another 12% of respondents said that such contact with a pharmacy was a monthly occurrence.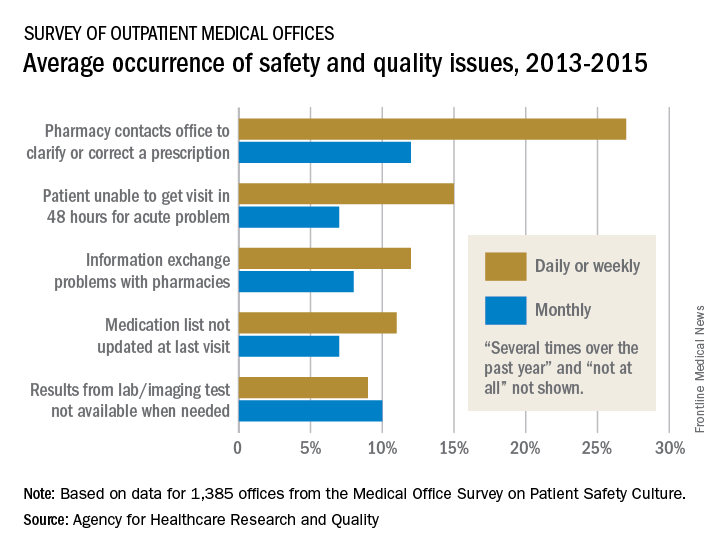
Information exchange problems with pharmacies occurred daily or weekly in 12% of offices and monthly in 8%, while the occurrence of medication lists not being updated at the last visit was 11% daily/weekly and 7% monthly. Additionally, 9% of offices reported that results from laboratory or imaging tests were not available when needed on a daily/weekly basis and 10% on a monthly basis, the AHRQ reported.
“Lack of access to care and lack of access to timely and accurate medical information and test results may contribute to patient safety events such as missed or delayed diagnoses, medication errors, failure to order appropriate diagnostic or laboratory tests, incorrect interpretation of tests, and inadequate follow-up on results,” the AHRQ said in the report.
More than a quarter of medical offices report that they are contacted by pharmacies on a daily or weekly basis to clarify or correct prescriptions, according to the Agency for Healthcare Research and Quality.
That safety issue – reported by 27% of outpatient medical offices – was the most common among those included in the Medical Office Survey on Patient Safety Culture from November 2013 to November 2015, the AHRQ said in its annual National Healthcare Quality and Disparities Report. Another 12% of respondents said that such contact with a pharmacy was a monthly occurrence.
Information exchange problems with pharmacies occurred daily or weekly in 12% of offices and monthly in 8%, while the occurrence of medication lists not being updated at the last visit was 11% daily/weekly and 7% monthly. Additionally, 9% of offices reported that results from laboratory or imaging tests were not available when needed on a daily/weekly basis and 10% on a monthly basis, the AHRQ reported.
“Lack of access to care and lack of access to timely and accurate medical information and test results may contribute to patient safety events such as missed or delayed diagnoses, medication errors, failure to order appropriate diagnostic or laboratory tests, incorrect interpretation of tests, and inadequate follow-up on results,” the AHRQ said in the report.
More than a quarter of medical offices report that they are contacted by pharmacies on a daily or weekly basis to clarify or correct prescriptions, according to the Agency for Healthcare Research and Quality.
That safety issue – reported by 27% of outpatient medical offices – was the most common among those included in the Medical Office Survey on Patient Safety Culture from November 2013 to November 2015, the AHRQ said in its annual National Healthcare Quality and Disparities Report. Another 12% of respondents said that such contact with a pharmacy was a monthly occurrence.
Information exchange problems with pharmacies occurred daily or weekly in 12% of offices and monthly in 8%, while the occurrence of medication lists not being updated at the last visit was 11% daily/weekly and 7% monthly. Additionally, 9% of offices reported that results from laboratory or imaging tests were not available when needed on a daily/weekly basis and 10% on a monthly basis, the AHRQ reported.
“Lack of access to care and lack of access to timely and accurate medical information and test results may contribute to patient safety events such as missed or delayed diagnoses, medication errors, failure to order appropriate diagnostic or laboratory tests, incorrect interpretation of tests, and inadequate follow-up on results,” the AHRQ said in the report.
Study reveals limits of 4-D CT scanning for parathyroid disease
Preoperative four-dimensional computed tomography imaging and intraoperative findings for parathyroid disease are not always in agreement, a retrospective study has found.
Among patients with primary hyperparathyroidism who underwent preoperative four-dimensional computed tomography (4-D CT) followed by parathyroidectomy, multigland disease was the most strongly associated with discordance between the scan and the intraoperative findings, according to the study.
“Parathyroid 4-D CTs have emerged as one of the most accurate preoperative imaging modalities to localize abnormal parathyroid glands,” wrote researchers led by Shonan Sho, MD (JAMA Surg. 2017 Aug 9. doi: 10.1001/jamasurg.2017.2649). “Despite this use, missed lesions and incorrect localization still occur.”
In what is believed to be the first study of its kind, Dr. Sho of the section of endocrine surgery at the University of California, Los Angeles, and his associates prospectively evaluated factors associated with discordance between preoperative four-dimensional computed tomographic scans and intraoperative findings. They examined data from 411 patients with primary hyperparathyroidism who underwent 4-D CTs followed by parathyroidectomy at UCLA from Sept. 1, 2011, through Oct. 31, 2016. The mean age of patients was 59, 79% were female, and 30% had discordance between preoperative 4-D CTs and intraoperative findings.
When the researchers compared concordant cases with discordant cases, they found that discordant cases had higher frequencies of multigland disease (24.3% vs. 66.7%, respectively; P less than .001) and multinodular goiter or thyroid nodule (29.2% vs. 40.7%; P = .02). “Thyroid nodules can mimic parathyroid adenomas because they can occur in similar locations and appear oval or round, and they can have enhancement characteristics similar to those of parathyroid adenomas,” Dr. Sho and his associates wrote. “The addition of ultrasound may enable correct identification of abnormal parathyroid glands in a patient with thyroid nodules.”
The investigators also found that missed parathyroid lesions tended to be smaller than 10 mm in size and were more likely to be in the inferior position.
Multivariable analysis revealed the analysis risk factors for discordant 4-D CT findings: multigland disease (odds ratio, 7.63), parathyroid lesion in the inferior position (OR, 6.82), parathyroid lesion size of 10 mm or less (OR, 4.37), and multinodular goiter or thyroid nodule (OR, 1.82). The researchers concluded, “In the case of a negative 4-D CT, the surgeon may elect to allot additional operative time for what may be a more difficult case. Or, after considering the likelihood of MGD [multigland disease] based on biochemical values and the 4-D CT result, the surgeon may consider having a more detailed discussion with the patient regarding the potential need for subtotal parathyroidectomy. During surgery, if the surgeon is not finding the culprit glands or if the PTH [parathyroid hormone] level is not dropping, he or she should recall that discordance between intraoperative findings and the 4-D CT results is likely to be explained by MGD, an inferior gland that is flattened against the surface of the thyroid gland, or, less commonly, an intrathyroidal gland.”
They acknowledged certain limitations of the study, including its single-center, retrospective design; the fact that calcium levels were not available in all patients; and the fact that the 4-D CT technique remains novel.
The investigators reported having no relevant financial disclosures.
This study highlights the fact that no imaging for parathyroid disease is perfect. The diagnosis of hyperparathyroidism is based on laboratory testing, not on imaging studies.

Dr. Rebecca S. Sippel is chief of endocrine surgery at the University of Wisconsin–Madison.
This study highlights the fact that no imaging for parathyroid disease is perfect. The diagnosis of hyperparathyroidism is based on laboratory testing, not on imaging studies.
Dr. Rebecca S. Sippel is chief of endocrine surgery at the University of Wisconsin–Madison.
This study highlights the fact that no imaging for parathyroid disease is perfect. The diagnosis of hyperparathyroidism is based on laboratory testing, not on imaging studies.
Dr. Rebecca S. Sippel is chief of endocrine surgery at the University of Wisconsin–Madison.
Preoperative four-dimensional computed tomography imaging and intraoperative findings for parathyroid disease are not always in agreement, a retrospective study has found.
Among patients with primary hyperparathyroidism who underwent preoperative four-dimensional computed tomography (4-D CT) followed by parathyroidectomy, multigland disease was the most strongly associated with discordance between the scan and the intraoperative findings, according to the study.
“Parathyroid 4-D CTs have emerged as one of the most accurate preoperative imaging modalities to localize abnormal parathyroid glands,” wrote researchers led by Shonan Sho, MD (JAMA Surg. 2017 Aug 9. doi: 10.1001/jamasurg.2017.2649). “Despite this use, missed lesions and incorrect localization still occur.”
In what is believed to be the first study of its kind, Dr. Sho of the section of endocrine surgery at the University of California, Los Angeles, and his associates prospectively evaluated factors associated with discordance between preoperative four-dimensional computed tomographic scans and intraoperative findings. They examined data from 411 patients with primary hyperparathyroidism who underwent 4-D CTs followed by parathyroidectomy at UCLA from Sept. 1, 2011, through Oct. 31, 2016. The mean age of patients was 59, 79% were female, and 30% had discordance between preoperative 4-D CTs and intraoperative findings.
When the researchers compared concordant cases with discordant cases, they found that discordant cases had higher frequencies of multigland disease (24.3% vs. 66.7%, respectively; P less than .001) and multinodular goiter or thyroid nodule (29.2% vs. 40.7%; P = .02). “Thyroid nodules can mimic parathyroid adenomas because they can occur in similar locations and appear oval or round, and they can have enhancement characteristics similar to those of parathyroid adenomas,” Dr. Sho and his associates wrote. “The addition of ultrasound may enable correct identification of abnormal parathyroid glands in a patient with thyroid nodules.”
The investigators also found that missed parathyroid lesions tended to be smaller than 10 mm in size and were more likely to be in the inferior position.
Multivariable analysis revealed the analysis risk factors for discordant 4-D CT findings: multigland disease (odds ratio, 7.63), parathyroid lesion in the inferior position (OR, 6.82), parathyroid lesion size of 10 mm or less (OR, 4.37), and multinodular goiter or thyroid nodule (OR, 1.82). The researchers concluded, “In the case of a negative 4-D CT, the surgeon may elect to allot additional operative time for what may be a more difficult case. Or, after considering the likelihood of MGD [multigland disease] based on biochemical values and the 4-D CT result, the surgeon may consider having a more detailed discussion with the patient regarding the potential need for subtotal parathyroidectomy. During surgery, if the surgeon is not finding the culprit glands or if the PTH [parathyroid hormone] level is not dropping, he or she should recall that discordance between intraoperative findings and the 4-D CT results is likely to be explained by MGD, an inferior gland that is flattened against the surface of the thyroid gland, or, less commonly, an intrathyroidal gland.”
They acknowledged certain limitations of the study, including its single-center, retrospective design; the fact that calcium levels were not available in all patients; and the fact that the 4-D CT technique remains novel.
The investigators reported having no relevant financial disclosures.
Preoperative four-dimensional computed tomography imaging and intraoperative findings for parathyroid disease are not always in agreement, a retrospective study has found.
Among patients with primary hyperparathyroidism who underwent preoperative four-dimensional computed tomography (4-D CT) followed by parathyroidectomy, multigland disease was the most strongly associated with discordance between the scan and the intraoperative findings, according to the study.
“Parathyroid 4-D CTs have emerged as one of the most accurate preoperative imaging modalities to localize abnormal parathyroid glands,” wrote researchers led by Shonan Sho, MD (JAMA Surg. 2017 Aug 9. doi: 10.1001/jamasurg.2017.2649). “Despite this use, missed lesions and incorrect localization still occur.”
In what is believed to be the first study of its kind, Dr. Sho of the section of endocrine surgery at the University of California, Los Angeles, and his associates prospectively evaluated factors associated with discordance between preoperative four-dimensional computed tomographic scans and intraoperative findings. They examined data from 411 patients with primary hyperparathyroidism who underwent 4-D CTs followed by parathyroidectomy at UCLA from Sept. 1, 2011, through Oct. 31, 2016. The mean age of patients was 59, 79% were female, and 30% had discordance between preoperative 4-D CTs and intraoperative findings.
When the researchers compared concordant cases with discordant cases, they found that discordant cases had higher frequencies of multigland disease (24.3% vs. 66.7%, respectively; P less than .001) and multinodular goiter or thyroid nodule (29.2% vs. 40.7%; P = .02). “Thyroid nodules can mimic parathyroid adenomas because they can occur in similar locations and appear oval or round, and they can have enhancement characteristics similar to those of parathyroid adenomas,” Dr. Sho and his associates wrote. “The addition of ultrasound may enable correct identification of abnormal parathyroid glands in a patient with thyroid nodules.”
The investigators also found that missed parathyroid lesions tended to be smaller than 10 mm in size and were more likely to be in the inferior position.
Multivariable analysis revealed the analysis risk factors for discordant 4-D CT findings: multigland disease (odds ratio, 7.63), parathyroid lesion in the inferior position (OR, 6.82), parathyroid lesion size of 10 mm or less (OR, 4.37), and multinodular goiter or thyroid nodule (OR, 1.82). The researchers concluded, “In the case of a negative 4-D CT, the surgeon may elect to allot additional operative time for what may be a more difficult case. Or, after considering the likelihood of MGD [multigland disease] based on biochemical values and the 4-D CT result, the surgeon may consider having a more detailed discussion with the patient regarding the potential need for subtotal parathyroidectomy. During surgery, if the surgeon is not finding the culprit glands or if the PTH [parathyroid hormone] level is not dropping, he or she should recall that discordance between intraoperative findings and the 4-D CT results is likely to be explained by MGD, an inferior gland that is flattened against the surface of the thyroid gland, or, less commonly, an intrathyroidal gland.”
They acknowledged certain limitations of the study, including its single-center, retrospective design; the fact that calcium levels were not available in all patients; and the fact that the 4-D CT technique remains novel.
The investigators reported having no relevant financial disclosures.
FROM JAMA SURGERY
Key clinical point:
Major finding: Compared with cases that showed concordance between the 4-D CT scan and the intraoperative findings, discordant cases had higher frequencies of multigland disease (24.3% vs. 66.7%, respectively; P less than .001) and multinodular goiter or thyroid nodule (29.2% vs. 40.7%; P = .02).
Data source: A retrospective analysis of 411 patients with primary hyperparathyroidism who underwent preoperative 4-D CT scans followed by parathyroidectomy.
Disclosures: The researchers reported having no relevant financial disclosures.
Deutetrabenazine Improves Tardive Dyskinesia
VANCOUVER—Deutetrabenazine provides clinically significant reductions in involuntary movements of tardive dyskinesia, according to a study described at the 21st International Congress of Parkinson’s Disease and Movement Disorders. The treatment yields benefits regardless of patients’ concomitant use of dopamine-receptor antagonists. In addition, the drug is safe and well tolerated.
Tardive dyskinesia often results from exposure to dopamine-receptor antagonists. Clinicians sometimes manage the disorder by lowering the dose of the causative agent, but this tactic may increase the burden of the underlying disease.
Deutetrabenazine is a novel, highly selective vesicular monoamine transporter type 2 (VMAT2) inhibitor. The drug has been approved for the treatment of Huntington disease chorea and is under investigation as a treatment for tardive dyskinesia. A randomized, double-blind, placebo-controlled trial suggested that deutetrabenazine reduced abnormal involuntary movements, compared with placebo, in patients with tardive dyskinesia.
Comparing Three Doses With Placebo
Karen E. Anderson, MD, Director of the Huntington’s Disease Care, Education, and Research Center at MedStar Georgetown University Hospital in Washington, DC, and colleagues conducted a phase III, double-blind, parallel-group study to evaluate the efficacy, safety, and tolerability of three fixed doses of deutetrabenazine in patients with tardive dyskinesia. Eligible patients had a history of dopamine-receptor antagonist use, stable psychiatric illness on stable psychoactive medication, and an Abnormal Involuntary Movement Scale (AIMS) score of 6 or higher at baseline. Patients with a history of depression or suicidal behavior and those with neurologic conditions that may interfere with the assessment of tardive dyskinesia severity were excluded.

The investigators randomized patients in equal groups to deutetrabenazine (12 mg/day, 24 mg/day, or 36 mg/day) or placebo. At study initiation, all patients randomized to deutetrabenazine received 12 mg/day. Patients randomized to 24 mg/day or to 36 mg/day underwent a four-week dose-escalation period, at the end of which they reached their assigned doses. An eight-week maintenance period followed for all patients, and the subsequent washout period lasted for one week. Patients were followed up by telephone at week 16.
The study’s primary efficacy end point was change in AIMS score from baseline to week 12. The secondary end point was treatment success, which the investigators defined as the proportion of patients who were “much improved” or “very much improved” on the Clinical Global Impression of Change (CGIC), at week 12.
Benefits Persisted for 10 Weeks
The study included 298 participants. The population’s mean age was 57, and approximately 52% of participants were female. At week 12, AIMS score improved significantly from baseline by 3.2 points for patients receiving 24 mg/day of deutetrabenazine and by 3.3 points for patients receiving 36 mg/day of deutetrabenazine. AIMS score improved by 2.1 points for patients randomized to 12 mg/day of treatment, and by 1.4 points for controls, but these changes were not statistically significant. Clinically meaningful reductions in AIMS score were observed at week 2 and persisted throughout the treatment period for the 24-mg/day and 36-mg/day doses, compared with placebo. AIMS score improved in patients receiving the two higher doses regardless of patients’ use of dopamine-receptor antagonists at baseline.
At week 12, the proportion of patients who had treatment success was greater in those treated with deutetrabenazine, compared with controls. Also, all three doses of deutetrabenazine had clinically meaningful least-squares mean treatment differences on the CGIC at week 12, compared with placebo. The proportion of patients with treatment success was greater for patients who had not received dopamine-receptor antagonists at baseline than for those who had (58% vs 46% for the 24-mg/day dose and 60% vs 34% for the 36-mg/day dose).
The rates of adverse events and discontinuations were similar between the deutetrabenazine and placebo groups. Common adverse events included headache, diarrhea, nausea, nasopharyngitis, and somnolence. Serious adverse events included appendicitis, cardiorespiratory arrest, cellulitis, depression, sudden cardiac death, and psychotic disorders, but none of these was determined to be related to the study drug.
The study was funded by Teva Pharmaceutical Industries.
—Erik Greb
Suggested Reading
Anderson KE, Stamler D, Davis MD, et al. Deutetrabenazine for treatment of involuntary movements in patients with tardive dyskinesia (AIM-TD): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Psychiatry. 2017 Jun 28 [Epub ahead of print].
Fernandez HH, Factor SA, Hauser RA, et al. Randomized controlled trial of deutetrabenazine for tardive dyskinesia: The ARM-TD study. Neurology. 2017;88(21):2003-2010.
VANCOUVER—Deutetrabenazine provides clinically significant reductions in involuntary movements of tardive dyskinesia, according to a study described at the 21st International Congress of Parkinson’s Disease and Movement Disorders. The treatment yields benefits regardless of patients’ concomitant use of dopamine-receptor antagonists. In addition, the drug is safe and well tolerated.
Tardive dyskinesia often results from exposure to dopamine-receptor antagonists. Clinicians sometimes manage the disorder by lowering the dose of the causative agent, but this tactic may increase the burden of the underlying disease.
Deutetrabenazine is a novel, highly selective vesicular monoamine transporter type 2 (VMAT2) inhibitor. The drug has been approved for the treatment of Huntington disease chorea and is under investigation as a treatment for tardive dyskinesia. A randomized, double-blind, placebo-controlled trial suggested that deutetrabenazine reduced abnormal involuntary movements, compared with placebo, in patients with tardive dyskinesia.
Comparing Three Doses With Placebo
Karen E. Anderson, MD, Director of the Huntington’s Disease Care, Education, and Research Center at MedStar Georgetown University Hospital in Washington, DC, and colleagues conducted a phase III, double-blind, parallel-group study to evaluate the efficacy, safety, and tolerability of three fixed doses of deutetrabenazine in patients with tardive dyskinesia. Eligible patients had a history of dopamine-receptor antagonist use, stable psychiatric illness on stable psychoactive medication, and an Abnormal Involuntary Movement Scale (AIMS) score of 6 or higher at baseline. Patients with a history of depression or suicidal behavior and those with neurologic conditions that may interfere with the assessment of tardive dyskinesia severity were excluded.
The investigators randomized patients in equal groups to deutetrabenazine (12 mg/day, 24 mg/day, or 36 mg/day) or placebo. At study initiation, all patients randomized to deutetrabenazine received 12 mg/day. Patients randomized to 24 mg/day or to 36 mg/day underwent a four-week dose-escalation period, at the end of which they reached their assigned doses. An eight-week maintenance period followed for all patients, and the subsequent washout period lasted for one week. Patients were followed up by telephone at week 16.
The study’s primary efficacy end point was change in AIMS score from baseline to week 12. The secondary end point was treatment success, which the investigators defined as the proportion of patients who were “much improved” or “very much improved” on the Clinical Global Impression of Change (CGIC), at week 12.
Benefits Persisted for 10 Weeks
The study included 298 participants. The population’s mean age was 57, and approximately 52% of participants were female. At week 12, AIMS score improved significantly from baseline by 3.2 points for patients receiving 24 mg/day of deutetrabenazine and by 3.3 points for patients receiving 36 mg/day of deutetrabenazine. AIMS score improved by 2.1 points for patients randomized to 12 mg/day of treatment, and by 1.4 points for controls, but these changes were not statistically significant. Clinically meaningful reductions in AIMS score were observed at week 2 and persisted throughout the treatment period for the 24-mg/day and 36-mg/day doses, compared with placebo. AIMS score improved in patients receiving the two higher doses regardless of patients’ use of dopamine-receptor antagonists at baseline.
At week 12, the proportion of patients who had treatment success was greater in those treated with deutetrabenazine, compared with controls. Also, all three doses of deutetrabenazine had clinically meaningful least-squares mean treatment differences on the CGIC at week 12, compared with placebo. The proportion of patients with treatment success was greater for patients who had not received dopamine-receptor antagonists at baseline than for those who had (58% vs 46% for the 24-mg/day dose and 60% vs 34% for the 36-mg/day dose).
The rates of adverse events and discontinuations were similar between the deutetrabenazine and placebo groups. Common adverse events included headache, diarrhea, nausea, nasopharyngitis, and somnolence. Serious adverse events included appendicitis, cardiorespiratory arrest, cellulitis, depression, sudden cardiac death, and psychotic disorders, but none of these was determined to be related to the study drug.
The study was funded by Teva Pharmaceutical Industries.
—Erik Greb
Suggested Reading
Anderson KE, Stamler D, Davis MD, et al. Deutetrabenazine for treatment of involuntary movements in patients with tardive dyskinesia (AIM-TD): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Psychiatry. 2017 Jun 28 [Epub ahead of print].
Fernandez HH, Factor SA, Hauser RA, et al. Randomized controlled trial of deutetrabenazine for tardive dyskinesia: The ARM-TD study. Neurology. 2017;88(21):2003-2010.
VANCOUVER—Deutetrabenazine provides clinically significant reductions in involuntary movements of tardive dyskinesia, according to a study described at the 21st International Congress of Parkinson’s Disease and Movement Disorders. The treatment yields benefits regardless of patients’ concomitant use of dopamine-receptor antagonists. In addition, the drug is safe and well tolerated.
Tardive dyskinesia often results from exposure to dopamine-receptor antagonists. Clinicians sometimes manage the disorder by lowering the dose of the causative agent, but this tactic may increase the burden of the underlying disease.
Deutetrabenazine is a novel, highly selective vesicular monoamine transporter type 2 (VMAT2) inhibitor. The drug has been approved for the treatment of Huntington disease chorea and is under investigation as a treatment for tardive dyskinesia. A randomized, double-blind, placebo-controlled trial suggested that deutetrabenazine reduced abnormal involuntary movements, compared with placebo, in patients with tardive dyskinesia.
Comparing Three Doses With Placebo
Karen E. Anderson, MD, Director of the Huntington’s Disease Care, Education, and Research Center at MedStar Georgetown University Hospital in Washington, DC, and colleagues conducted a phase III, double-blind, parallel-group study to evaluate the efficacy, safety, and tolerability of three fixed doses of deutetrabenazine in patients with tardive dyskinesia. Eligible patients had a history of dopamine-receptor antagonist use, stable psychiatric illness on stable psychoactive medication, and an Abnormal Involuntary Movement Scale (AIMS) score of 6 or higher at baseline. Patients with a history of depression or suicidal behavior and those with neurologic conditions that may interfere with the assessment of tardive dyskinesia severity were excluded.
The investigators randomized patients in equal groups to deutetrabenazine (12 mg/day, 24 mg/day, or 36 mg/day) or placebo. At study initiation, all patients randomized to deutetrabenazine received 12 mg/day. Patients randomized to 24 mg/day or to 36 mg/day underwent a four-week dose-escalation period, at the end of which they reached their assigned doses. An eight-week maintenance period followed for all patients, and the subsequent washout period lasted for one week. Patients were followed up by telephone at week 16.
The study’s primary efficacy end point was change in AIMS score from baseline to week 12. The secondary end point was treatment success, which the investigators defined as the proportion of patients who were “much improved” or “very much improved” on the Clinical Global Impression of Change (CGIC), at week 12.
Benefits Persisted for 10 Weeks
The study included 298 participants. The population’s mean age was 57, and approximately 52% of participants were female. At week 12, AIMS score improved significantly from baseline by 3.2 points for patients receiving 24 mg/day of deutetrabenazine and by 3.3 points for patients receiving 36 mg/day of deutetrabenazine. AIMS score improved by 2.1 points for patients randomized to 12 mg/day of treatment, and by 1.4 points for controls, but these changes were not statistically significant. Clinically meaningful reductions in AIMS score were observed at week 2 and persisted throughout the treatment period for the 24-mg/day and 36-mg/day doses, compared with placebo. AIMS score improved in patients receiving the two higher doses regardless of patients’ use of dopamine-receptor antagonists at baseline.
At week 12, the proportion of patients who had treatment success was greater in those treated with deutetrabenazine, compared with controls. Also, all three doses of deutetrabenazine had clinically meaningful least-squares mean treatment differences on the CGIC at week 12, compared with placebo. The proportion of patients with treatment success was greater for patients who had not received dopamine-receptor antagonists at baseline than for those who had (58% vs 46% for the 24-mg/day dose and 60% vs 34% for the 36-mg/day dose).
The rates of adverse events and discontinuations were similar between the deutetrabenazine and placebo groups. Common adverse events included headache, diarrhea, nausea, nasopharyngitis, and somnolence. Serious adverse events included appendicitis, cardiorespiratory arrest, cellulitis, depression, sudden cardiac death, and psychotic disorders, but none of these was determined to be related to the study drug.
The study was funded by Teva Pharmaceutical Industries.
—Erik Greb
Suggested Reading
Anderson KE, Stamler D, Davis MD, et al. Deutetrabenazine for treatment of involuntary movements in patients with tardive dyskinesia (AIM-TD): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Psychiatry. 2017 Jun 28 [Epub ahead of print].
Fernandez HH, Factor SA, Hauser RA, et al. Randomized controlled trial of deutetrabenazine for tardive dyskinesia: The ARM-TD study. Neurology. 2017;88(21):2003-2010.
Insurance coverage gainers outnumber coverage losers
Fewer nonelderly adults lost their health insurance in 2015 than in 2013, while more gained coverage, according to the Agency for Healthcare Research and Quality.
The presence of chronic conditions played a part for those who lost coverage. From 2012 to 2013, 2.9% of adults aged 18-64 years with one or more chronic conditions lost their insurance, compared with 1.5% who lost coverage from 2014 to 2015. Those with no chronic conditions saw a corresponding drop from 4% to 3.2%, but that change was not significant, AHRQ investigators reported.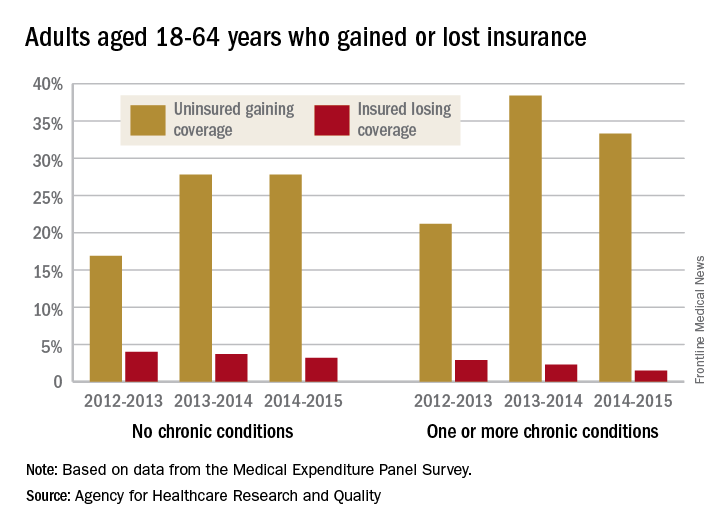
For this analysis, the chronic conditions were active asthma, arthritis, diabetes, emphysema, heart disease, high blood pressure, high cholesterol, bronchitis, and stroke. The source of the data was the Medical Expenditure Panel Survey.
Fewer nonelderly adults lost their health insurance in 2015 than in 2013, while more gained coverage, according to the Agency for Healthcare Research and Quality.
The presence of chronic conditions played a part for those who lost coverage. From 2012 to 2013, 2.9% of adults aged 18-64 years with one or more chronic conditions lost their insurance, compared with 1.5% who lost coverage from 2014 to 2015. Those with no chronic conditions saw a corresponding drop from 4% to 3.2%, but that change was not significant, AHRQ investigators reported.
For this analysis, the chronic conditions were active asthma, arthritis, diabetes, emphysema, heart disease, high blood pressure, high cholesterol, bronchitis, and stroke. The source of the data was the Medical Expenditure Panel Survey.
Fewer nonelderly adults lost their health insurance in 2015 than in 2013, while more gained coverage, according to the Agency for Healthcare Research and Quality.
The presence of chronic conditions played a part for those who lost coverage. From 2012 to 2013, 2.9% of adults aged 18-64 years with one or more chronic conditions lost their insurance, compared with 1.5% who lost coverage from 2014 to 2015. Those with no chronic conditions saw a corresponding drop from 4% to 3.2%, but that change was not significant, AHRQ investigators reported.
For this analysis, the chronic conditions were active asthma, arthritis, diabetes, emphysema, heart disease, high blood pressure, high cholesterol, bronchitis, and stroke. The source of the data was the Medical Expenditure Panel Survey.
Noninvasive NASH test could help monitor hepatotoxicity in patients on methotrexate
A noninvasive test for nonalcoholic steatohepatitis (NASH) and hepatic fibrosis could be used to help detect worsening hepatic fibrosis in psoriasis patients who are on long-term methotrexate therapy, according to the authors of a retrospective study published online Aug. 23.
To evaluate the use of the noninvasive test to monitor for hepatic fibrosis in this group of patients and guide the management of methotrexate (MTX) without a liver biopsy, investigators conducted an analysis of 107 patients with psoriasis who were on long-term MTX treatment, for whom the NASH FibroSure test was used between January 2007 and December 2013. All the patients were white, fifty were men, the mean age was 83 years, and almost all of the patients had a body mass index of 28 or more (16% had a BMI between 28 and 30, and 81% had a BMI over 30).
The NASH FibroSure test, which was developed for use in patients suspected of having nonalcoholic fatty liver disease (NAFLD), combines analyses of 10 biochemical markers combined with age, sex, height, and weight to calculate the degree of hepatic fibrosis. The test has a reported sensitivity of 83% and a specificity of 78% in detecting risk of significant fibrosis, according to Bruce Bauer, MD, of Pariser Dermatology Specialists, Norfolk, Va., and his coinvestigators (JAMA Dermatol. 2017 Aug 23. doi: 10.1001/jamadermatol.2017.2083).
Among the 107 patients, the investigators found a statistically significant correlation “between worsening fibrosis scores and cumulative methotrexate” dose among women (P = .02), but not among men (P = .11). In addition, women with a BMI of 28 or more were more likely to have worsening fibrosis scores (P = .03). “There were no differences between men and women with regard to prevalence of a BMI of 28 or more, diabetes, age older than 65 years, or chronic kidney disease,” which they said, suggests that among women, “obesity influences the progression of fibrosis scores.”
The investigators advised providers not to disregard any potential warning signs when using FibroSure on men. “No differences between the cohorts were observed that would explain the association of worsening fibrosis scores and cumulative MTX dose among women but not men,” they wrote. “However, given the implications of the progression of hepatic fibrosis, we still recommend discontinuing MTX for male patients who demonstrate worsening fibrosis scores.”
While the test may not be able to replace liver biopsy, based on these results, the investigators noted that noninvasive tests such as this one could help significantly reduce the number of liver biopsies needed.
They pointed out that because the study was conducted at one center, the next step is to conduct “a prospective, randomized, multi-institutional analysis of NASH FibroSure and liver biopsies for patients with psoriasis receiving MTX vs. other treatments, including a larger cohort of men and women with different racial and ethnic backgrounds.”
One of the four authors reported receiving research funding from T2 Biosystems. Dr. Bauer and the two other authors reported no relevant financial disclosures. The study was funded by the Marshfield Clinic Resident Research Program.
[email protected]
On Twitter @eaztweets
A noninvasive test for nonalcoholic steatohepatitis (NASH) and hepatic fibrosis could be used to help detect worsening hepatic fibrosis in psoriasis patients who are on long-term methotrexate therapy, according to the authors of a retrospective study published online Aug. 23.
To evaluate the use of the noninvasive test to monitor for hepatic fibrosis in this group of patients and guide the management of methotrexate (MTX) without a liver biopsy, investigators conducted an analysis of 107 patients with psoriasis who were on long-term MTX treatment, for whom the NASH FibroSure test was used between January 2007 and December 2013. All the patients were white, fifty were men, the mean age was 83 years, and almost all of the patients had a body mass index of 28 or more (16% had a BMI between 28 and 30, and 81% had a BMI over 30).
The NASH FibroSure test, which was developed for use in patients suspected of having nonalcoholic fatty liver disease (NAFLD), combines analyses of 10 biochemical markers combined with age, sex, height, and weight to calculate the degree of hepatic fibrosis. The test has a reported sensitivity of 83% and a specificity of 78% in detecting risk of significant fibrosis, according to Bruce Bauer, MD, of Pariser Dermatology Specialists, Norfolk, Va., and his coinvestigators (JAMA Dermatol. 2017 Aug 23. doi: 10.1001/jamadermatol.2017.2083).
Among the 107 patients, the investigators found a statistically significant correlation “between worsening fibrosis scores and cumulative methotrexate” dose among women (P = .02), but not among men (P = .11). In addition, women with a BMI of 28 or more were more likely to have worsening fibrosis scores (P = .03). “There were no differences between men and women with regard to prevalence of a BMI of 28 or more, diabetes, age older than 65 years, or chronic kidney disease,” which they said, suggests that among women, “obesity influences the progression of fibrosis scores.”
The investigators advised providers not to disregard any potential warning signs when using FibroSure on men. “No differences between the cohorts were observed that would explain the association of worsening fibrosis scores and cumulative MTX dose among women but not men,” they wrote. “However, given the implications of the progression of hepatic fibrosis, we still recommend discontinuing MTX for male patients who demonstrate worsening fibrosis scores.”
While the test may not be able to replace liver biopsy, based on these results, the investigators noted that noninvasive tests such as this one could help significantly reduce the number of liver biopsies needed.
They pointed out that because the study was conducted at one center, the next step is to conduct “a prospective, randomized, multi-institutional analysis of NASH FibroSure and liver biopsies for patients with psoriasis receiving MTX vs. other treatments, including a larger cohort of men and women with different racial and ethnic backgrounds.”
One of the four authors reported receiving research funding from T2 Biosystems. Dr. Bauer and the two other authors reported no relevant financial disclosures. The study was funded by the Marshfield Clinic Resident Research Program.
[email protected]
On Twitter @eaztweets
A noninvasive test for nonalcoholic steatohepatitis (NASH) and hepatic fibrosis could be used to help detect worsening hepatic fibrosis in psoriasis patients who are on long-term methotrexate therapy, according to the authors of a retrospective study published online Aug. 23.
To evaluate the use of the noninvasive test to monitor for hepatic fibrosis in this group of patients and guide the management of methotrexate (MTX) without a liver biopsy, investigators conducted an analysis of 107 patients with psoriasis who were on long-term MTX treatment, for whom the NASH FibroSure test was used between January 2007 and December 2013. All the patients were white, fifty were men, the mean age was 83 years, and almost all of the patients had a body mass index of 28 or more (16% had a BMI between 28 and 30, and 81% had a BMI over 30).
The NASH FibroSure test, which was developed for use in patients suspected of having nonalcoholic fatty liver disease (NAFLD), combines analyses of 10 biochemical markers combined with age, sex, height, and weight to calculate the degree of hepatic fibrosis. The test has a reported sensitivity of 83% and a specificity of 78% in detecting risk of significant fibrosis, according to Bruce Bauer, MD, of Pariser Dermatology Specialists, Norfolk, Va., and his coinvestigators (JAMA Dermatol. 2017 Aug 23. doi: 10.1001/jamadermatol.2017.2083).
Among the 107 patients, the investigators found a statistically significant correlation “between worsening fibrosis scores and cumulative methotrexate” dose among women (P = .02), but not among men (P = .11). In addition, women with a BMI of 28 or more were more likely to have worsening fibrosis scores (P = .03). “There were no differences between men and women with regard to prevalence of a BMI of 28 or more, diabetes, age older than 65 years, or chronic kidney disease,” which they said, suggests that among women, “obesity influences the progression of fibrosis scores.”
The investigators advised providers not to disregard any potential warning signs when using FibroSure on men. “No differences between the cohorts were observed that would explain the association of worsening fibrosis scores and cumulative MTX dose among women but not men,” they wrote. “However, given the implications of the progression of hepatic fibrosis, we still recommend discontinuing MTX for male patients who demonstrate worsening fibrosis scores.”
While the test may not be able to replace liver biopsy, based on these results, the investigators noted that noninvasive tests such as this one could help significantly reduce the number of liver biopsies needed.
They pointed out that because the study was conducted at one center, the next step is to conduct “a prospective, randomized, multi-institutional analysis of NASH FibroSure and liver biopsies for patients with psoriasis receiving MTX vs. other treatments, including a larger cohort of men and women with different racial and ethnic backgrounds.”
One of the four authors reported receiving research funding from T2 Biosystems. Dr. Bauer and the two other authors reported no relevant financial disclosures. The study was funded by the Marshfield Clinic Resident Research Program.
[email protected]
On Twitter @eaztweets
FROM JAMA DERMATOLOGY
Key clinical point:
Major finding: There was a significant correlation between worsening fibrosis scores on the test and cumulative methotrexate dose among women (P = .02), but not among men (P = .11).
Data source: A retrospective single-center study analyzing the test in 107 psoriasis patients on methotrexate, collected between January 2007 and December 2013.
Disclosures: One of the four authors received research funding from T2 Biosystems. There were no other financial disclosures.
National Trends (2007-2013) of Clostridium difficile Infection in Patients with Septic Shock: Impact on Outcome
Clostridium difficile infection (CDI) is the most common infectious cause of healthcare-associated diarrhea.1 Development of a CDI during hospitalization is associated with increases in morbidity, mortality, length of stay (LOS), and cost.2-5 The prevalence of CDI in hospitalized patients has increased dramatically from the mid-1990s to the mid-2000s to almost 9 cases per 1000 discharges; however, the CDI rate since 2007 appears to have plateaued.6,7 Antibiotic use has historically been the most important risk factor for acquiring CDI; however, use of acid-suppressing agents, chemotherapy, chronic comorbidities, and healthcare exposure all also increase the risk of CDI.7-10 The elderly (> 65 years of age) are particularly at risk for developing CDI and having worse clinical outcomes with CDI.6,7
Patients with septic shock (SS) often have multiple CDI risk factors (in particular, extensive antibiotic exposure) and thus, represent a population at a particularly high risk for acquiring a CDI during hospitalization. However, little data are available on the prevalence of CDI acquired in patients hospitalized with SS. We sought to determine the national-level temporal trends in the prevalence of CDI in patients with SS and the impact of CDI complicating SS on clinical outcomes between 2007 and 2013.
METHODS
Data Source
We used the National Inpatient Sample (NIS) and Nationwide Readmissions Database (NRD) for this study. The NIS is a database developed by the Agency of Healthcare Research and Quality for the Healthcare Cost and Utilization Project (HCUP).11 It is the largest all-payer inpatient database in the United States and has been used by researchers and policy makers to analyze national trends in outcomes and healthcare utilization. The NIS database now approximates a 20% stratified sample of all discharges from all participating US hospitals. Sampling weights are provided by the manufacturer and can be used to produce national-level estimates. Following the redesign of the NIS in 2012, new sampling weights were provided for trend analysis for the years prior to 2012 to account for the new design. Every hospitalization is deidentified and converted into one unique entry that provides information on demographics, hospital characteristics, 1 primary and up to 24 secondary discharge diagnoses, comorbidities, LOS, in-hospital mortality, and procedures performed during stay. The discharge diagnoses are provided in the form of the International Classification of Diseases, 9th Revision-Clinical Modification (ICD-9-CM) codes.
The NRD is a database developed for HCUP that contains about 35 million discharges each year and supports readmission data analyses. In 2013, the NRD contained data from 21 geographically diverse states, accounting for 49.1% of all US hospitalizations. Diagnosis, comorbidities, and outcomes are presented in a similar manner to NIS.
Study Design
This was a retrospective cohort study. Data from the NIS between 2007 and 2013 were used for the analysis. Demographic data obtained included age, gender, race, Charlson-Deyo Comorbidity Index,12 hospital characteristics (hospital region, hospital-bed size, urban versus rural location, and teaching status), calendar year, and use of mechanical ventilation. Cases with information missing on key demographic variables (age, gender, and race) were excluded. Only adults (>18 years of age) were included for the analysis.
SS was identified by either (1) ICD-9-CM diagnosis code for SS (785.52) or (2) presence of vasopressor use (00.17) along with ICD-9-CM codes of sepsis, severe sepsis, septicemia, bacteremia, or fungemia. This approach is consistent with what has been utilized in other studies to identify cases of sepsis or SS from administrative databases.13-15 The appendix provides a complete list of ICD-9-CM codes used in the study. CDI was identified by ICD-9-CM code 008.45 among the secondary diagnosis. This code has been shown to have good accuracy for identifying CDI using administrative data.16 To minimize the inclusion of cases in which a CDI was present at admission, hospitalizations with a primary diagnosis of CDI were not included as cases of CDI complicating SS.
We used NRD 2013 for estimating the effect of CDI on 30-day readmission after initial hospitalizations with SS. We used the criteria for index admissions and 30-day readmissions as defined by the Centers for Medicare and Medicaid Services. We excluded patients who died during their index admission, patients with index discharges in December due to a lack of sufficient time to capture 30-day readmissions, and patients with missing information on key variables. We also excluded patients who were not a resident of the state of index hospitalization since readmission across state boundaries could not be identified in NRD. Manufacturer provided sampling weights were used to produce national level estimates. The cases of SS and CDI were identified by ICD-9-CM codes using the methodology described above.
Outcomes
Our primary outcome of interest was the total and yearly prevalence of CDI in patients with SS from 2007 to 2013. The secondary outcomes were mortality, LOS, and 30-day readmissions in patients with SS with and without CDI.
Statistical Analysis
Weighted data from NIS were used for all analyses. Demographics, hospital characteristics, and outcomes of all patients with SS were obtained. The prevalence of CDI was calculated for each calendar year. The temporal trends of outcomes (LOS and in-hospital mortality) of patients were plotted for patients with SS with and without CDI. A χ2 test of trend for proportions was used with the Cochran-Armitage test to calculate statistical significance of changes in prevalence. To test for statistical significance of the temporal trends of LOS, a univariate linear regression was used, with calendar year as a covariate. Independent samples t test, a Mann-Whitney U test, and a χ2 test were used to determine statistical significance of parameters between the group with CDI and the group without CDI.
Prolonged LOS was defined either as a LOS > 75th or > 90th percentile of LOS among all patients with SS. To identify if CDI was associated with a prolonged LOS after adjusting for patient and hospital characteristics, a multivariate logistic regression analysis was used. Variables included in the regression model were age, gender, race, Charlson-Deyo Comorbidity Index, hospital characteristics (hospital region, hospital-bed size, urban versus rural location, and teaching status), calendar year, and use of mechanical ventilation. Data on cases were available for all the above covariates except hospital characteristics, such as teaching status, location, and bed size (these were missing for 0.7% of hospitals).
Stata 13.1.0 (Stata Corp, College Station, TX) and SPSS 23.0 (SPSS Inc., Chicago, IL) were used to perform statistical analyses. A P value of <0.05 was considered statistically significant.
RESULTS
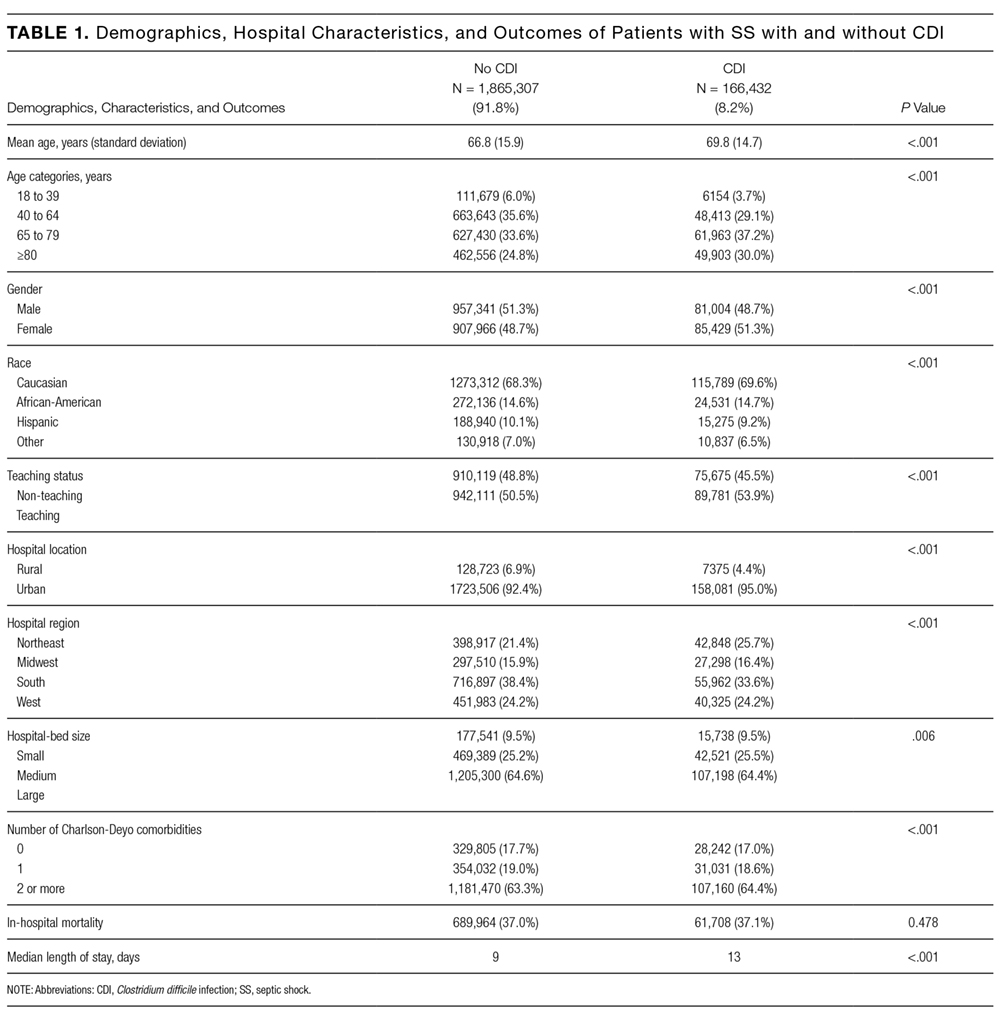
Demographics
A total of 2,031,739 hospitalizations of adults with SS were identified between 2007 and 2013. CDI was present in 166,432 (8.2%) of these patients. Demographic data are displayed in Table 1. CDI was more commonly observed in elderly patients (> 65 years) with SS; 9.3% among the elderly versus 6.6% among individuals < 65 years; P < 0.001. The prevalence of CDI was greater in urban than in rural hospitals (8.4% vs 5.4%; P < 0.001) and greater in teaching than in nonteaching hospitals (8.7% vs 7.7%; P < 0.001). The prevalence of CDI in SS remained stable between 2007 and 2013 (Table 2).
Mortality

In the overall study cohort, the in-hospital mortality for SS was 37%. The in-hospital mortality rate of patients with SS complicated by a CDI was comparable to the mortality rate of patients without a CDI (37.1% vs 37.0%; P = 0.48). The mortality of patients with SS, with or without CDI, progressively decreased from 2007 to 2013 (P value for trend < 0.001 for each group; Figure 1).
Length of Stay
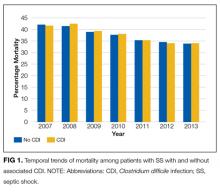
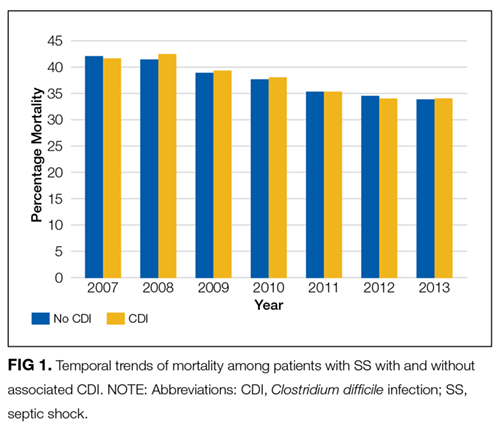
The median LOS for all patients with SS was 9 days. Patients with CDI had a longer median LOS than did those without CDI (13 vs 9 days; P < 0.001). Between 2007 and 2013, the median LOS of CDI group decreased from 14 to 12 days (P < 0.001) while that of non-CDI group decreased from 9 to 8 days (P < 0.001; Figure 2). We also examined LOS among subgroups who were discharged alive and those who died during hospitalization. For patients who were discharged alive, the LOS with and without CDI was 15 days versus 10 days, respectively (P < 0.001). For patients who died during hospitalization, LOS with and without CDI was 10 days versus 6 days, respectively (P < 0.001).
The 75th percentile of LOS of the total SS cohort was 17 days. An LOS > 17 days was observed in 36.9% of SS patients with CDI versus 22.7% without CDI (P < 0.001). After adjusting for patient and provider level variables, the odds of a LOS > 17 days were significantly greater for SS patients with CDI (odds ratio [OR] 2.11; 95% confidence interval [CI], 2.06-2.15; P < 0.001).
The 90th percentile of LOS of the total SS cohort was 29 days. An LOS > 29 days was observed in 17.5% of SS patients with a CDI versus 9.1% without a CDI (P < 0.001). After adjustment for patient and provider level variables, the odds of a LOS > 29 days were significantly greater for SS patients with a CDI (OR 2.25; 95% CI, 2.22-2.28; P < 0.001).
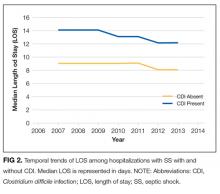
Hospital Readmission
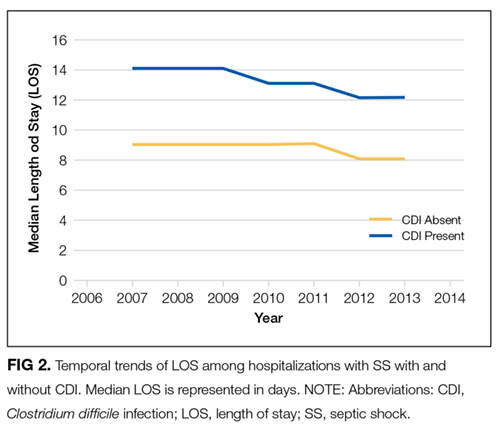
In 2013, patients with SS and CDI had a higher rate of 30-day readmission as compared to patients with SS without CDI (9.8% vs 7.4% respectively; P < 0.001). The multivariate adjusted OR for 30-day readmission for patients with SS and a CDI was 1.26 (95% CI, 1.22-1.31; P < 0.001).
Additional Analyses
Lastly, we performed an additional analysis to confirm our hypothesis that a CDI by itself is rarely a cause of SS, and that CDI as the principal diagnosis would constitute an extremely low number of patients with SS in an administrative dataset. In NIS 2013, there were 105,750 cases with CDI as the primary diagnosis. A total of 4470 (4.2%) had a secondary diagnosis of sepsis and only 930 (0.9%) cases had a secondary diagnosis of SS.
DISCUSSION
This is the first study to report on the prevalence and outcome of CDI complicating SS. By using a large nationally representative sample, we found CDI was very prevalent among individuals hospitalized with SS and, at a level in excess of that seen in other populations. Of interest, we did not observe an increase in mortality of SS when complicated by CDI. On the other hand, patients with SS complicated by CDI were more much likely to have a prolonged hospital LOS and a higher risk of 30-day hospital readmission.
The prevalence of CDI exploded between the mid-1990s and mid-2000s, including community, hospital, and intensive care unit (ICU)–related disease.6,7,17-20 Patients with SS often have multiple risk factors associated with CDI and thus represent a high-risk population for developing CDI.7 Our findings are consistent with the suggestion that individuals with SS are at a higher risk of developing CDI. Compared to the rate of CDI in all hospitalized patients, our data suggest an almost 10-fold increase in CDI rate for patients with SS.6 Patients with SS and CDI may account for as much as 10% of total CDIs.6,7 As has been reported for CDI in general, we observed that CDI complicating SS was more common in those > 65 years of age.4,21 The prevalence of CDI we observed in patients with SS was also higher than has been reported in ICU patients in general (1%), and higher than reported for patients requiring mechanical ventilation (6.6%), including prolonged mechanical ventilation (5.3%); further supporting the conclusion that patients with SS are a particularly high-risk group for acquiring CDI, even compared with other ICU patients.20,22,23 Similarly, the rate of CDI among SS was 8 times higher than that of recently reported hospital-onset CDI among patients with sepsis in general (incidence 1.08%).24 We have no data regarding why patients with SS have a higher rate of CDI; however, the intensity and duration of antibiotic treatment of these patients may certainly play a role.25 It has recently been reported that CDI in itself can be a precursor leading to intestinal dysbiosis that can increase the risk of subsequent sepsis. Similarly, patients with SS may have higher prevalence of dysbiosis that, in turn, might predispose them to CDI at a higher rate than other individuals.
Following the increase in CDIs in the mid-1990s and the mid-2000s, since 2007 the overall prevalence of CDIs has been stable, albeit at the higher rate. More recently, the Centers for Disease Control and Prevention (CDC) has reported a decrease in hospital onset CDI after 2011.26
The finding that CDI in SS patients was not associated with an increase in mortality is consistent with other reports of CDI in ICU patients in general as well as higher-risk ICU populations such as patients requiring mechanical ventilation, including those on long-term mechanical ventilator support.17,18,20,22,23 Why the mortality of ICU patients with CDI is not increased is not completely clear. It has been suggested that this may be related to early recognition and treatment of CDI developing in the ICU.22 Along these lines, it has been previously observed that for patients with CDI on mechanical ventilation, patients who were transferred to the ICU from the ward had worse clinical outcomes compared to patients directly admitted to the ICU, likely due to delayed recognition and treatment in the former.22 Similarly, ICU patients in whom CDI was identified prior to ICU admission had more severe CDI, and mortality that was directly related to CDI was only observed in patients who had CDI identified pre-ICU transfer.18 The increase in mortality observed in patients with sepsis in general with CDI may reflect similar factors.24 We observed a trend of decreasing mortality in SS patients with or without CDI during 2007 to 2013 consistent to what has been generally reported in SS.13,14
The increase in LOS observed in SS patients with CDI is also consistent with what has been observed in other ICU populations, as well as in patients with sepsis in general.17,22-24 Of note, in addition to the increase in median LOS, we found a significant increase in the number of patients with a prolonged LOS associated with having SS with CDI. It is important to note that development of CDI during hospitalization is affected by pre-CDI hospital LOS, so prolonged LOS may not be solely attributable to CDI. The interaction between LOS and CDI remains complex in which higher LOS might be associated with higher incidence of CDI occurrence, and once established, CDI might be associated with changes in LOS for the remaining hospitalization.
Hospitalized patients with CDI have an overall higher resource utilization than those without CDI.27 A recent review has estimated the overall attributable cost of CDI to be $6.3 billion; the attributable cost per case of hospital acquired CDI being 1.5 times the cost of community-acquired CDI.5 We did not look at cost directly. However, in the high-CDI risk ICU population requiring prolonged mechanical ventilation, those with CDI had a substantial increase in total costs.23 Given the substantial increase in LOS associated with CDI complicating SS, there would likely be a significant increase in hospital costs related to providing care for these patients. Further adding to the potential burden of CDI is our finding that CDI and SS was associated with an increase in 30-day hospital readmission rate. This is consistent with a recent report that ICU patients with CDI who are discharged from the hospital have a 25% 30-day hospital readmission rate.28 However, we do not have data either as to the reason for hospital readmission or whether the initial CDI or CDI recurrence played a role. This suggests that, in addition to intervention directed toward preventing CDI, efforts should be directed towards identifying factors that can be modified in CDI patients prior to or after hospital discharge.
This study has several limitations. Using an administrative database (such as NIS) has an inherent limitation of coding errors and reporting bias can lead to misclassification of cohort definition (SS) and outcome (CDI). To minimize bias due to coding errors, we used previously validated ICD-9-CM codes and approach to identify individuals with SS and CDI.13-15 Although the SS population was identified with ICD-9-CM codes using an administrative database, the in-hospital mortality for our septic population was similar to previously reported mortality of SS, suggesting the population selected was appropriate.13 SS due to CDI could not be identified; however, CDI by itself causing SS is rare, as described in recent literature.29,30 An important potential bias that needs to be acknowledged is the immortal time bias. The occurrence of CDI in itself can be influenced by pre-CDI hospital LOS. Patients who were extremely sick could have died early in their hospital course before they could acquire CDI, which would influence the mortality difference between the group with CDI and group without CDI. Furthermore, we did not have information on either the treatment of CDI or SS or any measures of severity of illness, which could lead to residual confounding despite adjusting for multiple variables. In terms of readmission data, it was necessary to exclude nonresidents of a state for the 30-day readmission analysis, as readmissions could not be tracked across state boundaries by using the NRD. This might have resulted in an underrepresentation of the readmission burden. Lastly, it was not possible to identify mortality after hospital discharge as the NIS provides only in-hospital mortality.
In conclusion, CDI is more prevalent in SS than are other ICU populations or the hospital population in general, and CDI complicating SS is associated with significant increase in LOS and risk of 30-day hospital readmission. How much of the increase in resource utilization and cost are in fact attributable to CDI in this population remains to be studied. Our finding of high prevalence of CDI in the SS population further emphasizes the importance of maintaining and furthering approaches to reduce incidence of hospital acquired CDI. While reducing unnecessary antibiotics is important, a multipronged approach that includes education and infection control interventions has also been shown to reduce the incidence of CDI in the ICU.31 Given the economic burden of CDI, implementing these strategies to reduce CDI is warranted. Similarly, the risk of 30-day hospital readmission with CDI highlights the importance of identifying the factors that contribute to hospital readmission prior to initial hospital discharge. Programs to reduce CDI will not only improve outcomes directly attributable to CDI but also decrease the reservoir of CDI. Finally, to the extent that CDI can be reduced in the ICU, the utilization of ICU resources will be more effective.
Disclosure
No conflicts of interest or financial disclosures to report. Author Contributions: KC had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis, including and especially any adverse effects. KC, AG, AC, KK, and HC contributed to study design, data analysis, interpretation, and the writing of the manuscript. Guarantor statement: Kshitij Chatterjee takes responsibility for (is the guarantor of) the content of the manuscript, including the data and analysis.
1. Polage CR, Solnick JV, Cohen SH. Nosocomial diarrhea: evaluation and treatment of causes other than Clostridium difficile. Clin Infect Dis. 2012;55(7):982-989. Doi: 10.1093/cid/cis551. PubMed
2. Kyne L, Hamel MB, Polavaram R, Kelly CP. Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile. Clin Infect Dis. 2002;34(3):346-353. Doi: 10.1086/338260. PubMed
3. Dubberke ER, Olsen MA. Burden of Clostridium difficile on the healthcare system. Clin Infect Dis. 2012;55(Suppl 2):S88-S92. Doi: 10.1093/cid/cis335. PubMed
4. Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med. 2015;372(9):825-834. Doi: 10.1056/NEJMoa1408913. PubMed
5. Zhang S, Palazuelos-Munoz S, Balsells EM, Nair H, Chit A, Kyaw MH. Cost of hospital management of Clostridium difficile infection in United States-a meta-analysis and modelling study. BMC Infect Dis. 2016;16(1):447. Doi: 10.1186/s12879-016-1786-6. PubMed
6. Lessa FC, Gould CV, McDonald LC. Current status of Clostridium difficile infection epidemiology. Clin Infect Dis. 2012;55(Suppl 2):S65-S70. Doi: 10.1093/cid/cis319. PubMed
7. Depestel DD, Aronoff DM. Epidemiology of Clostridium difficile infection. J Pharm Pract. 2013;26(5):464-475. Doi: 10.1177/0897190013499521. PubMed
8. Dial S., Delaney JAC, Barkun AN, Suissa S. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA. 2005;294(23):2989-2995. Doi: 10.1001/jama.294.23.2989. PubMed
9. Aseeri M., Schroeder T, Kramer J, Zackula R. Gastric acid suppression by proton pump inhibitors as a risk factor for clostridium difficile-associated diarrhea in hospitalized patients. Am J Gastroenterol. 2008;103(9):2308-2313. Doi: 10.1111/j.1572-0241.2008.01975.x. PubMed
10. Cunningham R, Dial S. Is over-use of proton pump inhibitors fuelling the current epidemic of Clostridium difficile-associated diarrhoea? J Hosp Infect. 2008;70(1):1-6. Doi: 10.1016/j.jhin.2008.04.023. PubMed
11. HCUP-US NIS Overview. https://www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed on April 23, 2016.
12. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613-619. PubMed
13. Goto T, Yoshida K, Tsugawa Y, Filbin MR, Camargo CA, Hasegawa K. Mortality trends in U.S. adults with septic shock, 2005-2011: a serial cross-sectional analysis of nationally-representative data. BMC Infect Dis. 2016;16:294. Doi: 10.1186/s12879-016-1620-1. PubMed
14. Kumar G, Kumar N, Taneja A, et al. Nationwide trends of severe sepsis in the 21st century (2000-2007). Chest. 2011;140(5):1223-1231. Doi: 10.1378/chest.11-0352. PubMed
15. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546-1554. Doi: 10.1056/NEJMoa022139. PubMed
16. Scheurer DB, Hicks LS, Cook EF, Schnipper JL. Accuracy of ICD-9 coding for Clostridium difficile infections: a retrospective cohort. Epidemiol Infect. 2007;135(6):1010-1013. Doi: 10.1017/S0950268806007655. PubMed
17. Dodek PM, Norena M, Ayas NT, Romney M, Wong H. Length of stay and mortality due to Clostridium difficile infection acquired in the intensive care unit. J Crit Care. 2013;28(4):335-340. Doi: 10.1016/j.jcrc.2012.11.008. PubMed
18. Bouza E, Rodríguez-Créixems M, Alcalá L, et al. Is Clostridium difficile infection an increasingly common severe disease in adult intensive care units? A 10-year experience. J Crit Care. 2015;30(3):543-549. Doi: 10.1016/j.jcrc.2015.02.011. PubMed
19. Karanika S, Paudel S, Zervou FN, Grigoras C, Zacharioudakis IM, Mylonakis E. Prevalence and clinical outcomes of Clostridium difficile infection in the intensive care unit: a systematic review and meta-analysis. Open Forum Infect Dis. 2016;3(1):ofv186. Doi: 10.1093/ofid/ofv186. PubMed
20. Zahar JR, Schwebel C, Adrie C, et al. Outcome of ICU patients with Clostridium difficile infection. Crit Care. 2012;16(6):R215. Doi: 10.1186/cc11852. PubMed
21. Shorr AF, Zilberberg MD, Wang L, Baser O, Yu H. Mortality and costs in clostridium difficile infection among the elderly in the United States. Infect Control Hosp Epidemiol. 2016;37(11):1331-1336. Doi: 10.1017/ice.2016.188. PubMed
22. Micek ST, Schramm G, Morrow L, et al. Clostridium difficile infection: a multicenter study of epidemiology and outcomes in mechanically ventilated patients. Crit Care Med. 2013;41(8):1968-1975. Doi: 10.1097/CCM.0b013e31828a40d5. PubMed
23. Zilberberg MD, Nathanson BH, Sadigov S, Higgins TL, Kollef MH, Shorr AF. Epidemiology and outcomes of clostridium difficile-associated disease among patients on prolonged acute mechanical ventilation. Chest. 2009;136(3):752-758. Doi: 10.1378/chest.09-0596. PubMed
24. Lagu T, Stefan MS, Haessler S, et al. The impact of hospital-onset Clostridium difficile infection on outcomes of hospitalized patients with sepsis. J Hosp Med. 2014;9(7):411-417. Doi: 10.1002/jhm.2199. PubMed
25. Prescott HC, Dickson RP, Rogers MA, Langa KM, Iwashyna TJ. Hospitalization type and subsequent severe sepsis. Am J Respir Crit Care Med. 2015;192(5):581-588. Doi: 10.1164/rccm.201503-0483OC. PubMed
26. Healthcare-associated Infections (HAI) Progress Report. Centers for Disease Control and Prevention. http://www.cdc.gov/hai/surveillance/progress-report/index.html. Accessed on July 29, 2017.
27. Song X, Bartlett JG, Speck K, Naegeli A, Carroll K, Perl TM. Rising economic impact of clostridium difficile-associated disease in adult hospitalized patient population. Infect Control Hosp Epidemiol. 2008;29(9):823-828. Doi: 10.1086/588756. PubMed
28. Zilberberg MD, Shorr AF, Micek ST, et al. Clostridium difficile recurrence is a strong predictor of 30-day rehospitalization among patients in intensive care. Infect Control Hosp Epidemiol. 2015;36(3):273-279. Doi: 10.1017/ice.2014.47. PubMed
29. Loftus KV, Wilson PM. A curiously rare case of septic shock from Clostridium difficile colitis. Pediatr Emerg Care. 2015. [Epub ahead of print]. Doi: 10.1097/PEC.0000000000000496. PubMed
30. Bermejo C, Maseda E, Salgado P, Gabilondo G., Gilsanz F. Septic shock due to a community acquired Clostridium difficile infection. A case study and a review of the literature. Rev Esp Anestesiol Reanimvol. 2014;61(4):219-222. PubMed
31. You E, Song H, Cho J, Lee J. Reduction in the incidence of hospital-acquired Clostridium difficile infection through infection control interventions other than the restriction of antimicrobial use. Int J Infect Dis. 2014;22:9-10. 2014. PubMed
Clostridium difficile infection (CDI) is the most common infectious cause of healthcare-associated diarrhea.1 Development of a CDI during hospitalization is associated with increases in morbidity, mortality, length of stay (LOS), and cost.2-5 The prevalence of CDI in hospitalized patients has increased dramatically from the mid-1990s to the mid-2000s to almost 9 cases per 1000 discharges; however, the CDI rate since 2007 appears to have plateaued.6,7 Antibiotic use has historically been the most important risk factor for acquiring CDI; however, use of acid-suppressing agents, chemotherapy, chronic comorbidities, and healthcare exposure all also increase the risk of CDI.7-10 The elderly (> 65 years of age) are particularly at risk for developing CDI and having worse clinical outcomes with CDI.6,7
Patients with septic shock (SS) often have multiple CDI risk factors (in particular, extensive antibiotic exposure) and thus, represent a population at a particularly high risk for acquiring a CDI during hospitalization. However, little data are available on the prevalence of CDI acquired in patients hospitalized with SS. We sought to determine the national-level temporal trends in the prevalence of CDI in patients with SS and the impact of CDI complicating SS on clinical outcomes between 2007 and 2013.
METHODS
Data Source
We used the National Inpatient Sample (NIS) and Nationwide Readmissions Database (NRD) for this study. The NIS is a database developed by the Agency of Healthcare Research and Quality for the Healthcare Cost and Utilization Project (HCUP).11 It is the largest all-payer inpatient database in the United States and has been used by researchers and policy makers to analyze national trends in outcomes and healthcare utilization. The NIS database now approximates a 20% stratified sample of all discharges from all participating US hospitals. Sampling weights are provided by the manufacturer and can be used to produce national-level estimates. Following the redesign of the NIS in 2012, new sampling weights were provided for trend analysis for the years prior to 2012 to account for the new design. Every hospitalization is deidentified and converted into one unique entry that provides information on demographics, hospital characteristics, 1 primary and up to 24 secondary discharge diagnoses, comorbidities, LOS, in-hospital mortality, and procedures performed during stay. The discharge diagnoses are provided in the form of the International Classification of Diseases, 9th Revision-Clinical Modification (ICD-9-CM) codes.
The NRD is a database developed for HCUP that contains about 35 million discharges each year and supports readmission data analyses. In 2013, the NRD contained data from 21 geographically diverse states, accounting for 49.1% of all US hospitalizations. Diagnosis, comorbidities, and outcomes are presented in a similar manner to NIS.
Study Design
This was a retrospective cohort study. Data from the NIS between 2007 and 2013 were used for the analysis. Demographic data obtained included age, gender, race, Charlson-Deyo Comorbidity Index,12 hospital characteristics (hospital region, hospital-bed size, urban versus rural location, and teaching status), calendar year, and use of mechanical ventilation. Cases with information missing on key demographic variables (age, gender, and race) were excluded. Only adults (>18 years of age) were included for the analysis.
SS was identified by either (1) ICD-9-CM diagnosis code for SS (785.52) or (2) presence of vasopressor use (00.17) along with ICD-9-CM codes of sepsis, severe sepsis, septicemia, bacteremia, or fungemia. This approach is consistent with what has been utilized in other studies to identify cases of sepsis or SS from administrative databases.13-15 The appendix provides a complete list of ICD-9-CM codes used in the study. CDI was identified by ICD-9-CM code 008.45 among the secondary diagnosis. This code has been shown to have good accuracy for identifying CDI using administrative data.16 To minimize the inclusion of cases in which a CDI was present at admission, hospitalizations with a primary diagnosis of CDI were not included as cases of CDI complicating SS.
We used NRD 2013 for estimating the effect of CDI on 30-day readmission after initial hospitalizations with SS. We used the criteria for index admissions and 30-day readmissions as defined by the Centers for Medicare and Medicaid Services. We excluded patients who died during their index admission, patients with index discharges in December due to a lack of sufficient time to capture 30-day readmissions, and patients with missing information on key variables. We also excluded patients who were not a resident of the state of index hospitalization since readmission across state boundaries could not be identified in NRD. Manufacturer provided sampling weights were used to produce national level estimates. The cases of SS and CDI were identified by ICD-9-CM codes using the methodology described above.
Outcomes
Our primary outcome of interest was the total and yearly prevalence of CDI in patients with SS from 2007 to 2013. The secondary outcomes were mortality, LOS, and 30-day readmissions in patients with SS with and without CDI.
Statistical Analysis
Weighted data from NIS were used for all analyses. Demographics, hospital characteristics, and outcomes of all patients with SS were obtained. The prevalence of CDI was calculated for each calendar year. The temporal trends of outcomes (LOS and in-hospital mortality) of patients were plotted for patients with SS with and without CDI. A χ2 test of trend for proportions was used with the Cochran-Armitage test to calculate statistical significance of changes in prevalence. To test for statistical significance of the temporal trends of LOS, a univariate linear regression was used, with calendar year as a covariate. Independent samples t test, a Mann-Whitney U test, and a χ2 test were used to determine statistical significance of parameters between the group with CDI and the group without CDI.
Prolonged LOS was defined either as a LOS > 75th or > 90th percentile of LOS among all patients with SS. To identify if CDI was associated with a prolonged LOS after adjusting for patient and hospital characteristics, a multivariate logistic regression analysis was used. Variables included in the regression model were age, gender, race, Charlson-Deyo Comorbidity Index, hospital characteristics (hospital region, hospital-bed size, urban versus rural location, and teaching status), calendar year, and use of mechanical ventilation. Data on cases were available for all the above covariates except hospital characteristics, such as teaching status, location, and bed size (these were missing for 0.7% of hospitals).
Stata 13.1.0 (Stata Corp, College Station, TX) and SPSS 23.0 (SPSS Inc., Chicago, IL) were used to perform statistical analyses. A P value of <0.05 was considered statistically significant.
RESULTS
Demographics
A total of 2,031,739 hospitalizations of adults with SS were identified between 2007 and 2013. CDI was present in 166,432 (8.2%) of these patients. Demographic data are displayed in Table 1. CDI was more commonly observed in elderly patients (> 65 years) with SS; 9.3% among the elderly versus 6.6% among individuals < 65 years; P < 0.001. The prevalence of CDI was greater in urban than in rural hospitals (8.4% vs 5.4%; P < 0.001) and greater in teaching than in nonteaching hospitals (8.7% vs 7.7%; P < 0.001). The prevalence of CDI in SS remained stable between 2007 and 2013 (Table 2).
Mortality
In the overall study cohort, the in-hospital mortality for SS was 37%. The in-hospital mortality rate of patients with SS complicated by a CDI was comparable to the mortality rate of patients without a CDI (37.1% vs 37.0%; P = 0.48). The mortality of patients with SS, with or without CDI, progressively decreased from 2007 to 2013 (P value for trend < 0.001 for each group; Figure 1).
Length of Stay
The median LOS for all patients with SS was 9 days. Patients with CDI had a longer median LOS than did those without CDI (13 vs 9 days; P < 0.001). Between 2007 and 2013, the median LOS of CDI group decreased from 14 to 12 days (P < 0.001) while that of non-CDI group decreased from 9 to 8 days (P < 0.001; Figure 2). We also examined LOS among subgroups who were discharged alive and those who died during hospitalization. For patients who were discharged alive, the LOS with and without CDI was 15 days versus 10 days, respectively (P < 0.001). For patients who died during hospitalization, LOS with and without CDI was 10 days versus 6 days, respectively (P < 0.001).
The 75th percentile of LOS of the total SS cohort was 17 days. An LOS > 17 days was observed in 36.9% of SS patients with CDI versus 22.7% without CDI (P < 0.001). After adjusting for patient and provider level variables, the odds of a LOS > 17 days were significantly greater for SS patients with CDI (odds ratio [OR] 2.11; 95% confidence interval [CI], 2.06-2.15; P < 0.001).
The 90th percentile of LOS of the total SS cohort was 29 days. An LOS > 29 days was observed in 17.5% of SS patients with a CDI versus 9.1% without a CDI (P < 0.001). After adjustment for patient and provider level variables, the odds of a LOS > 29 days were significantly greater for SS patients with a CDI (OR 2.25; 95% CI, 2.22-2.28; P < 0.001).
Hospital Readmission
In 2013, patients with SS and CDI had a higher rate of 30-day readmission as compared to patients with SS without CDI (9.8% vs 7.4% respectively; P < 0.001). The multivariate adjusted OR for 30-day readmission for patients with SS and a CDI was 1.26 (95% CI, 1.22-1.31; P < 0.001).
Additional Analyses
Lastly, we performed an additional analysis to confirm our hypothesis that a CDI by itself is rarely a cause of SS, and that CDI as the principal diagnosis would constitute an extremely low number of patients with SS in an administrative dataset. In NIS 2013, there were 105,750 cases with CDI as the primary diagnosis. A total of 4470 (4.2%) had a secondary diagnosis of sepsis and only 930 (0.9%) cases had a secondary diagnosis of SS.
DISCUSSION
This is the first study to report on the prevalence and outcome of CDI complicating SS. By using a large nationally representative sample, we found CDI was very prevalent among individuals hospitalized with SS and, at a level in excess of that seen in other populations. Of interest, we did not observe an increase in mortality of SS when complicated by CDI. On the other hand, patients with SS complicated by CDI were more much likely to have a prolonged hospital LOS and a higher risk of 30-day hospital readmission.
The prevalence of CDI exploded between the mid-1990s and mid-2000s, including community, hospital, and intensive care unit (ICU)–related disease.6,7,17-20 Patients with SS often have multiple risk factors associated with CDI and thus represent a high-risk population for developing CDI.7 Our findings are consistent with the suggestion that individuals with SS are at a higher risk of developing CDI. Compared to the rate of CDI in all hospitalized patients, our data suggest an almost 10-fold increase in CDI rate for patients with SS.6 Patients with SS and CDI may account for as much as 10% of total CDIs.6,7 As has been reported for CDI in general, we observed that CDI complicating SS was more common in those > 65 years of age.4,21 The prevalence of CDI we observed in patients with SS was also higher than has been reported in ICU patients in general (1%), and higher than reported for patients requiring mechanical ventilation (6.6%), including prolonged mechanical ventilation (5.3%); further supporting the conclusion that patients with SS are a particularly high-risk group for acquiring CDI, even compared with other ICU patients.20,22,23 Similarly, the rate of CDI among SS was 8 times higher than that of recently reported hospital-onset CDI among patients with sepsis in general (incidence 1.08%).24 We have no data regarding why patients with SS have a higher rate of CDI; however, the intensity and duration of antibiotic treatment of these patients may certainly play a role.25 It has recently been reported that CDI in itself can be a precursor leading to intestinal dysbiosis that can increase the risk of subsequent sepsis. Similarly, patients with SS may have higher prevalence of dysbiosis that, in turn, might predispose them to CDI at a higher rate than other individuals.
Following the increase in CDIs in the mid-1990s and the mid-2000s, since 2007 the overall prevalence of CDIs has been stable, albeit at the higher rate. More recently, the Centers for Disease Control and Prevention (CDC) has reported a decrease in hospital onset CDI after 2011.26
The finding that CDI in SS patients was not associated with an increase in mortality is consistent with other reports of CDI in ICU patients in general as well as higher-risk ICU populations such as patients requiring mechanical ventilation, including those on long-term mechanical ventilator support.17,18,20,22,23 Why the mortality of ICU patients with CDI is not increased is not completely clear. It has been suggested that this may be related to early recognition and treatment of CDI developing in the ICU.22 Along these lines, it has been previously observed that for patients with CDI on mechanical ventilation, patients who were transferred to the ICU from the ward had worse clinical outcomes compared to patients directly admitted to the ICU, likely due to delayed recognition and treatment in the former.22 Similarly, ICU patients in whom CDI was identified prior to ICU admission had more severe CDI, and mortality that was directly related to CDI was only observed in patients who had CDI identified pre-ICU transfer.18 The increase in mortality observed in patients with sepsis in general with CDI may reflect similar factors.24 We observed a trend of decreasing mortality in SS patients with or without CDI during 2007 to 2013 consistent to what has been generally reported in SS.13,14
The increase in LOS observed in SS patients with CDI is also consistent with what has been observed in other ICU populations, as well as in patients with sepsis in general.17,22-24 Of note, in addition to the increase in median LOS, we found a significant increase in the number of patients with a prolonged LOS associated with having SS with CDI. It is important to note that development of CDI during hospitalization is affected by pre-CDI hospital LOS, so prolonged LOS may not be solely attributable to CDI. The interaction between LOS and CDI remains complex in which higher LOS might be associated with higher incidence of CDI occurrence, and once established, CDI might be associated with changes in LOS for the remaining hospitalization.
Hospitalized patients with CDI have an overall higher resource utilization than those without CDI.27 A recent review has estimated the overall attributable cost of CDI to be $6.3 billion; the attributable cost per case of hospital acquired CDI being 1.5 times the cost of community-acquired CDI.5 We did not look at cost directly. However, in the high-CDI risk ICU population requiring prolonged mechanical ventilation, those with CDI had a substantial increase in total costs.23 Given the substantial increase in LOS associated with CDI complicating SS, there would likely be a significant increase in hospital costs related to providing care for these patients. Further adding to the potential burden of CDI is our finding that CDI and SS was associated with an increase in 30-day hospital readmission rate. This is consistent with a recent report that ICU patients with CDI who are discharged from the hospital have a 25% 30-day hospital readmission rate.28 However, we do not have data either as to the reason for hospital readmission or whether the initial CDI or CDI recurrence played a role. This suggests that, in addition to intervention directed toward preventing CDI, efforts should be directed towards identifying factors that can be modified in CDI patients prior to or after hospital discharge.
This study has several limitations. Using an administrative database (such as NIS) has an inherent limitation of coding errors and reporting bias can lead to misclassification of cohort definition (SS) and outcome (CDI). To minimize bias due to coding errors, we used previously validated ICD-9-CM codes and approach to identify individuals with SS and CDI.13-15 Although the SS population was identified with ICD-9-CM codes using an administrative database, the in-hospital mortality for our septic population was similar to previously reported mortality of SS, suggesting the population selected was appropriate.13 SS due to CDI could not be identified; however, CDI by itself causing SS is rare, as described in recent literature.29,30 An important potential bias that needs to be acknowledged is the immortal time bias. The occurrence of CDI in itself can be influenced by pre-CDI hospital LOS. Patients who were extremely sick could have died early in their hospital course before they could acquire CDI, which would influence the mortality difference between the group with CDI and group without CDI. Furthermore, we did not have information on either the treatment of CDI or SS or any measures of severity of illness, which could lead to residual confounding despite adjusting for multiple variables. In terms of readmission data, it was necessary to exclude nonresidents of a state for the 30-day readmission analysis, as readmissions could not be tracked across state boundaries by using the NRD. This might have resulted in an underrepresentation of the readmission burden. Lastly, it was not possible to identify mortality after hospital discharge as the NIS provides only in-hospital mortality.
In conclusion, CDI is more prevalent in SS than are other ICU populations or the hospital population in general, and CDI complicating SS is associated with significant increase in LOS and risk of 30-day hospital readmission. How much of the increase in resource utilization and cost are in fact attributable to CDI in this population remains to be studied. Our finding of high prevalence of CDI in the SS population further emphasizes the importance of maintaining and furthering approaches to reduce incidence of hospital acquired CDI. While reducing unnecessary antibiotics is important, a multipronged approach that includes education and infection control interventions has also been shown to reduce the incidence of CDI in the ICU.31 Given the economic burden of CDI, implementing these strategies to reduce CDI is warranted. Similarly, the risk of 30-day hospital readmission with CDI highlights the importance of identifying the factors that contribute to hospital readmission prior to initial hospital discharge. Programs to reduce CDI will not only improve outcomes directly attributable to CDI but also decrease the reservoir of CDI. Finally, to the extent that CDI can be reduced in the ICU, the utilization of ICU resources will be more effective.
Disclosure
No conflicts of interest or financial disclosures to report. Author Contributions: KC had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis, including and especially any adverse effects. KC, AG, AC, KK, and HC contributed to study design, data analysis, interpretation, and the writing of the manuscript. Guarantor statement: Kshitij Chatterjee takes responsibility for (is the guarantor of) the content of the manuscript, including the data and analysis.
Clostridium difficile infection (CDI) is the most common infectious cause of healthcare-associated diarrhea.1 Development of a CDI during hospitalization is associated with increases in morbidity, mortality, length of stay (LOS), and cost.2-5 The prevalence of CDI in hospitalized patients has increased dramatically from the mid-1990s to the mid-2000s to almost 9 cases per 1000 discharges; however, the CDI rate since 2007 appears to have plateaued.6,7 Antibiotic use has historically been the most important risk factor for acquiring CDI; however, use of acid-suppressing agents, chemotherapy, chronic comorbidities, and healthcare exposure all also increase the risk of CDI.7-10 The elderly (> 65 years of age) are particularly at risk for developing CDI and having worse clinical outcomes with CDI.6,7
Patients with septic shock (SS) often have multiple CDI risk factors (in particular, extensive antibiotic exposure) and thus, represent a population at a particularly high risk for acquiring a CDI during hospitalization. However, little data are available on the prevalence of CDI acquired in patients hospitalized with SS. We sought to determine the national-level temporal trends in the prevalence of CDI in patients with SS and the impact of CDI complicating SS on clinical outcomes between 2007 and 2013.
METHODS
Data Source
We used the National Inpatient Sample (NIS) and Nationwide Readmissions Database (NRD) for this study. The NIS is a database developed by the Agency of Healthcare Research and Quality for the Healthcare Cost and Utilization Project (HCUP).11 It is the largest all-payer inpatient database in the United States and has been used by researchers and policy makers to analyze national trends in outcomes and healthcare utilization. The NIS database now approximates a 20% stratified sample of all discharges from all participating US hospitals. Sampling weights are provided by the manufacturer and can be used to produce national-level estimates. Following the redesign of the NIS in 2012, new sampling weights were provided for trend analysis for the years prior to 2012 to account for the new design. Every hospitalization is deidentified and converted into one unique entry that provides information on demographics, hospital characteristics, 1 primary and up to 24 secondary discharge diagnoses, comorbidities, LOS, in-hospital mortality, and procedures performed during stay. The discharge diagnoses are provided in the form of the International Classification of Diseases, 9th Revision-Clinical Modification (ICD-9-CM) codes.
The NRD is a database developed for HCUP that contains about 35 million discharges each year and supports readmission data analyses. In 2013, the NRD contained data from 21 geographically diverse states, accounting for 49.1% of all US hospitalizations. Diagnosis, comorbidities, and outcomes are presented in a similar manner to NIS.
Study Design
This was a retrospective cohort study. Data from the NIS between 2007 and 2013 were used for the analysis. Demographic data obtained included age, gender, race, Charlson-Deyo Comorbidity Index,12 hospital characteristics (hospital region, hospital-bed size, urban versus rural location, and teaching status), calendar year, and use of mechanical ventilation. Cases with information missing on key demographic variables (age, gender, and race) were excluded. Only adults (>18 years of age) were included for the analysis.
SS was identified by either (1) ICD-9-CM diagnosis code for SS (785.52) or (2) presence of vasopressor use (00.17) along with ICD-9-CM codes of sepsis, severe sepsis, septicemia, bacteremia, or fungemia. This approach is consistent with what has been utilized in other studies to identify cases of sepsis or SS from administrative databases.13-15 The appendix provides a complete list of ICD-9-CM codes used in the study. CDI was identified by ICD-9-CM code 008.45 among the secondary diagnosis. This code has been shown to have good accuracy for identifying CDI using administrative data.16 To minimize the inclusion of cases in which a CDI was present at admission, hospitalizations with a primary diagnosis of CDI were not included as cases of CDI complicating SS.
We used NRD 2013 for estimating the effect of CDI on 30-day readmission after initial hospitalizations with SS. We used the criteria for index admissions and 30-day readmissions as defined by the Centers for Medicare and Medicaid Services. We excluded patients who died during their index admission, patients with index discharges in December due to a lack of sufficient time to capture 30-day readmissions, and patients with missing information on key variables. We also excluded patients who were not a resident of the state of index hospitalization since readmission across state boundaries could not be identified in NRD. Manufacturer provided sampling weights were used to produce national level estimates. The cases of SS and CDI were identified by ICD-9-CM codes using the methodology described above.
Outcomes
Our primary outcome of interest was the total and yearly prevalence of CDI in patients with SS from 2007 to 2013. The secondary outcomes were mortality, LOS, and 30-day readmissions in patients with SS with and without CDI.
Statistical Analysis
Weighted data from NIS were used for all analyses. Demographics, hospital characteristics, and outcomes of all patients with SS were obtained. The prevalence of CDI was calculated for each calendar year. The temporal trends of outcomes (LOS and in-hospital mortality) of patients were plotted for patients with SS with and without CDI. A χ2 test of trend for proportions was used with the Cochran-Armitage test to calculate statistical significance of changes in prevalence. To test for statistical significance of the temporal trends of LOS, a univariate linear regression was used, with calendar year as a covariate. Independent samples t test, a Mann-Whitney U test, and a χ2 test were used to determine statistical significance of parameters between the group with CDI and the group without CDI.
Prolonged LOS was defined either as a LOS > 75th or > 90th percentile of LOS among all patients with SS. To identify if CDI was associated with a prolonged LOS after adjusting for patient and hospital characteristics, a multivariate logistic regression analysis was used. Variables included in the regression model were age, gender, race, Charlson-Deyo Comorbidity Index, hospital characteristics (hospital region, hospital-bed size, urban versus rural location, and teaching status), calendar year, and use of mechanical ventilation. Data on cases were available for all the above covariates except hospital characteristics, such as teaching status, location, and bed size (these were missing for 0.7% of hospitals).
Stata 13.1.0 (Stata Corp, College Station, TX) and SPSS 23.0 (SPSS Inc., Chicago, IL) were used to perform statistical analyses. A P value of <0.05 was considered statistically significant.
RESULTS
Demographics
A total of 2,031,739 hospitalizations of adults with SS were identified between 2007 and 2013. CDI was present in 166,432 (8.2%) of these patients. Demographic data are displayed in Table 1. CDI was more commonly observed in elderly patients (> 65 years) with SS; 9.3% among the elderly versus 6.6% among individuals < 65 years; P < 0.001. The prevalence of CDI was greater in urban than in rural hospitals (8.4% vs 5.4%; P < 0.001) and greater in teaching than in nonteaching hospitals (8.7% vs 7.7%; P < 0.001). The prevalence of CDI in SS remained stable between 2007 and 2013 (Table 2).
Mortality
In the overall study cohort, the in-hospital mortality for SS was 37%. The in-hospital mortality rate of patients with SS complicated by a CDI was comparable to the mortality rate of patients without a CDI (37.1% vs 37.0%; P = 0.48). The mortality of patients with SS, with or without CDI, progressively decreased from 2007 to 2013 (P value for trend < 0.001 for each group; Figure 1).
Length of Stay
The median LOS for all patients with SS was 9 days. Patients with CDI had a longer median LOS than did those without CDI (13 vs 9 days; P < 0.001). Between 2007 and 2013, the median LOS of CDI group decreased from 14 to 12 days (P < 0.001) while that of non-CDI group decreased from 9 to 8 days (P < 0.001; Figure 2). We also examined LOS among subgroups who were discharged alive and those who died during hospitalization. For patients who were discharged alive, the LOS with and without CDI was 15 days versus 10 days, respectively (P < 0.001). For patients who died during hospitalization, LOS with and without CDI was 10 days versus 6 days, respectively (P < 0.001).
The 75th percentile of LOS of the total SS cohort was 17 days. An LOS > 17 days was observed in 36.9% of SS patients with CDI versus 22.7% without CDI (P < 0.001). After adjusting for patient and provider level variables, the odds of a LOS > 17 days were significantly greater for SS patients with CDI (odds ratio [OR] 2.11; 95% confidence interval [CI], 2.06-2.15; P < 0.001).
The 90th percentile of LOS of the total SS cohort was 29 days. An LOS > 29 days was observed in 17.5% of SS patients with a CDI versus 9.1% without a CDI (P < 0.001). After adjustment for patient and provider level variables, the odds of a LOS > 29 days were significantly greater for SS patients with a CDI (OR 2.25; 95% CI, 2.22-2.28; P < 0.001).
Hospital Readmission
In 2013, patients with SS and CDI had a higher rate of 30-day readmission as compared to patients with SS without CDI (9.8% vs 7.4% respectively; P < 0.001). The multivariate adjusted OR for 30-day readmission for patients with SS and a CDI was 1.26 (95% CI, 1.22-1.31; P < 0.001).
Additional Analyses
Lastly, we performed an additional analysis to confirm our hypothesis that a CDI by itself is rarely a cause of SS, and that CDI as the principal diagnosis would constitute an extremely low number of patients with SS in an administrative dataset. In NIS 2013, there were 105,750 cases with CDI as the primary diagnosis. A total of 4470 (4.2%) had a secondary diagnosis of sepsis and only 930 (0.9%) cases had a secondary diagnosis of SS.
DISCUSSION
This is the first study to report on the prevalence and outcome of CDI complicating SS. By using a large nationally representative sample, we found CDI was very prevalent among individuals hospitalized with SS and, at a level in excess of that seen in other populations. Of interest, we did not observe an increase in mortality of SS when complicated by CDI. On the other hand, patients with SS complicated by CDI were more much likely to have a prolonged hospital LOS and a higher risk of 30-day hospital readmission.
The prevalence of CDI exploded between the mid-1990s and mid-2000s, including community, hospital, and intensive care unit (ICU)–related disease.6,7,17-20 Patients with SS often have multiple risk factors associated with CDI and thus represent a high-risk population for developing CDI.7 Our findings are consistent with the suggestion that individuals with SS are at a higher risk of developing CDI. Compared to the rate of CDI in all hospitalized patients, our data suggest an almost 10-fold increase in CDI rate for patients with SS.6 Patients with SS and CDI may account for as much as 10% of total CDIs.6,7 As has been reported for CDI in general, we observed that CDI complicating SS was more common in those > 65 years of age.4,21 The prevalence of CDI we observed in patients with SS was also higher than has been reported in ICU patients in general (1%), and higher than reported for patients requiring mechanical ventilation (6.6%), including prolonged mechanical ventilation (5.3%); further supporting the conclusion that patients with SS are a particularly high-risk group for acquiring CDI, even compared with other ICU patients.20,22,23 Similarly, the rate of CDI among SS was 8 times higher than that of recently reported hospital-onset CDI among patients with sepsis in general (incidence 1.08%).24 We have no data regarding why patients with SS have a higher rate of CDI; however, the intensity and duration of antibiotic treatment of these patients may certainly play a role.25 It has recently been reported that CDI in itself can be a precursor leading to intestinal dysbiosis that can increase the risk of subsequent sepsis. Similarly, patients with SS may have higher prevalence of dysbiosis that, in turn, might predispose them to CDI at a higher rate than other individuals.
Following the increase in CDIs in the mid-1990s and the mid-2000s, since 2007 the overall prevalence of CDIs has been stable, albeit at the higher rate. More recently, the Centers for Disease Control and Prevention (CDC) has reported a decrease in hospital onset CDI after 2011.26
The finding that CDI in SS patients was not associated with an increase in mortality is consistent with other reports of CDI in ICU patients in general as well as higher-risk ICU populations such as patients requiring mechanical ventilation, including those on long-term mechanical ventilator support.17,18,20,22,23 Why the mortality of ICU patients with CDI is not increased is not completely clear. It has been suggested that this may be related to early recognition and treatment of CDI developing in the ICU.22 Along these lines, it has been previously observed that for patients with CDI on mechanical ventilation, patients who were transferred to the ICU from the ward had worse clinical outcomes compared to patients directly admitted to the ICU, likely due to delayed recognition and treatment in the former.22 Similarly, ICU patients in whom CDI was identified prior to ICU admission had more severe CDI, and mortality that was directly related to CDI was only observed in patients who had CDI identified pre-ICU transfer.18 The increase in mortality observed in patients with sepsis in general with CDI may reflect similar factors.24 We observed a trend of decreasing mortality in SS patients with or without CDI during 2007 to 2013 consistent to what has been generally reported in SS.13,14
The increase in LOS observed in SS patients with CDI is also consistent with what has been observed in other ICU populations, as well as in patients with sepsis in general.17,22-24 Of note, in addition to the increase in median LOS, we found a significant increase in the number of patients with a prolonged LOS associated with having SS with CDI. It is important to note that development of CDI during hospitalization is affected by pre-CDI hospital LOS, so prolonged LOS may not be solely attributable to CDI. The interaction between LOS and CDI remains complex in which higher LOS might be associated with higher incidence of CDI occurrence, and once established, CDI might be associated with changes in LOS for the remaining hospitalization.
Hospitalized patients with CDI have an overall higher resource utilization than those without CDI.27 A recent review has estimated the overall attributable cost of CDI to be $6.3 billion; the attributable cost per case of hospital acquired CDI being 1.5 times the cost of community-acquired CDI.5 We did not look at cost directly. However, in the high-CDI risk ICU population requiring prolonged mechanical ventilation, those with CDI had a substantial increase in total costs.23 Given the substantial increase in LOS associated with CDI complicating SS, there would likely be a significant increase in hospital costs related to providing care for these patients. Further adding to the potential burden of CDI is our finding that CDI and SS was associated with an increase in 30-day hospital readmission rate. This is consistent with a recent report that ICU patients with CDI who are discharged from the hospital have a 25% 30-day hospital readmission rate.28 However, we do not have data either as to the reason for hospital readmission or whether the initial CDI or CDI recurrence played a role. This suggests that, in addition to intervention directed toward preventing CDI, efforts should be directed towards identifying factors that can be modified in CDI patients prior to or after hospital discharge.
This study has several limitations. Using an administrative database (such as NIS) has an inherent limitation of coding errors and reporting bias can lead to misclassification of cohort definition (SS) and outcome (CDI). To minimize bias due to coding errors, we used previously validated ICD-9-CM codes and approach to identify individuals with SS and CDI.13-15 Although the SS population was identified with ICD-9-CM codes using an administrative database, the in-hospital mortality for our septic population was similar to previously reported mortality of SS, suggesting the population selected was appropriate.13 SS due to CDI could not be identified; however, CDI by itself causing SS is rare, as described in recent literature.29,30 An important potential bias that needs to be acknowledged is the immortal time bias. The occurrence of CDI in itself can be influenced by pre-CDI hospital LOS. Patients who were extremely sick could have died early in their hospital course before they could acquire CDI, which would influence the mortality difference between the group with CDI and group without CDI. Furthermore, we did not have information on either the treatment of CDI or SS or any measures of severity of illness, which could lead to residual confounding despite adjusting for multiple variables. In terms of readmission data, it was necessary to exclude nonresidents of a state for the 30-day readmission analysis, as readmissions could not be tracked across state boundaries by using the NRD. This might have resulted in an underrepresentation of the readmission burden. Lastly, it was not possible to identify mortality after hospital discharge as the NIS provides only in-hospital mortality.
In conclusion, CDI is more prevalent in SS than are other ICU populations or the hospital population in general, and CDI complicating SS is associated with significant increase in LOS and risk of 30-day hospital readmission. How much of the increase in resource utilization and cost are in fact attributable to CDI in this population remains to be studied. Our finding of high prevalence of CDI in the SS population further emphasizes the importance of maintaining and furthering approaches to reduce incidence of hospital acquired CDI. While reducing unnecessary antibiotics is important, a multipronged approach that includes education and infection control interventions has also been shown to reduce the incidence of CDI in the ICU.31 Given the economic burden of CDI, implementing these strategies to reduce CDI is warranted. Similarly, the risk of 30-day hospital readmission with CDI highlights the importance of identifying the factors that contribute to hospital readmission prior to initial hospital discharge. Programs to reduce CDI will not only improve outcomes directly attributable to CDI but also decrease the reservoir of CDI. Finally, to the extent that CDI can be reduced in the ICU, the utilization of ICU resources will be more effective.
Disclosure
No conflicts of interest or financial disclosures to report. Author Contributions: KC had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis, including and especially any adverse effects. KC, AG, AC, KK, and HC contributed to study design, data analysis, interpretation, and the writing of the manuscript. Guarantor statement: Kshitij Chatterjee takes responsibility for (is the guarantor of) the content of the manuscript, including the data and analysis.
1. Polage CR, Solnick JV, Cohen SH. Nosocomial diarrhea: evaluation and treatment of causes other than Clostridium difficile. Clin Infect Dis. 2012;55(7):982-989. Doi: 10.1093/cid/cis551. PubMed
2. Kyne L, Hamel MB, Polavaram R, Kelly CP. Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile. Clin Infect Dis. 2002;34(3):346-353. Doi: 10.1086/338260. PubMed
3. Dubberke ER, Olsen MA. Burden of Clostridium difficile on the healthcare system. Clin Infect Dis. 2012;55(Suppl 2):S88-S92. Doi: 10.1093/cid/cis335. PubMed
4. Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med. 2015;372(9):825-834. Doi: 10.1056/NEJMoa1408913. PubMed
5. Zhang S, Palazuelos-Munoz S, Balsells EM, Nair H, Chit A, Kyaw MH. Cost of hospital management of Clostridium difficile infection in United States-a meta-analysis and modelling study. BMC Infect Dis. 2016;16(1):447. Doi: 10.1186/s12879-016-1786-6. PubMed
6. Lessa FC, Gould CV, McDonald LC. Current status of Clostridium difficile infection epidemiology. Clin Infect Dis. 2012;55(Suppl 2):S65-S70. Doi: 10.1093/cid/cis319. PubMed
7. Depestel DD, Aronoff DM. Epidemiology of Clostridium difficile infection. J Pharm Pract. 2013;26(5):464-475. Doi: 10.1177/0897190013499521. PubMed
8. Dial S., Delaney JAC, Barkun AN, Suissa S. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA. 2005;294(23):2989-2995. Doi: 10.1001/jama.294.23.2989. PubMed
9. Aseeri M., Schroeder T, Kramer J, Zackula R. Gastric acid suppression by proton pump inhibitors as a risk factor for clostridium difficile-associated diarrhea in hospitalized patients. Am J Gastroenterol. 2008;103(9):2308-2313. Doi: 10.1111/j.1572-0241.2008.01975.x. PubMed
10. Cunningham R, Dial S. Is over-use of proton pump inhibitors fuelling the current epidemic of Clostridium difficile-associated diarrhoea? J Hosp Infect. 2008;70(1):1-6. Doi: 10.1016/j.jhin.2008.04.023. PubMed
11. HCUP-US NIS Overview. https://www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed on April 23, 2016.
12. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613-619. PubMed
13. Goto T, Yoshida K, Tsugawa Y, Filbin MR, Camargo CA, Hasegawa K. Mortality trends in U.S. adults with septic shock, 2005-2011: a serial cross-sectional analysis of nationally-representative data. BMC Infect Dis. 2016;16:294. Doi: 10.1186/s12879-016-1620-1. PubMed
14. Kumar G, Kumar N, Taneja A, et al. Nationwide trends of severe sepsis in the 21st century (2000-2007). Chest. 2011;140(5):1223-1231. Doi: 10.1378/chest.11-0352. PubMed
15. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546-1554. Doi: 10.1056/NEJMoa022139. PubMed
16. Scheurer DB, Hicks LS, Cook EF, Schnipper JL. Accuracy of ICD-9 coding for Clostridium difficile infections: a retrospective cohort. Epidemiol Infect. 2007;135(6):1010-1013. Doi: 10.1017/S0950268806007655. PubMed
17. Dodek PM, Norena M, Ayas NT, Romney M, Wong H. Length of stay and mortality due to Clostridium difficile infection acquired in the intensive care unit. J Crit Care. 2013;28(4):335-340. Doi: 10.1016/j.jcrc.2012.11.008. PubMed
18. Bouza E, Rodríguez-Créixems M, Alcalá L, et al. Is Clostridium difficile infection an increasingly common severe disease in adult intensive care units? A 10-year experience. J Crit Care. 2015;30(3):543-549. Doi: 10.1016/j.jcrc.2015.02.011. PubMed
19. Karanika S, Paudel S, Zervou FN, Grigoras C, Zacharioudakis IM, Mylonakis E. Prevalence and clinical outcomes of Clostridium difficile infection in the intensive care unit: a systematic review and meta-analysis. Open Forum Infect Dis. 2016;3(1):ofv186. Doi: 10.1093/ofid/ofv186. PubMed
20. Zahar JR, Schwebel C, Adrie C, et al. Outcome of ICU patients with Clostridium difficile infection. Crit Care. 2012;16(6):R215. Doi: 10.1186/cc11852. PubMed
21. Shorr AF, Zilberberg MD, Wang L, Baser O, Yu H. Mortality and costs in clostridium difficile infection among the elderly in the United States. Infect Control Hosp Epidemiol. 2016;37(11):1331-1336. Doi: 10.1017/ice.2016.188. PubMed
22. Micek ST, Schramm G, Morrow L, et al. Clostridium difficile infection: a multicenter study of epidemiology and outcomes in mechanically ventilated patients. Crit Care Med. 2013;41(8):1968-1975. Doi: 10.1097/CCM.0b013e31828a40d5. PubMed
23. Zilberberg MD, Nathanson BH, Sadigov S, Higgins TL, Kollef MH, Shorr AF. Epidemiology and outcomes of clostridium difficile-associated disease among patients on prolonged acute mechanical ventilation. Chest. 2009;136(3):752-758. Doi: 10.1378/chest.09-0596. PubMed
24. Lagu T, Stefan MS, Haessler S, et al. The impact of hospital-onset Clostridium difficile infection on outcomes of hospitalized patients with sepsis. J Hosp Med. 2014;9(7):411-417. Doi: 10.1002/jhm.2199. PubMed
25. Prescott HC, Dickson RP, Rogers MA, Langa KM, Iwashyna TJ. Hospitalization type and subsequent severe sepsis. Am J Respir Crit Care Med. 2015;192(5):581-588. Doi: 10.1164/rccm.201503-0483OC. PubMed
26. Healthcare-associated Infections (HAI) Progress Report. Centers for Disease Control and Prevention. http://www.cdc.gov/hai/surveillance/progress-report/index.html. Accessed on July 29, 2017.
27. Song X, Bartlett JG, Speck K, Naegeli A, Carroll K, Perl TM. Rising economic impact of clostridium difficile-associated disease in adult hospitalized patient population. Infect Control Hosp Epidemiol. 2008;29(9):823-828. Doi: 10.1086/588756. PubMed
28. Zilberberg MD, Shorr AF, Micek ST, et al. Clostridium difficile recurrence is a strong predictor of 30-day rehospitalization among patients in intensive care. Infect Control Hosp Epidemiol. 2015;36(3):273-279. Doi: 10.1017/ice.2014.47. PubMed
29. Loftus KV, Wilson PM. A curiously rare case of septic shock from Clostridium difficile colitis. Pediatr Emerg Care. 2015. [Epub ahead of print]. Doi: 10.1097/PEC.0000000000000496. PubMed
30. Bermejo C, Maseda E, Salgado P, Gabilondo G., Gilsanz F. Septic shock due to a community acquired Clostridium difficile infection. A case study and a review of the literature. Rev Esp Anestesiol Reanimvol. 2014;61(4):219-222. PubMed
31. You E, Song H, Cho J, Lee J. Reduction in the incidence of hospital-acquired Clostridium difficile infection through infection control interventions other than the restriction of antimicrobial use. Int J Infect Dis. 2014;22:9-10. 2014. PubMed
1. Polage CR, Solnick JV, Cohen SH. Nosocomial diarrhea: evaluation and treatment of causes other than Clostridium difficile. Clin Infect Dis. 2012;55(7):982-989. Doi: 10.1093/cid/cis551. PubMed
2. Kyne L, Hamel MB, Polavaram R, Kelly CP. Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile. Clin Infect Dis. 2002;34(3):346-353. Doi: 10.1086/338260. PubMed
3. Dubberke ER, Olsen MA. Burden of Clostridium difficile on the healthcare system. Clin Infect Dis. 2012;55(Suppl 2):S88-S92. Doi: 10.1093/cid/cis335. PubMed
4. Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med. 2015;372(9):825-834. Doi: 10.1056/NEJMoa1408913. PubMed
5. Zhang S, Palazuelos-Munoz S, Balsells EM, Nair H, Chit A, Kyaw MH. Cost of hospital management of Clostridium difficile infection in United States-a meta-analysis and modelling study. BMC Infect Dis. 2016;16(1):447. Doi: 10.1186/s12879-016-1786-6. PubMed
6. Lessa FC, Gould CV, McDonald LC. Current status of Clostridium difficile infection epidemiology. Clin Infect Dis. 2012;55(Suppl 2):S65-S70. Doi: 10.1093/cid/cis319. PubMed
7. Depestel DD, Aronoff DM. Epidemiology of Clostridium difficile infection. J Pharm Pract. 2013;26(5):464-475. Doi: 10.1177/0897190013499521. PubMed
8. Dial S., Delaney JAC, Barkun AN, Suissa S. Use of gastric acid-suppressive agents and the risk of community-acquired Clostridium difficile-associated disease. JAMA. 2005;294(23):2989-2995. Doi: 10.1001/jama.294.23.2989. PubMed
9. Aseeri M., Schroeder T, Kramer J, Zackula R. Gastric acid suppression by proton pump inhibitors as a risk factor for clostridium difficile-associated diarrhea in hospitalized patients. Am J Gastroenterol. 2008;103(9):2308-2313. Doi: 10.1111/j.1572-0241.2008.01975.x. PubMed
10. Cunningham R, Dial S. Is over-use of proton pump inhibitors fuelling the current epidemic of Clostridium difficile-associated diarrhoea? J Hosp Infect. 2008;70(1):1-6. Doi: 10.1016/j.jhin.2008.04.023. PubMed
11. HCUP-US NIS Overview. https://www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed on April 23, 2016.
12. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613-619. PubMed
13. Goto T, Yoshida K, Tsugawa Y, Filbin MR, Camargo CA, Hasegawa K. Mortality trends in U.S. adults with septic shock, 2005-2011: a serial cross-sectional analysis of nationally-representative data. BMC Infect Dis. 2016;16:294. Doi: 10.1186/s12879-016-1620-1. PubMed
14. Kumar G, Kumar N, Taneja A, et al. Nationwide trends of severe sepsis in the 21st century (2000-2007). Chest. 2011;140(5):1223-1231. Doi: 10.1378/chest.11-0352. PubMed
15. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546-1554. Doi: 10.1056/NEJMoa022139. PubMed
16. Scheurer DB, Hicks LS, Cook EF, Schnipper JL. Accuracy of ICD-9 coding for Clostridium difficile infections: a retrospective cohort. Epidemiol Infect. 2007;135(6):1010-1013. Doi: 10.1017/S0950268806007655. PubMed
17. Dodek PM, Norena M, Ayas NT, Romney M, Wong H. Length of stay and mortality due to Clostridium difficile infection acquired in the intensive care unit. J Crit Care. 2013;28(4):335-340. Doi: 10.1016/j.jcrc.2012.11.008. PubMed
18. Bouza E, Rodríguez-Créixems M, Alcalá L, et al. Is Clostridium difficile infection an increasingly common severe disease in adult intensive care units? A 10-year experience. J Crit Care. 2015;30(3):543-549. Doi: 10.1016/j.jcrc.2015.02.011. PubMed
19. Karanika S, Paudel S, Zervou FN, Grigoras C, Zacharioudakis IM, Mylonakis E. Prevalence and clinical outcomes of Clostridium difficile infection in the intensive care unit: a systematic review and meta-analysis. Open Forum Infect Dis. 2016;3(1):ofv186. Doi: 10.1093/ofid/ofv186. PubMed
20. Zahar JR, Schwebel C, Adrie C, et al. Outcome of ICU patients with Clostridium difficile infection. Crit Care. 2012;16(6):R215. Doi: 10.1186/cc11852. PubMed
21. Shorr AF, Zilberberg MD, Wang L, Baser O, Yu H. Mortality and costs in clostridium difficile infection among the elderly in the United States. Infect Control Hosp Epidemiol. 2016;37(11):1331-1336. Doi: 10.1017/ice.2016.188. PubMed
22. Micek ST, Schramm G, Morrow L, et al. Clostridium difficile infection: a multicenter study of epidemiology and outcomes in mechanically ventilated patients. Crit Care Med. 2013;41(8):1968-1975. Doi: 10.1097/CCM.0b013e31828a40d5. PubMed
23. Zilberberg MD, Nathanson BH, Sadigov S, Higgins TL, Kollef MH, Shorr AF. Epidemiology and outcomes of clostridium difficile-associated disease among patients on prolonged acute mechanical ventilation. Chest. 2009;136(3):752-758. Doi: 10.1378/chest.09-0596. PubMed
24. Lagu T, Stefan MS, Haessler S, et al. The impact of hospital-onset Clostridium difficile infection on outcomes of hospitalized patients with sepsis. J Hosp Med. 2014;9(7):411-417. Doi: 10.1002/jhm.2199. PubMed
25. Prescott HC, Dickson RP, Rogers MA, Langa KM, Iwashyna TJ. Hospitalization type and subsequent severe sepsis. Am J Respir Crit Care Med. 2015;192(5):581-588. Doi: 10.1164/rccm.201503-0483OC. PubMed
26. Healthcare-associated Infections (HAI) Progress Report. Centers for Disease Control and Prevention. http://www.cdc.gov/hai/surveillance/progress-report/index.html. Accessed on July 29, 2017.
27. Song X, Bartlett JG, Speck K, Naegeli A, Carroll K, Perl TM. Rising economic impact of clostridium difficile-associated disease in adult hospitalized patient population. Infect Control Hosp Epidemiol. 2008;29(9):823-828. Doi: 10.1086/588756. PubMed
28. Zilberberg MD, Shorr AF, Micek ST, et al. Clostridium difficile recurrence is a strong predictor of 30-day rehospitalization among patients in intensive care. Infect Control Hosp Epidemiol. 2015;36(3):273-279. Doi: 10.1017/ice.2014.47. PubMed
29. Loftus KV, Wilson PM. A curiously rare case of septic shock from Clostridium difficile colitis. Pediatr Emerg Care. 2015. [Epub ahead of print]. Doi: 10.1097/PEC.0000000000000496. PubMed
30. Bermejo C, Maseda E, Salgado P, Gabilondo G., Gilsanz F. Septic shock due to a community acquired Clostridium difficile infection. A case study and a review of the literature. Rev Esp Anestesiol Reanimvol. 2014;61(4):219-222. PubMed
31. You E, Song H, Cho J, Lee J. Reduction in the incidence of hospital-acquired Clostridium difficile infection through infection control interventions other than the restriction of antimicrobial use. Int J Infect Dis. 2014;22:9-10. 2014. PubMed
© 2017 Society of Hospital Medicine