User login
VAM Registration Now Open
Registration and housing for the 2018 Vascular Annual Meeting are now open. Register today for VAM, June 20 to 23 in Boston, including looking over housing options. Following a full day of postgraduate courses, VESS abstracts, workshops and international programming on Wednesday, June 20, abstract-based scientific sessions will open June 21 and continue to June 23. The Exhibit Hall will be open June 21 to 22.
Catch the highlights of this year's annual meeting here.
Registration and housing for the 2018 Vascular Annual Meeting are now open. Register today for VAM, June 20 to 23 in Boston, including looking over housing options. Following a full day of postgraduate courses, VESS abstracts, workshops and international programming on Wednesday, June 20, abstract-based scientific sessions will open June 21 and continue to June 23. The Exhibit Hall will be open June 21 to 22.
Catch the highlights of this year's annual meeting here.
Registration and housing for the 2018 Vascular Annual Meeting are now open. Register today for VAM, June 20 to 23 in Boston, including looking over housing options. Following a full day of postgraduate courses, VESS abstracts, workshops and international programming on Wednesday, June 20, abstract-based scientific sessions will open June 21 and continue to June 23. The Exhibit Hall will be open June 21 to 22.
Catch the highlights of this year's annual meeting here.
Medical Marijuana Redux
There were so many developments that occurred in the first months of 2018 that could potentially affect federal health care—the government shutdown, the proposed change in rights of conscience protections for federal health care professionals (HCPs), and more debate about medical marijuana in the VA—that it was hard to pick just one topic to discuss this month. In the end I felt it was time to examine how and in what ways the new VA policy on medical marijuana may have changed.
In 2014, before I became editor-in-chief of Federal Practitioner, I wrote an article analyzing the legal and ethical conflicts that arise for VA clinicians who practice under the federal regulations that prohibit them from prescribing medical marijuana or from completing forms or providing referrals for their patients who live in states where medical marijuana is legal.2 The article summarized the events and issues that led to the VA issuing a policy on medical marijuana in 2011. When that article was written, medical marijuana had been legalized in 20 states.
Now in March 2018, 29 states have passed legislation to permit marijuana use for medical purposes.3 Prior to issuing the revised version of its medical marijuana policy, the VA rumor mill went into high gear. Anticipatory stories predicted dramatic changes from the extreme of the VA penalizing veterans who used medical marijuana to allowing doctors to prescribe it. Such massive shifts are not typical of any bureaucracy, and indeed some VA officials denied that the revision represented any substantive movement in either direction.4
VHA Directive 1315, Access to Clinical Programs for Veterans Participating in State Medical Marijuana Programs was issued December 8, 2017.5 In accordance with federal regulation, its issuance superceded VHA Directive 2011-04 of the same title.6 According to the directive, its emphasis on discussion with veterans was a significant policy shift. “Major changes include adding policy to support the Veteran-provider relationship when discussing the use of medical marijuana and its impact on health including Veteran-specific treatment plans.” It should be noted that the prior directive did not prohibit or even discourage such conversations, and accompanying less official guidance actually promoted them.7
Interestingly, the new directive does not instruct HCPs to ask about medical marijuana in the way questions about alcohol, tobacco, and drug use as well as many other lifestyle factors are mandated. Asking a veteran about marijuana use would be a step toward medical mainstreaming. The burden is still on the veteran to bring up the subject—not an easy thing to do in light of the fear among some veterans that the VA will curtail benefits for a veteran caught using medical marijuana.
The new directive is a minor move toward appropriate medicalization. Practitioners are advised to discuss medical marijuana use with any veteran for whom it “may have clinical relevance” or who asks about medical marijuana. This underscores the need for VA practitioners to have access to up-to-date information in order to keep up with their Internet savvy patients and combat ever proliferating myths about the panacea-like properties of medical marijuana.
But when it comes down to the devilish details, the primary rules provide no deliverance from the impasse between state and federal law. Marijuana remains a Schedule I drug under the Controlled Substances Act. For purposes of federal health care, it still is, “a substance with a high potential for abuse without a currently acceptable medical use in treatment in the United States, and lacking accepted safety for use under medical supervision.”8 Although many vocal veterans as well as some federal practitioners, HCPs in the wider medical community, and more recently a number of politicians would challenge this regulation, federal lawprohibits prescribing medical marijuana. The new VA directive is more explicit in stating that VA practitioners cannot complete forms enrolling veterans or permitting their registration in state-approved medical marijuana programs. This restriction was implicit in the prior directive but has been a continuing source of confusion for HCPs. The new directive at least clarifies these restrictions.
Another point of clinical misunderstanding had been about whether HCPs in the VA could refer patients to state-approved medical marijuana programs and what exactly referral entails. There is a direct prohibition in the new directive on making referrals, yet the term remains undefined. Nothing in the directive contradicts the right of a veteran to access their medical records for purposes of registering for state-approved programs. But the directive does forcefully restate that if a veteran appears in an HCP’s office or at the pharmacy with an authorization or registration for medical marijuana from a state-approved program, the VA will neither provide the product nor pay for its purchase elsewhere. The more rules-based form of this directive also strongly states that possession of marijuana on VA grounds even for medical purposes and with state approval is a violation of federal regulation that may be prosecuted under the Controlled Substance Act.
The new directive does clarify a question that had arisen about VA employees’ participation in state-approved medical marijuana programs. VA employees, even those who do not receive their care at the VA, are prohibited from using medical marijuana. Individuals who use marijuana for medical indications often do so daily. Considering that a person may test positive for marijuana months after regular use, a segment of VA staff may be at risk for violating federal drug-free workplace regulations.9,10
The administrative aspects of the directive are tightened, which will help clinicians know what they are supposed to do when a veteran reports medical marijuana use; it is hoped that this will bring more consistency and fairness to the process. Practitioners continue to be required to enter a veteran’s reported use of medical marijuana in the electronic medical record under the section Non-VA/Herbal Medication/Over the Counter. When HCPs discuss the use of medical marijuana with patients, the requirement to document those discussions is instructive.
Those looking for a relaxation in the VA’s clinical approach will find little to cheer about. But there are a few rays of hope for those HCPs and patients trying to do the best they can in this catch-22 situation. First, the VA has stood firm that veterans cannot be excluded from other types of VA medical care due to their use of medical marijuana. “Veterans must not be denied VHA services solely because they are participating in State-approved marijuana programs.”5 The directive specifically acknowledges the clinical areas in which veteran medical marijuana use has been the most contentious: PTSD, substance use, and pain management. It also encourages HCPs to review potential drug interactions and how marijuana use may affect other types of medical or psychiatric care. These 3 areas also are the object of intensified congressional pressure and veteran service organization lobbying for the VA to not only incorporate these modalities into VA care, but also to expand research.11
Second, the phrase “modifying treatment plans,” which understandably makes patients and their advocates apprehensive, is qualified. To those clinicians who would prefer, either because of concerns of professional liability or personal belief, to have a black-and-white stance on the use of medical marijuana, the directive mandates that they must deal with the gray. “Providers need to make decisions to modify treatment plans based on marijuana use on a case-by-case basis.”5
Third, those modifications cannot be unilateral pronouncements, but must be the result of shared decisions making and mutual discussion. The only ground on which a practitioner can exercise any degree of soft paternalism is when the use of medical marijuana and treatment for another condition represents an evidence-based threat to the health and safety of the veteran. “Providers need to
Overall the policy has no big surprises, leaving those who hoped the revision would bring a softening of the VA’s institutional position and federal law frustrated. Those who sought a strengthening of VA policy based on those same regulations regarding the use of medical marijuana will be equally thwarted. And those clinicians who are just trying to do the right thing as HCPs who work for the federal government and for their patients who are interested only in relief from their most troubling ailments, will stay right where they were, suspended over the ethical chasm that medical marijuana generates between state and federal law.
1. Curie M. Pierre Curie With Autobiographical Notes. Kellogg C, Kellogg V, trans. New York: Macmillan; 1923.
2. Geppert CMA. Legal and clinical evolution of Veterans Health Administration policy on medical marijuana. Fed Pract. 2014;31(3):6-12.
3. National Conference of State Legislators. State Medical Marijuana Laws. http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx Updated February 15, 2018. Accessed March 2, 2018.
4. Shane L. VA refutes rumors of new policy on medical marijuana. https://www.militarytimes.com/veterans/2017/12/19/va-refutes-rumors-of-a-new-policy-on-medical-marijuana. Published December 19, 2017. Accessed March 2, 2018.
5. U.S. Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1315, Access to Clinical Programs for Veterans Participating in State Medical Marijuana Programs. December 8, 2017.
6. U.S. Department of Veterans Affairs, Veterans Health Administration. VHA Directive 2011-004, Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs, dated January 31, 2011 (rescinded).
7. U.S. Department of Veterans Affairs, Veterans Health Administration. Clinical considerations regarding veteran patients who participate in state-approved medical marijuana programs. Washington, DC; 2010. [Nonpublic document.]
8. 21 U.S.C. 801 et al, the Controlled Substances Act.
9. Welch SA. The pharmacology of cannabinoids. In: Principles of Addiction Medicine: The Essentials. Cavacuiti CA, ed. Philadelphia, PA: Lippincott-Williams & Wilkins; 2011:62.
10. U.S. Department of Veterans Affairs. VA Handbook 5383.2, VA drug-free workplace plan. https://www.va.gov/vapubs/search_action.cfm?dType=2. Published April 11, 1997. Accessed March 2, 2018.
11. Zezima K. VA says it won’t study medical marijuana’s effect on veterans. The Washington Post. https://www.washingtonpost.com/news/post-nation/wp/2018/01/16/va-says-it-wont-study-medical-marijuanas-effect-on-veterans/?utm_term=.9d554109d135. Published January 16, 2018. Accessed March 2, 2018.
There were so many developments that occurred in the first months of 2018 that could potentially affect federal health care—the government shutdown, the proposed change in rights of conscience protections for federal health care professionals (HCPs), and more debate about medical marijuana in the VA—that it was hard to pick just one topic to discuss this month. In the end I felt it was time to examine how and in what ways the new VA policy on medical marijuana may have changed.
In 2014, before I became editor-in-chief of Federal Practitioner, I wrote an article analyzing the legal and ethical conflicts that arise for VA clinicians who practice under the federal regulations that prohibit them from prescribing medical marijuana or from completing forms or providing referrals for their patients who live in states where medical marijuana is legal.2 The article summarized the events and issues that led to the VA issuing a policy on medical marijuana in 2011. When that article was written, medical marijuana had been legalized in 20 states.
Now in March 2018, 29 states have passed legislation to permit marijuana use for medical purposes.3 Prior to issuing the revised version of its medical marijuana policy, the VA rumor mill went into high gear. Anticipatory stories predicted dramatic changes from the extreme of the VA penalizing veterans who used medical marijuana to allowing doctors to prescribe it. Such massive shifts are not typical of any bureaucracy, and indeed some VA officials denied that the revision represented any substantive movement in either direction.4
VHA Directive 1315, Access to Clinical Programs for Veterans Participating in State Medical Marijuana Programs was issued December 8, 2017.5 In accordance with federal regulation, its issuance superceded VHA Directive 2011-04 of the same title.6 According to the directive, its emphasis on discussion with veterans was a significant policy shift. “Major changes include adding policy to support the Veteran-provider relationship when discussing the use of medical marijuana and its impact on health including Veteran-specific treatment plans.” It should be noted that the prior directive did not prohibit or even discourage such conversations, and accompanying less official guidance actually promoted them.7
Interestingly, the new directive does not instruct HCPs to ask about medical marijuana in the way questions about alcohol, tobacco, and drug use as well as many other lifestyle factors are mandated. Asking a veteran about marijuana use would be a step toward medical mainstreaming. The burden is still on the veteran to bring up the subject—not an easy thing to do in light of the fear among some veterans that the VA will curtail benefits for a veteran caught using medical marijuana.
The new directive is a minor move toward appropriate medicalization. Practitioners are advised to discuss medical marijuana use with any veteran for whom it “may have clinical relevance” or who asks about medical marijuana. This underscores the need for VA practitioners to have access to up-to-date information in order to keep up with their Internet savvy patients and combat ever proliferating myths about the panacea-like properties of medical marijuana.
But when it comes down to the devilish details, the primary rules provide no deliverance from the impasse between state and federal law. Marijuana remains a Schedule I drug under the Controlled Substances Act. For purposes of federal health care, it still is, “a substance with a high potential for abuse without a currently acceptable medical use in treatment in the United States, and lacking accepted safety for use under medical supervision.”8 Although many vocal veterans as well as some federal practitioners, HCPs in the wider medical community, and more recently a number of politicians would challenge this regulation, federal lawprohibits prescribing medical marijuana. The new VA directive is more explicit in stating that VA practitioners cannot complete forms enrolling veterans or permitting their registration in state-approved medical marijuana programs. This restriction was implicit in the prior directive but has been a continuing source of confusion for HCPs. The new directive at least clarifies these restrictions.
Another point of clinical misunderstanding had been about whether HCPs in the VA could refer patients to state-approved medical marijuana programs and what exactly referral entails. There is a direct prohibition in the new directive on making referrals, yet the term remains undefined. Nothing in the directive contradicts the right of a veteran to access their medical records for purposes of registering for state-approved programs. But the directive does forcefully restate that if a veteran appears in an HCP’s office or at the pharmacy with an authorization or registration for medical marijuana from a state-approved program, the VA will neither provide the product nor pay for its purchase elsewhere. The more rules-based form of this directive also strongly states that possession of marijuana on VA grounds even for medical purposes and with state approval is a violation of federal regulation that may be prosecuted under the Controlled Substance Act.
The new directive does clarify a question that had arisen about VA employees’ participation in state-approved medical marijuana programs. VA employees, even those who do not receive their care at the VA, are prohibited from using medical marijuana. Individuals who use marijuana for medical indications often do so daily. Considering that a person may test positive for marijuana months after regular use, a segment of VA staff may be at risk for violating federal drug-free workplace regulations.9,10
The administrative aspects of the directive are tightened, which will help clinicians know what they are supposed to do when a veteran reports medical marijuana use; it is hoped that this will bring more consistency and fairness to the process. Practitioners continue to be required to enter a veteran’s reported use of medical marijuana in the electronic medical record under the section Non-VA/Herbal Medication/Over the Counter. When HCPs discuss the use of medical marijuana with patients, the requirement to document those discussions is instructive.
Those looking for a relaxation in the VA’s clinical approach will find little to cheer about. But there are a few rays of hope for those HCPs and patients trying to do the best they can in this catch-22 situation. First, the VA has stood firm that veterans cannot be excluded from other types of VA medical care due to their use of medical marijuana. “Veterans must not be denied VHA services solely because they are participating in State-approved marijuana programs.”5 The directive specifically acknowledges the clinical areas in which veteran medical marijuana use has been the most contentious: PTSD, substance use, and pain management. It also encourages HCPs to review potential drug interactions and how marijuana use may affect other types of medical or psychiatric care. These 3 areas also are the object of intensified congressional pressure and veteran service organization lobbying for the VA to not only incorporate these modalities into VA care, but also to expand research.11
Second, the phrase “modifying treatment plans,” which understandably makes patients and their advocates apprehensive, is qualified. To those clinicians who would prefer, either because of concerns of professional liability or personal belief, to have a black-and-white stance on the use of medical marijuana, the directive mandates that they must deal with the gray. “Providers need to make decisions to modify treatment plans based on marijuana use on a case-by-case basis.”5
Third, those modifications cannot be unilateral pronouncements, but must be the result of shared decisions making and mutual discussion. The only ground on which a practitioner can exercise any degree of soft paternalism is when the use of medical marijuana and treatment for another condition represents an evidence-based threat to the health and safety of the veteran. “Providers need to
Overall the policy has no big surprises, leaving those who hoped the revision would bring a softening of the VA’s institutional position and federal law frustrated. Those who sought a strengthening of VA policy based on those same regulations regarding the use of medical marijuana will be equally thwarted. And those clinicians who are just trying to do the right thing as HCPs who work for the federal government and for their patients who are interested only in relief from their most troubling ailments, will stay right where they were, suspended over the ethical chasm that medical marijuana generates between state and federal law.
There were so many developments that occurred in the first months of 2018 that could potentially affect federal health care—the government shutdown, the proposed change in rights of conscience protections for federal health care professionals (HCPs), and more debate about medical marijuana in the VA—that it was hard to pick just one topic to discuss this month. In the end I felt it was time to examine how and in what ways the new VA policy on medical marijuana may have changed.
In 2014, before I became editor-in-chief of Federal Practitioner, I wrote an article analyzing the legal and ethical conflicts that arise for VA clinicians who practice under the federal regulations that prohibit them from prescribing medical marijuana or from completing forms or providing referrals for their patients who live in states where medical marijuana is legal.2 The article summarized the events and issues that led to the VA issuing a policy on medical marijuana in 2011. When that article was written, medical marijuana had been legalized in 20 states.
Now in March 2018, 29 states have passed legislation to permit marijuana use for medical purposes.3 Prior to issuing the revised version of its medical marijuana policy, the VA rumor mill went into high gear. Anticipatory stories predicted dramatic changes from the extreme of the VA penalizing veterans who used medical marijuana to allowing doctors to prescribe it. Such massive shifts are not typical of any bureaucracy, and indeed some VA officials denied that the revision represented any substantive movement in either direction.4
VHA Directive 1315, Access to Clinical Programs for Veterans Participating in State Medical Marijuana Programs was issued December 8, 2017.5 In accordance with federal regulation, its issuance superceded VHA Directive 2011-04 of the same title.6 According to the directive, its emphasis on discussion with veterans was a significant policy shift. “Major changes include adding policy to support the Veteran-provider relationship when discussing the use of medical marijuana and its impact on health including Veteran-specific treatment plans.” It should be noted that the prior directive did not prohibit or even discourage such conversations, and accompanying less official guidance actually promoted them.7
Interestingly, the new directive does not instruct HCPs to ask about medical marijuana in the way questions about alcohol, tobacco, and drug use as well as many other lifestyle factors are mandated. Asking a veteran about marijuana use would be a step toward medical mainstreaming. The burden is still on the veteran to bring up the subject—not an easy thing to do in light of the fear among some veterans that the VA will curtail benefits for a veteran caught using medical marijuana.
The new directive is a minor move toward appropriate medicalization. Practitioners are advised to discuss medical marijuana use with any veteran for whom it “may have clinical relevance” or who asks about medical marijuana. This underscores the need for VA practitioners to have access to up-to-date information in order to keep up with their Internet savvy patients and combat ever proliferating myths about the panacea-like properties of medical marijuana.
But when it comes down to the devilish details, the primary rules provide no deliverance from the impasse between state and federal law. Marijuana remains a Schedule I drug under the Controlled Substances Act. For purposes of federal health care, it still is, “a substance with a high potential for abuse without a currently acceptable medical use in treatment in the United States, and lacking accepted safety for use under medical supervision.”8 Although many vocal veterans as well as some federal practitioners, HCPs in the wider medical community, and more recently a number of politicians would challenge this regulation, federal lawprohibits prescribing medical marijuana. The new VA directive is more explicit in stating that VA practitioners cannot complete forms enrolling veterans or permitting their registration in state-approved medical marijuana programs. This restriction was implicit in the prior directive but has been a continuing source of confusion for HCPs. The new directive at least clarifies these restrictions.
Another point of clinical misunderstanding had been about whether HCPs in the VA could refer patients to state-approved medical marijuana programs and what exactly referral entails. There is a direct prohibition in the new directive on making referrals, yet the term remains undefined. Nothing in the directive contradicts the right of a veteran to access their medical records for purposes of registering for state-approved programs. But the directive does forcefully restate that if a veteran appears in an HCP’s office or at the pharmacy with an authorization or registration for medical marijuana from a state-approved program, the VA will neither provide the product nor pay for its purchase elsewhere. The more rules-based form of this directive also strongly states that possession of marijuana on VA grounds even for medical purposes and with state approval is a violation of federal regulation that may be prosecuted under the Controlled Substance Act.
The new directive does clarify a question that had arisen about VA employees’ participation in state-approved medical marijuana programs. VA employees, even those who do not receive their care at the VA, are prohibited from using medical marijuana. Individuals who use marijuana for medical indications often do so daily. Considering that a person may test positive for marijuana months after regular use, a segment of VA staff may be at risk for violating federal drug-free workplace regulations.9,10
The administrative aspects of the directive are tightened, which will help clinicians know what they are supposed to do when a veteran reports medical marijuana use; it is hoped that this will bring more consistency and fairness to the process. Practitioners continue to be required to enter a veteran’s reported use of medical marijuana in the electronic medical record under the section Non-VA/Herbal Medication/Over the Counter. When HCPs discuss the use of medical marijuana with patients, the requirement to document those discussions is instructive.
Those looking for a relaxation in the VA’s clinical approach will find little to cheer about. But there are a few rays of hope for those HCPs and patients trying to do the best they can in this catch-22 situation. First, the VA has stood firm that veterans cannot be excluded from other types of VA medical care due to their use of medical marijuana. “Veterans must not be denied VHA services solely because they are participating in State-approved marijuana programs.”5 The directive specifically acknowledges the clinical areas in which veteran medical marijuana use has been the most contentious: PTSD, substance use, and pain management. It also encourages HCPs to review potential drug interactions and how marijuana use may affect other types of medical or psychiatric care. These 3 areas also are the object of intensified congressional pressure and veteran service organization lobbying for the VA to not only incorporate these modalities into VA care, but also to expand research.11
Second, the phrase “modifying treatment plans,” which understandably makes patients and their advocates apprehensive, is qualified. To those clinicians who would prefer, either because of concerns of professional liability or personal belief, to have a black-and-white stance on the use of medical marijuana, the directive mandates that they must deal with the gray. “Providers need to make decisions to modify treatment plans based on marijuana use on a case-by-case basis.”5
Third, those modifications cannot be unilateral pronouncements, but must be the result of shared decisions making and mutual discussion. The only ground on which a practitioner can exercise any degree of soft paternalism is when the use of medical marijuana and treatment for another condition represents an evidence-based threat to the health and safety of the veteran. “Providers need to
Overall the policy has no big surprises, leaving those who hoped the revision would bring a softening of the VA’s institutional position and federal law frustrated. Those who sought a strengthening of VA policy based on those same regulations regarding the use of medical marijuana will be equally thwarted. And those clinicians who are just trying to do the right thing as HCPs who work for the federal government and for their patients who are interested only in relief from their most troubling ailments, will stay right where they were, suspended over the ethical chasm that medical marijuana generates between state and federal law.
1. Curie M. Pierre Curie With Autobiographical Notes. Kellogg C, Kellogg V, trans. New York: Macmillan; 1923.
2. Geppert CMA. Legal and clinical evolution of Veterans Health Administration policy on medical marijuana. Fed Pract. 2014;31(3):6-12.
3. National Conference of State Legislators. State Medical Marijuana Laws. http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx Updated February 15, 2018. Accessed March 2, 2018.
4. Shane L. VA refutes rumors of new policy on medical marijuana. https://www.militarytimes.com/veterans/2017/12/19/va-refutes-rumors-of-a-new-policy-on-medical-marijuana. Published December 19, 2017. Accessed March 2, 2018.
5. U.S. Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1315, Access to Clinical Programs for Veterans Participating in State Medical Marijuana Programs. December 8, 2017.
6. U.S. Department of Veterans Affairs, Veterans Health Administration. VHA Directive 2011-004, Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs, dated January 31, 2011 (rescinded).
7. U.S. Department of Veterans Affairs, Veterans Health Administration. Clinical considerations regarding veteran patients who participate in state-approved medical marijuana programs. Washington, DC; 2010. [Nonpublic document.]
8. 21 U.S.C. 801 et al, the Controlled Substances Act.
9. Welch SA. The pharmacology of cannabinoids. In: Principles of Addiction Medicine: The Essentials. Cavacuiti CA, ed. Philadelphia, PA: Lippincott-Williams & Wilkins; 2011:62.
10. U.S. Department of Veterans Affairs. VA Handbook 5383.2, VA drug-free workplace plan. https://www.va.gov/vapubs/search_action.cfm?dType=2. Published April 11, 1997. Accessed March 2, 2018.
11. Zezima K. VA says it won’t study medical marijuana’s effect on veterans. The Washington Post. https://www.washingtonpost.com/news/post-nation/wp/2018/01/16/va-says-it-wont-study-medical-marijuanas-effect-on-veterans/?utm_term=.9d554109d135. Published January 16, 2018. Accessed March 2, 2018.
1. Curie M. Pierre Curie With Autobiographical Notes. Kellogg C, Kellogg V, trans. New York: Macmillan; 1923.
2. Geppert CMA. Legal and clinical evolution of Veterans Health Administration policy on medical marijuana. Fed Pract. 2014;31(3):6-12.
3. National Conference of State Legislators. State Medical Marijuana Laws. http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx Updated February 15, 2018. Accessed March 2, 2018.
4. Shane L. VA refutes rumors of new policy on medical marijuana. https://www.militarytimes.com/veterans/2017/12/19/va-refutes-rumors-of-a-new-policy-on-medical-marijuana. Published December 19, 2017. Accessed March 2, 2018.
5. U.S. Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1315, Access to Clinical Programs for Veterans Participating in State Medical Marijuana Programs. December 8, 2017.
6. U.S. Department of Veterans Affairs, Veterans Health Administration. VHA Directive 2011-004, Access to Clinical Programs for Veterans Participating in State-Approved Marijuana Programs, dated January 31, 2011 (rescinded).
7. U.S. Department of Veterans Affairs, Veterans Health Administration. Clinical considerations regarding veteran patients who participate in state-approved medical marijuana programs. Washington, DC; 2010. [Nonpublic document.]
8. 21 U.S.C. 801 et al, the Controlled Substances Act.
9. Welch SA. The pharmacology of cannabinoids. In: Principles of Addiction Medicine: The Essentials. Cavacuiti CA, ed. Philadelphia, PA: Lippincott-Williams & Wilkins; 2011:62.
10. U.S. Department of Veterans Affairs. VA Handbook 5383.2, VA drug-free workplace plan. https://www.va.gov/vapubs/search_action.cfm?dType=2. Published April 11, 1997. Accessed March 2, 2018.
11. Zezima K. VA says it won’t study medical marijuana’s effect on veterans. The Washington Post. https://www.washingtonpost.com/news/post-nation/wp/2018/01/16/va-says-it-wont-study-medical-marijuanas-effect-on-veterans/?utm_term=.9d554109d135. Published January 16, 2018. Accessed March 2, 2018.

Approaches to Enhancing Patient-Centered Communication In Caring For Hispanic/Latino Patients With Diabetes
From the University of Texas at El Paso, El Paso, TX.
Abstract
- Objective: To demonstrate the applied use of recommended cultural competency communication tools.
- Methods: An overview of several cultural competency tools is presented and vignettes are used to demonstrate the use of these tools with Hispanic patients with diabetes.
- Results: Three communication mnemonic instruments, ie, BELIEF, ETHNIC, and BATHE, may be useful for engaging health professionals in patient-centered communication with their Hispanic patients and shared decision making. Health professionals can also employ nonjudgmental probing as part of engaging patients in setting diabetes treatment goals.
- Conclusion: Health professionals are in an influential position to leverage a patient- and culture-centered communication style to improve communication with Hispanic patients. Using mnemonic tools can help facilitate this communication and improve health professionals’ understanding on how cultural and social factors influence diabetes management in this population.
Key words: Hispanic/Latino; diabetes; patient-centered communication; cultural-competency.
The 2017 American Diabetes Association (ADA) Standards of Medical Care recommend that health professionals engage in a patient-centered communication style with patient to facilitate shared decision-making and improve diabetes outcomes. The ADA defines patient-centered communication as “a style that uses active listening, elicits patient preferences and beliefs, and assesses literacy, numeracy, and potential barriers to care” [1]. One of the main goals of using patient-centered communication is to create a collaborative, personal, and non-judgmental relationship with patients. These guidelines, however, provide less direction on the type of communication skills training that would facilitate this type of communication, particularly as it relates to ethnic/racial minority groups most at risk for diabetes and related complications.
The US Hispanic/Latino population, in particular, is a group that is burdened by the diabetes epidemic, with a prevalence that is 130% higher than non-Hispanic whites [2]. It is widely known that certain social determinants of health, like socioeconomic status, social injustices, poor access to health care, food insecurity, or living in environments that do not support health behaviors, all contribute to health disparities for Hispanics/Latinos [3]. Understanding how Hispanics/Latinos cope with these social determinants of health is important for health care professionals, and a patient-centered communication style is an ideal approach for active listening and eliciting information about the social barriers/challenges that may influence diabetes self-care. However, there is some evidence that suggests this approach is not fully used by health care professionals when communicating with Hispanics/Latinos with diabetes, and Hispanics/Latinos continue to be more likely to experience disparities in the quality of diabetes care they receive compared to non-Hispanic whites [4–9]. One of the identified contributors to these disparities is the poor communication between physicians and Hispanic/Latino patients [10–16]. Given that health care professionals are the primary source of health care and diabetes information for Hispanics/Latinos, it is important for health professionals to enhance their patient-centered communications skills to improve the quality of care that is provided to this population [12].
Cultural Competence and Patient-Centered Communication
Not all health professional communication skills are perceived as unsatisfactory by Hispanic/Latino patients with diabetes. In fact, Hispanics/Latinos report a positive provider-patient clinical interaction when health professionals display cultural competency skills [15,17–20]. Moreover, evidence suggest that Hispanic/Latino patients with diabetes reported better quality of care and improved self-management behaviors with a culturally competent provider [18–20]. Cultural competency is described as “understanding and responding effectively to the cultural and linguistic needs brought by the patient to the health care encounter” and “valuing diversity, provider self-assessment, managing dynamics of differences, acquiring and institutionalizing knowledge, and adapting to diversity and the cultural context of individuals served” [9,11,12]. One approach for gaining cultural competency skills is to understand how the disease process is conceptualized within a culture and how that influences a patient’s own theory about their disease etiology, prognosis, and outcome [21]. This approach is known as culture-centered in the health communications literature and may be useful when communicating with Hispanic/Latino patients with diabetes because there is extensive literature describing unique indigenous Latin American explanatory models for diabetes [22–26].
Language Discordance in Physician-Patient Communication
The process of patient-physician communication includes “attending to one another and begin interpreting one another’s verbal and nonverbal” interactions [9]. A conventional assumption regarding the disparities in diabetes care quality for Hispanic/Latino patients is that it stems from language discordant patient-physician interactions, which result in errors in the provision of diabetes information and treatment instructions regarding medications and self-care behaviors [9]. While language is a contributing factor, the US Census reports that over half of US Hispanics/Latinos are bilingual and speak English “very well” [27]. Thus, other underlying mechanisms must be contributing to patient-physician miscommunication and suboptimal diabetes outcomes. Moreover, the findings from studies of patient-physician language concordance and diabetes management are inconsistent. For example, language concordance between Hispanic/Latino patients and physicians is associated with improvement in HbA1c but not self-care behaviors (ie, healthy eating, self-monitoring, medicine adherence, exercise) [20]. Thus, there is need to move beyond spoken language to address elements of interpersonal communication around diabetes care through addressing cultural health beliefs and explanatory models of diabetes.
Cultural Explanatory Models of Diabetes
Explanatory models for diabetes among Hispanics/Latinos are diverse and often include a biomedical framework (eg, obesity, unhealthy eating, sedentary lifestyle, genetics); however, there is one unique indigenous belief that continues to be held within this population. Specifically, there is a cultural belief that diabetes is caused by strong or negative emotions, like fright sickness (susto), stress (estres), anger (coraje), or nerves (nervios) [22–26]. Although this cultural belief has been in existence long before scientific evidence has shown the bi-directional relationship between stress/depression and diabetes, the integration of emotions in diabetes self-management in patient-provider communication has not been standardized [28–31]. Health professionals’ interest in how patients view their own disease process may help build rapport with patients. Enhancing health professionals’ cultural competency skills can be a critical first step for improving patient-provider communication. For instance, it can (1) present an opportunity to integrate cultural belief systems into diabetes care for Hispanics/Latinos, (2) open the door for other important conversations about Hispanic/Latino patients’ psychosocial and familial environment and identify barriers or motivators in diabetes self-management, and (3) build rapport and trust between the health professional and patient.
Additionally, inquiring about emotional beliefs or emotions about diabetes in general can help improve the patient-provider relationship, giving Hispanic/Latino patients a sense that their provider cares about their feelings and emotional well-being. For example, in a study conducted by Concha et al, a Hispanic/Latino male patient with diabetes expresses his appreciation of his doctor for attending to his emotional problems and suggests that his diabetes is in control because of the encouragement he receives from the doctor [22].
…I believe the doctors..can encourage one with ..diabetes… I am very grateful to God before anything that till today I have my sugar controlled. I am a diabetic, but controlled. And Dr. [name omitted], he’s a blessing from God. He knows my body like my mother….Because whatever little thing, he attends to me, he gives me a lot of encouragement with my emotional problems. He sent me to a counselor, I have a specialist for my problem with my urinary tracts. I have attention, I have all the attention from the doctor…
Inquiring about emotional well-being may also be beneficial because Hispanics/Latinos with diabetes have reported that they would feel more comfortable talking to a professional about personal problems compared to Hispanics/Latinos without diabetes [32]. Having a physical illness may provide an opportunity for these patients to discuss stress or depression in tandem with diabetes to diminish any possible stigma or shame associated with having a mental health problem. It is important for health care providers to be aware of emotional or social problems that may be negatively influencing diabetes self-care behaviors.
Models of Effective Cross-Cultural Communication
Cultural competency training for health professionals is one strategy for reducing health disparities and ensuring that racial/ethnic populations receive “equitable, effective, and culturally appropriate clinical care” [9,11,12,33]. The Association of American Medical Colleges’ guide for cultural competence education in medical school cites several models of effective cross-cultural communication for physicians and/or physician assistants [34]. I describe 3 communication tools below that may help health care professionals initiate conversations and aid them in understanding how to better manage sociocultural and environmental issues that may impede patients’ ability to manage diabetes. For each tool, a vignette is offered that illustrates how the tool may be used in communicating with Hispanic/Latino patients.
BELIEF
The BELIEF instrument (Dobbie 2003) is a teaching tool designed to elicit patients’ health beliefs and to assist preclinical medical students or medical professionals in understanding how explanatory models of a disease influence patient engagement in care. The BELIEF instrument is straightforward and can be easily implemented into clinical case vignettes and or role-play as part of cultural competency training [35]. The specific questions corresponding to the BELIEF prompts are
- B: Beliefs about health (What caused your illness/problem?)
- E: Explanation (Why did it happen at this time?)
- L: Learn (Help me understand your belief/opinion)
- I: Impact (How is this illness/problem impacting your life?)
- E: Empathy (This must be very hard for you)
- F: Feelings (How are you feeling about it?)
Vignette 1
The following vignette is a conversation between a Spanish-speaking Hispanic women, a language interpreter, and medical professional. The patient, Mrs. Chavez, has come into the clinic for the third time after experiencing symptoms due to hypoglycemia. Mrs. Chavez believes stress may have something to do with her hypoglycemia but is not quite sure how. By using the BELIEF mnemonic, the medical professional is able to ask more about the stress that led into a discussion about how stress actually influenced her eating and medication intake behaviors. Through this probing, the medical professional was able to identify the possible cause of her hypoglycemia and work with Mrs. Chavez on finding a solution every time she experiences the stressful event. The vignette also demonstrates how interpreters may share cultural information that may clarify problems.
Medical Professional: Mrs. Chavez, I see you are here again for hypoglycemia. Can you tell me what has happened? Do you have your medications with you today?
Interpreter: Sra. Chavez, entiendo que está aquí nuevamente por hipoglucemia. ¿Puedes decirme qué ha pasado? ¿Tiene sus medicamentos con usted hoy?
Mrs. Chavez: Si, me ha sentido débil y mareado.
Interpreter: Yes I have felt faint and dizzy?
Medical Professional: Have you been taking your metformin as prescribed?
Interpreter: ¿Ha estado tomando su metformin según lo recetado?
Mrs. Chavez: Si (YES).
Medical Professional: We might have to consider adjusting your dosage.
Interpreter: Es posible que tengamos que considerar ajustar su dosis.
Mrs. Chavez privately to the Interpreter: ¿no es posible que las emociones o nervios puedan causar algo? He escuchado que este puede ser el problema?
Interpreter to Mrs. Chavez: Déjame preguntarle al doctor, si?
Let me ask the doctor, yes? (Mrs. Chavez, nods in agreement)
Interpreter to Medical Professional: She is asking if emotions or nervousness could be the cause. She has heard that this could be the problem.
Medical Profesional to Interpreter: What does she mean?
Interpreter: There is a cultural belief that stress or nerves can cause diabetes or affect diabetes. You may want to ask about this.
Medical Professional: Yes emotions like stress can cause changes in you glucose. (Beliefs) Do you believe that some emotions are causing your hypoglycemia?
Interpreter: Sí, las emociones como el estrés pueden provocar cambios en la glucosa. ¿Crees que algunas emociones están causando tu hipoglucemia?
Mrs. Chavez: (Shrugs shoulders).
Medical Professional: I see here in your records, that the other two times you had hypoglycemica were 1 month and 3 months ago. (Beliefs) What do you think caused these events and (Explanation) why do you think it happened during these times?
Interpreter: Veo aquí en sus registros que las otras dos veces que tuvo hipoglucemia fueron hace 1 mes y 3 meses. ¿Qué crees que causó estos eventos y por qué crees que sucedió durante estos tiempos?
Mrs. Chavez: Pues, no sé.
Interpreter: Well I don’t know.
Medical Professional: (Learn) Help me understand what you think happened 3 and 1 month ago and this month that may have caused your glucose to drop. What was happening emotionally during these times? Do you remember?
Interpreter: Ayúdame a entender lo que piensas que sucedió hace 3 y 1 meses y este mes, puede haber causado que tu glucosa baje. ¿Qué estaba pasando emocionalmente durante este tiempo? ¿Te acuerdas?
Mrs. Chavez: Hmm. Pues, hace 3 meses fui a visitar a mi madre y hace 1 meses fui a visitar a mi hermano al norte.
Interpreter: Hmm. Well 3 months ago I went to visit my mother and 1 months ago I went to visit my brother up north.
Medical Professional: (Learn) How were those trips for you. Did you have fun? What types of emotions were you feeling during these trips?
Interpreter: ¿Cómo fueron esos viajes para ti? ¿Te divertiste? ¿Qué tipo de emociones sentías durante estos viajes?
Mrs. Chavez: Pues, yo estaba muy estresado durante mis viajes.
Interpreter: Well, I was very stressed during my trips.
Medical Professional: (Learn) Would you like to share why you were stressed? What was happening for you to feel so stressed?
Interpreter: ¿Te gustaría compartir por qué estabas estresado? ¿Qué estaba pasando para que te sientas tan estresado?
Mrs. Chavez: Bueno, tenemos muchos problemas familiares y conflictos. Hay muchos argumentos familiares y se vuelve estresante.
Interpreter: Well we have a lot of family problems and conflict. There are a lot of family arguments and it gets stressful.
Medical Professional: (Impact) How do you think this has affected your glucose?
Interpreter: ¿Cómo crees que esto ha afectado tu glucosa?
Mrs. Chavez: No lo sé.
Interpreter: I don’t know.
Medical Professional: (Learn) Do you think the stress maybe led you to forget to take your medication or affected your eating?
Interprter: ¿Crees que el estrés puede llevarte a olvidarte de tomar tu medicación o afectó su alimentación?
Mrs. Chavez: Pues si y no comí. Estaba demasiado estresado para comer. Raramente comí mientras estaba allí. Estaba tan estresado que no tenía apetito.
Interpreter: Well yes and I didn’t eat. I was too stressed to eat. I rarely ate while I was there. I was so stressed i did not have an appetite.
Medical Professional: (Empathy) Mrs. Chavez, that must have been very hard for you. I’m sorry you have had to feel this way. (Feelings) Is this how you feel everytime you visit your family?
Interpreter: Sra. Chávez, eso debe haber sido muy difícil para usted. Lamento que hayas tenido que sentirte de esta manera. ¿Es así como te sientes cada vez que visitas a tu familia?
Mrs. Chavez: Sí, todos se involucran en los problemas familiares y es muy estresante visitarlos, pero tengo que ir a ayudar a mi madre porque mi hermano está enfermo y no puede ayudarla. Soy el único que está cerca y mis otros hermanos discuten sobre lo que debería hacer. Tengo que estar ahí. Tengo que visitar.
Interpreter: Yes, everyone gets involved in the family problems and it is very stressful to visit but I have to go to help my mom because my brother is sick and can’t help her. I’m the only one close by and my other siblings argue about what I should do. I have to be there. I have to visit.
Medical Profesional: (Empathy) Yes, that must be very difficult for you. Okay, now I understand what is happening. Your visits are necessary but it seems like the stress is affecting your eating patterns and whether you remember to take your metformin. How do you feel if we come up with a plan for when you visit your family now that we know what might be causing your hypoglycemia? Do you think it is a good idea to take high glucose snacks or candy and have them with you on the trip so when you feel dizzy or faint you can eat them?
Interpreter: Sí, eso debe ser muy difícil para ti. De acuerdo, ahora entiendo lo que está pasando. Sus visitas son necesarias, pero parece que el estrés está afectando sus patrones de alimentación y si recuerda tomar su metformina. ¿Cómo se siente si elaboramos un plan para su familia ahora que sabemos lo que podría estar causando su hipoglucemia? ¿Cree que es una buena idea tomar refrigerios con alto contenido de glucosa o dulces y llevarlos consigo durante el viaje para que cuando se sienta mareado o desmayado pueda comerlos?
Mrs. Chavez: Sí, por supuesto. Ni siquiera me di cuenta de eso hasta ahora que hablamos sobre eso. Tienes razón, no he estado comiendo bien cuando lo visito. Me siento terrible cuando estoy allí como si quisiera desmayarme.
Interpreter: Yes of course. I didn’t even really realize that until now that we talked about it. You are right, I haven’t been eating right when I visit. I feel terrible when I am there like I want to faint.
Medical Professional: Mrs. Chavez, sometimes it is helpful to talk about our stress and problems we encournter in life, just to talk through it. Is this something you would be interested in? If so, we can arrange for you to come talk to the social worker.
Interpreter: Sra. Chavez, a veces es útil hablar sobre nuestro estrés y los problemas que alegramos en la vida, solo para hablar sobre ello. ¿Esto es algo que te interesaría? Si tu quieres, podemos hacer arreglos para que vengas a hablar con el trabajador social.
Mrs. Chavez: Tal vez, no estoy seguro, pero tal vez
Interpreter: Maybe, I’m not sure but maybe.
Medical Professional: Okay, you let me know if this is something you would like to do. You can call and let us know and I’ll ask again during our next visit and see how you are dealing with the stress when you visit your family.
Interpreter: De acuerdo, dime si esto es algo que te gustaría hacer. Puede llamar y dejarnos saber, y volveré a preguntar durante nuestra próxima visita y verá cómo lidia con el estrés cuando visita a su familia.
ETHNIC
The ETHNIC interviewing tool (Levin SJ 2000) can be used to explore cross cultural issues and facilitate collaboration during clinical encounters and is designed for clinical students or health professionals permitted to diagnose and provide therapeutic interventions [36]. The specific questions corresponding to the ETHNIC prompts:
- E: Explanation (How do you explain your illness?)
- T: Treatment (What treatment have you tried?)
- H: Healers (Have you sought any advice from folk healers?)
- N: Negotiate (mutually acceptable options)
- I: Intervention (agreed on)
- C: Collaboration (with patient, family, and healers)
Vignette 2
The second vignette is a discussion between a conscientious patient, Mrs. Rodriguez, and her doctor. Mrs. Rodriguez is determined to keep her glucose levels within optimal range by eating healthy and living a natural lifestyle. Included in her natural lifestyle is the use of herbs from her garden and herbal supplements sold to her by her neighbor. Because her numbers have been in the normal range she discontinues her prescribed medication to rely on natural products. However, a trip with family members interrupts her daily routine, which is replaced with fast foods and little rest. Upon returning from her trip her glucose levels increase and she cannot decrease her glucose numbers.
Medical Professional: Good morning Mrs. Rodriguez. I see you are here today for high blood sugar because of your diabetes. (Explanation) Can you share why you think you have recently had higher numbers than normal?
Mrs. Rodriguez: Good morning Doctor. Yes, I am usually very good with my numbers but lately they have gone up and I know why.
Medical Professional: Yes, that is good that you have had your glucose managed. (Explanation) What has caused your numbers to go up Mrs. Rodriguez?
Mrs. Rodriguez: All this American food. I went on a trip to visit my daughter and all we did was eat out, hamburgers, fast food restaurants. They do not cook at home and we were always doing something so I could not cook. It was terrible, all we did was keep busy out and about, I was tired. I spent so much money on food that has chemicals. Look at me now. I can’t seem to get my numbers down.
Medical Professional: Oh, I understand. Yes, a trip can sometimes mess with our routine. (Treatment) Since you have been good at managing your glucose in the past what have you been doing now to get your glucose in normal range?
Mrs. Rodriguez: Well I have been doing the same thing I have always been doing. Eating healthy, resting, gardening, and praying.
Medical Professional: Gardening? That’s really nice. What do you garden?
Mrs. Rodriguez: Oh I love gardening. I plant all types of herbs, vegetables, flowers.
Medical Professional: That is so good Mrs. Rodriguez. I wish I had more time to garden. Do you use your own vegetable and herbs when you cook?
Mrs. Rodriguez: Haha. Yes of course. That is why my sugar was fine before I went on this trip. I rely on my garden to keep me healthy.
Medical Professional: There are so many herbs that are helpful for diabetes. (Treatment) Do you use any to help with your diabetes?
Mrs. Rodriguez: Well yes, in fact, I do. I know you doctors don’t like us to use our herbs but I do. And that was what keeps my sugars normal.
Medical Professional: Oh Mrs. Rodriguez, yes sometimes you hear doctors say this but some herbs are helpful. We just like to know what other things our patients do so we know how to make sure your medications work with certain herbs. (Treatment) I know many people use nopal (cactus), do you eat nopal?
Mrs. Rodriguez: ¿Como no? (of course). I eat them all the time. I make my morning licuado (drink); a little bit of parsley, oregano, oatmeal, lemon, nopal mixed with milk and yogurt.
Medical Professional: (Treatment) Sounds good, what else do you use?
Mrs. Rodriguez: Oh you know other things. Apple cider, cinnamon, cayenne.
Medical Professional: All from your garden?
Mrs. Rodriguez: Yes.
Medical Professional: (Treatment) Do you use any type of herbal supplements from stores or online?
Mrs. Rodriguez: My neighbor sells supplements specifically for diabetes. I started to use a natural supplement with cinnamon, vitamin D, and fish oil. All very natural.
Medical Professional: (Healer) Oh does your neighbor also have diabetes?
Mrs. Rodriguez: No, she sells products. But she sells to many people with diabetes and the supplement works. We get together and she tells us about how they work.
Medical Professional: Do you know the name of this supplement Mrs. Rodriguez?
Mrs. Rodriguez: Oh, gluco…something, it has a heart in the name. But I read the ingredients and it has only natural ingredients. (An FDA banned supplement for false claims)
Medical Professional: Oh I see. I may be familiar with that. Can you bring the supplement along with the medications I have prescribed? I just want to make sure there is not interaction between the two. To get your glucose back to normal I want to make sure we think of every possible situation that could be causing your high numbers. (Treatment) How have you been taking the supplement and the prescribed medications?
Mrs. Rodriguez: Well, I have not refilled your prescription. I was doing so well with my numbers, I’d rather go natural than take all those chemicals.
Medical Professional: Oh, I see Mrs. Rodriguez. Okay, you have done so well controlling your glucose before your trip and now we are in a situation where your numbers are not coming down so let’s try to figure this out. I’d like to learn more about this supplement, so for our next visit can you bring in your supplements so I can take a look at it? (Negotiate) We can then talk about the benefits or cautions. But in the meantime I’d like you to refill your medication and take as followed to see if that helps your sugars. (Negotiate) What do you think? Is this possible?
Mrs. Rodriguez: Oh Doctor, I just don’t like taking chemicals.
Medical Professional: I understand Mrs. Rodriguez. You did take them to start when you first came in for diabetes, is this correct?
Mrs. Rodriguez: Well yes but, I slowly got off them.
Medical Professional: I know it’s difficult to take medications every day but they can help in addition to your healthy eating. I know you are concerned about medications but for now we have to focus on getting your numbers down or your diabetes could become worse and we don’t want you to get there. Do you agree? (Negotiating process)
Mrs. Rodriguez: Well, I am concerned about my numbers.
Medical Professional: (Intervention) Okay well let’s try to get back to where you were before the trip. Let’s get you back on the medication and let’s see if this helps. (Negotiate) For the next visit would you be willing to bring any supplements you are taking along with the medication? (Collaboration) We can talk about the benefits and cautions for the medications and supplements. How does this sound?
Mrs. Rodriguez: Well, I am here to fix my numbers. I have everything I take in a box so I can bring that.
Medical Professional: Yes that would be great. (Collaboration) We can both talk about your daily routine and what have you learned about the supplement, any information or papers that you have, in addition to the medication I prescribed.
Mrs. Rodriguez: Yes I can do that.
Medical Professional: Thank you Mrs. Rodriguez. (Intervention) Also, I’ll have the nurse call you today or tomorrow and you can give her the name of the supplement and she’ll make sure the drug store has a refill for you. Would this work for you Mrs. Rodriguez?
Mrs. Rodriguez: Yes Doctor. You can call me. I’ll have the list ready.
BATHE
Unlike the BELIEF and ETHNIC instruments, the BATHE mnemonic (Lieberman 1999)
- B: Background (What is going on in your life?)
- A: Affect (How do you feel about what is going on?)
- T: Trouble (What troubles you most?)
- H: Handling (How are you handling that?)
- E: Empathy (This must be very difficult for you)
Vignette 3
The last vignette features Mr. Gonzalez, who typically shows a positive outlook on life when visiting his doctor. He is a patient who would not necessarily discuss his emotions if not asked specific questions about his emotional well-being.
Medical Professional: Hello Mr. Gonzalez. (Background) How are you doing today? What’s new? What’s going on in your life lately?
Mr. Gonzalez: Hey, Doctor! I’m good you know just living day to day.
Medical Professional: Good. (Affect) So how is your diabetes treating you day to day? How are you feeling with life and managing your diabetes?
Mr. Gonzalez: Ah well you know, just dealing with it as best as I can.
Medical Professional: Ah okay. As best as you can. (Troubles) What troubles you the most about managing diabetes?
Mr. Gonzalez: Well you know the aches and pains. But what can I do.
Medical Professional: (Affect) How do you feel about those aches and pains?
Mr. Gonzalez: Well it does limit me. I can’t move as well as I use to.
Medical Professional: (Handling) Hmm. I see. How are you handling those aches and pains? What are you doing to relieve it?
Mr. Gonzalez: I do my best with pain cream.
Medical Professional: (Empathy) Pains and aches, that must be difficult. (Affect) How do the aches and pains make you feel?
Mr. Gonzalez: Ahh, Doc, it’s not the same. You know I can’t do the same things anymore.
Medical Professional: (Background) What do you mean? What is not the same anymore?
Mr. Gonzalez: This diabetes, I’m not the same person. I use to be able to be there for my family and community and now I feel like I can’t be there for them the way I use to. I use to be the strong one for my family, helping those in need, and now I’m limited, my body is limited.
Medical Professional: (Affect) How do you feel about that? How does it make you feel emotionally and physically?
Mr. Gonzalez: Bad. I feel bad about it.
Medical Professional: Bad emotionally or physically?
Mr. Gonzalez: Both
Medical Professional: I see. (Handling) How are you dealing with the emotional part of it?
Mr. Gonzalez: I don’t know. I don’t know how.
Medical Professional: (Empathy) Dealing with diabetes and how it makes your body feel can be very emotionally distressing. It is common to feel this way but I want to make sure we also work on how you feel emotionally or how your emotions is affecting your diabetes.
Conclusion
Three mnemonic tools have been suggested to initiate patient-centered and culture-centered communication with patients. Beyond the use of these instruments, there are 2 key skills that are essential for engaging a Hispanic/Latino patient. The first is a non-judgmental, warm communication approach, and the second is astute probing. Once when I was interpreting for a Spanish-speaking Hispanic/Latino patient and English-speaking doctor, the patient expressed to me that she felt that the medical professionals “tienen una cultura fría” (“have a cold culture”), and she did not feel comfortable sharing more about herself because of it. It is also important for medical professionals to be aware of a patient’s doublespeak as a way to share enough information but not all information to keep from being judged by medical professionals. Thus, non-judgmental probing can uncover important information that may be useful for collaborative goal setting and treatment decisions.
The management of diabetes is multifaceted and complex, particularly for populations who face social barriers and challenges. The Hispanic/Latino population is more likely to encounter disparities in access to quality health care and disparities in social determinants of health compared to non-Hispanic whites [4–9]. Therefore, it is important for health professionals to engage Hispanic/Latino patients in self-care by eliciting information that best facilitates collaborative goal setting. Health professionals are in an influential position to leverage a communication style that is empathetic, trusting, and open, setting the tone for a positive patient-physician encounter and, in turn, positive patient outcomes [18–20].
Corresponding author: Jeannie Belinda Concha, PhD, MPH, Dept. of Public Health Sciences, The University of Texas at El Paso, 500 W. University Ave., El Paso, TX 79968, [email protected].
Funding support: Support for this research was provided by the Office of Research and Sponsored Projects at The University of Texas at El Paso.
Financial disclosures: None.
1. American Diabetes Association. American Diabetes Association Standards of Medical Care in Diabetes. Diabetes Care 2017; 40: Suppl 1.
2. Dominguez K, Penman-Aguilar A, Chang MH, et al. Vital signs: Leading causes of death, prevalence of diseases and risk factors, and use of health services among Hispanics in the United States, 2009–2013. MMWR 2015;64:1–10.
3. Commission on Social Determinants of Heath. Closing the gap in a generation: health equity through action on the social determinants of health. Final report on the Commission on Social Determinants of Health. Geneva, World Health Organization. Accessed 10 Sept 2017 at http://apps.who.int/iris/bitstream/10665/43943/1/9789241563703_eng.pdf.
4. Laiterapong N, Fairchild PC, Chou CH, et al. Revisiting disparities in quality of care among US adults with diabetes in the era of individualized care, NHANES 2007-2010. Med Care 2015;53:25–31.
5. Vaccaro JA, Feaster DJ, Lobar SL, et al. Medical advice and diabetes self-management reported by Mexican-American, Black, and White-non-Hispanic adults across the United States. BMC Public Health 2012;12:185.
6. Correa-de-Araujo R, McDermott K, Moy E. Gender differences across racial and ethnic groups in quality of care for diabetes. Women Health Iss 2006;16:56–65.
7. Chawla N, Rodriguez MA, Babey SH, Brown ER. Health policy fact sheet: diabetes among Latinos in California; disparities in access and management. UCLA Center for Health Policy Research. Accessed 1 Aug 2017 at http://healthpolicy.ucla.edu/publications/Documents/PDF/Diabetes%20among%20Latinos%20in%20California%20Disparities%20in%20Access%20and%20Management.pdf.
8. Pu J, Chewning B. Racial differences in diabetes preventive care. Res Social Adm Pharm 2013;9:790–6.
9. Institute of Medicine. Unequal treatment: Confronting racial and ethnic disparities in healthcare. Washington, DC: National Academies Press; 2003.
10. Saha S, Arbeaez JJ, Cooper LA. Patient-physician relationships and racial disparities in the quality of care. Am J Public Health 2003;93:1713–9.
11. What is cultural and linguistic competence?: Definitions, February 2003. Agency for Healthcare Research and Quality, Rockville, MD. Accessed 28 Aug 2017 at http://www.ahrq.gov/pprofessionals/systems/primary -care/cultural-competence-mco/cultcompdef.html.
12. U.S. Department of Health and Human Services, Office of Minority Health. 2000. Assuring cultural competence in health care: Recommendations for National Standards and an outcomes-focused research agenda. Accessed 17 August 2017 at http://www.omhrc.gov/clas/finalpo.htm.
13. Zhao X. Relationships between sources of health information and diabetes knowledge in the US Hispanic population. Health Commun 2014;29:574–85.
14. Perchman ML, Flannagan D, Ferrer RL, Matamoras M. Communication compete c e, self-care behaviors, and glucose control in patients with type 2 diabetes. Patient Educ Couns 2009;77:55–9.
15. Reimann JOF, Talavera GA, Salmon M, et al. Cultural competence among physicians treating Mexican Americans who have diabetes: a structural model. Soc Sci Med 2004;59:2195–205.
16. Gordon HS, Gerber BS. What we’ve got here is a failure to communication. J Gen Intern Med 2011;26:104–6.
17. Gonzalez A, Salas D, Umpierrez GE. Special considerations on the management of Latino patients with type 2 diabetes mellitus. Curr Med Res Opin 2011;27:969–79.
18. Peek ME, Cargill A, Juang ES. Diabetes health disparities: A systematic review of health care interventions. Med Care Res Rev 2007;64(5 Supp):101S–156S.
19. Kutob RM, Bormanis J, Crago M, et al. Assessing culturally competent diabetes care with unannounced standardized patients. Fam Med 2013;45:400–8.
20. Weller SC, Baer RD, Garcia de Alba Garcia J, Salcedo Rocha AL. Are differences between patient and provider explanatory models of diabetes associated with patient self-management and glycemic control? J Health Care Poor Underserved 2013:24;1498–510.
21. Duta MJ. Communicating about culture and health: Theorizing culture-centered and cultural sensitivity approaches. Commun Theory 2007;17:304–28.
22. Concha JB, Mayer SD, Mezuk B, Avula D. Diabetes causation beliefs among Spanish speaking patients. Diabetes Educ 2015:42:116–25.
23. Arcury TA, Skelly AH, Gesler WM, et al. Diabetes meanings among those without diabetes: explanatory models of immigrant Latinos in rural North Carolina. Soc Sci Med 2004;59:2183–3.
24. Daniulaityte R. Making sense of diabetes: cultural models, gender and individual adjustment to type 2 diabetes in a Mexican community. Soc Sci Med 2004;59:1899–912.
25. Poss J, Jezewski MA. The role and meaning of susto in Mexican American’s explanatory model of type 2 diabetes. Med Anthropol Q 2002;16:360–77.
26. Weller SC, Baer RD, Pachter LM, et al. Latino beliefs about diabetes. Diabetes Care 1999;22:722–8.
27. United States Census Bureau. Language use. Accessed Sept 2017 at https://www.census.gov/topics/population/language-use/about.html.
28. Mezuk B, Albrecht S, Eaton WW, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care 2008;31:2383–90.
29. Li C, Ford ES, Strine TW, Mokdad AH. Prevalence of depression among US adults with diabetes. Diabetes Care 2007;31:105–7.
30. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2006;24:1069–78.
31. Li C, Barker L, Ford ES, et al. Diabetes and anxiety In US adults: findings from the 2006 Behavioral Risk Factor Surveillance System. Diabetes Med 2008;25:878–81.
32. Concha JB, Mezuk B, Duran B. Culture-centered approaches: the relevance of assessing emotional health for Latinos with type 2 diabetes. BMJ Open Diab Res Care 2015;3.
33. Bentancourt JR, Green AR, Carillo Je, Park ER. Cultural competence and health care: Key perspectives and trends. Health Affairs 2015;24:499–506.
34. Association of American Medical Colleges. Cultural Competence Education 2005. Accessed Feb 2016 at https://www.aamc.org/download/54338/data/.
35. Dobbie AE, Medrano M, Tysinger J, Olney C. The BELIEF Instrument: A preclinical teaching tool to elicit patients’ health beliefs. Family Med 2003;35:316–9.
36. Levin SJ, Like RC, Gottlieb JE. ETHNIC: A framework for culturally competent ethical practice. Patient Care 2003;34:188–9.
37. Stuart MR, Leibermann JR. The fifteen-minute hour: applied psychotherapy for the primary care physician. New York: Praeger.
38. Pace EJ, Somerville NJ, Enyoha C, et al. Effects of a brief psychosocial intervention on inpatient satisfaction: a randomized control trial. Fam Med 2017;49:675–8.
From the University of Texas at El Paso, El Paso, TX.
Abstract
- Objective: To demonstrate the applied use of recommended cultural competency communication tools.
- Methods: An overview of several cultural competency tools is presented and vignettes are used to demonstrate the use of these tools with Hispanic patients with diabetes.
- Results: Three communication mnemonic instruments, ie, BELIEF, ETHNIC, and BATHE, may be useful for engaging health professionals in patient-centered communication with their Hispanic patients and shared decision making. Health professionals can also employ nonjudgmental probing as part of engaging patients in setting diabetes treatment goals.
- Conclusion: Health professionals are in an influential position to leverage a patient- and culture-centered communication style to improve communication with Hispanic patients. Using mnemonic tools can help facilitate this communication and improve health professionals’ understanding on how cultural and social factors influence diabetes management in this population.
Key words: Hispanic/Latino; diabetes; patient-centered communication; cultural-competency.
The 2017 American Diabetes Association (ADA) Standards of Medical Care recommend that health professionals engage in a patient-centered communication style with patient to facilitate shared decision-making and improve diabetes outcomes. The ADA defines patient-centered communication as “a style that uses active listening, elicits patient preferences and beliefs, and assesses literacy, numeracy, and potential barriers to care” [1]. One of the main goals of using patient-centered communication is to create a collaborative, personal, and non-judgmental relationship with patients. These guidelines, however, provide less direction on the type of communication skills training that would facilitate this type of communication, particularly as it relates to ethnic/racial minority groups most at risk for diabetes and related complications.
The US Hispanic/Latino population, in particular, is a group that is burdened by the diabetes epidemic, with a prevalence that is 130% higher than non-Hispanic whites [2]. It is widely known that certain social determinants of health, like socioeconomic status, social injustices, poor access to health care, food insecurity, or living in environments that do not support health behaviors, all contribute to health disparities for Hispanics/Latinos [3]. Understanding how Hispanics/Latinos cope with these social determinants of health is important for health care professionals, and a patient-centered communication style is an ideal approach for active listening and eliciting information about the social barriers/challenges that may influence diabetes self-care. However, there is some evidence that suggests this approach is not fully used by health care professionals when communicating with Hispanics/Latinos with diabetes, and Hispanics/Latinos continue to be more likely to experience disparities in the quality of diabetes care they receive compared to non-Hispanic whites [4–9]. One of the identified contributors to these disparities is the poor communication between physicians and Hispanic/Latino patients [10–16]. Given that health care professionals are the primary source of health care and diabetes information for Hispanics/Latinos, it is important for health professionals to enhance their patient-centered communications skills to improve the quality of care that is provided to this population [12].
Cultural Competence and Patient-Centered Communication
Not all health professional communication skills are perceived as unsatisfactory by Hispanic/Latino patients with diabetes. In fact, Hispanics/Latinos report a positive provider-patient clinical interaction when health professionals display cultural competency skills [15,17–20]. Moreover, evidence suggest that Hispanic/Latino patients with diabetes reported better quality of care and improved self-management behaviors with a culturally competent provider [18–20]. Cultural competency is described as “understanding and responding effectively to the cultural and linguistic needs brought by the patient to the health care encounter” and “valuing diversity, provider self-assessment, managing dynamics of differences, acquiring and institutionalizing knowledge, and adapting to diversity and the cultural context of individuals served” [9,11,12]. One approach for gaining cultural competency skills is to understand how the disease process is conceptualized within a culture and how that influences a patient’s own theory about their disease etiology, prognosis, and outcome [21]. This approach is known as culture-centered in the health communications literature and may be useful when communicating with Hispanic/Latino patients with diabetes because there is extensive literature describing unique indigenous Latin American explanatory models for diabetes [22–26].
Language Discordance in Physician-Patient Communication
The process of patient-physician communication includes “attending to one another and begin interpreting one another’s verbal and nonverbal” interactions [9]. A conventional assumption regarding the disparities in diabetes care quality for Hispanic/Latino patients is that it stems from language discordant patient-physician interactions, which result in errors in the provision of diabetes information and treatment instructions regarding medications and self-care behaviors [9]. While language is a contributing factor, the US Census reports that over half of US Hispanics/Latinos are bilingual and speak English “very well” [27]. Thus, other underlying mechanisms must be contributing to patient-physician miscommunication and suboptimal diabetes outcomes. Moreover, the findings from studies of patient-physician language concordance and diabetes management are inconsistent. For example, language concordance between Hispanic/Latino patients and physicians is associated with improvement in HbA1c but not self-care behaviors (ie, healthy eating, self-monitoring, medicine adherence, exercise) [20]. Thus, there is need to move beyond spoken language to address elements of interpersonal communication around diabetes care through addressing cultural health beliefs and explanatory models of diabetes.
Cultural Explanatory Models of Diabetes
Explanatory models for diabetes among Hispanics/Latinos are diverse and often include a biomedical framework (eg, obesity, unhealthy eating, sedentary lifestyle, genetics); however, there is one unique indigenous belief that continues to be held within this population. Specifically, there is a cultural belief that diabetes is caused by strong or negative emotions, like fright sickness (susto), stress (estres), anger (coraje), or nerves (nervios) [22–26]. Although this cultural belief has been in existence long before scientific evidence has shown the bi-directional relationship between stress/depression and diabetes, the integration of emotions in diabetes self-management in patient-provider communication has not been standardized [28–31]. Health professionals’ interest in how patients view their own disease process may help build rapport with patients. Enhancing health professionals’ cultural competency skills can be a critical first step for improving patient-provider communication. For instance, it can (1) present an opportunity to integrate cultural belief systems into diabetes care for Hispanics/Latinos, (2) open the door for other important conversations about Hispanic/Latino patients’ psychosocial and familial environment and identify barriers or motivators in diabetes self-management, and (3) build rapport and trust between the health professional and patient.
Additionally, inquiring about emotional beliefs or emotions about diabetes in general can help improve the patient-provider relationship, giving Hispanic/Latino patients a sense that their provider cares about their feelings and emotional well-being. For example, in a study conducted by Concha et al, a Hispanic/Latino male patient with diabetes expresses his appreciation of his doctor for attending to his emotional problems and suggests that his diabetes is in control because of the encouragement he receives from the doctor [22].
…I believe the doctors..can encourage one with ..diabetes… I am very grateful to God before anything that till today I have my sugar controlled. I am a diabetic, but controlled. And Dr. [name omitted], he’s a blessing from God. He knows my body like my mother….Because whatever little thing, he attends to me, he gives me a lot of encouragement with my emotional problems. He sent me to a counselor, I have a specialist for my problem with my urinary tracts. I have attention, I have all the attention from the doctor…
Inquiring about emotional well-being may also be beneficial because Hispanics/Latinos with diabetes have reported that they would feel more comfortable talking to a professional about personal problems compared to Hispanics/Latinos without diabetes [32]. Having a physical illness may provide an opportunity for these patients to discuss stress or depression in tandem with diabetes to diminish any possible stigma or shame associated with having a mental health problem. It is important for health care providers to be aware of emotional or social problems that may be negatively influencing diabetes self-care behaviors.
Models of Effective Cross-Cultural Communication
Cultural competency training for health professionals is one strategy for reducing health disparities and ensuring that racial/ethnic populations receive “equitable, effective, and culturally appropriate clinical care” [9,11,12,33]. The Association of American Medical Colleges’ guide for cultural competence education in medical school cites several models of effective cross-cultural communication for physicians and/or physician assistants [34]. I describe 3 communication tools below that may help health care professionals initiate conversations and aid them in understanding how to better manage sociocultural and environmental issues that may impede patients’ ability to manage diabetes. For each tool, a vignette is offered that illustrates how the tool may be used in communicating with Hispanic/Latino patients.
BELIEF
The BELIEF instrument (Dobbie 2003) is a teaching tool designed to elicit patients’ health beliefs and to assist preclinical medical students or medical professionals in understanding how explanatory models of a disease influence patient engagement in care. The BELIEF instrument is straightforward and can be easily implemented into clinical case vignettes and or role-play as part of cultural competency training [35]. The specific questions corresponding to the BELIEF prompts are
- B: Beliefs about health (What caused your illness/problem?)
- E: Explanation (Why did it happen at this time?)
- L: Learn (Help me understand your belief/opinion)
- I: Impact (How is this illness/problem impacting your life?)
- E: Empathy (This must be very hard for you)
- F: Feelings (How are you feeling about it?)
Vignette 1
The following vignette is a conversation between a Spanish-speaking Hispanic women, a language interpreter, and medical professional. The patient, Mrs. Chavez, has come into the clinic for the third time after experiencing symptoms due to hypoglycemia. Mrs. Chavez believes stress may have something to do with her hypoglycemia but is not quite sure how. By using the BELIEF mnemonic, the medical professional is able to ask more about the stress that led into a discussion about how stress actually influenced her eating and medication intake behaviors. Through this probing, the medical professional was able to identify the possible cause of her hypoglycemia and work with Mrs. Chavez on finding a solution every time she experiences the stressful event. The vignette also demonstrates how interpreters may share cultural information that may clarify problems.
Medical Professional: Mrs. Chavez, I see you are here again for hypoglycemia. Can you tell me what has happened? Do you have your medications with you today?
Interpreter: Sra. Chavez, entiendo que está aquí nuevamente por hipoglucemia. ¿Puedes decirme qué ha pasado? ¿Tiene sus medicamentos con usted hoy?
Mrs. Chavez: Si, me ha sentido débil y mareado.
Interpreter: Yes I have felt faint and dizzy?
Medical Professional: Have you been taking your metformin as prescribed?
Interpreter: ¿Ha estado tomando su metformin según lo recetado?
Mrs. Chavez: Si (YES).
Medical Professional: We might have to consider adjusting your dosage.
Interpreter: Es posible que tengamos que considerar ajustar su dosis.
Mrs. Chavez privately to the Interpreter: ¿no es posible que las emociones o nervios puedan causar algo? He escuchado que este puede ser el problema?
Interpreter to Mrs. Chavez: Déjame preguntarle al doctor, si?
Let me ask the doctor, yes? (Mrs. Chavez, nods in agreement)
Interpreter to Medical Professional: She is asking if emotions or nervousness could be the cause. She has heard that this could be the problem.
Medical Profesional to Interpreter: What does she mean?
Interpreter: There is a cultural belief that stress or nerves can cause diabetes or affect diabetes. You may want to ask about this.
Medical Professional: Yes emotions like stress can cause changes in you glucose. (Beliefs) Do you believe that some emotions are causing your hypoglycemia?
Interpreter: Sí, las emociones como el estrés pueden provocar cambios en la glucosa. ¿Crees que algunas emociones están causando tu hipoglucemia?
Mrs. Chavez: (Shrugs shoulders).
Medical Professional: I see here in your records, that the other two times you had hypoglycemica were 1 month and 3 months ago. (Beliefs) What do you think caused these events and (Explanation) why do you think it happened during these times?
Interpreter: Veo aquí en sus registros que las otras dos veces que tuvo hipoglucemia fueron hace 1 mes y 3 meses. ¿Qué crees que causó estos eventos y por qué crees que sucedió durante estos tiempos?
Mrs. Chavez: Pues, no sé.
Interpreter: Well I don’t know.
Medical Professional: (Learn) Help me understand what you think happened 3 and 1 month ago and this month that may have caused your glucose to drop. What was happening emotionally during these times? Do you remember?
Interpreter: Ayúdame a entender lo que piensas que sucedió hace 3 y 1 meses y este mes, puede haber causado que tu glucosa baje. ¿Qué estaba pasando emocionalmente durante este tiempo? ¿Te acuerdas?
Mrs. Chavez: Hmm. Pues, hace 3 meses fui a visitar a mi madre y hace 1 meses fui a visitar a mi hermano al norte.
Interpreter: Hmm. Well 3 months ago I went to visit my mother and 1 months ago I went to visit my brother up north.
Medical Professional: (Learn) How were those trips for you. Did you have fun? What types of emotions were you feeling during these trips?
Interpreter: ¿Cómo fueron esos viajes para ti? ¿Te divertiste? ¿Qué tipo de emociones sentías durante estos viajes?
Mrs. Chavez: Pues, yo estaba muy estresado durante mis viajes.
Interpreter: Well, I was very stressed during my trips.
Medical Professional: (Learn) Would you like to share why you were stressed? What was happening for you to feel so stressed?
Interpreter: ¿Te gustaría compartir por qué estabas estresado? ¿Qué estaba pasando para que te sientas tan estresado?
Mrs. Chavez: Bueno, tenemos muchos problemas familiares y conflictos. Hay muchos argumentos familiares y se vuelve estresante.
Interpreter: Well we have a lot of family problems and conflict. There are a lot of family arguments and it gets stressful.
Medical Professional: (Impact) How do you think this has affected your glucose?
Interpreter: ¿Cómo crees que esto ha afectado tu glucosa?
Mrs. Chavez: No lo sé.
Interpreter: I don’t know.
Medical Professional: (Learn) Do you think the stress maybe led you to forget to take your medication or affected your eating?
Interprter: ¿Crees que el estrés puede llevarte a olvidarte de tomar tu medicación o afectó su alimentación?
Mrs. Chavez: Pues si y no comí. Estaba demasiado estresado para comer. Raramente comí mientras estaba allí. Estaba tan estresado que no tenía apetito.
Interpreter: Well yes and I didn’t eat. I was too stressed to eat. I rarely ate while I was there. I was so stressed i did not have an appetite.
Medical Professional: (Empathy) Mrs. Chavez, that must have been very hard for you. I’m sorry you have had to feel this way. (Feelings) Is this how you feel everytime you visit your family?
Interpreter: Sra. Chávez, eso debe haber sido muy difícil para usted. Lamento que hayas tenido que sentirte de esta manera. ¿Es así como te sientes cada vez que visitas a tu familia?
Mrs. Chavez: Sí, todos se involucran en los problemas familiares y es muy estresante visitarlos, pero tengo que ir a ayudar a mi madre porque mi hermano está enfermo y no puede ayudarla. Soy el único que está cerca y mis otros hermanos discuten sobre lo que debería hacer. Tengo que estar ahí. Tengo que visitar.
Interpreter: Yes, everyone gets involved in the family problems and it is very stressful to visit but I have to go to help my mom because my brother is sick and can’t help her. I’m the only one close by and my other siblings argue about what I should do. I have to be there. I have to visit.
Medical Profesional: (Empathy) Yes, that must be very difficult for you. Okay, now I understand what is happening. Your visits are necessary but it seems like the stress is affecting your eating patterns and whether you remember to take your metformin. How do you feel if we come up with a plan for when you visit your family now that we know what might be causing your hypoglycemia? Do you think it is a good idea to take high glucose snacks or candy and have them with you on the trip so when you feel dizzy or faint you can eat them?
Interpreter: Sí, eso debe ser muy difícil para ti. De acuerdo, ahora entiendo lo que está pasando. Sus visitas son necesarias, pero parece que el estrés está afectando sus patrones de alimentación y si recuerda tomar su metformina. ¿Cómo se siente si elaboramos un plan para su familia ahora que sabemos lo que podría estar causando su hipoglucemia? ¿Cree que es una buena idea tomar refrigerios con alto contenido de glucosa o dulces y llevarlos consigo durante el viaje para que cuando se sienta mareado o desmayado pueda comerlos?
Mrs. Chavez: Sí, por supuesto. Ni siquiera me di cuenta de eso hasta ahora que hablamos sobre eso. Tienes razón, no he estado comiendo bien cuando lo visito. Me siento terrible cuando estoy allí como si quisiera desmayarme.
Interpreter: Yes of course. I didn’t even really realize that until now that we talked about it. You are right, I haven’t been eating right when I visit. I feel terrible when I am there like I want to faint.
Medical Professional: Mrs. Chavez, sometimes it is helpful to talk about our stress and problems we encournter in life, just to talk through it. Is this something you would be interested in? If so, we can arrange for you to come talk to the social worker.
Interpreter: Sra. Chavez, a veces es útil hablar sobre nuestro estrés y los problemas que alegramos en la vida, solo para hablar sobre ello. ¿Esto es algo que te interesaría? Si tu quieres, podemos hacer arreglos para que vengas a hablar con el trabajador social.
Mrs. Chavez: Tal vez, no estoy seguro, pero tal vez
Interpreter: Maybe, I’m not sure but maybe.
Medical Professional: Okay, you let me know if this is something you would like to do. You can call and let us know and I’ll ask again during our next visit and see how you are dealing with the stress when you visit your family.
Interpreter: De acuerdo, dime si esto es algo que te gustaría hacer. Puede llamar y dejarnos saber, y volveré a preguntar durante nuestra próxima visita y verá cómo lidia con el estrés cuando visita a su familia.
ETHNIC
The ETHNIC interviewing tool (Levin SJ 2000) can be used to explore cross cultural issues and facilitate collaboration during clinical encounters and is designed for clinical students or health professionals permitted to diagnose and provide therapeutic interventions [36]. The specific questions corresponding to the ETHNIC prompts:
- E: Explanation (How do you explain your illness?)
- T: Treatment (What treatment have you tried?)
- H: Healers (Have you sought any advice from folk healers?)
- N: Negotiate (mutually acceptable options)
- I: Intervention (agreed on)
- C: Collaboration (with patient, family, and healers)
Vignette 2
The second vignette is a discussion between a conscientious patient, Mrs. Rodriguez, and her doctor. Mrs. Rodriguez is determined to keep her glucose levels within optimal range by eating healthy and living a natural lifestyle. Included in her natural lifestyle is the use of herbs from her garden and herbal supplements sold to her by her neighbor. Because her numbers have been in the normal range she discontinues her prescribed medication to rely on natural products. However, a trip with family members interrupts her daily routine, which is replaced with fast foods and little rest. Upon returning from her trip her glucose levels increase and she cannot decrease her glucose numbers.
Medical Professional: Good morning Mrs. Rodriguez. I see you are here today for high blood sugar because of your diabetes. (Explanation) Can you share why you think you have recently had higher numbers than normal?
Mrs. Rodriguez: Good morning Doctor. Yes, I am usually very good with my numbers but lately they have gone up and I know why.
Medical Professional: Yes, that is good that you have had your glucose managed. (Explanation) What has caused your numbers to go up Mrs. Rodriguez?
Mrs. Rodriguez: All this American food. I went on a trip to visit my daughter and all we did was eat out, hamburgers, fast food restaurants. They do not cook at home and we were always doing something so I could not cook. It was terrible, all we did was keep busy out and about, I was tired. I spent so much money on food that has chemicals. Look at me now. I can’t seem to get my numbers down.
Medical Professional: Oh, I understand. Yes, a trip can sometimes mess with our routine. (Treatment) Since you have been good at managing your glucose in the past what have you been doing now to get your glucose in normal range?
Mrs. Rodriguez: Well I have been doing the same thing I have always been doing. Eating healthy, resting, gardening, and praying.
Medical Professional: Gardening? That’s really nice. What do you garden?
Mrs. Rodriguez: Oh I love gardening. I plant all types of herbs, vegetables, flowers.
Medical Professional: That is so good Mrs. Rodriguez. I wish I had more time to garden. Do you use your own vegetable and herbs when you cook?
Mrs. Rodriguez: Haha. Yes of course. That is why my sugar was fine before I went on this trip. I rely on my garden to keep me healthy.
Medical Professional: There are so many herbs that are helpful for diabetes. (Treatment) Do you use any to help with your diabetes?
Mrs. Rodriguez: Well yes, in fact, I do. I know you doctors don’t like us to use our herbs but I do. And that was what keeps my sugars normal.
Medical Professional: Oh Mrs. Rodriguez, yes sometimes you hear doctors say this but some herbs are helpful. We just like to know what other things our patients do so we know how to make sure your medications work with certain herbs. (Treatment) I know many people use nopal (cactus), do you eat nopal?
Mrs. Rodriguez: ¿Como no? (of course). I eat them all the time. I make my morning licuado (drink); a little bit of parsley, oregano, oatmeal, lemon, nopal mixed with milk and yogurt.
Medical Professional: (Treatment) Sounds good, what else do you use?
Mrs. Rodriguez: Oh you know other things. Apple cider, cinnamon, cayenne.
Medical Professional: All from your garden?
Mrs. Rodriguez: Yes.
Medical Professional: (Treatment) Do you use any type of herbal supplements from stores or online?
Mrs. Rodriguez: My neighbor sells supplements specifically for diabetes. I started to use a natural supplement with cinnamon, vitamin D, and fish oil. All very natural.
Medical Professional: (Healer) Oh does your neighbor also have diabetes?
Mrs. Rodriguez: No, she sells products. But she sells to many people with diabetes and the supplement works. We get together and she tells us about how they work.
Medical Professional: Do you know the name of this supplement Mrs. Rodriguez?
Mrs. Rodriguez: Oh, gluco…something, it has a heart in the name. But I read the ingredients and it has only natural ingredients. (An FDA banned supplement for false claims)
Medical Professional: Oh I see. I may be familiar with that. Can you bring the supplement along with the medications I have prescribed? I just want to make sure there is not interaction between the two. To get your glucose back to normal I want to make sure we think of every possible situation that could be causing your high numbers. (Treatment) How have you been taking the supplement and the prescribed medications?
Mrs. Rodriguez: Well, I have not refilled your prescription. I was doing so well with my numbers, I’d rather go natural than take all those chemicals.
Medical Professional: Oh, I see Mrs. Rodriguez. Okay, you have done so well controlling your glucose before your trip and now we are in a situation where your numbers are not coming down so let’s try to figure this out. I’d like to learn more about this supplement, so for our next visit can you bring in your supplements so I can take a look at it? (Negotiate) We can then talk about the benefits or cautions. But in the meantime I’d like you to refill your medication and take as followed to see if that helps your sugars. (Negotiate) What do you think? Is this possible?
Mrs. Rodriguez: Oh Doctor, I just don’t like taking chemicals.
Medical Professional: I understand Mrs. Rodriguez. You did take them to start when you first came in for diabetes, is this correct?
Mrs. Rodriguez: Well yes but, I slowly got off them.
Medical Professional: I know it’s difficult to take medications every day but they can help in addition to your healthy eating. I know you are concerned about medications but for now we have to focus on getting your numbers down or your diabetes could become worse and we don’t want you to get there. Do you agree? (Negotiating process)
Mrs. Rodriguez: Well, I am concerned about my numbers.
Medical Professional: (Intervention) Okay well let’s try to get back to where you were before the trip. Let’s get you back on the medication and let’s see if this helps. (Negotiate) For the next visit would you be willing to bring any supplements you are taking along with the medication? (Collaboration) We can talk about the benefits and cautions for the medications and supplements. How does this sound?
Mrs. Rodriguez: Well, I am here to fix my numbers. I have everything I take in a box so I can bring that.
Medical Professional: Yes that would be great. (Collaboration) We can both talk about your daily routine and what have you learned about the supplement, any information or papers that you have, in addition to the medication I prescribed.
Mrs. Rodriguez: Yes I can do that.
Medical Professional: Thank you Mrs. Rodriguez. (Intervention) Also, I’ll have the nurse call you today or tomorrow and you can give her the name of the supplement and she’ll make sure the drug store has a refill for you. Would this work for you Mrs. Rodriguez?
Mrs. Rodriguez: Yes Doctor. You can call me. I’ll have the list ready.
BATHE
Unlike the BELIEF and ETHNIC instruments, the BATHE mnemonic (Lieberman 1999)
- B: Background (What is going on in your life?)
- A: Affect (How do you feel about what is going on?)
- T: Trouble (What troubles you most?)
- H: Handling (How are you handling that?)
- E: Empathy (This must be very difficult for you)
Vignette 3
The last vignette features Mr. Gonzalez, who typically shows a positive outlook on life when visiting his doctor. He is a patient who would not necessarily discuss his emotions if not asked specific questions about his emotional well-being.
Medical Professional: Hello Mr. Gonzalez. (Background) How are you doing today? What’s new? What’s going on in your life lately?
Mr. Gonzalez: Hey, Doctor! I’m good you know just living day to day.
Medical Professional: Good. (Affect) So how is your diabetes treating you day to day? How are you feeling with life and managing your diabetes?
Mr. Gonzalez: Ah well you know, just dealing with it as best as I can.
Medical Professional: Ah okay. As best as you can. (Troubles) What troubles you the most about managing diabetes?
Mr. Gonzalez: Well you know the aches and pains. But what can I do.
Medical Professional: (Affect) How do you feel about those aches and pains?
Mr. Gonzalez: Well it does limit me. I can’t move as well as I use to.
Medical Professional: (Handling) Hmm. I see. How are you handling those aches and pains? What are you doing to relieve it?
Mr. Gonzalez: I do my best with pain cream.
Medical Professional: (Empathy) Pains and aches, that must be difficult. (Affect) How do the aches and pains make you feel?
Mr. Gonzalez: Ahh, Doc, it’s not the same. You know I can’t do the same things anymore.
Medical Professional: (Background) What do you mean? What is not the same anymore?
Mr. Gonzalez: This diabetes, I’m not the same person. I use to be able to be there for my family and community and now I feel like I can’t be there for them the way I use to. I use to be the strong one for my family, helping those in need, and now I’m limited, my body is limited.
Medical Professional: (Affect) How do you feel about that? How does it make you feel emotionally and physically?
Mr. Gonzalez: Bad. I feel bad about it.
Medical Professional: Bad emotionally or physically?
Mr. Gonzalez: Both
Medical Professional: I see. (Handling) How are you dealing with the emotional part of it?
Mr. Gonzalez: I don’t know. I don’t know how.
Medical Professional: (Empathy) Dealing with diabetes and how it makes your body feel can be very emotionally distressing. It is common to feel this way but I want to make sure we also work on how you feel emotionally or how your emotions is affecting your diabetes.
Conclusion
Three mnemonic tools have been suggested to initiate patient-centered and culture-centered communication with patients. Beyond the use of these instruments, there are 2 key skills that are essential for engaging a Hispanic/Latino patient. The first is a non-judgmental, warm communication approach, and the second is astute probing. Once when I was interpreting for a Spanish-speaking Hispanic/Latino patient and English-speaking doctor, the patient expressed to me that she felt that the medical professionals “tienen una cultura fría” (“have a cold culture”), and she did not feel comfortable sharing more about herself because of it. It is also important for medical professionals to be aware of a patient’s doublespeak as a way to share enough information but not all information to keep from being judged by medical professionals. Thus, non-judgmental probing can uncover important information that may be useful for collaborative goal setting and treatment decisions.
The management of diabetes is multifaceted and complex, particularly for populations who face social barriers and challenges. The Hispanic/Latino population is more likely to encounter disparities in access to quality health care and disparities in social determinants of health compared to non-Hispanic whites [4–9]. Therefore, it is important for health professionals to engage Hispanic/Latino patients in self-care by eliciting information that best facilitates collaborative goal setting. Health professionals are in an influential position to leverage a communication style that is empathetic, trusting, and open, setting the tone for a positive patient-physician encounter and, in turn, positive patient outcomes [18–20].
Corresponding author: Jeannie Belinda Concha, PhD, MPH, Dept. of Public Health Sciences, The University of Texas at El Paso, 500 W. University Ave., El Paso, TX 79968, [email protected].
Funding support: Support for this research was provided by the Office of Research and Sponsored Projects at The University of Texas at El Paso.
Financial disclosures: None.
From the University of Texas at El Paso, El Paso, TX.
Abstract
- Objective: To demonstrate the applied use of recommended cultural competency communication tools.
- Methods: An overview of several cultural competency tools is presented and vignettes are used to demonstrate the use of these tools with Hispanic patients with diabetes.
- Results: Three communication mnemonic instruments, ie, BELIEF, ETHNIC, and BATHE, may be useful for engaging health professionals in patient-centered communication with their Hispanic patients and shared decision making. Health professionals can also employ nonjudgmental probing as part of engaging patients in setting diabetes treatment goals.
- Conclusion: Health professionals are in an influential position to leverage a patient- and culture-centered communication style to improve communication with Hispanic patients. Using mnemonic tools can help facilitate this communication and improve health professionals’ understanding on how cultural and social factors influence diabetes management in this population.
Key words: Hispanic/Latino; diabetes; patient-centered communication; cultural-competency.
The 2017 American Diabetes Association (ADA) Standards of Medical Care recommend that health professionals engage in a patient-centered communication style with patient to facilitate shared decision-making and improve diabetes outcomes. The ADA defines patient-centered communication as “a style that uses active listening, elicits patient preferences and beliefs, and assesses literacy, numeracy, and potential barriers to care” [1]. One of the main goals of using patient-centered communication is to create a collaborative, personal, and non-judgmental relationship with patients. These guidelines, however, provide less direction on the type of communication skills training that would facilitate this type of communication, particularly as it relates to ethnic/racial minority groups most at risk for diabetes and related complications.
The US Hispanic/Latino population, in particular, is a group that is burdened by the diabetes epidemic, with a prevalence that is 130% higher than non-Hispanic whites [2]. It is widely known that certain social determinants of health, like socioeconomic status, social injustices, poor access to health care, food insecurity, or living in environments that do not support health behaviors, all contribute to health disparities for Hispanics/Latinos [3]. Understanding how Hispanics/Latinos cope with these social determinants of health is important for health care professionals, and a patient-centered communication style is an ideal approach for active listening and eliciting information about the social barriers/challenges that may influence diabetes self-care. However, there is some evidence that suggests this approach is not fully used by health care professionals when communicating with Hispanics/Latinos with diabetes, and Hispanics/Latinos continue to be more likely to experience disparities in the quality of diabetes care they receive compared to non-Hispanic whites [4–9]. One of the identified contributors to these disparities is the poor communication between physicians and Hispanic/Latino patients [10–16]. Given that health care professionals are the primary source of health care and diabetes information for Hispanics/Latinos, it is important for health professionals to enhance their patient-centered communications skills to improve the quality of care that is provided to this population [12].
Cultural Competence and Patient-Centered Communication
Not all health professional communication skills are perceived as unsatisfactory by Hispanic/Latino patients with diabetes. In fact, Hispanics/Latinos report a positive provider-patient clinical interaction when health professionals display cultural competency skills [15,17–20]. Moreover, evidence suggest that Hispanic/Latino patients with diabetes reported better quality of care and improved self-management behaviors with a culturally competent provider [18–20]. Cultural competency is described as “understanding and responding effectively to the cultural and linguistic needs brought by the patient to the health care encounter” and “valuing diversity, provider self-assessment, managing dynamics of differences, acquiring and institutionalizing knowledge, and adapting to diversity and the cultural context of individuals served” [9,11,12]. One approach for gaining cultural competency skills is to understand how the disease process is conceptualized within a culture and how that influences a patient’s own theory about their disease etiology, prognosis, and outcome [21]. This approach is known as culture-centered in the health communications literature and may be useful when communicating with Hispanic/Latino patients with diabetes because there is extensive literature describing unique indigenous Latin American explanatory models for diabetes [22–26].
Language Discordance in Physician-Patient Communication
The process of patient-physician communication includes “attending to one another and begin interpreting one another’s verbal and nonverbal” interactions [9]. A conventional assumption regarding the disparities in diabetes care quality for Hispanic/Latino patients is that it stems from language discordant patient-physician interactions, which result in errors in the provision of diabetes information and treatment instructions regarding medications and self-care behaviors [9]. While language is a contributing factor, the US Census reports that over half of US Hispanics/Latinos are bilingual and speak English “very well” [27]. Thus, other underlying mechanisms must be contributing to patient-physician miscommunication and suboptimal diabetes outcomes. Moreover, the findings from studies of patient-physician language concordance and diabetes management are inconsistent. For example, language concordance between Hispanic/Latino patients and physicians is associated with improvement in HbA1c but not self-care behaviors (ie, healthy eating, self-monitoring, medicine adherence, exercise) [20]. Thus, there is need to move beyond spoken language to address elements of interpersonal communication around diabetes care through addressing cultural health beliefs and explanatory models of diabetes.
Cultural Explanatory Models of Diabetes
Explanatory models for diabetes among Hispanics/Latinos are diverse and often include a biomedical framework (eg, obesity, unhealthy eating, sedentary lifestyle, genetics); however, there is one unique indigenous belief that continues to be held within this population. Specifically, there is a cultural belief that diabetes is caused by strong or negative emotions, like fright sickness (susto), stress (estres), anger (coraje), or nerves (nervios) [22–26]. Although this cultural belief has been in existence long before scientific evidence has shown the bi-directional relationship between stress/depression and diabetes, the integration of emotions in diabetes self-management in patient-provider communication has not been standardized [28–31]. Health professionals’ interest in how patients view their own disease process may help build rapport with patients. Enhancing health professionals’ cultural competency skills can be a critical first step for improving patient-provider communication. For instance, it can (1) present an opportunity to integrate cultural belief systems into diabetes care for Hispanics/Latinos, (2) open the door for other important conversations about Hispanic/Latino patients’ psychosocial and familial environment and identify barriers or motivators in diabetes self-management, and (3) build rapport and trust between the health professional and patient.
Additionally, inquiring about emotional beliefs or emotions about diabetes in general can help improve the patient-provider relationship, giving Hispanic/Latino patients a sense that their provider cares about their feelings and emotional well-being. For example, in a study conducted by Concha et al, a Hispanic/Latino male patient with diabetes expresses his appreciation of his doctor for attending to his emotional problems and suggests that his diabetes is in control because of the encouragement he receives from the doctor [22].
…I believe the doctors..can encourage one with ..diabetes… I am very grateful to God before anything that till today I have my sugar controlled. I am a diabetic, but controlled. And Dr. [name omitted], he’s a blessing from God. He knows my body like my mother….Because whatever little thing, he attends to me, he gives me a lot of encouragement with my emotional problems. He sent me to a counselor, I have a specialist for my problem with my urinary tracts. I have attention, I have all the attention from the doctor…
Inquiring about emotional well-being may also be beneficial because Hispanics/Latinos with diabetes have reported that they would feel more comfortable talking to a professional about personal problems compared to Hispanics/Latinos without diabetes [32]. Having a physical illness may provide an opportunity for these patients to discuss stress or depression in tandem with diabetes to diminish any possible stigma or shame associated with having a mental health problem. It is important for health care providers to be aware of emotional or social problems that may be negatively influencing diabetes self-care behaviors.
Models of Effective Cross-Cultural Communication
Cultural competency training for health professionals is one strategy for reducing health disparities and ensuring that racial/ethnic populations receive “equitable, effective, and culturally appropriate clinical care” [9,11,12,33]. The Association of American Medical Colleges’ guide for cultural competence education in medical school cites several models of effective cross-cultural communication for physicians and/or physician assistants [34]. I describe 3 communication tools below that may help health care professionals initiate conversations and aid them in understanding how to better manage sociocultural and environmental issues that may impede patients’ ability to manage diabetes. For each tool, a vignette is offered that illustrates how the tool may be used in communicating with Hispanic/Latino patients.
BELIEF
The BELIEF instrument (Dobbie 2003) is a teaching tool designed to elicit patients’ health beliefs and to assist preclinical medical students or medical professionals in understanding how explanatory models of a disease influence patient engagement in care. The BELIEF instrument is straightforward and can be easily implemented into clinical case vignettes and or role-play as part of cultural competency training [35]. The specific questions corresponding to the BELIEF prompts are
- B: Beliefs about health (What caused your illness/problem?)
- E: Explanation (Why did it happen at this time?)
- L: Learn (Help me understand your belief/opinion)
- I: Impact (How is this illness/problem impacting your life?)
- E: Empathy (This must be very hard for you)
- F: Feelings (How are you feeling about it?)
Vignette 1
The following vignette is a conversation between a Spanish-speaking Hispanic women, a language interpreter, and medical professional. The patient, Mrs. Chavez, has come into the clinic for the third time after experiencing symptoms due to hypoglycemia. Mrs. Chavez believes stress may have something to do with her hypoglycemia but is not quite sure how. By using the BELIEF mnemonic, the medical professional is able to ask more about the stress that led into a discussion about how stress actually influenced her eating and medication intake behaviors. Through this probing, the medical professional was able to identify the possible cause of her hypoglycemia and work with Mrs. Chavez on finding a solution every time she experiences the stressful event. The vignette also demonstrates how interpreters may share cultural information that may clarify problems.
Medical Professional: Mrs. Chavez, I see you are here again for hypoglycemia. Can you tell me what has happened? Do you have your medications with you today?
Interpreter: Sra. Chavez, entiendo que está aquí nuevamente por hipoglucemia. ¿Puedes decirme qué ha pasado? ¿Tiene sus medicamentos con usted hoy?
Mrs. Chavez: Si, me ha sentido débil y mareado.
Interpreter: Yes I have felt faint and dizzy?
Medical Professional: Have you been taking your metformin as prescribed?
Interpreter: ¿Ha estado tomando su metformin según lo recetado?
Mrs. Chavez: Si (YES).
Medical Professional: We might have to consider adjusting your dosage.
Interpreter: Es posible que tengamos que considerar ajustar su dosis.
Mrs. Chavez privately to the Interpreter: ¿no es posible que las emociones o nervios puedan causar algo? He escuchado que este puede ser el problema?
Interpreter to Mrs. Chavez: Déjame preguntarle al doctor, si?
Let me ask the doctor, yes? (Mrs. Chavez, nods in agreement)
Interpreter to Medical Professional: She is asking if emotions or nervousness could be the cause. She has heard that this could be the problem.
Medical Profesional to Interpreter: What does she mean?
Interpreter: There is a cultural belief that stress or nerves can cause diabetes or affect diabetes. You may want to ask about this.
Medical Professional: Yes emotions like stress can cause changes in you glucose. (Beliefs) Do you believe that some emotions are causing your hypoglycemia?
Interpreter: Sí, las emociones como el estrés pueden provocar cambios en la glucosa. ¿Crees que algunas emociones están causando tu hipoglucemia?
Mrs. Chavez: (Shrugs shoulders).
Medical Professional: I see here in your records, that the other two times you had hypoglycemica were 1 month and 3 months ago. (Beliefs) What do you think caused these events and (Explanation) why do you think it happened during these times?
Interpreter: Veo aquí en sus registros que las otras dos veces que tuvo hipoglucemia fueron hace 1 mes y 3 meses. ¿Qué crees que causó estos eventos y por qué crees que sucedió durante estos tiempos?
Mrs. Chavez: Pues, no sé.
Interpreter: Well I don’t know.
Medical Professional: (Learn) Help me understand what you think happened 3 and 1 month ago and this month that may have caused your glucose to drop. What was happening emotionally during these times? Do you remember?
Interpreter: Ayúdame a entender lo que piensas que sucedió hace 3 y 1 meses y este mes, puede haber causado que tu glucosa baje. ¿Qué estaba pasando emocionalmente durante este tiempo? ¿Te acuerdas?
Mrs. Chavez: Hmm. Pues, hace 3 meses fui a visitar a mi madre y hace 1 meses fui a visitar a mi hermano al norte.
Interpreter: Hmm. Well 3 months ago I went to visit my mother and 1 months ago I went to visit my brother up north.
Medical Professional: (Learn) How were those trips for you. Did you have fun? What types of emotions were you feeling during these trips?
Interpreter: ¿Cómo fueron esos viajes para ti? ¿Te divertiste? ¿Qué tipo de emociones sentías durante estos viajes?
Mrs. Chavez: Pues, yo estaba muy estresado durante mis viajes.
Interpreter: Well, I was very stressed during my trips.
Medical Professional: (Learn) Would you like to share why you were stressed? What was happening for you to feel so stressed?
Interpreter: ¿Te gustaría compartir por qué estabas estresado? ¿Qué estaba pasando para que te sientas tan estresado?
Mrs. Chavez: Bueno, tenemos muchos problemas familiares y conflictos. Hay muchos argumentos familiares y se vuelve estresante.
Interpreter: Well we have a lot of family problems and conflict. There are a lot of family arguments and it gets stressful.
Medical Professional: (Impact) How do you think this has affected your glucose?
Interpreter: ¿Cómo crees que esto ha afectado tu glucosa?
Mrs. Chavez: No lo sé.
Interpreter: I don’t know.
Medical Professional: (Learn) Do you think the stress maybe led you to forget to take your medication or affected your eating?
Interprter: ¿Crees que el estrés puede llevarte a olvidarte de tomar tu medicación o afectó su alimentación?
Mrs. Chavez: Pues si y no comí. Estaba demasiado estresado para comer. Raramente comí mientras estaba allí. Estaba tan estresado que no tenía apetito.
Interpreter: Well yes and I didn’t eat. I was too stressed to eat. I rarely ate while I was there. I was so stressed i did not have an appetite.
Medical Professional: (Empathy) Mrs. Chavez, that must have been very hard for you. I’m sorry you have had to feel this way. (Feelings) Is this how you feel everytime you visit your family?
Interpreter: Sra. Chávez, eso debe haber sido muy difícil para usted. Lamento que hayas tenido que sentirte de esta manera. ¿Es así como te sientes cada vez que visitas a tu familia?
Mrs. Chavez: Sí, todos se involucran en los problemas familiares y es muy estresante visitarlos, pero tengo que ir a ayudar a mi madre porque mi hermano está enfermo y no puede ayudarla. Soy el único que está cerca y mis otros hermanos discuten sobre lo que debería hacer. Tengo que estar ahí. Tengo que visitar.
Interpreter: Yes, everyone gets involved in the family problems and it is very stressful to visit but I have to go to help my mom because my brother is sick and can’t help her. I’m the only one close by and my other siblings argue about what I should do. I have to be there. I have to visit.
Medical Profesional: (Empathy) Yes, that must be very difficult for you. Okay, now I understand what is happening. Your visits are necessary but it seems like the stress is affecting your eating patterns and whether you remember to take your metformin. How do you feel if we come up with a plan for when you visit your family now that we know what might be causing your hypoglycemia? Do you think it is a good idea to take high glucose snacks or candy and have them with you on the trip so when you feel dizzy or faint you can eat them?
Interpreter: Sí, eso debe ser muy difícil para ti. De acuerdo, ahora entiendo lo que está pasando. Sus visitas son necesarias, pero parece que el estrés está afectando sus patrones de alimentación y si recuerda tomar su metformina. ¿Cómo se siente si elaboramos un plan para su familia ahora que sabemos lo que podría estar causando su hipoglucemia? ¿Cree que es una buena idea tomar refrigerios con alto contenido de glucosa o dulces y llevarlos consigo durante el viaje para que cuando se sienta mareado o desmayado pueda comerlos?
Mrs. Chavez: Sí, por supuesto. Ni siquiera me di cuenta de eso hasta ahora que hablamos sobre eso. Tienes razón, no he estado comiendo bien cuando lo visito. Me siento terrible cuando estoy allí como si quisiera desmayarme.
Interpreter: Yes of course. I didn’t even really realize that until now that we talked about it. You are right, I haven’t been eating right when I visit. I feel terrible when I am there like I want to faint.
Medical Professional: Mrs. Chavez, sometimes it is helpful to talk about our stress and problems we encournter in life, just to talk through it. Is this something you would be interested in? If so, we can arrange for you to come talk to the social worker.
Interpreter: Sra. Chavez, a veces es útil hablar sobre nuestro estrés y los problemas que alegramos en la vida, solo para hablar sobre ello. ¿Esto es algo que te interesaría? Si tu quieres, podemos hacer arreglos para que vengas a hablar con el trabajador social.
Mrs. Chavez: Tal vez, no estoy seguro, pero tal vez
Interpreter: Maybe, I’m not sure but maybe.
Medical Professional: Okay, you let me know if this is something you would like to do. You can call and let us know and I’ll ask again during our next visit and see how you are dealing with the stress when you visit your family.
Interpreter: De acuerdo, dime si esto es algo que te gustaría hacer. Puede llamar y dejarnos saber, y volveré a preguntar durante nuestra próxima visita y verá cómo lidia con el estrés cuando visita a su familia.
ETHNIC
The ETHNIC interviewing tool (Levin SJ 2000) can be used to explore cross cultural issues and facilitate collaboration during clinical encounters and is designed for clinical students or health professionals permitted to diagnose and provide therapeutic interventions [36]. The specific questions corresponding to the ETHNIC prompts:
- E: Explanation (How do you explain your illness?)
- T: Treatment (What treatment have you tried?)
- H: Healers (Have you sought any advice from folk healers?)
- N: Negotiate (mutually acceptable options)
- I: Intervention (agreed on)
- C: Collaboration (with patient, family, and healers)
Vignette 2
The second vignette is a discussion between a conscientious patient, Mrs. Rodriguez, and her doctor. Mrs. Rodriguez is determined to keep her glucose levels within optimal range by eating healthy and living a natural lifestyle. Included in her natural lifestyle is the use of herbs from her garden and herbal supplements sold to her by her neighbor. Because her numbers have been in the normal range she discontinues her prescribed medication to rely on natural products. However, a trip with family members interrupts her daily routine, which is replaced with fast foods and little rest. Upon returning from her trip her glucose levels increase and she cannot decrease her glucose numbers.
Medical Professional: Good morning Mrs. Rodriguez. I see you are here today for high blood sugar because of your diabetes. (Explanation) Can you share why you think you have recently had higher numbers than normal?
Mrs. Rodriguez: Good morning Doctor. Yes, I am usually very good with my numbers but lately they have gone up and I know why.
Medical Professional: Yes, that is good that you have had your glucose managed. (Explanation) What has caused your numbers to go up Mrs. Rodriguez?
Mrs. Rodriguez: All this American food. I went on a trip to visit my daughter and all we did was eat out, hamburgers, fast food restaurants. They do not cook at home and we were always doing something so I could not cook. It was terrible, all we did was keep busy out and about, I was tired. I spent so much money on food that has chemicals. Look at me now. I can’t seem to get my numbers down.
Medical Professional: Oh, I understand. Yes, a trip can sometimes mess with our routine. (Treatment) Since you have been good at managing your glucose in the past what have you been doing now to get your glucose in normal range?
Mrs. Rodriguez: Well I have been doing the same thing I have always been doing. Eating healthy, resting, gardening, and praying.
Medical Professional: Gardening? That’s really nice. What do you garden?
Mrs. Rodriguez: Oh I love gardening. I plant all types of herbs, vegetables, flowers.
Medical Professional: That is so good Mrs. Rodriguez. I wish I had more time to garden. Do you use your own vegetable and herbs when you cook?
Mrs. Rodriguez: Haha. Yes of course. That is why my sugar was fine before I went on this trip. I rely on my garden to keep me healthy.
Medical Professional: There are so many herbs that are helpful for diabetes. (Treatment) Do you use any to help with your diabetes?
Mrs. Rodriguez: Well yes, in fact, I do. I know you doctors don’t like us to use our herbs but I do. And that was what keeps my sugars normal.
Medical Professional: Oh Mrs. Rodriguez, yes sometimes you hear doctors say this but some herbs are helpful. We just like to know what other things our patients do so we know how to make sure your medications work with certain herbs. (Treatment) I know many people use nopal (cactus), do you eat nopal?
Mrs. Rodriguez: ¿Como no? (of course). I eat them all the time. I make my morning licuado (drink); a little bit of parsley, oregano, oatmeal, lemon, nopal mixed with milk and yogurt.
Medical Professional: (Treatment) Sounds good, what else do you use?
Mrs. Rodriguez: Oh you know other things. Apple cider, cinnamon, cayenne.
Medical Professional: All from your garden?
Mrs. Rodriguez: Yes.
Medical Professional: (Treatment) Do you use any type of herbal supplements from stores or online?
Mrs. Rodriguez: My neighbor sells supplements specifically for diabetes. I started to use a natural supplement with cinnamon, vitamin D, and fish oil. All very natural.
Medical Professional: (Healer) Oh does your neighbor also have diabetes?
Mrs. Rodriguez: No, she sells products. But she sells to many people with diabetes and the supplement works. We get together and she tells us about how they work.
Medical Professional: Do you know the name of this supplement Mrs. Rodriguez?
Mrs. Rodriguez: Oh, gluco…something, it has a heart in the name. But I read the ingredients and it has only natural ingredients. (An FDA banned supplement for false claims)
Medical Professional: Oh I see. I may be familiar with that. Can you bring the supplement along with the medications I have prescribed? I just want to make sure there is not interaction between the two. To get your glucose back to normal I want to make sure we think of every possible situation that could be causing your high numbers. (Treatment) How have you been taking the supplement and the prescribed medications?
Mrs. Rodriguez: Well, I have not refilled your prescription. I was doing so well with my numbers, I’d rather go natural than take all those chemicals.
Medical Professional: Oh, I see Mrs. Rodriguez. Okay, you have done so well controlling your glucose before your trip and now we are in a situation where your numbers are not coming down so let’s try to figure this out. I’d like to learn more about this supplement, so for our next visit can you bring in your supplements so I can take a look at it? (Negotiate) We can then talk about the benefits or cautions. But in the meantime I’d like you to refill your medication and take as followed to see if that helps your sugars. (Negotiate) What do you think? Is this possible?
Mrs. Rodriguez: Oh Doctor, I just don’t like taking chemicals.
Medical Professional: I understand Mrs. Rodriguez. You did take them to start when you first came in for diabetes, is this correct?
Mrs. Rodriguez: Well yes but, I slowly got off them.
Medical Professional: I know it’s difficult to take medications every day but they can help in addition to your healthy eating. I know you are concerned about medications but for now we have to focus on getting your numbers down or your diabetes could become worse and we don’t want you to get there. Do you agree? (Negotiating process)
Mrs. Rodriguez: Well, I am concerned about my numbers.
Medical Professional: (Intervention) Okay well let’s try to get back to where you were before the trip. Let’s get you back on the medication and let’s see if this helps. (Negotiate) For the next visit would you be willing to bring any supplements you are taking along with the medication? (Collaboration) We can talk about the benefits and cautions for the medications and supplements. How does this sound?
Mrs. Rodriguez: Well, I am here to fix my numbers. I have everything I take in a box so I can bring that.
Medical Professional: Yes that would be great. (Collaboration) We can both talk about your daily routine and what have you learned about the supplement, any information or papers that you have, in addition to the medication I prescribed.
Mrs. Rodriguez: Yes I can do that.
Medical Professional: Thank you Mrs. Rodriguez. (Intervention) Also, I’ll have the nurse call you today or tomorrow and you can give her the name of the supplement and she’ll make sure the drug store has a refill for you. Would this work for you Mrs. Rodriguez?
Mrs. Rodriguez: Yes Doctor. You can call me. I’ll have the list ready.
BATHE
Unlike the BELIEF and ETHNIC instruments, the BATHE mnemonic (Lieberman 1999)
- B: Background (What is going on in your life?)
- A: Affect (How do you feel about what is going on?)
- T: Trouble (What troubles you most?)
- H: Handling (How are you handling that?)
- E: Empathy (This must be very difficult for you)
Vignette 3
The last vignette features Mr. Gonzalez, who typically shows a positive outlook on life when visiting his doctor. He is a patient who would not necessarily discuss his emotions if not asked specific questions about his emotional well-being.
Medical Professional: Hello Mr. Gonzalez. (Background) How are you doing today? What’s new? What’s going on in your life lately?
Mr. Gonzalez: Hey, Doctor! I’m good you know just living day to day.
Medical Professional: Good. (Affect) So how is your diabetes treating you day to day? How are you feeling with life and managing your diabetes?
Mr. Gonzalez: Ah well you know, just dealing with it as best as I can.
Medical Professional: Ah okay. As best as you can. (Troubles) What troubles you the most about managing diabetes?
Mr. Gonzalez: Well you know the aches and pains. But what can I do.
Medical Professional: (Affect) How do you feel about those aches and pains?
Mr. Gonzalez: Well it does limit me. I can’t move as well as I use to.
Medical Professional: (Handling) Hmm. I see. How are you handling those aches and pains? What are you doing to relieve it?
Mr. Gonzalez: I do my best with pain cream.
Medical Professional: (Empathy) Pains and aches, that must be difficult. (Affect) How do the aches and pains make you feel?
Mr. Gonzalez: Ahh, Doc, it’s not the same. You know I can’t do the same things anymore.
Medical Professional: (Background) What do you mean? What is not the same anymore?
Mr. Gonzalez: This diabetes, I’m not the same person. I use to be able to be there for my family and community and now I feel like I can’t be there for them the way I use to. I use to be the strong one for my family, helping those in need, and now I’m limited, my body is limited.
Medical Professional: (Affect) How do you feel about that? How does it make you feel emotionally and physically?
Mr. Gonzalez: Bad. I feel bad about it.
Medical Professional: Bad emotionally or physically?
Mr. Gonzalez: Both
Medical Professional: I see. (Handling) How are you dealing with the emotional part of it?
Mr. Gonzalez: I don’t know. I don’t know how.
Medical Professional: (Empathy) Dealing with diabetes and how it makes your body feel can be very emotionally distressing. It is common to feel this way but I want to make sure we also work on how you feel emotionally or how your emotions is affecting your diabetes.
Conclusion
Three mnemonic tools have been suggested to initiate patient-centered and culture-centered communication with patients. Beyond the use of these instruments, there are 2 key skills that are essential for engaging a Hispanic/Latino patient. The first is a non-judgmental, warm communication approach, and the second is astute probing. Once when I was interpreting for a Spanish-speaking Hispanic/Latino patient and English-speaking doctor, the patient expressed to me that she felt that the medical professionals “tienen una cultura fría” (“have a cold culture”), and she did not feel comfortable sharing more about herself because of it. It is also important for medical professionals to be aware of a patient’s doublespeak as a way to share enough information but not all information to keep from being judged by medical professionals. Thus, non-judgmental probing can uncover important information that may be useful for collaborative goal setting and treatment decisions.
The management of diabetes is multifaceted and complex, particularly for populations who face social barriers and challenges. The Hispanic/Latino population is more likely to encounter disparities in access to quality health care and disparities in social determinants of health compared to non-Hispanic whites [4–9]. Therefore, it is important for health professionals to engage Hispanic/Latino patients in self-care by eliciting information that best facilitates collaborative goal setting. Health professionals are in an influential position to leverage a communication style that is empathetic, trusting, and open, setting the tone for a positive patient-physician encounter and, in turn, positive patient outcomes [18–20].
Corresponding author: Jeannie Belinda Concha, PhD, MPH, Dept. of Public Health Sciences, The University of Texas at El Paso, 500 W. University Ave., El Paso, TX 79968, [email protected].
Funding support: Support for this research was provided by the Office of Research and Sponsored Projects at The University of Texas at El Paso.
Financial disclosures: None.
1. American Diabetes Association. American Diabetes Association Standards of Medical Care in Diabetes. Diabetes Care 2017; 40: Suppl 1.
2. Dominguez K, Penman-Aguilar A, Chang MH, et al. Vital signs: Leading causes of death, prevalence of diseases and risk factors, and use of health services among Hispanics in the United States, 2009–2013. MMWR 2015;64:1–10.
3. Commission on Social Determinants of Heath. Closing the gap in a generation: health equity through action on the social determinants of health. Final report on the Commission on Social Determinants of Health. Geneva, World Health Organization. Accessed 10 Sept 2017 at http://apps.who.int/iris/bitstream/10665/43943/1/9789241563703_eng.pdf.
4. Laiterapong N, Fairchild PC, Chou CH, et al. Revisiting disparities in quality of care among US adults with diabetes in the era of individualized care, NHANES 2007-2010. Med Care 2015;53:25–31.
5. Vaccaro JA, Feaster DJ, Lobar SL, et al. Medical advice and diabetes self-management reported by Mexican-American, Black, and White-non-Hispanic adults across the United States. BMC Public Health 2012;12:185.
6. Correa-de-Araujo R, McDermott K, Moy E. Gender differences across racial and ethnic groups in quality of care for diabetes. Women Health Iss 2006;16:56–65.
7. Chawla N, Rodriguez MA, Babey SH, Brown ER. Health policy fact sheet: diabetes among Latinos in California; disparities in access and management. UCLA Center for Health Policy Research. Accessed 1 Aug 2017 at http://healthpolicy.ucla.edu/publications/Documents/PDF/Diabetes%20among%20Latinos%20in%20California%20Disparities%20in%20Access%20and%20Management.pdf.
8. Pu J, Chewning B. Racial differences in diabetes preventive care. Res Social Adm Pharm 2013;9:790–6.
9. Institute of Medicine. Unequal treatment: Confronting racial and ethnic disparities in healthcare. Washington, DC: National Academies Press; 2003.
10. Saha S, Arbeaez JJ, Cooper LA. Patient-physician relationships and racial disparities in the quality of care. Am J Public Health 2003;93:1713–9.
11. What is cultural and linguistic competence?: Definitions, February 2003. Agency for Healthcare Research and Quality, Rockville, MD. Accessed 28 Aug 2017 at http://www.ahrq.gov/pprofessionals/systems/primary -care/cultural-competence-mco/cultcompdef.html.
12. U.S. Department of Health and Human Services, Office of Minority Health. 2000. Assuring cultural competence in health care: Recommendations for National Standards and an outcomes-focused research agenda. Accessed 17 August 2017 at http://www.omhrc.gov/clas/finalpo.htm.
13. Zhao X. Relationships between sources of health information and diabetes knowledge in the US Hispanic population. Health Commun 2014;29:574–85.
14. Perchman ML, Flannagan D, Ferrer RL, Matamoras M. Communication compete c e, self-care behaviors, and glucose control in patients with type 2 diabetes. Patient Educ Couns 2009;77:55–9.
15. Reimann JOF, Talavera GA, Salmon M, et al. Cultural competence among physicians treating Mexican Americans who have diabetes: a structural model. Soc Sci Med 2004;59:2195–205.
16. Gordon HS, Gerber BS. What we’ve got here is a failure to communication. J Gen Intern Med 2011;26:104–6.
17. Gonzalez A, Salas D, Umpierrez GE. Special considerations on the management of Latino patients with type 2 diabetes mellitus. Curr Med Res Opin 2011;27:969–79.
18. Peek ME, Cargill A, Juang ES. Diabetes health disparities: A systematic review of health care interventions. Med Care Res Rev 2007;64(5 Supp):101S–156S.
19. Kutob RM, Bormanis J, Crago M, et al. Assessing culturally competent diabetes care with unannounced standardized patients. Fam Med 2013;45:400–8.
20. Weller SC, Baer RD, Garcia de Alba Garcia J, Salcedo Rocha AL. Are differences between patient and provider explanatory models of diabetes associated with patient self-management and glycemic control? J Health Care Poor Underserved 2013:24;1498–510.
21. Duta MJ. Communicating about culture and health: Theorizing culture-centered and cultural sensitivity approaches. Commun Theory 2007;17:304–28.
22. Concha JB, Mayer SD, Mezuk B, Avula D. Diabetes causation beliefs among Spanish speaking patients. Diabetes Educ 2015:42:116–25.
23. Arcury TA, Skelly AH, Gesler WM, et al. Diabetes meanings among those without diabetes: explanatory models of immigrant Latinos in rural North Carolina. Soc Sci Med 2004;59:2183–3.
24. Daniulaityte R. Making sense of diabetes: cultural models, gender and individual adjustment to type 2 diabetes in a Mexican community. Soc Sci Med 2004;59:1899–912.
25. Poss J, Jezewski MA. The role and meaning of susto in Mexican American’s explanatory model of type 2 diabetes. Med Anthropol Q 2002;16:360–77.
26. Weller SC, Baer RD, Pachter LM, et al. Latino beliefs about diabetes. Diabetes Care 1999;22:722–8.
27. United States Census Bureau. Language use. Accessed Sept 2017 at https://www.census.gov/topics/population/language-use/about.html.
28. Mezuk B, Albrecht S, Eaton WW, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care 2008;31:2383–90.
29. Li C, Ford ES, Strine TW, Mokdad AH. Prevalence of depression among US adults with diabetes. Diabetes Care 2007;31:105–7.
30. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2006;24:1069–78.
31. Li C, Barker L, Ford ES, et al. Diabetes and anxiety In US adults: findings from the 2006 Behavioral Risk Factor Surveillance System. Diabetes Med 2008;25:878–81.
32. Concha JB, Mezuk B, Duran B. Culture-centered approaches: the relevance of assessing emotional health for Latinos with type 2 diabetes. BMJ Open Diab Res Care 2015;3.
33. Bentancourt JR, Green AR, Carillo Je, Park ER. Cultural competence and health care: Key perspectives and trends. Health Affairs 2015;24:499–506.
34. Association of American Medical Colleges. Cultural Competence Education 2005. Accessed Feb 2016 at https://www.aamc.org/download/54338/data/.
35. Dobbie AE, Medrano M, Tysinger J, Olney C. The BELIEF Instrument: A preclinical teaching tool to elicit patients’ health beliefs. Family Med 2003;35:316–9.
36. Levin SJ, Like RC, Gottlieb JE. ETHNIC: A framework for culturally competent ethical practice. Patient Care 2003;34:188–9.
37. Stuart MR, Leibermann JR. The fifteen-minute hour: applied psychotherapy for the primary care physician. New York: Praeger.
38. Pace EJ, Somerville NJ, Enyoha C, et al. Effects of a brief psychosocial intervention on inpatient satisfaction: a randomized control trial. Fam Med 2017;49:675–8.
1. American Diabetes Association. American Diabetes Association Standards of Medical Care in Diabetes. Diabetes Care 2017; 40: Suppl 1.
2. Dominguez K, Penman-Aguilar A, Chang MH, et al. Vital signs: Leading causes of death, prevalence of diseases and risk factors, and use of health services among Hispanics in the United States, 2009–2013. MMWR 2015;64:1–10.
3. Commission on Social Determinants of Heath. Closing the gap in a generation: health equity through action on the social determinants of health. Final report on the Commission on Social Determinants of Health. Geneva, World Health Organization. Accessed 10 Sept 2017 at http://apps.who.int/iris/bitstream/10665/43943/1/9789241563703_eng.pdf.
4. Laiterapong N, Fairchild PC, Chou CH, et al. Revisiting disparities in quality of care among US adults with diabetes in the era of individualized care, NHANES 2007-2010. Med Care 2015;53:25–31.
5. Vaccaro JA, Feaster DJ, Lobar SL, et al. Medical advice and diabetes self-management reported by Mexican-American, Black, and White-non-Hispanic adults across the United States. BMC Public Health 2012;12:185.
6. Correa-de-Araujo R, McDermott K, Moy E. Gender differences across racial and ethnic groups in quality of care for diabetes. Women Health Iss 2006;16:56–65.
7. Chawla N, Rodriguez MA, Babey SH, Brown ER. Health policy fact sheet: diabetes among Latinos in California; disparities in access and management. UCLA Center for Health Policy Research. Accessed 1 Aug 2017 at http://healthpolicy.ucla.edu/publications/Documents/PDF/Diabetes%20among%20Latinos%20in%20California%20Disparities%20in%20Access%20and%20Management.pdf.
8. Pu J, Chewning B. Racial differences in diabetes preventive care. Res Social Adm Pharm 2013;9:790–6.
9. Institute of Medicine. Unequal treatment: Confronting racial and ethnic disparities in healthcare. Washington, DC: National Academies Press; 2003.
10. Saha S, Arbeaez JJ, Cooper LA. Patient-physician relationships and racial disparities in the quality of care. Am J Public Health 2003;93:1713–9.
11. What is cultural and linguistic competence?: Definitions, February 2003. Agency for Healthcare Research and Quality, Rockville, MD. Accessed 28 Aug 2017 at http://www.ahrq.gov/pprofessionals/systems/primary -care/cultural-competence-mco/cultcompdef.html.
12. U.S. Department of Health and Human Services, Office of Minority Health. 2000. Assuring cultural competence in health care: Recommendations for National Standards and an outcomes-focused research agenda. Accessed 17 August 2017 at http://www.omhrc.gov/clas/finalpo.htm.
13. Zhao X. Relationships between sources of health information and diabetes knowledge in the US Hispanic population. Health Commun 2014;29:574–85.
14. Perchman ML, Flannagan D, Ferrer RL, Matamoras M. Communication compete c e, self-care behaviors, and glucose control in patients with type 2 diabetes. Patient Educ Couns 2009;77:55–9.
15. Reimann JOF, Talavera GA, Salmon M, et al. Cultural competence among physicians treating Mexican Americans who have diabetes: a structural model. Soc Sci Med 2004;59:2195–205.
16. Gordon HS, Gerber BS. What we’ve got here is a failure to communication. J Gen Intern Med 2011;26:104–6.
17. Gonzalez A, Salas D, Umpierrez GE. Special considerations on the management of Latino patients with type 2 diabetes mellitus. Curr Med Res Opin 2011;27:969–79.
18. Peek ME, Cargill A, Juang ES. Diabetes health disparities: A systematic review of health care interventions. Med Care Res Rev 2007;64(5 Supp):101S–156S.
19. Kutob RM, Bormanis J, Crago M, et al. Assessing culturally competent diabetes care with unannounced standardized patients. Fam Med 2013;45:400–8.
20. Weller SC, Baer RD, Garcia de Alba Garcia J, Salcedo Rocha AL. Are differences between patient and provider explanatory models of diabetes associated with patient self-management and glycemic control? J Health Care Poor Underserved 2013:24;1498–510.
21. Duta MJ. Communicating about culture and health: Theorizing culture-centered and cultural sensitivity approaches. Commun Theory 2007;17:304–28.
22. Concha JB, Mayer SD, Mezuk B, Avula D. Diabetes causation beliefs among Spanish speaking patients. Diabetes Educ 2015:42:116–25.
23. Arcury TA, Skelly AH, Gesler WM, et al. Diabetes meanings among those without diabetes: explanatory models of immigrant Latinos in rural North Carolina. Soc Sci Med 2004;59:2183–3.
24. Daniulaityte R. Making sense of diabetes: cultural models, gender and individual adjustment to type 2 diabetes in a Mexican community. Soc Sci Med 2004;59:1899–912.
25. Poss J, Jezewski MA. The role and meaning of susto in Mexican American’s explanatory model of type 2 diabetes. Med Anthropol Q 2002;16:360–77.
26. Weller SC, Baer RD, Pachter LM, et al. Latino beliefs about diabetes. Diabetes Care 1999;22:722–8.
27. United States Census Bureau. Language use. Accessed Sept 2017 at https://www.census.gov/topics/population/language-use/about.html.
28. Mezuk B, Albrecht S, Eaton WW, Golden SH. Depression and type 2 diabetes over the lifespan: a meta-analysis. Diabetes Care 2008;31:2383–90.
29. Li C, Ford ES, Strine TW, Mokdad AH. Prevalence of depression among US adults with diabetes. Diabetes Care 2007;31:105–7.
30. Ali S, Stone MA, Peters JL, Davies MJ, Khunti K. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2006;24:1069–78.
31. Li C, Barker L, Ford ES, et al. Diabetes and anxiety In US adults: findings from the 2006 Behavioral Risk Factor Surveillance System. Diabetes Med 2008;25:878–81.
32. Concha JB, Mezuk B, Duran B. Culture-centered approaches: the relevance of assessing emotional health for Latinos with type 2 diabetes. BMJ Open Diab Res Care 2015;3.
33. Bentancourt JR, Green AR, Carillo Je, Park ER. Cultural competence and health care: Key perspectives and trends. Health Affairs 2015;24:499–506.
34. Association of American Medical Colleges. Cultural Competence Education 2005. Accessed Feb 2016 at https://www.aamc.org/download/54338/data/.
35. Dobbie AE, Medrano M, Tysinger J, Olney C. The BELIEF Instrument: A preclinical teaching tool to elicit patients’ health beliefs. Family Med 2003;35:316–9.
36. Levin SJ, Like RC, Gottlieb JE. ETHNIC: A framework for culturally competent ethical practice. Patient Care 2003;34:188–9.
37. Stuart MR, Leibermann JR. The fifteen-minute hour: applied psychotherapy for the primary care physician. New York: Praeger.
38. Pace EJ, Somerville NJ, Enyoha C, et al. Effects of a brief psychosocial intervention on inpatient satisfaction: a randomized control trial. Fam Med 2017;49:675–8.
Update on Management of Barrett’s Esophagus for Primary Care Providers
From the Gastroenterology and Hepatology Section, Baylor College of Medicine, Houston, TX.
Abstract
- Objective: To provide an update on management of Barrett’s esophagus.
- Methods: Review of the literature.
- Results: Management of Barrett’s esophagus depends on the degree of dysplasia. Surveillance by endoscopy every 3–5 years is recommended in patients with Barrett’s esophagus without dysplasia. Patients with Barrett’s esophagus and low-grade dysplasia should undergo surveillance by endoscopy in 3 months for confirmation of the diagnosis; if the diagnosis is confirmed then surveillance by endoscopy or eradication of Barrett’s epithelium by ablation or endoscopic resection are recommended. There is a sufficient evidence to recommend radiofrequency ablation of high-grade dysplasia within Barrett’s esophagus or to perform endoscopic mucosal resection of nodular Barrett’s esophagus with any degree of dysplasia. Early esophageal cancers that are limited to the mucosa can be treated by endoscopic resection, while cancer invading into the deep submucosa or muscularis propria may need esophagectomy with or without chemoradiation.
- Conclusion: The management of Barrett’s esophagus depends on the degree of dysplasia. Radiofrequency ablation and endoscopic mucosal resection are the most commonly used treatment for Barrett’s esophagus with dysplasia.
Keywords: Barrett’s esophagus; radiofrequency ablation; endoscopic submucosal dissection; endoscopic mucosal resection; early esophageal cancer.
Barrett’s esophagus is a common complication of chronic reflux disease [1]. Metaplastic changes that occur at the distal esophageal epithelium are usually asymptomatic [2,3] and occur as reparative adaptations to the insult of the gastric acid [4]. The management of Barrett’s esophagus after diagnosis is currently debated amongst experts without a clear consensus [5,6]. This review is generally consistent with the 2016 guidelines from the American College of Gastroenterology [1], a 2012 guideline from the American Society of Gastrointestinal Endoscopy [7], a 2011 guideline, and a 2016 expert review from the American Gastroenterological Association [8,9].
D efinition
Barrett’s esophagus is a metaplasia of the stratified squamous epithelium to a specialized columnar intestinal epithelium of mucus cells and goblet cells at the distal esophagus secondary to gastroesophageal reflux disease (GERD) [7,10]. Barrett’s esophagus is unstable tissue which can progress to esophageal adenocarcinoma. When unmanaged, the risk of cancer in dysplastic mucosa is at least thirty-fold greater than that for the general population [11–14], with recent studies suggesting a 0.4–0.7 occurrence rate per year [11,15]. With no dysplasia, the risk is low [16].
Epidemiology
The prevalence of Barrett’s esophagus is ~10% in patients with GERD [11–13,17], an estimate tied to the prevalence of GERD. However, due to the lack of symptoms of Barrett’s esophagus, no solid data supports this assumption [18–20]. A European study estimated the prevalence of Barrett’s esophagus to be 1.6% among the general population [21,22]. Barrett’s esophagus is usually diagnosed during endoscopic examinations of middle-aged and older adults, with the mean age being 55 years of age. It is most commonly found in Caucasian males and associated with the use of smoking tobacco. The male-to-female ratio is approximately 2:1 [1] and it appears to be uncommon in African Americans [23,24]. Abdominal obesity as measured by an increased waist-to-hip ratio is associated with an increased risk of Barrett’s esophagus [25,26]. Germline mutations in the MSR1, ASCC1, and CTHRC1 genes have been associated with the presence of Barrett’s esophagus and esophageal adenocarcinoma [27]. Risk factors are listed in Table 1. 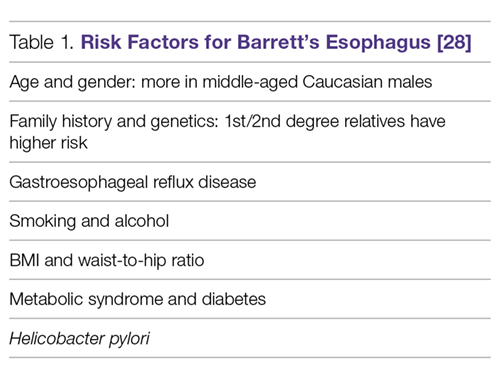
Clinical Symptoms
Columnar metaplasia itself does not cause any symptoms but is merely the adaptation of the cells to the repeated effect of the acid. The main clinical symptoms of the disease would initially be symptoms associated with GERD, such as heartburn, water brash, and dysphagia [1]. Severe presentations of GERD, such as esophageal ulceration, stricture, and hemorrhage, usually occur with long-segment Barrett’s esophagus [29,30]. However, 40% of patients presenting with adenocarcinoma had no history of GERD or symptoms of heartburn [13]. Furthermore, as few as 5% of those presenting with adenocarcinoma were known to have Barrett’s esophagus [31].
D iagnosis
Barrett’s esophagus generally requires an endoscopic examination with biopsy confirmation from the distal esophagus showing specialized intestinal columnar epithelium [32]. The biopsy specimen is acquired from the cellular lining proximal to gastroesophageal junction [5,33]. Barrett’s esophagus is classified into long- and short-segment based on the length of salmon-colored mucosa in the distal esophagus. A distance longer than 3 cm is 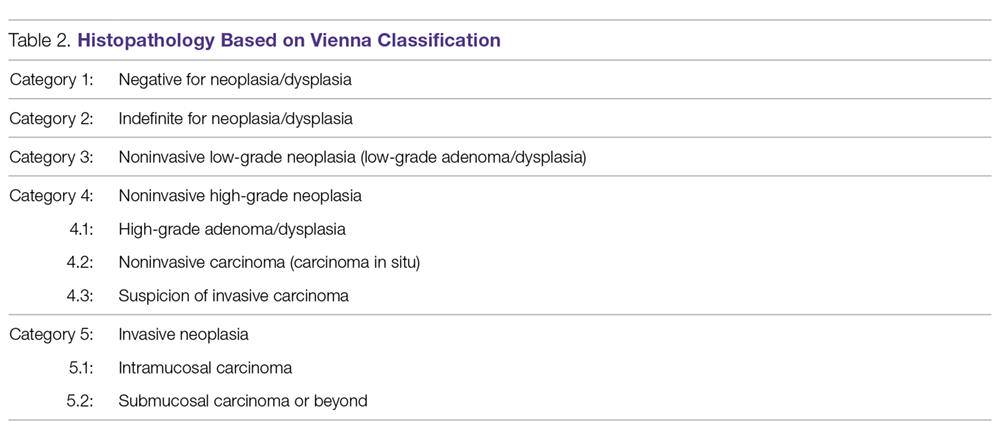
The Prague classification was presented by an international research group in 2006 and is regarded as the standard for measuring the length of Barrett’s esophagus. The lower measurement boundary is formed by the proximal cardial notch, and the 2 upper measurement boundaries are marked by the proximal limit of the circumferential Barrett’s segment and the longest tongue of Barrett’s [37].Confirmation of the diagnosis of dysplastic 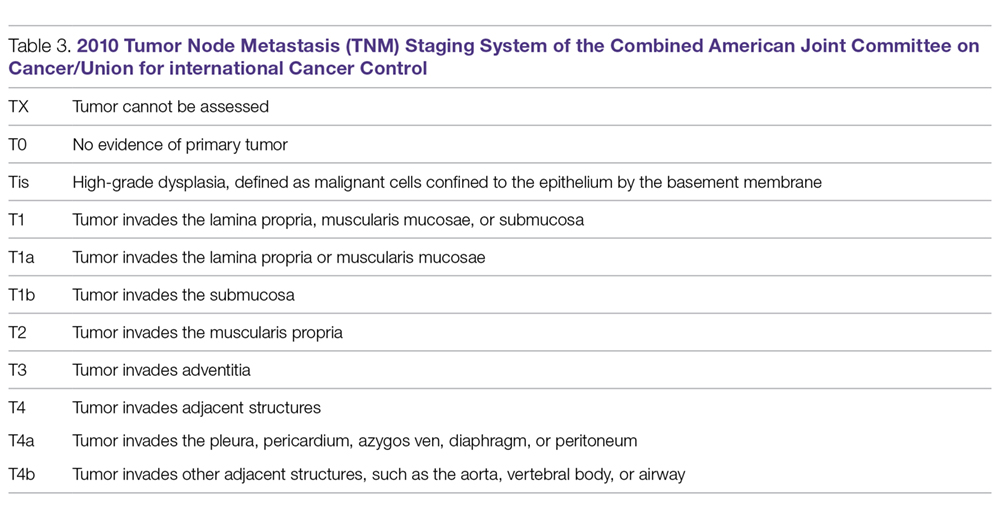
Once the initial diagnosis of Barrett’s esophagus is made, we recommend referring the patient to a Barrett’s esophagus specialized center in order to offer the patient a second opinion from a team of experts in Barrett’s esophagus. This would avoid possible false-positive results, which can be as high as 40% [1,8]. It would also offer the patient a comprehensive multidisciplinary approach and adequate long-term management. It is further preferred if an advanced intervention is offered to the patient such as endoscopic mucosal resection or endoscopic submucosal dissection. Expert endoscopists 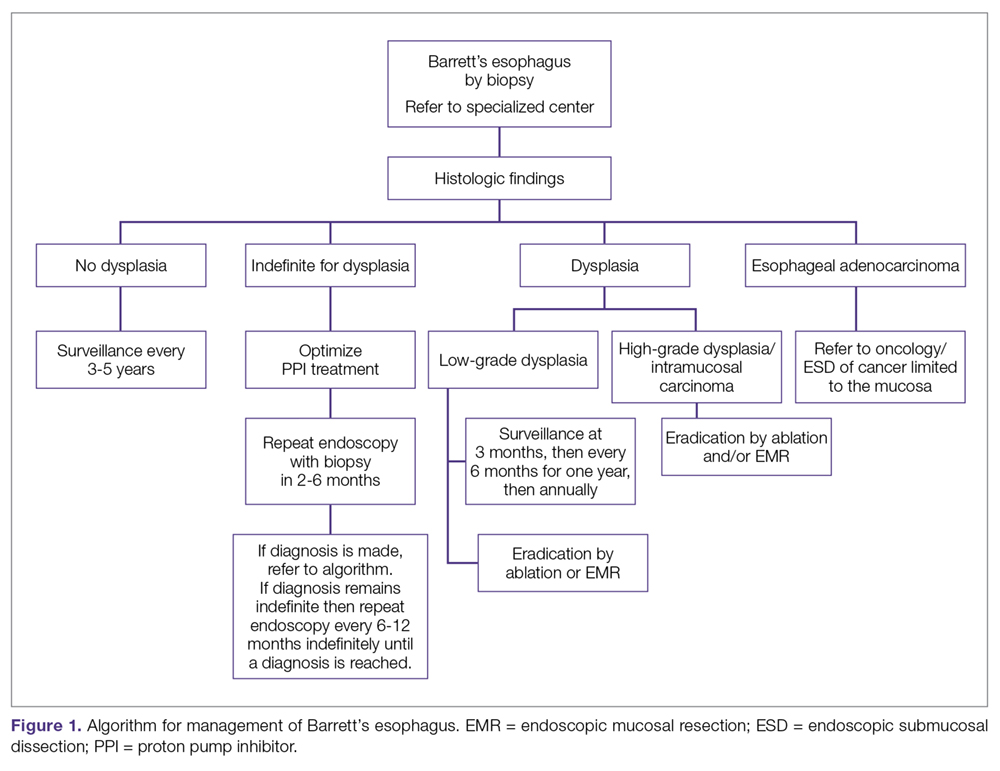
The availability of advanced endoscopic tools improves diagnostic yield. Adopting advanced techniques can reduce errors during biopsy sampling [40–42]. Some of the newer advanced imaging endoscopic tools include chromoendoscopy, optical coherence tomography, confocal microendoscopy, autofluorescence endoscopy, narrow band imaging (NBI), and Fujinon intelligent chromoendoscopy (FICE) [43,44]. In a meta-analysis examining whether advanced techniques improved diagnostic yield, it was found that advanced imaging increased the diagnostic yield by 34%. Advanced technology mentioned here is not mandated in current guidelines [5,45].
Histopathology categories and TNM staging system for Barrett’s esophagus are shown in Table 2 and Table 3. A management algorithm based on histologic findings is presented in Figure 1.
S creening
Logically, Barrett’s esophagus screening should be offered to every patient with GERD; however, this is against current recommendations because it is cost-prohibitive [46,47]. It is a given that the rationale behind the screening is to decrease morbidity and mortality from esophageal adenocarcinoma by offering early and definitive intervention [14,48,49]. The gold standard for screening is upper endoscopy, although nonendoscopic methods are being studied [1]. For example, a capsule attached to a string can be swallowed by the patient, the capsule is then deployed and pulled through the esophagus to obtains a brush sample of the cells. It is a promising technology due to high sensitivity and specificity [50]; however, it is not regularly utilized in practice.
Approaches to screening for Barrett’s esophagus has been addressed by multiple societies with several guidelines currently available [51]. None of these approaches have been proven to be superior in clinical studies. The American Gastroenterological Association (AGA) recommends screening patients with multiple risk factors associated with esophageal adenocarcinoma for Barrett’s esophagus. Risk factors listed by the AGA include white patients, male patients, patients above the age of 50 with a history of chronic GERD, hiatal hernia, elevated body mass index, and certain body fat distribution. The AGA recommends against screening the general population with GERD [9]. The American College of Gastroenterology (ACG) recommends upper endoscopy only in the presence of alarm symptoms (eg, dysphagia, weight loss, gastrointestinal bleeding) and for screening of patients at high risk for complications [52]. The American College of Physicians recommends upper endoscopy for screening for Barrett’s esophagus in men older than 50 years with GERD symptoms for more than 5 years with any risk factors like nocturnal reflux symptoms, hiatus hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat [1].
Overall, the sensitivity of endoscopy to diagnose Barrett’s esophagus, as seen in a Veterans Affairs (VA) cohort study for the detection of Barrett’s, is about 80%. The concluded 80% sensitivity rate was based on the performance of 2 endoscopies, 6 weeks apart for each patient, with subsequent labeling of the diagnosis if intestinal metaplasia was found in either of the 2 biopsy samples taken from the 2 procedures [53].
Promising molecular biomarkers have been associated with Barrett’s esophagus including p53 and cyclin D1 expression. However, additional studies are needed before they are incorporated as part of screening practices [5].
General Management
Medical Management of GERD
All patients with Barrett’s esophagus should be treated with a proton pump inhibitor (PPI) indefinitely based on multiple studies [54–56]. Effective control of GERD was associated with a decreased risk of dysplasia and adenocarcinoma (adjusted odds ratio 0.29, 95% CI 0.12–0.79) [57].
Effective control of GERD decreases chronic esophageal inflammation, which could progress to Barrett’s esophagus and has a risk of possible progression to adenocarcinoma. In one study, patients with proven Barrett’s esophagus showed partial regression of the intestinal metaplasia with aggressive PPI therapy [57–59]. Despite this, it is not clear whether the regression decreased risk of malignant progression [58,60,61]. In a study of 68 patients, aggressive acid reduction with omeprazole 40 mg twice a day lead to partial regression of Barrett’s esophagus when compared to mild suppression with ranitidine 150 mg twice a day. However, there was no reduction in the risk of cancer [59].
Surveillance
The reasoning behind surveillance is to detect dysplasia or adenocarcinoma in patients known to have Barrett’s esophagus early enough to provide early and efficient treatment to improve the outcome. Surveillance is done by endoscopy with biopsies in addition to sampling any irregularity [1,62,63]; however, the evidence to back up the benefit of surveillance is not clear [5,64]. It should be noted that surveillance carries risks, and morbidity associated with repeated procedures may affect patients psychologically and financially. Patients who have Barrett’s esophagus are more likely to die from other more common diseases, such as coronary heart disease, prior to developing adenocarcinoma [65]. In a recent meta-analysis, the mortality rate due to esophageal adenocarcinoma was 3.0 per 1000 person-years, whereas the mortality rate due to other causes was 37.1 per 1000 person-years [65]. An ongoing randomized, multicenter trial which assesses scheduled endoscopy every 2 years will shed more light on the overall survival after applying surveillance recommendations for each grade of dysplasia [66].
The following are ACG recommendations for surveillance of Barrett’s esophagus based on the histopathology report. The histopathology report delineates 1 of 3 types of columnar epithelium [68]: cardiac epithelium of mucus-secreting cells, atrophic gastric fundic type epithelium, or specialized columnar cells with goblet cells. The latter type is the most common with high potential for cancer [32]. Degrees of dysplasia and possible adenocarcinoma is usually described in the report as well. The degree of dysplasia if found helps the endoscopist plan the next step in management. It is worth mentioning that sampling errors can lead to missing a diagnosis. In a meta-analysis, 13% of patients diagnosed with high-grade dysplasia who underwent resection were found to have invasive cancer [69].
Surveillance for Patients with No Dysplasia
We suggest surveillance every 3 to 5 years since the rate of neoplasia is low [14]. For management of select patients with no dysplasia and with additional risk factors, radiofrequency ablation (RFA) may be an option, although it remains a controversial approach. For example, in a patient under 50 years of age, family history would be an argument for proceeding with RFA instead of prolonged surveillance. In a prospective cohort study of 139 patients with 10-year follow-up after ablation, recurrent Barrett’s occurred in less than 5% of the patients. [70]
Surveillance for Patients with Biopsy Showing “Indefinite for Dysplasia”
Aggressive treatment with PPI twice daily is recommended to avoid the misinterpretation of reactive esophageal changes secondary to reflux as dysplasia on the following endoscopy with biopsy. These patients will require a repeat endoscopy with biopsies after 3 months of aggressive treatment with PPI. Biopsies should be taken every 1 centimeter within Barrett’s epithelium [1].
If it remains indefinite, biopsies should be examined by a second pathologist with expertise in Barrett’s esophagus. If the second pathologist agrees on the indefinite diagnosis for dysplasia, then endoscopy every 12 months is recommended [1]. Treatment versus surveillance after repeat endoscopy and biopsy should be tailored to the new histopathology results on the most recent exam.
Surveillance for Patients with Biopsy Results showing Low-Grade Dysplasia (LGD), High-Grade Dysplasia (HGD), or Intramucosal Carcinoma
Surveillance recommendations are discussed under Management of Dysplasia or Intramucosal Carcinoma, below.
Efficacy of Surveillance
Asymptomatic adenocarcinoma could be discovered during surveillance, and neoplasia detected during surveillance is usually less advanced than those found after development of symptoms such as dysphagia, bleeding or weight loss [2,3,71–75]. These studies obviously had lead–time bias and did not document terminal cancer in patients adherent to surveillance protocol.
Management of Dysplasia or Intramucosal Carcinoma
Overview
Historically, dysplasia was managed with esophagectomy, which was associated with high morbidity and mortality. With advancement in the field of endoscopy, dysplasia is managed quite differently today, with endoscopic eradication therapy, which includes the use of endoscopic ablation techniques and endoscopic resection. The advantage of endoscopic resection is preservation of resected tissue for further examination, thus providing valuable information regarding the stage of the tumor (depth). Histological examination is not possible with photo or thermal ablation techniques as destroyed mucosa cannot be submitted for tissue analysis.
Low-Grade Dysplasia
If low-grade dysplasia is found, it is followed by a repeat endoscopy 8 weeks after aggressive PPI therapy. The repeat endoscopy should be performed with high definition/high-resolution endoscopy. The rationale of a second endoscopy is to ensure that the metaplastic mucosa was adequately inspected and biopsied prior to further intervention [1,9]. If the diagnosis is confirmed as low-grade dysplasia, and the patient prefers to go with the path of intervention instead of conservative management (endoscopic surveillance every 6 months for 1 year then annually with biopsies), then multiple options are available for the patient, including RFA or cryotherapy [8] [76]. In a randomized clinical trial in patients with Barrett’s esophagus and LGD, RFA was shown to reduce risk of neoplastic progression over a 3-year follow-up. The study included 136 patients randomized to receive ablation and 68 patients who underwent endoscopic surveillance. In the ablation group, the risk of progression to HGD or esophageal adenocarcinoma was reduced by 25% and the risk of progression to adenocarcinoma was reduced by 7.4%. In the ablation group, complete eradication of dysplasia and intestinal metaplasia occurred in 92.6% and 88.2% of patients respectively. In the endoscopic surveillance group, complete eradication of dysplasia and intestinal metaplasia was seen in 27.9% and 0.0% of patients respectively. [76]. Treatment-related adverse events occurred in 19.1% of patients receiving ablation (P < 0.001). The most common adverse event was stricture, occurring in 8 patients receiving ablation (11.8%), all resolved by endoscopic dilation [76,78].
Surveillance after ablation of LGD is still an ongoing debate, and further evidence is needed to establish guidelines [8]. Due to lack of evidence, we would lean towards surveillance for those patients with an annual esophagogastroduodenoscopy with biopsy examination (author’s opinion, no associated level of evidence).
High-Grade Dysplasia or Intramucosal Carcinoma
For patients with HGD or intramucosal carcinoma without submucosal invasion, eradication is the treatment of choice. Current guidelines advocate for endoscopic eradication therapy for most if not all patients with HGD or intramucosal carcinoma with a goal of removing all metaplastic and dysplastic tissue [1,5,62,64]. It should be noted that the biopsy specimen should be extensive to decrease the error margin. If the diagnosis were made on endoscopy without procuring extensive biopsies, then repeat endoscopy with extensive biopsies is needed prior to deciding the treatment path. The rationale behind extensive biopsies is to confirm the diagnosis and to determine the extent of dysplasia. Other factors potentially influencing the treatment path include the patient’s age, comorbid conditions, quality of life, and available access to an advanced endoscopist or specialized surgeon. Patient’s preferences and adherence to follow-up visits should also be a consideration.
The long-term benefits of endoscopic intervention versus surgical intervention are not well established. Esophagectomy is no longer a preferred method of treatment due to high morbidity and mortality associated with the procedure when compared to endoscopic interventions. However, it is still a preferred choice amongst a select group of patients unwilling to follow-up. A cost-effective analysis found that endoscopic ablation provided the longest quality adjusted life expectancy for Barrett’s esophagus with HGD [79,80].
Endoscopic Therapy in Barrett’s Esophagus
Endoscopic Ablative Therapies
With the advancement of endoscopic intervention, we now have multiple tools to ablate abnormal epithelium in Barrett’s esophagus. Examples of ablation techniques include thermal, photochemical, and mechanical techniques [81,82]. RFA is the treatment of choice for ablation [83]. However, non-contact ablative therapy, such as cryoablation, may be prefered if topography of the esophagus doesn’t allow contact ablation.
Radiofrequency Ablation (Figure 2). RFA is a procedure in which heat is generated from medium frequency alternating current and leads to thermal injury [84]. In Barrett’s esophagus, RFA uses radiofrequency energy delivered by a balloon that has a series of closely spaced electrodes in a 
Most patients will require multiple sessions of RFA to achieve eradication. It is very rarely a one-time procedure. In a meta-analysis of 18 studies including 3082 patients, the most common adverse effects of RFA were stricture in 5% [76,98], bleeding in 1%, and pain in 3% of patients [99].
It is crucial for successful RFA to continue medical treatment for acid suppression, in order to allow healthy regeneration of the squamous cell lining. It is suggested to use PPI twice a day with sucralfate and ranitidine after the intervention [100,101]. Adhering to a liquid diet for 24 hours is needed, followed by a soft diet to allow faster regeneration of the epithelium.
The caveat with RFA is that new evidence shows a higher rate of recurrence than previously thought. In one study of 246 patients, recurrence of dysplasia occurred in 25% of patients at 48 months after eradication in 80% of the patients, and metaplasia occurred in 50% at 60 months [102]. The other risk is buried Barrett’s, a condition occurring after incomplete ablation, in which squamous cell epithelium covers patches of incompletely destroyed intestinal lining, leading to possible progression of the disease to adenocarcinoma under the surface [103].
It has been reported that patients who underwent RFA had remarkable improvement in quality of life even if RFA did not achieve eradication. Patients reported less depression, less stress and better quality of life [104].
Based on a survey of experts, follow-up at 3 months, 6 months, and then annually is recommended after ablation [1,105]. Biopsies should be taken distal to neosquamous epithelium and from suspicious areas [97,106].
Endoscopic Spray Cryotherapy. This technique involves application of liquid nitrogen or carbon dioxide gas by endoscope on the tissue to freeze it off. Although it has been shown to eliminate HGD in over 95% of the cases and all dysplasia in over 85% of the cases, it was effective in eradicating intestinal metaplasia in only 55% of patients [103,108,109]. Thus, RFA as ablation therapy is still superior to cryotherapy and is still the first-line treatment for dysplastic Barrett’s esophagus. In comparison to cryotherapy, RFA efficacy has been studied extensively with well documented outcomes. However, there is a role for cryotherapy over RFA in certain clinical situations (such as severe chest pain from RFA or lack of efficacy in eradicating intestinal metaplasia or dysplasia by RFA).
Similar to RFA, on occasions of partial ablation, the remaining metaplastic tissue may get buried beneath a layer of squamous epithelium and can possibly progress to adenocarcinoma [110].
Photodynamic Therapy (PDT). This technique works by producing cytotoxicity at the cellular level by exposure to light at a specific wavelength in the presence of a chemical agent known as photosensitize [107]. Although superior to omeprazole, PDT has a significant rate of complications, mainly stricture, and a high occurrence of esophageal cancer during follow-up. For this reason, it is less favorable compared to RFA [107] and mentioned here as a historical therapy.
Endoscopic Resection Techniques: Endoscopic Mucosal Resection (EMR) and Endoscopic Submucosal Dissection (ESD)
Unlike flat mucosa in Barrett’s esophagus, which respond to ablative techniques such as RFA or cryotherapy, nodular Barrett’s esophagus is hard to treat and requires endoscopic resection prior to ablation. Endoscopic mucosal resection (EMR) is the most widely used technique and it is available in most tertiary referral centers. Another technique named endoscopic submucosal dissection (ESD) allows the removal of large nodular areas of Barrett’s esophagus in one piece to ensure complete removal of nodular dysplasia. ESD is technically challenging and it is only available in a handful of centers in the US. Endoscopic resection techniques are the preferred interventions for nodular dysplasia due to their ability to provide valuable information for staging the lesion [111–113]. Endoscopic resection techniques are safer and more effective with similar or better results when compared with other approaches [114].
EMR is completed by the excision of esophageal mucosa down to the submucosa and submitting a large tissue specimen to the pathologist. It additionally serves as a therapeutic measure in cases of no submucosal extension. Another advantage of EMR is the ability to predict lymph node metastasis. The rationale is based on the fact that the most important predictor of lymph node metastasis is the depth of the tumor; hence, invasive tumors would likely be associated with lymph node metastasis [115,116].
In a systematic review of 11 studies, complete EMR was as equally effective in the short-term treatment of dysplastic Barrett’s esophagus when compared to RFA, but adverse event rates were greater with complete EMR (mainly strictures). Strictures are more likely to occur in patients undergoing extensive EMR. In another meta-analysis of 22 studies comparing the efficacy of EMR to RFA, both techniques were effective in eradicating dysplasia (95% in EMR group and 92% in RFA group). However, extensive EMR was associated with higher complication rates suggesting that a combined endoscopic approach of focal EMR followed by RFA is preferred over extensive EMR alone [86].
It should be noted that EMR and ESD information were derived from highly specialized center and these results may not be duplicated in community settings [113,117].
Efficacy of Endoscopic Resection. Endoscopic resection has a success rate comparable to surgical esophagectomy with fewer complications [113,114,118–121] in patients with HGD and early stages of esophageal cancer [122]. Complete remission can be as high as 89%. Recurrence occurred in 6% to 30% of patients [114,118,119], which was attributed to incomplete removal, large lesions, failure to use adjunct therapy, or lack of follow-up [123]. Even when recurrence occurred, it was successfully managed by endoscopic intervention [124].
In a large cohort study of 1000 patients with early mucosal adenocarcinoma who were treated with endoscopic resection, long-term complete remission occurred in 94% of patients. There was no mortality and less than 2% of patients had major complications. Infrequent complications include bleeding, perforations, and strictures [123,125,126]. The rate of complications is lower in highly specialized centers [127–129].
Surgery was necessary in 12 patients (3.7%) after endoscopic therapy failed [123]. Post-resection care and follow-up is similar to the post-RFA care discussed above.
Management of Invasive Esophageal Adenocarcinoma
Patients diagnosed with an invasive adenocarcinoma need to be referred to an oncologist for staging and to discuss treatment options. A select number of patients may be referred by oncology for endoscopic resection, yet the need for a multidisciplinary approach in these situations is absolutely necessary [1].
Esophagectomy
Esophagectomy offers the complete removal of the HGD along with any adenocarcinoma in the regional lymph nodes. However, mortality rates are as high as 12% immediately after the procedure [130]. The multitude of short- and long-term morbidity has significant effects on quality of life. Short-term morbidity is as high as 30%. Patients may develop serious postoperative complications such as myocardial infarction, hospital associated pneumonia, or anatomic leak [131].
Examples of long-term morbidity include dysphagia, transection of vagal nerve, and dumping syndrome. Recent development in minimally invasive surgeries for esophagectomy has not reduced postoperative morbidity rates [132].
Advocates of esophagectomy illustrate the advantage of eradication of occult lymph node metastasis. The counter argument has been established by a systemic review in which occult lymph node metastasis occurred in less than 2% of patients with HGD and intramucosal carcinoma; whereas the mortality rate after esophagectomy is substantially higher with no guarantee of curing metastatic disease [133].
Prevention of Barrett’s Esophagus
Since Barrett’s esophagus precedes most of the cases of EAC if not all [1,134], methods that aim at decreasing the incidence of Barrett’s esophagus could help in prevention. The modifiable risk factors listed by the AGA include BMI, GERD, and hiatal hernia management. Along with diet and exercise, the advent of new therapies to help patients manage their weight could in return help in avoiding a plethora of medical conditions including Barrett’s esophagus. Hiatal hernia management could lower the risk of Barrett’s by restoring normal anatomy. Lastly, proper management of GERD would lower the risk of developing Barrett’s esophagus as discussed in this article [1,9].
It is worth noting that a large trial on the efficacy and safety of aspirin for prevention of adenocarcinoma progression in Barrett’s esophagus is ongoing in the UK (AspECT trial). The AspECT trial examines the efficacy of low dose vs. high dose PPI with or without aspirin for the chemoprevention of esophageal adenocarcinoma. The theory behind the study is the inhibition of COX 2 receptors in Barrett’s cells can decrease tissue progression to cancer. This chempreventive effect of nonsteroidal anti-inflammatory drugs was shown to be augmented when combined with statin intake [56,135–138].
Conclusion
Barrett’s esophagus is usually diagnosed during routine endoscopic examination. The initial symptoms are those associated with GERD, like heartburn, dyspepsia, and regurgitation. Specialized columnar epithelium is the hallmark of histopathological diagnosis. Recommendations of the ACG and AGA suggest treatment based on biopsy results. The intervention would vary on a wide spectrum starting from acid suppression, radiofrequency ablation, endoscopic resection therapy, and rarely, esophagectomy.
Corresponding author: Mohamed O. Othman, MD, Gastroenterology and Hepatology Section, Baylor College of Medicine, 7200 Cambridge St., Suite 8C, Houston, TX 77030, [email protected].
Financial disclosures: Dr. Othman has received grant support from Abbvie and has served as a consultant for Olympus.
1. Shaheen NJ, Falk GW, Iyer PG, Gerson LB; American College of Gastroenterology. ACG Clinical Guideline: diagnosis and management of Barrett’s esophagus. Am J Gastroenterol 2016;111:30–50; quiz 51.
2. Peters JH, Clark GW, Ireland AP. Outcome of adenocarcinoma arising in Barrett’s esophagus in endoscopically surveyed and nonsurveyed patients. J Thorac Cardiovasc Surg 1994;108:813–21; discussion 821–2.
3. Streitz JM Jr, Andrews CW Jr, Ellis FH Jr. Endoscopic surveillance of Barrett’s esophagus. Does it help? J Thorac Cardiovasc Surg 1993;105:383–7; discussion 387–8.
4. Spechler SJ, Souza RF. Barrett’s esophagus. N Engl J Med 2014;371:836–45.
5. Spechler SJ, Sharma P, Souza RF, et al; American Gastroenterological Association. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology 2011;140:1084–91.
6. Sharma P, McQuaid K, Dent J, et al; AGA Chicago Workshop. A critical review of the diagnosis and management of Barrett’s esophagus: the AGA Chicago Workshop. Gastroenterology 2004;127:310–30.
7. ASGE Standards of Practice Committee, Evans JA, Early DS; Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. The role of endoscopy in Barrett’s esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc 2012;76(6):1087–94.
8. Wani S, Rubenstein JH, Vieth M, Bergman J. Diagnosis and management of low–grade dysplasia in Barrett’s esophagus: Expert review from the clinical practice updates Committee of the American Gastroenterological Association. Gastroenterology 2016;151:822–835.
9. American Gastroenterological, A., et al., American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology, 2011. 140(3): p. 1084–91. [Same as #5]
10. Van Eyken P. Definition of Barrett’s oesophagus. Acta Gastroenterol Belg 2000;63:10–2.
11. Hirota WK, Loughney TM, Lazas DJ, et al. Specialized intestinal metaplasia, dysplasia, and cancer of the esophagus and esophagogastric junction: prevalence and clinical data. Gastroenterology 1999;116(2):277–85.
12. Cameron AJ, Zinsmeister AR, Ballard DJ, Carney JA. Prevalence of columnar–lined (Barrett’s) esophagus. Comparison of population–based clinical and autopsy findings. Gastroenterology 1990;99:918–22.
13. Gerson LB, Shetler K, Triadafilopoulos G. Prevalence of Barrett’s esophagus in asymptomatic individuals. Gastroenterology 2002;123:461–7.
14. Van der Veen AH, Dees J, Blankensteijn JD, Van Blankenstein M. Adenocarcinoma in Barrett’s oesophagus: an overrated risk. Gut 1989;30:14–8.
15. Winters C Jr, Spurling TJ, Chobanian SJ, et al. Barrett’s esophagus. A prevalent, occult complication of gastroesophageal reflux disease. Gastroenterology 1987;92:118–24.
16. Wani S, Falk G, Hall M, et al. Patients with nondysplastic Barrett’s esophagus have low risks for developing dysplasia or esophageal adenocarcinoma. Clin Gastroenterol Hepatol 2011;9:220–7;quiz e26.
17. Ward EM, Wolfsen HC, Achem SR, et al. Barrett’s esophagus is common in older men and women undergoing screening colonoscopy regardless of reflux symptoms. Am J Gastroenterol 2006;101:12–7.
18. Rex DK, Cummings OW, Shaw M. Screening for Barrett’s esophagus in colonoscopy patients with and without heartburn. Gastroenterology 2003;125:1670–7.
19. Rubenstein JH, Taylor JB. Meta–analysis: the association of oesophageal adenocarcinoma with symptoms of gastro–oesophageal reflux. Aliment Pharmacol Ther 2010;32:1222–7.
20. Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 1999;340:825–31.
21. Ronkainen J, Aro P, Storskrubb T, et al. Prevalence of Barrett’s esophagus in the general population: an endoscopic study. Gastroenterology, 2005;129:1825–31.
22. Sampliner RE. A population prevalence of Barrett’s esophagus––finally. Gastroenterology 2005; 129:2101–3.
23. Abrams JA, Fields S, Lightdale CJ, Neugut AI. Racial and ethnic disparities in the prevalence of Barrett’s esophagus among patients who undergo upper endoscopy. Clin Gastroenterol Hepatol 2008;6:30–4.
24. Corley DA, Kubo A, Levin TR, et al. Race, ethnicity, sex and temporal differences in Barrett’s oesophagus diagnosis: a large community–based study, 1994–2006. Gut 2009;58:182–8.
25. Kamat P, Wen S, Morris J, Anandasabapathy S. Exploring the association between elevated body mass index and Barrett’s esophagus: a systematic review and meta–analysis. Ann Thorac Surg 2009;87:655–62.
26. Jacobson BC, Chan AT, Giovannucci EL, Fuchs CS. Body mass index and Barrett’s oesophagus in women. Gut 2009;58:1460–6.
27. Orloff M, Peterson C, He X, et al. Germline mutations in MSR1, ASCC1, and CTHRC1 in patients with Barrett esophagus and esophageal adenocarcinoma. JAMA 2011;306:410–9.
28. Sharma N, Ho KY. Risk Factors for Barrett’s oesophagus. Gastrointest Tumors 2016;3:103–8.
29. Spechler SJ. Barrett’s esophagus. Semin Gastrointest Dis 1996;7:51–60.
30. Ronkainen J, Talley NJ, Storskrubb T. Erosive esophagitis is a risk factor for Barrett’s esophagus: a community–based endoscopic follow–up study. Am J Gastroenterol 2011;106:1946–52.
31. Kim SL, Wo JM, Hunter JG. The prevalence of intestinal metaplasia in patients with and without peptic strictures. Am J Gastroenterol 1998;93:53–5.
32. Spechler SJ. Clinical practice. Barrett’s esophagus. N Engl J Med 2002;346:836–42.
33. Riddell RH, Odze RD. Definition of Barrett’s esophagus: time for a rethink––is intestinal metaplasia dead? Am J Gastroenterol 2009;104:2588–94.
34. Sharma P, Morales TG, Sampliner RE. Short segment Barrett’s esophagus––the need for standardization of the definition and of endoscopic criteria. Am J Gastroenterol 1998;93:1033–6.
35. Eloubeidi MA, Provenzale D. Does this patient have Barrett’s esophagus? The utility of predicting Barrett’s esophagus at the index endoscopy. Am J Gastroenterol 1999;94:937–43.
36. Rudolph RE, Vaughan TL, Storer BE, et al. Effect of segment length on risk for neoplastic progression in patients with Barrett esophagus. Ann Intern Med 2000;132:612–20.
37. Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett’s esophagus: the Prague C & M criteria. Gastroenterology 2006;131:1392–9.
38. Bhat S, Coleman HG, Yousef F, et al. Risk of malignant progression in Barrett’s esophagus patients: results from a large population–based study. J Natl Cancer Inst 2011;103:1049–57.
39. Shaheen NJ, Dulai GS, Ascher B, et al. Effect of a new diagnosis of Barrett’s esophagus on insurance status. Am J Gastroenterol 2005;100:577–80.
40. Canto MI, Setrakian S, Willis J, et al. Methylene blue–directed biopsies improve detection of intestinal metaplasia and dysplasia in Barrett’s esophagus. Gastrointest Endosc 2000;51:560–8.
41. Scotiniotis IA, Kochman ML, Lewis JD. Accuracy of EUS in the evaluation of Barrett’s esophagus and high–grade dysplasia or intramucosal carcinoma. Gastrointest Endosc 2001;54:689–96.
42. Kobayashi K, Izatt JA, Kulkarni MD, et al. High–resolution cross–sectional imaging of the gastrointestinal tract using optical coherence tomography: preliminary results. Gastrointest Endosc 1998;47:515–23.
43. Georgakoudi I, Jacobson BC, Van Dam J, et al. Fluorescence, reflectance, and light–scattering spectroscopy for evaluating dysplasia in patients with Barrett’s esophagus. Gastroenterology 2001. 120: 1620–9.
44. Wallace MB, Sharma P, Lightdale C, et al. Preliminary accuracy and interobserver agreement for the detection of intraepithelial neoplasia in Barrett’s esophagus with probe–based confocal laser endomicroscopy. Gastrointest Endosc 2010;72:19–24.
45. Qumseya BJ, Wang H, Badie N, et al. Advanced imaging technologies increase detection of dysplasia and neoplasia in patients with Barrett’s esophagus: a meta–analysis and systematic review. Clin Gastroenterol Hepatol 2013;11:1562–70.e1–2.–
46. DeVault KR, Castell DO. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. The Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol 1999;94:1434–42.
47. Inadomi JM, Sampliner R, Lagergren J. Screening and surveillance for Barrett esophagus in high–risk groups: a cost–utility analysis. Ann Intern Med 2003;138:176–86.
48. Conio M, Blanchi S, Lapertosa G, et al. Long–term endoscopic surveillance of patients with Barrett’s esophagus. Incidence of dysplasia and adenocarcinoma: a prospective study. Am J Gastroenterol 2003;98:1931–9.
49. Rastogi A, Puli S, El–Serag HB, et al. Incidence of esophageal adenocarcinoma in patients with Barrett’s esophagus and high–grade dysplasia: a meta–analysis. Gastrointest Endosc 2008;67:394–8.
50. Kadri SR, Lao–Sirieix P, O’Donovan M, et al. Acceptability and accuracy of a non–endoscopic screening test for Barrett’s oesophagus in primary care: cohort study. BMJ 2010;341:c4372.
51. Sharma, P., et al., A critical review of the diagnosis and management of Barrett’s esophagus: the AGA Chicago Workshop. Gastroenterology, 2004. 127(1): p. 310–30. [Same as #6]
52. Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 2013;108:308–28; quiz 329.
53. Kim SL, Waring JP, Spechler SJ, et al. Diagnostic inconsistencies in Barrett’s esophagus. Department of Veterans Affairs Gastroesophageal Reflux Study Group. Gastroenterology 1994;107:945–9.
54. Kastelein F, Spaander MC, Steyerberg EW, et al; ProBar Study Group. Proton pump inhibitors reduce the risk of neoplastic progression in patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 2013;11:382–8.
55. El–Serag HB, Aguirre TV, Davis S, et al. Proton pump inhibitors are associated with reduced incidence of dysplasia in Barrett’s esophagus. Am J Gastroenterol 2004;99:1877–83.
56. Nguyen DM, El–Serag HB, Henderson L, et al. Medication usage and the risk of neoplasia in patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 2009;7:1299–304.
57. Singh S, Garg SK, Singh PP, et al. Acid–suppressive medications and risk of oesophageal adenocarcinoma in patients with Barrett’s oesophagus: a systematic review and meta–analysis. Gut 2014;63:1229–37.
58. Spechler SJ, Lee E, Ahnen D, et al. Long–term outcome of medical and surgical therapies for gastroesophageal reflux disease: follow–up of a randomized controlled trial. JAMA 2001;285:2331–8.
59. Peters FT, Ganesh S, Kuipers EJ, et al. Endoscopic regression of Barrett’s oesophagus during omeprazole treatment; a randomised double blind study. Gut 1999;45:489–94.
60. Ouatu–Lascar R, Triadafilopoulos G. –Complete elimination of reflux symptoms does not guarantee normalization of intraesophageal acid reflux in patients with Barrett’s esophagus. Am J Gastroenterol 1998;93:711–6.
61. Maret–Ouda J, Konings P, Lagergren J, Brusselaers N. Antireflux surgery and risk of esophageal adenocarcinoma: A systematic review and meta–analysis. Ann Surg 2016;263:251–7.
62. Evans, J.A., et al., The role of endoscopy in Barrett’s esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc, 2012. 76(6): p. 1087–94. [Same as #7]
63. ASGE Standards of Practice Committee, Evans JA, Early DS,et al; American Society for Gastrointestinal Endoscopy. The role of endoscopy in the assessment and treatment of esophageal cancer. Gastrointest Endosc 2013;77:328–34.
64. Bennett C, Moayyedi P, Corley DA, et al; BOB CAT Consortium. BOB CAT: A large–scale review and delphi consensus for ,anagement of Barrett’s esophagus with no dysplasia, indefinite for, or low–grade dysplasia. Am J Gastroenterol 2015;110:662–82; quiz 683.
65. Sikkema M, de Jonge PJ, Steyerberg EW, Kuipers EJ. Risk of esophageal adenocarcinoma and mortality in patients with Barrett’s esophagus: a systematic review and meta–analysis. Clin Gastroenterol Hepatol 2010;8:235–44; quiz e32.
66. Old O, Moayyedi P, Love S, et al; BOSS Trial Team. Barrett’s Oesophagus Surveillance versus endoscopy at need Study (BOSS): protocol and analysis plan for a multicentre randomized controlled trial. J Med Screen 2015;22:158–64.
67. Weston AP, Sharma P, Topalovski M, et al. Long–term follow–up of Barrett’s high–grade dysplasia. Am J Gastroenterol 2000;95:1888–93.
68. Paull A, Trier JS, Dalton MD, et al. The histologic spectrum of Barrett’s esophagus. N Engl J Med 1976;295:476–80.
69. Konda VJ, Ross AS, Ferguson MK, et al. Is the risk of concomitant invasive esophageal cancer in high–grade dysplasia in Barrett’s esophagus overestimated? Clin Gastroenterol Hepatol 2008;6:159–64.
70. Allison H, Banchs MA, Bonis PA, Guelrud M. Long–term remission of nondysplastic Barrett’s esophagus after multipolar electrocoagulation ablation: report of 139 patients with 10 years of follow–up. Gastrointest Endosc 2011;73:651–8.
71. Corley DA, Levin TR, Habel LA, Weiss NS, et al. Surveillance and survival in Barrett’s adenocarcinomas: a population–based study. Gastroenterology 2002;122:633–40.
72. Wong T, Tian J, Nagar AB. Barrett’s surveillance identifies patients with early esophageal adenocarcinoma. Am J Med 2010;123:462–7.
73. Fountoulakis A, Zafirellis KD, Dolan K, et al. Effect of surveillance of Barrett’s oesophagus on the clinical outcome of oesophageal cancer. Br J Surg 2004;91:997–1003.
74. Verbeek RE, Leenders M, Ten Kate FJ, et al. Surveillance of Barrett’s esophagus and mortality from esophageal adenocarcinoma: a population–based cohort study. Am J Gastroenterol 2014;109:1215–22.
75. Kastelein F, van Olphen SH, Steyerberg EW, et al. Impact of surveillance for Barrett’s oesophagus on tumour stage and survival of patients with neoplastic progression. Gut 2016;65:548–54.
76. Phoa KN, van Vilsteren FG, Weusten BL, et al. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low–grade dysplasia: a randomized clinical trial. JAMA 2014;311: 1209–17.
77. Wang WL, Chang IW, Chen CC, et al. Radiofrequency ablation versus endoscopic submucosal dissection in treating large early esophageal squamous cell neoplasia. Medicine (Baltimore) 2015;94:e2240.
78. Lim CH, Treanor D, Dixon MF, Axon AT. Low–grade dysplasia in Barrett’s esophagus has a high risk of progression. Endoscopy 2007;39:581–7.
79. Shaheen NJ, Inadomi JM, Overholt BF, Sharma P. What is the best management strategy for high grade dysplasia in Barrett’s oesophagus? A cost effectiveness analysis. Gut 2004;53:1736–44.
80. Vij R, Triadafilopoulos G, Owens DK, et al. Cost–effectiveness of photodynamic therapy for high–grade dysplasia in Barrett’s esophagus. Gastrointest Endosc 2004;60:739–56.
81. van den Boogert J, v an Hillegersberg R, Siersema PD, et al. Endoscopic ablation therapy for Barrett’s esophagus with high–grade dysplasia: a review. Am J Gastroenterol 1999;94:1153–60.
82. Sampliner RE. Endoscopic ablative therapy for Barrett’s esophagus: current status. Gastrointest Endosc 2004;59:66–9.
83. Sharma VK, Wang KK, Overholt BF, et al. Balloon–based, circumferential, endoscopic radiofrequency ablation of Barrett’s esophagus: 1–year follow–up of 100 patients. Gastrointest Endosc 2007;65:185–95.
84. Hanlon CR. Textbook of surgery: The biological basis of modern surgical practice, 14th edition. Ann Surg 1992;216:94.
85. Bright T, Watson DI, Tam W, et al. Randomized trial of argon plasma coagulation versus endoscopic surveillance for barrett esophagus after antireflux surgery: late results. Ann Surg 2007;246:1016–20.
86. Chadwick G, Groene O, Markar SR, et al. Systematic review comparing radiofrequency ablation and complete endoscopic resection in treating dysplastic Barrett’s esophagus: a critical assessment of histologic outcomes and adverse events. Gastrointest Endosc 2014;79:718–31.e3.
87. Gondrie JJ, Pouw RE, Sondermeijer CM, et al. Effective treatment of early Barrett’s neoplasia with stepwise circumferential and focal ablation using the HALO system. Endoscopy 2008;40:370–9.
88. Pouw RE, Wirths K, Eisendrath P, et al. Efficacy of radiofrequency ablation combined with endoscopic resection for barrett’s esophagus with early neoplasia. Clin Gastroenterol Hepatol 2010;8:23–9.
89. Kim HP, Bulsiewicz WJ, Cotton CC, et al. Focal endoscopic mucosal resection before radiofrequency ablation is equally effective and safe compared with radiofrequency ablation alone for the eradication of Barrett’s esophagus with advanced neoplasia. Gastrointest Endosc 2012;76:733–9.
90. Fleischer DE, Overholt BF, Sharma VK, et al. Endoscopic ablation of Barrett’s esophagus: a multicenter study with 2.5–year follow–up. Gastrointest Endosc 2008;68:867–76.
91. Sharma VK, Jae Kim H, Das A, et al. Circumferential and focal ablation of Barrett’s esophagus containing dysplasia. Am J Gastroenterol 2009;104:310–7.
92. Ganz RA, Overholt BF, Sharma VK, et al. Circumferential ablation of Barrett’s esophagus that contains high–grade dysplasia: a U.S. multicenter registry. Gastrointest Endosc 2008;68:35–40.
93. Gupta M, Iyer PG, Lutzke L, et al. Recurrence of esophageal intestinal metaplasia after endoscopic mucosal resection and radiofrequency ablation of Barrett’s esophagus: results from a US Multicenter Consortium. Gastroenterology 2013;145:79–86.e1.
94. Lyday WD, Corbett FS, Kuperman DA, et al. Radiofrequency ablation of Barrett’s esophagus: outcomes of 429 patients from a multicenter community practice registry. Endoscopy 2010;42:272–8.
95. Pasricha S, Bulsiewicz WJ, Hathorn KE, et al. Durability and predictors of successful radiofrequency ablation for Barrett’s esophagus. Clin Gastroenterol Hepatol 2014;12:1840–7.e1.
96. Fleischer DE, Overholt BF, Sharma VK, et al. Endoscopic radiofrequency ablation for Barrett’s esophagus: 5–year outcomes from a prospective multicenter trial. Endoscopy 2010;42:781–9.
97. Weston AP, Sharma P, Banerjee S, et al. Visible endoscopic and histologic changes in the cardia, before and after complete Barrett’s esophagus ablation. Gastrointest Endosc 2005;61:515–21.
98. Beaumont H, Gondrie JJ, McMahon BP, et al. Stepwise radiofrequency ablation of Barrett’s esophagus preserves esophageal inner diameter, compliance, and motility. Endoscopy 2009;41:2–8.
99. Orman ES, Li N, Shaheen NJ.Efficacy and durability of radiofrequency ablation for Barrett’s Esophagus: systematic review and meta–analysis. Clin Gastroenterol Hepatol 2013;11:1245–55.
100. Krishnan K, Pandolfino JE, Kahrilas PJ, et al. Increased risk for persistent intestinal metaplasia in patients with Barrett’s esophagus and uncontrolled reflux exposure before radiofrequency ablation. Gastroenterology 2012;143:576–81.
101. Akiyama J, Marcus SN, Triadafilopoulos G. Effective intra–esophageal acid control is associated with improved radiofrequency ablation outcomes in Barrett’s esophagus. Dig Dis Sci 2012;57:2625–32.
102. Small AJ, Sutherland SE, Hightower JS, et al. Comparative risk of recurrence of dysplasia and carcinoma after endoluminal eradication therapy of high–grade dysplasia versus intramucosal carcinoma in Barrett’s esophagus. Gastrointest Endosc 2015;81:1158–66.e1–4.
103. Shaheen NJ, Greenwald BD, Peery AF, et al. Safety and efficacy of endoscopic spray cryotherapy for Barrett’s esophagus with high–grade dysplasia. Gastrointest Endosc 2010;71:680–5.
104. Shaheen NJ, Peery AF, Hawes RH, et al. Quality of life following radiofrequency ablation of dysplastic Barrett’s esophagus. Endoscopy 2010;42:790–9.
105. Bedi AO, Kwon RS, Rubenstein JH, et al. A survey of expert follow–up practices after successful endoscopic eradication therapy for Barrett’s esophagus with high–grade dysplasia and intramucosal adenocarcinoma. Gastrointest Endosc 2013;78:696–701.
106. Sampliner RE, Camargo E, Prasad AR. Prasad, Association of ablation of Barrett’s esophagus with high grade dysplasia and adenocarcinoma of the gastric cardia. Dis Esophagus 2006;19:277–9.
107. Overholt BF, Panjehpour M, Halberg DL. Photodynamic therapy for Barrett’s esophagus with dysplasia and/or early stage carcinoma: long–term results. Gastrointest Endosc 2003;58:183–8.
108. Gosain S, Mercer K, Twaddell WS, et al. Liquid nitrogen spray cryotherapy in Barrett’s esophagus with high–grade dysplasia: long–term results. Gastrointest Endosc 2013;78:260–5.
109. Canto MI, Shin EJ, Khashab MA, et al. Safety and efficacy of carbon dioxide cryotherapy for treatment of neoplastic Barrett’s esophagus. Endoscopy 2015;47:582–91.
110. Van Laethem JL, Peny MO, Salmon I, et al. Intramucosal adenocarcinoma arising under squamous re–epithelialisation of Barrett’s oesophagus. Gut 2000;46:574–7.
111. Pech O, May A, Gossner L, et al. Management of pre–malignant and malignant lesions by endoscopic resection. Best Pract Res Clin Gastroenterol 2004;18:61–76.
112. Soetikno RM, Gotoda T, Nakanishi Y, Soehendra N. Endoscopic mucosal resection. Gastrointest Endosc 2003;57:567–79.
113. Ell C, May A, Gossner L, et al. Endoscopic mucosal resection of early cancer and high–grade dysplasia in Barrett’s esophagus. Gastroenterology 2000;118:670–7.
114. Pech O, Behrens A, May A, et al. Long–term results and risk factor analysis for recurrence after curative endoscopic therapy in 349 patients with high–grade intraepithelial neoplasia and mucosal adenocarcinoma in Barrett’s oesophagus. Gut 2008;57:1200–6.
115. Vieth M, Ell C, Gossner L, et al. Histological analysis of endoscopic resection specimens from 326 patients with Barrett’s esophagus and early neoplasia. Endoscopy 2004;36:776–81.
116. Buskens CJ, Westerterp M, Lagarde SM, et al. Prediction of appropriateness of local endoscopic treatment for high–grade dysplasia and early adenocarcinoma by EUS and histopathologic features. Gastrointest Endosc 2004;60:703–10.
117. Nijhawan PK, Wang KK. Endoscopic mucosal resection for lesions with endoscopic features suggestive of malignancy and high–grade dysplasia within Barrett’s esophagus. Gastrointest Endosc 2000;52:328–32.
118. Esaki M, Matsumoto T, Hirakawa K, et al. Risk factors for local recurrence of superficial esophageal cancer after treatment by endoscopic mucosal resection. Endoscopy 2007;39:41–5.
119. Ell C, May A, Pech O, et al. Curative endoscopic resection of early esophageal adenocarcinomas (Barrett’s cancer). Gastrointest Endosc 2007;65:3–10.
120. Chennat J, Konda VJ, Ross AS, et al. Complete Barrett’s eradication endoscopic mucosal resection: an effective treatment modality for high–grade dysplasia and intramucosal carcinoma––an American single–center experience. Am J Gastroenterol 2009;104:2684–92.
121. Pech O, Bollschweiler E, Manner H, et al. Comparison between endoscopic and surgical resection of mucosal esophageal adenocarcinoma in Barrett’s esophagus at two high–volume centers. Ann Surg 2011;254:67–72.
122. Wu J, Pan YM, Wang TT, et al. Endotherapy versus surgery for early neoplasia in Barrett’s esophagus: a meta–analysis. Gastrointest Endosc 2014;79:233–241.e2.
123. Pech O, May A, Manner H, et al. Long–term efficacy and safety of endoscopic resection for patients with mucosal adenocarcinoma of the esophagus. Gastroenterology 2014;146:652–660.e1.
124. Prasad GA, Wu TT, Wigle DA, et al. Endoscopic and surgical treatment of mucosal (T1a) esophageal adenocarcinoma in Barrett’s esophagus. Gastroenterology 2009;137:815–23.
125. May A, Gossner L, Pech O, et al. Local endoscopic therapy for intraepithelial high–grade neoplasia and early adenocarcinoma in Barrett’s oesophagus: acute–phase and intermediate results of a new treatment approach. Eur J Gastroenterol Hepatol 2002;14(10):1085–91.
126. Gerke H, Siddiqui J, Nasr I, et al. Efficacy and safety of EMR to completely remove Barrett’s esophagus: experience in 41 patients. Gastrointest Endosc 2011;74:761–71.
127. Lewis JJ, Rubenstein JH, Singal AG, et al. Factors associated with esophageal stricture formation after endoscopic mucosal resection for neoplastic Barrett’s esophagus. Gastrointest Endosc 2011;74:753–60.
128. Choi IJ, Kim CG, Chang HJ, et al. The learning curve for EMR with circumferential mucosal incision in treating intramucosal gastric neoplasm. Gastrointest Endosc 2005;62:860–5.
129. Deprez PH, Bergman JJ, Meisner S, et al. Current practice with endoscopic submucosal dissection in Europe: position statement from a panel of experts. Endoscopy 2010;42:853–8.
130. van Lanschot JJ, Hulscher JB, Buskens CJ, et al. Hospital volume and hospital mortality for esophagectomy. Cancer 2001;91:1574–8.
131. Karl RC, Schreiber R, Boulware D, et al. Factors affecting morbidity, mortality, and survival in patients undergoing Ivor Lewis esophagogastrectomy. Ann Surg 2000;231:635–43.
132. Young MM, Deschamps C, Trastek VF, et al. Esophageal reconstruction for benign disease: early morbidity, mortality, and functional results. Ann Thorac Surg 2000;70:1651–5.
133. Dunbar KB, Spechler SJ. The risk of lymph–node metastases in patients with high–grade dysplasia or intramucosal carcinoma in Barrett’s esophagus: a systematic review. Am J Gastroenterol 2012;107:850–62; quiz 863.
134. Morales CP, Souza RF, Spechler SJ. Hallmarks of cancer progression in Barrett’s oesophagus. Lancet 2002;360:1587–9.
135. Omer ZB, Ananthakrishnan AN, Nattinger KJ, et al. Aspirin protects against Barrett’s esophagus in a multivariate logistic regression analysis. Clin Gastroenterol Hepatol 2012;10:722–7.
136. Abnet CC, Freedman ND, Kamangar F, et al. Non–steroidal anti–inflammatory drugs and risk of gastric and oesophageal adenocarcinomas: results from a cohort study and a meta–analysis. Br J Cancer 2009;100:551–7.
137. Kastelein F, Spaander MC, Biermann K, et al. Nonsteroidal anti–inflammatory drugs and statins have chemopreventative effects in patients with Barrett’s esophagus. Gastroenterology 2011;141:2000–8; quiz e13–4.
138. Zhang S, Zhang XQ, Ding XW, et al. Cyclooxygenase inhibitors use is associated with reduced risk of esophageal adenocarcinoma in patients with Barrett’s esophagus: a meta–analysis. Br J Cancer 2014;110: 2378–88.
From the Gastroenterology and Hepatology Section, Baylor College of Medicine, Houston, TX.
Abstract
- Objective: To provide an update on management of Barrett’s esophagus.
- Methods: Review of the literature.
- Results: Management of Barrett’s esophagus depends on the degree of dysplasia. Surveillance by endoscopy every 3–5 years is recommended in patients with Barrett’s esophagus without dysplasia. Patients with Barrett’s esophagus and low-grade dysplasia should undergo surveillance by endoscopy in 3 months for confirmation of the diagnosis; if the diagnosis is confirmed then surveillance by endoscopy or eradication of Barrett’s epithelium by ablation or endoscopic resection are recommended. There is a sufficient evidence to recommend radiofrequency ablation of high-grade dysplasia within Barrett’s esophagus or to perform endoscopic mucosal resection of nodular Barrett’s esophagus with any degree of dysplasia. Early esophageal cancers that are limited to the mucosa can be treated by endoscopic resection, while cancer invading into the deep submucosa or muscularis propria may need esophagectomy with or without chemoradiation.
- Conclusion: The management of Barrett’s esophagus depends on the degree of dysplasia. Radiofrequency ablation and endoscopic mucosal resection are the most commonly used treatment for Barrett’s esophagus with dysplasia.
Keywords: Barrett’s esophagus; radiofrequency ablation; endoscopic submucosal dissection; endoscopic mucosal resection; early esophageal cancer.
Barrett’s esophagus is a common complication of chronic reflux disease [1]. Metaplastic changes that occur at the distal esophageal epithelium are usually asymptomatic [2,3] and occur as reparative adaptations to the insult of the gastric acid [4]. The management of Barrett’s esophagus after diagnosis is currently debated amongst experts without a clear consensus [5,6]. This review is generally consistent with the 2016 guidelines from the American College of Gastroenterology [1], a 2012 guideline from the American Society of Gastrointestinal Endoscopy [7], a 2011 guideline, and a 2016 expert review from the American Gastroenterological Association [8,9].
D efinition
Barrett’s esophagus is a metaplasia of the stratified squamous epithelium to a specialized columnar intestinal epithelium of mucus cells and goblet cells at the distal esophagus secondary to gastroesophageal reflux disease (GERD) [7,10]. Barrett’s esophagus is unstable tissue which can progress to esophageal adenocarcinoma. When unmanaged, the risk of cancer in dysplastic mucosa is at least thirty-fold greater than that for the general population [11–14], with recent studies suggesting a 0.4–0.7 occurrence rate per year [11,15]. With no dysplasia, the risk is low [16].
Epidemiology
The prevalence of Barrett’s esophagus is ~10% in patients with GERD [11–13,17], an estimate tied to the prevalence of GERD. However, due to the lack of symptoms of Barrett’s esophagus, no solid data supports this assumption [18–20]. A European study estimated the prevalence of Barrett’s esophagus to be 1.6% among the general population [21,22]. Barrett’s esophagus is usually diagnosed during endoscopic examinations of middle-aged and older adults, with the mean age being 55 years of age. It is most commonly found in Caucasian males and associated with the use of smoking tobacco. The male-to-female ratio is approximately 2:1 [1] and it appears to be uncommon in African Americans [23,24]. Abdominal obesity as measured by an increased waist-to-hip ratio is associated with an increased risk of Barrett’s esophagus [25,26]. Germline mutations in the MSR1, ASCC1, and CTHRC1 genes have been associated with the presence of Barrett’s esophagus and esophageal adenocarcinoma [27]. Risk factors are listed in Table 1.
Clinical Symptoms
Columnar metaplasia itself does not cause any symptoms but is merely the adaptation of the cells to the repeated effect of the acid. The main clinical symptoms of the disease would initially be symptoms associated with GERD, such as heartburn, water brash, and dysphagia [1]. Severe presentations of GERD, such as esophageal ulceration, stricture, and hemorrhage, usually occur with long-segment Barrett’s esophagus [29,30]. However, 40% of patients presenting with adenocarcinoma had no history of GERD or symptoms of heartburn [13]. Furthermore, as few as 5% of those presenting with adenocarcinoma were known to have Barrett’s esophagus [31].
D iagnosis
Barrett’s esophagus generally requires an endoscopic examination with biopsy confirmation from the distal esophagus showing specialized intestinal columnar epithelium [32]. The biopsy specimen is acquired from the cellular lining proximal to gastroesophageal junction [5,33]. Barrett’s esophagus is classified into long- and short-segment based on the length of salmon-colored mucosa in the distal esophagus. A distance longer than 3 cm is
The Prague classification was presented by an international research group in 2006 and is regarded as the standard for measuring the length of Barrett’s esophagus. The lower measurement boundary is formed by the proximal cardial notch, and the 2 upper measurement boundaries are marked by the proximal limit of the circumferential Barrett’s segment and the longest tongue of Barrett’s [37].Confirmation of the diagnosis of dysplastic
Once the initial diagnosis of Barrett’s esophagus is made, we recommend referring the patient to a Barrett’s esophagus specialized center in order to offer the patient a second opinion from a team of experts in Barrett’s esophagus. This would avoid possible false-positive results, which can be as high as 40% [1,8]. It would also offer the patient a comprehensive multidisciplinary approach and adequate long-term management. It is further preferred if an advanced intervention is offered to the patient such as endoscopic mucosal resection or endoscopic submucosal dissection. Expert endoscopists
The availability of advanced endoscopic tools improves diagnostic yield. Adopting advanced techniques can reduce errors during biopsy sampling [40–42]. Some of the newer advanced imaging endoscopic tools include chromoendoscopy, optical coherence tomography, confocal microendoscopy, autofluorescence endoscopy, narrow band imaging (NBI), and Fujinon intelligent chromoendoscopy (FICE) [43,44]. In a meta-analysis examining whether advanced techniques improved diagnostic yield, it was found that advanced imaging increased the diagnostic yield by 34%. Advanced technology mentioned here is not mandated in current guidelines [5,45].
Histopathology categories and TNM staging system for Barrett’s esophagus are shown in Table 2 and Table 3. A management algorithm based on histologic findings is presented in Figure 1.
S creening
Logically, Barrett’s esophagus screening should be offered to every patient with GERD; however, this is against current recommendations because it is cost-prohibitive [46,47]. It is a given that the rationale behind the screening is to decrease morbidity and mortality from esophageal adenocarcinoma by offering early and definitive intervention [14,48,49]. The gold standard for screening is upper endoscopy, although nonendoscopic methods are being studied [1]. For example, a capsule attached to a string can be swallowed by the patient, the capsule is then deployed and pulled through the esophagus to obtains a brush sample of the cells. It is a promising technology due to high sensitivity and specificity [50]; however, it is not regularly utilized in practice.
Approaches to screening for Barrett’s esophagus has been addressed by multiple societies with several guidelines currently available [51]. None of these approaches have been proven to be superior in clinical studies. The American Gastroenterological Association (AGA) recommends screening patients with multiple risk factors associated with esophageal adenocarcinoma for Barrett’s esophagus. Risk factors listed by the AGA include white patients, male patients, patients above the age of 50 with a history of chronic GERD, hiatal hernia, elevated body mass index, and certain body fat distribution. The AGA recommends against screening the general population with GERD [9]. The American College of Gastroenterology (ACG) recommends upper endoscopy only in the presence of alarm symptoms (eg, dysphagia, weight loss, gastrointestinal bleeding) and for screening of patients at high risk for complications [52]. The American College of Physicians recommends upper endoscopy for screening for Barrett’s esophagus in men older than 50 years with GERD symptoms for more than 5 years with any risk factors like nocturnal reflux symptoms, hiatus hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat [1].
Overall, the sensitivity of endoscopy to diagnose Barrett’s esophagus, as seen in a Veterans Affairs (VA) cohort study for the detection of Barrett’s, is about 80%. The concluded 80% sensitivity rate was based on the performance of 2 endoscopies, 6 weeks apart for each patient, with subsequent labeling of the diagnosis if intestinal metaplasia was found in either of the 2 biopsy samples taken from the 2 procedures [53].
Promising molecular biomarkers have been associated with Barrett’s esophagus including p53 and cyclin D1 expression. However, additional studies are needed before they are incorporated as part of screening practices [5].
General Management
Medical Management of GERD
All patients with Barrett’s esophagus should be treated with a proton pump inhibitor (PPI) indefinitely based on multiple studies [54–56]. Effective control of GERD was associated with a decreased risk of dysplasia and adenocarcinoma (adjusted odds ratio 0.29, 95% CI 0.12–0.79) [57].
Effective control of GERD decreases chronic esophageal inflammation, which could progress to Barrett’s esophagus and has a risk of possible progression to adenocarcinoma. In one study, patients with proven Barrett’s esophagus showed partial regression of the intestinal metaplasia with aggressive PPI therapy [57–59]. Despite this, it is not clear whether the regression decreased risk of malignant progression [58,60,61]. In a study of 68 patients, aggressive acid reduction with omeprazole 40 mg twice a day lead to partial regression of Barrett’s esophagus when compared to mild suppression with ranitidine 150 mg twice a day. However, there was no reduction in the risk of cancer [59].
Surveillance
The reasoning behind surveillance is to detect dysplasia or adenocarcinoma in patients known to have Barrett’s esophagus early enough to provide early and efficient treatment to improve the outcome. Surveillance is done by endoscopy with biopsies in addition to sampling any irregularity [1,62,63]; however, the evidence to back up the benefit of surveillance is not clear [5,64]. It should be noted that surveillance carries risks, and morbidity associated with repeated procedures may affect patients psychologically and financially. Patients who have Barrett’s esophagus are more likely to die from other more common diseases, such as coronary heart disease, prior to developing adenocarcinoma [65]. In a recent meta-analysis, the mortality rate due to esophageal adenocarcinoma was 3.0 per 1000 person-years, whereas the mortality rate due to other causes was 37.1 per 1000 person-years [65]. An ongoing randomized, multicenter trial which assesses scheduled endoscopy every 2 years will shed more light on the overall survival after applying surveillance recommendations for each grade of dysplasia [66].
The following are ACG recommendations for surveillance of Barrett’s esophagus based on the histopathology report. The histopathology report delineates 1 of 3 types of columnar epithelium [68]: cardiac epithelium of mucus-secreting cells, atrophic gastric fundic type epithelium, or specialized columnar cells with goblet cells. The latter type is the most common with high potential for cancer [32]. Degrees of dysplasia and possible adenocarcinoma is usually described in the report as well. The degree of dysplasia if found helps the endoscopist plan the next step in management. It is worth mentioning that sampling errors can lead to missing a diagnosis. In a meta-analysis, 13% of patients diagnosed with high-grade dysplasia who underwent resection were found to have invasive cancer [69].
Surveillance for Patients with No Dysplasia
We suggest surveillance every 3 to 5 years since the rate of neoplasia is low [14]. For management of select patients with no dysplasia and with additional risk factors, radiofrequency ablation (RFA) may be an option, although it remains a controversial approach. For example, in a patient under 50 years of age, family history would be an argument for proceeding with RFA instead of prolonged surveillance. In a prospective cohort study of 139 patients with 10-year follow-up after ablation, recurrent Barrett’s occurred in less than 5% of the patients. [70]
Surveillance for Patients with Biopsy Showing “Indefinite for Dysplasia”
Aggressive treatment with PPI twice daily is recommended to avoid the misinterpretation of reactive esophageal changes secondary to reflux as dysplasia on the following endoscopy with biopsy. These patients will require a repeat endoscopy with biopsies after 3 months of aggressive treatment with PPI. Biopsies should be taken every 1 centimeter within Barrett’s epithelium [1].
If it remains indefinite, biopsies should be examined by a second pathologist with expertise in Barrett’s esophagus. If the second pathologist agrees on the indefinite diagnosis for dysplasia, then endoscopy every 12 months is recommended [1]. Treatment versus surveillance after repeat endoscopy and biopsy should be tailored to the new histopathology results on the most recent exam.
Surveillance for Patients with Biopsy Results showing Low-Grade Dysplasia (LGD), High-Grade Dysplasia (HGD), or Intramucosal Carcinoma
Surveillance recommendations are discussed under Management of Dysplasia or Intramucosal Carcinoma, below.
Efficacy of Surveillance
Asymptomatic adenocarcinoma could be discovered during surveillance, and neoplasia detected during surveillance is usually less advanced than those found after development of symptoms such as dysphagia, bleeding or weight loss [2,3,71–75]. These studies obviously had lead–time bias and did not document terminal cancer in patients adherent to surveillance protocol.
Management of Dysplasia or Intramucosal Carcinoma
Overview
Historically, dysplasia was managed with esophagectomy, which was associated with high morbidity and mortality. With advancement in the field of endoscopy, dysplasia is managed quite differently today, with endoscopic eradication therapy, which includes the use of endoscopic ablation techniques and endoscopic resection. The advantage of endoscopic resection is preservation of resected tissue for further examination, thus providing valuable information regarding the stage of the tumor (depth). Histological examination is not possible with photo or thermal ablation techniques as destroyed mucosa cannot be submitted for tissue analysis.
Low-Grade Dysplasia
If low-grade dysplasia is found, it is followed by a repeat endoscopy 8 weeks after aggressive PPI therapy. The repeat endoscopy should be performed with high definition/high-resolution endoscopy. The rationale of a second endoscopy is to ensure that the metaplastic mucosa was adequately inspected and biopsied prior to further intervention [1,9]. If the diagnosis is confirmed as low-grade dysplasia, and the patient prefers to go with the path of intervention instead of conservative management (endoscopic surveillance every 6 months for 1 year then annually with biopsies), then multiple options are available for the patient, including RFA or cryotherapy [8] [76]. In a randomized clinical trial in patients with Barrett’s esophagus and LGD, RFA was shown to reduce risk of neoplastic progression over a 3-year follow-up. The study included 136 patients randomized to receive ablation and 68 patients who underwent endoscopic surveillance. In the ablation group, the risk of progression to HGD or esophageal adenocarcinoma was reduced by 25% and the risk of progression to adenocarcinoma was reduced by 7.4%. In the ablation group, complete eradication of dysplasia and intestinal metaplasia occurred in 92.6% and 88.2% of patients respectively. In the endoscopic surveillance group, complete eradication of dysplasia and intestinal metaplasia was seen in 27.9% and 0.0% of patients respectively. [76]. Treatment-related adverse events occurred in 19.1% of patients receiving ablation (P < 0.001). The most common adverse event was stricture, occurring in 8 patients receiving ablation (11.8%), all resolved by endoscopic dilation [76,78].
Surveillance after ablation of LGD is still an ongoing debate, and further evidence is needed to establish guidelines [8]. Due to lack of evidence, we would lean towards surveillance for those patients with an annual esophagogastroduodenoscopy with biopsy examination (author’s opinion, no associated level of evidence).
High-Grade Dysplasia or Intramucosal Carcinoma
For patients with HGD or intramucosal carcinoma without submucosal invasion, eradication is the treatment of choice. Current guidelines advocate for endoscopic eradication therapy for most if not all patients with HGD or intramucosal carcinoma with a goal of removing all metaplastic and dysplastic tissue [1,5,62,64]. It should be noted that the biopsy specimen should be extensive to decrease the error margin. If the diagnosis were made on endoscopy without procuring extensive biopsies, then repeat endoscopy with extensive biopsies is needed prior to deciding the treatment path. The rationale behind extensive biopsies is to confirm the diagnosis and to determine the extent of dysplasia. Other factors potentially influencing the treatment path include the patient’s age, comorbid conditions, quality of life, and available access to an advanced endoscopist or specialized surgeon. Patient’s preferences and adherence to follow-up visits should also be a consideration.
The long-term benefits of endoscopic intervention versus surgical intervention are not well established. Esophagectomy is no longer a preferred method of treatment due to high morbidity and mortality associated with the procedure when compared to endoscopic interventions. However, it is still a preferred choice amongst a select group of patients unwilling to follow-up. A cost-effective analysis found that endoscopic ablation provided the longest quality adjusted life expectancy for Barrett’s esophagus with HGD [79,80].
Endoscopic Therapy in Barrett’s Esophagus
Endoscopic Ablative Therapies
With the advancement of endoscopic intervention, we now have multiple tools to ablate abnormal epithelium in Barrett’s esophagus. Examples of ablation techniques include thermal, photochemical, and mechanical techniques [81,82]. RFA is the treatment of choice for ablation [83]. However, non-contact ablative therapy, such as cryoablation, may be prefered if topography of the esophagus doesn’t allow contact ablation.
Radiofrequency Ablation (Figure 2). RFA is a procedure in which heat is generated from medium frequency alternating current and leads to thermal injury [84]. In Barrett’s esophagus, RFA uses radiofrequency energy delivered by a balloon that has a series of closely spaced electrodes in a
Most patients will require multiple sessions of RFA to achieve eradication. It is very rarely a one-time procedure. In a meta-analysis of 18 studies including 3082 patients, the most common adverse effects of RFA were stricture in 5% [76,98], bleeding in 1%, and pain in 3% of patients [99].
It is crucial for successful RFA to continue medical treatment for acid suppression, in order to allow healthy regeneration of the squamous cell lining. It is suggested to use PPI twice a day with sucralfate and ranitidine after the intervention [100,101]. Adhering to a liquid diet for 24 hours is needed, followed by a soft diet to allow faster regeneration of the epithelium.
The caveat with RFA is that new evidence shows a higher rate of recurrence than previously thought. In one study of 246 patients, recurrence of dysplasia occurred in 25% of patients at 48 months after eradication in 80% of the patients, and metaplasia occurred in 50% at 60 months [102]. The other risk is buried Barrett’s, a condition occurring after incomplete ablation, in which squamous cell epithelium covers patches of incompletely destroyed intestinal lining, leading to possible progression of the disease to adenocarcinoma under the surface [103].
It has been reported that patients who underwent RFA had remarkable improvement in quality of life even if RFA did not achieve eradication. Patients reported less depression, less stress and better quality of life [104].
Based on a survey of experts, follow-up at 3 months, 6 months, and then annually is recommended after ablation [1,105]. Biopsies should be taken distal to neosquamous epithelium and from suspicious areas [97,106].
Endoscopic Spray Cryotherapy. This technique involves application of liquid nitrogen or carbon dioxide gas by endoscope on the tissue to freeze it off. Although it has been shown to eliminate HGD in over 95% of the cases and all dysplasia in over 85% of the cases, it was effective in eradicating intestinal metaplasia in only 55% of patients [103,108,109]. Thus, RFA as ablation therapy is still superior to cryotherapy and is still the first-line treatment for dysplastic Barrett’s esophagus. In comparison to cryotherapy, RFA efficacy has been studied extensively with well documented outcomes. However, there is a role for cryotherapy over RFA in certain clinical situations (such as severe chest pain from RFA or lack of efficacy in eradicating intestinal metaplasia or dysplasia by RFA).
Similar to RFA, on occasions of partial ablation, the remaining metaplastic tissue may get buried beneath a layer of squamous epithelium and can possibly progress to adenocarcinoma [110].
Photodynamic Therapy (PDT). This technique works by producing cytotoxicity at the cellular level by exposure to light at a specific wavelength in the presence of a chemical agent known as photosensitize [107]. Although superior to omeprazole, PDT has a significant rate of complications, mainly stricture, and a high occurrence of esophageal cancer during follow-up. For this reason, it is less favorable compared to RFA [107] and mentioned here as a historical therapy.
Endoscopic Resection Techniques: Endoscopic Mucosal Resection (EMR) and Endoscopic Submucosal Dissection (ESD)
Unlike flat mucosa in Barrett’s esophagus, which respond to ablative techniques such as RFA or cryotherapy, nodular Barrett’s esophagus is hard to treat and requires endoscopic resection prior to ablation. Endoscopic mucosal resection (EMR) is the most widely used technique and it is available in most tertiary referral centers. Another technique named endoscopic submucosal dissection (ESD) allows the removal of large nodular areas of Barrett’s esophagus in one piece to ensure complete removal of nodular dysplasia. ESD is technically challenging and it is only available in a handful of centers in the US. Endoscopic resection techniques are the preferred interventions for nodular dysplasia due to their ability to provide valuable information for staging the lesion [111–113]. Endoscopic resection techniques are safer and more effective with similar or better results when compared with other approaches [114].
EMR is completed by the excision of esophageal mucosa down to the submucosa and submitting a large tissue specimen to the pathologist. It additionally serves as a therapeutic measure in cases of no submucosal extension. Another advantage of EMR is the ability to predict lymph node metastasis. The rationale is based on the fact that the most important predictor of lymph node metastasis is the depth of the tumor; hence, invasive tumors would likely be associated with lymph node metastasis [115,116].
In a systematic review of 11 studies, complete EMR was as equally effective in the short-term treatment of dysplastic Barrett’s esophagus when compared to RFA, but adverse event rates were greater with complete EMR (mainly strictures). Strictures are more likely to occur in patients undergoing extensive EMR. In another meta-analysis of 22 studies comparing the efficacy of EMR to RFA, both techniques were effective in eradicating dysplasia (95% in EMR group and 92% in RFA group). However, extensive EMR was associated with higher complication rates suggesting that a combined endoscopic approach of focal EMR followed by RFA is preferred over extensive EMR alone [86].
It should be noted that EMR and ESD information were derived from highly specialized center and these results may not be duplicated in community settings [113,117].
Efficacy of Endoscopic Resection. Endoscopic resection has a success rate comparable to surgical esophagectomy with fewer complications [113,114,118–121] in patients with HGD and early stages of esophageal cancer [122]. Complete remission can be as high as 89%. Recurrence occurred in 6% to 30% of patients [114,118,119], which was attributed to incomplete removal, large lesions, failure to use adjunct therapy, or lack of follow-up [123]. Even when recurrence occurred, it was successfully managed by endoscopic intervention [124].
In a large cohort study of 1000 patients with early mucosal adenocarcinoma who were treated with endoscopic resection, long-term complete remission occurred in 94% of patients. There was no mortality and less than 2% of patients had major complications. Infrequent complications include bleeding, perforations, and strictures [123,125,126]. The rate of complications is lower in highly specialized centers [127–129].
Surgery was necessary in 12 patients (3.7%) after endoscopic therapy failed [123]. Post-resection care and follow-up is similar to the post-RFA care discussed above.
Management of Invasive Esophageal Adenocarcinoma
Patients diagnosed with an invasive adenocarcinoma need to be referred to an oncologist for staging and to discuss treatment options. A select number of patients may be referred by oncology for endoscopic resection, yet the need for a multidisciplinary approach in these situations is absolutely necessary [1].
Esophagectomy
Esophagectomy offers the complete removal of the HGD along with any adenocarcinoma in the regional lymph nodes. However, mortality rates are as high as 12% immediately after the procedure [130]. The multitude of short- and long-term morbidity has significant effects on quality of life. Short-term morbidity is as high as 30%. Patients may develop serious postoperative complications such as myocardial infarction, hospital associated pneumonia, or anatomic leak [131].
Examples of long-term morbidity include dysphagia, transection of vagal nerve, and dumping syndrome. Recent development in minimally invasive surgeries for esophagectomy has not reduced postoperative morbidity rates [132].
Advocates of esophagectomy illustrate the advantage of eradication of occult lymph node metastasis. The counter argument has been established by a systemic review in which occult lymph node metastasis occurred in less than 2% of patients with HGD and intramucosal carcinoma; whereas the mortality rate after esophagectomy is substantially higher with no guarantee of curing metastatic disease [133].
Prevention of Barrett’s Esophagus
Since Barrett’s esophagus precedes most of the cases of EAC if not all [1,134], methods that aim at decreasing the incidence of Barrett’s esophagus could help in prevention. The modifiable risk factors listed by the AGA include BMI, GERD, and hiatal hernia management. Along with diet and exercise, the advent of new therapies to help patients manage their weight could in return help in avoiding a plethora of medical conditions including Barrett’s esophagus. Hiatal hernia management could lower the risk of Barrett’s by restoring normal anatomy. Lastly, proper management of GERD would lower the risk of developing Barrett’s esophagus as discussed in this article [1,9].
It is worth noting that a large trial on the efficacy and safety of aspirin for prevention of adenocarcinoma progression in Barrett’s esophagus is ongoing in the UK (AspECT trial). The AspECT trial examines the efficacy of low dose vs. high dose PPI with or without aspirin for the chemoprevention of esophageal adenocarcinoma. The theory behind the study is the inhibition of COX 2 receptors in Barrett’s cells can decrease tissue progression to cancer. This chempreventive effect of nonsteroidal anti-inflammatory drugs was shown to be augmented when combined with statin intake [56,135–138].
Conclusion
Barrett’s esophagus is usually diagnosed during routine endoscopic examination. The initial symptoms are those associated with GERD, like heartburn, dyspepsia, and regurgitation. Specialized columnar epithelium is the hallmark of histopathological diagnosis. Recommendations of the ACG and AGA suggest treatment based on biopsy results. The intervention would vary on a wide spectrum starting from acid suppression, radiofrequency ablation, endoscopic resection therapy, and rarely, esophagectomy.
Corresponding author: Mohamed O. Othman, MD, Gastroenterology and Hepatology Section, Baylor College of Medicine, 7200 Cambridge St., Suite 8C, Houston, TX 77030, [email protected].
Financial disclosures: Dr. Othman has received grant support from Abbvie and has served as a consultant for Olympus.
From the Gastroenterology and Hepatology Section, Baylor College of Medicine, Houston, TX.
Abstract
- Objective: To provide an update on management of Barrett’s esophagus.
- Methods: Review of the literature.
- Results: Management of Barrett’s esophagus depends on the degree of dysplasia. Surveillance by endoscopy every 3–5 years is recommended in patients with Barrett’s esophagus without dysplasia. Patients with Barrett’s esophagus and low-grade dysplasia should undergo surveillance by endoscopy in 3 months for confirmation of the diagnosis; if the diagnosis is confirmed then surveillance by endoscopy or eradication of Barrett’s epithelium by ablation or endoscopic resection are recommended. There is a sufficient evidence to recommend radiofrequency ablation of high-grade dysplasia within Barrett’s esophagus or to perform endoscopic mucosal resection of nodular Barrett’s esophagus with any degree of dysplasia. Early esophageal cancers that are limited to the mucosa can be treated by endoscopic resection, while cancer invading into the deep submucosa or muscularis propria may need esophagectomy with or without chemoradiation.
- Conclusion: The management of Barrett’s esophagus depends on the degree of dysplasia. Radiofrequency ablation and endoscopic mucosal resection are the most commonly used treatment for Barrett’s esophagus with dysplasia.
Keywords: Barrett’s esophagus; radiofrequency ablation; endoscopic submucosal dissection; endoscopic mucosal resection; early esophageal cancer.
Barrett’s esophagus is a common complication of chronic reflux disease [1]. Metaplastic changes that occur at the distal esophageal epithelium are usually asymptomatic [2,3] and occur as reparative adaptations to the insult of the gastric acid [4]. The management of Barrett’s esophagus after diagnosis is currently debated amongst experts without a clear consensus [5,6]. This review is generally consistent with the 2016 guidelines from the American College of Gastroenterology [1], a 2012 guideline from the American Society of Gastrointestinal Endoscopy [7], a 2011 guideline, and a 2016 expert review from the American Gastroenterological Association [8,9].
D efinition
Barrett’s esophagus is a metaplasia of the stratified squamous epithelium to a specialized columnar intestinal epithelium of mucus cells and goblet cells at the distal esophagus secondary to gastroesophageal reflux disease (GERD) [7,10]. Barrett’s esophagus is unstable tissue which can progress to esophageal adenocarcinoma. When unmanaged, the risk of cancer in dysplastic mucosa is at least thirty-fold greater than that for the general population [11–14], with recent studies suggesting a 0.4–0.7 occurrence rate per year [11,15]. With no dysplasia, the risk is low [16].
Epidemiology
The prevalence of Barrett’s esophagus is ~10% in patients with GERD [11–13,17], an estimate tied to the prevalence of GERD. However, due to the lack of symptoms of Barrett’s esophagus, no solid data supports this assumption [18–20]. A European study estimated the prevalence of Barrett’s esophagus to be 1.6% among the general population [21,22]. Barrett’s esophagus is usually diagnosed during endoscopic examinations of middle-aged and older adults, with the mean age being 55 years of age. It is most commonly found in Caucasian males and associated with the use of smoking tobacco. The male-to-female ratio is approximately 2:1 [1] and it appears to be uncommon in African Americans [23,24]. Abdominal obesity as measured by an increased waist-to-hip ratio is associated with an increased risk of Barrett’s esophagus [25,26]. Germline mutations in the MSR1, ASCC1, and CTHRC1 genes have been associated with the presence of Barrett’s esophagus and esophageal adenocarcinoma [27]. Risk factors are listed in Table 1.
Clinical Symptoms
Columnar metaplasia itself does not cause any symptoms but is merely the adaptation of the cells to the repeated effect of the acid. The main clinical symptoms of the disease would initially be symptoms associated with GERD, such as heartburn, water brash, and dysphagia [1]. Severe presentations of GERD, such as esophageal ulceration, stricture, and hemorrhage, usually occur with long-segment Barrett’s esophagus [29,30]. However, 40% of patients presenting with adenocarcinoma had no history of GERD or symptoms of heartburn [13]. Furthermore, as few as 5% of those presenting with adenocarcinoma were known to have Barrett’s esophagus [31].
D iagnosis
Barrett’s esophagus generally requires an endoscopic examination with biopsy confirmation from the distal esophagus showing specialized intestinal columnar epithelium [32]. The biopsy specimen is acquired from the cellular lining proximal to gastroesophageal junction [5,33]. Barrett’s esophagus is classified into long- and short-segment based on the length of salmon-colored mucosa in the distal esophagus. A distance longer than 3 cm is
The Prague classification was presented by an international research group in 2006 and is regarded as the standard for measuring the length of Barrett’s esophagus. The lower measurement boundary is formed by the proximal cardial notch, and the 2 upper measurement boundaries are marked by the proximal limit of the circumferential Barrett’s segment and the longest tongue of Barrett’s [37].Confirmation of the diagnosis of dysplastic
Once the initial diagnosis of Barrett’s esophagus is made, we recommend referring the patient to a Barrett’s esophagus specialized center in order to offer the patient a second opinion from a team of experts in Barrett’s esophagus. This would avoid possible false-positive results, which can be as high as 40% [1,8]. It would also offer the patient a comprehensive multidisciplinary approach and adequate long-term management. It is further preferred if an advanced intervention is offered to the patient such as endoscopic mucosal resection or endoscopic submucosal dissection. Expert endoscopists
The availability of advanced endoscopic tools improves diagnostic yield. Adopting advanced techniques can reduce errors during biopsy sampling [40–42]. Some of the newer advanced imaging endoscopic tools include chromoendoscopy, optical coherence tomography, confocal microendoscopy, autofluorescence endoscopy, narrow band imaging (NBI), and Fujinon intelligent chromoendoscopy (FICE) [43,44]. In a meta-analysis examining whether advanced techniques improved diagnostic yield, it was found that advanced imaging increased the diagnostic yield by 34%. Advanced technology mentioned here is not mandated in current guidelines [5,45].
Histopathology categories and TNM staging system for Barrett’s esophagus are shown in Table 2 and Table 3. A management algorithm based on histologic findings is presented in Figure 1.
S creening
Logically, Barrett’s esophagus screening should be offered to every patient with GERD; however, this is against current recommendations because it is cost-prohibitive [46,47]. It is a given that the rationale behind the screening is to decrease morbidity and mortality from esophageal adenocarcinoma by offering early and definitive intervention [14,48,49]. The gold standard for screening is upper endoscopy, although nonendoscopic methods are being studied [1]. For example, a capsule attached to a string can be swallowed by the patient, the capsule is then deployed and pulled through the esophagus to obtains a brush sample of the cells. It is a promising technology due to high sensitivity and specificity [50]; however, it is not regularly utilized in practice.
Approaches to screening for Barrett’s esophagus has been addressed by multiple societies with several guidelines currently available [51]. None of these approaches have been proven to be superior in clinical studies. The American Gastroenterological Association (AGA) recommends screening patients with multiple risk factors associated with esophageal adenocarcinoma for Barrett’s esophagus. Risk factors listed by the AGA include white patients, male patients, patients above the age of 50 with a history of chronic GERD, hiatal hernia, elevated body mass index, and certain body fat distribution. The AGA recommends against screening the general population with GERD [9]. The American College of Gastroenterology (ACG) recommends upper endoscopy only in the presence of alarm symptoms (eg, dysphagia, weight loss, gastrointestinal bleeding) and for screening of patients at high risk for complications [52]. The American College of Physicians recommends upper endoscopy for screening for Barrett’s esophagus in men older than 50 years with GERD symptoms for more than 5 years with any risk factors like nocturnal reflux symptoms, hiatus hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat [1].
Overall, the sensitivity of endoscopy to diagnose Barrett’s esophagus, as seen in a Veterans Affairs (VA) cohort study for the detection of Barrett’s, is about 80%. The concluded 80% sensitivity rate was based on the performance of 2 endoscopies, 6 weeks apart for each patient, with subsequent labeling of the diagnosis if intestinal metaplasia was found in either of the 2 biopsy samples taken from the 2 procedures [53].
Promising molecular biomarkers have been associated with Barrett’s esophagus including p53 and cyclin D1 expression. However, additional studies are needed before they are incorporated as part of screening practices [5].
General Management
Medical Management of GERD
All patients with Barrett’s esophagus should be treated with a proton pump inhibitor (PPI) indefinitely based on multiple studies [54–56]. Effective control of GERD was associated with a decreased risk of dysplasia and adenocarcinoma (adjusted odds ratio 0.29, 95% CI 0.12–0.79) [57].
Effective control of GERD decreases chronic esophageal inflammation, which could progress to Barrett’s esophagus and has a risk of possible progression to adenocarcinoma. In one study, patients with proven Barrett’s esophagus showed partial regression of the intestinal metaplasia with aggressive PPI therapy [57–59]. Despite this, it is not clear whether the regression decreased risk of malignant progression [58,60,61]. In a study of 68 patients, aggressive acid reduction with omeprazole 40 mg twice a day lead to partial regression of Barrett’s esophagus when compared to mild suppression with ranitidine 150 mg twice a day. However, there was no reduction in the risk of cancer [59].
Surveillance
The reasoning behind surveillance is to detect dysplasia or adenocarcinoma in patients known to have Barrett’s esophagus early enough to provide early and efficient treatment to improve the outcome. Surveillance is done by endoscopy with biopsies in addition to sampling any irregularity [1,62,63]; however, the evidence to back up the benefit of surveillance is not clear [5,64]. It should be noted that surveillance carries risks, and morbidity associated with repeated procedures may affect patients psychologically and financially. Patients who have Barrett’s esophagus are more likely to die from other more common diseases, such as coronary heart disease, prior to developing adenocarcinoma [65]. In a recent meta-analysis, the mortality rate due to esophageal adenocarcinoma was 3.0 per 1000 person-years, whereas the mortality rate due to other causes was 37.1 per 1000 person-years [65]. An ongoing randomized, multicenter trial which assesses scheduled endoscopy every 2 years will shed more light on the overall survival after applying surveillance recommendations for each grade of dysplasia [66].
The following are ACG recommendations for surveillance of Barrett’s esophagus based on the histopathology report. The histopathology report delineates 1 of 3 types of columnar epithelium [68]: cardiac epithelium of mucus-secreting cells, atrophic gastric fundic type epithelium, or specialized columnar cells with goblet cells. The latter type is the most common with high potential for cancer [32]. Degrees of dysplasia and possible adenocarcinoma is usually described in the report as well. The degree of dysplasia if found helps the endoscopist plan the next step in management. It is worth mentioning that sampling errors can lead to missing a diagnosis. In a meta-analysis, 13% of patients diagnosed with high-grade dysplasia who underwent resection were found to have invasive cancer [69].
Surveillance for Patients with No Dysplasia
We suggest surveillance every 3 to 5 years since the rate of neoplasia is low [14]. For management of select patients with no dysplasia and with additional risk factors, radiofrequency ablation (RFA) may be an option, although it remains a controversial approach. For example, in a patient under 50 years of age, family history would be an argument for proceeding with RFA instead of prolonged surveillance. In a prospective cohort study of 139 patients with 10-year follow-up after ablation, recurrent Barrett’s occurred in less than 5% of the patients. [70]
Surveillance for Patients with Biopsy Showing “Indefinite for Dysplasia”
Aggressive treatment with PPI twice daily is recommended to avoid the misinterpretation of reactive esophageal changes secondary to reflux as dysplasia on the following endoscopy with biopsy. These patients will require a repeat endoscopy with biopsies after 3 months of aggressive treatment with PPI. Biopsies should be taken every 1 centimeter within Barrett’s epithelium [1].
If it remains indefinite, biopsies should be examined by a second pathologist with expertise in Barrett’s esophagus. If the second pathologist agrees on the indefinite diagnosis for dysplasia, then endoscopy every 12 months is recommended [1]. Treatment versus surveillance after repeat endoscopy and biopsy should be tailored to the new histopathology results on the most recent exam.
Surveillance for Patients with Biopsy Results showing Low-Grade Dysplasia (LGD), High-Grade Dysplasia (HGD), or Intramucosal Carcinoma
Surveillance recommendations are discussed under Management of Dysplasia or Intramucosal Carcinoma, below.
Efficacy of Surveillance
Asymptomatic adenocarcinoma could be discovered during surveillance, and neoplasia detected during surveillance is usually less advanced than those found after development of symptoms such as dysphagia, bleeding or weight loss [2,3,71–75]. These studies obviously had lead–time bias and did not document terminal cancer in patients adherent to surveillance protocol.
Management of Dysplasia or Intramucosal Carcinoma
Overview
Historically, dysplasia was managed with esophagectomy, which was associated with high morbidity and mortality. With advancement in the field of endoscopy, dysplasia is managed quite differently today, with endoscopic eradication therapy, which includes the use of endoscopic ablation techniques and endoscopic resection. The advantage of endoscopic resection is preservation of resected tissue for further examination, thus providing valuable information regarding the stage of the tumor (depth). Histological examination is not possible with photo or thermal ablation techniques as destroyed mucosa cannot be submitted for tissue analysis.
Low-Grade Dysplasia
If low-grade dysplasia is found, it is followed by a repeat endoscopy 8 weeks after aggressive PPI therapy. The repeat endoscopy should be performed with high definition/high-resolution endoscopy. The rationale of a second endoscopy is to ensure that the metaplastic mucosa was adequately inspected and biopsied prior to further intervention [1,9]. If the diagnosis is confirmed as low-grade dysplasia, and the patient prefers to go with the path of intervention instead of conservative management (endoscopic surveillance every 6 months for 1 year then annually with biopsies), then multiple options are available for the patient, including RFA or cryotherapy [8] [76]. In a randomized clinical trial in patients with Barrett’s esophagus and LGD, RFA was shown to reduce risk of neoplastic progression over a 3-year follow-up. The study included 136 patients randomized to receive ablation and 68 patients who underwent endoscopic surveillance. In the ablation group, the risk of progression to HGD or esophageal adenocarcinoma was reduced by 25% and the risk of progression to adenocarcinoma was reduced by 7.4%. In the ablation group, complete eradication of dysplasia and intestinal metaplasia occurred in 92.6% and 88.2% of patients respectively. In the endoscopic surveillance group, complete eradication of dysplasia and intestinal metaplasia was seen in 27.9% and 0.0% of patients respectively. [76]. Treatment-related adverse events occurred in 19.1% of patients receiving ablation (P < 0.001). The most common adverse event was stricture, occurring in 8 patients receiving ablation (11.8%), all resolved by endoscopic dilation [76,78].
Surveillance after ablation of LGD is still an ongoing debate, and further evidence is needed to establish guidelines [8]. Due to lack of evidence, we would lean towards surveillance for those patients with an annual esophagogastroduodenoscopy with biopsy examination (author’s opinion, no associated level of evidence).
High-Grade Dysplasia or Intramucosal Carcinoma
For patients with HGD or intramucosal carcinoma without submucosal invasion, eradication is the treatment of choice. Current guidelines advocate for endoscopic eradication therapy for most if not all patients with HGD or intramucosal carcinoma with a goal of removing all metaplastic and dysplastic tissue [1,5,62,64]. It should be noted that the biopsy specimen should be extensive to decrease the error margin. If the diagnosis were made on endoscopy without procuring extensive biopsies, then repeat endoscopy with extensive biopsies is needed prior to deciding the treatment path. The rationale behind extensive biopsies is to confirm the diagnosis and to determine the extent of dysplasia. Other factors potentially influencing the treatment path include the patient’s age, comorbid conditions, quality of life, and available access to an advanced endoscopist or specialized surgeon. Patient’s preferences and adherence to follow-up visits should also be a consideration.
The long-term benefits of endoscopic intervention versus surgical intervention are not well established. Esophagectomy is no longer a preferred method of treatment due to high morbidity and mortality associated with the procedure when compared to endoscopic interventions. However, it is still a preferred choice amongst a select group of patients unwilling to follow-up. A cost-effective analysis found that endoscopic ablation provided the longest quality adjusted life expectancy for Barrett’s esophagus with HGD [79,80].
Endoscopic Therapy in Barrett’s Esophagus
Endoscopic Ablative Therapies
With the advancement of endoscopic intervention, we now have multiple tools to ablate abnormal epithelium in Barrett’s esophagus. Examples of ablation techniques include thermal, photochemical, and mechanical techniques [81,82]. RFA is the treatment of choice for ablation [83]. However, non-contact ablative therapy, such as cryoablation, may be prefered if topography of the esophagus doesn’t allow contact ablation.
Radiofrequency Ablation (Figure 2). RFA is a procedure in which heat is generated from medium frequency alternating current and leads to thermal injury [84]. In Barrett’s esophagus, RFA uses radiofrequency energy delivered by a balloon that has a series of closely spaced electrodes in a
Most patients will require multiple sessions of RFA to achieve eradication. It is very rarely a one-time procedure. In a meta-analysis of 18 studies including 3082 patients, the most common adverse effects of RFA were stricture in 5% [76,98], bleeding in 1%, and pain in 3% of patients [99].
It is crucial for successful RFA to continue medical treatment for acid suppression, in order to allow healthy regeneration of the squamous cell lining. It is suggested to use PPI twice a day with sucralfate and ranitidine after the intervention [100,101]. Adhering to a liquid diet for 24 hours is needed, followed by a soft diet to allow faster regeneration of the epithelium.
The caveat with RFA is that new evidence shows a higher rate of recurrence than previously thought. In one study of 246 patients, recurrence of dysplasia occurred in 25% of patients at 48 months after eradication in 80% of the patients, and metaplasia occurred in 50% at 60 months [102]. The other risk is buried Barrett’s, a condition occurring after incomplete ablation, in which squamous cell epithelium covers patches of incompletely destroyed intestinal lining, leading to possible progression of the disease to adenocarcinoma under the surface [103].
It has been reported that patients who underwent RFA had remarkable improvement in quality of life even if RFA did not achieve eradication. Patients reported less depression, less stress and better quality of life [104].
Based on a survey of experts, follow-up at 3 months, 6 months, and then annually is recommended after ablation [1,105]. Biopsies should be taken distal to neosquamous epithelium and from suspicious areas [97,106].
Endoscopic Spray Cryotherapy. This technique involves application of liquid nitrogen or carbon dioxide gas by endoscope on the tissue to freeze it off. Although it has been shown to eliminate HGD in over 95% of the cases and all dysplasia in over 85% of the cases, it was effective in eradicating intestinal metaplasia in only 55% of patients [103,108,109]. Thus, RFA as ablation therapy is still superior to cryotherapy and is still the first-line treatment for dysplastic Barrett’s esophagus. In comparison to cryotherapy, RFA efficacy has been studied extensively with well documented outcomes. However, there is a role for cryotherapy over RFA in certain clinical situations (such as severe chest pain from RFA or lack of efficacy in eradicating intestinal metaplasia or dysplasia by RFA).
Similar to RFA, on occasions of partial ablation, the remaining metaplastic tissue may get buried beneath a layer of squamous epithelium and can possibly progress to adenocarcinoma [110].
Photodynamic Therapy (PDT). This technique works by producing cytotoxicity at the cellular level by exposure to light at a specific wavelength in the presence of a chemical agent known as photosensitize [107]. Although superior to omeprazole, PDT has a significant rate of complications, mainly stricture, and a high occurrence of esophageal cancer during follow-up. For this reason, it is less favorable compared to RFA [107] and mentioned here as a historical therapy.
Endoscopic Resection Techniques: Endoscopic Mucosal Resection (EMR) and Endoscopic Submucosal Dissection (ESD)
Unlike flat mucosa in Barrett’s esophagus, which respond to ablative techniques such as RFA or cryotherapy, nodular Barrett’s esophagus is hard to treat and requires endoscopic resection prior to ablation. Endoscopic mucosal resection (EMR) is the most widely used technique and it is available in most tertiary referral centers. Another technique named endoscopic submucosal dissection (ESD) allows the removal of large nodular areas of Barrett’s esophagus in one piece to ensure complete removal of nodular dysplasia. ESD is technically challenging and it is only available in a handful of centers in the US. Endoscopic resection techniques are the preferred interventions for nodular dysplasia due to their ability to provide valuable information for staging the lesion [111–113]. Endoscopic resection techniques are safer and more effective with similar or better results when compared with other approaches [114].
EMR is completed by the excision of esophageal mucosa down to the submucosa and submitting a large tissue specimen to the pathologist. It additionally serves as a therapeutic measure in cases of no submucosal extension. Another advantage of EMR is the ability to predict lymph node metastasis. The rationale is based on the fact that the most important predictor of lymph node metastasis is the depth of the tumor; hence, invasive tumors would likely be associated with lymph node metastasis [115,116].
In a systematic review of 11 studies, complete EMR was as equally effective in the short-term treatment of dysplastic Barrett’s esophagus when compared to RFA, but adverse event rates were greater with complete EMR (mainly strictures). Strictures are more likely to occur in patients undergoing extensive EMR. In another meta-analysis of 22 studies comparing the efficacy of EMR to RFA, both techniques were effective in eradicating dysplasia (95% in EMR group and 92% in RFA group). However, extensive EMR was associated with higher complication rates suggesting that a combined endoscopic approach of focal EMR followed by RFA is preferred over extensive EMR alone [86].
It should be noted that EMR and ESD information were derived from highly specialized center and these results may not be duplicated in community settings [113,117].
Efficacy of Endoscopic Resection. Endoscopic resection has a success rate comparable to surgical esophagectomy with fewer complications [113,114,118–121] in patients with HGD and early stages of esophageal cancer [122]. Complete remission can be as high as 89%. Recurrence occurred in 6% to 30% of patients [114,118,119], which was attributed to incomplete removal, large lesions, failure to use adjunct therapy, or lack of follow-up [123]. Even when recurrence occurred, it was successfully managed by endoscopic intervention [124].
In a large cohort study of 1000 patients with early mucosal adenocarcinoma who were treated with endoscopic resection, long-term complete remission occurred in 94% of patients. There was no mortality and less than 2% of patients had major complications. Infrequent complications include bleeding, perforations, and strictures [123,125,126]. The rate of complications is lower in highly specialized centers [127–129].
Surgery was necessary in 12 patients (3.7%) after endoscopic therapy failed [123]. Post-resection care and follow-up is similar to the post-RFA care discussed above.
Management of Invasive Esophageal Adenocarcinoma
Patients diagnosed with an invasive adenocarcinoma need to be referred to an oncologist for staging and to discuss treatment options. A select number of patients may be referred by oncology for endoscopic resection, yet the need for a multidisciplinary approach in these situations is absolutely necessary [1].
Esophagectomy
Esophagectomy offers the complete removal of the HGD along with any adenocarcinoma in the regional lymph nodes. However, mortality rates are as high as 12% immediately after the procedure [130]. The multitude of short- and long-term morbidity has significant effects on quality of life. Short-term morbidity is as high as 30%. Patients may develop serious postoperative complications such as myocardial infarction, hospital associated pneumonia, or anatomic leak [131].
Examples of long-term morbidity include dysphagia, transection of vagal nerve, and dumping syndrome. Recent development in minimally invasive surgeries for esophagectomy has not reduced postoperative morbidity rates [132].
Advocates of esophagectomy illustrate the advantage of eradication of occult lymph node metastasis. The counter argument has been established by a systemic review in which occult lymph node metastasis occurred in less than 2% of patients with HGD and intramucosal carcinoma; whereas the mortality rate after esophagectomy is substantially higher with no guarantee of curing metastatic disease [133].
Prevention of Barrett’s Esophagus
Since Barrett’s esophagus precedes most of the cases of EAC if not all [1,134], methods that aim at decreasing the incidence of Barrett’s esophagus could help in prevention. The modifiable risk factors listed by the AGA include BMI, GERD, and hiatal hernia management. Along with diet and exercise, the advent of new therapies to help patients manage their weight could in return help in avoiding a plethora of medical conditions including Barrett’s esophagus. Hiatal hernia management could lower the risk of Barrett’s by restoring normal anatomy. Lastly, proper management of GERD would lower the risk of developing Barrett’s esophagus as discussed in this article [1,9].
It is worth noting that a large trial on the efficacy and safety of aspirin for prevention of adenocarcinoma progression in Barrett’s esophagus is ongoing in the UK (AspECT trial). The AspECT trial examines the efficacy of low dose vs. high dose PPI with or without aspirin for the chemoprevention of esophageal adenocarcinoma. The theory behind the study is the inhibition of COX 2 receptors in Barrett’s cells can decrease tissue progression to cancer. This chempreventive effect of nonsteroidal anti-inflammatory drugs was shown to be augmented when combined with statin intake [56,135–138].
Conclusion
Barrett’s esophagus is usually diagnosed during routine endoscopic examination. The initial symptoms are those associated with GERD, like heartburn, dyspepsia, and regurgitation. Specialized columnar epithelium is the hallmark of histopathological diagnosis. Recommendations of the ACG and AGA suggest treatment based on biopsy results. The intervention would vary on a wide spectrum starting from acid suppression, radiofrequency ablation, endoscopic resection therapy, and rarely, esophagectomy.
Corresponding author: Mohamed O. Othman, MD, Gastroenterology and Hepatology Section, Baylor College of Medicine, 7200 Cambridge St., Suite 8C, Houston, TX 77030, [email protected].
Financial disclosures: Dr. Othman has received grant support from Abbvie and has served as a consultant for Olympus.
1. Shaheen NJ, Falk GW, Iyer PG, Gerson LB; American College of Gastroenterology. ACG Clinical Guideline: diagnosis and management of Barrett’s esophagus. Am J Gastroenterol 2016;111:30–50; quiz 51.
2. Peters JH, Clark GW, Ireland AP. Outcome of adenocarcinoma arising in Barrett’s esophagus in endoscopically surveyed and nonsurveyed patients. J Thorac Cardiovasc Surg 1994;108:813–21; discussion 821–2.
3. Streitz JM Jr, Andrews CW Jr, Ellis FH Jr. Endoscopic surveillance of Barrett’s esophagus. Does it help? J Thorac Cardiovasc Surg 1993;105:383–7; discussion 387–8.
4. Spechler SJ, Souza RF. Barrett’s esophagus. N Engl J Med 2014;371:836–45.
5. Spechler SJ, Sharma P, Souza RF, et al; American Gastroenterological Association. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology 2011;140:1084–91.
6. Sharma P, McQuaid K, Dent J, et al; AGA Chicago Workshop. A critical review of the diagnosis and management of Barrett’s esophagus: the AGA Chicago Workshop. Gastroenterology 2004;127:310–30.
7. ASGE Standards of Practice Committee, Evans JA, Early DS; Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. The role of endoscopy in Barrett’s esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc 2012;76(6):1087–94.
8. Wani S, Rubenstein JH, Vieth M, Bergman J. Diagnosis and management of low–grade dysplasia in Barrett’s esophagus: Expert review from the clinical practice updates Committee of the American Gastroenterological Association. Gastroenterology 2016;151:822–835.
9. American Gastroenterological, A., et al., American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology, 2011. 140(3): p. 1084–91. [Same as #5]
10. Van Eyken P. Definition of Barrett’s oesophagus. Acta Gastroenterol Belg 2000;63:10–2.
11. Hirota WK, Loughney TM, Lazas DJ, et al. Specialized intestinal metaplasia, dysplasia, and cancer of the esophagus and esophagogastric junction: prevalence and clinical data. Gastroenterology 1999;116(2):277–85.
12. Cameron AJ, Zinsmeister AR, Ballard DJ, Carney JA. Prevalence of columnar–lined (Barrett’s) esophagus. Comparison of population–based clinical and autopsy findings. Gastroenterology 1990;99:918–22.
13. Gerson LB, Shetler K, Triadafilopoulos G. Prevalence of Barrett’s esophagus in asymptomatic individuals. Gastroenterology 2002;123:461–7.
14. Van der Veen AH, Dees J, Blankensteijn JD, Van Blankenstein M. Adenocarcinoma in Barrett’s oesophagus: an overrated risk. Gut 1989;30:14–8.
15. Winters C Jr, Spurling TJ, Chobanian SJ, et al. Barrett’s esophagus. A prevalent, occult complication of gastroesophageal reflux disease. Gastroenterology 1987;92:118–24.
16. Wani S, Falk G, Hall M, et al. Patients with nondysplastic Barrett’s esophagus have low risks for developing dysplasia or esophageal adenocarcinoma. Clin Gastroenterol Hepatol 2011;9:220–7;quiz e26.
17. Ward EM, Wolfsen HC, Achem SR, et al. Barrett’s esophagus is common in older men and women undergoing screening colonoscopy regardless of reflux symptoms. Am J Gastroenterol 2006;101:12–7.
18. Rex DK, Cummings OW, Shaw M. Screening for Barrett’s esophagus in colonoscopy patients with and without heartburn. Gastroenterology 2003;125:1670–7.
19. Rubenstein JH, Taylor JB. Meta–analysis: the association of oesophageal adenocarcinoma with symptoms of gastro–oesophageal reflux. Aliment Pharmacol Ther 2010;32:1222–7.
20. Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 1999;340:825–31.
21. Ronkainen J, Aro P, Storskrubb T, et al. Prevalence of Barrett’s esophagus in the general population: an endoscopic study. Gastroenterology, 2005;129:1825–31.
22. Sampliner RE. A population prevalence of Barrett’s esophagus––finally. Gastroenterology 2005; 129:2101–3.
23. Abrams JA, Fields S, Lightdale CJ, Neugut AI. Racial and ethnic disparities in the prevalence of Barrett’s esophagus among patients who undergo upper endoscopy. Clin Gastroenterol Hepatol 2008;6:30–4.
24. Corley DA, Kubo A, Levin TR, et al. Race, ethnicity, sex and temporal differences in Barrett’s oesophagus diagnosis: a large community–based study, 1994–2006. Gut 2009;58:182–8.
25. Kamat P, Wen S, Morris J, Anandasabapathy S. Exploring the association between elevated body mass index and Barrett’s esophagus: a systematic review and meta–analysis. Ann Thorac Surg 2009;87:655–62.
26. Jacobson BC, Chan AT, Giovannucci EL, Fuchs CS. Body mass index and Barrett’s oesophagus in women. Gut 2009;58:1460–6.
27. Orloff M, Peterson C, He X, et al. Germline mutations in MSR1, ASCC1, and CTHRC1 in patients with Barrett esophagus and esophageal adenocarcinoma. JAMA 2011;306:410–9.
28. Sharma N, Ho KY. Risk Factors for Barrett’s oesophagus. Gastrointest Tumors 2016;3:103–8.
29. Spechler SJ. Barrett’s esophagus. Semin Gastrointest Dis 1996;7:51–60.
30. Ronkainen J, Talley NJ, Storskrubb T. Erosive esophagitis is a risk factor for Barrett’s esophagus: a community–based endoscopic follow–up study. Am J Gastroenterol 2011;106:1946–52.
31. Kim SL, Wo JM, Hunter JG. The prevalence of intestinal metaplasia in patients with and without peptic strictures. Am J Gastroenterol 1998;93:53–5.
32. Spechler SJ. Clinical practice. Barrett’s esophagus. N Engl J Med 2002;346:836–42.
33. Riddell RH, Odze RD. Definition of Barrett’s esophagus: time for a rethink––is intestinal metaplasia dead? Am J Gastroenterol 2009;104:2588–94.
34. Sharma P, Morales TG, Sampliner RE. Short segment Barrett’s esophagus––the need for standardization of the definition and of endoscopic criteria. Am J Gastroenterol 1998;93:1033–6.
35. Eloubeidi MA, Provenzale D. Does this patient have Barrett’s esophagus? The utility of predicting Barrett’s esophagus at the index endoscopy. Am J Gastroenterol 1999;94:937–43.
36. Rudolph RE, Vaughan TL, Storer BE, et al. Effect of segment length on risk for neoplastic progression in patients with Barrett esophagus. Ann Intern Med 2000;132:612–20.
37. Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett’s esophagus: the Prague C & M criteria. Gastroenterology 2006;131:1392–9.
38. Bhat S, Coleman HG, Yousef F, et al. Risk of malignant progression in Barrett’s esophagus patients: results from a large population–based study. J Natl Cancer Inst 2011;103:1049–57.
39. Shaheen NJ, Dulai GS, Ascher B, et al. Effect of a new diagnosis of Barrett’s esophagus on insurance status. Am J Gastroenterol 2005;100:577–80.
40. Canto MI, Setrakian S, Willis J, et al. Methylene blue–directed biopsies improve detection of intestinal metaplasia and dysplasia in Barrett’s esophagus. Gastrointest Endosc 2000;51:560–8.
41. Scotiniotis IA, Kochman ML, Lewis JD. Accuracy of EUS in the evaluation of Barrett’s esophagus and high–grade dysplasia or intramucosal carcinoma. Gastrointest Endosc 2001;54:689–96.
42. Kobayashi K, Izatt JA, Kulkarni MD, et al. High–resolution cross–sectional imaging of the gastrointestinal tract using optical coherence tomography: preliminary results. Gastrointest Endosc 1998;47:515–23.
43. Georgakoudi I, Jacobson BC, Van Dam J, et al. Fluorescence, reflectance, and light–scattering spectroscopy for evaluating dysplasia in patients with Barrett’s esophagus. Gastroenterology 2001. 120: 1620–9.
44. Wallace MB, Sharma P, Lightdale C, et al. Preliminary accuracy and interobserver agreement for the detection of intraepithelial neoplasia in Barrett’s esophagus with probe–based confocal laser endomicroscopy. Gastrointest Endosc 2010;72:19–24.
45. Qumseya BJ, Wang H, Badie N, et al. Advanced imaging technologies increase detection of dysplasia and neoplasia in patients with Barrett’s esophagus: a meta–analysis and systematic review. Clin Gastroenterol Hepatol 2013;11:1562–70.e1–2.–
46. DeVault KR, Castell DO. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. The Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol 1999;94:1434–42.
47. Inadomi JM, Sampliner R, Lagergren J. Screening and surveillance for Barrett esophagus in high–risk groups: a cost–utility analysis. Ann Intern Med 2003;138:176–86.
48. Conio M, Blanchi S, Lapertosa G, et al. Long–term endoscopic surveillance of patients with Barrett’s esophagus. Incidence of dysplasia and adenocarcinoma: a prospective study. Am J Gastroenterol 2003;98:1931–9.
49. Rastogi A, Puli S, El–Serag HB, et al. Incidence of esophageal adenocarcinoma in patients with Barrett’s esophagus and high–grade dysplasia: a meta–analysis. Gastrointest Endosc 2008;67:394–8.
50. Kadri SR, Lao–Sirieix P, O’Donovan M, et al. Acceptability and accuracy of a non–endoscopic screening test for Barrett’s oesophagus in primary care: cohort study. BMJ 2010;341:c4372.
51. Sharma, P., et al., A critical review of the diagnosis and management of Barrett’s esophagus: the AGA Chicago Workshop. Gastroenterology, 2004. 127(1): p. 310–30. [Same as #6]
52. Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 2013;108:308–28; quiz 329.
53. Kim SL, Waring JP, Spechler SJ, et al. Diagnostic inconsistencies in Barrett’s esophagus. Department of Veterans Affairs Gastroesophageal Reflux Study Group. Gastroenterology 1994;107:945–9.
54. Kastelein F, Spaander MC, Steyerberg EW, et al; ProBar Study Group. Proton pump inhibitors reduce the risk of neoplastic progression in patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 2013;11:382–8.
55. El–Serag HB, Aguirre TV, Davis S, et al. Proton pump inhibitors are associated with reduced incidence of dysplasia in Barrett’s esophagus. Am J Gastroenterol 2004;99:1877–83.
56. Nguyen DM, El–Serag HB, Henderson L, et al. Medication usage and the risk of neoplasia in patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 2009;7:1299–304.
57. Singh S, Garg SK, Singh PP, et al. Acid–suppressive medications and risk of oesophageal adenocarcinoma in patients with Barrett’s oesophagus: a systematic review and meta–analysis. Gut 2014;63:1229–37.
58. Spechler SJ, Lee E, Ahnen D, et al. Long–term outcome of medical and surgical therapies for gastroesophageal reflux disease: follow–up of a randomized controlled trial. JAMA 2001;285:2331–8.
59. Peters FT, Ganesh S, Kuipers EJ, et al. Endoscopic regression of Barrett’s oesophagus during omeprazole treatment; a randomised double blind study. Gut 1999;45:489–94.
60. Ouatu–Lascar R, Triadafilopoulos G. –Complete elimination of reflux symptoms does not guarantee normalization of intraesophageal acid reflux in patients with Barrett’s esophagus. Am J Gastroenterol 1998;93:711–6.
61. Maret–Ouda J, Konings P, Lagergren J, Brusselaers N. Antireflux surgery and risk of esophageal adenocarcinoma: A systematic review and meta–analysis. Ann Surg 2016;263:251–7.
62. Evans, J.A., et al., The role of endoscopy in Barrett’s esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc, 2012. 76(6): p. 1087–94. [Same as #7]
63. ASGE Standards of Practice Committee, Evans JA, Early DS,et al; American Society for Gastrointestinal Endoscopy. The role of endoscopy in the assessment and treatment of esophageal cancer. Gastrointest Endosc 2013;77:328–34.
64. Bennett C, Moayyedi P, Corley DA, et al; BOB CAT Consortium. BOB CAT: A large–scale review and delphi consensus for ,anagement of Barrett’s esophagus with no dysplasia, indefinite for, or low–grade dysplasia. Am J Gastroenterol 2015;110:662–82; quiz 683.
65. Sikkema M, de Jonge PJ, Steyerberg EW, Kuipers EJ. Risk of esophageal adenocarcinoma and mortality in patients with Barrett’s esophagus: a systematic review and meta–analysis. Clin Gastroenterol Hepatol 2010;8:235–44; quiz e32.
66. Old O, Moayyedi P, Love S, et al; BOSS Trial Team. Barrett’s Oesophagus Surveillance versus endoscopy at need Study (BOSS): protocol and analysis plan for a multicentre randomized controlled trial. J Med Screen 2015;22:158–64.
67. Weston AP, Sharma P, Topalovski M, et al. Long–term follow–up of Barrett’s high–grade dysplasia. Am J Gastroenterol 2000;95:1888–93.
68. Paull A, Trier JS, Dalton MD, et al. The histologic spectrum of Barrett’s esophagus. N Engl J Med 1976;295:476–80.
69. Konda VJ, Ross AS, Ferguson MK, et al. Is the risk of concomitant invasive esophageal cancer in high–grade dysplasia in Barrett’s esophagus overestimated? Clin Gastroenterol Hepatol 2008;6:159–64.
70. Allison H, Banchs MA, Bonis PA, Guelrud M. Long–term remission of nondysplastic Barrett’s esophagus after multipolar electrocoagulation ablation: report of 139 patients with 10 years of follow–up. Gastrointest Endosc 2011;73:651–8.
71. Corley DA, Levin TR, Habel LA, Weiss NS, et al. Surveillance and survival in Barrett’s adenocarcinomas: a population–based study. Gastroenterology 2002;122:633–40.
72. Wong T, Tian J, Nagar AB. Barrett’s surveillance identifies patients with early esophageal adenocarcinoma. Am J Med 2010;123:462–7.
73. Fountoulakis A, Zafirellis KD, Dolan K, et al. Effect of surveillance of Barrett’s oesophagus on the clinical outcome of oesophageal cancer. Br J Surg 2004;91:997–1003.
74. Verbeek RE, Leenders M, Ten Kate FJ, et al. Surveillance of Barrett’s esophagus and mortality from esophageal adenocarcinoma: a population–based cohort study. Am J Gastroenterol 2014;109:1215–22.
75. Kastelein F, van Olphen SH, Steyerberg EW, et al. Impact of surveillance for Barrett’s oesophagus on tumour stage and survival of patients with neoplastic progression. Gut 2016;65:548–54.
76. Phoa KN, van Vilsteren FG, Weusten BL, et al. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low–grade dysplasia: a randomized clinical trial. JAMA 2014;311: 1209–17.
77. Wang WL, Chang IW, Chen CC, et al. Radiofrequency ablation versus endoscopic submucosal dissection in treating large early esophageal squamous cell neoplasia. Medicine (Baltimore) 2015;94:e2240.
78. Lim CH, Treanor D, Dixon MF, Axon AT. Low–grade dysplasia in Barrett’s esophagus has a high risk of progression. Endoscopy 2007;39:581–7.
79. Shaheen NJ, Inadomi JM, Overholt BF, Sharma P. What is the best management strategy for high grade dysplasia in Barrett’s oesophagus? A cost effectiveness analysis. Gut 2004;53:1736–44.
80. Vij R, Triadafilopoulos G, Owens DK, et al. Cost–effectiveness of photodynamic therapy for high–grade dysplasia in Barrett’s esophagus. Gastrointest Endosc 2004;60:739–56.
81. van den Boogert J, v an Hillegersberg R, Siersema PD, et al. Endoscopic ablation therapy for Barrett’s esophagus with high–grade dysplasia: a review. Am J Gastroenterol 1999;94:1153–60.
82. Sampliner RE. Endoscopic ablative therapy for Barrett’s esophagus: current status. Gastrointest Endosc 2004;59:66–9.
83. Sharma VK, Wang KK, Overholt BF, et al. Balloon–based, circumferential, endoscopic radiofrequency ablation of Barrett’s esophagus: 1–year follow–up of 100 patients. Gastrointest Endosc 2007;65:185–95.
84. Hanlon CR. Textbook of surgery: The biological basis of modern surgical practice, 14th edition. Ann Surg 1992;216:94.
85. Bright T, Watson DI, Tam W, et al. Randomized trial of argon plasma coagulation versus endoscopic surveillance for barrett esophagus after antireflux surgery: late results. Ann Surg 2007;246:1016–20.
86. Chadwick G, Groene O, Markar SR, et al. Systematic review comparing radiofrequency ablation and complete endoscopic resection in treating dysplastic Barrett’s esophagus: a critical assessment of histologic outcomes and adverse events. Gastrointest Endosc 2014;79:718–31.e3.
87. Gondrie JJ, Pouw RE, Sondermeijer CM, et al. Effective treatment of early Barrett’s neoplasia with stepwise circumferential and focal ablation using the HALO system. Endoscopy 2008;40:370–9.
88. Pouw RE, Wirths K, Eisendrath P, et al. Efficacy of radiofrequency ablation combined with endoscopic resection for barrett’s esophagus with early neoplasia. Clin Gastroenterol Hepatol 2010;8:23–9.
89. Kim HP, Bulsiewicz WJ, Cotton CC, et al. Focal endoscopic mucosal resection before radiofrequency ablation is equally effective and safe compared with radiofrequency ablation alone for the eradication of Barrett’s esophagus with advanced neoplasia. Gastrointest Endosc 2012;76:733–9.
90. Fleischer DE, Overholt BF, Sharma VK, et al. Endoscopic ablation of Barrett’s esophagus: a multicenter study with 2.5–year follow–up. Gastrointest Endosc 2008;68:867–76.
91. Sharma VK, Jae Kim H, Das A, et al. Circumferential and focal ablation of Barrett’s esophagus containing dysplasia. Am J Gastroenterol 2009;104:310–7.
92. Ganz RA, Overholt BF, Sharma VK, et al. Circumferential ablation of Barrett’s esophagus that contains high–grade dysplasia: a U.S. multicenter registry. Gastrointest Endosc 2008;68:35–40.
93. Gupta M, Iyer PG, Lutzke L, et al. Recurrence of esophageal intestinal metaplasia after endoscopic mucosal resection and radiofrequency ablation of Barrett’s esophagus: results from a US Multicenter Consortium. Gastroenterology 2013;145:79–86.e1.
94. Lyday WD, Corbett FS, Kuperman DA, et al. Radiofrequency ablation of Barrett’s esophagus: outcomes of 429 patients from a multicenter community practice registry. Endoscopy 2010;42:272–8.
95. Pasricha S, Bulsiewicz WJ, Hathorn KE, et al. Durability and predictors of successful radiofrequency ablation for Barrett’s esophagus. Clin Gastroenterol Hepatol 2014;12:1840–7.e1.
96. Fleischer DE, Overholt BF, Sharma VK, et al. Endoscopic radiofrequency ablation for Barrett’s esophagus: 5–year outcomes from a prospective multicenter trial. Endoscopy 2010;42:781–9.
97. Weston AP, Sharma P, Banerjee S, et al. Visible endoscopic and histologic changes in the cardia, before and after complete Barrett’s esophagus ablation. Gastrointest Endosc 2005;61:515–21.
98. Beaumont H, Gondrie JJ, McMahon BP, et al. Stepwise radiofrequency ablation of Barrett’s esophagus preserves esophageal inner diameter, compliance, and motility. Endoscopy 2009;41:2–8.
99. Orman ES, Li N, Shaheen NJ.Efficacy and durability of radiofrequency ablation for Barrett’s Esophagus: systematic review and meta–analysis. Clin Gastroenterol Hepatol 2013;11:1245–55.
100. Krishnan K, Pandolfino JE, Kahrilas PJ, et al. Increased risk for persistent intestinal metaplasia in patients with Barrett’s esophagus and uncontrolled reflux exposure before radiofrequency ablation. Gastroenterology 2012;143:576–81.
101. Akiyama J, Marcus SN, Triadafilopoulos G. Effective intra–esophageal acid control is associated with improved radiofrequency ablation outcomes in Barrett’s esophagus. Dig Dis Sci 2012;57:2625–32.
102. Small AJ, Sutherland SE, Hightower JS, et al. Comparative risk of recurrence of dysplasia and carcinoma after endoluminal eradication therapy of high–grade dysplasia versus intramucosal carcinoma in Barrett’s esophagus. Gastrointest Endosc 2015;81:1158–66.e1–4.
103. Shaheen NJ, Greenwald BD, Peery AF, et al. Safety and efficacy of endoscopic spray cryotherapy for Barrett’s esophagus with high–grade dysplasia. Gastrointest Endosc 2010;71:680–5.
104. Shaheen NJ, Peery AF, Hawes RH, et al. Quality of life following radiofrequency ablation of dysplastic Barrett’s esophagus. Endoscopy 2010;42:790–9.
105. Bedi AO, Kwon RS, Rubenstein JH, et al. A survey of expert follow–up practices after successful endoscopic eradication therapy for Barrett’s esophagus with high–grade dysplasia and intramucosal adenocarcinoma. Gastrointest Endosc 2013;78:696–701.
106. Sampliner RE, Camargo E, Prasad AR. Prasad, Association of ablation of Barrett’s esophagus with high grade dysplasia and adenocarcinoma of the gastric cardia. Dis Esophagus 2006;19:277–9.
107. Overholt BF, Panjehpour M, Halberg DL. Photodynamic therapy for Barrett’s esophagus with dysplasia and/or early stage carcinoma: long–term results. Gastrointest Endosc 2003;58:183–8.
108. Gosain S, Mercer K, Twaddell WS, et al. Liquid nitrogen spray cryotherapy in Barrett’s esophagus with high–grade dysplasia: long–term results. Gastrointest Endosc 2013;78:260–5.
109. Canto MI, Shin EJ, Khashab MA, et al. Safety and efficacy of carbon dioxide cryotherapy for treatment of neoplastic Barrett’s esophagus. Endoscopy 2015;47:582–91.
110. Van Laethem JL, Peny MO, Salmon I, et al. Intramucosal adenocarcinoma arising under squamous re–epithelialisation of Barrett’s oesophagus. Gut 2000;46:574–7.
111. Pech O, May A, Gossner L, et al. Management of pre–malignant and malignant lesions by endoscopic resection. Best Pract Res Clin Gastroenterol 2004;18:61–76.
112. Soetikno RM, Gotoda T, Nakanishi Y, Soehendra N. Endoscopic mucosal resection. Gastrointest Endosc 2003;57:567–79.
113. Ell C, May A, Gossner L, et al. Endoscopic mucosal resection of early cancer and high–grade dysplasia in Barrett’s esophagus. Gastroenterology 2000;118:670–7.
114. Pech O, Behrens A, May A, et al. Long–term results and risk factor analysis for recurrence after curative endoscopic therapy in 349 patients with high–grade intraepithelial neoplasia and mucosal adenocarcinoma in Barrett’s oesophagus. Gut 2008;57:1200–6.
115. Vieth M, Ell C, Gossner L, et al. Histological analysis of endoscopic resection specimens from 326 patients with Barrett’s esophagus and early neoplasia. Endoscopy 2004;36:776–81.
116. Buskens CJ, Westerterp M, Lagarde SM, et al. Prediction of appropriateness of local endoscopic treatment for high–grade dysplasia and early adenocarcinoma by EUS and histopathologic features. Gastrointest Endosc 2004;60:703–10.
117. Nijhawan PK, Wang KK. Endoscopic mucosal resection for lesions with endoscopic features suggestive of malignancy and high–grade dysplasia within Barrett’s esophagus. Gastrointest Endosc 2000;52:328–32.
118. Esaki M, Matsumoto T, Hirakawa K, et al. Risk factors for local recurrence of superficial esophageal cancer after treatment by endoscopic mucosal resection. Endoscopy 2007;39:41–5.
119. Ell C, May A, Pech O, et al. Curative endoscopic resection of early esophageal adenocarcinomas (Barrett’s cancer). Gastrointest Endosc 2007;65:3–10.
120. Chennat J, Konda VJ, Ross AS, et al. Complete Barrett’s eradication endoscopic mucosal resection: an effective treatment modality for high–grade dysplasia and intramucosal carcinoma––an American single–center experience. Am J Gastroenterol 2009;104:2684–92.
121. Pech O, Bollschweiler E, Manner H, et al. Comparison between endoscopic and surgical resection of mucosal esophageal adenocarcinoma in Barrett’s esophagus at two high–volume centers. Ann Surg 2011;254:67–72.
122. Wu J, Pan YM, Wang TT, et al. Endotherapy versus surgery for early neoplasia in Barrett’s esophagus: a meta–analysis. Gastrointest Endosc 2014;79:233–241.e2.
123. Pech O, May A, Manner H, et al. Long–term efficacy and safety of endoscopic resection for patients with mucosal adenocarcinoma of the esophagus. Gastroenterology 2014;146:652–660.e1.
124. Prasad GA, Wu TT, Wigle DA, et al. Endoscopic and surgical treatment of mucosal (T1a) esophageal adenocarcinoma in Barrett’s esophagus. Gastroenterology 2009;137:815–23.
125. May A, Gossner L, Pech O, et al. Local endoscopic therapy for intraepithelial high–grade neoplasia and early adenocarcinoma in Barrett’s oesophagus: acute–phase and intermediate results of a new treatment approach. Eur J Gastroenterol Hepatol 2002;14(10):1085–91.
126. Gerke H, Siddiqui J, Nasr I, et al. Efficacy and safety of EMR to completely remove Barrett’s esophagus: experience in 41 patients. Gastrointest Endosc 2011;74:761–71.
127. Lewis JJ, Rubenstein JH, Singal AG, et al. Factors associated with esophageal stricture formation after endoscopic mucosal resection for neoplastic Barrett’s esophagus. Gastrointest Endosc 2011;74:753–60.
128. Choi IJ, Kim CG, Chang HJ, et al. The learning curve for EMR with circumferential mucosal incision in treating intramucosal gastric neoplasm. Gastrointest Endosc 2005;62:860–5.
129. Deprez PH, Bergman JJ, Meisner S, et al. Current practice with endoscopic submucosal dissection in Europe: position statement from a panel of experts. Endoscopy 2010;42:853–8.
130. van Lanschot JJ, Hulscher JB, Buskens CJ, et al. Hospital volume and hospital mortality for esophagectomy. Cancer 2001;91:1574–8.
131. Karl RC, Schreiber R, Boulware D, et al. Factors affecting morbidity, mortality, and survival in patients undergoing Ivor Lewis esophagogastrectomy. Ann Surg 2000;231:635–43.
132. Young MM, Deschamps C, Trastek VF, et al. Esophageal reconstruction for benign disease: early morbidity, mortality, and functional results. Ann Thorac Surg 2000;70:1651–5.
133. Dunbar KB, Spechler SJ. The risk of lymph–node metastases in patients with high–grade dysplasia or intramucosal carcinoma in Barrett’s esophagus: a systematic review. Am J Gastroenterol 2012;107:850–62; quiz 863.
134. Morales CP, Souza RF, Spechler SJ. Hallmarks of cancer progression in Barrett’s oesophagus. Lancet 2002;360:1587–9.
135. Omer ZB, Ananthakrishnan AN, Nattinger KJ, et al. Aspirin protects against Barrett’s esophagus in a multivariate logistic regression analysis. Clin Gastroenterol Hepatol 2012;10:722–7.
136. Abnet CC, Freedman ND, Kamangar F, et al. Non–steroidal anti–inflammatory drugs and risk of gastric and oesophageal adenocarcinomas: results from a cohort study and a meta–analysis. Br J Cancer 2009;100:551–7.
137. Kastelein F, Spaander MC, Biermann K, et al. Nonsteroidal anti–inflammatory drugs and statins have chemopreventative effects in patients with Barrett’s esophagus. Gastroenterology 2011;141:2000–8; quiz e13–4.
138. Zhang S, Zhang XQ, Ding XW, et al. Cyclooxygenase inhibitors use is associated with reduced risk of esophageal adenocarcinoma in patients with Barrett’s esophagus: a meta–analysis. Br J Cancer 2014;110: 2378–88.
1. Shaheen NJ, Falk GW, Iyer PG, Gerson LB; American College of Gastroenterology. ACG Clinical Guideline: diagnosis and management of Barrett’s esophagus. Am J Gastroenterol 2016;111:30–50; quiz 51.
2. Peters JH, Clark GW, Ireland AP. Outcome of adenocarcinoma arising in Barrett’s esophagus in endoscopically surveyed and nonsurveyed patients. J Thorac Cardiovasc Surg 1994;108:813–21; discussion 821–2.
3. Streitz JM Jr, Andrews CW Jr, Ellis FH Jr. Endoscopic surveillance of Barrett’s esophagus. Does it help? J Thorac Cardiovasc Surg 1993;105:383–7; discussion 387–8.
4. Spechler SJ, Souza RF. Barrett’s esophagus. N Engl J Med 2014;371:836–45.
5. Spechler SJ, Sharma P, Souza RF, et al; American Gastroenterological Association. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology 2011;140:1084–91.
6. Sharma P, McQuaid K, Dent J, et al; AGA Chicago Workshop. A critical review of the diagnosis and management of Barrett’s esophagus: the AGA Chicago Workshop. Gastroenterology 2004;127:310–30.
7. ASGE Standards of Practice Committee, Evans JA, Early DS; Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. The role of endoscopy in Barrett’s esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc 2012;76(6):1087–94.
8. Wani S, Rubenstein JH, Vieth M, Bergman J. Diagnosis and management of low–grade dysplasia in Barrett’s esophagus: Expert review from the clinical practice updates Committee of the American Gastroenterological Association. Gastroenterology 2016;151:822–835.
9. American Gastroenterological, A., et al., American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology, 2011. 140(3): p. 1084–91. [Same as #5]
10. Van Eyken P. Definition of Barrett’s oesophagus. Acta Gastroenterol Belg 2000;63:10–2.
11. Hirota WK, Loughney TM, Lazas DJ, et al. Specialized intestinal metaplasia, dysplasia, and cancer of the esophagus and esophagogastric junction: prevalence and clinical data. Gastroenterology 1999;116(2):277–85.
12. Cameron AJ, Zinsmeister AR, Ballard DJ, Carney JA. Prevalence of columnar–lined (Barrett’s) esophagus. Comparison of population–based clinical and autopsy findings. Gastroenterology 1990;99:918–22.
13. Gerson LB, Shetler K, Triadafilopoulos G. Prevalence of Barrett’s esophagus in asymptomatic individuals. Gastroenterology 2002;123:461–7.
14. Van der Veen AH, Dees J, Blankensteijn JD, Van Blankenstein M. Adenocarcinoma in Barrett’s oesophagus: an overrated risk. Gut 1989;30:14–8.
15. Winters C Jr, Spurling TJ, Chobanian SJ, et al. Barrett’s esophagus. A prevalent, occult complication of gastroesophageal reflux disease. Gastroenterology 1987;92:118–24.
16. Wani S, Falk G, Hall M, et al. Patients with nondysplastic Barrett’s esophagus have low risks for developing dysplasia or esophageal adenocarcinoma. Clin Gastroenterol Hepatol 2011;9:220–7;quiz e26.
17. Ward EM, Wolfsen HC, Achem SR, et al. Barrett’s esophagus is common in older men and women undergoing screening colonoscopy regardless of reflux symptoms. Am J Gastroenterol 2006;101:12–7.
18. Rex DK, Cummings OW, Shaw M. Screening for Barrett’s esophagus in colonoscopy patients with and without heartburn. Gastroenterology 2003;125:1670–7.
19. Rubenstein JH, Taylor JB. Meta–analysis: the association of oesophageal adenocarcinoma with symptoms of gastro–oesophageal reflux. Aliment Pharmacol Ther 2010;32:1222–7.
20. Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 1999;340:825–31.
21. Ronkainen J, Aro P, Storskrubb T, et al. Prevalence of Barrett’s esophagus in the general population: an endoscopic study. Gastroenterology, 2005;129:1825–31.
22. Sampliner RE. A population prevalence of Barrett’s esophagus––finally. Gastroenterology 2005; 129:2101–3.
23. Abrams JA, Fields S, Lightdale CJ, Neugut AI. Racial and ethnic disparities in the prevalence of Barrett’s esophagus among patients who undergo upper endoscopy. Clin Gastroenterol Hepatol 2008;6:30–4.
24. Corley DA, Kubo A, Levin TR, et al. Race, ethnicity, sex and temporal differences in Barrett’s oesophagus diagnosis: a large community–based study, 1994–2006. Gut 2009;58:182–8.
25. Kamat P, Wen S, Morris J, Anandasabapathy S. Exploring the association between elevated body mass index and Barrett’s esophagus: a systematic review and meta–analysis. Ann Thorac Surg 2009;87:655–62.
26. Jacobson BC, Chan AT, Giovannucci EL, Fuchs CS. Body mass index and Barrett’s oesophagus in women. Gut 2009;58:1460–6.
27. Orloff M, Peterson C, He X, et al. Germline mutations in MSR1, ASCC1, and CTHRC1 in patients with Barrett esophagus and esophageal adenocarcinoma. JAMA 2011;306:410–9.
28. Sharma N, Ho KY. Risk Factors for Barrett’s oesophagus. Gastrointest Tumors 2016;3:103–8.
29. Spechler SJ. Barrett’s esophagus. Semin Gastrointest Dis 1996;7:51–60.
30. Ronkainen J, Talley NJ, Storskrubb T. Erosive esophagitis is a risk factor for Barrett’s esophagus: a community–based endoscopic follow–up study. Am J Gastroenterol 2011;106:1946–52.
31. Kim SL, Wo JM, Hunter JG. The prevalence of intestinal metaplasia in patients with and without peptic strictures. Am J Gastroenterol 1998;93:53–5.
32. Spechler SJ. Clinical practice. Barrett’s esophagus. N Engl J Med 2002;346:836–42.
33. Riddell RH, Odze RD. Definition of Barrett’s esophagus: time for a rethink––is intestinal metaplasia dead? Am J Gastroenterol 2009;104:2588–94.
34. Sharma P, Morales TG, Sampliner RE. Short segment Barrett’s esophagus––the need for standardization of the definition and of endoscopic criteria. Am J Gastroenterol 1998;93:1033–6.
35. Eloubeidi MA, Provenzale D. Does this patient have Barrett’s esophagus? The utility of predicting Barrett’s esophagus at the index endoscopy. Am J Gastroenterol 1999;94:937–43.
36. Rudolph RE, Vaughan TL, Storer BE, et al. Effect of segment length on risk for neoplastic progression in patients with Barrett esophagus. Ann Intern Med 2000;132:612–20.
37. Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett’s esophagus: the Prague C & M criteria. Gastroenterology 2006;131:1392–9.
38. Bhat S, Coleman HG, Yousef F, et al. Risk of malignant progression in Barrett’s esophagus patients: results from a large population–based study. J Natl Cancer Inst 2011;103:1049–57.
39. Shaheen NJ, Dulai GS, Ascher B, et al. Effect of a new diagnosis of Barrett’s esophagus on insurance status. Am J Gastroenterol 2005;100:577–80.
40. Canto MI, Setrakian S, Willis J, et al. Methylene blue–directed biopsies improve detection of intestinal metaplasia and dysplasia in Barrett’s esophagus. Gastrointest Endosc 2000;51:560–8.
41. Scotiniotis IA, Kochman ML, Lewis JD. Accuracy of EUS in the evaluation of Barrett’s esophagus and high–grade dysplasia or intramucosal carcinoma. Gastrointest Endosc 2001;54:689–96.
42. Kobayashi K, Izatt JA, Kulkarni MD, et al. High–resolution cross–sectional imaging of the gastrointestinal tract using optical coherence tomography: preliminary results. Gastrointest Endosc 1998;47:515–23.
43. Georgakoudi I, Jacobson BC, Van Dam J, et al. Fluorescence, reflectance, and light–scattering spectroscopy for evaluating dysplasia in patients with Barrett’s esophagus. Gastroenterology 2001. 120: 1620–9.
44. Wallace MB, Sharma P, Lightdale C, et al. Preliminary accuracy and interobserver agreement for the detection of intraepithelial neoplasia in Barrett’s esophagus with probe–based confocal laser endomicroscopy. Gastrointest Endosc 2010;72:19–24.
45. Qumseya BJ, Wang H, Badie N, et al. Advanced imaging technologies increase detection of dysplasia and neoplasia in patients with Barrett’s esophagus: a meta–analysis and systematic review. Clin Gastroenterol Hepatol 2013;11:1562–70.e1–2.–
46. DeVault KR, Castell DO. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. The Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol 1999;94:1434–42.
47. Inadomi JM, Sampliner R, Lagergren J. Screening and surveillance for Barrett esophagus in high–risk groups: a cost–utility analysis. Ann Intern Med 2003;138:176–86.
48. Conio M, Blanchi S, Lapertosa G, et al. Long–term endoscopic surveillance of patients with Barrett’s esophagus. Incidence of dysplasia and adenocarcinoma: a prospective study. Am J Gastroenterol 2003;98:1931–9.
49. Rastogi A, Puli S, El–Serag HB, et al. Incidence of esophageal adenocarcinoma in patients with Barrett’s esophagus and high–grade dysplasia: a meta–analysis. Gastrointest Endosc 2008;67:394–8.
50. Kadri SR, Lao–Sirieix P, O’Donovan M, et al. Acceptability and accuracy of a non–endoscopic screening test for Barrett’s oesophagus in primary care: cohort study. BMJ 2010;341:c4372.
51. Sharma, P., et al., A critical review of the diagnosis and management of Barrett’s esophagus: the AGA Chicago Workshop. Gastroenterology, 2004. 127(1): p. 310–30. [Same as #6]
52. Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol 2013;108:308–28; quiz 329.
53. Kim SL, Waring JP, Spechler SJ, et al. Diagnostic inconsistencies in Barrett’s esophagus. Department of Veterans Affairs Gastroesophageal Reflux Study Group. Gastroenterology 1994;107:945–9.
54. Kastelein F, Spaander MC, Steyerberg EW, et al; ProBar Study Group. Proton pump inhibitors reduce the risk of neoplastic progression in patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 2013;11:382–8.
55. El–Serag HB, Aguirre TV, Davis S, et al. Proton pump inhibitors are associated with reduced incidence of dysplasia in Barrett’s esophagus. Am J Gastroenterol 2004;99:1877–83.
56. Nguyen DM, El–Serag HB, Henderson L, et al. Medication usage and the risk of neoplasia in patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 2009;7:1299–304.
57. Singh S, Garg SK, Singh PP, et al. Acid–suppressive medications and risk of oesophageal adenocarcinoma in patients with Barrett’s oesophagus: a systematic review and meta–analysis. Gut 2014;63:1229–37.
58. Spechler SJ, Lee E, Ahnen D, et al. Long–term outcome of medical and surgical therapies for gastroesophageal reflux disease: follow–up of a randomized controlled trial. JAMA 2001;285:2331–8.
59. Peters FT, Ganesh S, Kuipers EJ, et al. Endoscopic regression of Barrett’s oesophagus during omeprazole treatment; a randomised double blind study. Gut 1999;45:489–94.
60. Ouatu–Lascar R, Triadafilopoulos G. –Complete elimination of reflux symptoms does not guarantee normalization of intraesophageal acid reflux in patients with Barrett’s esophagus. Am J Gastroenterol 1998;93:711–6.
61. Maret–Ouda J, Konings P, Lagergren J, Brusselaers N. Antireflux surgery and risk of esophageal adenocarcinoma: A systematic review and meta–analysis. Ann Surg 2016;263:251–7.
62. Evans, J.A., et al., The role of endoscopy in Barrett’s esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc, 2012. 76(6): p. 1087–94. [Same as #7]
63. ASGE Standards of Practice Committee, Evans JA, Early DS,et al; American Society for Gastrointestinal Endoscopy. The role of endoscopy in the assessment and treatment of esophageal cancer. Gastrointest Endosc 2013;77:328–34.
64. Bennett C, Moayyedi P, Corley DA, et al; BOB CAT Consortium. BOB CAT: A large–scale review and delphi consensus for ,anagement of Barrett’s esophagus with no dysplasia, indefinite for, or low–grade dysplasia. Am J Gastroenterol 2015;110:662–82; quiz 683.
65. Sikkema M, de Jonge PJ, Steyerberg EW, Kuipers EJ. Risk of esophageal adenocarcinoma and mortality in patients with Barrett’s esophagus: a systematic review and meta–analysis. Clin Gastroenterol Hepatol 2010;8:235–44; quiz e32.
66. Old O, Moayyedi P, Love S, et al; BOSS Trial Team. Barrett’s Oesophagus Surveillance versus endoscopy at need Study (BOSS): protocol and analysis plan for a multicentre randomized controlled trial. J Med Screen 2015;22:158–64.
67. Weston AP, Sharma P, Topalovski M, et al. Long–term follow–up of Barrett’s high–grade dysplasia. Am J Gastroenterol 2000;95:1888–93.
68. Paull A, Trier JS, Dalton MD, et al. The histologic spectrum of Barrett’s esophagus. N Engl J Med 1976;295:476–80.
69. Konda VJ, Ross AS, Ferguson MK, et al. Is the risk of concomitant invasive esophageal cancer in high–grade dysplasia in Barrett’s esophagus overestimated? Clin Gastroenterol Hepatol 2008;6:159–64.
70. Allison H, Banchs MA, Bonis PA, Guelrud M. Long–term remission of nondysplastic Barrett’s esophagus after multipolar electrocoagulation ablation: report of 139 patients with 10 years of follow–up. Gastrointest Endosc 2011;73:651–8.
71. Corley DA, Levin TR, Habel LA, Weiss NS, et al. Surveillance and survival in Barrett’s adenocarcinomas: a population–based study. Gastroenterology 2002;122:633–40.
72. Wong T, Tian J, Nagar AB. Barrett’s surveillance identifies patients with early esophageal adenocarcinoma. Am J Med 2010;123:462–7.
73. Fountoulakis A, Zafirellis KD, Dolan K, et al. Effect of surveillance of Barrett’s oesophagus on the clinical outcome of oesophageal cancer. Br J Surg 2004;91:997–1003.
74. Verbeek RE, Leenders M, Ten Kate FJ, et al. Surveillance of Barrett’s esophagus and mortality from esophageal adenocarcinoma: a population–based cohort study. Am J Gastroenterol 2014;109:1215–22.
75. Kastelein F, van Olphen SH, Steyerberg EW, et al. Impact of surveillance for Barrett’s oesophagus on tumour stage and survival of patients with neoplastic progression. Gut 2016;65:548–54.
76. Phoa KN, van Vilsteren FG, Weusten BL, et al. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low–grade dysplasia: a randomized clinical trial. JAMA 2014;311: 1209–17.
77. Wang WL, Chang IW, Chen CC, et al. Radiofrequency ablation versus endoscopic submucosal dissection in treating large early esophageal squamous cell neoplasia. Medicine (Baltimore) 2015;94:e2240.
78. Lim CH, Treanor D, Dixon MF, Axon AT. Low–grade dysplasia in Barrett’s esophagus has a high risk of progression. Endoscopy 2007;39:581–7.
79. Shaheen NJ, Inadomi JM, Overholt BF, Sharma P. What is the best management strategy for high grade dysplasia in Barrett’s oesophagus? A cost effectiveness analysis. Gut 2004;53:1736–44.
80. Vij R, Triadafilopoulos G, Owens DK, et al. Cost–effectiveness of photodynamic therapy for high–grade dysplasia in Barrett’s esophagus. Gastrointest Endosc 2004;60:739–56.
81. van den Boogert J, v an Hillegersberg R, Siersema PD, et al. Endoscopic ablation therapy for Barrett’s esophagus with high–grade dysplasia: a review. Am J Gastroenterol 1999;94:1153–60.
82. Sampliner RE. Endoscopic ablative therapy for Barrett’s esophagus: current status. Gastrointest Endosc 2004;59:66–9.
83. Sharma VK, Wang KK, Overholt BF, et al. Balloon–based, circumferential, endoscopic radiofrequency ablation of Barrett’s esophagus: 1–year follow–up of 100 patients. Gastrointest Endosc 2007;65:185–95.
84. Hanlon CR. Textbook of surgery: The biological basis of modern surgical practice, 14th edition. Ann Surg 1992;216:94.
85. Bright T, Watson DI, Tam W, et al. Randomized trial of argon plasma coagulation versus endoscopic surveillance for barrett esophagus after antireflux surgery: late results. Ann Surg 2007;246:1016–20.
86. Chadwick G, Groene O, Markar SR, et al. Systematic review comparing radiofrequency ablation and complete endoscopic resection in treating dysplastic Barrett’s esophagus: a critical assessment of histologic outcomes and adverse events. Gastrointest Endosc 2014;79:718–31.e3.
87. Gondrie JJ, Pouw RE, Sondermeijer CM, et al. Effective treatment of early Barrett’s neoplasia with stepwise circumferential and focal ablation using the HALO system. Endoscopy 2008;40:370–9.
88. Pouw RE, Wirths K, Eisendrath P, et al. Efficacy of radiofrequency ablation combined with endoscopic resection for barrett’s esophagus with early neoplasia. Clin Gastroenterol Hepatol 2010;8:23–9.
89. Kim HP, Bulsiewicz WJ, Cotton CC, et al. Focal endoscopic mucosal resection before radiofrequency ablation is equally effective and safe compared with radiofrequency ablation alone for the eradication of Barrett’s esophagus with advanced neoplasia. Gastrointest Endosc 2012;76:733–9.
90. Fleischer DE, Overholt BF, Sharma VK, et al. Endoscopic ablation of Barrett’s esophagus: a multicenter study with 2.5–year follow–up. Gastrointest Endosc 2008;68:867–76.
91. Sharma VK, Jae Kim H, Das A, et al. Circumferential and focal ablation of Barrett’s esophagus containing dysplasia. Am J Gastroenterol 2009;104:310–7.
92. Ganz RA, Overholt BF, Sharma VK, et al. Circumferential ablation of Barrett’s esophagus that contains high–grade dysplasia: a U.S. multicenter registry. Gastrointest Endosc 2008;68:35–40.
93. Gupta M, Iyer PG, Lutzke L, et al. Recurrence of esophageal intestinal metaplasia after endoscopic mucosal resection and radiofrequency ablation of Barrett’s esophagus: results from a US Multicenter Consortium. Gastroenterology 2013;145:79–86.e1.
94. Lyday WD, Corbett FS, Kuperman DA, et al. Radiofrequency ablation of Barrett’s esophagus: outcomes of 429 patients from a multicenter community practice registry. Endoscopy 2010;42:272–8.
95. Pasricha S, Bulsiewicz WJ, Hathorn KE, et al. Durability and predictors of successful radiofrequency ablation for Barrett’s esophagus. Clin Gastroenterol Hepatol 2014;12:1840–7.e1.
96. Fleischer DE, Overholt BF, Sharma VK, et al. Endoscopic radiofrequency ablation for Barrett’s esophagus: 5–year outcomes from a prospective multicenter trial. Endoscopy 2010;42:781–9.
97. Weston AP, Sharma P, Banerjee S, et al. Visible endoscopic and histologic changes in the cardia, before and after complete Barrett’s esophagus ablation. Gastrointest Endosc 2005;61:515–21.
98. Beaumont H, Gondrie JJ, McMahon BP, et al. Stepwise radiofrequency ablation of Barrett’s esophagus preserves esophageal inner diameter, compliance, and motility. Endoscopy 2009;41:2–8.
99. Orman ES, Li N, Shaheen NJ.Efficacy and durability of radiofrequency ablation for Barrett’s Esophagus: systematic review and meta–analysis. Clin Gastroenterol Hepatol 2013;11:1245–55.
100. Krishnan K, Pandolfino JE, Kahrilas PJ, et al. Increased risk for persistent intestinal metaplasia in patients with Barrett’s esophagus and uncontrolled reflux exposure before radiofrequency ablation. Gastroenterology 2012;143:576–81.
101. Akiyama J, Marcus SN, Triadafilopoulos G. Effective intra–esophageal acid control is associated with improved radiofrequency ablation outcomes in Barrett’s esophagus. Dig Dis Sci 2012;57:2625–32.
102. Small AJ, Sutherland SE, Hightower JS, et al. Comparative risk of recurrence of dysplasia and carcinoma after endoluminal eradication therapy of high–grade dysplasia versus intramucosal carcinoma in Barrett’s esophagus. Gastrointest Endosc 2015;81:1158–66.e1–4.
103. Shaheen NJ, Greenwald BD, Peery AF, et al. Safety and efficacy of endoscopic spray cryotherapy for Barrett’s esophagus with high–grade dysplasia. Gastrointest Endosc 2010;71:680–5.
104. Shaheen NJ, Peery AF, Hawes RH, et al. Quality of life following radiofrequency ablation of dysplastic Barrett’s esophagus. Endoscopy 2010;42:790–9.
105. Bedi AO, Kwon RS, Rubenstein JH, et al. A survey of expert follow–up practices after successful endoscopic eradication therapy for Barrett’s esophagus with high–grade dysplasia and intramucosal adenocarcinoma. Gastrointest Endosc 2013;78:696–701.
106. Sampliner RE, Camargo E, Prasad AR. Prasad, Association of ablation of Barrett’s esophagus with high grade dysplasia and adenocarcinoma of the gastric cardia. Dis Esophagus 2006;19:277–9.
107. Overholt BF, Panjehpour M, Halberg DL. Photodynamic therapy for Barrett’s esophagus with dysplasia and/or early stage carcinoma: long–term results. Gastrointest Endosc 2003;58:183–8.
108. Gosain S, Mercer K, Twaddell WS, et al. Liquid nitrogen spray cryotherapy in Barrett’s esophagus with high–grade dysplasia: long–term results. Gastrointest Endosc 2013;78:260–5.
109. Canto MI, Shin EJ, Khashab MA, et al. Safety and efficacy of carbon dioxide cryotherapy for treatment of neoplastic Barrett’s esophagus. Endoscopy 2015;47:582–91.
110. Van Laethem JL, Peny MO, Salmon I, et al. Intramucosal adenocarcinoma arising under squamous re–epithelialisation of Barrett’s oesophagus. Gut 2000;46:574–7.
111. Pech O, May A, Gossner L, et al. Management of pre–malignant and malignant lesions by endoscopic resection. Best Pract Res Clin Gastroenterol 2004;18:61–76.
112. Soetikno RM, Gotoda T, Nakanishi Y, Soehendra N. Endoscopic mucosal resection. Gastrointest Endosc 2003;57:567–79.
113. Ell C, May A, Gossner L, et al. Endoscopic mucosal resection of early cancer and high–grade dysplasia in Barrett’s esophagus. Gastroenterology 2000;118:670–7.
114. Pech O, Behrens A, May A, et al. Long–term results and risk factor analysis for recurrence after curative endoscopic therapy in 349 patients with high–grade intraepithelial neoplasia and mucosal adenocarcinoma in Barrett’s oesophagus. Gut 2008;57:1200–6.
115. Vieth M, Ell C, Gossner L, et al. Histological analysis of endoscopic resection specimens from 326 patients with Barrett’s esophagus and early neoplasia. Endoscopy 2004;36:776–81.
116. Buskens CJ, Westerterp M, Lagarde SM, et al. Prediction of appropriateness of local endoscopic treatment for high–grade dysplasia and early adenocarcinoma by EUS and histopathologic features. Gastrointest Endosc 2004;60:703–10.
117. Nijhawan PK, Wang KK. Endoscopic mucosal resection for lesions with endoscopic features suggestive of malignancy and high–grade dysplasia within Barrett’s esophagus. Gastrointest Endosc 2000;52:328–32.
118. Esaki M, Matsumoto T, Hirakawa K, et al. Risk factors for local recurrence of superficial esophageal cancer after treatment by endoscopic mucosal resection. Endoscopy 2007;39:41–5.
119. Ell C, May A, Pech O, et al. Curative endoscopic resection of early esophageal adenocarcinomas (Barrett’s cancer). Gastrointest Endosc 2007;65:3–10.
120. Chennat J, Konda VJ, Ross AS, et al. Complete Barrett’s eradication endoscopic mucosal resection: an effective treatment modality for high–grade dysplasia and intramucosal carcinoma––an American single–center experience. Am J Gastroenterol 2009;104:2684–92.
121. Pech O, Bollschweiler E, Manner H, et al. Comparison between endoscopic and surgical resection of mucosal esophageal adenocarcinoma in Barrett’s esophagus at two high–volume centers. Ann Surg 2011;254:67–72.
122. Wu J, Pan YM, Wang TT, et al. Endotherapy versus surgery for early neoplasia in Barrett’s esophagus: a meta–analysis. Gastrointest Endosc 2014;79:233–241.e2.
123. Pech O, May A, Manner H, et al. Long–term efficacy and safety of endoscopic resection for patients with mucosal adenocarcinoma of the esophagus. Gastroenterology 2014;146:652–660.e1.
124. Prasad GA, Wu TT, Wigle DA, et al. Endoscopic and surgical treatment of mucosal (T1a) esophageal adenocarcinoma in Barrett’s esophagus. Gastroenterology 2009;137:815–23.
125. May A, Gossner L, Pech O, et al. Local endoscopic therapy for intraepithelial high–grade neoplasia and early adenocarcinoma in Barrett’s oesophagus: acute–phase and intermediate results of a new treatment approach. Eur J Gastroenterol Hepatol 2002;14(10):1085–91.
126. Gerke H, Siddiqui J, Nasr I, et al. Efficacy and safety of EMR to completely remove Barrett’s esophagus: experience in 41 patients. Gastrointest Endosc 2011;74:761–71.
127. Lewis JJ, Rubenstein JH, Singal AG, et al. Factors associated with esophageal stricture formation after endoscopic mucosal resection for neoplastic Barrett’s esophagus. Gastrointest Endosc 2011;74:753–60.
128. Choi IJ, Kim CG, Chang HJ, et al. The learning curve for EMR with circumferential mucosal incision in treating intramucosal gastric neoplasm. Gastrointest Endosc 2005;62:860–5.
129. Deprez PH, Bergman JJ, Meisner S, et al. Current practice with endoscopic submucosal dissection in Europe: position statement from a panel of experts. Endoscopy 2010;42:853–8.
130. van Lanschot JJ, Hulscher JB, Buskens CJ, et al. Hospital volume and hospital mortality for esophagectomy. Cancer 2001;91:1574–8.
131. Karl RC, Schreiber R, Boulware D, et al. Factors affecting morbidity, mortality, and survival in patients undergoing Ivor Lewis esophagogastrectomy. Ann Surg 2000;231:635–43.
132. Young MM, Deschamps C, Trastek VF, et al. Esophageal reconstruction for benign disease: early morbidity, mortality, and functional results. Ann Thorac Surg 2000;70:1651–5.
133. Dunbar KB, Spechler SJ. The risk of lymph–node metastases in patients with high–grade dysplasia or intramucosal carcinoma in Barrett’s esophagus: a systematic review. Am J Gastroenterol 2012;107:850–62; quiz 863.
134. Morales CP, Souza RF, Spechler SJ. Hallmarks of cancer progression in Barrett’s oesophagus. Lancet 2002;360:1587–9.
135. Omer ZB, Ananthakrishnan AN, Nattinger KJ, et al. Aspirin protects against Barrett’s esophagus in a multivariate logistic regression analysis. Clin Gastroenterol Hepatol 2012;10:722–7.
136. Abnet CC, Freedman ND, Kamangar F, et al. Non–steroidal anti–inflammatory drugs and risk of gastric and oesophageal adenocarcinomas: results from a cohort study and a meta–analysis. Br J Cancer 2009;100:551–7.
137. Kastelein F, Spaander MC, Biermann K, et al. Nonsteroidal anti–inflammatory drugs and statins have chemopreventative effects in patients with Barrett’s esophagus. Gastroenterology 2011;141:2000–8; quiz e13–4.
138. Zhang S, Zhang XQ, Ding XW, et al. Cyclooxygenase inhibitors use is associated with reduced risk of esophageal adenocarcinoma in patients with Barrett’s esophagus: a meta–analysis. Br J Cancer 2014;110: 2378–88.
Reducing Deep Joint Infection in Hip Hemiarthroplasty—A Quality Improvement Project
From the Department of Trauma and Orthopaedics, Royal Victoria Hospital, Belfast, N. Ireland.
Abstract
- Objective: To improve the deep wound infection rate in patients undergoing hip hemiarthroplasty in our regional trauma center.
- Methods: We conducted a retrospective audit of patients who had undergone hip hemiarthroplasty between January 2013 and July 2014 and found that in 750 hip hemiarthroplasties performed, 20 (2.7%) developed a deep infection, a figure in excess of the literature standard. In line with international consensus recommendations, 4 changes to our perioperative practice were implemented: standardized draping of the affected extremity, improved skin preparation using a 2% chlorhexidine gluconate solution, change of incision drapes to iodophor-impregnated adhesive film drapes, and the use of interactive wound dressing. We conducted staff education to highlight the impact of deep wound infection, introduce the changes, and underscore the importance of strict adherence to intraoperative sterility.
- Results: One year after introducing the changes, we audited the period April 2015 to March 2016, during which time 457 hip hemiarthoplasties were performed. Five (1.1%) deep infections were identified.
- Conclusion: Improvement in the perioperative care of our hip hemiarthroplasty patients has resulted in a reduced risk of the development of deep wound infection. This improvement was maintained in a third audit period, with continued implementation of these changes in practice.
Keywords: deep infection; hip hemiarthroplasty; quality improvement; proximal femoral fracture; risk reduction strategies.
Deep wound infection following hip hemiarthroplasty is a catastrophic outcome for the patient, resulting in a prolonged stay in hospital, a poor outcome and increased costs. There is limited evidence in the literature reporting early deep infection rates specific to hip hemiarthroplasty. A number of studies describe the incidence of deep infection in proximal femur fractures treated by arthroplasty and fixation [1], with only a single study reporting on solely hip hemiarthroplasty [2]. The reported incidence of early deep infection following hip hemiarthroplasty specifically varies from 1.6% [1] to 4.9% [2,3]. These figures are primarily provided by retrospective, descriptive studies, with variable lengths of follow-up.
Early deep infection occurs more frequently in hip hemiarthroplasty for trauma than elective total hip arthroplasty. This is thought to be due to several factors including the advanced age of hip hemiarthroplasty patients and their comorbid status, in addition to the shorter time frame in which to medically optimize trauma patients, including less opportunity to address nutritional elements known to impact recovery.
A number of prognostic factors have been identified as increasing the chance of developing a deep periprosthetic infection following hip hemiarthroplasty. Although these are debated they include cognitive impairment, high body mass index, development of wound hematoma post-operatively and increased operating time [8].
Many of the measures taken to reduce the risk of deep infection in arthroplasty have a limited evidence base, with a significant amount of practice based on expert opinion [10]. This is due to the difficulty in designing robust randomized controlled trials with sufficient numbers to identify significant trends. It is generally accepted that parenteral antibiotic prophylaxis [4] and antibiotic-loaded cement reduce the incidence of infection [5]. Increased theatre traffic has long been accepted as increasing bacterial counts in theatre [6]. Sterile skin preparation and draping with impermeable drapes and an iodophor-impregnated adhesive skin drape have been shown to reduce bacterial contamination and recolonization rates in vitro [4], although this has not resulted in a clinical reduction in deep periprosthetic joint infections. Other practices such as the use of laminar flow theatres are less well evidenced [7].
Following concerns regarding a perceived spike in infection rates in our hip hemiarthroplasty patients, the senior author, who is the training liaison officer for trauma and orthopedics in the hospital, convened a meeting with the first 2 authors regarding how best to investigate this potential issue. It was decided that an audit of practice should be conducted, as well as a literature review to assess acceptable infection rates within the literature and any potential areas for improvement.
Setting
The Royal Victoria Hospital in Belfast is one of the UK’s largest dedicated trauma units, treating over 900 proximal femur fractures per year. Of these, approximately 500 are displaced intracapsular neck of femur fractures requiring hip hemiarthroplasty. Patients are managed on dedicated trauma wards, and in accordance with British Orthopaedic Association guidelines there is a focus on multidisciplinary rehabilitation including a fully integrated orthogeriatric service [8]. We routinely use a modular Exeter trauma stem (Stryker, Kalamazoo MI) prosthesis with gentamycin-loaded cement and an antibiotic prophylaxis regimen of flucloxacillin and gentamicin prior to incision, followed by 2 further doses of flucloxacillin over 24 hours. A preoperative checklist is conducted to ensure that antibiotics are administered prior to skin incision and that there are no concerns regarding equipment sterility. Four trauma theatres are run each weekday, prioritizing medically optimized proximal femoral fracture patients.
Quality Improvement Project
Pre-intervention Audit
A retrospective audit was carried out via interrogation of the Fracture Outcome Research Database (FORD) between January 2013 and July 2014. This is a prospectively collected database of demographic data and outcome measurements that is managed by a dedicated team employed by the institution. This ensures accurate documentation of hospital admissions for trauma, operations conducted, and outcomes, such as discharge destination and further procedures.
The search terms used were wound washout, irrigation and debridement, first stage revision, girdlestone, and excision arthroplasty. Exclusion criteria included washouts for septic arthritis of a native hip joint, open injuries, and repeated washouts on the same patient. Data were collected including demographics, comorbidities, surgeon level, ward, theatre and causative organism by reviewing the electronic and written records.
725 patients were identified who met the inclusion criteria and underwent a hip hemiarthroplasty. Of these, 20 had undergone a washout procedure for deep infection, a rate of 2.7%. There were 14 females, nine males, 12 were right hips, 8 left, with a mean age of 81 years (range, 66–92). The mean American Society of Anesthetists (ASA) score was 3.2 (range, 2–4). Fourteen infections were identified within 4 weeks postoperatively, 6 within 8 weeks. Nineteen out of 20 of the causative organisms isolated were sensitive to the standard prophylactic antibiotic regimen. There was no association identified with a particular theatre, presence of laminar flow, ward, or grade of operating surgeon.
Changes to Perioperative Practice
We met on 2 further occasions to discuss the findings of the literature review and strategy for improvement prior to institution of changes.
We reviewed the National Institute for Clinical Excellence (NICE) Clinical Guideline [9] and the “International Consensus on Periprosthetic Joint Infection” [10] to compare our perioperative practice to national and international recommendations. We identified that we were compliant with a large majority of recommended practices, for example using antibiotic prophylaxis, laminar flow theatres, and sterile disposable drapes. We defined an acceptable infection rate to be 1.6% following a comprehensive literature review [1–3].
Four potential changes to our perioperative practice were chosen based on our review of the clinical guidelines and consensus document. These were chosen due to the strong expert opinion that they commanded within the consensus document and their relative ease and speed of implementation.
- Standardized draping of the affected extremity using stockinette isolation and windowed drape towards patient’s upper body.
- Use of a chlorhexidine gluconate (2% [w/v] in 70% [v/v] isopropyl alcohol) preoperative skin solution in theatre as a preliminary antiseptic skin preparation prior to formal preparation with povidone-iodine. Darouiche et al [11] demonstrated that preoperative cleansing of the patient’s skin with chlorhexidine-alcohol is superior to cleansing with povidone-iodine for preventing surgical site infection. Subsequent studies have suggested that concurrent application of the 2 antiseptic agents confer a further potential benefit by reducing the number of viable colony forming organisms and, subsequently, deep surgical site infection [12,13].
- Change from non-impregnated adhesive incision drapes to Ioban (3M, St Paul, MN) (other manufacturers available) iodophor-impregnated adhesive incision drapes. Experimental studies have demonstrated a lower rate of skin recolonization with bacteria following the use of impregnated drapes compared to non-impregnated drapes [14,15] although this has not been correlated to rates of deep infection.
- Change from simple absorbent dressings to interactive wound dressings (Aquacel and Duoderm; ConvaTec Ltd., Flintshire, UK) (alternative manufacturers available). There is evidence to show that Aquacel and Duoderm dressings were associated with reduced rates of skin blistering and infection in elective arthroplasty [16].
We also felt that staff education would be important for implementing change. We presented the results of the initial audit at departmental and regional quality improvement meetings, demonstrating the need for change in practice. Following the literature search and decision to implement 4 changes, medical staff were re-educated at the departmental audit meeting on the rationale behind the changes being made. Via liaison with the nurse lead of trauma theatres, nursing and auxiliary staff underwent education sessions. These were small group sessions, with visual aids, designed to fit in to staff breaks to reduce disruption of their work. Groups consisted of 4 to 6 people per session. They were led by the authors and focused on highlighting the reasoning behind the changes in practices and answering any questions that staff had. During these sessions, a revision of good theatre etiquette was conducted. This included reinforcing basic theatre principles, for example, reducing theatre traffic, ensuring correct theatre dress and head coverings are worn at all times, highlighting the need to regularly wash hands and wear gloves when required, and to respect the sterile areas and instruments appropriately.
Results
A re-audit of hip hemiarthroplasties was conducted after a 12-month interval to allow proposed changes to become routine practice. Re-audit was undertaken retrospectively from April 2015 to March 2016 using the same methods and search strategy as before. 457 (male 43.3%, female 56.7%) hip hemiarthroplasty procedures were carried out in this time period with 5 deep infections occurring, a rate of 1.1%, demonstrating a statistically significant reduction in periprosthetic joint infection rate (P = 0.03, chi square test). There were 3 males and 4 females, with a mean age of 79 years (range 57–91), and mean ASA of 3.1 (range, 2–4). Two were right hips, 3 were left hips. Four infections occurred within 4 weeks and one at day 50. The overall mortality rate for those patients who developed deep periprosthetic infection within our study time frame was 28%.
Findings were presented at the regional audit meeting. This highlighted the positive impact of the changes to practice and stimulated discussion on further improvements to practice that could be instituted. Prior to implementation of any further changes to practice a re-audit was conducted over a further 12-month period. This demonstrated maintenance of an infection rate below the literature standard of 1.6% and a continued reduction in the initial audit rate of 2.7%
Lessons and Limitations
This quality improvement project demonstrates how simple changes can deliver large benefits to both patients and the health system. There is considerable variability in worldwide orthopedic practice, due in part to the limited evidence base for some perioperative infection precautions. This was the first attempt in Northern Ireland to quantify the effect of some of these precautions and to contribute to the evidence in support of their implementation. We acknowledge that the numbers involved in our project are small, and the effect size is likely to be overestimated. Factors contributing to this include the Hawthorne effect, improved staff awareness of postoperative infection, and that patients who either died or were treated conservatively did not undergo a washout procedure and therefore would not have been identified.
Institutional change is challenging. We selected the changes to practice that we felt would likely provide the largest benefit, with minimal cultural resistance. All materials (eg, Ioban drapes and Chloraprep skin solution) were already stocked in theatre suite and therefore did not have to undergo procurement procedures. Junior medical staff were instructed on strict standardised draping technique, as agreed by revision arthroplasty surgeons working within the unit.
We would advocate that theatre staff at every level are involved in this process from the outset in order to maximise the overall benefit. It is important that medical, nursing, and auxiliary staff are involved in decision making and implementation to facilitate uptake of new practices. All staff were re-educated on the impact of deep infections in these patients and the importance of perioperative practice in minimising these. Whenever resistance was met we addressed with open discussion and answering all questions to ensure staff understanding and acceptance.
Conclusion
Deep joint infection represents a significant cause of morbidity and mortality in the elderly population and a financial burden on the health service. The implementation of these simple perioperative interventions has achieved a significantly reduced rate of infection in a regional trauma center. Our interventions have been straightforward to implement, cost-effective and, most importantly, have demonstrated a significant, tangible benefit to our patients.
Corresponding author: Mr. Brendan Gallagher, Department of Trauma and Orthopedics, Royal Victoria Hospital, 274 Grosvenor Road, Belfast, N. Ireland, BT12 6BA, [email protected] .
Financial disclosures: None.
1. Duckworth AD, Phillips S-A, Stone O, et al. Deep infection after hip fracture surgery: predictors of early mortality. Injury 2012;43:1182–6.
2. de Jong L, Klem TMAL, Kuijper TM, Roukema GR. Factors affecting the rate of surgical site infection in patients after hemiarthroplasty of the hip following a fracture of the neck of the femur. Bone Joint J 2017;99-B:1088–94
3. Ridgeway S, Wilson J, Charlet A, et al. Infection of the surgical site after arthroplasty of the hip. J Bone Joint Surg [Br] 2005;87–B(6):844–50.
4. Matar WY, Jafari SM, Restrepo C, et al. Preventing Infection in Total Joint Arthroplasty. J Bone Joint Surg [Am] 2010;92(Suppl 2):36–46.
5. Parvizi J, Saleh KJ, Ragland PS, et al. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop 2008;79:335–41.
6. Ritter MA, Eitzen H, French ML, Hart JB. The operating room environment as affected by people and the surgical face mask. Clin Orthop Rel Res 1975;:147–50.
7. Hooper GJ, Rothwell a G, Frampton C, Wyatt MC. Does the use of laminar flow and space suits reduce early deep infection after total hip and knee replacement?: the ten-year results of the New Zealand Joint Registry. J Bone Joint Surg [Br] 2011;93:85–90.
8. British Orthopaedic Association. British Orthopaedic Association standards for trauma. 2012. Available at www.boa.ac.uk/wpcontent/uploads/2014/12/BOAST-1.pdf.
9. NICE. Hip fracture: management | 1-Guidance | Guidance and guidelines | NICE. Health Technol Assess (Rockv). NICE; 2014. Available at www.nice.org.uk/guidance/cg124/chapter/1-guidance.
10. Parvizi J, Gehrke T. International consensus on periprosthetic joint infection. J Bone Joint Surg [Am] 2014;96:441.
11. Darouiche RO, Wall Jr MJ, Itani KMF, et al. Chlorhexidine–alcohol versus povidone–iodine for surgical-site antisepsis. N Engl J Med 2010;362:18–26.
12. Anderson MJ, Horn ME, Lin YC et al. Efficacy of concurrent application of chlorhexidine gluconate and povidone iodine against six nosocomial pathogens. Am J Infect Control 2010;38:826–31.
13. Patrick S, McDowell A, Lee A et al. Antisepsis of the skin before spinal surgery with povidone iodine-alcohol followed by chlorhexidine gluconate-alcohol versus povidone iodine-alcohol applied twice for the prevention of contamination of the wound by bacteria. Bone Joint J 2017;99-B:1354–65.
14. Johnston DH, Fairclough JA, Brown EM, Morris R. Rate of bacterial recolonization of the skin after preparation: four methods compared. Br J Surg 1987;74:64.
15. Dewan PA, Van Rij AM, Robinson RG, et al. The use of an iodophor-impregnated plastic incise drape in abdominal surgery--a controlled clinical trial. Aust N Z J Surg 1987;57:859–63.
16. Clarke JV, Deakin AH, Dillon JM, et al. A prospective clinical audit of a new dressing design for lower limb arthroplasty wounds. J Wound Care 2009;18:5–8, 10–11.
From the Department of Trauma and Orthopaedics, Royal Victoria Hospital, Belfast, N. Ireland.
Abstract
- Objective: To improve the deep wound infection rate in patients undergoing hip hemiarthroplasty in our regional trauma center.
- Methods: We conducted a retrospective audit of patients who had undergone hip hemiarthroplasty between January 2013 and July 2014 and found that in 750 hip hemiarthroplasties performed, 20 (2.7%) developed a deep infection, a figure in excess of the literature standard. In line with international consensus recommendations, 4 changes to our perioperative practice were implemented: standardized draping of the affected extremity, improved skin preparation using a 2% chlorhexidine gluconate solution, change of incision drapes to iodophor-impregnated adhesive film drapes, and the use of interactive wound dressing. We conducted staff education to highlight the impact of deep wound infection, introduce the changes, and underscore the importance of strict adherence to intraoperative sterility.
- Results: One year after introducing the changes, we audited the period April 2015 to March 2016, during which time 457 hip hemiarthoplasties were performed. Five (1.1%) deep infections were identified.
- Conclusion: Improvement in the perioperative care of our hip hemiarthroplasty patients has resulted in a reduced risk of the development of deep wound infection. This improvement was maintained in a third audit period, with continued implementation of these changes in practice.
Keywords: deep infection; hip hemiarthroplasty; quality improvement; proximal femoral fracture; risk reduction strategies.
Deep wound infection following hip hemiarthroplasty is a catastrophic outcome for the patient, resulting in a prolonged stay in hospital, a poor outcome and increased costs. There is limited evidence in the literature reporting early deep infection rates specific to hip hemiarthroplasty. A number of studies describe the incidence of deep infection in proximal femur fractures treated by arthroplasty and fixation [1], with only a single study reporting on solely hip hemiarthroplasty [2]. The reported incidence of early deep infection following hip hemiarthroplasty specifically varies from 1.6% [1] to 4.9% [2,3]. These figures are primarily provided by retrospective, descriptive studies, with variable lengths of follow-up.
Early deep infection occurs more frequently in hip hemiarthroplasty for trauma than elective total hip arthroplasty. This is thought to be due to several factors including the advanced age of hip hemiarthroplasty patients and their comorbid status, in addition to the shorter time frame in which to medically optimize trauma patients, including less opportunity to address nutritional elements known to impact recovery.
A number of prognostic factors have been identified as increasing the chance of developing a deep periprosthetic infection following hip hemiarthroplasty. Although these are debated they include cognitive impairment, high body mass index, development of wound hematoma post-operatively and increased operating time [8].
Many of the measures taken to reduce the risk of deep infection in arthroplasty have a limited evidence base, with a significant amount of practice based on expert opinion [10]. This is due to the difficulty in designing robust randomized controlled trials with sufficient numbers to identify significant trends. It is generally accepted that parenteral antibiotic prophylaxis [4] and antibiotic-loaded cement reduce the incidence of infection [5]. Increased theatre traffic has long been accepted as increasing bacterial counts in theatre [6]. Sterile skin preparation and draping with impermeable drapes and an iodophor-impregnated adhesive skin drape have been shown to reduce bacterial contamination and recolonization rates in vitro [4], although this has not resulted in a clinical reduction in deep periprosthetic joint infections. Other practices such as the use of laminar flow theatres are less well evidenced [7].
Following concerns regarding a perceived spike in infection rates in our hip hemiarthroplasty patients, the senior author, who is the training liaison officer for trauma and orthopedics in the hospital, convened a meeting with the first 2 authors regarding how best to investigate this potential issue. It was decided that an audit of practice should be conducted, as well as a literature review to assess acceptable infection rates within the literature and any potential areas for improvement.
Setting
The Royal Victoria Hospital in Belfast is one of the UK’s largest dedicated trauma units, treating over 900 proximal femur fractures per year. Of these, approximately 500 are displaced intracapsular neck of femur fractures requiring hip hemiarthroplasty. Patients are managed on dedicated trauma wards, and in accordance with British Orthopaedic Association guidelines there is a focus on multidisciplinary rehabilitation including a fully integrated orthogeriatric service [8]. We routinely use a modular Exeter trauma stem (Stryker, Kalamazoo MI) prosthesis with gentamycin-loaded cement and an antibiotic prophylaxis regimen of flucloxacillin and gentamicin prior to incision, followed by 2 further doses of flucloxacillin over 24 hours. A preoperative checklist is conducted to ensure that antibiotics are administered prior to skin incision and that there are no concerns regarding equipment sterility. Four trauma theatres are run each weekday, prioritizing medically optimized proximal femoral fracture patients.
Quality Improvement Project
Pre-intervention Audit
A retrospective audit was carried out via interrogation of the Fracture Outcome Research Database (FORD) between January 2013 and July 2014. This is a prospectively collected database of demographic data and outcome measurements that is managed by a dedicated team employed by the institution. This ensures accurate documentation of hospital admissions for trauma, operations conducted, and outcomes, such as discharge destination and further procedures.
The search terms used were wound washout, irrigation and debridement, first stage revision, girdlestone, and excision arthroplasty. Exclusion criteria included washouts for septic arthritis of a native hip joint, open injuries, and repeated washouts on the same patient. Data were collected including demographics, comorbidities, surgeon level, ward, theatre and causative organism by reviewing the electronic and written records.
725 patients were identified who met the inclusion criteria and underwent a hip hemiarthroplasty. Of these, 20 had undergone a washout procedure for deep infection, a rate of 2.7%. There were 14 females, nine males, 12 were right hips, 8 left, with a mean age of 81 years (range, 66–92). The mean American Society of Anesthetists (ASA) score was 3.2 (range, 2–4). Fourteen infections were identified within 4 weeks postoperatively, 6 within 8 weeks. Nineteen out of 20 of the causative organisms isolated were sensitive to the standard prophylactic antibiotic regimen. There was no association identified with a particular theatre, presence of laminar flow, ward, or grade of operating surgeon.
Changes to Perioperative Practice
We met on 2 further occasions to discuss the findings of the literature review and strategy for improvement prior to institution of changes.
We reviewed the National Institute for Clinical Excellence (NICE) Clinical Guideline [9] and the “International Consensus on Periprosthetic Joint Infection” [10] to compare our perioperative practice to national and international recommendations. We identified that we were compliant with a large majority of recommended practices, for example using antibiotic prophylaxis, laminar flow theatres, and sterile disposable drapes. We defined an acceptable infection rate to be 1.6% following a comprehensive literature review [1–3].
Four potential changes to our perioperative practice were chosen based on our review of the clinical guidelines and consensus document. These were chosen due to the strong expert opinion that they commanded within the consensus document and their relative ease and speed of implementation.
- Standardized draping of the affected extremity using stockinette isolation and windowed drape towards patient’s upper body.
- Use of a chlorhexidine gluconate (2% [w/v] in 70% [v/v] isopropyl alcohol) preoperative skin solution in theatre as a preliminary antiseptic skin preparation prior to formal preparation with povidone-iodine. Darouiche et al [11] demonstrated that preoperative cleansing of the patient’s skin with chlorhexidine-alcohol is superior to cleansing with povidone-iodine for preventing surgical site infection. Subsequent studies have suggested that concurrent application of the 2 antiseptic agents confer a further potential benefit by reducing the number of viable colony forming organisms and, subsequently, deep surgical site infection [12,13].
- Change from non-impregnated adhesive incision drapes to Ioban (3M, St Paul, MN) (other manufacturers available) iodophor-impregnated adhesive incision drapes. Experimental studies have demonstrated a lower rate of skin recolonization with bacteria following the use of impregnated drapes compared to non-impregnated drapes [14,15] although this has not been correlated to rates of deep infection.
- Change from simple absorbent dressings to interactive wound dressings (Aquacel and Duoderm; ConvaTec Ltd., Flintshire, UK) (alternative manufacturers available). There is evidence to show that Aquacel and Duoderm dressings were associated with reduced rates of skin blistering and infection in elective arthroplasty [16].
We also felt that staff education would be important for implementing change. We presented the results of the initial audit at departmental and regional quality improvement meetings, demonstrating the need for change in practice. Following the literature search and decision to implement 4 changes, medical staff were re-educated at the departmental audit meeting on the rationale behind the changes being made. Via liaison with the nurse lead of trauma theatres, nursing and auxiliary staff underwent education sessions. These were small group sessions, with visual aids, designed to fit in to staff breaks to reduce disruption of their work. Groups consisted of 4 to 6 people per session. They were led by the authors and focused on highlighting the reasoning behind the changes in practices and answering any questions that staff had. During these sessions, a revision of good theatre etiquette was conducted. This included reinforcing basic theatre principles, for example, reducing theatre traffic, ensuring correct theatre dress and head coverings are worn at all times, highlighting the need to regularly wash hands and wear gloves when required, and to respect the sterile areas and instruments appropriately.
Results
A re-audit of hip hemiarthroplasties was conducted after a 12-month interval to allow proposed changes to become routine practice. Re-audit was undertaken retrospectively from April 2015 to March 2016 using the same methods and search strategy as before. 457 (male 43.3%, female 56.7%) hip hemiarthroplasty procedures were carried out in this time period with 5 deep infections occurring, a rate of 1.1%, demonstrating a statistically significant reduction in periprosthetic joint infection rate (P = 0.03, chi square test). There were 3 males and 4 females, with a mean age of 79 years (range 57–91), and mean ASA of 3.1 (range, 2–4). Two were right hips, 3 were left hips. Four infections occurred within 4 weeks and one at day 50. The overall mortality rate for those patients who developed deep periprosthetic infection within our study time frame was 28%.
Findings were presented at the regional audit meeting. This highlighted the positive impact of the changes to practice and stimulated discussion on further improvements to practice that could be instituted. Prior to implementation of any further changes to practice a re-audit was conducted over a further 12-month period. This demonstrated maintenance of an infection rate below the literature standard of 1.6% and a continued reduction in the initial audit rate of 2.7%
Lessons and Limitations
This quality improvement project demonstrates how simple changes can deliver large benefits to both patients and the health system. There is considerable variability in worldwide orthopedic practice, due in part to the limited evidence base for some perioperative infection precautions. This was the first attempt in Northern Ireland to quantify the effect of some of these precautions and to contribute to the evidence in support of their implementation. We acknowledge that the numbers involved in our project are small, and the effect size is likely to be overestimated. Factors contributing to this include the Hawthorne effect, improved staff awareness of postoperative infection, and that patients who either died or were treated conservatively did not undergo a washout procedure and therefore would not have been identified.
Institutional change is challenging. We selected the changes to practice that we felt would likely provide the largest benefit, with minimal cultural resistance. All materials (eg, Ioban drapes and Chloraprep skin solution) were already stocked in theatre suite and therefore did not have to undergo procurement procedures. Junior medical staff were instructed on strict standardised draping technique, as agreed by revision arthroplasty surgeons working within the unit.
We would advocate that theatre staff at every level are involved in this process from the outset in order to maximise the overall benefit. It is important that medical, nursing, and auxiliary staff are involved in decision making and implementation to facilitate uptake of new practices. All staff were re-educated on the impact of deep infections in these patients and the importance of perioperative practice in minimising these. Whenever resistance was met we addressed with open discussion and answering all questions to ensure staff understanding and acceptance.
Conclusion
Deep joint infection represents a significant cause of morbidity and mortality in the elderly population and a financial burden on the health service. The implementation of these simple perioperative interventions has achieved a significantly reduced rate of infection in a regional trauma center. Our interventions have been straightforward to implement, cost-effective and, most importantly, have demonstrated a significant, tangible benefit to our patients.
Corresponding author: Mr. Brendan Gallagher, Department of Trauma and Orthopedics, Royal Victoria Hospital, 274 Grosvenor Road, Belfast, N. Ireland, BT12 6BA, [email protected] .
Financial disclosures: None.
From the Department of Trauma and Orthopaedics, Royal Victoria Hospital, Belfast, N. Ireland.
Abstract
- Objective: To improve the deep wound infection rate in patients undergoing hip hemiarthroplasty in our regional trauma center.
- Methods: We conducted a retrospective audit of patients who had undergone hip hemiarthroplasty between January 2013 and July 2014 and found that in 750 hip hemiarthroplasties performed, 20 (2.7%) developed a deep infection, a figure in excess of the literature standard. In line with international consensus recommendations, 4 changes to our perioperative practice were implemented: standardized draping of the affected extremity, improved skin preparation using a 2% chlorhexidine gluconate solution, change of incision drapes to iodophor-impregnated adhesive film drapes, and the use of interactive wound dressing. We conducted staff education to highlight the impact of deep wound infection, introduce the changes, and underscore the importance of strict adherence to intraoperative sterility.
- Results: One year after introducing the changes, we audited the period April 2015 to March 2016, during which time 457 hip hemiarthoplasties were performed. Five (1.1%) deep infections were identified.
- Conclusion: Improvement in the perioperative care of our hip hemiarthroplasty patients has resulted in a reduced risk of the development of deep wound infection. This improvement was maintained in a third audit period, with continued implementation of these changes in practice.
Keywords: deep infection; hip hemiarthroplasty; quality improvement; proximal femoral fracture; risk reduction strategies.
Deep wound infection following hip hemiarthroplasty is a catastrophic outcome for the patient, resulting in a prolonged stay in hospital, a poor outcome and increased costs. There is limited evidence in the literature reporting early deep infection rates specific to hip hemiarthroplasty. A number of studies describe the incidence of deep infection in proximal femur fractures treated by arthroplasty and fixation [1], with only a single study reporting on solely hip hemiarthroplasty [2]. The reported incidence of early deep infection following hip hemiarthroplasty specifically varies from 1.6% [1] to 4.9% [2,3]. These figures are primarily provided by retrospective, descriptive studies, with variable lengths of follow-up.
Early deep infection occurs more frequently in hip hemiarthroplasty for trauma than elective total hip arthroplasty. This is thought to be due to several factors including the advanced age of hip hemiarthroplasty patients and their comorbid status, in addition to the shorter time frame in which to medically optimize trauma patients, including less opportunity to address nutritional elements known to impact recovery.
A number of prognostic factors have been identified as increasing the chance of developing a deep periprosthetic infection following hip hemiarthroplasty. Although these are debated they include cognitive impairment, high body mass index, development of wound hematoma post-operatively and increased operating time [8].
Many of the measures taken to reduce the risk of deep infection in arthroplasty have a limited evidence base, with a significant amount of practice based on expert opinion [10]. This is due to the difficulty in designing robust randomized controlled trials with sufficient numbers to identify significant trends. It is generally accepted that parenteral antibiotic prophylaxis [4] and antibiotic-loaded cement reduce the incidence of infection [5]. Increased theatre traffic has long been accepted as increasing bacterial counts in theatre [6]. Sterile skin preparation and draping with impermeable drapes and an iodophor-impregnated adhesive skin drape have been shown to reduce bacterial contamination and recolonization rates in vitro [4], although this has not resulted in a clinical reduction in deep periprosthetic joint infections. Other practices such as the use of laminar flow theatres are less well evidenced [7].
Following concerns regarding a perceived spike in infection rates in our hip hemiarthroplasty patients, the senior author, who is the training liaison officer for trauma and orthopedics in the hospital, convened a meeting with the first 2 authors regarding how best to investigate this potential issue. It was decided that an audit of practice should be conducted, as well as a literature review to assess acceptable infection rates within the literature and any potential areas for improvement.
Setting
The Royal Victoria Hospital in Belfast is one of the UK’s largest dedicated trauma units, treating over 900 proximal femur fractures per year. Of these, approximately 500 are displaced intracapsular neck of femur fractures requiring hip hemiarthroplasty. Patients are managed on dedicated trauma wards, and in accordance with British Orthopaedic Association guidelines there is a focus on multidisciplinary rehabilitation including a fully integrated orthogeriatric service [8]. We routinely use a modular Exeter trauma stem (Stryker, Kalamazoo MI) prosthesis with gentamycin-loaded cement and an antibiotic prophylaxis regimen of flucloxacillin and gentamicin prior to incision, followed by 2 further doses of flucloxacillin over 24 hours. A preoperative checklist is conducted to ensure that antibiotics are administered prior to skin incision and that there are no concerns regarding equipment sterility. Four trauma theatres are run each weekday, prioritizing medically optimized proximal femoral fracture patients.
Quality Improvement Project
Pre-intervention Audit
A retrospective audit was carried out via interrogation of the Fracture Outcome Research Database (FORD) between January 2013 and July 2014. This is a prospectively collected database of demographic data and outcome measurements that is managed by a dedicated team employed by the institution. This ensures accurate documentation of hospital admissions for trauma, operations conducted, and outcomes, such as discharge destination and further procedures.
The search terms used were wound washout, irrigation and debridement, first stage revision, girdlestone, and excision arthroplasty. Exclusion criteria included washouts for septic arthritis of a native hip joint, open injuries, and repeated washouts on the same patient. Data were collected including demographics, comorbidities, surgeon level, ward, theatre and causative organism by reviewing the electronic and written records.
725 patients were identified who met the inclusion criteria and underwent a hip hemiarthroplasty. Of these, 20 had undergone a washout procedure for deep infection, a rate of 2.7%. There were 14 females, nine males, 12 were right hips, 8 left, with a mean age of 81 years (range, 66–92). The mean American Society of Anesthetists (ASA) score was 3.2 (range, 2–4). Fourteen infections were identified within 4 weeks postoperatively, 6 within 8 weeks. Nineteen out of 20 of the causative organisms isolated were sensitive to the standard prophylactic antibiotic regimen. There was no association identified with a particular theatre, presence of laminar flow, ward, or grade of operating surgeon.
Changes to Perioperative Practice
We met on 2 further occasions to discuss the findings of the literature review and strategy for improvement prior to institution of changes.
We reviewed the National Institute for Clinical Excellence (NICE) Clinical Guideline [9] and the “International Consensus on Periprosthetic Joint Infection” [10] to compare our perioperative practice to national and international recommendations. We identified that we were compliant with a large majority of recommended practices, for example using antibiotic prophylaxis, laminar flow theatres, and sterile disposable drapes. We defined an acceptable infection rate to be 1.6% following a comprehensive literature review [1–3].
Four potential changes to our perioperative practice were chosen based on our review of the clinical guidelines and consensus document. These were chosen due to the strong expert opinion that they commanded within the consensus document and their relative ease and speed of implementation.
- Standardized draping of the affected extremity using stockinette isolation and windowed drape towards patient’s upper body.
- Use of a chlorhexidine gluconate (2% [w/v] in 70% [v/v] isopropyl alcohol) preoperative skin solution in theatre as a preliminary antiseptic skin preparation prior to formal preparation with povidone-iodine. Darouiche et al [11] demonstrated that preoperative cleansing of the patient’s skin with chlorhexidine-alcohol is superior to cleansing with povidone-iodine for preventing surgical site infection. Subsequent studies have suggested that concurrent application of the 2 antiseptic agents confer a further potential benefit by reducing the number of viable colony forming organisms and, subsequently, deep surgical site infection [12,13].
- Change from non-impregnated adhesive incision drapes to Ioban (3M, St Paul, MN) (other manufacturers available) iodophor-impregnated adhesive incision drapes. Experimental studies have demonstrated a lower rate of skin recolonization with bacteria following the use of impregnated drapes compared to non-impregnated drapes [14,15] although this has not been correlated to rates of deep infection.
- Change from simple absorbent dressings to interactive wound dressings (Aquacel and Duoderm; ConvaTec Ltd., Flintshire, UK) (alternative manufacturers available). There is evidence to show that Aquacel and Duoderm dressings were associated with reduced rates of skin blistering and infection in elective arthroplasty [16].
We also felt that staff education would be important for implementing change. We presented the results of the initial audit at departmental and regional quality improvement meetings, demonstrating the need for change in practice. Following the literature search and decision to implement 4 changes, medical staff were re-educated at the departmental audit meeting on the rationale behind the changes being made. Via liaison with the nurse lead of trauma theatres, nursing and auxiliary staff underwent education sessions. These were small group sessions, with visual aids, designed to fit in to staff breaks to reduce disruption of their work. Groups consisted of 4 to 6 people per session. They were led by the authors and focused on highlighting the reasoning behind the changes in practices and answering any questions that staff had. During these sessions, a revision of good theatre etiquette was conducted. This included reinforcing basic theatre principles, for example, reducing theatre traffic, ensuring correct theatre dress and head coverings are worn at all times, highlighting the need to regularly wash hands and wear gloves when required, and to respect the sterile areas and instruments appropriately.
Results
A re-audit of hip hemiarthroplasties was conducted after a 12-month interval to allow proposed changes to become routine practice. Re-audit was undertaken retrospectively from April 2015 to March 2016 using the same methods and search strategy as before. 457 (male 43.3%, female 56.7%) hip hemiarthroplasty procedures were carried out in this time period with 5 deep infections occurring, a rate of 1.1%, demonstrating a statistically significant reduction in periprosthetic joint infection rate (P = 0.03, chi square test). There were 3 males and 4 females, with a mean age of 79 years (range 57–91), and mean ASA of 3.1 (range, 2–4). Two were right hips, 3 were left hips. Four infections occurred within 4 weeks and one at day 50. The overall mortality rate for those patients who developed deep periprosthetic infection within our study time frame was 28%.
Findings were presented at the regional audit meeting. This highlighted the positive impact of the changes to practice and stimulated discussion on further improvements to practice that could be instituted. Prior to implementation of any further changes to practice a re-audit was conducted over a further 12-month period. This demonstrated maintenance of an infection rate below the literature standard of 1.6% and a continued reduction in the initial audit rate of 2.7%
Lessons and Limitations
This quality improvement project demonstrates how simple changes can deliver large benefits to both patients and the health system. There is considerable variability in worldwide orthopedic practice, due in part to the limited evidence base for some perioperative infection precautions. This was the first attempt in Northern Ireland to quantify the effect of some of these precautions and to contribute to the evidence in support of their implementation. We acknowledge that the numbers involved in our project are small, and the effect size is likely to be overestimated. Factors contributing to this include the Hawthorne effect, improved staff awareness of postoperative infection, and that patients who either died or were treated conservatively did not undergo a washout procedure and therefore would not have been identified.
Institutional change is challenging. We selected the changes to practice that we felt would likely provide the largest benefit, with minimal cultural resistance. All materials (eg, Ioban drapes and Chloraprep skin solution) were already stocked in theatre suite and therefore did not have to undergo procurement procedures. Junior medical staff were instructed on strict standardised draping technique, as agreed by revision arthroplasty surgeons working within the unit.
We would advocate that theatre staff at every level are involved in this process from the outset in order to maximise the overall benefit. It is important that medical, nursing, and auxiliary staff are involved in decision making and implementation to facilitate uptake of new practices. All staff were re-educated on the impact of deep infections in these patients and the importance of perioperative practice in minimising these. Whenever resistance was met we addressed with open discussion and answering all questions to ensure staff understanding and acceptance.
Conclusion
Deep joint infection represents a significant cause of morbidity and mortality in the elderly population and a financial burden on the health service. The implementation of these simple perioperative interventions has achieved a significantly reduced rate of infection in a regional trauma center. Our interventions have been straightforward to implement, cost-effective and, most importantly, have demonstrated a significant, tangible benefit to our patients.
Corresponding author: Mr. Brendan Gallagher, Department of Trauma and Orthopedics, Royal Victoria Hospital, 274 Grosvenor Road, Belfast, N. Ireland, BT12 6BA, [email protected] .
Financial disclosures: None.
1. Duckworth AD, Phillips S-A, Stone O, et al. Deep infection after hip fracture surgery: predictors of early mortality. Injury 2012;43:1182–6.
2. de Jong L, Klem TMAL, Kuijper TM, Roukema GR. Factors affecting the rate of surgical site infection in patients after hemiarthroplasty of the hip following a fracture of the neck of the femur. Bone Joint J 2017;99-B:1088–94
3. Ridgeway S, Wilson J, Charlet A, et al. Infection of the surgical site after arthroplasty of the hip. J Bone Joint Surg [Br] 2005;87–B(6):844–50.
4. Matar WY, Jafari SM, Restrepo C, et al. Preventing Infection in Total Joint Arthroplasty. J Bone Joint Surg [Am] 2010;92(Suppl 2):36–46.
5. Parvizi J, Saleh KJ, Ragland PS, et al. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop 2008;79:335–41.
6. Ritter MA, Eitzen H, French ML, Hart JB. The operating room environment as affected by people and the surgical face mask. Clin Orthop Rel Res 1975;:147–50.
7. Hooper GJ, Rothwell a G, Frampton C, Wyatt MC. Does the use of laminar flow and space suits reduce early deep infection after total hip and knee replacement?: the ten-year results of the New Zealand Joint Registry. J Bone Joint Surg [Br] 2011;93:85–90.
8. British Orthopaedic Association. British Orthopaedic Association standards for trauma. 2012. Available at www.boa.ac.uk/wpcontent/uploads/2014/12/BOAST-1.pdf.
9. NICE. Hip fracture: management | 1-Guidance | Guidance and guidelines | NICE. Health Technol Assess (Rockv). NICE; 2014. Available at www.nice.org.uk/guidance/cg124/chapter/1-guidance.
10. Parvizi J, Gehrke T. International consensus on periprosthetic joint infection. J Bone Joint Surg [Am] 2014;96:441.
11. Darouiche RO, Wall Jr MJ, Itani KMF, et al. Chlorhexidine–alcohol versus povidone–iodine for surgical-site antisepsis. N Engl J Med 2010;362:18–26.
12. Anderson MJ, Horn ME, Lin YC et al. Efficacy of concurrent application of chlorhexidine gluconate and povidone iodine against six nosocomial pathogens. Am J Infect Control 2010;38:826–31.
13. Patrick S, McDowell A, Lee A et al. Antisepsis of the skin before spinal surgery with povidone iodine-alcohol followed by chlorhexidine gluconate-alcohol versus povidone iodine-alcohol applied twice for the prevention of contamination of the wound by bacteria. Bone Joint J 2017;99-B:1354–65.
14. Johnston DH, Fairclough JA, Brown EM, Morris R. Rate of bacterial recolonization of the skin after preparation: four methods compared. Br J Surg 1987;74:64.
15. Dewan PA, Van Rij AM, Robinson RG, et al. The use of an iodophor-impregnated plastic incise drape in abdominal surgery--a controlled clinical trial. Aust N Z J Surg 1987;57:859–63.
16. Clarke JV, Deakin AH, Dillon JM, et al. A prospective clinical audit of a new dressing design for lower limb arthroplasty wounds. J Wound Care 2009;18:5–8, 10–11.
1. Duckworth AD, Phillips S-A, Stone O, et al. Deep infection after hip fracture surgery: predictors of early mortality. Injury 2012;43:1182–6.
2. de Jong L, Klem TMAL, Kuijper TM, Roukema GR. Factors affecting the rate of surgical site infection in patients after hemiarthroplasty of the hip following a fracture of the neck of the femur. Bone Joint J 2017;99-B:1088–94
3. Ridgeway S, Wilson J, Charlet A, et al. Infection of the surgical site after arthroplasty of the hip. J Bone Joint Surg [Br] 2005;87–B(6):844–50.
4. Matar WY, Jafari SM, Restrepo C, et al. Preventing Infection in Total Joint Arthroplasty. J Bone Joint Surg [Am] 2010;92(Suppl 2):36–46.
5. Parvizi J, Saleh KJ, Ragland PS, et al. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop 2008;79:335–41.
6. Ritter MA, Eitzen H, French ML, Hart JB. The operating room environment as affected by people and the surgical face mask. Clin Orthop Rel Res 1975;:147–50.
7. Hooper GJ, Rothwell a G, Frampton C, Wyatt MC. Does the use of laminar flow and space suits reduce early deep infection after total hip and knee replacement?: the ten-year results of the New Zealand Joint Registry. J Bone Joint Surg [Br] 2011;93:85–90.
8. British Orthopaedic Association. British Orthopaedic Association standards for trauma. 2012. Available at www.boa.ac.uk/wpcontent/uploads/2014/12/BOAST-1.pdf.
9. NICE. Hip fracture: management | 1-Guidance | Guidance and guidelines | NICE. Health Technol Assess (Rockv). NICE; 2014. Available at www.nice.org.uk/guidance/cg124/chapter/1-guidance.
10. Parvizi J, Gehrke T. International consensus on periprosthetic joint infection. J Bone Joint Surg [Am] 2014;96:441.
11. Darouiche RO, Wall Jr MJ, Itani KMF, et al. Chlorhexidine–alcohol versus povidone–iodine for surgical-site antisepsis. N Engl J Med 2010;362:18–26.
12. Anderson MJ, Horn ME, Lin YC et al. Efficacy of concurrent application of chlorhexidine gluconate and povidone iodine against six nosocomial pathogens. Am J Infect Control 2010;38:826–31.
13. Patrick S, McDowell A, Lee A et al. Antisepsis of the skin before spinal surgery with povidone iodine-alcohol followed by chlorhexidine gluconate-alcohol versus povidone iodine-alcohol applied twice for the prevention of contamination of the wound by bacteria. Bone Joint J 2017;99-B:1354–65.
14. Johnston DH, Fairclough JA, Brown EM, Morris R. Rate of bacterial recolonization of the skin after preparation: four methods compared. Br J Surg 1987;74:64.
15. Dewan PA, Van Rij AM, Robinson RG, et al. The use of an iodophor-impregnated plastic incise drape in abdominal surgery--a controlled clinical trial. Aust N Z J Surg 1987;57:859–63.
16. Clarke JV, Deakin AH, Dillon JM, et al. A prospective clinical audit of a new dressing design for lower limb arthroplasty wounds. J Wound Care 2009;18:5–8, 10–11.
Outcomes After Endoscopic Dilation of Laryngotracheal Stenosis: An Analysis of ACS-NSQIP
From the Northwestern University, Feinberg School of Medicine, Chicago, IL (Mr. Bavishi, Dr. Lavin), the Johns Hopkins University, Baltimore, MD (Dr. Boss), Children’s National Medical Center, Washington, DC (Dr. Shah), and Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL (Dr. Lavin).
Abstract
- Background: Endoscopic management of pediatric subglottic stenosis is common; however, no multiinstitutional studies have assessed its perioperative outcomes. The American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS-NSQIP-P) represents a source of such data.
- Objective: To investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to those seen with open reconstruction techniques.
- Methods: Current procedural terminology (CPT) codes were queried for endoscopic or open airway reconstruction in the 2015 ACS-NSQIP-P Public Use File (PUF). Demographics and 30-day events were abstracted to compare open to endoscopic techniques and to assess for risk factors for varied outcomes after endoscopic dilation. Outcome measures included length of stay (LOS), 30-day rates of reintubation, readmission, and reoperation.
- Results: 171 endoscopic and 116 open procedures were identified. Mean age at endoscopic and open procedures was 4.1 (SEM = 0.37) and 5.4 years (SEM = 0.40). Mean LOS was shorter after endoscopic procedures (5.5 days, SEM = 1.13 vs. 11.3 days SEM = 1.01, P < 0.001). Open procedures had higher rates of reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009). In patients undergoing endoscopic dilation, children < 1 year were more likely to require readmission (OR = 4.21, P = 0.03) and reoperation (OR = 4.39, P = 0.03) when compared with older children.
- Conclusion: Open airway reconstruction is associated with longer LOS and increased reintubations and reoperations, suggesting a possible opportunity to improve value in health care in the appropriately selected patient. Reoperations and readmissions following endoscopic dilation are more prevalent in children younger than 1 year.
Keywords: airway stenosis; subglottic stenosis; endoscopic dilation; pediatrics; outcomes.
Historically, pediatric laryngotracheal stenosis was managed using open reconstruction techniques, including laryngoplasty, tracheal resection, and cervical tracheoplasty. Initial reports of endoscopic dilation were described in the 1980s as a means to salvage re-stenosis after open reconstruction [1]. Currently, primary endoscopic dilation has become commonplace in otolaryngology due to its less invasive nature as well as—in cases of balloon dilation—minimization of tissue damage [2]. The advancements made in endoscopic balloon dilation have reduced the frequency with which open reconstruction is performed.
Systematic reviews and case series investigating endoscopic dilation indicate a 70% to 80% success rate in preventing future open surgery or tracheostomy [2–5]. While increased severity of stenosis has been associated with poorer outcomes in endoscopic procedures, few other risk factors that influence surgical success have been identified [4,5]. In a single study in the adult literature, open surgical management of idiopathic subglottic stenosis was associated with improved outcomes when compared to endoscopic techniques [5]. Such findings suggest a need to identify these factors for the purpose of optimizing clinical decision-making.
As laryngotracheal stenosis is rare, postoperative outcomes and risk factors are best identified on a multiinstitutional level. Due to its participation from 80 hospitals and its accurate and reliable reporting of both demographic and risk-stratified 30-day outcomes data, the American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS NSQIP-P) provides such a platform [6–8]. Thirty-day outcomes and risk factors for open reconstruction utilizing the ACS NSQIP-P database have previously been reported; however, no such outcomes for endoscopic dilation have been described, and no comparison between endoscopic and open procedures has been made [9]. The purpose of this study was to utilize the 2015 ACS-NSQIP-P database to investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to open reconstruction techniques. Secondarily, we aimed to determine if any demographic factors or medical comorbidities are associated with varied outcomes in endoscopic reconstruction. While these data reflect safety and quality of this procedure in the United States, findings may potentially be applied across international settings.
Methods
Data Source
Data was obtained from the 2015 ACS-NSQIP-P Public Use File (PUF). Due to the de-identified and public nature of these data, this research was exempt from review by the Ann & Robert H. Lurie Children’s Hospital of Chicago review board. Data collection methods for ACS-NSQIP-P have previously been described [10]. In brief, data was collected from 80 hospitals on approximately 120 preoperative, intraoperative, and postoperative variables. Cases are systematically sampled on an 8-day cycle basis, where the first 35 cases meeting the inclusion criteria in each hospital in each cycle are submitted to ACS-NSQIP-P.
Variables and Outcomes
Airway procedures for endoscopic dilations and open reconstructions were obtained by CPT code. Endoscopic dilations (CPT 31528) were compared to open reconstructions, which included laryngoplasty (31580, 31582), cervical tracheoplasty (31750), cricoid split (31587), and tracheal resection (31780). Demographic variables included age, sex, race, and history of prematurity. Presence of specific comorbid diseases were also collected and tested for significance.
Dependent outcomes of interest were unplanned 30-day postoperative events grouped as reoperation, unplanned readmission, and postoperative reintubation. In the case of endoscopic procedures, the presence of salvage open reconstruction or tracheostomy within 30 days of surgery was also recorded. Length of stay (LOS) after the procedure was collected. Specific postoperative complications and reasons for readmission were recorded within the limitations of data available in the PUF.
Analysis
Analysis was performed using descriptive statistics and frequency analysis where appropriate. Chi-square analysis was used to compare adverse events between open and endoscopic procedures. Logistic regression with calculation of odds ratio (OR) was performed to determine predictive factors for reoperation, readmission, and reintubation in all pediatric airway reconstructive procedures in adjusted and unadjusted models. T-test and linear regression was performed on the continuous outcome of length of stay. For all analyses, a p value of < 0.05 was considered statistically significant. All variable recoding and statistical analyses were performed in SAS/STAT software (Cary, NC).
Results
A total of 84,056 pediatric procedures were extracted from the 2015 NSQIP-P PUFs. Using the above CPT codes, 171 endoscopic dilations and 116 open airway reconstructions were identified, with patient age ranging from 0 days to 17.6 years. Average age of patients undergoing endoscopic dilation and open reconstruction was 4.1 and 5.4 years, respectively (Table 1). 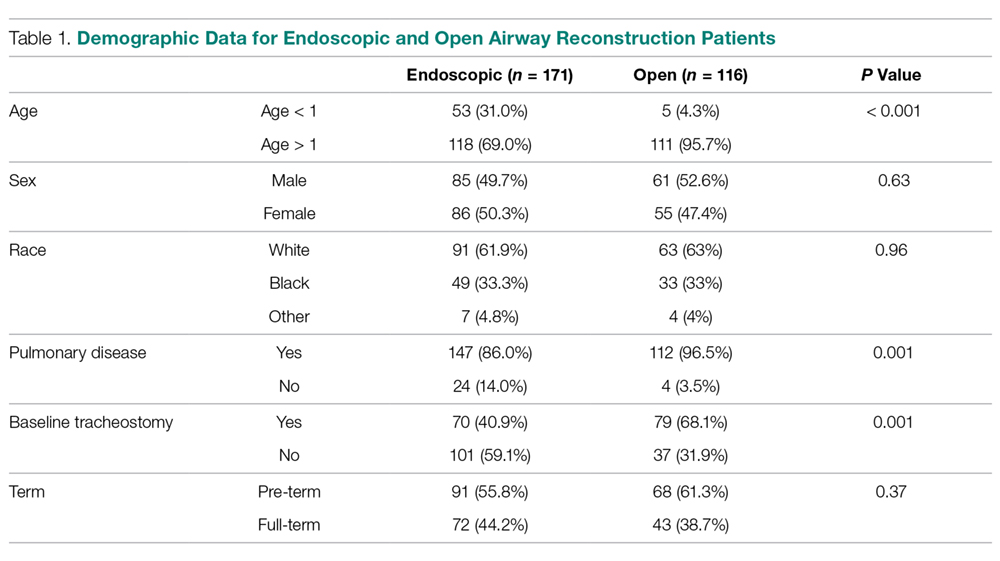
Potential confounders were tested with univariate logistic regression to determine if they had a significant impact on readmission, reintubation, or reoperation rates. These variables (Table 2) 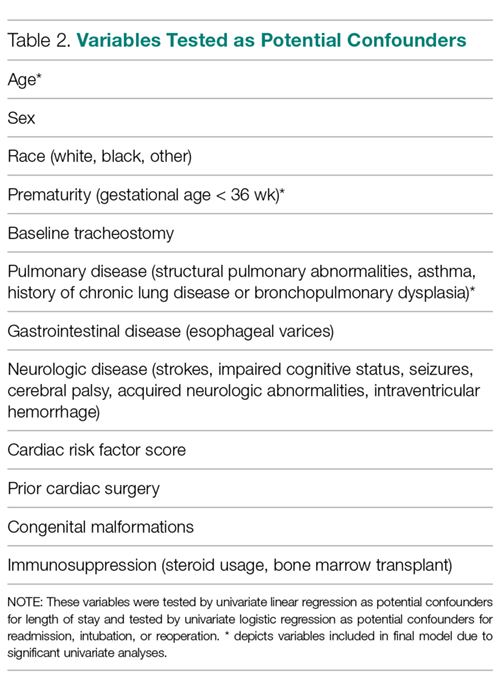
In patients undergoing endoscopic dilation, average length of stay was 5.5 days (SEM = 1.13), with 79 (48.5%) patients having a length of stay of zero days. Of all patients who had endoscopic dilations, 70 (40.1%) had a pre-existing tracheostomy and these accounted for the majority (73%) of patients who had zero days as their LOS. LOS after endoscopic management was significantly shorter than the mean of 11.3 days (SEM = 1.01) reported in those undergoing open reconstruction (P < 0.001).
With respect to 30-day adverse events, 2 patients in the endoscopic group (1.1%) required reintubation. Thirteen endoscopic dilation cases (7.6%) had an unplanned readmission, four (2.3%) of which were associated with reoperation within 30 days of the primary surgical procedure. There were 9 other reoperations unassociated with unplanned readmission. Three of these reoperations were due to failed endoscopic dilations, resulting in 2 tracheostomies and one open airway reconstruction. There was one patient death, in a 0-day old with tetralogy of Fallot, trachea-esophageal fistula, and ventilator dependence who underwent emergent endoscopic dilation and died the same day.
Open procedures were associated with 11 unplanned readmissions (9.5%), 7 re-intubations (6%) and 18 reoperations (15.5%). Of patents undergoing reoperation, one patient undergoing open reconstruction underwent tracheostomy within 30 days of surgery.
When comparing open reconstruction to endoscopic dilation, there was a significant increase in reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009) for open procedures, even with adjustment for age, tracheostomy status, and pulmonary disease. There was no significant difference between the two for unplanned readmissions (OR = 1.19, P = 0.79) (Figure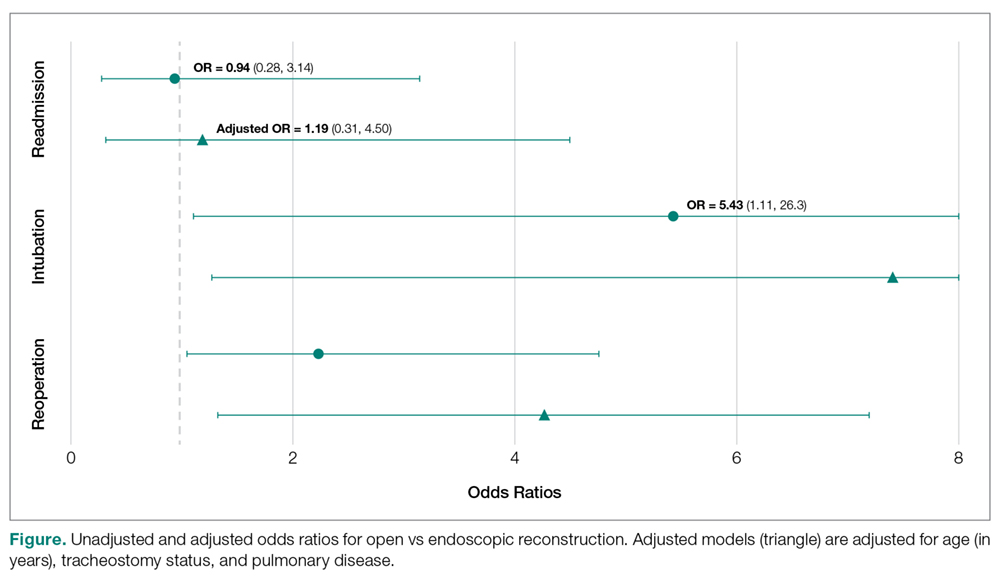
Younger age was also found to be significantly associated with reoperation rates, in an adjusted logistic model that accounted for tracheostomy status, type of surgery, and pulmonary disease. Per year of life, younger children had higher reoperation rates than older children (OR = 1.91, P = 0.017). When endoscopic dilation was individually examined, children younger than 1 year of age were more likely to undergo reoperation after an endoscopic dilation than children older than 1 (OR = 4.39, P = 0.03). Children under age 1 were also more likely to have an unplanned readmission after an endoscopic dilation (OR = 4.21, P = 0.03). The relationship between age and re-intubation was not significant (OR = 0, P = 0.95). For open reconstruction, this age dichotomization was not associated with any increased reoperation (OR = 2.3, P = 0.52), readmission (OR = 0, P = 0.97), or reintubation (OR = 0, P = 0.94).
T-test analysis was performed to determine if children < 1 year old also had significantly longer hospital stays after endoscopic dilation than older children (mean 14.1 days vs 1.9 days, P < 0.001). This relationship held true in a linear regression after adjustment for pulmonary disease and tracheostomy, with length of stay decreasing by 0.48 days per year of life (P = 0.03). For endoscopic dilations, the same relationship held true, where length of stay decreased by 0.75 days per year of life.
Discussion
Endoscopic dilation for primary management of pediatric laryngotracheal stenosis has become commonplace. Despite this, outcomes of this procedure have only been described in case series and meta-analyses [2–5]. The relative rarity of pediatric laryngotracheal stenosis suggests the need for large, multi-institutional data for purposes of patient selection and medical decision-making.
This study utilized the ACS-NSQIP-Pediatric database to highlight 30-day outcomes of endoscopic dilation and to compare these outcomes to those of open airway reconstruction procedures. The ACS-NSQIP database has been endorsed by multiple organizations, including the Center for Medicare and Medicaid Services, the Joint Commission, and the American Medical Association. It has been shown to have higher sensitivity and a lower false-positive rate when compared to administrative data, in part due to data collection from trained personnel [11]. Furthermore, ACS-NSQIP use has the additional benefit of reporting an unplanned admission—a feature unavailable in review of claims data [12].
With respect to adverse events, our study demonstrates that endoscopic dilation is associated with an equally high rate of unplanned readmission when compared to open reconstruction. The high prevalence of comorbid disease such as chronic lung disease (32% of endoscopic dilation and 43% of open reconstruction) can account for some of the morbidity associated with any airway procedures.
Despite high rates of unplanned readmission, patients undergoing endoscopic dilation were less likely to have reoperations within 30 days of initial surgery when compared to those undergoing open reconstruction. While differences in disease severity may be partially responsible for this difference in the reoperation rate, this finding is notable given the health care costs associated with multiple operations as well as safety concerns with multiple anesthetics in the very young [13,14].
The ACS-NSQIP platform does not distinguish unplanned from planned reoperations. In the setting of airway surgery, where multiple planned reoperations are commonplace, this metric is a suboptimal stand-alone indicator of adverse outcomes. Other markers available in the database—such as reintubations and performance of tracheostomy or open airway reconstruction within 30-days of surgery—are more indicative of surgical outcome in the setting of airway surgery. We found that both reintubations and salvage open reconstruction within 30-days were rare. It should be noted that the ACS-NSQIP data does not report any events occurring outside of the 30-day postoperative period, representing potential limitation of the use of this database. As was previously advocated by Roxbury and colleagues, procedure/subspecialty specific outcome data collection would also improve outcome analysis of airway and other otolaryngologic procedures [9]. In the setting of airway reconstruction, this would include data pertaining to Cotton-Meyer grading systems well as postoperative voice and swallow outcomes.
In addition to safety profile, endoscopic procedures were associated with shorter LOS when compared with open reconstruction, representing another potential source of cost savings with this less invasive method. This is especially significant given that open reconstruction patients spend much of their inpatient stay in an ICU setting. In patients who are candidates for endoscopic procedures, this lower-risk, lower-cost profile of endoscopic dilation has the opportunity to improve value in health care and may be the source of future improvement initiatives.
In addition to comparing overall outcomes between endoscopic and open management of laryngotracheal stenosis, our study aimed to identify factors that were associated with varied outcomes in patients undergoing primary endoscopic dilation. We found that children younger than 1 year of age were 5.8 times more likely to undergo an unplanned reoperation after an endoscopic dilation than children over 1 year. A similar finding was reported in open airway surgeries, with increased reoperation rates in children < 3 years old [9]. The justification of a dichotomization at 1 year was made as expert opinion recognizes that the infant airway is less forgiving to intervention given its small size. Young age was also a factor in prolonged LOS as was determined by linear regression. It is likely that this increased LOS may be in part due to associations of young age and the neonatal ICU population. One must balance the increased risk of surgery in the young with that of tracheostomy, which has a published complication rate of 18% to 50% and direct mortality rate of 1% to 2% in the pediatric population [15–18]. Understanding these relative risks may help guide the airway surgeon in preoperative counseling with families and medical decision-making.
As discussed above, the limitation of data to a 30-day period is a relative weakness of ACS-NSQIP database use for studies of airway reconstruction, as the ultimate outcome—a stable, decannulated airway—may occur outside of this time period. As many quality metrics utilize data from the 30-day postoperative period, knowledge of these outcomes remains valuable in surgical decision-making. Ultimately, collection of data in a large, long-term dataset would allow broader generalizations to be made about the differences between open and endoscopic procedures and would also give a more comprehensive picture of the outcomes of endoscopic dilation.
In conclusion, this study is the first to analyze 30-day postoperative outcomes in pediatric endoscopic airway dilations using data aggregated by ACS-NSQIP from institutions across the United States. This data indicates that endoscopic airway dilation is a relatively safe procedure, especially compared with open reconstruction; however, additional data on disease severity and other outcomes is necessary to draw final conclusions of superiority of technique. Future improvement initiatives could be aimed at the impact of this lower-risk, lower-cost procedure in the appropriately selected patient. Outcomes of endoscopic dilation are poorer in those less than 1 year of age, as they are associated with increased reoperation rates and increased length of stay compared to older children. One must balance these risks in the very young with the risks associated with tracheostomy and other alternative airway management modalities.
Note: This work was presented in a paper at the AAO-HNS 2017 meeting, Chicago, IL, 10 Sep 2017.
Corresponding author: Jennifer Lavin, MD, MS, 225 E Chicago Ave., Box 25, Chicago, IL 60611, [email protected].
Financial disclosures: None.
1. Cohen MD, Weber TR, Rao CC. Balloon dilatation of tracheal and bronchial stenosis. AJR Am J Roentgenol 1984;142:477–8.
2. Chueng K, Chadha NK. Primary dilatation as a treatment for pediatric laryngotracheal stenosis: a systematic review. Int J Pediatr Otorhinolaryngol 2013;77:623–8.
3. Hautefort C, Teissier N, Viala P, Van Den Abbeele T. Balloon dilation laryngoplasty for subglottic stenosis in children: eight years’ experience. Arch Otolaryngol Head Neck Surg 2012;138:235–40.
4. Lang M, Brietzke SE. A systematic review and meta-analysis of endoscopic balloon dilation of pediatric subglottic stenosis. Otolaryngol Head Neck Surg 2014;150:174–9.
5. Maresh A, Preciado DA, O’Connell AP, Zalzal GH. A comparative analysis of open surgery vs endoscopic balloon dilation for pediatric subglottic stenosis. JAMA Otolaryngol Head Neck Surg 2014;140:901–5.
6. Gelbard A, Donovan DT, Ongkasuwan J, et al. Disease homogeneity and treatment heterogeneity in idiopathic subglottic stenosis. Laryngoscope 2016;126:1390–6.
7. ACS-NSQIP. ACS National Surgical Quality Improvement Program® (ACS NSQIP®). 2017. Available at: http://site.acsnsqip.org/program-specifics/scr-training-and-resources. Accessed June 2 2017.
8. Shiloach M, Frencher SK Jr, Steeger JE, et al. Toward robust information: data quality and inter-rater reliability in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2010;210:6–16.
9. Roxbury CR, Jatana KR, Shah RK, Boss EF. Safety and postoperative adverse events in pediatric airway reconstruction: Analysis of ACS-NSQIP-P 30-day outcomes. Laryngoscope 2017;127:504–8.
10. Raval MV, Dillon PW, Bruny JL, et al. Pediatric American College of Surgeons National Surgical Quality Improvement Program: feasibility of a novel, prospective assessment of surgical outcomes. J Pediatr Surg 2011;46:115–21.
11. Lawson EH, Louie R, Zingmond DS, et al. A comparison of clinical registry versus administrative claims data for reporting of 30-day surgical complications. Ann Surg 2012;256:973–81.
12. Sellers MM, Merkow RP, Halverson A, et al. Validation of new readmission data in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2013;216:420–7.
13. Jevtovic-Todorovic V, Hartman RE, Izumi Y, et al. Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. J Neurosci 2003;23:876–82.
14. Patel P, Sun L. Update on neonatal anesthetic neurotoxicity: insight into molecular mechanisms and relevance to humans. Anesthesiology 2009;110:703–8.
15. Crysdale WS, Feldman RI, Naito K. Tracheotomies: a 10-year experience in 319 children. Ann Otol Rhinol Laryngol 1988;97(5 Pt 1):439–43.
16. Goldenberg D, Ari EG, Golz A, et al. Tracheotomy complications: a retrospective study of 1130 cases. Otolaryngol Head Neck Surg 2000;123:495–500.
17. Mahadevan M, Barber C, Salkeld L, et al N. Pediatric tracheotomy: 17 year review. Int J Pediatr Otorhinolaryngol 2007;71:1829–35.
18. Ozmen S, Ozmen OA, Unal OF. Pediatric tracheotomies: a 37-year experience in 282 children. Int J Pediatr Otorhinolaryngol 2009;73:959–61.
From the Northwestern University, Feinberg School of Medicine, Chicago, IL (Mr. Bavishi, Dr. Lavin), the Johns Hopkins University, Baltimore, MD (Dr. Boss), Children’s National Medical Center, Washington, DC (Dr. Shah), and Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL (Dr. Lavin).
Abstract
- Background: Endoscopic management of pediatric subglottic stenosis is common; however, no multiinstitutional studies have assessed its perioperative outcomes. The American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS-NSQIP-P) represents a source of such data.
- Objective: To investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to those seen with open reconstruction techniques.
- Methods: Current procedural terminology (CPT) codes were queried for endoscopic or open airway reconstruction in the 2015 ACS-NSQIP-P Public Use File (PUF). Demographics and 30-day events were abstracted to compare open to endoscopic techniques and to assess for risk factors for varied outcomes after endoscopic dilation. Outcome measures included length of stay (LOS), 30-day rates of reintubation, readmission, and reoperation.
- Results: 171 endoscopic and 116 open procedures were identified. Mean age at endoscopic and open procedures was 4.1 (SEM = 0.37) and 5.4 years (SEM = 0.40). Mean LOS was shorter after endoscopic procedures (5.5 days, SEM = 1.13 vs. 11.3 days SEM = 1.01, P < 0.001). Open procedures had higher rates of reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009). In patients undergoing endoscopic dilation, children < 1 year were more likely to require readmission (OR = 4.21, P = 0.03) and reoperation (OR = 4.39, P = 0.03) when compared with older children.
- Conclusion: Open airway reconstruction is associated with longer LOS and increased reintubations and reoperations, suggesting a possible opportunity to improve value in health care in the appropriately selected patient. Reoperations and readmissions following endoscopic dilation are more prevalent in children younger than 1 year.
Keywords: airway stenosis; subglottic stenosis; endoscopic dilation; pediatrics; outcomes.
Historically, pediatric laryngotracheal stenosis was managed using open reconstruction techniques, including laryngoplasty, tracheal resection, and cervical tracheoplasty. Initial reports of endoscopic dilation were described in the 1980s as a means to salvage re-stenosis after open reconstruction [1]. Currently, primary endoscopic dilation has become commonplace in otolaryngology due to its less invasive nature as well as—in cases of balloon dilation—minimization of tissue damage [2]. The advancements made in endoscopic balloon dilation have reduced the frequency with which open reconstruction is performed.
Systematic reviews and case series investigating endoscopic dilation indicate a 70% to 80% success rate in preventing future open surgery or tracheostomy [2–5]. While increased severity of stenosis has been associated with poorer outcomes in endoscopic procedures, few other risk factors that influence surgical success have been identified [4,5]. In a single study in the adult literature, open surgical management of idiopathic subglottic stenosis was associated with improved outcomes when compared to endoscopic techniques [5]. Such findings suggest a need to identify these factors for the purpose of optimizing clinical decision-making.
As laryngotracheal stenosis is rare, postoperative outcomes and risk factors are best identified on a multiinstitutional level. Due to its participation from 80 hospitals and its accurate and reliable reporting of both demographic and risk-stratified 30-day outcomes data, the American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS NSQIP-P) provides such a platform [6–8]. Thirty-day outcomes and risk factors for open reconstruction utilizing the ACS NSQIP-P database have previously been reported; however, no such outcomes for endoscopic dilation have been described, and no comparison between endoscopic and open procedures has been made [9]. The purpose of this study was to utilize the 2015 ACS-NSQIP-P database to investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to open reconstruction techniques. Secondarily, we aimed to determine if any demographic factors or medical comorbidities are associated with varied outcomes in endoscopic reconstruction. While these data reflect safety and quality of this procedure in the United States, findings may potentially be applied across international settings.
Methods
Data Source
Data was obtained from the 2015 ACS-NSQIP-P Public Use File (PUF). Due to the de-identified and public nature of these data, this research was exempt from review by the Ann & Robert H. Lurie Children’s Hospital of Chicago review board. Data collection methods for ACS-NSQIP-P have previously been described [10]. In brief, data was collected from 80 hospitals on approximately 120 preoperative, intraoperative, and postoperative variables. Cases are systematically sampled on an 8-day cycle basis, where the first 35 cases meeting the inclusion criteria in each hospital in each cycle are submitted to ACS-NSQIP-P.
Variables and Outcomes
Airway procedures for endoscopic dilations and open reconstructions were obtained by CPT code. Endoscopic dilations (CPT 31528) were compared to open reconstructions, which included laryngoplasty (31580, 31582), cervical tracheoplasty (31750), cricoid split (31587), and tracheal resection (31780). Demographic variables included age, sex, race, and history of prematurity. Presence of specific comorbid diseases were also collected and tested for significance.
Dependent outcomes of interest were unplanned 30-day postoperative events grouped as reoperation, unplanned readmission, and postoperative reintubation. In the case of endoscopic procedures, the presence of salvage open reconstruction or tracheostomy within 30 days of surgery was also recorded. Length of stay (LOS) after the procedure was collected. Specific postoperative complications and reasons for readmission were recorded within the limitations of data available in the PUF.
Analysis
Analysis was performed using descriptive statistics and frequency analysis where appropriate. Chi-square analysis was used to compare adverse events between open and endoscopic procedures. Logistic regression with calculation of odds ratio (OR) was performed to determine predictive factors for reoperation, readmission, and reintubation in all pediatric airway reconstructive procedures in adjusted and unadjusted models. T-test and linear regression was performed on the continuous outcome of length of stay. For all analyses, a p value of < 0.05 was considered statistically significant. All variable recoding and statistical analyses were performed in SAS/STAT software (Cary, NC).
Results
A total of 84,056 pediatric procedures were extracted from the 2015 NSQIP-P PUFs. Using the above CPT codes, 171 endoscopic dilations and 116 open airway reconstructions were identified, with patient age ranging from 0 days to 17.6 years. Average age of patients undergoing endoscopic dilation and open reconstruction was 4.1 and 5.4 years, respectively (Table 1).
Potential confounders were tested with univariate logistic regression to determine if they had a significant impact on readmission, reintubation, or reoperation rates. These variables (Table 2)
In patients undergoing endoscopic dilation, average length of stay was 5.5 days (SEM = 1.13), with 79 (48.5%) patients having a length of stay of zero days. Of all patients who had endoscopic dilations, 70 (40.1%) had a pre-existing tracheostomy and these accounted for the majority (73%) of patients who had zero days as their LOS. LOS after endoscopic management was significantly shorter than the mean of 11.3 days (SEM = 1.01) reported in those undergoing open reconstruction (P < 0.001).
With respect to 30-day adverse events, 2 patients in the endoscopic group (1.1%) required reintubation. Thirteen endoscopic dilation cases (7.6%) had an unplanned readmission, four (2.3%) of which were associated with reoperation within 30 days of the primary surgical procedure. There were 9 other reoperations unassociated with unplanned readmission. Three of these reoperations were due to failed endoscopic dilations, resulting in 2 tracheostomies and one open airway reconstruction. There was one patient death, in a 0-day old with tetralogy of Fallot, trachea-esophageal fistula, and ventilator dependence who underwent emergent endoscopic dilation and died the same day.
Open procedures were associated with 11 unplanned readmissions (9.5%), 7 re-intubations (6%) and 18 reoperations (15.5%). Of patents undergoing reoperation, one patient undergoing open reconstruction underwent tracheostomy within 30 days of surgery.
When comparing open reconstruction to endoscopic dilation, there was a significant increase in reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009) for open procedures, even with adjustment for age, tracheostomy status, and pulmonary disease. There was no significant difference between the two for unplanned readmissions (OR = 1.19, P = 0.79) (Figure
Younger age was also found to be significantly associated with reoperation rates, in an adjusted logistic model that accounted for tracheostomy status, type of surgery, and pulmonary disease. Per year of life, younger children had higher reoperation rates than older children (OR = 1.91, P = 0.017). When endoscopic dilation was individually examined, children younger than 1 year of age were more likely to undergo reoperation after an endoscopic dilation than children older than 1 (OR = 4.39, P = 0.03). Children under age 1 were also more likely to have an unplanned readmission after an endoscopic dilation (OR = 4.21, P = 0.03). The relationship between age and re-intubation was not significant (OR = 0, P = 0.95). For open reconstruction, this age dichotomization was not associated with any increased reoperation (OR = 2.3, P = 0.52), readmission (OR = 0, P = 0.97), or reintubation (OR = 0, P = 0.94).
T-test analysis was performed to determine if children < 1 year old also had significantly longer hospital stays after endoscopic dilation than older children (mean 14.1 days vs 1.9 days, P < 0.001). This relationship held true in a linear regression after adjustment for pulmonary disease and tracheostomy, with length of stay decreasing by 0.48 days per year of life (P = 0.03). For endoscopic dilations, the same relationship held true, where length of stay decreased by 0.75 days per year of life.
Discussion
Endoscopic dilation for primary management of pediatric laryngotracheal stenosis has become commonplace. Despite this, outcomes of this procedure have only been described in case series and meta-analyses [2–5]. The relative rarity of pediatric laryngotracheal stenosis suggests the need for large, multi-institutional data for purposes of patient selection and medical decision-making.
This study utilized the ACS-NSQIP-Pediatric database to highlight 30-day outcomes of endoscopic dilation and to compare these outcomes to those of open airway reconstruction procedures. The ACS-NSQIP database has been endorsed by multiple organizations, including the Center for Medicare and Medicaid Services, the Joint Commission, and the American Medical Association. It has been shown to have higher sensitivity and a lower false-positive rate when compared to administrative data, in part due to data collection from trained personnel [11]. Furthermore, ACS-NSQIP use has the additional benefit of reporting an unplanned admission—a feature unavailable in review of claims data [12].
With respect to adverse events, our study demonstrates that endoscopic dilation is associated with an equally high rate of unplanned readmission when compared to open reconstruction. The high prevalence of comorbid disease such as chronic lung disease (32% of endoscopic dilation and 43% of open reconstruction) can account for some of the morbidity associated with any airway procedures.
Despite high rates of unplanned readmission, patients undergoing endoscopic dilation were less likely to have reoperations within 30 days of initial surgery when compared to those undergoing open reconstruction. While differences in disease severity may be partially responsible for this difference in the reoperation rate, this finding is notable given the health care costs associated with multiple operations as well as safety concerns with multiple anesthetics in the very young [13,14].
The ACS-NSQIP platform does not distinguish unplanned from planned reoperations. In the setting of airway surgery, where multiple planned reoperations are commonplace, this metric is a suboptimal stand-alone indicator of adverse outcomes. Other markers available in the database—such as reintubations and performance of tracheostomy or open airway reconstruction within 30-days of surgery—are more indicative of surgical outcome in the setting of airway surgery. We found that both reintubations and salvage open reconstruction within 30-days were rare. It should be noted that the ACS-NSQIP data does not report any events occurring outside of the 30-day postoperative period, representing potential limitation of the use of this database. As was previously advocated by Roxbury and colleagues, procedure/subspecialty specific outcome data collection would also improve outcome analysis of airway and other otolaryngologic procedures [9]. In the setting of airway reconstruction, this would include data pertaining to Cotton-Meyer grading systems well as postoperative voice and swallow outcomes.
In addition to safety profile, endoscopic procedures were associated with shorter LOS when compared with open reconstruction, representing another potential source of cost savings with this less invasive method. This is especially significant given that open reconstruction patients spend much of their inpatient stay in an ICU setting. In patients who are candidates for endoscopic procedures, this lower-risk, lower-cost profile of endoscopic dilation has the opportunity to improve value in health care and may be the source of future improvement initiatives.
In addition to comparing overall outcomes between endoscopic and open management of laryngotracheal stenosis, our study aimed to identify factors that were associated with varied outcomes in patients undergoing primary endoscopic dilation. We found that children younger than 1 year of age were 5.8 times more likely to undergo an unplanned reoperation after an endoscopic dilation than children over 1 year. A similar finding was reported in open airway surgeries, with increased reoperation rates in children < 3 years old [9]. The justification of a dichotomization at 1 year was made as expert opinion recognizes that the infant airway is less forgiving to intervention given its small size. Young age was also a factor in prolonged LOS as was determined by linear regression. It is likely that this increased LOS may be in part due to associations of young age and the neonatal ICU population. One must balance the increased risk of surgery in the young with that of tracheostomy, which has a published complication rate of 18% to 50% and direct mortality rate of 1% to 2% in the pediatric population [15–18]. Understanding these relative risks may help guide the airway surgeon in preoperative counseling with families and medical decision-making.
As discussed above, the limitation of data to a 30-day period is a relative weakness of ACS-NSQIP database use for studies of airway reconstruction, as the ultimate outcome—a stable, decannulated airway—may occur outside of this time period. As many quality metrics utilize data from the 30-day postoperative period, knowledge of these outcomes remains valuable in surgical decision-making. Ultimately, collection of data in a large, long-term dataset would allow broader generalizations to be made about the differences between open and endoscopic procedures and would also give a more comprehensive picture of the outcomes of endoscopic dilation.
In conclusion, this study is the first to analyze 30-day postoperative outcomes in pediatric endoscopic airway dilations using data aggregated by ACS-NSQIP from institutions across the United States. This data indicates that endoscopic airway dilation is a relatively safe procedure, especially compared with open reconstruction; however, additional data on disease severity and other outcomes is necessary to draw final conclusions of superiority of technique. Future improvement initiatives could be aimed at the impact of this lower-risk, lower-cost procedure in the appropriately selected patient. Outcomes of endoscopic dilation are poorer in those less than 1 year of age, as they are associated with increased reoperation rates and increased length of stay compared to older children. One must balance these risks in the very young with the risks associated with tracheostomy and other alternative airway management modalities.
Note: This work was presented in a paper at the AAO-HNS 2017 meeting, Chicago, IL, 10 Sep 2017.
Corresponding author: Jennifer Lavin, MD, MS, 225 E Chicago Ave., Box 25, Chicago, IL 60611, [email protected].
Financial disclosures: None.
From the Northwestern University, Feinberg School of Medicine, Chicago, IL (Mr. Bavishi, Dr. Lavin), the Johns Hopkins University, Baltimore, MD (Dr. Boss), Children’s National Medical Center, Washington, DC (Dr. Shah), and Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL (Dr. Lavin).
Abstract
- Background: Endoscopic management of pediatric subglottic stenosis is common; however, no multiinstitutional studies have assessed its perioperative outcomes. The American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS-NSQIP-P) represents a source of such data.
- Objective: To investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to those seen with open reconstruction techniques.
- Methods: Current procedural terminology (CPT) codes were queried for endoscopic or open airway reconstruction in the 2015 ACS-NSQIP-P Public Use File (PUF). Demographics and 30-day events were abstracted to compare open to endoscopic techniques and to assess for risk factors for varied outcomes after endoscopic dilation. Outcome measures included length of stay (LOS), 30-day rates of reintubation, readmission, and reoperation.
- Results: 171 endoscopic and 116 open procedures were identified. Mean age at endoscopic and open procedures was 4.1 (SEM = 0.37) and 5.4 years (SEM = 0.40). Mean LOS was shorter after endoscopic procedures (5.5 days, SEM = 1.13 vs. 11.3 days SEM = 1.01, P < 0.001). Open procedures had higher rates of reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009). In patients undergoing endoscopic dilation, children < 1 year were more likely to require readmission (OR = 4.21, P = 0.03) and reoperation (OR = 4.39, P = 0.03) when compared with older children.
- Conclusion: Open airway reconstruction is associated with longer LOS and increased reintubations and reoperations, suggesting a possible opportunity to improve value in health care in the appropriately selected patient. Reoperations and readmissions following endoscopic dilation are more prevalent in children younger than 1 year.
Keywords: airway stenosis; subglottic stenosis; endoscopic dilation; pediatrics; outcomes.
Historically, pediatric laryngotracheal stenosis was managed using open reconstruction techniques, including laryngoplasty, tracheal resection, and cervical tracheoplasty. Initial reports of endoscopic dilation were described in the 1980s as a means to salvage re-stenosis after open reconstruction [1]. Currently, primary endoscopic dilation has become commonplace in otolaryngology due to its less invasive nature as well as—in cases of balloon dilation—minimization of tissue damage [2]. The advancements made in endoscopic balloon dilation have reduced the frequency with which open reconstruction is performed.
Systematic reviews and case series investigating endoscopic dilation indicate a 70% to 80% success rate in preventing future open surgery or tracheostomy [2–5]. While increased severity of stenosis has been associated with poorer outcomes in endoscopic procedures, few other risk factors that influence surgical success have been identified [4,5]. In a single study in the adult literature, open surgical management of idiopathic subglottic stenosis was associated with improved outcomes when compared to endoscopic techniques [5]. Such findings suggest a need to identify these factors for the purpose of optimizing clinical decision-making.
As laryngotracheal stenosis is rare, postoperative outcomes and risk factors are best identified on a multiinstitutional level. Due to its participation from 80 hospitals and its accurate and reliable reporting of both demographic and risk-stratified 30-day outcomes data, the American College of Surgeon’s National Surgical Quality Improvement Program – Pediatric (ACS NSQIP-P) provides such a platform [6–8]. Thirty-day outcomes and risk factors for open reconstruction utilizing the ACS NSQIP-P database have previously been reported; however, no such outcomes for endoscopic dilation have been described, and no comparison between endoscopic and open procedures has been made [9]. The purpose of this study was to utilize the 2015 ACS-NSQIP-P database to investigate 30-day outcomes of endoscopic dilation of the pediatric airway and to compare these outcomes to open reconstruction techniques. Secondarily, we aimed to determine if any demographic factors or medical comorbidities are associated with varied outcomes in endoscopic reconstruction. While these data reflect safety and quality of this procedure in the United States, findings may potentially be applied across international settings.
Methods
Data Source
Data was obtained from the 2015 ACS-NSQIP-P Public Use File (PUF). Due to the de-identified and public nature of these data, this research was exempt from review by the Ann & Robert H. Lurie Children’s Hospital of Chicago review board. Data collection methods for ACS-NSQIP-P have previously been described [10]. In brief, data was collected from 80 hospitals on approximately 120 preoperative, intraoperative, and postoperative variables. Cases are systematically sampled on an 8-day cycle basis, where the first 35 cases meeting the inclusion criteria in each hospital in each cycle are submitted to ACS-NSQIP-P.
Variables and Outcomes
Airway procedures for endoscopic dilations and open reconstructions were obtained by CPT code. Endoscopic dilations (CPT 31528) were compared to open reconstructions, which included laryngoplasty (31580, 31582), cervical tracheoplasty (31750), cricoid split (31587), and tracheal resection (31780). Demographic variables included age, sex, race, and history of prematurity. Presence of specific comorbid diseases were also collected and tested for significance.
Dependent outcomes of interest were unplanned 30-day postoperative events grouped as reoperation, unplanned readmission, and postoperative reintubation. In the case of endoscopic procedures, the presence of salvage open reconstruction or tracheostomy within 30 days of surgery was also recorded. Length of stay (LOS) after the procedure was collected. Specific postoperative complications and reasons for readmission were recorded within the limitations of data available in the PUF.
Analysis
Analysis was performed using descriptive statistics and frequency analysis where appropriate. Chi-square analysis was used to compare adverse events between open and endoscopic procedures. Logistic regression with calculation of odds ratio (OR) was performed to determine predictive factors for reoperation, readmission, and reintubation in all pediatric airway reconstructive procedures in adjusted and unadjusted models. T-test and linear regression was performed on the continuous outcome of length of stay. For all analyses, a p value of < 0.05 was considered statistically significant. All variable recoding and statistical analyses were performed in SAS/STAT software (Cary, NC).
Results
A total of 84,056 pediatric procedures were extracted from the 2015 NSQIP-P PUFs. Using the above CPT codes, 171 endoscopic dilations and 116 open airway reconstructions were identified, with patient age ranging from 0 days to 17.6 years. Average age of patients undergoing endoscopic dilation and open reconstruction was 4.1 and 5.4 years, respectively (Table 1).
Potential confounders were tested with univariate logistic regression to determine if they had a significant impact on readmission, reintubation, or reoperation rates. These variables (Table 2)
In patients undergoing endoscopic dilation, average length of stay was 5.5 days (SEM = 1.13), with 79 (48.5%) patients having a length of stay of zero days. Of all patients who had endoscopic dilations, 70 (40.1%) had a pre-existing tracheostomy and these accounted for the majority (73%) of patients who had zero days as their LOS. LOS after endoscopic management was significantly shorter than the mean of 11.3 days (SEM = 1.01) reported in those undergoing open reconstruction (P < 0.001).
With respect to 30-day adverse events, 2 patients in the endoscopic group (1.1%) required reintubation. Thirteen endoscopic dilation cases (7.6%) had an unplanned readmission, four (2.3%) of which were associated with reoperation within 30 days of the primary surgical procedure. There were 9 other reoperations unassociated with unplanned readmission. Three of these reoperations were due to failed endoscopic dilations, resulting in 2 tracheostomies and one open airway reconstruction. There was one patient death, in a 0-day old with tetralogy of Fallot, trachea-esophageal fistula, and ventilator dependence who underwent emergent endoscopic dilation and died the same day.
Open procedures were associated with 11 unplanned readmissions (9.5%), 7 re-intubations (6%) and 18 reoperations (15.5%). Of patents undergoing reoperation, one patient undergoing open reconstruction underwent tracheostomy within 30 days of surgery.
When comparing open reconstruction to endoscopic dilation, there was a significant increase in reintubation (OR = 7.41, P = 0.026) and reoperation (OR = 3.09, P = 0.009) for open procedures, even with adjustment for age, tracheostomy status, and pulmonary disease. There was no significant difference between the two for unplanned readmissions (OR = 1.19, P = 0.79) (Figure
Younger age was also found to be significantly associated with reoperation rates, in an adjusted logistic model that accounted for tracheostomy status, type of surgery, and pulmonary disease. Per year of life, younger children had higher reoperation rates than older children (OR = 1.91, P = 0.017). When endoscopic dilation was individually examined, children younger than 1 year of age were more likely to undergo reoperation after an endoscopic dilation than children older than 1 (OR = 4.39, P = 0.03). Children under age 1 were also more likely to have an unplanned readmission after an endoscopic dilation (OR = 4.21, P = 0.03). The relationship between age and re-intubation was not significant (OR = 0, P = 0.95). For open reconstruction, this age dichotomization was not associated with any increased reoperation (OR = 2.3, P = 0.52), readmission (OR = 0, P = 0.97), or reintubation (OR = 0, P = 0.94).
T-test analysis was performed to determine if children < 1 year old also had significantly longer hospital stays after endoscopic dilation than older children (mean 14.1 days vs 1.9 days, P < 0.001). This relationship held true in a linear regression after adjustment for pulmonary disease and tracheostomy, with length of stay decreasing by 0.48 days per year of life (P = 0.03). For endoscopic dilations, the same relationship held true, where length of stay decreased by 0.75 days per year of life.
Discussion
Endoscopic dilation for primary management of pediatric laryngotracheal stenosis has become commonplace. Despite this, outcomes of this procedure have only been described in case series and meta-analyses [2–5]. The relative rarity of pediatric laryngotracheal stenosis suggests the need for large, multi-institutional data for purposes of patient selection and medical decision-making.
This study utilized the ACS-NSQIP-Pediatric database to highlight 30-day outcomes of endoscopic dilation and to compare these outcomes to those of open airway reconstruction procedures. The ACS-NSQIP database has been endorsed by multiple organizations, including the Center for Medicare and Medicaid Services, the Joint Commission, and the American Medical Association. It has been shown to have higher sensitivity and a lower false-positive rate when compared to administrative data, in part due to data collection from trained personnel [11]. Furthermore, ACS-NSQIP use has the additional benefit of reporting an unplanned admission—a feature unavailable in review of claims data [12].
With respect to adverse events, our study demonstrates that endoscopic dilation is associated with an equally high rate of unplanned readmission when compared to open reconstruction. The high prevalence of comorbid disease such as chronic lung disease (32% of endoscopic dilation and 43% of open reconstruction) can account for some of the morbidity associated with any airway procedures.
Despite high rates of unplanned readmission, patients undergoing endoscopic dilation were less likely to have reoperations within 30 days of initial surgery when compared to those undergoing open reconstruction. While differences in disease severity may be partially responsible for this difference in the reoperation rate, this finding is notable given the health care costs associated with multiple operations as well as safety concerns with multiple anesthetics in the very young [13,14].
The ACS-NSQIP platform does not distinguish unplanned from planned reoperations. In the setting of airway surgery, where multiple planned reoperations are commonplace, this metric is a suboptimal stand-alone indicator of adverse outcomes. Other markers available in the database—such as reintubations and performance of tracheostomy or open airway reconstruction within 30-days of surgery—are more indicative of surgical outcome in the setting of airway surgery. We found that both reintubations and salvage open reconstruction within 30-days were rare. It should be noted that the ACS-NSQIP data does not report any events occurring outside of the 30-day postoperative period, representing potential limitation of the use of this database. As was previously advocated by Roxbury and colleagues, procedure/subspecialty specific outcome data collection would also improve outcome analysis of airway and other otolaryngologic procedures [9]. In the setting of airway reconstruction, this would include data pertaining to Cotton-Meyer grading systems well as postoperative voice and swallow outcomes.
In addition to safety profile, endoscopic procedures were associated with shorter LOS when compared with open reconstruction, representing another potential source of cost savings with this less invasive method. This is especially significant given that open reconstruction patients spend much of their inpatient stay in an ICU setting. In patients who are candidates for endoscopic procedures, this lower-risk, lower-cost profile of endoscopic dilation has the opportunity to improve value in health care and may be the source of future improvement initiatives.
In addition to comparing overall outcomes between endoscopic and open management of laryngotracheal stenosis, our study aimed to identify factors that were associated with varied outcomes in patients undergoing primary endoscopic dilation. We found that children younger than 1 year of age were 5.8 times more likely to undergo an unplanned reoperation after an endoscopic dilation than children over 1 year. A similar finding was reported in open airway surgeries, with increased reoperation rates in children < 3 years old [9]. The justification of a dichotomization at 1 year was made as expert opinion recognizes that the infant airway is less forgiving to intervention given its small size. Young age was also a factor in prolonged LOS as was determined by linear regression. It is likely that this increased LOS may be in part due to associations of young age and the neonatal ICU population. One must balance the increased risk of surgery in the young with that of tracheostomy, which has a published complication rate of 18% to 50% and direct mortality rate of 1% to 2% in the pediatric population [15–18]. Understanding these relative risks may help guide the airway surgeon in preoperative counseling with families and medical decision-making.
As discussed above, the limitation of data to a 30-day period is a relative weakness of ACS-NSQIP database use for studies of airway reconstruction, as the ultimate outcome—a stable, decannulated airway—may occur outside of this time period. As many quality metrics utilize data from the 30-day postoperative period, knowledge of these outcomes remains valuable in surgical decision-making. Ultimately, collection of data in a large, long-term dataset would allow broader generalizations to be made about the differences between open and endoscopic procedures and would also give a more comprehensive picture of the outcomes of endoscopic dilation.
In conclusion, this study is the first to analyze 30-day postoperative outcomes in pediatric endoscopic airway dilations using data aggregated by ACS-NSQIP from institutions across the United States. This data indicates that endoscopic airway dilation is a relatively safe procedure, especially compared with open reconstruction; however, additional data on disease severity and other outcomes is necessary to draw final conclusions of superiority of technique. Future improvement initiatives could be aimed at the impact of this lower-risk, lower-cost procedure in the appropriately selected patient. Outcomes of endoscopic dilation are poorer in those less than 1 year of age, as they are associated with increased reoperation rates and increased length of stay compared to older children. One must balance these risks in the very young with the risks associated with tracheostomy and other alternative airway management modalities.
Note: This work was presented in a paper at the AAO-HNS 2017 meeting, Chicago, IL, 10 Sep 2017.
Corresponding author: Jennifer Lavin, MD, MS, 225 E Chicago Ave., Box 25, Chicago, IL 60611, [email protected].
Financial disclosures: None.
1. Cohen MD, Weber TR, Rao CC. Balloon dilatation of tracheal and bronchial stenosis. AJR Am J Roentgenol 1984;142:477–8.
2. Chueng K, Chadha NK. Primary dilatation as a treatment for pediatric laryngotracheal stenosis: a systematic review. Int J Pediatr Otorhinolaryngol 2013;77:623–8.
3. Hautefort C, Teissier N, Viala P, Van Den Abbeele T. Balloon dilation laryngoplasty for subglottic stenosis in children: eight years’ experience. Arch Otolaryngol Head Neck Surg 2012;138:235–40.
4. Lang M, Brietzke SE. A systematic review and meta-analysis of endoscopic balloon dilation of pediatric subglottic stenosis. Otolaryngol Head Neck Surg 2014;150:174–9.
5. Maresh A, Preciado DA, O’Connell AP, Zalzal GH. A comparative analysis of open surgery vs endoscopic balloon dilation for pediatric subglottic stenosis. JAMA Otolaryngol Head Neck Surg 2014;140:901–5.
6. Gelbard A, Donovan DT, Ongkasuwan J, et al. Disease homogeneity and treatment heterogeneity in idiopathic subglottic stenosis. Laryngoscope 2016;126:1390–6.
7. ACS-NSQIP. ACS National Surgical Quality Improvement Program® (ACS NSQIP®). 2017. Available at: http://site.acsnsqip.org/program-specifics/scr-training-and-resources. Accessed June 2 2017.
8. Shiloach M, Frencher SK Jr, Steeger JE, et al. Toward robust information: data quality and inter-rater reliability in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2010;210:6–16.
9. Roxbury CR, Jatana KR, Shah RK, Boss EF. Safety and postoperative adverse events in pediatric airway reconstruction: Analysis of ACS-NSQIP-P 30-day outcomes. Laryngoscope 2017;127:504–8.
10. Raval MV, Dillon PW, Bruny JL, et al. Pediatric American College of Surgeons National Surgical Quality Improvement Program: feasibility of a novel, prospective assessment of surgical outcomes. J Pediatr Surg 2011;46:115–21.
11. Lawson EH, Louie R, Zingmond DS, et al. A comparison of clinical registry versus administrative claims data for reporting of 30-day surgical complications. Ann Surg 2012;256:973–81.
12. Sellers MM, Merkow RP, Halverson A, et al. Validation of new readmission data in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2013;216:420–7.
13. Jevtovic-Todorovic V, Hartman RE, Izumi Y, et al. Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. J Neurosci 2003;23:876–82.
14. Patel P, Sun L. Update on neonatal anesthetic neurotoxicity: insight into molecular mechanisms and relevance to humans. Anesthesiology 2009;110:703–8.
15. Crysdale WS, Feldman RI, Naito K. Tracheotomies: a 10-year experience in 319 children. Ann Otol Rhinol Laryngol 1988;97(5 Pt 1):439–43.
16. Goldenberg D, Ari EG, Golz A, et al. Tracheotomy complications: a retrospective study of 1130 cases. Otolaryngol Head Neck Surg 2000;123:495–500.
17. Mahadevan M, Barber C, Salkeld L, et al N. Pediatric tracheotomy: 17 year review. Int J Pediatr Otorhinolaryngol 2007;71:1829–35.
18. Ozmen S, Ozmen OA, Unal OF. Pediatric tracheotomies: a 37-year experience in 282 children. Int J Pediatr Otorhinolaryngol 2009;73:959–61.
1. Cohen MD, Weber TR, Rao CC. Balloon dilatation of tracheal and bronchial stenosis. AJR Am J Roentgenol 1984;142:477–8.
2. Chueng K, Chadha NK. Primary dilatation as a treatment for pediatric laryngotracheal stenosis: a systematic review. Int J Pediatr Otorhinolaryngol 2013;77:623–8.
3. Hautefort C, Teissier N, Viala P, Van Den Abbeele T. Balloon dilation laryngoplasty for subglottic stenosis in children: eight years’ experience. Arch Otolaryngol Head Neck Surg 2012;138:235–40.
4. Lang M, Brietzke SE. A systematic review and meta-analysis of endoscopic balloon dilation of pediatric subglottic stenosis. Otolaryngol Head Neck Surg 2014;150:174–9.
5. Maresh A, Preciado DA, O’Connell AP, Zalzal GH. A comparative analysis of open surgery vs endoscopic balloon dilation for pediatric subglottic stenosis. JAMA Otolaryngol Head Neck Surg 2014;140:901–5.
6. Gelbard A, Donovan DT, Ongkasuwan J, et al. Disease homogeneity and treatment heterogeneity in idiopathic subglottic stenosis. Laryngoscope 2016;126:1390–6.
7. ACS-NSQIP. ACS National Surgical Quality Improvement Program® (ACS NSQIP®). 2017. Available at: http://site.acsnsqip.org/program-specifics/scr-training-and-resources. Accessed June 2 2017.
8. Shiloach M, Frencher SK Jr, Steeger JE, et al. Toward robust information: data quality and inter-rater reliability in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2010;210:6–16.
9. Roxbury CR, Jatana KR, Shah RK, Boss EF. Safety and postoperative adverse events in pediatric airway reconstruction: Analysis of ACS-NSQIP-P 30-day outcomes. Laryngoscope 2017;127:504–8.
10. Raval MV, Dillon PW, Bruny JL, et al. Pediatric American College of Surgeons National Surgical Quality Improvement Program: feasibility of a novel, prospective assessment of surgical outcomes. J Pediatr Surg 2011;46:115–21.
11. Lawson EH, Louie R, Zingmond DS, et al. A comparison of clinical registry versus administrative claims data for reporting of 30-day surgical complications. Ann Surg 2012;256:973–81.
12. Sellers MM, Merkow RP, Halverson A, et al. Validation of new readmission data in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2013;216:420–7.
13. Jevtovic-Todorovic V, Hartman RE, Izumi Y, et al. Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. J Neurosci 2003;23:876–82.
14. Patel P, Sun L. Update on neonatal anesthetic neurotoxicity: insight into molecular mechanisms and relevance to humans. Anesthesiology 2009;110:703–8.
15. Crysdale WS, Feldman RI, Naito K. Tracheotomies: a 10-year experience in 319 children. Ann Otol Rhinol Laryngol 1988;97(5 Pt 1):439–43.
16. Goldenberg D, Ari EG, Golz A, et al. Tracheotomy complications: a retrospective study of 1130 cases. Otolaryngol Head Neck Surg 2000;123:495–500.
17. Mahadevan M, Barber C, Salkeld L, et al N. Pediatric tracheotomy: 17 year review. Int J Pediatr Otorhinolaryngol 2007;71:1829–35.
18. Ozmen S, Ozmen OA, Unal OF. Pediatric tracheotomies: a 37-year experience in 282 children. Int J Pediatr Otorhinolaryngol 2009;73:959–61.
HIPEC for Ovarian Cancer: Standard of Care or Experimental Approach?
Study Overview
Objective. To evaluate whether the addition of hyperthermic intraperotoneal chemotherapy (HIPEC) to interval cytoreductive surgery would improve outcomes among patients who were receiving neoadjuvant chemotherapy for stage III epithelial ovarian cancer.
Design. Phase 3 prospective randomized clinical trial.
Setting and participants. The trial was conducted at 8 hospitals in the Netherlands and Belgium at which medical personnel had experience in administering HIPEC in patients with peritoneal disease from colon cancer or from pseudomyxoma perotinei. Eligible patients had newly diagnosed stage III epithelial ovarian, fallopian tube, or peritoneal cancer and were referred for neoadjuvant chemotherapy because of extensive abdominal disease or incomplete cytoreductive surgery (one or more residual tumors measuring > 1 cm in diameter). Eligibility criteria also including performance status score of 0 to 2, normal blood counts, and adequate renal function.
Intervention. At the time of surgery, patients were randomly assigned in a 1:1 ratio to undergo interval cytoreductive surgery either with HIPEC (surgery-plus-HIPEC group) or without HIPEC (surgery group). HIPEC was administered at the end of the cytoreductive surgical procedure. The abdomen was filled with saline that circulated continuously with the use of a roller pump through a heat exchanger. Perfusion with cisplatin at a dose of 100 mg per square meter and at a flow rate of 1 liter per minute was then initiated. The procedure took 120 minutes in total. To prevent nephrotoxicity, sodium thiosulphate was administered at the start of perfusion as an intravenous bolus (9 g per square meter in 200 mL), followed by a continuous infusion (12 g per square meter in 1000 mL) over 6 hours. Patient received in addition 3 cycles of carboplatin and paclitaxel after surgery. During follow-up, physical examinations and measurement of CA-125 level were repeated every 3 months for 2 years and then every 6 months until 5 years after the completion of chemotherapy. Computed tomography was performed at 1, 6, 12, and 24 months after the last cycle of chemotherapy.
Main outcome measure. The primary endpoint was recurrence-free survival in the intent-to-treat population. Secondary endpoints included overall survival, the side-effect profile, and health-related quality of life.
Main results. A total of 245 women were randomized between April 2007 and April 2016. The median follow-up at the time of recurrence-free survival analysis was 4.7 years. Recurrence-free survival events occurred in 81% of the HIPEC group vs 89% of the control group; median recurrence-free survival was 14.2 months vs 10.7 months, respectively (hazard ratio [HR] 0.66, P = 0.003). The benefit of HIPEC was consistent across stratification factors and post hoc subgroups. Hazard ratios (none reaching statistical significance) were 0.63 and 0.72 for those aged ≥ 65 and < 65 years; 0.69 and 0.56 for those with high-grade serous and other histology; 0.71 and 0.47 for those with no previous surgery and previous surgery; 0.64 and 0.66 for those with 0 to 5 and 6 to 8 involved regions; and 0.69 and 0.61 for those with no laparoscopy vs laparoscopy before surgery. Death occurred in 50% of the hyperthermic intraperitoneal chemotherapy group vs 62% of the control group; median overall survival was 45.7 vs 33.9 months (HR 0.67, P = 0.02).
No significant differences between the HIPEC and control groups were observed in the incidence of adverse events of any grade. The most common adverse events of any grade in the HIPEC group were nausea (63% vs 57%), abdominal pain (60% vs 575), and fatigue (37% vs 30%). Grade ≥ 3 adverse events occurred in 27% vs 25% of patients (P = 0.76). The most common grade 3 or 4 adverse events in the HIPEC group were infection (6% vs 2%), abdominal pain (5% vs 6%), and ileus (4% vs 2%). Among the patients who underwent bowel resection, a colostomy or ileostomy was performed more commonly among patients in the surgery-plus-HIPEC group (21 of 29 patients [72%]) than among those in the surgery group (13 of 30 patients [43%]) (P = 0.04).
Conclusion. Among patients with stage III epithelial ovarian cancer, the addition of hyperthermic intraperitoneal chemotherapy to interval cytoreductive surgery resulted in longer recurrence-free survival and overall survival than surgery alone and did not result in higher rates of side effects.
Commentary
Ovarian cancer is associated with the highest mortality of all gynecologic cancers in the Western world [1].The majority of the patients have advanced disease at diagnosis and the most effective treatment for advanced disease involved maximum debulking surgery followed by chemotherapy. For those patients for whom primary surgery is not feasible, primary chemotherapy is given, which is followed by interval debulking after 3 courses of chemotherapy [2].However, outcome remains dismal for patients with advanced disease. Regional (intraperitoneal) chemotherapy theoretically results in a decreased rate of systemic toxic effects and may improve outcomes by eliminating residual microscopic disease more effectively than intravenous chemotherapy [3].
Intraperitoneal chemotherapy during surgery that can be delivered under hyperthermic conditions is termed hyperthermic intraperitoneal chemotherapy. Rationale for using hyperthermic conditions when delivering intraperitoneal chemotherapy is multifactorial. Clinical hyperthermia is defined as the use of temperatures of 41oC and higher. Hyperthermia itself has a direct cytotoxic effects on cells caused by impaired DNA repair, denaturation of proteins, inductions of heat-shock proteins which may serve as receptors for natural killer-cells, induction of apoptosis, and inhibition of angiogenesis. In addition to its intrinsic cytotoxic effect, hyperthermia acts in synergy with some chemotherapeutics agents and increase peritoneal and tumour drug penetration [4].
The study by van Driel et al evaluates the impact of addition of HIPEC to interval cytoreductive surgery in patients who received neoadjuvant chemotherapy for stage III epithelial ovarian cancer. Authors found that addition of HIPEC resulted in 11.8 months improvement in overall survival compared to surgery alone without increased rate of side effects.
The outcomes of the trial by van Driel et al are encouraging, but questions remain about how to apply these results in everyday clinical practice. First, with the extensive reported experience with HIPEC in select single center or multicenter trials, it is reasonable to conclude the procedure can be successfully undertaken by well-trained surgical/gynecologic oncologists and at institutions experienced in the approach. However, clinical trials have limited external validity, and while providing evidence regarding efficacy (ie, the effect of the intervention under highly selected conditions), they generally do not provide evidence of effectiveness (ie, the benefit to the general population of patients with the disease). Can the same results be reproduced in hospitals across the country? Second, what part of HIPEC was responsible for benefit? Was it merely administration of chemotherapy through intraperitoneal route? Is hyperthermia necessary to see the observed benefit in this trial? The answers to these questions are not known. Third, the assessment of cost-benefit ratio warrants serious consideration as well. As authors pointed, the addition of HIPEC resulted in extension of duration of surgery by 2 hours and a perfusionist was needed. Additional standard costs are incurred due to the use of HIPEC machine, the disposable products needed to administer HIPEC, and the 1-day stay in the ICU. Increased use of diverting colostomy and ileostomy will also increase the overall cost of the treatment.
Applications for Clinical Practice
This trial is an important step in establishing the efficacy of adding HIPEC to interval cytoreductive surgery without increasing the side effects. However, whether the same results can be reproduced at centers at which surgeons do not have as much expertise in administering HIPEC remains to be seen. New confirmatory clinical trials of HIPEC are needed before it can be recommended as a common treatment strategy.
—Deval Rajyaguru, MD, Gundersen Health System, La Crosse, WI
1. Levi F, Lucchini F, Negri E, La Vecchia C. Trends in mortality from major cancers in the European Union, including acceding countries, in 2004. Cancer 2006;101:2843–50.
2. van der Burg MEL, van Lent M, Buyse M, et al. The effect of debulking surgery after induction chemotherapy on the prognosis in advanced epithelial ovarian cancer. N Engl J Med 1995;332:629–34.
3. Armstrong DK, Bundy B, Wenzel L, et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006;354:34–43.
4. Ohno S, Siddik ZH, Kido Y, et al. Thermal enhancement of drug uptake and DNA adducts as a possible mechanism for the effect of sequencing hyperthermia on cisplatin-induced cytotoxicity in L1210 cells. Cancer Chemother Pharmacol 1994;34:302–6.
Study Overview
Objective. To evaluate whether the addition of hyperthermic intraperotoneal chemotherapy (HIPEC) to interval cytoreductive surgery would improve outcomes among patients who were receiving neoadjuvant chemotherapy for stage III epithelial ovarian cancer.
Design. Phase 3 prospective randomized clinical trial.
Setting and participants. The trial was conducted at 8 hospitals in the Netherlands and Belgium at which medical personnel had experience in administering HIPEC in patients with peritoneal disease from colon cancer or from pseudomyxoma perotinei. Eligible patients had newly diagnosed stage III epithelial ovarian, fallopian tube, or peritoneal cancer and were referred for neoadjuvant chemotherapy because of extensive abdominal disease or incomplete cytoreductive surgery (one or more residual tumors measuring > 1 cm in diameter). Eligibility criteria also including performance status score of 0 to 2, normal blood counts, and adequate renal function.
Intervention. At the time of surgery, patients were randomly assigned in a 1:1 ratio to undergo interval cytoreductive surgery either with HIPEC (surgery-plus-HIPEC group) or without HIPEC (surgery group). HIPEC was administered at the end of the cytoreductive surgical procedure. The abdomen was filled with saline that circulated continuously with the use of a roller pump through a heat exchanger. Perfusion with cisplatin at a dose of 100 mg per square meter and at a flow rate of 1 liter per minute was then initiated. The procedure took 120 minutes in total. To prevent nephrotoxicity, sodium thiosulphate was administered at the start of perfusion as an intravenous bolus (9 g per square meter in 200 mL), followed by a continuous infusion (12 g per square meter in 1000 mL) over 6 hours. Patient received in addition 3 cycles of carboplatin and paclitaxel after surgery. During follow-up, physical examinations and measurement of CA-125 level were repeated every 3 months for 2 years and then every 6 months until 5 years after the completion of chemotherapy. Computed tomography was performed at 1, 6, 12, and 24 months after the last cycle of chemotherapy.
Main outcome measure. The primary endpoint was recurrence-free survival in the intent-to-treat population. Secondary endpoints included overall survival, the side-effect profile, and health-related quality of life.
Main results. A total of 245 women were randomized between April 2007 and April 2016. The median follow-up at the time of recurrence-free survival analysis was 4.7 years. Recurrence-free survival events occurred in 81% of the HIPEC group vs 89% of the control group; median recurrence-free survival was 14.2 months vs 10.7 months, respectively (hazard ratio [HR] 0.66, P = 0.003). The benefit of HIPEC was consistent across stratification factors and post hoc subgroups. Hazard ratios (none reaching statistical significance) were 0.63 and 0.72 for those aged ≥ 65 and < 65 years; 0.69 and 0.56 for those with high-grade serous and other histology; 0.71 and 0.47 for those with no previous surgery and previous surgery; 0.64 and 0.66 for those with 0 to 5 and 6 to 8 involved regions; and 0.69 and 0.61 for those with no laparoscopy vs laparoscopy before surgery. Death occurred in 50% of the hyperthermic intraperitoneal chemotherapy group vs 62% of the control group; median overall survival was 45.7 vs 33.9 months (HR 0.67, P = 0.02).
No significant differences between the HIPEC and control groups were observed in the incidence of adverse events of any grade. The most common adverse events of any grade in the HIPEC group were nausea (63% vs 57%), abdominal pain (60% vs 575), and fatigue (37% vs 30%). Grade ≥ 3 adverse events occurred in 27% vs 25% of patients (P = 0.76). The most common grade 3 or 4 adverse events in the HIPEC group were infection (6% vs 2%), abdominal pain (5% vs 6%), and ileus (4% vs 2%). Among the patients who underwent bowel resection, a colostomy or ileostomy was performed more commonly among patients in the surgery-plus-HIPEC group (21 of 29 patients [72%]) than among those in the surgery group (13 of 30 patients [43%]) (P = 0.04).
Conclusion. Among patients with stage III epithelial ovarian cancer, the addition of hyperthermic intraperitoneal chemotherapy to interval cytoreductive surgery resulted in longer recurrence-free survival and overall survival than surgery alone and did not result in higher rates of side effects.
Commentary
Ovarian cancer is associated with the highest mortality of all gynecologic cancers in the Western world [1].The majority of the patients have advanced disease at diagnosis and the most effective treatment for advanced disease involved maximum debulking surgery followed by chemotherapy. For those patients for whom primary surgery is not feasible, primary chemotherapy is given, which is followed by interval debulking after 3 courses of chemotherapy [2].However, outcome remains dismal for patients with advanced disease. Regional (intraperitoneal) chemotherapy theoretically results in a decreased rate of systemic toxic effects and may improve outcomes by eliminating residual microscopic disease more effectively than intravenous chemotherapy [3].
Intraperitoneal chemotherapy during surgery that can be delivered under hyperthermic conditions is termed hyperthermic intraperitoneal chemotherapy. Rationale for using hyperthermic conditions when delivering intraperitoneal chemotherapy is multifactorial. Clinical hyperthermia is defined as the use of temperatures of 41oC and higher. Hyperthermia itself has a direct cytotoxic effects on cells caused by impaired DNA repair, denaturation of proteins, inductions of heat-shock proteins which may serve as receptors for natural killer-cells, induction of apoptosis, and inhibition of angiogenesis. In addition to its intrinsic cytotoxic effect, hyperthermia acts in synergy with some chemotherapeutics agents and increase peritoneal and tumour drug penetration [4].
The study by van Driel et al evaluates the impact of addition of HIPEC to interval cytoreductive surgery in patients who received neoadjuvant chemotherapy for stage III epithelial ovarian cancer. Authors found that addition of HIPEC resulted in 11.8 months improvement in overall survival compared to surgery alone without increased rate of side effects.
The outcomes of the trial by van Driel et al are encouraging, but questions remain about how to apply these results in everyday clinical practice. First, with the extensive reported experience with HIPEC in select single center or multicenter trials, it is reasonable to conclude the procedure can be successfully undertaken by well-trained surgical/gynecologic oncologists and at institutions experienced in the approach. However, clinical trials have limited external validity, and while providing evidence regarding efficacy (ie, the effect of the intervention under highly selected conditions), they generally do not provide evidence of effectiveness (ie, the benefit to the general population of patients with the disease). Can the same results be reproduced in hospitals across the country? Second, what part of HIPEC was responsible for benefit? Was it merely administration of chemotherapy through intraperitoneal route? Is hyperthermia necessary to see the observed benefit in this trial? The answers to these questions are not known. Third, the assessment of cost-benefit ratio warrants serious consideration as well. As authors pointed, the addition of HIPEC resulted in extension of duration of surgery by 2 hours and a perfusionist was needed. Additional standard costs are incurred due to the use of HIPEC machine, the disposable products needed to administer HIPEC, and the 1-day stay in the ICU. Increased use of diverting colostomy and ileostomy will also increase the overall cost of the treatment.
Applications for Clinical Practice
This trial is an important step in establishing the efficacy of adding HIPEC to interval cytoreductive surgery without increasing the side effects. However, whether the same results can be reproduced at centers at which surgeons do not have as much expertise in administering HIPEC remains to be seen. New confirmatory clinical trials of HIPEC are needed before it can be recommended as a common treatment strategy.
—Deval Rajyaguru, MD, Gundersen Health System, La Crosse, WI
Study Overview
Objective. To evaluate whether the addition of hyperthermic intraperotoneal chemotherapy (HIPEC) to interval cytoreductive surgery would improve outcomes among patients who were receiving neoadjuvant chemotherapy for stage III epithelial ovarian cancer.
Design. Phase 3 prospective randomized clinical trial.
Setting and participants. The trial was conducted at 8 hospitals in the Netherlands and Belgium at which medical personnel had experience in administering HIPEC in patients with peritoneal disease from colon cancer or from pseudomyxoma perotinei. Eligible patients had newly diagnosed stage III epithelial ovarian, fallopian tube, or peritoneal cancer and were referred for neoadjuvant chemotherapy because of extensive abdominal disease or incomplete cytoreductive surgery (one or more residual tumors measuring > 1 cm in diameter). Eligibility criteria also including performance status score of 0 to 2, normal blood counts, and adequate renal function.
Intervention. At the time of surgery, patients were randomly assigned in a 1:1 ratio to undergo interval cytoreductive surgery either with HIPEC (surgery-plus-HIPEC group) or without HIPEC (surgery group). HIPEC was administered at the end of the cytoreductive surgical procedure. The abdomen was filled with saline that circulated continuously with the use of a roller pump through a heat exchanger. Perfusion with cisplatin at a dose of 100 mg per square meter and at a flow rate of 1 liter per minute was then initiated. The procedure took 120 minutes in total. To prevent nephrotoxicity, sodium thiosulphate was administered at the start of perfusion as an intravenous bolus (9 g per square meter in 200 mL), followed by a continuous infusion (12 g per square meter in 1000 mL) over 6 hours. Patient received in addition 3 cycles of carboplatin and paclitaxel after surgery. During follow-up, physical examinations and measurement of CA-125 level were repeated every 3 months for 2 years and then every 6 months until 5 years after the completion of chemotherapy. Computed tomography was performed at 1, 6, 12, and 24 months after the last cycle of chemotherapy.
Main outcome measure. The primary endpoint was recurrence-free survival in the intent-to-treat population. Secondary endpoints included overall survival, the side-effect profile, and health-related quality of life.
Main results. A total of 245 women were randomized between April 2007 and April 2016. The median follow-up at the time of recurrence-free survival analysis was 4.7 years. Recurrence-free survival events occurred in 81% of the HIPEC group vs 89% of the control group; median recurrence-free survival was 14.2 months vs 10.7 months, respectively (hazard ratio [HR] 0.66, P = 0.003). The benefit of HIPEC was consistent across stratification factors and post hoc subgroups. Hazard ratios (none reaching statistical significance) were 0.63 and 0.72 for those aged ≥ 65 and < 65 years; 0.69 and 0.56 for those with high-grade serous and other histology; 0.71 and 0.47 for those with no previous surgery and previous surgery; 0.64 and 0.66 for those with 0 to 5 and 6 to 8 involved regions; and 0.69 and 0.61 for those with no laparoscopy vs laparoscopy before surgery. Death occurred in 50% of the hyperthermic intraperitoneal chemotherapy group vs 62% of the control group; median overall survival was 45.7 vs 33.9 months (HR 0.67, P = 0.02).
No significant differences between the HIPEC and control groups were observed in the incidence of adverse events of any grade. The most common adverse events of any grade in the HIPEC group were nausea (63% vs 57%), abdominal pain (60% vs 575), and fatigue (37% vs 30%). Grade ≥ 3 adverse events occurred in 27% vs 25% of patients (P = 0.76). The most common grade 3 or 4 adverse events in the HIPEC group were infection (6% vs 2%), abdominal pain (5% vs 6%), and ileus (4% vs 2%). Among the patients who underwent bowel resection, a colostomy or ileostomy was performed more commonly among patients in the surgery-plus-HIPEC group (21 of 29 patients [72%]) than among those in the surgery group (13 of 30 patients [43%]) (P = 0.04).
Conclusion. Among patients with stage III epithelial ovarian cancer, the addition of hyperthermic intraperitoneal chemotherapy to interval cytoreductive surgery resulted in longer recurrence-free survival and overall survival than surgery alone and did not result in higher rates of side effects.
Commentary
Ovarian cancer is associated with the highest mortality of all gynecologic cancers in the Western world [1].The majority of the patients have advanced disease at diagnosis and the most effective treatment for advanced disease involved maximum debulking surgery followed by chemotherapy. For those patients for whom primary surgery is not feasible, primary chemotherapy is given, which is followed by interval debulking after 3 courses of chemotherapy [2].However, outcome remains dismal for patients with advanced disease. Regional (intraperitoneal) chemotherapy theoretically results in a decreased rate of systemic toxic effects and may improve outcomes by eliminating residual microscopic disease more effectively than intravenous chemotherapy [3].
Intraperitoneal chemotherapy during surgery that can be delivered under hyperthermic conditions is termed hyperthermic intraperitoneal chemotherapy. Rationale for using hyperthermic conditions when delivering intraperitoneal chemotherapy is multifactorial. Clinical hyperthermia is defined as the use of temperatures of 41oC and higher. Hyperthermia itself has a direct cytotoxic effects on cells caused by impaired DNA repair, denaturation of proteins, inductions of heat-shock proteins which may serve as receptors for natural killer-cells, induction of apoptosis, and inhibition of angiogenesis. In addition to its intrinsic cytotoxic effect, hyperthermia acts in synergy with some chemotherapeutics agents and increase peritoneal and tumour drug penetration [4].
The study by van Driel et al evaluates the impact of addition of HIPEC to interval cytoreductive surgery in patients who received neoadjuvant chemotherapy for stage III epithelial ovarian cancer. Authors found that addition of HIPEC resulted in 11.8 months improvement in overall survival compared to surgery alone without increased rate of side effects.
The outcomes of the trial by van Driel et al are encouraging, but questions remain about how to apply these results in everyday clinical practice. First, with the extensive reported experience with HIPEC in select single center or multicenter trials, it is reasonable to conclude the procedure can be successfully undertaken by well-trained surgical/gynecologic oncologists and at institutions experienced in the approach. However, clinical trials have limited external validity, and while providing evidence regarding efficacy (ie, the effect of the intervention under highly selected conditions), they generally do not provide evidence of effectiveness (ie, the benefit to the general population of patients with the disease). Can the same results be reproduced in hospitals across the country? Second, what part of HIPEC was responsible for benefit? Was it merely administration of chemotherapy through intraperitoneal route? Is hyperthermia necessary to see the observed benefit in this trial? The answers to these questions are not known. Third, the assessment of cost-benefit ratio warrants serious consideration as well. As authors pointed, the addition of HIPEC resulted in extension of duration of surgery by 2 hours and a perfusionist was needed. Additional standard costs are incurred due to the use of HIPEC machine, the disposable products needed to administer HIPEC, and the 1-day stay in the ICU. Increased use of diverting colostomy and ileostomy will also increase the overall cost of the treatment.
Applications for Clinical Practice
This trial is an important step in establishing the efficacy of adding HIPEC to interval cytoreductive surgery without increasing the side effects. However, whether the same results can be reproduced at centers at which surgeons do not have as much expertise in administering HIPEC remains to be seen. New confirmatory clinical trials of HIPEC are needed before it can be recommended as a common treatment strategy.
—Deval Rajyaguru, MD, Gundersen Health System, La Crosse, WI
1. Levi F, Lucchini F, Negri E, La Vecchia C. Trends in mortality from major cancers in the European Union, including acceding countries, in 2004. Cancer 2006;101:2843–50.
2. van der Burg MEL, van Lent M, Buyse M, et al. The effect of debulking surgery after induction chemotherapy on the prognosis in advanced epithelial ovarian cancer. N Engl J Med 1995;332:629–34.
3. Armstrong DK, Bundy B, Wenzel L, et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006;354:34–43.
4. Ohno S, Siddik ZH, Kido Y, et al. Thermal enhancement of drug uptake and DNA adducts as a possible mechanism for the effect of sequencing hyperthermia on cisplatin-induced cytotoxicity in L1210 cells. Cancer Chemother Pharmacol 1994;34:302–6.
1. Levi F, Lucchini F, Negri E, La Vecchia C. Trends in mortality from major cancers in the European Union, including acceding countries, in 2004. Cancer 2006;101:2843–50.
2. van der Burg MEL, van Lent M, Buyse M, et al. The effect of debulking surgery after induction chemotherapy on the prognosis in advanced epithelial ovarian cancer. N Engl J Med 1995;332:629–34.
3. Armstrong DK, Bundy B, Wenzel L, et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006;354:34–43.
4. Ohno S, Siddik ZH, Kido Y, et al. Thermal enhancement of drug uptake and DNA adducts as a possible mechanism for the effect of sequencing hyperthermia on cisplatin-induced cytotoxicity in L1210 cells. Cancer Chemother Pharmacol 1994;34:302–6.
Effect of Romosozumab vs. Alendronate on Osteoporosis Fracture Risk
Study Overview
Objective. To determine if romosuzumab, an antisclerostin antibody, is superior to alendronate in reducing the incidence of fracture in postmenopausal women with osteoporosis at high-risk for fracture.
Design. Multicenter, international, double-blind, randomized clinical trial.
Setting and participants. 4093 postmenopausal women with osteoporosis and a previous fragility fracture were enrolled from over 40 countries worldwide. Patients were eligible for the study if they were 55 to 90 years old and were deemed at high risk for future fracture based on bone mineral density (BMD) T score at the total hip or femoral neck and fracture history. This included T score ≤ –2.5 and ≥ 1 moderate or severe vertebral fractures or ≥ 2 mild vertebral fractures; T score ≤ –2.0 and either ≥ 2 moderate or severe vertebral fractures or proximal femur fracture within 3 to 24 months before randomization. Subjects with a history of prior use of medications that affect bone metabolism were excluded, as were those with other metabolic bone disease, vitamin D deficiency, uncontrolled metabolic disease, malabsorption syndromes, history of transplant, severe renal insufficiency, malignancy or severe illness.
Intervention. Patients were randomized to either subcutaneous romosuzumab 210 mg monthly or oral alendronate 70 mg weekly for 12 months. Following the 12-month double-blind period, all patients received open-label weekly alendronate until the end of the trial, with maintenance of blinding to the initial treatment assignment. Primary analysis occurred when all subjects had completed the 24-month visit and clinical fractures had been confirmed in at least 330 patients. All patients received daily calcium and vitamin D. Lateral radiographs of the thoracic and lumbar spine were obtained at screening and months 12 and 24. The BMD at the lumbar spine and proximal femur was evaluated by dual-energy x-ray absorptiometry at baseline and every 12 months thereafter. Serum concentrations of bone-turnover markers were measured in a subgroup of patients.
Main outcome measures. The primary outcomes were the incidence of new vertebral fracture and the incidence of clinical fracture at 24 months. Clinical fractures included symptomatic vertebral fracture and nonvertebral fractures. The secondary outcomes were the BMD at the lumbar spine, total hip, and femoral neck at 12 and 24 months, the incidence of nonvertebral fracture, and fracture category. Safety outcomes included the incidence of adjudicated clinical events, including serious cardiovascular adverse events, osteonecrosis of the jaw, and atypical femoral fracture. Serious cardiovascular events were defined as cardiac ischemic event, cerebrovascular event, heart failure, death, non-coronary revascularization and peripheral vascular ischemic event not requiring revascularization.
Analysis. An intention to treat approach was used for data analysis. For the incidence of fractures, the treatment groups were compared using a Cox proportional-hazards model and the Mantel-Haenszel method with adjustment for age (< 75 vs ≥ 75 years), the presence or absence of severe vertebral fracture at baseline, and baseline BMD T score at the total hip. Between-group comparisons of the percentage change in BMD from baseline were analyzed by means of a repeated-measures model with adjustment for treatment, age category, baseline severe vertebral fracture, visit, treatment-by-visit interaction, and baseline BMD. Percentage changes from baseline in bone turnover were assessed using a Wilcoxon rank-sum test. The safety analysis included cumulated incidence rates of adverse outcomes. Odds ratios and confidence intervals were estimated for serious cardiovascular adverse events with the use of a logistic regression model.
Main results. 2046 participants were randomized to the romosozumab group and 2047 to the alendronate group. A total of 3654 participants from both groups (89.3%) completed 12 months of the trial, and 3150 (77.0%) completed the primary analysis period. The treatment groups were similar in baseline age, ethnicity, and fracture history. The majority of patients in both groups were non-Hispanic (> 60%) and ≥ 75 years old (> 50%). The mean age of the patients was 74.3 years. Baseline mean bone mineral density T scores were –2.96 at the lumbar spine, –2.8 at the total hip, and –2.9 at the femoral neck.
After 24 months of treatment, 6.2% of patients in the romosozumab-alendronate group had a new vertebral fracture as compared to 11.9% in the alendronate-alendronate group. This represents a 48% lower risk (risk ratio 0.52, 95% confidence interval [CI] 0.4–0.66; P < 0.001) of new vertebral fractures with romosozumab. At the time of the primary analysis, romosozumab followed by alendronate resulted in a 27% lower risk of clinical fracture than alendronate alone (hazard ratio 0.73, 95% CI 0.61–0.88; P < 0.001). 8.7% of the romosozumab-alendronate group had a nonvertebral fracture versus 10.6% in the alendronate-alendronate group, representing a 19% lower risk with romosozumab (hazard ratio 0.81, 95% CI 0.66–0.99; P = 0.04). Hip fractures occurred in 2.0% of the romosozumab-alendronate group as compared with 3.2% in the alendronate-alendronate group, representing a 38% lower risk with romosozumab (hazard ratio 0.62, 95% CI 0.42–0.92; P
Patients in the romosozumab-alendronate group had greater gains in BMD from baseline at the lumbar spine (14.9% vs 8.5%) and total hip (7% vs 3.6%) compared to the alendronate-alendronate group. (P < 0.001 for all comparisons). At 12 months, romosozumab treatment resulted in decreased levels of bone resorption marker β-CTX and increased levels of bone formation marker P1NP. β-CTX and P1NP decreased and remained below baseline levels after transitioning to alendronate. In the alendronate-alendronate group, P1NP and β-CTX decreased within 1 month and remained below baseline levels at 36 months.
Overall, the adverse events and serious event rates were similar between the 2 treatment groups during the double-blind period with 2 exceptions. In the first 12 months, injection-site reactions were reported in 4.4% of patients receiving romosozumab compared to 2.6% in those receiving alendronate. Patients in the romosozumab group had an increased incidence of adjudicated serious cardiovascular outcomes during the double-blind period, 2.5% (50 of 2040 patients) compared to 1.9% (38 of 2014 patients) in the alendronate group. During the open-label period, osteonecrosis of the jaw occurred in one patient in each group. Two atypical femoral fractures occurred in the romosozumab-alendronate group, compared to 4 in the alendronate-alendronate group. During the first 18 months of the study, binding anti-romosozumab antibodies were observed in 15.3% of the romosozumab group, with neutralizing antibodies in 0.6%.
Conclusion. In postmenopausal woman with osteoporosis and high fracture risk, 12 months of romosozumab treatment followed by alendronate resulted in significantly lower risk of fracture than use of alendronate alone.
Commentary
Osteoporosis-related fragility fractures carry a substantial risk of morbidity and mortality [1]. The goal of osteoporosis treatment is to ameliorate this risk. The current FDA-approved medications for osteoporosis can be divided into anabolic (teriparatide, abaloparatide) and anti-resorptive (bisphosphonate, denosumab, selective estrogen receptor modulators) categories. Sclerostin is a glycoprotein produced by osteocytes that inhibits the Wnt signaling pathway, thereby impeding osteoblast proliferation and activity. Romosozumab is a monoclonal antisclerostin antibody that results in both increased bone formation and decreased bone resorption [1]. By apparently uncoupling bone formation and resorption to increase bone mass, this medication holds promise to become the ideal osteoporosis drug.
Initial studies have shown that 12 months of romosozumab treatment significantly increased BMD at the lumbar spine (+11.3%), as compared to placebo (–0.1%), alendronate (+4.1%), and teriparatide (+7.1%) [2]. The Fracture Study in Postmenopausal Women with Osteoporosis (FRAME) was a large (7180 patients) randomized controlled trial that demonstrated that 12 months of romosozumab resulted in a 73% lower risk of vertebral fracture and 36% lower risk of clinical fracture compared to placebo [3]. However, there was no significant reduction in non-vertebral facture [3]. This may be due to the fact that FRAME excluded women at the highest risk for fracture. That is, exclusion criteria included history of hip fracture, any severe vertebral facture, or more than 2 moderate vertebral fractures. The current phase 3 ARCH trial (Active-Controlled Fracture Study in Postmenopausal Women with Osteoporosis at High Risk) attempts to clarify the potential benefit of romosozumab treatment in this very high-risk patient population, compared to a common first-line osteoporosis treatment, alendronate.
Indeed, ARCH demonstrates that sequential therapy with romosozumab followed by alendronate is superior to alendronate alone in improving BMD at all sites and preventing new vertebral, clinical, and non-vertebral fractures in postmenopausal women with osteoporosis and a history of fragility fracture. While ARCH was not designed as a cardiovascular outcomes trial, the higher rate of serious cardiovascular adverse events in the romosozumab group raises concern that romosozumab may have a negative effect on vascular tissue. Sclerostin is expressed in vascular smooth muscle [4] and upregulated at sites of vascular calcification [5]. It is possible that inhibiting sclerostin activity could alter vascular remodeling or increase vascular calcification. However, it is interesting that in the larger FRAME trial, no increase in adverse cardiovascular events was seen in the romosozumab group compared to placebo. This may be due to the fact that the average age of patients in FRAME was lower than ARCH. However, it also raises the hypothesis that alendronate itself may be protective in terms of cardiovascular risk. It has been postulated that bisphosphonates may have cardiovascular protective effects, given animal studies have demonstrated that alendronate downregulates monocyte chemoattractant protein 1 and macrophage inflammatory protein 1 [6]. However no cardioprotective benefit was seen in meta-analysis [7].
ARCH has several strengths, including its design as an international, double-blind, and randomized clinical trial. The primary outcome of cumulative fracture incidence is a hard endpoint and is clinically relevant. The intervention is simple and the results are clearly defined. The statistical assessment yields significant results. However, there are some limitations to the study. The lead author has received research support from Amgen and UCB Pharma, the makers of romosuzumab. Amgen and UCB Pharma designed the trial, and Amgen was responsible for trial oversight and data analyses per a pre-specified statistical analysis plan. An external independent data monitoring committee monitored unblinded safety data. Because there was no placebo-controlled arm, it is difficult to determine whether the unexpected cardiovascular signal was due to romosuzumab itself or a protective effect of alendronate. In addition, the majority of study participants were non-Hispanic from Central or Eastern Europe and Latin America, with only ~2% of patients from North America. As a result, ARCH findings may not be generalizable to other regional or ethnic populations. Furthermore, the majority of the patients were ≥ 75 years of age and were at very high fracture risk. It is unclear if younger patients or those with lower risk of fracture would see the same fracture prevention and BMD gain. In addition, because of the relatively short length of the trial, the durability of the metabolic bone benefit and cardiovascular risk is unknown. While the authors reported the increased anti-romosozumab antibodies in the romosozumab group had no detectable effect on efficacy or safety, given the short duration of the trial, this has not been proven.
Applications for Clinical Practice
The dual anti-resorptive and anabolic effect of romosozumab makes it an attractive and promising new osteoporosis therapy. ARCH suggests that sequential therapy with romosuzumab and alendronate is superior in terms of fracture prevention to alendronate alone in elderly postmenopausal women with osteoporosis and a history of fragility fractures, although longer term studies are needed to define the durability of this effect. While the absolute number of serious adjudicated cardiovascular events was low, the increased incidence in the romosuzumab group will likely prevent the FDA from approving this medication for widespread use at this time. Additional studies are needed to clarify the cause and magnitude of this cardiovascular risk and to determine whether prevention of fracture-associated morbidity and mortality is enough to mitigate it.
—Simona Frunza-Stefan, MD, and Hillary B. Whitlach, MD, University of Maryland School of Medicine, Baltimore, MD
1. Cummings SR, Melton IJ. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002; 359:176107.
2. McClung MR, Grauer A, Boonen S, et al. Romosozumab in postmenopausal women with low bone mineral density. N Engl J Med 2014;370:412–20.
3. Cosman F, Crittenden DB, Adachi JD, et al. Romosozumab treatment in postmenopausal women with osteoporosis. N Engl J Med 2016;375:1532–43.
4. Zhu D, Mackenzie NCW, Millán JL, et al. The appearance and modulation of osteocyte marker expres- sion during calcification of vascular smooth muscle cells. PLoS One 2011;6:e19595.
5. Evenepoel P, Goffin E, Meijers B, et al. Sclerostin serum levels and vascular calcification progression in prevalent renal transplant recipients. J Clin Endocrinol Metab 2015;100:4669–76.
6. Masuda T, Deng X, Tamai R. Mouse macrophages primed with alendronate down-regulate monocyte chemoattractant protein-1 (MCP-1) and macrophage inflammatory protein-1alpha (MIP-1alpha) production in response to Toll-like receptor (TLR) 2 and TLR4 agonist via Smad3 activation. Int Immunopharmacol 2009;9:1115–21.
7. Kim DH, Rogers JR, Fulchino LA, et al. Bisphosphonates and risk of cardiovascular events: a meta-analysis. PLoS One 2015;10:e0122646.
Study Overview
Objective. To determine if romosuzumab, an antisclerostin antibody, is superior to alendronate in reducing the incidence of fracture in postmenopausal women with osteoporosis at high-risk for fracture.
Design. Multicenter, international, double-blind, randomized clinical trial.
Setting and participants. 4093 postmenopausal women with osteoporosis and a previous fragility fracture were enrolled from over 40 countries worldwide. Patients were eligible for the study if they were 55 to 90 years old and were deemed at high risk for future fracture based on bone mineral density (BMD) T score at the total hip or femoral neck and fracture history. This included T score ≤ –2.5 and ≥ 1 moderate or severe vertebral fractures or ≥ 2 mild vertebral fractures; T score ≤ –2.0 and either ≥ 2 moderate or severe vertebral fractures or proximal femur fracture within 3 to 24 months before randomization. Subjects with a history of prior use of medications that affect bone metabolism were excluded, as were those with other metabolic bone disease, vitamin D deficiency, uncontrolled metabolic disease, malabsorption syndromes, history of transplant, severe renal insufficiency, malignancy or severe illness.
Intervention. Patients were randomized to either subcutaneous romosuzumab 210 mg monthly or oral alendronate 70 mg weekly for 12 months. Following the 12-month double-blind period, all patients received open-label weekly alendronate until the end of the trial, with maintenance of blinding to the initial treatment assignment. Primary analysis occurred when all subjects had completed the 24-month visit and clinical fractures had been confirmed in at least 330 patients. All patients received daily calcium and vitamin D. Lateral radiographs of the thoracic and lumbar spine were obtained at screening and months 12 and 24. The BMD at the lumbar spine and proximal femur was evaluated by dual-energy x-ray absorptiometry at baseline and every 12 months thereafter. Serum concentrations of bone-turnover markers were measured in a subgroup of patients.
Main outcome measures. The primary outcomes were the incidence of new vertebral fracture and the incidence of clinical fracture at 24 months. Clinical fractures included symptomatic vertebral fracture and nonvertebral fractures. The secondary outcomes were the BMD at the lumbar spine, total hip, and femoral neck at 12 and 24 months, the incidence of nonvertebral fracture, and fracture category. Safety outcomes included the incidence of adjudicated clinical events, including serious cardiovascular adverse events, osteonecrosis of the jaw, and atypical femoral fracture. Serious cardiovascular events were defined as cardiac ischemic event, cerebrovascular event, heart failure, death, non-coronary revascularization and peripheral vascular ischemic event not requiring revascularization.
Analysis. An intention to treat approach was used for data analysis. For the incidence of fractures, the treatment groups were compared using a Cox proportional-hazards model and the Mantel-Haenszel method with adjustment for age (< 75 vs ≥ 75 years), the presence or absence of severe vertebral fracture at baseline, and baseline BMD T score at the total hip. Between-group comparisons of the percentage change in BMD from baseline were analyzed by means of a repeated-measures model with adjustment for treatment, age category, baseline severe vertebral fracture, visit, treatment-by-visit interaction, and baseline BMD. Percentage changes from baseline in bone turnover were assessed using a Wilcoxon rank-sum test. The safety analysis included cumulated incidence rates of adverse outcomes. Odds ratios and confidence intervals were estimated for serious cardiovascular adverse events with the use of a logistic regression model.
Main results. 2046 participants were randomized to the romosozumab group and 2047 to the alendronate group. A total of 3654 participants from both groups (89.3%) completed 12 months of the trial, and 3150 (77.0%) completed the primary analysis period. The treatment groups were similar in baseline age, ethnicity, and fracture history. The majority of patients in both groups were non-Hispanic (> 60%) and ≥ 75 years old (> 50%). The mean age of the patients was 74.3 years. Baseline mean bone mineral density T scores were –2.96 at the lumbar spine, –2.8 at the total hip, and –2.9 at the femoral neck.
After 24 months of treatment, 6.2% of patients in the romosozumab-alendronate group had a new vertebral fracture as compared to 11.9% in the alendronate-alendronate group. This represents a 48% lower risk (risk ratio 0.52, 95% confidence interval [CI] 0.4–0.66; P < 0.001) of new vertebral fractures with romosozumab. At the time of the primary analysis, romosozumab followed by alendronate resulted in a 27% lower risk of clinical fracture than alendronate alone (hazard ratio 0.73, 95% CI 0.61–0.88; P < 0.001). 8.7% of the romosozumab-alendronate group had a nonvertebral fracture versus 10.6% in the alendronate-alendronate group, representing a 19% lower risk with romosozumab (hazard ratio 0.81, 95% CI 0.66–0.99; P = 0.04). Hip fractures occurred in 2.0% of the romosozumab-alendronate group as compared with 3.2% in the alendronate-alendronate group, representing a 38% lower risk with romosozumab (hazard ratio 0.62, 95% CI 0.42–0.92; P
Patients in the romosozumab-alendronate group had greater gains in BMD from baseline at the lumbar spine (14.9% vs 8.5%) and total hip (7% vs 3.6%) compared to the alendronate-alendronate group. (P < 0.001 for all comparisons). At 12 months, romosozumab treatment resulted in decreased levels of bone resorption marker β-CTX and increased levels of bone formation marker P1NP. β-CTX and P1NP decreased and remained below baseline levels after transitioning to alendronate. In the alendronate-alendronate group, P1NP and β-CTX decreased within 1 month and remained below baseline levels at 36 months.
Overall, the adverse events and serious event rates were similar between the 2 treatment groups during the double-blind period with 2 exceptions. In the first 12 months, injection-site reactions were reported in 4.4% of patients receiving romosozumab compared to 2.6% in those receiving alendronate. Patients in the romosozumab group had an increased incidence of adjudicated serious cardiovascular outcomes during the double-blind period, 2.5% (50 of 2040 patients) compared to 1.9% (38 of 2014 patients) in the alendronate group. During the open-label period, osteonecrosis of the jaw occurred in one patient in each group. Two atypical femoral fractures occurred in the romosozumab-alendronate group, compared to 4 in the alendronate-alendronate group. During the first 18 months of the study, binding anti-romosozumab antibodies were observed in 15.3% of the romosozumab group, with neutralizing antibodies in 0.6%.
Conclusion. In postmenopausal woman with osteoporosis and high fracture risk, 12 months of romosozumab treatment followed by alendronate resulted in significantly lower risk of fracture than use of alendronate alone.
Commentary
Osteoporosis-related fragility fractures carry a substantial risk of morbidity and mortality [1]. The goal of osteoporosis treatment is to ameliorate this risk. The current FDA-approved medications for osteoporosis can be divided into anabolic (teriparatide, abaloparatide) and anti-resorptive (bisphosphonate, denosumab, selective estrogen receptor modulators) categories. Sclerostin is a glycoprotein produced by osteocytes that inhibits the Wnt signaling pathway, thereby impeding osteoblast proliferation and activity. Romosozumab is a monoclonal antisclerostin antibody that results in both increased bone formation and decreased bone resorption [1]. By apparently uncoupling bone formation and resorption to increase bone mass, this medication holds promise to become the ideal osteoporosis drug.
Initial studies have shown that 12 months of romosozumab treatment significantly increased BMD at the lumbar spine (+11.3%), as compared to placebo (–0.1%), alendronate (+4.1%), and teriparatide (+7.1%) [2]. The Fracture Study in Postmenopausal Women with Osteoporosis (FRAME) was a large (7180 patients) randomized controlled trial that demonstrated that 12 months of romosozumab resulted in a 73% lower risk of vertebral fracture and 36% lower risk of clinical fracture compared to placebo [3]. However, there was no significant reduction in non-vertebral facture [3]. This may be due to the fact that FRAME excluded women at the highest risk for fracture. That is, exclusion criteria included history of hip fracture, any severe vertebral facture, or more than 2 moderate vertebral fractures. The current phase 3 ARCH trial (Active-Controlled Fracture Study in Postmenopausal Women with Osteoporosis at High Risk) attempts to clarify the potential benefit of romosozumab treatment in this very high-risk patient population, compared to a common first-line osteoporosis treatment, alendronate.
Indeed, ARCH demonstrates that sequential therapy with romosozumab followed by alendronate is superior to alendronate alone in improving BMD at all sites and preventing new vertebral, clinical, and non-vertebral fractures in postmenopausal women with osteoporosis and a history of fragility fracture. While ARCH was not designed as a cardiovascular outcomes trial, the higher rate of serious cardiovascular adverse events in the romosozumab group raises concern that romosozumab may have a negative effect on vascular tissue. Sclerostin is expressed in vascular smooth muscle [4] and upregulated at sites of vascular calcification [5]. It is possible that inhibiting sclerostin activity could alter vascular remodeling or increase vascular calcification. However, it is interesting that in the larger FRAME trial, no increase in adverse cardiovascular events was seen in the romosozumab group compared to placebo. This may be due to the fact that the average age of patients in FRAME was lower than ARCH. However, it also raises the hypothesis that alendronate itself may be protective in terms of cardiovascular risk. It has been postulated that bisphosphonates may have cardiovascular protective effects, given animal studies have demonstrated that alendronate downregulates monocyte chemoattractant protein 1 and macrophage inflammatory protein 1 [6]. However no cardioprotective benefit was seen in meta-analysis [7].
ARCH has several strengths, including its design as an international, double-blind, and randomized clinical trial. The primary outcome of cumulative fracture incidence is a hard endpoint and is clinically relevant. The intervention is simple and the results are clearly defined. The statistical assessment yields significant results. However, there are some limitations to the study. The lead author has received research support from Amgen and UCB Pharma, the makers of romosuzumab. Amgen and UCB Pharma designed the trial, and Amgen was responsible for trial oversight and data analyses per a pre-specified statistical analysis plan. An external independent data monitoring committee monitored unblinded safety data. Because there was no placebo-controlled arm, it is difficult to determine whether the unexpected cardiovascular signal was due to romosuzumab itself or a protective effect of alendronate. In addition, the majority of study participants were non-Hispanic from Central or Eastern Europe and Latin America, with only ~2% of patients from North America. As a result, ARCH findings may not be generalizable to other regional or ethnic populations. Furthermore, the majority of the patients were ≥ 75 years of age and were at very high fracture risk. It is unclear if younger patients or those with lower risk of fracture would see the same fracture prevention and BMD gain. In addition, because of the relatively short length of the trial, the durability of the metabolic bone benefit and cardiovascular risk is unknown. While the authors reported the increased anti-romosozumab antibodies in the romosozumab group had no detectable effect on efficacy or safety, given the short duration of the trial, this has not been proven.
Applications for Clinical Practice
The dual anti-resorptive and anabolic effect of romosozumab makes it an attractive and promising new osteoporosis therapy. ARCH suggests that sequential therapy with romosuzumab and alendronate is superior in terms of fracture prevention to alendronate alone in elderly postmenopausal women with osteoporosis and a history of fragility fractures, although longer term studies are needed to define the durability of this effect. While the absolute number of serious adjudicated cardiovascular events was low, the increased incidence in the romosuzumab group will likely prevent the FDA from approving this medication for widespread use at this time. Additional studies are needed to clarify the cause and magnitude of this cardiovascular risk and to determine whether prevention of fracture-associated morbidity and mortality is enough to mitigate it.
—Simona Frunza-Stefan, MD, and Hillary B. Whitlach, MD, University of Maryland School of Medicine, Baltimore, MD
Study Overview
Objective. To determine if romosuzumab, an antisclerostin antibody, is superior to alendronate in reducing the incidence of fracture in postmenopausal women with osteoporosis at high-risk for fracture.
Design. Multicenter, international, double-blind, randomized clinical trial.
Setting and participants. 4093 postmenopausal women with osteoporosis and a previous fragility fracture were enrolled from over 40 countries worldwide. Patients were eligible for the study if they were 55 to 90 years old and were deemed at high risk for future fracture based on bone mineral density (BMD) T score at the total hip or femoral neck and fracture history. This included T score ≤ –2.5 and ≥ 1 moderate or severe vertebral fractures or ≥ 2 mild vertebral fractures; T score ≤ –2.0 and either ≥ 2 moderate or severe vertebral fractures or proximal femur fracture within 3 to 24 months before randomization. Subjects with a history of prior use of medications that affect bone metabolism were excluded, as were those with other metabolic bone disease, vitamin D deficiency, uncontrolled metabolic disease, malabsorption syndromes, history of transplant, severe renal insufficiency, malignancy or severe illness.
Intervention. Patients were randomized to either subcutaneous romosuzumab 210 mg monthly or oral alendronate 70 mg weekly for 12 months. Following the 12-month double-blind period, all patients received open-label weekly alendronate until the end of the trial, with maintenance of blinding to the initial treatment assignment. Primary analysis occurred when all subjects had completed the 24-month visit and clinical fractures had been confirmed in at least 330 patients. All patients received daily calcium and vitamin D. Lateral radiographs of the thoracic and lumbar spine were obtained at screening and months 12 and 24. The BMD at the lumbar spine and proximal femur was evaluated by dual-energy x-ray absorptiometry at baseline and every 12 months thereafter. Serum concentrations of bone-turnover markers were measured in a subgroup of patients.
Main outcome measures. The primary outcomes were the incidence of new vertebral fracture and the incidence of clinical fracture at 24 months. Clinical fractures included symptomatic vertebral fracture and nonvertebral fractures. The secondary outcomes were the BMD at the lumbar spine, total hip, and femoral neck at 12 and 24 months, the incidence of nonvertebral fracture, and fracture category. Safety outcomes included the incidence of adjudicated clinical events, including serious cardiovascular adverse events, osteonecrosis of the jaw, and atypical femoral fracture. Serious cardiovascular events were defined as cardiac ischemic event, cerebrovascular event, heart failure, death, non-coronary revascularization and peripheral vascular ischemic event not requiring revascularization.
Analysis. An intention to treat approach was used for data analysis. For the incidence of fractures, the treatment groups were compared using a Cox proportional-hazards model and the Mantel-Haenszel method with adjustment for age (< 75 vs ≥ 75 years), the presence or absence of severe vertebral fracture at baseline, and baseline BMD T score at the total hip. Between-group comparisons of the percentage change in BMD from baseline were analyzed by means of a repeated-measures model with adjustment for treatment, age category, baseline severe vertebral fracture, visit, treatment-by-visit interaction, and baseline BMD. Percentage changes from baseline in bone turnover were assessed using a Wilcoxon rank-sum test. The safety analysis included cumulated incidence rates of adverse outcomes. Odds ratios and confidence intervals were estimated for serious cardiovascular adverse events with the use of a logistic regression model.
Main results. 2046 participants were randomized to the romosozumab group and 2047 to the alendronate group. A total of 3654 participants from both groups (89.3%) completed 12 months of the trial, and 3150 (77.0%) completed the primary analysis period. The treatment groups were similar in baseline age, ethnicity, and fracture history. The majority of patients in both groups were non-Hispanic (> 60%) and ≥ 75 years old (> 50%). The mean age of the patients was 74.3 years. Baseline mean bone mineral density T scores were –2.96 at the lumbar spine, –2.8 at the total hip, and –2.9 at the femoral neck.
After 24 months of treatment, 6.2% of patients in the romosozumab-alendronate group had a new vertebral fracture as compared to 11.9% in the alendronate-alendronate group. This represents a 48% lower risk (risk ratio 0.52, 95% confidence interval [CI] 0.4–0.66; P < 0.001) of new vertebral fractures with romosozumab. At the time of the primary analysis, romosozumab followed by alendronate resulted in a 27% lower risk of clinical fracture than alendronate alone (hazard ratio 0.73, 95% CI 0.61–0.88; P < 0.001). 8.7% of the romosozumab-alendronate group had a nonvertebral fracture versus 10.6% in the alendronate-alendronate group, representing a 19% lower risk with romosozumab (hazard ratio 0.81, 95% CI 0.66–0.99; P = 0.04). Hip fractures occurred in 2.0% of the romosozumab-alendronate group as compared with 3.2% in the alendronate-alendronate group, representing a 38% lower risk with romosozumab (hazard ratio 0.62, 95% CI 0.42–0.92; P
Patients in the romosozumab-alendronate group had greater gains in BMD from baseline at the lumbar spine (14.9% vs 8.5%) and total hip (7% vs 3.6%) compared to the alendronate-alendronate group. (P < 0.001 for all comparisons). At 12 months, romosozumab treatment resulted in decreased levels of bone resorption marker β-CTX and increased levels of bone formation marker P1NP. β-CTX and P1NP decreased and remained below baseline levels after transitioning to alendronate. In the alendronate-alendronate group, P1NP and β-CTX decreased within 1 month and remained below baseline levels at 36 months.
Overall, the adverse events and serious event rates were similar between the 2 treatment groups during the double-blind period with 2 exceptions. In the first 12 months, injection-site reactions were reported in 4.4% of patients receiving romosozumab compared to 2.6% in those receiving alendronate. Patients in the romosozumab group had an increased incidence of adjudicated serious cardiovascular outcomes during the double-blind period, 2.5% (50 of 2040 patients) compared to 1.9% (38 of 2014 patients) in the alendronate group. During the open-label period, osteonecrosis of the jaw occurred in one patient in each group. Two atypical femoral fractures occurred in the romosozumab-alendronate group, compared to 4 in the alendronate-alendronate group. During the first 18 months of the study, binding anti-romosozumab antibodies were observed in 15.3% of the romosozumab group, with neutralizing antibodies in 0.6%.
Conclusion. In postmenopausal woman with osteoporosis and high fracture risk, 12 months of romosozumab treatment followed by alendronate resulted in significantly lower risk of fracture than use of alendronate alone.
Commentary
Osteoporosis-related fragility fractures carry a substantial risk of morbidity and mortality [1]. The goal of osteoporosis treatment is to ameliorate this risk. The current FDA-approved medications for osteoporosis can be divided into anabolic (teriparatide, abaloparatide) and anti-resorptive (bisphosphonate, denosumab, selective estrogen receptor modulators) categories. Sclerostin is a glycoprotein produced by osteocytes that inhibits the Wnt signaling pathway, thereby impeding osteoblast proliferation and activity. Romosozumab is a monoclonal antisclerostin antibody that results in both increased bone formation and decreased bone resorption [1]. By apparently uncoupling bone formation and resorption to increase bone mass, this medication holds promise to become the ideal osteoporosis drug.
Initial studies have shown that 12 months of romosozumab treatment significantly increased BMD at the lumbar spine (+11.3%), as compared to placebo (–0.1%), alendronate (+4.1%), and teriparatide (+7.1%) [2]. The Fracture Study in Postmenopausal Women with Osteoporosis (FRAME) was a large (7180 patients) randomized controlled trial that demonstrated that 12 months of romosozumab resulted in a 73% lower risk of vertebral fracture and 36% lower risk of clinical fracture compared to placebo [3]. However, there was no significant reduction in non-vertebral facture [3]. This may be due to the fact that FRAME excluded women at the highest risk for fracture. That is, exclusion criteria included history of hip fracture, any severe vertebral facture, or more than 2 moderate vertebral fractures. The current phase 3 ARCH trial (Active-Controlled Fracture Study in Postmenopausal Women with Osteoporosis at High Risk) attempts to clarify the potential benefit of romosozumab treatment in this very high-risk patient population, compared to a common first-line osteoporosis treatment, alendronate.
Indeed, ARCH demonstrates that sequential therapy with romosozumab followed by alendronate is superior to alendronate alone in improving BMD at all sites and preventing new vertebral, clinical, and non-vertebral fractures in postmenopausal women with osteoporosis and a history of fragility fracture. While ARCH was not designed as a cardiovascular outcomes trial, the higher rate of serious cardiovascular adverse events in the romosozumab group raises concern that romosozumab may have a negative effect on vascular tissue. Sclerostin is expressed in vascular smooth muscle [4] and upregulated at sites of vascular calcification [5]. It is possible that inhibiting sclerostin activity could alter vascular remodeling or increase vascular calcification. However, it is interesting that in the larger FRAME trial, no increase in adverse cardiovascular events was seen in the romosozumab group compared to placebo. This may be due to the fact that the average age of patients in FRAME was lower than ARCH. However, it also raises the hypothesis that alendronate itself may be protective in terms of cardiovascular risk. It has been postulated that bisphosphonates may have cardiovascular protective effects, given animal studies have demonstrated that alendronate downregulates monocyte chemoattractant protein 1 and macrophage inflammatory protein 1 [6]. However no cardioprotective benefit was seen in meta-analysis [7].
ARCH has several strengths, including its design as an international, double-blind, and randomized clinical trial. The primary outcome of cumulative fracture incidence is a hard endpoint and is clinically relevant. The intervention is simple and the results are clearly defined. The statistical assessment yields significant results. However, there are some limitations to the study. The lead author has received research support from Amgen and UCB Pharma, the makers of romosuzumab. Amgen and UCB Pharma designed the trial, and Amgen was responsible for trial oversight and data analyses per a pre-specified statistical analysis plan. An external independent data monitoring committee monitored unblinded safety data. Because there was no placebo-controlled arm, it is difficult to determine whether the unexpected cardiovascular signal was due to romosuzumab itself or a protective effect of alendronate. In addition, the majority of study participants were non-Hispanic from Central or Eastern Europe and Latin America, with only ~2% of patients from North America. As a result, ARCH findings may not be generalizable to other regional or ethnic populations. Furthermore, the majority of the patients were ≥ 75 years of age and were at very high fracture risk. It is unclear if younger patients or those with lower risk of fracture would see the same fracture prevention and BMD gain. In addition, because of the relatively short length of the trial, the durability of the metabolic bone benefit and cardiovascular risk is unknown. While the authors reported the increased anti-romosozumab antibodies in the romosozumab group had no detectable effect on efficacy or safety, given the short duration of the trial, this has not been proven.
Applications for Clinical Practice
The dual anti-resorptive and anabolic effect of romosozumab makes it an attractive and promising new osteoporosis therapy. ARCH suggests that sequential therapy with romosuzumab and alendronate is superior in terms of fracture prevention to alendronate alone in elderly postmenopausal women with osteoporosis and a history of fragility fractures, although longer term studies are needed to define the durability of this effect. While the absolute number of serious adjudicated cardiovascular events was low, the increased incidence in the romosuzumab group will likely prevent the FDA from approving this medication for widespread use at this time. Additional studies are needed to clarify the cause and magnitude of this cardiovascular risk and to determine whether prevention of fracture-associated morbidity and mortality is enough to mitigate it.
—Simona Frunza-Stefan, MD, and Hillary B. Whitlach, MD, University of Maryland School of Medicine, Baltimore, MD
1. Cummings SR, Melton IJ. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002; 359:176107.
2. McClung MR, Grauer A, Boonen S, et al. Romosozumab in postmenopausal women with low bone mineral density. N Engl J Med 2014;370:412–20.
3. Cosman F, Crittenden DB, Adachi JD, et al. Romosozumab treatment in postmenopausal women with osteoporosis. N Engl J Med 2016;375:1532–43.
4. Zhu D, Mackenzie NCW, Millán JL, et al. The appearance and modulation of osteocyte marker expres- sion during calcification of vascular smooth muscle cells. PLoS One 2011;6:e19595.
5. Evenepoel P, Goffin E, Meijers B, et al. Sclerostin serum levels and vascular calcification progression in prevalent renal transplant recipients. J Clin Endocrinol Metab 2015;100:4669–76.
6. Masuda T, Deng X, Tamai R. Mouse macrophages primed with alendronate down-regulate monocyte chemoattractant protein-1 (MCP-1) and macrophage inflammatory protein-1alpha (MIP-1alpha) production in response to Toll-like receptor (TLR) 2 and TLR4 agonist via Smad3 activation. Int Immunopharmacol 2009;9:1115–21.
7. Kim DH, Rogers JR, Fulchino LA, et al. Bisphosphonates and risk of cardiovascular events: a meta-analysis. PLoS One 2015;10:e0122646.
1. Cummings SR, Melton IJ. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002; 359:176107.
2. McClung MR, Grauer A, Boonen S, et al. Romosozumab in postmenopausal women with low bone mineral density. N Engl J Med 2014;370:412–20.
3. Cosman F, Crittenden DB, Adachi JD, et al. Romosozumab treatment in postmenopausal women with osteoporosis. N Engl J Med 2016;375:1532–43.
4. Zhu D, Mackenzie NCW, Millán JL, et al. The appearance and modulation of osteocyte marker expres- sion during calcification of vascular smooth muscle cells. PLoS One 2011;6:e19595.
5. Evenepoel P, Goffin E, Meijers B, et al. Sclerostin serum levels and vascular calcification progression in prevalent renal transplant recipients. J Clin Endocrinol Metab 2015;100:4669–76.
6. Masuda T, Deng X, Tamai R. Mouse macrophages primed with alendronate down-regulate monocyte chemoattractant protein-1 (MCP-1) and macrophage inflammatory protein-1alpha (MIP-1alpha) production in response to Toll-like receptor (TLR) 2 and TLR4 agonist via Smad3 activation. Int Immunopharmacol 2009;9:1115–21.
7. Kim DH, Rogers JR, Fulchino LA, et al. Bisphosphonates and risk of cardiovascular events: a meta-analysis. PLoS One 2015;10:e0122646.
Which Herpes Zoster Vaccine is Most Cost-Effective?
Study Overview
Objective. To assess the cost-effectiveness of the new adjuvanted herpes zoster subunit vaccine (HZ/su) as compared with that of the current live attenuated herpes zoster vaccine (ZVL), or no vaccine.
Design. Markov decision model evaluating 3 strategies from a societal perspective: (1) no vaccination, (2) vaccination with single dose ZVL, and (3) vaccination with 2-dose series of HZ/su.
Setting and participants. Data for the model were extracted from the US medical literature using PubMed through January 2015. Data were derived from studies of fewer than 100 patients to more than 30,000 patients, depending on the variable assessed. Variables included epidemiologic parameters, vaccine efficacy and adverse events, quality-adjusted life-years (QALYs), and costs. Because there is no standard willingness-to-pay (WTP) threshold for cost-effectiveness in the United States, $50,000 per QALY was chosen.
Main outcome measures. Total costs and QALYs.
Main results. At all ages, no vaccination was always the least expensive and least effective option, while HZ/su was always the most effective and less expensive than ZVL. At a proposed price of $280 per series ($140 per dose), HZ/su was more effective and less expensive than ZVL at all ages. The incremental cost-effectiveness ratios compared with no vaccination ranged from $20,038 to $30,084 per QALY, depending on vaccination age. The cost-effectiveness of HZ/su was insensitive to the waning rate of either vaccine due to its high efficacy, with initial level of protection close to 90% even among people 70 years or older.
Conclusion. At a manufacturer suggested price of $280 per series ($140 per dose), HZ/su would cost less than ZVL and has a high probability of offering good value.
Commentary
Herpes zosters is a localized, usually painful, cutaneous eruption resulting from reactivation of latent varicella zoster virus. It is a common disease with approximately one million cases occurring each year in the United States [1]. The incidence increases with age, from 5 cases per 1000 population in adults aged 50–59 years to 11 cases per 1000 population in persons aged ≥ 80 years. Postherpetic neuralgia, commonly defined as persistent pain for at least 90 days following the resolution of the herpes zoster rash, is the most common complication and occurs in 10% to 13% of herpes zoster cases in persons aged > 50 years [2,3].
In 2006, the US Food and Drug Administration (FDA) approved the ZVL vaccine Zostavax (Merck) for prevention of postherpetic neuralgia. By 2016, 33% of adults aged ≥ 60 years reported receipt of the vaccine [4]. However, ZVL does not prevent all herpes zoster, particularly among the elderly. Moreover, the efficacy wanes completely after approximately 10 years [5]. To address these shortcomings, a 2-dose HZ/su (Shingrix; GlaxoSmithKline) containing recombinant glycoprotein E in combination with a novel adjuvant (AS01B) was approved by the FDA in adults aged ≥ 50 years. In randomized controlled trials, HZ/su has an efficacy of close to 97%, even after age 70 years [6].
With the approval of the new attenuated herpes zoster vaccine, clinicians and patients face the question of which vaccine to get and when. The cost-effectiveness analysis published by Le and Rothberg in this study compare the value of HZ/su with ZVL vaccine and a no-vaccine strategy for individuals 60 years or older from the US societal perspective. The results suggest that, at $140 per dose, using HZ/su vaccine compared with no vaccine would cost between $20,038 and $30,084 per QALY and thus is a cost-effective strategy. The deterministic sensitivity analysis indicates that the overall results do not change under different assumptions about model input parameters, even if patients are nonadherent to the second dose of HZ/su vaccine.
As with any simulation study, the major limitation of this study is the accuracy of the model and the assumptions on which it is based. The body of evidence for benefits of ZVL was large, including multiple pre-licensure and post-licensure RCTs, as well as observational studies of effectiveness. On the other hand, the body of evidence for benefits of RZV was primarily informed by one high-quality RCT that studied vaccine efficacy through 4 years post-vaccination [4,6]. Currently, 3 other independent cost-effectiveness analysis are available. The Centers for Disease Control and Prevention model estimated HZ/su vaccine cost per QALY of $31,000 when vaccination occurred at age ≥ 50 years. The GlaxoSmithKline model, manufacturer of HZ/su vaccine, estimated a HZ/su vaccine cost per QALY of $12,000. While the Merck model, manufacturer of the ZVL vaccine, estimated a HZ/su vaccine cost per QALY of $107,000 [4]. In addition to model variables, the key assumption by Le and Rothberg are based on the HZ/su vaccine cost at $140 per dose and ZVL at $213. The study results need to be interpreted carefully if the vaccine prices turn out to be different in the future.
Applications for Clinical Practice
The current study by Le and Rothberg demonstrated the cost-effectiveness of the new HZ/su vaccine. Since the study’s publication, the CDC has updated their recommendations on immunization practices for use of herpes zoster vaccine [4]. HZ/su vaccine, also known as the recombinant zoster vaccine (RZV), is now preferred over ZVL for the prevention of herpes zoster and related complications. RZV is recommended for immunocompetent adults age 50 or older, 10 years earlier than previously for the ZVL. In addition, RZV is recommended for adults who previously received ZVL. Finally, RZV can be administered concomitantly with other adult vaccines, does not require screening for a history of varicella, and is likely safe for immunocompromised persons.
—Ka Ming Gordon Ngai, MD, MPH
1. Insinga RP, Itzler RF, Pellissier JM, et al. The incidence of herpes zoster in a United States administrative database. J Gen Intern Med 2005;20:748–53.
2. Yawn BP, Saddier P, Wollan PC, et al. A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc 2007;82:1341–9.
3. Oxman MN, Levin MJ, Johnson GR, et al. Shingles Prevention Study Group. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Eng J Med 2005;352:2271-84.
4. Dooling KL, Guo A, Patel M, et al. Recommendations of the Advisory Committee on Immunization Practices for use of herpes zoster vaccines. MMWR Morb Mortal Wkly Rep 2018;67:103–8.
5. Morrison VA, Johnson GR, Schmader KE, et al; Shingles Prevention Study Group. Long-term persistence of zoster vaccine efficacy. Clin Infect Dis 2015;60:900–9.
6. Lai H, Cunningham AL, Godeaux O, et al; ZOE-50 Study Group. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med 2015;372:2087–96.
Study Overview
Objective. To assess the cost-effectiveness of the new adjuvanted herpes zoster subunit vaccine (HZ/su) as compared with that of the current live attenuated herpes zoster vaccine (ZVL), or no vaccine.
Design. Markov decision model evaluating 3 strategies from a societal perspective: (1) no vaccination, (2) vaccination with single dose ZVL, and (3) vaccination with 2-dose series of HZ/su.
Setting and participants. Data for the model were extracted from the US medical literature using PubMed through January 2015. Data were derived from studies of fewer than 100 patients to more than 30,000 patients, depending on the variable assessed. Variables included epidemiologic parameters, vaccine efficacy and adverse events, quality-adjusted life-years (QALYs), and costs. Because there is no standard willingness-to-pay (WTP) threshold for cost-effectiveness in the United States, $50,000 per QALY was chosen.
Main outcome measures. Total costs and QALYs.
Main results. At all ages, no vaccination was always the least expensive and least effective option, while HZ/su was always the most effective and less expensive than ZVL. At a proposed price of $280 per series ($140 per dose), HZ/su was more effective and less expensive than ZVL at all ages. The incremental cost-effectiveness ratios compared with no vaccination ranged from $20,038 to $30,084 per QALY, depending on vaccination age. The cost-effectiveness of HZ/su was insensitive to the waning rate of either vaccine due to its high efficacy, with initial level of protection close to 90% even among people 70 years or older.
Conclusion. At a manufacturer suggested price of $280 per series ($140 per dose), HZ/su would cost less than ZVL and has a high probability of offering good value.
Commentary
Herpes zosters is a localized, usually painful, cutaneous eruption resulting from reactivation of latent varicella zoster virus. It is a common disease with approximately one million cases occurring each year in the United States [1]. The incidence increases with age, from 5 cases per 1000 population in adults aged 50–59 years to 11 cases per 1000 population in persons aged ≥ 80 years. Postherpetic neuralgia, commonly defined as persistent pain for at least 90 days following the resolution of the herpes zoster rash, is the most common complication and occurs in 10% to 13% of herpes zoster cases in persons aged > 50 years [2,3].
In 2006, the US Food and Drug Administration (FDA) approved the ZVL vaccine Zostavax (Merck) for prevention of postherpetic neuralgia. By 2016, 33% of adults aged ≥ 60 years reported receipt of the vaccine [4]. However, ZVL does not prevent all herpes zoster, particularly among the elderly. Moreover, the efficacy wanes completely after approximately 10 years [5]. To address these shortcomings, a 2-dose HZ/su (Shingrix; GlaxoSmithKline) containing recombinant glycoprotein E in combination with a novel adjuvant (AS01B) was approved by the FDA in adults aged ≥ 50 years. In randomized controlled trials, HZ/su has an efficacy of close to 97%, even after age 70 years [6].
With the approval of the new attenuated herpes zoster vaccine, clinicians and patients face the question of which vaccine to get and when. The cost-effectiveness analysis published by Le and Rothberg in this study compare the value of HZ/su with ZVL vaccine and a no-vaccine strategy for individuals 60 years or older from the US societal perspective. The results suggest that, at $140 per dose, using HZ/su vaccine compared with no vaccine would cost between $20,038 and $30,084 per QALY and thus is a cost-effective strategy. The deterministic sensitivity analysis indicates that the overall results do not change under different assumptions about model input parameters, even if patients are nonadherent to the second dose of HZ/su vaccine.
As with any simulation study, the major limitation of this study is the accuracy of the model and the assumptions on which it is based. The body of evidence for benefits of ZVL was large, including multiple pre-licensure and post-licensure RCTs, as well as observational studies of effectiveness. On the other hand, the body of evidence for benefits of RZV was primarily informed by one high-quality RCT that studied vaccine efficacy through 4 years post-vaccination [4,6]. Currently, 3 other independent cost-effectiveness analysis are available. The Centers for Disease Control and Prevention model estimated HZ/su vaccine cost per QALY of $31,000 when vaccination occurred at age ≥ 50 years. The GlaxoSmithKline model, manufacturer of HZ/su vaccine, estimated a HZ/su vaccine cost per QALY of $12,000. While the Merck model, manufacturer of the ZVL vaccine, estimated a HZ/su vaccine cost per QALY of $107,000 [4]. In addition to model variables, the key assumption by Le and Rothberg are based on the HZ/su vaccine cost at $140 per dose and ZVL at $213. The study results need to be interpreted carefully if the vaccine prices turn out to be different in the future.
Applications for Clinical Practice
The current study by Le and Rothberg demonstrated the cost-effectiveness of the new HZ/su vaccine. Since the study’s publication, the CDC has updated their recommendations on immunization practices for use of herpes zoster vaccine [4]. HZ/su vaccine, also known as the recombinant zoster vaccine (RZV), is now preferred over ZVL for the prevention of herpes zoster and related complications. RZV is recommended for immunocompetent adults age 50 or older, 10 years earlier than previously for the ZVL. In addition, RZV is recommended for adults who previously received ZVL. Finally, RZV can be administered concomitantly with other adult vaccines, does not require screening for a history of varicella, and is likely safe for immunocompromised persons.
—Ka Ming Gordon Ngai, MD, MPH
Study Overview
Objective. To assess the cost-effectiveness of the new adjuvanted herpes zoster subunit vaccine (HZ/su) as compared with that of the current live attenuated herpes zoster vaccine (ZVL), or no vaccine.
Design. Markov decision model evaluating 3 strategies from a societal perspective: (1) no vaccination, (2) vaccination with single dose ZVL, and (3) vaccination with 2-dose series of HZ/su.
Setting and participants. Data for the model were extracted from the US medical literature using PubMed through January 2015. Data were derived from studies of fewer than 100 patients to more than 30,000 patients, depending on the variable assessed. Variables included epidemiologic parameters, vaccine efficacy and adverse events, quality-adjusted life-years (QALYs), and costs. Because there is no standard willingness-to-pay (WTP) threshold for cost-effectiveness in the United States, $50,000 per QALY was chosen.
Main outcome measures. Total costs and QALYs.
Main results. At all ages, no vaccination was always the least expensive and least effective option, while HZ/su was always the most effective and less expensive than ZVL. At a proposed price of $280 per series ($140 per dose), HZ/su was more effective and less expensive than ZVL at all ages. The incremental cost-effectiveness ratios compared with no vaccination ranged from $20,038 to $30,084 per QALY, depending on vaccination age. The cost-effectiveness of HZ/su was insensitive to the waning rate of either vaccine due to its high efficacy, with initial level of protection close to 90% even among people 70 years or older.
Conclusion. At a manufacturer suggested price of $280 per series ($140 per dose), HZ/su would cost less than ZVL and has a high probability of offering good value.
Commentary
Herpes zosters is a localized, usually painful, cutaneous eruption resulting from reactivation of latent varicella zoster virus. It is a common disease with approximately one million cases occurring each year in the United States [1]. The incidence increases with age, from 5 cases per 1000 population in adults aged 50–59 years to 11 cases per 1000 population in persons aged ≥ 80 years. Postherpetic neuralgia, commonly defined as persistent pain for at least 90 days following the resolution of the herpes zoster rash, is the most common complication and occurs in 10% to 13% of herpes zoster cases in persons aged > 50 years [2,3].
In 2006, the US Food and Drug Administration (FDA) approved the ZVL vaccine Zostavax (Merck) for prevention of postherpetic neuralgia. By 2016, 33% of adults aged ≥ 60 years reported receipt of the vaccine [4]. However, ZVL does not prevent all herpes zoster, particularly among the elderly. Moreover, the efficacy wanes completely after approximately 10 years [5]. To address these shortcomings, a 2-dose HZ/su (Shingrix; GlaxoSmithKline) containing recombinant glycoprotein E in combination with a novel adjuvant (AS01B) was approved by the FDA in adults aged ≥ 50 years. In randomized controlled trials, HZ/su has an efficacy of close to 97%, even after age 70 years [6].
With the approval of the new attenuated herpes zoster vaccine, clinicians and patients face the question of which vaccine to get and when. The cost-effectiveness analysis published by Le and Rothberg in this study compare the value of HZ/su with ZVL vaccine and a no-vaccine strategy for individuals 60 years or older from the US societal perspective. The results suggest that, at $140 per dose, using HZ/su vaccine compared with no vaccine would cost between $20,038 and $30,084 per QALY and thus is a cost-effective strategy. The deterministic sensitivity analysis indicates that the overall results do not change under different assumptions about model input parameters, even if patients are nonadherent to the second dose of HZ/su vaccine.
As with any simulation study, the major limitation of this study is the accuracy of the model and the assumptions on which it is based. The body of evidence for benefits of ZVL was large, including multiple pre-licensure and post-licensure RCTs, as well as observational studies of effectiveness. On the other hand, the body of evidence for benefits of RZV was primarily informed by one high-quality RCT that studied vaccine efficacy through 4 years post-vaccination [4,6]. Currently, 3 other independent cost-effectiveness analysis are available. The Centers for Disease Control and Prevention model estimated HZ/su vaccine cost per QALY of $31,000 when vaccination occurred at age ≥ 50 years. The GlaxoSmithKline model, manufacturer of HZ/su vaccine, estimated a HZ/su vaccine cost per QALY of $12,000. While the Merck model, manufacturer of the ZVL vaccine, estimated a HZ/su vaccine cost per QALY of $107,000 [4]. In addition to model variables, the key assumption by Le and Rothberg are based on the HZ/su vaccine cost at $140 per dose and ZVL at $213. The study results need to be interpreted carefully if the vaccine prices turn out to be different in the future.
Applications for Clinical Practice
The current study by Le and Rothberg demonstrated the cost-effectiveness of the new HZ/su vaccine. Since the study’s publication, the CDC has updated their recommendations on immunization practices for use of herpes zoster vaccine [4]. HZ/su vaccine, also known as the recombinant zoster vaccine (RZV), is now preferred over ZVL for the prevention of herpes zoster and related complications. RZV is recommended for immunocompetent adults age 50 or older, 10 years earlier than previously for the ZVL. In addition, RZV is recommended for adults who previously received ZVL. Finally, RZV can be administered concomitantly with other adult vaccines, does not require screening for a history of varicella, and is likely safe for immunocompromised persons.
—Ka Ming Gordon Ngai, MD, MPH
1. Insinga RP, Itzler RF, Pellissier JM, et al. The incidence of herpes zoster in a United States administrative database. J Gen Intern Med 2005;20:748–53.
2. Yawn BP, Saddier P, Wollan PC, et al. A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc 2007;82:1341–9.
3. Oxman MN, Levin MJ, Johnson GR, et al. Shingles Prevention Study Group. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Eng J Med 2005;352:2271-84.
4. Dooling KL, Guo A, Patel M, et al. Recommendations of the Advisory Committee on Immunization Practices for use of herpes zoster vaccines. MMWR Morb Mortal Wkly Rep 2018;67:103–8.
5. Morrison VA, Johnson GR, Schmader KE, et al; Shingles Prevention Study Group. Long-term persistence of zoster vaccine efficacy. Clin Infect Dis 2015;60:900–9.
6. Lai H, Cunningham AL, Godeaux O, et al; ZOE-50 Study Group. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med 2015;372:2087–96.
1. Insinga RP, Itzler RF, Pellissier JM, et al. The incidence of herpes zoster in a United States administrative database. J Gen Intern Med 2005;20:748–53.
2. Yawn BP, Saddier P, Wollan PC, et al. A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc 2007;82:1341–9.
3. Oxman MN, Levin MJ, Johnson GR, et al. Shingles Prevention Study Group. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Eng J Med 2005;352:2271-84.
4. Dooling KL, Guo A, Patel M, et al. Recommendations of the Advisory Committee on Immunization Practices for use of herpes zoster vaccines. MMWR Morb Mortal Wkly Rep 2018;67:103–8.
5. Morrison VA, Johnson GR, Schmader KE, et al; Shingles Prevention Study Group. Long-term persistence of zoster vaccine efficacy. Clin Infect Dis 2015;60:900–9.
6. Lai H, Cunningham AL, Godeaux O, et al; ZOE-50 Study Group. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med 2015;372:2087–96.
Non-Culprit Lesion PCI Strategies in Patients with Acute Myocardial Infarction and Cardiogenic Shock
Study Overview
Objective. To determine if percutaneous coronary intervention (PCI) of non-culprit vessels should be performed in patients with acute myocardial infarction and cardiogenic shock.
Design. Multicenter randomized controlled trial.
Setting and participants. 706 patients who had multivessel disease, acute myocardial infarction, and cardiogenic shock were assigned to one of 2 revascularization strategies: PCI of the culprit lesion only with the option of staged revascularization of non-culprit lesions, or immediate multivessel PCI.
Main outcome measures. The primary endpoint was the composite of death or severe renal failure leading to renal replacement therapy within 30 days after randomization. Safety endpoints included bleeding and stroke.
Main results. The primary endpoint of death or renal replacement therapy occurred in 158 /344 patients (45.9%) in the culprit lesion–only PCI group and 189/341 patients (55.4%) in the multivessel PCI group (relative risk [RR] 0.83, 95% CI 0.72–0.96, P = 0.01). The rate of death from any cause was lower in the culprit lesion–only PCI group compared to multivessel PCI group (RR 0.84, 95% CI 0.72–0.98, P = 0.03). There was no difference in stroke and numerically lower risk of bleeding in culprit lesion–only PCI group (RR 0.75, 95% CI 0.55–1.03).
Conclusion. Among patients who had multivessel coronary artery disease and acute myocardial infarction with cardiogenic shock, the 30-day risk of death or severe renal failure leading to renal replacement therapy was lower in patients who initially underwent PCI of the culprit lesion only compared with patients who underwent immediate multivessel PCI.
Commentary
Patients presenting with cardiogenic shock at the time of acute myocardial infarction have the highest mortality—up to 50%. Since the original SHOCK trial in 1999, it is known that the mortality can be reduced by early revascularization of the culprit vessel [1]. However, whether the non-culprit vessel should be revascularized at the time of presentation with acute myocardial infarction is unknown.
Recently, there have been multiple trials suggesting the benefit of non-culprit vessel revascularization in patients with acute myocardial infarction who are hemodynamically stable at the time of their presentation. Three recent trials—PRAMI, CvPRIT and DANAMI-PRIMULTI—investigated this clinical question and found benefit of non-culprit vessel revascularization [2–4]. The results of these trials led to a focused update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention in 2015 [5]. Noninfarct-related artery PCI in hemodynamically stable patients presenting with acute myocardial infarction was upgraded to class IIb from class III [5]. Whether these findings can be extended to hemodynamically unstable (cardiogenic shock) patients is not mentioned in the guidelines.
In the current CULPRIT-SHOCK trial, Thiele et al investigated this clinical question by performing a well-designed clinical trial in patients with acute myocardial infarction and cardiogenic shock. They found that the composite endpoint of death and renal replacement therapy at 30 days occurred more frequently in the multivessel PCI group compared with the culprit lesion–only group (relative risk [RR] 0.83, 95% CI 0.71–0.96, P = 0.01). The composite endpoint was mainly driven by death (43.3% vs 51.6%, RR 0.84, 95% CI 0.72–0.98, P = 0.03), and the rate of renal replacement therapy was numerically higher in the mutivessel PCI group (11.6% vs 16.4%, P = 0.07). The study was conducted in the sickest population compared to prior trials as evidenced by high rate of mechanical ventilation (~80%), requirement of catecholamine support (~90%), and long ICU stay (median 5 days). The significance of non-culprit lesion was determined by angiogram (stenosis > 70%). The culprit vessel–only group had treatment of the culprit vessel only initially, but the staged intervention for non-culprit vessel was encouraged.
A unique point of this trial is that patients with chronic total occlusion (CTO) were included in the study and it was encouraged to attempt revascularization of CTO lesions, contrary to previous trials. Although CTO intervention improves angina and ejection fraction [6,7], whether CTO intervention has a mortality benefit needs further investigation. In the CULPRIT-SHOCK trial, 24% of patients had one or more CTO lesions. This most likely contributed to the increased contrast use in the multivessel PCI group (250 vs 190 mL, P < 0.01). CTO is considered a most challenging lesion to treat, and expertise and skill level vary among operators. In the hybrid CTO intervention model, it is recommended to stage the intervention as much as possible, as this type of intervention requires meticulous planning [8]. There is a possibility that attempting CTO intervention in this acute setting caused more harm than benefit. Furthermore, the investigators did not report the success rate of CTO intervention.
Another interesting finding of this trial is that the mortality of both groups was high (43.3% vs 51.6%). The revascularization arm of the original shock trial almost 20 years ago had a 30-day mortality of 46.7%, which is almost identical with the current CULPRIT-SHOCK study. Despite improvement in hemodynamic support such as Impella, TandemHeart, extracorporeal membrane oxygenation device, and improvement in medical therapy over the years, patients with cardiogenic shock with acute myocardial infarction have a dismal prognosis.
The CULPRIT-SHOCK trial has number of strengths, including low drop-out rate (3%) and adequate power, however, there are some limitations. Some patients crossed over from culprit-vessel only to multivessel PCI group due to lack of hemodynamic improvement, plaque shifts, and newly detected lesions after treatment of the culprit lesion. On the other hand, some patients crossed over from multivessel PCI from culprit lesion only due to multiple reasons, including technical difficulty of intervention.
Applications for Clinical Practice
In patients presenting with cardiogenic shock and acute myocardial infarction, culprit lesion–only intervention and focusing on hemodynamic support with a staged intervention if necessary seems to be better strategy than immediate multivessel PCI, including non-culprit vessel PCI.
—Taishi Hirai, MD, University of Chicago Medical Center, Chicago, IL
1. Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should we emergently revascularize occluded coronaries for cardiogenic shock. N Engl J Med 1999;341:625–34.
2. Wald DS, Morris JK, Wald NJ, et al. Randomized trial of preventive angioplasty in myocardial infarction. N Engl J Med 2013;369:1115–23.
3. Gershlick AH, Khan JN, Kelly DJ, et al. Randomized trial of complete versus lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol 2015;65:963–72.
4. Engstrom T, Kelbaek H, Helqvist S, et al. Complete revasculari Outcomes Research in Review www.mdedge.com/jcomjournal Vol. 25, No. 3 March 2018 JCOM 103 sation versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3-PRIMULTI): an open-label, randomised controlled trial. Lancet 2015;386:665–71.
5. Levine GN, Bates ER, Blankenship JC, et al. 2015 ACC/AHA/SCAI Focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol 2016;67:1235–50.
6. Sapontis J, Salisbury AC, Yeh RW, et al. Early procedural and health status outcomes after chronic total occlusion angioplasty: a report from the OPEN-CTO Registry (Outcomes, Patient Health Status, and Efficiency in Chronic Total Occlusion Hybrid Procedures). JACC Cardiovasc Interv 2017;10:1523–34.
7. Henriques JP, Hoebers LP, Ramunddal T, et al. Percutaneous intervention for concurrent chronic total occlusions in patients with STEMI: the EXPLORE trial. J Am Coll Cardiol 2016;68:1622–32.
8. Brilakis ES, Grantham JA, Rinfret S, et al. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv 2012;5:367–79.
Study Overview
Objective. To determine if percutaneous coronary intervention (PCI) of non-culprit vessels should be performed in patients with acute myocardial infarction and cardiogenic shock.
Design. Multicenter randomized controlled trial.
Setting and participants. 706 patients who had multivessel disease, acute myocardial infarction, and cardiogenic shock were assigned to one of 2 revascularization strategies: PCI of the culprit lesion only with the option of staged revascularization of non-culprit lesions, or immediate multivessel PCI.
Main outcome measures. The primary endpoint was the composite of death or severe renal failure leading to renal replacement therapy within 30 days after randomization. Safety endpoints included bleeding and stroke.
Main results. The primary endpoint of death or renal replacement therapy occurred in 158 /344 patients (45.9%) in the culprit lesion–only PCI group and 189/341 patients (55.4%) in the multivessel PCI group (relative risk [RR] 0.83, 95% CI 0.72–0.96, P = 0.01). The rate of death from any cause was lower in the culprit lesion–only PCI group compared to multivessel PCI group (RR 0.84, 95% CI 0.72–0.98, P = 0.03). There was no difference in stroke and numerically lower risk of bleeding in culprit lesion–only PCI group (RR 0.75, 95% CI 0.55–1.03).
Conclusion. Among patients who had multivessel coronary artery disease and acute myocardial infarction with cardiogenic shock, the 30-day risk of death or severe renal failure leading to renal replacement therapy was lower in patients who initially underwent PCI of the culprit lesion only compared with patients who underwent immediate multivessel PCI.
Commentary
Patients presenting with cardiogenic shock at the time of acute myocardial infarction have the highest mortality—up to 50%. Since the original SHOCK trial in 1999, it is known that the mortality can be reduced by early revascularization of the culprit vessel [1]. However, whether the non-culprit vessel should be revascularized at the time of presentation with acute myocardial infarction is unknown.
Recently, there have been multiple trials suggesting the benefit of non-culprit vessel revascularization in patients with acute myocardial infarction who are hemodynamically stable at the time of their presentation. Three recent trials—PRAMI, CvPRIT and DANAMI-PRIMULTI—investigated this clinical question and found benefit of non-culprit vessel revascularization [2–4]. The results of these trials led to a focused update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention in 2015 [5]. Noninfarct-related artery PCI in hemodynamically stable patients presenting with acute myocardial infarction was upgraded to class IIb from class III [5]. Whether these findings can be extended to hemodynamically unstable (cardiogenic shock) patients is not mentioned in the guidelines.
In the current CULPRIT-SHOCK trial, Thiele et al investigated this clinical question by performing a well-designed clinical trial in patients with acute myocardial infarction and cardiogenic shock. They found that the composite endpoint of death and renal replacement therapy at 30 days occurred more frequently in the multivessel PCI group compared with the culprit lesion–only group (relative risk [RR] 0.83, 95% CI 0.71–0.96, P = 0.01). The composite endpoint was mainly driven by death (43.3% vs 51.6%, RR 0.84, 95% CI 0.72–0.98, P = 0.03), and the rate of renal replacement therapy was numerically higher in the mutivessel PCI group (11.6% vs 16.4%, P = 0.07). The study was conducted in the sickest population compared to prior trials as evidenced by high rate of mechanical ventilation (~80%), requirement of catecholamine support (~90%), and long ICU stay (median 5 days). The significance of non-culprit lesion was determined by angiogram (stenosis > 70%). The culprit vessel–only group had treatment of the culprit vessel only initially, but the staged intervention for non-culprit vessel was encouraged.
A unique point of this trial is that patients with chronic total occlusion (CTO) were included in the study and it was encouraged to attempt revascularization of CTO lesions, contrary to previous trials. Although CTO intervention improves angina and ejection fraction [6,7], whether CTO intervention has a mortality benefit needs further investigation. In the CULPRIT-SHOCK trial, 24% of patients had one or more CTO lesions. This most likely contributed to the increased contrast use in the multivessel PCI group (250 vs 190 mL, P < 0.01). CTO is considered a most challenging lesion to treat, and expertise and skill level vary among operators. In the hybrid CTO intervention model, it is recommended to stage the intervention as much as possible, as this type of intervention requires meticulous planning [8]. There is a possibility that attempting CTO intervention in this acute setting caused more harm than benefit. Furthermore, the investigators did not report the success rate of CTO intervention.
Another interesting finding of this trial is that the mortality of both groups was high (43.3% vs 51.6%). The revascularization arm of the original shock trial almost 20 years ago had a 30-day mortality of 46.7%, which is almost identical with the current CULPRIT-SHOCK study. Despite improvement in hemodynamic support such as Impella, TandemHeart, extracorporeal membrane oxygenation device, and improvement in medical therapy over the years, patients with cardiogenic shock with acute myocardial infarction have a dismal prognosis.
The CULPRIT-SHOCK trial has number of strengths, including low drop-out rate (3%) and adequate power, however, there are some limitations. Some patients crossed over from culprit-vessel only to multivessel PCI group due to lack of hemodynamic improvement, plaque shifts, and newly detected lesions after treatment of the culprit lesion. On the other hand, some patients crossed over from multivessel PCI from culprit lesion only due to multiple reasons, including technical difficulty of intervention.
Applications for Clinical Practice
In patients presenting with cardiogenic shock and acute myocardial infarction, culprit lesion–only intervention and focusing on hemodynamic support with a staged intervention if necessary seems to be better strategy than immediate multivessel PCI, including non-culprit vessel PCI.
—Taishi Hirai, MD, University of Chicago Medical Center, Chicago, IL
Study Overview
Objective. To determine if percutaneous coronary intervention (PCI) of non-culprit vessels should be performed in patients with acute myocardial infarction and cardiogenic shock.
Design. Multicenter randomized controlled trial.
Setting and participants. 706 patients who had multivessel disease, acute myocardial infarction, and cardiogenic shock were assigned to one of 2 revascularization strategies: PCI of the culprit lesion only with the option of staged revascularization of non-culprit lesions, or immediate multivessel PCI.
Main outcome measures. The primary endpoint was the composite of death or severe renal failure leading to renal replacement therapy within 30 days after randomization. Safety endpoints included bleeding and stroke.
Main results. The primary endpoint of death or renal replacement therapy occurred in 158 /344 patients (45.9%) in the culprit lesion–only PCI group and 189/341 patients (55.4%) in the multivessel PCI group (relative risk [RR] 0.83, 95% CI 0.72–0.96, P = 0.01). The rate of death from any cause was lower in the culprit lesion–only PCI group compared to multivessel PCI group (RR 0.84, 95% CI 0.72–0.98, P = 0.03). There was no difference in stroke and numerically lower risk of bleeding in culprit lesion–only PCI group (RR 0.75, 95% CI 0.55–1.03).
Conclusion. Among patients who had multivessel coronary artery disease and acute myocardial infarction with cardiogenic shock, the 30-day risk of death or severe renal failure leading to renal replacement therapy was lower in patients who initially underwent PCI of the culprit lesion only compared with patients who underwent immediate multivessel PCI.
Commentary
Patients presenting with cardiogenic shock at the time of acute myocardial infarction have the highest mortality—up to 50%. Since the original SHOCK trial in 1999, it is known that the mortality can be reduced by early revascularization of the culprit vessel [1]. However, whether the non-culprit vessel should be revascularized at the time of presentation with acute myocardial infarction is unknown.
Recently, there have been multiple trials suggesting the benefit of non-culprit vessel revascularization in patients with acute myocardial infarction who are hemodynamically stable at the time of their presentation. Three recent trials—PRAMI, CvPRIT and DANAMI-PRIMULTI—investigated this clinical question and found benefit of non-culprit vessel revascularization [2–4]. The results of these trials led to a focused update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention in 2015 [5]. Noninfarct-related artery PCI in hemodynamically stable patients presenting with acute myocardial infarction was upgraded to class IIb from class III [5]. Whether these findings can be extended to hemodynamically unstable (cardiogenic shock) patients is not mentioned in the guidelines.
In the current CULPRIT-SHOCK trial, Thiele et al investigated this clinical question by performing a well-designed clinical trial in patients with acute myocardial infarction and cardiogenic shock. They found that the composite endpoint of death and renal replacement therapy at 30 days occurred more frequently in the multivessel PCI group compared with the culprit lesion–only group (relative risk [RR] 0.83, 95% CI 0.71–0.96, P = 0.01). The composite endpoint was mainly driven by death (43.3% vs 51.6%, RR 0.84, 95% CI 0.72–0.98, P = 0.03), and the rate of renal replacement therapy was numerically higher in the mutivessel PCI group (11.6% vs 16.4%, P = 0.07). The study was conducted in the sickest population compared to prior trials as evidenced by high rate of mechanical ventilation (~80%), requirement of catecholamine support (~90%), and long ICU stay (median 5 days). The significance of non-culprit lesion was determined by angiogram (stenosis > 70%). The culprit vessel–only group had treatment of the culprit vessel only initially, but the staged intervention for non-culprit vessel was encouraged.
A unique point of this trial is that patients with chronic total occlusion (CTO) were included in the study and it was encouraged to attempt revascularization of CTO lesions, contrary to previous trials. Although CTO intervention improves angina and ejection fraction [6,7], whether CTO intervention has a mortality benefit needs further investigation. In the CULPRIT-SHOCK trial, 24% of patients had one or more CTO lesions. This most likely contributed to the increased contrast use in the multivessel PCI group (250 vs 190 mL, P < 0.01). CTO is considered a most challenging lesion to treat, and expertise and skill level vary among operators. In the hybrid CTO intervention model, it is recommended to stage the intervention as much as possible, as this type of intervention requires meticulous planning [8]. There is a possibility that attempting CTO intervention in this acute setting caused more harm than benefit. Furthermore, the investigators did not report the success rate of CTO intervention.
Another interesting finding of this trial is that the mortality of both groups was high (43.3% vs 51.6%). The revascularization arm of the original shock trial almost 20 years ago had a 30-day mortality of 46.7%, which is almost identical with the current CULPRIT-SHOCK study. Despite improvement in hemodynamic support such as Impella, TandemHeart, extracorporeal membrane oxygenation device, and improvement in medical therapy over the years, patients with cardiogenic shock with acute myocardial infarction have a dismal prognosis.
The CULPRIT-SHOCK trial has number of strengths, including low drop-out rate (3%) and adequate power, however, there are some limitations. Some patients crossed over from culprit-vessel only to multivessel PCI group due to lack of hemodynamic improvement, plaque shifts, and newly detected lesions after treatment of the culprit lesion. On the other hand, some patients crossed over from multivessel PCI from culprit lesion only due to multiple reasons, including technical difficulty of intervention.
Applications for Clinical Practice
In patients presenting with cardiogenic shock and acute myocardial infarction, culprit lesion–only intervention and focusing on hemodynamic support with a staged intervention if necessary seems to be better strategy than immediate multivessel PCI, including non-culprit vessel PCI.
—Taishi Hirai, MD, University of Chicago Medical Center, Chicago, IL
1. Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should we emergently revascularize occluded coronaries for cardiogenic shock. N Engl J Med 1999;341:625–34.
2. Wald DS, Morris JK, Wald NJ, et al. Randomized trial of preventive angioplasty in myocardial infarction. N Engl J Med 2013;369:1115–23.
3. Gershlick AH, Khan JN, Kelly DJ, et al. Randomized trial of complete versus lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol 2015;65:963–72.
4. Engstrom T, Kelbaek H, Helqvist S, et al. Complete revasculari Outcomes Research in Review www.mdedge.com/jcomjournal Vol. 25, No. 3 March 2018 JCOM 103 sation versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3-PRIMULTI): an open-label, randomised controlled trial. Lancet 2015;386:665–71.
5. Levine GN, Bates ER, Blankenship JC, et al. 2015 ACC/AHA/SCAI Focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol 2016;67:1235–50.
6. Sapontis J, Salisbury AC, Yeh RW, et al. Early procedural and health status outcomes after chronic total occlusion angioplasty: a report from the OPEN-CTO Registry (Outcomes, Patient Health Status, and Efficiency in Chronic Total Occlusion Hybrid Procedures). JACC Cardiovasc Interv 2017;10:1523–34.
7. Henriques JP, Hoebers LP, Ramunddal T, et al. Percutaneous intervention for concurrent chronic total occlusions in patients with STEMI: the EXPLORE trial. J Am Coll Cardiol 2016;68:1622–32.
8. Brilakis ES, Grantham JA, Rinfret S, et al. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv 2012;5:367–79.
1. Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should we emergently revascularize occluded coronaries for cardiogenic shock. N Engl J Med 1999;341:625–34.
2. Wald DS, Morris JK, Wald NJ, et al. Randomized trial of preventive angioplasty in myocardial infarction. N Engl J Med 2013;369:1115–23.
3. Gershlick AH, Khan JN, Kelly DJ, et al. Randomized trial of complete versus lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol 2015;65:963–72.
4. Engstrom T, Kelbaek H, Helqvist S, et al. Complete revasculari Outcomes Research in Review www.mdedge.com/jcomjournal Vol. 25, No. 3 March 2018 JCOM 103 sation versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3-PRIMULTI): an open-label, randomised controlled trial. Lancet 2015;386:665–71.
5. Levine GN, Bates ER, Blankenship JC, et al. 2015 ACC/AHA/SCAI Focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol 2016;67:1235–50.
6. Sapontis J, Salisbury AC, Yeh RW, et al. Early procedural and health status outcomes after chronic total occlusion angioplasty: a report from the OPEN-CTO Registry (Outcomes, Patient Health Status, and Efficiency in Chronic Total Occlusion Hybrid Procedures). JACC Cardiovasc Interv 2017;10:1523–34.
7. Henriques JP, Hoebers LP, Ramunddal T, et al. Percutaneous intervention for concurrent chronic total occlusions in patients with STEMI: the EXPLORE trial. J Am Coll Cardiol 2016;68:1622–32.
8. Brilakis ES, Grantham JA, Rinfret S, et al. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv 2012;5:367–79.