User login
App monitoring improves quality of IBD care
WASHINGTON – in a single-center randomized study with 320 patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Based on this success, the app will soon be made available to all of the roughly 5,000 inflammatory bowel disease (IBD) patients managed at Mount Sinai Medical Center in New York as well as IBD patients at several other North American centers that plan to adopt the app, Ashish Atreja, MD, said at the annual Digestive Disease Week.®
Home monitoring of IBD patients “is feasible with high adoption,” said Dr. Atreja, a gastroenterologist at Mount Sinai who directs the Sinai AppLab. The 162 IBD patients randomized to regularly use the HealthPROMISE app had their quality-of-care metric rise from 50% at baseline to 84% after an average follow-up of 575 days (19 months), a statistically significant improvement over the 158 control patients whose metric rose from 50% to 65% for the study’s primary endpoint, he reported. The results also showed a trend toward improved quality of life among the patients using the HealthPROMISE app, compared with the controls, who used an IBD educational app that produced less patient engagement than did the HealthPROMISE app, Dr Atreja said.
Dr. Atreja and his associates modeled the app on remote monitoring methods developed for patients with other types of chronic disease, such as diabetes and heart failure.
“You can’t provide proactive IBD care without remote monitoring,” Dr. Atreja explained in a video interview. “Reactive care is not best practice anymore. The only way to do treat-to-target is with remote monitoring.”
Care coordinators monitor the entries that IBD patients send in via the app. Dr. Atreja estimated that about five care coordinators will be able to track the inputs from the roughly 5,000 IBD patients at Mount Sinai who will soon begin using the app. The financial feasibility of this approach depends in part on the $45/patient per month reimbursement that U.S. health insurers now provide to centers that run remote monitoring programs, he said.
“The direction for managing chronic diseases is increasingly looking at home monitoring as a way to streamline costs and improve patient care,” commented Gil Y. Melmed, MD, director of Clinical Inflammatory Bowel Disease at Cedars-Sinai Medical Center in Los Angeles. The results that Dr. Atreja reported came from “a highly selected population that was well educated and largely white.” The study needs replication in different patient groups to establish its reproducibility and generalizability, Dr. Melmed said in an interview.
Dr. Melmed had no relevant disclosures.
[email protected]
On Twitter @mitchelzoler
SOURCE: Atreja A et al. Digestive Disease Week 2018 abstract 17.
*This story was updated on June 7, 2018.
WASHINGTON – in a single-center randomized study with 320 patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Based on this success, the app will soon be made available to all of the roughly 5,000 inflammatory bowel disease (IBD) patients managed at Mount Sinai Medical Center in New York as well as IBD patients at several other North American centers that plan to adopt the app, Ashish Atreja, MD, said at the annual Digestive Disease Week.®
Home monitoring of IBD patients “is feasible with high adoption,” said Dr. Atreja, a gastroenterologist at Mount Sinai who directs the Sinai AppLab. The 162 IBD patients randomized to regularly use the HealthPROMISE app had their quality-of-care metric rise from 50% at baseline to 84% after an average follow-up of 575 days (19 months), a statistically significant improvement over the 158 control patients whose metric rose from 50% to 65% for the study’s primary endpoint, he reported. The results also showed a trend toward improved quality of life among the patients using the HealthPROMISE app, compared with the controls, who used an IBD educational app that produced less patient engagement than did the HealthPROMISE app, Dr Atreja said.
Dr. Atreja and his associates modeled the app on remote monitoring methods developed for patients with other types of chronic disease, such as diabetes and heart failure.
“You can’t provide proactive IBD care without remote monitoring,” Dr. Atreja explained in a video interview. “Reactive care is not best practice anymore. The only way to do treat-to-target is with remote monitoring.”
Care coordinators monitor the entries that IBD patients send in via the app. Dr. Atreja estimated that about five care coordinators will be able to track the inputs from the roughly 5,000 IBD patients at Mount Sinai who will soon begin using the app. The financial feasibility of this approach depends in part on the $45/patient per month reimbursement that U.S. health insurers now provide to centers that run remote monitoring programs, he said.
“The direction for managing chronic diseases is increasingly looking at home monitoring as a way to streamline costs and improve patient care,” commented Gil Y. Melmed, MD, director of Clinical Inflammatory Bowel Disease at Cedars-Sinai Medical Center in Los Angeles. The results that Dr. Atreja reported came from “a highly selected population that was well educated and largely white.” The study needs replication in different patient groups to establish its reproducibility and generalizability, Dr. Melmed said in an interview.
Dr. Melmed had no relevant disclosures.
[email protected]
On Twitter @mitchelzoler
SOURCE: Atreja A et al. Digestive Disease Week 2018 abstract 17.
*This story was updated on June 7, 2018.
WASHINGTON – in a single-center randomized study with 320 patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Based on this success, the app will soon be made available to all of the roughly 5,000 inflammatory bowel disease (IBD) patients managed at Mount Sinai Medical Center in New York as well as IBD patients at several other North American centers that plan to adopt the app, Ashish Atreja, MD, said at the annual Digestive Disease Week.®
Home monitoring of IBD patients “is feasible with high adoption,” said Dr. Atreja, a gastroenterologist at Mount Sinai who directs the Sinai AppLab. The 162 IBD patients randomized to regularly use the HealthPROMISE app had their quality-of-care metric rise from 50% at baseline to 84% after an average follow-up of 575 days (19 months), a statistically significant improvement over the 158 control patients whose metric rose from 50% to 65% for the study’s primary endpoint, he reported. The results also showed a trend toward improved quality of life among the patients using the HealthPROMISE app, compared with the controls, who used an IBD educational app that produced less patient engagement than did the HealthPROMISE app, Dr Atreja said.
Dr. Atreja and his associates modeled the app on remote monitoring methods developed for patients with other types of chronic disease, such as diabetes and heart failure.
“You can’t provide proactive IBD care without remote monitoring,” Dr. Atreja explained in a video interview. “Reactive care is not best practice anymore. The only way to do treat-to-target is with remote monitoring.”
Care coordinators monitor the entries that IBD patients send in via the app. Dr. Atreja estimated that about five care coordinators will be able to track the inputs from the roughly 5,000 IBD patients at Mount Sinai who will soon begin using the app. The financial feasibility of this approach depends in part on the $45/patient per month reimbursement that U.S. health insurers now provide to centers that run remote monitoring programs, he said.
“The direction for managing chronic diseases is increasingly looking at home monitoring as a way to streamline costs and improve patient care,” commented Gil Y. Melmed, MD, director of Clinical Inflammatory Bowel Disease at Cedars-Sinai Medical Center in Los Angeles. The results that Dr. Atreja reported came from “a highly selected population that was well educated and largely white.” The study needs replication in different patient groups to establish its reproducibility and generalizability, Dr. Melmed said in an interview.
Dr. Melmed had no relevant disclosures.
[email protected]
On Twitter @mitchelzoler
SOURCE: Atreja A et al. Digestive Disease Week 2018 abstract 17.
*This story was updated on June 7, 2018.
REPORTING FROM DDW 2018
Key clinical point: Regular remote monitoring of IBD patients improved the medical care they received.
Major finding: Quality of care rose from 50% at baseline to 84% in app-monitored patients and to 65% in controls.
Study details: A single-center randomized study with 320 IBD patients.
Disclosures: The study had no commercial funding. Dr. Atreja had no disclosures.
Source: Atreja A et al. Digestive Disease Week 2018 abstract 17.

Timely dermatomyositis diagnosis, treatment remain elusive
ORLANDO – There was a median 1-year delay between the onset of symptoms and diagnosis of classic dermatomyositis, and a 17-month delay before diagnosis of amyopathic dermatomyositis, based on a review of 232 dermatomyositis patients seen at the University of Pennsylvania, Philadelphia.
Just 103 (44.4%) patients were diagnosed with dermatomyositis (DM) right out of the gate. Among the other 129, 48 (37.2%) were diagnosed with lupus, 38 (29.5%) with undifferentiated connective tissue disease, 10 (7.8%) went undiagnosed, and 33 (25.5%) were diagnosed with rosacea, psoriasis, rheumatoid arthritis, fibromyalgia, lichen planus, and a number of other conditions. By the time the DM diagnosis was finally confirmed, almost every patient had Gottron’s papules or sign.
Misdiagnosis of dermatomyositis (DM) is nothing new, but the study brings home just how common the problem is, even at a major academic medical institution.
One of the take homes is that , and remain vigilant for erythema on the lateral thighs or nasolabial fold, Gottron’s papules, and other diagnostic giveaways, the researchers said.

Interface dermatitis, in particular, can’t be relied on to differentiate the conditions. A better option is checking for lupus bands and membrane attack complexes on direct immunofluorescence.
There’s also just not enough awareness that dermatomyositis can present without the classic muscle symptoms and findings, i.e. clinically amyopathic DM. While 49 of 120 patients with classic dermatomyositis (40.8%) were misdiagnosed or undiagnosed in the study, the number rose to 80 of 112 (71.4%) among amyopathic patients.
“We saw that there was a much higher rate of misdiagnosis in patients who didn’t have any muscle disease. We have to raise awareness that amyopathic dermatomyositis is a very prevalent condition,” Dr. Patel said at the International Conference on Cutaneous Lupus Erythematosus.
“There might be some level of subclinical muscle activity where, if you did an MRI, you might see inflammation, but the patient doesn’t report any symptoms. There are also patients that don’t have any muscle findings on MRI, or elevated muscle enzymes, but still have the skin findings,” he said.
Perhaps the markedly increased risk of cancer in DM, especially within a year or 2 of symptom onset, is the strongest argument for earlier diagnosis. “There’s also a risk of interstitial lung disease, so making sure that you’re getting pulmonary function tests and age-appropriate malignancy screening in a timely fashion is very important,” Dr. Patel said.
Also, although many of the initial treatments for DM – sun protection and topical steroids and calcineurin inhibitors, for instance – are the same as for cutaneous lupus, medications like mycophenolate mofetil and methotrexate are used more readily. The sooner DM is recognized for what it is, the sooner patients can get relief, he said.
Almost all the patients were white women. The majority were 40-80 years old.
There was no industry funding for the work, and Dr. Patel didn’t have any disclosures.
SOURCE: da Silva DM et al. Presented at the 2018 International Conference on Cutaneous Lupus Erythematosus
ORLANDO – There was a median 1-year delay between the onset of symptoms and diagnosis of classic dermatomyositis, and a 17-month delay before diagnosis of amyopathic dermatomyositis, based on a review of 232 dermatomyositis patients seen at the University of Pennsylvania, Philadelphia.
Just 103 (44.4%) patients were diagnosed with dermatomyositis (DM) right out of the gate. Among the other 129, 48 (37.2%) were diagnosed with lupus, 38 (29.5%) with undifferentiated connective tissue disease, 10 (7.8%) went undiagnosed, and 33 (25.5%) were diagnosed with rosacea, psoriasis, rheumatoid arthritis, fibromyalgia, lichen planus, and a number of other conditions. By the time the DM diagnosis was finally confirmed, almost every patient had Gottron’s papules or sign.
Misdiagnosis of dermatomyositis (DM) is nothing new, but the study brings home just how common the problem is, even at a major academic medical institution.
One of the take homes is that , and remain vigilant for erythema on the lateral thighs or nasolabial fold, Gottron’s papules, and other diagnostic giveaways, the researchers said.
Interface dermatitis, in particular, can’t be relied on to differentiate the conditions. A better option is checking for lupus bands and membrane attack complexes on direct immunofluorescence.
There’s also just not enough awareness that dermatomyositis can present without the classic muscle symptoms and findings, i.e. clinically amyopathic DM. While 49 of 120 patients with classic dermatomyositis (40.8%) were misdiagnosed or undiagnosed in the study, the number rose to 80 of 112 (71.4%) among amyopathic patients.
“We saw that there was a much higher rate of misdiagnosis in patients who didn’t have any muscle disease. We have to raise awareness that amyopathic dermatomyositis is a very prevalent condition,” Dr. Patel said at the International Conference on Cutaneous Lupus Erythematosus.
“There might be some level of subclinical muscle activity where, if you did an MRI, you might see inflammation, but the patient doesn’t report any symptoms. There are also patients that don’t have any muscle findings on MRI, or elevated muscle enzymes, but still have the skin findings,” he said.
Perhaps the markedly increased risk of cancer in DM, especially within a year or 2 of symptom onset, is the strongest argument for earlier diagnosis. “There’s also a risk of interstitial lung disease, so making sure that you’re getting pulmonary function tests and age-appropriate malignancy screening in a timely fashion is very important,” Dr. Patel said.
Also, although many of the initial treatments for DM – sun protection and topical steroids and calcineurin inhibitors, for instance – are the same as for cutaneous lupus, medications like mycophenolate mofetil and methotrexate are used more readily. The sooner DM is recognized for what it is, the sooner patients can get relief, he said.
Almost all the patients were white women. The majority were 40-80 years old.
There was no industry funding for the work, and Dr. Patel didn’t have any disclosures.
SOURCE: da Silva DM et al. Presented at the 2018 International Conference on Cutaneous Lupus Erythematosus
ORLANDO – There was a median 1-year delay between the onset of symptoms and diagnosis of classic dermatomyositis, and a 17-month delay before diagnosis of amyopathic dermatomyositis, based on a review of 232 dermatomyositis patients seen at the University of Pennsylvania, Philadelphia.
Just 103 (44.4%) patients were diagnosed with dermatomyositis (DM) right out of the gate. Among the other 129, 48 (37.2%) were diagnosed with lupus, 38 (29.5%) with undifferentiated connective tissue disease, 10 (7.8%) went undiagnosed, and 33 (25.5%) were diagnosed with rosacea, psoriasis, rheumatoid arthritis, fibromyalgia, lichen planus, and a number of other conditions. By the time the DM diagnosis was finally confirmed, almost every patient had Gottron’s papules or sign.
Misdiagnosis of dermatomyositis (DM) is nothing new, but the study brings home just how common the problem is, even at a major academic medical institution.
One of the take homes is that , and remain vigilant for erythema on the lateral thighs or nasolabial fold, Gottron’s papules, and other diagnostic giveaways, the researchers said.
Interface dermatitis, in particular, can’t be relied on to differentiate the conditions. A better option is checking for lupus bands and membrane attack complexes on direct immunofluorescence.
There’s also just not enough awareness that dermatomyositis can present without the classic muscle symptoms and findings, i.e. clinically amyopathic DM. While 49 of 120 patients with classic dermatomyositis (40.8%) were misdiagnosed or undiagnosed in the study, the number rose to 80 of 112 (71.4%) among amyopathic patients.
“We saw that there was a much higher rate of misdiagnosis in patients who didn’t have any muscle disease. We have to raise awareness that amyopathic dermatomyositis is a very prevalent condition,” Dr. Patel said at the International Conference on Cutaneous Lupus Erythematosus.
“There might be some level of subclinical muscle activity where, if you did an MRI, you might see inflammation, but the patient doesn’t report any symptoms. There are also patients that don’t have any muscle findings on MRI, or elevated muscle enzymes, but still have the skin findings,” he said.
Perhaps the markedly increased risk of cancer in DM, especially within a year or 2 of symptom onset, is the strongest argument for earlier diagnosis. “There’s also a risk of interstitial lung disease, so making sure that you’re getting pulmonary function tests and age-appropriate malignancy screening in a timely fashion is very important,” Dr. Patel said.
Also, although many of the initial treatments for DM – sun protection and topical steroids and calcineurin inhibitors, for instance – are the same as for cutaneous lupus, medications like mycophenolate mofetil and methotrexate are used more readily. The sooner DM is recognized for what it is, the sooner patients can get relief, he said.
Almost all the patients were white women. The majority were 40-80 years old.
There was no industry funding for the work, and Dr. Patel didn’t have any disclosures.
SOURCE: da Silva DM et al. Presented at the 2018 International Conference on Cutaneous Lupus Erythematosus
REPORTING FROM ICCLE 2018
Key clinical point: Clinicians need to do a better job of catching DM early.
Major finding: It took a median of 12.2 months after the start of symptoms to diagnose classic dermatomyositis, and 17.1 months to diagnose amyopathic dermatomyositis.
Study details: Review of 232 patients
Disclosures: There was no industry funding, and the presenter didn’t have any disclosures.
Source: da Silva DM et al. Presented at the 2018 International Conference on Cutaneous Lupus Erythematosus
Ivosidenib leads to complete responses in 32% of IDH1-mutated relapsed/refractory AML
CHICAGO – The investigational drug ivosidenib was associated with durable responses, transfusion independence, and a low rate of serious adverse events in patients with IDH1-mutated relapsed/refractory acute myeloid leukemia (AML), based on results of a phase 1 study presented at the annual meeting of the American Society of Clinical Oncology (ASCO).
Daily oral ivosidenib, which inhibits mutant IDH1 the gene that encodes for isocitrate dehydrogenase 1 and is present in 6%-10% of AML patients, was associated with a complete response rate of nearly 32%. In patients who achieved a complete response, median duration of response was 8.2 months and median overall survival was 18.8 months, Daniel A. Pollyea, MD, University of Colorado School of Medicine, Aurora, reported at the meeting.
A wide variety of study participants achieved transfusion independence, even patients who had lesser and no discernable responses, Dr. Pollyea said. “A significant minority of these patients (with lesser or no response) were able to achieve transfusion independence which is obviously a big achievement with respect to quality of life, and suggestive of the mechanism of action here with respect to differentiation.”
The conclusions of this study are “striking,” with response rates and tolerability “very similar” to results seen with the IDH2 inhibitor enasidenib, said Eunice S. Wang, MD, of Roswell Park Comprehensive Cancer Center, Buffalo, N.Y.
Ivosidenib is “likely to become the new standard of care treatment” for IDH1-mutant patients in the relapsed-refractory setting based on the data presented at ASCO, Dr. Wang said in a presentation commenting on the results.
“Given the development of ivosidenib and enasidenib, I think we should all carefully consider whether testing of IDH1 and IDH2 mutational status should also become standard of care in all relapsed and refractory patients, in order to offer them these novel and highly effective as well as well-tolerated targeted therapies,” she said.
Enasidenib was approved by the U.S. Food and Drug Administration (FDA) in 2017 for relapsed or refractory AML with an IDH2 mutation.
Here at ASCO, Dr. Pollyea reported results based on 179 patients with relapsed/refractory IDH1-mutant AML who received 500 mg of ivosidenib daily.
The overall response rate was 41.9% (75 patients), he said. The rate of complete remission (CR) or CR with partial hematologic recovery (CRh) was 31.8% (57 patients), with a median of 2.0 months to CR/CRh and a median duration of CR/CRh of 8.2 months, he said.
Grade 3 or greater leukocytosis was seen in 8% of patients, and grade 3 or greater QT prolongation was seen in 10% of patients, Dr. Pollyea reported.
IHD differentiation syndrome of any grade was seen in 19 patients (10.6%), and about half of those cases (5%) were grade 3 or greater. However, cases were managed with supportive care, and there were no dose reductions, permanent treatment discontinuations, or deaths due to the condition, Dr. Pollyea said.
Moreover, the majority of those patients (10 out of 19) went on to have a response. “Supportive care and continued treatment can allow for patients ultimately to respond who are experiencing differentiation syndrome,” Dr. Pollyea said.
Results of the phase 1 study were published simultaneously in the New England Journal of Medicine.The trial was sponsored by Agios. Dr. Pollyea reported disclosures related to Agios, as well as Abbvie, argenx, Celgene, Celyad, Curis, Pfizer, and Servier.
SOURCE: Pollyea DA, et al. J Clin Oncol36, 2018 (suppl; abstr 7000).
CHICAGO – The investigational drug ivosidenib was associated with durable responses, transfusion independence, and a low rate of serious adverse events in patients with IDH1-mutated relapsed/refractory acute myeloid leukemia (AML), based on results of a phase 1 study presented at the annual meeting of the American Society of Clinical Oncology (ASCO).
Daily oral ivosidenib, which inhibits mutant IDH1 the gene that encodes for isocitrate dehydrogenase 1 and is present in 6%-10% of AML patients, was associated with a complete response rate of nearly 32%. In patients who achieved a complete response, median duration of response was 8.2 months and median overall survival was 18.8 months, Daniel A. Pollyea, MD, University of Colorado School of Medicine, Aurora, reported at the meeting.
A wide variety of study participants achieved transfusion independence, even patients who had lesser and no discernable responses, Dr. Pollyea said. “A significant minority of these patients (with lesser or no response) were able to achieve transfusion independence which is obviously a big achievement with respect to quality of life, and suggestive of the mechanism of action here with respect to differentiation.”
The conclusions of this study are “striking,” with response rates and tolerability “very similar” to results seen with the IDH2 inhibitor enasidenib, said Eunice S. Wang, MD, of Roswell Park Comprehensive Cancer Center, Buffalo, N.Y.
Ivosidenib is “likely to become the new standard of care treatment” for IDH1-mutant patients in the relapsed-refractory setting based on the data presented at ASCO, Dr. Wang said in a presentation commenting on the results.
“Given the development of ivosidenib and enasidenib, I think we should all carefully consider whether testing of IDH1 and IDH2 mutational status should also become standard of care in all relapsed and refractory patients, in order to offer them these novel and highly effective as well as well-tolerated targeted therapies,” she said.
Enasidenib was approved by the U.S. Food and Drug Administration (FDA) in 2017 for relapsed or refractory AML with an IDH2 mutation.
Here at ASCO, Dr. Pollyea reported results based on 179 patients with relapsed/refractory IDH1-mutant AML who received 500 mg of ivosidenib daily.
The overall response rate was 41.9% (75 patients), he said. The rate of complete remission (CR) or CR with partial hematologic recovery (CRh) was 31.8% (57 patients), with a median of 2.0 months to CR/CRh and a median duration of CR/CRh of 8.2 months, he said.
Grade 3 or greater leukocytosis was seen in 8% of patients, and grade 3 or greater QT prolongation was seen in 10% of patients, Dr. Pollyea reported.
IHD differentiation syndrome of any grade was seen in 19 patients (10.6%), and about half of those cases (5%) were grade 3 or greater. However, cases were managed with supportive care, and there were no dose reductions, permanent treatment discontinuations, or deaths due to the condition, Dr. Pollyea said.
Moreover, the majority of those patients (10 out of 19) went on to have a response. “Supportive care and continued treatment can allow for patients ultimately to respond who are experiencing differentiation syndrome,” Dr. Pollyea said.
Results of the phase 1 study were published simultaneously in the New England Journal of Medicine.The trial was sponsored by Agios. Dr. Pollyea reported disclosures related to Agios, as well as Abbvie, argenx, Celgene, Celyad, Curis, Pfizer, and Servier.
SOURCE: Pollyea DA, et al. J Clin Oncol36, 2018 (suppl; abstr 7000).
CHICAGO – The investigational drug ivosidenib was associated with durable responses, transfusion independence, and a low rate of serious adverse events in patients with IDH1-mutated relapsed/refractory acute myeloid leukemia (AML), based on results of a phase 1 study presented at the annual meeting of the American Society of Clinical Oncology (ASCO).
Daily oral ivosidenib, which inhibits mutant IDH1 the gene that encodes for isocitrate dehydrogenase 1 and is present in 6%-10% of AML patients, was associated with a complete response rate of nearly 32%. In patients who achieved a complete response, median duration of response was 8.2 months and median overall survival was 18.8 months, Daniel A. Pollyea, MD, University of Colorado School of Medicine, Aurora, reported at the meeting.
A wide variety of study participants achieved transfusion independence, even patients who had lesser and no discernable responses, Dr. Pollyea said. “A significant minority of these patients (with lesser or no response) were able to achieve transfusion independence which is obviously a big achievement with respect to quality of life, and suggestive of the mechanism of action here with respect to differentiation.”
The conclusions of this study are “striking,” with response rates and tolerability “very similar” to results seen with the IDH2 inhibitor enasidenib, said Eunice S. Wang, MD, of Roswell Park Comprehensive Cancer Center, Buffalo, N.Y.
Ivosidenib is “likely to become the new standard of care treatment” for IDH1-mutant patients in the relapsed-refractory setting based on the data presented at ASCO, Dr. Wang said in a presentation commenting on the results.
“Given the development of ivosidenib and enasidenib, I think we should all carefully consider whether testing of IDH1 and IDH2 mutational status should also become standard of care in all relapsed and refractory patients, in order to offer them these novel and highly effective as well as well-tolerated targeted therapies,” she said.
Enasidenib was approved by the U.S. Food and Drug Administration (FDA) in 2017 for relapsed or refractory AML with an IDH2 mutation.
Here at ASCO, Dr. Pollyea reported results based on 179 patients with relapsed/refractory IDH1-mutant AML who received 500 mg of ivosidenib daily.
The overall response rate was 41.9% (75 patients), he said. The rate of complete remission (CR) or CR with partial hematologic recovery (CRh) was 31.8% (57 patients), with a median of 2.0 months to CR/CRh and a median duration of CR/CRh of 8.2 months, he said.
Grade 3 or greater leukocytosis was seen in 8% of patients, and grade 3 or greater QT prolongation was seen in 10% of patients, Dr. Pollyea reported.
IHD differentiation syndrome of any grade was seen in 19 patients (10.6%), and about half of those cases (5%) were grade 3 or greater. However, cases were managed with supportive care, and there were no dose reductions, permanent treatment discontinuations, or deaths due to the condition, Dr. Pollyea said.
Moreover, the majority of those patients (10 out of 19) went on to have a response. “Supportive care and continued treatment can allow for patients ultimately to respond who are experiencing differentiation syndrome,” Dr. Pollyea said.
Results of the phase 1 study were published simultaneously in the New England Journal of Medicine.The trial was sponsored by Agios. Dr. Pollyea reported disclosures related to Agios, as well as Abbvie, argenx, Celgene, Celyad, Curis, Pfizer, and Servier.
SOURCE: Pollyea DA, et al. J Clin Oncol36, 2018 (suppl; abstr 7000).
REPORTING FROM ASCO 2018
Key clinical point: Daily oral ivosidenib was associated with a complete response rate of nearly 32% and a low rate of serious adverse events in patients with IDH1-mutated relapsed/refractory acute myeloid leukemia (AML).
Major finding: Patients with complete responses had an 8.2-month duration of response, and a median overall survival of 18.8 months.
Study details: A phase 1 study including 179 patients who received 500 mg of ivosidenib daily.
Disclosures: Daniel A. Pollyea, MD, who presented the study, reported disclosures related to Abbvie, Agios, argenx, Celgene, Celyad, Curis, Pfizer, and Servier.
Source: Pollyea DA, et al. J Clin Oncol 36, 2018 (suppl; abstr 7000).
Tumor analysis: Test all MSI-high patients for Lynch Syndrome
CHICAGO – , according to “absolutely practice changing” findings from a prospective analysis of more than 15,000 tumor samples.

“The impact of these findings cannot be understated,” ASCO expert Shannon N. Westin, MD, said during a discussion of the findings presented by Zsofia K. Stadler, MD, at a press briefing at the annual meeting of the American Society of Clinical Oncology.
Lynch Syndrome (LS), an autosomal dominant inherited cancer predisposition syndrome caused by germline mutation in the DNA mismatch repair genes, is responsible for about 3% of colorectal and endometrial cancers; universal testing for tumor markers of LS is recommended in all patients with these types of cancers, said Dr. Stadler, director of the Clinical Genetics Service at Memorial Sloan Kettering Cancer Center, New York.
“This is usually done either via MSI analysis or immunohistochemical staining for the DNA mismatch repair proteins,” she said, noting that genetic testing and counseling is recommended in patients with tumors suggestive of LS, and increased surveillance and/or risk-reducing surgery is recommended in those recognized as having LS.
MSI-high is a hallmark of LS-associated cancers and has recently been implicated as a marker for response to immunotherapy. This has led to increased MSI testing in metastatic cancer regardless of cancer type.
However, the prevalence of germline mutations in the DNA mismatch repair genes diagnostic of LS across all MSI-high tumors is unknown, she said.
In 15,045 tumor samples across more than 50 cancer types, germline mutations were analyzed across tumor types and according to MSI status.
As expected, the highest level of MSI-high was seen in small bowel cancer (25%), followed by endometrial, colorectal, and gastric cancer (16%, 14%, and 6%, respectively), Dr. Stadler said.
“High frequency MSI was also seen in a number of other tumors as suggested by other papers previously,” she noted.
LS was present in 16.3% of MSI-high tumors vs. 1.9% of MSI-indeterminate (moderate MSI level) tumors, and 0.3% of microsatellite stable (MSS) tumors, she added.
Additional tumor evaluations, including immunohistochemical staining for the mismatch repair genes, were also performed.
“Our analysis corroborated the finding that in these Lynch patients, the MSI-high and MSI-indeterminate tumors were caused by Lynch Syndrome. This is in contrast to our Lynch Syndrome patients with microsatellite stable tumors; their tumor signature suggested that the Lynch Syndrome did not cause these cancers,” she said. “In fact, the prevalence of Lynch Syndrome in the MSS cohort of 0.3% is equivalent to the presence of Lynch Syndrome in the general at-large population.”
Of note, 50% of LS patients with MSI-high and indeterminate tumors had cancers other than colorectal or endometrial cancer, including prostate, sarcoma, mesothelioma, adrenocortical carcinoma, and ovarian germ cell carcinoma, which have been rarely or not previously associated with LS, and 45% of those patients did not meet clinical testing criteria for LS and would not have undergone LS testing.
This finding underscores the previously unknown heterogeneity of the phenotype.
“Our study supports that MSI-high is predictive of LS across tumor types...and also supports that the spectrum of cancers associated with Lynch Syndrome seems to be much broader that previously thought, she said, concluding that “MSI-high tumor signature, regardless of cancer subtype and irrespective of the family cancer history, should prompt germline genetic assessment for the evaluation of Lynch [Syndrome].
“This will result in an increased ability to recognize Lynch Syndrome not only in cancer patients, but also in at-risk family members who will benefit from genetic testing for Lynch [Syndrome] and subsequent enhanced cancer surveillance and risk reduction measures.”
In emphasizing the practice-changing nature of these findings, Dr. Westin, a gynecologic oncologist at MD Anderson Cancer Center, Houston, said that with the rise of precision medicine, increasing numbers of patients are undergoing testing for microsatellite instability, mainly to determine if their tumor can be affected by an-approved therapy.
“What we’ve learned is that MSI not only has therapeutic implications, it also has cancer prevention implications,” she said. “We’ve only been testing the tip of the iceberg of patients who are affected by Lynch Syndrome, and what we now know is that under the surface there is a larger number of patients with specific cancer types that should be tested for Lynch Syndrome.”
She added that this is “a straightforward testing strategy which can be immediately implemented to impact not only the patients themselves and their risk of cancer, but also their family members and their risk of cancer.”
This study was funded by Romeo Milio Lynch Syndrome Foundation, the Marie-Josee and Henry R. Kravis Center for Molecular Oncology, the Robert and Kate Niehaus Center for Inherited Cancer Genomics, the Fieldstone Family Fund, Stand Up to Cancer Colorectal Cancer Dream Team Translational Research Grant and the NIH/NCI Cancer Center Support Grant. Dr. Stadler reported consulting or advisory roles on the part of an immediate family member for Allergan, Genentech/Roche, Regeneron, Optos, and Adverum.
SOURCE: Schwark A et al., ASCO 2018 LBA1509.
CHICAGO – , according to “absolutely practice changing” findings from a prospective analysis of more than 15,000 tumor samples.
“The impact of these findings cannot be understated,” ASCO expert Shannon N. Westin, MD, said during a discussion of the findings presented by Zsofia K. Stadler, MD, at a press briefing at the annual meeting of the American Society of Clinical Oncology.
Lynch Syndrome (LS), an autosomal dominant inherited cancer predisposition syndrome caused by germline mutation in the DNA mismatch repair genes, is responsible for about 3% of colorectal and endometrial cancers; universal testing for tumor markers of LS is recommended in all patients with these types of cancers, said Dr. Stadler, director of the Clinical Genetics Service at Memorial Sloan Kettering Cancer Center, New York.
“This is usually done either via MSI analysis or immunohistochemical staining for the DNA mismatch repair proteins,” she said, noting that genetic testing and counseling is recommended in patients with tumors suggestive of LS, and increased surveillance and/or risk-reducing surgery is recommended in those recognized as having LS.
MSI-high is a hallmark of LS-associated cancers and has recently been implicated as a marker for response to immunotherapy. This has led to increased MSI testing in metastatic cancer regardless of cancer type.
However, the prevalence of germline mutations in the DNA mismatch repair genes diagnostic of LS across all MSI-high tumors is unknown, she said.
In 15,045 tumor samples across more than 50 cancer types, germline mutations were analyzed across tumor types and according to MSI status.
As expected, the highest level of MSI-high was seen in small bowel cancer (25%), followed by endometrial, colorectal, and gastric cancer (16%, 14%, and 6%, respectively), Dr. Stadler said.
“High frequency MSI was also seen in a number of other tumors as suggested by other papers previously,” she noted.
LS was present in 16.3% of MSI-high tumors vs. 1.9% of MSI-indeterminate (moderate MSI level) tumors, and 0.3% of microsatellite stable (MSS) tumors, she added.
Additional tumor evaluations, including immunohistochemical staining for the mismatch repair genes, were also performed.
“Our analysis corroborated the finding that in these Lynch patients, the MSI-high and MSI-indeterminate tumors were caused by Lynch Syndrome. This is in contrast to our Lynch Syndrome patients with microsatellite stable tumors; their tumor signature suggested that the Lynch Syndrome did not cause these cancers,” she said. “In fact, the prevalence of Lynch Syndrome in the MSS cohort of 0.3% is equivalent to the presence of Lynch Syndrome in the general at-large population.”
Of note, 50% of LS patients with MSI-high and indeterminate tumors had cancers other than colorectal or endometrial cancer, including prostate, sarcoma, mesothelioma, adrenocortical carcinoma, and ovarian germ cell carcinoma, which have been rarely or not previously associated with LS, and 45% of those patients did not meet clinical testing criteria for LS and would not have undergone LS testing.
This finding underscores the previously unknown heterogeneity of the phenotype.
“Our study supports that MSI-high is predictive of LS across tumor types...and also supports that the spectrum of cancers associated with Lynch Syndrome seems to be much broader that previously thought, she said, concluding that “MSI-high tumor signature, regardless of cancer subtype and irrespective of the family cancer history, should prompt germline genetic assessment for the evaluation of Lynch [Syndrome].
“This will result in an increased ability to recognize Lynch Syndrome not only in cancer patients, but also in at-risk family members who will benefit from genetic testing for Lynch [Syndrome] and subsequent enhanced cancer surveillance and risk reduction measures.”
In emphasizing the practice-changing nature of these findings, Dr. Westin, a gynecologic oncologist at MD Anderson Cancer Center, Houston, said that with the rise of precision medicine, increasing numbers of patients are undergoing testing for microsatellite instability, mainly to determine if their tumor can be affected by an-approved therapy.
“What we’ve learned is that MSI not only has therapeutic implications, it also has cancer prevention implications,” she said. “We’ve only been testing the tip of the iceberg of patients who are affected by Lynch Syndrome, and what we now know is that under the surface there is a larger number of patients with specific cancer types that should be tested for Lynch Syndrome.”
She added that this is “a straightforward testing strategy which can be immediately implemented to impact not only the patients themselves and their risk of cancer, but also their family members and their risk of cancer.”
This study was funded by Romeo Milio Lynch Syndrome Foundation, the Marie-Josee and Henry R. Kravis Center for Molecular Oncology, the Robert and Kate Niehaus Center for Inherited Cancer Genomics, the Fieldstone Family Fund, Stand Up to Cancer Colorectal Cancer Dream Team Translational Research Grant and the NIH/NCI Cancer Center Support Grant. Dr. Stadler reported consulting or advisory roles on the part of an immediate family member for Allergan, Genentech/Roche, Regeneron, Optos, and Adverum.
SOURCE: Schwark A et al., ASCO 2018 LBA1509.
CHICAGO – , according to “absolutely practice changing” findings from a prospective analysis of more than 15,000 tumor samples.
“The impact of these findings cannot be understated,” ASCO expert Shannon N. Westin, MD, said during a discussion of the findings presented by Zsofia K. Stadler, MD, at a press briefing at the annual meeting of the American Society of Clinical Oncology.
Lynch Syndrome (LS), an autosomal dominant inherited cancer predisposition syndrome caused by germline mutation in the DNA mismatch repair genes, is responsible for about 3% of colorectal and endometrial cancers; universal testing for tumor markers of LS is recommended in all patients with these types of cancers, said Dr. Stadler, director of the Clinical Genetics Service at Memorial Sloan Kettering Cancer Center, New York.
“This is usually done either via MSI analysis or immunohistochemical staining for the DNA mismatch repair proteins,” she said, noting that genetic testing and counseling is recommended in patients with tumors suggestive of LS, and increased surveillance and/or risk-reducing surgery is recommended in those recognized as having LS.
MSI-high is a hallmark of LS-associated cancers and has recently been implicated as a marker for response to immunotherapy. This has led to increased MSI testing in metastatic cancer regardless of cancer type.
However, the prevalence of germline mutations in the DNA mismatch repair genes diagnostic of LS across all MSI-high tumors is unknown, she said.
In 15,045 tumor samples across more than 50 cancer types, germline mutations were analyzed across tumor types and according to MSI status.
As expected, the highest level of MSI-high was seen in small bowel cancer (25%), followed by endometrial, colorectal, and gastric cancer (16%, 14%, and 6%, respectively), Dr. Stadler said.
“High frequency MSI was also seen in a number of other tumors as suggested by other papers previously,” she noted.
LS was present in 16.3% of MSI-high tumors vs. 1.9% of MSI-indeterminate (moderate MSI level) tumors, and 0.3% of microsatellite stable (MSS) tumors, she added.
Additional tumor evaluations, including immunohistochemical staining for the mismatch repair genes, were also performed.
“Our analysis corroborated the finding that in these Lynch patients, the MSI-high and MSI-indeterminate tumors were caused by Lynch Syndrome. This is in contrast to our Lynch Syndrome patients with microsatellite stable tumors; their tumor signature suggested that the Lynch Syndrome did not cause these cancers,” she said. “In fact, the prevalence of Lynch Syndrome in the MSS cohort of 0.3% is equivalent to the presence of Lynch Syndrome in the general at-large population.”
Of note, 50% of LS patients with MSI-high and indeterminate tumors had cancers other than colorectal or endometrial cancer, including prostate, sarcoma, mesothelioma, adrenocortical carcinoma, and ovarian germ cell carcinoma, which have been rarely or not previously associated with LS, and 45% of those patients did not meet clinical testing criteria for LS and would not have undergone LS testing.
This finding underscores the previously unknown heterogeneity of the phenotype.
“Our study supports that MSI-high is predictive of LS across tumor types...and also supports that the spectrum of cancers associated with Lynch Syndrome seems to be much broader that previously thought, she said, concluding that “MSI-high tumor signature, regardless of cancer subtype and irrespective of the family cancer history, should prompt germline genetic assessment for the evaluation of Lynch [Syndrome].
“This will result in an increased ability to recognize Lynch Syndrome not only in cancer patients, but also in at-risk family members who will benefit from genetic testing for Lynch [Syndrome] and subsequent enhanced cancer surveillance and risk reduction measures.”
In emphasizing the practice-changing nature of these findings, Dr. Westin, a gynecologic oncologist at MD Anderson Cancer Center, Houston, said that with the rise of precision medicine, increasing numbers of patients are undergoing testing for microsatellite instability, mainly to determine if their tumor can be affected by an-approved therapy.
“What we’ve learned is that MSI not only has therapeutic implications, it also has cancer prevention implications,” she said. “We’ve only been testing the tip of the iceberg of patients who are affected by Lynch Syndrome, and what we now know is that under the surface there is a larger number of patients with specific cancer types that should be tested for Lynch Syndrome.”
She added that this is “a straightforward testing strategy which can be immediately implemented to impact not only the patients themselves and their risk of cancer, but also their family members and their risk of cancer.”
This study was funded by Romeo Milio Lynch Syndrome Foundation, the Marie-Josee and Henry R. Kravis Center for Molecular Oncology, the Robert and Kate Niehaus Center for Inherited Cancer Genomics, the Fieldstone Family Fund, Stand Up to Cancer Colorectal Cancer Dream Team Translational Research Grant and the NIH/NCI Cancer Center Support Grant. Dr. Stadler reported consulting or advisory roles on the part of an immediate family member for Allergan, Genentech/Roche, Regeneron, Optos, and Adverum.
SOURCE: Schwark A et al., ASCO 2018 LBA1509.
REPORTING FROM ASCO 2018
Key clinical point: All MSI-high patients should be tested for LS regardless of cancer type or family history.
Major finding: LS was present in 16.3% of MSI-high tumors vs. 1.9% and 0.3% of MSI-indeterminate and stable tumors, respectively.
Study details: An analysis of 15,045 tumor samples.
Disclosures: This study was funded by Romeo Milio Lynch Syndrome Foundation, the Marie-Josee and Henry R. Kravis Center for Molecular Oncology, the Robert and Kate Niehaus Center for Inherited Cancer Genomics, the Fieldstone Family Fund, Stand Up to Cancer Colorectal Cancer Dream Team Translational Research Grant, and the NIH/NCI Cancer Center Support Grant. Dr. Stadler reported consulting or advisory roles on the part of an immediate family member for Allergan, Genentech/Roche, Regeneron, Optos, and Adverum.
Source: Schwark A et al. ASCO 2018 LBA 1509.
Setting and Method of Measurement Affect Blood Pressure Readings in Older Veterans
Seventy-five percent of adults aged >75 years have hypertension.1-3 According to the Joint National Commission 8 (JNC 8), the recommended target blood pressure (BP) is < 150/80 mm Hg for adults aged > 60 years.4 In 2016 the Systolic Blood Pressure Intervention Trial (SPRINT) suggested that more aggressive BP control with a goal of < 120/80 mm Hg reduced rates of cardiovascular disease and lowered the risk of death in adults aged > 50 years with hypertension.5 It is anticipated that as a result of the landmark SPRINT results, clinicians may attempt to treat hypertension more intensely in older patients with an increased risk of adverse consequences if BPs are not appropriately measured.
There is a standardized protocol for BP measurement, but these recommendations typically are not followed in routine office visits.6,7 Some studies have noted that home BP measurement may be more accurate than office measurement.8 However, clinicians may not always trust the accuracy of home BP readings, and many patients are not adherent with home measurement. As a result, physicians usually manage hypertension in older patients based on office readings, though it is likely that most office measurements do not follow protocol on proper measurement. Office measurements have been noted to be inaccurate with high likelihood of overestimating or underestimating BP control.9
Office BP measurements demonstrate poor correlation with home measurements and have not been shown to be as good of a predictor for target organ damage or long-term cardiovascular outcomes compared with that of home measurements.10,11 Although there have been studies comparing home and office BP measurements and comparing office and ambulatory BP measurement, no literature has been found that reports on the difference between routine office and standardized measurement of BP.9,12-14
This study seeks to identify the magnitude of difference among BP measured according to a standardized protocol, routine clinical, and home BP. The authors hypothesized that there would be a significant, clinically relevant difference among the 3 BP measurement methods, especially between the routine office and standardized office measurements. This study has implications for implementing intensive treatment of hypertension based on office measurements.
Methods
Participants included 30 male veterans aged > 65 years who were actively participating in the Gerofit program at the VA Greater Los Angeles Healthcare System (VAGLAHS). The Gerofit program is a model clinical demonstration exercise and health promotion program targeting older and veterans at risk for falls or institutionalization. Gerofit was established in 1987 at the Durham VA Health System and successfully implemented in 2014 at VAGLAHS. Supervised exercise is offered 3 times per week and consists of individually tailored exercises aimed at reducing functional deficits that are identified and monitored by an initial and quarterly functional assessment. Blood pressures are checked routinely once a week as a part of the program. Gerofit was reviewed and approved by the institutional review board at VAGLAHS as a quality improvement/quality assurance project.
Data
Routine office and standardized protocol measurements were obtained by a single CasMED 740 (Branford, CT) automated BP machine and were conducted separately on different days. The CasMED 740 machine was not otherwise calibrated; however, a one-time correlation was performed between the CasMED 740 and the home BP monitor for each participant, when it was brought to VAGLAHS. Two measurements were made with the CasMed 740 automated BP machine on the arm that gave the higher BP reading throughout the standardized and routine protocol. Two subsequent measurements were made with the participant’s home automated BP cuff. Averages for the CasMED 740 and the home BP monitoring device were compared and assessed for significance by paired t test. No rest was scheduled prior to the first measurement, but there was a 1-minute rest after each subsequent measurement.
Mean values (SD) were used for participant characteristics and mean values (standard error [SE]) were used for BP measurements. Data were analyzed using Microsoft Excel (Redmond, WA) and GraphPad Prism version 7.03 (San Diego, CA). T tests were used for analysis of home BP measurements due to low sample size. Values of P < .05 were considered to be statistically significant.
Routine office protocol. Automated BP was measured to mimic routine office visits. Upon arrival, participants sat down, and the BP cuff was placed around their arm. Any rest before a measurement was incidental and not intentionally structured. Appropriate cuff size was determined by visual estimation of arm circumference. Only 1 measurement was made unless BP was > 150/90 mm Hg, in which case a repeat measurement was made after 2 to 4 minutes of rest. The BP was then determined based on the average of 2 or more readings. The BPs were recorded by hand in a weekly log. Participants had at least 12 weeks of BP readings measured by the routine method, and these BPs were averaged over 12 weeks to yield their average routine measured BP.
Standardized protocol. Automated BP was measured according to the 2015 USPSTF Guidelines and Look AHEAD trial protocol.7,15 A participant’s arm circumference was measured, and appropriate cuff size was determined. The participant rested quietly in a chair for at least 5 minutes with feet flat on the floor and back supported. The cuff was snugly placed 2 to 3 cm above the antecubital fossa, and the arm was supported at the level of the right atrium during the measurement. Blood pressure was determined using the mean of 4 automated cuff readings, 2 on each arm, taken 1 minute apart. Participants did not necessarily have their BP measured by the standardized method immediately following the routine method but all measurements were performed during the same 12-week time period.
Home blood pressure protocol. Participants were given instructions according to the American Heart Association (AHA) recommendations for measuring home BP. Patients were instructed to use a calibrated, automated arm BP cuff. Home BP machines were not provided in advance, and each individual’s BP machine was not calibrated. They also were instructed to rest at least 5 minutes before measuring their BP. The mean home BP was determined by the cumulative average of 3 readings in the morning and evening, taken 1 minute between each reading, for a total of 6 readings/d. Participants recorded home BPs for 2 weeks before submitting their readings. Each participant affirmed clear understanding of how to measure BP by correctly demonstrating placement of the cuff 1 time under supervision.
Results
Thirty veterans aged > 65 years participated in the study. The average age (SD) was 82.7 (9.3) years. The average BMI (SD) was overweight at 29.7 kg/m2 (5.7). Most (87.6%) of the study participants had been diagnosed with hypertension prior to the study, and no new diagnoses were made as a result of the study. 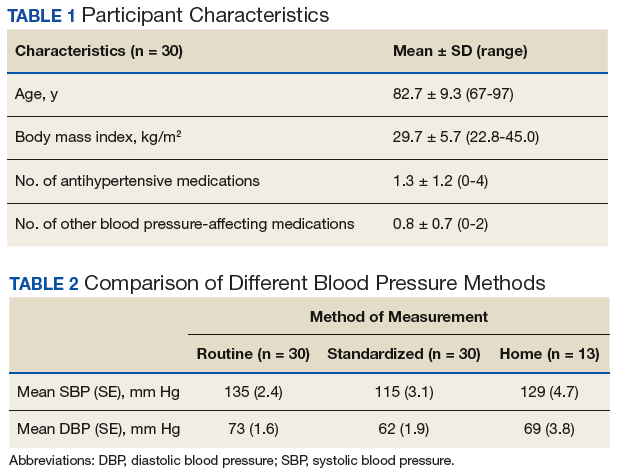
Both systolic BP (SBP) and diastolic BPs (DBP) measured by the standardized method were significantly lower than those by the routine method (P < .01 and P < .01, respectively) (Figure 1). 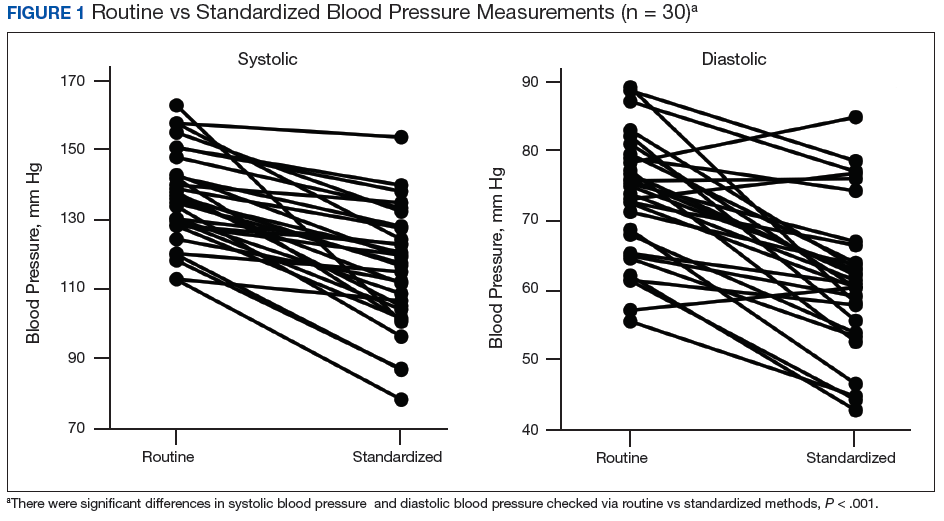
To determine the accuracy of the home BP monitors, the average routine VAGLAHS BP measure was compared with home BP results. For SBPs, there was a significant correlation coefficient of 0.91 (P < .01). 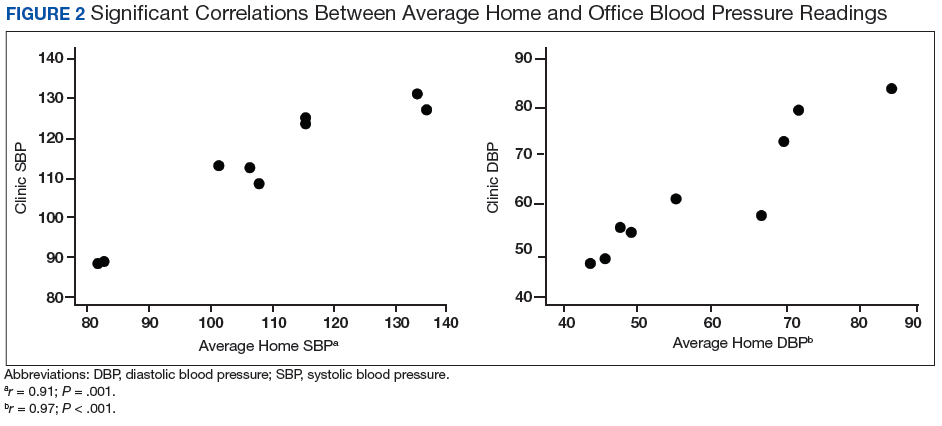
Discussion
The present study demonstrated that standardized measurements of BP were lower than that of the routine method used in most office settings. These results suggest that there could be a risk of overtreatment for some patients those of whose results are higher than the SPRINT BP target of < 120/80 mm Hg. Clinicians might be treating BPs that are elevated due to improper measurement, which can lead to deleterious consequences in older adults, such as syncope and falls.16
Each participant exhibited a significantly lower BP reading with the standardized method than the routine method. The 20-point decrease in SBP and 10-point decrease in DBP are clinically significant. The routine method of measurement was intended to simulate BP measurement in outpatient settings. There is usually little time structured for rest, and because the protocol established by the AHA and other professional organizations is time consuming, it usually is not strictly followed. With guidelines proposed by JNC 8 and new findings from SPRINT, the method of BP readings should be reviewed in all clinical settings.
While changes in BP management are not necessarily immediate, the differences in recommendations proposed by SPRINT and JNC 8 can lead to confusion regarding how intensely to treat BP. These recommendations guide clinical practice, but clinicians’ best judgment ultimately determines BP management. Physicians who utilize routine office measurements likely rely on BP readings that are higher on average than are readings done under proper conditions. This leads to the prospect of overtreatment, where physicians attempt to control hypertension too aggressively, potentially leading to orthostatic hypotension, syncope, and increased risk for falls.16 With findings from SPRINT recommending even lower BPs than that by JNC 8, overtreatment risk becomes especially relevant. While BP protocol was strictly followed in SPRINT, some clinicians may not necessarily follow the same fastidious protocol.
The average differences between the home and standardized BPs were not statistically significant possibly due to the small sample size in the home BP measurements; however, the difference might represent some clinical relevance. There was a 15-point difference in SBP results between home (129 mm Hg) and standardized (115 mm Hg) measures. There also was a difference in DBP between home (69 mm Hg) and standardized (62 mm Hg) results. The close correlation between both home and BPs measured in VAGLAHS demonstrated that any difference was not due to variability in the measurement devices. Previous studies have demonstrated that home BPs are better indicators of cardiovascular risk than office BP.8
Despite lack of statistical significance, home BPs were lower than routine, which suggests that they still may be more reliable than routine office measurements. Definitive conclusions regarding the accuracy of the home BPs in the present study cannot be drawn due to the small sample size (n = 13). Further exploration with comparisons to ambulatory BP monitoring could yield more information on accuracy of home BP monitoring.
In this study’s cohort of older veterans, the average BMI was between 25 and 30 (overweight), which is a risk factor for hypertension.17 Every participant with hypertension was taking at least 1 antihypertensive medication and being actively managed. In this study, the authors accounted for other medications that may affect BP, such as α blockers used in patients with benign prostatic hyperplasia.18 These could have potential elevating or lowering effects on BP measurements.
An issue in this study was the lack of adherence to home BP monitoring. Many patients forgot to bring in their records or to measure their BPs at home. The difficulties highlight real-life issues. Clinicians often request that patients monitor their BP at home, but few may actually remember, let alone keep diligent records. There are many barriers between measuring and reporting home BPs, which may prevent the usefulness of monitoring BP at home.
Limitations
There were several limitations to the study. There was no specific protocol for the routine method of BP measurement, as it was intended to simulate the haphazard nature of office measurements. However, this approach limits its reproducibility. For home BP monitoring, it would have been ideal to provide the same calibrated, automated BP device to each participant. This study of older veterans may not be applicable to the general population. Finally, the relatively small number of participants in the study (n = 30) may have limited power in drawing definitive conclusions.
Future Directions
For future studies, comparing the standardized method to ambulatory BP monitoring would provide more information on accuracy. In addition, the authors would like to evaluate the effect of exercise on BP measurements in the different settings: home, standardized, and routine methods.
1. Mozaffarian D, Benjamin EJ, Go AS, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29-e322.
2. Benjamin EJ, Blaha MJ, Chiuve SE, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146-e603.
3. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;(133):1-8.
4. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
5. Williamson JD, Supiano MA, Applegate WB, et al; SPRINT Research Group. Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged ≥ 75 years: a randomized clinical trial. JAMA. 2016;315(24):2673-2682.
6. Pickering TG, Hall JE, Appel LJ, et al; Council on High Blood Pressure Research Professional and Public Education Subcommittee, American Heart Association. Recommendations for blood pressure measurement in humans: an AHA scientific statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee. J Clin Hypertens (Greenwich). 2005;7(2):102-109.
7. Siu AL; U.S. Preventive Services Task Force. Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;163(10):778-786.
8. Niiranen TJ, Hänninen MR, Johansson J, Reunanen A, Jula AM. Home-measured blood pressure is a stronger predictor of cardiovascular risk than office blood pressure: the Finn-Home study. Hypertension. 2010;55(6):1346-1351.
9. Reino-Gonzalez S, Pita-Fernández S, Seoane-Pillado T, López-Calviño B, Pértega Díaz S. How in-office and ambulatory BP monitoring compare: a systematic review and meta-analysis. J Fam Pract. 2017;66(1):E5-E12.
10. Cohen JB, Cohen DL. Integrating out-of-office blood pressure in the diagnosis and management of hypertension. Curr Cardiol Rep. 2016;18(11):112.
11. Fuchs SC, Mello RB, Fuchs FC. Home blood pressure monitoring is better predictor of cardiovascular disease and target organ damage than office blood pressure: a systematic review and meta-analysis. Curr Cardiol Rep. 2013;15(11):413.
12. Imai Y, Obara T, Asamaya K, Ohkubo T. The reason why home blood pressure measurements are preferred over clinic or ambulatory blood pressure in Japan. Hypertens Res. 2013;36(8):661-672.
13. Bliziotis IA, Destounis A, Stergiou GS. Home versus ambulatory and office blood pressure in predicting target organ damage in hypertension: a systematic review and meta-analysis. J Hypertens. 2012;30(7):1289-1299.
14. Yang Y, Xu JZ, Wang Y, Gao PJ. Ambulatory versus clinic blood pressure in predicting overall subclinical target organ damage progression in essential hypertensive patients: a 3-year follow-up study. Blood Press Monit. 2016;21(6):319-326.
15. Espeland MA, Probstfield J, Hire D, et al; Look AHEAD Research Group; ACCORD Study Group. Systolic blood pressure control among individuals with type 2 diabetes: a comparative effectiveness analysis of three interventions. Am J Hypertens. 2015;28(8):995-1009.
16. Weiss J, Freeman M, Low A, et al. Benefits and harms of intensive blood pressure treatment in adults aged 60 years or older: a systematic review and meta-analysis. Ann Intern Med. 2017;166(6):419-429.
17. Nagai M, Ohkubo T, Murakami Y, et al; NIPPON DATA80/90/2010 Research Group. Secular trends of the impact of overweight and obesity on hypertension in Japan, 1980-2010. Hypertens Res. 2015;38(11):790-795.
18. Press Y, Punchik B, Freud T. Orthostatic hypotension and drug therapy in patients at an outpatient comprehensive geriatric assessment unit. J Hypertens. 2016;34(2):351-358.
Seventy-five percent of adults aged >75 years have hypertension.1-3 According to the Joint National Commission 8 (JNC 8), the recommended target blood pressure (BP) is < 150/80 mm Hg for adults aged > 60 years.4 In 2016 the Systolic Blood Pressure Intervention Trial (SPRINT) suggested that more aggressive BP control with a goal of < 120/80 mm Hg reduced rates of cardiovascular disease and lowered the risk of death in adults aged > 50 years with hypertension.5 It is anticipated that as a result of the landmark SPRINT results, clinicians may attempt to treat hypertension more intensely in older patients with an increased risk of adverse consequences if BPs are not appropriately measured.
There is a standardized protocol for BP measurement, but these recommendations typically are not followed in routine office visits.6,7 Some studies have noted that home BP measurement may be more accurate than office measurement.8 However, clinicians may not always trust the accuracy of home BP readings, and many patients are not adherent with home measurement. As a result, physicians usually manage hypertension in older patients based on office readings, though it is likely that most office measurements do not follow protocol on proper measurement. Office measurements have been noted to be inaccurate with high likelihood of overestimating or underestimating BP control.9
Office BP measurements demonstrate poor correlation with home measurements and have not been shown to be as good of a predictor for target organ damage or long-term cardiovascular outcomes compared with that of home measurements.10,11 Although there have been studies comparing home and office BP measurements and comparing office and ambulatory BP measurement, no literature has been found that reports on the difference between routine office and standardized measurement of BP.9,12-14
This study seeks to identify the magnitude of difference among BP measured according to a standardized protocol, routine clinical, and home BP. The authors hypothesized that there would be a significant, clinically relevant difference among the 3 BP measurement methods, especially between the routine office and standardized office measurements. This study has implications for implementing intensive treatment of hypertension based on office measurements.
Methods
Participants included 30 male veterans aged > 65 years who were actively participating in the Gerofit program at the VA Greater Los Angeles Healthcare System (VAGLAHS). The Gerofit program is a model clinical demonstration exercise and health promotion program targeting older and veterans at risk for falls or institutionalization. Gerofit was established in 1987 at the Durham VA Health System and successfully implemented in 2014 at VAGLAHS. Supervised exercise is offered 3 times per week and consists of individually tailored exercises aimed at reducing functional deficits that are identified and monitored by an initial and quarterly functional assessment. Blood pressures are checked routinely once a week as a part of the program. Gerofit was reviewed and approved by the institutional review board at VAGLAHS as a quality improvement/quality assurance project.
Data
Routine office and standardized protocol measurements were obtained by a single CasMED 740 (Branford, CT) automated BP machine and were conducted separately on different days. The CasMED 740 machine was not otherwise calibrated; however, a one-time correlation was performed between the CasMED 740 and the home BP monitor for each participant, when it was brought to VAGLAHS. Two measurements were made with the CasMed 740 automated BP machine on the arm that gave the higher BP reading throughout the standardized and routine protocol. Two subsequent measurements were made with the participant’s home automated BP cuff. Averages for the CasMED 740 and the home BP monitoring device were compared and assessed for significance by paired t test. No rest was scheduled prior to the first measurement, but there was a 1-minute rest after each subsequent measurement.
Mean values (SD) were used for participant characteristics and mean values (standard error [SE]) were used for BP measurements. Data were analyzed using Microsoft Excel (Redmond, WA) and GraphPad Prism version 7.03 (San Diego, CA). T tests were used for analysis of home BP measurements due to low sample size. Values of P < .05 were considered to be statistically significant.
Routine office protocol. Automated BP was measured to mimic routine office visits. Upon arrival, participants sat down, and the BP cuff was placed around their arm. Any rest before a measurement was incidental and not intentionally structured. Appropriate cuff size was determined by visual estimation of arm circumference. Only 1 measurement was made unless BP was > 150/90 mm Hg, in which case a repeat measurement was made after 2 to 4 minutes of rest. The BP was then determined based on the average of 2 or more readings. The BPs were recorded by hand in a weekly log. Participants had at least 12 weeks of BP readings measured by the routine method, and these BPs were averaged over 12 weeks to yield their average routine measured BP.
Standardized protocol. Automated BP was measured according to the 2015 USPSTF Guidelines and Look AHEAD trial protocol.7,15 A participant’s arm circumference was measured, and appropriate cuff size was determined. The participant rested quietly in a chair for at least 5 minutes with feet flat on the floor and back supported. The cuff was snugly placed 2 to 3 cm above the antecubital fossa, and the arm was supported at the level of the right atrium during the measurement. Blood pressure was determined using the mean of 4 automated cuff readings, 2 on each arm, taken 1 minute apart. Participants did not necessarily have their BP measured by the standardized method immediately following the routine method but all measurements were performed during the same 12-week time period.
Home blood pressure protocol. Participants were given instructions according to the American Heart Association (AHA) recommendations for measuring home BP. Patients were instructed to use a calibrated, automated arm BP cuff. Home BP machines were not provided in advance, and each individual’s BP machine was not calibrated. They also were instructed to rest at least 5 minutes before measuring their BP. The mean home BP was determined by the cumulative average of 3 readings in the morning and evening, taken 1 minute between each reading, for a total of 6 readings/d. Participants recorded home BPs for 2 weeks before submitting their readings. Each participant affirmed clear understanding of how to measure BP by correctly demonstrating placement of the cuff 1 time under supervision.
Results
Thirty veterans aged > 65 years participated in the study. The average age (SD) was 82.7 (9.3) years. The average BMI (SD) was overweight at 29.7 kg/m2 (5.7). Most (87.6%) of the study participants had been diagnosed with hypertension prior to the study, and no new diagnoses were made as a result of the study.
Both systolic BP (SBP) and diastolic BPs (DBP) measured by the standardized method were significantly lower than those by the routine method (P < .01 and P < .01, respectively) (Figure 1).
To determine the accuracy of the home BP monitors, the average routine VAGLAHS BP measure was compared with home BP results. For SBPs, there was a significant correlation coefficient of 0.91 (P < .01).
Discussion
The present study demonstrated that standardized measurements of BP were lower than that of the routine method used in most office settings. These results suggest that there could be a risk of overtreatment for some patients those of whose results are higher than the SPRINT BP target of < 120/80 mm Hg. Clinicians might be treating BPs that are elevated due to improper measurement, which can lead to deleterious consequences in older adults, such as syncope and falls.16
Each participant exhibited a significantly lower BP reading with the standardized method than the routine method. The 20-point decrease in SBP and 10-point decrease in DBP are clinically significant. The routine method of measurement was intended to simulate BP measurement in outpatient settings. There is usually little time structured for rest, and because the protocol established by the AHA and other professional organizations is time consuming, it usually is not strictly followed. With guidelines proposed by JNC 8 and new findings from SPRINT, the method of BP readings should be reviewed in all clinical settings.
While changes in BP management are not necessarily immediate, the differences in recommendations proposed by SPRINT and JNC 8 can lead to confusion regarding how intensely to treat BP. These recommendations guide clinical practice, but clinicians’ best judgment ultimately determines BP management. Physicians who utilize routine office measurements likely rely on BP readings that are higher on average than are readings done under proper conditions. This leads to the prospect of overtreatment, where physicians attempt to control hypertension too aggressively, potentially leading to orthostatic hypotension, syncope, and increased risk for falls.16 With findings from SPRINT recommending even lower BPs than that by JNC 8, overtreatment risk becomes especially relevant. While BP protocol was strictly followed in SPRINT, some clinicians may not necessarily follow the same fastidious protocol.
The average differences between the home and standardized BPs were not statistically significant possibly due to the small sample size in the home BP measurements; however, the difference might represent some clinical relevance. There was a 15-point difference in SBP results between home (129 mm Hg) and standardized (115 mm Hg) measures. There also was a difference in DBP between home (69 mm Hg) and standardized (62 mm Hg) results. The close correlation between both home and BPs measured in VAGLAHS demonstrated that any difference was not due to variability in the measurement devices. Previous studies have demonstrated that home BPs are better indicators of cardiovascular risk than office BP.8
Despite lack of statistical significance, home BPs were lower than routine, which suggests that they still may be more reliable than routine office measurements. Definitive conclusions regarding the accuracy of the home BPs in the present study cannot be drawn due to the small sample size (n = 13). Further exploration with comparisons to ambulatory BP monitoring could yield more information on accuracy of home BP monitoring.
In this study’s cohort of older veterans, the average BMI was between 25 and 30 (overweight), which is a risk factor for hypertension.17 Every participant with hypertension was taking at least 1 antihypertensive medication and being actively managed. In this study, the authors accounted for other medications that may affect BP, such as α blockers used in patients with benign prostatic hyperplasia.18 These could have potential elevating or lowering effects on BP measurements.
An issue in this study was the lack of adherence to home BP monitoring. Many patients forgot to bring in their records or to measure their BPs at home. The difficulties highlight real-life issues. Clinicians often request that patients monitor their BP at home, but few may actually remember, let alone keep diligent records. There are many barriers between measuring and reporting home BPs, which may prevent the usefulness of monitoring BP at home.
Limitations
There were several limitations to the study. There was no specific protocol for the routine method of BP measurement, as it was intended to simulate the haphazard nature of office measurements. However, this approach limits its reproducibility. For home BP monitoring, it would have been ideal to provide the same calibrated, automated BP device to each participant. This study of older veterans may not be applicable to the general population. Finally, the relatively small number of participants in the study (n = 30) may have limited power in drawing definitive conclusions.
Future Directions
For future studies, comparing the standardized method to ambulatory BP monitoring would provide more information on accuracy. In addition, the authors would like to evaluate the effect of exercise on BP measurements in the different settings: home, standardized, and routine methods.
Seventy-five percent of adults aged >75 years have hypertension.1-3 According to the Joint National Commission 8 (JNC 8), the recommended target blood pressure (BP) is < 150/80 mm Hg for adults aged > 60 years.4 In 2016 the Systolic Blood Pressure Intervention Trial (SPRINT) suggested that more aggressive BP control with a goal of < 120/80 mm Hg reduced rates of cardiovascular disease and lowered the risk of death in adults aged > 50 years with hypertension.5 It is anticipated that as a result of the landmark SPRINT results, clinicians may attempt to treat hypertension more intensely in older patients with an increased risk of adverse consequences if BPs are not appropriately measured.
There is a standardized protocol for BP measurement, but these recommendations typically are not followed in routine office visits.6,7 Some studies have noted that home BP measurement may be more accurate than office measurement.8 However, clinicians may not always trust the accuracy of home BP readings, and many patients are not adherent with home measurement. As a result, physicians usually manage hypertension in older patients based on office readings, though it is likely that most office measurements do not follow protocol on proper measurement. Office measurements have been noted to be inaccurate with high likelihood of overestimating or underestimating BP control.9
Office BP measurements demonstrate poor correlation with home measurements and have not been shown to be as good of a predictor for target organ damage or long-term cardiovascular outcomes compared with that of home measurements.10,11 Although there have been studies comparing home and office BP measurements and comparing office and ambulatory BP measurement, no literature has been found that reports on the difference between routine office and standardized measurement of BP.9,12-14
This study seeks to identify the magnitude of difference among BP measured according to a standardized protocol, routine clinical, and home BP. The authors hypothesized that there would be a significant, clinically relevant difference among the 3 BP measurement methods, especially between the routine office and standardized office measurements. This study has implications for implementing intensive treatment of hypertension based on office measurements.
Methods
Participants included 30 male veterans aged > 65 years who were actively participating in the Gerofit program at the VA Greater Los Angeles Healthcare System (VAGLAHS). The Gerofit program is a model clinical demonstration exercise and health promotion program targeting older and veterans at risk for falls or institutionalization. Gerofit was established in 1987 at the Durham VA Health System and successfully implemented in 2014 at VAGLAHS. Supervised exercise is offered 3 times per week and consists of individually tailored exercises aimed at reducing functional deficits that are identified and monitored by an initial and quarterly functional assessment. Blood pressures are checked routinely once a week as a part of the program. Gerofit was reviewed and approved by the institutional review board at VAGLAHS as a quality improvement/quality assurance project.
Data
Routine office and standardized protocol measurements were obtained by a single CasMED 740 (Branford, CT) automated BP machine and were conducted separately on different days. The CasMED 740 machine was not otherwise calibrated; however, a one-time correlation was performed between the CasMED 740 and the home BP monitor for each participant, when it was brought to VAGLAHS. Two measurements were made with the CasMed 740 automated BP machine on the arm that gave the higher BP reading throughout the standardized and routine protocol. Two subsequent measurements were made with the participant’s home automated BP cuff. Averages for the CasMED 740 and the home BP monitoring device were compared and assessed for significance by paired t test. No rest was scheduled prior to the first measurement, but there was a 1-minute rest after each subsequent measurement.
Mean values (SD) were used for participant characteristics and mean values (standard error [SE]) were used for BP measurements. Data were analyzed using Microsoft Excel (Redmond, WA) and GraphPad Prism version 7.03 (San Diego, CA). T tests were used for analysis of home BP measurements due to low sample size. Values of P < .05 were considered to be statistically significant.
Routine office protocol. Automated BP was measured to mimic routine office visits. Upon arrival, participants sat down, and the BP cuff was placed around their arm. Any rest before a measurement was incidental and not intentionally structured. Appropriate cuff size was determined by visual estimation of arm circumference. Only 1 measurement was made unless BP was > 150/90 mm Hg, in which case a repeat measurement was made after 2 to 4 minutes of rest. The BP was then determined based on the average of 2 or more readings. The BPs were recorded by hand in a weekly log. Participants had at least 12 weeks of BP readings measured by the routine method, and these BPs were averaged over 12 weeks to yield their average routine measured BP.
Standardized protocol. Automated BP was measured according to the 2015 USPSTF Guidelines and Look AHEAD trial protocol.7,15 A participant’s arm circumference was measured, and appropriate cuff size was determined. The participant rested quietly in a chair for at least 5 minutes with feet flat on the floor and back supported. The cuff was snugly placed 2 to 3 cm above the antecubital fossa, and the arm was supported at the level of the right atrium during the measurement. Blood pressure was determined using the mean of 4 automated cuff readings, 2 on each arm, taken 1 minute apart. Participants did not necessarily have their BP measured by the standardized method immediately following the routine method but all measurements were performed during the same 12-week time period.
Home blood pressure protocol. Participants were given instructions according to the American Heart Association (AHA) recommendations for measuring home BP. Patients were instructed to use a calibrated, automated arm BP cuff. Home BP machines were not provided in advance, and each individual’s BP machine was not calibrated. They also were instructed to rest at least 5 minutes before measuring their BP. The mean home BP was determined by the cumulative average of 3 readings in the morning and evening, taken 1 minute between each reading, for a total of 6 readings/d. Participants recorded home BPs for 2 weeks before submitting their readings. Each participant affirmed clear understanding of how to measure BP by correctly demonstrating placement of the cuff 1 time under supervision.
Results
Thirty veterans aged > 65 years participated in the study. The average age (SD) was 82.7 (9.3) years. The average BMI (SD) was overweight at 29.7 kg/m2 (5.7). Most (87.6%) of the study participants had been diagnosed with hypertension prior to the study, and no new diagnoses were made as a result of the study.
Both systolic BP (SBP) and diastolic BPs (DBP) measured by the standardized method were significantly lower than those by the routine method (P < .01 and P < .01, respectively) (Figure 1).
To determine the accuracy of the home BP monitors, the average routine VAGLAHS BP measure was compared with home BP results. For SBPs, there was a significant correlation coefficient of 0.91 (P < .01).
Discussion
The present study demonstrated that standardized measurements of BP were lower than that of the routine method used in most office settings. These results suggest that there could be a risk of overtreatment for some patients those of whose results are higher than the SPRINT BP target of < 120/80 mm Hg. Clinicians might be treating BPs that are elevated due to improper measurement, which can lead to deleterious consequences in older adults, such as syncope and falls.16
Each participant exhibited a significantly lower BP reading with the standardized method than the routine method. The 20-point decrease in SBP and 10-point decrease in DBP are clinically significant. The routine method of measurement was intended to simulate BP measurement in outpatient settings. There is usually little time structured for rest, and because the protocol established by the AHA and other professional organizations is time consuming, it usually is not strictly followed. With guidelines proposed by JNC 8 and new findings from SPRINT, the method of BP readings should be reviewed in all clinical settings.
While changes in BP management are not necessarily immediate, the differences in recommendations proposed by SPRINT and JNC 8 can lead to confusion regarding how intensely to treat BP. These recommendations guide clinical practice, but clinicians’ best judgment ultimately determines BP management. Physicians who utilize routine office measurements likely rely on BP readings that are higher on average than are readings done under proper conditions. This leads to the prospect of overtreatment, where physicians attempt to control hypertension too aggressively, potentially leading to orthostatic hypotension, syncope, and increased risk for falls.16 With findings from SPRINT recommending even lower BPs than that by JNC 8, overtreatment risk becomes especially relevant. While BP protocol was strictly followed in SPRINT, some clinicians may not necessarily follow the same fastidious protocol.
The average differences between the home and standardized BPs were not statistically significant possibly due to the small sample size in the home BP measurements; however, the difference might represent some clinical relevance. There was a 15-point difference in SBP results between home (129 mm Hg) and standardized (115 mm Hg) measures. There also was a difference in DBP between home (69 mm Hg) and standardized (62 mm Hg) results. The close correlation between both home and BPs measured in VAGLAHS demonstrated that any difference was not due to variability in the measurement devices. Previous studies have demonstrated that home BPs are better indicators of cardiovascular risk than office BP.8
Despite lack of statistical significance, home BPs were lower than routine, which suggests that they still may be more reliable than routine office measurements. Definitive conclusions regarding the accuracy of the home BPs in the present study cannot be drawn due to the small sample size (n = 13). Further exploration with comparisons to ambulatory BP monitoring could yield more information on accuracy of home BP monitoring.
In this study’s cohort of older veterans, the average BMI was between 25 and 30 (overweight), which is a risk factor for hypertension.17 Every participant with hypertension was taking at least 1 antihypertensive medication and being actively managed. In this study, the authors accounted for other medications that may affect BP, such as α blockers used in patients with benign prostatic hyperplasia.18 These could have potential elevating or lowering effects on BP measurements.
An issue in this study was the lack of adherence to home BP monitoring. Many patients forgot to bring in their records or to measure their BPs at home. The difficulties highlight real-life issues. Clinicians often request that patients monitor their BP at home, but few may actually remember, let alone keep diligent records. There are many barriers between measuring and reporting home BPs, which may prevent the usefulness of monitoring BP at home.
Limitations
There were several limitations to the study. There was no specific protocol for the routine method of BP measurement, as it was intended to simulate the haphazard nature of office measurements. However, this approach limits its reproducibility. For home BP monitoring, it would have been ideal to provide the same calibrated, automated BP device to each participant. This study of older veterans may not be applicable to the general population. Finally, the relatively small number of participants in the study (n = 30) may have limited power in drawing definitive conclusions.
Future Directions
For future studies, comparing the standardized method to ambulatory BP monitoring would provide more information on accuracy. In addition, the authors would like to evaluate the effect of exercise on BP measurements in the different settings: home, standardized, and routine methods.
1. Mozaffarian D, Benjamin EJ, Go AS, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29-e322.
2. Benjamin EJ, Blaha MJ, Chiuve SE, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146-e603.
3. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;(133):1-8.
4. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
5. Williamson JD, Supiano MA, Applegate WB, et al; SPRINT Research Group. Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged ≥ 75 years: a randomized clinical trial. JAMA. 2016;315(24):2673-2682.
6. Pickering TG, Hall JE, Appel LJ, et al; Council on High Blood Pressure Research Professional and Public Education Subcommittee, American Heart Association. Recommendations for blood pressure measurement in humans: an AHA scientific statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee. J Clin Hypertens (Greenwich). 2005;7(2):102-109.
7. Siu AL; U.S. Preventive Services Task Force. Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;163(10):778-786.
8. Niiranen TJ, Hänninen MR, Johansson J, Reunanen A, Jula AM. Home-measured blood pressure is a stronger predictor of cardiovascular risk than office blood pressure: the Finn-Home study. Hypertension. 2010;55(6):1346-1351.
9. Reino-Gonzalez S, Pita-Fernández S, Seoane-Pillado T, López-Calviño B, Pértega Díaz S. How in-office and ambulatory BP monitoring compare: a systematic review and meta-analysis. J Fam Pract. 2017;66(1):E5-E12.
10. Cohen JB, Cohen DL. Integrating out-of-office blood pressure in the diagnosis and management of hypertension. Curr Cardiol Rep. 2016;18(11):112.
11. Fuchs SC, Mello RB, Fuchs FC. Home blood pressure monitoring is better predictor of cardiovascular disease and target organ damage than office blood pressure: a systematic review and meta-analysis. Curr Cardiol Rep. 2013;15(11):413.
12. Imai Y, Obara T, Asamaya K, Ohkubo T. The reason why home blood pressure measurements are preferred over clinic or ambulatory blood pressure in Japan. Hypertens Res. 2013;36(8):661-672.
13. Bliziotis IA, Destounis A, Stergiou GS. Home versus ambulatory and office blood pressure in predicting target organ damage in hypertension: a systematic review and meta-analysis. J Hypertens. 2012;30(7):1289-1299.
14. Yang Y, Xu JZ, Wang Y, Gao PJ. Ambulatory versus clinic blood pressure in predicting overall subclinical target organ damage progression in essential hypertensive patients: a 3-year follow-up study. Blood Press Monit. 2016;21(6):319-326.
15. Espeland MA, Probstfield J, Hire D, et al; Look AHEAD Research Group; ACCORD Study Group. Systolic blood pressure control among individuals with type 2 diabetes: a comparative effectiveness analysis of three interventions. Am J Hypertens. 2015;28(8):995-1009.
16. Weiss J, Freeman M, Low A, et al. Benefits and harms of intensive blood pressure treatment in adults aged 60 years or older: a systematic review and meta-analysis. Ann Intern Med. 2017;166(6):419-429.
17. Nagai M, Ohkubo T, Murakami Y, et al; NIPPON DATA80/90/2010 Research Group. Secular trends of the impact of overweight and obesity on hypertension in Japan, 1980-2010. Hypertens Res. 2015;38(11):790-795.
18. Press Y, Punchik B, Freud T. Orthostatic hypotension and drug therapy in patients at an outpatient comprehensive geriatric assessment unit. J Hypertens. 2016;34(2):351-358.
1. Mozaffarian D, Benjamin EJ, Go AS, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29-e322.
2. Benjamin EJ, Blaha MJ, Chiuve SE, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146-e603.
3. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011-2012. NCHS Data Brief. 2013;(133):1-8.
4. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
5. Williamson JD, Supiano MA, Applegate WB, et al; SPRINT Research Group. Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged ≥ 75 years: a randomized clinical trial. JAMA. 2016;315(24):2673-2682.
6. Pickering TG, Hall JE, Appel LJ, et al; Council on High Blood Pressure Research Professional and Public Education Subcommittee, American Heart Association. Recommendations for blood pressure measurement in humans: an AHA scientific statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee. J Clin Hypertens (Greenwich). 2005;7(2):102-109.
7. Siu AL; U.S. Preventive Services Task Force. Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2015;163(10):778-786.
8. Niiranen TJ, Hänninen MR, Johansson J, Reunanen A, Jula AM. Home-measured blood pressure is a stronger predictor of cardiovascular risk than office blood pressure: the Finn-Home study. Hypertension. 2010;55(6):1346-1351.
9. Reino-Gonzalez S, Pita-Fernández S, Seoane-Pillado T, López-Calviño B, Pértega Díaz S. How in-office and ambulatory BP monitoring compare: a systematic review and meta-analysis. J Fam Pract. 2017;66(1):E5-E12.
10. Cohen JB, Cohen DL. Integrating out-of-office blood pressure in the diagnosis and management of hypertension. Curr Cardiol Rep. 2016;18(11):112.
11. Fuchs SC, Mello RB, Fuchs FC. Home blood pressure monitoring is better predictor of cardiovascular disease and target organ damage than office blood pressure: a systematic review and meta-analysis. Curr Cardiol Rep. 2013;15(11):413.
12. Imai Y, Obara T, Asamaya K, Ohkubo T. The reason why home blood pressure measurements are preferred over clinic or ambulatory blood pressure in Japan. Hypertens Res. 2013;36(8):661-672.
13. Bliziotis IA, Destounis A, Stergiou GS. Home versus ambulatory and office blood pressure in predicting target organ damage in hypertension: a systematic review and meta-analysis. J Hypertens. 2012;30(7):1289-1299.
14. Yang Y, Xu JZ, Wang Y, Gao PJ. Ambulatory versus clinic blood pressure in predicting overall subclinical target organ damage progression in essential hypertensive patients: a 3-year follow-up study. Blood Press Monit. 2016;21(6):319-326.
15. Espeland MA, Probstfield J, Hire D, et al; Look AHEAD Research Group; ACCORD Study Group. Systolic blood pressure control among individuals with type 2 diabetes: a comparative effectiveness analysis of three interventions. Am J Hypertens. 2015;28(8):995-1009.
16. Weiss J, Freeman M, Low A, et al. Benefits and harms of intensive blood pressure treatment in adults aged 60 years or older: a systematic review and meta-analysis. Ann Intern Med. 2017;166(6):419-429.
17. Nagai M, Ohkubo T, Murakami Y, et al; NIPPON DATA80/90/2010 Research Group. Secular trends of the impact of overweight and obesity on hypertension in Japan, 1980-2010. Hypertens Res. 2015;38(11):790-795.
18. Press Y, Punchik B, Freud T. Orthostatic hypotension and drug therapy in patients at an outpatient comprehensive geriatric assessment unit. J Hypertens. 2016;34(2):351-358.

Eltrombopag receives priority review designation for SAA

Eltrombopag (Promacta®) in combination with standard immunosuppressive therapy (IST) has received priority review designation from the US Food and Drug Administration (FDA) for first-line treatment of severe aplastic anemia (SAA).
The drug is already approved for SAA in the refractory setting for patients who have had an insufficient response to IST.
And it is approved for adults and children with chronic immune thrombocytopenia (ITP) who are refractory to other treatments and for patients with chronic hepatitis C virus infection who are thrombocytopenic.
Eltrombopag, an oral thrombopoietin receptor agonist, had received breakthrough therapy designation from the FDA earlier this year for use in combination with IST as first-line treatment of SAA.
The priority review designation for the agent as a first-line treatment for SAA is supported by data from a phase 1/2 trial published in NEJM in April 2017 and subsequent data on file with Novartis.
The FDA intends to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The agency grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
Trial data
Ninety-two patients with previously untreated SAA were enrolled on the trial and received IST and eltrombopag in 3 different cohorts.
Cohorts varied by start day of eltrombopag and duration of eltrombopag therapy. Patients in cohort 1 received eltrombopag from day 14 to 6 months. Patients in cohort 2 received the drug from day 14 to 3 months. And patients in cohort 3 received eltrombopag from day 1 to 6 months.
The overall response rate (ORR) at 6 months was 80% (cohort 1), 87% (cohort 2), and 94% (cohort 3).
The complete response rate at 6 months was 33%, 26%, and 58% in the 3 cohorts, respectively.
At a median follow-up of 2 years, the overall survival rate was 97%.
In the corporate announcement of the priority review designation, Novartis reported an ORR of 85% at 6 months.
Adverse events included transient elevations in liver enzyme levels (7 patients) and 2 severe adverse events—grades 2 and 3 cutaneous eruption—related to eltrombopag that resulted in patients stopping the drug.
Eltrombopag is marketed as Revolade in countries outside the US.
Eltrombopag (Promacta®) in combination with standard immunosuppressive therapy (IST) has received priority review designation from the US Food and Drug Administration (FDA) for first-line treatment of severe aplastic anemia (SAA).
The drug is already approved for SAA in the refractory setting for patients who have had an insufficient response to IST.
And it is approved for adults and children with chronic immune thrombocytopenia (ITP) who are refractory to other treatments and for patients with chronic hepatitis C virus infection who are thrombocytopenic.
Eltrombopag, an oral thrombopoietin receptor agonist, had received breakthrough therapy designation from the FDA earlier this year for use in combination with IST as first-line treatment of SAA.
The priority review designation for the agent as a first-line treatment for SAA is supported by data from a phase 1/2 trial published in NEJM in April 2017 and subsequent data on file with Novartis.
The FDA intends to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The agency grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
Trial data
Ninety-two patients with previously untreated SAA were enrolled on the trial and received IST and eltrombopag in 3 different cohorts.
Cohorts varied by start day of eltrombopag and duration of eltrombopag therapy. Patients in cohort 1 received eltrombopag from day 14 to 6 months. Patients in cohort 2 received the drug from day 14 to 3 months. And patients in cohort 3 received eltrombopag from day 1 to 6 months.
The overall response rate (ORR) at 6 months was 80% (cohort 1), 87% (cohort 2), and 94% (cohort 3).
The complete response rate at 6 months was 33%, 26%, and 58% in the 3 cohorts, respectively.
At a median follow-up of 2 years, the overall survival rate was 97%.
In the corporate announcement of the priority review designation, Novartis reported an ORR of 85% at 6 months.
Adverse events included transient elevations in liver enzyme levels (7 patients) and 2 severe adverse events—grades 2 and 3 cutaneous eruption—related to eltrombopag that resulted in patients stopping the drug.
Eltrombopag is marketed as Revolade in countries outside the US.
Eltrombopag (Promacta®) in combination with standard immunosuppressive therapy (IST) has received priority review designation from the US Food and Drug Administration (FDA) for first-line treatment of severe aplastic anemia (SAA).
The drug is already approved for SAA in the refractory setting for patients who have had an insufficient response to IST.
And it is approved for adults and children with chronic immune thrombocytopenia (ITP) who are refractory to other treatments and for patients with chronic hepatitis C virus infection who are thrombocytopenic.
Eltrombopag, an oral thrombopoietin receptor agonist, had received breakthrough therapy designation from the FDA earlier this year for use in combination with IST as first-line treatment of SAA.
The priority review designation for the agent as a first-line treatment for SAA is supported by data from a phase 1/2 trial published in NEJM in April 2017 and subsequent data on file with Novartis.
The FDA intends to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The agency grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
Trial data
Ninety-two patients with previously untreated SAA were enrolled on the trial and received IST and eltrombopag in 3 different cohorts.
Cohorts varied by start day of eltrombopag and duration of eltrombopag therapy. Patients in cohort 1 received eltrombopag from day 14 to 6 months. Patients in cohort 2 received the drug from day 14 to 3 months. And patients in cohort 3 received eltrombopag from day 1 to 6 months.
The overall response rate (ORR) at 6 months was 80% (cohort 1), 87% (cohort 2), and 94% (cohort 3).
The complete response rate at 6 months was 33%, 26%, and 58% in the 3 cohorts, respectively.
At a median follow-up of 2 years, the overall survival rate was 97%.
In the corporate announcement of the priority review designation, Novartis reported an ORR of 85% at 6 months.
Adverse events included transient elevations in liver enzyme levels (7 patients) and 2 severe adverse events—grades 2 and 3 cutaneous eruption—related to eltrombopag that resulted in patients stopping the drug.
Eltrombopag is marketed as Revolade in countries outside the US.
Equal treatment, equal or better prostate cancer outcomes for black men
CHICAGO – Black men with advanced prostate cancer have survival with chemotherapy that rivals or surpasses that of white men with advanced disease, and black men with castration-resistant prostate cancer have better outcomes with abiraterone than white men.
Those conclusions come from two studies presented here at the annual meeting of the American Society of Clinical Oncology. Taken together, they suggest that although there may be genetic or biologic differences in cancer presentation among different racial groups, receiving the appropriate care can level out those differences.

In the first study, Susan Halabi, PhD, from Duke University in Durham, N.C., and colleagues pooled data from nine randomized phase 3 chemotherapy trials in men with advanced prostate cancer and found that black and white men had the same median survival, 21 months, but black men had an adjusted hazard ratio [HR} for death of 0.81, compared with white men.
For the subpopulation of African Americans who were enrolled in trials funded by the National Cancer Institute (NCI), the HR for death was 0.76 (P less than .0001).
“The bottom line, in a sense, is that African American men with advanced prostate cancer need to get to an oncologist and ideally need to get on a clinical trial, and if they do, their outcomes are every bit as good as Caucasian men, if not even a little bit better,” Richard Schilsky, MD, chief medical officer of ASCO, said at a briefing prior to presentation of the studies.

In the second study, a prospective clinical trial of abiraterone (Zytiga) in 100 men with metastatic castration-resistant prostate cancer (mCRPC), black men were more likely to have a decline in prostate-specific antigen (PSA), and a longer median time to PSA rise than white men (16.6 vs. 11.5 months), reported Daniel George, MD, also from Duke.
“There’s a 1.6 times greater likelihood that African Americans are diagnosed with prostate cancer, but a 2.4 times greater chance they die from that disease, and although there very well may be multi-factorial reasons for that, I think some of this is genetic,” he said.
Pooled analysis
In the United States, black men are more likely to be diagnosed with prostate cancer in their 40s and 50s than white men and are often diagnosed with advanced-stage and higher grade cancers. Black men also have double the rate of prostate cancer-specific deaths as white men.

Black men, however, are underrepresented in clinical trials, making it difficult to draw firm conclusions about racial differences due to small sample sizes.
To overcome this problem, Dr. Halabi and colleagues pooled data on 8,452 patients with mCRPC - including 7,528 white men and 500 African American men – from nine randomized phase 3 trials of docetaxel and prednisone or a regimen containing those agents.
Median overall survival, the primary endpoint, was 21.0 months for black men and 21.2 months for white men.
In multivariate analysis adjusted for age, PSA, performance status, alkaline phosphatase, hemoglobin, and metastatic sites, the pooled hazard ratio (HR) for black vs. white men was 0.81 (P = .001) for all patients in the study, and when the analysis was restricted to those patients who received only docetaxel and prednisone (4,172), the results were similar, Dr. Halabi said.

“I would argue that what this tells us is pretty striking: that African-American men have potentially better survival by getting conventional therapy,” commented ASCO expert Robert Dreicer, MD, MS, from the University of Virginia in Charlottesville.
“The nihilism associated with prostate cancer in African-American men is not supported by this really interesting work,” he continued. “What it says to us is when we treat those with bad prostate cancer, African Americans, they do well.”
Abiraterone Study
In the abiraterone study, 50 men who self-identified as white and 50 as black were enrolled and treated with abiraterone acetate and prednisone until disease progression or intolerable toxicity.
Radiographic progression-free survival, the primary endpoint, was 16.8 months in each group. As previously noted, however, median PFS was 16.6 months for black patients, vs. 11.5 months for white men. Black men also had a longer median PSA PFS, with 82% of black men having a 30% or greater PSA decline, compared with 78% of white patients. Respective proportions of men having higher declines were 74% vs. 66% experiencing a PSA decline of at least 50%, and 48% vs. 38% having a decline of at least 90%.
Rates of tumor flare, however, were higher among African Americans, at 16% vs. 4%.
Adverse event rates were generally similar between the study arms, although more white than black patients experienced fatigue, and more black than white patients had hypokalemia.
Single-nucletoide polymorphism (SNP) profiling showed differences between the two groups in key genes involved in androgen metabolism and transport, which may explain the improved responses to abiraterone among African Americans.
“We talk about access to care; we have now demonstrated that if you treat African Americans with standard-of-care drugs for advanced prostate cancer, there’s compelling evidence that they respond as well or maybe better than white men,” Dr. Dreicer commented.
“[We are] beginning to understand the differences that drive differential responses,” he continued. “When African-American men are under-represented in clinical trials, the trial outcomes might be different, frankly, because people respond differently to drugs. I think those are the take homes.”
SOURCE: Halabi et al, George et al. ASCO 2018 Abstracts LBA5005 and LBA5009
CHICAGO – Black men with advanced prostate cancer have survival with chemotherapy that rivals or surpasses that of white men with advanced disease, and black men with castration-resistant prostate cancer have better outcomes with abiraterone than white men.
Those conclusions come from two studies presented here at the annual meeting of the American Society of Clinical Oncology. Taken together, they suggest that although there may be genetic or biologic differences in cancer presentation among different racial groups, receiving the appropriate care can level out those differences.
In the first study, Susan Halabi, PhD, from Duke University in Durham, N.C., and colleagues pooled data from nine randomized phase 3 chemotherapy trials in men with advanced prostate cancer and found that black and white men had the same median survival, 21 months, but black men had an adjusted hazard ratio [HR} for death of 0.81, compared with white men.
For the subpopulation of African Americans who were enrolled in trials funded by the National Cancer Institute (NCI), the HR for death was 0.76 (P less than .0001).
“The bottom line, in a sense, is that African American men with advanced prostate cancer need to get to an oncologist and ideally need to get on a clinical trial, and if they do, their outcomes are every bit as good as Caucasian men, if not even a little bit better,” Richard Schilsky, MD, chief medical officer of ASCO, said at a briefing prior to presentation of the studies.
In the second study, a prospective clinical trial of abiraterone (Zytiga) in 100 men with metastatic castration-resistant prostate cancer (mCRPC), black men were more likely to have a decline in prostate-specific antigen (PSA), and a longer median time to PSA rise than white men (16.6 vs. 11.5 months), reported Daniel George, MD, also from Duke.
“There’s a 1.6 times greater likelihood that African Americans are diagnosed with prostate cancer, but a 2.4 times greater chance they die from that disease, and although there very well may be multi-factorial reasons for that, I think some of this is genetic,” he said.
Pooled analysis
In the United States, black men are more likely to be diagnosed with prostate cancer in their 40s and 50s than white men and are often diagnosed with advanced-stage and higher grade cancers. Black men also have double the rate of prostate cancer-specific deaths as white men.
Black men, however, are underrepresented in clinical trials, making it difficult to draw firm conclusions about racial differences due to small sample sizes.
To overcome this problem, Dr. Halabi and colleagues pooled data on 8,452 patients with mCRPC - including 7,528 white men and 500 African American men – from nine randomized phase 3 trials of docetaxel and prednisone or a regimen containing those agents.
Median overall survival, the primary endpoint, was 21.0 months for black men and 21.2 months for white men.
In multivariate analysis adjusted for age, PSA, performance status, alkaline phosphatase, hemoglobin, and metastatic sites, the pooled hazard ratio (HR) for black vs. white men was 0.81 (P = .001) for all patients in the study, and when the analysis was restricted to those patients who received only docetaxel and prednisone (4,172), the results were similar, Dr. Halabi said.
“I would argue that what this tells us is pretty striking: that African-American men have potentially better survival by getting conventional therapy,” commented ASCO expert Robert Dreicer, MD, MS, from the University of Virginia in Charlottesville.
“The nihilism associated with prostate cancer in African-American men is not supported by this really interesting work,” he continued. “What it says to us is when we treat those with bad prostate cancer, African Americans, they do well.”
Abiraterone Study
In the abiraterone study, 50 men who self-identified as white and 50 as black were enrolled and treated with abiraterone acetate and prednisone until disease progression or intolerable toxicity.
Radiographic progression-free survival, the primary endpoint, was 16.8 months in each group. As previously noted, however, median PFS was 16.6 months for black patients, vs. 11.5 months for white men. Black men also had a longer median PSA PFS, with 82% of black men having a 30% or greater PSA decline, compared with 78% of white patients. Respective proportions of men having higher declines were 74% vs. 66% experiencing a PSA decline of at least 50%, and 48% vs. 38% having a decline of at least 90%.
Rates of tumor flare, however, were higher among African Americans, at 16% vs. 4%.
Adverse event rates were generally similar between the study arms, although more white than black patients experienced fatigue, and more black than white patients had hypokalemia.
Single-nucletoide polymorphism (SNP) profiling showed differences between the two groups in key genes involved in androgen metabolism and transport, which may explain the improved responses to abiraterone among African Americans.
“We talk about access to care; we have now demonstrated that if you treat African Americans with standard-of-care drugs for advanced prostate cancer, there’s compelling evidence that they respond as well or maybe better than white men,” Dr. Dreicer commented.
“[We are] beginning to understand the differences that drive differential responses,” he continued. “When African-American men are under-represented in clinical trials, the trial outcomes might be different, frankly, because people respond differently to drugs. I think those are the take homes.”
SOURCE: Halabi et al, George et al. ASCO 2018 Abstracts LBA5005 and LBA5009
CHICAGO – Black men with advanced prostate cancer have survival with chemotherapy that rivals or surpasses that of white men with advanced disease, and black men with castration-resistant prostate cancer have better outcomes with abiraterone than white men.
Those conclusions come from two studies presented here at the annual meeting of the American Society of Clinical Oncology. Taken together, they suggest that although there may be genetic or biologic differences in cancer presentation among different racial groups, receiving the appropriate care can level out those differences.
In the first study, Susan Halabi, PhD, from Duke University in Durham, N.C., and colleagues pooled data from nine randomized phase 3 chemotherapy trials in men with advanced prostate cancer and found that black and white men had the same median survival, 21 months, but black men had an adjusted hazard ratio [HR} for death of 0.81, compared with white men.
For the subpopulation of African Americans who were enrolled in trials funded by the National Cancer Institute (NCI), the HR for death was 0.76 (P less than .0001).
“The bottom line, in a sense, is that African American men with advanced prostate cancer need to get to an oncologist and ideally need to get on a clinical trial, and if they do, their outcomes are every bit as good as Caucasian men, if not even a little bit better,” Richard Schilsky, MD, chief medical officer of ASCO, said at a briefing prior to presentation of the studies.
In the second study, a prospective clinical trial of abiraterone (Zytiga) in 100 men with metastatic castration-resistant prostate cancer (mCRPC), black men were more likely to have a decline in prostate-specific antigen (PSA), and a longer median time to PSA rise than white men (16.6 vs. 11.5 months), reported Daniel George, MD, also from Duke.
“There’s a 1.6 times greater likelihood that African Americans are diagnosed with prostate cancer, but a 2.4 times greater chance they die from that disease, and although there very well may be multi-factorial reasons for that, I think some of this is genetic,” he said.
Pooled analysis
In the United States, black men are more likely to be diagnosed with prostate cancer in their 40s and 50s than white men and are often diagnosed with advanced-stage and higher grade cancers. Black men also have double the rate of prostate cancer-specific deaths as white men.
Black men, however, are underrepresented in clinical trials, making it difficult to draw firm conclusions about racial differences due to small sample sizes.
To overcome this problem, Dr. Halabi and colleagues pooled data on 8,452 patients with mCRPC - including 7,528 white men and 500 African American men – from nine randomized phase 3 trials of docetaxel and prednisone or a regimen containing those agents.
Median overall survival, the primary endpoint, was 21.0 months for black men and 21.2 months for white men.
In multivariate analysis adjusted for age, PSA, performance status, alkaline phosphatase, hemoglobin, and metastatic sites, the pooled hazard ratio (HR) for black vs. white men was 0.81 (P = .001) for all patients in the study, and when the analysis was restricted to those patients who received only docetaxel and prednisone (4,172), the results were similar, Dr. Halabi said.
“I would argue that what this tells us is pretty striking: that African-American men have potentially better survival by getting conventional therapy,” commented ASCO expert Robert Dreicer, MD, MS, from the University of Virginia in Charlottesville.
“The nihilism associated with prostate cancer in African-American men is not supported by this really interesting work,” he continued. “What it says to us is when we treat those with bad prostate cancer, African Americans, they do well.”
Abiraterone Study
In the abiraterone study, 50 men who self-identified as white and 50 as black were enrolled and treated with abiraterone acetate and prednisone until disease progression or intolerable toxicity.
Radiographic progression-free survival, the primary endpoint, was 16.8 months in each group. As previously noted, however, median PFS was 16.6 months for black patients, vs. 11.5 months for white men. Black men also had a longer median PSA PFS, with 82% of black men having a 30% or greater PSA decline, compared with 78% of white patients. Respective proportions of men having higher declines were 74% vs. 66% experiencing a PSA decline of at least 50%, and 48% vs. 38% having a decline of at least 90%.
Rates of tumor flare, however, were higher among African Americans, at 16% vs. 4%.
Adverse event rates were generally similar between the study arms, although more white than black patients experienced fatigue, and more black than white patients had hypokalemia.
Single-nucletoide polymorphism (SNP) profiling showed differences between the two groups in key genes involved in androgen metabolism and transport, which may explain the improved responses to abiraterone among African Americans.
“We talk about access to care; we have now demonstrated that if you treat African Americans with standard-of-care drugs for advanced prostate cancer, there’s compelling evidence that they respond as well or maybe better than white men,” Dr. Dreicer commented.
“[We are] beginning to understand the differences that drive differential responses,” he continued. “When African-American men are under-represented in clinical trials, the trial outcomes might be different, frankly, because people respond differently to drugs. I think those are the take homes.”
SOURCE: Halabi et al, George et al. ASCO 2018 Abstracts LBA5005 and LBA5009
REPORTING FROM ASCO 2018
Key clinical point: Apparent racial disparities in prostate cancer care may be reduced or eliminated with proper care and access to clinical trials.
Major finding: In a pooled analysis, black men with advanced prostate cancer treated with docetaxel prednisone had a 19% lower risk for death than white men,
Study details: Pooled analysis of 9 randomized phase III trials with a total of 8,452 men and a prospective trial with 100 men with advanced prostate cancer.
Disclosures: The study by Halabi et al was funded by Congressionally Directed Medical Research Programs. The study by George et al was funded by Janssen. Dr. Halabi disclosed a consulting or advisory role with Tokai Pharmaceuticals, Eisai, and Bayer, and travel expenses from Bayer. Dr. George disclosed consulting/advising with Janssen and several other pharmaceutical companies, in addition to speakers’ bureau, travel expenses, and honoraria from various companies. He has also received institutional research funding from Exelixis, Genentech/Roche, Janssen Oncology, Novartis, Pfizer, Astellas Pharma, Bristol-Myers Squibb, Millennium, Acerta Pharma, Bayer, Dendreon, and Innocrin Pharma.
Source: Halabi et al, George et al. ASCO 2018 Abstracts LBA5005 and LBA5009.
Post-traumatic osteoarthritis needs to be prevention focus
, Jackie Whittaker, PT, PhD, said at the World Congress of Osteoarthritis.
“We all know that the burden of this disease is enormous and it’s expanding at an alarming rate,” she said at the congress, sponsored by the Osteoarthritis Research Society International.
“The only way that we have at this moment to try to reduce the burden of this disease is to shift our approach to management upstream and focus on prevention,” said Dr. Whittaker, who is an associate professor and research director at the University of Alberta, Edmonton, Canada.
According to the World Health Organization, OA is expected to become the fourth leading cause of disability worldwide by 2020. Furthermore, there will be a projected rise in prevalence from 12% to 25% in North America by 2030.
Dr. Whittaker suggested that it was time to try to identify those at risk of developing OA, such as after a joint injury, and ran through some suggestions on how posttraumatic OA (PTOA) might be preventable.
Secondary prevention of posttraumatic osteoarthritis
The prevention of PTOA can be split into primary, secondary and tertiary prevention, with primary prevention trying to prevent injuries from occurring in the first place.
“Strategies aimed at identifying and slowing down the onset of symptomatic osteoarthritis in preclinical populations would be referred to as secondary prevention,” Dr. Whittaker explained, adding that tertiary prevention would then be strategies aimed at improving function and reducing disability in those who already have symptomatic PTOA.
While there are programs that address primary and tertiary prevention – such as Footy First, an exercise training program adopted by the Australian Football League to reduce the risk of common leg injuries and the Good Life with osteoArthritis in Denmark (GLA:D®) education and supervised exercise program for those with symptomatic OA – there is more of a gap for secondary prevention.
Some of the first steps to developing a secondary prevention model would be to determine the extent of PTOA after joint injury and then identify risk factors or causal mechanisms. Then, prevention strategies could be developed and tested before implementation and effectiveness studies are performed.
Performing the necessary prospective cohort studies, however, is when things get challenging – PTOA can take 10–15 years to manifest and studies would potentially need to run for long periods of time, which comes at a cost. Other challenges are that there is no commonly agree definition. PTOA is multifactorial, and because people may be in their 20s, there could be other contributing factors to the disease course.
Identifying modifiable risk factors
There are a “fair number” of prospective and retrospective studies that have been done to try to identify patients at risk for OA after joint injury. Several have looked at unmodifiable risk factors, such as age and sex, and the type of injury. Others have looked at potentially modifiable factors such as the treatment approach and avoiding re-injury, joint mechanics and strength, body composition and aerobic fitness and behavioral characteristics such as physical activity and return to sport.
Data from the Alberta Youth PrE-OA Study, an ongoing longitudinal cohort study, have shown that structural changes consistent with OA are not unique to tears in the anterior cruciate ligament or to meniscal tears, which are known to up the risk of PTOA. Furthermore, the odds of having MRI-defined OA 3–10 years after a knee injury varies by the injury history, type, and surgery.
Other findings from the Alberta Youth PrE-OA Study data have shown that previously injured subjects have a 30% risk for re-injury, with weaker knee extensors and flexors and poorer dynamic balance than uninjured study participants. The results have also shown that there is reduced physical activity and avoidance in those who have been injured.
Who is the population at risk?
“Although the supporting evidence and the level of evidence for some of the risk factors is not as thorough as we would like it, there are some common themes across the literature, that are consistent to what we see in clinical practice, and what we know from primary and tertiary prevention,” Dr. Whittaker said. “Based upon that, we can start to hypothesize who’s at greatest risk of developing posttraumatic osteoarthritis and what we might start doing about it right now.”
Dr. Whittaker proposed the following risk factors could be used to “build a profile” of someone at risk of PTOA:
- Having sustained an anterior cruciate ligament (ACL) tear with or without a damaged meniscus
- Elevated body mass index (BMI) or adiposity, and low grade systemic inflammation
- Weak knee muscles, and poor dynamic balance
- Reduced or disengaged from physical activity
- Insufficient rehabilitation, pain or stiffness, or fear of movement
There is also an argument for nutrition being involved, Dr. Whittaker said, with levels of micronutrients such as vitamins D and K and calcium playing an integral role in bone health.
What could secondary prevention look like?
“So, with this risk profile, what can be done?” Dr. Whittaker asked rhetorically. Exercise therapy is key, and increasing the muscle strength of the knee and lower extremity are an important component of this strategy. Strength alone may not be enough, so exercise programs will need to increase the neuromuscular control of functional movements. Tackling people’s fear of movement will also be a priority. “I think it’s very important that we promote, if not implement, physical activity guidelines.”
Education is also going to be an important part of any secondary prevention program for PTOA, ensuring that people have realistic expectations about re-injury and their risk of developing osteoarthritis and the importance of remaining physically active. Balancing physical activity against their likelihood of flare-ups and learning how to avoid re-injury if at all possible. Weight control and diet will also be a component to include.
One final component is how clinicians work with patients to minimize their risk of PTOA. “We need to co-manage these patients,” Dr. Whittaker said. “We need to have difficult conversations with them and really balance giving them a picture of reality without over medicalizing the situation.”
Dr. Whitaker stated that she had no financial relationships or commercial interests to disclose.
SOURCE: Whittaker J, et al. Osteoarthritis Cartilage 2018:26(1):S7-8. Abstract I-22.
, Jackie Whittaker, PT, PhD, said at the World Congress of Osteoarthritis.
“We all know that the burden of this disease is enormous and it’s expanding at an alarming rate,” she said at the congress, sponsored by the Osteoarthritis Research Society International.
“The only way that we have at this moment to try to reduce the burden of this disease is to shift our approach to management upstream and focus on prevention,” said Dr. Whittaker, who is an associate professor and research director at the University of Alberta, Edmonton, Canada.
According to the World Health Organization, OA is expected to become the fourth leading cause of disability worldwide by 2020. Furthermore, there will be a projected rise in prevalence from 12% to 25% in North America by 2030.
Dr. Whittaker suggested that it was time to try to identify those at risk of developing OA, such as after a joint injury, and ran through some suggestions on how posttraumatic OA (PTOA) might be preventable.
Secondary prevention of posttraumatic osteoarthritis
The prevention of PTOA can be split into primary, secondary and tertiary prevention, with primary prevention trying to prevent injuries from occurring in the first place.
“Strategies aimed at identifying and slowing down the onset of symptomatic osteoarthritis in preclinical populations would be referred to as secondary prevention,” Dr. Whittaker explained, adding that tertiary prevention would then be strategies aimed at improving function and reducing disability in those who already have symptomatic PTOA.
While there are programs that address primary and tertiary prevention – such as Footy First, an exercise training program adopted by the Australian Football League to reduce the risk of common leg injuries and the Good Life with osteoArthritis in Denmark (GLA:D®) education and supervised exercise program for those with symptomatic OA – there is more of a gap for secondary prevention.
Some of the first steps to developing a secondary prevention model would be to determine the extent of PTOA after joint injury and then identify risk factors or causal mechanisms. Then, prevention strategies could be developed and tested before implementation and effectiveness studies are performed.
Performing the necessary prospective cohort studies, however, is when things get challenging – PTOA can take 10–15 years to manifest and studies would potentially need to run for long periods of time, which comes at a cost. Other challenges are that there is no commonly agree definition. PTOA is multifactorial, and because people may be in their 20s, there could be other contributing factors to the disease course.
Identifying modifiable risk factors
There are a “fair number” of prospective and retrospective studies that have been done to try to identify patients at risk for OA after joint injury. Several have looked at unmodifiable risk factors, such as age and sex, and the type of injury. Others have looked at potentially modifiable factors such as the treatment approach and avoiding re-injury, joint mechanics and strength, body composition and aerobic fitness and behavioral characteristics such as physical activity and return to sport.
Data from the Alberta Youth PrE-OA Study, an ongoing longitudinal cohort study, have shown that structural changes consistent with OA are not unique to tears in the anterior cruciate ligament or to meniscal tears, which are known to up the risk of PTOA. Furthermore, the odds of having MRI-defined OA 3–10 years after a knee injury varies by the injury history, type, and surgery.
Other findings from the Alberta Youth PrE-OA Study data have shown that previously injured subjects have a 30% risk for re-injury, with weaker knee extensors and flexors and poorer dynamic balance than uninjured study participants. The results have also shown that there is reduced physical activity and avoidance in those who have been injured.
Who is the population at risk?
“Although the supporting evidence and the level of evidence for some of the risk factors is not as thorough as we would like it, there are some common themes across the literature, that are consistent to what we see in clinical practice, and what we know from primary and tertiary prevention,” Dr. Whittaker said. “Based upon that, we can start to hypothesize who’s at greatest risk of developing posttraumatic osteoarthritis and what we might start doing about it right now.”
Dr. Whittaker proposed the following risk factors could be used to “build a profile” of someone at risk of PTOA:
- Having sustained an anterior cruciate ligament (ACL) tear with or without a damaged meniscus
- Elevated body mass index (BMI) or adiposity, and low grade systemic inflammation
- Weak knee muscles, and poor dynamic balance
- Reduced or disengaged from physical activity
- Insufficient rehabilitation, pain or stiffness, or fear of movement
There is also an argument for nutrition being involved, Dr. Whittaker said, with levels of micronutrients such as vitamins D and K and calcium playing an integral role in bone health.
What could secondary prevention look like?
“So, with this risk profile, what can be done?” Dr. Whittaker asked rhetorically. Exercise therapy is key, and increasing the muscle strength of the knee and lower extremity are an important component of this strategy. Strength alone may not be enough, so exercise programs will need to increase the neuromuscular control of functional movements. Tackling people’s fear of movement will also be a priority. “I think it’s very important that we promote, if not implement, physical activity guidelines.”
Education is also going to be an important part of any secondary prevention program for PTOA, ensuring that people have realistic expectations about re-injury and their risk of developing osteoarthritis and the importance of remaining physically active. Balancing physical activity against their likelihood of flare-ups and learning how to avoid re-injury if at all possible. Weight control and diet will also be a component to include.
One final component is how clinicians work with patients to minimize their risk of PTOA. “We need to co-manage these patients,” Dr. Whittaker said. “We need to have difficult conversations with them and really balance giving them a picture of reality without over medicalizing the situation.”
Dr. Whitaker stated that she had no financial relationships or commercial interests to disclose.
SOURCE: Whittaker J, et al. Osteoarthritis Cartilage 2018:26(1):S7-8. Abstract I-22.
, Jackie Whittaker, PT, PhD, said at the World Congress of Osteoarthritis.
“We all know that the burden of this disease is enormous and it’s expanding at an alarming rate,” she said at the congress, sponsored by the Osteoarthritis Research Society International.
“The only way that we have at this moment to try to reduce the burden of this disease is to shift our approach to management upstream and focus on prevention,” said Dr. Whittaker, who is an associate professor and research director at the University of Alberta, Edmonton, Canada.
According to the World Health Organization, OA is expected to become the fourth leading cause of disability worldwide by 2020. Furthermore, there will be a projected rise in prevalence from 12% to 25% in North America by 2030.
Dr. Whittaker suggested that it was time to try to identify those at risk of developing OA, such as after a joint injury, and ran through some suggestions on how posttraumatic OA (PTOA) might be preventable.
Secondary prevention of posttraumatic osteoarthritis
The prevention of PTOA can be split into primary, secondary and tertiary prevention, with primary prevention trying to prevent injuries from occurring in the first place.
“Strategies aimed at identifying and slowing down the onset of symptomatic osteoarthritis in preclinical populations would be referred to as secondary prevention,” Dr. Whittaker explained, adding that tertiary prevention would then be strategies aimed at improving function and reducing disability in those who already have symptomatic PTOA.
While there are programs that address primary and tertiary prevention – such as Footy First, an exercise training program adopted by the Australian Football League to reduce the risk of common leg injuries and the Good Life with osteoArthritis in Denmark (GLA:D®) education and supervised exercise program for those with symptomatic OA – there is more of a gap for secondary prevention.
Some of the first steps to developing a secondary prevention model would be to determine the extent of PTOA after joint injury and then identify risk factors or causal mechanisms. Then, prevention strategies could be developed and tested before implementation and effectiveness studies are performed.
Performing the necessary prospective cohort studies, however, is when things get challenging – PTOA can take 10–15 years to manifest and studies would potentially need to run for long periods of time, which comes at a cost. Other challenges are that there is no commonly agree definition. PTOA is multifactorial, and because people may be in their 20s, there could be other contributing factors to the disease course.
Identifying modifiable risk factors
There are a “fair number” of prospective and retrospective studies that have been done to try to identify patients at risk for OA after joint injury. Several have looked at unmodifiable risk factors, such as age and sex, and the type of injury. Others have looked at potentially modifiable factors such as the treatment approach and avoiding re-injury, joint mechanics and strength, body composition and aerobic fitness and behavioral characteristics such as physical activity and return to sport.
Data from the Alberta Youth PrE-OA Study, an ongoing longitudinal cohort study, have shown that structural changes consistent with OA are not unique to tears in the anterior cruciate ligament or to meniscal tears, which are known to up the risk of PTOA. Furthermore, the odds of having MRI-defined OA 3–10 years after a knee injury varies by the injury history, type, and surgery.
Other findings from the Alberta Youth PrE-OA Study data have shown that previously injured subjects have a 30% risk for re-injury, with weaker knee extensors and flexors and poorer dynamic balance than uninjured study participants. The results have also shown that there is reduced physical activity and avoidance in those who have been injured.
Who is the population at risk?
“Although the supporting evidence and the level of evidence for some of the risk factors is not as thorough as we would like it, there are some common themes across the literature, that are consistent to what we see in clinical practice, and what we know from primary and tertiary prevention,” Dr. Whittaker said. “Based upon that, we can start to hypothesize who’s at greatest risk of developing posttraumatic osteoarthritis and what we might start doing about it right now.”
Dr. Whittaker proposed the following risk factors could be used to “build a profile” of someone at risk of PTOA:
- Having sustained an anterior cruciate ligament (ACL) tear with or without a damaged meniscus
- Elevated body mass index (BMI) or adiposity, and low grade systemic inflammation
- Weak knee muscles, and poor dynamic balance
- Reduced or disengaged from physical activity
- Insufficient rehabilitation, pain or stiffness, or fear of movement
There is also an argument for nutrition being involved, Dr. Whittaker said, with levels of micronutrients such as vitamins D and K and calcium playing an integral role in bone health.
What could secondary prevention look like?
“So, with this risk profile, what can be done?” Dr. Whittaker asked rhetorically. Exercise therapy is key, and increasing the muscle strength of the knee and lower extremity are an important component of this strategy. Strength alone may not be enough, so exercise programs will need to increase the neuromuscular control of functional movements. Tackling people’s fear of movement will also be a priority. “I think it’s very important that we promote, if not implement, physical activity guidelines.”
Education is also going to be an important part of any secondary prevention program for PTOA, ensuring that people have realistic expectations about re-injury and their risk of developing osteoarthritis and the importance of remaining physically active. Balancing physical activity against their likelihood of flare-ups and learning how to avoid re-injury if at all possible. Weight control and diet will also be a component to include.
One final component is how clinicians work with patients to minimize their risk of PTOA. “We need to co-manage these patients,” Dr. Whittaker said. “We need to have difficult conversations with them and really balance giving them a picture of reality without over medicalizing the situation.”
Dr. Whitaker stated that she had no financial relationships or commercial interests to disclose.
SOURCE: Whittaker J, et al. Osteoarthritis Cartilage 2018:26(1):S7-8. Abstract I-22.
REPORTING FROM OARSI 2018
A blood test to detect lung cancer inches toward the clinic
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO - Uptake of recommended low-dose CT for lung cancer screening has been dismal. Blood-based assays are an attractive alternative being explored by the Circulating Cell–Free Genome Atlas (CCGA) project. Interim results of a CCGA study of 561 individuals without cancer and 118 patients with lung cancers of all stages have found that a trio of assays searching for molecular signatures in plasma cell-free DNA achieved roughly 50% sensitivity for detection of early-stage (stage I-IIIA) lung cancers and 91% sensitivity for detection of late-stage (stage IIIB-IV) lung cancers.
In this video interview from the annual meeting of the American Society of Clinical Oncology, lead study author Geoffrey R. Oxnard, MD, of the Dana-Farber Cancer Institute, Boston, discusses the science behind these assays, how they may fill an unmet medical need, and ongoing work to bring them into the clinic.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO - Uptake of recommended low-dose CT for lung cancer screening has been dismal. Blood-based assays are an attractive alternative being explored by the Circulating Cell–Free Genome Atlas (CCGA) project. Interim results of a CCGA study of 561 individuals without cancer and 118 patients with lung cancers of all stages have found that a trio of assays searching for molecular signatures in plasma cell-free DNA achieved roughly 50% sensitivity for detection of early-stage (stage I-IIIA) lung cancers and 91% sensitivity for detection of late-stage (stage IIIB-IV) lung cancers.
In this video interview from the annual meeting of the American Society of Clinical Oncology, lead study author Geoffrey R. Oxnard, MD, of the Dana-Farber Cancer Institute, Boston, discusses the science behind these assays, how they may fill an unmet medical need, and ongoing work to bring them into the clinic.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO - Uptake of recommended low-dose CT for lung cancer screening has been dismal. Blood-based assays are an attractive alternative being explored by the Circulating Cell–Free Genome Atlas (CCGA) project. Interim results of a CCGA study of 561 individuals without cancer and 118 patients with lung cancers of all stages have found that a trio of assays searching for molecular signatures in plasma cell-free DNA achieved roughly 50% sensitivity for detection of early-stage (stage I-IIIA) lung cancers and 91% sensitivity for detection of late-stage (stage IIIB-IV) lung cancers.
In this video interview from the annual meeting of the American Society of Clinical Oncology, lead study author Geoffrey R. Oxnard, MD, of the Dana-Farber Cancer Institute, Boston, discusses the science behind these assays, how they may fill an unmet medical need, and ongoing work to bring them into the clinic.
REPORTING FROM ASCO 2018

Heading down the wrong pathway in advanced breast cancer?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – In the SANDPIPER trial, the combination of the phosphatidylinositol 3-kinase (PI3K) inhibitor taselisib and the selective estrogen receptor modifier fulvestrant (Faslodex) was associated with a small but significant progression-free survival (PFS) benefit, compared with fulvestrant alone in women with advanced estrogen-receptor positive, HER2-negative breast cancer.
That 2-month PFS benefit, described as “modest” by investigators, came at the cost of significant toxicities, with nearly 50% of patients treated with the combination having grade 3 or greater toxicities, compared with 16% of patients treated with fulvestrant alone.
In this video interview from the annual meeting of the American Society of Clinical Oncology, ASCO expert Harold Burstein, MD, PhD, from the Dana-Farber Cancer Institute in Boston, questions whether the PI3K pathway, shown to be targetable in hematologic malignancies, is worth continuing to pursue in breast cancer.
Dr. Burstein had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – In the SANDPIPER trial, the combination of the phosphatidylinositol 3-kinase (PI3K) inhibitor taselisib and the selective estrogen receptor modifier fulvestrant (Faslodex) was associated with a small but significant progression-free survival (PFS) benefit, compared with fulvestrant alone in women with advanced estrogen-receptor positive, HER2-negative breast cancer.
That 2-month PFS benefit, described as “modest” by investigators, came at the cost of significant toxicities, with nearly 50% of patients treated with the combination having grade 3 or greater toxicities, compared with 16% of patients treated with fulvestrant alone.
In this video interview from the annual meeting of the American Society of Clinical Oncology, ASCO expert Harold Burstein, MD, PhD, from the Dana-Farber Cancer Institute in Boston, questions whether the PI3K pathway, shown to be targetable in hematologic malignancies, is worth continuing to pursue in breast cancer.
Dr. Burstein had no disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – In the SANDPIPER trial, the combination of the phosphatidylinositol 3-kinase (PI3K) inhibitor taselisib and the selective estrogen receptor modifier fulvestrant (Faslodex) was associated with a small but significant progression-free survival (PFS) benefit, compared with fulvestrant alone in women with advanced estrogen-receptor positive, HER2-negative breast cancer.
That 2-month PFS benefit, described as “modest” by investigators, came at the cost of significant toxicities, with nearly 50% of patients treated with the combination having grade 3 or greater toxicities, compared with 16% of patients treated with fulvestrant alone.
In this video interview from the annual meeting of the American Society of Clinical Oncology, ASCO expert Harold Burstein, MD, PhD, from the Dana-Farber Cancer Institute in Boston, questions whether the PI3K pathway, shown to be targetable in hematologic malignancies, is worth continuing to pursue in breast cancer.
Dr. Burstein had no disclosures.
REPORTING FROM ASCO 2018
