User login
Thrown Off Track

ANSWER
The radiograph shows rib fractures on the left side (arrows); on the same side, there is a moderate-sized pleural effusion—presumably a hemothorax from the trauma.
A closer look at the mid-thoracic spine reveals some irregularity and possible deformity—note the slight offset. This finding is strongly suspicious for a fracture.
A subsequent CT revealed a thoracic burst fracture with retropulsion into the spinal canal.
ANSWER
The radiograph shows rib fractures on the left side (arrows); on the same side, there is a moderate-sized pleural effusion—presumably a hemothorax from the trauma.
A closer look at the mid-thoracic spine reveals some irregularity and possible deformity—note the slight offset. This finding is strongly suspicious for a fracture.
A subsequent CT revealed a thoracic burst fracture with retropulsion into the spinal canal.
ANSWER
The radiograph shows rib fractures on the left side (arrows); on the same side, there is a moderate-sized pleural effusion—presumably a hemothorax from the trauma.
A closer look at the mid-thoracic spine reveals some irregularity and possible deformity—note the slight offset. This finding is strongly suspicious for a fracture.
A subsequent CT revealed a thoracic burst fracture with retropulsion into the spinal canal.

A 20-year-old man is riding a four-wheel all-terrain vehicle at a high rate of speed when he loses control and is thrown off. He is not wearin
As you begin your primary survey, you note a young male who is anxious but awake and able to converse. He is receiving 100% oxygen via a non-rebreather mask. His heart rate is 130 beats/min and his blood pressure, 80/40 mm Hg. Breath sounds are somewhat decreased on the left side. The patient can move both arms, and his strength is normal. However, he is insensate from his mid-chest down and is unable to move his legs at all.
Portable radiographs are obtained, including a chest radiograph (shown). What is your impression?

From the EVP/CEO
As we wrap up CHEST’s fiscal year 2017-18 (our fiscal year runs July 1 – June 30), it has been an incredibly positive and productive year, on all fronts. We have educated more learners than ever before, expanded our educational offerings, increased our collaboration with other organizations, grown our CHEST Foundation activities, and are in excellent financial shape to continue our commitment to clinical chest medicine education.
As we prepare for fiscal year 2018-19, I want to highlight some of the key programs, events, and projects we will be undertaking that will support our strategic plan (http://www.chestnet.org/About/Overview/Strategic-Plan) and achieve our mission to champion the prevention, diagnosis, and treatment of chest diseases through education, communication, and research.
Our organization goals are primarily focused on (but are not limited to) the following broad achievements:
a. Increasing the number of learners that CHEST engages (and increasing their engagement with our content) and assessing the results of our educational interactions
b. Keeping our journal CHEST® among the top Pulmonary, Critical Care, and Sleep peer review journals in the world
c. Expanding domestic and global access to CHEST guidelines and other relevant clinical content
d. Continuing to offer a positive and inclusive culture and work environment at CHEST, for our volunteers, world-class faculty, members, and staff
e. Meeting or exceeding our budget, reserve policy, and grant funding targets to ensure delivery of our mission-based educational efforts and programs
Because our mission as a 501(c)3 not-for-profit is education, I’ll start with those key programs that are driving our budget for FY2018-19 and will also cover publishing and membership.
Education – Clinical
• Increased global activity due to global partnerships with several key international educational providers
• Holding April 2019 CHEST World Congress in Bangkok
• Planning June 2019 Board Review conference in Athens, Greece
• 21 total international courses planned
• Increased Live Learning courses, simulation, and hands-on skills training
• 21 courses planned (including 3 new courses)
• Holding two Fellows courses at CHEST HQ (up to 80 fellows)
• Annual Meeting includes 11 postgraduate programs and 24 simulation courses (including more cadaver courses)
• Includes more Fellows courses (up to 240 Fellows)
• Board Courses include two half-day simulation courses; more sponsorship/exhibits, games, and virtual patient tours (VPTs)
• Continuing to build Board Review on-demand and e-learning content packages for those who cannot attend live events
• Launching inaugural e-Learning program with Elsevier
Education – Patient
• Developing multiple CHEST Foundation disease awareness campaigns and patient education resources
• New patient education guides
• Increased visual content (infographics, graphically based materials)
• Increased use of multimedia and video content
• Increased funding for clinical research grants, community service programs and lung health events, and fund-raising through cause marketing (i.e., Feldman Family Poker Night, NYC events, and other local fund raising events)
• Expanding awareness and access of our patient education materials
• Institutions, large group practices
• International reach
• Digital distribution via social media and online campaigns
Education – Industry
• Projecting seven new live clinical immersion courses
• Two new proposed PREP courses with CTS
• Expansion of educational games, VPTs, and e-learning
• Expanded CHEST Analytics Product Lines
• View Points (3 focus groups, 4-5 KOL panels, 4 pulse surveys)
• Deep Dives (3 advanced analytics projects, 5 premium research projects, 2 ethnography studies, and 4-6 Clinical Perspectives)
• Data Lab (looking to launch beta partner)
• Booth IQ (increasing capacity for booth flow and booth intel reports)
Publications, Guidelines and Digital Content
• CHEST® Journal
• Elsevier partnership remains strong; leveraging key data and Elsevier offerings, will be announcing the next Editor in Chief
• CHEST Physician
• New content and delivery mechanisms
• Supplements
• Electronic features
• CHEST SEEK
• Publish Volume 28 (Critical Care)
• Continue development of SEEK online library
• Guidelines
• Completions: Antithrombotic therapy, cough, ILD diagnosis, hypersensitivity pneumonitis, lung cancer, and PAH
• Updates: Antithrombotic therapy, lung cancer, cough, neuromuscular weakness, EBUS needle sampling, and blood transfusions in critical care setting (doing more in critical care)
• Piloting use of DoctorEvidence methodology services and platform for “living guidelines”
Membership
• Focusing on adding value to CHEST membership for key segments
• Bundling e-learning packages with membership
• Exploring international group/society memberships and group practice/institutional memberships
• Working to attract advanced practice providers
• Performing member market research, including member satisfaction, net promoter scores, and other key metrics
Supporting Divisions (Finance, Marketing, IT, Capital expenses)
• Have more visibility (booth presence) at more meetings (AACN, AARC (new), ALAT, APSR, ATS, CTS, ERS, SCCM, and more)
• Develop and execute comprehensive marketing and branding strategies for all business units
• Clinical Education (CHEST annual meeting, Board Reviews, all int’l meetings and live learning, simulation)
• Industry Education (PREP, CHEST Analytics)
• Patient Education
• Foundation Fundraising
• Publishing and Content Strategy
• Membership
• Support new IT platforms and bolster security (HR, Finance, Board Effect, Tableau, CHEST analytics, LMS, CMS, NetForum AMS), as well as marketing and social interaction tools (HubSpot)
• Maintain Capital Budget for building, infrastructure, technology, etc

All in all, CHEST has a very active fiscal year planned, with a number of new educational programs and e-learning opportunities showcasing CHEST’s unique brand of innovative clinical education. We look forward to connecting with you and impacting health-care delivery and patient outcomes. It is an honor and a privilege to be able to lead this organization, and all of this news is directly attributable to our dedicated volunteer leadership, faculty, content expertise, staff, and valuable time that you all contribute to make this organization great. Thank you for your ongoing support of CHEST.
.
As we wrap up CHEST’s fiscal year 2017-18 (our fiscal year runs July 1 – June 30), it has been an incredibly positive and productive year, on all fronts. We have educated more learners than ever before, expanded our educational offerings, increased our collaboration with other organizations, grown our CHEST Foundation activities, and are in excellent financial shape to continue our commitment to clinical chest medicine education.
As we prepare for fiscal year 2018-19, I want to highlight some of the key programs, events, and projects we will be undertaking that will support our strategic plan (http://www.chestnet.org/About/Overview/Strategic-Plan) and achieve our mission to champion the prevention, diagnosis, and treatment of chest diseases through education, communication, and research.
Our organization goals are primarily focused on (but are not limited to) the following broad achievements:
a. Increasing the number of learners that CHEST engages (and increasing their engagement with our content) and assessing the results of our educational interactions
b. Keeping our journal CHEST® among the top Pulmonary, Critical Care, and Sleep peer review journals in the world
c. Expanding domestic and global access to CHEST guidelines and other relevant clinical content
d. Continuing to offer a positive and inclusive culture and work environment at CHEST, for our volunteers, world-class faculty, members, and staff
e. Meeting or exceeding our budget, reserve policy, and grant funding targets to ensure delivery of our mission-based educational efforts and programs
Because our mission as a 501(c)3 not-for-profit is education, I’ll start with those key programs that are driving our budget for FY2018-19 and will also cover publishing and membership.
Education – Clinical
• Increased global activity due to global partnerships with several key international educational providers
• Holding April 2019 CHEST World Congress in Bangkok
• Planning June 2019 Board Review conference in Athens, Greece
• 21 total international courses planned
• Increased Live Learning courses, simulation, and hands-on skills training
• 21 courses planned (including 3 new courses)
• Holding two Fellows courses at CHEST HQ (up to 80 fellows)
• Annual Meeting includes 11 postgraduate programs and 24 simulation courses (including more cadaver courses)
• Includes more Fellows courses (up to 240 Fellows)
• Board Courses include two half-day simulation courses; more sponsorship/exhibits, games, and virtual patient tours (VPTs)
• Continuing to build Board Review on-demand and e-learning content packages for those who cannot attend live events
• Launching inaugural e-Learning program with Elsevier
Education – Patient
• Developing multiple CHEST Foundation disease awareness campaigns and patient education resources
• New patient education guides
• Increased visual content (infographics, graphically based materials)
• Increased use of multimedia and video content
• Increased funding for clinical research grants, community service programs and lung health events, and fund-raising through cause marketing (i.e., Feldman Family Poker Night, NYC events, and other local fund raising events)
• Expanding awareness and access of our patient education materials
• Institutions, large group practices
• International reach
• Digital distribution via social media and online campaigns
Education – Industry
• Projecting seven new live clinical immersion courses
• Two new proposed PREP courses with CTS
• Expansion of educational games, VPTs, and e-learning
• Expanded CHEST Analytics Product Lines
• View Points (3 focus groups, 4-5 KOL panels, 4 pulse surveys)
• Deep Dives (3 advanced analytics projects, 5 premium research projects, 2 ethnography studies, and 4-6 Clinical Perspectives)
• Data Lab (looking to launch beta partner)
• Booth IQ (increasing capacity for booth flow and booth intel reports)
Publications, Guidelines and Digital Content
• CHEST® Journal
• Elsevier partnership remains strong; leveraging key data and Elsevier offerings, will be announcing the next Editor in Chief
• CHEST Physician
• New content and delivery mechanisms
• Supplements
• Electronic features
• CHEST SEEK
• Publish Volume 28 (Critical Care)
• Continue development of SEEK online library
• Guidelines
• Completions: Antithrombotic therapy, cough, ILD diagnosis, hypersensitivity pneumonitis, lung cancer, and PAH
• Updates: Antithrombotic therapy, lung cancer, cough, neuromuscular weakness, EBUS needle sampling, and blood transfusions in critical care setting (doing more in critical care)
• Piloting use of DoctorEvidence methodology services and platform for “living guidelines”
Membership
• Focusing on adding value to CHEST membership for key segments
• Bundling e-learning packages with membership
• Exploring international group/society memberships and group practice/institutional memberships
• Working to attract advanced practice providers
• Performing member market research, including member satisfaction, net promoter scores, and other key metrics
Supporting Divisions (Finance, Marketing, IT, Capital expenses)
• Have more visibility (booth presence) at more meetings (AACN, AARC (new), ALAT, APSR, ATS, CTS, ERS, SCCM, and more)
• Develop and execute comprehensive marketing and branding strategies for all business units
• Clinical Education (CHEST annual meeting, Board Reviews, all int’l meetings and live learning, simulation)
• Industry Education (PREP, CHEST Analytics)
• Patient Education
• Foundation Fundraising
• Publishing and Content Strategy
• Membership
• Support new IT platforms and bolster security (HR, Finance, Board Effect, Tableau, CHEST analytics, LMS, CMS, NetForum AMS), as well as marketing and social interaction tools (HubSpot)
• Maintain Capital Budget for building, infrastructure, technology, etc
All in all, CHEST has a very active fiscal year planned, with a number of new educational programs and e-learning opportunities showcasing CHEST’s unique brand of innovative clinical education. We look forward to connecting with you and impacting health-care delivery and patient outcomes. It is an honor and a privilege to be able to lead this organization, and all of this news is directly attributable to our dedicated volunteer leadership, faculty, content expertise, staff, and valuable time that you all contribute to make this organization great. Thank you for your ongoing support of CHEST.
.
As we wrap up CHEST’s fiscal year 2017-18 (our fiscal year runs July 1 – June 30), it has been an incredibly positive and productive year, on all fronts. We have educated more learners than ever before, expanded our educational offerings, increased our collaboration with other organizations, grown our CHEST Foundation activities, and are in excellent financial shape to continue our commitment to clinical chest medicine education.
As we prepare for fiscal year 2018-19, I want to highlight some of the key programs, events, and projects we will be undertaking that will support our strategic plan (http://www.chestnet.org/About/Overview/Strategic-Plan) and achieve our mission to champion the prevention, diagnosis, and treatment of chest diseases through education, communication, and research.
Our organization goals are primarily focused on (but are not limited to) the following broad achievements:
a. Increasing the number of learners that CHEST engages (and increasing their engagement with our content) and assessing the results of our educational interactions
b. Keeping our journal CHEST® among the top Pulmonary, Critical Care, and Sleep peer review journals in the world
c. Expanding domestic and global access to CHEST guidelines and other relevant clinical content
d. Continuing to offer a positive and inclusive culture and work environment at CHEST, for our volunteers, world-class faculty, members, and staff
e. Meeting or exceeding our budget, reserve policy, and grant funding targets to ensure delivery of our mission-based educational efforts and programs
Because our mission as a 501(c)3 not-for-profit is education, I’ll start with those key programs that are driving our budget for FY2018-19 and will also cover publishing and membership.
Education – Clinical
• Increased global activity due to global partnerships with several key international educational providers
• Holding April 2019 CHEST World Congress in Bangkok
• Planning June 2019 Board Review conference in Athens, Greece
• 21 total international courses planned
• Increased Live Learning courses, simulation, and hands-on skills training
• 21 courses planned (including 3 new courses)
• Holding two Fellows courses at CHEST HQ (up to 80 fellows)
• Annual Meeting includes 11 postgraduate programs and 24 simulation courses (including more cadaver courses)
• Includes more Fellows courses (up to 240 Fellows)
• Board Courses include two half-day simulation courses; more sponsorship/exhibits, games, and virtual patient tours (VPTs)
• Continuing to build Board Review on-demand and e-learning content packages for those who cannot attend live events
• Launching inaugural e-Learning program with Elsevier
Education – Patient
• Developing multiple CHEST Foundation disease awareness campaigns and patient education resources
• New patient education guides
• Increased visual content (infographics, graphically based materials)
• Increased use of multimedia and video content
• Increased funding for clinical research grants, community service programs and lung health events, and fund-raising through cause marketing (i.e., Feldman Family Poker Night, NYC events, and other local fund raising events)
• Expanding awareness and access of our patient education materials
• Institutions, large group practices
• International reach
• Digital distribution via social media and online campaigns
Education – Industry
• Projecting seven new live clinical immersion courses
• Two new proposed PREP courses with CTS
• Expansion of educational games, VPTs, and e-learning
• Expanded CHEST Analytics Product Lines
• View Points (3 focus groups, 4-5 KOL panels, 4 pulse surveys)
• Deep Dives (3 advanced analytics projects, 5 premium research projects, 2 ethnography studies, and 4-6 Clinical Perspectives)
• Data Lab (looking to launch beta partner)
• Booth IQ (increasing capacity for booth flow and booth intel reports)
Publications, Guidelines and Digital Content
• CHEST® Journal
• Elsevier partnership remains strong; leveraging key data and Elsevier offerings, will be announcing the next Editor in Chief
• CHEST Physician
• New content and delivery mechanisms
• Supplements
• Electronic features
• CHEST SEEK
• Publish Volume 28 (Critical Care)
• Continue development of SEEK online library
• Guidelines
• Completions: Antithrombotic therapy, cough, ILD diagnosis, hypersensitivity pneumonitis, lung cancer, and PAH
• Updates: Antithrombotic therapy, lung cancer, cough, neuromuscular weakness, EBUS needle sampling, and blood transfusions in critical care setting (doing more in critical care)
• Piloting use of DoctorEvidence methodology services and platform for “living guidelines”
Membership
• Focusing on adding value to CHEST membership for key segments
• Bundling e-learning packages with membership
• Exploring international group/society memberships and group practice/institutional memberships
• Working to attract advanced practice providers
• Performing member market research, including member satisfaction, net promoter scores, and other key metrics
Supporting Divisions (Finance, Marketing, IT, Capital expenses)
• Have more visibility (booth presence) at more meetings (AACN, AARC (new), ALAT, APSR, ATS, CTS, ERS, SCCM, and more)
• Develop and execute comprehensive marketing and branding strategies for all business units
• Clinical Education (CHEST annual meeting, Board Reviews, all int’l meetings and live learning, simulation)
• Industry Education (PREP, CHEST Analytics)
• Patient Education
• Foundation Fundraising
• Publishing and Content Strategy
• Membership
• Support new IT platforms and bolster security (HR, Finance, Board Effect, Tableau, CHEST analytics, LMS, CMS, NetForum AMS), as well as marketing and social interaction tools (HubSpot)
• Maintain Capital Budget for building, infrastructure, technology, etc
All in all, CHEST has a very active fiscal year planned, with a number of new educational programs and e-learning opportunities showcasing CHEST’s unique brand of innovative clinical education. We look forward to connecting with you and impacting health-care delivery and patient outcomes. It is an honor and a privilege to be able to lead this organization, and all of this news is directly attributable to our dedicated volunteer leadership, faculty, content expertise, staff, and valuable time that you all contribute to make this organization great. Thank you for your ongoing support of CHEST.
.
Airways, Consent, Fluid Resuscitation, Home Ventilation
Airways Disorders
Quadrupling the inhaled glucocorticoid dose in those with deteriorating asthma control: Zone 2 asthma
Asthma exacerbations account for most asthma-associated health-care costs and are a key outcome for successful asthma management programs. Inhaled corticosteroid (ICS) forms the cornerstone of asthma maintenance therapy.
Previously published data show that:
Most therapeutic benefit of budesonide was achieved at dose range of 400-1000 µg/day (Masoli et al. Eur Respir J. 2004;23:552).
Doubling ICS dose was ineffective in preventing acute asthma exacerbations (Harrison et al. Lancet. 2004;363:271. FitzGerald et al. Thorax. 2004;59: 550).
Increasing ICS dose was unlikely to reduce systemic glucocorticoid use or hospitalization for asthma exacerbations(Kew et al. Cochrane Database Syst Rev. 2016;6:CD007524).
A recent open-label pragmatic study, published in the New England Journal of Medicine, included 1,922 adolescents and adults with asthma. The authors observed a small reduction in severe asthma exacerbations (Hazard ratio 0.81 for time to first severe exacerbation) by quadrupling the dose of ICS during periods of worsening asthma control (McKeever et al. N Engl J Med. 2018;378:902).
This study does create opportunities for cost-benefit by decreasing health-care utilization, decrease in systemic steroid exposure in some patients, and increase in patient awareness of asthma control allowing self-management. Although statistically significant, the treatment effect was small, with 45% of subjects in the ‘quadrupling dose’ arm still experiencing severe exacerbations. Intervention arm also experienced increased rate of adverse effects.
Additional studies are needed before this strategy can be broadly applied. In the same issue of NEJM, quintupling the dose of ICS in children was not associated with decrease in exacerbations (Jackson et al. N Engl J Med. 2018;378:891). The fact that nearly half of asthmatics who quadrupled ICS dose had exacerbations is disconcerting. This highlights an urgent need to understand treatment-responsive phenotypes, mechanisms of steroid sensitivity, and modalities to improve them, if we are to reduce asthma morbidity in the community.
Navitha Ramesh, MD
Steering Committee Member
Mahesh Padukudru Anand, MBBS, FCCP
Steering Committee Member
Clinical Research
Informed consent: Do we need to change our practice?
Informed consent is the keystone of clinical research and helps respect and protect the rights of the participants/subjects. While the informed consent process has been standardized, some challenges still remain, such as pieces of information that should be disclosed, how to disclose information and document understanding of participants, and how detailed that disclosure should be (Grady, N Engl J Med. 2015;372:855). Digital technology can and has been used to improve the process of obtaining informed consent.
Substituting long and complex written forms with electronic consent (e-consent), however, has issues. Few people read through online agreements before clicking “agree,” which may lead to participants consenting without a clear understanding of what they are consenting to. On the other hand, it is also possible to use e-consent to improve comprehension by including videos and graphics. Interactive quizzes can assess the understanding of the participants, embedded links to audios or videos can further enhance the grasp of information. With e-consents, queries from participants can be answered via phone call or email. When e-consent is obtained remotely, the identity can be confirmed by electronic signatures, username, password, or biometrics.
E-consent has advantages, can be done remotely, no paper is needed, etc. It has potential disadvantages like being costly, videos can add time to the process, and multicenter international trials can be difficult (Grady, et al. N Engl J Med, 2017; 376:e43). Studying e-consents to identify gaps in communication between the researcher and the participant in the digitalized world may help improve the process and allow research to proceed with better understanding of the risks and benefits of involvement in clinical research.
Mohsin Ijaz, MD, FCCP
Steering Committee Member
Critical Care
Fluid Resuscitation in ICU Patients With Sepsis
Appropriate fluid resuscitation is a major goal in sepsis management. Debate remains regarding fluid choice and the impact on acute kidney injury (AKI), renal replacement therapy (RRT), and mortality. Normal saline solution (NS) may be associated with hyperchloremic metabolic acidosis, AKI, and death, but study results have been inconsistent. A large before-after study revealed that balanced crystalloids (BC) were associated with lower rates of AKI and RRT but did not impact mortality (Yunos et al. JAMA. 2012;308:1566). A meta-analysis specifically examining patients with sepsis failed to find a significant difference in RRT or mortality, although this conclusion was of low certainty (Rochwerg, et al., Intensive Care Med. 2015;41:1561).
Earlier this year, a large RCT comparing NS vs BC demonstrated a reduction in major adverse kidney events using BC. Independent rates of new RRT, mortality, and persistent renal dysfunction were not significant, but when combined as a composite outcome, the difference was significant. A 30-day mortality reduction was significant in patients with sepsis (25.2% BC vs 29.4% NS) and in patients with large infusions of NS (Semler et al., N Engl J Med. 2018;378:829). Given these results, a move toward a “balanced approach” to fluid resuscitation seems prudent and may be the next step toward improving outcomes in sepsis. These results are likely related to the large infusions of fluid in patients with sepsis or to the inflammatory effects of the disease. Finally, the applicability of these outcomes to the overall critically ill population is still open to debate.
Margaret Disselkamp, MD
Steering Committee Member
Home-Based Mechanical Ventilation and Neuromuscular Disease
Transcutaneous Carbon Dioxide Monitoring: New Era for Home Ventilation
A primary objective of noninvasive home ventilation is normalization of arterial blood gas tensions, night and day. Pulse oximetry has long enabled estimation of arterial oxygen saturation (SpO2) in outpatient offices and overnight at home; however, until recently, measurement of the partial pressure of carbon dioxide (PCO2) has been limited to invasive arterial blood gas testing (PaCO2) or end-tidal CO2 (PetCO2) measurements. Assessment of PetCO2 has been limited by challenges in accessing true end-tidal exhaled gas under a face mask during noninvasive ventilation, particularly for patients with parenchymal lung diseases such as COPD.
Thanks to recent technological advances, transcutaneous measurement of carbon dioxide (PtcCO2) is emerging as the method of choice for assessing the adequacy of noninvasive ventilation. PtcCO2 monitoring is a standard assessment for pediatric patients in the sleep lab, and it is increasingly being utilized in adults to complement diagnostic and treatment purposes. The transcutaneous CO2 sensors work by heating underlying skin to approximately 43° C, increasing blood flow through the underlying dermal capillary bed. Within 2 to 5 minutes, the “arteriolized” capillary PtcCO2 approximates PaCO2. Commercially available devices for measuring PtcCO2 reliably estimate PaCO2 in patients undergoing noninvasive ventilation to within 5 mm Hg (95% CI) (Storre et al. Respir Med. 2010;105:143).
PtcCO2 measurement has limitations. Measured PtcCO2 can drift upward (i.e., technical drift) during continuous monitoring; however, currently available devices adequately adjust for this phenomenon. Arterialization may be limited by thickened skin, edema, or hypoperfusion.
Currently, U.S. insurance companies do not accept PtcCO2 for documentation of hypercapnia, and the cost of measuring PtcCO2 is not reimbursed. Nevertheless, PtcCO2 technology promises a new era for home mechanical ventilation guided by accurate and practical assessment of PCO2, in particular for chronic respiratory failure syndromes. In this setting, home PtcCO2 monitoring potentially can be utilized in place of in-laboratory sleep studies for assessment of nocturnal hypoventilation and optimizing home mechanical ventilation.
Jason Ackrivo, MD
Steering Committee Member
Interstitial and Diffuse Lung Disease
Electronic Patient Education
The management of patients with an interstitial lung disease (ILD) is challenging. A provider must examine the fine details about current and prior medication history, explore various occupational and environmental exposures, perform a thorough physical examination that includes a careful dermatologic and rheumatologic review, and peruse the objective data, such as the high-resolution CT scan of the chest and pulmonary function tests. Then, the pulmonologist and the patient (plus often multiple family members) discuss diagnostic possibilities, any future testing for confirmation, and prognostic implications. Understandably, the patient may leave the office bewildered, overwhelmed, and in search of clarification.
Bewilderment may lead to the internet. In 2001, 4.5% of all internet searches were determined to be health-care-related (Eysenbach et al. AMIA Annu Symp Proc. 2003;225). It is reasonable to presume the percentage is higher today. Just as with any nonmedical website, the choices for digital health-care information are sometimes not contemporaneous and vary in quality. By exploring the most common “hits” on popular search engines when searching for idiopathic pulmonary fibrosis, a 2016 study found that not only is information presented at a high reading level – 12th grade – but often outdated or simply wrong (Fisher, et al. Am J Respir Crit Care Med. 2016;194[2)]:218). Adding to a patient’s possible confusion is that websites expected to be the most helpful, foundation or advocacy websites, were more likely to suggest disproven and even harmful therapies years after those conclusions were published.
CHEST and the Interstitial and Diffuse Lung Disease NetWork are committed to patient education both in and out of the clinical setting. An ongoing redesign of ILD patient education on the CHEST Foundation website is nearing completion and will ensure patients have the most accurate and understandable information available.
Corey Kershaw, MD
Steering Committee Member
Airways Disorders
Quadrupling the inhaled glucocorticoid dose in those with deteriorating asthma control: Zone 2 asthma
Asthma exacerbations account for most asthma-associated health-care costs and are a key outcome for successful asthma management programs. Inhaled corticosteroid (ICS) forms the cornerstone of asthma maintenance therapy.
Previously published data show that:
Most therapeutic benefit of budesonide was achieved at dose range of 400-1000 µg/day (Masoli et al. Eur Respir J. 2004;23:552).
Doubling ICS dose was ineffective in preventing acute asthma exacerbations (Harrison et al. Lancet. 2004;363:271. FitzGerald et al. Thorax. 2004;59: 550).
Increasing ICS dose was unlikely to reduce systemic glucocorticoid use or hospitalization for asthma exacerbations(Kew et al. Cochrane Database Syst Rev. 2016;6:CD007524).
A recent open-label pragmatic study, published in the New England Journal of Medicine, included 1,922 adolescents and adults with asthma. The authors observed a small reduction in severe asthma exacerbations (Hazard ratio 0.81 for time to first severe exacerbation) by quadrupling the dose of ICS during periods of worsening asthma control (McKeever et al. N Engl J Med. 2018;378:902).
This study does create opportunities for cost-benefit by decreasing health-care utilization, decrease in systemic steroid exposure in some patients, and increase in patient awareness of asthma control allowing self-management. Although statistically significant, the treatment effect was small, with 45% of subjects in the ‘quadrupling dose’ arm still experiencing severe exacerbations. Intervention arm also experienced increased rate of adverse effects.
Additional studies are needed before this strategy can be broadly applied. In the same issue of NEJM, quintupling the dose of ICS in children was not associated with decrease in exacerbations (Jackson et al. N Engl J Med. 2018;378:891). The fact that nearly half of asthmatics who quadrupled ICS dose had exacerbations is disconcerting. This highlights an urgent need to understand treatment-responsive phenotypes, mechanisms of steroid sensitivity, and modalities to improve them, if we are to reduce asthma morbidity in the community.
Navitha Ramesh, MD
Steering Committee Member
Mahesh Padukudru Anand, MBBS, FCCP
Steering Committee Member
Clinical Research
Informed consent: Do we need to change our practice?
Informed consent is the keystone of clinical research and helps respect and protect the rights of the participants/subjects. While the informed consent process has been standardized, some challenges still remain, such as pieces of information that should be disclosed, how to disclose information and document understanding of participants, and how detailed that disclosure should be (Grady, N Engl J Med. 2015;372:855). Digital technology can and has been used to improve the process of obtaining informed consent.
Substituting long and complex written forms with electronic consent (e-consent), however, has issues. Few people read through online agreements before clicking “agree,” which may lead to participants consenting without a clear understanding of what they are consenting to. On the other hand, it is also possible to use e-consent to improve comprehension by including videos and graphics. Interactive quizzes can assess the understanding of the participants, embedded links to audios or videos can further enhance the grasp of information. With e-consents, queries from participants can be answered via phone call or email. When e-consent is obtained remotely, the identity can be confirmed by electronic signatures, username, password, or biometrics.
E-consent has advantages, can be done remotely, no paper is needed, etc. It has potential disadvantages like being costly, videos can add time to the process, and multicenter international trials can be difficult (Grady, et al. N Engl J Med, 2017; 376:e43). Studying e-consents to identify gaps in communication between the researcher and the participant in the digitalized world may help improve the process and allow research to proceed with better understanding of the risks and benefits of involvement in clinical research.
Mohsin Ijaz, MD, FCCP
Steering Committee Member
Critical Care
Fluid Resuscitation in ICU Patients With Sepsis
Appropriate fluid resuscitation is a major goal in sepsis management. Debate remains regarding fluid choice and the impact on acute kidney injury (AKI), renal replacement therapy (RRT), and mortality. Normal saline solution (NS) may be associated with hyperchloremic metabolic acidosis, AKI, and death, but study results have been inconsistent. A large before-after study revealed that balanced crystalloids (BC) were associated with lower rates of AKI and RRT but did not impact mortality (Yunos et al. JAMA. 2012;308:1566). A meta-analysis specifically examining patients with sepsis failed to find a significant difference in RRT or mortality, although this conclusion was of low certainty (Rochwerg, et al., Intensive Care Med. 2015;41:1561).
Earlier this year, a large RCT comparing NS vs BC demonstrated a reduction in major adverse kidney events using BC. Independent rates of new RRT, mortality, and persistent renal dysfunction were not significant, but when combined as a composite outcome, the difference was significant. A 30-day mortality reduction was significant in patients with sepsis (25.2% BC vs 29.4% NS) and in patients with large infusions of NS (Semler et al., N Engl J Med. 2018;378:829). Given these results, a move toward a “balanced approach” to fluid resuscitation seems prudent and may be the next step toward improving outcomes in sepsis. These results are likely related to the large infusions of fluid in patients with sepsis or to the inflammatory effects of the disease. Finally, the applicability of these outcomes to the overall critically ill population is still open to debate.
Margaret Disselkamp, MD
Steering Committee Member
Home-Based Mechanical Ventilation and Neuromuscular Disease
Transcutaneous Carbon Dioxide Monitoring: New Era for Home Ventilation
A primary objective of noninvasive home ventilation is normalization of arterial blood gas tensions, night and day. Pulse oximetry has long enabled estimation of arterial oxygen saturation (SpO2) in outpatient offices and overnight at home; however, until recently, measurement of the partial pressure of carbon dioxide (PCO2) has been limited to invasive arterial blood gas testing (PaCO2) or end-tidal CO2 (PetCO2) measurements. Assessment of PetCO2 has been limited by challenges in accessing true end-tidal exhaled gas under a face mask during noninvasive ventilation, particularly for patients with parenchymal lung diseases such as COPD.
Thanks to recent technological advances, transcutaneous measurement of carbon dioxide (PtcCO2) is emerging as the method of choice for assessing the adequacy of noninvasive ventilation. PtcCO2 monitoring is a standard assessment for pediatric patients in the sleep lab, and it is increasingly being utilized in adults to complement diagnostic and treatment purposes. The transcutaneous CO2 sensors work by heating underlying skin to approximately 43° C, increasing blood flow through the underlying dermal capillary bed. Within 2 to 5 minutes, the “arteriolized” capillary PtcCO2 approximates PaCO2. Commercially available devices for measuring PtcCO2 reliably estimate PaCO2 in patients undergoing noninvasive ventilation to within 5 mm Hg (95% CI) (Storre et al. Respir Med. 2010;105:143).
PtcCO2 measurement has limitations. Measured PtcCO2 can drift upward (i.e., technical drift) during continuous monitoring; however, currently available devices adequately adjust for this phenomenon. Arterialization may be limited by thickened skin, edema, or hypoperfusion.
Currently, U.S. insurance companies do not accept PtcCO2 for documentation of hypercapnia, and the cost of measuring PtcCO2 is not reimbursed. Nevertheless, PtcCO2 technology promises a new era for home mechanical ventilation guided by accurate and practical assessment of PCO2, in particular for chronic respiratory failure syndromes. In this setting, home PtcCO2 monitoring potentially can be utilized in place of in-laboratory sleep studies for assessment of nocturnal hypoventilation and optimizing home mechanical ventilation.
Jason Ackrivo, MD
Steering Committee Member
Interstitial and Diffuse Lung Disease
Electronic Patient Education
The management of patients with an interstitial lung disease (ILD) is challenging. A provider must examine the fine details about current and prior medication history, explore various occupational and environmental exposures, perform a thorough physical examination that includes a careful dermatologic and rheumatologic review, and peruse the objective data, such as the high-resolution CT scan of the chest and pulmonary function tests. Then, the pulmonologist and the patient (plus often multiple family members) discuss diagnostic possibilities, any future testing for confirmation, and prognostic implications. Understandably, the patient may leave the office bewildered, overwhelmed, and in search of clarification.
Bewilderment may lead to the internet. In 2001, 4.5% of all internet searches were determined to be health-care-related (Eysenbach et al. AMIA Annu Symp Proc. 2003;225). It is reasonable to presume the percentage is higher today. Just as with any nonmedical website, the choices for digital health-care information are sometimes not contemporaneous and vary in quality. By exploring the most common “hits” on popular search engines when searching for idiopathic pulmonary fibrosis, a 2016 study found that not only is information presented at a high reading level – 12th grade – but often outdated or simply wrong (Fisher, et al. Am J Respir Crit Care Med. 2016;194[2)]:218). Adding to a patient’s possible confusion is that websites expected to be the most helpful, foundation or advocacy websites, were more likely to suggest disproven and even harmful therapies years after those conclusions were published.
CHEST and the Interstitial and Diffuse Lung Disease NetWork are committed to patient education both in and out of the clinical setting. An ongoing redesign of ILD patient education on the CHEST Foundation website is nearing completion and will ensure patients have the most accurate and understandable information available.
Corey Kershaw, MD
Steering Committee Member
Airways Disorders
Quadrupling the inhaled glucocorticoid dose in those with deteriorating asthma control: Zone 2 asthma
Asthma exacerbations account for most asthma-associated health-care costs and are a key outcome for successful asthma management programs. Inhaled corticosteroid (ICS) forms the cornerstone of asthma maintenance therapy.
Previously published data show that:
Most therapeutic benefit of budesonide was achieved at dose range of 400-1000 µg/day (Masoli et al. Eur Respir J. 2004;23:552).
Doubling ICS dose was ineffective in preventing acute asthma exacerbations (Harrison et al. Lancet. 2004;363:271. FitzGerald et al. Thorax. 2004;59: 550).
Increasing ICS dose was unlikely to reduce systemic glucocorticoid use or hospitalization for asthma exacerbations(Kew et al. Cochrane Database Syst Rev. 2016;6:CD007524).
A recent open-label pragmatic study, published in the New England Journal of Medicine, included 1,922 adolescents and adults with asthma. The authors observed a small reduction in severe asthma exacerbations (Hazard ratio 0.81 for time to first severe exacerbation) by quadrupling the dose of ICS during periods of worsening asthma control (McKeever et al. N Engl J Med. 2018;378:902).
This study does create opportunities for cost-benefit by decreasing health-care utilization, decrease in systemic steroid exposure in some patients, and increase in patient awareness of asthma control allowing self-management. Although statistically significant, the treatment effect was small, with 45% of subjects in the ‘quadrupling dose’ arm still experiencing severe exacerbations. Intervention arm also experienced increased rate of adverse effects.
Additional studies are needed before this strategy can be broadly applied. In the same issue of NEJM, quintupling the dose of ICS in children was not associated with decrease in exacerbations (Jackson et al. N Engl J Med. 2018;378:891). The fact that nearly half of asthmatics who quadrupled ICS dose had exacerbations is disconcerting. This highlights an urgent need to understand treatment-responsive phenotypes, mechanisms of steroid sensitivity, and modalities to improve them, if we are to reduce asthma morbidity in the community.
Navitha Ramesh, MD
Steering Committee Member
Mahesh Padukudru Anand, MBBS, FCCP
Steering Committee Member
Clinical Research
Informed consent: Do we need to change our practice?
Informed consent is the keystone of clinical research and helps respect and protect the rights of the participants/subjects. While the informed consent process has been standardized, some challenges still remain, such as pieces of information that should be disclosed, how to disclose information and document understanding of participants, and how detailed that disclosure should be (Grady, N Engl J Med. 2015;372:855). Digital technology can and has been used to improve the process of obtaining informed consent.
Substituting long and complex written forms with electronic consent (e-consent), however, has issues. Few people read through online agreements before clicking “agree,” which may lead to participants consenting without a clear understanding of what they are consenting to. On the other hand, it is also possible to use e-consent to improve comprehension by including videos and graphics. Interactive quizzes can assess the understanding of the participants, embedded links to audios or videos can further enhance the grasp of information. With e-consents, queries from participants can be answered via phone call or email. When e-consent is obtained remotely, the identity can be confirmed by electronic signatures, username, password, or biometrics.
E-consent has advantages, can be done remotely, no paper is needed, etc. It has potential disadvantages like being costly, videos can add time to the process, and multicenter international trials can be difficult (Grady, et al. N Engl J Med, 2017; 376:e43). Studying e-consents to identify gaps in communication between the researcher and the participant in the digitalized world may help improve the process and allow research to proceed with better understanding of the risks and benefits of involvement in clinical research.
Mohsin Ijaz, MD, FCCP
Steering Committee Member
Critical Care
Fluid Resuscitation in ICU Patients With Sepsis
Appropriate fluid resuscitation is a major goal in sepsis management. Debate remains regarding fluid choice and the impact on acute kidney injury (AKI), renal replacement therapy (RRT), and mortality. Normal saline solution (NS) may be associated with hyperchloremic metabolic acidosis, AKI, and death, but study results have been inconsistent. A large before-after study revealed that balanced crystalloids (BC) were associated with lower rates of AKI and RRT but did not impact mortality (Yunos et al. JAMA. 2012;308:1566). A meta-analysis specifically examining patients with sepsis failed to find a significant difference in RRT or mortality, although this conclusion was of low certainty (Rochwerg, et al., Intensive Care Med. 2015;41:1561).
Earlier this year, a large RCT comparing NS vs BC demonstrated a reduction in major adverse kidney events using BC. Independent rates of new RRT, mortality, and persistent renal dysfunction were not significant, but when combined as a composite outcome, the difference was significant. A 30-day mortality reduction was significant in patients with sepsis (25.2% BC vs 29.4% NS) and in patients with large infusions of NS (Semler et al., N Engl J Med. 2018;378:829). Given these results, a move toward a “balanced approach” to fluid resuscitation seems prudent and may be the next step toward improving outcomes in sepsis. These results are likely related to the large infusions of fluid in patients with sepsis or to the inflammatory effects of the disease. Finally, the applicability of these outcomes to the overall critically ill population is still open to debate.
Margaret Disselkamp, MD
Steering Committee Member
Home-Based Mechanical Ventilation and Neuromuscular Disease
Transcutaneous Carbon Dioxide Monitoring: New Era for Home Ventilation
A primary objective of noninvasive home ventilation is normalization of arterial blood gas tensions, night and day. Pulse oximetry has long enabled estimation of arterial oxygen saturation (SpO2) in outpatient offices and overnight at home; however, until recently, measurement of the partial pressure of carbon dioxide (PCO2) has been limited to invasive arterial blood gas testing (PaCO2) or end-tidal CO2 (PetCO2) measurements. Assessment of PetCO2 has been limited by challenges in accessing true end-tidal exhaled gas under a face mask during noninvasive ventilation, particularly for patients with parenchymal lung diseases such as COPD.
Thanks to recent technological advances, transcutaneous measurement of carbon dioxide (PtcCO2) is emerging as the method of choice for assessing the adequacy of noninvasive ventilation. PtcCO2 monitoring is a standard assessment for pediatric patients in the sleep lab, and it is increasingly being utilized in adults to complement diagnostic and treatment purposes. The transcutaneous CO2 sensors work by heating underlying skin to approximately 43° C, increasing blood flow through the underlying dermal capillary bed. Within 2 to 5 minutes, the “arteriolized” capillary PtcCO2 approximates PaCO2. Commercially available devices for measuring PtcCO2 reliably estimate PaCO2 in patients undergoing noninvasive ventilation to within 5 mm Hg (95% CI) (Storre et al. Respir Med. 2010;105:143).
PtcCO2 measurement has limitations. Measured PtcCO2 can drift upward (i.e., technical drift) during continuous monitoring; however, currently available devices adequately adjust for this phenomenon. Arterialization may be limited by thickened skin, edema, or hypoperfusion.
Currently, U.S. insurance companies do not accept PtcCO2 for documentation of hypercapnia, and the cost of measuring PtcCO2 is not reimbursed. Nevertheless, PtcCO2 technology promises a new era for home mechanical ventilation guided by accurate and practical assessment of PCO2, in particular for chronic respiratory failure syndromes. In this setting, home PtcCO2 monitoring potentially can be utilized in place of in-laboratory sleep studies for assessment of nocturnal hypoventilation and optimizing home mechanical ventilation.
Jason Ackrivo, MD
Steering Committee Member
Interstitial and Diffuse Lung Disease
Electronic Patient Education
The management of patients with an interstitial lung disease (ILD) is challenging. A provider must examine the fine details about current and prior medication history, explore various occupational and environmental exposures, perform a thorough physical examination that includes a careful dermatologic and rheumatologic review, and peruse the objective data, such as the high-resolution CT scan of the chest and pulmonary function tests. Then, the pulmonologist and the patient (plus often multiple family members) discuss diagnostic possibilities, any future testing for confirmation, and prognostic implications. Understandably, the patient may leave the office bewildered, overwhelmed, and in search of clarification.
Bewilderment may lead to the internet. In 2001, 4.5% of all internet searches were determined to be health-care-related (Eysenbach et al. AMIA Annu Symp Proc. 2003;225). It is reasonable to presume the percentage is higher today. Just as with any nonmedical website, the choices for digital health-care information are sometimes not contemporaneous and vary in quality. By exploring the most common “hits” on popular search engines when searching for idiopathic pulmonary fibrosis, a 2016 study found that not only is information presented at a high reading level – 12th grade – but often outdated or simply wrong (Fisher, et al. Am J Respir Crit Care Med. 2016;194[2)]:218). Adding to a patient’s possible confusion is that websites expected to be the most helpful, foundation or advocacy websites, were more likely to suggest disproven and even harmful therapies years after those conclusions were published.
CHEST and the Interstitial and Diffuse Lung Disease NetWork are committed to patient education both in and out of the clinical setting. An ongoing redesign of ILD patient education on the CHEST Foundation website is nearing completion and will ensure patients have the most accurate and understandable information available.
Corey Kershaw, MD
Steering Committee Member
Mentors Creating Mentors
Upon wrapping up a successful 2018 NetWorks Challenge Giving campaign – supporting travel grants to CHEST 2018 for early career and diverse clinicians, CHEST Foundation staff sat down with one of our champions, Demondes Haynes, MD, FCCP. Our conversation focused heavily on the role of mentorship in the development of early career clinicians and his own experience as both a mentor and mentee.
Dr. Haynes has had several mentors over the course of his career, but one stands out to him in particular: Doug Campbell, MD, FCCP. Dr. Campbell is a pulmonary and critical care physician who was the division chief at the University of Mississippi Medical Center in Jackson. “When I was finishing my chief residency, the entire pulmonary division imploded. All of the faculty left, except one or two professors, and all those who were going to become fellows here started looking for other places to go. I was actively looking as well…planning to leave my home state, which was not my initial plan. Dr. Campbell came in about that time and promised me that if I gave him some time, we could rebuild the division. He told me if I stayed for my fellowship, I could really help rebuild it. From that day forward, he was my mentor. I stayed for my fellowship under Dr. Campbell.
He delivered on all of those promises. He taught pulmonary medicine extremely well. Not only was a he a great clinician, but he built up the faculty – started a telemedicine program for the ICU and brought in a diverse set of faculty who had all trained at other institutions. He really helped build the program up to be a strong program. I was very happy I chose to stay and learn under his leadership.”
Doug Campbell not only had an impact on Dr. Haynes’ professional life, but also his personal life. “When I agreed to stay for my fellowship, he sent a beautiful handwritten note to my mother, thanking her for raising me to be respectful. She was amazed.” Dr. Haynes mother passed 10 years ago. The night before the funeral at the visitation, Dr. Campbell brought the card his mother sent back – an exchange that Dr. Haynes never knew took place. “It really meant the world to me, not only had he mentored me in my academic career, but he made those personal touches. Those moments are very special to me.”
Dr. Haynes is now mentoring residents and feels it is even more rewarding being a mentor. “You actually get to invest in others, and when you invest in others, the best comes out in them. Sometimes, in this mentoring role, you’re helping people uncover what their qualities are. Sometimes they don’t even know what they are capable of until you push them just a little bit. That’s been so rewarding. I have been blessed, my mentors have invested so much in me, and I am able to pay it forward and give back.”
Dr. Haynes chose to honor Dr. Campbell through giving during the NetWorks Challenge Giving Month. “The NetWork Challenge is great because part of our mission as an organization is philanthropy. We are an education organization, and, in medicine in general, we should support philanthropy. We talk a lot about empathy for our patients… and giving back is just a small part of that. There is a scripture that says, ‘To whom much is given, much is required.’ I truly believe that. I believe that it should just be an ingrained part of our calling as physicians.”
Your generosity funds young clinicians’ learning opportunities that will change the future of patient outcomes and lung diseases. Thank you for making these opportunities possible.
Your continued support will support the next generation of mentees launching their careers (with the proper hands-on training). You can be a Champion for Lung Health and DONATE today through a new gift to the CHEST Foundation by going to chestfoundation.org/donate or calling 224/521-9527.
Again, thank you for all you do to improve patient outcomes. You are the lung health champions who patients and families count on to positively impact lung health.
Upon wrapping up a successful 2018 NetWorks Challenge Giving campaign – supporting travel grants to CHEST 2018 for early career and diverse clinicians, CHEST Foundation staff sat down with one of our champions, Demondes Haynes, MD, FCCP. Our conversation focused heavily on the role of mentorship in the development of early career clinicians and his own experience as both a mentor and mentee.
Dr. Haynes has had several mentors over the course of his career, but one stands out to him in particular: Doug Campbell, MD, FCCP. Dr. Campbell is a pulmonary and critical care physician who was the division chief at the University of Mississippi Medical Center in Jackson. “When I was finishing my chief residency, the entire pulmonary division imploded. All of the faculty left, except one or two professors, and all those who were going to become fellows here started looking for other places to go. I was actively looking as well…planning to leave my home state, which was not my initial plan. Dr. Campbell came in about that time and promised me that if I gave him some time, we could rebuild the division. He told me if I stayed for my fellowship, I could really help rebuild it. From that day forward, he was my mentor. I stayed for my fellowship under Dr. Campbell.
He delivered on all of those promises. He taught pulmonary medicine extremely well. Not only was a he a great clinician, but he built up the faculty – started a telemedicine program for the ICU and brought in a diverse set of faculty who had all trained at other institutions. He really helped build the program up to be a strong program. I was very happy I chose to stay and learn under his leadership.”
Doug Campbell not only had an impact on Dr. Haynes’ professional life, but also his personal life. “When I agreed to stay for my fellowship, he sent a beautiful handwritten note to my mother, thanking her for raising me to be respectful. She was amazed.” Dr. Haynes mother passed 10 years ago. The night before the funeral at the visitation, Dr. Campbell brought the card his mother sent back – an exchange that Dr. Haynes never knew took place. “It really meant the world to me, not only had he mentored me in my academic career, but he made those personal touches. Those moments are very special to me.”
Dr. Haynes is now mentoring residents and feels it is even more rewarding being a mentor. “You actually get to invest in others, and when you invest in others, the best comes out in them. Sometimes, in this mentoring role, you’re helping people uncover what their qualities are. Sometimes they don’t even know what they are capable of until you push them just a little bit. That’s been so rewarding. I have been blessed, my mentors have invested so much in me, and I am able to pay it forward and give back.”
Dr. Haynes chose to honor Dr. Campbell through giving during the NetWorks Challenge Giving Month. “The NetWork Challenge is great because part of our mission as an organization is philanthropy. We are an education organization, and, in medicine in general, we should support philanthropy. We talk a lot about empathy for our patients… and giving back is just a small part of that. There is a scripture that says, ‘To whom much is given, much is required.’ I truly believe that. I believe that it should just be an ingrained part of our calling as physicians.”
Your generosity funds young clinicians’ learning opportunities that will change the future of patient outcomes and lung diseases. Thank you for making these opportunities possible.
Your continued support will support the next generation of mentees launching their careers (with the proper hands-on training). You can be a Champion for Lung Health and DONATE today through a new gift to the CHEST Foundation by going to chestfoundation.org/donate or calling 224/521-9527.
Again, thank you for all you do to improve patient outcomes. You are the lung health champions who patients and families count on to positively impact lung health.
Upon wrapping up a successful 2018 NetWorks Challenge Giving campaign – supporting travel grants to CHEST 2018 for early career and diverse clinicians, CHEST Foundation staff sat down with one of our champions, Demondes Haynes, MD, FCCP. Our conversation focused heavily on the role of mentorship in the development of early career clinicians and his own experience as both a mentor and mentee.
Dr. Haynes has had several mentors over the course of his career, but one stands out to him in particular: Doug Campbell, MD, FCCP. Dr. Campbell is a pulmonary and critical care physician who was the division chief at the University of Mississippi Medical Center in Jackson. “When I was finishing my chief residency, the entire pulmonary division imploded. All of the faculty left, except one or two professors, and all those who were going to become fellows here started looking for other places to go. I was actively looking as well…planning to leave my home state, which was not my initial plan. Dr. Campbell came in about that time and promised me that if I gave him some time, we could rebuild the division. He told me if I stayed for my fellowship, I could really help rebuild it. From that day forward, he was my mentor. I stayed for my fellowship under Dr. Campbell.
He delivered on all of those promises. He taught pulmonary medicine extremely well. Not only was a he a great clinician, but he built up the faculty – started a telemedicine program for the ICU and brought in a diverse set of faculty who had all trained at other institutions. He really helped build the program up to be a strong program. I was very happy I chose to stay and learn under his leadership.”
Doug Campbell not only had an impact on Dr. Haynes’ professional life, but also his personal life. “When I agreed to stay for my fellowship, he sent a beautiful handwritten note to my mother, thanking her for raising me to be respectful. She was amazed.” Dr. Haynes mother passed 10 years ago. The night before the funeral at the visitation, Dr. Campbell brought the card his mother sent back – an exchange that Dr. Haynes never knew took place. “It really meant the world to me, not only had he mentored me in my academic career, but he made those personal touches. Those moments are very special to me.”
Dr. Haynes is now mentoring residents and feels it is even more rewarding being a mentor. “You actually get to invest in others, and when you invest in others, the best comes out in them. Sometimes, in this mentoring role, you’re helping people uncover what their qualities are. Sometimes they don’t even know what they are capable of until you push them just a little bit. That’s been so rewarding. I have been blessed, my mentors have invested so much in me, and I am able to pay it forward and give back.”
Dr. Haynes chose to honor Dr. Campbell through giving during the NetWorks Challenge Giving Month. “The NetWork Challenge is great because part of our mission as an organization is philanthropy. We are an education organization, and, in medicine in general, we should support philanthropy. We talk a lot about empathy for our patients… and giving back is just a small part of that. There is a scripture that says, ‘To whom much is given, much is required.’ I truly believe that. I believe that it should just be an ingrained part of our calling as physicians.”
Your generosity funds young clinicians’ learning opportunities that will change the future of patient outcomes and lung diseases. Thank you for making these opportunities possible.
Your continued support will support the next generation of mentees launching their careers (with the proper hands-on training). You can be a Champion for Lung Health and DONATE today through a new gift to the CHEST Foundation by going to chestfoundation.org/donate or calling 224/521-9527.
Again, thank you for all you do to improve patient outcomes. You are the lung health champions who patients and families count on to positively impact lung health.
This month in the journal CHEST®
Editor’s Picks
Editor in Chief, CHEST
Giants in CHEST Medicine –Arthur S. Slutsky, MD, MASc, BASc
By Dr. Eliot A. Phillipson
Original Research
A Longitudinal Cohort Study of Aspirin Use and Progression of Emphysema-like Lung
Characteristics on CT Imaging: The MESA Lung Study
By Dr. C. P. Aaron, et al.
The Effect of Alcohol Consumption on the Risk of ARDS: A Systematic Review and
Meta-analysis
By Dr. E. Simou, et al.
The Relationship Between COPD and Frailty: A Systematic Review and Meta-Analysis of
Observational Studies
By Dr. A. Marengoni, et al.
Editor’s Picks
Editor in Chief, CHEST
Giants in CHEST Medicine –Arthur S. Slutsky, MD, MASc, BASc
By Dr. Eliot A. Phillipson
Original Research
A Longitudinal Cohort Study of Aspirin Use and Progression of Emphysema-like Lung
Characteristics on CT Imaging: The MESA Lung Study
By Dr. C. P. Aaron, et al.
The Effect of Alcohol Consumption on the Risk of ARDS: A Systematic Review and
Meta-analysis
By Dr. E. Simou, et al.
The Relationship Between COPD and Frailty: A Systematic Review and Meta-Analysis of
Observational Studies
By Dr. A. Marengoni, et al.
Editor’s Picks
Editor in Chief, CHEST
Giants in CHEST Medicine –Arthur S. Slutsky, MD, MASc, BASc
By Dr. Eliot A. Phillipson
Original Research
A Longitudinal Cohort Study of Aspirin Use and Progression of Emphysema-like Lung
Characteristics on CT Imaging: The MESA Lung Study
By Dr. C. P. Aaron, et al.
The Effect of Alcohol Consumption on the Risk of ARDS: A Systematic Review and
Meta-analysis
By Dr. E. Simou, et al.
The Relationship Between COPD and Frailty: A Systematic Review and Meta-Analysis of
Observational Studies
By Dr. A. Marengoni, et al.
Family Fun in San Antonio During CHEST 2018
Planning on bringing your family with you to CHEST 2018 in San Antonio? Well, we’ve got you covered on ways to have some family fun when you’re not immersed in learning at the convention center. Here are a few activities you can take part in:
San Antonio Missions National Historical Park
There are four San Antonio Missions you can visit: San José, Espada, Concepción, and San Juan. Explore the missions on your own, or join a park ranger or volunteer for a free, 45- to 60- minute guided tour of your chosen mission. While Mission San José is the most popular tour with ranger-led tours between 10:00 am and 3:00 pm, make sure to stop at the visitor center or information center of the other missions you want to tour to check available tour times.
World’s Largest Cowboy Boots
Just outside Saks Fifth Avenue at North Star Mall, you can take a selfie next to the World’s Largest Cowboy Boots. These 35-foot tall and 30-foot long boots shouldn’t be too hard to spot. Originally the boots were built by Bob “Daddy-O” Wade in Washington, DC, in 1979 and moved to San Antonio just 1 year later.
Natural Bridge Caverns
Explore the Natural Bridge Caverns, the largest caverns in Texas. This family-owned and family-operated attraction offers guided and adventure tours, and outdoor maze, mining for gems and fossils, and more! When you’re done, you can visit the Shops of Discovery Village where you’ll find treats, a general store, and souvenirs to take home.
The Alamo Trolley
Need a captivating-yet-low impact activity? Ride the Alamo Trolley. This “hop-on, hop-off” trolley allows you to explore San Antonio at your own pace. With 10 stops around town, this entirely narrated tour includes The Alamo, Hemisfair Park, River Walk, the Mission Trail, and more.
Clyde and Seamore’s Sea Lion High
If you go to SeaWorld San Antonio, kids will love attending the sea lion show called “Clyde and Seamore’s Sea Lion High.” The sea lions perform tricks and interact with the audience as Clyde and Seamore go back to school in search of their diplomas.
Cool Off at a Waterpark
While October weather in San Antonio may be slightly cooler than in the summer, it still averages in the mid-80 degrees Fahrenheit, so you’ll want to cool off at the pool or a waterpark. Take some downtime with the family and head to one of the several waterparks in the area, including Schlitterbahn, Splashtown San Antonio, and Aquatica at SeaWorld.
Brackenridge Park
Spend the day at one of San Antonio’s most popular parks, Brackenridge Park. Hike or bike along one of the nature trails, have a picnic, play with your kids at the Kiddie Park, or find the Japanese Tea Garden. Want to add something a little more exciting to your day? The San Antonio Zoo is also on the grounds, where there are lots of animals, experiences, and events.
Planning on bringing your family with you to CHEST 2018 in San Antonio? Well, we’ve got you covered on ways to have some family fun when you’re not immersed in learning at the convention center. Here are a few activities you can take part in:
San Antonio Missions National Historical Park
There are four San Antonio Missions you can visit: San José, Espada, Concepción, and San Juan. Explore the missions on your own, or join a park ranger or volunteer for a free, 45- to 60- minute guided tour of your chosen mission. While Mission San José is the most popular tour with ranger-led tours between 10:00 am and 3:00 pm, make sure to stop at the visitor center or information center of the other missions you want to tour to check available tour times.
World’s Largest Cowboy Boots
Just outside Saks Fifth Avenue at North Star Mall, you can take a selfie next to the World’s Largest Cowboy Boots. These 35-foot tall and 30-foot long boots shouldn’t be too hard to spot. Originally the boots were built by Bob “Daddy-O” Wade in Washington, DC, in 1979 and moved to San Antonio just 1 year later.
Natural Bridge Caverns
Explore the Natural Bridge Caverns, the largest caverns in Texas. This family-owned and family-operated attraction offers guided and adventure tours, and outdoor maze, mining for gems and fossils, and more! When you’re done, you can visit the Shops of Discovery Village where you’ll find treats, a general store, and souvenirs to take home.
The Alamo Trolley
Need a captivating-yet-low impact activity? Ride the Alamo Trolley. This “hop-on, hop-off” trolley allows you to explore San Antonio at your own pace. With 10 stops around town, this entirely narrated tour includes The Alamo, Hemisfair Park, River Walk, the Mission Trail, and more.
Clyde and Seamore’s Sea Lion High
If you go to SeaWorld San Antonio, kids will love attending the sea lion show called “Clyde and Seamore’s Sea Lion High.” The sea lions perform tricks and interact with the audience as Clyde and Seamore go back to school in search of their diplomas.
Cool Off at a Waterpark
While October weather in San Antonio may be slightly cooler than in the summer, it still averages in the mid-80 degrees Fahrenheit, so you’ll want to cool off at the pool or a waterpark. Take some downtime with the family and head to one of the several waterparks in the area, including Schlitterbahn, Splashtown San Antonio, and Aquatica at SeaWorld.
Brackenridge Park
Spend the day at one of San Antonio’s most popular parks, Brackenridge Park. Hike or bike along one of the nature trails, have a picnic, play with your kids at the Kiddie Park, or find the Japanese Tea Garden. Want to add something a little more exciting to your day? The San Antonio Zoo is also on the grounds, where there are lots of animals, experiences, and events.
Planning on bringing your family with you to CHEST 2018 in San Antonio? Well, we’ve got you covered on ways to have some family fun when you’re not immersed in learning at the convention center. Here are a few activities you can take part in:
San Antonio Missions National Historical Park
There are four San Antonio Missions you can visit: San José, Espada, Concepción, and San Juan. Explore the missions on your own, or join a park ranger or volunteer for a free, 45- to 60- minute guided tour of your chosen mission. While Mission San José is the most popular tour with ranger-led tours between 10:00 am and 3:00 pm, make sure to stop at the visitor center or information center of the other missions you want to tour to check available tour times.
World’s Largest Cowboy Boots
Just outside Saks Fifth Avenue at North Star Mall, you can take a selfie next to the World’s Largest Cowboy Boots. These 35-foot tall and 30-foot long boots shouldn’t be too hard to spot. Originally the boots were built by Bob “Daddy-O” Wade in Washington, DC, in 1979 and moved to San Antonio just 1 year later.
Natural Bridge Caverns
Explore the Natural Bridge Caverns, the largest caverns in Texas. This family-owned and family-operated attraction offers guided and adventure tours, and outdoor maze, mining for gems and fossils, and more! When you’re done, you can visit the Shops of Discovery Village where you’ll find treats, a general store, and souvenirs to take home.
The Alamo Trolley
Need a captivating-yet-low impact activity? Ride the Alamo Trolley. This “hop-on, hop-off” trolley allows you to explore San Antonio at your own pace. With 10 stops around town, this entirely narrated tour includes The Alamo, Hemisfair Park, River Walk, the Mission Trail, and more.
Clyde and Seamore’s Sea Lion High
If you go to SeaWorld San Antonio, kids will love attending the sea lion show called “Clyde and Seamore’s Sea Lion High.” The sea lions perform tricks and interact with the audience as Clyde and Seamore go back to school in search of their diplomas.
Cool Off at a Waterpark
While October weather in San Antonio may be slightly cooler than in the summer, it still averages in the mid-80 degrees Fahrenheit, so you’ll want to cool off at the pool or a waterpark. Take some downtime with the family and head to one of the several waterparks in the area, including Schlitterbahn, Splashtown San Antonio, and Aquatica at SeaWorld.
Brackenridge Park
Spend the day at one of San Antonio’s most popular parks, Brackenridge Park. Hike or bike along one of the nature trails, have a picnic, play with your kids at the Kiddie Park, or find the Japanese Tea Garden. Want to add something a little more exciting to your day? The San Antonio Zoo is also on the grounds, where there are lots of animals, experiences, and events.
Launching the Moderate to Severe Asthma Center of Excellence
The American College of Chest Physicians (CHEST) announces a new partnership with Medscape focused on supporting physicians in addressing the challenges of diagnosing and treating moderate to severe asthma. The Moderate to Severe Asthma Center of Excellence (https://www.medscape.com/resource/moderate-severe-asthma) will provide news, expert commentary, and insights on challenging cases to physicians specializing in chest medicine, allergy, primary care, pediatrics, and emergency medicine.
Medscape is a leading source of clinical news, health information, and point-of-care tools for physicians and health-care professionals. This new Center of Excellence available on Medscape.com will explore the diagnostic, therapeutic, and prevention strategies associated with moderate to severe asthma, including the latest research and breakthroughs. Topics will include challenges in classifying and diagnosing disease; risks, benefits, and barriers to treatment; and impact on patients’ quality of life.
“We look forward to working with Medscape on the Center of Excellence to ensure that all physicians treating patients with asthma have access to the latest information and research on managing this pervasive and challenging disease,” said John Studdard, MD, FCCP, President, American College of Chest Physicians.
“The Moderate to Severe Asthma Center of Excellence with CHEST provides a new, accessible channel for information, practical insights, and commentary to the thousands of physicians and health-care professionals who visit Medscape daily,” said Jo-Ann Strangis, Senior Vice President, Editorial for Medscape. “We are privileged to be working with CHEST and look forward to the Center of Excellence making a meaningful difference in patient care.”
Don’t miss Dr. Aaron Holley’s video on “Diagnosing Severe Asthma: ‘Not as Easy as It Sounds” (https://www.medscape.com/viewarticle/896135?src=dpcs).
Visit the Moderate to Severe Asthma Center of Excellence: https://www.medscape.com/resource/moderate-severe-asthma
The American College of Chest Physicians (CHEST) announces a new partnership with Medscape focused on supporting physicians in addressing the challenges of diagnosing and treating moderate to severe asthma. The Moderate to Severe Asthma Center of Excellence (https://www.medscape.com/resource/moderate-severe-asthma) will provide news, expert commentary, and insights on challenging cases to physicians specializing in chest medicine, allergy, primary care, pediatrics, and emergency medicine.
Medscape is a leading source of clinical news, health information, and point-of-care tools for physicians and health-care professionals. This new Center of Excellence available on Medscape.com will explore the diagnostic, therapeutic, and prevention strategies associated with moderate to severe asthma, including the latest research and breakthroughs. Topics will include challenges in classifying and diagnosing disease; risks, benefits, and barriers to treatment; and impact on patients’ quality of life.
“We look forward to working with Medscape on the Center of Excellence to ensure that all physicians treating patients with asthma have access to the latest information and research on managing this pervasive and challenging disease,” said John Studdard, MD, FCCP, President, American College of Chest Physicians.
“The Moderate to Severe Asthma Center of Excellence with CHEST provides a new, accessible channel for information, practical insights, and commentary to the thousands of physicians and health-care professionals who visit Medscape daily,” said Jo-Ann Strangis, Senior Vice President, Editorial for Medscape. “We are privileged to be working with CHEST and look forward to the Center of Excellence making a meaningful difference in patient care.”
Don’t miss Dr. Aaron Holley’s video on “Diagnosing Severe Asthma: ‘Not as Easy as It Sounds” (https://www.medscape.com/viewarticle/896135?src=dpcs).
Visit the Moderate to Severe Asthma Center of Excellence: https://www.medscape.com/resource/moderate-severe-asthma
The American College of Chest Physicians (CHEST) announces a new partnership with Medscape focused on supporting physicians in addressing the challenges of diagnosing and treating moderate to severe asthma. The Moderate to Severe Asthma Center of Excellence (https://www.medscape.com/resource/moderate-severe-asthma) will provide news, expert commentary, and insights on challenging cases to physicians specializing in chest medicine, allergy, primary care, pediatrics, and emergency medicine.
Medscape is a leading source of clinical news, health information, and point-of-care tools for physicians and health-care professionals. This new Center of Excellence available on Medscape.com will explore the diagnostic, therapeutic, and prevention strategies associated with moderate to severe asthma, including the latest research and breakthroughs. Topics will include challenges in classifying and diagnosing disease; risks, benefits, and barriers to treatment; and impact on patients’ quality of life.
“We look forward to working with Medscape on the Center of Excellence to ensure that all physicians treating patients with asthma have access to the latest information and research on managing this pervasive and challenging disease,” said John Studdard, MD, FCCP, President, American College of Chest Physicians.
“The Moderate to Severe Asthma Center of Excellence with CHEST provides a new, accessible channel for information, practical insights, and commentary to the thousands of physicians and health-care professionals who visit Medscape daily,” said Jo-Ann Strangis, Senior Vice President, Editorial for Medscape. “We are privileged to be working with CHEST and look forward to the Center of Excellence making a meaningful difference in patient care.”
Don’t miss Dr. Aaron Holley’s video on “Diagnosing Severe Asthma: ‘Not as Easy as It Sounds” (https://www.medscape.com/viewarticle/896135?src=dpcs).
Visit the Moderate to Severe Asthma Center of Excellence: https://www.medscape.com/resource/moderate-severe-asthma
Diabetes risk may rise with work hours
Men have a higher risk overall for developing diabetes, 12.2%, compared with 7.5% for women, but the risk for women increases as they work more hours per week, which is not the case for men, according to the results of a 12-year Canadian study that included over 7,000 workers.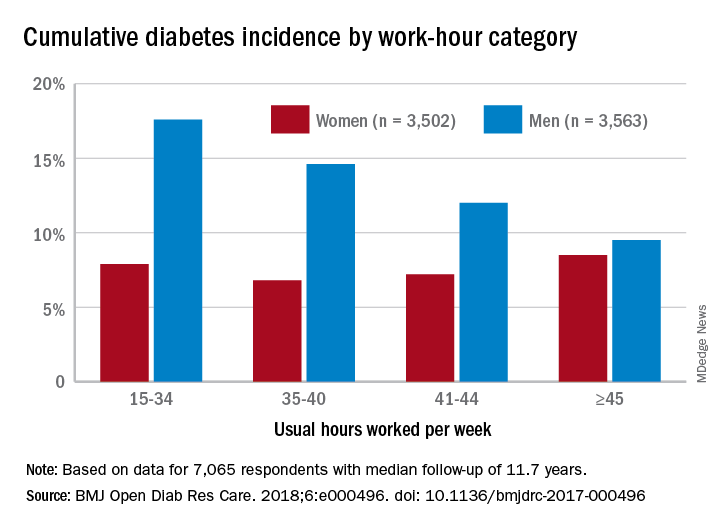
Among the 3,502 women in the study, those who worked 45 or more hours per week had a cumulative diabetes incidence of 8.5% over the median 11.7 years of follow-up. Diabetes incidence was 7.2% for women who worked 41-44 hours a week, 6.8% for those who worked 35-40 hours, and 7.9% among women who worked 15-34 hours weekly, Mahée Gilbert-Ouimet, PhD, of the Institute for Work & Health, Toronto, and her associates reported in BMJ Open Diabetes Research & Care.
For the 3,563 men included in the study, diabetes incidence was 9.5% for those who worked at least 45 hours a week versus 12% for those who worked 41-44 hours, 14.6% for men working 35-40 hours weekly, and 17.6% among those who put in 15-34 hours, the investigators wrote.
Hazard ratios for working 45 or more hours, compared with 35-40 hours, were 1.63 for women and 0.81 for men after adjustment for age, level of education, working conditions, and other factors, although the effect was significant only for women, they noted.
“Considering the rapid and substantial increase of diabetes prevalence in Canada and worldwide, identifying modifiable risk factors, such as long work hours, is of major importance to improve prevention and orient policy making as it could prevent numerous cases of diabetes and diabetes-related chronic diseases,” Dr. Gilbert-Ouimet and her associates wrote.
The study was supported by the Canadian Institutes of Health Research and by the Institute for Clinical Evaluative Sciences, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. None of the investigators declared any conflicts of interest.
SOURCE: Gilbert-Ouimet M et al. BMJ Open Diab Res Care. 2018. doi: 10.1136/bmjdrc-2017-000496.
Men have a higher risk overall for developing diabetes, 12.2%, compared with 7.5% for women, but the risk for women increases as they work more hours per week, which is not the case for men, according to the results of a 12-year Canadian study that included over 7,000 workers.
Among the 3,502 women in the study, those who worked 45 or more hours per week had a cumulative diabetes incidence of 8.5% over the median 11.7 years of follow-up. Diabetes incidence was 7.2% for women who worked 41-44 hours a week, 6.8% for those who worked 35-40 hours, and 7.9% among women who worked 15-34 hours weekly, Mahée Gilbert-Ouimet, PhD, of the Institute for Work & Health, Toronto, and her associates reported in BMJ Open Diabetes Research & Care.
For the 3,563 men included in the study, diabetes incidence was 9.5% for those who worked at least 45 hours a week versus 12% for those who worked 41-44 hours, 14.6% for men working 35-40 hours weekly, and 17.6% among those who put in 15-34 hours, the investigators wrote.
Hazard ratios for working 45 or more hours, compared with 35-40 hours, were 1.63 for women and 0.81 for men after adjustment for age, level of education, working conditions, and other factors, although the effect was significant only for women, they noted.
“Considering the rapid and substantial increase of diabetes prevalence in Canada and worldwide, identifying modifiable risk factors, such as long work hours, is of major importance to improve prevention and orient policy making as it could prevent numerous cases of diabetes and diabetes-related chronic diseases,” Dr. Gilbert-Ouimet and her associates wrote.
The study was supported by the Canadian Institutes of Health Research and by the Institute for Clinical Evaluative Sciences, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. None of the investigators declared any conflicts of interest.
SOURCE: Gilbert-Ouimet M et al. BMJ Open Diab Res Care. 2018. doi: 10.1136/bmjdrc-2017-000496.
Men have a higher risk overall for developing diabetes, 12.2%, compared with 7.5% for women, but the risk for women increases as they work more hours per week, which is not the case for men, according to the results of a 12-year Canadian study that included over 7,000 workers.
Among the 3,502 women in the study, those who worked 45 or more hours per week had a cumulative diabetes incidence of 8.5% over the median 11.7 years of follow-up. Diabetes incidence was 7.2% for women who worked 41-44 hours a week, 6.8% for those who worked 35-40 hours, and 7.9% among women who worked 15-34 hours weekly, Mahée Gilbert-Ouimet, PhD, of the Institute for Work & Health, Toronto, and her associates reported in BMJ Open Diabetes Research & Care.
For the 3,563 men included in the study, diabetes incidence was 9.5% for those who worked at least 45 hours a week versus 12% for those who worked 41-44 hours, 14.6% for men working 35-40 hours weekly, and 17.6% among those who put in 15-34 hours, the investigators wrote.
Hazard ratios for working 45 or more hours, compared with 35-40 hours, were 1.63 for women and 0.81 for men after adjustment for age, level of education, working conditions, and other factors, although the effect was significant only for women, they noted.
“Considering the rapid and substantial increase of diabetes prevalence in Canada and worldwide, identifying modifiable risk factors, such as long work hours, is of major importance to improve prevention and orient policy making as it could prevent numerous cases of diabetes and diabetes-related chronic diseases,” Dr. Gilbert-Ouimet and her associates wrote.
The study was supported by the Canadian Institutes of Health Research and by the Institute for Clinical Evaluative Sciences, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. None of the investigators declared any conflicts of interest.
SOURCE: Gilbert-Ouimet M et al. BMJ Open Diab Res Care. 2018. doi: 10.1136/bmjdrc-2017-000496.
FROM BMJ OPEN DIABETES RESEARCH & CARE
High risk of low glucose? Hospital alerts promise a crucial heads-up
ORLANDO – Researchers have been able to sustain a dramatic reduction in hypoglycemia incidents at nine St. Louis–area hospitals, thanks to a computer algorithm that warns medical staff when patients appear to be on the road to dangerously low blood sugar levels.

The 6-year retrospective system-wide study, which was released at the annual scientific sessions of the American Diabetes Association, found that the use of the alert system lowered the annual occurrence of severe hypoglycemia events by 41% at the hospitals.
In at-risk patients – those with blood glucose levels under 90 mg/dL – the system considers several variables, such as their weight, creatinine clearance, insulin therapy, and basal insulin doses. If the algorithm considers that a patient is at high risk of a sub–40-mg/dL glucose level – dangerously low – it sends a single alert to medical staff during the patient’s stay.
The idea is that the real-time alerts will go to nurses or pharmacists who will review patient charts and then contact physicians. The doctors are expected to “make clinically appropriate changes,” Dr. Tobin said.
Earlier, Dr. Tobin and colleagues prospectively analyzed the alert system’s effectiveness at a single hospital for 5 months. The trial, a cohort intervention study, tracked 655 patients with a blood glucose level under 90 mg/dL.
In 2014, the researchers reported the results of that trial: The alert identified 390 of the patients as being at high risk for severe hypoglycemia (blood glucose under 40 mg/dL). The frequency of severe hypoglycemia events was just 3.1% in this population vs. 9.7% in unalerted patients who were also deemed to be at high risk (J Hosp Med. 2014[9]: 621-6).
For the new study, researchers extended the alert system to nine hospitals and tracked its use from 2011 to 2017.
During all visits, the number of severe hypoglycemic events fell from 2.9 to 1.7 per 1,000 at-risk patient days. (P less than .001)
At one hospital, Dr. Tobin said, the average monthly number of severe hypoglycemia incidents fell from 40 to 12.
Researchers found that the average blood glucose level post alert was 93 mg/dL vs. 74 mg/dL before alert. They also reported that the system-wide total of alerts per year ranged from 4,142 to 5,649.
“The current data reflected in our poster show that the alert process is sustainable over a wide range of clinical settings, including community hospitals of various size and complexity, as well as academic medical centers,” Dr. Tobin said.
The alert system had no effect on hyperglycemia, Dr. Tobin said.
In regard to expense, Dr. Tobin said it’s small because the alert system uses existing current staff and computer systems. Setup costs, he said, included programming, creating the alert infrastructure, and staff training
No study funding is reported. Dr. Tobin reports relationships with Novo Nordisk (advisory board, speaker’s bureau) and MannKind (speaker’s bureau). The other authors report no relevant disclosures.
SOURCE: Tobin G et al. ADA 2018. Abstract 397-P.
ORLANDO – Researchers have been able to sustain a dramatic reduction in hypoglycemia incidents at nine St. Louis–area hospitals, thanks to a computer algorithm that warns medical staff when patients appear to be on the road to dangerously low blood sugar levels.
The 6-year retrospective system-wide study, which was released at the annual scientific sessions of the American Diabetes Association, found that the use of the alert system lowered the annual occurrence of severe hypoglycemia events by 41% at the hospitals.
In at-risk patients – those with blood glucose levels under 90 mg/dL – the system considers several variables, such as their weight, creatinine clearance, insulin therapy, and basal insulin doses. If the algorithm considers that a patient is at high risk of a sub–40-mg/dL glucose level – dangerously low – it sends a single alert to medical staff during the patient’s stay.
The idea is that the real-time alerts will go to nurses or pharmacists who will review patient charts and then contact physicians. The doctors are expected to “make clinically appropriate changes,” Dr. Tobin said.
Earlier, Dr. Tobin and colleagues prospectively analyzed the alert system’s effectiveness at a single hospital for 5 months. The trial, a cohort intervention study, tracked 655 patients with a blood glucose level under 90 mg/dL.
In 2014, the researchers reported the results of that trial: The alert identified 390 of the patients as being at high risk for severe hypoglycemia (blood glucose under 40 mg/dL). The frequency of severe hypoglycemia events was just 3.1% in this population vs. 9.7% in unalerted patients who were also deemed to be at high risk (J Hosp Med. 2014[9]: 621-6).
For the new study, researchers extended the alert system to nine hospitals and tracked its use from 2011 to 2017.
During all visits, the number of severe hypoglycemic events fell from 2.9 to 1.7 per 1,000 at-risk patient days. (P less than .001)
At one hospital, Dr. Tobin said, the average monthly number of severe hypoglycemia incidents fell from 40 to 12.
Researchers found that the average blood glucose level post alert was 93 mg/dL vs. 74 mg/dL before alert. They also reported that the system-wide total of alerts per year ranged from 4,142 to 5,649.
“The current data reflected in our poster show that the alert process is sustainable over a wide range of clinical settings, including community hospitals of various size and complexity, as well as academic medical centers,” Dr. Tobin said.
The alert system had no effect on hyperglycemia, Dr. Tobin said.
In regard to expense, Dr. Tobin said it’s small because the alert system uses existing current staff and computer systems. Setup costs, he said, included programming, creating the alert infrastructure, and staff training
No study funding is reported. Dr. Tobin reports relationships with Novo Nordisk (advisory board, speaker’s bureau) and MannKind (speaker’s bureau). The other authors report no relevant disclosures.
SOURCE: Tobin G et al. ADA 2018. Abstract 397-P.
ORLANDO – Researchers have been able to sustain a dramatic reduction in hypoglycemia incidents at nine St. Louis–area hospitals, thanks to a computer algorithm that warns medical staff when patients appear to be on the road to dangerously low blood sugar levels.
The 6-year retrospective system-wide study, which was released at the annual scientific sessions of the American Diabetes Association, found that the use of the alert system lowered the annual occurrence of severe hypoglycemia events by 41% at the hospitals.
In at-risk patients – those with blood glucose levels under 90 mg/dL – the system considers several variables, such as their weight, creatinine clearance, insulin therapy, and basal insulin doses. If the algorithm considers that a patient is at high risk of a sub–40-mg/dL glucose level – dangerously low – it sends a single alert to medical staff during the patient’s stay.
The idea is that the real-time alerts will go to nurses or pharmacists who will review patient charts and then contact physicians. The doctors are expected to “make clinically appropriate changes,” Dr. Tobin said.
Earlier, Dr. Tobin and colleagues prospectively analyzed the alert system’s effectiveness at a single hospital for 5 months. The trial, a cohort intervention study, tracked 655 patients with a blood glucose level under 90 mg/dL.
In 2014, the researchers reported the results of that trial: The alert identified 390 of the patients as being at high risk for severe hypoglycemia (blood glucose under 40 mg/dL). The frequency of severe hypoglycemia events was just 3.1% in this population vs. 9.7% in unalerted patients who were also deemed to be at high risk (J Hosp Med. 2014[9]: 621-6).
For the new study, researchers extended the alert system to nine hospitals and tracked its use from 2011 to 2017.
During all visits, the number of severe hypoglycemic events fell from 2.9 to 1.7 per 1,000 at-risk patient days. (P less than .001)
At one hospital, Dr. Tobin said, the average monthly number of severe hypoglycemia incidents fell from 40 to 12.
Researchers found that the average blood glucose level post alert was 93 mg/dL vs. 74 mg/dL before alert. They also reported that the system-wide total of alerts per year ranged from 4,142 to 5,649.
“The current data reflected in our poster show that the alert process is sustainable over a wide range of clinical settings, including community hospitals of various size and complexity, as well as academic medical centers,” Dr. Tobin said.
The alert system had no effect on hyperglycemia, Dr. Tobin said.
In regard to expense, Dr. Tobin said it’s small because the alert system uses existing current staff and computer systems. Setup costs, he said, included programming, creating the alert infrastructure, and staff training
No study funding is reported. Dr. Tobin reports relationships with Novo Nordisk (advisory board, speaker’s bureau) and MannKind (speaker’s bureau). The other authors report no relevant disclosures.
SOURCE: Tobin G et al. ADA 2018. Abstract 397-P.
REPORTING FROM ADA 2018
Key clinical point: Hospitals were able to sustain lower numbers of severe hypoglycemia events over 6 years by using a prewarning alert system.
Major finding: The number of severe hypoglycemic events (below 40 mg/dL) fell from 2.9 per 1,000 at-risk patient-days to 1.7 per 1,000 at-risk patient-days.
Study details: Retrospective, system-wide study of nine hospitals with alert system in place from 2011 to 2017.
Disclosures: No funding is reported. One author reports relationships with Novo Nordisk and MannKind. The other authors report no relevant disclosures.
Source: Tobin G et al. ADA 2018. Abstract 397-P.
Data Indicate Disparities in IV t-PA Administration
Women are more likely than men, and African Americans are less likely than Caucasians, to receive IV t-PA.
LOS ANGELES—Variables such as age, sex, race, and insurance status predict whether a patient with ischemic stroke will receive IV t-PA, according to an analysis presented at the 70th Annual Meeting of the American Academy of Neurology. The results provide “compelling evidence” of disparities, despite increased use of IV thrombolysis over time, said F. Stephen Benesh, MD, Chief Resident at the University of Alabama at Birmingham School of Medicine.

Stroke is the leading cause of mortality and morbidity in the United States and has an economic impact of more than $34 billion annually, said Dr. Benesh. IV t-PA has been available since the 1990s, but not all eligible patients have access to this treatment. Dr. Benesh and colleagues examined data from the National Inpatient Sample to find emerging trends and predictors of IV t-PA administration in the clinical setting.
The National Inpatient Sample is a stratified sample of all discharges from US community hospitals. The investigators analyzed data from 2003 through 2013 and identified 1,168,847 patients who had been discharged with a primary diagnosis of ischemic stroke. They ascertained whether patients had received thrombolytic infusion by looking at medical coding. A bimodal logistic regression analysis was performed to identify differences between patients who received t-PA and those who did not. Variables included age, sex, race, teaching status of the treating institution, and patient’s insurance type.
During the period examined, 3.2% of patients with ischemic stroke received thrombolytic treatment. The annual rate of IV t-PA administration increased during the period to approximately 6% in 2013.
Women were slightly more likely to receive IV t-PA than men (odds ratio [OR], 1.036). African Americans (OR, 0.884) were less likely than Caucasians to receive IV t-PA.
Patients insured with Medicare were less likely to receive t-PA than patients insured with Medicaid (OR, 1.128), patients with private insurance (OR, 1.216), and self-paying patients (OR, 1.162). Dr. Benesh and colleagues found no statistically significant difference in the rate of t-PA administration between patients with Medicaid, those with private insurance, and self-paying patients.
In addition, teaching hospitals were more likely than nonteaching hospitals to administer IV t-PA (OR, 1.685).
Various factors may account for the discrepancies in IV t-PA administration. For example, a recent study found that African Americans are more likely to refuse t-PA than patients of other ethnicities. This research reveals “ongoing problems with education and socioeconomic disparities,” said Dr. Benesh.
—Erik Greb
Women are more likely than men, and African Americans are less likely than Caucasians, to receive IV t-PA.
Women are more likely than men, and African Americans are less likely than Caucasians, to receive IV t-PA.
LOS ANGELES—Variables such as age, sex, race, and insurance status predict whether a patient with ischemic stroke will receive IV t-PA, according to an analysis presented at the 70th Annual Meeting of the American Academy of Neurology. The results provide “compelling evidence” of disparities, despite increased use of IV thrombolysis over time, said F. Stephen Benesh, MD, Chief Resident at the University of Alabama at Birmingham School of Medicine.
Stroke is the leading cause of mortality and morbidity in the United States and has an economic impact of more than $34 billion annually, said Dr. Benesh. IV t-PA has been available since the 1990s, but not all eligible patients have access to this treatment. Dr. Benesh and colleagues examined data from the National Inpatient Sample to find emerging trends and predictors of IV t-PA administration in the clinical setting.
The National Inpatient Sample is a stratified sample of all discharges from US community hospitals. The investigators analyzed data from 2003 through 2013 and identified 1,168,847 patients who had been discharged with a primary diagnosis of ischemic stroke. They ascertained whether patients had received thrombolytic infusion by looking at medical coding. A bimodal logistic regression analysis was performed to identify differences between patients who received t-PA and those who did not. Variables included age, sex, race, teaching status of the treating institution, and patient’s insurance type.
During the period examined, 3.2% of patients with ischemic stroke received thrombolytic treatment. The annual rate of IV t-PA administration increased during the period to approximately 6% in 2013.
Women were slightly more likely to receive IV t-PA than men (odds ratio [OR], 1.036). African Americans (OR, 0.884) were less likely than Caucasians to receive IV t-PA.
Patients insured with Medicare were less likely to receive t-PA than patients insured with Medicaid (OR, 1.128), patients with private insurance (OR, 1.216), and self-paying patients (OR, 1.162). Dr. Benesh and colleagues found no statistically significant difference in the rate of t-PA administration between patients with Medicaid, those with private insurance, and self-paying patients.
In addition, teaching hospitals were more likely than nonteaching hospitals to administer IV t-PA (OR, 1.685).
Various factors may account for the discrepancies in IV t-PA administration. For example, a recent study found that African Americans are more likely to refuse t-PA than patients of other ethnicities. This research reveals “ongoing problems with education and socioeconomic disparities,” said Dr. Benesh.
—Erik Greb
LOS ANGELES—Variables such as age, sex, race, and insurance status predict whether a patient with ischemic stroke will receive IV t-PA, according to an analysis presented at the 70th Annual Meeting of the American Academy of Neurology. The results provide “compelling evidence” of disparities, despite increased use of IV thrombolysis over time, said F. Stephen Benesh, MD, Chief Resident at the University of Alabama at Birmingham School of Medicine.
Stroke is the leading cause of mortality and morbidity in the United States and has an economic impact of more than $34 billion annually, said Dr. Benesh. IV t-PA has been available since the 1990s, but not all eligible patients have access to this treatment. Dr. Benesh and colleagues examined data from the National Inpatient Sample to find emerging trends and predictors of IV t-PA administration in the clinical setting.
The National Inpatient Sample is a stratified sample of all discharges from US community hospitals. The investigators analyzed data from 2003 through 2013 and identified 1,168,847 patients who had been discharged with a primary diagnosis of ischemic stroke. They ascertained whether patients had received thrombolytic infusion by looking at medical coding. A bimodal logistic regression analysis was performed to identify differences between patients who received t-PA and those who did not. Variables included age, sex, race, teaching status of the treating institution, and patient’s insurance type.
During the period examined, 3.2% of patients with ischemic stroke received thrombolytic treatment. The annual rate of IV t-PA administration increased during the period to approximately 6% in 2013.
Women were slightly more likely to receive IV t-PA than men (odds ratio [OR], 1.036). African Americans (OR, 0.884) were less likely than Caucasians to receive IV t-PA.
Patients insured with Medicare were less likely to receive t-PA than patients insured with Medicaid (OR, 1.128), patients with private insurance (OR, 1.216), and self-paying patients (OR, 1.162). Dr. Benesh and colleagues found no statistically significant difference in the rate of t-PA administration between patients with Medicaid, those with private insurance, and self-paying patients.
In addition, teaching hospitals were more likely than nonteaching hospitals to administer IV t-PA (OR, 1.685).
Various factors may account for the discrepancies in IV t-PA administration. For example, a recent study found that African Americans are more likely to refuse t-PA than patients of other ethnicities. This research reveals “ongoing problems with education and socioeconomic disparities,” said Dr. Benesh.
—Erik Greb