User login
2018 Update on abnormal uterine bleeding
Over the past year, a few gems have been published to help us manage and treat abnormal uterine bleeding (AUB). One study suggests an order of performing hysteroscopy and endometrial biopsy, another emphasizes the continued cost-effectiveness of the levonorgestrel-releasing intrauterine system (LNG-IUS), while a third provides more evidence that ulipristal acetate is effective in the management of leiomyomas.
Optimal order of office hysteroscopy and endometrial biopsy?
Sarkar P, Mikhail E, Schickler R, Plosker S, Imudia AN. Optimal order of successive office hysteroscopy and endometrial biopsy for the evaluation of abnormal uterine bleeding: a randomized controlled trial. Obstet Gynecol. 2017;130(3):565-572.
Office hysteroscopy and endometrial biopsy are frequently used in the evaluation of women presenting with AUB. Sarkar and colleagues conducted a study aimed at estimating the optimal order of office hysteroscopy and endometrial biopsy when performed successively among premenopausal women.
Pain perception, procedure duration, and other outcomes
This prospective single-blind randomized trial included 78 consecutive patients. The primary outcome was detection of any difference in patients' global pain perception based on the order of the procedures. Secondary outcome measures included determining whether the procedure order affected the duration of the procedures, the adequacy of the endometrial biopsy sample, the number of attempts to obtain an adequate tissue sample, and optimal visualization of the endometrial cavity during office hysteroscopy.
Order not important, but other factors may be
Not surprisingly, the results showed that the order in which the procedures were performed had no effect on patients' pain perception or on the overall procedure duration. Assessed using a visual analog scale scored from 1 to 10, global pain perception in the hysteroscopy-first patients (group A, n = 40) compared with the biopsy-first patients (group B, n = 38) was similar (7 vs 7, P = .57; 95% confidence interval [CI], 5.8-7.1). Procedure duration also was similar in group A and group B (3 vs 3, P = .32; 95% CI, 3.3-4.1).
However, when hysteroscopy was performed first, the quality of endometrial cavity images was superior compared with images from patients in whom biopsy was performed first. The number of endometrial biopsy curette passes required to obtain an adequate tissue sample was lower in the biopsy-first patients. The endometrial biopsy specimen was adequate for histologic evaluation regardless of whether hysteroscopy or biopsy was performed first.
Sarkar and colleagues suggested that their study findings emphasize the importance of individualizing the order of successive procedures to achieve the most clinically relevant result with maximum ease and comfort. They proposed that patients who have a high index of suspicion for occult malignancy or endometrial hyperplasia should have a biopsy procedure first so that adequate tissue samples can be obtained with fewer attempts. In patients with underlying uterine anatomic defects, performing hysteroscopy first would be clinically relevant to obtain the best images for optimal surgical planning.
Read next: Which treatment for AUB is most cost-effective?
Which treatment for AUB is most cost-effective?
Spencer JC, Louie M, Moulder JK, et al. Cost-effectiveness of treatments for heavy menstrual bleeding. Am J Obstet Gynecol. 2017;217(5):574.e1-574e.9.
The costs associated with heavy menstrual bleeding are significant. Spencer and colleagues sought to evaluate the relative cost-effectiveness of 4 treatment options for heavy menstrual bleeding: hysterectomy, resectoscopic endometrial ablation, nonresectoscopic endometrial ablation, and the LNG-IUS in a hypothetical cohort of 100,000 premenopausal women. No previous studies have examined the cost-effectiveness of these options in the context of the US health care setting.
Decision tree used for analysis
The authors formulated a decision tree to evaluate private payer costs and quality-adjusted life-years over a 5-year time horizon for premenopausal women with heavy menstrual bleeding and no suspected malignancy. For each treatment option, the authors used probabilities to estimate frequencies of complications and treatment failure leading to additional therapies. They compared the treatments in terms of total average costs, quality-adjusted life years, and incremental cost-effectiveness ratios.
Comparing costs, quality of life, and complications
Quality of life was fairly high for all treatment options; however, the estimated costs and the complications of each treatment were markedly different between treatment options. The LNG-IUS was superior to all alternatives in terms of both cost and quality, making it the dominant strategy. The 5-year cost for the LNG-IUS was $4,500, about half the cost of endometrial ablation ($9,500) and about one-third the cost of hysterectomy ($13,500). When examined over a range of possible values, the LNG-IUS was cost-effective compared with hysterectomy in the large majority of scenarios (90%).
If the LNG-IUS is removed from consideration because of either patient preference or clinical judgment, the decision between hysterectomy and ablation is more complex. Hysterectomy results in better quality of life in the majority of simulations, but it is cost-effective in just more than half of the simulations compared with either resectoscopic or nonresectoscopic ablation. Therefore, consideration of cost, procedure-specific complications, and patient preferences may guide the therapeutic decision between hysterectomy and endometrial ablation.
The 52-mg LNG-IUS was superior to all treatment alternatives in both cost and quality, making it the dominant strategy for the treatment of heavy menstrual bleeding.
Ulipristal may be useful for managing AUB associated with uterine leiomyomas
Simon JA, Catherino W, Segars JH, et al. Ulipristal acetate for treatment of symptomatic uterine leiomyomas: a randomized controlled trial. Obstet Gynecol. 2018;131(3):431-439.
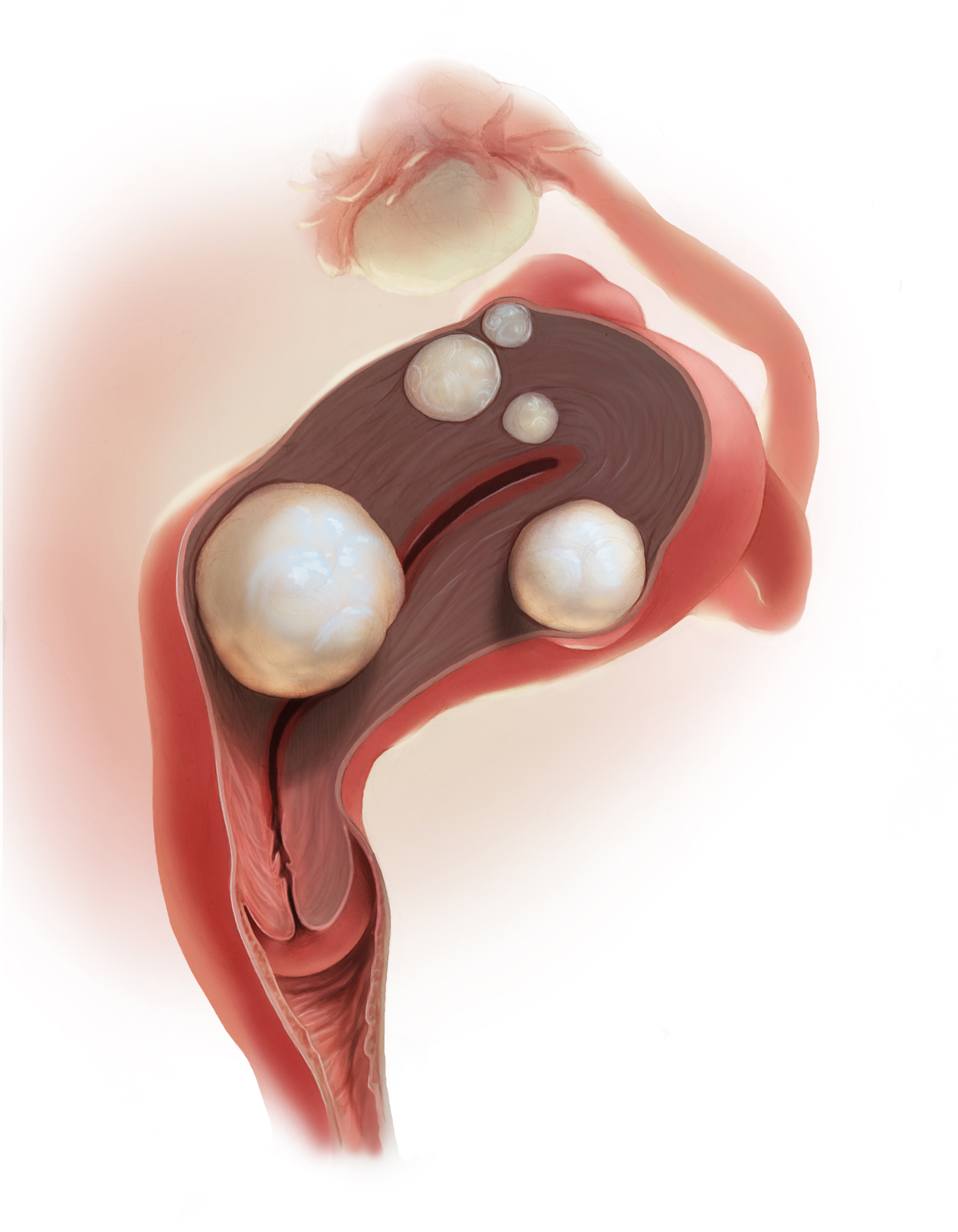
Managing uterine leiomyomas is a common issue for gynecologists, as up to 70% of white women and more than 80% of black women of reproductive age in the United States have leiomyomas.
Ulipristal acetate is an orally administered selective progesterone-receptor modulator that decreases bleeding and reduces leiomyoma size. Although trials conducted in Europe found ulipristal to be superior to placebo and noninferior to leuprolide acetate in controlling bleeding and reducing leiomyoma size, those initial trials were conducted in a predominantly white population.
Study assessed efficacy and safety
Simon and colleagues recently conducted a randomized double-blind, placebo-controlled trial designed to assess the safety and efficacy of ulipristal in a more diverse population, such as patients in the United States. The 148 participants included in the study were randomly assigned on a 1:1:1 basis to once-daily oral ulipristal 5 mg, ulipristal 10 mg, or placebo for 12 weeks, with a 12-week drug-free follow-up.
Amenorrhea achieved and quality of life improved
The investigators found that ulipristal in 5-mg and 10-mg doses was well tolerated and superior to placebo in both the rate of and the time to amenorrhea (the coprimary end points) in women with symptomatic leiomyomas. In women treated with ulipristal 5 mg, amenorrhea was achieved in 25 of 53 (47.2%; 97.5% CI, 31.6-63.2), and of those treated with the 10-mg dose, 28 of 48 (58.3%; 97.5% CI, 41.2-74.1) achieved amenorrhea (P<.001 for both groups), compared with 1 of 56 (1.8%; 97.5% CI, 0.0-10.9) in the placebo group.
AUB continues to be a significant issue for many women. As women's health care providers, it is important that we deliver care with high value (Quality ÷ Cost). Therefore, consider these takeaway points:
- The LNG-IUS consistently delivers high value by affecting both sides of this equation. We should use it more.
- Although we do not yet know what ulipristal acetate will cost in the United States, effective medical treatments usually affect both sides of the Quality ÷ Cost equation, and new medications on the horizon are worth knowing about.
- Last, efficiency with office-based hysteroscopy is also an opportunity to increase value by improving biopsy and visualization quality.
Ulipristal treatment also was shown to improve health-related quality of life, including physical and social activities. No patient discontinued ulipristal because of lack of efficacy, and 1 patient in the placebo group stopped taking the drug because of an adverse event. Estradiol levels were maintained at midfollicular levels during ulipristal treatment, and endometrial biopsies did not show any atypical or malignant changes. These results are consistent with those of the studies conducted in Europe in a predominantly white, nonobese population.
Results of this study help to define a niche for ulipristal when hysterectomy is not an option for women who wish to preserve fertility. Further, although leuprolide is used for preoperative hematologic improvement of anemia, its use results in hypoestrogenic adverse effects.
The findings from this and other studies suggest that ulipristal may be useful for the medical management of AUB associated with uterine leiomyomas, especially for patients desiring uterine- and fertility-sparing treatment. Hopefully, this treatment will be available soon in the United States.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Howard T. Sharp, MD
Dr. Sharp is Professor and Vice Chair for Clinical and Quality Activities, Department of Obstetrics and Gynecology, University of Utah Health Sciences Center, Salt Lake City.
Marisa R. Adelman, MD
Dr. Adelman is Assistant Professor, Department of Obstetrics and Gynecology, University of Utah Health Sciences Center, Salt Lake City.
The authors report no financial relationships relevant to this article.
Howard T. Sharp, MD
Dr. Sharp is Professor and Vice Chair for Clinical and Quality Activities, Department of Obstetrics and Gynecology, University of Utah Health Sciences Center, Salt Lake City.
Marisa R. Adelman, MD
Dr. Adelman is Assistant Professor, Department of Obstetrics and Gynecology, University of Utah Health Sciences Center, Salt Lake City.
The authors report no financial relationships relevant to this article.
Howard T. Sharp, MD
Dr. Sharp is Professor and Vice Chair for Clinical and Quality Activities, Department of Obstetrics and Gynecology, University of Utah Health Sciences Center, Salt Lake City.
Marisa R. Adelman, MD
Dr. Adelman is Assistant Professor, Department of Obstetrics and Gynecology, University of Utah Health Sciences Center, Salt Lake City.
The authors report no financial relationships relevant to this article.
Over the past year, a few gems have been published to help us manage and treat abnormal uterine bleeding (AUB). One study suggests an order of performing hysteroscopy and endometrial biopsy, another emphasizes the continued cost-effectiveness of the levonorgestrel-releasing intrauterine system (LNG-IUS), while a third provides more evidence that ulipristal acetate is effective in the management of leiomyomas.
Optimal order of office hysteroscopy and endometrial biopsy?
Sarkar P, Mikhail E, Schickler R, Plosker S, Imudia AN. Optimal order of successive office hysteroscopy and endometrial biopsy for the evaluation of abnormal uterine bleeding: a randomized controlled trial. Obstet Gynecol. 2017;130(3):565-572.
Office hysteroscopy and endometrial biopsy are frequently used in the evaluation of women presenting with AUB. Sarkar and colleagues conducted a study aimed at estimating the optimal order of office hysteroscopy and endometrial biopsy when performed successively among premenopausal women.
Pain perception, procedure duration, and other outcomes
This prospective single-blind randomized trial included 78 consecutive patients. The primary outcome was detection of any difference in patients' global pain perception based on the order of the procedures. Secondary outcome measures included determining whether the procedure order affected the duration of the procedures, the adequacy of the endometrial biopsy sample, the number of attempts to obtain an adequate tissue sample, and optimal visualization of the endometrial cavity during office hysteroscopy.
Order not important, but other factors may be
Not surprisingly, the results showed that the order in which the procedures were performed had no effect on patients' pain perception or on the overall procedure duration. Assessed using a visual analog scale scored from 1 to 10, global pain perception in the hysteroscopy-first patients (group A, n = 40) compared with the biopsy-first patients (group B, n = 38) was similar (7 vs 7, P = .57; 95% confidence interval [CI], 5.8-7.1). Procedure duration also was similar in group A and group B (3 vs 3, P = .32; 95% CI, 3.3-4.1).
However, when hysteroscopy was performed first, the quality of endometrial cavity images was superior compared with images from patients in whom biopsy was performed first. The number of endometrial biopsy curette passes required to obtain an adequate tissue sample was lower in the biopsy-first patients. The endometrial biopsy specimen was adequate for histologic evaluation regardless of whether hysteroscopy or biopsy was performed first.
Sarkar and colleagues suggested that their study findings emphasize the importance of individualizing the order of successive procedures to achieve the most clinically relevant result with maximum ease and comfort. They proposed that patients who have a high index of suspicion for occult malignancy or endometrial hyperplasia should have a biopsy procedure first so that adequate tissue samples can be obtained with fewer attempts. In patients with underlying uterine anatomic defects, performing hysteroscopy first would be clinically relevant to obtain the best images for optimal surgical planning.
Read next: Which treatment for AUB is most cost-effective?
Which treatment for AUB is most cost-effective?
Spencer JC, Louie M, Moulder JK, et al. Cost-effectiveness of treatments for heavy menstrual bleeding. Am J Obstet Gynecol. 2017;217(5):574.e1-574e.9.
The costs associated with heavy menstrual bleeding are significant. Spencer and colleagues sought to evaluate the relative cost-effectiveness of 4 treatment options for heavy menstrual bleeding: hysterectomy, resectoscopic endometrial ablation, nonresectoscopic endometrial ablation, and the LNG-IUS in a hypothetical cohort of 100,000 premenopausal women. No previous studies have examined the cost-effectiveness of these options in the context of the US health care setting.
Decision tree used for analysis
The authors formulated a decision tree to evaluate private payer costs and quality-adjusted life-years over a 5-year time horizon for premenopausal women with heavy menstrual bleeding and no suspected malignancy. For each treatment option, the authors used probabilities to estimate frequencies of complications and treatment failure leading to additional therapies. They compared the treatments in terms of total average costs, quality-adjusted life years, and incremental cost-effectiveness ratios.
Comparing costs, quality of life, and complications
Quality of life was fairly high for all treatment options; however, the estimated costs and the complications of each treatment were markedly different between treatment options. The LNG-IUS was superior to all alternatives in terms of both cost and quality, making it the dominant strategy. The 5-year cost for the LNG-IUS was $4,500, about half the cost of endometrial ablation ($9,500) and about one-third the cost of hysterectomy ($13,500). When examined over a range of possible values, the LNG-IUS was cost-effective compared with hysterectomy in the large majority of scenarios (90%).
If the LNG-IUS is removed from consideration because of either patient preference or clinical judgment, the decision between hysterectomy and ablation is more complex. Hysterectomy results in better quality of life in the majority of simulations, but it is cost-effective in just more than half of the simulations compared with either resectoscopic or nonresectoscopic ablation. Therefore, consideration of cost, procedure-specific complications, and patient preferences may guide the therapeutic decision between hysterectomy and endometrial ablation.
The 52-mg LNG-IUS was superior to all treatment alternatives in both cost and quality, making it the dominant strategy for the treatment of heavy menstrual bleeding.
Ulipristal may be useful for managing AUB associated with uterine leiomyomas
Simon JA, Catherino W, Segars JH, et al. Ulipristal acetate for treatment of symptomatic uterine leiomyomas: a randomized controlled trial. Obstet Gynecol. 2018;131(3):431-439.
Managing uterine leiomyomas is a common issue for gynecologists, as up to 70% of white women and more than 80% of black women of reproductive age in the United States have leiomyomas.
Ulipristal acetate is an orally administered selective progesterone-receptor modulator that decreases bleeding and reduces leiomyoma size. Although trials conducted in Europe found ulipristal to be superior to placebo and noninferior to leuprolide acetate in controlling bleeding and reducing leiomyoma size, those initial trials were conducted in a predominantly white population.
Study assessed efficacy and safety
Simon and colleagues recently conducted a randomized double-blind, placebo-controlled trial designed to assess the safety and efficacy of ulipristal in a more diverse population, such as patients in the United States. The 148 participants included in the study were randomly assigned on a 1:1:1 basis to once-daily oral ulipristal 5 mg, ulipristal 10 mg, or placebo for 12 weeks, with a 12-week drug-free follow-up.
Amenorrhea achieved and quality of life improved
The investigators found that ulipristal in 5-mg and 10-mg doses was well tolerated and superior to placebo in both the rate of and the time to amenorrhea (the coprimary end points) in women with symptomatic leiomyomas. In women treated with ulipristal 5 mg, amenorrhea was achieved in 25 of 53 (47.2%; 97.5% CI, 31.6-63.2), and of those treated with the 10-mg dose, 28 of 48 (58.3%; 97.5% CI, 41.2-74.1) achieved amenorrhea (P<.001 for both groups), compared with 1 of 56 (1.8%; 97.5% CI, 0.0-10.9) in the placebo group.
AUB continues to be a significant issue for many women. As women's health care providers, it is important that we deliver care with high value (Quality ÷ Cost). Therefore, consider these takeaway points:
- The LNG-IUS consistently delivers high value by affecting both sides of this equation. We should use it more.
- Although we do not yet know what ulipristal acetate will cost in the United States, effective medical treatments usually affect both sides of the Quality ÷ Cost equation, and new medications on the horizon are worth knowing about.
- Last, efficiency with office-based hysteroscopy is also an opportunity to increase value by improving biopsy and visualization quality.
Ulipristal treatment also was shown to improve health-related quality of life, including physical and social activities. No patient discontinued ulipristal because of lack of efficacy, and 1 patient in the placebo group stopped taking the drug because of an adverse event. Estradiol levels were maintained at midfollicular levels during ulipristal treatment, and endometrial biopsies did not show any atypical or malignant changes. These results are consistent with those of the studies conducted in Europe in a predominantly white, nonobese population.
Results of this study help to define a niche for ulipristal when hysterectomy is not an option for women who wish to preserve fertility. Further, although leuprolide is used for preoperative hematologic improvement of anemia, its use results in hypoestrogenic adverse effects.
The findings from this and other studies suggest that ulipristal may be useful for the medical management of AUB associated with uterine leiomyomas, especially for patients desiring uterine- and fertility-sparing treatment. Hopefully, this treatment will be available soon in the United States.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Over the past year, a few gems have been published to help us manage and treat abnormal uterine bleeding (AUB). One study suggests an order of performing hysteroscopy and endometrial biopsy, another emphasizes the continued cost-effectiveness of the levonorgestrel-releasing intrauterine system (LNG-IUS), while a third provides more evidence that ulipristal acetate is effective in the management of leiomyomas.
Optimal order of office hysteroscopy and endometrial biopsy?
Sarkar P, Mikhail E, Schickler R, Plosker S, Imudia AN. Optimal order of successive office hysteroscopy and endometrial biopsy for the evaluation of abnormal uterine bleeding: a randomized controlled trial. Obstet Gynecol. 2017;130(3):565-572.
Office hysteroscopy and endometrial biopsy are frequently used in the evaluation of women presenting with AUB. Sarkar and colleagues conducted a study aimed at estimating the optimal order of office hysteroscopy and endometrial biopsy when performed successively among premenopausal women.
Pain perception, procedure duration, and other outcomes
This prospective single-blind randomized trial included 78 consecutive patients. The primary outcome was detection of any difference in patients' global pain perception based on the order of the procedures. Secondary outcome measures included determining whether the procedure order affected the duration of the procedures, the adequacy of the endometrial biopsy sample, the number of attempts to obtain an adequate tissue sample, and optimal visualization of the endometrial cavity during office hysteroscopy.
Order not important, but other factors may be
Not surprisingly, the results showed that the order in which the procedures were performed had no effect on patients' pain perception or on the overall procedure duration. Assessed using a visual analog scale scored from 1 to 10, global pain perception in the hysteroscopy-first patients (group A, n = 40) compared with the biopsy-first patients (group B, n = 38) was similar (7 vs 7, P = .57; 95% confidence interval [CI], 5.8-7.1). Procedure duration also was similar in group A and group B (3 vs 3, P = .32; 95% CI, 3.3-4.1).
However, when hysteroscopy was performed first, the quality of endometrial cavity images was superior compared with images from patients in whom biopsy was performed first. The number of endometrial biopsy curette passes required to obtain an adequate tissue sample was lower in the biopsy-first patients. The endometrial biopsy specimen was adequate for histologic evaluation regardless of whether hysteroscopy or biopsy was performed first.
Sarkar and colleagues suggested that their study findings emphasize the importance of individualizing the order of successive procedures to achieve the most clinically relevant result with maximum ease and comfort. They proposed that patients who have a high index of suspicion for occult malignancy or endometrial hyperplasia should have a biopsy procedure first so that adequate tissue samples can be obtained with fewer attempts. In patients with underlying uterine anatomic defects, performing hysteroscopy first would be clinically relevant to obtain the best images for optimal surgical planning.
Read next: Which treatment for AUB is most cost-effective?
Which treatment for AUB is most cost-effective?
Spencer JC, Louie M, Moulder JK, et al. Cost-effectiveness of treatments for heavy menstrual bleeding. Am J Obstet Gynecol. 2017;217(5):574.e1-574e.9.
The costs associated with heavy menstrual bleeding are significant. Spencer and colleagues sought to evaluate the relative cost-effectiveness of 4 treatment options for heavy menstrual bleeding: hysterectomy, resectoscopic endometrial ablation, nonresectoscopic endometrial ablation, and the LNG-IUS in a hypothetical cohort of 100,000 premenopausal women. No previous studies have examined the cost-effectiveness of these options in the context of the US health care setting.
Decision tree used for analysis
The authors formulated a decision tree to evaluate private payer costs and quality-adjusted life-years over a 5-year time horizon for premenopausal women with heavy menstrual bleeding and no suspected malignancy. For each treatment option, the authors used probabilities to estimate frequencies of complications and treatment failure leading to additional therapies. They compared the treatments in terms of total average costs, quality-adjusted life years, and incremental cost-effectiveness ratios.
Comparing costs, quality of life, and complications
Quality of life was fairly high for all treatment options; however, the estimated costs and the complications of each treatment were markedly different between treatment options. The LNG-IUS was superior to all alternatives in terms of both cost and quality, making it the dominant strategy. The 5-year cost for the LNG-IUS was $4,500, about half the cost of endometrial ablation ($9,500) and about one-third the cost of hysterectomy ($13,500). When examined over a range of possible values, the LNG-IUS was cost-effective compared with hysterectomy in the large majority of scenarios (90%).
If the LNG-IUS is removed from consideration because of either patient preference or clinical judgment, the decision between hysterectomy and ablation is more complex. Hysterectomy results in better quality of life in the majority of simulations, but it is cost-effective in just more than half of the simulations compared with either resectoscopic or nonresectoscopic ablation. Therefore, consideration of cost, procedure-specific complications, and patient preferences may guide the therapeutic decision between hysterectomy and endometrial ablation.
The 52-mg LNG-IUS was superior to all treatment alternatives in both cost and quality, making it the dominant strategy for the treatment of heavy menstrual bleeding.
Ulipristal may be useful for managing AUB associated with uterine leiomyomas
Simon JA, Catherino W, Segars JH, et al. Ulipristal acetate for treatment of symptomatic uterine leiomyomas: a randomized controlled trial. Obstet Gynecol. 2018;131(3):431-439.
Managing uterine leiomyomas is a common issue for gynecologists, as up to 70% of white women and more than 80% of black women of reproductive age in the United States have leiomyomas.
Ulipristal acetate is an orally administered selective progesterone-receptor modulator that decreases bleeding and reduces leiomyoma size. Although trials conducted in Europe found ulipristal to be superior to placebo and noninferior to leuprolide acetate in controlling bleeding and reducing leiomyoma size, those initial trials were conducted in a predominantly white population.
Study assessed efficacy and safety
Simon and colleagues recently conducted a randomized double-blind, placebo-controlled trial designed to assess the safety and efficacy of ulipristal in a more diverse population, such as patients in the United States. The 148 participants included in the study were randomly assigned on a 1:1:1 basis to once-daily oral ulipristal 5 mg, ulipristal 10 mg, or placebo for 12 weeks, with a 12-week drug-free follow-up.
Amenorrhea achieved and quality of life improved
The investigators found that ulipristal in 5-mg and 10-mg doses was well tolerated and superior to placebo in both the rate of and the time to amenorrhea (the coprimary end points) in women with symptomatic leiomyomas. In women treated with ulipristal 5 mg, amenorrhea was achieved in 25 of 53 (47.2%; 97.5% CI, 31.6-63.2), and of those treated with the 10-mg dose, 28 of 48 (58.3%; 97.5% CI, 41.2-74.1) achieved amenorrhea (P<.001 for both groups), compared with 1 of 56 (1.8%; 97.5% CI, 0.0-10.9) in the placebo group.
AUB continues to be a significant issue for many women. As women's health care providers, it is important that we deliver care with high value (Quality ÷ Cost). Therefore, consider these takeaway points:
- The LNG-IUS consistently delivers high value by affecting both sides of this equation. We should use it more.
- Although we do not yet know what ulipristal acetate will cost in the United States, effective medical treatments usually affect both sides of the Quality ÷ Cost equation, and new medications on the horizon are worth knowing about.
- Last, efficiency with office-based hysteroscopy is also an opportunity to increase value by improving biopsy and visualization quality.
Ulipristal treatment also was shown to improve health-related quality of life, including physical and social activities. No patient discontinued ulipristal because of lack of efficacy, and 1 patient in the placebo group stopped taking the drug because of an adverse event. Estradiol levels were maintained at midfollicular levels during ulipristal treatment, and endometrial biopsies did not show any atypical or malignant changes. These results are consistent with those of the studies conducted in Europe in a predominantly white, nonobese population.
Results of this study help to define a niche for ulipristal when hysterectomy is not an option for women who wish to preserve fertility. Further, although leuprolide is used for preoperative hematologic improvement of anemia, its use results in hypoestrogenic adverse effects.
The findings from this and other studies suggest that ulipristal may be useful for the medical management of AUB associated with uterine leiomyomas, especially for patients desiring uterine- and fertility-sparing treatment. Hopefully, this treatment will be available soon in the United States.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Endoscopic screening tied to significantly lower risk of death from gastric cancer
Endoscopic screening was associated with an approximately 40% reduction in risk of death from gastric cancer in a systematic review and meta-analysis of studies from Asian countries.
The study is the first systematic review and meta-analysis of gastric cancer mortality and incidence after endoscopic screening, wrote Xing Zhang, MD, of the China Academy of Chinese Medical Sciences in Beijing with his associates. “Population-based prospective cohort studies are warranted to confirm our findings,” the reviewers wrote in the August issue of Gastroenterology.
In general, the rates of gastric cancer and related mortality in East Asian countries are significantly higher than global averages. As a result, countries in this region have implemented a variety of national and opportunistic screening programs that vary from country to country. Japan, for example, has a national screening program based on photofluorography. “Although data are inconsistent, most studies have shown a 40%-60% decrease in the mortality of gastric cancer in those who have been screened using photofluorography,” the reviewers noted. When findings are positive, follow-up endoscopy is recommended. However, debates persist about whether population-level endoscopy significantly improves hard endpoints in gastric cancer, such as incidence and mortality.
To help clarify the population-level benefits of endoscopic screening, Dr. Zhang and his associates searched PubMed and EMBASE; they identified six cohort studies and four nested case-control studies that included approximately 342,000 adults from Asia who did not have baseline gastric cancer but did undergo surveillance endoscopy at least once. Studies of both mass and opportunistic screening were included. Each study included a comparator; reported incidence, mortality, or both; and was published by March 8, 2018.
Endoscopic screening was tied to a 40% reduction in the relative risk of death from gastric cancer (risk ratio, 0.60; 95% confidence interval, 0.49-0.73). There also was a slight trend toward increased incidence of gastric cancer, which was not statistically significant (RR, 1.14; 95% CI, 0.93-1.40). However, only two studies examined the incidence of gastric cancer, so this outcome “should be interpreted with caution,” the reviewers wrote. Endoscopic screening also was associated with a significantly lower risk of death from gastric cancer, compared with radiographic screening (RR, 0.33; 95% CI, 0.12-0.91).
Endoscopic screening did not significantly reduce mortality, compared with expected deaths (RR, 0.67; 95% CI, 0.38-1.16), the reviewers reported. This might be because the reviewers included an outlier study conducted in Linqu County, China, which has some of the highest rates of gastric cancer death in the world, they noted. Endoscopic surveillance did not reduce mortality in the Linqu County study, but screenings were spaced by 4.5 years, which was probably too long to show an effect, especially in a high-risk region, they added. The study in Linqu County accounted for most of the heterogeneity among studies, and removing it from the pooled analysis produced a “slightly more pronounced reduction in gastric cancer mortality,” with an RR of 0.56, they noted.
Funders included the National Natural Science Foundation and the National Twelfth Five-Year Plan for Science and Technology Support Program of China. The reviewers reported having no relevant conflicts of interest.
SOURCE: Zhang X, et al. Gastroenterology. 2018 Apr 30. doi: 10.1053/j.gastro.2018.04.026.
Gastric cancer remains the third most common cause of cancer death worldwide, although incidence and mortality rates have been declining for several years. For populations in eastern Asia – a region that carries the unenviable tag of having the highest gastric cancer mortality rates in the world – finding ways to reduce the burden of this disease remains a key priority.
New findings reported by Zhang and his colleagues have highlighted a strong evidence base for one mode of gastric cancer control in eastern Asia. The systematic review team demonstrated a significant 40% reduction in the risk of death from gastric cancer when screening was conducted in general populations. The magnitude of this benefit likely reflects the appropriateness of screening in such high-incidence areas, although this finding might not necessarily be extrapolated to other regions.
The authors cautioned that screening did not reduce gastric cancer incidence, although only two studies were included. However, reduced incidence is often not an aim of screening programs; indeed, to detect more gastric cancers at an earlier stage can be an intentional outcome.
The observed benefits might be somewhat attributed to lead time bias (whereby individuals are diagnosed at a younger age than they would have presented symptomatically but still die at the same age) or length time bias (detecting only the slower-growing biological tumors). Further refinement of optimal screening intervals is also required. Nevertheless, public health policy makers in Japan and Korea, where national screening programs already exist, should be reassured by these review findings.
Helen Coleman, PhD, BSc(Hons), is a senior lecturer and lead of the Cancer Epidemiology Research Group at the Centre for Public Health and Centre for Cancer Research and Cell Biology at Queen’s University Belfast. She has no conflicts of interest.
Gastric cancer remains the third most common cause of cancer death worldwide, although incidence and mortality rates have been declining for several years. For populations in eastern Asia – a region that carries the unenviable tag of having the highest gastric cancer mortality rates in the world – finding ways to reduce the burden of this disease remains a key priority.
New findings reported by Zhang and his colleagues have highlighted a strong evidence base for one mode of gastric cancer control in eastern Asia. The systematic review team demonstrated a significant 40% reduction in the risk of death from gastric cancer when screening was conducted in general populations. The magnitude of this benefit likely reflects the appropriateness of screening in such high-incidence areas, although this finding might not necessarily be extrapolated to other regions.
The authors cautioned that screening did not reduce gastric cancer incidence, although only two studies were included. However, reduced incidence is often not an aim of screening programs; indeed, to detect more gastric cancers at an earlier stage can be an intentional outcome.
The observed benefits might be somewhat attributed to lead time bias (whereby individuals are diagnosed at a younger age than they would have presented symptomatically but still die at the same age) or length time bias (detecting only the slower-growing biological tumors). Further refinement of optimal screening intervals is also required. Nevertheless, public health policy makers in Japan and Korea, where national screening programs already exist, should be reassured by these review findings.
Helen Coleman, PhD, BSc(Hons), is a senior lecturer and lead of the Cancer Epidemiology Research Group at the Centre for Public Health and Centre for Cancer Research and Cell Biology at Queen’s University Belfast. She has no conflicts of interest.
Gastric cancer remains the third most common cause of cancer death worldwide, although incidence and mortality rates have been declining for several years. For populations in eastern Asia – a region that carries the unenviable tag of having the highest gastric cancer mortality rates in the world – finding ways to reduce the burden of this disease remains a key priority.
New findings reported by Zhang and his colleagues have highlighted a strong evidence base for one mode of gastric cancer control in eastern Asia. The systematic review team demonstrated a significant 40% reduction in the risk of death from gastric cancer when screening was conducted in general populations. The magnitude of this benefit likely reflects the appropriateness of screening in such high-incidence areas, although this finding might not necessarily be extrapolated to other regions.
The authors cautioned that screening did not reduce gastric cancer incidence, although only two studies were included. However, reduced incidence is often not an aim of screening programs; indeed, to detect more gastric cancers at an earlier stage can be an intentional outcome.
The observed benefits might be somewhat attributed to lead time bias (whereby individuals are diagnosed at a younger age than they would have presented symptomatically but still die at the same age) or length time bias (detecting only the slower-growing biological tumors). Further refinement of optimal screening intervals is also required. Nevertheless, public health policy makers in Japan and Korea, where national screening programs already exist, should be reassured by these review findings.
Helen Coleman, PhD, BSc(Hons), is a senior lecturer and lead of the Cancer Epidemiology Research Group at the Centre for Public Health and Centre for Cancer Research and Cell Biology at Queen’s University Belfast. She has no conflicts of interest.
Endoscopic screening was associated with an approximately 40% reduction in risk of death from gastric cancer in a systematic review and meta-analysis of studies from Asian countries.
The study is the first systematic review and meta-analysis of gastric cancer mortality and incidence after endoscopic screening, wrote Xing Zhang, MD, of the China Academy of Chinese Medical Sciences in Beijing with his associates. “Population-based prospective cohort studies are warranted to confirm our findings,” the reviewers wrote in the August issue of Gastroenterology.
In general, the rates of gastric cancer and related mortality in East Asian countries are significantly higher than global averages. As a result, countries in this region have implemented a variety of national and opportunistic screening programs that vary from country to country. Japan, for example, has a national screening program based on photofluorography. “Although data are inconsistent, most studies have shown a 40%-60% decrease in the mortality of gastric cancer in those who have been screened using photofluorography,” the reviewers noted. When findings are positive, follow-up endoscopy is recommended. However, debates persist about whether population-level endoscopy significantly improves hard endpoints in gastric cancer, such as incidence and mortality.
To help clarify the population-level benefits of endoscopic screening, Dr. Zhang and his associates searched PubMed and EMBASE; they identified six cohort studies and four nested case-control studies that included approximately 342,000 adults from Asia who did not have baseline gastric cancer but did undergo surveillance endoscopy at least once. Studies of both mass and opportunistic screening were included. Each study included a comparator; reported incidence, mortality, or both; and was published by March 8, 2018.
Endoscopic screening was tied to a 40% reduction in the relative risk of death from gastric cancer (risk ratio, 0.60; 95% confidence interval, 0.49-0.73). There also was a slight trend toward increased incidence of gastric cancer, which was not statistically significant (RR, 1.14; 95% CI, 0.93-1.40). However, only two studies examined the incidence of gastric cancer, so this outcome “should be interpreted with caution,” the reviewers wrote. Endoscopic screening also was associated with a significantly lower risk of death from gastric cancer, compared with radiographic screening (RR, 0.33; 95% CI, 0.12-0.91).
Endoscopic screening did not significantly reduce mortality, compared with expected deaths (RR, 0.67; 95% CI, 0.38-1.16), the reviewers reported. This might be because the reviewers included an outlier study conducted in Linqu County, China, which has some of the highest rates of gastric cancer death in the world, they noted. Endoscopic surveillance did not reduce mortality in the Linqu County study, but screenings were spaced by 4.5 years, which was probably too long to show an effect, especially in a high-risk region, they added. The study in Linqu County accounted for most of the heterogeneity among studies, and removing it from the pooled analysis produced a “slightly more pronounced reduction in gastric cancer mortality,” with an RR of 0.56, they noted.
Funders included the National Natural Science Foundation and the National Twelfth Five-Year Plan for Science and Technology Support Program of China. The reviewers reported having no relevant conflicts of interest.
SOURCE: Zhang X, et al. Gastroenterology. 2018 Apr 30. doi: 10.1053/j.gastro.2018.04.026.
Endoscopic screening was associated with an approximately 40% reduction in risk of death from gastric cancer in a systematic review and meta-analysis of studies from Asian countries.
The study is the first systematic review and meta-analysis of gastric cancer mortality and incidence after endoscopic screening, wrote Xing Zhang, MD, of the China Academy of Chinese Medical Sciences in Beijing with his associates. “Population-based prospective cohort studies are warranted to confirm our findings,” the reviewers wrote in the August issue of Gastroenterology.
In general, the rates of gastric cancer and related mortality in East Asian countries are significantly higher than global averages. As a result, countries in this region have implemented a variety of national and opportunistic screening programs that vary from country to country. Japan, for example, has a national screening program based on photofluorography. “Although data are inconsistent, most studies have shown a 40%-60% decrease in the mortality of gastric cancer in those who have been screened using photofluorography,” the reviewers noted. When findings are positive, follow-up endoscopy is recommended. However, debates persist about whether population-level endoscopy significantly improves hard endpoints in gastric cancer, such as incidence and mortality.
To help clarify the population-level benefits of endoscopic screening, Dr. Zhang and his associates searched PubMed and EMBASE; they identified six cohort studies and four nested case-control studies that included approximately 342,000 adults from Asia who did not have baseline gastric cancer but did undergo surveillance endoscopy at least once. Studies of both mass and opportunistic screening were included. Each study included a comparator; reported incidence, mortality, or both; and was published by March 8, 2018.
Endoscopic screening was tied to a 40% reduction in the relative risk of death from gastric cancer (risk ratio, 0.60; 95% confidence interval, 0.49-0.73). There also was a slight trend toward increased incidence of gastric cancer, which was not statistically significant (RR, 1.14; 95% CI, 0.93-1.40). However, only two studies examined the incidence of gastric cancer, so this outcome “should be interpreted with caution,” the reviewers wrote. Endoscopic screening also was associated with a significantly lower risk of death from gastric cancer, compared with radiographic screening (RR, 0.33; 95% CI, 0.12-0.91).
Endoscopic screening did not significantly reduce mortality, compared with expected deaths (RR, 0.67; 95% CI, 0.38-1.16), the reviewers reported. This might be because the reviewers included an outlier study conducted in Linqu County, China, which has some of the highest rates of gastric cancer death in the world, they noted. Endoscopic surveillance did not reduce mortality in the Linqu County study, but screenings were spaced by 4.5 years, which was probably too long to show an effect, especially in a high-risk region, they added. The study in Linqu County accounted for most of the heterogeneity among studies, and removing it from the pooled analysis produced a “slightly more pronounced reduction in gastric cancer mortality,” with an RR of 0.56, they noted.
Funders included the National Natural Science Foundation and the National Twelfth Five-Year Plan for Science and Technology Support Program of China. The reviewers reported having no relevant conflicts of interest.
SOURCE: Zhang X, et al. Gastroenterology. 2018 Apr 30. doi: 10.1053/j.gastro.2018.04.026.
FROM GASTROENTEROLOGY
Key clinical point: Endoscopic screening was associated with a significant decrease in risk of death from gastric cancer.
Major finding: Compared with no screening, the reduction in risk was 40% (risk ratio, 0.60; 95% confidence interval, 0.49-0.73).
Study details: Systematic review and meta-analysis of six cohort studies and four nested case-control studies of approximately 342,000 adults.
Disclosures: Funders included the National Natural Science Foundation and the National Twelfth Five-Year Plan for Science and Technology Support Program of China. The reviewers reported having no relevant conflicts of interest.
Source: Zhang X et al. Gastroenterology. 2018 Apr 30. doi: 10.1053/j.gastro.2018.04.026.
Investigators Describe the MS Prodrome
Patients who later develop MS are more likely than others to consult physicians for nervous system and genitourinary symptoms.
The prodrome of multiple sclerosis (MS) may include an increased risk of nervous system, sensory, and musculoskeletal disorders, according to research published online ahead of print July 1 in Multiple Sclerosis Journal. Patients who later develop MS also may be more likely to have genitourinary and psychiatric symptoms in the five years before diagnosis.

“The existence of such warning signs is well-accepted for Alzheimer’s disease and Parkinson’s disease, but there has been little investigation into a similar pattern for MS,” said Helen Tremlett, PhD, Professor in the Division of Neurology at the University of British Columbia in Canada. “We now need to delve deeper into this phenomenon, perhaps using data-mining techniques. We want to see if there are discernible patterns related to sex, age, or the type of MS they eventually develop.”
Clinical and Administrative Matched Cohorts
Dr. Tremlett and colleagues analyzed data from a matched-cohort record-linkage study to examine the MS prodrome. The investigators used population-based health administrative data and clinical data from the Canadian provinces of British Columbia, Saskatchewan, Manitoba, and Nova Scotia. The information included demographics, hospital visits, physician encounters, and prescriptions filled. Clinical data were for patients diagnosed by a neurologist at an MS clinic and included first clinical visit (or date of diagnosis) and date of symptom onset. Data were collected from April 1984 to April 2014.
Using the data, Dr. Tremlett and colleagues created a health-administrative cohort and a clinical cohort. The clinical cohort did not include data from Saskatchewan. To create the cohorts, the investigators identified patients with MS and matched them by sex, year of birth, and postal code with as many as five controls. The index date was the earliest recorded claim for a demyelinating disease for the health-administrative cohort and the date of MS symptom onset for the clinical cohort. Study outcomes were the number of physician and hospital encounters per ICD-10 chapter, the number of physician encounters per physician specialty, and the percentage of people with one or more prescriptions per drug class in the five years before the index date.
Clinical Cohort Results May Be More Accurate
The administrative cohort included 13,951 cases and 66,940 controls. The clinical cohort included 3,202 cases and 16,006 controls. Compared with controls, people with MS had more physician and hospital encounters for the nervous (rate ratio [RR], 2.31 to 4.75), sensory (RR, 1.40 to 2.28), musculoskeletal (RR, 1.19 to 1.70), and genitourinary systems (RR, 1.17 to 1.59) in the five years before the first demyelinating claim or symptom onset. Cases had more visits with psychiatrists and urologists (RR, 1.48 to 1.80) and higher proportions of musculoskeletal, genitourinary, or hormonal-related prescriptions (1.1–1.5 times higher), compared with controls. People with MS had fewer pregnancy-related encounters than controls, however (RR, 0.78 to 0.88).
The “more conservative” results for the clinical cohort are more likely to reflect the MS prodrome accurately because they are “unlikely to be influenced by a physician’s suspicion or consideration of MS,” said Dr. Tremlett and colleagues. “Although not all individuals with MS attend an MS specialty clinic, the clinical cohort represents a subgroup of the population that may differ with respect to demographic and clinical characteristics from nonclinic attendees (eg, have fewer comorbidities),” they added. NR
—Erik Greb
Suggested Reading
Wijnands JM, Zhu F, Kingwell E, et al. Five years before multiple sclerosis onset: Phenotyping the prodrome. Mult Scler. 2018 Jul 1 [Epub ahead of print].
Patients who later develop MS are more likely than others to consult physicians for nervous system and genitourinary symptoms.
Patients who later develop MS are more likely than others to consult physicians for nervous system and genitourinary symptoms.
The prodrome of multiple sclerosis (MS) may include an increased risk of nervous system, sensory, and musculoskeletal disorders, according to research published online ahead of print July 1 in Multiple Sclerosis Journal. Patients who later develop MS also may be more likely to have genitourinary and psychiatric symptoms in the five years before diagnosis.
“The existence of such warning signs is well-accepted for Alzheimer’s disease and Parkinson’s disease, but there has been little investigation into a similar pattern for MS,” said Helen Tremlett, PhD, Professor in the Division of Neurology at the University of British Columbia in Canada. “We now need to delve deeper into this phenomenon, perhaps using data-mining techniques. We want to see if there are discernible patterns related to sex, age, or the type of MS they eventually develop.”
Clinical and Administrative Matched Cohorts
Dr. Tremlett and colleagues analyzed data from a matched-cohort record-linkage study to examine the MS prodrome. The investigators used population-based health administrative data and clinical data from the Canadian provinces of British Columbia, Saskatchewan, Manitoba, and Nova Scotia. The information included demographics, hospital visits, physician encounters, and prescriptions filled. Clinical data were for patients diagnosed by a neurologist at an MS clinic and included first clinical visit (or date of diagnosis) and date of symptom onset. Data were collected from April 1984 to April 2014.
Using the data, Dr. Tremlett and colleagues created a health-administrative cohort and a clinical cohort. The clinical cohort did not include data from Saskatchewan. To create the cohorts, the investigators identified patients with MS and matched them by sex, year of birth, and postal code with as many as five controls. The index date was the earliest recorded claim for a demyelinating disease for the health-administrative cohort and the date of MS symptom onset for the clinical cohort. Study outcomes were the number of physician and hospital encounters per ICD-10 chapter, the number of physician encounters per physician specialty, and the percentage of people with one or more prescriptions per drug class in the five years before the index date.
Clinical Cohort Results May Be More Accurate
The administrative cohort included 13,951 cases and 66,940 controls. The clinical cohort included 3,202 cases and 16,006 controls. Compared with controls, people with MS had more physician and hospital encounters for the nervous (rate ratio [RR], 2.31 to 4.75), sensory (RR, 1.40 to 2.28), musculoskeletal (RR, 1.19 to 1.70), and genitourinary systems (RR, 1.17 to 1.59) in the five years before the first demyelinating claim or symptom onset. Cases had more visits with psychiatrists and urologists (RR, 1.48 to 1.80) and higher proportions of musculoskeletal, genitourinary, or hormonal-related prescriptions (1.1–1.5 times higher), compared with controls. People with MS had fewer pregnancy-related encounters than controls, however (RR, 0.78 to 0.88).
The “more conservative” results for the clinical cohort are more likely to reflect the MS prodrome accurately because they are “unlikely to be influenced by a physician’s suspicion or consideration of MS,” said Dr. Tremlett and colleagues. “Although not all individuals with MS attend an MS specialty clinic, the clinical cohort represents a subgroup of the population that may differ with respect to demographic and clinical characteristics from nonclinic attendees (eg, have fewer comorbidities),” they added. NR
—Erik Greb
Suggested Reading
Wijnands JM, Zhu F, Kingwell E, et al. Five years before multiple sclerosis onset: Phenotyping the prodrome. Mult Scler. 2018 Jul 1 [Epub ahead of print].
The prodrome of multiple sclerosis (MS) may include an increased risk of nervous system, sensory, and musculoskeletal disorders, according to research published online ahead of print July 1 in Multiple Sclerosis Journal. Patients who later develop MS also may be more likely to have genitourinary and psychiatric symptoms in the five years before diagnosis.
“The existence of such warning signs is well-accepted for Alzheimer’s disease and Parkinson’s disease, but there has been little investigation into a similar pattern for MS,” said Helen Tremlett, PhD, Professor in the Division of Neurology at the University of British Columbia in Canada. “We now need to delve deeper into this phenomenon, perhaps using data-mining techniques. We want to see if there are discernible patterns related to sex, age, or the type of MS they eventually develop.”
Clinical and Administrative Matched Cohorts
Dr. Tremlett and colleagues analyzed data from a matched-cohort record-linkage study to examine the MS prodrome. The investigators used population-based health administrative data and clinical data from the Canadian provinces of British Columbia, Saskatchewan, Manitoba, and Nova Scotia. The information included demographics, hospital visits, physician encounters, and prescriptions filled. Clinical data were for patients diagnosed by a neurologist at an MS clinic and included first clinical visit (or date of diagnosis) and date of symptom onset. Data were collected from April 1984 to April 2014.
Using the data, Dr. Tremlett and colleagues created a health-administrative cohort and a clinical cohort. The clinical cohort did not include data from Saskatchewan. To create the cohorts, the investigators identified patients with MS and matched them by sex, year of birth, and postal code with as many as five controls. The index date was the earliest recorded claim for a demyelinating disease for the health-administrative cohort and the date of MS symptom onset for the clinical cohort. Study outcomes were the number of physician and hospital encounters per ICD-10 chapter, the number of physician encounters per physician specialty, and the percentage of people with one or more prescriptions per drug class in the five years before the index date.
Clinical Cohort Results May Be More Accurate
The administrative cohort included 13,951 cases and 66,940 controls. The clinical cohort included 3,202 cases and 16,006 controls. Compared with controls, people with MS had more physician and hospital encounters for the nervous (rate ratio [RR], 2.31 to 4.75), sensory (RR, 1.40 to 2.28), musculoskeletal (RR, 1.19 to 1.70), and genitourinary systems (RR, 1.17 to 1.59) in the five years before the first demyelinating claim or symptom onset. Cases had more visits with psychiatrists and urologists (RR, 1.48 to 1.80) and higher proportions of musculoskeletal, genitourinary, or hormonal-related prescriptions (1.1–1.5 times higher), compared with controls. People with MS had fewer pregnancy-related encounters than controls, however (RR, 0.78 to 0.88).
The “more conservative” results for the clinical cohort are more likely to reflect the MS prodrome accurately because they are “unlikely to be influenced by a physician’s suspicion or consideration of MS,” said Dr. Tremlett and colleagues. “Although not all individuals with MS attend an MS specialty clinic, the clinical cohort represents a subgroup of the population that may differ with respect to demographic and clinical characteristics from nonclinic attendees (eg, have fewer comorbidities),” they added. NR
—Erik Greb
Suggested Reading
Wijnands JM, Zhu F, Kingwell E, et al. Five years before multiple sclerosis onset: Phenotyping the prodrome. Mult Scler. 2018 Jul 1 [Epub ahead of print].
Contraceptive considerations for women with headache and migraine
The use of hormonal contraception in women with headaches, especially migraine headaches, is an important topic. Approximately 43% of women in the United States report migraines.1 Roughly the same percentage of reproductive-aged women use hormonal contraception.2 Data suggest that all migraineurs have some increased risk of stroke. Therefore, can women with migraine headaches use combination hormonal contraception? And can women with severe headaches that are nonmigrainous use combination hormonal contraception? Let’s examine available data to help us answer these questions.
Risk factors for stroke
Migraine without aura is the most common subset, but migraine with aura is more problematic relative to the increased incidence of stroke.1
A migraine aura is visual 90% of the time.1 Symptoms can include flickering lights, spots, zigzag lines, a sense of pins and needles, or dysphasic speech. Aura precedes the headache and usually resolves within 1 hour after the aura begins.
In addition to migraine headaches, risk factors for stroke include increasing age, hypertension, the use of combination oral contraceptives (COCs), the contraceptive patch and ring, and smoking.1
Data indicate that the risk for ischemic stroke is increased in women with migraines even without the presence of other risk factors. In a meta-analysis of 14 observational studies, the risk of ischemic stroke among all migraineurs was about 2-fold (relative risk [RR], 2.2; 95% confidence interval [CI], 1.9–2.5) compared with the risk of ischemic stroke in women of the same age group who did not have migraine headaches. When there is migraine without aura, it was slightly less than 2-fold (RR, 1.8; 95% CI, 1.1–3.2). The risk of ischemic stroke among migraineurs with aura is increased more than 2 times compared with women without migraine (RR, 2.27; 95% CI, 1.61–3.19).3 However, the absolute risk of ischemic stroke among reproductive-aged women is 11 per 100,000 women years.4
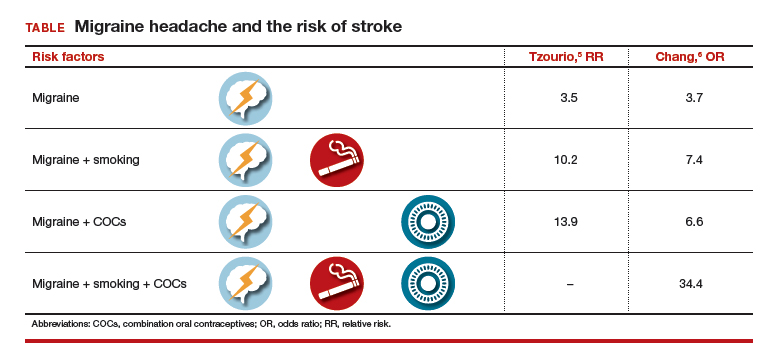
Two observational studies show how additional risk factors increase that risk (TABLE).5,6 There are similar trends in terms of overall risk of stroke among women with all types of migraine. However, when you add smoking as an additional risk factor for women with migraine headaches, there is a substantial increase in the risk of stroke. When a woman who has migraines uses COCs, there is increased risk varying from 2-fold to almost 4-fold. When you combine migraine, smoking, and COCs, a very, very large risk factor (odds ratio [OR], 34.4; 95% CI, 3.27–3.61) was reported by Chang and colleagues.6
Although these risks are impressive, it is important to keep in mind that even with a 10-fold increase, we are only talking about 1 case per 1,000 migraineurs.4 Unfortunately, stroke often leads to major disability and even death, such that any reduction in risk is still important.
Preventing estrogen withdrawal or menstrual migraines
How should we treat a woman who uses hormonal contraception and reports estrogen withdrawal or menstrual migraines? Based on clinical evidence, there are 2 ways to reduce her symptoms:
- COCs. Reduce the hormone-free interval by having her take COCs for 3 to 4 days instead of 7 days, or eliminate the hormone-free interval altogether by continuous use of COCs, usually 3 months at a time.7
- NSAIDs. For those who do not want to alter how they take their hormonal product, use nonsteroidal anti-inflammatory drugs (NSAIDs) starting 7 days before the onset of menses and continuing for 13 days. In a clinical trial by Sances and colleagues, this plan reduced the frequency, duration, and severity of menstrual migraines.8
Probably altering how she takes the COC would make the most sense for most individuals instead of taking NSAIDs for 75% of each month.
Recommendations from the US MEC
The US Medical Eligibility Criteria (US MEC) from the Centers for Disease Control and Prevention (CDC) offers recommendations for contraceptive use9:
- For nonmigrainous headache, the CDC suggests that the benefits of using COCs outweigh the risks unless the headaches persist after 3 months of COC use.
- For migraine without aura, the benefits outweigh the risks in starting women who are younger than age 35 years on oral contraceptives. However, the risks of COCs outweigh the benefits in women who are age 35 years and older who develop migraine headache while on COCs, or who have risk factors for stroke.
- For migraine with aura, COCs are contraindicated.
- Progestin-only contraceptives. The CDC considers that the benefits of COC use outweigh any theoretical risk of stroke, even in women with risk factors or in women who have migraine with aura. Progestin-only contraceptives do not alter one’s risk of stroke, unlike contraceptives that contain estrogen.
My bottom line
Can women with migraine headaches begin the use of combination hormonal methods? Yes, if there is no aura in their migraines and they are not older than age 35.
Can women with severe headaches that are nonmigrainous use combination hormonal methods? Possibly, but you should discontinue COCs if headache severity persists or worsens, using a 3-month time period for evaluation.
How do you manage women with migraines during the hormone-free interval? Consider the continuous method or shorten the hormone-free interval.
Recommendations for complicated patients. Consulting the CDC’s US MEC database7 can provide assistance in your care of more complicated patients requesting contraception. I also recommend the book, “Contraception for the Medically Challenging Patient,” edited by Rebecca Allen and Carrie Cwiak.10 It links nicely with the CDC guidelines and presents more detail on each subject.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Stewart WF, Wood C, Reed MD, et al. Cumulative lifetime migraine incidence in women and men. Cephalalgia. 2008;28(11):1170–1178.
- Finer LB, Frohwirth LF, Dauphinee LA, Singh S, Moore AM. Reasons U.S. women have abortions: quantitative and qualitative perspectives. Perspect Sex Reprod Health. 2005;37(3):110–118.
- Etminan M, Takkouche B, Isorna FC, Samii A. Risk of ischemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ. 2005;330(7482):63–66.
- Petitti DB, Sydney S, Bernstein A, Wolf S, Quesenberry C, Ziel HK. Stoke in users of low-dose oral contraceptives. N Engl J Med. 1996;335(1):8–15.
- Tzourio C, Tehindrazanarivelo A, Iglesias S, et al. Case-control study of migraine and risk of ischemic stroke in young women. BMJ. 1995;310:830–833.
- Chang CL, Donaghy M, Poulter N. Migraine and stroke in young women: case-control study. The World Health Organisation Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. BMJ. 1999;318(7175):13–18.
- Edelman A, Gallo MF, Nichols MD, Jensen JT, Schulz KF, Grimes DA. Continuous versus cyclic use of combined oral contraceptives for contraception: systematic Cochrane review of randomized controlled trials. Hum Reprod. 2006;21(3):573–578.
- Sances G, Martignoni E, Fioroni L, Blandini F, Facchinetti F, Nappi G. Naproxen sodium in menstrual migraine prophylaxis: a double-blind placebo controlled study. Headache. 1990;30(11):705–709.
- US Medical Eligibility Criteria for Contraceptive Use, 2010. MMWR Recomm Rep. 2010;59(RR-4):1–86. https://www.cdc .gov/mmwr/pdf/rr/rr59e0528.pdf. Accessed October 4, 2016.
- Allen RH, Cwiak CA, eds. Contraception for the medically challenging patient. New York, New York: Springer New York; 2014.

At the time of this writing, Dr. Burkman was Professor, Department of Obstetrics and Gynecology, Tufts University School of Medicine, Boston, Massachusetts, and an obstetrician-gynecologist at Baystate Medical Center, Springfield. He is an OBG Management Contributing Editor.
The author reports no financial relationships relevant to this article.
At the time of this writing, Dr. Burkman was Professor, Department of Obstetrics and Gynecology, Tufts University School of Medicine, Boston, Massachusetts, and an obstetrician-gynecologist at Baystate Medical Center, Springfield. He is an OBG Management Contributing Editor.
The author reports no financial relationships relevant to this article.
At the time of this writing, Dr. Burkman was Professor, Department of Obstetrics and Gynecology, Tufts University School of Medicine, Boston, Massachusetts, and an obstetrician-gynecologist at Baystate Medical Center, Springfield. He is an OBG Management Contributing Editor.
The author reports no financial relationships relevant to this article.
The use of hormonal contraception in women with headaches, especially migraine headaches, is an important topic. Approximately 43% of women in the United States report migraines.1 Roughly the same percentage of reproductive-aged women use hormonal contraception.2 Data suggest that all migraineurs have some increased risk of stroke. Therefore, can women with migraine headaches use combination hormonal contraception? And can women with severe headaches that are nonmigrainous use combination hormonal contraception? Let’s examine available data to help us answer these questions.
Risk factors for stroke
Migraine without aura is the most common subset, but migraine with aura is more problematic relative to the increased incidence of stroke.1
A migraine aura is visual 90% of the time.1 Symptoms can include flickering lights, spots, zigzag lines, a sense of pins and needles, or dysphasic speech. Aura precedes the headache and usually resolves within 1 hour after the aura begins.
In addition to migraine headaches, risk factors for stroke include increasing age, hypertension, the use of combination oral contraceptives (COCs), the contraceptive patch and ring, and smoking.1
Data indicate that the risk for ischemic stroke is increased in women with migraines even without the presence of other risk factors. In a meta-analysis of 14 observational studies, the risk of ischemic stroke among all migraineurs was about 2-fold (relative risk [RR], 2.2; 95% confidence interval [CI], 1.9–2.5) compared with the risk of ischemic stroke in women of the same age group who did not have migraine headaches. When there is migraine without aura, it was slightly less than 2-fold (RR, 1.8; 95% CI, 1.1–3.2). The risk of ischemic stroke among migraineurs with aura is increased more than 2 times compared with women without migraine (RR, 2.27; 95% CI, 1.61–3.19).3 However, the absolute risk of ischemic stroke among reproductive-aged women is 11 per 100,000 women years.4
Two observational studies show how additional risk factors increase that risk (TABLE).5,6 There are similar trends in terms of overall risk of stroke among women with all types of migraine. However, when you add smoking as an additional risk factor for women with migraine headaches, there is a substantial increase in the risk of stroke. When a woman who has migraines uses COCs, there is increased risk varying from 2-fold to almost 4-fold. When you combine migraine, smoking, and COCs, a very, very large risk factor (odds ratio [OR], 34.4; 95% CI, 3.27–3.61) was reported by Chang and colleagues.6
Although these risks are impressive, it is important to keep in mind that even with a 10-fold increase, we are only talking about 1 case per 1,000 migraineurs.4 Unfortunately, stroke often leads to major disability and even death, such that any reduction in risk is still important.
Preventing estrogen withdrawal or menstrual migraines
How should we treat a woman who uses hormonal contraception and reports estrogen withdrawal or menstrual migraines? Based on clinical evidence, there are 2 ways to reduce her symptoms:
- COCs. Reduce the hormone-free interval by having her take COCs for 3 to 4 days instead of 7 days, or eliminate the hormone-free interval altogether by continuous use of COCs, usually 3 months at a time.7
- NSAIDs. For those who do not want to alter how they take their hormonal product, use nonsteroidal anti-inflammatory drugs (NSAIDs) starting 7 days before the onset of menses and continuing for 13 days. In a clinical trial by Sances and colleagues, this plan reduced the frequency, duration, and severity of menstrual migraines.8
Probably altering how she takes the COC would make the most sense for most individuals instead of taking NSAIDs for 75% of each month.
Recommendations from the US MEC
The US Medical Eligibility Criteria (US MEC) from the Centers for Disease Control and Prevention (CDC) offers recommendations for contraceptive use9:
- For nonmigrainous headache, the CDC suggests that the benefits of using COCs outweigh the risks unless the headaches persist after 3 months of COC use.
- For migraine without aura, the benefits outweigh the risks in starting women who are younger than age 35 years on oral contraceptives. However, the risks of COCs outweigh the benefits in women who are age 35 years and older who develop migraine headache while on COCs, or who have risk factors for stroke.
- For migraine with aura, COCs are contraindicated.
- Progestin-only contraceptives. The CDC considers that the benefits of COC use outweigh any theoretical risk of stroke, even in women with risk factors or in women who have migraine with aura. Progestin-only contraceptives do not alter one’s risk of stroke, unlike contraceptives that contain estrogen.
My bottom line
Can women with migraine headaches begin the use of combination hormonal methods? Yes, if there is no aura in their migraines and they are not older than age 35.
Can women with severe headaches that are nonmigrainous use combination hormonal methods? Possibly, but you should discontinue COCs if headache severity persists or worsens, using a 3-month time period for evaluation.
How do you manage women with migraines during the hormone-free interval? Consider the continuous method or shorten the hormone-free interval.
Recommendations for complicated patients. Consulting the CDC’s US MEC database7 can provide assistance in your care of more complicated patients requesting contraception. I also recommend the book, “Contraception for the Medically Challenging Patient,” edited by Rebecca Allen and Carrie Cwiak.10 It links nicely with the CDC guidelines and presents more detail on each subject.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The use of hormonal contraception in women with headaches, especially migraine headaches, is an important topic. Approximately 43% of women in the United States report migraines.1 Roughly the same percentage of reproductive-aged women use hormonal contraception.2 Data suggest that all migraineurs have some increased risk of stroke. Therefore, can women with migraine headaches use combination hormonal contraception? And can women with severe headaches that are nonmigrainous use combination hormonal contraception? Let’s examine available data to help us answer these questions.
Risk factors for stroke
Migraine without aura is the most common subset, but migraine with aura is more problematic relative to the increased incidence of stroke.1
A migraine aura is visual 90% of the time.1 Symptoms can include flickering lights, spots, zigzag lines, a sense of pins and needles, or dysphasic speech. Aura precedes the headache and usually resolves within 1 hour after the aura begins.
In addition to migraine headaches, risk factors for stroke include increasing age, hypertension, the use of combination oral contraceptives (COCs), the contraceptive patch and ring, and smoking.1
Data indicate that the risk for ischemic stroke is increased in women with migraines even without the presence of other risk factors. In a meta-analysis of 14 observational studies, the risk of ischemic stroke among all migraineurs was about 2-fold (relative risk [RR], 2.2; 95% confidence interval [CI], 1.9–2.5) compared with the risk of ischemic stroke in women of the same age group who did not have migraine headaches. When there is migraine without aura, it was slightly less than 2-fold (RR, 1.8; 95% CI, 1.1–3.2). The risk of ischemic stroke among migraineurs with aura is increased more than 2 times compared with women without migraine (RR, 2.27; 95% CI, 1.61–3.19).3 However, the absolute risk of ischemic stroke among reproductive-aged women is 11 per 100,000 women years.4
Two observational studies show how additional risk factors increase that risk (TABLE).5,6 There are similar trends in terms of overall risk of stroke among women with all types of migraine. However, when you add smoking as an additional risk factor for women with migraine headaches, there is a substantial increase in the risk of stroke. When a woman who has migraines uses COCs, there is increased risk varying from 2-fold to almost 4-fold. When you combine migraine, smoking, and COCs, a very, very large risk factor (odds ratio [OR], 34.4; 95% CI, 3.27–3.61) was reported by Chang and colleagues.6
Although these risks are impressive, it is important to keep in mind that even with a 10-fold increase, we are only talking about 1 case per 1,000 migraineurs.4 Unfortunately, stroke often leads to major disability and even death, such that any reduction in risk is still important.
Preventing estrogen withdrawal or menstrual migraines
How should we treat a woman who uses hormonal contraception and reports estrogen withdrawal or menstrual migraines? Based on clinical evidence, there are 2 ways to reduce her symptoms:
- COCs. Reduce the hormone-free interval by having her take COCs for 3 to 4 days instead of 7 days, or eliminate the hormone-free interval altogether by continuous use of COCs, usually 3 months at a time.7
- NSAIDs. For those who do not want to alter how they take their hormonal product, use nonsteroidal anti-inflammatory drugs (NSAIDs) starting 7 days before the onset of menses and continuing for 13 days. In a clinical trial by Sances and colleagues, this plan reduced the frequency, duration, and severity of menstrual migraines.8
Probably altering how she takes the COC would make the most sense for most individuals instead of taking NSAIDs for 75% of each month.
Recommendations from the US MEC
The US Medical Eligibility Criteria (US MEC) from the Centers for Disease Control and Prevention (CDC) offers recommendations for contraceptive use9:
- For nonmigrainous headache, the CDC suggests that the benefits of using COCs outweigh the risks unless the headaches persist after 3 months of COC use.
- For migraine without aura, the benefits outweigh the risks in starting women who are younger than age 35 years on oral contraceptives. However, the risks of COCs outweigh the benefits in women who are age 35 years and older who develop migraine headache while on COCs, or who have risk factors for stroke.
- For migraine with aura, COCs are contraindicated.
- Progestin-only contraceptives. The CDC considers that the benefits of COC use outweigh any theoretical risk of stroke, even in women with risk factors or in women who have migraine with aura. Progestin-only contraceptives do not alter one’s risk of stroke, unlike contraceptives that contain estrogen.
My bottom line
Can women with migraine headaches begin the use of combination hormonal methods? Yes, if there is no aura in their migraines and they are not older than age 35.
Can women with severe headaches that are nonmigrainous use combination hormonal methods? Possibly, but you should discontinue COCs if headache severity persists or worsens, using a 3-month time period for evaluation.
How do you manage women with migraines during the hormone-free interval? Consider the continuous method or shorten the hormone-free interval.
Recommendations for complicated patients. Consulting the CDC’s US MEC database7 can provide assistance in your care of more complicated patients requesting contraception. I also recommend the book, “Contraception for the Medically Challenging Patient,” edited by Rebecca Allen and Carrie Cwiak.10 It links nicely with the CDC guidelines and presents more detail on each subject.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Stewart WF, Wood C, Reed MD, et al. Cumulative lifetime migraine incidence in women and men. Cephalalgia. 2008;28(11):1170–1178.
- Finer LB, Frohwirth LF, Dauphinee LA, Singh S, Moore AM. Reasons U.S. women have abortions: quantitative and qualitative perspectives. Perspect Sex Reprod Health. 2005;37(3):110–118.
- Etminan M, Takkouche B, Isorna FC, Samii A. Risk of ischemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ. 2005;330(7482):63–66.
- Petitti DB, Sydney S, Bernstein A, Wolf S, Quesenberry C, Ziel HK. Stoke in users of low-dose oral contraceptives. N Engl J Med. 1996;335(1):8–15.
- Tzourio C, Tehindrazanarivelo A, Iglesias S, et al. Case-control study of migraine and risk of ischemic stroke in young women. BMJ. 1995;310:830–833.
- Chang CL, Donaghy M, Poulter N. Migraine and stroke in young women: case-control study. The World Health Organisation Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. BMJ. 1999;318(7175):13–18.
- Edelman A, Gallo MF, Nichols MD, Jensen JT, Schulz KF, Grimes DA. Continuous versus cyclic use of combined oral contraceptives for contraception: systematic Cochrane review of randomized controlled trials. Hum Reprod. 2006;21(3):573–578.
- Sances G, Martignoni E, Fioroni L, Blandini F, Facchinetti F, Nappi G. Naproxen sodium in menstrual migraine prophylaxis: a double-blind placebo controlled study. Headache. 1990;30(11):705–709.
- US Medical Eligibility Criteria for Contraceptive Use, 2010. MMWR Recomm Rep. 2010;59(RR-4):1–86. https://www.cdc .gov/mmwr/pdf/rr/rr59e0528.pdf. Accessed October 4, 2016.
- Allen RH, Cwiak CA, eds. Contraception for the medically challenging patient. New York, New York: Springer New York; 2014.
- Stewart WF, Wood C, Reed MD, et al. Cumulative lifetime migraine incidence in women and men. Cephalalgia. 2008;28(11):1170–1178.
- Finer LB, Frohwirth LF, Dauphinee LA, Singh S, Moore AM. Reasons U.S. women have abortions: quantitative and qualitative perspectives. Perspect Sex Reprod Health. 2005;37(3):110–118.
- Etminan M, Takkouche B, Isorna FC, Samii A. Risk of ischemic stroke in people with migraine: systematic review and meta-analysis of observational studies. BMJ. 2005;330(7482):63–66.
- Petitti DB, Sydney S, Bernstein A, Wolf S, Quesenberry C, Ziel HK. Stoke in users of low-dose oral contraceptives. N Engl J Med. 1996;335(1):8–15.
- Tzourio C, Tehindrazanarivelo A, Iglesias S, et al. Case-control study of migraine and risk of ischemic stroke in young women. BMJ. 1995;310:830–833.
- Chang CL, Donaghy M, Poulter N. Migraine and stroke in young women: case-control study. The World Health Organisation Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. BMJ. 1999;318(7175):13–18.
- Edelman A, Gallo MF, Nichols MD, Jensen JT, Schulz KF, Grimes DA. Continuous versus cyclic use of combined oral contraceptives for contraception: systematic Cochrane review of randomized controlled trials. Hum Reprod. 2006;21(3):573–578.
- Sances G, Martignoni E, Fioroni L, Blandini F, Facchinetti F, Nappi G. Naproxen sodium in menstrual migraine prophylaxis: a double-blind placebo controlled study. Headache. 1990;30(11):705–709.
- US Medical Eligibility Criteria for Contraceptive Use, 2010. MMWR Recomm Rep. 2010;59(RR-4):1–86. https://www.cdc .gov/mmwr/pdf/rr/rr59e0528.pdf. Accessed October 4, 2016.
- Allen RH, Cwiak CA, eds. Contraception for the medically challenging patient. New York, New York: Springer New York; 2014.

How Does Migraine Change During the Menopausal Transition?
Migraine may worsen or change its pattern for many women approaching menopause.
SAN FRANCISCO—Most women with migraine develop migraine pattern change, worsening migraine, or new-onset migraine at the age of menopause, according to a study presented at the 60th Annual Scientific Meeting of the American Headache Society. These changes most often occur during the perimenopausal or postmenopausal stages.
Previous research indicates that the prevalence and frequency of migraine are higher in perimenopausal women than in other women. Yu-Chen Cheng, MD, MPH, a postdoctoral fellow at Massachusetts General Hospital in Boston, and colleagues investigated patterns of migraine in women at menopausal age (ie, age 40–60) with migraine who presented to the Partners Healthcare Hospitals. The investigators reviewed participants’ medical records, brain image reports, and laboratory data, including levels of estradiol and follicle-stimulating hormone (FSH).
In their retrospective study, Dr. Cheng and colleagues identified 81 patients with concurrent diagnoses of migraine and menopause who had clinical data available. They excluded patients with missing or inaccessible data, as well as patients with organic brain lesions such as those associated with multiple sclerosis or brain tumor. The researchers included 69 patients in the study.
Sixty patients (86.96%) had a history of migraine, and the other nine patients (13.04%) had new-onset migraine. Among participants with a history of migraine, 35 (58.33%) had a change in migraine pattern or worsening of their migraine headaches. The investigators categorized patients in this group as having migraine worsening (60.00%), migraine pattern change (28.57%), worsening related to other cause (8.57%), and not sure (2.86%). Twenty-five patients with migraine history were stable and had no change in the pattern of their headaches.
Dr. Cheng and colleagues also examined the population’s menopausal status when they had migraine change or worsening or new migraine. Among patients with migraine history, nine of 35 (25.71%) were at the perimenopausal stage, 12 (34.29%) were postmenopausal, five (14.29%) were premenopausal, three (8.57%) had worsening because of other causes, and three (8.57%) did not have records on their menopausal status. For patients with new-onset migraine, three of nine (33%) were perimenopausal, three (33%) were postmenopausal, and one (11.11%) was premenopausal.
Among patients with new-onset migraine, brain MRI was normal in 44.44%, showed pituitary abnormality in 22.22%, and showed other brain lesion in 33.33%. In patients with migraine history, brain MRI was normal in 45%, showed pituitary abnormality in 8.3%, showed nonspecific T2 high white matter lesion in 16.67%, and showed other brain lesion in 11.67%.
“Identifying migraine worsening or new-onset migraine during the menopausal transition age may help the diagnosis and treatment optimization of migraine for women during the menopausal age,” said Dr. Cheng.
Migraine may worsen or change its pattern for many women approaching menopause.
Migraine may worsen or change its pattern for many women approaching menopause.
SAN FRANCISCO—Most women with migraine develop migraine pattern change, worsening migraine, or new-onset migraine at the age of menopause, according to a study presented at the 60th Annual Scientific Meeting of the American Headache Society. These changes most often occur during the perimenopausal or postmenopausal stages.
Previous research indicates that the prevalence and frequency of migraine are higher in perimenopausal women than in other women. Yu-Chen Cheng, MD, MPH, a postdoctoral fellow at Massachusetts General Hospital in Boston, and colleagues investigated patterns of migraine in women at menopausal age (ie, age 40–60) with migraine who presented to the Partners Healthcare Hospitals. The investigators reviewed participants’ medical records, brain image reports, and laboratory data, including levels of estradiol and follicle-stimulating hormone (FSH).
In their retrospective study, Dr. Cheng and colleagues identified 81 patients with concurrent diagnoses of migraine and menopause who had clinical data available. They excluded patients with missing or inaccessible data, as well as patients with organic brain lesions such as those associated with multiple sclerosis or brain tumor. The researchers included 69 patients in the study.
Sixty patients (86.96%) had a history of migraine, and the other nine patients (13.04%) had new-onset migraine. Among participants with a history of migraine, 35 (58.33%) had a change in migraine pattern or worsening of their migraine headaches. The investigators categorized patients in this group as having migraine worsening (60.00%), migraine pattern change (28.57%), worsening related to other cause (8.57%), and not sure (2.86%). Twenty-five patients with migraine history were stable and had no change in the pattern of their headaches.
Dr. Cheng and colleagues also examined the population’s menopausal status when they had migraine change or worsening or new migraine. Among patients with migraine history, nine of 35 (25.71%) were at the perimenopausal stage, 12 (34.29%) were postmenopausal, five (14.29%) were premenopausal, three (8.57%) had worsening because of other causes, and three (8.57%) did not have records on their menopausal status. For patients with new-onset migraine, three of nine (33%) were perimenopausal, three (33%) were postmenopausal, and one (11.11%) was premenopausal.
Among patients with new-onset migraine, brain MRI was normal in 44.44%, showed pituitary abnormality in 22.22%, and showed other brain lesion in 33.33%. In patients with migraine history, brain MRI was normal in 45%, showed pituitary abnormality in 8.3%, showed nonspecific T2 high white matter lesion in 16.67%, and showed other brain lesion in 11.67%.
“Identifying migraine worsening or new-onset migraine during the menopausal transition age may help the diagnosis and treatment optimization of migraine for women during the menopausal age,” said Dr. Cheng.
SAN FRANCISCO—Most women with migraine develop migraine pattern change, worsening migraine, or new-onset migraine at the age of menopause, according to a study presented at the 60th Annual Scientific Meeting of the American Headache Society. These changes most often occur during the perimenopausal or postmenopausal stages.
Previous research indicates that the prevalence and frequency of migraine are higher in perimenopausal women than in other women. Yu-Chen Cheng, MD, MPH, a postdoctoral fellow at Massachusetts General Hospital in Boston, and colleagues investigated patterns of migraine in women at menopausal age (ie, age 40–60) with migraine who presented to the Partners Healthcare Hospitals. The investigators reviewed participants’ medical records, brain image reports, and laboratory data, including levels of estradiol and follicle-stimulating hormone (FSH).
In their retrospective study, Dr. Cheng and colleagues identified 81 patients with concurrent diagnoses of migraine and menopause who had clinical data available. They excluded patients with missing or inaccessible data, as well as patients with organic brain lesions such as those associated with multiple sclerosis or brain tumor. The researchers included 69 patients in the study.
Sixty patients (86.96%) had a history of migraine, and the other nine patients (13.04%) had new-onset migraine. Among participants with a history of migraine, 35 (58.33%) had a change in migraine pattern or worsening of their migraine headaches. The investigators categorized patients in this group as having migraine worsening (60.00%), migraine pattern change (28.57%), worsening related to other cause (8.57%), and not sure (2.86%). Twenty-five patients with migraine history were stable and had no change in the pattern of their headaches.
Dr. Cheng and colleagues also examined the population’s menopausal status when they had migraine change or worsening or new migraine. Among patients with migraine history, nine of 35 (25.71%) were at the perimenopausal stage, 12 (34.29%) were postmenopausal, five (14.29%) were premenopausal, three (8.57%) had worsening because of other causes, and three (8.57%) did not have records on their menopausal status. For patients with new-onset migraine, three of nine (33%) were perimenopausal, three (33%) were postmenopausal, and one (11.11%) was premenopausal.
Among patients with new-onset migraine, brain MRI was normal in 44.44%, showed pituitary abnormality in 22.22%, and showed other brain lesion in 33.33%. In patients with migraine history, brain MRI was normal in 45%, showed pituitary abnormality in 8.3%, showed nonspecific T2 high white matter lesion in 16.67%, and showed other brain lesion in 11.67%.
“Identifying migraine worsening or new-onset migraine during the menopausal transition age may help the diagnosis and treatment optimization of migraine for women during the menopausal age,” said Dr. Cheng.
Study supports meningococcal B vaccine in children with rare diseases
A new study, the first of its kind, provided support for guidelines suggesting that the capsular meningococcal B vaccine be given to children with three rare conditions that boost infection risk.

For children with terminal chain complement deficiencies or who are undergoing treatment with eculizumab, “it is important that these patients are identified, receive education about sepsis management plans, and are prescribed prophylactic antibiotics according to local guidelines, along with vaccination, to provide every chance for them to be protected against this deadly disease,” the researchers wrote in Pediatrics.
While some countries suggest that the vaccine be given to all healthy infants, U.S. guidelines advise that the vaccine be given to preteenagers, teenagers, and adults who are considered at special risk. These include those with terminal chain complement deficiencies, who are believed to be up to 10,000 times more likely than healthy children to develop invasive meningococcal disease, and those who take eculizumab (Soliris). The risk groups recommended for vaccinations also include those with asplenia and splenic dysfunction, although their excess risk, if any, is unknown.
The new study of the capsular group meningococcal B vaccine, led by Federico Martinón-Torres, PhD, of the Hospital Clinico Universitario de Santiago de Compostela, Spain, adds to previous research that confirmed the effectiveness of vaccinating complement-deficient patients with capsular group A, C, W, and Y meningococcal vaccines.
For the open-label, phase 3b study, researchers in Italy, Spain, Poland, and Russia gave two doses of the vaccine 2 months apart to 239 children aged 2-17 years with an average age of 10 years. Nearly all were white, and 45% were female.
A total of 40 children had complement deficiency, 112 had asplenia or splenic dysfunction, and 87 children in the control group also received the vaccine.
Following vaccination, the percentages of children with exogenous complement serum bactericidal activity titers greater than or equal to 1:5 to the four test strains were similar in the healthy children and those with asplenia/splenic dysfunction. “It is reasonable to expect that this vaccine will be as effective in children with asplenia or splenic deficiency as in children in the control category,” the researchers wrote.
However, these levels were lower in the complement-deficient children, particularly in those with terminal chain complement deficiency and those who took eculizumab.
The proportions of children with exogenous complement serum bactericidal activity titers greater than or equal to 1:5 against the four test strains were 87% (H44/76), 95% (5/99), 68% (NZ98/254), and 73% (M10713) in complement-deficient children, compared with 98%, 99%, 83%, and 99%, respectively, in the healthy controls.
“Ongoing surveillance for vaccine failures is required to determine the significance of the trend to reduced immune response in children with terminal chain complement deficiencies or undergoing treatment with eculizumab,” the researchers wrote.
Eculizumab’s manufacturer has noted the risk of serious meningococcal infections and warned physicians to “immunize patients with meningococcal vaccines at least 2 weeks prior to administering the first dose of Soliris, unless the risks of delaying Soliris therapy outweigh the risk of developing a meningococcal infection,” according to the website.
The study was funded by Novartis Vaccines and Diagnostics (now GlaxoSmithKline Biologicals). Some of the study authors reported various disclosures, including financial relationships with Novartis and GlaxoSmithKline outside the submitted work. Dr. Kaplan reported no relevant financial disclosures.
SOURCE: Martinón-Torres F et al. Pediatrics. 2018 Aug 1. doi: 10.1542/peds.2017-4250.
The Centers for Disease Control and Prevention reported an annual average of 792 cases of meningococcal disease and 98 deaths in the United States from 2006 to 2015 with serotype B isolates causing the highest numbers of cases. In a recent development, two vaccines against this strain have become available in the United States in the past 3 years for people aged 10-25 years. But officials don’t recommend their routine use, instead, guidelines suggest they be given to those at high risk only.
There’s a gap in knowledge because vaccine researchers didn’t include people with complement deficiency (either congenital or related to eculizumab), asplenia, or splenic dysfunction in studies that led to approval. Now, the new study offers reassuring findings regarding the latter two conditions, as bactericidal antibody responses were equal to those in healthy controls.
The findings regarding complement deficiency aren’t surprising, and suggest that vaccine strength in children with the condition only reached the levels in healthy children when an exogenous complement was added.
The study supports guidelines suggesting antibiotic prophylaxis in patients receiving eculizumab even if they already underwent meningococcal vaccination. It’s not clear if this approach also will be effective in those with congenital complement deficiencies (except for complement component 6 deficiency).
It is hoped that surveillance studies will show that use of serogroup B vaccines will prevent invasive meningococcal infections in these high-risk populations for which they are recommended.
Sheldon L. Kaplan, MD, is a pediatrician at Baylor College of Medicine and Texas Children’s Hospital, both in Houston. These comments are summarized from an editorial accompanying the article by Martinón-Torres et al. (Pediatrics. 2018 Aug 1. doi: 10.1542/peds.2018-0554).
The Centers for Disease Control and Prevention reported an annual average of 792 cases of meningococcal disease and 98 deaths in the United States from 2006 to 2015 with serotype B isolates causing the highest numbers of cases. In a recent development, two vaccines against this strain have become available in the United States in the past 3 years for people aged 10-25 years. But officials don’t recommend their routine use, instead, guidelines suggest they be given to those at high risk only.
There’s a gap in knowledge because vaccine researchers didn’t include people with complement deficiency (either congenital or related to eculizumab), asplenia, or splenic dysfunction in studies that led to approval. Now, the new study offers reassuring findings regarding the latter two conditions, as bactericidal antibody responses were equal to those in healthy controls.
The findings regarding complement deficiency aren’t surprising, and suggest that vaccine strength in children with the condition only reached the levels in healthy children when an exogenous complement was added.
The study supports guidelines suggesting antibiotic prophylaxis in patients receiving eculizumab even if they already underwent meningococcal vaccination. It’s not clear if this approach also will be effective in those with congenital complement deficiencies (except for complement component 6 deficiency).
It is hoped that surveillance studies will show that use of serogroup B vaccines will prevent invasive meningococcal infections in these high-risk populations for which they are recommended.
Sheldon L. Kaplan, MD, is a pediatrician at Baylor College of Medicine and Texas Children’s Hospital, both in Houston. These comments are summarized from an editorial accompanying the article by Martinón-Torres et al. (Pediatrics. 2018 Aug 1. doi: 10.1542/peds.2018-0554).
The Centers for Disease Control and Prevention reported an annual average of 792 cases of meningococcal disease and 98 deaths in the United States from 2006 to 2015 with serotype B isolates causing the highest numbers of cases. In a recent development, two vaccines against this strain have become available in the United States in the past 3 years for people aged 10-25 years. But officials don’t recommend their routine use, instead, guidelines suggest they be given to those at high risk only.
There’s a gap in knowledge because vaccine researchers didn’t include people with complement deficiency (either congenital or related to eculizumab), asplenia, or splenic dysfunction in studies that led to approval. Now, the new study offers reassuring findings regarding the latter two conditions, as bactericidal antibody responses were equal to those in healthy controls.
The findings regarding complement deficiency aren’t surprising, and suggest that vaccine strength in children with the condition only reached the levels in healthy children when an exogenous complement was added.
The study supports guidelines suggesting antibiotic prophylaxis in patients receiving eculizumab even if they already underwent meningococcal vaccination. It’s not clear if this approach also will be effective in those with congenital complement deficiencies (except for complement component 6 deficiency).
It is hoped that surveillance studies will show that use of serogroup B vaccines will prevent invasive meningococcal infections in these high-risk populations for which they are recommended.
Sheldon L. Kaplan, MD, is a pediatrician at Baylor College of Medicine and Texas Children’s Hospital, both in Houston. These comments are summarized from an editorial accompanying the article by Martinón-Torres et al. (Pediatrics. 2018 Aug 1. doi: 10.1542/peds.2018-0554).
A new study, the first of its kind, provided support for guidelines suggesting that the capsular meningococcal B vaccine be given to children with three rare conditions that boost infection risk.
For children with terminal chain complement deficiencies or who are undergoing treatment with eculizumab, “it is important that these patients are identified, receive education about sepsis management plans, and are prescribed prophylactic antibiotics according to local guidelines, along with vaccination, to provide every chance for them to be protected against this deadly disease,” the researchers wrote in Pediatrics.
While some countries suggest that the vaccine be given to all healthy infants, U.S. guidelines advise that the vaccine be given to preteenagers, teenagers, and adults who are considered at special risk. These include those with terminal chain complement deficiencies, who are believed to be up to 10,000 times more likely than healthy children to develop invasive meningococcal disease, and those who take eculizumab (Soliris). The risk groups recommended for vaccinations also include those with asplenia and splenic dysfunction, although their excess risk, if any, is unknown.
The new study of the capsular group meningococcal B vaccine, led by Federico Martinón-Torres, PhD, of the Hospital Clinico Universitario de Santiago de Compostela, Spain, adds to previous research that confirmed the effectiveness of vaccinating complement-deficient patients with capsular group A, C, W, and Y meningococcal vaccines.
For the open-label, phase 3b study, researchers in Italy, Spain, Poland, and Russia gave two doses of the vaccine 2 months apart to 239 children aged 2-17 years with an average age of 10 years. Nearly all were white, and 45% were female.
A total of 40 children had complement deficiency, 112 had asplenia or splenic dysfunction, and 87 children in the control group also received the vaccine.
Following vaccination, the percentages of children with exogenous complement serum bactericidal activity titers greater than or equal to 1:5 to the four test strains were similar in the healthy children and those with asplenia/splenic dysfunction. “It is reasonable to expect that this vaccine will be as effective in children with asplenia or splenic deficiency as in children in the control category,” the researchers wrote.
However, these levels were lower in the complement-deficient children, particularly in those with terminal chain complement deficiency and those who took eculizumab.
The proportions of children with exogenous complement serum bactericidal activity titers greater than or equal to 1:5 against the four test strains were 87% (H44/76), 95% (5/99), 68% (NZ98/254), and 73% (M10713) in complement-deficient children, compared with 98%, 99%, 83%, and 99%, respectively, in the healthy controls.
“Ongoing surveillance for vaccine failures is required to determine the significance of the trend to reduced immune response in children with terminal chain complement deficiencies or undergoing treatment with eculizumab,” the researchers wrote.
Eculizumab’s manufacturer has noted the risk of serious meningococcal infections and warned physicians to “immunize patients with meningococcal vaccines at least 2 weeks prior to administering the first dose of Soliris, unless the risks of delaying Soliris therapy outweigh the risk of developing a meningococcal infection,” according to the website.
The study was funded by Novartis Vaccines and Diagnostics (now GlaxoSmithKline Biologicals). Some of the study authors reported various disclosures, including financial relationships with Novartis and GlaxoSmithKline outside the submitted work. Dr. Kaplan reported no relevant financial disclosures.
SOURCE: Martinón-Torres F et al. Pediatrics. 2018 Aug 1. doi: 10.1542/peds.2017-4250.
A new study, the first of its kind, provided support for guidelines suggesting that the capsular meningococcal B vaccine be given to children with three rare conditions that boost infection risk.
For children with terminal chain complement deficiencies or who are undergoing treatment with eculizumab, “it is important that these patients are identified, receive education about sepsis management plans, and are prescribed prophylactic antibiotics according to local guidelines, along with vaccination, to provide every chance for them to be protected against this deadly disease,” the researchers wrote in Pediatrics.
While some countries suggest that the vaccine be given to all healthy infants, U.S. guidelines advise that the vaccine be given to preteenagers, teenagers, and adults who are considered at special risk. These include those with terminal chain complement deficiencies, who are believed to be up to 10,000 times more likely than healthy children to develop invasive meningococcal disease, and those who take eculizumab (Soliris). The risk groups recommended for vaccinations also include those with asplenia and splenic dysfunction, although their excess risk, if any, is unknown.
The new study of the capsular group meningococcal B vaccine, led by Federico Martinón-Torres, PhD, of the Hospital Clinico Universitario de Santiago de Compostela, Spain, adds to previous research that confirmed the effectiveness of vaccinating complement-deficient patients with capsular group A, C, W, and Y meningococcal vaccines.
For the open-label, phase 3b study, researchers in Italy, Spain, Poland, and Russia gave two doses of the vaccine 2 months apart to 239 children aged 2-17 years with an average age of 10 years. Nearly all were white, and 45% were female.
A total of 40 children had complement deficiency, 112 had asplenia or splenic dysfunction, and 87 children in the control group also received the vaccine.
Following vaccination, the percentages of children with exogenous complement serum bactericidal activity titers greater than or equal to 1:5 to the four test strains were similar in the healthy children and those with asplenia/splenic dysfunction. “It is reasonable to expect that this vaccine will be as effective in children with asplenia or splenic deficiency as in children in the control category,” the researchers wrote.
However, these levels were lower in the complement-deficient children, particularly in those with terminal chain complement deficiency and those who took eculizumab.
The proportions of children with exogenous complement serum bactericidal activity titers greater than or equal to 1:5 against the four test strains were 87% (H44/76), 95% (5/99), 68% (NZ98/254), and 73% (M10713) in complement-deficient children, compared with 98%, 99%, 83%, and 99%, respectively, in the healthy controls.
“Ongoing surveillance for vaccine failures is required to determine the significance of the trend to reduced immune response in children with terminal chain complement deficiencies or undergoing treatment with eculizumab,” the researchers wrote.
Eculizumab’s manufacturer has noted the risk of serious meningococcal infections and warned physicians to “immunize patients with meningococcal vaccines at least 2 weeks prior to administering the first dose of Soliris, unless the risks of delaying Soliris therapy outweigh the risk of developing a meningococcal infection,” according to the website.
The study was funded by Novartis Vaccines and Diagnostics (now GlaxoSmithKline Biologicals). Some of the study authors reported various disclosures, including financial relationships with Novartis and GlaxoSmithKline outside the submitted work. Dr. Kaplan reported no relevant financial disclosures.
SOURCE: Martinón-Torres F et al. Pediatrics. 2018 Aug 1. doi: 10.1542/peds.2017-4250.
FROM PEDIATRICS
Key clinical point: The meningococcal B vaccine retained its strength in kids with two rare immunosuppressive diseases, but may be weaker in a third group.
Major finding: The vaccine’s effectiveness was roughly the same in healthy controls and in those with asplenia and splenic dysfunction, but it dipped in those with complement deficiency.
Study details: An open-label, multicenter analysis of children aged 2-17 years who received two doses over 2 months.
Disclosures: The study was funded by Novartis Vaccines and Diagnostics (now GlaxoSmithKline Biologicals). Some of the study authors reported various disclosures, including financial relationships with Novartis and GlaxoSmithKline outside the submitted work. Dr. Kaplan reported no relevant financial disclosures.
Source: Martinón-Torres F et al. Pediatrics. 2018 Aug 1. doi: 10.1542/peds.2017-4250.
OnabotulinumtoxinA Versus Topiramate for Prevention of Chronic Migraine: The FORWARD Study
A randomized trial examines discontinuations, efficacy, cognition, and depressive symptoms over 36 weeks of treatment.
SAN FRANCISCO—For the prevention of chronic migraine, onabotulinumtoxinA has a superior tolerability profile versus topiramate based on treatment-related adverse events and overall discontinuations, according to data presented at the 60th Annual Scientific Meeting of the American Headache Society. In addition, “patient-reported outcomes data suggest that changes in cognition, an important adverse event leading to treatment discontinuation with topiramate, may be seen as early as week 12,” said Andrew M. Blumenfeld, MD, Director of the Headache Center of Southern California in Oceanside, and colleagues. Dr. Blumenfeld also reported that onabotulinumtoxinA has a more favorable effect on depressive symptoms than does topiramate.

According to Dr. Blumenfeld and colleagues, many adults with chronic migraine are not receiving appropriate preventive treatment and when prescribed, adherence to treatment is relatively low. To address this problem, he and his colleagues conducted a multicenter, prospective, randomized, parallel-group, open-label study to compare onabotulinumtoxinA and topiramate for headache prevention in adults with chronic migraine (the FORWARD study).
The study assessed the effectiveness of onabotulinumtoxinA 155 U administered to 31 sites across seven head and neck muscles, fixed-site, fixed-dose, every 12 weeks for three cycles versus topiramate 50 to 100 mg/day up to week 36. The primary efficacy measure was the proportion of patients with a 50% or greater reduction in headache days versus baseline in the 28 days before week 32. Safety and tolerability were assessed; adverse events were monitored. Patient-reported outcomes collected from questionnaires at day 1 and weeks 12, 24, and 36 included the Controlled Oral Word Association Test (COWAT) and the nine-item Patient Health Questionnaire (PHQ-9). Baseline observation carried forward (BLOCF) was used to impute missing values at primary time points, followed by questionnaire guidelines for missing questionnaire data.
A total of 282 patients were enrolled—140 in the onabotulinumtoxinA arm and 142 in the topiramate arm. Mean baseline headache days (onabotulinumtoxinA, 22.1; topiramate, 21.8) were similar. Of the patients enrolled, 148 completed randomized treatment (onabotulinumtoxinA, 85.7%; topiramate, 19.7%). Primary reasons for withdrawal were ineffective treatment (onabotulinumtoxinA, 5.0%; topiramate, 19.0%) and adverse events (onabotulinumtoxinA, 3.6%; topiramate, 50.7%). Based on BLOCF, more patients on onabotulinumtoxinA had a 50% or greater reduction in headache frequency compared with baseline versus topiramate (40.0% vs 12.0%). Adverse events were reported by 45.5% of patients who received onabotulinumtoxinA and 76.8% of patients who received topiramate; treatment-related adverse events were reported by 17.3% and 69.0%, respectively. No new safety signals were identified for onabotulinumtoxinA. Adverse events relating to nervous system disorders most commonly led to treatment discontinuation for topiramate. Topiramate reduced mean COWAT scores from as early as week 12, suggesting cognitive changes occurred early in treatment with topiramate. As the study progressed, topiramate’s effect may have been obscured by the BLOCF imputation methodology due to the large proportion of patients withdrawing from topiramate, the investigators said. In contrast, onabotulinumtoxinA resulted in a small increase in COWAT scores from week 12 to week 36. OnabotulinumtoxinA had a significantly greater effect on mean PHQ-9 scores at week 36 (4.4), compared with topiramate (7.1; estimated mean difference, –1.86).
A randomized trial examines discontinuations, efficacy, cognition, and depressive symptoms over 36 weeks of treatment.
A randomized trial examines discontinuations, efficacy, cognition, and depressive symptoms over 36 weeks of treatment.
SAN FRANCISCO—For the prevention of chronic migraine, onabotulinumtoxinA has a superior tolerability profile versus topiramate based on treatment-related adverse events and overall discontinuations, according to data presented at the 60th Annual Scientific Meeting of the American Headache Society. In addition, “patient-reported outcomes data suggest that changes in cognition, an important adverse event leading to treatment discontinuation with topiramate, may be seen as early as week 12,” said Andrew M. Blumenfeld, MD, Director of the Headache Center of Southern California in Oceanside, and colleagues. Dr. Blumenfeld also reported that onabotulinumtoxinA has a more favorable effect on depressive symptoms than does topiramate.
According to Dr. Blumenfeld and colleagues, many adults with chronic migraine are not receiving appropriate preventive treatment and when prescribed, adherence to treatment is relatively low. To address this problem, he and his colleagues conducted a multicenter, prospective, randomized, parallel-group, open-label study to compare onabotulinumtoxinA and topiramate for headache prevention in adults with chronic migraine (the FORWARD study).
The study assessed the effectiveness of onabotulinumtoxinA 155 U administered to 31 sites across seven head and neck muscles, fixed-site, fixed-dose, every 12 weeks for three cycles versus topiramate 50 to 100 mg/day up to week 36. The primary efficacy measure was the proportion of patients with a 50% or greater reduction in headache days versus baseline in the 28 days before week 32. Safety and tolerability were assessed; adverse events were monitored. Patient-reported outcomes collected from questionnaires at day 1 and weeks 12, 24, and 36 included the Controlled Oral Word Association Test (COWAT) and the nine-item Patient Health Questionnaire (PHQ-9). Baseline observation carried forward (BLOCF) was used to impute missing values at primary time points, followed by questionnaire guidelines for missing questionnaire data.
A total of 282 patients were enrolled—140 in the onabotulinumtoxinA arm and 142 in the topiramate arm. Mean baseline headache days (onabotulinumtoxinA, 22.1; topiramate, 21.8) were similar. Of the patients enrolled, 148 completed randomized treatment (onabotulinumtoxinA, 85.7%; topiramate, 19.7%). Primary reasons for withdrawal were ineffective treatment (onabotulinumtoxinA, 5.0%; topiramate, 19.0%) and adverse events (onabotulinumtoxinA, 3.6%; topiramate, 50.7%). Based on BLOCF, more patients on onabotulinumtoxinA had a 50% or greater reduction in headache frequency compared with baseline versus topiramate (40.0% vs 12.0%). Adverse events were reported by 45.5% of patients who received onabotulinumtoxinA and 76.8% of patients who received topiramate; treatment-related adverse events were reported by 17.3% and 69.0%, respectively. No new safety signals were identified for onabotulinumtoxinA. Adverse events relating to nervous system disorders most commonly led to treatment discontinuation for topiramate. Topiramate reduced mean COWAT scores from as early as week 12, suggesting cognitive changes occurred early in treatment with topiramate. As the study progressed, topiramate’s effect may have been obscured by the BLOCF imputation methodology due to the large proportion of patients withdrawing from topiramate, the investigators said. In contrast, onabotulinumtoxinA resulted in a small increase in COWAT scores from week 12 to week 36. OnabotulinumtoxinA had a significantly greater effect on mean PHQ-9 scores at week 36 (4.4), compared with topiramate (7.1; estimated mean difference, –1.86).
SAN FRANCISCO—For the prevention of chronic migraine, onabotulinumtoxinA has a superior tolerability profile versus topiramate based on treatment-related adverse events and overall discontinuations, according to data presented at the 60th Annual Scientific Meeting of the American Headache Society. In addition, “patient-reported outcomes data suggest that changes in cognition, an important adverse event leading to treatment discontinuation with topiramate, may be seen as early as week 12,” said Andrew M. Blumenfeld, MD, Director of the Headache Center of Southern California in Oceanside, and colleagues. Dr. Blumenfeld also reported that onabotulinumtoxinA has a more favorable effect on depressive symptoms than does topiramate.
According to Dr. Blumenfeld and colleagues, many adults with chronic migraine are not receiving appropriate preventive treatment and when prescribed, adherence to treatment is relatively low. To address this problem, he and his colleagues conducted a multicenter, prospective, randomized, parallel-group, open-label study to compare onabotulinumtoxinA and topiramate for headache prevention in adults with chronic migraine (the FORWARD study).
The study assessed the effectiveness of onabotulinumtoxinA 155 U administered to 31 sites across seven head and neck muscles, fixed-site, fixed-dose, every 12 weeks for three cycles versus topiramate 50 to 100 mg/day up to week 36. The primary efficacy measure was the proportion of patients with a 50% or greater reduction in headache days versus baseline in the 28 days before week 32. Safety and tolerability were assessed; adverse events were monitored. Patient-reported outcomes collected from questionnaires at day 1 and weeks 12, 24, and 36 included the Controlled Oral Word Association Test (COWAT) and the nine-item Patient Health Questionnaire (PHQ-9). Baseline observation carried forward (BLOCF) was used to impute missing values at primary time points, followed by questionnaire guidelines for missing questionnaire data.
A total of 282 patients were enrolled—140 in the onabotulinumtoxinA arm and 142 in the topiramate arm. Mean baseline headache days (onabotulinumtoxinA, 22.1; topiramate, 21.8) were similar. Of the patients enrolled, 148 completed randomized treatment (onabotulinumtoxinA, 85.7%; topiramate, 19.7%). Primary reasons for withdrawal were ineffective treatment (onabotulinumtoxinA, 5.0%; topiramate, 19.0%) and adverse events (onabotulinumtoxinA, 3.6%; topiramate, 50.7%). Based on BLOCF, more patients on onabotulinumtoxinA had a 50% or greater reduction in headache frequency compared with baseline versus topiramate (40.0% vs 12.0%). Adverse events were reported by 45.5% of patients who received onabotulinumtoxinA and 76.8% of patients who received topiramate; treatment-related adverse events were reported by 17.3% and 69.0%, respectively. No new safety signals were identified for onabotulinumtoxinA. Adverse events relating to nervous system disorders most commonly led to treatment discontinuation for topiramate. Topiramate reduced mean COWAT scores from as early as week 12, suggesting cognitive changes occurred early in treatment with topiramate. As the study progressed, topiramate’s effect may have been obscured by the BLOCF imputation methodology due to the large proportion of patients withdrawing from topiramate, the investigators said. In contrast, onabotulinumtoxinA resulted in a small increase in COWAT scores from week 12 to week 36. OnabotulinumtoxinA had a significantly greater effect on mean PHQ-9 scores at week 36 (4.4), compared with topiramate (7.1; estimated mean difference, –1.86).
Droxidopa May Reduce Neurogenic Orthostatic Hypotension Symptoms in Patients Taking DDCIs
The number of patients experiencing falls significantly decreased after six months of droxidopa treatment, regardless of whether patients were on dopa decarboxylase inhibitors.
MIAMI—Droxidopa is associated with reductions in fall risk and dizziness or lightheadedness among users and nonusers of dopamine decarboxylase inhibitors (DDCIs), according to research described at the Second Pan American Parkinson’s Disease and Movement Disorders Congress. These findings from an open-label, observational study “support previous data showing the efficacy of droxidopa for neurogenic orthostatic hypotension symptom reduction, even with concomitant DDCI use,” said the researchers.
Neurogenic orthostatic hypotension—a sustained blood pressure drop upon standing due to deficient norepinephrine release—is common among patients with disorders associated with autonomic nervous system dysfunction (eg, Parkinson’s disease, multiple system atrophy, and pure autonomic failure). Symptoms include lightheadedness or dizziness, presyncope, syncope, and falls.
Droxidopa, a prodrug of norepinephrine, is approved to treat symptomatic neurogenic orthostatic hypotension. Droxidopa is converted to norepinephrine by dopamine decarboxylase, which also converts levodopa to dopamine. Patients with Parkinson’s disease are commonly treated with DDCIs in conjunction with levodopa treatment. DDCIs did not appear to interfere with the therapeutic efficacy of droxidopa in clinical studies, but “high doses of DDCIs (8- to 10-fold higher than clinical doses) have been shown to blunt the effects of droxidopa,” said Steven Kymes, PhD, Director of Health Economics and Outcomes Research at Lundbeck in Deerfield, Illinois, and colleagues.
A Post Hoc Analysis
To assess the long-term efficacy of droxidopa for the treatment of neurogenic orthostatic hypotension in patients concomitantly receiving DDCIs, Dr. Kymes and colleagues conducted a post hoc analysis of outcomes related to falls and neurogenic orthostatic hypotension symptoms in patients using DDCIs versus patients not using them. The researchers used data from a six-month open-label, prospective, observational study of patients newly initiating droxidopa.
Eligible participants were 18 and older; had underlying Parkinson’s disease, multiple system atrophy, pure autonomic failure, dopamine beta-hydroxylase deficiency, or nondiabetic autonomic neuropathy; were newly initiating droxidopa; and were able to speak and understand English. The researchers excluded patients with a self-reported diagnosis of dementia, Alzheimer disease, schizophrenia, or other psychiatric disorder, as well as those who were nonambulatory or confined to a wheelchair.
Researchers used a patient falls questionnaire to record the number of falls in the past month at baseline and at one, three, and six months. They also used the Orthostatic Hypotension Symptom Assessment (OHSA) Item I test to assess dizziness or lightheadedness. All outcomes were self-reported.
Investigators then compared baseline differences using chi-square tests for categorical variables and t-tests for continuous variables. “The influence of DDCIs on risk of falling and OHSA Item I scores was compared across time points using generalized linear mixed models (logistic for risk of falling) adjusting for repeated measures within individuals,” said the researchers.
Droxidopa Treatment Was Associated With Reduced Falls
A total of 168 patients were included in this study; 55 were DDCI users, and 113 were non-DDCI users. The mean age in the DDCI group was 75, and the mean age in the non-DDCI group was 57. There were 19 women (34.5%) in the DDCI user group and 68 (60.2%) in non-DDCI user group. Most participants were white in both groups (92.7% in the DDCI group and 81.4% in the non-DDCI group).
“There were significant differences in the primary diagnoses between the groups. Parkinson’s disease was the most frequent diagnosis in the DDCI group (89.1%), and autonomic failure with no cause identified was the most frequent diagnosis in the non-DDCI group (92.9%),” Dr. Kymes and colleagues said. “At baseline, 61.8% of patients receiving DDCIs and 46.9 % of patients not receiving DDCI reported at least one fall in the last month.” The mean OHSA Item I scores at baseline were 5 in the DDCI group and 6 in the non-DDCI group.
The proportion of patients receiving DDCIs who experienced one or more falls in the past month after six months of droxidopa treatment significantly decreased from baseline, with a 36.5% reduction over the course of the study.
Among patients not receiving a DDCI, there was a 6.2% reduction in falls over the course of the study, but the reduction was not significant. Changes in the proportion of patients reporting one or more falls in the past month from baseline to six months did not differ significantly between the groups.
In addition, patients receiving DDCIs and nonusers showed significant improvement in OHSA Item I scores from baseline after six months of droxidopa treatment (change of 1.5 and 1.9 units, respectively). The difference between groups was not statistically significant.
“Specifically designed studies are needed to further examine the impact of DDCIs on droxidopa because the current study sample was not powered for subgroup analyses and all data were self-reported by patients,” the researchers concluded.
—Erica Tricarico
The number of patients experiencing falls significantly decreased after six months of droxidopa treatment, regardless of whether patients were on dopa decarboxylase inhibitors.
The number of patients experiencing falls significantly decreased after six months of droxidopa treatment, regardless of whether patients were on dopa decarboxylase inhibitors.
MIAMI—Droxidopa is associated with reductions in fall risk and dizziness or lightheadedness among users and nonusers of dopamine decarboxylase inhibitors (DDCIs), according to research described at the Second Pan American Parkinson’s Disease and Movement Disorders Congress. These findings from an open-label, observational study “support previous data showing the efficacy of droxidopa for neurogenic orthostatic hypotension symptom reduction, even with concomitant DDCI use,” said the researchers.
Neurogenic orthostatic hypotension—a sustained blood pressure drop upon standing due to deficient norepinephrine release—is common among patients with disorders associated with autonomic nervous system dysfunction (eg, Parkinson’s disease, multiple system atrophy, and pure autonomic failure). Symptoms include lightheadedness or dizziness, presyncope, syncope, and falls.
Droxidopa, a prodrug of norepinephrine, is approved to treat symptomatic neurogenic orthostatic hypotension. Droxidopa is converted to norepinephrine by dopamine decarboxylase, which also converts levodopa to dopamine. Patients with Parkinson’s disease are commonly treated with DDCIs in conjunction with levodopa treatment. DDCIs did not appear to interfere with the therapeutic efficacy of droxidopa in clinical studies, but “high doses of DDCIs (8- to 10-fold higher than clinical doses) have been shown to blunt the effects of droxidopa,” said Steven Kymes, PhD, Director of Health Economics and Outcomes Research at Lundbeck in Deerfield, Illinois, and colleagues.
A Post Hoc Analysis
To assess the long-term efficacy of droxidopa for the treatment of neurogenic orthostatic hypotension in patients concomitantly receiving DDCIs, Dr. Kymes and colleagues conducted a post hoc analysis of outcomes related to falls and neurogenic orthostatic hypotension symptoms in patients using DDCIs versus patients not using them. The researchers used data from a six-month open-label, prospective, observational study of patients newly initiating droxidopa.
Eligible participants were 18 and older; had underlying Parkinson’s disease, multiple system atrophy, pure autonomic failure, dopamine beta-hydroxylase deficiency, or nondiabetic autonomic neuropathy; were newly initiating droxidopa; and were able to speak and understand English. The researchers excluded patients with a self-reported diagnosis of dementia, Alzheimer disease, schizophrenia, or other psychiatric disorder, as well as those who were nonambulatory or confined to a wheelchair.
Researchers used a patient falls questionnaire to record the number of falls in the past month at baseline and at one, three, and six months. They also used the Orthostatic Hypotension Symptom Assessment (OHSA) Item I test to assess dizziness or lightheadedness. All outcomes were self-reported.
Investigators then compared baseline differences using chi-square tests for categorical variables and t-tests for continuous variables. “The influence of DDCIs on risk of falling and OHSA Item I scores was compared across time points using generalized linear mixed models (logistic for risk of falling) adjusting for repeated measures within individuals,” said the researchers.
Droxidopa Treatment Was Associated With Reduced Falls
A total of 168 patients were included in this study; 55 were DDCI users, and 113 were non-DDCI users. The mean age in the DDCI group was 75, and the mean age in the non-DDCI group was 57. There were 19 women (34.5%) in the DDCI user group and 68 (60.2%) in non-DDCI user group. Most participants were white in both groups (92.7% in the DDCI group and 81.4% in the non-DDCI group).
“There were significant differences in the primary diagnoses between the groups. Parkinson’s disease was the most frequent diagnosis in the DDCI group (89.1%), and autonomic failure with no cause identified was the most frequent diagnosis in the non-DDCI group (92.9%),” Dr. Kymes and colleagues said. “At baseline, 61.8% of patients receiving DDCIs and 46.9 % of patients not receiving DDCI reported at least one fall in the last month.” The mean OHSA Item I scores at baseline were 5 in the DDCI group and 6 in the non-DDCI group.
The proportion of patients receiving DDCIs who experienced one or more falls in the past month after six months of droxidopa treatment significantly decreased from baseline, with a 36.5% reduction over the course of the study.
Among patients not receiving a DDCI, there was a 6.2% reduction in falls over the course of the study, but the reduction was not significant. Changes in the proportion of patients reporting one or more falls in the past month from baseline to six months did not differ significantly between the groups.
In addition, patients receiving DDCIs and nonusers showed significant improvement in OHSA Item I scores from baseline after six months of droxidopa treatment (change of 1.5 and 1.9 units, respectively). The difference between groups was not statistically significant.
“Specifically designed studies are needed to further examine the impact of DDCIs on droxidopa because the current study sample was not powered for subgroup analyses and all data were self-reported by patients,” the researchers concluded.
—Erica Tricarico
MIAMI—Droxidopa is associated with reductions in fall risk and dizziness or lightheadedness among users and nonusers of dopamine decarboxylase inhibitors (DDCIs), according to research described at the Second Pan American Parkinson’s Disease and Movement Disorders Congress. These findings from an open-label, observational study “support previous data showing the efficacy of droxidopa for neurogenic orthostatic hypotension symptom reduction, even with concomitant DDCI use,” said the researchers.
Neurogenic orthostatic hypotension—a sustained blood pressure drop upon standing due to deficient norepinephrine release—is common among patients with disorders associated with autonomic nervous system dysfunction (eg, Parkinson’s disease, multiple system atrophy, and pure autonomic failure). Symptoms include lightheadedness or dizziness, presyncope, syncope, and falls.
Droxidopa, a prodrug of norepinephrine, is approved to treat symptomatic neurogenic orthostatic hypotension. Droxidopa is converted to norepinephrine by dopamine decarboxylase, which also converts levodopa to dopamine. Patients with Parkinson’s disease are commonly treated with DDCIs in conjunction with levodopa treatment. DDCIs did not appear to interfere with the therapeutic efficacy of droxidopa in clinical studies, but “high doses of DDCIs (8- to 10-fold higher than clinical doses) have been shown to blunt the effects of droxidopa,” said Steven Kymes, PhD, Director of Health Economics and Outcomes Research at Lundbeck in Deerfield, Illinois, and colleagues.
A Post Hoc Analysis
To assess the long-term efficacy of droxidopa for the treatment of neurogenic orthostatic hypotension in patients concomitantly receiving DDCIs, Dr. Kymes and colleagues conducted a post hoc analysis of outcomes related to falls and neurogenic orthostatic hypotension symptoms in patients using DDCIs versus patients not using them. The researchers used data from a six-month open-label, prospective, observational study of patients newly initiating droxidopa.
Eligible participants were 18 and older; had underlying Parkinson’s disease, multiple system atrophy, pure autonomic failure, dopamine beta-hydroxylase deficiency, or nondiabetic autonomic neuropathy; were newly initiating droxidopa; and were able to speak and understand English. The researchers excluded patients with a self-reported diagnosis of dementia, Alzheimer disease, schizophrenia, or other psychiatric disorder, as well as those who were nonambulatory or confined to a wheelchair.
Researchers used a patient falls questionnaire to record the number of falls in the past month at baseline and at one, three, and six months. They also used the Orthostatic Hypotension Symptom Assessment (OHSA) Item I test to assess dizziness or lightheadedness. All outcomes were self-reported.
Investigators then compared baseline differences using chi-square tests for categorical variables and t-tests for continuous variables. “The influence of DDCIs on risk of falling and OHSA Item I scores was compared across time points using generalized linear mixed models (logistic for risk of falling) adjusting for repeated measures within individuals,” said the researchers.
Droxidopa Treatment Was Associated With Reduced Falls
A total of 168 patients were included in this study; 55 were DDCI users, and 113 were non-DDCI users. The mean age in the DDCI group was 75, and the mean age in the non-DDCI group was 57. There were 19 women (34.5%) in the DDCI user group and 68 (60.2%) in non-DDCI user group. Most participants were white in both groups (92.7% in the DDCI group and 81.4% in the non-DDCI group).
“There were significant differences in the primary diagnoses between the groups. Parkinson’s disease was the most frequent diagnosis in the DDCI group (89.1%), and autonomic failure with no cause identified was the most frequent diagnosis in the non-DDCI group (92.9%),” Dr. Kymes and colleagues said. “At baseline, 61.8% of patients receiving DDCIs and 46.9 % of patients not receiving DDCI reported at least one fall in the last month.” The mean OHSA Item I scores at baseline were 5 in the DDCI group and 6 in the non-DDCI group.
The proportion of patients receiving DDCIs who experienced one or more falls in the past month after six months of droxidopa treatment significantly decreased from baseline, with a 36.5% reduction over the course of the study.
Among patients not receiving a DDCI, there was a 6.2% reduction in falls over the course of the study, but the reduction was not significant. Changes in the proportion of patients reporting one or more falls in the past month from baseline to six months did not differ significantly between the groups.
In addition, patients receiving DDCIs and nonusers showed significant improvement in OHSA Item I scores from baseline after six months of droxidopa treatment (change of 1.5 and 1.9 units, respectively). The difference between groups was not statistically significant.
“Specifically designed studies are needed to further examine the impact of DDCIs on droxidopa because the current study sample was not powered for subgroup analyses and all data were self-reported by patients,” the researchers concluded.
—Erica Tricarico
Ch4 Density Is a Potential Imaging Biomarker of Cognition in Early Parkinson’s Disease
Increasing Ch4 density is associated with higher scores on various cognitive measurements.
MIAMI—Reduced cholinergic nucleus 4 (Ch4) density in Parkinson’s disease, as measured with MRI, is associated with deficits in attention, processing speed, and visuospatial function, according to research described at the Second Pan American Parkinson’s Disease and Movement Disorders Congress. Ch4 density may serve as a surrogate imaging biomarker of cognition in early Parkinson’s disease, said the researchers.
Degeneration of the nucleus basalis of Meynert (NBM) contributes to dementia in Parkinson’s disease through a loss of cholinergic innervation to the neocortex. Cholinergic neurons of the NBM are in Ch4, a structure that can be measured with MRI techniques using cytoarchitectonic maps.
Evaluating Ch4 Density and Cognitive Performance
To determine whether Ch4 density, a proxy measure for NBM volume, is associated with cognitive test performance in de novo Parkinson’s disease, Cody S. Freeman, MD, a fellow at the University of Virginia School of Medicine in Charlottesville, and colleagues analyzed baseline brain MRIs and neuropsychologic test scores for 228 patients with Parkinson’s disease and 101 healthy controls from the Parkinson’s Progression Markers Initiative (PPMI). They also analyzed brain MRIs and neuropsychologic test scores at four years for a subset of 92 participants with Parkinson’s disease in the PPMI.

Neuropsychologic testing included the Montreal Cognitive Assessment (MoCA), Hopkins Verbal Learning Test (HVLT), Judgment of Line Orientation (JLO), Letter Number Sequencing (LNS), Symbol Digit Modalities Test (SDMT), and semantic fluency (animals).
The researchers used MP-RAGE T1 sequences and a probabilistic atlas from the reference Montreal Neurological Institute single subject brain to apply voxel-based morphometry methods to determine Ch4 density. In addition, they used correlation coefficients and linear regression models to analyze relationships between Ch4 density and cognitive scores.
Ch4 Density Was Significantly Associated With Higher MoCA Scores
At baseline, 33.7% of healthy controls and 38.2% of patients with Parkinson’s disease were female. The mean age at neurologic testing was 59.5 among healthy controls and 61.0 in the Parkinson’s disease cohort. The median MoCA score was 28 for controls and patients with Parkinson’s disease at baseline. The mean Ch4 density was 87.9 in the control group and 86.4 in the Parkinson’s disease cohort.
At baseline, Ch4 density was significantly correlated with MoCA, JLO, LNS, and SDMT scores. In a linear regression model adjusted for age and sex, Ch4 density was significantly associated with higher MoCA scores in patients with Parkinson’s disease. In linear regression models adjusted for sex, increasing Ch4 density was associated with higher JLO, LNS, and SDMT scores. The researchers observed no associations between Ch4 density and JLO and semantic fluency in linear regression models adjusted for sex.
For the subset of participants with Parkinson’s disease with brain MRI and neuropsychologic testing available at four years, Ch4 density was significantly correlated with MoCA, JLO, LNS, and SDMT. In a linear regression model adjusted for age and sex, increasing Ch4 density was associated with higher MoCA scores in patients with Parkinson’s disease. In linear regression models adjusted for sex, increasing Ch4 density was associated with higher JLO, LNS, and SDMT scores.
Increasing Ch4 density is associated with higher scores on various cognitive measurements.
Increasing Ch4 density is associated with higher scores on various cognitive measurements.
MIAMI—Reduced cholinergic nucleus 4 (Ch4) density in Parkinson’s disease, as measured with MRI, is associated with deficits in attention, processing speed, and visuospatial function, according to research described at the Second Pan American Parkinson’s Disease and Movement Disorders Congress. Ch4 density may serve as a surrogate imaging biomarker of cognition in early Parkinson’s disease, said the researchers.
Degeneration of the nucleus basalis of Meynert (NBM) contributes to dementia in Parkinson’s disease through a loss of cholinergic innervation to the neocortex. Cholinergic neurons of the NBM are in Ch4, a structure that can be measured with MRI techniques using cytoarchitectonic maps.
Evaluating Ch4 Density and Cognitive Performance
To determine whether Ch4 density, a proxy measure for NBM volume, is associated with cognitive test performance in de novo Parkinson’s disease, Cody S. Freeman, MD, a fellow at the University of Virginia School of Medicine in Charlottesville, and colleagues analyzed baseline brain MRIs and neuropsychologic test scores for 228 patients with Parkinson’s disease and 101 healthy controls from the Parkinson’s Progression Markers Initiative (PPMI). They also analyzed brain MRIs and neuropsychologic test scores at four years for a subset of 92 participants with Parkinson’s disease in the PPMI.
Neuropsychologic testing included the Montreal Cognitive Assessment (MoCA), Hopkins Verbal Learning Test (HVLT), Judgment of Line Orientation (JLO), Letter Number Sequencing (LNS), Symbol Digit Modalities Test (SDMT), and semantic fluency (animals).
The researchers used MP-RAGE T1 sequences and a probabilistic atlas from the reference Montreal Neurological Institute single subject brain to apply voxel-based morphometry methods to determine Ch4 density. In addition, they used correlation coefficients and linear regression models to analyze relationships between Ch4 density and cognitive scores.
Ch4 Density Was Significantly Associated With Higher MoCA Scores
At baseline, 33.7% of healthy controls and 38.2% of patients with Parkinson’s disease were female. The mean age at neurologic testing was 59.5 among healthy controls and 61.0 in the Parkinson’s disease cohort. The median MoCA score was 28 for controls and patients with Parkinson’s disease at baseline. The mean Ch4 density was 87.9 in the control group and 86.4 in the Parkinson’s disease cohort.
At baseline, Ch4 density was significantly correlated with MoCA, JLO, LNS, and SDMT scores. In a linear regression model adjusted for age and sex, Ch4 density was significantly associated with higher MoCA scores in patients with Parkinson’s disease. In linear regression models adjusted for sex, increasing Ch4 density was associated with higher JLO, LNS, and SDMT scores. The researchers observed no associations between Ch4 density and JLO and semantic fluency in linear regression models adjusted for sex.
For the subset of participants with Parkinson’s disease with brain MRI and neuropsychologic testing available at four years, Ch4 density was significantly correlated with MoCA, JLO, LNS, and SDMT. In a linear regression model adjusted for age and sex, increasing Ch4 density was associated with higher MoCA scores in patients with Parkinson’s disease. In linear regression models adjusted for sex, increasing Ch4 density was associated with higher JLO, LNS, and SDMT scores.
MIAMI—Reduced cholinergic nucleus 4 (Ch4) density in Parkinson’s disease, as measured with MRI, is associated with deficits in attention, processing speed, and visuospatial function, according to research described at the Second Pan American Parkinson’s Disease and Movement Disorders Congress. Ch4 density may serve as a surrogate imaging biomarker of cognition in early Parkinson’s disease, said the researchers.
Degeneration of the nucleus basalis of Meynert (NBM) contributes to dementia in Parkinson’s disease through a loss of cholinergic innervation to the neocortex. Cholinergic neurons of the NBM are in Ch4, a structure that can be measured with MRI techniques using cytoarchitectonic maps.
Evaluating Ch4 Density and Cognitive Performance
To determine whether Ch4 density, a proxy measure for NBM volume, is associated with cognitive test performance in de novo Parkinson’s disease, Cody S. Freeman, MD, a fellow at the University of Virginia School of Medicine in Charlottesville, and colleagues analyzed baseline brain MRIs and neuropsychologic test scores for 228 patients with Parkinson’s disease and 101 healthy controls from the Parkinson’s Progression Markers Initiative (PPMI). They also analyzed brain MRIs and neuropsychologic test scores at four years for a subset of 92 participants with Parkinson’s disease in the PPMI.
Neuropsychologic testing included the Montreal Cognitive Assessment (MoCA), Hopkins Verbal Learning Test (HVLT), Judgment of Line Orientation (JLO), Letter Number Sequencing (LNS), Symbol Digit Modalities Test (SDMT), and semantic fluency (animals).
The researchers used MP-RAGE T1 sequences and a probabilistic atlas from the reference Montreal Neurological Institute single subject brain to apply voxel-based morphometry methods to determine Ch4 density. In addition, they used correlation coefficients and linear regression models to analyze relationships between Ch4 density and cognitive scores.
Ch4 Density Was Significantly Associated With Higher MoCA Scores
At baseline, 33.7% of healthy controls and 38.2% of patients with Parkinson’s disease were female. The mean age at neurologic testing was 59.5 among healthy controls and 61.0 in the Parkinson’s disease cohort. The median MoCA score was 28 for controls and patients with Parkinson’s disease at baseline. The mean Ch4 density was 87.9 in the control group and 86.4 in the Parkinson’s disease cohort.
At baseline, Ch4 density was significantly correlated with MoCA, JLO, LNS, and SDMT scores. In a linear regression model adjusted for age and sex, Ch4 density was significantly associated with higher MoCA scores in patients with Parkinson’s disease. In linear regression models adjusted for sex, increasing Ch4 density was associated with higher JLO, LNS, and SDMT scores. The researchers observed no associations between Ch4 density and JLO and semantic fluency in linear regression models adjusted for sex.
For the subset of participants with Parkinson’s disease with brain MRI and neuropsychologic testing available at four years, Ch4 density was significantly correlated with MoCA, JLO, LNS, and SDMT. In a linear regression model adjusted for age and sex, increasing Ch4 density was associated with higher MoCA scores in patients with Parkinson’s disease. In linear regression models adjusted for sex, increasing Ch4 density was associated with higher JLO, LNS, and SDMT scores.
Strategies for Treating Motor Fluctuations in Parkinson’s Disease
Improved delivery of levodopa and new therapies may help to reduce off time.
MIAMI—Motor fluctuations in Parkinson’s disease can arise from more than one cause, and a clinician needs to consider a range of possibilities. Most commonly, motor fluctuations arise as a consequence of chronic levodopa therapy, though the progression of parkinsonism is a contributing factor, according to an overview presented at the Second Pan American Parkinson’s Disease and Movement Disorders Congress. The pharmacokinetics of levodopa provide the basis for studying most clinical patterns of motor fluctuations, and new pharmacologic strategies are under development to improve upon existing treatment options.
“In recent years, there have been some exciting and novel directions of Parkinson’s disease therapeutics for motor fluctuations,” said Peter A. LeWitt, MD, Director of the Parkinson’s Disease and Movement Disorder Program at Henry Ford Hospital in West Bloomfield, Michigan.
A Need to Improve Levodopa Delivery
Beyond irregular effects of levodopa, motor fluctuations may be intrinsic to Parkinson’s disease, said Dr. LeWitt. One problem experienced by some patients is freezing of gait, immobility that is often situation-specific irrespective of medication dosing, he added. The sleep-benefit phenomenon, stress-exacerbated tremors and dyskinesias, and end-of-day medication unresponsiveness are further examples. “But for the most part, most motor fluctuations tend to be closely linked to the variable delivery of levodopa to the brain, where, after a short delay, it undergoes conversion to dopamine. This neurotransmitter does not have long to carry out its intended signaling because enzymes and re-uptake mechanisms quickly dispose of it. So, consistent delivery is the key for averting dose-by-dose motor fluctuations.”
During its 50 years of service to the Parkinson’s disease patient, levodopa has revolutionized the identity of this disorder. It has improved longevity, disability, and overall quality of life, and it inspired
Because the short-duration response pattern is associated with benefits as brief as two to three hours per oral immediate-release dose, the focus for improving levodopa has been the use of extension therapies. Blocking the breakdown of peripheral levodopa metabolism (the mechanism for catechol-O-methyltransferase inhibition) or slowing the central metabolism of dopamine (by inhibiting monoamine oxidase-type B) join extended-release carbidopa-levodopa preparations as ways to improve upon the immediate-release product. “While these strategies do provide some level of effectiveness, the problems of irregular responsiveness and up to several hours of daily ‘off’ time haven’t been solved. ‘Off’ time still imposes a major burden on many patients living with Parkinson’s disease,” said Dr. LeWitt. Like delayed onset of effect and rapid wearing-off, levodopa-induced dyskinesias present another challenge for understanding their origin and optimal control. While new mechanisms of blocking dyskinesia are being sought, a simpler solution can be more continuous levodopa delivery so that drug concentration peaks causing involuntary movements are averted.
Future Therapies Undergoing Trials Today
Several new therapeutic approaches have been developed for dealing with the shortcomings of current therapies, especially levodopa. “The first of these options was a tube inserted through the stomach into the upper small intestine for continuous pumping of a carbidopa-levodopa microsuspension gel –quite effective but not an easy choice for most patients,” said Dr. LeWitt. Less cumbersome ways to extend levodopa effects have been the several sustained-release formulations now under development. One is a gastric-retention product, termed the “Accordion Pill,” which slowly leaches carbidopa and levodopa to enhance their pharmacokinetic absorption profile. Another treatment strategy for motor fluctuations that, like the Accordion Pill, is also in worldwide clinical trials, involves continuous subcutaneous infusion of solubilized levodopa and carbidopa. With the latter approach, the drug is administered by a small pump adjusted to optimized rate of delivery. Dr. LeWitt also described another novel way for administering levodopa for rapid entry into the bloodstream for treating “off” states. This involves an inhalation device for pulmonary uptake of a micro-particulate levodopa formulation. In a recently completed study, “off” states were reversed rapidly with this approach.
Subcutaneous apomorphine infusion has already been used for more than 30 years in treating motor fluctuations. However, just recently, a more complete story of what this adjunctive therapy offers was reported from a large-scale randomized clinical trial in Europe. A similar study is underway in the United States and might lead to availability of apomorphine infusion in the near future, said Dr. LeWitt. Another approach to motor fluctuations can be found in a drug for motor fluctuations that does not act on dopaminergic pathways. This medication is istradefylline, a selective inhibitor of adenosine A2a receptors (which are located in the same pathway targeted by deep brain stimulation). In Japan, istradefylline is marketed for reducing “off” time, and studies with this drug are planned for review in the US, said Dr. LeWitt.
For a nonpharmacologic approach to managing motor fluctuations, neurosurgical targeting of brain circuitry with deep brain electrical stimulation has had several decades of experience. Another direction of neurosurgical intervention is under investigation; this involves gene therapy to improve the efficacy of oral levodopa therapy. “Inserting into the putamen a gene for producing an increase of L-aromatic amino acid decarboxylase appears to offer a way for enhancing dopamine formation. The clinical investigation currently underway is testing whether producing this localized alteration of brain neurochemistry might succeed at attenuating motor fluctuations,” said Dr. LeWitt
“In talking to patients about their experiences with motor fluctuations, my advice is to think both about levodopa pharmacokinetics and how the patient uses levodopa (since schedule compliance, the interaction of meals, and drinking sufficient water with medications commonly contribute to these problems). Fortunately, new treatment options are on their way to help in fighting back against the limitations of levodopa therapy,” Dr. LeWitt concluded.
—Erica Tricarico
Suggested Reading
Anderson E, Nutt J. The long-duration response to levodopa: phenomenology, potential mechanisms and clinical implications. Parkinsonism Relat Disord. 2011;17:587-592.
Cilia R, Akpalu A, Sarfo FS, et al. The modern pre-levodopa era of Parkinson’s disease: insights into motor complications from sub-Saharan Africa. Brain. 2014;137(10);2731-2742.
LeWitt PA. Levodopa therapy for Parkinson’s disease: Pharmacokinetics and pharmacodynamics. Mov Disord. 2015;30(1):64-72.
Improved delivery of levodopa and new therapies may help to reduce off time.
Improved delivery of levodopa and new therapies may help to reduce off time.
MIAMI—Motor fluctuations in Parkinson’s disease can arise from more than one cause, and a clinician needs to consider a range of possibilities. Most commonly, motor fluctuations arise as a consequence of chronic levodopa therapy, though the progression of parkinsonism is a contributing factor, according to an overview presented at the Second Pan American Parkinson’s Disease and Movement Disorders Congress. The pharmacokinetics of levodopa provide the basis for studying most clinical patterns of motor fluctuations, and new pharmacologic strategies are under development to improve upon existing treatment options.
“In recent years, there have been some exciting and novel directions of Parkinson’s disease therapeutics for motor fluctuations,” said Peter A. LeWitt, MD, Director of the Parkinson’s Disease and Movement Disorder Program at Henry Ford Hospital in West Bloomfield, Michigan.
A Need to Improve Levodopa Delivery
Beyond irregular effects of levodopa, motor fluctuations may be intrinsic to Parkinson’s disease, said Dr. LeWitt. One problem experienced by some patients is freezing of gait, immobility that is often situation-specific irrespective of medication dosing, he added. The sleep-benefit phenomenon, stress-exacerbated tremors and dyskinesias, and end-of-day medication unresponsiveness are further examples. “But for the most part, most motor fluctuations tend to be closely linked to the variable delivery of levodopa to the brain, where, after a short delay, it undergoes conversion to dopamine. This neurotransmitter does not have long to carry out its intended signaling because enzymes and re-uptake mechanisms quickly dispose of it. So, consistent delivery is the key for averting dose-by-dose motor fluctuations.”
During its 50 years of service to the Parkinson’s disease patient, levodopa has revolutionized the identity of this disorder. It has improved longevity, disability, and overall quality of life, and it inspired
Because the short-duration response pattern is associated with benefits as brief as two to three hours per oral immediate-release dose, the focus for improving levodopa has been the use of extension therapies. Blocking the breakdown of peripheral levodopa metabolism (the mechanism for catechol-O-methyltransferase inhibition) or slowing the central metabolism of dopamine (by inhibiting monoamine oxidase-type B) join extended-release carbidopa-levodopa preparations as ways to improve upon the immediate-release product. “While these strategies do provide some level of effectiveness, the problems of irregular responsiveness and up to several hours of daily ‘off’ time haven’t been solved. ‘Off’ time still imposes a major burden on many patients living with Parkinson’s disease,” said Dr. LeWitt. Like delayed onset of effect and rapid wearing-off, levodopa-induced dyskinesias present another challenge for understanding their origin and optimal control. While new mechanisms of blocking dyskinesia are being sought, a simpler solution can be more continuous levodopa delivery so that drug concentration peaks causing involuntary movements are averted.
Future Therapies Undergoing Trials Today
Several new therapeutic approaches have been developed for dealing with the shortcomings of current therapies, especially levodopa. “The first of these options was a tube inserted through the stomach into the upper small intestine for continuous pumping of a carbidopa-levodopa microsuspension gel –quite effective but not an easy choice for most patients,” said Dr. LeWitt. Less cumbersome ways to extend levodopa effects have been the several sustained-release formulations now under development. One is a gastric-retention product, termed the “Accordion Pill,” which slowly leaches carbidopa and levodopa to enhance their pharmacokinetic absorption profile. Another treatment strategy for motor fluctuations that, like the Accordion Pill, is also in worldwide clinical trials, involves continuous subcutaneous infusion of solubilized levodopa and carbidopa. With the latter approach, the drug is administered by a small pump adjusted to optimized rate of delivery. Dr. LeWitt also described another novel way for administering levodopa for rapid entry into the bloodstream for treating “off” states. This involves an inhalation device for pulmonary uptake of a micro-particulate levodopa formulation. In a recently completed study, “off” states were reversed rapidly with this approach.
Subcutaneous apomorphine infusion has already been used for more than 30 years in treating motor fluctuations. However, just recently, a more complete story of what this adjunctive therapy offers was reported from a large-scale randomized clinical trial in Europe. A similar study is underway in the United States and might lead to availability of apomorphine infusion in the near future, said Dr. LeWitt. Another approach to motor fluctuations can be found in a drug for motor fluctuations that does not act on dopaminergic pathways. This medication is istradefylline, a selective inhibitor of adenosine A2a receptors (which are located in the same pathway targeted by deep brain stimulation). In Japan, istradefylline is marketed for reducing “off” time, and studies with this drug are planned for review in the US, said Dr. LeWitt.
For a nonpharmacologic approach to managing motor fluctuations, neurosurgical targeting of brain circuitry with deep brain electrical stimulation has had several decades of experience. Another direction of neurosurgical intervention is under investigation; this involves gene therapy to improve the efficacy of oral levodopa therapy. “Inserting into the putamen a gene for producing an increase of L-aromatic amino acid decarboxylase appears to offer a way for enhancing dopamine formation. The clinical investigation currently underway is testing whether producing this localized alteration of brain neurochemistry might succeed at attenuating motor fluctuations,” said Dr. LeWitt
“In talking to patients about their experiences with motor fluctuations, my advice is to think both about levodopa pharmacokinetics and how the patient uses levodopa (since schedule compliance, the interaction of meals, and drinking sufficient water with medications commonly contribute to these problems). Fortunately, new treatment options are on their way to help in fighting back against the limitations of levodopa therapy,” Dr. LeWitt concluded.
—Erica Tricarico
Suggested Reading
Anderson E, Nutt J. The long-duration response to levodopa: phenomenology, potential mechanisms and clinical implications. Parkinsonism Relat Disord. 2011;17:587-592.
Cilia R, Akpalu A, Sarfo FS, et al. The modern pre-levodopa era of Parkinson’s disease: insights into motor complications from sub-Saharan Africa. Brain. 2014;137(10);2731-2742.
LeWitt PA. Levodopa therapy for Parkinson’s disease: Pharmacokinetics and pharmacodynamics. Mov Disord. 2015;30(1):64-72.
MIAMI—Motor fluctuations in Parkinson’s disease can arise from more than one cause, and a clinician needs to consider a range of possibilities. Most commonly, motor fluctuations arise as a consequence of chronic levodopa therapy, though the progression of parkinsonism is a contributing factor, according to an overview presented at the Second Pan American Parkinson’s Disease and Movement Disorders Congress. The pharmacokinetics of levodopa provide the basis for studying most clinical patterns of motor fluctuations, and new pharmacologic strategies are under development to improve upon existing treatment options.
“In recent years, there have been some exciting and novel directions of Parkinson’s disease therapeutics for motor fluctuations,” said Peter A. LeWitt, MD, Director of the Parkinson’s Disease and Movement Disorder Program at Henry Ford Hospital in West Bloomfield, Michigan.
A Need to Improve Levodopa Delivery
Beyond irregular effects of levodopa, motor fluctuations may be intrinsic to Parkinson’s disease, said Dr. LeWitt. One problem experienced by some patients is freezing of gait, immobility that is often situation-specific irrespective of medication dosing, he added. The sleep-benefit phenomenon, stress-exacerbated tremors and dyskinesias, and end-of-day medication unresponsiveness are further examples. “But for the most part, most motor fluctuations tend to be closely linked to the variable delivery of levodopa to the brain, where, after a short delay, it undergoes conversion to dopamine. This neurotransmitter does not have long to carry out its intended signaling because enzymes and re-uptake mechanisms quickly dispose of it. So, consistent delivery is the key for averting dose-by-dose motor fluctuations.”
During its 50 years of service to the Parkinson’s disease patient, levodopa has revolutionized the identity of this disorder. It has improved longevity, disability, and overall quality of life, and it inspired
Because the short-duration response pattern is associated with benefits as brief as two to three hours per oral immediate-release dose, the focus for improving levodopa has been the use of extension therapies. Blocking the breakdown of peripheral levodopa metabolism (the mechanism for catechol-O-methyltransferase inhibition) or slowing the central metabolism of dopamine (by inhibiting monoamine oxidase-type B) join extended-release carbidopa-levodopa preparations as ways to improve upon the immediate-release product. “While these strategies do provide some level of effectiveness, the problems of irregular responsiveness and up to several hours of daily ‘off’ time haven’t been solved. ‘Off’ time still imposes a major burden on many patients living with Parkinson’s disease,” said Dr. LeWitt. Like delayed onset of effect and rapid wearing-off, levodopa-induced dyskinesias present another challenge for understanding their origin and optimal control. While new mechanisms of blocking dyskinesia are being sought, a simpler solution can be more continuous levodopa delivery so that drug concentration peaks causing involuntary movements are averted.
Future Therapies Undergoing Trials Today
Several new therapeutic approaches have been developed for dealing with the shortcomings of current therapies, especially levodopa. “The first of these options was a tube inserted through the stomach into the upper small intestine for continuous pumping of a carbidopa-levodopa microsuspension gel –quite effective but not an easy choice for most patients,” said Dr. LeWitt. Less cumbersome ways to extend levodopa effects have been the several sustained-release formulations now under development. One is a gastric-retention product, termed the “Accordion Pill,” which slowly leaches carbidopa and levodopa to enhance their pharmacokinetic absorption profile. Another treatment strategy for motor fluctuations that, like the Accordion Pill, is also in worldwide clinical trials, involves continuous subcutaneous infusion of solubilized levodopa and carbidopa. With the latter approach, the drug is administered by a small pump adjusted to optimized rate of delivery. Dr. LeWitt also described another novel way for administering levodopa for rapid entry into the bloodstream for treating “off” states. This involves an inhalation device for pulmonary uptake of a micro-particulate levodopa formulation. In a recently completed study, “off” states were reversed rapidly with this approach.
Subcutaneous apomorphine infusion has already been used for more than 30 years in treating motor fluctuations. However, just recently, a more complete story of what this adjunctive therapy offers was reported from a large-scale randomized clinical trial in Europe. A similar study is underway in the United States and might lead to availability of apomorphine infusion in the near future, said Dr. LeWitt. Another approach to motor fluctuations can be found in a drug for motor fluctuations that does not act on dopaminergic pathways. This medication is istradefylline, a selective inhibitor of adenosine A2a receptors (which are located in the same pathway targeted by deep brain stimulation). In Japan, istradefylline is marketed for reducing “off” time, and studies with this drug are planned for review in the US, said Dr. LeWitt.
For a nonpharmacologic approach to managing motor fluctuations, neurosurgical targeting of brain circuitry with deep brain electrical stimulation has had several decades of experience. Another direction of neurosurgical intervention is under investigation; this involves gene therapy to improve the efficacy of oral levodopa therapy. “Inserting into the putamen a gene for producing an increase of L-aromatic amino acid decarboxylase appears to offer a way for enhancing dopamine formation. The clinical investigation currently underway is testing whether producing this localized alteration of brain neurochemistry might succeed at attenuating motor fluctuations,” said Dr. LeWitt
“In talking to patients about their experiences with motor fluctuations, my advice is to think both about levodopa pharmacokinetics and how the patient uses levodopa (since schedule compliance, the interaction of meals, and drinking sufficient water with medications commonly contribute to these problems). Fortunately, new treatment options are on their way to help in fighting back against the limitations of levodopa therapy,” Dr. LeWitt concluded.
—Erica Tricarico
Suggested Reading
Anderson E, Nutt J. The long-duration response to levodopa: phenomenology, potential mechanisms and clinical implications. Parkinsonism Relat Disord. 2011;17:587-592.
Cilia R, Akpalu A, Sarfo FS, et al. The modern pre-levodopa era of Parkinson’s disease: insights into motor complications from sub-Saharan Africa. Brain. 2014;137(10);2731-2742.
LeWitt PA. Levodopa therapy for Parkinson’s disease: Pharmacokinetics and pharmacodynamics. Mov Disord. 2015;30(1):64-72.