User login
Risk of ALS May Increase With Greater Exposure to Diesel Exhaust
In men, an association exists between risk of ALS and occupational exposure to diesel exhaust.
LOS ANGELES—People with consistently high occupational exposures to diesel exhaust may have a higher risk of amyotrophic lateral sclerosis (ALS), and that risk may increase with greater exposure, according to a preliminary study presented at the American Academy of Neurology’s 70th Annual Meeting.
“There is some suggestion from previous studies of occupation that workers in jobs with higher exposure to diesel exhaust may have a higher risk of ALS. However, no studies have directly looked at the relationship between diesel exhaust exposure during different time points in life and ALS,” said lead study author Aisha Dickerson, PhD, a postdoctoral fellow in the Departments of Environmental Health and Epidemiology at the Harvard T.H. Chan School of Public Health in Boston. “The overall risk of developing ALS is low, but our findings suggest that the greater the exposure to diesel exhaust, the greater the risk of developing ALS.”

For this study, researchers identified 1,639 people with an average age of 56 from the Danish National Patient Registry who were diagnosed with ALS between 1982 and 2013. For each case, 100 birth year- and sex-matched controls were selected using the Danish Central Person Registry. Employment history since 1964 was acquired from the nationwide Danish Pension Fund.
Cumulative diesel exhaust exposures prior to index dates (the date of ALS diagnosis in the ALS case) were estimated using a job exposure matrix. The estimated exposure was based on potential hazards for specific jobs, including service station attendants, bus drivers, and construction workers. Cumulative exposure was calculated for up to five and 10 years before the diagnosis time period, allowing for the time it may take diesel exhaust to have an effect on the body. Subjects who were older than age 25 in 1964 were excluded to diminish exposure misclassification.
The participants were divided into quartiles based on the amount of exposure to diesel exhaust. Men with any exposure to diesel exhaust at jobs held at least 10 years prior to their date of inclusion in the study were 20% more likely to have ALS than men with no exposure to exhaust during the same time period. For men who had a greater than 50% likelihood of being exposed to exhaust based on their occupation, the link was stronger. That group was 45% more likely to develop ALS than those with no exhaust exposure at both five and 10 years prior to study inclusion. No associations were observed among women, although the types of jobs and even tasks performed in the same job can differ substantially for men and women.
The results were adjusted for other factors that could affect risk of ALS including socioeconomic status and the region of Denmark where a participant lived.
“This type of exposure deserves more attention and study as we work to develop a better understanding of what causes ALS,” Dr. Dickerson said. “Importantly, the general population can be exposed to diesel exhaust from traffic pollution. Understanding whether that exposure increases ALS risk is also an important question to pursue.”
This study does not show that diesel exhaust causes ALS; it only shows an association, the researchers said. One study limitation was that investigators used a job exposure matrix to estimate occupational diesel exhaust levels and could not directly measure personal exposures. However, any potential misclassification caused by this would likely have diminished the observed associations, the researchers noted.
The study was supported by the National Institute of Environmental Health Sciences and the National Institutes of Health.
In men, an association exists between risk of ALS and occupational exposure to diesel exhaust.
In men, an association exists between risk of ALS and occupational exposure to diesel exhaust.
LOS ANGELES—People with consistently high occupational exposures to diesel exhaust may have a higher risk of amyotrophic lateral sclerosis (ALS), and that risk may increase with greater exposure, according to a preliminary study presented at the American Academy of Neurology’s 70th Annual Meeting.
“There is some suggestion from previous studies of occupation that workers in jobs with higher exposure to diesel exhaust may have a higher risk of ALS. However, no studies have directly looked at the relationship between diesel exhaust exposure during different time points in life and ALS,” said lead study author Aisha Dickerson, PhD, a postdoctoral fellow in the Departments of Environmental Health and Epidemiology at the Harvard T.H. Chan School of Public Health in Boston. “The overall risk of developing ALS is low, but our findings suggest that the greater the exposure to diesel exhaust, the greater the risk of developing ALS.”
For this study, researchers identified 1,639 people with an average age of 56 from the Danish National Patient Registry who were diagnosed with ALS between 1982 and 2013. For each case, 100 birth year- and sex-matched controls were selected using the Danish Central Person Registry. Employment history since 1964 was acquired from the nationwide Danish Pension Fund.
Cumulative diesel exhaust exposures prior to index dates (the date of ALS diagnosis in the ALS case) were estimated using a job exposure matrix. The estimated exposure was based on potential hazards for specific jobs, including service station attendants, bus drivers, and construction workers. Cumulative exposure was calculated for up to five and 10 years before the diagnosis time period, allowing for the time it may take diesel exhaust to have an effect on the body. Subjects who were older than age 25 in 1964 were excluded to diminish exposure misclassification.
The participants were divided into quartiles based on the amount of exposure to diesel exhaust. Men with any exposure to diesel exhaust at jobs held at least 10 years prior to their date of inclusion in the study were 20% more likely to have ALS than men with no exposure to exhaust during the same time period. For men who had a greater than 50% likelihood of being exposed to exhaust based on their occupation, the link was stronger. That group was 45% more likely to develop ALS than those with no exhaust exposure at both five and 10 years prior to study inclusion. No associations were observed among women, although the types of jobs and even tasks performed in the same job can differ substantially for men and women.
The results were adjusted for other factors that could affect risk of ALS including socioeconomic status and the region of Denmark where a participant lived.
“This type of exposure deserves more attention and study as we work to develop a better understanding of what causes ALS,” Dr. Dickerson said. “Importantly, the general population can be exposed to diesel exhaust from traffic pollution. Understanding whether that exposure increases ALS risk is also an important question to pursue.”
This study does not show that diesel exhaust causes ALS; it only shows an association, the researchers said. One study limitation was that investigators used a job exposure matrix to estimate occupational diesel exhaust levels and could not directly measure personal exposures. However, any potential misclassification caused by this would likely have diminished the observed associations, the researchers noted.
The study was supported by the National Institute of Environmental Health Sciences and the National Institutes of Health.
LOS ANGELES—People with consistently high occupational exposures to diesel exhaust may have a higher risk of amyotrophic lateral sclerosis (ALS), and that risk may increase with greater exposure, according to a preliminary study presented at the American Academy of Neurology’s 70th Annual Meeting.
“There is some suggestion from previous studies of occupation that workers in jobs with higher exposure to diesel exhaust may have a higher risk of ALS. However, no studies have directly looked at the relationship between diesel exhaust exposure during different time points in life and ALS,” said lead study author Aisha Dickerson, PhD, a postdoctoral fellow in the Departments of Environmental Health and Epidemiology at the Harvard T.H. Chan School of Public Health in Boston. “The overall risk of developing ALS is low, but our findings suggest that the greater the exposure to diesel exhaust, the greater the risk of developing ALS.”
For this study, researchers identified 1,639 people with an average age of 56 from the Danish National Patient Registry who were diagnosed with ALS between 1982 and 2013. For each case, 100 birth year- and sex-matched controls were selected using the Danish Central Person Registry. Employment history since 1964 was acquired from the nationwide Danish Pension Fund.
Cumulative diesel exhaust exposures prior to index dates (the date of ALS diagnosis in the ALS case) were estimated using a job exposure matrix. The estimated exposure was based on potential hazards for specific jobs, including service station attendants, bus drivers, and construction workers. Cumulative exposure was calculated for up to five and 10 years before the diagnosis time period, allowing for the time it may take diesel exhaust to have an effect on the body. Subjects who were older than age 25 in 1964 were excluded to diminish exposure misclassification.
The participants were divided into quartiles based on the amount of exposure to diesel exhaust. Men with any exposure to diesel exhaust at jobs held at least 10 years prior to their date of inclusion in the study were 20% more likely to have ALS than men with no exposure to exhaust during the same time period. For men who had a greater than 50% likelihood of being exposed to exhaust based on their occupation, the link was stronger. That group was 45% more likely to develop ALS than those with no exhaust exposure at both five and 10 years prior to study inclusion. No associations were observed among women, although the types of jobs and even tasks performed in the same job can differ substantially for men and women.
The results were adjusted for other factors that could affect risk of ALS including socioeconomic status and the region of Denmark where a participant lived.
“This type of exposure deserves more attention and study as we work to develop a better understanding of what causes ALS,” Dr. Dickerson said. “Importantly, the general population can be exposed to diesel exhaust from traffic pollution. Understanding whether that exposure increases ALS risk is also an important question to pursue.”
This study does not show that diesel exhaust causes ALS; it only shows an association, the researchers said. One study limitation was that investigators used a job exposure matrix to estimate occupational diesel exhaust levels and could not directly measure personal exposures. However, any potential misclassification caused by this would likely have diminished the observed associations, the researchers noted.
The study was supported by the National Institute of Environmental Health Sciences and the National Institutes of Health.
PhRMA spending leads health-sector lobbying efforts
The Pharmaceutical Research and Manufacturers of America (PhRMA) led the way on health-sector lobbying in the first half of 2018 with spending that’s on pace to top its previous 1-year high, according to the Center for Responsive Politics.
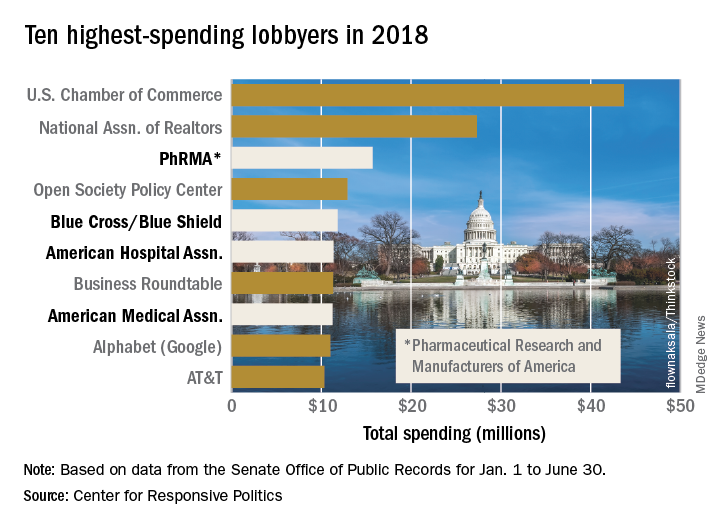
PhRMA spent over $15.7 million on lobbying through the end of June, and equaling that amount over the second half of the year would eclipse the $27.4 million the organization spent in 2009. PhRMA’s total for the year so far puts it third among all entities: The U.S. Chamber of Commerce was first with $43.7 million and the National Association of Realtors was second at $27.3 million, the center reported on OpenSecrets.org. The National Association of Realtors has been second in spending every year since 2012, and the chamber has been first every year since 2001.
The health sector’s three other representatives in the lobbying Top 10 for the first half of this year are Blue Cross/Blue Shield in fifth with $11.8 million in spending, the American Hospital Association in sixth ($11.4 million), and the American Medical Association in eighth ($11.2 million), based on the center’s analysis of data from the Senate Office of Public Records. The four current health sector representatives have all been in the top 10 every year since 2013.
Total spending for the health sector through June was $290.3 million, which was first among the 13 sectors into which the center separates the U.S. economy; spending for lobbying among all sectors was $1.69 billion. The health sector was ranked first in spending each of the 2 previous years and has never been lower than third since the center’s record keeping began in 2000, according to OpenSecrets.org.
The Pharmaceutical Research and Manufacturers of America (PhRMA) led the way on health-sector lobbying in the first half of 2018 with spending that’s on pace to top its previous 1-year high, according to the Center for Responsive Politics.
PhRMA spent over $15.7 million on lobbying through the end of June, and equaling that amount over the second half of the year would eclipse the $27.4 million the organization spent in 2009. PhRMA’s total for the year so far puts it third among all entities: The U.S. Chamber of Commerce was first with $43.7 million and the National Association of Realtors was second at $27.3 million, the center reported on OpenSecrets.org. The National Association of Realtors has been second in spending every year since 2012, and the chamber has been first every year since 2001.
The health sector’s three other representatives in the lobbying Top 10 for the first half of this year are Blue Cross/Blue Shield in fifth with $11.8 million in spending, the American Hospital Association in sixth ($11.4 million), and the American Medical Association in eighth ($11.2 million), based on the center’s analysis of data from the Senate Office of Public Records. The four current health sector representatives have all been in the top 10 every year since 2013.
Total spending for the health sector through June was $290.3 million, which was first among the 13 sectors into which the center separates the U.S. economy; spending for lobbying among all sectors was $1.69 billion. The health sector was ranked first in spending each of the 2 previous years and has never been lower than third since the center’s record keeping began in 2000, according to OpenSecrets.org.
The Pharmaceutical Research and Manufacturers of America (PhRMA) led the way on health-sector lobbying in the first half of 2018 with spending that’s on pace to top its previous 1-year high, according to the Center for Responsive Politics.
PhRMA spent over $15.7 million on lobbying through the end of June, and equaling that amount over the second half of the year would eclipse the $27.4 million the organization spent in 2009. PhRMA’s total for the year so far puts it third among all entities: The U.S. Chamber of Commerce was first with $43.7 million and the National Association of Realtors was second at $27.3 million, the center reported on OpenSecrets.org. The National Association of Realtors has been second in spending every year since 2012, and the chamber has been first every year since 2001.
The health sector’s three other representatives in the lobbying Top 10 for the first half of this year are Blue Cross/Blue Shield in fifth with $11.8 million in spending, the American Hospital Association in sixth ($11.4 million), and the American Medical Association in eighth ($11.2 million), based on the center’s analysis of data from the Senate Office of Public Records. The four current health sector representatives have all been in the top 10 every year since 2013.
Total spending for the health sector through June was $290.3 million, which was first among the 13 sectors into which the center separates the U.S. economy; spending for lobbying among all sectors was $1.69 billion. The health sector was ranked first in spending each of the 2 previous years and has never been lower than third since the center’s record keeping began in 2000, according to OpenSecrets.org.
New and Noteworthy Information—August 2018
Practice Effects May Influence MCI Detection
Failing to account for practice effects may lead to underdiagnosis of mild cognitive impairment (MCI), according to a study published May 14 in Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring. In an approximately six-year follow-up of the Vietnam Era Twin Study of Aging, researchers retested the cognitive function of 995 late-middle-aged men. In addition, the researchers tested 170 age-matched study replacements for the first time. The investigators used group differences to calculate practice effects after controlling for attrition effects and generated MCI diagnoses from practice-adjusted scores. There were significant practice effects on most cognitive domains, even though participants’ uncorrected scores may have declined. Conversion to MCI doubled after correcting for practice effects, from 4.5% to 9%.
Elman JA, Jak AJ, Panizzon MS, et al. Underdiagnosis of mild cognitive impairment: a consequence of ignoring practice effects. Alzheimers Dement (Amst). 2018;10:372-381.
Brain Iron Levels Predict Disability in Patients With MS
Iron levels in the brains of patients with multiple sclerosis (MS) measured using quantitative susceptibility mapping (QSM) may help identify people at a higher risk of physical disability, according to a study published online ahead of print July 17 in Radiology. In this prospective study, 600 participants with MS and 250 age- and sex-matched healthy controls were imaged with 3.0-T MRI. The researchers assessed QSM and MRI volumetric differences between study groups and associations with clinical outcomes using analysis of covariance, multivariable linear regression, and voxelwise analyses, controlling for age and sex. Compared with controls, participants with MS had lower thalamic susceptibility and higher susceptibility of basal ganglia. Lower thalamic susceptibility was associated with longer disease duration, greater disability, and secondary-progressive disease course.
Zivadinov R, Tavazzi E, Bergsland N, et al. Brain iron at quantitative MRI is associated with disability in multiple sclerosis. Radiology. 2018 Jul 17 [Epub ahead of print].
Concussion and ADHD May Increase Depression and Anxiety
Athletes with attention deficit hyperactivity disorder (ADHD) may be at greater risk of persistent anxiety and depression after a concussion, compared with athletes without ADHD, according to a study presented at the American Academy of Neurology’s Sports Concussion Conference. The study included 979 NCAA Division I college athletes. Researchers gathered information on ADHD diagnosis and history of concussion, and athletes completed questionnaires measuring anxiety and depression symptoms before the start of their sporting seasons. The investigators divided athletes into four groups—those with ADHD who had had a concussion, those with ADHD who had not had a concussion, those without ADHD who had had a concussion, and those without a history of concussion or ADHD. Athletes with ADHD and concussion had significantly higher anxiety and depression scores, compared with the other groups.
Late-Life Blood Pressure Is Associated With Brain Lesions
Higher average late-life systolic blood pressure and diastolic blood pressure are associated with an increasing number of brain infarcts, including gross and microinfarcts, according to a study published online ahead of print July 11 in Neurology. In addition, faster decline in systolic blood pressure increases the likelihood of an infarct. This clinical-pathologic study included data from 1,288 people who participated in prospective, community-based cohort studies of aging with similar designs and data collection. Blood pressure measurements were obtained annually. Participants were followed for an average of eight years, and the average age at death was 89. The mean standardized person-specific systolic blood pressure was 134 mm Hg and diastolic blood pressure was 71 mm Hg. Alzheimer’s disease pathology analyses found that systolic blood pressure was associated with the number of tangles but not plaques or other pathology.
Arvanitakis Z, Capuano AW, Lamar M, et al. Late-life blood pressure association with cerebrovascular and Alzheimer disease pathology. Neurology. 2018 Jul 11 [Epub ahead of print].
Is t-PA Beneficial for Minor Stroke?
Among patients with mild acute ischemic stroke, treatment with alteplase does not increase the likelihood of favorable functional outcome at 90 days, compared with treatment with aspirin, according to a study published July 10 in JAMA. The PRISMS trial, a phase IIIb, double-blind, double-placebo, randomized clinical trial, compared alteplase with aspirin for the treatment of emergent stroke. The study enrolled patients with NIH Stroke Scale scores of 0 to 5 and deficits that were not clearly disabling. Eligible patients were able to receive treatment within three hours of onset. Participants were randomized to receive IV alteplase (0.9 mg/kg) with oral placebo (n = 156) or oral aspirin (325 mg) with IV placebo (n = 157). At 90 days, 78.2% of patients in the alteplase group and 81.5% of patients in the aspirin group had a favorable outcome (ie, a modified Rankin Scale score of 0 or 1). The trial originally was designed to enroll 948 patients but was ended early because of slow enrollment. The early study termination precludes definitive conclusions, the investigators said.
Khatri P, Kleindorfer DO, Devlin T, et al. Effect of alteplase vs aspirin on functional outcome for patients with acute ischemic stroke and minor nondisabling neurologic deficits: the PRISMS randomized clinical trial. JAMA. 2018 Jul 10;320(2):156-166.
FDA Approves Xeomin for Adults With Sialorrhea
The FDA has approved the supplemental Biologics License Application for Xeomin (incobotulinumtoxinA) for the treatment of chronic sialorrhea in adult patients. The approval was based on a phase III, randomized, double-blind, placebo-controlled, multicenter trial that included 184 patients. The coprimary end points of change in unstimulated salivary flow rate and Global Impression of Change Scale at week four as compared with baseline significantly improved for participants administered 100 U incobotulinumtoxinA versus placebo. The overall frequency of adverse events was similar between placebo and treatment groups with no new or unexpected adverse events reported. Participants in the study received placebo, incobotulinumtoxinA 75 U, or incobotulinumtoxinA 100 U. Merz North America, which markets Xeomin, is headquartered in Raleigh, North Carolina.
Does Exposure to Organic Solvents Heighten the Risk of MS?
People who are exposed to organic solvents and carry genes that make them more susceptible to developing multiple sclerosis (MS) may be at greater risk of the disease than people who have only the exposure to solvents or the MS risk genes, according to a study published online ahead of print July 3 in Neurology. Using a Swedish population-based case–control study of 2,042 incident cases of MS and 2,947 controls, investigators compared the occurrence of MS in participants with different genotypes, smoking habits, and exposures to organic solvents such as paint and varnish. A potential interaction between exposure to organic solvents and MS risk human leukocyte antigen genes was evaluated by calculating the attributable proportion due to interaction. The MS genes and exposure to solvents combined were responsible for an estimated 60% of the risk of developing MS.
Hedström AK, Hössjer O, Katsoulis M, et al. Organic solvents and MS susceptibility: interaction with MS risk HLA genes. Neurology. 2018 Jul 3 [Epub ahead of print].
Epidiolex Approved for the Treatment of Seizures
The FDA approved Epidiolex (cannabidiol) oral solution for the treatment of seizures associated with Lennox-Gastaut syndrome and Dravet syndrome in patients age 2 and older. Epidiolex is the first FDA-approved drug that contains a purified drug substance derived from marijuana. It also is the first FDA approval of a drug for the treatment of patients with Dravet syndrome. The drug’s effectiveness was studied in three randomized, double-blind, placebo-controlled clinical trials that included 516 patients with Lennox-Gastaut syndrome or Dravet syndrome. Taken with other medications, cannabidiol reduced the frequency of seizures, compared with placebo. Epidiolex must be dispensed with a patient medication guide that describes the drug’s uses and risks. GW Pharmaceuticals, located in the United Kingdom, markets Epidiolex.
FDA Approves Nuplazid Capsule Formulation and 10-mg Tablet
The FDA approved a new capsule dose formulation and tablet strength of Nuplazid (pimavanserin), a treatment for hallucinations and delusions associated with Parkinson’s disease psychosis. The 34-mg capsule formulation provides the recommended once daily dose in one capsule, versus the current administration of two 17-mg tablets. The 10-mg tablet provides a lower dosage strength for patients who are concomitantly receiving strong cytochrome 3A4 inhibitors, which can inhibit the metabolism of Nuplazid. The drug is a nondopaminergic, selective serotonin inverse agonist preferentially targeting 5-HT2A receptors. Acadia Pharmaceuticals, which markets the therapy, is headquartered in San Diego.
Mild Sleep Problems May Elevate Blood Pressure in Women
Mild sleep problems such as trouble falling asleep are associated with increased blood pressure and vascular inflammation in women, according to a study published June 9 in the Journal of the American Heart Association. Researchers examined blood pressure and sleep habits in 323 women in the ongoing American Heart Association Go Red for Women Strategically Focused Research Network. Investigators assessed participant’s sleep quality, obstructive sleep apnea risk, and insomnia severity. In a subset of women, sleep duration was assessed using actigraphy, and endothelial inflammation was assessed directly in harvested endothelial cells. Systolic blood pressure was associated with poor sleep quality. Poor sleep quality, insomnia, and longer sleep onset latency were associated with endothelial inflammation.
Aggarwal B, Makarem N, Shah R, et al. Effects of inadequate sleep on blood pressure and endothelial inflammation in women: findings from the American Heart Association Go Red for Women Strategically Focused Research Network. J Am Heart Assoc. 2018;7(12):e008590.
DBS May Slow Tremor Progression in Early Parkinson’s Disease
Deep brain stimulation (DBS) in the early stage of Parkinson’s disease may slow tremor progression, according to a study published online ahead of print June 29 in Neurology. The prospective pilot trial enrolled patients with Parkinson’s disease who were ages 50 to 75, had been treated with Parkinson’s disease medications for six months to four years, and had no history of dyskinesia or other motor fluctuations. Participants were randomized to receive optimal drug therapy (ODT) or DBS and ODT. At baseline and six, 12, 18, and 24 months, all patients stopped all Parkinson’s disease therapy for one week. Unified Parkinson’s Disease Rating Scale-III scores were compared between the ODT and DBS and ODT groups (n = 28). Rest tremor slopes from baseline to 24 months favored DBS plus ODT off and on therapy, compared with ODT alone.
Hacker ML, DeLong MR, Turchan M, et al. Effects of deep brain stimulation on rest tremor progression in early stage Parkinson disease. Neurology. 2018 Jun 29 [Epub ahead of print].
—Kimberly Williams
Practice Effects May Influence MCI Detection
Failing to account for practice effects may lead to underdiagnosis of mild cognitive impairment (MCI), according to a study published May 14 in Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring. In an approximately six-year follow-up of the Vietnam Era Twin Study of Aging, researchers retested the cognitive function of 995 late-middle-aged men. In addition, the researchers tested 170 age-matched study replacements for the first time. The investigators used group differences to calculate practice effects after controlling for attrition effects and generated MCI diagnoses from practice-adjusted scores. There were significant practice effects on most cognitive domains, even though participants’ uncorrected scores may have declined. Conversion to MCI doubled after correcting for practice effects, from 4.5% to 9%.
Elman JA, Jak AJ, Panizzon MS, et al. Underdiagnosis of mild cognitive impairment: a consequence of ignoring practice effects. Alzheimers Dement (Amst). 2018;10:372-381.
Brain Iron Levels Predict Disability in Patients With MS
Iron levels in the brains of patients with multiple sclerosis (MS) measured using quantitative susceptibility mapping (QSM) may help identify people at a higher risk of physical disability, according to a study published online ahead of print July 17 in Radiology. In this prospective study, 600 participants with MS and 250 age- and sex-matched healthy controls were imaged with 3.0-T MRI. The researchers assessed QSM and MRI volumetric differences between study groups and associations with clinical outcomes using analysis of covariance, multivariable linear regression, and voxelwise analyses, controlling for age and sex. Compared with controls, participants with MS had lower thalamic susceptibility and higher susceptibility of basal ganglia. Lower thalamic susceptibility was associated with longer disease duration, greater disability, and secondary-progressive disease course.
Zivadinov R, Tavazzi E, Bergsland N, et al. Brain iron at quantitative MRI is associated with disability in multiple sclerosis. Radiology. 2018 Jul 17 [Epub ahead of print].
Concussion and ADHD May Increase Depression and Anxiety
Athletes with attention deficit hyperactivity disorder (ADHD) may be at greater risk of persistent anxiety and depression after a concussion, compared with athletes without ADHD, according to a study presented at the American Academy of Neurology’s Sports Concussion Conference. The study included 979 NCAA Division I college athletes. Researchers gathered information on ADHD diagnosis and history of concussion, and athletes completed questionnaires measuring anxiety and depression symptoms before the start of their sporting seasons. The investigators divided athletes into four groups—those with ADHD who had had a concussion, those with ADHD who had not had a concussion, those without ADHD who had had a concussion, and those without a history of concussion or ADHD. Athletes with ADHD and concussion had significantly higher anxiety and depression scores, compared with the other groups.
Late-Life Blood Pressure Is Associated With Brain Lesions
Higher average late-life systolic blood pressure and diastolic blood pressure are associated with an increasing number of brain infarcts, including gross and microinfarcts, according to a study published online ahead of print July 11 in Neurology. In addition, faster decline in systolic blood pressure increases the likelihood of an infarct. This clinical-pathologic study included data from 1,288 people who participated in prospective, community-based cohort studies of aging with similar designs and data collection. Blood pressure measurements were obtained annually. Participants were followed for an average of eight years, and the average age at death was 89. The mean standardized person-specific systolic blood pressure was 134 mm Hg and diastolic blood pressure was 71 mm Hg. Alzheimer’s disease pathology analyses found that systolic blood pressure was associated with the number of tangles but not plaques or other pathology.
Arvanitakis Z, Capuano AW, Lamar M, et al. Late-life blood pressure association with cerebrovascular and Alzheimer disease pathology. Neurology. 2018 Jul 11 [Epub ahead of print].
Is t-PA Beneficial for Minor Stroke?
Among patients with mild acute ischemic stroke, treatment with alteplase does not increase the likelihood of favorable functional outcome at 90 days, compared with treatment with aspirin, according to a study published July 10 in JAMA. The PRISMS trial, a phase IIIb, double-blind, double-placebo, randomized clinical trial, compared alteplase with aspirin for the treatment of emergent stroke. The study enrolled patients with NIH Stroke Scale scores of 0 to 5 and deficits that were not clearly disabling. Eligible patients were able to receive treatment within three hours of onset. Participants were randomized to receive IV alteplase (0.9 mg/kg) with oral placebo (n = 156) or oral aspirin (325 mg) with IV placebo (n = 157). At 90 days, 78.2% of patients in the alteplase group and 81.5% of patients in the aspirin group had a favorable outcome (ie, a modified Rankin Scale score of 0 or 1). The trial originally was designed to enroll 948 patients but was ended early because of slow enrollment. The early study termination precludes definitive conclusions, the investigators said.
Khatri P, Kleindorfer DO, Devlin T, et al. Effect of alteplase vs aspirin on functional outcome for patients with acute ischemic stroke and minor nondisabling neurologic deficits: the PRISMS randomized clinical trial. JAMA. 2018 Jul 10;320(2):156-166.
FDA Approves Xeomin for Adults With Sialorrhea
The FDA has approved the supplemental Biologics License Application for Xeomin (incobotulinumtoxinA) for the treatment of chronic sialorrhea in adult patients. The approval was based on a phase III, randomized, double-blind, placebo-controlled, multicenter trial that included 184 patients. The coprimary end points of change in unstimulated salivary flow rate and Global Impression of Change Scale at week four as compared with baseline significantly improved for participants administered 100 U incobotulinumtoxinA versus placebo. The overall frequency of adverse events was similar between placebo and treatment groups with no new or unexpected adverse events reported. Participants in the study received placebo, incobotulinumtoxinA 75 U, or incobotulinumtoxinA 100 U. Merz North America, which markets Xeomin, is headquartered in Raleigh, North Carolina.
Does Exposure to Organic Solvents Heighten the Risk of MS?
People who are exposed to organic solvents and carry genes that make them more susceptible to developing multiple sclerosis (MS) may be at greater risk of the disease than people who have only the exposure to solvents or the MS risk genes, according to a study published online ahead of print July 3 in Neurology. Using a Swedish population-based case–control study of 2,042 incident cases of MS and 2,947 controls, investigators compared the occurrence of MS in participants with different genotypes, smoking habits, and exposures to organic solvents such as paint and varnish. A potential interaction between exposure to organic solvents and MS risk human leukocyte antigen genes was evaluated by calculating the attributable proportion due to interaction. The MS genes and exposure to solvents combined were responsible for an estimated 60% of the risk of developing MS.
Hedström AK, Hössjer O, Katsoulis M, et al. Organic solvents and MS susceptibility: interaction with MS risk HLA genes. Neurology. 2018 Jul 3 [Epub ahead of print].
Epidiolex Approved for the Treatment of Seizures
The FDA approved Epidiolex (cannabidiol) oral solution for the treatment of seizures associated with Lennox-Gastaut syndrome and Dravet syndrome in patients age 2 and older. Epidiolex is the first FDA-approved drug that contains a purified drug substance derived from marijuana. It also is the first FDA approval of a drug for the treatment of patients with Dravet syndrome. The drug’s effectiveness was studied in three randomized, double-blind, placebo-controlled clinical trials that included 516 patients with Lennox-Gastaut syndrome or Dravet syndrome. Taken with other medications, cannabidiol reduced the frequency of seizures, compared with placebo. Epidiolex must be dispensed with a patient medication guide that describes the drug’s uses and risks. GW Pharmaceuticals, located in the United Kingdom, markets Epidiolex.
FDA Approves Nuplazid Capsule Formulation and 10-mg Tablet
The FDA approved a new capsule dose formulation and tablet strength of Nuplazid (pimavanserin), a treatment for hallucinations and delusions associated with Parkinson’s disease psychosis. The 34-mg capsule formulation provides the recommended once daily dose in one capsule, versus the current administration of two 17-mg tablets. The 10-mg tablet provides a lower dosage strength for patients who are concomitantly receiving strong cytochrome 3A4 inhibitors, which can inhibit the metabolism of Nuplazid. The drug is a nondopaminergic, selective serotonin inverse agonist preferentially targeting 5-HT2A receptors. Acadia Pharmaceuticals, which markets the therapy, is headquartered in San Diego.
Mild Sleep Problems May Elevate Blood Pressure in Women
Mild sleep problems such as trouble falling asleep are associated with increased blood pressure and vascular inflammation in women, according to a study published June 9 in the Journal of the American Heart Association. Researchers examined blood pressure and sleep habits in 323 women in the ongoing American Heart Association Go Red for Women Strategically Focused Research Network. Investigators assessed participant’s sleep quality, obstructive sleep apnea risk, and insomnia severity. In a subset of women, sleep duration was assessed using actigraphy, and endothelial inflammation was assessed directly in harvested endothelial cells. Systolic blood pressure was associated with poor sleep quality. Poor sleep quality, insomnia, and longer sleep onset latency were associated with endothelial inflammation.
Aggarwal B, Makarem N, Shah R, et al. Effects of inadequate sleep on blood pressure and endothelial inflammation in women: findings from the American Heart Association Go Red for Women Strategically Focused Research Network. J Am Heart Assoc. 2018;7(12):e008590.
DBS May Slow Tremor Progression in Early Parkinson’s Disease
Deep brain stimulation (DBS) in the early stage of Parkinson’s disease may slow tremor progression, according to a study published online ahead of print June 29 in Neurology. The prospective pilot trial enrolled patients with Parkinson’s disease who were ages 50 to 75, had been treated with Parkinson’s disease medications for six months to four years, and had no history of dyskinesia or other motor fluctuations. Participants were randomized to receive optimal drug therapy (ODT) or DBS and ODT. At baseline and six, 12, 18, and 24 months, all patients stopped all Parkinson’s disease therapy for one week. Unified Parkinson’s Disease Rating Scale-III scores were compared between the ODT and DBS and ODT groups (n = 28). Rest tremor slopes from baseline to 24 months favored DBS plus ODT off and on therapy, compared with ODT alone.
Hacker ML, DeLong MR, Turchan M, et al. Effects of deep brain stimulation on rest tremor progression in early stage Parkinson disease. Neurology. 2018 Jun 29 [Epub ahead of print].
—Kimberly Williams
Practice Effects May Influence MCI Detection
Failing to account for practice effects may lead to underdiagnosis of mild cognitive impairment (MCI), according to a study published May 14 in Alzheimer’s & Dementia: Diagnosis, Assessment & Disease Monitoring. In an approximately six-year follow-up of the Vietnam Era Twin Study of Aging, researchers retested the cognitive function of 995 late-middle-aged men. In addition, the researchers tested 170 age-matched study replacements for the first time. The investigators used group differences to calculate practice effects after controlling for attrition effects and generated MCI diagnoses from practice-adjusted scores. There were significant practice effects on most cognitive domains, even though participants’ uncorrected scores may have declined. Conversion to MCI doubled after correcting for practice effects, from 4.5% to 9%.
Elman JA, Jak AJ, Panizzon MS, et al. Underdiagnosis of mild cognitive impairment: a consequence of ignoring practice effects. Alzheimers Dement (Amst). 2018;10:372-381.
Brain Iron Levels Predict Disability in Patients With MS
Iron levels in the brains of patients with multiple sclerosis (MS) measured using quantitative susceptibility mapping (QSM) may help identify people at a higher risk of physical disability, according to a study published online ahead of print July 17 in Radiology. In this prospective study, 600 participants with MS and 250 age- and sex-matched healthy controls were imaged with 3.0-T MRI. The researchers assessed QSM and MRI volumetric differences between study groups and associations with clinical outcomes using analysis of covariance, multivariable linear regression, and voxelwise analyses, controlling for age and sex. Compared with controls, participants with MS had lower thalamic susceptibility and higher susceptibility of basal ganglia. Lower thalamic susceptibility was associated with longer disease duration, greater disability, and secondary-progressive disease course.
Zivadinov R, Tavazzi E, Bergsland N, et al. Brain iron at quantitative MRI is associated with disability in multiple sclerosis. Radiology. 2018 Jul 17 [Epub ahead of print].
Concussion and ADHD May Increase Depression and Anxiety
Athletes with attention deficit hyperactivity disorder (ADHD) may be at greater risk of persistent anxiety and depression after a concussion, compared with athletes without ADHD, according to a study presented at the American Academy of Neurology’s Sports Concussion Conference. The study included 979 NCAA Division I college athletes. Researchers gathered information on ADHD diagnosis and history of concussion, and athletes completed questionnaires measuring anxiety and depression symptoms before the start of their sporting seasons. The investigators divided athletes into four groups—those with ADHD who had had a concussion, those with ADHD who had not had a concussion, those without ADHD who had had a concussion, and those without a history of concussion or ADHD. Athletes with ADHD and concussion had significantly higher anxiety and depression scores, compared with the other groups.
Late-Life Blood Pressure Is Associated With Brain Lesions
Higher average late-life systolic blood pressure and diastolic blood pressure are associated with an increasing number of brain infarcts, including gross and microinfarcts, according to a study published online ahead of print July 11 in Neurology. In addition, faster decline in systolic blood pressure increases the likelihood of an infarct. This clinical-pathologic study included data from 1,288 people who participated in prospective, community-based cohort studies of aging with similar designs and data collection. Blood pressure measurements were obtained annually. Participants were followed for an average of eight years, and the average age at death was 89. The mean standardized person-specific systolic blood pressure was 134 mm Hg and diastolic blood pressure was 71 mm Hg. Alzheimer’s disease pathology analyses found that systolic blood pressure was associated with the number of tangles but not plaques or other pathology.
Arvanitakis Z, Capuano AW, Lamar M, et al. Late-life blood pressure association with cerebrovascular and Alzheimer disease pathology. Neurology. 2018 Jul 11 [Epub ahead of print].
Is t-PA Beneficial for Minor Stroke?
Among patients with mild acute ischemic stroke, treatment with alteplase does not increase the likelihood of favorable functional outcome at 90 days, compared with treatment with aspirin, according to a study published July 10 in JAMA. The PRISMS trial, a phase IIIb, double-blind, double-placebo, randomized clinical trial, compared alteplase with aspirin for the treatment of emergent stroke. The study enrolled patients with NIH Stroke Scale scores of 0 to 5 and deficits that were not clearly disabling. Eligible patients were able to receive treatment within three hours of onset. Participants were randomized to receive IV alteplase (0.9 mg/kg) with oral placebo (n = 156) or oral aspirin (325 mg) with IV placebo (n = 157). At 90 days, 78.2% of patients in the alteplase group and 81.5% of patients in the aspirin group had a favorable outcome (ie, a modified Rankin Scale score of 0 or 1). The trial originally was designed to enroll 948 patients but was ended early because of slow enrollment. The early study termination precludes definitive conclusions, the investigators said.
Khatri P, Kleindorfer DO, Devlin T, et al. Effect of alteplase vs aspirin on functional outcome for patients with acute ischemic stroke and minor nondisabling neurologic deficits: the PRISMS randomized clinical trial. JAMA. 2018 Jul 10;320(2):156-166.
FDA Approves Xeomin for Adults With Sialorrhea
The FDA has approved the supplemental Biologics License Application for Xeomin (incobotulinumtoxinA) for the treatment of chronic sialorrhea in adult patients. The approval was based on a phase III, randomized, double-blind, placebo-controlled, multicenter trial that included 184 patients. The coprimary end points of change in unstimulated salivary flow rate and Global Impression of Change Scale at week four as compared with baseline significantly improved for participants administered 100 U incobotulinumtoxinA versus placebo. The overall frequency of adverse events was similar between placebo and treatment groups with no new or unexpected adverse events reported. Participants in the study received placebo, incobotulinumtoxinA 75 U, or incobotulinumtoxinA 100 U. Merz North America, which markets Xeomin, is headquartered in Raleigh, North Carolina.
Does Exposure to Organic Solvents Heighten the Risk of MS?
People who are exposed to organic solvents and carry genes that make them more susceptible to developing multiple sclerosis (MS) may be at greater risk of the disease than people who have only the exposure to solvents or the MS risk genes, according to a study published online ahead of print July 3 in Neurology. Using a Swedish population-based case–control study of 2,042 incident cases of MS and 2,947 controls, investigators compared the occurrence of MS in participants with different genotypes, smoking habits, and exposures to organic solvents such as paint and varnish. A potential interaction between exposure to organic solvents and MS risk human leukocyte antigen genes was evaluated by calculating the attributable proportion due to interaction. The MS genes and exposure to solvents combined were responsible for an estimated 60% of the risk of developing MS.
Hedström AK, Hössjer O, Katsoulis M, et al. Organic solvents and MS susceptibility: interaction with MS risk HLA genes. Neurology. 2018 Jul 3 [Epub ahead of print].
Epidiolex Approved for the Treatment of Seizures
The FDA approved Epidiolex (cannabidiol) oral solution for the treatment of seizures associated with Lennox-Gastaut syndrome and Dravet syndrome in patients age 2 and older. Epidiolex is the first FDA-approved drug that contains a purified drug substance derived from marijuana. It also is the first FDA approval of a drug for the treatment of patients with Dravet syndrome. The drug’s effectiveness was studied in three randomized, double-blind, placebo-controlled clinical trials that included 516 patients with Lennox-Gastaut syndrome or Dravet syndrome. Taken with other medications, cannabidiol reduced the frequency of seizures, compared with placebo. Epidiolex must be dispensed with a patient medication guide that describes the drug’s uses and risks. GW Pharmaceuticals, located in the United Kingdom, markets Epidiolex.
FDA Approves Nuplazid Capsule Formulation and 10-mg Tablet
The FDA approved a new capsule dose formulation and tablet strength of Nuplazid (pimavanserin), a treatment for hallucinations and delusions associated with Parkinson’s disease psychosis. The 34-mg capsule formulation provides the recommended once daily dose in one capsule, versus the current administration of two 17-mg tablets. The 10-mg tablet provides a lower dosage strength for patients who are concomitantly receiving strong cytochrome 3A4 inhibitors, which can inhibit the metabolism of Nuplazid. The drug is a nondopaminergic, selective serotonin inverse agonist preferentially targeting 5-HT2A receptors. Acadia Pharmaceuticals, which markets the therapy, is headquartered in San Diego.
Mild Sleep Problems May Elevate Blood Pressure in Women
Mild sleep problems such as trouble falling asleep are associated with increased blood pressure and vascular inflammation in women, according to a study published June 9 in the Journal of the American Heart Association. Researchers examined blood pressure and sleep habits in 323 women in the ongoing American Heart Association Go Red for Women Strategically Focused Research Network. Investigators assessed participant’s sleep quality, obstructive sleep apnea risk, and insomnia severity. In a subset of women, sleep duration was assessed using actigraphy, and endothelial inflammation was assessed directly in harvested endothelial cells. Systolic blood pressure was associated with poor sleep quality. Poor sleep quality, insomnia, and longer sleep onset latency were associated with endothelial inflammation.
Aggarwal B, Makarem N, Shah R, et al. Effects of inadequate sleep on blood pressure and endothelial inflammation in women: findings from the American Heart Association Go Red for Women Strategically Focused Research Network. J Am Heart Assoc. 2018;7(12):e008590.
DBS May Slow Tremor Progression in Early Parkinson’s Disease
Deep brain stimulation (DBS) in the early stage of Parkinson’s disease may slow tremor progression, according to a study published online ahead of print June 29 in Neurology. The prospective pilot trial enrolled patients with Parkinson’s disease who were ages 50 to 75, had been treated with Parkinson’s disease medications for six months to four years, and had no history of dyskinesia or other motor fluctuations. Participants were randomized to receive optimal drug therapy (ODT) or DBS and ODT. At baseline and six, 12, 18, and 24 months, all patients stopped all Parkinson’s disease therapy for one week. Unified Parkinson’s Disease Rating Scale-III scores were compared between the ODT and DBS and ODT groups (n = 28). Rest tremor slopes from baseline to 24 months favored DBS plus ODT off and on therapy, compared with ODT alone.
Hacker ML, DeLong MR, Turchan M, et al. Effects of deep brain stimulation on rest tremor progression in early stage Parkinson disease. Neurology. 2018 Jun 29 [Epub ahead of print].
—Kimberly Williams

Black Esophagus: A Rare Cause of Gastrointestinal Hemorrhage in the Emergency Department
In this case presentation of a 65-year-old man who presented to the ED for evaluation of a 1-week history of intermittent coffee-ground emesis and syncope, the authors review the literature about a rare, but potentially fatal diagnosis.
Case
A 65-year-old man presented to the ED for evaluation of a 1-week history of intermittent, exertional syncope and coffee ground emesis. His medical history was significant for hypertension, peripheral vascular disease, hyperlipidemia, and peptic ulcer disease. Although his social history was positive for alcohol use and abuse, the patient stated that he had not consumed any alcoholic beverages since the onset of nausea and vomiting.
A review of the patient’s systems was positive for lightheadedness upon standing and for palpitations. He had no prior history of melena, hematochezia, or syncope, but did report a previous history of upper gastrointestinal (GI) bleeding due to peptic ulcer disease and alcohol abuse.
The patient’s vital signs at presentation were: blood pressure (BP), 114/74 mm Hg; heart rate, 112 beats/min; respiratory rate, 15 breaths/min; and temperature, 97.7°F. Oxygen saturation was 97% on room air. On examination, the patient was conversant and oriented. He had dried blood around his mouth and chin from vomiting and appeared ill but nontoxic. His mucous membranes were pale. The cardiopulmonary examination was remarkable for tachycardia; however, the patient’s extremities were warm and his capillary refill time was normal. The rectal examination was notable for melenic stool, which was guaiac positive. During the patient’s course in the ED, he passed a large, melenic stool. The remainder of the physical examination was normal.
The chest X-ray was normal, but the electrocardiogram demonstrated sinus tachycardia. Laboratory studies were remarkable for the following:
hemoglobin (Hgb), 12.7 g/dL;
platelet count, 97 x 109/L;
sodium, 122 mmol/L;
chloride, 73 mmol/L;
potassium, 2.9 mmol/L;
blood urea nitrogen, 121 mg/dL;
creatinine, 1.89 mg/dL;
glucose, 297 mg/dL;
calcium, 7.9 mg/dL;
anion gap, 27 mmol/L;
total bilirubin, 1.6 mg/dL (mildly elevated);
direct bilirubin, 0.5 mg/dL;
aspartate aminotransferase, 41 IU/L; and
lactic acid, 5.5 mmol/L (elevated).
The patient’s international normalized ratio and activated partial thromboplastin time were normal. There were no recent prior laboratory studies available for comparison with current findings.

Two large bore intravenous (IV) lines were placed, and the patient was resuscitated with a bolus of 20 mL/kg of isotonic fluids. He was given 1 g of ceftriaxone and 80 mg of pantoprazole IV and was started on an infusion of octreotide. Meanwhile, the patient was consented for blood products and 2 U of packed red blood cells were crossmatched and held in reserve. He received potassium repletion of 60 mEq IV potassium chloride.

The emergency physician (EP) consulted with gastroenterology services. Due to concern for variceal bleeding and to control hemorrhaging, the gastroenterologist recommended emergent upper endoscopy. The upper endoscopy revealed circumferential necrosis of the distal third of the esophagus, which stopped abruptly at the gastroesophageal junction (Figures 1-3). Since no varices were demonstrated on endoscopy, octreotide was discontinued. The gastroenterologist recommended the patient receive nothing orally for 24 hours and that he continue to receive IV proton pump inhibitors (PPIs) and empiric antibiotics. The patient was admitted to the medical intensive care unit (ICU) for further care.

Following admission to the ICU, the patient did not have any additional episodes of hematemesis or melenic or bloody stools. However, his Hgb levels down-trended to 8.6 g/dL and his BP decreased to 84/63 mm Hg. He was transfused a single unit of packed red blood cells, after which BP normalized and Hgb stabilized at 9.5 g/dL. The patient’s diet was advanced on hospital day 1 to clear liquids and then solid foods, and he was discharged home on hospital day 2 with prescriptions for pantoprazole 40 mg twice daily and ranitidine 300 mg nightly and with close primary care and gastroenterology follow-up.
Discussion
Black esophagus, also referred to as acute esophageal necrosis (AEN) or necrotizing esophagitis, is an uncommon, but life-threatening cause of GI bleeding.1 First described by Brennan2 during a patient autopsy in 1967, black esophagus remained a postmortem finding until its first description on endoscopy by Goldenberg et al3 in 1990.With the increased use of endoscopy, black esophagus has been more commonly described in case reports and case series but remains an extremely rare diagnosis, with an incidence of 0.008% to 0.2%.4-7 A single study by Yasuda et al8 demonstrated a surprising incidence of AEN in 6% of patients undergoing upper endoscopy for upper GI hemorrhage.
Patients with black esophagus typically present for evaluation as a result of GI bleeding, which occurs in 65% to 90% of cases.9,10 This condition is more common in elderly patients with a disproportionately higher incidence in men, who represent approximately 80% of cases. A variety of comorbidities are associated with AEN, most commonly diabetes mellitus, malignancy, hypertension, renal insufficiency, heart disease, and duodenal ulcer.5,10 In a recent case series by Gurvits et al,11 tachycardia or hypotension was observed in 90% of cases.
Diagnosis
Black esophagus is defined by diffuse, circumferential necrosis of the esophagus with preferential involvement of the distal third of the esophagus that abruptly stops at the gastroesophageal junction, and in the absence of caustic ingestion.12 The predilection toward involvement of the distal esophagus is thought to be due to its relatively poor perfusion. Blood flow to the distal esophagus is highly variable, but typically occurs through the left gastric and left inferior phrenic arteries. This is believed to result in a “watershed region” that creates a susceptibility to insult.7,13 Histologically, there is necrosis of the mucosa and submucosa, inflammation of the muscle fibers, and occasional thrombosis of blood vessels.4 However, gross findings alone are sufficient for diagnosis, and biopsy is not mandatory.1,14
Etiology
The etiology of acute esophageal necrosis is not well understood. The prevailing theory is that the combination of an ischemic insult and reflux of gastric contents leads to mucosal destruction. The watershed distribution of blood flow to the distal esophagus is thought to predispose patients to ischemia or thrombosis.5,7,10 As previously mentioned, a recent series by Gurvits et al11 demonstrated that 90% of patients with black esophagus also develop tachycardia or hypotension. Further, many of the comorbid conditions noted in cases of AEN are characterized by a tendency toward malperfusion or thrombosis.
Management
The mainstay of managing black esophagus in the ED is aggressive fluid resuscitation, bowel rest, and treatment with IV PPIs. Antibiotics are not indicated unless the patient has an infection, is immunocompromised, continues to decompensate despite adequate IV fluid resuscitation, or has an esophageal perforation.7,11 In practice, the necessity of early antibiotic therapy may be unclear in the ED due to other considerations in the differential diagnosis; therefore, it is prudent to treat the patient empirically until these etiologies can be ruled out. Some clinicians recommend sucralfate due to its ability to bind pepsin and stimulate mucus secretion which theoretically prevents further esophageal injury.4 The initiation of sucralfate should be deferred until after endoscopy.
Esophageal strictures are the most common complication of black esophagus, developing in 16% to 25% of cases. Due to underlying disease, AEN is associated with a high-mortality of 12.5% to 36%.4,11 Mortality as a direct result of esophageal necrosis is less than 6%.10 Complications of black esophagus include perforation and mediastinitis, both of which are indications for emergent surgical intervention.1,15Emergency physicians traditionally manage GI bleeding with conservative measures and early involvement of gastroenterology services. Failure of patients to respond to traditional resuscitative measures may signal mediastinitis and require immediate surgical intervention. This infrequent diagnosis represents a significant deviation from the typical presentations seen by EPs in standard practice; for this reason, EPs should be aware of the signs and symptoms associated with black esophagus and consider it in the differential diagnosis of patients presenting with GI bleeding.
Summary
Emergency physicians are often the first providers to care for patients with an upper GI hemorrhage. While the mainstay of treatment of hematemesis is resuscitation with intravenous fluids and blood products, EPs must be aware of the potential etiologies that may change management. Black esophagus is a rare but important cause of hematemesis—a condition that can lead to esophageal perforation and mediastinitis. In cases wherein patients fail to respond to appropriate resuscitation, subsequently decompensate despite resuscitation, or appear septic, EPs should consider IV broad-spectrum antibiotics and surgical consultation.
1. Shafa S, Sharma N, Keshishian J, Dellon ES. The black esophagus: a rare but deadly disease. ACG Case Rep J. 2016;3(2):88-91. doi:10.14309/crj.2016.9.
2. Brennan JL. Case of extensive necrosis of the oesophageal mucosa following hypothermia. J Clin Pathol. 1967;20(4):581-584.
3. Goldenberg SP, Wain SL, Marignani P. Acute necrotizing esophagitis. Gastroenterology. 1990;98(2):493-496.
4. Lacy BE, Toor A, Bensen SP, Rothstein RI, Maheshwari Y. Acute esophageal necrosis: report of two cases and a review of the literature. Gastrointest Endosc. 1999;49(4 Pt 1):527-532.
5. Grudell ABM, Mueller PS, Viggiano TR. Black esophagus: report of six cases and review of the literature, 1963-2003. Dis Esophagus. 2006;19(2):105-110. doi:10.1111/j.1442-2050.2006.00549.x.
6. Moretó M, Ojembarrena E, Zaballa M, Tánago JG, Ibánez S. Idiopathic acute esophageal necrosis: not necessarily a terminal event. Endoscopy. 1993;25(8):534-538.
7. Gurvits GE. Black esophagus: acute esophageal necrosis syndrome. World J Gastroenterol. 2010;16(26):3219-3225.
8. Yasuda H, Yamada M, Endo Y, Inoue K, Yoshiba M. Acute necrotizing esophagitis: role of nonsteroidal anti-inflammatory drugs. J Gastroenterol. 2006;41(3):193-197. doi:10.1007/s00535-005-1741-6.
9. Zacharia GS, Sandesh K, Ramachandran T. Acute esophageal necrosis: an uncommon cause of hematemesis. Oman Med J. 2014;29(4):302-304. doi:10.5001/omj.2014.79.
10. Gurvits GE, Shapsis A, Lau N, Gualtieri N, Robilotti JG. Acute esophageal necrosis: a rare syndrome. J Gastroenterol. 2007;42(1):29-38. doi:10.1007/s00535-006-1974-z.
11. Gurvits GE, Cherian K, Shami MN, et al. Black esophagus: new insights and multicenter international experience in 2014. Dig Dis Sci. 2015;60(2):444-453. doi:10.1007/s10620-014-3382-1.
12. Burtally A, Gregoire P. Acute esophageal necrosis and low-flow state. Can J Gastroenterol. 2007;21(4):245-247.
13. Bear BC, Mathew J, Parker CW III. Acute esophageal necrosis: black esophagus in setting of diabetic ketoacidosis. J Case Rep Images Med. 2015;1:18-21.
14. Altenburger DL, Wagner AS, Li S, Garavaglia J. A case of black esophagus with histopathologic description and characterization. Arch Pathol Lab Med. 2011;135(6):797-798. doi:10.1043/2010-0128-C.1.
15. Hwang J, Weigel TL. Acute esophageal necrosis: “black esophagus.” JSLS. 2007;11(1):165-167.
In this case presentation of a 65-year-old man who presented to the ED for evaluation of a 1-week history of intermittent coffee-ground emesis and syncope, the authors review the literature about a rare, but potentially fatal diagnosis.
In this case presentation of a 65-year-old man who presented to the ED for evaluation of a 1-week history of intermittent coffee-ground emesis and syncope, the authors review the literature about a rare, but potentially fatal diagnosis.
Case
A 65-year-old man presented to the ED for evaluation of a 1-week history of intermittent, exertional syncope and coffee ground emesis. His medical history was significant for hypertension, peripheral vascular disease, hyperlipidemia, and peptic ulcer disease. Although his social history was positive for alcohol use and abuse, the patient stated that he had not consumed any alcoholic beverages since the onset of nausea and vomiting.
A review of the patient’s systems was positive for lightheadedness upon standing and for palpitations. He had no prior history of melena, hematochezia, or syncope, but did report a previous history of upper gastrointestinal (GI) bleeding due to peptic ulcer disease and alcohol abuse.
The patient’s vital signs at presentation were: blood pressure (BP), 114/74 mm Hg; heart rate, 112 beats/min; respiratory rate, 15 breaths/min; and temperature, 97.7°F. Oxygen saturation was 97% on room air. On examination, the patient was conversant and oriented. He had dried blood around his mouth and chin from vomiting and appeared ill but nontoxic. His mucous membranes were pale. The cardiopulmonary examination was remarkable for tachycardia; however, the patient’s extremities were warm and his capillary refill time was normal. The rectal examination was notable for melenic stool, which was guaiac positive. During the patient’s course in the ED, he passed a large, melenic stool. The remainder of the physical examination was normal.
The chest X-ray was normal, but the electrocardiogram demonstrated sinus tachycardia. Laboratory studies were remarkable for the following:
hemoglobin (Hgb), 12.7 g/dL;
platelet count, 97 x 109/L;
sodium, 122 mmol/L;
chloride, 73 mmol/L;
potassium, 2.9 mmol/L;
blood urea nitrogen, 121 mg/dL;
creatinine, 1.89 mg/dL;
glucose, 297 mg/dL;
calcium, 7.9 mg/dL;
anion gap, 27 mmol/L;
total bilirubin, 1.6 mg/dL (mildly elevated);
direct bilirubin, 0.5 mg/dL;
aspartate aminotransferase, 41 IU/L; and
lactic acid, 5.5 mmol/L (elevated).
The patient’s international normalized ratio and activated partial thromboplastin time were normal. There were no recent prior laboratory studies available for comparison with current findings.
Two large bore intravenous (IV) lines were placed, and the patient was resuscitated with a bolus of 20 mL/kg of isotonic fluids. He was given 1 g of ceftriaxone and 80 mg of pantoprazole IV and was started on an infusion of octreotide. Meanwhile, the patient was consented for blood products and 2 U of packed red blood cells were crossmatched and held in reserve. He received potassium repletion of 60 mEq IV potassium chloride.
The emergency physician (EP) consulted with gastroenterology services. Due to concern for variceal bleeding and to control hemorrhaging, the gastroenterologist recommended emergent upper endoscopy. The upper endoscopy revealed circumferential necrosis of the distal third of the esophagus, which stopped abruptly at the gastroesophageal junction (Figures 1-3). Since no varices were demonstrated on endoscopy, octreotide was discontinued. The gastroenterologist recommended the patient receive nothing orally for 24 hours and that he continue to receive IV proton pump inhibitors (PPIs) and empiric antibiotics. The patient was admitted to the medical intensive care unit (ICU) for further care.
Following admission to the ICU, the patient did not have any additional episodes of hematemesis or melenic or bloody stools. However, his Hgb levels down-trended to 8.6 g/dL and his BP decreased to 84/63 mm Hg. He was transfused a single unit of packed red blood cells, after which BP normalized and Hgb stabilized at 9.5 g/dL. The patient’s diet was advanced on hospital day 1 to clear liquids and then solid foods, and he was discharged home on hospital day 2 with prescriptions for pantoprazole 40 mg twice daily and ranitidine 300 mg nightly and with close primary care and gastroenterology follow-up.
Discussion
Black esophagus, also referred to as acute esophageal necrosis (AEN) or necrotizing esophagitis, is an uncommon, but life-threatening cause of GI bleeding.1 First described by Brennan2 during a patient autopsy in 1967, black esophagus remained a postmortem finding until its first description on endoscopy by Goldenberg et al3 in 1990.With the increased use of endoscopy, black esophagus has been more commonly described in case reports and case series but remains an extremely rare diagnosis, with an incidence of 0.008% to 0.2%.4-7 A single study by Yasuda et al8 demonstrated a surprising incidence of AEN in 6% of patients undergoing upper endoscopy for upper GI hemorrhage.
Patients with black esophagus typically present for evaluation as a result of GI bleeding, which occurs in 65% to 90% of cases.9,10 This condition is more common in elderly patients with a disproportionately higher incidence in men, who represent approximately 80% of cases. A variety of comorbidities are associated with AEN, most commonly diabetes mellitus, malignancy, hypertension, renal insufficiency, heart disease, and duodenal ulcer.5,10 In a recent case series by Gurvits et al,11 tachycardia or hypotension was observed in 90% of cases.
Diagnosis
Black esophagus is defined by diffuse, circumferential necrosis of the esophagus with preferential involvement of the distal third of the esophagus that abruptly stops at the gastroesophageal junction, and in the absence of caustic ingestion.12 The predilection toward involvement of the distal esophagus is thought to be due to its relatively poor perfusion. Blood flow to the distal esophagus is highly variable, but typically occurs through the left gastric and left inferior phrenic arteries. This is believed to result in a “watershed region” that creates a susceptibility to insult.7,13 Histologically, there is necrosis of the mucosa and submucosa, inflammation of the muscle fibers, and occasional thrombosis of blood vessels.4 However, gross findings alone are sufficient for diagnosis, and biopsy is not mandatory.1,14
Etiology
The etiology of acute esophageal necrosis is not well understood. The prevailing theory is that the combination of an ischemic insult and reflux of gastric contents leads to mucosal destruction. The watershed distribution of blood flow to the distal esophagus is thought to predispose patients to ischemia or thrombosis.5,7,10 As previously mentioned, a recent series by Gurvits et al11 demonstrated that 90% of patients with black esophagus also develop tachycardia or hypotension. Further, many of the comorbid conditions noted in cases of AEN are characterized by a tendency toward malperfusion or thrombosis.
Management
The mainstay of managing black esophagus in the ED is aggressive fluid resuscitation, bowel rest, and treatment with IV PPIs. Antibiotics are not indicated unless the patient has an infection, is immunocompromised, continues to decompensate despite adequate IV fluid resuscitation, or has an esophageal perforation.7,11 In practice, the necessity of early antibiotic therapy may be unclear in the ED due to other considerations in the differential diagnosis; therefore, it is prudent to treat the patient empirically until these etiologies can be ruled out. Some clinicians recommend sucralfate due to its ability to bind pepsin and stimulate mucus secretion which theoretically prevents further esophageal injury.4 The initiation of sucralfate should be deferred until after endoscopy.
Esophageal strictures are the most common complication of black esophagus, developing in 16% to 25% of cases. Due to underlying disease, AEN is associated with a high-mortality of 12.5% to 36%.4,11 Mortality as a direct result of esophageal necrosis is less than 6%.10 Complications of black esophagus include perforation and mediastinitis, both of which are indications for emergent surgical intervention.1,15Emergency physicians traditionally manage GI bleeding with conservative measures and early involvement of gastroenterology services. Failure of patients to respond to traditional resuscitative measures may signal mediastinitis and require immediate surgical intervention. This infrequent diagnosis represents a significant deviation from the typical presentations seen by EPs in standard practice; for this reason, EPs should be aware of the signs and symptoms associated with black esophagus and consider it in the differential diagnosis of patients presenting with GI bleeding.
Summary
Emergency physicians are often the first providers to care for patients with an upper GI hemorrhage. While the mainstay of treatment of hematemesis is resuscitation with intravenous fluids and blood products, EPs must be aware of the potential etiologies that may change management. Black esophagus is a rare but important cause of hematemesis—a condition that can lead to esophageal perforation and mediastinitis. In cases wherein patients fail to respond to appropriate resuscitation, subsequently decompensate despite resuscitation, or appear septic, EPs should consider IV broad-spectrum antibiotics and surgical consultation.
Case
A 65-year-old man presented to the ED for evaluation of a 1-week history of intermittent, exertional syncope and coffee ground emesis. His medical history was significant for hypertension, peripheral vascular disease, hyperlipidemia, and peptic ulcer disease. Although his social history was positive for alcohol use and abuse, the patient stated that he had not consumed any alcoholic beverages since the onset of nausea and vomiting.
A review of the patient’s systems was positive for lightheadedness upon standing and for palpitations. He had no prior history of melena, hematochezia, or syncope, but did report a previous history of upper gastrointestinal (GI) bleeding due to peptic ulcer disease and alcohol abuse.
The patient’s vital signs at presentation were: blood pressure (BP), 114/74 mm Hg; heart rate, 112 beats/min; respiratory rate, 15 breaths/min; and temperature, 97.7°F. Oxygen saturation was 97% on room air. On examination, the patient was conversant and oriented. He had dried blood around his mouth and chin from vomiting and appeared ill but nontoxic. His mucous membranes were pale. The cardiopulmonary examination was remarkable for tachycardia; however, the patient’s extremities were warm and his capillary refill time was normal. The rectal examination was notable for melenic stool, which was guaiac positive. During the patient’s course in the ED, he passed a large, melenic stool. The remainder of the physical examination was normal.
The chest X-ray was normal, but the electrocardiogram demonstrated sinus tachycardia. Laboratory studies were remarkable for the following:
hemoglobin (Hgb), 12.7 g/dL;
platelet count, 97 x 109/L;
sodium, 122 mmol/L;
chloride, 73 mmol/L;
potassium, 2.9 mmol/L;
blood urea nitrogen, 121 mg/dL;
creatinine, 1.89 mg/dL;
glucose, 297 mg/dL;
calcium, 7.9 mg/dL;
anion gap, 27 mmol/L;
total bilirubin, 1.6 mg/dL (mildly elevated);
direct bilirubin, 0.5 mg/dL;
aspartate aminotransferase, 41 IU/L; and
lactic acid, 5.5 mmol/L (elevated).
The patient’s international normalized ratio and activated partial thromboplastin time were normal. There were no recent prior laboratory studies available for comparison with current findings.
Two large bore intravenous (IV) lines were placed, and the patient was resuscitated with a bolus of 20 mL/kg of isotonic fluids. He was given 1 g of ceftriaxone and 80 mg of pantoprazole IV and was started on an infusion of octreotide. Meanwhile, the patient was consented for blood products and 2 U of packed red blood cells were crossmatched and held in reserve. He received potassium repletion of 60 mEq IV potassium chloride.
The emergency physician (EP) consulted with gastroenterology services. Due to concern for variceal bleeding and to control hemorrhaging, the gastroenterologist recommended emergent upper endoscopy. The upper endoscopy revealed circumferential necrosis of the distal third of the esophagus, which stopped abruptly at the gastroesophageal junction (Figures 1-3). Since no varices were demonstrated on endoscopy, octreotide was discontinued. The gastroenterologist recommended the patient receive nothing orally for 24 hours and that he continue to receive IV proton pump inhibitors (PPIs) and empiric antibiotics. The patient was admitted to the medical intensive care unit (ICU) for further care.
Following admission to the ICU, the patient did not have any additional episodes of hematemesis or melenic or bloody stools. However, his Hgb levels down-trended to 8.6 g/dL and his BP decreased to 84/63 mm Hg. He was transfused a single unit of packed red blood cells, after which BP normalized and Hgb stabilized at 9.5 g/dL. The patient’s diet was advanced on hospital day 1 to clear liquids and then solid foods, and he was discharged home on hospital day 2 with prescriptions for pantoprazole 40 mg twice daily and ranitidine 300 mg nightly and with close primary care and gastroenterology follow-up.
Discussion
Black esophagus, also referred to as acute esophageal necrosis (AEN) or necrotizing esophagitis, is an uncommon, but life-threatening cause of GI bleeding.1 First described by Brennan2 during a patient autopsy in 1967, black esophagus remained a postmortem finding until its first description on endoscopy by Goldenberg et al3 in 1990.With the increased use of endoscopy, black esophagus has been more commonly described in case reports and case series but remains an extremely rare diagnosis, with an incidence of 0.008% to 0.2%.4-7 A single study by Yasuda et al8 demonstrated a surprising incidence of AEN in 6% of patients undergoing upper endoscopy for upper GI hemorrhage.
Patients with black esophagus typically present for evaluation as a result of GI bleeding, which occurs in 65% to 90% of cases.9,10 This condition is more common in elderly patients with a disproportionately higher incidence in men, who represent approximately 80% of cases. A variety of comorbidities are associated with AEN, most commonly diabetes mellitus, malignancy, hypertension, renal insufficiency, heart disease, and duodenal ulcer.5,10 In a recent case series by Gurvits et al,11 tachycardia or hypotension was observed in 90% of cases.
Diagnosis
Black esophagus is defined by diffuse, circumferential necrosis of the esophagus with preferential involvement of the distal third of the esophagus that abruptly stops at the gastroesophageal junction, and in the absence of caustic ingestion.12 The predilection toward involvement of the distal esophagus is thought to be due to its relatively poor perfusion. Blood flow to the distal esophagus is highly variable, but typically occurs through the left gastric and left inferior phrenic arteries. This is believed to result in a “watershed region” that creates a susceptibility to insult.7,13 Histologically, there is necrosis of the mucosa and submucosa, inflammation of the muscle fibers, and occasional thrombosis of blood vessels.4 However, gross findings alone are sufficient for diagnosis, and biopsy is not mandatory.1,14
Etiology
The etiology of acute esophageal necrosis is not well understood. The prevailing theory is that the combination of an ischemic insult and reflux of gastric contents leads to mucosal destruction. The watershed distribution of blood flow to the distal esophagus is thought to predispose patients to ischemia or thrombosis.5,7,10 As previously mentioned, a recent series by Gurvits et al11 demonstrated that 90% of patients with black esophagus also develop tachycardia or hypotension. Further, many of the comorbid conditions noted in cases of AEN are characterized by a tendency toward malperfusion or thrombosis.
Management
The mainstay of managing black esophagus in the ED is aggressive fluid resuscitation, bowel rest, and treatment with IV PPIs. Antibiotics are not indicated unless the patient has an infection, is immunocompromised, continues to decompensate despite adequate IV fluid resuscitation, or has an esophageal perforation.7,11 In practice, the necessity of early antibiotic therapy may be unclear in the ED due to other considerations in the differential diagnosis; therefore, it is prudent to treat the patient empirically until these etiologies can be ruled out. Some clinicians recommend sucralfate due to its ability to bind pepsin and stimulate mucus secretion which theoretically prevents further esophageal injury.4 The initiation of sucralfate should be deferred until after endoscopy.
Esophageal strictures are the most common complication of black esophagus, developing in 16% to 25% of cases. Due to underlying disease, AEN is associated with a high-mortality of 12.5% to 36%.4,11 Mortality as a direct result of esophageal necrosis is less than 6%.10 Complications of black esophagus include perforation and mediastinitis, both of which are indications for emergent surgical intervention.1,15Emergency physicians traditionally manage GI bleeding with conservative measures and early involvement of gastroenterology services. Failure of patients to respond to traditional resuscitative measures may signal mediastinitis and require immediate surgical intervention. This infrequent diagnosis represents a significant deviation from the typical presentations seen by EPs in standard practice; for this reason, EPs should be aware of the signs and symptoms associated with black esophagus and consider it in the differential diagnosis of patients presenting with GI bleeding.
Summary
Emergency physicians are often the first providers to care for patients with an upper GI hemorrhage. While the mainstay of treatment of hematemesis is resuscitation with intravenous fluids and blood products, EPs must be aware of the potential etiologies that may change management. Black esophagus is a rare but important cause of hematemesis—a condition that can lead to esophageal perforation and mediastinitis. In cases wherein patients fail to respond to appropriate resuscitation, subsequently decompensate despite resuscitation, or appear septic, EPs should consider IV broad-spectrum antibiotics and surgical consultation.
1. Shafa S, Sharma N, Keshishian J, Dellon ES. The black esophagus: a rare but deadly disease. ACG Case Rep J. 2016;3(2):88-91. doi:10.14309/crj.2016.9.
2. Brennan JL. Case of extensive necrosis of the oesophageal mucosa following hypothermia. J Clin Pathol. 1967;20(4):581-584.
3. Goldenberg SP, Wain SL, Marignani P. Acute necrotizing esophagitis. Gastroenterology. 1990;98(2):493-496.
4. Lacy BE, Toor A, Bensen SP, Rothstein RI, Maheshwari Y. Acute esophageal necrosis: report of two cases and a review of the literature. Gastrointest Endosc. 1999;49(4 Pt 1):527-532.
5. Grudell ABM, Mueller PS, Viggiano TR. Black esophagus: report of six cases and review of the literature, 1963-2003. Dis Esophagus. 2006;19(2):105-110. doi:10.1111/j.1442-2050.2006.00549.x.
6. Moretó M, Ojembarrena E, Zaballa M, Tánago JG, Ibánez S. Idiopathic acute esophageal necrosis: not necessarily a terminal event. Endoscopy. 1993;25(8):534-538.
7. Gurvits GE. Black esophagus: acute esophageal necrosis syndrome. World J Gastroenterol. 2010;16(26):3219-3225.
8. Yasuda H, Yamada M, Endo Y, Inoue K, Yoshiba M. Acute necrotizing esophagitis: role of nonsteroidal anti-inflammatory drugs. J Gastroenterol. 2006;41(3):193-197. doi:10.1007/s00535-005-1741-6.
9. Zacharia GS, Sandesh K, Ramachandran T. Acute esophageal necrosis: an uncommon cause of hematemesis. Oman Med J. 2014;29(4):302-304. doi:10.5001/omj.2014.79.
10. Gurvits GE, Shapsis A, Lau N, Gualtieri N, Robilotti JG. Acute esophageal necrosis: a rare syndrome. J Gastroenterol. 2007;42(1):29-38. doi:10.1007/s00535-006-1974-z.
11. Gurvits GE, Cherian K, Shami MN, et al. Black esophagus: new insights and multicenter international experience in 2014. Dig Dis Sci. 2015;60(2):444-453. doi:10.1007/s10620-014-3382-1.
12. Burtally A, Gregoire P. Acute esophageal necrosis and low-flow state. Can J Gastroenterol. 2007;21(4):245-247.
13. Bear BC, Mathew J, Parker CW III. Acute esophageal necrosis: black esophagus in setting of diabetic ketoacidosis. J Case Rep Images Med. 2015;1:18-21.
14. Altenburger DL, Wagner AS, Li S, Garavaglia J. A case of black esophagus with histopathologic description and characterization. Arch Pathol Lab Med. 2011;135(6):797-798. doi:10.1043/2010-0128-C.1.
15. Hwang J, Weigel TL. Acute esophageal necrosis: “black esophagus.” JSLS. 2007;11(1):165-167.
1. Shafa S, Sharma N, Keshishian J, Dellon ES. The black esophagus: a rare but deadly disease. ACG Case Rep J. 2016;3(2):88-91. doi:10.14309/crj.2016.9.
2. Brennan JL. Case of extensive necrosis of the oesophageal mucosa following hypothermia. J Clin Pathol. 1967;20(4):581-584.
3. Goldenberg SP, Wain SL, Marignani P. Acute necrotizing esophagitis. Gastroenterology. 1990;98(2):493-496.
4. Lacy BE, Toor A, Bensen SP, Rothstein RI, Maheshwari Y. Acute esophageal necrosis: report of two cases and a review of the literature. Gastrointest Endosc. 1999;49(4 Pt 1):527-532.
5. Grudell ABM, Mueller PS, Viggiano TR. Black esophagus: report of six cases and review of the literature, 1963-2003. Dis Esophagus. 2006;19(2):105-110. doi:10.1111/j.1442-2050.2006.00549.x.
6. Moretó M, Ojembarrena E, Zaballa M, Tánago JG, Ibánez S. Idiopathic acute esophageal necrosis: not necessarily a terminal event. Endoscopy. 1993;25(8):534-538.
7. Gurvits GE. Black esophagus: acute esophageal necrosis syndrome. World J Gastroenterol. 2010;16(26):3219-3225.
8. Yasuda H, Yamada M, Endo Y, Inoue K, Yoshiba M. Acute necrotizing esophagitis: role of nonsteroidal anti-inflammatory drugs. J Gastroenterol. 2006;41(3):193-197. doi:10.1007/s00535-005-1741-6.
9. Zacharia GS, Sandesh K, Ramachandran T. Acute esophageal necrosis: an uncommon cause of hematemesis. Oman Med J. 2014;29(4):302-304. doi:10.5001/omj.2014.79.
10. Gurvits GE, Shapsis A, Lau N, Gualtieri N, Robilotti JG. Acute esophageal necrosis: a rare syndrome. J Gastroenterol. 2007;42(1):29-38. doi:10.1007/s00535-006-1974-z.
11. Gurvits GE, Cherian K, Shami MN, et al. Black esophagus: new insights and multicenter international experience in 2014. Dig Dis Sci. 2015;60(2):444-453. doi:10.1007/s10620-014-3382-1.
12. Burtally A, Gregoire P. Acute esophageal necrosis and low-flow state. Can J Gastroenterol. 2007;21(4):245-247.
13. Bear BC, Mathew J, Parker CW III. Acute esophageal necrosis: black esophagus in setting of diabetic ketoacidosis. J Case Rep Images Med. 2015;1:18-21.
14. Altenburger DL, Wagner AS, Li S, Garavaglia J. A case of black esophagus with histopathologic description and characterization. Arch Pathol Lab Med. 2011;135(6):797-798. doi:10.1043/2010-0128-C.1.
15. Hwang J, Weigel TL. Acute esophageal necrosis: “black esophagus.” JSLS. 2007;11(1):165-167.

FDA warns against azithromycin in blood or lymph node cancers
The Food and Drug Administration has issued a in patients with blood or lymph node cancers who have received donor stem cell transplants.

This use of azithromycin can lead to increased risk of cancer relapse and death in this population. The FDA is continuing to review data and is expected to issue further recommendations.
Patients with blood or lymph node cancers are at an increased risk of bronchiolitis obliterans syndrome after donor stem cell transplant; although azithromycin is not approved for prevention of this condition, the antibiotic is sometimes prescribed for that purpose.
A French study of 480 patients was undertaken to assess the effectiveness of this prophylaxis but revealed the increased risk of relapse and death and was halted 13 months after completing enrollment. The rate of cancer relapse was 32.9% in the azithromycin group and just 20.8% in the placebo group; the 2-year survival rate was 56.6% in the azithromycin group and 70.1% in the placebo group (JAMA 2017;318[6]:557-66).
Bronchiolitis obliterans syndrome is marked by inflammation and scarring of the airways that leads to severe shortness of breath and dry cough. There are no known effective antibiotic treatments for prophylaxis of the condition, according to the FDA.
FDA officials are advising physicians not to prescribe long-term azithromycin in this population. Patients who have had a stem cell transplant and are already taking the antibiotic, should consult a doctor before discontinuing.
The manufacturer of brand name azithromycin (Zithromax) has issued a Dear Healthcare Provider letter about the safety issue, and more information can be found in the FDA’s safety announcement.
The Food and Drug Administration has issued a in patients with blood or lymph node cancers who have received donor stem cell transplants.
This use of azithromycin can lead to increased risk of cancer relapse and death in this population. The FDA is continuing to review data and is expected to issue further recommendations.
Patients with blood or lymph node cancers are at an increased risk of bronchiolitis obliterans syndrome after donor stem cell transplant; although azithromycin is not approved for prevention of this condition, the antibiotic is sometimes prescribed for that purpose.
A French study of 480 patients was undertaken to assess the effectiveness of this prophylaxis but revealed the increased risk of relapse and death and was halted 13 months after completing enrollment. The rate of cancer relapse was 32.9% in the azithromycin group and just 20.8% in the placebo group; the 2-year survival rate was 56.6% in the azithromycin group and 70.1% in the placebo group (JAMA 2017;318[6]:557-66).
Bronchiolitis obliterans syndrome is marked by inflammation and scarring of the airways that leads to severe shortness of breath and dry cough. There are no known effective antibiotic treatments for prophylaxis of the condition, according to the FDA.
FDA officials are advising physicians not to prescribe long-term azithromycin in this population. Patients who have had a stem cell transplant and are already taking the antibiotic, should consult a doctor before discontinuing.
The manufacturer of brand name azithromycin (Zithromax) has issued a Dear Healthcare Provider letter about the safety issue, and more information can be found in the FDA’s safety announcement.
The Food and Drug Administration has issued a in patients with blood or lymph node cancers who have received donor stem cell transplants.
This use of azithromycin can lead to increased risk of cancer relapse and death in this population. The FDA is continuing to review data and is expected to issue further recommendations.
Patients with blood or lymph node cancers are at an increased risk of bronchiolitis obliterans syndrome after donor stem cell transplant; although azithromycin is not approved for prevention of this condition, the antibiotic is sometimes prescribed for that purpose.
A French study of 480 patients was undertaken to assess the effectiveness of this prophylaxis but revealed the increased risk of relapse and death and was halted 13 months after completing enrollment. The rate of cancer relapse was 32.9% in the azithromycin group and just 20.8% in the placebo group; the 2-year survival rate was 56.6% in the azithromycin group and 70.1% in the placebo group (JAMA 2017;318[6]:557-66).
Bronchiolitis obliterans syndrome is marked by inflammation and scarring of the airways that leads to severe shortness of breath and dry cough. There are no known effective antibiotic treatments for prophylaxis of the condition, according to the FDA.
FDA officials are advising physicians not to prescribe long-term azithromycin in this population. Patients who have had a stem cell transplant and are already taking the antibiotic, should consult a doctor before discontinuing.
The manufacturer of brand name azithromycin (Zithromax) has issued a Dear Healthcare Provider letter about the safety issue, and more information can be found in the FDA’s safety announcement.
Documentation and billing: Tips for hospitalists
Is it AMS, Delirium, or Encephalopathy?
During residency, physicians are trained to care for patients and write notes that are clinically useful. However, physicians are often not taught about how documentation affects reimbursement and quality measures. Our purpose here, and in articles to follow, is to give readers tools to enable them to more accurately reflect the complexity and work that is done for accurate reimbursements.
If you were to get in a car accident, the body shop would document the damage done and submit it to the insurance company. It’s the body shop’s responsibility to record the damage, not the insurance company’s. So while documentation can seem onerous, the insurance company is not going to scour the chart to find diagnoses missed in the note. That would be like the body shop doing repair work without documenting the damage but then somehow expecting to get paid.
For the insurance company, “If you didn’t document it, it didn’t happen.” The body shop should not underdocument and say there were only a few scratches on the right rear panel if it was severely damaged. Likewise, it should not overbill and say the front bumper was damaged if it was not. The goal is not to bill as much as possible but rather to document appropriately.
Terminology
The expected length of stay (LOS) and the expected mortality for a particular patient is determined by how sick the patient appears to be based on the medical record documentation. So documenting all the appropriate diagnoses makes the LOS index (actual LOS divided by expected LOS) and mortality index more accurate as well. It is particularly important to document when a condition is (or is not) “present on admission”.
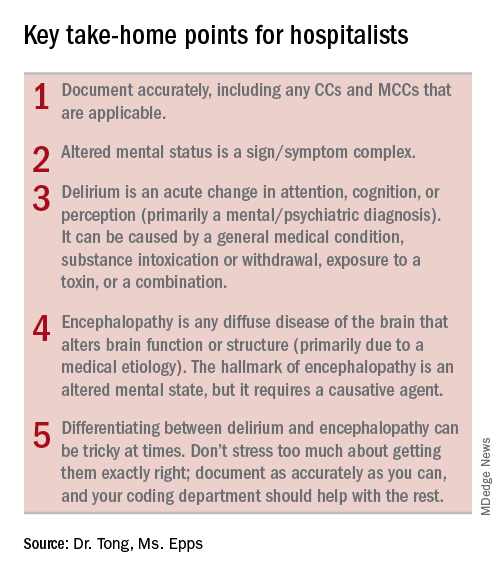
While physician payments can be based on evaluation and management coding, the hospital’s reimbursement is largely determined by physician documentation. Hospitals are paid by Medicare on a capitated basis according to the Acute Inpatient Prospective Payment System. The amount paid is determined by the base rate of the hospital multiplied by the relative weight (RW) of the Medicare Severity Diagnosis Related Group (MS-DRG).
The base rate is adjusted by the wage index of the hospital location. Hospitals that serve a high proportion of low income patients receive a Disproportionate Share Hospital adjustment. The base rate is not something hospitalists have control over.
The RW, however, is determined by the primary diagnosis (reason for admission) and whether or not there are complications or comorbidities (CCs) or major complications or comorbidities (MCCs). The more CCs and MCCs a patient has, the higher the severity of illness and expected increased resources needed to care for that patient.
Diagnoses are currently coded using ICD-10 used by the World Health Organization. The ICD-10 of the primary diagnosis is mapped to an MS-DRG. Many, but not all, MS-DRGs have increasing reimbursements for CCs and MCCs. Coders map the ICD-10 of the principal diagnosis along with any associated CCs or MCCs to the MS-DRG code. The relative weights for different DRGs can found on table 5 of the Medicare website (see reference 1).
Altered mental status versus delirium versus encephalopathy
As an example, let’s look at the difference in RW, LOS, and reimbursement in an otherwise identical patient based on documenting altered mental status (AMS), delirium, or encephalopathy. (see Table 1)
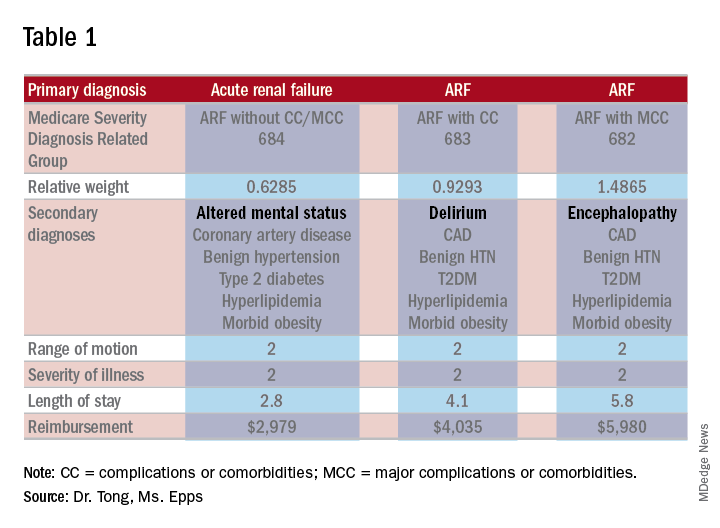
As one can see, RW, estimated LOS, and reimbursement would significantly increase for the patient with delirium (CC) or encephalopathy (MCC) versus AMS (no CC/MCC). A list of which diagnoses are considered CC’s versus MCC’s are on tables 6J and 6I, respectively, on the same Medicare website as table 5.
The difference between AMS, delirium, and encephalopathy
AMS is a sign/symptom complex similar to shortness of breath before an etiology is found. AMS can be the presenting symptom; when a specific etiology is found, however, a more specific diagnosis should be used such as delirium or encephalopathy.
Delirium, according to the DSM-5, is an acute change in the level of attention, cognition, or perception from baseline that developed over hours or days and tends to fluctuate during the course of a day. The change described is not better explained by a preexisting or evolving neurocognitive disorder and does not occur in the context of a severely reduced level of arousal, such as coma. There is evidence from the history, physical examination, or laboratory findings that the disturbance is a direct consequence of a general medical condition, substance intoxication or withdrawal, exposure to a toxin, or more than one cause.
The National Institute of Neurological Diseases and Stroke defines encephalopathy as “any diffuse disease of the brain that alters brain function or structure. Encephalopathy may be caused by an infectious agent, metabolic or mitochondrial dysfunction, brain tumor or increased intracranial pressure, prolonged exposure to toxic elements, chronic progressive trauma, poor nutrition, or lack of oxygen or blood flow to the brain. The hallmark of encephalopathy is an altered mental state.”
It is confusing since there is a lot of overlap in the definitions of delirium and encephalopathy. One way to tease this out conceptually is noting that delirium is listed under mental, behavioral, and neurodevelopmental disorders, while encephalopathy appears under disorders of the nervous system. One can think of delirium as more of a “mental/psychiatric” diagnosis, while encephalopathy is caused by more “medical” causes.
If a patient who is normally not altered presents with confusion because of an infection or metabolic derangement, one can diagnose and document the cause of an acute encephalopathy. However, let’s say a patient is admitted in the morning with an infection, is started on treatment, but is not initially confused. If he/she later becomes confused at night, one could err conservatively and document delirium caused by sundowning.
Differentiating delirium and encephalopathy can be especially difficult in patients who have dementia with episodic confusion when they present with an infection and confusion. If the confusion is within what family members/caretakers say is “normal,” then one shouldn’t document encephalopathy. As a provider, one shouldn’t focus on all the rules and exceptions, just document as specifically and accurately as possible and the coders should take care of the rest.
Dr. Tong is an assistant professor of hospital medicine and an assistant director of the clinical research program at Emory University, Atlanta. Ms. Epps is director of clinical documentation improvement at Emory Healthcare, Atlanta.
References
1. “Acute Inpatient PPS.” Centers for Medicare and Medicaid Services. Accessed 2/17/18. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/index.html.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing, 2013.
3. “Details for title: FY 2018 Final Rule and Correction Notice Tables.” Centers for Medicare and Medicaid Services Accessed 2/17/18. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/FY2018-IPPS-Final-Rule-Home-Page-Items/FY2018-IPPS-Final-Rule-Tables.html.
4. “Encephalopathy Information Page.” National Institute of Neurologic Disorders and Stroke. Accessed on 2/17/18. https://www.ninds.nih.gov/Disorders/All-Disorders/Encephalopathy-Information-Page.
5. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organization, 1992. http://apps.who.int/iris/handle/10665/37958.
Is it AMS, Delirium, or Encephalopathy?
Is it AMS, Delirium, or Encephalopathy?
During residency, physicians are trained to care for patients and write notes that are clinically useful. However, physicians are often not taught about how documentation affects reimbursement and quality measures. Our purpose here, and in articles to follow, is to give readers tools to enable them to more accurately reflect the complexity and work that is done for accurate reimbursements.
If you were to get in a car accident, the body shop would document the damage done and submit it to the insurance company. It’s the body shop’s responsibility to record the damage, not the insurance company’s. So while documentation can seem onerous, the insurance company is not going to scour the chart to find diagnoses missed in the note. That would be like the body shop doing repair work without documenting the damage but then somehow expecting to get paid.
For the insurance company, “If you didn’t document it, it didn’t happen.” The body shop should not underdocument and say there were only a few scratches on the right rear panel if it was severely damaged. Likewise, it should not overbill and say the front bumper was damaged if it was not. The goal is not to bill as much as possible but rather to document appropriately.
Terminology
The expected length of stay (LOS) and the expected mortality for a particular patient is determined by how sick the patient appears to be based on the medical record documentation. So documenting all the appropriate diagnoses makes the LOS index (actual LOS divided by expected LOS) and mortality index more accurate as well. It is particularly important to document when a condition is (or is not) “present on admission”.
While physician payments can be based on evaluation and management coding, the hospital’s reimbursement is largely determined by physician documentation. Hospitals are paid by Medicare on a capitated basis according to the Acute Inpatient Prospective Payment System. The amount paid is determined by the base rate of the hospital multiplied by the relative weight (RW) of the Medicare Severity Diagnosis Related Group (MS-DRG).
The base rate is adjusted by the wage index of the hospital location. Hospitals that serve a high proportion of low income patients receive a Disproportionate Share Hospital adjustment. The base rate is not something hospitalists have control over.
The RW, however, is determined by the primary diagnosis (reason for admission) and whether or not there are complications or comorbidities (CCs) or major complications or comorbidities (MCCs). The more CCs and MCCs a patient has, the higher the severity of illness and expected increased resources needed to care for that patient.
Diagnoses are currently coded using ICD-10 used by the World Health Organization. The ICD-10 of the primary diagnosis is mapped to an MS-DRG. Many, but not all, MS-DRGs have increasing reimbursements for CCs and MCCs. Coders map the ICD-10 of the principal diagnosis along with any associated CCs or MCCs to the MS-DRG code. The relative weights for different DRGs can found on table 5 of the Medicare website (see reference 1).
Altered mental status versus delirium versus encephalopathy
As an example, let’s look at the difference in RW, LOS, and reimbursement in an otherwise identical patient based on documenting altered mental status (AMS), delirium, or encephalopathy. (see Table 1)
As one can see, RW, estimated LOS, and reimbursement would significantly increase for the patient with delirium (CC) or encephalopathy (MCC) versus AMS (no CC/MCC). A list of which diagnoses are considered CC’s versus MCC’s are on tables 6J and 6I, respectively, on the same Medicare website as table 5.
The difference between AMS, delirium, and encephalopathy
AMS is a sign/symptom complex similar to shortness of breath before an etiology is found. AMS can be the presenting symptom; when a specific etiology is found, however, a more specific diagnosis should be used such as delirium or encephalopathy.
Delirium, according to the DSM-5, is an acute change in the level of attention, cognition, or perception from baseline that developed over hours or days and tends to fluctuate during the course of a day. The change described is not better explained by a preexisting or evolving neurocognitive disorder and does not occur in the context of a severely reduced level of arousal, such as coma. There is evidence from the history, physical examination, or laboratory findings that the disturbance is a direct consequence of a general medical condition, substance intoxication or withdrawal, exposure to a toxin, or more than one cause.
The National Institute of Neurological Diseases and Stroke defines encephalopathy as “any diffuse disease of the brain that alters brain function or structure. Encephalopathy may be caused by an infectious agent, metabolic or mitochondrial dysfunction, brain tumor or increased intracranial pressure, prolonged exposure to toxic elements, chronic progressive trauma, poor nutrition, or lack of oxygen or blood flow to the brain. The hallmark of encephalopathy is an altered mental state.”
It is confusing since there is a lot of overlap in the definitions of delirium and encephalopathy. One way to tease this out conceptually is noting that delirium is listed under mental, behavioral, and neurodevelopmental disorders, while encephalopathy appears under disorders of the nervous system. One can think of delirium as more of a “mental/psychiatric” diagnosis, while encephalopathy is caused by more “medical” causes.
If a patient who is normally not altered presents with confusion because of an infection or metabolic derangement, one can diagnose and document the cause of an acute encephalopathy. However, let’s say a patient is admitted in the morning with an infection, is started on treatment, but is not initially confused. If he/she later becomes confused at night, one could err conservatively and document delirium caused by sundowning.
Differentiating delirium and encephalopathy can be especially difficult in patients who have dementia with episodic confusion when they present with an infection and confusion. If the confusion is within what family members/caretakers say is “normal,” then one shouldn’t document encephalopathy. As a provider, one shouldn’t focus on all the rules and exceptions, just document as specifically and accurately as possible and the coders should take care of the rest.
Dr. Tong is an assistant professor of hospital medicine and an assistant director of the clinical research program at Emory University, Atlanta. Ms. Epps is director of clinical documentation improvement at Emory Healthcare, Atlanta.
References
1. “Acute Inpatient PPS.” Centers for Medicare and Medicaid Services. Accessed 2/17/18. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/index.html.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing, 2013.
3. “Details for title: FY 2018 Final Rule and Correction Notice Tables.” Centers for Medicare and Medicaid Services Accessed 2/17/18. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/FY2018-IPPS-Final-Rule-Home-Page-Items/FY2018-IPPS-Final-Rule-Tables.html.
4. “Encephalopathy Information Page.” National Institute of Neurologic Disorders and Stroke. Accessed on 2/17/18. https://www.ninds.nih.gov/Disorders/All-Disorders/Encephalopathy-Information-Page.
5. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organization, 1992. http://apps.who.int/iris/handle/10665/37958.
During residency, physicians are trained to care for patients and write notes that are clinically useful. However, physicians are often not taught about how documentation affects reimbursement and quality measures. Our purpose here, and in articles to follow, is to give readers tools to enable them to more accurately reflect the complexity and work that is done for accurate reimbursements.
If you were to get in a car accident, the body shop would document the damage done and submit it to the insurance company. It’s the body shop’s responsibility to record the damage, not the insurance company’s. So while documentation can seem onerous, the insurance company is not going to scour the chart to find diagnoses missed in the note. That would be like the body shop doing repair work without documenting the damage but then somehow expecting to get paid.
For the insurance company, “If you didn’t document it, it didn’t happen.” The body shop should not underdocument and say there were only a few scratches on the right rear panel if it was severely damaged. Likewise, it should not overbill and say the front bumper was damaged if it was not. The goal is not to bill as much as possible but rather to document appropriately.
Terminology
The expected length of stay (LOS) and the expected mortality for a particular patient is determined by how sick the patient appears to be based on the medical record documentation. So documenting all the appropriate diagnoses makes the LOS index (actual LOS divided by expected LOS) and mortality index more accurate as well. It is particularly important to document when a condition is (or is not) “present on admission”.
While physician payments can be based on evaluation and management coding, the hospital’s reimbursement is largely determined by physician documentation. Hospitals are paid by Medicare on a capitated basis according to the Acute Inpatient Prospective Payment System. The amount paid is determined by the base rate of the hospital multiplied by the relative weight (RW) of the Medicare Severity Diagnosis Related Group (MS-DRG).
The base rate is adjusted by the wage index of the hospital location. Hospitals that serve a high proportion of low income patients receive a Disproportionate Share Hospital adjustment. The base rate is not something hospitalists have control over.
The RW, however, is determined by the primary diagnosis (reason for admission) and whether or not there are complications or comorbidities (CCs) or major complications or comorbidities (MCCs). The more CCs and MCCs a patient has, the higher the severity of illness and expected increased resources needed to care for that patient.
Diagnoses are currently coded using ICD-10 used by the World Health Organization. The ICD-10 of the primary diagnosis is mapped to an MS-DRG. Many, but not all, MS-DRGs have increasing reimbursements for CCs and MCCs. Coders map the ICD-10 of the principal diagnosis along with any associated CCs or MCCs to the MS-DRG code. The relative weights for different DRGs can found on table 5 of the Medicare website (see reference 1).
Altered mental status versus delirium versus encephalopathy
As an example, let’s look at the difference in RW, LOS, and reimbursement in an otherwise identical patient based on documenting altered mental status (AMS), delirium, or encephalopathy. (see Table 1)
As one can see, RW, estimated LOS, and reimbursement would significantly increase for the patient with delirium (CC) or encephalopathy (MCC) versus AMS (no CC/MCC). A list of which diagnoses are considered CC’s versus MCC’s are on tables 6J and 6I, respectively, on the same Medicare website as table 5.
The difference between AMS, delirium, and encephalopathy
AMS is a sign/symptom complex similar to shortness of breath before an etiology is found. AMS can be the presenting symptom; when a specific etiology is found, however, a more specific diagnosis should be used such as delirium or encephalopathy.
Delirium, according to the DSM-5, is an acute change in the level of attention, cognition, or perception from baseline that developed over hours or days and tends to fluctuate during the course of a day. The change described is not better explained by a preexisting or evolving neurocognitive disorder and does not occur in the context of a severely reduced level of arousal, such as coma. There is evidence from the history, physical examination, or laboratory findings that the disturbance is a direct consequence of a general medical condition, substance intoxication or withdrawal, exposure to a toxin, or more than one cause.
The National Institute of Neurological Diseases and Stroke defines encephalopathy as “any diffuse disease of the brain that alters brain function or structure. Encephalopathy may be caused by an infectious agent, metabolic or mitochondrial dysfunction, brain tumor or increased intracranial pressure, prolonged exposure to toxic elements, chronic progressive trauma, poor nutrition, or lack of oxygen or blood flow to the brain. The hallmark of encephalopathy is an altered mental state.”
It is confusing since there is a lot of overlap in the definitions of delirium and encephalopathy. One way to tease this out conceptually is noting that delirium is listed under mental, behavioral, and neurodevelopmental disorders, while encephalopathy appears under disorders of the nervous system. One can think of delirium as more of a “mental/psychiatric” diagnosis, while encephalopathy is caused by more “medical” causes.
If a patient who is normally not altered presents with confusion because of an infection or metabolic derangement, one can diagnose and document the cause of an acute encephalopathy. However, let’s say a patient is admitted in the morning with an infection, is started on treatment, but is not initially confused. If he/she later becomes confused at night, one could err conservatively and document delirium caused by sundowning.
Differentiating delirium and encephalopathy can be especially difficult in patients who have dementia with episodic confusion when they present with an infection and confusion. If the confusion is within what family members/caretakers say is “normal,” then one shouldn’t document encephalopathy. As a provider, one shouldn’t focus on all the rules and exceptions, just document as specifically and accurately as possible and the coders should take care of the rest.
Dr. Tong is an assistant professor of hospital medicine and an assistant director of the clinical research program at Emory University, Atlanta. Ms. Epps is director of clinical documentation improvement at Emory Healthcare, Atlanta.
References
1. “Acute Inpatient PPS.” Centers for Medicare and Medicaid Services. Accessed 2/17/18. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/index.html.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing, 2013.
3. “Details for title: FY 2018 Final Rule and Correction Notice Tables.” Centers for Medicare and Medicaid Services Accessed 2/17/18. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/FY2018-IPPS-Final-Rule-Home-Page-Items/FY2018-IPPS-Final-Rule-Tables.html.
4. “Encephalopathy Information Page.” National Institute of Neurologic Disorders and Stroke. Accessed on 2/17/18. https://www.ninds.nih.gov/Disorders/All-Disorders/Encephalopathy-Information-Page.
5. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organization, 1992. http://apps.who.int/iris/handle/10665/37958.
Positive change through advocacy
SHM seen as an ‘honest broker’ on Capitol Hill
Editor’s note: The “Legacies of Hospital Medicine” is a recurring opinion column submitted by some of the best and brightest hospitalists in the field, who have helped shape our specialty into what it is today. It is a series of articles that reflect on Hospital Medicine and its evolution over time, from a variety of unique and innovative perspectives.
Medical professional societies have many goals and serve numerous functions. Some of these include education and training, professional development, and shaping the perception of their specialty both in the medical world and the public arena. Advocacy and governmental affairs are also on that list. SHM is no exception to that rule, although we have taken what is clearly an unorthodox approach to those efforts and our strategy has resulted in an unusual amount of success for a society of our size and age.

As my contribution to the “Legacies” series, I am calling upon my 20-year history of participation in SHM’s advocacy and policy efforts to describe that approach, recount some of the history of our efforts, and to talk a bit about our current activities, goals, and strategies.
In 1999 the leadership of SHM decided to create the Public Policy Committee and to provide resources for what was, at the time, a single dedicated staff position to support the work of the committee. As nascent as our efforts were, the strategy for entering into the Washington fray was clear. We decided our priorities were first and foremost to educate our “targets” on exactly what a hospitalist was and on the increasing role hospitalists were playing in the American health care system.
The target audience was (and has remained) Congress, the Centers for Medicare and Medicaid Services, and the Medicare Payment Advisory Committee, which is the advisory board tasked to recommend to Congress how Medicare should spend its resources. The goal of this education was to establish our credibility and to advance the notion that we were the experts on care design for acutely ill patients in the inpatient setting. To this end, we decided that, when we met with folks on the Hill, we would ask for nothing for ourselves or our members, an approach that was virtually unheard of in the halls of Congress.
When responding to questions as to why we were not bringing “asks” to our Hill meetings, we would simply comment that we were only offering our services. And whenever they decided to try to make the health care system better and expertise was required regarding redesign of care in the hospital, they should think about us. Our stated goal: improve the delivery system and provide better and more cost-effective care for our patients.
We also exercised what I will call “issue discipline.” With very limited resources it was critical that we limit our issues to ones on which we could have significant impact, and had enough expertise to shape an effective argument. In addition, as we were going to be operating within a highly partisan system and representing members with varying political views, it was highly important that we did not approach issues in a way that resulted in our appearing politically motivated.
That approach took a lot of time and patience. But as a small and relatively under-resourced organization, we saw it as the only way that we could eventually have our message heard. So for many years the small contingent of SHM staff and the members of the Public Policy Committee (PPC) worked quietly to have our specialty and society recognized by policy makers in Washington and Baltimore (where CMS resides). But in the years just prior to and since the passage of the Affordable Care Act, when serious redesign of the American health care system began, our patience started to pay dividends and policy makers actually reached out for our input on issues related to the care of patients admitted to acute care hospitals. In addition, our advocacy efforts started to gain more traction.
Today, our specialty and society are well known by the key health care policymakers at CMS, MedPAC, and the Center for Medicare and Medicaid Innovation (CMMI), the latter of which was created by the ACA and whose role is to test the new alternative payment models (like accountable care organizations and bundled payments) to find out if they actually lead to better outcomes and lower costs. In the halls of Congress, especially with the health care staff for the committees of jurisdiction for federal health care legislation, our society is seen as an “honest broker” and as an organization committed not just to the issues that impact our members, but one that has the improvement of the entire health care system at the top of its priority list. We have been told that this perception gives us a voice that is much more influential than would be expected for a society of our age, size, and resources.
Along the way, the PPC has grown to a committee of 20 select members led by committee chair Joshua Lenchus, DO, RPh, SFHM. The committee is known to be among the most difficult committees to get on, and members commit to hours of work monthly to support our efforts. Our government relations staff in Philadelphia is still small at just three, but they are extremely bright and productive. Director Josh Boswell serves as their extremely capable leader. Josh Lapps and Ellen Boyer round out the incredibly strong team. Recently, my role evolved from being the long-term chairman of the PPC to one of volunteer staff, as the senior advisor for government relations. In this role I hope to support our full time staff, especially in our Washington-facing efforts.
The SHM staff has brought several systemic improvements to our advocacy work, including execution of several highly successful “Hill Days” and, more recently, the establishment of our “Grassroots Network” that allows a wider swath of our membership to get involved in the field. The Hill Days occur during years when the SHM Annual Conference is in Washington, and one of the days includes busing hundreds of hospitalists to Capitol Hill for meetings with their representatives to discuss our advocacy issues. Our next Hill Day will be at the 2019 annual conference, and we will be signing up volunteer members for this unique experience.
The success of our advocacy can be seen in several high-level “wins” over the last few years. Some of the more notable include:
- Successful application to CMS for a specialty code for Hospital Medicine (the C6 designation), so that performance data for hospitalists will be fairly compared with other hospitalists and not with our outpatient colleagues’ performance.
- Successful support of risk adjustment of readmission rates for safety net hospitals.
- Creation of a hardship exemption of Meaningful Use penalties for hospitalists, an initiative that saved our membership approximately $37 million of unfair penalties per year; this ensured a permanent exemption from these penalties within the Medicare Access and CHIP Reauthorization Act.
- Implementation of Advanced Care Planning CPT codes to encourage appropriate use of “end of life” discussions.
- Establishment of a Hospitalist Measure set with CMS.
- Repeal of the Independent Advisory Board earlier this year.
- Creation of the “Facility Based Option” to replace Merit-Based Incentive Payment System reporting for hospital-based physicians including hospitalists. This voluntary method to replace MIPS reporting was first suggested to CMS by SHM, was developed in partnership with CMS, and will be available in 2019.
SHM continues to take the lead on issues that impact the U.S. health care system and our patients. For several years we have been explaining to CMS and Congress the complete dysfunction of observation status, and its negative impact on elderly patients and hospitals. We have taken advantage of the expertise of several members of the PPC, including research currently being done by member Ann Sheehy, MD, SFHM, to publish two iterations of a white paper on the subject, which was widely read by Hill staff and resulted in Dr. Sheehy testifying on the subject to Congress.
More recently, SHM released a consensus statement on the use of opioids in the inpatient setting, along with a policy statement on opioid abuse, both of which have been widely lauded after being distributed to key committees of both chambers of Congress. Our recommendations will undoubtedly be addressed in an opioid bill which, at the time of this writing, is moving to a vote on the Hill.
As the U.S. health care system undergoes a necessary transformation to one in which value creation is tantamount, hospitalists – by the nature of our work – are in a propitious position to guide the development of better federal policy. We still must be judicious in the use of our limited resources and circumspect in our selection of issues. And we must jealously guard the reputation we have cultivated as a medical society that is looking out for the entire health care system and its patients, while we also support our members and their work.
We want to continue to be an organization that, rather than resisting change, is focused on driving positive change through better ideas and intelligent advocacy.
Dr. Greeno is senior advisor for government affairs and past president of the Society of Hospital Medicine.
SHM seen as an ‘honest broker’ on Capitol Hill
SHM seen as an ‘honest broker’ on Capitol Hill
Editor’s note: The “Legacies of Hospital Medicine” is a recurring opinion column submitted by some of the best and brightest hospitalists in the field, who have helped shape our specialty into what it is today. It is a series of articles that reflect on Hospital Medicine and its evolution over time, from a variety of unique and innovative perspectives.
Medical professional societies have many goals and serve numerous functions. Some of these include education and training, professional development, and shaping the perception of their specialty both in the medical world and the public arena. Advocacy and governmental affairs are also on that list. SHM is no exception to that rule, although we have taken what is clearly an unorthodox approach to those efforts and our strategy has resulted in an unusual amount of success for a society of our size and age.
As my contribution to the “Legacies” series, I am calling upon my 20-year history of participation in SHM’s advocacy and policy efforts to describe that approach, recount some of the history of our efforts, and to talk a bit about our current activities, goals, and strategies.
In 1999 the leadership of SHM decided to create the Public Policy Committee and to provide resources for what was, at the time, a single dedicated staff position to support the work of the committee. As nascent as our efforts were, the strategy for entering into the Washington fray was clear. We decided our priorities were first and foremost to educate our “targets” on exactly what a hospitalist was and on the increasing role hospitalists were playing in the American health care system.
The target audience was (and has remained) Congress, the Centers for Medicare and Medicaid Services, and the Medicare Payment Advisory Committee, which is the advisory board tasked to recommend to Congress how Medicare should spend its resources. The goal of this education was to establish our credibility and to advance the notion that we were the experts on care design for acutely ill patients in the inpatient setting. To this end, we decided that, when we met with folks on the Hill, we would ask for nothing for ourselves or our members, an approach that was virtually unheard of in the halls of Congress.
When responding to questions as to why we were not bringing “asks” to our Hill meetings, we would simply comment that we were only offering our services. And whenever they decided to try to make the health care system better and expertise was required regarding redesign of care in the hospital, they should think about us. Our stated goal: improve the delivery system and provide better and more cost-effective care for our patients.
We also exercised what I will call “issue discipline.” With very limited resources it was critical that we limit our issues to ones on which we could have significant impact, and had enough expertise to shape an effective argument. In addition, as we were going to be operating within a highly partisan system and representing members with varying political views, it was highly important that we did not approach issues in a way that resulted in our appearing politically motivated.
That approach took a lot of time and patience. But as a small and relatively under-resourced organization, we saw it as the only way that we could eventually have our message heard. So for many years the small contingent of SHM staff and the members of the Public Policy Committee (PPC) worked quietly to have our specialty and society recognized by policy makers in Washington and Baltimore (where CMS resides). But in the years just prior to and since the passage of the Affordable Care Act, when serious redesign of the American health care system began, our patience started to pay dividends and policy makers actually reached out for our input on issues related to the care of patients admitted to acute care hospitals. In addition, our advocacy efforts started to gain more traction.
Today, our specialty and society are well known by the key health care policymakers at CMS, MedPAC, and the Center for Medicare and Medicaid Innovation (CMMI), the latter of which was created by the ACA and whose role is to test the new alternative payment models (like accountable care organizations and bundled payments) to find out if they actually lead to better outcomes and lower costs. In the halls of Congress, especially with the health care staff for the committees of jurisdiction for federal health care legislation, our society is seen as an “honest broker” and as an organization committed not just to the issues that impact our members, but one that has the improvement of the entire health care system at the top of its priority list. We have been told that this perception gives us a voice that is much more influential than would be expected for a society of our age, size, and resources.
Along the way, the PPC has grown to a committee of 20 select members led by committee chair Joshua Lenchus, DO, RPh, SFHM. The committee is known to be among the most difficult committees to get on, and members commit to hours of work monthly to support our efforts. Our government relations staff in Philadelphia is still small at just three, but they are extremely bright and productive. Director Josh Boswell serves as their extremely capable leader. Josh Lapps and Ellen Boyer round out the incredibly strong team. Recently, my role evolved from being the long-term chairman of the PPC to one of volunteer staff, as the senior advisor for government relations. In this role I hope to support our full time staff, especially in our Washington-facing efforts.
The SHM staff has brought several systemic improvements to our advocacy work, including execution of several highly successful “Hill Days” and, more recently, the establishment of our “Grassroots Network” that allows a wider swath of our membership to get involved in the field. The Hill Days occur during years when the SHM Annual Conference is in Washington, and one of the days includes busing hundreds of hospitalists to Capitol Hill for meetings with their representatives to discuss our advocacy issues. Our next Hill Day will be at the 2019 annual conference, and we will be signing up volunteer members for this unique experience.
The success of our advocacy can be seen in several high-level “wins” over the last few years. Some of the more notable include:
- Successful application to CMS for a specialty code for Hospital Medicine (the C6 designation), so that performance data for hospitalists will be fairly compared with other hospitalists and not with our outpatient colleagues’ performance.
- Successful support of risk adjustment of readmission rates for safety net hospitals.
- Creation of a hardship exemption of Meaningful Use penalties for hospitalists, an initiative that saved our membership approximately $37 million of unfair penalties per year; this ensured a permanent exemption from these penalties within the Medicare Access and CHIP Reauthorization Act.
- Implementation of Advanced Care Planning CPT codes to encourage appropriate use of “end of life” discussions.
- Establishment of a Hospitalist Measure set with CMS.
- Repeal of the Independent Advisory Board earlier this year.
- Creation of the “Facility Based Option” to replace Merit-Based Incentive Payment System reporting for hospital-based physicians including hospitalists. This voluntary method to replace MIPS reporting was first suggested to CMS by SHM, was developed in partnership with CMS, and will be available in 2019.
SHM continues to take the lead on issues that impact the U.S. health care system and our patients. For several years we have been explaining to CMS and Congress the complete dysfunction of observation status, and its negative impact on elderly patients and hospitals. We have taken advantage of the expertise of several members of the PPC, including research currently being done by member Ann Sheehy, MD, SFHM, to publish two iterations of a white paper on the subject, which was widely read by Hill staff and resulted in Dr. Sheehy testifying on the subject to Congress.
More recently, SHM released a consensus statement on the use of opioids in the inpatient setting, along with a policy statement on opioid abuse, both of which have been widely lauded after being distributed to key committees of both chambers of Congress. Our recommendations will undoubtedly be addressed in an opioid bill which, at the time of this writing, is moving to a vote on the Hill.
As the U.S. health care system undergoes a necessary transformation to one in which value creation is tantamount, hospitalists – by the nature of our work – are in a propitious position to guide the development of better federal policy. We still must be judicious in the use of our limited resources and circumspect in our selection of issues. And we must jealously guard the reputation we have cultivated as a medical society that is looking out for the entire health care system and its patients, while we also support our members and their work.
We want to continue to be an organization that, rather than resisting change, is focused on driving positive change through better ideas and intelligent advocacy.
Dr. Greeno is senior advisor for government affairs and past president of the Society of Hospital Medicine.
Editor’s note: The “Legacies of Hospital Medicine” is a recurring opinion column submitted by some of the best and brightest hospitalists in the field, who have helped shape our specialty into what it is today. It is a series of articles that reflect on Hospital Medicine and its evolution over time, from a variety of unique and innovative perspectives.
Medical professional societies have many goals and serve numerous functions. Some of these include education and training, professional development, and shaping the perception of their specialty both in the medical world and the public arena. Advocacy and governmental affairs are also on that list. SHM is no exception to that rule, although we have taken what is clearly an unorthodox approach to those efforts and our strategy has resulted in an unusual amount of success for a society of our size and age.
As my contribution to the “Legacies” series, I am calling upon my 20-year history of participation in SHM’s advocacy and policy efforts to describe that approach, recount some of the history of our efforts, and to talk a bit about our current activities, goals, and strategies.
In 1999 the leadership of SHM decided to create the Public Policy Committee and to provide resources for what was, at the time, a single dedicated staff position to support the work of the committee. As nascent as our efforts were, the strategy for entering into the Washington fray was clear. We decided our priorities were first and foremost to educate our “targets” on exactly what a hospitalist was and on the increasing role hospitalists were playing in the American health care system.
The target audience was (and has remained) Congress, the Centers for Medicare and Medicaid Services, and the Medicare Payment Advisory Committee, which is the advisory board tasked to recommend to Congress how Medicare should spend its resources. The goal of this education was to establish our credibility and to advance the notion that we were the experts on care design for acutely ill patients in the inpatient setting. To this end, we decided that, when we met with folks on the Hill, we would ask for nothing for ourselves or our members, an approach that was virtually unheard of in the halls of Congress.
When responding to questions as to why we were not bringing “asks” to our Hill meetings, we would simply comment that we were only offering our services. And whenever they decided to try to make the health care system better and expertise was required regarding redesign of care in the hospital, they should think about us. Our stated goal: improve the delivery system and provide better and more cost-effective care for our patients.
We also exercised what I will call “issue discipline.” With very limited resources it was critical that we limit our issues to ones on which we could have significant impact, and had enough expertise to shape an effective argument. In addition, as we were going to be operating within a highly partisan system and representing members with varying political views, it was highly important that we did not approach issues in a way that resulted in our appearing politically motivated.
That approach took a lot of time and patience. But as a small and relatively under-resourced organization, we saw it as the only way that we could eventually have our message heard. So for many years the small contingent of SHM staff and the members of the Public Policy Committee (PPC) worked quietly to have our specialty and society recognized by policy makers in Washington and Baltimore (where CMS resides). But in the years just prior to and since the passage of the Affordable Care Act, when serious redesign of the American health care system began, our patience started to pay dividends and policy makers actually reached out for our input on issues related to the care of patients admitted to acute care hospitals. In addition, our advocacy efforts started to gain more traction.
Today, our specialty and society are well known by the key health care policymakers at CMS, MedPAC, and the Center for Medicare and Medicaid Innovation (CMMI), the latter of which was created by the ACA and whose role is to test the new alternative payment models (like accountable care organizations and bundled payments) to find out if they actually lead to better outcomes and lower costs. In the halls of Congress, especially with the health care staff for the committees of jurisdiction for federal health care legislation, our society is seen as an “honest broker” and as an organization committed not just to the issues that impact our members, but one that has the improvement of the entire health care system at the top of its priority list. We have been told that this perception gives us a voice that is much more influential than would be expected for a society of our age, size, and resources.
Along the way, the PPC has grown to a committee of 20 select members led by committee chair Joshua Lenchus, DO, RPh, SFHM. The committee is known to be among the most difficult committees to get on, and members commit to hours of work monthly to support our efforts. Our government relations staff in Philadelphia is still small at just three, but they are extremely bright and productive. Director Josh Boswell serves as their extremely capable leader. Josh Lapps and Ellen Boyer round out the incredibly strong team. Recently, my role evolved from being the long-term chairman of the PPC to one of volunteer staff, as the senior advisor for government relations. In this role I hope to support our full time staff, especially in our Washington-facing efforts.
The SHM staff has brought several systemic improvements to our advocacy work, including execution of several highly successful “Hill Days” and, more recently, the establishment of our “Grassroots Network” that allows a wider swath of our membership to get involved in the field. The Hill Days occur during years when the SHM Annual Conference is in Washington, and one of the days includes busing hundreds of hospitalists to Capitol Hill for meetings with their representatives to discuss our advocacy issues. Our next Hill Day will be at the 2019 annual conference, and we will be signing up volunteer members for this unique experience.
The success of our advocacy can be seen in several high-level “wins” over the last few years. Some of the more notable include:
- Successful application to CMS for a specialty code for Hospital Medicine (the C6 designation), so that performance data for hospitalists will be fairly compared with other hospitalists and not with our outpatient colleagues’ performance.
- Successful support of risk adjustment of readmission rates for safety net hospitals.
- Creation of a hardship exemption of Meaningful Use penalties for hospitalists, an initiative that saved our membership approximately $37 million of unfair penalties per year; this ensured a permanent exemption from these penalties within the Medicare Access and CHIP Reauthorization Act.
- Implementation of Advanced Care Planning CPT codes to encourage appropriate use of “end of life” discussions.
- Establishment of a Hospitalist Measure set with CMS.
- Repeal of the Independent Advisory Board earlier this year.
- Creation of the “Facility Based Option” to replace Merit-Based Incentive Payment System reporting for hospital-based physicians including hospitalists. This voluntary method to replace MIPS reporting was first suggested to CMS by SHM, was developed in partnership with CMS, and will be available in 2019.
SHM continues to take the lead on issues that impact the U.S. health care system and our patients. For several years we have been explaining to CMS and Congress the complete dysfunction of observation status, and its negative impact on elderly patients and hospitals. We have taken advantage of the expertise of several members of the PPC, including research currently being done by member Ann Sheehy, MD, SFHM, to publish two iterations of a white paper on the subject, which was widely read by Hill staff and resulted in Dr. Sheehy testifying on the subject to Congress.
More recently, SHM released a consensus statement on the use of opioids in the inpatient setting, along with a policy statement on opioid abuse, both of which have been widely lauded after being distributed to key committees of both chambers of Congress. Our recommendations will undoubtedly be addressed in an opioid bill which, at the time of this writing, is moving to a vote on the Hill.
As the U.S. health care system undergoes a necessary transformation to one in which value creation is tantamount, hospitalists – by the nature of our work – are in a propitious position to guide the development of better federal policy. We still must be judicious in the use of our limited resources and circumspect in our selection of issues. And we must jealously guard the reputation we have cultivated as a medical society that is looking out for the entire health care system and its patients, while we also support our members and their work.
We want to continue to be an organization that, rather than resisting change, is focused on driving positive change through better ideas and intelligent advocacy.
Dr. Greeno is senior advisor for government affairs and past president of the Society of Hospital Medicine.
Conference News Roundup—European Academy of Neurology
Thrombectomy Is Feasible for the Elderly, but Entails Risks
Mechanical thrombectomy is an increasingly important therapy for acute stroke that can benefit the very old, assuming a careful selection of patients and risk assessment, according to a Portuguese study.
For several years, endovascular thrombectomy has been a way of removing larger vascular obstructions. In this procedure, the thrombus is extracted from the cerebral vessel via a catheter inserted in the groin. Numerous international studies have shown that endovascular treatment is a substantial improvement over purely drug-based therapy. The procedure is especially effective in dealing with extremely long blood clots and large obstructions of the cerebral arteries and often yields positive results. Thanks to this procedure, more than 60% of patients treated survive the stroke with no or minor subsequent impairment.
“More and more study results show the high effectiveness of mechanical removal of blood clots after a stroke. But researchers are still trying to determine the type of patient for whom this relatively new procedure is the best treatment option,” said Ary Lopes de Sousa, MD, a neurology resident at Central Lisbon Hospital Center.
Dr. de Sousa and his colleagues reviewed the treatment success of thrombectomy in more than 200 patients with anterior acute ischemic stroke and no or slight disability prior to this event. The researchers separated patients into two groups: one with individuals younger than 80 and one with individuals age 80 and older.
In the group of patients age 80 and older, hypertension and transient ischemic attacks were more frequent. The treatment did not differ between the two groups (eg, in terms of the time frame of the revascularization). But in the older group, two-thirds of the patients exhibited a poor functional outcome at three months after the treatment (ie, they were moderately or severely limited in their ability to handle their daily tasks). The number of impaired individuals in that group was substantially larger than in the younger group, where 46% faced limitations in their everyday lives. On the other hand, one-third of the patients age 80 and older were able to handle their everyday lives three months after the treatment with no or mild impairments from the stroke. No difference in mortality was observed between the two age groups.
“For patients over 80, thrombectomy appears to be riskier than for younger patients,” said Dr. de Sousa. “But one third of the patients over 80 can be fully functional in their everyday lives after the procedure, so we must identify the factors associated with this favorable outcome. This [step] will support us applying this modern procedure efficiently to those individuals among the very old who can benefit from it.”
Studies Gauge the Cost of Migraine
A pair of studies have evaluated the cost of migraine to individuals, society, and businesses. A French study looked at the socioeconomic impact of the condition. In a survey of more than 7,700 people, a representative sample of the general population, 3.8% indicated that they experienced severe migraines on at least eight days per month. “Two-thirds of those [patients] were women, and the average age of those affected was 41, meaning that migraines significantly affect people at the peak of their careers, and who have families to provide for. These regular attacks represent a serious problem as far as keeping their jobs is concerned,” said Dr. Guillaume Leiba, Pricing and Market Access Manager at Novartis in Paris. In the current study, patients with severe migraine reported missing 33 working days per year because of their condition. This absence translates into a cost to society of approximately EUR 3.8 billion. Migraine also has an impact on patients’ social environment: 14% of respondents indicated that family members had to adjust their working hours because of patients’ migraine headaches. The study also quantified the financial burden placed on migraineurs: 58% reported an average monthly cost of more than EUR 30 per month for nonreimbursed medicines. Approximately 43% spent more than EUR 50 each month on other, nonpharmaceutical therapies. Despite the high level of public and private spending associated with the condition, quality of life for migraineurs remains far from satisfactory. More than three-quarters have sleep disorders and benefit less from their free time than healthy controls.
A Swiss study obtained more detailed results regarding absenteeism in the workplace. A group of 700 working migraineurs reported losing an average of 32 days per year because of migraine. This rate is similar to that reported in the French study. But there were significant differences depending on the specific type of headache, according to study author François Cadiou, CEO of Healint in Singapore. “With an average of more than 56 working days missed per year, patients with chronic migraine had the highest rate of absenteeism. People with episodic migraine were unable to go to work on 33 days of the year, while those with low-frequency episodic migraine took an average of 15 days off because of their condition.” Another finding has implications for preventive measures: the number of sick days was not always constant. In fact, the total steadily increased, and with it the amount of medication taken if patients indicated anxiety or depression as a symptom or trigger at least once within the 28-day observation period. In light of the outcomes presented, experts at the EAN Congress have issued a call for increased investment in migraine research and prevention, citing the advantages to society.
Both studies were funded by Novartis Pharma.
Parkinson’s Disease Progression Varies by Gender
A current study has now furnished the first neurophysiologic evidence that Parkinson’s disease progresses differently in women than in men. “Numerous demographic studies have provided evidence that men contract Parkinson’s disease nearly twice as often as women. What was unclear, however, was whether a gender-specific pathophysiology exists as soon as the first symptoms appear,” said Maja Kojovic, MD, PhD, a consultant neurologist at Ljubljana University Medical Center in Slovenia.
The international research team proceeded from the concept that in early Parkinson’s disease, functional changes can be detected in the primary motor cortex (M1) using transcranial magnetic stimulation (TMS). If pathophysiology differs between genders in Parkinson’s disease, they hypothesized, it will be reflected in differences of M1 TMS measurements.
Thirty-nine newly diagnosed and untreated patients with Parkinson’s disease (23 males) were assessed using the Unified Parkinson’s Disease Rating Scale (UPDRS). Then the patients and a group of healthy controls underwent TMS measurements of motor thresholds of the brain, input–output curve, short interval intracortical inhibition, cortical silent period, and intracortical facilitation. Brain plasticity was also measured using paired associative stimulation.
The UPDRS tests did not yield any differences in motor scores between the genders. However, the female patients had a less steep input–output curve than the male patients on the side of the brain more affected by Parkinson’s disease.
The women with Parkinson’s disease also exhibited better preserved short interval intracortical inhibition in both hemispheres, compared with affected men, and tended to have a better response to the paired associative stimulation protocol on the side less affected by symptoms. No gender-specific differences were determined, however, in the motor thresholds, intracortical facilitation, and the cortical silent period. The healthy control group did not show any gender or interhemispheric differences for any of the TMS parameters measured. “The detected gender differences in corticospinal and intracortical excitability in patients with early untreated Parkinson’s disease represent differences in disease pathophysiology. Gender may also prove to be a relevant factor when choosing appropriate treatment,” said Dr. Kojovic.
EAN Develops Guideline on Palliative Care of Patients With Severe MS
A cohort of 934 individuals affected by multiple sclerosis (MS) from seven European countries played an instrumental part in developing the European Academy of Neurology’s (EAN) new guideline on palliative care for people with severe MS. “There were 751 MS patients and 183 caregiver relatives involved,” said Sascha Köpke, PhD, Professor of Nursing Research at the University of Lübeck in Germany.
With the involvement of patients and their families in a new guideline, the EAN is emphasizing shared decision-making as an increasingly important concept that underscores patient autonomy and promotes the individualization of diagnosis and therapy. According to this approach, patients and physicians undergo a detailed consultation and then choose the medical treatment. The EAN has supported this patient-centered approach for a long time, and it is becoming increasingly established in other medical areas as well.
“It was resource- and time-intensive to include consumers in the guideline process, but also highly rewarding,” said Prof. Köpke. “Patients and caregivers really helped us to formulate the guideline in a way that was in line with actual practice and their own needs. We were able to see clearly which of our ideas met with approval or rejection.” The comments were also instructive for the group of EAN experts. They raised new aspects as well as sensitive issues that had been left out of the first draft.
Two approaches were chosen to ensure that consumers would participate. “First, there was an international online survey launched by national MS societies following a trial run involving 20 patients and 18 caregivers. Second, we invited MS patients and caregiver relatives to focus group meetings,” said Prof. Köpke. The majority of participants approved the topics proposed by the EAN group of experts. About 98% agreed to incorporate the subject of multidisciplinary rehabilitation in the guideline. There were 569 free comments, of which 182 (32%) pertained to the specified topics. A further 227 comments (40%) addressed additional topics, of which 16 were pertinent to the guideline. Five of the focus group meetings corroborated the results of the online survey and helped to work out important issues for the individuals affected. “The involvement of patients and caregivers increases the reliability and relevance of the guideline for clinical practice,” said Prof. Köpke.
Thrombectomy Is Feasible for the Elderly, but Entails Risks
Mechanical thrombectomy is an increasingly important therapy for acute stroke that can benefit the very old, assuming a careful selection of patients and risk assessment, according to a Portuguese study.
For several years, endovascular thrombectomy has been a way of removing larger vascular obstructions. In this procedure, the thrombus is extracted from the cerebral vessel via a catheter inserted in the groin. Numerous international studies have shown that endovascular treatment is a substantial improvement over purely drug-based therapy. The procedure is especially effective in dealing with extremely long blood clots and large obstructions of the cerebral arteries and often yields positive results. Thanks to this procedure, more than 60% of patients treated survive the stroke with no or minor subsequent impairment.
“More and more study results show the high effectiveness of mechanical removal of blood clots after a stroke. But researchers are still trying to determine the type of patient for whom this relatively new procedure is the best treatment option,” said Ary Lopes de Sousa, MD, a neurology resident at Central Lisbon Hospital Center.
Dr. de Sousa and his colleagues reviewed the treatment success of thrombectomy in more than 200 patients with anterior acute ischemic stroke and no or slight disability prior to this event. The researchers separated patients into two groups: one with individuals younger than 80 and one with individuals age 80 and older.
In the group of patients age 80 and older, hypertension and transient ischemic attacks were more frequent. The treatment did not differ between the two groups (eg, in terms of the time frame of the revascularization). But in the older group, two-thirds of the patients exhibited a poor functional outcome at three months after the treatment (ie, they were moderately or severely limited in their ability to handle their daily tasks). The number of impaired individuals in that group was substantially larger than in the younger group, where 46% faced limitations in their everyday lives. On the other hand, one-third of the patients age 80 and older were able to handle their everyday lives three months after the treatment with no or mild impairments from the stroke. No difference in mortality was observed between the two age groups.
“For patients over 80, thrombectomy appears to be riskier than for younger patients,” said Dr. de Sousa. “But one third of the patients over 80 can be fully functional in their everyday lives after the procedure, so we must identify the factors associated with this favorable outcome. This [step] will support us applying this modern procedure efficiently to those individuals among the very old who can benefit from it.”
Studies Gauge the Cost of Migraine
A pair of studies have evaluated the cost of migraine to individuals, society, and businesses. A French study looked at the socioeconomic impact of the condition. In a survey of more than 7,700 people, a representative sample of the general population, 3.8% indicated that they experienced severe migraines on at least eight days per month. “Two-thirds of those [patients] were women, and the average age of those affected was 41, meaning that migraines significantly affect people at the peak of their careers, and who have families to provide for. These regular attacks represent a serious problem as far as keeping their jobs is concerned,” said Dr. Guillaume Leiba, Pricing and Market Access Manager at Novartis in Paris. In the current study, patients with severe migraine reported missing 33 working days per year because of their condition. This absence translates into a cost to society of approximately EUR 3.8 billion. Migraine also has an impact on patients’ social environment: 14% of respondents indicated that family members had to adjust their working hours because of patients’ migraine headaches. The study also quantified the financial burden placed on migraineurs: 58% reported an average monthly cost of more than EUR 30 per month for nonreimbursed medicines. Approximately 43% spent more than EUR 50 each month on other, nonpharmaceutical therapies. Despite the high level of public and private spending associated with the condition, quality of life for migraineurs remains far from satisfactory. More than three-quarters have sleep disorders and benefit less from their free time than healthy controls.
A Swiss study obtained more detailed results regarding absenteeism in the workplace. A group of 700 working migraineurs reported losing an average of 32 days per year because of migraine. This rate is similar to that reported in the French study. But there were significant differences depending on the specific type of headache, according to study author François Cadiou, CEO of Healint in Singapore. “With an average of more than 56 working days missed per year, patients with chronic migraine had the highest rate of absenteeism. People with episodic migraine were unable to go to work on 33 days of the year, while those with low-frequency episodic migraine took an average of 15 days off because of their condition.” Another finding has implications for preventive measures: the number of sick days was not always constant. In fact, the total steadily increased, and with it the amount of medication taken if patients indicated anxiety or depression as a symptom or trigger at least once within the 28-day observation period. In light of the outcomes presented, experts at the EAN Congress have issued a call for increased investment in migraine research and prevention, citing the advantages to society.
Both studies were funded by Novartis Pharma.
Parkinson’s Disease Progression Varies by Gender
A current study has now furnished the first neurophysiologic evidence that Parkinson’s disease progresses differently in women than in men. “Numerous demographic studies have provided evidence that men contract Parkinson’s disease nearly twice as often as women. What was unclear, however, was whether a gender-specific pathophysiology exists as soon as the first symptoms appear,” said Maja Kojovic, MD, PhD, a consultant neurologist at Ljubljana University Medical Center in Slovenia.
The international research team proceeded from the concept that in early Parkinson’s disease, functional changes can be detected in the primary motor cortex (M1) using transcranial magnetic stimulation (TMS). If pathophysiology differs between genders in Parkinson’s disease, they hypothesized, it will be reflected in differences of M1 TMS measurements.
Thirty-nine newly diagnosed and untreated patients with Parkinson’s disease (23 males) were assessed using the Unified Parkinson’s Disease Rating Scale (UPDRS). Then the patients and a group of healthy controls underwent TMS measurements of motor thresholds of the brain, input–output curve, short interval intracortical inhibition, cortical silent period, and intracortical facilitation. Brain plasticity was also measured using paired associative stimulation.
The UPDRS tests did not yield any differences in motor scores between the genders. However, the female patients had a less steep input–output curve than the male patients on the side of the brain more affected by Parkinson’s disease.
The women with Parkinson’s disease also exhibited better preserved short interval intracortical inhibition in both hemispheres, compared with affected men, and tended to have a better response to the paired associative stimulation protocol on the side less affected by symptoms. No gender-specific differences were determined, however, in the motor thresholds, intracortical facilitation, and the cortical silent period. The healthy control group did not show any gender or interhemispheric differences for any of the TMS parameters measured. “The detected gender differences in corticospinal and intracortical excitability in patients with early untreated Parkinson’s disease represent differences in disease pathophysiology. Gender may also prove to be a relevant factor when choosing appropriate treatment,” said Dr. Kojovic.
EAN Develops Guideline on Palliative Care of Patients With Severe MS
A cohort of 934 individuals affected by multiple sclerosis (MS) from seven European countries played an instrumental part in developing the European Academy of Neurology’s (EAN) new guideline on palliative care for people with severe MS. “There were 751 MS patients and 183 caregiver relatives involved,” said Sascha Köpke, PhD, Professor of Nursing Research at the University of Lübeck in Germany.
With the involvement of patients and their families in a new guideline, the EAN is emphasizing shared decision-making as an increasingly important concept that underscores patient autonomy and promotes the individualization of diagnosis and therapy. According to this approach, patients and physicians undergo a detailed consultation and then choose the medical treatment. The EAN has supported this patient-centered approach for a long time, and it is becoming increasingly established in other medical areas as well.
“It was resource- and time-intensive to include consumers in the guideline process, but also highly rewarding,” said Prof. Köpke. “Patients and caregivers really helped us to formulate the guideline in a way that was in line with actual practice and their own needs. We were able to see clearly which of our ideas met with approval or rejection.” The comments were also instructive for the group of EAN experts. They raised new aspects as well as sensitive issues that had been left out of the first draft.
Two approaches were chosen to ensure that consumers would participate. “First, there was an international online survey launched by national MS societies following a trial run involving 20 patients and 18 caregivers. Second, we invited MS patients and caregiver relatives to focus group meetings,” said Prof. Köpke. The majority of participants approved the topics proposed by the EAN group of experts. About 98% agreed to incorporate the subject of multidisciplinary rehabilitation in the guideline. There were 569 free comments, of which 182 (32%) pertained to the specified topics. A further 227 comments (40%) addressed additional topics, of which 16 were pertinent to the guideline. Five of the focus group meetings corroborated the results of the online survey and helped to work out important issues for the individuals affected. “The involvement of patients and caregivers increases the reliability and relevance of the guideline for clinical practice,” said Prof. Köpke.
Thrombectomy Is Feasible for the Elderly, but Entails Risks
Mechanical thrombectomy is an increasingly important therapy for acute stroke that can benefit the very old, assuming a careful selection of patients and risk assessment, according to a Portuguese study.
For several years, endovascular thrombectomy has been a way of removing larger vascular obstructions. In this procedure, the thrombus is extracted from the cerebral vessel via a catheter inserted in the groin. Numerous international studies have shown that endovascular treatment is a substantial improvement over purely drug-based therapy. The procedure is especially effective in dealing with extremely long blood clots and large obstructions of the cerebral arteries and often yields positive results. Thanks to this procedure, more than 60% of patients treated survive the stroke with no or minor subsequent impairment.
“More and more study results show the high effectiveness of mechanical removal of blood clots after a stroke. But researchers are still trying to determine the type of patient for whom this relatively new procedure is the best treatment option,” said Ary Lopes de Sousa, MD, a neurology resident at Central Lisbon Hospital Center.
Dr. de Sousa and his colleagues reviewed the treatment success of thrombectomy in more than 200 patients with anterior acute ischemic stroke and no or slight disability prior to this event. The researchers separated patients into two groups: one with individuals younger than 80 and one with individuals age 80 and older.
In the group of patients age 80 and older, hypertension and transient ischemic attacks were more frequent. The treatment did not differ between the two groups (eg, in terms of the time frame of the revascularization). But in the older group, two-thirds of the patients exhibited a poor functional outcome at three months after the treatment (ie, they were moderately or severely limited in their ability to handle their daily tasks). The number of impaired individuals in that group was substantially larger than in the younger group, where 46% faced limitations in their everyday lives. On the other hand, one-third of the patients age 80 and older were able to handle their everyday lives three months after the treatment with no or mild impairments from the stroke. No difference in mortality was observed between the two age groups.
“For patients over 80, thrombectomy appears to be riskier than for younger patients,” said Dr. de Sousa. “But one third of the patients over 80 can be fully functional in their everyday lives after the procedure, so we must identify the factors associated with this favorable outcome. This [step] will support us applying this modern procedure efficiently to those individuals among the very old who can benefit from it.”
Studies Gauge the Cost of Migraine
A pair of studies have evaluated the cost of migraine to individuals, society, and businesses. A French study looked at the socioeconomic impact of the condition. In a survey of more than 7,700 people, a representative sample of the general population, 3.8% indicated that they experienced severe migraines on at least eight days per month. “Two-thirds of those [patients] were women, and the average age of those affected was 41, meaning that migraines significantly affect people at the peak of their careers, and who have families to provide for. These regular attacks represent a serious problem as far as keeping their jobs is concerned,” said Dr. Guillaume Leiba, Pricing and Market Access Manager at Novartis in Paris. In the current study, patients with severe migraine reported missing 33 working days per year because of their condition. This absence translates into a cost to society of approximately EUR 3.8 billion. Migraine also has an impact on patients’ social environment: 14% of respondents indicated that family members had to adjust their working hours because of patients’ migraine headaches. The study also quantified the financial burden placed on migraineurs: 58% reported an average monthly cost of more than EUR 30 per month for nonreimbursed medicines. Approximately 43% spent more than EUR 50 each month on other, nonpharmaceutical therapies. Despite the high level of public and private spending associated with the condition, quality of life for migraineurs remains far from satisfactory. More than three-quarters have sleep disorders and benefit less from their free time than healthy controls.
A Swiss study obtained more detailed results regarding absenteeism in the workplace. A group of 700 working migraineurs reported losing an average of 32 days per year because of migraine. This rate is similar to that reported in the French study. But there were significant differences depending on the specific type of headache, according to study author François Cadiou, CEO of Healint in Singapore. “With an average of more than 56 working days missed per year, patients with chronic migraine had the highest rate of absenteeism. People with episodic migraine were unable to go to work on 33 days of the year, while those with low-frequency episodic migraine took an average of 15 days off because of their condition.” Another finding has implications for preventive measures: the number of sick days was not always constant. In fact, the total steadily increased, and with it the amount of medication taken if patients indicated anxiety or depression as a symptom or trigger at least once within the 28-day observation period. In light of the outcomes presented, experts at the EAN Congress have issued a call for increased investment in migraine research and prevention, citing the advantages to society.
Both studies were funded by Novartis Pharma.
Parkinson’s Disease Progression Varies by Gender
A current study has now furnished the first neurophysiologic evidence that Parkinson’s disease progresses differently in women than in men. “Numerous demographic studies have provided evidence that men contract Parkinson’s disease nearly twice as often as women. What was unclear, however, was whether a gender-specific pathophysiology exists as soon as the first symptoms appear,” said Maja Kojovic, MD, PhD, a consultant neurologist at Ljubljana University Medical Center in Slovenia.
The international research team proceeded from the concept that in early Parkinson’s disease, functional changes can be detected in the primary motor cortex (M1) using transcranial magnetic stimulation (TMS). If pathophysiology differs between genders in Parkinson’s disease, they hypothesized, it will be reflected in differences of M1 TMS measurements.
Thirty-nine newly diagnosed and untreated patients with Parkinson’s disease (23 males) were assessed using the Unified Parkinson’s Disease Rating Scale (UPDRS). Then the patients and a group of healthy controls underwent TMS measurements of motor thresholds of the brain, input–output curve, short interval intracortical inhibition, cortical silent period, and intracortical facilitation. Brain plasticity was also measured using paired associative stimulation.
The UPDRS tests did not yield any differences in motor scores between the genders. However, the female patients had a less steep input–output curve than the male patients on the side of the brain more affected by Parkinson’s disease.
The women with Parkinson’s disease also exhibited better preserved short interval intracortical inhibition in both hemispheres, compared with affected men, and tended to have a better response to the paired associative stimulation protocol on the side less affected by symptoms. No gender-specific differences were determined, however, in the motor thresholds, intracortical facilitation, and the cortical silent period. The healthy control group did not show any gender or interhemispheric differences for any of the TMS parameters measured. “The detected gender differences in corticospinal and intracortical excitability in patients with early untreated Parkinson’s disease represent differences in disease pathophysiology. Gender may also prove to be a relevant factor when choosing appropriate treatment,” said Dr. Kojovic.
EAN Develops Guideline on Palliative Care of Patients With Severe MS
A cohort of 934 individuals affected by multiple sclerosis (MS) from seven European countries played an instrumental part in developing the European Academy of Neurology’s (EAN) new guideline on palliative care for people with severe MS. “There were 751 MS patients and 183 caregiver relatives involved,” said Sascha Köpke, PhD, Professor of Nursing Research at the University of Lübeck in Germany.
With the involvement of patients and their families in a new guideline, the EAN is emphasizing shared decision-making as an increasingly important concept that underscores patient autonomy and promotes the individualization of diagnosis and therapy. According to this approach, patients and physicians undergo a detailed consultation and then choose the medical treatment. The EAN has supported this patient-centered approach for a long time, and it is becoming increasingly established in other medical areas as well.
“It was resource- and time-intensive to include consumers in the guideline process, but also highly rewarding,” said Prof. Köpke. “Patients and caregivers really helped us to formulate the guideline in a way that was in line with actual practice and their own needs. We were able to see clearly which of our ideas met with approval or rejection.” The comments were also instructive for the group of EAN experts. They raised new aspects as well as sensitive issues that had been left out of the first draft.
Two approaches were chosen to ensure that consumers would participate. “First, there was an international online survey launched by national MS societies following a trial run involving 20 patients and 18 caregivers. Second, we invited MS patients and caregiver relatives to focus group meetings,” said Prof. Köpke. The majority of participants approved the topics proposed by the EAN group of experts. About 98% agreed to incorporate the subject of multidisciplinary rehabilitation in the guideline. There were 569 free comments, of which 182 (32%) pertained to the specified topics. A further 227 comments (40%) addressed additional topics, of which 16 were pertinent to the guideline. Five of the focus group meetings corroborated the results of the online survey and helped to work out important issues for the individuals affected. “The involvement of patients and caregivers increases the reliability and relevance of the guideline for clinical practice,” said Prof. Köpke.

Childhood Neuromuscular Disease as a Metaphor for the Scientific Advances in Child Neurology of the Last Quarter Century
John B. Bodensteiner, MD
Dr. Bodensteiner is Director of the American Board of Psychiatry and Neurology, Founding Editor and Senior Associate Editor of Seminars in Pediatric Neurology, and Senior Associate Editor of the Journal of Child Neurology.
The impetus for this article is the celebration of 25 years of publication of Neurology Reviews. Child neurology has advanced so much in these years that it is hardly recognizable from the previous state of our understanding. Many components of the discipline include, but are not limited to, epilepsy, headache, demyelinating diseases, autoimmune diseases, neoplastic, neonatal, neuromuscular disease, and developmental conditions. My interest has been related to the neuromuscular diseases of childhood. Thus, I have chosen to describe some of the ways the advances in basic medical science and our understanding of the genetic and molecular mechanisms of disease have altered the way we think about these conditions. For the first time, this knowledge has allowed us to identify targets and techniques for effective intervention and disease modification.
Myotonic Muscular Dystrophy
One example of how the advancement in the discipline of genetics has changed our understanding of disease would be myotonic muscular dystrophy (MyoD1). When I started seeing patients in the mid 1960s, MyoD1, particularly as seen in children, was recognized as an example of autosomal dominant inheritance. The tendency for subsequent generations to be more severely affected than their parents is a phenomenon known as anticipation. Anticipation was recognized, though not explained, with the understanding of the genetic mechanisms of the time. The fact that when the disease affected an infant or newborn it was almost always inherited from the mother was also well established, though the reason for this was also not understood. Actually, during the late 1970s and early 1980s the existence of the phenomenon of anticipation was widely questioned and some publications proposed that anticipation was just an artifact of observation due to the fact that we (medical clinicians) were getting better and thus identifying the disease earlier than in past years. The recognition of the importance of repeated segments of DNA in the pathogenesis of human disease and the subsequent development of the technology to study the phenomenon allowed recognition of this previously unappreciated mechanism of genetic disease causation. This new genetic mechanism explained how anticipation could occur and confirmed it as a real phenomenon. Expanded numbers of tandem repeats probably allowed the explanation of the difference in gene transmission related to the parental gender as well.1

Genetic Insights
Advancements in the understanding of genetic mechanisms of disease have made it possible to begin to identify the molecular mechanisms operating in many previously incomprehensible diseases. The development of laboratory techniques necessary for the identification of these genetic abnormalities has brought the recognition of these disease mechanisms into clinical practice. Twenty-five years ago, the ability to identify alterations in DNA sequences, the presence of deletions/duplications and expansion of trinucleotide repeats, as well as the determination (and recognition of the significance) of gene copy number, was not available to the clinician. This advancement in genetic understanding has, in turn, allowed the identification of therapeutic targets in the hope of being able to moderate or eliminate the consequence of the defective gene.
Spinal Muscular Atrophy
In the last few years, the use of relatively small molecules such as oligonucleotides to alter the transcription of mutated RNA to produce a functioning protein has been developed. Because they are small molecules, they can be delivered with relative ease to the desired site. This technology has been applied to the treatment of spinal muscular atrophy (SMA) with considerable success.
Survival motor neuron gene product is essential for the health of the anterior horn cells of the spinal cord of the central nervous system. In the human genome there are two copies of the survival motor neuron gene, labeled SMN1 and SMN2. SMN1 normally produces a functional protein that is stable and necessary for the anterior horn survival. All patients with SMA have mutations in SMN1 that result in the gene being inactive. The protein product of SMN2 is usually truncated and not very stable, though it has some function. The severity of the resulting disease is influenced by the number of copies of the SMN2 gene present, and thus the available amount of partially functional SMN2 product. The oligonucleotide, in this case delivered via lumbar puncture, serves to alter the splicing of the protein product from SMN2, allowing the production of the more effective and stable protein with properties more similar to the SMN1 protein, thus ameliorating the effect of the SMN1 mutation. The patient, however, requires the administration of the therapeutic oligonucleotide indefinitely.
Gene Editing
The Gold Ring of therapeutic intervention, being able to actually correct the gene defect in any given disease, is still a goal of medical science. For the first time, this is a realistic aspiration due to the identification, development, and application of the gene editing tool Cas9 and CRISPR-Cas9 techniques.2 This new technology allows the production of a custom piece of DNA (cassette) that can repair the defective gene if incorporated into the DNA sequence of the host. The techniques necessary to introduce the therapeutic cassette to the affected cell and encourage the incorporation of the new material into the DNA have largely been developed already. The hurdle has always been the difficulty producing the therapeutic cassette for the given defect. The application of the CRISPR-Cas9 technology offers the promise of being able to produce a custom cassette specific for the given mutation, and thus potentially correcting the mutation involved in a wide variety of diseases.
The last quarter century has seen the expansion of the genetic techniques to allow the recognition and diagnosis of diseases that had resisted definitive diagnosis up to this time. These techniques have also led to the uncovering of disease mechanisms previously opaque to our understanding. The next quarter century promises to produce an explosion of therapeutic possibilities on a scale previously unimaginable. Despite the considerable initial expense of these new therapies, I believe they will be of incalculable value going forward.
References
1. de Koning AP, Gu W, Castoe TA, et al. Repetitive elements may comprise over two-thirds of the human genome. PLoS Genet. 2011;7(12):e1002384.
2. Adli M. The CRISPR tool kit for genome editing and beyond. Nat Commun. 2018;9(1):1911.
John B. Bodensteiner, MD
Dr. Bodensteiner is Director of the American Board of Psychiatry and Neurology, Founding Editor and Senior Associate Editor of Seminars in Pediatric Neurology, and Senior Associate Editor of the Journal of Child Neurology.
The impetus for this article is the celebration of 25 years of publication of Neurology Reviews. Child neurology has advanced so much in these years that it is hardly recognizable from the previous state of our understanding. Many components of the discipline include, but are not limited to, epilepsy, headache, demyelinating diseases, autoimmune diseases, neoplastic, neonatal, neuromuscular disease, and developmental conditions. My interest has been related to the neuromuscular diseases of childhood. Thus, I have chosen to describe some of the ways the advances in basic medical science and our understanding of the genetic and molecular mechanisms of disease have altered the way we think about these conditions. For the first time, this knowledge has allowed us to identify targets and techniques for effective intervention and disease modification.
Myotonic Muscular Dystrophy
One example of how the advancement in the discipline of genetics has changed our understanding of disease would be myotonic muscular dystrophy (MyoD1). When I started seeing patients in the mid 1960s, MyoD1, particularly as seen in children, was recognized as an example of autosomal dominant inheritance. The tendency for subsequent generations to be more severely affected than their parents is a phenomenon known as anticipation. Anticipation was recognized, though not explained, with the understanding of the genetic mechanisms of the time. The fact that when the disease affected an infant or newborn it was almost always inherited from the mother was also well established, though the reason for this was also not understood. Actually, during the late 1970s and early 1980s the existence of the phenomenon of anticipation was widely questioned and some publications proposed that anticipation was just an artifact of observation due to the fact that we (medical clinicians) were getting better and thus identifying the disease earlier than in past years. The recognition of the importance of repeated segments of DNA in the pathogenesis of human disease and the subsequent development of the technology to study the phenomenon allowed recognition of this previously unappreciated mechanism of genetic disease causation. This new genetic mechanism explained how anticipation could occur and confirmed it as a real phenomenon. Expanded numbers of tandem repeats probably allowed the explanation of the difference in gene transmission related to the parental gender as well.1
Genetic Insights
Advancements in the understanding of genetic mechanisms of disease have made it possible to begin to identify the molecular mechanisms operating in many previously incomprehensible diseases. The development of laboratory techniques necessary for the identification of these genetic abnormalities has brought the recognition of these disease mechanisms into clinical practice. Twenty-five years ago, the ability to identify alterations in DNA sequences, the presence of deletions/duplications and expansion of trinucleotide repeats, as well as the determination (and recognition of the significance) of gene copy number, was not available to the clinician. This advancement in genetic understanding has, in turn, allowed the identification of therapeutic targets in the hope of being able to moderate or eliminate the consequence of the defective gene.
Spinal Muscular Atrophy
In the last few years, the use of relatively small molecules such as oligonucleotides to alter the transcription of mutated RNA to produce a functioning protein has been developed. Because they are small molecules, they can be delivered with relative ease to the desired site. This technology has been applied to the treatment of spinal muscular atrophy (SMA) with considerable success.
Survival motor neuron gene product is essential for the health of the anterior horn cells of the spinal cord of the central nervous system. In the human genome there are two copies of the survival motor neuron gene, labeled SMN1 and SMN2. SMN1 normally produces a functional protein that is stable and necessary for the anterior horn survival. All patients with SMA have mutations in SMN1 that result in the gene being inactive. The protein product of SMN2 is usually truncated and not very stable, though it has some function. The severity of the resulting disease is influenced by the number of copies of the SMN2 gene present, and thus the available amount of partially functional SMN2 product. The oligonucleotide, in this case delivered via lumbar puncture, serves to alter the splicing of the protein product from SMN2, allowing the production of the more effective and stable protein with properties more similar to the SMN1 protein, thus ameliorating the effect of the SMN1 mutation. The patient, however, requires the administration of the therapeutic oligonucleotide indefinitely.
Gene Editing
The Gold Ring of therapeutic intervention, being able to actually correct the gene defect in any given disease, is still a goal of medical science. For the first time, this is a realistic aspiration due to the identification, development, and application of the gene editing tool Cas9 and CRISPR-Cas9 techniques.2 This new technology allows the production of a custom piece of DNA (cassette) that can repair the defective gene if incorporated into the DNA sequence of the host. The techniques necessary to introduce the therapeutic cassette to the affected cell and encourage the incorporation of the new material into the DNA have largely been developed already. The hurdle has always been the difficulty producing the therapeutic cassette for the given defect. The application of the CRISPR-Cas9 technology offers the promise of being able to produce a custom cassette specific for the given mutation, and thus potentially correcting the mutation involved in a wide variety of diseases.
The last quarter century has seen the expansion of the genetic techniques to allow the recognition and diagnosis of diseases that had resisted definitive diagnosis up to this time. These techniques have also led to the uncovering of disease mechanisms previously opaque to our understanding. The next quarter century promises to produce an explosion of therapeutic possibilities on a scale previously unimaginable. Despite the considerable initial expense of these new therapies, I believe they will be of incalculable value going forward.
References
1. de Koning AP, Gu W, Castoe TA, et al. Repetitive elements may comprise over two-thirds of the human genome. PLoS Genet. 2011;7(12):e1002384.
2. Adli M. The CRISPR tool kit for genome editing and beyond. Nat Commun. 2018;9(1):1911.
John B. Bodensteiner, MD
Dr. Bodensteiner is Director of the American Board of Psychiatry and Neurology, Founding Editor and Senior Associate Editor of Seminars in Pediatric Neurology, and Senior Associate Editor of the Journal of Child Neurology.
The impetus for this article is the celebration of 25 years of publication of Neurology Reviews. Child neurology has advanced so much in these years that it is hardly recognizable from the previous state of our understanding. Many components of the discipline include, but are not limited to, epilepsy, headache, demyelinating diseases, autoimmune diseases, neoplastic, neonatal, neuromuscular disease, and developmental conditions. My interest has been related to the neuromuscular diseases of childhood. Thus, I have chosen to describe some of the ways the advances in basic medical science and our understanding of the genetic and molecular mechanisms of disease have altered the way we think about these conditions. For the first time, this knowledge has allowed us to identify targets and techniques for effective intervention and disease modification.
Myotonic Muscular Dystrophy
One example of how the advancement in the discipline of genetics has changed our understanding of disease would be myotonic muscular dystrophy (MyoD1). When I started seeing patients in the mid 1960s, MyoD1, particularly as seen in children, was recognized as an example of autosomal dominant inheritance. The tendency for subsequent generations to be more severely affected than their parents is a phenomenon known as anticipation. Anticipation was recognized, though not explained, with the understanding of the genetic mechanisms of the time. The fact that when the disease affected an infant or newborn it was almost always inherited from the mother was also well established, though the reason for this was also not understood. Actually, during the late 1970s and early 1980s the existence of the phenomenon of anticipation was widely questioned and some publications proposed that anticipation was just an artifact of observation due to the fact that we (medical clinicians) were getting better and thus identifying the disease earlier than in past years. The recognition of the importance of repeated segments of DNA in the pathogenesis of human disease and the subsequent development of the technology to study the phenomenon allowed recognition of this previously unappreciated mechanism of genetic disease causation. This new genetic mechanism explained how anticipation could occur and confirmed it as a real phenomenon. Expanded numbers of tandem repeats probably allowed the explanation of the difference in gene transmission related to the parental gender as well.1
Genetic Insights
Advancements in the understanding of genetic mechanisms of disease have made it possible to begin to identify the molecular mechanisms operating in many previously incomprehensible diseases. The development of laboratory techniques necessary for the identification of these genetic abnormalities has brought the recognition of these disease mechanisms into clinical practice. Twenty-five years ago, the ability to identify alterations in DNA sequences, the presence of deletions/duplications and expansion of trinucleotide repeats, as well as the determination (and recognition of the significance) of gene copy number, was not available to the clinician. This advancement in genetic understanding has, in turn, allowed the identification of therapeutic targets in the hope of being able to moderate or eliminate the consequence of the defective gene.
Spinal Muscular Atrophy
In the last few years, the use of relatively small molecules such as oligonucleotides to alter the transcription of mutated RNA to produce a functioning protein has been developed. Because they are small molecules, they can be delivered with relative ease to the desired site. This technology has been applied to the treatment of spinal muscular atrophy (SMA) with considerable success.
Survival motor neuron gene product is essential for the health of the anterior horn cells of the spinal cord of the central nervous system. In the human genome there are two copies of the survival motor neuron gene, labeled SMN1 and SMN2. SMN1 normally produces a functional protein that is stable and necessary for the anterior horn survival. All patients with SMA have mutations in SMN1 that result in the gene being inactive. The protein product of SMN2 is usually truncated and not very stable, though it has some function. The severity of the resulting disease is influenced by the number of copies of the SMN2 gene present, and thus the available amount of partially functional SMN2 product. The oligonucleotide, in this case delivered via lumbar puncture, serves to alter the splicing of the protein product from SMN2, allowing the production of the more effective and stable protein with properties more similar to the SMN1 protein, thus ameliorating the effect of the SMN1 mutation. The patient, however, requires the administration of the therapeutic oligonucleotide indefinitely.
Gene Editing
The Gold Ring of therapeutic intervention, being able to actually correct the gene defect in any given disease, is still a goal of medical science. For the first time, this is a realistic aspiration due to the identification, development, and application of the gene editing tool Cas9 and CRISPR-Cas9 techniques.2 This new technology allows the production of a custom piece of DNA (cassette) that can repair the defective gene if incorporated into the DNA sequence of the host. The techniques necessary to introduce the therapeutic cassette to the affected cell and encourage the incorporation of the new material into the DNA have largely been developed already. The hurdle has always been the difficulty producing the therapeutic cassette for the given defect. The application of the CRISPR-Cas9 technology offers the promise of being able to produce a custom cassette specific for the given mutation, and thus potentially correcting the mutation involved in a wide variety of diseases.
The last quarter century has seen the expansion of the genetic techniques to allow the recognition and diagnosis of diseases that had resisted definitive diagnosis up to this time. These techniques have also led to the uncovering of disease mechanisms previously opaque to our understanding. The next quarter century promises to produce an explosion of therapeutic possibilities on a scale previously unimaginable. Despite the considerable initial expense of these new therapies, I believe they will be of incalculable value going forward.
References
1. de Koning AP, Gu W, Castoe TA, et al. Repetitive elements may comprise over two-thirds of the human genome. PLoS Genet. 2011;7(12):e1002384.
2. Adli M. The CRISPR tool kit for genome editing and beyond. Nat Commun. 2018;9(1):1911.
Tasimelteon May Be Effective for Jet Lag Disorder
The drug increased total sleep time by about an hour and a half.
BALTIMORE—Tasimelteon, a drug approved for non–24-hour sleep-wake disorder, has been shown to increase sleep times in travelers with jet lag, according to results from a phase III trial. “Tasimelteon demonstrated an increase in total sleep time of 85 minutes versus placebo and also demonstrated improvement in next-day alertness versus placebo,” said Christoph Polymeropoulos, MD, Medical Director of Vanda Pharmaceuticals, and colleagues at the 32nd Annual Meeting of the Associated Professional Sleep Societies.
Tasimelteon, sold under the trade name Hetlioz, is a melatonin receptor agonist that is FDA-approved for non–24-hour sleep-wake disorder but not for the treatment of
“Jet lag disorder is a circadian disorder frequently observed in millions of travelers who cross multiple time zones,” Dr. Polymeropoulos said. “Jet lag disorder is characterized by nighttime sleep disruption, decrease in daytime alertness, and impairment in social and occupational function.”
The JET8 trial induced the circadian challenge equivalent to crossing eight time zones. The study involved 318 individuals randomized evenly to 20 mg tasimelteon or placebo 30 minutes before bedtime. The primary end point of the study was total sleep time in the first two-thirds of sleep time, as measured by polysomnography.
Those on tasimelteon averaged 216.4 minutes of total sleep time in the first two-thirds of their sleep time versus 156.1 minutes for those on placebo, Dr. Polymeropoulos said. Total sleep times were 315.8 minutes versus 230.3 minutes, respectively. “For total sleep time, the tasimelteon subjects gained about an hour and a half, as measured by polysomnography,” Dr. Polymeropoulos said.
Other key markers the trial measured were latency to persistent sleep and wakefulness after sleep onset. They measured 15 minutes less and 74.6 minutes less, respectively, in the tasimelteon arm.
Dr. Polymeropoulos also disclosed early results of a second trial of tasimelteon in jet lag disorder: the JET Study, a two-phase transatlantic travel study of 25 patients. The subjects flew from four US cities to London for three nights, receiving tasimelteon or placebo each night in London. The study was terminated before reaching its enrollment goal of 90 patients because of its complexity, Vanda said in a separate press release. Over three nights of study, participants in the tasimelteon arm gained a total of about 130 minutes of sleep versus 40 minutes for those in the placebo arm, Dr. Polymeropoulos said.
Vanda plans to file a supplemental new drug application for tasimelteon for the treatment of jet lag disorder in the second half of this year.
Suggested Reading
Herxheimer A. Jet lag. BMJ Clin Evid. 2014 Apr 29;pii2303.
Srinivasan V, Singh J, Pandi-Perumal SR, et al. Jet lag, circadian rhythm sleep disturbances, and depression: the role of melatonin and its analogs. Adv Ther. 2010;27(11):796-813.
The drug increased total sleep time by about an hour and a half.
The drug increased total sleep time by about an hour and a half.
BALTIMORE—Tasimelteon, a drug approved for non–24-hour sleep-wake disorder, has been shown to increase sleep times in travelers with jet lag, according to results from a phase III trial. “Tasimelteon demonstrated an increase in total sleep time of 85 minutes versus placebo and also demonstrated improvement in next-day alertness versus placebo,” said Christoph Polymeropoulos, MD, Medical Director of Vanda Pharmaceuticals, and colleagues at the 32nd Annual Meeting of the Associated Professional Sleep Societies.
Tasimelteon, sold under the trade name Hetlioz, is a melatonin receptor agonist that is FDA-approved for non–24-hour sleep-wake disorder but not for the treatment of
“Jet lag disorder is a circadian disorder frequently observed in millions of travelers who cross multiple time zones,” Dr. Polymeropoulos said. “Jet lag disorder is characterized by nighttime sleep disruption, decrease in daytime alertness, and impairment in social and occupational function.”
The JET8 trial induced the circadian challenge equivalent to crossing eight time zones. The study involved 318 individuals randomized evenly to 20 mg tasimelteon or placebo 30 minutes before bedtime. The primary end point of the study was total sleep time in the first two-thirds of sleep time, as measured by polysomnography.
Those on tasimelteon averaged 216.4 minutes of total sleep time in the first two-thirds of their sleep time versus 156.1 minutes for those on placebo, Dr. Polymeropoulos said. Total sleep times were 315.8 minutes versus 230.3 minutes, respectively. “For total sleep time, the tasimelteon subjects gained about an hour and a half, as measured by polysomnography,” Dr. Polymeropoulos said.
Other key markers the trial measured were latency to persistent sleep and wakefulness after sleep onset. They measured 15 minutes less and 74.6 minutes less, respectively, in the tasimelteon arm.
Dr. Polymeropoulos also disclosed early results of a second trial of tasimelteon in jet lag disorder: the JET Study, a two-phase transatlantic travel study of 25 patients. The subjects flew from four US cities to London for three nights, receiving tasimelteon or placebo each night in London. The study was terminated before reaching its enrollment goal of 90 patients because of its complexity, Vanda said in a separate press release. Over three nights of study, participants in the tasimelteon arm gained a total of about 130 minutes of sleep versus 40 minutes for those in the placebo arm, Dr. Polymeropoulos said.
Vanda plans to file a supplemental new drug application for tasimelteon for the treatment of jet lag disorder in the second half of this year.
Suggested Reading
Herxheimer A. Jet lag. BMJ Clin Evid. 2014 Apr 29;pii2303.
Srinivasan V, Singh J, Pandi-Perumal SR, et al. Jet lag, circadian rhythm sleep disturbances, and depression: the role of melatonin and its analogs. Adv Ther. 2010;27(11):796-813.
BALTIMORE—Tasimelteon, a drug approved for non–24-hour sleep-wake disorder, has been shown to increase sleep times in travelers with jet lag, according to results from a phase III trial. “Tasimelteon demonstrated an increase in total sleep time of 85 minutes versus placebo and also demonstrated improvement in next-day alertness versus placebo,” said Christoph Polymeropoulos, MD, Medical Director of Vanda Pharmaceuticals, and colleagues at the 32nd Annual Meeting of the Associated Professional Sleep Societies.
Tasimelteon, sold under the trade name Hetlioz, is a melatonin receptor agonist that is FDA-approved for non–24-hour sleep-wake disorder but not for the treatment of
“Jet lag disorder is a circadian disorder frequently observed in millions of travelers who cross multiple time zones,” Dr. Polymeropoulos said. “Jet lag disorder is characterized by nighttime sleep disruption, decrease in daytime alertness, and impairment in social and occupational function.”
The JET8 trial induced the circadian challenge equivalent to crossing eight time zones. The study involved 318 individuals randomized evenly to 20 mg tasimelteon or placebo 30 minutes before bedtime. The primary end point of the study was total sleep time in the first two-thirds of sleep time, as measured by polysomnography.
Those on tasimelteon averaged 216.4 minutes of total sleep time in the first two-thirds of their sleep time versus 156.1 minutes for those on placebo, Dr. Polymeropoulos said. Total sleep times were 315.8 minutes versus 230.3 minutes, respectively. “For total sleep time, the tasimelteon subjects gained about an hour and a half, as measured by polysomnography,” Dr. Polymeropoulos said.
Other key markers the trial measured were latency to persistent sleep and wakefulness after sleep onset. They measured 15 minutes less and 74.6 minutes less, respectively, in the tasimelteon arm.
Dr. Polymeropoulos also disclosed early results of a second trial of tasimelteon in jet lag disorder: the JET Study, a two-phase transatlantic travel study of 25 patients. The subjects flew from four US cities to London for three nights, receiving tasimelteon or placebo each night in London. The study was terminated before reaching its enrollment goal of 90 patients because of its complexity, Vanda said in a separate press release. Over three nights of study, participants in the tasimelteon arm gained a total of about 130 minutes of sleep versus 40 minutes for those in the placebo arm, Dr. Polymeropoulos said.
Vanda plans to file a supplemental new drug application for tasimelteon for the treatment of jet lag disorder in the second half of this year.
Suggested Reading
Herxheimer A. Jet lag. BMJ Clin Evid. 2014 Apr 29;pii2303.
Srinivasan V, Singh J, Pandi-Perumal SR, et al. Jet lag, circadian rhythm sleep disturbances, and depression: the role of melatonin and its analogs. Adv Ther. 2010;27(11):796-813.