User login
Should PCPs take over chronic HCV treatment?
ESTES PARK, COLO. – Direct-acting antiviral (DAA) therapy for chronic hepatitis C virus (HCV) infection has progressed to the point that it’s time for primary care physicians to take on the treatment of all affected patients who don’t have advanced fibrosis or other complex forms of the disease, Michael Kriss, MD, asserted at a conference on internal medicine sponsored by the University of Colorado.

declared Dr. Kriss, a gastroenterologist at the university.
Referral to a specialist should be reserved for those more complex patients with stage 3 or 4 fibrosis, hepatocellular carcinoma, coinfection with HIV or hepatitis B virus, end-stage organ disease being considered for transplantation, prior exposure to an NS5A inhibitor, or concomitant secondary liver disease, such as nonalcoholic steatohepatitis, he continued.
Treatment of chronic HCV now entails just 8-12 weeks of DAA therapy, with a cure rate greater than 95% and almost no side effects. The costs have come down, too, because of increased competition.
The epidemiology of HCV infection is changing. The opioid epidemic is driving an increased incidence of acute infection, with nearly 34,000 new cases per year, most of which will go on to chronic infection. Moreover, 93% of acutely infected individuals and half of the estimated 3.5 million Americans with chronic HCV are unaware they are infected. The scope of the problem is too big for gastroenterologists and infectious disease specialists to handle alone, according to Dr. Kriss.
Contemporary treatment of HCV involves a 6-step program that’s simpler than that of many of the diseases primary care physicians currently manage.
1) Confirm chronicity by two measurements of HCV RNA obtained 6 months apart.
2) Stage the patient’s fibrosis.
3) Order a baseline cross-sectional ultrasound to exclude cirrhosis or hepatocellular carcinoma, since the fibrosis staging methods aren’t foolproof.
4) Make sure the patient is still positive for HCV RNA prior to therapy.
5) Commence DAA therapy. The simplest regimen is 8 weeks of glecaprevir/pibrentasvir (Mavyret), provided it’s approved by the patient’s insurance.
6) Get a repeat HCV RNA 12 weeks after conclusion of treatment to confirm there is a sustained virologic response.
The critical part is step 2 because that’s how primary care physicians will decide which patients to treat in their office and which to refer to a specialist. Many biomarkers are available, some proprietary and others gratis. Dr. Kriss is particularly partial to the free Fibrosis-4 (Fib-4) calculator, which provides an estimate of the amount of liver scarring based upon the patient’s age, liver enzyme levels, and platelet count.
“This is really a valuable, extremely well-validated tool that any of you can use in your clinic,” he said.
The American Association for the Study of Liver Disease/Infectious Diseases Society of America hepatitis C guidelines state that the nonproprietary biomarker assays are equivalent to transient elastography for staging fibrosis. Those guidelines are an “outstanding” and extremely user-friendly resource for primary care physicians interested in taking on the treatment of chronic HCV, Dr. Kriss added.
In selecting a DAA, another key resource is the HEP Drug Interactions website, which enables physicians to identify potentially problematic drug-drug interactions. The two most important interactions involve statins or proton pump inhibitors.
Recent studies have shown that the benefits of achieving a sustained virologic response include a clinically meaningful regression of advanced fibrosis at 1 year after treatment in roughly half of patients (Dig Dis Sci. 2018 Feb;63[2]:486-92) and a reduced risk of developing hepatocellular carcinoma (Hepatology. 2018 Jun;67[6]:2244-53).
Models of remote consultation pathways to link primary care providers with consultant HCV specialists are being developed. In a study of 600 patients at federally qualified community health centers in Washington, the risk-adjusted cure rate was 90.4% among patients assigned to a nurse practitioner, 87.6% if DAA therapy was prescribed by a primary care physician, and 84.8% if treated by a specialist. Treatment visit adherence followed the same pattern and correlated with cure rates (Ann Intern Med. 2017 Sep 5;167[5]:311-8).
“Patients might be better off seeing someone they know instead of somebody like me who they’re only going to see one time,” Dr. Kriss observed.
Turning to a couple of controversial expansions of DAA into new populations, Dr. Kriss noted that the AASLD/IDSA guidelines state that active intravenous drug use should not be considered a contraindication to HCV therapy.
“Scaling up HCV treatment in persons who inject drugs is necessary to positively impact the HCV epidemic in the U.S. and globally,” according to the guidelines.
This message was recently underscored by the positive results of the seven-country SIMPLIFY trial, in which 12 weeks of velpatasvir-sofosbuvir (Epclusa) in a population of recent IV drug users achieved a 97% cure rate, with only one reinfection in this high-risk population (Lancet Gastroenterol Hepatol. 2018 Mar;3[3]:153-61).
The hottest controversy in hepatology has been whether to place HCV-positive donor organs in HCV-negative recipients.
“This is intentionally giving hepatitis C to the recipient knowing that he can be cured. Because treatment cure rates are so high, I predict this will become the standard of care in the next year or two,” Dr. Kriss said.
He reported having no financial conflicts regarding his presentation.
.
ESTES PARK, COLO. – Direct-acting antiviral (DAA) therapy for chronic hepatitis C virus (HCV) infection has progressed to the point that it’s time for primary care physicians to take on the treatment of all affected patients who don’t have advanced fibrosis or other complex forms of the disease, Michael Kriss, MD, asserted at a conference on internal medicine sponsored by the University of Colorado.
declared Dr. Kriss, a gastroenterologist at the university.
Referral to a specialist should be reserved for those more complex patients with stage 3 or 4 fibrosis, hepatocellular carcinoma, coinfection with HIV or hepatitis B virus, end-stage organ disease being considered for transplantation, prior exposure to an NS5A inhibitor, or concomitant secondary liver disease, such as nonalcoholic steatohepatitis, he continued.
Treatment of chronic HCV now entails just 8-12 weeks of DAA therapy, with a cure rate greater than 95% and almost no side effects. The costs have come down, too, because of increased competition.
The epidemiology of HCV infection is changing. The opioid epidemic is driving an increased incidence of acute infection, with nearly 34,000 new cases per year, most of which will go on to chronic infection. Moreover, 93% of acutely infected individuals and half of the estimated 3.5 million Americans with chronic HCV are unaware they are infected. The scope of the problem is too big for gastroenterologists and infectious disease specialists to handle alone, according to Dr. Kriss.
Contemporary treatment of HCV involves a 6-step program that’s simpler than that of many of the diseases primary care physicians currently manage.
1) Confirm chronicity by two measurements of HCV RNA obtained 6 months apart.
2) Stage the patient’s fibrosis.
3) Order a baseline cross-sectional ultrasound to exclude cirrhosis or hepatocellular carcinoma, since the fibrosis staging methods aren’t foolproof.
4) Make sure the patient is still positive for HCV RNA prior to therapy.
5) Commence DAA therapy. The simplest regimen is 8 weeks of glecaprevir/pibrentasvir (Mavyret), provided it’s approved by the patient’s insurance.
6) Get a repeat HCV RNA 12 weeks after conclusion of treatment to confirm there is a sustained virologic response.
The critical part is step 2 because that’s how primary care physicians will decide which patients to treat in their office and which to refer to a specialist. Many biomarkers are available, some proprietary and others gratis. Dr. Kriss is particularly partial to the free Fibrosis-4 (Fib-4) calculator, which provides an estimate of the amount of liver scarring based upon the patient’s age, liver enzyme levels, and platelet count.
“This is really a valuable, extremely well-validated tool that any of you can use in your clinic,” he said.
The American Association for the Study of Liver Disease/Infectious Diseases Society of America hepatitis C guidelines state that the nonproprietary biomarker assays are equivalent to transient elastography for staging fibrosis. Those guidelines are an “outstanding” and extremely user-friendly resource for primary care physicians interested in taking on the treatment of chronic HCV, Dr. Kriss added.
In selecting a DAA, another key resource is the HEP Drug Interactions website, which enables physicians to identify potentially problematic drug-drug interactions. The two most important interactions involve statins or proton pump inhibitors.
Recent studies have shown that the benefits of achieving a sustained virologic response include a clinically meaningful regression of advanced fibrosis at 1 year after treatment in roughly half of patients (Dig Dis Sci. 2018 Feb;63[2]:486-92) and a reduced risk of developing hepatocellular carcinoma (Hepatology. 2018 Jun;67[6]:2244-53).
Models of remote consultation pathways to link primary care providers with consultant HCV specialists are being developed. In a study of 600 patients at federally qualified community health centers in Washington, the risk-adjusted cure rate was 90.4% among patients assigned to a nurse practitioner, 87.6% if DAA therapy was prescribed by a primary care physician, and 84.8% if treated by a specialist. Treatment visit adherence followed the same pattern and correlated with cure rates (Ann Intern Med. 2017 Sep 5;167[5]:311-8).
“Patients might be better off seeing someone they know instead of somebody like me who they’re only going to see one time,” Dr. Kriss observed.
Turning to a couple of controversial expansions of DAA into new populations, Dr. Kriss noted that the AASLD/IDSA guidelines state that active intravenous drug use should not be considered a contraindication to HCV therapy.
“Scaling up HCV treatment in persons who inject drugs is necessary to positively impact the HCV epidemic in the U.S. and globally,” according to the guidelines.
This message was recently underscored by the positive results of the seven-country SIMPLIFY trial, in which 12 weeks of velpatasvir-sofosbuvir (Epclusa) in a population of recent IV drug users achieved a 97% cure rate, with only one reinfection in this high-risk population (Lancet Gastroenterol Hepatol. 2018 Mar;3[3]:153-61).
The hottest controversy in hepatology has been whether to place HCV-positive donor organs in HCV-negative recipients.
“This is intentionally giving hepatitis C to the recipient knowing that he can be cured. Because treatment cure rates are so high, I predict this will become the standard of care in the next year or two,” Dr. Kriss said.
He reported having no financial conflicts regarding his presentation.
.
ESTES PARK, COLO. – Direct-acting antiviral (DAA) therapy for chronic hepatitis C virus (HCV) infection has progressed to the point that it’s time for primary care physicians to take on the treatment of all affected patients who don’t have advanced fibrosis or other complex forms of the disease, Michael Kriss, MD, asserted at a conference on internal medicine sponsored by the University of Colorado.
declared Dr. Kriss, a gastroenterologist at the university.
Referral to a specialist should be reserved for those more complex patients with stage 3 or 4 fibrosis, hepatocellular carcinoma, coinfection with HIV or hepatitis B virus, end-stage organ disease being considered for transplantation, prior exposure to an NS5A inhibitor, or concomitant secondary liver disease, such as nonalcoholic steatohepatitis, he continued.
Treatment of chronic HCV now entails just 8-12 weeks of DAA therapy, with a cure rate greater than 95% and almost no side effects. The costs have come down, too, because of increased competition.
The epidemiology of HCV infection is changing. The opioid epidemic is driving an increased incidence of acute infection, with nearly 34,000 new cases per year, most of which will go on to chronic infection. Moreover, 93% of acutely infected individuals and half of the estimated 3.5 million Americans with chronic HCV are unaware they are infected. The scope of the problem is too big for gastroenterologists and infectious disease specialists to handle alone, according to Dr. Kriss.
Contemporary treatment of HCV involves a 6-step program that’s simpler than that of many of the diseases primary care physicians currently manage.
1) Confirm chronicity by two measurements of HCV RNA obtained 6 months apart.
2) Stage the patient’s fibrosis.
3) Order a baseline cross-sectional ultrasound to exclude cirrhosis or hepatocellular carcinoma, since the fibrosis staging methods aren’t foolproof.
4) Make sure the patient is still positive for HCV RNA prior to therapy.
5) Commence DAA therapy. The simplest regimen is 8 weeks of glecaprevir/pibrentasvir (Mavyret), provided it’s approved by the patient’s insurance.
6) Get a repeat HCV RNA 12 weeks after conclusion of treatment to confirm there is a sustained virologic response.
The critical part is step 2 because that’s how primary care physicians will decide which patients to treat in their office and which to refer to a specialist. Many biomarkers are available, some proprietary and others gratis. Dr. Kriss is particularly partial to the free Fibrosis-4 (Fib-4) calculator, which provides an estimate of the amount of liver scarring based upon the patient’s age, liver enzyme levels, and platelet count.
“This is really a valuable, extremely well-validated tool that any of you can use in your clinic,” he said.
The American Association for the Study of Liver Disease/Infectious Diseases Society of America hepatitis C guidelines state that the nonproprietary biomarker assays are equivalent to transient elastography for staging fibrosis. Those guidelines are an “outstanding” and extremely user-friendly resource for primary care physicians interested in taking on the treatment of chronic HCV, Dr. Kriss added.
In selecting a DAA, another key resource is the HEP Drug Interactions website, which enables physicians to identify potentially problematic drug-drug interactions. The two most important interactions involve statins or proton pump inhibitors.
Recent studies have shown that the benefits of achieving a sustained virologic response include a clinically meaningful regression of advanced fibrosis at 1 year after treatment in roughly half of patients (Dig Dis Sci. 2018 Feb;63[2]:486-92) and a reduced risk of developing hepatocellular carcinoma (Hepatology. 2018 Jun;67[6]:2244-53).
Models of remote consultation pathways to link primary care providers with consultant HCV specialists are being developed. In a study of 600 patients at federally qualified community health centers in Washington, the risk-adjusted cure rate was 90.4% among patients assigned to a nurse practitioner, 87.6% if DAA therapy was prescribed by a primary care physician, and 84.8% if treated by a specialist. Treatment visit adherence followed the same pattern and correlated with cure rates (Ann Intern Med. 2017 Sep 5;167[5]:311-8).
“Patients might be better off seeing someone they know instead of somebody like me who they’re only going to see one time,” Dr. Kriss observed.
Turning to a couple of controversial expansions of DAA into new populations, Dr. Kriss noted that the AASLD/IDSA guidelines state that active intravenous drug use should not be considered a contraindication to HCV therapy.
“Scaling up HCV treatment in persons who inject drugs is necessary to positively impact the HCV epidemic in the U.S. and globally,” according to the guidelines.
This message was recently underscored by the positive results of the seven-country SIMPLIFY trial, in which 12 weeks of velpatasvir-sofosbuvir (Epclusa) in a population of recent IV drug users achieved a 97% cure rate, with only one reinfection in this high-risk population (Lancet Gastroenterol Hepatol. 2018 Mar;3[3]:153-61).
The hottest controversy in hepatology has been whether to place HCV-positive donor organs in HCV-negative recipients.
“This is intentionally giving hepatitis C to the recipient knowing that he can be cured. Because treatment cure rates are so high, I predict this will become the standard of care in the next year or two,” Dr. Kriss said.
He reported having no financial conflicts regarding his presentation.
.
REPORTING FROM COLORADO IM
Marzeptacog alfa reduces bleeding episodes in hemophilia with inhibitors
The activated factor VIIa variant according to researchers.
To date, the trial has enrolled five patients with hemophilia A or B and inhibitors. Catalyst would not disclose how many patients have hemophilia A and how many have hemophilia B. Three patients have completed dosing with marzeptacog alfa in a phase 2/3 study. None of these patients experienced bleeding during treatment, and none have developed antidrug antibodies or reported injection site reactions. As for the other two patients enrolled in this study, one withdrew consent, and one died of an adverse event unrelated to marzeptacog alfa.
Howard Levy, chief medical officer of Catalyst Biosciences, which has been developing this drug and sponsored the trial, presented these data at the 2018 Hemophilia Drug Development Summit in Boston.
The goal of this ongoing trial is to determine whether daily subcutaneous injections of marzeptacog alfa can eliminate or minimize spontaneous bleeding episodes. The primary endpoint is a reduction in annualized bleed rate (ABR), compared with each individual’s recorded historical ABR.
One patient with a historic ABR of 26.7 experienced a bleed on day 46 when receiving marzeptacog alfa at 30 mcg/kg but then had no bleeds after 50 days of treatment with marzeptacog alfa at 60 mcg/kg. This patient did experience a bleed 16 days after the end of dosing at 60 mcg/kg.
A second patient with a historic ABR of 16.6 had no bleeds when receiving marzeptacog alfa at 30 mcg/kg for 50 days.
And a third patient with a historic ABR of 15.9 had no bleeds when receiving marzeptacog alfa at 30 mcg/kg for 44 days.
“The data from these 3 individuals support the efficacy of [marzeptacog alfa] to reduce annualized bleed rates after daily subcutaneous injections,” said Nassim Usman, PhD, chief executive officer of Catalyst Biosciences. “Importantly, to date, we have not observed any injection site reactions nor any antidrug antibodies after more than 200 subcutaneous doses of [marzeptacog alfa].”
A fourth patient with a historic ABR of 18.3 had a fatal hemorrhagic stroke on day 11 that was considered unrelated to marzeptacog alfa. The patient had previously treated hypertension that was going untreated at the time of death.
A fifth patient with a historic ABR of 12.2 withdrew consent.
The activated factor VIIa variant according to researchers.
To date, the trial has enrolled five patients with hemophilia A or B and inhibitors. Catalyst would not disclose how many patients have hemophilia A and how many have hemophilia B. Three patients have completed dosing with marzeptacog alfa in a phase 2/3 study. None of these patients experienced bleeding during treatment, and none have developed antidrug antibodies or reported injection site reactions. As for the other two patients enrolled in this study, one withdrew consent, and one died of an adverse event unrelated to marzeptacog alfa.
Howard Levy, chief medical officer of Catalyst Biosciences, which has been developing this drug and sponsored the trial, presented these data at the 2018 Hemophilia Drug Development Summit in Boston.
The goal of this ongoing trial is to determine whether daily subcutaneous injections of marzeptacog alfa can eliminate or minimize spontaneous bleeding episodes. The primary endpoint is a reduction in annualized bleed rate (ABR), compared with each individual’s recorded historical ABR.
One patient with a historic ABR of 26.7 experienced a bleed on day 46 when receiving marzeptacog alfa at 30 mcg/kg but then had no bleeds after 50 days of treatment with marzeptacog alfa at 60 mcg/kg. This patient did experience a bleed 16 days after the end of dosing at 60 mcg/kg.
A second patient with a historic ABR of 16.6 had no bleeds when receiving marzeptacog alfa at 30 mcg/kg for 50 days.
And a third patient with a historic ABR of 15.9 had no bleeds when receiving marzeptacog alfa at 30 mcg/kg for 44 days.
“The data from these 3 individuals support the efficacy of [marzeptacog alfa] to reduce annualized bleed rates after daily subcutaneous injections,” said Nassim Usman, PhD, chief executive officer of Catalyst Biosciences. “Importantly, to date, we have not observed any injection site reactions nor any antidrug antibodies after more than 200 subcutaneous doses of [marzeptacog alfa].”
A fourth patient with a historic ABR of 18.3 had a fatal hemorrhagic stroke on day 11 that was considered unrelated to marzeptacog alfa. The patient had previously treated hypertension that was going untreated at the time of death.
A fifth patient with a historic ABR of 12.2 withdrew consent.
The activated factor VIIa variant according to researchers.
To date, the trial has enrolled five patients with hemophilia A or B and inhibitors. Catalyst would not disclose how many patients have hemophilia A and how many have hemophilia B. Three patients have completed dosing with marzeptacog alfa in a phase 2/3 study. None of these patients experienced bleeding during treatment, and none have developed antidrug antibodies or reported injection site reactions. As for the other two patients enrolled in this study, one withdrew consent, and one died of an adverse event unrelated to marzeptacog alfa.
Howard Levy, chief medical officer of Catalyst Biosciences, which has been developing this drug and sponsored the trial, presented these data at the 2018 Hemophilia Drug Development Summit in Boston.
The goal of this ongoing trial is to determine whether daily subcutaneous injections of marzeptacog alfa can eliminate or minimize spontaneous bleeding episodes. The primary endpoint is a reduction in annualized bleed rate (ABR), compared with each individual’s recorded historical ABR.
One patient with a historic ABR of 26.7 experienced a bleed on day 46 when receiving marzeptacog alfa at 30 mcg/kg but then had no bleeds after 50 days of treatment with marzeptacog alfa at 60 mcg/kg. This patient did experience a bleed 16 days after the end of dosing at 60 mcg/kg.
A second patient with a historic ABR of 16.6 had no bleeds when receiving marzeptacog alfa at 30 mcg/kg for 50 days.
And a third patient with a historic ABR of 15.9 had no bleeds when receiving marzeptacog alfa at 30 mcg/kg for 44 days.
“The data from these 3 individuals support the efficacy of [marzeptacog alfa] to reduce annualized bleed rates after daily subcutaneous injections,” said Nassim Usman, PhD, chief executive officer of Catalyst Biosciences. “Importantly, to date, we have not observed any injection site reactions nor any antidrug antibodies after more than 200 subcutaneous doses of [marzeptacog alfa].”
A fourth patient with a historic ABR of 18.3 had a fatal hemorrhagic stroke on day 11 that was considered unrelated to marzeptacog alfa. The patient had previously treated hypertension that was going untreated at the time of death.
A fifth patient with a historic ABR of 12.2 withdrew consent.
How Does Provider Attire Impact Perceived Care and Infection Risk in the Clinical Setting?


Schools’ cell phone policies: What’s best for students?
Schools across the country – or around the world, for that matter – are grappling with policies and regulations tied to their students’ use of cell phones during school hours.

These policies run the gamut, from allowing students to use smartphones as learning tools to requiring them to keep the devices turned off. One public high school’s action on cell phones, initiated this year by a parent, has prompted one parent’s thumbs-up. This school is phasing in a lock-up-your-cell-phone policy.
NPR reporter Jennifer Ludden said that when the idea was first floated toward the end of the last school year, it provoked a parental outcry at her sons’ school. “My generation is used to 24/7 access to our kids, wherever they are. I confess, I’ve texted mine at school. It was about a doctor’s appointment,” Ms. Ludden says.
Meanwhile, she says, some asked: “ ‘What if there’s an emergency?’ It’s a fair question. We’ve all heard about students hiding from a gunman, posting updates, and texting to let friends and family know they’re safe,” she says.
Yet, evidence suggests that a cell-free classroom is a safer classroom, without the distraction of that screen to divert attention instructions that come in the wake of a school emergency. And, in a chilling mental image, a phone’s ringtone or vibration on a desk could be a beacon for a shooter.
Putting aside the horrific potential of school violence, a no-phone policy could have other tangible benefits that would help students in real life. The rejigging of adolescent brains away from the umbilical cord of their phone would be welcome. Imagine social interactions, instead of that face-down, thumbs-poised posture that is everywhere! And it could also help curb the electronic version of passing notes during tests.
Ms. Ludden mentions another benefit. “ Invaluable time to relax, and connect, without phones. I’m grateful to see some schools investing in that,” Ms. Ludden says.
Click here to listen to Ms. Ludden’s take.
Schools across the country – or around the world, for that matter – are grappling with policies and regulations tied to their students’ use of cell phones during school hours.
These policies run the gamut, from allowing students to use smartphones as learning tools to requiring them to keep the devices turned off. One public high school’s action on cell phones, initiated this year by a parent, has prompted one parent’s thumbs-up. This school is phasing in a lock-up-your-cell-phone policy.
NPR reporter Jennifer Ludden said that when the idea was first floated toward the end of the last school year, it provoked a parental outcry at her sons’ school. “My generation is used to 24/7 access to our kids, wherever they are. I confess, I’ve texted mine at school. It was about a doctor’s appointment,” Ms. Ludden says.
Meanwhile, she says, some asked: “ ‘What if there’s an emergency?’ It’s a fair question. We’ve all heard about students hiding from a gunman, posting updates, and texting to let friends and family know they’re safe,” she says.
Yet, evidence suggests that a cell-free classroom is a safer classroom, without the distraction of that screen to divert attention instructions that come in the wake of a school emergency. And, in a chilling mental image, a phone’s ringtone or vibration on a desk could be a beacon for a shooter.
Putting aside the horrific potential of school violence, a no-phone policy could have other tangible benefits that would help students in real life. The rejigging of adolescent brains away from the umbilical cord of their phone would be welcome. Imagine social interactions, instead of that face-down, thumbs-poised posture that is everywhere! And it could also help curb the electronic version of passing notes during tests.
Ms. Ludden mentions another benefit. “ Invaluable time to relax, and connect, without phones. I’m grateful to see some schools investing in that,” Ms. Ludden says.
Click here to listen to Ms. Ludden’s take.
Schools across the country – or around the world, for that matter – are grappling with policies and regulations tied to their students’ use of cell phones during school hours.
These policies run the gamut, from allowing students to use smartphones as learning tools to requiring them to keep the devices turned off. One public high school’s action on cell phones, initiated this year by a parent, has prompted one parent’s thumbs-up. This school is phasing in a lock-up-your-cell-phone policy.
NPR reporter Jennifer Ludden said that when the idea was first floated toward the end of the last school year, it provoked a parental outcry at her sons’ school. “My generation is used to 24/7 access to our kids, wherever they are. I confess, I’ve texted mine at school. It was about a doctor’s appointment,” Ms. Ludden says.
Meanwhile, she says, some asked: “ ‘What if there’s an emergency?’ It’s a fair question. We’ve all heard about students hiding from a gunman, posting updates, and texting to let friends and family know they’re safe,” she says.
Yet, evidence suggests that a cell-free classroom is a safer classroom, without the distraction of that screen to divert attention instructions that come in the wake of a school emergency. And, in a chilling mental image, a phone’s ringtone or vibration on a desk could be a beacon for a shooter.
Putting aside the horrific potential of school violence, a no-phone policy could have other tangible benefits that would help students in real life. The rejigging of adolescent brains away from the umbilical cord of their phone would be welcome. Imagine social interactions, instead of that face-down, thumbs-poised posture that is everywhere! And it could also help curb the electronic version of passing notes during tests.
Ms. Ludden mentions another benefit. “ Invaluable time to relax, and connect, without phones. I’m grateful to see some schools investing in that,” Ms. Ludden says.
Click here to listen to Ms. Ludden’s take.
Hypofractionated radiation has untapped potential as RCC mets therapy
Hypofractionated radiation therapy (RT) may be a more viable treatment option for oligometastatic renal cell carcinoma (RCC) than is generally recognized, a recent literature review has suggested.
Advances in stereotactic RT offer “new opportunities in RCC management” with limited toxicity, reported Francesca De Felice, PhD, of Sapienza University in Rome and her coauthor. The authors suggested that future studies investigate RT in combination with immunotherapy.
“Due to the assumption that RCC is a radioresistant tumor,” the authors wrote in Critical Reviews in Oncology/Hematology, “RT has long been considered a futile approach to manage primary disease” and is predominantly used for treatment of distant metastases with palliative intent. “This review provides highlights in current RCC strategies to potentially suggest a more tailored treatment approach in clinical daily practice.”
The investigators concluded that hypofractionated RT (greater than 3 Gy/fraction) deserves more serious consideration. “It has enormous advantages,” the authors wrote, “assuring ablative doses to the target meanwhile preserving surrounding normal tissues. Using stereotactic technique, surprising high local control rates have been achieved in several tumors (such as lung, liver, and bone), in both primary and oligometastatic setting[s].”
In five studies, single-dose RT (ranging from 8 to 24 Gy) was used to treat patients with RCC and extracranial metastases. Of the patients in these studies, 89% of them achieved local control, median overall survival (OS) ranged from 11.7 months to 21 months, and severe RT-related toxicity occurred 0%-4% of the time.
“Although [there is a] high level of data heterogeneity,” the authors wrote, “this systematic review suggested that stereotactic RT is associated with excellent local control rates and low toxicity incidence. Thus, if feasible, stereotactic RT represents an effective and safe approach to treat RCC metastasis.”
The authors cautioned that “the optimal high dose required for local tumor control has not yet been defined.”
The authors suggested that, in the future, immunotherapy in combination with RT may “produce synergistic effects, resulting in better response rate and duration, given the known immune-modulated abscopal effect of RT.” First, questions about treatment sequencing, dosing, and patient selection would need to be answered. “Further research should be aimed at these clinical needs in order to achieve the maximum benefit to RCC patient[s].”
This study did not receive specific funding.
SOURCE: Felice F et al. Crit Rev Oncol Hematol. 2018 Aug 1. doi: 10.1016/j.critrevonc.2018.06.002
Hypofractionated radiation therapy (RT) may be a more viable treatment option for oligometastatic renal cell carcinoma (RCC) than is generally recognized, a recent literature review has suggested.
Advances in stereotactic RT offer “new opportunities in RCC management” with limited toxicity, reported Francesca De Felice, PhD, of Sapienza University in Rome and her coauthor. The authors suggested that future studies investigate RT in combination with immunotherapy.
“Due to the assumption that RCC is a radioresistant tumor,” the authors wrote in Critical Reviews in Oncology/Hematology, “RT has long been considered a futile approach to manage primary disease” and is predominantly used for treatment of distant metastases with palliative intent. “This review provides highlights in current RCC strategies to potentially suggest a more tailored treatment approach in clinical daily practice.”
The investigators concluded that hypofractionated RT (greater than 3 Gy/fraction) deserves more serious consideration. “It has enormous advantages,” the authors wrote, “assuring ablative doses to the target meanwhile preserving surrounding normal tissues. Using stereotactic technique, surprising high local control rates have been achieved in several tumors (such as lung, liver, and bone), in both primary and oligometastatic setting[s].”
In five studies, single-dose RT (ranging from 8 to 24 Gy) was used to treat patients with RCC and extracranial metastases. Of the patients in these studies, 89% of them achieved local control, median overall survival (OS) ranged from 11.7 months to 21 months, and severe RT-related toxicity occurred 0%-4% of the time.
“Although [there is a] high level of data heterogeneity,” the authors wrote, “this systematic review suggested that stereotactic RT is associated with excellent local control rates and low toxicity incidence. Thus, if feasible, stereotactic RT represents an effective and safe approach to treat RCC metastasis.”
The authors cautioned that “the optimal high dose required for local tumor control has not yet been defined.”
The authors suggested that, in the future, immunotherapy in combination with RT may “produce synergistic effects, resulting in better response rate and duration, given the known immune-modulated abscopal effect of RT.” First, questions about treatment sequencing, dosing, and patient selection would need to be answered. “Further research should be aimed at these clinical needs in order to achieve the maximum benefit to RCC patient[s].”
This study did not receive specific funding.
SOURCE: Felice F et al. Crit Rev Oncol Hematol. 2018 Aug 1. doi: 10.1016/j.critrevonc.2018.06.002
Hypofractionated radiation therapy (RT) may be a more viable treatment option for oligometastatic renal cell carcinoma (RCC) than is generally recognized, a recent literature review has suggested.
Advances in stereotactic RT offer “new opportunities in RCC management” with limited toxicity, reported Francesca De Felice, PhD, of Sapienza University in Rome and her coauthor. The authors suggested that future studies investigate RT in combination with immunotherapy.
“Due to the assumption that RCC is a radioresistant tumor,” the authors wrote in Critical Reviews in Oncology/Hematology, “RT has long been considered a futile approach to manage primary disease” and is predominantly used for treatment of distant metastases with palliative intent. “This review provides highlights in current RCC strategies to potentially suggest a more tailored treatment approach in clinical daily practice.”
The investigators concluded that hypofractionated RT (greater than 3 Gy/fraction) deserves more serious consideration. “It has enormous advantages,” the authors wrote, “assuring ablative doses to the target meanwhile preserving surrounding normal tissues. Using stereotactic technique, surprising high local control rates have been achieved in several tumors (such as lung, liver, and bone), in both primary and oligometastatic setting[s].”
In five studies, single-dose RT (ranging from 8 to 24 Gy) was used to treat patients with RCC and extracranial metastases. Of the patients in these studies, 89% of them achieved local control, median overall survival (OS) ranged from 11.7 months to 21 months, and severe RT-related toxicity occurred 0%-4% of the time.
“Although [there is a] high level of data heterogeneity,” the authors wrote, “this systematic review suggested that stereotactic RT is associated with excellent local control rates and low toxicity incidence. Thus, if feasible, stereotactic RT represents an effective and safe approach to treat RCC metastasis.”
The authors cautioned that “the optimal high dose required for local tumor control has not yet been defined.”
The authors suggested that, in the future, immunotherapy in combination with RT may “produce synergistic effects, resulting in better response rate and duration, given the known immune-modulated abscopal effect of RT.” First, questions about treatment sequencing, dosing, and patient selection would need to be answered. “Further research should be aimed at these clinical needs in order to achieve the maximum benefit to RCC patient[s].”
This study did not receive specific funding.
SOURCE: Felice F et al. Crit Rev Oncol Hematol. 2018 Aug 1. doi: 10.1016/j.critrevonc.2018.06.002
FROM CRITICAL REVIEWS IN ONCOLOGY/HEMATOLOGY
Key clinical point: Hypofractionated radiation therapy (RT) is a safe and efficient treatment strategy in patients with oligometastatic renal cell carcinoma (RCC).
Major finding: In five studies, single-dose RT was used to treat patients with RCC and extracranial metastases; 89% of patients achieved local control, median overall survival (OS) was as high as 21 months, and severe RT-related toxicity occurred 0%-4% of the time.
Study details: A literature review of radiation therapy for RCC.
Disclosures: None.
Source: Felice F et al. Crit Rev Oncol Hematol. 2018 Aug 1. doi: 10.1016/j.critrevonc.2018.06.002.
Blood disorders researcher is finalist for Trailblazer Prize
Daniel Bauer, MD, PhD, a pediatric hematologist and blood disorders researcher in Boston, is one of three finalists for the inaugural Trailblazer Prize for Clinician-Scientists, which is awarded by the Foundation for the National Institutes of Health.

Dr. Bauer, of Dana-Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard Medical School, was selected based on his research using genome editing to tease out the causes of blood disorders, such as sickle cell disease and beta-thalassemia.
All three finalists for the Trailblazer Prize are early career clinician-scientists whose work has the potential to or has led to innovations in patient care, according to the Foundation for the National Institutes of Health.
The other two finalists are Jaehyuk Choi, MD, PhD, of Northwestern University in Chicago and Michael Fox, MD, PhD, of Beth Israel Deaconess Medical Center in Boston.
Dr. Choi was selected for using genomics to identify mutations in skin cells that can lead to autoinflammatory diseases and cancer. Dr. Fox was selected for the development of innovative techniques to map human brain connectivity that can be used in novel treatments for Parkinson’s disease and depression.
The winner will be announced during a ceremony in Washington on Oct. 24, 2018, and will receive a $10,000 honorarium.
Daniel Bauer, MD, PhD, a pediatric hematologist and blood disorders researcher in Boston, is one of three finalists for the inaugural Trailblazer Prize for Clinician-Scientists, which is awarded by the Foundation for the National Institutes of Health.
Dr. Bauer, of Dana-Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard Medical School, was selected based on his research using genome editing to tease out the causes of blood disorders, such as sickle cell disease and beta-thalassemia.
All three finalists for the Trailblazer Prize are early career clinician-scientists whose work has the potential to or has led to innovations in patient care, according to the Foundation for the National Institutes of Health.
The other two finalists are Jaehyuk Choi, MD, PhD, of Northwestern University in Chicago and Michael Fox, MD, PhD, of Beth Israel Deaconess Medical Center in Boston.
Dr. Choi was selected for using genomics to identify mutations in skin cells that can lead to autoinflammatory diseases and cancer. Dr. Fox was selected for the development of innovative techniques to map human brain connectivity that can be used in novel treatments for Parkinson’s disease and depression.
The winner will be announced during a ceremony in Washington on Oct. 24, 2018, and will receive a $10,000 honorarium.
Daniel Bauer, MD, PhD, a pediatric hematologist and blood disorders researcher in Boston, is one of three finalists for the inaugural Trailblazer Prize for Clinician-Scientists, which is awarded by the Foundation for the National Institutes of Health.
Dr. Bauer, of Dana-Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard Medical School, was selected based on his research using genome editing to tease out the causes of blood disorders, such as sickle cell disease and beta-thalassemia.
All three finalists for the Trailblazer Prize are early career clinician-scientists whose work has the potential to or has led to innovations in patient care, according to the Foundation for the National Institutes of Health.
The other two finalists are Jaehyuk Choi, MD, PhD, of Northwestern University in Chicago and Michael Fox, MD, PhD, of Beth Israel Deaconess Medical Center in Boston.
Dr. Choi was selected for using genomics to identify mutations in skin cells that can lead to autoinflammatory diseases and cancer. Dr. Fox was selected for the development of innovative techniques to map human brain connectivity that can be used in novel treatments for Parkinson’s disease and depression.
The winner will be announced during a ceremony in Washington on Oct. 24, 2018, and will receive a $10,000 honorarium.
Increasing incidence of metastatic RCC raises concerns for SREs
The incidence of metastatic renal cell carcinoma (RCC) continues to rise, according to a recent study. In turn, skeletal-related events are also becoming more common.
Many patients with metastatic disease have skeletal involvement, so knowledge of skeletal-related events (SREs) is more important than ever, reported Masood Umer, MD, of Aga Khan University Hospital in Karachi, Pakistan, and his coauthors. SREs include nerve compression, hypercalcemia, impending fractures, and pathological fractures, any one of which may require medical or surgical intervention.
Beyond SREs, “bone metastases in RCC [have a] negative impact on progression-free survival and overall survival of patients treated with systemic therapies,” the authors wrote in Annals of Medicine and Surgery.
The authors conducted a literature review of skeletal metastasis in RCC, which included 947 patients, assessing incidence and discussing appropriate medical and surgical interventions.
A total of 26.7% of patients with RCC also had skeletal metastasis. The most common sites of metastasis were the proximal femur, pelvis, and spine. It was estimated that 85% of patients with metastatic RCC may experience SREs and related complications, with an average of more than two events per individual.
A multimodal approach is required, potentially involving surgical and medical interventions. For isolated bony metastases and fractures, surgery is often beneficial. Denosumab is the leading medical treatment; compared with zoledronic acid, denosumab prolongs time to first SRE by a median of approximately 8 months and reduces risk of first SRE by almost 20%. Risks of osteonecrosis are similar between agents.
The authors noted that research concerning the impact of targeted therapies on rates of bone metastasis and SREs is limited by patient exclusions in clinical trials. Granted, these agents have likely made for better outcomes.
“Advancement in targeted therapy in recent decades [has] made some improvement in treatment of SREs and has helped in improving patent’s quality of life, but still we are in need of further improvement in treatment modalities,” they concluded
This study did not receive specific funding.
SOURCE: Umer M et al. Ann Med Surg. 2018 Jan 21. doi: 10.1016/j.amsu.2018.01.002.
The incidence of metastatic renal cell carcinoma (RCC) continues to rise, according to a recent study. In turn, skeletal-related events are also becoming more common.
Many patients with metastatic disease have skeletal involvement, so knowledge of skeletal-related events (SREs) is more important than ever, reported Masood Umer, MD, of Aga Khan University Hospital in Karachi, Pakistan, and his coauthors. SREs include nerve compression, hypercalcemia, impending fractures, and pathological fractures, any one of which may require medical or surgical intervention.
Beyond SREs, “bone metastases in RCC [have a] negative impact on progression-free survival and overall survival of patients treated with systemic therapies,” the authors wrote in Annals of Medicine and Surgery.
The authors conducted a literature review of skeletal metastasis in RCC, which included 947 patients, assessing incidence and discussing appropriate medical and surgical interventions.
A total of 26.7% of patients with RCC also had skeletal metastasis. The most common sites of metastasis were the proximal femur, pelvis, and spine. It was estimated that 85% of patients with metastatic RCC may experience SREs and related complications, with an average of more than two events per individual.
A multimodal approach is required, potentially involving surgical and medical interventions. For isolated bony metastases and fractures, surgery is often beneficial. Denosumab is the leading medical treatment; compared with zoledronic acid, denosumab prolongs time to first SRE by a median of approximately 8 months and reduces risk of first SRE by almost 20%. Risks of osteonecrosis are similar between agents.
The authors noted that research concerning the impact of targeted therapies on rates of bone metastasis and SREs is limited by patient exclusions in clinical trials. Granted, these agents have likely made for better outcomes.
“Advancement in targeted therapy in recent decades [has] made some improvement in treatment of SREs and has helped in improving patent’s quality of life, but still we are in need of further improvement in treatment modalities,” they concluded
This study did not receive specific funding.
SOURCE: Umer M et al. Ann Med Surg. 2018 Jan 21. doi: 10.1016/j.amsu.2018.01.002.
The incidence of metastatic renal cell carcinoma (RCC) continues to rise, according to a recent study. In turn, skeletal-related events are also becoming more common.
Many patients with metastatic disease have skeletal involvement, so knowledge of skeletal-related events (SREs) is more important than ever, reported Masood Umer, MD, of Aga Khan University Hospital in Karachi, Pakistan, and his coauthors. SREs include nerve compression, hypercalcemia, impending fractures, and pathological fractures, any one of which may require medical or surgical intervention.
Beyond SREs, “bone metastases in RCC [have a] negative impact on progression-free survival and overall survival of patients treated with systemic therapies,” the authors wrote in Annals of Medicine and Surgery.
The authors conducted a literature review of skeletal metastasis in RCC, which included 947 patients, assessing incidence and discussing appropriate medical and surgical interventions.
A total of 26.7% of patients with RCC also had skeletal metastasis. The most common sites of metastasis were the proximal femur, pelvis, and spine. It was estimated that 85% of patients with metastatic RCC may experience SREs and related complications, with an average of more than two events per individual.
A multimodal approach is required, potentially involving surgical and medical interventions. For isolated bony metastases and fractures, surgery is often beneficial. Denosumab is the leading medical treatment; compared with zoledronic acid, denosumab prolongs time to first SRE by a median of approximately 8 months and reduces risk of first SRE by almost 20%. Risks of osteonecrosis are similar between agents.
The authors noted that research concerning the impact of targeted therapies on rates of bone metastasis and SREs is limited by patient exclusions in clinical trials. Granted, these agents have likely made for better outcomes.
“Advancement in targeted therapy in recent decades [has] made some improvement in treatment of SREs and has helped in improving patent’s quality of life, but still we are in need of further improvement in treatment modalities,” they concluded
This study did not receive specific funding.
SOURCE: Umer M et al. Ann Med Surg. 2018 Jan 21. doi: 10.1016/j.amsu.2018.01.002.
FROM ANNALS OF MEDICINE AND SURGERY
Key clinical point: As the incidence of metastatic renal cell carcinoma (RCC) continues to rise, knowledge of skeletal-related events and appropriate interventions is essential.
Major finding: About 85% of patients with metastatic RCC experience skeletal-related events and associated complications.
Study details: A literature review of skeletal metastasis in RCC.
Disclosures: The study did not receive specific funding.
Source: Umer M et al. Ann Med Surg. 2018 Jan 21. doi: 10.1016/j.amsu.2018.01.002.
Dr. Eric Howell joins SHM as chief operating officer
Veteran hospitalist will help define organizational goals
The Society of Hospital Medicine has announced the appointment of Eric Howell, MD, MHM, to the position of chief operating officer (COO).

“Having been involved with SHM in many capacities since first joining, I am honored to now transition to chief operating officer,” Dr. Howell said. “I always tell everyone that my goal is to make the world a better place, and I know that SHM’s staff will be able to do just that through the development and deployment of a variety of products, tools, and services to help hospitalists improve patient care.”
In his new role as COO at SHM, Dr. Howell will lead senior management’s strategic planning as well as define organizational goals to drive extensive, sustainable growth. In addition to serving as SHM’s COO, Dr. Howell will continue his role as director of the hospital medicine division of Johns Hopkins Bayview Medical Center in Baltimore and professor of medicine in the department of medicine at Johns Hopkins University, also in Baltimore. Dr. Howell joined the Johns Hopkins Bayview hospitalist program in 2000, began the Howard County (Md.) General Hospital hospitalist program in 2010, and now oversees more than 200 physicians and clinical staff providing patient care in three hospitals.
“Eric has the perfect background to take SHM, its staff, and its membership to the next level,” said Laurence Wellikson, MD, MHM, chief executive officer of SHM. “His foundational leadership in the hospital medicine movement makes him the ideal person to lead SHM forward in its quest to provide hospitalists with the tools necessary to make a noteworthy difference in their institutions and in the lives of their patients.”
Dr. Howell is also a past president of SHM, the course director for the SHM Leadership Academies, and most recently, served as the senior physician advisor to SHM’s Center for Quality Improvement, which conducts quality improvement programs for hospitalist teams. He received his electrical engineering degree from the University of Maryland, which he said has served as an instrumental piece of his background for managing and implementing change in the hospital. His research has focused on the relationship between the emergency department and medicine floors, improving communication, throughput, and patient outcomes.
Veteran hospitalist will help define organizational goals
Veteran hospitalist will help define organizational goals
The Society of Hospital Medicine has announced the appointment of Eric Howell, MD, MHM, to the position of chief operating officer (COO).
“Having been involved with SHM in many capacities since first joining, I am honored to now transition to chief operating officer,” Dr. Howell said. “I always tell everyone that my goal is to make the world a better place, and I know that SHM’s staff will be able to do just that through the development and deployment of a variety of products, tools, and services to help hospitalists improve patient care.”
In his new role as COO at SHM, Dr. Howell will lead senior management’s strategic planning as well as define organizational goals to drive extensive, sustainable growth. In addition to serving as SHM’s COO, Dr. Howell will continue his role as director of the hospital medicine division of Johns Hopkins Bayview Medical Center in Baltimore and professor of medicine in the department of medicine at Johns Hopkins University, also in Baltimore. Dr. Howell joined the Johns Hopkins Bayview hospitalist program in 2000, began the Howard County (Md.) General Hospital hospitalist program in 2010, and now oversees more than 200 physicians and clinical staff providing patient care in three hospitals.
“Eric has the perfect background to take SHM, its staff, and its membership to the next level,” said Laurence Wellikson, MD, MHM, chief executive officer of SHM. “His foundational leadership in the hospital medicine movement makes him the ideal person to lead SHM forward in its quest to provide hospitalists with the tools necessary to make a noteworthy difference in their institutions and in the lives of their patients.”
Dr. Howell is also a past president of SHM, the course director for the SHM Leadership Academies, and most recently, served as the senior physician advisor to SHM’s Center for Quality Improvement, which conducts quality improvement programs for hospitalist teams. He received his electrical engineering degree from the University of Maryland, which he said has served as an instrumental piece of his background for managing and implementing change in the hospital. His research has focused on the relationship between the emergency department and medicine floors, improving communication, throughput, and patient outcomes.
The Society of Hospital Medicine has announced the appointment of Eric Howell, MD, MHM, to the position of chief operating officer (COO).
“Having been involved with SHM in many capacities since first joining, I am honored to now transition to chief operating officer,” Dr. Howell said. “I always tell everyone that my goal is to make the world a better place, and I know that SHM’s staff will be able to do just that through the development and deployment of a variety of products, tools, and services to help hospitalists improve patient care.”
In his new role as COO at SHM, Dr. Howell will lead senior management’s strategic planning as well as define organizational goals to drive extensive, sustainable growth. In addition to serving as SHM’s COO, Dr. Howell will continue his role as director of the hospital medicine division of Johns Hopkins Bayview Medical Center in Baltimore and professor of medicine in the department of medicine at Johns Hopkins University, also in Baltimore. Dr. Howell joined the Johns Hopkins Bayview hospitalist program in 2000, began the Howard County (Md.) General Hospital hospitalist program in 2010, and now oversees more than 200 physicians and clinical staff providing patient care in three hospitals.
“Eric has the perfect background to take SHM, its staff, and its membership to the next level,” said Laurence Wellikson, MD, MHM, chief executive officer of SHM. “His foundational leadership in the hospital medicine movement makes him the ideal person to lead SHM forward in its quest to provide hospitalists with the tools necessary to make a noteworthy difference in their institutions and in the lives of their patients.”
Dr. Howell is also a past president of SHM, the course director for the SHM Leadership Academies, and most recently, served as the senior physician advisor to SHM’s Center for Quality Improvement, which conducts quality improvement programs for hospitalist teams. He received his electrical engineering degree from the University of Maryland, which he said has served as an instrumental piece of his background for managing and implementing change in the hospital. His research has focused on the relationship between the emergency department and medicine floors, improving communication, throughput, and patient outcomes.
Little overlap between surgical M&M and AHRQ on adverse events
Limited overlap in adverse events identified by surgical morbidity and mortality (M&M) conferences and by Agency for Healthcare Research and Quality patient safety indicators (PSIs) demonstrates that the two processes tend to capture different, but equally important, measures, according to study results published in the Journal of the American College of Surgeons.

Just 18 of 149 (12.1%) PSI-defined events were identified by both processes in a retrospective, observational study of complications at the UC Davis Medical Center’s department of surgery. Most events (62.4%) were identified by only the M&M review, while 25.5% were identified by only the PSIs, reported Jamie E. Anderson, MD, MPH, of the department of surgery at UC Davis Medical Center in Sacramento and coauthors.
The study authors identified 6,563 surgical hospitalizations in the year 2016, of which 647 (9.9%) had at least one event that was either submitted for review for a departmental M&M conference, identified as a PSI event from administrative data, or both. Cases in patients aged less than 18 years were excluded.
Hospital administrative data were reported using ICD-10 CM/PCS codes. Investigators identified all PSI cases, which included pressure ulcer, retained surgical item, iatrogenic pneumothorax, central venous catheter–related blood stream infection, postoperative hip fracture, perioperative hematoma or hemorrhage requiring a procedure, postoperative acute kidney injury requiring dialysis, postoperative respiratory failure, perioperative pulmonary embolism or deep venous thrombosis, postoperative sepsis, postoperative wound dehiscence, and unrecognized abdominopelvic accidental puncture or laceration.
Complications submitted to the M&M conference were reviewed for PSI-defined events, and included events from general surgery, bariatric surgery, burn, cardiothoracic, colorectal, surgical oncology, plastic, vascular, transplant, and trauma. PSI-defined events were then reviewed to verify whether they counted as “true” PSI events and further classified as a documentation error, intentional exclusion, or inherent limitation of the PSI, the authors reported.
Of 6,563 surgical hospitalizations, 647 had at least one complication identified by M&M, PSI, or both. Of these, 116 had at least one PSI-defined event identified by either M&M or PSI. The remaining hospitalizations had unrelated complications and were excluded from analysis.
Of the 116 hospitalizations, there were 149 PSI-defined events, of which 18 (12.1%) were identified by both methods. Most events (62.4%) were identified by only the M&M review, and 25.5% were identified by only the PSIs. Perioperative hemorrhage/hematoma and postoperative sepsis were most likely to be identified by both.
Of the 93 PSI-defined events captured by only M&M, 11 (11.8%) met AHRQ criteria and were considered “true” events, or “false negatives.” All 38 events identified by PSI alone were correctly identified as true PSI events, Dr. Anderson and colleagues reported.
The findings indicate that the AHRQ PSI and surgical M&M conference “should be considered complementary approaches for identifying complications,” the authors wrote.
The PSI data captured central venous catheter–related blood stream infection and pressure ulcers, but the M&M conferences did not include these outcomes. The M&M reviewed more cases of postoperative sepsis, abdominopelvic accidental laceration, and the one case of retained surgical item.
“These two processes of identifying complications have different purposes, and each approach captured different events,” they added.
The M&M conference “balances clinician education and quality improvement with an underlying theme of accountability,” they said, with increased emphasis on examining adverse events in the context of systems-based practices. PSI, on the other hand, is intended as a “resource-nonintensive means” to help hospitals identify preventable events and facilitate quality improvement, they said.
“In an era in which there are numerous mechanisms to measure surgical quality, the traditional M&M conference is still relevant for identifying and discussing surgical complications,” the authors concluded. “We believe that our center’s existing M&M case-finding process is fundamentally sound, but it could be improved by including all PSI-flagged hospitalizations in our M&M process. This may result in review of some false-positive records, but it will enable our department to address certain potentially preventable complications that are currently overlooked.”
Two of the study coauthors received salary support from the AHRQ to support the agency’s Quality Indicator Program, one of whom serves on the agency’s Quality Indicators Expert Workgroup. No other disclosures were reported.
SOURCE: Anderson J et al. J Am Coll Surg. 2018 Jul 5. doi: 10.1016/j.jamcollsurg.2018.06.008.
Limited overlap in adverse events identified by surgical morbidity and mortality (M&M) conferences and by Agency for Healthcare Research and Quality patient safety indicators (PSIs) demonstrates that the two processes tend to capture different, but equally important, measures, according to study results published in the Journal of the American College of Surgeons.
Just 18 of 149 (12.1%) PSI-defined events were identified by both processes in a retrospective, observational study of complications at the UC Davis Medical Center’s department of surgery. Most events (62.4%) were identified by only the M&M review, while 25.5% were identified by only the PSIs, reported Jamie E. Anderson, MD, MPH, of the department of surgery at UC Davis Medical Center in Sacramento and coauthors.
The study authors identified 6,563 surgical hospitalizations in the year 2016, of which 647 (9.9%) had at least one event that was either submitted for review for a departmental M&M conference, identified as a PSI event from administrative data, or both. Cases in patients aged less than 18 years were excluded.
Hospital administrative data were reported using ICD-10 CM/PCS codes. Investigators identified all PSI cases, which included pressure ulcer, retained surgical item, iatrogenic pneumothorax, central venous catheter–related blood stream infection, postoperative hip fracture, perioperative hematoma or hemorrhage requiring a procedure, postoperative acute kidney injury requiring dialysis, postoperative respiratory failure, perioperative pulmonary embolism or deep venous thrombosis, postoperative sepsis, postoperative wound dehiscence, and unrecognized abdominopelvic accidental puncture or laceration.
Complications submitted to the M&M conference were reviewed for PSI-defined events, and included events from general surgery, bariatric surgery, burn, cardiothoracic, colorectal, surgical oncology, plastic, vascular, transplant, and trauma. PSI-defined events were then reviewed to verify whether they counted as “true” PSI events and further classified as a documentation error, intentional exclusion, or inherent limitation of the PSI, the authors reported.
Of 6,563 surgical hospitalizations, 647 had at least one complication identified by M&M, PSI, or both. Of these, 116 had at least one PSI-defined event identified by either M&M or PSI. The remaining hospitalizations had unrelated complications and were excluded from analysis.
Of the 116 hospitalizations, there were 149 PSI-defined events, of which 18 (12.1%) were identified by both methods. Most events (62.4%) were identified by only the M&M review, and 25.5% were identified by only the PSIs. Perioperative hemorrhage/hematoma and postoperative sepsis were most likely to be identified by both.
Of the 93 PSI-defined events captured by only M&M, 11 (11.8%) met AHRQ criteria and were considered “true” events, or “false negatives.” All 38 events identified by PSI alone were correctly identified as true PSI events, Dr. Anderson and colleagues reported.
The findings indicate that the AHRQ PSI and surgical M&M conference “should be considered complementary approaches for identifying complications,” the authors wrote.
The PSI data captured central venous catheter–related blood stream infection and pressure ulcers, but the M&M conferences did not include these outcomes. The M&M reviewed more cases of postoperative sepsis, abdominopelvic accidental laceration, and the one case of retained surgical item.
“These two processes of identifying complications have different purposes, and each approach captured different events,” they added.
The M&M conference “balances clinician education and quality improvement with an underlying theme of accountability,” they said, with increased emphasis on examining adverse events in the context of systems-based practices. PSI, on the other hand, is intended as a “resource-nonintensive means” to help hospitals identify preventable events and facilitate quality improvement, they said.
“In an era in which there are numerous mechanisms to measure surgical quality, the traditional M&M conference is still relevant for identifying and discussing surgical complications,” the authors concluded. “We believe that our center’s existing M&M case-finding process is fundamentally sound, but it could be improved by including all PSI-flagged hospitalizations in our M&M process. This may result in review of some false-positive records, but it will enable our department to address certain potentially preventable complications that are currently overlooked.”
Two of the study coauthors received salary support from the AHRQ to support the agency’s Quality Indicator Program, one of whom serves on the agency’s Quality Indicators Expert Workgroup. No other disclosures were reported.
SOURCE: Anderson J et al. J Am Coll Surg. 2018 Jul 5. doi: 10.1016/j.jamcollsurg.2018.06.008.
Limited overlap in adverse events identified by surgical morbidity and mortality (M&M) conferences and by Agency for Healthcare Research and Quality patient safety indicators (PSIs) demonstrates that the two processes tend to capture different, but equally important, measures, according to study results published in the Journal of the American College of Surgeons.
Just 18 of 149 (12.1%) PSI-defined events were identified by both processes in a retrospective, observational study of complications at the UC Davis Medical Center’s department of surgery. Most events (62.4%) were identified by only the M&M review, while 25.5% were identified by only the PSIs, reported Jamie E. Anderson, MD, MPH, of the department of surgery at UC Davis Medical Center in Sacramento and coauthors.
The study authors identified 6,563 surgical hospitalizations in the year 2016, of which 647 (9.9%) had at least one event that was either submitted for review for a departmental M&M conference, identified as a PSI event from administrative data, or both. Cases in patients aged less than 18 years were excluded.
Hospital administrative data were reported using ICD-10 CM/PCS codes. Investigators identified all PSI cases, which included pressure ulcer, retained surgical item, iatrogenic pneumothorax, central venous catheter–related blood stream infection, postoperative hip fracture, perioperative hematoma or hemorrhage requiring a procedure, postoperative acute kidney injury requiring dialysis, postoperative respiratory failure, perioperative pulmonary embolism or deep venous thrombosis, postoperative sepsis, postoperative wound dehiscence, and unrecognized abdominopelvic accidental puncture or laceration.
Complications submitted to the M&M conference were reviewed for PSI-defined events, and included events from general surgery, bariatric surgery, burn, cardiothoracic, colorectal, surgical oncology, plastic, vascular, transplant, and trauma. PSI-defined events were then reviewed to verify whether they counted as “true” PSI events and further classified as a documentation error, intentional exclusion, or inherent limitation of the PSI, the authors reported.
Of 6,563 surgical hospitalizations, 647 had at least one complication identified by M&M, PSI, or both. Of these, 116 had at least one PSI-defined event identified by either M&M or PSI. The remaining hospitalizations had unrelated complications and were excluded from analysis.
Of the 116 hospitalizations, there were 149 PSI-defined events, of which 18 (12.1%) were identified by both methods. Most events (62.4%) were identified by only the M&M review, and 25.5% were identified by only the PSIs. Perioperative hemorrhage/hematoma and postoperative sepsis were most likely to be identified by both.
Of the 93 PSI-defined events captured by only M&M, 11 (11.8%) met AHRQ criteria and were considered “true” events, or “false negatives.” All 38 events identified by PSI alone were correctly identified as true PSI events, Dr. Anderson and colleagues reported.
The findings indicate that the AHRQ PSI and surgical M&M conference “should be considered complementary approaches for identifying complications,” the authors wrote.
The PSI data captured central venous catheter–related blood stream infection and pressure ulcers, but the M&M conferences did not include these outcomes. The M&M reviewed more cases of postoperative sepsis, abdominopelvic accidental laceration, and the one case of retained surgical item.
“These two processes of identifying complications have different purposes, and each approach captured different events,” they added.
The M&M conference “balances clinician education and quality improvement with an underlying theme of accountability,” they said, with increased emphasis on examining adverse events in the context of systems-based practices. PSI, on the other hand, is intended as a “resource-nonintensive means” to help hospitals identify preventable events and facilitate quality improvement, they said.
“In an era in which there are numerous mechanisms to measure surgical quality, the traditional M&M conference is still relevant for identifying and discussing surgical complications,” the authors concluded. “We believe that our center’s existing M&M case-finding process is fundamentally sound, but it could be improved by including all PSI-flagged hospitalizations in our M&M process. This may result in review of some false-positive records, but it will enable our department to address certain potentially preventable complications that are currently overlooked.”
Two of the study coauthors received salary support from the AHRQ to support the agency’s Quality Indicator Program, one of whom serves on the agency’s Quality Indicators Expert Workgroup. No other disclosures were reported.
SOURCE: Anderson J et al. J Am Coll Surg. 2018 Jul 5. doi: 10.1016/j.jamcollsurg.2018.06.008.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: Surgical morbidity and mortality conferences and AHRQ patient safety indicators should be considered complementary measures of adverse events because of a limited overlap in identifying adverse events.
Major finding: Eighteen of 149 (12.1%) PSI-defined events were identified by both processes; most (62.4%) were identified by only M&M review, and 25.5% by only PSI.
Study details: A retrospective observational study of all complications in 2016 at the UC Davis Medical Center department of surgery.
Disclosures: Two of the study coauthors received salary support from the AHRQ to support the agency’s Quality Indicator Program, one of whom serves on the agency’s Quality Indicators Expert Workgroup. No other disclosures were reported.
Source: Anderson J et al. J Am Coll Surg. 2018 Jul 5. doi: 10.1016/j.jamcollsurg.2018.06.008.

Is the most effective emergency contraception easily obtained at US pharmacies?
EXPERT COMMENTARY
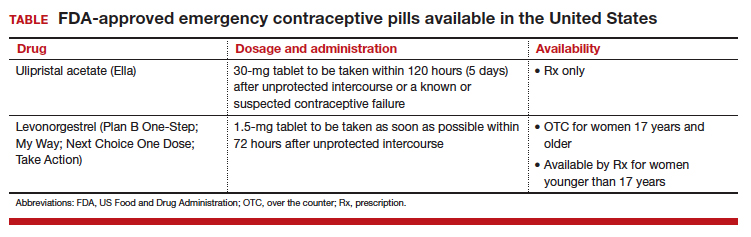
Although it is available only by prescription, ulipristal acetate provides emergency contraception that is more effective than the emergency contraception provided by levonorgestrel (LNG), which is available without a prescription (TABLE). In addition, ulipristal acetate appears more effective than LNG in obese and overweight women.1,2 Package labeling for ulipristal acetate indicates that a single 30-mg tablet should be taken orally within 5 days of unprotected sex.
According to a survey of pharmacy availability of ulipristal acetate in Hawaii, 2.6% of retail pharmacies had the drug immediately available, compared with 82.4% for LNG, and 22.8% reported the ability to order it.3 To assess pharmacy availability of ulipristal acetate on a nationwide scale, Shigesato and colleagues conducted a national “secret shopper” telephone survey in 10 cities (each with a population of at least 500,000) in all major regions of the United States.
Details of the study
Independent pharmacies (defined as having fewer than 5 locations within the city) and chain pharmacies were included in the survey. The survey callers, representing themselves as uninsured 18-year-old women attempting to fill a prescription for ulipristal acetate, followed a semistructured questionnaire and recorded the responses. They asked about the immediate availability of ulipristal acetate and LNG, the pharmacy’s ability to order ulipristal acetate if not immediately available, out-of-pocket costs, instructions for use, and the differences between ulipristal acetate and LNG. Questions were directed to whichever pharmacy staff member answered the phone; callers did not specifically ask to speak to a pharmacist.
Of the 344 pharmacies included in this analysis, 10% (33) indicated that they could fill a prescription for ulipristal acetate immediately. While availability did not vary by region, there was a difference in immediate availability by city.
Almost three-quarters of pharmacies without immediate drug availability indicated that they could order ulipristal acetate, with a median predicted time for availability of 24 hours. Of the chain pharmacies, 81% (167 of 205) reported the ability to order ulipristal acetate, compared with 55% (57 of 106) of independent pharmacies.
When asked if ulipristal acetate was different from LNG, more than one-third of pharmacy personnel contacted stated either that there was no difference between ulipristal acetate and LNG or that they were not sure of a difference.
Study strengths and weaknesses
The authors noted that the secret shopper methodology, along with having callers speak to the pharmacy staff person who answered the call (rather than asking for the pharmacist), provided data that closely approximates real-world patient experiences.
Since more pharmacies than anticipated met exclusion criteria for the study, the estimate of ulipristal acetate immediate availability was less precise than the power analysis predicted. Further, results from the 10 large, geographically diverse cities may not be representative of all similarly sized cities nationally or all areas of the United States.
As the authors point out, a low prevalence of pharmacies stock ulipristal acetate, and more than 25% are not able to order this emergency contraception. This underscores the fact that access to the most effective oral emergency contraception is limited for US women. I agree with the authors’ speculation that access to ulipristal acetate may be even lower in rural areas. In many European countries, ulipristal acetate is available without a prescription. Clinicians caring for women who may benefit from emergency contraception, particularly those using short-acting or less effective contraceptives, may wish to prescribe ulipristal acetate in advance of need.
—Andrew M. Kaunitz, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Kapp N, Abitbol JL, Mathé H, et al. Effect of body weight and BMI on the efficacy of levonorgestrel emergency contraception. Contraception. 2015;91(2):97–104.
- Glasier A, Cameron ST, Blithe D, et al. Can we identify women at risk of pregnancy despite using emergency contraception? Data from randomized trials of ulipristal acetate and levonorgestrel. Contraception. 2011;84(4):363–367.
- Bullock H, Steele S, Kurata N, et al. Pharmacy access to ulipristal acetate in Hawaii: is a prescription enough? Contraception. 2016;93(5):452–454.
EXPERT COMMENTARY
Although it is available only by prescription, ulipristal acetate provides emergency contraception that is more effective than the emergency contraception provided by levonorgestrel (LNG), which is available without a prescription (TABLE). In addition, ulipristal acetate appears more effective than LNG in obese and overweight women.1,2 Package labeling for ulipristal acetate indicates that a single 30-mg tablet should be taken orally within 5 days of unprotected sex.
According to a survey of pharmacy availability of ulipristal acetate in Hawaii, 2.6% of retail pharmacies had the drug immediately available, compared with 82.4% for LNG, and 22.8% reported the ability to order it.3 To assess pharmacy availability of ulipristal acetate on a nationwide scale, Shigesato and colleagues conducted a national “secret shopper” telephone survey in 10 cities (each with a population of at least 500,000) in all major regions of the United States.
Details of the study
Independent pharmacies (defined as having fewer than 5 locations within the city) and chain pharmacies were included in the survey. The survey callers, representing themselves as uninsured 18-year-old women attempting to fill a prescription for ulipristal acetate, followed a semistructured questionnaire and recorded the responses. They asked about the immediate availability of ulipristal acetate and LNG, the pharmacy’s ability to order ulipristal acetate if not immediately available, out-of-pocket costs, instructions for use, and the differences between ulipristal acetate and LNG. Questions were directed to whichever pharmacy staff member answered the phone; callers did not specifically ask to speak to a pharmacist.
Of the 344 pharmacies included in this analysis, 10% (33) indicated that they could fill a prescription for ulipristal acetate immediately. While availability did not vary by region, there was a difference in immediate availability by city.
Almost three-quarters of pharmacies without immediate drug availability indicated that they could order ulipristal acetate, with a median predicted time for availability of 24 hours. Of the chain pharmacies, 81% (167 of 205) reported the ability to order ulipristal acetate, compared with 55% (57 of 106) of independent pharmacies.
When asked if ulipristal acetate was different from LNG, more than one-third of pharmacy personnel contacted stated either that there was no difference between ulipristal acetate and LNG or that they were not sure of a difference.
Study strengths and weaknesses
The authors noted that the secret shopper methodology, along with having callers speak to the pharmacy staff person who answered the call (rather than asking for the pharmacist), provided data that closely approximates real-world patient experiences.
Since more pharmacies than anticipated met exclusion criteria for the study, the estimate of ulipristal acetate immediate availability was less precise than the power analysis predicted. Further, results from the 10 large, geographically diverse cities may not be representative of all similarly sized cities nationally or all areas of the United States.
As the authors point out, a low prevalence of pharmacies stock ulipristal acetate, and more than 25% are not able to order this emergency contraception. This underscores the fact that access to the most effective oral emergency contraception is limited for US women. I agree with the authors’ speculation that access to ulipristal acetate may be even lower in rural areas. In many European countries, ulipristal acetate is available without a prescription. Clinicians caring for women who may benefit from emergency contraception, particularly those using short-acting or less effective contraceptives, may wish to prescribe ulipristal acetate in advance of need.
—Andrew M. Kaunitz, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
EXPERT COMMENTARY
Although it is available only by prescription, ulipristal acetate provides emergency contraception that is more effective than the emergency contraception provided by levonorgestrel (LNG), which is available without a prescription (TABLE). In addition, ulipristal acetate appears more effective than LNG in obese and overweight women.1,2 Package labeling for ulipristal acetate indicates that a single 30-mg tablet should be taken orally within 5 days of unprotected sex.
According to a survey of pharmacy availability of ulipristal acetate in Hawaii, 2.6% of retail pharmacies had the drug immediately available, compared with 82.4% for LNG, and 22.8% reported the ability to order it.3 To assess pharmacy availability of ulipristal acetate on a nationwide scale, Shigesato and colleagues conducted a national “secret shopper” telephone survey in 10 cities (each with a population of at least 500,000) in all major regions of the United States.
Details of the study
Independent pharmacies (defined as having fewer than 5 locations within the city) and chain pharmacies were included in the survey. The survey callers, representing themselves as uninsured 18-year-old women attempting to fill a prescription for ulipristal acetate, followed a semistructured questionnaire and recorded the responses. They asked about the immediate availability of ulipristal acetate and LNG, the pharmacy’s ability to order ulipristal acetate if not immediately available, out-of-pocket costs, instructions for use, and the differences between ulipristal acetate and LNG. Questions were directed to whichever pharmacy staff member answered the phone; callers did not specifically ask to speak to a pharmacist.
Of the 344 pharmacies included in this analysis, 10% (33) indicated that they could fill a prescription for ulipristal acetate immediately. While availability did not vary by region, there was a difference in immediate availability by city.
Almost three-quarters of pharmacies without immediate drug availability indicated that they could order ulipristal acetate, with a median predicted time for availability of 24 hours. Of the chain pharmacies, 81% (167 of 205) reported the ability to order ulipristal acetate, compared with 55% (57 of 106) of independent pharmacies.
When asked if ulipristal acetate was different from LNG, more than one-third of pharmacy personnel contacted stated either that there was no difference between ulipristal acetate and LNG or that they were not sure of a difference.
Study strengths and weaknesses
The authors noted that the secret shopper methodology, along with having callers speak to the pharmacy staff person who answered the call (rather than asking for the pharmacist), provided data that closely approximates real-world patient experiences.
Since more pharmacies than anticipated met exclusion criteria for the study, the estimate of ulipristal acetate immediate availability was less precise than the power analysis predicted. Further, results from the 10 large, geographically diverse cities may not be representative of all similarly sized cities nationally or all areas of the United States.
As the authors point out, a low prevalence of pharmacies stock ulipristal acetate, and more than 25% are not able to order this emergency contraception. This underscores the fact that access to the most effective oral emergency contraception is limited for US women. I agree with the authors’ speculation that access to ulipristal acetate may be even lower in rural areas. In many European countries, ulipristal acetate is available without a prescription. Clinicians caring for women who may benefit from emergency contraception, particularly those using short-acting or less effective contraceptives, may wish to prescribe ulipristal acetate in advance of need.
—Andrew M. Kaunitz, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Kapp N, Abitbol JL, Mathé H, et al. Effect of body weight and BMI on the efficacy of levonorgestrel emergency contraception. Contraception. 2015;91(2):97–104.
- Glasier A, Cameron ST, Blithe D, et al. Can we identify women at risk of pregnancy despite using emergency contraception? Data from randomized trials of ulipristal acetate and levonorgestrel. Contraception. 2011;84(4):363–367.
- Bullock H, Steele S, Kurata N, et al. Pharmacy access to ulipristal acetate in Hawaii: is a prescription enough? Contraception. 2016;93(5):452–454.
- Kapp N, Abitbol JL, Mathé H, et al. Effect of body weight and BMI on the efficacy of levonorgestrel emergency contraception. Contraception. 2015;91(2):97–104.
- Glasier A, Cameron ST, Blithe D, et al. Can we identify women at risk of pregnancy despite using emergency contraception? Data from randomized trials of ulipristal acetate and levonorgestrel. Contraception. 2011;84(4):363–367.
- Bullock H, Steele S, Kurata N, et al. Pharmacy access to ulipristal acetate in Hawaii: is a prescription enough? Contraception. 2016;93(5):452–454.