User login
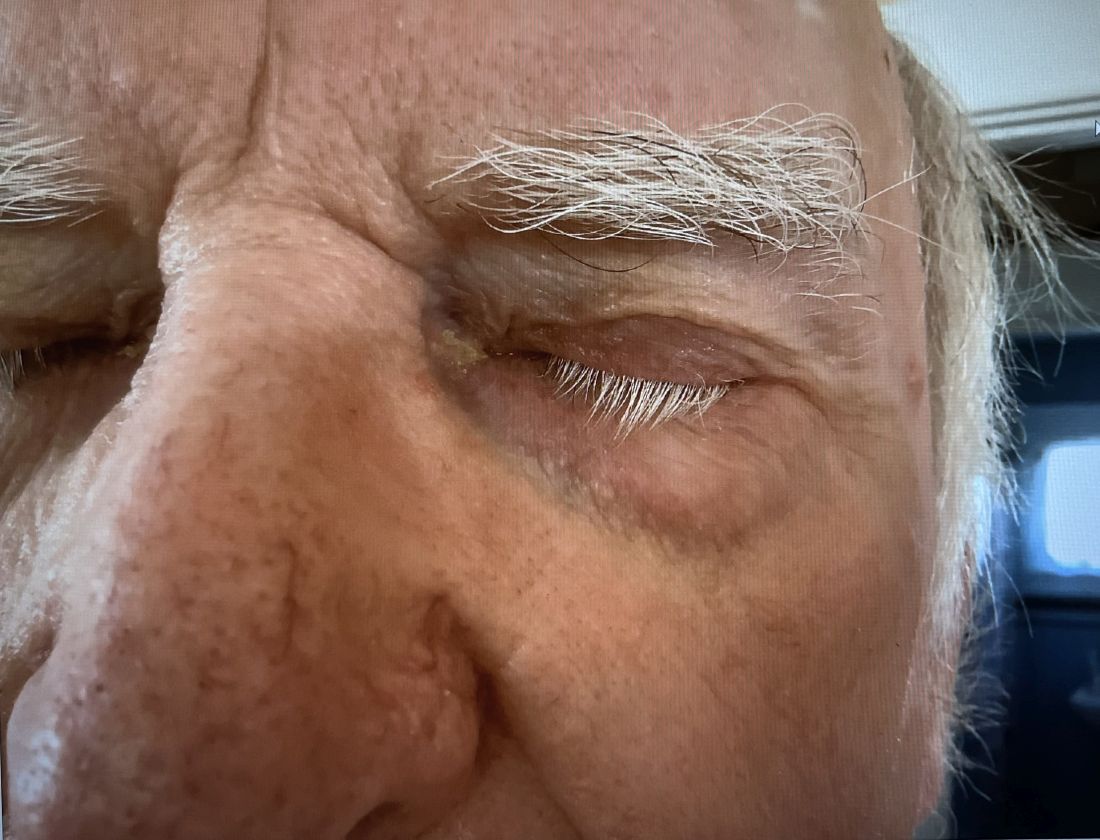
A 74-year-old White male presented with a 1-year history of depigmented patches on the hands, arms, and face, as well as white eyelashes and eyebrows
This patient showed no evidence of recurrence in the scar where the melanoma was excised, and had no enlarged lymph nodes on palpation. His complete blood count and liver function tests were normal. A positron emission tomography (PET) scan was ordered by Dr. Nasser that revealed hypermetabolic right paratracheal, right hilar, and subcarinal lymph nodes, highly suspicious for malignant lymph nodes. The patient was referred to oncology for metastatic melanoma treatment and has been doing well on ipilimumab and nivolumab.
Vitiligo is an autoimmune condition characterized by the progressive destruction of melanocytes resulting in hypopigmentation or depigmentation of the skin. Vitiligo has been associated with cutaneous melanoma. Melanoma-associated leukoderma occurs in a portion of patients with melanoma and is correlated with a favorable prognosis. Additionally, leukoderma has been described as a side effect of melanoma treatment itself. However, cases such as this one have also been reported of vitiligo-like depigmentation presenting prior to the diagnosis of metastatic melanoma.
Melanoma, like vitiligo, is considered highly immunogenic, and cytotoxic T lymphocytes (CTLs) can recognize antigens in melanoma. Furthermore, studies have shown a vitiligo-like halo around melanoma tumors, likely caused by T-cell recruitment, and this may lead to tumor destruction, but rarely total clearance. It seems that the CTL infiltrate in both diseases is similar, but regulatory T cells are decreased in vitiligo, whereas they are present in melanomas and may contribute to the immunosuppressive tumor microenvironment found at the margin of these lesions.
Leukoderma is also associated with melanoma immunotherapy which may be described as drug-induced leukoderma. Additionally, the frequency of recognition of melanoma cells by CTLs leading to hypopigmentation appears to be higher in those with metastatic disease. High immune infiltrate with CTLs and interferon-gamma (IFN-gamma) expression by type 1 T helper cells is associated with favorable prognosis. Immunotherapy with checkpoint inhibitors has shown promise in treatment augmentation for melanoma, but not all patients fully respond to therapy. Nonetheless, development of leukoderma with these treatments has been significantly associated with good therapeutic response. Depigmentation of hair and retinal epithelium has also been reported. However, drug-induced leukoderma and vitiligo seem to have clinical and biological differences, including family history of disease and serum chemokine levels. Vaccines are in production to aid in the treatment of melanoma, but researchers must first identify the appropriate antigen(s) to include.

Conversely, vitiligo-like depigmentation has been reported as a harbinger of metastatic melanoma. Patients with previous excision of primary melanoma have presented months or years later with depigmentation and, upon further evaluation, have been diagnosed with metastatic melanoma. The prevalence of depigmentation in melanoma patients is about 3%-6%, and is estimated to be 7-10 times more common in those with melanoma than in the general population. In most cases, hypopigmentation follows the diagnosis of melanoma, with an average of 4.8 years after the initial diagnosis and 1-2 years after lymph node or distant metastases. It is unclear whether hypopigmentation occurs before or after the growth of metastatic lesions, but this clinical finding in a patient with previous melanoma may serve as an important clue to conduct further investigation for metastasis.
This case and the photos were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Natalie Y. Nasser, MD, Kaiser Permanente Riverside Medical Center; Riverside, California. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Cerci FB et al. Cutis. 2017 Jun;99(6):E1-E2. PMID: 28686764.
Cho EA et al. Ann Dermatol. 2009 May;21(2):178-181.
Failla CM et al. Int J Mol Sci. 2019 Nov 15;20(22):5731.
This patient showed no evidence of recurrence in the scar where the melanoma was excised, and had no enlarged lymph nodes on palpation. His complete blood count and liver function tests were normal. A positron emission tomography (PET) scan was ordered by Dr. Nasser that revealed hypermetabolic right paratracheal, right hilar, and subcarinal lymph nodes, highly suspicious for malignant lymph nodes. The patient was referred to oncology for metastatic melanoma treatment and has been doing well on ipilimumab and nivolumab.
Vitiligo is an autoimmune condition characterized by the progressive destruction of melanocytes resulting in hypopigmentation or depigmentation of the skin. Vitiligo has been associated with cutaneous melanoma. Melanoma-associated leukoderma occurs in a portion of patients with melanoma and is correlated with a favorable prognosis. Additionally, leukoderma has been described as a side effect of melanoma treatment itself. However, cases such as this one have also been reported of vitiligo-like depigmentation presenting prior to the diagnosis of metastatic melanoma.
Melanoma, like vitiligo, is considered highly immunogenic, and cytotoxic T lymphocytes (CTLs) can recognize antigens in melanoma. Furthermore, studies have shown a vitiligo-like halo around melanoma tumors, likely caused by T-cell recruitment, and this may lead to tumor destruction, but rarely total clearance. It seems that the CTL infiltrate in both diseases is similar, but regulatory T cells are decreased in vitiligo, whereas they are present in melanomas and may contribute to the immunosuppressive tumor microenvironment found at the margin of these lesions.
Leukoderma is also associated with melanoma immunotherapy which may be described as drug-induced leukoderma. Additionally, the frequency of recognition of melanoma cells by CTLs leading to hypopigmentation appears to be higher in those with metastatic disease. High immune infiltrate with CTLs and interferon-gamma (IFN-gamma) expression by type 1 T helper cells is associated with favorable prognosis. Immunotherapy with checkpoint inhibitors has shown promise in treatment augmentation for melanoma, but not all patients fully respond to therapy. Nonetheless, development of leukoderma with these treatments has been significantly associated with good therapeutic response. Depigmentation of hair and retinal epithelium has also been reported. However, drug-induced leukoderma and vitiligo seem to have clinical and biological differences, including family history of disease and serum chemokine levels. Vaccines are in production to aid in the treatment of melanoma, but researchers must first identify the appropriate antigen(s) to include.
Conversely, vitiligo-like depigmentation has been reported as a harbinger of metastatic melanoma. Patients with previous excision of primary melanoma have presented months or years later with depigmentation and, upon further evaluation, have been diagnosed with metastatic melanoma. The prevalence of depigmentation in melanoma patients is about 3%-6%, and is estimated to be 7-10 times more common in those with melanoma than in the general population. In most cases, hypopigmentation follows the diagnosis of melanoma, with an average of 4.8 years after the initial diagnosis and 1-2 years after lymph node or distant metastases. It is unclear whether hypopigmentation occurs before or after the growth of metastatic lesions, but this clinical finding in a patient with previous melanoma may serve as an important clue to conduct further investigation for metastasis.
This case and the photos were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Natalie Y. Nasser, MD, Kaiser Permanente Riverside Medical Center; Riverside, California. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Cerci FB et al. Cutis. 2017 Jun;99(6):E1-E2. PMID: 28686764.
Cho EA et al. Ann Dermatol. 2009 May;21(2):178-181.
Failla CM et al. Int J Mol Sci. 2019 Nov 15;20(22):5731.
This patient showed no evidence of recurrence in the scar where the melanoma was excised, and had no enlarged lymph nodes on palpation. His complete blood count and liver function tests were normal. A positron emission tomography (PET) scan was ordered by Dr. Nasser that revealed hypermetabolic right paratracheal, right hilar, and subcarinal lymph nodes, highly suspicious for malignant lymph nodes. The patient was referred to oncology for metastatic melanoma treatment and has been doing well on ipilimumab and nivolumab.
Vitiligo is an autoimmune condition characterized by the progressive destruction of melanocytes resulting in hypopigmentation or depigmentation of the skin. Vitiligo has been associated with cutaneous melanoma. Melanoma-associated leukoderma occurs in a portion of patients with melanoma and is correlated with a favorable prognosis. Additionally, leukoderma has been described as a side effect of melanoma treatment itself. However, cases such as this one have also been reported of vitiligo-like depigmentation presenting prior to the diagnosis of metastatic melanoma.
Melanoma, like vitiligo, is considered highly immunogenic, and cytotoxic T lymphocytes (CTLs) can recognize antigens in melanoma. Furthermore, studies have shown a vitiligo-like halo around melanoma tumors, likely caused by T-cell recruitment, and this may lead to tumor destruction, but rarely total clearance. It seems that the CTL infiltrate in both diseases is similar, but regulatory T cells are decreased in vitiligo, whereas they are present in melanomas and may contribute to the immunosuppressive tumor microenvironment found at the margin of these lesions.
Leukoderma is also associated with melanoma immunotherapy which may be described as drug-induced leukoderma. Additionally, the frequency of recognition of melanoma cells by CTLs leading to hypopigmentation appears to be higher in those with metastatic disease. High immune infiltrate with CTLs and interferon-gamma (IFN-gamma) expression by type 1 T helper cells is associated with favorable prognosis. Immunotherapy with checkpoint inhibitors has shown promise in treatment augmentation for melanoma, but not all patients fully respond to therapy. Nonetheless, development of leukoderma with these treatments has been significantly associated with good therapeutic response. Depigmentation of hair and retinal epithelium has also been reported. However, drug-induced leukoderma and vitiligo seem to have clinical and biological differences, including family history of disease and serum chemokine levels. Vaccines are in production to aid in the treatment of melanoma, but researchers must first identify the appropriate antigen(s) to include.
Conversely, vitiligo-like depigmentation has been reported as a harbinger of metastatic melanoma. Patients with previous excision of primary melanoma have presented months or years later with depigmentation and, upon further evaluation, have been diagnosed with metastatic melanoma. The prevalence of depigmentation in melanoma patients is about 3%-6%, and is estimated to be 7-10 times more common in those with melanoma than in the general population. In most cases, hypopigmentation follows the diagnosis of melanoma, with an average of 4.8 years after the initial diagnosis and 1-2 years after lymph node or distant metastases. It is unclear whether hypopigmentation occurs before or after the growth of metastatic lesions, but this clinical finding in a patient with previous melanoma may serve as an important clue to conduct further investigation for metastasis.
This case and the photos were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Natalie Y. Nasser, MD, Kaiser Permanente Riverside Medical Center; Riverside, California. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
Cerci FB et al. Cutis. 2017 Jun;99(6):E1-E2. PMID: 28686764.
Cho EA et al. Ann Dermatol. 2009 May;21(2):178-181.
Failla CM et al. Int J Mol Sci. 2019 Nov 15;20(22):5731.

Switching From IV to Oral Antibiotics Safe for Patients, Study Shows
TOPLINE:
, according to a recent observational study published in JAMA Network Open.
METHODOLOGY:
- Patients receiving antibiotics through an IV line risk developing a secondary infection; antibiotics received orally are considered safer.
- Researchers analyzed observational data from 914 adults with uncomplicated gram-negative bacteremia who received care in four hospitals in Denmark between 2018 and 2021.
- The outcomes of patients who were switched to oral antibiotics within 4 days after a positive blood culture were compared with those who continued to receive IV antibiotics for at least 5 days after the blood culture; participants in both groups received antibiotics for 7-14 days.
- Researchers assessed mortality rates over a 90-day window and used a target trial emulation method to conduct the study.
TAKEAWAY:
- Overall, 14.3% of patients who received prolonged IV treatment died, compared with 6.9% in the oral antibiotics group.
- In an intention-to-treat analysis, patients who were switched to oral antibiotics had a 22% lower risk for death within 90 days of initiation of treatment (relative risk [RR], 0.78; 95% CI, 0.60-1.10).
- In a per-protocol analysis, patients who switched to the oral route had a 1% lower odds of dying within 90 days (RR, 0.99; 95% CI, 0.70-1.40).
- Individuals who were switched to oral antibiotic treatment were younger than those who continued to receive antibiotics via the IV route (median age, 73 vs 76 years, respectively), had fewer comorbidities (four vs five), and were more likely to have community-acquired gram-negative bacteremia (89.4% vs 80.9%).
IN PRACTICE:
“These findings suggest that the mortality associated with early antibiotic stepdown treatment is comparable to that associated with receiving prolonged IV antibiotic treatment for individuals with uncomplicated gram-negative bacteremia,” the authors of the study wrote.
SOURCE:
The study was led by Sandra Tingsgård, MD, of the Center of Research & Department of Infectious Diseases at Copenhagen University Hospital–Amager and Hvidovre in Denmark.
LIMITATIONS:
The study was based on data from electronic health records, so some factors may not have been recorded or considered. The researchers identified few cases of multidrug-resistant infections, and the findings may not apply to those cases. Complicated cases and people who were not stabilized by day 4 were excluded from the analysis.
DISCLOSURES:
The authors report no disclosures or sources of funding.
A version of this article appeared on Medscape.com.
TOPLINE:
, according to a recent observational study published in JAMA Network Open.
METHODOLOGY:
- Patients receiving antibiotics through an IV line risk developing a secondary infection; antibiotics received orally are considered safer.
- Researchers analyzed observational data from 914 adults with uncomplicated gram-negative bacteremia who received care in four hospitals in Denmark between 2018 and 2021.
- The outcomes of patients who were switched to oral antibiotics within 4 days after a positive blood culture were compared with those who continued to receive IV antibiotics for at least 5 days after the blood culture; participants in both groups received antibiotics for 7-14 days.
- Researchers assessed mortality rates over a 90-day window and used a target trial emulation method to conduct the study.
TAKEAWAY:
- Overall, 14.3% of patients who received prolonged IV treatment died, compared with 6.9% in the oral antibiotics group.
- In an intention-to-treat analysis, patients who were switched to oral antibiotics had a 22% lower risk for death within 90 days of initiation of treatment (relative risk [RR], 0.78; 95% CI, 0.60-1.10).
- In a per-protocol analysis, patients who switched to the oral route had a 1% lower odds of dying within 90 days (RR, 0.99; 95% CI, 0.70-1.40).
- Individuals who were switched to oral antibiotic treatment were younger than those who continued to receive antibiotics via the IV route (median age, 73 vs 76 years, respectively), had fewer comorbidities (four vs five), and were more likely to have community-acquired gram-negative bacteremia (89.4% vs 80.9%).
IN PRACTICE:
“These findings suggest that the mortality associated with early antibiotic stepdown treatment is comparable to that associated with receiving prolonged IV antibiotic treatment for individuals with uncomplicated gram-negative bacteremia,” the authors of the study wrote.
SOURCE:
The study was led by Sandra Tingsgård, MD, of the Center of Research & Department of Infectious Diseases at Copenhagen University Hospital–Amager and Hvidovre in Denmark.
LIMITATIONS:
The study was based on data from electronic health records, so some factors may not have been recorded or considered. The researchers identified few cases of multidrug-resistant infections, and the findings may not apply to those cases. Complicated cases and people who were not stabilized by day 4 were excluded from the analysis.
DISCLOSURES:
The authors report no disclosures or sources of funding.
A version of this article appeared on Medscape.com.
TOPLINE:
, according to a recent observational study published in JAMA Network Open.
METHODOLOGY:
- Patients receiving antibiotics through an IV line risk developing a secondary infection; antibiotics received orally are considered safer.
- Researchers analyzed observational data from 914 adults with uncomplicated gram-negative bacteremia who received care in four hospitals in Denmark between 2018 and 2021.
- The outcomes of patients who were switched to oral antibiotics within 4 days after a positive blood culture were compared with those who continued to receive IV antibiotics for at least 5 days after the blood culture; participants in both groups received antibiotics for 7-14 days.
- Researchers assessed mortality rates over a 90-day window and used a target trial emulation method to conduct the study.
TAKEAWAY:
- Overall, 14.3% of patients who received prolonged IV treatment died, compared with 6.9% in the oral antibiotics group.
- In an intention-to-treat analysis, patients who were switched to oral antibiotics had a 22% lower risk for death within 90 days of initiation of treatment (relative risk [RR], 0.78; 95% CI, 0.60-1.10).
- In a per-protocol analysis, patients who switched to the oral route had a 1% lower odds of dying within 90 days (RR, 0.99; 95% CI, 0.70-1.40).
- Individuals who were switched to oral antibiotic treatment were younger than those who continued to receive antibiotics via the IV route (median age, 73 vs 76 years, respectively), had fewer comorbidities (four vs five), and were more likely to have community-acquired gram-negative bacteremia (89.4% vs 80.9%).
IN PRACTICE:
“These findings suggest that the mortality associated with early antibiotic stepdown treatment is comparable to that associated with receiving prolonged IV antibiotic treatment for individuals with uncomplicated gram-negative bacteremia,” the authors of the study wrote.
SOURCE:
The study was led by Sandra Tingsgård, MD, of the Center of Research & Department of Infectious Diseases at Copenhagen University Hospital–Amager and Hvidovre in Denmark.
LIMITATIONS:
The study was based on data from electronic health records, so some factors may not have been recorded or considered. The researchers identified few cases of multidrug-resistant infections, and the findings may not apply to those cases. Complicated cases and people who were not stabilized by day 4 were excluded from the analysis.
DISCLOSURES:
The authors report no disclosures or sources of funding.
A version of this article appeared on Medscape.com.
Higher Dose of Naloxone Has No Impact on Overdose Survival; Increases Withdrawal Symptoms
TOPLINE:
A new report from the US Centers for Disease Control and Prevention (CDC) showed that administering an 8 mg dose of intranasal naloxone does not increase the odds of surviving an opioid overdose; a higher dose than the usual 4 mg may result in a greater risk for onset of opioid withdrawal symptoms.
METHODOLOGY:
- The Morbidity and Mortality Weekly Report from the CDC presents data from a New York State Department of Health initiative.
- New York State Police troops administered either 8-mg or 4-mg doses of intranasal naloxone in response to suspected opiate overdose cases between March 2022 and August 2023.
- People who had died before the administration of the naloxone were excluded from the study.
- A total of 354 people were included in the study, 101 of whom received an 8-mg dose, while the others received the usual 4-mg dosage.
- Police officers documented the behavior and symptoms of people after receiving each dose, which could have included vomiting, disorientation, refusal to be transported to an emergency department, lethargy, and anger or combativeness.
TAKEAWAY:
- Survival rates were nearly identical regardless of intranasal naloxone dosage: 99% of people who received 8 mg compared with 99.2% of those who received 4 mg of the drug.
- Opioid withdrawal signs, including vomiting, were more prevalent among 8 mg naloxone recipients (37.6%) than among 4 mg recipients (19.4%) (risk ratio [RR], 2.51; P < .001).
- Police officers documented that people who received 8 mg were more frequently displayed anger or combativeness after revival than those who received the lower dose (RR, 1.42; P = .37).
IN PRACTICE:
The study “suggests that there are no benefits to law enforcement administration of higher-dose naloxone ... even in light of the increased prevalence of synthetic opioids, including fentanyl, in the drug supply.”
SOURCE:
Emily R. Payne, MSPH, of the New York State Department of Health, was the lead author of the study published in the Morbidity and Mortality Weekly Report on February 8, 2024.
LIMITATIONS:
The sample size of people receiving 8-mg doses was not equal to that of those receiving the usual dosage. Medical professionals did not report on the symptoms and behavior of people after receiving naloxone, law enforcement workers did, and may not have accurately captured what was occurring. In addition, researchers lacked complete data on the substances people used before an overdose, and the results may only be generalizable to New York State.
DISCLOSURES:
Study author Sharon Stancliff reported institutional support from the New York State Stewardship Funding Harm Reduction. No other potential conflicts of interest were disclosed.
A version of this article appeared on Medscape.com.
TOPLINE:
A new report from the US Centers for Disease Control and Prevention (CDC) showed that administering an 8 mg dose of intranasal naloxone does not increase the odds of surviving an opioid overdose; a higher dose than the usual 4 mg may result in a greater risk for onset of opioid withdrawal symptoms.
METHODOLOGY:
- The Morbidity and Mortality Weekly Report from the CDC presents data from a New York State Department of Health initiative.
- New York State Police troops administered either 8-mg or 4-mg doses of intranasal naloxone in response to suspected opiate overdose cases between March 2022 and August 2023.
- People who had died before the administration of the naloxone were excluded from the study.
- A total of 354 people were included in the study, 101 of whom received an 8-mg dose, while the others received the usual 4-mg dosage.
- Police officers documented the behavior and symptoms of people after receiving each dose, which could have included vomiting, disorientation, refusal to be transported to an emergency department, lethargy, and anger or combativeness.
TAKEAWAY:
- Survival rates were nearly identical regardless of intranasal naloxone dosage: 99% of people who received 8 mg compared with 99.2% of those who received 4 mg of the drug.
- Opioid withdrawal signs, including vomiting, were more prevalent among 8 mg naloxone recipients (37.6%) than among 4 mg recipients (19.4%) (risk ratio [RR], 2.51; P < .001).
- Police officers documented that people who received 8 mg were more frequently displayed anger or combativeness after revival than those who received the lower dose (RR, 1.42; P = .37).
IN PRACTICE:
The study “suggests that there are no benefits to law enforcement administration of higher-dose naloxone ... even in light of the increased prevalence of synthetic opioids, including fentanyl, in the drug supply.”
SOURCE:
Emily R. Payne, MSPH, of the New York State Department of Health, was the lead author of the study published in the Morbidity and Mortality Weekly Report on February 8, 2024.
LIMITATIONS:
The sample size of people receiving 8-mg doses was not equal to that of those receiving the usual dosage. Medical professionals did not report on the symptoms and behavior of people after receiving naloxone, law enforcement workers did, and may not have accurately captured what was occurring. In addition, researchers lacked complete data on the substances people used before an overdose, and the results may only be generalizable to New York State.
DISCLOSURES:
Study author Sharon Stancliff reported institutional support from the New York State Stewardship Funding Harm Reduction. No other potential conflicts of interest were disclosed.
A version of this article appeared on Medscape.com.
TOPLINE:
A new report from the US Centers for Disease Control and Prevention (CDC) showed that administering an 8 mg dose of intranasal naloxone does not increase the odds of surviving an opioid overdose; a higher dose than the usual 4 mg may result in a greater risk for onset of opioid withdrawal symptoms.
METHODOLOGY:
- The Morbidity and Mortality Weekly Report from the CDC presents data from a New York State Department of Health initiative.
- New York State Police troops administered either 8-mg or 4-mg doses of intranasal naloxone in response to suspected opiate overdose cases between March 2022 and August 2023.
- People who had died before the administration of the naloxone were excluded from the study.
- A total of 354 people were included in the study, 101 of whom received an 8-mg dose, while the others received the usual 4-mg dosage.
- Police officers documented the behavior and symptoms of people after receiving each dose, which could have included vomiting, disorientation, refusal to be transported to an emergency department, lethargy, and anger or combativeness.
TAKEAWAY:
- Survival rates were nearly identical regardless of intranasal naloxone dosage: 99% of people who received 8 mg compared with 99.2% of those who received 4 mg of the drug.
- Opioid withdrawal signs, including vomiting, were more prevalent among 8 mg naloxone recipients (37.6%) than among 4 mg recipients (19.4%) (risk ratio [RR], 2.51; P < .001).
- Police officers documented that people who received 8 mg were more frequently displayed anger or combativeness after revival than those who received the lower dose (RR, 1.42; P = .37).
IN PRACTICE:
The study “suggests that there are no benefits to law enforcement administration of higher-dose naloxone ... even in light of the increased prevalence of synthetic opioids, including fentanyl, in the drug supply.”
SOURCE:
Emily R. Payne, MSPH, of the New York State Department of Health, was the lead author of the study published in the Morbidity and Mortality Weekly Report on February 8, 2024.
LIMITATIONS:
The sample size of people receiving 8-mg doses was not equal to that of those receiving the usual dosage. Medical professionals did not report on the symptoms and behavior of people after receiving naloxone, law enforcement workers did, and may not have accurately captured what was occurring. In addition, researchers lacked complete data on the substances people used before an overdose, and the results may only be generalizable to New York State.
DISCLOSURES:
Study author Sharon Stancliff reported institutional support from the New York State Stewardship Funding Harm Reduction. No other potential conflicts of interest were disclosed.
A version of this article appeared on Medscape.com.
When Babies ‘Stop Breathing,’ Who Needs Admission and a Workup?
Many infants have experienced an episode of apnea, defined as a pause in respiration of 20 seconds or more. Most episodes remain unexplained, and no underlying cause can be found. Historically, these were referred to as “near-miss SIDS,” episodes, but that label suggested that all of these events would have ended in death had someone not intervened. New descriptive terminology was needed.
In the mid-1980s, the term “apparent life-threatening event” (ALTE) was adopted. But that term, too, was an overstatement, because although scary for parents, these brief apnea episodes were not, in most cases, truly life-threatening.
In 2013, authors of a systematic review coined the term “brief resolved unexplained event” (BRUE). This review also addressed the history and physical exam features associated with risk for a subsequent episode. It was felt that hospitalization and testing might be warranted if certain infants could be identified as high risk for recurrence.
What Is Considered a BRUE?
In the current working definition of BRUE, the child must be < 1 year old. The episode must be a sudden, brief, and resolved, with one or more of these characteristics:
- Cyanosis or pallor (but not turning red)
- A change in breathing (absent, decreased, or irregular)
- A change in tone (hypertonia or hypotonia)
- A change in responsiveness.
Furthermore, to qualify as a BRUE, no explanation can be found for the event based on the history and physical examination but before any laboratory testing is done. The definition also excludes children with known potential explanatory diagnoses (such as gastroesophageal reflux or bronchiolitis) and those who are otherwise symptomatically ill at the time of the event.
Decision to Admit and Recurrence Risk
An apnea event in an otherwise healthy infant, regardless of what it’s called, puts providers and parents in a difficult position. Should the infant be hospitalized for further monitoring and potentially more invasive testing to determine the cause of the episode? And what are the chances that the episode will be repeated?
A clinical practice guideline (CPG) for BRUE, widely adopted in 2016, resulted in significant reductions in healthcare utilization. The CPG attempted to identify low-risk infants who could safely be discharged from the emergency department. Although the CPG improved outcomes, experts acknowledged that an underlying problem was not likely to be identified even among infants deemed high risk, and these infants would be hospitalized unnecessarily.
Available data were simply insufficient to support this decision. So, with the goal of identifying factors that could help predict recurrent BRUE risk, a 15-hospital collaborative study was undertaken, followed by the development and validation of a clinical decision rule for predicting the risk for a serious underlying diagnosis or event recurrence among infants presenting with BRUE.
Here’s what we learned from more than 3000 cases of BRUE.
First, it turns out that it’s not easy to determine whether an infant is at low or high risk for recurrence of BRUE. Initially, 91.5% of patients enrolled in the study would have been labeled high risk.
Furthermore, a BRUE recurred in 14.3% of the cohort, and 4.8% of high-risk infants were found to have a serious undiagnosed condition. Seizures, airway anomalies, and gastroesophageal reflux were the top three causes of BRUE, but the spectrum of underlying pathology was quite considerable.
The problem was that 4.6% of the entire cohort were found to have a serious underlying condition, nearly identical to the proportion of high-risk infants with these conditions. This prompted the question of whether simply labeling infants “high risk” was really appropriate any longer.
Revised BRUE Management
Although it hasn’t been possible to group infants neatly in low and high-risk categories, the data from that large cohort led to the development of the BRUE 2.0 criteria, which enabled more focused risk assessment of an infant who experienced a BRUE. With an app on MDCalc, these criteria allow providers to ascertain, and show families, a visual representation of their infant’s individualized risk for a subsequent BRUE and of having a serious underlying condition.
The cohort study also identified red flags from the history or physical exam of infants who experienced a BRUE: weight loss, failure to thrive, or a history of feeding problems. Exam findings such as a bulging fontanelle, forceful or bilious emesis, and evidence of gastrointestinal (GI) bleeding suggest a medical diagnosis rather than a BRUE. If GI-related causes are high on the differential, a feeding evaluation can be helpful. A feeding evaluation can be done in the outpatient setting and does not require hospitalization.
For suspicion of an underlying neurological condition (such as seizures), experts recommend obtaining a short EEG, which is highly sensitive for detecting infantile spasms and encephalopathy. They recommend reserving MRI for infants with abnormalities on EEG or physical exam. Metabolic or genetic testing should be done only if the infant looks ill, because most patients with genetic or inborn errors of metabolism will continue to have symptoms as they become older.
The approach to BRUE has moved into the realm of shared decision-making with families. The likelihood of identifying a serious diagnosis is low for most of these children. And unfortunately, no single test can diagnose the full spectrum of potential explanatory diagnoses. For example, data from 2023 demonstrate that only 1.1% of lab tests following a BRUE contributed to a diagnosis, and most of the time that was a positive viral test. Similarly, imaging was helpful in only 1.5% of cases. So, explaining the evidence and deciding along with parents what is reasonable to do (or not do) is the current state of affairs.
My Take
As I reflect back on two and a half decades of caring for these patients, I believe that recent data have helped us a great deal. We do less testing and admit fewer infants to the hospital than we did 20 years ago, and that’s a good thing. Nevertheless, looking for a few red flags, having a high index of suspicion when the clinical exam is abnormal, and engaging in shared decision-making with families can help make the caring for these challenging patients more bearable and lead to better outcomes for all involved.
Dr. Basco is Professor, Department of Pediatrics, Medical University of South Carolina (MUSC); Director, Division of General Pediatrics, Department of Pediatrics, MUSC Children’s Hospital, Charleston, South Carolina. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Many infants have experienced an episode of apnea, defined as a pause in respiration of 20 seconds or more. Most episodes remain unexplained, and no underlying cause can be found. Historically, these were referred to as “near-miss SIDS,” episodes, but that label suggested that all of these events would have ended in death had someone not intervened. New descriptive terminology was needed.
In the mid-1980s, the term “apparent life-threatening event” (ALTE) was adopted. But that term, too, was an overstatement, because although scary for parents, these brief apnea episodes were not, in most cases, truly life-threatening.
In 2013, authors of a systematic review coined the term “brief resolved unexplained event” (BRUE). This review also addressed the history and physical exam features associated with risk for a subsequent episode. It was felt that hospitalization and testing might be warranted if certain infants could be identified as high risk for recurrence.
What Is Considered a BRUE?
In the current working definition of BRUE, the child must be < 1 year old. The episode must be a sudden, brief, and resolved, with one or more of these characteristics:
- Cyanosis or pallor (but not turning red)
- A change in breathing (absent, decreased, or irregular)
- A change in tone (hypertonia or hypotonia)
- A change in responsiveness.
Furthermore, to qualify as a BRUE, no explanation can be found for the event based on the history and physical examination but before any laboratory testing is done. The definition also excludes children with known potential explanatory diagnoses (such as gastroesophageal reflux or bronchiolitis) and those who are otherwise symptomatically ill at the time of the event.
Decision to Admit and Recurrence Risk
An apnea event in an otherwise healthy infant, regardless of what it’s called, puts providers and parents in a difficult position. Should the infant be hospitalized for further monitoring and potentially more invasive testing to determine the cause of the episode? And what are the chances that the episode will be repeated?
A clinical practice guideline (CPG) for BRUE, widely adopted in 2016, resulted in significant reductions in healthcare utilization. The CPG attempted to identify low-risk infants who could safely be discharged from the emergency department. Although the CPG improved outcomes, experts acknowledged that an underlying problem was not likely to be identified even among infants deemed high risk, and these infants would be hospitalized unnecessarily.
Available data were simply insufficient to support this decision. So, with the goal of identifying factors that could help predict recurrent BRUE risk, a 15-hospital collaborative study was undertaken, followed by the development and validation of a clinical decision rule for predicting the risk for a serious underlying diagnosis or event recurrence among infants presenting with BRUE.
Here’s what we learned from more than 3000 cases of BRUE.
First, it turns out that it’s not easy to determine whether an infant is at low or high risk for recurrence of BRUE. Initially, 91.5% of patients enrolled in the study would have been labeled high risk.
Furthermore, a BRUE recurred in 14.3% of the cohort, and 4.8% of high-risk infants were found to have a serious undiagnosed condition. Seizures, airway anomalies, and gastroesophageal reflux were the top three causes of BRUE, but the spectrum of underlying pathology was quite considerable.
The problem was that 4.6% of the entire cohort were found to have a serious underlying condition, nearly identical to the proportion of high-risk infants with these conditions. This prompted the question of whether simply labeling infants “high risk” was really appropriate any longer.
Revised BRUE Management
Although it hasn’t been possible to group infants neatly in low and high-risk categories, the data from that large cohort led to the development of the BRUE 2.0 criteria, which enabled more focused risk assessment of an infant who experienced a BRUE. With an app on MDCalc, these criteria allow providers to ascertain, and show families, a visual representation of their infant’s individualized risk for a subsequent BRUE and of having a serious underlying condition.
The cohort study also identified red flags from the history or physical exam of infants who experienced a BRUE: weight loss, failure to thrive, or a history of feeding problems. Exam findings such as a bulging fontanelle, forceful or bilious emesis, and evidence of gastrointestinal (GI) bleeding suggest a medical diagnosis rather than a BRUE. If GI-related causes are high on the differential, a feeding evaluation can be helpful. A feeding evaluation can be done in the outpatient setting and does not require hospitalization.
For suspicion of an underlying neurological condition (such as seizures), experts recommend obtaining a short EEG, which is highly sensitive for detecting infantile spasms and encephalopathy. They recommend reserving MRI for infants with abnormalities on EEG or physical exam. Metabolic or genetic testing should be done only if the infant looks ill, because most patients with genetic or inborn errors of metabolism will continue to have symptoms as they become older.
The approach to BRUE has moved into the realm of shared decision-making with families. The likelihood of identifying a serious diagnosis is low for most of these children. And unfortunately, no single test can diagnose the full spectrum of potential explanatory diagnoses. For example, data from 2023 demonstrate that only 1.1% of lab tests following a BRUE contributed to a diagnosis, and most of the time that was a positive viral test. Similarly, imaging was helpful in only 1.5% of cases. So, explaining the evidence and deciding along with parents what is reasonable to do (or not do) is the current state of affairs.
My Take
As I reflect back on two and a half decades of caring for these patients, I believe that recent data have helped us a great deal. We do less testing and admit fewer infants to the hospital than we did 20 years ago, and that’s a good thing. Nevertheless, looking for a few red flags, having a high index of suspicion when the clinical exam is abnormal, and engaging in shared decision-making with families can help make the caring for these challenging patients more bearable and lead to better outcomes for all involved.
Dr. Basco is Professor, Department of Pediatrics, Medical University of South Carolina (MUSC); Director, Division of General Pediatrics, Department of Pediatrics, MUSC Children’s Hospital, Charleston, South Carolina. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Many infants have experienced an episode of apnea, defined as a pause in respiration of 20 seconds or more. Most episodes remain unexplained, and no underlying cause can be found. Historically, these were referred to as “near-miss SIDS,” episodes, but that label suggested that all of these events would have ended in death had someone not intervened. New descriptive terminology was needed.
In the mid-1980s, the term “apparent life-threatening event” (ALTE) was adopted. But that term, too, was an overstatement, because although scary for parents, these brief apnea episodes were not, in most cases, truly life-threatening.
In 2013, authors of a systematic review coined the term “brief resolved unexplained event” (BRUE). This review also addressed the history and physical exam features associated with risk for a subsequent episode. It was felt that hospitalization and testing might be warranted if certain infants could be identified as high risk for recurrence.
What Is Considered a BRUE?
In the current working definition of BRUE, the child must be < 1 year old. The episode must be a sudden, brief, and resolved, with one or more of these characteristics:
- Cyanosis or pallor (but not turning red)
- A change in breathing (absent, decreased, or irregular)
- A change in tone (hypertonia or hypotonia)
- A change in responsiveness.
Furthermore, to qualify as a BRUE, no explanation can be found for the event based on the history and physical examination but before any laboratory testing is done. The definition also excludes children with known potential explanatory diagnoses (such as gastroesophageal reflux or bronchiolitis) and those who are otherwise symptomatically ill at the time of the event.
Decision to Admit and Recurrence Risk
An apnea event in an otherwise healthy infant, regardless of what it’s called, puts providers and parents in a difficult position. Should the infant be hospitalized for further monitoring and potentially more invasive testing to determine the cause of the episode? And what are the chances that the episode will be repeated?
A clinical practice guideline (CPG) for BRUE, widely adopted in 2016, resulted in significant reductions in healthcare utilization. The CPG attempted to identify low-risk infants who could safely be discharged from the emergency department. Although the CPG improved outcomes, experts acknowledged that an underlying problem was not likely to be identified even among infants deemed high risk, and these infants would be hospitalized unnecessarily.
Available data were simply insufficient to support this decision. So, with the goal of identifying factors that could help predict recurrent BRUE risk, a 15-hospital collaborative study was undertaken, followed by the development and validation of a clinical decision rule for predicting the risk for a serious underlying diagnosis or event recurrence among infants presenting with BRUE.
Here’s what we learned from more than 3000 cases of BRUE.
First, it turns out that it’s not easy to determine whether an infant is at low or high risk for recurrence of BRUE. Initially, 91.5% of patients enrolled in the study would have been labeled high risk.
Furthermore, a BRUE recurred in 14.3% of the cohort, and 4.8% of high-risk infants were found to have a serious undiagnosed condition. Seizures, airway anomalies, and gastroesophageal reflux were the top three causes of BRUE, but the spectrum of underlying pathology was quite considerable.
The problem was that 4.6% of the entire cohort were found to have a serious underlying condition, nearly identical to the proportion of high-risk infants with these conditions. This prompted the question of whether simply labeling infants “high risk” was really appropriate any longer.
Revised BRUE Management
Although it hasn’t been possible to group infants neatly in low and high-risk categories, the data from that large cohort led to the development of the BRUE 2.0 criteria, which enabled more focused risk assessment of an infant who experienced a BRUE. With an app on MDCalc, these criteria allow providers to ascertain, and show families, a visual representation of their infant’s individualized risk for a subsequent BRUE and of having a serious underlying condition.
The cohort study also identified red flags from the history or physical exam of infants who experienced a BRUE: weight loss, failure to thrive, or a history of feeding problems. Exam findings such as a bulging fontanelle, forceful or bilious emesis, and evidence of gastrointestinal (GI) bleeding suggest a medical diagnosis rather than a BRUE. If GI-related causes are high on the differential, a feeding evaluation can be helpful. A feeding evaluation can be done in the outpatient setting and does not require hospitalization.
For suspicion of an underlying neurological condition (such as seizures), experts recommend obtaining a short EEG, which is highly sensitive for detecting infantile spasms and encephalopathy. They recommend reserving MRI for infants with abnormalities on EEG or physical exam. Metabolic or genetic testing should be done only if the infant looks ill, because most patients with genetic or inborn errors of metabolism will continue to have symptoms as they become older.
The approach to BRUE has moved into the realm of shared decision-making with families. The likelihood of identifying a serious diagnosis is low for most of these children. And unfortunately, no single test can diagnose the full spectrum of potential explanatory diagnoses. For example, data from 2023 demonstrate that only 1.1% of lab tests following a BRUE contributed to a diagnosis, and most of the time that was a positive viral test. Similarly, imaging was helpful in only 1.5% of cases. So, explaining the evidence and deciding along with parents what is reasonable to do (or not do) is the current state of affairs.
My Take
As I reflect back on two and a half decades of caring for these patients, I believe that recent data have helped us a great deal. We do less testing and admit fewer infants to the hospital than we did 20 years ago, and that’s a good thing. Nevertheless, looking for a few red flags, having a high index of suspicion when the clinical exam is abnormal, and engaging in shared decision-making with families can help make the caring for these challenging patients more bearable and lead to better outcomes for all involved.
Dr. Basco is Professor, Department of Pediatrics, Medical University of South Carolina (MUSC); Director, Division of General Pediatrics, Department of Pediatrics, MUSC Children’s Hospital, Charleston, South Carolina. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Tirofiban Reduces Early Neurologic Deterioration After Stroke
Intravenous (IV) administration of the antiplatelet agent tirofiban for 72 hours was associated with a reduction in early neurologic deterioration compared with oral aspirin therapy in patients with acute ischemic stroke, in the randomized TREND trial.
The results were presented at the International Stroke Conference 2024, held on February 7-9 in Phoenix, Arizona.
Lead author Zhao Wenbo, MD, Xuanwu Hospital, Beijing, China, noted that neurologic deterioration, characterized by a sudden onset and quick peak of neurologic deficits, is a common phenomenon in acute ischemic stroke and is strongly associated with poor clinical outcomes.
Ischemic stroke progression is the main cause of neurologic deterioration, especially during the first few days after onset, Dr. Wenbo said. , but administering oral antiplatelet agents can be difficult because of dysphagia, he reported.
The TREND trial was conducted to investigate whether IV tirofiban could prevent early neurologic deterioration without increasing the risk for symptomatic intracerebral hemorrhage in acute ischemic stroke.
The study included 426 patients with acute ischemic stroke within 24 hours of symptom onset who had a neurologic deficit attributed to focal cerebral ischemia and a National Institutes of Health Stroke Scale (NIHSS) score between 4 and 20 points and who were not treated with thrombolysis or endovascular thrombectomy. Patients with cardioembolic stroke were also excluded.
Patients were a median of 10-12 hours from symptom onset and had a baseline NIHSS score of 5.
They were randomized to IV tirofiban or oral aspirin for 72 hours. All patients were then continued on oral antiplatelet therapy.
The primary efficacy outcome was neurologic deterioration within 72 hours after randomization, defined as an increase in NIHSS score of 4 points or more.
This occurred in nine patients (4.2%) in the tirofiban group vs 28 (13.2%) in the control group (relative risk, 0.32; 95% CI, 0.15-0.66; P = .002).
A consistent benefit of IV tirofiban was seen across all subgroups.
The secondary endpoint of neurologic deterioration within 72 hours after randomization, defined as an increase of NIHSS score of 2 points or more, was also significantly reduced. This occurred in 11.7% of the tirofiban group vs 23.6% of the aspirin group (RR, 0.49; 95% CI, 0.32-0.75; P = .001).
An excellent outcome on the modified Rankin Scale (mRS) disability score (mRS, 0-1) at 90 days was seen in 75% of tirofiban vs 68% of aspirin patients, a nonsignificant difference.
A good outcome (mRS, 0-2) occurred in 89% of tirofiban vs 86% of aspirin patients, again a nonsignificant difference.
There were no symptomatic intracerebral hemorrhages within 72 hours after randomization (the primary safety endpoint) in either group, and the incidence of systemic bleeding also did not differ significantly between the groups.
Dr. Wenbo concluded that further randomized clinical trials are needed to determine the efficacy of tirofiban on functional outcomes.
‘Promising Results’
Commenting on the study for this news organization, conference chair, Tudor Jovin, MD, Cooper Medical School of Rowan University, Camden, New Jersey, and vice-chair, Lauren Sansing, MD, Yale School of Medicine, New Haven, Connecticut, both said they thought the results were promising.
“This study didn’t show any long-term outcome benefit, but this was a smaller study, and the results need to be replicated in a larger study with sufficient power to look at longer-term outcomes,” Sansing noted. “But we don’t have anything better than aspirin at present for these patients, so it’s exciting that there may be something in the pipeline for this group.”
Dr. Jovin pointed out that the TREND trial selected patients on the cause of their stroke, in line with the practice of precision medicine.
“By excluding patients who received thrombolysis or thrombectomy and those who had cardioembolic strokes, we are left with a population who we don’t have many treatment options for,” he said. “These are patients with smaller or moderate strokes who may arrive too late for thrombolysis. It would be great to be able to do something more than just aspirin for these patients.”
Dr. Jovin noted that the study was underpowered to show long-term benefits, but there were some promising trends.
“It stands to reason that if neurologic function does not get worse in the early hours and days after stroke, then the long-term outcomes are likely to be better,” he noted. “But this needs to be confirmed in larger trials.”
Interestingly, another study, the MOST trial, also presented at the ISC-24 meeting, showed no benefit with the IV antithrombotic agents argatroban or eptifibatide on 90-day functional outcomes when added to thrombolysis in acute ischemic stroke.
Dr. Jovin pointed out that the MOST and TREND trials included different populations of patients — the MOST patients received thrombolysis, while the TREND patients did not. And in the MOST trial, about half the patients had a large vessel occlusion and underwent thrombectomy, whereas these patients were excluded in TREND.
Dr. Sansing added that patients in the TREND trial may have had small vessel disease or other atherosclerotic disease, or strokes due to the narrowing of vessels or due to an unknown cause. They were also given 3 days of IV tirofiban, whereas the duration of antithrombotic treatment in MOST was shorter.
The TREND study was funded by the National Key Research and Development Program of China, the National Science Foundation of Beijing Municipality, and the Beijing Municipal Science and Technology Commission.
A version of this article appeared on Medscape.com.
Intravenous (IV) administration of the antiplatelet agent tirofiban for 72 hours was associated with a reduction in early neurologic deterioration compared with oral aspirin therapy in patients with acute ischemic stroke, in the randomized TREND trial.
The results were presented at the International Stroke Conference 2024, held on February 7-9 in Phoenix, Arizona.
Lead author Zhao Wenbo, MD, Xuanwu Hospital, Beijing, China, noted that neurologic deterioration, characterized by a sudden onset and quick peak of neurologic deficits, is a common phenomenon in acute ischemic stroke and is strongly associated with poor clinical outcomes.
Ischemic stroke progression is the main cause of neurologic deterioration, especially during the first few days after onset, Dr. Wenbo said. , but administering oral antiplatelet agents can be difficult because of dysphagia, he reported.
The TREND trial was conducted to investigate whether IV tirofiban could prevent early neurologic deterioration without increasing the risk for symptomatic intracerebral hemorrhage in acute ischemic stroke.
The study included 426 patients with acute ischemic stroke within 24 hours of symptom onset who had a neurologic deficit attributed to focal cerebral ischemia and a National Institutes of Health Stroke Scale (NIHSS) score between 4 and 20 points and who were not treated with thrombolysis or endovascular thrombectomy. Patients with cardioembolic stroke were also excluded.
Patients were a median of 10-12 hours from symptom onset and had a baseline NIHSS score of 5.
They were randomized to IV tirofiban or oral aspirin for 72 hours. All patients were then continued on oral antiplatelet therapy.
The primary efficacy outcome was neurologic deterioration within 72 hours after randomization, defined as an increase in NIHSS score of 4 points or more.
This occurred in nine patients (4.2%) in the tirofiban group vs 28 (13.2%) in the control group (relative risk, 0.32; 95% CI, 0.15-0.66; P = .002).
A consistent benefit of IV tirofiban was seen across all subgroups.
The secondary endpoint of neurologic deterioration within 72 hours after randomization, defined as an increase of NIHSS score of 2 points or more, was also significantly reduced. This occurred in 11.7% of the tirofiban group vs 23.6% of the aspirin group (RR, 0.49; 95% CI, 0.32-0.75; P = .001).
An excellent outcome on the modified Rankin Scale (mRS) disability score (mRS, 0-1) at 90 days was seen in 75% of tirofiban vs 68% of aspirin patients, a nonsignificant difference.
A good outcome (mRS, 0-2) occurred in 89% of tirofiban vs 86% of aspirin patients, again a nonsignificant difference.
There were no symptomatic intracerebral hemorrhages within 72 hours after randomization (the primary safety endpoint) in either group, and the incidence of systemic bleeding also did not differ significantly between the groups.
Dr. Wenbo concluded that further randomized clinical trials are needed to determine the efficacy of tirofiban on functional outcomes.
‘Promising Results’
Commenting on the study for this news organization, conference chair, Tudor Jovin, MD, Cooper Medical School of Rowan University, Camden, New Jersey, and vice-chair, Lauren Sansing, MD, Yale School of Medicine, New Haven, Connecticut, both said they thought the results were promising.
“This study didn’t show any long-term outcome benefit, but this was a smaller study, and the results need to be replicated in a larger study with sufficient power to look at longer-term outcomes,” Sansing noted. “But we don’t have anything better than aspirin at present for these patients, so it’s exciting that there may be something in the pipeline for this group.”
Dr. Jovin pointed out that the TREND trial selected patients on the cause of their stroke, in line with the practice of precision medicine.
“By excluding patients who received thrombolysis or thrombectomy and those who had cardioembolic strokes, we are left with a population who we don’t have many treatment options for,” he said. “These are patients with smaller or moderate strokes who may arrive too late for thrombolysis. It would be great to be able to do something more than just aspirin for these patients.”
Dr. Jovin noted that the study was underpowered to show long-term benefits, but there were some promising trends.
“It stands to reason that if neurologic function does not get worse in the early hours and days after stroke, then the long-term outcomes are likely to be better,” he noted. “But this needs to be confirmed in larger trials.”
Interestingly, another study, the MOST trial, also presented at the ISC-24 meeting, showed no benefit with the IV antithrombotic agents argatroban or eptifibatide on 90-day functional outcomes when added to thrombolysis in acute ischemic stroke.
Dr. Jovin pointed out that the MOST and TREND trials included different populations of patients — the MOST patients received thrombolysis, while the TREND patients did not. And in the MOST trial, about half the patients had a large vessel occlusion and underwent thrombectomy, whereas these patients were excluded in TREND.
Dr. Sansing added that patients in the TREND trial may have had small vessel disease or other atherosclerotic disease, or strokes due to the narrowing of vessels or due to an unknown cause. They were also given 3 days of IV tirofiban, whereas the duration of antithrombotic treatment in MOST was shorter.
The TREND study was funded by the National Key Research and Development Program of China, the National Science Foundation of Beijing Municipality, and the Beijing Municipal Science and Technology Commission.
A version of this article appeared on Medscape.com.
Intravenous (IV) administration of the antiplatelet agent tirofiban for 72 hours was associated with a reduction in early neurologic deterioration compared with oral aspirin therapy in patients with acute ischemic stroke, in the randomized TREND trial.
The results were presented at the International Stroke Conference 2024, held on February 7-9 in Phoenix, Arizona.
Lead author Zhao Wenbo, MD, Xuanwu Hospital, Beijing, China, noted that neurologic deterioration, characterized by a sudden onset and quick peak of neurologic deficits, is a common phenomenon in acute ischemic stroke and is strongly associated with poor clinical outcomes.
Ischemic stroke progression is the main cause of neurologic deterioration, especially during the first few days after onset, Dr. Wenbo said. , but administering oral antiplatelet agents can be difficult because of dysphagia, he reported.
The TREND trial was conducted to investigate whether IV tirofiban could prevent early neurologic deterioration without increasing the risk for symptomatic intracerebral hemorrhage in acute ischemic stroke.
The study included 426 patients with acute ischemic stroke within 24 hours of symptom onset who had a neurologic deficit attributed to focal cerebral ischemia and a National Institutes of Health Stroke Scale (NIHSS) score between 4 and 20 points and who were not treated with thrombolysis or endovascular thrombectomy. Patients with cardioembolic stroke were also excluded.
Patients were a median of 10-12 hours from symptom onset and had a baseline NIHSS score of 5.
They were randomized to IV tirofiban or oral aspirin for 72 hours. All patients were then continued on oral antiplatelet therapy.
The primary efficacy outcome was neurologic deterioration within 72 hours after randomization, defined as an increase in NIHSS score of 4 points or more.
This occurred in nine patients (4.2%) in the tirofiban group vs 28 (13.2%) in the control group (relative risk, 0.32; 95% CI, 0.15-0.66; P = .002).
A consistent benefit of IV tirofiban was seen across all subgroups.
The secondary endpoint of neurologic deterioration within 72 hours after randomization, defined as an increase of NIHSS score of 2 points or more, was also significantly reduced. This occurred in 11.7% of the tirofiban group vs 23.6% of the aspirin group (RR, 0.49; 95% CI, 0.32-0.75; P = .001).
An excellent outcome on the modified Rankin Scale (mRS) disability score (mRS, 0-1) at 90 days was seen in 75% of tirofiban vs 68% of aspirin patients, a nonsignificant difference.
A good outcome (mRS, 0-2) occurred in 89% of tirofiban vs 86% of aspirin patients, again a nonsignificant difference.
There were no symptomatic intracerebral hemorrhages within 72 hours after randomization (the primary safety endpoint) in either group, and the incidence of systemic bleeding also did not differ significantly between the groups.
Dr. Wenbo concluded that further randomized clinical trials are needed to determine the efficacy of tirofiban on functional outcomes.
‘Promising Results’
Commenting on the study for this news organization, conference chair, Tudor Jovin, MD, Cooper Medical School of Rowan University, Camden, New Jersey, and vice-chair, Lauren Sansing, MD, Yale School of Medicine, New Haven, Connecticut, both said they thought the results were promising.
“This study didn’t show any long-term outcome benefit, but this was a smaller study, and the results need to be replicated in a larger study with sufficient power to look at longer-term outcomes,” Sansing noted. “But we don’t have anything better than aspirin at present for these patients, so it’s exciting that there may be something in the pipeline for this group.”
Dr. Jovin pointed out that the TREND trial selected patients on the cause of their stroke, in line with the practice of precision medicine.
“By excluding patients who received thrombolysis or thrombectomy and those who had cardioembolic strokes, we are left with a population who we don’t have many treatment options for,” he said. “These are patients with smaller or moderate strokes who may arrive too late for thrombolysis. It would be great to be able to do something more than just aspirin for these patients.”
Dr. Jovin noted that the study was underpowered to show long-term benefits, but there were some promising trends.
“It stands to reason that if neurologic function does not get worse in the early hours and days after stroke, then the long-term outcomes are likely to be better,” he noted. “But this needs to be confirmed in larger trials.”
Interestingly, another study, the MOST trial, also presented at the ISC-24 meeting, showed no benefit with the IV antithrombotic agents argatroban or eptifibatide on 90-day functional outcomes when added to thrombolysis in acute ischemic stroke.
Dr. Jovin pointed out that the MOST and TREND trials included different populations of patients — the MOST patients received thrombolysis, while the TREND patients did not. And in the MOST trial, about half the patients had a large vessel occlusion and underwent thrombectomy, whereas these patients were excluded in TREND.
Dr. Sansing added that patients in the TREND trial may have had small vessel disease or other atherosclerotic disease, or strokes due to the narrowing of vessels or due to an unknown cause. They were also given 3 days of IV tirofiban, whereas the duration of antithrombotic treatment in MOST was shorter.
The TREND study was funded by the National Key Research and Development Program of China, the National Science Foundation of Beijing Municipality, and the Beijing Municipal Science and Technology Commission.
A version of this article appeared on Medscape.com.
Study Suggests Mind-Body Benefits of GLP-1s
, according to an analysis of millions of people’s health records.
The findings were published this week by researchers from the electronic health record company Epic. Researchers looked for new diagnoses of depression or anxiety among people who started taking drugs from a class called GLP-1 agonists that can help manage blood sugar or treat obesity by mimicking hormone levels in the body that can affect appetite and blood sugar. Many people who take the drugs experience significant weight loss.
The researchers found that people with diabetes who started taking most versions of GLP-1 agonists were between 11% and 65% less likely to be newly diagnosed with depression than people with diabetes who didn’t take one of the drugs. The greatest reduction in likelihood of a new depression diagnosis was observed among people taking tirzepatide, which is sold under the brand names Mounjaro and Zepbound.
A reduced likelihood of being diagnosed with anxiety was also observed among people with diabetes after they started taking a GLP-1 agonist, compared to people with diabetes who didn’t take one of the drugs. Again, tirzepatide showed the greatest reduction in odds, with people taking that drug experiencing a 60% reduced likelihood of being newly diagnosed with anxiety.
Similar reductions in the likelihood of new depression or anxiety diagnoses were observed among people who didn’t have diabetes but were taking GLP-1 agonists, such as for weight loss.
The mind-body connection has been well established by research.
“Thoughts, feelings, beliefs, and attitudes can affect how healthy your body is,” according to a summary from the CDC about the connection between diabetes and depression. “Untreated mental health issues can make diabetes worse, and problems with diabetes can make mental health issues worse. But fortunately if one gets better, the other tends to get better, too.”
This latest analysis included the drugs dulaglutide, exenatide, liraglutide, semaglutide, and tirzepatide. The medicines, used for weight loss or to manage diabetes, include the brand names Byetta, Ozempic, Mounjaro, Trulicity, Wegovy, and Zepbound. The researchers also looked for links between depression or anxiety diagnoses among people taking liraglutide (sold under brand names Saxenda and Victoza), but found that there was little to no change in the likelihood of being diagnosed with depression or anxiety after starting liraglutide.
The findings are timely as regulators in the U.S. and Europe are investigating reports of suicidal thoughts among people using the drugs. In January, the FDA announced that a preliminary investigation showed no increased risk of suicidal thoughts or actions, but the agency could not “definitively rule out that a small risk may exist; therefore, FDA is continuing to look into this issue.”
This latest analysis from Epic Research only looked at health records, was not published in a peer-reviewed journal, nor could it establish a definitive role the medications may have played in whether or not someone was diagnosed with depression or anxiety. It’s unknown whether people in the study had symptoms of depression or anxiety before starting the medications.
“These results show that these medications may serve a dual purpose for patients, but we do not understand them well enough yet to say these medications should be given as a treatment for anxiety or depression outside of diabetes or weight management,” Kersten Bartelt, a researcher employed by Epic, told ABC News.
A version of this article appeared on WebMD.com.
, according to an analysis of millions of people’s health records.
The findings were published this week by researchers from the electronic health record company Epic. Researchers looked for new diagnoses of depression or anxiety among people who started taking drugs from a class called GLP-1 agonists that can help manage blood sugar or treat obesity by mimicking hormone levels in the body that can affect appetite and blood sugar. Many people who take the drugs experience significant weight loss.
The researchers found that people with diabetes who started taking most versions of GLP-1 agonists were between 11% and 65% less likely to be newly diagnosed with depression than people with diabetes who didn’t take one of the drugs. The greatest reduction in likelihood of a new depression diagnosis was observed among people taking tirzepatide, which is sold under the brand names Mounjaro and Zepbound.
A reduced likelihood of being diagnosed with anxiety was also observed among people with diabetes after they started taking a GLP-1 agonist, compared to people with diabetes who didn’t take one of the drugs. Again, tirzepatide showed the greatest reduction in odds, with people taking that drug experiencing a 60% reduced likelihood of being newly diagnosed with anxiety.
Similar reductions in the likelihood of new depression or anxiety diagnoses were observed among people who didn’t have diabetes but were taking GLP-1 agonists, such as for weight loss.
The mind-body connection has been well established by research.
“Thoughts, feelings, beliefs, and attitudes can affect how healthy your body is,” according to a summary from the CDC about the connection between diabetes and depression. “Untreated mental health issues can make diabetes worse, and problems with diabetes can make mental health issues worse. But fortunately if one gets better, the other tends to get better, too.”
This latest analysis included the drugs dulaglutide, exenatide, liraglutide, semaglutide, and tirzepatide. The medicines, used for weight loss or to manage diabetes, include the brand names Byetta, Ozempic, Mounjaro, Trulicity, Wegovy, and Zepbound. The researchers also looked for links between depression or anxiety diagnoses among people taking liraglutide (sold under brand names Saxenda and Victoza), but found that there was little to no change in the likelihood of being diagnosed with depression or anxiety after starting liraglutide.
The findings are timely as regulators in the U.S. and Europe are investigating reports of suicidal thoughts among people using the drugs. In January, the FDA announced that a preliminary investigation showed no increased risk of suicidal thoughts or actions, but the agency could not “definitively rule out that a small risk may exist; therefore, FDA is continuing to look into this issue.”
This latest analysis from Epic Research only looked at health records, was not published in a peer-reviewed journal, nor could it establish a definitive role the medications may have played in whether or not someone was diagnosed with depression or anxiety. It’s unknown whether people in the study had symptoms of depression or anxiety before starting the medications.
“These results show that these medications may serve a dual purpose for patients, but we do not understand them well enough yet to say these medications should be given as a treatment for anxiety or depression outside of diabetes or weight management,” Kersten Bartelt, a researcher employed by Epic, told ABC News.
A version of this article appeared on WebMD.com.
, according to an analysis of millions of people’s health records.
The findings were published this week by researchers from the electronic health record company Epic. Researchers looked for new diagnoses of depression or anxiety among people who started taking drugs from a class called GLP-1 agonists that can help manage blood sugar or treat obesity by mimicking hormone levels in the body that can affect appetite and blood sugar. Many people who take the drugs experience significant weight loss.
The researchers found that people with diabetes who started taking most versions of GLP-1 agonists were between 11% and 65% less likely to be newly diagnosed with depression than people with diabetes who didn’t take one of the drugs. The greatest reduction in likelihood of a new depression diagnosis was observed among people taking tirzepatide, which is sold under the brand names Mounjaro and Zepbound.
A reduced likelihood of being diagnosed with anxiety was also observed among people with diabetes after they started taking a GLP-1 agonist, compared to people with diabetes who didn’t take one of the drugs. Again, tirzepatide showed the greatest reduction in odds, with people taking that drug experiencing a 60% reduced likelihood of being newly diagnosed with anxiety.
Similar reductions in the likelihood of new depression or anxiety diagnoses were observed among people who didn’t have diabetes but were taking GLP-1 agonists, such as for weight loss.
The mind-body connection has been well established by research.
“Thoughts, feelings, beliefs, and attitudes can affect how healthy your body is,” according to a summary from the CDC about the connection between diabetes and depression. “Untreated mental health issues can make diabetes worse, and problems with diabetes can make mental health issues worse. But fortunately if one gets better, the other tends to get better, too.”
This latest analysis included the drugs dulaglutide, exenatide, liraglutide, semaglutide, and tirzepatide. The medicines, used for weight loss or to manage diabetes, include the brand names Byetta, Ozempic, Mounjaro, Trulicity, Wegovy, and Zepbound. The researchers also looked for links between depression or anxiety diagnoses among people taking liraglutide (sold under brand names Saxenda and Victoza), but found that there was little to no change in the likelihood of being diagnosed with depression or anxiety after starting liraglutide.
The findings are timely as regulators in the U.S. and Europe are investigating reports of suicidal thoughts among people using the drugs. In January, the FDA announced that a preliminary investigation showed no increased risk of suicidal thoughts or actions, but the agency could not “definitively rule out that a small risk may exist; therefore, FDA is continuing to look into this issue.”
This latest analysis from Epic Research only looked at health records, was not published in a peer-reviewed journal, nor could it establish a definitive role the medications may have played in whether or not someone was diagnosed with depression or anxiety. It’s unknown whether people in the study had symptoms of depression or anxiety before starting the medications.
“These results show that these medications may serve a dual purpose for patients, but we do not understand them well enough yet to say these medications should be given as a treatment for anxiety or depression outside of diabetes or weight management,” Kersten Bartelt, a researcher employed by Epic, told ABC News.
A version of this article appeared on WebMD.com.
New Guidelines: Brain Death Is Equal to Heart Death, Says Ethicist
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the Division of Medical Ethics at the New York University Grossman School of Medicine in New York City.
I think we had a breakthrough on a very controversial subject over the past month. Over and over again, debates have been breaking out, cases have been going to court, and fights have been coming to ethics committees about brain death. How do we know what brain death is, how do we diagnose it, and what rights do families have with respect to the diagnosis?
The American Academy of Neurology decided to form a task force, and they just issued guidelines on the definition, tests to use it, and the rights of families. They did a wonderful job, in my view. They›ve achieved clarity.
First, they tried to handle both adults and children. Children are, if you will, more difficult — and that’s been known — to test for brain death. Their brains are smaller. You get more interference and false signals coming from muscle or nerve activity that might be going on elsewhere in their bodies.
The guidelines say we’re going to try to see whether a person can breathe without support. If it’s an adult, one test over a 24-hour period would be sufficient. If you had them off the ventilator and they can’t breathe and show no signs of being able to do that, that’s a very fundamental test for brain death. For children, you’re going to have to do it twice. The guidelines are saying to be cautious.
Second, they say it’s very important to know the cause of the suspected brain death condition. If someone has a massive head injury, that’s different from a situation in which someone overdoses from drugs or drowns. Those conditions can be a little deceptive. In the case of drowning, sometimes the brain has protective mechanisms to protect circulation to the brain naturally for a little bit of time. I’m talking about minutes, not hours.
You want to be careful to make sure that you know the cause of the massive brain injury or insult that makes someone believe that the patient is brain-dead, whether it’s a stroke, an embolism, a bleed, a gunshot wound, or trauma to the head. Those factors really drive the certainty with which brain death should be pronounced. I think that’s very, very important.
They also said that brain death means the permanent loss of brain function. You may get a few cells still firing or you may be in a situation, because the life support is still there, where the body looks pink and perhaps might appear to still be alive to someone. When you know that the damage to the brain is so severe that there’s nothing that can be done to bring back the support of heart function, breathing, and most likely any ability to sense or feel anything, that is death.
I believe it’s very important, when talking to families, to say there are two ways that we pronounce people dead, and they’re equal: One is to say their heart has stopped, their breathing has stopped, and there’s nothing we can do to resuscitate them, which is cardiac death. The other is to say their brain has permanently ceased to function in any kind of integrated way. That means no heartbeat, no breathing, and no mental sensations. That is death.
In approaching families, it is critical that doctors and nurses don’t say, “Your relative is brain-dead.” That gives the family a sense that maybe they’re only “partially dead” or maybe there’s one key organ that has stopped working but maybe you can bring it back. Death is death. The law recognizes both cardiac death and brain death as death.
When you approach a family, if you believe that death has occurred, you say, “I’m very sorry. With regret, I have to tell you, your loved one is dead.” If they ask how you know, you can say, “We’ve determined it through brain death or through cardiac death.” You don’t give them a sense that people could be kind of dead, sort of dead, or nearly dead. Those states are comas or permanent vegetative states; they’re not the same as death.
What if the family says, “I don’t want you to do any testing. I don’t want to find out whether my relative is dead”? The American Academy of Neurology looked at this carefully and said that any test for death can be done without the permission or consent of the family. They said that because doctors need to know what steps to take to treat someone.
If a person is dead, then treatment is going to stop. It may not stop immediately. There may be issues about organ donation. There may be issues about gathering the family to come to the bedside to say goodbye, because many people think that’s more humane than saying goodbye at the morgue or in another setting.
This is all well and good, but patients cannot protect against bad news when it comes to death. We don’t want to be doing things to the dead that cost money or are futile because of death and using resources that might go to others.
We’ve got much more clarity than we have ever had with respect to the issue of brain death and how it works in any hospital. We have certain tests, including being off the ventilator and some other tests, that the guidelines supply. We know we have to be more careful with children. We want to know the etiology of the cause of the brain trauma, the devastating brain injury, to be sure that this is something that really is permanent cessation of integrated brain function.
We know that if you believe the person has died, you don’t need the consent of the family in order to do a brain-death test. You have to do it because there is no point in continuing treatment in expensive ICU settings and denying resources to others who might want to use those resources. The family can’t hold the medical team hostage.
We do know that when we approach someone with the determination, whatever it is, we should lead by saying that the person has died and then explain how that was determined, whether it be by cardiac death pronouncement — where you tried to resuscitate and the heart’s not beating — or brain-death analysis.
I’m Art Caplan at the Division of Medical Ethics at the NYU Grossman School of Medicine. Thanks for watching.
Dr. Caplan has disclosed the following relevant financial relationships: Served as a director, officer, partner, employee, advisor, consultant, or trustee for: Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position); serves as a contributing author and adviser for this news organization.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the Division of Medical Ethics at the New York University Grossman School of Medicine in New York City.
I think we had a breakthrough on a very controversial subject over the past month. Over and over again, debates have been breaking out, cases have been going to court, and fights have been coming to ethics committees about brain death. How do we know what brain death is, how do we diagnose it, and what rights do families have with respect to the diagnosis?
The American Academy of Neurology decided to form a task force, and they just issued guidelines on the definition, tests to use it, and the rights of families. They did a wonderful job, in my view. They›ve achieved clarity.
First, they tried to handle both adults and children. Children are, if you will, more difficult — and that’s been known — to test for brain death. Their brains are smaller. You get more interference and false signals coming from muscle or nerve activity that might be going on elsewhere in their bodies.
The guidelines say we’re going to try to see whether a person can breathe without support. If it’s an adult, one test over a 24-hour period would be sufficient. If you had them off the ventilator and they can’t breathe and show no signs of being able to do that, that’s a very fundamental test for brain death. For children, you’re going to have to do it twice. The guidelines are saying to be cautious.
Second, they say it’s very important to know the cause of the suspected brain death condition. If someone has a massive head injury, that’s different from a situation in which someone overdoses from drugs or drowns. Those conditions can be a little deceptive. In the case of drowning, sometimes the brain has protective mechanisms to protect circulation to the brain naturally for a little bit of time. I’m talking about minutes, not hours.
You want to be careful to make sure that you know the cause of the massive brain injury or insult that makes someone believe that the patient is brain-dead, whether it’s a stroke, an embolism, a bleed, a gunshot wound, or trauma to the head. Those factors really drive the certainty with which brain death should be pronounced. I think that’s very, very important.
They also said that brain death means the permanent loss of brain function. You may get a few cells still firing or you may be in a situation, because the life support is still there, where the body looks pink and perhaps might appear to still be alive to someone. When you know that the damage to the brain is so severe that there’s nothing that can be done to bring back the support of heart function, breathing, and most likely any ability to sense or feel anything, that is death.
I believe it’s very important, when talking to families, to say there are two ways that we pronounce people dead, and they’re equal: One is to say their heart has stopped, their breathing has stopped, and there’s nothing we can do to resuscitate them, which is cardiac death. The other is to say their brain has permanently ceased to function in any kind of integrated way. That means no heartbeat, no breathing, and no mental sensations. That is death.
In approaching families, it is critical that doctors and nurses don’t say, “Your relative is brain-dead.” That gives the family a sense that maybe they’re only “partially dead” or maybe there’s one key organ that has stopped working but maybe you can bring it back. Death is death. The law recognizes both cardiac death and brain death as death.
When you approach a family, if you believe that death has occurred, you say, “I’m very sorry. With regret, I have to tell you, your loved one is dead.” If they ask how you know, you can say, “We’ve determined it through brain death or through cardiac death.” You don’t give them a sense that people could be kind of dead, sort of dead, or nearly dead. Those states are comas or permanent vegetative states; they’re not the same as death.
What if the family says, “I don’t want you to do any testing. I don’t want to find out whether my relative is dead”? The American Academy of Neurology looked at this carefully and said that any test for death can be done without the permission or consent of the family. They said that because doctors need to know what steps to take to treat someone.
If a person is dead, then treatment is going to stop. It may not stop immediately. There may be issues about organ donation. There may be issues about gathering the family to come to the bedside to say goodbye, because many people think that’s more humane than saying goodbye at the morgue or in another setting.
This is all well and good, but patients cannot protect against bad news when it comes to death. We don’t want to be doing things to the dead that cost money or are futile because of death and using resources that might go to others.
We’ve got much more clarity than we have ever had with respect to the issue of brain death and how it works in any hospital. We have certain tests, including being off the ventilator and some other tests, that the guidelines supply. We know we have to be more careful with children. We want to know the etiology of the cause of the brain trauma, the devastating brain injury, to be sure that this is something that really is permanent cessation of integrated brain function.
We know that if you believe the person has died, you don’t need the consent of the family in order to do a brain-death test. You have to do it because there is no point in continuing treatment in expensive ICU settings and denying resources to others who might want to use those resources. The family can’t hold the medical team hostage.
We do know that when we approach someone with the determination, whatever it is, we should lead by saying that the person has died and then explain how that was determined, whether it be by cardiac death pronouncement — where you tried to resuscitate and the heart’s not beating — or brain-death analysis.
I’m Art Caplan at the Division of Medical Ethics at the NYU Grossman School of Medicine. Thanks for watching.
Dr. Caplan has disclosed the following relevant financial relationships: Served as a director, officer, partner, employee, advisor, consultant, or trustee for: Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position); serves as a contributing author and adviser for this news organization.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the Division of Medical Ethics at the New York University Grossman School of Medicine in New York City.
I think we had a breakthrough on a very controversial subject over the past month. Over and over again, debates have been breaking out, cases have been going to court, and fights have been coming to ethics committees about brain death. How do we know what brain death is, how do we diagnose it, and what rights do families have with respect to the diagnosis?
The American Academy of Neurology decided to form a task force, and they just issued guidelines on the definition, tests to use it, and the rights of families. They did a wonderful job, in my view. They›ve achieved clarity.
First, they tried to handle both adults and children. Children are, if you will, more difficult — and that’s been known — to test for brain death. Their brains are smaller. You get more interference and false signals coming from muscle or nerve activity that might be going on elsewhere in their bodies.
The guidelines say we’re going to try to see whether a person can breathe without support. If it’s an adult, one test over a 24-hour period would be sufficient. If you had them off the ventilator and they can’t breathe and show no signs of being able to do that, that’s a very fundamental test for brain death. For children, you’re going to have to do it twice. The guidelines are saying to be cautious.
Second, they say it’s very important to know the cause of the suspected brain death condition. If someone has a massive head injury, that’s different from a situation in which someone overdoses from drugs or drowns. Those conditions can be a little deceptive. In the case of drowning, sometimes the brain has protective mechanisms to protect circulation to the brain naturally for a little bit of time. I’m talking about minutes, not hours.
You want to be careful to make sure that you know the cause of the massive brain injury or insult that makes someone believe that the patient is brain-dead, whether it’s a stroke, an embolism, a bleed, a gunshot wound, or trauma to the head. Those factors really drive the certainty with which brain death should be pronounced. I think that’s very, very important.
They also said that brain death means the permanent loss of brain function. You may get a few cells still firing or you may be in a situation, because the life support is still there, where the body looks pink and perhaps might appear to still be alive to someone. When you know that the damage to the brain is so severe that there’s nothing that can be done to bring back the support of heart function, breathing, and most likely any ability to sense or feel anything, that is death.
I believe it’s very important, when talking to families, to say there are two ways that we pronounce people dead, and they’re equal: One is to say their heart has stopped, their breathing has stopped, and there’s nothing we can do to resuscitate them, which is cardiac death. The other is to say their brain has permanently ceased to function in any kind of integrated way. That means no heartbeat, no breathing, and no mental sensations. That is death.
In approaching families, it is critical that doctors and nurses don’t say, “Your relative is brain-dead.” That gives the family a sense that maybe they’re only “partially dead” or maybe there’s one key organ that has stopped working but maybe you can bring it back. Death is death. The law recognizes both cardiac death and brain death as death.
When you approach a family, if you believe that death has occurred, you say, “I’m very sorry. With regret, I have to tell you, your loved one is dead.” If they ask how you know, you can say, “We’ve determined it through brain death or through cardiac death.” You don’t give them a sense that people could be kind of dead, sort of dead, or nearly dead. Those states are comas or permanent vegetative states; they’re not the same as death.
What if the family says, “I don’t want you to do any testing. I don’t want to find out whether my relative is dead”? The American Academy of Neurology looked at this carefully and said that any test for death can be done without the permission or consent of the family. They said that because doctors need to know what steps to take to treat someone.
If a person is dead, then treatment is going to stop. It may not stop immediately. There may be issues about organ donation. There may be issues about gathering the family to come to the bedside to say goodbye, because many people think that’s more humane than saying goodbye at the morgue or in another setting.
This is all well and good, but patients cannot protect against bad news when it comes to death. We don’t want to be doing things to the dead that cost money or are futile because of death and using resources that might go to others.
We’ve got much more clarity than we have ever had with respect to the issue of brain death and how it works in any hospital. We have certain tests, including being off the ventilator and some other tests, that the guidelines supply. We know we have to be more careful with children. We want to know the etiology of the cause of the brain trauma, the devastating brain injury, to be sure that this is something that really is permanent cessation of integrated brain function.
We know that if you believe the person has died, you don’t need the consent of the family in order to do a brain-death test. You have to do it because there is no point in continuing treatment in expensive ICU settings and denying resources to others who might want to use those resources. The family can’t hold the medical team hostage.
We do know that when we approach someone with the determination, whatever it is, we should lead by saying that the person has died and then explain how that was determined, whether it be by cardiac death pronouncement — where you tried to resuscitate and the heart’s not beating — or brain-death analysis.
I’m Art Caplan at the Division of Medical Ethics at the NYU Grossman School of Medicine. Thanks for watching.
Dr. Caplan has disclosed the following relevant financial relationships: Served as a director, officer, partner, employee, advisor, consultant, or trustee for: Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position); serves as a contributing author and adviser for this news organization.
A version of this article appeared on Medscape.com.
Weighing the Big Decisions
In my mind’s calendar, two dates stand out. Both far enough away that I don’t have to think about them too much right now, but near enough that they can’t be forgotten about, either.
On September 30, 2028, my office lease ends, and in 2029 my neurology board certification has to be renewed. I’ll be in my early 60s then and I’ve been a practicing neurologist for 30 years.

I have no idea what I’m going to do. Of course, a lot can happen between now and then, and a lot of variables come into the calculus of when to retire.
After all these years, I still enjoy my job. It gives me the purpose that I wanted so long ago when I applied to medical school. The late William Pancoe, associate dean when I was at Creighton, always told us to remember how we felt when we got that acceptance letter — we’d need it to keep us going through medical school.
And, even now, I still remember the call from my dad that it had arrived. What a moment that was. I have no regrets. I can’t imagine doing anything else.
But in 4 years how much longer will I want to practice? Hopefully I’ll be faced with that decision. Will I want to renew the lease for 2 years? 5 years? I like my little office. It’s far from gleaming, there’s no TV or Keurig in the lobby, the carpet, paint, and furnishings are still from the early 90s when the place was built. But it’s my home away from home. I spend anywhere from 40-60 hours/week there. It’s quiet and (at least for me) cozy. Would I want to give that up and move to a smaller, shared place, for the remainder of my career? Or just close down?
Likewise, will I want to renew my board certification? Granted, that isn’t necessary to practice, but it certainly looks better to have it. To do that I’ll have to fork over a decent chunk of change to take the test, more money for a review course, and spend some time studying. Strange to think that at 63 I might be back at my desk (same desk, by the way) studying for a test like I did in college and medical school. But, if I want to keep playing doctor, that’s what I’ll have to do.
Four years to think about this. The same amount of time I spent each in high school, medical school, and residency. For that matter, the same amount of time since we all went into quarantine.
Doesn’t seem that long, does it?
I guess I’ve got some thinking to do.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In my mind’s calendar, two dates stand out. Both far enough away that I don’t have to think about them too much right now, but near enough that they can’t be forgotten about, either.
On September 30, 2028, my office lease ends, and in 2029 my neurology board certification has to be renewed. I’ll be in my early 60s then and I’ve been a practicing neurologist for 30 years.
I have no idea what I’m going to do. Of course, a lot can happen between now and then, and a lot of variables come into the calculus of when to retire.
After all these years, I still enjoy my job. It gives me the purpose that I wanted so long ago when I applied to medical school. The late William Pancoe, associate dean when I was at Creighton, always told us to remember how we felt when we got that acceptance letter — we’d need it to keep us going through medical school.
And, even now, I still remember the call from my dad that it had arrived. What a moment that was. I have no regrets. I can’t imagine doing anything else.
But in 4 years how much longer will I want to practice? Hopefully I’ll be faced with that decision. Will I want to renew the lease for 2 years? 5 years? I like my little office. It’s far from gleaming, there’s no TV or Keurig in the lobby, the carpet, paint, and furnishings are still from the early 90s when the place was built. But it’s my home away from home. I spend anywhere from 40-60 hours/week there. It’s quiet and (at least for me) cozy. Would I want to give that up and move to a smaller, shared place, for the remainder of my career? Or just close down?
Likewise, will I want to renew my board certification? Granted, that isn’t necessary to practice, but it certainly looks better to have it. To do that I’ll have to fork over a decent chunk of change to take the test, more money for a review course, and spend some time studying. Strange to think that at 63 I might be back at my desk (same desk, by the way) studying for a test like I did in college and medical school. But, if I want to keep playing doctor, that’s what I’ll have to do.
Four years to think about this. The same amount of time I spent each in high school, medical school, and residency. For that matter, the same amount of time since we all went into quarantine.
Doesn’t seem that long, does it?
I guess I’ve got some thinking to do.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In my mind’s calendar, two dates stand out. Both far enough away that I don’t have to think about them too much right now, but near enough that they can’t be forgotten about, either.
On September 30, 2028, my office lease ends, and in 2029 my neurology board certification has to be renewed. I’ll be in my early 60s then and I’ve been a practicing neurologist for 30 years.
I have no idea what I’m going to do. Of course, a lot can happen between now and then, and a lot of variables come into the calculus of when to retire.
After all these years, I still enjoy my job. It gives me the purpose that I wanted so long ago when I applied to medical school. The late William Pancoe, associate dean when I was at Creighton, always told us to remember how we felt when we got that acceptance letter — we’d need it to keep us going through medical school.
And, even now, I still remember the call from my dad that it had arrived. What a moment that was. I have no regrets. I can’t imagine doing anything else.
But in 4 years how much longer will I want to practice? Hopefully I’ll be faced with that decision. Will I want to renew the lease for 2 years? 5 years? I like my little office. It’s far from gleaming, there’s no TV or Keurig in the lobby, the carpet, paint, and furnishings are still from the early 90s when the place was built. But it’s my home away from home. I spend anywhere from 40-60 hours/week there. It’s quiet and (at least for me) cozy. Would I want to give that up and move to a smaller, shared place, for the remainder of my career? Or just close down?
Likewise, will I want to renew my board certification? Granted, that isn’t necessary to practice, but it certainly looks better to have it. To do that I’ll have to fork over a decent chunk of change to take the test, more money for a review course, and spend some time studying. Strange to think that at 63 I might be back at my desk (same desk, by the way) studying for a test like I did in college and medical school. But, if I want to keep playing doctor, that’s what I’ll have to do.
Four years to think about this. The same amount of time I spent each in high school, medical school, and residency. For that matter, the same amount of time since we all went into quarantine.
Doesn’t seem that long, does it?
I guess I’ve got some thinking to do.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Long COVID: Another Great Pretender
Has COVID replaced syphilis as the great imitator? At the turn of the 20th century, Sir William Osler was quoted as saying, “He who knows syphilis knows medicine.”
If you have any doubts about the “imitator” analogy, simply use any broad search engine or AI portal and enter “what is the differential diagnosis of primary syphilis, or secondary syphilis, or tertiary syphilis?” A plethora of diseases across many body systems appears.
Another Great Pretender?
Did you or do you now have long COVID? How do you know? Do you even know what long COVID is? How would you diagnosis it?
When asked about long COVID, this is what large language model source bard.google.com had to say:
Long COVID, also known as post-COVID conditions or PASC, is a complex condition that can occur in people who have had COVID-19, even if their initial illness was mild or even asymptomatic. It’s characterized by a wide range of symptoms that can last for weeks, months, or even years after the initial infection.
Symptoms of long COVID can include: fatigue, shortness of breath, brain fog (trouble thinking or concentrating), loss of smell or taste, sleep problems, muscle pain, joint pain, headache, dizziness, depression or anxiety, heart palpitations, gastrointestinal problems.
Duh!!! It reads much like a continuation of the symptoms of acute COVID. Bard continued:
The exact cause of long COVID is still unknown, but there are several theories. One possibility is that the virus itself can damage organs and tissues, leading to ongoing symptoms. Another possibility is that the immune system’s response to the virus can continue to cause inflammation even after the virus is gone.
Human intelligence source Wikipedia says this:
Long COVID or long-haul COVID is a group of health problems persisting or developing after an initial COVID-19 infection. Symptoms can last weeks, months or years and are often debilitating. The World Health Organization defines long COVID as starting three months after infection, but other definitions put the start of long COVID at four weeks.
Highly varied, including post-exertional malaise (symptoms made worse with effort), fatigue, muscle pain, shortness of breath, chest pain, and cognitive dysfunction (brain fog).
Acute COVID to Long COVID
The World Health Organization estimates that 36 million people in the European region have developed long COVID in the first 3 years of the pandemic. That›s a lot.
We all know that the common signs and symptoms of acute COVID-19 include fever or chills, a dry cough and shortness of breath, feeling very tired, muscle or body aches, headache, loss of taste or smell, sore throat, congestion, runny nose, nausea, vomiting, and diarrhea. Except for the taste and smell findings, every one of these symptoms or signs could indicate a different virus infection or even some type of allergy. My point is the nonspecificity in this list.
Uncommon signs and symptoms of acute COVID include a flat skin rash covered with small bumps, discolored swollen areas on the fingers and toes (COVID toes), and hives. The skin of hands, wrists, or ankles also can be affected. Blisters, itchiness, rough skin, or pus can be seen.
Severe confusion (delirium) might be the main or only symptom of COVID-19 in older people. This COVID-19 symptom is linked with a high risk for poor outcomes, including death. Pink eye (conjunctivitis) can be a COVID-19 symptom. Other eye problems linked to COVID-19 are light sensitivity, sore eyes, and itchy eyes. Acute myocarditis, tinnitus, vertigo, and hearing loss have been reported. And 1-4 weeks after the onset of COVID-19 infection, a patient may experience de novo reactive synovitis and arthritis of any joints.
So, take your pick. Myriad symptoms, signs, diseases, diagnoses, and organ systems — still present, recurring, just appearing, apparently de novo, or after asymptomatic infection. We have so much still to learn.
What big-time symptoms, signs, and major diseases are not on any of these lists? Obviously, cancer, atherosclerotic cardiovascular diseases, obesity, bone diseases, and competitive infections. But be patient; the lingering effects of direct tissue invasion by the virus as well as a wide range of immunologic reactions may just be getting started. Mitochondrial damage, especially in muscles, is increasingly a pathophysiologic suspect.
Human diseases can be physical or mental; and in COVID, that twain not only meet but mix and mingle freely, and may even merge into psychosoma. Don’t ever forget that. Consider “fatigue.” Who among us, COVID or NOVID, does not experience that from time to time?
Or consider brain fog as a common reported symptom of COVID. What on earth is that actually? How can a person know they have brain fog, or whether they had it and are over it?
We need one or more lab or other diagnostic tests that can objectively confirm the diagnosis of long COVID.
Useful Progress?
A recent research paper in Science reported intriguing chemical findings that seemed to point a finger at some form of complement dysregulation as a potential disease marker for long COVID. Unfortunately, some critics have pointed out that this entire study may be invalid or irrelevant because the New York cohort was recruited in 2020, before vaccines were available. The Zurich cohort was recruited up until April 2021, so some may have been vaccinated.
Then this news organization came along in early January 2024 with an article about COVID causing not only more than a million American deaths but also more than 5000 deaths from long COVID. We physicians don’t really know what long COVID even is, but we have to sign death certificates blaming thousands of deaths on it anyway? And rolling back the clock to 2020: Are patients dying from COVID or with COVID, according to death certificates?Now, armed with the knowledge that “documented serious post–COVID-19 conditions include cardiovascular, pulmonary, neurological, renal, endocrine, hematological, and gastrointestinal complications, as well as death,” CDC has published clear and fairly concise instructions on how to address post-acute COVID sequelae on death certificates.
In late January, this news organization painted a hopeful picture by naming four phenotypes of long COVID, suggesting that such divisions might further our understanding, including prognosis, and even therapy for this condition. Among the clinical phenotypes of (1) chronic fatigue–like syndrome, headache, and memory loss; (2) respiratory syndrome (which includes cough and difficulty breathing); (3) chronic pain; and (4) neurosensorial syndrome (which causes an altered sense of taste and smell), overlap is clearly possible but isn›t addressed.
I see these recent developments as needed and useful progress, but we are still left with…not much. So, when you tell me that you do or do not have long COVID, I will say to you, “How do you know?”
I also say: She/he/they who know COVID know medicine.
A version of this article first appeared on Medscape.com.
Has COVID replaced syphilis as the great imitator? At the turn of the 20th century, Sir William Osler was quoted as saying, “He who knows syphilis knows medicine.”
If you have any doubts about the “imitator” analogy, simply use any broad search engine or AI portal and enter “what is the differential diagnosis of primary syphilis, or secondary syphilis, or tertiary syphilis?” A plethora of diseases across many body systems appears.
Another Great Pretender?
Did you or do you now have long COVID? How do you know? Do you even know what long COVID is? How would you diagnosis it?
When asked about long COVID, this is what large language model source bard.google.com had to say:
Long COVID, also known as post-COVID conditions or PASC, is a complex condition that can occur in people who have had COVID-19, even if their initial illness was mild or even asymptomatic. It’s characterized by a wide range of symptoms that can last for weeks, months, or even years after the initial infection.
Symptoms of long COVID can include: fatigue, shortness of breath, brain fog (trouble thinking or concentrating), loss of smell or taste, sleep problems, muscle pain, joint pain, headache, dizziness, depression or anxiety, heart palpitations, gastrointestinal problems.
Duh!!! It reads much like a continuation of the symptoms of acute COVID. Bard continued:
The exact cause of long COVID is still unknown, but there are several theories. One possibility is that the virus itself can damage organs and tissues, leading to ongoing symptoms. Another possibility is that the immune system’s response to the virus can continue to cause inflammation even after the virus is gone.
Human intelligence source Wikipedia says this:
Long COVID or long-haul COVID is a group of health problems persisting or developing after an initial COVID-19 infection. Symptoms can last weeks, months or years and are often debilitating. The World Health Organization defines long COVID as starting three months after infection, but other definitions put the start of long COVID at four weeks.
Highly varied, including post-exertional malaise (symptoms made worse with effort), fatigue, muscle pain, shortness of breath, chest pain, and cognitive dysfunction (brain fog).
Acute COVID to Long COVID
The World Health Organization estimates that 36 million people in the European region have developed long COVID in the first 3 years of the pandemic. That›s a lot.
We all know that the common signs and symptoms of acute COVID-19 include fever or chills, a dry cough and shortness of breath, feeling very tired, muscle or body aches, headache, loss of taste or smell, sore throat, congestion, runny nose, nausea, vomiting, and diarrhea. Except for the taste and smell findings, every one of these symptoms or signs could indicate a different virus infection or even some type of allergy. My point is the nonspecificity in this list.
Uncommon signs and symptoms of acute COVID include a flat skin rash covered with small bumps, discolored swollen areas on the fingers and toes (COVID toes), and hives. The skin of hands, wrists, or ankles also can be affected. Blisters, itchiness, rough skin, or pus can be seen.
Severe confusion (delirium) might be the main or only symptom of COVID-19 in older people. This COVID-19 symptom is linked with a high risk for poor outcomes, including death. Pink eye (conjunctivitis) can be a COVID-19 symptom. Other eye problems linked to COVID-19 are light sensitivity, sore eyes, and itchy eyes. Acute myocarditis, tinnitus, vertigo, and hearing loss have been reported. And 1-4 weeks after the onset of COVID-19 infection, a patient may experience de novo reactive synovitis and arthritis of any joints.
So, take your pick. Myriad symptoms, signs, diseases, diagnoses, and organ systems — still present, recurring, just appearing, apparently de novo, or after asymptomatic infection. We have so much still to learn.
What big-time symptoms, signs, and major diseases are not on any of these lists? Obviously, cancer, atherosclerotic cardiovascular diseases, obesity, bone diseases, and competitive infections. But be patient; the lingering effects of direct tissue invasion by the virus as well as a wide range of immunologic reactions may just be getting started. Mitochondrial damage, especially in muscles, is increasingly a pathophysiologic suspect.
Human diseases can be physical or mental; and in COVID, that twain not only meet but mix and mingle freely, and may even merge into psychosoma. Don’t ever forget that. Consider “fatigue.” Who among us, COVID or NOVID, does not experience that from time to time?
Or consider brain fog as a common reported symptom of COVID. What on earth is that actually? How can a person know they have brain fog, or whether they had it and are over it?
We need one or more lab or other diagnostic tests that can objectively confirm the diagnosis of long COVID.
Useful Progress?
A recent research paper in Science reported intriguing chemical findings that seemed to point a finger at some form of complement dysregulation as a potential disease marker for long COVID. Unfortunately, some critics have pointed out that this entire study may be invalid or irrelevant because the New York cohort was recruited in 2020, before vaccines were available. The Zurich cohort was recruited up until April 2021, so some may have been vaccinated.
Then this news organization came along in early January 2024 with an article about COVID causing not only more than a million American deaths but also more than 5000 deaths from long COVID. We physicians don’t really know what long COVID even is, but we have to sign death certificates blaming thousands of deaths on it anyway? And rolling back the clock to 2020: Are patients dying from COVID or with COVID, according to death certificates?Now, armed with the knowledge that “documented serious post–COVID-19 conditions include cardiovascular, pulmonary, neurological, renal, endocrine, hematological, and gastrointestinal complications, as well as death,” CDC has published clear and fairly concise instructions on how to address post-acute COVID sequelae on death certificates.
In late January, this news organization painted a hopeful picture by naming four phenotypes of long COVID, suggesting that such divisions might further our understanding, including prognosis, and even therapy for this condition. Among the clinical phenotypes of (1) chronic fatigue–like syndrome, headache, and memory loss; (2) respiratory syndrome (which includes cough and difficulty breathing); (3) chronic pain; and (4) neurosensorial syndrome (which causes an altered sense of taste and smell), overlap is clearly possible but isn›t addressed.
I see these recent developments as needed and useful progress, but we are still left with…not much. So, when you tell me that you do or do not have long COVID, I will say to you, “How do you know?”
I also say: She/he/they who know COVID know medicine.
A version of this article first appeared on Medscape.com.
Has COVID replaced syphilis as the great imitator? At the turn of the 20th century, Sir William Osler was quoted as saying, “He who knows syphilis knows medicine.”
If you have any doubts about the “imitator” analogy, simply use any broad search engine or AI portal and enter “what is the differential diagnosis of primary syphilis, or secondary syphilis, or tertiary syphilis?” A plethora of diseases across many body systems appears.
Another Great Pretender?
Did you or do you now have long COVID? How do you know? Do you even know what long COVID is? How would you diagnosis it?
When asked about long COVID, this is what large language model source bard.google.com had to say:
Long COVID, also known as post-COVID conditions or PASC, is a complex condition that can occur in people who have had COVID-19, even if their initial illness was mild or even asymptomatic. It’s characterized by a wide range of symptoms that can last for weeks, months, or even years after the initial infection.
Symptoms of long COVID can include: fatigue, shortness of breath, brain fog (trouble thinking or concentrating), loss of smell or taste, sleep problems, muscle pain, joint pain, headache, dizziness, depression or anxiety, heart palpitations, gastrointestinal problems.
Duh!!! It reads much like a continuation of the symptoms of acute COVID. Bard continued:
The exact cause of long COVID is still unknown, but there are several theories. One possibility is that the virus itself can damage organs and tissues, leading to ongoing symptoms. Another possibility is that the immune system’s response to the virus can continue to cause inflammation even after the virus is gone.
Human intelligence source Wikipedia says this:
Long COVID or long-haul COVID is a group of health problems persisting or developing after an initial COVID-19 infection. Symptoms can last weeks, months or years and are often debilitating. The World Health Organization defines long COVID as starting three months after infection, but other definitions put the start of long COVID at four weeks.
Highly varied, including post-exertional malaise (symptoms made worse with effort), fatigue, muscle pain, shortness of breath, chest pain, and cognitive dysfunction (brain fog).
Acute COVID to Long COVID
The World Health Organization estimates that 36 million people in the European region have developed long COVID in the first 3 years of the pandemic. That›s a lot.
We all know that the common signs and symptoms of acute COVID-19 include fever or chills, a dry cough and shortness of breath, feeling very tired, muscle or body aches, headache, loss of taste or smell, sore throat, congestion, runny nose, nausea, vomiting, and diarrhea. Except for the taste and smell findings, every one of these symptoms or signs could indicate a different virus infection or even some type of allergy. My point is the nonspecificity in this list.
Uncommon signs and symptoms of acute COVID include a flat skin rash covered with small bumps, discolored swollen areas on the fingers and toes (COVID toes), and hives. The skin of hands, wrists, or ankles also can be affected. Blisters, itchiness, rough skin, or pus can be seen.
Severe confusion (delirium) might be the main or only symptom of COVID-19 in older people. This COVID-19 symptom is linked with a high risk for poor outcomes, including death. Pink eye (conjunctivitis) can be a COVID-19 symptom. Other eye problems linked to COVID-19 are light sensitivity, sore eyes, and itchy eyes. Acute myocarditis, tinnitus, vertigo, and hearing loss have been reported. And 1-4 weeks after the onset of COVID-19 infection, a patient may experience de novo reactive synovitis and arthritis of any joints.
So, take your pick. Myriad symptoms, signs, diseases, diagnoses, and organ systems — still present, recurring, just appearing, apparently de novo, or after asymptomatic infection. We have so much still to learn.
What big-time symptoms, signs, and major diseases are not on any of these lists? Obviously, cancer, atherosclerotic cardiovascular diseases, obesity, bone diseases, and competitive infections. But be patient; the lingering effects of direct tissue invasion by the virus as well as a wide range of immunologic reactions may just be getting started. Mitochondrial damage, especially in muscles, is increasingly a pathophysiologic suspect.
Human diseases can be physical or mental; and in COVID, that twain not only meet but mix and mingle freely, and may even merge into psychosoma. Don’t ever forget that. Consider “fatigue.” Who among us, COVID or NOVID, does not experience that from time to time?
Or consider brain fog as a common reported symptom of COVID. What on earth is that actually? How can a person know they have brain fog, or whether they had it and are over it?
We need one or more lab or other diagnostic tests that can objectively confirm the diagnosis of long COVID.
Useful Progress?
A recent research paper in Science reported intriguing chemical findings that seemed to point a finger at some form of complement dysregulation as a potential disease marker for long COVID. Unfortunately, some critics have pointed out that this entire study may be invalid or irrelevant because the New York cohort was recruited in 2020, before vaccines were available. The Zurich cohort was recruited up until April 2021, so some may have been vaccinated.
Then this news organization came along in early January 2024 with an article about COVID causing not only more than a million American deaths but also more than 5000 deaths from long COVID. We physicians don’t really know what long COVID even is, but we have to sign death certificates blaming thousands of deaths on it anyway? And rolling back the clock to 2020: Are patients dying from COVID or with COVID, according to death certificates?Now, armed with the knowledge that “documented serious post–COVID-19 conditions include cardiovascular, pulmonary, neurological, renal, endocrine, hematological, and gastrointestinal complications, as well as death,” CDC has published clear and fairly concise instructions on how to address post-acute COVID sequelae on death certificates.
In late January, this news organization painted a hopeful picture by naming four phenotypes of long COVID, suggesting that such divisions might further our understanding, including prognosis, and even therapy for this condition. Among the clinical phenotypes of (1) chronic fatigue–like syndrome, headache, and memory loss; (2) respiratory syndrome (which includes cough and difficulty breathing); (3) chronic pain; and (4) neurosensorial syndrome (which causes an altered sense of taste and smell), overlap is clearly possible but isn›t addressed.
I see these recent developments as needed and useful progress, but we are still left with…not much. So, when you tell me that you do or do not have long COVID, I will say to you, “How do you know?”
I also say: She/he/they who know COVID know medicine.
A version of this article first appeared on Medscape.com.
Biosimilars Have Driven Down Cost of Infliximab
LAS VEGAS — , according to two new retrospective analyses that separately looked at private insurance and Medicare patients.
“It is interesting to see that biosimilar use is increasing in patients with Medicare insurance in the U.S. since introduction into the market. This shows that clinicians are getting more comfortable with their use in clinical practice,” said Sara Horst, MD, associate professor of gastroenterology, hepatology, and nutrition at Vanderbilt University Medical Center in Nashville, Tennessee. That “is a continued important question in use, especially in the older population,” Dr. Horst said at the poster session where the two studies were presented, at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.

One study examined Medicare part D participants. The researchers included infliximab prescriptions between 2013 and 2021, with a break in 2017 when biosimilars were first introduced. Between 2013 and 2017, there was a 93.7% annual increase in infliximab cost, and a 29.0% increase in annual claims. Between 2017 and 2021, those numbers declined to 23.9% and 12.1%, respectively. The researchers also examined trends by individual states and found a wide range of results. “Nationwide, it seems to be doing exactly what you’d expect, and I’d say it’s encouraging. This is exactly what you want with the introduction of biosimilars, and this is what you want for the patient population. But there are some states that have not really kept up with the rest of the country, and may need to look further into what types of trends are there,” said Modan Goldman, who presented the study. He is a medical student at Carle Illinois College of Medicine in Urbana, Illinois.
The other study looked at use of infliximab versus a biosimilar between 2015 and 2021 in 42,009 patients 64 or younger, drawing data from Merative Marketscan Commercial Claims and Encounters Database. They excluded government-funded insurance. Between January 2015 and December 2017, the cost of a vial of infliximab increased by $6.31 per month, reaching a maxim cost of $1,491 per vial. In January 2018, the cost decreased by $62 per vial, with a downward trend after that of $12.93 per vial per month.

“[Getting] access to these drugs, especially for pediatric IBD, has been an uphill battle with insurance companies and getting the medication and the doses we want,” said Samantha Paglinco, DO, who presented the Marketscan study.
The findings demonstrated clear cost reductions. “At the beginning of our period, infliximab originator Remicade was a little over $1,200 per vial, and at the end of our period of 2021, we expected it to be around $1,800 per vial. However, with the introduction of multiple infliximab biosimilars, we did see it come down to $800 per vial, which generated a savings of $1,000, which is pretty significant. We’re hoping that by generating overall cost savings to insurance companies, this will allow for greater access, because we know infliximab is such a good medication for pediatric IBD and for many other autoimmune conditions,” said Dr. Paglinco, a pediatric GI fellow at Nationwide Children’s Hospital in Columbus, Ohio.
The decrease in the cost of medication per vial in both the originator and biosimilar is an important finding in light of cost containment strategies, although Dr. Horst pointed out that the study didn’t determine if there were any savings to patients. “That is what clinicians and patients care about the most. I worry that while these savings were seen at insurance and health care organizational levels, patients may not have experienced any cost savings, and this is something we need to consider in the future,” she said.
The FDA created the biosimilar regulatory pathway in 2010 in an effort to reduce costs. “And they have. The cost savings however, has not directly translated to the individual patient in their copays or necessarily in changes to access when prescribing. Nor has it allowed dose escalation more easily, which is frequently needed,” said David T. Rubin, MD, AGAF, who was asked for comment.

Although the changes in prescribing patterns may reflect cost savings to patients, there are some limits to this interpretation, according to Dr. Rubin, of the University of Chicago. Payers are often the ones who determine a switch to biosimilar. The study also does not account for disease activity or phenotype, which can be an important confounder. Newer biologics that have come on to the market in recent years may also have affected the prescribing patterns for infliximab.
Nevertheless, an association between introduction of biosimilars and declining cost in the originator product (Remicade) is welcome, according to Dr. Rubin. “This is nice to see and we have seen it in our practices,” he said.
Unfortunately, “it has also not been seen to translate into reduced costs for patients nor has it been associated with increased access or changes in payer policies to allow these drugs to be used, or dose escalations to occur,” Dr. Rubin added.
Dr. Paglinco and Mr. Goldman have no relevant financial disclosures. Dr. Horst has consulted for Janssen, Takeda, Bristol-Myers Squibb, and Abbvie. Dr. Rubin has received grant support from Takeda and has consulted for Abbvie, Bristol-Myers Squibb, Janssen Pharmaceuticals, Lilly, Pfizer, and Takeda.
LAS VEGAS — , according to two new retrospective analyses that separately looked at private insurance and Medicare patients.
“It is interesting to see that biosimilar use is increasing in patients with Medicare insurance in the U.S. since introduction into the market. This shows that clinicians are getting more comfortable with their use in clinical practice,” said Sara Horst, MD, associate professor of gastroenterology, hepatology, and nutrition at Vanderbilt University Medical Center in Nashville, Tennessee. That “is a continued important question in use, especially in the older population,” Dr. Horst said at the poster session where the two studies were presented, at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
One study examined Medicare part D participants. The researchers included infliximab prescriptions between 2013 and 2021, with a break in 2017 when biosimilars were first introduced. Between 2013 and 2017, there was a 93.7% annual increase in infliximab cost, and a 29.0% increase in annual claims. Between 2017 and 2021, those numbers declined to 23.9% and 12.1%, respectively. The researchers also examined trends by individual states and found a wide range of results. “Nationwide, it seems to be doing exactly what you’d expect, and I’d say it’s encouraging. This is exactly what you want with the introduction of biosimilars, and this is what you want for the patient population. But there are some states that have not really kept up with the rest of the country, and may need to look further into what types of trends are there,” said Modan Goldman, who presented the study. He is a medical student at Carle Illinois College of Medicine in Urbana, Illinois.
The other study looked at use of infliximab versus a biosimilar between 2015 and 2021 in 42,009 patients 64 or younger, drawing data from Merative Marketscan Commercial Claims and Encounters Database. They excluded government-funded insurance. Between January 2015 and December 2017, the cost of a vial of infliximab increased by $6.31 per month, reaching a maxim cost of $1,491 per vial. In January 2018, the cost decreased by $62 per vial, with a downward trend after that of $12.93 per vial per month.
“[Getting] access to these drugs, especially for pediatric IBD, has been an uphill battle with insurance companies and getting the medication and the doses we want,” said Samantha Paglinco, DO, who presented the Marketscan study.
The findings demonstrated clear cost reductions. “At the beginning of our period, infliximab originator Remicade was a little over $1,200 per vial, and at the end of our period of 2021, we expected it to be around $1,800 per vial. However, with the introduction of multiple infliximab biosimilars, we did see it come down to $800 per vial, which generated a savings of $1,000, which is pretty significant. We’re hoping that by generating overall cost savings to insurance companies, this will allow for greater access, because we know infliximab is such a good medication for pediatric IBD and for many other autoimmune conditions,” said Dr. Paglinco, a pediatric GI fellow at Nationwide Children’s Hospital in Columbus, Ohio.
The decrease in the cost of medication per vial in both the originator and biosimilar is an important finding in light of cost containment strategies, although Dr. Horst pointed out that the study didn’t determine if there were any savings to patients. “That is what clinicians and patients care about the most. I worry that while these savings were seen at insurance and health care organizational levels, patients may not have experienced any cost savings, and this is something we need to consider in the future,” she said.
The FDA created the biosimilar regulatory pathway in 2010 in an effort to reduce costs. “And they have. The cost savings however, has not directly translated to the individual patient in their copays or necessarily in changes to access when prescribing. Nor has it allowed dose escalation more easily, which is frequently needed,” said David T. Rubin, MD, AGAF, who was asked for comment.
Although the changes in prescribing patterns may reflect cost savings to patients, there are some limits to this interpretation, according to Dr. Rubin, of the University of Chicago. Payers are often the ones who determine a switch to biosimilar. The study also does not account for disease activity or phenotype, which can be an important confounder. Newer biologics that have come on to the market in recent years may also have affected the prescribing patterns for infliximab.
Nevertheless, an association between introduction of biosimilars and declining cost in the originator product (Remicade) is welcome, according to Dr. Rubin. “This is nice to see and we have seen it in our practices,” he said.
Unfortunately, “it has also not been seen to translate into reduced costs for patients nor has it been associated with increased access or changes in payer policies to allow these drugs to be used, or dose escalations to occur,” Dr. Rubin added.
Dr. Paglinco and Mr. Goldman have no relevant financial disclosures. Dr. Horst has consulted for Janssen, Takeda, Bristol-Myers Squibb, and Abbvie. Dr. Rubin has received grant support from Takeda and has consulted for Abbvie, Bristol-Myers Squibb, Janssen Pharmaceuticals, Lilly, Pfizer, and Takeda.
LAS VEGAS — , according to two new retrospective analyses that separately looked at private insurance and Medicare patients.
“It is interesting to see that biosimilar use is increasing in patients with Medicare insurance in the U.S. since introduction into the market. This shows that clinicians are getting more comfortable with their use in clinical practice,” said Sara Horst, MD, associate professor of gastroenterology, hepatology, and nutrition at Vanderbilt University Medical Center in Nashville, Tennessee. That “is a continued important question in use, especially in the older population,” Dr. Horst said at the poster session where the two studies were presented, at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
One study examined Medicare part D participants. The researchers included infliximab prescriptions between 2013 and 2021, with a break in 2017 when biosimilars were first introduced. Between 2013 and 2017, there was a 93.7% annual increase in infliximab cost, and a 29.0% increase in annual claims. Between 2017 and 2021, those numbers declined to 23.9% and 12.1%, respectively. The researchers also examined trends by individual states and found a wide range of results. “Nationwide, it seems to be doing exactly what you’d expect, and I’d say it’s encouraging. This is exactly what you want with the introduction of biosimilars, and this is what you want for the patient population. But there are some states that have not really kept up with the rest of the country, and may need to look further into what types of trends are there,” said Modan Goldman, who presented the study. He is a medical student at Carle Illinois College of Medicine in Urbana, Illinois.
The other study looked at use of infliximab versus a biosimilar between 2015 and 2021 in 42,009 patients 64 or younger, drawing data from Merative Marketscan Commercial Claims and Encounters Database. They excluded government-funded insurance. Between January 2015 and December 2017, the cost of a vial of infliximab increased by $6.31 per month, reaching a maxim cost of $1,491 per vial. In January 2018, the cost decreased by $62 per vial, with a downward trend after that of $12.93 per vial per month.
“[Getting] access to these drugs, especially for pediatric IBD, has been an uphill battle with insurance companies and getting the medication and the doses we want,” said Samantha Paglinco, DO, who presented the Marketscan study.
The findings demonstrated clear cost reductions. “At the beginning of our period, infliximab originator Remicade was a little over $1,200 per vial, and at the end of our period of 2021, we expected it to be around $1,800 per vial. However, with the introduction of multiple infliximab biosimilars, we did see it come down to $800 per vial, which generated a savings of $1,000, which is pretty significant. We’re hoping that by generating overall cost savings to insurance companies, this will allow for greater access, because we know infliximab is such a good medication for pediatric IBD and for many other autoimmune conditions,” said Dr. Paglinco, a pediatric GI fellow at Nationwide Children’s Hospital in Columbus, Ohio.
The decrease in the cost of medication per vial in both the originator and biosimilar is an important finding in light of cost containment strategies, although Dr. Horst pointed out that the study didn’t determine if there were any savings to patients. “That is what clinicians and patients care about the most. I worry that while these savings were seen at insurance and health care organizational levels, patients may not have experienced any cost savings, and this is something we need to consider in the future,” she said.
The FDA created the biosimilar regulatory pathway in 2010 in an effort to reduce costs. “And they have. The cost savings however, has not directly translated to the individual patient in their copays or necessarily in changes to access when prescribing. Nor has it allowed dose escalation more easily, which is frequently needed,” said David T. Rubin, MD, AGAF, who was asked for comment.
Although the changes in prescribing patterns may reflect cost savings to patients, there are some limits to this interpretation, according to Dr. Rubin, of the University of Chicago. Payers are often the ones who determine a switch to biosimilar. The study also does not account for disease activity or phenotype, which can be an important confounder. Newer biologics that have come on to the market in recent years may also have affected the prescribing patterns for infliximab.
Nevertheless, an association between introduction of biosimilars and declining cost in the originator product (Remicade) is welcome, according to Dr. Rubin. “This is nice to see and we have seen it in our practices,” he said.
Unfortunately, “it has also not been seen to translate into reduced costs for patients nor has it been associated with increased access or changes in payer policies to allow these drugs to be used, or dose escalations to occur,” Dr. Rubin added.
Dr. Paglinco and Mr. Goldman have no relevant financial disclosures. Dr. Horst has consulted for Janssen, Takeda, Bristol-Myers Squibb, and Abbvie. Dr. Rubin has received grant support from Takeda and has consulted for Abbvie, Bristol-Myers Squibb, Janssen Pharmaceuticals, Lilly, Pfizer, and Takeda.
FROM CROHN’S AND COLITIS CONGRESS