User login
Virus and Booster Apathy Could Be Fueling Long COVID
A celebrity makeup artist, the 55-year-old New Yorker had been boosted and vaccinated at every opportunity since vaccines were approved at the end of 2020, until the fall of 2023, when she skipped the shot.
“I really started subscribing to the mindset that you have an immune system and your immune system is supposed to work for you,” she said. “That was the stupidest thing I’ve ever done.”
Maio was not the only person to skip the latest booster: A recent study reported that while nearly 80% of adults in the United States said they’d received their first series of vaccines, barely 20% were up to date on boosters. Nor was Maio alone in getting long COVID 4 years after the start of the deadliest pandemic in a century.
It’s tempting, this far out from the shutdowns of 2020, to think the virus is over, that we’re immune, and nobody’s going to get sick anymore. But while fewer people are getting COVID, it is still very much a part of our lives. And as Maio and others are learning the hard way, long COVID is, too — and it can be deadly.
For those who have recently contracted long COVID, it can feel as if the whole world has moved on from the pandemic, and they are being left behind.
Too Easy to Let Our Guard Down
“It’s really difficult to prevent exposure to COVID no matter how careful you are and no matter how many times you are vaccinated,” said Akiko Iwasaki, an immunology professor at Yale School of Medicine, New Haven, Connecticut, and pioneer in long COVID research. Iwasaki was quick to point out that “we should never blame anybody for getting long COVID because there is no bulletproof way of preventing long COVID from happening” — although research shows you can increase your protection through vaccination, masking, and increasing ventilation indoors.
Also, just because you didn’t get long COVID after catching the virus once, doesn’t mean you’ll dodge the bullet if you get sick again, as Maio has now learned twice. She had long COVID in 2022 after her second bout with the virus, with breathing problems and brain fog that lasted for several months.
Subsequent long COVID experiences won’t necessarily mimic previous ones. Although Maio developed brain fog again, this time she didn’t have the breathing problems that plagued her in 2022. Instead, she had headaches so excruciating she thought she was dying of a brain aneurysm.
A Journal of the American Medical Association study released in May identified the 37 most common symptoms of long COVID, including symptom subgroups that occurred in 80% of the nearly 10,000 study participants. But the symptoms that patients with long COVID are experiencing now are slightly different from earlier in the pandemic or at least that’s what doctors are finding at the Post-COVID Recovery Clinic affiliated with the University of Pittsburgh Medical Center.
Michael Risbano, MD, the clinic’s codirector, said fewer patients have pulmonary or lung damage now than in the past, but a steady stream report problems with brain fog, forgetfulness, exercise intolerance (shortness of breath and fatigue with exercise and difficulty performing any kind of exertional activity), and post-exertional malaise (feeling wiped out or fatigued for hours or even days after physical or mental activity).
Long COVID Treatments Showing Improvement — Slowly
“There still isn’t a great way to treat any of this,” said Risbano, whose clinic is involved with the National Institute of Health’s RECOVER-VITAL trial, which is evaluating potential treatments including Paxlovid and exercise to treat autonomic dysfunction with similarities to myalgic encephalomyelitis/chronic fatigue syndrome and POTS, exercise intolerance, and neurocognitive effects such as brain fog.
Risbano and colleagues have found that physical therapy and exercise training have helped patients with exercise intolerance and neurocognitive problems. “It’s not a quick thing where they go through one visit and are better the next day,” he stressed. “It takes a little bit of time, a little bit of effort, a little bit of homework — there are no silver bullets, no magic medications.”
A quick fix was definitely not in the cards for Dean Jones, PhD, who could barely move when he developed long COVID in May 2023. A 74-year-old biochemist and professor of medicine at Emory University in Atlanta, Georgia, he’d recovered fully the first time he had COVID, in August 2022, but had a completely different experience the second time. He had been vaccinated four times when he began experiencing chronic fatigue, intense exertion-induced migraines, severe airway congestion, brain fog, and shortness of breath. The symptoms began after Memorial Day and worsened over the next month.
His resting heart rate began racing even when he was sleeping, jumping from 53 to 70 beats per minute. “It was almost as though the virus had hit my heart rather than the lungs alone,” he said.
Doctors prescribed multiple inhalers and glucocorticoids to calm Jones’s immune system. The worst symptoms began to abate after a few weeks. The bad ones continued for fully 2 months, severely limiting Jones’s activity. Although he no longer slept all day, just walking from one room to another was exhausting. A dedicated scientist who typically worked 10-15 hours a day before getting sick, he was lucky to focus on work-related tasks for a fraction of that time.
Although the migraines went away early on, the headaches remained until well into the fall. Jones’s energy level gradually returned, and by Christmas, he was beginning to feel as healthy as he had before getting COVID in May.
Still, he’s not complaining that it took so long to get better. “At 74, there’s a lot of colleagues who have already passed away,” he said. “I respect the realities of my age. There are so many people who died from COVID that I’m thankful I had those vaccines. I’m thankful that I pulled through it and was able to rebound.”
Time Helps Healing — But Prompt Care Still Needed
Recovery is the case for most patients with long COVID, said Lisa Sanders, MD, medical director of the Yale New Haven Health Systems Long COVID Consultation Clinic, which opened in March 2023. Although the clinic has a small segment of patients who have had the condition since 2020, “people who recover, who are most people, move on,” she said. “Even the patients who sometimes have to wait a month or so to see me, some of them say, ‘I’m already starting to get better. I wasn’t sure I should come.’”
Maio, too, is recovering but only after multiple visits to the emergency room and a neurologist in late December and early January. The third emergency room trip was prompted after a brief episode in which she lost the feeling in her legs, which began convulsing. A CAT scan showed severely constricted blood vessels in her brain, leading the medical team to speculate she might have reversible cerebral vasoconstriction syndrome (RCVS), which can trigger the thunderclap headaches that had been causing her such misery.
After her third such headache prompted a fourth emergency room visit, further tests confirmed RCVS, which doctors said was related to inflammation caused by COVID. Maio was then admitted to the hospital, where she spent 4 days starting on a regimen of blood pressure medication, magnesium for the headaches, and oxycodone for pain management.
The TV show Maio works on went back into production after the holidays. She went back at the end of January. She’s still having headaches, though they’re less intense, and she’s still taking medication. She was scheduled for another test to look at her blood vessels in February.
Maio has yet to forgive herself for skipping the last booster, even though there’s no guarantee it would have prevented her from getting sick. Her message for others: it’s better to be safe than to be as sorry as she is.
“I’ll never, ever be persuaded by people who don’t believe in vaccines because I believe in science, and I believe in vaccines — that’s why people don’t die at the age of 30 anymore,” she said. “I really think that people need to know about this and what to expect. Because it is horrendous. It is very painful. I would never want anyone to go through this. Ever.”
A version of this article appeared on Medscape.com.
A celebrity makeup artist, the 55-year-old New Yorker had been boosted and vaccinated at every opportunity since vaccines were approved at the end of 2020, until the fall of 2023, when she skipped the shot.
“I really started subscribing to the mindset that you have an immune system and your immune system is supposed to work for you,” she said. “That was the stupidest thing I’ve ever done.”
Maio was not the only person to skip the latest booster: A recent study reported that while nearly 80% of adults in the United States said they’d received their first series of vaccines, barely 20% were up to date on boosters. Nor was Maio alone in getting long COVID 4 years after the start of the deadliest pandemic in a century.
It’s tempting, this far out from the shutdowns of 2020, to think the virus is over, that we’re immune, and nobody’s going to get sick anymore. But while fewer people are getting COVID, it is still very much a part of our lives. And as Maio and others are learning the hard way, long COVID is, too — and it can be deadly.
For those who have recently contracted long COVID, it can feel as if the whole world has moved on from the pandemic, and they are being left behind.
Too Easy to Let Our Guard Down
“It’s really difficult to prevent exposure to COVID no matter how careful you are and no matter how many times you are vaccinated,” said Akiko Iwasaki, an immunology professor at Yale School of Medicine, New Haven, Connecticut, and pioneer in long COVID research. Iwasaki was quick to point out that “we should never blame anybody for getting long COVID because there is no bulletproof way of preventing long COVID from happening” — although research shows you can increase your protection through vaccination, masking, and increasing ventilation indoors.
Also, just because you didn’t get long COVID after catching the virus once, doesn’t mean you’ll dodge the bullet if you get sick again, as Maio has now learned twice. She had long COVID in 2022 after her second bout with the virus, with breathing problems and brain fog that lasted for several months.
Subsequent long COVID experiences won’t necessarily mimic previous ones. Although Maio developed brain fog again, this time she didn’t have the breathing problems that plagued her in 2022. Instead, she had headaches so excruciating she thought she was dying of a brain aneurysm.
A Journal of the American Medical Association study released in May identified the 37 most common symptoms of long COVID, including symptom subgroups that occurred in 80% of the nearly 10,000 study participants. But the symptoms that patients with long COVID are experiencing now are slightly different from earlier in the pandemic or at least that’s what doctors are finding at the Post-COVID Recovery Clinic affiliated with the University of Pittsburgh Medical Center.
Michael Risbano, MD, the clinic’s codirector, said fewer patients have pulmonary or lung damage now than in the past, but a steady stream report problems with brain fog, forgetfulness, exercise intolerance (shortness of breath and fatigue with exercise and difficulty performing any kind of exertional activity), and post-exertional malaise (feeling wiped out or fatigued for hours or even days after physical or mental activity).
Long COVID Treatments Showing Improvement — Slowly
“There still isn’t a great way to treat any of this,” said Risbano, whose clinic is involved with the National Institute of Health’s RECOVER-VITAL trial, which is evaluating potential treatments including Paxlovid and exercise to treat autonomic dysfunction with similarities to myalgic encephalomyelitis/chronic fatigue syndrome and POTS, exercise intolerance, and neurocognitive effects such as brain fog.
Risbano and colleagues have found that physical therapy and exercise training have helped patients with exercise intolerance and neurocognitive problems. “It’s not a quick thing where they go through one visit and are better the next day,” he stressed. “It takes a little bit of time, a little bit of effort, a little bit of homework — there are no silver bullets, no magic medications.”
A quick fix was definitely not in the cards for Dean Jones, PhD, who could barely move when he developed long COVID in May 2023. A 74-year-old biochemist and professor of medicine at Emory University in Atlanta, Georgia, he’d recovered fully the first time he had COVID, in August 2022, but had a completely different experience the second time. He had been vaccinated four times when he began experiencing chronic fatigue, intense exertion-induced migraines, severe airway congestion, brain fog, and shortness of breath. The symptoms began after Memorial Day and worsened over the next month.
His resting heart rate began racing even when he was sleeping, jumping from 53 to 70 beats per minute. “It was almost as though the virus had hit my heart rather than the lungs alone,” he said.
Doctors prescribed multiple inhalers and glucocorticoids to calm Jones’s immune system. The worst symptoms began to abate after a few weeks. The bad ones continued for fully 2 months, severely limiting Jones’s activity. Although he no longer slept all day, just walking from one room to another was exhausting. A dedicated scientist who typically worked 10-15 hours a day before getting sick, he was lucky to focus on work-related tasks for a fraction of that time.
Although the migraines went away early on, the headaches remained until well into the fall. Jones’s energy level gradually returned, and by Christmas, he was beginning to feel as healthy as he had before getting COVID in May.
Still, he’s not complaining that it took so long to get better. “At 74, there’s a lot of colleagues who have already passed away,” he said. “I respect the realities of my age. There are so many people who died from COVID that I’m thankful I had those vaccines. I’m thankful that I pulled through it and was able to rebound.”
Time Helps Healing — But Prompt Care Still Needed
Recovery is the case for most patients with long COVID, said Lisa Sanders, MD, medical director of the Yale New Haven Health Systems Long COVID Consultation Clinic, which opened in March 2023. Although the clinic has a small segment of patients who have had the condition since 2020, “people who recover, who are most people, move on,” she said. “Even the patients who sometimes have to wait a month or so to see me, some of them say, ‘I’m already starting to get better. I wasn’t sure I should come.’”
Maio, too, is recovering but only after multiple visits to the emergency room and a neurologist in late December and early January. The third emergency room trip was prompted after a brief episode in which she lost the feeling in her legs, which began convulsing. A CAT scan showed severely constricted blood vessels in her brain, leading the medical team to speculate she might have reversible cerebral vasoconstriction syndrome (RCVS), which can trigger the thunderclap headaches that had been causing her such misery.
After her third such headache prompted a fourth emergency room visit, further tests confirmed RCVS, which doctors said was related to inflammation caused by COVID. Maio was then admitted to the hospital, where she spent 4 days starting on a regimen of blood pressure medication, magnesium for the headaches, and oxycodone for pain management.
The TV show Maio works on went back into production after the holidays. She went back at the end of January. She’s still having headaches, though they’re less intense, and she’s still taking medication. She was scheduled for another test to look at her blood vessels in February.
Maio has yet to forgive herself for skipping the last booster, even though there’s no guarantee it would have prevented her from getting sick. Her message for others: it’s better to be safe than to be as sorry as she is.
“I’ll never, ever be persuaded by people who don’t believe in vaccines because I believe in science, and I believe in vaccines — that’s why people don’t die at the age of 30 anymore,” she said. “I really think that people need to know about this and what to expect. Because it is horrendous. It is very painful. I would never want anyone to go through this. Ever.”
A version of this article appeared on Medscape.com.
A celebrity makeup artist, the 55-year-old New Yorker had been boosted and vaccinated at every opportunity since vaccines were approved at the end of 2020, until the fall of 2023, when she skipped the shot.
“I really started subscribing to the mindset that you have an immune system and your immune system is supposed to work for you,” she said. “That was the stupidest thing I’ve ever done.”
Maio was not the only person to skip the latest booster: A recent study reported that while nearly 80% of adults in the United States said they’d received their first series of vaccines, barely 20% were up to date on boosters. Nor was Maio alone in getting long COVID 4 years after the start of the deadliest pandemic in a century.
It’s tempting, this far out from the shutdowns of 2020, to think the virus is over, that we’re immune, and nobody’s going to get sick anymore. But while fewer people are getting COVID, it is still very much a part of our lives. And as Maio and others are learning the hard way, long COVID is, too — and it can be deadly.
For those who have recently contracted long COVID, it can feel as if the whole world has moved on from the pandemic, and they are being left behind.
Too Easy to Let Our Guard Down
“It’s really difficult to prevent exposure to COVID no matter how careful you are and no matter how many times you are vaccinated,” said Akiko Iwasaki, an immunology professor at Yale School of Medicine, New Haven, Connecticut, and pioneer in long COVID research. Iwasaki was quick to point out that “we should never blame anybody for getting long COVID because there is no bulletproof way of preventing long COVID from happening” — although research shows you can increase your protection through vaccination, masking, and increasing ventilation indoors.
Also, just because you didn’t get long COVID after catching the virus once, doesn’t mean you’ll dodge the bullet if you get sick again, as Maio has now learned twice. She had long COVID in 2022 after her second bout with the virus, with breathing problems and brain fog that lasted for several months.
Subsequent long COVID experiences won’t necessarily mimic previous ones. Although Maio developed brain fog again, this time she didn’t have the breathing problems that plagued her in 2022. Instead, she had headaches so excruciating she thought she was dying of a brain aneurysm.
A Journal of the American Medical Association study released in May identified the 37 most common symptoms of long COVID, including symptom subgroups that occurred in 80% of the nearly 10,000 study participants. But the symptoms that patients with long COVID are experiencing now are slightly different from earlier in the pandemic or at least that’s what doctors are finding at the Post-COVID Recovery Clinic affiliated with the University of Pittsburgh Medical Center.
Michael Risbano, MD, the clinic’s codirector, said fewer patients have pulmonary or lung damage now than in the past, but a steady stream report problems with brain fog, forgetfulness, exercise intolerance (shortness of breath and fatigue with exercise and difficulty performing any kind of exertional activity), and post-exertional malaise (feeling wiped out or fatigued for hours or even days after physical or mental activity).
Long COVID Treatments Showing Improvement — Slowly
“There still isn’t a great way to treat any of this,” said Risbano, whose clinic is involved with the National Institute of Health’s RECOVER-VITAL trial, which is evaluating potential treatments including Paxlovid and exercise to treat autonomic dysfunction with similarities to myalgic encephalomyelitis/chronic fatigue syndrome and POTS, exercise intolerance, and neurocognitive effects such as brain fog.
Risbano and colleagues have found that physical therapy and exercise training have helped patients with exercise intolerance and neurocognitive problems. “It’s not a quick thing where they go through one visit and are better the next day,” he stressed. “It takes a little bit of time, a little bit of effort, a little bit of homework — there are no silver bullets, no magic medications.”
A quick fix was definitely not in the cards for Dean Jones, PhD, who could barely move when he developed long COVID in May 2023. A 74-year-old biochemist and professor of medicine at Emory University in Atlanta, Georgia, he’d recovered fully the first time he had COVID, in August 2022, but had a completely different experience the second time. He had been vaccinated four times when he began experiencing chronic fatigue, intense exertion-induced migraines, severe airway congestion, brain fog, and shortness of breath. The symptoms began after Memorial Day and worsened over the next month.
His resting heart rate began racing even when he was sleeping, jumping from 53 to 70 beats per minute. “It was almost as though the virus had hit my heart rather than the lungs alone,” he said.
Doctors prescribed multiple inhalers and glucocorticoids to calm Jones’s immune system. The worst symptoms began to abate after a few weeks. The bad ones continued for fully 2 months, severely limiting Jones’s activity. Although he no longer slept all day, just walking from one room to another was exhausting. A dedicated scientist who typically worked 10-15 hours a day before getting sick, he was lucky to focus on work-related tasks for a fraction of that time.
Although the migraines went away early on, the headaches remained until well into the fall. Jones’s energy level gradually returned, and by Christmas, he was beginning to feel as healthy as he had before getting COVID in May.
Still, he’s not complaining that it took so long to get better. “At 74, there’s a lot of colleagues who have already passed away,” he said. “I respect the realities of my age. There are so many people who died from COVID that I’m thankful I had those vaccines. I’m thankful that I pulled through it and was able to rebound.”
Time Helps Healing — But Prompt Care Still Needed
Recovery is the case for most patients with long COVID, said Lisa Sanders, MD, medical director of the Yale New Haven Health Systems Long COVID Consultation Clinic, which opened in March 2023. Although the clinic has a small segment of patients who have had the condition since 2020, “people who recover, who are most people, move on,” she said. “Even the patients who sometimes have to wait a month or so to see me, some of them say, ‘I’m already starting to get better. I wasn’t sure I should come.’”
Maio, too, is recovering but only after multiple visits to the emergency room and a neurologist in late December and early January. The third emergency room trip was prompted after a brief episode in which she lost the feeling in her legs, which began convulsing. A CAT scan showed severely constricted blood vessels in her brain, leading the medical team to speculate she might have reversible cerebral vasoconstriction syndrome (RCVS), which can trigger the thunderclap headaches that had been causing her such misery.
After her third such headache prompted a fourth emergency room visit, further tests confirmed RCVS, which doctors said was related to inflammation caused by COVID. Maio was then admitted to the hospital, where she spent 4 days starting on a regimen of blood pressure medication, magnesium for the headaches, and oxycodone for pain management.
The TV show Maio works on went back into production after the holidays. She went back at the end of January. She’s still having headaches, though they’re less intense, and she’s still taking medication. She was scheduled for another test to look at her blood vessels in February.
Maio has yet to forgive herself for skipping the last booster, even though there’s no guarantee it would have prevented her from getting sick. Her message for others: it’s better to be safe than to be as sorry as she is.
“I’ll never, ever be persuaded by people who don’t believe in vaccines because I believe in science, and I believe in vaccines — that’s why people don’t die at the age of 30 anymore,” she said. “I really think that people need to know about this and what to expect. Because it is horrendous. It is very painful. I would never want anyone to go through this. Ever.”
A version of this article appeared on Medscape.com.
Plant-Based Diet a Boon for Men With Prostate Cancer
, new research showed.
The findings, published on February 13, 2024, in the journal Cancer, bolster previous research showing plant-based diets can reduce the risk for recurrence and improve survivorship in men with prostate cancer.
“The current study shows for the first time an association between eating more plant-based food with better scores for quality of life among patients diagnosed with prostate cancer,” Stacy Loeb, MD, a urologist in the departments of Urology and Population Health at NYU Langone Health, in New York City, who led the research.
For the new study, Dr. Loeb and her colleagues looked at data from more than 3500 men with prostate cancer in the Health Professionals Follow-Up Study, an ongoing investigation begun in 1986 and sponsored by Harvard T.H. Chan School of Public Health. The dataset included more than 50,000 male dentists, pharmacists, optometrists, osteopaths, podiatrists, and veterinarians.
The median age of prostate cancer diagnosis was 68 years; 48% of patients underwent radical prostatectomy and 35% had radiation as primary therapy. None of the patients were known to have had metastatic disease.
Men in the study answered a questionnaire every 4 years about the kinds of foods they ate and in what proportions. Another survey, administered every 2 years, assessed the frequency of incontinence, difficulties maintaining an erection, and problems with bowels, energy, and mood, among many other health concerns.
Dr. Loeb and her colleagues sorted patients into quintiles based on the proportion of plant vs animal foods the men said they eat. The authors found those who consumed the most plant-based foods scored 8%-11% better in measures of sexual function than the group that consumed the least of these products.
These men also reported up to 14% better scores for urinary health, with fewer instances of incontinence, obstruction, and irritation, and up to 13% better scores in hormonal health, marked by symptoms like low energy, depression, and hot flashes.
Justin Gregg, MD, a urology researcher at the University of Texas MD Anderson Cancer Center, in Houston, Texas, whose research has found the Mediterranean diet can slow tumor progression among men with localized prostate cancer on active surveillance, called the results “not entirely surprising, as prior studies have shown associations between plant-based diet and outcomes like erectile function among men who do not have prostate cancer.”
But Kenneth Jacobsohn, MD, professor of urology and director of lifestyle medicine at the Medical College of Wisconsin, in Milwaukee, said the new findings help establish “the positive role of diet quality and plant-based diets, specifically on quality of life after prostate cancer diagnosis and treatment for men with nonmetastatic prostate cancer.”
Dr. Jacobsohn said the study was limited by its retrospective nature and the manner of the dietary assessment.
“As the authors point out, a plant-based diet may be helpful, though it’s important to keep in mind the strong data for its protective effect in terms of cardiovascular disease risk, which is very important for men who have a history of prostate cancer as many will die of cardiovascular disease,” Dr. Gregg added.
Dr. Loeb, Dr. Gregg, and Dr. Jacobsohn reported no conflicts of interest. Some of the study authors reported a variety of potential conflicts.
A version of this article appeared on Medscape.com .
, new research showed.
The findings, published on February 13, 2024, in the journal Cancer, bolster previous research showing plant-based diets can reduce the risk for recurrence and improve survivorship in men with prostate cancer.
“The current study shows for the first time an association between eating more plant-based food with better scores for quality of life among patients diagnosed with prostate cancer,” Stacy Loeb, MD, a urologist in the departments of Urology and Population Health at NYU Langone Health, in New York City, who led the research.
For the new study, Dr. Loeb and her colleagues looked at data from more than 3500 men with prostate cancer in the Health Professionals Follow-Up Study, an ongoing investigation begun in 1986 and sponsored by Harvard T.H. Chan School of Public Health. The dataset included more than 50,000 male dentists, pharmacists, optometrists, osteopaths, podiatrists, and veterinarians.
The median age of prostate cancer diagnosis was 68 years; 48% of patients underwent radical prostatectomy and 35% had radiation as primary therapy. None of the patients were known to have had metastatic disease.
Men in the study answered a questionnaire every 4 years about the kinds of foods they ate and in what proportions. Another survey, administered every 2 years, assessed the frequency of incontinence, difficulties maintaining an erection, and problems with bowels, energy, and mood, among many other health concerns.
Dr. Loeb and her colleagues sorted patients into quintiles based on the proportion of plant vs animal foods the men said they eat. The authors found those who consumed the most plant-based foods scored 8%-11% better in measures of sexual function than the group that consumed the least of these products.
These men also reported up to 14% better scores for urinary health, with fewer instances of incontinence, obstruction, and irritation, and up to 13% better scores in hormonal health, marked by symptoms like low energy, depression, and hot flashes.
Justin Gregg, MD, a urology researcher at the University of Texas MD Anderson Cancer Center, in Houston, Texas, whose research has found the Mediterranean diet can slow tumor progression among men with localized prostate cancer on active surveillance, called the results “not entirely surprising, as prior studies have shown associations between plant-based diet and outcomes like erectile function among men who do not have prostate cancer.”
But Kenneth Jacobsohn, MD, professor of urology and director of lifestyle medicine at the Medical College of Wisconsin, in Milwaukee, said the new findings help establish “the positive role of diet quality and plant-based diets, specifically on quality of life after prostate cancer diagnosis and treatment for men with nonmetastatic prostate cancer.”
Dr. Jacobsohn said the study was limited by its retrospective nature and the manner of the dietary assessment.
“As the authors point out, a plant-based diet may be helpful, though it’s important to keep in mind the strong data for its protective effect in terms of cardiovascular disease risk, which is very important for men who have a history of prostate cancer as many will die of cardiovascular disease,” Dr. Gregg added.
Dr. Loeb, Dr. Gregg, and Dr. Jacobsohn reported no conflicts of interest. Some of the study authors reported a variety of potential conflicts.
A version of this article appeared on Medscape.com .
, new research showed.
The findings, published on February 13, 2024, in the journal Cancer, bolster previous research showing plant-based diets can reduce the risk for recurrence and improve survivorship in men with prostate cancer.
“The current study shows for the first time an association between eating more plant-based food with better scores for quality of life among patients diagnosed with prostate cancer,” Stacy Loeb, MD, a urologist in the departments of Urology and Population Health at NYU Langone Health, in New York City, who led the research.
For the new study, Dr. Loeb and her colleagues looked at data from more than 3500 men with prostate cancer in the Health Professionals Follow-Up Study, an ongoing investigation begun in 1986 and sponsored by Harvard T.H. Chan School of Public Health. The dataset included more than 50,000 male dentists, pharmacists, optometrists, osteopaths, podiatrists, and veterinarians.
The median age of prostate cancer diagnosis was 68 years; 48% of patients underwent radical prostatectomy and 35% had radiation as primary therapy. None of the patients were known to have had metastatic disease.
Men in the study answered a questionnaire every 4 years about the kinds of foods they ate and in what proportions. Another survey, administered every 2 years, assessed the frequency of incontinence, difficulties maintaining an erection, and problems with bowels, energy, and mood, among many other health concerns.
Dr. Loeb and her colleagues sorted patients into quintiles based on the proportion of plant vs animal foods the men said they eat. The authors found those who consumed the most plant-based foods scored 8%-11% better in measures of sexual function than the group that consumed the least of these products.
These men also reported up to 14% better scores for urinary health, with fewer instances of incontinence, obstruction, and irritation, and up to 13% better scores in hormonal health, marked by symptoms like low energy, depression, and hot flashes.
Justin Gregg, MD, a urology researcher at the University of Texas MD Anderson Cancer Center, in Houston, Texas, whose research has found the Mediterranean diet can slow tumor progression among men with localized prostate cancer on active surveillance, called the results “not entirely surprising, as prior studies have shown associations between plant-based diet and outcomes like erectile function among men who do not have prostate cancer.”
But Kenneth Jacobsohn, MD, professor of urology and director of lifestyle medicine at the Medical College of Wisconsin, in Milwaukee, said the new findings help establish “the positive role of diet quality and plant-based diets, specifically on quality of life after prostate cancer diagnosis and treatment for men with nonmetastatic prostate cancer.”
Dr. Jacobsohn said the study was limited by its retrospective nature and the manner of the dietary assessment.
“As the authors point out, a plant-based diet may be helpful, though it’s important to keep in mind the strong data for its protective effect in terms of cardiovascular disease risk, which is very important for men who have a history of prostate cancer as many will die of cardiovascular disease,” Dr. Gregg added.
Dr. Loeb, Dr. Gregg, and Dr. Jacobsohn reported no conflicts of interest. Some of the study authors reported a variety of potential conflicts.
A version of this article appeared on Medscape.com .
Exercising With Osteoarthritis: Five Things to Know
It’s no secret that regular exercise is important. But for patients with painful joints, it can be the last thing they want to do. Exercise is one of the cornerstones of managing arthritis, yet nearly one third of patients with arthritis are inactive.
This news organization recently spoke to experts on what resources are available, how much exercise is ideal, and how to motivate patients to move more.
What Are the Benefits of Exercise in Osteoarthritis?
Nearly all professional societies agree that exercise is one of the hallmarks of managing osteoarthritis (OA). According to two Cochrane reviews, there is high-equality evidence that exercise can help reduce pain as well as improve physical function in both hip and knee OA. In fact, physical activity can decrease pain and improve function by 40% in adults with arthritis, according to the Centers for Disease Control and Prevention.
Exercise also plays a large role in preventing disability by improving joint range of motion as well as maintaining muscle mass that supports joints.
There is also preliminary evidence that exercise could have a structural benefit to osteoarthritic joints. In a study of about 1200 individuals with knee OA, those who walked for exercise not only had reduced frequent knee pain, compared with non-walkers, but also were 20% less likely to have worsening of medial joint space narrowing.
Beyond symptom and impairment improvements, exercise can also play a role in staving off other chronic diseases linked to OA, such as cardiovascular disease and type 2 diabetes. Physical activity and exercise “are effective in preventing at least 35 chronic conditions and treating at least 26 chronic conditions, with one of the potential working mechanisms being exercise-induced anti-inflammatory effects,” wrote the authors of a commentary in the Journal of Orthopaedic & Sports Physical Therapy.
The known mental health benefits of exercise can also be beneficial for patients, as rates of depression and anxiety can be higher in people with arthritis than in the general population.
What Is the Ideal Amount of Exercise for Patients?
Current guidelines recommend that adults should get 150 minutes of moderate physical activity each week. But for patients with chronic pain, that may seem unachievable, Kelli Allen, PhD, professor of medicine and exercise physiologist at the University of North Carolina School of Medicine in Chapel Hill, said during a presentation at the American College of Rheumatology 2023 annual meeting in San Diego. Promisingly, research has shown that some exercise is better than none.
One study looking at over 1500 adults with lower extremity joint symptoms suggested that approximately 1 hour of physical activity per week increased the likelihood that participants remained disability-free over 4 years. In another analysis looking at 280 studies, researchers concluded that resistance training programs lasting 3-6 months resulted in moderate improvements in pain and physical function, but these benefits did not depend on exercise volume or participant adherence.
“These findings highlight the flexibility available for clinicians in the prescription of resistance exercise for knee and hip OA without compromising improvements in pain and physical function,” the authors wrote.
Step counts can be another way to measure activity, with 10,000 steps being a common target. But fewer steps a day can also yield health benefits. One study found that among nearly 1800 participants with knee OA, each additional 1000 steps per day was associated with a 16%-18% reduced risk of developing functional limitations 2 years later. Walking 6000 steps a day was the threshold that best determined who would develop functional limitations and who would not.
“I think it’s really a helpful message to encourage people with chronic pain that if you can get to 6000, maybe that’s a good goal,” Dr. Allen said.
Going for a 20-minute walk three times a week can be a good place to start, said Grace H. Lo, MD, associate professor in the Division of Immunology, Allergy, and Rheumatology at Baylor College of Medicine in Houston, Texas. For people who currently do not do any activity, Dr. Lo recommends starting small, like walking to get the mail every day. “Do something practical that is something they can sustain and keep in their daily activities that will help to increase their function and hopefully lessen some of their symptoms.”
Are Certain Types of Exercise More Beneficial?
There is no specific type of exercise that is best for OA, so it comes down to patient preference. The best exercise is “whatever somebody is actually going to do,” Dr. Allen noted.
Una Makris, MD, associate professor of internal medicine in the Division of Rheumatic Disease at the University of Texas Southwestern Medical Center and rheumatologist at the North Texas VA Health Care System in Dallas, Texas, said that her practice focuses on a combination of aerobic activity, functional balance, and strength training, as recommended by the World Health Organization.
“It’s not clear to me that one type of exercise is better than another; it’s more about what does this patient enjoy, and how can we make this a routine, so it is a sustainable behavior,” she told this news organization.
Generally, lower-impact exercises like biking, walking, or swimming tend to be better for OA, Dr. Lo added. Several studies have also shown tai chi to be beneficial in patients with OA, she said. More recently, Dr. Lo has conducted research on gardening as an exercise intervention for OA.
“It’s a great way to encourage people to exercise,” she said in an interview. “Besides the fact that they’re physically active, they can also be outside. There are a lot of mental health benefits to doing gardening as well.”
Dr. Allen added that certain exercises should be considered on the basis of an individual’s goals and physical needs. If someone has balance issues, for example, then yoga or tai chi could be useful to add to their exercise program, she said.
What Resources Are Available?
The Osteoarthritis Action Alliance has a list of 23 evidence-based exercise programs that have been shown to improve arthritis symptoms. These arthritis-appropriate, evidence-based interventions vary from instructor-led, in-person sessions to self-directed programs.
Walk with Ease (or Camine Con Gusto in Spanish) is one popular program, noted Dr. Allen. The program can be in-person or self-directed, with a required booklet that costs $11.95. However, there are discounted books for community-based organizations. The My Knee Exercise program, created by the University of Melbourne, Australia, provides a free, self-directed, 6-month strengthening program. The availability and cost of other programs are dependent on the format and location, the guide noted.
But understanding what programs are available in certain communities takes time, which can be a barrier to clinician referrals, noted Katie Huffman, director of education and outreach at OA Action Alliance.
“We would love to see these programs being covered by payers and health plans so that there’s incentive for providers to refer and patients to participate in the programs,” she noted.
While some states do cover a limited number of programs under Medicaid, coverage across states and payers is not yet universal.
In addition to these programs, the alliance has a simple guide to help plan workouts based on current activity level. The guide links to free exercises from CreakyJoints, an online community for people with arthritis, and the Arthritis Foundation.
Dr. Lo noted that the Veterans Affairs program, “VA Whole Health,” has free resources that are available to anyone. The provided videos offer tai chi, chair exercises, and guided meditations.
“It’s thoughtful to people who have some limitations in their physical activity,” she said.
Because the program is online, it could be difficult to access for those who are not comfortable with electronics, she said, “but if you can find a way to pass that, I think that this is an amazing resource,” she said.
How Do You Motivate Patients to Move?
“When it comes to motivation, I don’t think there is a one-size-fits-all approach,” said Dr. Makris. She tries to identify what matters most for each patient as a starting point. “When they can identify something in their day-to-day life that they value, then I like to link a physical activity-based goal to that,” she said. Setting physical activity goals using the mnemonic SMART (Specific, Measurable, Attainable, Realistic, and Timely) can be useful, she advised.
The OA Action Alliance also provides additional tools for clinicians on how to counsel patients on behavior change.
Understanding the patient’s lifestyle is also crucial when discussing physical activity, Dr. Lo added. “You have to give them practical solutions that they can actually incorporate into their lives,” she said.
Discussions around physical activity should be an ongoing part of clinic visits, both Dr. Lo and Dr. Makris agreed, to celebrate achievements and revise goals.
“I’m kind of notorious for being really slow in clinic because I just let people talk,” Dr. Lo said. “I do feel like these extra moments, when you spend time talking about these things, allow your recommendations to be more customized for the patients” and make the biggest impact.
Dr. Allen, Dr. Lo, and Dr. Makris reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
It’s no secret that regular exercise is important. But for patients with painful joints, it can be the last thing they want to do. Exercise is one of the cornerstones of managing arthritis, yet nearly one third of patients with arthritis are inactive.
This news organization recently spoke to experts on what resources are available, how much exercise is ideal, and how to motivate patients to move more.
What Are the Benefits of Exercise in Osteoarthritis?
Nearly all professional societies agree that exercise is one of the hallmarks of managing osteoarthritis (OA). According to two Cochrane reviews, there is high-equality evidence that exercise can help reduce pain as well as improve physical function in both hip and knee OA. In fact, physical activity can decrease pain and improve function by 40% in adults with arthritis, according to the Centers for Disease Control and Prevention.
Exercise also plays a large role in preventing disability by improving joint range of motion as well as maintaining muscle mass that supports joints.
There is also preliminary evidence that exercise could have a structural benefit to osteoarthritic joints. In a study of about 1200 individuals with knee OA, those who walked for exercise not only had reduced frequent knee pain, compared with non-walkers, but also were 20% less likely to have worsening of medial joint space narrowing.
Beyond symptom and impairment improvements, exercise can also play a role in staving off other chronic diseases linked to OA, such as cardiovascular disease and type 2 diabetes. Physical activity and exercise “are effective in preventing at least 35 chronic conditions and treating at least 26 chronic conditions, with one of the potential working mechanisms being exercise-induced anti-inflammatory effects,” wrote the authors of a commentary in the Journal of Orthopaedic & Sports Physical Therapy.
The known mental health benefits of exercise can also be beneficial for patients, as rates of depression and anxiety can be higher in people with arthritis than in the general population.
What Is the Ideal Amount of Exercise for Patients?
Current guidelines recommend that adults should get 150 minutes of moderate physical activity each week. But for patients with chronic pain, that may seem unachievable, Kelli Allen, PhD, professor of medicine and exercise physiologist at the University of North Carolina School of Medicine in Chapel Hill, said during a presentation at the American College of Rheumatology 2023 annual meeting in San Diego. Promisingly, research has shown that some exercise is better than none.
One study looking at over 1500 adults with lower extremity joint symptoms suggested that approximately 1 hour of physical activity per week increased the likelihood that participants remained disability-free over 4 years. In another analysis looking at 280 studies, researchers concluded that resistance training programs lasting 3-6 months resulted in moderate improvements in pain and physical function, but these benefits did not depend on exercise volume or participant adherence.
“These findings highlight the flexibility available for clinicians in the prescription of resistance exercise for knee and hip OA without compromising improvements in pain and physical function,” the authors wrote.
Step counts can be another way to measure activity, with 10,000 steps being a common target. But fewer steps a day can also yield health benefits. One study found that among nearly 1800 participants with knee OA, each additional 1000 steps per day was associated with a 16%-18% reduced risk of developing functional limitations 2 years later. Walking 6000 steps a day was the threshold that best determined who would develop functional limitations and who would not.
“I think it’s really a helpful message to encourage people with chronic pain that if you can get to 6000, maybe that’s a good goal,” Dr. Allen said.
Going for a 20-minute walk three times a week can be a good place to start, said Grace H. Lo, MD, associate professor in the Division of Immunology, Allergy, and Rheumatology at Baylor College of Medicine in Houston, Texas. For people who currently do not do any activity, Dr. Lo recommends starting small, like walking to get the mail every day. “Do something practical that is something they can sustain and keep in their daily activities that will help to increase their function and hopefully lessen some of their symptoms.”
Are Certain Types of Exercise More Beneficial?
There is no specific type of exercise that is best for OA, so it comes down to patient preference. The best exercise is “whatever somebody is actually going to do,” Dr. Allen noted.
Una Makris, MD, associate professor of internal medicine in the Division of Rheumatic Disease at the University of Texas Southwestern Medical Center and rheumatologist at the North Texas VA Health Care System in Dallas, Texas, said that her practice focuses on a combination of aerobic activity, functional balance, and strength training, as recommended by the World Health Organization.
“It’s not clear to me that one type of exercise is better than another; it’s more about what does this patient enjoy, and how can we make this a routine, so it is a sustainable behavior,” she told this news organization.
Generally, lower-impact exercises like biking, walking, or swimming tend to be better for OA, Dr. Lo added. Several studies have also shown tai chi to be beneficial in patients with OA, she said. More recently, Dr. Lo has conducted research on gardening as an exercise intervention for OA.
“It’s a great way to encourage people to exercise,” she said in an interview. “Besides the fact that they’re physically active, they can also be outside. There are a lot of mental health benefits to doing gardening as well.”
Dr. Allen added that certain exercises should be considered on the basis of an individual’s goals and physical needs. If someone has balance issues, for example, then yoga or tai chi could be useful to add to their exercise program, she said.
What Resources Are Available?
The Osteoarthritis Action Alliance has a list of 23 evidence-based exercise programs that have been shown to improve arthritis symptoms. These arthritis-appropriate, evidence-based interventions vary from instructor-led, in-person sessions to self-directed programs.
Walk with Ease (or Camine Con Gusto in Spanish) is one popular program, noted Dr. Allen. The program can be in-person or self-directed, with a required booklet that costs $11.95. However, there are discounted books for community-based organizations. The My Knee Exercise program, created by the University of Melbourne, Australia, provides a free, self-directed, 6-month strengthening program. The availability and cost of other programs are dependent on the format and location, the guide noted.
But understanding what programs are available in certain communities takes time, which can be a barrier to clinician referrals, noted Katie Huffman, director of education and outreach at OA Action Alliance.
“We would love to see these programs being covered by payers and health plans so that there’s incentive for providers to refer and patients to participate in the programs,” she noted.
While some states do cover a limited number of programs under Medicaid, coverage across states and payers is not yet universal.
In addition to these programs, the alliance has a simple guide to help plan workouts based on current activity level. The guide links to free exercises from CreakyJoints, an online community for people with arthritis, and the Arthritis Foundation.
Dr. Lo noted that the Veterans Affairs program, “VA Whole Health,” has free resources that are available to anyone. The provided videos offer tai chi, chair exercises, and guided meditations.
“It’s thoughtful to people who have some limitations in their physical activity,” she said.
Because the program is online, it could be difficult to access for those who are not comfortable with electronics, she said, “but if you can find a way to pass that, I think that this is an amazing resource,” she said.
How Do You Motivate Patients to Move?
“When it comes to motivation, I don’t think there is a one-size-fits-all approach,” said Dr. Makris. She tries to identify what matters most for each patient as a starting point. “When they can identify something in their day-to-day life that they value, then I like to link a physical activity-based goal to that,” she said. Setting physical activity goals using the mnemonic SMART (Specific, Measurable, Attainable, Realistic, and Timely) can be useful, she advised.
The OA Action Alliance also provides additional tools for clinicians on how to counsel patients on behavior change.
Understanding the patient’s lifestyle is also crucial when discussing physical activity, Dr. Lo added. “You have to give them practical solutions that they can actually incorporate into their lives,” she said.
Discussions around physical activity should be an ongoing part of clinic visits, both Dr. Lo and Dr. Makris agreed, to celebrate achievements and revise goals.
“I’m kind of notorious for being really slow in clinic because I just let people talk,” Dr. Lo said. “I do feel like these extra moments, when you spend time talking about these things, allow your recommendations to be more customized for the patients” and make the biggest impact.
Dr. Allen, Dr. Lo, and Dr. Makris reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
It’s no secret that regular exercise is important. But for patients with painful joints, it can be the last thing they want to do. Exercise is one of the cornerstones of managing arthritis, yet nearly one third of patients with arthritis are inactive.
This news organization recently spoke to experts on what resources are available, how much exercise is ideal, and how to motivate patients to move more.
What Are the Benefits of Exercise in Osteoarthritis?
Nearly all professional societies agree that exercise is one of the hallmarks of managing osteoarthritis (OA). According to two Cochrane reviews, there is high-equality evidence that exercise can help reduce pain as well as improve physical function in both hip and knee OA. In fact, physical activity can decrease pain and improve function by 40% in adults with arthritis, according to the Centers for Disease Control and Prevention.
Exercise also plays a large role in preventing disability by improving joint range of motion as well as maintaining muscle mass that supports joints.
There is also preliminary evidence that exercise could have a structural benefit to osteoarthritic joints. In a study of about 1200 individuals with knee OA, those who walked for exercise not only had reduced frequent knee pain, compared with non-walkers, but also were 20% less likely to have worsening of medial joint space narrowing.
Beyond symptom and impairment improvements, exercise can also play a role in staving off other chronic diseases linked to OA, such as cardiovascular disease and type 2 diabetes. Physical activity and exercise “are effective in preventing at least 35 chronic conditions and treating at least 26 chronic conditions, with one of the potential working mechanisms being exercise-induced anti-inflammatory effects,” wrote the authors of a commentary in the Journal of Orthopaedic & Sports Physical Therapy.
The known mental health benefits of exercise can also be beneficial for patients, as rates of depression and anxiety can be higher in people with arthritis than in the general population.
What Is the Ideal Amount of Exercise for Patients?
Current guidelines recommend that adults should get 150 minutes of moderate physical activity each week. But for patients with chronic pain, that may seem unachievable, Kelli Allen, PhD, professor of medicine and exercise physiologist at the University of North Carolina School of Medicine in Chapel Hill, said during a presentation at the American College of Rheumatology 2023 annual meeting in San Diego. Promisingly, research has shown that some exercise is better than none.
One study looking at over 1500 adults with lower extremity joint symptoms suggested that approximately 1 hour of physical activity per week increased the likelihood that participants remained disability-free over 4 years. In another analysis looking at 280 studies, researchers concluded that resistance training programs lasting 3-6 months resulted in moderate improvements in pain and physical function, but these benefits did not depend on exercise volume or participant adherence.
“These findings highlight the flexibility available for clinicians in the prescription of resistance exercise for knee and hip OA without compromising improvements in pain and physical function,” the authors wrote.
Step counts can be another way to measure activity, with 10,000 steps being a common target. But fewer steps a day can also yield health benefits. One study found that among nearly 1800 participants with knee OA, each additional 1000 steps per day was associated with a 16%-18% reduced risk of developing functional limitations 2 years later. Walking 6000 steps a day was the threshold that best determined who would develop functional limitations and who would not.
“I think it’s really a helpful message to encourage people with chronic pain that if you can get to 6000, maybe that’s a good goal,” Dr. Allen said.
Going for a 20-minute walk three times a week can be a good place to start, said Grace H. Lo, MD, associate professor in the Division of Immunology, Allergy, and Rheumatology at Baylor College of Medicine in Houston, Texas. For people who currently do not do any activity, Dr. Lo recommends starting small, like walking to get the mail every day. “Do something practical that is something they can sustain and keep in their daily activities that will help to increase their function and hopefully lessen some of their symptoms.”
Are Certain Types of Exercise More Beneficial?
There is no specific type of exercise that is best for OA, so it comes down to patient preference. The best exercise is “whatever somebody is actually going to do,” Dr. Allen noted.
Una Makris, MD, associate professor of internal medicine in the Division of Rheumatic Disease at the University of Texas Southwestern Medical Center and rheumatologist at the North Texas VA Health Care System in Dallas, Texas, said that her practice focuses on a combination of aerobic activity, functional balance, and strength training, as recommended by the World Health Organization.
“It’s not clear to me that one type of exercise is better than another; it’s more about what does this patient enjoy, and how can we make this a routine, so it is a sustainable behavior,” she told this news organization.
Generally, lower-impact exercises like biking, walking, or swimming tend to be better for OA, Dr. Lo added. Several studies have also shown tai chi to be beneficial in patients with OA, she said. More recently, Dr. Lo has conducted research on gardening as an exercise intervention for OA.
“It’s a great way to encourage people to exercise,” she said in an interview. “Besides the fact that they’re physically active, they can also be outside. There are a lot of mental health benefits to doing gardening as well.”
Dr. Allen added that certain exercises should be considered on the basis of an individual’s goals and physical needs. If someone has balance issues, for example, then yoga or tai chi could be useful to add to their exercise program, she said.
What Resources Are Available?
The Osteoarthritis Action Alliance has a list of 23 evidence-based exercise programs that have been shown to improve arthritis symptoms. These arthritis-appropriate, evidence-based interventions vary from instructor-led, in-person sessions to self-directed programs.
Walk with Ease (or Camine Con Gusto in Spanish) is one popular program, noted Dr. Allen. The program can be in-person or self-directed, with a required booklet that costs $11.95. However, there are discounted books for community-based organizations. The My Knee Exercise program, created by the University of Melbourne, Australia, provides a free, self-directed, 6-month strengthening program. The availability and cost of other programs are dependent on the format and location, the guide noted.
But understanding what programs are available in certain communities takes time, which can be a barrier to clinician referrals, noted Katie Huffman, director of education and outreach at OA Action Alliance.
“We would love to see these programs being covered by payers and health plans so that there’s incentive for providers to refer and patients to participate in the programs,” she noted.
While some states do cover a limited number of programs under Medicaid, coverage across states and payers is not yet universal.
In addition to these programs, the alliance has a simple guide to help plan workouts based on current activity level. The guide links to free exercises from CreakyJoints, an online community for people with arthritis, and the Arthritis Foundation.
Dr. Lo noted that the Veterans Affairs program, “VA Whole Health,” has free resources that are available to anyone. The provided videos offer tai chi, chair exercises, and guided meditations.
“It’s thoughtful to people who have some limitations in their physical activity,” she said.
Because the program is online, it could be difficult to access for those who are not comfortable with electronics, she said, “but if you can find a way to pass that, I think that this is an amazing resource,” she said.
How Do You Motivate Patients to Move?
“When it comes to motivation, I don’t think there is a one-size-fits-all approach,” said Dr. Makris. She tries to identify what matters most for each patient as a starting point. “When they can identify something in their day-to-day life that they value, then I like to link a physical activity-based goal to that,” she said. Setting physical activity goals using the mnemonic SMART (Specific, Measurable, Attainable, Realistic, and Timely) can be useful, she advised.
The OA Action Alliance also provides additional tools for clinicians on how to counsel patients on behavior change.
Understanding the patient’s lifestyle is also crucial when discussing physical activity, Dr. Lo added. “You have to give them practical solutions that they can actually incorporate into their lives,” she said.
Discussions around physical activity should be an ongoing part of clinic visits, both Dr. Lo and Dr. Makris agreed, to celebrate achievements and revise goals.
“I’m kind of notorious for being really slow in clinic because I just let people talk,” Dr. Lo said. “I do feel like these extra moments, when you spend time talking about these things, allow your recommendations to be more customized for the patients” and make the biggest impact.
Dr. Allen, Dr. Lo, and Dr. Makris reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
CAR T-Cell: Do Benefits Still Outweigh Risks?
Importantly, most specialists agree, so far the risk appears no greater than the known risk of secondary primary malignancies that is well established with other cancer therapies.
“The data that we have so far suggest that the risk of secondary T-cell lymphoma in patients treated with CAR T-cells is similar to [that] of patients treated with other cancer therapies, [including] chemotherapy, radiation, transplantation,” Marco Ruella, MD, said in an interview. He reported on a case of a T-cell lymphoma occurring following CAR-T therapy at the University of Pennsylvania.
While his team is still investigating the development of such malignancies, “the FDA notice does not change our clinical practice and patients should be reassured that the benefit of CAR-T therapy significantly outweighs the potential risk of secondary malignancies including T-cell lymphoma,” said Dr. Ruella, scientific director of the Lymphoma Program, Division of Hematology and Oncology and Center for Cellular Immunotherapies, at the University of Pennsylvania, Philadelphia.
FDA: 28 Reports of Malignancies; 3 with Evidence of ‘Likely’ CAR T Involvement
Concerns were raised last November when the FDA announced in a safety communication that it was investigating the “serious risk of T-cell malignancy” following B-cell maturation antigen (BCMA)-directed or CD19-directed CAR T-cell immunotherapies, citing reports from clinical trials and/or postmarketing adverse event data sources. Subsequently, in January, the FDA called for the boxed warning on all approved BCMA- and CD19-targeted genetically modified autologous T-cell immunotherapies, which include: Abecma (idecabtagene vicleucel); Breyanzi (lisocabtagene maraleucel); Carvykti (ciltacabtagene autoleucel); Kymriah (tisagenlecleucel); Tecartus (brexucabtagene autoleucel); and Yescarta (axicabtagene ciloleucel).
“Although the overall benefits of these products continue to outweigh their potential risks for their approved uses, the FDA continues to investigate the identified risk of T-cell malignancy with serious outcomes, including hospitalization and death,” the FDA reported in discussing the safety warnings.
The cases were detailed in a report from FDA researchers published in the New England Journal of Medicine, noting that as of December 31, 2023, the FDA had become aware of 22 cases of T-cell cancers occurring following CAR T-cell treatment, including T-cell lymphoma, T-cell large granular lymphocytosis, peripheral T-cell lymphoma, and cutaneous T-cell lymphoma.
Report coauthor Peter Marks, MD, PhD, of the FDA’s Center for Biologics Evaluation and Research in Silver Spring, Maryland, said in an interview that since the publication of their report, six new cases have emerged.
“As reported in the NEJM Perspective, there were 22 cases of T-cell malignancy after treatment with CAR T-cell immunotherapies as of December 31, 2023, but we have received additional reports and, as of February 9, 2024, FDA has now received 28 reports,” he said. “Note that as new cases are being reported, there will be updates to the total number of cases under ongoing review by FDA.”
The initial 22 cases all occurred relatively soon after treatment. Of 14 cases with sufficient data, all developed within 2 years of the CAR-T therapy, ranging from 1 to 19 months, with about half occurring in the first year after administration.
The cases involved five of the six FDA-approved CAR-T products, with the numbers too low to suggest an association with any particular product.
In three of the cases, the lymphoma was found in genetic testing to contain the CAR construction, “indicating that the CAR-T product was most likely involved in the development of the T-cell cancer,” according to the FDA researchers.
With inadequate genetic sampling in most of the remaining 19 cases, the association is less clear, however “the timing of several of the cases makes association a possibility,” Dr. Marks said. In their report, Dr. Marks and colleagues added that “determination of whether the T-cell cancer is associated with the CAR construct ... most likely won’t be possible for every case reported to date.”
Even if all the reported cases are assumed to be related to CAR-T treatment, the numbers still represent a very small proportion of the more than 27,000 doses of the six CAR-T therapies approved in the United States, the authors noted, but they cautioned that the numbers could indeed be higher than reported.
“Relying on postmarketing reporting may lead to underestimates of such cases,” they said.
Life-Long Monitoring Recommended
In response to the reports, the FDA is urging that clinicians’ monitoring of patients treated with CAR-T therapy should be lifelong.
“Patients and clinical trial participants receiving treatment with these products should be monitored lifelong for new malignancies,” Dr. Marks said.
“In the event that a new malignancy occurs following treatment with these products, contact the manufacturer to report the event and obtain instructions on collection of patient samples for testing for the presence of the CAR transgene.”
In addition, cases should be reported to the FDA, either by calling or through the FDA’s medical product safety reporting program.
T-Cell Malignancy Case Report
In describing the case at their medical center in the report in Nature Medicine, Dr. Ruella and colleagues said a T-cell lymphoma occurred in a patient with non-Hodgkin B-cell lymphoma 3 months after an anti-CD19 CAR T-cell treatment.
As a result, the team conducted a subsequent analysis of 449 patients treated with CAR-T therapy at the University of Pennsylvania center, and with a median follow-up of 10.3 months, 16 patients (3.6%) had developed a secondary primary malignancy, with a median onset time of 26.4 months for solid and 9.7 months for hematological malignancies.
The patient who had developed a T-cell lymphoma tested negative for CAR integration upon diagnosis, and regarding the other cancers, Dr. Ruella noted that “we have no indication that the secondary malignancies are directly caused by the CAR-T therapy.
“We have many patients with a very long follow-up beyond 5 and even 10 years,” he said. “In these patients, we don’t see an increased risk of T-cell lymphoma.”
‘Cautious Reassurance’ Urged in Discussion with Patients
With alarming headlines on the findings suggesting that CAR-T therapy may cause cancer, Rahul Banerjee, MD, and colleagues at the University of Washington, Seattle, recommend the use of “cautious reassurance” in discussing the issue with patients. In a paper published in January in Blood Advances, they suggest a three-part response: underscoring that the benefits of CAR T “far outweigh” the risks in relapsed/refractory malignancies, that the ‘one-and-done’ nature of CAR-T infusions provide meaningful improvements in quality of life, and that the active cancer at hand is “a much larger threat than a hypothetical cancer years later.”
In many cases, patients may only have months to live without CAR-T therapy and will have already had multiple prior lines of therapy, therefore the CAR-T treatment itself may provide time for the secondary primary cancers from any of the treatments to emerge, as experts have noted.
“One has to be alive to be diagnosed with a secondary primary malignancy, and it’s thus very possible that CAR-T may be creating a type of ‘immortal time bias’ wherein patients live long enough to experience the unfortunate sequelae of their previous therapies,” Dr. Banerjee explained in an interview.
Nevertheless, the potential for substantial improvements in quality of life with CAR-T therapy compared with traditional treatments addresses a top priority for patients, he added.
“For most patients with [for instance], myeloma, the ability of CAR-T to put them rapidly into a deep remission without the need for maintenance is an unheard-of potential for them,” Dr. Banerjee said.
“In multiple myeloma, no CAR-T therapy has (yet) demonstrated an overall survival benefit — but I think the substantial quality-of-life benefit stands by itself as a big reason why patients continue to prefer CAR-T.”
Keep Patients In Touch with CAR T Centers
In light of the concerns regarding the secondary malignancies, Dr. Banerjee underscored that CAR-T patients should be kept in close touch with centers that have CAR-T treatment expertise.
With most patients followed primarily at community practices where CAR-T therapy is not administered, “I’d strongly encourage my colleagues in community practices to refer all eligible patients to a CAR-T-capable center for evaluation regardless of what their risk of post-CAR-T secondary primary malignancies may be,” Dr. Banerjee urged.
“Based on the evidence we have currently, which includes the FDA’s updated information, there are many more unknowns about this potential secondary primary malignancy risk than knowns,” he said. “This is of course a much more nuanced issue than any one package insert can convey, and CAR-T experts at treating centers can have these conversations at length with eligible patients who are nervous about these recent updates.”
Dr. Ruella disclosed that he holds patents related to CD19 CAR T cells, as well as relationships with NanoString, Bristol Myers Squibb, GlaxoSmithKline, Scailyte, Bayer, AbClon, Oxford NanoImaging, CURIOX, and Beckman Coulter, and he was the scientific founder of viTToria Biotherapeutics. Dr. Banerjee reported ties with BMS, Caribou Biosciences, Genentech, Janssen, Karyopharm, Pfizer, Sanofi, SparkCures, Novartis, and Pack Health.
Importantly, most specialists agree, so far the risk appears no greater than the known risk of secondary primary malignancies that is well established with other cancer therapies.
“The data that we have so far suggest that the risk of secondary T-cell lymphoma in patients treated with CAR T-cells is similar to [that] of patients treated with other cancer therapies, [including] chemotherapy, radiation, transplantation,” Marco Ruella, MD, said in an interview. He reported on a case of a T-cell lymphoma occurring following CAR-T therapy at the University of Pennsylvania.
While his team is still investigating the development of such malignancies, “the FDA notice does not change our clinical practice and patients should be reassured that the benefit of CAR-T therapy significantly outweighs the potential risk of secondary malignancies including T-cell lymphoma,” said Dr. Ruella, scientific director of the Lymphoma Program, Division of Hematology and Oncology and Center for Cellular Immunotherapies, at the University of Pennsylvania, Philadelphia.
FDA: 28 Reports of Malignancies; 3 with Evidence of ‘Likely’ CAR T Involvement
Concerns were raised last November when the FDA announced in a safety communication that it was investigating the “serious risk of T-cell malignancy” following B-cell maturation antigen (BCMA)-directed or CD19-directed CAR T-cell immunotherapies, citing reports from clinical trials and/or postmarketing adverse event data sources. Subsequently, in January, the FDA called for the boxed warning on all approved BCMA- and CD19-targeted genetically modified autologous T-cell immunotherapies, which include: Abecma (idecabtagene vicleucel); Breyanzi (lisocabtagene maraleucel); Carvykti (ciltacabtagene autoleucel); Kymriah (tisagenlecleucel); Tecartus (brexucabtagene autoleucel); and Yescarta (axicabtagene ciloleucel).
“Although the overall benefits of these products continue to outweigh their potential risks for their approved uses, the FDA continues to investigate the identified risk of T-cell malignancy with serious outcomes, including hospitalization and death,” the FDA reported in discussing the safety warnings.
The cases were detailed in a report from FDA researchers published in the New England Journal of Medicine, noting that as of December 31, 2023, the FDA had become aware of 22 cases of T-cell cancers occurring following CAR T-cell treatment, including T-cell lymphoma, T-cell large granular lymphocytosis, peripheral T-cell lymphoma, and cutaneous T-cell lymphoma.
Report coauthor Peter Marks, MD, PhD, of the FDA’s Center for Biologics Evaluation and Research in Silver Spring, Maryland, said in an interview that since the publication of their report, six new cases have emerged.
“As reported in the NEJM Perspective, there were 22 cases of T-cell malignancy after treatment with CAR T-cell immunotherapies as of December 31, 2023, but we have received additional reports and, as of February 9, 2024, FDA has now received 28 reports,” he said. “Note that as new cases are being reported, there will be updates to the total number of cases under ongoing review by FDA.”
The initial 22 cases all occurred relatively soon after treatment. Of 14 cases with sufficient data, all developed within 2 years of the CAR-T therapy, ranging from 1 to 19 months, with about half occurring in the first year after administration.
The cases involved five of the six FDA-approved CAR-T products, with the numbers too low to suggest an association with any particular product.
In three of the cases, the lymphoma was found in genetic testing to contain the CAR construction, “indicating that the CAR-T product was most likely involved in the development of the T-cell cancer,” according to the FDA researchers.
With inadequate genetic sampling in most of the remaining 19 cases, the association is less clear, however “the timing of several of the cases makes association a possibility,” Dr. Marks said. In their report, Dr. Marks and colleagues added that “determination of whether the T-cell cancer is associated with the CAR construct ... most likely won’t be possible for every case reported to date.”
Even if all the reported cases are assumed to be related to CAR-T treatment, the numbers still represent a very small proportion of the more than 27,000 doses of the six CAR-T therapies approved in the United States, the authors noted, but they cautioned that the numbers could indeed be higher than reported.
“Relying on postmarketing reporting may lead to underestimates of such cases,” they said.
Life-Long Monitoring Recommended
In response to the reports, the FDA is urging that clinicians’ monitoring of patients treated with CAR-T therapy should be lifelong.
“Patients and clinical trial participants receiving treatment with these products should be monitored lifelong for new malignancies,” Dr. Marks said.
“In the event that a new malignancy occurs following treatment with these products, contact the manufacturer to report the event and obtain instructions on collection of patient samples for testing for the presence of the CAR transgene.”
In addition, cases should be reported to the FDA, either by calling or through the FDA’s medical product safety reporting program.
T-Cell Malignancy Case Report
In describing the case at their medical center in the report in Nature Medicine, Dr. Ruella and colleagues said a T-cell lymphoma occurred in a patient with non-Hodgkin B-cell lymphoma 3 months after an anti-CD19 CAR T-cell treatment.
As a result, the team conducted a subsequent analysis of 449 patients treated with CAR-T therapy at the University of Pennsylvania center, and with a median follow-up of 10.3 months, 16 patients (3.6%) had developed a secondary primary malignancy, with a median onset time of 26.4 months for solid and 9.7 months for hematological malignancies.
The patient who had developed a T-cell lymphoma tested negative for CAR integration upon diagnosis, and regarding the other cancers, Dr. Ruella noted that “we have no indication that the secondary malignancies are directly caused by the CAR-T therapy.
“We have many patients with a very long follow-up beyond 5 and even 10 years,” he said. “In these patients, we don’t see an increased risk of T-cell lymphoma.”
‘Cautious Reassurance’ Urged in Discussion with Patients
With alarming headlines on the findings suggesting that CAR-T therapy may cause cancer, Rahul Banerjee, MD, and colleagues at the University of Washington, Seattle, recommend the use of “cautious reassurance” in discussing the issue with patients. In a paper published in January in Blood Advances, they suggest a three-part response: underscoring that the benefits of CAR T “far outweigh” the risks in relapsed/refractory malignancies, that the ‘one-and-done’ nature of CAR-T infusions provide meaningful improvements in quality of life, and that the active cancer at hand is “a much larger threat than a hypothetical cancer years later.”
In many cases, patients may only have months to live without CAR-T therapy and will have already had multiple prior lines of therapy, therefore the CAR-T treatment itself may provide time for the secondary primary cancers from any of the treatments to emerge, as experts have noted.
“One has to be alive to be diagnosed with a secondary primary malignancy, and it’s thus very possible that CAR-T may be creating a type of ‘immortal time bias’ wherein patients live long enough to experience the unfortunate sequelae of their previous therapies,” Dr. Banerjee explained in an interview.
Nevertheless, the potential for substantial improvements in quality of life with CAR-T therapy compared with traditional treatments addresses a top priority for patients, he added.
“For most patients with [for instance], myeloma, the ability of CAR-T to put them rapidly into a deep remission without the need for maintenance is an unheard-of potential for them,” Dr. Banerjee said.
“In multiple myeloma, no CAR-T therapy has (yet) demonstrated an overall survival benefit — but I think the substantial quality-of-life benefit stands by itself as a big reason why patients continue to prefer CAR-T.”
Keep Patients In Touch with CAR T Centers
In light of the concerns regarding the secondary malignancies, Dr. Banerjee underscored that CAR-T patients should be kept in close touch with centers that have CAR-T treatment expertise.
With most patients followed primarily at community practices where CAR-T therapy is not administered, “I’d strongly encourage my colleagues in community practices to refer all eligible patients to a CAR-T-capable center for evaluation regardless of what their risk of post-CAR-T secondary primary malignancies may be,” Dr. Banerjee urged.
“Based on the evidence we have currently, which includes the FDA’s updated information, there are many more unknowns about this potential secondary primary malignancy risk than knowns,” he said. “This is of course a much more nuanced issue than any one package insert can convey, and CAR-T experts at treating centers can have these conversations at length with eligible patients who are nervous about these recent updates.”
Dr. Ruella disclosed that he holds patents related to CD19 CAR T cells, as well as relationships with NanoString, Bristol Myers Squibb, GlaxoSmithKline, Scailyte, Bayer, AbClon, Oxford NanoImaging, CURIOX, and Beckman Coulter, and he was the scientific founder of viTToria Biotherapeutics. Dr. Banerjee reported ties with BMS, Caribou Biosciences, Genentech, Janssen, Karyopharm, Pfizer, Sanofi, SparkCures, Novartis, and Pack Health.
Importantly, most specialists agree, so far the risk appears no greater than the known risk of secondary primary malignancies that is well established with other cancer therapies.
“The data that we have so far suggest that the risk of secondary T-cell lymphoma in patients treated with CAR T-cells is similar to [that] of patients treated with other cancer therapies, [including] chemotherapy, radiation, transplantation,” Marco Ruella, MD, said in an interview. He reported on a case of a T-cell lymphoma occurring following CAR-T therapy at the University of Pennsylvania.
While his team is still investigating the development of such malignancies, “the FDA notice does not change our clinical practice and patients should be reassured that the benefit of CAR-T therapy significantly outweighs the potential risk of secondary malignancies including T-cell lymphoma,” said Dr. Ruella, scientific director of the Lymphoma Program, Division of Hematology and Oncology and Center for Cellular Immunotherapies, at the University of Pennsylvania, Philadelphia.
FDA: 28 Reports of Malignancies; 3 with Evidence of ‘Likely’ CAR T Involvement
Concerns were raised last November when the FDA announced in a safety communication that it was investigating the “serious risk of T-cell malignancy” following B-cell maturation antigen (BCMA)-directed or CD19-directed CAR T-cell immunotherapies, citing reports from clinical trials and/or postmarketing adverse event data sources. Subsequently, in January, the FDA called for the boxed warning on all approved BCMA- and CD19-targeted genetically modified autologous T-cell immunotherapies, which include: Abecma (idecabtagene vicleucel); Breyanzi (lisocabtagene maraleucel); Carvykti (ciltacabtagene autoleucel); Kymriah (tisagenlecleucel); Tecartus (brexucabtagene autoleucel); and Yescarta (axicabtagene ciloleucel).
“Although the overall benefits of these products continue to outweigh their potential risks for their approved uses, the FDA continues to investigate the identified risk of T-cell malignancy with serious outcomes, including hospitalization and death,” the FDA reported in discussing the safety warnings.
The cases were detailed in a report from FDA researchers published in the New England Journal of Medicine, noting that as of December 31, 2023, the FDA had become aware of 22 cases of T-cell cancers occurring following CAR T-cell treatment, including T-cell lymphoma, T-cell large granular lymphocytosis, peripheral T-cell lymphoma, and cutaneous T-cell lymphoma.
Report coauthor Peter Marks, MD, PhD, of the FDA’s Center for Biologics Evaluation and Research in Silver Spring, Maryland, said in an interview that since the publication of their report, six new cases have emerged.
“As reported in the NEJM Perspective, there were 22 cases of T-cell malignancy after treatment with CAR T-cell immunotherapies as of December 31, 2023, but we have received additional reports and, as of February 9, 2024, FDA has now received 28 reports,” he said. “Note that as new cases are being reported, there will be updates to the total number of cases under ongoing review by FDA.”
The initial 22 cases all occurred relatively soon after treatment. Of 14 cases with sufficient data, all developed within 2 years of the CAR-T therapy, ranging from 1 to 19 months, with about half occurring in the first year after administration.
The cases involved five of the six FDA-approved CAR-T products, with the numbers too low to suggest an association with any particular product.
In three of the cases, the lymphoma was found in genetic testing to contain the CAR construction, “indicating that the CAR-T product was most likely involved in the development of the T-cell cancer,” according to the FDA researchers.
With inadequate genetic sampling in most of the remaining 19 cases, the association is less clear, however “the timing of several of the cases makes association a possibility,” Dr. Marks said. In their report, Dr. Marks and colleagues added that “determination of whether the T-cell cancer is associated with the CAR construct ... most likely won’t be possible for every case reported to date.”
Even if all the reported cases are assumed to be related to CAR-T treatment, the numbers still represent a very small proportion of the more than 27,000 doses of the six CAR-T therapies approved in the United States, the authors noted, but they cautioned that the numbers could indeed be higher than reported.
“Relying on postmarketing reporting may lead to underestimates of such cases,” they said.
Life-Long Monitoring Recommended
In response to the reports, the FDA is urging that clinicians’ monitoring of patients treated with CAR-T therapy should be lifelong.
“Patients and clinical trial participants receiving treatment with these products should be monitored lifelong for new malignancies,” Dr. Marks said.
“In the event that a new malignancy occurs following treatment with these products, contact the manufacturer to report the event and obtain instructions on collection of patient samples for testing for the presence of the CAR transgene.”
In addition, cases should be reported to the FDA, either by calling or through the FDA’s medical product safety reporting program.
T-Cell Malignancy Case Report
In describing the case at their medical center in the report in Nature Medicine, Dr. Ruella and colleagues said a T-cell lymphoma occurred in a patient with non-Hodgkin B-cell lymphoma 3 months after an anti-CD19 CAR T-cell treatment.
As a result, the team conducted a subsequent analysis of 449 patients treated with CAR-T therapy at the University of Pennsylvania center, and with a median follow-up of 10.3 months, 16 patients (3.6%) had developed a secondary primary malignancy, with a median onset time of 26.4 months for solid and 9.7 months for hematological malignancies.
The patient who had developed a T-cell lymphoma tested negative for CAR integration upon diagnosis, and regarding the other cancers, Dr. Ruella noted that “we have no indication that the secondary malignancies are directly caused by the CAR-T therapy.
“We have many patients with a very long follow-up beyond 5 and even 10 years,” he said. “In these patients, we don’t see an increased risk of T-cell lymphoma.”
‘Cautious Reassurance’ Urged in Discussion with Patients
With alarming headlines on the findings suggesting that CAR-T therapy may cause cancer, Rahul Banerjee, MD, and colleagues at the University of Washington, Seattle, recommend the use of “cautious reassurance” in discussing the issue with patients. In a paper published in January in Blood Advances, they suggest a three-part response: underscoring that the benefits of CAR T “far outweigh” the risks in relapsed/refractory malignancies, that the ‘one-and-done’ nature of CAR-T infusions provide meaningful improvements in quality of life, and that the active cancer at hand is “a much larger threat than a hypothetical cancer years later.”
In many cases, patients may only have months to live without CAR-T therapy and will have already had multiple prior lines of therapy, therefore the CAR-T treatment itself may provide time for the secondary primary cancers from any of the treatments to emerge, as experts have noted.
“One has to be alive to be diagnosed with a secondary primary malignancy, and it’s thus very possible that CAR-T may be creating a type of ‘immortal time bias’ wherein patients live long enough to experience the unfortunate sequelae of their previous therapies,” Dr. Banerjee explained in an interview.
Nevertheless, the potential for substantial improvements in quality of life with CAR-T therapy compared with traditional treatments addresses a top priority for patients, he added.
“For most patients with [for instance], myeloma, the ability of CAR-T to put them rapidly into a deep remission without the need for maintenance is an unheard-of potential for them,” Dr. Banerjee said.
“In multiple myeloma, no CAR-T therapy has (yet) demonstrated an overall survival benefit — but I think the substantial quality-of-life benefit stands by itself as a big reason why patients continue to prefer CAR-T.”
Keep Patients In Touch with CAR T Centers
In light of the concerns regarding the secondary malignancies, Dr. Banerjee underscored that CAR-T patients should be kept in close touch with centers that have CAR-T treatment expertise.
With most patients followed primarily at community practices where CAR-T therapy is not administered, “I’d strongly encourage my colleagues in community practices to refer all eligible patients to a CAR-T-capable center for evaluation regardless of what their risk of post-CAR-T secondary primary malignancies may be,” Dr. Banerjee urged.
“Based on the evidence we have currently, which includes the FDA’s updated information, there are many more unknowns about this potential secondary primary malignancy risk than knowns,” he said. “This is of course a much more nuanced issue than any one package insert can convey, and CAR-T experts at treating centers can have these conversations at length with eligible patients who are nervous about these recent updates.”
Dr. Ruella disclosed that he holds patents related to CD19 CAR T cells, as well as relationships with NanoString, Bristol Myers Squibb, GlaxoSmithKline, Scailyte, Bayer, AbClon, Oxford NanoImaging, CURIOX, and Beckman Coulter, and he was the scientific founder of viTToria Biotherapeutics. Dr. Banerjee reported ties with BMS, Caribou Biosciences, Genentech, Janssen, Karyopharm, Pfizer, Sanofi, SparkCures, Novartis, and Pack Health.
Expert Hopes to Expand Ohio Model of Melanoma Case Reporting
SAN DIEGO – Soon after Brett M. Coldiron, MD, launched his Cincinnati-based dermatology and Mohs surgery practice more than 20 years ago, he reported his first three cases of thin melanomas to the Ohio Department of Health, as mandated by state law.
“I got sent reams of paperwork to fill out that I did not understand,” Dr. Coldiron, a past president of the American College of Mohs Surgery and the American Academy of Dermatology, recalled at the annual Cutaneous Malignancy Update. “Then, I got chewed out for not reporting sooner and threatened with thousands of dollars in fines if I did not promptly report the forms in the future. It was an obnoxious experience.”

About 15 years later, while testifying at the Ohio Legislature on medical reasons to restrict the use of tanning beds, a lobbyist for the tanning bed industry told him that the melanoma rates had been stable in Ohio for the previous 5 years. “It turns out they were cherry picking certain segments of data to fit their narrative,” Dr. Coldiron said. “I was stunned and it kind of deflated me. I thought about this for a long time, and thought, ‘how do we solve this issue of reporting melanoma cases without adding work to existing staff if you’re a small practice and without spending significant amounts of money? Let’s make this easier.’ ”
In addition to reducing the use of tanning beds, proper reporting of melanoma cases is important for reasons that include efforts to increase sunscreen use and to be counted in ongoing research efforts to obtain a realistic snapshot of melanoma prevalence and incidence, he said.
Quality of melanoma case reporting relies on the Centers for Disease Control and Prevention’s National Program of Cancer Registries (NPCR), and the National Cancer Institute’s Surveillance Epidemiology and End Results (SEER) Program, which collects data on the incidence, treatment, staging, and survival for 28% of the US population. All 50 states and US territories require melanoma to be reported to the NPCR, but while most hospital systems have reporting protocols and dedicated data registrars, private practices may not.
Also, many dermatopathology practices operate independently and do not have dedicated registrars and may not report cases. “Melanoma is unique in that it is often completely managed in outpatient settings and these melanomas may never be reported,” said Dr. Coldiron, current president of the Ohio Dermatological Foundation. “That’s the practice gap.” One study published in 2018 found that only 49% of dermatologists knew that melanoma was a reportable disease and only 34% routinely reported newly diagnosed cases to their state’s cancer registry. He characterized melanoma reporting as an unfunded mandate.
“Hospitals are doing the most of them, because they have a registrar,” he said. “Small practices have to assign someone to do this, and it can be difficult to train that person. It’s time consuming. The first time we did it, it took an hour,” but, he said, taking a 2-hour tutorial from the Ohio Department of Health helped.
He noted that there is a lack of awareness and clinicians think it’s the dermatopathologist’s job to report cases, “while the dermatopathologist thinks it’s the clinician’s job,” and many of the entry fields are not applicable to thinner melanomas.
There is also a “patchwork” of ways that state departments of health accept the information, not all electronically, he continued. For example, those in Arizona, Montana, West Virginia, Delaware, Vermont, and Maine accept paper copies only, “meaning you have to download a PDF, fill it out, and fax it back to them,” Dr. Coldiron said at the meeting, which was hosted by Scripps Cancer Center.
“We have them sign a HIPAA form and take the two-hour online tutorial,” he said. They download data that Ohio dermatologists have faxed to a dedicated secure HIPAA-compliant cloud-based fax line that Dr. Coldiron has set up, and the cases are then sent to the Ohio Department of Health.
Dr. Coldiron and colleagues have also partnered with the University of Cincinnati Clermont, which offers a National Cancer Registries Association–accredited certificate program — one of several nationwide. Students in this program are trained to become cancer registrars. “The university staff are gung-ho about it because they are looking for easy cases to train the students on. Also, the Ohio Department of Health staff are keen to help train the students and even help them find jobs or hire them after they complete the degree. Staff from the department of health and college faculty are fully engaged and supervising. It’s a win-win for all.”
According to Dr. Coldiron, in 2023, 8 Ohio dermatology practices were sending their reports to the fax line he set up and 7 more have signed up in recent months, making 15 practices to date. “It’s self-perpetuating at this point,” he said. “The Ohio Department of Health and the University of Cincinnati are invested in this program long-term.” The fax service costs Dr. Coldiron $42 per month — a small price to pay, he said, for being a clearinghouse for private Ohio dermatology practices looking for a practical way to report their melanoma cases. The model has increased melanoma reporting in Ohio by 2.8% in the last 2 years, “which doesn’t seem like that many, but if there are 6500 cases of melanoma, and you can increase reporting by a couple hundred cases, that’s a lot,” he said.
His goal is to expand this model to more states. “Dermatologists, surgical oncologists, and cancer center administrators should embrace this opportunity to make their practices a clearinghouse for their state,” he said. “This is an opportunity to improve state health, quality improvement projects, help providers, and gain recognition as a center of excellence. The increase in incidence of melanoma will lend great clout to public and legislative requests for prevention, treatment, and research dollars.”
In an interview, Hugh Greenway, MD, the head of Mohs and dermatologic surgery at Scripps Clinic in San Diego, also noted that cutaneous melanoma is significantly underreported in spite of individual state requirements. “As Dr. Coldiron reminds us, the main reason is that in many cases the pathology diagnosis and report come from the dermatologist’s/dermatopathologist’s office,” Dr. Greenway said. “With no hospital or large multispecialty laboratory involved, the reporting may be incomplete or not done. This is not the case with almost all other cancers where a hospital laboratory is involved.”
If widespread adoption of Dr. Coldiron’s model can occur, he added, “then we will have much better melanoma reporting data on which to both help our patients and specialty. He is to be applauded for producing a workable solution to the problem of underreporting.”
Dr. Coldiron reported having no relevant disclosures. Dr. Greenway reported that he conducts research for Castle Biosciences. He is also course director of the annual Cutaneous Malignancy Update.
SAN DIEGO – Soon after Brett M. Coldiron, MD, launched his Cincinnati-based dermatology and Mohs surgery practice more than 20 years ago, he reported his first three cases of thin melanomas to the Ohio Department of Health, as mandated by state law.
“I got sent reams of paperwork to fill out that I did not understand,” Dr. Coldiron, a past president of the American College of Mohs Surgery and the American Academy of Dermatology, recalled at the annual Cutaneous Malignancy Update. “Then, I got chewed out for not reporting sooner and threatened with thousands of dollars in fines if I did not promptly report the forms in the future. It was an obnoxious experience.”
About 15 years later, while testifying at the Ohio Legislature on medical reasons to restrict the use of tanning beds, a lobbyist for the tanning bed industry told him that the melanoma rates had been stable in Ohio for the previous 5 years. “It turns out they were cherry picking certain segments of data to fit their narrative,” Dr. Coldiron said. “I was stunned and it kind of deflated me. I thought about this for a long time, and thought, ‘how do we solve this issue of reporting melanoma cases without adding work to existing staff if you’re a small practice and without spending significant amounts of money? Let’s make this easier.’ ”
In addition to reducing the use of tanning beds, proper reporting of melanoma cases is important for reasons that include efforts to increase sunscreen use and to be counted in ongoing research efforts to obtain a realistic snapshot of melanoma prevalence and incidence, he said.
Quality of melanoma case reporting relies on the Centers for Disease Control and Prevention’s National Program of Cancer Registries (NPCR), and the National Cancer Institute’s Surveillance Epidemiology and End Results (SEER) Program, which collects data on the incidence, treatment, staging, and survival for 28% of the US population. All 50 states and US territories require melanoma to be reported to the NPCR, but while most hospital systems have reporting protocols and dedicated data registrars, private practices may not.
Also, many dermatopathology practices operate independently and do not have dedicated registrars and may not report cases. “Melanoma is unique in that it is often completely managed in outpatient settings and these melanomas may never be reported,” said Dr. Coldiron, current president of the Ohio Dermatological Foundation. “That’s the practice gap.” One study published in 2018 found that only 49% of dermatologists knew that melanoma was a reportable disease and only 34% routinely reported newly diagnosed cases to their state’s cancer registry. He characterized melanoma reporting as an unfunded mandate.
“Hospitals are doing the most of them, because they have a registrar,” he said. “Small practices have to assign someone to do this, and it can be difficult to train that person. It’s time consuming. The first time we did it, it took an hour,” but, he said, taking a 2-hour tutorial from the Ohio Department of Health helped.
He noted that there is a lack of awareness and clinicians think it’s the dermatopathologist’s job to report cases, “while the dermatopathologist thinks it’s the clinician’s job,” and many of the entry fields are not applicable to thinner melanomas.
There is also a “patchwork” of ways that state departments of health accept the information, not all electronically, he continued. For example, those in Arizona, Montana, West Virginia, Delaware, Vermont, and Maine accept paper copies only, “meaning you have to download a PDF, fill it out, and fax it back to them,” Dr. Coldiron said at the meeting, which was hosted by Scripps Cancer Center.
“We have them sign a HIPAA form and take the two-hour online tutorial,” he said. They download data that Ohio dermatologists have faxed to a dedicated secure HIPAA-compliant cloud-based fax line that Dr. Coldiron has set up, and the cases are then sent to the Ohio Department of Health.
Dr. Coldiron and colleagues have also partnered with the University of Cincinnati Clermont, which offers a National Cancer Registries Association–accredited certificate program — one of several nationwide. Students in this program are trained to become cancer registrars. “The university staff are gung-ho about it because they are looking for easy cases to train the students on. Also, the Ohio Department of Health staff are keen to help train the students and even help them find jobs or hire them after they complete the degree. Staff from the department of health and college faculty are fully engaged and supervising. It’s a win-win for all.”
According to Dr. Coldiron, in 2023, 8 Ohio dermatology practices were sending their reports to the fax line he set up and 7 more have signed up in recent months, making 15 practices to date. “It’s self-perpetuating at this point,” he said. “The Ohio Department of Health and the University of Cincinnati are invested in this program long-term.” The fax service costs Dr. Coldiron $42 per month — a small price to pay, he said, for being a clearinghouse for private Ohio dermatology practices looking for a practical way to report their melanoma cases. The model has increased melanoma reporting in Ohio by 2.8% in the last 2 years, “which doesn’t seem like that many, but if there are 6500 cases of melanoma, and you can increase reporting by a couple hundred cases, that’s a lot,” he said.
His goal is to expand this model to more states. “Dermatologists, surgical oncologists, and cancer center administrators should embrace this opportunity to make their practices a clearinghouse for their state,” he said. “This is an opportunity to improve state health, quality improvement projects, help providers, and gain recognition as a center of excellence. The increase in incidence of melanoma will lend great clout to public and legislative requests for prevention, treatment, and research dollars.”
In an interview, Hugh Greenway, MD, the head of Mohs and dermatologic surgery at Scripps Clinic in San Diego, also noted that cutaneous melanoma is significantly underreported in spite of individual state requirements. “As Dr. Coldiron reminds us, the main reason is that in many cases the pathology diagnosis and report come from the dermatologist’s/dermatopathologist’s office,” Dr. Greenway said. “With no hospital or large multispecialty laboratory involved, the reporting may be incomplete or not done. This is not the case with almost all other cancers where a hospital laboratory is involved.”
If widespread adoption of Dr. Coldiron’s model can occur, he added, “then we will have much better melanoma reporting data on which to both help our patients and specialty. He is to be applauded for producing a workable solution to the problem of underreporting.”
Dr. Coldiron reported having no relevant disclosures. Dr. Greenway reported that he conducts research for Castle Biosciences. He is also course director of the annual Cutaneous Malignancy Update.
SAN DIEGO – Soon after Brett M. Coldiron, MD, launched his Cincinnati-based dermatology and Mohs surgery practice more than 20 years ago, he reported his first three cases of thin melanomas to the Ohio Department of Health, as mandated by state law.
“I got sent reams of paperwork to fill out that I did not understand,” Dr. Coldiron, a past president of the American College of Mohs Surgery and the American Academy of Dermatology, recalled at the annual Cutaneous Malignancy Update. “Then, I got chewed out for not reporting sooner and threatened with thousands of dollars in fines if I did not promptly report the forms in the future. It was an obnoxious experience.”
About 15 years later, while testifying at the Ohio Legislature on medical reasons to restrict the use of tanning beds, a lobbyist for the tanning bed industry told him that the melanoma rates had been stable in Ohio for the previous 5 years. “It turns out they were cherry picking certain segments of data to fit their narrative,” Dr. Coldiron said. “I was stunned and it kind of deflated me. I thought about this for a long time, and thought, ‘how do we solve this issue of reporting melanoma cases without adding work to existing staff if you’re a small practice and without spending significant amounts of money? Let’s make this easier.’ ”
In addition to reducing the use of tanning beds, proper reporting of melanoma cases is important for reasons that include efforts to increase sunscreen use and to be counted in ongoing research efforts to obtain a realistic snapshot of melanoma prevalence and incidence, he said.
Quality of melanoma case reporting relies on the Centers for Disease Control and Prevention’s National Program of Cancer Registries (NPCR), and the National Cancer Institute’s Surveillance Epidemiology and End Results (SEER) Program, which collects data on the incidence, treatment, staging, and survival for 28% of the US population. All 50 states and US territories require melanoma to be reported to the NPCR, but while most hospital systems have reporting protocols and dedicated data registrars, private practices may not.
Also, many dermatopathology practices operate independently and do not have dedicated registrars and may not report cases. “Melanoma is unique in that it is often completely managed in outpatient settings and these melanomas may never be reported,” said Dr. Coldiron, current president of the Ohio Dermatological Foundation. “That’s the practice gap.” One study published in 2018 found that only 49% of dermatologists knew that melanoma was a reportable disease and only 34% routinely reported newly diagnosed cases to their state’s cancer registry. He characterized melanoma reporting as an unfunded mandate.
“Hospitals are doing the most of them, because they have a registrar,” he said. “Small practices have to assign someone to do this, and it can be difficult to train that person. It’s time consuming. The first time we did it, it took an hour,” but, he said, taking a 2-hour tutorial from the Ohio Department of Health helped.
He noted that there is a lack of awareness and clinicians think it’s the dermatopathologist’s job to report cases, “while the dermatopathologist thinks it’s the clinician’s job,” and many of the entry fields are not applicable to thinner melanomas.
There is also a “patchwork” of ways that state departments of health accept the information, not all electronically, he continued. For example, those in Arizona, Montana, West Virginia, Delaware, Vermont, and Maine accept paper copies only, “meaning you have to download a PDF, fill it out, and fax it back to them,” Dr. Coldiron said at the meeting, which was hosted by Scripps Cancer Center.
“We have them sign a HIPAA form and take the two-hour online tutorial,” he said. They download data that Ohio dermatologists have faxed to a dedicated secure HIPAA-compliant cloud-based fax line that Dr. Coldiron has set up, and the cases are then sent to the Ohio Department of Health.
Dr. Coldiron and colleagues have also partnered with the University of Cincinnati Clermont, which offers a National Cancer Registries Association–accredited certificate program — one of several nationwide. Students in this program are trained to become cancer registrars. “The university staff are gung-ho about it because they are looking for easy cases to train the students on. Also, the Ohio Department of Health staff are keen to help train the students and even help them find jobs or hire them after they complete the degree. Staff from the department of health and college faculty are fully engaged and supervising. It’s a win-win for all.”
According to Dr. Coldiron, in 2023, 8 Ohio dermatology practices were sending their reports to the fax line he set up and 7 more have signed up in recent months, making 15 practices to date. “It’s self-perpetuating at this point,” he said. “The Ohio Department of Health and the University of Cincinnati are invested in this program long-term.” The fax service costs Dr. Coldiron $42 per month — a small price to pay, he said, for being a clearinghouse for private Ohio dermatology practices looking for a practical way to report their melanoma cases. The model has increased melanoma reporting in Ohio by 2.8% in the last 2 years, “which doesn’t seem like that many, but if there are 6500 cases of melanoma, and you can increase reporting by a couple hundred cases, that’s a lot,” he said.
His goal is to expand this model to more states. “Dermatologists, surgical oncologists, and cancer center administrators should embrace this opportunity to make their practices a clearinghouse for their state,” he said. “This is an opportunity to improve state health, quality improvement projects, help providers, and gain recognition as a center of excellence. The increase in incidence of melanoma will lend great clout to public and legislative requests for prevention, treatment, and research dollars.”
In an interview, Hugh Greenway, MD, the head of Mohs and dermatologic surgery at Scripps Clinic in San Diego, also noted that cutaneous melanoma is significantly underreported in spite of individual state requirements. “As Dr. Coldiron reminds us, the main reason is that in many cases the pathology diagnosis and report come from the dermatologist’s/dermatopathologist’s office,” Dr. Greenway said. “With no hospital or large multispecialty laboratory involved, the reporting may be incomplete or not done. This is not the case with almost all other cancers where a hospital laboratory is involved.”
If widespread adoption of Dr. Coldiron’s model can occur, he added, “then we will have much better melanoma reporting data on which to both help our patients and specialty. He is to be applauded for producing a workable solution to the problem of underreporting.”
Dr. Coldiron reported having no relevant disclosures. Dr. Greenway reported that he conducts research for Castle Biosciences. He is also course director of the annual Cutaneous Malignancy Update.
FROM MELANOMA 2024
Genetic Biomarker May Predict Pancreatic Adenocarcinoma Outcomes
These were the main findings of a new study of more than 300 individuals.
Previous studies have shown an association between widespread disease and loss of SMAD4 immunolabeling, according to the paper. Biomarkers to predict which pancreatic adenocarcinoma patients may benefit from more aggressive therapy are lacking, wrote Emily J. Anstadt, MD, of the University of Pennsylvania, Philadelphia, and colleagues, in their paper published in Cancer.
The human transcription factor and tumor suppressor, mothers against decapentaplegic homolog 4 (SMAD4), “may be a promising biomarker for predicting the likelihood of experiencing distant failure in patients with pancreatic cancer,” the researchers wrote.
“For patients with pancreatic cancer, improving treatments and overall outcomes remains invaluable,” Dr. Anstadt said in an interview. However, the disparate clinical courses make studies of this patient population challenging.
“As with much of medicine and oncology at this time, we feel the key to better outcomes lies in personalizing treatment strategies and relying on tumor genetics to predict tumor behavior and guide us towards individualized optimal treatments,” she added.
Study Methods and Results
The researchers identified 322 patients with resected stage I–III pancreatic adenocarcinoma from The Cancer Genome Atlas (TCGA) and the International Cancer Genome Consortium (ICGC). The study population included 165 patients from the TCGA who served as the training set and 157 patients from the ICGC who served as the validation set.
The primary outcomes were overall survival (OS) and distant metastasis-free survival (DMFS).
A total of 50 patients in the TCGA group (30%) had at least one of the three identified SMAD4 genomic aberrations.
Using the TCGA group, the researchers conducted a regression analysis on the survival outcomes as a function of either the presence of an SMAD4 genomic aberration or the expression of messenger RNA sequencing (RNA-seq). They then used the ICGC to validate whether SMAD4 RNA-seq expression improved risk stratification for OS and DMFS in a separate group of patients.
In the TCGA group, 3-year OS for patients with any SMAD4 aberrations vs no SMAD4 aberrations was 18% vs 36% (hazard ratio, 1.55; P = .048). However, the 3-year DMFS for patients with and without SMAD4 aberrations was 14% vs 23%, a nonsignificant difference (HR, 1.33; P = .19).
In a multivariate analysis, SMAD4 aberrations also were associated with increased risk of stage III disease (HR, 1.89; P = .003). The researchers noted that adjuvant radiotherapy and adjuvant chemotherapy were significantly associated with a decreased risk of death in these patients (HR, 0.53 and HR, 0.28, respectively).
In addition, low SMAD4 RNA-seq expression was associated with worse OS and DMFS, (HR, 1.83 and HR, 1.70, respectively) in the TCGA group.
In the ICGC validation group, increased SMAD4 RNA‐seq expression correlated with improved OS (area under the curve .92) and DMFS (AUC, .84).
Dr. Anstadt said she and her colleagues were not surprised by any of their findings, given earlier research’s suggestions of SMAD4 loss having been associated with poor outcomes for pancreatic cancer.
“Prior studies determined SMAD4 status based on immunohistochemistry and different investigators used different scoring systems,” Dr. Anstadt noted, in an interview. “The results of those studies were conflicting, and consequently SMAD4 has not been adopted clinically as part of the work-up or to aid in treatment decisions.”
“It is essential to find robust, reliable, and cost-effective methods for implementing this in the clinic. As such, we were happy to find that expression of SMAD4 by mRNA sequencing may be that method,” she added.
Not Quite Clinic-Ready
“While we are hopeful that this tool will be a reliable method for use in the clinic, it has yet to be validated in a prospective manner,” Dr. Anstadt said in an interview. “In addition, this study showed that [genetic] expression levels are correlated with worse outcomes and can be of prognostic use; however, we have not directly studied whether expression levels can be predictive of treatment response,” she said.
“Practicing oncologists often have to make difficult decisions in situations where there are no clear answers,” Dr. Anstadt continued. “When considering gray-zone treatment recommendations, we often integrate multiple factors to form an opinion. The reality of cancer medicine is that not all those factors we consider have been validated in prospective studies, but together they produce a picture that is clinically useful. We would submit that SMAD4 status should be one of those factors taken into consideration in forming a comprehensive opinion about suitability for resection or radiotherapy.”
In practice, “if this test is prospectively validated in a future study and will impact clinical decision-making, then this cost will be similar to other genetic tests that have been adopted and have been practice-changing in other oncologic fields,” said Dr. Anstadt. “Being able to individualize treatment can also save overall cost; for instance, predicting which patients would not benefit from local radiation or surgery could decrease use and cost in that population,” she said.
Limitations of the current study included the inability to examine interactions between SMAD4 and radiotherapy because of the sample size and the potential for selection bias, the researchers wrote.
Potential Predictive Value
“A major challenge in the management of patients with pancreatic cancer is the difficulty in predicting which patients will develop metastasis early,” said Jatin Roper, MD, a gastroenterologist at Duke University, Durham, North Carolina, in an interview.
“SMAD4 has previously been evaluated as a prognostic marker in pancreatic cancer, but the association between SMAD4 gene expression, gene mutations, and cancer metastasis has not yet been systematically evaluated in patients, said Dr. Roper, who was not involved in the study.
The new study’s main findings that SMAD4 genomic alterations are associated with worse overall survival, but not distant metastasis-free survival, and that increased SMAD4 expression is associated with improved overall survival and distant metastasis-free survival, suggest that SMAD4 gene expression may be a useful marker in predicting clinical outcomes in pancreatic cancer, Dr. Roper said.
In the future the current study may prompt prospective research to determine a potential association between clinical assessment of SMAD4 gene expression at the time of surgical cancer resection and worse overall survival and distant metastasis-free survival, he said.
The study received no outside funding. Dr. Anstadt and Dr. Roper had no financial conflicts to disclose.
These were the main findings of a new study of more than 300 individuals.
Previous studies have shown an association between widespread disease and loss of SMAD4 immunolabeling, according to the paper. Biomarkers to predict which pancreatic adenocarcinoma patients may benefit from more aggressive therapy are lacking, wrote Emily J. Anstadt, MD, of the University of Pennsylvania, Philadelphia, and colleagues, in their paper published in Cancer.
The human transcription factor and tumor suppressor, mothers against decapentaplegic homolog 4 (SMAD4), “may be a promising biomarker for predicting the likelihood of experiencing distant failure in patients with pancreatic cancer,” the researchers wrote.
“For patients with pancreatic cancer, improving treatments and overall outcomes remains invaluable,” Dr. Anstadt said in an interview. However, the disparate clinical courses make studies of this patient population challenging.
“As with much of medicine and oncology at this time, we feel the key to better outcomes lies in personalizing treatment strategies and relying on tumor genetics to predict tumor behavior and guide us towards individualized optimal treatments,” she added.
Study Methods and Results
The researchers identified 322 patients with resected stage I–III pancreatic adenocarcinoma from The Cancer Genome Atlas (TCGA) and the International Cancer Genome Consortium (ICGC). The study population included 165 patients from the TCGA who served as the training set and 157 patients from the ICGC who served as the validation set.
The primary outcomes were overall survival (OS) and distant metastasis-free survival (DMFS).
A total of 50 patients in the TCGA group (30%) had at least one of the three identified SMAD4 genomic aberrations.
Using the TCGA group, the researchers conducted a regression analysis on the survival outcomes as a function of either the presence of an SMAD4 genomic aberration or the expression of messenger RNA sequencing (RNA-seq). They then used the ICGC to validate whether SMAD4 RNA-seq expression improved risk stratification for OS and DMFS in a separate group of patients.
In the TCGA group, 3-year OS for patients with any SMAD4 aberrations vs no SMAD4 aberrations was 18% vs 36% (hazard ratio, 1.55; P = .048). However, the 3-year DMFS for patients with and without SMAD4 aberrations was 14% vs 23%, a nonsignificant difference (HR, 1.33; P = .19).
In a multivariate analysis, SMAD4 aberrations also were associated with increased risk of stage III disease (HR, 1.89; P = .003). The researchers noted that adjuvant radiotherapy and adjuvant chemotherapy were significantly associated with a decreased risk of death in these patients (HR, 0.53 and HR, 0.28, respectively).
In addition, low SMAD4 RNA-seq expression was associated with worse OS and DMFS, (HR, 1.83 and HR, 1.70, respectively) in the TCGA group.
In the ICGC validation group, increased SMAD4 RNA‐seq expression correlated with improved OS (area under the curve .92) and DMFS (AUC, .84).
Dr. Anstadt said she and her colleagues were not surprised by any of their findings, given earlier research’s suggestions of SMAD4 loss having been associated with poor outcomes for pancreatic cancer.
“Prior studies determined SMAD4 status based on immunohistochemistry and different investigators used different scoring systems,” Dr. Anstadt noted, in an interview. “The results of those studies were conflicting, and consequently SMAD4 has not been adopted clinically as part of the work-up or to aid in treatment decisions.”
“It is essential to find robust, reliable, and cost-effective methods for implementing this in the clinic. As such, we were happy to find that expression of SMAD4 by mRNA sequencing may be that method,” she added.
Not Quite Clinic-Ready
“While we are hopeful that this tool will be a reliable method for use in the clinic, it has yet to be validated in a prospective manner,” Dr. Anstadt said in an interview. “In addition, this study showed that [genetic] expression levels are correlated with worse outcomes and can be of prognostic use; however, we have not directly studied whether expression levels can be predictive of treatment response,” she said.
“Practicing oncologists often have to make difficult decisions in situations where there are no clear answers,” Dr. Anstadt continued. “When considering gray-zone treatment recommendations, we often integrate multiple factors to form an opinion. The reality of cancer medicine is that not all those factors we consider have been validated in prospective studies, but together they produce a picture that is clinically useful. We would submit that SMAD4 status should be one of those factors taken into consideration in forming a comprehensive opinion about suitability for resection or radiotherapy.”
In practice, “if this test is prospectively validated in a future study and will impact clinical decision-making, then this cost will be similar to other genetic tests that have been adopted and have been practice-changing in other oncologic fields,” said Dr. Anstadt. “Being able to individualize treatment can also save overall cost; for instance, predicting which patients would not benefit from local radiation or surgery could decrease use and cost in that population,” she said.
Limitations of the current study included the inability to examine interactions between SMAD4 and radiotherapy because of the sample size and the potential for selection bias, the researchers wrote.
Potential Predictive Value
“A major challenge in the management of patients with pancreatic cancer is the difficulty in predicting which patients will develop metastasis early,” said Jatin Roper, MD, a gastroenterologist at Duke University, Durham, North Carolina, in an interview.
“SMAD4 has previously been evaluated as a prognostic marker in pancreatic cancer, but the association between SMAD4 gene expression, gene mutations, and cancer metastasis has not yet been systematically evaluated in patients, said Dr. Roper, who was not involved in the study.
The new study’s main findings that SMAD4 genomic alterations are associated with worse overall survival, but not distant metastasis-free survival, and that increased SMAD4 expression is associated with improved overall survival and distant metastasis-free survival, suggest that SMAD4 gene expression may be a useful marker in predicting clinical outcomes in pancreatic cancer, Dr. Roper said.
In the future the current study may prompt prospective research to determine a potential association between clinical assessment of SMAD4 gene expression at the time of surgical cancer resection and worse overall survival and distant metastasis-free survival, he said.
The study received no outside funding. Dr. Anstadt and Dr. Roper had no financial conflicts to disclose.
These were the main findings of a new study of more than 300 individuals.
Previous studies have shown an association between widespread disease and loss of SMAD4 immunolabeling, according to the paper. Biomarkers to predict which pancreatic adenocarcinoma patients may benefit from more aggressive therapy are lacking, wrote Emily J. Anstadt, MD, of the University of Pennsylvania, Philadelphia, and colleagues, in their paper published in Cancer.
The human transcription factor and tumor suppressor, mothers against decapentaplegic homolog 4 (SMAD4), “may be a promising biomarker for predicting the likelihood of experiencing distant failure in patients with pancreatic cancer,” the researchers wrote.
“For patients with pancreatic cancer, improving treatments and overall outcomes remains invaluable,” Dr. Anstadt said in an interview. However, the disparate clinical courses make studies of this patient population challenging.
“As with much of medicine and oncology at this time, we feel the key to better outcomes lies in personalizing treatment strategies and relying on tumor genetics to predict tumor behavior and guide us towards individualized optimal treatments,” she added.
Study Methods and Results
The researchers identified 322 patients with resected stage I–III pancreatic adenocarcinoma from The Cancer Genome Atlas (TCGA) and the International Cancer Genome Consortium (ICGC). The study population included 165 patients from the TCGA who served as the training set and 157 patients from the ICGC who served as the validation set.
The primary outcomes were overall survival (OS) and distant metastasis-free survival (DMFS).
A total of 50 patients in the TCGA group (30%) had at least one of the three identified SMAD4 genomic aberrations.
Using the TCGA group, the researchers conducted a regression analysis on the survival outcomes as a function of either the presence of an SMAD4 genomic aberration or the expression of messenger RNA sequencing (RNA-seq). They then used the ICGC to validate whether SMAD4 RNA-seq expression improved risk stratification for OS and DMFS in a separate group of patients.
In the TCGA group, 3-year OS for patients with any SMAD4 aberrations vs no SMAD4 aberrations was 18% vs 36% (hazard ratio, 1.55; P = .048). However, the 3-year DMFS for patients with and without SMAD4 aberrations was 14% vs 23%, a nonsignificant difference (HR, 1.33; P = .19).
In a multivariate analysis, SMAD4 aberrations also were associated with increased risk of stage III disease (HR, 1.89; P = .003). The researchers noted that adjuvant radiotherapy and adjuvant chemotherapy were significantly associated with a decreased risk of death in these patients (HR, 0.53 and HR, 0.28, respectively).
In addition, low SMAD4 RNA-seq expression was associated with worse OS and DMFS, (HR, 1.83 and HR, 1.70, respectively) in the TCGA group.
In the ICGC validation group, increased SMAD4 RNA‐seq expression correlated with improved OS (area under the curve .92) and DMFS (AUC, .84).
Dr. Anstadt said she and her colleagues were not surprised by any of their findings, given earlier research’s suggestions of SMAD4 loss having been associated with poor outcomes for pancreatic cancer.
“Prior studies determined SMAD4 status based on immunohistochemistry and different investigators used different scoring systems,” Dr. Anstadt noted, in an interview. “The results of those studies were conflicting, and consequently SMAD4 has not been adopted clinically as part of the work-up or to aid in treatment decisions.”
“It is essential to find robust, reliable, and cost-effective methods for implementing this in the clinic. As such, we were happy to find that expression of SMAD4 by mRNA sequencing may be that method,” she added.
Not Quite Clinic-Ready
“While we are hopeful that this tool will be a reliable method for use in the clinic, it has yet to be validated in a prospective manner,” Dr. Anstadt said in an interview. “In addition, this study showed that [genetic] expression levels are correlated with worse outcomes and can be of prognostic use; however, we have not directly studied whether expression levels can be predictive of treatment response,” she said.
“Practicing oncologists often have to make difficult decisions in situations where there are no clear answers,” Dr. Anstadt continued. “When considering gray-zone treatment recommendations, we often integrate multiple factors to form an opinion. The reality of cancer medicine is that not all those factors we consider have been validated in prospective studies, but together they produce a picture that is clinically useful. We would submit that SMAD4 status should be one of those factors taken into consideration in forming a comprehensive opinion about suitability for resection or radiotherapy.”
In practice, “if this test is prospectively validated in a future study and will impact clinical decision-making, then this cost will be similar to other genetic tests that have been adopted and have been practice-changing in other oncologic fields,” said Dr. Anstadt. “Being able to individualize treatment can also save overall cost; for instance, predicting which patients would not benefit from local radiation or surgery could decrease use and cost in that population,” she said.
Limitations of the current study included the inability to examine interactions between SMAD4 and radiotherapy because of the sample size and the potential for selection bias, the researchers wrote.
Potential Predictive Value
“A major challenge in the management of patients with pancreatic cancer is the difficulty in predicting which patients will develop metastasis early,” said Jatin Roper, MD, a gastroenterologist at Duke University, Durham, North Carolina, in an interview.
“SMAD4 has previously been evaluated as a prognostic marker in pancreatic cancer, but the association between SMAD4 gene expression, gene mutations, and cancer metastasis has not yet been systematically evaluated in patients, said Dr. Roper, who was not involved in the study.
The new study’s main findings that SMAD4 genomic alterations are associated with worse overall survival, but not distant metastasis-free survival, and that increased SMAD4 expression is associated with improved overall survival and distant metastasis-free survival, suggest that SMAD4 gene expression may be a useful marker in predicting clinical outcomes in pancreatic cancer, Dr. Roper said.
In the future the current study may prompt prospective research to determine a potential association between clinical assessment of SMAD4 gene expression at the time of surgical cancer resection and worse overall survival and distant metastasis-free survival, he said.
The study received no outside funding. Dr. Anstadt and Dr. Roper had no financial conflicts to disclose.
FROM CANCER
Do Multivitamin Supplements Lower Mortality Risk in CRC?
TOPLINE:
METHODOLOGY:
- Some studies suggest that multivitamin supplements might increase a person’s risk for CRC, and other research indicates that certain components of multivitamins, such as vitamins C and D, may have anti-CRC properties.
- Because as many as half of CRC survivors take a multivitamin, researchers wanted to assess whether multivitamin use affects overall survival among people with CRC.
- In the current prospective cohort study, researchers evaluated the use and dose of multivitamin supplements in 2424 patients with stages I-III CRC, using detailed information from patients in the Nurses’ Health Study and Health Professionals Follow‐Up Study.
- The participants completed a mailed questionnaire every 2 years, which included questions about the current use of multivitamin supplements as well as doses per week (0, 1-2, 3-5, 6-9, and ≥ 10 tablets).
- The researchers assessed the potential association between multivitamin use and CRC-related as well as all‐cause mortality.
TAKEAWAY:
- Over a median follow-up period of 11 years, 1512 deaths and 343 cancer-specific deaths occurred.
- For patients diagnosed with CRC, a moderate dose of multivitamins (three to five tablets per week) vs no multivitamin use was associated with a 45% lower risk for cancer-related mortality (adjusted hazard ratio [aHR], 0.55; P = .005).
- Moderate multivitamin use was also associated with a lower risk for all-cause mortality (aHR, 0.81; P = .04) as was a higher dose of six to nine tablets per week (aHR, 0.79; P < .001).
- However, high doses of 10 or more tablets per week were associated with a 60% higher risk for cancer-related mortality (aHR, 1.60; P = .02).
IN PRACTICE:
The study findings suggested that moderate multivitamin supplement use may come with a survival benefit in patients with CRC, while high doses may not, but “further studies are needed before making clinical recommendations for multivitamin use in patients with CRC,” the authors said.
SOURCE:
This work, led by Ming‐ming He of Sun Yat‐sen University Cancer Center, Guangzhou, China, was published in Cancer.
LIMITATIONS:
Given the study’s observational design, residual confounding may be possible. Reverse causation and recall bias are also possible limitations.
DISCLOSURES:
This study was funded by the National Institutes of Health, American Institute for Cancer Research, Wellesley College, Dana‐Farber Cancer Institute, and the Entertainment Industry Foundation. Three study authors reported financial relationships outside this work.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Some studies suggest that multivitamin supplements might increase a person’s risk for CRC, and other research indicates that certain components of multivitamins, such as vitamins C and D, may have anti-CRC properties.
- Because as many as half of CRC survivors take a multivitamin, researchers wanted to assess whether multivitamin use affects overall survival among people with CRC.
- In the current prospective cohort study, researchers evaluated the use and dose of multivitamin supplements in 2424 patients with stages I-III CRC, using detailed information from patients in the Nurses’ Health Study and Health Professionals Follow‐Up Study.
- The participants completed a mailed questionnaire every 2 years, which included questions about the current use of multivitamin supplements as well as doses per week (0, 1-2, 3-5, 6-9, and ≥ 10 tablets).
- The researchers assessed the potential association between multivitamin use and CRC-related as well as all‐cause mortality.
TAKEAWAY:
- Over a median follow-up period of 11 years, 1512 deaths and 343 cancer-specific deaths occurred.
- For patients diagnosed with CRC, a moderate dose of multivitamins (three to five tablets per week) vs no multivitamin use was associated with a 45% lower risk for cancer-related mortality (adjusted hazard ratio [aHR], 0.55; P = .005).
- Moderate multivitamin use was also associated with a lower risk for all-cause mortality (aHR, 0.81; P = .04) as was a higher dose of six to nine tablets per week (aHR, 0.79; P < .001).
- However, high doses of 10 or more tablets per week were associated with a 60% higher risk for cancer-related mortality (aHR, 1.60; P = .02).
IN PRACTICE:
The study findings suggested that moderate multivitamin supplement use may come with a survival benefit in patients with CRC, while high doses may not, but “further studies are needed before making clinical recommendations for multivitamin use in patients with CRC,” the authors said.
SOURCE:
This work, led by Ming‐ming He of Sun Yat‐sen University Cancer Center, Guangzhou, China, was published in Cancer.
LIMITATIONS:
Given the study’s observational design, residual confounding may be possible. Reverse causation and recall bias are also possible limitations.
DISCLOSURES:
This study was funded by the National Institutes of Health, American Institute for Cancer Research, Wellesley College, Dana‐Farber Cancer Institute, and the Entertainment Industry Foundation. Three study authors reported financial relationships outside this work.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Some studies suggest that multivitamin supplements might increase a person’s risk for CRC, and other research indicates that certain components of multivitamins, such as vitamins C and D, may have anti-CRC properties.
- Because as many as half of CRC survivors take a multivitamin, researchers wanted to assess whether multivitamin use affects overall survival among people with CRC.
- In the current prospective cohort study, researchers evaluated the use and dose of multivitamin supplements in 2424 patients with stages I-III CRC, using detailed information from patients in the Nurses’ Health Study and Health Professionals Follow‐Up Study.
- The participants completed a mailed questionnaire every 2 years, which included questions about the current use of multivitamin supplements as well as doses per week (0, 1-2, 3-5, 6-9, and ≥ 10 tablets).
- The researchers assessed the potential association between multivitamin use and CRC-related as well as all‐cause mortality.
TAKEAWAY:
- Over a median follow-up period of 11 years, 1512 deaths and 343 cancer-specific deaths occurred.
- For patients diagnosed with CRC, a moderate dose of multivitamins (three to five tablets per week) vs no multivitamin use was associated with a 45% lower risk for cancer-related mortality (adjusted hazard ratio [aHR], 0.55; P = .005).
- Moderate multivitamin use was also associated with a lower risk for all-cause mortality (aHR, 0.81; P = .04) as was a higher dose of six to nine tablets per week (aHR, 0.79; P < .001).
- However, high doses of 10 or more tablets per week were associated with a 60% higher risk for cancer-related mortality (aHR, 1.60; P = .02).
IN PRACTICE:
The study findings suggested that moderate multivitamin supplement use may come with a survival benefit in patients with CRC, while high doses may not, but “further studies are needed before making clinical recommendations for multivitamin use in patients with CRC,” the authors said.
SOURCE:
This work, led by Ming‐ming He of Sun Yat‐sen University Cancer Center, Guangzhou, China, was published in Cancer.
LIMITATIONS:
Given the study’s observational design, residual confounding may be possible. Reverse causation and recall bias are also possible limitations.
DISCLOSURES:
This study was funded by the National Institutes of Health, American Institute for Cancer Research, Wellesley College, Dana‐Farber Cancer Institute, and the Entertainment Industry Foundation. Three study authors reported financial relationships outside this work.
A version of this article appeared on Medscape.com.
Diabetes Tech Falls Short as Hypoglycemic Challenges Persist
TOPLINE:
Despite diabetes technology, many with type 1 diabetes (T1D) miss glycemic targets and experience severe hypoglycemia and impaired awareness of hypoglycemia (IAH).
METHODOLOGY:
- The clinical management of T1D through technology is now recognized as the standard of care, but its real-world impact on glycemic targets and severe hypoglycemic events and IAH is unclear.
- Researchers assessed the self-reported prevalence of glycemic metrics, severe hypoglycemia, and hypoglycemia awareness according to the use of continuous glucose monitoring (CGM) and automated insulin delivery (AID) systems.
- They enrolled 2044 individuals diagnosed with T1D for at least 2 years (mean age, 43.0 years; 72.1% women; 95.4% White) from the T1D Exchange Registry and online communities who filled an online survey.
- Participants were stratified on the basis of the presence or absence of CGM and different insulin delivery methods (multiple daily injections, conventional pumps, or AID systems).
- The primary outcome was the proportion of participants who achieved glycemic targets (self-reported A1c), had severe hypoglycemia (any low glucose incidence in 12 months), and/or IAH (a modified Gold score on a seven-point Likert scale).
TAKEAWAY:
- Most participants (91.7%) used CGM, and 50.8% of CGM users used an AID system.
- Despite advanced interventions, only 59.6% (95% CI, 57.3%-61.8%) of CGM users met the glycemic target (A1c < 7%), while nearly 40% of CGM users and 35.6% of AID users didn’t reach the target.
- At least one event of severe hypoglycemia in the previous 12 months was reported in 10.8% of CGM users and 16.6% of those using an AID system.
- IAH prevalence was seen in 31.1% (95% CI, 29.0%-33.2%) and 30.3% (95% CI, 17.5%-33.3%) of participants using CGM and CGM + AID, respectively.
IN PRACTICE:
“Educational initiatives continue to be important for all individuals with type 1 diabetes, and the development of novel therapeutic options and strategies, including bihormonal AID systems and beta-cell replacement, will be required to enable more of these individuals to meet treatment goals,” the authors wrote.
SOURCE:
The study, published online in Diabetes Care, was led by Jennifer L. Sherr, MD, PhD, Yale School of Medicine, New Haven, Connecticut.
LIMITATIONS:
The survey participants in this study were from the T1D Exchange online community, who tend to be highly involved, have technology experience, and are more likely to achieve glycemic targets. The data reported as part of the survey were based on self-reports by participants and may be subject to recall bias. Notably, severe hypoglycemic events may be overreported by individuals using CGM and AID systems due to sensor alarms.
DISCLOSURES:
The study was funded by Vertex Pharmaceuticals. Several authors disclosed financial relationships, including grants, consulting fees, honoraria, stock ownership, and employment with pharmaceutical and device companies and other entities.
A version of this article appeared on Medscape.com.
TOPLINE:
Despite diabetes technology, many with type 1 diabetes (T1D) miss glycemic targets and experience severe hypoglycemia and impaired awareness of hypoglycemia (IAH).
METHODOLOGY:
- The clinical management of T1D through technology is now recognized as the standard of care, but its real-world impact on glycemic targets and severe hypoglycemic events and IAH is unclear.
- Researchers assessed the self-reported prevalence of glycemic metrics, severe hypoglycemia, and hypoglycemia awareness according to the use of continuous glucose monitoring (CGM) and automated insulin delivery (AID) systems.
- They enrolled 2044 individuals diagnosed with T1D for at least 2 years (mean age, 43.0 years; 72.1% women; 95.4% White) from the T1D Exchange Registry and online communities who filled an online survey.
- Participants were stratified on the basis of the presence or absence of CGM and different insulin delivery methods (multiple daily injections, conventional pumps, or AID systems).
- The primary outcome was the proportion of participants who achieved glycemic targets (self-reported A1c), had severe hypoglycemia (any low glucose incidence in 12 months), and/or IAH (a modified Gold score on a seven-point Likert scale).
TAKEAWAY:
- Most participants (91.7%) used CGM, and 50.8% of CGM users used an AID system.
- Despite advanced interventions, only 59.6% (95% CI, 57.3%-61.8%) of CGM users met the glycemic target (A1c < 7%), while nearly 40% of CGM users and 35.6% of AID users didn’t reach the target.
- At least one event of severe hypoglycemia in the previous 12 months was reported in 10.8% of CGM users and 16.6% of those using an AID system.
- IAH prevalence was seen in 31.1% (95% CI, 29.0%-33.2%) and 30.3% (95% CI, 17.5%-33.3%) of participants using CGM and CGM + AID, respectively.
IN PRACTICE:
“Educational initiatives continue to be important for all individuals with type 1 diabetes, and the development of novel therapeutic options and strategies, including bihormonal AID systems and beta-cell replacement, will be required to enable more of these individuals to meet treatment goals,” the authors wrote.
SOURCE:
The study, published online in Diabetes Care, was led by Jennifer L. Sherr, MD, PhD, Yale School of Medicine, New Haven, Connecticut.
LIMITATIONS:
The survey participants in this study were from the T1D Exchange online community, who tend to be highly involved, have technology experience, and are more likely to achieve glycemic targets. The data reported as part of the survey were based on self-reports by participants and may be subject to recall bias. Notably, severe hypoglycemic events may be overreported by individuals using CGM and AID systems due to sensor alarms.
DISCLOSURES:
The study was funded by Vertex Pharmaceuticals. Several authors disclosed financial relationships, including grants, consulting fees, honoraria, stock ownership, and employment with pharmaceutical and device companies and other entities.
A version of this article appeared on Medscape.com.
TOPLINE:
Despite diabetes technology, many with type 1 diabetes (T1D) miss glycemic targets and experience severe hypoglycemia and impaired awareness of hypoglycemia (IAH).
METHODOLOGY:
- The clinical management of T1D through technology is now recognized as the standard of care, but its real-world impact on glycemic targets and severe hypoglycemic events and IAH is unclear.
- Researchers assessed the self-reported prevalence of glycemic metrics, severe hypoglycemia, and hypoglycemia awareness according to the use of continuous glucose monitoring (CGM) and automated insulin delivery (AID) systems.
- They enrolled 2044 individuals diagnosed with T1D for at least 2 years (mean age, 43.0 years; 72.1% women; 95.4% White) from the T1D Exchange Registry and online communities who filled an online survey.
- Participants were stratified on the basis of the presence or absence of CGM and different insulin delivery methods (multiple daily injections, conventional pumps, or AID systems).
- The primary outcome was the proportion of participants who achieved glycemic targets (self-reported A1c), had severe hypoglycemia (any low glucose incidence in 12 months), and/or IAH (a modified Gold score on a seven-point Likert scale).
TAKEAWAY:
- Most participants (91.7%) used CGM, and 50.8% of CGM users used an AID system.
- Despite advanced interventions, only 59.6% (95% CI, 57.3%-61.8%) of CGM users met the glycemic target (A1c < 7%), while nearly 40% of CGM users and 35.6% of AID users didn’t reach the target.
- At least one event of severe hypoglycemia in the previous 12 months was reported in 10.8% of CGM users and 16.6% of those using an AID system.
- IAH prevalence was seen in 31.1% (95% CI, 29.0%-33.2%) and 30.3% (95% CI, 17.5%-33.3%) of participants using CGM and CGM + AID, respectively.
IN PRACTICE:
“Educational initiatives continue to be important for all individuals with type 1 diabetes, and the development of novel therapeutic options and strategies, including bihormonal AID systems and beta-cell replacement, will be required to enable more of these individuals to meet treatment goals,” the authors wrote.
SOURCE:
The study, published online in Diabetes Care, was led by Jennifer L. Sherr, MD, PhD, Yale School of Medicine, New Haven, Connecticut.
LIMITATIONS:
The survey participants in this study were from the T1D Exchange online community, who tend to be highly involved, have technology experience, and are more likely to achieve glycemic targets. The data reported as part of the survey were based on self-reports by participants and may be subject to recall bias. Notably, severe hypoglycemic events may be overreported by individuals using CGM and AID systems due to sensor alarms.
DISCLOSURES:
The study was funded by Vertex Pharmaceuticals. Several authors disclosed financial relationships, including grants, consulting fees, honoraria, stock ownership, and employment with pharmaceutical and device companies and other entities.
A version of this article appeared on Medscape.com.
Bivalent Vaccines Protect Even Children Who’ve Had COVID
This transcript has been edited for clarity.
It was only 3 years ago when we called the pathogen we now refer to as the coronavirus “nCOV-19.” It was, in many ways, more descriptive than what we have today. The little “n” there stood for “novel” — and it was really that little “n” that caused us all the trouble.
You see, coronaviruses themselves were not really new to us. Understudied, perhaps, but with four strains running around the globe at any time giving rise to the common cold, these were viruses our bodies understood.
But Instead of acting like a cold, it acted like nothing we had seen before, at least in our lifetime. The story of the pandemic is very much a bildungsroman of our immune systems — a story of how our immunity grew up.
The difference between the start of 2020 and now, when infections with the coronavirus remain common but not as deadly, can be measured in terms of immune education. Some of our immune systems were educated by infection, some by vaccination, and many by both.
When the first vaccines emerged in December 2020, the opportunity to educate our immune systems was still huge. Though, at the time, an estimated 20 million had been infected in the US and 350,000 had died, there was a large population that remained immunologically naive. I was one of them.
If 2020 into early 2021 was the era of immune education, the postvaccine period was the era of the variant. From one COVID strain to two, to five, to innumerable, our immune memory — trained on a specific version of the virus or its spike protein — became imperfect again. Not naive; these variants were not “novel” in the way COVID-19 was novel, but they were different. And different enough to cause infection.
Following the playbook of another virus that loves to come dressed up in different outfits, the flu virus, we find ourselves in the booster era — a world where yearly doses of a vaccine, ideally matched to the variants circulating when the vaccine is given, are the recommendation if not the norm.
But questions remain about the vaccination program, particularly around who should get it. And two populations with big question marks over their heads are (1) people who have already been infected and (2) kids, because their risk for bad outcomes is so much lower.
This week, we finally have some evidence that can shed light on these questions. The study under the spotlight is this one, appearing in JAMA, which tries to analyze the ability of the bivalent vaccine — that’s the second one to come out, around September 2022 — to protect kids from COVID-19.
Now, right off the bat, this was not a randomized trial. The studies that established the viability of the mRNA vaccine platform were; they happened before the vaccine was authorized. But trials of the bivalent vaccine were mostly limited to proving immune response, not protection from disease.
Nevertheless, with some good observational methods and some statistics, we can try to tease out whether bivalent vaccines in kids worked.
The study combines three prospective cohort studies. The details are in the paper, but what you need to know is that the special sauce of these studies was that the kids were tested for COVID-19 on a weekly basis, whether they had symptoms or not. This is critical because asymptomatic infections can transmit COVID-19.
Let’s do the variables of interest. First and foremost, the bivalent vaccine. Some of these kids got the bivalent vaccine, some didn’t. Other key variables include prior vaccination with the monovalent vaccine. Some had been vaccinated with the monovalent vaccine before, some hadn’t. And, of course, prior infection. Some had been infected before (based on either nasal swabs or blood tests).
Let’s focus first on the primary exposure of interest: getting that bivalent vaccine. Again, this was not randomly assigned; kids who got the bivalent vaccine were different from those who did not. In general, they lived in smaller households, they were more likely to be White, less likely to have had a prior COVID infection, and quite a bit more likely to have at least one chronic condition.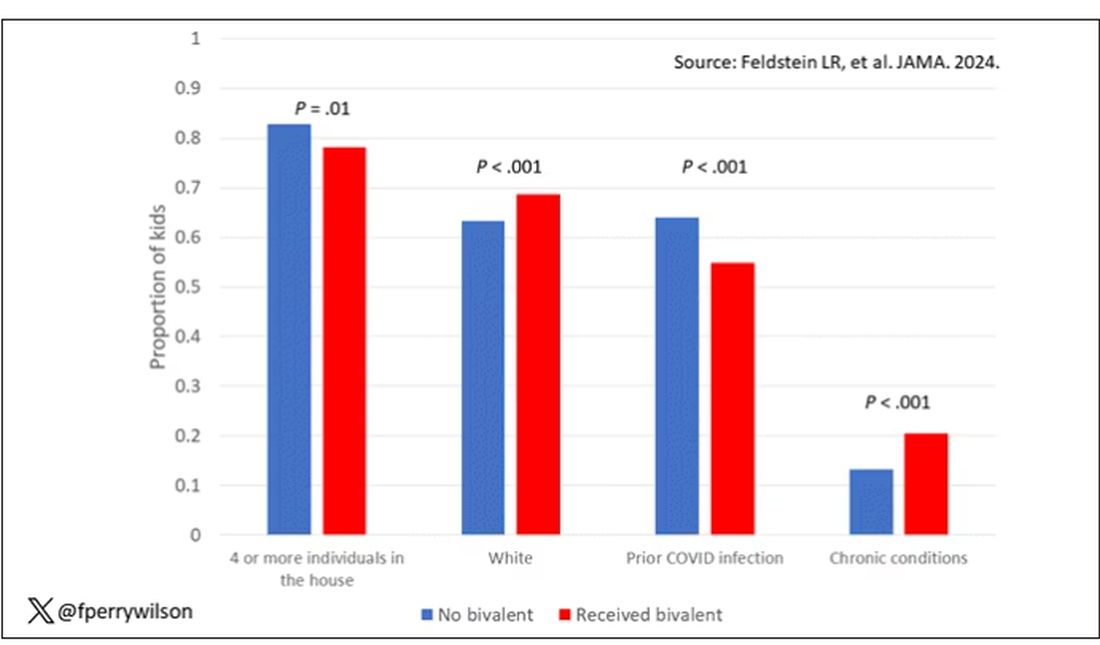
To me, this constellation of factors describes a slightly higher-risk group; it makes sense that they were more likely to get the second vaccine.
Given those factors, what were the rates of COVID infection? After nearly a year of follow-up, around 15% of the kids who hadn’t received the bivalent vaccine got infected compared with 5% of the vaccinated kids. Symptomatic infections represented roughly half of all infections in both groups.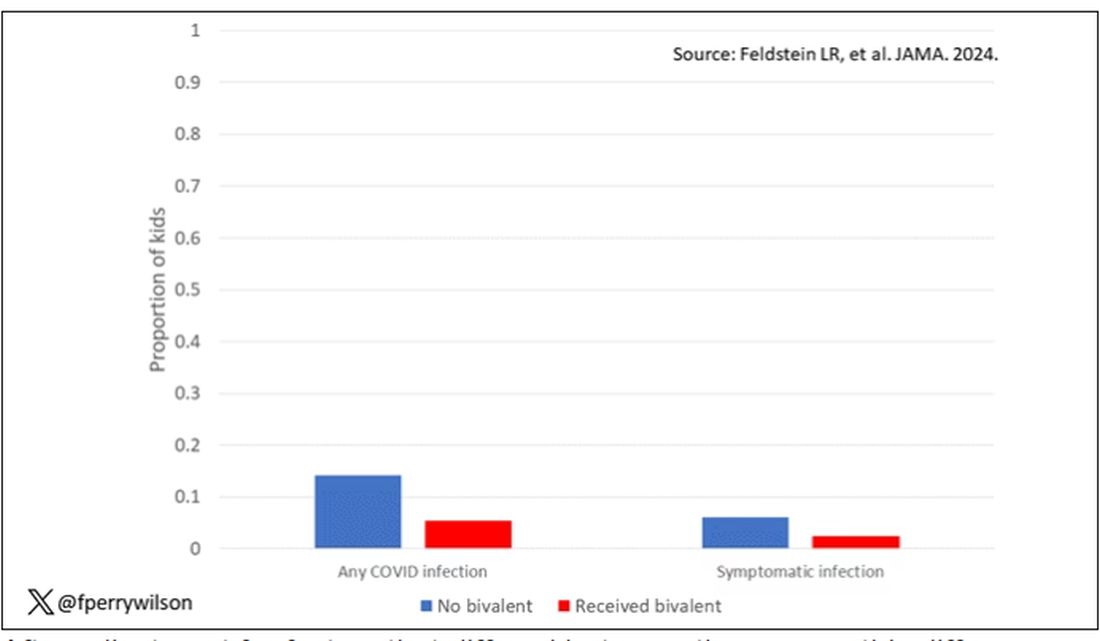
After adjustment for factors that differed between the groups, this difference translated into a vaccine efficacy of about 50% in this population. That’s our first data point. Yes, the bivalent vaccine worked. Not amazingly, of course. But it worked.
What about the kids who had had a prior COVID infection? Somewhat surprisingly, the vaccine was just as effective in this population, despite the fact that their immune systems already had some knowledge of COVID. Ten percent of unvaccinated kids got infected, even though they had been infected before. Just 2.5% of kids who received the bivalent vaccine got infected, suggesting some synergy between prior infection and vaccination.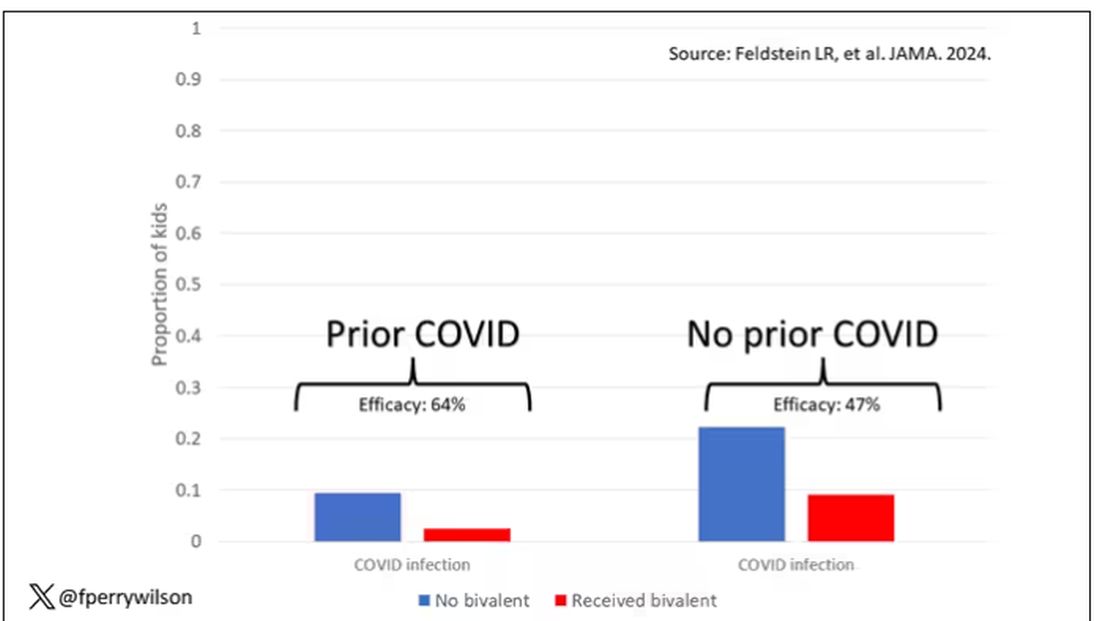
These data suggest that the bivalent vaccine did reduce the risk for COVID infection in kids. All good. But the piece still missing is how severe these infections were. It doesn’t appear that any of the 426 infections documented in this study resulted in hospitalization or death, fortunately. And no data are presented on the incidence of multisystem inflammatory syndrome of children, though given the rarity, I’d be surprised if any of these kids have this either.
So where are we? Well, it seems that the narrative out there that says “the vaccines don’t work” or “the vaccines don’t work if you’ve already been infected” is probably not true. They do work. This study and others in adults show that. If they work to reduce infections, as this study shows, they will also work to reduce deaths. It’s just that death is fortunately so rare in children that the number needed to vaccinate to prevent one death is very large. In that situation, the decision to vaccinate comes down to the risks associated with vaccination. So far, those risk seem very minimal.
Perhaps falling into a flu-like yearly vaccination schedule is not simply the result of old habits dying hard. Maybe it’s actually not a bad idea.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It was only 3 years ago when we called the pathogen we now refer to as the coronavirus “nCOV-19.” It was, in many ways, more descriptive than what we have today. The little “n” there stood for “novel” — and it was really that little “n” that caused us all the trouble.
You see, coronaviruses themselves were not really new to us. Understudied, perhaps, but with four strains running around the globe at any time giving rise to the common cold, these were viruses our bodies understood.
But Instead of acting like a cold, it acted like nothing we had seen before, at least in our lifetime. The story of the pandemic is very much a bildungsroman of our immune systems — a story of how our immunity grew up.
The difference between the start of 2020 and now, when infections with the coronavirus remain common but not as deadly, can be measured in terms of immune education. Some of our immune systems were educated by infection, some by vaccination, and many by both.
When the first vaccines emerged in December 2020, the opportunity to educate our immune systems was still huge. Though, at the time, an estimated 20 million had been infected in the US and 350,000 had died, there was a large population that remained immunologically naive. I was one of them.
If 2020 into early 2021 was the era of immune education, the postvaccine period was the era of the variant. From one COVID strain to two, to five, to innumerable, our immune memory — trained on a specific version of the virus or its spike protein — became imperfect again. Not naive; these variants were not “novel” in the way COVID-19 was novel, but they were different. And different enough to cause infection.
Following the playbook of another virus that loves to come dressed up in different outfits, the flu virus, we find ourselves in the booster era — a world where yearly doses of a vaccine, ideally matched to the variants circulating when the vaccine is given, are the recommendation if not the norm.
But questions remain about the vaccination program, particularly around who should get it. And two populations with big question marks over their heads are (1) people who have already been infected and (2) kids, because their risk for bad outcomes is so much lower.
This week, we finally have some evidence that can shed light on these questions. The study under the spotlight is this one, appearing in JAMA, which tries to analyze the ability of the bivalent vaccine — that’s the second one to come out, around September 2022 — to protect kids from COVID-19.
Now, right off the bat, this was not a randomized trial. The studies that established the viability of the mRNA vaccine platform were; they happened before the vaccine was authorized. But trials of the bivalent vaccine were mostly limited to proving immune response, not protection from disease.
Nevertheless, with some good observational methods and some statistics, we can try to tease out whether bivalent vaccines in kids worked.
The study combines three prospective cohort studies. The details are in the paper, but what you need to know is that the special sauce of these studies was that the kids were tested for COVID-19 on a weekly basis, whether they had symptoms or not. This is critical because asymptomatic infections can transmit COVID-19.
Let’s do the variables of interest. First and foremost, the bivalent vaccine. Some of these kids got the bivalent vaccine, some didn’t. Other key variables include prior vaccination with the monovalent vaccine. Some had been vaccinated with the monovalent vaccine before, some hadn’t. And, of course, prior infection. Some had been infected before (based on either nasal swabs or blood tests).
Let’s focus first on the primary exposure of interest: getting that bivalent vaccine. Again, this was not randomly assigned; kids who got the bivalent vaccine were different from those who did not. In general, they lived in smaller households, they were more likely to be White, less likely to have had a prior COVID infection, and quite a bit more likely to have at least one chronic condition.
To me, this constellation of factors describes a slightly higher-risk group; it makes sense that they were more likely to get the second vaccine.
Given those factors, what were the rates of COVID infection? After nearly a year of follow-up, around 15% of the kids who hadn’t received the bivalent vaccine got infected compared with 5% of the vaccinated kids. Symptomatic infections represented roughly half of all infections in both groups.
After adjustment for factors that differed between the groups, this difference translated into a vaccine efficacy of about 50% in this population. That’s our first data point. Yes, the bivalent vaccine worked. Not amazingly, of course. But it worked.
What about the kids who had had a prior COVID infection? Somewhat surprisingly, the vaccine was just as effective in this population, despite the fact that their immune systems already had some knowledge of COVID. Ten percent of unvaccinated kids got infected, even though they had been infected before. Just 2.5% of kids who received the bivalent vaccine got infected, suggesting some synergy between prior infection and vaccination.
These data suggest that the bivalent vaccine did reduce the risk for COVID infection in kids. All good. But the piece still missing is how severe these infections were. It doesn’t appear that any of the 426 infections documented in this study resulted in hospitalization or death, fortunately. And no data are presented on the incidence of multisystem inflammatory syndrome of children, though given the rarity, I’d be surprised if any of these kids have this either.
So where are we? Well, it seems that the narrative out there that says “the vaccines don’t work” or “the vaccines don’t work if you’ve already been infected” is probably not true. They do work. This study and others in adults show that. If they work to reduce infections, as this study shows, they will also work to reduce deaths. It’s just that death is fortunately so rare in children that the number needed to vaccinate to prevent one death is very large. In that situation, the decision to vaccinate comes down to the risks associated with vaccination. So far, those risk seem very minimal.
Perhaps falling into a flu-like yearly vaccination schedule is not simply the result of old habits dying hard. Maybe it’s actually not a bad idea.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It was only 3 years ago when we called the pathogen we now refer to as the coronavirus “nCOV-19.” It was, in many ways, more descriptive than what we have today. The little “n” there stood for “novel” — and it was really that little “n” that caused us all the trouble.
You see, coronaviruses themselves were not really new to us. Understudied, perhaps, but with four strains running around the globe at any time giving rise to the common cold, these were viruses our bodies understood.
But Instead of acting like a cold, it acted like nothing we had seen before, at least in our lifetime. The story of the pandemic is very much a bildungsroman of our immune systems — a story of how our immunity grew up.
The difference between the start of 2020 and now, when infections with the coronavirus remain common but not as deadly, can be measured in terms of immune education. Some of our immune systems were educated by infection, some by vaccination, and many by both.
When the first vaccines emerged in December 2020, the opportunity to educate our immune systems was still huge. Though, at the time, an estimated 20 million had been infected in the US and 350,000 had died, there was a large population that remained immunologically naive. I was one of them.
If 2020 into early 2021 was the era of immune education, the postvaccine period was the era of the variant. From one COVID strain to two, to five, to innumerable, our immune memory — trained on a specific version of the virus or its spike protein — became imperfect again. Not naive; these variants were not “novel” in the way COVID-19 was novel, but they were different. And different enough to cause infection.
Following the playbook of another virus that loves to come dressed up in different outfits, the flu virus, we find ourselves in the booster era — a world where yearly doses of a vaccine, ideally matched to the variants circulating when the vaccine is given, are the recommendation if not the norm.
But questions remain about the vaccination program, particularly around who should get it. And two populations with big question marks over their heads are (1) people who have already been infected and (2) kids, because their risk for bad outcomes is so much lower.
This week, we finally have some evidence that can shed light on these questions. The study under the spotlight is this one, appearing in JAMA, which tries to analyze the ability of the bivalent vaccine — that’s the second one to come out, around September 2022 — to protect kids from COVID-19.
Now, right off the bat, this was not a randomized trial. The studies that established the viability of the mRNA vaccine platform were; they happened before the vaccine was authorized. But trials of the bivalent vaccine were mostly limited to proving immune response, not protection from disease.
Nevertheless, with some good observational methods and some statistics, we can try to tease out whether bivalent vaccines in kids worked.
The study combines three prospective cohort studies. The details are in the paper, but what you need to know is that the special sauce of these studies was that the kids were tested for COVID-19 on a weekly basis, whether they had symptoms or not. This is critical because asymptomatic infections can transmit COVID-19.
Let’s do the variables of interest. First and foremost, the bivalent vaccine. Some of these kids got the bivalent vaccine, some didn’t. Other key variables include prior vaccination with the monovalent vaccine. Some had been vaccinated with the monovalent vaccine before, some hadn’t. And, of course, prior infection. Some had been infected before (based on either nasal swabs or blood tests).
Let’s focus first on the primary exposure of interest: getting that bivalent vaccine. Again, this was not randomly assigned; kids who got the bivalent vaccine were different from those who did not. In general, they lived in smaller households, they were more likely to be White, less likely to have had a prior COVID infection, and quite a bit more likely to have at least one chronic condition.
To me, this constellation of factors describes a slightly higher-risk group; it makes sense that they were more likely to get the second vaccine.
Given those factors, what were the rates of COVID infection? After nearly a year of follow-up, around 15% of the kids who hadn’t received the bivalent vaccine got infected compared with 5% of the vaccinated kids. Symptomatic infections represented roughly half of all infections in both groups.
After adjustment for factors that differed between the groups, this difference translated into a vaccine efficacy of about 50% in this population. That’s our first data point. Yes, the bivalent vaccine worked. Not amazingly, of course. But it worked.
What about the kids who had had a prior COVID infection? Somewhat surprisingly, the vaccine was just as effective in this population, despite the fact that their immune systems already had some knowledge of COVID. Ten percent of unvaccinated kids got infected, even though they had been infected before. Just 2.5% of kids who received the bivalent vaccine got infected, suggesting some synergy between prior infection and vaccination.
These data suggest that the bivalent vaccine did reduce the risk for COVID infection in kids. All good. But the piece still missing is how severe these infections were. It doesn’t appear that any of the 426 infections documented in this study resulted in hospitalization or death, fortunately. And no data are presented on the incidence of multisystem inflammatory syndrome of children, though given the rarity, I’d be surprised if any of these kids have this either.
So where are we? Well, it seems that the narrative out there that says “the vaccines don’t work” or “the vaccines don’t work if you’ve already been infected” is probably not true. They do work. This study and others in adults show that. If they work to reduce infections, as this study shows, they will also work to reduce deaths. It’s just that death is fortunately so rare in children that the number needed to vaccinate to prevent one death is very large. In that situation, the decision to vaccinate comes down to the risks associated with vaccination. So far, those risk seem very minimal.
Perhaps falling into a flu-like yearly vaccination schedule is not simply the result of old habits dying hard. Maybe it’s actually not a bad idea.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Premeal Stomach-Filling Capsule Effective for Weight Loss
TOPLINE:
Oral intragastric expandable capsules taken twice daily before meals reduce body weight in adults with overweight or obesity compared with placebo, with mild gastrointestinal adverse events.
METHODOLOGY:
- Numerous anti-obesity pharmacotherapies have demonstrated effectiveness in reducing weight, but they may lead to side effects.
- This 24-week phase 3 randomized placebo-controlled study evaluated 2.24 g oral intragastric expandable capsules for weight loss in 280 adults (ages 18-60 years) with overweight or obesity (body mass index ≥ 24 kg/m2).
- One capsule, taken before lunch and dinner with water, expands to fill about one quarter of average stomach volume and then passes through the body, similar to the US Food and Drug Administration–cleared device Plenity.
- Primary endpoints were the percentage change in body weight from baseline and the weight loss response rate (weight loss of at least 5% of baseline body weight) at week 24.
- Researchers analyzed efficacy outcomes in two ways: Intention to treat (a full analysis based on groups to which they were randomly assigned) and per protocol (based on data from participants who follow the protocol).
TAKEAWAY:
- At 24 weeks, the change in mean body weight was higher with intragastric expandable capsules than with placebo using the per protocol set (estimated treatment difference [ETD], −3.6%; P < .001), with similar results using the full analysis set.
- The weight loss response rate at 24 weeks was higher with intragastric expandable capsules than with placebo using the per protocol set (ETD, 29.6%; P < .001), with similar results using the full analysis set.
- Reduction in fasting insulin levels was higher with intragastric expandable capsules than with placebo (P = .008), while improvements in the lipid profile, fasting plasma glucose levels, and heart rate were similar between the groups.
- Gastrointestinal disorders were reported in 25.0% of participants in the intragastric expandable capsule group compared with 21.9% in the placebo group, with most being transient and mild in severity.
IN PRACTICE:
“As a mild and safe anti-obesity medication, intragastric expandable capsules provide a new therapeutic choice for individuals with overweight or obesity, helping them to enhance and maintain the effect of diet restriction,” wrote the authors.
SOURCE:
Difei Lu, MD, Department of Endocrinology, Peking University First Hospital, Beijing, China, led the study, which was published online in Diabetes, Obesity and Metabolism.
LIMITATIONS:
The study included individuals who were overweight or obese, who might have been more willing to lose weight than the general population. Moreover, only 3.25% of the participants had type 2 diabetes, and participants were relatively young. This may have reduced the potential to discover metabolic or cardiovascular improvement by the product.
DISCLOSURES:
This study was funded by Xiamen Junde Pharmaceutical Technology. The authors disclosed no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Oral intragastric expandable capsules taken twice daily before meals reduce body weight in adults with overweight or obesity compared with placebo, with mild gastrointestinal adverse events.
METHODOLOGY:
- Numerous anti-obesity pharmacotherapies have demonstrated effectiveness in reducing weight, but they may lead to side effects.
- This 24-week phase 3 randomized placebo-controlled study evaluated 2.24 g oral intragastric expandable capsules for weight loss in 280 adults (ages 18-60 years) with overweight or obesity (body mass index ≥ 24 kg/m2).
- One capsule, taken before lunch and dinner with water, expands to fill about one quarter of average stomach volume and then passes through the body, similar to the US Food and Drug Administration–cleared device Plenity.
- Primary endpoints were the percentage change in body weight from baseline and the weight loss response rate (weight loss of at least 5% of baseline body weight) at week 24.
- Researchers analyzed efficacy outcomes in two ways: Intention to treat (a full analysis based on groups to which they were randomly assigned) and per protocol (based on data from participants who follow the protocol).
TAKEAWAY:
- At 24 weeks, the change in mean body weight was higher with intragastric expandable capsules than with placebo using the per protocol set (estimated treatment difference [ETD], −3.6%; P < .001), with similar results using the full analysis set.
- The weight loss response rate at 24 weeks was higher with intragastric expandable capsules than with placebo using the per protocol set (ETD, 29.6%; P < .001), with similar results using the full analysis set.
- Reduction in fasting insulin levels was higher with intragastric expandable capsules than with placebo (P = .008), while improvements in the lipid profile, fasting plasma glucose levels, and heart rate were similar between the groups.
- Gastrointestinal disorders were reported in 25.0% of participants in the intragastric expandable capsule group compared with 21.9% in the placebo group, with most being transient and mild in severity.
IN PRACTICE:
“As a mild and safe anti-obesity medication, intragastric expandable capsules provide a new therapeutic choice for individuals with overweight or obesity, helping them to enhance and maintain the effect of diet restriction,” wrote the authors.
SOURCE:
Difei Lu, MD, Department of Endocrinology, Peking University First Hospital, Beijing, China, led the study, which was published online in Diabetes, Obesity and Metabolism.
LIMITATIONS:
The study included individuals who were overweight or obese, who might have been more willing to lose weight than the general population. Moreover, only 3.25% of the participants had type 2 diabetes, and participants were relatively young. This may have reduced the potential to discover metabolic or cardiovascular improvement by the product.
DISCLOSURES:
This study was funded by Xiamen Junde Pharmaceutical Technology. The authors disclosed no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Oral intragastric expandable capsules taken twice daily before meals reduce body weight in adults with overweight or obesity compared with placebo, with mild gastrointestinal adverse events.
METHODOLOGY:
- Numerous anti-obesity pharmacotherapies have demonstrated effectiveness in reducing weight, but they may lead to side effects.
- This 24-week phase 3 randomized placebo-controlled study evaluated 2.24 g oral intragastric expandable capsules for weight loss in 280 adults (ages 18-60 years) with overweight or obesity (body mass index ≥ 24 kg/m2).
- One capsule, taken before lunch and dinner with water, expands to fill about one quarter of average stomach volume and then passes through the body, similar to the US Food and Drug Administration–cleared device Plenity.
- Primary endpoints were the percentage change in body weight from baseline and the weight loss response rate (weight loss of at least 5% of baseline body weight) at week 24.
- Researchers analyzed efficacy outcomes in two ways: Intention to treat (a full analysis based on groups to which they were randomly assigned) and per protocol (based on data from participants who follow the protocol).
TAKEAWAY:
- At 24 weeks, the change in mean body weight was higher with intragastric expandable capsules than with placebo using the per protocol set (estimated treatment difference [ETD], −3.6%; P < .001), with similar results using the full analysis set.
- The weight loss response rate at 24 weeks was higher with intragastric expandable capsules than with placebo using the per protocol set (ETD, 29.6%; P < .001), with similar results using the full analysis set.
- Reduction in fasting insulin levels was higher with intragastric expandable capsules than with placebo (P = .008), while improvements in the lipid profile, fasting plasma glucose levels, and heart rate were similar between the groups.
- Gastrointestinal disorders were reported in 25.0% of participants in the intragastric expandable capsule group compared with 21.9% in the placebo group, with most being transient and mild in severity.
IN PRACTICE:
“As a mild and safe anti-obesity medication, intragastric expandable capsules provide a new therapeutic choice for individuals with overweight or obesity, helping them to enhance and maintain the effect of diet restriction,” wrote the authors.
SOURCE:
Difei Lu, MD, Department of Endocrinology, Peking University First Hospital, Beijing, China, led the study, which was published online in Diabetes, Obesity and Metabolism.
LIMITATIONS:
The study included individuals who were overweight or obese, who might have been more willing to lose weight than the general population. Moreover, only 3.25% of the participants had type 2 diabetes, and participants were relatively young. This may have reduced the potential to discover metabolic or cardiovascular improvement by the product.
DISCLOSURES:
This study was funded by Xiamen Junde Pharmaceutical Technology. The authors disclosed no conflicts of interest.
A version of this article appeared on Medscape.com.