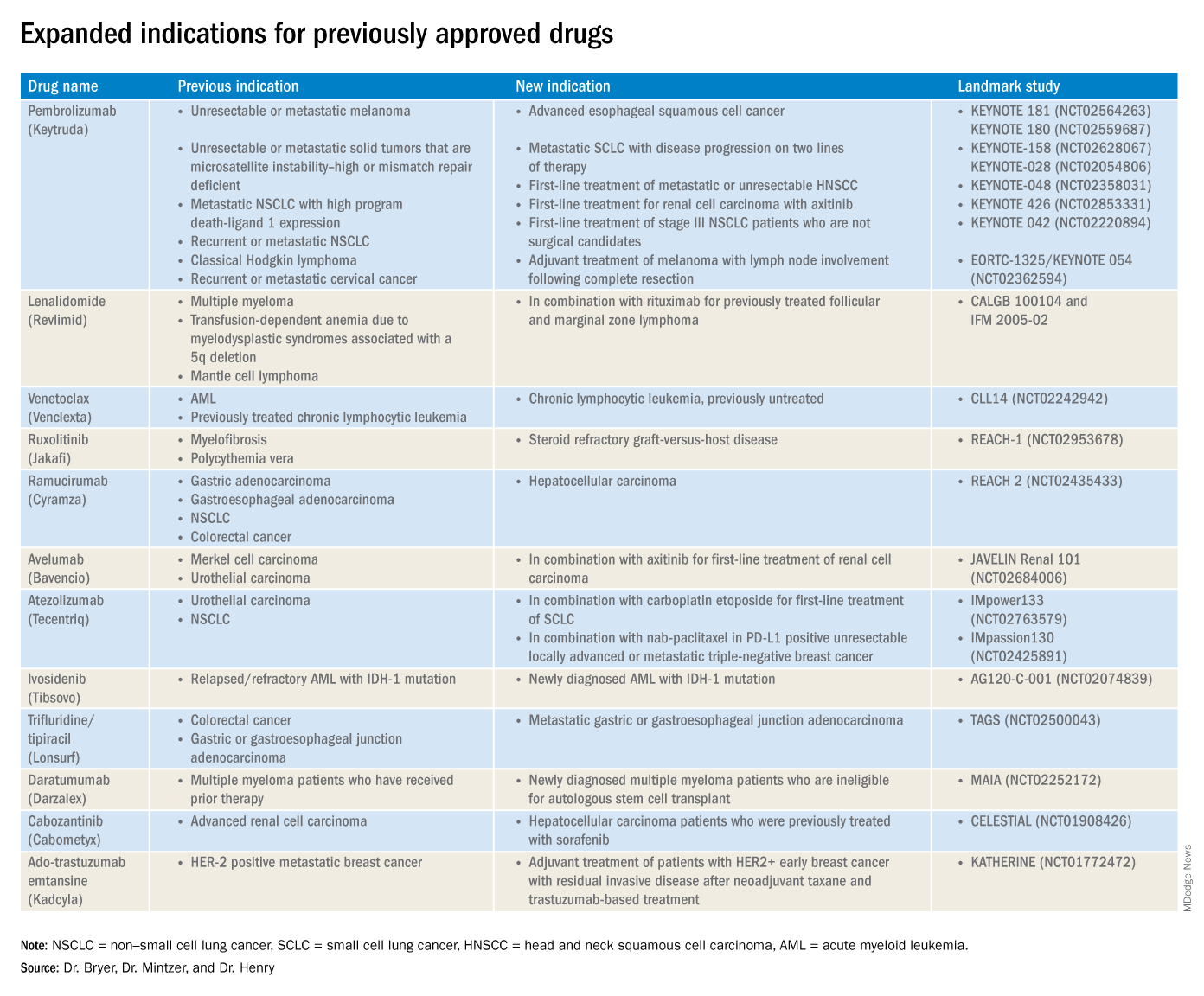
The rapid development and identification of novel drugs has translated into innovative therapies in hematology and oncology. The aim of this piece is to present newly approved drugs and expanded indications to serve as a reference guide for practicing clinicians.
This article reviews therapies that were newly approved so far in 2019, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
New approvals
Fedratinib (Inrebic)
Class: JAK2 and FLT3 selective kinase inhibitor.
Disease: Intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis.
Dose: 400 mg orally once daily, with or without food.
Adverse events (AEs): Black box warning: Fatal encephalopathy, including Wernicke’s (thiamine level monitoring suggested).
Trials: In JAKARTA (NCT01437787), 37% of patients achieved a 35% or greater reduction in spleen volume and 40% received a 50% or greater reduction in myelofibrosis-related symptoms. In Jakarta-2, there was a 55% spleen response in patients resistant or intolerant to ruxolitinib.
Disease: Solid tumors that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion and for ROS-1 positive non–small cell lung cancer (NSCLC).
Dose: 600 mg orally once daily.
AEs: Heart failure, QT prolongation, skeletal fractures, hepatotoxicity, central nervous system effects, and hyperuricemia.
Trial: ALKA, STARTRK-1 (NCT02097810) and STARTRK-2 (NCT02568267): Overall response rate of 57% for NTRK positive patients; response rate of 77% in ROS-1 positive NSCLC.
Pexidartinib (Turalio)
Class: Small molecule tyrosine kinase inhibitor targeting CSF1R.
Dose: 600 mg orally twice daily with food with concomitant androgen deprivation therapy.
AEs: Fatigue, extremity pain, and rash.
Trial: ARAMIS (NCT02200614): Median metastasis free survival was 40.4 months for patients with darolutamide, compared with 18.4 months for controls.
Selinexor (Xpovio)
Class: Reversible inhibitor of nuclear export of tumor suppressor proteins, growth regulators, and mRNAs of oncogenic proteins.
Disease: Relapsed or refractory multiple myeloma. Indicated for patients who have received at least four prior therapies, including at least two immunomodulatory agents and an anti-CD38 monoclonal antibody.
Dose: 80 mg orally in combination with oral dexamethasone on days 1 and 3 of each week.
AEs: Thrombocytopenia, fatigue, pancytopenia, and hyponatremia.
Trial: STORM (NCT02336815): Overall response rate 25.3% with a median time to first response of 4 weeks and 3.8-month median duration of response.
Polatuzumab vedotin-piiq (Polivy)
Class: CD79b-directed antibody-drug conjugate.
Disease: Relapsed or refractory diffuse large B-cell lymphoma. Indicated for patients who have had at least two prior therapies.
Dose: 1.8 mg/kg intravenous infusion every 21 days for six cycles in combination with bendamustine and a rituximab product.
AEs: Pancytopenia, peripheral neuropathy.
Trial: GO29365 (NCT02257567): Complete response rate was 40% for polatuzumab vedotin-piiq plus bendamustine/rituximab, compared with 18% with bendamustine/rituximab alone.*
Caplacizumab-yhdp (Cablivi)
Class: Monoclonal antibody fragment directed against von Willebrand factor.
Disease: Thrombotic thrombocytopenic purpura.
Dose: 11 mg IV initially, then daily subcutaneously; in combination with plasma exchange and immunosuppressive therapy.
AEs: Epistaxis, headache, and gingival bleeding.
Trial: Hercules trial (NCT02553317): More rapid normalization of platelets, lower incidence of composite TTP-related death, and lower rate of recurrence when added to plasma exchange and steroids.
Disease: Hormone receptor positive HER2-negative PIK3CA-mutated, advanced or metastatic breast cancer.
Dose: 300 mg orally once daily with food with concomitant fulvestrant.
AEs: Hyperglycemia, pancytopenia.
Trial: SOLAR-1 (NCT02437318): 11-month progression-free survival among patients treated with alpelisib and fulvestrant, compared with 5.7 months in fulvestrant alone control arm; overall response rate of 36% versus 16%, respectively.
Disease: Locally advanced or metastatic urothelial carcinoma with FGFR3 or FGFR2 mutations.
Dose: 8 mg orally once daily, with or without food.
AEs: Ocular disorders including retinopathy or retinal detachment.
Trial: BLC2001 (NCT02365597): Objective response rate of 32.2%, with a complete response in 2.3% of patients and partial response in 29.9% of patients.
Biosimilar approvals
Trastuzumab and hyaluronidase-oysk (Herceptin Hylecta)
Biosimilar to: Trastuzumab.
Indication: HER2-overexpressing breast cancer.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mintzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania.
*Correction, 11/7/2019: An earlier version of this article misstated the drug combination in the GO29365 trial.
The rapid development and identification of novel drugs has translated into innovative therapies in hematology and oncology. The aim of this piece is to present newly approved drugs and expanded indications to serve as a reference guide for practicing clinicians.
This article reviews therapies that were newly approved so far in 2019, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
New approvals
Fedratinib (Inrebic)
Class: JAK2 and FLT3 selective kinase inhibitor.
Disease: Intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis.
Dose: 400 mg orally once daily, with or without food.
Adverse events (AEs): Black box warning: Fatal encephalopathy, including Wernicke’s (thiamine level monitoring suggested).
Trials: In JAKARTA (NCT01437787), 37% of patients achieved a 35% or greater reduction in spleen volume and 40% received a 50% or greater reduction in myelofibrosis-related symptoms. In Jakarta-2, there was a 55% spleen response in patients resistant or intolerant to ruxolitinib.
Disease: Solid tumors that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion and for ROS-1 positive non–small cell lung cancer (NSCLC).
Dose: 600 mg orally once daily.
AEs: Heart failure, QT prolongation, skeletal fractures, hepatotoxicity, central nervous system effects, and hyperuricemia.
Trial: ALKA, STARTRK-1 (NCT02097810) and STARTRK-2 (NCT02568267): Overall response rate of 57% for NTRK positive patients; response rate of 77% in ROS-1 positive NSCLC.
Pexidartinib (Turalio)
Class: Small molecule tyrosine kinase inhibitor targeting CSF1R.
Dose: 600 mg orally twice daily with food with concomitant androgen deprivation therapy.
AEs: Fatigue, extremity pain, and rash.
Trial: ARAMIS (NCT02200614): Median metastasis free survival was 40.4 months for patients with darolutamide, compared with 18.4 months for controls.
Selinexor (Xpovio)
Class: Reversible inhibitor of nuclear export of tumor suppressor proteins, growth regulators, and mRNAs of oncogenic proteins.
Disease: Relapsed or refractory multiple myeloma. Indicated for patients who have received at least four prior therapies, including at least two immunomodulatory agents and an anti-CD38 monoclonal antibody.
Dose: 80 mg orally in combination with oral dexamethasone on days 1 and 3 of each week.
AEs: Thrombocytopenia, fatigue, pancytopenia, and hyponatremia.
Trial: STORM (NCT02336815): Overall response rate 25.3% with a median time to first response of 4 weeks and 3.8-month median duration of response.
Polatuzumab vedotin-piiq (Polivy)
Class: CD79b-directed antibody-drug conjugate.
Disease: Relapsed or refractory diffuse large B-cell lymphoma. Indicated for patients who have had at least two prior therapies.
Dose: 1.8 mg/kg intravenous infusion every 21 days for six cycles in combination with bendamustine and a rituximab product.
AEs: Pancytopenia, peripheral neuropathy.
Trial: GO29365 (NCT02257567): Complete response rate was 40% for polatuzumab vedotin-piiq plus bendamustine/rituximab, compared with 18% with bendamustine/rituximab alone.*
Caplacizumab-yhdp (Cablivi)
Class: Monoclonal antibody fragment directed against von Willebrand factor.
Disease: Thrombotic thrombocytopenic purpura.
Dose: 11 mg IV initially, then daily subcutaneously; in combination with plasma exchange and immunosuppressive therapy.
AEs: Epistaxis, headache, and gingival bleeding.
Trial: Hercules trial (NCT02553317): More rapid normalization of platelets, lower incidence of composite TTP-related death, and lower rate of recurrence when added to plasma exchange and steroids.
Disease: Hormone receptor positive HER2-negative PIK3CA-mutated, advanced or metastatic breast cancer.
Dose: 300 mg orally once daily with food with concomitant fulvestrant.
AEs: Hyperglycemia, pancytopenia.
Trial: SOLAR-1 (NCT02437318): 11-month progression-free survival among patients treated with alpelisib and fulvestrant, compared with 5.7 months in fulvestrant alone control arm; overall response rate of 36% versus 16%, respectively.
Disease: Locally advanced or metastatic urothelial carcinoma with FGFR3 or FGFR2 mutations.
Dose: 8 mg orally once daily, with or without food.
AEs: Ocular disorders including retinopathy or retinal detachment.
Trial: BLC2001 (NCT02365597): Objective response rate of 32.2%, with a complete response in 2.3% of patients and partial response in 29.9% of patients.
Biosimilar approvals
Trastuzumab and hyaluronidase-oysk (Herceptin Hylecta)
Biosimilar to: Trastuzumab.
Indication: HER2-overexpressing breast cancer.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mintzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania.
*Correction, 11/7/2019: An earlier version of this article misstated the drug combination in the GO29365 trial.
The rapid development and identification of novel drugs has translated into innovative therapies in hematology and oncology. The aim of this piece is to present newly approved drugs and expanded indications to serve as a reference guide for practicing clinicians.
This article reviews therapies that were newly approved so far in 2019, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
New approvals
Fedratinib (Inrebic)
Class: JAK2 and FLT3 selective kinase inhibitor.
Disease: Intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis.
Dose: 400 mg orally once daily, with or without food.
Adverse events (AEs): Black box warning: Fatal encephalopathy, including Wernicke’s (thiamine level monitoring suggested).
Trials: In JAKARTA (NCT01437787), 37% of patients achieved a 35% or greater reduction in spleen volume and 40% received a 50% or greater reduction in myelofibrosis-related symptoms. In Jakarta-2, there was a 55% spleen response in patients resistant or intolerant to ruxolitinib.
Disease: Solid tumors that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion and for ROS-1 positive non–small cell lung cancer (NSCLC).
Dose: 600 mg orally once daily.
AEs: Heart failure, QT prolongation, skeletal fractures, hepatotoxicity, central nervous system effects, and hyperuricemia.
Trial: ALKA, STARTRK-1 (NCT02097810) and STARTRK-2 (NCT02568267): Overall response rate of 57% for NTRK positive patients; response rate of 77% in ROS-1 positive NSCLC.
Pexidartinib (Turalio)
Class: Small molecule tyrosine kinase inhibitor targeting CSF1R.
Dose: 600 mg orally twice daily with food with concomitant androgen deprivation therapy.
AEs: Fatigue, extremity pain, and rash.
Trial: ARAMIS (NCT02200614): Median metastasis free survival was 40.4 months for patients with darolutamide, compared with 18.4 months for controls.
Selinexor (Xpovio)
Class: Reversible inhibitor of nuclear export of tumor suppressor proteins, growth regulators, and mRNAs of oncogenic proteins.
Disease: Relapsed or refractory multiple myeloma. Indicated for patients who have received at least four prior therapies, including at least two immunomodulatory agents and an anti-CD38 monoclonal antibody.
Dose: 80 mg orally in combination with oral dexamethasone on days 1 and 3 of each week.
AEs: Thrombocytopenia, fatigue, pancytopenia, and hyponatremia.
Trial: STORM (NCT02336815): Overall response rate 25.3% with a median time to first response of 4 weeks and 3.8-month median duration of response.
Polatuzumab vedotin-piiq (Polivy)
Class: CD79b-directed antibody-drug conjugate.
Disease: Relapsed or refractory diffuse large B-cell lymphoma. Indicated for patients who have had at least two prior therapies.
Dose: 1.8 mg/kg intravenous infusion every 21 days for six cycles in combination with bendamustine and a rituximab product.
AEs: Pancytopenia, peripheral neuropathy.
Trial: GO29365 (NCT02257567): Complete response rate was 40% for polatuzumab vedotin-piiq plus bendamustine/rituximab, compared with 18% with bendamustine/rituximab alone.*
Caplacizumab-yhdp (Cablivi)
Class: Monoclonal antibody fragment directed against von Willebrand factor.
Disease: Thrombotic thrombocytopenic purpura.
Dose: 11 mg IV initially, then daily subcutaneously; in combination with plasma exchange and immunosuppressive therapy.
AEs: Epistaxis, headache, and gingival bleeding.
Trial: Hercules trial (NCT02553317): More rapid normalization of platelets, lower incidence of composite TTP-related death, and lower rate of recurrence when added to plasma exchange and steroids.
Disease: Hormone receptor positive HER2-negative PIK3CA-mutated, advanced or metastatic breast cancer.
Dose: 300 mg orally once daily with food with concomitant fulvestrant.
AEs: Hyperglycemia, pancytopenia.
Trial: SOLAR-1 (NCT02437318): 11-month progression-free survival among patients treated with alpelisib and fulvestrant, compared with 5.7 months in fulvestrant alone control arm; overall response rate of 36% versus 16%, respectively.
Disease: Locally advanced or metastatic urothelial carcinoma with FGFR3 or FGFR2 mutations.
Dose: 8 mg orally once daily, with or without food.
AEs: Ocular disorders including retinopathy or retinal detachment.
Trial: BLC2001 (NCT02365597): Objective response rate of 32.2%, with a complete response in 2.3% of patients and partial response in 29.9% of patients.
Biosimilar approvals
Trastuzumab and hyaluronidase-oysk (Herceptin Hylecta)
Biosimilar to: Trastuzumab.
Indication: HER2-overexpressing breast cancer.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mintzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania.
*Correction, 11/7/2019: An earlier version of this article misstated the drug combination in the GO29365 trial.
Patients whose clear cell renal cell carcinoma (RCC) tumors lack the cytoskeleton linker protein ezrin have a poorer prognosis, finds a single-center retrospective cohort study.
The number of small renal masses discovered incidentally is rising, and some of these tumors can or must be treated less aggressively, according to lead investigator Marcos Vinicius O. Ferrari, MD, urology division, A.C. Camargo Cancer Center, São Paulo, and coinvestigators. “Thus, it is important to identify molecular markers that have prognostic value that can assist physicians in therapeutic strategies.”
The investigators studied 575 consecutive patients who underwent radical or partial nephrectomy for clear cell RCC during 1985-2016. A single pathologist reclassified all cases and determined the most representative tumor areas for tissue immunohistochemistry for ezrin and moesin, proteins that link the actin cytoskeleton to the cell membrane and that play roles in cell adhesion, migration, and growth.
Results reported in Urologic Oncology showed that 18.3% of tumors were negative for ezrin and 2.8% were negative for moesin.
Compared with counterparts who had ezrin-positive tumors, patients with ezrin-negative tumors had higher pathologic T stage (P less than .001); were less likely to have incidentally discovered tumors (P = .007); and were more likely to have clinical stage III or IV disease (P = .012), synchronous metastasis (P less than .001), and an International Society of Urological Pathology histologic grade of 3 or 4 (P = .025).
Similarly, compared with counterparts who had moesin-positive tumors, patients with moesin-negative tumors had higher pathologic T stage (P = .025) and pathologic N stage (P = .007), and were more likely to have clinical stage III or IV disease (P = .027).
The 10-year rate of disease-specific survival was poorer for patients with ezrin-negative vs. ezrin-positive tumors (70% vs. 88%; P less than .001) and for patients with moesin-negative vs. moesin-positive tumors (68% vs. 86%; P = .065). Similarly, the 10-year rate of overall survival was poorer for patients with ezrin-negative vs. ezrin-positive tumors (68% vs. 86%; P = .001) and for patients with moesin-negative vs. moesin-positive tumors (68% vs. 84%; P = .142).
In multivariate analyses, ezrin negativity was associated with a near doubling of the risk of disease-specific survival events (hazard ratio, 1.89; 95% confidence interval, 1.11-3.20) and with a trend toward poorer overall survival. Moesin negativity was not independently associated with either outcome.
“Negative expression of ezrin was associated with major prognostic factors in renal cancer and significantly influenced tumor-related death,” Dr. Ferrari and coinvestigators summarize, noting that this aligns with the pattern seen in bladder and ovarian cancers, but contrasts with the pattern seen in head and neck, colorectal, cervical, and breast cancers.
“The exact mechanism by which negative ezrin expression influences tumor progression and survival rates is unknown,” they conclude. “We encourage further prospective studies to analyze ezrin to determine its value in the prognosis of clear cell RCC.”
Dr. Ferrari disclosed that he had no relevant conflicts of interest. The study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.
Patients whose clear cell renal cell carcinoma (RCC) tumors lack the cytoskeleton linker protein ezrin have a poorer prognosis, finds a single-center retrospective cohort study.
The number of small renal masses discovered incidentally is rising, and some of these tumors can or must be treated less aggressively, according to lead investigator Marcos Vinicius O. Ferrari, MD, urology division, A.C. Camargo Cancer Center, São Paulo, and coinvestigators. “Thus, it is important to identify molecular markers that have prognostic value that can assist physicians in therapeutic strategies.”
The investigators studied 575 consecutive patients who underwent radical or partial nephrectomy for clear cell RCC during 1985-2016. A single pathologist reclassified all cases and determined the most representative tumor areas for tissue immunohistochemistry for ezrin and moesin, proteins that link the actin cytoskeleton to the cell membrane and that play roles in cell adhesion, migration, and growth.
Results reported in Urologic Oncology showed that 18.3% of tumors were negative for ezrin and 2.8% were negative for moesin.
Compared with counterparts who had ezrin-positive tumors, patients with ezrin-negative tumors had higher pathologic T stage (P less than .001); were less likely to have incidentally discovered tumors (P = .007); and were more likely to have clinical stage III or IV disease (P = .012), synchronous metastasis (P less than .001), and an International Society of Urological Pathology histologic grade of 3 or 4 (P = .025).
Similarly, compared with counterparts who had moesin-positive tumors, patients with moesin-negative tumors had higher pathologic T stage (P = .025) and pathologic N stage (P = .007), and were more likely to have clinical stage III or IV disease (P = .027).
The 10-year rate of disease-specific survival was poorer for patients with ezrin-negative vs. ezrin-positive tumors (70% vs. 88%; P less than .001) and for patients with moesin-negative vs. moesin-positive tumors (68% vs. 86%; P = .065). Similarly, the 10-year rate of overall survival was poorer for patients with ezrin-negative vs. ezrin-positive tumors (68% vs. 86%; P = .001) and for patients with moesin-negative vs. moesin-positive tumors (68% vs. 84%; P = .142).
In multivariate analyses, ezrin negativity was associated with a near doubling of the risk of disease-specific survival events (hazard ratio, 1.89; 95% confidence interval, 1.11-3.20) and with a trend toward poorer overall survival. Moesin negativity was not independently associated with either outcome.
“Negative expression of ezrin was associated with major prognostic factors in renal cancer and significantly influenced tumor-related death,” Dr. Ferrari and coinvestigators summarize, noting that this aligns with the pattern seen in bladder and ovarian cancers, but contrasts with the pattern seen in head and neck, colorectal, cervical, and breast cancers.
“The exact mechanism by which negative ezrin expression influences tumor progression and survival rates is unknown,” they conclude. “We encourage further prospective studies to analyze ezrin to determine its value in the prognosis of clear cell RCC.”
Dr. Ferrari disclosed that he had no relevant conflicts of interest. The study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.
Patients whose clear cell renal cell carcinoma (RCC) tumors lack the cytoskeleton linker protein ezrin have a poorer prognosis, finds a single-center retrospective cohort study.
The number of small renal masses discovered incidentally is rising, and some of these tumors can or must be treated less aggressively, according to lead investigator Marcos Vinicius O. Ferrari, MD, urology division, A.C. Camargo Cancer Center, São Paulo, and coinvestigators. “Thus, it is important to identify molecular markers that have prognostic value that can assist physicians in therapeutic strategies.”
The investigators studied 575 consecutive patients who underwent radical or partial nephrectomy for clear cell RCC during 1985-2016. A single pathologist reclassified all cases and determined the most representative tumor areas for tissue immunohistochemistry for ezrin and moesin, proteins that link the actin cytoskeleton to the cell membrane and that play roles in cell adhesion, migration, and growth.
Results reported in Urologic Oncology showed that 18.3% of tumors were negative for ezrin and 2.8% were negative for moesin.
Compared with counterparts who had ezrin-positive tumors, patients with ezrin-negative tumors had higher pathologic T stage (P less than .001); were less likely to have incidentally discovered tumors (P = .007); and were more likely to have clinical stage III or IV disease (P = .012), synchronous metastasis (P less than .001), and an International Society of Urological Pathology histologic grade of 3 or 4 (P = .025).
Similarly, compared with counterparts who had moesin-positive tumors, patients with moesin-negative tumors had higher pathologic T stage (P = .025) and pathologic N stage (P = .007), and were more likely to have clinical stage III or IV disease (P = .027).
The 10-year rate of disease-specific survival was poorer for patients with ezrin-negative vs. ezrin-positive tumors (70% vs. 88%; P less than .001) and for patients with moesin-negative vs. moesin-positive tumors (68% vs. 86%; P = .065). Similarly, the 10-year rate of overall survival was poorer for patients with ezrin-negative vs. ezrin-positive tumors (68% vs. 86%; P = .001) and for patients with moesin-negative vs. moesin-positive tumors (68% vs. 84%; P = .142).
In multivariate analyses, ezrin negativity was associated with a near doubling of the risk of disease-specific survival events (hazard ratio, 1.89; 95% confidence interval, 1.11-3.20) and with a trend toward poorer overall survival. Moesin negativity was not independently associated with either outcome.
“Negative expression of ezrin was associated with major prognostic factors in renal cancer and significantly influenced tumor-related death,” Dr. Ferrari and coinvestigators summarize, noting that this aligns with the pattern seen in bladder and ovarian cancers, but contrasts with the pattern seen in head and neck, colorectal, cervical, and breast cancers.
“The exact mechanism by which negative ezrin expression influences tumor progression and survival rates is unknown,” they conclude. “We encourage further prospective studies to analyze ezrin to determine its value in the prognosis of clear cell RCC.”
Dr. Ferrari disclosed that he had no relevant conflicts of interest. The study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector.
Although most neonatal vascular lumps, bumps, and tumors are benign, proper diagnosis is important for prognosis and management. Therefore, knowledge of both common and rare conditions is important when evaluating a neonatal nodule. Differential diagnosis of neonatal vascular nodules must focus on important diagnostic clues that should prompt consideration and evaluation for less common and/or potentially threatening conditions. Infantile hemangioma (IH), congenital hemangioma (CH), venous malformation (VM), lymphatic malformation (LM), kaposiform hemangioendothelioma (KHE) and tufted angioma, and malignant tumors are reviewed here.
Infantile Hemangioma
Infantile hemangioma, a benign proliferation of capillaries, is the most common tumor of infancy with reported incidence of up to 5% in neonates.1 As such, suspicion for less common lesions is often predicated on identifying features that would be atypical for an IH. A superficial IH presents as a bright red papule, nodule, or plaque, while a deep IH presents as a flesh-colored to bluish nodule. Mixed IHs combine features of both superficial and deep lesions. The distribution may be focal or segmental, with segmental lesions encompassing a larger territory–like distribution and frequently displaying a thin, coarsely telangiectatic appearance.
Knowledge of the natural history of IH generally is crucial in differentiating it from other neonatal lesions. Infantile hemangiomas display a natural history that is distinct and predictable. They typically manifest within the first few weeks of life, though up to 30% present at birth with a premonitory mark, which may be a light red, pink, bluish, or vasoconstricted patch. Thus, mere presence of a lesion at birth is not the feature that distinguishes other congenital lesions from an IH. After initial appearance, IHs undergo a period of proliferation that occurs over 4 to 6 months in most patients. In some cases, areas of proliferation may be subtle, but nonetheless the presence of some areas of increased redness and/or volumetric growth generally is required to firmly establish the diagnosis of IH. Thereafter, IH will involute, a process that begins before 1 year of age in most cases and continues over years. Although IHs undergo involution, complete clearance may not occur, as nearly 70% will leave permanent residua such as fibrofatty masses or anetodermic skin.2 Nevertheless, the presence of a proliferative phase followed by a slower period of involution is a hallmark feature of the IH.
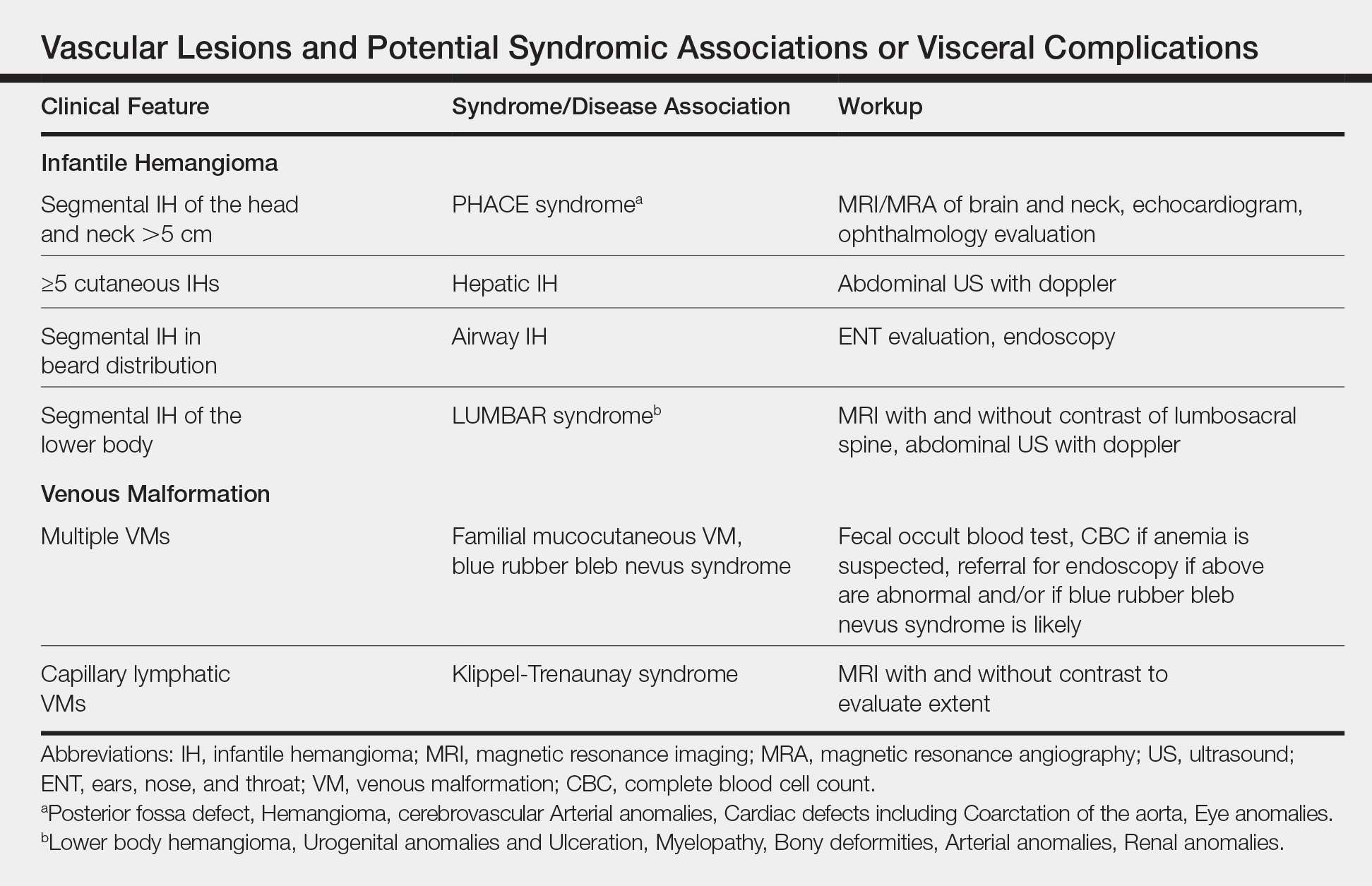
Biopsy and imaging rarely are required for establishing diagnosis of an IH. Histopathology showing a proliferation of capillaries with positive glucose transporter 1 (GLUT-1) staining is characteristic. Imaging with ultrasound reveals a fast-flow lesion. Apart from exceptionally rare cases, a cutaneous IH typically does not cross muscle fascia, and thus alternative diagnoses should be considered for a cutaneous lesion that demonstrates infiltration into nerve, bone, joint, or other deeper tissues. Most IHs do not require treatment; however, a small subset may be associated with complications and thus require intervention. Complications of IH may include impairment of function (eg, vision, feeding, respiratory), ulceration, and risk for permanent disfigurement. When treatment is indicated, the most commonly employed options during the proliferative phase are the topical beta-blocker timolol and the oral beta-blocker propranolol. In addition, certain IHs may be associated with either syndromic presentations and/or visceral involvement, thus requiring further workup (Table).
Congenital Hemangioma
A CH is an uncommon benign neonatal tumor that is distinct from an IH in behavior, biology, and treatment. Congenital hemangiomas may have a rapidly involuting course, referred to as RICH (rapidly involuting congenital hemangioma), or a noninvoluting course, referred to as NICH (noninvoluting congenital hemangioma). Partially involuting types also have been described.3 A RICH typically presents as a highly vascular, red-violaceous or bluish plaque, nodule, or large mass at birth. An NICH presents as a red-violaceous or bluish, coarsely telangiectatic patch, plaque, or nodule. A characteristic feature of the CH is the rim of vasoconstriction around the lesion, which is an important diagnostic clue (Figure 1). In contrast to IH, multifocal lesions are highly unlikely in CH, though it rarely has been reported.4
Figure 1. A rapidly involuting congenital hemangioma with a rim of pallor that is a characteristic feature.
Regardless of subtype, CHs are fully developed at birth. Infantile hemangiomas, on the other hand, are either minimally present or not present at birth and thereafter proliferate. After birth, a RICH rapidly involutes over the first 9 to 12 months of life. This process generally is evident even in the first few weeks of life, which would not be expected of an IH and is therefore a major distinguishing factor. A NICH, on the other hand, is expected to be persistent, for the most part neither showing signs of proliferation nor involution.
Complications of CHs may include ulceration, functional impairment, or risk for permanent disfigurement depending on location. In addition, due to their fast-flow state and potential large size, some CHs may be complicated by high-output heart failure in the neonate. Distinguishing an IH from a CH is important not only for prognosis but also treatment. Beta-blocker therapy generally is not useful for CHs, and management usually is supportive in the neonatal period.
In the majority of cases, diagnosis can be achieved solely on clinical features. Biopsy with immunohistochemistry shows negative GLUT-1 staining, which will distinguish this lesion from an IH. At times, the highly vascular nature and/or striking size of a CH may lead some to consider the potential diagnosis of an arteriovenous malformation. However, soft-tissue arteriovenous malformations involving the skin are almost never fully developed in the neonatal period and generally take years to evolve from a quiescent state to a destructive lesion.
Venous Malformation
Venous malformations are congenital malformations of veins that may be apparent at birth or later. They appear as bluish to flesh-colored, compressible nodules or plaques. They tend to increase in size when the affected body part is in a dependent position, and this maneuver can be a helpful distinguishing clue. Although the majority of patients have a single lesion, multifocal involvement may occur uncommonly (Table). The diagnosis of VM usually is clinical, though at times, a VM may be difficult to distinguish from a purely deep IH. However, a VM will persist over time, growing in proportion to the patient. In addition, a VM displays low flow on ultrasound, a distinguishing feature from the fast-flow IH. Magnetic resonance imaging with and without contrast is the imaging study of choice. At times, cutaneous VMs will demonstrate infiltration into other tissue planes such as muscle and joint. Pain may occur secondary to thrombus formation within the malformation. In extensive lesions, intravascular coagulation may be notable, as reflected in elevated D-dimer and decreased fibrinogen levels. Treatment with sclerotherapy or surgery may be considered in select cases during infancy; however, in general, an asymptomatic VM may be observed early on in life.
Lymphatic Malformation
A lymphatic malformation (LM) is a congenital malformation of lymphatic vessels and may be further differentiated into microcystic, macrocystic, or mixed types depending on the size of the channels. An LM may present at birth or later and persists over time. Superficial microcystic LMs, synonymous with the term lymphangioma circumscriptum, characteristically appear as a group of clear and violaceous hemorrhagic vesicles on the skin. Deeper LMs appear as a tense or spongy, flesh-colored nodule or mass. Involvement of the head and neck is common. Complications frequently occur in LMs. Cutaneous LMs may ooze or bleed. Infection and hemorrhage into cysts may occur, which will cause acute pain, redness, swelling, and induration. Cervicofacial lesions may result in respiratory distress. Thus, the majority of LMs require treatment, though asymptomatic lesions may be observed in the neonate. An ultrasound will demonstrate a low-flow lesion, and magnetic resonance imaging is the diagnostic modality of choice for diagnosis and definition of extent.
KHE and Tufted Angioma
Kaposiform hemangioendothelioma is a rare, locally aggressive, vascular tumor that is frequently associated with a potentially life-threatening coagulopathy, Kasabach-Merritt phenomenon. Tufted angiomas are now understood to belong on a spectrum with KHEs, which usually present in the neonatal period or infancy as firm, red-violaceous plaques, nodules, or large tumors. Infiltration into nerve, muscle, and bone may occur. The firm/hard nature and deep violaceous appearance generally are initial clues that it is not an IH. Kasabach-Merritt phenomenon manifests as thrombocytopenia as well as low fibrinogen and elevated D-dimer levels. Thrombocytopenia is generally profound in Kasabach-Merritt phenomenon and results from platelet trapping within the vascular tumor. Given these potential complications, KHEs generally require immediate medical attention, and various treatment protocols including prednisone, vincristine, and sirolimus are utilized for complicated cases.5 The diagnosis may require biopsy to distinguish it from malignant tumors, particularly sarcomas.
Malignant Tumors
Various malignancies, including congenital leukemia, neuroblastoma, Langerhans cell histiocytosis, infantile fibrosarcoma, and rhabdomyosarcoma, rarely may present as cutaneous nodules or masses in a neonate mimicking hemangiomas or other vascular lesions (Figure 2). Neonates may present with multiple bluish papules and nodules resembling a blueberry muffin baby; multiple violaceous-red nodules; or a single red-violaceous, highly vascular–appearing mass mimicking hemangiomas. Malignant tumors may display vascularity on imaging, and thus the presence of vascular flow on ultrasound should not dissuade one from the possibility of a malignancy if other clinical features are atypical or unusual for a hemangioma. When a neonatal malignancy is suspected, a large punch biopsy or incisional biopsy is required for workup.
Figure 2. A vascular-appearing nodule with infiltrative edges in an infant. Biopsy showed a spindle cell sarcoma.
Final Thoughts
Although IHs are the most common vascular nodules in neonates and young infants, other conditions such as VMs, LMs, CHs, KHEs, and malignancy may occur less commonly. Identifying features that would be considered atypical for IH is crucial to recognize these less common possibilities.
References
Kanada KN, Merin MR, Munden A, et al. A prospective study of cutaneous findings in newborns in the United States: correlation with race, ethnicity, and gestational status using updated classification and nomenclature. J Pediatr. 2012;161:240-245.
Darrow DH, Greene AK, Mancini AJ, et al. Diagnosis and management of infantile hemangioma. Pediatrics. 2015;136:E1060-E1104.
Nasseri E, Piram M, McCuaig CC, et al. Partially involuting congenital hemangiomas: a report of 8 cases and review of the literature. J Am Acad Dermatol. 2014;70:75-79.
Blumenthal S, Stefanko N, Cossio M, et al. Multifocal congenital hemangioma: expanding the pathogenesis of “neonatal hemangiomatosis.” Pediatr Dermatol. 2019;36:720-722.
Croteau SE, Gupta D. The clinical spectrum of kaposiform hemangioendothelioma and tufted angioma. Semin Cutan Med Surg. 2016;35:147-152.
Although most neonatal vascular lumps, bumps, and tumors are benign, proper diagnosis is important for prognosis and management. Therefore, knowledge of both common and rare conditions is important when evaluating a neonatal nodule. Differential diagnosis of neonatal vascular nodules must focus on important diagnostic clues that should prompt consideration and evaluation for less common and/or potentially threatening conditions. Infantile hemangioma (IH), congenital hemangioma (CH), venous malformation (VM), lymphatic malformation (LM), kaposiform hemangioendothelioma (KHE) and tufted angioma, and malignant tumors are reviewed here.
Infantile Hemangioma
Infantile hemangioma, a benign proliferation of capillaries, is the most common tumor of infancy with reported incidence of up to 5% in neonates.1 As such, suspicion for less common lesions is often predicated on identifying features that would be atypical for an IH. A superficial IH presents as a bright red papule, nodule, or plaque, while a deep IH presents as a flesh-colored to bluish nodule. Mixed IHs combine features of both superficial and deep lesions. The distribution may be focal or segmental, with segmental lesions encompassing a larger territory–like distribution and frequently displaying a thin, coarsely telangiectatic appearance.
Knowledge of the natural history of IH generally is crucial in differentiating it from other neonatal lesions. Infantile hemangiomas display a natural history that is distinct and predictable. They typically manifest within the first few weeks of life, though up to 30% present at birth with a premonitory mark, which may be a light red, pink, bluish, or vasoconstricted patch. Thus, mere presence of a lesion at birth is not the feature that distinguishes other congenital lesions from an IH. After initial appearance, IHs undergo a period of proliferation that occurs over 4 to 6 months in most patients. In some cases, areas of proliferation may be subtle, but nonetheless the presence of some areas of increased redness and/or volumetric growth generally is required to firmly establish the diagnosis of IH. Thereafter, IH will involute, a process that begins before 1 year of age in most cases and continues over years. Although IHs undergo involution, complete clearance may not occur, as nearly 70% will leave permanent residua such as fibrofatty masses or anetodermic skin.2 Nevertheless, the presence of a proliferative phase followed by a slower period of involution is a hallmark feature of the IH.
Biopsy and imaging rarely are required for establishing diagnosis of an IH. Histopathology showing a proliferation of capillaries with positive glucose transporter 1 (GLUT-1) staining is characteristic. Imaging with ultrasound reveals a fast-flow lesion. Apart from exceptionally rare cases, a cutaneous IH typically does not cross muscle fascia, and thus alternative diagnoses should be considered for a cutaneous lesion that demonstrates infiltration into nerve, bone, joint, or other deeper tissues. Most IHs do not require treatment; however, a small subset may be associated with complications and thus require intervention. Complications of IH may include impairment of function (eg, vision, feeding, respiratory), ulceration, and risk for permanent disfigurement. When treatment is indicated, the most commonly employed options during the proliferative phase are the topical beta-blocker timolol and the oral beta-blocker propranolol. In addition, certain IHs may be associated with either syndromic presentations and/or visceral involvement, thus requiring further workup (Table).
Congenital Hemangioma
A CH is an uncommon benign neonatal tumor that is distinct from an IH in behavior, biology, and treatment. Congenital hemangiomas may have a rapidly involuting course, referred to as RICH (rapidly involuting congenital hemangioma), or a noninvoluting course, referred to as NICH (noninvoluting congenital hemangioma). Partially involuting types also have been described.3 A RICH typically presents as a highly vascular, red-violaceous or bluish plaque, nodule, or large mass at birth. An NICH presents as a red-violaceous or bluish, coarsely telangiectatic patch, plaque, or nodule. A characteristic feature of the CH is the rim of vasoconstriction around the lesion, which is an important diagnostic clue (Figure 1). In contrast to IH, multifocal lesions are highly unlikely in CH, though it rarely has been reported.4
Figure 1. A rapidly involuting congenital hemangioma with a rim of pallor that is a characteristic feature.
Regardless of subtype, CHs are fully developed at birth. Infantile hemangiomas, on the other hand, are either minimally present or not present at birth and thereafter proliferate. After birth, a RICH rapidly involutes over the first 9 to 12 months of life. This process generally is evident even in the first few weeks of life, which would not be expected of an IH and is therefore a major distinguishing factor. A NICH, on the other hand, is expected to be persistent, for the most part neither showing signs of proliferation nor involution.
Complications of CHs may include ulceration, functional impairment, or risk for permanent disfigurement depending on location. In addition, due to their fast-flow state and potential large size, some CHs may be complicated by high-output heart failure in the neonate. Distinguishing an IH from a CH is important not only for prognosis but also treatment. Beta-blocker therapy generally is not useful for CHs, and management usually is supportive in the neonatal period.
In the majority of cases, diagnosis can be achieved solely on clinical features. Biopsy with immunohistochemistry shows negative GLUT-1 staining, which will distinguish this lesion from an IH. At times, the highly vascular nature and/or striking size of a CH may lead some to consider the potential diagnosis of an arteriovenous malformation. However, soft-tissue arteriovenous malformations involving the skin are almost never fully developed in the neonatal period and generally take years to evolve from a quiescent state to a destructive lesion.
Venous Malformation
Venous malformations are congenital malformations of veins that may be apparent at birth or later. They appear as bluish to flesh-colored, compressible nodules or plaques. They tend to increase in size when the affected body part is in a dependent position, and this maneuver can be a helpful distinguishing clue. Although the majority of patients have a single lesion, multifocal involvement may occur uncommonly (Table). The diagnosis of VM usually is clinical, though at times, a VM may be difficult to distinguish from a purely deep IH. However, a VM will persist over time, growing in proportion to the patient. In addition, a VM displays low flow on ultrasound, a distinguishing feature from the fast-flow IH. Magnetic resonance imaging with and without contrast is the imaging study of choice. At times, cutaneous VMs will demonstrate infiltration into other tissue planes such as muscle and joint. Pain may occur secondary to thrombus formation within the malformation. In extensive lesions, intravascular coagulation may be notable, as reflected in elevated D-dimer and decreased fibrinogen levels. Treatment with sclerotherapy or surgery may be considered in select cases during infancy; however, in general, an asymptomatic VM may be observed early on in life.
Lymphatic Malformation
A lymphatic malformation (LM) is a congenital malformation of lymphatic vessels and may be further differentiated into microcystic, macrocystic, or mixed types depending on the size of the channels. An LM may present at birth or later and persists over time. Superficial microcystic LMs, synonymous with the term lymphangioma circumscriptum, characteristically appear as a group of clear and violaceous hemorrhagic vesicles on the skin. Deeper LMs appear as a tense or spongy, flesh-colored nodule or mass. Involvement of the head and neck is common. Complications frequently occur in LMs. Cutaneous LMs may ooze or bleed. Infection and hemorrhage into cysts may occur, which will cause acute pain, redness, swelling, and induration. Cervicofacial lesions may result in respiratory distress. Thus, the majority of LMs require treatment, though asymptomatic lesions may be observed in the neonate. An ultrasound will demonstrate a low-flow lesion, and magnetic resonance imaging is the diagnostic modality of choice for diagnosis and definition of extent.
KHE and Tufted Angioma
Kaposiform hemangioendothelioma is a rare, locally aggressive, vascular tumor that is frequently associated with a potentially life-threatening coagulopathy, Kasabach-Merritt phenomenon. Tufted angiomas are now understood to belong on a spectrum with KHEs, which usually present in the neonatal period or infancy as firm, red-violaceous plaques, nodules, or large tumors. Infiltration into nerve, muscle, and bone may occur. The firm/hard nature and deep violaceous appearance generally are initial clues that it is not an IH. Kasabach-Merritt phenomenon manifests as thrombocytopenia as well as low fibrinogen and elevated D-dimer levels. Thrombocytopenia is generally profound in Kasabach-Merritt phenomenon and results from platelet trapping within the vascular tumor. Given these potential complications, KHEs generally require immediate medical attention, and various treatment protocols including prednisone, vincristine, and sirolimus are utilized for complicated cases.5 The diagnosis may require biopsy to distinguish it from malignant tumors, particularly sarcomas.
Malignant Tumors
Various malignancies, including congenital leukemia, neuroblastoma, Langerhans cell histiocytosis, infantile fibrosarcoma, and rhabdomyosarcoma, rarely may present as cutaneous nodules or masses in a neonate mimicking hemangiomas or other vascular lesions (Figure 2). Neonates may present with multiple bluish papules and nodules resembling a blueberry muffin baby; multiple violaceous-red nodules; or a single red-violaceous, highly vascular–appearing mass mimicking hemangiomas. Malignant tumors may display vascularity on imaging, and thus the presence of vascular flow on ultrasound should not dissuade one from the possibility of a malignancy if other clinical features are atypical or unusual for a hemangioma. When a neonatal malignancy is suspected, a large punch biopsy or incisional biopsy is required for workup.
Figure 2. A vascular-appearing nodule with infiltrative edges in an infant. Biopsy showed a spindle cell sarcoma.
Final Thoughts
Although IHs are the most common vascular nodules in neonates and young infants, other conditions such as VMs, LMs, CHs, KHEs, and malignancy may occur less commonly. Identifying features that would be considered atypical for IH is crucial to recognize these less common possibilities.
Although most neonatal vascular lumps, bumps, and tumors are benign, proper diagnosis is important for prognosis and management. Therefore, knowledge of both common and rare conditions is important when evaluating a neonatal nodule. Differential diagnosis of neonatal vascular nodules must focus on important diagnostic clues that should prompt consideration and evaluation for less common and/or potentially threatening conditions. Infantile hemangioma (IH), congenital hemangioma (CH), venous malformation (VM), lymphatic malformation (LM), kaposiform hemangioendothelioma (KHE) and tufted angioma, and malignant tumors are reviewed here.
Infantile Hemangioma
Infantile hemangioma, a benign proliferation of capillaries, is the most common tumor of infancy with reported incidence of up to 5% in neonates.1 As such, suspicion for less common lesions is often predicated on identifying features that would be atypical for an IH. A superficial IH presents as a bright red papule, nodule, or plaque, while a deep IH presents as a flesh-colored to bluish nodule. Mixed IHs combine features of both superficial and deep lesions. The distribution may be focal or segmental, with segmental lesions encompassing a larger territory–like distribution and frequently displaying a thin, coarsely telangiectatic appearance.
Knowledge of the natural history of IH generally is crucial in differentiating it from other neonatal lesions. Infantile hemangiomas display a natural history that is distinct and predictable. They typically manifest within the first few weeks of life, though up to 30% present at birth with a premonitory mark, which may be a light red, pink, bluish, or vasoconstricted patch. Thus, mere presence of a lesion at birth is not the feature that distinguishes other congenital lesions from an IH. After initial appearance, IHs undergo a period of proliferation that occurs over 4 to 6 months in most patients. In some cases, areas of proliferation may be subtle, but nonetheless the presence of some areas of increased redness and/or volumetric growth generally is required to firmly establish the diagnosis of IH. Thereafter, IH will involute, a process that begins before 1 year of age in most cases and continues over years. Although IHs undergo involution, complete clearance may not occur, as nearly 70% will leave permanent residua such as fibrofatty masses or anetodermic skin.2 Nevertheless, the presence of a proliferative phase followed by a slower period of involution is a hallmark feature of the IH.
Biopsy and imaging rarely are required for establishing diagnosis of an IH. Histopathology showing a proliferation of capillaries with positive glucose transporter 1 (GLUT-1) staining is characteristic. Imaging with ultrasound reveals a fast-flow lesion. Apart from exceptionally rare cases, a cutaneous IH typically does not cross muscle fascia, and thus alternative diagnoses should be considered for a cutaneous lesion that demonstrates infiltration into nerve, bone, joint, or other deeper tissues. Most IHs do not require treatment; however, a small subset may be associated with complications and thus require intervention. Complications of IH may include impairment of function (eg, vision, feeding, respiratory), ulceration, and risk for permanent disfigurement. When treatment is indicated, the most commonly employed options during the proliferative phase are the topical beta-blocker timolol and the oral beta-blocker propranolol. In addition, certain IHs may be associated with either syndromic presentations and/or visceral involvement, thus requiring further workup (Table).
Congenital Hemangioma
A CH is an uncommon benign neonatal tumor that is distinct from an IH in behavior, biology, and treatment. Congenital hemangiomas may have a rapidly involuting course, referred to as RICH (rapidly involuting congenital hemangioma), or a noninvoluting course, referred to as NICH (noninvoluting congenital hemangioma). Partially involuting types also have been described.3 A RICH typically presents as a highly vascular, red-violaceous or bluish plaque, nodule, or large mass at birth. An NICH presents as a red-violaceous or bluish, coarsely telangiectatic patch, plaque, or nodule. A characteristic feature of the CH is the rim of vasoconstriction around the lesion, which is an important diagnostic clue (Figure 1). In contrast to IH, multifocal lesions are highly unlikely in CH, though it rarely has been reported.4
Figure 1. A rapidly involuting congenital hemangioma with a rim of pallor that is a characteristic feature.
Regardless of subtype, CHs are fully developed at birth. Infantile hemangiomas, on the other hand, are either minimally present or not present at birth and thereafter proliferate. After birth, a RICH rapidly involutes over the first 9 to 12 months of life. This process generally is evident even in the first few weeks of life, which would not be expected of an IH and is therefore a major distinguishing factor. A NICH, on the other hand, is expected to be persistent, for the most part neither showing signs of proliferation nor involution.
Complications of CHs may include ulceration, functional impairment, or risk for permanent disfigurement depending on location. In addition, due to their fast-flow state and potential large size, some CHs may be complicated by high-output heart failure in the neonate. Distinguishing an IH from a CH is important not only for prognosis but also treatment. Beta-blocker therapy generally is not useful for CHs, and management usually is supportive in the neonatal period.
In the majority of cases, diagnosis can be achieved solely on clinical features. Biopsy with immunohistochemistry shows negative GLUT-1 staining, which will distinguish this lesion from an IH. At times, the highly vascular nature and/or striking size of a CH may lead some to consider the potential diagnosis of an arteriovenous malformation. However, soft-tissue arteriovenous malformations involving the skin are almost never fully developed in the neonatal period and generally take years to evolve from a quiescent state to a destructive lesion.
Venous Malformation
Venous malformations are congenital malformations of veins that may be apparent at birth or later. They appear as bluish to flesh-colored, compressible nodules or plaques. They tend to increase in size when the affected body part is in a dependent position, and this maneuver can be a helpful distinguishing clue. Although the majority of patients have a single lesion, multifocal involvement may occur uncommonly (Table). The diagnosis of VM usually is clinical, though at times, a VM may be difficult to distinguish from a purely deep IH. However, a VM will persist over time, growing in proportion to the patient. In addition, a VM displays low flow on ultrasound, a distinguishing feature from the fast-flow IH. Magnetic resonance imaging with and without contrast is the imaging study of choice. At times, cutaneous VMs will demonstrate infiltration into other tissue planes such as muscle and joint. Pain may occur secondary to thrombus formation within the malformation. In extensive lesions, intravascular coagulation may be notable, as reflected in elevated D-dimer and decreased fibrinogen levels. Treatment with sclerotherapy or surgery may be considered in select cases during infancy; however, in general, an asymptomatic VM may be observed early on in life.
Lymphatic Malformation
A lymphatic malformation (LM) is a congenital malformation of lymphatic vessels and may be further differentiated into microcystic, macrocystic, or mixed types depending on the size of the channels. An LM may present at birth or later and persists over time. Superficial microcystic LMs, synonymous with the term lymphangioma circumscriptum, characteristically appear as a group of clear and violaceous hemorrhagic vesicles on the skin. Deeper LMs appear as a tense or spongy, flesh-colored nodule or mass. Involvement of the head and neck is common. Complications frequently occur in LMs. Cutaneous LMs may ooze or bleed. Infection and hemorrhage into cysts may occur, which will cause acute pain, redness, swelling, and induration. Cervicofacial lesions may result in respiratory distress. Thus, the majority of LMs require treatment, though asymptomatic lesions may be observed in the neonate. An ultrasound will demonstrate a low-flow lesion, and magnetic resonance imaging is the diagnostic modality of choice for diagnosis and definition of extent.
KHE and Tufted Angioma
Kaposiform hemangioendothelioma is a rare, locally aggressive, vascular tumor that is frequently associated with a potentially life-threatening coagulopathy, Kasabach-Merritt phenomenon. Tufted angiomas are now understood to belong on a spectrum with KHEs, which usually present in the neonatal period or infancy as firm, red-violaceous plaques, nodules, or large tumors. Infiltration into nerve, muscle, and bone may occur. The firm/hard nature and deep violaceous appearance generally are initial clues that it is not an IH. Kasabach-Merritt phenomenon manifests as thrombocytopenia as well as low fibrinogen and elevated D-dimer levels. Thrombocytopenia is generally profound in Kasabach-Merritt phenomenon and results from platelet trapping within the vascular tumor. Given these potential complications, KHEs generally require immediate medical attention, and various treatment protocols including prednisone, vincristine, and sirolimus are utilized for complicated cases.5 The diagnosis may require biopsy to distinguish it from malignant tumors, particularly sarcomas.
Malignant Tumors
Various malignancies, including congenital leukemia, neuroblastoma, Langerhans cell histiocytosis, infantile fibrosarcoma, and rhabdomyosarcoma, rarely may present as cutaneous nodules or masses in a neonate mimicking hemangiomas or other vascular lesions (Figure 2). Neonates may present with multiple bluish papules and nodules resembling a blueberry muffin baby; multiple violaceous-red nodules; or a single red-violaceous, highly vascular–appearing mass mimicking hemangiomas. Malignant tumors may display vascularity on imaging, and thus the presence of vascular flow on ultrasound should not dissuade one from the possibility of a malignancy if other clinical features are atypical or unusual for a hemangioma. When a neonatal malignancy is suspected, a large punch biopsy or incisional biopsy is required for workup.
Figure 2. A vascular-appearing nodule with infiltrative edges in an infant. Biopsy showed a spindle cell sarcoma.
Final Thoughts
Although IHs are the most common vascular nodules in neonates and young infants, other conditions such as VMs, LMs, CHs, KHEs, and malignancy may occur less commonly. Identifying features that would be considered atypical for IH is crucial to recognize these less common possibilities.
References
Kanada KN, Merin MR, Munden A, et al. A prospective study of cutaneous findings in newborns in the United States: correlation with race, ethnicity, and gestational status using updated classification and nomenclature. J Pediatr. 2012;161:240-245.
Darrow DH, Greene AK, Mancini AJ, et al. Diagnosis and management of infantile hemangioma. Pediatrics. 2015;136:E1060-E1104.
Nasseri E, Piram M, McCuaig CC, et al. Partially involuting congenital hemangiomas: a report of 8 cases and review of the literature. J Am Acad Dermatol. 2014;70:75-79.
Blumenthal S, Stefanko N, Cossio M, et al. Multifocal congenital hemangioma: expanding the pathogenesis of “neonatal hemangiomatosis.” Pediatr Dermatol. 2019;36:720-722.
Croteau SE, Gupta D. The clinical spectrum of kaposiform hemangioendothelioma and tufted angioma. Semin Cutan Med Surg. 2016;35:147-152.
References
Kanada KN, Merin MR, Munden A, et al. A prospective study of cutaneous findings in newborns in the United States: correlation with race, ethnicity, and gestational status using updated classification and nomenclature. J Pediatr. 2012;161:240-245.
Darrow DH, Greene AK, Mancini AJ, et al. Diagnosis and management of infantile hemangioma. Pediatrics. 2015;136:E1060-E1104.
Nasseri E, Piram M, McCuaig CC, et al. Partially involuting congenital hemangiomas: a report of 8 cases and review of the literature. J Am Acad Dermatol. 2014;70:75-79.
Blumenthal S, Stefanko N, Cossio M, et al. Multifocal congenital hemangioma: expanding the pathogenesis of “neonatal hemangiomatosis.” Pediatr Dermatol. 2019;36:720-722.
Croteau SE, Gupta D. The clinical spectrum of kaposiform hemangioendothelioma and tufted angioma. Semin Cutan Med Surg. 2016;35:147-152.
While the symptoms of Takayasu’s and giant cell arteritis do not differ greatly, they are associated with different imaging findings of vascular inflammation and luminal damage, a retrospective cohort study has found.
“Clinical symptoms were not sensitive markers of underlying vascular pathology but were specific when present,” Despina Michailidou, MD, PhD, and colleagues wrote in Annals of the Rheumatic Diseases. “Vascular imaging should be considered in the management of these patients since reliance on the presence of clinical symptoms may not be sensitive to detect vascular pathology within an acceptable window to prevent or minimize damage.”
Dr. Michailidou and coauthors in the Systemic Autoimmunity Branch of the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) examined the relationships between clinical presentation and imaging findings in 110 patients involved in an ongoing observational cohort study at the National Institutes of Health, including 56 with Takayasu’s arteritis (TAK) and 54 with giant cell arteritis (GCA). The study included data from 270 visits. Dr. Michailidou conducted the study while she was a research fellow at NIAMS, and she is now a rheumatology fellow at the University of Washington, Seattle.
The team looked at 11 symptoms (lightheadedness, positional lightheadedness, carotidynia, arm claudication vertigo, frontotemporal and posterior headache, posterior neck pain, blurred vision, vision loss, and major CNS events, including stroke, transient ischemic attack, or syncope). These were related to findings on MR angiography (MRA) and 18F-fluorodeoxyglucose PET (FDG-PET).
There were no significant between-group differences in six of the symptoms. However, those with TAK had significantly higher rates of carotidynia (21% vs. 0%), lightheadedness (30% vs. 9%), positional lightheadedness (29% vs. 5%), major CNS events (25% vs. 9%), and arm claudication (52% vs. 28%). Arm claudication was the most common symptom in those with TAK (52%), and blurred vision the most common in patients with GCA (37%).
On the day of evaluation, 8% of patients with TAK reported carotidynia; none of the GCA patients reported this. On FDG-PET, carotidynia was more strongly associated with inflammation of the carotid artery than with damage of the carotid artery on MRA.
The sensitivity of this association was low, which indicates “that an absence of carotidynia could still be associated with imaging abnormalities in the carotid artery, particularly on MRA compared with FDG-PET,” the authors wrote. But specificity was high for both FDG-PET and MRA, suggesting that carotidynia was strongly associated with corresponding carotid artery abnormalities on both FDG-PET and MRA.
More of those with GCA than those with TAK reported posterior neck pain (18% vs. 7%). It was significantly associated with vertebral artery inflammation in those with GCA, but not in those with TAK. There was no significant association with vertebral artery damage in either group.
While sensitivity was low for posterior neck pain and imaging abnormalities, specificity was very high in both groups, which indicates “the presence of posterior neck pain was strongly associated with corresponding vertebral artery abnormalities on both FDG-PET and MRA.”
Posterior headache was present in 5% of GCA patients and was significantly associated with vertebral artery damage, but it was not associated with such damage in patients with TAK.
“While posterior headaches in the occipital region are uncommon in patients with GCA, this study emphasizes that presence of a posterior headache should alert the clinician to the likelihood of associated vascular inflammation and damage in the corresponding vertebral artery,” the researchers wrote.
About 6% of patients with TAK and 10% of those with GCA reported frontotemporal headache. The headache was not associated with carotid PET activity or damage in either group of patients.
“While frontotemporal headaches frequently occur in patients with TAK, and are a cardinal feature of GCA, headaches in this region may reflect inflammation in smaller branches of cranial arteries, rather than the corresponding larger arteries of the neck,” the investigators wrote.
Arm claudication was the most commonly reported symptom overall, present in 52% of those with TAK and 28% of those with GCA. It was more strongly associated with subclavian artery damage on MRA than with inflammation on FDG-PET.
The investigators also assessed the association between specific clinical symptoms and the number of affected neck arteries. Patients with large vessel vasculitis and an increased number of damaged neck arteries on MRA were significantly more likely to experience lightheadedness (odds ratio, 2.61), positional lightheadedness (OR, 3.51), or a major CNS event (OR, 3.23). But those with large vessel vasculitis and inflamed neck arteries on FDG-PET were more likely to experience posterior headache (OR, 2.84).
The study isn’t intended to dictate how MRA and FDG-PET should be employed with these patients, the authors noted.
“Rather, these findings may help clinicians predict imaging pathology in specific vascular territories based on patient-reported symptoms and may inform which type of imaging modality would be the most useful to obtain in certain clinical scenarios, recognizing that additional sequences to detect wall morphology may augment the ability of MR-based assessments to detect vascular inflammation in addition to luminal damage.”
The Division of Intramural Research at NIAMS funded the research. The authors had no financial disclosures.
While the symptoms of Takayasu’s and giant cell arteritis do not differ greatly, they are associated with different imaging findings of vascular inflammation and luminal damage, a retrospective cohort study has found.
“Clinical symptoms were not sensitive markers of underlying vascular pathology but were specific when present,” Despina Michailidou, MD, PhD, and colleagues wrote in Annals of the Rheumatic Diseases. “Vascular imaging should be considered in the management of these patients since reliance on the presence of clinical symptoms may not be sensitive to detect vascular pathology within an acceptable window to prevent or minimize damage.”
Dr. Michailidou and coauthors in the Systemic Autoimmunity Branch of the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) examined the relationships between clinical presentation and imaging findings in 110 patients involved in an ongoing observational cohort study at the National Institutes of Health, including 56 with Takayasu’s arteritis (TAK) and 54 with giant cell arteritis (GCA). The study included data from 270 visits. Dr. Michailidou conducted the study while she was a research fellow at NIAMS, and she is now a rheumatology fellow at the University of Washington, Seattle.
The team looked at 11 symptoms (lightheadedness, positional lightheadedness, carotidynia, arm claudication vertigo, frontotemporal and posterior headache, posterior neck pain, blurred vision, vision loss, and major CNS events, including stroke, transient ischemic attack, or syncope). These were related to findings on MR angiography (MRA) and 18F-fluorodeoxyglucose PET (FDG-PET).
There were no significant between-group differences in six of the symptoms. However, those with TAK had significantly higher rates of carotidynia (21% vs. 0%), lightheadedness (30% vs. 9%), positional lightheadedness (29% vs. 5%), major CNS events (25% vs. 9%), and arm claudication (52% vs. 28%). Arm claudication was the most common symptom in those with TAK (52%), and blurred vision the most common in patients with GCA (37%).
On the day of evaluation, 8% of patients with TAK reported carotidynia; none of the GCA patients reported this. On FDG-PET, carotidynia was more strongly associated with inflammation of the carotid artery than with damage of the carotid artery on MRA.
The sensitivity of this association was low, which indicates “that an absence of carotidynia could still be associated with imaging abnormalities in the carotid artery, particularly on MRA compared with FDG-PET,” the authors wrote. But specificity was high for both FDG-PET and MRA, suggesting that carotidynia was strongly associated with corresponding carotid artery abnormalities on both FDG-PET and MRA.
More of those with GCA than those with TAK reported posterior neck pain (18% vs. 7%). It was significantly associated with vertebral artery inflammation in those with GCA, but not in those with TAK. There was no significant association with vertebral artery damage in either group.
While sensitivity was low for posterior neck pain and imaging abnormalities, specificity was very high in both groups, which indicates “the presence of posterior neck pain was strongly associated with corresponding vertebral artery abnormalities on both FDG-PET and MRA.”
Posterior headache was present in 5% of GCA patients and was significantly associated with vertebral artery damage, but it was not associated with such damage in patients with TAK.
“While posterior headaches in the occipital region are uncommon in patients with GCA, this study emphasizes that presence of a posterior headache should alert the clinician to the likelihood of associated vascular inflammation and damage in the corresponding vertebral artery,” the researchers wrote.
About 6% of patients with TAK and 10% of those with GCA reported frontotemporal headache. The headache was not associated with carotid PET activity or damage in either group of patients.
“While frontotemporal headaches frequently occur in patients with TAK, and are a cardinal feature of GCA, headaches in this region may reflect inflammation in smaller branches of cranial arteries, rather than the corresponding larger arteries of the neck,” the investigators wrote.
Arm claudication was the most commonly reported symptom overall, present in 52% of those with TAK and 28% of those with GCA. It was more strongly associated with subclavian artery damage on MRA than with inflammation on FDG-PET.
The investigators also assessed the association between specific clinical symptoms and the number of affected neck arteries. Patients with large vessel vasculitis and an increased number of damaged neck arteries on MRA were significantly more likely to experience lightheadedness (odds ratio, 2.61), positional lightheadedness (OR, 3.51), or a major CNS event (OR, 3.23). But those with large vessel vasculitis and inflamed neck arteries on FDG-PET were more likely to experience posterior headache (OR, 2.84).
The study isn’t intended to dictate how MRA and FDG-PET should be employed with these patients, the authors noted.
“Rather, these findings may help clinicians predict imaging pathology in specific vascular territories based on patient-reported symptoms and may inform which type of imaging modality would be the most useful to obtain in certain clinical scenarios, recognizing that additional sequences to detect wall morphology may augment the ability of MR-based assessments to detect vascular inflammation in addition to luminal damage.”
The Division of Intramural Research at NIAMS funded the research. The authors had no financial disclosures.
While the symptoms of Takayasu’s and giant cell arteritis do not differ greatly, they are associated with different imaging findings of vascular inflammation and luminal damage, a retrospective cohort study has found.
“Clinical symptoms were not sensitive markers of underlying vascular pathology but were specific when present,” Despina Michailidou, MD, PhD, and colleagues wrote in Annals of the Rheumatic Diseases. “Vascular imaging should be considered in the management of these patients since reliance on the presence of clinical symptoms may not be sensitive to detect vascular pathology within an acceptable window to prevent or minimize damage.”
Dr. Michailidou and coauthors in the Systemic Autoimmunity Branch of the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) examined the relationships between clinical presentation and imaging findings in 110 patients involved in an ongoing observational cohort study at the National Institutes of Health, including 56 with Takayasu’s arteritis (TAK) and 54 with giant cell arteritis (GCA). The study included data from 270 visits. Dr. Michailidou conducted the study while she was a research fellow at NIAMS, and she is now a rheumatology fellow at the University of Washington, Seattle.
The team looked at 11 symptoms (lightheadedness, positional lightheadedness, carotidynia, arm claudication vertigo, frontotemporal and posterior headache, posterior neck pain, blurred vision, vision loss, and major CNS events, including stroke, transient ischemic attack, or syncope). These were related to findings on MR angiography (MRA) and 18F-fluorodeoxyglucose PET (FDG-PET).
There were no significant between-group differences in six of the symptoms. However, those with TAK had significantly higher rates of carotidynia (21% vs. 0%), lightheadedness (30% vs. 9%), positional lightheadedness (29% vs. 5%), major CNS events (25% vs. 9%), and arm claudication (52% vs. 28%). Arm claudication was the most common symptom in those with TAK (52%), and blurred vision the most common in patients with GCA (37%).
On the day of evaluation, 8% of patients with TAK reported carotidynia; none of the GCA patients reported this. On FDG-PET, carotidynia was more strongly associated with inflammation of the carotid artery than with damage of the carotid artery on MRA.
The sensitivity of this association was low, which indicates “that an absence of carotidynia could still be associated with imaging abnormalities in the carotid artery, particularly on MRA compared with FDG-PET,” the authors wrote. But specificity was high for both FDG-PET and MRA, suggesting that carotidynia was strongly associated with corresponding carotid artery abnormalities on both FDG-PET and MRA.
More of those with GCA than those with TAK reported posterior neck pain (18% vs. 7%). It was significantly associated with vertebral artery inflammation in those with GCA, but not in those with TAK. There was no significant association with vertebral artery damage in either group.
While sensitivity was low for posterior neck pain and imaging abnormalities, specificity was very high in both groups, which indicates “the presence of posterior neck pain was strongly associated with corresponding vertebral artery abnormalities on both FDG-PET and MRA.”
Posterior headache was present in 5% of GCA patients and was significantly associated with vertebral artery damage, but it was not associated with such damage in patients with TAK.
“While posterior headaches in the occipital region are uncommon in patients with GCA, this study emphasizes that presence of a posterior headache should alert the clinician to the likelihood of associated vascular inflammation and damage in the corresponding vertebral artery,” the researchers wrote.
About 6% of patients with TAK and 10% of those with GCA reported frontotemporal headache. The headache was not associated with carotid PET activity or damage in either group of patients.
“While frontotemporal headaches frequently occur in patients with TAK, and are a cardinal feature of GCA, headaches in this region may reflect inflammation in smaller branches of cranial arteries, rather than the corresponding larger arteries of the neck,” the investigators wrote.
Arm claudication was the most commonly reported symptom overall, present in 52% of those with TAK and 28% of those with GCA. It was more strongly associated with subclavian artery damage on MRA than with inflammation on FDG-PET.
The investigators also assessed the association between specific clinical symptoms and the number of affected neck arteries. Patients with large vessel vasculitis and an increased number of damaged neck arteries on MRA were significantly more likely to experience lightheadedness (odds ratio, 2.61), positional lightheadedness (OR, 3.51), or a major CNS event (OR, 3.23). But those with large vessel vasculitis and inflamed neck arteries on FDG-PET were more likely to experience posterior headache (OR, 2.84).
The study isn’t intended to dictate how MRA and FDG-PET should be employed with these patients, the authors noted.
“Rather, these findings may help clinicians predict imaging pathology in specific vascular territories based on patient-reported symptoms and may inform which type of imaging modality would be the most useful to obtain in certain clinical scenarios, recognizing that additional sequences to detect wall morphology may augment the ability of MR-based assessments to detect vascular inflammation in addition to luminal damage.”
The Division of Intramural Research at NIAMS funded the research. The authors had no financial disclosures.
Key clinical point: The associations between findings on MR angiography (MRA) and 18F-fluorodeoxyglucose (FDG) PET and differing clinical symptom presentations in patients with Takayasu’s arteritis and those with giant cell arteritis may be used to predict imaging pathology.
Major finding: Arm claudication was the most commonly reported symptom overall, present in 52% of those with Takayasu’s arteritis and 28% of those with giant cell arteritis. It was more strongly associated with subclavian artery damage on MRA than with inflammation on FDG-PET.
Study details: The cohort comprised 56 patients with Takayasu’s arteritis and 54 with giant cell arteritis who together had made 270 visits.
Disclosures: The Division of Intramural Research at the National Institute of Arthritis and Musculoskeletal and Skin Diseases funded the research. The investigators had no financial disclosures.
Background: Prior studies have suggested that NOACs have a favorable risk-benefit profile when compared with warfarin, but it is unclear if this advantage also is present for those high-risk patients for whom NOAC dose reduction is recommended.
Study design: A meta-analysis.
Setting: Three phase 3 randomized, control trials.
Synopsis: From the three randomized, control trials, the authors identified 7,351 of the 46,426 patients as being eligible for dose-reduced NOACs. Of these patients, 3,702 were randomized to take a NOAC and 3,649 were randomized to take warfarin. For the primary outcomes of stroke or systemic embolism, there was no significant difference between patients randomized to receive dose-reduced NOAC versus warfarin. For outcomes of major bleeding, hemorrhagic stroke, intracranial hemorrhage, and fatal bleeding, dose-reduced NOACs had a significantly lower risk, compared with warfarin.
Bottom line: In patients eligible for dose-reduced NOACs, the use of dose-reduced NOACs may have a better safety profile without significant difference in the rate of ischemic stroke or systemic embolism.
Citation: Wang KL et al. Efficacy and safety of reduced-dose non–vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: A meta-analysis of randomized controlled trials. Eur Heart J. 2018 Dec 22. doi: 10.1093/eurheartj/ehy802.
Dr. Biddick is a hospitalist at Beth Israel Deaconess Medical Center and instructor in medicine Harvard Medical School.
Background: Prior studies have suggested that NOACs have a favorable risk-benefit profile when compared with warfarin, but it is unclear if this advantage also is present for those high-risk patients for whom NOAC dose reduction is recommended.
Study design: A meta-analysis.
Setting: Three phase 3 randomized, control trials.
Synopsis: From the three randomized, control trials, the authors identified 7,351 of the 46,426 patients as being eligible for dose-reduced NOACs. Of these patients, 3,702 were randomized to take a NOAC and 3,649 were randomized to take warfarin. For the primary outcomes of stroke or systemic embolism, there was no significant difference between patients randomized to receive dose-reduced NOAC versus warfarin. For outcomes of major bleeding, hemorrhagic stroke, intracranial hemorrhage, and fatal bleeding, dose-reduced NOACs had a significantly lower risk, compared with warfarin.
Bottom line: In patients eligible for dose-reduced NOACs, the use of dose-reduced NOACs may have a better safety profile without significant difference in the rate of ischemic stroke or systemic embolism.
Citation: Wang KL et al. Efficacy and safety of reduced-dose non–vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: A meta-analysis of randomized controlled trials. Eur Heart J. 2018 Dec 22. doi: 10.1093/eurheartj/ehy802.
Dr. Biddick is a hospitalist at Beth Israel Deaconess Medical Center and instructor in medicine Harvard Medical School.
Background: Prior studies have suggested that NOACs have a favorable risk-benefit profile when compared with warfarin, but it is unclear if this advantage also is present for those high-risk patients for whom NOAC dose reduction is recommended.
Study design: A meta-analysis.
Setting: Three phase 3 randomized, control trials.
Synopsis: From the three randomized, control trials, the authors identified 7,351 of the 46,426 patients as being eligible for dose-reduced NOACs. Of these patients, 3,702 were randomized to take a NOAC and 3,649 were randomized to take warfarin. For the primary outcomes of stroke or systemic embolism, there was no significant difference between patients randomized to receive dose-reduced NOAC versus warfarin. For outcomes of major bleeding, hemorrhagic stroke, intracranial hemorrhage, and fatal bleeding, dose-reduced NOACs had a significantly lower risk, compared with warfarin.
Bottom line: In patients eligible for dose-reduced NOACs, the use of dose-reduced NOACs may have a better safety profile without significant difference in the rate of ischemic stroke or systemic embolism.
Citation: Wang KL et al. Efficacy and safety of reduced-dose non–vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: A meta-analysis of randomized controlled trials. Eur Heart J. 2018 Dec 22. doi: 10.1093/eurheartj/ehy802.
Dr. Biddick is a hospitalist at Beth Israel Deaconess Medical Center and instructor in medicine Harvard Medical School.
Combination pertuzumab, trastuzumab, and docetaxel provided better responses than did placebo, trastuzumab, and docetaxel in Asian patients with ERBB2-positive early or locally advanced breast cancer, according to a phase 3 trial.
The safety profile of the combination regimen was similar between the treatment arms and in accordance with that of pertuzumab alone, reported Zhimin Shao, MD, of Fudan (Shanghai) University Cancer Center, and colleagues. The study was published in JAMA Oncology.
The randomized, placebo-controlled, phase 3 PEONY study included 329 women with ERBB2-positive early or locally advanced disease. The effects of adding pertuzumab to trastuzumab and docetaxel was studied in 23 centers throughout Asia.
Prior to surgery, study subjects in the treatment arm received intravenous pertuzumab at a loading dose of 840 mg followed by 420 mg, trastuzumab at a loading dose of 8 mg/kg followed by 6 mg/kg, and 75 mg/m2 of docetaxel, while patients in the placebo arm received placebo, trastuzumab, and docetaxel. Both regimens were administered every 3 weeks for a total of four cycles.
Post surgery, study patients received intravenous fluorouracil, cyclophosphamide, and epirubicin for a total of 3 cycles, followed by pertuzumab plus trastuzumab or placebo plus trastuzumab for a total of 13 cycles.
The primary outcome was the total pathologic complete response rate assessed at the completion of surgery.
After analysis, the researchers found that total pathologic complete response rates were significantly higher for patients in the pertuzumab arm (39.3%) compared with the placebo arm (21.8%) (difference, 17.5%; P = .001).
With respect to safety, the rates of common adverse events were similar between the groups, with the exception of diarrhea (38.5% in the pertuzumab arm vs. 16.4% in the placebo arm). The incidences of serious toxicities were slightly higher in the pertuzumab arm (10.1%) compared with the placebo arm (8.2%).
“Of the most common grade 3 or higher adverse events, there was a higher incidence of neutropenia in the pertuzumab group (38.1% vs. 32.7%),” they reported.
The researchers acknowledged a key limitation of the study was the short duration of follow-up. As a result, some secondary outcome data were immature at the time of the analysis.
“The PEONY trial adds to the totality of the data showing the benefit of pertuzumab and trastuzumab with chemotherapy in ERBB2-positive early breast cancer,” they concluded.
The authors reported financial affiliations with F. Hoffmann-La Roche Ltd., which funded the study, and Genentech.
Combination pertuzumab, trastuzumab, and docetaxel provided better responses than did placebo, trastuzumab, and docetaxel in Asian patients with ERBB2-positive early or locally advanced breast cancer, according to a phase 3 trial.
The safety profile of the combination regimen was similar between the treatment arms and in accordance with that of pertuzumab alone, reported Zhimin Shao, MD, of Fudan (Shanghai) University Cancer Center, and colleagues. The study was published in JAMA Oncology.
The randomized, placebo-controlled, phase 3 PEONY study included 329 women with ERBB2-positive early or locally advanced disease. The effects of adding pertuzumab to trastuzumab and docetaxel was studied in 23 centers throughout Asia.
Prior to surgery, study subjects in the treatment arm received intravenous pertuzumab at a loading dose of 840 mg followed by 420 mg, trastuzumab at a loading dose of 8 mg/kg followed by 6 mg/kg, and 75 mg/m2 of docetaxel, while patients in the placebo arm received placebo, trastuzumab, and docetaxel. Both regimens were administered every 3 weeks for a total of four cycles.
Post surgery, study patients received intravenous fluorouracil, cyclophosphamide, and epirubicin for a total of 3 cycles, followed by pertuzumab plus trastuzumab or placebo plus trastuzumab for a total of 13 cycles.
The primary outcome was the total pathologic complete response rate assessed at the completion of surgery.
After analysis, the researchers found that total pathologic complete response rates were significantly higher for patients in the pertuzumab arm (39.3%) compared with the placebo arm (21.8%) (difference, 17.5%; P = .001).
With respect to safety, the rates of common adverse events were similar between the groups, with the exception of diarrhea (38.5% in the pertuzumab arm vs. 16.4% in the placebo arm). The incidences of serious toxicities were slightly higher in the pertuzumab arm (10.1%) compared with the placebo arm (8.2%).
“Of the most common grade 3 or higher adverse events, there was a higher incidence of neutropenia in the pertuzumab group (38.1% vs. 32.7%),” they reported.
The researchers acknowledged a key limitation of the study was the short duration of follow-up. As a result, some secondary outcome data were immature at the time of the analysis.
“The PEONY trial adds to the totality of the data showing the benefit of pertuzumab and trastuzumab with chemotherapy in ERBB2-positive early breast cancer,” they concluded.
The authors reported financial affiliations with F. Hoffmann-La Roche Ltd., which funded the study, and Genentech.
Combination pertuzumab, trastuzumab, and docetaxel provided better responses than did placebo, trastuzumab, and docetaxel in Asian patients with ERBB2-positive early or locally advanced breast cancer, according to a phase 3 trial.
The safety profile of the combination regimen was similar between the treatment arms and in accordance with that of pertuzumab alone, reported Zhimin Shao, MD, of Fudan (Shanghai) University Cancer Center, and colleagues. The study was published in JAMA Oncology.
The randomized, placebo-controlled, phase 3 PEONY study included 329 women with ERBB2-positive early or locally advanced disease. The effects of adding pertuzumab to trastuzumab and docetaxel was studied in 23 centers throughout Asia.
Prior to surgery, study subjects in the treatment arm received intravenous pertuzumab at a loading dose of 840 mg followed by 420 mg, trastuzumab at a loading dose of 8 mg/kg followed by 6 mg/kg, and 75 mg/m2 of docetaxel, while patients in the placebo arm received placebo, trastuzumab, and docetaxel. Both regimens were administered every 3 weeks for a total of four cycles.
Post surgery, study patients received intravenous fluorouracil, cyclophosphamide, and epirubicin for a total of 3 cycles, followed by pertuzumab plus trastuzumab or placebo plus trastuzumab for a total of 13 cycles.
The primary outcome was the total pathologic complete response rate assessed at the completion of surgery.
After analysis, the researchers found that total pathologic complete response rates were significantly higher for patients in the pertuzumab arm (39.3%) compared with the placebo arm (21.8%) (difference, 17.5%; P = .001).
With respect to safety, the rates of common adverse events were similar between the groups, with the exception of diarrhea (38.5% in the pertuzumab arm vs. 16.4% in the placebo arm). The incidences of serious toxicities were slightly higher in the pertuzumab arm (10.1%) compared with the placebo arm (8.2%).
“Of the most common grade 3 or higher adverse events, there was a higher incidence of neutropenia in the pertuzumab group (38.1% vs. 32.7%),” they reported.
The researchers acknowledged a key limitation of the study was the short duration of follow-up. As a result, some secondary outcome data were immature at the time of the analysis.
“The PEONY trial adds to the totality of the data showing the benefit of pertuzumab and trastuzumab with chemotherapy in ERBB2-positive early breast cancer,” they concluded.
The authors reported financial affiliations with F. Hoffmann-La Roche Ltd., which funded the study, and Genentech.
NEW ORLEANS – Single ventricle congenital heart disease (CHD) and worse social determinants of health are associated with more behavior problems and less total competency in children, and this relationship is mediated by disease-related chronic stress, self-perception, and family environment.
Dr. Asad Qadir
Those are key findings from a large analysis of existing cross-sectional data presented at the annual meeting of the American Academy of Pediatrics. The study set out to assess what factors mediate the relationship between CHD severity, social determinants of health, and behavioral and emotional outcomes.
“We know that worse CHD severity is associated with worse parent-reported and self-reported behavioral and emotional functioning in children and adolescents survivors,” lead author Asad Qadir, MD, said in an interview. “We may be able to improve and optimize behavioral and emotional outcomes in children with congenital heart disease by taking measures that would decrease their and their caregivers’ disease-related chronic stress, improve family functioning, and improve the self-perception of the child. While social determinants of health are not modifiable, they are important for predicting which children may be at risk for behavior problems.”
Dr. Qadir, a cardiology fellow in the department of pediatrics at Northwestern University, Chicago, and colleagues performed a corollary analysis of the Pediatric Cardiac Quality of Life Inventory Testing study, an international, multicenter, cross-sectional study in which parents and patients with CHD completed questionnaires measuring behavioral and emotional functioning, self-perception, family environment, family coping, posttraumatic stress, and illness-related parenting stress (see Qual Life Res. 2008;17:613-26, Pediatrics. 2010;126[3]:498-508, and Cardiol Young. 2014;[2]:220-8). They assessed the relationships between CHD severity and social determinants of health (predictors), disease-related stress and psychosocial adaptation (mediators), and behavioral and emotional outcomes. They used structural equation modeling to determine the effects of predictors and mediators on outcomes, and created multivariable models for each patient- and parent-reported outcome.
The analysis included 981 patient-parent dyads. Of these, 210 patients had mild biventricular CHD, 620 had moderate biventricular CHD, and 151 had single ventricle CHD. The mean age of patients was 13 years and 55% were male. The researchers found that single ventricle CHD and worse social determinants of health were significant predictors of greater disease-related chronic stress for patients and caregivers and worse psychosocial adaptation in CHD survivors, including self-perception and family functioning constructs of cohesion and expressiveness (P less than .001 for all associations). In addition, single ventricle CHD and worse social determinants of health were associated with worse behavioral and emotional outcomes as reported by patients and parents, including internalizing behaviors, externalizing behaviors, and total competency (P less than .001 for all associations).
In multivariable models for all parent-reported outcomes, significant associations were observed between single ventricle CHD, social determinants of health, disease-related stress, child receiving mental health services, and cohesion/conflict in the family environment (P less than .001). In multivariable models for all patient-reported outcomes, significant associations were seen between single ventricle CHD, self-perception, and cohesion/conflict in the family environment (P less than 0.001).
Patient disease-related stress had the strongest association with externalizing problems, and worse social determinants of health significantly lowered patient-reported total competency.
“Many of the relationships found in the study make intuitive sense,” Dr. Qadir said. “For example, less favorable social determinants of health were associated with more parent disease-related chronic stress, which in turn was associated with parent-reported behavior problems in children. What was surprising was that worse behavioral outcomes were specifically associated with single ventricle disease only. Complex biventricular congenital heart disease patients (CHD that required a surgical- or catheter-based intervention) often have worse behavioral and emotional outcomes, similar to single ventricle patients. However, our model would argue that biventricular congenital heart disease complexity patients have more behavioral and emotional issues not because of their disease complexity, but due to their social determinants of health and the amount of disease-related chronic stress in the child and the parent and the amount of psychosocial adaptation found in the child and parent.”
Parent and patient disease-related chronic stress was not only an important mediator of the effect of CHD severity and social determinants of health on behavioral and emotional outcomes, he added, but it also had indirect effects that were mediated by family cohesion/conflict and patient self-perception.
“These data suggest that for those children with worse social determinants of health and single ventricle congenital heart disease, interventions that mitigate disease-related chronic stress, promote family functioning, and promote self-perception in the child may improve or optimize behavioral and emotional functioning during childhood and adolescence in CHD surgical survivors,” Dr. Qadir concluded.
He acknowledged certain limitations of the analysis, including the fact that it was a corollary cross-sectional analysis of an existing data set. “The results do not reflect possible changes over time,” he added. “There was also selection bias as non-English speakers were excluded, and the study population had a greater percentage of Caucasian and highly educated parents with higher income than the general population, which may affect the generalizability of our results.”
The researchers reported having no relevant financial disclosures.
NEW ORLEANS – Single ventricle congenital heart disease (CHD) and worse social determinants of health are associated with more behavior problems and less total competency in children, and this relationship is mediated by disease-related chronic stress, self-perception, and family environment.
Dr. Asad Qadir
Those are key findings from a large analysis of existing cross-sectional data presented at the annual meeting of the American Academy of Pediatrics. The study set out to assess what factors mediate the relationship between CHD severity, social determinants of health, and behavioral and emotional outcomes.
“We know that worse CHD severity is associated with worse parent-reported and self-reported behavioral and emotional functioning in children and adolescents survivors,” lead author Asad Qadir, MD, said in an interview. “We may be able to improve and optimize behavioral and emotional outcomes in children with congenital heart disease by taking measures that would decrease their and their caregivers’ disease-related chronic stress, improve family functioning, and improve the self-perception of the child. While social determinants of health are not modifiable, they are important for predicting which children may be at risk for behavior problems.”
Dr. Qadir, a cardiology fellow in the department of pediatrics at Northwestern University, Chicago, and colleagues performed a corollary analysis of the Pediatric Cardiac Quality of Life Inventory Testing study, an international, multicenter, cross-sectional study in which parents and patients with CHD completed questionnaires measuring behavioral and emotional functioning, self-perception, family environment, family coping, posttraumatic stress, and illness-related parenting stress (see Qual Life Res. 2008;17:613-26, Pediatrics. 2010;126[3]:498-508, and Cardiol Young. 2014;[2]:220-8). They assessed the relationships between CHD severity and social determinants of health (predictors), disease-related stress and psychosocial adaptation (mediators), and behavioral and emotional outcomes. They used structural equation modeling to determine the effects of predictors and mediators on outcomes, and created multivariable models for each patient- and parent-reported outcome.
The analysis included 981 patient-parent dyads. Of these, 210 patients had mild biventricular CHD, 620 had moderate biventricular CHD, and 151 had single ventricle CHD. The mean age of patients was 13 years and 55% were male. The researchers found that single ventricle CHD and worse social determinants of health were significant predictors of greater disease-related chronic stress for patients and caregivers and worse psychosocial adaptation in CHD survivors, including self-perception and family functioning constructs of cohesion and expressiveness (P less than .001 for all associations). In addition, single ventricle CHD and worse social determinants of health were associated with worse behavioral and emotional outcomes as reported by patients and parents, including internalizing behaviors, externalizing behaviors, and total competency (P less than .001 for all associations).
In multivariable models for all parent-reported outcomes, significant associations were observed between single ventricle CHD, social determinants of health, disease-related stress, child receiving mental health services, and cohesion/conflict in the family environment (P less than .001). In multivariable models for all patient-reported outcomes, significant associations were seen between single ventricle CHD, self-perception, and cohesion/conflict in the family environment (P less than 0.001).
Patient disease-related stress had the strongest association with externalizing problems, and worse social determinants of health significantly lowered patient-reported total competency.
“Many of the relationships found in the study make intuitive sense,” Dr. Qadir said. “For example, less favorable social determinants of health were associated with more parent disease-related chronic stress, which in turn was associated with parent-reported behavior problems in children. What was surprising was that worse behavioral outcomes were specifically associated with single ventricle disease only. Complex biventricular congenital heart disease patients (CHD that required a surgical- or catheter-based intervention) often have worse behavioral and emotional outcomes, similar to single ventricle patients. However, our model would argue that biventricular congenital heart disease complexity patients have more behavioral and emotional issues not because of their disease complexity, but due to their social determinants of health and the amount of disease-related chronic stress in the child and the parent and the amount of psychosocial adaptation found in the child and parent.”
Parent and patient disease-related chronic stress was not only an important mediator of the effect of CHD severity and social determinants of health on behavioral and emotional outcomes, he added, but it also had indirect effects that were mediated by family cohesion/conflict and patient self-perception.
“These data suggest that for those children with worse social determinants of health and single ventricle congenital heart disease, interventions that mitigate disease-related chronic stress, promote family functioning, and promote self-perception in the child may improve or optimize behavioral and emotional functioning during childhood and adolescence in CHD surgical survivors,” Dr. Qadir concluded.
He acknowledged certain limitations of the analysis, including the fact that it was a corollary cross-sectional analysis of an existing data set. “The results do not reflect possible changes over time,” he added. “There was also selection bias as non-English speakers were excluded, and the study population had a greater percentage of Caucasian and highly educated parents with higher income than the general population, which may affect the generalizability of our results.”
The researchers reported having no relevant financial disclosures.
NEW ORLEANS – Single ventricle congenital heart disease (CHD) and worse social determinants of health are associated with more behavior problems and less total competency in children, and this relationship is mediated by disease-related chronic stress, self-perception, and family environment.
Dr. Asad Qadir
Those are key findings from a large analysis of existing cross-sectional data presented at the annual meeting of the American Academy of Pediatrics. The study set out to assess what factors mediate the relationship between CHD severity, social determinants of health, and behavioral and emotional outcomes.
“We know that worse CHD severity is associated with worse parent-reported and self-reported behavioral and emotional functioning in children and adolescents survivors,” lead author Asad Qadir, MD, said in an interview. “We may be able to improve and optimize behavioral and emotional outcomes in children with congenital heart disease by taking measures that would decrease their and their caregivers’ disease-related chronic stress, improve family functioning, and improve the self-perception of the child. While social determinants of health are not modifiable, they are important for predicting which children may be at risk for behavior problems.”
Dr. Qadir, a cardiology fellow in the department of pediatrics at Northwestern University, Chicago, and colleagues performed a corollary analysis of the Pediatric Cardiac Quality of Life Inventory Testing study, an international, multicenter, cross-sectional study in which parents and patients with CHD completed questionnaires measuring behavioral and emotional functioning, self-perception, family environment, family coping, posttraumatic stress, and illness-related parenting stress (see Qual Life Res. 2008;17:613-26, Pediatrics. 2010;126[3]:498-508, and Cardiol Young. 2014;[2]:220-8). They assessed the relationships between CHD severity and social determinants of health (predictors), disease-related stress and psychosocial adaptation (mediators), and behavioral and emotional outcomes. They used structural equation modeling to determine the effects of predictors and mediators on outcomes, and created multivariable models for each patient- and parent-reported outcome.
The analysis included 981 patient-parent dyads. Of these, 210 patients had mild biventricular CHD, 620 had moderate biventricular CHD, and 151 had single ventricle CHD. The mean age of patients was 13 years and 55% were male. The researchers found that single ventricle CHD and worse social determinants of health were significant predictors of greater disease-related chronic stress for patients and caregivers and worse psychosocial adaptation in CHD survivors, including self-perception and family functioning constructs of cohesion and expressiveness (P less than .001 for all associations). In addition, single ventricle CHD and worse social determinants of health were associated with worse behavioral and emotional outcomes as reported by patients and parents, including internalizing behaviors, externalizing behaviors, and total competency (P less than .001 for all associations).
In multivariable models for all parent-reported outcomes, significant associations were observed between single ventricle CHD, social determinants of health, disease-related stress, child receiving mental health services, and cohesion/conflict in the family environment (P less than .001). In multivariable models for all patient-reported outcomes, significant associations were seen between single ventricle CHD, self-perception, and cohesion/conflict in the family environment (P less than 0.001).
Patient disease-related stress had the strongest association with externalizing problems, and worse social determinants of health significantly lowered patient-reported total competency.
“Many of the relationships found in the study make intuitive sense,” Dr. Qadir said. “For example, less favorable social determinants of health were associated with more parent disease-related chronic stress, which in turn was associated with parent-reported behavior problems in children. What was surprising was that worse behavioral outcomes were specifically associated with single ventricle disease only. Complex biventricular congenital heart disease patients (CHD that required a surgical- or catheter-based intervention) often have worse behavioral and emotional outcomes, similar to single ventricle patients. However, our model would argue that biventricular congenital heart disease complexity patients have more behavioral and emotional issues not because of their disease complexity, but due to their social determinants of health and the amount of disease-related chronic stress in the child and the parent and the amount of psychosocial adaptation found in the child and parent.”
Parent and patient disease-related chronic stress was not only an important mediator of the effect of CHD severity and social determinants of health on behavioral and emotional outcomes, he added, but it also had indirect effects that were mediated by family cohesion/conflict and patient self-perception.
“These data suggest that for those children with worse social determinants of health and single ventricle congenital heart disease, interventions that mitigate disease-related chronic stress, promote family functioning, and promote self-perception in the child may improve or optimize behavioral and emotional functioning during childhood and adolescence in CHD surgical survivors,” Dr. Qadir concluded.
He acknowledged certain limitations of the analysis, including the fact that it was a corollary cross-sectional analysis of an existing data set. “The results do not reflect possible changes over time,” he added. “There was also selection bias as non-English speakers were excluded, and the study population had a greater percentage of Caucasian and highly educated parents with higher income than the general population, which may affect the generalizability of our results.”
The researchers reported having no relevant financial disclosures.
Minimally invasive surgical techniques, which have revolutionized modern-day surgery, are the current standard of care for benign hysterectomies.1-4 Many surgeons use a video-laparoscopic approach, with or without robotic assistance, to perform a hysterectomy. The development of a bladder flap or vesicovaginal surgical space is a critical step for mobilizing the bladder. When properly performed, it allows for appropriate closure of the vaginal cuff while mitigating the risk of urinary bladder damage.
In patients with no prior pelvic surgeries, this vesicovaginal anatomic space is typically developed with ease. However, in patients who have had prior cesarean deliveries (CDs), the presence of vesicouterine adhesions could make this step significantly more challenging. As a result, the risk of bladder injury is higher.5-8
With the current tide of cesarean birth rates approaching 33% on a national scale, the presence of vesicouterine adhesions is commonly encountered.9 These adhesions can distort the anatomy and thereby create more difficult dissections and increase operative time, conversion to laparotomy, and inadvertent cystotomy. Such a challenge also presents an increased risk of injuring adjacent structures.
In this article, we describe an effective method of dissection that is especially useful in the setting of prior CDs. This method involves developing a "new" surgical space lateral and caudal to the vesicocervical space.
Steps in operative planning
Preoperative evaluation.A thorough preoperative evaluation should be performed for patients planning to undergo a laparoscopic hysterectomy. This includes obtaining details of their medical and surgical history. Access to prior surgical records may help to facilitate planning of the surgical approach. Previous pelvic surgery, such as CD, anterior myomectomy, cesarean scar defect repair, endometriosis treatment, or exploratory laparotomy, may predispose these patients to develop adhesions in the anterior cul-de-sac. Our method of reverse vesicouterine fold dissection can be particularly efficacious in these settings.
Surgical preparation and laparoscopic port placement.In the operative suite, the patient is placed under general anesthesia and positioned in the dorsal lithotomy position.10 Sterile prep and drapes are used in the standard fashion. A urinary catheter is inserted to maintain a decompressed bladder. A uterine manipulator is inserted with good placement ensured.
Per our practice, we introduce laparoscopic ports in 4 locations. The first incision is made in the umbilicus for the introduction of a 10-mm laparoscope. Three subsequent 5-mm incisions are made in the left and right lower lateral quadrants and medially at the level of the suprapubic region.10 Upon laparoscopic entry, we perform a comprehensive survey of the abdominopelvic cavity. Adequate mobility of the uterus is confirmed.11 Any posterior uterine adhesions or endometriosis are treated appropriately.12
First step in the surgical technique: Lateral dissection
We proceed by first desiccating and cutting the round ligament laterally near the inguinal canal. This technique is carried forward in a caudal direction as the areolar tissue near the obliterated umbilical artery is expanded by the pneumoperitoneum. With a vessel sealing-cutting device, we address the attachments to the adnexa. If the ovaries are to be retained, the utero-ovarian ligament is dessicated and cut. If an oophorectomy is indicated, the infundibulopelvic ligament is dessicated and cut.
Continue to: Using the tip of the vessel sealing...
Using the tip of the vessel sealing-cutting device, the space between the anterior and posterior leaves of the broad ligament is developed and opened. A grasping forceps is then used to elevate the anterior leaf of the broad ligament and maintain medial traction. A space parallel and lateral to the cervix and bladder is then created with blunt dissection.
The inferior and medial direction of this dissection is paramount to avoid injury to nearby structures in the pelvic sidewall. Gradually, this will lead to the identification of the vesciovaginal ligament and then the vesicocervical ligament. The development of these spaces allows for the lateral and inferior displacement of the ureter. These maneuvers can mitigate ureter injury by pushing it away from the planes of dissection during the hysterectomy.
Continued traction is maintained by keeping the medial aspect of the anterior leaf of the broad ligament intact. However, the posterior leaf is dissected next, which further lateralizes the ureter. Now, with the uterine vessels fully exposed, they are thoroughly dessicated and ligated. The same procedure is then performed on the contralateral side.11 (See the box below for links to videos that demonstrate the techniques described here.)
Creating the “new” space
In the “new” space that was partially developed during the lateral dissection, blunt dissection is continued, using a sweeping motion from an inferior-to-superior direction, to extend this avascular space. This is performed bilaterally until both sides are connected from the inferior aspect of the vesicouterine adhesions, if present. This thorough dissection creates what we refer to as a “new” space11 (FIGURE 1).
Medially, the new space is bordered by the vesicocervical-vaginal ligament, also known as the bladder pillar. Its distal landmark is the bladder. The remaining intact anterior leaf of the broad ligament lies adjacent to the space anteriorly. The inner aspect of the obliterated umbilical artery neighbors it laterally. Lastly, the vesicovaginal plane’s posterior margin is the parametrium, which is the region where the ureter courses into the bladder. The paravesical space lies lateral to the obliterated umbilical ligament.
Visualization of this new space is made possible in the laparoscopic setting. The pneumoperitoneum allows for better demarcation of the space. Additionally, laparoscopic views of the anatomic spaces differ from those of the laparotomy view because of the magnification and the insufflation of carbon dioxide gas in the spaces.13,14 In our experience, approaching the surgery from the “new” space could significantly decrease the risk of genitourinary injuries in patients with anterior cul-de-sac adhesions (FIGURE 2).
Using the reverse vesicouterine fold dissection technique
Among patients with prior CDs, adhesions often are at the level of or superior to the prior CD scar. By creating the new space, safe dissection from a previously untouched area can be accomplished and injury to the urinary bladder can be avoided.
The reverse vesicouterine fold dissection can be performed from this space. Using the previously described blunt sweeping motion from an inferior-to-superior direction, the vesicovaginal and vesicocervical space is further developed from an unscarred plane. This will separate the lowest portion of the bladder from the vagina, cervix, and uterus in a safe manner. Similar to the technique performed during a vaginal hysterectomy, this reverse motion of developing the bladder flap avoids erroneous and blind dissection through the vesicouterine adhesions (FIGURES 3–5).
Once the bladder adhesions are well delineated and separated from the uterus by the reverse vesicouterine fold dissection technique, it is safe to proceed with complete bladder mobilization. Sharp dissection can be used to dissect the remaining scarred bladder at its most superior attachments. Avoid the use of thermal energy to prevent heat injury to the bladder. Carefully dissect the bladder adhesions from the cervicouterine junction. Additional inferior bladder mobilization should be performed up to 3 cm past the leading edge of the cervicovaginal junction to ensure sufficient vaginal tissue for cuff closure. Note that the bladder pillars occasionally may be trapped inside a CD scar. This surgical technique could make it easier to release the pillars from inside the adhesions and penetrating into the scar.15
Continue to: Completing the surgery...
Completing the surgery
Once the bladder is freely mobilized and all adhesions have been dissected, the cervix is circumferentially amputated using monopolar cautery. The vaginal cuff can then be closed from either a laparoscopic or vaginal approach using polyglactin 910 (0-Vicryl) or barbed (V-Loc) suture in a running or interrupted fashion. Our practice uses a 1.5-cm margin depth with each suture. At the end of the surgery, routine cystoscopy is performed to verify distal ureteral patency.16 Postoperatively, we manage these patients using a fast-track, or enhanced recovery, model.17
These videos demonstrate the reverse vesicouterine fold dissection technique
From the Center for Special Minimally Invasive and Robotic Surgery
https://youtu.be/wgGssnd1JAo
Reverse vesicouterine fold dissection for total laparoscopic hysterectomy
Case 1: TLH with development of the "new space": The technique with prior C-section
Case 2: A straightforward case: Dysmenorrhea and menorrhagia
Case 3: History of multiple C-sections with adhesions and fibroids
https://youtu.be/6vHamfPZhdY
Reverse vesicouterine fold dissection for total laparoscopic hysterectomy after prior cesarean delivery
An effective technique in challenging situations
Genitourinary injury is a common complication of hysterectomy.18 The proximity of the bladder and ureters to the field of dissection during a hysterectomy can be especially challenging when the anatomy is distorted by adhesion formation from prior surgeries. One study demonstrated a 1.3% incidence of urinary tract injuries during laparoscopic hysterectomy.6 This included 0.54% ureteral injuries, 0.71% urinary bladder injuries, and 0.06% combined bladder and ureteral injuries.6 Particularly among patients with a prior CD, the risk of bladder injury can be significantly heightened.18
The reverse vesicouterine fold dissection technique that we described offers multiple benefits. By starting the procedure from an untouched and avascular plane, dissection into the plane of the prior adhesions can be circumvented; thus, bleeding is limited and injury to the bladder and ureters is avoided or minimized. By using blunt and sharp dissection, thermal injury and delayed necrosis can be mitigated. Finally, with bladder mobilization well below the colpotomy site, more adequate vaginal tissue is free to be incorporated into the vaginal cuff closure, thereby limiting the risk of cuff dehiscence.16
While we have found this technique effective for patients with prior cesarean deliveries, it also may be applied to any patient who has a scarred anterior cul-de-sac. This could include patients with prior myomectomy, cesarean scar defect, or endometriosis. Despite the technique being a safeguard against bladder injury, surgeons must still use care in developing the spaces to avoid ureteral injury, especially in a setting of distorted anatomy.
References
Page B. Nezhat & the advent of advanced operative video-laparoscopy. In: Nezhat C. Nezhat's History of Endoscopy. Tuttlingen, Germany: Endo Press; 2011:159-179. https://laparoscopy.blogs.com/endoscopyhistory/chapter_22. Accessed October 23, 2019.
Podratz KC. Degrees of freedom: advances in gynecological and obstetric surgery. In: American College of Surgeons. Remembering Milestones and Achievements in Surgery: Inspiring Quality for a Hundred Years, 1913-2012. Tampa, FL: Faircount Media Group; 2013:113-119. http://endometriosisspecialists.com/wp-content/uploads/pdfs/Degrees-of-Freedom-Advances-in-Gynecological-and-Obstetrical-Surgery.pdf. Accessed October 31, 2019.
Kelley WE Jr. The evolution of laparoscopy and the revolution in surgery in the decade of the 1990s. JSLS. 2008;12:351-357.
Tokunaga T. Video surgery expands its scope. Stanford Med. 1993/1994;11(2)12-16.
Rooney CM, Crawford AT, Vassallo BJ, et al. Is previous cesarean section a risk for incidental cystotomy at the time of hysterectomy? A case-controlled study. Am J Obstet Gynecol. 2005;193:2041-2044.
Tan-Kim J, Menefee SA, Reinsch CS, et al. Laparoscopic hysterectomy and urinary tract injury: experience in a health maintenance organization. J Minim Invasive Gynecol. 2015;22:1278-1286.
Sinha R, Sundaram M, Lakhotia S, et al. Total laparoscopic hysterectomy in women with previous cesarean sections. J Minim Invasive Gynecol. 2010;17:513-517.
O'Hanlan KA. Cystosufflation to prevent bladder injury. J Minim Invasive Gynecol. 2009;16:195-197.
Martin JA, Hamilton BE, Osterman MJ, et al. Births: final data for 2013. Natl Vital Stat Rep. 2015;64:1-65.
Nezhat C, Nezhat F, Nezhat C, eds. Nezhat's Video-Assisted and Robotic-Assisted Laparoscopy and Hysteroscopy with DVD, 4th ed. New York, NY: Cambridge University Press; 2013.
Nezhat C, Grace LA, Razavi GM, et al. Reverse vesicouterine fold dissection for laparoscopic hysterectomy after prior cesarean deliveries. Obstet Gynecol. 2016;128:629-633.
Nezhat C, Xie J, Aldape D, et al. Use of laparoscopic modified nerve-sparing radical hysterectomy for the treatment of extensive endometriosis. Cureus. 2014;6:e159.
Yabuki Y, Sasaki H, Hatakeyama N, et al. Discrepancies between classic anatomy and modern gynecologic surgery on pelvic connective tissue structure: harmonization of those concepts by collaborative cadaver dissection. Am J Obstet Gynecol. 2005;193:7-15.
Uhlenhuth E. Problems in the Anatomy of the Pelvis: An Atlas. Philadelphia, PA: JB Lippincott Co; 1953.
Nezhat C, Grace, L, Soliemannjad, et al. Cesarean scar defect: what is it and how should it be treated? OBG Manag. 2016;28(4):32,34,36,38-39,53.
Nezhat C, Kennedy Burns M, Wood M, et al. Vaginal cuff dehiscence and evisceration: a review. Obstet Gynecol. 2018;132:972-985.
Nezhat C, Main J, Paka C, et al. Advanced gynecologic laparoscopy in a fast-track ambulatory surgery center. JSLS. 2014;18:pii:e2014.00291.
Nezhat C, Falik R, McKinney S, et al. Pathophysiology and management of urinary tract endometriosis. Nat Rev Urol. 2017;14:359-372.
Minimally invasive surgical techniques, which have revolutionized modern-day surgery, are the current standard of care for benign hysterectomies.1-4 Many surgeons use a video-laparoscopic approach, with or without robotic assistance, to perform a hysterectomy. The development of a bladder flap or vesicovaginal surgical space is a critical step for mobilizing the bladder. When properly performed, it allows for appropriate closure of the vaginal cuff while mitigating the risk of urinary bladder damage.
In patients with no prior pelvic surgeries, this vesicovaginal anatomic space is typically developed with ease. However, in patients who have had prior cesarean deliveries (CDs), the presence of vesicouterine adhesions could make this step significantly more challenging. As a result, the risk of bladder injury is higher.5-8
With the current tide of cesarean birth rates approaching 33% on a national scale, the presence of vesicouterine adhesions is commonly encountered.9 These adhesions can distort the anatomy and thereby create more difficult dissections and increase operative time, conversion to laparotomy, and inadvertent cystotomy. Such a challenge also presents an increased risk of injuring adjacent structures.
In this article, we describe an effective method of dissection that is especially useful in the setting of prior CDs. This method involves developing a "new" surgical space lateral and caudal to the vesicocervical space.
Steps in operative planning
Preoperative evaluation.A thorough preoperative evaluation should be performed for patients planning to undergo a laparoscopic hysterectomy. This includes obtaining details of their medical and surgical history. Access to prior surgical records may help to facilitate planning of the surgical approach. Previous pelvic surgery, such as CD, anterior myomectomy, cesarean scar defect repair, endometriosis treatment, or exploratory laparotomy, may predispose these patients to develop adhesions in the anterior cul-de-sac. Our method of reverse vesicouterine fold dissection can be particularly efficacious in these settings.
Surgical preparation and laparoscopic port placement.In the operative suite, the patient is placed under general anesthesia and positioned in the dorsal lithotomy position.10 Sterile prep and drapes are used in the standard fashion. A urinary catheter is inserted to maintain a decompressed bladder. A uterine manipulator is inserted with good placement ensured.
Per our practice, we introduce laparoscopic ports in 4 locations. The first incision is made in the umbilicus for the introduction of a 10-mm laparoscope. Three subsequent 5-mm incisions are made in the left and right lower lateral quadrants and medially at the level of the suprapubic region.10 Upon laparoscopic entry, we perform a comprehensive survey of the abdominopelvic cavity. Adequate mobility of the uterus is confirmed.11 Any posterior uterine adhesions or endometriosis are treated appropriately.12
First step in the surgical technique: Lateral dissection
We proceed by first desiccating and cutting the round ligament laterally near the inguinal canal. This technique is carried forward in a caudal direction as the areolar tissue near the obliterated umbilical artery is expanded by the pneumoperitoneum. With a vessel sealing-cutting device, we address the attachments to the adnexa. If the ovaries are to be retained, the utero-ovarian ligament is dessicated and cut. If an oophorectomy is indicated, the infundibulopelvic ligament is dessicated and cut.
Continue to: Using the tip of the vessel sealing...
Using the tip of the vessel sealing-cutting device, the space between the anterior and posterior leaves of the broad ligament is developed and opened. A grasping forceps is then used to elevate the anterior leaf of the broad ligament and maintain medial traction. A space parallel and lateral to the cervix and bladder is then created with blunt dissection.
The inferior and medial direction of this dissection is paramount to avoid injury to nearby structures in the pelvic sidewall. Gradually, this will lead to the identification of the vesciovaginal ligament and then the vesicocervical ligament. The development of these spaces allows for the lateral and inferior displacement of the ureter. These maneuvers can mitigate ureter injury by pushing it away from the planes of dissection during the hysterectomy.
Continued traction is maintained by keeping the medial aspect of the anterior leaf of the broad ligament intact. However, the posterior leaf is dissected next, which further lateralizes the ureter. Now, with the uterine vessels fully exposed, they are thoroughly dessicated and ligated. The same procedure is then performed on the contralateral side.11 (See the box below for links to videos that demonstrate the techniques described here.)
Creating the “new” space
In the “new” space that was partially developed during the lateral dissection, blunt dissection is continued, using a sweeping motion from an inferior-to-superior direction, to extend this avascular space. This is performed bilaterally until both sides are connected from the inferior aspect of the vesicouterine adhesions, if present. This thorough dissection creates what we refer to as a “new” space11 (FIGURE 1).
Medially, the new space is bordered by the vesicocervical-vaginal ligament, also known as the bladder pillar. Its distal landmark is the bladder. The remaining intact anterior leaf of the broad ligament lies adjacent to the space anteriorly. The inner aspect of the obliterated umbilical artery neighbors it laterally. Lastly, the vesicovaginal plane’s posterior margin is the parametrium, which is the region where the ureter courses into the bladder. The paravesical space lies lateral to the obliterated umbilical ligament.
Visualization of this new space is made possible in the laparoscopic setting. The pneumoperitoneum allows for better demarcation of the space. Additionally, laparoscopic views of the anatomic spaces differ from those of the laparotomy view because of the magnification and the insufflation of carbon dioxide gas in the spaces.13,14 In our experience, approaching the surgery from the “new” space could significantly decrease the risk of genitourinary injuries in patients with anterior cul-de-sac adhesions (FIGURE 2).
Using the reverse vesicouterine fold dissection technique
Among patients with prior CDs, adhesions often are at the level of or superior to the prior CD scar. By creating the new space, safe dissection from a previously untouched area can be accomplished and injury to the urinary bladder can be avoided.
The reverse vesicouterine fold dissection can be performed from this space. Using the previously described blunt sweeping motion from an inferior-to-superior direction, the vesicovaginal and vesicocervical space is further developed from an unscarred plane. This will separate the lowest portion of the bladder from the vagina, cervix, and uterus in a safe manner. Similar to the technique performed during a vaginal hysterectomy, this reverse motion of developing the bladder flap avoids erroneous and blind dissection through the vesicouterine adhesions (FIGURES 3–5).
Once the bladder adhesions are well delineated and separated from the uterus by the reverse vesicouterine fold dissection technique, it is safe to proceed with complete bladder mobilization. Sharp dissection can be used to dissect the remaining scarred bladder at its most superior attachments. Avoid the use of thermal energy to prevent heat injury to the bladder. Carefully dissect the bladder adhesions from the cervicouterine junction. Additional inferior bladder mobilization should be performed up to 3 cm past the leading edge of the cervicovaginal junction to ensure sufficient vaginal tissue for cuff closure. Note that the bladder pillars occasionally may be trapped inside a CD scar. This surgical technique could make it easier to release the pillars from inside the adhesions and penetrating into the scar.15
Continue to: Completing the surgery...
Completing the surgery
Once the bladder is freely mobilized and all adhesions have been dissected, the cervix is circumferentially amputated using monopolar cautery. The vaginal cuff can then be closed from either a laparoscopic or vaginal approach using polyglactin 910 (0-Vicryl) or barbed (V-Loc) suture in a running or interrupted fashion. Our practice uses a 1.5-cm margin depth with each suture. At the end of the surgery, routine cystoscopy is performed to verify distal ureteral patency.16 Postoperatively, we manage these patients using a fast-track, or enhanced recovery, model.17
These videos demonstrate the reverse vesicouterine fold dissection technique
From the Center for Special Minimally Invasive and Robotic Surgery
https://youtu.be/wgGssnd1JAo
Reverse vesicouterine fold dissection for total laparoscopic hysterectomy
Case 1: TLH with development of the "new space": The technique with prior C-section
Case 2: A straightforward case: Dysmenorrhea and menorrhagia
Case 3: History of multiple C-sections with adhesions and fibroids
https://youtu.be/6vHamfPZhdY
Reverse vesicouterine fold dissection for total laparoscopic hysterectomy after prior cesarean delivery
An effective technique in challenging situations
Genitourinary injury is a common complication of hysterectomy.18 The proximity of the bladder and ureters to the field of dissection during a hysterectomy can be especially challenging when the anatomy is distorted by adhesion formation from prior surgeries. One study demonstrated a 1.3% incidence of urinary tract injuries during laparoscopic hysterectomy.6 This included 0.54% ureteral injuries, 0.71% urinary bladder injuries, and 0.06% combined bladder and ureteral injuries.6 Particularly among patients with a prior CD, the risk of bladder injury can be significantly heightened.18
The reverse vesicouterine fold dissection technique that we described offers multiple benefits. By starting the procedure from an untouched and avascular plane, dissection into the plane of the prior adhesions can be circumvented; thus, bleeding is limited and injury to the bladder and ureters is avoided or minimized. By using blunt and sharp dissection, thermal injury and delayed necrosis can be mitigated. Finally, with bladder mobilization well below the colpotomy site, more adequate vaginal tissue is free to be incorporated into the vaginal cuff closure, thereby limiting the risk of cuff dehiscence.16
While we have found this technique effective for patients with prior cesarean deliveries, it also may be applied to any patient who has a scarred anterior cul-de-sac. This could include patients with prior myomectomy, cesarean scar defect, or endometriosis. Despite the technique being a safeguard against bladder injury, surgeons must still use care in developing the spaces to avoid ureteral injury, especially in a setting of distorted anatomy.
Minimally invasive surgical techniques, which have revolutionized modern-day surgery, are the current standard of care for benign hysterectomies.1-4 Many surgeons use a video-laparoscopic approach, with or without robotic assistance, to perform a hysterectomy. The development of a bladder flap or vesicovaginal surgical space is a critical step for mobilizing the bladder. When properly performed, it allows for appropriate closure of the vaginal cuff while mitigating the risk of urinary bladder damage.
In patients with no prior pelvic surgeries, this vesicovaginal anatomic space is typically developed with ease. However, in patients who have had prior cesarean deliveries (CDs), the presence of vesicouterine adhesions could make this step significantly more challenging. As a result, the risk of bladder injury is higher.5-8
With the current tide of cesarean birth rates approaching 33% on a national scale, the presence of vesicouterine adhesions is commonly encountered.9 These adhesions can distort the anatomy and thereby create more difficult dissections and increase operative time, conversion to laparotomy, and inadvertent cystotomy. Such a challenge also presents an increased risk of injuring adjacent structures.
In this article, we describe an effective method of dissection that is especially useful in the setting of prior CDs. This method involves developing a "new" surgical space lateral and caudal to the vesicocervical space.
Steps in operative planning
Preoperative evaluation.A thorough preoperative evaluation should be performed for patients planning to undergo a laparoscopic hysterectomy. This includes obtaining details of their medical and surgical history. Access to prior surgical records may help to facilitate planning of the surgical approach. Previous pelvic surgery, such as CD, anterior myomectomy, cesarean scar defect repair, endometriosis treatment, or exploratory laparotomy, may predispose these patients to develop adhesions in the anterior cul-de-sac. Our method of reverse vesicouterine fold dissection can be particularly efficacious in these settings.
Surgical preparation and laparoscopic port placement.In the operative suite, the patient is placed under general anesthesia and positioned in the dorsal lithotomy position.10 Sterile prep and drapes are used in the standard fashion. A urinary catheter is inserted to maintain a decompressed bladder. A uterine manipulator is inserted with good placement ensured.
Per our practice, we introduce laparoscopic ports in 4 locations. The first incision is made in the umbilicus for the introduction of a 10-mm laparoscope. Three subsequent 5-mm incisions are made in the left and right lower lateral quadrants and medially at the level of the suprapubic region.10 Upon laparoscopic entry, we perform a comprehensive survey of the abdominopelvic cavity. Adequate mobility of the uterus is confirmed.11 Any posterior uterine adhesions or endometriosis are treated appropriately.12
First step in the surgical technique: Lateral dissection
We proceed by first desiccating and cutting the round ligament laterally near the inguinal canal. This technique is carried forward in a caudal direction as the areolar tissue near the obliterated umbilical artery is expanded by the pneumoperitoneum. With a vessel sealing-cutting device, we address the attachments to the adnexa. If the ovaries are to be retained, the utero-ovarian ligament is dessicated and cut. If an oophorectomy is indicated, the infundibulopelvic ligament is dessicated and cut.
Continue to: Using the tip of the vessel sealing...
Using the tip of the vessel sealing-cutting device, the space between the anterior and posterior leaves of the broad ligament is developed and opened. A grasping forceps is then used to elevate the anterior leaf of the broad ligament and maintain medial traction. A space parallel and lateral to the cervix and bladder is then created with blunt dissection.
The inferior and medial direction of this dissection is paramount to avoid injury to nearby structures in the pelvic sidewall. Gradually, this will lead to the identification of the vesciovaginal ligament and then the vesicocervical ligament. The development of these spaces allows for the lateral and inferior displacement of the ureter. These maneuvers can mitigate ureter injury by pushing it away from the planes of dissection during the hysterectomy.
Continued traction is maintained by keeping the medial aspect of the anterior leaf of the broad ligament intact. However, the posterior leaf is dissected next, which further lateralizes the ureter. Now, with the uterine vessels fully exposed, they are thoroughly dessicated and ligated. The same procedure is then performed on the contralateral side.11 (See the box below for links to videos that demonstrate the techniques described here.)
Creating the “new” space
In the “new” space that was partially developed during the lateral dissection, blunt dissection is continued, using a sweeping motion from an inferior-to-superior direction, to extend this avascular space. This is performed bilaterally until both sides are connected from the inferior aspect of the vesicouterine adhesions, if present. This thorough dissection creates what we refer to as a “new” space11 (FIGURE 1).
Medially, the new space is bordered by the vesicocervical-vaginal ligament, also known as the bladder pillar. Its distal landmark is the bladder. The remaining intact anterior leaf of the broad ligament lies adjacent to the space anteriorly. The inner aspect of the obliterated umbilical artery neighbors it laterally. Lastly, the vesicovaginal plane’s posterior margin is the parametrium, which is the region where the ureter courses into the bladder. The paravesical space lies lateral to the obliterated umbilical ligament.
Visualization of this new space is made possible in the laparoscopic setting. The pneumoperitoneum allows for better demarcation of the space. Additionally, laparoscopic views of the anatomic spaces differ from those of the laparotomy view because of the magnification and the insufflation of carbon dioxide gas in the spaces.13,14 In our experience, approaching the surgery from the “new” space could significantly decrease the risk of genitourinary injuries in patients with anterior cul-de-sac adhesions (FIGURE 2).
Using the reverse vesicouterine fold dissection technique
Among patients with prior CDs, adhesions often are at the level of or superior to the prior CD scar. By creating the new space, safe dissection from a previously untouched area can be accomplished and injury to the urinary bladder can be avoided.
The reverse vesicouterine fold dissection can be performed from this space. Using the previously described blunt sweeping motion from an inferior-to-superior direction, the vesicovaginal and vesicocervical space is further developed from an unscarred plane. This will separate the lowest portion of the bladder from the vagina, cervix, and uterus in a safe manner. Similar to the technique performed during a vaginal hysterectomy, this reverse motion of developing the bladder flap avoids erroneous and blind dissection through the vesicouterine adhesions (FIGURES 3–5).
Once the bladder adhesions are well delineated and separated from the uterus by the reverse vesicouterine fold dissection technique, it is safe to proceed with complete bladder mobilization. Sharp dissection can be used to dissect the remaining scarred bladder at its most superior attachments. Avoid the use of thermal energy to prevent heat injury to the bladder. Carefully dissect the bladder adhesions from the cervicouterine junction. Additional inferior bladder mobilization should be performed up to 3 cm past the leading edge of the cervicovaginal junction to ensure sufficient vaginal tissue for cuff closure. Note that the bladder pillars occasionally may be trapped inside a CD scar. This surgical technique could make it easier to release the pillars from inside the adhesions and penetrating into the scar.15
Continue to: Completing the surgery...
Completing the surgery
Once the bladder is freely mobilized and all adhesions have been dissected, the cervix is circumferentially amputated using monopolar cautery. The vaginal cuff can then be closed from either a laparoscopic or vaginal approach using polyglactin 910 (0-Vicryl) or barbed (V-Loc) suture in a running or interrupted fashion. Our practice uses a 1.5-cm margin depth with each suture. At the end of the surgery, routine cystoscopy is performed to verify distal ureteral patency.16 Postoperatively, we manage these patients using a fast-track, or enhanced recovery, model.17
These videos demonstrate the reverse vesicouterine fold dissection technique
From the Center for Special Minimally Invasive and Robotic Surgery
https://youtu.be/wgGssnd1JAo
Reverse vesicouterine fold dissection for total laparoscopic hysterectomy
Case 1: TLH with development of the "new space": The technique with prior C-section
Case 2: A straightforward case: Dysmenorrhea and menorrhagia
Case 3: History of multiple C-sections with adhesions and fibroids
https://youtu.be/6vHamfPZhdY
Reverse vesicouterine fold dissection for total laparoscopic hysterectomy after prior cesarean delivery
An effective technique in challenging situations
Genitourinary injury is a common complication of hysterectomy.18 The proximity of the bladder and ureters to the field of dissection during a hysterectomy can be especially challenging when the anatomy is distorted by adhesion formation from prior surgeries. One study demonstrated a 1.3% incidence of urinary tract injuries during laparoscopic hysterectomy.6 This included 0.54% ureteral injuries, 0.71% urinary bladder injuries, and 0.06% combined bladder and ureteral injuries.6 Particularly among patients with a prior CD, the risk of bladder injury can be significantly heightened.18
The reverse vesicouterine fold dissection technique that we described offers multiple benefits. By starting the procedure from an untouched and avascular plane, dissection into the plane of the prior adhesions can be circumvented; thus, bleeding is limited and injury to the bladder and ureters is avoided or minimized. By using blunt and sharp dissection, thermal injury and delayed necrosis can be mitigated. Finally, with bladder mobilization well below the colpotomy site, more adequate vaginal tissue is free to be incorporated into the vaginal cuff closure, thereby limiting the risk of cuff dehiscence.16
While we have found this technique effective for patients with prior cesarean deliveries, it also may be applied to any patient who has a scarred anterior cul-de-sac. This could include patients with prior myomectomy, cesarean scar defect, or endometriosis. Despite the technique being a safeguard against bladder injury, surgeons must still use care in developing the spaces to avoid ureteral injury, especially in a setting of distorted anatomy.
References
Page B. Nezhat & the advent of advanced operative video-laparoscopy. In: Nezhat C. Nezhat's History of Endoscopy. Tuttlingen, Germany: Endo Press; 2011:159-179. https://laparoscopy.blogs.com/endoscopyhistory/chapter_22. Accessed October 23, 2019.
Podratz KC. Degrees of freedom: advances in gynecological and obstetric surgery. In: American College of Surgeons. Remembering Milestones and Achievements in Surgery: Inspiring Quality for a Hundred Years, 1913-2012. Tampa, FL: Faircount Media Group; 2013:113-119. http://endometriosisspecialists.com/wp-content/uploads/pdfs/Degrees-of-Freedom-Advances-in-Gynecological-and-Obstetrical-Surgery.pdf. Accessed October 31, 2019.
Kelley WE Jr. The evolution of laparoscopy and the revolution in surgery in the decade of the 1990s. JSLS. 2008;12:351-357.
Tokunaga T. Video surgery expands its scope. Stanford Med. 1993/1994;11(2)12-16.
Rooney CM, Crawford AT, Vassallo BJ, et al. Is previous cesarean section a risk for incidental cystotomy at the time of hysterectomy? A case-controlled study. Am J Obstet Gynecol. 2005;193:2041-2044.
Tan-Kim J, Menefee SA, Reinsch CS, et al. Laparoscopic hysterectomy and urinary tract injury: experience in a health maintenance organization. J Minim Invasive Gynecol. 2015;22:1278-1286.
Sinha R, Sundaram M, Lakhotia S, et al. Total laparoscopic hysterectomy in women with previous cesarean sections. J Minim Invasive Gynecol. 2010;17:513-517.
O'Hanlan KA. Cystosufflation to prevent bladder injury. J Minim Invasive Gynecol. 2009;16:195-197.
Martin JA, Hamilton BE, Osterman MJ, et al. Births: final data for 2013. Natl Vital Stat Rep. 2015;64:1-65.
Nezhat C, Nezhat F, Nezhat C, eds. Nezhat's Video-Assisted and Robotic-Assisted Laparoscopy and Hysteroscopy with DVD, 4th ed. New York, NY: Cambridge University Press; 2013.
Nezhat C, Grace LA, Razavi GM, et al. Reverse vesicouterine fold dissection for laparoscopic hysterectomy after prior cesarean deliveries. Obstet Gynecol. 2016;128:629-633.
Nezhat C, Xie J, Aldape D, et al. Use of laparoscopic modified nerve-sparing radical hysterectomy for the treatment of extensive endometriosis. Cureus. 2014;6:e159.
Yabuki Y, Sasaki H, Hatakeyama N, et al. Discrepancies between classic anatomy and modern gynecologic surgery on pelvic connective tissue structure: harmonization of those concepts by collaborative cadaver dissection. Am J Obstet Gynecol. 2005;193:7-15.
Uhlenhuth E. Problems in the Anatomy of the Pelvis: An Atlas. Philadelphia, PA: JB Lippincott Co; 1953.
Nezhat C, Grace, L, Soliemannjad, et al. Cesarean scar defect: what is it and how should it be treated? OBG Manag. 2016;28(4):32,34,36,38-39,53.
Nezhat C, Kennedy Burns M, Wood M, et al. Vaginal cuff dehiscence and evisceration: a review. Obstet Gynecol. 2018;132:972-985.
Nezhat C, Main J, Paka C, et al. Advanced gynecologic laparoscopy in a fast-track ambulatory surgery center. JSLS. 2014;18:pii:e2014.00291.
Nezhat C, Falik R, McKinney S, et al. Pathophysiology and management of urinary tract endometriosis. Nat Rev Urol. 2017;14:359-372.
References
Page B. Nezhat & the advent of advanced operative video-laparoscopy. In: Nezhat C. Nezhat's History of Endoscopy. Tuttlingen, Germany: Endo Press; 2011:159-179. https://laparoscopy.blogs.com/endoscopyhistory/chapter_22. Accessed October 23, 2019.
Podratz KC. Degrees of freedom: advances in gynecological and obstetric surgery. In: American College of Surgeons. Remembering Milestones and Achievements in Surgery: Inspiring Quality for a Hundred Years, 1913-2012. Tampa, FL: Faircount Media Group; 2013:113-119. http://endometriosisspecialists.com/wp-content/uploads/pdfs/Degrees-of-Freedom-Advances-in-Gynecological-and-Obstetrical-Surgery.pdf. Accessed October 31, 2019.
Kelley WE Jr. The evolution of laparoscopy and the revolution in surgery in the decade of the 1990s. JSLS. 2008;12:351-357.
Tokunaga T. Video surgery expands its scope. Stanford Med. 1993/1994;11(2)12-16.
Rooney CM, Crawford AT, Vassallo BJ, et al. Is previous cesarean section a risk for incidental cystotomy at the time of hysterectomy? A case-controlled study. Am J Obstet Gynecol. 2005;193:2041-2044.
Tan-Kim J, Menefee SA, Reinsch CS, et al. Laparoscopic hysterectomy and urinary tract injury: experience in a health maintenance organization. J Minim Invasive Gynecol. 2015;22:1278-1286.
Sinha R, Sundaram M, Lakhotia S, et al. Total laparoscopic hysterectomy in women with previous cesarean sections. J Minim Invasive Gynecol. 2010;17:513-517.
O'Hanlan KA. Cystosufflation to prevent bladder injury. J Minim Invasive Gynecol. 2009;16:195-197.
Martin JA, Hamilton BE, Osterman MJ, et al. Births: final data for 2013. Natl Vital Stat Rep. 2015;64:1-65.
Nezhat C, Nezhat F, Nezhat C, eds. Nezhat's Video-Assisted and Robotic-Assisted Laparoscopy and Hysteroscopy with DVD, 4th ed. New York, NY: Cambridge University Press; 2013.
Nezhat C, Grace LA, Razavi GM, et al. Reverse vesicouterine fold dissection for laparoscopic hysterectomy after prior cesarean deliveries. Obstet Gynecol. 2016;128:629-633.
Nezhat C, Xie J, Aldape D, et al. Use of laparoscopic modified nerve-sparing radical hysterectomy for the treatment of extensive endometriosis. Cureus. 2014;6:e159.
Yabuki Y, Sasaki H, Hatakeyama N, et al. Discrepancies between classic anatomy and modern gynecologic surgery on pelvic connective tissue structure: harmonization of those concepts by collaborative cadaver dissection. Am J Obstet Gynecol. 2005;193:7-15.
Uhlenhuth E. Problems in the Anatomy of the Pelvis: An Atlas. Philadelphia, PA: JB Lippincott Co; 1953.
Nezhat C, Grace, L, Soliemannjad, et al. Cesarean scar defect: what is it and how should it be treated? OBG Manag. 2016;28(4):32,34,36,38-39,53.
Nezhat C, Kennedy Burns M, Wood M, et al. Vaginal cuff dehiscence and evisceration: a review. Obstet Gynecol. 2018;132:972-985.
Nezhat C, Main J, Paka C, et al. Advanced gynecologic laparoscopy in a fast-track ambulatory surgery center. JSLS. 2014;18:pii:e2014.00291.
Nezhat C, Falik R, McKinney S, et al. Pathophysiology and management of urinary tract endometriosis. Nat Rev Urol. 2017;14:359-372.
Reducing Cardiovascular Events in Patients with Type 2 Diabetes Mellitus
This supplement offers the opportunity to earn a total of 1 CME credit.
Credit is awarded for successful completion of the online evaluation at the link below. This link may also be found within the supplement on the first page of the article.
To receive CME credit, please read the journal article and, upon completion, go to www.pceconsortium.org/CVEvents to complete the online post-test and receive your certificate of credit.
Sponsor
This supplement was sponsored by Primary Care Education Consortium and Primary …
Reducing Cardiovascular Events in Patients with Type 2 Diabetes Mellitus
This supplement offers the opportunity to earn a total of 1 CME credit.
Credit is awarded for successful completion of the online evaluation at the link below. This link may also be found within the supplement on the first page of the article.
To receive CME credit, please read the journal article and, upon completion, go to www.pceconsortium.org/CVEvents to complete the online post-test and receive your certificate of credit.
Reducing Cardiovascular Events in Patients with Type 2 Diabetes Mellitus
This supplement offers the opportunity to earn a total of 1 CME credit.
Credit is awarded for successful completion of the online evaluation at the link below. This link may also be found within the supplement on the first page of the article.
To receive CME credit, please read the journal article and, upon completion, go to www.pceconsortium.org/CVEvents to complete the online post-test and receive your certificate of credit.
Traumatic microbleeds (TMBs) may indicate vascular injury and predict worse outcomes after even minor brain injury, according to a study at the National Institute of Neurological Disorders and Stroke.
The study involved 439 adults with head injuries treated in the emergency department. The participants had magnetic resonance imaging (MRI) scans within 48 hours of the injury and again during 4 subsequent visits. They also completed behavioral and outcome questionnaires.
Microbleeds appear as small dark lesions on MRI scans but are usually too small to be seen on computer tomography (CT) scans. Sometimes they appear as dots (punctate), sometimes they are linear. In previous studies, researchers examined TMBs in the acute phase of traumatic brain injury (TBI) and stroke and found linear-appearing TMBs only in patients with TBI, suggesting that at least linear TMBs are consistent with trauma and might be the result of injured vessels. They conjectured that TMBs seen on MRI might be a form of traumatic vascular injury distinct from primary injury to the axons.
In this study, one-third of the patients had TMBs. More than half (58%) of the participants with severe head injury showed microbleeds, as did 27% of patients with mild injuries. In most patients with microbleeds, they appeared as linear streaks or dotted lesions. The study also revealed that the frontal lobes were the region most likely to show microbleeds.
The researchers controlled for variables known to predict poor outcome, such as trauma level and trauma-related injury on CT. Even so, microbleeds significantly predicted worse outcome. Patients with both punctate and linear TMBs were twice as likely to have disability (Glasgow Outcome Scale-Extended ≤6) on follow-up.
One participant’s family donated his brain for further analysis after he died. Imaging with a more powerful MRI scanner and a detailed histologic analysis allowed the researchers to better understand the pathology.
The researchers found that what appeared as a punctate TMB on MRI corresponded to iron-laden macrophages in the perivascular space surrounding a vascular tree that extended over centimeters. That was surprising, the researchers say. They expected to see iron within the parenchyma, but they also found iron inside macrophages outside of the parenchyma between the vessel and neuropil, tracking alongside vessels.
The researchers say that finding signified that the extent of injury was more extensive than indicated on MRI and had consequences to cellular function over a larger area of brain. In fact, they suggest, punctate and linear TMBs may not be distinct entities: The difference in shape may be “an issue of resolution.”
The researchers conclude that TMBs could be biomarkers for vascular injury. They also note that the leakage of blood from damaged blood vessels can trigger an inflammatory response. The damage to vessels, the disruption of normal pathways of blood flow, and the influx of inflammatory cells could result in secondary injury to the brain tissue due to ischemia.
Thus, TMBs may also be useful biomarkers for identifying which patients are candidates for treatments that reduce ischemic damage or improve microvascular cerebral blood flow.
Researchers discover certain “dots” on the brain may be a biomarker for vascular injury and aid in predicting outcomes after injury.
Researchers discover certain “dots” on the brain may be a biomarker for vascular injury and aid in predicting outcomes after injury.
Traumatic microbleeds (TMBs) may indicate vascular injury and predict worse outcomes after even minor brain injury, according to a study at the National Institute of Neurological Disorders and Stroke.
The study involved 439 adults with head injuries treated in the emergency department. The participants had magnetic resonance imaging (MRI) scans within 48 hours of the injury and again during 4 subsequent visits. They also completed behavioral and outcome questionnaires.
Microbleeds appear as small dark lesions on MRI scans but are usually too small to be seen on computer tomography (CT) scans. Sometimes they appear as dots (punctate), sometimes they are linear. In previous studies, researchers examined TMBs in the acute phase of traumatic brain injury (TBI) and stroke and found linear-appearing TMBs only in patients with TBI, suggesting that at least linear TMBs are consistent with trauma and might be the result of injured vessels. They conjectured that TMBs seen on MRI might be a form of traumatic vascular injury distinct from primary injury to the axons.
In this study, one-third of the patients had TMBs. More than half (58%) of the participants with severe head injury showed microbleeds, as did 27% of patients with mild injuries. In most patients with microbleeds, they appeared as linear streaks or dotted lesions. The study also revealed that the frontal lobes were the region most likely to show microbleeds.
The researchers controlled for variables known to predict poor outcome, such as trauma level and trauma-related injury on CT. Even so, microbleeds significantly predicted worse outcome. Patients with both punctate and linear TMBs were twice as likely to have disability (Glasgow Outcome Scale-Extended ≤6) on follow-up.
One participant’s family donated his brain for further analysis after he died. Imaging with a more powerful MRI scanner and a detailed histologic analysis allowed the researchers to better understand the pathology.
The researchers found that what appeared as a punctate TMB on MRI corresponded to iron-laden macrophages in the perivascular space surrounding a vascular tree that extended over centimeters. That was surprising, the researchers say. They expected to see iron within the parenchyma, but they also found iron inside macrophages outside of the parenchyma between the vessel and neuropil, tracking alongside vessels.
The researchers say that finding signified that the extent of injury was more extensive than indicated on MRI and had consequences to cellular function over a larger area of brain. In fact, they suggest, punctate and linear TMBs may not be distinct entities: The difference in shape may be “an issue of resolution.”
The researchers conclude that TMBs could be biomarkers for vascular injury. They also note that the leakage of blood from damaged blood vessels can trigger an inflammatory response. The damage to vessels, the disruption of normal pathways of blood flow, and the influx of inflammatory cells could result in secondary injury to the brain tissue due to ischemia.
Thus, TMBs may also be useful biomarkers for identifying which patients are candidates for treatments that reduce ischemic damage or improve microvascular cerebral blood flow.
Traumatic microbleeds (TMBs) may indicate vascular injury and predict worse outcomes after even minor brain injury, according to a study at the National Institute of Neurological Disorders and Stroke.
The study involved 439 adults with head injuries treated in the emergency department. The participants had magnetic resonance imaging (MRI) scans within 48 hours of the injury and again during 4 subsequent visits. They also completed behavioral and outcome questionnaires.
Microbleeds appear as small dark lesions on MRI scans but are usually too small to be seen on computer tomography (CT) scans. Sometimes they appear as dots (punctate), sometimes they are linear. In previous studies, researchers examined TMBs in the acute phase of traumatic brain injury (TBI) and stroke and found linear-appearing TMBs only in patients with TBI, suggesting that at least linear TMBs are consistent with trauma and might be the result of injured vessels. They conjectured that TMBs seen on MRI might be a form of traumatic vascular injury distinct from primary injury to the axons.
In this study, one-third of the patients had TMBs. More than half (58%) of the participants with severe head injury showed microbleeds, as did 27% of patients with mild injuries. In most patients with microbleeds, they appeared as linear streaks or dotted lesions. The study also revealed that the frontal lobes were the region most likely to show microbleeds.
The researchers controlled for variables known to predict poor outcome, such as trauma level and trauma-related injury on CT. Even so, microbleeds significantly predicted worse outcome. Patients with both punctate and linear TMBs were twice as likely to have disability (Glasgow Outcome Scale-Extended ≤6) on follow-up.
One participant’s family donated his brain for further analysis after he died. Imaging with a more powerful MRI scanner and a detailed histologic analysis allowed the researchers to better understand the pathology.
The researchers found that what appeared as a punctate TMB on MRI corresponded to iron-laden macrophages in the perivascular space surrounding a vascular tree that extended over centimeters. That was surprising, the researchers say. They expected to see iron within the parenchyma, but they also found iron inside macrophages outside of the parenchyma between the vessel and neuropil, tracking alongside vessels.
The researchers say that finding signified that the extent of injury was more extensive than indicated on MRI and had consequences to cellular function over a larger area of brain. In fact, they suggest, punctate and linear TMBs may not be distinct entities: The difference in shape may be “an issue of resolution.”
The researchers conclude that TMBs could be biomarkers for vascular injury. They also note that the leakage of blood from damaged blood vessels can trigger an inflammatory response. The damage to vessels, the disruption of normal pathways of blood flow, and the influx of inflammatory cells could result in secondary injury to the brain tissue due to ischemia.
Thus, TMBs may also be useful biomarkers for identifying which patients are candidates for treatments that reduce ischemic damage or improve microvascular cerebral blood flow.