User login
Endoscopic myotomy for achalasia
Dear colleagues and friends,

In this edition of Perspectives, Dr. Mouen Khashab and Dr. Robert Siwiec tackle an exciting and constantly evolving topic, which is the optimal approach to myotomy for patients with achalasia. Dr. Khashab makes the case for endoscopic myotomy, while Dr. Siwiec argues that surgical myotomy remains the gold standard. I hope that you will find this debate as useful and thought provoking as I did. As always, I welcome your comments and suggestions for future topics at [email protected].
Charles Kahi, MD, MS, AGAF, is a professor of medicine at Indiana University, Indianapolis. He is also an associate editor for GI & Hepatology News.
Endoscopic myotomy for achalasia is ready for prime time
BY MOUEN A. KHASHAB, MD
When I encounter a symptomatic patient with manometrically confirmed achalasia, I discuss three effective treatment modalities: pneumatic dilation (PD), peroral endoscopic myotomy (POEM), and laparoscopic Heller myotomy (LHM). I recommend against botulinum toxin injection and reserve it for patients who are not candidates for the aforementioned definitive therapies. I also present to the patient the current level I evidence from randomized, controlled trials (RCTs) comparing achalasia treatment modalities.

One landmark RCT reported comparative outcomes at 2 years following POEM and PD and found higher treatment success at the 2-year follow-up in the POEM group (92% vs. 54%; P < .001).1 Reflux esophagitis was observed significantly more frequently in patients treated with POEM (41% in the POEM group, of whom 35% were assigned Los Angeles grade A-B and 6% were assigned LA grade C versus 7% in the PD group, all of whom were assigned LA grade A; P = .002).1
Another milestone RCT included 221 patients and compared outcomes of POEM and LHM plus Dor fundoplication.2 Clinical success at the 2-year follow-up was observed in 83.0% of patients in the POEM group, and was noninferior to the LHM group (81.7%). Serious adverse events occurred in 2.7% of patients in the POEM group and in 7.3% of patients in the LHM group. Although 57% of patients in the POEM group and 20% of patients in the LHM group had reflux esophagitis as assessed by endoscopy at 3 months, the corresponding proportions were 44% and 29% at 24 months. Importantly, the rate of severe esophagitis was not different between both groups (6% vs. 3% at 3 months, and 5% vs. 6% at 24 months).2
I summarize these results by stating that POEM seems to be superior to PD and equivalent to LHM in terms of clinical success. Nonetheless, POEM also seems to be associated with increased risk of early gastroesophageal reflux disease.
POEM is now a ubiquitous procedure performed worldwide and is endorsed as a primary achalasia treatment by multiple society guidelines.3 It is a minimally invasive, effective, and safe therapeutic option for patients with all types of achalasia and is considered the treatment of choice for achalasia type III. POEM has also been shown to be effective in the treatment of spastic esophageal disorders (e.g. Jackhammer esophagus, diffuse esophageal spasm) and esophagogastric junction outflow obstruction. It can be performed in the endoscopy unit or operating theater either by experienced therapeutic endoscopists or surgical endoscopists in less than an hour. The procedure can be performed on an outpatient basis in appropriate individuals and allows tailoring the myotomy length to specific clinical scenarios. For example, patients with type III achalasia (and those with spastic esophageal disorders) typically require a long myotomy and that can be readily accomplished during POEM as opposed to LHM. POEM has also proven effective in children; octogenarians; and patients with sigmoid esophagus, epiphrenic diverticula, and those who had undergone prior interventions for achalasia, including LHM and PD. In experienced hands, the rate of adverse events is low and serious events are rare and occur in 0.5% of cases. Perforations/leakage are also uncommon and occur in 0.7% of patients. It is an incisionless procedure that eliminates the risk of wound infection and shortens postprocedural recovery. Patients are typically admitted for an overnight observation postprocedure, discharged home the following day, and back to activities of daily living (including work) within a few days. Postprocedural pain is minimal in most patients and narcotics are rarely needed. Resumption of a soft diet is carried out on the first postoperative day and normal diet 1 week later.
LHM is an established procedure with proven long-term efficacy in the treatment of achalasia. Nonetheless, it is invasive and requires placement of multiple trocars. The procedure is more time consuming than POEM and length of hospital stay can also be longer. This results in possibly higher cost than POEM. Importantly, recovery of dysphagia and resumption of normal diet is significantly delayed and is likely the result of the partial concomitant fundoplication procedure. Finally, LHM is not appropriate for the treatment of spastic esophageal disorders, including type III achalasia.
A major advantage of LHM plus partial fundoplication over POEM is the diminished risk of gastroesophageal reflux disease (GERD). However, this advantage seems short lived as the risk of GERD increases over time after surgery, likely because of the loosening of the wrap over time. From the New England Journal of Medicine paper mentioned earlier, it seems that the increased risk of GERD after POEM as compared with LHM diminishes over time.2 Importantly, it also appears that the rate of significant esophagitis (LA grade C-D) is similar between both procedures.2
In an effort to assess the long-term antireflux efficacy of surgical partial fundoplication, one study noted that 12% of 182 patients who had surgical myotomy with partial fundoplication continued to have occasional or continuous heartburn symptoms at a median of 18 years after surgery. Esophagitis and Barrett’s esophagus were found in 14.5% and 0.8% of patients, respectively. De novo esophageal adenocarcinoma has been reported after both POEM and LHM.4
Therefore, GERD and its complications can occur after any procedure that disrupts the lower esophageal sphincter (POEM, LHM, and PD) and postprocedural management of patients should include long-term testing and management of possible GERD. Different strategies have been proposed and include objective periodic testing for esophageal acid exposure, long-term and possible lifelong proton pump inhibitor use, and surveillance for long-term consequences of GER via periodic upper endoscopy.3
It is important to acknowledge that the lack of symptoms or the absence of endoscopic evidence of GER on initial endoscopy does not necessarily rule out GER. Approximately a third of post-POEM patients with clinically successful outcome and absence of reflux esophagitis on their first surveillance endoscopy eventually develop esophagitis at subsequent surveillance endoscopy.5
In summary, POEM has deservingly taken a prime time spot in the management of patients with achalasia. It is an efficient, efficacious and safe treatment modality that results in rapid resolution of achalasia symptoms in the majority of patients. Research should focus on technical modifications (e.g., short gastric myotomy; addition of endoscopic fundoplication) that reduce the incidence of postprocedural GERD.
References
1. Ponds FA et al. Effect of peroral endoscopic myotomy versus pneumatic dilation on symptom severity and treatment outcomes among treatment-naive patients with achalasia: A randomized clinical trial. JAMA. 2019;322:134-44.
2. Werner YB et al. Endoscopic or surgical myotomy in patients with idiopathic achalasia. N Engl J Med. 2019;381:2219-29.
3. Khashab MA et al. ASGE guideline on the management of achalasia. Gastrointest Endosc. 2020;91:213-27 e6.
4. Ichkhanian Y et al. Case of early Barrett cancer following peroral endoscopic myotomy. Gut. 2019;68:2107-110.
5. Werner YB et al. Clinical response to peroral endoscopic myotomy in patients with idiopathic achalasia at a minimum follow-up of 2 years. Gut. 2016;65:899-906.
Dr. Khashab is associate professor of medicine, director of therapeutic endoscopy, division of gastroenterology and hepatology, Johns Hopkins Hospital, Baltimore. He is a consultant for BSCI, Olympus, and Medtronic.
Heller myotomy is still the gold standard
BY ROBERT M. SIWIEC, MD
Achalasia is a rare, primary esophageal motor disorder characterized by ineffective relaxation of the lower esophageal sphincter (LES) and concomitant loss of esophageal peristalsis. High-resolution esophageal manometry has allowed for the diagnosis and classification of achalasia into relevant clinical subtypes which become important when discussing and considering treatment options. Confirmatory studies (e.g., timed barium esophagram) and provocative manometric maneuvers (e.g., upright swallows, rapid swallow sequence, and/or rapid drink challenge) can be helpful when distinguishing between true achalasia versus achalasia variants and esophagogastric junction outflow obstruction.

Treatment options only provide palliation by eliminating outflow obstruction caused by a nonrelaxing and often times hypertensive LES. Pharmacotherapy (e.g., oral nitrates, 5-phosphodiesterase inhibitors, anticholinergics) is the least effective option because of medication side effects and short-acting duration. I only consider it for patients who are either unwilling or unable to tolerate invasive therapies. Botulinum toxin injection into the LES can be considered in patients who are not good candidates for more definitive therapy with PD or myotomy (endoscopic or surgical). Although the success rates with botulinum toxin are comparable with PD and surgical myotomy, patients treated with botulinum toxin require retreatment. Furthermore, continued botulinum toxin injections can compromise tissue planes making myotomy complex and challenging.
During the 1970s and 1980s, PD was the primary treatment modality for achalasia. Surgical myotomy was reserved for patients who suffered a perforation during PD or developed recurrent symptoms after multiple dilations. Minimally invasive surgery (left thoracoscopic approach) for achalasia was first introduced in the early 1990s and was shown to be a feasible, safe, and effective procedure, becoming the primary treatment approach in most centers. Patients fared well; however, it was soon discovered that >50% had pathological reflux based on pH monitoring. A few centers then began to perform a Heller myotomy through a laparoscopic approach with the addition of a fundoplication resulting in significant reductions in pathological reflux by pH monitoring. Eventually, a seminal RCT confirmed the importance of fundoplication with laparoscopic Heller myotomy (LHM) – resolution of dysphagia was unaffected and pathological reflux was avoided in most patients.1 Overall, clinical success rates for LHM with fundoplication are typically >90% and reflux incidence rates <10% with the overall complication rate being about 5% with reported mortality <0.1%.
PD remains appealing in that it is cost effective and less invasive, compared with POEM and LHM. Initial success rates and short-term efficacy are comparable with LHM but unfortunately PD’s efficacy significantly wanes over time. POEM, introduced by Inoue et al. in 2010, is a novel endoscopic technique with an excellent safety profile that provides good symptom relief while avoiding abdominal wall scars for patients. It has been shown to have a distinct advantage in patients with type III achalasia by nature of the longer myotomy not achievable by LHM.2 POEM has seen increasing enthusiasm and acceptance as a standard treatment option for achalasia largely because of the fact that its safety and efficacy have been shown to be comparable and in most cases equal with LHM. However, in 2020, direct comparison with LHM is challenging given that the follow-up in the majority of studies is either short or incomplete. The most recent multicenter, randomized trial comparing POEM with LHM plus Dor fundoplication showed POEM’s noninferiority in controlling symptoms of achalasia, but only after a 24 month follow-up.3 A recent report included one of the largest cohorts of post-POEM patients (500), but the 36-month data were based on the follow-up of only 61 patients (about 12%).4
Once the muscle fibers of the LES are disrupted, reflux will occur in the majority of patients. Unlike LHM, no concomitant fundoplication is performed during POEM and this increases the incidence of GERD and its long-term sequelae including peptic strictures, Barrett’s esophagus, and adenocarcinoma. A meta-analysis from 2018 looked at published series of POEM and LHM with fundoplication and found that GERD symptoms were present in 19% of POEM patients, compared with 8.8% of LHM patients. Worse yet, esophagitis was seen in 29.4% of the POEM group and 7.6% of the LHM group, with more individuals in the POEM group also having abnormal acid exposure based on ambulatory pH monitoring (39.0% vs. 16.8%).5
Proponents of POEM will argue that proton pump inhibitors (PPIs) are the panacea for post-POEM GERD. Unfortunately, this approach has its own problems. PPIs are very effective at reducing acid secretion by parietal cells, but do not block reflux through an iatrogenically incompetent LES. The drumbeat of publications on potential complications from chronic PPI use has greatly contributed to patients’ reluctance to commit to long-term PPI use. Lastly, the first case of early Barrett’s cancer was recently reported in a patient 4 years post-POEM despite adherence to an aggressive antisecretory regimen (b.i.d. PPI and H2 blocker at bedtime).6 LHM with fundoplication significantly reduces the risk of pathological GERD and spares patients from committing to lifelong PPI therapy and routine endoscopic surveillance (appropriate interval yet to be determined) and needing to consider additional procedures (i.e., endoscopic or surgical fundoplication).
Despite POEM’s well established efficacy and safety, the development of post-POEM GERD is a major concern that has yet to be adequately addressed. A significant number of post-POEM patients with pathological reflux have asymptomatic and unrecognized GERD and current management and monitoring strategies for post-POEM GERD are anemic and poorly established. Without question, there are individual patients who are clearly better served with POEM (type III achalasia and other spastic esophageal disorders). However, as we continue to learn more about post-POEM GERD and how to better prevent, manage, and monitor it, LHM with fundoplication for the time being remains the tried-and-tested treatment option for patients with non–type III achalasia.
References
1. Richards WO et al. Heller myotomy versus Heller myotomy with Dor fundoplication for achalasia: A prospective randomized double-blind clinical trial. Ann Surg. 2004;240:405-12.
2. Podboy AJ et al. Long-term outcomes of peroral endoscopic myotomy compared to laparoscopic Heller myotomy for achalasia: A single-center experience. Surg Endosc. 2020. doi: 10.1007/s00464-020-07450-6.
3. Werner YB et al. Endoscopic or surgical myotomy in patients with idiopathic achalasia. N Engl J Med. 2019;381(23):2219-29.
4. Inoue H et al. Peroral endoscopic myotomy: A series of 500 patients. J Am Coll Surg. 2015;221:256-64.
5. Repici A et al. GERD after peroral endoscopic myotomy as compared with Heller’s myotomy with fundoplication: A systematic review with meta-analysis. Gastrointest Endosc. 2018;87(4):934-43.
6. Ichkhanian Y et al. Case of early Barrett cancer following peroral endoscopic myotomy. Gut. 2019;68:2107-10.
Dr. Siwiec is assistant professor of clinical medicine, division of gastroenterology and hepatology, GI motility and neurogastroenterology unit, Indiana University, Indianapolis. He has no conflicts of interest.
Dear colleagues and friends,
In this edition of Perspectives, Dr. Mouen Khashab and Dr. Robert Siwiec tackle an exciting and constantly evolving topic, which is the optimal approach to myotomy for patients with achalasia. Dr. Khashab makes the case for endoscopic myotomy, while Dr. Siwiec argues that surgical myotomy remains the gold standard. I hope that you will find this debate as useful and thought provoking as I did. As always, I welcome your comments and suggestions for future topics at [email protected].
Charles Kahi, MD, MS, AGAF, is a professor of medicine at Indiana University, Indianapolis. He is also an associate editor for GI & Hepatology News.
Endoscopic myotomy for achalasia is ready for prime time
BY MOUEN A. KHASHAB, MD
When I encounter a symptomatic patient with manometrically confirmed achalasia, I discuss three effective treatment modalities: pneumatic dilation (PD), peroral endoscopic myotomy (POEM), and laparoscopic Heller myotomy (LHM). I recommend against botulinum toxin injection and reserve it for patients who are not candidates for the aforementioned definitive therapies. I also present to the patient the current level I evidence from randomized, controlled trials (RCTs) comparing achalasia treatment modalities.
One landmark RCT reported comparative outcomes at 2 years following POEM and PD and found higher treatment success at the 2-year follow-up in the POEM group (92% vs. 54%; P < .001).1 Reflux esophagitis was observed significantly more frequently in patients treated with POEM (41% in the POEM group, of whom 35% were assigned Los Angeles grade A-B and 6% were assigned LA grade C versus 7% in the PD group, all of whom were assigned LA grade A; P = .002).1
Another milestone RCT included 221 patients and compared outcomes of POEM and LHM plus Dor fundoplication.2 Clinical success at the 2-year follow-up was observed in 83.0% of patients in the POEM group, and was noninferior to the LHM group (81.7%). Serious adverse events occurred in 2.7% of patients in the POEM group and in 7.3% of patients in the LHM group. Although 57% of patients in the POEM group and 20% of patients in the LHM group had reflux esophagitis as assessed by endoscopy at 3 months, the corresponding proportions were 44% and 29% at 24 months. Importantly, the rate of severe esophagitis was not different between both groups (6% vs. 3% at 3 months, and 5% vs. 6% at 24 months).2
I summarize these results by stating that POEM seems to be superior to PD and equivalent to LHM in terms of clinical success. Nonetheless, POEM also seems to be associated with increased risk of early gastroesophageal reflux disease.
POEM is now a ubiquitous procedure performed worldwide and is endorsed as a primary achalasia treatment by multiple society guidelines.3 It is a minimally invasive, effective, and safe therapeutic option for patients with all types of achalasia and is considered the treatment of choice for achalasia type III. POEM has also been shown to be effective in the treatment of spastic esophageal disorders (e.g. Jackhammer esophagus, diffuse esophageal spasm) and esophagogastric junction outflow obstruction. It can be performed in the endoscopy unit or operating theater either by experienced therapeutic endoscopists or surgical endoscopists in less than an hour. The procedure can be performed on an outpatient basis in appropriate individuals and allows tailoring the myotomy length to specific clinical scenarios. For example, patients with type III achalasia (and those with spastic esophageal disorders) typically require a long myotomy and that can be readily accomplished during POEM as opposed to LHM. POEM has also proven effective in children; octogenarians; and patients with sigmoid esophagus, epiphrenic diverticula, and those who had undergone prior interventions for achalasia, including LHM and PD. In experienced hands, the rate of adverse events is low and serious events are rare and occur in 0.5% of cases. Perforations/leakage are also uncommon and occur in 0.7% of patients. It is an incisionless procedure that eliminates the risk of wound infection and shortens postprocedural recovery. Patients are typically admitted for an overnight observation postprocedure, discharged home the following day, and back to activities of daily living (including work) within a few days. Postprocedural pain is minimal in most patients and narcotics are rarely needed. Resumption of a soft diet is carried out on the first postoperative day and normal diet 1 week later.
LHM is an established procedure with proven long-term efficacy in the treatment of achalasia. Nonetheless, it is invasive and requires placement of multiple trocars. The procedure is more time consuming than POEM and length of hospital stay can also be longer. This results in possibly higher cost than POEM. Importantly, recovery of dysphagia and resumption of normal diet is significantly delayed and is likely the result of the partial concomitant fundoplication procedure. Finally, LHM is not appropriate for the treatment of spastic esophageal disorders, including type III achalasia.
A major advantage of LHM plus partial fundoplication over POEM is the diminished risk of gastroesophageal reflux disease (GERD). However, this advantage seems short lived as the risk of GERD increases over time after surgery, likely because of the loosening of the wrap over time. From the New England Journal of Medicine paper mentioned earlier, it seems that the increased risk of GERD after POEM as compared with LHM diminishes over time.2 Importantly, it also appears that the rate of significant esophagitis (LA grade C-D) is similar between both procedures.2
In an effort to assess the long-term antireflux efficacy of surgical partial fundoplication, one study noted that 12% of 182 patients who had surgical myotomy with partial fundoplication continued to have occasional or continuous heartburn symptoms at a median of 18 years after surgery. Esophagitis and Barrett’s esophagus were found in 14.5% and 0.8% of patients, respectively. De novo esophageal adenocarcinoma has been reported after both POEM and LHM.4
Therefore, GERD and its complications can occur after any procedure that disrupts the lower esophageal sphincter (POEM, LHM, and PD) and postprocedural management of patients should include long-term testing and management of possible GERD. Different strategies have been proposed and include objective periodic testing for esophageal acid exposure, long-term and possible lifelong proton pump inhibitor use, and surveillance for long-term consequences of GER via periodic upper endoscopy.3
It is important to acknowledge that the lack of symptoms or the absence of endoscopic evidence of GER on initial endoscopy does not necessarily rule out GER. Approximately a third of post-POEM patients with clinically successful outcome and absence of reflux esophagitis on their first surveillance endoscopy eventually develop esophagitis at subsequent surveillance endoscopy.5
In summary, POEM has deservingly taken a prime time spot in the management of patients with achalasia. It is an efficient, efficacious and safe treatment modality that results in rapid resolution of achalasia symptoms in the majority of patients. Research should focus on technical modifications (e.g., short gastric myotomy; addition of endoscopic fundoplication) that reduce the incidence of postprocedural GERD.
References
1. Ponds FA et al. Effect of peroral endoscopic myotomy versus pneumatic dilation on symptom severity and treatment outcomes among treatment-naive patients with achalasia: A randomized clinical trial. JAMA. 2019;322:134-44.
2. Werner YB et al. Endoscopic or surgical myotomy in patients with idiopathic achalasia. N Engl J Med. 2019;381:2219-29.
3. Khashab MA et al. ASGE guideline on the management of achalasia. Gastrointest Endosc. 2020;91:213-27 e6.
4. Ichkhanian Y et al. Case of early Barrett cancer following peroral endoscopic myotomy. Gut. 2019;68:2107-110.
5. Werner YB et al. Clinical response to peroral endoscopic myotomy in patients with idiopathic achalasia at a minimum follow-up of 2 years. Gut. 2016;65:899-906.
Dr. Khashab is associate professor of medicine, director of therapeutic endoscopy, division of gastroenterology and hepatology, Johns Hopkins Hospital, Baltimore. He is a consultant for BSCI, Olympus, and Medtronic.
Heller myotomy is still the gold standard
BY ROBERT M. SIWIEC, MD
Achalasia is a rare, primary esophageal motor disorder characterized by ineffective relaxation of the lower esophageal sphincter (LES) and concomitant loss of esophageal peristalsis. High-resolution esophageal manometry has allowed for the diagnosis and classification of achalasia into relevant clinical subtypes which become important when discussing and considering treatment options. Confirmatory studies (e.g., timed barium esophagram) and provocative manometric maneuvers (e.g., upright swallows, rapid swallow sequence, and/or rapid drink challenge) can be helpful when distinguishing between true achalasia versus achalasia variants and esophagogastric junction outflow obstruction.
Treatment options only provide palliation by eliminating outflow obstruction caused by a nonrelaxing and often times hypertensive LES. Pharmacotherapy (e.g., oral nitrates, 5-phosphodiesterase inhibitors, anticholinergics) is the least effective option because of medication side effects and short-acting duration. I only consider it for patients who are either unwilling or unable to tolerate invasive therapies. Botulinum toxin injection into the LES can be considered in patients who are not good candidates for more definitive therapy with PD or myotomy (endoscopic or surgical). Although the success rates with botulinum toxin are comparable with PD and surgical myotomy, patients treated with botulinum toxin require retreatment. Furthermore, continued botulinum toxin injections can compromise tissue planes making myotomy complex and challenging.
During the 1970s and 1980s, PD was the primary treatment modality for achalasia. Surgical myotomy was reserved for patients who suffered a perforation during PD or developed recurrent symptoms after multiple dilations. Minimally invasive surgery (left thoracoscopic approach) for achalasia was first introduced in the early 1990s and was shown to be a feasible, safe, and effective procedure, becoming the primary treatment approach in most centers. Patients fared well; however, it was soon discovered that >50% had pathological reflux based on pH monitoring. A few centers then began to perform a Heller myotomy through a laparoscopic approach with the addition of a fundoplication resulting in significant reductions in pathological reflux by pH monitoring. Eventually, a seminal RCT confirmed the importance of fundoplication with laparoscopic Heller myotomy (LHM) – resolution of dysphagia was unaffected and pathological reflux was avoided in most patients.1 Overall, clinical success rates for LHM with fundoplication are typically >90% and reflux incidence rates <10% with the overall complication rate being about 5% with reported mortality <0.1%.
PD remains appealing in that it is cost effective and less invasive, compared with POEM and LHM. Initial success rates and short-term efficacy are comparable with LHM but unfortunately PD’s efficacy significantly wanes over time. POEM, introduced by Inoue et al. in 2010, is a novel endoscopic technique with an excellent safety profile that provides good symptom relief while avoiding abdominal wall scars for patients. It has been shown to have a distinct advantage in patients with type III achalasia by nature of the longer myotomy not achievable by LHM.2 POEM has seen increasing enthusiasm and acceptance as a standard treatment option for achalasia largely because of the fact that its safety and efficacy have been shown to be comparable and in most cases equal with LHM. However, in 2020, direct comparison with LHM is challenging given that the follow-up in the majority of studies is either short or incomplete. The most recent multicenter, randomized trial comparing POEM with LHM plus Dor fundoplication showed POEM’s noninferiority in controlling symptoms of achalasia, but only after a 24 month follow-up.3 A recent report included one of the largest cohorts of post-POEM patients (500), but the 36-month data were based on the follow-up of only 61 patients (about 12%).4
Once the muscle fibers of the LES are disrupted, reflux will occur in the majority of patients. Unlike LHM, no concomitant fundoplication is performed during POEM and this increases the incidence of GERD and its long-term sequelae including peptic strictures, Barrett’s esophagus, and adenocarcinoma. A meta-analysis from 2018 looked at published series of POEM and LHM with fundoplication and found that GERD symptoms were present in 19% of POEM patients, compared with 8.8% of LHM patients. Worse yet, esophagitis was seen in 29.4% of the POEM group and 7.6% of the LHM group, with more individuals in the POEM group also having abnormal acid exposure based on ambulatory pH monitoring (39.0% vs. 16.8%).5
Proponents of POEM will argue that proton pump inhibitors (PPIs) are the panacea for post-POEM GERD. Unfortunately, this approach has its own problems. PPIs are very effective at reducing acid secretion by parietal cells, but do not block reflux through an iatrogenically incompetent LES. The drumbeat of publications on potential complications from chronic PPI use has greatly contributed to patients’ reluctance to commit to long-term PPI use. Lastly, the first case of early Barrett’s cancer was recently reported in a patient 4 years post-POEM despite adherence to an aggressive antisecretory regimen (b.i.d. PPI and H2 blocker at bedtime).6 LHM with fundoplication significantly reduces the risk of pathological GERD and spares patients from committing to lifelong PPI therapy and routine endoscopic surveillance (appropriate interval yet to be determined) and needing to consider additional procedures (i.e., endoscopic or surgical fundoplication).
Despite POEM’s well established efficacy and safety, the development of post-POEM GERD is a major concern that has yet to be adequately addressed. A significant number of post-POEM patients with pathological reflux have asymptomatic and unrecognized GERD and current management and monitoring strategies for post-POEM GERD are anemic and poorly established. Without question, there are individual patients who are clearly better served with POEM (type III achalasia and other spastic esophageal disorders). However, as we continue to learn more about post-POEM GERD and how to better prevent, manage, and monitor it, LHM with fundoplication for the time being remains the tried-and-tested treatment option for patients with non–type III achalasia.
References
1. Richards WO et al. Heller myotomy versus Heller myotomy with Dor fundoplication for achalasia: A prospective randomized double-blind clinical trial. Ann Surg. 2004;240:405-12.
2. Podboy AJ et al. Long-term outcomes of peroral endoscopic myotomy compared to laparoscopic Heller myotomy for achalasia: A single-center experience. Surg Endosc. 2020. doi: 10.1007/s00464-020-07450-6.
3. Werner YB et al. Endoscopic or surgical myotomy in patients with idiopathic achalasia. N Engl J Med. 2019;381(23):2219-29.
4. Inoue H et al. Peroral endoscopic myotomy: A series of 500 patients. J Am Coll Surg. 2015;221:256-64.
5. Repici A et al. GERD after peroral endoscopic myotomy as compared with Heller’s myotomy with fundoplication: A systematic review with meta-analysis. Gastrointest Endosc. 2018;87(4):934-43.
6. Ichkhanian Y et al. Case of early Barrett cancer following peroral endoscopic myotomy. Gut. 2019;68:2107-10.
Dr. Siwiec is assistant professor of clinical medicine, division of gastroenterology and hepatology, GI motility and neurogastroenterology unit, Indiana University, Indianapolis. He has no conflicts of interest.
Dear colleagues and friends,
In this edition of Perspectives, Dr. Mouen Khashab and Dr. Robert Siwiec tackle an exciting and constantly evolving topic, which is the optimal approach to myotomy for patients with achalasia. Dr. Khashab makes the case for endoscopic myotomy, while Dr. Siwiec argues that surgical myotomy remains the gold standard. I hope that you will find this debate as useful and thought provoking as I did. As always, I welcome your comments and suggestions for future topics at [email protected].
Charles Kahi, MD, MS, AGAF, is a professor of medicine at Indiana University, Indianapolis. He is also an associate editor for GI & Hepatology News.
Endoscopic myotomy for achalasia is ready for prime time
BY MOUEN A. KHASHAB, MD
When I encounter a symptomatic patient with manometrically confirmed achalasia, I discuss three effective treatment modalities: pneumatic dilation (PD), peroral endoscopic myotomy (POEM), and laparoscopic Heller myotomy (LHM). I recommend against botulinum toxin injection and reserve it for patients who are not candidates for the aforementioned definitive therapies. I also present to the patient the current level I evidence from randomized, controlled trials (RCTs) comparing achalasia treatment modalities.
One landmark RCT reported comparative outcomes at 2 years following POEM and PD and found higher treatment success at the 2-year follow-up in the POEM group (92% vs. 54%; P < .001).1 Reflux esophagitis was observed significantly more frequently in patients treated with POEM (41% in the POEM group, of whom 35% were assigned Los Angeles grade A-B and 6% were assigned LA grade C versus 7% in the PD group, all of whom were assigned LA grade A; P = .002).1
Another milestone RCT included 221 patients and compared outcomes of POEM and LHM plus Dor fundoplication.2 Clinical success at the 2-year follow-up was observed in 83.0% of patients in the POEM group, and was noninferior to the LHM group (81.7%). Serious adverse events occurred in 2.7% of patients in the POEM group and in 7.3% of patients in the LHM group. Although 57% of patients in the POEM group and 20% of patients in the LHM group had reflux esophagitis as assessed by endoscopy at 3 months, the corresponding proportions were 44% and 29% at 24 months. Importantly, the rate of severe esophagitis was not different between both groups (6% vs. 3% at 3 months, and 5% vs. 6% at 24 months).2
I summarize these results by stating that POEM seems to be superior to PD and equivalent to LHM in terms of clinical success. Nonetheless, POEM also seems to be associated with increased risk of early gastroesophageal reflux disease.
POEM is now a ubiquitous procedure performed worldwide and is endorsed as a primary achalasia treatment by multiple society guidelines.3 It is a minimally invasive, effective, and safe therapeutic option for patients with all types of achalasia and is considered the treatment of choice for achalasia type III. POEM has also been shown to be effective in the treatment of spastic esophageal disorders (e.g. Jackhammer esophagus, diffuse esophageal spasm) and esophagogastric junction outflow obstruction. It can be performed in the endoscopy unit or operating theater either by experienced therapeutic endoscopists or surgical endoscopists in less than an hour. The procedure can be performed on an outpatient basis in appropriate individuals and allows tailoring the myotomy length to specific clinical scenarios. For example, patients with type III achalasia (and those with spastic esophageal disorders) typically require a long myotomy and that can be readily accomplished during POEM as opposed to LHM. POEM has also proven effective in children; octogenarians; and patients with sigmoid esophagus, epiphrenic diverticula, and those who had undergone prior interventions for achalasia, including LHM and PD. In experienced hands, the rate of adverse events is low and serious events are rare and occur in 0.5% of cases. Perforations/leakage are also uncommon and occur in 0.7% of patients. It is an incisionless procedure that eliminates the risk of wound infection and shortens postprocedural recovery. Patients are typically admitted for an overnight observation postprocedure, discharged home the following day, and back to activities of daily living (including work) within a few days. Postprocedural pain is minimal in most patients and narcotics are rarely needed. Resumption of a soft diet is carried out on the first postoperative day and normal diet 1 week later.
LHM is an established procedure with proven long-term efficacy in the treatment of achalasia. Nonetheless, it is invasive and requires placement of multiple trocars. The procedure is more time consuming than POEM and length of hospital stay can also be longer. This results in possibly higher cost than POEM. Importantly, recovery of dysphagia and resumption of normal diet is significantly delayed and is likely the result of the partial concomitant fundoplication procedure. Finally, LHM is not appropriate for the treatment of spastic esophageal disorders, including type III achalasia.
A major advantage of LHM plus partial fundoplication over POEM is the diminished risk of gastroesophageal reflux disease (GERD). However, this advantage seems short lived as the risk of GERD increases over time after surgery, likely because of the loosening of the wrap over time. From the New England Journal of Medicine paper mentioned earlier, it seems that the increased risk of GERD after POEM as compared with LHM diminishes over time.2 Importantly, it also appears that the rate of significant esophagitis (LA grade C-D) is similar between both procedures.2
In an effort to assess the long-term antireflux efficacy of surgical partial fundoplication, one study noted that 12% of 182 patients who had surgical myotomy with partial fundoplication continued to have occasional or continuous heartburn symptoms at a median of 18 years after surgery. Esophagitis and Barrett’s esophagus were found in 14.5% and 0.8% of patients, respectively. De novo esophageal adenocarcinoma has been reported after both POEM and LHM.4
Therefore, GERD and its complications can occur after any procedure that disrupts the lower esophageal sphincter (POEM, LHM, and PD) and postprocedural management of patients should include long-term testing and management of possible GERD. Different strategies have been proposed and include objective periodic testing for esophageal acid exposure, long-term and possible lifelong proton pump inhibitor use, and surveillance for long-term consequences of GER via periodic upper endoscopy.3
It is important to acknowledge that the lack of symptoms or the absence of endoscopic evidence of GER on initial endoscopy does not necessarily rule out GER. Approximately a third of post-POEM patients with clinically successful outcome and absence of reflux esophagitis on their first surveillance endoscopy eventually develop esophagitis at subsequent surveillance endoscopy.5
In summary, POEM has deservingly taken a prime time spot in the management of patients with achalasia. It is an efficient, efficacious and safe treatment modality that results in rapid resolution of achalasia symptoms in the majority of patients. Research should focus on technical modifications (e.g., short gastric myotomy; addition of endoscopic fundoplication) that reduce the incidence of postprocedural GERD.
References
1. Ponds FA et al. Effect of peroral endoscopic myotomy versus pneumatic dilation on symptom severity and treatment outcomes among treatment-naive patients with achalasia: A randomized clinical trial. JAMA. 2019;322:134-44.
2. Werner YB et al. Endoscopic or surgical myotomy in patients with idiopathic achalasia. N Engl J Med. 2019;381:2219-29.
3. Khashab MA et al. ASGE guideline on the management of achalasia. Gastrointest Endosc. 2020;91:213-27 e6.
4. Ichkhanian Y et al. Case of early Barrett cancer following peroral endoscopic myotomy. Gut. 2019;68:2107-110.
5. Werner YB et al. Clinical response to peroral endoscopic myotomy in patients with idiopathic achalasia at a minimum follow-up of 2 years. Gut. 2016;65:899-906.
Dr. Khashab is associate professor of medicine, director of therapeutic endoscopy, division of gastroenterology and hepatology, Johns Hopkins Hospital, Baltimore. He is a consultant for BSCI, Olympus, and Medtronic.
Heller myotomy is still the gold standard
BY ROBERT M. SIWIEC, MD
Achalasia is a rare, primary esophageal motor disorder characterized by ineffective relaxation of the lower esophageal sphincter (LES) and concomitant loss of esophageal peristalsis. High-resolution esophageal manometry has allowed for the diagnosis and classification of achalasia into relevant clinical subtypes which become important when discussing and considering treatment options. Confirmatory studies (e.g., timed barium esophagram) and provocative manometric maneuvers (e.g., upright swallows, rapid swallow sequence, and/or rapid drink challenge) can be helpful when distinguishing between true achalasia versus achalasia variants and esophagogastric junction outflow obstruction.
Treatment options only provide palliation by eliminating outflow obstruction caused by a nonrelaxing and often times hypertensive LES. Pharmacotherapy (e.g., oral nitrates, 5-phosphodiesterase inhibitors, anticholinergics) is the least effective option because of medication side effects and short-acting duration. I only consider it for patients who are either unwilling or unable to tolerate invasive therapies. Botulinum toxin injection into the LES can be considered in patients who are not good candidates for more definitive therapy with PD or myotomy (endoscopic or surgical). Although the success rates with botulinum toxin are comparable with PD and surgical myotomy, patients treated with botulinum toxin require retreatment. Furthermore, continued botulinum toxin injections can compromise tissue planes making myotomy complex and challenging.
During the 1970s and 1980s, PD was the primary treatment modality for achalasia. Surgical myotomy was reserved for patients who suffered a perforation during PD or developed recurrent symptoms after multiple dilations. Minimally invasive surgery (left thoracoscopic approach) for achalasia was first introduced in the early 1990s and was shown to be a feasible, safe, and effective procedure, becoming the primary treatment approach in most centers. Patients fared well; however, it was soon discovered that >50% had pathological reflux based on pH monitoring. A few centers then began to perform a Heller myotomy through a laparoscopic approach with the addition of a fundoplication resulting in significant reductions in pathological reflux by pH monitoring. Eventually, a seminal RCT confirmed the importance of fundoplication with laparoscopic Heller myotomy (LHM) – resolution of dysphagia was unaffected and pathological reflux was avoided in most patients.1 Overall, clinical success rates for LHM with fundoplication are typically >90% and reflux incidence rates <10% with the overall complication rate being about 5% with reported mortality <0.1%.
PD remains appealing in that it is cost effective and less invasive, compared with POEM and LHM. Initial success rates and short-term efficacy are comparable with LHM but unfortunately PD’s efficacy significantly wanes over time. POEM, introduced by Inoue et al. in 2010, is a novel endoscopic technique with an excellent safety profile that provides good symptom relief while avoiding abdominal wall scars for patients. It has been shown to have a distinct advantage in patients with type III achalasia by nature of the longer myotomy not achievable by LHM.2 POEM has seen increasing enthusiasm and acceptance as a standard treatment option for achalasia largely because of the fact that its safety and efficacy have been shown to be comparable and in most cases equal with LHM. However, in 2020, direct comparison with LHM is challenging given that the follow-up in the majority of studies is either short or incomplete. The most recent multicenter, randomized trial comparing POEM with LHM plus Dor fundoplication showed POEM’s noninferiority in controlling symptoms of achalasia, but only after a 24 month follow-up.3 A recent report included one of the largest cohorts of post-POEM patients (500), but the 36-month data were based on the follow-up of only 61 patients (about 12%).4
Once the muscle fibers of the LES are disrupted, reflux will occur in the majority of patients. Unlike LHM, no concomitant fundoplication is performed during POEM and this increases the incidence of GERD and its long-term sequelae including peptic strictures, Barrett’s esophagus, and adenocarcinoma. A meta-analysis from 2018 looked at published series of POEM and LHM with fundoplication and found that GERD symptoms were present in 19% of POEM patients, compared with 8.8% of LHM patients. Worse yet, esophagitis was seen in 29.4% of the POEM group and 7.6% of the LHM group, with more individuals in the POEM group also having abnormal acid exposure based on ambulatory pH monitoring (39.0% vs. 16.8%).5
Proponents of POEM will argue that proton pump inhibitors (PPIs) are the panacea for post-POEM GERD. Unfortunately, this approach has its own problems. PPIs are very effective at reducing acid secretion by parietal cells, but do not block reflux through an iatrogenically incompetent LES. The drumbeat of publications on potential complications from chronic PPI use has greatly contributed to patients’ reluctance to commit to long-term PPI use. Lastly, the first case of early Barrett’s cancer was recently reported in a patient 4 years post-POEM despite adherence to an aggressive antisecretory regimen (b.i.d. PPI and H2 blocker at bedtime).6 LHM with fundoplication significantly reduces the risk of pathological GERD and spares patients from committing to lifelong PPI therapy and routine endoscopic surveillance (appropriate interval yet to be determined) and needing to consider additional procedures (i.e., endoscopic or surgical fundoplication).
Despite POEM’s well established efficacy and safety, the development of post-POEM GERD is a major concern that has yet to be adequately addressed. A significant number of post-POEM patients with pathological reflux have asymptomatic and unrecognized GERD and current management and monitoring strategies for post-POEM GERD are anemic and poorly established. Without question, there are individual patients who are clearly better served with POEM (type III achalasia and other spastic esophageal disorders). However, as we continue to learn more about post-POEM GERD and how to better prevent, manage, and monitor it, LHM with fundoplication for the time being remains the tried-and-tested treatment option for patients with non–type III achalasia.
References
1. Richards WO et al. Heller myotomy versus Heller myotomy with Dor fundoplication for achalasia: A prospective randomized double-blind clinical trial. Ann Surg. 2004;240:405-12.
2. Podboy AJ et al. Long-term outcomes of peroral endoscopic myotomy compared to laparoscopic Heller myotomy for achalasia: A single-center experience. Surg Endosc. 2020. doi: 10.1007/s00464-020-07450-6.
3. Werner YB et al. Endoscopic or surgical myotomy in patients with idiopathic achalasia. N Engl J Med. 2019;381(23):2219-29.
4. Inoue H et al. Peroral endoscopic myotomy: A series of 500 patients. J Am Coll Surg. 2015;221:256-64.
5. Repici A et al. GERD after peroral endoscopic myotomy as compared with Heller’s myotomy with fundoplication: A systematic review with meta-analysis. Gastrointest Endosc. 2018;87(4):934-43.
6. Ichkhanian Y et al. Case of early Barrett cancer following peroral endoscopic myotomy. Gut. 2019;68:2107-10.
Dr. Siwiec is assistant professor of clinical medicine, division of gastroenterology and hepatology, GI motility and neurogastroenterology unit, Indiana University, Indianapolis. He has no conflicts of interest.
A tribute to Edward Ross Ritvo, MD, 1930-2020
Reflections on loss amid COVID-19
I sit here on Father’s Day during a global pandemic and can’t help but think of Mark Twain’s quote, “Truth is stranger than fiction.” Isn’t that what calls us to our profession? When friends ask if I have watched a particular movie or TV show, I almost always say no. Why would I? Day after day at “work” I am hearing the most remarkable stories – many unfolding right before my eyes.
My Dad’s story is no less remarkable. As he was a pioneer in our field, I hope you will allow me to share a few recollections.
June 10, just 10 days after turning 90, Dad died peacefully in his home. His obituary, written by James McCracken, MD, says: “He was an internationally known child psychiatrist who, with colleagues, formed the vanguard of UCLA researchers establishing the biomedical basis of autism in the 1960s despite the prevailing psychological theories of the day ... who would later break new ground in identifying the role of genetics, sleep, and neurophysiological differences, perinatal risk factors, and biomarkers relating to autism and autism risk.”
Dad had extensive training in psychoanalysis and worked hard to maintain expertise in both the psychological and biological arenas. While he helped established autism as a neurologic disease and advocated for DSM criteria changes, he continued teaching Psychodynamic Theory of Personality to the UCLA medical students and maintained a clinical practice based in psychotherapeutic techniques. He was practicing biopsychosocial medicine long before the concept was articulated.

He conducted the first epidemiologic survey of autism in the state of Utah. He chose Utah because the Mormons keep perfect genealogical records. He identified multiple families with more than one child affected as well as examining, pre-, peri-, and postnatal factors affecting these families. Being a maverick has its challenges. One paper about parents with mild autism was rejected from publication seven times before a watered-down version of clinical vignettes finally got accepted. In collaboration with his wife, Riva Ariella Ritvo, he developed the Ritvo Autism Asperger Diagnostic Scale–Revised, (RAADS-R) still in use today.
Dad’s career was complicated by medical issues beginning in his 40s when he had a near-fatal heart attack at the top of Mammoth Mountain while skiing. After struggling for 20 years, he ultimately had a heart transplant at Cedars-Sinai Medical Center at 69 years old. Months after the transplant, he was back at work. He was unstoppable and maintained his optimism and great sense of humor throughout this complicated ordeal. He always remembered his commitment to his donor and his new heart, and worked out every day. Living to 90 was against all the odds.
Dad also persevered throughout his youngest son’s 10-year battle with Ewing’s sarcoma. Despite losing Max in 2016, Dad was active in research and clinical practice until the very end. He was doing telepsychiatry with patients in prisons and rehabilitation hospitals the last few years because he was too weak to travel to an office. He continued his research, and his last paper on eye movement responses as a possible biological marker of autism was published in February 2020.
Although Dad did not have COVID-19, the social isolation and stress of the last few months hastened his decline. The last week in the hospital with no visitors was too much for such a social man, and he died days after he was discharged. Always a trailblazer, Dad’s Zoom funeral was watched across the country by his children, grandchildren, extended family, and friends. Choosing to honor his wish to be cautious in this pandemic, we remained sheltering in place.

As Dad was the ultimate professor, I know he would want us to learn from his life and his passing. We are in an accelerated growth phase now as our lives and the lives of our patients are radically altered.
I hope, like Dad, we can choose to feel nourished by our meaningful work as we travel through life’s ups and downs. We must learn new ways to care for ourselves, our families, and our patients during these challenging times. We must find ways to mourn and celebrate those lost during the pandemic.
I know Dad would love synchronicity that I spent Father’s Day writing about him for Clinical Psychiatry News! Thank you for giving me this gift of reflection on this special day.
Dr. Ritvo, a psychiatrist with more than 25 years’ experience, practices in Miami Beach. She is the author of “Bekindr – The Transformative Power of Kindness” (Hellertown, Pa.: Momosa Publishing, 2018) and is the founder of the Bekindr Global Initiative, a movement aimed at cultivating kindness in the world. Dr. Ritvo also is the cofounder of the Bold Beauty Project, a nonprofit group that pairs women with disabilities with photographers who create art exhibitions to raise awareness.
Reflections on loss amid COVID-19
Reflections on loss amid COVID-19
I sit here on Father’s Day during a global pandemic and can’t help but think of Mark Twain’s quote, “Truth is stranger than fiction.” Isn’t that what calls us to our profession? When friends ask if I have watched a particular movie or TV show, I almost always say no. Why would I? Day after day at “work” I am hearing the most remarkable stories – many unfolding right before my eyes.
My Dad’s story is no less remarkable. As he was a pioneer in our field, I hope you will allow me to share a few recollections.
June 10, just 10 days after turning 90, Dad died peacefully in his home. His obituary, written by James McCracken, MD, says: “He was an internationally known child psychiatrist who, with colleagues, formed the vanguard of UCLA researchers establishing the biomedical basis of autism in the 1960s despite the prevailing psychological theories of the day ... who would later break new ground in identifying the role of genetics, sleep, and neurophysiological differences, perinatal risk factors, and biomarkers relating to autism and autism risk.”
Dad had extensive training in psychoanalysis and worked hard to maintain expertise in both the psychological and biological arenas. While he helped established autism as a neurologic disease and advocated for DSM criteria changes, he continued teaching Psychodynamic Theory of Personality to the UCLA medical students and maintained a clinical practice based in psychotherapeutic techniques. He was practicing biopsychosocial medicine long before the concept was articulated.
He conducted the first epidemiologic survey of autism in the state of Utah. He chose Utah because the Mormons keep perfect genealogical records. He identified multiple families with more than one child affected as well as examining, pre-, peri-, and postnatal factors affecting these families. Being a maverick has its challenges. One paper about parents with mild autism was rejected from publication seven times before a watered-down version of clinical vignettes finally got accepted. In collaboration with his wife, Riva Ariella Ritvo, he developed the Ritvo Autism Asperger Diagnostic Scale–Revised, (RAADS-R) still in use today.
Dad’s career was complicated by medical issues beginning in his 40s when he had a near-fatal heart attack at the top of Mammoth Mountain while skiing. After struggling for 20 years, he ultimately had a heart transplant at Cedars-Sinai Medical Center at 69 years old. Months after the transplant, he was back at work. He was unstoppable and maintained his optimism and great sense of humor throughout this complicated ordeal. He always remembered his commitment to his donor and his new heart, and worked out every day. Living to 90 was against all the odds.
Dad also persevered throughout his youngest son’s 10-year battle with Ewing’s sarcoma. Despite losing Max in 2016, Dad was active in research and clinical practice until the very end. He was doing telepsychiatry with patients in prisons and rehabilitation hospitals the last few years because he was too weak to travel to an office. He continued his research, and his last paper on eye movement responses as a possible biological marker of autism was published in February 2020.
Although Dad did not have COVID-19, the social isolation and stress of the last few months hastened his decline. The last week in the hospital with no visitors was too much for such a social man, and he died days after he was discharged. Always a trailblazer, Dad’s Zoom funeral was watched across the country by his children, grandchildren, extended family, and friends. Choosing to honor his wish to be cautious in this pandemic, we remained sheltering in place.
As Dad was the ultimate professor, I know he would want us to learn from his life and his passing. We are in an accelerated growth phase now as our lives and the lives of our patients are radically altered.
I hope, like Dad, we can choose to feel nourished by our meaningful work as we travel through life’s ups and downs. We must learn new ways to care for ourselves, our families, and our patients during these challenging times. We must find ways to mourn and celebrate those lost during the pandemic.
I know Dad would love synchronicity that I spent Father’s Day writing about him for Clinical Psychiatry News! Thank you for giving me this gift of reflection on this special day.
Dr. Ritvo, a psychiatrist with more than 25 years’ experience, practices in Miami Beach. She is the author of “Bekindr – The Transformative Power of Kindness” (Hellertown, Pa.: Momosa Publishing, 2018) and is the founder of the Bekindr Global Initiative, a movement aimed at cultivating kindness in the world. Dr. Ritvo also is the cofounder of the Bold Beauty Project, a nonprofit group that pairs women with disabilities with photographers who create art exhibitions to raise awareness.
I sit here on Father’s Day during a global pandemic and can’t help but think of Mark Twain’s quote, “Truth is stranger than fiction.” Isn’t that what calls us to our profession? When friends ask if I have watched a particular movie or TV show, I almost always say no. Why would I? Day after day at “work” I am hearing the most remarkable stories – many unfolding right before my eyes.
My Dad’s story is no less remarkable. As he was a pioneer in our field, I hope you will allow me to share a few recollections.
June 10, just 10 days after turning 90, Dad died peacefully in his home. His obituary, written by James McCracken, MD, says: “He was an internationally known child psychiatrist who, with colleagues, formed the vanguard of UCLA researchers establishing the biomedical basis of autism in the 1960s despite the prevailing psychological theories of the day ... who would later break new ground in identifying the role of genetics, sleep, and neurophysiological differences, perinatal risk factors, and biomarkers relating to autism and autism risk.”
Dad had extensive training in psychoanalysis and worked hard to maintain expertise in both the psychological and biological arenas. While he helped established autism as a neurologic disease and advocated for DSM criteria changes, he continued teaching Psychodynamic Theory of Personality to the UCLA medical students and maintained a clinical practice based in psychotherapeutic techniques. He was practicing biopsychosocial medicine long before the concept was articulated.
He conducted the first epidemiologic survey of autism in the state of Utah. He chose Utah because the Mormons keep perfect genealogical records. He identified multiple families with more than one child affected as well as examining, pre-, peri-, and postnatal factors affecting these families. Being a maverick has its challenges. One paper about parents with mild autism was rejected from publication seven times before a watered-down version of clinical vignettes finally got accepted. In collaboration with his wife, Riva Ariella Ritvo, he developed the Ritvo Autism Asperger Diagnostic Scale–Revised, (RAADS-R) still in use today.
Dad’s career was complicated by medical issues beginning in his 40s when he had a near-fatal heart attack at the top of Mammoth Mountain while skiing. After struggling for 20 years, he ultimately had a heart transplant at Cedars-Sinai Medical Center at 69 years old. Months after the transplant, he was back at work. He was unstoppable and maintained his optimism and great sense of humor throughout this complicated ordeal. He always remembered his commitment to his donor and his new heart, and worked out every day. Living to 90 was against all the odds.
Dad also persevered throughout his youngest son’s 10-year battle with Ewing’s sarcoma. Despite losing Max in 2016, Dad was active in research and clinical practice until the very end. He was doing telepsychiatry with patients in prisons and rehabilitation hospitals the last few years because he was too weak to travel to an office. He continued his research, and his last paper on eye movement responses as a possible biological marker of autism was published in February 2020.
Although Dad did not have COVID-19, the social isolation and stress of the last few months hastened his decline. The last week in the hospital with no visitors was too much for such a social man, and he died days after he was discharged. Always a trailblazer, Dad’s Zoom funeral was watched across the country by his children, grandchildren, extended family, and friends. Choosing to honor his wish to be cautious in this pandemic, we remained sheltering in place.
As Dad was the ultimate professor, I know he would want us to learn from his life and his passing. We are in an accelerated growth phase now as our lives and the lives of our patients are radically altered.
I hope, like Dad, we can choose to feel nourished by our meaningful work as we travel through life’s ups and downs. We must learn new ways to care for ourselves, our families, and our patients during these challenging times. We must find ways to mourn and celebrate those lost during the pandemic.
I know Dad would love synchronicity that I spent Father’s Day writing about him for Clinical Psychiatry News! Thank you for giving me this gift of reflection on this special day.
Dr. Ritvo, a psychiatrist with more than 25 years’ experience, practices in Miami Beach. She is the author of “Bekindr – The Transformative Power of Kindness” (Hellertown, Pa.: Momosa Publishing, 2018) and is the founder of the Bekindr Global Initiative, a movement aimed at cultivating kindness in the world. Dr. Ritvo also is the cofounder of the Bold Beauty Project, a nonprofit group that pairs women with disabilities with photographers who create art exhibitions to raise awareness.
Isa-Kd improves PFS in relapsed/refractory multiple myeloma
The risk of progression or death for patients with relapsed or refractory multiple myeloma was nearly halved with the addition of isatuximab to carfilzomib and dexamethasone, according to an interim analysis of the phase 3 IKEMA trial (NCT03275285).
After a median follow-up of 20.7 months, the median progression-free survival had not been reached for 179 patients treated with isatuximab (Sarclisa), carfilzomib (Kyprolis), and dexamethasone (together, known as Isa-Kd), compared with 19.5 months for 123 patients treated with carfilzomib and dexamethasone alone (Kd). The hazard ratio for progression free survival with the triple combination was 0.531 (P = .0007), reported coprincipal investigator Phillipe Moreau, MD, from the University Hospital Hôtel-Dieu in Nantes, France.
“The benefit of the triplet combination was observed across subgroups, including patients difficult to treat, such as [those with] high-risk cytogenetics or elderly patients,” he said in a late-breaking abstract presentation during the virtual annual congress of the European Hematology Association.
Isatuximab is an immunoglobulin G1 monoclonal antibody targeting a CD38 transmembrane glycoprotein on multiple myeloma cells, with a mechanism of action similar to that of another anti-CD38 antibody, daratumumab (Darzalex). Isatuximab is approved in the United States and Europe in combination with pomalidomide and dexamethasone for patients with relapsed/refractory multiple myeloma after at least two prior lines of therapy.
A ‘me too’ agent?
It’s unclear, however, whether isatuximab offers any additional benefit over daratumumab, an agent approved for use both in front line therapy combinations and for patients with relapsed/refractory disease, said Brea C. Lipe, MD, a multiple myeloma specialist at the University of Rochester (N.Y.) Wilmot Cancer Institute, who was not involved in the study.
“Every time we get a new drug it’s nice to have another option, but it doesn’t really add anything different from daratumumab at this point,” she said in an interview.
Dr. Lipe noted the IKEMA results are similar to those seen in the phase 3 CANDOR trial, comparing carfilzomib, dexamethasone, and daratumumab to carfilzomib/dexamethasone alone in patients with relapsed/refractory myeloma. In addition, it’s unknown whether patients with disease that is refractory to daratumumab could benefit from isatuximab, she said.
Although isatuximab has been touted as offering more rapid and more convenient dosing than daratumumab, the introduction of rapid infusion and subcutaneous administration of daratumumab has negated any theoretical advantage of the newcomer, Dr. Lipe added.
Study details
In the IKEMA trial, 302 patients with relapsed/refractory multiple myeloma who’d received one to three prior lines of therapy were stratified by the number of prior lines and by revised Multiple Myeloma International Staging System (R-ISS) and were then randomized on a 3:2 basis to treatment with carfilzomib 20 mg/m2 on days 1, 2, 8, 9, 15, and 16 of cycle 1 and 56 mg/m2 on the corresponding days of each subsequent cycle plus dexamethasone 20 mg on days 1, 2, 8, 9, 15, 16, 22, and 23 of each cycle, with or without isatuximab. The antibody was dosed 10 mg/kg on days 1, 8, 15, and 22 in cycle 1 then every 2 weeks thereafter.
Treatments were continued until disease progression, unacceptable toxicity, or patient choice intervened.
At a prespecified interim analysis, the trial met its primary endpoint of a minimum 41% risk reduction in the hazard rate for progression free survival (PFS), with an actual risk reduction of 47%.
An analysis of PFS by subgroup showed significant benefits with the triple combination for patients aged 65 years and older, those with baseline estimated glomerular filtration rates below 60 mL/min per 1.73 m2, those with more than one prior line of therapy, those who had not previously received a proteasome inhibitor (e.g., bortezomib) or immunomodulatory agent (e.g., lenalidomide), those with high-risk cytogenetic status, and those with R-ISS stage II at study entry.
Overall response rates were similar between the study arms, at 86.6% with Isa-Kd and 82.9% with Kd, but the rate of very good partial responses or better was significantly higher with the triplet, at 72.6% versus 56.1% (P = .0011). The rate of minimal residual disease negativity was also significantly lower with Isa-Kd in the intent-to-treat population, at 29.6% versus 13%, respectively (P = .0004).
Overall survival data were not mature at the time of data cutoff and will be reported later, Dr. Moreau said.
Grade 3 or greater treatment-emergent adverse events (TEAEs) occurred in 76.8% of patients on the triplet and 67.2% of those on Kd. The incidences of death, serious TEAEs, or adverse events leading to discontinuation of therapy did not differ markedly between the treatment arms, however. Grade 3 or greater cardiac failure occurred in seven patients treated with the triplet (4%) and five treated with Kd (4.1%); respective rates of grade 3 or greater hematologic abnormalities included anemia in 22% and 19.7%, neutropenia in 19.2% and 7.4%, and thrombocytopenia in 29.9% and 23.8%.
The primary completion date for the trial is estimated to occur in November 2020, with final results in November 2023.
The study was sponsored by Sanofi. Dr. Moreau disclosed honoraria and a consulting or advisory role with several companies, not including Sanofi. Dr. Lipe disclosed impending advisory board activity for Janssen.
SOURCE: Moreau P et al. EHA Congress, Abstract LB2603.
The risk of progression or death for patients with relapsed or refractory multiple myeloma was nearly halved with the addition of isatuximab to carfilzomib and dexamethasone, according to an interim analysis of the phase 3 IKEMA trial (NCT03275285).
After a median follow-up of 20.7 months, the median progression-free survival had not been reached for 179 patients treated with isatuximab (Sarclisa), carfilzomib (Kyprolis), and dexamethasone (together, known as Isa-Kd), compared with 19.5 months for 123 patients treated with carfilzomib and dexamethasone alone (Kd). The hazard ratio for progression free survival with the triple combination was 0.531 (P = .0007), reported coprincipal investigator Phillipe Moreau, MD, from the University Hospital Hôtel-Dieu in Nantes, France.
“The benefit of the triplet combination was observed across subgroups, including patients difficult to treat, such as [those with] high-risk cytogenetics or elderly patients,” he said in a late-breaking abstract presentation during the virtual annual congress of the European Hematology Association.
Isatuximab is an immunoglobulin G1 monoclonal antibody targeting a CD38 transmembrane glycoprotein on multiple myeloma cells, with a mechanism of action similar to that of another anti-CD38 antibody, daratumumab (Darzalex). Isatuximab is approved in the United States and Europe in combination with pomalidomide and dexamethasone for patients with relapsed/refractory multiple myeloma after at least two prior lines of therapy.
A ‘me too’ agent?
It’s unclear, however, whether isatuximab offers any additional benefit over daratumumab, an agent approved for use both in front line therapy combinations and for patients with relapsed/refractory disease, said Brea C. Lipe, MD, a multiple myeloma specialist at the University of Rochester (N.Y.) Wilmot Cancer Institute, who was not involved in the study.
“Every time we get a new drug it’s nice to have another option, but it doesn’t really add anything different from daratumumab at this point,” she said in an interview.
Dr. Lipe noted the IKEMA results are similar to those seen in the phase 3 CANDOR trial, comparing carfilzomib, dexamethasone, and daratumumab to carfilzomib/dexamethasone alone in patients with relapsed/refractory myeloma. In addition, it’s unknown whether patients with disease that is refractory to daratumumab could benefit from isatuximab, she said.
Although isatuximab has been touted as offering more rapid and more convenient dosing than daratumumab, the introduction of rapid infusion and subcutaneous administration of daratumumab has negated any theoretical advantage of the newcomer, Dr. Lipe added.
Study details
In the IKEMA trial, 302 patients with relapsed/refractory multiple myeloma who’d received one to three prior lines of therapy were stratified by the number of prior lines and by revised Multiple Myeloma International Staging System (R-ISS) and were then randomized on a 3:2 basis to treatment with carfilzomib 20 mg/m2 on days 1, 2, 8, 9, 15, and 16 of cycle 1 and 56 mg/m2 on the corresponding days of each subsequent cycle plus dexamethasone 20 mg on days 1, 2, 8, 9, 15, 16, 22, and 23 of each cycle, with or without isatuximab. The antibody was dosed 10 mg/kg on days 1, 8, 15, and 22 in cycle 1 then every 2 weeks thereafter.
Treatments were continued until disease progression, unacceptable toxicity, or patient choice intervened.
At a prespecified interim analysis, the trial met its primary endpoint of a minimum 41% risk reduction in the hazard rate for progression free survival (PFS), with an actual risk reduction of 47%.
An analysis of PFS by subgroup showed significant benefits with the triple combination for patients aged 65 years and older, those with baseline estimated glomerular filtration rates below 60 mL/min per 1.73 m2, those with more than one prior line of therapy, those who had not previously received a proteasome inhibitor (e.g., bortezomib) or immunomodulatory agent (e.g., lenalidomide), those with high-risk cytogenetic status, and those with R-ISS stage II at study entry.
Overall response rates were similar between the study arms, at 86.6% with Isa-Kd and 82.9% with Kd, but the rate of very good partial responses or better was significantly higher with the triplet, at 72.6% versus 56.1% (P = .0011). The rate of minimal residual disease negativity was also significantly lower with Isa-Kd in the intent-to-treat population, at 29.6% versus 13%, respectively (P = .0004).
Overall survival data were not mature at the time of data cutoff and will be reported later, Dr. Moreau said.
Grade 3 or greater treatment-emergent adverse events (TEAEs) occurred in 76.8% of patients on the triplet and 67.2% of those on Kd. The incidences of death, serious TEAEs, or adverse events leading to discontinuation of therapy did not differ markedly between the treatment arms, however. Grade 3 or greater cardiac failure occurred in seven patients treated with the triplet (4%) and five treated with Kd (4.1%); respective rates of grade 3 or greater hematologic abnormalities included anemia in 22% and 19.7%, neutropenia in 19.2% and 7.4%, and thrombocytopenia in 29.9% and 23.8%.
The primary completion date for the trial is estimated to occur in November 2020, with final results in November 2023.
The study was sponsored by Sanofi. Dr. Moreau disclosed honoraria and a consulting or advisory role with several companies, not including Sanofi. Dr. Lipe disclosed impending advisory board activity for Janssen.
SOURCE: Moreau P et al. EHA Congress, Abstract LB2603.
The risk of progression or death for patients with relapsed or refractory multiple myeloma was nearly halved with the addition of isatuximab to carfilzomib and dexamethasone, according to an interim analysis of the phase 3 IKEMA trial (NCT03275285).
After a median follow-up of 20.7 months, the median progression-free survival had not been reached for 179 patients treated with isatuximab (Sarclisa), carfilzomib (Kyprolis), and dexamethasone (together, known as Isa-Kd), compared with 19.5 months for 123 patients treated with carfilzomib and dexamethasone alone (Kd). The hazard ratio for progression free survival with the triple combination was 0.531 (P = .0007), reported coprincipal investigator Phillipe Moreau, MD, from the University Hospital Hôtel-Dieu in Nantes, France.
“The benefit of the triplet combination was observed across subgroups, including patients difficult to treat, such as [those with] high-risk cytogenetics or elderly patients,” he said in a late-breaking abstract presentation during the virtual annual congress of the European Hematology Association.
Isatuximab is an immunoglobulin G1 monoclonal antibody targeting a CD38 transmembrane glycoprotein on multiple myeloma cells, with a mechanism of action similar to that of another anti-CD38 antibody, daratumumab (Darzalex). Isatuximab is approved in the United States and Europe in combination with pomalidomide and dexamethasone for patients with relapsed/refractory multiple myeloma after at least two prior lines of therapy.
A ‘me too’ agent?
It’s unclear, however, whether isatuximab offers any additional benefit over daratumumab, an agent approved for use both in front line therapy combinations and for patients with relapsed/refractory disease, said Brea C. Lipe, MD, a multiple myeloma specialist at the University of Rochester (N.Y.) Wilmot Cancer Institute, who was not involved in the study.
“Every time we get a new drug it’s nice to have another option, but it doesn’t really add anything different from daratumumab at this point,” she said in an interview.
Dr. Lipe noted the IKEMA results are similar to those seen in the phase 3 CANDOR trial, comparing carfilzomib, dexamethasone, and daratumumab to carfilzomib/dexamethasone alone in patients with relapsed/refractory myeloma. In addition, it’s unknown whether patients with disease that is refractory to daratumumab could benefit from isatuximab, she said.
Although isatuximab has been touted as offering more rapid and more convenient dosing than daratumumab, the introduction of rapid infusion and subcutaneous administration of daratumumab has negated any theoretical advantage of the newcomer, Dr. Lipe added.
Study details
In the IKEMA trial, 302 patients with relapsed/refractory multiple myeloma who’d received one to three prior lines of therapy were stratified by the number of prior lines and by revised Multiple Myeloma International Staging System (R-ISS) and were then randomized on a 3:2 basis to treatment with carfilzomib 20 mg/m2 on days 1, 2, 8, 9, 15, and 16 of cycle 1 and 56 mg/m2 on the corresponding days of each subsequent cycle plus dexamethasone 20 mg on days 1, 2, 8, 9, 15, 16, 22, and 23 of each cycle, with or without isatuximab. The antibody was dosed 10 mg/kg on days 1, 8, 15, and 22 in cycle 1 then every 2 weeks thereafter.
Treatments were continued until disease progression, unacceptable toxicity, or patient choice intervened.
At a prespecified interim analysis, the trial met its primary endpoint of a minimum 41% risk reduction in the hazard rate for progression free survival (PFS), with an actual risk reduction of 47%.
An analysis of PFS by subgroup showed significant benefits with the triple combination for patients aged 65 years and older, those with baseline estimated glomerular filtration rates below 60 mL/min per 1.73 m2, those with more than one prior line of therapy, those who had not previously received a proteasome inhibitor (e.g., bortezomib) or immunomodulatory agent (e.g., lenalidomide), those with high-risk cytogenetic status, and those with R-ISS stage II at study entry.
Overall response rates were similar between the study arms, at 86.6% with Isa-Kd and 82.9% with Kd, but the rate of very good partial responses or better was significantly higher with the triplet, at 72.6% versus 56.1% (P = .0011). The rate of minimal residual disease negativity was also significantly lower with Isa-Kd in the intent-to-treat population, at 29.6% versus 13%, respectively (P = .0004).
Overall survival data were not mature at the time of data cutoff and will be reported later, Dr. Moreau said.
Grade 3 or greater treatment-emergent adverse events (TEAEs) occurred in 76.8% of patients on the triplet and 67.2% of those on Kd. The incidences of death, serious TEAEs, or adverse events leading to discontinuation of therapy did not differ markedly between the treatment arms, however. Grade 3 or greater cardiac failure occurred in seven patients treated with the triplet (4%) and five treated with Kd (4.1%); respective rates of grade 3 or greater hematologic abnormalities included anemia in 22% and 19.7%, neutropenia in 19.2% and 7.4%, and thrombocytopenia in 29.9% and 23.8%.
The primary completion date for the trial is estimated to occur in November 2020, with final results in November 2023.
The study was sponsored by Sanofi. Dr. Moreau disclosed honoraria and a consulting or advisory role with several companies, not including Sanofi. Dr. Lipe disclosed impending advisory board activity for Janssen.
SOURCE: Moreau P et al. EHA Congress, Abstract LB2603.
FROM EHA CONGRESS
Microneedling plus 10% TCA peels bests CO2 laser alone for infraorbital dark circles
In a study of patients with mild to moderate infraorbital dark circles, treatment with carbon dioxide laser resurfacing did not produce a significant improvement in infraorbital hyperpigmentation. However, the combination of microneedling and 10% trichloroacetic acid peels did.

The finding comes from what is believed to be the first head-to-head comparison of the two procedures for infraorbital dark circles, which are a common cosmetic concern with increased age.
During a late-breaking abstract session at the virtual annual meeting of the American Academy of Dermatology, lead study author Banu Farabi, MD, said that dark circles seen in the periorbital area are defined as bilateral, round homogeneous pigmented macules whose etiology is thought to be multifactorial. Available treatments include bleaching creams, topical retinoids, chemical peels, lasers, autologous fat transplantation, injectable fillers, and blepharoplasty.
“Microneedling has been recently suggested as an effective and efficient method for reducing infraorbital dark circles,” Dr. Farabi said. “This technique is based on creating microchannels that can stimulate the production of subcutaneous collagen and elastin. It also enhances the revascularization and fibroblast activity, which increases the skin thickness and gives a shiny appearance to the skin. The fractional CO2 has also been introduced as an effective procedure to remove infraorbital dark circles. However, there are some potential complications with that therapy.”
For the current study, Dr. Farabi, of the department of dermatology at Ankara (Turkey) University, and Mohamad Goldust, MD, of University Hospital Basel (Switzerland), They used the handheld Automatic Microneedle Therapy System-Handhold from MCure. After creating microchannels, the investigators topically applied 10% trichloroacetic acid peels to each infraorbital area and waited for 5 minutes.
In the carbon dioxide laser group, a Lutronic CO2 laser was used with a pulse energy of 10 J/cm2, a 100-microsecond pulse rate, 30 W of power, and a pulse width of 4 mm. The treatment outcome was assessed with the patient’s satisfaction and the physician’s judgment, which were no response, partial response, and complete response. Patients in both study groups were followed up for blinded-investigator assessment of infraorbital hyperpigmentation, adverse events, and improvement, compared with baseline.
The mean age of patients was 40 years, with a range between 27 and 58 years. About one-third of patients in each group had Fitzpatrick skin types II, III, and IV, respectively. In the blinded investigator assessment, the laser-resurfacing procedure did not demonstrate a significant improvement in infraorbital hyperpigmentation at day 90 (P = .24). However, the combination of microneedling and 10% trichloroacetic acid peels significantly improved infraorbital hyperpigmentation by day 90, with improvement maintained through day 180 (P = .012 and .002, respectively).
Adverse events were mild and temporary in both groups. In the laser-resurfacing group, 7 of the patients (22.5%) developed transient infraorbital hyperpigmentation postoperatively that lasted 4 weeks. In the combination treatment group, 18 patients (58%) developed transient erythema that lasted for up to 1 week.
“We suggest using microneedling plus 10% [trichloroacetic acid] as a cost-effective and efficient method for reducing infraorbital dark circles,” Dr. Farabi concluded.
The researchers reported having no financial disclosures.
In a study of patients with mild to moderate infraorbital dark circles, treatment with carbon dioxide laser resurfacing did not produce a significant improvement in infraorbital hyperpigmentation. However, the combination of microneedling and 10% trichloroacetic acid peels did.
The finding comes from what is believed to be the first head-to-head comparison of the two procedures for infraorbital dark circles, which are a common cosmetic concern with increased age.
During a late-breaking abstract session at the virtual annual meeting of the American Academy of Dermatology, lead study author Banu Farabi, MD, said that dark circles seen in the periorbital area are defined as bilateral, round homogeneous pigmented macules whose etiology is thought to be multifactorial. Available treatments include bleaching creams, topical retinoids, chemical peels, lasers, autologous fat transplantation, injectable fillers, and blepharoplasty.
“Microneedling has been recently suggested as an effective and efficient method for reducing infraorbital dark circles,” Dr. Farabi said. “This technique is based on creating microchannels that can stimulate the production of subcutaneous collagen and elastin. It also enhances the revascularization and fibroblast activity, which increases the skin thickness and gives a shiny appearance to the skin. The fractional CO2 has also been introduced as an effective procedure to remove infraorbital dark circles. However, there are some potential complications with that therapy.”
For the current study, Dr. Farabi, of the department of dermatology at Ankara (Turkey) University, and Mohamad Goldust, MD, of University Hospital Basel (Switzerland), They used the handheld Automatic Microneedle Therapy System-Handhold from MCure. After creating microchannels, the investigators topically applied 10% trichloroacetic acid peels to each infraorbital area and waited for 5 minutes.
In the carbon dioxide laser group, a Lutronic CO2 laser was used with a pulse energy of 10 J/cm2, a 100-microsecond pulse rate, 30 W of power, and a pulse width of 4 mm. The treatment outcome was assessed with the patient’s satisfaction and the physician’s judgment, which were no response, partial response, and complete response. Patients in both study groups were followed up for blinded-investigator assessment of infraorbital hyperpigmentation, adverse events, and improvement, compared with baseline.
The mean age of patients was 40 years, with a range between 27 and 58 years. About one-third of patients in each group had Fitzpatrick skin types II, III, and IV, respectively. In the blinded investigator assessment, the laser-resurfacing procedure did not demonstrate a significant improvement in infraorbital hyperpigmentation at day 90 (P = .24). However, the combination of microneedling and 10% trichloroacetic acid peels significantly improved infraorbital hyperpigmentation by day 90, with improvement maintained through day 180 (P = .012 and .002, respectively).
Adverse events were mild and temporary in both groups. In the laser-resurfacing group, 7 of the patients (22.5%) developed transient infraorbital hyperpigmentation postoperatively that lasted 4 weeks. In the combination treatment group, 18 patients (58%) developed transient erythema that lasted for up to 1 week.
“We suggest using microneedling plus 10% [trichloroacetic acid] as a cost-effective and efficient method for reducing infraorbital dark circles,” Dr. Farabi concluded.
The researchers reported having no financial disclosures.
In a study of patients with mild to moderate infraorbital dark circles, treatment with carbon dioxide laser resurfacing did not produce a significant improvement in infraorbital hyperpigmentation. However, the combination of microneedling and 10% trichloroacetic acid peels did.
The finding comes from what is believed to be the first head-to-head comparison of the two procedures for infraorbital dark circles, which are a common cosmetic concern with increased age.
During a late-breaking abstract session at the virtual annual meeting of the American Academy of Dermatology, lead study author Banu Farabi, MD, said that dark circles seen in the periorbital area are defined as bilateral, round homogeneous pigmented macules whose etiology is thought to be multifactorial. Available treatments include bleaching creams, topical retinoids, chemical peels, lasers, autologous fat transplantation, injectable fillers, and blepharoplasty.
“Microneedling has been recently suggested as an effective and efficient method for reducing infraorbital dark circles,” Dr. Farabi said. “This technique is based on creating microchannels that can stimulate the production of subcutaneous collagen and elastin. It also enhances the revascularization and fibroblast activity, which increases the skin thickness and gives a shiny appearance to the skin. The fractional CO2 has also been introduced as an effective procedure to remove infraorbital dark circles. However, there are some potential complications with that therapy.”
For the current study, Dr. Farabi, of the department of dermatology at Ankara (Turkey) University, and Mohamad Goldust, MD, of University Hospital Basel (Switzerland), They used the handheld Automatic Microneedle Therapy System-Handhold from MCure. After creating microchannels, the investigators topically applied 10% trichloroacetic acid peels to each infraorbital area and waited for 5 minutes.
In the carbon dioxide laser group, a Lutronic CO2 laser was used with a pulse energy of 10 J/cm2, a 100-microsecond pulse rate, 30 W of power, and a pulse width of 4 mm. The treatment outcome was assessed with the patient’s satisfaction and the physician’s judgment, which were no response, partial response, and complete response. Patients in both study groups were followed up for blinded-investigator assessment of infraorbital hyperpigmentation, adverse events, and improvement, compared with baseline.
The mean age of patients was 40 years, with a range between 27 and 58 years. About one-third of patients in each group had Fitzpatrick skin types II, III, and IV, respectively. In the blinded investigator assessment, the laser-resurfacing procedure did not demonstrate a significant improvement in infraorbital hyperpigmentation at day 90 (P = .24). However, the combination of microneedling and 10% trichloroacetic acid peels significantly improved infraorbital hyperpigmentation by day 90, with improvement maintained through day 180 (P = .012 and .002, respectively).
Adverse events were mild and temporary in both groups. In the laser-resurfacing group, 7 of the patients (22.5%) developed transient infraorbital hyperpigmentation postoperatively that lasted 4 weeks. In the combination treatment group, 18 patients (58%) developed transient erythema that lasted for up to 1 week.
“We suggest using microneedling plus 10% [trichloroacetic acid] as a cost-effective and efficient method for reducing infraorbital dark circles,” Dr. Farabi concluded.
The researchers reported having no financial disclosures.
FROM AAD 20
Women thrive on baroreflex activation for heart failure
The striking gains in functional capacity and quality of life conferred by baroreflex activation therapy in patients with heart failure, as shown in the pivotal phase 3 clinical trial for this novel intervention, were at least as great in women as in men, JoAnn Lindenfeld, MD, said at the European Society of Cardiology Heart Failure Discoveries virtual meeting.

The results of the multicenter, prospective, randomized BeAT-HF trial led to marketing approval of the BaroStim Neo system for improvement in symptoms of heart failure with reduced ejection fraction (HFrEF) by the Food and Drug Administration in August 2019. Dr. Lindenfeld presented a fresh breakdown of the results by gender which showed, intriguingly, that the improvement in all study endpoints was consistently numerically greater in the women – sometimes startlingly so – although these gender differences in response didn’t achieve statistical significance. The 6-month randomized trial was underpowered for drawing definitive conclusions on that score, with a study population of only 53 women and 211 men. So the investigator remained circumspect.
“We think that what this study shows us is that women have at least equivalent improvement as men in this population. I don’t think we can conclude from this study yet that it’s better, but it’s certainly in all these parameters as least as good. And I think this is a population in which we’ve seen that improving symptoms and functional capacity is very important,” said Dr. Lindenfeld, professor of medicine and director of advanced heart failure/cardiac transplantation at Vanderbilt University, Nashville, Tenn.
The FDA approval was restricted to patients like those enrolled in BeAT-HF: that is, individuals with New York Heart Association functional class III heart failure, a left ventricular ejection fraction of 35% or less while on stable optimal medical therapy, and ineligibility for cardiac resynchronization therapy according to current guidelines. Seventy-eight percent of BeAT-HF participants had an implantable cardioverter-defibrillator.
Participants were randomized to baroreflex activation therapy (BAT) plus optimal medical therapy or to optimal medical therapy alone. The three coprimary endpoints were change from baseline to 6 months in 6-minute hall walk distance (6MHW), scores on the Minnesota Living with Heart Failure Questionnaire (MLHF), and N-terminal pro-B-type natriuretic peptide (NT-proBNP).
In the overall study population, 6MHW increased by 60 m in the BAT group and decreased by 8 m in controls; MLHF scores dropped by 14 and 6 points, respectively; and NT-proBNP fell by an average of 25% with BAT while rising by 3% in controls.
Very often, just a 5-point reduction in MLHF score is considered a clinically meaningful improvement in quality of life, the cardiologist noted.
The gender-based analysis is where things got particularly interesting.
The investigators defined a clinically relevant response as a greater than 10% increase from baseline on the 6MHW, at least a one-class improvement in NYHA class, or a reduction of 5 points or more on the MLHF. Among subjects in the BAT group, 70% of women and 60% of men met the clinically relevant response standard in terms of 6MHW, as did 70% of women and 64% of men for improvement in NYHA class, and 78% of women and 66% of men for MLHF score.
Eighty-seven percent of women and 68% of men on BAT had a clinically relevant response on at least one of these endpoints, as did about 28% of controls. Moreover, 31% of women in the BAT group were clinically relevant responders on at least two endpoints, compared with 19% of BAT men and 4% and 9% of controls.
Women dominate super-responder category
In order to be classified as a super responder, a patient had to demonstrate a greater than 20% increase in 6MHW, improvement in NYHA class I status, or at least a 10-point improvement in MLHF score. Ninety-one percent of women on BAT achieved super-responder status for at least one of these endpoints, compared with 76% of men. Forty-three percent of women and 24% of men in the BAT group were super responders in at least two domains, as were 8% and 11% of female and male controls, Dr. Lindenfeld continued.
Discussant Ewa Anita Jankowska, MD, PhD, deemed the BeAT-HF results on the therapeutic benefits of this autonomic modulation strategy “quite convincing.”
“We need to acknowledge that in recent years we have been spoiled a bit by the huge trials in heart failure where the ultimate goal was a reduction in mortality. But I think this is the time when we should think about the patients who want to live – here, now – with a better life. Patients expect symptomatic benefits. There is a substantial group of patients who are symptomatic even though they receive quite extensive neurohormonal blockage and who are not suitable for CRT. This study demonstrates that, for this group of patients, BAT can bring really significant symptomatic benefits,” she said.
“If you think about a treatment that provides patients who are NYHA class III an increase in 6MHW of 60 meters, that’s really something. And 20% of patients went from NYHA class III to class I – that’s really something, too,” added Dr. Jankowska, professor of medicine and head of the laboratory of applied research on the cardiovascular system at Wroclaw (Poland) University.
How baroreflex activation therapy works
The BaroStim system consists of a 2-mm unipolar electrode on a 7-mm backer that is placed over the carotid sinus. It is supported by a small generator with a 4- to 5-year battery life implanted under the collarbone, along with radiofrequency telemetry capability and programming flexibility.
Stimulation of the carotid baroreceptor promotes an integrated autonomic nervous system response which enhances parasympathetic activity and inhibits sympathetic nervous system activity. The result, as shown in numerous earlier proof-of-concept studies, is a reduced heart rate, decreased ventricular remodeling, enhanced diuresis, increased vasodilation, a drop in elevated blood pressure, and decreased renin secretion – all achieved nonpharmacologically.
The study was sponsored by CVRx. Dr. Lindenfeld reported serving as a consultant to CVRx, Abbott, AstraZeneca, Boehringer Ingelheim, Edwards Lifesciences, Impulse Dynamics, and VWave.
The striking gains in functional capacity and quality of life conferred by baroreflex activation therapy in patients with heart failure, as shown in the pivotal phase 3 clinical trial for this novel intervention, were at least as great in women as in men, JoAnn Lindenfeld, MD, said at the European Society of Cardiology Heart Failure Discoveries virtual meeting.
The results of the multicenter, prospective, randomized BeAT-HF trial led to marketing approval of the BaroStim Neo system for improvement in symptoms of heart failure with reduced ejection fraction (HFrEF) by the Food and Drug Administration in August 2019. Dr. Lindenfeld presented a fresh breakdown of the results by gender which showed, intriguingly, that the improvement in all study endpoints was consistently numerically greater in the women – sometimes startlingly so – although these gender differences in response didn’t achieve statistical significance. The 6-month randomized trial was underpowered for drawing definitive conclusions on that score, with a study population of only 53 women and 211 men. So the investigator remained circumspect.
“We think that what this study shows us is that women have at least equivalent improvement as men in this population. I don’t think we can conclude from this study yet that it’s better, but it’s certainly in all these parameters as least as good. And I think this is a population in which we’ve seen that improving symptoms and functional capacity is very important,” said Dr. Lindenfeld, professor of medicine and director of advanced heart failure/cardiac transplantation at Vanderbilt University, Nashville, Tenn.
The FDA approval was restricted to patients like those enrolled in BeAT-HF: that is, individuals with New York Heart Association functional class III heart failure, a left ventricular ejection fraction of 35% or less while on stable optimal medical therapy, and ineligibility for cardiac resynchronization therapy according to current guidelines. Seventy-eight percent of BeAT-HF participants had an implantable cardioverter-defibrillator.
Participants were randomized to baroreflex activation therapy (BAT) plus optimal medical therapy or to optimal medical therapy alone. The three coprimary endpoints were change from baseline to 6 months in 6-minute hall walk distance (6MHW), scores on the Minnesota Living with Heart Failure Questionnaire (MLHF), and N-terminal pro-B-type natriuretic peptide (NT-proBNP).
In the overall study population, 6MHW increased by 60 m in the BAT group and decreased by 8 m in controls; MLHF scores dropped by 14 and 6 points, respectively; and NT-proBNP fell by an average of 25% with BAT while rising by 3% in controls.
Very often, just a 5-point reduction in MLHF score is considered a clinically meaningful improvement in quality of life, the cardiologist noted.
The gender-based analysis is where things got particularly interesting.
The investigators defined a clinically relevant response as a greater than 10% increase from baseline on the 6MHW, at least a one-class improvement in NYHA class, or a reduction of 5 points or more on the MLHF. Among subjects in the BAT group, 70% of women and 60% of men met the clinically relevant response standard in terms of 6MHW, as did 70% of women and 64% of men for improvement in NYHA class, and 78% of women and 66% of men for MLHF score.
Eighty-seven percent of women and 68% of men on BAT had a clinically relevant response on at least one of these endpoints, as did about 28% of controls. Moreover, 31% of women in the BAT group were clinically relevant responders on at least two endpoints, compared with 19% of BAT men and 4% and 9% of controls.
Women dominate super-responder category
In order to be classified as a super responder, a patient had to demonstrate a greater than 20% increase in 6MHW, improvement in NYHA class I status, or at least a 10-point improvement in MLHF score. Ninety-one percent of women on BAT achieved super-responder status for at least one of these endpoints, compared with 76% of men. Forty-three percent of women and 24% of men in the BAT group were super responders in at least two domains, as were 8% and 11% of female and male controls, Dr. Lindenfeld continued.
Discussant Ewa Anita Jankowska, MD, PhD, deemed the BeAT-HF results on the therapeutic benefits of this autonomic modulation strategy “quite convincing.”
“We need to acknowledge that in recent years we have been spoiled a bit by the huge trials in heart failure where the ultimate goal was a reduction in mortality. But I think this is the time when we should think about the patients who want to live – here, now – with a better life. Patients expect symptomatic benefits. There is a substantial group of patients who are symptomatic even though they receive quite extensive neurohormonal blockage and who are not suitable for CRT. This study demonstrates that, for this group of patients, BAT can bring really significant symptomatic benefits,” she said.
“If you think about a treatment that provides patients who are NYHA class III an increase in 6MHW of 60 meters, that’s really something. And 20% of patients went from NYHA class III to class I – that’s really something, too,” added Dr. Jankowska, professor of medicine and head of the laboratory of applied research on the cardiovascular system at Wroclaw (Poland) University.
How baroreflex activation therapy works
The BaroStim system consists of a 2-mm unipolar electrode on a 7-mm backer that is placed over the carotid sinus. It is supported by a small generator with a 4- to 5-year battery life implanted under the collarbone, along with radiofrequency telemetry capability and programming flexibility.
Stimulation of the carotid baroreceptor promotes an integrated autonomic nervous system response which enhances parasympathetic activity and inhibits sympathetic nervous system activity. The result, as shown in numerous earlier proof-of-concept studies, is a reduced heart rate, decreased ventricular remodeling, enhanced diuresis, increased vasodilation, a drop in elevated blood pressure, and decreased renin secretion – all achieved nonpharmacologically.
The study was sponsored by CVRx. Dr. Lindenfeld reported serving as a consultant to CVRx, Abbott, AstraZeneca, Boehringer Ingelheim, Edwards Lifesciences, Impulse Dynamics, and VWave.
The striking gains in functional capacity and quality of life conferred by baroreflex activation therapy in patients with heart failure, as shown in the pivotal phase 3 clinical trial for this novel intervention, were at least as great in women as in men, JoAnn Lindenfeld, MD, said at the European Society of Cardiology Heart Failure Discoveries virtual meeting.
The results of the multicenter, prospective, randomized BeAT-HF trial led to marketing approval of the BaroStim Neo system for improvement in symptoms of heart failure with reduced ejection fraction (HFrEF) by the Food and Drug Administration in August 2019. Dr. Lindenfeld presented a fresh breakdown of the results by gender which showed, intriguingly, that the improvement in all study endpoints was consistently numerically greater in the women – sometimes startlingly so – although these gender differences in response didn’t achieve statistical significance. The 6-month randomized trial was underpowered for drawing definitive conclusions on that score, with a study population of only 53 women and 211 men. So the investigator remained circumspect.
“We think that what this study shows us is that women have at least equivalent improvement as men in this population. I don’t think we can conclude from this study yet that it’s better, but it’s certainly in all these parameters as least as good. And I think this is a population in which we’ve seen that improving symptoms and functional capacity is very important,” said Dr. Lindenfeld, professor of medicine and director of advanced heart failure/cardiac transplantation at Vanderbilt University, Nashville, Tenn.
The FDA approval was restricted to patients like those enrolled in BeAT-HF: that is, individuals with New York Heart Association functional class III heart failure, a left ventricular ejection fraction of 35% or less while on stable optimal medical therapy, and ineligibility for cardiac resynchronization therapy according to current guidelines. Seventy-eight percent of BeAT-HF participants had an implantable cardioverter-defibrillator.
Participants were randomized to baroreflex activation therapy (BAT) plus optimal medical therapy or to optimal medical therapy alone. The three coprimary endpoints were change from baseline to 6 months in 6-minute hall walk distance (6MHW), scores on the Minnesota Living with Heart Failure Questionnaire (MLHF), and N-terminal pro-B-type natriuretic peptide (NT-proBNP).
In the overall study population, 6MHW increased by 60 m in the BAT group and decreased by 8 m in controls; MLHF scores dropped by 14 and 6 points, respectively; and NT-proBNP fell by an average of 25% with BAT while rising by 3% in controls.
Very often, just a 5-point reduction in MLHF score is considered a clinically meaningful improvement in quality of life, the cardiologist noted.
The gender-based analysis is where things got particularly interesting.
The investigators defined a clinically relevant response as a greater than 10% increase from baseline on the 6MHW, at least a one-class improvement in NYHA class, or a reduction of 5 points or more on the MLHF. Among subjects in the BAT group, 70% of women and 60% of men met the clinically relevant response standard in terms of 6MHW, as did 70% of women and 64% of men for improvement in NYHA class, and 78% of women and 66% of men for MLHF score.
Eighty-seven percent of women and 68% of men on BAT had a clinically relevant response on at least one of these endpoints, as did about 28% of controls. Moreover, 31% of women in the BAT group were clinically relevant responders on at least two endpoints, compared with 19% of BAT men and 4% and 9% of controls.
Women dominate super-responder category
In order to be classified as a super responder, a patient had to demonstrate a greater than 20% increase in 6MHW, improvement in NYHA class I status, or at least a 10-point improvement in MLHF score. Ninety-one percent of women on BAT achieved super-responder status for at least one of these endpoints, compared with 76% of men. Forty-three percent of women and 24% of men in the BAT group were super responders in at least two domains, as were 8% and 11% of female and male controls, Dr. Lindenfeld continued.
Discussant Ewa Anita Jankowska, MD, PhD, deemed the BeAT-HF results on the therapeutic benefits of this autonomic modulation strategy “quite convincing.”
“We need to acknowledge that in recent years we have been spoiled a bit by the huge trials in heart failure where the ultimate goal was a reduction in mortality. But I think this is the time when we should think about the patients who want to live – here, now – with a better life. Patients expect symptomatic benefits. There is a substantial group of patients who are symptomatic even though they receive quite extensive neurohormonal blockage and who are not suitable for CRT. This study demonstrates that, for this group of patients, BAT can bring really significant symptomatic benefits,” she said.
“If you think about a treatment that provides patients who are NYHA class III an increase in 6MHW of 60 meters, that’s really something. And 20% of patients went from NYHA class III to class I – that’s really something, too,” added Dr. Jankowska, professor of medicine and head of the laboratory of applied research on the cardiovascular system at Wroclaw (Poland) University.
How baroreflex activation therapy works
The BaroStim system consists of a 2-mm unipolar electrode on a 7-mm backer that is placed over the carotid sinus. It is supported by a small generator with a 4- to 5-year battery life implanted under the collarbone, along with radiofrequency telemetry capability and programming flexibility.
Stimulation of the carotid baroreceptor promotes an integrated autonomic nervous system response which enhances parasympathetic activity and inhibits sympathetic nervous system activity. The result, as shown in numerous earlier proof-of-concept studies, is a reduced heart rate, decreased ventricular remodeling, enhanced diuresis, increased vasodilation, a drop in elevated blood pressure, and decreased renin secretion – all achieved nonpharmacologically.
The study was sponsored by CVRx. Dr. Lindenfeld reported serving as a consultant to CVRx, Abbott, AstraZeneca, Boehringer Ingelheim, Edwards Lifesciences, Impulse Dynamics, and VWave.
FROM ESC HEART FAILURE 2020
School daze
A few weeks ago I was asked by the head of our local parks and recreation department for my opinion on whether the town should open its summer recreation camps program. He had been receiving multiple inquiries from parents who in the past had relied on the day camps for day care. The director already had surveyed health care administrators and other providers in the town and his team had crafted a plan based on what guidelines they could glean from state and federal advisory groups. The feedback he had received from town officials and health care representatives was that they felt opening would be a bad decision. One physician observed that there is just “so much we don’t know about the virus at this point.”
I certainly agreed that we still have much to learn about COVID-19, but I told the director that we know enough that I would feel comfortable with opening the day camps, which have traditionally been held outdoors under open-sided tents. If group sizes were kept small, staff personnel were dedicated to just one group, and temperatures were taken at the beginning and at the midpoint of each daily session, I felt that the risk of triggering an outbreak was small. I told him that in my mind the Achilles heel of the plan was whether the camp staff, who are generally high school and college-age young people, could be trusted to follow rigorous social distancing in their off-work hours.
Eventually the decision was made by the traditionally risk-averse town officials to open the camps. I hope that this step forward will spur the process of reopening the schools in the fall by demonstrating that, at least in an open-air environment, some simple common sense measures could create a safe environment for children to congregate in. Unfortunately, the long delay in formulating the plan and a basic hesitancy on the part of some parents has resulted in disappointing enrollment figures so far.
I suspect that many of you have been asked to participate in the planning and decision-making processes for opening the school systems in your community or at least have some thoughts of your own about how best to begin the reopening process.
I suspect you agree that, if the number of new cases detected each day in your state is still rising and/or your state’s ability to test, track, case find, and quarantine is inadequate, reopening schools is probably just asking for trouble. However, a recent study has found that children and young adults under the age of 20 years were almost half as likely to become infected as those over the age of 20 (Nat Med. 2020 Jun 16. doi: 10.1038/s41591-020-0962-9). We already know that, in general, children are presenting with less severe illness. Although the authors observe that we still need to learn more about the transmissibility of subclinical infections, particularly in children, they suggest that “interventions aimed at children might have relatively little impact on reducing SARS-CoV-2 transmission.” It is sounding like reopening schools will place the children at relatively low risk. However, until we know more about transmissibility we have to assume reopening schools may place the community at an increased risk.

If this new information is confirmed by other studies, how would this change the recommendations you would make to the community about reopening its schools? What about masks? We are learning that they make a difference for adults, but is this true for very young children as well? Masks should probably remain part of the hygiene education program as well for at least the foreseeable future.
Do you think your school system can broaden its focus beyond surface cleaning to air handling and ventilation? Here in Maine, keeping the windows open for more than a few weeks a year is going to present problems that may be expensive to remedy.
There are always more questions than answers, but my hope is that here in Maine our apparent success on a state level will allow us to reopen the schools as long as we remain vigilant for the first signs that we need to return to lock down. How do you feel about your community’s situation?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
A few weeks ago I was asked by the head of our local parks and recreation department for my opinion on whether the town should open its summer recreation camps program. He had been receiving multiple inquiries from parents who in the past had relied on the day camps for day care. The director already had surveyed health care administrators and other providers in the town and his team had crafted a plan based on what guidelines they could glean from state and federal advisory groups. The feedback he had received from town officials and health care representatives was that they felt opening would be a bad decision. One physician observed that there is just “so much we don’t know about the virus at this point.”
I certainly agreed that we still have much to learn about COVID-19, but I told the director that we know enough that I would feel comfortable with opening the day camps, which have traditionally been held outdoors under open-sided tents. If group sizes were kept small, staff personnel were dedicated to just one group, and temperatures were taken at the beginning and at the midpoint of each daily session, I felt that the risk of triggering an outbreak was small. I told him that in my mind the Achilles heel of the plan was whether the camp staff, who are generally high school and college-age young people, could be trusted to follow rigorous social distancing in their off-work hours.
Eventually the decision was made by the traditionally risk-averse town officials to open the camps. I hope that this step forward will spur the process of reopening the schools in the fall by demonstrating that, at least in an open-air environment, some simple common sense measures could create a safe environment for children to congregate in. Unfortunately, the long delay in formulating the plan and a basic hesitancy on the part of some parents has resulted in disappointing enrollment figures so far.
I suspect that many of you have been asked to participate in the planning and decision-making processes for opening the school systems in your community or at least have some thoughts of your own about how best to begin the reopening process.
I suspect you agree that, if the number of new cases detected each day in your state is still rising and/or your state’s ability to test, track, case find, and quarantine is inadequate, reopening schools is probably just asking for trouble. However, a recent study has found that children and young adults under the age of 20 years were almost half as likely to become infected as those over the age of 20 (Nat Med. 2020 Jun 16. doi: 10.1038/s41591-020-0962-9). We already know that, in general, children are presenting with less severe illness. Although the authors observe that we still need to learn more about the transmissibility of subclinical infections, particularly in children, they suggest that “interventions aimed at children might have relatively little impact on reducing SARS-CoV-2 transmission.” It is sounding like reopening schools will place the children at relatively low risk. However, until we know more about transmissibility we have to assume reopening schools may place the community at an increased risk.
If this new information is confirmed by other studies, how would this change the recommendations you would make to the community about reopening its schools? What about masks? We are learning that they make a difference for adults, but is this true for very young children as well? Masks should probably remain part of the hygiene education program as well for at least the foreseeable future.
Do you think your school system can broaden its focus beyond surface cleaning to air handling and ventilation? Here in Maine, keeping the windows open for more than a few weeks a year is going to present problems that may be expensive to remedy.
There are always more questions than answers, but my hope is that here in Maine our apparent success on a state level will allow us to reopen the schools as long as we remain vigilant for the first signs that we need to return to lock down. How do you feel about your community’s situation?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
A few weeks ago I was asked by the head of our local parks and recreation department for my opinion on whether the town should open its summer recreation camps program. He had been receiving multiple inquiries from parents who in the past had relied on the day camps for day care. The director already had surveyed health care administrators and other providers in the town and his team had crafted a plan based on what guidelines they could glean from state and federal advisory groups. The feedback he had received from town officials and health care representatives was that they felt opening would be a bad decision. One physician observed that there is just “so much we don’t know about the virus at this point.”
I certainly agreed that we still have much to learn about COVID-19, but I told the director that we know enough that I would feel comfortable with opening the day camps, which have traditionally been held outdoors under open-sided tents. If group sizes were kept small, staff personnel were dedicated to just one group, and temperatures were taken at the beginning and at the midpoint of each daily session, I felt that the risk of triggering an outbreak was small. I told him that in my mind the Achilles heel of the plan was whether the camp staff, who are generally high school and college-age young people, could be trusted to follow rigorous social distancing in their off-work hours.
Eventually the decision was made by the traditionally risk-averse town officials to open the camps. I hope that this step forward will spur the process of reopening the schools in the fall by demonstrating that, at least in an open-air environment, some simple common sense measures could create a safe environment for children to congregate in. Unfortunately, the long delay in formulating the plan and a basic hesitancy on the part of some parents has resulted in disappointing enrollment figures so far.
I suspect that many of you have been asked to participate in the planning and decision-making processes for opening the school systems in your community or at least have some thoughts of your own about how best to begin the reopening process.
I suspect you agree that, if the number of new cases detected each day in your state is still rising and/or your state’s ability to test, track, case find, and quarantine is inadequate, reopening schools is probably just asking for trouble. However, a recent study has found that children and young adults under the age of 20 years were almost half as likely to become infected as those over the age of 20 (Nat Med. 2020 Jun 16. doi: 10.1038/s41591-020-0962-9). We already know that, in general, children are presenting with less severe illness. Although the authors observe that we still need to learn more about the transmissibility of subclinical infections, particularly in children, they suggest that “interventions aimed at children might have relatively little impact on reducing SARS-CoV-2 transmission.” It is sounding like reopening schools will place the children at relatively low risk. However, until we know more about transmissibility we have to assume reopening schools may place the community at an increased risk.
If this new information is confirmed by other studies, how would this change the recommendations you would make to the community about reopening its schools? What about masks? We are learning that they make a difference for adults, but is this true for very young children as well? Masks should probably remain part of the hygiene education program as well for at least the foreseeable future.
Do you think your school system can broaden its focus beyond surface cleaning to air handling and ventilation? Here in Maine, keeping the windows open for more than a few weeks a year is going to present problems that may be expensive to remedy.
There are always more questions than answers, but my hope is that here in Maine our apparent success on a state level will allow us to reopen the schools as long as we remain vigilant for the first signs that we need to return to lock down. How do you feel about your community’s situation?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Telehealth and medical liability
The COVID-19 pandemic has led to the rapid uptake of telehealth nationwide in primary care and specialty practices. Over the last few months many practices have actually performed more telehealth visits than traditional in-person visits. The use of telehealth, which had been increasing slowly for the last few years, accelerated rapidly during the pandemic. Long term, telehealth has the potential to increase access to primary care and specialists, and make follow-up easier for many patients, changing how health care is delivered to millions of patients throughout the world.

Since telehealth will be a regular part of our practices from now on, it is important for clinicians to recognize how telehealth visits are viewed in a legal arena.
As is often the case with technological advances, the law needs time to adapt. Will a health care provider treating a patient using telemedicine be held to the same standard of care applicable to an in-person encounter? Stated differently, will consideration be given to the obvious limitations imposed by a telemedicine exam?
Standard of care in medical malpractice cases
The central question in most medical malpractice cases is whether the provider complied with the generally accepted standard of care when evaluating, diagnosing, or treating a patient. This standard typically takes into consideration the provider’s particular specialty as well as all the circumstances surrounding the encounter.1 Medical providers, not state legislators, usually define the standard of care for medical professionals. In malpractice cases, medical experts explain the applicable standard of care to the jury and guide its determination of whether, in the particular case, the standard of care was met. In this way, the law has long recognized that the medical profession itself is best suited to establish the appropriate standards of care under any particular set of circumstances. This standard of care is often referred to as the “reasonable professional under the circumstances” standard of care.
Telemedicine standard of care
Despite the fact that the complex and often nebulous concept of standard of care has been traditionally left to the medical experts to define, state legislators and regulators throughout the nation have chosen to weigh in on this issue in the context of telemedicine. Most states with telemedicine regulations have followed the model policy adopted by the Federation of State Medical Boards in April 2014 which states that “[t]reatment and consultation recommendations made in an online setting … will be held to the same standards of appropriate practice as those in traditional (in-person) settings.”2 States that have adopted this model policy have effectively created a “legal fiction” requiring a jury to ignore the fact that the care was provided virtually by telemedicine technologies and instead assume that the physician treated the patient in person, i.e, applying an “in-person” standard of care. Hawaii appears to be the lone notable exception. Its telemedicine law recognizes that an in-person standard of care should not be applied if there was not a face-to-face visit.3

Proponents of the in-person telemedicine standard claim that it is necessary to ensure patient safety, thus justifying the “legal fiction.” Holding the provider to the in-person standard, it is argued, forces the physician to err on the side of caution and require an actual in-person encounter to ensure the advantages of sight, touch, and sense of things are fully available.4 This discourages the use of telemedicine and deprives the population of its many benefits.
Telemedicine can overcome geographical barriers, increase clinical support, improve health outcomes, reduce health care costs, encourage patient input, reduce travel, and foster continuity of care. The pandemic, which has significantly limited the ability of providers to see patients in person, only underscores the benefits of telemedicine.
The legislatively imposed in-person telemedicine standard of care should be replaced with the “reasonable professional under the circumstances” standard in order to fairly judge physicians’ care and promote overall population health. The “reasonable professional under the circumstances” standard has applied to physicians and other health care professionals outside of telemedicine for decades, and it has served the medical community and public well. It is unfortunate that legislators felt the need to weigh in and define a distinctly different standard of care for telemedicine than for the rest of medicine, as this may present unforeseen obstacles to the use of telemedicine.
The in-person telemedicine standard of care remains a significant barrier for long-term telemedicine. Eliminating this legal fiction has the potential to further expand physicians’ use of telemedicine and fulfill its promise of improving access to care and improving population health.
Mr. Horner (partner), Mr. Milewski (partner), and Mr. Gajer (associate) are attorneys with White and Williams. They specialize in defending health care providers in medical malpractice lawsuits and other health care–related matters. Dr. Skolnik is professor of family and community Medicine at the Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Follow Dr. Skolnik, and feel free to submit questions to him on Twitter: @neilskolnik. The authors have no financial conflicts related to the content of this piece.
References
1. Cowan v. Doering, 111 N.J. 451-62,.1988.
2. Model Policy For The Appropriate Use Of Telemedicine Technologies In The Practice Of Medicine. State Medical Boards Appropriate Regulation of Telemedicine. April 2014..
3. Haw. Rev. Stat. Ann. § 453-1.3(c).
4. Kaspar BJ. Iowa Law Review. 2014 Jan;99:839-59.
The COVID-19 pandemic has led to the rapid uptake of telehealth nationwide in primary care and specialty practices. Over the last few months many practices have actually performed more telehealth visits than traditional in-person visits. The use of telehealth, which had been increasing slowly for the last few years, accelerated rapidly during the pandemic. Long term, telehealth has the potential to increase access to primary care and specialists, and make follow-up easier for many patients, changing how health care is delivered to millions of patients throughout the world.
Since telehealth will be a regular part of our practices from now on, it is important for clinicians to recognize how telehealth visits are viewed in a legal arena.
As is often the case with technological advances, the law needs time to adapt. Will a health care provider treating a patient using telemedicine be held to the same standard of care applicable to an in-person encounter? Stated differently, will consideration be given to the obvious limitations imposed by a telemedicine exam?
Standard of care in medical malpractice cases
The central question in most medical malpractice cases is whether the provider complied with the generally accepted standard of care when evaluating, diagnosing, or treating a patient. This standard typically takes into consideration the provider’s particular specialty as well as all the circumstances surrounding the encounter.1 Medical providers, not state legislators, usually define the standard of care for medical professionals. In malpractice cases, medical experts explain the applicable standard of care to the jury and guide its determination of whether, in the particular case, the standard of care was met. In this way, the law has long recognized that the medical profession itself is best suited to establish the appropriate standards of care under any particular set of circumstances. This standard of care is often referred to as the “reasonable professional under the circumstances” standard of care.
Telemedicine standard of care
Despite the fact that the complex and often nebulous concept of standard of care has been traditionally left to the medical experts to define, state legislators and regulators throughout the nation have chosen to weigh in on this issue in the context of telemedicine. Most states with telemedicine regulations have followed the model policy adopted by the Federation of State Medical Boards in April 2014 which states that “[t]reatment and consultation recommendations made in an online setting … will be held to the same standards of appropriate practice as those in traditional (in-person) settings.”2 States that have adopted this model policy have effectively created a “legal fiction” requiring a jury to ignore the fact that the care was provided virtually by telemedicine technologies and instead assume that the physician treated the patient in person, i.e, applying an “in-person” standard of care. Hawaii appears to be the lone notable exception. Its telemedicine law recognizes that an in-person standard of care should not be applied if there was not a face-to-face visit.3
Proponents of the in-person telemedicine standard claim that it is necessary to ensure patient safety, thus justifying the “legal fiction.” Holding the provider to the in-person standard, it is argued, forces the physician to err on the side of caution and require an actual in-person encounter to ensure the advantages of sight, touch, and sense of things are fully available.4 This discourages the use of telemedicine and deprives the population of its many benefits.
Telemedicine can overcome geographical barriers, increase clinical support, improve health outcomes, reduce health care costs, encourage patient input, reduce travel, and foster continuity of care. The pandemic, which has significantly limited the ability of providers to see patients in person, only underscores the benefits of telemedicine.
The legislatively imposed in-person telemedicine standard of care should be replaced with the “reasonable professional under the circumstances” standard in order to fairly judge physicians’ care and promote overall population health. The “reasonable professional under the circumstances” standard has applied to physicians and other health care professionals outside of telemedicine for decades, and it has served the medical community and public well. It is unfortunate that legislators felt the need to weigh in and define a distinctly different standard of care for telemedicine than for the rest of medicine, as this may present unforeseen obstacles to the use of telemedicine.
The in-person telemedicine standard of care remains a significant barrier for long-term telemedicine. Eliminating this legal fiction has the potential to further expand physicians’ use of telemedicine and fulfill its promise of improving access to care and improving population health.
Mr. Horner (partner), Mr. Milewski (partner), and Mr. Gajer (associate) are attorneys with White and Williams. They specialize in defending health care providers in medical malpractice lawsuits and other health care–related matters. Dr. Skolnik is professor of family and community Medicine at the Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Follow Dr. Skolnik, and feel free to submit questions to him on Twitter: @neilskolnik. The authors have no financial conflicts related to the content of this piece.
References
1. Cowan v. Doering, 111 N.J. 451-62,.1988.
2. Model Policy For The Appropriate Use Of Telemedicine Technologies In The Practice Of Medicine. State Medical Boards Appropriate Regulation of Telemedicine. April 2014..
3. Haw. Rev. Stat. Ann. § 453-1.3(c).
4. Kaspar BJ. Iowa Law Review. 2014 Jan;99:839-59.
The COVID-19 pandemic has led to the rapid uptake of telehealth nationwide in primary care and specialty practices. Over the last few months many practices have actually performed more telehealth visits than traditional in-person visits. The use of telehealth, which had been increasing slowly for the last few years, accelerated rapidly during the pandemic. Long term, telehealth has the potential to increase access to primary care and specialists, and make follow-up easier for many patients, changing how health care is delivered to millions of patients throughout the world.
Since telehealth will be a regular part of our practices from now on, it is important for clinicians to recognize how telehealth visits are viewed in a legal arena.
As is often the case with technological advances, the law needs time to adapt. Will a health care provider treating a patient using telemedicine be held to the same standard of care applicable to an in-person encounter? Stated differently, will consideration be given to the obvious limitations imposed by a telemedicine exam?
Standard of care in medical malpractice cases
The central question in most medical malpractice cases is whether the provider complied with the generally accepted standard of care when evaluating, diagnosing, or treating a patient. This standard typically takes into consideration the provider’s particular specialty as well as all the circumstances surrounding the encounter.1 Medical providers, not state legislators, usually define the standard of care for medical professionals. In malpractice cases, medical experts explain the applicable standard of care to the jury and guide its determination of whether, in the particular case, the standard of care was met. In this way, the law has long recognized that the medical profession itself is best suited to establish the appropriate standards of care under any particular set of circumstances. This standard of care is often referred to as the “reasonable professional under the circumstances” standard of care.
Telemedicine standard of care
Despite the fact that the complex and often nebulous concept of standard of care has been traditionally left to the medical experts to define, state legislators and regulators throughout the nation have chosen to weigh in on this issue in the context of telemedicine. Most states with telemedicine regulations have followed the model policy adopted by the Federation of State Medical Boards in April 2014 which states that “[t]reatment and consultation recommendations made in an online setting … will be held to the same standards of appropriate practice as those in traditional (in-person) settings.”2 States that have adopted this model policy have effectively created a “legal fiction” requiring a jury to ignore the fact that the care was provided virtually by telemedicine technologies and instead assume that the physician treated the patient in person, i.e, applying an “in-person” standard of care. Hawaii appears to be the lone notable exception. Its telemedicine law recognizes that an in-person standard of care should not be applied if there was not a face-to-face visit.3
Proponents of the in-person telemedicine standard claim that it is necessary to ensure patient safety, thus justifying the “legal fiction.” Holding the provider to the in-person standard, it is argued, forces the physician to err on the side of caution and require an actual in-person encounter to ensure the advantages of sight, touch, and sense of things are fully available.4 This discourages the use of telemedicine and deprives the population of its many benefits.
Telemedicine can overcome geographical barriers, increase clinical support, improve health outcomes, reduce health care costs, encourage patient input, reduce travel, and foster continuity of care. The pandemic, which has significantly limited the ability of providers to see patients in person, only underscores the benefits of telemedicine.
The legislatively imposed in-person telemedicine standard of care should be replaced with the “reasonable professional under the circumstances” standard in order to fairly judge physicians’ care and promote overall population health. The “reasonable professional under the circumstances” standard has applied to physicians and other health care professionals outside of telemedicine for decades, and it has served the medical community and public well. It is unfortunate that legislators felt the need to weigh in and define a distinctly different standard of care for telemedicine than for the rest of medicine, as this may present unforeseen obstacles to the use of telemedicine.
The in-person telemedicine standard of care remains a significant barrier for long-term telemedicine. Eliminating this legal fiction has the potential to further expand physicians’ use of telemedicine and fulfill its promise of improving access to care and improving population health.
Mr. Horner (partner), Mr. Milewski (partner), and Mr. Gajer (associate) are attorneys with White and Williams. They specialize in defending health care providers in medical malpractice lawsuits and other health care–related matters. Dr. Skolnik is professor of family and community Medicine at the Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Follow Dr. Skolnik, and feel free to submit questions to him on Twitter: @neilskolnik. The authors have no financial conflicts related to the content of this piece.
References
1. Cowan v. Doering, 111 N.J. 451-62,.1988.
2. Model Policy For The Appropriate Use Of Telemedicine Technologies In The Practice Of Medicine. State Medical Boards Appropriate Regulation of Telemedicine. April 2014..
3. Haw. Rev. Stat. Ann. § 453-1.3(c).
4. Kaspar BJ. Iowa Law Review. 2014 Jan;99:839-59.
COVID-19: Medicare data show long hospital stays, disparities
according to a new analysis by the Centers for Medicare & Medicaid Services.
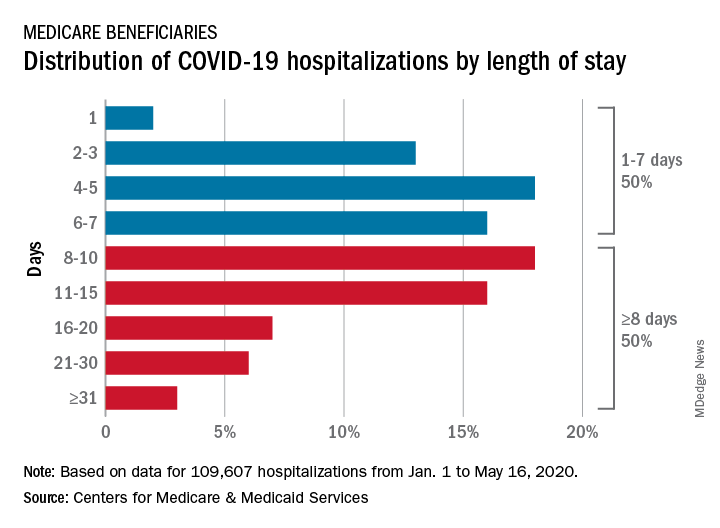
CMS encounter and claims data show almost 110,000 hospital stays for COVID-19 from Jan. 1 to May 16, 2020. Of the longer admissions, 18% were 8-10 days, 16% were 11-15 days, and another 16% were 16 days or longer, the CMS reported in a preliminary data snapshot released June 22.
The hospitalization rate for the Medicare population was 175 per 100,000 as of May 16, but the CMS data show a number of disparities involving race/ethnicity and other demographic characteristics were uncovered, such as the following:
- Black patients were hospitalized for COVID-19 at a much higher rate, at 465 per 100,000 beneficiaries, than were Hispanics (258), Asians (187), and whites (123).
- Residents of urban/suburban areas had a much higher hospitalization rate than did those living in rural areas: 205 versus 57 per 100,000.
- Beneficiaries enrolled in both Medicare and Medicaid had 473 hospitalizations per 100,000, but the rate for those with Medicare only was 112.
“The disparities in the data reflect longstanding challenges facing minority communities and low-income older adults, many of whom face structural challenges to their health that go far beyond what is traditionally considered ‘medical,’ ” CMS Administrator Seema Verma said in a separate statement.
according to a new analysis by the Centers for Medicare & Medicaid Services.
CMS encounter and claims data show almost 110,000 hospital stays for COVID-19 from Jan. 1 to May 16, 2020. Of the longer admissions, 18% were 8-10 days, 16% were 11-15 days, and another 16% were 16 days or longer, the CMS reported in a preliminary data snapshot released June 22.
The hospitalization rate for the Medicare population was 175 per 100,000 as of May 16, but the CMS data show a number of disparities involving race/ethnicity and other demographic characteristics were uncovered, such as the following:
- Black patients were hospitalized for COVID-19 at a much higher rate, at 465 per 100,000 beneficiaries, than were Hispanics (258), Asians (187), and whites (123).
- Residents of urban/suburban areas had a much higher hospitalization rate than did those living in rural areas: 205 versus 57 per 100,000.
- Beneficiaries enrolled in both Medicare and Medicaid had 473 hospitalizations per 100,000, but the rate for those with Medicare only was 112.
“The disparities in the data reflect longstanding challenges facing minority communities and low-income older adults, many of whom face structural challenges to their health that go far beyond what is traditionally considered ‘medical,’ ” CMS Administrator Seema Verma said in a separate statement.
according to a new analysis by the Centers for Medicare & Medicaid Services.
CMS encounter and claims data show almost 110,000 hospital stays for COVID-19 from Jan. 1 to May 16, 2020. Of the longer admissions, 18% were 8-10 days, 16% were 11-15 days, and another 16% were 16 days or longer, the CMS reported in a preliminary data snapshot released June 22.
The hospitalization rate for the Medicare population was 175 per 100,000 as of May 16, but the CMS data show a number of disparities involving race/ethnicity and other demographic characteristics were uncovered, such as the following:
- Black patients were hospitalized for COVID-19 at a much higher rate, at 465 per 100,000 beneficiaries, than were Hispanics (258), Asians (187), and whites (123).
- Residents of urban/suburban areas had a much higher hospitalization rate than did those living in rural areas: 205 versus 57 per 100,000.
- Beneficiaries enrolled in both Medicare and Medicaid had 473 hospitalizations per 100,000, but the rate for those with Medicare only was 112.
“The disparities in the data reflect longstanding challenges facing minority communities and low-income older adults, many of whom face structural challenges to their health that go far beyond what is traditionally considered ‘medical,’ ” CMS Administrator Seema Verma said in a separate statement.
Could jump in opioid overdoses be linked to COVID?
Early evidence suggests that opioid overdoses and deaths are on the rise this year, the director of the National Institute on Drug Abuse warned colleagues, although it’s not clear whether the coronavirus pandemic is responsible for the trend.

The picture is complicated since COVID-19 could have both positive and negative effects on substance use, Nora D. Volkow, MD, said in a plenary session at the virtual annual meeting of the College on Problems of Drug Dependence. However, she said, one thing is clear: The pandemic marks an opportunity to investigate new strategies and potentially reform treatment.
“We are being faced with an unknown world, and the lack of information curtails our capacity to implement interventions in the most effective way,” Dr. Volkow said. “There’s an urgency to obtain these data. All of you out there in the trenches have an opportunity to help gather this information in a way that can be integrated and deployed rapidly for us to guide practices and treatment.”
It’s too early to know for certain how the pandemic is affecting substance use in the United States, since statistics are sparse and COVID-19 is still relatively new. Still, local news reports have suggested overdose deaths have risen, Dr. Volkow said.
And, she noted, the Office of National Drug Control Policy’s Overdose Detection Mapping Application Program – which tracks overdoses nationwide – issued 191% more “spike alerts” from January to April this year, compared with the same time period in 2019. However, the spike alerts started going up in January, several weeks before mass numbers of COVID-19 cases began to be diagnosed.
Dr. Volkow noted the uncertainty about the numbers but said several factors could cause the pandemic to boost overdoses:
- Stress and isolation. “My first fear was that overdoses are going to go up because the stress is actually extraordinarily difficult,” she said. “Social distancing is making it very difficult for individuals with substance use disorder or opioid use disorder to get the community support that keeps them from relapsing,” such as methadone clinics and syringe exchange programs.
- Unwitnessed opioid overdoses. Social distancing could “lead to overdoses that nobody has observed, so no one can administer naloxone,” she said.
- Treatment decisions affected by stigma. “Our health systems will be overburdened, and they have to make decisions about which patients to treat,” she said. Stigma could play a very important role in interfering with the treatment of individuals with substance use disorders.”
- Drug-related vulnerabilities. On another front, she said, substance users may be especially vulnerable to the pandemic, because the drugs target multiple body systems that worsen COVID-19 outcomes. These include not only the lungs but also the cardiac and metabolic systems, she said.
For example, “if you have a long history of drug use, you’re going to be much more likely to have a pulmonary disease,” she said. “We know that pulmonary disease is a risk factor for getting COVID and for much worse outcomes.”
But the pandemic could also help in the fight against substance use. For one thing, she said, the pandemic could disrupt drug markets and make it harder for users to get illicit products.
In yet another complication, there is an ongoing debate over whether tobacco use could actually be protective against COVID-19. Research into nicotine patches as a treatment is in the works, she said.
What now? Dr. Volkow said one priority going forward should be an evaluation of virtual medicine. “We have virtual technologies that have enabled us to do telemedicine to provide mental health support and hotlines, as well as virtual support meetings,” she said. “These have proliferated and have served to a certain extent to compensate for some of the deficit from the erosion of the community support systems that exist.”
Now, she said, we should evaluate which interventions are effective, which patients they help, and the components that make them work.
There are other opportunities for useful investigations, she said. For example, researchers could examine the effects of COVID-related changes in policy, such as the federal government allowing more methadone users to take doses home and expanded telemedicine policy allowing more remote prescriptions.
“If we can show that the outcomes are as good or better [than before] then we may be able to transform these practices that make it so very difficult for so many patients to get access to treatment and to sustain treatment – but have not been questioned for years and years.”
Dr. Volkow reported no relevant disclosures.
Early evidence suggests that opioid overdoses and deaths are on the rise this year, the director of the National Institute on Drug Abuse warned colleagues, although it’s not clear whether the coronavirus pandemic is responsible for the trend.
The picture is complicated since COVID-19 could have both positive and negative effects on substance use, Nora D. Volkow, MD, said in a plenary session at the virtual annual meeting of the College on Problems of Drug Dependence. However, she said, one thing is clear: The pandemic marks an opportunity to investigate new strategies and potentially reform treatment.
“We are being faced with an unknown world, and the lack of information curtails our capacity to implement interventions in the most effective way,” Dr. Volkow said. “There’s an urgency to obtain these data. All of you out there in the trenches have an opportunity to help gather this information in a way that can be integrated and deployed rapidly for us to guide practices and treatment.”
It’s too early to know for certain how the pandemic is affecting substance use in the United States, since statistics are sparse and COVID-19 is still relatively new. Still, local news reports have suggested overdose deaths have risen, Dr. Volkow said.
And, she noted, the Office of National Drug Control Policy’s Overdose Detection Mapping Application Program – which tracks overdoses nationwide – issued 191% more “spike alerts” from January to April this year, compared with the same time period in 2019. However, the spike alerts started going up in January, several weeks before mass numbers of COVID-19 cases began to be diagnosed.
Dr. Volkow noted the uncertainty about the numbers but said several factors could cause the pandemic to boost overdoses:
- Stress and isolation. “My first fear was that overdoses are going to go up because the stress is actually extraordinarily difficult,” she said. “Social distancing is making it very difficult for individuals with substance use disorder or opioid use disorder to get the community support that keeps them from relapsing,” such as methadone clinics and syringe exchange programs.
- Unwitnessed opioid overdoses. Social distancing could “lead to overdoses that nobody has observed, so no one can administer naloxone,” she said.
- Treatment decisions affected by stigma. “Our health systems will be overburdened, and they have to make decisions about which patients to treat,” she said. Stigma could play a very important role in interfering with the treatment of individuals with substance use disorders.”
- Drug-related vulnerabilities. On another front, she said, substance users may be especially vulnerable to the pandemic, because the drugs target multiple body systems that worsen COVID-19 outcomes. These include not only the lungs but also the cardiac and metabolic systems, she said.
For example, “if you have a long history of drug use, you’re going to be much more likely to have a pulmonary disease,” she said. “We know that pulmonary disease is a risk factor for getting COVID and for much worse outcomes.”
But the pandemic could also help in the fight against substance use. For one thing, she said, the pandemic could disrupt drug markets and make it harder for users to get illicit products.
In yet another complication, there is an ongoing debate over whether tobacco use could actually be protective against COVID-19. Research into nicotine patches as a treatment is in the works, she said.
What now? Dr. Volkow said one priority going forward should be an evaluation of virtual medicine. “We have virtual technologies that have enabled us to do telemedicine to provide mental health support and hotlines, as well as virtual support meetings,” she said. “These have proliferated and have served to a certain extent to compensate for some of the deficit from the erosion of the community support systems that exist.”
Now, she said, we should evaluate which interventions are effective, which patients they help, and the components that make them work.
There are other opportunities for useful investigations, she said. For example, researchers could examine the effects of COVID-related changes in policy, such as the federal government allowing more methadone users to take doses home and expanded telemedicine policy allowing more remote prescriptions.
“If we can show that the outcomes are as good or better [than before] then we may be able to transform these practices that make it so very difficult for so many patients to get access to treatment and to sustain treatment – but have not been questioned for years and years.”
Dr. Volkow reported no relevant disclosures.
Early evidence suggests that opioid overdoses and deaths are on the rise this year, the director of the National Institute on Drug Abuse warned colleagues, although it’s not clear whether the coronavirus pandemic is responsible for the trend.
The picture is complicated since COVID-19 could have both positive and negative effects on substance use, Nora D. Volkow, MD, said in a plenary session at the virtual annual meeting of the College on Problems of Drug Dependence. However, she said, one thing is clear: The pandemic marks an opportunity to investigate new strategies and potentially reform treatment.
“We are being faced with an unknown world, and the lack of information curtails our capacity to implement interventions in the most effective way,” Dr. Volkow said. “There’s an urgency to obtain these data. All of you out there in the trenches have an opportunity to help gather this information in a way that can be integrated and deployed rapidly for us to guide practices and treatment.”
It’s too early to know for certain how the pandemic is affecting substance use in the United States, since statistics are sparse and COVID-19 is still relatively new. Still, local news reports have suggested overdose deaths have risen, Dr. Volkow said.
And, she noted, the Office of National Drug Control Policy’s Overdose Detection Mapping Application Program – which tracks overdoses nationwide – issued 191% more “spike alerts” from January to April this year, compared with the same time period in 2019. However, the spike alerts started going up in January, several weeks before mass numbers of COVID-19 cases began to be diagnosed.
Dr. Volkow noted the uncertainty about the numbers but said several factors could cause the pandemic to boost overdoses:
- Stress and isolation. “My first fear was that overdoses are going to go up because the stress is actually extraordinarily difficult,” she said. “Social distancing is making it very difficult for individuals with substance use disorder or opioid use disorder to get the community support that keeps them from relapsing,” such as methadone clinics and syringe exchange programs.
- Unwitnessed opioid overdoses. Social distancing could “lead to overdoses that nobody has observed, so no one can administer naloxone,” she said.
- Treatment decisions affected by stigma. “Our health systems will be overburdened, and they have to make decisions about which patients to treat,” she said. Stigma could play a very important role in interfering with the treatment of individuals with substance use disorders.”
- Drug-related vulnerabilities. On another front, she said, substance users may be especially vulnerable to the pandemic, because the drugs target multiple body systems that worsen COVID-19 outcomes. These include not only the lungs but also the cardiac and metabolic systems, she said.
For example, “if you have a long history of drug use, you’re going to be much more likely to have a pulmonary disease,” she said. “We know that pulmonary disease is a risk factor for getting COVID and for much worse outcomes.”
But the pandemic could also help in the fight against substance use. For one thing, she said, the pandemic could disrupt drug markets and make it harder for users to get illicit products.
In yet another complication, there is an ongoing debate over whether tobacco use could actually be protective against COVID-19. Research into nicotine patches as a treatment is in the works, she said.
What now? Dr. Volkow said one priority going forward should be an evaluation of virtual medicine. “We have virtual technologies that have enabled us to do telemedicine to provide mental health support and hotlines, as well as virtual support meetings,” she said. “These have proliferated and have served to a certain extent to compensate for some of the deficit from the erosion of the community support systems that exist.”
Now, she said, we should evaluate which interventions are effective, which patients they help, and the components that make them work.
There are other opportunities for useful investigations, she said. For example, researchers could examine the effects of COVID-related changes in policy, such as the federal government allowing more methadone users to take doses home and expanded telemedicine policy allowing more remote prescriptions.
“If we can show that the outcomes are as good or better [than before] then we may be able to transform these practices that make it so very difficult for so many patients to get access to treatment and to sustain treatment – but have not been questioned for years and years.”
Dr. Volkow reported no relevant disclosures.
FROM CPDD 2020
Inside Mercy’s mission to care for non-COVID patients in Los Angeles
When the hospital ship USNS Mercy departed San Diego’s Naval Station North Island on March 23, 2020, to support the Department of Defense efforts in Los Angeles during the coronavirus outbreak, Commander Erin Blevins remembers the crew’s excitement was palpable.

“We normally do partnerships abroad and respond to tsunamis and earthquakes,” said Cdr. Blevins, MD, a pediatric hematologist-oncologist who served as director of medical services for the mission. “This was a slight change in situation, but still disaster relief in the form of a pandemic. We switched our mindset to putting together the best experts for an infectious disease pandemic versus an earthquake disaster relief.”
A new mission

The 1,000-bed Mercy ship – a converted San Clemente–class oil tanker that was delivered in 1986 – spent nearly 50 days pier side in Los Angeles as a referral hospital for non–COVID-19 patients, so that clinicians at Los Angeles area hospitals could care for an anticipated surge of COVID-19 patients. “We went into it with expectations of, ‘We’ll treat as many patients as you need us to take,” Cdr. Blevins recalled. “I don’t even think Los Angeles [health officials] knew exactly where they were going to peak and what the need was going to be.”
Between March 29 and May 15, about 1,071 medical personnel aboard the Mercy cared for 77 patients with an average age of 53 years who were referred from 11 Los Angeles area hospitals. The physicians, nurses, and other medical support personnel were drawn from military treatment facilities across the country. “We had additional people join us as we scoped the mission to be more medically heavy and surgically light,” said Captain John Rotruck, MD, an anesthesiologist who is commanding officer of Mercy’s medical treatment facility. “We did adjust to make sure that we had the right staffing mix to meet the parameters that we were assigned. That was the crux of the change: a change in flavors of staffing to ensure that we focused on ICU and ward medical care as opposed to very heavy surgical care in support of a combat operation.”

About 10% of the team consisted of reservists who volunteered for the mission. “There’s no way you could have walked around the ship and known who was active duty and who was reservist,” said Capt. Rotruck, who was formerly chief of staff at Walter Reed National Military Medical Center, Bethesda, Md. “They worked together so well, and I think that marriage of active duty who are used to working in a military medical treatment facility – in our case, a Navy medical treatment facility – together with our reservist physician colleagues who work in civilian facilities around the country, was beneficial. It was a synergistic relationship. I think both sides walked away learning quite a bit from each other.”
Start with screening
All crew members underwent a temperature check and completed a health screening questionnaire: once before departing their home of record and again before boarding Mercy. Based on those results, crew members and medical staff were screened for COVID-19 and tested as needed in order to minimize the risk of an outbreak aboard the ship.
Fewer than 1% of crew members developed COVID-19 or tested positive for the virus during the mission, according to Capt. Rotruck. Affected individuals were isolated and quarantined. “All staff have recovered and are doing well,” he said.
Mercy personnel worked with local health officials to ensure that all patients transferred to the ship tested negative for COVID-19. Physicians aboard the Mercy then worked directly with the patients’ civilian physician to ensure a safe and thorough turnover process before the patients were transferred.
From basic medical to trauma care

Care aboard the ship, which consists of open-bay medical wards, ranged from basic medical and surgical care to critical care and trauma. The most common procedures were cholecystectomies and orthopedic procedures, and the average length of stay was 4-5 days, according to Cdr. Blevins. Over the course of the mission, the medical professionals conducted 36 surgeries, 77 x-ray exams, 26 CT scans, and administered hundreds of ancillary studies ranging from routine labs to high-end x-rays and blood transfusion support.
“Within our ICU, we did have some end-of-life patients who ended up dying on our ship in comfort care,” Cdr. Blevins said. “Fortunately, we had a wonderful ICU team who had a great deal of experience with end-of-life care and were able to take care of these patients very comfortably and ensure good communication with family and loved ones during that time. In most instances we tried to make sure that people got to FaceTime or video chat with their loved one before they passed away.”

The Mercy, which includes 12 operating rooms, four x-ray units, and one CAT-scan unit, was not equipped to deliver pediatric or obstetrical care. Other unavailable services included psychiatry, oncology, cardiac and thoracic surgery, nuclear medicine, MRI, mammography, electrophysiology, cardiac catheterization, negative-pressure isolation, speech therapy, and occupational therapy.
Not your typical hospital experience
But for patients who did receive medical care aboard the Mercy – which made three 150-day deployments in recent years for the military-led humanitarian response known as Pacific Partnership in 2015, 2016, and 2018 – it was an experience that they are unlikely to forget.
“Every time a patient left the ship, our team on the ground surveyed them to see how their experience was and see what we could do to improve,” Cdr. Blevins said. “Across the board, they were all very appreciative of the medical care. We had a couple of veterans on board. They got [USNS Mercy] hats on their way out and seemed to very much enjoy a slightly different experience than they would get at a regular hospital.”
Capt. Rotruck added that the enthusiasm crew members had for supporting fellow Americans “really energized our team and really saturated that caring aspect of the people who interacted directly with patients,” he said. “It wasn’t just the physicians and nurses, but it was the staff delivering the food and coming to take blood samples and every other interaction that the patients had with our team. I think they really felt that enthusiasm for being there and supporting our neighbors in LA [Los Angeles].”
Crew life aboard the Mercy
Just as with any hospital on shore, personnel aboard the Mercy practiced preventive hygiene measures recommended by the Centers for Disease Control and Prevention to help prevent the spread of COVID-19, such as wearing cloth face masks, spacing out tables in the dining hall, closing indoor gyms, and devising creative ways to stay physically fit. Popular options included jogging around the perimeter of the ship and practicing yoga and calisthenics on the deck, “making sure you were physically distanced appropriately, and when you were done, putting your mask back on,” Cdr. Blevins said. Others supplemented their workouts with a pull-up bar on the deck. “In addition, we have a series of ramps that run on the starboard side of the ship that we can use for patient movement with litters on wheels or patient beds,” Capt. Rotruck said. “The uphill portion of those ramps represents a good workout opportunity as well.”
Downtime in an era of physical distancing also afforded crew members the opportunity to call or FaceTime with loved ones, watch streamed TV shows and movies, and work on their own professional development. Some continued with coursework for online degree programs offered by colleges and universities they were enrolled in, while some enlisted personnel used the time to complete the Navy Enlisted Warfare Qualification Programs Instruction, which issues the basic overarching requirements for the qualification and designation of all enlisted warfare programs.
“As you can imagine, people spend a lot of time learning how the ship works and how it integrates into larger naval forces and so forth,” Capt. Rotruck said. “Not just our ship but also other ships: their weapons systems and defense mechanisms and navigation systems. We had people spending a significant amount of time working on that. We had people complete their Enlisted Surface Warfare qualification while we were on the mission.”
End of the mission
Mercy returned to its home base in San Diego on May 15, but about 60 medical personnel stayed behind in Los Angeles to support Federal Emergency Management Agency (FEMA), state, and local health care professionals. Some worked at a site where clinicians provided care for COVID-19–positive patients who had been transferred from area skilled nursing facilities.
In addition, a team consisting of one nurse and five corpsmen “would go out to individual skilled nursing facilities and mainly conduct assessments and training, such as training in donning proper PPE [personal protective equipment] and determining what needs they had,” Capt. Rotruck said. “They met those needs if possible or [communicated with California officials] and let them know what the requirements were and what the needs were in that facility.” The assignment for those who stayed behind ended on May 31.
On the opposite coast, Mercy’s sister ship, USNS Comfort, arrived in New York Harbor from Norfolk, Va., on March 30 and spent 3½ weeks assisting area hospitals in the COVID-19 pandemic fight. A few days into the mission, Comfort’s internal spaces were reconfigured to create separate COVID-negative and COVID-positive sections. Medical teams aboard the ship cared for a total of 182 patients during the assignment.
Looking back on Mercy’s mission, Cdr. Blevins marveled at the sense of teamwork that unfolded. “We have quarterly training exercises with a core set of personnel, [and] we train getting ready for activation in 5 days,” she said. “All of that training kicks in and it comes to fruition in a mission like this. It was terrific to see a group of very disparate subject matter experts from all over the country come together with one purpose: which was to serve our own country during the pandemic.”
Capt. Rotruck pointed out that the experience enabled enlisted and nonenlisted physicians to maintain their skill sets during a time when military and civilian hospitals had stopped doing elective procedures and routine appointments. “The fact that those people were able to come on board the ship and continue to conduct their medical practice and maintain their skills and competencies in an environment that they weren’t quite used to is great,” he said. “Otherwise, some of those medical personnel would have been sitting idle, wherever they were from. This is the power of Navy medicine on behalf of our country.”
When the hospital ship USNS Mercy departed San Diego’s Naval Station North Island on March 23, 2020, to support the Department of Defense efforts in Los Angeles during the coronavirus outbreak, Commander Erin Blevins remembers the crew’s excitement was palpable.
“We normally do partnerships abroad and respond to tsunamis and earthquakes,” said Cdr. Blevins, MD, a pediatric hematologist-oncologist who served as director of medical services for the mission. “This was a slight change in situation, but still disaster relief in the form of a pandemic. We switched our mindset to putting together the best experts for an infectious disease pandemic versus an earthquake disaster relief.”
A new mission
The 1,000-bed Mercy ship – a converted San Clemente–class oil tanker that was delivered in 1986 – spent nearly 50 days pier side in Los Angeles as a referral hospital for non–COVID-19 patients, so that clinicians at Los Angeles area hospitals could care for an anticipated surge of COVID-19 patients. “We went into it with expectations of, ‘We’ll treat as many patients as you need us to take,” Cdr. Blevins recalled. “I don’t even think Los Angeles [health officials] knew exactly where they were going to peak and what the need was going to be.”
Between March 29 and May 15, about 1,071 medical personnel aboard the Mercy cared for 77 patients with an average age of 53 years who were referred from 11 Los Angeles area hospitals. The physicians, nurses, and other medical support personnel were drawn from military treatment facilities across the country. “We had additional people join us as we scoped the mission to be more medically heavy and surgically light,” said Captain John Rotruck, MD, an anesthesiologist who is commanding officer of Mercy’s medical treatment facility. “We did adjust to make sure that we had the right staffing mix to meet the parameters that we were assigned. That was the crux of the change: a change in flavors of staffing to ensure that we focused on ICU and ward medical care as opposed to very heavy surgical care in support of a combat operation.”
About 10% of the team consisted of reservists who volunteered for the mission. “There’s no way you could have walked around the ship and known who was active duty and who was reservist,” said Capt. Rotruck, who was formerly chief of staff at Walter Reed National Military Medical Center, Bethesda, Md. “They worked together so well, and I think that marriage of active duty who are used to working in a military medical treatment facility – in our case, a Navy medical treatment facility – together with our reservist physician colleagues who work in civilian facilities around the country, was beneficial. It was a synergistic relationship. I think both sides walked away learning quite a bit from each other.”
Start with screening
All crew members underwent a temperature check and completed a health screening questionnaire: once before departing their home of record and again before boarding Mercy. Based on those results, crew members and medical staff were screened for COVID-19 and tested as needed in order to minimize the risk of an outbreak aboard the ship.
Fewer than 1% of crew members developed COVID-19 or tested positive for the virus during the mission, according to Capt. Rotruck. Affected individuals were isolated and quarantined. “All staff have recovered and are doing well,” he said.
Mercy personnel worked with local health officials to ensure that all patients transferred to the ship tested negative for COVID-19. Physicians aboard the Mercy then worked directly with the patients’ civilian physician to ensure a safe and thorough turnover process before the patients were transferred.
From basic medical to trauma care
Care aboard the ship, which consists of open-bay medical wards, ranged from basic medical and surgical care to critical care and trauma. The most common procedures were cholecystectomies and orthopedic procedures, and the average length of stay was 4-5 days, according to Cdr. Blevins. Over the course of the mission, the medical professionals conducted 36 surgeries, 77 x-ray exams, 26 CT scans, and administered hundreds of ancillary studies ranging from routine labs to high-end x-rays and blood transfusion support.
“Within our ICU, we did have some end-of-life patients who ended up dying on our ship in comfort care,” Cdr. Blevins said. “Fortunately, we had a wonderful ICU team who had a great deal of experience with end-of-life care and were able to take care of these patients very comfortably and ensure good communication with family and loved ones during that time. In most instances we tried to make sure that people got to FaceTime or video chat with their loved one before they passed away.”
The Mercy, which includes 12 operating rooms, four x-ray units, and one CAT-scan unit, was not equipped to deliver pediatric or obstetrical care. Other unavailable services included psychiatry, oncology, cardiac and thoracic surgery, nuclear medicine, MRI, mammography, electrophysiology, cardiac catheterization, negative-pressure isolation, speech therapy, and occupational therapy.
Not your typical hospital experience
But for patients who did receive medical care aboard the Mercy – which made three 150-day deployments in recent years for the military-led humanitarian response known as Pacific Partnership in 2015, 2016, and 2018 – it was an experience that they are unlikely to forget.
“Every time a patient left the ship, our team on the ground surveyed them to see how their experience was and see what we could do to improve,” Cdr. Blevins said. “Across the board, they were all very appreciative of the medical care. We had a couple of veterans on board. They got [USNS Mercy] hats on their way out and seemed to very much enjoy a slightly different experience than they would get at a regular hospital.”
Capt. Rotruck added that the enthusiasm crew members had for supporting fellow Americans “really energized our team and really saturated that caring aspect of the people who interacted directly with patients,” he said. “It wasn’t just the physicians and nurses, but it was the staff delivering the food and coming to take blood samples and every other interaction that the patients had with our team. I think they really felt that enthusiasm for being there and supporting our neighbors in LA [Los Angeles].”
Crew life aboard the Mercy
Just as with any hospital on shore, personnel aboard the Mercy practiced preventive hygiene measures recommended by the Centers for Disease Control and Prevention to help prevent the spread of COVID-19, such as wearing cloth face masks, spacing out tables in the dining hall, closing indoor gyms, and devising creative ways to stay physically fit. Popular options included jogging around the perimeter of the ship and practicing yoga and calisthenics on the deck, “making sure you were physically distanced appropriately, and when you were done, putting your mask back on,” Cdr. Blevins said. Others supplemented their workouts with a pull-up bar on the deck. “In addition, we have a series of ramps that run on the starboard side of the ship that we can use for patient movement with litters on wheels or patient beds,” Capt. Rotruck said. “The uphill portion of those ramps represents a good workout opportunity as well.”
Downtime in an era of physical distancing also afforded crew members the opportunity to call or FaceTime with loved ones, watch streamed TV shows and movies, and work on their own professional development. Some continued with coursework for online degree programs offered by colleges and universities they were enrolled in, while some enlisted personnel used the time to complete the Navy Enlisted Warfare Qualification Programs Instruction, which issues the basic overarching requirements for the qualification and designation of all enlisted warfare programs.
“As you can imagine, people spend a lot of time learning how the ship works and how it integrates into larger naval forces and so forth,” Capt. Rotruck said. “Not just our ship but also other ships: their weapons systems and defense mechanisms and navigation systems. We had people spending a significant amount of time working on that. We had people complete their Enlisted Surface Warfare qualification while we were on the mission.”
End of the mission
Mercy returned to its home base in San Diego on May 15, but about 60 medical personnel stayed behind in Los Angeles to support Federal Emergency Management Agency (FEMA), state, and local health care professionals. Some worked at a site where clinicians provided care for COVID-19–positive patients who had been transferred from area skilled nursing facilities.
In addition, a team consisting of one nurse and five corpsmen “would go out to individual skilled nursing facilities and mainly conduct assessments and training, such as training in donning proper PPE [personal protective equipment] and determining what needs they had,” Capt. Rotruck said. “They met those needs if possible or [communicated with California officials] and let them know what the requirements were and what the needs were in that facility.” The assignment for those who stayed behind ended on May 31.
On the opposite coast, Mercy’s sister ship, USNS Comfort, arrived in New York Harbor from Norfolk, Va., on March 30 and spent 3½ weeks assisting area hospitals in the COVID-19 pandemic fight. A few days into the mission, Comfort’s internal spaces were reconfigured to create separate COVID-negative and COVID-positive sections. Medical teams aboard the ship cared for a total of 182 patients during the assignment.
Looking back on Mercy’s mission, Cdr. Blevins marveled at the sense of teamwork that unfolded. “We have quarterly training exercises with a core set of personnel, [and] we train getting ready for activation in 5 days,” she said. “All of that training kicks in and it comes to fruition in a mission like this. It was terrific to see a group of very disparate subject matter experts from all over the country come together with one purpose: which was to serve our own country during the pandemic.”
Capt. Rotruck pointed out that the experience enabled enlisted and nonenlisted physicians to maintain their skill sets during a time when military and civilian hospitals had stopped doing elective procedures and routine appointments. “The fact that those people were able to come on board the ship and continue to conduct their medical practice and maintain their skills and competencies in an environment that they weren’t quite used to is great,” he said. “Otherwise, some of those medical personnel would have been sitting idle, wherever they were from. This is the power of Navy medicine on behalf of our country.”
When the hospital ship USNS Mercy departed San Diego’s Naval Station North Island on March 23, 2020, to support the Department of Defense efforts in Los Angeles during the coronavirus outbreak, Commander Erin Blevins remembers the crew’s excitement was palpable.
“We normally do partnerships abroad and respond to tsunamis and earthquakes,” said Cdr. Blevins, MD, a pediatric hematologist-oncologist who served as director of medical services for the mission. “This was a slight change in situation, but still disaster relief in the form of a pandemic. We switched our mindset to putting together the best experts for an infectious disease pandemic versus an earthquake disaster relief.”
A new mission
The 1,000-bed Mercy ship – a converted San Clemente–class oil tanker that was delivered in 1986 – spent nearly 50 days pier side in Los Angeles as a referral hospital for non–COVID-19 patients, so that clinicians at Los Angeles area hospitals could care for an anticipated surge of COVID-19 patients. “We went into it with expectations of, ‘We’ll treat as many patients as you need us to take,” Cdr. Blevins recalled. “I don’t even think Los Angeles [health officials] knew exactly where they were going to peak and what the need was going to be.”
Between March 29 and May 15, about 1,071 medical personnel aboard the Mercy cared for 77 patients with an average age of 53 years who were referred from 11 Los Angeles area hospitals. The physicians, nurses, and other medical support personnel were drawn from military treatment facilities across the country. “We had additional people join us as we scoped the mission to be more medically heavy and surgically light,” said Captain John Rotruck, MD, an anesthesiologist who is commanding officer of Mercy’s medical treatment facility. “We did adjust to make sure that we had the right staffing mix to meet the parameters that we were assigned. That was the crux of the change: a change in flavors of staffing to ensure that we focused on ICU and ward medical care as opposed to very heavy surgical care in support of a combat operation.”
About 10% of the team consisted of reservists who volunteered for the mission. “There’s no way you could have walked around the ship and known who was active duty and who was reservist,” said Capt. Rotruck, who was formerly chief of staff at Walter Reed National Military Medical Center, Bethesda, Md. “They worked together so well, and I think that marriage of active duty who are used to working in a military medical treatment facility – in our case, a Navy medical treatment facility – together with our reservist physician colleagues who work in civilian facilities around the country, was beneficial. It was a synergistic relationship. I think both sides walked away learning quite a bit from each other.”
Start with screening
All crew members underwent a temperature check and completed a health screening questionnaire: once before departing their home of record and again before boarding Mercy. Based on those results, crew members and medical staff were screened for COVID-19 and tested as needed in order to minimize the risk of an outbreak aboard the ship.
Fewer than 1% of crew members developed COVID-19 or tested positive for the virus during the mission, according to Capt. Rotruck. Affected individuals were isolated and quarantined. “All staff have recovered and are doing well,” he said.
Mercy personnel worked with local health officials to ensure that all patients transferred to the ship tested negative for COVID-19. Physicians aboard the Mercy then worked directly with the patients’ civilian physician to ensure a safe and thorough turnover process before the patients were transferred.
From basic medical to trauma care
Care aboard the ship, which consists of open-bay medical wards, ranged from basic medical and surgical care to critical care and trauma. The most common procedures were cholecystectomies and orthopedic procedures, and the average length of stay was 4-5 days, according to Cdr. Blevins. Over the course of the mission, the medical professionals conducted 36 surgeries, 77 x-ray exams, 26 CT scans, and administered hundreds of ancillary studies ranging from routine labs to high-end x-rays and blood transfusion support.
“Within our ICU, we did have some end-of-life patients who ended up dying on our ship in comfort care,” Cdr. Blevins said. “Fortunately, we had a wonderful ICU team who had a great deal of experience with end-of-life care and were able to take care of these patients very comfortably and ensure good communication with family and loved ones during that time. In most instances we tried to make sure that people got to FaceTime or video chat with their loved one before they passed away.”
The Mercy, which includes 12 operating rooms, four x-ray units, and one CAT-scan unit, was not equipped to deliver pediatric or obstetrical care. Other unavailable services included psychiatry, oncology, cardiac and thoracic surgery, nuclear medicine, MRI, mammography, electrophysiology, cardiac catheterization, negative-pressure isolation, speech therapy, and occupational therapy.
Not your typical hospital experience
But for patients who did receive medical care aboard the Mercy – which made three 150-day deployments in recent years for the military-led humanitarian response known as Pacific Partnership in 2015, 2016, and 2018 – it was an experience that they are unlikely to forget.
“Every time a patient left the ship, our team on the ground surveyed them to see how their experience was and see what we could do to improve,” Cdr. Blevins said. “Across the board, they were all very appreciative of the medical care. We had a couple of veterans on board. They got [USNS Mercy] hats on their way out and seemed to very much enjoy a slightly different experience than they would get at a regular hospital.”
Capt. Rotruck added that the enthusiasm crew members had for supporting fellow Americans “really energized our team and really saturated that caring aspect of the people who interacted directly with patients,” he said. “It wasn’t just the physicians and nurses, but it was the staff delivering the food and coming to take blood samples and every other interaction that the patients had with our team. I think they really felt that enthusiasm for being there and supporting our neighbors in LA [Los Angeles].”
Crew life aboard the Mercy
Just as with any hospital on shore, personnel aboard the Mercy practiced preventive hygiene measures recommended by the Centers for Disease Control and Prevention to help prevent the spread of COVID-19, such as wearing cloth face masks, spacing out tables in the dining hall, closing indoor gyms, and devising creative ways to stay physically fit. Popular options included jogging around the perimeter of the ship and practicing yoga and calisthenics on the deck, “making sure you were physically distanced appropriately, and when you were done, putting your mask back on,” Cdr. Blevins said. Others supplemented their workouts with a pull-up bar on the deck. “In addition, we have a series of ramps that run on the starboard side of the ship that we can use for patient movement with litters on wheels or patient beds,” Capt. Rotruck said. “The uphill portion of those ramps represents a good workout opportunity as well.”
Downtime in an era of physical distancing also afforded crew members the opportunity to call or FaceTime with loved ones, watch streamed TV shows and movies, and work on their own professional development. Some continued with coursework for online degree programs offered by colleges and universities they were enrolled in, while some enlisted personnel used the time to complete the Navy Enlisted Warfare Qualification Programs Instruction, which issues the basic overarching requirements for the qualification and designation of all enlisted warfare programs.
“As you can imagine, people spend a lot of time learning how the ship works and how it integrates into larger naval forces and so forth,” Capt. Rotruck said. “Not just our ship but also other ships: their weapons systems and defense mechanisms and navigation systems. We had people spending a significant amount of time working on that. We had people complete their Enlisted Surface Warfare qualification while we were on the mission.”
End of the mission
Mercy returned to its home base in San Diego on May 15, but about 60 medical personnel stayed behind in Los Angeles to support Federal Emergency Management Agency (FEMA), state, and local health care professionals. Some worked at a site where clinicians provided care for COVID-19–positive patients who had been transferred from area skilled nursing facilities.
In addition, a team consisting of one nurse and five corpsmen “would go out to individual skilled nursing facilities and mainly conduct assessments and training, such as training in donning proper PPE [personal protective equipment] and determining what needs they had,” Capt. Rotruck said. “They met those needs if possible or [communicated with California officials] and let them know what the requirements were and what the needs were in that facility.” The assignment for those who stayed behind ended on May 31.
On the opposite coast, Mercy’s sister ship, USNS Comfort, arrived in New York Harbor from Norfolk, Va., on March 30 and spent 3½ weeks assisting area hospitals in the COVID-19 pandemic fight. A few days into the mission, Comfort’s internal spaces were reconfigured to create separate COVID-negative and COVID-positive sections. Medical teams aboard the ship cared for a total of 182 patients during the assignment.
Looking back on Mercy’s mission, Cdr. Blevins marveled at the sense of teamwork that unfolded. “We have quarterly training exercises with a core set of personnel, [and] we train getting ready for activation in 5 days,” she said. “All of that training kicks in and it comes to fruition in a mission like this. It was terrific to see a group of very disparate subject matter experts from all over the country come together with one purpose: which was to serve our own country during the pandemic.”
Capt. Rotruck pointed out that the experience enabled enlisted and nonenlisted physicians to maintain their skill sets during a time when military and civilian hospitals had stopped doing elective procedures and routine appointments. “The fact that those people were able to come on board the ship and continue to conduct their medical practice and maintain their skills and competencies in an environment that they weren’t quite used to is great,” he said. “Otherwise, some of those medical personnel would have been sitting idle, wherever they were from. This is the power of Navy medicine on behalf of our country.”