User login
Holistic HIV care broadens scope to noncommunicable diseases
Several HIV management efforts in African groups have developed differentiated service delivery models for people living with HIV who also have noncommunicable diseases, offering diagnostic and management strategies that can treat HIV patients holistically and address their range of health issues.
These efforts allow “countries with effective HIV programs to leverage lessons learned and best practices to enhance chronic noncommunicable disease” management, Miriam Rabkin, MD, said at the virtual meeting of the International AIDS conference. This approach aims to address the “growing prevalence of chronic noncommunicable diseases in low- and middle-income countries,” and the recognition that ”people living with HIV have the same or higher prevalence” of chronic noncommunicable diseases as that of others in the region where they live, said Dr. Rabkin, an epidemiologist at Columbia University in New York and director for health systems strengthening at ICAP, an international AIDS care program run at Columbia. The differentiated service delivery model derived from the premise that “one size does not fit all,” and that effective interventions must be “tailored” to the social and clinical circumstances of specific regions, she explained.
One program has focused on introducing more contemporary methods for diagnosing leukemias, lymphomas, and melanomas using flow cytometry at the Uganda National Health Laboratory Service in Kampala. This change in testing, which became available to patients starting in February 2019, has allowed diagnostics with fresh specimens that require minimal processing and results returned to referring physicians within 48 hours, a significant upgrade from the 1- to 4-week delay that was typical in the past, said Steven J. Kussick, MD, a hematopathologist and associate medical director of PhenoPath, a commercial pathology laboratory in Seattle.
The idea was to “leverage existing HIV laboratory capabilities to transform cancer diagnosis in sub-Saharan Africa,” he said during his talk at the conference. The flow cytometry approach allows an experienced pathologist like Dr. Kussick to diagnose clearcut cases in “5 seconds,” he said. The lab has already run specimens from more than 200 patients, and estimates an ability to handle specimens from about 250 patients per year at a total annual cost of roughly $60,000, an apparently sustainable operating model, said Dr. Kussick, who serves as a full-time consultant to the operation and was also instrumental in the 5-year process that created the diagnostic program. Future improvements planned for this program include bringing on-line a higher complexity diagnostic assay that’s closer to what is currently standard U.S. testing, digital imaging to facilitate consultation with remote experts, adding immunochemistry assays to allow diagnosis of solid tumors, and opening of a second laboratory in Kenya.
Another noncommunicable disease intervention in Africa that’s building on existing infrastructure for dealing with HIV infection is targeting hypertension, the most lethal risk factor globally for preventable deaths, said Jennifer Cohn, MD, senior vice president for cardiovascular health at the New York–based Resolve to Save Lives initiative. “We need to learn from what’s been done for HIV to rapidly incorporate and scale differentiated service models,” she said.
HIV and hypertension, along with diabetes, “are beginning to be recognized as ‘syndemics,’ ”synergistic pandemics, that need a holistic approach. A recent review of the topic reported that in the seven sub-Saharan countries with the highest HIV infection prevalence the percentage of adults with hypertension ranged from 20% to 24% (Curr Opin HIV AIDS. 2020 Jul;15[4]:356-60). Projections call for a “dramatic” increase in the prevalence of hypertension in both the general population and among people living with HIV, Dr. Cohn said.
As an example of the potential for combining HIV and antihypertensive care into a one-stop protocol, she cited a model program launched at Makarere University in Kampala, Uganda, that integrates HIV and antihypertensive treatment. Recent data from the program showed that among HIV-infected individuals 24% also had hypertension, and while the program lagged in putting only 28% of these hypertensive patients on a blood pressure-lowering regimen, more than three quarters of these patients on treatment successfully reached their goal blood pressure, proving the feasibility of the combined approach, Dr. Cohn said.
“Starting and scaling with differentiated service delivery models for noncommunicable diseases can help overcome barriers to uptake of care,” concluded Dr. Cohn. “As HIV cohorts age, we have to adapt and ensure we are providing quality, holistic care, including care for high impact noncommunicable diseases such as hypertension.”
Dr. Rabkin and Dr. Cohn had no disclosures.
Several HIV management efforts in African groups have developed differentiated service delivery models for people living with HIV who also have noncommunicable diseases, offering diagnostic and management strategies that can treat HIV patients holistically and address their range of health issues.
These efforts allow “countries with effective HIV programs to leverage lessons learned and best practices to enhance chronic noncommunicable disease” management, Miriam Rabkin, MD, said at the virtual meeting of the International AIDS conference. This approach aims to address the “growing prevalence of chronic noncommunicable diseases in low- and middle-income countries,” and the recognition that ”people living with HIV have the same or higher prevalence” of chronic noncommunicable diseases as that of others in the region where they live, said Dr. Rabkin, an epidemiologist at Columbia University in New York and director for health systems strengthening at ICAP, an international AIDS care program run at Columbia. The differentiated service delivery model derived from the premise that “one size does not fit all,” and that effective interventions must be “tailored” to the social and clinical circumstances of specific regions, she explained.
One program has focused on introducing more contemporary methods for diagnosing leukemias, lymphomas, and melanomas using flow cytometry at the Uganda National Health Laboratory Service in Kampala. This change in testing, which became available to patients starting in February 2019, has allowed diagnostics with fresh specimens that require minimal processing and results returned to referring physicians within 48 hours, a significant upgrade from the 1- to 4-week delay that was typical in the past, said Steven J. Kussick, MD, a hematopathologist and associate medical director of PhenoPath, a commercial pathology laboratory in Seattle.
The idea was to “leverage existing HIV laboratory capabilities to transform cancer diagnosis in sub-Saharan Africa,” he said during his talk at the conference. The flow cytometry approach allows an experienced pathologist like Dr. Kussick to diagnose clearcut cases in “5 seconds,” he said. The lab has already run specimens from more than 200 patients, and estimates an ability to handle specimens from about 250 patients per year at a total annual cost of roughly $60,000, an apparently sustainable operating model, said Dr. Kussick, who serves as a full-time consultant to the operation and was also instrumental in the 5-year process that created the diagnostic program. Future improvements planned for this program include bringing on-line a higher complexity diagnostic assay that’s closer to what is currently standard U.S. testing, digital imaging to facilitate consultation with remote experts, adding immunochemistry assays to allow diagnosis of solid tumors, and opening of a second laboratory in Kenya.
Another noncommunicable disease intervention in Africa that’s building on existing infrastructure for dealing with HIV infection is targeting hypertension, the most lethal risk factor globally for preventable deaths, said Jennifer Cohn, MD, senior vice president for cardiovascular health at the New York–based Resolve to Save Lives initiative. “We need to learn from what’s been done for HIV to rapidly incorporate and scale differentiated service models,” she said.
HIV and hypertension, along with diabetes, “are beginning to be recognized as ‘syndemics,’ ”synergistic pandemics, that need a holistic approach. A recent review of the topic reported that in the seven sub-Saharan countries with the highest HIV infection prevalence the percentage of adults with hypertension ranged from 20% to 24% (Curr Opin HIV AIDS. 2020 Jul;15[4]:356-60). Projections call for a “dramatic” increase in the prevalence of hypertension in both the general population and among people living with HIV, Dr. Cohn said.
As an example of the potential for combining HIV and antihypertensive care into a one-stop protocol, she cited a model program launched at Makarere University in Kampala, Uganda, that integrates HIV and antihypertensive treatment. Recent data from the program showed that among HIV-infected individuals 24% also had hypertension, and while the program lagged in putting only 28% of these hypertensive patients on a blood pressure-lowering regimen, more than three quarters of these patients on treatment successfully reached their goal blood pressure, proving the feasibility of the combined approach, Dr. Cohn said.
“Starting and scaling with differentiated service delivery models for noncommunicable diseases can help overcome barriers to uptake of care,” concluded Dr. Cohn. “As HIV cohorts age, we have to adapt and ensure we are providing quality, holistic care, including care for high impact noncommunicable diseases such as hypertension.”
Dr. Rabkin and Dr. Cohn had no disclosures.
Several HIV management efforts in African groups have developed differentiated service delivery models for people living with HIV who also have noncommunicable diseases, offering diagnostic and management strategies that can treat HIV patients holistically and address their range of health issues.
These efforts allow “countries with effective HIV programs to leverage lessons learned and best practices to enhance chronic noncommunicable disease” management, Miriam Rabkin, MD, said at the virtual meeting of the International AIDS conference. This approach aims to address the “growing prevalence of chronic noncommunicable diseases in low- and middle-income countries,” and the recognition that ”people living with HIV have the same or higher prevalence” of chronic noncommunicable diseases as that of others in the region where they live, said Dr. Rabkin, an epidemiologist at Columbia University in New York and director for health systems strengthening at ICAP, an international AIDS care program run at Columbia. The differentiated service delivery model derived from the premise that “one size does not fit all,” and that effective interventions must be “tailored” to the social and clinical circumstances of specific regions, she explained.
One program has focused on introducing more contemporary methods for diagnosing leukemias, lymphomas, and melanomas using flow cytometry at the Uganda National Health Laboratory Service in Kampala. This change in testing, which became available to patients starting in February 2019, has allowed diagnostics with fresh specimens that require minimal processing and results returned to referring physicians within 48 hours, a significant upgrade from the 1- to 4-week delay that was typical in the past, said Steven J. Kussick, MD, a hematopathologist and associate medical director of PhenoPath, a commercial pathology laboratory in Seattle.
The idea was to “leverage existing HIV laboratory capabilities to transform cancer diagnosis in sub-Saharan Africa,” he said during his talk at the conference. The flow cytometry approach allows an experienced pathologist like Dr. Kussick to diagnose clearcut cases in “5 seconds,” he said. The lab has already run specimens from more than 200 patients, and estimates an ability to handle specimens from about 250 patients per year at a total annual cost of roughly $60,000, an apparently sustainable operating model, said Dr. Kussick, who serves as a full-time consultant to the operation and was also instrumental in the 5-year process that created the diagnostic program. Future improvements planned for this program include bringing on-line a higher complexity diagnostic assay that’s closer to what is currently standard U.S. testing, digital imaging to facilitate consultation with remote experts, adding immunochemistry assays to allow diagnosis of solid tumors, and opening of a second laboratory in Kenya.
Another noncommunicable disease intervention in Africa that’s building on existing infrastructure for dealing with HIV infection is targeting hypertension, the most lethal risk factor globally for preventable deaths, said Jennifer Cohn, MD, senior vice president for cardiovascular health at the New York–based Resolve to Save Lives initiative. “We need to learn from what’s been done for HIV to rapidly incorporate and scale differentiated service models,” she said.
HIV and hypertension, along with diabetes, “are beginning to be recognized as ‘syndemics,’ ”synergistic pandemics, that need a holistic approach. A recent review of the topic reported that in the seven sub-Saharan countries with the highest HIV infection prevalence the percentage of adults with hypertension ranged from 20% to 24% (Curr Opin HIV AIDS. 2020 Jul;15[4]:356-60). Projections call for a “dramatic” increase in the prevalence of hypertension in both the general population and among people living with HIV, Dr. Cohn said.
As an example of the potential for combining HIV and antihypertensive care into a one-stop protocol, she cited a model program launched at Makarere University in Kampala, Uganda, that integrates HIV and antihypertensive treatment. Recent data from the program showed that among HIV-infected individuals 24% also had hypertension, and while the program lagged in putting only 28% of these hypertensive patients on a blood pressure-lowering regimen, more than three quarters of these patients on treatment successfully reached their goal blood pressure, proving the feasibility of the combined approach, Dr. Cohn said.
“Starting and scaling with differentiated service delivery models for noncommunicable diseases can help overcome barriers to uptake of care,” concluded Dr. Cohn. “As HIV cohorts age, we have to adapt and ensure we are providing quality, holistic care, including care for high impact noncommunicable diseases such as hypertension.”
Dr. Rabkin and Dr. Cohn had no disclosures.
FROM AIDS 2020
COVID-19 disruptions ‘life threatening’ for people with HIV
When the COVID-19 pandemic led to a blanket shelter-in-place order in California in March, it did more than shut down in-person visits at Ward 86, the HIV clinic for publicly insured patients at San Francisco General Hospital. It also led to a decrease in viral suppression among the clinic›s clients. By the end of June, the percentage of patients with an undetectable viral load had dropped by nearly one-third.
This is exactly what Monica Gandhi, MD, associate division chief of HIV, infectious diseases, and global medicine at the University of California, San Francisco, and medical director of the clinic, was afraid of.
“We’re profoundly worried about the impact of COVID-19 on actual treatment outcomes,” said Dr. Gandhi, cochair of the virtual International AIDS Conference (AIDS) 2020.
And it’s not just the clinic’s clients at risk. Of the 106 countries served by the Global Fund to Fight HIV, Tuberculosis, and Malaria, 85% saw disruptions in HIV programs, according to a report released last month.
These service disruptions are considerable and “life threatening,” affecting some of the people at greatest risk for HIV acquisition and poor outcomes – such as people engaged in transactional sex (40%), men who have sex with men (37%), and transgender people (31%) – the 2020 Global AIDS Update, released today by UNAIDS, reports.
“In sub-Saharan Africa alone, if there is a 6-month interruption in HIV treatment services, it will account for an additional 500,000 deaths. That doubles the number of deaths in sub-Saharan Africa alone and brings us back to 2008 mortality levels,” said Shannon Hader, MD, deputy executive director of UNAIDS. “We just can’t allow that to happen.”
In addition, 73 countries are at risk of running out of HIV medications, according to a World Health Organization report, also released today.
Quantifying the impact
The impact is not the same for all patients, said Anton Pozniak, MD, consulting physician in HIV medicine at the Chelsea and Westminster Hospital in London, and international cochair of AIDS 2020.
For some, COVID-19 has not changed much. Their viral loads remain undetectable and all they need is multimonth supplies of their antiretroviral therapy (ART) medications, he told Medscape Medical News. Still, he said he worries about the well-documented effects that social isolation is having on the mental health of these patients, and the increase in substance use associated with the pandemic.
Then there is a small group of patients with HIV who had put off starting ART before the pandemic, but now want to start, he reported.
And finally, there are the people for whom the fear of COVID-19 has crippled their ability to get care.
There are people who have decided they don’t want to come to the hospital or come to the clinic because they’re scared of getting COVID-19.
“It’s really very striking,” said Dr. Pozniak. “There are people who have decided they don’t want to come to the hospital or come to the clinic because they’re scared of getting COVID-19. We’ve offered to deliver treatment, but they don’t want the stigma of parcels of drugs arriving.”
In a study presented at the conference, four of 12 care and substance-use treatment facilities in Europe and North America – including Seattle and Philadelphia – reported patients taking longer to fill ART prescriptions. And four of the 12 also reported that clients who injected drugs and were at risk for or living with HIV were having trouble adhering to prescribed therapies. In addition, at 11 of the sites, HIV testing has either nearly or completely shut down.
Structural barriers to telemedicine
And then there are structural barriers to care – poverty, lack of transportation, lack of or slow internet access, and lack of insurance – which affect 10% to 20% of the people with HIV that Jodie Dionne-Odom, MD, sees at the 1917 Ryan White HIV clinic at the University of Alabama at Birmingham.
These are the patients she said she worries about most, the ones who, even before COVID-19, were barely managing to pay their rent, car payments, and cell phone bills.
“With COVID-19 and being at home or being laid off, those things could no longer be paid. They’ve lost their phone, they’ve lost their car,” said Dionne-Odom, chief of women’s health services for the clinic. “That’s a really significant impact, because that’s exactly the group you can’t reach by telemedicine.”
In March, when the 1917 Clinic began providing the majority of services online, these people fell off the radar, said Aadia Rana, MD, associate professor of infectious diseases at the University of Alabama at Birmingham, who also works at the clinic.
This is not for lack of trying, she explained. Staff called patients weekly to check in and reschedule appointments, but there were some they just couldn’t reach.
Although the data for the second quarter have not yet been analyzed, “I would expect that our typically close to 90% viral suppression rate is going to decrease,” she said.
This decrease is likely widespread, said Rana, who is principle investigator of the Long-Acting Therapy to Improve Treatment Success in Daily Life (LATITUDE) study.
Many of the 33 sites involved in LATITUDE shut down in the early months of the pandemic, but some are now coming back online. In fact, “we are getting all these pleas from sites around the country saying, ‘Hey, once LATITUDE is open for enrollment, we have so many people who would now be eligible’,” she told Medscape Medical News.
“Why are they now eligible and they weren’t eligible before? I’m assuming it’s because they now have a detectable viral load,” which is one of the requirements for enrollment in LATITUDE, she explained.
Impact on the LGBTI community
At the onset of the COVID-19 pandemic, Erik Lamontagne, senior economist at UNAIDS, wondered how the quarantine was affecting LGBTI people.
To find out, he and his colleagues launched a survey asking just that. He is also coprinciple investigator of the LGBT Happiness Survey, a multicountry survey of LGBTI people launched last year.
The 13,562 LGBTI respondents came from 138 countries or territories. Of the 1,140 respondents living with HIV, 26% had seen their HIV care disrupted or restricted in some way during the pandemic, and 55% of those had no more than a month’s worth of HIV medications on hand.
But the pandemic hasn’t just affected people already living with HIV, Mr. Lamontagne reported. Nine of 10 respondents were living under some form of stay-at-home order, 73% were not meeting their basic needs, 37% had missed meals as a result of economic hardship, and half of those who were still working expected to lose their jobs.
Many could not afford to quarantine, Mr. Lamontagne told Medscape Medical News. And financial resources were stretched so thin that about 1% of respondents reported engaging in transactional sex for the first time. Some reported that their economic circumstances were so dire that they couldn’t require clients to wear condoms, increasing their risk for both COVID-19 and HIV.
“What they can eat in the evening is what they can earn during the day,” Mr. Lamontagne explained.
Unfortunately, it is the people already in a situation of economic vulnerability – often those from the LGBTI community – who are most affected by COVID-19, he added.
PrEP use changing
The pandemic has also affected the use of pre-exposure prophylaxis (PrEP).
South African women taking PrEP to protect themselves from HIV during pregnancy were 2.36 times more likely to miss a clinic visit to refill their prescription after COVID-19 lockdowns began than before, data presented at the conference showed. The women cited fear of acquiring COVID-19 at the medical facility, fear of police, transportation barriers, and long clinic wait times to explain the missed visits.
A study on the use of PrEP at Fenway Health, a sexual health clinic in Boston, showed a 278% increase in unfilled PrEP prescriptions after stay-at-home orders and a 72.1% drop in new PrEP prescriptions.
It’s unclear what these data, which will be presented at the conference later this week, mean, said Douglas Krakower, MD, assistant professor of medicine and population medicine at Harvard Medical School in Boston.
“We don’t know whether this represents people having trouble accessing PrEP” out of concern about getting COVID “or concerns about financial implications,” he explained.
“They may have had hardships from unemployment or other financial constraints” and have lost insurance or are still having to pay copays, he told Medscape Medical News. Or it could just be that they’re not going out or having sex, so they’ve discontinued the medication.
“Anecdotally we’ve heard that some patients are sheltering in place and not having sex and so have chosen not to use PrEP,” he added.
It’s also possible that people are rationing pills or have moved themselves to the PrEP 2-1-1 protocol, which is used only when someone is having sex, said Dr. Krakower, citing a study showing that sexual behavior is continuing as usual during quarantine for about half the gay men in the United States.
Resilience and fragility
It’s not just people living with HIV whose routines have changed during the pandemic. A survey of HIV clinicians around the world conducted by the International Association of Providers of AIDS Care showed that 88% of HIV clinicians have been pulled away from their regular work to manage COVID-19 in their communities.
But the COVID-19 pandemic shows no signs of stopping, and clinicians are now having to re-engage with their HIV patients.
“What COVID-19 has represented for us is a looking glass to see the resilience, but also the fragility, in HIV responses, not just in the global south, but also in the global north,” José Zuniga, PhD, IAPAC president and chief executive officer, said during a preconference session on controlling the HIV epidemic.
For Dr. Dionne-Odom, reopening the 1917 Clinic in Alabama meant tracking down patients who could not participate in telemedicine. Fortunately (or unfortunately, depending on how you look at it), the clinic, which serves a population with a high level of economic insecurity, has worked to get as many phone numbers as possible for each patient. So when the clinic opened back up, staff was able to call family members, friends, and trusted contacts to bring their patients back into the clinic.
“No one wanted to reopen too quickly,” said Dr. Dionne-Odom. “But having people come in allowed us to do all the other things that are the key part of HIV care: getting them connected with a social worker and making sure they have enough food, helping them with their electricity bills and their housing issues, all the wrap-around services that are so crucial for these patients.”
This article first appeared on Medscape.com.
When the COVID-19 pandemic led to a blanket shelter-in-place order in California in March, it did more than shut down in-person visits at Ward 86, the HIV clinic for publicly insured patients at San Francisco General Hospital. It also led to a decrease in viral suppression among the clinic›s clients. By the end of June, the percentage of patients with an undetectable viral load had dropped by nearly one-third.
This is exactly what Monica Gandhi, MD, associate division chief of HIV, infectious diseases, and global medicine at the University of California, San Francisco, and medical director of the clinic, was afraid of.
“We’re profoundly worried about the impact of COVID-19 on actual treatment outcomes,” said Dr. Gandhi, cochair of the virtual International AIDS Conference (AIDS) 2020.
And it’s not just the clinic’s clients at risk. Of the 106 countries served by the Global Fund to Fight HIV, Tuberculosis, and Malaria, 85% saw disruptions in HIV programs, according to a report released last month.
These service disruptions are considerable and “life threatening,” affecting some of the people at greatest risk for HIV acquisition and poor outcomes – such as people engaged in transactional sex (40%), men who have sex with men (37%), and transgender people (31%) – the 2020 Global AIDS Update, released today by UNAIDS, reports.
“In sub-Saharan Africa alone, if there is a 6-month interruption in HIV treatment services, it will account for an additional 500,000 deaths. That doubles the number of deaths in sub-Saharan Africa alone and brings us back to 2008 mortality levels,” said Shannon Hader, MD, deputy executive director of UNAIDS. “We just can’t allow that to happen.”
In addition, 73 countries are at risk of running out of HIV medications, according to a World Health Organization report, also released today.
Quantifying the impact
The impact is not the same for all patients, said Anton Pozniak, MD, consulting physician in HIV medicine at the Chelsea and Westminster Hospital in London, and international cochair of AIDS 2020.
For some, COVID-19 has not changed much. Their viral loads remain undetectable and all they need is multimonth supplies of their antiretroviral therapy (ART) medications, he told Medscape Medical News. Still, he said he worries about the well-documented effects that social isolation is having on the mental health of these patients, and the increase in substance use associated with the pandemic.
Then there is a small group of patients with HIV who had put off starting ART before the pandemic, but now want to start, he reported.
And finally, there are the people for whom the fear of COVID-19 has crippled their ability to get care.
There are people who have decided they don’t want to come to the hospital or come to the clinic because they’re scared of getting COVID-19.
“It’s really very striking,” said Dr. Pozniak. “There are people who have decided they don’t want to come to the hospital or come to the clinic because they’re scared of getting COVID-19. We’ve offered to deliver treatment, but they don’t want the stigma of parcels of drugs arriving.”
In a study presented at the conference, four of 12 care and substance-use treatment facilities in Europe and North America – including Seattle and Philadelphia – reported patients taking longer to fill ART prescriptions. And four of the 12 also reported that clients who injected drugs and were at risk for or living with HIV were having trouble adhering to prescribed therapies. In addition, at 11 of the sites, HIV testing has either nearly or completely shut down.
Structural barriers to telemedicine
And then there are structural barriers to care – poverty, lack of transportation, lack of or slow internet access, and lack of insurance – which affect 10% to 20% of the people with HIV that Jodie Dionne-Odom, MD, sees at the 1917 Ryan White HIV clinic at the University of Alabama at Birmingham.
These are the patients she said she worries about most, the ones who, even before COVID-19, were barely managing to pay their rent, car payments, and cell phone bills.
“With COVID-19 and being at home or being laid off, those things could no longer be paid. They’ve lost their phone, they’ve lost their car,” said Dionne-Odom, chief of women’s health services for the clinic. “That’s a really significant impact, because that’s exactly the group you can’t reach by telemedicine.”
In March, when the 1917 Clinic began providing the majority of services online, these people fell off the radar, said Aadia Rana, MD, associate professor of infectious diseases at the University of Alabama at Birmingham, who also works at the clinic.
This is not for lack of trying, she explained. Staff called patients weekly to check in and reschedule appointments, but there were some they just couldn’t reach.
Although the data for the second quarter have not yet been analyzed, “I would expect that our typically close to 90% viral suppression rate is going to decrease,” she said.
This decrease is likely widespread, said Rana, who is principle investigator of the Long-Acting Therapy to Improve Treatment Success in Daily Life (LATITUDE) study.
Many of the 33 sites involved in LATITUDE shut down in the early months of the pandemic, but some are now coming back online. In fact, “we are getting all these pleas from sites around the country saying, ‘Hey, once LATITUDE is open for enrollment, we have so many people who would now be eligible’,” she told Medscape Medical News.
“Why are they now eligible and they weren’t eligible before? I’m assuming it’s because they now have a detectable viral load,” which is one of the requirements for enrollment in LATITUDE, she explained.
Impact on the LGBTI community
At the onset of the COVID-19 pandemic, Erik Lamontagne, senior economist at UNAIDS, wondered how the quarantine was affecting LGBTI people.
To find out, he and his colleagues launched a survey asking just that. He is also coprinciple investigator of the LGBT Happiness Survey, a multicountry survey of LGBTI people launched last year.
The 13,562 LGBTI respondents came from 138 countries or territories. Of the 1,140 respondents living with HIV, 26% had seen their HIV care disrupted or restricted in some way during the pandemic, and 55% of those had no more than a month’s worth of HIV medications on hand.
But the pandemic hasn’t just affected people already living with HIV, Mr. Lamontagne reported. Nine of 10 respondents were living under some form of stay-at-home order, 73% were not meeting their basic needs, 37% had missed meals as a result of economic hardship, and half of those who were still working expected to lose their jobs.
Many could not afford to quarantine, Mr. Lamontagne told Medscape Medical News. And financial resources were stretched so thin that about 1% of respondents reported engaging in transactional sex for the first time. Some reported that their economic circumstances were so dire that they couldn’t require clients to wear condoms, increasing their risk for both COVID-19 and HIV.
“What they can eat in the evening is what they can earn during the day,” Mr. Lamontagne explained.
Unfortunately, it is the people already in a situation of economic vulnerability – often those from the LGBTI community – who are most affected by COVID-19, he added.
PrEP use changing
The pandemic has also affected the use of pre-exposure prophylaxis (PrEP).
South African women taking PrEP to protect themselves from HIV during pregnancy were 2.36 times more likely to miss a clinic visit to refill their prescription after COVID-19 lockdowns began than before, data presented at the conference showed. The women cited fear of acquiring COVID-19 at the medical facility, fear of police, transportation barriers, and long clinic wait times to explain the missed visits.
A study on the use of PrEP at Fenway Health, a sexual health clinic in Boston, showed a 278% increase in unfilled PrEP prescriptions after stay-at-home orders and a 72.1% drop in new PrEP prescriptions.
It’s unclear what these data, which will be presented at the conference later this week, mean, said Douglas Krakower, MD, assistant professor of medicine and population medicine at Harvard Medical School in Boston.
“We don’t know whether this represents people having trouble accessing PrEP” out of concern about getting COVID “or concerns about financial implications,” he explained.
“They may have had hardships from unemployment or other financial constraints” and have lost insurance or are still having to pay copays, he told Medscape Medical News. Or it could just be that they’re not going out or having sex, so they’ve discontinued the medication.
“Anecdotally we’ve heard that some patients are sheltering in place and not having sex and so have chosen not to use PrEP,” he added.
It’s also possible that people are rationing pills or have moved themselves to the PrEP 2-1-1 protocol, which is used only when someone is having sex, said Dr. Krakower, citing a study showing that sexual behavior is continuing as usual during quarantine for about half the gay men in the United States.
Resilience and fragility
It’s not just people living with HIV whose routines have changed during the pandemic. A survey of HIV clinicians around the world conducted by the International Association of Providers of AIDS Care showed that 88% of HIV clinicians have been pulled away from their regular work to manage COVID-19 in their communities.
But the COVID-19 pandemic shows no signs of stopping, and clinicians are now having to re-engage with their HIV patients.
“What COVID-19 has represented for us is a looking glass to see the resilience, but also the fragility, in HIV responses, not just in the global south, but also in the global north,” José Zuniga, PhD, IAPAC president and chief executive officer, said during a preconference session on controlling the HIV epidemic.
For Dr. Dionne-Odom, reopening the 1917 Clinic in Alabama meant tracking down patients who could not participate in telemedicine. Fortunately (or unfortunately, depending on how you look at it), the clinic, which serves a population with a high level of economic insecurity, has worked to get as many phone numbers as possible for each patient. So when the clinic opened back up, staff was able to call family members, friends, and trusted contacts to bring their patients back into the clinic.
“No one wanted to reopen too quickly,” said Dr. Dionne-Odom. “But having people come in allowed us to do all the other things that are the key part of HIV care: getting them connected with a social worker and making sure they have enough food, helping them with their electricity bills and their housing issues, all the wrap-around services that are so crucial for these patients.”
This article first appeared on Medscape.com.
When the COVID-19 pandemic led to a blanket shelter-in-place order in California in March, it did more than shut down in-person visits at Ward 86, the HIV clinic for publicly insured patients at San Francisco General Hospital. It also led to a decrease in viral suppression among the clinic›s clients. By the end of June, the percentage of patients with an undetectable viral load had dropped by nearly one-third.
This is exactly what Monica Gandhi, MD, associate division chief of HIV, infectious diseases, and global medicine at the University of California, San Francisco, and medical director of the clinic, was afraid of.
“We’re profoundly worried about the impact of COVID-19 on actual treatment outcomes,” said Dr. Gandhi, cochair of the virtual International AIDS Conference (AIDS) 2020.
And it’s not just the clinic’s clients at risk. Of the 106 countries served by the Global Fund to Fight HIV, Tuberculosis, and Malaria, 85% saw disruptions in HIV programs, according to a report released last month.
These service disruptions are considerable and “life threatening,” affecting some of the people at greatest risk for HIV acquisition and poor outcomes – such as people engaged in transactional sex (40%), men who have sex with men (37%), and transgender people (31%) – the 2020 Global AIDS Update, released today by UNAIDS, reports.
“In sub-Saharan Africa alone, if there is a 6-month interruption in HIV treatment services, it will account for an additional 500,000 deaths. That doubles the number of deaths in sub-Saharan Africa alone and brings us back to 2008 mortality levels,” said Shannon Hader, MD, deputy executive director of UNAIDS. “We just can’t allow that to happen.”
In addition, 73 countries are at risk of running out of HIV medications, according to a World Health Organization report, also released today.
Quantifying the impact
The impact is not the same for all patients, said Anton Pozniak, MD, consulting physician in HIV medicine at the Chelsea and Westminster Hospital in London, and international cochair of AIDS 2020.
For some, COVID-19 has not changed much. Their viral loads remain undetectable and all they need is multimonth supplies of their antiretroviral therapy (ART) medications, he told Medscape Medical News. Still, he said he worries about the well-documented effects that social isolation is having on the mental health of these patients, and the increase in substance use associated with the pandemic.
Then there is a small group of patients with HIV who had put off starting ART before the pandemic, but now want to start, he reported.
And finally, there are the people for whom the fear of COVID-19 has crippled their ability to get care.
There are people who have decided they don’t want to come to the hospital or come to the clinic because they’re scared of getting COVID-19.
“It’s really very striking,” said Dr. Pozniak. “There are people who have decided they don’t want to come to the hospital or come to the clinic because they’re scared of getting COVID-19. We’ve offered to deliver treatment, but they don’t want the stigma of parcels of drugs arriving.”
In a study presented at the conference, four of 12 care and substance-use treatment facilities in Europe and North America – including Seattle and Philadelphia – reported patients taking longer to fill ART prescriptions. And four of the 12 also reported that clients who injected drugs and were at risk for or living with HIV were having trouble adhering to prescribed therapies. In addition, at 11 of the sites, HIV testing has either nearly or completely shut down.
Structural barriers to telemedicine
And then there are structural barriers to care – poverty, lack of transportation, lack of or slow internet access, and lack of insurance – which affect 10% to 20% of the people with HIV that Jodie Dionne-Odom, MD, sees at the 1917 Ryan White HIV clinic at the University of Alabama at Birmingham.
These are the patients she said she worries about most, the ones who, even before COVID-19, were barely managing to pay their rent, car payments, and cell phone bills.
“With COVID-19 and being at home or being laid off, those things could no longer be paid. They’ve lost their phone, they’ve lost their car,” said Dionne-Odom, chief of women’s health services for the clinic. “That’s a really significant impact, because that’s exactly the group you can’t reach by telemedicine.”
In March, when the 1917 Clinic began providing the majority of services online, these people fell off the radar, said Aadia Rana, MD, associate professor of infectious diseases at the University of Alabama at Birmingham, who also works at the clinic.
This is not for lack of trying, she explained. Staff called patients weekly to check in and reschedule appointments, but there were some they just couldn’t reach.
Although the data for the second quarter have not yet been analyzed, “I would expect that our typically close to 90% viral suppression rate is going to decrease,” she said.
This decrease is likely widespread, said Rana, who is principle investigator of the Long-Acting Therapy to Improve Treatment Success in Daily Life (LATITUDE) study.
Many of the 33 sites involved in LATITUDE shut down in the early months of the pandemic, but some are now coming back online. In fact, “we are getting all these pleas from sites around the country saying, ‘Hey, once LATITUDE is open for enrollment, we have so many people who would now be eligible’,” she told Medscape Medical News.
“Why are they now eligible and they weren’t eligible before? I’m assuming it’s because they now have a detectable viral load,” which is one of the requirements for enrollment in LATITUDE, she explained.
Impact on the LGBTI community
At the onset of the COVID-19 pandemic, Erik Lamontagne, senior economist at UNAIDS, wondered how the quarantine was affecting LGBTI people.
To find out, he and his colleagues launched a survey asking just that. He is also coprinciple investigator of the LGBT Happiness Survey, a multicountry survey of LGBTI people launched last year.
The 13,562 LGBTI respondents came from 138 countries or territories. Of the 1,140 respondents living with HIV, 26% had seen their HIV care disrupted or restricted in some way during the pandemic, and 55% of those had no more than a month’s worth of HIV medications on hand.
But the pandemic hasn’t just affected people already living with HIV, Mr. Lamontagne reported. Nine of 10 respondents were living under some form of stay-at-home order, 73% were not meeting their basic needs, 37% had missed meals as a result of economic hardship, and half of those who were still working expected to lose their jobs.
Many could not afford to quarantine, Mr. Lamontagne told Medscape Medical News. And financial resources were stretched so thin that about 1% of respondents reported engaging in transactional sex for the first time. Some reported that their economic circumstances were so dire that they couldn’t require clients to wear condoms, increasing their risk for both COVID-19 and HIV.
“What they can eat in the evening is what they can earn during the day,” Mr. Lamontagne explained.
Unfortunately, it is the people already in a situation of economic vulnerability – often those from the LGBTI community – who are most affected by COVID-19, he added.
PrEP use changing
The pandemic has also affected the use of pre-exposure prophylaxis (PrEP).
South African women taking PrEP to protect themselves from HIV during pregnancy were 2.36 times more likely to miss a clinic visit to refill their prescription after COVID-19 lockdowns began than before, data presented at the conference showed. The women cited fear of acquiring COVID-19 at the medical facility, fear of police, transportation barriers, and long clinic wait times to explain the missed visits.
A study on the use of PrEP at Fenway Health, a sexual health clinic in Boston, showed a 278% increase in unfilled PrEP prescriptions after stay-at-home orders and a 72.1% drop in new PrEP prescriptions.
It’s unclear what these data, which will be presented at the conference later this week, mean, said Douglas Krakower, MD, assistant professor of medicine and population medicine at Harvard Medical School in Boston.
“We don’t know whether this represents people having trouble accessing PrEP” out of concern about getting COVID “or concerns about financial implications,” he explained.
“They may have had hardships from unemployment or other financial constraints” and have lost insurance or are still having to pay copays, he told Medscape Medical News. Or it could just be that they’re not going out or having sex, so they’ve discontinued the medication.
“Anecdotally we’ve heard that some patients are sheltering in place and not having sex and so have chosen not to use PrEP,” he added.
It’s also possible that people are rationing pills or have moved themselves to the PrEP 2-1-1 protocol, which is used only when someone is having sex, said Dr. Krakower, citing a study showing that sexual behavior is continuing as usual during quarantine for about half the gay men in the United States.
Resilience and fragility
It’s not just people living with HIV whose routines have changed during the pandemic. A survey of HIV clinicians around the world conducted by the International Association of Providers of AIDS Care showed that 88% of HIV clinicians have been pulled away from their regular work to manage COVID-19 in their communities.
But the COVID-19 pandemic shows no signs of stopping, and clinicians are now having to re-engage with their HIV patients.
“What COVID-19 has represented for us is a looking glass to see the resilience, but also the fragility, in HIV responses, not just in the global south, but also in the global north,” José Zuniga, PhD, IAPAC president and chief executive officer, said during a preconference session on controlling the HIV epidemic.
For Dr. Dionne-Odom, reopening the 1917 Clinic in Alabama meant tracking down patients who could not participate in telemedicine. Fortunately (or unfortunately, depending on how you look at it), the clinic, which serves a population with a high level of economic insecurity, has worked to get as many phone numbers as possible for each patient. So when the clinic opened back up, staff was able to call family members, friends, and trusted contacts to bring their patients back into the clinic.
“No one wanted to reopen too quickly,” said Dr. Dionne-Odom. “But having people come in allowed us to do all the other things that are the key part of HIV care: getting them connected with a social worker and making sure they have enough food, helping them with their electricity bills and their housing issues, all the wrap-around services that are so crucial for these patients.”
This article first appeared on Medscape.com.
Epilepsy after TBI linked to worse 12-month outcomes
findings from an analysis of a large, prospective database suggest. “We found that patients essentially have a 10-times greater risk of developing posttraumatic epilepsy and seizures at 12 months [post injury] if the presenting Glasgow Coma Scale GCS) is less than 8,” said lead author John F. Burke, MD, PhD, University of California, San Francisco, in presenting the findings as part of the virtual annual meeting of the American Association of Neurological Surgeons.
Assessing risk factors
While posttraumatic epilepsy represents an estimated 20% of all cases of symptomatic epilepsy, many questions remain on those most at risk and on the long-term effects of posttraumatic epilepsy on TBI outcomes. To probe those issues, Dr. Burke and colleagues turned to the multicenter TRACK-TBI database, which has prospective, longitudinal data on more than 2,700 patients with traumatic brain injuries and is considered the largest source of prospective data on posttraumatic epilepsy.
Using the criteria of no previous epilepsy and having 12 months of follow-up, the team identified 1,493 patients with TBI. In addition, investigators identified 182 orthopedic controls (included and prospectively followed because they have injuries but not specifically head trauma) and 210 controls who are friends of the patients and who do not have injuries but allow researchers to control for socioeconomic and environmental factors.
Of the 1,493 patients with TBI, 41 (2.7%) were determined to have posttraumatic epilepsy, assessed according to a National Institute of Neurological Disorders and Stroke epilepsy screening questionnaire, which is designed to identify patients with posttraumatic epilepsy symptoms. There were no reports of epilepsy symptoms using the screening tool among the controls. Dr. Burke noted that the 2.7% was in agreement with historical reports.
In comparing patients with TBI who did and did not have posttraumatic epilepsy, no differences were observed in the groups in terms of gender, although there was a trend toward younger age among those with PTE (mean age, 35.4 years with posttraumatic injury vs. 41.5 without; P = .05).
A major risk factor for the development of posttraumatic epilepsy was presenting GCS scores. Among those with scores of less than 8, indicative of severe injury, the rate of posttraumatic epilepsy was 6% at 6 months and 12.5% at 12 months. In contrast, those with TBI presenting with GCS scores between 13 and 15, indicative of minor injury, had an incidence of posttraumatic epilepsy of 0.9% at 6 months and 1.4% at 12 months.
Imaging findings in the two groups showed that hemorrhage detected on CT imaging was associated with a significantly higher risk for posttraumatic epilepsy (P < .001).
“The main takeaway is that any hemorrhage in the brain is a major risk factor for developing seizures,” Dr. Burke said. “Whether it is subdural, epidural blood, subarachnoid or contusion, any blood confers a very [high] risk for developing seizures.”
Posttraumatic epilepsy was linked to poorer longer-term outcomes even for patients with lesser injury: Among those with TBI and GCS of 13-15, the mean Glasgow Outcome Scale Extended (GOSE) score at 12 months among those without posttraumatic epilepsy was 7, indicative of a good recovery with minor defects, whereas the mean GOSE score for those with PTE was 4.6, indicative of moderate to severe disability (P < .001).
“It was surprising to us that PTE-positive patients had a very significant decrease in GOSE, compared to PTE-negative patients,” Dr. Burke said. “There was a nearly 2-point drop in the GOSE and that was extremely significant.”
A multivariate analysis showed there was still a significant independent risk for a poor GOSE score with posttraumatic epilepsy after controlling for GCS score, head CT findings, and age (P < .001).
The authors also looked at mood outcomes using the Brief Symptom Inventory–18, which showed significant worse effect in those with posttraumatic epilepsy after multivariate adjustment (P = .01). Additionally, a highly significant worse effect in cognitive outcomes on the Rivermead cognitive metric was observed with posttraumatic epilepsy (P = .001).
“On all metrics tested, posttraumatic epilepsy worsened outcomes,” Dr. Burke said.
He noted that the study has some key limitations, including the 12-month follow-up. A previous study showed a linear increase in posttraumatic follow-up up to 30 years. “The fact that we found 41 patients at 12 months indicates there are probably more that are out there who are going to develop seizures, but because we don’t have the follow-up we can’t look at that.”
Although the screening questionnaires are effective, “the issue is these people are not being seen by an epileptologist or having scalp EEG done, and we need a more accurate way to do this,” he said. A new study, TRACK-TBI EPI, will address those limitations and a host of other issues with a 5-year follow-up.
Capturing the nuances of brain injury
Commenting on the study as a discussant, neurosurgeon Uzma Samadani, MD, PhD, of the Minneapolis Veterans Affairs Medical Center and CentraCare in Minneapolis, suggested that the future work should focus on issues including the wide-ranging mechanisms that could explain the seizure activity.
“For example, it’s known that posttraumatic epilepsy or seizures can be triggered by abnormal conductivity due to multiple different mechanisms associated with brain injury, such as endocrine dysfunction, cortical-spreading depression, and many others,” said Dr. Samadani, who has been a researcher on the TRACK-TBI study.
Factors ranging from genetic differences to comorbid conditions such as alcoholism can play a role in brain injury susceptibility, Dr. Samadani added. Furthermore, outcome measures currently available simply may not capture the unknown nuances of brain injury.
“We have to ask, are these an all-or-none phenomena, or is aberrant electrical activity after brain injury a continuum of dysfunction?” Dr. Samadani speculated.
“I would caution that we are likely underestimating the non–easily measurable consequences of brain injury,” she said. “And the better we can quantitate susceptibility, classify the nature of injury and target acute management, the less posttraumatic epilepsy/aberrant electrical activity our patients will have.”
Dr. Burke and Dr. Samadani disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
findings from an analysis of a large, prospective database suggest. “We found that patients essentially have a 10-times greater risk of developing posttraumatic epilepsy and seizures at 12 months [post injury] if the presenting Glasgow Coma Scale GCS) is less than 8,” said lead author John F. Burke, MD, PhD, University of California, San Francisco, in presenting the findings as part of the virtual annual meeting of the American Association of Neurological Surgeons.
Assessing risk factors
While posttraumatic epilepsy represents an estimated 20% of all cases of symptomatic epilepsy, many questions remain on those most at risk and on the long-term effects of posttraumatic epilepsy on TBI outcomes. To probe those issues, Dr. Burke and colleagues turned to the multicenter TRACK-TBI database, which has prospective, longitudinal data on more than 2,700 patients with traumatic brain injuries and is considered the largest source of prospective data on posttraumatic epilepsy.
Using the criteria of no previous epilepsy and having 12 months of follow-up, the team identified 1,493 patients with TBI. In addition, investigators identified 182 orthopedic controls (included and prospectively followed because they have injuries but not specifically head trauma) and 210 controls who are friends of the patients and who do not have injuries but allow researchers to control for socioeconomic and environmental factors.
Of the 1,493 patients with TBI, 41 (2.7%) were determined to have posttraumatic epilepsy, assessed according to a National Institute of Neurological Disorders and Stroke epilepsy screening questionnaire, which is designed to identify patients with posttraumatic epilepsy symptoms. There were no reports of epilepsy symptoms using the screening tool among the controls. Dr. Burke noted that the 2.7% was in agreement with historical reports.
In comparing patients with TBI who did and did not have posttraumatic epilepsy, no differences were observed in the groups in terms of gender, although there was a trend toward younger age among those with PTE (mean age, 35.4 years with posttraumatic injury vs. 41.5 without; P = .05).
A major risk factor for the development of posttraumatic epilepsy was presenting GCS scores. Among those with scores of less than 8, indicative of severe injury, the rate of posttraumatic epilepsy was 6% at 6 months and 12.5% at 12 months. In contrast, those with TBI presenting with GCS scores between 13 and 15, indicative of minor injury, had an incidence of posttraumatic epilepsy of 0.9% at 6 months and 1.4% at 12 months.
Imaging findings in the two groups showed that hemorrhage detected on CT imaging was associated with a significantly higher risk for posttraumatic epilepsy (P < .001).
“The main takeaway is that any hemorrhage in the brain is a major risk factor for developing seizures,” Dr. Burke said. “Whether it is subdural, epidural blood, subarachnoid or contusion, any blood confers a very [high] risk for developing seizures.”
Posttraumatic epilepsy was linked to poorer longer-term outcomes even for patients with lesser injury: Among those with TBI and GCS of 13-15, the mean Glasgow Outcome Scale Extended (GOSE) score at 12 months among those without posttraumatic epilepsy was 7, indicative of a good recovery with minor defects, whereas the mean GOSE score for those with PTE was 4.6, indicative of moderate to severe disability (P < .001).
“It was surprising to us that PTE-positive patients had a very significant decrease in GOSE, compared to PTE-negative patients,” Dr. Burke said. “There was a nearly 2-point drop in the GOSE and that was extremely significant.”
A multivariate analysis showed there was still a significant independent risk for a poor GOSE score with posttraumatic epilepsy after controlling for GCS score, head CT findings, and age (P < .001).
The authors also looked at mood outcomes using the Brief Symptom Inventory–18, which showed significant worse effect in those with posttraumatic epilepsy after multivariate adjustment (P = .01). Additionally, a highly significant worse effect in cognitive outcomes on the Rivermead cognitive metric was observed with posttraumatic epilepsy (P = .001).
“On all metrics tested, posttraumatic epilepsy worsened outcomes,” Dr. Burke said.
He noted that the study has some key limitations, including the 12-month follow-up. A previous study showed a linear increase in posttraumatic follow-up up to 30 years. “The fact that we found 41 patients at 12 months indicates there are probably more that are out there who are going to develop seizures, but because we don’t have the follow-up we can’t look at that.”
Although the screening questionnaires are effective, “the issue is these people are not being seen by an epileptologist or having scalp EEG done, and we need a more accurate way to do this,” he said. A new study, TRACK-TBI EPI, will address those limitations and a host of other issues with a 5-year follow-up.
Capturing the nuances of brain injury
Commenting on the study as a discussant, neurosurgeon Uzma Samadani, MD, PhD, of the Minneapolis Veterans Affairs Medical Center and CentraCare in Minneapolis, suggested that the future work should focus on issues including the wide-ranging mechanisms that could explain the seizure activity.
“For example, it’s known that posttraumatic epilepsy or seizures can be triggered by abnormal conductivity due to multiple different mechanisms associated with brain injury, such as endocrine dysfunction, cortical-spreading depression, and many others,” said Dr. Samadani, who has been a researcher on the TRACK-TBI study.
Factors ranging from genetic differences to comorbid conditions such as alcoholism can play a role in brain injury susceptibility, Dr. Samadani added. Furthermore, outcome measures currently available simply may not capture the unknown nuances of brain injury.
“We have to ask, are these an all-or-none phenomena, or is aberrant electrical activity after brain injury a continuum of dysfunction?” Dr. Samadani speculated.
“I would caution that we are likely underestimating the non–easily measurable consequences of brain injury,” she said. “And the better we can quantitate susceptibility, classify the nature of injury and target acute management, the less posttraumatic epilepsy/aberrant electrical activity our patients will have.”
Dr. Burke and Dr. Samadani disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
findings from an analysis of a large, prospective database suggest. “We found that patients essentially have a 10-times greater risk of developing posttraumatic epilepsy and seizures at 12 months [post injury] if the presenting Glasgow Coma Scale GCS) is less than 8,” said lead author John F. Burke, MD, PhD, University of California, San Francisco, in presenting the findings as part of the virtual annual meeting of the American Association of Neurological Surgeons.
Assessing risk factors
While posttraumatic epilepsy represents an estimated 20% of all cases of symptomatic epilepsy, many questions remain on those most at risk and on the long-term effects of posttraumatic epilepsy on TBI outcomes. To probe those issues, Dr. Burke and colleagues turned to the multicenter TRACK-TBI database, which has prospective, longitudinal data on more than 2,700 patients with traumatic brain injuries and is considered the largest source of prospective data on posttraumatic epilepsy.
Using the criteria of no previous epilepsy and having 12 months of follow-up, the team identified 1,493 patients with TBI. In addition, investigators identified 182 orthopedic controls (included and prospectively followed because they have injuries but not specifically head trauma) and 210 controls who are friends of the patients and who do not have injuries but allow researchers to control for socioeconomic and environmental factors.
Of the 1,493 patients with TBI, 41 (2.7%) were determined to have posttraumatic epilepsy, assessed according to a National Institute of Neurological Disorders and Stroke epilepsy screening questionnaire, which is designed to identify patients with posttraumatic epilepsy symptoms. There were no reports of epilepsy symptoms using the screening tool among the controls. Dr. Burke noted that the 2.7% was in agreement with historical reports.
In comparing patients with TBI who did and did not have posttraumatic epilepsy, no differences were observed in the groups in terms of gender, although there was a trend toward younger age among those with PTE (mean age, 35.4 years with posttraumatic injury vs. 41.5 without; P = .05).
A major risk factor for the development of posttraumatic epilepsy was presenting GCS scores. Among those with scores of less than 8, indicative of severe injury, the rate of posttraumatic epilepsy was 6% at 6 months and 12.5% at 12 months. In contrast, those with TBI presenting with GCS scores between 13 and 15, indicative of minor injury, had an incidence of posttraumatic epilepsy of 0.9% at 6 months and 1.4% at 12 months.
Imaging findings in the two groups showed that hemorrhage detected on CT imaging was associated with a significantly higher risk for posttraumatic epilepsy (P < .001).
“The main takeaway is that any hemorrhage in the brain is a major risk factor for developing seizures,” Dr. Burke said. “Whether it is subdural, epidural blood, subarachnoid or contusion, any blood confers a very [high] risk for developing seizures.”
Posttraumatic epilepsy was linked to poorer longer-term outcomes even for patients with lesser injury: Among those with TBI and GCS of 13-15, the mean Glasgow Outcome Scale Extended (GOSE) score at 12 months among those without posttraumatic epilepsy was 7, indicative of a good recovery with minor defects, whereas the mean GOSE score for those with PTE was 4.6, indicative of moderate to severe disability (P < .001).
“It was surprising to us that PTE-positive patients had a very significant decrease in GOSE, compared to PTE-negative patients,” Dr. Burke said. “There was a nearly 2-point drop in the GOSE and that was extremely significant.”
A multivariate analysis showed there was still a significant independent risk for a poor GOSE score with posttraumatic epilepsy after controlling for GCS score, head CT findings, and age (P < .001).
The authors also looked at mood outcomes using the Brief Symptom Inventory–18, which showed significant worse effect in those with posttraumatic epilepsy after multivariate adjustment (P = .01). Additionally, a highly significant worse effect in cognitive outcomes on the Rivermead cognitive metric was observed with posttraumatic epilepsy (P = .001).
“On all metrics tested, posttraumatic epilepsy worsened outcomes,” Dr. Burke said.
He noted that the study has some key limitations, including the 12-month follow-up. A previous study showed a linear increase in posttraumatic follow-up up to 30 years. “The fact that we found 41 patients at 12 months indicates there are probably more that are out there who are going to develop seizures, but because we don’t have the follow-up we can’t look at that.”
Although the screening questionnaires are effective, “the issue is these people are not being seen by an epileptologist or having scalp EEG done, and we need a more accurate way to do this,” he said. A new study, TRACK-TBI EPI, will address those limitations and a host of other issues with a 5-year follow-up.
Capturing the nuances of brain injury
Commenting on the study as a discussant, neurosurgeon Uzma Samadani, MD, PhD, of the Minneapolis Veterans Affairs Medical Center and CentraCare in Minneapolis, suggested that the future work should focus on issues including the wide-ranging mechanisms that could explain the seizure activity.
“For example, it’s known that posttraumatic epilepsy or seizures can be triggered by abnormal conductivity due to multiple different mechanisms associated with brain injury, such as endocrine dysfunction, cortical-spreading depression, and many others,” said Dr. Samadani, who has been a researcher on the TRACK-TBI study.
Factors ranging from genetic differences to comorbid conditions such as alcoholism can play a role in brain injury susceptibility, Dr. Samadani added. Furthermore, outcome measures currently available simply may not capture the unknown nuances of brain injury.
“We have to ask, are these an all-or-none phenomena, or is aberrant electrical activity after brain injury a continuum of dysfunction?” Dr. Samadani speculated.
“I would caution that we are likely underestimating the non–easily measurable consequences of brain injury,” she said. “And the better we can quantitate susceptibility, classify the nature of injury and target acute management, the less posttraumatic epilepsy/aberrant electrical activity our patients will have.”
Dr. Burke and Dr. Samadani disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM AANS 2020
Beefed up inpatient/outpatient care transition is key to suicide prevention
The care transition period between inpatient psychiatric hospitalization and initiation of outpatient mental health services is a time of extraordinarily heightened suicide risk that has been woefully neglected, according to speakers from the National Action Alliance for Suicide Prevention at the virtual annual meeting of the American Association of Suicidology.
This transition period traditionally has been a time when nobody really takes responsibility for patient care. In an effort to close this potentially deadly gap in services, the alliance recently has issued a report entitled, “Best Practices in Care Transitions for Individuals with Suicide Risk: Inpatient Care to Outpatient Care.” The recommendations focus on specific, innovative, evidence-based strategies that health care systems can use to prevent patients from falling through the cracks in care, mainly by implementing protocols aimed at fostering interorganizational teamwork between inpatient and outpatient behavioral health services.
“I believe that improving care transitions in the United States is the area where we can likely save the most lives. It’s within our grasp if we can just do this better,” declared Richard McKeon, PhD, MPH, chief of the Suicide Prevention Branch at the Center for Mental Health Services within SAMHSA, the Substance Abuse and Mental Health Services Administration.
He cited a recent meta-analysis that concluded that the risk of suicide during the first week post discharge after psychiatric hospitalization is a staggering 300 times greater than in the general population, while in the first month, the risk is increased 200-fold. The meta-analysis included 29 studies encompassing 3,551 suicides during the first month and 24 studies reporting 1,928 suicides during the first week post discharge (BMJ Open. 2019 Mar 23;9[3]:e023883. doi: 10.1136/bmjopen-2018-023883).
Everyone in the mental health field as well as patients and their families should know those statistics, but they don’t.
“I think it’s natural for people to think someone who’s been discharged from an inpatient unit or the emergency department is not at risk, when in reality it’s still a high-risk time. Suicide risk is not like a light switch that you can just switch off,” the clinical psychologist observed.
He cited other harrowing statistics that underscore the vast problem of poor care transitions. Nationally, fully one-third of patients don’t complete a single outpatient visit within the first 30 days after discharge from inpatient behavioral health care. And one in seven people who die by suicide have had contact with inpatient mental health services in the year before they died.
“That doesn’t mean that inpatient care did not do everything that they could do. What it does reflect is the need to make sure that there’s follow-up care after inpatient discharge. Too often, people don’t get the follow-up care that they need. And the research literature is clear that intervention can save lives,” Dr. McKeon said.
Panelist Becky Stoll, LCSW, vice president for crisis and disaster management at Centerstone Health in Nashville, Tenn., noted, “We see a lot of no-shows on the outpatient side, because nobody ever asked the patients if they can actually get to the outpatient appointment that’s been made.
“We have got to figure out this care transition and do better. The road to mental health is paved with Swiss cheese. There are so many holes to fall into, even if you know how to navigate the system – and most of the people we’re serving don’t know how,” observed Ms. Stoll, who, like Dr. McKeon, was among the coauthors of the alliance’s guidelines on best practices in care transitions. Ms. Stoll also serves on the AAS board as crisis services division chair.*
The National Action Alliance for Suicide Prevention is a public/private partnership whose goal is to advance the National Strategy for Suicide Prevention, which was developed by the alliance and the U.S. Surgeon General. The alliance includes mental health professionals as well as influential leaders from the military, journalism, entertainment, railroad, health insurance, law enforcement, defense, education, technology, and other industries.
Dr. McKeon and Ms. Stall were joined by Karen Johnson, MSW, another coauthor of the guidelines. They shared highlights of the report.
Inpatient provider strategies
Discharge and crisis safety planning should begin upon admission, according to Ms. Johnson, senior vice president for clinical services and division compliance at Universal Health Services, which owns and operates more than 200 behavioral health facilities across the United States.
Inpatient and outpatient care providers need to sit down and develop collaborative protocols and negotiate a memorandum of understanding regarding expectations, which absolutely must include procedures to ensure timely electronic delivery of medical records and other key documents to the outpatient care providers. The inpatient providers need to work collaboratively with the patient, family, and community support resources to develop a safety plan – including reduced access to lethal mean – as part of predischarge planning.
Among the strategies routinely employed on the inpatient side at Universal Health Services are advance scheduling of an initial outpatient appointment within 24-72 hours post discharge. Also, someone on the inpatient team is tasked with connecting with the outpatient provider prior to discharge to develop rapport.
“If our outpatient providers are located in our facility, as many of them are, we ask them to come in and attend inpatient team meetings to identify and meet with patients who are appropriate for continuing care in outpatient settings,” she explained. “A soft, warm handoff is critical.”
At these team meetings, the appropriateness of step-down care in the form of partial hospitalization or intensive outpatient care is weighed. Someone from the inpatient side is charged with maintaining contact with the patient until after the first outpatient appointment. Ongoing caring contact in the form of brief, encouraging postcards, emails, or texts that do not require a response from the patient should be maintained for several months.
Strategies for outpatient providers
Ms. Stoll is a big believer in the guideline-recommended practice of notifying the inpatient provider that the patient kept the outpatient appointment, along with having a system for red-flagging no-shows for prompt follow-up by a crisis management team.
She and her colleagues at Centerstone Health have conducted two studies of an intensive patient outreach program designed for the first 30 days of the care transition. The program included many elements of the alliance’s best practices guidelines. The yearlong first study, funded by Blue Cross/Blue Shield of Tennessee, documented zero suicides and 92% freedom from emergency department visits during the care transition period, along with greater than $400,000 savings in health care costs, compared with usual care. The second study, funded by SAMHSA, showed much the same over a 2-year period.
She emphasized that this was not a high-tech, intensive intervention. She characterized it, instead as “high-touch follow-up.
“It’s some staff and a phone and a laptop, nothing fancy, just a person who’s competent and confident and skilled with a laptop. With that, you can do some pretty amazing stuff: Get people what they need, keep them alive, and oh, guess what? You can also save a lot of health care dollars that can be put back into the system,” Ms. Stoll said.
She recognizes that it’s a lot to ask busy outpatient providers to leave their practice during the workday to participate in inpatient team meetings addressing discharge planning, as recommended in the alliance guidelines. But in this regard, she sees a silver lining to the COVID-19 pandemic, in that it forces health professionals to rely upon newly opened channels of telemedicine.
“COVID-19 is giving us an opportunity to do things in a different way. Things don’t just have to be done in person. , where we can do things in a more innovative way,” she said.
Dr. McKeon agreed that reimbursement issues have long impeded efforts to improve the inpatient to outpatient care transition. He added that it will be really important that adequate reimbursement of remote forms of care remain in place after COVID-19 fades.
“This is exactly the kind of thing that’s needed to improve care transitions,” according to Dr. McKeon.
*This story was updated 7/9/2020.
The care transition period between inpatient psychiatric hospitalization and initiation of outpatient mental health services is a time of extraordinarily heightened suicide risk that has been woefully neglected, according to speakers from the National Action Alliance for Suicide Prevention at the virtual annual meeting of the American Association of Suicidology.
This transition period traditionally has been a time when nobody really takes responsibility for patient care. In an effort to close this potentially deadly gap in services, the alliance recently has issued a report entitled, “Best Practices in Care Transitions for Individuals with Suicide Risk: Inpatient Care to Outpatient Care.” The recommendations focus on specific, innovative, evidence-based strategies that health care systems can use to prevent patients from falling through the cracks in care, mainly by implementing protocols aimed at fostering interorganizational teamwork between inpatient and outpatient behavioral health services.
“I believe that improving care transitions in the United States is the area where we can likely save the most lives. It’s within our grasp if we can just do this better,” declared Richard McKeon, PhD, MPH, chief of the Suicide Prevention Branch at the Center for Mental Health Services within SAMHSA, the Substance Abuse and Mental Health Services Administration.
He cited a recent meta-analysis that concluded that the risk of suicide during the first week post discharge after psychiatric hospitalization is a staggering 300 times greater than in the general population, while in the first month, the risk is increased 200-fold. The meta-analysis included 29 studies encompassing 3,551 suicides during the first month and 24 studies reporting 1,928 suicides during the first week post discharge (BMJ Open. 2019 Mar 23;9[3]:e023883. doi: 10.1136/bmjopen-2018-023883).
Everyone in the mental health field as well as patients and their families should know those statistics, but they don’t.
“I think it’s natural for people to think someone who’s been discharged from an inpatient unit or the emergency department is not at risk, when in reality it’s still a high-risk time. Suicide risk is not like a light switch that you can just switch off,” the clinical psychologist observed.
He cited other harrowing statistics that underscore the vast problem of poor care transitions. Nationally, fully one-third of patients don’t complete a single outpatient visit within the first 30 days after discharge from inpatient behavioral health care. And one in seven people who die by suicide have had contact with inpatient mental health services in the year before they died.
“That doesn’t mean that inpatient care did not do everything that they could do. What it does reflect is the need to make sure that there’s follow-up care after inpatient discharge. Too often, people don’t get the follow-up care that they need. And the research literature is clear that intervention can save lives,” Dr. McKeon said.
Panelist Becky Stoll, LCSW, vice president for crisis and disaster management at Centerstone Health in Nashville, Tenn., noted, “We see a lot of no-shows on the outpatient side, because nobody ever asked the patients if they can actually get to the outpatient appointment that’s been made.
“We have got to figure out this care transition and do better. The road to mental health is paved with Swiss cheese. There are so many holes to fall into, even if you know how to navigate the system – and most of the people we’re serving don’t know how,” observed Ms. Stoll, who, like Dr. McKeon, was among the coauthors of the alliance’s guidelines on best practices in care transitions. Ms. Stoll also serves on the AAS board as crisis services division chair.*
The National Action Alliance for Suicide Prevention is a public/private partnership whose goal is to advance the National Strategy for Suicide Prevention, which was developed by the alliance and the U.S. Surgeon General. The alliance includes mental health professionals as well as influential leaders from the military, journalism, entertainment, railroad, health insurance, law enforcement, defense, education, technology, and other industries.
Dr. McKeon and Ms. Stall were joined by Karen Johnson, MSW, another coauthor of the guidelines. They shared highlights of the report.
Inpatient provider strategies
Discharge and crisis safety planning should begin upon admission, according to Ms. Johnson, senior vice president for clinical services and division compliance at Universal Health Services, which owns and operates more than 200 behavioral health facilities across the United States.
Inpatient and outpatient care providers need to sit down and develop collaborative protocols and negotiate a memorandum of understanding regarding expectations, which absolutely must include procedures to ensure timely electronic delivery of medical records and other key documents to the outpatient care providers. The inpatient providers need to work collaboratively with the patient, family, and community support resources to develop a safety plan – including reduced access to lethal mean – as part of predischarge planning.
Among the strategies routinely employed on the inpatient side at Universal Health Services are advance scheduling of an initial outpatient appointment within 24-72 hours post discharge. Also, someone on the inpatient team is tasked with connecting with the outpatient provider prior to discharge to develop rapport.
“If our outpatient providers are located in our facility, as many of them are, we ask them to come in and attend inpatient team meetings to identify and meet with patients who are appropriate for continuing care in outpatient settings,” she explained. “A soft, warm handoff is critical.”
At these team meetings, the appropriateness of step-down care in the form of partial hospitalization or intensive outpatient care is weighed. Someone from the inpatient side is charged with maintaining contact with the patient until after the first outpatient appointment. Ongoing caring contact in the form of brief, encouraging postcards, emails, or texts that do not require a response from the patient should be maintained for several months.
Strategies for outpatient providers
Ms. Stoll is a big believer in the guideline-recommended practice of notifying the inpatient provider that the patient kept the outpatient appointment, along with having a system for red-flagging no-shows for prompt follow-up by a crisis management team.
She and her colleagues at Centerstone Health have conducted two studies of an intensive patient outreach program designed for the first 30 days of the care transition. The program included many elements of the alliance’s best practices guidelines. The yearlong first study, funded by Blue Cross/Blue Shield of Tennessee, documented zero suicides and 92% freedom from emergency department visits during the care transition period, along with greater than $400,000 savings in health care costs, compared with usual care. The second study, funded by SAMHSA, showed much the same over a 2-year period.
She emphasized that this was not a high-tech, intensive intervention. She characterized it, instead as “high-touch follow-up.
“It’s some staff and a phone and a laptop, nothing fancy, just a person who’s competent and confident and skilled with a laptop. With that, you can do some pretty amazing stuff: Get people what they need, keep them alive, and oh, guess what? You can also save a lot of health care dollars that can be put back into the system,” Ms. Stoll said.
She recognizes that it’s a lot to ask busy outpatient providers to leave their practice during the workday to participate in inpatient team meetings addressing discharge planning, as recommended in the alliance guidelines. But in this regard, she sees a silver lining to the COVID-19 pandemic, in that it forces health professionals to rely upon newly opened channels of telemedicine.
“COVID-19 is giving us an opportunity to do things in a different way. Things don’t just have to be done in person. , where we can do things in a more innovative way,” she said.
Dr. McKeon agreed that reimbursement issues have long impeded efforts to improve the inpatient to outpatient care transition. He added that it will be really important that adequate reimbursement of remote forms of care remain in place after COVID-19 fades.
“This is exactly the kind of thing that’s needed to improve care transitions,” according to Dr. McKeon.
*This story was updated 7/9/2020.
The care transition period between inpatient psychiatric hospitalization and initiation of outpatient mental health services is a time of extraordinarily heightened suicide risk that has been woefully neglected, according to speakers from the National Action Alliance for Suicide Prevention at the virtual annual meeting of the American Association of Suicidology.
This transition period traditionally has been a time when nobody really takes responsibility for patient care. In an effort to close this potentially deadly gap in services, the alliance recently has issued a report entitled, “Best Practices in Care Transitions for Individuals with Suicide Risk: Inpatient Care to Outpatient Care.” The recommendations focus on specific, innovative, evidence-based strategies that health care systems can use to prevent patients from falling through the cracks in care, mainly by implementing protocols aimed at fostering interorganizational teamwork between inpatient and outpatient behavioral health services.
“I believe that improving care transitions in the United States is the area where we can likely save the most lives. It’s within our grasp if we can just do this better,” declared Richard McKeon, PhD, MPH, chief of the Suicide Prevention Branch at the Center for Mental Health Services within SAMHSA, the Substance Abuse and Mental Health Services Administration.
He cited a recent meta-analysis that concluded that the risk of suicide during the first week post discharge after psychiatric hospitalization is a staggering 300 times greater than in the general population, while in the first month, the risk is increased 200-fold. The meta-analysis included 29 studies encompassing 3,551 suicides during the first month and 24 studies reporting 1,928 suicides during the first week post discharge (BMJ Open. 2019 Mar 23;9[3]:e023883. doi: 10.1136/bmjopen-2018-023883).
Everyone in the mental health field as well as patients and their families should know those statistics, but they don’t.
“I think it’s natural for people to think someone who’s been discharged from an inpatient unit or the emergency department is not at risk, when in reality it’s still a high-risk time. Suicide risk is not like a light switch that you can just switch off,” the clinical psychologist observed.
He cited other harrowing statistics that underscore the vast problem of poor care transitions. Nationally, fully one-third of patients don’t complete a single outpatient visit within the first 30 days after discharge from inpatient behavioral health care. And one in seven people who die by suicide have had contact with inpatient mental health services in the year before they died.
“That doesn’t mean that inpatient care did not do everything that they could do. What it does reflect is the need to make sure that there’s follow-up care after inpatient discharge. Too often, people don’t get the follow-up care that they need. And the research literature is clear that intervention can save lives,” Dr. McKeon said.
Panelist Becky Stoll, LCSW, vice president for crisis and disaster management at Centerstone Health in Nashville, Tenn., noted, “We see a lot of no-shows on the outpatient side, because nobody ever asked the patients if they can actually get to the outpatient appointment that’s been made.
“We have got to figure out this care transition and do better. The road to mental health is paved with Swiss cheese. There are so many holes to fall into, even if you know how to navigate the system – and most of the people we’re serving don’t know how,” observed Ms. Stoll, who, like Dr. McKeon, was among the coauthors of the alliance’s guidelines on best practices in care transitions. Ms. Stoll also serves on the AAS board as crisis services division chair.*
The National Action Alliance for Suicide Prevention is a public/private partnership whose goal is to advance the National Strategy for Suicide Prevention, which was developed by the alliance and the U.S. Surgeon General. The alliance includes mental health professionals as well as influential leaders from the military, journalism, entertainment, railroad, health insurance, law enforcement, defense, education, technology, and other industries.
Dr. McKeon and Ms. Stall were joined by Karen Johnson, MSW, another coauthor of the guidelines. They shared highlights of the report.
Inpatient provider strategies
Discharge and crisis safety planning should begin upon admission, according to Ms. Johnson, senior vice president for clinical services and division compliance at Universal Health Services, which owns and operates more than 200 behavioral health facilities across the United States.
Inpatient and outpatient care providers need to sit down and develop collaborative protocols and negotiate a memorandum of understanding regarding expectations, which absolutely must include procedures to ensure timely electronic delivery of medical records and other key documents to the outpatient care providers. The inpatient providers need to work collaboratively with the patient, family, and community support resources to develop a safety plan – including reduced access to lethal mean – as part of predischarge planning.
Among the strategies routinely employed on the inpatient side at Universal Health Services are advance scheduling of an initial outpatient appointment within 24-72 hours post discharge. Also, someone on the inpatient team is tasked with connecting with the outpatient provider prior to discharge to develop rapport.
“If our outpatient providers are located in our facility, as many of them are, we ask them to come in and attend inpatient team meetings to identify and meet with patients who are appropriate for continuing care in outpatient settings,” she explained. “A soft, warm handoff is critical.”
At these team meetings, the appropriateness of step-down care in the form of partial hospitalization or intensive outpatient care is weighed. Someone from the inpatient side is charged with maintaining contact with the patient until after the first outpatient appointment. Ongoing caring contact in the form of brief, encouraging postcards, emails, or texts that do not require a response from the patient should be maintained for several months.
Strategies for outpatient providers
Ms. Stoll is a big believer in the guideline-recommended practice of notifying the inpatient provider that the patient kept the outpatient appointment, along with having a system for red-flagging no-shows for prompt follow-up by a crisis management team.
She and her colleagues at Centerstone Health have conducted two studies of an intensive patient outreach program designed for the first 30 days of the care transition. The program included many elements of the alliance’s best practices guidelines. The yearlong first study, funded by Blue Cross/Blue Shield of Tennessee, documented zero suicides and 92% freedom from emergency department visits during the care transition period, along with greater than $400,000 savings in health care costs, compared with usual care. The second study, funded by SAMHSA, showed much the same over a 2-year period.
She emphasized that this was not a high-tech, intensive intervention. She characterized it, instead as “high-touch follow-up.
“It’s some staff and a phone and a laptop, nothing fancy, just a person who’s competent and confident and skilled with a laptop. With that, you can do some pretty amazing stuff: Get people what they need, keep them alive, and oh, guess what? You can also save a lot of health care dollars that can be put back into the system,” Ms. Stoll said.
She recognizes that it’s a lot to ask busy outpatient providers to leave their practice during the workday to participate in inpatient team meetings addressing discharge planning, as recommended in the alliance guidelines. But in this regard, she sees a silver lining to the COVID-19 pandemic, in that it forces health professionals to rely upon newly opened channels of telemedicine.
“COVID-19 is giving us an opportunity to do things in a different way. Things don’t just have to be done in person. , where we can do things in a more innovative way,” she said.
Dr. McKeon agreed that reimbursement issues have long impeded efforts to improve the inpatient to outpatient care transition. He added that it will be really important that adequate reimbursement of remote forms of care remain in place after COVID-19 fades.
“This is exactly the kind of thing that’s needed to improve care transitions,” according to Dr. McKeon.
*This story was updated 7/9/2020.
FROM AAS20
Amid pandemic, Virginia hospital’s opioid overdoses up nearly 10-fold
Opioid overdoses have shot up by almost 10-fold at a Virginia ED since March, a new report finds. The report provides more evidence that the coronavirus pandemic is sparking a severe medical crisis among illicit drug users.
“Health care providers should closely monitor the number of overdoses coming into their hospitals and in the surrounding community during this time,” study lead author and postdoctoral research fellow Taylor Ochalek, PhD, said in an interview. “If they do notice an increasing trend of overdoses, they should spread awareness in the community to the general public, and offer resources and information for those that may be seeking help and/or may be at a high risk of overdosing.”
Dr. Ochalek presented the study findings at the virtual annual meeting of the College on Problems of Drug Dependence.
According to the report, opioid overdoses at the VCU Medical Center in Richmond, Va., grew from an average of six a month from February to December 2019 to 50, 57, and 63 in March, April, and May 2020. Of the 171 cases in the later time frame, the average age was 44 years, 72% were male, and 82% were African American.
“The steep increase in overdoses began primarily in March,” said Dr. Ochalek, of Virginia Commonwealth University in Richmond. “This timing coincides with the Virginia governor’s state of emergency declaration, stay-at-home order, and closure of nonessential businesses order.”
The researchers did not provide details about the types of opioids used, the patient outcomes, or whether the patients tested positive for COVID-19. It’s unclear whether the pandemic directly spawned a higher number of overdoses, but there are growing signs of a stark nationwide trend.
“Nationwide, federal and local officials are reporting alarming spikes in drug overdoses – a hidden epidemic within the coronavirus pandemic,” the Washington Post reported on July 1, pointing to increases in Kentucky, Virginia, and the Chicago area.
Meanwhile, the federal Overdose Detection Mapping Application Program, which tracks overdoses nationwide, issued 191% more “spike alerts” in January to April 2020 than in the same time period in 2019. However, the spike alerts began to increase in January, weeks before the pandemic began to take hold.
The findings are consistent with trends in Houston, where overdose calls were up 31% in the first 3 months of 2020, compared with 2019, said psychologist James Bray, PhD, of the University of Texas, San Antonio, in an interview. More recent data suggest that the numbers are rising even higher, said Dr. Bray, who works with Houston first responders and has analyzed data.
Dr. Bray said.
Another potential factor is the disruption in the illicit drug supply chain because of limits on crossings at the southern border, said ED physician Scott Weiner, MD, MPH, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston. “As a result, opioids of extremely variable potency have infiltrated markets, and people using drugs may not be used to the new doses, especially if they are high-potency fentanyl analogues.”
Moving forward, Dr. Bray said, “people need continued access to treatment. Telehealth and other virtual services need to be provided so that people can continue to have access to treatment even during the pandemic.”
Dr. Weiner also emphasized the importance of treatment for patients who overdose on opioids. “In my previous work, we discovered that about 1 in 20 patients who are treated in an emergency department and survive would die within 1 year. That number will likely increase drastically during COVID,” he said. “When a patient presents after overdose, we must intervene aggressively with buprenorphine and other harm-reduction techniques to save these lives.”
The study was funded by the National Institutes of Health. Dr. Ochalek, Dr. Weiner, and Dr. Bray reported no relevant disclosures.
Opioid overdoses have shot up by almost 10-fold at a Virginia ED since March, a new report finds. The report provides more evidence that the coronavirus pandemic is sparking a severe medical crisis among illicit drug users.
“Health care providers should closely monitor the number of overdoses coming into their hospitals and in the surrounding community during this time,” study lead author and postdoctoral research fellow Taylor Ochalek, PhD, said in an interview. “If they do notice an increasing trend of overdoses, they should spread awareness in the community to the general public, and offer resources and information for those that may be seeking help and/or may be at a high risk of overdosing.”
Dr. Ochalek presented the study findings at the virtual annual meeting of the College on Problems of Drug Dependence.
According to the report, opioid overdoses at the VCU Medical Center in Richmond, Va., grew from an average of six a month from February to December 2019 to 50, 57, and 63 in March, April, and May 2020. Of the 171 cases in the later time frame, the average age was 44 years, 72% were male, and 82% were African American.
“The steep increase in overdoses began primarily in March,” said Dr. Ochalek, of Virginia Commonwealth University in Richmond. “This timing coincides with the Virginia governor’s state of emergency declaration, stay-at-home order, and closure of nonessential businesses order.”
The researchers did not provide details about the types of opioids used, the patient outcomes, or whether the patients tested positive for COVID-19. It’s unclear whether the pandemic directly spawned a higher number of overdoses, but there are growing signs of a stark nationwide trend.
“Nationwide, federal and local officials are reporting alarming spikes in drug overdoses – a hidden epidemic within the coronavirus pandemic,” the Washington Post reported on July 1, pointing to increases in Kentucky, Virginia, and the Chicago area.
Meanwhile, the federal Overdose Detection Mapping Application Program, which tracks overdoses nationwide, issued 191% more “spike alerts” in January to April 2020 than in the same time period in 2019. However, the spike alerts began to increase in January, weeks before the pandemic began to take hold.
The findings are consistent with trends in Houston, where overdose calls were up 31% in the first 3 months of 2020, compared with 2019, said psychologist James Bray, PhD, of the University of Texas, San Antonio, in an interview. More recent data suggest that the numbers are rising even higher, said Dr. Bray, who works with Houston first responders and has analyzed data.
Dr. Bray said.
Another potential factor is the disruption in the illicit drug supply chain because of limits on crossings at the southern border, said ED physician Scott Weiner, MD, MPH, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston. “As a result, opioids of extremely variable potency have infiltrated markets, and people using drugs may not be used to the new doses, especially if they are high-potency fentanyl analogues.”
Moving forward, Dr. Bray said, “people need continued access to treatment. Telehealth and other virtual services need to be provided so that people can continue to have access to treatment even during the pandemic.”
Dr. Weiner also emphasized the importance of treatment for patients who overdose on opioids. “In my previous work, we discovered that about 1 in 20 patients who are treated in an emergency department and survive would die within 1 year. That number will likely increase drastically during COVID,” he said. “When a patient presents after overdose, we must intervene aggressively with buprenorphine and other harm-reduction techniques to save these lives.”
The study was funded by the National Institutes of Health. Dr. Ochalek, Dr. Weiner, and Dr. Bray reported no relevant disclosures.
Opioid overdoses have shot up by almost 10-fold at a Virginia ED since March, a new report finds. The report provides more evidence that the coronavirus pandemic is sparking a severe medical crisis among illicit drug users.
“Health care providers should closely monitor the number of overdoses coming into their hospitals and in the surrounding community during this time,” study lead author and postdoctoral research fellow Taylor Ochalek, PhD, said in an interview. “If they do notice an increasing trend of overdoses, they should spread awareness in the community to the general public, and offer resources and information for those that may be seeking help and/or may be at a high risk of overdosing.”
Dr. Ochalek presented the study findings at the virtual annual meeting of the College on Problems of Drug Dependence.
According to the report, opioid overdoses at the VCU Medical Center in Richmond, Va., grew from an average of six a month from February to December 2019 to 50, 57, and 63 in March, April, and May 2020. Of the 171 cases in the later time frame, the average age was 44 years, 72% were male, and 82% were African American.
“The steep increase in overdoses began primarily in March,” said Dr. Ochalek, of Virginia Commonwealth University in Richmond. “This timing coincides with the Virginia governor’s state of emergency declaration, stay-at-home order, and closure of nonessential businesses order.”
The researchers did not provide details about the types of opioids used, the patient outcomes, or whether the patients tested positive for COVID-19. It’s unclear whether the pandemic directly spawned a higher number of overdoses, but there are growing signs of a stark nationwide trend.
“Nationwide, federal and local officials are reporting alarming spikes in drug overdoses – a hidden epidemic within the coronavirus pandemic,” the Washington Post reported on July 1, pointing to increases in Kentucky, Virginia, and the Chicago area.
Meanwhile, the federal Overdose Detection Mapping Application Program, which tracks overdoses nationwide, issued 191% more “spike alerts” in January to April 2020 than in the same time period in 2019. However, the spike alerts began to increase in January, weeks before the pandemic began to take hold.
The findings are consistent with trends in Houston, where overdose calls were up 31% in the first 3 months of 2020, compared with 2019, said psychologist James Bray, PhD, of the University of Texas, San Antonio, in an interview. More recent data suggest that the numbers are rising even higher, said Dr. Bray, who works with Houston first responders and has analyzed data.
Dr. Bray said.
Another potential factor is the disruption in the illicit drug supply chain because of limits on crossings at the southern border, said ED physician Scott Weiner, MD, MPH, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston. “As a result, opioids of extremely variable potency have infiltrated markets, and people using drugs may not be used to the new doses, especially if they are high-potency fentanyl analogues.”
Moving forward, Dr. Bray said, “people need continued access to treatment. Telehealth and other virtual services need to be provided so that people can continue to have access to treatment even during the pandemic.”
Dr. Weiner also emphasized the importance of treatment for patients who overdose on opioids. “In my previous work, we discovered that about 1 in 20 patients who are treated in an emergency department and survive would die within 1 year. That number will likely increase drastically during COVID,” he said. “When a patient presents after overdose, we must intervene aggressively with buprenorphine and other harm-reduction techniques to save these lives.”
The study was funded by the National Institutes of Health. Dr. Ochalek, Dr. Weiner, and Dr. Bray reported no relevant disclosures.
FROM CPDD 2020
Study highlights benefits of integrating dermatology into oncology centers
, according to the results of a retrospective study of 208 adults treated at the Dana-Farber Cancer Institute in Boston, or affiliated sites.
The benefits of prophylactic treatment for treatment-related skin rash in cancer patients are well established, based largely on the Skin Toxicity Evaluation Protocol With Panitumumab (STEPP) trial published in 2012, which led to the development of guidelines for preventing and managing skin toxicity associated with epidermal growth factor receptor inhibitor (EGFRi) treatment, wrote Zizi Yu of Harvard Medical School, Boston, and coauthors. However, they added, “awareness of and adherence to these guidelines among oncology clinicians are thus far poorly understood.” They pointed out that 90% of patients treated with an EGFRi develop cutaneous toxicities, which can affect quality of life, increase the risk of infection, and require dose modification, interruption, or discontinuation of treatment.
In the study, published in JAMA Dermatology, the researchers compared adherence to protocols at Dana-Farber before and after the 2014-2015 initiation of a Skin Toxicities from Anticancer Therapies (STAT) program at Dana-Farber established in 2014 by the department of dermatology.
The study population included 208 adult cancer patients with colorectal cancer, head and neck cancer, or cutaneous squamous cell cancer, treated with at least one dose of cetuximab (Erbitux); the average age of the patients was 62 years and the majority were men. Most had stage IV disease. The STAT program included the integration of 9 oncodermatologists in the head and neck, genitourinary, and cutaneous oncology clinics for 7 of 10 cancer treatment sessions per week, as well as the creation of urgent access time slots in oncodermatology clinics for 10 of 10 sessions per week.
Overall, significantly more patients were treated prophylactically for skin toxicity at the start of cetuximab treatment in 2017 vs. 2012 (47% vs. 25%, P less than .001) after the initiation of a dermatology protocol.
In addition, the preemptive use of tetracycline increased significantly from 45% to 71% (P = .02) between the two time periods, as did the use of topical corticosteroids (from 7% to 57%, P less than .001), while the use of topical antibiotics decreased from 79% to 43% (P = .02). Rates of dose changes or interruptions were significantly lower among those on prophylaxis (5% vs. 19%, P =.01), a 79% lower risk. Patients treated prophylactically were 94% less likely to need a first rescue treatment and 74% less likely to need a second rescue treatment for rash.
The study findings were limited by several factors including the retrospective design, use of data from a single institution, and incomplete documentation of some patients, the researchers noted. However, the results “highlight the value of integrating dermatologic care and education into oncology centers by increasing adherence to evidence-based prophylaxis protocols for rash and appropriate treatment agent selection, which may minimize toxicity-associated chemotherapy interruptions and improve quality of life,” they concluded.
“As novel cancer treatment options for patients continue to develop, and as patients with cancer live longer, the spectrum and prevalence of dermatologic toxic effects will continue to expand,” Bernice Y. Kwong, MD, director of the supportive dermato-oncology program at Stanford (Calif.) University, wrote in an accompanying editorial.
“Dermatologists have a critical and growing opportunity and role to engage in multidisciplinary efforts to provide expert guidance to best manage these cutaneous adverse events to achieve the best outcome for patients with cancer,” she said.
Although the prophylaxis rates at Dana-Farber improved after the establishment of the oncodermatology program, they remained relatively low, “underscoring an opportunity to improve on how to teach, execute, and improve access to oncodermatologic care for patients with cancer,” said Dr. Kwong. Knowledge gaps in the nature of skin toxicity for newer cancer drugs poses another challenge for skin toxicity management in these patients, she added.
However, “timely and consistent access to dermatologic expertise in oncology practices is critical to prevent unnecessary discontinuation of life-saving anticancer therapy, especially as multiple studies have demonstrated that anticancer therapy–associated skin toxicity may be associated with a positive response to anticancer therapy,” she emphasized.
Ms. Yu and one coauthor had no financial conflicts to disclose, the two other authors had several disclosures, outside of the submitted work. Dr. Kwong disclosed serving as a consultant for Genentech and Oncoderm and serving on the advisory board for Kyowa Kirin.
SOURCE: Yu Z et al. JAMA Dermatol. 2020 July 1. doi: 10.1001/jamadermatol.2020.1795. Kwong BY. JAMA Dermatol. 2020 Jul 1. doi: 10.1001/jamadermatol.2020.1794.
, according to the results of a retrospective study of 208 adults treated at the Dana-Farber Cancer Institute in Boston, or affiliated sites.
The benefits of prophylactic treatment for treatment-related skin rash in cancer patients are well established, based largely on the Skin Toxicity Evaluation Protocol With Panitumumab (STEPP) trial published in 2012, which led to the development of guidelines for preventing and managing skin toxicity associated with epidermal growth factor receptor inhibitor (EGFRi) treatment, wrote Zizi Yu of Harvard Medical School, Boston, and coauthors. However, they added, “awareness of and adherence to these guidelines among oncology clinicians are thus far poorly understood.” They pointed out that 90% of patients treated with an EGFRi develop cutaneous toxicities, which can affect quality of life, increase the risk of infection, and require dose modification, interruption, or discontinuation of treatment.
In the study, published in JAMA Dermatology, the researchers compared adherence to protocols at Dana-Farber before and after the 2014-2015 initiation of a Skin Toxicities from Anticancer Therapies (STAT) program at Dana-Farber established in 2014 by the department of dermatology.
The study population included 208 adult cancer patients with colorectal cancer, head and neck cancer, or cutaneous squamous cell cancer, treated with at least one dose of cetuximab (Erbitux); the average age of the patients was 62 years and the majority were men. Most had stage IV disease. The STAT program included the integration of 9 oncodermatologists in the head and neck, genitourinary, and cutaneous oncology clinics for 7 of 10 cancer treatment sessions per week, as well as the creation of urgent access time slots in oncodermatology clinics for 10 of 10 sessions per week.
Overall, significantly more patients were treated prophylactically for skin toxicity at the start of cetuximab treatment in 2017 vs. 2012 (47% vs. 25%, P less than .001) after the initiation of a dermatology protocol.
In addition, the preemptive use of tetracycline increased significantly from 45% to 71% (P = .02) between the two time periods, as did the use of topical corticosteroids (from 7% to 57%, P less than .001), while the use of topical antibiotics decreased from 79% to 43% (P = .02). Rates of dose changes or interruptions were significantly lower among those on prophylaxis (5% vs. 19%, P =.01), a 79% lower risk. Patients treated prophylactically were 94% less likely to need a first rescue treatment and 74% less likely to need a second rescue treatment for rash.
The study findings were limited by several factors including the retrospective design, use of data from a single institution, and incomplete documentation of some patients, the researchers noted. However, the results “highlight the value of integrating dermatologic care and education into oncology centers by increasing adherence to evidence-based prophylaxis protocols for rash and appropriate treatment agent selection, which may minimize toxicity-associated chemotherapy interruptions and improve quality of life,” they concluded.
“As novel cancer treatment options for patients continue to develop, and as patients with cancer live longer, the spectrum and prevalence of dermatologic toxic effects will continue to expand,” Bernice Y. Kwong, MD, director of the supportive dermato-oncology program at Stanford (Calif.) University, wrote in an accompanying editorial.
“Dermatologists have a critical and growing opportunity and role to engage in multidisciplinary efforts to provide expert guidance to best manage these cutaneous adverse events to achieve the best outcome for patients with cancer,” she said.
Although the prophylaxis rates at Dana-Farber improved after the establishment of the oncodermatology program, they remained relatively low, “underscoring an opportunity to improve on how to teach, execute, and improve access to oncodermatologic care for patients with cancer,” said Dr. Kwong. Knowledge gaps in the nature of skin toxicity for newer cancer drugs poses another challenge for skin toxicity management in these patients, she added.
However, “timely and consistent access to dermatologic expertise in oncology practices is critical to prevent unnecessary discontinuation of life-saving anticancer therapy, especially as multiple studies have demonstrated that anticancer therapy–associated skin toxicity may be associated with a positive response to anticancer therapy,” she emphasized.
Ms. Yu and one coauthor had no financial conflicts to disclose, the two other authors had several disclosures, outside of the submitted work. Dr. Kwong disclosed serving as a consultant for Genentech and Oncoderm and serving on the advisory board for Kyowa Kirin.
SOURCE: Yu Z et al. JAMA Dermatol. 2020 July 1. doi: 10.1001/jamadermatol.2020.1795. Kwong BY. JAMA Dermatol. 2020 Jul 1. doi: 10.1001/jamadermatol.2020.1794.
, according to the results of a retrospective study of 208 adults treated at the Dana-Farber Cancer Institute in Boston, or affiliated sites.
The benefits of prophylactic treatment for treatment-related skin rash in cancer patients are well established, based largely on the Skin Toxicity Evaluation Protocol With Panitumumab (STEPP) trial published in 2012, which led to the development of guidelines for preventing and managing skin toxicity associated with epidermal growth factor receptor inhibitor (EGFRi) treatment, wrote Zizi Yu of Harvard Medical School, Boston, and coauthors. However, they added, “awareness of and adherence to these guidelines among oncology clinicians are thus far poorly understood.” They pointed out that 90% of patients treated with an EGFRi develop cutaneous toxicities, which can affect quality of life, increase the risk of infection, and require dose modification, interruption, or discontinuation of treatment.
In the study, published in JAMA Dermatology, the researchers compared adherence to protocols at Dana-Farber before and after the 2014-2015 initiation of a Skin Toxicities from Anticancer Therapies (STAT) program at Dana-Farber established in 2014 by the department of dermatology.
The study population included 208 adult cancer patients with colorectal cancer, head and neck cancer, or cutaneous squamous cell cancer, treated with at least one dose of cetuximab (Erbitux); the average age of the patients was 62 years and the majority were men. Most had stage IV disease. The STAT program included the integration of 9 oncodermatologists in the head and neck, genitourinary, and cutaneous oncology clinics for 7 of 10 cancer treatment sessions per week, as well as the creation of urgent access time slots in oncodermatology clinics for 10 of 10 sessions per week.
Overall, significantly more patients were treated prophylactically for skin toxicity at the start of cetuximab treatment in 2017 vs. 2012 (47% vs. 25%, P less than .001) after the initiation of a dermatology protocol.
In addition, the preemptive use of tetracycline increased significantly from 45% to 71% (P = .02) between the two time periods, as did the use of topical corticosteroids (from 7% to 57%, P less than .001), while the use of topical antibiotics decreased from 79% to 43% (P = .02). Rates of dose changes or interruptions were significantly lower among those on prophylaxis (5% vs. 19%, P =.01), a 79% lower risk. Patients treated prophylactically were 94% less likely to need a first rescue treatment and 74% less likely to need a second rescue treatment for rash.
The study findings were limited by several factors including the retrospective design, use of data from a single institution, and incomplete documentation of some patients, the researchers noted. However, the results “highlight the value of integrating dermatologic care and education into oncology centers by increasing adherence to evidence-based prophylaxis protocols for rash and appropriate treatment agent selection, which may minimize toxicity-associated chemotherapy interruptions and improve quality of life,” they concluded.
“As novel cancer treatment options for patients continue to develop, and as patients with cancer live longer, the spectrum and prevalence of dermatologic toxic effects will continue to expand,” Bernice Y. Kwong, MD, director of the supportive dermato-oncology program at Stanford (Calif.) University, wrote in an accompanying editorial.
“Dermatologists have a critical and growing opportunity and role to engage in multidisciplinary efforts to provide expert guidance to best manage these cutaneous adverse events to achieve the best outcome for patients with cancer,” she said.
Although the prophylaxis rates at Dana-Farber improved after the establishment of the oncodermatology program, they remained relatively low, “underscoring an opportunity to improve on how to teach, execute, and improve access to oncodermatologic care for patients with cancer,” said Dr. Kwong. Knowledge gaps in the nature of skin toxicity for newer cancer drugs poses another challenge for skin toxicity management in these patients, she added.
However, “timely and consistent access to dermatologic expertise in oncology practices is critical to prevent unnecessary discontinuation of life-saving anticancer therapy, especially as multiple studies have demonstrated that anticancer therapy–associated skin toxicity may be associated with a positive response to anticancer therapy,” she emphasized.
Ms. Yu and one coauthor had no financial conflicts to disclose, the two other authors had several disclosures, outside of the submitted work. Dr. Kwong disclosed serving as a consultant for Genentech and Oncoderm and serving on the advisory board for Kyowa Kirin.
SOURCE: Yu Z et al. JAMA Dermatol. 2020 July 1. doi: 10.1001/jamadermatol.2020.1795. Kwong BY. JAMA Dermatol. 2020 Jul 1. doi: 10.1001/jamadermatol.2020.1794.
FROM JAMA DERMATOLOGY
Expert shares his approach to treating warts in children
In the clinical experience of Anthony J. Mancini, MD, one option for children and adolescents who present with common warts is to do nothing, since they may resolve on their own.

“Many effective treatments that we have are painful and poorly tolerated, especially in younger children,” Dr. Mancini, professor of pediatrics and dermatology at Northwestern University, Chicago, said during the virtual Pediatric Dermatology 2020: Best Practices and Innovations Conference. “However, while they’re harmless and often self-limited, warts often form a social stigma, and parents often desire therapy.”
Even though warts may spontaneously resolve in up to 65% of patients at 2 years and 80% at 4 years, the goals of treatment are to eradicate them, minimize pain, avoid scarring, and help prevent recurrence.
One effective topical therapy he highlighted is WartPEEL cream, which is a proprietary, compounded formulation of 17% salicylic acid and 2% 5-fluorouracil. “It’s in a sustained release vehicle called Remedium, and is available from a compounding pharmacy, but not FDA approved,” said Dr. Mancini, who is also head of pediatric dermatology at Lurie Children’s Hospital of Chicago. “It’s applied nightly with plastic tape occlusion and rinsed off each morning.”
WartPEEL is available through NuCara Pharmacy at 877-268-2272. It is not covered by most insurance plans and it costs around $80. “It is very effective, tends to be totally painless, and has a much quicker response than over-the-counter salicylic acid-based treatments for warts,” he said.
Another treatment option is oral cimetidine, especially in patients who have multiple or recalcitrant warts. The recommended dosing is 30-40 mg/kg per day, divided into twice-daily dosing. “You have to give it for at least 8-12 weeks to determine whether it’s working or not,” Dr. Mancini said. “In the initial report, [investigators] described an 81% complete response rate, but subsequent randomized, controlled trials were not able to confirm that data against placebo or topical treatments. I will say, though, that cimetidine is well tolerated. It’s always worth a try but, if you do use it, always consider other medications the patient may be taking and potential drug-drug interactions.”
For flat warts, verrucous papules that commonly occur on the face, Dr. Mancini recommends off-label treatment with 5% 5-fluorouracil cream (Efudex), which is normally indicated for actinic keratoses in adults. “I have patients apply this for 3 nights per week and work their way up gradually to nightly application,” he said. “It’s really important that parents and patients understand the importance of sun protection when they’re using Efudex, and they need to know that some irritation is possible. Overall, this treatment seems to be very well tolerated.”
Other treatment options for common warts, in addition to over-the-counter products that contain salicylic acid, are home cryotherapy kits that contain a mixture of diethyl ether and propane. “These can be effective for small warts,” Dr. Mancini said. “But for larger, thicker lesions, they’re not going to quite as effective.”
Treatment options best reserved for dermatologists, he continued, include in-office liquid nitrogen cryotherapy, “if it’s tolerated,” he said. “I have a no-hold policy, so if we have to hold a child down who’s flailing and crying and screaming during treatment, we’re probably not going to use liquid nitrogen.” He also mentioned topical immunotherapy with agents like squaric acid dibutylester. “This is almost like putting poison ivy on your warts to get the immune system revved up,” he said. “It can be very effective.” Other treatment options include intralesional immune therapy, topical cidofovir, and even pulsed-dye laser.
Dr. Mancini disclosed that he is a consultant to and a member of the scientific advisory board for Verrica Pharmaceuticals.
In the clinical experience of Anthony J. Mancini, MD, one option for children and adolescents who present with common warts is to do nothing, since they may resolve on their own.
“Many effective treatments that we have are painful and poorly tolerated, especially in younger children,” Dr. Mancini, professor of pediatrics and dermatology at Northwestern University, Chicago, said during the virtual Pediatric Dermatology 2020: Best Practices and Innovations Conference. “However, while they’re harmless and often self-limited, warts often form a social stigma, and parents often desire therapy.”
Even though warts may spontaneously resolve in up to 65% of patients at 2 years and 80% at 4 years, the goals of treatment are to eradicate them, minimize pain, avoid scarring, and help prevent recurrence.
One effective topical therapy he highlighted is WartPEEL cream, which is a proprietary, compounded formulation of 17% salicylic acid and 2% 5-fluorouracil. “It’s in a sustained release vehicle called Remedium, and is available from a compounding pharmacy, but not FDA approved,” said Dr. Mancini, who is also head of pediatric dermatology at Lurie Children’s Hospital of Chicago. “It’s applied nightly with plastic tape occlusion and rinsed off each morning.”
WartPEEL is available through NuCara Pharmacy at 877-268-2272. It is not covered by most insurance plans and it costs around $80. “It is very effective, tends to be totally painless, and has a much quicker response than over-the-counter salicylic acid-based treatments for warts,” he said.
Another treatment option is oral cimetidine, especially in patients who have multiple or recalcitrant warts. The recommended dosing is 30-40 mg/kg per day, divided into twice-daily dosing. “You have to give it for at least 8-12 weeks to determine whether it’s working or not,” Dr. Mancini said. “In the initial report, [investigators] described an 81% complete response rate, but subsequent randomized, controlled trials were not able to confirm that data against placebo or topical treatments. I will say, though, that cimetidine is well tolerated. It’s always worth a try but, if you do use it, always consider other medications the patient may be taking and potential drug-drug interactions.”
For flat warts, verrucous papules that commonly occur on the face, Dr. Mancini recommends off-label treatment with 5% 5-fluorouracil cream (Efudex), which is normally indicated for actinic keratoses in adults. “I have patients apply this for 3 nights per week and work their way up gradually to nightly application,” he said. “It’s really important that parents and patients understand the importance of sun protection when they’re using Efudex, and they need to know that some irritation is possible. Overall, this treatment seems to be very well tolerated.”
Other treatment options for common warts, in addition to over-the-counter products that contain salicylic acid, are home cryotherapy kits that contain a mixture of diethyl ether and propane. “These can be effective for small warts,” Dr. Mancini said. “But for larger, thicker lesions, they’re not going to quite as effective.”
Treatment options best reserved for dermatologists, he continued, include in-office liquid nitrogen cryotherapy, “if it’s tolerated,” he said. “I have a no-hold policy, so if we have to hold a child down who’s flailing and crying and screaming during treatment, we’re probably not going to use liquid nitrogen.” He also mentioned topical immunotherapy with agents like squaric acid dibutylester. “This is almost like putting poison ivy on your warts to get the immune system revved up,” he said. “It can be very effective.” Other treatment options include intralesional immune therapy, topical cidofovir, and even pulsed-dye laser.
Dr. Mancini disclosed that he is a consultant to and a member of the scientific advisory board for Verrica Pharmaceuticals.
In the clinical experience of Anthony J. Mancini, MD, one option for children and adolescents who present with common warts is to do nothing, since they may resolve on their own.
“Many effective treatments that we have are painful and poorly tolerated, especially in younger children,” Dr. Mancini, professor of pediatrics and dermatology at Northwestern University, Chicago, said during the virtual Pediatric Dermatology 2020: Best Practices and Innovations Conference. “However, while they’re harmless and often self-limited, warts often form a social stigma, and parents often desire therapy.”
Even though warts may spontaneously resolve in up to 65% of patients at 2 years and 80% at 4 years, the goals of treatment are to eradicate them, minimize pain, avoid scarring, and help prevent recurrence.
One effective topical therapy he highlighted is WartPEEL cream, which is a proprietary, compounded formulation of 17% salicylic acid and 2% 5-fluorouracil. “It’s in a sustained release vehicle called Remedium, and is available from a compounding pharmacy, but not FDA approved,” said Dr. Mancini, who is also head of pediatric dermatology at Lurie Children’s Hospital of Chicago. “It’s applied nightly with plastic tape occlusion and rinsed off each morning.”
WartPEEL is available through NuCara Pharmacy at 877-268-2272. It is not covered by most insurance plans and it costs around $80. “It is very effective, tends to be totally painless, and has a much quicker response than over-the-counter salicylic acid-based treatments for warts,” he said.
Another treatment option is oral cimetidine, especially in patients who have multiple or recalcitrant warts. The recommended dosing is 30-40 mg/kg per day, divided into twice-daily dosing. “You have to give it for at least 8-12 weeks to determine whether it’s working or not,” Dr. Mancini said. “In the initial report, [investigators] described an 81% complete response rate, but subsequent randomized, controlled trials were not able to confirm that data against placebo or topical treatments. I will say, though, that cimetidine is well tolerated. It’s always worth a try but, if you do use it, always consider other medications the patient may be taking and potential drug-drug interactions.”
For flat warts, verrucous papules that commonly occur on the face, Dr. Mancini recommends off-label treatment with 5% 5-fluorouracil cream (Efudex), which is normally indicated for actinic keratoses in adults. “I have patients apply this for 3 nights per week and work their way up gradually to nightly application,” he said. “It’s really important that parents and patients understand the importance of sun protection when they’re using Efudex, and they need to know that some irritation is possible. Overall, this treatment seems to be very well tolerated.”
Other treatment options for common warts, in addition to over-the-counter products that contain salicylic acid, are home cryotherapy kits that contain a mixture of diethyl ether and propane. “These can be effective for small warts,” Dr. Mancini said. “But for larger, thicker lesions, they’re not going to quite as effective.”
Treatment options best reserved for dermatologists, he continued, include in-office liquid nitrogen cryotherapy, “if it’s tolerated,” he said. “I have a no-hold policy, so if we have to hold a child down who’s flailing and crying and screaming during treatment, we’re probably not going to use liquid nitrogen.” He also mentioned topical immunotherapy with agents like squaric acid dibutylester. “This is almost like putting poison ivy on your warts to get the immune system revved up,” he said. “It can be very effective.” Other treatment options include intralesional immune therapy, topical cidofovir, and even pulsed-dye laser.
Dr. Mancini disclosed that he is a consultant to and a member of the scientific advisory board for Verrica Pharmaceuticals.
FROM PEDIATRIC DERMATOLOGY 2020
Geographical hot spots for early-onset colon cancer
The incidence of colorectal cancer (CRC) in adults younger than 55 years has been increasing in recent years ― a “dramatic increase” was noted in the United States in 2017, and an increase in incidence has subsequently been seen in many other countries across Europe, as well as Australia, New Zealand, and Canada.
A new study has identified geographic hot spots across the United States, characterized by distinct patterns of early-onset CRC with worse survival among men. The hot spots primarily include counties in the lower Mississippi Delta, west-central Appalachia, and eastern Virginia/North Carolina.
The study was published online on May 15 in the American Journal of Cancer Research.
These data can help to identify some of the risk factors associated with early-onset CRC/mortality, commented lead author Charles Rogers, PhD, MPH, a researcher at the Huntsman Cancer Institute and assistant professor of public health at the University of Utah, Salt Lake City.
“We noted potential explanations for the hot spots,” he told Medscape Medical News. “These include an enduring history of unique challenges, such as inadequate access to care, poor health literacy, and low educational attainment.”
Within hot-spot counties there were also higher rates of poverty, a lack of health insurance, and fewer primary care physicians.
“The disproportionate burden of early-onset colorectal cancer among non-Hispanic black men may result from distinctive stressors coupled with cultural and social expectations that impact screening and care behaviors,” said Rogers. “And while it’s estimated that approximately 14% of all US adults are current smokers, we observed that 24% of the adult population residing in hot-spot counties reported currently smoking and having smoked at least 100 cigarettes in their lifetime.”
Lifestyle and screening
Elements relating to the increase in early-onset CRC include environmental and geographical factors, as well as lifestyle factors, such as diet, obesity, and sedentary behaviors, Rogers commented.
“I think lifestyle factors are huge,” he said. “Consumption of high-fructose corn syrup and charred meat, for example, are worth considering and deserve more attention.”
He emphasized the importance of screening. Most health organizations in the United States recommend that screening start at age 50 years, but the American Cancer Society lowered this to 45 years, and the issue has been hotly debated. Rogers said that adults younger than 50 should be having conversations with their clinicians about screening for CRC. He noted that this is particularly important if they have any symptoms of CRC, have a family history of the disease, or reside in one of the hot spots that were identified in their study.
An expert who was approached for outside comment agreed. Chyke Doubeni, MBBS, MPH, director of the Center for Health Equity and Community Engagement Research at the Mayo Clinic in Rochester, Minnesota, said that anyone with health concerns should discuss preventive measures with their primary care physician.
“Screening for people younger than the age of 50 is currently controversial, as it is not recommended by some guidelines,” he said. “Recommendations for screening are different for people with a family history or certain genetic conditions.”
Such people include those younger than 50 years who have a family history of CRC or advanced adenomas. These patients should share that history with their primary care physician in order to determine when to begin screening and how often to be screened.
“People under the age of 50 who have symptoms such as unexplained rectal bleeding or iron deficiency anemia that may suggest the presence of colorectal cancer should be promptly evaluated for that possibility,” Doubeni added.
Hot spots versus other counties
The goal of the study was to identify mortality hot spots specific to men with early-onset CRC and to evaluate disparities while controlling for sex-specific differences. Rogers and colleagues identified counties with high early-onset CRC mortality rates using data from the Centers for Disease Control and Prevention (1999–2017) and linked them to data from the Surveillance, Epidemiology, and End Results (SEER) for men aged 15 to 49 years.
The team identified 232 US counties (7% of the total) as hot spots. The majority (214 of 232, 92%) were located in the South, and the remainder (18 of 232, 8%) were in the Midwest P < .01).
As compared to men living in other counties, those residing in hot-spot counties were more likely to be non-Hispanic blacks (30.82% vs 13.06%), less likely to be Hispanic (1.68% vs 16.65%; P < .01), and more likely to be diagnosed with metastatic disease (stage IV CRC) (2.58% vs 1.94%; P < .01).
Among men who lived in hot spots, CRC survival was poorer than was seen elsewhere (113.76 vs 129.04 months, respectively; P < .001). Among those with early-onset CRC, the risk for CRC-specific death was 24% higher (hazard ratio [HR], 1.24) than for men living outside of the hot-spot counties. However, that figure dropped to 12% after adjustment for county-level smoking (HR, 1.12).
With respect to racial/ethnic differences, non-Hispanic black (HR, 1.31) and Hispanic (HR, 1.12) patients had a 31% and 12% increased risk for CRC-specific death as compared to non-Hispanic white men (HR, 1.01) after adjusting for smoking status.
The authors note that among all determinants, “clinical stage explained the largest proportion of the variance” in early-onset CRC survival for men living in hot spots and other locations combined.
In the hot-spot counties, severe tumor grade was associated with greater CRC-specific mortality risk. Among patients with poorly differentiated tumors (HR, 1.87) and undifferentiated tumors (HR, 2.60), the mortality risk was nearly 2 times and 2.6 times greater, respectively, than those with well-differentiated tumors.
Compared to other counties, hot-spot counties were characterized by demographics that have been linked to poorer health outcomes, such as higher poverty rates (26.57% vs 16.77%), greater prevalence of adult obesity (34.94% vs 25.89%), higher adult smoking rates (23.97% vs 15.44%), higher uninsured rates (20.06% vs 17.91%), and fewer primary care physicians (58.28 vs 75.45 per 100,000 population).
Geographic distribution of CRC
Commenting to Medscape Medical News, Doubeni pointed out that the identified hot spots are similar to previously reported overall CRC hot spots.
“It shows the same patterns of geographic distribution of colorectal cancer in the United States,” he said. “These patterns tend to be associated with areas with high levels of poverty, as is the case with other chronic diseases, and may be related to clustering of risk factors and limited access to care in those areas.”
The research was supported by the National Cancer Institute of the National Institutes of Health, the Huntsman Cancer Foundation, and the Health Studies Fund of the Department of Family and Preventative Medicine at the University of Utah. The authors and Doubeni have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The incidence of colorectal cancer (CRC) in adults younger than 55 years has been increasing in recent years ― a “dramatic increase” was noted in the United States in 2017, and an increase in incidence has subsequently been seen in many other countries across Europe, as well as Australia, New Zealand, and Canada.
A new study has identified geographic hot spots across the United States, characterized by distinct patterns of early-onset CRC with worse survival among men. The hot spots primarily include counties in the lower Mississippi Delta, west-central Appalachia, and eastern Virginia/North Carolina.
The study was published online on May 15 in the American Journal of Cancer Research.
These data can help to identify some of the risk factors associated with early-onset CRC/mortality, commented lead author Charles Rogers, PhD, MPH, a researcher at the Huntsman Cancer Institute and assistant professor of public health at the University of Utah, Salt Lake City.
“We noted potential explanations for the hot spots,” he told Medscape Medical News. “These include an enduring history of unique challenges, such as inadequate access to care, poor health literacy, and low educational attainment.”
Within hot-spot counties there were also higher rates of poverty, a lack of health insurance, and fewer primary care physicians.
“The disproportionate burden of early-onset colorectal cancer among non-Hispanic black men may result from distinctive stressors coupled with cultural and social expectations that impact screening and care behaviors,” said Rogers. “And while it’s estimated that approximately 14% of all US adults are current smokers, we observed that 24% of the adult population residing in hot-spot counties reported currently smoking and having smoked at least 100 cigarettes in their lifetime.”
Lifestyle and screening
Elements relating to the increase in early-onset CRC include environmental and geographical factors, as well as lifestyle factors, such as diet, obesity, and sedentary behaviors, Rogers commented.
“I think lifestyle factors are huge,” he said. “Consumption of high-fructose corn syrup and charred meat, for example, are worth considering and deserve more attention.”
He emphasized the importance of screening. Most health organizations in the United States recommend that screening start at age 50 years, but the American Cancer Society lowered this to 45 years, and the issue has been hotly debated. Rogers said that adults younger than 50 should be having conversations with their clinicians about screening for CRC. He noted that this is particularly important if they have any symptoms of CRC, have a family history of the disease, or reside in one of the hot spots that were identified in their study.
An expert who was approached for outside comment agreed. Chyke Doubeni, MBBS, MPH, director of the Center for Health Equity and Community Engagement Research at the Mayo Clinic in Rochester, Minnesota, said that anyone with health concerns should discuss preventive measures with their primary care physician.
“Screening for people younger than the age of 50 is currently controversial, as it is not recommended by some guidelines,” he said. “Recommendations for screening are different for people with a family history or certain genetic conditions.”
Such people include those younger than 50 years who have a family history of CRC or advanced adenomas. These patients should share that history with their primary care physician in order to determine when to begin screening and how often to be screened.
“People under the age of 50 who have symptoms such as unexplained rectal bleeding or iron deficiency anemia that may suggest the presence of colorectal cancer should be promptly evaluated for that possibility,” Doubeni added.
Hot spots versus other counties
The goal of the study was to identify mortality hot spots specific to men with early-onset CRC and to evaluate disparities while controlling for sex-specific differences. Rogers and colleagues identified counties with high early-onset CRC mortality rates using data from the Centers for Disease Control and Prevention (1999–2017) and linked them to data from the Surveillance, Epidemiology, and End Results (SEER) for men aged 15 to 49 years.
The team identified 232 US counties (7% of the total) as hot spots. The majority (214 of 232, 92%) were located in the South, and the remainder (18 of 232, 8%) were in the Midwest P < .01).
As compared to men living in other counties, those residing in hot-spot counties were more likely to be non-Hispanic blacks (30.82% vs 13.06%), less likely to be Hispanic (1.68% vs 16.65%; P < .01), and more likely to be diagnosed with metastatic disease (stage IV CRC) (2.58% vs 1.94%; P < .01).
Among men who lived in hot spots, CRC survival was poorer than was seen elsewhere (113.76 vs 129.04 months, respectively; P < .001). Among those with early-onset CRC, the risk for CRC-specific death was 24% higher (hazard ratio [HR], 1.24) than for men living outside of the hot-spot counties. However, that figure dropped to 12% after adjustment for county-level smoking (HR, 1.12).
With respect to racial/ethnic differences, non-Hispanic black (HR, 1.31) and Hispanic (HR, 1.12) patients had a 31% and 12% increased risk for CRC-specific death as compared to non-Hispanic white men (HR, 1.01) after adjusting for smoking status.
The authors note that among all determinants, “clinical stage explained the largest proportion of the variance” in early-onset CRC survival for men living in hot spots and other locations combined.
In the hot-spot counties, severe tumor grade was associated with greater CRC-specific mortality risk. Among patients with poorly differentiated tumors (HR, 1.87) and undifferentiated tumors (HR, 2.60), the mortality risk was nearly 2 times and 2.6 times greater, respectively, than those with well-differentiated tumors.
Compared to other counties, hot-spot counties were characterized by demographics that have been linked to poorer health outcomes, such as higher poverty rates (26.57% vs 16.77%), greater prevalence of adult obesity (34.94% vs 25.89%), higher adult smoking rates (23.97% vs 15.44%), higher uninsured rates (20.06% vs 17.91%), and fewer primary care physicians (58.28 vs 75.45 per 100,000 population).
Geographic distribution of CRC
Commenting to Medscape Medical News, Doubeni pointed out that the identified hot spots are similar to previously reported overall CRC hot spots.
“It shows the same patterns of geographic distribution of colorectal cancer in the United States,” he said. “These patterns tend to be associated with areas with high levels of poverty, as is the case with other chronic diseases, and may be related to clustering of risk factors and limited access to care in those areas.”
The research was supported by the National Cancer Institute of the National Institutes of Health, the Huntsman Cancer Foundation, and the Health Studies Fund of the Department of Family and Preventative Medicine at the University of Utah. The authors and Doubeni have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The incidence of colorectal cancer (CRC) in adults younger than 55 years has been increasing in recent years ― a “dramatic increase” was noted in the United States in 2017, and an increase in incidence has subsequently been seen in many other countries across Europe, as well as Australia, New Zealand, and Canada.
A new study has identified geographic hot spots across the United States, characterized by distinct patterns of early-onset CRC with worse survival among men. The hot spots primarily include counties in the lower Mississippi Delta, west-central Appalachia, and eastern Virginia/North Carolina.
The study was published online on May 15 in the American Journal of Cancer Research.
These data can help to identify some of the risk factors associated with early-onset CRC/mortality, commented lead author Charles Rogers, PhD, MPH, a researcher at the Huntsman Cancer Institute and assistant professor of public health at the University of Utah, Salt Lake City.
“We noted potential explanations for the hot spots,” he told Medscape Medical News. “These include an enduring history of unique challenges, such as inadequate access to care, poor health literacy, and low educational attainment.”
Within hot-spot counties there were also higher rates of poverty, a lack of health insurance, and fewer primary care physicians.
“The disproportionate burden of early-onset colorectal cancer among non-Hispanic black men may result from distinctive stressors coupled with cultural and social expectations that impact screening and care behaviors,” said Rogers. “And while it’s estimated that approximately 14% of all US adults are current smokers, we observed that 24% of the adult population residing in hot-spot counties reported currently smoking and having smoked at least 100 cigarettes in their lifetime.”
Lifestyle and screening
Elements relating to the increase in early-onset CRC include environmental and geographical factors, as well as lifestyle factors, such as diet, obesity, and sedentary behaviors, Rogers commented.
“I think lifestyle factors are huge,” he said. “Consumption of high-fructose corn syrup and charred meat, for example, are worth considering and deserve more attention.”
He emphasized the importance of screening. Most health organizations in the United States recommend that screening start at age 50 years, but the American Cancer Society lowered this to 45 years, and the issue has been hotly debated. Rogers said that adults younger than 50 should be having conversations with their clinicians about screening for CRC. He noted that this is particularly important if they have any symptoms of CRC, have a family history of the disease, or reside in one of the hot spots that were identified in their study.
An expert who was approached for outside comment agreed. Chyke Doubeni, MBBS, MPH, director of the Center for Health Equity and Community Engagement Research at the Mayo Clinic in Rochester, Minnesota, said that anyone with health concerns should discuss preventive measures with their primary care physician.
“Screening for people younger than the age of 50 is currently controversial, as it is not recommended by some guidelines,” he said. “Recommendations for screening are different for people with a family history or certain genetic conditions.”
Such people include those younger than 50 years who have a family history of CRC or advanced adenomas. These patients should share that history with their primary care physician in order to determine when to begin screening and how often to be screened.
“People under the age of 50 who have symptoms such as unexplained rectal bleeding or iron deficiency anemia that may suggest the presence of colorectal cancer should be promptly evaluated for that possibility,” Doubeni added.
Hot spots versus other counties
The goal of the study was to identify mortality hot spots specific to men with early-onset CRC and to evaluate disparities while controlling for sex-specific differences. Rogers and colleagues identified counties with high early-onset CRC mortality rates using data from the Centers for Disease Control and Prevention (1999–2017) and linked them to data from the Surveillance, Epidemiology, and End Results (SEER) for men aged 15 to 49 years.
The team identified 232 US counties (7% of the total) as hot spots. The majority (214 of 232, 92%) were located in the South, and the remainder (18 of 232, 8%) were in the Midwest P < .01).
As compared to men living in other counties, those residing in hot-spot counties were more likely to be non-Hispanic blacks (30.82% vs 13.06%), less likely to be Hispanic (1.68% vs 16.65%; P < .01), and more likely to be diagnosed with metastatic disease (stage IV CRC) (2.58% vs 1.94%; P < .01).
Among men who lived in hot spots, CRC survival was poorer than was seen elsewhere (113.76 vs 129.04 months, respectively; P < .001). Among those with early-onset CRC, the risk for CRC-specific death was 24% higher (hazard ratio [HR], 1.24) than for men living outside of the hot-spot counties. However, that figure dropped to 12% after adjustment for county-level smoking (HR, 1.12).
With respect to racial/ethnic differences, non-Hispanic black (HR, 1.31) and Hispanic (HR, 1.12) patients had a 31% and 12% increased risk for CRC-specific death as compared to non-Hispanic white men (HR, 1.01) after adjusting for smoking status.
The authors note that among all determinants, “clinical stage explained the largest proportion of the variance” in early-onset CRC survival for men living in hot spots and other locations combined.
In the hot-spot counties, severe tumor grade was associated with greater CRC-specific mortality risk. Among patients with poorly differentiated tumors (HR, 1.87) and undifferentiated tumors (HR, 2.60), the mortality risk was nearly 2 times and 2.6 times greater, respectively, than those with well-differentiated tumors.
Compared to other counties, hot-spot counties were characterized by demographics that have been linked to poorer health outcomes, such as higher poverty rates (26.57% vs 16.77%), greater prevalence of adult obesity (34.94% vs 25.89%), higher adult smoking rates (23.97% vs 15.44%), higher uninsured rates (20.06% vs 17.91%), and fewer primary care physicians (58.28 vs 75.45 per 100,000 population).
Geographic distribution of CRC
Commenting to Medscape Medical News, Doubeni pointed out that the identified hot spots are similar to previously reported overall CRC hot spots.
“It shows the same patterns of geographic distribution of colorectal cancer in the United States,” he said. “These patterns tend to be associated with areas with high levels of poverty, as is the case with other chronic diseases, and may be related to clustering of risk factors and limited access to care in those areas.”
The research was supported by the National Cancer Institute of the National Institutes of Health, the Huntsman Cancer Foundation, and the Health Studies Fund of the Department of Family and Preventative Medicine at the University of Utah. The authors and Doubeni have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Use of nonopioid pain meds is on the rise
Opioid and nonopioid prescription pain medications have taken different journeys since 2009, but they ended up in the same place in 2018, according to a recent report from the National Center for Health Statistics.
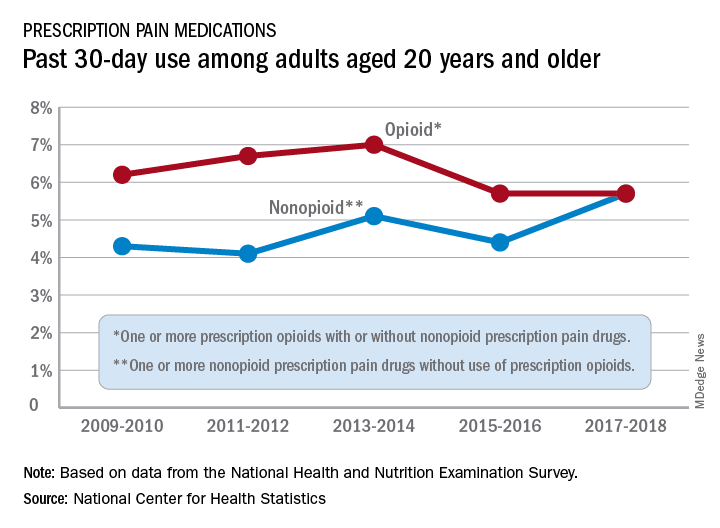
At least by one measure, anyway. Survey data from 2009 to 2010 show that 6.2% of adults aged 20 years and older had taken at least one prescription opioid in the last 30 days and 4.3% had used a prescription nonopioid without an opioid. By 2017-2018, past 30-day use of both drug groups was 5.7%, Craig M. Hales, MD, and associates said in an NCHS data brief.
“Opioids may be prescribed together with nonopioid pain medications, [but] nonpharmacologic and nonopioid-containing pharmacologic therapies are preferred for management of chronic pain,” the NCHS researchers noted.
as did the short-term increase in nonopioids from 2015-2016 to 2017-2018, but the 10-year trend for opioids was not significant, based on data from the National Health and Nutrition Examination Survey.
Much of the analysis focused on 2015-2018, when 30-day use of any prescription pain medication was reported by 10.7% of adults aged 20 years and older, with use of opioids at 5.7% and nonopioids at 5.0%. For women, use of any pain drug was 12.6% (6.4% opioid, 6.2% nonopioid) from 2015 to 2018, compared with 8.7% for men (4.9%, 3.8%), Dr. Hales and associates reported.
Past 30-day use of both opioids and nonopioids over those 4 years was highest for non-Hispanic whites and lowest, by a significant margin for both drug groups, among non-Hispanic Asian adults, a pattern that held for both men and women, they said.
Opioid and nonopioid prescription pain medications have taken different journeys since 2009, but they ended up in the same place in 2018, according to a recent report from the National Center for Health Statistics.
At least by one measure, anyway. Survey data from 2009 to 2010 show that 6.2% of adults aged 20 years and older had taken at least one prescription opioid in the last 30 days and 4.3% had used a prescription nonopioid without an opioid. By 2017-2018, past 30-day use of both drug groups was 5.7%, Craig M. Hales, MD, and associates said in an NCHS data brief.
“Opioids may be prescribed together with nonopioid pain medications, [but] nonpharmacologic and nonopioid-containing pharmacologic therapies are preferred for management of chronic pain,” the NCHS researchers noted.
as did the short-term increase in nonopioids from 2015-2016 to 2017-2018, but the 10-year trend for opioids was not significant, based on data from the National Health and Nutrition Examination Survey.
Much of the analysis focused on 2015-2018, when 30-day use of any prescription pain medication was reported by 10.7% of adults aged 20 years and older, with use of opioids at 5.7% and nonopioids at 5.0%. For women, use of any pain drug was 12.6% (6.4% opioid, 6.2% nonopioid) from 2015 to 2018, compared with 8.7% for men (4.9%, 3.8%), Dr. Hales and associates reported.
Past 30-day use of both opioids and nonopioids over those 4 years was highest for non-Hispanic whites and lowest, by a significant margin for both drug groups, among non-Hispanic Asian adults, a pattern that held for both men and women, they said.
Opioid and nonopioid prescription pain medications have taken different journeys since 2009, but they ended up in the same place in 2018, according to a recent report from the National Center for Health Statistics.
At least by one measure, anyway. Survey data from 2009 to 2010 show that 6.2% of adults aged 20 years and older had taken at least one prescription opioid in the last 30 days and 4.3% had used a prescription nonopioid without an opioid. By 2017-2018, past 30-day use of both drug groups was 5.7%, Craig M. Hales, MD, and associates said in an NCHS data brief.
“Opioids may be prescribed together with nonopioid pain medications, [but] nonpharmacologic and nonopioid-containing pharmacologic therapies are preferred for management of chronic pain,” the NCHS researchers noted.
as did the short-term increase in nonopioids from 2015-2016 to 2017-2018, but the 10-year trend for opioids was not significant, based on data from the National Health and Nutrition Examination Survey.
Much of the analysis focused on 2015-2018, when 30-day use of any prescription pain medication was reported by 10.7% of adults aged 20 years and older, with use of opioids at 5.7% and nonopioids at 5.0%. For women, use of any pain drug was 12.6% (6.4% opioid, 6.2% nonopioid) from 2015 to 2018, compared with 8.7% for men (4.9%, 3.8%), Dr. Hales and associates reported.
Past 30-day use of both opioids and nonopioids over those 4 years was highest for non-Hispanic whites and lowest, by a significant margin for both drug groups, among non-Hispanic Asian adults, a pattern that held for both men and women, they said.
HIV does not appear to worsen COVID-19 outcomes
People living with HIV who are admitted to the hospital with COVID-19 are no more likely to die than those without HIV, an analysis conducted in New York City shows. This is despite the fact that comorbidities associated with worse COVID-19 outcomes were more common in the HIV group.
“We don’t see any signs that people with HIV should take extra precautions” to protect themselves from COVID-19, said Keith Sigel, MD, associate professor of medicine and infectious diseases at the Icahn School of Medicine at Mount Sinai, New York, and the lead researcher on the study, published online June 28 in Clinical Infectious Diseases.
“We still don’t have a great explanation for why we’re seeing what we’re seeing,” he added. “But we’re glad we’re seeing it.”
The findings have changed how Dr. Sigel talks to his patients with HIV about protecting themselves from COVID-19. Some patients have so curtailed their behavior for fear of acquiring COVID-19 that they aren’t buying groceries or attending needed medical appointments. With these data, Dr. Sigel said he’s comfortable telling his patients, “COVID-19 is bad all by itself, but you don’t need to go crazy. Wear a mask, practice appropriate social distancing and hygiene, but your risk doesn’t appear to be greater.”
The findings conform with those on the lack of association between HIV and COVID-19 severity seen in a cohort study from Spain, a case study from China, and case series from New Jersey, New York City, and Spain.
One of the only regions reporting something different so far is South Africa. There, HIV is the third most common comorbidity associated with death from COVID-19, according to a cohort analysis conducted in the province of Western Cape.
Along with data from HIV prevention and treatment trials, the conference will feature updates on where the world stands in the control of HIV during the COVID-19 pandemic. And for an even more focused look, the IAS COVID-19 Conference will immediately follow that meeting.
The New York City cohort
For their study, Dr. Sigel and colleagues examined the 4402 COVID-19 cases at the Mount Sinai Health System’s five hospitals between March 12 and April 23.
They found 88 people with COVID-19 whose charts showed codes indicating they were living with HIV. All 88 were receiving treatment, and 81% of them had undetectable viral loads documented at COVID admission or in the 12 months prior to admission.
The median age was 61 years, and 40% of the cohort was black and 30% was Hispanic.
Patients in the comparison group – 405 people without HIV from the Veterans Aging Cohort Study who had been admitted to the hospital for COVID-19 – were matched in terms of age, race, and stage of COVID-19.
The study had an 80% power to detect a 15% increase in the absolute risk for death in people with COVID-19, with or without HIV.
Patients with HIV were almost three times as likely to have smoked and were more likely to have chronic obstructive pulmonary disease, cirrhosis, and a history of cancer.
“This was a group of patients that one might suspect would do worse,” Dr. Sigel said. And yet, “we didn’t see any difference in deaths. We didn’t see any difference in respiratory failure.”
In fact, people with HIV required mechanical ventilation less often than those without HIV (18% vs. 23%). And when it came to mortality, one in five people died from COVID-19 during follow-up whether they had HIV or not (21% vs. 20%).
The only factor associated with significantly worse outcomes was a history of organ transplantation, “suggesting that non-HIV causes of immunodeficiency may be more prominent risks for severe outcomes,” Dr. Sigel and colleagues explained.
A surprise association
What’s more, the researchers found a slight association between the use of nucleoside reverse-transcriptase inhibitors (NRTI) by people with HIV and better outcomes in COVID-19. That echoes findings published June 26 in Annals of Internal Medicine, which showed that people with HIV taking the combination of tenofovir disoproxil fumarate plus emtricitabine (Truvada, Gilead Sciences) were less likely to be diagnosed with COVID-19, less likely to be hospitalized, and less likely to die.
This has led some to wonder whether NRTIs have some effect on SARS-CoV-2, the virus that causes COVID-19. Dr. Sigel said he wonders that too, but right now, it’s just musings.
“These studies are not even remotely designed” to show that NRTIs are protective against COVID-19, he explained. “Ours was extremely underpowered to detect that and there was a high potential for confounding.”
“I’d be wary of any study in a subpopulation – which is what we’re dealing with here – that is looking for signals of protection with certain medications,” he added.
A “modest” increase
Using the South African data, released on June 22, public health officials estimate that people with HIV are 2.75 times more likely to die from COVID-19 than those without HIV, making it the third most common comorbidity in people who died from COVID-19, behind diabetes and hypertension. This held true regardless of whether the people with HIV were on treatment.
But when they looked at COVID-19 deaths in the sickest of the sick – those hospitalized with COVID-19 symptoms – HIV was associated with just a 28% increase in the risk for death. The South African researchers called this risk “modest.”
“While these findings may overestimate the effect of HIV on COVID-19 death due to the presence of residual confounding, people living with HIV should be considered a high-risk group for COVID-19 management, with modestly elevated risk of poor outcomes, irrespective of viral suppression,” they wrote.
Epidemiologist Gregorio Millett, MPH, has been tracking the effect of HIV on COVID-19 outcomes since the start of the pandemic in his role as vice president and head of policy at the American Foundation for AIDS Research (amFAR).
Back in April, he and his colleagues looked at rates of COVID-19 deaths and hospitalizations in counties with disproportionate levels of black residents. These areas often overlapped with the communities selected for the Ending the HIV Epidemic plan to control HIV by 2030. What they found was that there was more HIV and COVID-19 in those communities.
What they didn’t find was that people with HIV in those communities had worse outcomes with COVID-19. This remained true even when they reran the analysis after the number of cases of COVID-19 in the United States surpassed 100,000. Those data have yet to be published, Mr. Millett reported.
“HIV does not pop out,” he said. “It’s still social determinants of health. It’s still underlying conditions. It’s still age as a primary factor.”
“People living with HIV are mainly dying of underlying conditions – so all the things associated with COVID-19 – rather than the association being with HIV itself,” he added.
Although he’s not ruling out the possibility that an association like the one in South Africa could emerge, Mr. Millett, who will present a plenary on the context of the HIV epidemic at the IAS conference, said he suspects we won’t see one.
“If we didn’t see an association with the counties that are disproportionately African American, in the black belt where we see high rates of HIV, particularly where we see the social determinants of health that definitely make a difference – if we’re not seeing that association there, where we have a high proportion of African Americans who are at risk both for HIV and COVID-19 – I just don’t think it’s going to emerge,” he said.
This article first appeared on Medscape.com.
People living with HIV who are admitted to the hospital with COVID-19 are no more likely to die than those without HIV, an analysis conducted in New York City shows. This is despite the fact that comorbidities associated with worse COVID-19 outcomes were more common in the HIV group.
“We don’t see any signs that people with HIV should take extra precautions” to protect themselves from COVID-19, said Keith Sigel, MD, associate professor of medicine and infectious diseases at the Icahn School of Medicine at Mount Sinai, New York, and the lead researcher on the study, published online June 28 in Clinical Infectious Diseases.
“We still don’t have a great explanation for why we’re seeing what we’re seeing,” he added. “But we’re glad we’re seeing it.”
The findings have changed how Dr. Sigel talks to his patients with HIV about protecting themselves from COVID-19. Some patients have so curtailed their behavior for fear of acquiring COVID-19 that they aren’t buying groceries or attending needed medical appointments. With these data, Dr. Sigel said he’s comfortable telling his patients, “COVID-19 is bad all by itself, but you don’t need to go crazy. Wear a mask, practice appropriate social distancing and hygiene, but your risk doesn’t appear to be greater.”
The findings conform with those on the lack of association between HIV and COVID-19 severity seen in a cohort study from Spain, a case study from China, and case series from New Jersey, New York City, and Spain.
One of the only regions reporting something different so far is South Africa. There, HIV is the third most common comorbidity associated with death from COVID-19, according to a cohort analysis conducted in the province of Western Cape.
Along with data from HIV prevention and treatment trials, the conference will feature updates on where the world stands in the control of HIV during the COVID-19 pandemic. And for an even more focused look, the IAS COVID-19 Conference will immediately follow that meeting.
The New York City cohort
For their study, Dr. Sigel and colleagues examined the 4402 COVID-19 cases at the Mount Sinai Health System’s five hospitals between March 12 and April 23.
They found 88 people with COVID-19 whose charts showed codes indicating they were living with HIV. All 88 were receiving treatment, and 81% of them had undetectable viral loads documented at COVID admission or in the 12 months prior to admission.
The median age was 61 years, and 40% of the cohort was black and 30% was Hispanic.
Patients in the comparison group – 405 people without HIV from the Veterans Aging Cohort Study who had been admitted to the hospital for COVID-19 – were matched in terms of age, race, and stage of COVID-19.
The study had an 80% power to detect a 15% increase in the absolute risk for death in people with COVID-19, with or without HIV.
Patients with HIV were almost three times as likely to have smoked and were more likely to have chronic obstructive pulmonary disease, cirrhosis, and a history of cancer.
“This was a group of patients that one might suspect would do worse,” Dr. Sigel said. And yet, “we didn’t see any difference in deaths. We didn’t see any difference in respiratory failure.”
In fact, people with HIV required mechanical ventilation less often than those without HIV (18% vs. 23%). And when it came to mortality, one in five people died from COVID-19 during follow-up whether they had HIV or not (21% vs. 20%).
The only factor associated with significantly worse outcomes was a history of organ transplantation, “suggesting that non-HIV causes of immunodeficiency may be more prominent risks for severe outcomes,” Dr. Sigel and colleagues explained.
A surprise association
What’s more, the researchers found a slight association between the use of nucleoside reverse-transcriptase inhibitors (NRTI) by people with HIV and better outcomes in COVID-19. That echoes findings published June 26 in Annals of Internal Medicine, which showed that people with HIV taking the combination of tenofovir disoproxil fumarate plus emtricitabine (Truvada, Gilead Sciences) were less likely to be diagnosed with COVID-19, less likely to be hospitalized, and less likely to die.
This has led some to wonder whether NRTIs have some effect on SARS-CoV-2, the virus that causes COVID-19. Dr. Sigel said he wonders that too, but right now, it’s just musings.
“These studies are not even remotely designed” to show that NRTIs are protective against COVID-19, he explained. “Ours was extremely underpowered to detect that and there was a high potential for confounding.”
“I’d be wary of any study in a subpopulation – which is what we’re dealing with here – that is looking for signals of protection with certain medications,” he added.
A “modest” increase
Using the South African data, released on June 22, public health officials estimate that people with HIV are 2.75 times more likely to die from COVID-19 than those without HIV, making it the third most common comorbidity in people who died from COVID-19, behind diabetes and hypertension. This held true regardless of whether the people with HIV were on treatment.
But when they looked at COVID-19 deaths in the sickest of the sick – those hospitalized with COVID-19 symptoms – HIV was associated with just a 28% increase in the risk for death. The South African researchers called this risk “modest.”
“While these findings may overestimate the effect of HIV on COVID-19 death due to the presence of residual confounding, people living with HIV should be considered a high-risk group for COVID-19 management, with modestly elevated risk of poor outcomes, irrespective of viral suppression,” they wrote.
Epidemiologist Gregorio Millett, MPH, has been tracking the effect of HIV on COVID-19 outcomes since the start of the pandemic in his role as vice president and head of policy at the American Foundation for AIDS Research (amFAR).
Back in April, he and his colleagues looked at rates of COVID-19 deaths and hospitalizations in counties with disproportionate levels of black residents. These areas often overlapped with the communities selected for the Ending the HIV Epidemic plan to control HIV by 2030. What they found was that there was more HIV and COVID-19 in those communities.
What they didn’t find was that people with HIV in those communities had worse outcomes with COVID-19. This remained true even when they reran the analysis after the number of cases of COVID-19 in the United States surpassed 100,000. Those data have yet to be published, Mr. Millett reported.
“HIV does not pop out,” he said. “It’s still social determinants of health. It’s still underlying conditions. It’s still age as a primary factor.”
“People living with HIV are mainly dying of underlying conditions – so all the things associated with COVID-19 – rather than the association being with HIV itself,” he added.
Although he’s not ruling out the possibility that an association like the one in South Africa could emerge, Mr. Millett, who will present a plenary on the context of the HIV epidemic at the IAS conference, said he suspects we won’t see one.
“If we didn’t see an association with the counties that are disproportionately African American, in the black belt where we see high rates of HIV, particularly where we see the social determinants of health that definitely make a difference – if we’re not seeing that association there, where we have a high proportion of African Americans who are at risk both for HIV and COVID-19 – I just don’t think it’s going to emerge,” he said.
This article first appeared on Medscape.com.
People living with HIV who are admitted to the hospital with COVID-19 are no more likely to die than those without HIV, an analysis conducted in New York City shows. This is despite the fact that comorbidities associated with worse COVID-19 outcomes were more common in the HIV group.
“We don’t see any signs that people with HIV should take extra precautions” to protect themselves from COVID-19, said Keith Sigel, MD, associate professor of medicine and infectious diseases at the Icahn School of Medicine at Mount Sinai, New York, and the lead researcher on the study, published online June 28 in Clinical Infectious Diseases.
“We still don’t have a great explanation for why we’re seeing what we’re seeing,” he added. “But we’re glad we’re seeing it.”
The findings have changed how Dr. Sigel talks to his patients with HIV about protecting themselves from COVID-19. Some patients have so curtailed their behavior for fear of acquiring COVID-19 that they aren’t buying groceries or attending needed medical appointments. With these data, Dr. Sigel said he’s comfortable telling his patients, “COVID-19 is bad all by itself, but you don’t need to go crazy. Wear a mask, practice appropriate social distancing and hygiene, but your risk doesn’t appear to be greater.”
The findings conform with those on the lack of association between HIV and COVID-19 severity seen in a cohort study from Spain, a case study from China, and case series from New Jersey, New York City, and Spain.
One of the only regions reporting something different so far is South Africa. There, HIV is the third most common comorbidity associated with death from COVID-19, according to a cohort analysis conducted in the province of Western Cape.
Along with data from HIV prevention and treatment trials, the conference will feature updates on where the world stands in the control of HIV during the COVID-19 pandemic. And for an even more focused look, the IAS COVID-19 Conference will immediately follow that meeting.
The New York City cohort
For their study, Dr. Sigel and colleagues examined the 4402 COVID-19 cases at the Mount Sinai Health System’s five hospitals between March 12 and April 23.
They found 88 people with COVID-19 whose charts showed codes indicating they were living with HIV. All 88 were receiving treatment, and 81% of them had undetectable viral loads documented at COVID admission or in the 12 months prior to admission.
The median age was 61 years, and 40% of the cohort was black and 30% was Hispanic.
Patients in the comparison group – 405 people without HIV from the Veterans Aging Cohort Study who had been admitted to the hospital for COVID-19 – were matched in terms of age, race, and stage of COVID-19.
The study had an 80% power to detect a 15% increase in the absolute risk for death in people with COVID-19, with or without HIV.
Patients with HIV were almost three times as likely to have smoked and were more likely to have chronic obstructive pulmonary disease, cirrhosis, and a history of cancer.
“This was a group of patients that one might suspect would do worse,” Dr. Sigel said. And yet, “we didn’t see any difference in deaths. We didn’t see any difference in respiratory failure.”
In fact, people with HIV required mechanical ventilation less often than those without HIV (18% vs. 23%). And when it came to mortality, one in five people died from COVID-19 during follow-up whether they had HIV or not (21% vs. 20%).
The only factor associated with significantly worse outcomes was a history of organ transplantation, “suggesting that non-HIV causes of immunodeficiency may be more prominent risks for severe outcomes,” Dr. Sigel and colleagues explained.
A surprise association
What’s more, the researchers found a slight association between the use of nucleoside reverse-transcriptase inhibitors (NRTI) by people with HIV and better outcomes in COVID-19. That echoes findings published June 26 in Annals of Internal Medicine, which showed that people with HIV taking the combination of tenofovir disoproxil fumarate plus emtricitabine (Truvada, Gilead Sciences) were less likely to be diagnosed with COVID-19, less likely to be hospitalized, and less likely to die.
This has led some to wonder whether NRTIs have some effect on SARS-CoV-2, the virus that causes COVID-19. Dr. Sigel said he wonders that too, but right now, it’s just musings.
“These studies are not even remotely designed” to show that NRTIs are protective against COVID-19, he explained. “Ours was extremely underpowered to detect that and there was a high potential for confounding.”
“I’d be wary of any study in a subpopulation – which is what we’re dealing with here – that is looking for signals of protection with certain medications,” he added.
A “modest” increase
Using the South African data, released on June 22, public health officials estimate that people with HIV are 2.75 times more likely to die from COVID-19 than those without HIV, making it the third most common comorbidity in people who died from COVID-19, behind diabetes and hypertension. This held true regardless of whether the people with HIV were on treatment.
But when they looked at COVID-19 deaths in the sickest of the sick – those hospitalized with COVID-19 symptoms – HIV was associated with just a 28% increase in the risk for death. The South African researchers called this risk “modest.”
“While these findings may overestimate the effect of HIV on COVID-19 death due to the presence of residual confounding, people living with HIV should be considered a high-risk group for COVID-19 management, with modestly elevated risk of poor outcomes, irrespective of viral suppression,” they wrote.
Epidemiologist Gregorio Millett, MPH, has been tracking the effect of HIV on COVID-19 outcomes since the start of the pandemic in his role as vice president and head of policy at the American Foundation for AIDS Research (amFAR).
Back in April, he and his colleagues looked at rates of COVID-19 deaths and hospitalizations in counties with disproportionate levels of black residents. These areas often overlapped with the communities selected for the Ending the HIV Epidemic plan to control HIV by 2030. What they found was that there was more HIV and COVID-19 in those communities.
What they didn’t find was that people with HIV in those communities had worse outcomes with COVID-19. This remained true even when they reran the analysis after the number of cases of COVID-19 in the United States surpassed 100,000. Those data have yet to be published, Mr. Millett reported.
“HIV does not pop out,” he said. “It’s still social determinants of health. It’s still underlying conditions. It’s still age as a primary factor.”
“People living with HIV are mainly dying of underlying conditions – so all the things associated with COVID-19 – rather than the association being with HIV itself,” he added.
Although he’s not ruling out the possibility that an association like the one in South Africa could emerge, Mr. Millett, who will present a plenary on the context of the HIV epidemic at the IAS conference, said he suspects we won’t see one.
“If we didn’t see an association with the counties that are disproportionately African American, in the black belt where we see high rates of HIV, particularly where we see the social determinants of health that definitely make a difference – if we’re not seeing that association there, where we have a high proportion of African Americans who are at risk both for HIV and COVID-19 – I just don’t think it’s going to emerge,” he said.
This article first appeared on Medscape.com.
FROM AIDS 2020