User login
Brensocatib reduced bronchiectasis exacerbations
Brensocatib, an experimental small-molecule inhibitor targeted to inflammation-regulating neutrophil serine proteases, may be a novel, nonantibiotic option for reducing exacerbations in patients with bronchiectasis, investigators in the phase 2 WILLOW study said.
Among 256 adults with a recent history of bronchiectasis exacerbations, oral brensocatib at doses of both 10 mg and 25 mg daily for 24 weeks was associated with significantly longer time to first exacerbation than placebo, and the 10-mg dose was associated with a significant reduction in the annualized rate of exacerbations, reported James Chalmers, MB, ChB, PhD of Ninewells Hospital and Medical School in Dundee (England).
“We also observed a dose-dependent reduction in neutrophil elastase levels in sputum, which supports the mechanism of action of this drug, and importantly showed a link between reducing neutrophil serine protease activity and clinical benefits in people with bronchiectasis,” he said in at the American Thoracic Society’s virtual clinical trial session.
“This is a very important trial, a landmark trial for people with bronchiectasis, because this is a drug that for the first time appears to be able to target directly neutrophilic inflammation, resulting in clinical benefit,” he said.
Pulmonologist Jennifer L. Taylor-Cousar, MD, MSCS, of National Jewish Health in Denver, who was facilitator for the online presentation but was not involved in the study, said that it offered welcome news.
“For those of us who treat bronchiectasis, a safe and effective anti-inflammatory has really been the Holy Grail, so this is really exciting,” she said.
Novel mechanism of action
Frequent exacerbations in bronchiectasis are related to uncontrolled neutrophilic inflammation, and proinflammatory neutrophil serine proteases (NSPs), including neutrophil elastase, are seen at increased levels in sputum of patients with bronchiectasis. In addition, the presence in sputum of elevated NSPs are associated with exacerbations and poor quality of life, Dr. Chalmers said.
Brensocatib is an inhibitor of dipeptidyl peptidase 1 (DPP1), a lysosomal cysteine protease that is responsible for NSP activation in bone marrow during the neutrophil maturation cycle.
In phase 1 trials, brensocatib was associated with a dose-dependent reduction in neutrophil elastase in healthy volunteers.
Three WILLOW branches
In the phase 2 WILLOW trial, patients with bronchiectasis not related to cystic fibrosis were screened and stratified by Pseudomonas aeruginosa on sputum culture and use of macrolide antibiotics and then randomized in equal proportions to receive either brensocatib at daily oral doses of 25 mg or 10 mg, or placebo for 24 weeks, followed by a 4-week off-treatment period.
Both doses of brensocatib met the primary endpoint of time to first exacerbation, compared with placebo. The hazard ratio (HR) for the 10-mg brensocatib dose, compared with placebo was 0.58 (P = .029), and the HR for the 25-mg dose was 0.62 (P = .046).
The exacerbation rate over 24 weeks among patients on placebo was 48.3%, compared with 31.7% of patients on 10 mg brensocatib (P = .033) and 33.3% of patients on the 25 mg dose (P = .038).
The annualized exacerbation rate was 1.37 for patients on placebo, compared with 0.88 with 10 mg brensocatib (P = .041) and 1.03 with 25 mg brensocatib (nonsignificant).
In both brensocatib groups there were significant reductions from baseline neutrophil elastase concentrations in sputum, compared with placebo (P = .034 for 10 mg and .021 for 25 mg). During the 4-week period following treatment neutrophil elastase levels in both active drug arms rose rapidly and returned to baseline.
The importance of these reductions was reflected in pooled data from the two brensocatib cohorts, which showed that patients who achieved neutrophil elastase levels below the limit of quantification had a significantly lower incidence of bronchiectasis exacerbations (HR 0.28, P < .0001).
Although the study was not powered to compare changes in postbronchodilator forced expiratory volume in 1 second (FEV1) levels, placebo-treated patients had a numerically larger decline in lung function from baseline, compared with brensocatib-treated patients.
Safety
Expected adverse events with brensocatib included those associated with Papillon-Lefèvre syndrome, a rare congenital condition caused by the absence of the gene coding for DPP1, resulting in keratinization leading to redness, thickening of soles and palms, and severe, destructive periodontal disease, as well as reduced immune response to bacterial infection.
Treatment-emergent adverse events (TEAEs) resulting in study discontinuation occurred in only three patients on placebo and 10 mg brensocatib, and four on the 25-mg dose. TEAEs resulting in treatment discontinuation were more common in the placebo arm, occurring in nine patients compared with six each in the brensocatib arms.
Serious TEAEs occurring in more than 3% of patients in any group included infective exacerbations in three patients on placebo, none on the 10-mg dose, and four on the 25-mg dose of brensocatib. Respective numbers of patients with treatment-emergent pneumonia were three, zero, and four.
Other TEAEs included cough, headache, sputum increase, dyspnea, and diarrhea.
Adverse events of special interest included skin events in 10 patients on placebo, 12 on the 10-mg dose, and 21 on the 25-mg brensocatib dose. Dental changes occurred in 3, 13, and 9 patients, and infections in 9, 12, and 14 patients, respectively.
A phase 3 study to confirm efficacy and establish the optimal dose of brensocatib is planned for the end of 2020, “COVID willing,” Dr. Chalmers said.
Dr. Chalmers disclosed consultancy with and research funding from Insmed, which funded the study. Dr. Taylor-Cousar has disclosed grants and/or personal fees from various companies.
Brensocatib, an experimental small-molecule inhibitor targeted to inflammation-regulating neutrophil serine proteases, may be a novel, nonantibiotic option for reducing exacerbations in patients with bronchiectasis, investigators in the phase 2 WILLOW study said.
Among 256 adults with a recent history of bronchiectasis exacerbations, oral brensocatib at doses of both 10 mg and 25 mg daily for 24 weeks was associated with significantly longer time to first exacerbation than placebo, and the 10-mg dose was associated with a significant reduction in the annualized rate of exacerbations, reported James Chalmers, MB, ChB, PhD of Ninewells Hospital and Medical School in Dundee (England).
“We also observed a dose-dependent reduction in neutrophil elastase levels in sputum, which supports the mechanism of action of this drug, and importantly showed a link between reducing neutrophil serine protease activity and clinical benefits in people with bronchiectasis,” he said in at the American Thoracic Society’s virtual clinical trial session.
“This is a very important trial, a landmark trial for people with bronchiectasis, because this is a drug that for the first time appears to be able to target directly neutrophilic inflammation, resulting in clinical benefit,” he said.
Pulmonologist Jennifer L. Taylor-Cousar, MD, MSCS, of National Jewish Health in Denver, who was facilitator for the online presentation but was not involved in the study, said that it offered welcome news.
“For those of us who treat bronchiectasis, a safe and effective anti-inflammatory has really been the Holy Grail, so this is really exciting,” she said.
Novel mechanism of action
Frequent exacerbations in bronchiectasis are related to uncontrolled neutrophilic inflammation, and proinflammatory neutrophil serine proteases (NSPs), including neutrophil elastase, are seen at increased levels in sputum of patients with bronchiectasis. In addition, the presence in sputum of elevated NSPs are associated with exacerbations and poor quality of life, Dr. Chalmers said.
Brensocatib is an inhibitor of dipeptidyl peptidase 1 (DPP1), a lysosomal cysteine protease that is responsible for NSP activation in bone marrow during the neutrophil maturation cycle.
In phase 1 trials, brensocatib was associated with a dose-dependent reduction in neutrophil elastase in healthy volunteers.
Three WILLOW branches
In the phase 2 WILLOW trial, patients with bronchiectasis not related to cystic fibrosis were screened and stratified by Pseudomonas aeruginosa on sputum culture and use of macrolide antibiotics and then randomized in equal proportions to receive either brensocatib at daily oral doses of 25 mg or 10 mg, or placebo for 24 weeks, followed by a 4-week off-treatment period.
Both doses of brensocatib met the primary endpoint of time to first exacerbation, compared with placebo. The hazard ratio (HR) for the 10-mg brensocatib dose, compared with placebo was 0.58 (P = .029), and the HR for the 25-mg dose was 0.62 (P = .046).
The exacerbation rate over 24 weeks among patients on placebo was 48.3%, compared with 31.7% of patients on 10 mg brensocatib (P = .033) and 33.3% of patients on the 25 mg dose (P = .038).
The annualized exacerbation rate was 1.37 for patients on placebo, compared with 0.88 with 10 mg brensocatib (P = .041) and 1.03 with 25 mg brensocatib (nonsignificant).
In both brensocatib groups there were significant reductions from baseline neutrophil elastase concentrations in sputum, compared with placebo (P = .034 for 10 mg and .021 for 25 mg). During the 4-week period following treatment neutrophil elastase levels in both active drug arms rose rapidly and returned to baseline.
The importance of these reductions was reflected in pooled data from the two brensocatib cohorts, which showed that patients who achieved neutrophil elastase levels below the limit of quantification had a significantly lower incidence of bronchiectasis exacerbations (HR 0.28, P < .0001).
Although the study was not powered to compare changes in postbronchodilator forced expiratory volume in 1 second (FEV1) levels, placebo-treated patients had a numerically larger decline in lung function from baseline, compared with brensocatib-treated patients.
Safety
Expected adverse events with brensocatib included those associated with Papillon-Lefèvre syndrome, a rare congenital condition caused by the absence of the gene coding for DPP1, resulting in keratinization leading to redness, thickening of soles and palms, and severe, destructive periodontal disease, as well as reduced immune response to bacterial infection.
Treatment-emergent adverse events (TEAEs) resulting in study discontinuation occurred in only three patients on placebo and 10 mg brensocatib, and four on the 25-mg dose. TEAEs resulting in treatment discontinuation were more common in the placebo arm, occurring in nine patients compared with six each in the brensocatib arms.
Serious TEAEs occurring in more than 3% of patients in any group included infective exacerbations in three patients on placebo, none on the 10-mg dose, and four on the 25-mg dose of brensocatib. Respective numbers of patients with treatment-emergent pneumonia were three, zero, and four.
Other TEAEs included cough, headache, sputum increase, dyspnea, and diarrhea.
Adverse events of special interest included skin events in 10 patients on placebo, 12 on the 10-mg dose, and 21 on the 25-mg brensocatib dose. Dental changes occurred in 3, 13, and 9 patients, and infections in 9, 12, and 14 patients, respectively.
A phase 3 study to confirm efficacy and establish the optimal dose of brensocatib is planned for the end of 2020, “COVID willing,” Dr. Chalmers said.
Dr. Chalmers disclosed consultancy with and research funding from Insmed, which funded the study. Dr. Taylor-Cousar has disclosed grants and/or personal fees from various companies.
Brensocatib, an experimental small-molecule inhibitor targeted to inflammation-regulating neutrophil serine proteases, may be a novel, nonantibiotic option for reducing exacerbations in patients with bronchiectasis, investigators in the phase 2 WILLOW study said.
Among 256 adults with a recent history of bronchiectasis exacerbations, oral brensocatib at doses of both 10 mg and 25 mg daily for 24 weeks was associated with significantly longer time to first exacerbation than placebo, and the 10-mg dose was associated with a significant reduction in the annualized rate of exacerbations, reported James Chalmers, MB, ChB, PhD of Ninewells Hospital and Medical School in Dundee (England).
“We also observed a dose-dependent reduction in neutrophil elastase levels in sputum, which supports the mechanism of action of this drug, and importantly showed a link between reducing neutrophil serine protease activity and clinical benefits in people with bronchiectasis,” he said in at the American Thoracic Society’s virtual clinical trial session.
“This is a very important trial, a landmark trial for people with bronchiectasis, because this is a drug that for the first time appears to be able to target directly neutrophilic inflammation, resulting in clinical benefit,” he said.
Pulmonologist Jennifer L. Taylor-Cousar, MD, MSCS, of National Jewish Health in Denver, who was facilitator for the online presentation but was not involved in the study, said that it offered welcome news.
“For those of us who treat bronchiectasis, a safe and effective anti-inflammatory has really been the Holy Grail, so this is really exciting,” she said.
Novel mechanism of action
Frequent exacerbations in bronchiectasis are related to uncontrolled neutrophilic inflammation, and proinflammatory neutrophil serine proteases (NSPs), including neutrophil elastase, are seen at increased levels in sputum of patients with bronchiectasis. In addition, the presence in sputum of elevated NSPs are associated with exacerbations and poor quality of life, Dr. Chalmers said.
Brensocatib is an inhibitor of dipeptidyl peptidase 1 (DPP1), a lysosomal cysteine protease that is responsible for NSP activation in bone marrow during the neutrophil maturation cycle.
In phase 1 trials, brensocatib was associated with a dose-dependent reduction in neutrophil elastase in healthy volunteers.
Three WILLOW branches
In the phase 2 WILLOW trial, patients with bronchiectasis not related to cystic fibrosis were screened and stratified by Pseudomonas aeruginosa on sputum culture and use of macrolide antibiotics and then randomized in equal proportions to receive either brensocatib at daily oral doses of 25 mg or 10 mg, or placebo for 24 weeks, followed by a 4-week off-treatment period.
Both doses of brensocatib met the primary endpoint of time to first exacerbation, compared with placebo. The hazard ratio (HR) for the 10-mg brensocatib dose, compared with placebo was 0.58 (P = .029), and the HR for the 25-mg dose was 0.62 (P = .046).
The exacerbation rate over 24 weeks among patients on placebo was 48.3%, compared with 31.7% of patients on 10 mg brensocatib (P = .033) and 33.3% of patients on the 25 mg dose (P = .038).
The annualized exacerbation rate was 1.37 for patients on placebo, compared with 0.88 with 10 mg brensocatib (P = .041) and 1.03 with 25 mg brensocatib (nonsignificant).
In both brensocatib groups there were significant reductions from baseline neutrophil elastase concentrations in sputum, compared with placebo (P = .034 for 10 mg and .021 for 25 mg). During the 4-week period following treatment neutrophil elastase levels in both active drug arms rose rapidly and returned to baseline.
The importance of these reductions was reflected in pooled data from the two brensocatib cohorts, which showed that patients who achieved neutrophil elastase levels below the limit of quantification had a significantly lower incidence of bronchiectasis exacerbations (HR 0.28, P < .0001).
Although the study was not powered to compare changes in postbronchodilator forced expiratory volume in 1 second (FEV1) levels, placebo-treated patients had a numerically larger decline in lung function from baseline, compared with brensocatib-treated patients.
Safety
Expected adverse events with brensocatib included those associated with Papillon-Lefèvre syndrome, a rare congenital condition caused by the absence of the gene coding for DPP1, resulting in keratinization leading to redness, thickening of soles and palms, and severe, destructive periodontal disease, as well as reduced immune response to bacterial infection.
Treatment-emergent adverse events (TEAEs) resulting in study discontinuation occurred in only three patients on placebo and 10 mg brensocatib, and four on the 25-mg dose. TEAEs resulting in treatment discontinuation were more common in the placebo arm, occurring in nine patients compared with six each in the brensocatib arms.
Serious TEAEs occurring in more than 3% of patients in any group included infective exacerbations in three patients on placebo, none on the 10-mg dose, and four on the 25-mg dose of brensocatib. Respective numbers of patients with treatment-emergent pneumonia were three, zero, and four.
Other TEAEs included cough, headache, sputum increase, dyspnea, and diarrhea.
Adverse events of special interest included skin events in 10 patients on placebo, 12 on the 10-mg dose, and 21 on the 25-mg brensocatib dose. Dental changes occurred in 3, 13, and 9 patients, and infections in 9, 12, and 14 patients, respectively.
A phase 3 study to confirm efficacy and establish the optimal dose of brensocatib is planned for the end of 2020, “COVID willing,” Dr. Chalmers said.
Dr. Chalmers disclosed consultancy with and research funding from Insmed, which funded the study. Dr. Taylor-Cousar has disclosed grants and/or personal fees from various companies.
FROM ATS 2020
Breast density asymmetry might increase breast cancer risk
The 854 women in the study had been referred for biopsy after an abnormal mammogram.
Researchers used the mammograms to assess global bilateral asymmetry, which was the overall absolute difference in percent fibroglandular tissue volume (%FGV) between the ipsilateral (biopsied) breast and the contralateral (unaffected) breast.
The researchers also assessed local bilateral asymmetry, which was the perilesional %FGV difference in an area twice the size of, but excluding, the biopsy target, and the corresponding area in the unaffected breast.
The women were then divided into quartiles based on breast density asymmetry.
Most of the women had benign breast disease, including proliferative (43%) and nonproliferative (33%) disease, but 23% had carcinoma in situ or invasive breast cancer.
The trend for higher risk of in situ or invasive cancer with increasing breast density asymmetry was observed only in the local analysis. The odds ratio was 1.59 (95% confidence interval, 0.94-2.69) for women in the highest quartile of breast density asymmetry (absolute difference, > 8.23) versus those in the lowest quartile (absolute difference, ≤ –5.55; P = .067).
When compared with women who had proliferative benign disease, women with carcinoma in situ or invasive breast cancer “were more likely to be in the higher than lower quartiles,” said lead investigator Maeve Mullooly, PhD, a research fellow at the Royal College of Surgeons in Dublin.
There was no association between breast density asymmetry and traditional breast cancer risk factors such as age, body mass index, race, and hormone therapy. However, among women diagnosed with benign nonproliferative disease, women with a breast cancer family history were more likely to have higher overall breast density asymmetry.
Study rationale and details
Higher breast density is a known risk factor for breast cancer. Breast asymmetry also has been reported as a possible risk factor (Breast Cancer Res. 2006;8[2]:R14), and incorporation of breast density asymmetry into traditional risk factors in one study improved risk prediction (Breast Cancer Res. 2017 Mar 14;19[1]:29).
Building on that work, the goal of Dr. Mullooly’s study was to “learn how to better use breast density to inform breast cancer risk prediction,” she said.
To that end, her team turned to 854 women enrolled from 2007-2010 in the National Cancer Institute’s Breast Radiology Evaluation and Study of Tissues Project, a cross-sectional molecular epidemiologic study designed to understand how breast density measures are related to breast cancer etiology.
Most of the women were non-Hispanic white. The mean age was 51 years (range, 40-65), and the median body mass index was 25 kg/m2.
About three-quarters of the women (76%) had a breast density asymmetry of at least 2% on the global analysis, with 43% having higher %FGV in the biopsied breast and 33% having higher %FGV in the unaffected breast. In all, 89% of women had local breast density asymmetry, with higher density in the biopsied breast in 61% of women and higher density in the contralateral breast in 28%.
Next steps
This research is ongoing, and additional follow-up is planned, according to Dr. Mullooly. She said the researchers hope to apply more recent analytical techniques to the mammograms and to study the histologic differences in their breast biopsy specimens, among other steps, to see if stronger relationships with greater clinical utility emerge.
It was a “very well done study” with “very provocative data,” said presentation moderator Jennifer Wargo, MD, professor of genomic medicine and surgical oncology at the University of Texas MD Anderson Cancer Center in Houston.
She was interested in the planned next steps, particularly the histologic analysis of dense versus less dense breast tissue. There could be “differences in stroma or hormonal levels even at the microenvironmental level” that “represent a potential field defect, which later puts someone at risk,” she said, adding that it’s “great” that the work is continuing.
The National Cancer Institute funded the research. Dr. Mullooly reported no relevant disclosures. Dr. Wargo disclosed relationships with Bristol-Myers Squibb, Roche/Genentech, Novartis, GlaxoSmithKline, AstraZeneca, Imedex, Dava Oncology, Omniprex, Illumina, Gilead, PeerView, Physician Education Resource, MedImmune, Merck, Biothera Pharmaceuticals, and Microbiome DX.
SOURCE: Mullooly M et al. AACR 2020, Abstract NG15.
The 854 women in the study had been referred for biopsy after an abnormal mammogram.
Researchers used the mammograms to assess global bilateral asymmetry, which was the overall absolute difference in percent fibroglandular tissue volume (%FGV) between the ipsilateral (biopsied) breast and the contralateral (unaffected) breast.
The researchers also assessed local bilateral asymmetry, which was the perilesional %FGV difference in an area twice the size of, but excluding, the biopsy target, and the corresponding area in the unaffected breast.
The women were then divided into quartiles based on breast density asymmetry.
Most of the women had benign breast disease, including proliferative (43%) and nonproliferative (33%) disease, but 23% had carcinoma in situ or invasive breast cancer.
The trend for higher risk of in situ or invasive cancer with increasing breast density asymmetry was observed only in the local analysis. The odds ratio was 1.59 (95% confidence interval, 0.94-2.69) for women in the highest quartile of breast density asymmetry (absolute difference, > 8.23) versus those in the lowest quartile (absolute difference, ≤ –5.55; P = .067).
When compared with women who had proliferative benign disease, women with carcinoma in situ or invasive breast cancer “were more likely to be in the higher than lower quartiles,” said lead investigator Maeve Mullooly, PhD, a research fellow at the Royal College of Surgeons in Dublin.
There was no association between breast density asymmetry and traditional breast cancer risk factors such as age, body mass index, race, and hormone therapy. However, among women diagnosed with benign nonproliferative disease, women with a breast cancer family history were more likely to have higher overall breast density asymmetry.
Study rationale and details
Higher breast density is a known risk factor for breast cancer. Breast asymmetry also has been reported as a possible risk factor (Breast Cancer Res. 2006;8[2]:R14), and incorporation of breast density asymmetry into traditional risk factors in one study improved risk prediction (Breast Cancer Res. 2017 Mar 14;19[1]:29).
Building on that work, the goal of Dr. Mullooly’s study was to “learn how to better use breast density to inform breast cancer risk prediction,” she said.
To that end, her team turned to 854 women enrolled from 2007-2010 in the National Cancer Institute’s Breast Radiology Evaluation and Study of Tissues Project, a cross-sectional molecular epidemiologic study designed to understand how breast density measures are related to breast cancer etiology.
Most of the women were non-Hispanic white. The mean age was 51 years (range, 40-65), and the median body mass index was 25 kg/m2.
About three-quarters of the women (76%) had a breast density asymmetry of at least 2% on the global analysis, with 43% having higher %FGV in the biopsied breast and 33% having higher %FGV in the unaffected breast. In all, 89% of women had local breast density asymmetry, with higher density in the biopsied breast in 61% of women and higher density in the contralateral breast in 28%.
Next steps
This research is ongoing, and additional follow-up is planned, according to Dr. Mullooly. She said the researchers hope to apply more recent analytical techniques to the mammograms and to study the histologic differences in their breast biopsy specimens, among other steps, to see if stronger relationships with greater clinical utility emerge.
It was a “very well done study” with “very provocative data,” said presentation moderator Jennifer Wargo, MD, professor of genomic medicine and surgical oncology at the University of Texas MD Anderson Cancer Center in Houston.
She was interested in the planned next steps, particularly the histologic analysis of dense versus less dense breast tissue. There could be “differences in stroma or hormonal levels even at the microenvironmental level” that “represent a potential field defect, which later puts someone at risk,” she said, adding that it’s “great” that the work is continuing.
The National Cancer Institute funded the research. Dr. Mullooly reported no relevant disclosures. Dr. Wargo disclosed relationships with Bristol-Myers Squibb, Roche/Genentech, Novartis, GlaxoSmithKline, AstraZeneca, Imedex, Dava Oncology, Omniprex, Illumina, Gilead, PeerView, Physician Education Resource, MedImmune, Merck, Biothera Pharmaceuticals, and Microbiome DX.
SOURCE: Mullooly M et al. AACR 2020, Abstract NG15.
The 854 women in the study had been referred for biopsy after an abnormal mammogram.
Researchers used the mammograms to assess global bilateral asymmetry, which was the overall absolute difference in percent fibroglandular tissue volume (%FGV) between the ipsilateral (biopsied) breast and the contralateral (unaffected) breast.
The researchers also assessed local bilateral asymmetry, which was the perilesional %FGV difference in an area twice the size of, but excluding, the biopsy target, and the corresponding area in the unaffected breast.
The women were then divided into quartiles based on breast density asymmetry.
Most of the women had benign breast disease, including proliferative (43%) and nonproliferative (33%) disease, but 23% had carcinoma in situ or invasive breast cancer.
The trend for higher risk of in situ or invasive cancer with increasing breast density asymmetry was observed only in the local analysis. The odds ratio was 1.59 (95% confidence interval, 0.94-2.69) for women in the highest quartile of breast density asymmetry (absolute difference, > 8.23) versus those in the lowest quartile (absolute difference, ≤ –5.55; P = .067).
When compared with women who had proliferative benign disease, women with carcinoma in situ or invasive breast cancer “were more likely to be in the higher than lower quartiles,” said lead investigator Maeve Mullooly, PhD, a research fellow at the Royal College of Surgeons in Dublin.
There was no association between breast density asymmetry and traditional breast cancer risk factors such as age, body mass index, race, and hormone therapy. However, among women diagnosed with benign nonproliferative disease, women with a breast cancer family history were more likely to have higher overall breast density asymmetry.
Study rationale and details
Higher breast density is a known risk factor for breast cancer. Breast asymmetry also has been reported as a possible risk factor (Breast Cancer Res. 2006;8[2]:R14), and incorporation of breast density asymmetry into traditional risk factors in one study improved risk prediction (Breast Cancer Res. 2017 Mar 14;19[1]:29).
Building on that work, the goal of Dr. Mullooly’s study was to “learn how to better use breast density to inform breast cancer risk prediction,” she said.
To that end, her team turned to 854 women enrolled from 2007-2010 in the National Cancer Institute’s Breast Radiology Evaluation and Study of Tissues Project, a cross-sectional molecular epidemiologic study designed to understand how breast density measures are related to breast cancer etiology.
Most of the women were non-Hispanic white. The mean age was 51 years (range, 40-65), and the median body mass index was 25 kg/m2.
About three-quarters of the women (76%) had a breast density asymmetry of at least 2% on the global analysis, with 43% having higher %FGV in the biopsied breast and 33% having higher %FGV in the unaffected breast. In all, 89% of women had local breast density asymmetry, with higher density in the biopsied breast in 61% of women and higher density in the contralateral breast in 28%.
Next steps
This research is ongoing, and additional follow-up is planned, according to Dr. Mullooly. She said the researchers hope to apply more recent analytical techniques to the mammograms and to study the histologic differences in their breast biopsy specimens, among other steps, to see if stronger relationships with greater clinical utility emerge.
It was a “very well done study” with “very provocative data,” said presentation moderator Jennifer Wargo, MD, professor of genomic medicine and surgical oncology at the University of Texas MD Anderson Cancer Center in Houston.
She was interested in the planned next steps, particularly the histologic analysis of dense versus less dense breast tissue. There could be “differences in stroma or hormonal levels even at the microenvironmental level” that “represent a potential field defect, which later puts someone at risk,” she said, adding that it’s “great” that the work is continuing.
The National Cancer Institute funded the research. Dr. Mullooly reported no relevant disclosures. Dr. Wargo disclosed relationships with Bristol-Myers Squibb, Roche/Genentech, Novartis, GlaxoSmithKline, AstraZeneca, Imedex, Dava Oncology, Omniprex, Illumina, Gilead, PeerView, Physician Education Resource, MedImmune, Merck, Biothera Pharmaceuticals, and Microbiome DX.
SOURCE: Mullooly M et al. AACR 2020, Abstract NG15.
FROM AACR 2020
Asymptomatic Plaque on the Scalp
The Diagnosis: Nevus Comedonicus
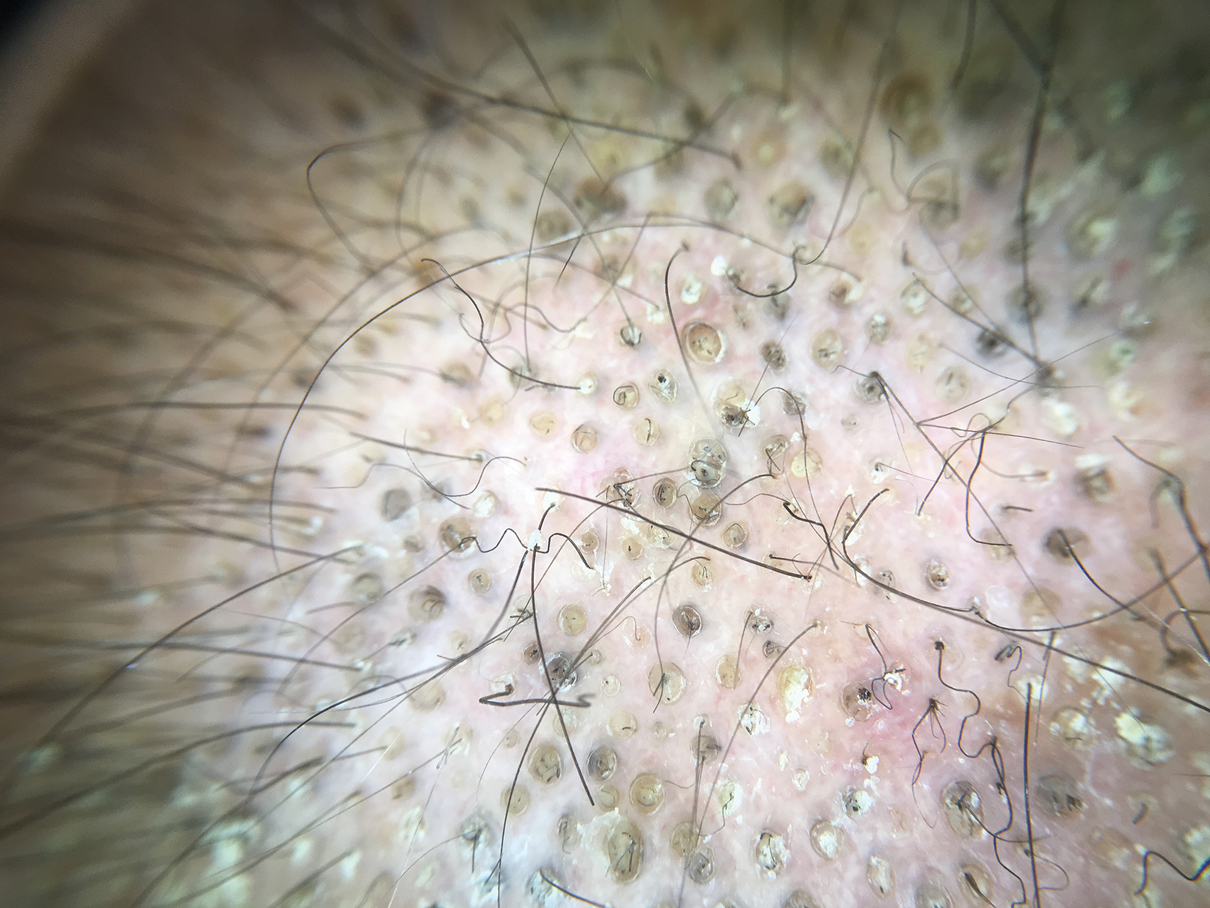
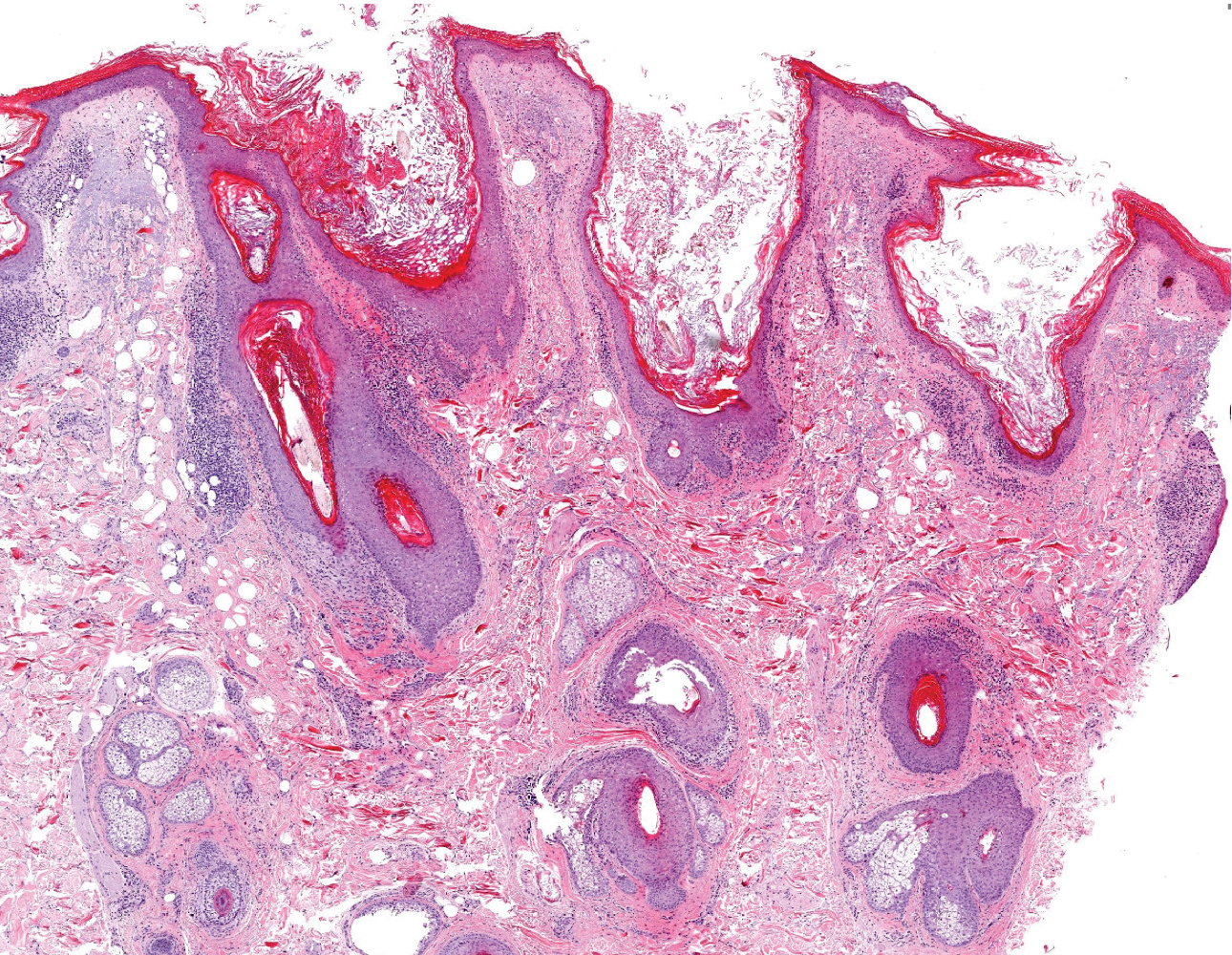
Dermoscopy showed multiple dilated follicular openings plugged with keratinous material (Figure 1). Histopathology revealed dilated follicular infundibula with dilation and orthokeratotic plugging (Figure 2). Routine laboratory tests including complete blood cell count and blood chemistry were within reference range. Thus, on the basis of clinical, dermoscopy, and histopathological findings, a diagnosis of nevus comedonicus (NC) was made. The patient refused treatment for cosmetic reasons.
Nevus comedonicus is a rare hamartoma first described by Kofmann1 in 1895. It is thought to be a developmental defect of the pilosebaceous unit; the resulting structure is unable to produce mature hairs, matrix cells, or sebaceous glands and is capable only of forming soft keratin.2 Clinically, it is characterized by closely grouped papules with hyperkeratotic plugs that mimic comedones. It has a predilection for the face, neck, and trunk area. Nevertheless, scalp involvement rarely has been reported in the literature.2-4 Nevus comedonicus usually appears at birth or during childhood and generally is asymptomatic; however, an inflammatory variant of NC with cyst formation and recurrent infections also has been described.5 Moreover, a syndromic variant was reported and characterized by a combination of NC with ocular, skeletal, or neurological defects.5 Most lesions grow proportionately with age and usually stabilize by late adolescence.2 Our patient's plaque increased in size with age. No triggering factors were found. Although NC usually has a benign course, squamous cell carcinoma arising in NC has been reported.6 Consequently, routine surveillance is necessary.
Diagnosis often is easily made by considering the characteristic morphology of the lesions and the early age of its appearance. However, in atypical NC presentations, acne, seborrheic keratosis, porokeratotic eccrine ostial and dermal duct nevus, folliculotropic mycosis fungoides, Favre-Racouchot syndrome, or familial dyskeratotic comedones should be considered. Dermoscopy has been reported to be useful in the diagnosis of NC. Typical dermoscopy findings are numerous circular and barrel-shaped homogenous areas in light and dark brown shades with remarkable keratin plugs.7,8
Folliculotropic mycosis fungoides is a variant of mycosis fungoides characterized by hair follicle invasion of mature, CD4+, small, lymphoid cells with cerebriform nuclei.9 Patients may present with grouped follicular papules that preferentially involve the head and neck area. It typically occurs in adults but occasionally may affect children. Histopathology is characterized by the presence of folliculotropic infiltrates with variable infiltration of the follicular epithelium, often with sparing of the epidermis. Familial dyskeratotic comedones, rare autosomal-dominant genodermatoses, clinically are characterized by symmetrically scattered comedonelike hyperkeratotic papules. These lesions appear around puberty and show a predilection for the trunk, arms, and face. Histopathology reveals craterlike invaginations filled with keratinous material and evidence of dyskeratosis. Porokeratotic eccrine ostial and dermal duct nevus is a rare adnexal hamartoma with eccrine differentiation. It is characterized by asymptomatic grouped keratotic papules and plaques. The lesions usually present at birth or in childhood and favor the palms and soles. Widespread involvement along Blaschko lines also can occur. Cornoid lamella involving an eccrine duct is the characteristic histopathologic feature of this condition.9
Treatment of NC is essentially reserved for cosmetic reasons or when there are complications such as discomfort or infection. Treatment options include topical corticosteroids, topical retinoids, and keratolytic agents such as ammonium lactate or salicylic acid.10 The use of oral isotretinoin is controversial.2 Surgical excision is useful for localized lesions. Nevus comedonicus, especially occurring at unusual sites such as the scalp, is uncommon. Therefore, a high index of suspicion is required to reach a diagnosis.
- Kofmann S. Ein fall von seltener localisation und verbreitiing von comedonen. Arch Derm Syph. 1895;32:177-178.
- Sikorski D, Parker J, Shwayder T. A boy with an unusual scalp birthmark. Int J Dermatol. 2011;50:670-672.
- Ghaninezhad H, Ehsani AH, Mansoori P, et al. Naevus comedonicus of the scalp. J Eur Acad Dermatol Venereol. 2006;20:184-185.
- Kikkeri N, Priyanka R, Parshawanath H. Nevus comedonicus on scalp: a rare site. Indian J Dermatol. 2015;60:105.
- Happle R. The group of epidermal nevus syndromes. J Am Acad Dermatol. 2010;63:1-22.
- Walling HW, Swick BL. Squamous cell carcinoma arising in nevus comedonicus. Dermatol Surg. 2009;35:144-146.
- Kamin´ska-Winciorek G, S´piewak R. Dermoscopy on nevus comedonicus: a case report and review of the literature. Postepy Dermatol Alergol. 2013;30:252-254.
- Vora R, Kota R, Sheth N. Dermoscopy of nevus comedonicus. Indian Dermatol Online J. 2017;8:388.
- Wang NS, Meola T, Orlow SJ, et al. Porokeratotic eccrine ostial and dermal duct nevus: a report of 2 cases and review of the literature. Am J Dermatopathol. 2009;31:582-586.
- Ferrari B, Taliercio V, Restrepo P, et al. Nevus comedonicus: a case series. Pediatr Dermatol. 2015;32:216-219
The Diagnosis: Nevus Comedonicus
Dermoscopy showed multiple dilated follicular openings plugged with keratinous material (Figure 1). Histopathology revealed dilated follicular infundibula with dilation and orthokeratotic plugging (Figure 2). Routine laboratory tests including complete blood cell count and blood chemistry were within reference range. Thus, on the basis of clinical, dermoscopy, and histopathological findings, a diagnosis of nevus comedonicus (NC) was made. The patient refused treatment for cosmetic reasons.
Nevus comedonicus is a rare hamartoma first described by Kofmann1 in 1895. It is thought to be a developmental defect of the pilosebaceous unit; the resulting structure is unable to produce mature hairs, matrix cells, or sebaceous glands and is capable only of forming soft keratin.2 Clinically, it is characterized by closely grouped papules with hyperkeratotic plugs that mimic comedones. It has a predilection for the face, neck, and trunk area. Nevertheless, scalp involvement rarely has been reported in the literature.2-4 Nevus comedonicus usually appears at birth or during childhood and generally is asymptomatic; however, an inflammatory variant of NC with cyst formation and recurrent infections also has been described.5 Moreover, a syndromic variant was reported and characterized by a combination of NC with ocular, skeletal, or neurological defects.5 Most lesions grow proportionately with age and usually stabilize by late adolescence.2 Our patient's plaque increased in size with age. No triggering factors were found. Although NC usually has a benign course, squamous cell carcinoma arising in NC has been reported.6 Consequently, routine surveillance is necessary.
Diagnosis often is easily made by considering the characteristic morphology of the lesions and the early age of its appearance. However, in atypical NC presentations, acne, seborrheic keratosis, porokeratotic eccrine ostial and dermal duct nevus, folliculotropic mycosis fungoides, Favre-Racouchot syndrome, or familial dyskeratotic comedones should be considered. Dermoscopy has been reported to be useful in the diagnosis of NC. Typical dermoscopy findings are numerous circular and barrel-shaped homogenous areas in light and dark brown shades with remarkable keratin plugs.7,8
Folliculotropic mycosis fungoides is a variant of mycosis fungoides characterized by hair follicle invasion of mature, CD4+, small, lymphoid cells with cerebriform nuclei.9 Patients may present with grouped follicular papules that preferentially involve the head and neck area. It typically occurs in adults but occasionally may affect children. Histopathology is characterized by the presence of folliculotropic infiltrates with variable infiltration of the follicular epithelium, often with sparing of the epidermis. Familial dyskeratotic comedones, rare autosomal-dominant genodermatoses, clinically are characterized by symmetrically scattered comedonelike hyperkeratotic papules. These lesions appear around puberty and show a predilection for the trunk, arms, and face. Histopathology reveals craterlike invaginations filled with keratinous material and evidence of dyskeratosis. Porokeratotic eccrine ostial and dermal duct nevus is a rare adnexal hamartoma with eccrine differentiation. It is characterized by asymptomatic grouped keratotic papules and plaques. The lesions usually present at birth or in childhood and favor the palms and soles. Widespread involvement along Blaschko lines also can occur. Cornoid lamella involving an eccrine duct is the characteristic histopathologic feature of this condition.9
Treatment of NC is essentially reserved for cosmetic reasons or when there are complications such as discomfort or infection. Treatment options include topical corticosteroids, topical retinoids, and keratolytic agents such as ammonium lactate or salicylic acid.10 The use of oral isotretinoin is controversial.2 Surgical excision is useful for localized lesions. Nevus comedonicus, especially occurring at unusual sites such as the scalp, is uncommon. Therefore, a high index of suspicion is required to reach a diagnosis.
The Diagnosis: Nevus Comedonicus
Dermoscopy showed multiple dilated follicular openings plugged with keratinous material (Figure 1). Histopathology revealed dilated follicular infundibula with dilation and orthokeratotic plugging (Figure 2). Routine laboratory tests including complete blood cell count and blood chemistry were within reference range. Thus, on the basis of clinical, dermoscopy, and histopathological findings, a diagnosis of nevus comedonicus (NC) was made. The patient refused treatment for cosmetic reasons.
Nevus comedonicus is a rare hamartoma first described by Kofmann1 in 1895. It is thought to be a developmental defect of the pilosebaceous unit; the resulting structure is unable to produce mature hairs, matrix cells, or sebaceous glands and is capable only of forming soft keratin.2 Clinically, it is characterized by closely grouped papules with hyperkeratotic plugs that mimic comedones. It has a predilection for the face, neck, and trunk area. Nevertheless, scalp involvement rarely has been reported in the literature.2-4 Nevus comedonicus usually appears at birth or during childhood and generally is asymptomatic; however, an inflammatory variant of NC with cyst formation and recurrent infections also has been described.5 Moreover, a syndromic variant was reported and characterized by a combination of NC with ocular, skeletal, or neurological defects.5 Most lesions grow proportionately with age and usually stabilize by late adolescence.2 Our patient's plaque increased in size with age. No triggering factors were found. Although NC usually has a benign course, squamous cell carcinoma arising in NC has been reported.6 Consequently, routine surveillance is necessary.
Diagnosis often is easily made by considering the characteristic morphology of the lesions and the early age of its appearance. However, in atypical NC presentations, acne, seborrheic keratosis, porokeratotic eccrine ostial and dermal duct nevus, folliculotropic mycosis fungoides, Favre-Racouchot syndrome, or familial dyskeratotic comedones should be considered. Dermoscopy has been reported to be useful in the diagnosis of NC. Typical dermoscopy findings are numerous circular and barrel-shaped homogenous areas in light and dark brown shades with remarkable keratin plugs.7,8
Folliculotropic mycosis fungoides is a variant of mycosis fungoides characterized by hair follicle invasion of mature, CD4+, small, lymphoid cells with cerebriform nuclei.9 Patients may present with grouped follicular papules that preferentially involve the head and neck area. It typically occurs in adults but occasionally may affect children. Histopathology is characterized by the presence of folliculotropic infiltrates with variable infiltration of the follicular epithelium, often with sparing of the epidermis. Familial dyskeratotic comedones, rare autosomal-dominant genodermatoses, clinically are characterized by symmetrically scattered comedonelike hyperkeratotic papules. These lesions appear around puberty and show a predilection for the trunk, arms, and face. Histopathology reveals craterlike invaginations filled with keratinous material and evidence of dyskeratosis. Porokeratotic eccrine ostial and dermal duct nevus is a rare adnexal hamartoma with eccrine differentiation. It is characterized by asymptomatic grouped keratotic papules and plaques. The lesions usually present at birth or in childhood and favor the palms and soles. Widespread involvement along Blaschko lines also can occur. Cornoid lamella involving an eccrine duct is the characteristic histopathologic feature of this condition.9
Treatment of NC is essentially reserved for cosmetic reasons or when there are complications such as discomfort or infection. Treatment options include topical corticosteroids, topical retinoids, and keratolytic agents such as ammonium lactate or salicylic acid.10 The use of oral isotretinoin is controversial.2 Surgical excision is useful for localized lesions. Nevus comedonicus, especially occurring at unusual sites such as the scalp, is uncommon. Therefore, a high index of suspicion is required to reach a diagnosis.
- Kofmann S. Ein fall von seltener localisation und verbreitiing von comedonen. Arch Derm Syph. 1895;32:177-178.
- Sikorski D, Parker J, Shwayder T. A boy with an unusual scalp birthmark. Int J Dermatol. 2011;50:670-672.
- Ghaninezhad H, Ehsani AH, Mansoori P, et al. Naevus comedonicus of the scalp. J Eur Acad Dermatol Venereol. 2006;20:184-185.
- Kikkeri N, Priyanka R, Parshawanath H. Nevus comedonicus on scalp: a rare site. Indian J Dermatol. 2015;60:105.
- Happle R. The group of epidermal nevus syndromes. J Am Acad Dermatol. 2010;63:1-22.
- Walling HW, Swick BL. Squamous cell carcinoma arising in nevus comedonicus. Dermatol Surg. 2009;35:144-146.
- Kamin´ska-Winciorek G, S´piewak R. Dermoscopy on nevus comedonicus: a case report and review of the literature. Postepy Dermatol Alergol. 2013;30:252-254.
- Vora R, Kota R, Sheth N. Dermoscopy of nevus comedonicus. Indian Dermatol Online J. 2017;8:388.
- Wang NS, Meola T, Orlow SJ, et al. Porokeratotic eccrine ostial and dermal duct nevus: a report of 2 cases and review of the literature. Am J Dermatopathol. 2009;31:582-586.
- Ferrari B, Taliercio V, Restrepo P, et al. Nevus comedonicus: a case series. Pediatr Dermatol. 2015;32:216-219
- Kofmann S. Ein fall von seltener localisation und verbreitiing von comedonen. Arch Derm Syph. 1895;32:177-178.
- Sikorski D, Parker J, Shwayder T. A boy with an unusual scalp birthmark. Int J Dermatol. 2011;50:670-672.
- Ghaninezhad H, Ehsani AH, Mansoori P, et al. Naevus comedonicus of the scalp. J Eur Acad Dermatol Venereol. 2006;20:184-185.
- Kikkeri N, Priyanka R, Parshawanath H. Nevus comedonicus on scalp: a rare site. Indian J Dermatol. 2015;60:105.
- Happle R. The group of epidermal nevus syndromes. J Am Acad Dermatol. 2010;63:1-22.
- Walling HW, Swick BL. Squamous cell carcinoma arising in nevus comedonicus. Dermatol Surg. 2009;35:144-146.
- Kamin´ska-Winciorek G, S´piewak R. Dermoscopy on nevus comedonicus: a case report and review of the literature. Postepy Dermatol Alergol. 2013;30:252-254.
- Vora R, Kota R, Sheth N. Dermoscopy of nevus comedonicus. Indian Dermatol Online J. 2017;8:388.
- Wang NS, Meola T, Orlow SJ, et al. Porokeratotic eccrine ostial and dermal duct nevus: a report of 2 cases and review of the literature. Am J Dermatopathol. 2009;31:582-586.
- Ferrari B, Taliercio V, Restrepo P, et al. Nevus comedonicus: a case series. Pediatr Dermatol. 2015;32:216-219

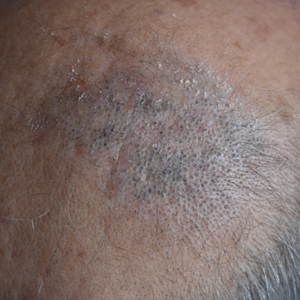
A 50-year-old man presented to the dermatology department with an asymptomatic plaque on the scalp that had been present since childhood. The size of the plaque gradually progressed initially but had notably increased in size in the last 6 months. There was no association with trauma or irritation. There was no family history of similar lesions. Physical examination revealed a 3.0×2.5-cm plaque on the vertex of the scalp consisting of aggregated pits plugged with keratinous material resembling comedones. There were no lesions elsewhere on the body. Dermoscopy and a 4-mm punch biopsy were performed.
Neural tube defect risk from dolutegravir drops as clinical experience grows

The newest data, based on 3,591 deliveries among women in Botswana infected by HIV and treated with dolutegravir at the time of conception during a little more than 5.5 years through April 2020, showed that dolutegravir use at conception linked with 7 cases of neonatal neural tube defects (NTDs), a 0.19% rate that exceeded comparator rates by about 1 in every 1,000 deliveries, far below the 0.94% rate initially found and that raised a red flag 2 years ago (New Engl J Med. 2018 Sep 6;379[10]:979-81). “The prevalence of NTDs among infants born to women on dolutegravir at conception may be stabilizing at approximately 2 per 1,000,” said Rebecca Zash, MD, during the virtual meeting of the International AIDS conference.
“This small absolute risk for neural tube defects is far outweighed by the potential benefits from dolutegravir” for better tolerability than alternative drugs and fewer drug-drug interactions. “This should allow for broader use of dolutegravir in women,” added Dr. Zash, an HIV specialist at Beth Israel Deaconess Medical Center and codirector of the Placental Scientific Working Group of the Harvard University Center for AIDS Research, both in Boston.
“What this has taught us is that women are not a niche population” of people infected with HIV, but rather constitute about half of HIV patients worldwide. “Maintaining gender equity in HIV treatment requires safety data for treatments during pregnancy,” she said during a press briefing.

The new findings mean that it’s “time to lay to rest” concerns about neural tube defects (NTDs) in infants born to women treated with dolutegravir, “given the incredible benefits of dolutegravir,” commented Monica Gandhi, MD, professor of medicine and associate chief of the division of HIV, infectious disease, and global medicine at the University of California, San Francisco. Another benefit from removing any caveats about use of dolutegravir in women who could become pregnant is that it would simplify treatment recommendations and make dolutegravir the unqualified first-line agent for treating HIV infection, Dr. Gandhi said during the briefing. “It’s super reassuring to have these data, as the incidence of NTDs goes down and down,” she added.
Following the alarm raised by initial findings from the Tsepamo study in 2018, Dr. Zash and associates first updated their data through March 2019, when they reported a revised cumulative NTD incidence rate of 0.3% (New Engl J Med. 2019 Aug 29;381[9]:827-40). The Tsepamo study began by following the pregnancy outcomes of women at eight Botswana sites during August 2014–July 2018, representing 45% of the country’s deliveries. This expanded to 18 sites and 72% of deliveries during July-September 2018, and then starting in September 2019 the scope slightly reduced to 16 Botswana sites with 70% of the nation’s deliveries.
Folate supplementation to women who might conceive is vital, but remains spotty in Botswana. “Folate supplementation is a no-brainer, but has had really slow adoption in many countries,” Dr. Zash said. “Folate supplementation, especially in food so that everyone gets it, will reduce NTDs by half.” The two most recent cases of infants born with a NTD to mothers who had been on dolutegravir at conception occurred in mothers who had received no folate supplementation, Dr. Zash reported.
The most recent HIV treatment guidelines for adults from the Department of Health & Human Services, which date from late 2019, designated dolutegravir plus lamivudine as a first-line regimen for most, but flagged it as an “alternative” antiretroviral drug when treating women who have childbearing potential and are either trying to conceive or are sexually active but not using contraception.
The study had no commercial funding. Dr. Zash has been a researcher in studies funded by CytoDyn, Fulcrum, and Gilead. Dr. Gandhi had no commercial disclosures.
The newest data, based on 3,591 deliveries among women in Botswana infected by HIV and treated with dolutegravir at the time of conception during a little more than 5.5 years through April 2020, showed that dolutegravir use at conception linked with 7 cases of neonatal neural tube defects (NTDs), a 0.19% rate that exceeded comparator rates by about 1 in every 1,000 deliveries, far below the 0.94% rate initially found and that raised a red flag 2 years ago (New Engl J Med. 2018 Sep 6;379[10]:979-81). “The prevalence of NTDs among infants born to women on dolutegravir at conception may be stabilizing at approximately 2 per 1,000,” said Rebecca Zash, MD, during the virtual meeting of the International AIDS conference.
“This small absolute risk for neural tube defects is far outweighed by the potential benefits from dolutegravir” for better tolerability than alternative drugs and fewer drug-drug interactions. “This should allow for broader use of dolutegravir in women,” added Dr. Zash, an HIV specialist at Beth Israel Deaconess Medical Center and codirector of the Placental Scientific Working Group of the Harvard University Center for AIDS Research, both in Boston.
“What this has taught us is that women are not a niche population” of people infected with HIV, but rather constitute about half of HIV patients worldwide. “Maintaining gender equity in HIV treatment requires safety data for treatments during pregnancy,” she said during a press briefing.
The new findings mean that it’s “time to lay to rest” concerns about neural tube defects (NTDs) in infants born to women treated with dolutegravir, “given the incredible benefits of dolutegravir,” commented Monica Gandhi, MD, professor of medicine and associate chief of the division of HIV, infectious disease, and global medicine at the University of California, San Francisco. Another benefit from removing any caveats about use of dolutegravir in women who could become pregnant is that it would simplify treatment recommendations and make dolutegravir the unqualified first-line agent for treating HIV infection, Dr. Gandhi said during the briefing. “It’s super reassuring to have these data, as the incidence of NTDs goes down and down,” she added.
Following the alarm raised by initial findings from the Tsepamo study in 2018, Dr. Zash and associates first updated their data through March 2019, when they reported a revised cumulative NTD incidence rate of 0.3% (New Engl J Med. 2019 Aug 29;381[9]:827-40). The Tsepamo study began by following the pregnancy outcomes of women at eight Botswana sites during August 2014–July 2018, representing 45% of the country’s deliveries. This expanded to 18 sites and 72% of deliveries during July-September 2018, and then starting in September 2019 the scope slightly reduced to 16 Botswana sites with 70% of the nation’s deliveries.
Folate supplementation to women who might conceive is vital, but remains spotty in Botswana. “Folate supplementation is a no-brainer, but has had really slow adoption in many countries,” Dr. Zash said. “Folate supplementation, especially in food so that everyone gets it, will reduce NTDs by half.” The two most recent cases of infants born with a NTD to mothers who had been on dolutegravir at conception occurred in mothers who had received no folate supplementation, Dr. Zash reported.
The most recent HIV treatment guidelines for adults from the Department of Health & Human Services, which date from late 2019, designated dolutegravir plus lamivudine as a first-line regimen for most, but flagged it as an “alternative” antiretroviral drug when treating women who have childbearing potential and are either trying to conceive or are sexually active but not using contraception.
The study had no commercial funding. Dr. Zash has been a researcher in studies funded by CytoDyn, Fulcrum, and Gilead. Dr. Gandhi had no commercial disclosures.
The newest data, based on 3,591 deliveries among women in Botswana infected by HIV and treated with dolutegravir at the time of conception during a little more than 5.5 years through April 2020, showed that dolutegravir use at conception linked with 7 cases of neonatal neural tube defects (NTDs), a 0.19% rate that exceeded comparator rates by about 1 in every 1,000 deliveries, far below the 0.94% rate initially found and that raised a red flag 2 years ago (New Engl J Med. 2018 Sep 6;379[10]:979-81). “The prevalence of NTDs among infants born to women on dolutegravir at conception may be stabilizing at approximately 2 per 1,000,” said Rebecca Zash, MD, during the virtual meeting of the International AIDS conference.
“This small absolute risk for neural tube defects is far outweighed by the potential benefits from dolutegravir” for better tolerability than alternative drugs and fewer drug-drug interactions. “This should allow for broader use of dolutegravir in women,” added Dr. Zash, an HIV specialist at Beth Israel Deaconess Medical Center and codirector of the Placental Scientific Working Group of the Harvard University Center for AIDS Research, both in Boston.
“What this has taught us is that women are not a niche population” of people infected with HIV, but rather constitute about half of HIV patients worldwide. “Maintaining gender equity in HIV treatment requires safety data for treatments during pregnancy,” she said during a press briefing.
The new findings mean that it’s “time to lay to rest” concerns about neural tube defects (NTDs) in infants born to women treated with dolutegravir, “given the incredible benefits of dolutegravir,” commented Monica Gandhi, MD, professor of medicine and associate chief of the division of HIV, infectious disease, and global medicine at the University of California, San Francisco. Another benefit from removing any caveats about use of dolutegravir in women who could become pregnant is that it would simplify treatment recommendations and make dolutegravir the unqualified first-line agent for treating HIV infection, Dr. Gandhi said during the briefing. “It’s super reassuring to have these data, as the incidence of NTDs goes down and down,” she added.
Following the alarm raised by initial findings from the Tsepamo study in 2018, Dr. Zash and associates first updated their data through March 2019, when they reported a revised cumulative NTD incidence rate of 0.3% (New Engl J Med. 2019 Aug 29;381[9]:827-40). The Tsepamo study began by following the pregnancy outcomes of women at eight Botswana sites during August 2014–July 2018, representing 45% of the country’s deliveries. This expanded to 18 sites and 72% of deliveries during July-September 2018, and then starting in September 2019 the scope slightly reduced to 16 Botswana sites with 70% of the nation’s deliveries.
Folate supplementation to women who might conceive is vital, but remains spotty in Botswana. “Folate supplementation is a no-brainer, but has had really slow adoption in many countries,” Dr. Zash said. “Folate supplementation, especially in food so that everyone gets it, will reduce NTDs by half.” The two most recent cases of infants born with a NTD to mothers who had been on dolutegravir at conception occurred in mothers who had received no folate supplementation, Dr. Zash reported.
The most recent HIV treatment guidelines for adults from the Department of Health & Human Services, which date from late 2019, designated dolutegravir plus lamivudine as a first-line regimen for most, but flagged it as an “alternative” antiretroviral drug when treating women who have childbearing potential and are either trying to conceive or are sexually active but not using contraception.
The study had no commercial funding. Dr. Zash has been a researcher in studies funded by CytoDyn, Fulcrum, and Gilead. Dr. Gandhi had no commercial disclosures.
FROM AIDS 2020
FDA approves oral therapy for myelodysplastic syndromes, CMML
The Food and Drug Administration has approved Inqovi (decitabine and cedazuridine tablets, Astex Pharmaceuticals) to treat adults with myelodysplastic syndromes (MDS) or chronic myelomonocytic leukemia (CMML).
Approval of the tablets could obviate the need for some patients to come to healthcare settings for intravenous therapy, a consideration that goes beyond patient convenience. “The FDA remains committed to providing additional treatments to patients during the coronavirus pandemic. In this case, the FDA is making available an oral outpatient treatment option that can reduce the need for frequent visits to health care facilities,” Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence, stated in a news release.
“At this critical time, we continue to focus on providing options to patients with cancer, including regimens that can be taken at home,” added Dr. Pazdur, who is also acting director of the office of oncologic diseases in the FDA’s Center for Drug Evaluation and Research.
Inqovi received an Orphan Drug designation and a Priority Review from the agency.
The FDA based the new formulation approval on clinical trials that showed patients taking Inqovi had similar drug concentrations, compared with others receiving intravenous decitabine.
The two therapies also had similar safety profiles. Fatigue, constipation, hemorrhage, muscle pain, mucositis, arthralgia, nausea, and fever with low white blood cell count were common side effects reported in people taking Inqovi. The agency noted that Inqovi can cause fetal harm, and that both male and female patients of reproductive age are advised to use effective contraception.
In the clinical trials, approximately half of the patients formerly dependent on transfusions no longer required them during an 8-week period.
Inqovi is taken as one tablet by mouth once daily for 5 consecutive days of each 28-day cycle.
The Food and Drug Administration has approved Inqovi (decitabine and cedazuridine tablets, Astex Pharmaceuticals) to treat adults with myelodysplastic syndromes (MDS) or chronic myelomonocytic leukemia (CMML).
Approval of the tablets could obviate the need for some patients to come to healthcare settings for intravenous therapy, a consideration that goes beyond patient convenience. “The FDA remains committed to providing additional treatments to patients during the coronavirus pandemic. In this case, the FDA is making available an oral outpatient treatment option that can reduce the need for frequent visits to health care facilities,” Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence, stated in a news release.
“At this critical time, we continue to focus on providing options to patients with cancer, including regimens that can be taken at home,” added Dr. Pazdur, who is also acting director of the office of oncologic diseases in the FDA’s Center for Drug Evaluation and Research.
Inqovi received an Orphan Drug designation and a Priority Review from the agency.
The FDA based the new formulation approval on clinical trials that showed patients taking Inqovi had similar drug concentrations, compared with others receiving intravenous decitabine.
The two therapies also had similar safety profiles. Fatigue, constipation, hemorrhage, muscle pain, mucositis, arthralgia, nausea, and fever with low white blood cell count were common side effects reported in people taking Inqovi. The agency noted that Inqovi can cause fetal harm, and that both male and female patients of reproductive age are advised to use effective contraception.
In the clinical trials, approximately half of the patients formerly dependent on transfusions no longer required them during an 8-week period.
Inqovi is taken as one tablet by mouth once daily for 5 consecutive days of each 28-day cycle.
The Food and Drug Administration has approved Inqovi (decitabine and cedazuridine tablets, Astex Pharmaceuticals) to treat adults with myelodysplastic syndromes (MDS) or chronic myelomonocytic leukemia (CMML).
Approval of the tablets could obviate the need for some patients to come to healthcare settings for intravenous therapy, a consideration that goes beyond patient convenience. “The FDA remains committed to providing additional treatments to patients during the coronavirus pandemic. In this case, the FDA is making available an oral outpatient treatment option that can reduce the need for frequent visits to health care facilities,” Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence, stated in a news release.
“At this critical time, we continue to focus on providing options to patients with cancer, including regimens that can be taken at home,” added Dr. Pazdur, who is also acting director of the office of oncologic diseases in the FDA’s Center for Drug Evaluation and Research.
Inqovi received an Orphan Drug designation and a Priority Review from the agency.
The FDA based the new formulation approval on clinical trials that showed patients taking Inqovi had similar drug concentrations, compared with others receiving intravenous decitabine.
The two therapies also had similar safety profiles. Fatigue, constipation, hemorrhage, muscle pain, mucositis, arthralgia, nausea, and fever with low white blood cell count were common side effects reported in people taking Inqovi. The agency noted that Inqovi can cause fetal harm, and that both male and female patients of reproductive age are advised to use effective contraception.
In the clinical trials, approximately half of the patients formerly dependent on transfusions no longer required them during an 8-week period.
Inqovi is taken as one tablet by mouth once daily for 5 consecutive days of each 28-day cycle.
Is your job performance being evaluated for the wrong factors?
Most physicians get an annual performance review, and may be either elated, disappointed, or confused with their rating.
But some physicians say the right factors aren’t being evaluated or, in many cases, the performance measures promote efforts that are counterproductive.
“Bonuses are a behaviorist approach,” said Richard Gunderman, MD, professor in the schools of medicine, liberal arts, and philanthropy at Indiana University, Indianapolis. “The presumption is that people will change if they get some money – that they will do what the incentive wants them to do and refrain from what it doesn’t want them to do.”
Dr. Gunderman said this often means just going through the motions to get the bonus, and not sharing goals that only the administration cares about. “The goals might be to lower costs, ensure compliance with regulations or billing requirements, or make patterns of care more uniform. These are not changes that are well tailored to what patients want or how doctors think.”
The bonus is a central feature of the annual review. Merritt Hawkins, the physician search firm, reported that 75% of the physician jobs that it searches for involve some kind of production bonus. Bonuses often make up at least 5% of total compensation, but they can be quite hefty in some specialties.
Having to fulfill measures that they’re not excited about can lead physicians to feel disengaged from their work, Dr. Gunderman said. And this disengagement can contribute to physician burnout, which has climbed to very high rates in recent years.
A 2018 paper by two physician leadership experts explored this problem with bonuses. “A growing consensus [of experts] suggests that quality-incentive pay isn’t paying the dividends first envisioned,” they wrote.
The problem is that the measurements tied to a bonus represent an extrinsic motivation – involving goals that doctors don’t really believe in. Instead, physicians need to be intrinsically motivated. They need to be inspired “to manage their own lives,” “to get better at something,” and “to be a part of a larger cause,” they wrote.
How to develop a better review process
“The best way to motivate improved performance is through purpose and mission,” said Robert Pearl, MD, former CEO of the Permanente Medical Group in California and now a lecturer on strategy at Stanford (Calif.) University.
The review process, Dr. Pearl said, should inspire physicians to do better. The doctors should be asking themselves: “How well did we do in helping maximize the health of all of our patients? And how well did we do in avoiding medical errors, preventing complications, meeting the needs of our patients, and achieving superior quality outcomes?”
When he was CEO of Permanente, the huge physician group that works exclusively for health maintenance organization Kaiser, Dr. Pearl and fellow leaders revamped the review system that all Permanente physicians undergo.
First, the Permanente executives provided all physicians with everyone’s patient-satisfaction data, including their own. That way, each physician could compare performance with others and assess strengths and weaknesses. Then Permanente offered educational programs so that physicians could get help in meeting their goals.
“This approach helped improve quality of care, patient satisfaction, and fulfillment of physicians,” Dr. Pearl said. Kaiser Permanente earned the highest health plan member satisfaction rating by J.D. Power and higher rankings by the National Committee for Quality Assurance.
Permanente does not base the bonus on relative value units but on performance measures that are carefully balanced to avoid too much focus on certain measures. “There needs to be an array of quality measures because doctors deal with a complex set of problems,” Dr. Pearl said. For example, a primary care physician at Permanente is assessed on about 30 different measures.
Physicians are more likely to be successful when you emphasize collaboration. Dr. Pearl said.
Although Permanente physicians are compared with each other, they are not pitted against each other but rather are asked to collaborate. “Physicians are more likely to be successful when you emphasize collaboration,” he said. “They can teach each other. You can be good at some things, and your colleague can be good at others.”
Permanente still has one-on-one yearly evaluations, but much of the assessment work is done in monthly meetings within each department. “There, small groups of doctors look at their data and discuss how each of them can improve,” Dr. Pearl noted.
The 360-degree review is valuable but has some problems
Physicians should be getting a lot more feedback about their behavior than they are actually getting, according to Milton Hammerly, MD, chief medical officer at QualChoice Health Insurance in Little Rock, Ark.
“After residency, you get very little feedback on your work,” said Dr. Hammerly, who used to work for a hospital system. “Annual reviews for physicians focus almost exclusively on outcomes, productivity, and quality metrics, but not on people skills, what is called ‘emotional intelligence.’ ”
Dr. Hammerly said he saw the consequence of this lack of education when he was vice president for medical affairs at the hospital system. He was constantly dealing with physicians who exhibited serious disruptive behavior and had to be disciplined. “If only they had gotten a little help earlier on,” he noted.
Dr. Hammerly said that 360-degree evaluations, which are common in corporations but rarely used for physicians, could benefit the profession. He discovered the 360-degree evaluation when it was used for him at QualChoice, and he has been a fan ever since.
The approach involves collecting evaluations of you from your boss, your peers, and from people who work for you. That is, from 360 degrees around you. These people are asked to rate your strengths and weaknesses in a variety of competencies. In this way, you get feedback from all of your work relationships, not just from your boss.
Ideally, the evaluators are anonymous, and the subject works with a facilitator to process the information. But 360-degree evaluations can be done in all kinds of ways.
Critics of the 360-degree evaluations say the usual anonymity of evaluators allows them to be too harsh. Also, evaluators may be too subjective: What they say about you says more about their own perspective than anything about you.
But many people think 360-degree evaluations are at least going in the right direction, because they focus on people skills rather than just meeting metrics.
Robert Centor, MD, an internist in Birmingham, Ala., and a member of the performance measures committee of the American College of Physicians, said the best way to improve performance is to have conversations about your work with colleagues on the department level. “For example, 20 doctors could meet to discuss a certain issue, such as the need for more vaccinations. That doesn’t have to get rewarded with a bonus payment.”
Dr. Pearl said that “doctors need feedback from their colleagues. Without feedback, how else do you get better? You can only improve if you can know how you’re performing, compared to others.”
A version of this article originally appeared on Medscape.com.
Most physicians get an annual performance review, and may be either elated, disappointed, or confused with their rating.
But some physicians say the right factors aren’t being evaluated or, in many cases, the performance measures promote efforts that are counterproductive.
“Bonuses are a behaviorist approach,” said Richard Gunderman, MD, professor in the schools of medicine, liberal arts, and philanthropy at Indiana University, Indianapolis. “The presumption is that people will change if they get some money – that they will do what the incentive wants them to do and refrain from what it doesn’t want them to do.”
Dr. Gunderman said this often means just going through the motions to get the bonus, and not sharing goals that only the administration cares about. “The goals might be to lower costs, ensure compliance with regulations or billing requirements, or make patterns of care more uniform. These are not changes that are well tailored to what patients want or how doctors think.”
The bonus is a central feature of the annual review. Merritt Hawkins, the physician search firm, reported that 75% of the physician jobs that it searches for involve some kind of production bonus. Bonuses often make up at least 5% of total compensation, but they can be quite hefty in some specialties.
Having to fulfill measures that they’re not excited about can lead physicians to feel disengaged from their work, Dr. Gunderman said. And this disengagement can contribute to physician burnout, which has climbed to very high rates in recent years.
A 2018 paper by two physician leadership experts explored this problem with bonuses. “A growing consensus [of experts] suggests that quality-incentive pay isn’t paying the dividends first envisioned,” they wrote.
The problem is that the measurements tied to a bonus represent an extrinsic motivation – involving goals that doctors don’t really believe in. Instead, physicians need to be intrinsically motivated. They need to be inspired “to manage their own lives,” “to get better at something,” and “to be a part of a larger cause,” they wrote.
How to develop a better review process
“The best way to motivate improved performance is through purpose and mission,” said Robert Pearl, MD, former CEO of the Permanente Medical Group in California and now a lecturer on strategy at Stanford (Calif.) University.
The review process, Dr. Pearl said, should inspire physicians to do better. The doctors should be asking themselves: “How well did we do in helping maximize the health of all of our patients? And how well did we do in avoiding medical errors, preventing complications, meeting the needs of our patients, and achieving superior quality outcomes?”
When he was CEO of Permanente, the huge physician group that works exclusively for health maintenance organization Kaiser, Dr. Pearl and fellow leaders revamped the review system that all Permanente physicians undergo.
First, the Permanente executives provided all physicians with everyone’s patient-satisfaction data, including their own. That way, each physician could compare performance with others and assess strengths and weaknesses. Then Permanente offered educational programs so that physicians could get help in meeting their goals.
“This approach helped improve quality of care, patient satisfaction, and fulfillment of physicians,” Dr. Pearl said. Kaiser Permanente earned the highest health plan member satisfaction rating by J.D. Power and higher rankings by the National Committee for Quality Assurance.
Permanente does not base the bonus on relative value units but on performance measures that are carefully balanced to avoid too much focus on certain measures. “There needs to be an array of quality measures because doctors deal with a complex set of problems,” Dr. Pearl said. For example, a primary care physician at Permanente is assessed on about 30 different measures.
Physicians are more likely to be successful when you emphasize collaboration. Dr. Pearl said.
Although Permanente physicians are compared with each other, they are not pitted against each other but rather are asked to collaborate. “Physicians are more likely to be successful when you emphasize collaboration,” he said. “They can teach each other. You can be good at some things, and your colleague can be good at others.”
Permanente still has one-on-one yearly evaluations, but much of the assessment work is done in monthly meetings within each department. “There, small groups of doctors look at their data and discuss how each of them can improve,” Dr. Pearl noted.
The 360-degree review is valuable but has some problems
Physicians should be getting a lot more feedback about their behavior than they are actually getting, according to Milton Hammerly, MD, chief medical officer at QualChoice Health Insurance in Little Rock, Ark.
“After residency, you get very little feedback on your work,” said Dr. Hammerly, who used to work for a hospital system. “Annual reviews for physicians focus almost exclusively on outcomes, productivity, and quality metrics, but not on people skills, what is called ‘emotional intelligence.’ ”
Dr. Hammerly said he saw the consequence of this lack of education when he was vice president for medical affairs at the hospital system. He was constantly dealing with physicians who exhibited serious disruptive behavior and had to be disciplined. “If only they had gotten a little help earlier on,” he noted.
Dr. Hammerly said that 360-degree evaluations, which are common in corporations but rarely used for physicians, could benefit the profession. He discovered the 360-degree evaluation when it was used for him at QualChoice, and he has been a fan ever since.
The approach involves collecting evaluations of you from your boss, your peers, and from people who work for you. That is, from 360 degrees around you. These people are asked to rate your strengths and weaknesses in a variety of competencies. In this way, you get feedback from all of your work relationships, not just from your boss.
Ideally, the evaluators are anonymous, and the subject works with a facilitator to process the information. But 360-degree evaluations can be done in all kinds of ways.
Critics of the 360-degree evaluations say the usual anonymity of evaluators allows them to be too harsh. Also, evaluators may be too subjective: What they say about you says more about their own perspective than anything about you.
But many people think 360-degree evaluations are at least going in the right direction, because they focus on people skills rather than just meeting metrics.
Robert Centor, MD, an internist in Birmingham, Ala., and a member of the performance measures committee of the American College of Physicians, said the best way to improve performance is to have conversations about your work with colleagues on the department level. “For example, 20 doctors could meet to discuss a certain issue, such as the need for more vaccinations. That doesn’t have to get rewarded with a bonus payment.”
Dr. Pearl said that “doctors need feedback from their colleagues. Without feedback, how else do you get better? You can only improve if you can know how you’re performing, compared to others.”
A version of this article originally appeared on Medscape.com.
Most physicians get an annual performance review, and may be either elated, disappointed, or confused with their rating.
But some physicians say the right factors aren’t being evaluated or, in many cases, the performance measures promote efforts that are counterproductive.
“Bonuses are a behaviorist approach,” said Richard Gunderman, MD, professor in the schools of medicine, liberal arts, and philanthropy at Indiana University, Indianapolis. “The presumption is that people will change if they get some money – that they will do what the incentive wants them to do and refrain from what it doesn’t want them to do.”
Dr. Gunderman said this often means just going through the motions to get the bonus, and not sharing goals that only the administration cares about. “The goals might be to lower costs, ensure compliance with regulations or billing requirements, or make patterns of care more uniform. These are not changes that are well tailored to what patients want or how doctors think.”
The bonus is a central feature of the annual review. Merritt Hawkins, the physician search firm, reported that 75% of the physician jobs that it searches for involve some kind of production bonus. Bonuses often make up at least 5% of total compensation, but they can be quite hefty in some specialties.
Having to fulfill measures that they’re not excited about can lead physicians to feel disengaged from their work, Dr. Gunderman said. And this disengagement can contribute to physician burnout, which has climbed to very high rates in recent years.
A 2018 paper by two physician leadership experts explored this problem with bonuses. “A growing consensus [of experts] suggests that quality-incentive pay isn’t paying the dividends first envisioned,” they wrote.
The problem is that the measurements tied to a bonus represent an extrinsic motivation – involving goals that doctors don’t really believe in. Instead, physicians need to be intrinsically motivated. They need to be inspired “to manage their own lives,” “to get better at something,” and “to be a part of a larger cause,” they wrote.
How to develop a better review process
“The best way to motivate improved performance is through purpose and mission,” said Robert Pearl, MD, former CEO of the Permanente Medical Group in California and now a lecturer on strategy at Stanford (Calif.) University.
The review process, Dr. Pearl said, should inspire physicians to do better. The doctors should be asking themselves: “How well did we do in helping maximize the health of all of our patients? And how well did we do in avoiding medical errors, preventing complications, meeting the needs of our patients, and achieving superior quality outcomes?”
When he was CEO of Permanente, the huge physician group that works exclusively for health maintenance organization Kaiser, Dr. Pearl and fellow leaders revamped the review system that all Permanente physicians undergo.
First, the Permanente executives provided all physicians with everyone’s patient-satisfaction data, including their own. That way, each physician could compare performance with others and assess strengths and weaknesses. Then Permanente offered educational programs so that physicians could get help in meeting their goals.
“This approach helped improve quality of care, patient satisfaction, and fulfillment of physicians,” Dr. Pearl said. Kaiser Permanente earned the highest health plan member satisfaction rating by J.D. Power and higher rankings by the National Committee for Quality Assurance.
Permanente does not base the bonus on relative value units but on performance measures that are carefully balanced to avoid too much focus on certain measures. “There needs to be an array of quality measures because doctors deal with a complex set of problems,” Dr. Pearl said. For example, a primary care physician at Permanente is assessed on about 30 different measures.
Physicians are more likely to be successful when you emphasize collaboration. Dr. Pearl said.
Although Permanente physicians are compared with each other, they are not pitted against each other but rather are asked to collaborate. “Physicians are more likely to be successful when you emphasize collaboration,” he said. “They can teach each other. You can be good at some things, and your colleague can be good at others.”
Permanente still has one-on-one yearly evaluations, but much of the assessment work is done in monthly meetings within each department. “There, small groups of doctors look at their data and discuss how each of them can improve,” Dr. Pearl noted.
The 360-degree review is valuable but has some problems
Physicians should be getting a lot more feedback about their behavior than they are actually getting, according to Milton Hammerly, MD, chief medical officer at QualChoice Health Insurance in Little Rock, Ark.
“After residency, you get very little feedback on your work,” said Dr. Hammerly, who used to work for a hospital system. “Annual reviews for physicians focus almost exclusively on outcomes, productivity, and quality metrics, but not on people skills, what is called ‘emotional intelligence.’ ”
Dr. Hammerly said he saw the consequence of this lack of education when he was vice president for medical affairs at the hospital system. He was constantly dealing with physicians who exhibited serious disruptive behavior and had to be disciplined. “If only they had gotten a little help earlier on,” he noted.
Dr. Hammerly said that 360-degree evaluations, which are common in corporations but rarely used for physicians, could benefit the profession. He discovered the 360-degree evaluation when it was used for him at QualChoice, and he has been a fan ever since.
The approach involves collecting evaluations of you from your boss, your peers, and from people who work for you. That is, from 360 degrees around you. These people are asked to rate your strengths and weaknesses in a variety of competencies. In this way, you get feedback from all of your work relationships, not just from your boss.
Ideally, the evaluators are anonymous, and the subject works with a facilitator to process the information. But 360-degree evaluations can be done in all kinds of ways.
Critics of the 360-degree evaluations say the usual anonymity of evaluators allows them to be too harsh. Also, evaluators may be too subjective: What they say about you says more about their own perspective than anything about you.
But many people think 360-degree evaluations are at least going in the right direction, because they focus on people skills rather than just meeting metrics.
Robert Centor, MD, an internist in Birmingham, Ala., and a member of the performance measures committee of the American College of Physicians, said the best way to improve performance is to have conversations about your work with colleagues on the department level. “For example, 20 doctors could meet to discuss a certain issue, such as the need for more vaccinations. That doesn’t have to get rewarded with a bonus payment.”
Dr. Pearl said that “doctors need feedback from their colleagues. Without feedback, how else do you get better? You can only improve if you can know how you’re performing, compared to others.”
A version of this article originally appeared on Medscape.com.
Brazilian patient in HIV remission, negative antibody test
A 35-year-old Brazilian man who participated in a trial in which he received an intensified antiretroviral regimen plus supplemental vitamin B3 for 48 weeks has joined the short list of patients who have experienced a period of remission from HIV in the absence of effective treatment.
Along with the Mississippi baby, a San Francisco man, a 24-year-old Thai man, a 9-year-old South African child, and the London and Berlin patients, the Brazilian man has an undetectable viral load and, more than a year after stopping treatment, his HIV antibody test is negative.
But as with the Berlin and London patients, it seems unlikely that – even if the man remains HIV free into the future – the circumstances of his remission will be broadly applicable to other people with HIV, said Carl Dieffenbach, PhD, director of the Division of AIDS at the National Institute of Allergy and Infectious Diseases, National Institutes of Health.
“I don’t think it’s replicable,” Dieffenbach told Medscape Medical News. Researchers should still try to confirm the finding, but they will probably learn more by studying the man’s unique genetic characteristics and immune system “than to go out and treat another 200 people with the same protocol.”
‘Shock-and-kill strategy’
The man had been on treatment since his HIV diagnosis in 2012, and was one of 30 people to enroll in a Brazilian study – the Multi Interventional Study Exploring HIV-1 Residual Replication: A Step Toward HIV Eradication and Sterilizing Cure – in 2016. At that point, his regimen consisted of the combination of efavirenz, lamivudine, and tenofovir disoproxil fumarate (Symfi, Mylan Pharmaceuticals) and his viral load was undetectable.
He was one of five people in the study to be randomized to receive the integrase inhibitor dolutegravir (Tivicay, ViiV Healthcare), the CCR5 receptor inhibitor maraviroc (Selzentry, ViiV Healthcare), and twice-daily nicotinamide 500 mg, a form of vitamin B3, in addition to his regular regimen for 48 weeks.
Nicotinamide has been used for decades because of its anti-infective properties, particularly in tuberculosis. In vitro, it also works to reverse HIV latency, said study investigator Ricardo Diaz, MD, from the Federal University of São Paulo, who presented the data at a press conference for the International AIDS Conference (AIDS) 2020.
“This is a shock-and-kill strategy,” said Leila Giron, PhD, from the Wistar Institute in Philadelphia, who was one of the study investigators. “We did in vitro studies to make sure nicotinamide took HIV out of the cells.”
“The cell machinery changed a lot,” she told Medscape Medical News. “And because it’s a B vitamin, all five participants didn’t have any side effects.”
But the patient was the only person in his treatment group to experience viral load “blips” during treatment – at weeks 16 and 24. And viral DNA was present at low levels in his peripheral blood spots and rectal tissue at baseline and at 48 weeks, and his HIV antibodies dropped from 91.8 RLU at baseline to 58.0 RLU at week 48.
“He had a decline in cell activation, inflammation, and a very deep decline in antibody titers,” Diaz reported.
After 48 weeks of the intensified treatment, the patient returned to his usual regimen for 3 years. Then, in March 2019, he agreed to try an analytical treatment interruption and discontinued all HIV treatment.
“What’s interesting is right before the analytical treatment interruption, the HIV DNA sequences were completely negative,” said Diaz.
Every 3 weeks for the next 64.7 weeks, his viral load came back undetectable, and so did HIV DNA in blood spots. One thing did change, though: in February 2020, the man’s HIV antibody test came back negative.
The team checked that he wasn’t still taking his antiretroviral medication, which might have explained the undetectable viral load, and he wasn’t.
Surprise, skepticism, and hope
The results have prompted surprise, skepticism, and questions from clinicians and researchers.
said Anton Pozniak, MD, from Chelsea and Westminster Hospital in London, who is cochair of AIDS 2020.
“They need a bigger study to see whether or not [the participant] is one of these guys who stopped treatment and might take a year or two, or four, to rebound,” he said. But if other studies replicate the results, the control of HIV in “one in five people would still be huge.”
The rationale behind treatment intensification for HIV remission is that “the three-drug ART regimen was perhaps insufficient to completely block HIV replication” in the reservoirs, even though that replication could be happening below levels detectable with current tests, said Laura Persaud, MD, from the Johns Hopkins University School of Medicine in Baltimore, who is chair of the International Maternal Pediatric Adolescent AIDS Clinical Trial Network (IMPAACT) HIV Cure Committee and was not involved in the study.
“The idea was to see if you could accelerate the decay of the reservoir” if you added medications that targeted different parts of the HIV lifecycle. Symfi, for instance, targets just one step in the viral replication process: the point where HIV RNA reverse transcribes itself into DNA so it can integrate into immune cells. But CCR5 inhibitors block entry of HIV into the cell in the first place, and integrase inhibitors, like raltegravir (Isentress, Merck) and dolutegravir, prevent HIV DNA from integrating into the host chromosome after it has reverse transcribed itself.
Still, recent data suggest that treatment intensification might not be as effective as hypothesized, she said. And the nicotinamide study was in vitro. To what extent this is a direct result of this treatment strategy is unclear.
“It’s hard to believe, in this small study, that this agent [nicotinamide] would have such a striking effect on DNA proviral levels,” she said. “We learn from each of these cases. But this is a single case, with multiple mechanisms that may have contributed to the outcome here. To what extent this is a direct result of this treatment strategy is unclear.”
Only time will tell, and Persaud knows this first hand. Back in 2014, she presented data at another HIV conference on the Mississippi baby who, after 21 months of no treatment, still didn›t have an HIV viral load.
At the time, the baby was hailed as “functionally cured,” but just 6 months later, the virus returned.
Dieffenbach agrees. “There are 10,000 genetic variations that need to be considered, and it all adds up to a unique individual,” he said of the Brazilian patient. “This one is one person, and it’s still early days.”
Counseling patients on niacin supplementation
Some clinicians are already bracing for the flood of people with HIV now wanting to take, or who are already taking, a niacin supplement because of this case, said Laura Waters, MD, from Mortimer Market Centre in London, who is chair of the British HIV Association.
But nicotinamide is different than nicotinic acid, which is what many people mean when they talk about niacin supplementation, according to data from the Office of Dietary Supplements (ODS) at the National Institutes of Health. Nicotinic acid has been used as a supplement for people with high cholesterol for years. Most Americans get more than the recommended daily intake of both types of niacin – 16 mg for adult men and 14 mg for adult women – in their regular diet, according to the 2015/16 National Health and Nutrition Examination Survey.
The Brazilian patient received a total daily dose of nicotinamide of 1000 mg, which is not associated with any adverse effects. Doses above 3000 mg daily can lead to diarrhea and a decrease in platelet count, according to the ODS.
Although Diaz said he doesn’t think people with HIV should run out and start taking a supplement right away, Waters said she sees it as inevitable.
The good news is that if people really are taking nicotinamide – not nicotinic acid – it seems “fairly well tolerated without many side effects,” she said, but added: “I expect shortages of nicotinamide from tomorrow.”
This story first appeared on Medscape.com.
A 35-year-old Brazilian man who participated in a trial in which he received an intensified antiretroviral regimen plus supplemental vitamin B3 for 48 weeks has joined the short list of patients who have experienced a period of remission from HIV in the absence of effective treatment.
Along with the Mississippi baby, a San Francisco man, a 24-year-old Thai man, a 9-year-old South African child, and the London and Berlin patients, the Brazilian man has an undetectable viral load and, more than a year after stopping treatment, his HIV antibody test is negative.
But as with the Berlin and London patients, it seems unlikely that – even if the man remains HIV free into the future – the circumstances of his remission will be broadly applicable to other people with HIV, said Carl Dieffenbach, PhD, director of the Division of AIDS at the National Institute of Allergy and Infectious Diseases, National Institutes of Health.
“I don’t think it’s replicable,” Dieffenbach told Medscape Medical News. Researchers should still try to confirm the finding, but they will probably learn more by studying the man’s unique genetic characteristics and immune system “than to go out and treat another 200 people with the same protocol.”
‘Shock-and-kill strategy’
The man had been on treatment since his HIV diagnosis in 2012, and was one of 30 people to enroll in a Brazilian study – the Multi Interventional Study Exploring HIV-1 Residual Replication: A Step Toward HIV Eradication and Sterilizing Cure – in 2016. At that point, his regimen consisted of the combination of efavirenz, lamivudine, and tenofovir disoproxil fumarate (Symfi, Mylan Pharmaceuticals) and his viral load was undetectable.
He was one of five people in the study to be randomized to receive the integrase inhibitor dolutegravir (Tivicay, ViiV Healthcare), the CCR5 receptor inhibitor maraviroc (Selzentry, ViiV Healthcare), and twice-daily nicotinamide 500 mg, a form of vitamin B3, in addition to his regular regimen for 48 weeks.
Nicotinamide has been used for decades because of its anti-infective properties, particularly in tuberculosis. In vitro, it also works to reverse HIV latency, said study investigator Ricardo Diaz, MD, from the Federal University of São Paulo, who presented the data at a press conference for the International AIDS Conference (AIDS) 2020.
“This is a shock-and-kill strategy,” said Leila Giron, PhD, from the Wistar Institute in Philadelphia, who was one of the study investigators. “We did in vitro studies to make sure nicotinamide took HIV out of the cells.”
“The cell machinery changed a lot,” she told Medscape Medical News. “And because it’s a B vitamin, all five participants didn’t have any side effects.”
But the patient was the only person in his treatment group to experience viral load “blips” during treatment – at weeks 16 and 24. And viral DNA was present at low levels in his peripheral blood spots and rectal tissue at baseline and at 48 weeks, and his HIV antibodies dropped from 91.8 RLU at baseline to 58.0 RLU at week 48.
“He had a decline in cell activation, inflammation, and a very deep decline in antibody titers,” Diaz reported.
After 48 weeks of the intensified treatment, the patient returned to his usual regimen for 3 years. Then, in March 2019, he agreed to try an analytical treatment interruption and discontinued all HIV treatment.
“What’s interesting is right before the analytical treatment interruption, the HIV DNA sequences were completely negative,” said Diaz.
Every 3 weeks for the next 64.7 weeks, his viral load came back undetectable, and so did HIV DNA in blood spots. One thing did change, though: in February 2020, the man’s HIV antibody test came back negative.
The team checked that he wasn’t still taking his antiretroviral medication, which might have explained the undetectable viral load, and he wasn’t.
Surprise, skepticism, and hope
The results have prompted surprise, skepticism, and questions from clinicians and researchers.
said Anton Pozniak, MD, from Chelsea and Westminster Hospital in London, who is cochair of AIDS 2020.
“They need a bigger study to see whether or not [the participant] is one of these guys who stopped treatment and might take a year or two, or four, to rebound,” he said. But if other studies replicate the results, the control of HIV in “one in five people would still be huge.”
The rationale behind treatment intensification for HIV remission is that “the three-drug ART regimen was perhaps insufficient to completely block HIV replication” in the reservoirs, even though that replication could be happening below levels detectable with current tests, said Laura Persaud, MD, from the Johns Hopkins University School of Medicine in Baltimore, who is chair of the International Maternal Pediatric Adolescent AIDS Clinical Trial Network (IMPAACT) HIV Cure Committee and was not involved in the study.
“The idea was to see if you could accelerate the decay of the reservoir” if you added medications that targeted different parts of the HIV lifecycle. Symfi, for instance, targets just one step in the viral replication process: the point where HIV RNA reverse transcribes itself into DNA so it can integrate into immune cells. But CCR5 inhibitors block entry of HIV into the cell in the first place, and integrase inhibitors, like raltegravir (Isentress, Merck) and dolutegravir, prevent HIV DNA from integrating into the host chromosome after it has reverse transcribed itself.
Still, recent data suggest that treatment intensification might not be as effective as hypothesized, she said. And the nicotinamide study was in vitro. To what extent this is a direct result of this treatment strategy is unclear.
“It’s hard to believe, in this small study, that this agent [nicotinamide] would have such a striking effect on DNA proviral levels,” she said. “We learn from each of these cases. But this is a single case, with multiple mechanisms that may have contributed to the outcome here. To what extent this is a direct result of this treatment strategy is unclear.”
Only time will tell, and Persaud knows this first hand. Back in 2014, she presented data at another HIV conference on the Mississippi baby who, after 21 months of no treatment, still didn›t have an HIV viral load.
At the time, the baby was hailed as “functionally cured,” but just 6 months later, the virus returned.
Dieffenbach agrees. “There are 10,000 genetic variations that need to be considered, and it all adds up to a unique individual,” he said of the Brazilian patient. “This one is one person, and it’s still early days.”
Counseling patients on niacin supplementation
Some clinicians are already bracing for the flood of people with HIV now wanting to take, or who are already taking, a niacin supplement because of this case, said Laura Waters, MD, from Mortimer Market Centre in London, who is chair of the British HIV Association.
But nicotinamide is different than nicotinic acid, which is what many people mean when they talk about niacin supplementation, according to data from the Office of Dietary Supplements (ODS) at the National Institutes of Health. Nicotinic acid has been used as a supplement for people with high cholesterol for years. Most Americans get more than the recommended daily intake of both types of niacin – 16 mg for adult men and 14 mg for adult women – in their regular diet, according to the 2015/16 National Health and Nutrition Examination Survey.
The Brazilian patient received a total daily dose of nicotinamide of 1000 mg, which is not associated with any adverse effects. Doses above 3000 mg daily can lead to diarrhea and a decrease in platelet count, according to the ODS.
Although Diaz said he doesn’t think people with HIV should run out and start taking a supplement right away, Waters said she sees it as inevitable.
The good news is that if people really are taking nicotinamide – not nicotinic acid – it seems “fairly well tolerated without many side effects,” she said, but added: “I expect shortages of nicotinamide from tomorrow.”
This story first appeared on Medscape.com.
A 35-year-old Brazilian man who participated in a trial in which he received an intensified antiretroviral regimen plus supplemental vitamin B3 for 48 weeks has joined the short list of patients who have experienced a period of remission from HIV in the absence of effective treatment.
Along with the Mississippi baby, a San Francisco man, a 24-year-old Thai man, a 9-year-old South African child, and the London and Berlin patients, the Brazilian man has an undetectable viral load and, more than a year after stopping treatment, his HIV antibody test is negative.
But as with the Berlin and London patients, it seems unlikely that – even if the man remains HIV free into the future – the circumstances of his remission will be broadly applicable to other people with HIV, said Carl Dieffenbach, PhD, director of the Division of AIDS at the National Institute of Allergy and Infectious Diseases, National Institutes of Health.
“I don’t think it’s replicable,” Dieffenbach told Medscape Medical News. Researchers should still try to confirm the finding, but they will probably learn more by studying the man’s unique genetic characteristics and immune system “than to go out and treat another 200 people with the same protocol.”
‘Shock-and-kill strategy’
The man had been on treatment since his HIV diagnosis in 2012, and was one of 30 people to enroll in a Brazilian study – the Multi Interventional Study Exploring HIV-1 Residual Replication: A Step Toward HIV Eradication and Sterilizing Cure – in 2016. At that point, his regimen consisted of the combination of efavirenz, lamivudine, and tenofovir disoproxil fumarate (Symfi, Mylan Pharmaceuticals) and his viral load was undetectable.
He was one of five people in the study to be randomized to receive the integrase inhibitor dolutegravir (Tivicay, ViiV Healthcare), the CCR5 receptor inhibitor maraviroc (Selzentry, ViiV Healthcare), and twice-daily nicotinamide 500 mg, a form of vitamin B3, in addition to his regular regimen for 48 weeks.
Nicotinamide has been used for decades because of its anti-infective properties, particularly in tuberculosis. In vitro, it also works to reverse HIV latency, said study investigator Ricardo Diaz, MD, from the Federal University of São Paulo, who presented the data at a press conference for the International AIDS Conference (AIDS) 2020.
“This is a shock-and-kill strategy,” said Leila Giron, PhD, from the Wistar Institute in Philadelphia, who was one of the study investigators. “We did in vitro studies to make sure nicotinamide took HIV out of the cells.”
“The cell machinery changed a lot,” she told Medscape Medical News. “And because it’s a B vitamin, all five participants didn’t have any side effects.”
But the patient was the only person in his treatment group to experience viral load “blips” during treatment – at weeks 16 and 24. And viral DNA was present at low levels in his peripheral blood spots and rectal tissue at baseline and at 48 weeks, and his HIV antibodies dropped from 91.8 RLU at baseline to 58.0 RLU at week 48.
“He had a decline in cell activation, inflammation, and a very deep decline in antibody titers,” Diaz reported.
After 48 weeks of the intensified treatment, the patient returned to his usual regimen for 3 years. Then, in March 2019, he agreed to try an analytical treatment interruption and discontinued all HIV treatment.
“What’s interesting is right before the analytical treatment interruption, the HIV DNA sequences were completely negative,” said Diaz.
Every 3 weeks for the next 64.7 weeks, his viral load came back undetectable, and so did HIV DNA in blood spots. One thing did change, though: in February 2020, the man’s HIV antibody test came back negative.
The team checked that he wasn’t still taking his antiretroviral medication, which might have explained the undetectable viral load, and he wasn’t.
Surprise, skepticism, and hope
The results have prompted surprise, skepticism, and questions from clinicians and researchers.
said Anton Pozniak, MD, from Chelsea and Westminster Hospital in London, who is cochair of AIDS 2020.
“They need a bigger study to see whether or not [the participant] is one of these guys who stopped treatment and might take a year or two, or four, to rebound,” he said. But if other studies replicate the results, the control of HIV in “one in five people would still be huge.”
The rationale behind treatment intensification for HIV remission is that “the three-drug ART regimen was perhaps insufficient to completely block HIV replication” in the reservoirs, even though that replication could be happening below levels detectable with current tests, said Laura Persaud, MD, from the Johns Hopkins University School of Medicine in Baltimore, who is chair of the International Maternal Pediatric Adolescent AIDS Clinical Trial Network (IMPAACT) HIV Cure Committee and was not involved in the study.
“The idea was to see if you could accelerate the decay of the reservoir” if you added medications that targeted different parts of the HIV lifecycle. Symfi, for instance, targets just one step in the viral replication process: the point where HIV RNA reverse transcribes itself into DNA so it can integrate into immune cells. But CCR5 inhibitors block entry of HIV into the cell in the first place, and integrase inhibitors, like raltegravir (Isentress, Merck) and dolutegravir, prevent HIV DNA from integrating into the host chromosome after it has reverse transcribed itself.
Still, recent data suggest that treatment intensification might not be as effective as hypothesized, she said. And the nicotinamide study was in vitro. To what extent this is a direct result of this treatment strategy is unclear.
“It’s hard to believe, in this small study, that this agent [nicotinamide] would have such a striking effect on DNA proviral levels,” she said. “We learn from each of these cases. But this is a single case, with multiple mechanisms that may have contributed to the outcome here. To what extent this is a direct result of this treatment strategy is unclear.”
Only time will tell, and Persaud knows this first hand. Back in 2014, she presented data at another HIV conference on the Mississippi baby who, after 21 months of no treatment, still didn›t have an HIV viral load.
At the time, the baby was hailed as “functionally cured,” but just 6 months later, the virus returned.
Dieffenbach agrees. “There are 10,000 genetic variations that need to be considered, and it all adds up to a unique individual,” he said of the Brazilian patient. “This one is one person, and it’s still early days.”
Counseling patients on niacin supplementation
Some clinicians are already bracing for the flood of people with HIV now wanting to take, or who are already taking, a niacin supplement because of this case, said Laura Waters, MD, from Mortimer Market Centre in London, who is chair of the British HIV Association.
But nicotinamide is different than nicotinic acid, which is what many people mean when they talk about niacin supplementation, according to data from the Office of Dietary Supplements (ODS) at the National Institutes of Health. Nicotinic acid has been used as a supplement for people with high cholesterol for years. Most Americans get more than the recommended daily intake of both types of niacin – 16 mg for adult men and 14 mg for adult women – in their regular diet, according to the 2015/16 National Health and Nutrition Examination Survey.
The Brazilian patient received a total daily dose of nicotinamide of 1000 mg, which is not associated with any adverse effects. Doses above 3000 mg daily can lead to diarrhea and a decrease in platelet count, according to the ODS.
Although Diaz said he doesn’t think people with HIV should run out and start taking a supplement right away, Waters said she sees it as inevitable.
The good news is that if people really are taking nicotinamide – not nicotinic acid – it seems “fairly well tolerated without many side effects,” she said, but added: “I expect shortages of nicotinamide from tomorrow.”
This story first appeared on Medscape.com.
Would you be happier in a leadership position? This hospitalist wasn’t
After practicing clinical care for 4 years, hospitalist Suneel Dhand, MD, was ready for a change and eager for the chance to help improve the broader health care system.

So when the opportunity arose to direct an internal medicine program at a large hospital, Dr. Dhand gladly accepted the role. He aimed to enhance frontline staffing, expand his hospital medicine team’s influence, and raise the standard of care for patients.
Almost immediately, however, Dr. Dhand knew the administrative route was the wrong path for him.
“I realized very quickly that initiating change and being a positive force, while working with multiple competing interests, is far from easy,” said Dr. Dhand. “I didn’t particularly feel well supported by the high-level administrators. Without resources, it’s extra difficult to make things happen.”
A year and half into the role, Dr. Dhand left the position and returned to purely clinical work. He now practices as a Boston-area hospitalist while writing, filming, and podcasting about medicine on the side.
“I have no intention of leaving clinical medicine,” he said. “If somebody gave me a very highly compensated offer right now to come and be a hospital leader, I wouldn’t do it. It’s not me, and I wouldn’t enjoy it.”
Taking on an administrative or executive role can sound appealing to many clinicians. The Medscape Physician Compensation Report 2018 found that 42% of employed physicians were aiming for a promotion. Another physician survey by The Physicians Foundation found that 46% planned to change career paths in 2018 and that more than 12% planned to seek a nonclinical job in the next 1-3 years.
Interest in executive and leadership roles has also increased because of the COVID-19 pandemic, particularly as more physicians struggle financially and search for alternative compensation, said Peter B. Angood, MD, CEO and president for the American Association for Physician Leadership.
“Because of the COVID-19 impacts on health care and our country as a whole, the strengths of physician leadership have been better recognized at multiple levels,” Dr. Angood said. “As a result, there is definitely early interest as the ongoing impacts of COVID-19 are appreciated in how to further integrate physicians as leaders within the health care industry as a whole.”
Administration: Not for everyone
But as Dr. Dhand’s experience highlights, administration is not the right direction for every physician. Take the case of prominent surgeon and Harvard University professor Atul Gawande, MD, who in May stepped down as chief executive for Haven, the health care venture backed by Amazon, after just 2 years. In a statement, Dr. Gawande indicated he would be taking a less operational role with the company to devote more time to policy and activities associated with COVID-19.
Although the details of Dr. Gawande’s departure are unclear, his abrupt exit raises questions. Are physicians prepared for executive positions before making the move? Who makes the best fit for an administrative job?
“It’s certainly something most folks should not just jump into,” said Dr. Angood. “In the same way that physicians spend an awful lot of time developing their expertise to become an expert clinician, the same philosophy for becoming an expert administrative leader should be applied. You need to put in the same amount of energy and effort to truly be effective.”
The motivations behind moving to an administrative role vary among physicians, said Carson F. Dye, fellow and faculty member at the American College of Healthcare Executives and a leadership consultant. Some doctors make the shift because they have a natural proclivity for leading, whereas others want to make a greater impact on patient care and quality, Mr. Dye said. Still other physicians simply want a greater say in the everyday areas that affect them.
At the same time, there are more physician leadership opportunities than before. Positions such as chief quality officer, chief medical information officer, president of the employed medical group, and chief population health officer rarely existed 20 or 30 years ago, Mr. Dye noted.
“Moreover, nonclinical executives have begun to see the great value in having more physician leaders involved because it enhances physician engagement and provides valuable input for strategic change,” Mr. Dye said. “As a result, more physicians are coaxed into considering leadership roles.”
North Carolina internist Michael Lalor, MD, says leadership responsibilities landed in his lap early in his career and led to his ultimate post as a full-time administrator. Dr. Lalor was a couple years out of residency and working for a small private practice when the owner decided to retire early and asked him to take over the group, he explained.
After accepting, Dr. Lalor hired another physician, expanded the group, and later merged with a larger network.
“I loved it from the perspective of the intersection of business and medicine,” he said. “It really gave me experience you don’t get in training, such as the actual operations of running a medical group, contract negotiations, expansion plans, payroll, accounting. It was an entirely new experience that I really enjoyed.”
Dr. Lalor also served as a medical director for a small, nonprofit hospice in the area, which spurred him to become board certified in hospice and palliative medicine. He now acts as chief medical officer for a large hospice and palliative care organization based in North Carolina.
Chicago-area family physician John Jurica, MD, made his way up the executive ladder through a series of steps. Dr. Jurica said he felt drawn to committees and projects that addressed population health and quality issues. Tapping into this interest, he became medical director for Riverside Medical Center in Kankakee, Ill., followed by vice president of medical affairs and then chief medical officer for the hospital.
Along the way, Dr. Jurica volunteered with nonprofit organizations, served on hospital boards, and completed a master’s degree in public health.
“The more I got into it, the more I liked it,” he said. “I was wanting to be involved in helping larger numbers of patients in a different way, work on big problems, affect the community, and work on multidisciplinary teams.”
Today, Dr. Jurica is medical director and part owner of two urgent care centers. His career journey inspired him to create the VITAL Physician Executive blog, which offers advice about becoming a physician executive. He also hosts a podcast devoted to nonclinical careers for physicians.
Dr. Jurica said he hears a range of reasons for seeking a change from clinical care, including disillusionment with medicine; high debt; outside interests; and burnout.
“A number of physicians have said, ‘I really don’t enjoy medicine anymore,’ ” Dr. Jurica said. “ ‘The paperwork is onerous, I’m working long hours, I have to see more patients, and I’m getting paid the same or less. It’s just not what I thought it would be.’ ”
Although burnout prompts some physicians to pursue administrative roles, Dr. Angood cautions that this is like entering a rebound relationship after leaving a bad relationship. Making the move merely because of dissatisfaction with your current position can set you up for disappointment, he said.
“Too often, physicians who are frustrated with the complexities of clinical care will view administrative roles as a parachute for themselves out of that situation,” he said. “If they don’t understand the nuances of administrative work, they run the risk of moving into a role that will ultimately provide them a different level of dissatisfaction, rather than the higher level of satisfaction they were seeking. It is all about trying to ensure a good match in terms of expectations in order to obtain optimal outcomes.”
Who’s right for an administrative job?
Nearly any type of personality can make a good fit for an administrative post, said Dr. Jurica.

“If you look at most leadership teams, they usually have a team of people that have different personality types that complement one another,” he said. “You can be an extrovert, an introvert, Whatever kind of breakdown in personality you have can be successful.”
Certain attributes, however, are more helpful for executive positions, according to Mr. Dye, including comfort in dealing with ambiguity, a willingness to make difficult decisions, an aptitude for interpreting nonverbal cues, and the ability to demonstrate confidence, but not arrogance.
“Someone who is collaborative and cooperative, a good listener, and has a compelling vision for change in health care also makes a great leader,” he said.
The ability to balance and manage the needs of different groups is also key, said Heidi Moawad, MD, a neurologist, career consultant, and author of “Careers Beyond Clinical Medicine” (New York: Oxford University Press, 2013).
“Sometimes the needs of one group steps on the toes of the needs of another group,” said Dr. Moawad, who provides career resources for physicians at nonclinicaldoctors.com. “You have to be someone who isn’t so overwhelmed by pleasing everyone. You have to think fairly about the needs of all the groups involved, not just the loudest group.”
Is there a specialty best suited to an administrative role? Executive recruiters typically encounter more primary care physician candidates when conducting physician executive searches, according to Mr. Dye. This is likely because primary care doctors are usually the lowest paid of all specialties, and their pay scale may better fit with that of hiring organizations, he said. Higher-paid specialists, on the other hand, may be deterred from pursuing executive roles because of the possibility of lower pay. In addition, primary care physicians typically have traits that align well with administrative/executive functions.
“The nature of their clinical practice means that they are able to see the broad spectrum of the continuum of care and understand the system better,” he said.
Dr. Jurica stressed, however, that strong leaders can come from any specialty and that many medical backgrounds can fit an administrative or executive position.
“It’s more related to interests, desires, personality, and experiences over time as to whether they fit that role or mature into that role,” he said.
Just because you’re a great clinician doesn’t mean you’ll make a good administrative leader, Dr. Lalor said. Physicians can often fall into executive or leadership positions because they’re considered the best or most productive clinician in a group, he explained.
“The skill set is not 100% the same,” he said. “Not everybody is necessarily suited for it. They kind of fall into it and then have great missteps in their earliest experiences.”
Will you miss your former responsibilities?
Some physicians who enter the administrative realm really miss the clinical world and the satisfaction of helping patients directly, added Mr. Dye. He hears from many physicians who miss the “short-term nature” of clinical practice, meaning encountering a patient, determining an intervention, and moving on to another patient.
“Decisions are made, and the physician gets to see the result of those decisions,” he said. “One physician remarked to me that she lived her clinical life in ‘15-minute segments’ and that her executive world had many issues that went on for years, making it very frustrating to her that she was not really making progress.”
For physicians such as family physician Krista Skorupa, MD, who straddle both the clinical and administrative spheres, obstacles can arise in the form of time and balance. Dr. Skorupa splits her time between practicing family medicine and acting as vice president of medical practice for the M Health Fairview Primary Care Service Line in St. Paul, Minn.
“Most people will tell you it’s the balance that’s one of the hardest things,” she said. “You always feel like you’re doing one job not as well as you could because you’re trying to do two jobs at 100%.”
Dr. Skorupa said she has been fortunate to work for organizations that have provided the time and compensation for both jobs. But she warns that some institutions expect physicians to excel at dual clinical and administrative roles, yet fail to allot enough time or compensation for both.
Doctors going the executive route should also prepare for their work relationships to change – some for the worse.
Some peers may perceive a physician’s trek into administration as going to “the dark side,” Dr. Angood said. Attitudes from colleagues may change, and not everyone may be accepting of your new role, he advised.
And as Dr. Dhand experienced, conflict can stem from having to act as an intermediary between staff physicians and administrators. In his director position, Dr. Dhand had to relay administrative policies to his physician colleagues. The task was challenging because Dr. Dhand did not necessarily agree with the policies and felt they burdened already overworked physicians.
“I believe almost all physician leaders feel this way,” he said. “They walk in the same shoes as clinicians and know what a tough job it is. Yet, we are part of the system and have to follow rules and protocols. When you are the one giving bad news, you frequently become the fall guy.”
Is administration right for me?
To decide whether administration is right for you, start by talking to other physicians in the industry and asking questions, said Dr. Skorupa.
“I strongly encourage mentorship and network,” she said. “I learned a lot by just asking physicians who were in different leadership roles, to ‘Tell me your story. How did you get to where you’re at?’ It’s been hearing those stories that helped me craft my own.”
Consider joining committees within your local hospital or among your national specialty organization to evaluate whether the work interests you, Dr. Moawad advises.
“Getting some experience is important to see if it’s right for you,” she said.
Another way to measure your interest is by taking on a part-time job in physician leadership, Mr. Dye said. This allows physicians to try out leadership without leaving clinical practice behind.
“Dyad roles where physicians are paired with a nonphysician partner can also be helpful to physicians who are wanting to move slowly into leadership,” he said. “Typically, the physician partner in a dyad model also continues to practice clinically part time and thus does not lose that connection with medicine.”
In addition to getting some leadership experience, you may want to consider formal training in executive leadership. Many specialty societies offer formal coursework related to leadership, as do some hospital organizations.
The Society of Hospital Medicine offers a 3-course Leadership Academy that prepares clinical and academic leaders with skills traditionally not taught in medical school or typical residency programs. The society also offers a Leadership Capstone program for hospitalists with 3 or more years of experience, who are already leading or preparing to lead an academic, business, or clinical change initiative at their institution.
Physicians can find numerous courses and programs through AAPL, including the organization’s certified physician executive credential. The ACHE has a spectrum of career resources for health care professionals, including courses, competency assessments, and executive career coaches. Medscape’s Physician Business Academy also offers a course in leadership called “How to Become an Effective Leader,” which covers the attributes needed to become an effective leader and how to learn and develop relevant skills and traits.
Some physicians heading down the administrative road pursue more formal degrees, such as an MBA, MHA, or MMM, added Dr. Jurica. A business degree is not required, but degrees do have advantages, he said.
“The most important factor in preparing a physician for this career shift is taking on progressively more challenging duties managing people, running important projects, working with budgets, and honing your leadership skills,” he said. “However, there are benefits to having a degree. It provides formal education in these areas. Pursuing such a degree demonstrates a commitment to your leadership career and can be helpful when competing with other physician leaders for an attractive position.”
The reality is that more hospitals and health systems are recognizing the value of having physicians in leadership and executive functions, Dr. Angood said. Data show that health systems and hospitals with physician leaders perform better.
“This is because physicians not only have strong leadership and administrative capabilities, but they already have a strong sense of the clinical environment and how best to deliver good clinical care. It’s a double benefit nonclinical administrators are unable to match.”
As for Dr. Dhand, he doesn’t regret his stint in administration, despite finding out the path was not his calling.
“My experience was an eye-opener; I’m glad I did it,” he said. “I would change certain things looking back, like having lower expectations and understanding that change takes time. It’s also okay to be unpopular. I’m much happier now, though, only doing clinical medicine, and have found fulfillment through other nonclinical ventures.”
A version of this article originally appeared on Medscape.com.
After practicing clinical care for 4 years, hospitalist Suneel Dhand, MD, was ready for a change and eager for the chance to help improve the broader health care system.
So when the opportunity arose to direct an internal medicine program at a large hospital, Dr. Dhand gladly accepted the role. He aimed to enhance frontline staffing, expand his hospital medicine team’s influence, and raise the standard of care for patients.
Almost immediately, however, Dr. Dhand knew the administrative route was the wrong path for him.
“I realized very quickly that initiating change and being a positive force, while working with multiple competing interests, is far from easy,” said Dr. Dhand. “I didn’t particularly feel well supported by the high-level administrators. Without resources, it’s extra difficult to make things happen.”
A year and half into the role, Dr. Dhand left the position and returned to purely clinical work. He now practices as a Boston-area hospitalist while writing, filming, and podcasting about medicine on the side.
“I have no intention of leaving clinical medicine,” he said. “If somebody gave me a very highly compensated offer right now to come and be a hospital leader, I wouldn’t do it. It’s not me, and I wouldn’t enjoy it.”
Taking on an administrative or executive role can sound appealing to many clinicians. The Medscape Physician Compensation Report 2018 found that 42% of employed physicians were aiming for a promotion. Another physician survey by The Physicians Foundation found that 46% planned to change career paths in 2018 and that more than 12% planned to seek a nonclinical job in the next 1-3 years.
Interest in executive and leadership roles has also increased because of the COVID-19 pandemic, particularly as more physicians struggle financially and search for alternative compensation, said Peter B. Angood, MD, CEO and president for the American Association for Physician Leadership.
“Because of the COVID-19 impacts on health care and our country as a whole, the strengths of physician leadership have been better recognized at multiple levels,” Dr. Angood said. “As a result, there is definitely early interest as the ongoing impacts of COVID-19 are appreciated in how to further integrate physicians as leaders within the health care industry as a whole.”
Administration: Not for everyone
But as Dr. Dhand’s experience highlights, administration is not the right direction for every physician. Take the case of prominent surgeon and Harvard University professor Atul Gawande, MD, who in May stepped down as chief executive for Haven, the health care venture backed by Amazon, after just 2 years. In a statement, Dr. Gawande indicated he would be taking a less operational role with the company to devote more time to policy and activities associated with COVID-19.
Although the details of Dr. Gawande’s departure are unclear, his abrupt exit raises questions. Are physicians prepared for executive positions before making the move? Who makes the best fit for an administrative job?
“It’s certainly something most folks should not just jump into,” said Dr. Angood. “In the same way that physicians spend an awful lot of time developing their expertise to become an expert clinician, the same philosophy for becoming an expert administrative leader should be applied. You need to put in the same amount of energy and effort to truly be effective.”
The motivations behind moving to an administrative role vary among physicians, said Carson F. Dye, fellow and faculty member at the American College of Healthcare Executives and a leadership consultant. Some doctors make the shift because they have a natural proclivity for leading, whereas others want to make a greater impact on patient care and quality, Mr. Dye said. Still other physicians simply want a greater say in the everyday areas that affect them.
At the same time, there are more physician leadership opportunities than before. Positions such as chief quality officer, chief medical information officer, president of the employed medical group, and chief population health officer rarely existed 20 or 30 years ago, Mr. Dye noted.
“Moreover, nonclinical executives have begun to see the great value in having more physician leaders involved because it enhances physician engagement and provides valuable input for strategic change,” Mr. Dye said. “As a result, more physicians are coaxed into considering leadership roles.”
North Carolina internist Michael Lalor, MD, says leadership responsibilities landed in his lap early in his career and led to his ultimate post as a full-time administrator. Dr. Lalor was a couple years out of residency and working for a small private practice when the owner decided to retire early and asked him to take over the group, he explained.
After accepting, Dr. Lalor hired another physician, expanded the group, and later merged with a larger network.
“I loved it from the perspective of the intersection of business and medicine,” he said. “It really gave me experience you don’t get in training, such as the actual operations of running a medical group, contract negotiations, expansion plans, payroll, accounting. It was an entirely new experience that I really enjoyed.”
Dr. Lalor also served as a medical director for a small, nonprofit hospice in the area, which spurred him to become board certified in hospice and palliative medicine. He now acts as chief medical officer for a large hospice and palliative care organization based in North Carolina.
Chicago-area family physician John Jurica, MD, made his way up the executive ladder through a series of steps. Dr. Jurica said he felt drawn to committees and projects that addressed population health and quality issues. Tapping into this interest, he became medical director for Riverside Medical Center in Kankakee, Ill., followed by vice president of medical affairs and then chief medical officer for the hospital.
Along the way, Dr. Jurica volunteered with nonprofit organizations, served on hospital boards, and completed a master’s degree in public health.
“The more I got into it, the more I liked it,” he said. “I was wanting to be involved in helping larger numbers of patients in a different way, work on big problems, affect the community, and work on multidisciplinary teams.”
Today, Dr. Jurica is medical director and part owner of two urgent care centers. His career journey inspired him to create the VITAL Physician Executive blog, which offers advice about becoming a physician executive. He also hosts a podcast devoted to nonclinical careers for physicians.
Dr. Jurica said he hears a range of reasons for seeking a change from clinical care, including disillusionment with medicine; high debt; outside interests; and burnout.
“A number of physicians have said, ‘I really don’t enjoy medicine anymore,’ ” Dr. Jurica said. “ ‘The paperwork is onerous, I’m working long hours, I have to see more patients, and I’m getting paid the same or less. It’s just not what I thought it would be.’ ”
Although burnout prompts some physicians to pursue administrative roles, Dr. Angood cautions that this is like entering a rebound relationship after leaving a bad relationship. Making the move merely because of dissatisfaction with your current position can set you up for disappointment, he said.
“Too often, physicians who are frustrated with the complexities of clinical care will view administrative roles as a parachute for themselves out of that situation,” he said. “If they don’t understand the nuances of administrative work, they run the risk of moving into a role that will ultimately provide them a different level of dissatisfaction, rather than the higher level of satisfaction they were seeking. It is all about trying to ensure a good match in terms of expectations in order to obtain optimal outcomes.”
Who’s right for an administrative job?
Nearly any type of personality can make a good fit for an administrative post, said Dr. Jurica.
“If you look at most leadership teams, they usually have a team of people that have different personality types that complement one another,” he said. “You can be an extrovert, an introvert, Whatever kind of breakdown in personality you have can be successful.”
Certain attributes, however, are more helpful for executive positions, according to Mr. Dye, including comfort in dealing with ambiguity, a willingness to make difficult decisions, an aptitude for interpreting nonverbal cues, and the ability to demonstrate confidence, but not arrogance.
“Someone who is collaborative and cooperative, a good listener, and has a compelling vision for change in health care also makes a great leader,” he said.
The ability to balance and manage the needs of different groups is also key, said Heidi Moawad, MD, a neurologist, career consultant, and author of “Careers Beyond Clinical Medicine” (New York: Oxford University Press, 2013).
“Sometimes the needs of one group steps on the toes of the needs of another group,” said Dr. Moawad, who provides career resources for physicians at nonclinicaldoctors.com. “You have to be someone who isn’t so overwhelmed by pleasing everyone. You have to think fairly about the needs of all the groups involved, not just the loudest group.”
Is there a specialty best suited to an administrative role? Executive recruiters typically encounter more primary care physician candidates when conducting physician executive searches, according to Mr. Dye. This is likely because primary care doctors are usually the lowest paid of all specialties, and their pay scale may better fit with that of hiring organizations, he said. Higher-paid specialists, on the other hand, may be deterred from pursuing executive roles because of the possibility of lower pay. In addition, primary care physicians typically have traits that align well with administrative/executive functions.
“The nature of their clinical practice means that they are able to see the broad spectrum of the continuum of care and understand the system better,” he said.
Dr. Jurica stressed, however, that strong leaders can come from any specialty and that many medical backgrounds can fit an administrative or executive position.
“It’s more related to interests, desires, personality, and experiences over time as to whether they fit that role or mature into that role,” he said.
Just because you’re a great clinician doesn’t mean you’ll make a good administrative leader, Dr. Lalor said. Physicians can often fall into executive or leadership positions because they’re considered the best or most productive clinician in a group, he explained.
“The skill set is not 100% the same,” he said. “Not everybody is necessarily suited for it. They kind of fall into it and then have great missteps in their earliest experiences.”
Will you miss your former responsibilities?
Some physicians who enter the administrative realm really miss the clinical world and the satisfaction of helping patients directly, added Mr. Dye. He hears from many physicians who miss the “short-term nature” of clinical practice, meaning encountering a patient, determining an intervention, and moving on to another patient.
“Decisions are made, and the physician gets to see the result of those decisions,” he said. “One physician remarked to me that she lived her clinical life in ‘15-minute segments’ and that her executive world had many issues that went on for years, making it very frustrating to her that she was not really making progress.”
For physicians such as family physician Krista Skorupa, MD, who straddle both the clinical and administrative spheres, obstacles can arise in the form of time and balance. Dr. Skorupa splits her time between practicing family medicine and acting as vice president of medical practice for the M Health Fairview Primary Care Service Line in St. Paul, Minn.
“Most people will tell you it’s the balance that’s one of the hardest things,” she said. “You always feel like you’re doing one job not as well as you could because you’re trying to do two jobs at 100%.”
Dr. Skorupa said she has been fortunate to work for organizations that have provided the time and compensation for both jobs. But she warns that some institutions expect physicians to excel at dual clinical and administrative roles, yet fail to allot enough time or compensation for both.
Doctors going the executive route should also prepare for their work relationships to change – some for the worse.
Some peers may perceive a physician’s trek into administration as going to “the dark side,” Dr. Angood said. Attitudes from colleagues may change, and not everyone may be accepting of your new role, he advised.
And as Dr. Dhand experienced, conflict can stem from having to act as an intermediary between staff physicians and administrators. In his director position, Dr. Dhand had to relay administrative policies to his physician colleagues. The task was challenging because Dr. Dhand did not necessarily agree with the policies and felt they burdened already overworked physicians.
“I believe almost all physician leaders feel this way,” he said. “They walk in the same shoes as clinicians and know what a tough job it is. Yet, we are part of the system and have to follow rules and protocols. When you are the one giving bad news, you frequently become the fall guy.”
Is administration right for me?
To decide whether administration is right for you, start by talking to other physicians in the industry and asking questions, said Dr. Skorupa.
“I strongly encourage mentorship and network,” she said. “I learned a lot by just asking physicians who were in different leadership roles, to ‘Tell me your story. How did you get to where you’re at?’ It’s been hearing those stories that helped me craft my own.”
Consider joining committees within your local hospital or among your national specialty organization to evaluate whether the work interests you, Dr. Moawad advises.
“Getting some experience is important to see if it’s right for you,” she said.
Another way to measure your interest is by taking on a part-time job in physician leadership, Mr. Dye said. This allows physicians to try out leadership without leaving clinical practice behind.
“Dyad roles where physicians are paired with a nonphysician partner can also be helpful to physicians who are wanting to move slowly into leadership,” he said. “Typically, the physician partner in a dyad model also continues to practice clinically part time and thus does not lose that connection with medicine.”
In addition to getting some leadership experience, you may want to consider formal training in executive leadership. Many specialty societies offer formal coursework related to leadership, as do some hospital organizations.
The Society of Hospital Medicine offers a 3-course Leadership Academy that prepares clinical and academic leaders with skills traditionally not taught in medical school or typical residency programs. The society also offers a Leadership Capstone program for hospitalists with 3 or more years of experience, who are already leading or preparing to lead an academic, business, or clinical change initiative at their institution.
Physicians can find numerous courses and programs through AAPL, including the organization’s certified physician executive credential. The ACHE has a spectrum of career resources for health care professionals, including courses, competency assessments, and executive career coaches. Medscape’s Physician Business Academy also offers a course in leadership called “How to Become an Effective Leader,” which covers the attributes needed to become an effective leader and how to learn and develop relevant skills and traits.
Some physicians heading down the administrative road pursue more formal degrees, such as an MBA, MHA, or MMM, added Dr. Jurica. A business degree is not required, but degrees do have advantages, he said.
“The most important factor in preparing a physician for this career shift is taking on progressively more challenging duties managing people, running important projects, working with budgets, and honing your leadership skills,” he said. “However, there are benefits to having a degree. It provides formal education in these areas. Pursuing such a degree demonstrates a commitment to your leadership career and can be helpful when competing with other physician leaders for an attractive position.”
The reality is that more hospitals and health systems are recognizing the value of having physicians in leadership and executive functions, Dr. Angood said. Data show that health systems and hospitals with physician leaders perform better.
“This is because physicians not only have strong leadership and administrative capabilities, but they already have a strong sense of the clinical environment and how best to deliver good clinical care. It’s a double benefit nonclinical administrators are unable to match.”
As for Dr. Dhand, he doesn’t regret his stint in administration, despite finding out the path was not his calling.
“My experience was an eye-opener; I’m glad I did it,” he said. “I would change certain things looking back, like having lower expectations and understanding that change takes time. It’s also okay to be unpopular. I’m much happier now, though, only doing clinical medicine, and have found fulfillment through other nonclinical ventures.”
A version of this article originally appeared on Medscape.com.
After practicing clinical care for 4 years, hospitalist Suneel Dhand, MD, was ready for a change and eager for the chance to help improve the broader health care system.
So when the opportunity arose to direct an internal medicine program at a large hospital, Dr. Dhand gladly accepted the role. He aimed to enhance frontline staffing, expand his hospital medicine team’s influence, and raise the standard of care for patients.
Almost immediately, however, Dr. Dhand knew the administrative route was the wrong path for him.
“I realized very quickly that initiating change and being a positive force, while working with multiple competing interests, is far from easy,” said Dr. Dhand. “I didn’t particularly feel well supported by the high-level administrators. Without resources, it’s extra difficult to make things happen.”
A year and half into the role, Dr. Dhand left the position and returned to purely clinical work. He now practices as a Boston-area hospitalist while writing, filming, and podcasting about medicine on the side.
“I have no intention of leaving clinical medicine,” he said. “If somebody gave me a very highly compensated offer right now to come and be a hospital leader, I wouldn’t do it. It’s not me, and I wouldn’t enjoy it.”
Taking on an administrative or executive role can sound appealing to many clinicians. The Medscape Physician Compensation Report 2018 found that 42% of employed physicians were aiming for a promotion. Another physician survey by The Physicians Foundation found that 46% planned to change career paths in 2018 and that more than 12% planned to seek a nonclinical job in the next 1-3 years.
Interest in executive and leadership roles has also increased because of the COVID-19 pandemic, particularly as more physicians struggle financially and search for alternative compensation, said Peter B. Angood, MD, CEO and president for the American Association for Physician Leadership.
“Because of the COVID-19 impacts on health care and our country as a whole, the strengths of physician leadership have been better recognized at multiple levels,” Dr. Angood said. “As a result, there is definitely early interest as the ongoing impacts of COVID-19 are appreciated in how to further integrate physicians as leaders within the health care industry as a whole.”
Administration: Not for everyone
But as Dr. Dhand’s experience highlights, administration is not the right direction for every physician. Take the case of prominent surgeon and Harvard University professor Atul Gawande, MD, who in May stepped down as chief executive for Haven, the health care venture backed by Amazon, after just 2 years. In a statement, Dr. Gawande indicated he would be taking a less operational role with the company to devote more time to policy and activities associated with COVID-19.
Although the details of Dr. Gawande’s departure are unclear, his abrupt exit raises questions. Are physicians prepared for executive positions before making the move? Who makes the best fit for an administrative job?
“It’s certainly something most folks should not just jump into,” said Dr. Angood. “In the same way that physicians spend an awful lot of time developing their expertise to become an expert clinician, the same philosophy for becoming an expert administrative leader should be applied. You need to put in the same amount of energy and effort to truly be effective.”
The motivations behind moving to an administrative role vary among physicians, said Carson F. Dye, fellow and faculty member at the American College of Healthcare Executives and a leadership consultant. Some doctors make the shift because they have a natural proclivity for leading, whereas others want to make a greater impact on patient care and quality, Mr. Dye said. Still other physicians simply want a greater say in the everyday areas that affect them.
At the same time, there are more physician leadership opportunities than before. Positions such as chief quality officer, chief medical information officer, president of the employed medical group, and chief population health officer rarely existed 20 or 30 years ago, Mr. Dye noted.
“Moreover, nonclinical executives have begun to see the great value in having more physician leaders involved because it enhances physician engagement and provides valuable input for strategic change,” Mr. Dye said. “As a result, more physicians are coaxed into considering leadership roles.”
North Carolina internist Michael Lalor, MD, says leadership responsibilities landed in his lap early in his career and led to his ultimate post as a full-time administrator. Dr. Lalor was a couple years out of residency and working for a small private practice when the owner decided to retire early and asked him to take over the group, he explained.
After accepting, Dr. Lalor hired another physician, expanded the group, and later merged with a larger network.
“I loved it from the perspective of the intersection of business and medicine,” he said. “It really gave me experience you don’t get in training, such as the actual operations of running a medical group, contract negotiations, expansion plans, payroll, accounting. It was an entirely new experience that I really enjoyed.”
Dr. Lalor also served as a medical director for a small, nonprofit hospice in the area, which spurred him to become board certified in hospice and palliative medicine. He now acts as chief medical officer for a large hospice and palliative care organization based in North Carolina.
Chicago-area family physician John Jurica, MD, made his way up the executive ladder through a series of steps. Dr. Jurica said he felt drawn to committees and projects that addressed population health and quality issues. Tapping into this interest, he became medical director for Riverside Medical Center in Kankakee, Ill., followed by vice president of medical affairs and then chief medical officer for the hospital.
Along the way, Dr. Jurica volunteered with nonprofit organizations, served on hospital boards, and completed a master’s degree in public health.
“The more I got into it, the more I liked it,” he said. “I was wanting to be involved in helping larger numbers of patients in a different way, work on big problems, affect the community, and work on multidisciplinary teams.”
Today, Dr. Jurica is medical director and part owner of two urgent care centers. His career journey inspired him to create the VITAL Physician Executive blog, which offers advice about becoming a physician executive. He also hosts a podcast devoted to nonclinical careers for physicians.
Dr. Jurica said he hears a range of reasons for seeking a change from clinical care, including disillusionment with medicine; high debt; outside interests; and burnout.
“A number of physicians have said, ‘I really don’t enjoy medicine anymore,’ ” Dr. Jurica said. “ ‘The paperwork is onerous, I’m working long hours, I have to see more patients, and I’m getting paid the same or less. It’s just not what I thought it would be.’ ”
Although burnout prompts some physicians to pursue administrative roles, Dr. Angood cautions that this is like entering a rebound relationship after leaving a bad relationship. Making the move merely because of dissatisfaction with your current position can set you up for disappointment, he said.
“Too often, physicians who are frustrated with the complexities of clinical care will view administrative roles as a parachute for themselves out of that situation,” he said. “If they don’t understand the nuances of administrative work, they run the risk of moving into a role that will ultimately provide them a different level of dissatisfaction, rather than the higher level of satisfaction they were seeking. It is all about trying to ensure a good match in terms of expectations in order to obtain optimal outcomes.”
Who’s right for an administrative job?
Nearly any type of personality can make a good fit for an administrative post, said Dr. Jurica.
“If you look at most leadership teams, they usually have a team of people that have different personality types that complement one another,” he said. “You can be an extrovert, an introvert, Whatever kind of breakdown in personality you have can be successful.”
Certain attributes, however, are more helpful for executive positions, according to Mr. Dye, including comfort in dealing with ambiguity, a willingness to make difficult decisions, an aptitude for interpreting nonverbal cues, and the ability to demonstrate confidence, but not arrogance.
“Someone who is collaborative and cooperative, a good listener, and has a compelling vision for change in health care also makes a great leader,” he said.
The ability to balance and manage the needs of different groups is also key, said Heidi Moawad, MD, a neurologist, career consultant, and author of “Careers Beyond Clinical Medicine” (New York: Oxford University Press, 2013).
“Sometimes the needs of one group steps on the toes of the needs of another group,” said Dr. Moawad, who provides career resources for physicians at nonclinicaldoctors.com. “You have to be someone who isn’t so overwhelmed by pleasing everyone. You have to think fairly about the needs of all the groups involved, not just the loudest group.”
Is there a specialty best suited to an administrative role? Executive recruiters typically encounter more primary care physician candidates when conducting physician executive searches, according to Mr. Dye. This is likely because primary care doctors are usually the lowest paid of all specialties, and their pay scale may better fit with that of hiring organizations, he said. Higher-paid specialists, on the other hand, may be deterred from pursuing executive roles because of the possibility of lower pay. In addition, primary care physicians typically have traits that align well with administrative/executive functions.
“The nature of their clinical practice means that they are able to see the broad spectrum of the continuum of care and understand the system better,” he said.
Dr. Jurica stressed, however, that strong leaders can come from any specialty and that many medical backgrounds can fit an administrative or executive position.
“It’s more related to interests, desires, personality, and experiences over time as to whether they fit that role or mature into that role,” he said.
Just because you’re a great clinician doesn’t mean you’ll make a good administrative leader, Dr. Lalor said. Physicians can often fall into executive or leadership positions because they’re considered the best or most productive clinician in a group, he explained.
“The skill set is not 100% the same,” he said. “Not everybody is necessarily suited for it. They kind of fall into it and then have great missteps in their earliest experiences.”
Will you miss your former responsibilities?
Some physicians who enter the administrative realm really miss the clinical world and the satisfaction of helping patients directly, added Mr. Dye. He hears from many physicians who miss the “short-term nature” of clinical practice, meaning encountering a patient, determining an intervention, and moving on to another patient.
“Decisions are made, and the physician gets to see the result of those decisions,” he said. “One physician remarked to me that she lived her clinical life in ‘15-minute segments’ and that her executive world had many issues that went on for years, making it very frustrating to her that she was not really making progress.”
For physicians such as family physician Krista Skorupa, MD, who straddle both the clinical and administrative spheres, obstacles can arise in the form of time and balance. Dr. Skorupa splits her time between practicing family medicine and acting as vice president of medical practice for the M Health Fairview Primary Care Service Line in St. Paul, Minn.
“Most people will tell you it’s the balance that’s one of the hardest things,” she said. “You always feel like you’re doing one job not as well as you could because you’re trying to do two jobs at 100%.”
Dr. Skorupa said she has been fortunate to work for organizations that have provided the time and compensation for both jobs. But she warns that some institutions expect physicians to excel at dual clinical and administrative roles, yet fail to allot enough time or compensation for both.
Doctors going the executive route should also prepare for their work relationships to change – some for the worse.
Some peers may perceive a physician’s trek into administration as going to “the dark side,” Dr. Angood said. Attitudes from colleagues may change, and not everyone may be accepting of your new role, he advised.
And as Dr. Dhand experienced, conflict can stem from having to act as an intermediary between staff physicians and administrators. In his director position, Dr. Dhand had to relay administrative policies to his physician colleagues. The task was challenging because Dr. Dhand did not necessarily agree with the policies and felt they burdened already overworked physicians.
“I believe almost all physician leaders feel this way,” he said. “They walk in the same shoes as clinicians and know what a tough job it is. Yet, we are part of the system and have to follow rules and protocols. When you are the one giving bad news, you frequently become the fall guy.”
Is administration right for me?
To decide whether administration is right for you, start by talking to other physicians in the industry and asking questions, said Dr. Skorupa.
“I strongly encourage mentorship and network,” she said. “I learned a lot by just asking physicians who were in different leadership roles, to ‘Tell me your story. How did you get to where you’re at?’ It’s been hearing those stories that helped me craft my own.”
Consider joining committees within your local hospital or among your national specialty organization to evaluate whether the work interests you, Dr. Moawad advises.
“Getting some experience is important to see if it’s right for you,” she said.
Another way to measure your interest is by taking on a part-time job in physician leadership, Mr. Dye said. This allows physicians to try out leadership without leaving clinical practice behind.
“Dyad roles where physicians are paired with a nonphysician partner can also be helpful to physicians who are wanting to move slowly into leadership,” he said. “Typically, the physician partner in a dyad model also continues to practice clinically part time and thus does not lose that connection with medicine.”
In addition to getting some leadership experience, you may want to consider formal training in executive leadership. Many specialty societies offer formal coursework related to leadership, as do some hospital organizations.
The Society of Hospital Medicine offers a 3-course Leadership Academy that prepares clinical and academic leaders with skills traditionally not taught in medical school or typical residency programs. The society also offers a Leadership Capstone program for hospitalists with 3 or more years of experience, who are already leading or preparing to lead an academic, business, or clinical change initiative at their institution.
Physicians can find numerous courses and programs through AAPL, including the organization’s certified physician executive credential. The ACHE has a spectrum of career resources for health care professionals, including courses, competency assessments, and executive career coaches. Medscape’s Physician Business Academy also offers a course in leadership called “How to Become an Effective Leader,” which covers the attributes needed to become an effective leader and how to learn and develop relevant skills and traits.
Some physicians heading down the administrative road pursue more formal degrees, such as an MBA, MHA, or MMM, added Dr. Jurica. A business degree is not required, but degrees do have advantages, he said.
“The most important factor in preparing a physician for this career shift is taking on progressively more challenging duties managing people, running important projects, working with budgets, and honing your leadership skills,” he said. “However, there are benefits to having a degree. It provides formal education in these areas. Pursuing such a degree demonstrates a commitment to your leadership career and can be helpful when competing with other physician leaders for an attractive position.”
The reality is that more hospitals and health systems are recognizing the value of having physicians in leadership and executive functions, Dr. Angood said. Data show that health systems and hospitals with physician leaders perform better.
“This is because physicians not only have strong leadership and administrative capabilities, but they already have a strong sense of the clinical environment and how best to deliver good clinical care. It’s a double benefit nonclinical administrators are unable to match.”
As for Dr. Dhand, he doesn’t regret his stint in administration, despite finding out the path was not his calling.
“My experience was an eye-opener; I’m glad I did it,” he said. “I would change certain things looking back, like having lower expectations and understanding that change takes time. It’s also okay to be unpopular. I’m much happier now, though, only doing clinical medicine, and have found fulfillment through other nonclinical ventures.”
A version of this article originally appeared on Medscape.com.
WHO plans to address airborne COVID-19 transmission
WHO will likely address airborne transmission of the virus after a commentary from almost 240 multidisciplinary scientists raised the alarm that virus particles could remain airborne longer that previously appreciated, particularly in poorly ventilated indoor spaces.
“Airborne route of infection transmission is significant, but so far completely undermined, and not recognized by the decision makers and bodies responsible for infection control,” lead commentary author Lidia Morawska, PhD, told Medscape Medical News.
“This means that no control measures are taken to mitigate airborne transmission and, as a consequence, people are infected and can die,” said Morawska, director of the International Laboratory for Air Quality and Health at Queensland University of Technology in Brisbane, Australia. “We wanted to bring this to the attention of the world to prevent this from happening.”
The commentary was published July 6 in Clinical Infectious Diseases.
WHO leaders defended their progress in announcing any changes regarding how COVID-19 can be transmitted during a virtual press briefing today. They have collaborated since April with some of the scientists who coauthored the commentary, for example, said Maria Van Kerkhove, PhD, WHO technical lead on COVID-19.
“We have been working on a scientific brief ... to consolidate knowledge around transmission,” she added.
One focus will be on how masks protect healthcare workers. “We are also looking at the possible role of airborne transmission in other settings,” Van Kerkhove said. “We will be releasing our brief in the coming days.”
“We acknowledge there is emerging evidence in this field,” Benedetta Allegranzi, MD, WHO technical lead on COVID-19, said during the briefing from Geneva. “Therefore, we believe we have to be open to this evidence and its implications.”
WHO participated in an international research meeting last week that addressed means for controlling modes of COVID-19 transmission, Allegranzi said. “Our group and others really highlighted importance of research on different modes of transmission, including droplets of different sizes and their relative importance,” she said. Another aim was determining the dose of the virus required for airborne transmission.
“These fields of research are really growing but not definitive. More evidence needs to be gathered and evaluated,” she explained.
In the meantime, Allegranzi said, “the possibility of airborne transmission in public settings – especially closed, poorly ventilated settings – cannot be ruled out.”
Morawska said the evidence already exists. “A continuous surprise is that it takes the world such a long time to accept this, while this has such solid scientific foundation.” As an example, she cited an April report she coauthored in the journal Environment International. She and colleagues call for “national authorities to acknowledge the reality that the virus spreads through air and recommend that adequate control measures be implemented to prevent further spread of the SARS-CoV-2 virus, in particularly removal of the virus-laden droplets from indoor air by ventilation.”
The take-home message from the commentary, Morawska said, is a call to action. The authors state there is a need “to provide sufficient and effective ventilation (supply clean outdoor air, minimize recirculating air) particularly in public buildings, workplace environments, schools, hospitals, and aged care homes.”
WHO Chief Scientist Soumya Swaminathan, MD, explained why the organization remains cautious about making premature pronouncements regarding airborne transmission. “Any guidance we put out has implications for billions of people around the world, so we want to be as careful as possible,” she said during the press briefing. “We have to consider the weight of the evidence.”
“We are constantly looking for information on how we can do better,” Swaminathan added. WHO officials are reviewing hundreds of scientific reports every day, she said, and not all are of good quality. For this reason, she and other scientists at WHO perform a “living systematic review” – updating the consensus of evidence on a weekly basis.
“This process on COVID-19 will, I am sure, continue for the weeks and months to come,” she added.
This article first appeared on Medscape.com.
WHO will likely address airborne transmission of the virus after a commentary from almost 240 multidisciplinary scientists raised the alarm that virus particles could remain airborne longer that previously appreciated, particularly in poorly ventilated indoor spaces.
“Airborne route of infection transmission is significant, but so far completely undermined, and not recognized by the decision makers and bodies responsible for infection control,” lead commentary author Lidia Morawska, PhD, told Medscape Medical News.
“This means that no control measures are taken to mitigate airborne transmission and, as a consequence, people are infected and can die,” said Morawska, director of the International Laboratory for Air Quality and Health at Queensland University of Technology in Brisbane, Australia. “We wanted to bring this to the attention of the world to prevent this from happening.”
The commentary was published July 6 in Clinical Infectious Diseases.
WHO leaders defended their progress in announcing any changes regarding how COVID-19 can be transmitted during a virtual press briefing today. They have collaborated since April with some of the scientists who coauthored the commentary, for example, said Maria Van Kerkhove, PhD, WHO technical lead on COVID-19.
“We have been working on a scientific brief ... to consolidate knowledge around transmission,” she added.
One focus will be on how masks protect healthcare workers. “We are also looking at the possible role of airborne transmission in other settings,” Van Kerkhove said. “We will be releasing our brief in the coming days.”
“We acknowledge there is emerging evidence in this field,” Benedetta Allegranzi, MD, WHO technical lead on COVID-19, said during the briefing from Geneva. “Therefore, we believe we have to be open to this evidence and its implications.”
WHO participated in an international research meeting last week that addressed means for controlling modes of COVID-19 transmission, Allegranzi said. “Our group and others really highlighted importance of research on different modes of transmission, including droplets of different sizes and their relative importance,” she said. Another aim was determining the dose of the virus required for airborne transmission.
“These fields of research are really growing but not definitive. More evidence needs to be gathered and evaluated,” she explained.
In the meantime, Allegranzi said, “the possibility of airborne transmission in public settings – especially closed, poorly ventilated settings – cannot be ruled out.”
Morawska said the evidence already exists. “A continuous surprise is that it takes the world such a long time to accept this, while this has such solid scientific foundation.” As an example, she cited an April report she coauthored in the journal Environment International. She and colleagues call for “national authorities to acknowledge the reality that the virus spreads through air and recommend that adequate control measures be implemented to prevent further spread of the SARS-CoV-2 virus, in particularly removal of the virus-laden droplets from indoor air by ventilation.”
The take-home message from the commentary, Morawska said, is a call to action. The authors state there is a need “to provide sufficient and effective ventilation (supply clean outdoor air, minimize recirculating air) particularly in public buildings, workplace environments, schools, hospitals, and aged care homes.”
WHO Chief Scientist Soumya Swaminathan, MD, explained why the organization remains cautious about making premature pronouncements regarding airborne transmission. “Any guidance we put out has implications for billions of people around the world, so we want to be as careful as possible,” she said during the press briefing. “We have to consider the weight of the evidence.”
“We are constantly looking for information on how we can do better,” Swaminathan added. WHO officials are reviewing hundreds of scientific reports every day, she said, and not all are of good quality. For this reason, she and other scientists at WHO perform a “living systematic review” – updating the consensus of evidence on a weekly basis.
“This process on COVID-19 will, I am sure, continue for the weeks and months to come,” she added.
This article first appeared on Medscape.com.
WHO will likely address airborne transmission of the virus after a commentary from almost 240 multidisciplinary scientists raised the alarm that virus particles could remain airborne longer that previously appreciated, particularly in poorly ventilated indoor spaces.
“Airborne route of infection transmission is significant, but so far completely undermined, and not recognized by the decision makers and bodies responsible for infection control,” lead commentary author Lidia Morawska, PhD, told Medscape Medical News.
“This means that no control measures are taken to mitigate airborne transmission and, as a consequence, people are infected and can die,” said Morawska, director of the International Laboratory for Air Quality and Health at Queensland University of Technology in Brisbane, Australia. “We wanted to bring this to the attention of the world to prevent this from happening.”
The commentary was published July 6 in Clinical Infectious Diseases.
WHO leaders defended their progress in announcing any changes regarding how COVID-19 can be transmitted during a virtual press briefing today. They have collaborated since April with some of the scientists who coauthored the commentary, for example, said Maria Van Kerkhove, PhD, WHO technical lead on COVID-19.
“We have been working on a scientific brief ... to consolidate knowledge around transmission,” she added.
One focus will be on how masks protect healthcare workers. “We are also looking at the possible role of airborne transmission in other settings,” Van Kerkhove said. “We will be releasing our brief in the coming days.”
“We acknowledge there is emerging evidence in this field,” Benedetta Allegranzi, MD, WHO technical lead on COVID-19, said during the briefing from Geneva. “Therefore, we believe we have to be open to this evidence and its implications.”
WHO participated in an international research meeting last week that addressed means for controlling modes of COVID-19 transmission, Allegranzi said. “Our group and others really highlighted importance of research on different modes of transmission, including droplets of different sizes and their relative importance,” she said. Another aim was determining the dose of the virus required for airborne transmission.
“These fields of research are really growing but not definitive. More evidence needs to be gathered and evaluated,” she explained.
In the meantime, Allegranzi said, “the possibility of airborne transmission in public settings – especially closed, poorly ventilated settings – cannot be ruled out.”
Morawska said the evidence already exists. “A continuous surprise is that it takes the world such a long time to accept this, while this has such solid scientific foundation.” As an example, she cited an April report she coauthored in the journal Environment International. She and colleagues call for “national authorities to acknowledge the reality that the virus spreads through air and recommend that adequate control measures be implemented to prevent further spread of the SARS-CoV-2 virus, in particularly removal of the virus-laden droplets from indoor air by ventilation.”
The take-home message from the commentary, Morawska said, is a call to action. The authors state there is a need “to provide sufficient and effective ventilation (supply clean outdoor air, minimize recirculating air) particularly in public buildings, workplace environments, schools, hospitals, and aged care homes.”
WHO Chief Scientist Soumya Swaminathan, MD, explained why the organization remains cautious about making premature pronouncements regarding airborne transmission. “Any guidance we put out has implications for billions of people around the world, so we want to be as careful as possible,” she said during the press briefing. “We have to consider the weight of the evidence.”
“We are constantly looking for information on how we can do better,” Swaminathan added. WHO officials are reviewing hundreds of scientific reports every day, she said, and not all are of good quality. For this reason, she and other scientists at WHO perform a “living systematic review” – updating the consensus of evidence on a weekly basis.
“This process on COVID-19 will, I am sure, continue for the weeks and months to come,” she added.
This article first appeared on Medscape.com.
FDA approves Qwo for treatment of cellulite
. The drug is the first injectable treatment for cellulite to receive regulatory approval.

In cellulite, fibrous septae are a primary contributing factor. The septae make up the fibrous connective tissue that connects the skin perpendicularly to the fascia below and tether the skin, drawing it downward and leading to a mattress-like appearance, commonly referred to as “dimpling.” When injected into the treatment area, Qwo is thought to release the fibrous septae enzymatically by specifically targeting types 1 and 3 collagen, which may result in smoothing of the skin and an improved appearance of cellulite.
The most common side effects of Qwo include injection site bruising, pain, areas of hardness, itching, redness, discoloration, swelling, and warmth in the treatment area.
Qwo is expected to be available throughout the United States at aesthetic health care practitioner’s offices starting in Spring 2021.
“Qwo could be a game-changer for many women with cellulite,” Anne Chapas, MD, a board-certified dermatologist at Union Square Laser Dermatology in New York, said in a press release. “I am thrilled there will now be an FDA-approved injectable treatment option proven to address a root cause of cellulite. What is exciting about Qwo is that it is a cutting-edge cellulite treatment, without the cutting,” Dr. Chapas, said.
. The drug is the first injectable treatment for cellulite to receive regulatory approval.
In cellulite, fibrous septae are a primary contributing factor. The septae make up the fibrous connective tissue that connects the skin perpendicularly to the fascia below and tether the skin, drawing it downward and leading to a mattress-like appearance, commonly referred to as “dimpling.” When injected into the treatment area, Qwo is thought to release the fibrous septae enzymatically by specifically targeting types 1 and 3 collagen, which may result in smoothing of the skin and an improved appearance of cellulite.
The most common side effects of Qwo include injection site bruising, pain, areas of hardness, itching, redness, discoloration, swelling, and warmth in the treatment area.
Qwo is expected to be available throughout the United States at aesthetic health care practitioner’s offices starting in Spring 2021.
“Qwo could be a game-changer for many women with cellulite,” Anne Chapas, MD, a board-certified dermatologist at Union Square Laser Dermatology in New York, said in a press release. “I am thrilled there will now be an FDA-approved injectable treatment option proven to address a root cause of cellulite. What is exciting about Qwo is that it is a cutting-edge cellulite treatment, without the cutting,” Dr. Chapas, said.
. The drug is the first injectable treatment for cellulite to receive regulatory approval.
In cellulite, fibrous septae are a primary contributing factor. The septae make up the fibrous connective tissue that connects the skin perpendicularly to the fascia below and tether the skin, drawing it downward and leading to a mattress-like appearance, commonly referred to as “dimpling.” When injected into the treatment area, Qwo is thought to release the fibrous septae enzymatically by specifically targeting types 1 and 3 collagen, which may result in smoothing of the skin and an improved appearance of cellulite.
The most common side effects of Qwo include injection site bruising, pain, areas of hardness, itching, redness, discoloration, swelling, and warmth in the treatment area.
Qwo is expected to be available throughout the United States at aesthetic health care practitioner’s offices starting in Spring 2021.
“Qwo could be a game-changer for many women with cellulite,” Anne Chapas, MD, a board-certified dermatologist at Union Square Laser Dermatology in New York, said in a press release. “I am thrilled there will now be an FDA-approved injectable treatment option proven to address a root cause of cellulite. What is exciting about Qwo is that it is a cutting-edge cellulite treatment, without the cutting,” Dr. Chapas, said.