User login
Physician income drops, burnout spikes globally in pandemic
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
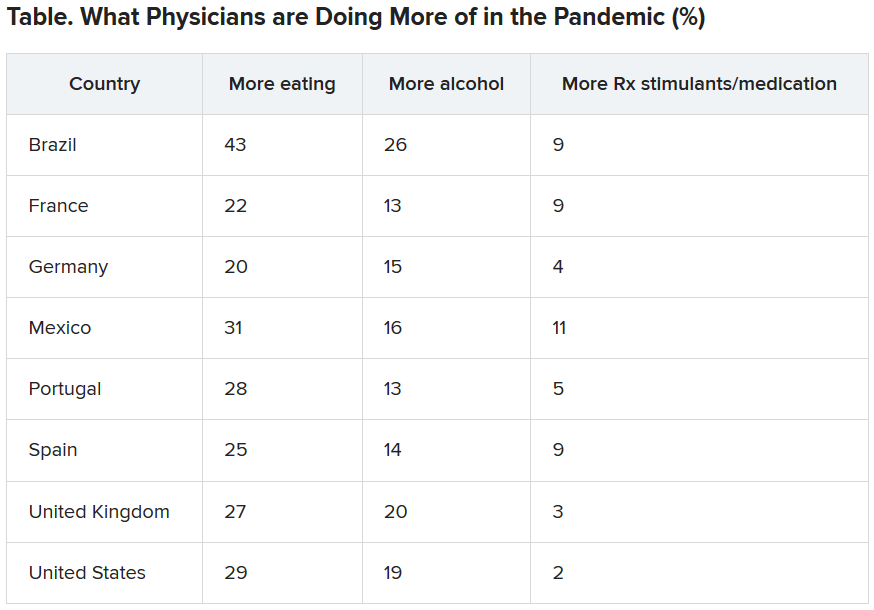
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
according to the results of a Medscape survey.
More than 7,500 physicians – nearly 5,000 in the United States, and others in Brazil, France, Germany, Mexico, Portugal, Spain, and the United Kingdom – responded to questions about their struggles to save patients and how the pandemic has changed their income and their lives at home and at work.
The pain was evident in this response from an emergency medicine physician in Spain: “It has been the worst time in my life ever, in both my personal and professional life.”
Conversely, some reported positive effects.
An internist in Brazil wrote: “I feel more proud of my career than ever before.”
One quarter of U.S. physicians considering earlier retirement
Physicians in the United States were asked what career changes, if any, they were considering in light of their experience with COVID-19. Although a little more than half (51%) said they were not planning any changes, 25% answered, “retiring earlier than previously planned,” and 12% answered, “a career change away from medicine.”
The number of physicians reporting an income drop was highest in Brazil (63% reported a drop), followed by the United States (62%), Mexico (56%), Portugal (49%), Germany (42%), France (41%), and Spain (31%). The question was not asked in the United Kingdom survey.
In the United States, the size of the drop has been substantial: 9% lost 76%-100% of their income; 14% lost 51%-75%; 28% lost 26%-50%; 33% lost 11%-25%; and 15% lost 1%-10%.
The U.S. specialists with the largest drop in income were ophthalmologists, who lost 51%, followed by allergists (46%), plastic surgeons (46%), and otolaryngologists (45%).
“I’m looking for a new profession due to economic impact,” an otolaryngologist in the United States said. “We are at risk while essentially using our private savings to keep our practice solvent.”
More than half of U.S. physicians (54%) have personally treated patients with COVID-19. Percentages were higher in France, Spain, and the United Kingdom (percentages ranged from 60%-68%).
The United States led all eight countries in treating patients with COVID-19 via telemedicine, at 26%. Germany had the lowest telemedicine percentage, at 10%.
Burnout intensifies
About two thirds of US physicians (64%) said that burnout had intensified during the crisis (70% of female physicians and 61% of male physicians said it had).
Many factors are feeding the burnout.
A critical care physician in the United States responded, “It is terrible to see people arriving at their rooms and assuming they were going to die soon; to see people saying goodbye to their families before dying or before being intubated.”
In all eight countries, a substantial percentage of physicians reported they “sometimes, often or always” treated patients with COVID-19 without the proper personal protective equipment. Spain had by far the largest percentage who answered that way (67%), followed by France (45%), Mexico (40%), the United Kingdom (34%), Brazil and Germany (28% each); and the United States and Portugal (23% each).
A U.S. rheumatologist wrote: “The fact that we were sent to take care of infectious patients without proper protection equipment made me feel we were betrayed in this fight.”
Sense of duty to volunteer to treat COVID-19 patients varied substantially among countries, from 69% who felt that way in Spain to 40% in Brazil. Half (50%) in the United States felt that way.
“Altruism must take second place where a real and present threat exists to my own personal existence,” one U.S. internist wrote.
Numbers personally infected
One fifth of physicians in Spain and the United Kingdom had personally been infected with the virus. Brazil, France, and Mexico had the next highest numbers, with 13%-15% of physicians infected; 5%-6% in the United States, Germany, and Portugal said they had been infected.
The percentage of physicians who reported that immediate family members had been infected ranged from 25% in Spain to 6% in Portugal. Among US physicians, 9% reported that family members had been diagnosed with COVID-19.
In the United States, 44% of respondents who had family living with them at home during the pandemic reported that relationships at home were more stressed because of stay-at-home guidelines and social distancing. Almost half (47%) said there had been no change, and 9% said relationships were less stressed.
Eating is coping mechanism of choice
Physicians were asked what they were doing more of during the pandemic, and food seemed to be the top source of comfort in all eight countries.
Loneliness reports differ across globe
Portugal had the highest percentage (51%) of physicians reporting increased loneliness. Next were Brazil (48%), the United States (46%), the United Kingdom (42%), France (41%), Spain and Mexico (40% each), and Germany (32%).
All eight countries lacked workplace activities to help physicians with grief. More than half (55%) of U.K. physicians reported having such activities available at their workplace, whereas only 25% of physicians in Germany did; 12%-24% of respondents across the countries were unsure about the offerings.
This article first appeared on Medscape.com.
The march of immunotherapy continues at ESMO 2020
The use of immunotherapy for upper gastrointestinal tumors and renal cancer, ALK- and EGFR-targeted agents in non–small cell lung cancer (NSCLC), and the next step in personalized prostate cancer management will all be subjects of headlining presentations at the ESMO Virtual Congress 2020.
The conference will, like so many other major events, be held online this year because of the COVID-19 pandemic.
John B. Haanen, PhD, ESMO 2020 scientific chair, who is from the Netherlands Cancer Institute, Amsterdam, the Netherlands, told Medscape Medical News that, because the congress is being held online this year, fewer abstracts were submitted; nevertheless, “We were very happy to see ... that the quality was very good.”
The number of submissions was not the only problem the organizing committee had to face in transforming the ESMO Congress into a virtual meeting.
They were unable to fit the scientific and educational programs together and so have had to split them over two consecutive weekends. Moreover, many of the sessions were highly interactive and needed to be either adapted or omitted.
“So the program is somewhat different,” Haanen said. He noted that “the presentations were also made shorter, especially on the educational sessions, because...we can’t expect people to sit behind screens for hours listening to long presentations.”
He added: “That was out of the question.”
Haanen is nevertheless hopeful that the virtual meeting will be “very exciting.”
Solange Peters, MD, PhD, ESMO president, who is also affiliated with the Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland, said in a press conference that it was a “sacrifice” to move ESMO 2020 online and that “there were very sad moments” when deciding on the content.
However, there were some benefits from the change.
She said that all of the ESMO meetings this year have seen “huge” increases in the number of attendees and the geographical span or reach of each of the conferences.
“So suddenly you also realize that, what is one of the missions of ESMO being to convey education globally ... was probably better reached, better achieved with the virtual format,” she commented.
Presidential symposia
Turning to the program, Haanen first picked out the third presidential symposium, which will be held on Monday, September 21. This will focus entirely on upper gastrointestinal tumors in both the adjuvant and metastatic setting.
He said that in recent years, “very little progress has been made” in this area, with treatment mostly consisting of chemotherapy and chemoradiotherapy.
However, this year’s presentations will explore the addition of immunotherapy either to chemotherapy or as an adjuvant treatment following completion of standard-of-care treatment for local disease.
Haanen said that the results will be “very interesting ... and may change current practice,” something that “is very important for both doctors and their patients.”
On Saturday, September 19, the first presidential symposium will include two presentations on lung cancer that Haanen said will offer some “exciting new [results] that I am sure will change clinical practice.”
One will be on the CROWN phase 3 trial comparing lorlatinib and crizotinib in the first-line treatment of patients with advanced ALK-positive NSCLC.
The other will present results on central nervous system disease recurrence from the ADAURA phase 3 trial of osimertinib adjuvant therapy in patients with resected EGFR-mutated NSCLC.
The same session will also see new data in advanced renal cell carcinoma from CheckMate 9ER, in which the c-Met and VEGFR2 inhibitor cabozantinib (Cabometyx) was combined with nivolumab (Opdivo) and compared to sunitinib (Sutent) in untreated patients.
“Last year, there were already some exciting results of the combination of axitinib [Inlyta], either with pembrolizumab [Keytruda] or with avelumab [Bavencio]...in the first-line setting in metastatic clear cell renal cell cancer,” Hannen said.
“Clearly there was a survival advantage over the standard of care, sunitinib,” he added.
This year, not only will efficacy data from CheckMate 9ER be presented but also quality-of-life results.
“That’s very important, because what everybody is afraid of is that, by adding drugs, you always get more impact on the quality of life, but you will see that the quality-of-life results are very exciting,” he said.
The second presidential symposium will feature studies on prostate cancer, notably the phase 3 IPATential150 trial of abiraterone (Zytiga) plus either ipatasertib or placebo in metastatic castration-resistant prostate cancer.
Ipatasertib targets Akt, and Haanen said that “by adding it to, let’s say, standard-of-care treatment ... the question of course of will be, Does that have a better outcome?”
He believes the results will be a “very nice illustration” that prostate cancer management is heading in the direction of personalized treatment.
Alongside the presidential symposia, there will be a number of proffered paper sessions on the latest results in all aspects of oncology, including results from the ASCENT trial in triple-negative breast cancer, as well as a dedicated COVID-19 track.
Haanen said that the ESMO Virtual Congress 2020, coming after the AACR and ASCO annual meetings, has the “advantage” of being able to present the latest outcomes of patients treated with chemotherapy and immunotherapy against the backdrop of the pandemic.
This will include a study from the ESMO Resilience Task Force on the impact of COVID-19 on oncology professionals both in terms of their personal distress and burnout and their job performance.
“I think that is very important,” Haanen said, “especially because the whole thing with COVID-19 is not yet over, and everybody is preparing for a second wave in the fall and winter.
“It may help us give us clues on how we can protect ourselves or each other to prevent burnout or other problems that we as healthcare caregivers face in this difficult period.”
Next year
For next year, Peters remains hopeful that the ESMO 2021 meeting will take place as planned in Paris.
She anticipates that, indeed, ESMO meetings will be able to take place from spring next year.
This will depend on a vaccine for COVID-19 becoming widely available, although oncologists in some countries may still not be able to travel.
This means “starting probably with hybrid formats, with some of the faculty being on site and some not, [and] the same thing for the attendees,” Peters said.
She suggested that, for ESMO Congress 2021 to work as an on-site meeting, it will require at least half or two-thirds of the originally anticipated number of attendees.
“I hope that Paris next year will happen,” Peters said, adding that it “will probably happen with less attendees – that’s fine, but [still] with a large number of faculty and attendees.”
The commentators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The use of immunotherapy for upper gastrointestinal tumors and renal cancer, ALK- and EGFR-targeted agents in non–small cell lung cancer (NSCLC), and the next step in personalized prostate cancer management will all be subjects of headlining presentations at the ESMO Virtual Congress 2020.
The conference will, like so many other major events, be held online this year because of the COVID-19 pandemic.
John B. Haanen, PhD, ESMO 2020 scientific chair, who is from the Netherlands Cancer Institute, Amsterdam, the Netherlands, told Medscape Medical News that, because the congress is being held online this year, fewer abstracts were submitted; nevertheless, “We were very happy to see ... that the quality was very good.”
The number of submissions was not the only problem the organizing committee had to face in transforming the ESMO Congress into a virtual meeting.
They were unable to fit the scientific and educational programs together and so have had to split them over two consecutive weekends. Moreover, many of the sessions were highly interactive and needed to be either adapted or omitted.
“So the program is somewhat different,” Haanen said. He noted that “the presentations were also made shorter, especially on the educational sessions, because...we can’t expect people to sit behind screens for hours listening to long presentations.”
He added: “That was out of the question.”
Haanen is nevertheless hopeful that the virtual meeting will be “very exciting.”
Solange Peters, MD, PhD, ESMO president, who is also affiliated with the Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland, said in a press conference that it was a “sacrifice” to move ESMO 2020 online and that “there were very sad moments” when deciding on the content.
However, there were some benefits from the change.
She said that all of the ESMO meetings this year have seen “huge” increases in the number of attendees and the geographical span or reach of each of the conferences.
“So suddenly you also realize that, what is one of the missions of ESMO being to convey education globally ... was probably better reached, better achieved with the virtual format,” she commented.
Presidential symposia
Turning to the program, Haanen first picked out the third presidential symposium, which will be held on Monday, September 21. This will focus entirely on upper gastrointestinal tumors in both the adjuvant and metastatic setting.
He said that in recent years, “very little progress has been made” in this area, with treatment mostly consisting of chemotherapy and chemoradiotherapy.
However, this year’s presentations will explore the addition of immunotherapy either to chemotherapy or as an adjuvant treatment following completion of standard-of-care treatment for local disease.
Haanen said that the results will be “very interesting ... and may change current practice,” something that “is very important for both doctors and their patients.”
On Saturday, September 19, the first presidential symposium will include two presentations on lung cancer that Haanen said will offer some “exciting new [results] that I am sure will change clinical practice.”
One will be on the CROWN phase 3 trial comparing lorlatinib and crizotinib in the first-line treatment of patients with advanced ALK-positive NSCLC.
The other will present results on central nervous system disease recurrence from the ADAURA phase 3 trial of osimertinib adjuvant therapy in patients with resected EGFR-mutated NSCLC.
The same session will also see new data in advanced renal cell carcinoma from CheckMate 9ER, in which the c-Met and VEGFR2 inhibitor cabozantinib (Cabometyx) was combined with nivolumab (Opdivo) and compared to sunitinib (Sutent) in untreated patients.
“Last year, there were already some exciting results of the combination of axitinib [Inlyta], either with pembrolizumab [Keytruda] or with avelumab [Bavencio]...in the first-line setting in metastatic clear cell renal cell cancer,” Hannen said.
“Clearly there was a survival advantage over the standard of care, sunitinib,” he added.
This year, not only will efficacy data from CheckMate 9ER be presented but also quality-of-life results.
“That’s very important, because what everybody is afraid of is that, by adding drugs, you always get more impact on the quality of life, but you will see that the quality-of-life results are very exciting,” he said.
The second presidential symposium will feature studies on prostate cancer, notably the phase 3 IPATential150 trial of abiraterone (Zytiga) plus either ipatasertib or placebo in metastatic castration-resistant prostate cancer.
Ipatasertib targets Akt, and Haanen said that “by adding it to, let’s say, standard-of-care treatment ... the question of course of will be, Does that have a better outcome?”
He believes the results will be a “very nice illustration” that prostate cancer management is heading in the direction of personalized treatment.
Alongside the presidential symposia, there will be a number of proffered paper sessions on the latest results in all aspects of oncology, including results from the ASCENT trial in triple-negative breast cancer, as well as a dedicated COVID-19 track.
Haanen said that the ESMO Virtual Congress 2020, coming after the AACR and ASCO annual meetings, has the “advantage” of being able to present the latest outcomes of patients treated with chemotherapy and immunotherapy against the backdrop of the pandemic.
This will include a study from the ESMO Resilience Task Force on the impact of COVID-19 on oncology professionals both in terms of their personal distress and burnout and their job performance.
“I think that is very important,” Haanen said, “especially because the whole thing with COVID-19 is not yet over, and everybody is preparing for a second wave in the fall and winter.
“It may help us give us clues on how we can protect ourselves or each other to prevent burnout or other problems that we as healthcare caregivers face in this difficult period.”
Next year
For next year, Peters remains hopeful that the ESMO 2021 meeting will take place as planned in Paris.
She anticipates that, indeed, ESMO meetings will be able to take place from spring next year.
This will depend on a vaccine for COVID-19 becoming widely available, although oncologists in some countries may still not be able to travel.
This means “starting probably with hybrid formats, with some of the faculty being on site and some not, [and] the same thing for the attendees,” Peters said.
She suggested that, for ESMO Congress 2021 to work as an on-site meeting, it will require at least half or two-thirds of the originally anticipated number of attendees.
“I hope that Paris next year will happen,” Peters said, adding that it “will probably happen with less attendees – that’s fine, but [still] with a large number of faculty and attendees.”
The commentators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The use of immunotherapy for upper gastrointestinal tumors and renal cancer, ALK- and EGFR-targeted agents in non–small cell lung cancer (NSCLC), and the next step in personalized prostate cancer management will all be subjects of headlining presentations at the ESMO Virtual Congress 2020.
The conference will, like so many other major events, be held online this year because of the COVID-19 pandemic.
John B. Haanen, PhD, ESMO 2020 scientific chair, who is from the Netherlands Cancer Institute, Amsterdam, the Netherlands, told Medscape Medical News that, because the congress is being held online this year, fewer abstracts were submitted; nevertheless, “We were very happy to see ... that the quality was very good.”
The number of submissions was not the only problem the organizing committee had to face in transforming the ESMO Congress into a virtual meeting.
They were unable to fit the scientific and educational programs together and so have had to split them over two consecutive weekends. Moreover, many of the sessions were highly interactive and needed to be either adapted or omitted.
“So the program is somewhat different,” Haanen said. He noted that “the presentations were also made shorter, especially on the educational sessions, because...we can’t expect people to sit behind screens for hours listening to long presentations.”
He added: “That was out of the question.”
Haanen is nevertheless hopeful that the virtual meeting will be “very exciting.”
Solange Peters, MD, PhD, ESMO president, who is also affiliated with the Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland, said in a press conference that it was a “sacrifice” to move ESMO 2020 online and that “there were very sad moments” when deciding on the content.
However, there were some benefits from the change.
She said that all of the ESMO meetings this year have seen “huge” increases in the number of attendees and the geographical span or reach of each of the conferences.
“So suddenly you also realize that, what is one of the missions of ESMO being to convey education globally ... was probably better reached, better achieved with the virtual format,” she commented.
Presidential symposia
Turning to the program, Haanen first picked out the third presidential symposium, which will be held on Monday, September 21. This will focus entirely on upper gastrointestinal tumors in both the adjuvant and metastatic setting.
He said that in recent years, “very little progress has been made” in this area, with treatment mostly consisting of chemotherapy and chemoradiotherapy.
However, this year’s presentations will explore the addition of immunotherapy either to chemotherapy or as an adjuvant treatment following completion of standard-of-care treatment for local disease.
Haanen said that the results will be “very interesting ... and may change current practice,” something that “is very important for both doctors and their patients.”
On Saturday, September 19, the first presidential symposium will include two presentations on lung cancer that Haanen said will offer some “exciting new [results] that I am sure will change clinical practice.”
One will be on the CROWN phase 3 trial comparing lorlatinib and crizotinib in the first-line treatment of patients with advanced ALK-positive NSCLC.
The other will present results on central nervous system disease recurrence from the ADAURA phase 3 trial of osimertinib adjuvant therapy in patients with resected EGFR-mutated NSCLC.
The same session will also see new data in advanced renal cell carcinoma from CheckMate 9ER, in which the c-Met and VEGFR2 inhibitor cabozantinib (Cabometyx) was combined with nivolumab (Opdivo) and compared to sunitinib (Sutent) in untreated patients.
“Last year, there were already some exciting results of the combination of axitinib [Inlyta], either with pembrolizumab [Keytruda] or with avelumab [Bavencio]...in the first-line setting in metastatic clear cell renal cell cancer,” Hannen said.
“Clearly there was a survival advantage over the standard of care, sunitinib,” he added.
This year, not only will efficacy data from CheckMate 9ER be presented but also quality-of-life results.
“That’s very important, because what everybody is afraid of is that, by adding drugs, you always get more impact on the quality of life, but you will see that the quality-of-life results are very exciting,” he said.
The second presidential symposium will feature studies on prostate cancer, notably the phase 3 IPATential150 trial of abiraterone (Zytiga) plus either ipatasertib or placebo in metastatic castration-resistant prostate cancer.
Ipatasertib targets Akt, and Haanen said that “by adding it to, let’s say, standard-of-care treatment ... the question of course of will be, Does that have a better outcome?”
He believes the results will be a “very nice illustration” that prostate cancer management is heading in the direction of personalized treatment.
Alongside the presidential symposia, there will be a number of proffered paper sessions on the latest results in all aspects of oncology, including results from the ASCENT trial in triple-negative breast cancer, as well as a dedicated COVID-19 track.
Haanen said that the ESMO Virtual Congress 2020, coming after the AACR and ASCO annual meetings, has the “advantage” of being able to present the latest outcomes of patients treated with chemotherapy and immunotherapy against the backdrop of the pandemic.
This will include a study from the ESMO Resilience Task Force on the impact of COVID-19 on oncology professionals both in terms of their personal distress and burnout and their job performance.
“I think that is very important,” Haanen said, “especially because the whole thing with COVID-19 is not yet over, and everybody is preparing for a second wave in the fall and winter.
“It may help us give us clues on how we can protect ourselves or each other to prevent burnout or other problems that we as healthcare caregivers face in this difficult period.”
Next year
For next year, Peters remains hopeful that the ESMO 2021 meeting will take place as planned in Paris.
She anticipates that, indeed, ESMO meetings will be able to take place from spring next year.
This will depend on a vaccine for COVID-19 becoming widely available, although oncologists in some countries may still not be able to travel.
This means “starting probably with hybrid formats, with some of the faculty being on site and some not, [and] the same thing for the attendees,” Peters said.
She suggested that, for ESMO Congress 2021 to work as an on-site meeting, it will require at least half or two-thirds of the originally anticipated number of attendees.
“I hope that Paris next year will happen,” Peters said, adding that it “will probably happen with less attendees – that’s fine, but [still] with a large number of faculty and attendees.”
The commentators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
FROM ESMO 2020
Lusutrombopag found safe, effective for severe thrombocytopenia in patients with hepatocellular carcinoma
For patients with severe thrombocytopenia and chronic liver diseases, including hepatocellular carcinoma, treatment with lusutrombopag prior to invasive procedures significantly decreased the need for platelet transfusions without increasing the need for rescue treatment for bleeding or the rate of thromboembolic events.
In a post hoc analysis of data from 270 patients in two manufacturer-sponsored, multicenter, randomized, double-blind, placebo-controlled, phase 3 trials, significantly more lusutrombopag recipients met the primary efficacy endpoint, including patients with hepatocellular carcinoma (68.0% vs. 8.9% in the placebo group; P < .0001) and those without it (77.0% vs. 21.6%; P < .0001). Rates of treatment-emergent adverse events were similar between the lusutrombopag and placebo groups, and patients with hepatocellular carcinoma were not at increased risk for thrombosis, Naim Alkhouri, MD, of Texas Liver Institute in San Antonio, and associates wrote in Clinical Gastroenterology and Hepatology.
Platelet transfusion is the treatment mainstay for patients with thrombocytopenia related to cirrhosis who are undergoing invasive procedures, but its effects are short-lived, and at least one in five transfusions fails. Thrombopoietin agonists such as lusutrombopag are efficacious and approved in this setting, but they can be prothrombotic, particularly in patients with hepatocellular carcinoma, who already are at heightened risk for portal vein thrombosis.
Dr. Alkhouri and associates performed an integrated analysis of the PLUS 1 trial (Japan, October 2013–May 2014) and the L-PLUS 2 (global, June 2015–April 2017). Participants were adults with Child-Pugh Class A or B chronic liver disease and baseline platelet counts under 50 x 109 per L who were scheduled for invasive procedures. Of the 270 patients, 95 had hepatocellular carcinoma. Patients were randomly assigned on a one-to-one basis to receive either lusutrombopag (3 mg) or placebo daily for up to 7 days before procedures. The primary endpoint was the percentage of patients in the per-protocol population who did not need a platelet transfusion before the invasive procedure or rescue therapy within 7 days afterward.
The treatment and placebo arms were similar except that patients with hepatocellular carcinoma were about 10 years older on average. In patients with hepatocellular carcinoma, 60.5% more lusutrombopag recipients than placebo recipients met the primary endpoint, and rates of bleeding-related adverse events were 9.1% and 15.7%, respectively. In patients with other chronic liver diseases, 52.6% more lusutrombopag recipients met the primary endpoint. Rates of bleeding-related adverse events were 5% and 10.6%.
“Approximately 88% of patients with hepatocellular carcinoma underwent a liver-related procedure, compared with approximately 10% of patients without hepatocellular carcinoma,” the investigators wrote. “This is significant because ablations or transcatheter arterial chemoembolizations can be associated with serious bleeding complications. It is clinically important that, given the greater number of liver-related procedures, the incidence of bleeding-related adverse events was lower in patients treated with lusutrombopag than placebo.”
Imaging after the procedures confirmed low rates of thromboses in both groups and subgroups. Four patients developed portal vein thromboses, including two lusutrombopag recipients (one of whom had hepatocellular carcinoma) and two placebo recipients without hepatocellular carcinoma.
These trials excluded patients undergoing major surgical procedures and those with decompensated cirrhosis; portal vein thrombosis; hematopoietic tumors; aplastic anemia; myelodysplastic syndrome; myelofibrosis; liver transplantation; splenectomy; and thrombocytopenia that was congenital, autoimmune, or drug induced. “A limitation of this study was the high rate of protocol violations related to platelet transfusions,” the researchers noted. “A number of patients [42 in all] were excluded from the per-protocol population owing to receipt of unnecessary platelet transfusions, or because they did not receive a needed platelet transfusion.”Shionogi makes lusutrombopag and sponsored the study. Dr. Alkhouri reported an advisory relationship with Shionogi and Dova Pharma. Two coinvestigators reported being employed by Shionogi. Three coinvestigators also disclosed ties to Shionogi and to several other pharmaceutical companies.
SOURCE: Alkhouri N et al. Clin Gastroenterol Hepatol. 2020 Mar 20. doi: 10.1016/j.cgh.2020.03.032.
Thrombocytopenia is of clinical concern in patients with cirrhosis, as it complicates routine patient care and results in delayed or canceled procedures due to concern for risk of bleeding. In the last few years, availability of thrombopoietin (TPO) receptor agonists have facilitated the performance of elective invasive procedures in cirrhotic patients with severe thrombocytopenia.

In this integrated analysis of data from two phase 3 studies, Alkhouri et al. demonstrated the efficacy of a novel TPO receptor agonist, lusutrombopag, in reducing bleeding events and need for platelet transfusion in cirrhotic patients undergoing invasive procedures. The risk for thrombosis-related adverse events was not increased in lusutrombopag recipients with or without HCC. Previous studies with another TPO, eltrombopag, resulted in high rate of symptomatic portal vein thrombosis. Avatrombopag, a recently approved TPO receptor agonist reported few thrombotic symptomatic events but no prospective imaging for evaluation of thrombotic events was included in the protocol. A unique strength of this study was inclusion of prospective imaging for evaluation of portal vein thrombosis. Strategic scheduling is required with use of TPO agonists. Lusutrombopag can be given orally in convenient daily doses and provides a 7-10-day procedural window for scheduling and performing elective invasive procedures. However, because of several days of lag period for platelet production, these agents cannot be used for emergent cases.
Gagan K. Sood, MD, AGAF, FAASLD, is an associate professor of medicine and surgery, division of gastroenterology and hepatology and division of abdominal transplantation, Baylor College of Medicine, Houston. He has no conflicts of interest.
Thrombocytopenia is of clinical concern in patients with cirrhosis, as it complicates routine patient care and results in delayed or canceled procedures due to concern for risk of bleeding. In the last few years, availability of thrombopoietin (TPO) receptor agonists have facilitated the performance of elective invasive procedures in cirrhotic patients with severe thrombocytopenia.
In this integrated analysis of data from two phase 3 studies, Alkhouri et al. demonstrated the efficacy of a novel TPO receptor agonist, lusutrombopag, in reducing bleeding events and need for platelet transfusion in cirrhotic patients undergoing invasive procedures. The risk for thrombosis-related adverse events was not increased in lusutrombopag recipients with or without HCC. Previous studies with another TPO, eltrombopag, resulted in high rate of symptomatic portal vein thrombosis. Avatrombopag, a recently approved TPO receptor agonist reported few thrombotic symptomatic events but no prospective imaging for evaluation of thrombotic events was included in the protocol. A unique strength of this study was inclusion of prospective imaging for evaluation of portal vein thrombosis. Strategic scheduling is required with use of TPO agonists. Lusutrombopag can be given orally in convenient daily doses and provides a 7-10-day procedural window for scheduling and performing elective invasive procedures. However, because of several days of lag period for platelet production, these agents cannot be used for emergent cases.
Gagan K. Sood, MD, AGAF, FAASLD, is an associate professor of medicine and surgery, division of gastroenterology and hepatology and division of abdominal transplantation, Baylor College of Medicine, Houston. He has no conflicts of interest.
Thrombocytopenia is of clinical concern in patients with cirrhosis, as it complicates routine patient care and results in delayed or canceled procedures due to concern for risk of bleeding. In the last few years, availability of thrombopoietin (TPO) receptor agonists have facilitated the performance of elective invasive procedures in cirrhotic patients with severe thrombocytopenia.
In this integrated analysis of data from two phase 3 studies, Alkhouri et al. demonstrated the efficacy of a novel TPO receptor agonist, lusutrombopag, in reducing bleeding events and need for platelet transfusion in cirrhotic patients undergoing invasive procedures. The risk for thrombosis-related adverse events was not increased in lusutrombopag recipients with or without HCC. Previous studies with another TPO, eltrombopag, resulted in high rate of symptomatic portal vein thrombosis. Avatrombopag, a recently approved TPO receptor agonist reported few thrombotic symptomatic events but no prospective imaging for evaluation of thrombotic events was included in the protocol. A unique strength of this study was inclusion of prospective imaging for evaluation of portal vein thrombosis. Strategic scheduling is required with use of TPO agonists. Lusutrombopag can be given orally in convenient daily doses and provides a 7-10-day procedural window for scheduling and performing elective invasive procedures. However, because of several days of lag period for platelet production, these agents cannot be used for emergent cases.
Gagan K. Sood, MD, AGAF, FAASLD, is an associate professor of medicine and surgery, division of gastroenterology and hepatology and division of abdominal transplantation, Baylor College of Medicine, Houston. He has no conflicts of interest.
For patients with severe thrombocytopenia and chronic liver diseases, including hepatocellular carcinoma, treatment with lusutrombopag prior to invasive procedures significantly decreased the need for platelet transfusions without increasing the need for rescue treatment for bleeding or the rate of thromboembolic events.
In a post hoc analysis of data from 270 patients in two manufacturer-sponsored, multicenter, randomized, double-blind, placebo-controlled, phase 3 trials, significantly more lusutrombopag recipients met the primary efficacy endpoint, including patients with hepatocellular carcinoma (68.0% vs. 8.9% in the placebo group; P < .0001) and those without it (77.0% vs. 21.6%; P < .0001). Rates of treatment-emergent adverse events were similar between the lusutrombopag and placebo groups, and patients with hepatocellular carcinoma were not at increased risk for thrombosis, Naim Alkhouri, MD, of Texas Liver Institute in San Antonio, and associates wrote in Clinical Gastroenterology and Hepatology.
Platelet transfusion is the treatment mainstay for patients with thrombocytopenia related to cirrhosis who are undergoing invasive procedures, but its effects are short-lived, and at least one in five transfusions fails. Thrombopoietin agonists such as lusutrombopag are efficacious and approved in this setting, but they can be prothrombotic, particularly in patients with hepatocellular carcinoma, who already are at heightened risk for portal vein thrombosis.
Dr. Alkhouri and associates performed an integrated analysis of the PLUS 1 trial (Japan, October 2013–May 2014) and the L-PLUS 2 (global, June 2015–April 2017). Participants were adults with Child-Pugh Class A or B chronic liver disease and baseline platelet counts under 50 x 109 per L who were scheduled for invasive procedures. Of the 270 patients, 95 had hepatocellular carcinoma. Patients were randomly assigned on a one-to-one basis to receive either lusutrombopag (3 mg) or placebo daily for up to 7 days before procedures. The primary endpoint was the percentage of patients in the per-protocol population who did not need a platelet transfusion before the invasive procedure or rescue therapy within 7 days afterward.
The treatment and placebo arms were similar except that patients with hepatocellular carcinoma were about 10 years older on average. In patients with hepatocellular carcinoma, 60.5% more lusutrombopag recipients than placebo recipients met the primary endpoint, and rates of bleeding-related adverse events were 9.1% and 15.7%, respectively. In patients with other chronic liver diseases, 52.6% more lusutrombopag recipients met the primary endpoint. Rates of bleeding-related adverse events were 5% and 10.6%.
“Approximately 88% of patients with hepatocellular carcinoma underwent a liver-related procedure, compared with approximately 10% of patients without hepatocellular carcinoma,” the investigators wrote. “This is significant because ablations or transcatheter arterial chemoembolizations can be associated with serious bleeding complications. It is clinically important that, given the greater number of liver-related procedures, the incidence of bleeding-related adverse events was lower in patients treated with lusutrombopag than placebo.”
Imaging after the procedures confirmed low rates of thromboses in both groups and subgroups. Four patients developed portal vein thromboses, including two lusutrombopag recipients (one of whom had hepatocellular carcinoma) and two placebo recipients without hepatocellular carcinoma.
These trials excluded patients undergoing major surgical procedures and those with decompensated cirrhosis; portal vein thrombosis; hematopoietic tumors; aplastic anemia; myelodysplastic syndrome; myelofibrosis; liver transplantation; splenectomy; and thrombocytopenia that was congenital, autoimmune, or drug induced. “A limitation of this study was the high rate of protocol violations related to platelet transfusions,” the researchers noted. “A number of patients [42 in all] were excluded from the per-protocol population owing to receipt of unnecessary platelet transfusions, or because they did not receive a needed platelet transfusion.”Shionogi makes lusutrombopag and sponsored the study. Dr. Alkhouri reported an advisory relationship with Shionogi and Dova Pharma. Two coinvestigators reported being employed by Shionogi. Three coinvestigators also disclosed ties to Shionogi and to several other pharmaceutical companies.
SOURCE: Alkhouri N et al. Clin Gastroenterol Hepatol. 2020 Mar 20. doi: 10.1016/j.cgh.2020.03.032.
For patients with severe thrombocytopenia and chronic liver diseases, including hepatocellular carcinoma, treatment with lusutrombopag prior to invasive procedures significantly decreased the need for platelet transfusions without increasing the need for rescue treatment for bleeding or the rate of thromboembolic events.
In a post hoc analysis of data from 270 patients in two manufacturer-sponsored, multicenter, randomized, double-blind, placebo-controlled, phase 3 trials, significantly more lusutrombopag recipients met the primary efficacy endpoint, including patients with hepatocellular carcinoma (68.0% vs. 8.9% in the placebo group; P < .0001) and those without it (77.0% vs. 21.6%; P < .0001). Rates of treatment-emergent adverse events were similar between the lusutrombopag and placebo groups, and patients with hepatocellular carcinoma were not at increased risk for thrombosis, Naim Alkhouri, MD, of Texas Liver Institute in San Antonio, and associates wrote in Clinical Gastroenterology and Hepatology.
Platelet transfusion is the treatment mainstay for patients with thrombocytopenia related to cirrhosis who are undergoing invasive procedures, but its effects are short-lived, and at least one in five transfusions fails. Thrombopoietin agonists such as lusutrombopag are efficacious and approved in this setting, but they can be prothrombotic, particularly in patients with hepatocellular carcinoma, who already are at heightened risk for portal vein thrombosis.
Dr. Alkhouri and associates performed an integrated analysis of the PLUS 1 trial (Japan, October 2013–May 2014) and the L-PLUS 2 (global, June 2015–April 2017). Participants were adults with Child-Pugh Class A or B chronic liver disease and baseline platelet counts under 50 x 109 per L who were scheduled for invasive procedures. Of the 270 patients, 95 had hepatocellular carcinoma. Patients were randomly assigned on a one-to-one basis to receive either lusutrombopag (3 mg) or placebo daily for up to 7 days before procedures. The primary endpoint was the percentage of patients in the per-protocol population who did not need a platelet transfusion before the invasive procedure or rescue therapy within 7 days afterward.
The treatment and placebo arms were similar except that patients with hepatocellular carcinoma were about 10 years older on average. In patients with hepatocellular carcinoma, 60.5% more lusutrombopag recipients than placebo recipients met the primary endpoint, and rates of bleeding-related adverse events were 9.1% and 15.7%, respectively. In patients with other chronic liver diseases, 52.6% more lusutrombopag recipients met the primary endpoint. Rates of bleeding-related adverse events were 5% and 10.6%.
“Approximately 88% of patients with hepatocellular carcinoma underwent a liver-related procedure, compared with approximately 10% of patients without hepatocellular carcinoma,” the investigators wrote. “This is significant because ablations or transcatheter arterial chemoembolizations can be associated with serious bleeding complications. It is clinically important that, given the greater number of liver-related procedures, the incidence of bleeding-related adverse events was lower in patients treated with lusutrombopag than placebo.”
Imaging after the procedures confirmed low rates of thromboses in both groups and subgroups. Four patients developed portal vein thromboses, including two lusutrombopag recipients (one of whom had hepatocellular carcinoma) and two placebo recipients without hepatocellular carcinoma.
These trials excluded patients undergoing major surgical procedures and those with decompensated cirrhosis; portal vein thrombosis; hematopoietic tumors; aplastic anemia; myelodysplastic syndrome; myelofibrosis; liver transplantation; splenectomy; and thrombocytopenia that was congenital, autoimmune, or drug induced. “A limitation of this study was the high rate of protocol violations related to platelet transfusions,” the researchers noted. “A number of patients [42 in all] were excluded from the per-protocol population owing to receipt of unnecessary platelet transfusions, or because they did not receive a needed platelet transfusion.”Shionogi makes lusutrombopag and sponsored the study. Dr. Alkhouri reported an advisory relationship with Shionogi and Dova Pharma. Two coinvestigators reported being employed by Shionogi. Three coinvestigators also disclosed ties to Shionogi and to several other pharmaceutical companies.
SOURCE: Alkhouri N et al. Clin Gastroenterol Hepatol. 2020 Mar 20. doi: 10.1016/j.cgh.2020.03.032.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Reworked OxyContin fails to cut overall opioid abuse, FDA panel says
The long-awaited postmarketing studies of the abuse-deterrent formulation (ADF) of OxyContin (Perdue Pharma) received mixed reviews from a Food and Drug Administration joint advisory committee.

After a 2-day discussion of new research submitted by Perdue, as well as other relevant published data, most members of the Drug Safety and Risk Management and Anesthetic and Analgesic Drug Products advisory committees came to the conclusion that the reformulated drug “meaningfully” reduced abuse via intranasal administration and intravenous injection, but not overall opioid abuse or overdose.
The reformulated OxyContin “was the first out of the gate,” and “has the greatest market penetration of any ADF” so “it gives us the greatest opportunity to measure change before and after reformulation,” said committee member Traci C. Green, PhD, MSc, professor and director of the Opioid Policy Research Collaborative at Brandeis University, Waltham, Mass.
The FDA approved the original formulation of OxyContin (oxycodone hydrochloride), a mu-receptor opioid agonist, in December 1995 for the management of pain requiring daily round-the-clock opioid treatment in cases where other treatments were inadequate. It approved an ADF version of the product in April 2010.
The updated formulation incorporates polyethylene oxide, an inactive polymer that makes the tablet harder and more crush resistant. The tablet turns into a gel or glue-like substance when wet.
At the request of the FDA, the company carried out four postmarketing studies, which the FDA also reviewed.
- A National Addictions Vigilance Intervention and Prevention Program study that included 66,897 assessments in patients undergoing evaluation for substance use or entering an opioid addiction program. Results showed a drop in up to 52% of self-reported past 30-day OxyContin injection and snorting versus comparators, including extended-release morphine and immediate-release hydrocodone.
- An analysis of 308,465 calls to U.S. poison centers showing a reduction of up to 28% for calls regarding intentional OxyContin-related exposures immediately following the drug’s reformulation. However, the FDA analysis concluded it is unclear whether the decline was attributable to the drug’s reformulation or co-occurring trends.
- A study of 63,528 individuals entering methadone clinics or treatment programs that showed a reduction of up to 27% in OxyContin abuse versus comparators. There was no information on route of abuse. Here, the FDA analysis determined the results were mixed and didn’t provide compelling evidence.
- A claims-based analysis of patients who were dispensed an opioid (297,836 OxyContin; 659,673 a comparator) that showed no evidence that the updated product affected the rate of fatal and nonfatal opioid overdoses.

During the meeting, committee members heard that opioid use in the United States peaked in 2012, with 260 million prescriptions dispensed, then declined by 41% by 2019. ADFs accounted for only 2% of prescriptions in 2019. They also heard that results of a wide variety of studies and surveys support the conclusion that misuse, abuse, and diversion of OxyContin decreased after it was reformulated.
Ultimately, the joint committee voted 20 to 7 (with 1 abstention) that the reformulated drug reduced nonoral abuse. Most members who voted in favor cited the NAVIPPRO study as a reason for their decision, but few found the strength of the evidence better than moderate.
Meeting chair Sonia Hernandez-Diaz, MD, professor of epidemiology, Harvard School of Public Health, Boston, noted the reduction in abuse may, in part, be a result of the overall reduction in opioid use.
Jon E. Zibbell, PhD, senior public health scientist, behavioral health research division, RTI International, Atlanta, who voted “no,” was disappointed there was not more data.
“We had a bunch of years for this and so many of us could have done some amazing studies” related to how abuse changed post reformulation, he said.
As for overall abuse deterrence, the committee believed the evidence was less compelling. Only two members voted that the reformulated version of the drug reduced overall abuse and only one member voted that the reformulated tablets reduced opioid overdose.
Members generally agreed that all of the studies had limitations, including retrospective designs, confounding, and potential misclassifications. Many noted the challenge of assessing abuse pre- and post reformulation given the evolving situation.
For instance, at the time the reformulated drug was launched, public health initiatives targeting opioid abuse were introduced, more treatment centers were opening, and there was a crackdown on “pill-mill” doctors.
In addition, prescribing and consumption habits were changing. Some doctors may have switched only “at-risk” patients to the reformulated opioid and there may have been “self-selection” among patients – with some potentially opting for another drug such as immediate-release oxycodone.
During the meeting, there was discussion about how to interpret a “meaningful” abuse reduction. However, there was no consensus of a percentage the reduction had to reach in order to be deemed meaningful.
Another issue discussed was the term “abuse deterrent,” which some members believed was stigmatizing and should be changed to crush resistant.

There was also concern that prescribers might consider the ADF a “safe” or less addictive opioid. Michael Sprintz, DO, clinical assistant professor, division of geriatric and palliative medicine, University of Texas Health Science Center, Houston, said ADFs might provide physicians with “a false sense of security.”
Dr. Sprintz, also founder of the Sprintz Center for Pain and Recovery, noted the importance of pain medicine physicians understanding addiction and addiction specialists understanding pain management.
Other committee members voiced concern that the reformulation results in patients switching from intravenous and intranasal abuse to oral abuse. Committed abusers can still swallow multiple pills.
Some members noted that reformulated OxyContin coincided with increased transition to heroin, which is relatively cheap and readily available. However, they recognized that proving causality is difficult.
The committee was reminded that the reformulated drug provides a significant barrier against, but doesn’t altogether eliminate, opioid abuse. With hot water and the right tools, the tablets can still be manipulated.
In addition, the reformulated drug will not solve the U.S. opioid epidemic, which requires a multifaceted approach. The opioid crisis, said Wilson Compton, MD, deputy director at the National Institute on Drug Abuse, has resulted in a “skyrocketing” of deaths linked to “tremendously potent” forms of fentanyl, emerging stimulant use issues, and the possible increase in drug overdoses linked to COVID-19.
A version of this article originally appeared on Medscape.com.
The long-awaited postmarketing studies of the abuse-deterrent formulation (ADF) of OxyContin (Perdue Pharma) received mixed reviews from a Food and Drug Administration joint advisory committee.
After a 2-day discussion of new research submitted by Perdue, as well as other relevant published data, most members of the Drug Safety and Risk Management and Anesthetic and Analgesic Drug Products advisory committees came to the conclusion that the reformulated drug “meaningfully” reduced abuse via intranasal administration and intravenous injection, but not overall opioid abuse or overdose.
The reformulated OxyContin “was the first out of the gate,” and “has the greatest market penetration of any ADF” so “it gives us the greatest opportunity to measure change before and after reformulation,” said committee member Traci C. Green, PhD, MSc, professor and director of the Opioid Policy Research Collaborative at Brandeis University, Waltham, Mass.
The FDA approved the original formulation of OxyContin (oxycodone hydrochloride), a mu-receptor opioid agonist, in December 1995 for the management of pain requiring daily round-the-clock opioid treatment in cases where other treatments were inadequate. It approved an ADF version of the product in April 2010.
The updated formulation incorporates polyethylene oxide, an inactive polymer that makes the tablet harder and more crush resistant. The tablet turns into a gel or glue-like substance when wet.
At the request of the FDA, the company carried out four postmarketing studies, which the FDA also reviewed.
- A National Addictions Vigilance Intervention and Prevention Program study that included 66,897 assessments in patients undergoing evaluation for substance use or entering an opioid addiction program. Results showed a drop in up to 52% of self-reported past 30-day OxyContin injection and snorting versus comparators, including extended-release morphine and immediate-release hydrocodone.
- An analysis of 308,465 calls to U.S. poison centers showing a reduction of up to 28% for calls regarding intentional OxyContin-related exposures immediately following the drug’s reformulation. However, the FDA analysis concluded it is unclear whether the decline was attributable to the drug’s reformulation or co-occurring trends.
- A study of 63,528 individuals entering methadone clinics or treatment programs that showed a reduction of up to 27% in OxyContin abuse versus comparators. There was no information on route of abuse. Here, the FDA analysis determined the results were mixed and didn’t provide compelling evidence.
- A claims-based analysis of patients who were dispensed an opioid (297,836 OxyContin; 659,673 a comparator) that showed no evidence that the updated product affected the rate of fatal and nonfatal opioid overdoses.
During the meeting, committee members heard that opioid use in the United States peaked in 2012, with 260 million prescriptions dispensed, then declined by 41% by 2019. ADFs accounted for only 2% of prescriptions in 2019. They also heard that results of a wide variety of studies and surveys support the conclusion that misuse, abuse, and diversion of OxyContin decreased after it was reformulated.
Ultimately, the joint committee voted 20 to 7 (with 1 abstention) that the reformulated drug reduced nonoral abuse. Most members who voted in favor cited the NAVIPPRO study as a reason for their decision, but few found the strength of the evidence better than moderate.
Meeting chair Sonia Hernandez-Diaz, MD, professor of epidemiology, Harvard School of Public Health, Boston, noted the reduction in abuse may, in part, be a result of the overall reduction in opioid use.
Jon E. Zibbell, PhD, senior public health scientist, behavioral health research division, RTI International, Atlanta, who voted “no,” was disappointed there was not more data.
“We had a bunch of years for this and so many of us could have done some amazing studies” related to how abuse changed post reformulation, he said.
As for overall abuse deterrence, the committee believed the evidence was less compelling. Only two members voted that the reformulated version of the drug reduced overall abuse and only one member voted that the reformulated tablets reduced opioid overdose.
Members generally agreed that all of the studies had limitations, including retrospective designs, confounding, and potential misclassifications. Many noted the challenge of assessing abuse pre- and post reformulation given the evolving situation.
For instance, at the time the reformulated drug was launched, public health initiatives targeting opioid abuse were introduced, more treatment centers were opening, and there was a crackdown on “pill-mill” doctors.
In addition, prescribing and consumption habits were changing. Some doctors may have switched only “at-risk” patients to the reformulated opioid and there may have been “self-selection” among patients – with some potentially opting for another drug such as immediate-release oxycodone.
During the meeting, there was discussion about how to interpret a “meaningful” abuse reduction. However, there was no consensus of a percentage the reduction had to reach in order to be deemed meaningful.
Another issue discussed was the term “abuse deterrent,” which some members believed was stigmatizing and should be changed to crush resistant.
There was also concern that prescribers might consider the ADF a “safe” or less addictive opioid. Michael Sprintz, DO, clinical assistant professor, division of geriatric and palliative medicine, University of Texas Health Science Center, Houston, said ADFs might provide physicians with “a false sense of security.”
Dr. Sprintz, also founder of the Sprintz Center for Pain and Recovery, noted the importance of pain medicine physicians understanding addiction and addiction specialists understanding pain management.
Other committee members voiced concern that the reformulation results in patients switching from intravenous and intranasal abuse to oral abuse. Committed abusers can still swallow multiple pills.
Some members noted that reformulated OxyContin coincided with increased transition to heroin, which is relatively cheap and readily available. However, they recognized that proving causality is difficult.
The committee was reminded that the reformulated drug provides a significant barrier against, but doesn’t altogether eliminate, opioid abuse. With hot water and the right tools, the tablets can still be manipulated.
In addition, the reformulated drug will not solve the U.S. opioid epidemic, which requires a multifaceted approach. The opioid crisis, said Wilson Compton, MD, deputy director at the National Institute on Drug Abuse, has resulted in a “skyrocketing” of deaths linked to “tremendously potent” forms of fentanyl, emerging stimulant use issues, and the possible increase in drug overdoses linked to COVID-19.
A version of this article originally appeared on Medscape.com.
The long-awaited postmarketing studies of the abuse-deterrent formulation (ADF) of OxyContin (Perdue Pharma) received mixed reviews from a Food and Drug Administration joint advisory committee.
After a 2-day discussion of new research submitted by Perdue, as well as other relevant published data, most members of the Drug Safety and Risk Management and Anesthetic and Analgesic Drug Products advisory committees came to the conclusion that the reformulated drug “meaningfully” reduced abuse via intranasal administration and intravenous injection, but not overall opioid abuse or overdose.
The reformulated OxyContin “was the first out of the gate,” and “has the greatest market penetration of any ADF” so “it gives us the greatest opportunity to measure change before and after reformulation,” said committee member Traci C. Green, PhD, MSc, professor and director of the Opioid Policy Research Collaborative at Brandeis University, Waltham, Mass.
The FDA approved the original formulation of OxyContin (oxycodone hydrochloride), a mu-receptor opioid agonist, in December 1995 for the management of pain requiring daily round-the-clock opioid treatment in cases where other treatments were inadequate. It approved an ADF version of the product in April 2010.
The updated formulation incorporates polyethylene oxide, an inactive polymer that makes the tablet harder and more crush resistant. The tablet turns into a gel or glue-like substance when wet.
At the request of the FDA, the company carried out four postmarketing studies, which the FDA also reviewed.
- A National Addictions Vigilance Intervention and Prevention Program study that included 66,897 assessments in patients undergoing evaluation for substance use or entering an opioid addiction program. Results showed a drop in up to 52% of self-reported past 30-day OxyContin injection and snorting versus comparators, including extended-release morphine and immediate-release hydrocodone.
- An analysis of 308,465 calls to U.S. poison centers showing a reduction of up to 28% for calls regarding intentional OxyContin-related exposures immediately following the drug’s reformulation. However, the FDA analysis concluded it is unclear whether the decline was attributable to the drug’s reformulation or co-occurring trends.
- A study of 63,528 individuals entering methadone clinics or treatment programs that showed a reduction of up to 27% in OxyContin abuse versus comparators. There was no information on route of abuse. Here, the FDA analysis determined the results were mixed and didn’t provide compelling evidence.
- A claims-based analysis of patients who were dispensed an opioid (297,836 OxyContin; 659,673 a comparator) that showed no evidence that the updated product affected the rate of fatal and nonfatal opioid overdoses.
During the meeting, committee members heard that opioid use in the United States peaked in 2012, with 260 million prescriptions dispensed, then declined by 41% by 2019. ADFs accounted for only 2% of prescriptions in 2019. They also heard that results of a wide variety of studies and surveys support the conclusion that misuse, abuse, and diversion of OxyContin decreased after it was reformulated.
Ultimately, the joint committee voted 20 to 7 (with 1 abstention) that the reformulated drug reduced nonoral abuse. Most members who voted in favor cited the NAVIPPRO study as a reason for their decision, but few found the strength of the evidence better than moderate.
Meeting chair Sonia Hernandez-Diaz, MD, professor of epidemiology, Harvard School of Public Health, Boston, noted the reduction in abuse may, in part, be a result of the overall reduction in opioid use.
Jon E. Zibbell, PhD, senior public health scientist, behavioral health research division, RTI International, Atlanta, who voted “no,” was disappointed there was not more data.
“We had a bunch of years for this and so many of us could have done some amazing studies” related to how abuse changed post reformulation, he said.
As for overall abuse deterrence, the committee believed the evidence was less compelling. Only two members voted that the reformulated version of the drug reduced overall abuse and only one member voted that the reformulated tablets reduced opioid overdose.
Members generally agreed that all of the studies had limitations, including retrospective designs, confounding, and potential misclassifications. Many noted the challenge of assessing abuse pre- and post reformulation given the evolving situation.
For instance, at the time the reformulated drug was launched, public health initiatives targeting opioid abuse were introduced, more treatment centers were opening, and there was a crackdown on “pill-mill” doctors.
In addition, prescribing and consumption habits were changing. Some doctors may have switched only “at-risk” patients to the reformulated opioid and there may have been “self-selection” among patients – with some potentially opting for another drug such as immediate-release oxycodone.
During the meeting, there was discussion about how to interpret a “meaningful” abuse reduction. However, there was no consensus of a percentage the reduction had to reach in order to be deemed meaningful.
Another issue discussed was the term “abuse deterrent,” which some members believed was stigmatizing and should be changed to crush resistant.
There was also concern that prescribers might consider the ADF a “safe” or less addictive opioid. Michael Sprintz, DO, clinical assistant professor, division of geriatric and palliative medicine, University of Texas Health Science Center, Houston, said ADFs might provide physicians with “a false sense of security.”
Dr. Sprintz, also founder of the Sprintz Center for Pain and Recovery, noted the importance of pain medicine physicians understanding addiction and addiction specialists understanding pain management.
Other committee members voiced concern that the reformulation results in patients switching from intravenous and intranasal abuse to oral abuse. Committed abusers can still swallow multiple pills.
Some members noted that reformulated OxyContin coincided with increased transition to heroin, which is relatively cheap and readily available. However, they recognized that proving causality is difficult.
The committee was reminded that the reformulated drug provides a significant barrier against, but doesn’t altogether eliminate, opioid abuse. With hot water and the right tools, the tablets can still be manipulated.
In addition, the reformulated drug will not solve the U.S. opioid epidemic, which requires a multifaceted approach. The opioid crisis, said Wilson Compton, MD, deputy director at the National Institute on Drug Abuse, has resulted in a “skyrocketing” of deaths linked to “tremendously potent” forms of fentanyl, emerging stimulant use issues, and the possible increase in drug overdoses linked to COVID-19.
A version of this article originally appeared on Medscape.com.
AGA Clinical Practice Update: Diagnosis and treatment of small intestinal bacterial overgrowth
Unexplained diarrhea may be the most reliable symptom of small intestinal bacterial overgrowth (SIBO) in at-risk patients, according to a new clinical practice update from the American Gastroenterological Association.
“In those predisposed to SIBO due to anatomical, pathological, pharmacological or other changes that promote stasis or recirculation of colonic contents and/or impaired resistance to bacteria, SIBO will lead to diarrhea and can progress to a full-blown malabsorption syndrome” marked by steatorrhea and vitamin deficiencies, wrote Eamonn M.M. Quigley, MD, of Houston Methodist Hospital and Weill Cornell Medical College in Houston together with his fellow experts in Gastroenterology. But malabsorption is uncommon in patients whose SIBO is not caused by structural abnormalities, and gastrointestinal symptoms are “weakly predictive at best” if patients lack clear risk factors for SIBO, the experts cautioned.
The growing availability of breath testing has fueled diagnoses of SIBO, which the lay press often implicates in various disorders even though SIBO has no clear clinical or laboratory definition. Recent progress in techniques to measure bacterial populations and their metabolic products “should provide much needed clarity,” but for now, a SIBO diagnosis simply means that a patient’s presenting symptoms or laboratory findings are attributed to bacterial changes in the small intestine, the experts wrote.
Detecting SIBO also remains challenging. Most patients have normal results on routine laboratory tests, and there is not enough evidence to support testing for inflammatory markers such as fecal calprotectin. Patients with SIBO may have increased folate levels because of bacterial production of folic acid. Vitamin B12 and other nutrient deficiencies also occur but are less common. The preferred diagnostic method is culture of a duodenal aspirate, and recent research supports a cutoff value of greater than 103 CFUs of coliform bacteria per mL. Breath testing is less invasive but “more complex than simply measuring hydrogen,” the experts stressed. Methane-producing microorganisms (methanogens) suppress hydrogen on a breath test (fortunately, standard breath tests measure methane). Furthermore, a positive methane breath test also has been linked to constipation-predominant irritable bowel syndrome (IBS). Recent studies also suggest that lactulose breath testing is more sensitive than glucose for identifying SIBO in patients with IBS.
Antibiotic therapy is the treatment mainstay but remains largely empiric. The goal is to improve SIBO symptoms, not eradicate bacteria from the small intestine. Ideally, the antimicrobial regimen should cover both aerobic and anaerobic bacteria, but clinicians should be mindful of the risks of chronic broad-spectrum antibiotic exposure. In studies, a single 7- to 10-day antibiotic course improved symptoms in approximately 45%-90% of patients with SIBO (rates of breath test response were lower). For patients with IBS and SIBO, rifaximin (which is poorly absorbed) produced encouraging results in two phase 3 studies, but most patients did not receive breath testing, the experts noted. Patients with recurrent SIBO symptoms may need multiple courses of antibiotics with specific regimens rotated to help prevent resistance. “Decisions on management should be individualized and also [should factor in] such risks as diarrhea, Clostridiodes difficile infection, intolerance, and cost,” the experts wrote. “It is not necessary to repeat diagnostic tests for SIBO following antibiotic therapy [if] gastrointestinal symptoms respond.”
Dr. Quigley disclosed financial ties to 4D Pharma, Alimentary Health, Allergan, Biocodex, Biomerica, Ironwood, Salix, Takeda, Vibrant, and Zealand. He also disclosed patents with and equity in Alimentary Health. Both of his coauthors also disclosed ties to various pharmaceutical companies.
SOURCE: Quigley EMM et al. Gastroenterology. 2020 Jun 1. doi: 10.1053/j.gastro.2020.06.090.
Unexplained diarrhea may be the most reliable symptom of small intestinal bacterial overgrowth (SIBO) in at-risk patients, according to a new clinical practice update from the American Gastroenterological Association.
“In those predisposed to SIBO due to anatomical, pathological, pharmacological or other changes that promote stasis or recirculation of colonic contents and/or impaired resistance to bacteria, SIBO will lead to diarrhea and can progress to a full-blown malabsorption syndrome” marked by steatorrhea and vitamin deficiencies, wrote Eamonn M.M. Quigley, MD, of Houston Methodist Hospital and Weill Cornell Medical College in Houston together with his fellow experts in Gastroenterology. But malabsorption is uncommon in patients whose SIBO is not caused by structural abnormalities, and gastrointestinal symptoms are “weakly predictive at best” if patients lack clear risk factors for SIBO, the experts cautioned.
The growing availability of breath testing has fueled diagnoses of SIBO, which the lay press often implicates in various disorders even though SIBO has no clear clinical or laboratory definition. Recent progress in techniques to measure bacterial populations and their metabolic products “should provide much needed clarity,” but for now, a SIBO diagnosis simply means that a patient’s presenting symptoms or laboratory findings are attributed to bacterial changes in the small intestine, the experts wrote.
Detecting SIBO also remains challenging. Most patients have normal results on routine laboratory tests, and there is not enough evidence to support testing for inflammatory markers such as fecal calprotectin. Patients with SIBO may have increased folate levels because of bacterial production of folic acid. Vitamin B12 and other nutrient deficiencies also occur but are less common. The preferred diagnostic method is culture of a duodenal aspirate, and recent research supports a cutoff value of greater than 103 CFUs of coliform bacteria per mL. Breath testing is less invasive but “more complex than simply measuring hydrogen,” the experts stressed. Methane-producing microorganisms (methanogens) suppress hydrogen on a breath test (fortunately, standard breath tests measure methane). Furthermore, a positive methane breath test also has been linked to constipation-predominant irritable bowel syndrome (IBS). Recent studies also suggest that lactulose breath testing is more sensitive than glucose for identifying SIBO in patients with IBS.
Antibiotic therapy is the treatment mainstay but remains largely empiric. The goal is to improve SIBO symptoms, not eradicate bacteria from the small intestine. Ideally, the antimicrobial regimen should cover both aerobic and anaerobic bacteria, but clinicians should be mindful of the risks of chronic broad-spectrum antibiotic exposure. In studies, a single 7- to 10-day antibiotic course improved symptoms in approximately 45%-90% of patients with SIBO (rates of breath test response were lower). For patients with IBS and SIBO, rifaximin (which is poorly absorbed) produced encouraging results in two phase 3 studies, but most patients did not receive breath testing, the experts noted. Patients with recurrent SIBO symptoms may need multiple courses of antibiotics with specific regimens rotated to help prevent resistance. “Decisions on management should be individualized and also [should factor in] such risks as diarrhea, Clostridiodes difficile infection, intolerance, and cost,” the experts wrote. “It is not necessary to repeat diagnostic tests for SIBO following antibiotic therapy [if] gastrointestinal symptoms respond.”
Dr. Quigley disclosed financial ties to 4D Pharma, Alimentary Health, Allergan, Biocodex, Biomerica, Ironwood, Salix, Takeda, Vibrant, and Zealand. He also disclosed patents with and equity in Alimentary Health. Both of his coauthors also disclosed ties to various pharmaceutical companies.
SOURCE: Quigley EMM et al. Gastroenterology. 2020 Jun 1. doi: 10.1053/j.gastro.2020.06.090.
Unexplained diarrhea may be the most reliable symptom of small intestinal bacterial overgrowth (SIBO) in at-risk patients, according to a new clinical practice update from the American Gastroenterological Association.
“In those predisposed to SIBO due to anatomical, pathological, pharmacological or other changes that promote stasis or recirculation of colonic contents and/or impaired resistance to bacteria, SIBO will lead to diarrhea and can progress to a full-blown malabsorption syndrome” marked by steatorrhea and vitamin deficiencies, wrote Eamonn M.M. Quigley, MD, of Houston Methodist Hospital and Weill Cornell Medical College in Houston together with his fellow experts in Gastroenterology. But malabsorption is uncommon in patients whose SIBO is not caused by structural abnormalities, and gastrointestinal symptoms are “weakly predictive at best” if patients lack clear risk factors for SIBO, the experts cautioned.
The growing availability of breath testing has fueled diagnoses of SIBO, which the lay press often implicates in various disorders even though SIBO has no clear clinical or laboratory definition. Recent progress in techniques to measure bacterial populations and their metabolic products “should provide much needed clarity,” but for now, a SIBO diagnosis simply means that a patient’s presenting symptoms or laboratory findings are attributed to bacterial changes in the small intestine, the experts wrote.
Detecting SIBO also remains challenging. Most patients have normal results on routine laboratory tests, and there is not enough evidence to support testing for inflammatory markers such as fecal calprotectin. Patients with SIBO may have increased folate levels because of bacterial production of folic acid. Vitamin B12 and other nutrient deficiencies also occur but are less common. The preferred diagnostic method is culture of a duodenal aspirate, and recent research supports a cutoff value of greater than 103 CFUs of coliform bacteria per mL. Breath testing is less invasive but “more complex than simply measuring hydrogen,” the experts stressed. Methane-producing microorganisms (methanogens) suppress hydrogen on a breath test (fortunately, standard breath tests measure methane). Furthermore, a positive methane breath test also has been linked to constipation-predominant irritable bowel syndrome (IBS). Recent studies also suggest that lactulose breath testing is more sensitive than glucose for identifying SIBO in patients with IBS.
Antibiotic therapy is the treatment mainstay but remains largely empiric. The goal is to improve SIBO symptoms, not eradicate bacteria from the small intestine. Ideally, the antimicrobial regimen should cover both aerobic and anaerobic bacteria, but clinicians should be mindful of the risks of chronic broad-spectrum antibiotic exposure. In studies, a single 7- to 10-day antibiotic course improved symptoms in approximately 45%-90% of patients with SIBO (rates of breath test response were lower). For patients with IBS and SIBO, rifaximin (which is poorly absorbed) produced encouraging results in two phase 3 studies, but most patients did not receive breath testing, the experts noted. Patients with recurrent SIBO symptoms may need multiple courses of antibiotics with specific regimens rotated to help prevent resistance. “Decisions on management should be individualized and also [should factor in] such risks as diarrhea, Clostridiodes difficile infection, intolerance, and cost,” the experts wrote. “It is not necessary to repeat diagnostic tests for SIBO following antibiotic therapy [if] gastrointestinal symptoms respond.”
Dr. Quigley disclosed financial ties to 4D Pharma, Alimentary Health, Allergan, Biocodex, Biomerica, Ironwood, Salix, Takeda, Vibrant, and Zealand. He also disclosed patents with and equity in Alimentary Health. Both of his coauthors also disclosed ties to various pharmaceutical companies.
SOURCE: Quigley EMM et al. Gastroenterology. 2020 Jun 1. doi: 10.1053/j.gastro.2020.06.090.
FROM GASTROENTEROLOGY
Mega vitamin D harms bone in women, not men, without osteoporosis
“More is not necessarily better” when it comes to vitamin D supplements for women with adequate serum levels, new research suggests.
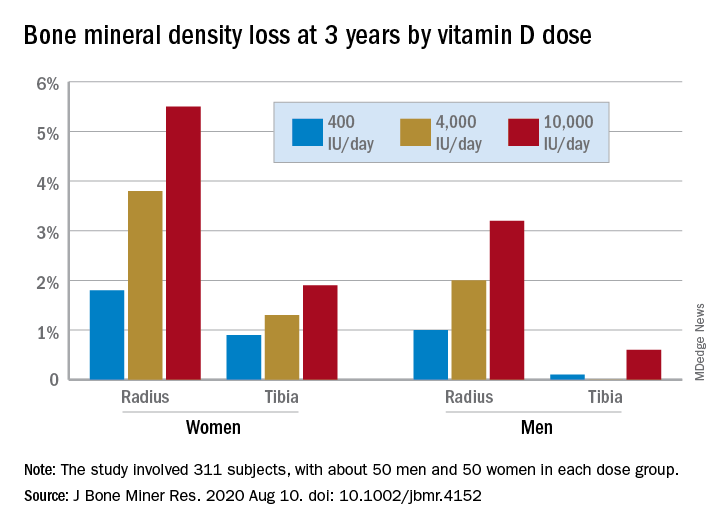
In a study of healthy 55- to 70-year-old women who took very-high-dose vitamin D supplements – either 4,000 IU/day or the previously identified “upper safe limit” of 10,000 IU/day – for 3 years had a significantly greater loss of total bone mineral density (BMD) at the radius and tibia than did women who took 400 IU/day. However, this effect was not seen in men. And the higher-dose vitamin D supplements did not improve bone strength in men or women.
But this was an exploratory post hoc analysis, and these were healthy community-dwelling adults with sufficient serum vitamin D levels (and no osteoporosis) at study entry, stressed lead researcher Lauren A. Burt, PhD, from the University of Calgary, in Alberta, Canada.
Dr. Burt presented these findings Sept. 11 at the virtual American Society of Bone and Mineral Research (ASBMR) 2020 annual meeting, and the study was also recently published online in the Journal of Bone and Mineral Research.
The results suggest that, “if you have normal bone density and adequate levels of vitamin D, there is no bone benefit in taking doses of vitamin D above the standard recommendations designed to prevent vitamin D deficiency, and doses at or above 4,000 IU/day might even be detrimental to bone, especially in females,” Dr. Burt said in an interview.
“These results are clinically relevant,” Dr. Burt and her coauthors wrote, “as vitamin D supplementation is widely administered to postmenopausal females for osteoporosis prevention.”
“Our findings do not support a benefit of high-dose vitamin D supplementation for bone health and raise the possibility of harm for females.”
Invited to comment, Meryl S. LeBoff, MD, of Harvard Medical School, Boston, said in an interview that this finding “warrants further research” because it is “important” to discover sex differences in bone responses to vitamin D.
“This doesn’t apply to osteoporosis”
Dr. LeBoff was lead author of a subanalysis of the Vitamin D and Omega-3 Trial (VITAL).
As she reported at last year’s ASBMR meeting, that analysis showed that, in healthy adults who did not have vitamin D insufficiency, taking vitamin D3 supplements for 2 years did not improve BMD, compared with placebo (recently published), nor was this linked with fewer fractures.
Dr. LeBoff pointed out that the current study investigated “very high doses of vitamin D” – at least double the 2,000 IU/day doses examined in VITAL.
Also, the serum vitamin D levels in this study were “above what we considered the upper normal limit for our assay in our hospital,” she noted, and there was no placebo control.
“We did not see any adverse effects of 2,000 IU/day vitamin D,” Dr. LeBoff stressed.
“At the same time, we didn’t see any significant benefits in terms of bone density because they already had achieved a normal level of vitamin D sufficient for bone.”
But “this doesn’t apply to patients with vitamin D deficiency, patients with osteoporosis, or low bone mass, in which case we would recommend vitamin D.”
Some patients take more vitamin D than they need because they think more is better, said LeBoff, but this study suggests “more is not necessarily better.”
“There’s been a concern for several years that too much vitamin D may be associated with increased fractures,” she emphasized.
Post hoc analysis
The current study analyzed new data from the Calgary Vitamin D study.
That study found no benefit in BMD or bone strength (JAMA. 2019;322[8]:736-45), contrary to the researchers’ hypothesis that high-dose vitamin D supplements would be associated with greater calcium absorption and parathyroid hormone suppression and, thus, reduced age-related bone loss (improved bone density and strength).
Instead, they found a negative dose-response relationship, which “should be regarded as hypothesis generating, requiring confirmation with further research,” they wrote.
The current study sought to determine if there were sex differences in the effect of vitamin D supplements on bone health in this population.
From October 2013 to December 2017, the Canada Vitamin D study enrolled 311 participants (53% male). To be eligible for the study, participants had to have serum 25-hydroxyvitamin D levels greater than 30 nmol/L and less than 125 nmol/L. They also needed to have adequate calcium intake (1,200 mg/day, as defined by the U.S. Institute of Medicine), or if not, they were instructed to take an appropriate calcium supplement dose.
Patients were randomized to receive 400, 4,000, or 10,000 IU/day of vitamin D3 cholecalciferol, given as 5 drops/day of liquid (Ddrops), with roughly 50 men and 50 women in each dose group.
Researchers selected the 400 IU/day dose as the comparator because the Institute of Medicine recommends a vitamin D intake of 600 IU/day for adults under age 70 years to provide the vitamin D needed for bone health. The typical Canadian diet includes 200-300 IU/day of vitamin D, so individuals would need a supplement of 400 IU/day to reach the recommended intake. The 4,000 IU/day dose is the recommended tolerable upper intake level, according to the Institute of Medicine. And the 10,000 IU/day dose is the tolerable upper intake level of vitamin D as identified in a review by Hathcock and colleagues (Am J Clin Nutr. 2007;85:6-18).
Participants underwent scans with high-resolution peripheral quantitative computed tomography (HR-pQCT) to measure total volumetric BMD at the radius and tibia at baseline, 6, 12, 24, and 36 months. Finite element analysis was used to estimate bone strength.
After 3 years, women had lost significantly more BMD at the radius after taking high-dose versus 400 IU/day of vitamin D. Losses in BMD at the tibia followed a similar trend but were smaller (Figure 1). There were no significant changes in this measure among men (Figure 2).
There were also no significant changes in bone strength among men or women.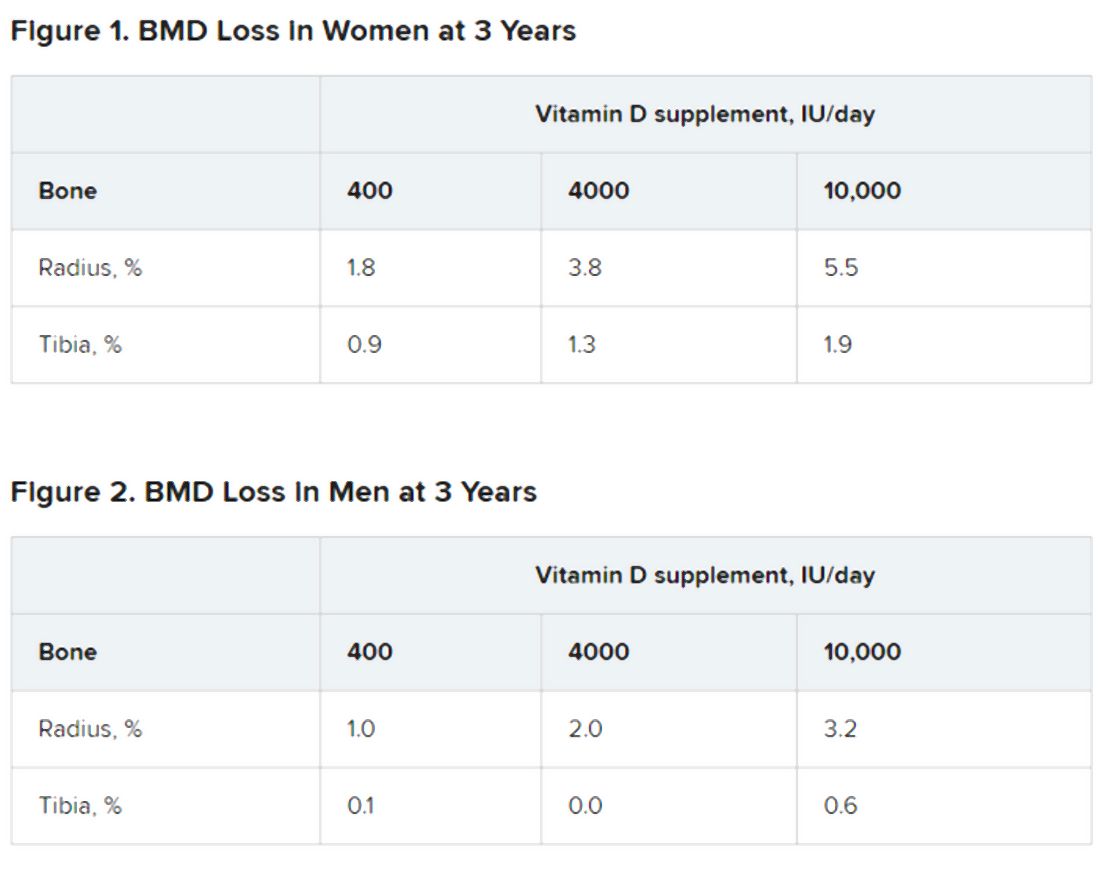
Biological mechanism remains to be determined
Dr. LeBoff said a “possible biological explanation” for the findings is that “women, particularly when they are younger, lose more bone than men.”
“Postmenopausal females do lose bone at an accelerated rate compared with males,” Dr. Burt agreed, “but at the time the study was designed, there was no reason to believe that high-dose vitamin D supplementation would accelerate the problem.”
“The biological mechanism of the vitamin D–related bone loss needs further investigation,” Dr. Burt added, “but there are laboratory data suggesting that supraphysiologic doses of active metabolites of vitamin D may stimulate bone resorption.”
The study was funded by the Pure North S’Energy Foundation. Dr. Burt has reported no relevant financial relationships. Disclosures for the other authors are listed with the article. Dr. LeBoff has reported receiving grants from the National Institutes of Health for the VITAL analysis.
A version of this article originally appeared on Medscape.com.
“More is not necessarily better” when it comes to vitamin D supplements for women with adequate serum levels, new research suggests.
In a study of healthy 55- to 70-year-old women who took very-high-dose vitamin D supplements – either 4,000 IU/day or the previously identified “upper safe limit” of 10,000 IU/day – for 3 years had a significantly greater loss of total bone mineral density (BMD) at the radius and tibia than did women who took 400 IU/day. However, this effect was not seen in men. And the higher-dose vitamin D supplements did not improve bone strength in men or women.
But this was an exploratory post hoc analysis, and these were healthy community-dwelling adults with sufficient serum vitamin D levels (and no osteoporosis) at study entry, stressed lead researcher Lauren A. Burt, PhD, from the University of Calgary, in Alberta, Canada.
Dr. Burt presented these findings Sept. 11 at the virtual American Society of Bone and Mineral Research (ASBMR) 2020 annual meeting, and the study was also recently published online in the Journal of Bone and Mineral Research.
The results suggest that, “if you have normal bone density and adequate levels of vitamin D, there is no bone benefit in taking doses of vitamin D above the standard recommendations designed to prevent vitamin D deficiency, and doses at or above 4,000 IU/day might even be detrimental to bone, especially in females,” Dr. Burt said in an interview.
“These results are clinically relevant,” Dr. Burt and her coauthors wrote, “as vitamin D supplementation is widely administered to postmenopausal females for osteoporosis prevention.”
“Our findings do not support a benefit of high-dose vitamin D supplementation for bone health and raise the possibility of harm for females.”
Invited to comment, Meryl S. LeBoff, MD, of Harvard Medical School, Boston, said in an interview that this finding “warrants further research” because it is “important” to discover sex differences in bone responses to vitamin D.
“This doesn’t apply to osteoporosis”
Dr. LeBoff was lead author of a subanalysis of the Vitamin D and Omega-3 Trial (VITAL).
As she reported at last year’s ASBMR meeting, that analysis showed that, in healthy adults who did not have vitamin D insufficiency, taking vitamin D3 supplements for 2 years did not improve BMD, compared with placebo (recently published), nor was this linked with fewer fractures.
Dr. LeBoff pointed out that the current study investigated “very high doses of vitamin D” – at least double the 2,000 IU/day doses examined in VITAL.
Also, the serum vitamin D levels in this study were “above what we considered the upper normal limit for our assay in our hospital,” she noted, and there was no placebo control.
“We did not see any adverse effects of 2,000 IU/day vitamin D,” Dr. LeBoff stressed.
“At the same time, we didn’t see any significant benefits in terms of bone density because they already had achieved a normal level of vitamin D sufficient for bone.”
But “this doesn’t apply to patients with vitamin D deficiency, patients with osteoporosis, or low bone mass, in which case we would recommend vitamin D.”
Some patients take more vitamin D than they need because they think more is better, said LeBoff, but this study suggests “more is not necessarily better.”
“There’s been a concern for several years that too much vitamin D may be associated with increased fractures,” she emphasized.
Post hoc analysis
The current study analyzed new data from the Calgary Vitamin D study.
That study found no benefit in BMD or bone strength (JAMA. 2019;322[8]:736-45), contrary to the researchers’ hypothesis that high-dose vitamin D supplements would be associated with greater calcium absorption and parathyroid hormone suppression and, thus, reduced age-related bone loss (improved bone density and strength).
Instead, they found a negative dose-response relationship, which “should be regarded as hypothesis generating, requiring confirmation with further research,” they wrote.
The current study sought to determine if there were sex differences in the effect of vitamin D supplements on bone health in this population.
From October 2013 to December 2017, the Canada Vitamin D study enrolled 311 participants (53% male). To be eligible for the study, participants had to have serum 25-hydroxyvitamin D levels greater than 30 nmol/L and less than 125 nmol/L. They also needed to have adequate calcium intake (1,200 mg/day, as defined by the U.S. Institute of Medicine), or if not, they were instructed to take an appropriate calcium supplement dose.
Patients were randomized to receive 400, 4,000, or 10,000 IU/day of vitamin D3 cholecalciferol, given as 5 drops/day of liquid (Ddrops), with roughly 50 men and 50 women in each dose group.
Researchers selected the 400 IU/day dose as the comparator because the Institute of Medicine recommends a vitamin D intake of 600 IU/day for adults under age 70 years to provide the vitamin D needed for bone health. The typical Canadian diet includes 200-300 IU/day of vitamin D, so individuals would need a supplement of 400 IU/day to reach the recommended intake. The 4,000 IU/day dose is the recommended tolerable upper intake level, according to the Institute of Medicine. And the 10,000 IU/day dose is the tolerable upper intake level of vitamin D as identified in a review by Hathcock and colleagues (Am J Clin Nutr. 2007;85:6-18).
Participants underwent scans with high-resolution peripheral quantitative computed tomography (HR-pQCT) to measure total volumetric BMD at the radius and tibia at baseline, 6, 12, 24, and 36 months. Finite element analysis was used to estimate bone strength.
After 3 years, women had lost significantly more BMD at the radius after taking high-dose versus 400 IU/day of vitamin D. Losses in BMD at the tibia followed a similar trend but were smaller (Figure 1). There were no significant changes in this measure among men (Figure 2).
There were also no significant changes in bone strength among men or women.
Biological mechanism remains to be determined
Dr. LeBoff said a “possible biological explanation” for the findings is that “women, particularly when they are younger, lose more bone than men.”
“Postmenopausal females do lose bone at an accelerated rate compared with males,” Dr. Burt agreed, “but at the time the study was designed, there was no reason to believe that high-dose vitamin D supplementation would accelerate the problem.”
“The biological mechanism of the vitamin D–related bone loss needs further investigation,” Dr. Burt added, “but there are laboratory data suggesting that supraphysiologic doses of active metabolites of vitamin D may stimulate bone resorption.”
The study was funded by the Pure North S’Energy Foundation. Dr. Burt has reported no relevant financial relationships. Disclosures for the other authors are listed with the article. Dr. LeBoff has reported receiving grants from the National Institutes of Health for the VITAL analysis.
A version of this article originally appeared on Medscape.com.
“More is not necessarily better” when it comes to vitamin D supplements for women with adequate serum levels, new research suggests.
In a study of healthy 55- to 70-year-old women who took very-high-dose vitamin D supplements – either 4,000 IU/day or the previously identified “upper safe limit” of 10,000 IU/day – for 3 years had a significantly greater loss of total bone mineral density (BMD) at the radius and tibia than did women who took 400 IU/day. However, this effect was not seen in men. And the higher-dose vitamin D supplements did not improve bone strength in men or women.
But this was an exploratory post hoc analysis, and these were healthy community-dwelling adults with sufficient serum vitamin D levels (and no osteoporosis) at study entry, stressed lead researcher Lauren A. Burt, PhD, from the University of Calgary, in Alberta, Canada.
Dr. Burt presented these findings Sept. 11 at the virtual American Society of Bone and Mineral Research (ASBMR) 2020 annual meeting, and the study was also recently published online in the Journal of Bone and Mineral Research.
The results suggest that, “if you have normal bone density and adequate levels of vitamin D, there is no bone benefit in taking doses of vitamin D above the standard recommendations designed to prevent vitamin D deficiency, and doses at or above 4,000 IU/day might even be detrimental to bone, especially in females,” Dr. Burt said in an interview.
“These results are clinically relevant,” Dr. Burt and her coauthors wrote, “as vitamin D supplementation is widely administered to postmenopausal females for osteoporosis prevention.”
“Our findings do not support a benefit of high-dose vitamin D supplementation for bone health and raise the possibility of harm for females.”
Invited to comment, Meryl S. LeBoff, MD, of Harvard Medical School, Boston, said in an interview that this finding “warrants further research” because it is “important” to discover sex differences in bone responses to vitamin D.
“This doesn’t apply to osteoporosis”
Dr. LeBoff was lead author of a subanalysis of the Vitamin D and Omega-3 Trial (VITAL).
As she reported at last year’s ASBMR meeting, that analysis showed that, in healthy adults who did not have vitamin D insufficiency, taking vitamin D3 supplements for 2 years did not improve BMD, compared with placebo (recently published), nor was this linked with fewer fractures.
Dr. LeBoff pointed out that the current study investigated “very high doses of vitamin D” – at least double the 2,000 IU/day doses examined in VITAL.
Also, the serum vitamin D levels in this study were “above what we considered the upper normal limit for our assay in our hospital,” she noted, and there was no placebo control.
“We did not see any adverse effects of 2,000 IU/day vitamin D,” Dr. LeBoff stressed.
“At the same time, we didn’t see any significant benefits in terms of bone density because they already had achieved a normal level of vitamin D sufficient for bone.”
But “this doesn’t apply to patients with vitamin D deficiency, patients with osteoporosis, or low bone mass, in which case we would recommend vitamin D.”
Some patients take more vitamin D than they need because they think more is better, said LeBoff, but this study suggests “more is not necessarily better.”
“There’s been a concern for several years that too much vitamin D may be associated with increased fractures,” she emphasized.
Post hoc analysis
The current study analyzed new data from the Calgary Vitamin D study.
That study found no benefit in BMD or bone strength (JAMA. 2019;322[8]:736-45), contrary to the researchers’ hypothesis that high-dose vitamin D supplements would be associated with greater calcium absorption and parathyroid hormone suppression and, thus, reduced age-related bone loss (improved bone density and strength).
Instead, they found a negative dose-response relationship, which “should be regarded as hypothesis generating, requiring confirmation with further research,” they wrote.
The current study sought to determine if there were sex differences in the effect of vitamin D supplements on bone health in this population.
From October 2013 to December 2017, the Canada Vitamin D study enrolled 311 participants (53% male). To be eligible for the study, participants had to have serum 25-hydroxyvitamin D levels greater than 30 nmol/L and less than 125 nmol/L. They also needed to have adequate calcium intake (1,200 mg/day, as defined by the U.S. Institute of Medicine), or if not, they were instructed to take an appropriate calcium supplement dose.
Patients were randomized to receive 400, 4,000, or 10,000 IU/day of vitamin D3 cholecalciferol, given as 5 drops/day of liquid (Ddrops), with roughly 50 men and 50 women in each dose group.
Researchers selected the 400 IU/day dose as the comparator because the Institute of Medicine recommends a vitamin D intake of 600 IU/day for adults under age 70 years to provide the vitamin D needed for bone health. The typical Canadian diet includes 200-300 IU/day of vitamin D, so individuals would need a supplement of 400 IU/day to reach the recommended intake. The 4,000 IU/day dose is the recommended tolerable upper intake level, according to the Institute of Medicine. And the 10,000 IU/day dose is the tolerable upper intake level of vitamin D as identified in a review by Hathcock and colleagues (Am J Clin Nutr. 2007;85:6-18).
Participants underwent scans with high-resolution peripheral quantitative computed tomography (HR-pQCT) to measure total volumetric BMD at the radius and tibia at baseline, 6, 12, 24, and 36 months. Finite element analysis was used to estimate bone strength.
After 3 years, women had lost significantly more BMD at the radius after taking high-dose versus 400 IU/day of vitamin D. Losses in BMD at the tibia followed a similar trend but were smaller (Figure 1). There were no significant changes in this measure among men (Figure 2).
There were also no significant changes in bone strength among men or women.
Biological mechanism remains to be determined
Dr. LeBoff said a “possible biological explanation” for the findings is that “women, particularly when they are younger, lose more bone than men.”
“Postmenopausal females do lose bone at an accelerated rate compared with males,” Dr. Burt agreed, “but at the time the study was designed, there was no reason to believe that high-dose vitamin D supplementation would accelerate the problem.”
“The biological mechanism of the vitamin D–related bone loss needs further investigation,” Dr. Burt added, “but there are laboratory data suggesting that supraphysiologic doses of active metabolites of vitamin D may stimulate bone resorption.”
The study was funded by the Pure North S’Energy Foundation. Dr. Burt has reported no relevant financial relationships. Disclosures for the other authors are listed with the article. Dr. LeBoff has reported receiving grants from the National Institutes of Health for the VITAL analysis.
A version of this article originally appeared on Medscape.com.
This month in the journal CHEST®
Editor’s picks
The burden of community-acquired pneumonia requiring admission to an intensive care unit in the United States.By Dr. R. Cavallazzi, et al.
Practical considerations for the diagnosis and treatment of fibrotic interstitial lung disease during the COVID-19 pandemic. By Dr. C. J. Ryerson, et al.
Pulmonary hypertension by the method of Paul Wood. By Dr. J. Newman.
Patient vs clinician perspectives on communication about results of lung cancer screening: A Qualitative Study. By Dr. R. Wiener, et al.
The Use of Bronchoscopy During the COVID-19 Pandemic: CHEST/AABIP Guideline and Expert Panel Report. By Dr. M. Wahidi, et al.
Editor’s picks
Editor’s picks
The burden of community-acquired pneumonia requiring admission to an intensive care unit in the United States.By Dr. R. Cavallazzi, et al.
Practical considerations for the diagnosis and treatment of fibrotic interstitial lung disease during the COVID-19 pandemic. By Dr. C. J. Ryerson, et al.
Pulmonary hypertension by the method of Paul Wood. By Dr. J. Newman.
Patient vs clinician perspectives on communication about results of lung cancer screening: A Qualitative Study. By Dr. R. Wiener, et al.
The Use of Bronchoscopy During the COVID-19 Pandemic: CHEST/AABIP Guideline and Expert Panel Report. By Dr. M. Wahidi, et al.
The burden of community-acquired pneumonia requiring admission to an intensive care unit in the United States.By Dr. R. Cavallazzi, et al.
Practical considerations for the diagnosis and treatment of fibrotic interstitial lung disease during the COVID-19 pandemic. By Dr. C. J. Ryerson, et al.
Pulmonary hypertension by the method of Paul Wood. By Dr. J. Newman.
Patient vs clinician perspectives on communication about results of lung cancer screening: A Qualitative Study. By Dr. R. Wiener, et al.
The Use of Bronchoscopy During the COVID-19 Pandemic: CHEST/AABIP Guideline and Expert Panel Report. By Dr. M. Wahidi, et al.
Occupations at risk for COVID-19. Palliative care and critical care mutualism. Safer mechanical ventilation. Treatment-emergent central apnea. Lung cancer outcomes improve.
Occupational and environmental health
Occupations at risk for COVID-19
As the COVID-19 pandemic has not yet ended, some occupational risks are faced day-to-day. Individuals have been practicing social distancing by working from home in recent months. While this arrangement can be a great way to reduce one’s exposure to COVID-19, it’s a luxury that’s available to just 29% of Americans. The situation for the remaining 71% is uncertain. The individuals on the front lines, whether they’re taking care of patients or stocking grocery shelves, may face a high risk of potential exposure to the virus (Baker et al. PLoS One. 2020; 15[4]:e0232452. doi: 10.1371/journal.pone.0232452).The high risk of the occupations lies in the close contact with people, such as pulmonologists, dentists, and ENT doctors and nurses using tools to lavage during aerosol-generating procedures (She et al. Clin Transl Med. 2020;9(1):19. doi: 10.1186/s40169-020-00271-z). Also, barbers, teachers, beauticians, fitness coaches, stewardesses, kindergarten teachers, chefs, waiters, etc, are required to be in contact with others facing the threat of infection.
Raising awareness of the issues will help avoid occupational transmission of COVID-19. Medical masks, N95 respirators, and hand hygiene are evidenced for high-risk, aerosol or non-aerosol-generating procedures offer protection against viral respiratory infection exposure in the pandemic (She et al. and Bartoszko et al. Influenza Other Respir Viruses. 2020;14(4):365. doi: 10.1111/irv.12745). In addition, using datasets to allow us to assign a more quantitative figure to each occupation’s level of risk to develop a protection strategy is imperative.
Mary Beth Scholand, MD, FCCP – Vice-Chair
Jun She, MD, PhD – Steering Committee Member
Palliative and end-of-life care
Palliative care and critical care mutualism: innovative support during the COVID-19 pandemic
The ICU is the epitome of a complex adaptive system (CAS), a highly organized and structured system that nonetheless is constantly evolving and adapting to changing needs and circumstances (Waldrom. Complexity: The Emerging Science at the Edge of Order and Chaos. Simon & Schuster, New York. 1992). This has never been more apparent than during the current novel coronavirus pandemic. Previously, medical advances and quality improvement projects were carefully vetted, slowly designed, willingly implemented. Today, health systems and society must take rapid and radical leaps to iterate policies and procedures in real time. Deeply embedding and consulting specialized palliative care teams early and often for hospitalized COVID-19 patients is a best practice strategy that benefits patients, families, and staff, and allows critical care teams to function at the top of their expertise. As one of our critical care physician colleagues noted, “Palliative care needs rise with critical care needs – we must help each other innovate practices.”
Beyond complex symptom management and relief of suffering, palliative care’s foundation is providing support during times of uncertainty and ambiguity. This proficiency is now an imperative. Here are some highly relevant examples of current palliative care initiatives within the ICU:
- Encouraging values assessment and goals of care for alignment of treatment plans.
- Advanced care planning with identification of primary and secondary health-care proxies in the setting of potential concurrent infections within families.
- Facilitating multidisciplinary video family meetings and clinical updates.
- Supporting ICU staff to alleviate moral distress and fatigue.
- Developing and distributing bereavement programs and remembrance rituals.
- Training and education on COVID-specific communication tools.
- Expanding outreach to patients/families through telehealth volunteer programs.
This is an opportunity to strengthen the multidisciplinary model of care in the ICU. It may appear that there is an abyss at the edge of chaos, but palliative care is helping engineer and build enduring bridges to help us all cross safely to the other side (Bilder and Knudsen. Front Psychol. 2014 Sep 30. doi: 10.3389/fpsyg.2014.01104).
Tara Coles, MD
Hunter Groninger, MD, Vice Chair
Cheryl Hughes, LICSW
Rachel Adams, MD
Respiratory care
Strategies and technology for safer mechanical ventilation
Clinicians often focus on safe practice as “vigilance in the moment” while interacting with patients and the health-care team and rightly so, especially with mechanical ventilation. New strategies for increasing safety include a more pre-emptive, technology-assisted approach. Alarm fatigue/flooding are serious concerns, and the ECRI found less than 15% of clinical alarms studied (including mechanical ventilation) were “clinically relevant” (eg, requiring some form of action) (ECRI Institute 2018; Plymouth Meeting, PA). Most alarms in health care are set to an “average” patient but as with tailored treatment in precision medicine, it is possible to tune alarm parameters to individual characteristics, including using patient trend data.

An excessive amount of alarms in a clinical environment is thought to be the largest contributing factor to alarm-related adverse events with rates sometimes exceeding 900 alarms per day (Graham et al. Am J Crit Care. 2010;19(1):28-34; quiz 35. doi: 10.4037/ajcc2010651). Human response to stimuli suggests response to alarms is closely matched to the perceived reliability of the alarm system. Instead of alarms based upon single physiological variables, the next generation of smart alarms is integrating much more information than previously possible to reduce false alarms and give more useful alerts. Trend data can better guide interpretation and activation of immediate alarm triggers. For example, a composite ventilation alarm could be created from the integration of trends of respiratory frequency, minute volume, oxygen saturation of hemoglobin, and end-tidal CO2. Fewer nonactionable alarms can result in greater attention when alarms do occur.

Integrated monitoring of patient data trends can also prompt clinicians when a different ventilation mode or setting combination should be considered, especially when indicated by consensus guidelines. The human factor of no-fault, peer audits can improve alarm policy compliance and guide the refinement of alarm policies. Most ventilator manufacturers are developing smart, precise patient monitoring and alarms, and their potential needs to be converted to practice as quickly as possible.
Brian Walsh, PhD, RRT, NetWork Member
Jonathan Waugh, PhD, RRT, Steering Committee Member
Sleep medicine
Treatment-emergent central apnea may be a frequent cause of PAP nonadherence
Treatment-emergent central apnea (TECSA) refers to new onset central-disordered breathing events after initiating treatment of obstructive sleep apnea (OSA), such as with positive airway pressure (PAP) therapy. The nature of the phenomenon is uncertain, but some theorize that in patients with ventilatory instability, CPAP intermittently lowers the partial pressure of PcCO2 below apneic threshold, causing a central apnea event (Gilmartin et al. Curr Opin Pulm Med. 2005;11[6]:485).

TECSA develops in 3.5% to 19.8% of patients starting PAP therapy for OSA. Risk factors include high baseline apnea or arousal index, higher CPAP pressure, older age, male sex, low BMI, and presence of heart failure or ischemic heart disease (Moro et al. Nat Sci Sleep. 2016;8:259; Nigam et al. Ann Thorac Med. 2016;11[3]:202). Most cases resolve in weeks to months; however, an estimated 14.3% to 46.2% evolve into treatment persistent central sleep apnea. Up to 4.2% of patients develop delayed TECSA (D-TECSA) or the emergence of central events after at least a month of PAP therapy (Nigam et al. Ann Thorac Med. 2018;13[2]:86).

TESCA can lead to PAP intolerance (discomfort, gasping, fragmented sleep), lower usage of PAP, and increased likelihood of discontinuing PAP therapy in the first 90 days (Liu et al. Chest. 2017;152[4]:751). When a patient presents with initial or delayed PAP intolerance or persistent symptoms, sleep providers should consider TECSA as a potential etiology. The diagnosis may be made by reviewing data from the patient’s PAP device, or by repeat testing. When encountering persistent TECSA, one can consider lowering the PAP pressure, or performing polysomnography with the goal of titrating the patient to an alternative PAP modality, such as bilevel ST or Adapto Servo Ventilation, which can stabilize breathing in patients with compromised ventilatory control (Morgenthaler et al. Sleep. 2014;37[5]:927).
Kara Dupuy-McCauley, MD
Fellow-in-Training Member
Caroline Okorie, MD, MPH
Steering Committee Member
Thoracic oncology
Times, they are a-changing: Lung cancer outcomes improve and the time for nihilism is past
The American Cancer Society 2020 Facts and Figures reported the largest single year drop in overall cancer mortality ever: 2.2% from 2016 to 2017. This record decrease was driven by the decline in lung cancer deaths thanks to treatment advances such as immunotherapy and targeted drugs for specific lung cancer mutations, combined with declining smoking rates. Lung cancer 5-year survival rates are 19% now and should continue rising, especially if screening rates increase. Immunotherapy has shown a 5-fold increase in survival for advanced non–small cell lung cancer (NSCLC) compared with chemotherapy (13.4% vs 2.6%) and half of metastatic NSCLC patients treated with first-line pembrolizumab were alive after 2 years (vs 34% of chemotherapy patients). Targeted therapies (eg, crizotinib) are similarly encouraging with half of stage IV, ALK-positive NSCLC patients diagnosed after 2009 alive 6.8 years later, compared with just 2% of those diagnosed between 1995 and 2001. Pulmonologists have an important role to play in early detection (screening) and identification of candidates for targeted therapy (ordering mutational analysis on diagnostic specimens).

Exciting treatment advances compel us to more aggressively diagnose lung cancer with early detection and offer diagnostic procedures, even for patients presenting with advanced disease. In fact, improving outcomes are opening the door to curative-intent treatment of oligometastatic lung cancer. In addition to improved disease outcomes, most new therapies are much better tolerated by patients than traditional cytotoxic chemotherapy. No longer is the appropriate response to an ugly-looking lung mass to “get your affairs in order.”
Abbie Begnaud, MD
Steering Committee Member
Reading list
Pacheco JM, Gao D, Smith D, et al. Natural history and factors associated with overall survival in stage IV ALK-rearranged non-small cell lung cancer. J Thorac Oncol. 2019;14(4):691. doi: 10.1016/j.jtho.2018.12.014.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7. doi: 10.3322/caac.21590.
Silvestri GA, Carpenter MJ. Smoking trends and lung cancer mortality: the good, the bad, and the ugly. Ann Intern Med. 2018;169(10):721-722. doi: 10.7326/M18-2775.
Stephens SJ, Moravan MJ, Salama JK. Managing patients with oligometastatic non-small-cell lung cancer. J Oncol Pract. 2018;14(1):23. doi: 10.1200/JOP.2017.026500.
Studies report prolonged long-term survival with immunotherapy vs chemotherapy in advanced NSCLC. ASCO Post October 10, 2019.
Occupational and environmental health
Occupations at risk for COVID-19
As the COVID-19 pandemic has not yet ended, some occupational risks are faced day-to-day. Individuals have been practicing social distancing by working from home in recent months. While this arrangement can be a great way to reduce one’s exposure to COVID-19, it’s a luxury that’s available to just 29% of Americans. The situation for the remaining 71% is uncertain. The individuals on the front lines, whether they’re taking care of patients or stocking grocery shelves, may face a high risk of potential exposure to the virus (Baker et al. PLoS One. 2020; 15[4]:e0232452. doi: 10.1371/journal.pone.0232452).The high risk of the occupations lies in the close contact with people, such as pulmonologists, dentists, and ENT doctors and nurses using tools to lavage during aerosol-generating procedures (She et al. Clin Transl Med. 2020;9(1):19. doi: 10.1186/s40169-020-00271-z). Also, barbers, teachers, beauticians, fitness coaches, stewardesses, kindergarten teachers, chefs, waiters, etc, are required to be in contact with others facing the threat of infection.
Raising awareness of the issues will help avoid occupational transmission of COVID-19. Medical masks, N95 respirators, and hand hygiene are evidenced for high-risk, aerosol or non-aerosol-generating procedures offer protection against viral respiratory infection exposure in the pandemic (She et al. and Bartoszko et al. Influenza Other Respir Viruses. 2020;14(4):365. doi: 10.1111/irv.12745). In addition, using datasets to allow us to assign a more quantitative figure to each occupation’s level of risk to develop a protection strategy is imperative.
Mary Beth Scholand, MD, FCCP – Vice-Chair
Jun She, MD, PhD – Steering Committee Member
Palliative and end-of-life care
Palliative care and critical care mutualism: innovative support during the COVID-19 pandemic
The ICU is the epitome of a complex adaptive system (CAS), a highly organized and structured system that nonetheless is constantly evolving and adapting to changing needs and circumstances (Waldrom. Complexity: The Emerging Science at the Edge of Order and Chaos. Simon & Schuster, New York. 1992). This has never been more apparent than during the current novel coronavirus pandemic. Previously, medical advances and quality improvement projects were carefully vetted, slowly designed, willingly implemented. Today, health systems and society must take rapid and radical leaps to iterate policies and procedures in real time. Deeply embedding and consulting specialized palliative care teams early and often for hospitalized COVID-19 patients is a best practice strategy that benefits patients, families, and staff, and allows critical care teams to function at the top of their expertise. As one of our critical care physician colleagues noted, “Palliative care needs rise with critical care needs – we must help each other innovate practices.”
Beyond complex symptom management and relief of suffering, palliative care’s foundation is providing support during times of uncertainty and ambiguity. This proficiency is now an imperative. Here are some highly relevant examples of current palliative care initiatives within the ICU:
- Encouraging values assessment and goals of care for alignment of treatment plans.
- Advanced care planning with identification of primary and secondary health-care proxies in the setting of potential concurrent infections within families.
- Facilitating multidisciplinary video family meetings and clinical updates.
- Supporting ICU staff to alleviate moral distress and fatigue.
- Developing and distributing bereavement programs and remembrance rituals.
- Training and education on COVID-specific communication tools.
- Expanding outreach to patients/families through telehealth volunteer programs.
This is an opportunity to strengthen the multidisciplinary model of care in the ICU. It may appear that there is an abyss at the edge of chaos, but palliative care is helping engineer and build enduring bridges to help us all cross safely to the other side (Bilder and Knudsen. Front Psychol. 2014 Sep 30. doi: 10.3389/fpsyg.2014.01104).
Tara Coles, MD
Hunter Groninger, MD, Vice Chair
Cheryl Hughes, LICSW
Rachel Adams, MD
Respiratory care
Strategies and technology for safer mechanical ventilation
Clinicians often focus on safe practice as “vigilance in the moment” while interacting with patients and the health-care team and rightly so, especially with mechanical ventilation. New strategies for increasing safety include a more pre-emptive, technology-assisted approach. Alarm fatigue/flooding are serious concerns, and the ECRI found less than 15% of clinical alarms studied (including mechanical ventilation) were “clinically relevant” (eg, requiring some form of action) (ECRI Institute 2018; Plymouth Meeting, PA). Most alarms in health care are set to an “average” patient but as with tailored treatment in precision medicine, it is possible to tune alarm parameters to individual characteristics, including using patient trend data.
An excessive amount of alarms in a clinical environment is thought to be the largest contributing factor to alarm-related adverse events with rates sometimes exceeding 900 alarms per day (Graham et al. Am J Crit Care. 2010;19(1):28-34; quiz 35. doi: 10.4037/ajcc2010651). Human response to stimuli suggests response to alarms is closely matched to the perceived reliability of the alarm system. Instead of alarms based upon single physiological variables, the next generation of smart alarms is integrating much more information than previously possible to reduce false alarms and give more useful alerts. Trend data can better guide interpretation and activation of immediate alarm triggers. For example, a composite ventilation alarm could be created from the integration of trends of respiratory frequency, minute volume, oxygen saturation of hemoglobin, and end-tidal CO2. Fewer nonactionable alarms can result in greater attention when alarms do occur.
Integrated monitoring of patient data trends can also prompt clinicians when a different ventilation mode or setting combination should be considered, especially when indicated by consensus guidelines. The human factor of no-fault, peer audits can improve alarm policy compliance and guide the refinement of alarm policies. Most ventilator manufacturers are developing smart, precise patient monitoring and alarms, and their potential needs to be converted to practice as quickly as possible.
Brian Walsh, PhD, RRT, NetWork Member
Jonathan Waugh, PhD, RRT, Steering Committee Member
Sleep medicine
Treatment-emergent central apnea may be a frequent cause of PAP nonadherence
Treatment-emergent central apnea (TECSA) refers to new onset central-disordered breathing events after initiating treatment of obstructive sleep apnea (OSA), such as with positive airway pressure (PAP) therapy. The nature of the phenomenon is uncertain, but some theorize that in patients with ventilatory instability, CPAP intermittently lowers the partial pressure of PcCO2 below apneic threshold, causing a central apnea event (Gilmartin et al. Curr Opin Pulm Med. 2005;11[6]:485).
TECSA develops in 3.5% to 19.8% of patients starting PAP therapy for OSA. Risk factors include high baseline apnea or arousal index, higher CPAP pressure, older age, male sex, low BMI, and presence of heart failure or ischemic heart disease (Moro et al. Nat Sci Sleep. 2016;8:259; Nigam et al. Ann Thorac Med. 2016;11[3]:202). Most cases resolve in weeks to months; however, an estimated 14.3% to 46.2% evolve into treatment persistent central sleep apnea. Up to 4.2% of patients develop delayed TECSA (D-TECSA) or the emergence of central events after at least a month of PAP therapy (Nigam et al. Ann Thorac Med. 2018;13[2]:86).
TESCA can lead to PAP intolerance (discomfort, gasping, fragmented sleep), lower usage of PAP, and increased likelihood of discontinuing PAP therapy in the first 90 days (Liu et al. Chest. 2017;152[4]:751). When a patient presents with initial or delayed PAP intolerance or persistent symptoms, sleep providers should consider TECSA as a potential etiology. The diagnosis may be made by reviewing data from the patient’s PAP device, or by repeat testing. When encountering persistent TECSA, one can consider lowering the PAP pressure, or performing polysomnography with the goal of titrating the patient to an alternative PAP modality, such as bilevel ST or Adapto Servo Ventilation, which can stabilize breathing in patients with compromised ventilatory control (Morgenthaler et al. Sleep. 2014;37[5]:927).
Kara Dupuy-McCauley, MD
Fellow-in-Training Member
Caroline Okorie, MD, MPH
Steering Committee Member
Thoracic oncology
Times, they are a-changing: Lung cancer outcomes improve and the time for nihilism is past
The American Cancer Society 2020 Facts and Figures reported the largest single year drop in overall cancer mortality ever: 2.2% from 2016 to 2017. This record decrease was driven by the decline in lung cancer deaths thanks to treatment advances such as immunotherapy and targeted drugs for specific lung cancer mutations, combined with declining smoking rates. Lung cancer 5-year survival rates are 19% now and should continue rising, especially if screening rates increase. Immunotherapy has shown a 5-fold increase in survival for advanced non–small cell lung cancer (NSCLC) compared with chemotherapy (13.4% vs 2.6%) and half of metastatic NSCLC patients treated with first-line pembrolizumab were alive after 2 years (vs 34% of chemotherapy patients). Targeted therapies (eg, crizotinib) are similarly encouraging with half of stage IV, ALK-positive NSCLC patients diagnosed after 2009 alive 6.8 years later, compared with just 2% of those diagnosed between 1995 and 2001. Pulmonologists have an important role to play in early detection (screening) and identification of candidates for targeted therapy (ordering mutational analysis on diagnostic specimens).
Exciting treatment advances compel us to more aggressively diagnose lung cancer with early detection and offer diagnostic procedures, even for patients presenting with advanced disease. In fact, improving outcomes are opening the door to curative-intent treatment of oligometastatic lung cancer. In addition to improved disease outcomes, most new therapies are much better tolerated by patients than traditional cytotoxic chemotherapy. No longer is the appropriate response to an ugly-looking lung mass to “get your affairs in order.”
Abbie Begnaud, MD
Steering Committee Member
Reading list
Pacheco JM, Gao D, Smith D, et al. Natural history and factors associated with overall survival in stage IV ALK-rearranged non-small cell lung cancer. J Thorac Oncol. 2019;14(4):691. doi: 10.1016/j.jtho.2018.12.014.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7. doi: 10.3322/caac.21590.
Silvestri GA, Carpenter MJ. Smoking trends and lung cancer mortality: the good, the bad, and the ugly. Ann Intern Med. 2018;169(10):721-722. doi: 10.7326/M18-2775.
Stephens SJ, Moravan MJ, Salama JK. Managing patients with oligometastatic non-small-cell lung cancer. J Oncol Pract. 2018;14(1):23. doi: 10.1200/JOP.2017.026500.
Studies report prolonged long-term survival with immunotherapy vs chemotherapy in advanced NSCLC. ASCO Post October 10, 2019.
Occupational and environmental health
Occupations at risk for COVID-19
As the COVID-19 pandemic has not yet ended, some occupational risks are faced day-to-day. Individuals have been practicing social distancing by working from home in recent months. While this arrangement can be a great way to reduce one’s exposure to COVID-19, it’s a luxury that’s available to just 29% of Americans. The situation for the remaining 71% is uncertain. The individuals on the front lines, whether they’re taking care of patients or stocking grocery shelves, may face a high risk of potential exposure to the virus (Baker et al. PLoS One. 2020; 15[4]:e0232452. doi: 10.1371/journal.pone.0232452).The high risk of the occupations lies in the close contact with people, such as pulmonologists, dentists, and ENT doctors and nurses using tools to lavage during aerosol-generating procedures (She et al. Clin Transl Med. 2020;9(1):19. doi: 10.1186/s40169-020-00271-z). Also, barbers, teachers, beauticians, fitness coaches, stewardesses, kindergarten teachers, chefs, waiters, etc, are required to be in contact with others facing the threat of infection.
Raising awareness of the issues will help avoid occupational transmission of COVID-19. Medical masks, N95 respirators, and hand hygiene are evidenced for high-risk, aerosol or non-aerosol-generating procedures offer protection against viral respiratory infection exposure in the pandemic (She et al. and Bartoszko et al. Influenza Other Respir Viruses. 2020;14(4):365. doi: 10.1111/irv.12745). In addition, using datasets to allow us to assign a more quantitative figure to each occupation’s level of risk to develop a protection strategy is imperative.
Mary Beth Scholand, MD, FCCP – Vice-Chair
Jun She, MD, PhD – Steering Committee Member
Palliative and end-of-life care
Palliative care and critical care mutualism: innovative support during the COVID-19 pandemic
The ICU is the epitome of a complex adaptive system (CAS), a highly organized and structured system that nonetheless is constantly evolving and adapting to changing needs and circumstances (Waldrom. Complexity: The Emerging Science at the Edge of Order and Chaos. Simon & Schuster, New York. 1992). This has never been more apparent than during the current novel coronavirus pandemic. Previously, medical advances and quality improvement projects were carefully vetted, slowly designed, willingly implemented. Today, health systems and society must take rapid and radical leaps to iterate policies and procedures in real time. Deeply embedding and consulting specialized palliative care teams early and often for hospitalized COVID-19 patients is a best practice strategy that benefits patients, families, and staff, and allows critical care teams to function at the top of their expertise. As one of our critical care physician colleagues noted, “Palliative care needs rise with critical care needs – we must help each other innovate practices.”
Beyond complex symptom management and relief of suffering, palliative care’s foundation is providing support during times of uncertainty and ambiguity. This proficiency is now an imperative. Here are some highly relevant examples of current palliative care initiatives within the ICU:
- Encouraging values assessment and goals of care for alignment of treatment plans.
- Advanced care planning with identification of primary and secondary health-care proxies in the setting of potential concurrent infections within families.
- Facilitating multidisciplinary video family meetings and clinical updates.
- Supporting ICU staff to alleviate moral distress and fatigue.
- Developing and distributing bereavement programs and remembrance rituals.
- Training and education on COVID-specific communication tools.
- Expanding outreach to patients/families through telehealth volunteer programs.
This is an opportunity to strengthen the multidisciplinary model of care in the ICU. It may appear that there is an abyss at the edge of chaos, but palliative care is helping engineer and build enduring bridges to help us all cross safely to the other side (Bilder and Knudsen. Front Psychol. 2014 Sep 30. doi: 10.3389/fpsyg.2014.01104).
Tara Coles, MD
Hunter Groninger, MD, Vice Chair
Cheryl Hughes, LICSW
Rachel Adams, MD
Respiratory care
Strategies and technology for safer mechanical ventilation
Clinicians often focus on safe practice as “vigilance in the moment” while interacting with patients and the health-care team and rightly so, especially with mechanical ventilation. New strategies for increasing safety include a more pre-emptive, technology-assisted approach. Alarm fatigue/flooding are serious concerns, and the ECRI found less than 15% of clinical alarms studied (including mechanical ventilation) were “clinically relevant” (eg, requiring some form of action) (ECRI Institute 2018; Plymouth Meeting, PA). Most alarms in health care are set to an “average” patient but as with tailored treatment in precision medicine, it is possible to tune alarm parameters to individual characteristics, including using patient trend data.
An excessive amount of alarms in a clinical environment is thought to be the largest contributing factor to alarm-related adverse events with rates sometimes exceeding 900 alarms per day (Graham et al. Am J Crit Care. 2010;19(1):28-34; quiz 35. doi: 10.4037/ajcc2010651). Human response to stimuli suggests response to alarms is closely matched to the perceived reliability of the alarm system. Instead of alarms based upon single physiological variables, the next generation of smart alarms is integrating much more information than previously possible to reduce false alarms and give more useful alerts. Trend data can better guide interpretation and activation of immediate alarm triggers. For example, a composite ventilation alarm could be created from the integration of trends of respiratory frequency, minute volume, oxygen saturation of hemoglobin, and end-tidal CO2. Fewer nonactionable alarms can result in greater attention when alarms do occur.
Integrated monitoring of patient data trends can also prompt clinicians when a different ventilation mode or setting combination should be considered, especially when indicated by consensus guidelines. The human factor of no-fault, peer audits can improve alarm policy compliance and guide the refinement of alarm policies. Most ventilator manufacturers are developing smart, precise patient monitoring and alarms, and their potential needs to be converted to practice as quickly as possible.
Brian Walsh, PhD, RRT, NetWork Member
Jonathan Waugh, PhD, RRT, Steering Committee Member
Sleep medicine
Treatment-emergent central apnea may be a frequent cause of PAP nonadherence
Treatment-emergent central apnea (TECSA) refers to new onset central-disordered breathing events after initiating treatment of obstructive sleep apnea (OSA), such as with positive airway pressure (PAP) therapy. The nature of the phenomenon is uncertain, but some theorize that in patients with ventilatory instability, CPAP intermittently lowers the partial pressure of PcCO2 below apneic threshold, causing a central apnea event (Gilmartin et al. Curr Opin Pulm Med. 2005;11[6]:485).
TECSA develops in 3.5% to 19.8% of patients starting PAP therapy for OSA. Risk factors include high baseline apnea or arousal index, higher CPAP pressure, older age, male sex, low BMI, and presence of heart failure or ischemic heart disease (Moro et al. Nat Sci Sleep. 2016;8:259; Nigam et al. Ann Thorac Med. 2016;11[3]:202). Most cases resolve in weeks to months; however, an estimated 14.3% to 46.2% evolve into treatment persistent central sleep apnea. Up to 4.2% of patients develop delayed TECSA (D-TECSA) or the emergence of central events after at least a month of PAP therapy (Nigam et al. Ann Thorac Med. 2018;13[2]:86).
TESCA can lead to PAP intolerance (discomfort, gasping, fragmented sleep), lower usage of PAP, and increased likelihood of discontinuing PAP therapy in the first 90 days (Liu et al. Chest. 2017;152[4]:751). When a patient presents with initial or delayed PAP intolerance or persistent symptoms, sleep providers should consider TECSA as a potential etiology. The diagnosis may be made by reviewing data from the patient’s PAP device, or by repeat testing. When encountering persistent TECSA, one can consider lowering the PAP pressure, or performing polysomnography with the goal of titrating the patient to an alternative PAP modality, such as bilevel ST or Adapto Servo Ventilation, which can stabilize breathing in patients with compromised ventilatory control (Morgenthaler et al. Sleep. 2014;37[5]:927).
Kara Dupuy-McCauley, MD
Fellow-in-Training Member
Caroline Okorie, MD, MPH
Steering Committee Member
Thoracic oncology
Times, they are a-changing: Lung cancer outcomes improve and the time for nihilism is past
The American Cancer Society 2020 Facts and Figures reported the largest single year drop in overall cancer mortality ever: 2.2% from 2016 to 2017. This record decrease was driven by the decline in lung cancer deaths thanks to treatment advances such as immunotherapy and targeted drugs for specific lung cancer mutations, combined with declining smoking rates. Lung cancer 5-year survival rates are 19% now and should continue rising, especially if screening rates increase. Immunotherapy has shown a 5-fold increase in survival for advanced non–small cell lung cancer (NSCLC) compared with chemotherapy (13.4% vs 2.6%) and half of metastatic NSCLC patients treated with first-line pembrolizumab were alive after 2 years (vs 34% of chemotherapy patients). Targeted therapies (eg, crizotinib) are similarly encouraging with half of stage IV, ALK-positive NSCLC patients diagnosed after 2009 alive 6.8 years later, compared with just 2% of those diagnosed between 1995 and 2001. Pulmonologists have an important role to play in early detection (screening) and identification of candidates for targeted therapy (ordering mutational analysis on diagnostic specimens).
Exciting treatment advances compel us to more aggressively diagnose lung cancer with early detection and offer diagnostic procedures, even for patients presenting with advanced disease. In fact, improving outcomes are opening the door to curative-intent treatment of oligometastatic lung cancer. In addition to improved disease outcomes, most new therapies are much better tolerated by patients than traditional cytotoxic chemotherapy. No longer is the appropriate response to an ugly-looking lung mass to “get your affairs in order.”
Abbie Begnaud, MD
Steering Committee Member
Reading list
Pacheco JM, Gao D, Smith D, et al. Natural history and factors associated with overall survival in stage IV ALK-rearranged non-small cell lung cancer. J Thorac Oncol. 2019;14(4):691. doi: 10.1016/j.jtho.2018.12.014.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7. doi: 10.3322/caac.21590.
Silvestri GA, Carpenter MJ. Smoking trends and lung cancer mortality: the good, the bad, and the ugly. Ann Intern Med. 2018;169(10):721-722. doi: 10.7326/M18-2775.
Stephens SJ, Moravan MJ, Salama JK. Managing patients with oligometastatic non-small-cell lung cancer. J Oncol Pract. 2018;14(1):23. doi: 10.1200/JOP.2017.026500.
Studies report prolonged long-term survival with immunotherapy vs chemotherapy in advanced NSCLC. ASCO Post October 10, 2019.
CHEST annual meeting 2020
Greetings,
As the Program Chair of CHEST Annual Meeting 2020, I’m excited to finally share the good news with all of you – our premiere educational event, CHEST 2020, will be taking place October 18-21! As you might have guessed, we’re migrating the meeting onto a virtual platform - not only will this change ensure your safety, it will enable so many more of you to attend. Colleagues who may have been excluded due to geographical restrictions in the past will now have the opportunity to experience all that we have to offer!
As always, we’ll be bringing you the latest, most relevant clinical topics in pulmonary, critical care, and sleep medicine. From COVID-19 to cultural diversity, we’ve carefully curated sessions to explore the issues that you want to learn about. Not to mention, our speakers are all experts in their field – at the forefront of the pandemic – and will bring a level of knowledge and insight to the meeting that is truly unparalleled. Afterall, that’s what our annual meeting is known for. Regardless of where or how it is taking place, it’s still “the very best of CHEST.”
Other highlights will include over 88 live sessions, including panel and case-based discussions, original investigation presentations with new, unpublished research, and CHEST Games.
Of course, we will have several networking opportunities where you will be able to connect with so many more of your colleagues because of the virtual nature of the meeting. While you may be sitting worlds apart, you’ll be socializing in an intimate online space.
While this isn’t exactly what we imagined for our meeting, it’s what we had to reimagine. Sometimes being pushed out of your comfort zone can lead to something extraordinary, and, in this instance, we think it did.
In closing, I’d like to acknowledge how challenging these past several months have been. For all the long hours, the time spent away from family, and the stress that continues to pile on – this is your chance to unplug and unwind.
We all need an event to look forward to right now, and at CHEST, we’ve worked hard to bring you one. I hope you’ll visit chestmeeting.chestnet.org to register for CHEST 2020.
Best,
Victor Test, MD, FCCP
Greetings,
As the Program Chair of CHEST Annual Meeting 2020, I’m excited to finally share the good news with all of you – our premiere educational event, CHEST 2020, will be taking place October 18-21! As you might have guessed, we’re migrating the meeting onto a virtual platform - not only will this change ensure your safety, it will enable so many more of you to attend. Colleagues who may have been excluded due to geographical restrictions in the past will now have the opportunity to experience all that we have to offer!
As always, we’ll be bringing you the latest, most relevant clinical topics in pulmonary, critical care, and sleep medicine. From COVID-19 to cultural diversity, we’ve carefully curated sessions to explore the issues that you want to learn about. Not to mention, our speakers are all experts in their field – at the forefront of the pandemic – and will bring a level of knowledge and insight to the meeting that is truly unparalleled. Afterall, that’s what our annual meeting is known for. Regardless of where or how it is taking place, it’s still “the very best of CHEST.”
Other highlights will include over 88 live sessions, including panel and case-based discussions, original investigation presentations with new, unpublished research, and CHEST Games.
Of course, we will have several networking opportunities where you will be able to connect with so many more of your colleagues because of the virtual nature of the meeting. While you may be sitting worlds apart, you’ll be socializing in an intimate online space.
While this isn’t exactly what we imagined for our meeting, it’s what we had to reimagine. Sometimes being pushed out of your comfort zone can lead to something extraordinary, and, in this instance, we think it did.
In closing, I’d like to acknowledge how challenging these past several months have been. For all the long hours, the time spent away from family, and the stress that continues to pile on – this is your chance to unplug and unwind.
We all need an event to look forward to right now, and at CHEST, we’ve worked hard to bring you one. I hope you’ll visit chestmeeting.chestnet.org to register for CHEST 2020.
Best,
Victor Test, MD, FCCP
Greetings,
As the Program Chair of CHEST Annual Meeting 2020, I’m excited to finally share the good news with all of you – our premiere educational event, CHEST 2020, will be taking place October 18-21! As you might have guessed, we’re migrating the meeting onto a virtual platform - not only will this change ensure your safety, it will enable so many more of you to attend. Colleagues who may have been excluded due to geographical restrictions in the past will now have the opportunity to experience all that we have to offer!
As always, we’ll be bringing you the latest, most relevant clinical topics in pulmonary, critical care, and sleep medicine. From COVID-19 to cultural diversity, we’ve carefully curated sessions to explore the issues that you want to learn about. Not to mention, our speakers are all experts in their field – at the forefront of the pandemic – and will bring a level of knowledge and insight to the meeting that is truly unparalleled. Afterall, that’s what our annual meeting is known for. Regardless of where or how it is taking place, it’s still “the very best of CHEST.”
Other highlights will include over 88 live sessions, including panel and case-based discussions, original investigation presentations with new, unpublished research, and CHEST Games.
Of course, we will have several networking opportunities where you will be able to connect with so many more of your colleagues because of the virtual nature of the meeting. While you may be sitting worlds apart, you’ll be socializing in an intimate online space.
While this isn’t exactly what we imagined for our meeting, it’s what we had to reimagine. Sometimes being pushed out of your comfort zone can lead to something extraordinary, and, in this instance, we think it did.
In closing, I’d like to acknowledge how challenging these past several months have been. For all the long hours, the time spent away from family, and the stress that continues to pile on – this is your chance to unplug and unwind.
We all need an event to look forward to right now, and at CHEST, we’ve worked hard to bring you one. I hope you’ll visit chestmeeting.chestnet.org to register for CHEST 2020.
Best,
Victor Test, MD, FCCP
News from your CHEST Foundation
As the NetWorks Challenge draws to a close, CHEST Foundation staff want to thank every member who donated to support this year’s drive for our COVID-19 Community Grants. When the fund was established in April, we started with a pool of $60,000 to award to patient support groups and small community organizations providing resources and interventions for those most vulnerable to develop severe complications from COVID-19 – American’s living with chronic lung disease. Within 2 months, we’d awarded all available funds to 25 organizations and had several others still seeking funding. The lion’s share of these groups were providing direct service to medically fragile and isolated patients – purchasing PPE, cleaning supplies, pulse oximeters, and even groceries to patients who otherwise wouldn’t have access to these critical supplies.
Because of YOUR support of the NetWorks Challenge, we are proud to share that we are providing an additional $43,850 in support of COVID-19 Community Grants. Because of you – we can continue to provide vital funding to support group members who lives’ you’ve changed forever.
“Receiving the CHEST Foundation grant for COVID-19 support was a real boost to all of our spirits. Our staff have been working tirelessly to care for our residents 24/7, and there have been some trying and exhausting moments. When we received the community-based grant, it reminded us that there are still people in our community cheering us on, and it’s an acknowledgment that our clients matter just as much to the community as they do to us, personally.” –– Katherine A. Brown, St. Coletta’s of Illinois
As the NetWorks Challenge draws to a close, CHEST Foundation staff want to thank every member who donated to support this year’s drive for our COVID-19 Community Grants. When the fund was established in April, we started with a pool of $60,000 to award to patient support groups and small community organizations providing resources and interventions for those most vulnerable to develop severe complications from COVID-19 – American’s living with chronic lung disease. Within 2 months, we’d awarded all available funds to 25 organizations and had several others still seeking funding. The lion’s share of these groups were providing direct service to medically fragile and isolated patients – purchasing PPE, cleaning supplies, pulse oximeters, and even groceries to patients who otherwise wouldn’t have access to these critical supplies.
Because of YOUR support of the NetWorks Challenge, we are proud to share that we are providing an additional $43,850 in support of COVID-19 Community Grants. Because of you – we can continue to provide vital funding to support group members who lives’ you’ve changed forever.
“Receiving the CHEST Foundation grant for COVID-19 support was a real boost to all of our spirits. Our staff have been working tirelessly to care for our residents 24/7, and there have been some trying and exhausting moments. When we received the community-based grant, it reminded us that there are still people in our community cheering us on, and it’s an acknowledgment that our clients matter just as much to the community as they do to us, personally.” –– Katherine A. Brown, St. Coletta’s of Illinois
As the NetWorks Challenge draws to a close, CHEST Foundation staff want to thank every member who donated to support this year’s drive for our COVID-19 Community Grants. When the fund was established in April, we started with a pool of $60,000 to award to patient support groups and small community organizations providing resources and interventions for those most vulnerable to develop severe complications from COVID-19 – American’s living with chronic lung disease. Within 2 months, we’d awarded all available funds to 25 organizations and had several others still seeking funding. The lion’s share of these groups were providing direct service to medically fragile and isolated patients – purchasing PPE, cleaning supplies, pulse oximeters, and even groceries to patients who otherwise wouldn’t have access to these critical supplies.
Because of YOUR support of the NetWorks Challenge, we are proud to share that we are providing an additional $43,850 in support of COVID-19 Community Grants. Because of you – we can continue to provide vital funding to support group members who lives’ you’ve changed forever.
“Receiving the CHEST Foundation grant for COVID-19 support was a real boost to all of our spirits. Our staff have been working tirelessly to care for our residents 24/7, and there have been some trying and exhausting moments. When we received the community-based grant, it reminded us that there are still people in our community cheering us on, and it’s an acknowledgment that our clients matter just as much to the community as they do to us, personally.” –– Katherine A. Brown, St. Coletta’s of Illinois