User login
5 Vaccinations Adults Need Beyond COVID and Flu
Many adults are complacent about vaccinations, believing that annual COVID and flu shots aside, they had all the immunizations they need as children and teens. But adults need vaccines as well, especially if they have missed earlier doses. And older and health-compromised adults, in particular, can benefit from newer vaccines that were not part of the childhood schedule.
“The question is whether adults had the vaccinations they need in the first place,” Sandra Adamson Fryhofer, MD, an internist in Atlanta and the American Medical Association’s liaison to the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention, said in an interview. “Many do not even have reliable records of vaccination.”

Primary care physicians are ideally positioned to get adult patients to update their vaccination status on older vaccines and obtain newer ones as needed. “ACIP recommendations for adult vaccines are getting longer and more complicated and the way they’re administered is more complex, too, in that they’re not all given in the primary care office but sometimes in pharmacies,” Dr. Fryhofer said.
Not all adult patients want to update their vaccinations. “Vaccine hesitancy among many adults is accelerated by the several new vaccines that have been recommended in recent years,” Lauren Block, MD, MPH, an internist at Northwell Health and assistant professor in the Institute of Health System Science at the Feinstein Institutes for Medical Research in metropolitan New York City, said in an interview.
Physicians are rightly concerned about the lagging rates of adult vaccination, Dr. Block said. “Given the prevalence of conditions like pneumonia and shingles and the morbidity associated with them, healthcare providers should take every opportunity to discuss vaccination with patients, from well visits to hospital visits,” Dr. Block added.

She pointed to several obstacles to broader uptake, including product shortages, financial barriers, and, increasingly, the negative vocal messaging from media outlets and social media.
Current Recommendations
The main vaccines recommended for adults, besides flu and COVID shots, are for respiratory syncytial virus (RVS); shingles; pneumococcal disease; measles, mumps, and rubella (MMR); and tetanus, diphtheria, and pertussis (Tdap). Less commonly, booster vaccines for MM, and hepatitis are recommended when titers are proven to be low.
ACIP’s updated 2024 Adult Immunization Schedule can be downloaded from the website of the CDC.
The newest additions to the schedule include RSV vaccines, the mpox vaccine (Jynneos), a new MenACWY-MenB combo vaccine (Penbraya), and the new 2023-2024 formulation of updated COVID vaccines (both mRNA and protein-based adjuvanted versions).
1. Respiratory Syncytial Virus Vaccines
There are two licensed RSV vaccines, Arexvy and Abrysvo. The CDC schedule recommends a single-dose RSV vaccine for adults age 60 years and older, especially those at high risk of contracting the virus — but after shared decision-making based on a discussion of the risk-harm balance since this vaccine carries a small increased chance of developing the neurological symptoms of Guillain-Barré syndrome.
Chronic health conditions associated with a higher risk of severe RVS include cardiopulmonary disease, diabetes, and kidney, liver, and hematologic disorders, as well as compromised immunity, older age, and frailty.
2. Shingles Vaccines
This painful disease carries the potential complication of postherpetic neuralgia (PHN), which leads to long-term nerve pain in 10%-18% of patients, especially those over age 40. ACIP recommends two doses of the recombinant zoster vaccine (Shingrix) for individuals 50 years and older. Those 19 years and older with weakened immune systems due to disease or medical treatments should get two doses of the recombinant vaccine, as they have a higher risk of getting shingles and its complications, including neurological problems and skin and eye infections.
3 Pneumococcal Vaccines
There are three approved pneumococcal vaccines: PCV15 (Vaxneuvance), PCV20 (Prevnar20), and PPSV23 (Pneumovax23).
“The pneumococcal vaccine schedule is the most complicated one as higher-valent products continue to become available,” Dr. Fryhofer said.
The two types are pneumococcal conjugate vaccines (PCVs, specifically PCV15 and PCV20) and the pneumococcal polysaccharide vaccine (PPSV23). “While PPSV23 covers 23 strains, it doesn’t give the long-term immunity of the conjugate vaccine,” said Dr. Fryhofer. “A patient may have completed their vaccination with the polysaccharide vaccine but 5 years out may no longer be protected. So we offer the option of getting a dose of PCV20 to round out the protection and confer greater immune memory.”
The ACIP schedule recommends immunization against the Streptococcus pneumoniae pathogen for all older and all at-risk adults. Routine administration of PCV15 or PCV20 is advised for those 65 years or older who have never received any pneumococcal conjugate vaccine or whose previous vaccination history is unknown. If PCV15 is used, it should be followed by PPSV23. Those 65 years or older should get PPSV23 even if they already had one or more doses of pneumococcal vaccine before turning 65.
Further vaccination is recommended for younger at-risk adults aged 19-64 years who have received both PCV13 and PPSV23 but have incomplete vaccination status. These individuals are advised to complete their pneumococcal series by receiving either a single dose of PCV20 at an interval of at least 5 years after the last pneumococcal vaccine dose or more than one dose of PPSV23.
See Pneumococcal Vaccination: Summary of Who and When to Vaccinate for CDC guidance on vaccination options for adults who have previously received a pneumococcal conjugate vaccine. Or, to sort out quickly who gets what and when based on their age, concurrent conditions, and vaccination history, the CDC offers a type-in app called the PneumoRecs VaxAdvisor.
4. Measles, Mumps, and Rubella, and Varicella Vaccines
The two approved MMR vaccines are M-M-R II and PRIORIX. A third vaccine, ProQuad, adds varicella.
Adults lacking presumptive evidence of immunity should get at least one dose of the MMR combination vaccine.
Those born before 1957 are deemed to be immune, Dr. Fryhofer noted.
Two doses are recommended for adults entering high-risk settings for measles or mumps transmission such as healthcare personnel, students away at college, and international travelers. The two doses should be separated by at least 28 days. It’s no secret that measles, though preventable, is making a comeback, with 146 reported cases (48 in adults) across 21 states as of May 31 — most linked to international travel.
Women who plan to get pregnant should be vaccinated before but not during each pregnancy. (The vaccine is safe during lactation.) And those of childbearing age with no presumptive evidence of immunity are advised to get at least one dose of the MMR vaccine.
5. Tetanus, Diphtheria, and Pertussis Vaccine
Adults with no previous Tdap vaccination should receive a single dose of Adacel or Boostrix followed by a booster every 10 years. Boostrix is recommended for adults over 64 years.
During every pregnancy, women should have a single dose of Tdap, preferably in gestational weeks 27 through 36.
As to the immediate postpartum period, Tdap is recommended only for mothers who did not receive it during their current pregnancy and never received a prior dose. If a woman did not receive Tdap during her current pregnancy but did receive a prior dose of Tdap, she does not need Tdap postpartum.
The Challenges
According to Dr. Fryhofer, widespread disinformation about the risks of immunization against vaccine-preventable diseases has brought us to a flashpoint. “It’s now more important than ever to keep telling patients that vaccination is one of the most effective tools for preventing individual illness and protecting public health.”
She recommends that doctors follow the National Institutes of Health’s AIMS method to broach the subject of adult vaccination and increase participation in an inquiring, reassuring, and low-pressure way. Standing for Announce, Inquire, Mirror, and Secure, AIMS structures a nonjudgmental, patient-friendly conversation around immunization to elicit and acknowledge the reasons for hesitancy while explaining the safety and efficacy of vaccines.
Dr. Fryhofer frequently uses AIMS to bring inoculation-averse patients around. “Keep the conversation open with reluctant patients but leave them where they are. They need to see you as a reliable source and nonjudgmental source of information,” she said.
Dr. Block recommends outlining the diseases that have been eliminated through vaccines, from polio to measles, as well as the dangers of vaccine refusal, as indicated by recent outbreaks of vaccine-preventable diseases in areas with low immunization rates. “This approach highlights the opportunity we all have to get vaccinated to protect ourselves and our communities,” she said.
In Dr. Fryhofer’s view, the situation is urgent and doctors need to be proactive. “We’re now at a public-health tipping point where we may see a sliding back and a reversing of many years of progress.”
Dr. Fryhofer and Dr. Block disclosed no competing interests relevant to their comments.
Many adults are complacent about vaccinations, believing that annual COVID and flu shots aside, they had all the immunizations they need as children and teens. But adults need vaccines as well, especially if they have missed earlier doses. And older and health-compromised adults, in particular, can benefit from newer vaccines that were not part of the childhood schedule.
“The question is whether adults had the vaccinations they need in the first place,” Sandra Adamson Fryhofer, MD, an internist in Atlanta and the American Medical Association’s liaison to the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention, said in an interview. “Many do not even have reliable records of vaccination.”
Primary care physicians are ideally positioned to get adult patients to update their vaccination status on older vaccines and obtain newer ones as needed. “ACIP recommendations for adult vaccines are getting longer and more complicated and the way they’re administered is more complex, too, in that they’re not all given in the primary care office but sometimes in pharmacies,” Dr. Fryhofer said.
Not all adult patients want to update their vaccinations. “Vaccine hesitancy among many adults is accelerated by the several new vaccines that have been recommended in recent years,” Lauren Block, MD, MPH, an internist at Northwell Health and assistant professor in the Institute of Health System Science at the Feinstein Institutes for Medical Research in metropolitan New York City, said in an interview.
Physicians are rightly concerned about the lagging rates of adult vaccination, Dr. Block said. “Given the prevalence of conditions like pneumonia and shingles and the morbidity associated with them, healthcare providers should take every opportunity to discuss vaccination with patients, from well visits to hospital visits,” Dr. Block added.
She pointed to several obstacles to broader uptake, including product shortages, financial barriers, and, increasingly, the negative vocal messaging from media outlets and social media.
Current Recommendations
The main vaccines recommended for adults, besides flu and COVID shots, are for respiratory syncytial virus (RVS); shingles; pneumococcal disease; measles, mumps, and rubella (MMR); and tetanus, diphtheria, and pertussis (Tdap). Less commonly, booster vaccines for MM, and hepatitis are recommended when titers are proven to be low.
ACIP’s updated 2024 Adult Immunization Schedule can be downloaded from the website of the CDC.
The newest additions to the schedule include RSV vaccines, the mpox vaccine (Jynneos), a new MenACWY-MenB combo vaccine (Penbraya), and the new 2023-2024 formulation of updated COVID vaccines (both mRNA and protein-based adjuvanted versions).
1. Respiratory Syncytial Virus Vaccines
There are two licensed RSV vaccines, Arexvy and Abrysvo. The CDC schedule recommends a single-dose RSV vaccine for adults age 60 years and older, especially those at high risk of contracting the virus — but after shared decision-making based on a discussion of the risk-harm balance since this vaccine carries a small increased chance of developing the neurological symptoms of Guillain-Barré syndrome.
Chronic health conditions associated with a higher risk of severe RVS include cardiopulmonary disease, diabetes, and kidney, liver, and hematologic disorders, as well as compromised immunity, older age, and frailty.
2. Shingles Vaccines
This painful disease carries the potential complication of postherpetic neuralgia (PHN), which leads to long-term nerve pain in 10%-18% of patients, especially those over age 40. ACIP recommends two doses of the recombinant zoster vaccine (Shingrix) for individuals 50 years and older. Those 19 years and older with weakened immune systems due to disease or medical treatments should get two doses of the recombinant vaccine, as they have a higher risk of getting shingles and its complications, including neurological problems and skin and eye infections.
3 Pneumococcal Vaccines
There are three approved pneumococcal vaccines: PCV15 (Vaxneuvance), PCV20 (Prevnar20), and PPSV23 (Pneumovax23).
“The pneumococcal vaccine schedule is the most complicated one as higher-valent products continue to become available,” Dr. Fryhofer said.
The two types are pneumococcal conjugate vaccines (PCVs, specifically PCV15 and PCV20) and the pneumococcal polysaccharide vaccine (PPSV23). “While PPSV23 covers 23 strains, it doesn’t give the long-term immunity of the conjugate vaccine,” said Dr. Fryhofer. “A patient may have completed their vaccination with the polysaccharide vaccine but 5 years out may no longer be protected. So we offer the option of getting a dose of PCV20 to round out the protection and confer greater immune memory.”
The ACIP schedule recommends immunization against the Streptococcus pneumoniae pathogen for all older and all at-risk adults. Routine administration of PCV15 or PCV20 is advised for those 65 years or older who have never received any pneumococcal conjugate vaccine or whose previous vaccination history is unknown. If PCV15 is used, it should be followed by PPSV23. Those 65 years or older should get PPSV23 even if they already had one or more doses of pneumococcal vaccine before turning 65.
Further vaccination is recommended for younger at-risk adults aged 19-64 years who have received both PCV13 and PPSV23 but have incomplete vaccination status. These individuals are advised to complete their pneumococcal series by receiving either a single dose of PCV20 at an interval of at least 5 years after the last pneumococcal vaccine dose or more than one dose of PPSV23.
See Pneumococcal Vaccination: Summary of Who and When to Vaccinate for CDC guidance on vaccination options for adults who have previously received a pneumococcal conjugate vaccine. Or, to sort out quickly who gets what and when based on their age, concurrent conditions, and vaccination history, the CDC offers a type-in app called the PneumoRecs VaxAdvisor.
4. Measles, Mumps, and Rubella, and Varicella Vaccines
The two approved MMR vaccines are M-M-R II and PRIORIX. A third vaccine, ProQuad, adds varicella.
Adults lacking presumptive evidence of immunity should get at least one dose of the MMR combination vaccine.
Those born before 1957 are deemed to be immune, Dr. Fryhofer noted.
Two doses are recommended for adults entering high-risk settings for measles or mumps transmission such as healthcare personnel, students away at college, and international travelers. The two doses should be separated by at least 28 days. It’s no secret that measles, though preventable, is making a comeback, with 146 reported cases (48 in adults) across 21 states as of May 31 — most linked to international travel.
Women who plan to get pregnant should be vaccinated before but not during each pregnancy. (The vaccine is safe during lactation.) And those of childbearing age with no presumptive evidence of immunity are advised to get at least one dose of the MMR vaccine.
5. Tetanus, Diphtheria, and Pertussis Vaccine
Adults with no previous Tdap vaccination should receive a single dose of Adacel or Boostrix followed by a booster every 10 years. Boostrix is recommended for adults over 64 years.
During every pregnancy, women should have a single dose of Tdap, preferably in gestational weeks 27 through 36.
As to the immediate postpartum period, Tdap is recommended only for mothers who did not receive it during their current pregnancy and never received a prior dose. If a woman did not receive Tdap during her current pregnancy but did receive a prior dose of Tdap, she does not need Tdap postpartum.
The Challenges
According to Dr. Fryhofer, widespread disinformation about the risks of immunization against vaccine-preventable diseases has brought us to a flashpoint. “It’s now more important than ever to keep telling patients that vaccination is one of the most effective tools for preventing individual illness and protecting public health.”
She recommends that doctors follow the National Institutes of Health’s AIMS method to broach the subject of adult vaccination and increase participation in an inquiring, reassuring, and low-pressure way. Standing for Announce, Inquire, Mirror, and Secure, AIMS structures a nonjudgmental, patient-friendly conversation around immunization to elicit and acknowledge the reasons for hesitancy while explaining the safety and efficacy of vaccines.
Dr. Fryhofer frequently uses AIMS to bring inoculation-averse patients around. “Keep the conversation open with reluctant patients but leave them where they are. They need to see you as a reliable source and nonjudgmental source of information,” she said.
Dr. Block recommends outlining the diseases that have been eliminated through vaccines, from polio to measles, as well as the dangers of vaccine refusal, as indicated by recent outbreaks of vaccine-preventable diseases in areas with low immunization rates. “This approach highlights the opportunity we all have to get vaccinated to protect ourselves and our communities,” she said.
In Dr. Fryhofer’s view, the situation is urgent and doctors need to be proactive. “We’re now at a public-health tipping point where we may see a sliding back and a reversing of many years of progress.”
Dr. Fryhofer and Dr. Block disclosed no competing interests relevant to their comments.
Many adults are complacent about vaccinations, believing that annual COVID and flu shots aside, they had all the immunizations they need as children and teens. But adults need vaccines as well, especially if they have missed earlier doses. And older and health-compromised adults, in particular, can benefit from newer vaccines that were not part of the childhood schedule.
“The question is whether adults had the vaccinations they need in the first place,” Sandra Adamson Fryhofer, MD, an internist in Atlanta and the American Medical Association’s liaison to the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention, said in an interview. “Many do not even have reliable records of vaccination.”
Primary care physicians are ideally positioned to get adult patients to update their vaccination status on older vaccines and obtain newer ones as needed. “ACIP recommendations for adult vaccines are getting longer and more complicated and the way they’re administered is more complex, too, in that they’re not all given in the primary care office but sometimes in pharmacies,” Dr. Fryhofer said.
Not all adult patients want to update their vaccinations. “Vaccine hesitancy among many adults is accelerated by the several new vaccines that have been recommended in recent years,” Lauren Block, MD, MPH, an internist at Northwell Health and assistant professor in the Institute of Health System Science at the Feinstein Institutes for Medical Research in metropolitan New York City, said in an interview.
Physicians are rightly concerned about the lagging rates of adult vaccination, Dr. Block said. “Given the prevalence of conditions like pneumonia and shingles and the morbidity associated with them, healthcare providers should take every opportunity to discuss vaccination with patients, from well visits to hospital visits,” Dr. Block added.
She pointed to several obstacles to broader uptake, including product shortages, financial barriers, and, increasingly, the negative vocal messaging from media outlets and social media.
Current Recommendations
The main vaccines recommended for adults, besides flu and COVID shots, are for respiratory syncytial virus (RVS); shingles; pneumococcal disease; measles, mumps, and rubella (MMR); and tetanus, diphtheria, and pertussis (Tdap). Less commonly, booster vaccines for MM, and hepatitis are recommended when titers are proven to be low.
ACIP’s updated 2024 Adult Immunization Schedule can be downloaded from the website of the CDC.
The newest additions to the schedule include RSV vaccines, the mpox vaccine (Jynneos), a new MenACWY-MenB combo vaccine (Penbraya), and the new 2023-2024 formulation of updated COVID vaccines (both mRNA and protein-based adjuvanted versions).
1. Respiratory Syncytial Virus Vaccines
There are two licensed RSV vaccines, Arexvy and Abrysvo. The CDC schedule recommends a single-dose RSV vaccine for adults age 60 years and older, especially those at high risk of contracting the virus — but after shared decision-making based on a discussion of the risk-harm balance since this vaccine carries a small increased chance of developing the neurological symptoms of Guillain-Barré syndrome.
Chronic health conditions associated with a higher risk of severe RVS include cardiopulmonary disease, diabetes, and kidney, liver, and hematologic disorders, as well as compromised immunity, older age, and frailty.
2. Shingles Vaccines
This painful disease carries the potential complication of postherpetic neuralgia (PHN), which leads to long-term nerve pain in 10%-18% of patients, especially those over age 40. ACIP recommends two doses of the recombinant zoster vaccine (Shingrix) for individuals 50 years and older. Those 19 years and older with weakened immune systems due to disease or medical treatments should get two doses of the recombinant vaccine, as they have a higher risk of getting shingles and its complications, including neurological problems and skin and eye infections.
3 Pneumococcal Vaccines
There are three approved pneumococcal vaccines: PCV15 (Vaxneuvance), PCV20 (Prevnar20), and PPSV23 (Pneumovax23).
“The pneumococcal vaccine schedule is the most complicated one as higher-valent products continue to become available,” Dr. Fryhofer said.
The two types are pneumococcal conjugate vaccines (PCVs, specifically PCV15 and PCV20) and the pneumococcal polysaccharide vaccine (PPSV23). “While PPSV23 covers 23 strains, it doesn’t give the long-term immunity of the conjugate vaccine,” said Dr. Fryhofer. “A patient may have completed their vaccination with the polysaccharide vaccine but 5 years out may no longer be protected. So we offer the option of getting a dose of PCV20 to round out the protection and confer greater immune memory.”
The ACIP schedule recommends immunization against the Streptococcus pneumoniae pathogen for all older and all at-risk adults. Routine administration of PCV15 or PCV20 is advised for those 65 years or older who have never received any pneumococcal conjugate vaccine or whose previous vaccination history is unknown. If PCV15 is used, it should be followed by PPSV23. Those 65 years or older should get PPSV23 even if they already had one or more doses of pneumococcal vaccine before turning 65.
Further vaccination is recommended for younger at-risk adults aged 19-64 years who have received both PCV13 and PPSV23 but have incomplete vaccination status. These individuals are advised to complete their pneumococcal series by receiving either a single dose of PCV20 at an interval of at least 5 years after the last pneumococcal vaccine dose or more than one dose of PPSV23.
See Pneumococcal Vaccination: Summary of Who and When to Vaccinate for CDC guidance on vaccination options for adults who have previously received a pneumococcal conjugate vaccine. Or, to sort out quickly who gets what and when based on their age, concurrent conditions, and vaccination history, the CDC offers a type-in app called the PneumoRecs VaxAdvisor.
4. Measles, Mumps, and Rubella, and Varicella Vaccines
The two approved MMR vaccines are M-M-R II and PRIORIX. A third vaccine, ProQuad, adds varicella.
Adults lacking presumptive evidence of immunity should get at least one dose of the MMR combination vaccine.
Those born before 1957 are deemed to be immune, Dr. Fryhofer noted.
Two doses are recommended for adults entering high-risk settings for measles or mumps transmission such as healthcare personnel, students away at college, and international travelers. The two doses should be separated by at least 28 days. It’s no secret that measles, though preventable, is making a comeback, with 146 reported cases (48 in adults) across 21 states as of May 31 — most linked to international travel.
Women who plan to get pregnant should be vaccinated before but not during each pregnancy. (The vaccine is safe during lactation.) And those of childbearing age with no presumptive evidence of immunity are advised to get at least one dose of the MMR vaccine.
5. Tetanus, Diphtheria, and Pertussis Vaccine
Adults with no previous Tdap vaccination should receive a single dose of Adacel or Boostrix followed by a booster every 10 years. Boostrix is recommended for adults over 64 years.
During every pregnancy, women should have a single dose of Tdap, preferably in gestational weeks 27 through 36.
As to the immediate postpartum period, Tdap is recommended only for mothers who did not receive it during their current pregnancy and never received a prior dose. If a woman did not receive Tdap during her current pregnancy but did receive a prior dose of Tdap, she does not need Tdap postpartum.
The Challenges
According to Dr. Fryhofer, widespread disinformation about the risks of immunization against vaccine-preventable diseases has brought us to a flashpoint. “It’s now more important than ever to keep telling patients that vaccination is one of the most effective tools for preventing individual illness and protecting public health.”
She recommends that doctors follow the National Institutes of Health’s AIMS method to broach the subject of adult vaccination and increase participation in an inquiring, reassuring, and low-pressure way. Standing for Announce, Inquire, Mirror, and Secure, AIMS structures a nonjudgmental, patient-friendly conversation around immunization to elicit and acknowledge the reasons for hesitancy while explaining the safety and efficacy of vaccines.
Dr. Fryhofer frequently uses AIMS to bring inoculation-averse patients around. “Keep the conversation open with reluctant patients but leave them where they are. They need to see you as a reliable source and nonjudgmental source of information,” she said.
Dr. Block recommends outlining the diseases that have been eliminated through vaccines, from polio to measles, as well as the dangers of vaccine refusal, as indicated by recent outbreaks of vaccine-preventable diseases in areas with low immunization rates. “This approach highlights the opportunity we all have to get vaccinated to protect ourselves and our communities,” she said.
In Dr. Fryhofer’s view, the situation is urgent and doctors need to be proactive. “We’re now at a public-health tipping point where we may see a sliding back and a reversing of many years of progress.”
Dr. Fryhofer and Dr. Block disclosed no competing interests relevant to their comments.
Vaginal Ring Use Raises Risk for Certain STIs
Use of combined contraceptive vaginal rings was associated with an increased risk for several types of sexually transmitted infections (STIs), based on data from a pair of studies presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists (ACOG).
Previous research has shown that the use of a combined contraceptive vaginal ring (CCVR) may promote changes in immunity in the female genital tract by upregulating immune-related genes in the endocervix and immune mediators within the cervicovaginal fluid, wrote Amy Arceneaux, BS, a medical student at the University of Texas Medical Branch John Sealy School of Medicine, Galveston, and colleagues.
The infection rates in the female genital tract can vary according to hormones in the local environment and continued safety analysis is needed as the use of CCVR continues to rise, the researchers noted.
In a retrospective chart review, the researchers assessed de-identified data from TriNetX, a patient database, including 30,796 women who received etonogestrel and ethinyl estradiol CCVRs without segesterone and an equal number who were using oral contraceptive pills (OCP) without vaginal hormones. Patients were matched for age, race, and ethnicity.
Overall use of CCVRs was significantly associated with an increased risk for Herpes simplex virus 2 (HSV-2; relative risk [RR], 1.790), acute vaginitis (RR, 1.722), subacute/chronic vaginitis (RR, 1.904), subacute/chronic vulvitis (RR, 1.969), acute vulvitis (RR, 1.894), candidiasis (RR, 1.464), trichomoniasis (RR, 2.162), and pelvic inflammatory disease (RR, 2.984; P < .0005 for all).
By contrast, use of CCVRs was significantly associated with a decreased risk for chlamydia (RR, 0.760; P = .047). No differences in risk appeared for gonorrhea, syphilis, HIV, or anogenital warts between the CCVR and OCP groups.
Another study presented at the meeting, led by Kathleen Karam, BS, also a medical student at the University of Texas Medical Branch John Sealy School of Medicine, Galveston, Texas, focused on outcomes on vaginal health and infection risk in women who used CCVRs compared with women who did not use hormones.
The study by Ms. Karam and colleagues included de-identified TriNetX data for two cohorts of 274,743 women.
Overall, the researchers found a significantly increased risk for gonorrhea, HSV-2, vaginitis, vulvitis, pelvic inflammatory disease, anogenital warts, and candidiasis in women using CCVR compared with those using no hormonal contraception, while the risk for chlamydia, syphilis, and HIV was decreased in women using CCVR compared with those using no hormonal contraception.
“I was pleasantly surprised by the finding that the group of women using the hormonal contraception vaginal ring had decreased risk for HIV and syphilis infections,” said Kathleen L. Vincent, MD, of the University of Texas Medical Branch John Sealy School of Medicine, Galveston, Texas, and senior author on both studies, in an interview. She hypothesized that the estrogen released from the ring might have contributed to the decreased risk for those infections.
The findings of both studies were limited primarily by the retrospective design, but the results suggest a need for further study of the effect of local hormone delivery on the vaginal mucosa, the researchers wrote.
Although the study population was large, the lack of randomization can allow for differences in the behaviors or risk-taking of the groups, Dr. Vincent said in an interview.
“The fact that there were STIs that were increased and some that were decreased with use of the vaginal ring tells us that there were women with similar behaviors in both groups, or we might have seen STIs only in one group,” she said. “Additional research could be done to look at varying time courses of outcomes after initiation of the vaginal ring or to go more in-depth with matching the groups at baseline based on a history of risky behaviors,” she noted.
Data Inform Multipurpose Prevention Technology
Dr. Vincent and her colleague, Richard Pyles, PhD, have a 15-year history of studying vaginal drug and hormone effects on the vaginal mucosa in women and preclinical and cell models. “Based on that work, it was plausible for estrogen to be protective for several types of infections,” she said. The availability of TriNetX allowed the researchers to explore these relationships in a large database of women in the studies presented at the meeting. “We began with a basic science observation in an animal model and grew it into this clinical study because of the available TriNetX system that supported extensive medical record review,” Dr. Pyles noted.
The take-home messages from the current research remain that vaginal rings delivering hormones are indicated only for contraception or birth control, not for protection against STIs or HIV, and women at an increased risk for these infections should protect themselves by using condoms, Dr. Vincent said.
However, “the real clinical implication is for the future for the drugs that we call MPTs or multi-purpose prevention technologies,” Dr. Vincent said.
“This could be a vaginal ring that releases medications for birth control and prevention of HIV or an STI,” she explained.
The findings from the studies presented at the meeting have great potential for an MPT on which Dr. Vincent and Dr. Pyles are working that would provide protection against both HIV and pregnancy. “For HIV prevention, the hormonal vaginal ring components have potential to work synergistically with the HIV prevention drug rather than working against each other, and this could be realized as a need for less HIV prevention drug, and subsequently fewer potential side effects from that drug,” said Dr. Vincent.
The studies received no outside funding. The researchers had no financial conflicts to disclose.
Use of combined contraceptive vaginal rings was associated with an increased risk for several types of sexually transmitted infections (STIs), based on data from a pair of studies presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists (ACOG).
Previous research has shown that the use of a combined contraceptive vaginal ring (CCVR) may promote changes in immunity in the female genital tract by upregulating immune-related genes in the endocervix and immune mediators within the cervicovaginal fluid, wrote Amy Arceneaux, BS, a medical student at the University of Texas Medical Branch John Sealy School of Medicine, Galveston, and colleagues.
The infection rates in the female genital tract can vary according to hormones in the local environment and continued safety analysis is needed as the use of CCVR continues to rise, the researchers noted.
In a retrospective chart review, the researchers assessed de-identified data from TriNetX, a patient database, including 30,796 women who received etonogestrel and ethinyl estradiol CCVRs without segesterone and an equal number who were using oral contraceptive pills (OCP) without vaginal hormones. Patients were matched for age, race, and ethnicity.
Overall use of CCVRs was significantly associated with an increased risk for Herpes simplex virus 2 (HSV-2; relative risk [RR], 1.790), acute vaginitis (RR, 1.722), subacute/chronic vaginitis (RR, 1.904), subacute/chronic vulvitis (RR, 1.969), acute vulvitis (RR, 1.894), candidiasis (RR, 1.464), trichomoniasis (RR, 2.162), and pelvic inflammatory disease (RR, 2.984; P < .0005 for all).
By contrast, use of CCVRs was significantly associated with a decreased risk for chlamydia (RR, 0.760; P = .047). No differences in risk appeared for gonorrhea, syphilis, HIV, or anogenital warts between the CCVR and OCP groups.
Another study presented at the meeting, led by Kathleen Karam, BS, also a medical student at the University of Texas Medical Branch John Sealy School of Medicine, Galveston, Texas, focused on outcomes on vaginal health and infection risk in women who used CCVRs compared with women who did not use hormones.
The study by Ms. Karam and colleagues included de-identified TriNetX data for two cohorts of 274,743 women.
Overall, the researchers found a significantly increased risk for gonorrhea, HSV-2, vaginitis, vulvitis, pelvic inflammatory disease, anogenital warts, and candidiasis in women using CCVR compared with those using no hormonal contraception, while the risk for chlamydia, syphilis, and HIV was decreased in women using CCVR compared with those using no hormonal contraception.
“I was pleasantly surprised by the finding that the group of women using the hormonal contraception vaginal ring had decreased risk for HIV and syphilis infections,” said Kathleen L. Vincent, MD, of the University of Texas Medical Branch John Sealy School of Medicine, Galveston, Texas, and senior author on both studies, in an interview. She hypothesized that the estrogen released from the ring might have contributed to the decreased risk for those infections.
The findings of both studies were limited primarily by the retrospective design, but the results suggest a need for further study of the effect of local hormone delivery on the vaginal mucosa, the researchers wrote.
Although the study population was large, the lack of randomization can allow for differences in the behaviors or risk-taking of the groups, Dr. Vincent said in an interview.
“The fact that there were STIs that were increased and some that were decreased with use of the vaginal ring tells us that there were women with similar behaviors in both groups, or we might have seen STIs only in one group,” she said. “Additional research could be done to look at varying time courses of outcomes after initiation of the vaginal ring or to go more in-depth with matching the groups at baseline based on a history of risky behaviors,” she noted.
Data Inform Multipurpose Prevention Technology
Dr. Vincent and her colleague, Richard Pyles, PhD, have a 15-year history of studying vaginal drug and hormone effects on the vaginal mucosa in women and preclinical and cell models. “Based on that work, it was plausible for estrogen to be protective for several types of infections,” she said. The availability of TriNetX allowed the researchers to explore these relationships in a large database of women in the studies presented at the meeting. “We began with a basic science observation in an animal model and grew it into this clinical study because of the available TriNetX system that supported extensive medical record review,” Dr. Pyles noted.
The take-home messages from the current research remain that vaginal rings delivering hormones are indicated only for contraception or birth control, not for protection against STIs or HIV, and women at an increased risk for these infections should protect themselves by using condoms, Dr. Vincent said.
However, “the real clinical implication is for the future for the drugs that we call MPTs or multi-purpose prevention technologies,” Dr. Vincent said.
“This could be a vaginal ring that releases medications for birth control and prevention of HIV or an STI,” she explained.
The findings from the studies presented at the meeting have great potential for an MPT on which Dr. Vincent and Dr. Pyles are working that would provide protection against both HIV and pregnancy. “For HIV prevention, the hormonal vaginal ring components have potential to work synergistically with the HIV prevention drug rather than working against each other, and this could be realized as a need for less HIV prevention drug, and subsequently fewer potential side effects from that drug,” said Dr. Vincent.
The studies received no outside funding. The researchers had no financial conflicts to disclose.
Use of combined contraceptive vaginal rings was associated with an increased risk for several types of sexually transmitted infections (STIs), based on data from a pair of studies presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists (ACOG).
Previous research has shown that the use of a combined contraceptive vaginal ring (CCVR) may promote changes in immunity in the female genital tract by upregulating immune-related genes in the endocervix and immune mediators within the cervicovaginal fluid, wrote Amy Arceneaux, BS, a medical student at the University of Texas Medical Branch John Sealy School of Medicine, Galveston, and colleagues.
The infection rates in the female genital tract can vary according to hormones in the local environment and continued safety analysis is needed as the use of CCVR continues to rise, the researchers noted.
In a retrospective chart review, the researchers assessed de-identified data from TriNetX, a patient database, including 30,796 women who received etonogestrel and ethinyl estradiol CCVRs without segesterone and an equal number who were using oral contraceptive pills (OCP) without vaginal hormones. Patients were matched for age, race, and ethnicity.
Overall use of CCVRs was significantly associated with an increased risk for Herpes simplex virus 2 (HSV-2; relative risk [RR], 1.790), acute vaginitis (RR, 1.722), subacute/chronic vaginitis (RR, 1.904), subacute/chronic vulvitis (RR, 1.969), acute vulvitis (RR, 1.894), candidiasis (RR, 1.464), trichomoniasis (RR, 2.162), and pelvic inflammatory disease (RR, 2.984; P < .0005 for all).
By contrast, use of CCVRs was significantly associated with a decreased risk for chlamydia (RR, 0.760; P = .047). No differences in risk appeared for gonorrhea, syphilis, HIV, or anogenital warts between the CCVR and OCP groups.
Another study presented at the meeting, led by Kathleen Karam, BS, also a medical student at the University of Texas Medical Branch John Sealy School of Medicine, Galveston, Texas, focused on outcomes on vaginal health and infection risk in women who used CCVRs compared with women who did not use hormones.
The study by Ms. Karam and colleagues included de-identified TriNetX data for two cohorts of 274,743 women.
Overall, the researchers found a significantly increased risk for gonorrhea, HSV-2, vaginitis, vulvitis, pelvic inflammatory disease, anogenital warts, and candidiasis in women using CCVR compared with those using no hormonal contraception, while the risk for chlamydia, syphilis, and HIV was decreased in women using CCVR compared with those using no hormonal contraception.
“I was pleasantly surprised by the finding that the group of women using the hormonal contraception vaginal ring had decreased risk for HIV and syphilis infections,” said Kathleen L. Vincent, MD, of the University of Texas Medical Branch John Sealy School of Medicine, Galveston, Texas, and senior author on both studies, in an interview. She hypothesized that the estrogen released from the ring might have contributed to the decreased risk for those infections.
The findings of both studies were limited primarily by the retrospective design, but the results suggest a need for further study of the effect of local hormone delivery on the vaginal mucosa, the researchers wrote.
Although the study population was large, the lack of randomization can allow for differences in the behaviors or risk-taking of the groups, Dr. Vincent said in an interview.
“The fact that there were STIs that were increased and some that were decreased with use of the vaginal ring tells us that there were women with similar behaviors in both groups, or we might have seen STIs only in one group,” she said. “Additional research could be done to look at varying time courses of outcomes after initiation of the vaginal ring or to go more in-depth with matching the groups at baseline based on a history of risky behaviors,” she noted.
Data Inform Multipurpose Prevention Technology
Dr. Vincent and her colleague, Richard Pyles, PhD, have a 15-year history of studying vaginal drug and hormone effects on the vaginal mucosa in women and preclinical and cell models. “Based on that work, it was plausible for estrogen to be protective for several types of infections,” she said. The availability of TriNetX allowed the researchers to explore these relationships in a large database of women in the studies presented at the meeting. “We began with a basic science observation in an animal model and grew it into this clinical study because of the available TriNetX system that supported extensive medical record review,” Dr. Pyles noted.
The take-home messages from the current research remain that vaginal rings delivering hormones are indicated only for contraception or birth control, not for protection against STIs or HIV, and women at an increased risk for these infections should protect themselves by using condoms, Dr. Vincent said.
However, “the real clinical implication is for the future for the drugs that we call MPTs or multi-purpose prevention technologies,” Dr. Vincent said.
“This could be a vaginal ring that releases medications for birth control and prevention of HIV or an STI,” she explained.
The findings from the studies presented at the meeting have great potential for an MPT on which Dr. Vincent and Dr. Pyles are working that would provide protection against both HIV and pregnancy. “For HIV prevention, the hormonal vaginal ring components have potential to work synergistically with the HIV prevention drug rather than working against each other, and this could be realized as a need for less HIV prevention drug, and subsequently fewer potential side effects from that drug,” said Dr. Vincent.
The studies received no outside funding. The researchers had no financial conflicts to disclose.
FROM ACOG 2024
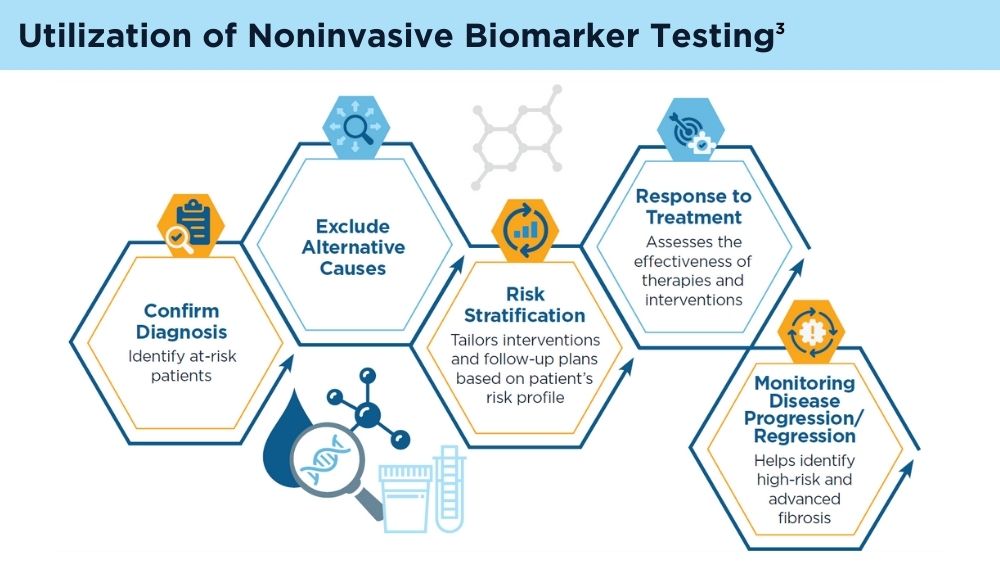
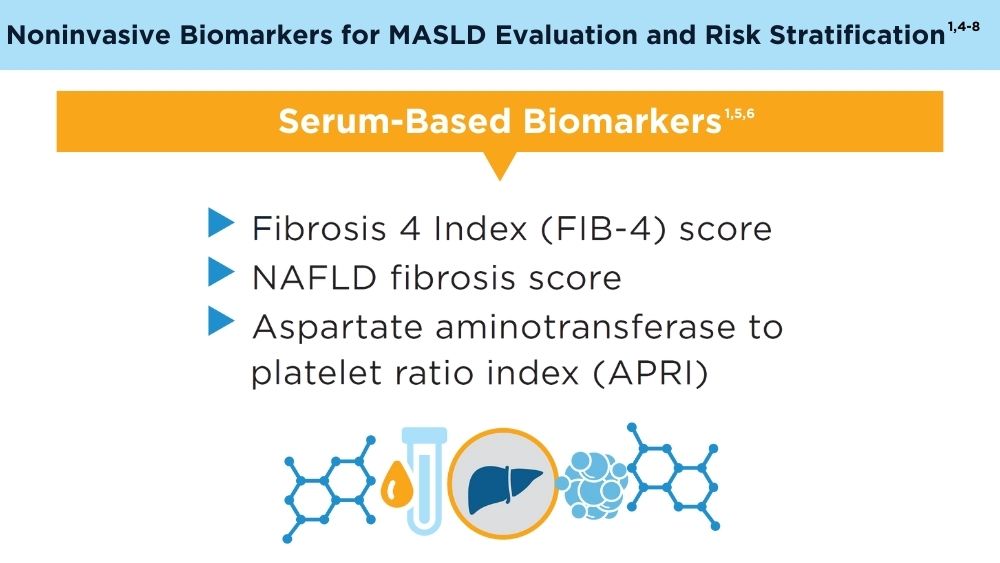
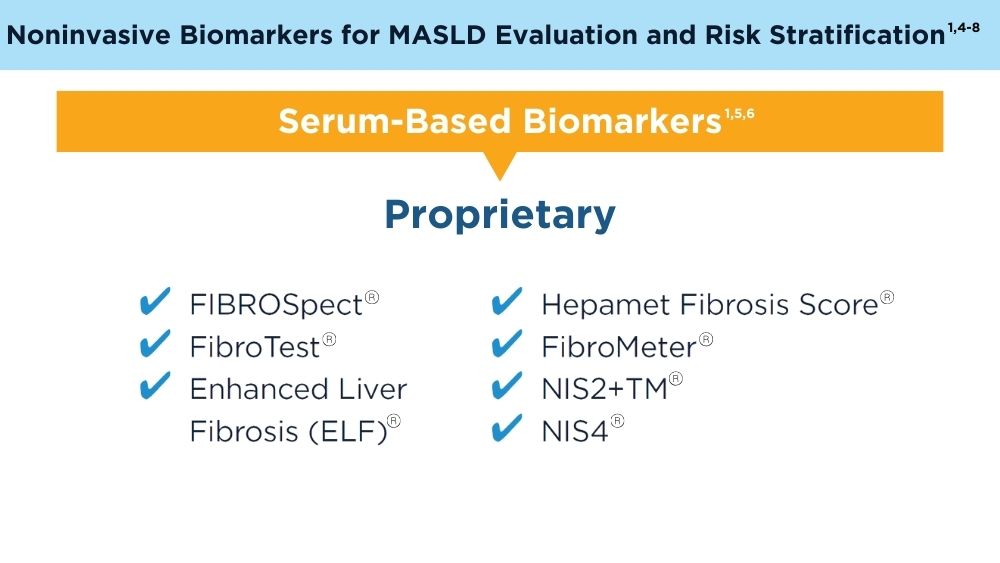
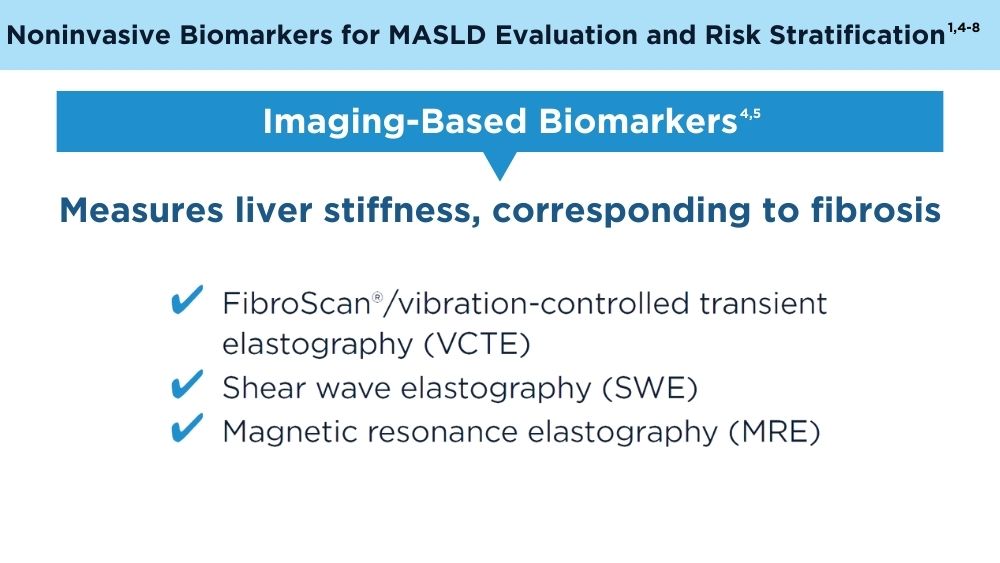
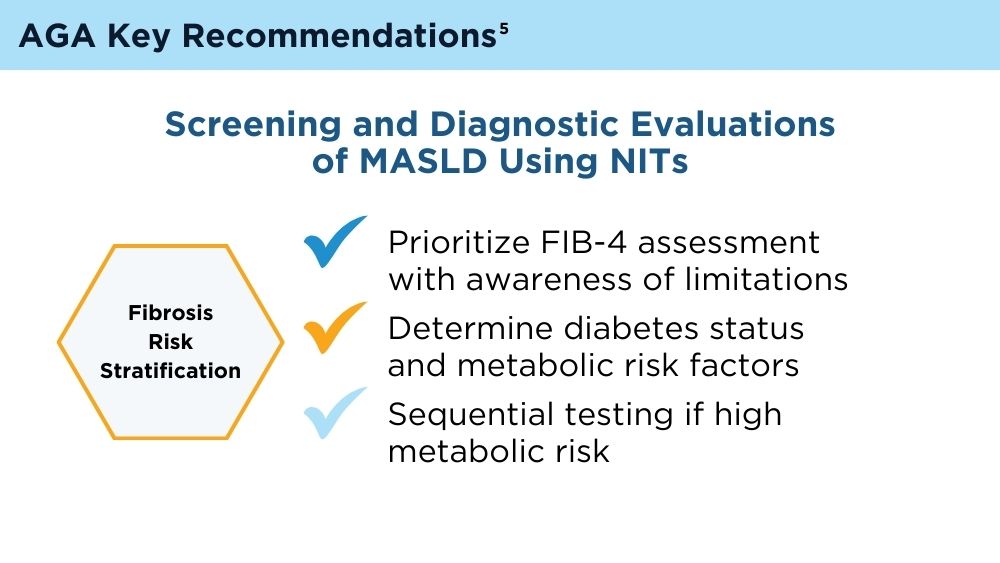
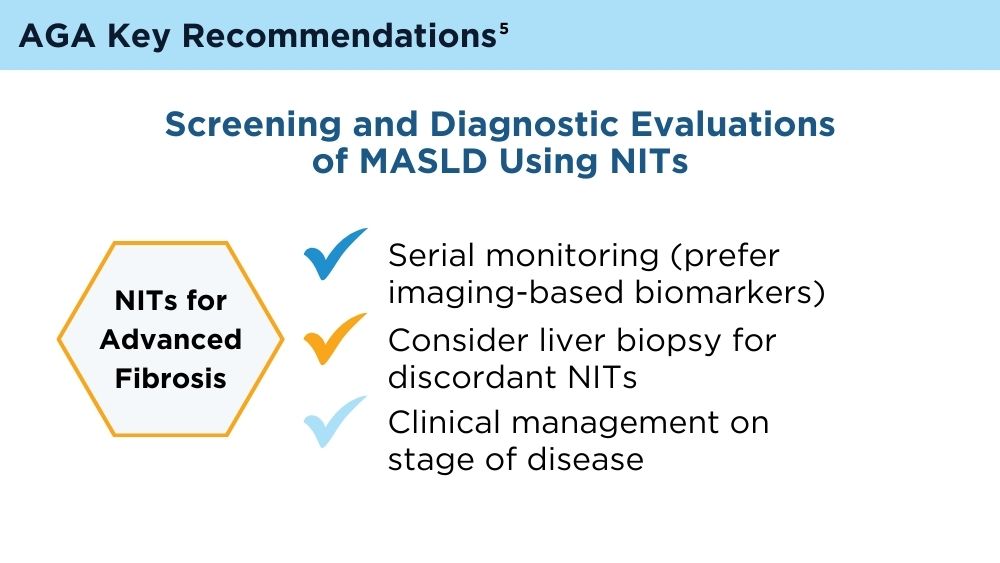
Role of Non-invasive Biomarkers in the Evaluation and Management of MASLD
Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023;78(6):1966-1986. doi:10.1097/HEP.0000000000000520
Wattacheril JJ, Abdelmalek MF, Lim JK, Sanyal AJ. AGA Clinical Practice Update on the Role of Noninvasive Biomarkers in the Evaluation and Management of Nonalcoholic Fatty Liver Disease: Expert Review. Gastroenterology. 2023;165(4):1080-1088. doi:10.1053/j.gastro.2023.06.013
Di Mauro S, Scamporrino A, Filippello A, et al. Clinical and Molecular Biomarkers for Diagnosis and Staging of NAFLD. Int J Mol Sci. 2021;22(21):11905. Published 2021 Nov 2. doi:10.3390/ijms222111905
Hsu C, Caussy C, Imajo K, et al. Magnetic Resonance vs Transient Elastography Analysis of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Pooled Analysis of Individual Participants. Clin Gastroenterol Hepatol. 2019;17(4):630-637.e8. doi:10.1016/j.cgh.2018.05.059
Ilagan-Ying YC, Banini BA, Do A, Lam R, Lim JK. Screening, Diagnosis, and Staging of Non-Alcoholic Fatty Liver Disease (NAFLD): Application of Society Guidelines to Clinical Practice. Curr Gastroenterol Rep. 2023;25(10):213-224. doi:10.1007/s11894-023-00883-8
Chen W, Gao Y, Xie W, et al. Genome-wide association analyses provide genetic and biochemical insights into natural variation in rice metabolism. Nat Genet. 2014;46(7):714-721. doi:10.1038/ng.3007
Wu YL, Kumar R, Wang MF, et al. Validation of conventional non-invasive fibrosis scoring systems in patients with metabolic associated fatty liver disease. World J Gastroenterol. 2021;27(34):5753-5763. doi:10.3748/wjg.v27.i34.5753
Kaneva AM, Bojko ER. Fatty liver index (FLI): more than a marker of hepatic steatosis. J Physiol Biochem. Published online October 25, 2023. doi:10.1007/s13105-023-00991-z
Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023;78(6):1966-1986. doi:10.1097/HEP.0000000000000520
Wattacheril JJ, Abdelmalek MF, Lim JK, Sanyal AJ. AGA Clinical Practice Update on the Role of Noninvasive Biomarkers in the Evaluation and Management of Nonalcoholic Fatty Liver Disease: Expert Review. Gastroenterology. 2023;165(4):1080-1088. doi:10.1053/j.gastro.2023.06.013
Di Mauro S, Scamporrino A, Filippello A, et al. Clinical and Molecular Biomarkers for Diagnosis and Staging of NAFLD. Int J Mol Sci. 2021;22(21):11905. Published 2021 Nov 2. doi:10.3390/ijms222111905
Hsu C, Caussy C, Imajo K, et al. Magnetic Resonance vs Transient Elastography Analysis of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Pooled Analysis of Individual Participants. Clin Gastroenterol Hepatol. 2019;17(4):630-637.e8. doi:10.1016/j.cgh.2018.05.059
Ilagan-Ying YC, Banini BA, Do A, Lam R, Lim JK. Screening, Diagnosis, and Staging of Non-Alcoholic Fatty Liver Disease (NAFLD): Application of Society Guidelines to Clinical Practice. Curr Gastroenterol Rep. 2023;25(10):213-224. doi:10.1007/s11894-023-00883-8
Chen W, Gao Y, Xie W, et al. Genome-wide association analyses provide genetic and biochemical insights into natural variation in rice metabolism. Nat Genet. 2014;46(7):714-721. doi:10.1038/ng.3007
Wu YL, Kumar R, Wang MF, et al. Validation of conventional non-invasive fibrosis scoring systems in patients with metabolic associated fatty liver disease. World J Gastroenterol. 2021;27(34):5753-5763. doi:10.3748/wjg.v27.i34.5753
Kaneva AM, Bojko ER. Fatty liver index (FLI): more than a marker of hepatic steatosis. J Physiol Biochem. Published online October 25, 2023. doi:10.1007/s13105-023-00991-z
Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023;78(6):1966-1986. doi:10.1097/HEP.0000000000000520
Wattacheril JJ, Abdelmalek MF, Lim JK, Sanyal AJ. AGA Clinical Practice Update on the Role of Noninvasive Biomarkers in the Evaluation and Management of Nonalcoholic Fatty Liver Disease: Expert Review. Gastroenterology. 2023;165(4):1080-1088. doi:10.1053/j.gastro.2023.06.013
Di Mauro S, Scamporrino A, Filippello A, et al. Clinical and Molecular Biomarkers for Diagnosis and Staging of NAFLD. Int J Mol Sci. 2021;22(21):11905. Published 2021 Nov 2. doi:10.3390/ijms222111905
Hsu C, Caussy C, Imajo K, et al. Magnetic Resonance vs Transient Elastography Analysis of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Pooled Analysis of Individual Participants. Clin Gastroenterol Hepatol. 2019;17(4):630-637.e8. doi:10.1016/j.cgh.2018.05.059
Ilagan-Ying YC, Banini BA, Do A, Lam R, Lim JK. Screening, Diagnosis, and Staging of Non-Alcoholic Fatty Liver Disease (NAFLD): Application of Society Guidelines to Clinical Practice. Curr Gastroenterol Rep. 2023;25(10):213-224. doi:10.1007/s11894-023-00883-8
Chen W, Gao Y, Xie W, et al. Genome-wide association analyses provide genetic and biochemical insights into natural variation in rice metabolism. Nat Genet. 2014;46(7):714-721. doi:10.1038/ng.3007
Wu YL, Kumar R, Wang MF, et al. Validation of conventional non-invasive fibrosis scoring systems in patients with metabolic associated fatty liver disease. World J Gastroenterol. 2021;27(34):5753-5763. doi:10.3748/wjg.v27.i34.5753
Kaneva AM, Bojko ER. Fatty liver index (FLI): more than a marker of hepatic steatosis. J Physiol Biochem. Published online October 25, 2023. doi:10.1007/s13105-023-00991-z
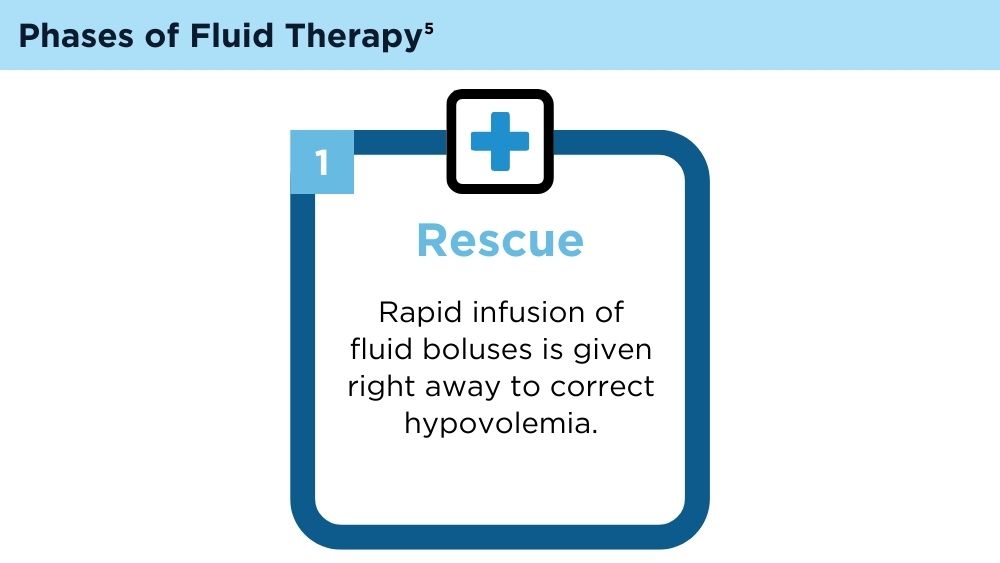
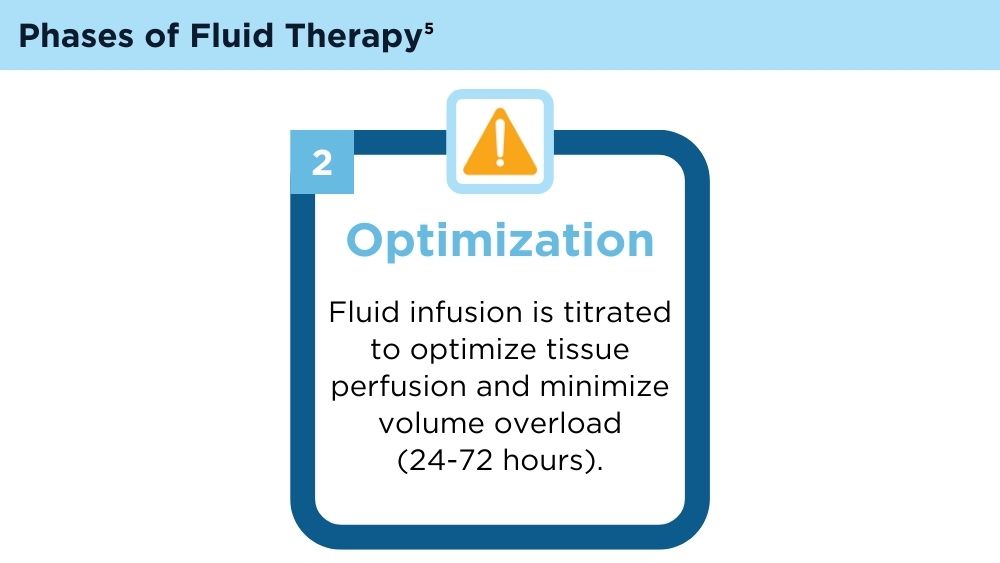
Fluid Management in Acute Pancreatitis
Tenner S, Baillie J, DeWitt J, Vege SS; American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014;109(2):302]. Am J Gastroenterol. 2013;108(9):1400-1415. doi:10.1038/ajg.2013.218
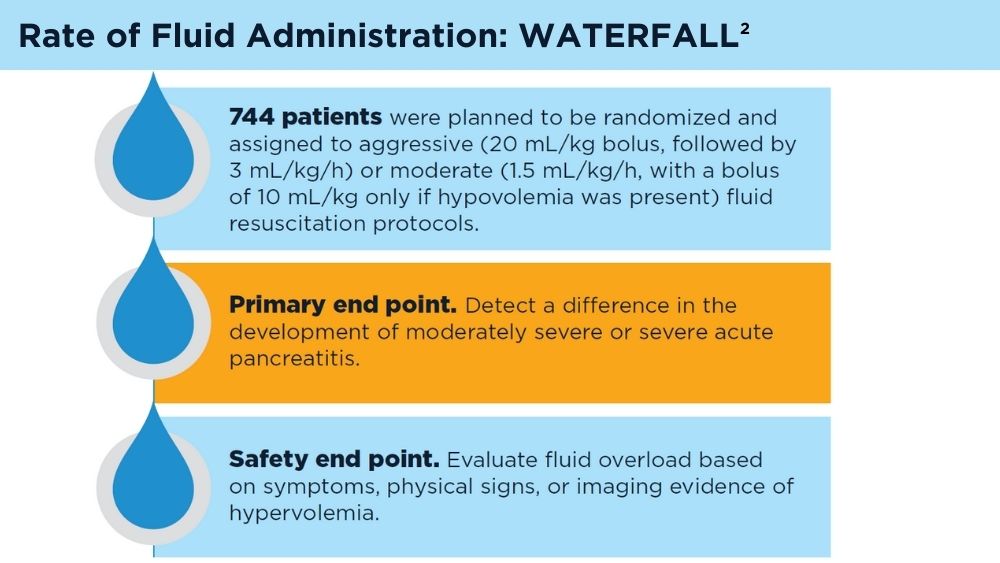
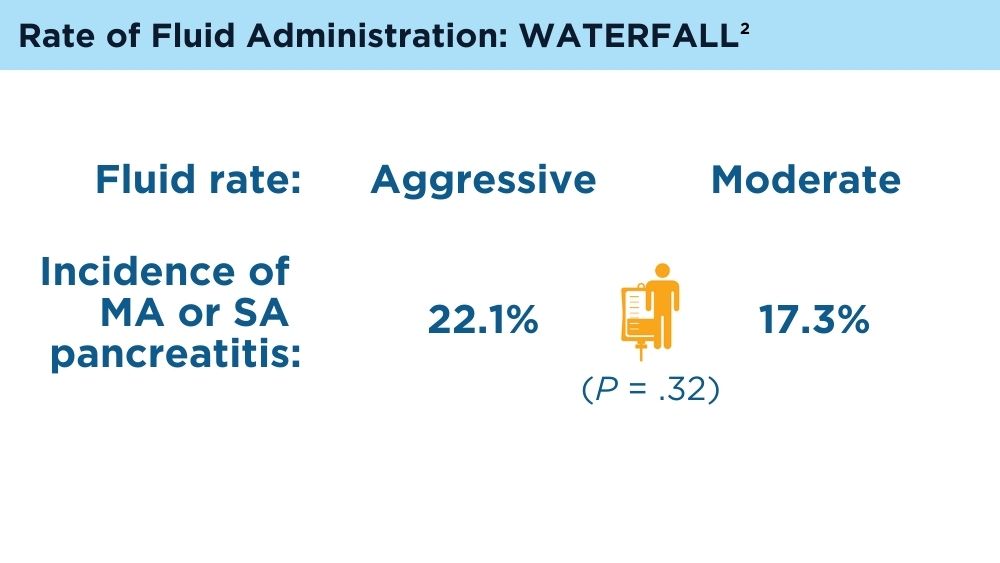
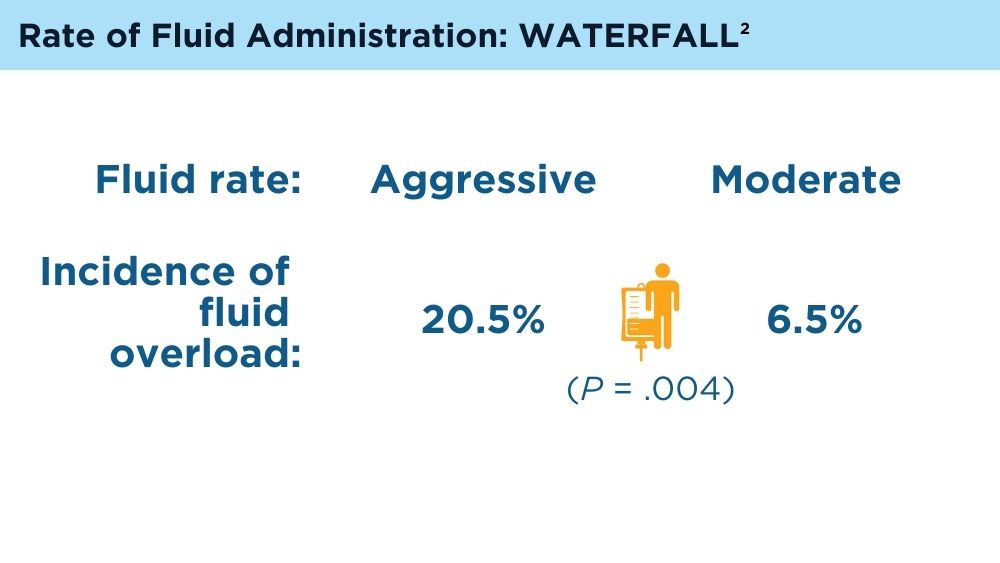
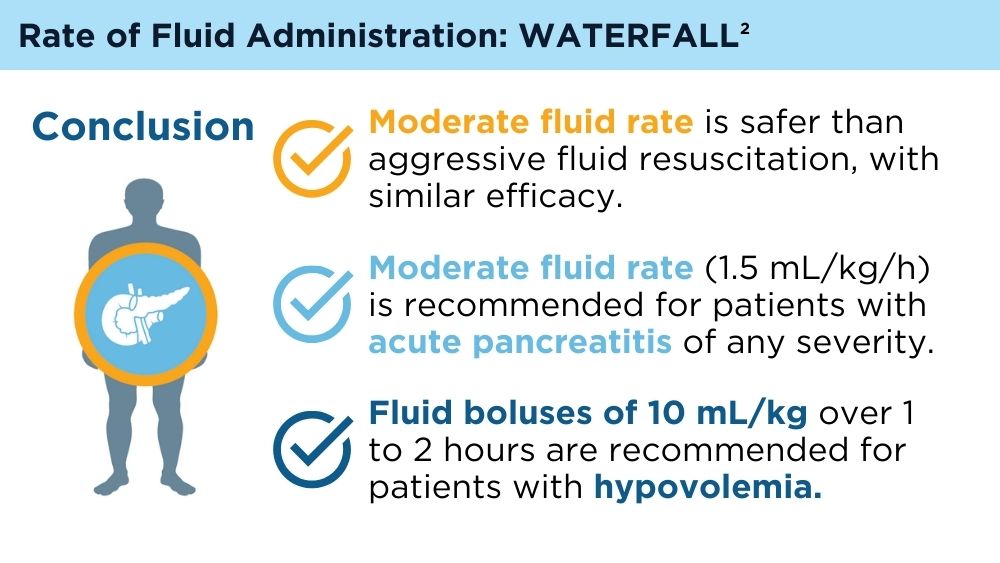
de-Madaria E, Buxbaum JL, Maisonneuve P, et al. Aggressive or moderate fluid resuscitation in acute pancreatitis. N Engl J Med. 2022;387(11):989-1000. doi:10.1056/NEJMoa2202884
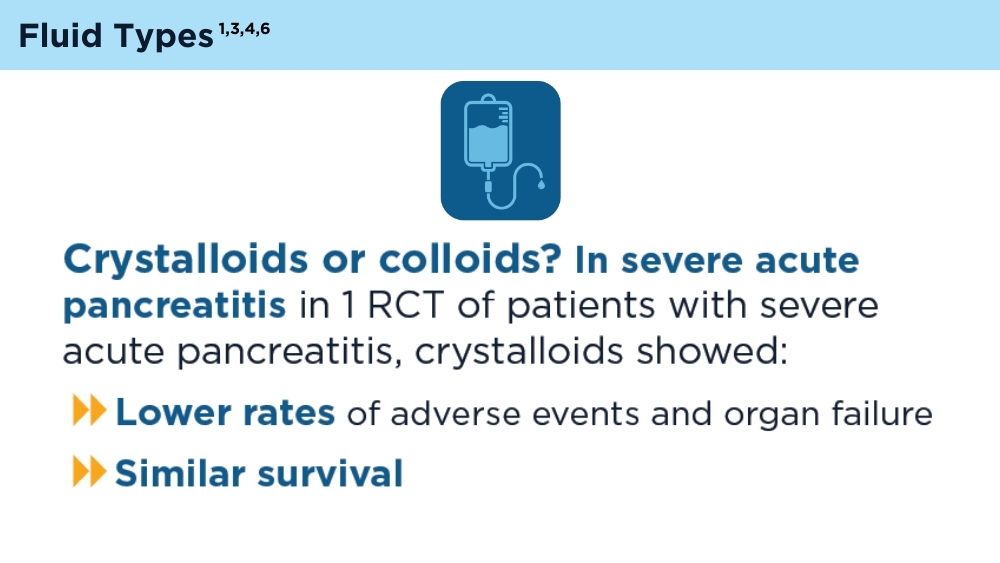
Zhao G, Zhang JG, Wu HS, et al. Effects of different resuscitation fluid on severe acute pancreatitis. World J Gastroenterol. 2013;19(13):2044-2052. doi:10.3748/wjg.v19.i13.2044
Guzmán-Calderón E, Diaz-Arocutipa C, Monge E. Lactate Ringer's versus normal saline in the management of acute pancreatitis: a systematic review and meta-analysis of randomized controlled trials. Dig Dis Sci. 2022;67(8):4131-4139. doi:10.1007/s10620-021-07269-8
Hoste EA, Maitland K, Brudney CS, et al; ADQI XII Investigators Group. Four phases of intravenous fluid therapy: a conceptual model. Br J Anaesth. 2014;113(5):740-747. doi:10.1093/bja/aeu300
Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13(4 suppl 2):e1-e15. doi:10.1016/j.pan.2013.07.063
Machicado JD, Papachristou GI. Pharmacologic management and prevention of acute pancreatitis. Curr Opin Gastroenterol. 2019;35(5):460-467. doi:10.1097/MOG.0000000000000563
Tenner S, Baillie J, DeWitt J, Vege SS; American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014;109(2):302]. Am J Gastroenterol. 2013;108(9):1400-1415. doi:10.1038/ajg.2013.218
de-Madaria E, Buxbaum JL, Maisonneuve P, et al. Aggressive or moderate fluid resuscitation in acute pancreatitis. N Engl J Med. 2022;387(11):989-1000. doi:10.1056/NEJMoa2202884
Zhao G, Zhang JG, Wu HS, et al. Effects of different resuscitation fluid on severe acute pancreatitis. World J Gastroenterol. 2013;19(13):2044-2052. doi:10.3748/wjg.v19.i13.2044
Guzmán-Calderón E, Diaz-Arocutipa C, Monge E. Lactate Ringer's versus normal saline in the management of acute pancreatitis: a systematic review and meta-analysis of randomized controlled trials. Dig Dis Sci. 2022;67(8):4131-4139. doi:10.1007/s10620-021-07269-8
Hoste EA, Maitland K, Brudney CS, et al; ADQI XII Investigators Group. Four phases of intravenous fluid therapy: a conceptual model. Br J Anaesth. 2014;113(5):740-747. doi:10.1093/bja/aeu300
Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13(4 suppl 2):e1-e15. doi:10.1016/j.pan.2013.07.063
Machicado JD, Papachristou GI. Pharmacologic management and prevention of acute pancreatitis. Curr Opin Gastroenterol. 2019;35(5):460-467. doi:10.1097/MOG.0000000000000563
Tenner S, Baillie J, DeWitt J, Vege SS; American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014;109(2):302]. Am J Gastroenterol. 2013;108(9):1400-1415. doi:10.1038/ajg.2013.218
de-Madaria E, Buxbaum JL, Maisonneuve P, et al. Aggressive or moderate fluid resuscitation in acute pancreatitis. N Engl J Med. 2022;387(11):989-1000. doi:10.1056/NEJMoa2202884
Zhao G, Zhang JG, Wu HS, et al. Effects of different resuscitation fluid on severe acute pancreatitis. World J Gastroenterol. 2013;19(13):2044-2052. doi:10.3748/wjg.v19.i13.2044
Guzmán-Calderón E, Diaz-Arocutipa C, Monge E. Lactate Ringer's versus normal saline in the management of acute pancreatitis: a systematic review and meta-analysis of randomized controlled trials. Dig Dis Sci. 2022;67(8):4131-4139. doi:10.1007/s10620-021-07269-8
Hoste EA, Maitland K, Brudney CS, et al; ADQI XII Investigators Group. Four phases of intravenous fluid therapy: a conceptual model. Br J Anaesth. 2014;113(5):740-747. doi:10.1093/bja/aeu300
Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13(4 suppl 2):e1-e15. doi:10.1016/j.pan.2013.07.063
Machicado JD, Papachristou GI. Pharmacologic management and prevention of acute pancreatitis. Curr Opin Gastroenterol. 2019;35(5):460-467. doi:10.1097/MOG.0000000000000563

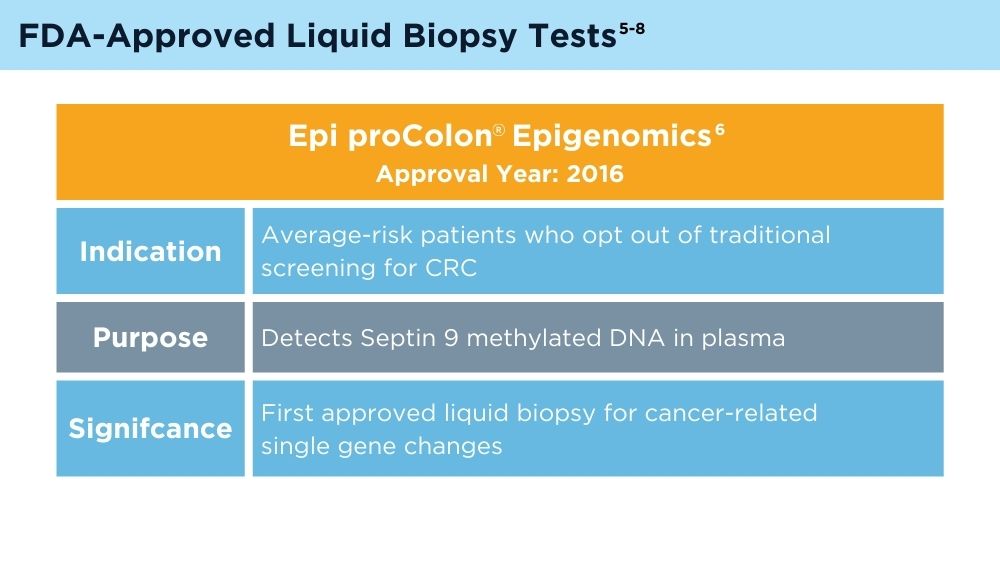
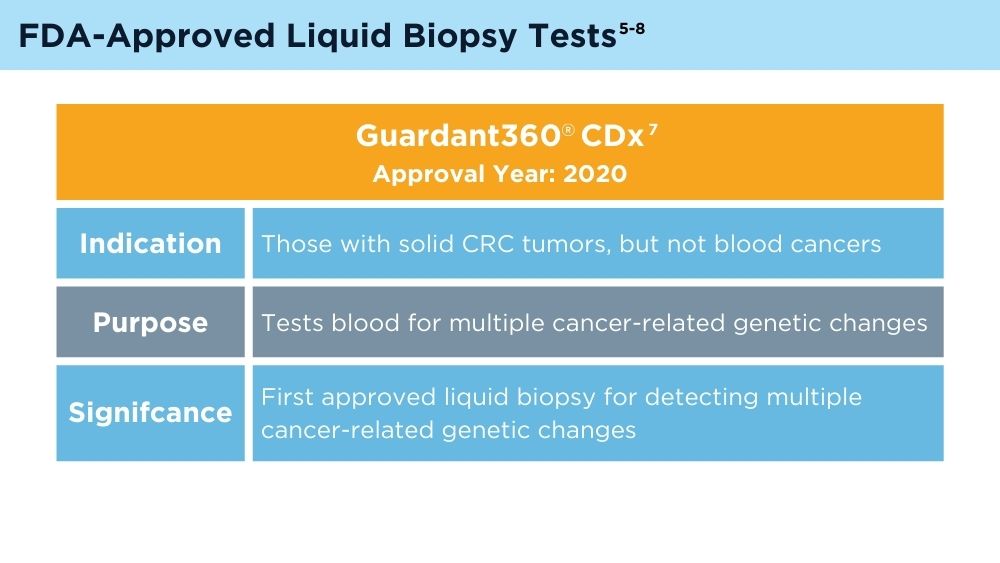
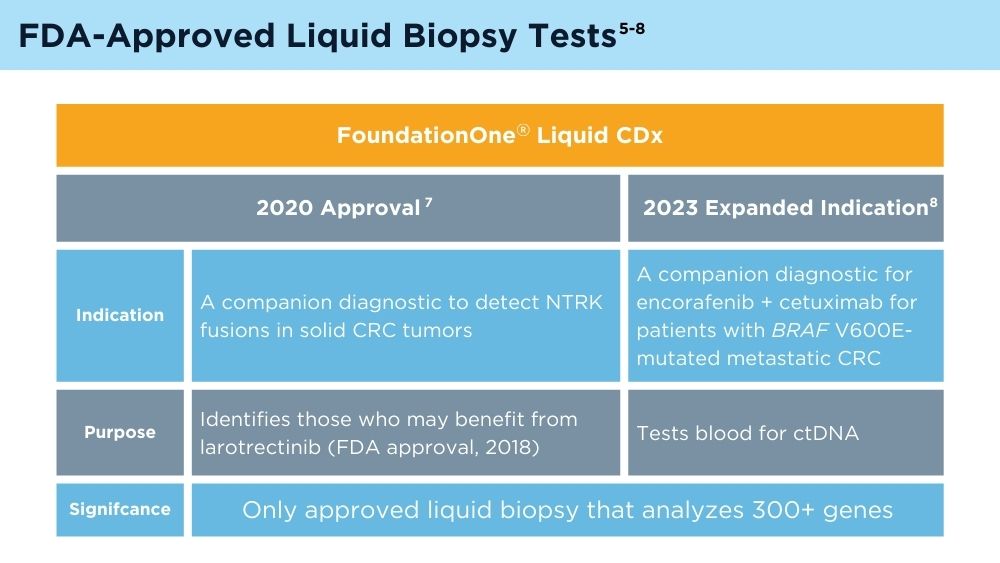
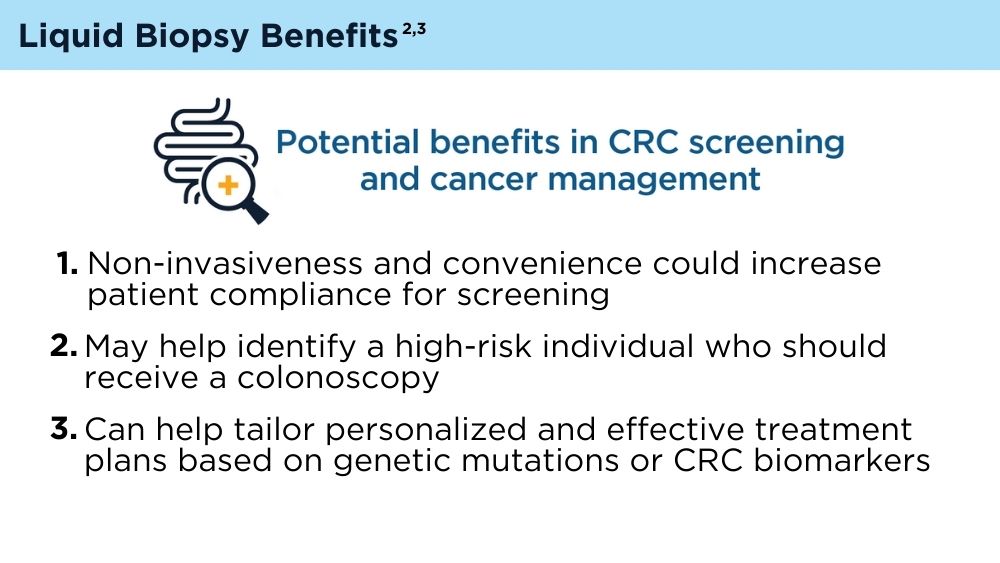
The Emerging Role of Liquid Biopsy in the Diagnosis and Management of CRC
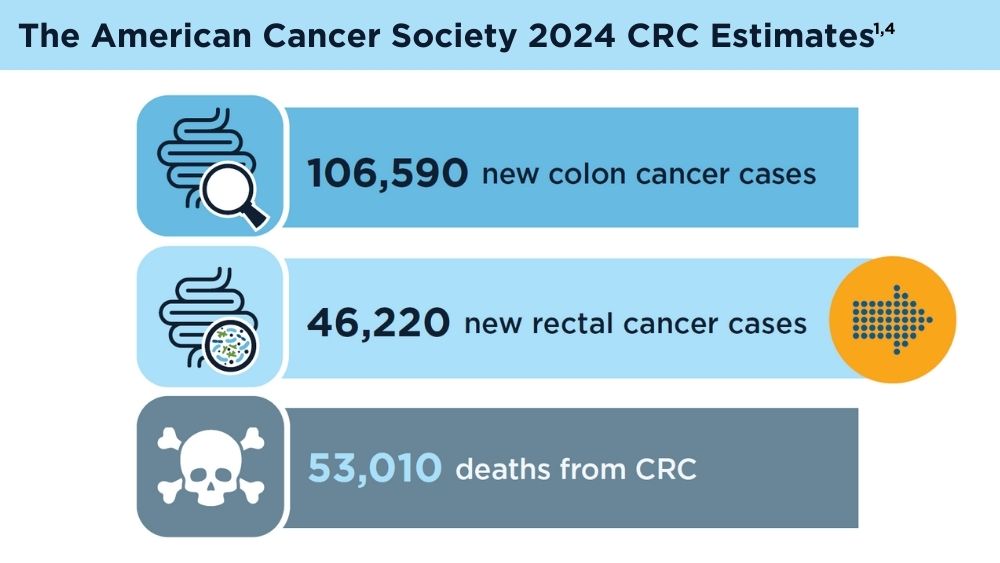
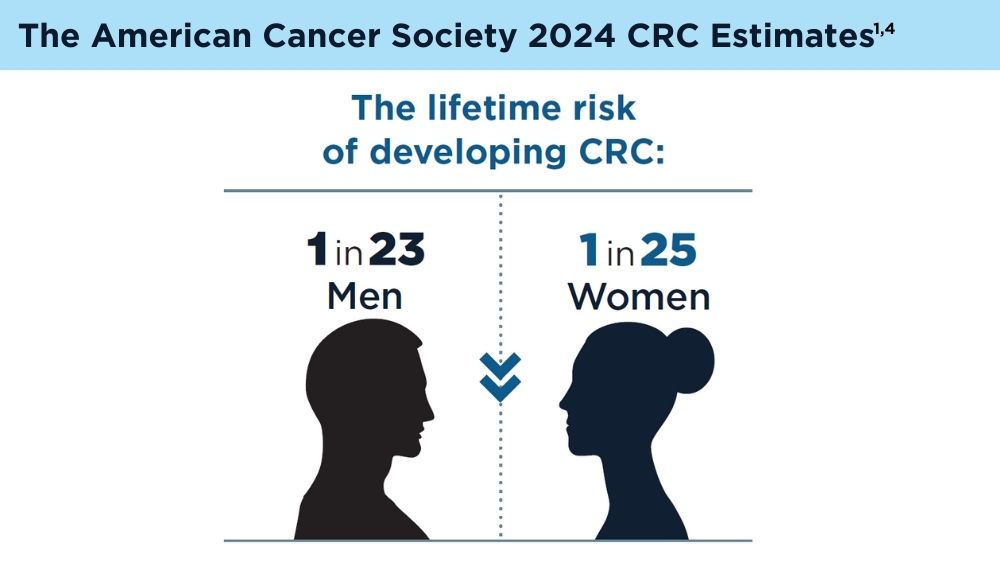
Key statistics for colorectal cancer. American Cancer Society. Revised January 13, 2023. Accessed November 30, 2023. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
Mazouji O, Ouhajjou A, Incitti R, Mansour H. Updates on clinical use of liquid biopsy in colorectal cancer screening, diagnosis, follow-up, and treatment guidance. Front Cell Dev Biol. 2021;9:660924. doi:10.3389/fcell.2021.660924
Vacante M, Ciuni R, Basile F, Biondi A. The liquid biopsy in the management of colorectal cancer: an overview. Biomedicines. 2020;8(9):308. doi:10.3390/biomedicines8090308
American Cancer Society. Colorectal cancer facts & figures 2020-2022. Published 2022. Accessed November 30, 2023. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/colorectal-cancer-facts-and-figures/colorectal-cancer-facts-and-figures-2020-2022.pdf
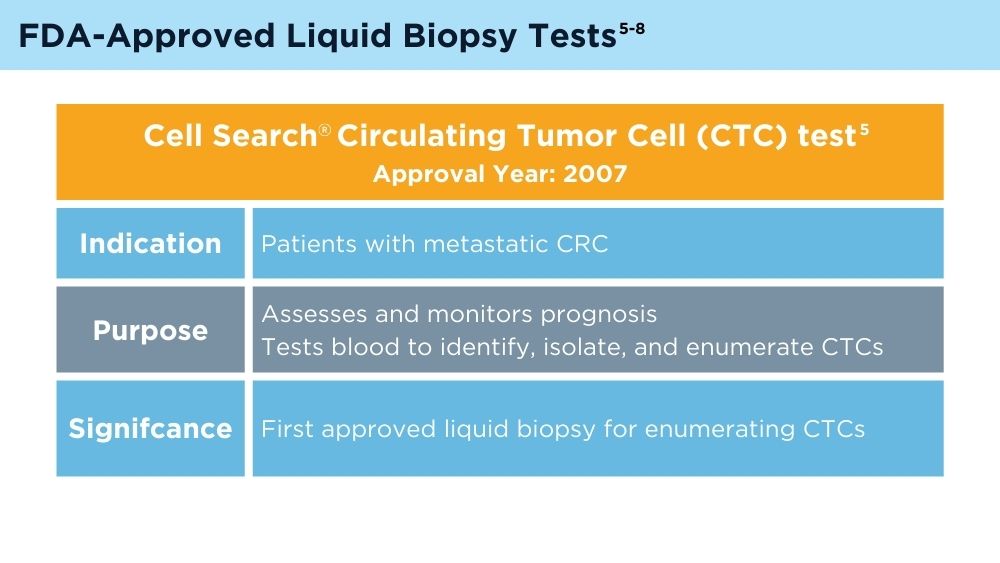
Johnson & Johnson. FDA clears Cellsearch™ circulating tumor cell test [news release]. Published February 27, 2008. Accessed November 30, 2023. https://johnsonandjohnson.gcs-web.com/news-releases/news-release-details/fda-clears-cellsearchtm-circulating-tumor-cell-test
US Food and Drug Administration. Summary of safety and effectiveness data, Epi proColon®. PMA number P130001. Published April 12, 2016. Accessed November 30, 2023. https://www.accessdata.fda.gov/cdrh_docs/pdf13/p130001b.pdf
FDA approves blood tests that can help guide cancer treatment. National Institutes of Health, National Cancer Institute. Published October 15, 2020. Accessed November 30, 2023. https://www.cancer.gov/news-events/cancer-currents-blog/2020/fda-guardant-360-foundation-one-cancer-liquid-biopsy
Foundation Medicine. US Food and Drug Administration (FDA) approves FoundationOne®LiquidCDx as a companion diagnostic for Pfizer’s BRAFTOVI® (encorafenib) in combination with cetuximab to identify patients with BRAF V600E alterations in metastatic colorectal cancer [press release]. Published June 10, 2023. Accessed November 30, 2023. https://www.foundationmedicine.com/press-releases/f9b285eb-db6d-4f61-856c-3f1edb803937
Key statistics for colorectal cancer. American Cancer Society. Revised January 13, 2023. Accessed November 30, 2023. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
Mazouji O, Ouhajjou A, Incitti R, Mansour H. Updates on clinical use of liquid biopsy in colorectal cancer screening, diagnosis, follow-up, and treatment guidance. Front Cell Dev Biol. 2021;9:660924. doi:10.3389/fcell.2021.660924
Vacante M, Ciuni R, Basile F, Biondi A. The liquid biopsy in the management of colorectal cancer: an overview. Biomedicines. 2020;8(9):308. doi:10.3390/biomedicines8090308
American Cancer Society. Colorectal cancer facts & figures 2020-2022. Published 2022. Accessed November 30, 2023. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/colorectal-cancer-facts-and-figures/colorectal-cancer-facts-and-figures-2020-2022.pdf
Johnson & Johnson. FDA clears Cellsearch™ circulating tumor cell test [news release]. Published February 27, 2008. Accessed November 30, 2023. https://johnsonandjohnson.gcs-web.com/news-releases/news-release-details/fda-clears-cellsearchtm-circulating-tumor-cell-test
US Food and Drug Administration. Summary of safety and effectiveness data, Epi proColon®. PMA number P130001. Published April 12, 2016. Accessed November 30, 2023. https://www.accessdata.fda.gov/cdrh_docs/pdf13/p130001b.pdf
FDA approves blood tests that can help guide cancer treatment. National Institutes of Health, National Cancer Institute. Published October 15, 2020. Accessed November 30, 2023. https://www.cancer.gov/news-events/cancer-currents-blog/2020/fda-guardant-360-foundation-one-cancer-liquid-biopsy
Foundation Medicine. US Food and Drug Administration (FDA) approves FoundationOne®LiquidCDx as a companion diagnostic for Pfizer’s BRAFTOVI® (encorafenib) in combination with cetuximab to identify patients with BRAF V600E alterations in metastatic colorectal cancer [press release]. Published June 10, 2023. Accessed November 30, 2023. https://www.foundationmedicine.com/press-releases/f9b285eb-db6d-4f61-856c-3f1edb803937
Key statistics for colorectal cancer. American Cancer Society. Revised January 13, 2023. Accessed November 30, 2023. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
Mazouji O, Ouhajjou A, Incitti R, Mansour H. Updates on clinical use of liquid biopsy in colorectal cancer screening, diagnosis, follow-up, and treatment guidance. Front Cell Dev Biol. 2021;9:660924. doi:10.3389/fcell.2021.660924
Vacante M, Ciuni R, Basile F, Biondi A. The liquid biopsy in the management of colorectal cancer: an overview. Biomedicines. 2020;8(9):308. doi:10.3390/biomedicines8090308
American Cancer Society. Colorectal cancer facts & figures 2020-2022. Published 2022. Accessed November 30, 2023. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/colorectal-cancer-facts-and-figures/colorectal-cancer-facts-and-figures-2020-2022.pdf
Johnson & Johnson. FDA clears Cellsearch™ circulating tumor cell test [news release]. Published February 27, 2008. Accessed November 30, 2023. https://johnsonandjohnson.gcs-web.com/news-releases/news-release-details/fda-clears-cellsearchtm-circulating-tumor-cell-test
US Food and Drug Administration. Summary of safety and effectiveness data, Epi proColon®. PMA number P130001. Published April 12, 2016. Accessed November 30, 2023. https://www.accessdata.fda.gov/cdrh_docs/pdf13/p130001b.pdf
FDA approves blood tests that can help guide cancer treatment. National Institutes of Health, National Cancer Institute. Published October 15, 2020. Accessed November 30, 2023. https://www.cancer.gov/news-events/cancer-currents-blog/2020/fda-guardant-360-foundation-one-cancer-liquid-biopsy
Foundation Medicine. US Food and Drug Administration (FDA) approves FoundationOne®LiquidCDx as a companion diagnostic for Pfizer’s BRAFTOVI® (encorafenib) in combination with cetuximab to identify patients with BRAF V600E alterations in metastatic colorectal cancer [press release]. Published June 10, 2023. Accessed November 30, 2023. https://www.foundationmedicine.com/press-releases/f9b285eb-db6d-4f61-856c-3f1edb803937
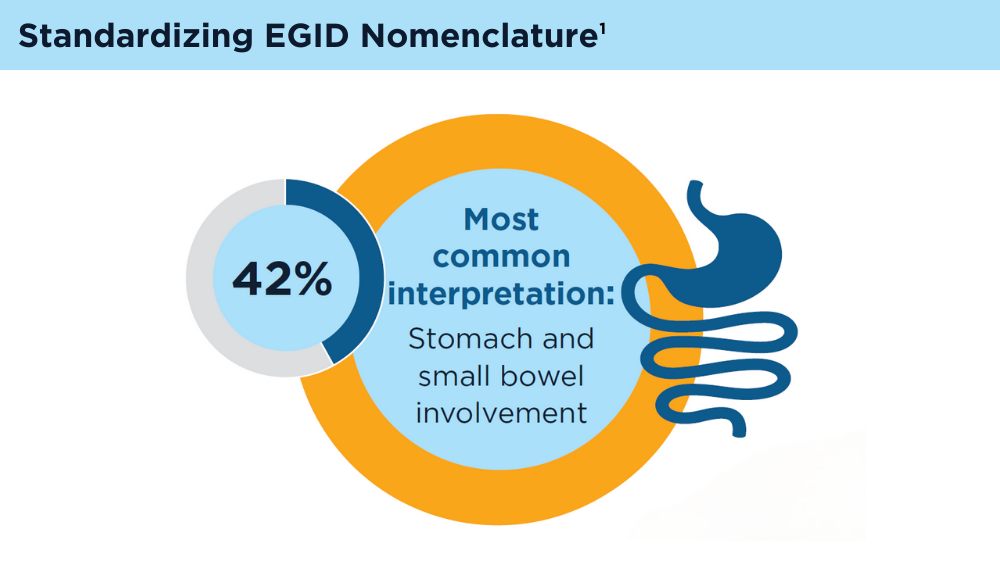
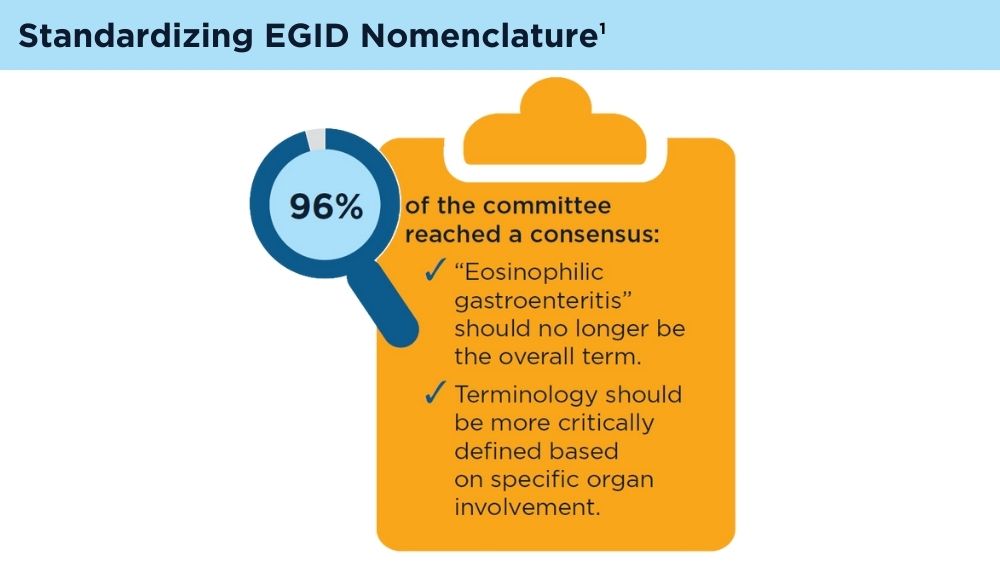
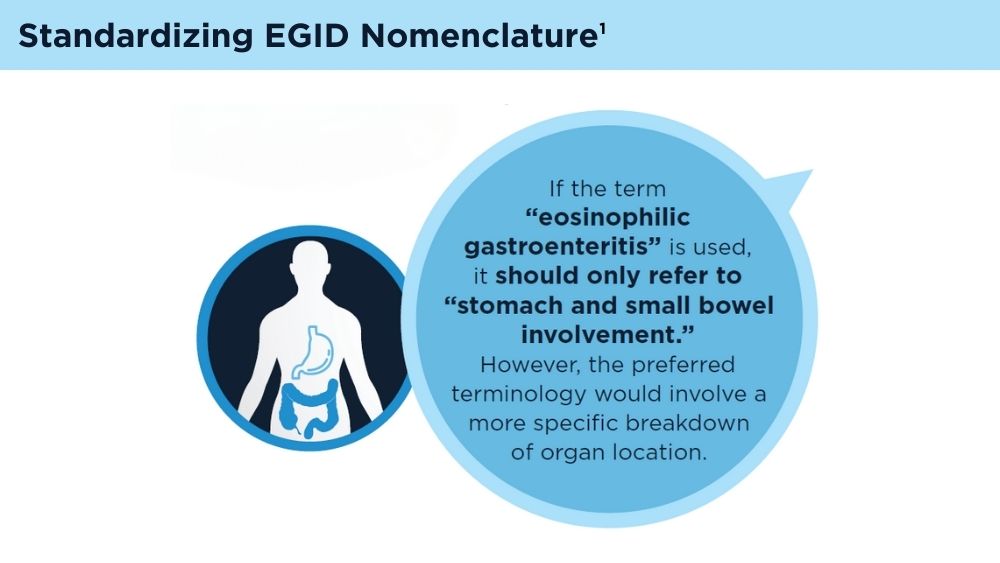
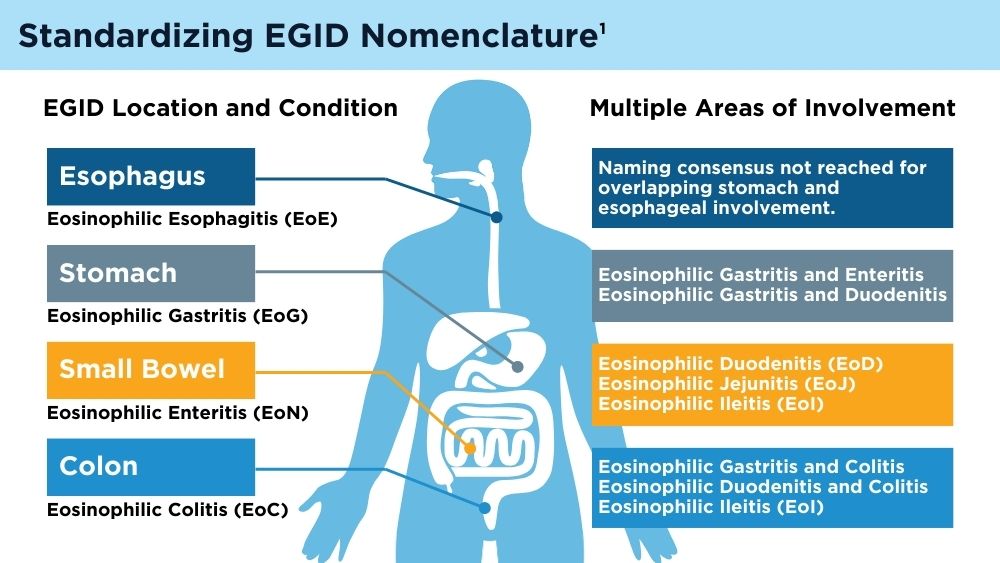
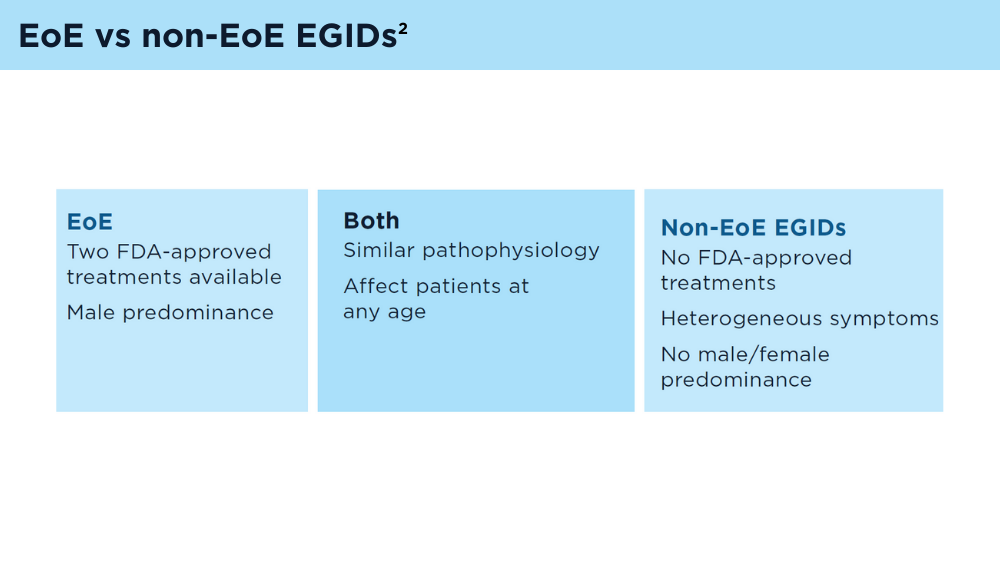
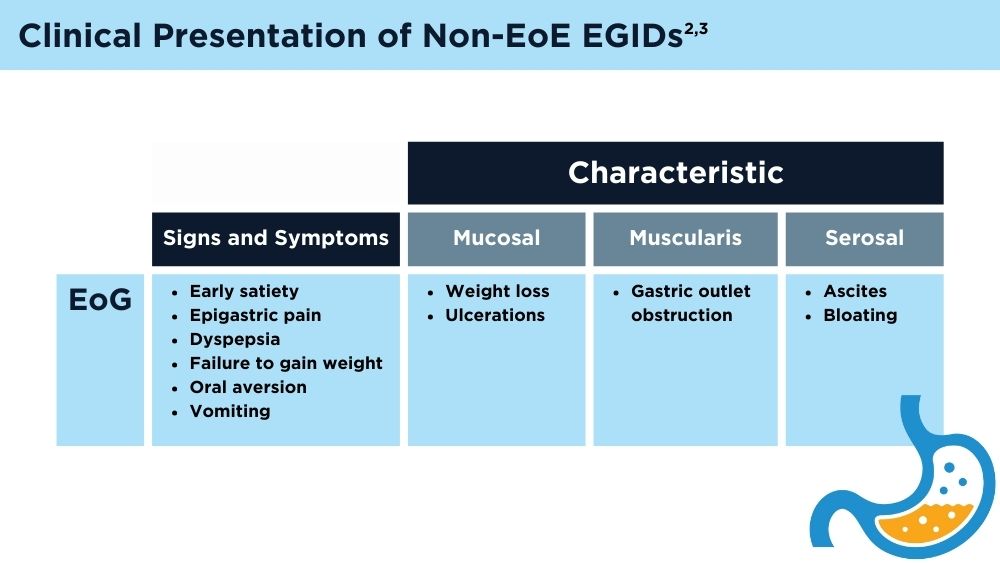
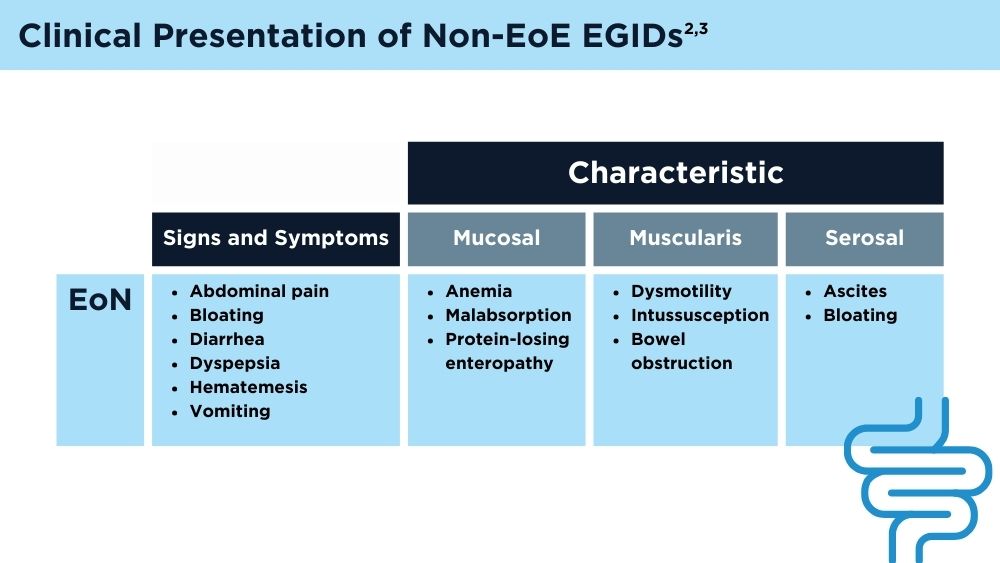
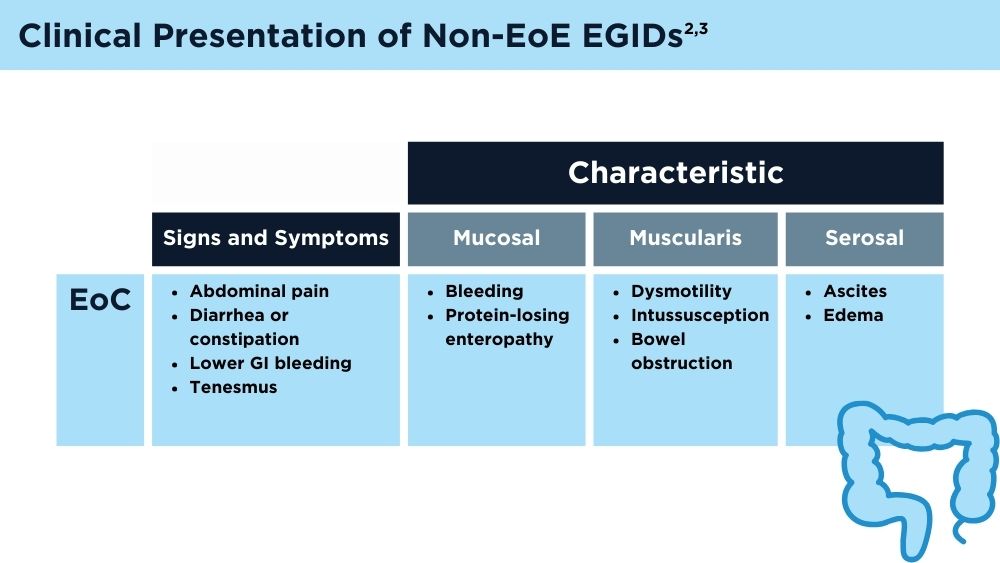
Eosinophilic Gastrointestinal Diseases: Beyond EoE
- Dellon ES, Gonsalves N, Abonia JP, et al. International consensus recommendations for eosinophilic gastrointestinal disease nomenclature. Clin Gastroenterol Hepatol. 2022;20(11):2474-2484.e3. doi:10.1016/j.cgh.2022.02.017
- Naramore S, Gupta SK. Nonesophageal eosinophilic gastrointestinal disorders: clinical care and future directions. J Pediatr Gastroenterol Nutr. 2018;67(3):318-321. doi:10.1097/MPG.0000000000002040
- Kinoshita Y, Sanuki T. Review of non-eosinophilic esophagitis-eosinophilic gastrointestinal disease (non-EoE-EGID) and a case series of twenty-eight affected patients. Biomolecules. 2023;13(9):1417. doi:10.3390/biom13091417
- Gonsalves N, Doerfler B, Zalewski A, et al. Prospective study of an amino acid-based elemental diet in an eosinophilic gastritis and gastroenteritis nutrition trial. J Allergy Clin Immunol. 2023;152(3):676-688. doi:10.1016/j.jaci.2023.05.024
- Oshima T. Biologic therapies targeting eosinophilic gastrointestinal diseases. Intern Med. 2023;62(23):3429-3430. doi:10.2169/internalmedicine.1911-23
- Pineton de Chambrun G, Gonzalez F, Canva JY, et al. Natural history of eosinophilic gastroenteritis. Clin Gastroenterol Hepatol. 2011;9(11):950-956.e1. doi:10.1016/j.cgh.2011.07.017
- Hirano I, Collins MH, King E, et al; CEGIR Investigators. Prospective endoscopic activity assessment for eosinophilic gastritis in a multi-site cohort. Am J Gastroenterol. 2022;117(3):413-423. doi:10.14309/ajg.0000000000001625
- Pesek RD, Reed CC, Muir AB, et al; Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR). Increasing rates of diagnosis, substantial co-occurrence, and variable treatment patterns of eosinophilic gastritis, gastroenteritis, and colitis based on 10-year data across a multicenter consortium. Am J Gastroenterol. 2019;114(6):984-994. doi:10.14309/ajg.0000000000000228
- Dellon ES, Gonsalves N, Abonia JP, et al. International consensus recommendations for eosinophilic gastrointestinal disease nomenclature. Clin Gastroenterol Hepatol. 2022;20(11):2474-2484.e3. doi:10.1016/j.cgh.2022.02.017
- Naramore S, Gupta SK. Nonesophageal eosinophilic gastrointestinal disorders: clinical care and future directions. J Pediatr Gastroenterol Nutr. 2018;67(3):318-321. doi:10.1097/MPG.0000000000002040
- Kinoshita Y, Sanuki T. Review of non-eosinophilic esophagitis-eosinophilic gastrointestinal disease (non-EoE-EGID) and a case series of twenty-eight affected patients. Biomolecules. 2023;13(9):1417. doi:10.3390/biom13091417
- Gonsalves N, Doerfler B, Zalewski A, et al. Prospective study of an amino acid-based elemental diet in an eosinophilic gastritis and gastroenteritis nutrition trial. J Allergy Clin Immunol. 2023;152(3):676-688. doi:10.1016/j.jaci.2023.05.024
- Oshima T. Biologic therapies targeting eosinophilic gastrointestinal diseases. Intern Med. 2023;62(23):3429-3430. doi:10.2169/internalmedicine.1911-23
- Pineton de Chambrun G, Gonzalez F, Canva JY, et al. Natural history of eosinophilic gastroenteritis. Clin Gastroenterol Hepatol. 2011;9(11):950-956.e1. doi:10.1016/j.cgh.2011.07.017
- Hirano I, Collins MH, King E, et al; CEGIR Investigators. Prospective endoscopic activity assessment for eosinophilic gastritis in a multi-site cohort. Am J Gastroenterol. 2022;117(3):413-423. doi:10.14309/ajg.0000000000001625
- Pesek RD, Reed CC, Muir AB, et al; Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR). Increasing rates of diagnosis, substantial co-occurrence, and variable treatment patterns of eosinophilic gastritis, gastroenteritis, and colitis based on 10-year data across a multicenter consortium. Am J Gastroenterol. 2019;114(6):984-994. doi:10.14309/ajg.0000000000000228
- Dellon ES, Gonsalves N, Abonia JP, et al. International consensus recommendations for eosinophilic gastrointestinal disease nomenclature. Clin Gastroenterol Hepatol. 2022;20(11):2474-2484.e3. doi:10.1016/j.cgh.2022.02.017
- Naramore S, Gupta SK. Nonesophageal eosinophilic gastrointestinal disorders: clinical care and future directions. J Pediatr Gastroenterol Nutr. 2018;67(3):318-321. doi:10.1097/MPG.0000000000002040
- Kinoshita Y, Sanuki T. Review of non-eosinophilic esophagitis-eosinophilic gastrointestinal disease (non-EoE-EGID) and a case series of twenty-eight affected patients. Biomolecules. 2023;13(9):1417. doi:10.3390/biom13091417
- Gonsalves N, Doerfler B, Zalewski A, et al. Prospective study of an amino acid-based elemental diet in an eosinophilic gastritis and gastroenteritis nutrition trial. J Allergy Clin Immunol. 2023;152(3):676-688. doi:10.1016/j.jaci.2023.05.024
- Oshima T. Biologic therapies targeting eosinophilic gastrointestinal diseases. Intern Med. 2023;62(23):3429-3430. doi:10.2169/internalmedicine.1911-23
- Pineton de Chambrun G, Gonzalez F, Canva JY, et al. Natural history of eosinophilic gastroenteritis. Clin Gastroenterol Hepatol. 2011;9(11):950-956.e1. doi:10.1016/j.cgh.2011.07.017
- Hirano I, Collins MH, King E, et al; CEGIR Investigators. Prospective endoscopic activity assessment for eosinophilic gastritis in a multi-site cohort. Am J Gastroenterol. 2022;117(3):413-423. doi:10.14309/ajg.0000000000001625
- Pesek RD, Reed CC, Muir AB, et al; Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR). Increasing rates of diagnosis, substantial co-occurrence, and variable treatment patterns of eosinophilic gastritis, gastroenteritis, and colitis based on 10-year data across a multicenter consortium. Am J Gastroenterol. 2019;114(6):984-994. doi:10.14309/ajg.0000000000000228
Emerging Evidence Supports Dietary Management of MASLD Through Gut-Liver Axis
WASHINGTON — , according to a study presented at the annual Digestive Disease Week® (DDW).
For instance, patients with MASLD had lower intake of fiber and omega-3 fatty acids but higher consumption of added sugars and ultraprocessed foods, which correlated with the associated bacterial species and functional pathways.
“MASLD is an escalating concern globally, which highlights the need for innovative targets for disease prevention and management,” said lead author Georgina Williams, PhD, a postdoctoral researcher in diet and gastroenterology at the University of Newcastle, Australia.
“Therapeutic options often rely on lifestyle modifications, with a focus on weight loss,” she said. “Diet is considered a key component of disease management.”
Although calorie restriction with a 3%-5% fat loss is associated with hepatic benefits in MASLD, Dr. Williams noted, researchers have considered whole dietary patterns and the best fit for patients. Aspects of the Mediterranean diet may be effective, as reflected in recommendations from the American Association for the Study of Liver Disease (AASLD), which highlight dietary components such as limited carbohydrates and saturated fat, along with high fiber and unsaturated fats. The gut microbiome may be essential to consider as well, she said, given MASLD-associated differences in bile acid metabolism, inflammation, and ethanol production.
Dr. Williams and colleagues conducted a retrospective case-control study in an outpatient liver clinic to understand diet and dysbiosis in MASLD, looking at differences in diet, gut microbiota composition, and functional pathways in those with and without MASLD. The researchers investigated daily average intake, serum, and stool samples among 50 people (25 per group) matched for age and gender, comparing fibrosis-4, MASLD severity scores, macronutrients, micronutrients, food groups, metagenomic sequencing, and inflammatory markers such as interleukin (IL)-1ß, IL-6, tumor necrosis factor (TNF)-α, cytokeratin (CK)-18, and high-sensitivity C-reactive protein (hsCRP).
Dietary Characteristics
At baseline, the groups differed by ethnicity, prescription medication use, and body mass index (BMI), where the MASLD group had greater ethnic diversity, medication use, and BMI. In addition, the MASLD group had a zero to mild score of fibrosis.
Overall, energy intake didn’t differ significantly between the two groups. The control group had higher alcohol intake, likely since the MASLD group was recommended to reduce alcohol intake, though the difference was about 5 grams per day. The MASLD group also had less caffeine intake than the control group, as well as slightly lower protein intake, though the differences weren’t statistically significant.
While consumption of total carbohydrates didn’t differ significantly between the groups, participants with MASLD consumed more calories from carbohydrates than did the controls. The MASLD group consumed more calories from added and free sugars and didn’t meet recommendations for dietary fiber.
With particular food groups, participants with MASLD ate significantly fewer whole grains, red and orange fruits, and leafy green vegetables. When consuming fruit, those with MASLD were more likely to drink juice than eat whole fruit. These findings could be relevant when considering high sugar intake and low dietary fiber, Dr. Williams said.
With dietary fat, there were no differences in total fat between the groups, but the fat profiles differed. The control group was significantly more likely to consume omega-3 fatty acids, including alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), docosapentaenoic acid (DPA), and docosahexaenoic acid (DHA). The MASLD group was less likely to consume seafood, nuts, seeds, avocado, and olive oil.
With inflammatory markers, hsCRP and CK-18 were increased in MASLD, while IL-1ß was increased in controls, which was consistently associated with higher alcohol intake among the control group. IL-6 and TNF-α didn’t differ between the groups.
Notably, dietary fats were most consistently associated with inflammatory markers, Dr. Williams said, with inflammation being positively associated with saturated fats and negatively associated with unsaturated fats.
Looking at microbiota, the alpha diversity was no different, but the beta diversity was across 162 taxa. Per bacterial species, there was an inverse relationship between MASLD and associations with unsaturated fat, as well as positive indicators of high sugar and fructose intake and low unsaturated fat and dietary fiber intake.
Beyond that, the functional pathways enriched in MASLD were associated with increased sugar and carbohydrates, reduced fiber, and reduced unsaturated fat. Lower butyrate production in MASLD was associated with low intake of nuts, seeds, and unsaturated fat.
In Clinical Practice
Dr. Williams suggested reinforcing AASLD guidelines and looking at diet quality, not just diet quantity. Although an energy deficit remains relevant in MASLD, macronutrient consumption matters across dietary fats, fibers, and sugars.
Future avenues for research include metabolomic pathways related to bile acids and fatty acids, she said, as well as disentangling metabolic syndrome from MASLD outcomes.
Session moderator Olivier Barbier, PhD, professor of pharmacy at Laval University in Quebec, Canada, asked about microbiome differences across countries. Dr. Williams noted the limitations in this study of looking at differences across geography and ethnicity, particularly in Australia, but said the species identified were consistent with those found in most literature globally.
In response to other questions after the presentation, Dr. Williams said supplements (such as omega-3 fatty acids) were included in total intake, and those taking prebiotics or probiotics were excluded from the study. In an upcoming clinical trial, she and colleagues plan to control for household microbiomes as well.
“The premise is that microbiomes are shared between households, so when you’re doing these sorts of large-scale clinical studies, if you’re going to look at the microbiome, then you should control for one of the major confounding variables,” said Mark Sundrud, PhD, professor of medicine at the Dartmouth Center for Digestive Health in Lebanon, New Hampshire. Dr. Sundrud, who wasn’t involved with this study, presented on the role of bile acids in mucosal immune cell function at DDW.
“We’ve done a collaborative study looking at microbiomes and bile acids in inflammatory bowel disease (IBD) patients versus controls,” which included consideration of households, he said. “We were able to see more intrinsic disease-specific changes.”
Dr. Williams declared no relevant disclosures. Dr. Sundrud has served as a scientific adviser to Sage Therapeutics.
WASHINGTON — , according to a study presented at the annual Digestive Disease Week® (DDW).
For instance, patients with MASLD had lower intake of fiber and omega-3 fatty acids but higher consumption of added sugars and ultraprocessed foods, which correlated with the associated bacterial species and functional pathways.
“MASLD is an escalating concern globally, which highlights the need for innovative targets for disease prevention and management,” said lead author Georgina Williams, PhD, a postdoctoral researcher in diet and gastroenterology at the University of Newcastle, Australia.
“Therapeutic options often rely on lifestyle modifications, with a focus on weight loss,” she said. “Diet is considered a key component of disease management.”
Although calorie restriction with a 3%-5% fat loss is associated with hepatic benefits in MASLD, Dr. Williams noted, researchers have considered whole dietary patterns and the best fit for patients. Aspects of the Mediterranean diet may be effective, as reflected in recommendations from the American Association for the Study of Liver Disease (AASLD), which highlight dietary components such as limited carbohydrates and saturated fat, along with high fiber and unsaturated fats. The gut microbiome may be essential to consider as well, she said, given MASLD-associated differences in bile acid metabolism, inflammation, and ethanol production.
Dr. Williams and colleagues conducted a retrospective case-control study in an outpatient liver clinic to understand diet and dysbiosis in MASLD, looking at differences in diet, gut microbiota composition, and functional pathways in those with and without MASLD. The researchers investigated daily average intake, serum, and stool samples among 50 people (25 per group) matched for age and gender, comparing fibrosis-4, MASLD severity scores, macronutrients, micronutrients, food groups, metagenomic sequencing, and inflammatory markers such as interleukin (IL)-1ß, IL-6, tumor necrosis factor (TNF)-α, cytokeratin (CK)-18, and high-sensitivity C-reactive protein (hsCRP).
Dietary Characteristics
At baseline, the groups differed by ethnicity, prescription medication use, and body mass index (BMI), where the MASLD group had greater ethnic diversity, medication use, and BMI. In addition, the MASLD group had a zero to mild score of fibrosis.
Overall, energy intake didn’t differ significantly between the two groups. The control group had higher alcohol intake, likely since the MASLD group was recommended to reduce alcohol intake, though the difference was about 5 grams per day. The MASLD group also had less caffeine intake than the control group, as well as slightly lower protein intake, though the differences weren’t statistically significant.
While consumption of total carbohydrates didn’t differ significantly between the groups, participants with MASLD consumed more calories from carbohydrates than did the controls. The MASLD group consumed more calories from added and free sugars and didn’t meet recommendations for dietary fiber.
With particular food groups, participants with MASLD ate significantly fewer whole grains, red and orange fruits, and leafy green vegetables. When consuming fruit, those with MASLD were more likely to drink juice than eat whole fruit. These findings could be relevant when considering high sugar intake and low dietary fiber, Dr. Williams said.
With dietary fat, there were no differences in total fat between the groups, but the fat profiles differed. The control group was significantly more likely to consume omega-3 fatty acids, including alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), docosapentaenoic acid (DPA), and docosahexaenoic acid (DHA). The MASLD group was less likely to consume seafood, nuts, seeds, avocado, and olive oil.
With inflammatory markers, hsCRP and CK-18 were increased in MASLD, while IL-1ß was increased in controls, which was consistently associated with higher alcohol intake among the control group. IL-6 and TNF-α didn’t differ between the groups.
Notably, dietary fats were most consistently associated with inflammatory markers, Dr. Williams said, with inflammation being positively associated with saturated fats and negatively associated with unsaturated fats.
Looking at microbiota, the alpha diversity was no different, but the beta diversity was across 162 taxa. Per bacterial species, there was an inverse relationship between MASLD and associations with unsaturated fat, as well as positive indicators of high sugar and fructose intake and low unsaturated fat and dietary fiber intake.
Beyond that, the functional pathways enriched in MASLD were associated with increased sugar and carbohydrates, reduced fiber, and reduced unsaturated fat. Lower butyrate production in MASLD was associated with low intake of nuts, seeds, and unsaturated fat.
In Clinical Practice
Dr. Williams suggested reinforcing AASLD guidelines and looking at diet quality, not just diet quantity. Although an energy deficit remains relevant in MASLD, macronutrient consumption matters across dietary fats, fibers, and sugars.
Future avenues for research include metabolomic pathways related to bile acids and fatty acids, she said, as well as disentangling metabolic syndrome from MASLD outcomes.
Session moderator Olivier Barbier, PhD, professor of pharmacy at Laval University in Quebec, Canada, asked about microbiome differences across countries. Dr. Williams noted the limitations in this study of looking at differences across geography and ethnicity, particularly in Australia, but said the species identified were consistent with those found in most literature globally.
In response to other questions after the presentation, Dr. Williams said supplements (such as omega-3 fatty acids) were included in total intake, and those taking prebiotics or probiotics were excluded from the study. In an upcoming clinical trial, she and colleagues plan to control for household microbiomes as well.
“The premise is that microbiomes are shared between households, so when you’re doing these sorts of large-scale clinical studies, if you’re going to look at the microbiome, then you should control for one of the major confounding variables,” said Mark Sundrud, PhD, professor of medicine at the Dartmouth Center for Digestive Health in Lebanon, New Hampshire. Dr. Sundrud, who wasn’t involved with this study, presented on the role of bile acids in mucosal immune cell function at DDW.
“We’ve done a collaborative study looking at microbiomes and bile acids in inflammatory bowel disease (IBD) patients versus controls,” which included consideration of households, he said. “We were able to see more intrinsic disease-specific changes.”
Dr. Williams declared no relevant disclosures. Dr. Sundrud has served as a scientific adviser to Sage Therapeutics.
WASHINGTON — , according to a study presented at the annual Digestive Disease Week® (DDW).
For instance, patients with MASLD had lower intake of fiber and omega-3 fatty acids but higher consumption of added sugars and ultraprocessed foods, which correlated with the associated bacterial species and functional pathways.
“MASLD is an escalating concern globally, which highlights the need for innovative targets for disease prevention and management,” said lead author Georgina Williams, PhD, a postdoctoral researcher in diet and gastroenterology at the University of Newcastle, Australia.
“Therapeutic options often rely on lifestyle modifications, with a focus on weight loss,” she said. “Diet is considered a key component of disease management.”
Although calorie restriction with a 3%-5% fat loss is associated with hepatic benefits in MASLD, Dr. Williams noted, researchers have considered whole dietary patterns and the best fit for patients. Aspects of the Mediterranean diet may be effective, as reflected in recommendations from the American Association for the Study of Liver Disease (AASLD), which highlight dietary components such as limited carbohydrates and saturated fat, along with high fiber and unsaturated fats. The gut microbiome may be essential to consider as well, she said, given MASLD-associated differences in bile acid metabolism, inflammation, and ethanol production.
Dr. Williams and colleagues conducted a retrospective case-control study in an outpatient liver clinic to understand diet and dysbiosis in MASLD, looking at differences in diet, gut microbiota composition, and functional pathways in those with and without MASLD. The researchers investigated daily average intake, serum, and stool samples among 50 people (25 per group) matched for age and gender, comparing fibrosis-4, MASLD severity scores, macronutrients, micronutrients, food groups, metagenomic sequencing, and inflammatory markers such as interleukin (IL)-1ß, IL-6, tumor necrosis factor (TNF)-α, cytokeratin (CK)-18, and high-sensitivity C-reactive protein (hsCRP).
Dietary Characteristics
At baseline, the groups differed by ethnicity, prescription medication use, and body mass index (BMI), where the MASLD group had greater ethnic diversity, medication use, and BMI. In addition, the MASLD group had a zero to mild score of fibrosis.
Overall, energy intake didn’t differ significantly between the two groups. The control group had higher alcohol intake, likely since the MASLD group was recommended to reduce alcohol intake, though the difference was about 5 grams per day. The MASLD group also had less caffeine intake than the control group, as well as slightly lower protein intake, though the differences weren’t statistically significant.
While consumption of total carbohydrates didn’t differ significantly between the groups, participants with MASLD consumed more calories from carbohydrates than did the controls. The MASLD group consumed more calories from added and free sugars and didn’t meet recommendations for dietary fiber.
With particular food groups, participants with MASLD ate significantly fewer whole grains, red and orange fruits, and leafy green vegetables. When consuming fruit, those with MASLD were more likely to drink juice than eat whole fruit. These findings could be relevant when considering high sugar intake and low dietary fiber, Dr. Williams said.
With dietary fat, there were no differences in total fat between the groups, but the fat profiles differed. The control group was significantly more likely to consume omega-3 fatty acids, including alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), docosapentaenoic acid (DPA), and docosahexaenoic acid (DHA). The MASLD group was less likely to consume seafood, nuts, seeds, avocado, and olive oil.
With inflammatory markers, hsCRP and CK-18 were increased in MASLD, while IL-1ß was increased in controls, which was consistently associated with higher alcohol intake among the control group. IL-6 and TNF-α didn’t differ between the groups.
Notably, dietary fats were most consistently associated with inflammatory markers, Dr. Williams said, with inflammation being positively associated with saturated fats and negatively associated with unsaturated fats.
Looking at microbiota, the alpha diversity was no different, but the beta diversity was across 162 taxa. Per bacterial species, there was an inverse relationship between MASLD and associations with unsaturated fat, as well as positive indicators of high sugar and fructose intake and low unsaturated fat and dietary fiber intake.
Beyond that, the functional pathways enriched in MASLD were associated with increased sugar and carbohydrates, reduced fiber, and reduced unsaturated fat. Lower butyrate production in MASLD was associated with low intake of nuts, seeds, and unsaturated fat.
In Clinical Practice
Dr. Williams suggested reinforcing AASLD guidelines and looking at diet quality, not just diet quantity. Although an energy deficit remains relevant in MASLD, macronutrient consumption matters across dietary fats, fibers, and sugars.
Future avenues for research include metabolomic pathways related to bile acids and fatty acids, she said, as well as disentangling metabolic syndrome from MASLD outcomes.
Session moderator Olivier Barbier, PhD, professor of pharmacy at Laval University in Quebec, Canada, asked about microbiome differences across countries. Dr. Williams noted the limitations in this study of looking at differences across geography and ethnicity, particularly in Australia, but said the species identified were consistent with those found in most literature globally.
In response to other questions after the presentation, Dr. Williams said supplements (such as omega-3 fatty acids) were included in total intake, and those taking prebiotics or probiotics were excluded from the study. In an upcoming clinical trial, she and colleagues plan to control for household microbiomes as well.
“The premise is that microbiomes are shared between households, so when you’re doing these sorts of large-scale clinical studies, if you’re going to look at the microbiome, then you should control for one of the major confounding variables,” said Mark Sundrud, PhD, professor of medicine at the Dartmouth Center for Digestive Health in Lebanon, New Hampshire. Dr. Sundrud, who wasn’t involved with this study, presented on the role of bile acids in mucosal immune cell function at DDW.
“We’ve done a collaborative study looking at microbiomes and bile acids in inflammatory bowel disease (IBD) patients versus controls,” which included consideration of households, he said. “We were able to see more intrinsic disease-specific changes.”
Dr. Williams declared no relevant disclosures. Dr. Sundrud has served as a scientific adviser to Sage Therapeutics.
FROM DDW 2024
Subungual Nodule in a Pediatric Patient
The Diagnosis: Subungual Exostosis
Subungual exostosis should be considered as a possible cause of an exophytic subungual nodule in a young active female. In our patient, the involvement of the great toe was a clue, as the hallux is the most common location of subungual exostosis. The patient’s age and sex also were supportive, as subungual exostosis is most common in female children and adolescents— particularly those who are active, as trauma is thought to play a possible role in development of this benign tumor.1-3 Radiography is the preferred modality for diagnosis; in our case, it showed a trabecular bony overgrowth (Figure 1), which confirmed the diagnosis. Subungual exostosis is a rare, benign, osteocartilaginous tumor of trabecular bone. The etiology is unknown but is hypothesized to be related to trauma, infection, or activation of a cartilaginous cyst.1,3 The subungual nodule may be asymptomatic or painful. Disruption and elevation of the nail plate is common.4 The differential diagnosis includes amelanotic melanoma, fibroma, fibrokeratoma, osteochondroma, pyogenic granuloma, squamous cell carcinoma, glomus tumor, and verruca vulgaris, among others.5

Physical examination demonstrates a firm, fixed, subungual nodule, often with an accompanying nail deformity. Further workup is required to confirm the benign nature of the lesion and exclude nail tumors such as melanoma or squamous cell carcinoma. Radiography is the gold standard for diagnosis, demonstrating a trabecular bony overgrowth.6 Performing a radiograph as the initial diagnostic test spares the patient from unnecessary procedures such as biopsy or expensive imaging techniques such as magnetic resonance imaging. Early lesions may not demonstrate sufficient bone formation shown on radiography. In these situations, a combination of dermoscopy and histopathologic examination may aid in diagnosis (Figure 2).4 Vascular ectasia, hyperkeratosis, onycholysis, and ulceration are the most common findings on dermoscopy (in ascending order).7 Histopathology typically demonstrates a base or stalk of normal-appearing trabecular bone with a fibrocartilage cap.8 However, initial clinical workup via radiography allows for the least-invasive and highest-yield intervention. Clinical suspicion for this condition is important, as it can be diagnosed with noninvasive inexpensive imaging rather than biopsy or more specialized imaging modalities. Appropriate recognition can save young patients from unnecessary and expensive procedures. Treatment typically involves surgical excision; to prevent regrowth, removal of the lesion at the base of the bone is recommended.2

Although amelanotic melanoma also can manifest as a subungual nail tumor, it would be unusual in a young child and would not be expected to show characteristic changes on radiography. A glomus tumor would be painful, is more common on the fingers than on the toes, and typically has a bluish hue.9 Verruca vulgaris can occur subungually but is more common around the nailfold and often has the characteristic dermoscopic finding of thrombosed capillaries. It also would not be expected to show characteristic radiographic findings. Osteochondroma can occur in young patients and can appear clinically similar to subungual exostosis; however, it typically is painful.10
- Pascoal D, Balaco I, Alves C, et al. Subungual exostosis—treatment results with preservation of the nail bed. J Pediatr Orthop B. 2020;29:382-386.
- Yousefian F, Davis B, Browning JC. Pediatric subungual exostosis. Cutis. 2021;108:256-257.
- Chiheb S, Slimani Y, Karam R, et al. Subungual exostosis: a case series of 48 patients. Skin Appendage Disord. 2021;7:475-479.
- Zhang W, Gu L, Fan H, et al. Subungual exostosis with an unusual dermoscopic feature. JAAD Case Rep. 2020;6:725-726.
- Demirdag HG, Tugrul Ayanoglu B, Akay BN. Dermoscopic features of subungual exostosis. Australas J Dermatol. 2019;60:E138-E141.
- Tritto M, Mirkin G, Hao X. Subungual exostosis on the right hallux. J Am Podiatr Med Assoc. 2021;111.
- Piccolo V, Argenziano G, Alessandrini AM, et al. Dermoscopy of subungual exostosis: a retrospective study of 10 patients. Dermatology. 2017;233:80-85.
- Lee SK, Jung MS, Lee YH, et al. Two distinctive subungual pathologies: subungual exostosis and subungual osteochondroma. Foot Ankle Int. 2007;28:595-601. doi:10.3113/FAI.2007.0595
- Samaniego E, Crespo A, Sanz A. Key diagnostic features and treatment of subungual glomus tumor. Actas Dermosifiliogr. 2009;100:875-882.
- Glick S. Subungual osteochondroma of the third toe. Consult.360. 2013;12.
The Diagnosis: Subungual Exostosis
Subungual exostosis should be considered as a possible cause of an exophytic subungual nodule in a young active female. In our patient, the involvement of the great toe was a clue, as the hallux is the most common location of subungual exostosis. The patient’s age and sex also were supportive, as subungual exostosis is most common in female children and adolescents— particularly those who are active, as trauma is thought to play a possible role in development of this benign tumor.1-3 Radiography is the preferred modality for diagnosis; in our case, it showed a trabecular bony overgrowth (Figure 1), which confirmed the diagnosis. Subungual exostosis is a rare, benign, osteocartilaginous tumor of trabecular bone. The etiology is unknown but is hypothesized to be related to trauma, infection, or activation of a cartilaginous cyst.1,3 The subungual nodule may be asymptomatic or painful. Disruption and elevation of the nail plate is common.4 The differential diagnosis includes amelanotic melanoma, fibroma, fibrokeratoma, osteochondroma, pyogenic granuloma, squamous cell carcinoma, glomus tumor, and verruca vulgaris, among others.5
Physical examination demonstrates a firm, fixed, subungual nodule, often with an accompanying nail deformity. Further workup is required to confirm the benign nature of the lesion and exclude nail tumors such as melanoma or squamous cell carcinoma. Radiography is the gold standard for diagnosis, demonstrating a trabecular bony overgrowth.6 Performing a radiograph as the initial diagnostic test spares the patient from unnecessary procedures such as biopsy or expensive imaging techniques such as magnetic resonance imaging. Early lesions may not demonstrate sufficient bone formation shown on radiography. In these situations, a combination of dermoscopy and histopathologic examination may aid in diagnosis (Figure 2).4 Vascular ectasia, hyperkeratosis, onycholysis, and ulceration are the most common findings on dermoscopy (in ascending order).7 Histopathology typically demonstrates a base or stalk of normal-appearing trabecular bone with a fibrocartilage cap.8 However, initial clinical workup via radiography allows for the least-invasive and highest-yield intervention. Clinical suspicion for this condition is important, as it can be diagnosed with noninvasive inexpensive imaging rather than biopsy or more specialized imaging modalities. Appropriate recognition can save young patients from unnecessary and expensive procedures. Treatment typically involves surgical excision; to prevent regrowth, removal of the lesion at the base of the bone is recommended.2
Although amelanotic melanoma also can manifest as a subungual nail tumor, it would be unusual in a young child and would not be expected to show characteristic changes on radiography. A glomus tumor would be painful, is more common on the fingers than on the toes, and typically has a bluish hue.9 Verruca vulgaris can occur subungually but is more common around the nailfold and often has the characteristic dermoscopic finding of thrombosed capillaries. It also would not be expected to show characteristic radiographic findings. Osteochondroma can occur in young patients and can appear clinically similar to subungual exostosis; however, it typically is painful.10
The Diagnosis: Subungual Exostosis
Subungual exostosis should be considered as a possible cause of an exophytic subungual nodule in a young active female. In our patient, the involvement of the great toe was a clue, as the hallux is the most common location of subungual exostosis. The patient’s age and sex also were supportive, as subungual exostosis is most common in female children and adolescents— particularly those who are active, as trauma is thought to play a possible role in development of this benign tumor.1-3 Radiography is the preferred modality for diagnosis; in our case, it showed a trabecular bony overgrowth (Figure 1), which confirmed the diagnosis. Subungual exostosis is a rare, benign, osteocartilaginous tumor of trabecular bone. The etiology is unknown but is hypothesized to be related to trauma, infection, or activation of a cartilaginous cyst.1,3 The subungual nodule may be asymptomatic or painful. Disruption and elevation of the nail plate is common.4 The differential diagnosis includes amelanotic melanoma, fibroma, fibrokeratoma, osteochondroma, pyogenic granuloma, squamous cell carcinoma, glomus tumor, and verruca vulgaris, among others.5
Physical examination demonstrates a firm, fixed, subungual nodule, often with an accompanying nail deformity. Further workup is required to confirm the benign nature of the lesion and exclude nail tumors such as melanoma or squamous cell carcinoma. Radiography is the gold standard for diagnosis, demonstrating a trabecular bony overgrowth.6 Performing a radiograph as the initial diagnostic test spares the patient from unnecessary procedures such as biopsy or expensive imaging techniques such as magnetic resonance imaging. Early lesions may not demonstrate sufficient bone formation shown on radiography. In these situations, a combination of dermoscopy and histopathologic examination may aid in diagnosis (Figure 2).4 Vascular ectasia, hyperkeratosis, onycholysis, and ulceration are the most common findings on dermoscopy (in ascending order).7 Histopathology typically demonstrates a base or stalk of normal-appearing trabecular bone with a fibrocartilage cap.8 However, initial clinical workup via radiography allows for the least-invasive and highest-yield intervention. Clinical suspicion for this condition is important, as it can be diagnosed with noninvasive inexpensive imaging rather than biopsy or more specialized imaging modalities. Appropriate recognition can save young patients from unnecessary and expensive procedures. Treatment typically involves surgical excision; to prevent regrowth, removal of the lesion at the base of the bone is recommended.2
Although amelanotic melanoma also can manifest as a subungual nail tumor, it would be unusual in a young child and would not be expected to show characteristic changes on radiography. A glomus tumor would be painful, is more common on the fingers than on the toes, and typically has a bluish hue.9 Verruca vulgaris can occur subungually but is more common around the nailfold and often has the characteristic dermoscopic finding of thrombosed capillaries. It also would not be expected to show characteristic radiographic findings. Osteochondroma can occur in young patients and can appear clinically similar to subungual exostosis; however, it typically is painful.10
- Pascoal D, Balaco I, Alves C, et al. Subungual exostosis—treatment results with preservation of the nail bed. J Pediatr Orthop B. 2020;29:382-386.
- Yousefian F, Davis B, Browning JC. Pediatric subungual exostosis. Cutis. 2021;108:256-257.
- Chiheb S, Slimani Y, Karam R, et al. Subungual exostosis: a case series of 48 patients. Skin Appendage Disord. 2021;7:475-479.
- Zhang W, Gu L, Fan H, et al. Subungual exostosis with an unusual dermoscopic feature. JAAD Case Rep. 2020;6:725-726.
- Demirdag HG, Tugrul Ayanoglu B, Akay BN. Dermoscopic features of subungual exostosis. Australas J Dermatol. 2019;60:E138-E141.
- Tritto M, Mirkin G, Hao X. Subungual exostosis on the right hallux. J Am Podiatr Med Assoc. 2021;111.
- Piccolo V, Argenziano G, Alessandrini AM, et al. Dermoscopy of subungual exostosis: a retrospective study of 10 patients. Dermatology. 2017;233:80-85.
- Lee SK, Jung MS, Lee YH, et al. Two distinctive subungual pathologies: subungual exostosis and subungual osteochondroma. Foot Ankle Int. 2007;28:595-601. doi:10.3113/FAI.2007.0595
- Samaniego E, Crespo A, Sanz A. Key diagnostic features and treatment of subungual glomus tumor. Actas Dermosifiliogr. 2009;100:875-882.
- Glick S. Subungual osteochondroma of the third toe. Consult.360. 2013;12.
- Pascoal D, Balaco I, Alves C, et al. Subungual exostosis—treatment results with preservation of the nail bed. J Pediatr Orthop B. 2020;29:382-386.
- Yousefian F, Davis B, Browning JC. Pediatric subungual exostosis. Cutis. 2021;108:256-257.
- Chiheb S, Slimani Y, Karam R, et al. Subungual exostosis: a case series of 48 patients. Skin Appendage Disord. 2021;7:475-479.
- Zhang W, Gu L, Fan H, et al. Subungual exostosis with an unusual dermoscopic feature. JAAD Case Rep. 2020;6:725-726.
- Demirdag HG, Tugrul Ayanoglu B, Akay BN. Dermoscopic features of subungual exostosis. Australas J Dermatol. 2019;60:E138-E141.
- Tritto M, Mirkin G, Hao X. Subungual exostosis on the right hallux. J Am Podiatr Med Assoc. 2021;111.
- Piccolo V, Argenziano G, Alessandrini AM, et al. Dermoscopy of subungual exostosis: a retrospective study of 10 patients. Dermatology. 2017;233:80-85.
- Lee SK, Jung MS, Lee YH, et al. Two distinctive subungual pathologies: subungual exostosis and subungual osteochondroma. Foot Ankle Int. 2007;28:595-601. doi:10.3113/FAI.2007.0595
- Samaniego E, Crespo A, Sanz A. Key diagnostic features and treatment of subungual glomus tumor. Actas Dermosifiliogr. 2009;100:875-882.
- Glick S. Subungual osteochondroma of the third toe. Consult.360. 2013;12.
A 13-year-old girl presented to her pediatrician with a small pink bump under the left great toenail of 8 months’ duration that was slowly growing. Months later, she developed an ingrown nail on the same toe, which was treated with partial nail avulsion by the pediatrician. Given continued nail dystrophy and a visible bump under the nail, the patient was referred to dermatology. Physical examination revealed a subungual, flesh-colored, sessile nodule causing distortion of the nail plate on the left great toe with associated intermittent redness and swelling. She denied wearing new shoes or experiencing any pain, pruritus, or purulent drainage or bleeding from the lesion. She reported being physically active and playing tennis.


Study Finds Mace Risk Remains High in Patients with Psoriasis, Dyslipidemia
Over a period of 5 years, the, even after adjusting for covariates, results from a large retrospective study showed.
“It is well-established that psoriasis is an independent risk factor for the development of MACE, with cardiometabolic risk factors being more prevalent and incident among patients with psoriasis,” the study’s first author Ana Ormaza Vera, MD, a dermatology research fellow at Eastern Virginia Medical School, Norfolk, said in an interview after the annual meeting of the Society for Investigational Dermatology, where the study was presented during a late-breaking abstract session.

Current guidelines from the joint American Academy of Dermatology/National Psoriasis Foundation and the American Academy of Cardiology/American Heart Association Task Force recommend statins, a lipid-lowering and anti-inflammatory therapy, “for patients with psoriasis who have additional risk-enhancing factors, similar to recommendations made for the general population without psoriasis,” she noted. But how the incidence of MACE differs between patients with and without psoriasis while on statin therapy “has not been explored in real-world settings,” she added.
To address this question, the researchers used real-world data from the TriNetX health research network to identify individuals aged 18-90 years with a diagnosis of both psoriasis and lipid disorders who were undergoing treatment with statins. Those with a prior history of MACE were excluded from the analysis. Patients with lipid disorders on statin therapy, but without psoriatic disease, were matched 1:1 by age, sex, race, ethnicity, common risk factors for MACE, and medications shown to reduce MACE risk. The researchers then assessed the cohorts 5 years following their first statin prescription and used the TriNetX analytics tool to calculate the odds ratio (OR) with 95% CI to evaluate the likelihood of MACE in the presence of statin therapy.
Dr. Ormaza Vera and colleagues identified 20,660 patients with psoriasis and 2,768,429 patients without psoriasis who met the criteria for analysis. After propensity score matching, each cohort included 20,660 patients with a mean age of 60 years. During the 5-year observation period, 2725 patients in the psoriasis cohort experienced MACE compared with 2203 patients in the non-psoriasis cohort (OR, 1.40; 95% CI, 1.317-1.488).
“This was an unexpected outcome that challenges the current understanding and highlights the need for further research into tailored treatments for cardiovascular risk in psoriasis patients,” Dr. Ormaza Vera told this news organization.
She acknowledged certain limitations of the study, including its retrospective design, the inherent limitations of an observational study, and the use of electronic medical record data.
Lawrence J. Green, MD, clinical professor of dermatology, George Washington University, Washington, who was asked to comment on the study results, said that the findings imply that there is more than statin use alone to protect someone with psoriasis from having an increased risk for MACE. “This is not really surprising because statin use alone is only part of a prevention strategy in someone with psoriasis who usually has multiple comorbidities,” Dr. Green said. “On the other hand, the study only went out for 5 years and cardiovascular disease is a long accumulating process, so it could also be too early to demonstrate MACE prevention.”
The study was funded by a grant from the American Skin Association. Dr. Ormaza Vera and her coauthors reported having no relevant disclosures. Dr. Green disclosed that he is a speaker, consultant, or investigator for many pharmaceutical companies.
A version of this article appeared on Medscape.com .
Over a period of 5 years, the, even after adjusting for covariates, results from a large retrospective study showed.
“It is well-established that psoriasis is an independent risk factor for the development of MACE, with cardiometabolic risk factors being more prevalent and incident among patients with psoriasis,” the study’s first author Ana Ormaza Vera, MD, a dermatology research fellow at Eastern Virginia Medical School, Norfolk, said in an interview after the annual meeting of the Society for Investigational Dermatology, where the study was presented during a late-breaking abstract session.
Current guidelines from the joint American Academy of Dermatology/National Psoriasis Foundation and the American Academy of Cardiology/American Heart Association Task Force recommend statins, a lipid-lowering and anti-inflammatory therapy, “for patients with psoriasis who have additional risk-enhancing factors, similar to recommendations made for the general population without psoriasis,” she noted. But how the incidence of MACE differs between patients with and without psoriasis while on statin therapy “has not been explored in real-world settings,” she added.
To address this question, the researchers used real-world data from the TriNetX health research network to identify individuals aged 18-90 years with a diagnosis of both psoriasis and lipid disorders who were undergoing treatment with statins. Those with a prior history of MACE were excluded from the analysis. Patients with lipid disorders on statin therapy, but without psoriatic disease, were matched 1:1 by age, sex, race, ethnicity, common risk factors for MACE, and medications shown to reduce MACE risk. The researchers then assessed the cohorts 5 years following their first statin prescription and used the TriNetX analytics tool to calculate the odds ratio (OR) with 95% CI to evaluate the likelihood of MACE in the presence of statin therapy.
Dr. Ormaza Vera and colleagues identified 20,660 patients with psoriasis and 2,768,429 patients without psoriasis who met the criteria for analysis. After propensity score matching, each cohort included 20,660 patients with a mean age of 60 years. During the 5-year observation period, 2725 patients in the psoriasis cohort experienced MACE compared with 2203 patients in the non-psoriasis cohort (OR, 1.40; 95% CI, 1.317-1.488).
“This was an unexpected outcome that challenges the current understanding and highlights the need for further research into tailored treatments for cardiovascular risk in psoriasis patients,” Dr. Ormaza Vera told this news organization.
She acknowledged certain limitations of the study, including its retrospective design, the inherent limitations of an observational study, and the use of electronic medical record data.
Lawrence J. Green, MD, clinical professor of dermatology, George Washington University, Washington, who was asked to comment on the study results, said that the findings imply that there is more than statin use alone to protect someone with psoriasis from having an increased risk for MACE. “This is not really surprising because statin use alone is only part of a prevention strategy in someone with psoriasis who usually has multiple comorbidities,” Dr. Green said. “On the other hand, the study only went out for 5 years and cardiovascular disease is a long accumulating process, so it could also be too early to demonstrate MACE prevention.”
The study was funded by a grant from the American Skin Association. Dr. Ormaza Vera and her coauthors reported having no relevant disclosures. Dr. Green disclosed that he is a speaker, consultant, or investigator for many pharmaceutical companies.
A version of this article appeared on Medscape.com .
Over a period of 5 years, the, even after adjusting for covariates, results from a large retrospective study showed.
“It is well-established that psoriasis is an independent risk factor for the development of MACE, with cardiometabolic risk factors being more prevalent and incident among patients with psoriasis,” the study’s first author Ana Ormaza Vera, MD, a dermatology research fellow at Eastern Virginia Medical School, Norfolk, said in an interview after the annual meeting of the Society for Investigational Dermatology, where the study was presented during a late-breaking abstract session.
Current guidelines from the joint American Academy of Dermatology/National Psoriasis Foundation and the American Academy of Cardiology/American Heart Association Task Force recommend statins, a lipid-lowering and anti-inflammatory therapy, “for patients with psoriasis who have additional risk-enhancing factors, similar to recommendations made for the general population without psoriasis,” she noted. But how the incidence of MACE differs between patients with and without psoriasis while on statin therapy “has not been explored in real-world settings,” she added.
To address this question, the researchers used real-world data from the TriNetX health research network to identify individuals aged 18-90 years with a diagnosis of both psoriasis and lipid disorders who were undergoing treatment with statins. Those with a prior history of MACE were excluded from the analysis. Patients with lipid disorders on statin therapy, but without psoriatic disease, were matched 1:1 by age, sex, race, ethnicity, common risk factors for MACE, and medications shown to reduce MACE risk. The researchers then assessed the cohorts 5 years following their first statin prescription and used the TriNetX analytics tool to calculate the odds ratio (OR) with 95% CI to evaluate the likelihood of MACE in the presence of statin therapy.
Dr. Ormaza Vera and colleagues identified 20,660 patients with psoriasis and 2,768,429 patients without psoriasis who met the criteria for analysis. After propensity score matching, each cohort included 20,660 patients with a mean age of 60 years. During the 5-year observation period, 2725 patients in the psoriasis cohort experienced MACE compared with 2203 patients in the non-psoriasis cohort (OR, 1.40; 95% CI, 1.317-1.488).
“This was an unexpected outcome that challenges the current understanding and highlights the need for further research into tailored treatments for cardiovascular risk in psoriasis patients,” Dr. Ormaza Vera told this news organization.
She acknowledged certain limitations of the study, including its retrospective design, the inherent limitations of an observational study, and the use of electronic medical record data.
Lawrence J. Green, MD, clinical professor of dermatology, George Washington University, Washington, who was asked to comment on the study results, said that the findings imply that there is more than statin use alone to protect someone with psoriasis from having an increased risk for MACE. “This is not really surprising because statin use alone is only part of a prevention strategy in someone with psoriasis who usually has multiple comorbidities,” Dr. Green said. “On the other hand, the study only went out for 5 years and cardiovascular disease is a long accumulating process, so it could also be too early to demonstrate MACE prevention.”
The study was funded by a grant from the American Skin Association. Dr. Ormaza Vera and her coauthors reported having no relevant disclosures. Dr. Green disclosed that he is a speaker, consultant, or investigator for many pharmaceutical companies.
A version of this article appeared on Medscape.com .
FROM SID 2024
Low-Field MRIs
Recently, “low field” MRIs have been in the news, with the promise that they’ll be safer and easier. People can go in them with their cell phones, car keys in pockets, no ear plugs needed for the noise, etc. They’re cheaper to build and can be plugged into a standard outlet.
That’s all well and good, but what about accuracy and image quality?

That’s a big question. Even proponents of the technology say it’s not as good as what we see with 3T MRI, so they’re trying to compensate by using AI and other software protocols to enhance the pictures. Allegedly it looks good, but so far only healthy volunteers have been scanned. How will it do with a small low-grade glioma or other subtle (but important) findings? We don’t know yet.
Personally, I think having to give up your iPhone and car keys for an hour, and put in foam ear plugs, are small trade-offs to get an accurate diagnosis.
Of course, I’m also approaching this as someone who deals with brain imaging. Maybe for other structures, like a knee, that kind of detail isn’t as necessary (or maybe it is. I’m definitely not in that field).
So, as with so many things that make it into the popular press, they likely have potential, but are still not ready for prime time.
This sort of stuff always gets my office phones ringing. Patients see a blurb about it on the news or Facebook and assume it’s available now, so they want one. They seem to think the new MRI is like Bones McCoy’s tricorder. I take the scanner off my belt, wave it over them, and the answer comes up on the screen. The fact that the unit still weighs over a ton is hidden at the bottom of the blurb, if it’s even mentioned at all.
There’s also the likelihood that this sort of thing is going to be taken to the public, in the same way carotid Dopplers have been. Marketed to the worried well with celebrity endorsements and taglines like “see what your doctor won’t look for.” Of course, MRIs are chock full of things like nonspecific white matter changes, disc bulges, tiny meningiomas, and a host of other incidental findings that cause panic in cyberchondriacs. Who then call us.
But that’s another story.
I understand that for some parts of the world a comparatively inexpensive, transportable, MRI that requires less shielding and power is a HUGE deal. Its availability can make the difference between life and death.
I’m not knocking the technology. I’m sure it will be useful. But, like so much in medicine, it’s not here yet.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Recently, “low field” MRIs have been in the news, with the promise that they’ll be safer and easier. People can go in them with their cell phones, car keys in pockets, no ear plugs needed for the noise, etc. They’re cheaper to build and can be plugged into a standard outlet.
That’s all well and good, but what about accuracy and image quality?
That’s a big question. Even proponents of the technology say it’s not as good as what we see with 3T MRI, so they’re trying to compensate by using AI and other software protocols to enhance the pictures. Allegedly it looks good, but so far only healthy volunteers have been scanned. How will it do with a small low-grade glioma or other subtle (but important) findings? We don’t know yet.
Personally, I think having to give up your iPhone and car keys for an hour, and put in foam ear plugs, are small trade-offs to get an accurate diagnosis.
Of course, I’m also approaching this as someone who deals with brain imaging. Maybe for other structures, like a knee, that kind of detail isn’t as necessary (or maybe it is. I’m definitely not in that field).
So, as with so many things that make it into the popular press, they likely have potential, but are still not ready for prime time.
This sort of stuff always gets my office phones ringing. Patients see a blurb about it on the news or Facebook and assume it’s available now, so they want one. They seem to think the new MRI is like Bones McCoy’s tricorder. I take the scanner off my belt, wave it over them, and the answer comes up on the screen. The fact that the unit still weighs over a ton is hidden at the bottom of the blurb, if it’s even mentioned at all.
There’s also the likelihood that this sort of thing is going to be taken to the public, in the same way carotid Dopplers have been. Marketed to the worried well with celebrity endorsements and taglines like “see what your doctor won’t look for.” Of course, MRIs are chock full of things like nonspecific white matter changes, disc bulges, tiny meningiomas, and a host of other incidental findings that cause panic in cyberchondriacs. Who then call us.
But that’s another story.
I understand that for some parts of the world a comparatively inexpensive, transportable, MRI that requires less shielding and power is a HUGE deal. Its availability can make the difference between life and death.
I’m not knocking the technology. I’m sure it will be useful. But, like so much in medicine, it’s not here yet.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
Recently, “low field” MRIs have been in the news, with the promise that they’ll be safer and easier. People can go in them with their cell phones, car keys in pockets, no ear plugs needed for the noise, etc. They’re cheaper to build and can be plugged into a standard outlet.
That’s all well and good, but what about accuracy and image quality?
That’s a big question. Even proponents of the technology say it’s not as good as what we see with 3T MRI, so they’re trying to compensate by using AI and other software protocols to enhance the pictures. Allegedly it looks good, but so far only healthy volunteers have been scanned. How will it do with a small low-grade glioma or other subtle (but important) findings? We don’t know yet.
Personally, I think having to give up your iPhone and car keys for an hour, and put in foam ear plugs, are small trade-offs to get an accurate diagnosis.
Of course, I’m also approaching this as someone who deals with brain imaging. Maybe for other structures, like a knee, that kind of detail isn’t as necessary (or maybe it is. I’m definitely not in that field).
So, as with so many things that make it into the popular press, they likely have potential, but are still not ready for prime time.
This sort of stuff always gets my office phones ringing. Patients see a blurb about it on the news or Facebook and assume it’s available now, so they want one. They seem to think the new MRI is like Bones McCoy’s tricorder. I take the scanner off my belt, wave it over them, and the answer comes up on the screen. The fact that the unit still weighs over a ton is hidden at the bottom of the blurb, if it’s even mentioned at all.
There’s also the likelihood that this sort of thing is going to be taken to the public, in the same way carotid Dopplers have been. Marketed to the worried well with celebrity endorsements and taglines like “see what your doctor won’t look for.” Of course, MRIs are chock full of things like nonspecific white matter changes, disc bulges, tiny meningiomas, and a host of other incidental findings that cause panic in cyberchondriacs. Who then call us.
But that’s another story.
I understand that for some parts of the world a comparatively inexpensive, transportable, MRI that requires less shielding and power is a HUGE deal. Its availability can make the difference between life and death.
I’m not knocking the technology. I’m sure it will be useful. But, like so much in medicine, it’s not here yet.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.