User login
2021 AMA Meeting of the AMA House of Delegates – Updates
The American Medical Association (AMA) conducted its June 2021 AMA Special Meeting of the AMA House of Delegates from June 11-16 virtually. Delegates from more than 170 societies (state societies, specialties, subspecialties, and uniformed services), comprised of nearly 700 physicians, residents, and medical students, gathered for the June 2021 AMA Special Meeting of the AMA House of Delegates (HOD) to consider a wide array of proposals.

CHEST is an active member, and through the HOD and Specialty and Service Society Caucus, CHEST has partnered with AMA and its sister societies to work with each other on important regulatory issues. Chest/Allergy Section Council (participants at this meeting were from the AAAAI, AAOA, AASM, ACAAI, ATS, CHEST, and SCCM) met before the proceedings of the House to discuss pending business. The meeting was hosted by the current CHEST/Allergy council chair Dr. Wesley Vander Ark (AMA Delegate AAOA) and Jami Lucas, CEO AAOA.
Brief updates on the Resolutions
Continuity of care of patients discharged from hospital settings (Adapted as a new policy)
The policy focuses on key issues around the continuity of care of patients. It includes protections of continuity of care for medical services and medications that are prescribed during patient hospitalizations, including when there are formulary or treatment coverage changes that have the potential to disrupt therapy following discharge.
Licensure and telehealth
The policy urges AMA to continue to support state efforts to expand physician licensure recognition across state lines in accordance with the standards and safeguards Coverage and Payment for Telemedicine. (New HOD Policy)
AMA to conduct or commission a study on the effect that telemedicine services have had on health insurance premiums, focusing on the differences between states that had telehealth payment parity provisions in effect prior to the pandemic vs those that did not, and report back at the 2021 Interim Meeting of the AMA House of Delegates. (Directive to Take Action). CHEST has taken an active role in supporting this resolution through advocating for telemedicine services and reimbursement, as well as leading the CHEST Clinician Matching Network that pairs volunteer doctors with hospitals based on their need throughout the country.
Vaccines (Adopted as a new policy)
The policy urges AMA to advocate for the prohibition of the use of patient/customer information collected by retail pharmacies for COVID-19 vaccination scheduling and/or the vaccine administration process for the purpose of commercial marketing or future patient recruiting purposes, especially any targeting based on medical history condition. AMA opposes the sale of medical history data and contact information accumulated through the scheduling or provision of government-funded vaccinations to third parties for use in marketing or advertising.
Additionally, as it relates to vaccines, CHEST has joined a joint society statement supporting a vaccine mandate for all health care workers.
Optimizing match outcomes (Directive to Take Action)
The policy urges AMA to encourage the Association of American Medical Colleges, American Association of Colleges of Osteopathic Medicine, National Resident Matching Program, and other key stakeholders to jointly create a no-fee, easily accessible clearinghouse of reliable and valid advice and tools for residency program applicants seeking cost-effective methods for applying to and successfully matching into residency.
Ensuring adequate health care resources to address the long COVID crisis and call for increased funding and research for post-viral syndromes
The policy directs AMA to support the development of an ICD-10 code or family of codes to recognize Post-Acute Sequelae of SARS-CoV-2 infection (“PASC” or “Long COVID”) and other novel post-viral syndromes as distinct diagnoses. (New HOD Policy). Further, the policy directs AMA to advocate for legislation to provide funding for research, prevention, control, and treatment of post-viral syndromes and long-term sequelae associated with viral infections, such as COVID-19 and AMA provide physicians and medical students with accurate and current information on post-viral syndromes and long-term sequelae associated with viral infections, such as COVID-19; and further that AMA collaborate with other medical and educational entities to promote education among patients about post-viral syndromes and long-term sequelae associated with viral infections, such as COVID-19, to minimize the harm and disability current and future patients face. (Directive to Take Action)
Medical misinformation in the age of social media (Directive to Take Action)
AMA encourage social media organizations to further strengthen their content moderation policies related to medical misinformation, including, but not limited to, enhanced content monitoring, augmentation of recommendation engines focused on false information, and stronger integration of verified health information. AMA should encourage social media organizations to recognize the spread of medical misinformation over dissemination networks and collaborate with relevant stakeholders, and work with public health agencies to establish relationships with journalists and news agencies to enhance the public reach in disseminating accurate medical information.
Promoting equity in global vaccine distribution
AMA call for the cooperation of all governments and international agencies to share data, research, and resources for the production and distribution of medicines, vaccines, and personal protective equipment (Directive to Take Action); and be it further, AMA promote and support efforts to supply COVID vaccines to 21health care agencies in other parts of the world to be administered to individuals who can’t afford them. (Directive to Take Action). AMA urge the US government to provide all possible assistance, including surplus vaccines and vaccines that have not had emergency use authorization, to the citizens of India and other countries in a similar situation in this humanitarian crisis (New HOD Policy).
CHEST has taken an active role in promoting equity in health care and vaccine distribution in partnership with the American Lung Association and the American Thoracic Society, including establishing a research grant program focused on this topic.
Addressing inflammatory and untruthful online ratings (Directive to Take Action)
AMA take action that would urge online review organizations to create internal mechanisms ensuring due process to physicians before the publication of negative reviews.
This is just a small sampling of the activities and more information, including reports from the various Councils, are available on the AMA website.
CHEST members interested in the AMA policy-making process may observe any AMA-HOD meeting or participate in the AMA’s democratic processes. Attendees will also be able to increase their knowledge and skills at no cost. They will also be able to connect with more than 1,500 peers and other meeting attendees from across the country. CHEST members with the time (there are two 5-day meetings each year) and interest are invited to apply to be an official CHEST delegate to the AMA. Contact Suzanne Sletto at [email protected] for details.
Delegates and alternate delegates to the House of Delegates (HOD) play a critical role in the democratic policy-making process that is the foundation of the AMA. Their role is multi-dimensional and includes:
- Advocacy for patients within the HOD to improve the health of the public and the health care system;
- Representation of the perspectives of their sponsoring organization to the HOD;
- Representation of their physician and medical student constituents in the decision-making process of the HOD;
- Representation of the AMA and its House of Delegates to member and nonmember physicians, medical associations, and others; and
- Solicitation of input from and provision of feedback to constituents.
Also, HOD delegates and alternate delegates are expected to foster a positive and useful two-way relationship between grassroots physicians and the CHEST leadership.
Dr. Desai is with the Chicago Chest Center and AMITA Health Suburban Lung Associates; and the Division of Pulmonary, Critical Care, Sleep and Allergy, University of Illinois at Chicago.
The American Medical Association (AMA) conducted its June 2021 AMA Special Meeting of the AMA House of Delegates from June 11-16 virtually. Delegates from more than 170 societies (state societies, specialties, subspecialties, and uniformed services), comprised of nearly 700 physicians, residents, and medical students, gathered for the June 2021 AMA Special Meeting of the AMA House of Delegates (HOD) to consider a wide array of proposals.
CHEST is an active member, and through the HOD and Specialty and Service Society Caucus, CHEST has partnered with AMA and its sister societies to work with each other on important regulatory issues. Chest/Allergy Section Council (participants at this meeting were from the AAAAI, AAOA, AASM, ACAAI, ATS, CHEST, and SCCM) met before the proceedings of the House to discuss pending business. The meeting was hosted by the current CHEST/Allergy council chair Dr. Wesley Vander Ark (AMA Delegate AAOA) and Jami Lucas, CEO AAOA.
Brief updates on the Resolutions
Continuity of care of patients discharged from hospital settings (Adapted as a new policy)
The policy focuses on key issues around the continuity of care of patients. It includes protections of continuity of care for medical services and medications that are prescribed during patient hospitalizations, including when there are formulary or treatment coverage changes that have the potential to disrupt therapy following discharge.
Licensure and telehealth
The policy urges AMA to continue to support state efforts to expand physician licensure recognition across state lines in accordance with the standards and safeguards Coverage and Payment for Telemedicine. (New HOD Policy)
AMA to conduct or commission a study on the effect that telemedicine services have had on health insurance premiums, focusing on the differences between states that had telehealth payment parity provisions in effect prior to the pandemic vs those that did not, and report back at the 2021 Interim Meeting of the AMA House of Delegates. (Directive to Take Action). CHEST has taken an active role in supporting this resolution through advocating for telemedicine services and reimbursement, as well as leading the CHEST Clinician Matching Network that pairs volunteer doctors with hospitals based on their need throughout the country.
Vaccines (Adopted as a new policy)
The policy urges AMA to advocate for the prohibition of the use of patient/customer information collected by retail pharmacies for COVID-19 vaccination scheduling and/or the vaccine administration process for the purpose of commercial marketing or future patient recruiting purposes, especially any targeting based on medical history condition. AMA opposes the sale of medical history data and contact information accumulated through the scheduling or provision of government-funded vaccinations to third parties for use in marketing or advertising.
Additionally, as it relates to vaccines, CHEST has joined a joint society statement supporting a vaccine mandate for all health care workers.
Optimizing match outcomes (Directive to Take Action)
The policy urges AMA to encourage the Association of American Medical Colleges, American Association of Colleges of Osteopathic Medicine, National Resident Matching Program, and other key stakeholders to jointly create a no-fee, easily accessible clearinghouse of reliable and valid advice and tools for residency program applicants seeking cost-effective methods for applying to and successfully matching into residency.
Ensuring adequate health care resources to address the long COVID crisis and call for increased funding and research for post-viral syndromes
The policy directs AMA to support the development of an ICD-10 code or family of codes to recognize Post-Acute Sequelae of SARS-CoV-2 infection (“PASC” or “Long COVID”) and other novel post-viral syndromes as distinct diagnoses. (New HOD Policy). Further, the policy directs AMA to advocate for legislation to provide funding for research, prevention, control, and treatment of post-viral syndromes and long-term sequelae associated with viral infections, such as COVID-19 and AMA provide physicians and medical students with accurate and current information on post-viral syndromes and long-term sequelae associated with viral infections, such as COVID-19; and further that AMA collaborate with other medical and educational entities to promote education among patients about post-viral syndromes and long-term sequelae associated with viral infections, such as COVID-19, to minimize the harm and disability current and future patients face. (Directive to Take Action)
Medical misinformation in the age of social media (Directive to Take Action)
AMA encourage social media organizations to further strengthen their content moderation policies related to medical misinformation, including, but not limited to, enhanced content monitoring, augmentation of recommendation engines focused on false information, and stronger integration of verified health information. AMA should encourage social media organizations to recognize the spread of medical misinformation over dissemination networks and collaborate with relevant stakeholders, and work with public health agencies to establish relationships with journalists and news agencies to enhance the public reach in disseminating accurate medical information.
Promoting equity in global vaccine distribution
AMA call for the cooperation of all governments and international agencies to share data, research, and resources for the production and distribution of medicines, vaccines, and personal protective equipment (Directive to Take Action); and be it further, AMA promote and support efforts to supply COVID vaccines to 21health care agencies in other parts of the world to be administered to individuals who can’t afford them. (Directive to Take Action). AMA urge the US government to provide all possible assistance, including surplus vaccines and vaccines that have not had emergency use authorization, to the citizens of India and other countries in a similar situation in this humanitarian crisis (New HOD Policy).
CHEST has taken an active role in promoting equity in health care and vaccine distribution in partnership with the American Lung Association and the American Thoracic Society, including establishing a research grant program focused on this topic.
Addressing inflammatory and untruthful online ratings (Directive to Take Action)
AMA take action that would urge online review organizations to create internal mechanisms ensuring due process to physicians before the publication of negative reviews.
This is just a small sampling of the activities and more information, including reports from the various Councils, are available on the AMA website.
CHEST members interested in the AMA policy-making process may observe any AMA-HOD meeting or participate in the AMA’s democratic processes. Attendees will also be able to increase their knowledge and skills at no cost. They will also be able to connect with more than 1,500 peers and other meeting attendees from across the country. CHEST members with the time (there are two 5-day meetings each year) and interest are invited to apply to be an official CHEST delegate to the AMA. Contact Suzanne Sletto at [email protected] for details.
Delegates and alternate delegates to the House of Delegates (HOD) play a critical role in the democratic policy-making process that is the foundation of the AMA. Their role is multi-dimensional and includes:
- Advocacy for patients within the HOD to improve the health of the public and the health care system;
- Representation of the perspectives of their sponsoring organization to the HOD;
- Representation of their physician and medical student constituents in the decision-making process of the HOD;
- Representation of the AMA and its House of Delegates to member and nonmember physicians, medical associations, and others; and
- Solicitation of input from and provision of feedback to constituents.
Also, HOD delegates and alternate delegates are expected to foster a positive and useful two-way relationship between grassroots physicians and the CHEST leadership.
Dr. Desai is with the Chicago Chest Center and AMITA Health Suburban Lung Associates; and the Division of Pulmonary, Critical Care, Sleep and Allergy, University of Illinois at Chicago.
The American Medical Association (AMA) conducted its June 2021 AMA Special Meeting of the AMA House of Delegates from June 11-16 virtually. Delegates from more than 170 societies (state societies, specialties, subspecialties, and uniformed services), comprised of nearly 700 physicians, residents, and medical students, gathered for the June 2021 AMA Special Meeting of the AMA House of Delegates (HOD) to consider a wide array of proposals.
CHEST is an active member, and through the HOD and Specialty and Service Society Caucus, CHEST has partnered with AMA and its sister societies to work with each other on important regulatory issues. Chest/Allergy Section Council (participants at this meeting were from the AAAAI, AAOA, AASM, ACAAI, ATS, CHEST, and SCCM) met before the proceedings of the House to discuss pending business. The meeting was hosted by the current CHEST/Allergy council chair Dr. Wesley Vander Ark (AMA Delegate AAOA) and Jami Lucas, CEO AAOA.
Brief updates on the Resolutions
Continuity of care of patients discharged from hospital settings (Adapted as a new policy)
The policy focuses on key issues around the continuity of care of patients. It includes protections of continuity of care for medical services and medications that are prescribed during patient hospitalizations, including when there are formulary or treatment coverage changes that have the potential to disrupt therapy following discharge.
Licensure and telehealth
The policy urges AMA to continue to support state efforts to expand physician licensure recognition across state lines in accordance with the standards and safeguards Coverage and Payment for Telemedicine. (New HOD Policy)
AMA to conduct or commission a study on the effect that telemedicine services have had on health insurance premiums, focusing on the differences between states that had telehealth payment parity provisions in effect prior to the pandemic vs those that did not, and report back at the 2021 Interim Meeting of the AMA House of Delegates. (Directive to Take Action). CHEST has taken an active role in supporting this resolution through advocating for telemedicine services and reimbursement, as well as leading the CHEST Clinician Matching Network that pairs volunteer doctors with hospitals based on their need throughout the country.
Vaccines (Adopted as a new policy)
The policy urges AMA to advocate for the prohibition of the use of patient/customer information collected by retail pharmacies for COVID-19 vaccination scheduling and/or the vaccine administration process for the purpose of commercial marketing or future patient recruiting purposes, especially any targeting based on medical history condition. AMA opposes the sale of medical history data and contact information accumulated through the scheduling or provision of government-funded vaccinations to third parties for use in marketing or advertising.
Additionally, as it relates to vaccines, CHEST has joined a joint society statement supporting a vaccine mandate for all health care workers.
Optimizing match outcomes (Directive to Take Action)
The policy urges AMA to encourage the Association of American Medical Colleges, American Association of Colleges of Osteopathic Medicine, National Resident Matching Program, and other key stakeholders to jointly create a no-fee, easily accessible clearinghouse of reliable and valid advice and tools for residency program applicants seeking cost-effective methods for applying to and successfully matching into residency.
Ensuring adequate health care resources to address the long COVID crisis and call for increased funding and research for post-viral syndromes
The policy directs AMA to support the development of an ICD-10 code or family of codes to recognize Post-Acute Sequelae of SARS-CoV-2 infection (“PASC” or “Long COVID”) and other novel post-viral syndromes as distinct diagnoses. (New HOD Policy). Further, the policy directs AMA to advocate for legislation to provide funding for research, prevention, control, and treatment of post-viral syndromes and long-term sequelae associated with viral infections, such as COVID-19 and AMA provide physicians and medical students with accurate and current information on post-viral syndromes and long-term sequelae associated with viral infections, such as COVID-19; and further that AMA collaborate with other medical and educational entities to promote education among patients about post-viral syndromes and long-term sequelae associated with viral infections, such as COVID-19, to minimize the harm and disability current and future patients face. (Directive to Take Action)
Medical misinformation in the age of social media (Directive to Take Action)
AMA encourage social media organizations to further strengthen their content moderation policies related to medical misinformation, including, but not limited to, enhanced content monitoring, augmentation of recommendation engines focused on false information, and stronger integration of verified health information. AMA should encourage social media organizations to recognize the spread of medical misinformation over dissemination networks and collaborate with relevant stakeholders, and work with public health agencies to establish relationships with journalists and news agencies to enhance the public reach in disseminating accurate medical information.
Promoting equity in global vaccine distribution
AMA call for the cooperation of all governments and international agencies to share data, research, and resources for the production and distribution of medicines, vaccines, and personal protective equipment (Directive to Take Action); and be it further, AMA promote and support efforts to supply COVID vaccines to 21health care agencies in other parts of the world to be administered to individuals who can’t afford them. (Directive to Take Action). AMA urge the US government to provide all possible assistance, including surplus vaccines and vaccines that have not had emergency use authorization, to the citizens of India and other countries in a similar situation in this humanitarian crisis (New HOD Policy).
CHEST has taken an active role in promoting equity in health care and vaccine distribution in partnership with the American Lung Association and the American Thoracic Society, including establishing a research grant program focused on this topic.
Addressing inflammatory and untruthful online ratings (Directive to Take Action)
AMA take action that would urge online review organizations to create internal mechanisms ensuring due process to physicians before the publication of negative reviews.
This is just a small sampling of the activities and more information, including reports from the various Councils, are available on the AMA website.
CHEST members interested in the AMA policy-making process may observe any AMA-HOD meeting or participate in the AMA’s democratic processes. Attendees will also be able to increase their knowledge and skills at no cost. They will also be able to connect with more than 1,500 peers and other meeting attendees from across the country. CHEST members with the time (there are two 5-day meetings each year) and interest are invited to apply to be an official CHEST delegate to the AMA. Contact Suzanne Sletto at [email protected] for details.
Delegates and alternate delegates to the House of Delegates (HOD) play a critical role in the democratic policy-making process that is the foundation of the AMA. Their role is multi-dimensional and includes:
- Advocacy for patients within the HOD to improve the health of the public and the health care system;
- Representation of the perspectives of their sponsoring organization to the HOD;
- Representation of their physician and medical student constituents in the decision-making process of the HOD;
- Representation of the AMA and its House of Delegates to member and nonmember physicians, medical associations, and others; and
- Solicitation of input from and provision of feedback to constituents.
Also, HOD delegates and alternate delegates are expected to foster a positive and useful two-way relationship between grassroots physicians and the CHEST leadership.
Dr. Desai is with the Chicago Chest Center and AMITA Health Suburban Lung Associates; and the Division of Pulmonary, Critical Care, Sleep and Allergy, University of Illinois at Chicago.
Destruction in the air; Empathy in the ICU; Respiratory therapist shortage; COPD and sleep disordered breathing; And more....
Occupational and environmental health
Destruction in the air
Building collapse, such as that of the Surfside condominiums in Miami, Florida, results not only in tragic loss of life but also leads to devastating effects on lung health. Following the World Trade Center collapse, a massive particle dust cloud of up to 11,000 tons of PM2.5 was dispersed, 90% of which was particles greater than 10 mcm (Rom et al. Proc Am Thorac Soc. 2010 May;7[2]:142-5).

Fine particulate matter has been associated with multiple lung conditions. Those who arrive on site in the first 24 hours may have immediate changes in FEV1 and FVC. Acute eosinophilic pneumonia has also been described in the initial aftermath (Rom et al. Am J Respir Crit Care Med. 2002;166(6):785).

Chronic lung diseases such as chronic obstructive pulmonary disease and asthma, may worsen with repeated exposure. One Swedish study demonstrated an increased incidence of chronic lower respiratory disease in cement and demolition workers compared with the general labor force (Purdue et al. Thorax. 2007 Jan;62[1]:51-6). Clean-up sites may contain a variety of materials associated with occupational lung diseases, like chrysolite asbestos, silica, and heavy metals.
Prevention remains key. In the United States, the Occupational Safety and Health Administration requires all construction and demolition sites to have a dust control plan. Primary prevention includes the use of N-95 masks and watering sites. N-95 masks protect against particulate matter PM2.5 and smaller (Zhou et al. J Thorac Dis. 2018 Mar;10[3]:2059-69. Watering sites, while useful, can be challenging depending on the size and temperature of the area. Workers in high-risk occupations should have prior screening with pulmonary function testing. After an exposure, it is recommended pulmonary function testing be repeated, with close interval monitoring.
Disclaimer: The views expressed in this article are those of the author(s) and do not reflect the official policy of the Department of Army/Navy/Air Force, Department of Defense, or U.S. Government.
Tyler Church, DO
Jason Unger, MD
Fellow-in-training Members
Bathmapriya Balakrishnan, MD
Steering Committee Member
Palliative care and end of life
Empathy in the ICU
The importance of empathetic patient care has never seemed so significant with patients isolated from the standard support systems in a pandemic that has pushed health care to its limits. While empathy can clearly impact patient outcomes (Rakel DP et al. Fam Med. 2009;41[7]:494-501), the practicality of delivering empathic care is less well defined. Into this void step Dr. Jessica Bunin and colleagues (Bunin J et al. J Crit Care. 2021;29;65:156-63), who present a scoping review of the limited literature in an effort to address gaps in the practice of empathy. Perhaps unsurprising but most critically, the authors found that far from being a dichotomous construct, empathy is a “complex phenomenon” that exists on a continuum. It is inconsistently defined in the existing literature, with the inclusion of cognitive, affective, and somatic processes variable. Equally important, they identified that practicing empathy carries risk in addition to its beneficial applications for both patients and intensivists.

Far from being easily identifiable, measured, and taught, this concept of empathy as a nuanced and contextually charged skill that requires practice and reflection aligns it with other skills and tools used in the care of our critically ill patients. This group has suggested that a clear definition of empathy, transparent discussion of the risks and benefits of using empathy, attention to developing environments that minimize barriers and facilitate the practice of empathy in clinical care, and the growth of educational practice to promote attention to self-care in the use of empathy will overall benefit both patient and physician well-being. At the very least, we need to allow ourselves grace to fail and learn as we strive to provide empathic care for our patients and ourselves.
Laura Johnson, MD, FCCP
NetWork Ex-Officio
Respiratory care network
National campaign to address respiratory therapist shortage
As our population grows, hospitals and physician practices face a rapidly growing need for more specialized, high-quality respiratory care; but the numbers of respiratory therapists are not keeping pace. (U.S. Bureau of Labor Statistics. Occupational Outlook Handbook. Respiratory Therapists).

To inspire a new generation of respiratory therapists and promote this lifesaving profession, the American Association for Respiratory Care (AARC), the Commission on Accreditation for Respiratory Care (CoARC), and The National Board for Respiratory Care (NBRC) are pursuing a multiyear, national campaign called The World Needs More RTs. This campaign has three primary goals:
1. Enhance the value of the respiratory care profession.
2. Recruit and retain more respiratory therapists.
3. Shape future leadership in respiratory care.

There are factors behind the current and impending future inadequate numbers of respiratory therapists:
- Decrease in undergraduate enrollment.
- Increase in retirements.
- Escalation of burnout in health care.
This campaign aims to address these factors, enhance interest in the profession, and prevent further decline in RT numbers.
Respiratory therapists make an invaluable impact on patient care, and simply put, the world needs more RTs. More RTs are needed to provide lifesaving care in the critical care units, emergency departments, and clinics (Shaw RC, Benavente JL. AARC Human Resources Survey of Acute Care Hospital Employers. NBRC 2020). More RTs are needed to educate the next RT generation (Shaw RC, Benavente JL. AARC Human Resources Survey of Education Programs. NBRC 2020). To see how you can champion the campaign, visit MoreRTs.com.
Lori Tinkler, MBA
CEO, NBRC
Steering Committee Member
De De Gardner, DrPH, RRT, FCCP
Vice-Chair
Sleep disorders
COPD and sleep-disordered breathing: Updates and steps forward
The presence of sleep breathing disorders in individuals with COPD, in the form of COPD and OSA overlap syndrome (OVS) or chronic hypercarbic respiratory failure (CHRF), portend poor outcomes when untreated. Treatment of OVS and CHRF are among few interventions that positively impact mortality, readmission rates, and quality of life in patients with COPD.

Higher mortality and readmission rates are seen in those admitted with COPD exacerbations who have OVS compared with COPD alone. Initiation and adherence to PAP therapy decreases mortality and COPD-related hospitalizations (Ioachimescu OC et al. J Clin Sleep Med. 2020;16[2]:267-77; Singh G et al. Sleep Breath. 2019;23[1]:193).

In CHRF, initiation of high intensity noninvasive ventilation (NIV) at least 2 weeks after resolution of acute respiratory failure reduces mortality and prolongs time to readmission (Murphy PB et al. JAMA. 2017;317[21]:2177-86; Kohnlein T et al. Lancet Respir Med. 2014;2:698-705). Initiating home NIV in individuals with acute hypercarbic respiratory failure does not improve readmission rates or time to readmission (Struik FM et al. Thorax. 2014;69:826-34). The new ATS guidelines, therefore, recommend NIV initiation for stable CHRF in COPD, screening for OVS prior to NIV initiation, and targeting PaCO2 normalization (Macrea M et al. Am J Respir Crit Care Med. 2020;202[4]:e74-e87).
Identification and treatment of OVS and CHRF pose unique challenges for clinicians, particularly when navigating current testing and reimbursement guidelines. A multisociety Technical Expert Panel, including members of CHEST, has recently published its recommendations for changes to CMS national coverage determinations for NIV to take the next steps forward (Gay PC et al. Chest. 2021;S0012-3692[21]01481-1).
Megan Lowery, MD
Sreelatha Naik, MD
Steering Committee Members
Thoracic oncology
CHEST releases its newest edition of the tobacco treatment toolkit
Tobacco remains the greatest single cause of morbidity and mortality. Left unaddressed, tobacco is projected to kill 1 billion people worldwide this century. Despite this, only 5% of all tobacco-dependent patients in the United States receive both a medication and even minimal counseling for their addiction.

Tobacco dependence is a severe chronic life-threatening disease. It is with this focus that CHEST released its latest iteration of the Tobacco Dependence Treatment Toolkit. This edition focuses on treating tobacco addiction as a chronic disease, titrating all seven FDA-approved medications toward tobacco abstinence, and medical practice/hospital reimbursement.
The CHEST toolkit is divided into eight sections: Motivational Interviewing, Testing/Diagnostics, Treatment Basics (pharmacologic and nonpharmacologic), Treatment Pearls, Clinical Vignettes and Studies, Special Populations, Treatment for e-Cigarettes and Other Tobacco Products, and Insurance Billing and Telehealth.
Special attention is given to tobacco addiction diagnostics and using these findings to treat the chronic disease of tobacco addiction just like any other chronic disease by aggressively and successfully titrating FDA-approved medications in various permutations and combinations, as needed. The therapeutic goal is assisting the patient to feel normal, minimizing withdrawal throughout the process, so that tobacco abstinence can ultimately be obtained and maintained.
Clinicians and medical centers can receive insurance reimbursement for these diagnostics and associated interventions. This includes both in-office procedures and via telehealth. The CHEST toolkit discusses both in-depth.
A new unique associated feature is our Clinician Interactive Toolkit. This multimedia interactive platform reviews clinician interactions with a tobacco-dependent patient via avatars and can be found here: Clinician Interactive Toolkit.
https://foundation.chestnet.org/lung-health-a-z/smoking-and-tobacco-use/?Item=For-Clinicians
The American College of Chest Physicians’ Tobacco Treatment Toolkit can be downloaded here.
The American College of Chest Physicians’ Tobacco Treatment Toolkit project also included the development of a new video game for tobacco users. Smoke Out: Tobacco Pirates is available for download for free to all at the Apple App Store for iPhones and iPads, and at Google Play (play.google.com/store/apps/details?id=com.gforcelearning.smokeout&hl=en_US&gl=US). The game is fun, the theme is immersive, and the educational content is specifically focused on tobacco users, although clinicians will enjoy it too.
Matthew Bars, MS
Steering Committee Member
Occupational and environmental health
Destruction in the air
Building collapse, such as that of the Surfside condominiums in Miami, Florida, results not only in tragic loss of life but also leads to devastating effects on lung health. Following the World Trade Center collapse, a massive particle dust cloud of up to 11,000 tons of PM2.5 was dispersed, 90% of which was particles greater than 10 mcm (Rom et al. Proc Am Thorac Soc. 2010 May;7[2]:142-5).
Fine particulate matter has been associated with multiple lung conditions. Those who arrive on site in the first 24 hours may have immediate changes in FEV1 and FVC. Acute eosinophilic pneumonia has also been described in the initial aftermath (Rom et al. Am J Respir Crit Care Med. 2002;166(6):785).
Chronic lung diseases such as chronic obstructive pulmonary disease and asthma, may worsen with repeated exposure. One Swedish study demonstrated an increased incidence of chronic lower respiratory disease in cement and demolition workers compared with the general labor force (Purdue et al. Thorax. 2007 Jan;62[1]:51-6). Clean-up sites may contain a variety of materials associated with occupational lung diseases, like chrysolite asbestos, silica, and heavy metals.
Prevention remains key. In the United States, the Occupational Safety and Health Administration requires all construction and demolition sites to have a dust control plan. Primary prevention includes the use of N-95 masks and watering sites. N-95 masks protect against particulate matter PM2.5 and smaller (Zhou et al. J Thorac Dis. 2018 Mar;10[3]:2059-69. Watering sites, while useful, can be challenging depending on the size and temperature of the area. Workers in high-risk occupations should have prior screening with pulmonary function testing. After an exposure, it is recommended pulmonary function testing be repeated, with close interval monitoring.
Disclaimer: The views expressed in this article are those of the author(s) and do not reflect the official policy of the Department of Army/Navy/Air Force, Department of Defense, or U.S. Government.
Tyler Church, DO
Jason Unger, MD
Fellow-in-training Members
Bathmapriya Balakrishnan, MD
Steering Committee Member
Palliative care and end of life
Empathy in the ICU
The importance of empathetic patient care has never seemed so significant with patients isolated from the standard support systems in a pandemic that has pushed health care to its limits. While empathy can clearly impact patient outcomes (Rakel DP et al. Fam Med. 2009;41[7]:494-501), the practicality of delivering empathic care is less well defined. Into this void step Dr. Jessica Bunin and colleagues (Bunin J et al. J Crit Care. 2021;29;65:156-63), who present a scoping review of the limited literature in an effort to address gaps in the practice of empathy. Perhaps unsurprising but most critically, the authors found that far from being a dichotomous construct, empathy is a “complex phenomenon” that exists on a continuum. It is inconsistently defined in the existing literature, with the inclusion of cognitive, affective, and somatic processes variable. Equally important, they identified that practicing empathy carries risk in addition to its beneficial applications for both patients and intensivists.
Far from being easily identifiable, measured, and taught, this concept of empathy as a nuanced and contextually charged skill that requires practice and reflection aligns it with other skills and tools used in the care of our critically ill patients. This group has suggested that a clear definition of empathy, transparent discussion of the risks and benefits of using empathy, attention to developing environments that minimize barriers and facilitate the practice of empathy in clinical care, and the growth of educational practice to promote attention to self-care in the use of empathy will overall benefit both patient and physician well-being. At the very least, we need to allow ourselves grace to fail and learn as we strive to provide empathic care for our patients and ourselves.
Laura Johnson, MD, FCCP
NetWork Ex-Officio
Respiratory care network
National campaign to address respiratory therapist shortage
As our population grows, hospitals and physician practices face a rapidly growing need for more specialized, high-quality respiratory care; but the numbers of respiratory therapists are not keeping pace. (U.S. Bureau of Labor Statistics. Occupational Outlook Handbook. Respiratory Therapists).
To inspire a new generation of respiratory therapists and promote this lifesaving profession, the American Association for Respiratory Care (AARC), the Commission on Accreditation for Respiratory Care (CoARC), and The National Board for Respiratory Care (NBRC) are pursuing a multiyear, national campaign called The World Needs More RTs. This campaign has three primary goals:
1. Enhance the value of the respiratory care profession.
2. Recruit and retain more respiratory therapists.
3. Shape future leadership in respiratory care.
There are factors behind the current and impending future inadequate numbers of respiratory therapists:
- Decrease in undergraduate enrollment.
- Increase in retirements.
- Escalation of burnout in health care.
This campaign aims to address these factors, enhance interest in the profession, and prevent further decline in RT numbers.
Respiratory therapists make an invaluable impact on patient care, and simply put, the world needs more RTs. More RTs are needed to provide lifesaving care in the critical care units, emergency departments, and clinics (Shaw RC, Benavente JL. AARC Human Resources Survey of Acute Care Hospital Employers. NBRC 2020). More RTs are needed to educate the next RT generation (Shaw RC, Benavente JL. AARC Human Resources Survey of Education Programs. NBRC 2020). To see how you can champion the campaign, visit MoreRTs.com.
Lori Tinkler, MBA
CEO, NBRC
Steering Committee Member
De De Gardner, DrPH, RRT, FCCP
Vice-Chair
Sleep disorders
COPD and sleep-disordered breathing: Updates and steps forward
The presence of sleep breathing disorders in individuals with COPD, in the form of COPD and OSA overlap syndrome (OVS) or chronic hypercarbic respiratory failure (CHRF), portend poor outcomes when untreated. Treatment of OVS and CHRF are among few interventions that positively impact mortality, readmission rates, and quality of life in patients with COPD.
Higher mortality and readmission rates are seen in those admitted with COPD exacerbations who have OVS compared with COPD alone. Initiation and adherence to PAP therapy decreases mortality and COPD-related hospitalizations (Ioachimescu OC et al. J Clin Sleep Med. 2020;16[2]:267-77; Singh G et al. Sleep Breath. 2019;23[1]:193).
In CHRF, initiation of high intensity noninvasive ventilation (NIV) at least 2 weeks after resolution of acute respiratory failure reduces mortality and prolongs time to readmission (Murphy PB et al. JAMA. 2017;317[21]:2177-86; Kohnlein T et al. Lancet Respir Med. 2014;2:698-705). Initiating home NIV in individuals with acute hypercarbic respiratory failure does not improve readmission rates or time to readmission (Struik FM et al. Thorax. 2014;69:826-34). The new ATS guidelines, therefore, recommend NIV initiation for stable CHRF in COPD, screening for OVS prior to NIV initiation, and targeting PaCO2 normalization (Macrea M et al. Am J Respir Crit Care Med. 2020;202[4]:e74-e87).
Identification and treatment of OVS and CHRF pose unique challenges for clinicians, particularly when navigating current testing and reimbursement guidelines. A multisociety Technical Expert Panel, including members of CHEST, has recently published its recommendations for changes to CMS national coverage determinations for NIV to take the next steps forward (Gay PC et al. Chest. 2021;S0012-3692[21]01481-1).
Megan Lowery, MD
Sreelatha Naik, MD
Steering Committee Members
Thoracic oncology
CHEST releases its newest edition of the tobacco treatment toolkit
Tobacco remains the greatest single cause of morbidity and mortality. Left unaddressed, tobacco is projected to kill 1 billion people worldwide this century. Despite this, only 5% of all tobacco-dependent patients in the United States receive both a medication and even minimal counseling for their addiction.
Tobacco dependence is a severe chronic life-threatening disease. It is with this focus that CHEST released its latest iteration of the Tobacco Dependence Treatment Toolkit. This edition focuses on treating tobacco addiction as a chronic disease, titrating all seven FDA-approved medications toward tobacco abstinence, and medical practice/hospital reimbursement.
The CHEST toolkit is divided into eight sections: Motivational Interviewing, Testing/Diagnostics, Treatment Basics (pharmacologic and nonpharmacologic), Treatment Pearls, Clinical Vignettes and Studies, Special Populations, Treatment for e-Cigarettes and Other Tobacco Products, and Insurance Billing and Telehealth.
Special attention is given to tobacco addiction diagnostics and using these findings to treat the chronic disease of tobacco addiction just like any other chronic disease by aggressively and successfully titrating FDA-approved medications in various permutations and combinations, as needed. The therapeutic goal is assisting the patient to feel normal, minimizing withdrawal throughout the process, so that tobacco abstinence can ultimately be obtained and maintained.
Clinicians and medical centers can receive insurance reimbursement for these diagnostics and associated interventions. This includes both in-office procedures and via telehealth. The CHEST toolkit discusses both in-depth.
A new unique associated feature is our Clinician Interactive Toolkit. This multimedia interactive platform reviews clinician interactions with a tobacco-dependent patient via avatars and can be found here: Clinician Interactive Toolkit.
https://foundation.chestnet.org/lung-health-a-z/smoking-and-tobacco-use/?Item=For-Clinicians
The American College of Chest Physicians’ Tobacco Treatment Toolkit can be downloaded here.
The American College of Chest Physicians’ Tobacco Treatment Toolkit project also included the development of a new video game for tobacco users. Smoke Out: Tobacco Pirates is available for download for free to all at the Apple App Store for iPhones and iPads, and at Google Play (play.google.com/store/apps/details?id=com.gforcelearning.smokeout&hl=en_US&gl=US). The game is fun, the theme is immersive, and the educational content is specifically focused on tobacco users, although clinicians will enjoy it too.
Matthew Bars, MS
Steering Committee Member
Occupational and environmental health
Destruction in the air
Building collapse, such as that of the Surfside condominiums in Miami, Florida, results not only in tragic loss of life but also leads to devastating effects on lung health. Following the World Trade Center collapse, a massive particle dust cloud of up to 11,000 tons of PM2.5 was dispersed, 90% of which was particles greater than 10 mcm (Rom et al. Proc Am Thorac Soc. 2010 May;7[2]:142-5).
Fine particulate matter has been associated with multiple lung conditions. Those who arrive on site in the first 24 hours may have immediate changes in FEV1 and FVC. Acute eosinophilic pneumonia has also been described in the initial aftermath (Rom et al. Am J Respir Crit Care Med. 2002;166(6):785).
Chronic lung diseases such as chronic obstructive pulmonary disease and asthma, may worsen with repeated exposure. One Swedish study demonstrated an increased incidence of chronic lower respiratory disease in cement and demolition workers compared with the general labor force (Purdue et al. Thorax. 2007 Jan;62[1]:51-6). Clean-up sites may contain a variety of materials associated with occupational lung diseases, like chrysolite asbestos, silica, and heavy metals.
Prevention remains key. In the United States, the Occupational Safety and Health Administration requires all construction and demolition sites to have a dust control plan. Primary prevention includes the use of N-95 masks and watering sites. N-95 masks protect against particulate matter PM2.5 and smaller (Zhou et al. J Thorac Dis. 2018 Mar;10[3]:2059-69. Watering sites, while useful, can be challenging depending on the size and temperature of the area. Workers in high-risk occupations should have prior screening with pulmonary function testing. After an exposure, it is recommended pulmonary function testing be repeated, with close interval monitoring.
Disclaimer: The views expressed in this article are those of the author(s) and do not reflect the official policy of the Department of Army/Navy/Air Force, Department of Defense, or U.S. Government.
Tyler Church, DO
Jason Unger, MD
Fellow-in-training Members
Bathmapriya Balakrishnan, MD
Steering Committee Member
Palliative care and end of life
Empathy in the ICU
The importance of empathetic patient care has never seemed so significant with patients isolated from the standard support systems in a pandemic that has pushed health care to its limits. While empathy can clearly impact patient outcomes (Rakel DP et al. Fam Med. 2009;41[7]:494-501), the practicality of delivering empathic care is less well defined. Into this void step Dr. Jessica Bunin and colleagues (Bunin J et al. J Crit Care. 2021;29;65:156-63), who present a scoping review of the limited literature in an effort to address gaps in the practice of empathy. Perhaps unsurprising but most critically, the authors found that far from being a dichotomous construct, empathy is a “complex phenomenon” that exists on a continuum. It is inconsistently defined in the existing literature, with the inclusion of cognitive, affective, and somatic processes variable. Equally important, they identified that practicing empathy carries risk in addition to its beneficial applications for both patients and intensivists.
Far from being easily identifiable, measured, and taught, this concept of empathy as a nuanced and contextually charged skill that requires practice and reflection aligns it with other skills and tools used in the care of our critically ill patients. This group has suggested that a clear definition of empathy, transparent discussion of the risks and benefits of using empathy, attention to developing environments that minimize barriers and facilitate the practice of empathy in clinical care, and the growth of educational practice to promote attention to self-care in the use of empathy will overall benefit both patient and physician well-being. At the very least, we need to allow ourselves grace to fail and learn as we strive to provide empathic care for our patients and ourselves.
Laura Johnson, MD, FCCP
NetWork Ex-Officio
Respiratory care network
National campaign to address respiratory therapist shortage
As our population grows, hospitals and physician practices face a rapidly growing need for more specialized, high-quality respiratory care; but the numbers of respiratory therapists are not keeping pace. (U.S. Bureau of Labor Statistics. Occupational Outlook Handbook. Respiratory Therapists).
To inspire a new generation of respiratory therapists and promote this lifesaving profession, the American Association for Respiratory Care (AARC), the Commission on Accreditation for Respiratory Care (CoARC), and The National Board for Respiratory Care (NBRC) are pursuing a multiyear, national campaign called The World Needs More RTs. This campaign has three primary goals:
1. Enhance the value of the respiratory care profession.
2. Recruit and retain more respiratory therapists.
3. Shape future leadership in respiratory care.
There are factors behind the current and impending future inadequate numbers of respiratory therapists:
- Decrease in undergraduate enrollment.
- Increase in retirements.
- Escalation of burnout in health care.
This campaign aims to address these factors, enhance interest in the profession, and prevent further decline in RT numbers.
Respiratory therapists make an invaluable impact on patient care, and simply put, the world needs more RTs. More RTs are needed to provide lifesaving care in the critical care units, emergency departments, and clinics (Shaw RC, Benavente JL. AARC Human Resources Survey of Acute Care Hospital Employers. NBRC 2020). More RTs are needed to educate the next RT generation (Shaw RC, Benavente JL. AARC Human Resources Survey of Education Programs. NBRC 2020). To see how you can champion the campaign, visit MoreRTs.com.
Lori Tinkler, MBA
CEO, NBRC
Steering Committee Member
De De Gardner, DrPH, RRT, FCCP
Vice-Chair
Sleep disorders
COPD and sleep-disordered breathing: Updates and steps forward
The presence of sleep breathing disorders in individuals with COPD, in the form of COPD and OSA overlap syndrome (OVS) or chronic hypercarbic respiratory failure (CHRF), portend poor outcomes when untreated. Treatment of OVS and CHRF are among few interventions that positively impact mortality, readmission rates, and quality of life in patients with COPD.
Higher mortality and readmission rates are seen in those admitted with COPD exacerbations who have OVS compared with COPD alone. Initiation and adherence to PAP therapy decreases mortality and COPD-related hospitalizations (Ioachimescu OC et al. J Clin Sleep Med. 2020;16[2]:267-77; Singh G et al. Sleep Breath. 2019;23[1]:193).
In CHRF, initiation of high intensity noninvasive ventilation (NIV) at least 2 weeks after resolution of acute respiratory failure reduces mortality and prolongs time to readmission (Murphy PB et al. JAMA. 2017;317[21]:2177-86; Kohnlein T et al. Lancet Respir Med. 2014;2:698-705). Initiating home NIV in individuals with acute hypercarbic respiratory failure does not improve readmission rates or time to readmission (Struik FM et al. Thorax. 2014;69:826-34). The new ATS guidelines, therefore, recommend NIV initiation for stable CHRF in COPD, screening for OVS prior to NIV initiation, and targeting PaCO2 normalization (Macrea M et al. Am J Respir Crit Care Med. 2020;202[4]:e74-e87).
Identification and treatment of OVS and CHRF pose unique challenges for clinicians, particularly when navigating current testing and reimbursement guidelines. A multisociety Technical Expert Panel, including members of CHEST, has recently published its recommendations for changes to CMS national coverage determinations for NIV to take the next steps forward (Gay PC et al. Chest. 2021;S0012-3692[21]01481-1).
Megan Lowery, MD
Sreelatha Naik, MD
Steering Committee Members
Thoracic oncology
CHEST releases its newest edition of the tobacco treatment toolkit
Tobacco remains the greatest single cause of morbidity and mortality. Left unaddressed, tobacco is projected to kill 1 billion people worldwide this century. Despite this, only 5% of all tobacco-dependent patients in the United States receive both a medication and even minimal counseling for their addiction.
Tobacco dependence is a severe chronic life-threatening disease. It is with this focus that CHEST released its latest iteration of the Tobacco Dependence Treatment Toolkit. This edition focuses on treating tobacco addiction as a chronic disease, titrating all seven FDA-approved medications toward tobacco abstinence, and medical practice/hospital reimbursement.
The CHEST toolkit is divided into eight sections: Motivational Interviewing, Testing/Diagnostics, Treatment Basics (pharmacologic and nonpharmacologic), Treatment Pearls, Clinical Vignettes and Studies, Special Populations, Treatment for e-Cigarettes and Other Tobacco Products, and Insurance Billing and Telehealth.
Special attention is given to tobacco addiction diagnostics and using these findings to treat the chronic disease of tobacco addiction just like any other chronic disease by aggressively and successfully titrating FDA-approved medications in various permutations and combinations, as needed. The therapeutic goal is assisting the patient to feel normal, minimizing withdrawal throughout the process, so that tobacco abstinence can ultimately be obtained and maintained.
Clinicians and medical centers can receive insurance reimbursement for these diagnostics and associated interventions. This includes both in-office procedures and via telehealth. The CHEST toolkit discusses both in-depth.
A new unique associated feature is our Clinician Interactive Toolkit. This multimedia interactive platform reviews clinician interactions with a tobacco-dependent patient via avatars and can be found here: Clinician Interactive Toolkit.
https://foundation.chestnet.org/lung-health-a-z/smoking-and-tobacco-use/?Item=For-Clinicians
The American College of Chest Physicians’ Tobacco Treatment Toolkit can be downloaded here.
The American College of Chest Physicians’ Tobacco Treatment Toolkit project also included the development of a new video game for tobacco users. Smoke Out: Tobacco Pirates is available for download for free to all at the Apple App Store for iPhones and iPads, and at Google Play (play.google.com/store/apps/details?id=com.gforcelearning.smokeout&hl=en_US&gl=US). The game is fun, the theme is immersive, and the educational content is specifically focused on tobacco users, although clinicians will enjoy it too.
Matthew Bars, MS
Steering Committee Member
This month in the journal CHEST®
Editor’s picks
Point: E-cigarettes for harm reduction in tobacco use disorder: Pro. By Dr. C. Bates.
Counterpoint: E-cigarettes for harm reduction in tobacco use disorder: Con. By Dr. H. Kathuria, et al.
Eosinophilic and non-eosinophilic asthma: an expert consensus framework to characterize phenotypes in a global real-life severe asthma cohort. By Dr. L. G. Heaney, et al.Symptoms of mental health disorders in critical care clinicians facing the COVID-19 second wave: A cross-sectional study. By Dr. E. Azoulay, et al.Tobacco smoking and risk for pulmonary fibrosis: A prospective cohort study in UK Biobank.By Dr. V. Bellow, et al.Sleep in the hospitalized child: A contemporary review. By Dr. J. Berger, et al.Avoid the Trap: Non-expanding Lung. By Dr. D. Gillett, et al.Resuscitation a la Carte: Ethical concerns about the practice and theory of partial codes. By Dr. B. Gremmels, et al.
Editor’s picks
Editor’s picks
Point: E-cigarettes for harm reduction in tobacco use disorder: Pro. By Dr. C. Bates.
Counterpoint: E-cigarettes for harm reduction in tobacco use disorder: Con. By Dr. H. Kathuria, et al.
Eosinophilic and non-eosinophilic asthma: an expert consensus framework to characterize phenotypes in a global real-life severe asthma cohort. By Dr. L. G. Heaney, et al.Symptoms of mental health disorders in critical care clinicians facing the COVID-19 second wave: A cross-sectional study. By Dr. E. Azoulay, et al.Tobacco smoking and risk for pulmonary fibrosis: A prospective cohort study in UK Biobank.By Dr. V. Bellow, et al.Sleep in the hospitalized child: A contemporary review. By Dr. J. Berger, et al.Avoid the Trap: Non-expanding Lung. By Dr. D. Gillett, et al.Resuscitation a la Carte: Ethical concerns about the practice and theory of partial codes. By Dr. B. Gremmels, et al.
Point: E-cigarettes for harm reduction in tobacco use disorder: Pro. By Dr. C. Bates.
Counterpoint: E-cigarettes for harm reduction in tobacco use disorder: Con. By Dr. H. Kathuria, et al.
Eosinophilic and non-eosinophilic asthma: an expert consensus framework to characterize phenotypes in a global real-life severe asthma cohort. By Dr. L. G. Heaney, et al.Symptoms of mental health disorders in critical care clinicians facing the COVID-19 second wave: A cross-sectional study. By Dr. E. Azoulay, et al.Tobacco smoking and risk for pulmonary fibrosis: A prospective cohort study in UK Biobank.By Dr. V. Bellow, et al.Sleep in the hospitalized child: A contemporary review. By Dr. J. Berger, et al.Avoid the Trap: Non-expanding Lung. By Dr. D. Gillett, et al.Resuscitation a la Carte: Ethical concerns about the practice and theory of partial codes. By Dr. B. Gremmels, et al.
Staying up to date with consumer sleep technology
With Siri and Alexa sitting at our kitchen tables and listening to our conversations, we have all but forgotten about the before times – when we had to use the Yellow Pages to look up a number or address and when we had no idea how many steps we took in a given day. Wearable technology has become ubiquitous and has us watching not only our step count but also our sleep. Did I get enough deep sleep? What does my sleep score of 82 mean? Should I be worried?

As clinicians, we must also navigate how this information impacts our clinical decision-making and consider how our patients are interpreting these data on a daily basis. There is an inherent assumption that we, as sleep clinicians, will understand the nuances of each consumer-facing sleep technology (CST) whether it is a wearable, a nearable (a device that sits near the body but not on the body), or an app. Very little validation data exist, as most of these technologies are marketed as wellness devices and are not intended to render a diagnosis. It therefore falls to us to determine how to utilize this information in an already busy clinic.
One strategy is to use these technologies as patient engagement tools – a way to increase public awareness of the importance of sleep. While this certainly should be beneficial, oftentimes, the data are confusing and can lead to misunderstandings about what normal sleep should look like. Approaching these data as partners to our patients allows us to set expectations around normal sleep cycles and sleep duration. It also allows us to discuss appropriate sleep timing and sleep hygiene.
Many wearable devices have incorporated oximetry into their metrics, and some claim to have accuracy that is better than hospital-grade oximeters. Many of these companies are no longer in business. Others specify higher accuracy in dark-skinned individuals (“CIRCUL Ring Pulse Oximeter in Dark-Pigmented Individuals: Clinical Study Validates Efficacy and Reliability,” Medical Device News Magazine, Feb. 26, 2021).
Despite these claims, they are registered as wellness devices with the FDA and are not diagnostic devices. Logically, if one of these devices demonstrates worrisome data, then it can prompt further clinical queries and, potentially, objective testing for obstructive sleep apnea (OSA). The reverse, however, cannot be claimed. A normal reading by CST does not obviate the need for objective testing if the clinical symptoms warrant it.
There are CSTs that have been created around very specific needs - such as jet lag- and provide guidance for how to quickly acclimate to the destination time zone by providing nudges for light exposure and timed melatonin or dark glasses (https://www.timeshifter.com/).
Others analyze the sleep space for extrinsic sounds (https://www.sleepcycle.com/), while a plethora of apps provides advice for how to optimize your sleep environment and wind-down routine. There is even a sleep robot designed to facilitate sleep onset (https://somnox.com/). This bean-shaped device is designed to “breathe” as you hold it, and the user is meant to emulate those same breathing patterns. It is a take on the 4-7-8 breathing pattern long endorsed by yogis.
Although validation data are lacking for the vast majority of CST, a recent study (www.ncbi.nlm.nih.gov/pmc/articles/PMC8120339/pdf/zsaa291.pdf).demonstrated that CST had high performance when compared with actigraphy in assessing sleep and wakefulness and, as such, may improve the evaluation of sleep and wake opportunities prior to MSLT or improve identification of circadian sleep-wake disorders. Many practices do not currently utilize actigraphy due to its expense and very limited potential for reimbursement. Using a patient’s sleep-tracking device may allow access to these data without financial outlay. While these data demonstrate the ability of CST to potentially differentiate sleep from wakefulness, it is notable that this study also found that the determination of individual sleep stages is less robust. In general, CST cannot identify an underlying sleep disorder, however, may raise awareness that a disorder might be present.
This leads to more reflection on the role of CST in a typical sleep clinic. Many years ago, discussion around this technology was primarily patient-initiated and often times met with skepticism on the part of the clinician. As technology has improved and has become more accessible, there appears to be more acceptance among our colleagues – not, perhaps, in terms of absolute actionable data, but rather as an opportunity to discuss sleep with our patients and to support their own efforts at improving their sleep. Trends in the data in response to CBT-I or medications can be observed. Abnormalities identified via CST often serve as the initial prompt for a clinical visit and, as such, should not be eschewed. Rather, reframing the use of this information while also addressing other sleep issues is likely to be the more appropriate path forward.
Assessing this information can be time-consuming, and best practice suggests establishing expectations around this process (J Clin Sleep Med 2018 May 15. doi: 10.5664/jcsm.7128).
Agreements can be made with patients that the data are reviewed in the context of a clinical visit rather than longitudinally as data are uploaded and then sent via messaging unless such an understanding has already been agreed upon. RPM billing codes may ultimately allow for reimbursement and recognition of this workload. At the present time, RPM billing is limited to FDA-cleared, prescription devices, and CST does not yet qualify.
There also needs to be recognition of potential harm from CST. Inevitably, some patients will develop orthosomnia, a term coined by Dr. Kelly Baron, where patients become so fixated on achieving perfect sleep scores that it contributes to insomnia. In this case, identification of orthosomnia is made via the clinical visit and patients are advised to stop tracking their sleep for a set period of time. This allows the anxiety around achieving “perfect sleep” to dissipate.
Google and the AASM recently announced a partnership. Essentially, the Google Nest Hub will serve to detect sleep concerns (such as timing of sleep, snoring, insufficient sleep, etc.) and will direct the user to educational resources such as www.sleepeducation.org. The idea behind this is that people are often unaware of an underlying sleep disorder such as OSA and don’t know what to search for. The Nest Hub uses information it collects and directs users to appropriate resources, thus obviating the need to know what to Google.
Clearly, big tech has invested heavily in our field. Between the copious wearables, nearables, and apps that are sleep-focused, these industry giants obviously believe that sleep is worthy of such a significant allocation of resources. This has improved the overall awareness of the importance of sleep and of identifying and treating sleep disorders. While these technologies are no replacement for a clinical evaluation, they can serve as patient engagement tools, as well as potentially large-scale OSA screening tools and may help us improve the percentage of patients with undiagnosed OSA, estimated to be 80% (Frost and Sullivan, “Hidden Health Crisis Costing America Billions,” American Academy of Sleep Medicine, 2016).
CST may allow us to better identify circadian sleep-wake disorders and evaluate sleep satiation prior to MLST that no longer requires investment in expensive actigraphy devices. They also allow us to partner with our patients by meeting them where they are and recognizing the efforts they have already made to improve their sleep before we even meet them.
Dr. Khosla is Medical Director, North Dakota Center for Sleep, Fargo, North Dakota.
With Siri and Alexa sitting at our kitchen tables and listening to our conversations, we have all but forgotten about the before times – when we had to use the Yellow Pages to look up a number or address and when we had no idea how many steps we took in a given day. Wearable technology has become ubiquitous and has us watching not only our step count but also our sleep. Did I get enough deep sleep? What does my sleep score of 82 mean? Should I be worried?
As clinicians, we must also navigate how this information impacts our clinical decision-making and consider how our patients are interpreting these data on a daily basis. There is an inherent assumption that we, as sleep clinicians, will understand the nuances of each consumer-facing sleep technology (CST) whether it is a wearable, a nearable (a device that sits near the body but not on the body), or an app. Very little validation data exist, as most of these technologies are marketed as wellness devices and are not intended to render a diagnosis. It therefore falls to us to determine how to utilize this information in an already busy clinic.
One strategy is to use these technologies as patient engagement tools – a way to increase public awareness of the importance of sleep. While this certainly should be beneficial, oftentimes, the data are confusing and can lead to misunderstandings about what normal sleep should look like. Approaching these data as partners to our patients allows us to set expectations around normal sleep cycles and sleep duration. It also allows us to discuss appropriate sleep timing and sleep hygiene.
Many wearable devices have incorporated oximetry into their metrics, and some claim to have accuracy that is better than hospital-grade oximeters. Many of these companies are no longer in business. Others specify higher accuracy in dark-skinned individuals (“CIRCUL Ring Pulse Oximeter in Dark-Pigmented Individuals: Clinical Study Validates Efficacy and Reliability,” Medical Device News Magazine, Feb. 26, 2021).
Despite these claims, they are registered as wellness devices with the FDA and are not diagnostic devices. Logically, if one of these devices demonstrates worrisome data, then it can prompt further clinical queries and, potentially, objective testing for obstructive sleep apnea (OSA). The reverse, however, cannot be claimed. A normal reading by CST does not obviate the need for objective testing if the clinical symptoms warrant it.
There are CSTs that have been created around very specific needs - such as jet lag- and provide guidance for how to quickly acclimate to the destination time zone by providing nudges for light exposure and timed melatonin or dark glasses (https://www.timeshifter.com/).
Others analyze the sleep space for extrinsic sounds (https://www.sleepcycle.com/), while a plethora of apps provides advice for how to optimize your sleep environment and wind-down routine. There is even a sleep robot designed to facilitate sleep onset (https://somnox.com/). This bean-shaped device is designed to “breathe” as you hold it, and the user is meant to emulate those same breathing patterns. It is a take on the 4-7-8 breathing pattern long endorsed by yogis.
Although validation data are lacking for the vast majority of CST, a recent study (www.ncbi.nlm.nih.gov/pmc/articles/PMC8120339/pdf/zsaa291.pdf).demonstrated that CST had high performance when compared with actigraphy in assessing sleep and wakefulness and, as such, may improve the evaluation of sleep and wake opportunities prior to MSLT or improve identification of circadian sleep-wake disorders. Many practices do not currently utilize actigraphy due to its expense and very limited potential for reimbursement. Using a patient’s sleep-tracking device may allow access to these data without financial outlay. While these data demonstrate the ability of CST to potentially differentiate sleep from wakefulness, it is notable that this study also found that the determination of individual sleep stages is less robust. In general, CST cannot identify an underlying sleep disorder, however, may raise awareness that a disorder might be present.
This leads to more reflection on the role of CST in a typical sleep clinic. Many years ago, discussion around this technology was primarily patient-initiated and often times met with skepticism on the part of the clinician. As technology has improved and has become more accessible, there appears to be more acceptance among our colleagues – not, perhaps, in terms of absolute actionable data, but rather as an opportunity to discuss sleep with our patients and to support their own efforts at improving their sleep. Trends in the data in response to CBT-I or medications can be observed. Abnormalities identified via CST often serve as the initial prompt for a clinical visit and, as such, should not be eschewed. Rather, reframing the use of this information while also addressing other sleep issues is likely to be the more appropriate path forward.
Assessing this information can be time-consuming, and best practice suggests establishing expectations around this process (J Clin Sleep Med 2018 May 15. doi: 10.5664/jcsm.7128).
Agreements can be made with patients that the data are reviewed in the context of a clinical visit rather than longitudinally as data are uploaded and then sent via messaging unless such an understanding has already been agreed upon. RPM billing codes may ultimately allow for reimbursement and recognition of this workload. At the present time, RPM billing is limited to FDA-cleared, prescription devices, and CST does not yet qualify.
There also needs to be recognition of potential harm from CST. Inevitably, some patients will develop orthosomnia, a term coined by Dr. Kelly Baron, where patients become so fixated on achieving perfect sleep scores that it contributes to insomnia. In this case, identification of orthosomnia is made via the clinical visit and patients are advised to stop tracking their sleep for a set period of time. This allows the anxiety around achieving “perfect sleep” to dissipate.
Google and the AASM recently announced a partnership. Essentially, the Google Nest Hub will serve to detect sleep concerns (such as timing of sleep, snoring, insufficient sleep, etc.) and will direct the user to educational resources such as www.sleepeducation.org. The idea behind this is that people are often unaware of an underlying sleep disorder such as OSA and don’t know what to search for. The Nest Hub uses information it collects and directs users to appropriate resources, thus obviating the need to know what to Google.
Clearly, big tech has invested heavily in our field. Between the copious wearables, nearables, and apps that are sleep-focused, these industry giants obviously believe that sleep is worthy of such a significant allocation of resources. This has improved the overall awareness of the importance of sleep and of identifying and treating sleep disorders. While these technologies are no replacement for a clinical evaluation, they can serve as patient engagement tools, as well as potentially large-scale OSA screening tools and may help us improve the percentage of patients with undiagnosed OSA, estimated to be 80% (Frost and Sullivan, “Hidden Health Crisis Costing America Billions,” American Academy of Sleep Medicine, 2016).
CST may allow us to better identify circadian sleep-wake disorders and evaluate sleep satiation prior to MLST that no longer requires investment in expensive actigraphy devices. They also allow us to partner with our patients by meeting them where they are and recognizing the efforts they have already made to improve their sleep before we even meet them.
Dr. Khosla is Medical Director, North Dakota Center for Sleep, Fargo, North Dakota.
With Siri and Alexa sitting at our kitchen tables and listening to our conversations, we have all but forgotten about the before times – when we had to use the Yellow Pages to look up a number or address and when we had no idea how many steps we took in a given day. Wearable technology has become ubiquitous and has us watching not only our step count but also our sleep. Did I get enough deep sleep? What does my sleep score of 82 mean? Should I be worried?
As clinicians, we must also navigate how this information impacts our clinical decision-making and consider how our patients are interpreting these data on a daily basis. There is an inherent assumption that we, as sleep clinicians, will understand the nuances of each consumer-facing sleep technology (CST) whether it is a wearable, a nearable (a device that sits near the body but not on the body), or an app. Very little validation data exist, as most of these technologies are marketed as wellness devices and are not intended to render a diagnosis. It therefore falls to us to determine how to utilize this information in an already busy clinic.
One strategy is to use these technologies as patient engagement tools – a way to increase public awareness of the importance of sleep. While this certainly should be beneficial, oftentimes, the data are confusing and can lead to misunderstandings about what normal sleep should look like. Approaching these data as partners to our patients allows us to set expectations around normal sleep cycles and sleep duration. It also allows us to discuss appropriate sleep timing and sleep hygiene.
Many wearable devices have incorporated oximetry into their metrics, and some claim to have accuracy that is better than hospital-grade oximeters. Many of these companies are no longer in business. Others specify higher accuracy in dark-skinned individuals (“CIRCUL Ring Pulse Oximeter in Dark-Pigmented Individuals: Clinical Study Validates Efficacy and Reliability,” Medical Device News Magazine, Feb. 26, 2021).
Despite these claims, they are registered as wellness devices with the FDA and are not diagnostic devices. Logically, if one of these devices demonstrates worrisome data, then it can prompt further clinical queries and, potentially, objective testing for obstructive sleep apnea (OSA). The reverse, however, cannot be claimed. A normal reading by CST does not obviate the need for objective testing if the clinical symptoms warrant it.
There are CSTs that have been created around very specific needs - such as jet lag- and provide guidance for how to quickly acclimate to the destination time zone by providing nudges for light exposure and timed melatonin or dark glasses (https://www.timeshifter.com/).
Others analyze the sleep space for extrinsic sounds (https://www.sleepcycle.com/), while a plethora of apps provides advice for how to optimize your sleep environment and wind-down routine. There is even a sleep robot designed to facilitate sleep onset (https://somnox.com/). This bean-shaped device is designed to “breathe” as you hold it, and the user is meant to emulate those same breathing patterns. It is a take on the 4-7-8 breathing pattern long endorsed by yogis.
Although validation data are lacking for the vast majority of CST, a recent study (www.ncbi.nlm.nih.gov/pmc/articles/PMC8120339/pdf/zsaa291.pdf).demonstrated that CST had high performance when compared with actigraphy in assessing sleep and wakefulness and, as such, may improve the evaluation of sleep and wake opportunities prior to MSLT or improve identification of circadian sleep-wake disorders. Many practices do not currently utilize actigraphy due to its expense and very limited potential for reimbursement. Using a patient’s sleep-tracking device may allow access to these data without financial outlay. While these data demonstrate the ability of CST to potentially differentiate sleep from wakefulness, it is notable that this study also found that the determination of individual sleep stages is less robust. In general, CST cannot identify an underlying sleep disorder, however, may raise awareness that a disorder might be present.
This leads to more reflection on the role of CST in a typical sleep clinic. Many years ago, discussion around this technology was primarily patient-initiated and often times met with skepticism on the part of the clinician. As technology has improved and has become more accessible, there appears to be more acceptance among our colleagues – not, perhaps, in terms of absolute actionable data, but rather as an opportunity to discuss sleep with our patients and to support their own efforts at improving their sleep. Trends in the data in response to CBT-I or medications can be observed. Abnormalities identified via CST often serve as the initial prompt for a clinical visit and, as such, should not be eschewed. Rather, reframing the use of this information while also addressing other sleep issues is likely to be the more appropriate path forward.
Assessing this information can be time-consuming, and best practice suggests establishing expectations around this process (J Clin Sleep Med 2018 May 15. doi: 10.5664/jcsm.7128).
Agreements can be made with patients that the data are reviewed in the context of a clinical visit rather than longitudinally as data are uploaded and then sent via messaging unless such an understanding has already been agreed upon. RPM billing codes may ultimately allow for reimbursement and recognition of this workload. At the present time, RPM billing is limited to FDA-cleared, prescription devices, and CST does not yet qualify.
There also needs to be recognition of potential harm from CST. Inevitably, some patients will develop orthosomnia, a term coined by Dr. Kelly Baron, where patients become so fixated on achieving perfect sleep scores that it contributes to insomnia. In this case, identification of orthosomnia is made via the clinical visit and patients are advised to stop tracking their sleep for a set period of time. This allows the anxiety around achieving “perfect sleep” to dissipate.
Google and the AASM recently announced a partnership. Essentially, the Google Nest Hub will serve to detect sleep concerns (such as timing of sleep, snoring, insufficient sleep, etc.) and will direct the user to educational resources such as www.sleepeducation.org. The idea behind this is that people are often unaware of an underlying sleep disorder such as OSA and don’t know what to search for. The Nest Hub uses information it collects and directs users to appropriate resources, thus obviating the need to know what to Google.
Clearly, big tech has invested heavily in our field. Between the copious wearables, nearables, and apps that are sleep-focused, these industry giants obviously believe that sleep is worthy of such a significant allocation of resources. This has improved the overall awareness of the importance of sleep and of identifying and treating sleep disorders. While these technologies are no replacement for a clinical evaluation, they can serve as patient engagement tools, as well as potentially large-scale OSA screening tools and may help us improve the percentage of patients with undiagnosed OSA, estimated to be 80% (Frost and Sullivan, “Hidden Health Crisis Costing America Billions,” American Academy of Sleep Medicine, 2016).
CST may allow us to better identify circadian sleep-wake disorders and evaluate sleep satiation prior to MLST that no longer requires investment in expensive actigraphy devices. They also allow us to partner with our patients by meeting them where they are and recognizing the efforts they have already made to improve their sleep before we even meet them.
Dr. Khosla is Medical Director, North Dakota Center for Sleep, Fargo, North Dakota.
CHEST 2021: The beginning of the rest of your career
Is this your first CHEST Annual Meeting? Co-Chair David Zielinski, MD, FCCP, shares some words of wisdom recounting his first experience at CHEST and what first-time attendees can expect from the annual meeting.
My very first CHEST meeting was 10 years ago at CHEST 2011 in Honolulu, Hawaii. I clearly remember my first session being a postgraduate course on Respiratory Management of Neuromuscular Disease and having the opportunity for hands-on teaching with devices and techniques.

Simulation was unique at medical conferences at that time and has continued to evolve at subsequent CHEST meetings.
Looking back, what really sticks out about this experience is what it started for me in terms of my career and learning. I was in a session with some of the biggest names in the field—people who I always looked up to as a relatively junior faculty. I was encouraged to get more involved at CHEST and with the committees. It put the bug in my ear.
A few years later, I started to get involved in the NetWorks. Eventually, I became a faculty member myself alongside these individuals at subsequent CHEST meetings. Meeting these chest medicine professionals also led to more collaborations with them outside of CHEST.
I never imagined this during my first meeting ten years ago. I have now been back to every meeting but one since that first one.
The CHEST Annual Meeting has always stood out for its focus on quality clinical teaching, being ahead of the curve on interactivity and adjusting to the audience’s learning needs.
For me personally, though, the three things that I have always enjoyed are as follows:
Simulation opportunities
One thing that sets apart CHEST 2021 from other conferences is the simulation sessions being offered online.
These sessions are an opportunity to practice your skills and techniques with some of the best educators anywhere in the world. I have always come out of these sessions impressed. I encourage you to try it at least once.
The fun
From the receptions, the meet-ups, pop-up events, CHEST Challenge, the games… the list goes on: the fun element of CHEST makes it a more immersive atmosphere. When the meeting was solely virtual last year, CHEST still aimed to provide fun and will continue to do the same this year. Challenge your colleagues and new friends to games at the CHEST Player Hub online to see which one of you rises to the top of the leaderboard.
The community
CHEST 2021 (and CHEST the organization) helps you make connections and provides opportunities for leadership involvement. CHEST committees are always looking for leaders at all stages of their careers. Attending satellite meetings, like the NetWork open forums that are occurring online before the meeting starts this year, will allow you to begin networking with those with similar interests to your own and hopefully will spark your interest in getting more involved in the future.
For many of us at CHEST, the NetWorks were a great place to start, and you can join one in the area that interests you most. Through my involvement in CHEST, I have become a part of the community, meeting so many other clinicians and educators in my field. I have made great friendships, which keep me coming back every year.
Moving forward
From the beginning, we have been planning CHEST 2021 so that if we needed to go entirely online, we could do so as seamlessly as possible. With the recent decision to cancel the in-person meeting and go fully online, plans are already underway to make CHEST 2021 just as successful as last year’s meeting.
We can give you our commitment that your CHEST 2021 experience will live up to being a world-class event that separates itself from other current online offerings. I will be in attendance and hope to see you online.
Start planning your days with the CHEST 2021 Schedule at A Glance at chestmeeting.chestnet.org.
Is this your first CHEST Annual Meeting? Co-Chair David Zielinski, MD, FCCP, shares some words of wisdom recounting his first experience at CHEST and what first-time attendees can expect from the annual meeting.
My very first CHEST meeting was 10 years ago at CHEST 2011 in Honolulu, Hawaii. I clearly remember my first session being a postgraduate course on Respiratory Management of Neuromuscular Disease and having the opportunity for hands-on teaching with devices and techniques.
Simulation was unique at medical conferences at that time and has continued to evolve at subsequent CHEST meetings.
Looking back, what really sticks out about this experience is what it started for me in terms of my career and learning. I was in a session with some of the biggest names in the field—people who I always looked up to as a relatively junior faculty. I was encouraged to get more involved at CHEST and with the committees. It put the bug in my ear.
A few years later, I started to get involved in the NetWorks. Eventually, I became a faculty member myself alongside these individuals at subsequent CHEST meetings. Meeting these chest medicine professionals also led to more collaborations with them outside of CHEST.
I never imagined this during my first meeting ten years ago. I have now been back to every meeting but one since that first one.
The CHEST Annual Meeting has always stood out for its focus on quality clinical teaching, being ahead of the curve on interactivity and adjusting to the audience’s learning needs.
For me personally, though, the three things that I have always enjoyed are as follows:
Simulation opportunities
One thing that sets apart CHEST 2021 from other conferences is the simulation sessions being offered online.
These sessions are an opportunity to practice your skills and techniques with some of the best educators anywhere in the world. I have always come out of these sessions impressed. I encourage you to try it at least once.
The fun
From the receptions, the meet-ups, pop-up events, CHEST Challenge, the games… the list goes on: the fun element of CHEST makes it a more immersive atmosphere. When the meeting was solely virtual last year, CHEST still aimed to provide fun and will continue to do the same this year. Challenge your colleagues and new friends to games at the CHEST Player Hub online to see which one of you rises to the top of the leaderboard.
The community
CHEST 2021 (and CHEST the organization) helps you make connections and provides opportunities for leadership involvement. CHEST committees are always looking for leaders at all stages of their careers. Attending satellite meetings, like the NetWork open forums that are occurring online before the meeting starts this year, will allow you to begin networking with those with similar interests to your own and hopefully will spark your interest in getting more involved in the future.
For many of us at CHEST, the NetWorks were a great place to start, and you can join one in the area that interests you most. Through my involvement in CHEST, I have become a part of the community, meeting so many other clinicians and educators in my field. I have made great friendships, which keep me coming back every year.
Moving forward
From the beginning, we have been planning CHEST 2021 so that if we needed to go entirely online, we could do so as seamlessly as possible. With the recent decision to cancel the in-person meeting and go fully online, plans are already underway to make CHEST 2021 just as successful as last year’s meeting.
We can give you our commitment that your CHEST 2021 experience will live up to being a world-class event that separates itself from other current online offerings. I will be in attendance and hope to see you online.
Start planning your days with the CHEST 2021 Schedule at A Glance at chestmeeting.chestnet.org.
Is this your first CHEST Annual Meeting? Co-Chair David Zielinski, MD, FCCP, shares some words of wisdom recounting his first experience at CHEST and what first-time attendees can expect from the annual meeting.
My very first CHEST meeting was 10 years ago at CHEST 2011 in Honolulu, Hawaii. I clearly remember my first session being a postgraduate course on Respiratory Management of Neuromuscular Disease and having the opportunity for hands-on teaching with devices and techniques.
Simulation was unique at medical conferences at that time and has continued to evolve at subsequent CHEST meetings.
Looking back, what really sticks out about this experience is what it started for me in terms of my career and learning. I was in a session with some of the biggest names in the field—people who I always looked up to as a relatively junior faculty. I was encouraged to get more involved at CHEST and with the committees. It put the bug in my ear.
A few years later, I started to get involved in the NetWorks. Eventually, I became a faculty member myself alongside these individuals at subsequent CHEST meetings. Meeting these chest medicine professionals also led to more collaborations with them outside of CHEST.
I never imagined this during my first meeting ten years ago. I have now been back to every meeting but one since that first one.
The CHEST Annual Meeting has always stood out for its focus on quality clinical teaching, being ahead of the curve on interactivity and adjusting to the audience’s learning needs.
For me personally, though, the three things that I have always enjoyed are as follows:
Simulation opportunities
One thing that sets apart CHEST 2021 from other conferences is the simulation sessions being offered online.
These sessions are an opportunity to practice your skills and techniques with some of the best educators anywhere in the world. I have always come out of these sessions impressed. I encourage you to try it at least once.
The fun
From the receptions, the meet-ups, pop-up events, CHEST Challenge, the games… the list goes on: the fun element of CHEST makes it a more immersive atmosphere. When the meeting was solely virtual last year, CHEST still aimed to provide fun and will continue to do the same this year. Challenge your colleagues and new friends to games at the CHEST Player Hub online to see which one of you rises to the top of the leaderboard.
The community
CHEST 2021 (and CHEST the organization) helps you make connections and provides opportunities for leadership involvement. CHEST committees are always looking for leaders at all stages of their careers. Attending satellite meetings, like the NetWork open forums that are occurring online before the meeting starts this year, will allow you to begin networking with those with similar interests to your own and hopefully will spark your interest in getting more involved in the future.
For many of us at CHEST, the NetWorks were a great place to start, and you can join one in the area that interests you most. Through my involvement in CHEST, I have become a part of the community, meeting so many other clinicians and educators in my field. I have made great friendships, which keep me coming back every year.
Moving forward
From the beginning, we have been planning CHEST 2021 so that if we needed to go entirely online, we could do so as seamlessly as possible. With the recent decision to cancel the in-person meeting and go fully online, plans are already underway to make CHEST 2021 just as successful as last year’s meeting.
We can give you our commitment that your CHEST 2021 experience will live up to being a world-class event that separates itself from other current online offerings. I will be in attendance and hope to see you online.
Start planning your days with the CHEST 2021 Schedule at A Glance at chestmeeting.chestnet.org.
Community service grants bedrock of support for communities in need
Community service grants are one way the Foundation strives to make a tangible, lasting impact on the lives of the patients we serve – they’re not just one-off projects with limited effects. But how do we really know that we’re making a difference?
For Dr. Roberta Kato, it’s when she gets to witness an “Aha!” moment – a time when everything clicks and a parent finally understands how to better care for their child. For Marina Lima, MD, MSc, it’s knowing that one more teen isn’t gasping for air. And for Dr. Joseph Huang, it’s seeing a country of 100 million people gain access to 14 pulmonologists when there was previously only one.

Whether it’s hosting family workshops in children’s museums across Los Angeles, developing a gaming app to help children in Brazil control their asthma symptoms, or establishing a pulmonary and critical care training program in Uganda, the Foundation community service grants all focus on the same goal: to enable our underserved patients gain access to the resources and care they need when they need it most.
Why community service grants?
The Foundation began giving community service grants in 1997 under the leadership of CHEST President D. Robert McCaffree, MD, Master FCCP. He believed the program would be the best way to support his colleagues in achieving their community service endeavors .To date, over $2 million has been given specifically to community service projects. “
Our physicians experience the limitations of our health care system first-hand – a system that isn’t built to assist the people who need help the most. Finding solutions requires a willingness to think and operate creatively. The funding the Foundation provides through our community service grants supplies the resources to do just that – implement real-world solutions that will help patients gain better access to care.
Cases in point
Marina Lima, MD, MSc, was seeing an inordinate number of children and teens with uncontrolled asthma symptoms in Brazil. She applied for and was awarded a grant to make Asthmaland, the first gamified pediatric asthma educational program in Portuguese.
Besides her “Aha!” moments, Dr. Roberta Kato revealed a way she knows her work is making a difference: the funding is helping to shift the nonprofit landscape in her community.
“Sometimes there is a rift between different organizations. When I ask them to collaborate or advertise together, I get resistance. However, when I’ve reached out and said that I’ve received funding for an initiative, all of a sudden, there is forward movement. That is how I am hoping to make the biggest difference,” explained Dr. Kato.
Dr. Joseph Huang, who received a grant to fund the East Africa Training Initiative (EATI), is faced with a different obstacle. “We’ve been awarded the grant many times, and I know the Foundation is focused on supporting new, up-and-coming programs. Therefore, I’m committed to ensuring that my program can continue even after we stop receiving funding.”
How is Dr. Huang going to do that? Besides procuring ICU equipment, EATI focuses on training pulmonology fellows in east Africa. The fellows who graduate will train other physicians and care team members across the continent, both in hospitals and rural clinics, safeguarding the future of his program.
A clear vision for the future
While the Foundation is ready to tackle new problems, community service grants will remain the constant thread woven throughout the work, and it’s obvious why. As Dr. Huang emphasized, his grant “will ensure that the people living in Africa have a better chance at getting access to the care they need.”
When you strip away everything else, community service grants boil down to one thing: helping people live healthier, more fulfilled lives. What can be more worthwhile?
Help us continue this important work
While we are privileged to award numerous grants over the past 2 decades, our community service grants have always held a special place in the hearts and minds of everyone involved with the CHEST Foundation. We hope they hold a special place in your heart too.
Please consider donating so that we can continue this work together.
Community service grants are one way the Foundation strives to make a tangible, lasting impact on the lives of the patients we serve – they’re not just one-off projects with limited effects. But how do we really know that we’re making a difference?
For Dr. Roberta Kato, it’s when she gets to witness an “Aha!” moment – a time when everything clicks and a parent finally understands how to better care for their child. For Marina Lima, MD, MSc, it’s knowing that one more teen isn’t gasping for air. And for Dr. Joseph Huang, it’s seeing a country of 100 million people gain access to 14 pulmonologists when there was previously only one.
Whether it’s hosting family workshops in children’s museums across Los Angeles, developing a gaming app to help children in Brazil control their asthma symptoms, or establishing a pulmonary and critical care training program in Uganda, the Foundation community service grants all focus on the same goal: to enable our underserved patients gain access to the resources and care they need when they need it most.
Why community service grants?
The Foundation began giving community service grants in 1997 under the leadership of CHEST President D. Robert McCaffree, MD, Master FCCP. He believed the program would be the best way to support his colleagues in achieving their community service endeavors .To date, over $2 million has been given specifically to community service projects. “
Our physicians experience the limitations of our health care system first-hand – a system that isn’t built to assist the people who need help the most. Finding solutions requires a willingness to think and operate creatively. The funding the Foundation provides through our community service grants supplies the resources to do just that – implement real-world solutions that will help patients gain better access to care.
Cases in point
Marina Lima, MD, MSc, was seeing an inordinate number of children and teens with uncontrolled asthma symptoms in Brazil. She applied for and was awarded a grant to make Asthmaland, the first gamified pediatric asthma educational program in Portuguese.
Besides her “Aha!” moments, Dr. Roberta Kato revealed a way she knows her work is making a difference: the funding is helping to shift the nonprofit landscape in her community.
“Sometimes there is a rift between different organizations. When I ask them to collaborate or advertise together, I get resistance. However, when I’ve reached out and said that I’ve received funding for an initiative, all of a sudden, there is forward movement. That is how I am hoping to make the biggest difference,” explained Dr. Kato.
Dr. Joseph Huang, who received a grant to fund the East Africa Training Initiative (EATI), is faced with a different obstacle. “We’ve been awarded the grant many times, and I know the Foundation is focused on supporting new, up-and-coming programs. Therefore, I’m committed to ensuring that my program can continue even after we stop receiving funding.”
How is Dr. Huang going to do that? Besides procuring ICU equipment, EATI focuses on training pulmonology fellows in east Africa. The fellows who graduate will train other physicians and care team members across the continent, both in hospitals and rural clinics, safeguarding the future of his program.
A clear vision for the future
While the Foundation is ready to tackle new problems, community service grants will remain the constant thread woven throughout the work, and it’s obvious why. As Dr. Huang emphasized, his grant “will ensure that the people living in Africa have a better chance at getting access to the care they need.”
When you strip away everything else, community service grants boil down to one thing: helping people live healthier, more fulfilled lives. What can be more worthwhile?
Help us continue this important work
While we are privileged to award numerous grants over the past 2 decades, our community service grants have always held a special place in the hearts and minds of everyone involved with the CHEST Foundation. We hope they hold a special place in your heart too.
Please consider donating so that we can continue this work together.
Community service grants are one way the Foundation strives to make a tangible, lasting impact on the lives of the patients we serve – they’re not just one-off projects with limited effects. But how do we really know that we’re making a difference?
For Dr. Roberta Kato, it’s when she gets to witness an “Aha!” moment – a time when everything clicks and a parent finally understands how to better care for their child. For Marina Lima, MD, MSc, it’s knowing that one more teen isn’t gasping for air. And for Dr. Joseph Huang, it’s seeing a country of 100 million people gain access to 14 pulmonologists when there was previously only one.
Whether it’s hosting family workshops in children’s museums across Los Angeles, developing a gaming app to help children in Brazil control their asthma symptoms, or establishing a pulmonary and critical care training program in Uganda, the Foundation community service grants all focus on the same goal: to enable our underserved patients gain access to the resources and care they need when they need it most.
Why community service grants?
The Foundation began giving community service grants in 1997 under the leadership of CHEST President D. Robert McCaffree, MD, Master FCCP. He believed the program would be the best way to support his colleagues in achieving their community service endeavors .To date, over $2 million has been given specifically to community service projects. “
Our physicians experience the limitations of our health care system first-hand – a system that isn’t built to assist the people who need help the most. Finding solutions requires a willingness to think and operate creatively. The funding the Foundation provides through our community service grants supplies the resources to do just that – implement real-world solutions that will help patients gain better access to care.
Cases in point
Marina Lima, MD, MSc, was seeing an inordinate number of children and teens with uncontrolled asthma symptoms in Brazil. She applied for and was awarded a grant to make Asthmaland, the first gamified pediatric asthma educational program in Portuguese.
Besides her “Aha!” moments, Dr. Roberta Kato revealed a way she knows her work is making a difference: the funding is helping to shift the nonprofit landscape in her community.
“Sometimes there is a rift between different organizations. When I ask them to collaborate or advertise together, I get resistance. However, when I’ve reached out and said that I’ve received funding for an initiative, all of a sudden, there is forward movement. That is how I am hoping to make the biggest difference,” explained Dr. Kato.
Dr. Joseph Huang, who received a grant to fund the East Africa Training Initiative (EATI), is faced with a different obstacle. “We’ve been awarded the grant many times, and I know the Foundation is focused on supporting new, up-and-coming programs. Therefore, I’m committed to ensuring that my program can continue even after we stop receiving funding.”
How is Dr. Huang going to do that? Besides procuring ICU equipment, EATI focuses on training pulmonology fellows in east Africa. The fellows who graduate will train other physicians and care team members across the continent, both in hospitals and rural clinics, safeguarding the future of his program.
A clear vision for the future
While the Foundation is ready to tackle new problems, community service grants will remain the constant thread woven throughout the work, and it’s obvious why. As Dr. Huang emphasized, his grant “will ensure that the people living in Africa have a better chance at getting access to the care they need.”
When you strip away everything else, community service grants boil down to one thing: helping people live healthier, more fulfilled lives. What can be more worthwhile?
Help us continue this important work
While we are privileged to award numerous grants over the past 2 decades, our community service grants have always held a special place in the hearts and minds of everyone involved with the CHEST Foundation. We hope they hold a special place in your heart too.
Please consider donating so that we can continue this work together.
Update – CHEST clinical practice guidelines
CHEST has a long history of developing high quality clinical practice guidelines based on rigorous methodology, particularly in Thoracic Oncology, Pulmonary Vascular/Venous Thromboembolic Disease, and Clinical Pulmonary Medicine/Cough. Using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach, CHEST guidelines aim to optimize patient care by providing evidence-based recommendations that are transparent and free from bias.

Recently, CHEST invested in reassessing how we could further enhance the relevance, timeliness, and impact of guidelines on patient care and outcomes. We re-evaluated how we prioritize guideline topics to ensure we identify conditions in which patient care might be significantly improved by the application of evidence-based recommendations. In addition to re-committing to the rigorous GRADE approach, we also committed to timelier guideline development that would cover a broader scope of clinical topics, better mirroring the needs of our membership.
Since resuming our guideline process last year, we completed four Expert Panel Reports covering COVID-19–related topics, as well as several CHEST clinical practice guidelines. This includes publications on the management of cough in various conditions and populations – chronic bronchitis, acute bronchitis in the immunocompromised adult, asthma and nonasthmatic eosinophilic bronchitis, and in children. We also published Diagnosis and Evaluation of Hypersensitivity Pneumonitis earlier this year. This guideline outlines a patient-centered and interdisciplinary diagnostic approach to aid clinicians and patients in navigating many of the uncertainties in the evaluation of this condition.
Updates from two of our guidelines following our ‘living guideline’ model were also recently published – Screening for Lung Cancer and Antithrombic Therapy for VTE Disease. The Screening for Lung Cancer update provides guidance on patient selection for lung cancer screening, updating the age and smoking history criteria based on new evidence published since the original CHEST guideline. The updated guideline also provides recommendations for implementing high-quality lung cancer screening programs to optimize the overall benefits of screening.
In Antithrombotic Therapy for VTE, the structure of recommendations follows the chronology of VTE management: ‘Whether to treat,’ ‘Interventional and adjunctive treatments,’ ‘Initiation phase,’ ‘Treatment phase,’ ‘Extended phase,’ and ‘Complications of VTE.’ This guideline was designed to provide a comprehensive reference for VTE management in patients at any stage of the disease. Several recommendations are new from prior versions of the guideline, including whether patients with cerebral venous sinus thrombosis should be treated with anticoagulation and the choice of anticoagulant therapy for patients with antiphospholipid syndrome and thrombosis.
As we look toward the future of guideline development at CHEST, we are excited by the opportunity to expand the CHEST guideline portfolio. Starting in 2022, we will be broadening the scope of CHEST guidelines to include topics in nine clinical domains: Airway Disorders, Chest Infections, Clinical Pulmonary Medicine, Critical Care, Interstitial Lung Disease, Interventional Pulmonology, Pulmonary Vascular Disease (including venous thromboembolic disease), Thoracic Oncology, and Sleep. We anticipate issuing a Request for Proposals in select areas from these domains in the Spring of 2022, allowing CHEST members the opportunity to propose topics for which clinical guidance is needed.
As we recommit to the rigorous guideline methodology for which CHEST is known and broaden our impact across the spectrum of chest disease, we seek to ensure CHEST remains the leading resource for evidence-based guidelines in the field of chest medicine.
CHEST has a long history of developing high quality clinical practice guidelines based on rigorous methodology, particularly in Thoracic Oncology, Pulmonary Vascular/Venous Thromboembolic Disease, and Clinical Pulmonary Medicine/Cough. Using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach, CHEST guidelines aim to optimize patient care by providing evidence-based recommendations that are transparent and free from bias.
Recently, CHEST invested in reassessing how we could further enhance the relevance, timeliness, and impact of guidelines on patient care and outcomes. We re-evaluated how we prioritize guideline topics to ensure we identify conditions in which patient care might be significantly improved by the application of evidence-based recommendations. In addition to re-committing to the rigorous GRADE approach, we also committed to timelier guideline development that would cover a broader scope of clinical topics, better mirroring the needs of our membership.
Since resuming our guideline process last year, we completed four Expert Panel Reports covering COVID-19–related topics, as well as several CHEST clinical practice guidelines. This includes publications on the management of cough in various conditions and populations – chronic bronchitis, acute bronchitis in the immunocompromised adult, asthma and nonasthmatic eosinophilic bronchitis, and in children. We also published Diagnosis and Evaluation of Hypersensitivity Pneumonitis earlier this year. This guideline outlines a patient-centered and interdisciplinary diagnostic approach to aid clinicians and patients in navigating many of the uncertainties in the evaluation of this condition.
Updates from two of our guidelines following our ‘living guideline’ model were also recently published – Screening for Lung Cancer and Antithrombic Therapy for VTE Disease. The Screening for Lung Cancer update provides guidance on patient selection for lung cancer screening, updating the age and smoking history criteria based on new evidence published since the original CHEST guideline. The updated guideline also provides recommendations for implementing high-quality lung cancer screening programs to optimize the overall benefits of screening.
In Antithrombotic Therapy for VTE, the structure of recommendations follows the chronology of VTE management: ‘Whether to treat,’ ‘Interventional and adjunctive treatments,’ ‘Initiation phase,’ ‘Treatment phase,’ ‘Extended phase,’ and ‘Complications of VTE.’ This guideline was designed to provide a comprehensive reference for VTE management in patients at any stage of the disease. Several recommendations are new from prior versions of the guideline, including whether patients with cerebral venous sinus thrombosis should be treated with anticoagulation and the choice of anticoagulant therapy for patients with antiphospholipid syndrome and thrombosis.
As we look toward the future of guideline development at CHEST, we are excited by the opportunity to expand the CHEST guideline portfolio. Starting in 2022, we will be broadening the scope of CHEST guidelines to include topics in nine clinical domains: Airway Disorders, Chest Infections, Clinical Pulmonary Medicine, Critical Care, Interstitial Lung Disease, Interventional Pulmonology, Pulmonary Vascular Disease (including venous thromboembolic disease), Thoracic Oncology, and Sleep. We anticipate issuing a Request for Proposals in select areas from these domains in the Spring of 2022, allowing CHEST members the opportunity to propose topics for which clinical guidance is needed.
As we recommit to the rigorous guideline methodology for which CHEST is known and broaden our impact across the spectrum of chest disease, we seek to ensure CHEST remains the leading resource for evidence-based guidelines in the field of chest medicine.
CHEST has a long history of developing high quality clinical practice guidelines based on rigorous methodology, particularly in Thoracic Oncology, Pulmonary Vascular/Venous Thromboembolic Disease, and Clinical Pulmonary Medicine/Cough. Using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach, CHEST guidelines aim to optimize patient care by providing evidence-based recommendations that are transparent and free from bias.
Recently, CHEST invested in reassessing how we could further enhance the relevance, timeliness, and impact of guidelines on patient care and outcomes. We re-evaluated how we prioritize guideline topics to ensure we identify conditions in which patient care might be significantly improved by the application of evidence-based recommendations. In addition to re-committing to the rigorous GRADE approach, we also committed to timelier guideline development that would cover a broader scope of clinical topics, better mirroring the needs of our membership.
Since resuming our guideline process last year, we completed four Expert Panel Reports covering COVID-19–related topics, as well as several CHEST clinical practice guidelines. This includes publications on the management of cough in various conditions and populations – chronic bronchitis, acute bronchitis in the immunocompromised adult, asthma and nonasthmatic eosinophilic bronchitis, and in children. We also published Diagnosis and Evaluation of Hypersensitivity Pneumonitis earlier this year. This guideline outlines a patient-centered and interdisciplinary diagnostic approach to aid clinicians and patients in navigating many of the uncertainties in the evaluation of this condition.
Updates from two of our guidelines following our ‘living guideline’ model were also recently published – Screening for Lung Cancer and Antithrombic Therapy for VTE Disease. The Screening for Lung Cancer update provides guidance on patient selection for lung cancer screening, updating the age and smoking history criteria based on new evidence published since the original CHEST guideline. The updated guideline also provides recommendations for implementing high-quality lung cancer screening programs to optimize the overall benefits of screening.
In Antithrombotic Therapy for VTE, the structure of recommendations follows the chronology of VTE management: ‘Whether to treat,’ ‘Interventional and adjunctive treatments,’ ‘Initiation phase,’ ‘Treatment phase,’ ‘Extended phase,’ and ‘Complications of VTE.’ This guideline was designed to provide a comprehensive reference for VTE management in patients at any stage of the disease. Several recommendations are new from prior versions of the guideline, including whether patients with cerebral venous sinus thrombosis should be treated with anticoagulation and the choice of anticoagulant therapy for patients with antiphospholipid syndrome and thrombosis.
As we look toward the future of guideline development at CHEST, we are excited by the opportunity to expand the CHEST guideline portfolio. Starting in 2022, we will be broadening the scope of CHEST guidelines to include topics in nine clinical domains: Airway Disorders, Chest Infections, Clinical Pulmonary Medicine, Critical Care, Interstitial Lung Disease, Interventional Pulmonology, Pulmonary Vascular Disease (including venous thromboembolic disease), Thoracic Oncology, and Sleep. We anticipate issuing a Request for Proposals in select areas from these domains in the Spring of 2022, allowing CHEST members the opportunity to propose topics for which clinical guidance is needed.
As we recommit to the rigorous guideline methodology for which CHEST is known and broaden our impact across the spectrum of chest disease, we seek to ensure CHEST remains the leading resource for evidence-based guidelines in the field of chest medicine.
New guidance on preventing cutaneous SCC in solid organ transplant patients
An expert panel of 48 dermatologists from 13 countries has developed recommendations to guide efforts aimed at preventing cutaneous squamous cell carcinoma (CSCC) in solid organ transplant recipients.
The recommendations were published online on Sept. 1 in JAMA Dermatology.
Because of lifelong immunosuppression, solid organ transplant recipients (SOTRs) have a risk of CSCC that is 20-200 times higher than in the general population and despite a growing literature on prevention of CSCC in these patients, uncertainty remains regarding best practices for various patient scenarios.
Paul Massey, MD, MPH, of the department of dermatology, Brigham and Women’s Hospital, Boston, and colleagues used a Delphi process to identify consensus-based medical management recommendations for prevention of CSCC in SOTRs.
The survey design was guided by a novel actinic damage and skin cancer index (AD-SCI) made up of six ordinal stages corresponding to an increasing burden of actinic damage and CSCC.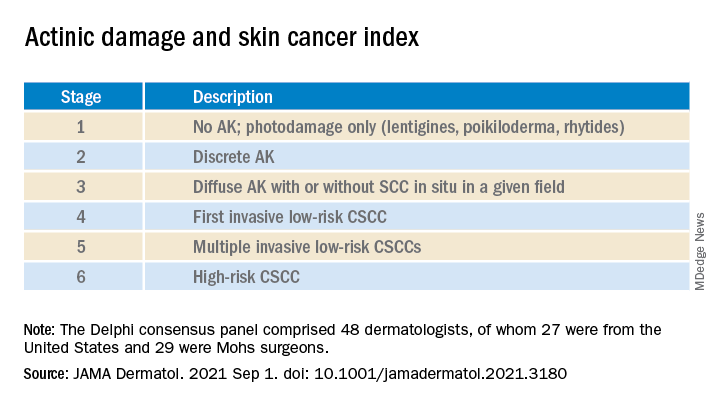
The AD-SCI stage-based recommendations were established when consensus was reached (80% or higher concordance) or near consensus was reached (70%-80% concordance) among panel members.
For five of the six AD-SCI stages, the panel was able to make recommendations. Key recommendations include:
- Cryotherapy for scattered AK.
- Field therapy for AK when grouped in one site, unless AKs are thick, in which case field therapy and cryotherapy are recommended.
- Combination lesion-directed and field therapy with fluorouracil for field cancerized skin.
- Initiation of acitretin therapy and discussion of immunosuppression reduction or modification for patients who develop multiple CSCCs at a high rate (10 per year) or develop high-risk CSCC (defined by a tumor with roughly ≥20% risk of nodal metastasis). The panel did not make a recommendation as to the best immunosuppression modification strategy to pursue.
Lingering questions
The panel was unable to reach consensus on a recommendation for SOTRs with a first low-risk CSCC, reflecting “clinical equipoise” in this situation and the need for further study in this clinical scenario, they say.
The panel did not make a recommendation for use of nicotinamide or capecitabine in any of the six stages, which is “notable,” they acknowledge, given results of a double-blind randomized controlled trial in immunocompetent patients demonstrating benefit in preventing AKs and CSCCs, as reported previously.
Nearly three-quarters of the panel felt that a lack of efficacy data specifically for the SOTR population limited their use of nicotinamide. “Given the low cost, high safety, and demonstration of CSCC reduction in non-SOTRs, nicotinamide administration may be an area for further consideration and expanded study,” the panel wrote.
As for capecitabine, the panel notes that case series in SOTRs have found efficacy for chemoprevention, but randomized controlled studies are lacking. More than half of the panel noted that they did not have routine access to capecitabine in their practice.
The panel recommended routine skin surveillance and sunscreen use for all patients.
“These recommendations reflect consensus among expert transplant dermatologists and the incorporation of limited and sometimes contradictory evidence into real-world clinical experience across a range of CSCC disease severity,” the panel said.
“Areas of consensus may aid physicians in establishing best practices regarding prevention of CSCC in SOTRs in the setting of limited high level of evidence data in this population,” they added.
This research had no specific funding. Author disclosures included serving as a consultant to Regeneron, Sanofi, and receiving research funding from Castle Biosciences, Regeneron, Novartis, and Genentech. A complete list of disclosures for panel members is available with the original article.
An expert panel of 48 dermatologists from 13 countries has developed recommendations to guide efforts aimed at preventing cutaneous squamous cell carcinoma (CSCC) in solid organ transplant recipients.
The recommendations were published online on Sept. 1 in JAMA Dermatology.
Because of lifelong immunosuppression, solid organ transplant recipients (SOTRs) have a risk of CSCC that is 20-200 times higher than in the general population and despite a growing literature on prevention of CSCC in these patients, uncertainty remains regarding best practices for various patient scenarios.
Paul Massey, MD, MPH, of the department of dermatology, Brigham and Women’s Hospital, Boston, and colleagues used a Delphi process to identify consensus-based medical management recommendations for prevention of CSCC in SOTRs.
The survey design was guided by a novel actinic damage and skin cancer index (AD-SCI) made up of six ordinal stages corresponding to an increasing burden of actinic damage and CSCC.
The AD-SCI stage-based recommendations were established when consensus was reached (80% or higher concordance) or near consensus was reached (70%-80% concordance) among panel members.
For five of the six AD-SCI stages, the panel was able to make recommendations. Key recommendations include:
- Cryotherapy for scattered AK.
- Field therapy for AK when grouped in one site, unless AKs are thick, in which case field therapy and cryotherapy are recommended.
- Combination lesion-directed and field therapy with fluorouracil for field cancerized skin.
- Initiation of acitretin therapy and discussion of immunosuppression reduction or modification for patients who develop multiple CSCCs at a high rate (10 per year) or develop high-risk CSCC (defined by a tumor with roughly ≥20% risk of nodal metastasis). The panel did not make a recommendation as to the best immunosuppression modification strategy to pursue.
Lingering questions
The panel was unable to reach consensus on a recommendation for SOTRs with a first low-risk CSCC, reflecting “clinical equipoise” in this situation and the need for further study in this clinical scenario, they say.
The panel did not make a recommendation for use of nicotinamide or capecitabine in any of the six stages, which is “notable,” they acknowledge, given results of a double-blind randomized controlled trial in immunocompetent patients demonstrating benefit in preventing AKs and CSCCs, as reported previously.
Nearly three-quarters of the panel felt that a lack of efficacy data specifically for the SOTR population limited their use of nicotinamide. “Given the low cost, high safety, and demonstration of CSCC reduction in non-SOTRs, nicotinamide administration may be an area for further consideration and expanded study,” the panel wrote.
As for capecitabine, the panel notes that case series in SOTRs have found efficacy for chemoprevention, but randomized controlled studies are lacking. More than half of the panel noted that they did not have routine access to capecitabine in their practice.
The panel recommended routine skin surveillance and sunscreen use for all patients.
“These recommendations reflect consensus among expert transplant dermatologists and the incorporation of limited and sometimes contradictory evidence into real-world clinical experience across a range of CSCC disease severity,” the panel said.
“Areas of consensus may aid physicians in establishing best practices regarding prevention of CSCC in SOTRs in the setting of limited high level of evidence data in this population,” they added.
This research had no specific funding. Author disclosures included serving as a consultant to Regeneron, Sanofi, and receiving research funding from Castle Biosciences, Regeneron, Novartis, and Genentech. A complete list of disclosures for panel members is available with the original article.
An expert panel of 48 dermatologists from 13 countries has developed recommendations to guide efforts aimed at preventing cutaneous squamous cell carcinoma (CSCC) in solid organ transplant recipients.
The recommendations were published online on Sept. 1 in JAMA Dermatology.
Because of lifelong immunosuppression, solid organ transplant recipients (SOTRs) have a risk of CSCC that is 20-200 times higher than in the general population and despite a growing literature on prevention of CSCC in these patients, uncertainty remains regarding best practices for various patient scenarios.
Paul Massey, MD, MPH, of the department of dermatology, Brigham and Women’s Hospital, Boston, and colleagues used a Delphi process to identify consensus-based medical management recommendations for prevention of CSCC in SOTRs.
The survey design was guided by a novel actinic damage and skin cancer index (AD-SCI) made up of six ordinal stages corresponding to an increasing burden of actinic damage and CSCC.
The AD-SCI stage-based recommendations were established when consensus was reached (80% or higher concordance) or near consensus was reached (70%-80% concordance) among panel members.
For five of the six AD-SCI stages, the panel was able to make recommendations. Key recommendations include:
- Cryotherapy for scattered AK.
- Field therapy for AK when grouped in one site, unless AKs are thick, in which case field therapy and cryotherapy are recommended.
- Combination lesion-directed and field therapy with fluorouracil for field cancerized skin.
- Initiation of acitretin therapy and discussion of immunosuppression reduction or modification for patients who develop multiple CSCCs at a high rate (10 per year) or develop high-risk CSCC (defined by a tumor with roughly ≥20% risk of nodal metastasis). The panel did not make a recommendation as to the best immunosuppression modification strategy to pursue.
Lingering questions
The panel was unable to reach consensus on a recommendation for SOTRs with a first low-risk CSCC, reflecting “clinical equipoise” in this situation and the need for further study in this clinical scenario, they say.
The panel did not make a recommendation for use of nicotinamide or capecitabine in any of the six stages, which is “notable,” they acknowledge, given results of a double-blind randomized controlled trial in immunocompetent patients demonstrating benefit in preventing AKs and CSCCs, as reported previously.
Nearly three-quarters of the panel felt that a lack of efficacy data specifically for the SOTR population limited their use of nicotinamide. “Given the low cost, high safety, and demonstration of CSCC reduction in non-SOTRs, nicotinamide administration may be an area for further consideration and expanded study,” the panel wrote.
As for capecitabine, the panel notes that case series in SOTRs have found efficacy for chemoprevention, but randomized controlled studies are lacking. More than half of the panel noted that they did not have routine access to capecitabine in their practice.
The panel recommended routine skin surveillance and sunscreen use for all patients.
“These recommendations reflect consensus among expert transplant dermatologists and the incorporation of limited and sometimes contradictory evidence into real-world clinical experience across a range of CSCC disease severity,” the panel said.
“Areas of consensus may aid physicians in establishing best practices regarding prevention of CSCC in SOTRs in the setting of limited high level of evidence data in this population,” they added.
This research had no specific funding. Author disclosures included serving as a consultant to Regeneron, Sanofi, and receiving research funding from Castle Biosciences, Regeneron, Novartis, and Genentech. A complete list of disclosures for panel members is available with the original article.
Even those who just test positive at more risk for long COVID: CDC
Long-term symptoms, like those linked with COVID-19, were common in people who had even just a single positive test, new Centers for Disease Control and Prevention data show.
The data show that symptoms in this group – including fatigue, cough, and headache – tended to last for more than a month.
Frequency of symptoms in people with a positive test was 1.5 times higher, compared with people whose tests had always been negative, according to the research published in the CDC’s latest Morbidity and Mortality Weekly Report.
Lead author Valentine Wanga, PhD, with the CDC’s COVID-19 response team, and colleagues conducted a non–probability-based internet panel survey of about 6,000 U.S. adults to assess long-term symptoms often associated with COVID-19 among those who had ever tested positive or always tested negative for COVID-19 between January 2020 and April 2021.
William Schaffner, MD, an infectious disease expert at Vanderbilt University, Nashville, Tenn., said in an interview that this research “establishes more securely than before that you don’t have to be hospitalized with COVID in order to develop long COVID symptoms.”
That’s better known among infectious disease experts, he said, but added that “this survey really gives a firm database for that.”
Study results
The study’s results showed that, compared with respondents who had a negative test result, those who received a positive result reported a significantly higher prevalence of any long-term symptom (65.9% vs. 42.9%), fatigue (22.5% vs. 12.0%), change in sense of smell or taste (17.3% vs. 1.7%), shortness of breath (15.5% vs. 5.2%), cough (14.5% vs. 4.9%), and headache (13.8% vs. 9.9%).
More people who had a positive test result (76.2%) reported persistence for more than a month of at least one initially occurring symptom, compared with those whose test results were always negative (69.6%).
The numbers are further proof, Dr. Schaffner said, that COVID not only will be an acute stressor on the health care system but patients with long COVID will need help with managing care for the long term.
“We still don’t know what the COVID virus does that results in these long COVID symptoms,” he said. Vanderbilt and many other institutions have developed “long COVID” centers as a testament to how important the problem is.
Long COVID symptoms are not well understood and most studies have looked at the effects from patients who had been hospitalized with COVID-19.
In this survey, respondents self-reported whether they had ever had a positive SARS-CoV-2 test result (698), always received a negative test result (2,437), or never were tested for SARS-CoV-2 (2,750).
Compared with those who always tested negative, a larger proportion of those who tested positive (28.7% vs. 15.7%) reported believing that receiving a COVID-19 vaccine made their long-term symptoms better. No difference was found in reported beliefs that a vaccine made long-term symptoms worse.
Dr. Schaffner said he found that survey result interesting, but said that is not backed up by current data and would need further study.
“I would treat that with great caution,” he said. “I’m not dismissing it, but you can’t take that at face value. All of us who get sick and those of us who care for people who are sick – if there’s an intervention, we all hope for the best. We’re being optimistic. It’s when you do a randomized, double-blind, placebo-controlled study that you can find out whether your instincts or hopes were correct.”
The authors said that findings can inform public health preparedness, help guide care for people with post-COVID conditions, and help make the case for vaccines.
The study authors and Dr. Schaffner disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Long-term symptoms, like those linked with COVID-19, were common in people who had even just a single positive test, new Centers for Disease Control and Prevention data show.
The data show that symptoms in this group – including fatigue, cough, and headache – tended to last for more than a month.
Frequency of symptoms in people with a positive test was 1.5 times higher, compared with people whose tests had always been negative, according to the research published in the CDC’s latest Morbidity and Mortality Weekly Report.
Lead author Valentine Wanga, PhD, with the CDC’s COVID-19 response team, and colleagues conducted a non–probability-based internet panel survey of about 6,000 U.S. adults to assess long-term symptoms often associated with COVID-19 among those who had ever tested positive or always tested negative for COVID-19 between January 2020 and April 2021.
William Schaffner, MD, an infectious disease expert at Vanderbilt University, Nashville, Tenn., said in an interview that this research “establishes more securely than before that you don’t have to be hospitalized with COVID in order to develop long COVID symptoms.”
That’s better known among infectious disease experts, he said, but added that “this survey really gives a firm database for that.”
Study results
The study’s results showed that, compared with respondents who had a negative test result, those who received a positive result reported a significantly higher prevalence of any long-term symptom (65.9% vs. 42.9%), fatigue (22.5% vs. 12.0%), change in sense of smell or taste (17.3% vs. 1.7%), shortness of breath (15.5% vs. 5.2%), cough (14.5% vs. 4.9%), and headache (13.8% vs. 9.9%).
More people who had a positive test result (76.2%) reported persistence for more than a month of at least one initially occurring symptom, compared with those whose test results were always negative (69.6%).
The numbers are further proof, Dr. Schaffner said, that COVID not only will be an acute stressor on the health care system but patients with long COVID will need help with managing care for the long term.
“We still don’t know what the COVID virus does that results in these long COVID symptoms,” he said. Vanderbilt and many other institutions have developed “long COVID” centers as a testament to how important the problem is.
Long COVID symptoms are not well understood and most studies have looked at the effects from patients who had been hospitalized with COVID-19.
In this survey, respondents self-reported whether they had ever had a positive SARS-CoV-2 test result (698), always received a negative test result (2,437), or never were tested for SARS-CoV-2 (2,750).
Compared with those who always tested negative, a larger proportion of those who tested positive (28.7% vs. 15.7%) reported believing that receiving a COVID-19 vaccine made their long-term symptoms better. No difference was found in reported beliefs that a vaccine made long-term symptoms worse.
Dr. Schaffner said he found that survey result interesting, but said that is not backed up by current data and would need further study.
“I would treat that with great caution,” he said. “I’m not dismissing it, but you can’t take that at face value. All of us who get sick and those of us who care for people who are sick – if there’s an intervention, we all hope for the best. We’re being optimistic. It’s when you do a randomized, double-blind, placebo-controlled study that you can find out whether your instincts or hopes were correct.”
The authors said that findings can inform public health preparedness, help guide care for people with post-COVID conditions, and help make the case for vaccines.
The study authors and Dr. Schaffner disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Long-term symptoms, like those linked with COVID-19, were common in people who had even just a single positive test, new Centers for Disease Control and Prevention data show.
The data show that symptoms in this group – including fatigue, cough, and headache – tended to last for more than a month.
Frequency of symptoms in people with a positive test was 1.5 times higher, compared with people whose tests had always been negative, according to the research published in the CDC’s latest Morbidity and Mortality Weekly Report.
Lead author Valentine Wanga, PhD, with the CDC’s COVID-19 response team, and colleagues conducted a non–probability-based internet panel survey of about 6,000 U.S. adults to assess long-term symptoms often associated with COVID-19 among those who had ever tested positive or always tested negative for COVID-19 between January 2020 and April 2021.
William Schaffner, MD, an infectious disease expert at Vanderbilt University, Nashville, Tenn., said in an interview that this research “establishes more securely than before that you don’t have to be hospitalized with COVID in order to develop long COVID symptoms.”
That’s better known among infectious disease experts, he said, but added that “this survey really gives a firm database for that.”
Study results
The study’s results showed that, compared with respondents who had a negative test result, those who received a positive result reported a significantly higher prevalence of any long-term symptom (65.9% vs. 42.9%), fatigue (22.5% vs. 12.0%), change in sense of smell or taste (17.3% vs. 1.7%), shortness of breath (15.5% vs. 5.2%), cough (14.5% vs. 4.9%), and headache (13.8% vs. 9.9%).
More people who had a positive test result (76.2%) reported persistence for more than a month of at least one initially occurring symptom, compared with those whose test results were always negative (69.6%).
The numbers are further proof, Dr. Schaffner said, that COVID not only will be an acute stressor on the health care system but patients with long COVID will need help with managing care for the long term.
“We still don’t know what the COVID virus does that results in these long COVID symptoms,” he said. Vanderbilt and many other institutions have developed “long COVID” centers as a testament to how important the problem is.
Long COVID symptoms are not well understood and most studies have looked at the effects from patients who had been hospitalized with COVID-19.
In this survey, respondents self-reported whether they had ever had a positive SARS-CoV-2 test result (698), always received a negative test result (2,437), or never were tested for SARS-CoV-2 (2,750).
Compared with those who always tested negative, a larger proportion of those who tested positive (28.7% vs. 15.7%) reported believing that receiving a COVID-19 vaccine made their long-term symptoms better. No difference was found in reported beliefs that a vaccine made long-term symptoms worse.
Dr. Schaffner said he found that survey result interesting, but said that is not backed up by current data and would need further study.
“I would treat that with great caution,” he said. “I’m not dismissing it, but you can’t take that at face value. All of us who get sick and those of us who care for people who are sick – if there’s an intervention, we all hope for the best. We’re being optimistic. It’s when you do a randomized, double-blind, placebo-controlled study that you can find out whether your instincts or hopes were correct.”
The authors said that findings can inform public health preparedness, help guide care for people with post-COVID conditions, and help make the case for vaccines.
The study authors and Dr. Schaffner disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Seizure a first sign of COVID in kids?
Unlike in adults, seizures, including status epilepticus (SE), may be the first and main manifestation of COVID-19 in children, new research suggests.
Seizures may occur even in children with no history of epilepsy and in the absence of fever or severe COVID-19 illness, necessitating a “high index” of suspicion for the virus to make an early diagnosis and allow for appropriate infection control measures, say the researchers.
“We hope to increase physicians’ awareness of noninfluenza-like presentations of COVID in children. In areas with a high prevalence of COVID, we suggest that children with seizures be tested for COVID,” Tal Gilboa, MD, director of the child neurology unit and codirector of epilepsy, Hadassah Medical Center, Jerusalem, told this news organization.
The study was published online August 27 in the journal Seizure.
Presenting symptom
Among 175 children diagnosed with acute SARS-CoV-2 infection in the emergency department over 10 months in 2020, 11 (6%) presented with seizures. Studies in adults with COVID-19 have reported seizures in 0% to 2% of cases, the investigators note.
The 11 children with seizures (seven boys) ranged in age from 6 months to 17 years (median age, 11.5 years). All of them had seizures as the presenting sign of infection and none had severe COVID-19 requiring ventilatory or hemodynamic support. Six of the 11 children presented with fever.
Seven of the children had a prior history of neurological disorder: Five had epilepsy, one had a single unprovoked seizure 3 years before admission, and one had an intellectual disability. Three of the children had uncontrolled seizures despite appropriate treatment with antiseizure medication.
Nine of the 11 children presented with generalized tonic-clonic seizures. One child with a prior history of uncontrolled epilepsy with multiple seizure types had a focal tonic seizure. The youngest patient, a 5-month-old infant, presented with bilateral asymmetrical tonic-clonic seizure.
Of note, say the investigators, five of the 11 children presented with convulsive SE; none had a history of prior SE, and one had no history of seizures.
Although young age, especially under 12 months, is a known risk factor for SE, four of the five patients with SE were between 5 and 17 years old. All five children with SE responded to treatment with antiseizure medications.
All 11 children made a full recovery while in hospital, although further follow-up is essential to determine long-term outcomes, the researchers report.
“Children with no prior history of epilepsy and those with well-controlled epilepsy who present with breakthrough seizures, regardless of their body temperature, should be considered as potentially infected by SARS-CoV-2,” said Dr. Gilboa.
“It is possible, however unlikely, that a child, especially with prior epilepsy, may have an unprovoked seizure while being asymptomatically infected by SARS-CoV-2; in any case, infection control measures should be taken,” Dr. Gilboa added.
Need for replication
Weighing in on the study, Carl E. Stafstrom, MD, PhD, professor of neurology and pediatrics, Johns Hopkins University, Baltimore, said it’s important to note that “about half of the children had had epilepsy already, and for whatever reason, had a seizure, which required an ED visit, and then they found COVID.”
“Nevertheless, this article is interesting and surprising in what they found because nobody else has found nearly as frequent a seizure presentation,” said Dr. Stafstrom, director of the John M. Freeman Pediatric Epilepsy Center, Johns Hopkins Medicine.
“We would want to see some replication from other institutions and other populations,” he added.
The study had no specific funding. Dr. Gilboa and Dr. Stafstrom have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Unlike in adults, seizures, including status epilepticus (SE), may be the first and main manifestation of COVID-19 in children, new research suggests.
Seizures may occur even in children with no history of epilepsy and in the absence of fever or severe COVID-19 illness, necessitating a “high index” of suspicion for the virus to make an early diagnosis and allow for appropriate infection control measures, say the researchers.
“We hope to increase physicians’ awareness of noninfluenza-like presentations of COVID in children. In areas with a high prevalence of COVID, we suggest that children with seizures be tested for COVID,” Tal Gilboa, MD, director of the child neurology unit and codirector of epilepsy, Hadassah Medical Center, Jerusalem, told this news organization.
The study was published online August 27 in the journal Seizure.
Presenting symptom
Among 175 children diagnosed with acute SARS-CoV-2 infection in the emergency department over 10 months in 2020, 11 (6%) presented with seizures. Studies in adults with COVID-19 have reported seizures in 0% to 2% of cases, the investigators note.
The 11 children with seizures (seven boys) ranged in age from 6 months to 17 years (median age, 11.5 years). All of them had seizures as the presenting sign of infection and none had severe COVID-19 requiring ventilatory or hemodynamic support. Six of the 11 children presented with fever.
Seven of the children had a prior history of neurological disorder: Five had epilepsy, one had a single unprovoked seizure 3 years before admission, and one had an intellectual disability. Three of the children had uncontrolled seizures despite appropriate treatment with antiseizure medication.
Nine of the 11 children presented with generalized tonic-clonic seizures. One child with a prior history of uncontrolled epilepsy with multiple seizure types had a focal tonic seizure. The youngest patient, a 5-month-old infant, presented with bilateral asymmetrical tonic-clonic seizure.
Of note, say the investigators, five of the 11 children presented with convulsive SE; none had a history of prior SE, and one had no history of seizures.
Although young age, especially under 12 months, is a known risk factor for SE, four of the five patients with SE were between 5 and 17 years old. All five children with SE responded to treatment with antiseizure medications.
All 11 children made a full recovery while in hospital, although further follow-up is essential to determine long-term outcomes, the researchers report.
“Children with no prior history of epilepsy and those with well-controlled epilepsy who present with breakthrough seizures, regardless of their body temperature, should be considered as potentially infected by SARS-CoV-2,” said Dr. Gilboa.
“It is possible, however unlikely, that a child, especially with prior epilepsy, may have an unprovoked seizure while being asymptomatically infected by SARS-CoV-2; in any case, infection control measures should be taken,” Dr. Gilboa added.
Need for replication
Weighing in on the study, Carl E. Stafstrom, MD, PhD, professor of neurology and pediatrics, Johns Hopkins University, Baltimore, said it’s important to note that “about half of the children had had epilepsy already, and for whatever reason, had a seizure, which required an ED visit, and then they found COVID.”
“Nevertheless, this article is interesting and surprising in what they found because nobody else has found nearly as frequent a seizure presentation,” said Dr. Stafstrom, director of the John M. Freeman Pediatric Epilepsy Center, Johns Hopkins Medicine.
“We would want to see some replication from other institutions and other populations,” he added.
The study had no specific funding. Dr. Gilboa and Dr. Stafstrom have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Unlike in adults, seizures, including status epilepticus (SE), may be the first and main manifestation of COVID-19 in children, new research suggests.
Seizures may occur even in children with no history of epilepsy and in the absence of fever or severe COVID-19 illness, necessitating a “high index” of suspicion for the virus to make an early diagnosis and allow for appropriate infection control measures, say the researchers.
“We hope to increase physicians’ awareness of noninfluenza-like presentations of COVID in children. In areas with a high prevalence of COVID, we suggest that children with seizures be tested for COVID,” Tal Gilboa, MD, director of the child neurology unit and codirector of epilepsy, Hadassah Medical Center, Jerusalem, told this news organization.
The study was published online August 27 in the journal Seizure.
Presenting symptom
Among 175 children diagnosed with acute SARS-CoV-2 infection in the emergency department over 10 months in 2020, 11 (6%) presented with seizures. Studies in adults with COVID-19 have reported seizures in 0% to 2% of cases, the investigators note.
The 11 children with seizures (seven boys) ranged in age from 6 months to 17 years (median age, 11.5 years). All of them had seizures as the presenting sign of infection and none had severe COVID-19 requiring ventilatory or hemodynamic support. Six of the 11 children presented with fever.
Seven of the children had a prior history of neurological disorder: Five had epilepsy, one had a single unprovoked seizure 3 years before admission, and one had an intellectual disability. Three of the children had uncontrolled seizures despite appropriate treatment with antiseizure medication.
Nine of the 11 children presented with generalized tonic-clonic seizures. One child with a prior history of uncontrolled epilepsy with multiple seizure types had a focal tonic seizure. The youngest patient, a 5-month-old infant, presented with bilateral asymmetrical tonic-clonic seizure.
Of note, say the investigators, five of the 11 children presented with convulsive SE; none had a history of prior SE, and one had no history of seizures.
Although young age, especially under 12 months, is a known risk factor for SE, four of the five patients with SE were between 5 and 17 years old. All five children with SE responded to treatment with antiseizure medications.
All 11 children made a full recovery while in hospital, although further follow-up is essential to determine long-term outcomes, the researchers report.
“Children with no prior history of epilepsy and those with well-controlled epilepsy who present with breakthrough seizures, regardless of their body temperature, should be considered as potentially infected by SARS-CoV-2,” said Dr. Gilboa.
“It is possible, however unlikely, that a child, especially with prior epilepsy, may have an unprovoked seizure while being asymptomatically infected by SARS-CoV-2; in any case, infection control measures should be taken,” Dr. Gilboa added.
Need for replication
Weighing in on the study, Carl E. Stafstrom, MD, PhD, professor of neurology and pediatrics, Johns Hopkins University, Baltimore, said it’s important to note that “about half of the children had had epilepsy already, and for whatever reason, had a seizure, which required an ED visit, and then they found COVID.”
“Nevertheless, this article is interesting and surprising in what they found because nobody else has found nearly as frequent a seizure presentation,” said Dr. Stafstrom, director of the John M. Freeman Pediatric Epilepsy Center, Johns Hopkins Medicine.
“We would want to see some replication from other institutions and other populations,” he added.
The study had no specific funding. Dr. Gilboa and Dr. Stafstrom have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.