User login
Telehealth apps in ObGyn practice
The COVID-19 pandemic has presented increasing demands on health care systems internationally. In addition to redistribution of inpatient health care resources, outpatient care practices evolved, with health care providers offering streamlined access to care to patients via telehealth.
Due to updated insurance practices, physicians now can receive reimbursement via private insurers, Medicare, and Medicaid (as determined by states) for telehealth visits both related and unrelated to COVID-19 care. Increased telehealth use has advantages, including increased health care access, reduced in-clinic wait times, and reduced patient and physician travel time. Within the field of obstetrics and gynecology, clinicians have used telehealth to maintain access to prenatal maternity care while redirecting resources and minimizing the risk of COVID-19 transmission. Additional advantages include provision of care during expanded hours, including evenings and weekends, to increase patient access without increasing the demand on office support staff and the ability to bill for 5- to 10-minute phone counseling encounters.1 Research shows that patients express satisfaction regarding the quality of telehealth care in the setting of prenatal care.2
In February 2020, the American College of Obstetricians and Gynecologists (ACOG) released a Committee Opinion regarding telehealth use in ObGyn, a sign of telehealth’s likely long-standing role within the field.3 Within the statement, ACOG commented on the increasing application of telemedicine in all aspects of obstetrics and gynecology and recommended that physicians become acquainted with new technologies and consider using them in their practice.
There is a large opportunity for development of mobile applications (apps) to further streamline telehealth-based medical care. During the pandemic, the Centers for Medicare and Medicaid Services instituted waivers for telemedicine use on non-HIPAA (Health Insurance Portability and Accountability Act) compliant video communications products, such as Google+ Hangout and Skype. However, HIPAA-compliant video services are preferred, and many virtual apps have released methods for patient communication that meet HIPAA guidelines.1,4 These apps offer services such as phone- and video-based patient visits, appointment scheduling, secure physician-patient messaging, and electronic health record (EHR) documentation.
App recommendations
To identify current mobile apps with clinical use for the ObGyn, we conducted a search of the Apple App Store using the term “telehealth” between December 1, 2021 and January 1, 2022. We limited search results to apps that had at least 1,000 user ratings and to HIPAA-compliant user communication apps. Based on our review, we selected 4 apps to highlight here: Doximity, OhMD, Spruce, and Telehealth by SimplePractice (TABLE). We excluded apps that were advertised as having internal medical clinicians with first patient encounter on-demand through the app or that were associated with a singular insurance company or hospital system.
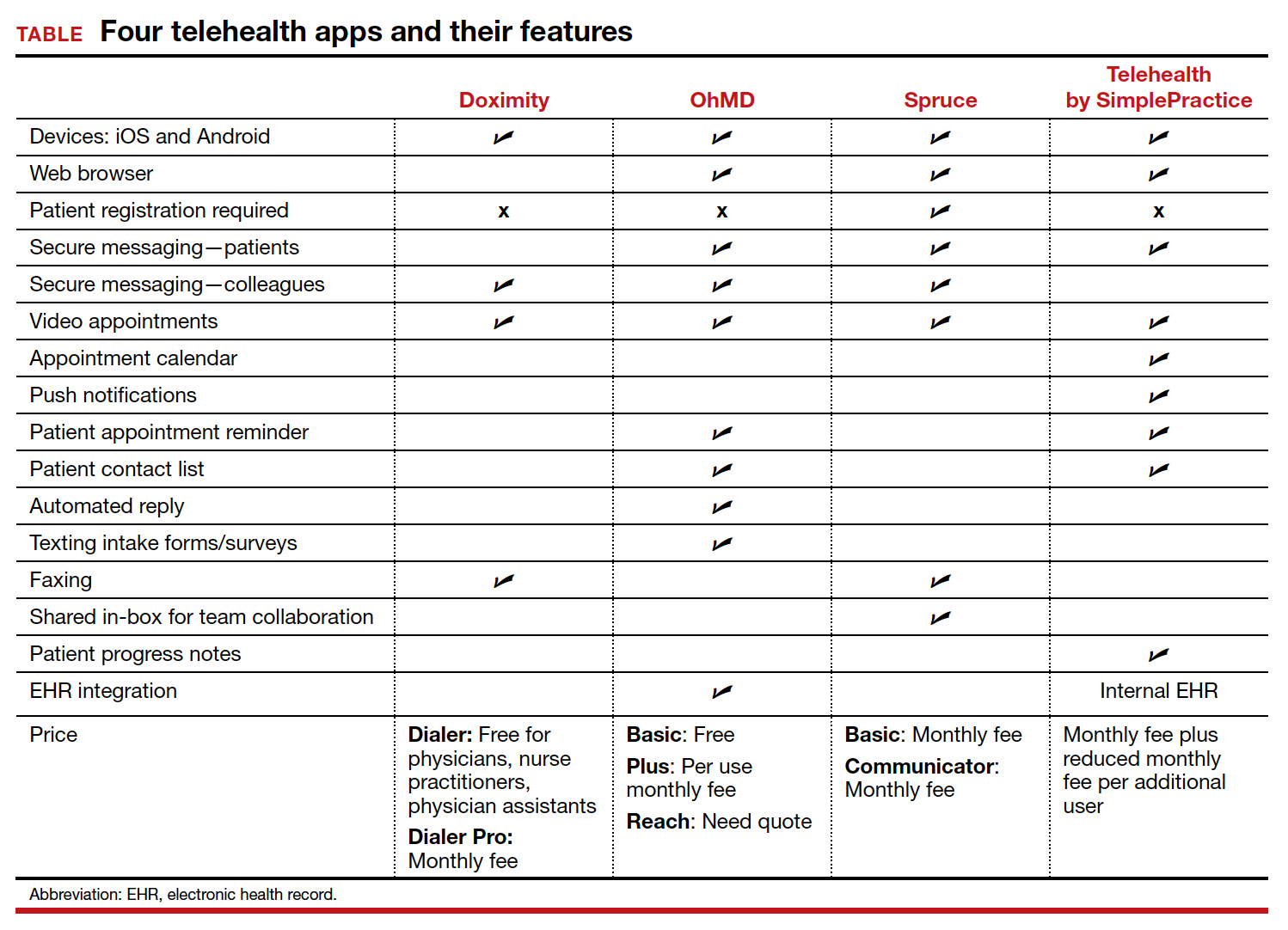
These apps are largely enabled for iOS and Android mobile devices and are offered at a range of price points for individual physician and practice-scale clinical implementation. Most apps offer secure messaging services between health care practitioners in addition to HIPAA-compliant patient messaging. Some apps offer additional features with the aim to increase patient attendance; these include push notifications, appointment reminders, and an option for automated replies with clinic information. For an additional fee, several apps offer integration to established EHR systems.
An additional tool
The COVID-19 pandemic caused health care systems and individual clinicians to rapidly evolve their practices to maintain patient access to essential health care. Notably, the pandemic led to accelerated implementation of virtual health care services. Telehealth apps likely will become another tool that ObGyns can use to improve the efficiency of their clinical practice and expand patient access to care. ●
- Karram M, Baum N. Telemedicine: a primer for today’s ObGyn. OBG Manag. 2020;32:28-32.
- Marko KI, Ganju N, Krapf JM, et al. A mobile prenatal care app to reduce in-person visits: prospective controlled trial. JMIR Mhealth Uhealth. 2019;7:e10520.
- American College of Obstetricians and Gynecologists. Implementing telehealth in practice: committee opinion no. 798. Obstet Gynecol. 2020;135:e73-e79.
- Karram M, Dooley A, de la Houssaye N, et al. Telemedicine: navigating legal issues. OBG Manag. 2020;32:18-24.

Dr. Warren is a second-year resident in the Department of Obstetrics, Gynecology, and Reproductive Science, Icahn School of Medicine at Mount Sinai, New York, New York.

Dr. Chen is Professor of Obstetrics, Gynecology, and Reproductive Science and Medical Education, Vice-Chair of Ob-Gyn Education for the Mount Sinai Health System, Icahn School of Medicine at Mount Sinai, New York. She is an OBG Management Contributing Editor.
Dr. Chen reports being an advisory board member and receiving royalties from UpToDate, Inc. and acting as a speaker for Sanofi Pasteur. Dr. Warren reports no financial relationships relevant to this article.
Dr. Warren is a second-year resident in the Department of Obstetrics, Gynecology, and Reproductive Science, Icahn School of Medicine at Mount Sinai, New York, New York.
Dr. Chen is Professor of Obstetrics, Gynecology, and Reproductive Science and Medical Education, Vice-Chair of Ob-Gyn Education for the Mount Sinai Health System, Icahn School of Medicine at Mount Sinai, New York. She is an OBG Management Contributing Editor.
Dr. Chen reports being an advisory board member and receiving royalties from UpToDate, Inc. and acting as a speaker for Sanofi Pasteur. Dr. Warren reports no financial relationships relevant to this article.
Dr. Warren is a second-year resident in the Department of Obstetrics, Gynecology, and Reproductive Science, Icahn School of Medicine at Mount Sinai, New York, New York.
Dr. Chen is Professor of Obstetrics, Gynecology, and Reproductive Science and Medical Education, Vice-Chair of Ob-Gyn Education for the Mount Sinai Health System, Icahn School of Medicine at Mount Sinai, New York. She is an OBG Management Contributing Editor.
Dr. Chen reports being an advisory board member and receiving royalties from UpToDate, Inc. and acting as a speaker for Sanofi Pasteur. Dr. Warren reports no financial relationships relevant to this article.
The COVID-19 pandemic has presented increasing demands on health care systems internationally. In addition to redistribution of inpatient health care resources, outpatient care practices evolved, with health care providers offering streamlined access to care to patients via telehealth.
Due to updated insurance practices, physicians now can receive reimbursement via private insurers, Medicare, and Medicaid (as determined by states) for telehealth visits both related and unrelated to COVID-19 care. Increased telehealth use has advantages, including increased health care access, reduced in-clinic wait times, and reduced patient and physician travel time. Within the field of obstetrics and gynecology, clinicians have used telehealth to maintain access to prenatal maternity care while redirecting resources and minimizing the risk of COVID-19 transmission. Additional advantages include provision of care during expanded hours, including evenings and weekends, to increase patient access without increasing the demand on office support staff and the ability to bill for 5- to 10-minute phone counseling encounters.1 Research shows that patients express satisfaction regarding the quality of telehealth care in the setting of prenatal care.2
In February 2020, the American College of Obstetricians and Gynecologists (ACOG) released a Committee Opinion regarding telehealth use in ObGyn, a sign of telehealth’s likely long-standing role within the field.3 Within the statement, ACOG commented on the increasing application of telemedicine in all aspects of obstetrics and gynecology and recommended that physicians become acquainted with new technologies and consider using them in their practice.
There is a large opportunity for development of mobile applications (apps) to further streamline telehealth-based medical care. During the pandemic, the Centers for Medicare and Medicaid Services instituted waivers for telemedicine use on non-HIPAA (Health Insurance Portability and Accountability Act) compliant video communications products, such as Google+ Hangout and Skype. However, HIPAA-compliant video services are preferred, and many virtual apps have released methods for patient communication that meet HIPAA guidelines.1,4 These apps offer services such as phone- and video-based patient visits, appointment scheduling, secure physician-patient messaging, and electronic health record (EHR) documentation.
App recommendations
To identify current mobile apps with clinical use for the ObGyn, we conducted a search of the Apple App Store using the term “telehealth” between December 1, 2021 and January 1, 2022. We limited search results to apps that had at least 1,000 user ratings and to HIPAA-compliant user communication apps. Based on our review, we selected 4 apps to highlight here: Doximity, OhMD, Spruce, and Telehealth by SimplePractice (TABLE). We excluded apps that were advertised as having internal medical clinicians with first patient encounter on-demand through the app or that were associated with a singular insurance company or hospital system.
These apps are largely enabled for iOS and Android mobile devices and are offered at a range of price points for individual physician and practice-scale clinical implementation. Most apps offer secure messaging services between health care practitioners in addition to HIPAA-compliant patient messaging. Some apps offer additional features with the aim to increase patient attendance; these include push notifications, appointment reminders, and an option for automated replies with clinic information. For an additional fee, several apps offer integration to established EHR systems.
An additional tool
The COVID-19 pandemic caused health care systems and individual clinicians to rapidly evolve their practices to maintain patient access to essential health care. Notably, the pandemic led to accelerated implementation of virtual health care services. Telehealth apps likely will become another tool that ObGyns can use to improve the efficiency of their clinical practice and expand patient access to care. ●
The COVID-19 pandemic has presented increasing demands on health care systems internationally. In addition to redistribution of inpatient health care resources, outpatient care practices evolved, with health care providers offering streamlined access to care to patients via telehealth.
Due to updated insurance practices, physicians now can receive reimbursement via private insurers, Medicare, and Medicaid (as determined by states) for telehealth visits both related and unrelated to COVID-19 care. Increased telehealth use has advantages, including increased health care access, reduced in-clinic wait times, and reduced patient and physician travel time. Within the field of obstetrics and gynecology, clinicians have used telehealth to maintain access to prenatal maternity care while redirecting resources and minimizing the risk of COVID-19 transmission. Additional advantages include provision of care during expanded hours, including evenings and weekends, to increase patient access without increasing the demand on office support staff and the ability to bill for 5- to 10-minute phone counseling encounters.1 Research shows that patients express satisfaction regarding the quality of telehealth care in the setting of prenatal care.2
In February 2020, the American College of Obstetricians and Gynecologists (ACOG) released a Committee Opinion regarding telehealth use in ObGyn, a sign of telehealth’s likely long-standing role within the field.3 Within the statement, ACOG commented on the increasing application of telemedicine in all aspects of obstetrics and gynecology and recommended that physicians become acquainted with new technologies and consider using them in their practice.
There is a large opportunity for development of mobile applications (apps) to further streamline telehealth-based medical care. During the pandemic, the Centers for Medicare and Medicaid Services instituted waivers for telemedicine use on non-HIPAA (Health Insurance Portability and Accountability Act) compliant video communications products, such as Google+ Hangout and Skype. However, HIPAA-compliant video services are preferred, and many virtual apps have released methods for patient communication that meet HIPAA guidelines.1,4 These apps offer services such as phone- and video-based patient visits, appointment scheduling, secure physician-patient messaging, and electronic health record (EHR) documentation.
App recommendations
To identify current mobile apps with clinical use for the ObGyn, we conducted a search of the Apple App Store using the term “telehealth” between December 1, 2021 and January 1, 2022. We limited search results to apps that had at least 1,000 user ratings and to HIPAA-compliant user communication apps. Based on our review, we selected 4 apps to highlight here: Doximity, OhMD, Spruce, and Telehealth by SimplePractice (TABLE). We excluded apps that were advertised as having internal medical clinicians with first patient encounter on-demand through the app or that were associated with a singular insurance company or hospital system.
These apps are largely enabled for iOS and Android mobile devices and are offered at a range of price points for individual physician and practice-scale clinical implementation. Most apps offer secure messaging services between health care practitioners in addition to HIPAA-compliant patient messaging. Some apps offer additional features with the aim to increase patient attendance; these include push notifications, appointment reminders, and an option for automated replies with clinic information. For an additional fee, several apps offer integration to established EHR systems.
An additional tool
The COVID-19 pandemic caused health care systems and individual clinicians to rapidly evolve their practices to maintain patient access to essential health care. Notably, the pandemic led to accelerated implementation of virtual health care services. Telehealth apps likely will become another tool that ObGyns can use to improve the efficiency of their clinical practice and expand patient access to care. ●
- Karram M, Baum N. Telemedicine: a primer for today’s ObGyn. OBG Manag. 2020;32:28-32.
- Marko KI, Ganju N, Krapf JM, et al. A mobile prenatal care app to reduce in-person visits: prospective controlled trial. JMIR Mhealth Uhealth. 2019;7:e10520.
- American College of Obstetricians and Gynecologists. Implementing telehealth in practice: committee opinion no. 798. Obstet Gynecol. 2020;135:e73-e79.
- Karram M, Dooley A, de la Houssaye N, et al. Telemedicine: navigating legal issues. OBG Manag. 2020;32:18-24.
- Karram M, Baum N. Telemedicine: a primer for today’s ObGyn. OBG Manag. 2020;32:28-32.
- Marko KI, Ganju N, Krapf JM, et al. A mobile prenatal care app to reduce in-person visits: prospective controlled trial. JMIR Mhealth Uhealth. 2019;7:e10520.
- American College of Obstetricians and Gynecologists. Implementing telehealth in practice: committee opinion no. 798. Obstet Gynecol. 2020;135:e73-e79.
- Karram M, Dooley A, de la Houssaye N, et al. Telemedicine: navigating legal issues. OBG Manag. 2020;32:18-24.

CPAP has only small effect on metabolic syndrome
Continuous positive airway pressure (CPAP) may be only modestly effective for ameliorating metabolic syndrome in patients with moderate to severe obstructive sleep apnea (OSA).
That conclusion comes from investigators in a randomized controlled, trial, who found that, among 100 patients with OSA and a recent diagnosis of metabolic syndrome (MS), 18% of those assigned to use CPAP at night had a reversal of MS at 6 months of follow-up, compared with 4% of controls who were assigned to use nasal strips at night (P = .04).
The majority of patients assigned to CPAP still retained their MS diagnoses at 6 months, and CPAP did not significantly reduce individual components of the syndrome. Use of CPAP was, however, associated with small reductions in visceral fat and improvement in endothelial function, reported Sara Q.C. Giampa, PhD, from the University of São Paulo, and colleagues.
“Despite a significant rate of MS reversibility after CPAP therapy, most of the patients maintained the MS diagnosis. The modest effects of CPAP on MS reversibility underscore the need for combined therapy with CPAP, aiming to maximize metabolic syndrome recovery in parallel with improvements in OSA severity and related symptoms,” according to their study, reported in the journal CHEST®.
Asked whether he still recommends CPAP to patients with OSA and the metabolic syndrome, given the findings, corresponding author Luciano F. Drager, MD, PhD, replied “yes, definitely.”
“Despite the modest rate in reversing metabolic syndrome after CPAP, the rate was 5-fold higher than non-effective treatment (18% vs. 4%),” he said in an interview.
Dr. Drager noted that studies of other single interventions such as physical exercise to reverse MS in patients with OSA also had modest results.
A researcher who studies the relationship between sleep, circadian rhythms, and metabolism commented that, although the patients in the CPAP group were compliant with the assigned equipment and had both reductions in apneic events and improvement in oxygen saturation, the effect of CPAP on the metabolic syndrome was rather small.
“The CPAP was doing what we thought it was supposed to do, but it didn’t have the magnitude of effect on the metabolic syndrome as I expected or I think as the authors expected,” said Deanna Arble, PhD, assistant professor of biological science at Marquette University, Milwaukee.
She noted that the study also failed to detect a significant improvement in the blood pressure component of metabolic syndrome.
“In my experience and my review of the literature, blood pressure tends to be the one that’s improved most dramatically with CPAP,” she said.
Dr. Arble was not involved in the study.
Study details
In the trial, titled TREATOSA-MS, the investigators enrolled 100 patients with a recent diagnosis of metabolic syndrome and moderate to severe OSA, defined as 15 or more apnea-hypopnea index events per hour. The patients were stratified by body mass index and then randomized to undergo therapeutic CPAP or to use nasal strips for 6 months.
At baseline and at the end of each intervention investigators measured anthropometric variables, blood pressure, glucose, and lipid profiles. They also leptin and adiponectin, body composition, food intake, physical activity, subcutaneous and abdominal fat (visceral and hepatic), and endothelial function to control for potential confounders.
As noted previously, they found that after 6 months “most patients with OSA randomized to CPAP retained the MS diagnosis, but the rate of MS reversibility was higher than observed in the placebo group.” The difference in metabolic syndrome reversal, 18% with CPAP versus 4% with nasal strips, translated into a hazard ratio favoring CPAP of 5.27 (P = .04).
Also as noted, in analyses adjusted for baseline values, CPAP did not significantly improve either weight, liver fat, lip profiles, or the adiposity biomarkers leptin and adiponectin, but did have “very modest” influence on reducing visceral fat and improving endothelial function.
Rigorous study
Dr. Arble said that most studies of the association between OSA and metabolic syndrome have focused on only one or two of the parameters that were included in the TREATOSA-MS study, giving the findings additional weight.
“This could potentially be a very good, carefully controlled first insight into how obstructive sleep apnea is related to the metabolic syndrome,” she said.
The study was funded by grants Fundação de Amparo Q22 à Pesquisa do Estado de São Paulo and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The authors and Dr. Arble reported having no conflicts of interest to disclose.
Continuous positive airway pressure (CPAP) may be only modestly effective for ameliorating metabolic syndrome in patients with moderate to severe obstructive sleep apnea (OSA).
That conclusion comes from investigators in a randomized controlled, trial, who found that, among 100 patients with OSA and a recent diagnosis of metabolic syndrome (MS), 18% of those assigned to use CPAP at night had a reversal of MS at 6 months of follow-up, compared with 4% of controls who were assigned to use nasal strips at night (P = .04).
The majority of patients assigned to CPAP still retained their MS diagnoses at 6 months, and CPAP did not significantly reduce individual components of the syndrome. Use of CPAP was, however, associated with small reductions in visceral fat and improvement in endothelial function, reported Sara Q.C. Giampa, PhD, from the University of São Paulo, and colleagues.
“Despite a significant rate of MS reversibility after CPAP therapy, most of the patients maintained the MS diagnosis. The modest effects of CPAP on MS reversibility underscore the need for combined therapy with CPAP, aiming to maximize metabolic syndrome recovery in parallel with improvements in OSA severity and related symptoms,” according to their study, reported in the journal CHEST®.
Asked whether he still recommends CPAP to patients with OSA and the metabolic syndrome, given the findings, corresponding author Luciano F. Drager, MD, PhD, replied “yes, definitely.”
“Despite the modest rate in reversing metabolic syndrome after CPAP, the rate was 5-fold higher than non-effective treatment (18% vs. 4%),” he said in an interview.
Dr. Drager noted that studies of other single interventions such as physical exercise to reverse MS in patients with OSA also had modest results.
A researcher who studies the relationship between sleep, circadian rhythms, and metabolism commented that, although the patients in the CPAP group were compliant with the assigned equipment and had both reductions in apneic events and improvement in oxygen saturation, the effect of CPAP on the metabolic syndrome was rather small.
“The CPAP was doing what we thought it was supposed to do, but it didn’t have the magnitude of effect on the metabolic syndrome as I expected or I think as the authors expected,” said Deanna Arble, PhD, assistant professor of biological science at Marquette University, Milwaukee.
She noted that the study also failed to detect a significant improvement in the blood pressure component of metabolic syndrome.
“In my experience and my review of the literature, blood pressure tends to be the one that’s improved most dramatically with CPAP,” she said.
Dr. Arble was not involved in the study.
Study details
In the trial, titled TREATOSA-MS, the investigators enrolled 100 patients with a recent diagnosis of metabolic syndrome and moderate to severe OSA, defined as 15 or more apnea-hypopnea index events per hour. The patients were stratified by body mass index and then randomized to undergo therapeutic CPAP or to use nasal strips for 6 months.
At baseline and at the end of each intervention investigators measured anthropometric variables, blood pressure, glucose, and lipid profiles. They also leptin and adiponectin, body composition, food intake, physical activity, subcutaneous and abdominal fat (visceral and hepatic), and endothelial function to control for potential confounders.
As noted previously, they found that after 6 months “most patients with OSA randomized to CPAP retained the MS diagnosis, but the rate of MS reversibility was higher than observed in the placebo group.” The difference in metabolic syndrome reversal, 18% with CPAP versus 4% with nasal strips, translated into a hazard ratio favoring CPAP of 5.27 (P = .04).
Also as noted, in analyses adjusted for baseline values, CPAP did not significantly improve either weight, liver fat, lip profiles, or the adiposity biomarkers leptin and adiponectin, but did have “very modest” influence on reducing visceral fat and improving endothelial function.
Rigorous study
Dr. Arble said that most studies of the association between OSA and metabolic syndrome have focused on only one or two of the parameters that were included in the TREATOSA-MS study, giving the findings additional weight.
“This could potentially be a very good, carefully controlled first insight into how obstructive sleep apnea is related to the metabolic syndrome,” she said.
The study was funded by grants Fundação de Amparo Q22 à Pesquisa do Estado de São Paulo and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The authors and Dr. Arble reported having no conflicts of interest to disclose.
Continuous positive airway pressure (CPAP) may be only modestly effective for ameliorating metabolic syndrome in patients with moderate to severe obstructive sleep apnea (OSA).
That conclusion comes from investigators in a randomized controlled, trial, who found that, among 100 patients with OSA and a recent diagnosis of metabolic syndrome (MS), 18% of those assigned to use CPAP at night had a reversal of MS at 6 months of follow-up, compared with 4% of controls who were assigned to use nasal strips at night (P = .04).
The majority of patients assigned to CPAP still retained their MS diagnoses at 6 months, and CPAP did not significantly reduce individual components of the syndrome. Use of CPAP was, however, associated with small reductions in visceral fat and improvement in endothelial function, reported Sara Q.C. Giampa, PhD, from the University of São Paulo, and colleagues.
“Despite a significant rate of MS reversibility after CPAP therapy, most of the patients maintained the MS diagnosis. The modest effects of CPAP on MS reversibility underscore the need for combined therapy with CPAP, aiming to maximize metabolic syndrome recovery in parallel with improvements in OSA severity and related symptoms,” according to their study, reported in the journal CHEST®.
Asked whether he still recommends CPAP to patients with OSA and the metabolic syndrome, given the findings, corresponding author Luciano F. Drager, MD, PhD, replied “yes, definitely.”
“Despite the modest rate in reversing metabolic syndrome after CPAP, the rate was 5-fold higher than non-effective treatment (18% vs. 4%),” he said in an interview.
Dr. Drager noted that studies of other single interventions such as physical exercise to reverse MS in patients with OSA also had modest results.
A researcher who studies the relationship between sleep, circadian rhythms, and metabolism commented that, although the patients in the CPAP group were compliant with the assigned equipment and had both reductions in apneic events and improvement in oxygen saturation, the effect of CPAP on the metabolic syndrome was rather small.
“The CPAP was doing what we thought it was supposed to do, but it didn’t have the magnitude of effect on the metabolic syndrome as I expected or I think as the authors expected,” said Deanna Arble, PhD, assistant professor of biological science at Marquette University, Milwaukee.
She noted that the study also failed to detect a significant improvement in the blood pressure component of metabolic syndrome.
“In my experience and my review of the literature, blood pressure tends to be the one that’s improved most dramatically with CPAP,” she said.
Dr. Arble was not involved in the study.
Study details
In the trial, titled TREATOSA-MS, the investigators enrolled 100 patients with a recent diagnosis of metabolic syndrome and moderate to severe OSA, defined as 15 or more apnea-hypopnea index events per hour. The patients were stratified by body mass index and then randomized to undergo therapeutic CPAP or to use nasal strips for 6 months.
At baseline and at the end of each intervention investigators measured anthropometric variables, blood pressure, glucose, and lipid profiles. They also leptin and adiponectin, body composition, food intake, physical activity, subcutaneous and abdominal fat (visceral and hepatic), and endothelial function to control for potential confounders.
As noted previously, they found that after 6 months “most patients with OSA randomized to CPAP retained the MS diagnosis, but the rate of MS reversibility was higher than observed in the placebo group.” The difference in metabolic syndrome reversal, 18% with CPAP versus 4% with nasal strips, translated into a hazard ratio favoring CPAP of 5.27 (P = .04).
Also as noted, in analyses adjusted for baseline values, CPAP did not significantly improve either weight, liver fat, lip profiles, or the adiposity biomarkers leptin and adiponectin, but did have “very modest” influence on reducing visceral fat and improving endothelial function.
Rigorous study
Dr. Arble said that most studies of the association between OSA and metabolic syndrome have focused on only one or two of the parameters that were included in the TREATOSA-MS study, giving the findings additional weight.
“This could potentially be a very good, carefully controlled first insight into how obstructive sleep apnea is related to the metabolic syndrome,” she said.
The study was funded by grants Fundação de Amparo Q22 à Pesquisa do Estado de São Paulo and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The authors and Dr. Arble reported having no conflicts of interest to disclose.
FROM CHEST
Lights on during sleep can play havoc with metabolism
“The most important finding” is that, compared with one night in a dim light environment, “one night of exposure to a moderate level of room light while sleeping with eyes closed increased heart rate and sympathetic [nervous system] activity during the entire sleep period,” said senior author Phyllis C. Zee, MD, PhD.
And on the morning following the moderate room light condition, a higher amount of insulin secretion was required to normalize glucose levels following ingestion of a bolus of glucose in an oral glucose tolerance test, consistent with higher insulin resistance, Dr. Zee, director of the center for circadian and sleep medicine at Northwestern University, Chicago, told this news organization in an email.
The study by Ivy C. Mason, PhD, also of Northwestern University, and colleagues was published March 14 in the Proceedings of the National Academy of Sciences.
Melatonin levels were similar under the two light conditions, Dr. Zee added, which “suggests that the effect of light during sleep on these cardiometabolic measures were more likely due to activation of the sympathetic [nervous] system and less likely due to changes in sleep or suppression of melatonin by light.”
“Attention to avoiding exposure to light at night during sleep may be beneficial for cardiometabolic health,” the researchers conclude.
That means “turn lights off before sleeping,” Dr. Zee elaborated. If a light is needed for safety reasons, keep it as dim as possible, she advises, and avoid exposure to blue or green light, but instead try red-amber colors.
How light during sleep may affect insulin, melatonin, heart rate
Several studies have investigated the effect of light on sleep and metabolic outcomes, the researchers explain.
In one study, light in the bedroom was associated with obesity in women, and in another study, it was associated with risk of type 2 diabetes in an elderly population.
Research has suggested that nighttime light exposure may alter glucose metabolism by increasing insulin resistance; lowering melatonin levels, which alters insulin secretion; and having an arousing effect on the sympathetic autonomic nervous system (increasing the stress hormone cortisol or heart rate, and decreasing heart rate variability).
However, the effect of a single night of moderate room light exposure across the entire nighttime sleep period has not been fully investigated.
The researchers enrolled and randomized 20 healthy young adults who were 18-40 years old and regularly went to sleep between 9 p.m. and 1 a.m. and slept 6.5-8.5 hours, to sleep 2 nights in the sleep laboratory under two conditions.
Ten participants (eight women, two men) slept in a dim light condition on night 1 and in a moderate light condition on night 2. The other 10 participants (six women, four men) slept 2 nights in the dim light condition.
The moderate light condition consisted of four 60-watt incandescent overhead ceiling light bulbs (a total of 100 lux), which “is bright enough to see, but not to read comfortably,” Dr. Zee explained. “It’s like hallway light in an apartment. But the people were sleeping, so about 90% of the light would be blocked by the eyelids.”
The dim light condition was less than 3 lux, which is dimmer than a night light.
When participants were awake, the room lighting was 240 lux.
Participants in each group were a mean age of 27 years and had a mean body mass index of 23 and 24 kg/m2.
The week before the study, participants went to bed at 11 p.m. and slept for 7 hours (based on actigraphy measures). During the laboratory stay, the participants were allowed to sleep 8 hours, during which polysomnography was performed.
They received standard meals at 2.5, 5, and 11 hours after waking and had 30 minutes to eat them. Snacking and caffeine were not permitted.
Participants were instructed to remain seated or standing in their room, but not exercise, when they were not sleeping. Blood samples to determine melatonin levels were collected hourly during wake and sleep via an intravenous line.
Participants slept for a similar time, around 7 hours, in both conditions.
Although melatonin levels were similar in both conditions, this was a relatively small sample, the researchers caution.
In the room light condition, participants spent proportionately more time in stage N2 sleep and less in slow-wave and rapid eye movement sleep. There was no increase in sleep fragmentation or arousals.
The research was partly supported by the Center for Circadian and Sleep Medicine at Northwestern University, the National Center for Advancing Translational Sciences, the National Institutes of Health, and the American Heart Association. The researchers have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“The most important finding” is that, compared with one night in a dim light environment, “one night of exposure to a moderate level of room light while sleeping with eyes closed increased heart rate and sympathetic [nervous system] activity during the entire sleep period,” said senior author Phyllis C. Zee, MD, PhD.
And on the morning following the moderate room light condition, a higher amount of insulin secretion was required to normalize glucose levels following ingestion of a bolus of glucose in an oral glucose tolerance test, consistent with higher insulin resistance, Dr. Zee, director of the center for circadian and sleep medicine at Northwestern University, Chicago, told this news organization in an email.
The study by Ivy C. Mason, PhD, also of Northwestern University, and colleagues was published March 14 in the Proceedings of the National Academy of Sciences.
Melatonin levels were similar under the two light conditions, Dr. Zee added, which “suggests that the effect of light during sleep on these cardiometabolic measures were more likely due to activation of the sympathetic [nervous] system and less likely due to changes in sleep or suppression of melatonin by light.”
“Attention to avoiding exposure to light at night during sleep may be beneficial for cardiometabolic health,” the researchers conclude.
That means “turn lights off before sleeping,” Dr. Zee elaborated. If a light is needed for safety reasons, keep it as dim as possible, she advises, and avoid exposure to blue or green light, but instead try red-amber colors.
How light during sleep may affect insulin, melatonin, heart rate
Several studies have investigated the effect of light on sleep and metabolic outcomes, the researchers explain.
In one study, light in the bedroom was associated with obesity in women, and in another study, it was associated with risk of type 2 diabetes in an elderly population.
Research has suggested that nighttime light exposure may alter glucose metabolism by increasing insulin resistance; lowering melatonin levels, which alters insulin secretion; and having an arousing effect on the sympathetic autonomic nervous system (increasing the stress hormone cortisol or heart rate, and decreasing heart rate variability).
However, the effect of a single night of moderate room light exposure across the entire nighttime sleep period has not been fully investigated.
The researchers enrolled and randomized 20 healthy young adults who were 18-40 years old and regularly went to sleep between 9 p.m. and 1 a.m. and slept 6.5-8.5 hours, to sleep 2 nights in the sleep laboratory under two conditions.
Ten participants (eight women, two men) slept in a dim light condition on night 1 and in a moderate light condition on night 2. The other 10 participants (six women, four men) slept 2 nights in the dim light condition.
The moderate light condition consisted of four 60-watt incandescent overhead ceiling light bulbs (a total of 100 lux), which “is bright enough to see, but not to read comfortably,” Dr. Zee explained. “It’s like hallway light in an apartment. But the people were sleeping, so about 90% of the light would be blocked by the eyelids.”
The dim light condition was less than 3 lux, which is dimmer than a night light.
When participants were awake, the room lighting was 240 lux.
Participants in each group were a mean age of 27 years and had a mean body mass index of 23 and 24 kg/m2.
The week before the study, participants went to bed at 11 p.m. and slept for 7 hours (based on actigraphy measures). During the laboratory stay, the participants were allowed to sleep 8 hours, during which polysomnography was performed.
They received standard meals at 2.5, 5, and 11 hours after waking and had 30 minutes to eat them. Snacking and caffeine were not permitted.
Participants were instructed to remain seated or standing in their room, but not exercise, when they were not sleeping. Blood samples to determine melatonin levels were collected hourly during wake and sleep via an intravenous line.
Participants slept for a similar time, around 7 hours, in both conditions.
Although melatonin levels were similar in both conditions, this was a relatively small sample, the researchers caution.
In the room light condition, participants spent proportionately more time in stage N2 sleep and less in slow-wave and rapid eye movement sleep. There was no increase in sleep fragmentation or arousals.
The research was partly supported by the Center for Circadian and Sleep Medicine at Northwestern University, the National Center for Advancing Translational Sciences, the National Institutes of Health, and the American Heart Association. The researchers have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“The most important finding” is that, compared with one night in a dim light environment, “one night of exposure to a moderate level of room light while sleeping with eyes closed increased heart rate and sympathetic [nervous system] activity during the entire sleep period,” said senior author Phyllis C. Zee, MD, PhD.
And on the morning following the moderate room light condition, a higher amount of insulin secretion was required to normalize glucose levels following ingestion of a bolus of glucose in an oral glucose tolerance test, consistent with higher insulin resistance, Dr. Zee, director of the center for circadian and sleep medicine at Northwestern University, Chicago, told this news organization in an email.
The study by Ivy C. Mason, PhD, also of Northwestern University, and colleagues was published March 14 in the Proceedings of the National Academy of Sciences.
Melatonin levels were similar under the two light conditions, Dr. Zee added, which “suggests that the effect of light during sleep on these cardiometabolic measures were more likely due to activation of the sympathetic [nervous] system and less likely due to changes in sleep or suppression of melatonin by light.”
“Attention to avoiding exposure to light at night during sleep may be beneficial for cardiometabolic health,” the researchers conclude.
That means “turn lights off before sleeping,” Dr. Zee elaborated. If a light is needed for safety reasons, keep it as dim as possible, she advises, and avoid exposure to blue or green light, but instead try red-amber colors.
How light during sleep may affect insulin, melatonin, heart rate
Several studies have investigated the effect of light on sleep and metabolic outcomes, the researchers explain.
In one study, light in the bedroom was associated with obesity in women, and in another study, it was associated with risk of type 2 diabetes in an elderly population.
Research has suggested that nighttime light exposure may alter glucose metabolism by increasing insulin resistance; lowering melatonin levels, which alters insulin secretion; and having an arousing effect on the sympathetic autonomic nervous system (increasing the stress hormone cortisol or heart rate, and decreasing heart rate variability).
However, the effect of a single night of moderate room light exposure across the entire nighttime sleep period has not been fully investigated.
The researchers enrolled and randomized 20 healthy young adults who were 18-40 years old and regularly went to sleep between 9 p.m. and 1 a.m. and slept 6.5-8.5 hours, to sleep 2 nights in the sleep laboratory under two conditions.
Ten participants (eight women, two men) slept in a dim light condition on night 1 and in a moderate light condition on night 2. The other 10 participants (six women, four men) slept 2 nights in the dim light condition.
The moderate light condition consisted of four 60-watt incandescent overhead ceiling light bulbs (a total of 100 lux), which “is bright enough to see, but not to read comfortably,” Dr. Zee explained. “It’s like hallway light in an apartment. But the people were sleeping, so about 90% of the light would be blocked by the eyelids.”
The dim light condition was less than 3 lux, which is dimmer than a night light.
When participants were awake, the room lighting was 240 lux.
Participants in each group were a mean age of 27 years and had a mean body mass index of 23 and 24 kg/m2.
The week before the study, participants went to bed at 11 p.m. and slept for 7 hours (based on actigraphy measures). During the laboratory stay, the participants were allowed to sleep 8 hours, during which polysomnography was performed.
They received standard meals at 2.5, 5, and 11 hours after waking and had 30 minutes to eat them. Snacking and caffeine were not permitted.
Participants were instructed to remain seated or standing in their room, but not exercise, when they were not sleeping. Blood samples to determine melatonin levels were collected hourly during wake and sleep via an intravenous line.
Participants slept for a similar time, around 7 hours, in both conditions.
Although melatonin levels were similar in both conditions, this was a relatively small sample, the researchers caution.
In the room light condition, participants spent proportionately more time in stage N2 sleep and less in slow-wave and rapid eye movement sleep. There was no increase in sleep fragmentation or arousals.
The research was partly supported by the Center for Circadian and Sleep Medicine at Northwestern University, the National Center for Advancing Translational Sciences, the National Institutes of Health, and the American Heart Association. The researchers have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PROCEEDINGS OF THE NATIONAL ACADEMY OF SCIENCES
Targeting the endocannabinoid system in migraine
, according to Italian researchers at the University of Pavia, and the C. Mondino National Institute of Neurology Foundation. “The complexity of the endocannabinoid system calls for accurate biochemical and pharmacological characterization of any new compounds undergoing testing and development,” noted Rosaria Greco, PhD. She and her colleagues authored a review on the topic that was published online Feb. 18, 2022, in Headache.
Although cannabis has been investigated for both the treatment and prevention of migraine, evidence for its benefit is weak because of lack of controlled studies, they explained. Archival data from a large database “showed greater improvements in men than in women and suggested that concentrated preparations were more effective than flower consumption.” In addition, a small single-center study linked nabilone, a synthetic cannabinoid, to reductions in pain duration, intensity, and daily intake of analgesics among patients with medication overuse headache. Finally, a pilot study reported a reduction in pain intensity among patients with chronic migraine treated with a combination of tested a combination of delta-9-tetrahydrocannabinol and cannabidiol. “Methodologically sound studies are now needed to investigate the possible effects of cannabis in migraine treatment and to define strains, formulations, and dosage,” they noted.
Not just cannabis
In addition to exogenous cannabis, there are now preclinical studies suggesting other compounds that interact with the endocannabinoid system “are also able to modulate the pathways involved in migraine-related pain,” the study authors wrote. “But the road ahead is still long. Multiple molecules linked to the endocannabinoid system have emerged as potential therapeutic targets.
The complexity of the system demands caution and precise biochemical and pharmacological characterization of the new compounds to be tested and developed.”
Among these compounds are endogenous ligands such as N-arachidonoylethanolamine (anandamide) and 2-arachidonoylglycerol that specifically target CB1 and CB2 receptors. Additionally, there are endocannabinoid-based drugs that also target the CB1/CB2 receptors, as well as other substances, such as lipids (palmitoylethanolamide [PEA]) and enzymes, that do not bind to the CB1/CB2 receptors but are responsible for endocannabinoid biosynthesis.
There is some evidence that the endocannabinoid system may be dysfunctional in patients with migraine, and the authors noted their work has shown that PEA plasma levels are increased during experimentally triggered migraine-like attacks. Thus, some preclinical and preliminary evidence suggests that administration of PEA or anandamide may have analgesic and anti-inflammatory effects in migraine.
Another approach is the inhibition of endocannabinoid catabolic enzymes, which could circumvent the adverse effects associated with direct activation of CB receptors. “Endocannabinoid tone enhancement has been proposed as an alternative modality of activation of CB receptors and is possibly devoid of the psychotropic effects reported with CB receptor agonists,” noted the authors, who have shown in animal and preclinical studies that inhibition of fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase can modulate migraine pain.
Yet another way of indirectly impacting CB receptors is through their allosteric ligands, an approach that “deserves further investigation”, and “might provide interesting leads for clinical development, given that it may have a favorable side-effect profile with limited psychomimetic and depressant effects,” wrote the authors. And finally, inhibition of N-acylethanolamine acid amide hydrolase, the enzyme that preferentially hydrolyzes PEA, might be a promising approach.
“The multiplicity of options and the wealth of data already obtained in animal models underscore the importance of further advancing research in this area,” the authors concluded.
Patients are taking cannabinoids; physicians should learn about them
Commenting on the paper, Alan Rapaport, MD, clinical professor of neurology at the University of California, Los Angeles, said “this well-done paper points out the complexity of the endocannabinoid system and the multiple ways of getting it to work for certain patients. It details some of the studies that show beneficial results in migraine, medication overuse headache, chronic migraine, and pain. Patients with headache, other types of pain, anxiety, nausea, sleep issues, and other symptoms are already taking cannabinoids, usually derived from the marijuana plant, that are not well regulated. A few are prescribed drugs which target CB1 and CB2 receptors. Patients often get relief of some of their symptoms, sometimes getting high and many times not.
“The paper makes the point that previous studies are often small, not carefully controlled, or well documented. We do need to start doing larger, properly designed studies and getting them into the literature. Doctors need to learn more about these treatments. The next step will be to get [Food and Drug Administration]–approved treatments, so physicians and nurses will know exactly what we are giving, the beneficial effects to expect in a certain percentage of patients, and the adverse events to warn our patients about. Cannabinoids have been tried by a large percentage of patients with headache and pain. Now we need to standardize the various treatments that are sure to be suggested in the future.”
The study was funded by the Migraine Research Foundation, and the Italian Ministry of Health. The study authors declared no conflicts of interest.
, according to Italian researchers at the University of Pavia, and the C. Mondino National Institute of Neurology Foundation. “The complexity of the endocannabinoid system calls for accurate biochemical and pharmacological characterization of any new compounds undergoing testing and development,” noted Rosaria Greco, PhD. She and her colleagues authored a review on the topic that was published online Feb. 18, 2022, in Headache.
Although cannabis has been investigated for both the treatment and prevention of migraine, evidence for its benefit is weak because of lack of controlled studies, they explained. Archival data from a large database “showed greater improvements in men than in women and suggested that concentrated preparations were more effective than flower consumption.” In addition, a small single-center study linked nabilone, a synthetic cannabinoid, to reductions in pain duration, intensity, and daily intake of analgesics among patients with medication overuse headache. Finally, a pilot study reported a reduction in pain intensity among patients with chronic migraine treated with a combination of tested a combination of delta-9-tetrahydrocannabinol and cannabidiol. “Methodologically sound studies are now needed to investigate the possible effects of cannabis in migraine treatment and to define strains, formulations, and dosage,” they noted.
Not just cannabis
In addition to exogenous cannabis, there are now preclinical studies suggesting other compounds that interact with the endocannabinoid system “are also able to modulate the pathways involved in migraine-related pain,” the study authors wrote. “But the road ahead is still long. Multiple molecules linked to the endocannabinoid system have emerged as potential therapeutic targets.
The complexity of the system demands caution and precise biochemical and pharmacological characterization of the new compounds to be tested and developed.”
Among these compounds are endogenous ligands such as N-arachidonoylethanolamine (anandamide) and 2-arachidonoylglycerol that specifically target CB1 and CB2 receptors. Additionally, there are endocannabinoid-based drugs that also target the CB1/CB2 receptors, as well as other substances, such as lipids (palmitoylethanolamide [PEA]) and enzymes, that do not bind to the CB1/CB2 receptors but are responsible for endocannabinoid biosynthesis.
There is some evidence that the endocannabinoid system may be dysfunctional in patients with migraine, and the authors noted their work has shown that PEA plasma levels are increased during experimentally triggered migraine-like attacks. Thus, some preclinical and preliminary evidence suggests that administration of PEA or anandamide may have analgesic and anti-inflammatory effects in migraine.
Another approach is the inhibition of endocannabinoid catabolic enzymes, which could circumvent the adverse effects associated with direct activation of CB receptors. “Endocannabinoid tone enhancement has been proposed as an alternative modality of activation of CB receptors and is possibly devoid of the psychotropic effects reported with CB receptor agonists,” noted the authors, who have shown in animal and preclinical studies that inhibition of fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase can modulate migraine pain.
Yet another way of indirectly impacting CB receptors is through their allosteric ligands, an approach that “deserves further investigation”, and “might provide interesting leads for clinical development, given that it may have a favorable side-effect profile with limited psychomimetic and depressant effects,” wrote the authors. And finally, inhibition of N-acylethanolamine acid amide hydrolase, the enzyme that preferentially hydrolyzes PEA, might be a promising approach.
“The multiplicity of options and the wealth of data already obtained in animal models underscore the importance of further advancing research in this area,” the authors concluded.
Patients are taking cannabinoids; physicians should learn about them
Commenting on the paper, Alan Rapaport, MD, clinical professor of neurology at the University of California, Los Angeles, said “this well-done paper points out the complexity of the endocannabinoid system and the multiple ways of getting it to work for certain patients. It details some of the studies that show beneficial results in migraine, medication overuse headache, chronic migraine, and pain. Patients with headache, other types of pain, anxiety, nausea, sleep issues, and other symptoms are already taking cannabinoids, usually derived from the marijuana plant, that are not well regulated. A few are prescribed drugs which target CB1 and CB2 receptors. Patients often get relief of some of their symptoms, sometimes getting high and many times not.
“The paper makes the point that previous studies are often small, not carefully controlled, or well documented. We do need to start doing larger, properly designed studies and getting them into the literature. Doctors need to learn more about these treatments. The next step will be to get [Food and Drug Administration]–approved treatments, so physicians and nurses will know exactly what we are giving, the beneficial effects to expect in a certain percentage of patients, and the adverse events to warn our patients about. Cannabinoids have been tried by a large percentage of patients with headache and pain. Now we need to standardize the various treatments that are sure to be suggested in the future.”
The study was funded by the Migraine Research Foundation, and the Italian Ministry of Health. The study authors declared no conflicts of interest.
, according to Italian researchers at the University of Pavia, and the C. Mondino National Institute of Neurology Foundation. “The complexity of the endocannabinoid system calls for accurate biochemical and pharmacological characterization of any new compounds undergoing testing and development,” noted Rosaria Greco, PhD. She and her colleagues authored a review on the topic that was published online Feb. 18, 2022, in Headache.
Although cannabis has been investigated for both the treatment and prevention of migraine, evidence for its benefit is weak because of lack of controlled studies, they explained. Archival data from a large database “showed greater improvements in men than in women and suggested that concentrated preparations were more effective than flower consumption.” In addition, a small single-center study linked nabilone, a synthetic cannabinoid, to reductions in pain duration, intensity, and daily intake of analgesics among patients with medication overuse headache. Finally, a pilot study reported a reduction in pain intensity among patients with chronic migraine treated with a combination of tested a combination of delta-9-tetrahydrocannabinol and cannabidiol. “Methodologically sound studies are now needed to investigate the possible effects of cannabis in migraine treatment and to define strains, formulations, and dosage,” they noted.
Not just cannabis
In addition to exogenous cannabis, there are now preclinical studies suggesting other compounds that interact with the endocannabinoid system “are also able to modulate the pathways involved in migraine-related pain,” the study authors wrote. “But the road ahead is still long. Multiple molecules linked to the endocannabinoid system have emerged as potential therapeutic targets.
The complexity of the system demands caution and precise biochemical and pharmacological characterization of the new compounds to be tested and developed.”
Among these compounds are endogenous ligands such as N-arachidonoylethanolamine (anandamide) and 2-arachidonoylglycerol that specifically target CB1 and CB2 receptors. Additionally, there are endocannabinoid-based drugs that also target the CB1/CB2 receptors, as well as other substances, such as lipids (palmitoylethanolamide [PEA]) and enzymes, that do not bind to the CB1/CB2 receptors but are responsible for endocannabinoid biosynthesis.
There is some evidence that the endocannabinoid system may be dysfunctional in patients with migraine, and the authors noted their work has shown that PEA plasma levels are increased during experimentally triggered migraine-like attacks. Thus, some preclinical and preliminary evidence suggests that administration of PEA or anandamide may have analgesic and anti-inflammatory effects in migraine.
Another approach is the inhibition of endocannabinoid catabolic enzymes, which could circumvent the adverse effects associated with direct activation of CB receptors. “Endocannabinoid tone enhancement has been proposed as an alternative modality of activation of CB receptors and is possibly devoid of the psychotropic effects reported with CB receptor agonists,” noted the authors, who have shown in animal and preclinical studies that inhibition of fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase can modulate migraine pain.
Yet another way of indirectly impacting CB receptors is through their allosteric ligands, an approach that “deserves further investigation”, and “might provide interesting leads for clinical development, given that it may have a favorable side-effect profile with limited psychomimetic and depressant effects,” wrote the authors. And finally, inhibition of N-acylethanolamine acid amide hydrolase, the enzyme that preferentially hydrolyzes PEA, might be a promising approach.
“The multiplicity of options and the wealth of data already obtained in animal models underscore the importance of further advancing research in this area,” the authors concluded.
Patients are taking cannabinoids; physicians should learn about them
Commenting on the paper, Alan Rapaport, MD, clinical professor of neurology at the University of California, Los Angeles, said “this well-done paper points out the complexity of the endocannabinoid system and the multiple ways of getting it to work for certain patients. It details some of the studies that show beneficial results in migraine, medication overuse headache, chronic migraine, and pain. Patients with headache, other types of pain, anxiety, nausea, sleep issues, and other symptoms are already taking cannabinoids, usually derived from the marijuana plant, that are not well regulated. A few are prescribed drugs which target CB1 and CB2 receptors. Patients often get relief of some of their symptoms, sometimes getting high and many times not.
“The paper makes the point that previous studies are often small, not carefully controlled, or well documented. We do need to start doing larger, properly designed studies and getting them into the literature. Doctors need to learn more about these treatments. The next step will be to get [Food and Drug Administration]–approved treatments, so physicians and nurses will know exactly what we are giving, the beneficial effects to expect in a certain percentage of patients, and the adverse events to warn our patients about. Cannabinoids have been tried by a large percentage of patients with headache and pain. Now we need to standardize the various treatments that are sure to be suggested in the future.”
The study was funded by the Migraine Research Foundation, and the Italian Ministry of Health. The study authors declared no conflicts of interest.
FROM HEADACHE
Real-world data support safety of newer LAA device
More than 18 months after the Watchman FLX device was licensed by the Food and Drug Administration for closure of the left atrial appendage (LAA), a prospective analysis of registry data presented at CRT 2022, sponsored by MedStar Heart & Vascular Institute, supports its safely outside of the clinical trial setting.
The data, drawn from the LAA occlusion registry of the National Cardiovascular Data Registry, showed a mortality rate at 45 days of under 1.0%, which was consistent with the acceptably low rate of other adverse events, according to Samir R. Kapadia, MD, chair of cardiovascular medicine at the Cleveland Clinic.

Only 0.5% had a pericardial effusion within 45 days of LAA closure that required intervention. Of those without effusion, 95% had a leak of less than 3 mm and 82% had no leak at all, according to Dr. Kapadia.
Patients enrolled in this analysis, called SURPASS (Surveillance Post Approval Analysis Plan), had undergone left atrial closure with the device from August 2020 to September 2022. There were no exclusion criteria. Ultimately, 2 years of follow-up is planned.
With more than 16,000 patients enrolled, the data on 14,363 patients in this initial 45-day analysis represents “the largest number of Watchman FLX patients evaluated to date,” Dr. Kapadia reported.
Device implantation success 97.5%
The Watchman FLX, which is delivered to the left atrial appendage by a transcatheter approach, was deployed successfully in 97.5% of all 16,048 patients enrolled in the registry. In the 398 cases without successful deployment, the anatomy was not conducive in nearly 70%. Other reasons included failure to meet device-release criteria and change in patient condition.
The outcomes of interest at 45 days were ischemic strokes, systemic emboli, device-related thrombi, device embolization, and bleeding. The primary endpoints at 2 years will be strokes and thrombotic events.
For stroke, the incidence within 45 days was 0.39%. About 25% of the strokes were hemorrhagic and the remainder were ischemic. There was 1 systemic embolism (0.01%), 5 device embolizations (0.03%), and 30 device-related thrombotic events (0.24%). Major bleeding occurred in 508 patients (3.55%).
For context, Dr. Kapadia compared these results to those observed in the PINNACLE FLX trial, which was a nonrandomized but prospective study of the Watchman FLX published about 1 year ago. In PINNACLE FLX, the enrollment was open to patients indicated for oral anticoagulation but who had an appropriate rationale for seeking a nonpharmacological alternative.
Taken from different studies, the outcomes at 45 days should not be construed as a direct comparison, but the similarity of the results can be considered reassuring, according to Dr. Kapadia.
For the composite safety endpoint of all-cause death, ischemic stroke, systemic embolism, or implantation-related events requiring intervention, the rates in SURPASS (0.4%) and PINNACLE FLX (0.5%) were nearly identical. Device leak rates (82.0% vs. 82.8%), stroke rates (0.4% vs. 0.7%), and all-cause death rates (0.9% vs. 0.5%) were also similar.
The similarity of the SURPASS and PINNACLE FLX data provides another level of reassurance.
“The SURPASS registry confirms the safety of the Watchman Flex in the real-world experience when the device is being used by many different operators in a large patient population,” Dr. Kapadia said in an interview.
In “appropriately selected patients,” the SURPASS data confirm that the Watchman FLX device “provides a safe and effective treatment option,” he added.
Relative to the PINNACLE FLX study, which enrolled 400 patients, it is noteworthy that the median age in SURPASS was older (76 vs. 73.8 years), a potential disadvantage in demonstrating comparable safety. The proportion of non-White patients was similar (6.7% vs. 6.3%). SURPASS had a higher proportion of women (40% vs. 35.5%).

The SURPASS data are credible, according to Vivek Y. Reddy, MD, director of cardiac arrhythmia services, Mount Sinai Health System, New York.
“While there are certainly limitations to registry data, I do feel pretty confident that these procedural complication and success rates [in SURPASS] do indeed reflect reality,” said Dr. Reddy, who was a coauthor of the PINNACLE FLX trial. In general, the SURPASS data “mirror most of our clinical experiences in routine clinical practice.”
With these registry data backing up multiple clinical studies, Dr. Reddy concluded, “I do believe that it is fair to say that Watchman-FLX implantation is a quite safe procedure.”
Dr. Kapadia reported no potential conflicts of interest. Dr. Reddy reported a financial relationship with Boston Scientific.
More than 18 months after the Watchman FLX device was licensed by the Food and Drug Administration for closure of the left atrial appendage (LAA), a prospective analysis of registry data presented at CRT 2022, sponsored by MedStar Heart & Vascular Institute, supports its safely outside of the clinical trial setting.
The data, drawn from the LAA occlusion registry of the National Cardiovascular Data Registry, showed a mortality rate at 45 days of under 1.0%, which was consistent with the acceptably low rate of other adverse events, according to Samir R. Kapadia, MD, chair of cardiovascular medicine at the Cleveland Clinic.
Only 0.5% had a pericardial effusion within 45 days of LAA closure that required intervention. Of those without effusion, 95% had a leak of less than 3 mm and 82% had no leak at all, according to Dr. Kapadia.
Patients enrolled in this analysis, called SURPASS (Surveillance Post Approval Analysis Plan), had undergone left atrial closure with the device from August 2020 to September 2022. There were no exclusion criteria. Ultimately, 2 years of follow-up is planned.
With more than 16,000 patients enrolled, the data on 14,363 patients in this initial 45-day analysis represents “the largest number of Watchman FLX patients evaluated to date,” Dr. Kapadia reported.
Device implantation success 97.5%
The Watchman FLX, which is delivered to the left atrial appendage by a transcatheter approach, was deployed successfully in 97.5% of all 16,048 patients enrolled in the registry. In the 398 cases without successful deployment, the anatomy was not conducive in nearly 70%. Other reasons included failure to meet device-release criteria and change in patient condition.
The outcomes of interest at 45 days were ischemic strokes, systemic emboli, device-related thrombi, device embolization, and bleeding. The primary endpoints at 2 years will be strokes and thrombotic events.
For stroke, the incidence within 45 days was 0.39%. About 25% of the strokes were hemorrhagic and the remainder were ischemic. There was 1 systemic embolism (0.01%), 5 device embolizations (0.03%), and 30 device-related thrombotic events (0.24%). Major bleeding occurred in 508 patients (3.55%).
For context, Dr. Kapadia compared these results to those observed in the PINNACLE FLX trial, which was a nonrandomized but prospective study of the Watchman FLX published about 1 year ago. In PINNACLE FLX, the enrollment was open to patients indicated for oral anticoagulation but who had an appropriate rationale for seeking a nonpharmacological alternative.
Taken from different studies, the outcomes at 45 days should not be construed as a direct comparison, but the similarity of the results can be considered reassuring, according to Dr. Kapadia.
For the composite safety endpoint of all-cause death, ischemic stroke, systemic embolism, or implantation-related events requiring intervention, the rates in SURPASS (0.4%) and PINNACLE FLX (0.5%) were nearly identical. Device leak rates (82.0% vs. 82.8%), stroke rates (0.4% vs. 0.7%), and all-cause death rates (0.9% vs. 0.5%) were also similar.
The similarity of the SURPASS and PINNACLE FLX data provides another level of reassurance.
“The SURPASS registry confirms the safety of the Watchman Flex in the real-world experience when the device is being used by many different operators in a large patient population,” Dr. Kapadia said in an interview.
In “appropriately selected patients,” the SURPASS data confirm that the Watchman FLX device “provides a safe and effective treatment option,” he added.
Relative to the PINNACLE FLX study, which enrolled 400 patients, it is noteworthy that the median age in SURPASS was older (76 vs. 73.8 years), a potential disadvantage in demonstrating comparable safety. The proportion of non-White patients was similar (6.7% vs. 6.3%). SURPASS had a higher proportion of women (40% vs. 35.5%).
The SURPASS data are credible, according to Vivek Y. Reddy, MD, director of cardiac arrhythmia services, Mount Sinai Health System, New York.
“While there are certainly limitations to registry data, I do feel pretty confident that these procedural complication and success rates [in SURPASS] do indeed reflect reality,” said Dr. Reddy, who was a coauthor of the PINNACLE FLX trial. In general, the SURPASS data “mirror most of our clinical experiences in routine clinical practice.”
With these registry data backing up multiple clinical studies, Dr. Reddy concluded, “I do believe that it is fair to say that Watchman-FLX implantation is a quite safe procedure.”
Dr. Kapadia reported no potential conflicts of interest. Dr. Reddy reported a financial relationship with Boston Scientific.
More than 18 months after the Watchman FLX device was licensed by the Food and Drug Administration for closure of the left atrial appendage (LAA), a prospective analysis of registry data presented at CRT 2022, sponsored by MedStar Heart & Vascular Institute, supports its safely outside of the clinical trial setting.
The data, drawn from the LAA occlusion registry of the National Cardiovascular Data Registry, showed a mortality rate at 45 days of under 1.0%, which was consistent with the acceptably low rate of other adverse events, according to Samir R. Kapadia, MD, chair of cardiovascular medicine at the Cleveland Clinic.
Only 0.5% had a pericardial effusion within 45 days of LAA closure that required intervention. Of those without effusion, 95% had a leak of less than 3 mm and 82% had no leak at all, according to Dr. Kapadia.
Patients enrolled in this analysis, called SURPASS (Surveillance Post Approval Analysis Plan), had undergone left atrial closure with the device from August 2020 to September 2022. There were no exclusion criteria. Ultimately, 2 years of follow-up is planned.
With more than 16,000 patients enrolled, the data on 14,363 patients in this initial 45-day analysis represents “the largest number of Watchman FLX patients evaluated to date,” Dr. Kapadia reported.
Device implantation success 97.5%
The Watchman FLX, which is delivered to the left atrial appendage by a transcatheter approach, was deployed successfully in 97.5% of all 16,048 patients enrolled in the registry. In the 398 cases without successful deployment, the anatomy was not conducive in nearly 70%. Other reasons included failure to meet device-release criteria and change in patient condition.
The outcomes of interest at 45 days were ischemic strokes, systemic emboli, device-related thrombi, device embolization, and bleeding. The primary endpoints at 2 years will be strokes and thrombotic events.
For stroke, the incidence within 45 days was 0.39%. About 25% of the strokes were hemorrhagic and the remainder were ischemic. There was 1 systemic embolism (0.01%), 5 device embolizations (0.03%), and 30 device-related thrombotic events (0.24%). Major bleeding occurred in 508 patients (3.55%).
For context, Dr. Kapadia compared these results to those observed in the PINNACLE FLX trial, which was a nonrandomized but prospective study of the Watchman FLX published about 1 year ago. In PINNACLE FLX, the enrollment was open to patients indicated for oral anticoagulation but who had an appropriate rationale for seeking a nonpharmacological alternative.
Taken from different studies, the outcomes at 45 days should not be construed as a direct comparison, but the similarity of the results can be considered reassuring, according to Dr. Kapadia.
For the composite safety endpoint of all-cause death, ischemic stroke, systemic embolism, or implantation-related events requiring intervention, the rates in SURPASS (0.4%) and PINNACLE FLX (0.5%) were nearly identical. Device leak rates (82.0% vs. 82.8%), stroke rates (0.4% vs. 0.7%), and all-cause death rates (0.9% vs. 0.5%) were also similar.
The similarity of the SURPASS and PINNACLE FLX data provides another level of reassurance.
“The SURPASS registry confirms the safety of the Watchman Flex in the real-world experience when the device is being used by many different operators in a large patient population,” Dr. Kapadia said in an interview.
In “appropriately selected patients,” the SURPASS data confirm that the Watchman FLX device “provides a safe and effective treatment option,” he added.
Relative to the PINNACLE FLX study, which enrolled 400 patients, it is noteworthy that the median age in SURPASS was older (76 vs. 73.8 years), a potential disadvantage in demonstrating comparable safety. The proportion of non-White patients was similar (6.7% vs. 6.3%). SURPASS had a higher proportion of women (40% vs. 35.5%).
The SURPASS data are credible, according to Vivek Y. Reddy, MD, director of cardiac arrhythmia services, Mount Sinai Health System, New York.
“While there are certainly limitations to registry data, I do feel pretty confident that these procedural complication and success rates [in SURPASS] do indeed reflect reality,” said Dr. Reddy, who was a coauthor of the PINNACLE FLX trial. In general, the SURPASS data “mirror most of our clinical experiences in routine clinical practice.”
With these registry data backing up multiple clinical studies, Dr. Reddy concluded, “I do believe that it is fair to say that Watchman-FLX implantation is a quite safe procedure.”
Dr. Kapadia reported no potential conflicts of interest. Dr. Reddy reported a financial relationship with Boston Scientific.
FROM CRT 2022
Can green tea extract protect against colorectal adenomas?
Green tea extract (GTE) does not appear to protect against colorectal adenoma recurrence, according to a study from Germany.
Preclinical, epidemiologic, and small clinical studies have suggested that GTE and its major active component, epigallocatechin gallate (EGCG), have antineoplastic effects in the colon and rectum.
But the new study found no statistically significant difference in adenoma recurrence in people who took GTE, standardized to 150 mg EGCG, twice daily for 3 years, relative to those who took matching placebo.
However, there was a suggestion of possible benefit in men but not women, which requires further study, Thomas Seufferlein, MD, with Ulm University Hospital, Baden-Württemberg, Germany, and colleagues write.
Their study was published online in The American Journal of Gastroenterology.
Largest trial to date
The MIRACLE trial (Minimizing the Risk of Metachronous Adenomas of the Colorectum With Green Tea Extract) included 879 adults aged 50-80 years. Participants had undergone removal of one or more histologically confirmed colorectal adenomas within 6 months prior to recruitment during colonoscopy, and there were no remaining colorectal adenomas.
There were 432 patients in the GTE group and 447 in the placebo group. Baseline characteristics were well balanced between the groups, and overall adherence to the study protocol was good.
After 3 years, adenomas were detected in 55.7% of participants in the placebo group and in 51.1% of those in the GTE group in the modified intention-to-treat population. This absolute difference of 4.6% in favor of GTE was not statistically significant.
The per protocol analysis also did not show a significant effect of GTE on new adenoma formation in the whole study population.
However, a preplanned subgroup analysis revealed a significant difference in the adenoma recurrence rate in favor of GTE in men but not women.
In men, GTE intake was associated with a significant 12.4% relative and 7.5% absolute reduction of metachronous adenomas, they report.
This potential gender-specific difference in chemoprevention “warrants further investigations,” the study team writes.
The safety profile of GTE as taken in this trial was good, with only grade 1/2 elevations in liver enzymes in the GTE group, compared with the placebo group. However, because the follow-up period was limited to 3 years, the long-term safety of GTE cannot be determined.
The researchers write that, to their knowledge, this study is the largest randomized trial to date of the effect of GTE on adenoma recurrence in a colorectal cancer screening population consisting of White patients.
Caveats and cautionary notes
Reached for comment, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, noted that “although the study showed no significant differences, the time horizon to show benefit may be longer than the 3-year duration of the study.”
“There are also methodologic issues with the readjustment of the target sample size, which may have led to a type II error, related to underpowering of the sample size,” said Dr. Johnson, who wasn’t involved in the study.
The researchers write that the study initially generated “great interest” and that many centers applied to participate. However, “quite a few” centers did not meet their promised recruitment targets and had to be replaced. Therefore, the statistical analysis plan had to be modified, and the number of participants had to be reduced over the course of the trial, they note.
Dr. Johnson also cautioned that while green tea is a popular drink, “there is strong evidence that green tea extract, found in many herbal and dietary supplements, is among the leading causes listed for drug-induced liver injury, including acute liver failure, urgent liver transplantation, and death.”
The study was fully funded by a grant from German Cancer Aid. The investigators and Dr. Johnson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Green tea extract (GTE) does not appear to protect against colorectal adenoma recurrence, according to a study from Germany.
Preclinical, epidemiologic, and small clinical studies have suggested that GTE and its major active component, epigallocatechin gallate (EGCG), have antineoplastic effects in the colon and rectum.
But the new study found no statistically significant difference in adenoma recurrence in people who took GTE, standardized to 150 mg EGCG, twice daily for 3 years, relative to those who took matching placebo.
However, there was a suggestion of possible benefit in men but not women, which requires further study, Thomas Seufferlein, MD, with Ulm University Hospital, Baden-Württemberg, Germany, and colleagues write.
Their study was published online in The American Journal of Gastroenterology.
Largest trial to date
The MIRACLE trial (Minimizing the Risk of Metachronous Adenomas of the Colorectum With Green Tea Extract) included 879 adults aged 50-80 years. Participants had undergone removal of one or more histologically confirmed colorectal adenomas within 6 months prior to recruitment during colonoscopy, and there were no remaining colorectal adenomas.
There were 432 patients in the GTE group and 447 in the placebo group. Baseline characteristics were well balanced between the groups, and overall adherence to the study protocol was good.
After 3 years, adenomas were detected in 55.7% of participants in the placebo group and in 51.1% of those in the GTE group in the modified intention-to-treat population. This absolute difference of 4.6% in favor of GTE was not statistically significant.
The per protocol analysis also did not show a significant effect of GTE on new adenoma formation in the whole study population.
However, a preplanned subgroup analysis revealed a significant difference in the adenoma recurrence rate in favor of GTE in men but not women.
In men, GTE intake was associated with a significant 12.4% relative and 7.5% absolute reduction of metachronous adenomas, they report.
This potential gender-specific difference in chemoprevention “warrants further investigations,” the study team writes.
The safety profile of GTE as taken in this trial was good, with only grade 1/2 elevations in liver enzymes in the GTE group, compared with the placebo group. However, because the follow-up period was limited to 3 years, the long-term safety of GTE cannot be determined.
The researchers write that, to their knowledge, this study is the largest randomized trial to date of the effect of GTE on adenoma recurrence in a colorectal cancer screening population consisting of White patients.
Caveats and cautionary notes
Reached for comment, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, noted that “although the study showed no significant differences, the time horizon to show benefit may be longer than the 3-year duration of the study.”
“There are also methodologic issues with the readjustment of the target sample size, which may have led to a type II error, related to underpowering of the sample size,” said Dr. Johnson, who wasn’t involved in the study.
The researchers write that the study initially generated “great interest” and that many centers applied to participate. However, “quite a few” centers did not meet their promised recruitment targets and had to be replaced. Therefore, the statistical analysis plan had to be modified, and the number of participants had to be reduced over the course of the trial, they note.
Dr. Johnson also cautioned that while green tea is a popular drink, “there is strong evidence that green tea extract, found in many herbal and dietary supplements, is among the leading causes listed for drug-induced liver injury, including acute liver failure, urgent liver transplantation, and death.”
The study was fully funded by a grant from German Cancer Aid. The investigators and Dr. Johnson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Green tea extract (GTE) does not appear to protect against colorectal adenoma recurrence, according to a study from Germany.
Preclinical, epidemiologic, and small clinical studies have suggested that GTE and its major active component, epigallocatechin gallate (EGCG), have antineoplastic effects in the colon and rectum.
But the new study found no statistically significant difference in adenoma recurrence in people who took GTE, standardized to 150 mg EGCG, twice daily for 3 years, relative to those who took matching placebo.
However, there was a suggestion of possible benefit in men but not women, which requires further study, Thomas Seufferlein, MD, with Ulm University Hospital, Baden-Württemberg, Germany, and colleagues write.
Their study was published online in The American Journal of Gastroenterology.
Largest trial to date
The MIRACLE trial (Minimizing the Risk of Metachronous Adenomas of the Colorectum With Green Tea Extract) included 879 adults aged 50-80 years. Participants had undergone removal of one or more histologically confirmed colorectal adenomas within 6 months prior to recruitment during colonoscopy, and there were no remaining colorectal adenomas.
There were 432 patients in the GTE group and 447 in the placebo group. Baseline characteristics were well balanced between the groups, and overall adherence to the study protocol was good.
After 3 years, adenomas were detected in 55.7% of participants in the placebo group and in 51.1% of those in the GTE group in the modified intention-to-treat population. This absolute difference of 4.6% in favor of GTE was not statistically significant.
The per protocol analysis also did not show a significant effect of GTE on new adenoma formation in the whole study population.
However, a preplanned subgroup analysis revealed a significant difference in the adenoma recurrence rate in favor of GTE in men but not women.
In men, GTE intake was associated with a significant 12.4% relative and 7.5% absolute reduction of metachronous adenomas, they report.
This potential gender-specific difference in chemoprevention “warrants further investigations,” the study team writes.
The safety profile of GTE as taken in this trial was good, with only grade 1/2 elevations in liver enzymes in the GTE group, compared with the placebo group. However, because the follow-up period was limited to 3 years, the long-term safety of GTE cannot be determined.
The researchers write that, to their knowledge, this study is the largest randomized trial to date of the effect of GTE on adenoma recurrence in a colorectal cancer screening population consisting of White patients.
Caveats and cautionary notes
Reached for comment, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, noted that “although the study showed no significant differences, the time horizon to show benefit may be longer than the 3-year duration of the study.”
“There are also methodologic issues with the readjustment of the target sample size, which may have led to a type II error, related to underpowering of the sample size,” said Dr. Johnson, who wasn’t involved in the study.
The researchers write that the study initially generated “great interest” and that many centers applied to participate. However, “quite a few” centers did not meet their promised recruitment targets and had to be replaced. Therefore, the statistical analysis plan had to be modified, and the number of participants had to be reduced over the course of the trial, they note.
Dr. Johnson also cautioned that while green tea is a popular drink, “there is strong evidence that green tea extract, found in many herbal and dietary supplements, is among the leading causes listed for drug-induced liver injury, including acute liver failure, urgent liver transplantation, and death.”
The study was fully funded by a grant from German Cancer Aid. The investigators and Dr. Johnson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Digital monitors can relieve asthma burden by boosting medication adherence and inhaler technique
PHOENIX – Before considering oral steroids or biologic therapies, many people with difficult-to-control asthma can reduce symptoms by addressing medication adherence and inhaler technique – and digital monitoring devices can play a key role.
Often physicians “will approach a patient about a biologic if they’re not responding to standard therapy. But we need to sometimes go back to those basic building blocks, like, are you taking the standard therapy?” William C. Anderson, MD, codirector of the multidisciplinary asthma clinic at Children’s Hospital Colorado, Aurora, said in an interview.
At the annual meeting of the American Academy of Allergy, Asthma, and Immunology, he and others presented data highlighting the diagnostic and therapeutic potential of digital monitoring devices for difficult-to-control asthma, the theme of the 2022s meeting.
The Global Initiative for Asthma (GINA) defines asthma as “difficult to control” if it remains uncontrolled despite medium- or high-dose inhaled corticosteroids with a second controller or with maintenance oral steroids, or if the asthma requires high-dose treatment to curb symptoms and exacerbations. About 17% of adult asthma patients have difficult-to-control asthma, according to the 2021 GINA report.
However, correcting for inhaling technique and adherence cuts the 17% down to just 3.7%, Giselle Mosnaim, MD, an allergist at NorthShore University HealthSystem outside Chicago and AAAAI immediate past president, told attendees at a Feb. 25 session on digital technologies for asthma management.
The CRITIKAL study, which reviewed data from more than 5,000 asthma patients, “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” Dr. Mosnaim said. Sadly, it also shows that, from 1975 to 2014, despite new devices and new technologies, “we still have poor inhaler technique.”
As for ways to measure adherence, physician judgments tend to be inaccurate, patient self-reporting has proved unreliable, and prescription refill data doesn’t indicate whether patients actually used the medications. “The ideal measure of adherence should be objective, accurate and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Tracking adherence
A closing afternoon session featured three presentations on research tracking adherence and outcomes in difficult-to-treat asthma patients – two pediatric cohorts and one across all ages. All studies used the Propeller Health sensor, a Food and Drug Administration–cleared device that attaches to the patient’s inhaler and automatically collects information on where, when, and how often they use their medication. The sensor then sends that information to a data cloud accessible to the patient and their health care professional.
Dr. Anderson’s team scoured a nationwide Propeller Health database for 8,000 patients using the digital monitors with controller therapies for asthma or chronic obstructive pulmonary disease (COPD). The study explored whether adherence differed for once-daily versus twice-daily medications, and if adherence differed based on patient age (4-60+ years).
For both asthma and COPD patients, those on once-daily regimens had higher medication adherence, compared with those who were prescribed twice-daily therapies. Plus, a greater proportion of once-daily patients met the prespecified 80% adherence threshold.
Looking across ages, medication use in the youngest group (aged 4-11 years) looked comparable with 30-somethings, “probably because parents are the ones giving the drug,” Dr. Anderson said. Mirroring patterns from other studies, adherence levels dipped in adolescents and young adults, relative to other age subsets.
Since this population-level analysis didn’t include individualized data on exacerbations or asthma control, “we can’t relate this to outcomes,” Dr. Anderson noted. But he said the data correlating medication use with adherence suggest that once-daily formulations may be the better option.
In one of the two pediatric studies, Matt McCulloch, MD, an allergy and immunology fellow working with Dr. Anderson, and colleagues reviewed charts of 40 children who received care at the Colorado Children’s multidisciplinary asthma clinic between 2018 and 2021. Half of these patients used Propeller Health sensors with their daily inhaled controller; the other patients were matched for age, ethnicity, sex, medication level, and disease control and severity – but had no electronic monitoring device.
On the whole, children who used digital monitoring for 12 months did not fare much better than matched controls on lung function (judged by forced expiratory volume) or asthma control (measured by Asthma Control Test scores).
However, within the digital monitoring group, patients who stayed on the Propeller system for 12 months did have better asthma control, fewer exacerbations, and improved asthma severity scores (measured by the Composite Asthma Severity Index), compared with when they first began digital monitoring. These children had all received care at the clinic for a while before their families opted for the electronic sensor, so “the effect wouldn’t have just been from starting in the clinic,” Dr. McCulloch said in an interview.
The gains came despite waning medication adherence. Similar to other digital monitoring studies, use of daily controller therapies in this retrospective analysis began at 50%-80% but dropped considerably during the first 4-5 months before settling into the 20%-30% range by 1 year.
Rachelle Ramsey, PhD, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center, presented data from 20 children with difficult-to-treat asthma who received 8 weeks of a digital adherence intervention during a 12-month treatment period. They analyzed three subsets – each with interventions based on how well the patients were managing daily controller therapy at baseline.
One patient with high (>80%) baseline adherence just received digital monitoring. The seven patients who began the study with intermediate (50%-80%) adherence received digital monitoring plus prescriptive text messaging. And the 12 children with poorest (<50%) baseline adherence received digital monitoring and a telehealth session in which a behavioral health specialist helped them set goals and create strategies to overcome barriers – for example, keeping the inhaler near their toothbrush in order to pair medication use with a daily habit.
“Overall, we found that matching Propeller with a behavioral intervention really improved adherence,” Dr. Ramsey said in an interview. While patients were receiving the intervention, adherence averaged across all groups increased from 39% to 76%. However, once the intervention period ended, the group’s adherence regressed toward baseline (36%).
Although adherence did not associate with clinical gains in this small study, the use of digital monitoring to improve medication adherence has translated to better outcomes in other recent efforts.
Remote monitoring
In a quality improvement project in the United Kingdom, nurses asked difficult-to-control asthma patients if they understood how to use their corticosteroid/long-acting beta2-agonist (LABA) inhalers and if they were adhering to treatment guidelines.
Those who answered yes to these questions were invited to a 28-day study that involved swapping their steroid/LABA inhalers for a different controller/bronchodilator (fluticasone/salmeterol) with INCA (Inhaler Compliance Assessment), a device that not only tracks adherence but also uses acoustics to gauge inhaler technique.
Among the 23 patients who participated, many had better clinical outcomes after 28 days of INCA monitoring. As Dr. Mosnaim told attendees, “what was amazing is so many of the patients that had been these difficult-to-control asthmatics who would have gone on to oral steroids or perhaps a biologic – lo and behold, you put them on a digital inhaler, and what do you see?” In two-thirds of the patients, “you see FeNo [a test that measures airway inflammation by detecting nitric oxide in exhalations] goes down. You see spirometry improve. You see the asthma control questionnaire improve. You see blood eosinophils go down.”
And in a 2020 randomized trial, Dr. Mosnaim and colleagues recruited 100 adults with uncontrolled asthma who had prescriptions for a daily inhaled corticosteroid and a short-acting beta-agonist (SABA) inhaler. Participants received Propeller sensors for their steroid and SABA inhalers. After a 2-week run-in period to calculate baseline corticosteroid adherence and SABA use for all participants, half the participants were randomly assigned to the control group, which had the app and sensor in silent mode, merely to collect data on medication use – whereas the treatment group received reminders, alerts, and monthly phone calls from providers who gave feedback on adherence and technique.
After 3 months of digital monitoring, patients didn’t use their rescue medication quite as often – as judged by a rise in the percentage of SABA-free days, compared with when they began the study. But the change in SABA-free days relative to baseline was more pronounced in the treatment group (19%) than in the control group (6%).
As seen in the other digital monitoring studies, adherence to daily corticosteroids fell with time, but the drop was milder in treated participants (2%) versus the control group (17%). So in this study, digital monitoring plus mobile app reminders and clinician feedback “prevented against fall in adherence to inhaled steroids over time,” Dr. Mosnaim said.
These results are “very encouraging” and offer “proof of concept that this type of remote monitoring could work,” Thanai Pongdee, MD, an allergist-immunologist with the Mayo Clinic in Rochester, Minn., said in an interview. One limitation was that the study was too short to measure exacerbation rates. A yearlong analysis would be “really fascinating because you’d catch all the seasons of the year – all the pollen seasons, all these things that could exacerbate you. Some people’s asthma can be quite seasonal.”
More important, the clinical utility of digital sensors will depend on how physicians choose to use them. If the doctor puts out a “blanket recommendation for using it but doesn’t ask you about it or doesn’t use the data to inform your care, then I think people just lose engagement and lose excitement over it,” Dr. Ramsey said. But if the health care team “asks you about the data or looks at the data with you or shows you how valuable this can be to your care, then I think that changes things.”
Building these analyses and interactions into the clinic workflow isn’t trivial. “If you have this wealth of data coming in, how are you going to look at it? Are you going to have an individual person assigned to this role? How are you going to respond to alerts?” Dr. Anderson asked.
In addition, because some digital monitors issue alerts when a patient’s asthma is not well controlled, some providers worry about liability if “something bad were to happen if you had that data but didn’t act upon it,” he said. Yet he noted that remote data monitoring is already used routinely in other areas of medicine, such as managing diabetes and heart conditions, “and it’s not like people are getting dinged for that stuff.”
Another issue is cost. Insurance only covers digital monitors in select cases, but it’s a bit of a catch-22. Insurers “don’t want to cover it until they get the data, but you can’t get the data until insurance covers it,” said Dr. Anderson, who added that “this year we finally got CPT reimbursement codes for monitoring devices.”
On the whole, studies of digital medication monitors suggest that better outcomes require “a good partnership between the health care provider and the patient,” Dr. Pongdee said. “It wasn’t like you could just put these things on and expect them to help. You still need that personal relationship to get the optimal results. We can have all this technology, but you still can’t take the people out of it.”
Dr. Mosnaim reported receiving current research grant support from GlaxoSmithKline, Novartis, Sanofi-Regeneron, and Teva; and past research grant support from AstraZeneca, Alk-Abello, and Genentech. She is immediate past president of the AAAAI, and directs the board of directors for the American Board of Allergy and Immunology. Dr. Anderson has served as a consultant for Regeneron, GlaxoSmithKline, and AstraZeneca, and has received research support from Colorado Medicaid. Dr. McCulloch and Dr. Ramsey disclosed no relevant financial relationships. Dr. Pongdee serves as an at-large director on the American Academy of Allergy, Asthma and Immunology board of directors. He receives grant funding from GlaxoSmithKline, and the Mayo Clinic is a trial site for GlaxoSmithKline and AstraZeneca.
A version of this article first appeared on Medscape.com.
PHOENIX – Before considering oral steroids or biologic therapies, many people with difficult-to-control asthma can reduce symptoms by addressing medication adherence and inhaler technique – and digital monitoring devices can play a key role.
Often physicians “will approach a patient about a biologic if they’re not responding to standard therapy. But we need to sometimes go back to those basic building blocks, like, are you taking the standard therapy?” William C. Anderson, MD, codirector of the multidisciplinary asthma clinic at Children’s Hospital Colorado, Aurora, said in an interview.
At the annual meeting of the American Academy of Allergy, Asthma, and Immunology, he and others presented data highlighting the diagnostic and therapeutic potential of digital monitoring devices for difficult-to-control asthma, the theme of the 2022s meeting.
The Global Initiative for Asthma (GINA) defines asthma as “difficult to control” if it remains uncontrolled despite medium- or high-dose inhaled corticosteroids with a second controller or with maintenance oral steroids, or if the asthma requires high-dose treatment to curb symptoms and exacerbations. About 17% of adult asthma patients have difficult-to-control asthma, according to the 2021 GINA report.
However, correcting for inhaling technique and adherence cuts the 17% down to just 3.7%, Giselle Mosnaim, MD, an allergist at NorthShore University HealthSystem outside Chicago and AAAAI immediate past president, told attendees at a Feb. 25 session on digital technologies for asthma management.
The CRITIKAL study, which reviewed data from more than 5,000 asthma patients, “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” Dr. Mosnaim said. Sadly, it also shows that, from 1975 to 2014, despite new devices and new technologies, “we still have poor inhaler technique.”
As for ways to measure adherence, physician judgments tend to be inaccurate, patient self-reporting has proved unreliable, and prescription refill data doesn’t indicate whether patients actually used the medications. “The ideal measure of adherence should be objective, accurate and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Tracking adherence
A closing afternoon session featured three presentations on research tracking adherence and outcomes in difficult-to-treat asthma patients – two pediatric cohorts and one across all ages. All studies used the Propeller Health sensor, a Food and Drug Administration–cleared device that attaches to the patient’s inhaler and automatically collects information on where, when, and how often they use their medication. The sensor then sends that information to a data cloud accessible to the patient and their health care professional.
Dr. Anderson’s team scoured a nationwide Propeller Health database for 8,000 patients using the digital monitors with controller therapies for asthma or chronic obstructive pulmonary disease (COPD). The study explored whether adherence differed for once-daily versus twice-daily medications, and if adherence differed based on patient age (4-60+ years).
For both asthma and COPD patients, those on once-daily regimens had higher medication adherence, compared with those who were prescribed twice-daily therapies. Plus, a greater proportion of once-daily patients met the prespecified 80% adherence threshold.
Looking across ages, medication use in the youngest group (aged 4-11 years) looked comparable with 30-somethings, “probably because parents are the ones giving the drug,” Dr. Anderson said. Mirroring patterns from other studies, adherence levels dipped in adolescents and young adults, relative to other age subsets.
Since this population-level analysis didn’t include individualized data on exacerbations or asthma control, “we can’t relate this to outcomes,” Dr. Anderson noted. But he said the data correlating medication use with adherence suggest that once-daily formulations may be the better option.
In one of the two pediatric studies, Matt McCulloch, MD, an allergy and immunology fellow working with Dr. Anderson, and colleagues reviewed charts of 40 children who received care at the Colorado Children’s multidisciplinary asthma clinic between 2018 and 2021. Half of these patients used Propeller Health sensors with their daily inhaled controller; the other patients were matched for age, ethnicity, sex, medication level, and disease control and severity – but had no electronic monitoring device.
On the whole, children who used digital monitoring for 12 months did not fare much better than matched controls on lung function (judged by forced expiratory volume) or asthma control (measured by Asthma Control Test scores).
However, within the digital monitoring group, patients who stayed on the Propeller system for 12 months did have better asthma control, fewer exacerbations, and improved asthma severity scores (measured by the Composite Asthma Severity Index), compared with when they first began digital monitoring. These children had all received care at the clinic for a while before their families opted for the electronic sensor, so “the effect wouldn’t have just been from starting in the clinic,” Dr. McCulloch said in an interview.
The gains came despite waning medication adherence. Similar to other digital monitoring studies, use of daily controller therapies in this retrospective analysis began at 50%-80% but dropped considerably during the first 4-5 months before settling into the 20%-30% range by 1 year.
Rachelle Ramsey, PhD, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center, presented data from 20 children with difficult-to-treat asthma who received 8 weeks of a digital adherence intervention during a 12-month treatment period. They analyzed three subsets – each with interventions based on how well the patients were managing daily controller therapy at baseline.
One patient with high (>80%) baseline adherence just received digital monitoring. The seven patients who began the study with intermediate (50%-80%) adherence received digital monitoring plus prescriptive text messaging. And the 12 children with poorest (<50%) baseline adherence received digital monitoring and a telehealth session in which a behavioral health specialist helped them set goals and create strategies to overcome barriers – for example, keeping the inhaler near their toothbrush in order to pair medication use with a daily habit.
“Overall, we found that matching Propeller with a behavioral intervention really improved adherence,” Dr. Ramsey said in an interview. While patients were receiving the intervention, adherence averaged across all groups increased from 39% to 76%. However, once the intervention period ended, the group’s adherence regressed toward baseline (36%).
Although adherence did not associate with clinical gains in this small study, the use of digital monitoring to improve medication adherence has translated to better outcomes in other recent efforts.
Remote monitoring
In a quality improvement project in the United Kingdom, nurses asked difficult-to-control asthma patients if they understood how to use their corticosteroid/long-acting beta2-agonist (LABA) inhalers and if they were adhering to treatment guidelines.
Those who answered yes to these questions were invited to a 28-day study that involved swapping their steroid/LABA inhalers for a different controller/bronchodilator (fluticasone/salmeterol) with INCA (Inhaler Compliance Assessment), a device that not only tracks adherence but also uses acoustics to gauge inhaler technique.
Among the 23 patients who participated, many had better clinical outcomes after 28 days of INCA monitoring. As Dr. Mosnaim told attendees, “what was amazing is so many of the patients that had been these difficult-to-control asthmatics who would have gone on to oral steroids or perhaps a biologic – lo and behold, you put them on a digital inhaler, and what do you see?” In two-thirds of the patients, “you see FeNo [a test that measures airway inflammation by detecting nitric oxide in exhalations] goes down. You see spirometry improve. You see the asthma control questionnaire improve. You see blood eosinophils go down.”
And in a 2020 randomized trial, Dr. Mosnaim and colleagues recruited 100 adults with uncontrolled asthma who had prescriptions for a daily inhaled corticosteroid and a short-acting beta-agonist (SABA) inhaler. Participants received Propeller sensors for their steroid and SABA inhalers. After a 2-week run-in period to calculate baseline corticosteroid adherence and SABA use for all participants, half the participants were randomly assigned to the control group, which had the app and sensor in silent mode, merely to collect data on medication use – whereas the treatment group received reminders, alerts, and monthly phone calls from providers who gave feedback on adherence and technique.
After 3 months of digital monitoring, patients didn’t use their rescue medication quite as often – as judged by a rise in the percentage of SABA-free days, compared with when they began the study. But the change in SABA-free days relative to baseline was more pronounced in the treatment group (19%) than in the control group (6%).
As seen in the other digital monitoring studies, adherence to daily corticosteroids fell with time, but the drop was milder in treated participants (2%) versus the control group (17%). So in this study, digital monitoring plus mobile app reminders and clinician feedback “prevented against fall in adherence to inhaled steroids over time,” Dr. Mosnaim said.
These results are “very encouraging” and offer “proof of concept that this type of remote monitoring could work,” Thanai Pongdee, MD, an allergist-immunologist with the Mayo Clinic in Rochester, Minn., said in an interview. One limitation was that the study was too short to measure exacerbation rates. A yearlong analysis would be “really fascinating because you’d catch all the seasons of the year – all the pollen seasons, all these things that could exacerbate you. Some people’s asthma can be quite seasonal.”
More important, the clinical utility of digital sensors will depend on how physicians choose to use them. If the doctor puts out a “blanket recommendation for using it but doesn’t ask you about it or doesn’t use the data to inform your care, then I think people just lose engagement and lose excitement over it,” Dr. Ramsey said. But if the health care team “asks you about the data or looks at the data with you or shows you how valuable this can be to your care, then I think that changes things.”
Building these analyses and interactions into the clinic workflow isn’t trivial. “If you have this wealth of data coming in, how are you going to look at it? Are you going to have an individual person assigned to this role? How are you going to respond to alerts?” Dr. Anderson asked.
In addition, because some digital monitors issue alerts when a patient’s asthma is not well controlled, some providers worry about liability if “something bad were to happen if you had that data but didn’t act upon it,” he said. Yet he noted that remote data monitoring is already used routinely in other areas of medicine, such as managing diabetes and heart conditions, “and it’s not like people are getting dinged for that stuff.”
Another issue is cost. Insurance only covers digital monitors in select cases, but it’s a bit of a catch-22. Insurers “don’t want to cover it until they get the data, but you can’t get the data until insurance covers it,” said Dr. Anderson, who added that “this year we finally got CPT reimbursement codes for monitoring devices.”
On the whole, studies of digital medication monitors suggest that better outcomes require “a good partnership between the health care provider and the patient,” Dr. Pongdee said. “It wasn’t like you could just put these things on and expect them to help. You still need that personal relationship to get the optimal results. We can have all this technology, but you still can’t take the people out of it.”
Dr. Mosnaim reported receiving current research grant support from GlaxoSmithKline, Novartis, Sanofi-Regeneron, and Teva; and past research grant support from AstraZeneca, Alk-Abello, and Genentech. She is immediate past president of the AAAAI, and directs the board of directors for the American Board of Allergy and Immunology. Dr. Anderson has served as a consultant for Regeneron, GlaxoSmithKline, and AstraZeneca, and has received research support from Colorado Medicaid. Dr. McCulloch and Dr. Ramsey disclosed no relevant financial relationships. Dr. Pongdee serves as an at-large director on the American Academy of Allergy, Asthma and Immunology board of directors. He receives grant funding from GlaxoSmithKline, and the Mayo Clinic is a trial site for GlaxoSmithKline and AstraZeneca.
A version of this article first appeared on Medscape.com.
PHOENIX – Before considering oral steroids or biologic therapies, many people with difficult-to-control asthma can reduce symptoms by addressing medication adherence and inhaler technique – and digital monitoring devices can play a key role.
Often physicians “will approach a patient about a biologic if they’re not responding to standard therapy. But we need to sometimes go back to those basic building blocks, like, are you taking the standard therapy?” William C. Anderson, MD, codirector of the multidisciplinary asthma clinic at Children’s Hospital Colorado, Aurora, said in an interview.
At the annual meeting of the American Academy of Allergy, Asthma, and Immunology, he and others presented data highlighting the diagnostic and therapeutic potential of digital monitoring devices for difficult-to-control asthma, the theme of the 2022s meeting.
The Global Initiative for Asthma (GINA) defines asthma as “difficult to control” if it remains uncontrolled despite medium- or high-dose inhaled corticosteroids with a second controller or with maintenance oral steroids, or if the asthma requires high-dose treatment to curb symptoms and exacerbations. About 17% of adult asthma patients have difficult-to-control asthma, according to the 2021 GINA report.
However, correcting for inhaling technique and adherence cuts the 17% down to just 3.7%, Giselle Mosnaim, MD, an allergist at NorthShore University HealthSystem outside Chicago and AAAAI immediate past president, told attendees at a Feb. 25 session on digital technologies for asthma management.
The CRITIKAL study, which reviewed data from more than 5,000 asthma patients, “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” Dr. Mosnaim said. Sadly, it also shows that, from 1975 to 2014, despite new devices and new technologies, “we still have poor inhaler technique.”
As for ways to measure adherence, physician judgments tend to be inaccurate, patient self-reporting has proved unreliable, and prescription refill data doesn’t indicate whether patients actually used the medications. “The ideal measure of adherence should be objective, accurate and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Tracking adherence
A closing afternoon session featured three presentations on research tracking adherence and outcomes in difficult-to-treat asthma patients – two pediatric cohorts and one across all ages. All studies used the Propeller Health sensor, a Food and Drug Administration–cleared device that attaches to the patient’s inhaler and automatically collects information on where, when, and how often they use their medication. The sensor then sends that information to a data cloud accessible to the patient and their health care professional.
Dr. Anderson’s team scoured a nationwide Propeller Health database for 8,000 patients using the digital monitors with controller therapies for asthma or chronic obstructive pulmonary disease (COPD). The study explored whether adherence differed for once-daily versus twice-daily medications, and if adherence differed based on patient age (4-60+ years).
For both asthma and COPD patients, those on once-daily regimens had higher medication adherence, compared with those who were prescribed twice-daily therapies. Plus, a greater proportion of once-daily patients met the prespecified 80% adherence threshold.
Looking across ages, medication use in the youngest group (aged 4-11 years) looked comparable with 30-somethings, “probably because parents are the ones giving the drug,” Dr. Anderson said. Mirroring patterns from other studies, adherence levels dipped in adolescents and young adults, relative to other age subsets.
Since this population-level analysis didn’t include individualized data on exacerbations or asthma control, “we can’t relate this to outcomes,” Dr. Anderson noted. But he said the data correlating medication use with adherence suggest that once-daily formulations may be the better option.
In one of the two pediatric studies, Matt McCulloch, MD, an allergy and immunology fellow working with Dr. Anderson, and colleagues reviewed charts of 40 children who received care at the Colorado Children’s multidisciplinary asthma clinic between 2018 and 2021. Half of these patients used Propeller Health sensors with their daily inhaled controller; the other patients were matched for age, ethnicity, sex, medication level, and disease control and severity – but had no electronic monitoring device.
On the whole, children who used digital monitoring for 12 months did not fare much better than matched controls on lung function (judged by forced expiratory volume) or asthma control (measured by Asthma Control Test scores).
However, within the digital monitoring group, patients who stayed on the Propeller system for 12 months did have better asthma control, fewer exacerbations, and improved asthma severity scores (measured by the Composite Asthma Severity Index), compared with when they first began digital monitoring. These children had all received care at the clinic for a while before their families opted for the electronic sensor, so “the effect wouldn’t have just been from starting in the clinic,” Dr. McCulloch said in an interview.
The gains came despite waning medication adherence. Similar to other digital monitoring studies, use of daily controller therapies in this retrospective analysis began at 50%-80% but dropped considerably during the first 4-5 months before settling into the 20%-30% range by 1 year.
Rachelle Ramsey, PhD, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center, presented data from 20 children with difficult-to-treat asthma who received 8 weeks of a digital adherence intervention during a 12-month treatment period. They analyzed three subsets – each with interventions based on how well the patients were managing daily controller therapy at baseline.
One patient with high (>80%) baseline adherence just received digital monitoring. The seven patients who began the study with intermediate (50%-80%) adherence received digital monitoring plus prescriptive text messaging. And the 12 children with poorest (<50%) baseline adherence received digital monitoring and a telehealth session in which a behavioral health specialist helped them set goals and create strategies to overcome barriers – for example, keeping the inhaler near their toothbrush in order to pair medication use with a daily habit.
“Overall, we found that matching Propeller with a behavioral intervention really improved adherence,” Dr. Ramsey said in an interview. While patients were receiving the intervention, adherence averaged across all groups increased from 39% to 76%. However, once the intervention period ended, the group’s adherence regressed toward baseline (36%).
Although adherence did not associate with clinical gains in this small study, the use of digital monitoring to improve medication adherence has translated to better outcomes in other recent efforts.
Remote monitoring
In a quality improvement project in the United Kingdom, nurses asked difficult-to-control asthma patients if they understood how to use their corticosteroid/long-acting beta2-agonist (LABA) inhalers and if they were adhering to treatment guidelines.
Those who answered yes to these questions were invited to a 28-day study that involved swapping their steroid/LABA inhalers for a different controller/bronchodilator (fluticasone/salmeterol) with INCA (Inhaler Compliance Assessment), a device that not only tracks adherence but also uses acoustics to gauge inhaler technique.
Among the 23 patients who participated, many had better clinical outcomes after 28 days of INCA monitoring. As Dr. Mosnaim told attendees, “what was amazing is so many of the patients that had been these difficult-to-control asthmatics who would have gone on to oral steroids or perhaps a biologic – lo and behold, you put them on a digital inhaler, and what do you see?” In two-thirds of the patients, “you see FeNo [a test that measures airway inflammation by detecting nitric oxide in exhalations] goes down. You see spirometry improve. You see the asthma control questionnaire improve. You see blood eosinophils go down.”
And in a 2020 randomized trial, Dr. Mosnaim and colleagues recruited 100 adults with uncontrolled asthma who had prescriptions for a daily inhaled corticosteroid and a short-acting beta-agonist (SABA) inhaler. Participants received Propeller sensors for their steroid and SABA inhalers. After a 2-week run-in period to calculate baseline corticosteroid adherence and SABA use for all participants, half the participants were randomly assigned to the control group, which had the app and sensor in silent mode, merely to collect data on medication use – whereas the treatment group received reminders, alerts, and monthly phone calls from providers who gave feedback on adherence and technique.
After 3 months of digital monitoring, patients didn’t use their rescue medication quite as often – as judged by a rise in the percentage of SABA-free days, compared with when they began the study. But the change in SABA-free days relative to baseline was more pronounced in the treatment group (19%) than in the control group (6%).
As seen in the other digital monitoring studies, adherence to daily corticosteroids fell with time, but the drop was milder in treated participants (2%) versus the control group (17%). So in this study, digital monitoring plus mobile app reminders and clinician feedback “prevented against fall in adherence to inhaled steroids over time,” Dr. Mosnaim said.
These results are “very encouraging” and offer “proof of concept that this type of remote monitoring could work,” Thanai Pongdee, MD, an allergist-immunologist with the Mayo Clinic in Rochester, Minn., said in an interview. One limitation was that the study was too short to measure exacerbation rates. A yearlong analysis would be “really fascinating because you’d catch all the seasons of the year – all the pollen seasons, all these things that could exacerbate you. Some people’s asthma can be quite seasonal.”
More important, the clinical utility of digital sensors will depend on how physicians choose to use them. If the doctor puts out a “blanket recommendation for using it but doesn’t ask you about it or doesn’t use the data to inform your care, then I think people just lose engagement and lose excitement over it,” Dr. Ramsey said. But if the health care team “asks you about the data or looks at the data with you or shows you how valuable this can be to your care, then I think that changes things.”
Building these analyses and interactions into the clinic workflow isn’t trivial. “If you have this wealth of data coming in, how are you going to look at it? Are you going to have an individual person assigned to this role? How are you going to respond to alerts?” Dr. Anderson asked.
In addition, because some digital monitors issue alerts when a patient’s asthma is not well controlled, some providers worry about liability if “something bad were to happen if you had that data but didn’t act upon it,” he said. Yet he noted that remote data monitoring is already used routinely in other areas of medicine, such as managing diabetes and heart conditions, “and it’s not like people are getting dinged for that stuff.”
Another issue is cost. Insurance only covers digital monitors in select cases, but it’s a bit of a catch-22. Insurers “don’t want to cover it until they get the data, but you can’t get the data until insurance covers it,” said Dr. Anderson, who added that “this year we finally got CPT reimbursement codes for monitoring devices.”
On the whole, studies of digital medication monitors suggest that better outcomes require “a good partnership between the health care provider and the patient,” Dr. Pongdee said. “It wasn’t like you could just put these things on and expect them to help. You still need that personal relationship to get the optimal results. We can have all this technology, but you still can’t take the people out of it.”
Dr. Mosnaim reported receiving current research grant support from GlaxoSmithKline, Novartis, Sanofi-Regeneron, and Teva; and past research grant support from AstraZeneca, Alk-Abello, and Genentech. She is immediate past president of the AAAAI, and directs the board of directors for the American Board of Allergy and Immunology. Dr. Anderson has served as a consultant for Regeneron, GlaxoSmithKline, and AstraZeneca, and has received research support from Colorado Medicaid. Dr. McCulloch and Dr. Ramsey disclosed no relevant financial relationships. Dr. Pongdee serves as an at-large director on the American Academy of Allergy, Asthma and Immunology board of directors. He receives grant funding from GlaxoSmithKline, and the Mayo Clinic is a trial site for GlaxoSmithKline and AstraZeneca.
A version of this article first appeared on Medscape.com.
AT AAAAI
FDA warns about off-label use of laparoscopic device for aesthetic procedures
The .
The device is cleared by the FDA for “general use of cutting, coagulation, and ablation of soft tissue during open and laparoscopic surgical procedures” but it “has not been determined to be safe or effective for any procedure intended to improve the appearance of the skin,” according to the March 14 statement from the FDA. The statement adds that the agency has received reports describing “serious and potentially life-threatening adverse events with use of this device for certain aesthetic procedures,” including some that have required treatment in an intensive care unit. The statement does not mention whether any cases were fatal.
Adverse events that have been reported include second- and third-degree burns, infections, changes in skin color, scars, nerve damage, “significant bleeding,” and “air or gas accumulation under the skin, in body cavities, and in blood vessels.”
Manufactured by Apyx medical, the device includes a hand piece and generator and uses radiofrequency energy and helium to generate plasma, which is used to “cut, coagulate ... and eliminate soft tissue with heat during surgery,” according to the FDA.
The FDA is advising health care providers not to use the device for dermal resurfacing or skin contraction “alone or in combination with liposuction.”
The statement also advises consumers who are considering an aesthetic skin treatment with this device to consult their health care providers regarding its use – and if they have any problems or are concerned after being treated with this device, to “seek care from a licensed health care provider.”
The FDA is working with Apyx to evaluate information about the use of the device for aesthetic skin procedures and to inform consumers and health care providers about the warning.
Health care providers and consumers should report problems or complications associated with the Renuvion/J-Plasma device to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
The .
The device is cleared by the FDA for “general use of cutting, coagulation, and ablation of soft tissue during open and laparoscopic surgical procedures” but it “has not been determined to be safe or effective for any procedure intended to improve the appearance of the skin,” according to the March 14 statement from the FDA. The statement adds that the agency has received reports describing “serious and potentially life-threatening adverse events with use of this device for certain aesthetic procedures,” including some that have required treatment in an intensive care unit. The statement does not mention whether any cases were fatal.
Adverse events that have been reported include second- and third-degree burns, infections, changes in skin color, scars, nerve damage, “significant bleeding,” and “air or gas accumulation under the skin, in body cavities, and in blood vessels.”
Manufactured by Apyx medical, the device includes a hand piece and generator and uses radiofrequency energy and helium to generate plasma, which is used to “cut, coagulate ... and eliminate soft tissue with heat during surgery,” according to the FDA.
The FDA is advising health care providers not to use the device for dermal resurfacing or skin contraction “alone or in combination with liposuction.”
The statement also advises consumers who are considering an aesthetic skin treatment with this device to consult their health care providers regarding its use – and if they have any problems or are concerned after being treated with this device, to “seek care from a licensed health care provider.”
The FDA is working with Apyx to evaluate information about the use of the device for aesthetic skin procedures and to inform consumers and health care providers about the warning.
Health care providers and consumers should report problems or complications associated with the Renuvion/J-Plasma device to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
The .
The device is cleared by the FDA for “general use of cutting, coagulation, and ablation of soft tissue during open and laparoscopic surgical procedures” but it “has not been determined to be safe or effective for any procedure intended to improve the appearance of the skin,” according to the March 14 statement from the FDA. The statement adds that the agency has received reports describing “serious and potentially life-threatening adverse events with use of this device for certain aesthetic procedures,” including some that have required treatment in an intensive care unit. The statement does not mention whether any cases were fatal.
Adverse events that have been reported include second- and third-degree burns, infections, changes in skin color, scars, nerve damage, “significant bleeding,” and “air or gas accumulation under the skin, in body cavities, and in blood vessels.”
Manufactured by Apyx medical, the device includes a hand piece and generator and uses radiofrequency energy and helium to generate plasma, which is used to “cut, coagulate ... and eliminate soft tissue with heat during surgery,” according to the FDA.
The FDA is advising health care providers not to use the device for dermal resurfacing or skin contraction “alone or in combination with liposuction.”
The statement also advises consumers who are considering an aesthetic skin treatment with this device to consult their health care providers regarding its use – and if they have any problems or are concerned after being treated with this device, to “seek care from a licensed health care provider.”
The FDA is working with Apyx to evaluate information about the use of the device for aesthetic skin procedures and to inform consumers and health care providers about the warning.
Health care providers and consumers should report problems or complications associated with the Renuvion/J-Plasma device to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
New 3D printable stent holds promise for tracheal tumors
Airflow obstruction caused by a malignant tracheal tumor may be managed with a uniquely designed, 3-dimensional (3D) drug-eluting tracheal stent that, at least in animal models so far, works well and may soon be ready for human trials, Chinese investigators are reporting.
The research was published online Jan. 29 in Materials Today Chemistry.
The problems with currently available stents used to treat airflow obstruction are considerable, corresponding author Shengrong Guo, PhD, professor of pharmaceutics, Shanghai Jiao Tong University, China, and colleagues observe. “Tracheal stents physically open up stenosis, recover airway patency, and promptly relieve symptoms, but [they] cannot treat the tumor,” they explain.
“Thus, tracheal restenosis always occurs soon [after], due to progressive tumor growth after stent placement,” they add. Moreover, implanted stents cover the entire tracheal mucosa, thus preventing mucus and sputum discharge, causing airway blockage, the investigators also note. Compounding these flaws is the unalterable fact that delivery of chemotherapy to a malignant tracheal tumor is inefficient, and systemic chemotherapy is always associated with systemic side effects.
All of these issues make it very challenging to treat these tumors, Dr. Guo noted. On the other hand, if there were a means to deliver a chemotherapeutic agent more directly to the disease site – as is done with drug-eluting beads, for example, in other tumor types – then at least drug delivery would be much more efficient. “In this study, a novel tracheal stent was designed with features of a C-shaped and trilayered wall,” the researchers explain.
The gap angle of the newly developed stent is 72°; the inner diameter is 0.5 cm, and it is 2.0 cm in length. The trilayered wall consists of an inner layer of poly (ε-caprolactone) (PCL), which is a biodegradable and implantable material used alone or compounded with other ingredients to print implants. The middle layer consists of magnetic nanoparticle (MNP)–loaded PCL. The authors explain that MNPs have been approved in the U.S. as contrast agents in MRI.
Combined with temperature-responsive materials, MNPs can serve as a source of magnetic thermotherapy as well, which can be used to control drug release and facilitate drug penetration into deeper tissues. The outer layer of the stent contains a paclitaxel-loaded ethylene-vinyl acetate copolymer layer.
“The C-shaped tracheal stents are easily fabricated on a roller by using a self-made specific three-dimensional printer,” the authors explain. They point out that the C-shaped tracheal stents do not cover the entire tracheal wall, and the uncovered gap in that wall allows for normal mucus and sputum discharge.
In vivo evaluation
Once the stents were printed, the researchers evaluated the biosafety and applicability of their C-shaped tracheal stents. Small rabbits weighing 2.5 to 3.0 kg were used as experimental models and were prepared for surgery. The stent was implanted in the rabbits’ tracheas through the use of a simple stent delivery device. During follow-up, the rabbits recovered well without any sign of infection or respiratory complications.
The animals were also eating well within about 5 days of the surgery, and their weight gradually increased, suggesting that the implantation of a stent with intermittent magnetic heating did not lead to any prominent systemic toxicities. “All rabbits were [euthanized] 30 days after the placement of the tracheal stents” and the stent was removed from the rabbits’ trachea, the researchers report.
Close observation of the trachea indicated that the gap left by the C-shaped stent could keep the airway patent without blocking either mucus or sputum discharge. “The stents have good biosafety in rabbits and keep airway patency for 1 month without the occurrence of mucus/sputum blockage after implantation in rabbit trachea,” Dr. Guo and colleagues conclude.
“These results provide a scientific basis for the development of novel self-expandable C-shaped tracheal stents with combinatorial tracheal support and local chemotherapy,” they affirm.
Pediatric airway obstruction
Thus far, the role of 3D printing seems to be most prominent in the treatment of pediatric airway obstruction, where it is used in the surgical planning stages and to create the implant itself. In a systematic review of its use for this, Joshua Stramiello, MD, University of California, San Diego, and colleagues identified 37 original articles, 11 of which discussed 3D printing for surgical planning, and 26 of which discussed 3D printing implants for interventions.
“3D printing for surgical planning not only improves preoperative assessment of surgical approach and stent customization but also helps facilitate patient/family education,” the authors observe. Most of the research so far has been focused on bioresorbable external airway splints and biological grafts, they add – “with both animal studies and human case reports showing good results in improving symptoms.” One clinical series focused on the use of a 3D-printed, patient-specific, bioresorbable airway splint in a cohort of critically ill children with severe tracheobronchomalacia. (Tracheobronchomalacia is the abnormal collapse of the windpipe).
When reported, 29 splints had been implanted in 15 children with intrathoracic tracheobronchomalacia. At a median follow-up of 8.5 months, 12 children were long-term survivors, and all but one lived at home. As recently discussed by George Cheng, MD, cofounder of restor3D, a Duke University startup that created the first 3D-printed airway stent using a compressible biocompatible material with properties similar to that of silicone, personalized airway stents have the potential for advance customization, minimize pressure points, and improve airflow dynamics to increase mucus clearance.
In fact, the U.S. Food and Drug Administration has already cleared patient-specific airway stents developed by Thomas Gildea, MD, of the Cleveland Clinic. Both the Duke University and Cleveland Clinic stents have been used in patients, with promising outcomes, Dr. Cheng noted.
The authors and Dr. Stramiello and colleagues have disclosed no relevant financial relationships. Dr. Cheng is the cofounder of restor3D.
A version of this article first appeared on Medscape.com.
Airflow obstruction caused by a malignant tracheal tumor may be managed with a uniquely designed, 3-dimensional (3D) drug-eluting tracheal stent that, at least in animal models so far, works well and may soon be ready for human trials, Chinese investigators are reporting.
The research was published online Jan. 29 in Materials Today Chemistry.
The problems with currently available stents used to treat airflow obstruction are considerable, corresponding author Shengrong Guo, PhD, professor of pharmaceutics, Shanghai Jiao Tong University, China, and colleagues observe. “Tracheal stents physically open up stenosis, recover airway patency, and promptly relieve symptoms, but [they] cannot treat the tumor,” they explain.
“Thus, tracheal restenosis always occurs soon [after], due to progressive tumor growth after stent placement,” they add. Moreover, implanted stents cover the entire tracheal mucosa, thus preventing mucus and sputum discharge, causing airway blockage, the investigators also note. Compounding these flaws is the unalterable fact that delivery of chemotherapy to a malignant tracheal tumor is inefficient, and systemic chemotherapy is always associated with systemic side effects.
All of these issues make it very challenging to treat these tumors, Dr. Guo noted. On the other hand, if there were a means to deliver a chemotherapeutic agent more directly to the disease site – as is done with drug-eluting beads, for example, in other tumor types – then at least drug delivery would be much more efficient. “In this study, a novel tracheal stent was designed with features of a C-shaped and trilayered wall,” the researchers explain.
The gap angle of the newly developed stent is 72°; the inner diameter is 0.5 cm, and it is 2.0 cm in length. The trilayered wall consists of an inner layer of poly (ε-caprolactone) (PCL), which is a biodegradable and implantable material used alone or compounded with other ingredients to print implants. The middle layer consists of magnetic nanoparticle (MNP)–loaded PCL. The authors explain that MNPs have been approved in the U.S. as contrast agents in MRI.
Combined with temperature-responsive materials, MNPs can serve as a source of magnetic thermotherapy as well, which can be used to control drug release and facilitate drug penetration into deeper tissues. The outer layer of the stent contains a paclitaxel-loaded ethylene-vinyl acetate copolymer layer.
“The C-shaped tracheal stents are easily fabricated on a roller by using a self-made specific three-dimensional printer,” the authors explain. They point out that the C-shaped tracheal stents do not cover the entire tracheal wall, and the uncovered gap in that wall allows for normal mucus and sputum discharge.
In vivo evaluation
Once the stents were printed, the researchers evaluated the biosafety and applicability of their C-shaped tracheal stents. Small rabbits weighing 2.5 to 3.0 kg were used as experimental models and were prepared for surgery. The stent was implanted in the rabbits’ tracheas through the use of a simple stent delivery device. During follow-up, the rabbits recovered well without any sign of infection or respiratory complications.
The animals were also eating well within about 5 days of the surgery, and their weight gradually increased, suggesting that the implantation of a stent with intermittent magnetic heating did not lead to any prominent systemic toxicities. “All rabbits were [euthanized] 30 days after the placement of the tracheal stents” and the stent was removed from the rabbits’ trachea, the researchers report.
Close observation of the trachea indicated that the gap left by the C-shaped stent could keep the airway patent without blocking either mucus or sputum discharge. “The stents have good biosafety in rabbits and keep airway patency for 1 month without the occurrence of mucus/sputum blockage after implantation in rabbit trachea,” Dr. Guo and colleagues conclude.
“These results provide a scientific basis for the development of novel self-expandable C-shaped tracheal stents with combinatorial tracheal support and local chemotherapy,” they affirm.
Pediatric airway obstruction
Thus far, the role of 3D printing seems to be most prominent in the treatment of pediatric airway obstruction, where it is used in the surgical planning stages and to create the implant itself. In a systematic review of its use for this, Joshua Stramiello, MD, University of California, San Diego, and colleagues identified 37 original articles, 11 of which discussed 3D printing for surgical planning, and 26 of which discussed 3D printing implants for interventions.
“3D printing for surgical planning not only improves preoperative assessment of surgical approach and stent customization but also helps facilitate patient/family education,” the authors observe. Most of the research so far has been focused on bioresorbable external airway splints and biological grafts, they add – “with both animal studies and human case reports showing good results in improving symptoms.” One clinical series focused on the use of a 3D-printed, patient-specific, bioresorbable airway splint in a cohort of critically ill children with severe tracheobronchomalacia. (Tracheobronchomalacia is the abnormal collapse of the windpipe).
When reported, 29 splints had been implanted in 15 children with intrathoracic tracheobronchomalacia. At a median follow-up of 8.5 months, 12 children were long-term survivors, and all but one lived at home. As recently discussed by George Cheng, MD, cofounder of restor3D, a Duke University startup that created the first 3D-printed airway stent using a compressible biocompatible material with properties similar to that of silicone, personalized airway stents have the potential for advance customization, minimize pressure points, and improve airflow dynamics to increase mucus clearance.
In fact, the U.S. Food and Drug Administration has already cleared patient-specific airway stents developed by Thomas Gildea, MD, of the Cleveland Clinic. Both the Duke University and Cleveland Clinic stents have been used in patients, with promising outcomes, Dr. Cheng noted.
The authors and Dr. Stramiello and colleagues have disclosed no relevant financial relationships. Dr. Cheng is the cofounder of restor3D.
A version of this article first appeared on Medscape.com.
Airflow obstruction caused by a malignant tracheal tumor may be managed with a uniquely designed, 3-dimensional (3D) drug-eluting tracheal stent that, at least in animal models so far, works well and may soon be ready for human trials, Chinese investigators are reporting.
The research was published online Jan. 29 in Materials Today Chemistry.
The problems with currently available stents used to treat airflow obstruction are considerable, corresponding author Shengrong Guo, PhD, professor of pharmaceutics, Shanghai Jiao Tong University, China, and colleagues observe. “Tracheal stents physically open up stenosis, recover airway patency, and promptly relieve symptoms, but [they] cannot treat the tumor,” they explain.
“Thus, tracheal restenosis always occurs soon [after], due to progressive tumor growth after stent placement,” they add. Moreover, implanted stents cover the entire tracheal mucosa, thus preventing mucus and sputum discharge, causing airway blockage, the investigators also note. Compounding these flaws is the unalterable fact that delivery of chemotherapy to a malignant tracheal tumor is inefficient, and systemic chemotherapy is always associated with systemic side effects.
All of these issues make it very challenging to treat these tumors, Dr. Guo noted. On the other hand, if there were a means to deliver a chemotherapeutic agent more directly to the disease site – as is done with drug-eluting beads, for example, in other tumor types – then at least drug delivery would be much more efficient. “In this study, a novel tracheal stent was designed with features of a C-shaped and trilayered wall,” the researchers explain.
The gap angle of the newly developed stent is 72°; the inner diameter is 0.5 cm, and it is 2.0 cm in length. The trilayered wall consists of an inner layer of poly (ε-caprolactone) (PCL), which is a biodegradable and implantable material used alone or compounded with other ingredients to print implants. The middle layer consists of magnetic nanoparticle (MNP)–loaded PCL. The authors explain that MNPs have been approved in the U.S. as contrast agents in MRI.
Combined with temperature-responsive materials, MNPs can serve as a source of magnetic thermotherapy as well, which can be used to control drug release and facilitate drug penetration into deeper tissues. The outer layer of the stent contains a paclitaxel-loaded ethylene-vinyl acetate copolymer layer.
“The C-shaped tracheal stents are easily fabricated on a roller by using a self-made specific three-dimensional printer,” the authors explain. They point out that the C-shaped tracheal stents do not cover the entire tracheal wall, and the uncovered gap in that wall allows for normal mucus and sputum discharge.
In vivo evaluation
Once the stents were printed, the researchers evaluated the biosafety and applicability of their C-shaped tracheal stents. Small rabbits weighing 2.5 to 3.0 kg were used as experimental models and were prepared for surgery. The stent was implanted in the rabbits’ tracheas through the use of a simple stent delivery device. During follow-up, the rabbits recovered well without any sign of infection or respiratory complications.
The animals were also eating well within about 5 days of the surgery, and their weight gradually increased, suggesting that the implantation of a stent with intermittent magnetic heating did not lead to any prominent systemic toxicities. “All rabbits were [euthanized] 30 days after the placement of the tracheal stents” and the stent was removed from the rabbits’ trachea, the researchers report.
Close observation of the trachea indicated that the gap left by the C-shaped stent could keep the airway patent without blocking either mucus or sputum discharge. “The stents have good biosafety in rabbits and keep airway patency for 1 month without the occurrence of mucus/sputum blockage after implantation in rabbit trachea,” Dr. Guo and colleagues conclude.
“These results provide a scientific basis for the development of novel self-expandable C-shaped tracheal stents with combinatorial tracheal support and local chemotherapy,” they affirm.
Pediatric airway obstruction
Thus far, the role of 3D printing seems to be most prominent in the treatment of pediatric airway obstruction, where it is used in the surgical planning stages and to create the implant itself. In a systematic review of its use for this, Joshua Stramiello, MD, University of California, San Diego, and colleagues identified 37 original articles, 11 of which discussed 3D printing for surgical planning, and 26 of which discussed 3D printing implants for interventions.
“3D printing for surgical planning not only improves preoperative assessment of surgical approach and stent customization but also helps facilitate patient/family education,” the authors observe. Most of the research so far has been focused on bioresorbable external airway splints and biological grafts, they add – “with both animal studies and human case reports showing good results in improving symptoms.” One clinical series focused on the use of a 3D-printed, patient-specific, bioresorbable airway splint in a cohort of critically ill children with severe tracheobronchomalacia. (Tracheobronchomalacia is the abnormal collapse of the windpipe).
When reported, 29 splints had been implanted in 15 children with intrathoracic tracheobronchomalacia. At a median follow-up of 8.5 months, 12 children were long-term survivors, and all but one lived at home. As recently discussed by George Cheng, MD, cofounder of restor3D, a Duke University startup that created the first 3D-printed airway stent using a compressible biocompatible material with properties similar to that of silicone, personalized airway stents have the potential for advance customization, minimize pressure points, and improve airflow dynamics to increase mucus clearance.
In fact, the U.S. Food and Drug Administration has already cleared patient-specific airway stents developed by Thomas Gildea, MD, of the Cleveland Clinic. Both the Duke University and Cleveland Clinic stents have been used in patients, with promising outcomes, Dr. Cheng noted.
The authors and Dr. Stramiello and colleagues have disclosed no relevant financial relationships. Dr. Cheng is the cofounder of restor3D.
A version of this article first appeared on Medscape.com.
New JIA guidelines emphasize earlier DMARD use
Treatment of systemic juvenile idiopathic arthritis (sJIA) should emphasize early use of conventional synthetic and biologic disease-modifying antirheumatic drugs (DMARDs), compared with the previous reliance on NSAIDs and glucocorticoids, according to new guidelines from the American College of Rheumatology. The recently published 2021 guidelines focus on therapeutic approaches for oligoarthritis, temporomandibular joint (TMJ) arthritis, and sJIA.
“Systemic JIA should be treated early with biologics to rapidly bring disease under control and to avoid long-term use of glucocorticoids,” Karen Onel, MD, chief of the division of pediatric rheumatology at Weill Cornell Medicine, New York, and lead author of the guidelines, told this news organization. “Unfortunately, biologics can and are frequently denied for first-line use. For this reason, the guidelines are critically important as they demonstrate that first-line use of biologics are standard of care for the treatment of sJIA.”

The new publication is the second part of the ACR’s process to update JIA guidelines that began in 2017 and complements the release in 2019 of guidelines on the management of nonsystemic polyarthritis, sacroiliitis, and enthesitis, as well as a separate guidance on JIA-associated uveitis. The new guidelines include a second publication focused on nonpharmacologic therapies, medication monitoring, immunizations, and imaging. Both sets of guidelines grew out of a 15-member panel that included young adults with JIA and caregivers of children with JIA, and which required at least 70% agreement on recommendations.
“Though the scope of the two guidelines differed, one thing they had in common is the recognition of the importance of shared decision-making with the patient/caregiver,” Dr. Onel said. “Not every decision will be appropriate for every patient, which is why it was so instrumental to receive input from both patients and caregivers when creating these recommendations.”
Oligoarticular and TMJ arthritis
Oligoarticular and TMJ arthritis have similar recommendations, beginning with NSAIDs conditionally recommended and intra-articular glucocorticoids (IAGCs) strongly recommended as part of initial therapy. For oligoarticular arthritis, the guidelines specifically include a strong recommendation of triamcinolone hexacetonide as the preferred agent; no preferred agent is recommended for TMJ arthritis.

“The one thing that the panel was unanimous about was the use of triamcinolone hexacetonide for intra-articular steroid injections in oligoarticular kids,” Susan Shenoi, MBBS, MS, an associate professor and clinical director of pediatric rheumatology at Seattle Children’s Hospital and Research Center, said in an interview. “Triamcinolone hexacetonide has not been available recently, and through advocacy efforts, there is now a pathway to get that medication,” added Dr. Shenoi, a coauthor on the guidelines.
Dr. Onel said that “triamcinolone hexacetonide has been shown to be superior to alternative injectable glucocorticoids in achieving and maintaining remission in children with JIA,” but its unavailability meant physicians had to consider less effective, more potent, or more costly alternatives.” To address the shortage, “the FDA allowed the importation of one particular formulation of triamcinolone hexacetonide [Hexatrione 2%] specifically for joint injections in patients with JIA.”
The guidelines conditionally recommend against oral glucocorticoids for initial therapy for both oligoarticular and TMJ arthritis. In fact, throughout the guidelines it’s clear that the authors emphasize using steroids as little as possible, Dr. Shenoi said.
“Steroids are great anti-inflammatories, but in kids we worry about the long-term effects on growth and metabolism, and now we have many more DMARDs available,” Dr. Shenoi said.
The guidelines strongly recommend conventional synthetic DMARDs for patients with either of these diseases who cannot tolerate or do not respond to NSAIDs or IAGCs, with methotrexate conditionally recommended over leflunomide (Arava) for TMJ and over leflunomide, sulfasalazine (Azulfidine, Sulfazine), and hydroxychloroquine, respectively, for oligoarticular arthritis.
“NSAIDs remain widely used despite evidence supporting early use of DMARDs,” Dr. Onel said. “NSAIDs are readily available and familiar; however, they will not prevent disease progression. These guidelines should encourage short courses of NSAIDs only.”
If patients do not respond to or cannot tolerate NSAIDs, IAGCs, and at least one conventional DMARD, the guidelines strongly recommend a biologic DMARD for oligoarticular arthritis and conditionally recommend one for TMJ arthritis, without any preferences to the specific agent.
The guidelines also advise using validated disease activity measures to guide treatment decisions.
“The most important thing when you’re looking at these patients is to determine, do they have active disease or not?” Dr. Shenoi said. “If they have active disease, then you really want to step up therapy.” Using the relatively new concept of treat-to-target, Dr. Shenoi added that a crucial part of shared decision-making with the family is identifying the most appropriate target for that family “and then really trying hard to achieve that target.”
The guidelines also list risk factors for poor outcome that can be used to guide treatment decisions.
“Specific involvement of key joints, such as TMJ, wrist, sacroiliac, hip, and ankle, and other features were considered reasonable justification for early escalation of therapy,” Dr. Onel said. Other features included presence of erosive disease or enthesitis, delay in diagnosis, elevated levels of inflammation markers, and symmetric disease. “Moving quickly may be needed for a patient who is rapidly worsening, while moving slower may be appropriate for somebody who has improved substantially, but not fully.”
Systemic JIA with and without macrophage activation syndrome
For systemic JIA without macrophage activation syndrome (MAS), the guidelines similarly advise against oral glucocorticoids as initial monotherapy while conditionally recommending NSAIDs for initial monotherapy. Where the guidelines differ most from those for oligoarticular and TMJ arthritis is in progression of DMARD use, with a strong recommendation against conventional synthetic DMARDs as an initial monotherapy and interleukin-1 and IL-6 inhibitors conditionally recommended for initial monotherapy.
For patients who don’t adequately respond to NSAIDs or glucocorticoids, IL-1 and IL-6 inhibitors are strongly recommended over a single or combination of conventional DMARDs. Residual arthritis or an incomplete response to IL-1 or IL-6 inhibitors should lead next to biologic or conventional DMARDs instead of long-term glucocorticoids.
For patients with MAS, the guidelines conditionally recommend IL-1 and IL-6 inhibitors over calcineurin inhibitor monotherapy to reach inactive disease and MAS resolution, with glucocorticoids conditionally recommended in initial treatment. Again, however, for patients with incomplete responses to IL-1 or IL-6 inhibitors or with residual arthritis, the guidelines advise biologic or conventional DMARDs over long-term glucocorticoids.
In patients with sJIA with or without a history of MAS who have inactive disease, practitioners should taper and discontinue glucocorticoids (a strong recommendation). A conditional recommendation for tapering and discontinuing biologic DMARDs follows attainment of inactive disease.
Beyond pharmacology
Although many of the nonpharmacologic recommendations did not have strong evidence based on assessment with Grading of Recommendations Assessment, Development, and Evaluation methodology, consensus was more often the case than not, Dr. Onel said, such as with vaccination.
“There was strong support for the use of immunizations in children with JIA and specific guidance for children with JIA receiving immunosuppression, not on immunosuppression, and children who are underimmunized or unimmunized,” she said. “Although the supportive evidence was very low as per GRADE, panel members were strongly in favor [of immunizations], given risk of infection for immunosuppressed children as well as the preponderance of evidence in similar disease states, such as IBD [inflammatory bowel disease].”
An area with less consensus was whether to check antibody titers for vaccine-preventable childhood infections before beginning immunosuppressive medication, but more panelists opposed the practice than supported it, Dr. Onel said.
“Some panelists felt that the information might be useful for risk management in case of an outbreak or exposure,” she said. “Most believed that screening a fully immunized child was of low benefit and might delay treatment and incur unnecessary cost.”
The process of developing the documents also reveals where the biggest gaps are in research.
“One of the things that we should strive for in the future is really to do more systematic studies so we have better quality of evidence going forward,” Dr. Shenoi said. Overall, however, the guidelines also reveal the progress made in treatment of JIA.
“We now know some of the key cytokines that are involved in the disease pathogenesis, and we have effective therapies for some of these pathways,” Dr. Shenoi said. “We used to use a lot more toxic medication for systemic JIA, and in past decades, these patients used to be on steroids forever. Now we have targeted therapies, and we have some patients who don’t ever need steroids because people are moving toward targeted therapies and having good results. That’s a huge step forward in the field.”
The research was funded by the ACR. Dr. Shenoi has been a consultant for Pfizer. Dr. Onel disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Treatment of systemic juvenile idiopathic arthritis (sJIA) should emphasize early use of conventional synthetic and biologic disease-modifying antirheumatic drugs (DMARDs), compared with the previous reliance on NSAIDs and glucocorticoids, according to new guidelines from the American College of Rheumatology. The recently published 2021 guidelines focus on therapeutic approaches for oligoarthritis, temporomandibular joint (TMJ) arthritis, and sJIA.
“Systemic JIA should be treated early with biologics to rapidly bring disease under control and to avoid long-term use of glucocorticoids,” Karen Onel, MD, chief of the division of pediatric rheumatology at Weill Cornell Medicine, New York, and lead author of the guidelines, told this news organization. “Unfortunately, biologics can and are frequently denied for first-line use. For this reason, the guidelines are critically important as they demonstrate that first-line use of biologics are standard of care for the treatment of sJIA.”
The new publication is the second part of the ACR’s process to update JIA guidelines that began in 2017 and complements the release in 2019 of guidelines on the management of nonsystemic polyarthritis, sacroiliitis, and enthesitis, as well as a separate guidance on JIA-associated uveitis. The new guidelines include a second publication focused on nonpharmacologic therapies, medication monitoring, immunizations, and imaging. Both sets of guidelines grew out of a 15-member panel that included young adults with JIA and caregivers of children with JIA, and which required at least 70% agreement on recommendations.
“Though the scope of the two guidelines differed, one thing they had in common is the recognition of the importance of shared decision-making with the patient/caregiver,” Dr. Onel said. “Not every decision will be appropriate for every patient, which is why it was so instrumental to receive input from both patients and caregivers when creating these recommendations.”
Oligoarticular and TMJ arthritis
Oligoarticular and TMJ arthritis have similar recommendations, beginning with NSAIDs conditionally recommended and intra-articular glucocorticoids (IAGCs) strongly recommended as part of initial therapy. For oligoarticular arthritis, the guidelines specifically include a strong recommendation of triamcinolone hexacetonide as the preferred agent; no preferred agent is recommended for TMJ arthritis.
“The one thing that the panel was unanimous about was the use of triamcinolone hexacetonide for intra-articular steroid injections in oligoarticular kids,” Susan Shenoi, MBBS, MS, an associate professor and clinical director of pediatric rheumatology at Seattle Children’s Hospital and Research Center, said in an interview. “Triamcinolone hexacetonide has not been available recently, and through advocacy efforts, there is now a pathway to get that medication,” added Dr. Shenoi, a coauthor on the guidelines.
Dr. Onel said that “triamcinolone hexacetonide has been shown to be superior to alternative injectable glucocorticoids in achieving and maintaining remission in children with JIA,” but its unavailability meant physicians had to consider less effective, more potent, or more costly alternatives.” To address the shortage, “the FDA allowed the importation of one particular formulation of triamcinolone hexacetonide [Hexatrione 2%] specifically for joint injections in patients with JIA.”
The guidelines conditionally recommend against oral glucocorticoids for initial therapy for both oligoarticular and TMJ arthritis. In fact, throughout the guidelines it’s clear that the authors emphasize using steroids as little as possible, Dr. Shenoi said.
“Steroids are great anti-inflammatories, but in kids we worry about the long-term effects on growth and metabolism, and now we have many more DMARDs available,” Dr. Shenoi said.
The guidelines strongly recommend conventional synthetic DMARDs for patients with either of these diseases who cannot tolerate or do not respond to NSAIDs or IAGCs, with methotrexate conditionally recommended over leflunomide (Arava) for TMJ and over leflunomide, sulfasalazine (Azulfidine, Sulfazine), and hydroxychloroquine, respectively, for oligoarticular arthritis.
“NSAIDs remain widely used despite evidence supporting early use of DMARDs,” Dr. Onel said. “NSAIDs are readily available and familiar; however, they will not prevent disease progression. These guidelines should encourage short courses of NSAIDs only.”
If patients do not respond to or cannot tolerate NSAIDs, IAGCs, and at least one conventional DMARD, the guidelines strongly recommend a biologic DMARD for oligoarticular arthritis and conditionally recommend one for TMJ arthritis, without any preferences to the specific agent.
The guidelines also advise using validated disease activity measures to guide treatment decisions.
“The most important thing when you’re looking at these patients is to determine, do they have active disease or not?” Dr. Shenoi said. “If they have active disease, then you really want to step up therapy.” Using the relatively new concept of treat-to-target, Dr. Shenoi added that a crucial part of shared decision-making with the family is identifying the most appropriate target for that family “and then really trying hard to achieve that target.”
The guidelines also list risk factors for poor outcome that can be used to guide treatment decisions.
“Specific involvement of key joints, such as TMJ, wrist, sacroiliac, hip, and ankle, and other features were considered reasonable justification for early escalation of therapy,” Dr. Onel said. Other features included presence of erosive disease or enthesitis, delay in diagnosis, elevated levels of inflammation markers, and symmetric disease. “Moving quickly may be needed for a patient who is rapidly worsening, while moving slower may be appropriate for somebody who has improved substantially, but not fully.”
Systemic JIA with and without macrophage activation syndrome
For systemic JIA without macrophage activation syndrome (MAS), the guidelines similarly advise against oral glucocorticoids as initial monotherapy while conditionally recommending NSAIDs for initial monotherapy. Where the guidelines differ most from those for oligoarticular and TMJ arthritis is in progression of DMARD use, with a strong recommendation against conventional synthetic DMARDs as an initial monotherapy and interleukin-1 and IL-6 inhibitors conditionally recommended for initial monotherapy.
For patients who don’t adequately respond to NSAIDs or glucocorticoids, IL-1 and IL-6 inhibitors are strongly recommended over a single or combination of conventional DMARDs. Residual arthritis or an incomplete response to IL-1 or IL-6 inhibitors should lead next to biologic or conventional DMARDs instead of long-term glucocorticoids.
For patients with MAS, the guidelines conditionally recommend IL-1 and IL-6 inhibitors over calcineurin inhibitor monotherapy to reach inactive disease and MAS resolution, with glucocorticoids conditionally recommended in initial treatment. Again, however, for patients with incomplete responses to IL-1 or IL-6 inhibitors or with residual arthritis, the guidelines advise biologic or conventional DMARDs over long-term glucocorticoids.
In patients with sJIA with or without a history of MAS who have inactive disease, practitioners should taper and discontinue glucocorticoids (a strong recommendation). A conditional recommendation for tapering and discontinuing biologic DMARDs follows attainment of inactive disease.
Beyond pharmacology
Although many of the nonpharmacologic recommendations did not have strong evidence based on assessment with Grading of Recommendations Assessment, Development, and Evaluation methodology, consensus was more often the case than not, Dr. Onel said, such as with vaccination.
“There was strong support for the use of immunizations in children with JIA and specific guidance for children with JIA receiving immunosuppression, not on immunosuppression, and children who are underimmunized or unimmunized,” she said. “Although the supportive evidence was very low as per GRADE, panel members were strongly in favor [of immunizations], given risk of infection for immunosuppressed children as well as the preponderance of evidence in similar disease states, such as IBD [inflammatory bowel disease].”
An area with less consensus was whether to check antibody titers for vaccine-preventable childhood infections before beginning immunosuppressive medication, but more panelists opposed the practice than supported it, Dr. Onel said.
“Some panelists felt that the information might be useful for risk management in case of an outbreak or exposure,” she said. “Most believed that screening a fully immunized child was of low benefit and might delay treatment and incur unnecessary cost.”
The process of developing the documents also reveals where the biggest gaps are in research.
“One of the things that we should strive for in the future is really to do more systematic studies so we have better quality of evidence going forward,” Dr. Shenoi said. Overall, however, the guidelines also reveal the progress made in treatment of JIA.
“We now know some of the key cytokines that are involved in the disease pathogenesis, and we have effective therapies for some of these pathways,” Dr. Shenoi said. “We used to use a lot more toxic medication for systemic JIA, and in past decades, these patients used to be on steroids forever. Now we have targeted therapies, and we have some patients who don’t ever need steroids because people are moving toward targeted therapies and having good results. That’s a huge step forward in the field.”
The research was funded by the ACR. Dr. Shenoi has been a consultant for Pfizer. Dr. Onel disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Treatment of systemic juvenile idiopathic arthritis (sJIA) should emphasize early use of conventional synthetic and biologic disease-modifying antirheumatic drugs (DMARDs), compared with the previous reliance on NSAIDs and glucocorticoids, according to new guidelines from the American College of Rheumatology. The recently published 2021 guidelines focus on therapeutic approaches for oligoarthritis, temporomandibular joint (TMJ) arthritis, and sJIA.
“Systemic JIA should be treated early with biologics to rapidly bring disease under control and to avoid long-term use of glucocorticoids,” Karen Onel, MD, chief of the division of pediatric rheumatology at Weill Cornell Medicine, New York, and lead author of the guidelines, told this news organization. “Unfortunately, biologics can and are frequently denied for first-line use. For this reason, the guidelines are critically important as they demonstrate that first-line use of biologics are standard of care for the treatment of sJIA.”
The new publication is the second part of the ACR’s process to update JIA guidelines that began in 2017 and complements the release in 2019 of guidelines on the management of nonsystemic polyarthritis, sacroiliitis, and enthesitis, as well as a separate guidance on JIA-associated uveitis. The new guidelines include a second publication focused on nonpharmacologic therapies, medication monitoring, immunizations, and imaging. Both sets of guidelines grew out of a 15-member panel that included young adults with JIA and caregivers of children with JIA, and which required at least 70% agreement on recommendations.
“Though the scope of the two guidelines differed, one thing they had in common is the recognition of the importance of shared decision-making with the patient/caregiver,” Dr. Onel said. “Not every decision will be appropriate for every patient, which is why it was so instrumental to receive input from both patients and caregivers when creating these recommendations.”
Oligoarticular and TMJ arthritis
Oligoarticular and TMJ arthritis have similar recommendations, beginning with NSAIDs conditionally recommended and intra-articular glucocorticoids (IAGCs) strongly recommended as part of initial therapy. For oligoarticular arthritis, the guidelines specifically include a strong recommendation of triamcinolone hexacetonide as the preferred agent; no preferred agent is recommended for TMJ arthritis.
“The one thing that the panel was unanimous about was the use of triamcinolone hexacetonide for intra-articular steroid injections in oligoarticular kids,” Susan Shenoi, MBBS, MS, an associate professor and clinical director of pediatric rheumatology at Seattle Children’s Hospital and Research Center, said in an interview. “Triamcinolone hexacetonide has not been available recently, and through advocacy efforts, there is now a pathway to get that medication,” added Dr. Shenoi, a coauthor on the guidelines.
Dr. Onel said that “triamcinolone hexacetonide has been shown to be superior to alternative injectable glucocorticoids in achieving and maintaining remission in children with JIA,” but its unavailability meant physicians had to consider less effective, more potent, or more costly alternatives.” To address the shortage, “the FDA allowed the importation of one particular formulation of triamcinolone hexacetonide [Hexatrione 2%] specifically for joint injections in patients with JIA.”
The guidelines conditionally recommend against oral glucocorticoids for initial therapy for both oligoarticular and TMJ arthritis. In fact, throughout the guidelines it’s clear that the authors emphasize using steroids as little as possible, Dr. Shenoi said.
“Steroids are great anti-inflammatories, but in kids we worry about the long-term effects on growth and metabolism, and now we have many more DMARDs available,” Dr. Shenoi said.
The guidelines strongly recommend conventional synthetic DMARDs for patients with either of these diseases who cannot tolerate or do not respond to NSAIDs or IAGCs, with methotrexate conditionally recommended over leflunomide (Arava) for TMJ and over leflunomide, sulfasalazine (Azulfidine, Sulfazine), and hydroxychloroquine, respectively, for oligoarticular arthritis.
“NSAIDs remain widely used despite evidence supporting early use of DMARDs,” Dr. Onel said. “NSAIDs are readily available and familiar; however, they will not prevent disease progression. These guidelines should encourage short courses of NSAIDs only.”
If patients do not respond to or cannot tolerate NSAIDs, IAGCs, and at least one conventional DMARD, the guidelines strongly recommend a biologic DMARD for oligoarticular arthritis and conditionally recommend one for TMJ arthritis, without any preferences to the specific agent.
The guidelines also advise using validated disease activity measures to guide treatment decisions.
“The most important thing when you’re looking at these patients is to determine, do they have active disease or not?” Dr. Shenoi said. “If they have active disease, then you really want to step up therapy.” Using the relatively new concept of treat-to-target, Dr. Shenoi added that a crucial part of shared decision-making with the family is identifying the most appropriate target for that family “and then really trying hard to achieve that target.”
The guidelines also list risk factors for poor outcome that can be used to guide treatment decisions.
“Specific involvement of key joints, such as TMJ, wrist, sacroiliac, hip, and ankle, and other features were considered reasonable justification for early escalation of therapy,” Dr. Onel said. Other features included presence of erosive disease or enthesitis, delay in diagnosis, elevated levels of inflammation markers, and symmetric disease. “Moving quickly may be needed for a patient who is rapidly worsening, while moving slower may be appropriate for somebody who has improved substantially, but not fully.”
Systemic JIA with and without macrophage activation syndrome
For systemic JIA without macrophage activation syndrome (MAS), the guidelines similarly advise against oral glucocorticoids as initial monotherapy while conditionally recommending NSAIDs for initial monotherapy. Where the guidelines differ most from those for oligoarticular and TMJ arthritis is in progression of DMARD use, with a strong recommendation against conventional synthetic DMARDs as an initial monotherapy and interleukin-1 and IL-6 inhibitors conditionally recommended for initial monotherapy.
For patients who don’t adequately respond to NSAIDs or glucocorticoids, IL-1 and IL-6 inhibitors are strongly recommended over a single or combination of conventional DMARDs. Residual arthritis or an incomplete response to IL-1 or IL-6 inhibitors should lead next to biologic or conventional DMARDs instead of long-term glucocorticoids.
For patients with MAS, the guidelines conditionally recommend IL-1 and IL-6 inhibitors over calcineurin inhibitor monotherapy to reach inactive disease and MAS resolution, with glucocorticoids conditionally recommended in initial treatment. Again, however, for patients with incomplete responses to IL-1 or IL-6 inhibitors or with residual arthritis, the guidelines advise biologic or conventional DMARDs over long-term glucocorticoids.
In patients with sJIA with or without a history of MAS who have inactive disease, practitioners should taper and discontinue glucocorticoids (a strong recommendation). A conditional recommendation for tapering and discontinuing biologic DMARDs follows attainment of inactive disease.
Beyond pharmacology
Although many of the nonpharmacologic recommendations did not have strong evidence based on assessment with Grading of Recommendations Assessment, Development, and Evaluation methodology, consensus was more often the case than not, Dr. Onel said, such as with vaccination.
“There was strong support for the use of immunizations in children with JIA and specific guidance for children with JIA receiving immunosuppression, not on immunosuppression, and children who are underimmunized or unimmunized,” she said. “Although the supportive evidence was very low as per GRADE, panel members were strongly in favor [of immunizations], given risk of infection for immunosuppressed children as well as the preponderance of evidence in similar disease states, such as IBD [inflammatory bowel disease].”
An area with less consensus was whether to check antibody titers for vaccine-preventable childhood infections before beginning immunosuppressive medication, but more panelists opposed the practice than supported it, Dr. Onel said.
“Some panelists felt that the information might be useful for risk management in case of an outbreak or exposure,” she said. “Most believed that screening a fully immunized child was of low benefit and might delay treatment and incur unnecessary cost.”
The process of developing the documents also reveals where the biggest gaps are in research.
“One of the things that we should strive for in the future is really to do more systematic studies so we have better quality of evidence going forward,” Dr. Shenoi said. Overall, however, the guidelines also reveal the progress made in treatment of JIA.
“We now know some of the key cytokines that are involved in the disease pathogenesis, and we have effective therapies for some of these pathways,” Dr. Shenoi said. “We used to use a lot more toxic medication for systemic JIA, and in past decades, these patients used to be on steroids forever. Now we have targeted therapies, and we have some patients who don’t ever need steroids because people are moving toward targeted therapies and having good results. That’s a huge step forward in the field.”
The research was funded by the ACR. Dr. Shenoi has been a consultant for Pfizer. Dr. Onel disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ARTHRITIS & RHEUMATOLOGY