User login
A 7-year-old with red bumps on her nose
The finding of individual, 1- to 4-mm firm, red papules depicted in the image are consistent with facial angiofibromas, which are most commonly seen in pediatric patients as a manifestation of tuberous sclerosis (TSC). Angiofibromas, previously called adenoma sebaceum, a misnomer, are seen in TSC as smooth papules, nodules, and occasionally plaques that typically involve the malar region of the face. These lesions usually develop in childhood and adolescence and can be misdiagnosed as lesions of acne. The number of lesions tend to increase with age, though there is no significant risk of malignant transformation. Ultraviolet-induced DNA damage is thought to play a role in the development of facial angiofibromas, so sun protection is called for.1 Patients may seek treatment to minimize deformity and the stigma of angiofibromas. Recently, the mammalian target of rapamycin inhibitor sirolimus (rapamycin) topical gel received Food and Drug Administration approval for the treatment of facial angiofibromas associated with TSC in patients age at least 6 years.2
The presence of angiofibromas should prompt consideration of TSC and as such, a thorough family history, medical history, and full-body skin examination. TSC is a rare autosomal-dominant genetic disorder, caused by a pathogenic variant in either the TSC1 or TSC2 gene. This neurocutaneous disorder is characterized by the development of multiple benign hamartomas across many organ systems including the brain, eyes, heart, lung, liver, kidney, and skin. The phenotypic expression of TSC is highly variable. Besides angiofibromas, some other characteristic dermatological findings in TSC include periungual fibromas, hypopigmented macules usually elliptical in shape (known as ash-leaf spots), and irregularly shaped elevated flesh-colored fibrous tissue most often found over the lower back (known as shagreen patches).3
What is on the differential?
Agminated spitz nevi refers to multiple spitz nevi in a localized area. Spitz nevi present as a well-circumscribed, dome-shaped, pink-red or brown papules, most commonly located on the face or lower extremities.4 The finding of agminated spitz nevi is very rare and less likely for this patient given the concomitant skin findings of dental pitting, renal cysts, and cortical tubers.

Juvenile xanthogranulomas are benign,proliferations of histiocytic cells that present as reddish or yellowish-to-brown papules, plaques, or nodules that typically develop in young children around the age of 1. With time, juvenile xanthogranulomas may flatten and become more yellow.
Basal cell carcinomas present as dome-shaped lesions with centralized erosions on sun-exposed areas of the skin. They are remarkably uncommon in children but are occasionally seen in basal cell nevus syndrome (also known as nevoid basal cell carcinoma syndrome or Gorlin syndrome). Affected patients may have other findings such as developmental anomalies, bifid ribs, palmar and plantar pitting, odontogenic keratocysts, and/or medulloblastomas.5
Flat warts commonly occur in children and occur by direct skin contact with human papillomavirus. Of the various types of warts, flat warts are smaller and tend to be smooth on top. The diagnosis of cutaneous warts is based on clinical appearance, showing thrombosed capillaries underneath the overlying hyperkeratotic debris. Our patient’s history of having a common wart on her hands raises suspicion for inoculation onto her face, but the morphology, distribution, and lack of response to tretinoin makes this diagnosis much less likely.

Disease workup and course
Our patient’s physical exam revealed dental pits but no evidence of hypopigmented macules, shagreen patches, or periungual lesions. Ultrasound of the kidney displayed renal cortical cysts and brain MRI showed cortical tubers, confirming extracutaneous TSC involvement. Over time, our patient developed angiofibromas on the forehead and was ultimately started on topical sirolimus, which led to marked improvement within months.
Ms. Kleinman is a pediatric dermatology research associate, division of pediatric and adolescent dermatology, University of California, San Diego, and Rady Children’s Hospital, also in San Diego. Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital. They have no relevant financial disclosures.
References
1. Tyburczy ME et al. Hum Molec Genet. 2014;23(8):2023-9.
2. Food & Drug Administration. New drug application (NDA) approval for Hyftor (sirolimus topical gel). https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2022/213478Orig1s000ltr.pdf.
3. Webb DW et al. Br J Dermatol. 1996;135(1):1-5.
4. Ricci F et al. Eur J Dermatol. 2017;27(1):59-62.
5. Evans DG and Farndon PA. Nevoid basal cell carcinoma syndrome, in “GeneReviews®.” Seattle: University of Washington, 2002.
The finding of individual, 1- to 4-mm firm, red papules depicted in the image are consistent with facial angiofibromas, which are most commonly seen in pediatric patients as a manifestation of tuberous sclerosis (TSC). Angiofibromas, previously called adenoma sebaceum, a misnomer, are seen in TSC as smooth papules, nodules, and occasionally plaques that typically involve the malar region of the face. These lesions usually develop in childhood and adolescence and can be misdiagnosed as lesions of acne. The number of lesions tend to increase with age, though there is no significant risk of malignant transformation. Ultraviolet-induced DNA damage is thought to play a role in the development of facial angiofibromas, so sun protection is called for.1 Patients may seek treatment to minimize deformity and the stigma of angiofibromas. Recently, the mammalian target of rapamycin inhibitor sirolimus (rapamycin) topical gel received Food and Drug Administration approval for the treatment of facial angiofibromas associated with TSC in patients age at least 6 years.2
The presence of angiofibromas should prompt consideration of TSC and as such, a thorough family history, medical history, and full-body skin examination. TSC is a rare autosomal-dominant genetic disorder, caused by a pathogenic variant in either the TSC1 or TSC2 gene. This neurocutaneous disorder is characterized by the development of multiple benign hamartomas across many organ systems including the brain, eyes, heart, lung, liver, kidney, and skin. The phenotypic expression of TSC is highly variable. Besides angiofibromas, some other characteristic dermatological findings in TSC include periungual fibromas, hypopigmented macules usually elliptical in shape (known as ash-leaf spots), and irregularly shaped elevated flesh-colored fibrous tissue most often found over the lower back (known as shagreen patches).3
What is on the differential?
Agminated spitz nevi refers to multiple spitz nevi in a localized area. Spitz nevi present as a well-circumscribed, dome-shaped, pink-red or brown papules, most commonly located on the face or lower extremities.4 The finding of agminated spitz nevi is very rare and less likely for this patient given the concomitant skin findings of dental pitting, renal cysts, and cortical tubers.
Juvenile xanthogranulomas are benign,proliferations of histiocytic cells that present as reddish or yellowish-to-brown papules, plaques, or nodules that typically develop in young children around the age of 1. With time, juvenile xanthogranulomas may flatten and become more yellow.
Basal cell carcinomas present as dome-shaped lesions with centralized erosions on sun-exposed areas of the skin. They are remarkably uncommon in children but are occasionally seen in basal cell nevus syndrome (also known as nevoid basal cell carcinoma syndrome or Gorlin syndrome). Affected patients may have other findings such as developmental anomalies, bifid ribs, palmar and plantar pitting, odontogenic keratocysts, and/or medulloblastomas.5
Flat warts commonly occur in children and occur by direct skin contact with human papillomavirus. Of the various types of warts, flat warts are smaller and tend to be smooth on top. The diagnosis of cutaneous warts is based on clinical appearance, showing thrombosed capillaries underneath the overlying hyperkeratotic debris. Our patient’s history of having a common wart on her hands raises suspicion for inoculation onto her face, but the morphology, distribution, and lack of response to tretinoin makes this diagnosis much less likely.
Disease workup and course
Our patient’s physical exam revealed dental pits but no evidence of hypopigmented macules, shagreen patches, or periungual lesions. Ultrasound of the kidney displayed renal cortical cysts and brain MRI showed cortical tubers, confirming extracutaneous TSC involvement. Over time, our patient developed angiofibromas on the forehead and was ultimately started on topical sirolimus, which led to marked improvement within months.
Ms. Kleinman is a pediatric dermatology research associate, division of pediatric and adolescent dermatology, University of California, San Diego, and Rady Children’s Hospital, also in San Diego. Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital. They have no relevant financial disclosures.
References
1. Tyburczy ME et al. Hum Molec Genet. 2014;23(8):2023-9.
2. Food & Drug Administration. New drug application (NDA) approval for Hyftor (sirolimus topical gel). https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2022/213478Orig1s000ltr.pdf.
3. Webb DW et al. Br J Dermatol. 1996;135(1):1-5.
4. Ricci F et al. Eur J Dermatol. 2017;27(1):59-62.
5. Evans DG and Farndon PA. Nevoid basal cell carcinoma syndrome, in “GeneReviews®.” Seattle: University of Washington, 2002.
The finding of individual, 1- to 4-mm firm, red papules depicted in the image are consistent with facial angiofibromas, which are most commonly seen in pediatric patients as a manifestation of tuberous sclerosis (TSC). Angiofibromas, previously called adenoma sebaceum, a misnomer, are seen in TSC as smooth papules, nodules, and occasionally plaques that typically involve the malar region of the face. These lesions usually develop in childhood and adolescence and can be misdiagnosed as lesions of acne. The number of lesions tend to increase with age, though there is no significant risk of malignant transformation. Ultraviolet-induced DNA damage is thought to play a role in the development of facial angiofibromas, so sun protection is called for.1 Patients may seek treatment to minimize deformity and the stigma of angiofibromas. Recently, the mammalian target of rapamycin inhibitor sirolimus (rapamycin) topical gel received Food and Drug Administration approval for the treatment of facial angiofibromas associated with TSC in patients age at least 6 years.2
The presence of angiofibromas should prompt consideration of TSC and as such, a thorough family history, medical history, and full-body skin examination. TSC is a rare autosomal-dominant genetic disorder, caused by a pathogenic variant in either the TSC1 or TSC2 gene. This neurocutaneous disorder is characterized by the development of multiple benign hamartomas across many organ systems including the brain, eyes, heart, lung, liver, kidney, and skin. The phenotypic expression of TSC is highly variable. Besides angiofibromas, some other characteristic dermatological findings in TSC include periungual fibromas, hypopigmented macules usually elliptical in shape (known as ash-leaf spots), and irregularly shaped elevated flesh-colored fibrous tissue most often found over the lower back (known as shagreen patches).3
What is on the differential?
Agminated spitz nevi refers to multiple spitz nevi in a localized area. Spitz nevi present as a well-circumscribed, dome-shaped, pink-red or brown papules, most commonly located on the face or lower extremities.4 The finding of agminated spitz nevi is very rare and less likely for this patient given the concomitant skin findings of dental pitting, renal cysts, and cortical tubers.
Juvenile xanthogranulomas are benign,proliferations of histiocytic cells that present as reddish or yellowish-to-brown papules, plaques, or nodules that typically develop in young children around the age of 1. With time, juvenile xanthogranulomas may flatten and become more yellow.
Basal cell carcinomas present as dome-shaped lesions with centralized erosions on sun-exposed areas of the skin. They are remarkably uncommon in children but are occasionally seen in basal cell nevus syndrome (also known as nevoid basal cell carcinoma syndrome or Gorlin syndrome). Affected patients may have other findings such as developmental anomalies, bifid ribs, palmar and plantar pitting, odontogenic keratocysts, and/or medulloblastomas.5
Flat warts commonly occur in children and occur by direct skin contact with human papillomavirus. Of the various types of warts, flat warts are smaller and tend to be smooth on top. The diagnosis of cutaneous warts is based on clinical appearance, showing thrombosed capillaries underneath the overlying hyperkeratotic debris. Our patient’s history of having a common wart on her hands raises suspicion for inoculation onto her face, but the morphology, distribution, and lack of response to tretinoin makes this diagnosis much less likely.
Disease workup and course
Our patient’s physical exam revealed dental pits but no evidence of hypopigmented macules, shagreen patches, or periungual lesions. Ultrasound of the kidney displayed renal cortical cysts and brain MRI showed cortical tubers, confirming extracutaneous TSC involvement. Over time, our patient developed angiofibromas on the forehead and was ultimately started on topical sirolimus, which led to marked improvement within months.
Ms. Kleinman is a pediatric dermatology research associate, division of pediatric and adolescent dermatology, University of California, San Diego, and Rady Children’s Hospital, also in San Diego. Dr. Eichenfield is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego, and Rady Children’s Hospital. They have no relevant financial disclosures.
References
1. Tyburczy ME et al. Hum Molec Genet. 2014;23(8):2023-9.
2. Food & Drug Administration. New drug application (NDA) approval for Hyftor (sirolimus topical gel). https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2022/213478Orig1s000ltr.pdf.
3. Webb DW et al. Br J Dermatol. 1996;135(1):1-5.
4. Ricci F et al. Eur J Dermatol. 2017;27(1):59-62.
5. Evans DG and Farndon PA. Nevoid basal cell carcinoma syndrome, in “GeneReviews®.” Seattle: University of Washington, 2002.
A 7-year-old female presented with a bump on the bridge of her nose that was present for 10 months, with subsequent development of multiple papules on the nose and cheeks.

A 7-year-old, previously healthy female presented with a bump on the bridge of her nose that was present for 10 months, with subsequent development of multiple papules on the nose and cheeks. She has no significant medical history aside from a wart on her hand that was recently frozen with liquid nitrogen and resolved. She denied pruritus, bumps, or skin changes elsewhere on the body. The patient was prescribed tretinoin 0.1% cream applied nightly for several months without response.
First fatty liver guidelines for endocrinology, primary care
New clinical practice guidelines for the diagnosis and management of nonalcoholic fatty liver disease (NAFLD) are the first to be targeted specifically to primary care and endocrinology clinical settings.
They include 34 evidence-based clinical practice recommendations for screening, diagnosis, management, and referral, presented in a table and an algorithm flow chart as well as detailed text.
The new guidelines are by the American Association of Clinical Endocrinology and cosponsored by the American Association for the Study of Liver Diseases. They were presented at the annual scientific & clinical congress of the AACE and simultaneously published in Endocrine Practice.
These are “the first of this type for this field of medicine. The vast majority of patients with NAFLD are being seen in the primary care and endocrinology settings. Only when they get to the more advanced disease are they being referred to the liver specialists. So, we need to be the ones who are diagnosing and managing these patients because there just aren’t enough liver specialists to do that,” Scott Isaacs, MD, cochair of the writing panel for the guidelines, said in an interview.
80 million Americans have NAFLD, but very few are aware
The spectrum of NAFLD ranges from nonprogressive steatosis to the progressive conditions nonalcoholic steatohepatitis, fibrotic NASH, and end-stage NASH cirrhosis. And NASH, in turn, is a major cause of liver cancer. NAFLD is also strongly associated with insulin resistance, type 2 diabetes, atherogenesis, and myocardial dysfunction.
The global prevalence of NAFLD is about 25% and NASH, about 12%-14%. However, a recent study found that, among patients in endocrine and primary care clinics, more than 70% of patients with type 2 diabetes and more than 90% with type 2 diabetes who had a body mass index above 35 kg/m2 also had NAFLD, and more than 20% of those patients had significant liver fibrosis.
Problematically, very few people are aware they have either. “It’s so common. At least 80 million Americans have this but only about 6% know they have it. We talk about it a lot, but it’s not talked about enough,” said Dr. Isaacs, an endocrinologist who practices in Atlanta.
In fact, most cases of NAFLD are diagnosed incidentally when people undergo an ultrasound or a CT scan for another reason. And, in about 70% of cases the liver enzymes are normal, and those patients rarely undergo liver workups, Dr. Isaacs noted.
In an accompanying editorial, Suthat Liangpunsakul, MD, wrote: “In my perspective, as a hepatologist, this AACE guideline is very practical and easy to incorporate into routine practice in primary care and endocrinology settings. ... Early identification and risk stratification of patients with NAFLD, especially the degree of hepatic fibrosis, are required to reduce downstream health care costs and triage unwarranted specialty care referrals.”
And “an effective screening strategy may also identify those in primary care and endocrinology settings who may benefit from an appropriate referral to hepatologists before the development of portal hypertension complications, decompensated liver disease, and hepatocellular carcinoma,” added Dr. Liangpunsakul, professor of medicine in the division of gastroenterology and hepatology at Indiana University, Indianapolis.
Screening advised using new FIB-4 test
The guideline calls for screening all patients at high risk for NAFLD, including those with prediabetes, type 2 diabetes, obesity, and/or two or more cardiometabolic risk factors, or those with hepatic steatosis found on imaging, and/or persistently elevated plasma aminotransferase levels (that is, for more than 6 months).
The recommended screening test is the Fibrosis-4 (FIB-4) index, calculated using the patient’s age, AST level, platelet count, and ALT level: FIB-4 score = age (years) x AST (U/L)/PLT (109/L) x ALT ½ (U/L).
Recently approved by the Food and Drug Administration, the FIB-4 has been demonstrated to help identify liver disease in primary care settings.
“We really want to encourage clinicians to do the screening. The first step is the FIB-4 test. It’s a mathematical calculation using blood tests that we do anyway,” Dr. Isaacs said in an interview.
The FIB-4 stratifies patients as being low, intermediate, or high risk for liver fibrosis. Those at low risk can be managed in primary care or endocrinology settings with a focus on obesity management and cardiovascular disease prevention. “Those at low risk on FIB-4 still have a high cardiovascular disease risk. They still need to be managed,” Dr. Isaacs observed.
For those at intermediate risk, a second noninvasive test – either a liver stiffness measurement by elastography or an enhanced liver fibrosis test – is advised. If the patient is found to be at high risk or is still indeterminant after two noninvasive tests, referral to a liver specialist for further testing, including possible biopsy, is advised.
Those found to be at high risk with the FIB-4 should also be referred to hepatology. In both the intermediate- and high-risk groups, management should be multidisciplinary, including a hepatologist, endocrinologist, and other professionals to prevent both cardiovascular disease and progression to cirrhosis, the guidelines say.
“The diagnosis isn’t about diagnosing liver fat. It’s about diagnosing fibrosis, or the risk for clinically significant fibrosis. That’s really where the challenge lies,” Dr. Isaacs commented.
NAFLD treatment in endocrinology and primary care: CVD prevention
During the presentation at the AACE meeting, guideline panel cochair Kenneth Cusi, MD, chief of endocrinology, diabetes, and metabolism at the University of Florida, Gainesville, summarized current and future treatments for NAFLD.
Lifestyle intervention, cardiovascular risk reduction, and weight loss for those who are overweight or obese are recommended for all patients with NAFLD, including structured weight-loss programs, antiobesity medications, and bariatric surgery if indicated.
There are currently no FDA-approved medications specifically for NASH, but pioglitazone, approved for type 2 diabetes, and glucagonlike peptide–1 agonists, approved for type 2 diabetes and weight loss, have been shown to be effective in treating the condition and preventing progression. Other treatments are in development, Dr. Cusi said.
The guideline also includes a section on diagnosis and management of NAFLD in children and adolescents. Here, the FIB-4 is not recommended because it isn’t accurate due to the age part of the equation, so liver enzyme tests are used in pediatric patients considered at high risk because of clinical factors. Management is similar to adults, except not all medications used in adults are approved for use in children.
In the editorial, Dr. Liangpunsakul cautioned that “the level of uptake and usage of the guideline may be an obstacle.”
To remedy that, he advised that “the next effort should gear toward distributing this guideline to the targeted providers and developing the ‘feedback platforms’ on its execution in the real-world. ... The successful implementation of this AACE guideline by the primary care providers and endocrinologists, hopefully, will deescalate the future burden of NAFLD-related morbidity and mortality.”
Dr. Isaacs and Dr. Liangpunsakul have reported no relevant financial relationships. Dr. Cusi has reported receiving research support towards the University of Florida as principal investigator from the National Institute of Health, Echosens, Inventiva, Nordic Bioscience, Novo Nordisk, Poxel, Labcorp, and Zydus, and is a consultant for Altimmune, Akero, Arrowhead, AstraZeneca, 89Bio, Bristol-Myers Squibb, Coherus, Intercept, Lilly, Madrigal, Merck, Novo Nordisk, Quest, Sagimet, Sonic Incytes, Terns, and Thera Technologies.
A version of this article first appeared on Medscape.com.
New clinical practice guidelines for the diagnosis and management of nonalcoholic fatty liver disease (NAFLD) are the first to be targeted specifically to primary care and endocrinology clinical settings.
They include 34 evidence-based clinical practice recommendations for screening, diagnosis, management, and referral, presented in a table and an algorithm flow chart as well as detailed text.
The new guidelines are by the American Association of Clinical Endocrinology and cosponsored by the American Association for the Study of Liver Diseases. They were presented at the annual scientific & clinical congress of the AACE and simultaneously published in Endocrine Practice.
These are “the first of this type for this field of medicine. The vast majority of patients with NAFLD are being seen in the primary care and endocrinology settings. Only when they get to the more advanced disease are they being referred to the liver specialists. So, we need to be the ones who are diagnosing and managing these patients because there just aren’t enough liver specialists to do that,” Scott Isaacs, MD, cochair of the writing panel for the guidelines, said in an interview.
80 million Americans have NAFLD, but very few are aware
The spectrum of NAFLD ranges from nonprogressive steatosis to the progressive conditions nonalcoholic steatohepatitis, fibrotic NASH, and end-stage NASH cirrhosis. And NASH, in turn, is a major cause of liver cancer. NAFLD is also strongly associated with insulin resistance, type 2 diabetes, atherogenesis, and myocardial dysfunction.
The global prevalence of NAFLD is about 25% and NASH, about 12%-14%. However, a recent study found that, among patients in endocrine and primary care clinics, more than 70% of patients with type 2 diabetes and more than 90% with type 2 diabetes who had a body mass index above 35 kg/m2 also had NAFLD, and more than 20% of those patients had significant liver fibrosis.
Problematically, very few people are aware they have either. “It’s so common. At least 80 million Americans have this but only about 6% know they have it. We talk about it a lot, but it’s not talked about enough,” said Dr. Isaacs, an endocrinologist who practices in Atlanta.
In fact, most cases of NAFLD are diagnosed incidentally when people undergo an ultrasound or a CT scan for another reason. And, in about 70% of cases the liver enzymes are normal, and those patients rarely undergo liver workups, Dr. Isaacs noted.
In an accompanying editorial, Suthat Liangpunsakul, MD, wrote: “In my perspective, as a hepatologist, this AACE guideline is very practical and easy to incorporate into routine practice in primary care and endocrinology settings. ... Early identification and risk stratification of patients with NAFLD, especially the degree of hepatic fibrosis, are required to reduce downstream health care costs and triage unwarranted specialty care referrals.”
And “an effective screening strategy may also identify those in primary care and endocrinology settings who may benefit from an appropriate referral to hepatologists before the development of portal hypertension complications, decompensated liver disease, and hepatocellular carcinoma,” added Dr. Liangpunsakul, professor of medicine in the division of gastroenterology and hepatology at Indiana University, Indianapolis.
Screening advised using new FIB-4 test
The guideline calls for screening all patients at high risk for NAFLD, including those with prediabetes, type 2 diabetes, obesity, and/or two or more cardiometabolic risk factors, or those with hepatic steatosis found on imaging, and/or persistently elevated plasma aminotransferase levels (that is, for more than 6 months).
The recommended screening test is the Fibrosis-4 (FIB-4) index, calculated using the patient’s age, AST level, platelet count, and ALT level: FIB-4 score = age (years) x AST (U/L)/PLT (109/L) x ALT ½ (U/L).
Recently approved by the Food and Drug Administration, the FIB-4 has been demonstrated to help identify liver disease in primary care settings.
“We really want to encourage clinicians to do the screening. The first step is the FIB-4 test. It’s a mathematical calculation using blood tests that we do anyway,” Dr. Isaacs said in an interview.
The FIB-4 stratifies patients as being low, intermediate, or high risk for liver fibrosis. Those at low risk can be managed in primary care or endocrinology settings with a focus on obesity management and cardiovascular disease prevention. “Those at low risk on FIB-4 still have a high cardiovascular disease risk. They still need to be managed,” Dr. Isaacs observed.
For those at intermediate risk, a second noninvasive test – either a liver stiffness measurement by elastography or an enhanced liver fibrosis test – is advised. If the patient is found to be at high risk or is still indeterminant after two noninvasive tests, referral to a liver specialist for further testing, including possible biopsy, is advised.
Those found to be at high risk with the FIB-4 should also be referred to hepatology. In both the intermediate- and high-risk groups, management should be multidisciplinary, including a hepatologist, endocrinologist, and other professionals to prevent both cardiovascular disease and progression to cirrhosis, the guidelines say.
“The diagnosis isn’t about diagnosing liver fat. It’s about diagnosing fibrosis, or the risk for clinically significant fibrosis. That’s really where the challenge lies,” Dr. Isaacs commented.
NAFLD treatment in endocrinology and primary care: CVD prevention
During the presentation at the AACE meeting, guideline panel cochair Kenneth Cusi, MD, chief of endocrinology, diabetes, and metabolism at the University of Florida, Gainesville, summarized current and future treatments for NAFLD.
Lifestyle intervention, cardiovascular risk reduction, and weight loss for those who are overweight or obese are recommended for all patients with NAFLD, including structured weight-loss programs, antiobesity medications, and bariatric surgery if indicated.
There are currently no FDA-approved medications specifically for NASH, but pioglitazone, approved for type 2 diabetes, and glucagonlike peptide–1 agonists, approved for type 2 diabetes and weight loss, have been shown to be effective in treating the condition and preventing progression. Other treatments are in development, Dr. Cusi said.
The guideline also includes a section on diagnosis and management of NAFLD in children and adolescents. Here, the FIB-4 is not recommended because it isn’t accurate due to the age part of the equation, so liver enzyme tests are used in pediatric patients considered at high risk because of clinical factors. Management is similar to adults, except not all medications used in adults are approved for use in children.
In the editorial, Dr. Liangpunsakul cautioned that “the level of uptake and usage of the guideline may be an obstacle.”
To remedy that, he advised that “the next effort should gear toward distributing this guideline to the targeted providers and developing the ‘feedback platforms’ on its execution in the real-world. ... The successful implementation of this AACE guideline by the primary care providers and endocrinologists, hopefully, will deescalate the future burden of NAFLD-related morbidity and mortality.”
Dr. Isaacs and Dr. Liangpunsakul have reported no relevant financial relationships. Dr. Cusi has reported receiving research support towards the University of Florida as principal investigator from the National Institute of Health, Echosens, Inventiva, Nordic Bioscience, Novo Nordisk, Poxel, Labcorp, and Zydus, and is a consultant for Altimmune, Akero, Arrowhead, AstraZeneca, 89Bio, Bristol-Myers Squibb, Coherus, Intercept, Lilly, Madrigal, Merck, Novo Nordisk, Quest, Sagimet, Sonic Incytes, Terns, and Thera Technologies.
A version of this article first appeared on Medscape.com.
New clinical practice guidelines for the diagnosis and management of nonalcoholic fatty liver disease (NAFLD) are the first to be targeted specifically to primary care and endocrinology clinical settings.
They include 34 evidence-based clinical practice recommendations for screening, diagnosis, management, and referral, presented in a table and an algorithm flow chart as well as detailed text.
The new guidelines are by the American Association of Clinical Endocrinology and cosponsored by the American Association for the Study of Liver Diseases. They were presented at the annual scientific & clinical congress of the AACE and simultaneously published in Endocrine Practice.
These are “the first of this type for this field of medicine. The vast majority of patients with NAFLD are being seen in the primary care and endocrinology settings. Only when they get to the more advanced disease are they being referred to the liver specialists. So, we need to be the ones who are diagnosing and managing these patients because there just aren’t enough liver specialists to do that,” Scott Isaacs, MD, cochair of the writing panel for the guidelines, said in an interview.
80 million Americans have NAFLD, but very few are aware
The spectrum of NAFLD ranges from nonprogressive steatosis to the progressive conditions nonalcoholic steatohepatitis, fibrotic NASH, and end-stage NASH cirrhosis. And NASH, in turn, is a major cause of liver cancer. NAFLD is also strongly associated with insulin resistance, type 2 diabetes, atherogenesis, and myocardial dysfunction.
The global prevalence of NAFLD is about 25% and NASH, about 12%-14%. However, a recent study found that, among patients in endocrine and primary care clinics, more than 70% of patients with type 2 diabetes and more than 90% with type 2 diabetes who had a body mass index above 35 kg/m2 also had NAFLD, and more than 20% of those patients had significant liver fibrosis.
Problematically, very few people are aware they have either. “It’s so common. At least 80 million Americans have this but only about 6% know they have it. We talk about it a lot, but it’s not talked about enough,” said Dr. Isaacs, an endocrinologist who practices in Atlanta.
In fact, most cases of NAFLD are diagnosed incidentally when people undergo an ultrasound or a CT scan for another reason. And, in about 70% of cases the liver enzymes are normal, and those patients rarely undergo liver workups, Dr. Isaacs noted.
In an accompanying editorial, Suthat Liangpunsakul, MD, wrote: “In my perspective, as a hepatologist, this AACE guideline is very practical and easy to incorporate into routine practice in primary care and endocrinology settings. ... Early identification and risk stratification of patients with NAFLD, especially the degree of hepatic fibrosis, are required to reduce downstream health care costs and triage unwarranted specialty care referrals.”
And “an effective screening strategy may also identify those in primary care and endocrinology settings who may benefit from an appropriate referral to hepatologists before the development of portal hypertension complications, decompensated liver disease, and hepatocellular carcinoma,” added Dr. Liangpunsakul, professor of medicine in the division of gastroenterology and hepatology at Indiana University, Indianapolis.
Screening advised using new FIB-4 test
The guideline calls for screening all patients at high risk for NAFLD, including those with prediabetes, type 2 diabetes, obesity, and/or two or more cardiometabolic risk factors, or those with hepatic steatosis found on imaging, and/or persistently elevated plasma aminotransferase levels (that is, for more than 6 months).
The recommended screening test is the Fibrosis-4 (FIB-4) index, calculated using the patient’s age, AST level, platelet count, and ALT level: FIB-4 score = age (years) x AST (U/L)/PLT (109/L) x ALT ½ (U/L).
Recently approved by the Food and Drug Administration, the FIB-4 has been demonstrated to help identify liver disease in primary care settings.
“We really want to encourage clinicians to do the screening. The first step is the FIB-4 test. It’s a mathematical calculation using blood tests that we do anyway,” Dr. Isaacs said in an interview.
The FIB-4 stratifies patients as being low, intermediate, or high risk for liver fibrosis. Those at low risk can be managed in primary care or endocrinology settings with a focus on obesity management and cardiovascular disease prevention. “Those at low risk on FIB-4 still have a high cardiovascular disease risk. They still need to be managed,” Dr. Isaacs observed.
For those at intermediate risk, a second noninvasive test – either a liver stiffness measurement by elastography or an enhanced liver fibrosis test – is advised. If the patient is found to be at high risk or is still indeterminant after two noninvasive tests, referral to a liver specialist for further testing, including possible biopsy, is advised.
Those found to be at high risk with the FIB-4 should also be referred to hepatology. In both the intermediate- and high-risk groups, management should be multidisciplinary, including a hepatologist, endocrinologist, and other professionals to prevent both cardiovascular disease and progression to cirrhosis, the guidelines say.
“The diagnosis isn’t about diagnosing liver fat. It’s about diagnosing fibrosis, or the risk for clinically significant fibrosis. That’s really where the challenge lies,” Dr. Isaacs commented.
NAFLD treatment in endocrinology and primary care: CVD prevention
During the presentation at the AACE meeting, guideline panel cochair Kenneth Cusi, MD, chief of endocrinology, diabetes, and metabolism at the University of Florida, Gainesville, summarized current and future treatments for NAFLD.
Lifestyle intervention, cardiovascular risk reduction, and weight loss for those who are overweight or obese are recommended for all patients with NAFLD, including structured weight-loss programs, antiobesity medications, and bariatric surgery if indicated.
There are currently no FDA-approved medications specifically for NASH, but pioglitazone, approved for type 2 diabetes, and glucagonlike peptide–1 agonists, approved for type 2 diabetes and weight loss, have been shown to be effective in treating the condition and preventing progression. Other treatments are in development, Dr. Cusi said.
The guideline also includes a section on diagnosis and management of NAFLD in children and adolescents. Here, the FIB-4 is not recommended because it isn’t accurate due to the age part of the equation, so liver enzyme tests are used in pediatric patients considered at high risk because of clinical factors. Management is similar to adults, except not all medications used in adults are approved for use in children.
In the editorial, Dr. Liangpunsakul cautioned that “the level of uptake and usage of the guideline may be an obstacle.”
To remedy that, he advised that “the next effort should gear toward distributing this guideline to the targeted providers and developing the ‘feedback platforms’ on its execution in the real-world. ... The successful implementation of this AACE guideline by the primary care providers and endocrinologists, hopefully, will deescalate the future burden of NAFLD-related morbidity and mortality.”
Dr. Isaacs and Dr. Liangpunsakul have reported no relevant financial relationships. Dr. Cusi has reported receiving research support towards the University of Florida as principal investigator from the National Institute of Health, Echosens, Inventiva, Nordic Bioscience, Novo Nordisk, Poxel, Labcorp, and Zydus, and is a consultant for Altimmune, Akero, Arrowhead, AstraZeneca, 89Bio, Bristol-Myers Squibb, Coherus, Intercept, Lilly, Madrigal, Merck, Novo Nordisk, Quest, Sagimet, Sonic Incytes, Terns, and Thera Technologies.
A version of this article first appeared on Medscape.com.
FROM AACE 2022
Mixing BP meds with NSAID may be ‘triple whammy’ for kidneys
The study also looked at risk factors associated with the effect of triple therapy with these agents, which has been called “triple whammy” AKI.
“It’s not that everyone who happens to take this combination of drugs is going to have problems,” Anita Layton, PhD, University of Waterloo, Ontario, said in a statement. “But the research shows it’s enough of a problem that you should exercise caution.”
The study was published online in Mathematical Biosciences.
In an earlier study, triple therapy with a diuretic, RAS inhibitor, and NSAID was associated with a 31% increased risk for AKI, relative to diuretic and RAS inhibitor therapy only.
However, the factors that predispose some patients to develop “triple whammy” AKI are unclear.
To better understand the mechanism by which triple therapy increases risk for AKI, Dr. Layton and colleagues used computational models to gauge interactions between concurrent use of a diuretic, a RAS inhibitor, and an NSAID.
They identified dehydration and high sensitivity to drug treatment as key contributing factors to the development of triple whammy AKI.
Their model simulations suggested that low water intake, the myogenic response (that is, the reflex response of arteries and arterioles to changes in blood pressure to maintain consistent blood flow), and drug sensitivity “may predispose patients with hypertension to develop triple whammy-induced AKI,” they wrote.
“We hypothesize that individuals with an impaired myogenic response may be particularly susceptible to triple whammy AKI. Additionally, increased drug sensitivity or low water intake can predispose patients to triple whammy AKI,” they added.
In the absence of additional risk factors, there was no indication of an elevated risk for AKI when an angiotensin-converting enzyme (ACE) inhibitor and NSAID are combined, the study team said.
In contrast, when an ACE inhibitor, diuretic, and NSAID are combined, critical blood pressure and glomerular filtration rate (GFR) regulatory mechanisms are simultaneously interrupted, they reported.
“Perhaps not unexpectedly, model simulations indicate that triple treatment reduces GFR more than single or double treatments in all individuals. However, under triple treatment, urine volume and GFR have not been predicted to fall sufficiently far to indicate AKI,” they wrote. “This result is consistent with the fact that only a fraction of individuals develop AKI following triple treatment.”
They expect, therefore, that hypertensive patients who are otherwise healthy will be able to withstand triple treatment, in the absence of these aggravating factors, the researchers concluded.
Nonetheless, it’s wise to “always be careful when mixing medications,” Dr. Layton told this news organization.
She noted that “triple whammy AKI is known among kidney researchers and nephrologists. To what extent nonspecialists are aware, it isn’t clear.
“More importantly,” Dr. Layton said, “NSAIDs can be obtained over the counter, and triple whammy AKI isn’t common knowledge outside of the medical community.”
This research was supported by the Canada 150 Research Chair program and by the Natural Sciences and Engineering Research Council of Canada. The authors have declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
The study also looked at risk factors associated with the effect of triple therapy with these agents, which has been called “triple whammy” AKI.
“It’s not that everyone who happens to take this combination of drugs is going to have problems,” Anita Layton, PhD, University of Waterloo, Ontario, said in a statement. “But the research shows it’s enough of a problem that you should exercise caution.”
The study was published online in Mathematical Biosciences.
In an earlier study, triple therapy with a diuretic, RAS inhibitor, and NSAID was associated with a 31% increased risk for AKI, relative to diuretic and RAS inhibitor therapy only.
However, the factors that predispose some patients to develop “triple whammy” AKI are unclear.
To better understand the mechanism by which triple therapy increases risk for AKI, Dr. Layton and colleagues used computational models to gauge interactions between concurrent use of a diuretic, a RAS inhibitor, and an NSAID.
They identified dehydration and high sensitivity to drug treatment as key contributing factors to the development of triple whammy AKI.
Their model simulations suggested that low water intake, the myogenic response (that is, the reflex response of arteries and arterioles to changes in blood pressure to maintain consistent blood flow), and drug sensitivity “may predispose patients with hypertension to develop triple whammy-induced AKI,” they wrote.
“We hypothesize that individuals with an impaired myogenic response may be particularly susceptible to triple whammy AKI. Additionally, increased drug sensitivity or low water intake can predispose patients to triple whammy AKI,” they added.
In the absence of additional risk factors, there was no indication of an elevated risk for AKI when an angiotensin-converting enzyme (ACE) inhibitor and NSAID are combined, the study team said.
In contrast, when an ACE inhibitor, diuretic, and NSAID are combined, critical blood pressure and glomerular filtration rate (GFR) regulatory mechanisms are simultaneously interrupted, they reported.
“Perhaps not unexpectedly, model simulations indicate that triple treatment reduces GFR more than single or double treatments in all individuals. However, under triple treatment, urine volume and GFR have not been predicted to fall sufficiently far to indicate AKI,” they wrote. “This result is consistent with the fact that only a fraction of individuals develop AKI following triple treatment.”
They expect, therefore, that hypertensive patients who are otherwise healthy will be able to withstand triple treatment, in the absence of these aggravating factors, the researchers concluded.
Nonetheless, it’s wise to “always be careful when mixing medications,” Dr. Layton told this news organization.
She noted that “triple whammy AKI is known among kidney researchers and nephrologists. To what extent nonspecialists are aware, it isn’t clear.
“More importantly,” Dr. Layton said, “NSAIDs can be obtained over the counter, and triple whammy AKI isn’t common knowledge outside of the medical community.”
This research was supported by the Canada 150 Research Chair program and by the Natural Sciences and Engineering Research Council of Canada. The authors have declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
The study also looked at risk factors associated with the effect of triple therapy with these agents, which has been called “triple whammy” AKI.
“It’s not that everyone who happens to take this combination of drugs is going to have problems,” Anita Layton, PhD, University of Waterloo, Ontario, said in a statement. “But the research shows it’s enough of a problem that you should exercise caution.”
The study was published online in Mathematical Biosciences.
In an earlier study, triple therapy with a diuretic, RAS inhibitor, and NSAID was associated with a 31% increased risk for AKI, relative to diuretic and RAS inhibitor therapy only.
However, the factors that predispose some patients to develop “triple whammy” AKI are unclear.
To better understand the mechanism by which triple therapy increases risk for AKI, Dr. Layton and colleagues used computational models to gauge interactions between concurrent use of a diuretic, a RAS inhibitor, and an NSAID.
They identified dehydration and high sensitivity to drug treatment as key contributing factors to the development of triple whammy AKI.
Their model simulations suggested that low water intake, the myogenic response (that is, the reflex response of arteries and arterioles to changes in blood pressure to maintain consistent blood flow), and drug sensitivity “may predispose patients with hypertension to develop triple whammy-induced AKI,” they wrote.
“We hypothesize that individuals with an impaired myogenic response may be particularly susceptible to triple whammy AKI. Additionally, increased drug sensitivity or low water intake can predispose patients to triple whammy AKI,” they added.
In the absence of additional risk factors, there was no indication of an elevated risk for AKI when an angiotensin-converting enzyme (ACE) inhibitor and NSAID are combined, the study team said.
In contrast, when an ACE inhibitor, diuretic, and NSAID are combined, critical blood pressure and glomerular filtration rate (GFR) regulatory mechanisms are simultaneously interrupted, they reported.
“Perhaps not unexpectedly, model simulations indicate that triple treatment reduces GFR more than single or double treatments in all individuals. However, under triple treatment, urine volume and GFR have not been predicted to fall sufficiently far to indicate AKI,” they wrote. “This result is consistent with the fact that only a fraction of individuals develop AKI following triple treatment.”
They expect, therefore, that hypertensive patients who are otherwise healthy will be able to withstand triple treatment, in the absence of these aggravating factors, the researchers concluded.
Nonetheless, it’s wise to “always be careful when mixing medications,” Dr. Layton told this news organization.
She noted that “triple whammy AKI is known among kidney researchers and nephrologists. To what extent nonspecialists are aware, it isn’t clear.
“More importantly,” Dr. Layton said, “NSAIDs can be obtained over the counter, and triple whammy AKI isn’t common knowledge outside of the medical community.”
This research was supported by the Canada 150 Research Chair program and by the Natural Sciences and Engineering Research Council of Canada. The authors have declared no conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM MATHEMATICAL BIOSCIENCES
Myositis guidelines aim to standardize adult and pediatric care
All patients with idiopathic inflammatory myopathies (IIM) should be screened for swallowing difficulties, according to the first evidence-based guideline to be produced.
The guideline, which has been developed by a working group of the British Society for Rheumatology (BSR), also advises that all diagnosed patients should have their myositis antibody levels checked and have their overall well-being assessed. Other recommendations for all patients include the use of glucocorticoids to reduce muscle inflammation and conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) for long-term treatment.
“Finally, now, we’re able to standardize the way we treat adults and children with IIM,” senior guideline author Hector Chinoy, PhD, said at the society’s annual meeting.
It has been a long labor of love, however, taking 4 years to get the guideline published, said Dr. Chinoy, professor of rheumatology and neuromuscular disease at the University of Manchester (England), and a consultant at Salford (England) Royal Hospital.
“We’re not covering diagnosis, classification, or the investigation of suspected IIM,” said Dr. Chinoy. Inclusion body myositis also is not included.
Altogether, there are 13 recommendations that have been developed using a PICO (patient or population, intervention, comparison, outcome) format, graded based on the quality of the available evidence, and then voted on by the working group members to give a score of the strength of agreement. Dr. Chinoy noted that there was a checklist included in the Supplementary Data section of the guideline to help follow the recommendations.
“The target audience for the guideline reflects the variety of clinicians caring for patients with IIM,” Dr. Chinoy said. So that is not just pediatric and adult rheumatologists, but also neurologists, dermatologists, respiratory physicians, oncologists, gastroenterologists, cardiologists, and of course other health care professionals. This includes rheumatology and neurology nurses, psychologists, speech and language therapists, and podiatrists, as well as rheumatology specialist pharmacists, physiotherapists, and occupational therapists.
With reference to the latter, Liza McCann, MBBS, who co-led the development of the guideline, said in a statement released by the BSR that the guideline “highlights the importance of exercise, led and monitored by specialist physiotherapists and occupational therapists.”
Dr. McCann, a consultant pediatric rheumatologist at Alder Hey Hospital, Liverpool, England, and Honorary Clinical Lecturer at the University of Liverpool, added that the guidelines also cover “the need to address psychological wellbeing as an integral part of treatment, in parallel with pharmacological therapies.”
Recommendation highlights
Some of the highlights of the recommendations include the use of high-dose glucocorticoids to manage skeletal muscle inflammation at the time of treatment induction, with specific guidance on the different doses to use in adults and in children. There also is guidance on the use of csDMARDs in both populations and what to use if there is refractory disease – with the strongest evidence supporting the use of intravenous immunoglobulin (IVIG) or cyclophosphamide, and possibly rituximab and abatacept.
“There is insufficient evidence to recommend JAK inhibition,” Dr. Chinoy said. The data search used to develop the guideline had a cutoff of October 2020, but even now there is only anecdotal evidence from case studies, he added.
Importantly, the guidelines recognize that childhood IIM differs from adult disease and call for children to be managed by pediatric specialists.
“Routine assessment of dysphagia should be considered in all patients,” Dr. Chinoy said, “so ask the question.” The recommendation is that a swallowing assessment should involve a speech and language therapist or gastroenterologist, and that IVIG be considered for active disease and dysphagia that is resistant to other treatments.
There also are recommendations to screen adult patients for interstitial lung disease, consider fracture risk, and screen adult patients for cancer if they have specific risk factors that include older age at onset, male gender, dysphagia, and rapid disease onset, among others.
Separate cancer screening guidelines on cards
“Around one in four patients with myositis will develop cancer within the 3 years either before or after myositis onset,” Alexander Oldroyd, MBChB, PhD, said in a separate presentation at the BSR annual meeting.
“It’s a hugely increased risk compared to the general population, and a great worry for patients,” he added. Exactly why there is an increased risk is not known, but “there’s a big link between the biological onset of cancer and myositis.”
Dr. Oldroyd, who is an NIHR Academic Clinical Lecturer at the University of Manchester in England and a coauthor of the BSR myositis guideline, is part of a special interest group set up by the International Myositis Assessment and Clinical Studies Group (IMACS) that is in the process of developing separate guidelines for cancer screening in people newly diagnosed with IIM.
The aim was to produce evidence-based recommendations that were both “pragmatic and practical,” that could help clinicians answer patient’s questions on their risk and how best and how often to screen them, Dr. Oldroyd explained. Importantly, IMACS has endeavored to create recommendations that should be applicable across different countries and health care systems.
“We had to acknowledge that there’s not a lot of evidence base there,” Dr. Oldroyd said, noting that he and colleagues conducted a systematic literature review and meta-analysis and used a Delphi process to draft 20 recommendations. These cover identifying risk factors for cancer in people with myositis and categorizing people into low, medium, and high-risk categories. The recommendations also cover what should constitute basic and enhanced screening, and how often someone should be screened.
Moreover, the authors make recommendations on the use of imaging modalities such as PET and CT scans, as well as upper and lower gastrointestinal endoscopy and naso-endoscopy.
“As rheumatologists, we don’t talk about cancer a lot,” Dr. Oldroyd said. “We pick up a lot of incidental cancers, but we don’t usually talk about cancer screening with patients.” That’s something that needs to change, he said.
“It’s important – just get it out in the open, talk to people about it,” Dr. Oldroyd said.
“Tell them what you’re wanting to do, how you’re wanting to investigate for it, clearly communicate their risk,” he said. “But also acknowledge the limited evidence as well, and clearly communicate the results.”
Dr. Chinoy acknowledged he had received fees for presentations (UCB, Biogen), consultancy (Alexion, Novartis, Eli Lilly, Orphazyme, AstraZeneca), or grant support (Eli Lilly, UCB) that had been paid via his institution for the purpose of furthering myositis research. Dr. Oldroyd had no conflicts of interest to disclose.
All patients with idiopathic inflammatory myopathies (IIM) should be screened for swallowing difficulties, according to the first evidence-based guideline to be produced.
The guideline, which has been developed by a working group of the British Society for Rheumatology (BSR), also advises that all diagnosed patients should have their myositis antibody levels checked and have their overall well-being assessed. Other recommendations for all patients include the use of glucocorticoids to reduce muscle inflammation and conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) for long-term treatment.
“Finally, now, we’re able to standardize the way we treat adults and children with IIM,” senior guideline author Hector Chinoy, PhD, said at the society’s annual meeting.
It has been a long labor of love, however, taking 4 years to get the guideline published, said Dr. Chinoy, professor of rheumatology and neuromuscular disease at the University of Manchester (England), and a consultant at Salford (England) Royal Hospital.
“We’re not covering diagnosis, classification, or the investigation of suspected IIM,” said Dr. Chinoy. Inclusion body myositis also is not included.
Altogether, there are 13 recommendations that have been developed using a PICO (patient or population, intervention, comparison, outcome) format, graded based on the quality of the available evidence, and then voted on by the working group members to give a score of the strength of agreement. Dr. Chinoy noted that there was a checklist included in the Supplementary Data section of the guideline to help follow the recommendations.
“The target audience for the guideline reflects the variety of clinicians caring for patients with IIM,” Dr. Chinoy said. So that is not just pediatric and adult rheumatologists, but also neurologists, dermatologists, respiratory physicians, oncologists, gastroenterologists, cardiologists, and of course other health care professionals. This includes rheumatology and neurology nurses, psychologists, speech and language therapists, and podiatrists, as well as rheumatology specialist pharmacists, physiotherapists, and occupational therapists.
With reference to the latter, Liza McCann, MBBS, who co-led the development of the guideline, said in a statement released by the BSR that the guideline “highlights the importance of exercise, led and monitored by specialist physiotherapists and occupational therapists.”
Dr. McCann, a consultant pediatric rheumatologist at Alder Hey Hospital, Liverpool, England, and Honorary Clinical Lecturer at the University of Liverpool, added that the guidelines also cover “the need to address psychological wellbeing as an integral part of treatment, in parallel with pharmacological therapies.”
Recommendation highlights
Some of the highlights of the recommendations include the use of high-dose glucocorticoids to manage skeletal muscle inflammation at the time of treatment induction, with specific guidance on the different doses to use in adults and in children. There also is guidance on the use of csDMARDs in both populations and what to use if there is refractory disease – with the strongest evidence supporting the use of intravenous immunoglobulin (IVIG) or cyclophosphamide, and possibly rituximab and abatacept.
“There is insufficient evidence to recommend JAK inhibition,” Dr. Chinoy said. The data search used to develop the guideline had a cutoff of October 2020, but even now there is only anecdotal evidence from case studies, he added.
Importantly, the guidelines recognize that childhood IIM differs from adult disease and call for children to be managed by pediatric specialists.
“Routine assessment of dysphagia should be considered in all patients,” Dr. Chinoy said, “so ask the question.” The recommendation is that a swallowing assessment should involve a speech and language therapist or gastroenterologist, and that IVIG be considered for active disease and dysphagia that is resistant to other treatments.
There also are recommendations to screen adult patients for interstitial lung disease, consider fracture risk, and screen adult patients for cancer if they have specific risk factors that include older age at onset, male gender, dysphagia, and rapid disease onset, among others.
Separate cancer screening guidelines on cards
“Around one in four patients with myositis will develop cancer within the 3 years either before or after myositis onset,” Alexander Oldroyd, MBChB, PhD, said in a separate presentation at the BSR annual meeting.
“It’s a hugely increased risk compared to the general population, and a great worry for patients,” he added. Exactly why there is an increased risk is not known, but “there’s a big link between the biological onset of cancer and myositis.”
Dr. Oldroyd, who is an NIHR Academic Clinical Lecturer at the University of Manchester in England and a coauthor of the BSR myositis guideline, is part of a special interest group set up by the International Myositis Assessment and Clinical Studies Group (IMACS) that is in the process of developing separate guidelines for cancer screening in people newly diagnosed with IIM.
The aim was to produce evidence-based recommendations that were both “pragmatic and practical,” that could help clinicians answer patient’s questions on their risk and how best and how often to screen them, Dr. Oldroyd explained. Importantly, IMACS has endeavored to create recommendations that should be applicable across different countries and health care systems.
“We had to acknowledge that there’s not a lot of evidence base there,” Dr. Oldroyd said, noting that he and colleagues conducted a systematic literature review and meta-analysis and used a Delphi process to draft 20 recommendations. These cover identifying risk factors for cancer in people with myositis and categorizing people into low, medium, and high-risk categories. The recommendations also cover what should constitute basic and enhanced screening, and how often someone should be screened.
Moreover, the authors make recommendations on the use of imaging modalities such as PET and CT scans, as well as upper and lower gastrointestinal endoscopy and naso-endoscopy.
“As rheumatologists, we don’t talk about cancer a lot,” Dr. Oldroyd said. “We pick up a lot of incidental cancers, but we don’t usually talk about cancer screening with patients.” That’s something that needs to change, he said.
“It’s important – just get it out in the open, talk to people about it,” Dr. Oldroyd said.
“Tell them what you’re wanting to do, how you’re wanting to investigate for it, clearly communicate their risk,” he said. “But also acknowledge the limited evidence as well, and clearly communicate the results.”
Dr. Chinoy acknowledged he had received fees for presentations (UCB, Biogen), consultancy (Alexion, Novartis, Eli Lilly, Orphazyme, AstraZeneca), or grant support (Eli Lilly, UCB) that had been paid via his institution for the purpose of furthering myositis research. Dr. Oldroyd had no conflicts of interest to disclose.
All patients with idiopathic inflammatory myopathies (IIM) should be screened for swallowing difficulties, according to the first evidence-based guideline to be produced.
The guideline, which has been developed by a working group of the British Society for Rheumatology (BSR), also advises that all diagnosed patients should have their myositis antibody levels checked and have their overall well-being assessed. Other recommendations for all patients include the use of glucocorticoids to reduce muscle inflammation and conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) for long-term treatment.
“Finally, now, we’re able to standardize the way we treat adults and children with IIM,” senior guideline author Hector Chinoy, PhD, said at the society’s annual meeting.
It has been a long labor of love, however, taking 4 years to get the guideline published, said Dr. Chinoy, professor of rheumatology and neuromuscular disease at the University of Manchester (England), and a consultant at Salford (England) Royal Hospital.
“We’re not covering diagnosis, classification, or the investigation of suspected IIM,” said Dr. Chinoy. Inclusion body myositis also is not included.
Altogether, there are 13 recommendations that have been developed using a PICO (patient or population, intervention, comparison, outcome) format, graded based on the quality of the available evidence, and then voted on by the working group members to give a score of the strength of agreement. Dr. Chinoy noted that there was a checklist included in the Supplementary Data section of the guideline to help follow the recommendations.
“The target audience for the guideline reflects the variety of clinicians caring for patients with IIM,” Dr. Chinoy said. So that is not just pediatric and adult rheumatologists, but also neurologists, dermatologists, respiratory physicians, oncologists, gastroenterologists, cardiologists, and of course other health care professionals. This includes rheumatology and neurology nurses, psychologists, speech and language therapists, and podiatrists, as well as rheumatology specialist pharmacists, physiotherapists, and occupational therapists.
With reference to the latter, Liza McCann, MBBS, who co-led the development of the guideline, said in a statement released by the BSR that the guideline “highlights the importance of exercise, led and monitored by specialist physiotherapists and occupational therapists.”
Dr. McCann, a consultant pediatric rheumatologist at Alder Hey Hospital, Liverpool, England, and Honorary Clinical Lecturer at the University of Liverpool, added that the guidelines also cover “the need to address psychological wellbeing as an integral part of treatment, in parallel with pharmacological therapies.”
Recommendation highlights
Some of the highlights of the recommendations include the use of high-dose glucocorticoids to manage skeletal muscle inflammation at the time of treatment induction, with specific guidance on the different doses to use in adults and in children. There also is guidance on the use of csDMARDs in both populations and what to use if there is refractory disease – with the strongest evidence supporting the use of intravenous immunoglobulin (IVIG) or cyclophosphamide, and possibly rituximab and abatacept.
“There is insufficient evidence to recommend JAK inhibition,” Dr. Chinoy said. The data search used to develop the guideline had a cutoff of October 2020, but even now there is only anecdotal evidence from case studies, he added.
Importantly, the guidelines recognize that childhood IIM differs from adult disease and call for children to be managed by pediatric specialists.
“Routine assessment of dysphagia should be considered in all patients,” Dr. Chinoy said, “so ask the question.” The recommendation is that a swallowing assessment should involve a speech and language therapist or gastroenterologist, and that IVIG be considered for active disease and dysphagia that is resistant to other treatments.
There also are recommendations to screen adult patients for interstitial lung disease, consider fracture risk, and screen adult patients for cancer if they have specific risk factors that include older age at onset, male gender, dysphagia, and rapid disease onset, among others.
Separate cancer screening guidelines on cards
“Around one in four patients with myositis will develop cancer within the 3 years either before or after myositis onset,” Alexander Oldroyd, MBChB, PhD, said in a separate presentation at the BSR annual meeting.
“It’s a hugely increased risk compared to the general population, and a great worry for patients,” he added. Exactly why there is an increased risk is not known, but “there’s a big link between the biological onset of cancer and myositis.”
Dr. Oldroyd, who is an NIHR Academic Clinical Lecturer at the University of Manchester in England and a coauthor of the BSR myositis guideline, is part of a special interest group set up by the International Myositis Assessment and Clinical Studies Group (IMACS) that is in the process of developing separate guidelines for cancer screening in people newly diagnosed with IIM.
The aim was to produce evidence-based recommendations that were both “pragmatic and practical,” that could help clinicians answer patient’s questions on their risk and how best and how often to screen them, Dr. Oldroyd explained. Importantly, IMACS has endeavored to create recommendations that should be applicable across different countries and health care systems.
“We had to acknowledge that there’s not a lot of evidence base there,” Dr. Oldroyd said, noting that he and colleagues conducted a systematic literature review and meta-analysis and used a Delphi process to draft 20 recommendations. These cover identifying risk factors for cancer in people with myositis and categorizing people into low, medium, and high-risk categories. The recommendations also cover what should constitute basic and enhanced screening, and how often someone should be screened.
Moreover, the authors make recommendations on the use of imaging modalities such as PET and CT scans, as well as upper and lower gastrointestinal endoscopy and naso-endoscopy.
“As rheumatologists, we don’t talk about cancer a lot,” Dr. Oldroyd said. “We pick up a lot of incidental cancers, but we don’t usually talk about cancer screening with patients.” That’s something that needs to change, he said.
“It’s important – just get it out in the open, talk to people about it,” Dr. Oldroyd said.
“Tell them what you’re wanting to do, how you’re wanting to investigate for it, clearly communicate their risk,” he said. “But also acknowledge the limited evidence as well, and clearly communicate the results.”
Dr. Chinoy acknowledged he had received fees for presentations (UCB, Biogen), consultancy (Alexion, Novartis, Eli Lilly, Orphazyme, AstraZeneca), or grant support (Eli Lilly, UCB) that had been paid via his institution for the purpose of furthering myositis research. Dr. Oldroyd had no conflicts of interest to disclose.
FROM BSR 2022
IUD cuts heavy menses in nulliparous patients with obesity
New phase 3 data support the use of the levonorgestrel 52-mg intrauterine device in nulliparous women with obesity and heavy menstrual bleeding. The findings, presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists, showed a 97% reduction in blood loss 6 months after placement of the device, which is sold as the contraceptive Liletta by Medicines360 and AbbVie.
Experts say the results fill a gap in research because prior clinical trials of the IUD and a competitor, Mirena (Bayer), excluded significantly obese as well as nulliparous populations.
William Schlaff, MD, professor and chairman of the department of obstetrics & gynecology, Thomas Jefferson University, Philadelphia, said the absence of confirmatory evidence in these women has meant that, although use of the IUD has been “pretty widespread,” clinicians have been uncertain about the efficacy of the approach.
“Now we have objective data from a well-designed study that supports a practice that many of us have felt is probably a good one,” Dr. Schlaff, who was not involved in the new study, said in an interview.
Lead researcher Mitchell Creinin, MD, professor of obstetrics and gynecology at UC Davis Health, Sacramento, and colleagues at several centers across the country provided treatment with Liletta to 105 individuals with proven heavy menstrual bleeding. The patients’ median blood loss during two menses prior to placement of the device was 165 mL (range, 73-520 mL).
Participant demographics were: 65% White, 24% Black, 10% Hispanic, 4% Asian, and 7% who identified with other racial groups. Mean body mass index was 30.9 kg/m2, and 45% of individuals met the criteria for obesity (BMI > 30), including 13% who had a BMI of at least 40. Nearly 30% of participants in the study had never given birth and none had known medical, anatomic, infectious, or neoplastic causes of bleeding.
According to Dr. Creinin, 86 women were assessed 3 months after device placement, and their median blood loss at the time was 9.5 mL (interquartile range, 2.5-22.9 mL), representing a median 93% decrease from baseline. Median blood loss 6 months after placement of the IUD was 3.8 mL (IQR, 0-10.1 mL), a 97% reduction from baseline.
Regardless of parity or BMI, blood loss at 6 months was 97%-97.5% lower than baseline, Dr. Creinin reported.
Among the 23% of participants who did not complete the study, 4% experienced expulsions of the device, which Dr. Creinin said is a rate twice as high as that seen in women using hormone-releasing IUDs for contraception. However, he said it “is consistent with other studies among patients with quantitatively proven heavy menstrual bleeding.”
Another 6% of women who did not complete the study removed the device owing to bleeding and cramping complaints, 9% were lost to follow-up or withdrew consent, and 5% discontinued treatment for unspecified reasons, Dr. Creinin said.
“Etiologies for heavy menstrual bleeding may be different in the individuals we studied, so our findings provide assurance that these populations with heavy menstrual bleeding are equally well treated” with the IUD, Dr. Creinin said.
Dr. Creinin reported study funding from Medicines360. Dr. Schlaff reported no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
New phase 3 data support the use of the levonorgestrel 52-mg intrauterine device in nulliparous women with obesity and heavy menstrual bleeding. The findings, presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists, showed a 97% reduction in blood loss 6 months after placement of the device, which is sold as the contraceptive Liletta by Medicines360 and AbbVie.
Experts say the results fill a gap in research because prior clinical trials of the IUD and a competitor, Mirena (Bayer), excluded significantly obese as well as nulliparous populations.
William Schlaff, MD, professor and chairman of the department of obstetrics & gynecology, Thomas Jefferson University, Philadelphia, said the absence of confirmatory evidence in these women has meant that, although use of the IUD has been “pretty widespread,” clinicians have been uncertain about the efficacy of the approach.
“Now we have objective data from a well-designed study that supports a practice that many of us have felt is probably a good one,” Dr. Schlaff, who was not involved in the new study, said in an interview.
Lead researcher Mitchell Creinin, MD, professor of obstetrics and gynecology at UC Davis Health, Sacramento, and colleagues at several centers across the country provided treatment with Liletta to 105 individuals with proven heavy menstrual bleeding. The patients’ median blood loss during two menses prior to placement of the device was 165 mL (range, 73-520 mL).
Participant demographics were: 65% White, 24% Black, 10% Hispanic, 4% Asian, and 7% who identified with other racial groups. Mean body mass index was 30.9 kg/m2, and 45% of individuals met the criteria for obesity (BMI > 30), including 13% who had a BMI of at least 40. Nearly 30% of participants in the study had never given birth and none had known medical, anatomic, infectious, or neoplastic causes of bleeding.
According to Dr. Creinin, 86 women were assessed 3 months after device placement, and their median blood loss at the time was 9.5 mL (interquartile range, 2.5-22.9 mL), representing a median 93% decrease from baseline. Median blood loss 6 months after placement of the IUD was 3.8 mL (IQR, 0-10.1 mL), a 97% reduction from baseline.
Regardless of parity or BMI, blood loss at 6 months was 97%-97.5% lower than baseline, Dr. Creinin reported.
Among the 23% of participants who did not complete the study, 4% experienced expulsions of the device, which Dr. Creinin said is a rate twice as high as that seen in women using hormone-releasing IUDs for contraception. However, he said it “is consistent with other studies among patients with quantitatively proven heavy menstrual bleeding.”
Another 6% of women who did not complete the study removed the device owing to bleeding and cramping complaints, 9% were lost to follow-up or withdrew consent, and 5% discontinued treatment for unspecified reasons, Dr. Creinin said.
“Etiologies for heavy menstrual bleeding may be different in the individuals we studied, so our findings provide assurance that these populations with heavy menstrual bleeding are equally well treated” with the IUD, Dr. Creinin said.
Dr. Creinin reported study funding from Medicines360. Dr. Schlaff reported no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
New phase 3 data support the use of the levonorgestrel 52-mg intrauterine device in nulliparous women with obesity and heavy menstrual bleeding. The findings, presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists, showed a 97% reduction in blood loss 6 months after placement of the device, which is sold as the contraceptive Liletta by Medicines360 and AbbVie.
Experts say the results fill a gap in research because prior clinical trials of the IUD and a competitor, Mirena (Bayer), excluded significantly obese as well as nulliparous populations.
William Schlaff, MD, professor and chairman of the department of obstetrics & gynecology, Thomas Jefferson University, Philadelphia, said the absence of confirmatory evidence in these women has meant that, although use of the IUD has been “pretty widespread,” clinicians have been uncertain about the efficacy of the approach.
“Now we have objective data from a well-designed study that supports a practice that many of us have felt is probably a good one,” Dr. Schlaff, who was not involved in the new study, said in an interview.
Lead researcher Mitchell Creinin, MD, professor of obstetrics and gynecology at UC Davis Health, Sacramento, and colleagues at several centers across the country provided treatment with Liletta to 105 individuals with proven heavy menstrual bleeding. The patients’ median blood loss during two menses prior to placement of the device was 165 mL (range, 73-520 mL).
Participant demographics were: 65% White, 24% Black, 10% Hispanic, 4% Asian, and 7% who identified with other racial groups. Mean body mass index was 30.9 kg/m2, and 45% of individuals met the criteria for obesity (BMI > 30), including 13% who had a BMI of at least 40. Nearly 30% of participants in the study had never given birth and none had known medical, anatomic, infectious, or neoplastic causes of bleeding.
According to Dr. Creinin, 86 women were assessed 3 months after device placement, and their median blood loss at the time was 9.5 mL (interquartile range, 2.5-22.9 mL), representing a median 93% decrease from baseline. Median blood loss 6 months after placement of the IUD was 3.8 mL (IQR, 0-10.1 mL), a 97% reduction from baseline.
Regardless of parity or BMI, blood loss at 6 months was 97%-97.5% lower than baseline, Dr. Creinin reported.
Among the 23% of participants who did not complete the study, 4% experienced expulsions of the device, which Dr. Creinin said is a rate twice as high as that seen in women using hormone-releasing IUDs for contraception. However, he said it “is consistent with other studies among patients with quantitatively proven heavy menstrual bleeding.”
Another 6% of women who did not complete the study removed the device owing to bleeding and cramping complaints, 9% were lost to follow-up or withdrew consent, and 5% discontinued treatment for unspecified reasons, Dr. Creinin said.
“Etiologies for heavy menstrual bleeding may be different in the individuals we studied, so our findings provide assurance that these populations with heavy menstrual bleeding are equally well treated” with the IUD, Dr. Creinin said.
Dr. Creinin reported study funding from Medicines360. Dr. Schlaff reported no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM ACOG 2022
Section reports
Pulmonary vascular & cardiovascular network: Cardiovascular medicine & surgery section
Targeted temperature management (TTM) after cardiac arrest: How cool?
Recent randomized control trials, TTM2 (Dankiewicz J. N Engl J Med. 2021;384:2283) and HYPERION (Lascarrou J-B. N Engl J Med. 2019;381:2327), of therapeutic hypothermia, as opposed to normothermia, in patients who remain comatose after return of spontaneous circulation (ROSC) after cardiac arrest have produced conflicting results regarding survival and neurologic benefit. TTM2 reported no benefit to cooling to 33°C, while HYPERION found improved neurologic outcome at 90 days in patients cooled to 33°C. The European Resuscitation Council (ERC) and European Society of Intensive Care Medicine (ESICM) recently released an evidence review and guideline for adults who remain comatose after cardiac arrest (Sandroni C. Intensive Care Med. 2022;48:261). These guidelines recommend continuous monitoring of core temperature in all patients who remain comatose after cardiac arrest, and preventing fever (>37.7°C) for 72 hours, but with no recommendation of target temperature of 32°C vs 36°C.
Differences in patient populations, presenting rhythm during arrest, duration of CPR, and time to target temperature likely each contribute to the disparate conclusions of previous trials. For example, HYPERION enrolled patients with out of hospital cardiac arrest with initial nonshockable rhythms and found benefit to cooling to 33°C. In comparison, TTM2 enrolled all patients with ROSC following arrest (regardless of rhythm), including patients with in-hospital cardiac arrest and found no benefit in therapeutic cooling. Differences in patient populations are underscored by the widely differing percentage of patients with good neurologic outcome in their respective control groups: approximately 30% in the TTM2 trial and 6% in HYPERION. The guidelines leave significant room for clinical judgment in employing therapeutic cooling but encourage the continuous monitoring of core temperature and active avoidance of fever.
Fiore Mastroianna, MD
Section Member-at-Large
Chest infections & disaster response network: Chest infections section
Update on LTBI treatment: Ensuring success by simplifying, shortening, and completing treatment
My patient has a positive IGRA test result – what’s next?
If TB disease is ruled out by clinical, radiographic, and microbiologic assessment (if indicated), then latent TB infection (LTBI) is established, and treatment should be offered, guided by shared-decision making between provider and patient.

What options are available?
While the former standard 9-month regimen of isoniazid-monotherapy can be shortened to 6 months, shorter rifamycin-based regimens are now preferred in most cases and include:
4 months rifampin daily, 3 months isoniazid plus rifampin daily, or 3 months isoniazid plus rifapentine weekly. In addition, 1 month of isoniazid plus rifapentine daily has recently been shown to be effective in people with HIV.

How to choose?
Rifamycin-based regimens have been shown to have less hepatotoxicity and higher completion rates. Drug-drug interactions are of potential concern, for example, in patients receiving anticoagulation or treatment for HIV. The clinician should be aware of rifamycins causing a flu-like illness that may be treatment-limiting. In patients with known contact to drug-resistant TB, regimens are individualized.
How to monitor?
Adherence and completion are the keys to success. Directly observed therapy may be indicated in certain scenarios. Baseline and monthly blood work is recommended for people with risk factors for hepatic or bone marrow toxicity. More importantly, patients should be instructed to discontinue LTBI medications and call the clinician with any new symptoms. HIV testing should be offered to all patients if status is unknown. Clinicians are encouraged to reach out to one of four regional TB Centers of Excellence for guidance.
Sebastian Kurz, MD, FCCP
Amee Patrawalla, MD, MPH, FCCP
Section Members-at-Large
References
Testing and Treatment of Latent Tuberculosis Infection in the United States: Clinical Recommendations. A Guide for Health Care Providers and Public Health Programs. Copyright © 2021 by the National Society of Tuberculosis Clinicians and National Tuberculosis Controllers Association
1. Shah, D. Latent tuberculosis infection. N Engl J Med. 2021;385:2271-80.
2. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of tuberculosis in adults and children. Clin Infect Dis. 2017 Jan 15;64(2):111-115.
3. Swindells et. al. One month of rifapentine plus isoniazid to prevent HIV-related tuberculosis. N Engl J Med. 2019;380:1001-11.
Thoracic oncology & chest procedures network: Lung cancer section
Adjuvant and neoadjuvant therapies in early stage lung cancer
Since the discovery of the epidermal growth factor receptor (EGFR) mutation in 2004 and the development of checkpoint blockade in 2006, personalized treatment options for non–small cell lung cancer (NSCLC) have exploded, but targeted systemic therapy medications were only recommended among patients with metastatic or locally advanced disease (Rivera MP, Matthay RA. Clin Chest Med. 2020;41[1]:ix-xi). However, in November 2020, the National Comprehensive Cancer Network (NCCN) updated guidelines to recommend EGFR testing in surgically resected stage IB-IIIA adenocarcinoma, and to consider adjuvant osimerintib in those who were mutation-positive (NCCN. Nov 2020). Interim analysis of an ongoing phase-3 trial showed 89% of patients in the osimertinib group were alive and disease-free at 24 months compared with 52% in the placebo group (hazard ratio 0.20, P < .001) (Wu YL, et al. N Engl J Med. 2020;383[18]:1711-23).

The FDA has also recently approved the use of neoadjuvant and adjuvant immunotherapy in combination with platinum-based chemotherapy. Nivolumab is now approved as neoadjuvant therapy in patients with resectable IB-IIIA NSCLC regardless of PDL-1 status. The Checkmate-816 trial showed increased median event-free survival in the immunotherapy plus chemotherapy group of 31.6 months vs 20.8 months in the chemotherapy-only group (FDA.gov. 2022, Mar 4). Atezolizumab is also now approved for adjuvant treatment following resection and platinum-based chemotherapy in patients with stage II to IIIA NSCLC whose tumors have PD-L1 expression on ≥ 1% of tumor cells. Median disease-free survival was not reached in patients in the atezolizumab groups vs 35.3 months in the best supportive care group (FDA.gov. 2021, Oct 15). With so many advances in the personalized treatment among all stages of NSCLC, this is a hopeful new chapter in the care of patients with NSCLC.
More information: https://www.nccn.org/guidelines/guidelines-process/transparency-process-and-recommendations/GetFileFromFileManager?fileManagerId=11259
Sohini Ghosh, MD
Section Member-at-Large
Diffuse lung disease and lung transplant network: Lung transplant section
Continuous distribution for lung transplant: Overhauling the wait list
Determining how to allocate the scarce resource of donor lungs to patients is a difficult task and evaluated continuously for potential improvement. Since 2005, in the United States, lung transplant recipients have been selected based primarily on location within a Donor Service Area and by lung allocation score (LAS), a composite score of urgency for transplant. This was updated in 2017 to an allocation by highest LAS within 250 nautical miles from the donor hospital. Factors such as blood type compatibility and height are also considered. Implementation of the LAS improved the sickest patients’ access to transplants while not worsening 1-year mortality (Egan TM. Semin Respir Crit Care Med. 2018;39[02]:126-37). Unfortunately, geographic hard boundaries mean a high proportion of low LAS (<50) patients receive local donors while high LAS patients receive national offers or die while on the waitlist (Iribarne A, et al. Clin Transplant. 2016:30:688-93).

A new model that employs continuous distribution has been developed based on concerns regarding equity and improving allocation. This model would prioritize patients based on factors including medical priority, efficient management of organ placement (distance), expected posttransplant outcomes, and patient access (equity). By creating a composite of these without a geographic boundary, patients would be considered more on urgency within realistic constraints of distance and outcomes.

The Organ Procurement and Transplantation Network has officially approved continuous distribution, with implementation planned for 2022; details regarding the new scoring system are to be published and further research will need to be undertaken to determine if it meets the goal of overall improvement in patient access, equity, and outcomes.
Grant A. Turner, MD, MHA
Laura Frye, MD
Section Members-at-Large
Critical care network: Non-respiratory critical care section
Update from the non-respiratory critical care section
As you’ve probably noticed, there have been some changes here at CHEST involving the Networks. Leadership here at CHEST has been hard at work restructuring the networks to make them more closely aligned with relevant clinical disciplines, and, ultimately, allow for greater participation. I am proud to have been given stewardship of the new Non-Respiratory Critical Care Section of the Critical Care Network.
So, what exactly is Non-Respiratory Critical Care? Well, that’s where I need your help. You see this network is meant to reflect the needs and wants of CHEST members like you. We need you, dear readers, to join in this venture and help us guide the content that this section will ultimately create for our members.
If you’re interested in critical care, but you don’t see your particular area of interest anywhere else in the current structure ... guess what? You’ve found the right place!
My Infectious Diseases and Nephro peeps? Welcome! Are you a surgical or anesthesia intensivist? Don’t be shy. ECMO people, let’s hear some chatter!Is therapeutic hypothermia your thing? Come on in. The water’s freezing. 33 degrees just like you folks like it. Or is it 36? Not sure. Anyway, see what I’m talking about? We really need your help!You can get involved by clicking on the Membership & Community tab at the CHEST website. Once you’re a member, you can even nominate yourself to run for the Steering Committee elections which are held periodically. Hope to see you soon!
Deep Ramachandran, MD, FCCP
Section Chair
Sleep medicine network: Non-respiratory sleep section
Unusual suspects? Breakthrough in the treatment of idiopathic hypersomnia
Idiopathic hypersomnia (IH) is a rare and debilitating disorder defined by its excessive daytime sleepiness, sleep inertia, prolonged nighttime sleep, and long, unrefreshing naps (AASM. ICSD 3rd ed. 2014). Gamma-aminobutyric acid (GABA) is one of the main inhibitory neurotransmitters in the nervous system. It is through the potentiation of GABA that substances such as alcohol and benzodiazepines yield their effects. It is also hypothesized that the “brain fog” experienced in IH may be a consequence of either higher levels of an endogenous benzodiazepines in the cerebral spinal fluid or the presence of a GABA-enhancing peptide (Rye DB. Science Transl Med. 2012;Med 4:161ra151).
Sodium oxybate (SXB), a compound that likely has its therapeutic effect through the potentiation of GABA receptors, is an effective treatment option for cataplexy and sleepiness in narcolepsy. Although there may be some overlap between narcolepsy and IH in both diagnosis and treatment (Bassetti C, et al. Brain. 1997;120:1423), it would perhaps be entirely counterintuitive (given SXB’s pharmacology) to imagine using SXB as a plausible treatment option in IH. It was, however, investigated in the treatment of refractory hypersomnia and IH. In the retrospective study looking at 46 subjects treated with SXB, 71% experienced improvement of their severe sleep inertia, 55% had a decrease in their excessive daytime sleepiness, and 52% reported a shortened nighttime sleep time (Leu-Semenescu S, et al. Sleep Med. 2016;17:38).
In a recent double-blind, randomized control trial, the lower-sodium oxybate (LXB) was trialed in 154 patients with IH. It demonstrated statistically significant and clinically meaningful improvements (compared with placebo) in the Epworth Sleepiness Scale score (P <.0001) and in the Idiopathic Hypersomnia Severity Scale (P <.0001). The effects were seen both during the up titration of LXB and the benefits were maintained during the stable phase of the intervention (Dauvilliers Y, et al. Lancet Neurol. 2022;21(1):53). In August 2021, LXB (initially launched in 2020 for the treatment of narcolepsy) is now the first FDA-approved medication to treat IH in adults. It is curious, however, that LXB’s understood therapeutic effects are secondary to the “potentiation” of the very GABA receptor we have believed to be the root cause of the debilitating symptoms in IH. Could this discovery lend to further insights into the origins of this condition?
Ruckshanda Majid, MD, FCCP
Pulmonary vascular & cardiovascular network: Cardiovascular medicine & surgery section
Targeted temperature management (TTM) after cardiac arrest: How cool?
Recent randomized control trials, TTM2 (Dankiewicz J. N Engl J Med. 2021;384:2283) and HYPERION (Lascarrou J-B. N Engl J Med. 2019;381:2327), of therapeutic hypothermia, as opposed to normothermia, in patients who remain comatose after return of spontaneous circulation (ROSC) after cardiac arrest have produced conflicting results regarding survival and neurologic benefit. TTM2 reported no benefit to cooling to 33°C, while HYPERION found improved neurologic outcome at 90 days in patients cooled to 33°C. The European Resuscitation Council (ERC) and European Society of Intensive Care Medicine (ESICM) recently released an evidence review and guideline for adults who remain comatose after cardiac arrest (Sandroni C. Intensive Care Med. 2022;48:261). These guidelines recommend continuous monitoring of core temperature in all patients who remain comatose after cardiac arrest, and preventing fever (>37.7°C) for 72 hours, but with no recommendation of target temperature of 32°C vs 36°C.
Differences in patient populations, presenting rhythm during arrest, duration of CPR, and time to target temperature likely each contribute to the disparate conclusions of previous trials. For example, HYPERION enrolled patients with out of hospital cardiac arrest with initial nonshockable rhythms and found benefit to cooling to 33°C. In comparison, TTM2 enrolled all patients with ROSC following arrest (regardless of rhythm), including patients with in-hospital cardiac arrest and found no benefit in therapeutic cooling. Differences in patient populations are underscored by the widely differing percentage of patients with good neurologic outcome in their respective control groups: approximately 30% in the TTM2 trial and 6% in HYPERION. The guidelines leave significant room for clinical judgment in employing therapeutic cooling but encourage the continuous monitoring of core temperature and active avoidance of fever.
Fiore Mastroianna, MD
Section Member-at-Large
Chest infections & disaster response network: Chest infections section
Update on LTBI treatment: Ensuring success by simplifying, shortening, and completing treatment
My patient has a positive IGRA test result – what’s next?
If TB disease is ruled out by clinical, radiographic, and microbiologic assessment (if indicated), then latent TB infection (LTBI) is established, and treatment should be offered, guided by shared-decision making between provider and patient.
What options are available?
While the former standard 9-month regimen of isoniazid-monotherapy can be shortened to 6 months, shorter rifamycin-based regimens are now preferred in most cases and include:
4 months rifampin daily, 3 months isoniazid plus rifampin daily, or 3 months isoniazid plus rifapentine weekly. In addition, 1 month of isoniazid plus rifapentine daily has recently been shown to be effective in people with HIV.
How to choose?
Rifamycin-based regimens have been shown to have less hepatotoxicity and higher completion rates. Drug-drug interactions are of potential concern, for example, in patients receiving anticoagulation or treatment for HIV. The clinician should be aware of rifamycins causing a flu-like illness that may be treatment-limiting. In patients with known contact to drug-resistant TB, regimens are individualized.
How to monitor?
Adherence and completion are the keys to success. Directly observed therapy may be indicated in certain scenarios. Baseline and monthly blood work is recommended for people with risk factors for hepatic or bone marrow toxicity. More importantly, patients should be instructed to discontinue LTBI medications and call the clinician with any new symptoms. HIV testing should be offered to all patients if status is unknown. Clinicians are encouraged to reach out to one of four regional TB Centers of Excellence for guidance.
Sebastian Kurz, MD, FCCP
Amee Patrawalla, MD, MPH, FCCP
Section Members-at-Large
References
Testing and Treatment of Latent Tuberculosis Infection in the United States: Clinical Recommendations. A Guide for Health Care Providers and Public Health Programs. Copyright © 2021 by the National Society of Tuberculosis Clinicians and National Tuberculosis Controllers Association
1. Shah, D. Latent tuberculosis infection. N Engl J Med. 2021;385:2271-80.
2. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of tuberculosis in adults and children. Clin Infect Dis. 2017 Jan 15;64(2):111-115.
3. Swindells et. al. One month of rifapentine plus isoniazid to prevent HIV-related tuberculosis. N Engl J Med. 2019;380:1001-11.
Thoracic oncology & chest procedures network: Lung cancer section
Adjuvant and neoadjuvant therapies in early stage lung cancer
Since the discovery of the epidermal growth factor receptor (EGFR) mutation in 2004 and the development of checkpoint blockade in 2006, personalized treatment options for non–small cell lung cancer (NSCLC) have exploded, but targeted systemic therapy medications were only recommended among patients with metastatic or locally advanced disease (Rivera MP, Matthay RA. Clin Chest Med. 2020;41[1]:ix-xi). However, in November 2020, the National Comprehensive Cancer Network (NCCN) updated guidelines to recommend EGFR testing in surgically resected stage IB-IIIA adenocarcinoma, and to consider adjuvant osimerintib in those who were mutation-positive (NCCN. Nov 2020). Interim analysis of an ongoing phase-3 trial showed 89% of patients in the osimertinib group were alive and disease-free at 24 months compared with 52% in the placebo group (hazard ratio 0.20, P < .001) (Wu YL, et al. N Engl J Med. 2020;383[18]:1711-23).
The FDA has also recently approved the use of neoadjuvant and adjuvant immunotherapy in combination with platinum-based chemotherapy. Nivolumab is now approved as neoadjuvant therapy in patients with resectable IB-IIIA NSCLC regardless of PDL-1 status. The Checkmate-816 trial showed increased median event-free survival in the immunotherapy plus chemotherapy group of 31.6 months vs 20.8 months in the chemotherapy-only group (FDA.gov. 2022, Mar 4). Atezolizumab is also now approved for adjuvant treatment following resection and platinum-based chemotherapy in patients with stage II to IIIA NSCLC whose tumors have PD-L1 expression on ≥ 1% of tumor cells. Median disease-free survival was not reached in patients in the atezolizumab groups vs 35.3 months in the best supportive care group (FDA.gov. 2021, Oct 15). With so many advances in the personalized treatment among all stages of NSCLC, this is a hopeful new chapter in the care of patients with NSCLC.
More information: https://www.nccn.org/guidelines/guidelines-process/transparency-process-and-recommendations/GetFileFromFileManager?fileManagerId=11259
Sohini Ghosh, MD
Section Member-at-Large
Diffuse lung disease and lung transplant network: Lung transplant section
Continuous distribution for lung transplant: Overhauling the wait list
Determining how to allocate the scarce resource of donor lungs to patients is a difficult task and evaluated continuously for potential improvement. Since 2005, in the United States, lung transplant recipients have been selected based primarily on location within a Donor Service Area and by lung allocation score (LAS), a composite score of urgency for transplant. This was updated in 2017 to an allocation by highest LAS within 250 nautical miles from the donor hospital. Factors such as blood type compatibility and height are also considered. Implementation of the LAS improved the sickest patients’ access to transplants while not worsening 1-year mortality (Egan TM. Semin Respir Crit Care Med. 2018;39[02]:126-37). Unfortunately, geographic hard boundaries mean a high proportion of low LAS (<50) patients receive local donors while high LAS patients receive national offers or die while on the waitlist (Iribarne A, et al. Clin Transplant. 2016:30:688-93).
A new model that employs continuous distribution has been developed based on concerns regarding equity and improving allocation. This model would prioritize patients based on factors including medical priority, efficient management of organ placement (distance), expected posttransplant outcomes, and patient access (equity). By creating a composite of these without a geographic boundary, patients would be considered more on urgency within realistic constraints of distance and outcomes.
The Organ Procurement and Transplantation Network has officially approved continuous distribution, with implementation planned for 2022; details regarding the new scoring system are to be published and further research will need to be undertaken to determine if it meets the goal of overall improvement in patient access, equity, and outcomes.
Grant A. Turner, MD, MHA
Laura Frye, MD
Section Members-at-Large
Critical care network: Non-respiratory critical care section
Update from the non-respiratory critical care section
As you’ve probably noticed, there have been some changes here at CHEST involving the Networks. Leadership here at CHEST has been hard at work restructuring the networks to make them more closely aligned with relevant clinical disciplines, and, ultimately, allow for greater participation. I am proud to have been given stewardship of the new Non-Respiratory Critical Care Section of the Critical Care Network.
So, what exactly is Non-Respiratory Critical Care? Well, that’s where I need your help. You see this network is meant to reflect the needs and wants of CHEST members like you. We need you, dear readers, to join in this venture and help us guide the content that this section will ultimately create for our members.
If you’re interested in critical care, but you don’t see your particular area of interest anywhere else in the current structure ... guess what? You’ve found the right place!
My Infectious Diseases and Nephro peeps? Welcome! Are you a surgical or anesthesia intensivist? Don’t be shy. ECMO people, let’s hear some chatter!Is therapeutic hypothermia your thing? Come on in. The water’s freezing. 33 degrees just like you folks like it. Or is it 36? Not sure. Anyway, see what I’m talking about? We really need your help!You can get involved by clicking on the Membership & Community tab at the CHEST website. Once you’re a member, you can even nominate yourself to run for the Steering Committee elections which are held periodically. Hope to see you soon!
Deep Ramachandran, MD, FCCP
Section Chair
Sleep medicine network: Non-respiratory sleep section
Unusual suspects? Breakthrough in the treatment of idiopathic hypersomnia
Idiopathic hypersomnia (IH) is a rare and debilitating disorder defined by its excessive daytime sleepiness, sleep inertia, prolonged nighttime sleep, and long, unrefreshing naps (AASM. ICSD 3rd ed. 2014). Gamma-aminobutyric acid (GABA) is one of the main inhibitory neurotransmitters in the nervous system. It is through the potentiation of GABA that substances such as alcohol and benzodiazepines yield their effects. It is also hypothesized that the “brain fog” experienced in IH may be a consequence of either higher levels of an endogenous benzodiazepines in the cerebral spinal fluid or the presence of a GABA-enhancing peptide (Rye DB. Science Transl Med. 2012;Med 4:161ra151).
Sodium oxybate (SXB), a compound that likely has its therapeutic effect through the potentiation of GABA receptors, is an effective treatment option for cataplexy and sleepiness in narcolepsy. Although there may be some overlap between narcolepsy and IH in both diagnosis and treatment (Bassetti C, et al. Brain. 1997;120:1423), it would perhaps be entirely counterintuitive (given SXB’s pharmacology) to imagine using SXB as a plausible treatment option in IH. It was, however, investigated in the treatment of refractory hypersomnia and IH. In the retrospective study looking at 46 subjects treated with SXB, 71% experienced improvement of their severe sleep inertia, 55% had a decrease in their excessive daytime sleepiness, and 52% reported a shortened nighttime sleep time (Leu-Semenescu S, et al. Sleep Med. 2016;17:38).
In a recent double-blind, randomized control trial, the lower-sodium oxybate (LXB) was trialed in 154 patients with IH. It demonstrated statistically significant and clinically meaningful improvements (compared with placebo) in the Epworth Sleepiness Scale score (P <.0001) and in the Idiopathic Hypersomnia Severity Scale (P <.0001). The effects were seen both during the up titration of LXB and the benefits were maintained during the stable phase of the intervention (Dauvilliers Y, et al. Lancet Neurol. 2022;21(1):53). In August 2021, LXB (initially launched in 2020 for the treatment of narcolepsy) is now the first FDA-approved medication to treat IH in adults. It is curious, however, that LXB’s understood therapeutic effects are secondary to the “potentiation” of the very GABA receptor we have believed to be the root cause of the debilitating symptoms in IH. Could this discovery lend to further insights into the origins of this condition?
Ruckshanda Majid, MD, FCCP
Pulmonary vascular & cardiovascular network: Cardiovascular medicine & surgery section
Targeted temperature management (TTM) after cardiac arrest: How cool?
Recent randomized control trials, TTM2 (Dankiewicz J. N Engl J Med. 2021;384:2283) and HYPERION (Lascarrou J-B. N Engl J Med. 2019;381:2327), of therapeutic hypothermia, as opposed to normothermia, in patients who remain comatose after return of spontaneous circulation (ROSC) after cardiac arrest have produced conflicting results regarding survival and neurologic benefit. TTM2 reported no benefit to cooling to 33°C, while HYPERION found improved neurologic outcome at 90 days in patients cooled to 33°C. The European Resuscitation Council (ERC) and European Society of Intensive Care Medicine (ESICM) recently released an evidence review and guideline for adults who remain comatose after cardiac arrest (Sandroni C. Intensive Care Med. 2022;48:261). These guidelines recommend continuous monitoring of core temperature in all patients who remain comatose after cardiac arrest, and preventing fever (>37.7°C) for 72 hours, but with no recommendation of target temperature of 32°C vs 36°C.
Differences in patient populations, presenting rhythm during arrest, duration of CPR, and time to target temperature likely each contribute to the disparate conclusions of previous trials. For example, HYPERION enrolled patients with out of hospital cardiac arrest with initial nonshockable rhythms and found benefit to cooling to 33°C. In comparison, TTM2 enrolled all patients with ROSC following arrest (regardless of rhythm), including patients with in-hospital cardiac arrest and found no benefit in therapeutic cooling. Differences in patient populations are underscored by the widely differing percentage of patients with good neurologic outcome in their respective control groups: approximately 30% in the TTM2 trial and 6% in HYPERION. The guidelines leave significant room for clinical judgment in employing therapeutic cooling but encourage the continuous monitoring of core temperature and active avoidance of fever.
Fiore Mastroianna, MD
Section Member-at-Large
Chest infections & disaster response network: Chest infections section
Update on LTBI treatment: Ensuring success by simplifying, shortening, and completing treatment
My patient has a positive IGRA test result – what’s next?
If TB disease is ruled out by clinical, radiographic, and microbiologic assessment (if indicated), then latent TB infection (LTBI) is established, and treatment should be offered, guided by shared-decision making between provider and patient.
What options are available?
While the former standard 9-month regimen of isoniazid-monotherapy can be shortened to 6 months, shorter rifamycin-based regimens are now preferred in most cases and include:
4 months rifampin daily, 3 months isoniazid plus rifampin daily, or 3 months isoniazid plus rifapentine weekly. In addition, 1 month of isoniazid plus rifapentine daily has recently been shown to be effective in people with HIV.
How to choose?
Rifamycin-based regimens have been shown to have less hepatotoxicity and higher completion rates. Drug-drug interactions are of potential concern, for example, in patients receiving anticoagulation or treatment for HIV. The clinician should be aware of rifamycins causing a flu-like illness that may be treatment-limiting. In patients with known contact to drug-resistant TB, regimens are individualized.
How to monitor?
Adherence and completion are the keys to success. Directly observed therapy may be indicated in certain scenarios. Baseline and monthly blood work is recommended for people with risk factors for hepatic or bone marrow toxicity. More importantly, patients should be instructed to discontinue LTBI medications and call the clinician with any new symptoms. HIV testing should be offered to all patients if status is unknown. Clinicians are encouraged to reach out to one of four regional TB Centers of Excellence for guidance.
Sebastian Kurz, MD, FCCP
Amee Patrawalla, MD, MPH, FCCP
Section Members-at-Large
References
Testing and Treatment of Latent Tuberculosis Infection in the United States: Clinical Recommendations. A Guide for Health Care Providers and Public Health Programs. Copyright © 2021 by the National Society of Tuberculosis Clinicians and National Tuberculosis Controllers Association
1. Shah, D. Latent tuberculosis infection. N Engl J Med. 2021;385:2271-80.
2. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of tuberculosis in adults and children. Clin Infect Dis. 2017 Jan 15;64(2):111-115.
3. Swindells et. al. One month of rifapentine plus isoniazid to prevent HIV-related tuberculosis. N Engl J Med. 2019;380:1001-11.
Thoracic oncology & chest procedures network: Lung cancer section
Adjuvant and neoadjuvant therapies in early stage lung cancer
Since the discovery of the epidermal growth factor receptor (EGFR) mutation in 2004 and the development of checkpoint blockade in 2006, personalized treatment options for non–small cell lung cancer (NSCLC) have exploded, but targeted systemic therapy medications were only recommended among patients with metastatic or locally advanced disease (Rivera MP, Matthay RA. Clin Chest Med. 2020;41[1]:ix-xi). However, in November 2020, the National Comprehensive Cancer Network (NCCN) updated guidelines to recommend EGFR testing in surgically resected stage IB-IIIA adenocarcinoma, and to consider adjuvant osimerintib in those who were mutation-positive (NCCN. Nov 2020). Interim analysis of an ongoing phase-3 trial showed 89% of patients in the osimertinib group were alive and disease-free at 24 months compared with 52% in the placebo group (hazard ratio 0.20, P < .001) (Wu YL, et al. N Engl J Med. 2020;383[18]:1711-23).
The FDA has also recently approved the use of neoadjuvant and adjuvant immunotherapy in combination with platinum-based chemotherapy. Nivolumab is now approved as neoadjuvant therapy in patients with resectable IB-IIIA NSCLC regardless of PDL-1 status. The Checkmate-816 trial showed increased median event-free survival in the immunotherapy plus chemotherapy group of 31.6 months vs 20.8 months in the chemotherapy-only group (FDA.gov. 2022, Mar 4). Atezolizumab is also now approved for adjuvant treatment following resection and platinum-based chemotherapy in patients with stage II to IIIA NSCLC whose tumors have PD-L1 expression on ≥ 1% of tumor cells. Median disease-free survival was not reached in patients in the atezolizumab groups vs 35.3 months in the best supportive care group (FDA.gov. 2021, Oct 15). With so many advances in the personalized treatment among all stages of NSCLC, this is a hopeful new chapter in the care of patients with NSCLC.
More information: https://www.nccn.org/guidelines/guidelines-process/transparency-process-and-recommendations/GetFileFromFileManager?fileManagerId=11259
Sohini Ghosh, MD
Section Member-at-Large
Diffuse lung disease and lung transplant network: Lung transplant section
Continuous distribution for lung transplant: Overhauling the wait list
Determining how to allocate the scarce resource of donor lungs to patients is a difficult task and evaluated continuously for potential improvement. Since 2005, in the United States, lung transplant recipients have been selected based primarily on location within a Donor Service Area and by lung allocation score (LAS), a composite score of urgency for transplant. This was updated in 2017 to an allocation by highest LAS within 250 nautical miles from the donor hospital. Factors such as blood type compatibility and height are also considered. Implementation of the LAS improved the sickest patients’ access to transplants while not worsening 1-year mortality (Egan TM. Semin Respir Crit Care Med. 2018;39[02]:126-37). Unfortunately, geographic hard boundaries mean a high proportion of low LAS (<50) patients receive local donors while high LAS patients receive national offers or die while on the waitlist (Iribarne A, et al. Clin Transplant. 2016:30:688-93).
A new model that employs continuous distribution has been developed based on concerns regarding equity and improving allocation. This model would prioritize patients based on factors including medical priority, efficient management of organ placement (distance), expected posttransplant outcomes, and patient access (equity). By creating a composite of these without a geographic boundary, patients would be considered more on urgency within realistic constraints of distance and outcomes.
The Organ Procurement and Transplantation Network has officially approved continuous distribution, with implementation planned for 2022; details regarding the new scoring system are to be published and further research will need to be undertaken to determine if it meets the goal of overall improvement in patient access, equity, and outcomes.
Grant A. Turner, MD, MHA
Laura Frye, MD
Section Members-at-Large
Critical care network: Non-respiratory critical care section
Update from the non-respiratory critical care section
As you’ve probably noticed, there have been some changes here at CHEST involving the Networks. Leadership here at CHEST has been hard at work restructuring the networks to make them more closely aligned with relevant clinical disciplines, and, ultimately, allow for greater participation. I am proud to have been given stewardship of the new Non-Respiratory Critical Care Section of the Critical Care Network.
So, what exactly is Non-Respiratory Critical Care? Well, that’s where I need your help. You see this network is meant to reflect the needs and wants of CHEST members like you. We need you, dear readers, to join in this venture and help us guide the content that this section will ultimately create for our members.
If you’re interested in critical care, but you don’t see your particular area of interest anywhere else in the current structure ... guess what? You’ve found the right place!
My Infectious Diseases and Nephro peeps? Welcome! Are you a surgical or anesthesia intensivist? Don’t be shy. ECMO people, let’s hear some chatter!Is therapeutic hypothermia your thing? Come on in. The water’s freezing. 33 degrees just like you folks like it. Or is it 36? Not sure. Anyway, see what I’m talking about? We really need your help!You can get involved by clicking on the Membership & Community tab at the CHEST website. Once you’re a member, you can even nominate yourself to run for the Steering Committee elections which are held periodically. Hope to see you soon!
Deep Ramachandran, MD, FCCP
Section Chair
Sleep medicine network: Non-respiratory sleep section
Unusual suspects? Breakthrough in the treatment of idiopathic hypersomnia
Idiopathic hypersomnia (IH) is a rare and debilitating disorder defined by its excessive daytime sleepiness, sleep inertia, prolonged nighttime sleep, and long, unrefreshing naps (AASM. ICSD 3rd ed. 2014). Gamma-aminobutyric acid (GABA) is one of the main inhibitory neurotransmitters in the nervous system. It is through the potentiation of GABA that substances such as alcohol and benzodiazepines yield their effects. It is also hypothesized that the “brain fog” experienced in IH may be a consequence of either higher levels of an endogenous benzodiazepines in the cerebral spinal fluid or the presence of a GABA-enhancing peptide (Rye DB. Science Transl Med. 2012;Med 4:161ra151).
Sodium oxybate (SXB), a compound that likely has its therapeutic effect through the potentiation of GABA receptors, is an effective treatment option for cataplexy and sleepiness in narcolepsy. Although there may be some overlap between narcolepsy and IH in both diagnosis and treatment (Bassetti C, et al. Brain. 1997;120:1423), it would perhaps be entirely counterintuitive (given SXB’s pharmacology) to imagine using SXB as a plausible treatment option in IH. It was, however, investigated in the treatment of refractory hypersomnia and IH. In the retrospective study looking at 46 subjects treated with SXB, 71% experienced improvement of their severe sleep inertia, 55% had a decrease in their excessive daytime sleepiness, and 52% reported a shortened nighttime sleep time (Leu-Semenescu S, et al. Sleep Med. 2016;17:38).
In a recent double-blind, randomized control trial, the lower-sodium oxybate (LXB) was trialed in 154 patients with IH. It demonstrated statistically significant and clinically meaningful improvements (compared with placebo) in the Epworth Sleepiness Scale score (P <.0001) and in the Idiopathic Hypersomnia Severity Scale (P <.0001). The effects were seen both during the up titration of LXB and the benefits were maintained during the stable phase of the intervention (Dauvilliers Y, et al. Lancet Neurol. 2022;21(1):53). In August 2021, LXB (initially launched in 2020 for the treatment of narcolepsy) is now the first FDA-approved medication to treat IH in adults. It is curious, however, that LXB’s understood therapeutic effects are secondary to the “potentiation” of the very GABA receptor we have believed to be the root cause of the debilitating symptoms in IH. Could this discovery lend to further insights into the origins of this condition?
Ruckshanda Majid, MD, FCCP
The quest for a good night’s sleep: An update on pharmacologic therapy for insomnia
Insomnia is one of the most common complaints in medicine, driving millions of clinic visits each year (Table 1). It is estimated that approximately 30% of individuals report at least short-term insomnia symptoms and 10% report chronic insomnia. These rates are even higher in groups that may be more susceptible to insomnia, including women, the elderly, and those of disadvantaged socioeconomic status (Ohayon MM. Sleep Med Rev. 2002;[2]:97-111). While most patients with insomnia find their sleep difficulties self-resolve within 3 months, a substantial number of patients will find their insomnia to persist for longer and require intervention (Sateia MJ et al. J Clin Sleep Med. 2017;13[2]:307-49).
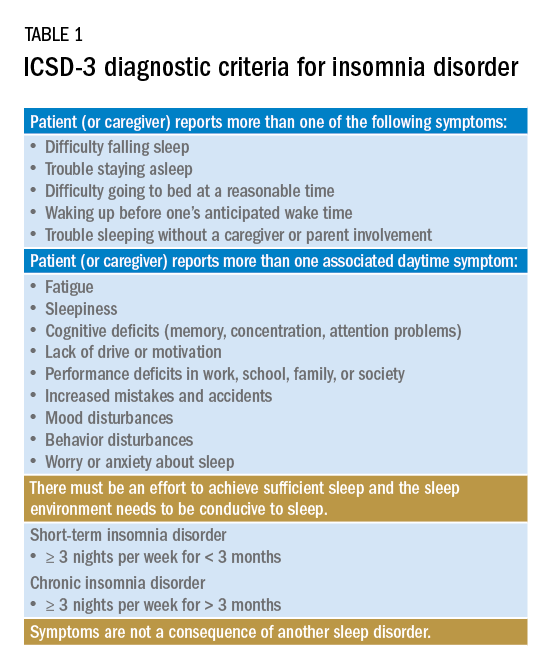
For individuals requiring treatment, cognitive behavioral therapy for insomnia (CBT-I) is considered first-line therapy by the American Academy of Sleep Medicine for both acute and chronic insomnia. Unfortunately, obtaining CBT-I for a patient is often a challenge as the number of trained therapists offering this service is limited, resulting in long wait times or, in some cases, a complete lack of access to this treatment option. Judicious use of sedative-hypnotic medications may be a reasonable alternative for patients with insomnia who are unable to undergo CBT-I, who are still symptomatic despite undergoing CBT-I, or, in some cases, as a temporary treatment (Sateia MJ et al. J Clin Sleep Med. 2017;13[2]:307-49).
Current medications used to treat insomnia are listed in Tables 2 and 3, some of which carry an FDA approval to be used as a hypnotic, while others are used in an off-label manner.
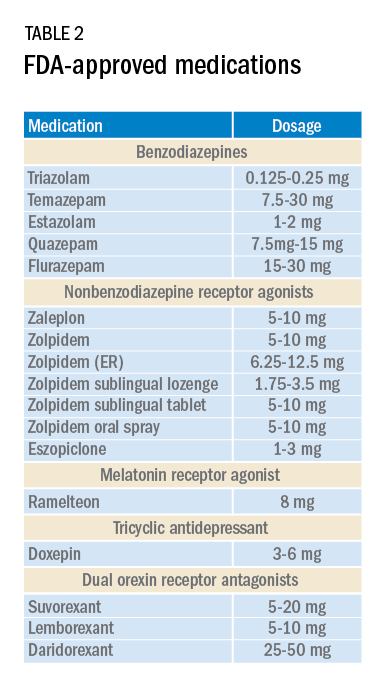
Cautions abound with use of many of these medications. Common concerns include safety, particularly for elderly patients and long-term use, and the potential for developing tolerance and dependence.
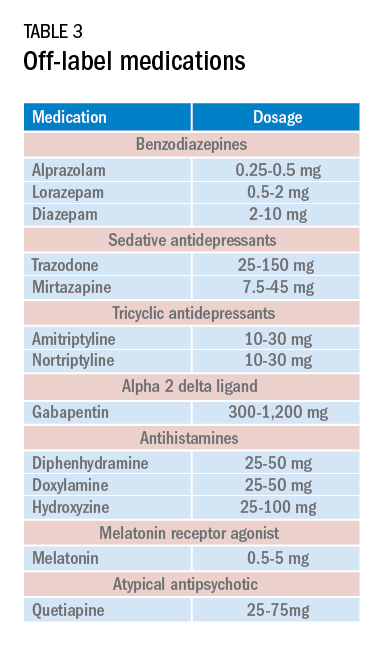
Most medications that have been used for insomnia have been available for decades, but, in recent years, a new class of hypnotics has emerged. Dual orexin receptor antagonists (DORAs) are the newest class of FDA-approved medications (Table 4).
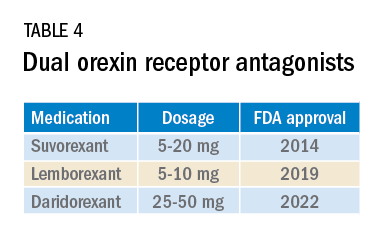
Orexin is a neuropeptide found primarily in the lateral hypothalamus and binds to the orexin 1 and orexin 2 receptors leading to a number of downstream effects, including stimulating wakefulness. Loss of orexin-generating neurons has been implicated as the cause of type 1 narcolepsy, and antagonism of their effects can facilitate sleep by suppressing wakefulness. The first medication in the DORA class to be FDA-approved was suvorexant in 2014, followed by lemborexant’s FDA approval in 2019. These are both indicated for treating sleep onset and sleep maintenance insomnia and have been shown to improve both subjective and objective measures of sleep. The most common side effects reported for both suvorexant and lemborexant are headache and somnolence, with morning-after sleepiness being a frequent complaint.
In January 2022, a new medication in the DORA class named daridorexant was approved by the FDA (Table 5).
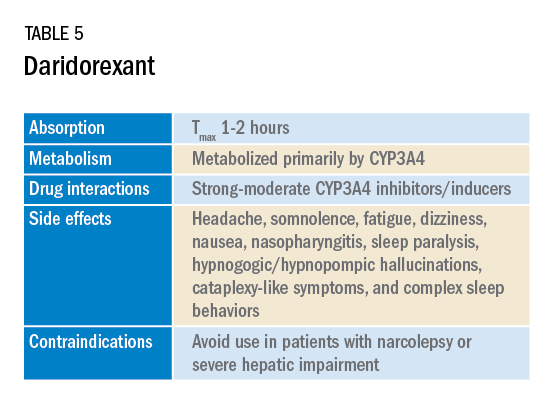
Daridorexant, like its DORA counterparts, has been shown to have efficacy in improving subjective and objective markers of insomnia. This has included polysomnographic measures of wake after sleep onset and latency to persistent sleep, as well as subjective total sleep time. Importantly, in addition to positive sleep outcomes, improvements with daytime function have also been observed with this medication (Mignot E et al. Lancet Neurol. 2022;21[2]:125-39). Daridorexant’s half-life of approximately 8 hours is shorter than that of the other available DORAs, leading to fewer day-after effects. The combination of effectiveness for sleep initiation and maintenance without daytime impairment distinguishes daridorexant from the other DORAs and even other classes of sleep medication.

Safety, especially in patients of age 65 and older, is an important concern with sleep medication, particularly with respect to polypharmacy, over-sedation, increased fall risk, and cognitive impairment, but daridorexant’s available safety data suggest a favorable safety profile (Zammit G et al. Neurology. 2020;94[21]:e2222-32).
Daridorexant at the highest dose available, 50 mg, did not worsen respiratory function, in terms of the apnea-hypopnea index and oxygen saturation in individuals with mild-moderate obstructive sleep apnea regardless of sleep stage (Boof ML et al. Sleep. 2021;44[6]:zsaa275). However, more safety and longitudinal data are needed to have a fuller understanding of any potential limitations of this medication.
While we continue to recommend CBT-I as the first-line treatment whenever possible for patients with insomnia, not all patients have access to this treatment and not all patients will respond satisfactorily to it. Thus, pharmacologic treatment can continue to play an important role in the management of some patients’ insomnia. Each class of medications used for treating insomnia features a unique constellation of advantages and limitations, meaning that the more available options, the greater the chances of finding an option that will be both effective and safe for a particular patient. The growing DORA class, especially its newest available entrant, daridorexant, represents a continued expansion of the armamentarium of options against insomnia.
Dr. Pelekanos and Dr. Sum-Ping are with the Division of Sleep Medicine, Department of Psychiatry & Behavioral Sciences, Stanford University, Stanford, California.
Insomnia is one of the most common complaints in medicine, driving millions of clinic visits each year (Table 1). It is estimated that approximately 30% of individuals report at least short-term insomnia symptoms and 10% report chronic insomnia. These rates are even higher in groups that may be more susceptible to insomnia, including women, the elderly, and those of disadvantaged socioeconomic status (Ohayon MM. Sleep Med Rev. 2002;[2]:97-111). While most patients with insomnia find their sleep difficulties self-resolve within 3 months, a substantial number of patients will find their insomnia to persist for longer and require intervention (Sateia MJ et al. J Clin Sleep Med. 2017;13[2]:307-49).
For individuals requiring treatment, cognitive behavioral therapy for insomnia (CBT-I) is considered first-line therapy by the American Academy of Sleep Medicine for both acute and chronic insomnia. Unfortunately, obtaining CBT-I for a patient is often a challenge as the number of trained therapists offering this service is limited, resulting in long wait times or, in some cases, a complete lack of access to this treatment option. Judicious use of sedative-hypnotic medications may be a reasonable alternative for patients with insomnia who are unable to undergo CBT-I, who are still symptomatic despite undergoing CBT-I, or, in some cases, as a temporary treatment (Sateia MJ et al. J Clin Sleep Med. 2017;13[2]:307-49).
Current medications used to treat insomnia are listed in Tables 2 and 3, some of which carry an FDA approval to be used as a hypnotic, while others are used in an off-label manner.
Cautions abound with use of many of these medications. Common concerns include safety, particularly for elderly patients and long-term use, and the potential for developing tolerance and dependence.
Most medications that have been used for insomnia have been available for decades, but, in recent years, a new class of hypnotics has emerged. Dual orexin receptor antagonists (DORAs) are the newest class of FDA-approved medications (Table 4).
Orexin is a neuropeptide found primarily in the lateral hypothalamus and binds to the orexin 1 and orexin 2 receptors leading to a number of downstream effects, including stimulating wakefulness. Loss of orexin-generating neurons has been implicated as the cause of type 1 narcolepsy, and antagonism of their effects can facilitate sleep by suppressing wakefulness. The first medication in the DORA class to be FDA-approved was suvorexant in 2014, followed by lemborexant’s FDA approval in 2019. These are both indicated for treating sleep onset and sleep maintenance insomnia and have been shown to improve both subjective and objective measures of sleep. The most common side effects reported for both suvorexant and lemborexant are headache and somnolence, with morning-after sleepiness being a frequent complaint.
In January 2022, a new medication in the DORA class named daridorexant was approved by the FDA (Table 5).
Daridorexant, like its DORA counterparts, has been shown to have efficacy in improving subjective and objective markers of insomnia. This has included polysomnographic measures of wake after sleep onset and latency to persistent sleep, as well as subjective total sleep time. Importantly, in addition to positive sleep outcomes, improvements with daytime function have also been observed with this medication (Mignot E et al. Lancet Neurol. 2022;21[2]:125-39). Daridorexant’s half-life of approximately 8 hours is shorter than that of the other available DORAs, leading to fewer day-after effects. The combination of effectiveness for sleep initiation and maintenance without daytime impairment distinguishes daridorexant from the other DORAs and even other classes of sleep medication.
Safety, especially in patients of age 65 and older, is an important concern with sleep medication, particularly with respect to polypharmacy, over-sedation, increased fall risk, and cognitive impairment, but daridorexant’s available safety data suggest a favorable safety profile (Zammit G et al. Neurology. 2020;94[21]:e2222-32).
Daridorexant at the highest dose available, 50 mg, did not worsen respiratory function, in terms of the apnea-hypopnea index and oxygen saturation in individuals with mild-moderate obstructive sleep apnea regardless of sleep stage (Boof ML et al. Sleep. 2021;44[6]:zsaa275). However, more safety and longitudinal data are needed to have a fuller understanding of any potential limitations of this medication.
While we continue to recommend CBT-I as the first-line treatment whenever possible for patients with insomnia, not all patients have access to this treatment and not all patients will respond satisfactorily to it. Thus, pharmacologic treatment can continue to play an important role in the management of some patients’ insomnia. Each class of medications used for treating insomnia features a unique constellation of advantages and limitations, meaning that the more available options, the greater the chances of finding an option that will be both effective and safe for a particular patient. The growing DORA class, especially its newest available entrant, daridorexant, represents a continued expansion of the armamentarium of options against insomnia.
Dr. Pelekanos and Dr. Sum-Ping are with the Division of Sleep Medicine, Department of Psychiatry & Behavioral Sciences, Stanford University, Stanford, California.
Insomnia is one of the most common complaints in medicine, driving millions of clinic visits each year (Table 1). It is estimated that approximately 30% of individuals report at least short-term insomnia symptoms and 10% report chronic insomnia. These rates are even higher in groups that may be more susceptible to insomnia, including women, the elderly, and those of disadvantaged socioeconomic status (Ohayon MM. Sleep Med Rev. 2002;[2]:97-111). While most patients with insomnia find their sleep difficulties self-resolve within 3 months, a substantial number of patients will find their insomnia to persist for longer and require intervention (Sateia MJ et al. J Clin Sleep Med. 2017;13[2]:307-49).
For individuals requiring treatment, cognitive behavioral therapy for insomnia (CBT-I) is considered first-line therapy by the American Academy of Sleep Medicine for both acute and chronic insomnia. Unfortunately, obtaining CBT-I for a patient is often a challenge as the number of trained therapists offering this service is limited, resulting in long wait times or, in some cases, a complete lack of access to this treatment option. Judicious use of sedative-hypnotic medications may be a reasonable alternative for patients with insomnia who are unable to undergo CBT-I, who are still symptomatic despite undergoing CBT-I, or, in some cases, as a temporary treatment (Sateia MJ et al. J Clin Sleep Med. 2017;13[2]:307-49).
Current medications used to treat insomnia are listed in Tables 2 and 3, some of which carry an FDA approval to be used as a hypnotic, while others are used in an off-label manner.
Cautions abound with use of many of these medications. Common concerns include safety, particularly for elderly patients and long-term use, and the potential for developing tolerance and dependence.
Most medications that have been used for insomnia have been available for decades, but, in recent years, a new class of hypnotics has emerged. Dual orexin receptor antagonists (DORAs) are the newest class of FDA-approved medications (Table 4).
Orexin is a neuropeptide found primarily in the lateral hypothalamus and binds to the orexin 1 and orexin 2 receptors leading to a number of downstream effects, including stimulating wakefulness. Loss of orexin-generating neurons has been implicated as the cause of type 1 narcolepsy, and antagonism of their effects can facilitate sleep by suppressing wakefulness. The first medication in the DORA class to be FDA-approved was suvorexant in 2014, followed by lemborexant’s FDA approval in 2019. These are both indicated for treating sleep onset and sleep maintenance insomnia and have been shown to improve both subjective and objective measures of sleep. The most common side effects reported for both suvorexant and lemborexant are headache and somnolence, with morning-after sleepiness being a frequent complaint.
In January 2022, a new medication in the DORA class named daridorexant was approved by the FDA (Table 5).
Daridorexant, like its DORA counterparts, has been shown to have efficacy in improving subjective and objective markers of insomnia. This has included polysomnographic measures of wake after sleep onset and latency to persistent sleep, as well as subjective total sleep time. Importantly, in addition to positive sleep outcomes, improvements with daytime function have also been observed with this medication (Mignot E et al. Lancet Neurol. 2022;21[2]:125-39). Daridorexant’s half-life of approximately 8 hours is shorter than that of the other available DORAs, leading to fewer day-after effects. The combination of effectiveness for sleep initiation and maintenance without daytime impairment distinguishes daridorexant from the other DORAs and even other classes of sleep medication.
Safety, especially in patients of age 65 and older, is an important concern with sleep medication, particularly with respect to polypharmacy, over-sedation, increased fall risk, and cognitive impairment, but daridorexant’s available safety data suggest a favorable safety profile (Zammit G et al. Neurology. 2020;94[21]:e2222-32).
Daridorexant at the highest dose available, 50 mg, did not worsen respiratory function, in terms of the apnea-hypopnea index and oxygen saturation in individuals with mild-moderate obstructive sleep apnea regardless of sleep stage (Boof ML et al. Sleep. 2021;44[6]:zsaa275). However, more safety and longitudinal data are needed to have a fuller understanding of any potential limitations of this medication.
While we continue to recommend CBT-I as the first-line treatment whenever possible for patients with insomnia, not all patients have access to this treatment and not all patients will respond satisfactorily to it. Thus, pharmacologic treatment can continue to play an important role in the management of some patients’ insomnia. Each class of medications used for treating insomnia features a unique constellation of advantages and limitations, meaning that the more available options, the greater the chances of finding an option that will be both effective and safe for a particular patient. The growing DORA class, especially its newest available entrant, daridorexant, represents a continued expansion of the armamentarium of options against insomnia.
Dr. Pelekanos and Dr. Sum-Ping are with the Division of Sleep Medicine, Department of Psychiatry & Behavioral Sciences, Stanford University, Stanford, California.