User login
Cognitive impairment may predict physical disability in MS
, new research suggests. In an analysis of more than 1,600 patients with secondary-progressive MS (SPMS), the likelihood of needing a wheelchair was almost doubled in those who had the worst scores on cognitive testing measures, compared with their counterparts who had the best scores.
“These findings should change our world view of MS,” study investigator Gavin Giovannoni, PhD, professor of neurology, Blizard Institute, Faculty of Medicine and Dentistry, Queen Mary University of London, told attendees at the Congress of the European Academy of Neurology.

On the basis of the results, clinicians should consider testing cognitive processing speed in patients with MS to identify those who are at increased risk for disease progression, Dr. Giovannoni noted. “I urge anybody who runs an MS service to think about putting in place mechanisms in their clinic” to measure cognition of patients over time, he said.
Expand data
Cognitive impairment occurs very early in the course of MS and is part of the disease, although to a greater or lesser degree depending on the patient, Dr. Giovannoni noted. Such impairment has a significant impact on quality of life for patients dealing with this disease, he added.
EXPAND was a phase 3 study of siponimod. Results showed the now-approved oral selective sphingosine 1–phosphate receptor modulator significantly reduced the risk for disability progression in patients with SPMS.
Using the EXPAND clinical trial database, the current researchers assessed 1,628 participants for an association between cognitive processing speed, as measured with the Symbol Digit Modality Test (SDMT), and physical disability progression, as measured with the Expanded Disability Status Scale (EDSS). A score of 7 or more on the EDSS indicates wheelchair dependence.
Dr. Giovannoni noted that cognitive processing speed is considered an indirect measure of thalamic network efficiency and functional brain reserve.
Investigators looked at both the core study, in which all patients continued on treatment or placebo for up to 37 months, and the core plus extension part, in which patients received treatment for up to 5 years.
They separated SDMT scores into quartiles: from worst (n = 435) to two intermediate quartiles (n = 808) to the best quartile (n = 385).
Wheelchair dependence
In addition, the researchers examined the predictive value by baseline SDMT, adjusting for treatment, age, gender, baseline EDSS score, baseline SCMT quartile, and treatment-by-baseline SCMT quartile interaction. On-study SDMT change (month 0-24) was also assessed after adjusting for treatment, age, gender, baseline EDS, baseline SCMT, and on-study change in SCMT quartile.
In the core study, those in the worst SDMT quartile at baseline were numerically more likely to reach deterioration to EDSS 7 or greater (wheelchair dependent), compared with patients in the best SDMT quartile (hazard ratio, 1.31; 95% confidence interval, .72-2.38; P = .371).
The short-term predictive value of baseline SDMT for reaching sustained EDSS of at least 7 was more obvious in the placebo arm than in the treatment arm.
Dr. Giovannoni said this is likely due to the treatment effect of siponimod preventing relatively more events in the worse quartile, and so reducing the risk for wheelchair dependency.
In the core plus extension part, there was an almost twofold increased risk for wheelchair dependence in the worse versus best SDMT groups (HR, 1.81; 95% CI, 1.17-2.78; P = .007).
Both baseline SDMT (HR, 1.81; P = .007) and on-study change in SDMT (HR, 1.73; P = .046) predicted wheelchair dependence in the long-term.
‘More important than a walking stick’
Measuring cognitive change over time “may be a more important predictor than a walking stick in terms of quality of life and outcomes, and it affects clinical decisionmaking,” said Dr. Giovannoni.
The findings are not novel, as post hoc analyses of other studies showed similar results. However, this new analysis adds more evidence to the importance of cognition in MS, Dr. Giovannoni noted.
“I have patients with EDSS of 0 or 1 who are profoundly disabled because of cognition. You shouldn’t just assume someone is not disabled because they don’t have physical disability,” he said.
However, Dr. Giovannoni noted that the study found an association and does not necessarily indicate a cause.
‘Valuable’ insights
Antonia Lefter, MD, of NeuroHope, Monza Oncologic Hospital, Bucharest, Romania, cochaired the session highlighting the research. Commenting on the study, she called this analysis from the “renowned” EXPAND study “valuable.”
In addition, it “underscores” the importance of assessing cognitive processing speed, as it may predict long-term disability progression in patients with SPMS, Dr. Lefter said.
The study was funded by Novartis Pharma AG, Basel, Switzerland. Dr. Giovannoni, a steering committee member of the EXPAND trial, reported receiving consulting fees from AbbVie, Actelion, Atara Bio, Biogen, Celgene, Sanofi-Genzyme, Genentech, GlaxoSmithKline, Merck-Serono, Novartis, Roche, and Reva. He has also received compensation for research from Biogen, Roche, Merck-Serono, Novartis, Sanofi-Genzyme, and Takeda. Dr. Lefter has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In an analysis of more than 1,600 patients with secondary-progressive MS (SPMS), the likelihood of needing a wheelchair was almost doubled in those who had the worst scores on cognitive testing measures, compared with their counterparts who had the best scores.
“These findings should change our world view of MS,” study investigator Gavin Giovannoni, PhD, professor of neurology, Blizard Institute, Faculty of Medicine and Dentistry, Queen Mary University of London, told attendees at the Congress of the European Academy of Neurology.
On the basis of the results, clinicians should consider testing cognitive processing speed in patients with MS to identify those who are at increased risk for disease progression, Dr. Giovannoni noted. “I urge anybody who runs an MS service to think about putting in place mechanisms in their clinic” to measure cognition of patients over time, he said.
Expand data
Cognitive impairment occurs very early in the course of MS and is part of the disease, although to a greater or lesser degree depending on the patient, Dr. Giovannoni noted. Such impairment has a significant impact on quality of life for patients dealing with this disease, he added.
EXPAND was a phase 3 study of siponimod. Results showed the now-approved oral selective sphingosine 1–phosphate receptor modulator significantly reduced the risk for disability progression in patients with SPMS.
Using the EXPAND clinical trial database, the current researchers assessed 1,628 participants for an association between cognitive processing speed, as measured with the Symbol Digit Modality Test (SDMT), and physical disability progression, as measured with the Expanded Disability Status Scale (EDSS). A score of 7 or more on the EDSS indicates wheelchair dependence.
Dr. Giovannoni noted that cognitive processing speed is considered an indirect measure of thalamic network efficiency and functional brain reserve.
Investigators looked at both the core study, in which all patients continued on treatment or placebo for up to 37 months, and the core plus extension part, in which patients received treatment for up to 5 years.
They separated SDMT scores into quartiles: from worst (n = 435) to two intermediate quartiles (n = 808) to the best quartile (n = 385).
Wheelchair dependence
In addition, the researchers examined the predictive value by baseline SDMT, adjusting for treatment, age, gender, baseline EDSS score, baseline SCMT quartile, and treatment-by-baseline SCMT quartile interaction. On-study SDMT change (month 0-24) was also assessed after adjusting for treatment, age, gender, baseline EDS, baseline SCMT, and on-study change in SCMT quartile.
In the core study, those in the worst SDMT quartile at baseline were numerically more likely to reach deterioration to EDSS 7 or greater (wheelchair dependent), compared with patients in the best SDMT quartile (hazard ratio, 1.31; 95% confidence interval, .72-2.38; P = .371).
The short-term predictive value of baseline SDMT for reaching sustained EDSS of at least 7 was more obvious in the placebo arm than in the treatment arm.
Dr. Giovannoni said this is likely due to the treatment effect of siponimod preventing relatively more events in the worse quartile, and so reducing the risk for wheelchair dependency.
In the core plus extension part, there was an almost twofold increased risk for wheelchair dependence in the worse versus best SDMT groups (HR, 1.81; 95% CI, 1.17-2.78; P = .007).
Both baseline SDMT (HR, 1.81; P = .007) and on-study change in SDMT (HR, 1.73; P = .046) predicted wheelchair dependence in the long-term.
‘More important than a walking stick’
Measuring cognitive change over time “may be a more important predictor than a walking stick in terms of quality of life and outcomes, and it affects clinical decisionmaking,” said Dr. Giovannoni.
The findings are not novel, as post hoc analyses of other studies showed similar results. However, this new analysis adds more evidence to the importance of cognition in MS, Dr. Giovannoni noted.
“I have patients with EDSS of 0 or 1 who are profoundly disabled because of cognition. You shouldn’t just assume someone is not disabled because they don’t have physical disability,” he said.
However, Dr. Giovannoni noted that the study found an association and does not necessarily indicate a cause.
‘Valuable’ insights
Antonia Lefter, MD, of NeuroHope, Monza Oncologic Hospital, Bucharest, Romania, cochaired the session highlighting the research. Commenting on the study, she called this analysis from the “renowned” EXPAND study “valuable.”
In addition, it “underscores” the importance of assessing cognitive processing speed, as it may predict long-term disability progression in patients with SPMS, Dr. Lefter said.
The study was funded by Novartis Pharma AG, Basel, Switzerland. Dr. Giovannoni, a steering committee member of the EXPAND trial, reported receiving consulting fees from AbbVie, Actelion, Atara Bio, Biogen, Celgene, Sanofi-Genzyme, Genentech, GlaxoSmithKline, Merck-Serono, Novartis, Roche, and Reva. He has also received compensation for research from Biogen, Roche, Merck-Serono, Novartis, Sanofi-Genzyme, and Takeda. Dr. Lefter has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In an analysis of more than 1,600 patients with secondary-progressive MS (SPMS), the likelihood of needing a wheelchair was almost doubled in those who had the worst scores on cognitive testing measures, compared with their counterparts who had the best scores.
“These findings should change our world view of MS,” study investigator Gavin Giovannoni, PhD, professor of neurology, Blizard Institute, Faculty of Medicine and Dentistry, Queen Mary University of London, told attendees at the Congress of the European Academy of Neurology.
On the basis of the results, clinicians should consider testing cognitive processing speed in patients with MS to identify those who are at increased risk for disease progression, Dr. Giovannoni noted. “I urge anybody who runs an MS service to think about putting in place mechanisms in their clinic” to measure cognition of patients over time, he said.
Expand data
Cognitive impairment occurs very early in the course of MS and is part of the disease, although to a greater or lesser degree depending on the patient, Dr. Giovannoni noted. Such impairment has a significant impact on quality of life for patients dealing with this disease, he added.
EXPAND was a phase 3 study of siponimod. Results showed the now-approved oral selective sphingosine 1–phosphate receptor modulator significantly reduced the risk for disability progression in patients with SPMS.
Using the EXPAND clinical trial database, the current researchers assessed 1,628 participants for an association between cognitive processing speed, as measured with the Symbol Digit Modality Test (SDMT), and physical disability progression, as measured with the Expanded Disability Status Scale (EDSS). A score of 7 or more on the EDSS indicates wheelchair dependence.
Dr. Giovannoni noted that cognitive processing speed is considered an indirect measure of thalamic network efficiency and functional brain reserve.
Investigators looked at both the core study, in which all patients continued on treatment or placebo for up to 37 months, and the core plus extension part, in which patients received treatment for up to 5 years.
They separated SDMT scores into quartiles: from worst (n = 435) to two intermediate quartiles (n = 808) to the best quartile (n = 385).
Wheelchair dependence
In addition, the researchers examined the predictive value by baseline SDMT, adjusting for treatment, age, gender, baseline EDSS score, baseline SCMT quartile, and treatment-by-baseline SCMT quartile interaction. On-study SDMT change (month 0-24) was also assessed after adjusting for treatment, age, gender, baseline EDS, baseline SCMT, and on-study change in SCMT quartile.
In the core study, those in the worst SDMT quartile at baseline were numerically more likely to reach deterioration to EDSS 7 or greater (wheelchair dependent), compared with patients in the best SDMT quartile (hazard ratio, 1.31; 95% confidence interval, .72-2.38; P = .371).
The short-term predictive value of baseline SDMT for reaching sustained EDSS of at least 7 was more obvious in the placebo arm than in the treatment arm.
Dr. Giovannoni said this is likely due to the treatment effect of siponimod preventing relatively more events in the worse quartile, and so reducing the risk for wheelchair dependency.
In the core plus extension part, there was an almost twofold increased risk for wheelchair dependence in the worse versus best SDMT groups (HR, 1.81; 95% CI, 1.17-2.78; P = .007).
Both baseline SDMT (HR, 1.81; P = .007) and on-study change in SDMT (HR, 1.73; P = .046) predicted wheelchair dependence in the long-term.
‘More important than a walking stick’
Measuring cognitive change over time “may be a more important predictor than a walking stick in terms of quality of life and outcomes, and it affects clinical decisionmaking,” said Dr. Giovannoni.
The findings are not novel, as post hoc analyses of other studies showed similar results. However, this new analysis adds more evidence to the importance of cognition in MS, Dr. Giovannoni noted.
“I have patients with EDSS of 0 or 1 who are profoundly disabled because of cognition. You shouldn’t just assume someone is not disabled because they don’t have physical disability,” he said.
However, Dr. Giovannoni noted that the study found an association and does not necessarily indicate a cause.
‘Valuable’ insights
Antonia Lefter, MD, of NeuroHope, Monza Oncologic Hospital, Bucharest, Romania, cochaired the session highlighting the research. Commenting on the study, she called this analysis from the “renowned” EXPAND study “valuable.”
In addition, it “underscores” the importance of assessing cognitive processing speed, as it may predict long-term disability progression in patients with SPMS, Dr. Lefter said.
The study was funded by Novartis Pharma AG, Basel, Switzerland. Dr. Giovannoni, a steering committee member of the EXPAND trial, reported receiving consulting fees from AbbVie, Actelion, Atara Bio, Biogen, Celgene, Sanofi-Genzyme, Genentech, GlaxoSmithKline, Merck-Serono, Novartis, Roche, and Reva. He has also received compensation for research from Biogen, Roche, Merck-Serono, Novartis, Sanofi-Genzyme, and Takeda. Dr. Lefter has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From EAN 2022
COPD predicts hospital readmission after fractures
Chronic obstructive pulmonary disease (COPD) was among the significant predictors of hospital readmission in older adults with fractures, based on data from nearly 400 individuals.
Fractures in the elderly remain a major health concern, and readmissions are common; however, Lara Cristina da Cunha Guimarães, MSN, of State School of Public Health Candido Santiago, State Department of Health of Goiás (Brazil), and colleagues wrote.
Previous research suggests that readmissions risk may be greater in patients with preadmission conditions including pulmonary and cardiac disease, history of stroke and other neurological conditions, and other factors associated with aging in general, they said.
In a study published in the journal Injury , the researchers reviewed data from 376 adults aged 60 years and older in a trauma referral hospital in Brazil who had suffered fractures and were hospitalized between Sept. 1, 2016, and Feb. 28, 2017. The primary outcome was readmission up to one year after discharge from the initial hospitalization for fracture.
Approximately half of the patients experienced femur fractures (53.2%), and the most frequent cause was falling from standing height (72.9%). The overall incidence of readmission was 20.7%. A total of 30.5% of readmissions were related to the fracture, and surgical-site infections were the most common cause of fracture-related complications.
More than half (58.3%) of the readmissions were related to clinical complications.
In a multivariate analysis, several clinical factors not related to fractures were independently associated with readmission, including a previous diagnosis of COPD, age between 60 and 69 years, a fracture of the femur, and delirium at the time of the first hospitalization for fracture.
Pneumonia was the most frequent cause of clinical complications, reflecting data from other recent studies, the researchers noted. “Elderly people with COPD are more susceptible to infections, such as pneumonia, which was a cause of frequent readmissions in the population studied. The presence of COPD can contribute to imbalance in the pulmonary microbiome, mucus production and persistent inflammation of the airways, and structural damage, which increases exposure of the pulmonary mucosa to pathogens.” COPD also can be associated with cardiovascular, mental, and musculoskeletal diseases that can further complicate and delay recovery from fractures.
The study findings were limited by the potential for incomplete information in medical records. However, the results indicate a range of causes and conditions associated with hospital readmission after fractures in older adults, they said. Recognizing these factors can guide plans for transitions from hospital to home care to reduce complications and readmissions.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Chronic obstructive pulmonary disease (COPD) was among the significant predictors of hospital readmission in older adults with fractures, based on data from nearly 400 individuals.
Fractures in the elderly remain a major health concern, and readmissions are common; however, Lara Cristina da Cunha Guimarães, MSN, of State School of Public Health Candido Santiago, State Department of Health of Goiás (Brazil), and colleagues wrote.
Previous research suggests that readmissions risk may be greater in patients with preadmission conditions including pulmonary and cardiac disease, history of stroke and other neurological conditions, and other factors associated with aging in general, they said.
In a study published in the journal Injury , the researchers reviewed data from 376 adults aged 60 years and older in a trauma referral hospital in Brazil who had suffered fractures and were hospitalized between Sept. 1, 2016, and Feb. 28, 2017. The primary outcome was readmission up to one year after discharge from the initial hospitalization for fracture.
Approximately half of the patients experienced femur fractures (53.2%), and the most frequent cause was falling from standing height (72.9%). The overall incidence of readmission was 20.7%. A total of 30.5% of readmissions were related to the fracture, and surgical-site infections were the most common cause of fracture-related complications.
More than half (58.3%) of the readmissions were related to clinical complications.
In a multivariate analysis, several clinical factors not related to fractures were independently associated with readmission, including a previous diagnosis of COPD, age between 60 and 69 years, a fracture of the femur, and delirium at the time of the first hospitalization for fracture.
Pneumonia was the most frequent cause of clinical complications, reflecting data from other recent studies, the researchers noted. “Elderly people with COPD are more susceptible to infections, such as pneumonia, which was a cause of frequent readmissions in the population studied. The presence of COPD can contribute to imbalance in the pulmonary microbiome, mucus production and persistent inflammation of the airways, and structural damage, which increases exposure of the pulmonary mucosa to pathogens.” COPD also can be associated with cardiovascular, mental, and musculoskeletal diseases that can further complicate and delay recovery from fractures.
The study findings were limited by the potential for incomplete information in medical records. However, the results indicate a range of causes and conditions associated with hospital readmission after fractures in older adults, they said. Recognizing these factors can guide plans for transitions from hospital to home care to reduce complications and readmissions.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Chronic obstructive pulmonary disease (COPD) was among the significant predictors of hospital readmission in older adults with fractures, based on data from nearly 400 individuals.
Fractures in the elderly remain a major health concern, and readmissions are common; however, Lara Cristina da Cunha Guimarães, MSN, of State School of Public Health Candido Santiago, State Department of Health of Goiás (Brazil), and colleagues wrote.
Previous research suggests that readmissions risk may be greater in patients with preadmission conditions including pulmonary and cardiac disease, history of stroke and other neurological conditions, and other factors associated with aging in general, they said.
In a study published in the journal Injury , the researchers reviewed data from 376 adults aged 60 years and older in a trauma referral hospital in Brazil who had suffered fractures and were hospitalized between Sept. 1, 2016, and Feb. 28, 2017. The primary outcome was readmission up to one year after discharge from the initial hospitalization for fracture.
Approximately half of the patients experienced femur fractures (53.2%), and the most frequent cause was falling from standing height (72.9%). The overall incidence of readmission was 20.7%. A total of 30.5% of readmissions were related to the fracture, and surgical-site infections were the most common cause of fracture-related complications.
More than half (58.3%) of the readmissions were related to clinical complications.
In a multivariate analysis, several clinical factors not related to fractures were independently associated with readmission, including a previous diagnosis of COPD, age between 60 and 69 years, a fracture of the femur, and delirium at the time of the first hospitalization for fracture.
Pneumonia was the most frequent cause of clinical complications, reflecting data from other recent studies, the researchers noted. “Elderly people with COPD are more susceptible to infections, such as pneumonia, which was a cause of frequent readmissions in the population studied. The presence of COPD can contribute to imbalance in the pulmonary microbiome, mucus production and persistent inflammation of the airways, and structural damage, which increases exposure of the pulmonary mucosa to pathogens.” COPD also can be associated with cardiovascular, mental, and musculoskeletal diseases that can further complicate and delay recovery from fractures.
The study findings were limited by the potential for incomplete information in medical records. However, the results indicate a range of causes and conditions associated with hospital readmission after fractures in older adults, they said. Recognizing these factors can guide plans for transitions from hospital to home care to reduce complications and readmissions.
The study received no outside funding. The researchers had no financial conflicts to disclose.
FROM INJURY
Insulin Injection-Site Acanthosis Nigricans: Skin Reactions and Clinical Implications
Insulin injection therapy is one of the most widely used health care interventions to manage both type 1 and type 2 diabetes mellitus (T1DM/T2DM). Globally, more than 150 to 200 million people inject insulin into their upper posterior arms, buttocks, anterior and lateral thighs, or abdomen.1,2 In an ideal world, every patient would be using the correct site and rotating their insulin injection sites in accordance with health care professional (HCP) recommendations—systematic injections in one general body location, at least 1 cm away from the previous injection.2 Unfortunately, same-site insulin injection (repeatedly in the same region within 1 cm of previous injections) is a common mistake made by patients with DM—in one study, 63% of participants either did not rotate sites correctly or failed to do so at all.
Insulin-resistant cutaneous complications may occur as a result of same-site insulin injections. The most common is lipohypertrophy, reported in some studies in nearly 50% of patients with DM on insulin therapy.4 Other common cutaneous complications include lipoatrophy and amyloidosis. Injection-site acanthosis nigricans, although uncommon, has been reported in 18 cases in the literature.
Most articles suggest that same-site insulin injections decrease local insulin sensitivity and result in tissue hypertrophy because of the anabolic properties of insulin and increase in insulin binding to insulin-like growth factor-1 (IGF-1) receptor.5-20 The hyperkeratotic growth and varying insulin absorption rates associated with these cutaneous complications increase chances of either hyper- or hypoglycemic episodes in patients.10,11,13 It is the responsibility of the DM care professional to provide proper insulin-injection technique education and perform routine inspection of injection sites to reduce cutaneous complications of insulin therapy. The purpose of this article is to (1) describe a case of acanthosis nigricans resulting from insulin injection at the same site; (2) review case reports
Case Presentation
A 75-year-old patient with an 8-year history of T2DM, as well as stable coronary artery disease, atrial fibrillation, hypertension, hyperlipidemia, chronic obstructive pulmonary disease, and stage 3 chronic kidney disease, presented with 2 discrete abdominal hyperpigmented plaques. At the time of the initial clinic visit, the patient was taking metformin 1000 mg twice daily and insulin glargine 40 units once daily. When insulin was initiated 7 years prior, the patient received
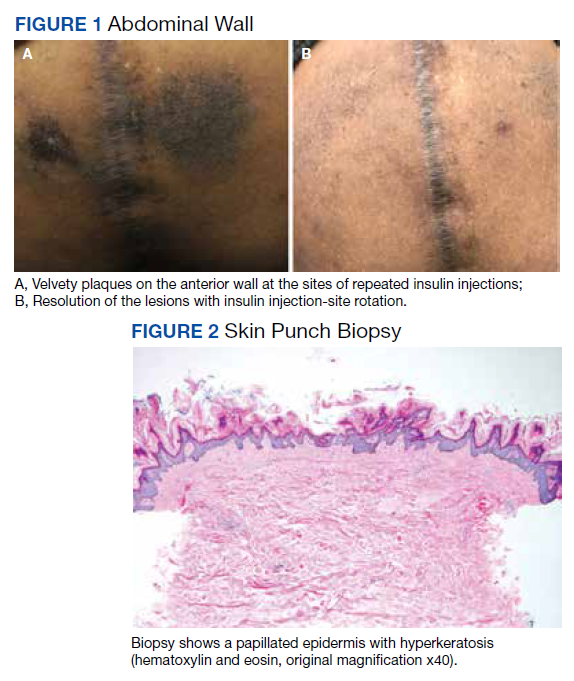
The patient reported 5 years of progressive, asymptomatic hyperpigmentation of the skin surrounding his insulin glargine injection sites and injecting in these same sites daily without rotation. He reported no additional skin changes or symptoms. He had noticed no skin changes while using NPH insulin during his first year of insulin therapy. On examination, the abdominal wall skin demonstrated 2 well-demarcated, nearly black, soft, velvety plaques, measuring 9 × 8 cm on the left side and 4 × 3.5 cm on the right, suggesting acanthosis nigricans (Figure 1A). The remainder of the skin examination, including the flexures, was normal. Of note, the patient received biweekly intramuscular testosterone injections in the gluteal region for secondary hypogonadism with no adverse dermatologic effects. A skin punch biopsy was performed and revealed epidermal papillomatosis and hyperkeratosis, confirming the clinical diagnosis of acanthosis nigricans (Figure 2).
After a review of insulin-injection technique at his clinic visit, the patient started rotating insulin injection sites over his entire abdomen, and the acanthosis nigricans partially improved. A few months later, the patient stopped rotating the insulin injection site, and the acanthosis nigricans worsened again. Because of worsening glycemic control, the patient was then started on insulin aspart. He did not develop any skin changes at the insulin aspart injection site, although he was not rotating its site of injection.
Subsequently, with reeducation and proper injection-site rotation, the patient had resolution of his acanthosis nigricans (Figure 1b).
Discussion
A review of the literature revealed 18 reported cases of acanthosis nigricans at sites of repeated insulin injection (Table).5-20 Acanthosis nigricans at the site of insulin injection afflicts patients of any age, with cases observed in patients aged 14 to 75 years. Sixteen (84%) of 19 cases were male. Fourteen cases (73%) had T2DM; the rest of the patients had T1DM. The duration of insulin injection therapy prior to onset ranged from immediate to 13 years (median 4 years). Fourteen cases (73%) were reported on the abdomen; however, other sites, such as thighs and upper arm, also were reported. Lesions size varied from 12 to 360 cm2. Two cases had associated amyloidosis. The average HbA1c reported at presentation was 10%. Following insulin injection-site rotation, most of the cases reported improvement of both glycemic control and acanthosis nigricans appearance.
In the case described by Kudo and colleagues, a 59-year-old male patient with T2DM had been injecting insulin into the same spot on his abdomen for 10 years. He developed acanthosis nigricans and an amyloidoma so large and firm that it bent the needle when he injected insulin.11
Most of the cases we found in the literature were after 2005 and associated with the use of human or analog insulin. These cases may be related to a bias, as cases may be easier to find in digital archives in the later years, when human or analog insulins have been in common use. Also noteworthy, in cases that reported dosage, most were not very high, and the highest daily dose was 240 IU/d. Ten reports of injection-site acanthosis nigricans were in dermatology journals; only 5 reports were in endocrinology journals and 3 in general medical journals, indicating possible less awareness of this phenomenon in other HCPs who care for patients with DM.
Complications of Same-Site Injections
Acanthosis nigricans. Commonly found in the armpits, neck folds, and groin, acanthosis nigricans is known as one of the calling cards for insulin resistance, obesity, and hyperinsulinemia.21 Acanthosis nigricans can be seen in people with or without DM and is not limited to those on insulin therapy. However, same-site insulin injections for 4 to 6 years also may result in injection-site acanthosis nigricans–like lesions because of factors such as insulin exposure at the local tissue level.16
Acanthosis nigricans development is characterized by hyperpigmented, hyperkeratotic, velvety, and sometimes verrucous plaques.6 Acanthosis nigricans surrounding repeated injection sites is hypothesized to develop as a result of localized hyperinsulinemia secondary to insulin resistance, which increases the stimulation of IGF, thereby causing epidermal hypertrophy.5-20 If insulin injection therapy continues to be administered through the acanthosis nigricans lesion, it results in decreased insulin absorption, leading to poor glycemic control.13
Acanthosis nigricans associated with insulin injection is reversible. After rotation of injection sites, lesions either decrease in size or severity of appearance.5-8,11 Also, by avoiding injection into the hyperkeratotic plaques and using normal subcutaneous tissue for injection, patients’ response to insulin improves, as measured by HbA1c and by decreased daily insulin requirement.6-8,10,12,18-20
Lipohypertrophy. This is characterized by an increase in localized adipose tissue and is the most common cutaneous complication of insulin therapy.2 Lipohypertrophy presents as a firm, rubbery mass in the location of same-site insulin injections.22 Development of lipohypertrophy is suspected to be the result of either (1) anabolic effect of insulin on local adipocytes, promoting fat and protein synthesis; (2) an autoimmune response by immunoglobulin (Ig) G or IgE antibodies to insulin, immune response to insulin of different species, or to insulin injection techniques; or (3) repeated trauma to the injection site from repeated needle usage.4,23
In a study assessing the prevalence of lipohypertrophy and its relation to insulin technique, 49.1% of participants with
Primary prevention measures include injection site inspection and patient education about rotation and abstaining from needle reuse.22 If a patient already has signs of lipohypertrophy, data supports education and insulin injection technique practice as simple and effective means to reduce insulin action variability and increase glycemic control.24
Lipoatrophy. Lipoatrophy is described as a local loss of subcutaneous adipose tissue often in the face, buttocks, legs and arm regions and can be rooted in genetic, immune, or drug-associated etiologies.25 Insulin-induced lipoatrophy is suspected to be the result of tumor necrosis factor-α hyperproduction in reaction to insulin crystal presence at the injection site.26,27 Overall, lipoatrophy development has decreased since the use of recombinant human insulin and analog insulin therapy.28 The decrease is hypothesized to be due to increased subcutaneous tissue absorption rate of human insulin and its analog, decreasing overall adipocyte exposure to localized high insulin concentration.27 Treatments for same-site insulin-derived lipoatrophy include changing injection sites and preparation of insulin.26 When injection into the lipoatrophic site was avoided, glycemic control and lipoatrophy appearance improved.26
Amyloidosis. Amyloidosis indicates the presence of an extracellular bundle of insoluble polymeric protein fibrils in tissues and organs.29 Insulin-induced amyloidosis presents as a hard mass or ball near the injection site.29 Insulin is one of many hormones that can form amyloid fibrils, and there have been several dozen cases reported of amyloid formation at the site of insulin injection.29-31 Although insulin-derived amyloidosis is rare, it may be misdiagnosed as lipohypertrophy due to a lack of histopathologic testing or general awareness of the complication.29
In a case series of 7 patients with amyloidosis, all patients had a mean HbA1c of 9.3% (range, 8.5-10.2%) and averaged 1 IU/kg bodyweight before intervention.30 After the discovery of the mass, participants were instructed to avoid injection into the amyloidoma, and average insulin requirements decreased to 0.48 IU/kg body weight (P = .40).30 Patients with amyloidosis who rotated their injection sites experienced better glycemic control and decreased insulin requirements.30
Pathophysiology of Localized Insulin Resistance
Insulin regulates glucose homeostasis in skeletal muscle and adipose tissue, increases hepatic and adipocyte lipid synthesis, and decreases adipocyte fatty acid release.32 Generalized insulin resistance occurs when target tissues have decreased glucose uptake in response to circulating insulin.32 Insulin resistance increases the amount of free insulin in surrounding tissues. At high concentrations, insulin fosters tissue growth by binding to IGF-1 receptors, stimulating hypertrophy and reproduction of keratinocytes and fibroblasts.33 This pathophysiology helps explain the origin of localized acanthosis nigricans at same-site insulin injections.
Conclusions
Cutaneous complications are a local adverse effect of long-term failure to rotate insulin injection sites. Our case serves as a call to action for HCPs to improve education regarding insulin injection-site rotation, conduct routine injection-site inspection, and actively document cases as they occur to increase public awareness of these important complications.
If a patient with DM presents with unexplained poor glycemic control, consider questioning the patient about injection-site location and how often they are rotating the insulin injection site. Inspect the site for cutaneous complications. Of note, if a patient has a cutaneous complication due to insulin injection, adjust or decrease the insulin dosage when rotating sites to mitigate the risk of hypoglycemic episodes.
Improvement of glycemic control, cosmetic appearance of injection site, and insulin use all begin with skin inspection, injection technique education, and periodic review by a HCP.
1. Foster NC, Beck RW, Miller KM, et al. State of type 1 diabetes management and outcomes from the T1D exchange in 2016-2018. Diabetes Technol Ther. 2019;21(2):66-72. doi:10.1089/dia.2018.0384
2. Frid AH, Kreugel G, Grassi G, et al. New insulin delivery recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. doi:10.1016/j.mayocp.2016.06.010
3. Blanco M, Hernández MT, Strauss KW, Amaya M. Prevalence and risk factors of lipohypertrophy in insulin-injecting patients with diabetes. Diabetes Metab. 2013;39(5):445-453. doi:10.1016/j.diabet.2013.05.006
4. Johansson UB, Amsberg S, Hannerz L, et al. Impaired absorption of insulin aspart from lipohypertrophic injection sites. Diabetes Care. 2005;28(8):2025-2027. doi:10.2337/diacare.28.8.2025
5. Erickson L, Lipschutz DE, Wrigley W, Kearse WO. A peculiar cutaneous reaction to repeated injections of insulin. JAMA. 1969;209(6):934-935. doi:10.1001/jama.1969.03160190056019
6. Fleming MG, Simon SI. Cutaneous insulin reaction resembling acanthosis nigricans. Arch Dermatol. 1986;122(9):1054-1056. doi:10.1001/archderm.1986.01660210104028 7. Gannon D, Ross MW, Mahajan T. Acanthosis nigricans-like plaque and lipohypertrophy in type 1 diabetes. Pract Diabetes International. 2005;22(6).
8. Mailler-Savage EA, Adams BB. Exogenous insulin-derived acanthosis nigricans. Arch Dermatol. 2008;144(1):126-127. doi:10.1001/archdermatol.2007.27
9. Pachón Burgos A, Chan Aguilar MP. Visual vignette. Hyperpigmented hyperkeratotic cutaneous insulin reaction that resembles acanthosis nigricans with lipohypertrophy. Endocr Pract. 2008;14(4):514. doi:10.4158/EP.14.4.514
10. Buzási K, Sápi Z, Jermendy G. Acanthosis nigricans as a local cutaneous side effect of repeated human insulin injections. Diabetes Res Clin Pract. 2011;94(2):e34-e36. doi:10.1016/j.diabres.2011.07.023
11. Kudo-Watanuki S, Kurihara E, Yamamoto K, Mukai K, Chen KR. Coexistence of insulin-derived amyloidosis and an overlying acanthosis nigricans-like lesion at the site of insulin injection. Clin Exp Dermatol. 2012;38(1):25-29. doi:10.1111/j.1365-2230.2012.04373.x
12. Brodell JD Jr, Cannella JD, Helms SE. Case report: acanthosis nigricans resulting from repetitive same-site insulin injections. J Drugs Dermatol. 2012;11(12):e85-e87.
13. Kanwar A, Sawatkar G, Dogra S, Bhadada S. Acanthosis nigricans—an uncommon cutaneous adverse effect of a common medication: report of two cases. Indian J Dermatol Venereol Leprol. 2013;79(4):553. doi:10.4103/0378-6323.113112
14. Dhingra M, Garg G, Gupta M, Khurana U, Thami GP. Exogenous insulin-derived acanthosis nigricans: could it be a cause of increased insulin requirement? Dermatol Online J. 2013;19(1):9. Published 2013 Jan 15.
15. Nandeesh BN, Rajalakshmi T, Shubha B. Cutaneous amyloidosis and insulin with coexistence of acanthosis nigricans. Indian J Pathol Microbiol. 2014;57(1):127-129. doi:10.4103/0377-4929.130920
16. Yahagi E, Mabuchi T, Nuruki H, et al. Case of exogenous insulin-derived acanthosis nigricans caused by insulin injections. Tokai J Exp Clin Med. 2014;39(1):5-9.
17. Chapman SE, Bandino JP. A verrucous plaque on the abdomen: challenge. Am J Dermatopathol. 2017;39(12):e163. doi:10.1097/DAD.0000000000000659
18. Huang Y, Hessami-Booshehri M. Acanthosis nigricans at sites of insulin injection in a man with diabetes. CMAJ. 2018;190(47):E1390. doi:10.1503/cmaj.180705
19. Pal R, Bhattacharjee R, Chatterjee D, Bhadada SK, Bhansali A, Dutta P. Exogenous insulin-induced localized acanthosis nigricans: a rare injection site complication. Can J Diabetes. 2020;44(3):219-221. doi:10.1016/j.jcjd.2019.08.010
20. Bomar L, Lewallen R, Jorizzo J. Localized acanthosis nigricans at the site of repetitive insulin injections. Cutis. 2020;105(2);E20-E22.
21. Karadağ AS, You Y, Danarti R, Al-Khuzaei S, Chen W. Acanthosis nigricans and the metabolic syndrome. Clin Dermatol. 2018;36(1):48-53. doi:10.1016/j.clindermatol.2017.09.008
22. Kalra S, Kumar A, Gupta Y. Prevention of lipohypertrophy. J Pak Med Assoc. 2016;66(7):910-911.
23. Singha A, Bhattarcharjee R, Ghosh S, Chakrabarti SK, Baidya A, Chowdhury S. Concurrence of lipoatrophy and lipohypertrophy in children with type 1 diabetes using recombinant human insulin: two case reports. Clin Diabetes. 2016;34(1):51-53. doi:10.2337/diaclin.34.1.51
24. Famulla S, Hövelmann U, Fischer A, et al. Insulin injection into lipohypertrophic tissue: blunted and more variable insulin absorption and action and impaired postprandial glucose control. Diabetes Care. 2016;39(9):1486-1492. doi:10.2337/dc16-0610.
25. Reitman ML, Arioglu E, Gavrilova O, Taylor SI. Lipoatrophy revisited. Trends Endocrinol Metab. 2000;11(10):410-416. doi:10.1016/s1043-2760(00)00309-x
26. Kondo A, Nakamura A, Takeuchi J, Miyoshi H, Atsumi T. Insulin-Induced Distant Site Lipoatrophy. Diabetes Care. 2017;40(6):e67-e68. doi:10.2337/dc16-2385
27. Jermendy G, Nádas J, Sápi Z. “Lipoblastoma-like” lipoatrophy induced by human insulin: morphological evidence for local dedifferentiation of adipocytes?. Diabetologia. 2000;43(7):955-956. doi:10.1007/s001250051476
28. Mokta JK, Mokta KK, Panda P. Insulin lipodystrophy and lipohypertrophy. Indian J Endocrinol Metab. 2013;17(4):773-774. doi:10.4103/2230-8210.113788
29. Gupta Y, Singla G, Singla R. Insulin-derived amyloidosis. Indian J Endocrinol Metab. 2015;19(1):174-177. doi:10.4103/2230-8210.146879
30. Nagase T, Iwaya K, Iwaki Y, et al. Insulin-derived amyloidosis and poor glycemic control: a case series. Am J Med. 2014;127(5):450-454. doi:10.1016/j.amjmed.2013.10.029
31. Swift B. Examination of insulin injection sites: an unexpected finding of localized amyloidosis. Diabet Med. 2002;19(10):881-882. doi:10.1046/j.1464-5491.2002.07581.x
32. Sesti G. Pathophysiology of insulin resistance. Best Pract Res Clin Endocrinol Metab. 2006;20(4):665-679. doi:10.1016/j.beem.2006.09.007
33. Phiske MM. An approach to acanthosis nigricans. Indian Dermatol Online J. 2014;5(3):239-249. doi:10.4103/2229-5178.137765
Insulin injection therapy is one of the most widely used health care interventions to manage both type 1 and type 2 diabetes mellitus (T1DM/T2DM). Globally, more than 150 to 200 million people inject insulin into their upper posterior arms, buttocks, anterior and lateral thighs, or abdomen.1,2 In an ideal world, every patient would be using the correct site and rotating their insulin injection sites in accordance with health care professional (HCP) recommendations—systematic injections in one general body location, at least 1 cm away from the previous injection.2 Unfortunately, same-site insulin injection (repeatedly in the same region within 1 cm of previous injections) is a common mistake made by patients with DM—in one study, 63% of participants either did not rotate sites correctly or failed to do so at all.
Insulin-resistant cutaneous complications may occur as a result of same-site insulin injections. The most common is lipohypertrophy, reported in some studies in nearly 50% of patients with DM on insulin therapy.4 Other common cutaneous complications include lipoatrophy and amyloidosis. Injection-site acanthosis nigricans, although uncommon, has been reported in 18 cases in the literature.
Most articles suggest that same-site insulin injections decrease local insulin sensitivity and result in tissue hypertrophy because of the anabolic properties of insulin and increase in insulin binding to insulin-like growth factor-1 (IGF-1) receptor.5-20 The hyperkeratotic growth and varying insulin absorption rates associated with these cutaneous complications increase chances of either hyper- or hypoglycemic episodes in patients.10,11,13 It is the responsibility of the DM care professional to provide proper insulin-injection technique education and perform routine inspection of injection sites to reduce cutaneous complications of insulin therapy. The purpose of this article is to (1) describe a case of acanthosis nigricans resulting from insulin injection at the same site; (2) review case reports
Case Presentation
A 75-year-old patient with an 8-year history of T2DM, as well as stable coronary artery disease, atrial fibrillation, hypertension, hyperlipidemia, chronic obstructive pulmonary disease, and stage 3 chronic kidney disease, presented with 2 discrete abdominal hyperpigmented plaques. At the time of the initial clinic visit, the patient was taking metformin 1000 mg twice daily and insulin glargine 40 units once daily. When insulin was initiated 7 years prior, the patient received
The patient reported 5 years of progressive, asymptomatic hyperpigmentation of the skin surrounding his insulin glargine injection sites and injecting in these same sites daily without rotation. He reported no additional skin changes or symptoms. He had noticed no skin changes while using NPH insulin during his first year of insulin therapy. On examination, the abdominal wall skin demonstrated 2 well-demarcated, nearly black, soft, velvety plaques, measuring 9 × 8 cm on the left side and 4 × 3.5 cm on the right, suggesting acanthosis nigricans (Figure 1A). The remainder of the skin examination, including the flexures, was normal. Of note, the patient received biweekly intramuscular testosterone injections in the gluteal region for secondary hypogonadism with no adverse dermatologic effects. A skin punch biopsy was performed and revealed epidermal papillomatosis and hyperkeratosis, confirming the clinical diagnosis of acanthosis nigricans (Figure 2).
After a review of insulin-injection technique at his clinic visit, the patient started rotating insulin injection sites over his entire abdomen, and the acanthosis nigricans partially improved. A few months later, the patient stopped rotating the insulin injection site, and the acanthosis nigricans worsened again. Because of worsening glycemic control, the patient was then started on insulin aspart. He did not develop any skin changes at the insulin aspart injection site, although he was not rotating its site of injection.
Subsequently, with reeducation and proper injection-site rotation, the patient had resolution of his acanthosis nigricans (Figure 1b).
Discussion
A review of the literature revealed 18 reported cases of acanthosis nigricans at sites of repeated insulin injection (Table).5-20 Acanthosis nigricans at the site of insulin injection afflicts patients of any age, with cases observed in patients aged 14 to 75 years. Sixteen (84%) of 19 cases were male. Fourteen cases (73%) had T2DM; the rest of the patients had T1DM. The duration of insulin injection therapy prior to onset ranged from immediate to 13 years (median 4 years). Fourteen cases (73%) were reported on the abdomen; however, other sites, such as thighs and upper arm, also were reported. Lesions size varied from 12 to 360 cm2. Two cases had associated amyloidosis. The average HbA1c reported at presentation was 10%. Following insulin injection-site rotation, most of the cases reported improvement of both glycemic control and acanthosis nigricans appearance.
In the case described by Kudo and colleagues, a 59-year-old male patient with T2DM had been injecting insulin into the same spot on his abdomen for 10 years. He developed acanthosis nigricans and an amyloidoma so large and firm that it bent the needle when he injected insulin.11
Most of the cases we found in the literature were after 2005 and associated with the use of human or analog insulin. These cases may be related to a bias, as cases may be easier to find in digital archives in the later years, when human or analog insulins have been in common use. Also noteworthy, in cases that reported dosage, most were not very high, and the highest daily dose was 240 IU/d. Ten reports of injection-site acanthosis nigricans were in dermatology journals; only 5 reports were in endocrinology journals and 3 in general medical journals, indicating possible less awareness of this phenomenon in other HCPs who care for patients with DM.
Complications of Same-Site Injections
Acanthosis nigricans. Commonly found in the armpits, neck folds, and groin, acanthosis nigricans is known as one of the calling cards for insulin resistance, obesity, and hyperinsulinemia.21 Acanthosis nigricans can be seen in people with or without DM and is not limited to those on insulin therapy. However, same-site insulin injections for 4 to 6 years also may result in injection-site acanthosis nigricans–like lesions because of factors such as insulin exposure at the local tissue level.16
Acanthosis nigricans development is characterized by hyperpigmented, hyperkeratotic, velvety, and sometimes verrucous plaques.6 Acanthosis nigricans surrounding repeated injection sites is hypothesized to develop as a result of localized hyperinsulinemia secondary to insulin resistance, which increases the stimulation of IGF, thereby causing epidermal hypertrophy.5-20 If insulin injection therapy continues to be administered through the acanthosis nigricans lesion, it results in decreased insulin absorption, leading to poor glycemic control.13
Acanthosis nigricans associated with insulin injection is reversible. After rotation of injection sites, lesions either decrease in size or severity of appearance.5-8,11 Also, by avoiding injection into the hyperkeratotic plaques and using normal subcutaneous tissue for injection, patients’ response to insulin improves, as measured by HbA1c and by decreased daily insulin requirement.6-8,10,12,18-20
Lipohypertrophy. This is characterized by an increase in localized adipose tissue and is the most common cutaneous complication of insulin therapy.2 Lipohypertrophy presents as a firm, rubbery mass in the location of same-site insulin injections.22 Development of lipohypertrophy is suspected to be the result of either (1) anabolic effect of insulin on local adipocytes, promoting fat and protein synthesis; (2) an autoimmune response by immunoglobulin (Ig) G or IgE antibodies to insulin, immune response to insulin of different species, or to insulin injection techniques; or (3) repeated trauma to the injection site from repeated needle usage.4,23
In a study assessing the prevalence of lipohypertrophy and its relation to insulin technique, 49.1% of participants with
Primary prevention measures include injection site inspection and patient education about rotation and abstaining from needle reuse.22 If a patient already has signs of lipohypertrophy, data supports education and insulin injection technique practice as simple and effective means to reduce insulin action variability and increase glycemic control.24
Lipoatrophy. Lipoatrophy is described as a local loss of subcutaneous adipose tissue often in the face, buttocks, legs and arm regions and can be rooted in genetic, immune, or drug-associated etiologies.25 Insulin-induced lipoatrophy is suspected to be the result of tumor necrosis factor-α hyperproduction in reaction to insulin crystal presence at the injection site.26,27 Overall, lipoatrophy development has decreased since the use of recombinant human insulin and analog insulin therapy.28 The decrease is hypothesized to be due to increased subcutaneous tissue absorption rate of human insulin and its analog, decreasing overall adipocyte exposure to localized high insulin concentration.27 Treatments for same-site insulin-derived lipoatrophy include changing injection sites and preparation of insulin.26 When injection into the lipoatrophic site was avoided, glycemic control and lipoatrophy appearance improved.26
Amyloidosis. Amyloidosis indicates the presence of an extracellular bundle of insoluble polymeric protein fibrils in tissues and organs.29 Insulin-induced amyloidosis presents as a hard mass or ball near the injection site.29 Insulin is one of many hormones that can form amyloid fibrils, and there have been several dozen cases reported of amyloid formation at the site of insulin injection.29-31 Although insulin-derived amyloidosis is rare, it may be misdiagnosed as lipohypertrophy due to a lack of histopathologic testing or general awareness of the complication.29
In a case series of 7 patients with amyloidosis, all patients had a mean HbA1c of 9.3% (range, 8.5-10.2%) and averaged 1 IU/kg bodyweight before intervention.30 After the discovery of the mass, participants were instructed to avoid injection into the amyloidoma, and average insulin requirements decreased to 0.48 IU/kg body weight (P = .40).30 Patients with amyloidosis who rotated their injection sites experienced better glycemic control and decreased insulin requirements.30
Pathophysiology of Localized Insulin Resistance
Insulin regulates glucose homeostasis in skeletal muscle and adipose tissue, increases hepatic and adipocyte lipid synthesis, and decreases adipocyte fatty acid release.32 Generalized insulin resistance occurs when target tissues have decreased glucose uptake in response to circulating insulin.32 Insulin resistance increases the amount of free insulin in surrounding tissues. At high concentrations, insulin fosters tissue growth by binding to IGF-1 receptors, stimulating hypertrophy and reproduction of keratinocytes and fibroblasts.33 This pathophysiology helps explain the origin of localized acanthosis nigricans at same-site insulin injections.
Conclusions
Cutaneous complications are a local adverse effect of long-term failure to rotate insulin injection sites. Our case serves as a call to action for HCPs to improve education regarding insulin injection-site rotation, conduct routine injection-site inspection, and actively document cases as they occur to increase public awareness of these important complications.
If a patient with DM presents with unexplained poor glycemic control, consider questioning the patient about injection-site location and how often they are rotating the insulin injection site. Inspect the site for cutaneous complications. Of note, if a patient has a cutaneous complication due to insulin injection, adjust or decrease the insulin dosage when rotating sites to mitigate the risk of hypoglycemic episodes.
Improvement of glycemic control, cosmetic appearance of injection site, and insulin use all begin with skin inspection, injection technique education, and periodic review by a HCP.
Insulin injection therapy is one of the most widely used health care interventions to manage both type 1 and type 2 diabetes mellitus (T1DM/T2DM). Globally, more than 150 to 200 million people inject insulin into their upper posterior arms, buttocks, anterior and lateral thighs, or abdomen.1,2 In an ideal world, every patient would be using the correct site and rotating their insulin injection sites in accordance with health care professional (HCP) recommendations—systematic injections in one general body location, at least 1 cm away from the previous injection.2 Unfortunately, same-site insulin injection (repeatedly in the same region within 1 cm of previous injections) is a common mistake made by patients with DM—in one study, 63% of participants either did not rotate sites correctly or failed to do so at all.
Insulin-resistant cutaneous complications may occur as a result of same-site insulin injections. The most common is lipohypertrophy, reported in some studies in nearly 50% of patients with DM on insulin therapy.4 Other common cutaneous complications include lipoatrophy and amyloidosis. Injection-site acanthosis nigricans, although uncommon, has been reported in 18 cases in the literature.
Most articles suggest that same-site insulin injections decrease local insulin sensitivity and result in tissue hypertrophy because of the anabolic properties of insulin and increase in insulin binding to insulin-like growth factor-1 (IGF-1) receptor.5-20 The hyperkeratotic growth and varying insulin absorption rates associated with these cutaneous complications increase chances of either hyper- or hypoglycemic episodes in patients.10,11,13 It is the responsibility of the DM care professional to provide proper insulin-injection technique education and perform routine inspection of injection sites to reduce cutaneous complications of insulin therapy. The purpose of this article is to (1) describe a case of acanthosis nigricans resulting from insulin injection at the same site; (2) review case reports
Case Presentation
A 75-year-old patient with an 8-year history of T2DM, as well as stable coronary artery disease, atrial fibrillation, hypertension, hyperlipidemia, chronic obstructive pulmonary disease, and stage 3 chronic kidney disease, presented with 2 discrete abdominal hyperpigmented plaques. At the time of the initial clinic visit, the patient was taking metformin 1000 mg twice daily and insulin glargine 40 units once daily. When insulin was initiated 7 years prior, the patient received
The patient reported 5 years of progressive, asymptomatic hyperpigmentation of the skin surrounding his insulin glargine injection sites and injecting in these same sites daily without rotation. He reported no additional skin changes or symptoms. He had noticed no skin changes while using NPH insulin during his first year of insulin therapy. On examination, the abdominal wall skin demonstrated 2 well-demarcated, nearly black, soft, velvety plaques, measuring 9 × 8 cm on the left side and 4 × 3.5 cm on the right, suggesting acanthosis nigricans (Figure 1A). The remainder of the skin examination, including the flexures, was normal. Of note, the patient received biweekly intramuscular testosterone injections in the gluteal region for secondary hypogonadism with no adverse dermatologic effects. A skin punch biopsy was performed and revealed epidermal papillomatosis and hyperkeratosis, confirming the clinical diagnosis of acanthosis nigricans (Figure 2).
After a review of insulin-injection technique at his clinic visit, the patient started rotating insulin injection sites over his entire abdomen, and the acanthosis nigricans partially improved. A few months later, the patient stopped rotating the insulin injection site, and the acanthosis nigricans worsened again. Because of worsening glycemic control, the patient was then started on insulin aspart. He did not develop any skin changes at the insulin aspart injection site, although he was not rotating its site of injection.
Subsequently, with reeducation and proper injection-site rotation, the patient had resolution of his acanthosis nigricans (Figure 1b).
Discussion
A review of the literature revealed 18 reported cases of acanthosis nigricans at sites of repeated insulin injection (Table).5-20 Acanthosis nigricans at the site of insulin injection afflicts patients of any age, with cases observed in patients aged 14 to 75 years. Sixteen (84%) of 19 cases were male. Fourteen cases (73%) had T2DM; the rest of the patients had T1DM. The duration of insulin injection therapy prior to onset ranged from immediate to 13 years (median 4 years). Fourteen cases (73%) were reported on the abdomen; however, other sites, such as thighs and upper arm, also were reported. Lesions size varied from 12 to 360 cm2. Two cases had associated amyloidosis. The average HbA1c reported at presentation was 10%. Following insulin injection-site rotation, most of the cases reported improvement of both glycemic control and acanthosis nigricans appearance.
In the case described by Kudo and colleagues, a 59-year-old male patient with T2DM had been injecting insulin into the same spot on his abdomen for 10 years. He developed acanthosis nigricans and an amyloidoma so large and firm that it bent the needle when he injected insulin.11
Most of the cases we found in the literature were after 2005 and associated with the use of human or analog insulin. These cases may be related to a bias, as cases may be easier to find in digital archives in the later years, when human or analog insulins have been in common use. Also noteworthy, in cases that reported dosage, most were not very high, and the highest daily dose was 240 IU/d. Ten reports of injection-site acanthosis nigricans were in dermatology journals; only 5 reports were in endocrinology journals and 3 in general medical journals, indicating possible less awareness of this phenomenon in other HCPs who care for patients with DM.
Complications of Same-Site Injections
Acanthosis nigricans. Commonly found in the armpits, neck folds, and groin, acanthosis nigricans is known as one of the calling cards for insulin resistance, obesity, and hyperinsulinemia.21 Acanthosis nigricans can be seen in people with or without DM and is not limited to those on insulin therapy. However, same-site insulin injections for 4 to 6 years also may result in injection-site acanthosis nigricans–like lesions because of factors such as insulin exposure at the local tissue level.16
Acanthosis nigricans development is characterized by hyperpigmented, hyperkeratotic, velvety, and sometimes verrucous plaques.6 Acanthosis nigricans surrounding repeated injection sites is hypothesized to develop as a result of localized hyperinsulinemia secondary to insulin resistance, which increases the stimulation of IGF, thereby causing epidermal hypertrophy.5-20 If insulin injection therapy continues to be administered through the acanthosis nigricans lesion, it results in decreased insulin absorption, leading to poor glycemic control.13
Acanthosis nigricans associated with insulin injection is reversible. After rotation of injection sites, lesions either decrease in size or severity of appearance.5-8,11 Also, by avoiding injection into the hyperkeratotic plaques and using normal subcutaneous tissue for injection, patients’ response to insulin improves, as measured by HbA1c and by decreased daily insulin requirement.6-8,10,12,18-20
Lipohypertrophy. This is characterized by an increase in localized adipose tissue and is the most common cutaneous complication of insulin therapy.2 Lipohypertrophy presents as a firm, rubbery mass in the location of same-site insulin injections.22 Development of lipohypertrophy is suspected to be the result of either (1) anabolic effect of insulin on local adipocytes, promoting fat and protein synthesis; (2) an autoimmune response by immunoglobulin (Ig) G or IgE antibodies to insulin, immune response to insulin of different species, or to insulin injection techniques; or (3) repeated trauma to the injection site from repeated needle usage.4,23
In a study assessing the prevalence of lipohypertrophy and its relation to insulin technique, 49.1% of participants with
Primary prevention measures include injection site inspection and patient education about rotation and abstaining from needle reuse.22 If a patient already has signs of lipohypertrophy, data supports education and insulin injection technique practice as simple and effective means to reduce insulin action variability and increase glycemic control.24
Lipoatrophy. Lipoatrophy is described as a local loss of subcutaneous adipose tissue often in the face, buttocks, legs and arm regions and can be rooted in genetic, immune, or drug-associated etiologies.25 Insulin-induced lipoatrophy is suspected to be the result of tumor necrosis factor-α hyperproduction in reaction to insulin crystal presence at the injection site.26,27 Overall, lipoatrophy development has decreased since the use of recombinant human insulin and analog insulin therapy.28 The decrease is hypothesized to be due to increased subcutaneous tissue absorption rate of human insulin and its analog, decreasing overall adipocyte exposure to localized high insulin concentration.27 Treatments for same-site insulin-derived lipoatrophy include changing injection sites and preparation of insulin.26 When injection into the lipoatrophic site was avoided, glycemic control and lipoatrophy appearance improved.26
Amyloidosis. Amyloidosis indicates the presence of an extracellular bundle of insoluble polymeric protein fibrils in tissues and organs.29 Insulin-induced amyloidosis presents as a hard mass or ball near the injection site.29 Insulin is one of many hormones that can form amyloid fibrils, and there have been several dozen cases reported of amyloid formation at the site of insulin injection.29-31 Although insulin-derived amyloidosis is rare, it may be misdiagnosed as lipohypertrophy due to a lack of histopathologic testing or general awareness of the complication.29
In a case series of 7 patients with amyloidosis, all patients had a mean HbA1c of 9.3% (range, 8.5-10.2%) and averaged 1 IU/kg bodyweight before intervention.30 After the discovery of the mass, participants were instructed to avoid injection into the amyloidoma, and average insulin requirements decreased to 0.48 IU/kg body weight (P = .40).30 Patients with amyloidosis who rotated their injection sites experienced better glycemic control and decreased insulin requirements.30
Pathophysiology of Localized Insulin Resistance
Insulin regulates glucose homeostasis in skeletal muscle and adipose tissue, increases hepatic and adipocyte lipid synthesis, and decreases adipocyte fatty acid release.32 Generalized insulin resistance occurs when target tissues have decreased glucose uptake in response to circulating insulin.32 Insulin resistance increases the amount of free insulin in surrounding tissues. At high concentrations, insulin fosters tissue growth by binding to IGF-1 receptors, stimulating hypertrophy and reproduction of keratinocytes and fibroblasts.33 This pathophysiology helps explain the origin of localized acanthosis nigricans at same-site insulin injections.
Conclusions
Cutaneous complications are a local adverse effect of long-term failure to rotate insulin injection sites. Our case serves as a call to action for HCPs to improve education regarding insulin injection-site rotation, conduct routine injection-site inspection, and actively document cases as they occur to increase public awareness of these important complications.
If a patient with DM presents with unexplained poor glycemic control, consider questioning the patient about injection-site location and how often they are rotating the insulin injection site. Inspect the site for cutaneous complications. Of note, if a patient has a cutaneous complication due to insulin injection, adjust or decrease the insulin dosage when rotating sites to mitigate the risk of hypoglycemic episodes.
Improvement of glycemic control, cosmetic appearance of injection site, and insulin use all begin with skin inspection, injection technique education, and periodic review by a HCP.
1. Foster NC, Beck RW, Miller KM, et al. State of type 1 diabetes management and outcomes from the T1D exchange in 2016-2018. Diabetes Technol Ther. 2019;21(2):66-72. doi:10.1089/dia.2018.0384
2. Frid AH, Kreugel G, Grassi G, et al. New insulin delivery recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. doi:10.1016/j.mayocp.2016.06.010
3. Blanco M, Hernández MT, Strauss KW, Amaya M. Prevalence and risk factors of lipohypertrophy in insulin-injecting patients with diabetes. Diabetes Metab. 2013;39(5):445-453. doi:10.1016/j.diabet.2013.05.006
4. Johansson UB, Amsberg S, Hannerz L, et al. Impaired absorption of insulin aspart from lipohypertrophic injection sites. Diabetes Care. 2005;28(8):2025-2027. doi:10.2337/diacare.28.8.2025
5. Erickson L, Lipschutz DE, Wrigley W, Kearse WO. A peculiar cutaneous reaction to repeated injections of insulin. JAMA. 1969;209(6):934-935. doi:10.1001/jama.1969.03160190056019
6. Fleming MG, Simon SI. Cutaneous insulin reaction resembling acanthosis nigricans. Arch Dermatol. 1986;122(9):1054-1056. doi:10.1001/archderm.1986.01660210104028 7. Gannon D, Ross MW, Mahajan T. Acanthosis nigricans-like plaque and lipohypertrophy in type 1 diabetes. Pract Diabetes International. 2005;22(6).
8. Mailler-Savage EA, Adams BB. Exogenous insulin-derived acanthosis nigricans. Arch Dermatol. 2008;144(1):126-127. doi:10.1001/archdermatol.2007.27
9. Pachón Burgos A, Chan Aguilar MP. Visual vignette. Hyperpigmented hyperkeratotic cutaneous insulin reaction that resembles acanthosis nigricans with lipohypertrophy. Endocr Pract. 2008;14(4):514. doi:10.4158/EP.14.4.514
10. Buzási K, Sápi Z, Jermendy G. Acanthosis nigricans as a local cutaneous side effect of repeated human insulin injections. Diabetes Res Clin Pract. 2011;94(2):e34-e36. doi:10.1016/j.diabres.2011.07.023
11. Kudo-Watanuki S, Kurihara E, Yamamoto K, Mukai K, Chen KR. Coexistence of insulin-derived amyloidosis and an overlying acanthosis nigricans-like lesion at the site of insulin injection. Clin Exp Dermatol. 2012;38(1):25-29. doi:10.1111/j.1365-2230.2012.04373.x
12. Brodell JD Jr, Cannella JD, Helms SE. Case report: acanthosis nigricans resulting from repetitive same-site insulin injections. J Drugs Dermatol. 2012;11(12):e85-e87.
13. Kanwar A, Sawatkar G, Dogra S, Bhadada S. Acanthosis nigricans—an uncommon cutaneous adverse effect of a common medication: report of two cases. Indian J Dermatol Venereol Leprol. 2013;79(4):553. doi:10.4103/0378-6323.113112
14. Dhingra M, Garg G, Gupta M, Khurana U, Thami GP. Exogenous insulin-derived acanthosis nigricans: could it be a cause of increased insulin requirement? Dermatol Online J. 2013;19(1):9. Published 2013 Jan 15.
15. Nandeesh BN, Rajalakshmi T, Shubha B. Cutaneous amyloidosis and insulin with coexistence of acanthosis nigricans. Indian J Pathol Microbiol. 2014;57(1):127-129. doi:10.4103/0377-4929.130920
16. Yahagi E, Mabuchi T, Nuruki H, et al. Case of exogenous insulin-derived acanthosis nigricans caused by insulin injections. Tokai J Exp Clin Med. 2014;39(1):5-9.
17. Chapman SE, Bandino JP. A verrucous plaque on the abdomen: challenge. Am J Dermatopathol. 2017;39(12):e163. doi:10.1097/DAD.0000000000000659
18. Huang Y, Hessami-Booshehri M. Acanthosis nigricans at sites of insulin injection in a man with diabetes. CMAJ. 2018;190(47):E1390. doi:10.1503/cmaj.180705
19. Pal R, Bhattacharjee R, Chatterjee D, Bhadada SK, Bhansali A, Dutta P. Exogenous insulin-induced localized acanthosis nigricans: a rare injection site complication. Can J Diabetes. 2020;44(3):219-221. doi:10.1016/j.jcjd.2019.08.010
20. Bomar L, Lewallen R, Jorizzo J. Localized acanthosis nigricans at the site of repetitive insulin injections. Cutis. 2020;105(2);E20-E22.
21. Karadağ AS, You Y, Danarti R, Al-Khuzaei S, Chen W. Acanthosis nigricans and the metabolic syndrome. Clin Dermatol. 2018;36(1):48-53. doi:10.1016/j.clindermatol.2017.09.008
22. Kalra S, Kumar A, Gupta Y. Prevention of lipohypertrophy. J Pak Med Assoc. 2016;66(7):910-911.
23. Singha A, Bhattarcharjee R, Ghosh S, Chakrabarti SK, Baidya A, Chowdhury S. Concurrence of lipoatrophy and lipohypertrophy in children with type 1 diabetes using recombinant human insulin: two case reports. Clin Diabetes. 2016;34(1):51-53. doi:10.2337/diaclin.34.1.51
24. Famulla S, Hövelmann U, Fischer A, et al. Insulin injection into lipohypertrophic tissue: blunted and more variable insulin absorption and action and impaired postprandial glucose control. Diabetes Care. 2016;39(9):1486-1492. doi:10.2337/dc16-0610.
25. Reitman ML, Arioglu E, Gavrilova O, Taylor SI. Lipoatrophy revisited. Trends Endocrinol Metab. 2000;11(10):410-416. doi:10.1016/s1043-2760(00)00309-x
26. Kondo A, Nakamura A, Takeuchi J, Miyoshi H, Atsumi T. Insulin-Induced Distant Site Lipoatrophy. Diabetes Care. 2017;40(6):e67-e68. doi:10.2337/dc16-2385
27. Jermendy G, Nádas J, Sápi Z. “Lipoblastoma-like” lipoatrophy induced by human insulin: morphological evidence for local dedifferentiation of adipocytes?. Diabetologia. 2000;43(7):955-956. doi:10.1007/s001250051476
28. Mokta JK, Mokta KK, Panda P. Insulin lipodystrophy and lipohypertrophy. Indian J Endocrinol Metab. 2013;17(4):773-774. doi:10.4103/2230-8210.113788
29. Gupta Y, Singla G, Singla R. Insulin-derived amyloidosis. Indian J Endocrinol Metab. 2015;19(1):174-177. doi:10.4103/2230-8210.146879
30. Nagase T, Iwaya K, Iwaki Y, et al. Insulin-derived amyloidosis and poor glycemic control: a case series. Am J Med. 2014;127(5):450-454. doi:10.1016/j.amjmed.2013.10.029
31. Swift B. Examination of insulin injection sites: an unexpected finding of localized amyloidosis. Diabet Med. 2002;19(10):881-882. doi:10.1046/j.1464-5491.2002.07581.x
32. Sesti G. Pathophysiology of insulin resistance. Best Pract Res Clin Endocrinol Metab. 2006;20(4):665-679. doi:10.1016/j.beem.2006.09.007
33. Phiske MM. An approach to acanthosis nigricans. Indian Dermatol Online J. 2014;5(3):239-249. doi:10.4103/2229-5178.137765
1. Foster NC, Beck RW, Miller KM, et al. State of type 1 diabetes management and outcomes from the T1D exchange in 2016-2018. Diabetes Technol Ther. 2019;21(2):66-72. doi:10.1089/dia.2018.0384
2. Frid AH, Kreugel G, Grassi G, et al. New insulin delivery recommendations. Mayo Clin Proc. 2016;91(9):1231-1255. doi:10.1016/j.mayocp.2016.06.010
3. Blanco M, Hernández MT, Strauss KW, Amaya M. Prevalence and risk factors of lipohypertrophy in insulin-injecting patients with diabetes. Diabetes Metab. 2013;39(5):445-453. doi:10.1016/j.diabet.2013.05.006
4. Johansson UB, Amsberg S, Hannerz L, et al. Impaired absorption of insulin aspart from lipohypertrophic injection sites. Diabetes Care. 2005;28(8):2025-2027. doi:10.2337/diacare.28.8.2025
5. Erickson L, Lipschutz DE, Wrigley W, Kearse WO. A peculiar cutaneous reaction to repeated injections of insulin. JAMA. 1969;209(6):934-935. doi:10.1001/jama.1969.03160190056019
6. Fleming MG, Simon SI. Cutaneous insulin reaction resembling acanthosis nigricans. Arch Dermatol. 1986;122(9):1054-1056. doi:10.1001/archderm.1986.01660210104028 7. Gannon D, Ross MW, Mahajan T. Acanthosis nigricans-like plaque and lipohypertrophy in type 1 diabetes. Pract Diabetes International. 2005;22(6).
8. Mailler-Savage EA, Adams BB. Exogenous insulin-derived acanthosis nigricans. Arch Dermatol. 2008;144(1):126-127. doi:10.1001/archdermatol.2007.27
9. Pachón Burgos A, Chan Aguilar MP. Visual vignette. Hyperpigmented hyperkeratotic cutaneous insulin reaction that resembles acanthosis nigricans with lipohypertrophy. Endocr Pract. 2008;14(4):514. doi:10.4158/EP.14.4.514
10. Buzási K, Sápi Z, Jermendy G. Acanthosis nigricans as a local cutaneous side effect of repeated human insulin injections. Diabetes Res Clin Pract. 2011;94(2):e34-e36. doi:10.1016/j.diabres.2011.07.023
11. Kudo-Watanuki S, Kurihara E, Yamamoto K, Mukai K, Chen KR. Coexistence of insulin-derived amyloidosis and an overlying acanthosis nigricans-like lesion at the site of insulin injection. Clin Exp Dermatol. 2012;38(1):25-29. doi:10.1111/j.1365-2230.2012.04373.x
12. Brodell JD Jr, Cannella JD, Helms SE. Case report: acanthosis nigricans resulting from repetitive same-site insulin injections. J Drugs Dermatol. 2012;11(12):e85-e87.
13. Kanwar A, Sawatkar G, Dogra S, Bhadada S. Acanthosis nigricans—an uncommon cutaneous adverse effect of a common medication: report of two cases. Indian J Dermatol Venereol Leprol. 2013;79(4):553. doi:10.4103/0378-6323.113112
14. Dhingra M, Garg G, Gupta M, Khurana U, Thami GP. Exogenous insulin-derived acanthosis nigricans: could it be a cause of increased insulin requirement? Dermatol Online J. 2013;19(1):9. Published 2013 Jan 15.
15. Nandeesh BN, Rajalakshmi T, Shubha B. Cutaneous amyloidosis and insulin with coexistence of acanthosis nigricans. Indian J Pathol Microbiol. 2014;57(1):127-129. doi:10.4103/0377-4929.130920
16. Yahagi E, Mabuchi T, Nuruki H, et al. Case of exogenous insulin-derived acanthosis nigricans caused by insulin injections. Tokai J Exp Clin Med. 2014;39(1):5-9.
17. Chapman SE, Bandino JP. A verrucous plaque on the abdomen: challenge. Am J Dermatopathol. 2017;39(12):e163. doi:10.1097/DAD.0000000000000659
18. Huang Y, Hessami-Booshehri M. Acanthosis nigricans at sites of insulin injection in a man with diabetes. CMAJ. 2018;190(47):E1390. doi:10.1503/cmaj.180705
19. Pal R, Bhattacharjee R, Chatterjee D, Bhadada SK, Bhansali A, Dutta P. Exogenous insulin-induced localized acanthosis nigricans: a rare injection site complication. Can J Diabetes. 2020;44(3):219-221. doi:10.1016/j.jcjd.2019.08.010
20. Bomar L, Lewallen R, Jorizzo J. Localized acanthosis nigricans at the site of repetitive insulin injections. Cutis. 2020;105(2);E20-E22.
21. Karadağ AS, You Y, Danarti R, Al-Khuzaei S, Chen W. Acanthosis nigricans and the metabolic syndrome. Clin Dermatol. 2018;36(1):48-53. doi:10.1016/j.clindermatol.2017.09.008
22. Kalra S, Kumar A, Gupta Y. Prevention of lipohypertrophy. J Pak Med Assoc. 2016;66(7):910-911.
23. Singha A, Bhattarcharjee R, Ghosh S, Chakrabarti SK, Baidya A, Chowdhury S. Concurrence of lipoatrophy and lipohypertrophy in children with type 1 diabetes using recombinant human insulin: two case reports. Clin Diabetes. 2016;34(1):51-53. doi:10.2337/diaclin.34.1.51
24. Famulla S, Hövelmann U, Fischer A, et al. Insulin injection into lipohypertrophic tissue: blunted and more variable insulin absorption and action and impaired postprandial glucose control. Diabetes Care. 2016;39(9):1486-1492. doi:10.2337/dc16-0610.
25. Reitman ML, Arioglu E, Gavrilova O, Taylor SI. Lipoatrophy revisited. Trends Endocrinol Metab. 2000;11(10):410-416. doi:10.1016/s1043-2760(00)00309-x
26. Kondo A, Nakamura A, Takeuchi J, Miyoshi H, Atsumi T. Insulin-Induced Distant Site Lipoatrophy. Diabetes Care. 2017;40(6):e67-e68. doi:10.2337/dc16-2385
27. Jermendy G, Nádas J, Sápi Z. “Lipoblastoma-like” lipoatrophy induced by human insulin: morphological evidence for local dedifferentiation of adipocytes?. Diabetologia. 2000;43(7):955-956. doi:10.1007/s001250051476
28. Mokta JK, Mokta KK, Panda P. Insulin lipodystrophy and lipohypertrophy. Indian J Endocrinol Metab. 2013;17(4):773-774. doi:10.4103/2230-8210.113788
29. Gupta Y, Singla G, Singla R. Insulin-derived amyloidosis. Indian J Endocrinol Metab. 2015;19(1):174-177. doi:10.4103/2230-8210.146879
30. Nagase T, Iwaya K, Iwaki Y, et al. Insulin-derived amyloidosis and poor glycemic control: a case series. Am J Med. 2014;127(5):450-454. doi:10.1016/j.amjmed.2013.10.029
31. Swift B. Examination of insulin injection sites: an unexpected finding of localized amyloidosis. Diabet Med. 2002;19(10):881-882. doi:10.1046/j.1464-5491.2002.07581.x
32. Sesti G. Pathophysiology of insulin resistance. Best Pract Res Clin Endocrinol Metab. 2006;20(4):665-679. doi:10.1016/j.beem.2006.09.007
33. Phiske MM. An approach to acanthosis nigricans. Indian Dermatol Online J. 2014;5(3):239-249. doi:10.4103/2229-5178.137765
This month in the journal CHEST®
Dupilumab Reduces Oral Corticosteroid Use in Patients With Corticosteroid-Dependent Severe Asthma. By Lawrence D. Sher, MD, et al.
Carriage and Transmission of Macrolide Resistance Genes in Patients With Chronic Respiratory Conditions and Their Close Contacts. By Yiming Wang, MSc, et al.
An Evaluation of Factors That Influence Referral to Pulmonary Rehabilitation Programs Among People With COPD. By Sarah Hug, BSc, et al.
Prevalence and Outcomes of Previously Healthy Adults Among Patients Hospitalized With Community-Onset Sepsis. By Mohammad Alrawashdeh, PhD, MSN, et al.
Screening Strategies for Pulmonary Hypertension in Patients With Interstitial Lung Disease: A Multidisciplinary Delphi Study. By Franck F. Rahaghi, MD, et al.
Race- and Ethnicity-Based Spirometry Reference Equations: Are They Accurate for Genetically Admixed Children? By Jonathan Witonsky, MD, et al.
No VTE Recurrence After 1-Year Follow Up of Hospitalized Patients With COVID-19 and a VTE Event: A Prospective Study. By Maxime Delrue, MD, PhD, et al.
Patient Perspectives on Longitudinal Adherence to Lung Cancer Screening. By Anna Holman, BS, et al.
Dupilumab Reduces Oral Corticosteroid Use in Patients With Corticosteroid-Dependent Severe Asthma. By Lawrence D. Sher, MD, et al.
Carriage and Transmission of Macrolide Resistance Genes in Patients With Chronic Respiratory Conditions and Their Close Contacts. By Yiming Wang, MSc, et al.
An Evaluation of Factors That Influence Referral to Pulmonary Rehabilitation Programs Among People With COPD. By Sarah Hug, BSc, et al.
Prevalence and Outcomes of Previously Healthy Adults Among Patients Hospitalized With Community-Onset Sepsis. By Mohammad Alrawashdeh, PhD, MSN, et al.
Screening Strategies for Pulmonary Hypertension in Patients With Interstitial Lung Disease: A Multidisciplinary Delphi Study. By Franck F. Rahaghi, MD, et al.
Race- and Ethnicity-Based Spirometry Reference Equations: Are They Accurate for Genetically Admixed Children? By Jonathan Witonsky, MD, et al.
No VTE Recurrence After 1-Year Follow Up of Hospitalized Patients With COVID-19 and a VTE Event: A Prospective Study. By Maxime Delrue, MD, PhD, et al.
Patient Perspectives on Longitudinal Adherence to Lung Cancer Screening. By Anna Holman, BS, et al.
Dupilumab Reduces Oral Corticosteroid Use in Patients With Corticosteroid-Dependent Severe Asthma. By Lawrence D. Sher, MD, et al.
Carriage and Transmission of Macrolide Resistance Genes in Patients With Chronic Respiratory Conditions and Their Close Contacts. By Yiming Wang, MSc, et al.
An Evaluation of Factors That Influence Referral to Pulmonary Rehabilitation Programs Among People With COPD. By Sarah Hug, BSc, et al.
Prevalence and Outcomes of Previously Healthy Adults Among Patients Hospitalized With Community-Onset Sepsis. By Mohammad Alrawashdeh, PhD, MSN, et al.
Screening Strategies for Pulmonary Hypertension in Patients With Interstitial Lung Disease: A Multidisciplinary Delphi Study. By Franck F. Rahaghi, MD, et al.
Race- and Ethnicity-Based Spirometry Reference Equations: Are They Accurate for Genetically Admixed Children? By Jonathan Witonsky, MD, et al.
No VTE Recurrence After 1-Year Follow Up of Hospitalized Patients With COVID-19 and a VTE Event: A Prospective Study. By Maxime Delrue, MD, PhD, et al.
Patient Perspectives on Longitudinal Adherence to Lung Cancer Screening. By Anna Holman, BS, et al.
Starting CHEST 2022 off with a step kick
, with a bang—or, more accurately, with a step kick, swivel, and stomp—at the Wildhorse Saloon.
The Wildhorse is famous for hosting daily line dancing lessons on the largest dance floor in the downtown area and for having a menu full of Nashville favorites, including Nashville hot chicken and a hearty selection of entrees (as well as a decadent bananas foster) with a “Jack Daniels” single barrel whiskey glaze.
The opening reception offers attendees the opportunity to relax and reconnect with their peers from across the fields of pulmonary, critical care, and sleep medicine before the jam-packed schedule of more than 300 educational sessions starts the following day.
But the fun doesn’t stop there. Attendees interested in exploring the city after hours have a host of options, from world-class music venues to iconic distilleries and restaurants. The Music City Center, where CHEST 2022 will be held, is located in the SoBro neighborhood of Nashville, not far from the Arts District, Downtown, and Music Row.
According to Nashville local and CHEST member Meredith Pugh, MD, MSCI, “it goes without saying that we have the best music scene in the country, but it’s a great place for outdoor activities and food.”
For those who don’t get their fill at the Wildhorse, Dr. Pugh recommends attendees check out the Assembly Food Hall (.3 miles from the convention center) to try the city’s famous Nashville Hot Chicken and a variety of other local options. And, don’t miss the many excellent options for BBQ. Fellow Nashville transplant and CHEST member Todd Rice, MD, FCCP, suggests Martin’s Bar-B-Que Joint and Jack’s Bar-B-Que—both within walking distance of the Music City Center—as well as other local options.
To learn more about everything Nashville has to offer, and get more recommendations from Drs. Rice and Pugh, check out the latest CHEST 2022 blog on chestnet.org
, with a bang—or, more accurately, with a step kick, swivel, and stomp—at the Wildhorse Saloon.
The Wildhorse is famous for hosting daily line dancing lessons on the largest dance floor in the downtown area and for having a menu full of Nashville favorites, including Nashville hot chicken and a hearty selection of entrees (as well as a decadent bananas foster) with a “Jack Daniels” single barrel whiskey glaze.
The opening reception offers attendees the opportunity to relax and reconnect with their peers from across the fields of pulmonary, critical care, and sleep medicine before the jam-packed schedule of more than 300 educational sessions starts the following day.
But the fun doesn’t stop there. Attendees interested in exploring the city after hours have a host of options, from world-class music venues to iconic distilleries and restaurants. The Music City Center, where CHEST 2022 will be held, is located in the SoBro neighborhood of Nashville, not far from the Arts District, Downtown, and Music Row.
According to Nashville local and CHEST member Meredith Pugh, MD, MSCI, “it goes without saying that we have the best music scene in the country, but it’s a great place for outdoor activities and food.”
For those who don’t get their fill at the Wildhorse, Dr. Pugh recommends attendees check out the Assembly Food Hall (.3 miles from the convention center) to try the city’s famous Nashville Hot Chicken and a variety of other local options. And, don’t miss the many excellent options for BBQ. Fellow Nashville transplant and CHEST member Todd Rice, MD, FCCP, suggests Martin’s Bar-B-Que Joint and Jack’s Bar-B-Que—both within walking distance of the Music City Center—as well as other local options.
To learn more about everything Nashville has to offer, and get more recommendations from Drs. Rice and Pugh, check out the latest CHEST 2022 blog on chestnet.org
, with a bang—or, more accurately, with a step kick, swivel, and stomp—at the Wildhorse Saloon.
The Wildhorse is famous for hosting daily line dancing lessons on the largest dance floor in the downtown area and for having a menu full of Nashville favorites, including Nashville hot chicken and a hearty selection of entrees (as well as a decadent bananas foster) with a “Jack Daniels” single barrel whiskey glaze.
The opening reception offers attendees the opportunity to relax and reconnect with their peers from across the fields of pulmonary, critical care, and sleep medicine before the jam-packed schedule of more than 300 educational sessions starts the following day.
But the fun doesn’t stop there. Attendees interested in exploring the city after hours have a host of options, from world-class music venues to iconic distilleries and restaurants. The Music City Center, where CHEST 2022 will be held, is located in the SoBro neighborhood of Nashville, not far from the Arts District, Downtown, and Music Row.
According to Nashville local and CHEST member Meredith Pugh, MD, MSCI, “it goes without saying that we have the best music scene in the country, but it’s a great place for outdoor activities and food.”
For those who don’t get their fill at the Wildhorse, Dr. Pugh recommends attendees check out the Assembly Food Hall (.3 miles from the convention center) to try the city’s famous Nashville Hot Chicken and a variety of other local options. And, don’t miss the many excellent options for BBQ. Fellow Nashville transplant and CHEST member Todd Rice, MD, FCCP, suggests Martin’s Bar-B-Que Joint and Jack’s Bar-B-Que—both within walking distance of the Music City Center—as well as other local options.
To learn more about everything Nashville has to offer, and get more recommendations from Drs. Rice and Pugh, check out the latest CHEST 2022 blog on chestnet.org
Beyond CPAP: Looking to alternative treatments for obstructive sleep apnea
Overview of the problem
Obstructive sleep apnea (OSA) is an extraordinarily common condition impacting nearly 1 billion individuals globally (Benjafield AV, et al. Lancet Respir Med. 2019;7[8]:687). For the past 40 years, the mainstay of treatment has been continuous positive airway pressure (CPAP). However, CPAP usage is highly variable, and not all sleep apnea is created the same with respect to underlying mechanism or patient symptoms. Currently, there is a global CPAP shortage, which has expedited the need for alternative therapies in OSA (Owens RL, et al. Am J Respir Crit Care Med. 2021;204[8]:887).
Characterizing OSA
First, it is important to understand that sleep apnea emerges for multiple reasons. Some examples include: an excessively collapsible airway, insufficient upper airway reflexes, low arousal threshold (awakening easily to ventilatory disturbance), as well as an unstable chemoreflex system. This list is not comprehensive. However, we believe that the future of OSA management will be targeted therapy for individual OSA traits.
Notably, the patient experience of OSA is also highly variable. Some individuals are excessively sleepy. Some individuals experience OSA as insomnia. Other patients are asymptomatic, but present to the sleep clinic at the behest of a disgruntled bed partner. These individual factors should all be kept in mind when deciding when and how to treat sleep apnea.
OSA scoring – past, present, and future
The traditional method for scoring sleep apnea severity is the apnea-hypopnea index (AHI), with mild, moderate, and severe OSA being stratified by the number of events per hour. This metric has shaped many of the modern sleep practices and consensus recommendations but is simply not sophisticated enough to capture the nuance of how or why an individual’s sleep is disrupted from flow-limited breathing. As such, there has been a push in recent times to tailor treatment for OSA to an individual’s physiology. Examples of alternative metrics which quantify sleep apnea traits include the apnea-hypopnea event duration, the sleep apnea-specific hypoxic burden (area under the SpO2 curve for flow-limited events), as well as the arousal intensity from sleep in the setting of flow-limited breathing. There are numerous other metrics that have been proposed but are beyond the scope of this review (Malhotra A, et al. Sleep. 2021;44[7]:zsab030).
What therapies are available and how can we individualize them to our patients?
As noted, CPAP has been the gold-standard for OSA treatment for 40 years but is not always accepted or tolerated (Malhotra A, et al. Chest. 2018;153[4]:843). Broad categories of OSA management are presented as follows.
Surgery for OSA
Upper airway surgery is effective for pediatric OSA treatment, where enlarged tonsils are often the culprit for flow-limited breathing in sleep. For adults, however, there is no one best surgery or surgical candidate. For instance, surgery can be used to improve CPAP tolerance or as a primary OSA treatment. Many individuals with sinus disease may require sinus surgery or septoplasty to improve CPAP tolerability by creating more space for airflow through the nasopharynx. Retrognathic individuals, on the other hand, may benefit from maxillomandibular advancement. Others may benefit from genioglossus advancement or hyoid suspension. The characteristics of the soft palate can be predictive of surgical success with respect to uvulopalatopharyngoplasty (UPPP), with longer uvulas and redundant soft palate tissue being attractive surgical targets. Obviously, this list is far from comprehensive, but Friedman tongue position, tonsil size, and body mass index also appear to be important in predicting surgical success (MacKay S, et al. JAMA. 2020;324[12]:1168).
Hypoglossal nerve stimulation is one surgical treatment option for patients with moderate-severe OSA who are unable or unwilling to use CPAP therapy, have a BMI <32-35 kg/m2 (center-dependent), no concentric velopharyngeal collapse on drug-induced sleep endoscopy, and fewer than 25% central/mixed apneas on their sleep study. Areas for further study are whether unilateral or bilateral stimulation are most effective, as well as which of the sleep apnea traits are most predictive of a treatment response (Strohl MM, et al. Curr Sleep Med Rep. 2017;3[3]:133).
Notably, surgical techniques are highly variable, and there are individual patient characteristics, such as lower loop gain (more stable ventilatory control), which may have a greater likelihood of successful upper airway surgery. This is likely because making the upper airway more patent allows for ventilatory overshoots and thereby airway collapse and cyclic, unstable breathing in those with an unstable ventilatory control system. Trials with prespecified surgical techniques based on individual traits are welcome. Additionally, the metrics of a successful surgical treatment for OSA, much like the AHI, are in need of evolution. The Sher criteria, for instance (50% AHI reduction to an AHI < 20/h), are arbitrary, and their clinical utility is unclear.
Oral appliances
Oral appliances fall into two broad categories – tongue-retaining devices and mandibular advancement splints (MAS). Of the two, MAS are much more commonly prescribed. Of the MAS devices, custom made devices by an American Academy of Dental Sleep Medicine (AADSM)–trained dentist are recommended over noncustom MAS in the treatment of primary snoring or OSA for those unwilling or unable to wear CPAP. Notably, the 2015 American Academy of Sleep Medicine (AASM) and AADSM shared guidelines were unable to make OSA treatment recommendations based on severity of disease as stratified by the AHI due to the limited quality of evidence. These devices are broadly thought to work by protruding the mandible/tongue and, in-turn, advancing multiple soft tissue components of the velopharynx. Relatively recent work suggests that the following OSA traits are associated with MAS efficacy: lower loop gain, higher arousal threshold, lower ventilatory response to arousal, moderate pharyngeal collapsibility, and weaker upper airway dilator muscle compensation. However, in order for these devices to be successful, close follow-up for titration with a AADSM-certified dentist, as well as a follow-up efficacy sleep study, are recommended. Adherence for custom device use appears to be about 70% use greater than 4 hours per night, with 35% to 40% of those prescribed a device achieving an AHI less than 5/h. Over the counter devices are not routinely recommended, though some practices do use these devices as a trial to see if patients may tolerate custom made devices (Ramar K, et al. J Clin Sleep Med. 2015;11[7]:773).
Upper airway training
Upper airway training has been shown possibly to be effective in treating OSA, though the ideal endotype is still being established. Upper airway training has taken many forms, from woodwind instrument playing, to nocturnal electrical stimulation of the tongue, and, more recently, daytime awake transoral neuromuscular stimulation. These interventions appear to be effective for mild sleep apnea and snoring, but the best training regimen has yet to be established. Equally, as with other routine exercise, there appears to be a “use it or lose it” component, and the ideal maintenance regimen for each of these therapies is yet to be determined.
Weight loss and bariatric surgery
Obesity is a common, reversible risk factor for OSA. However, not all obese individuals develop OSA (typically those with robust upper airway reflexes). Improvements in weight appear to correlate with reductions in tongue fat, which correlate to AHI reduction. Weight loss also creates lower CPAP requirements for many individuals, conceivably improving tolerability. Ongoing work is seeking to understand whether there are changes in upper airway muscle recruitability as well as other change in endotype traits following weight loss surgery.
Pharmacotherapy for OSA
There is a great deal of promise in tailoring pharmacotherapy to individual sleep traits. Acetazolamide, for instance, results in improvements an AHI for both obstructive and central sleep apnea through changes in chemosensitivity and is generally well-tolerated (Schmickl CN, et al. Physiol Rep. 2021;9[20]:e15071). Eszopiclone has been used to raise the arousal threshold for those who awaken from breathing events too easily. With added time, individuals with a low arousal threshold can more effectively recruit upper airway dilator muscles without waking up. Pharmacotherapy to improve upper airway recruitability with combination noradrenergic stimulation and antimuscarinic activity has limited data thus far but may be a useful part of the sleep armamentarium moving forward.
Summary
OSA is a public health priority, and the current global CPAP shortage emphasizes the need for alternative OSA therapies. The ideal therapy for a given patient requires a careful consideration of their individual traits and will be much more refined when endotyping is available in a routine clinical setting. Individualized sleep apnea treatment is the future of sleep medicine and a one-size fits all approach no longer meets the needs of our patients given the current state of sleep medicine knowledge.
Dr. Nokes, Dr. Schmickl, and Dr. Malhotra are with the University of California, San Diego, Division of Pulmonary, Critical Care, and Sleep Medicine, La, Jolla, CA. Dr. Nokes also is with the Veterans Affairs San Diego Healthcare System, sleep section, San Diego, CA. Dr. Vahabzadeh-Hagh is with the University of California, San Diego, Department of Otolaryngology, San Diego, CA.
Overview of the problem
Obstructive sleep apnea (OSA) is an extraordinarily common condition impacting nearly 1 billion individuals globally (Benjafield AV, et al. Lancet Respir Med. 2019;7[8]:687). For the past 40 years, the mainstay of treatment has been continuous positive airway pressure (CPAP). However, CPAP usage is highly variable, and not all sleep apnea is created the same with respect to underlying mechanism or patient symptoms. Currently, there is a global CPAP shortage, which has expedited the need for alternative therapies in OSA (Owens RL, et al. Am J Respir Crit Care Med. 2021;204[8]:887).
Characterizing OSA
First, it is important to understand that sleep apnea emerges for multiple reasons. Some examples include: an excessively collapsible airway, insufficient upper airway reflexes, low arousal threshold (awakening easily to ventilatory disturbance), as well as an unstable chemoreflex system. This list is not comprehensive. However, we believe that the future of OSA management will be targeted therapy for individual OSA traits.
Notably, the patient experience of OSA is also highly variable. Some individuals are excessively sleepy. Some individuals experience OSA as insomnia. Other patients are asymptomatic, but present to the sleep clinic at the behest of a disgruntled bed partner. These individual factors should all be kept in mind when deciding when and how to treat sleep apnea.
OSA scoring – past, present, and future
The traditional method for scoring sleep apnea severity is the apnea-hypopnea index (AHI), with mild, moderate, and severe OSA being stratified by the number of events per hour. This metric has shaped many of the modern sleep practices and consensus recommendations but is simply not sophisticated enough to capture the nuance of how or why an individual’s sleep is disrupted from flow-limited breathing. As such, there has been a push in recent times to tailor treatment for OSA to an individual’s physiology. Examples of alternative metrics which quantify sleep apnea traits include the apnea-hypopnea event duration, the sleep apnea-specific hypoxic burden (area under the SpO2 curve for flow-limited events), as well as the arousal intensity from sleep in the setting of flow-limited breathing. There are numerous other metrics that have been proposed but are beyond the scope of this review (Malhotra A, et al. Sleep. 2021;44[7]:zsab030).
What therapies are available and how can we individualize them to our patients?
As noted, CPAP has been the gold-standard for OSA treatment for 40 years but is not always accepted or tolerated (Malhotra A, et al. Chest. 2018;153[4]:843). Broad categories of OSA management are presented as follows.
Surgery for OSA
Upper airway surgery is effective for pediatric OSA treatment, where enlarged tonsils are often the culprit for flow-limited breathing in sleep. For adults, however, there is no one best surgery or surgical candidate. For instance, surgery can be used to improve CPAP tolerance or as a primary OSA treatment. Many individuals with sinus disease may require sinus surgery or septoplasty to improve CPAP tolerability by creating more space for airflow through the nasopharynx. Retrognathic individuals, on the other hand, may benefit from maxillomandibular advancement. Others may benefit from genioglossus advancement or hyoid suspension. The characteristics of the soft palate can be predictive of surgical success with respect to uvulopalatopharyngoplasty (UPPP), with longer uvulas and redundant soft palate tissue being attractive surgical targets. Obviously, this list is far from comprehensive, but Friedman tongue position, tonsil size, and body mass index also appear to be important in predicting surgical success (MacKay S, et al. JAMA. 2020;324[12]:1168).
Hypoglossal nerve stimulation is one surgical treatment option for patients with moderate-severe OSA who are unable or unwilling to use CPAP therapy, have a BMI <32-35 kg/m2 (center-dependent), no concentric velopharyngeal collapse on drug-induced sleep endoscopy, and fewer than 25% central/mixed apneas on their sleep study. Areas for further study are whether unilateral or bilateral stimulation are most effective, as well as which of the sleep apnea traits are most predictive of a treatment response (Strohl MM, et al. Curr Sleep Med Rep. 2017;3[3]:133).
Notably, surgical techniques are highly variable, and there are individual patient characteristics, such as lower loop gain (more stable ventilatory control), which may have a greater likelihood of successful upper airway surgery. This is likely because making the upper airway more patent allows for ventilatory overshoots and thereby airway collapse and cyclic, unstable breathing in those with an unstable ventilatory control system. Trials with prespecified surgical techniques based on individual traits are welcome. Additionally, the metrics of a successful surgical treatment for OSA, much like the AHI, are in need of evolution. The Sher criteria, for instance (50% AHI reduction to an AHI < 20/h), are arbitrary, and their clinical utility is unclear.
Oral appliances
Oral appliances fall into two broad categories – tongue-retaining devices and mandibular advancement splints (MAS). Of the two, MAS are much more commonly prescribed. Of the MAS devices, custom made devices by an American Academy of Dental Sleep Medicine (AADSM)–trained dentist are recommended over noncustom MAS in the treatment of primary snoring or OSA for those unwilling or unable to wear CPAP. Notably, the 2015 American Academy of Sleep Medicine (AASM) and AADSM shared guidelines were unable to make OSA treatment recommendations based on severity of disease as stratified by the AHI due to the limited quality of evidence. These devices are broadly thought to work by protruding the mandible/tongue and, in-turn, advancing multiple soft tissue components of the velopharynx. Relatively recent work suggests that the following OSA traits are associated with MAS efficacy: lower loop gain, higher arousal threshold, lower ventilatory response to arousal, moderate pharyngeal collapsibility, and weaker upper airway dilator muscle compensation. However, in order for these devices to be successful, close follow-up for titration with a AADSM-certified dentist, as well as a follow-up efficacy sleep study, are recommended. Adherence for custom device use appears to be about 70% use greater than 4 hours per night, with 35% to 40% of those prescribed a device achieving an AHI less than 5/h. Over the counter devices are not routinely recommended, though some practices do use these devices as a trial to see if patients may tolerate custom made devices (Ramar K, et al. J Clin Sleep Med. 2015;11[7]:773).
Upper airway training
Upper airway training has been shown possibly to be effective in treating OSA, though the ideal endotype is still being established. Upper airway training has taken many forms, from woodwind instrument playing, to nocturnal electrical stimulation of the tongue, and, more recently, daytime awake transoral neuromuscular stimulation. These interventions appear to be effective for mild sleep apnea and snoring, but the best training regimen has yet to be established. Equally, as with other routine exercise, there appears to be a “use it or lose it” component, and the ideal maintenance regimen for each of these therapies is yet to be determined.
Weight loss and bariatric surgery
Obesity is a common, reversible risk factor for OSA. However, not all obese individuals develop OSA (typically those with robust upper airway reflexes). Improvements in weight appear to correlate with reductions in tongue fat, which correlate to AHI reduction. Weight loss also creates lower CPAP requirements for many individuals, conceivably improving tolerability. Ongoing work is seeking to understand whether there are changes in upper airway muscle recruitability as well as other change in endotype traits following weight loss surgery.
Pharmacotherapy for OSA
There is a great deal of promise in tailoring pharmacotherapy to individual sleep traits. Acetazolamide, for instance, results in improvements an AHI for both obstructive and central sleep apnea through changes in chemosensitivity and is generally well-tolerated (Schmickl CN, et al. Physiol Rep. 2021;9[20]:e15071). Eszopiclone has been used to raise the arousal threshold for those who awaken from breathing events too easily. With added time, individuals with a low arousal threshold can more effectively recruit upper airway dilator muscles without waking up. Pharmacotherapy to improve upper airway recruitability with combination noradrenergic stimulation and antimuscarinic activity has limited data thus far but may be a useful part of the sleep armamentarium moving forward.
Summary
OSA is a public health priority, and the current global CPAP shortage emphasizes the need for alternative OSA therapies. The ideal therapy for a given patient requires a careful consideration of their individual traits and will be much more refined when endotyping is available in a routine clinical setting. Individualized sleep apnea treatment is the future of sleep medicine and a one-size fits all approach no longer meets the needs of our patients given the current state of sleep medicine knowledge.
Dr. Nokes, Dr. Schmickl, and Dr. Malhotra are with the University of California, San Diego, Division of Pulmonary, Critical Care, and Sleep Medicine, La, Jolla, CA. Dr. Nokes also is with the Veterans Affairs San Diego Healthcare System, sleep section, San Diego, CA. Dr. Vahabzadeh-Hagh is with the University of California, San Diego, Department of Otolaryngology, San Diego, CA.
Overview of the problem
Obstructive sleep apnea (OSA) is an extraordinarily common condition impacting nearly 1 billion individuals globally (Benjafield AV, et al. Lancet Respir Med. 2019;7[8]:687). For the past 40 years, the mainstay of treatment has been continuous positive airway pressure (CPAP). However, CPAP usage is highly variable, and not all sleep apnea is created the same with respect to underlying mechanism or patient symptoms. Currently, there is a global CPAP shortage, which has expedited the need for alternative therapies in OSA (Owens RL, et al. Am J Respir Crit Care Med. 2021;204[8]:887).
Characterizing OSA
First, it is important to understand that sleep apnea emerges for multiple reasons. Some examples include: an excessively collapsible airway, insufficient upper airway reflexes, low arousal threshold (awakening easily to ventilatory disturbance), as well as an unstable chemoreflex system. This list is not comprehensive. However, we believe that the future of OSA management will be targeted therapy for individual OSA traits.
Notably, the patient experience of OSA is also highly variable. Some individuals are excessively sleepy. Some individuals experience OSA as insomnia. Other patients are asymptomatic, but present to the sleep clinic at the behest of a disgruntled bed partner. These individual factors should all be kept in mind when deciding when and how to treat sleep apnea.
OSA scoring – past, present, and future
The traditional method for scoring sleep apnea severity is the apnea-hypopnea index (AHI), with mild, moderate, and severe OSA being stratified by the number of events per hour. This metric has shaped many of the modern sleep practices and consensus recommendations but is simply not sophisticated enough to capture the nuance of how or why an individual’s sleep is disrupted from flow-limited breathing. As such, there has been a push in recent times to tailor treatment for OSA to an individual’s physiology. Examples of alternative metrics which quantify sleep apnea traits include the apnea-hypopnea event duration, the sleep apnea-specific hypoxic burden (area under the SpO2 curve for flow-limited events), as well as the arousal intensity from sleep in the setting of flow-limited breathing. There are numerous other metrics that have been proposed but are beyond the scope of this review (Malhotra A, et al. Sleep. 2021;44[7]:zsab030).
What therapies are available and how can we individualize them to our patients?
As noted, CPAP has been the gold-standard for OSA treatment for 40 years but is not always accepted or tolerated (Malhotra A, et al. Chest. 2018;153[4]:843). Broad categories of OSA management are presented as follows.
Surgery for OSA
Upper airway surgery is effective for pediatric OSA treatment, where enlarged tonsils are often the culprit for flow-limited breathing in sleep. For adults, however, there is no one best surgery or surgical candidate. For instance, surgery can be used to improve CPAP tolerance or as a primary OSA treatment. Many individuals with sinus disease may require sinus surgery or septoplasty to improve CPAP tolerability by creating more space for airflow through the nasopharynx. Retrognathic individuals, on the other hand, may benefit from maxillomandibular advancement. Others may benefit from genioglossus advancement or hyoid suspension. The characteristics of the soft palate can be predictive of surgical success with respect to uvulopalatopharyngoplasty (UPPP), with longer uvulas and redundant soft palate tissue being attractive surgical targets. Obviously, this list is far from comprehensive, but Friedman tongue position, tonsil size, and body mass index also appear to be important in predicting surgical success (MacKay S, et al. JAMA. 2020;324[12]:1168).
Hypoglossal nerve stimulation is one surgical treatment option for patients with moderate-severe OSA who are unable or unwilling to use CPAP therapy, have a BMI <32-35 kg/m2 (center-dependent), no concentric velopharyngeal collapse on drug-induced sleep endoscopy, and fewer than 25% central/mixed apneas on their sleep study. Areas for further study are whether unilateral or bilateral stimulation are most effective, as well as which of the sleep apnea traits are most predictive of a treatment response (Strohl MM, et al. Curr Sleep Med Rep. 2017;3[3]:133).
Notably, surgical techniques are highly variable, and there are individual patient characteristics, such as lower loop gain (more stable ventilatory control), which may have a greater likelihood of successful upper airway surgery. This is likely because making the upper airway more patent allows for ventilatory overshoots and thereby airway collapse and cyclic, unstable breathing in those with an unstable ventilatory control system. Trials with prespecified surgical techniques based on individual traits are welcome. Additionally, the metrics of a successful surgical treatment for OSA, much like the AHI, are in need of evolution. The Sher criteria, for instance (50% AHI reduction to an AHI < 20/h), are arbitrary, and their clinical utility is unclear.
Oral appliances
Oral appliances fall into two broad categories – tongue-retaining devices and mandibular advancement splints (MAS). Of the two, MAS are much more commonly prescribed. Of the MAS devices, custom made devices by an American Academy of Dental Sleep Medicine (AADSM)–trained dentist are recommended over noncustom MAS in the treatment of primary snoring or OSA for those unwilling or unable to wear CPAP. Notably, the 2015 American Academy of Sleep Medicine (AASM) and AADSM shared guidelines were unable to make OSA treatment recommendations based on severity of disease as stratified by the AHI due to the limited quality of evidence. These devices are broadly thought to work by protruding the mandible/tongue and, in-turn, advancing multiple soft tissue components of the velopharynx. Relatively recent work suggests that the following OSA traits are associated with MAS efficacy: lower loop gain, higher arousal threshold, lower ventilatory response to arousal, moderate pharyngeal collapsibility, and weaker upper airway dilator muscle compensation. However, in order for these devices to be successful, close follow-up for titration with a AADSM-certified dentist, as well as a follow-up efficacy sleep study, are recommended. Adherence for custom device use appears to be about 70% use greater than 4 hours per night, with 35% to 40% of those prescribed a device achieving an AHI less than 5/h. Over the counter devices are not routinely recommended, though some practices do use these devices as a trial to see if patients may tolerate custom made devices (Ramar K, et al. J Clin Sleep Med. 2015;11[7]:773).
Upper airway training
Upper airway training has been shown possibly to be effective in treating OSA, though the ideal endotype is still being established. Upper airway training has taken many forms, from woodwind instrument playing, to nocturnal electrical stimulation of the tongue, and, more recently, daytime awake transoral neuromuscular stimulation. These interventions appear to be effective for mild sleep apnea and snoring, but the best training regimen has yet to be established. Equally, as with other routine exercise, there appears to be a “use it or lose it” component, and the ideal maintenance regimen for each of these therapies is yet to be determined.
Weight loss and bariatric surgery
Obesity is a common, reversible risk factor for OSA. However, not all obese individuals develop OSA (typically those with robust upper airway reflexes). Improvements in weight appear to correlate with reductions in tongue fat, which correlate to AHI reduction. Weight loss also creates lower CPAP requirements for many individuals, conceivably improving tolerability. Ongoing work is seeking to understand whether there are changes in upper airway muscle recruitability as well as other change in endotype traits following weight loss surgery.
Pharmacotherapy for OSA
There is a great deal of promise in tailoring pharmacotherapy to individual sleep traits. Acetazolamide, for instance, results in improvements an AHI for both obstructive and central sleep apnea through changes in chemosensitivity and is generally well-tolerated (Schmickl CN, et al. Physiol Rep. 2021;9[20]:e15071). Eszopiclone has been used to raise the arousal threshold for those who awaken from breathing events too easily. With added time, individuals with a low arousal threshold can more effectively recruit upper airway dilator muscles without waking up. Pharmacotherapy to improve upper airway recruitability with combination noradrenergic stimulation and antimuscarinic activity has limited data thus far but may be a useful part of the sleep armamentarium moving forward.
Summary
OSA is a public health priority, and the current global CPAP shortage emphasizes the need for alternative OSA therapies. The ideal therapy for a given patient requires a careful consideration of their individual traits and will be much more refined when endotyping is available in a routine clinical setting. Individualized sleep apnea treatment is the future of sleep medicine and a one-size fits all approach no longer meets the needs of our patients given the current state of sleep medicine knowledge.
Dr. Nokes, Dr. Schmickl, and Dr. Malhotra are with the University of California, San Diego, Division of Pulmonary, Critical Care, and Sleep Medicine, La, Jolla, CA. Dr. Nokes also is with the Veterans Affairs San Diego Healthcare System, sleep section, San Diego, CA. Dr. Vahabzadeh-Hagh is with the University of California, San Diego, Department of Otolaryngology, San Diego, CA.
From the President: A day in the life
For those of you in the Northern Hemisphere, like me, spring has transitioned into summer, allowing us all to spend more time outdoors, gathering again with family, friends, and colleagues. And, while people are always happy to hear about what’s going on with the family, or how things are going at Emory, the most common question I get is “So what’s it like to be President of CHEST?” Now that I’ve been on the job for 6 months, I thought it was well enough time to pull back the curtain on the role for all of you out in CHEST-land who might be interested, as well. For the purposes of this column, I’ll be incorporating things that occurred over the past week.

As I’ve previously reported, the most important decisions that relate to CHEST strategy are made by the Board of Regents. While I do have the privilege of organizing and running Board meetings, most presidential duties between these meetings focus on communication: with our members, our leaders, and other organizations. One of the best parts of the job is the opportunity to interact with our members; between the [email protected] account and my own, I receive a couple of emails each day with questions about navigating CHEST, or ideas about ways that things might be better accomplished. With our recent Network and section reorganization, many of those questions have focused on leadership opportunities, inquiring about whether the writer should apply, or asking for information about the qualities that might increase the odds of earning a position. My answer is almost always the same: go ahead and throw your name in the hat; for most members, the sections are the first place to start the journey in CHEST leadership. And I’m pleased to say that I’ve had the chance to see some of the members who’ve reached out to me in the past selected for the positions to which they’d applied (in full disclosure, I have little role in selecting leadership positions; Network and section positions are chosen by current members of those Networks and sections). I look forward to watching their progress in our organizational leadership.
While CHEST CEO Robert Musacchio and I communicate almost every day, Wednesday is our weekly meeting during which we review progress on our organizational goals, the status of ongoing projects, and concerns from our membership and leadership. I also have the pleasure of meeting with my co-Presidents every other week; though Jack, Doreen, and Steve have always been happy to offer their counsel on very short notice, this semimonthly meeting helps to provide continuity in leadership, as well as a more formal opportunity for me to meet with trusted advisors to get a sounding board on active issues that affect CHEST. And, this gets to the other main job of CHEST President, which is to facilitate the making of important decisions on behalf of the College. I receive sporadic emails from CHEST staff as we are approached by other organizations or international partners for input on or approval for statements that they wish to make. In the case where the topic is clearly in the CHEST wheelhouse and the statement is consistent with our organizational goals, I can unilaterally sign off; a common example of something that fits in this category is content related to tobacco cessation. In the more frequent situation where the statement for approval is a bit more complex, I will usually refer the request to one of our committee, Network, or section chairs for consideration. Since the turnaround time on these requests is usually pretty short, I may ask them to advise me on their own, although they sometimes opt to run things by their own membership for further input or to achieve consensus.
The CHEST President also serves as ambassador to other organizations; this week, I had the pleasure of participating in a meeting with the American Board of Internal Medicine and a number of medical specialty leaders focused on how professional societies can help to mitigate the spread of medical misinformation. I also interfaced with several of our international partners in the pulmonary space, as they plan their own international meetings, to see how CHEST can contribute to the success of those endeavors by contributing content, speakers, or both. At the time of this writing, the CHEST Congress in Bologna, Italy, is right around the corner, and so I also spent time working with our Italian partners and program co-chair William Kelly, MD, FCCP, to finalize the meeting’s opening session. Though our own international meeting is still months away, work continues with the annual meeting innovations group, and I’ve been working with my own small team on some special surprises that you’ll hear more about in the coming months! The other CHEST meeting-related item on the front burner is the selection of the keynote speaker. The way this works is that I outline in broad strokes a sense of the flavor I’m targeting, and the CHEST staff work with a consulting group to propose some options. They provide me with a brief biography in clips, and we narrow the list down. As I write, we are finalizing our invitation, and I look forward to formally announcing the CHEST 2022 keynote speaker shortly!
After I explain the breadth of duties involved in my role, the most common follow-up question asked of me is whether I am enjoying the position. I’ll concede that it’s not for everyone. There’s a lot less independent decision-making than people assume. But, if you like getting to meet and interact with people from around the globe, helping them to see how CHEST can help them in their pursuits or career goals (and how they can help CHEST in our mission), it’s a super fun job. And I’ll most definitely miss it when I’m done.
So that, in brief, is an overview of what the CHEST President does. But each week is different. And, I get better at the job each day, as I learn something new about the position, the organization, and our outstanding members, leaders, and staff. I look forward to continuing to represent each of you in making decisions and communicating on behalf of CHEST. As always, I remain interested in your input as to how things are going; please consider reaching out to me at [email protected] at your convenience. ... I expect to have a few minutes to write back sometime next Thursday.
Until next time,
David
For those of you in the Northern Hemisphere, like me, spring has transitioned into summer, allowing us all to spend more time outdoors, gathering again with family, friends, and colleagues. And, while people are always happy to hear about what’s going on with the family, or how things are going at Emory, the most common question I get is “So what’s it like to be President of CHEST?” Now that I’ve been on the job for 6 months, I thought it was well enough time to pull back the curtain on the role for all of you out in CHEST-land who might be interested, as well. For the purposes of this column, I’ll be incorporating things that occurred over the past week.
As I’ve previously reported, the most important decisions that relate to CHEST strategy are made by the Board of Regents. While I do have the privilege of organizing and running Board meetings, most presidential duties between these meetings focus on communication: with our members, our leaders, and other organizations. One of the best parts of the job is the opportunity to interact with our members; between the [email protected] account and my own, I receive a couple of emails each day with questions about navigating CHEST, or ideas about ways that things might be better accomplished. With our recent Network and section reorganization, many of those questions have focused on leadership opportunities, inquiring about whether the writer should apply, or asking for information about the qualities that might increase the odds of earning a position. My answer is almost always the same: go ahead and throw your name in the hat; for most members, the sections are the first place to start the journey in CHEST leadership. And I’m pleased to say that I’ve had the chance to see some of the members who’ve reached out to me in the past selected for the positions to which they’d applied (in full disclosure, I have little role in selecting leadership positions; Network and section positions are chosen by current members of those Networks and sections). I look forward to watching their progress in our organizational leadership.
While CHEST CEO Robert Musacchio and I communicate almost every day, Wednesday is our weekly meeting during which we review progress on our organizational goals, the status of ongoing projects, and concerns from our membership and leadership. I also have the pleasure of meeting with my co-Presidents every other week; though Jack, Doreen, and Steve have always been happy to offer their counsel on very short notice, this semimonthly meeting helps to provide continuity in leadership, as well as a more formal opportunity for me to meet with trusted advisors to get a sounding board on active issues that affect CHEST. And, this gets to the other main job of CHEST President, which is to facilitate the making of important decisions on behalf of the College. I receive sporadic emails from CHEST staff as we are approached by other organizations or international partners for input on or approval for statements that they wish to make. In the case where the topic is clearly in the CHEST wheelhouse and the statement is consistent with our organizational goals, I can unilaterally sign off; a common example of something that fits in this category is content related to tobacco cessation. In the more frequent situation where the statement for approval is a bit more complex, I will usually refer the request to one of our committee, Network, or section chairs for consideration. Since the turnaround time on these requests is usually pretty short, I may ask them to advise me on their own, although they sometimes opt to run things by their own membership for further input or to achieve consensus.
The CHEST President also serves as ambassador to other organizations; this week, I had the pleasure of participating in a meeting with the American Board of Internal Medicine and a number of medical specialty leaders focused on how professional societies can help to mitigate the spread of medical misinformation. I also interfaced with several of our international partners in the pulmonary space, as they plan their own international meetings, to see how CHEST can contribute to the success of those endeavors by contributing content, speakers, or both. At the time of this writing, the CHEST Congress in Bologna, Italy, is right around the corner, and so I also spent time working with our Italian partners and program co-chair William Kelly, MD, FCCP, to finalize the meeting’s opening session. Though our own international meeting is still months away, work continues with the annual meeting innovations group, and I’ve been working with my own small team on some special surprises that you’ll hear more about in the coming months! The other CHEST meeting-related item on the front burner is the selection of the keynote speaker. The way this works is that I outline in broad strokes a sense of the flavor I’m targeting, and the CHEST staff work with a consulting group to propose some options. They provide me with a brief biography in clips, and we narrow the list down. As I write, we are finalizing our invitation, and I look forward to formally announcing the CHEST 2022 keynote speaker shortly!
After I explain the breadth of duties involved in my role, the most common follow-up question asked of me is whether I am enjoying the position. I’ll concede that it’s not for everyone. There’s a lot less independent decision-making than people assume. But, if you like getting to meet and interact with people from around the globe, helping them to see how CHEST can help them in their pursuits or career goals (and how they can help CHEST in our mission), it’s a super fun job. And I’ll most definitely miss it when I’m done.
So that, in brief, is an overview of what the CHEST President does. But each week is different. And, I get better at the job each day, as I learn something new about the position, the organization, and our outstanding members, leaders, and staff. I look forward to continuing to represent each of you in making decisions and communicating on behalf of CHEST. As always, I remain interested in your input as to how things are going; please consider reaching out to me at [email protected] at your convenience. ... I expect to have a few minutes to write back sometime next Thursday.
Until next time,
David
For those of you in the Northern Hemisphere, like me, spring has transitioned into summer, allowing us all to spend more time outdoors, gathering again with family, friends, and colleagues. And, while people are always happy to hear about what’s going on with the family, or how things are going at Emory, the most common question I get is “So what’s it like to be President of CHEST?” Now that I’ve been on the job for 6 months, I thought it was well enough time to pull back the curtain on the role for all of you out in CHEST-land who might be interested, as well. For the purposes of this column, I’ll be incorporating things that occurred over the past week.
As I’ve previously reported, the most important decisions that relate to CHEST strategy are made by the Board of Regents. While I do have the privilege of organizing and running Board meetings, most presidential duties between these meetings focus on communication: with our members, our leaders, and other organizations. One of the best parts of the job is the opportunity to interact with our members; between the [email protected] account and my own, I receive a couple of emails each day with questions about navigating CHEST, or ideas about ways that things might be better accomplished. With our recent Network and section reorganization, many of those questions have focused on leadership opportunities, inquiring about whether the writer should apply, or asking for information about the qualities that might increase the odds of earning a position. My answer is almost always the same: go ahead and throw your name in the hat; for most members, the sections are the first place to start the journey in CHEST leadership. And I’m pleased to say that I’ve had the chance to see some of the members who’ve reached out to me in the past selected for the positions to which they’d applied (in full disclosure, I have little role in selecting leadership positions; Network and section positions are chosen by current members of those Networks and sections). I look forward to watching their progress in our organizational leadership.
While CHEST CEO Robert Musacchio and I communicate almost every day, Wednesday is our weekly meeting during which we review progress on our organizational goals, the status of ongoing projects, and concerns from our membership and leadership. I also have the pleasure of meeting with my co-Presidents every other week; though Jack, Doreen, and Steve have always been happy to offer their counsel on very short notice, this semimonthly meeting helps to provide continuity in leadership, as well as a more formal opportunity for me to meet with trusted advisors to get a sounding board on active issues that affect CHEST. And, this gets to the other main job of CHEST President, which is to facilitate the making of important decisions on behalf of the College. I receive sporadic emails from CHEST staff as we are approached by other organizations or international partners for input on or approval for statements that they wish to make. In the case where the topic is clearly in the CHEST wheelhouse and the statement is consistent with our organizational goals, I can unilaterally sign off; a common example of something that fits in this category is content related to tobacco cessation. In the more frequent situation where the statement for approval is a bit more complex, I will usually refer the request to one of our committee, Network, or section chairs for consideration. Since the turnaround time on these requests is usually pretty short, I may ask them to advise me on their own, although they sometimes opt to run things by their own membership for further input or to achieve consensus.
The CHEST President also serves as ambassador to other organizations; this week, I had the pleasure of participating in a meeting with the American Board of Internal Medicine and a number of medical specialty leaders focused on how professional societies can help to mitigate the spread of medical misinformation. I also interfaced with several of our international partners in the pulmonary space, as they plan their own international meetings, to see how CHEST can contribute to the success of those endeavors by contributing content, speakers, or both. At the time of this writing, the CHEST Congress in Bologna, Italy, is right around the corner, and so I also spent time working with our Italian partners and program co-chair William Kelly, MD, FCCP, to finalize the meeting’s opening session. Though our own international meeting is still months away, work continues with the annual meeting innovations group, and I’ve been working with my own small team on some special surprises that you’ll hear more about in the coming months! The other CHEST meeting-related item on the front burner is the selection of the keynote speaker. The way this works is that I outline in broad strokes a sense of the flavor I’m targeting, and the CHEST staff work with a consulting group to propose some options. They provide me with a brief biography in clips, and we narrow the list down. As I write, we are finalizing our invitation, and I look forward to formally announcing the CHEST 2022 keynote speaker shortly!
After I explain the breadth of duties involved in my role, the most common follow-up question asked of me is whether I am enjoying the position. I’ll concede that it’s not for everyone. There’s a lot less independent decision-making than people assume. But, if you like getting to meet and interact with people from around the globe, helping them to see how CHEST can help them in their pursuits or career goals (and how they can help CHEST in our mission), it’s a super fun job. And I’ll most definitely miss it when I’m done.
So that, in brief, is an overview of what the CHEST President does. But each week is different. And, I get better at the job each day, as I learn something new about the position, the organization, and our outstanding members, leaders, and staff. I look forward to continuing to represent each of you in making decisions and communicating on behalf of CHEST. As always, I remain interested in your input as to how things are going; please consider reaching out to me at [email protected] at your convenience. ... I expect to have a few minutes to write back sometime next Thursday.
Until next time,
David
And, they’re off! Belmont Stakes Dinner and Auction fundraises for patient education
For a night of fun and philanthropy, CHEST leadership and supporters of the CHEST Foundation came together in New York City to watch the Belmont Stakes race and raise money to support patient education.
What started 8 years ago as a brunch in the living room of Doreen Addrizzo-Harris, MD, FCCP, to support the initiatives of the CHEST Foundation.

Spearheaded by Dr. Addrizzo- Harris, President-Elect of the American College of Chest Physicians, this year’s event was focused entirely on patient education and advocacy. The attendees heard the moving stories of Betsy Glaeser and Fred Schick who are both patients living with lung disease and advocates for others living with like afflictions. Betsy is living with nontuberculous mycobacteria (NTM) disease and Fred with idiopathic pulmonary fibrosis (IPF). Betsy and Fred have used their experiences to serve as support for others in similar positions.
Betsy Glaeser, a longtime patient of Dr. Addrizzo-Harris, shared a story about the struggle of being one of the first cases of NTM bronchiectasis and helping to define the course of action. She shared that her original doctors gave her 5 years to live. The room erupted in applause when she shared that with the exceptional treatment she’s received, over 20 years later, she is standing in front of the supporters of the CHEST Foundation to share her story.
Because of the rarity of her disease, she was hospitalized multiple times with pneumonia before finally reaching her diagnosis of NTM disease. She channeled the accompanying frustrations into helping others who were recently diagnosed with the NTM disorder by sharing her experiences. “I would give them guidance on treatment options because in my years of living with the disease, I’d been there and tried almost everything,” said Betsy. “I would get calls from my doctor all of the time to speak with someone who just received an NTM disease diagnosis. I was happy to do so – at the time, the Internet didn’t exist, and firsthand experiences were all we had. Since forming our physical support group, the most memorable experience I can recall is when a woman, newly diagnosed with NTM, walked into the room and immediately burst into tears. She shared that she expected to see all of us on oxygen and wheelchair-bound, but that wasn’t the case at all. That day, we were able to give her hope. That’s why I do what I do, and I’m proud to do it.”
Fred Schick shared with the attendees his story of struggling to find his IPF diagnosis and how incredibly frustrating it was to be so short of breath that he needed to be rescued from the water while on vacation. With a history of cardiac complications, Fred’s doctors were looking at his heart.
For Fred to get to his IPF diagnosis, it took the careful ear of a primary care doctor Fred started to see when his previous doctor retired.
“It was almost like she was listening with different ears and was hearing what others didn’t. Once she recommended speaking with a pulmonologist, everything fell into place,” said Fred. “From my experience, IPF is best treated by a lot of pieces coming together and working together. It takes the dedication of a care team in the hospital, proper diet and exercise and, just as importantly, it takes a support group to guide you through the process. I’m grateful to my care team, but I’m equally thankful for the work I get to do as an advocate for others living with IPF.”
When she spoke to the attendees, Lisa Moores, MD, FCCP, reflected on what the patients shared. “We saw great examples of why we’re here tonight,” said Dr. Moores. “One of the things CHEST and the Foundation are focusing on is earlier diagnosis for interstitial lung diseases like pulmonary fibrosis and, with voices like Fred Schick, we’ll get there. The patients remind us why we’re here. We’re here for our patients; we’re here for Fred; and we’re here for Betsy.”
Laurence Feldman, Vice President of the Feldman Family Foundation that partners with the CHEST Foundation for their annual casino fundraiser benefiting pulmonary fibrosis, was able to participate in the dinner and theauction.
He shared, “Tonight, I was so impressed with the generosity of the attendees and the organization of this event. It reminded me that if you ask your supporters to give, they’ll be there for you. Almost like the ‘Field of Dreams’ quote of ‘if you build it, they will come.’ Being at the Belmont Stakes Dinner and Auction makes me that much more excited for our upcoming Irv Feldman Casino Night and Texas Hold ‘Em Tournament coming up in late August. Thanks to our corporate partners and the support of the CHEST Foundation, we’re able to produce an excellent event like the Belmont Stakes fundraiser that helps bring in donations that can make a difference in the lives of patients.”
At the end of the day, medicine is all about the patients and, by dedicating the night to patient education and patient advocates, the Belmont Stakes event brought the focus to where it should always be – improving care and helping patients.
To learn more and to support the various initiatives of the CHEST Foundation, visit foundation.chestnet.org/donate.
For a night of fun and philanthropy, CHEST leadership and supporters of the CHEST Foundation came together in New York City to watch the Belmont Stakes race and raise money to support patient education.
What started 8 years ago as a brunch in the living room of Doreen Addrizzo-Harris, MD, FCCP, to support the initiatives of the CHEST Foundation.
Spearheaded by Dr. Addrizzo- Harris, President-Elect of the American College of Chest Physicians, this year’s event was focused entirely on patient education and advocacy. The attendees heard the moving stories of Betsy Glaeser and Fred Schick who are both patients living with lung disease and advocates for others living with like afflictions. Betsy is living with nontuberculous mycobacteria (NTM) disease and Fred with idiopathic pulmonary fibrosis (IPF). Betsy and Fred have used their experiences to serve as support for others in similar positions.
Betsy Glaeser, a longtime patient of Dr. Addrizzo-Harris, shared a story about the struggle of being one of the first cases of NTM bronchiectasis and helping to define the course of action. She shared that her original doctors gave her 5 years to live. The room erupted in applause when she shared that with the exceptional treatment she’s received, over 20 years later, she is standing in front of the supporters of the CHEST Foundation to share her story.
Because of the rarity of her disease, she was hospitalized multiple times with pneumonia before finally reaching her diagnosis of NTM disease. She channeled the accompanying frustrations into helping others who were recently diagnosed with the NTM disorder by sharing her experiences. “I would give them guidance on treatment options because in my years of living with the disease, I’d been there and tried almost everything,” said Betsy. “I would get calls from my doctor all of the time to speak with someone who just received an NTM disease diagnosis. I was happy to do so – at the time, the Internet didn’t exist, and firsthand experiences were all we had. Since forming our physical support group, the most memorable experience I can recall is when a woman, newly diagnosed with NTM, walked into the room and immediately burst into tears. She shared that she expected to see all of us on oxygen and wheelchair-bound, but that wasn’t the case at all. That day, we were able to give her hope. That’s why I do what I do, and I’m proud to do it.”
Fred Schick shared with the attendees his story of struggling to find his IPF diagnosis and how incredibly frustrating it was to be so short of breath that he needed to be rescued from the water while on vacation. With a history of cardiac complications, Fred’s doctors were looking at his heart.
For Fred to get to his IPF diagnosis, it took the careful ear of a primary care doctor Fred started to see when his previous doctor retired.
“It was almost like she was listening with different ears and was hearing what others didn’t. Once she recommended speaking with a pulmonologist, everything fell into place,” said Fred. “From my experience, IPF is best treated by a lot of pieces coming together and working together. It takes the dedication of a care team in the hospital, proper diet and exercise and, just as importantly, it takes a support group to guide you through the process. I’m grateful to my care team, but I’m equally thankful for the work I get to do as an advocate for others living with IPF.”
When she spoke to the attendees, Lisa Moores, MD, FCCP, reflected on what the patients shared. “We saw great examples of why we’re here tonight,” said Dr. Moores. “One of the things CHEST and the Foundation are focusing on is earlier diagnosis for interstitial lung diseases like pulmonary fibrosis and, with voices like Fred Schick, we’ll get there. The patients remind us why we’re here. We’re here for our patients; we’re here for Fred; and we’re here for Betsy.”
Laurence Feldman, Vice President of the Feldman Family Foundation that partners with the CHEST Foundation for their annual casino fundraiser benefiting pulmonary fibrosis, was able to participate in the dinner and theauction.
He shared, “Tonight, I was so impressed with the generosity of the attendees and the organization of this event. It reminded me that if you ask your supporters to give, they’ll be there for you. Almost like the ‘Field of Dreams’ quote of ‘if you build it, they will come.’ Being at the Belmont Stakes Dinner and Auction makes me that much more excited for our upcoming Irv Feldman Casino Night and Texas Hold ‘Em Tournament coming up in late August. Thanks to our corporate partners and the support of the CHEST Foundation, we’re able to produce an excellent event like the Belmont Stakes fundraiser that helps bring in donations that can make a difference in the lives of patients.”
At the end of the day, medicine is all about the patients and, by dedicating the night to patient education and patient advocates, the Belmont Stakes event brought the focus to where it should always be – improving care and helping patients.
To learn more and to support the various initiatives of the CHEST Foundation, visit foundation.chestnet.org/donate.
For a night of fun and philanthropy, CHEST leadership and supporters of the CHEST Foundation came together in New York City to watch the Belmont Stakes race and raise money to support patient education.
What started 8 years ago as a brunch in the living room of Doreen Addrizzo-Harris, MD, FCCP, to support the initiatives of the CHEST Foundation.
Spearheaded by Dr. Addrizzo- Harris, President-Elect of the American College of Chest Physicians, this year’s event was focused entirely on patient education and advocacy. The attendees heard the moving stories of Betsy Glaeser and Fred Schick who are both patients living with lung disease and advocates for others living with like afflictions. Betsy is living with nontuberculous mycobacteria (NTM) disease and Fred with idiopathic pulmonary fibrosis (IPF). Betsy and Fred have used their experiences to serve as support for others in similar positions.
Betsy Glaeser, a longtime patient of Dr. Addrizzo-Harris, shared a story about the struggle of being one of the first cases of NTM bronchiectasis and helping to define the course of action. She shared that her original doctors gave her 5 years to live. The room erupted in applause when she shared that with the exceptional treatment she’s received, over 20 years later, she is standing in front of the supporters of the CHEST Foundation to share her story.
Because of the rarity of her disease, she was hospitalized multiple times with pneumonia before finally reaching her diagnosis of NTM disease. She channeled the accompanying frustrations into helping others who were recently diagnosed with the NTM disorder by sharing her experiences. “I would give them guidance on treatment options because in my years of living with the disease, I’d been there and tried almost everything,” said Betsy. “I would get calls from my doctor all of the time to speak with someone who just received an NTM disease diagnosis. I was happy to do so – at the time, the Internet didn’t exist, and firsthand experiences were all we had. Since forming our physical support group, the most memorable experience I can recall is when a woman, newly diagnosed with NTM, walked into the room and immediately burst into tears. She shared that she expected to see all of us on oxygen and wheelchair-bound, but that wasn’t the case at all. That day, we were able to give her hope. That’s why I do what I do, and I’m proud to do it.”
Fred Schick shared with the attendees his story of struggling to find his IPF diagnosis and how incredibly frustrating it was to be so short of breath that he needed to be rescued from the water while on vacation. With a history of cardiac complications, Fred’s doctors were looking at his heart.
For Fred to get to his IPF diagnosis, it took the careful ear of a primary care doctor Fred started to see when his previous doctor retired.
“It was almost like she was listening with different ears and was hearing what others didn’t. Once she recommended speaking with a pulmonologist, everything fell into place,” said Fred. “From my experience, IPF is best treated by a lot of pieces coming together and working together. It takes the dedication of a care team in the hospital, proper diet and exercise and, just as importantly, it takes a support group to guide you through the process. I’m grateful to my care team, but I’m equally thankful for the work I get to do as an advocate for others living with IPF.”
When she spoke to the attendees, Lisa Moores, MD, FCCP, reflected on what the patients shared. “We saw great examples of why we’re here tonight,” said Dr. Moores. “One of the things CHEST and the Foundation are focusing on is earlier diagnosis for interstitial lung diseases like pulmonary fibrosis and, with voices like Fred Schick, we’ll get there. The patients remind us why we’re here. We’re here for our patients; we’re here for Fred; and we’re here for Betsy.”
Laurence Feldman, Vice President of the Feldman Family Foundation that partners with the CHEST Foundation for their annual casino fundraiser benefiting pulmonary fibrosis, was able to participate in the dinner and theauction.
He shared, “Tonight, I was so impressed with the generosity of the attendees and the organization of this event. It reminded me that if you ask your supporters to give, they’ll be there for you. Almost like the ‘Field of Dreams’ quote of ‘if you build it, they will come.’ Being at the Belmont Stakes Dinner and Auction makes me that much more excited for our upcoming Irv Feldman Casino Night and Texas Hold ‘Em Tournament coming up in late August. Thanks to our corporate partners and the support of the CHEST Foundation, we’re able to produce an excellent event like the Belmont Stakes fundraiser that helps bring in donations that can make a difference in the lives of patients.”
At the end of the day, medicine is all about the patients and, by dedicating the night to patient education and patient advocates, the Belmont Stakes event brought the focus to where it should always be – improving care and helping patients.
To learn more and to support the various initiatives of the CHEST Foundation, visit foundation.chestnet.org/donate.