User login
EUS-guided gallbladder drainage for acute cholecystitis
Percutaneous transhepatic gallbladder drainage (PT-GBD) is the most common, nonoperative method for gallbladder decompression in patients unfit for cholecystectomy. However, drain-related complications (20%-75%), including tube changes, dyscosmesis, discomfort, and recurrent cholecystitis (up to 15%), limit its long-term use. Endoscopic transpapillary gallbladder drainage (ET-GBD) and now, endoscopic ultrasound–guided gallbladder drainage (EUS-GBD), have emerged as options.
ET-GBD is performed at endoscopic retrograde cholangiopancreatography (ERCP) by cannulating the cystic duct, allowing placement of a pigtail plastic stent into the gallbladder. However, obstructing pathology (stone, stricture, metal stent or mass) may result in lower technical and clinical success when compared with EUS-GBD (84% vs. 98% and 91% vs. 97%, respectively). Furthermore, it does not allow for treatment of gallstones, and may require stent exchanges.

EUS-GBD involves placing a stent from the duodenum/stomach into the gallbladder under EUS guidance. Initial use of pigtail plastic stents and biliary self-expandable metal stents were not ideal, because of their risk of leakage, longer length (contralateral wall injury, occlusions), and migration (lack of flanges). Lumen-apposing metal stents (LAMS) overcame these limitations because of their short length and large flanges, and their large diameters (up to 20 mm) aid passage of gallstones or cholecystoscopy. Several case series and comparative trials have been published on EUS-GBD including a randomized prospective trial of EUS-GBD vs. PT-GBD demonstrating its superiority. Adverse events are uncommon and include misdeployments, bleeding, perforation, bile leaks, occlusion (commonly with food, prompting some endoscopists to place pigtails stents through the LAMS and avoiding the stomach as a target), and migration.
EUS-GBD should be avoided in patients who have a perforated gallbladder, have large volume ascites, or are too sick to tolerate anesthesia. Although there are patients who have subsequently undergone cholecystectomy post EUS-GBD, a discussion with one’s surgeon must be had prior to choosing this approach over ET-GBD.
In conclusion, determining the ideal method for endoscopic GBD in high-surgical-risk patients requires consideration of comorbidities, anatomy (GB position, cystic duct characteristics), presence of ascites, future surgical candidacy, and local expertise. ET-GBD should be prioritized for patients requiring ERCP for alternative reasons, large volume ascites, and as a bridge to cholecystectomy. Conversely, EUS-GBD is preferred with indwelling metal biliary stents covering the cystic duct and/or high-volume cholelithiasis. LAMS can be left long term; however, in patients willing to undergo an additional procedure, exchanging the LAMS for plastic stents can be undertaken at 4-6 weeks. Ultimately, more randomized and prospective data are needed to compare ET- and EUS-GBD outcomes, including a formal cost analysis.
Dr. Irani is with Virginia Mason Medical Center, Seattle. He reports being a consultant for Boston Scientific and Gore, as well as remittance to his clinic. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
Percutaneous transhepatic gallbladder drainage (PT-GBD) is the most common, nonoperative method for gallbladder decompression in patients unfit for cholecystectomy. However, drain-related complications (20%-75%), including tube changes, dyscosmesis, discomfort, and recurrent cholecystitis (up to 15%), limit its long-term use. Endoscopic transpapillary gallbladder drainage (ET-GBD) and now, endoscopic ultrasound–guided gallbladder drainage (EUS-GBD), have emerged as options.
ET-GBD is performed at endoscopic retrograde cholangiopancreatography (ERCP) by cannulating the cystic duct, allowing placement of a pigtail plastic stent into the gallbladder. However, obstructing pathology (stone, stricture, metal stent or mass) may result in lower technical and clinical success when compared with EUS-GBD (84% vs. 98% and 91% vs. 97%, respectively). Furthermore, it does not allow for treatment of gallstones, and may require stent exchanges.
EUS-GBD involves placing a stent from the duodenum/stomach into the gallbladder under EUS guidance. Initial use of pigtail plastic stents and biliary self-expandable metal stents were not ideal, because of their risk of leakage, longer length (contralateral wall injury, occlusions), and migration (lack of flanges). Lumen-apposing metal stents (LAMS) overcame these limitations because of their short length and large flanges, and their large diameters (up to 20 mm) aid passage of gallstones or cholecystoscopy. Several case series and comparative trials have been published on EUS-GBD including a randomized prospective trial of EUS-GBD vs. PT-GBD demonstrating its superiority. Adverse events are uncommon and include misdeployments, bleeding, perforation, bile leaks, occlusion (commonly with food, prompting some endoscopists to place pigtails stents through the LAMS and avoiding the stomach as a target), and migration.
EUS-GBD should be avoided in patients who have a perforated gallbladder, have large volume ascites, or are too sick to tolerate anesthesia. Although there are patients who have subsequently undergone cholecystectomy post EUS-GBD, a discussion with one’s surgeon must be had prior to choosing this approach over ET-GBD.
In conclusion, determining the ideal method for endoscopic GBD in high-surgical-risk patients requires consideration of comorbidities, anatomy (GB position, cystic duct characteristics), presence of ascites, future surgical candidacy, and local expertise. ET-GBD should be prioritized for patients requiring ERCP for alternative reasons, large volume ascites, and as a bridge to cholecystectomy. Conversely, EUS-GBD is preferred with indwelling metal biliary stents covering the cystic duct and/or high-volume cholelithiasis. LAMS can be left long term; however, in patients willing to undergo an additional procedure, exchanging the LAMS for plastic stents can be undertaken at 4-6 weeks. Ultimately, more randomized and prospective data are needed to compare ET- and EUS-GBD outcomes, including a formal cost analysis.
Dr. Irani is with Virginia Mason Medical Center, Seattle. He reports being a consultant for Boston Scientific and Gore, as well as remittance to his clinic. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
Percutaneous transhepatic gallbladder drainage (PT-GBD) is the most common, nonoperative method for gallbladder decompression in patients unfit for cholecystectomy. However, drain-related complications (20%-75%), including tube changes, dyscosmesis, discomfort, and recurrent cholecystitis (up to 15%), limit its long-term use. Endoscopic transpapillary gallbladder drainage (ET-GBD) and now, endoscopic ultrasound–guided gallbladder drainage (EUS-GBD), have emerged as options.
ET-GBD is performed at endoscopic retrograde cholangiopancreatography (ERCP) by cannulating the cystic duct, allowing placement of a pigtail plastic stent into the gallbladder. However, obstructing pathology (stone, stricture, metal stent or mass) may result in lower technical and clinical success when compared with EUS-GBD (84% vs. 98% and 91% vs. 97%, respectively). Furthermore, it does not allow for treatment of gallstones, and may require stent exchanges.
EUS-GBD involves placing a stent from the duodenum/stomach into the gallbladder under EUS guidance. Initial use of pigtail plastic stents and biliary self-expandable metal stents were not ideal, because of their risk of leakage, longer length (contralateral wall injury, occlusions), and migration (lack of flanges). Lumen-apposing metal stents (LAMS) overcame these limitations because of their short length and large flanges, and their large diameters (up to 20 mm) aid passage of gallstones or cholecystoscopy. Several case series and comparative trials have been published on EUS-GBD including a randomized prospective trial of EUS-GBD vs. PT-GBD demonstrating its superiority. Adverse events are uncommon and include misdeployments, bleeding, perforation, bile leaks, occlusion (commonly with food, prompting some endoscopists to place pigtails stents through the LAMS and avoiding the stomach as a target), and migration.
EUS-GBD should be avoided in patients who have a perforated gallbladder, have large volume ascites, or are too sick to tolerate anesthesia. Although there are patients who have subsequently undergone cholecystectomy post EUS-GBD, a discussion with one’s surgeon must be had prior to choosing this approach over ET-GBD.
In conclusion, determining the ideal method for endoscopic GBD in high-surgical-risk patients requires consideration of comorbidities, anatomy (GB position, cystic duct characteristics), presence of ascites, future surgical candidacy, and local expertise. ET-GBD should be prioritized for patients requiring ERCP for alternative reasons, large volume ascites, and as a bridge to cholecystectomy. Conversely, EUS-GBD is preferred with indwelling metal biliary stents covering the cystic duct and/or high-volume cholelithiasis. LAMS can be left long term; however, in patients willing to undergo an additional procedure, exchanging the LAMS for plastic stents can be undertaken at 4-6 weeks. Ultimately, more randomized and prospective data are needed to compare ET- and EUS-GBD outcomes, including a formal cost analysis.
Dr. Irani is with Virginia Mason Medical Center, Seattle. He reports being a consultant for Boston Scientific and Gore, as well as remittance to his clinic. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
AT DDW 2022
An approach to germline genetic testing in your practice
Traditionally, a hereditary colorectal cancer syndrome (HCCS) was suspected in individuals with an obvious personal and/or family cancer phenotype informed by a three-generation family cancer history. Family history is still required to inform cancer risk. Documentation of age at cancer diagnosis, age of relatives’ deaths, and key intestinal and extraintestinal features of a HCCS (for example, macrocephaly, café au lait spots, polyp number, size, and histology) are requisite. Historically, Sanger sequencing was used to determine the presence of a suspected single pathogenic germline variant (PGV). If no PGV was detected, another PGV would be sought. This old “single gene/single syndrome” testing was expensive, time consuming, and inefficient, and has been supplanted by multigene cancer panel testing (MGPT). MGPT-driven low-cost, high-throughput testing has widespread insurance coverage in eligible patients. Since considerable clinical phenotypic overlap exists between HCCSs, casting a broader net for determining PGV, compared with a more limited approach, allows for greater identification of carriers of PGV as well as variants of uncertain significance.
The frequency of PGV detection by MGPT in individuals with CRC is dependent on age at diagnosis and presence of DNA mismatch repair (MMR) deficiency in the tumor. According to one review, PGVs on MGPT are detected in approximately 10% and 34% of individuals aged more than 50 and more than 35 years, respectively.1 Pearlman and colleagues performed MGPT in 450 patients with CRC less than 50 years.2 PGV were found in 8% and 83.3% of cases with MMR-proficient and -deficient tumors, respectively. Overall, 33.3% of patients did not meet genetic testing criteria for the gene in which a PGV was detected, raising the impetus to consider MGPT in all patients with CRC. The Collaborative Group of the Americas on Inherited Gastrointestinal Cancer and National Comprehensive Cancer Network provide guidance on who warrants PGV testing.3,4
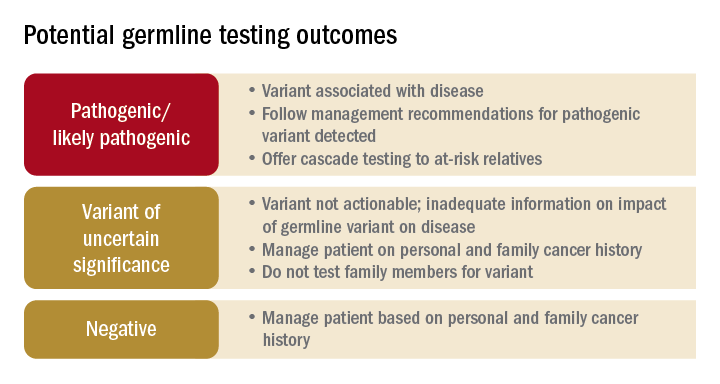
Germline testing outcomes and general approaches to patient management are provided in the graphic. HCCS are common and MGPT has broadened the identification of carriers of PGVs. In spite of advances in genetic testing technology, family history remains crucial to deploying risk-mitigation measures, regardless of the results of genetic testing.

Dr. Burke is in the department of gastroenterology, hepatology, and nutrition at the Cleveland Clinic. She disclosed ties to Janssen Pharma, Emtora Biosciences, Freenome, SLA Pharma, and Ambry Genetics. Dr. Burke is a member of the U.S. Multi-Society Task Force on Colorectal Cancer, National Comprehensive Cancer Network Guideline on Genetic/Familial High-Risk Assessment: Colorectal. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
References
1. Stoffel E and Murphy CC. Gastroenterology. 2020 Jan;158(2):341-353.
2. Pearlman R et al. JAMA Oncol. 2017 Apr 1;3(4):464-471.
3. Heald B et al. Fam Cancer. 2020 Jul;19(3):223-239.
4. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Colorectal Version 1.2022. 2022 Jun 8.
Traditionally, a hereditary colorectal cancer syndrome (HCCS) was suspected in individuals with an obvious personal and/or family cancer phenotype informed by a three-generation family cancer history. Family history is still required to inform cancer risk. Documentation of age at cancer diagnosis, age of relatives’ deaths, and key intestinal and extraintestinal features of a HCCS (for example, macrocephaly, café au lait spots, polyp number, size, and histology) are requisite. Historically, Sanger sequencing was used to determine the presence of a suspected single pathogenic germline variant (PGV). If no PGV was detected, another PGV would be sought. This old “single gene/single syndrome” testing was expensive, time consuming, and inefficient, and has been supplanted by multigene cancer panel testing (MGPT). MGPT-driven low-cost, high-throughput testing has widespread insurance coverage in eligible patients. Since considerable clinical phenotypic overlap exists between HCCSs, casting a broader net for determining PGV, compared with a more limited approach, allows for greater identification of carriers of PGV as well as variants of uncertain significance.
The frequency of PGV detection by MGPT in individuals with CRC is dependent on age at diagnosis and presence of DNA mismatch repair (MMR) deficiency in the tumor. According to one review, PGVs on MGPT are detected in approximately 10% and 34% of individuals aged more than 50 and more than 35 years, respectively.1 Pearlman and colleagues performed MGPT in 450 patients with CRC less than 50 years.2 PGV were found in 8% and 83.3% of cases with MMR-proficient and -deficient tumors, respectively. Overall, 33.3% of patients did not meet genetic testing criteria for the gene in which a PGV was detected, raising the impetus to consider MGPT in all patients with CRC. The Collaborative Group of the Americas on Inherited Gastrointestinal Cancer and National Comprehensive Cancer Network provide guidance on who warrants PGV testing.3,4
Germline testing outcomes and general approaches to patient management are provided in the graphic. HCCS are common and MGPT has broadened the identification of carriers of PGVs. In spite of advances in genetic testing technology, family history remains crucial to deploying risk-mitigation measures, regardless of the results of genetic testing.
Dr. Burke is in the department of gastroenterology, hepatology, and nutrition at the Cleveland Clinic. She disclosed ties to Janssen Pharma, Emtora Biosciences, Freenome, SLA Pharma, and Ambry Genetics. Dr. Burke is a member of the U.S. Multi-Society Task Force on Colorectal Cancer, National Comprehensive Cancer Network Guideline on Genetic/Familial High-Risk Assessment: Colorectal. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
References
1. Stoffel E and Murphy CC. Gastroenterology. 2020 Jan;158(2):341-353.
2. Pearlman R et al. JAMA Oncol. 2017 Apr 1;3(4):464-471.
3. Heald B et al. Fam Cancer. 2020 Jul;19(3):223-239.
4. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Colorectal Version 1.2022. 2022 Jun 8.
Traditionally, a hereditary colorectal cancer syndrome (HCCS) was suspected in individuals with an obvious personal and/or family cancer phenotype informed by a three-generation family cancer history. Family history is still required to inform cancer risk. Documentation of age at cancer diagnosis, age of relatives’ deaths, and key intestinal and extraintestinal features of a HCCS (for example, macrocephaly, café au lait spots, polyp number, size, and histology) are requisite. Historically, Sanger sequencing was used to determine the presence of a suspected single pathogenic germline variant (PGV). If no PGV was detected, another PGV would be sought. This old “single gene/single syndrome” testing was expensive, time consuming, and inefficient, and has been supplanted by multigene cancer panel testing (MGPT). MGPT-driven low-cost, high-throughput testing has widespread insurance coverage in eligible patients. Since considerable clinical phenotypic overlap exists between HCCSs, casting a broader net for determining PGV, compared with a more limited approach, allows for greater identification of carriers of PGV as well as variants of uncertain significance.
The frequency of PGV detection by MGPT in individuals with CRC is dependent on age at diagnosis and presence of DNA mismatch repair (MMR) deficiency in the tumor. According to one review, PGVs on MGPT are detected in approximately 10% and 34% of individuals aged more than 50 and more than 35 years, respectively.1 Pearlman and colleagues performed MGPT in 450 patients with CRC less than 50 years.2 PGV were found in 8% and 83.3% of cases with MMR-proficient and -deficient tumors, respectively. Overall, 33.3% of patients did not meet genetic testing criteria for the gene in which a PGV was detected, raising the impetus to consider MGPT in all patients with CRC. The Collaborative Group of the Americas on Inherited Gastrointestinal Cancer and National Comprehensive Cancer Network provide guidance on who warrants PGV testing.3,4
Germline testing outcomes and general approaches to patient management are provided in the graphic. HCCS are common and MGPT has broadened the identification of carriers of PGVs. In spite of advances in genetic testing technology, family history remains crucial to deploying risk-mitigation measures, regardless of the results of genetic testing.
Dr. Burke is in the department of gastroenterology, hepatology, and nutrition at the Cleveland Clinic. She disclosed ties to Janssen Pharma, Emtora Biosciences, Freenome, SLA Pharma, and Ambry Genetics. Dr. Burke is a member of the U.S. Multi-Society Task Force on Colorectal Cancer, National Comprehensive Cancer Network Guideline on Genetic/Familial High-Risk Assessment: Colorectal. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
References
1. Stoffel E and Murphy CC. Gastroenterology. 2020 Jan;158(2):341-353.
2. Pearlman R et al. JAMA Oncol. 2017 Apr 1;3(4):464-471.
3. Heald B et al. Fam Cancer. 2020 Jul;19(3):223-239.
4. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Colorectal Version 1.2022. 2022 Jun 8.
AT DDW 2022
What is new in cirrhosis management? From frailty to palliative care
There is a rich science around the management of the cirrhotic liver itself – for example, pragmatic prognostic markers such as MELDNa, data-driven strategies to prevent variceal bleeding, and well-utilized algorithms to manage ascites.

But what is new in cirrhosis management is an emerging science around the management of the person living with cirrhosis – a science that seeks to understand how these individuals function in their day-to-day lives, how they feel, and how they can best prepare for their future. What is so exciting is that the field is moving beyond simply understanding those complex aspects of the patient, which is important in and of itself, toward developing practical tools to help clinicians assess their patients’ symptoms and strategies to help improve their patients’ lived experience. Although terms such as “frailty,” “palliative care,” and “advance care planning” are not new in cirrhosis per se, they are now recognized as distinct patient-centered constructs that are highly relevant to the management of patients with cirrhosis. Furthermore, these constructs have been codified through two recent guidance statements sponsored by the American Association for the Study of Liver Diseases.1,2 Pragmatic tools are emerging to facilitate the integration of these patient-centered constructs into routine clinical practice, tools such as the Liver Frailty Index, the Edmonton Symptom Assessment System adapted for patients with cirrhosis, and structured frameworks for guiding goals-of-care discussions. The incorporation of these tools allows for new management strategies directed toward improving the patient’s experience such as timely initiation of nutrition and activity-based interventions, algorithms for pharmacologic and nonpharmacologic strategies for symptom management, and online/video-guided approaches to articulating one’s goals of care.
So, what is new in cirrhosis management is that we are moving beyond managing the cirrhotic liver itself to considering how cirrhosis and its complications impact the patient as a whole. In doing so, we are turning the art of hepatology care into science that can be applied systematically at the bedside for every patient, with the goal of improving care for all patients living with cirrhosis.
Dr. Lai holds the Endowed Professorship of Liver Health and Transplantation at the University of California, San Francisco. She reports having no conflicts of interest. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
References
1. Lai JC et al. Hepatology. 2021 Sep;74(3):1611-44.
2. Rogal S et al. Hepatology. 2022 Feb 1. doi: 10.1002/hep.32378.
There is a rich science around the management of the cirrhotic liver itself – for example, pragmatic prognostic markers such as MELDNa, data-driven strategies to prevent variceal bleeding, and well-utilized algorithms to manage ascites.
But what is new in cirrhosis management is an emerging science around the management of the person living with cirrhosis – a science that seeks to understand how these individuals function in their day-to-day lives, how they feel, and how they can best prepare for their future. What is so exciting is that the field is moving beyond simply understanding those complex aspects of the patient, which is important in and of itself, toward developing practical tools to help clinicians assess their patients’ symptoms and strategies to help improve their patients’ lived experience. Although terms such as “frailty,” “palliative care,” and “advance care planning” are not new in cirrhosis per se, they are now recognized as distinct patient-centered constructs that are highly relevant to the management of patients with cirrhosis. Furthermore, these constructs have been codified through two recent guidance statements sponsored by the American Association for the Study of Liver Diseases.1,2 Pragmatic tools are emerging to facilitate the integration of these patient-centered constructs into routine clinical practice, tools such as the Liver Frailty Index, the Edmonton Symptom Assessment System adapted for patients with cirrhosis, and structured frameworks for guiding goals-of-care discussions. The incorporation of these tools allows for new management strategies directed toward improving the patient’s experience such as timely initiation of nutrition and activity-based interventions, algorithms for pharmacologic and nonpharmacologic strategies for symptom management, and online/video-guided approaches to articulating one’s goals of care.
So, what is new in cirrhosis management is that we are moving beyond managing the cirrhotic liver itself to considering how cirrhosis and its complications impact the patient as a whole. In doing so, we are turning the art of hepatology care into science that can be applied systematically at the bedside for every patient, with the goal of improving care for all patients living with cirrhosis.
Dr. Lai holds the Endowed Professorship of Liver Health and Transplantation at the University of California, San Francisco. She reports having no conflicts of interest. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
References
1. Lai JC et al. Hepatology. 2021 Sep;74(3):1611-44.
2. Rogal S et al. Hepatology. 2022 Feb 1. doi: 10.1002/hep.32378.
There is a rich science around the management of the cirrhotic liver itself – for example, pragmatic prognostic markers such as MELDNa, data-driven strategies to prevent variceal bleeding, and well-utilized algorithms to manage ascites.
But what is new in cirrhosis management is an emerging science around the management of the person living with cirrhosis – a science that seeks to understand how these individuals function in their day-to-day lives, how they feel, and how they can best prepare for their future. What is so exciting is that the field is moving beyond simply understanding those complex aspects of the patient, which is important in and of itself, toward developing practical tools to help clinicians assess their patients’ symptoms and strategies to help improve their patients’ lived experience. Although terms such as “frailty,” “palliative care,” and “advance care planning” are not new in cirrhosis per se, they are now recognized as distinct patient-centered constructs that are highly relevant to the management of patients with cirrhosis. Furthermore, these constructs have been codified through two recent guidance statements sponsored by the American Association for the Study of Liver Diseases.1,2 Pragmatic tools are emerging to facilitate the integration of these patient-centered constructs into routine clinical practice, tools such as the Liver Frailty Index, the Edmonton Symptom Assessment System adapted for patients with cirrhosis, and structured frameworks for guiding goals-of-care discussions. The incorporation of these tools allows for new management strategies directed toward improving the patient’s experience such as timely initiation of nutrition and activity-based interventions, algorithms for pharmacologic and nonpharmacologic strategies for symptom management, and online/video-guided approaches to articulating one’s goals of care.
So, what is new in cirrhosis management is that we are moving beyond managing the cirrhotic liver itself to considering how cirrhosis and its complications impact the patient as a whole. In doing so, we are turning the art of hepatology care into science that can be applied systematically at the bedside for every patient, with the goal of improving care for all patients living with cirrhosis.
Dr. Lai holds the Endowed Professorship of Liver Health and Transplantation at the University of California, San Francisco. She reports having no conflicts of interest. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
References
1. Lai JC et al. Hepatology. 2021 Sep;74(3):1611-44.
2. Rogal S et al. Hepatology. 2022 Feb 1. doi: 10.1002/hep.32378.
AT DDW 2022
Barrett’s esophagus: Key new concepts
Barrett’s esophagus (BE) is the only known precursor of esophageal adenocarcinoma (EAC). The rationale for early detection of BE rests on the premise that, after the diagnosis of BE, patients can be placed under endoscopic surveillance to detect prevalent and incident dysplasia and EAC. Randomized controlled trials have demonstrated that endoscopic eradication therapy (EET) of low-grade dysplasia (LGD) and high-grade dysplasia (HGD) can reduce progression to EAC. Guidelines support endoscopic screening for BE in those with multiple (three or more) risk factors.
However, endoscopy is expensive, invasive, and not widely utilized (less than 10% of those eligible are screened). Most patients with BE are unaware of their diagnosis and hence not under surveillance. Nonendoscopic techniques of BE detection – swallowed cell collection devices providing rich esophageal cytology specimens combined with biomarkers – are being developed. Case-control studies have shown promising accuracy and a recent UK pragmatic primary care study showed the ability of this technology to increase BE detection safely.

Detection of dysplasia in endoscopic surveillance is critical and the neoplasia detection rate (NDR) has been recently proposed as a quality marker. The NDR is the ratio of HGD+EAC detected to all patients with BE undergoing their first surveillance endoscopy. A recent systematic review and meta-analysis showed an inverse association between NDR and postendoscopy BE neoplasia. Additional and prospective studies are required to further correlate NDR values to clinically relevant outcomes similar to the association between adenoma detection rate and postcolonoscopy colorectal cancer.
Detection of dysplasia with endoscopic surveillance is challenging because of sampling error inherent in the Seattle protocol. A recent technology, Wide Area Transepithelial Sampling–3D (WATS), combines the concept of increased sampling of the BE mucosa by using a stiff endoscopic brush followed by use of artificial intelligence neural network enabled selection of abnormal cells, which are presented to a pathologist. This technology has been shown to increase dysplasia and HGD detection, compared to endoscopic surveillance, in a systematic review and meta-analysis. However, WATS is negative in a substantial proportion of cases in which endoscopic Seattle protocol reveals dysplasia. In addition, only limited data are available on the natural history of WATS LGD or HGD. Confirmation of WATS-only dysplasia (LGD, HGD, or EAC) by endoscopic histology is also recommended before the institution of EET. Finally, assessment of progression risk in those with BE is critical to enable more personalized follow up recommendations. Clinical risk scores integrating age, sex, smoking history, and LGD have been proposed and validated. A recent tissue systems pathology test has been shown in multiple case-control studies to identify a subset of BE patients who are at higher risk of progression, independent of LGD. This test is highly specific but only modestly sensitive in identifying progressors.
Dr. Iyer is professor of medicine, director of the Esophageal Interest Group, and codirector of the Advanced Esophageal Fellowship at the Mayo Clinic College of Medicine and Science, Rochester, Minn. He reports relationships with Exact Sciences, Pentax Medical, and others. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
Barrett’s esophagus (BE) is the only known precursor of esophageal adenocarcinoma (EAC). The rationale for early detection of BE rests on the premise that, after the diagnosis of BE, patients can be placed under endoscopic surveillance to detect prevalent and incident dysplasia and EAC. Randomized controlled trials have demonstrated that endoscopic eradication therapy (EET) of low-grade dysplasia (LGD) and high-grade dysplasia (HGD) can reduce progression to EAC. Guidelines support endoscopic screening for BE in those with multiple (three or more) risk factors.
However, endoscopy is expensive, invasive, and not widely utilized (less than 10% of those eligible are screened). Most patients with BE are unaware of their diagnosis and hence not under surveillance. Nonendoscopic techniques of BE detection – swallowed cell collection devices providing rich esophageal cytology specimens combined with biomarkers – are being developed. Case-control studies have shown promising accuracy and a recent UK pragmatic primary care study showed the ability of this technology to increase BE detection safely.
Detection of dysplasia in endoscopic surveillance is critical and the neoplasia detection rate (NDR) has been recently proposed as a quality marker. The NDR is the ratio of HGD+EAC detected to all patients with BE undergoing their first surveillance endoscopy. A recent systematic review and meta-analysis showed an inverse association between NDR and postendoscopy BE neoplasia. Additional and prospective studies are required to further correlate NDR values to clinically relevant outcomes similar to the association between adenoma detection rate and postcolonoscopy colorectal cancer.
Detection of dysplasia with endoscopic surveillance is challenging because of sampling error inherent in the Seattle protocol. A recent technology, Wide Area Transepithelial Sampling–3D (WATS), combines the concept of increased sampling of the BE mucosa by using a stiff endoscopic brush followed by use of artificial intelligence neural network enabled selection of abnormal cells, which are presented to a pathologist. This technology has been shown to increase dysplasia and HGD detection, compared to endoscopic surveillance, in a systematic review and meta-analysis. However, WATS is negative in a substantial proportion of cases in which endoscopic Seattle protocol reveals dysplasia. In addition, only limited data are available on the natural history of WATS LGD or HGD. Confirmation of WATS-only dysplasia (LGD, HGD, or EAC) by endoscopic histology is also recommended before the institution of EET. Finally, assessment of progression risk in those with BE is critical to enable more personalized follow up recommendations. Clinical risk scores integrating age, sex, smoking history, and LGD have been proposed and validated. A recent tissue systems pathology test has been shown in multiple case-control studies to identify a subset of BE patients who are at higher risk of progression, independent of LGD. This test is highly specific but only modestly sensitive in identifying progressors.
Dr. Iyer is professor of medicine, director of the Esophageal Interest Group, and codirector of the Advanced Esophageal Fellowship at the Mayo Clinic College of Medicine and Science, Rochester, Minn. He reports relationships with Exact Sciences, Pentax Medical, and others. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
Barrett’s esophagus (BE) is the only known precursor of esophageal adenocarcinoma (EAC). The rationale for early detection of BE rests on the premise that, after the diagnosis of BE, patients can be placed under endoscopic surveillance to detect prevalent and incident dysplasia and EAC. Randomized controlled trials have demonstrated that endoscopic eradication therapy (EET) of low-grade dysplasia (LGD) and high-grade dysplasia (HGD) can reduce progression to EAC. Guidelines support endoscopic screening for BE in those with multiple (three or more) risk factors.
However, endoscopy is expensive, invasive, and not widely utilized (less than 10% of those eligible are screened). Most patients with BE are unaware of their diagnosis and hence not under surveillance. Nonendoscopic techniques of BE detection – swallowed cell collection devices providing rich esophageal cytology specimens combined with biomarkers – are being developed. Case-control studies have shown promising accuracy and a recent UK pragmatic primary care study showed the ability of this technology to increase BE detection safely.
Detection of dysplasia in endoscopic surveillance is critical and the neoplasia detection rate (NDR) has been recently proposed as a quality marker. The NDR is the ratio of HGD+EAC detected to all patients with BE undergoing their first surveillance endoscopy. A recent systematic review and meta-analysis showed an inverse association between NDR and postendoscopy BE neoplasia. Additional and prospective studies are required to further correlate NDR values to clinically relevant outcomes similar to the association between adenoma detection rate and postcolonoscopy colorectal cancer.
Detection of dysplasia with endoscopic surveillance is challenging because of sampling error inherent in the Seattle protocol. A recent technology, Wide Area Transepithelial Sampling–3D (WATS), combines the concept of increased sampling of the BE mucosa by using a stiff endoscopic brush followed by use of artificial intelligence neural network enabled selection of abnormal cells, which are presented to a pathologist. This technology has been shown to increase dysplasia and HGD detection, compared to endoscopic surveillance, in a systematic review and meta-analysis. However, WATS is negative in a substantial proportion of cases in which endoscopic Seattle protocol reveals dysplasia. In addition, only limited data are available on the natural history of WATS LGD or HGD. Confirmation of WATS-only dysplasia (LGD, HGD, or EAC) by endoscopic histology is also recommended before the institution of EET. Finally, assessment of progression risk in those with BE is critical to enable more personalized follow up recommendations. Clinical risk scores integrating age, sex, smoking history, and LGD have been proposed and validated. A recent tissue systems pathology test has been shown in multiple case-control studies to identify a subset of BE patients who are at higher risk of progression, independent of LGD. This test is highly specific but only modestly sensitive in identifying progressors.
Dr. Iyer is professor of medicine, director of the Esophageal Interest Group, and codirector of the Advanced Esophageal Fellowship at the Mayo Clinic College of Medicine and Science, Rochester, Minn. He reports relationships with Exact Sciences, Pentax Medical, and others. These remarks were made during one of the AGA Postgraduate Course sessions held at DDW 2022.
AT DDW 2022
Memorial and honorary gifts: A special tribute
Honor a family member, friend, or colleague while supporting the work of our mission through a gift to the AGA Research Foundation. Your gift will honor a loved one or yourself and support the AGA Research Awards Program, while giving you a tax benefit. The AGA Research Awards program recruits, retains, and supports the most promising investigators in gastroenterology and hepatology.
- Giving now or later. Any charitable gift can be made in honor or memory of someone.
- A gift today. An outright gift will help support researchers working toward developing new treatments and diagnostics for patients with GI conditions. Your gift will assist in fostering a new pipeline of scientists – the next generation of leaders in GI. The financial benefits include an income tax deduction and possible elimination of capital gains tax.
- A gift through your will or living trust. You can include a bequest in your will or living trust stating that a specific asset, certain dollar amount, or more commonly, a percentage of your estate will pass to the AGA Research Foundation at your death in honor of your loved one.
Conclusion
Your gift directly supports talented young researchers working to advance our understanding of digestive diseases. Make a tax-deductible donation to help spur innovation. Donate today at www.gastro.org/donateonline.
Honor a family member, friend, or colleague while supporting the work of our mission through a gift to the AGA Research Foundation. Your gift will honor a loved one or yourself and support the AGA Research Awards Program, while giving you a tax benefit. The AGA Research Awards program recruits, retains, and supports the most promising investigators in gastroenterology and hepatology.
- Giving now or later. Any charitable gift can be made in honor or memory of someone.
- A gift today. An outright gift will help support researchers working toward developing new treatments and diagnostics for patients with GI conditions. Your gift will assist in fostering a new pipeline of scientists – the next generation of leaders in GI. The financial benefits include an income tax deduction and possible elimination of capital gains tax.
- A gift through your will or living trust. You can include a bequest in your will or living trust stating that a specific asset, certain dollar amount, or more commonly, a percentage of your estate will pass to the AGA Research Foundation at your death in honor of your loved one.
Conclusion
Your gift directly supports talented young researchers working to advance our understanding of digestive diseases. Make a tax-deductible donation to help spur innovation. Donate today at www.gastro.org/donateonline.
Honor a family member, friend, or colleague while supporting the work of our mission through a gift to the AGA Research Foundation. Your gift will honor a loved one or yourself and support the AGA Research Awards Program, while giving you a tax benefit. The AGA Research Awards program recruits, retains, and supports the most promising investigators in gastroenterology and hepatology.
- Giving now or later. Any charitable gift can be made in honor or memory of someone.
- A gift today. An outright gift will help support researchers working toward developing new treatments and diagnostics for patients with GI conditions. Your gift will assist in fostering a new pipeline of scientists – the next generation of leaders in GI. The financial benefits include an income tax deduction and possible elimination of capital gains tax.
- A gift through your will or living trust. You can include a bequest in your will or living trust stating that a specific asset, certain dollar amount, or more commonly, a percentage of your estate will pass to the AGA Research Foundation at your death in honor of your loved one.
Conclusion
Your gift directly supports talented young researchers working to advance our understanding of digestive diseases. Make a tax-deductible donation to help spur innovation. Donate today at www.gastro.org/donateonline.
CMS releases proposed payment rule
On July 15, for calendar year 2023.
AGA, along with the American College of Gastroenterology and the American Society for Gastrointestinal Endoscopy, have identified the following top three takeaways:
Slight increase in ASC payments – The proposed ASC conversion factor increases 2.7% to $51.315 for ASCs that meet quality reporting requirements.
Slight increase in facility fees payments – Hospitals that meet quality reporting requirements also receive a 2.7% proposed increase, which translates to $86.785 – a stark difference from the ASC payment.
18% cuts to some motility and G-tube codes – Hospital outpatient facility payments for motility codes 91117 and 91122 and G-tube codes 43761-43763 could decrease by 18% because of proposed changes to their Ambulatory Payment Classification (APC) family.
On July 15, for calendar year 2023.
AGA, along with the American College of Gastroenterology and the American Society for Gastrointestinal Endoscopy, have identified the following top three takeaways:
Slight increase in ASC payments – The proposed ASC conversion factor increases 2.7% to $51.315 for ASCs that meet quality reporting requirements.
Slight increase in facility fees payments – Hospitals that meet quality reporting requirements also receive a 2.7% proposed increase, which translates to $86.785 – a stark difference from the ASC payment.
18% cuts to some motility and G-tube codes – Hospital outpatient facility payments for motility codes 91117 and 91122 and G-tube codes 43761-43763 could decrease by 18% because of proposed changes to their Ambulatory Payment Classification (APC) family.
On July 15, for calendar year 2023.
AGA, along with the American College of Gastroenterology and the American Society for Gastrointestinal Endoscopy, have identified the following top three takeaways:
Slight increase in ASC payments – The proposed ASC conversion factor increases 2.7% to $51.315 for ASCs that meet quality reporting requirements.
Slight increase in facility fees payments – Hospitals that meet quality reporting requirements also receive a 2.7% proposed increase, which translates to $86.785 – a stark difference from the ASC payment.
18% cuts to some motility and G-tube codes – Hospital outpatient facility payments for motility codes 91117 and 91122 and G-tube codes 43761-43763 could decrease by 18% because of proposed changes to their Ambulatory Payment Classification (APC) family.
FDA okays spesolimab, first treatment for generalized pustular psoriasis
The U.S. Food and Drug Administration has approved the biologic agent spesolimab (Spevigo) for the treatment of flares in adults with generalized pustular psoriasis (GPP), the company that manufactures the drug has announced.
Until this approval, “there were no FDA-approved options to treat patients experiencing a GPP flare,” Mark Lebwohl, MD, principal investigator in the pivotal spesolimab trial, told this news organization. The approval “is a turning point for dermatologists and clinicians who treat patients living with this devastating and debilitating disease,” he said. Treatment with spesolimab “rapidly improves the clinical symptoms of GPP flares and will greatly improve our ability to help our patients manage painful flares,” noted Dr. Lebwohl, dean of clinical therapeutics and professor of dermatology, Icahn School of Medicine at Mount Sinai, New York.
Spesolimab, manufactured by Boehringer Ingelheim, is a novel, selective monoclonal antibody that blocks interleukin-36 signaling known to be involved in GPP. It received priority review and had orphan drug and breakthrough therapy designation.
GPP affects an estimated 1 of every 10,000 people in the United States.
Though rare, GPP is a potentially life-threatening disease that is distinct from plaque psoriasis. GPP is caused by the accumulation of neutrophils in the skin. Throughout the course of the disease, patients may suffer recurring episodes of widespread eruptions of painful, sterile pustules across all parts of the body.
Spesolimab was evaluated in a global, 12-week, placebo-controlled clinical trial that involved 53 adults experiencing a GPP flare. After 1 week, significantly more patients treated with spesolimab than placebo showed no visible pustules (54% vs 6%), according to the company.
The most common adverse reactions, seen in at least 5% of patients treated with spesolimab, were asthenia and fatigue; nausea and vomiting; headache; pruritus and prurigo; hematoma and bruising at the infusion site; and urinary tract infection.
Dr. Lebwohl is a paid consultant to Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
This article was updated 9/6/22.
The U.S. Food and Drug Administration has approved the biologic agent spesolimab (Spevigo) for the treatment of flares in adults with generalized pustular psoriasis (GPP), the company that manufactures the drug has announced.
Until this approval, “there were no FDA-approved options to treat patients experiencing a GPP flare,” Mark Lebwohl, MD, principal investigator in the pivotal spesolimab trial, told this news organization. The approval “is a turning point for dermatologists and clinicians who treat patients living with this devastating and debilitating disease,” he said. Treatment with spesolimab “rapidly improves the clinical symptoms of GPP flares and will greatly improve our ability to help our patients manage painful flares,” noted Dr. Lebwohl, dean of clinical therapeutics and professor of dermatology, Icahn School of Medicine at Mount Sinai, New York.
Spesolimab, manufactured by Boehringer Ingelheim, is a novel, selective monoclonal antibody that blocks interleukin-36 signaling known to be involved in GPP. It received priority review and had orphan drug and breakthrough therapy designation.
GPP affects an estimated 1 of every 10,000 people in the United States.
Though rare, GPP is a potentially life-threatening disease that is distinct from plaque psoriasis. GPP is caused by the accumulation of neutrophils in the skin. Throughout the course of the disease, patients may suffer recurring episodes of widespread eruptions of painful, sterile pustules across all parts of the body.
Spesolimab was evaluated in a global, 12-week, placebo-controlled clinical trial that involved 53 adults experiencing a GPP flare. After 1 week, significantly more patients treated with spesolimab than placebo showed no visible pustules (54% vs 6%), according to the company.
The most common adverse reactions, seen in at least 5% of patients treated with spesolimab, were asthenia and fatigue; nausea and vomiting; headache; pruritus and prurigo; hematoma and bruising at the infusion site; and urinary tract infection.
Dr. Lebwohl is a paid consultant to Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
This article was updated 9/6/22.
The U.S. Food and Drug Administration has approved the biologic agent spesolimab (Spevigo) for the treatment of flares in adults with generalized pustular psoriasis (GPP), the company that manufactures the drug has announced.
Until this approval, “there were no FDA-approved options to treat patients experiencing a GPP flare,” Mark Lebwohl, MD, principal investigator in the pivotal spesolimab trial, told this news organization. The approval “is a turning point for dermatologists and clinicians who treat patients living with this devastating and debilitating disease,” he said. Treatment with spesolimab “rapidly improves the clinical symptoms of GPP flares and will greatly improve our ability to help our patients manage painful flares,” noted Dr. Lebwohl, dean of clinical therapeutics and professor of dermatology, Icahn School of Medicine at Mount Sinai, New York.
Spesolimab, manufactured by Boehringer Ingelheim, is a novel, selective monoclonal antibody that blocks interleukin-36 signaling known to be involved in GPP. It received priority review and had orphan drug and breakthrough therapy designation.
GPP affects an estimated 1 of every 10,000 people in the United States.
Though rare, GPP is a potentially life-threatening disease that is distinct from plaque psoriasis. GPP is caused by the accumulation of neutrophils in the skin. Throughout the course of the disease, patients may suffer recurring episodes of widespread eruptions of painful, sterile pustules across all parts of the body.
Spesolimab was evaluated in a global, 12-week, placebo-controlled clinical trial that involved 53 adults experiencing a GPP flare. After 1 week, significantly more patients treated with spesolimab than placebo showed no visible pustules (54% vs 6%), according to the company.
The most common adverse reactions, seen in at least 5% of patients treated with spesolimab, were asthenia and fatigue; nausea and vomiting; headache; pruritus and prurigo; hematoma and bruising at the infusion site; and urinary tract infection.
Dr. Lebwohl is a paid consultant to Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
This article was updated 9/6/22.
A case for when, how, and why to evaluate capacity
Case
Ms. F. is a 68-year-old woman who presented to the hospital with sepsis, developed delirium, and stopped eating. Her clinicians recommended a PEG tube. Although she was inconsistently oriented to self, time, and place, she reiterated the same decision across multiple discussions: She did not want the PEG tube. Her replies to what would happen if she didn’t have the procedure and continued not to eat were consistent, too: “I’ll wither away.”
Ms. F. had impaired cognition. Do these impairments mean her clinicians should over-rule her choice? What evidence indicates whether she lacks decision-making capacity? This case of a patient refusing a potentially life-saving procedure amplifies the importance of asking these questions and integrating capacity assessments into clinical care. In this article, we will describe what capacity is, when and how to assess it, and the alternatives when a patient does not have capacity.
The ethical background
Before starting a medical treatment or procedure, a physician must obtain the patient’s informed consent. This is a core ethic of medicine. Informed consent describes the voluntary decision made by a competent patient following the disclosure of necessary information. Informed consent is key to achieving a balance between promoting patient self-determination and protecting vulnerable patients from harm. In most clinical encounters, informed consent unfolds effortlessly. However, in the care of patients who are acutely ill, particularly those in hospitals, fulfilling the ethic can be challenging.

It is important to have skills to recognize and address these challenges. One of the most common challenges to practicing the ethic of informed consent is the impact of illness on a person’s decision-making capacity. A patient who retains capacity ought to make his or her decisions and does not need someone else (a friend or a family member) to help with the decision.
Incapacity is unfortunately common among the acutely ill medical inpatient population, which typically skews older with more comorbidities.1 Impairments frequently are overlooked for a variety of reasons,2-6 including that many hospitalized patients do not challenge their doctors’ decisions. Doctors may be reluctant to assess capacity because the assessment may medically, legally, or ethically complicate the patient’s care.
Two common terms describe the outcome of an assessment of a patient’s decision-making abilities: competency and capacity. Competency describes a legal principle. It is granted or withdrawn by judicial review. The consequences of a judge rescinding competency are severe: A patient would need a guardian to make choices on his or her behalf.

Capacity, on the other hand, is a clinical concept. A physician assesses whether the patient can make a specific decision in a specific context. The difference between the two terms – competency and capacity – delineates what are the consequences of the assessment and which authority, a judge or a physician, has the right to withdraw a person’s decision-making authority.
The judge offers a global assessment that can lead to a guardianship. The physician’s decision is temporal and situational. Patients can lack capacity when they are ill and recover it when they are healed. Capacity is specific to each medical decision that the patient makes and so a person can lack capacity to make some decisions but not others.
Ethical framework to make assessment
Capacity is described by four decisional abilities: 1) communicate a choice, 2) understand relevant information, 3) appreciation, and 4) reasoning.7
Communication of a choice may be verbal or nonverbal, but the patient must be able to indicate the treatment choice clearly and consistently. Understanding describes knowing essential information a physician has conveyed. This is assessed by having the patients say back what they were told, such as: “Can you tell me in your own words what is a PEG tube?”
The components of appreciation are: the diagnosis or disorder and the benefits and risks of the proposed intervention as it relates to the diagnosis or disorder. Patients who appreciate their disorder have insight into their condition: “I’m not eating because I have an infection.” This can be assessed with a question such as: “Can you tell me in your own words what are the risks or downsides to you?” This prompt assesses the patient’s appreciation of risk. Reframing the question to ask, “Can you tell me about the upsides of this intervention?” will assess the patient’s appreciation of benefit.
Reasoning assesses the thought process and rationale for a person’s decision. It has two components – comparative and consequential reasoning. The first compares the different choices presented about the proposed intervention: “How does having a PEG tube compare to not having it?” The second asks about the consequences of each choice: “What might happen to a person who has the PEG tube?”
The capacity assessment evaluates a patient's performance on these decision-making abilities. This informs the clinician’s judgment of whether the patient has the capacity to make a decision. A patient who has capacity makes the choice, regardless of the physician’s preference or recommendation.
The physician’s duty is to decide which decision-making abilities to assess. Choice and understanding are essential. In riskier or more consequential decisions, a physician may raise the rigor of the assessment to include appreciation and reasoning.8 It is common practice for physicians to raise the standard for when to evaluate and how extensive their evaluation is when the decision is life-altering, as with a PEG tube versus a more routine, non–life-altering decision such as drawing blood for a routine wellness visit.
A simple scoring rubric determines the patient’s ability to answer each question along a range from adequate = 2, marginal = 1, to inadequate = 0. The extremes or adequate or inadequate are straightforward. Judgment is needed when performance is marginal. In the case of repeated marginal answers, a physician must strongly consider whether the patient lacks capacity to make the decision in question.9
Who receives a capacity assessment and when?
A good doctor is a good teacher. A doctor should therefore check that patients understand what is happening with their health. Assessing understanding is simply good medicine; for example, a good teacher ought to be asking an unimpaired patient without impaired cognition, “Can you say back to me the key points of what I explained?” With this approach, every patient is effectively “screened” for a capacity impairment.
Certain patients ought to trigger a more thorough examination of decisional abilities. Across multiple articles, the strongest factors associated with incapacity are older age and diminished cognitive function (often detected by MMSE scores below the low 20s).1,7,10 Other factors that may amplify these deficits and thus should raise clinician concern would be patients with brain diseases such as Alzheimer’s or Parkinson’s, persons with lower education levels, or those who already have someone who helps them make decisions. To be sure, many older adults, even those with cognitive impairments, retain capacity, but extra protection should be in place to ensure their well-being.
Consequences of incapacity
If a careful assessment shows a patient has sound decision-making abilities, the patient is free to make the choice. On the other hand, a person does not have the capacity to make the decision at hand if he or she cannot communicate a choice or understand relevant information. Whether appreciation or reasoning ought to be assessed depends on the complexity and the significance of the decision. An assessment of decisional ability is not the end of the decision-making process. The goal is to maximize the patient’s autonomy.
Capacity can change over time. Factors that may inhibit capacity, such as medications, time of day, and even illness acuity, need to be accounted for and, if possible, addressed. The decision ought to be delayed, if possible, to a time when the patient has better chances of having capacity. If it is unlikely that patients’ status will change in the time frame needed to make the choice and they are found to not have capacity, then the decision making can be aided by advance directives or substitute decision makers such as family members or legal guardians.
Revisiting the case
Ms. F., who was delirious, retained notable decisional abilities. She understood the procedure of receiving the PEG tube and how the risk of continuing to not eat and not receive the PEG would result in dying by starvation. She appreciated her own diagnosis and how the proposed intervention could alter her condition. She appreciated how not having a PEG would lead to her death. Her choice to refuse the procedure was consistent. Ms. F. showed she retained capacity to make this decision. It was the physician’s duty to respect her autonomy and so to respect her refusal of the PEG.
Dr. Ney is a physician resident, department of psychiatry and human behavior, Thomas Jefferson University Hospital, Philadelphia. He has no conflicts to disclose. Dr. Karlawish is a professor in the departments of medicine, medical ethics and health policy, and neurology, University of Pennsylvania, Philadelphia. He is a site investigator for clinical trials sponsored by Biogen, Eisai, and Lilly.
References
1. Raymont V et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: Cross-sectional study. Lancet. 2004;364(9443):1421-7. doi: 10.1016/S0140-6736(04)17224-3.
2. Hanson M and Pitt D. Informed consent for surgery: risk discussion and documentation. Can J Surg. 2017;60(1):69-70. doi: 10.1503/cjs.004816.
3. Dahlberg J et al. Lack of informed consent for surgical procedures by elderly patients with inability to consent: A retrospective chart review from an academic medical center in Norway. Patient Saf Surg. 2019;13:24. doi: 10.1186/s13037-019-0205-5.
4. Sessums LL et al. Does this patient have medical decision-making capacity? JAMA. 2011;306(4):420-7. doi: 10.1001/jama.2011.1023.
5. Terranova C et al. Ethical and medicolegal implications of capacity of patients in geriatric surgery. Med Sci Law. 2013;53(3):166-71. doi: 10.1177/0025802412473963.
6. John S et al. Assessing patients decision-making capacity in the hospital setting: A literature review. Aust J Rural Health. 2020;28(2):141-8. doi: 10.1111/ajr.12592.
7. Kim SYH et al. Do clinicians follow a risk-sensitive model of capacity-determination? An experimental video survey. Psychosomatics. 2006;47(4):325-9. doi: 10.1176/appi.psy.47.4.325.
8. Appelbaum PS. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-40. doi: 10.1056/NEJMcp074045.
9. Karlawish J. Measuring decision-making capacity in cognitively impaired individuals. Neurosignals. 2008;16(1):91-8. doi: 10.1159/000109763.
10. Christensen K et al. Decision-making capacity for informed consent in the older population. Bull Am Acad Psychiatry Law. 1995;23(3):353-65.
Case
Ms. F. is a 68-year-old woman who presented to the hospital with sepsis, developed delirium, and stopped eating. Her clinicians recommended a PEG tube. Although she was inconsistently oriented to self, time, and place, she reiterated the same decision across multiple discussions: She did not want the PEG tube. Her replies to what would happen if she didn’t have the procedure and continued not to eat were consistent, too: “I’ll wither away.”
Ms. F. had impaired cognition. Do these impairments mean her clinicians should over-rule her choice? What evidence indicates whether she lacks decision-making capacity? This case of a patient refusing a potentially life-saving procedure amplifies the importance of asking these questions and integrating capacity assessments into clinical care. In this article, we will describe what capacity is, when and how to assess it, and the alternatives when a patient does not have capacity.
The ethical background
Before starting a medical treatment or procedure, a physician must obtain the patient’s informed consent. This is a core ethic of medicine. Informed consent describes the voluntary decision made by a competent patient following the disclosure of necessary information. Informed consent is key to achieving a balance between promoting patient self-determination and protecting vulnerable patients from harm. In most clinical encounters, informed consent unfolds effortlessly. However, in the care of patients who are acutely ill, particularly those in hospitals, fulfilling the ethic can be challenging.
It is important to have skills to recognize and address these challenges. One of the most common challenges to practicing the ethic of informed consent is the impact of illness on a person’s decision-making capacity. A patient who retains capacity ought to make his or her decisions and does not need someone else (a friend or a family member) to help with the decision.
Incapacity is unfortunately common among the acutely ill medical inpatient population, which typically skews older with more comorbidities.1 Impairments frequently are overlooked for a variety of reasons,2-6 including that many hospitalized patients do not challenge their doctors’ decisions. Doctors may be reluctant to assess capacity because the assessment may medically, legally, or ethically complicate the patient’s care.
Two common terms describe the outcome of an assessment of a patient’s decision-making abilities: competency and capacity. Competency describes a legal principle. It is granted or withdrawn by judicial review. The consequences of a judge rescinding competency are severe: A patient would need a guardian to make choices on his or her behalf.
Capacity, on the other hand, is a clinical concept. A physician assesses whether the patient can make a specific decision in a specific context. The difference between the two terms – competency and capacity – delineates what are the consequences of the assessment and which authority, a judge or a physician, has the right to withdraw a person’s decision-making authority.
The judge offers a global assessment that can lead to a guardianship. The physician’s decision is temporal and situational. Patients can lack capacity when they are ill and recover it when they are healed. Capacity is specific to each medical decision that the patient makes and so a person can lack capacity to make some decisions but not others.
Ethical framework to make assessment
Capacity is described by four decisional abilities: 1) communicate a choice, 2) understand relevant information, 3) appreciation, and 4) reasoning.7
Communication of a choice may be verbal or nonverbal, but the patient must be able to indicate the treatment choice clearly and consistently. Understanding describes knowing essential information a physician has conveyed. This is assessed by having the patients say back what they were told, such as: “Can you tell me in your own words what is a PEG tube?”
The components of appreciation are: the diagnosis or disorder and the benefits and risks of the proposed intervention as it relates to the diagnosis or disorder. Patients who appreciate their disorder have insight into their condition: “I’m not eating because I have an infection.” This can be assessed with a question such as: “Can you tell me in your own words what are the risks or downsides to you?” This prompt assesses the patient’s appreciation of risk. Reframing the question to ask, “Can you tell me about the upsides of this intervention?” will assess the patient’s appreciation of benefit.
Reasoning assesses the thought process and rationale for a person’s decision. It has two components – comparative and consequential reasoning. The first compares the different choices presented about the proposed intervention: “How does having a PEG tube compare to not having it?” The second asks about the consequences of each choice: “What might happen to a person who has the PEG tube?”
The capacity assessment evaluates a patient's performance on these decision-making abilities. This informs the clinician’s judgment of whether the patient has the capacity to make a decision. A patient who has capacity makes the choice, regardless of the physician’s preference or recommendation.
The physician’s duty is to decide which decision-making abilities to assess. Choice and understanding are essential. In riskier or more consequential decisions, a physician may raise the rigor of the assessment to include appreciation and reasoning.8 It is common practice for physicians to raise the standard for when to evaluate and how extensive their evaluation is when the decision is life-altering, as with a PEG tube versus a more routine, non–life-altering decision such as drawing blood for a routine wellness visit.
A simple scoring rubric determines the patient’s ability to answer each question along a range from adequate = 2, marginal = 1, to inadequate = 0. The extremes or adequate or inadequate are straightforward. Judgment is needed when performance is marginal. In the case of repeated marginal answers, a physician must strongly consider whether the patient lacks capacity to make the decision in question.9
Who receives a capacity assessment and when?
A good doctor is a good teacher. A doctor should therefore check that patients understand what is happening with their health. Assessing understanding is simply good medicine; for example, a good teacher ought to be asking an unimpaired patient without impaired cognition, “Can you say back to me the key points of what I explained?” With this approach, every patient is effectively “screened” for a capacity impairment.
Certain patients ought to trigger a more thorough examination of decisional abilities. Across multiple articles, the strongest factors associated with incapacity are older age and diminished cognitive function (often detected by MMSE scores below the low 20s).1,7,10 Other factors that may amplify these deficits and thus should raise clinician concern would be patients with brain diseases such as Alzheimer’s or Parkinson’s, persons with lower education levels, or those who already have someone who helps them make decisions. To be sure, many older adults, even those with cognitive impairments, retain capacity, but extra protection should be in place to ensure their well-being.
Consequences of incapacity
If a careful assessment shows a patient has sound decision-making abilities, the patient is free to make the choice. On the other hand, a person does not have the capacity to make the decision at hand if he or she cannot communicate a choice or understand relevant information. Whether appreciation or reasoning ought to be assessed depends on the complexity and the significance of the decision. An assessment of decisional ability is not the end of the decision-making process. The goal is to maximize the patient’s autonomy.
Capacity can change over time. Factors that may inhibit capacity, such as medications, time of day, and even illness acuity, need to be accounted for and, if possible, addressed. The decision ought to be delayed, if possible, to a time when the patient has better chances of having capacity. If it is unlikely that patients’ status will change in the time frame needed to make the choice and they are found to not have capacity, then the decision making can be aided by advance directives or substitute decision makers such as family members or legal guardians.
Revisiting the case
Ms. F., who was delirious, retained notable decisional abilities. She understood the procedure of receiving the PEG tube and how the risk of continuing to not eat and not receive the PEG would result in dying by starvation. She appreciated her own diagnosis and how the proposed intervention could alter her condition. She appreciated how not having a PEG would lead to her death. Her choice to refuse the procedure was consistent. Ms. F. showed she retained capacity to make this decision. It was the physician’s duty to respect her autonomy and so to respect her refusal of the PEG.
Dr. Ney is a physician resident, department of psychiatry and human behavior, Thomas Jefferson University Hospital, Philadelphia. He has no conflicts to disclose. Dr. Karlawish is a professor in the departments of medicine, medical ethics and health policy, and neurology, University of Pennsylvania, Philadelphia. He is a site investigator for clinical trials sponsored by Biogen, Eisai, and Lilly.
References
1. Raymont V et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: Cross-sectional study. Lancet. 2004;364(9443):1421-7. doi: 10.1016/S0140-6736(04)17224-3.
2. Hanson M and Pitt D. Informed consent for surgery: risk discussion and documentation. Can J Surg. 2017;60(1):69-70. doi: 10.1503/cjs.004816.
3. Dahlberg J et al. Lack of informed consent for surgical procedures by elderly patients with inability to consent: A retrospective chart review from an academic medical center in Norway. Patient Saf Surg. 2019;13:24. doi: 10.1186/s13037-019-0205-5.
4. Sessums LL et al. Does this patient have medical decision-making capacity? JAMA. 2011;306(4):420-7. doi: 10.1001/jama.2011.1023.
5. Terranova C et al. Ethical and medicolegal implications of capacity of patients in geriatric surgery. Med Sci Law. 2013;53(3):166-71. doi: 10.1177/0025802412473963.
6. John S et al. Assessing patients decision-making capacity in the hospital setting: A literature review. Aust J Rural Health. 2020;28(2):141-8. doi: 10.1111/ajr.12592.
7. Kim SYH et al. Do clinicians follow a risk-sensitive model of capacity-determination? An experimental video survey. Psychosomatics. 2006;47(4):325-9. doi: 10.1176/appi.psy.47.4.325.
8. Appelbaum PS. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-40. doi: 10.1056/NEJMcp074045.
9. Karlawish J. Measuring decision-making capacity in cognitively impaired individuals. Neurosignals. 2008;16(1):91-8. doi: 10.1159/000109763.
10. Christensen K et al. Decision-making capacity for informed consent in the older population. Bull Am Acad Psychiatry Law. 1995;23(3):353-65.
Case
Ms. F. is a 68-year-old woman who presented to the hospital with sepsis, developed delirium, and stopped eating. Her clinicians recommended a PEG tube. Although she was inconsistently oriented to self, time, and place, she reiterated the same decision across multiple discussions: She did not want the PEG tube. Her replies to what would happen if she didn’t have the procedure and continued not to eat were consistent, too: “I’ll wither away.”
Ms. F. had impaired cognition. Do these impairments mean her clinicians should over-rule her choice? What evidence indicates whether she lacks decision-making capacity? This case of a patient refusing a potentially life-saving procedure amplifies the importance of asking these questions and integrating capacity assessments into clinical care. In this article, we will describe what capacity is, when and how to assess it, and the alternatives when a patient does not have capacity.
The ethical background
Before starting a medical treatment or procedure, a physician must obtain the patient’s informed consent. This is a core ethic of medicine. Informed consent describes the voluntary decision made by a competent patient following the disclosure of necessary information. Informed consent is key to achieving a balance between promoting patient self-determination and protecting vulnerable patients from harm. In most clinical encounters, informed consent unfolds effortlessly. However, in the care of patients who are acutely ill, particularly those in hospitals, fulfilling the ethic can be challenging.
It is important to have skills to recognize and address these challenges. One of the most common challenges to practicing the ethic of informed consent is the impact of illness on a person’s decision-making capacity. A patient who retains capacity ought to make his or her decisions and does not need someone else (a friend or a family member) to help with the decision.
Incapacity is unfortunately common among the acutely ill medical inpatient population, which typically skews older with more comorbidities.1 Impairments frequently are overlooked for a variety of reasons,2-6 including that many hospitalized patients do not challenge their doctors’ decisions. Doctors may be reluctant to assess capacity because the assessment may medically, legally, or ethically complicate the patient’s care.
Two common terms describe the outcome of an assessment of a patient’s decision-making abilities: competency and capacity. Competency describes a legal principle. It is granted or withdrawn by judicial review. The consequences of a judge rescinding competency are severe: A patient would need a guardian to make choices on his or her behalf.
Capacity, on the other hand, is a clinical concept. A physician assesses whether the patient can make a specific decision in a specific context. The difference between the two terms – competency and capacity – delineates what are the consequences of the assessment and which authority, a judge or a physician, has the right to withdraw a person’s decision-making authority.
The judge offers a global assessment that can lead to a guardianship. The physician’s decision is temporal and situational. Patients can lack capacity when they are ill and recover it when they are healed. Capacity is specific to each medical decision that the patient makes and so a person can lack capacity to make some decisions but not others.
Ethical framework to make assessment
Capacity is described by four decisional abilities: 1) communicate a choice, 2) understand relevant information, 3) appreciation, and 4) reasoning.7
Communication of a choice may be verbal or nonverbal, but the patient must be able to indicate the treatment choice clearly and consistently. Understanding describes knowing essential information a physician has conveyed. This is assessed by having the patients say back what they were told, such as: “Can you tell me in your own words what is a PEG tube?”
The components of appreciation are: the diagnosis or disorder and the benefits and risks of the proposed intervention as it relates to the diagnosis or disorder. Patients who appreciate their disorder have insight into their condition: “I’m not eating because I have an infection.” This can be assessed with a question such as: “Can you tell me in your own words what are the risks or downsides to you?” This prompt assesses the patient’s appreciation of risk. Reframing the question to ask, “Can you tell me about the upsides of this intervention?” will assess the patient’s appreciation of benefit.
Reasoning assesses the thought process and rationale for a person’s decision. It has two components – comparative and consequential reasoning. The first compares the different choices presented about the proposed intervention: “How does having a PEG tube compare to not having it?” The second asks about the consequences of each choice: “What might happen to a person who has the PEG tube?”
The capacity assessment evaluates a patient's performance on these decision-making abilities. This informs the clinician’s judgment of whether the patient has the capacity to make a decision. A patient who has capacity makes the choice, regardless of the physician’s preference or recommendation.
The physician’s duty is to decide which decision-making abilities to assess. Choice and understanding are essential. In riskier or more consequential decisions, a physician may raise the rigor of the assessment to include appreciation and reasoning.8 It is common practice for physicians to raise the standard for when to evaluate and how extensive their evaluation is when the decision is life-altering, as with a PEG tube versus a more routine, non–life-altering decision such as drawing blood for a routine wellness visit.
A simple scoring rubric determines the patient’s ability to answer each question along a range from adequate = 2, marginal = 1, to inadequate = 0. The extremes or adequate or inadequate are straightforward. Judgment is needed when performance is marginal. In the case of repeated marginal answers, a physician must strongly consider whether the patient lacks capacity to make the decision in question.9
Who receives a capacity assessment and when?
A good doctor is a good teacher. A doctor should therefore check that patients understand what is happening with their health. Assessing understanding is simply good medicine; for example, a good teacher ought to be asking an unimpaired patient without impaired cognition, “Can you say back to me the key points of what I explained?” With this approach, every patient is effectively “screened” for a capacity impairment.
Certain patients ought to trigger a more thorough examination of decisional abilities. Across multiple articles, the strongest factors associated with incapacity are older age and diminished cognitive function (often detected by MMSE scores below the low 20s).1,7,10 Other factors that may amplify these deficits and thus should raise clinician concern would be patients with brain diseases such as Alzheimer’s or Parkinson’s, persons with lower education levels, or those who already have someone who helps them make decisions. To be sure, many older adults, even those with cognitive impairments, retain capacity, but extra protection should be in place to ensure their well-being.
Consequences of incapacity
If a careful assessment shows a patient has sound decision-making abilities, the patient is free to make the choice. On the other hand, a person does not have the capacity to make the decision at hand if he or she cannot communicate a choice or understand relevant information. Whether appreciation or reasoning ought to be assessed depends on the complexity and the significance of the decision. An assessment of decisional ability is not the end of the decision-making process. The goal is to maximize the patient’s autonomy.
Capacity can change over time. Factors that may inhibit capacity, such as medications, time of day, and even illness acuity, need to be accounted for and, if possible, addressed. The decision ought to be delayed, if possible, to a time when the patient has better chances of having capacity. If it is unlikely that patients’ status will change in the time frame needed to make the choice and they are found to not have capacity, then the decision making can be aided by advance directives or substitute decision makers such as family members or legal guardians.
Revisiting the case
Ms. F., who was delirious, retained notable decisional abilities. She understood the procedure of receiving the PEG tube and how the risk of continuing to not eat and not receive the PEG would result in dying by starvation. She appreciated her own diagnosis and how the proposed intervention could alter her condition. She appreciated how not having a PEG would lead to her death. Her choice to refuse the procedure was consistent. Ms. F. showed she retained capacity to make this decision. It was the physician’s duty to respect her autonomy and so to respect her refusal of the PEG.
Dr. Ney is a physician resident, department of psychiatry and human behavior, Thomas Jefferson University Hospital, Philadelphia. He has no conflicts to disclose. Dr. Karlawish is a professor in the departments of medicine, medical ethics and health policy, and neurology, University of Pennsylvania, Philadelphia. He is a site investigator for clinical trials sponsored by Biogen, Eisai, and Lilly.
References
1. Raymont V et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: Cross-sectional study. Lancet. 2004;364(9443):1421-7. doi: 10.1016/S0140-6736(04)17224-3.
2. Hanson M and Pitt D. Informed consent for surgery: risk discussion and documentation. Can J Surg. 2017;60(1):69-70. doi: 10.1503/cjs.004816.
3. Dahlberg J et al. Lack of informed consent for surgical procedures by elderly patients with inability to consent: A retrospective chart review from an academic medical center in Norway. Patient Saf Surg. 2019;13:24. doi: 10.1186/s13037-019-0205-5.
4. Sessums LL et al. Does this patient have medical decision-making capacity? JAMA. 2011;306(4):420-7. doi: 10.1001/jama.2011.1023.
5. Terranova C et al. Ethical and medicolegal implications of capacity of patients in geriatric surgery. Med Sci Law. 2013;53(3):166-71. doi: 10.1177/0025802412473963.
6. John S et al. Assessing patients decision-making capacity in the hospital setting: A literature review. Aust J Rural Health. 2020;28(2):141-8. doi: 10.1111/ajr.12592.
7. Kim SYH et al. Do clinicians follow a risk-sensitive model of capacity-determination? An experimental video survey. Psychosomatics. 2006;47(4):325-9. doi: 10.1176/appi.psy.47.4.325.
8. Appelbaum PS. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-40. doi: 10.1056/NEJMcp074045.
9. Karlawish J. Measuring decision-making capacity in cognitively impaired individuals. Neurosignals. 2008;16(1):91-8. doi: 10.1159/000109763.
10. Christensen K et al. Decision-making capacity for informed consent in the older population. Bull Am Acad Psychiatry Law. 1995;23(3):353-65.
Dolutegravir in pregnant patients with HIV showed more viral suppression at delivery vs. other treatments
“Dolutegravir is increasingly used in pregnancy in the United States,” Kunjal Patel, DSc, one of the investigators, said in an interview. “While its effectiveness and safety in pregnancy have been compared to efavirenz in previous studies, including three randomized trials, efavirenz isn’t really used in the United States and Europe for treatment of HIV; it is mainly used in Africa,” she said. Therefore, it was important to compare dolutegravir use in pregnancy to the other antiretroviral regimens that are listed as being preferred for use in pregnancy in the U.S., including atazanavir/ritonavir, darunavir/ritonavir, and raltegravir, and others often used in the U.S. and Europe, she said.
In the study published in the New England Journal of Medicine, Dr. Patel, of Harvard T.H. Chan School of Public Health, Boston, and colleagues analyzed data from kids enrolled in the Surveillance and Monitoring for ART Toxicities Dynamic (SMARTT) cohort. This group is part of an ongoing research project focused on evaluating ART toxicities during pregnancy in children who were exposed to HIV perinatally but not infected. It included pregnancies from 2007 until January 2020 that involved use of the ARTs listed.
The study population of 1,257 pregnancies with observed birth outcomes included 120 individuals with an initial ART of dolutegravir (DTG), 464 started on atazanavir–ritonavir (ATV/r), 185 on darunavir–ritonavir (DRV/r), 243 on oral rilpivirine (RPV), 86 on raltegravir (RAL), and 159 on elvitegravir–cobicistat (EVG/c). In approximately half of the pregnancies (51%), ART was started before conception, and the initial ART was changed in 27%.
The primary outcomes were viral suppression at delivery, and adverse birth outcomes, including preterm and very preterm birth, low and very low birth weight, and neonatal death within 14 days.
The median age of the patients at conception was 29 years, and 66% were non-Hispanic Black, representative of persons with HIV of childbearing age in the United States, the researchers noted. Overall, 96.7% of the patients who received dolutegravir showed viral suppression at delivery, compared to 90.1% for darunavir–ritonavir, 89.8% for elvitegravir–cobicistat, 89.2% for raltegravir, and 84.0% for atazanavir–ritonavir.
“We expected that dolutegravir to be similar with regards to viral suppression at delivery compared to raltegravir so were surprised that we observed less viral suppression with raltegravir compared to dolutegravir,” Dr. Patel said in an interview. “Our results may be due to the higher pill burden and lower barrier to resistance with RAL compared to dolutegravir, but we did not assess adherence or resistance in our study,” she noted.
Across ART regimens, the observed risks of preterm birth ranged from 13.6% to 17.6%, risks of low birth weight ranged from 11.9% to 16.7%, and risks of being small for gestational age ranged from 9.1% to 12.5%. For the composite of any adverse birth outcome and any severe adverse birth outcome, the observed risks ranged from 22.6% to 27.9% and 0% to 4.2%, respectively.
A total of 20 very preterm births, including 15 infants with very low birth weight, occurred across patients receiving all ART regimens, and no neonatal deaths occurred. The researchers found no apparent patterns of differences in the observed risk of adverse birth outcomes across all groups related to the timing of ART initiation in pregnancy, but the risks were greater among those who began the drugs during pregnancy compared to those who began before conception.
“Our results confirm the recommendation of DTG as “preferred” in U.S. perinatal guidelines, and provide evidence suggesting ATV/r and RAL provides lower HIV viral suppression at delivery compared to DTG, and support DRV/r as a reasonable alternative when DTG use is not feasible,” Dr. Patel said in an interview.
“With regards to next steps, we are interested in comparing the effectiveness and safety of dolutegravir-based regimens that include tenofovir alafenamide (TAF) vs. tenofovir disoproxil fumarate (TDF) in our U.S. setting,” she said.
The study findings were limited by several factors including the lack of data on predictors of preterm birth and low birth weight, such as previous preterm birth and prepregnancy body mass index, the researchers noted.
However, the results indicate that other common ARTs provide less HIV viral suppression at delivery than dolutegravir, with similar adverse birth outcomes; the results also support darunavir–ritonavir as a reasonable alternative when dolutegravir use is not feasible, as it showed the next highest level of viral suppression after dolutegravir, the researchers concluded.
Findings fill a key research gap
The current study is important given the limited data on effectiveness and outcomes in pregnancy with the use of contemporary HIV regimens in the United States, Martina L. Badell, MD, a maternal-fetal medicine specialist at Emory University, Atlanta, said in an interview.
“Pregnancy is still among exclusion criteria for most drug studies,” said Dr. Badell, who was not involved in the current study. “Dolutegravir-based ART is first line in the U.S. today because of its effectiveness, lower side effects, and higher barrier to resistance; therefore understanding the benefits and birth outcomes in pregnancy is critical,” she explained.
Dr. Badell said she was not surprised by the study findings. “However it is very reassuring to see in a large observational study comparing the dolutegravir regimens to other contemporary regimens in pregnancy, such a high level of viral suppression and no increased risk of adverse perinatal outcomes,” she said.
The study findings will impact clinical practice by reaffirming patient counseling regarding the use of dolutegravir in pregnancy, said Dr. Badell. “The use of ART in pregnancy is complex given the number of drug choices, whether the patient was on ART prior to pregnancy or initiated during pregnancy, and the various factors other than ART that affect perinatal outcomes, such as preterm birth and congenital anomalies, she explained.
The finding that the risk of adverse outcomes was higher for those who initiated ART during pregnancy vs. those who were already on ARTs when they became pregnant contradicts some previous research, said Dr. Badell. But this is “reassuring, as we highly recommend ART with viral suppression prior to pregnancy or to start as early as possible in pregnancy.”
Adverse birth outcomes can be affected by many variables such as age, substance abuse, prior adverse birth outcome and other factors, and larger studies that control for these variables will allow better evaluation of the effect of the ART drugs, Dr. Badell added.
The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, along with the Office of the Director, National Institutes of Health; National Institute of Dental and Craniofacial Research; National Institute of Allergy and Infectious Diseases; National Institute of Neurological Disorders and Stroke; National Institute on Deafness and Other Communication Disorders; National Institute of Mental Health; National Institute on Drug Abuse; National Cancer Institute; National Institute on Alcohol Abuse and Alcoholism; and National Heart, Lung, and Blood Institute through cooperative agreements with the Harvard T.H. Chan School of Public Health and the Tulane University School of Medicine.
The researchers and Dr. Badell had no financial conflicts to disclose.
“Dolutegravir is increasingly used in pregnancy in the United States,” Kunjal Patel, DSc, one of the investigators, said in an interview. “While its effectiveness and safety in pregnancy have been compared to efavirenz in previous studies, including three randomized trials, efavirenz isn’t really used in the United States and Europe for treatment of HIV; it is mainly used in Africa,” she said. Therefore, it was important to compare dolutegravir use in pregnancy to the other antiretroviral regimens that are listed as being preferred for use in pregnancy in the U.S., including atazanavir/ritonavir, darunavir/ritonavir, and raltegravir, and others often used in the U.S. and Europe, she said.
In the study published in the New England Journal of Medicine, Dr. Patel, of Harvard T.H. Chan School of Public Health, Boston, and colleagues analyzed data from kids enrolled in the Surveillance and Monitoring for ART Toxicities Dynamic (SMARTT) cohort. This group is part of an ongoing research project focused on evaluating ART toxicities during pregnancy in children who were exposed to HIV perinatally but not infected. It included pregnancies from 2007 until January 2020 that involved use of the ARTs listed.
The study population of 1,257 pregnancies with observed birth outcomes included 120 individuals with an initial ART of dolutegravir (DTG), 464 started on atazanavir–ritonavir (ATV/r), 185 on darunavir–ritonavir (DRV/r), 243 on oral rilpivirine (RPV), 86 on raltegravir (RAL), and 159 on elvitegravir–cobicistat (EVG/c). In approximately half of the pregnancies (51%), ART was started before conception, and the initial ART was changed in 27%.
The primary outcomes were viral suppression at delivery, and adverse birth outcomes, including preterm and very preterm birth, low and very low birth weight, and neonatal death within 14 days.
The median age of the patients at conception was 29 years, and 66% were non-Hispanic Black, representative of persons with HIV of childbearing age in the United States, the researchers noted. Overall, 96.7% of the patients who received dolutegravir showed viral suppression at delivery, compared to 90.1% for darunavir–ritonavir, 89.8% for elvitegravir–cobicistat, 89.2% for raltegravir, and 84.0% for atazanavir–ritonavir.
“We expected that dolutegravir to be similar with regards to viral suppression at delivery compared to raltegravir so were surprised that we observed less viral suppression with raltegravir compared to dolutegravir,” Dr. Patel said in an interview. “Our results may be due to the higher pill burden and lower barrier to resistance with RAL compared to dolutegravir, but we did not assess adherence or resistance in our study,” she noted.
Across ART regimens, the observed risks of preterm birth ranged from 13.6% to 17.6%, risks of low birth weight ranged from 11.9% to 16.7%, and risks of being small for gestational age ranged from 9.1% to 12.5%. For the composite of any adverse birth outcome and any severe adverse birth outcome, the observed risks ranged from 22.6% to 27.9% and 0% to 4.2%, respectively.
A total of 20 very preterm births, including 15 infants with very low birth weight, occurred across patients receiving all ART regimens, and no neonatal deaths occurred. The researchers found no apparent patterns of differences in the observed risk of adverse birth outcomes across all groups related to the timing of ART initiation in pregnancy, but the risks were greater among those who began the drugs during pregnancy compared to those who began before conception.
“Our results confirm the recommendation of DTG as “preferred” in U.S. perinatal guidelines, and provide evidence suggesting ATV/r and RAL provides lower HIV viral suppression at delivery compared to DTG, and support DRV/r as a reasonable alternative when DTG use is not feasible,” Dr. Patel said in an interview.
“With regards to next steps, we are interested in comparing the effectiveness and safety of dolutegravir-based regimens that include tenofovir alafenamide (TAF) vs. tenofovir disoproxil fumarate (TDF) in our U.S. setting,” she said.
The study findings were limited by several factors including the lack of data on predictors of preterm birth and low birth weight, such as previous preterm birth and prepregnancy body mass index, the researchers noted.
However, the results indicate that other common ARTs provide less HIV viral suppression at delivery than dolutegravir, with similar adverse birth outcomes; the results also support darunavir–ritonavir as a reasonable alternative when dolutegravir use is not feasible, as it showed the next highest level of viral suppression after dolutegravir, the researchers concluded.
Findings fill a key research gap
The current study is important given the limited data on effectiveness and outcomes in pregnancy with the use of contemporary HIV regimens in the United States, Martina L. Badell, MD, a maternal-fetal medicine specialist at Emory University, Atlanta, said in an interview.
“Pregnancy is still among exclusion criteria for most drug studies,” said Dr. Badell, who was not involved in the current study. “Dolutegravir-based ART is first line in the U.S. today because of its effectiveness, lower side effects, and higher barrier to resistance; therefore understanding the benefits and birth outcomes in pregnancy is critical,” she explained.
Dr. Badell said she was not surprised by the study findings. “However it is very reassuring to see in a large observational study comparing the dolutegravir regimens to other contemporary regimens in pregnancy, such a high level of viral suppression and no increased risk of adverse perinatal outcomes,” she said.
The study findings will impact clinical practice by reaffirming patient counseling regarding the use of dolutegravir in pregnancy, said Dr. Badell. “The use of ART in pregnancy is complex given the number of drug choices, whether the patient was on ART prior to pregnancy or initiated during pregnancy, and the various factors other than ART that affect perinatal outcomes, such as preterm birth and congenital anomalies, she explained.
The finding that the risk of adverse outcomes was higher for those who initiated ART during pregnancy vs. those who were already on ARTs when they became pregnant contradicts some previous research, said Dr. Badell. But this is “reassuring, as we highly recommend ART with viral suppression prior to pregnancy or to start as early as possible in pregnancy.”
Adverse birth outcomes can be affected by many variables such as age, substance abuse, prior adverse birth outcome and other factors, and larger studies that control for these variables will allow better evaluation of the effect of the ART drugs, Dr. Badell added.
The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, along with the Office of the Director, National Institutes of Health; National Institute of Dental and Craniofacial Research; National Institute of Allergy and Infectious Diseases; National Institute of Neurological Disorders and Stroke; National Institute on Deafness and Other Communication Disorders; National Institute of Mental Health; National Institute on Drug Abuse; National Cancer Institute; National Institute on Alcohol Abuse and Alcoholism; and National Heart, Lung, and Blood Institute through cooperative agreements with the Harvard T.H. Chan School of Public Health and the Tulane University School of Medicine.
The researchers and Dr. Badell had no financial conflicts to disclose.
“Dolutegravir is increasingly used in pregnancy in the United States,” Kunjal Patel, DSc, one of the investigators, said in an interview. “While its effectiveness and safety in pregnancy have been compared to efavirenz in previous studies, including three randomized trials, efavirenz isn’t really used in the United States and Europe for treatment of HIV; it is mainly used in Africa,” she said. Therefore, it was important to compare dolutegravir use in pregnancy to the other antiretroviral regimens that are listed as being preferred for use in pregnancy in the U.S., including atazanavir/ritonavir, darunavir/ritonavir, and raltegravir, and others often used in the U.S. and Europe, she said.
In the study published in the New England Journal of Medicine, Dr. Patel, of Harvard T.H. Chan School of Public Health, Boston, and colleagues analyzed data from kids enrolled in the Surveillance and Monitoring for ART Toxicities Dynamic (SMARTT) cohort. This group is part of an ongoing research project focused on evaluating ART toxicities during pregnancy in children who were exposed to HIV perinatally but not infected. It included pregnancies from 2007 until January 2020 that involved use of the ARTs listed.
The study population of 1,257 pregnancies with observed birth outcomes included 120 individuals with an initial ART of dolutegravir (DTG), 464 started on atazanavir–ritonavir (ATV/r), 185 on darunavir–ritonavir (DRV/r), 243 on oral rilpivirine (RPV), 86 on raltegravir (RAL), and 159 on elvitegravir–cobicistat (EVG/c). In approximately half of the pregnancies (51%), ART was started before conception, and the initial ART was changed in 27%.
The primary outcomes were viral suppression at delivery, and adverse birth outcomes, including preterm and very preterm birth, low and very low birth weight, and neonatal death within 14 days.
The median age of the patients at conception was 29 years, and 66% were non-Hispanic Black, representative of persons with HIV of childbearing age in the United States, the researchers noted. Overall, 96.7% of the patients who received dolutegravir showed viral suppression at delivery, compared to 90.1% for darunavir–ritonavir, 89.8% for elvitegravir–cobicistat, 89.2% for raltegravir, and 84.0% for atazanavir–ritonavir.
“We expected that dolutegravir to be similar with regards to viral suppression at delivery compared to raltegravir so were surprised that we observed less viral suppression with raltegravir compared to dolutegravir,” Dr. Patel said in an interview. “Our results may be due to the higher pill burden and lower barrier to resistance with RAL compared to dolutegravir, but we did not assess adherence or resistance in our study,” she noted.
Across ART regimens, the observed risks of preterm birth ranged from 13.6% to 17.6%, risks of low birth weight ranged from 11.9% to 16.7%, and risks of being small for gestational age ranged from 9.1% to 12.5%. For the composite of any adverse birth outcome and any severe adverse birth outcome, the observed risks ranged from 22.6% to 27.9% and 0% to 4.2%, respectively.
A total of 20 very preterm births, including 15 infants with very low birth weight, occurred across patients receiving all ART regimens, and no neonatal deaths occurred. The researchers found no apparent patterns of differences in the observed risk of adverse birth outcomes across all groups related to the timing of ART initiation in pregnancy, but the risks were greater among those who began the drugs during pregnancy compared to those who began before conception.
“Our results confirm the recommendation of DTG as “preferred” in U.S. perinatal guidelines, and provide evidence suggesting ATV/r and RAL provides lower HIV viral suppression at delivery compared to DTG, and support DRV/r as a reasonable alternative when DTG use is not feasible,” Dr. Patel said in an interview.
“With regards to next steps, we are interested in comparing the effectiveness and safety of dolutegravir-based regimens that include tenofovir alafenamide (TAF) vs. tenofovir disoproxil fumarate (TDF) in our U.S. setting,” she said.
The study findings were limited by several factors including the lack of data on predictors of preterm birth and low birth weight, such as previous preterm birth and prepregnancy body mass index, the researchers noted.
However, the results indicate that other common ARTs provide less HIV viral suppression at delivery than dolutegravir, with similar adverse birth outcomes; the results also support darunavir–ritonavir as a reasonable alternative when dolutegravir use is not feasible, as it showed the next highest level of viral suppression after dolutegravir, the researchers concluded.
Findings fill a key research gap
The current study is important given the limited data on effectiveness and outcomes in pregnancy with the use of contemporary HIV regimens in the United States, Martina L. Badell, MD, a maternal-fetal medicine specialist at Emory University, Atlanta, said in an interview.
“Pregnancy is still among exclusion criteria for most drug studies,” said Dr. Badell, who was not involved in the current study. “Dolutegravir-based ART is first line in the U.S. today because of its effectiveness, lower side effects, and higher barrier to resistance; therefore understanding the benefits and birth outcomes in pregnancy is critical,” she explained.
Dr. Badell said she was not surprised by the study findings. “However it is very reassuring to see in a large observational study comparing the dolutegravir regimens to other contemporary regimens in pregnancy, such a high level of viral suppression and no increased risk of adverse perinatal outcomes,” she said.
The study findings will impact clinical practice by reaffirming patient counseling regarding the use of dolutegravir in pregnancy, said Dr. Badell. “The use of ART in pregnancy is complex given the number of drug choices, whether the patient was on ART prior to pregnancy or initiated during pregnancy, and the various factors other than ART that affect perinatal outcomes, such as preterm birth and congenital anomalies, she explained.
The finding that the risk of adverse outcomes was higher for those who initiated ART during pregnancy vs. those who were already on ARTs when they became pregnant contradicts some previous research, said Dr. Badell. But this is “reassuring, as we highly recommend ART with viral suppression prior to pregnancy or to start as early as possible in pregnancy.”
Adverse birth outcomes can be affected by many variables such as age, substance abuse, prior adverse birth outcome and other factors, and larger studies that control for these variables will allow better evaluation of the effect of the ART drugs, Dr. Badell added.
The study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, along with the Office of the Director, National Institutes of Health; National Institute of Dental and Craniofacial Research; National Institute of Allergy and Infectious Diseases; National Institute of Neurological Disorders and Stroke; National Institute on Deafness and Other Communication Disorders; National Institute of Mental Health; National Institute on Drug Abuse; National Cancer Institute; National Institute on Alcohol Abuse and Alcoholism; and National Heart, Lung, and Blood Institute through cooperative agreements with the Harvard T.H. Chan School of Public Health and the Tulane University School of Medicine.
The researchers and Dr. Badell had no financial conflicts to disclose.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Implementation of a Pilot Study Evaluating the Feasibility of Delivery of Attune, a Digital Cognitive-Behavioral Stress Management (CBSM) Software Application for Treatment of Anxiety and Depressive Symptoms in Veterans with Cancer
Purpose
To assess promoters and obstacles of enrollment in a decentralized clinical research study, where veterans with cancer-related depressive symptoms are electronically prescribed a 10-session digitally administered Cognitive-Behavioral Stress Management (CBSM) program, called Attune.
Background
The US Department of Veterans Affairs (VA) National TeleOncology (NTO) Program has served 5688 veterans since inception, 3100 of which reside in rural areas (55%). Previous studies demonstrate clinically significant levels of psychosocial distress in up to 52% of patients with cancer. It is unknown if veterans with cancer experiencing psychosocial distress will benefit from a CBSM app. Traditional research studies often underrepresent rural cancer patients, so the VA-Attune clinical trial was designed for implementation in a decentralized fashion for NTO VA facilities serving a more predominant rural population.
Methods
We manually screened veteran appointments to identify potentially eligible veterans. NTO providers were notified if their patients were potentially eligible, providers asked patients if they wanted more information. Research staff then contacted veterans by telephone to confirm eligibility. Consent and HIPAA authorization were mailed to interested veterans and the consent process occurred via telephone. Descriptive statistics were used to summarize the patient population screened and consented.
Results
Between January and May 2022, there were 467 veterans screened and 15 veterans enrolled (mean [SD] age, 67.2 [8.28] years; 12 men and 3 women). 15 veterans received the electronic prescription of the Attune App and providers viewed the CBSM App as feasible. Promotors of implementation included convenience of a virtual format and use of the veteran’s mobile device to deliver the digital CBSM. Barriers identified by veterans were not having an appropriate mobile device, inadequate knowledge on using a mobile device, and insufficient time to commit to regularly using the Attune app.
Conclusions/Implications
This VA-Attune study demonstrated that clinical trials can be implemented in the VA in a decentralized fashion, enrolling rural and urban veterans. We identified significant barriers to enrollment and engagement despite our approach of remote consent. The VA-Attune research study continues to enroll veterans nationally, highlighting best practices and opportunities to improve the implementation of decentralized cancer clinical trials in the VA.
Purpose
To assess promoters and obstacles of enrollment in a decentralized clinical research study, where veterans with cancer-related depressive symptoms are electronically prescribed a 10-session digitally administered Cognitive-Behavioral Stress Management (CBSM) program, called Attune.
Background
The US Department of Veterans Affairs (VA) National TeleOncology (NTO) Program has served 5688 veterans since inception, 3100 of which reside in rural areas (55%). Previous studies demonstrate clinically significant levels of psychosocial distress in up to 52% of patients with cancer. It is unknown if veterans with cancer experiencing psychosocial distress will benefit from a CBSM app. Traditional research studies often underrepresent rural cancer patients, so the VA-Attune clinical trial was designed for implementation in a decentralized fashion for NTO VA facilities serving a more predominant rural population.
Methods
We manually screened veteran appointments to identify potentially eligible veterans. NTO providers were notified if their patients were potentially eligible, providers asked patients if they wanted more information. Research staff then contacted veterans by telephone to confirm eligibility. Consent and HIPAA authorization were mailed to interested veterans and the consent process occurred via telephone. Descriptive statistics were used to summarize the patient population screened and consented.
Results
Between January and May 2022, there were 467 veterans screened and 15 veterans enrolled (mean [SD] age, 67.2 [8.28] years; 12 men and 3 women). 15 veterans received the electronic prescription of the Attune App and providers viewed the CBSM App as feasible. Promotors of implementation included convenience of a virtual format and use of the veteran’s mobile device to deliver the digital CBSM. Barriers identified by veterans were not having an appropriate mobile device, inadequate knowledge on using a mobile device, and insufficient time to commit to regularly using the Attune app.
Conclusions/Implications
This VA-Attune study demonstrated that clinical trials can be implemented in the VA in a decentralized fashion, enrolling rural and urban veterans. We identified significant barriers to enrollment and engagement despite our approach of remote consent. The VA-Attune research study continues to enroll veterans nationally, highlighting best practices and opportunities to improve the implementation of decentralized cancer clinical trials in the VA.
Purpose
To assess promoters and obstacles of enrollment in a decentralized clinical research study, where veterans with cancer-related depressive symptoms are electronically prescribed a 10-session digitally administered Cognitive-Behavioral Stress Management (CBSM) program, called Attune.
Background
The US Department of Veterans Affairs (VA) National TeleOncology (NTO) Program has served 5688 veterans since inception, 3100 of which reside in rural areas (55%). Previous studies demonstrate clinically significant levels of psychosocial distress in up to 52% of patients with cancer. It is unknown if veterans with cancer experiencing psychosocial distress will benefit from a CBSM app. Traditional research studies often underrepresent rural cancer patients, so the VA-Attune clinical trial was designed for implementation in a decentralized fashion for NTO VA facilities serving a more predominant rural population.
Methods
We manually screened veteran appointments to identify potentially eligible veterans. NTO providers were notified if their patients were potentially eligible, providers asked patients if they wanted more information. Research staff then contacted veterans by telephone to confirm eligibility. Consent and HIPAA authorization were mailed to interested veterans and the consent process occurred via telephone. Descriptive statistics were used to summarize the patient population screened and consented.
Results
Between January and May 2022, there were 467 veterans screened and 15 veterans enrolled (mean [SD] age, 67.2 [8.28] years; 12 men and 3 women). 15 veterans received the electronic prescription of the Attune App and providers viewed the CBSM App as feasible. Promotors of implementation included convenience of a virtual format and use of the veteran’s mobile device to deliver the digital CBSM. Barriers identified by veterans were not having an appropriate mobile device, inadequate knowledge on using a mobile device, and insufficient time to commit to regularly using the Attune app.
Conclusions/Implications
This VA-Attune study demonstrated that clinical trials can be implemented in the VA in a decentralized fashion, enrolling rural and urban veterans. We identified significant barriers to enrollment and engagement despite our approach of remote consent. The VA-Attune research study continues to enroll veterans nationally, highlighting best practices and opportunities to improve the implementation of decentralized cancer clinical trials in the VA.