User login
RA in remission: Subclinical inflammation lower with cs/bDMARDs combination vs. monotherapy
Key clinical point: Ultrasound-detected subclinical inflammation of tendons and joints was better controlled in patients with rheumatoid arthritis (RA) in clinical remission who received the combination therapy of conventional synthetic and biologic disease-modifying antirheumatic drugs (csDMARD+bDMARD) vs csDMARD or bDMARD monotherapy.
Major finding: Grey-scale tenosynovitis (P = .025) and power Doppler (PD) tenosynovitis (P = .047) were better controlled with csDMARD+bDMARD than with csDMARD alone. csDMARD+bDMARD was also associated with better treatment results for PD synovitis vs csDMARD (P = .01) or bDMARD (P = .02) alone.
Study details: Findings are from a longitudinal analysis of the STARTER study including 256 patients with RA in clinical remission who received csDMARD alone, bDMARD alone, or csDMARD+bDMARD.
Disclosures: This study did not receive any specific funding. The authors declared no conflicts of interest.
Source: Parisi S et al. Relationship between the prevalence of subclinical tenosynovitis and treatment in patients with RA in clinical remission: STARTER study. Rheumatology (Oxford). 2022 (Sep 6). Doi: 10.1093/rheumatology/keac518
Key clinical point: Ultrasound-detected subclinical inflammation of tendons and joints was better controlled in patients with rheumatoid arthritis (RA) in clinical remission who received the combination therapy of conventional synthetic and biologic disease-modifying antirheumatic drugs (csDMARD+bDMARD) vs csDMARD or bDMARD monotherapy.
Major finding: Grey-scale tenosynovitis (P = .025) and power Doppler (PD) tenosynovitis (P = .047) were better controlled with csDMARD+bDMARD than with csDMARD alone. csDMARD+bDMARD was also associated with better treatment results for PD synovitis vs csDMARD (P = .01) or bDMARD (P = .02) alone.
Study details: Findings are from a longitudinal analysis of the STARTER study including 256 patients with RA in clinical remission who received csDMARD alone, bDMARD alone, or csDMARD+bDMARD.
Disclosures: This study did not receive any specific funding. The authors declared no conflicts of interest.
Source: Parisi S et al. Relationship between the prevalence of subclinical tenosynovitis and treatment in patients with RA in clinical remission: STARTER study. Rheumatology (Oxford). 2022 (Sep 6). Doi: 10.1093/rheumatology/keac518
Key clinical point: Ultrasound-detected subclinical inflammation of tendons and joints was better controlled in patients with rheumatoid arthritis (RA) in clinical remission who received the combination therapy of conventional synthetic and biologic disease-modifying antirheumatic drugs (csDMARD+bDMARD) vs csDMARD or bDMARD monotherapy.
Major finding: Grey-scale tenosynovitis (P = .025) and power Doppler (PD) tenosynovitis (P = .047) were better controlled with csDMARD+bDMARD than with csDMARD alone. csDMARD+bDMARD was also associated with better treatment results for PD synovitis vs csDMARD (P = .01) or bDMARD (P = .02) alone.
Study details: Findings are from a longitudinal analysis of the STARTER study including 256 patients with RA in clinical remission who received csDMARD alone, bDMARD alone, or csDMARD+bDMARD.
Disclosures: This study did not receive any specific funding. The authors declared no conflicts of interest.
Source: Parisi S et al. Relationship between the prevalence of subclinical tenosynovitis and treatment in patients with RA in clinical remission: STARTER study. Rheumatology (Oxford). 2022 (Sep 6). Doi: 10.1093/rheumatology/keac518
Increased risk for severe COVID-19 in rheumatoid arthritis and its phenotypic subgroups
Key clinical point: Patients with rheumatoid arthritis (RA), including those across different phenotypic subgroups, were at an increased risk for severe COVID-19 compared with patients without RA, with a pronounced association being observed in patients with RA-associated interstitial lung disease (RA-ILD).
Major finding: Risk for severe COVID-19 was significantly higher in patients with RA vs. those without RA (adjusted hazard ratio [aHR], 1.75; P < .0001). Risk was persistent among the sub-group of patients who were seropositive (aHR, 1.97; P < .0001) or had erosive disease (aHR, 1.93; P < .0001) and most prominent among patients with RA-ILD (aHR, 2.50; P < .0001).
Study details: Findings are from a retrospective study of 582 patients with RA and 2,875 matched comparators without RA, all of whom had COVID-19.
Disclosures: This study did not receive any funding. Some authors reported receiving research support, consulting fees, and/or grants unrelated to this study from various sources.
Source: Figueroa-Parra G et al. Risk of severe COVID-19 outcomes associated with rheumatoid arthritis and phenotypic subgroups: A retrospective, comparative, multicentre cohort study. Lancet Rheumatol. 2022 (Sep 13). Doi: 10.1016/S2665-9913(22)00227-2.
Key clinical point: Patients with rheumatoid arthritis (RA), including those across different phenotypic subgroups, were at an increased risk for severe COVID-19 compared with patients without RA, with a pronounced association being observed in patients with RA-associated interstitial lung disease (RA-ILD).
Major finding: Risk for severe COVID-19 was significantly higher in patients with RA vs. those without RA (adjusted hazard ratio [aHR], 1.75; P < .0001). Risk was persistent among the sub-group of patients who were seropositive (aHR, 1.97; P < .0001) or had erosive disease (aHR, 1.93; P < .0001) and most prominent among patients with RA-ILD (aHR, 2.50; P < .0001).
Study details: Findings are from a retrospective study of 582 patients with RA and 2,875 matched comparators without RA, all of whom had COVID-19.
Disclosures: This study did not receive any funding. Some authors reported receiving research support, consulting fees, and/or grants unrelated to this study from various sources.
Source: Figueroa-Parra G et al. Risk of severe COVID-19 outcomes associated with rheumatoid arthritis and phenotypic subgroups: A retrospective, comparative, multicentre cohort study. Lancet Rheumatol. 2022 (Sep 13). Doi: 10.1016/S2665-9913(22)00227-2.
Key clinical point: Patients with rheumatoid arthritis (RA), including those across different phenotypic subgroups, were at an increased risk for severe COVID-19 compared with patients without RA, with a pronounced association being observed in patients with RA-associated interstitial lung disease (RA-ILD).
Major finding: Risk for severe COVID-19 was significantly higher in patients with RA vs. those without RA (adjusted hazard ratio [aHR], 1.75; P < .0001). Risk was persistent among the sub-group of patients who were seropositive (aHR, 1.97; P < .0001) or had erosive disease (aHR, 1.93; P < .0001) and most prominent among patients with RA-ILD (aHR, 2.50; P < .0001).
Study details: Findings are from a retrospective study of 582 patients with RA and 2,875 matched comparators without RA, all of whom had COVID-19.
Disclosures: This study did not receive any funding. Some authors reported receiving research support, consulting fees, and/or grants unrelated to this study from various sources.
Source: Figueroa-Parra G et al. Risk of severe COVID-19 outcomes associated with rheumatoid arthritis and phenotypic subgroups: A retrospective, comparative, multicentre cohort study. Lancet Rheumatol. 2022 (Sep 13). Doi: 10.1016/S2665-9913(22)00227-2.
FDA OKs teclistamab for relapsed/refractory multiple myeloma
The results made the case for “teclistamab as a monotherapy for eligible patients with heavily pretreated multiple myeloma, in need of new treatment options,” investigator Maria-Victoria Mateos, MD, PhD, a hematologist at the University Hospital of Salamanca (Spain) said in a June press release from drug maker Janssen/Johnson & Johnson.
The approval was based on the phase 1-2 single-arm MajesTEC-1 trial. The MajesTEC-1 findings, published in August in the New England Journal of Medicine, included 165 patients with relapsed or refractory multiple myeloma after at least three therapy lines – including an immunomodulatory drug, a proteasome inhibitor, and an anti-CD38 antibody. These patients received a weekly subcutaneous 1.5 mg/kg injection of teclistamab after stepping up from 0.06 mg and 0.3 mg/kg doses.
According to the FDA announcement, the overall response rate was nearly 62%. And the estimated duration of response rate among responders was 90.6% at 6 months and 66.5% at 9 months.
The NEJM results also indicated that almost 40% of patients had a complete response to the therapy, over a median follow-up of 14.1 months. More than a quarter of patients (26.7%) had no minimal residual disease.
The study investigators concluded that “teclistamab resulted in a high rate of deep and durable response in patients with triple-class exposed relapsed or refractory multiple myeloma.”
In a press release, Michael Andreini, president and CEO of the Multiple Myeloma Research Foundation, commented that “teclistamab is an important new treatment option for patients who have faced multiple relapses.”
The recommended dose for teclistamab is 0.06 mg/kg via subcutaneous injection on day 1, 0.3 mg/kg on day 4, and 1.5 mg/kg on day 7, followed by 1.5 mg/kg once weekly until disease progression or unacceptable toxicity.
The FDA noted, however, that the prescribing information for teclistamab comes with a Boxed warning for “life-threatening or fatal cytokine-release syndrome (CRS) and neurologic toxicity, including immune effector cell–associated neurotoxicity (ICANS).”
CRS was reported in 72.1% of patients (grade 3 in one patient but no grade 4 cases), neurologic toxicity in 57%, and ICANS in 6%. Other common adverse events in the NEJM report included neutropenia in 71% of subjects (grade 3 or 4 in 64%); anemia in 52% (grade 3 or 4 in 37%), and thrombocytopenia in 40% (grade 3 or 4 in 21%). Overall, 45% of patients developed grade 3 or 4 infections.
“Because of the risks of CRS and neurologic toxicity, including ICANS, teclistamab-cqyv is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS), called the Tecvayli REMS,” according to the FDA’s press release.
Teclistamab is a T-cell–bispecific antibody that targets both CD3 expressed on the surface of T cells and B-cell maturation antigen (BCMA) expressed on the surface of myeloma cells, activating T-cells to kill cancer cells that express the antigen.
Three BCMA-directed therapies are already on the market in the United States that carry teclistamab’s indication: the antibody-drug conjugate belantamab mafodotin (Blenrep) and two chimeric antigen receptor (CAR) T-cell therapies, idecabtagene vicleucel (Abecma) and ciltacabtagene autoleucel (Carvykti).
The overall response rate is approximately 31% with belantamab mafodotin, 67% for idecabtagene vicleucel, and 83% for ciltacabtagene autoleucel.
Pfizer also has a bispecific BCMA-CD3–targeted antibody in development, elranatamab, for triple-class refractory multiple myeloma that is expected to compete with teclistamab.
MajesTEC-1 was funded by Janssen. Dr. Mateos is a paid speaker and consultant for the company.
A version of this article first appeared on Medscape.com.
The results made the case for “teclistamab as a monotherapy for eligible patients with heavily pretreated multiple myeloma, in need of new treatment options,” investigator Maria-Victoria Mateos, MD, PhD, a hematologist at the University Hospital of Salamanca (Spain) said in a June press release from drug maker Janssen/Johnson & Johnson.
The approval was based on the phase 1-2 single-arm MajesTEC-1 trial. The MajesTEC-1 findings, published in August in the New England Journal of Medicine, included 165 patients with relapsed or refractory multiple myeloma after at least three therapy lines – including an immunomodulatory drug, a proteasome inhibitor, and an anti-CD38 antibody. These patients received a weekly subcutaneous 1.5 mg/kg injection of teclistamab after stepping up from 0.06 mg and 0.3 mg/kg doses.
According to the FDA announcement, the overall response rate was nearly 62%. And the estimated duration of response rate among responders was 90.6% at 6 months and 66.5% at 9 months.
The NEJM results also indicated that almost 40% of patients had a complete response to the therapy, over a median follow-up of 14.1 months. More than a quarter of patients (26.7%) had no minimal residual disease.
The study investigators concluded that “teclistamab resulted in a high rate of deep and durable response in patients with triple-class exposed relapsed or refractory multiple myeloma.”
In a press release, Michael Andreini, president and CEO of the Multiple Myeloma Research Foundation, commented that “teclistamab is an important new treatment option for patients who have faced multiple relapses.”
The recommended dose for teclistamab is 0.06 mg/kg via subcutaneous injection on day 1, 0.3 mg/kg on day 4, and 1.5 mg/kg on day 7, followed by 1.5 mg/kg once weekly until disease progression or unacceptable toxicity.
The FDA noted, however, that the prescribing information for teclistamab comes with a Boxed warning for “life-threatening or fatal cytokine-release syndrome (CRS) and neurologic toxicity, including immune effector cell–associated neurotoxicity (ICANS).”
CRS was reported in 72.1% of patients (grade 3 in one patient but no grade 4 cases), neurologic toxicity in 57%, and ICANS in 6%. Other common adverse events in the NEJM report included neutropenia in 71% of subjects (grade 3 or 4 in 64%); anemia in 52% (grade 3 or 4 in 37%), and thrombocytopenia in 40% (grade 3 or 4 in 21%). Overall, 45% of patients developed grade 3 or 4 infections.
“Because of the risks of CRS and neurologic toxicity, including ICANS, teclistamab-cqyv is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS), called the Tecvayli REMS,” according to the FDA’s press release.
Teclistamab is a T-cell–bispecific antibody that targets both CD3 expressed on the surface of T cells and B-cell maturation antigen (BCMA) expressed on the surface of myeloma cells, activating T-cells to kill cancer cells that express the antigen.
Three BCMA-directed therapies are already on the market in the United States that carry teclistamab’s indication: the antibody-drug conjugate belantamab mafodotin (Blenrep) and two chimeric antigen receptor (CAR) T-cell therapies, idecabtagene vicleucel (Abecma) and ciltacabtagene autoleucel (Carvykti).
The overall response rate is approximately 31% with belantamab mafodotin, 67% for idecabtagene vicleucel, and 83% for ciltacabtagene autoleucel.
Pfizer also has a bispecific BCMA-CD3–targeted antibody in development, elranatamab, for triple-class refractory multiple myeloma that is expected to compete with teclistamab.
MajesTEC-1 was funded by Janssen. Dr. Mateos is a paid speaker and consultant for the company.
A version of this article first appeared on Medscape.com.
The results made the case for “teclistamab as a monotherapy for eligible patients with heavily pretreated multiple myeloma, in need of new treatment options,” investigator Maria-Victoria Mateos, MD, PhD, a hematologist at the University Hospital of Salamanca (Spain) said in a June press release from drug maker Janssen/Johnson & Johnson.
The approval was based on the phase 1-2 single-arm MajesTEC-1 trial. The MajesTEC-1 findings, published in August in the New England Journal of Medicine, included 165 patients with relapsed or refractory multiple myeloma after at least three therapy lines – including an immunomodulatory drug, a proteasome inhibitor, and an anti-CD38 antibody. These patients received a weekly subcutaneous 1.5 mg/kg injection of teclistamab after stepping up from 0.06 mg and 0.3 mg/kg doses.
According to the FDA announcement, the overall response rate was nearly 62%. And the estimated duration of response rate among responders was 90.6% at 6 months and 66.5% at 9 months.
The NEJM results also indicated that almost 40% of patients had a complete response to the therapy, over a median follow-up of 14.1 months. More than a quarter of patients (26.7%) had no minimal residual disease.
The study investigators concluded that “teclistamab resulted in a high rate of deep and durable response in patients with triple-class exposed relapsed or refractory multiple myeloma.”
In a press release, Michael Andreini, president and CEO of the Multiple Myeloma Research Foundation, commented that “teclistamab is an important new treatment option for patients who have faced multiple relapses.”
The recommended dose for teclistamab is 0.06 mg/kg via subcutaneous injection on day 1, 0.3 mg/kg on day 4, and 1.5 mg/kg on day 7, followed by 1.5 mg/kg once weekly until disease progression or unacceptable toxicity.
The FDA noted, however, that the prescribing information for teclistamab comes with a Boxed warning for “life-threatening or fatal cytokine-release syndrome (CRS) and neurologic toxicity, including immune effector cell–associated neurotoxicity (ICANS).”
CRS was reported in 72.1% of patients (grade 3 in one patient but no grade 4 cases), neurologic toxicity in 57%, and ICANS in 6%. Other common adverse events in the NEJM report included neutropenia in 71% of subjects (grade 3 or 4 in 64%); anemia in 52% (grade 3 or 4 in 37%), and thrombocytopenia in 40% (grade 3 or 4 in 21%). Overall, 45% of patients developed grade 3 or 4 infections.
“Because of the risks of CRS and neurologic toxicity, including ICANS, teclistamab-cqyv is available only through a restricted program under a Risk Evaluation and Mitigation Strategy (REMS), called the Tecvayli REMS,” according to the FDA’s press release.
Teclistamab is a T-cell–bispecific antibody that targets both CD3 expressed on the surface of T cells and B-cell maturation antigen (BCMA) expressed on the surface of myeloma cells, activating T-cells to kill cancer cells that express the antigen.
Three BCMA-directed therapies are already on the market in the United States that carry teclistamab’s indication: the antibody-drug conjugate belantamab mafodotin (Blenrep) and two chimeric antigen receptor (CAR) T-cell therapies, idecabtagene vicleucel (Abecma) and ciltacabtagene autoleucel (Carvykti).
The overall response rate is approximately 31% with belantamab mafodotin, 67% for idecabtagene vicleucel, and 83% for ciltacabtagene autoleucel.
Pfizer also has a bispecific BCMA-CD3–targeted antibody in development, elranatamab, for triple-class refractory multiple myeloma that is expected to compete with teclistamab.
MajesTEC-1 was funded by Janssen. Dr. Mateos is a paid speaker and consultant for the company.
A version of this article first appeared on Medscape.com.
Some young CRC patients are missing out on genetic counseling, testing
CHARLOTTE, N.C. – Nearly one-fourth of patients with early-onset colorectal cancer don’t get referrals for genetic counseling or testing, and although acceptance of genetic counseling has improved over the last 10 years, there is still a notable gap between referrals and uptake, investigators have found.
Among 791 patients with young- or early-onset colorectal cancer (YOCRC) seen at a large medical center from 2010 through 2019, 62.1% were referred for genetic counseling, but only 80.1% of this group followed through with the referrals by scheduling an appointment with a counselor or having genetic testing performed, reported Hareem Syed, MD, from the department of internal medicine at the Cleveland Clinic.
“Our findings highlight the need for health systems to implement care pathways to optimize genetic counseling referral and testing in all young-onset colorectal cancer patients,” she said at the annual meeting of the American College of Gastroenterology.
The incidence of CRC diagnosed in persons younger than 50 years is increasing and has been projected to double by 2030, Dr. Syed noted.
In 2009, the Eastern Cooperative Oncology Group recommended that all patients with colorectal cancer be screened for the Lynch syndrome, and earlier this year the National Comprehensive Cancer Network issued a recommendation that patients with YOCRC undergo germline multigene panel testing (MGPT). MGPT has shown that as many as 30% of patients with YOCRC carry a germline pathogenic variant that predisposes them to CRC, regardless of family history, she said.
“We hypothesized that the rate of referral to genetic counseling in this population is low despite the high incidence of pathogenic germline variants, but the uptake of genetic counseling is high [when referred],” Dr. Syed said.
How often, and who needs it?
The investigators sought to determine the frequency of referral to genetic counseling and patient uptake of referrals to assess factors associated with referrals and with uptake, and to evaluate the results of genetic testing.
They reviewed records on all patients younger than 50 years seen at the Cleveland Clinic for CRC from 2010 through 2019, excluding those with appendiceal cancers, a family history of a hereditary cancer syndrome, or irritable bowel syndrome.
The information they extracted from electronic medical records included patient age, sex, family history of CRC, income, tumor stage, and the location and time period of CRC diagnosis.
They considered a genetic counseling referral to be either an order for counseling in the record; clinical documentation of a referral in an office visit with colorectal surgery, oncology, or gastroenterology specialists; or documentation of a completed visit with a genetic counselor.
They considered patient uptake of a counseling referral as either a completed visit to the counselor or documentation of genetic testing results.
The mean patient age at diagnosis was 44 years, with 57.3% of patients male, and 42.7% female. The large majority of patients (86.5%) were White. In all, 40.2% of patients had a family history of CRC.
As noted above, 62.1% of the 791 patients included in the study were referred for counseling, and 80.1% of those referred followed through with uptake. Of this group, nearly all (97.1%) completed genetic testing.
In univariate analysis, factors associated with referral included older patient age at diagnosis, which showed that patients approaching 50 were less likely to receive a referral (odds ratio, 0.904), year of diagnosis with patients diagnosed in the most recent period more likely to receive a referral (OR, 1.247), and family history of CRC (OR, 2.195).
In multivariate analysis, factors significantly associated with referral were age at diagnosis (OR, 0.89), family history of CRC (OR, 2.112), and year of diagnosis (for 2017-19 vs. 2010-13, OR, 5.361).
Among 377 patients who completed genetic testing, 21% were found to have a pathogenic variant, 23% had variants of unknown significance, and 56% had no variants detected. The most commonly detected pathogenic variants were the Lynch syndrome and adenomatous polyposis.
Educate patients and physicians
In an interview, Daniel J. Pambianco, MD, from Charlottesville (Va.) Gastroenterology Associates, who was not involved in the study, commented that patient perceptions about the consequences of genetic testing may be a barrier to either getting a referral for counseling or following through on one.
“Oftentimes patients will perceive anything with ‘genetic’ in it as if their genes are somehow being manipulated, and we need to do a better job at educating patients in that regard,” he said.
Physicians, both primary care practitioners and gastroenterologists, also need to fully appreciate the importance of genetic testing in this population, “because in essence there may be a 4%, 5%, or 6% risk of genetic syndromes that we’re missing and cannot pick up just from getting patients’ histories,” he said.
The investigators did not report a study funding source. Dr. Syed and Dr. Pambianco reported having no relevant financial disclosures.
CHARLOTTE, N.C. – Nearly one-fourth of patients with early-onset colorectal cancer don’t get referrals for genetic counseling or testing, and although acceptance of genetic counseling has improved over the last 10 years, there is still a notable gap between referrals and uptake, investigators have found.
Among 791 patients with young- or early-onset colorectal cancer (YOCRC) seen at a large medical center from 2010 through 2019, 62.1% were referred for genetic counseling, but only 80.1% of this group followed through with the referrals by scheduling an appointment with a counselor or having genetic testing performed, reported Hareem Syed, MD, from the department of internal medicine at the Cleveland Clinic.
“Our findings highlight the need for health systems to implement care pathways to optimize genetic counseling referral and testing in all young-onset colorectal cancer patients,” she said at the annual meeting of the American College of Gastroenterology.
The incidence of CRC diagnosed in persons younger than 50 years is increasing and has been projected to double by 2030, Dr. Syed noted.
In 2009, the Eastern Cooperative Oncology Group recommended that all patients with colorectal cancer be screened for the Lynch syndrome, and earlier this year the National Comprehensive Cancer Network issued a recommendation that patients with YOCRC undergo germline multigene panel testing (MGPT). MGPT has shown that as many as 30% of patients with YOCRC carry a germline pathogenic variant that predisposes them to CRC, regardless of family history, she said.
“We hypothesized that the rate of referral to genetic counseling in this population is low despite the high incidence of pathogenic germline variants, but the uptake of genetic counseling is high [when referred],” Dr. Syed said.
How often, and who needs it?
The investigators sought to determine the frequency of referral to genetic counseling and patient uptake of referrals to assess factors associated with referrals and with uptake, and to evaluate the results of genetic testing.
They reviewed records on all patients younger than 50 years seen at the Cleveland Clinic for CRC from 2010 through 2019, excluding those with appendiceal cancers, a family history of a hereditary cancer syndrome, or irritable bowel syndrome.
The information they extracted from electronic medical records included patient age, sex, family history of CRC, income, tumor stage, and the location and time period of CRC diagnosis.
They considered a genetic counseling referral to be either an order for counseling in the record; clinical documentation of a referral in an office visit with colorectal surgery, oncology, or gastroenterology specialists; or documentation of a completed visit with a genetic counselor.
They considered patient uptake of a counseling referral as either a completed visit to the counselor or documentation of genetic testing results.
The mean patient age at diagnosis was 44 years, with 57.3% of patients male, and 42.7% female. The large majority of patients (86.5%) were White. In all, 40.2% of patients had a family history of CRC.
As noted above, 62.1% of the 791 patients included in the study were referred for counseling, and 80.1% of those referred followed through with uptake. Of this group, nearly all (97.1%) completed genetic testing.
In univariate analysis, factors associated with referral included older patient age at diagnosis, which showed that patients approaching 50 were less likely to receive a referral (odds ratio, 0.904), year of diagnosis with patients diagnosed in the most recent period more likely to receive a referral (OR, 1.247), and family history of CRC (OR, 2.195).
In multivariate analysis, factors significantly associated with referral were age at diagnosis (OR, 0.89), family history of CRC (OR, 2.112), and year of diagnosis (for 2017-19 vs. 2010-13, OR, 5.361).
Among 377 patients who completed genetic testing, 21% were found to have a pathogenic variant, 23% had variants of unknown significance, and 56% had no variants detected. The most commonly detected pathogenic variants were the Lynch syndrome and adenomatous polyposis.
Educate patients and physicians
In an interview, Daniel J. Pambianco, MD, from Charlottesville (Va.) Gastroenterology Associates, who was not involved in the study, commented that patient perceptions about the consequences of genetic testing may be a barrier to either getting a referral for counseling or following through on one.
“Oftentimes patients will perceive anything with ‘genetic’ in it as if their genes are somehow being manipulated, and we need to do a better job at educating patients in that regard,” he said.
Physicians, both primary care practitioners and gastroenterologists, also need to fully appreciate the importance of genetic testing in this population, “because in essence there may be a 4%, 5%, or 6% risk of genetic syndromes that we’re missing and cannot pick up just from getting patients’ histories,” he said.
The investigators did not report a study funding source. Dr. Syed and Dr. Pambianco reported having no relevant financial disclosures.
CHARLOTTE, N.C. – Nearly one-fourth of patients with early-onset colorectal cancer don’t get referrals for genetic counseling or testing, and although acceptance of genetic counseling has improved over the last 10 years, there is still a notable gap between referrals and uptake, investigators have found.
Among 791 patients with young- or early-onset colorectal cancer (YOCRC) seen at a large medical center from 2010 through 2019, 62.1% were referred for genetic counseling, but only 80.1% of this group followed through with the referrals by scheduling an appointment with a counselor or having genetic testing performed, reported Hareem Syed, MD, from the department of internal medicine at the Cleveland Clinic.
“Our findings highlight the need for health systems to implement care pathways to optimize genetic counseling referral and testing in all young-onset colorectal cancer patients,” she said at the annual meeting of the American College of Gastroenterology.
The incidence of CRC diagnosed in persons younger than 50 years is increasing and has been projected to double by 2030, Dr. Syed noted.
In 2009, the Eastern Cooperative Oncology Group recommended that all patients with colorectal cancer be screened for the Lynch syndrome, and earlier this year the National Comprehensive Cancer Network issued a recommendation that patients with YOCRC undergo germline multigene panel testing (MGPT). MGPT has shown that as many as 30% of patients with YOCRC carry a germline pathogenic variant that predisposes them to CRC, regardless of family history, she said.
“We hypothesized that the rate of referral to genetic counseling in this population is low despite the high incidence of pathogenic germline variants, but the uptake of genetic counseling is high [when referred],” Dr. Syed said.
How often, and who needs it?
The investigators sought to determine the frequency of referral to genetic counseling and patient uptake of referrals to assess factors associated with referrals and with uptake, and to evaluate the results of genetic testing.
They reviewed records on all patients younger than 50 years seen at the Cleveland Clinic for CRC from 2010 through 2019, excluding those with appendiceal cancers, a family history of a hereditary cancer syndrome, or irritable bowel syndrome.
The information they extracted from electronic medical records included patient age, sex, family history of CRC, income, tumor stage, and the location and time period of CRC diagnosis.
They considered a genetic counseling referral to be either an order for counseling in the record; clinical documentation of a referral in an office visit with colorectal surgery, oncology, or gastroenterology specialists; or documentation of a completed visit with a genetic counselor.
They considered patient uptake of a counseling referral as either a completed visit to the counselor or documentation of genetic testing results.
The mean patient age at diagnosis was 44 years, with 57.3% of patients male, and 42.7% female. The large majority of patients (86.5%) were White. In all, 40.2% of patients had a family history of CRC.
As noted above, 62.1% of the 791 patients included in the study were referred for counseling, and 80.1% of those referred followed through with uptake. Of this group, nearly all (97.1%) completed genetic testing.
In univariate analysis, factors associated with referral included older patient age at diagnosis, which showed that patients approaching 50 were less likely to receive a referral (odds ratio, 0.904), year of diagnosis with patients diagnosed in the most recent period more likely to receive a referral (OR, 1.247), and family history of CRC (OR, 2.195).
In multivariate analysis, factors significantly associated with referral were age at diagnosis (OR, 0.89), family history of CRC (OR, 2.112), and year of diagnosis (for 2017-19 vs. 2010-13, OR, 5.361).
Among 377 patients who completed genetic testing, 21% were found to have a pathogenic variant, 23% had variants of unknown significance, and 56% had no variants detected. The most commonly detected pathogenic variants were the Lynch syndrome and adenomatous polyposis.
Educate patients and physicians
In an interview, Daniel J. Pambianco, MD, from Charlottesville (Va.) Gastroenterology Associates, who was not involved in the study, commented that patient perceptions about the consequences of genetic testing may be a barrier to either getting a referral for counseling or following through on one.
“Oftentimes patients will perceive anything with ‘genetic’ in it as if their genes are somehow being manipulated, and we need to do a better job at educating patients in that regard,” he said.
Physicians, both primary care practitioners and gastroenterologists, also need to fully appreciate the importance of genetic testing in this population, “because in essence there may be a 4%, 5%, or 6% risk of genetic syndromes that we’re missing and cannot pick up just from getting patients’ histories,” he said.
The investigators did not report a study funding source. Dr. Syed and Dr. Pambianco reported having no relevant financial disclosures.
AT ACG 2022
Children and COVID: Weekly cases fall to lowest level in over a year
With the third autumn of the COVID era now upon us, the discussion has turned again to a possible influenza/COVID twindemic, as well as the new-for-2022 influenza/COVID/respiratory syncytial virus tripledemic. It appears, however, that COVID may have missed the memo.
For the sixth time in the last 7 weeks, the number of new COVID cases in children fell, with just under 23,000 reported during the week of Oct. 14-20, according to the American Academy of Pediatrics and the Children’s Hospital Association. That is the lowest weekly count so far this year, and the lowest since early July of 2021, just as the Delta surge was starting. New pediatric cases had dipped to 8,500, the lowest for any week during the pandemic, a couple of weeks before that, the AAP/CHA data show.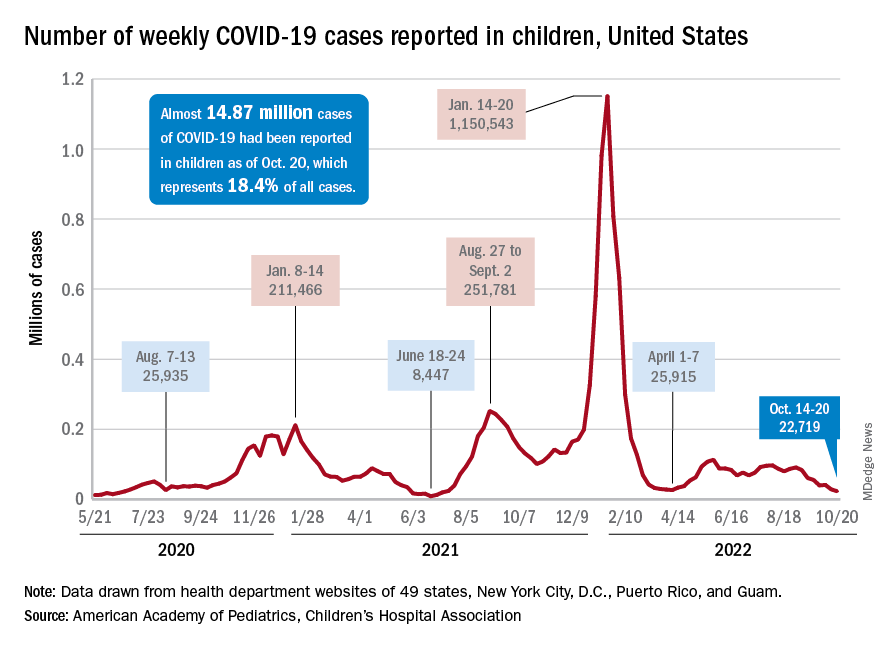
Weekly cases have fallen by almost 75% since over 90,000 were reported for the week of Aug. 26 to Sept. 1, even as children have returned to school and vaccine uptake remains slow in the youngest age groups. Rates of emergency department visits with diagnosed COVID also have continued to drop, as have new admissions, and both are nearing their 2021 lows, according to the Centers for Disease Control and Prevention.
New vaccinations in children under age 5 years were up slightly for the most recent week (Oct. 13-19), but total uptake for that age group is only 7.1% for an initial dose and 2.9% for full vaccination. Among children aged 5-11 years, 38.7% have received at least one dose and 31.6% have completed the primary series, with corresponding figures of 71.2% and 60.9% for those aged 12-17, the CDC said on its COVID Data Tracker.
Despite the low overall numbers, though, the youngest children are, in one respect, punching above their weight when it comes to vaccinations. In the 2 weeks from Oct. 6 to Oct. 19, children under 5 years of age, who represent 5.9% of the U.S. population, received 9.2% of the initial vaccine doses administered. Children aged 5-11 years, who represent 8.7% of the total population, got just 4.2% of all first doses over those same 2 weeks, while 12- to 17-year-olds, who make up 7.6% of the population, got 3.4% of the vaccine doses, the CDC reported.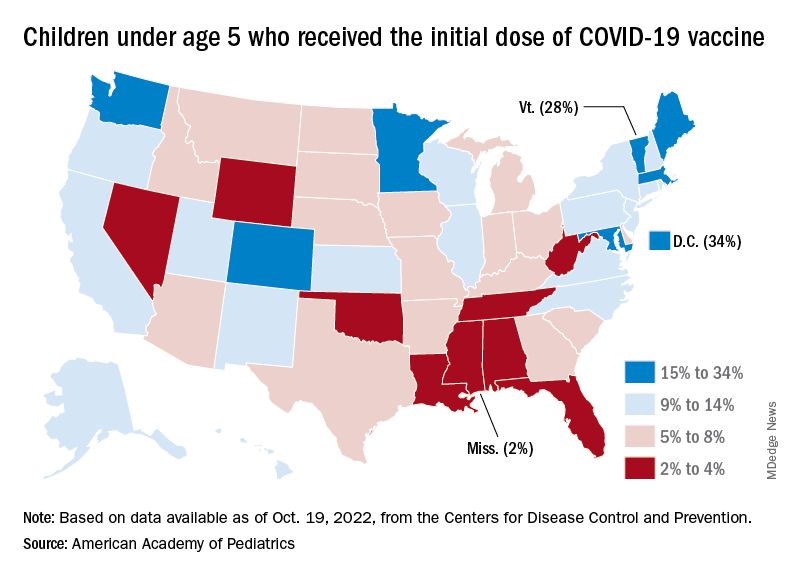
On the vaccine-approval front, the Food and Drug Administration recently announced that the new bivalent COVID-19 vaccines are now included in the emergency use authorizations for children who have completed primary or booster vaccination. The Moderna vaccine is authorized as a single-dose booster for children as young as 6 years and the Pfizer-BioNTech vaccine can be given as a single booster dose in children as young as 5 years, the FDA said.
“These bivalent COVID-19 vaccines include an mRNA component of the original strain to provide an immune response that is broadly protective against COVID-19 and an mRNA component in common between the omicron variant BA.4 and BA.5 lineages,” the FDA said.
With the third autumn of the COVID era now upon us, the discussion has turned again to a possible influenza/COVID twindemic, as well as the new-for-2022 influenza/COVID/respiratory syncytial virus tripledemic. It appears, however, that COVID may have missed the memo.
For the sixth time in the last 7 weeks, the number of new COVID cases in children fell, with just under 23,000 reported during the week of Oct. 14-20, according to the American Academy of Pediatrics and the Children’s Hospital Association. That is the lowest weekly count so far this year, and the lowest since early July of 2021, just as the Delta surge was starting. New pediatric cases had dipped to 8,500, the lowest for any week during the pandemic, a couple of weeks before that, the AAP/CHA data show.
Weekly cases have fallen by almost 75% since over 90,000 were reported for the week of Aug. 26 to Sept. 1, even as children have returned to school and vaccine uptake remains slow in the youngest age groups. Rates of emergency department visits with diagnosed COVID also have continued to drop, as have new admissions, and both are nearing their 2021 lows, according to the Centers for Disease Control and Prevention.
New vaccinations in children under age 5 years were up slightly for the most recent week (Oct. 13-19), but total uptake for that age group is only 7.1% for an initial dose and 2.9% for full vaccination. Among children aged 5-11 years, 38.7% have received at least one dose and 31.6% have completed the primary series, with corresponding figures of 71.2% and 60.9% for those aged 12-17, the CDC said on its COVID Data Tracker.
Despite the low overall numbers, though, the youngest children are, in one respect, punching above their weight when it comes to vaccinations. In the 2 weeks from Oct. 6 to Oct. 19, children under 5 years of age, who represent 5.9% of the U.S. population, received 9.2% of the initial vaccine doses administered. Children aged 5-11 years, who represent 8.7% of the total population, got just 4.2% of all first doses over those same 2 weeks, while 12- to 17-year-olds, who make up 7.6% of the population, got 3.4% of the vaccine doses, the CDC reported.
On the vaccine-approval front, the Food and Drug Administration recently announced that the new bivalent COVID-19 vaccines are now included in the emergency use authorizations for children who have completed primary or booster vaccination. The Moderna vaccine is authorized as a single-dose booster for children as young as 6 years and the Pfizer-BioNTech vaccine can be given as a single booster dose in children as young as 5 years, the FDA said.
“These bivalent COVID-19 vaccines include an mRNA component of the original strain to provide an immune response that is broadly protective against COVID-19 and an mRNA component in common between the omicron variant BA.4 and BA.5 lineages,” the FDA said.
With the third autumn of the COVID era now upon us, the discussion has turned again to a possible influenza/COVID twindemic, as well as the new-for-2022 influenza/COVID/respiratory syncytial virus tripledemic. It appears, however, that COVID may have missed the memo.
For the sixth time in the last 7 weeks, the number of new COVID cases in children fell, with just under 23,000 reported during the week of Oct. 14-20, according to the American Academy of Pediatrics and the Children’s Hospital Association. That is the lowest weekly count so far this year, and the lowest since early July of 2021, just as the Delta surge was starting. New pediatric cases had dipped to 8,500, the lowest for any week during the pandemic, a couple of weeks before that, the AAP/CHA data show.
Weekly cases have fallen by almost 75% since over 90,000 were reported for the week of Aug. 26 to Sept. 1, even as children have returned to school and vaccine uptake remains slow in the youngest age groups. Rates of emergency department visits with diagnosed COVID also have continued to drop, as have new admissions, and both are nearing their 2021 lows, according to the Centers for Disease Control and Prevention.
New vaccinations in children under age 5 years were up slightly for the most recent week (Oct. 13-19), but total uptake for that age group is only 7.1% for an initial dose and 2.9% for full vaccination. Among children aged 5-11 years, 38.7% have received at least one dose and 31.6% have completed the primary series, with corresponding figures of 71.2% and 60.9% for those aged 12-17, the CDC said on its COVID Data Tracker.
Despite the low overall numbers, though, the youngest children are, in one respect, punching above their weight when it comes to vaccinations. In the 2 weeks from Oct. 6 to Oct. 19, children under 5 years of age, who represent 5.9% of the U.S. population, received 9.2% of the initial vaccine doses administered. Children aged 5-11 years, who represent 8.7% of the total population, got just 4.2% of all first doses over those same 2 weeks, while 12- to 17-year-olds, who make up 7.6% of the population, got 3.4% of the vaccine doses, the CDC reported.
On the vaccine-approval front, the Food and Drug Administration recently announced that the new bivalent COVID-19 vaccines are now included in the emergency use authorizations for children who have completed primary or booster vaccination. The Moderna vaccine is authorized as a single-dose booster for children as young as 6 years and the Pfizer-BioNTech vaccine can be given as a single booster dose in children as young as 5 years, the FDA said.
“These bivalent COVID-19 vaccines include an mRNA component of the original strain to provide an immune response that is broadly protective against COVID-19 and an mRNA component in common between the omicron variant BA.4 and BA.5 lineages,” the FDA said.
EUS-guided RF ablation doubles survival for unresectable pancreatic cancer
CHARLOTTE, N.C. – In a small proof-of-concept study, patients with small unresectable pancreatic cancers treated with endoscopic ultrasound–guided radiofrequency ablation (EUS-RFA) had a more than twofold improvement in overall survival compared with historical controls with a similar disease history, investigators in Thailand found.
In a weighted analysis, median weighted overall survival – the primary outcome – was 14 months among 11 patients who underwent EUS-RFA, compared with 6.1 months for 35 matched controls, translating into a hazard ratio for death with EUS-RFA of 0.38 (P = .016), reported Chawin Lopimpisuth, MD, from King Chulalongkorn Memorial Hospital in Bangkok, Thailand.
Median weighted progression-free survival (PFS) was longer among cases than controls, but did not differ significantly, at 6.1 months and 3.9 months, respectively.
“In patients with unresectable pancreatic ductal adenocarcinomas that are less than 4 cm, EUS-RFA alone or combined with chemotherapy resulted in significantly improved overall survival and tended to improve progression-free survival with minimal adverse events,” Dr. Lopimpisuth reported at the annual meeting of the American College of Gastroenterology.
Small but unresectable tumors
Endoscopically guided radiofrequency ablation of pancreatic ductal tumors has been shown to be both feasible and safe in previous studies, he said, prompting his group to explore whether EUS-RFA could help to control the primary tumor and improve survival outcomes.
They enrolled 11 patients with primary pancreatic ductal adenocarcinoma tumors less than 4 cm in diameter that were unresectable due to blood vessel involvement or distant metastasis, and used propensity-score matching to pair them with a total of 35 controls. Controls were matched by tumor size, staging, age-adjusted Charlson Comorbidity Index, chemotherapy regimen received, and interactions between CCI, regimen, and staging.
The results were weighted to assure that covariate distribution among patients treated with chemotherapy only equaled that of patients who underwent EUS-RFA.
Patients underwent EUS-RFA with a 19-gauge needle, with 50 watts of energy delivered with an impedance of 100 ohms. Those patients deemed able to tolerate chemotherapy received that as well.
After a minimum of 1 year of follow-up, the median weighted survival, as noted before, was 14 months for patients who received EUS-RFA, compared with 6.1 months for controls.
Adjusted survival probabilities at 6 and 12 months were 73% and 64%, respectively, for patients in the EUS-RFA group, compared with 69% and 17% for controls. Adjusted PFS rates at 6 and 12 months were 55% and 36% in the EUS-RFA group, compared with 28% and 4% in the control group.
The only adverse event of significance was mild abdominal pain, reported by 8.3% of total EUS-RFA procedures.
Promising but preliminary
In an interview with this news organization, ACG President Samir A. Shah, MD, from Brown University and Miriam Hospital in Providence, R.I., who was not involved in the study, commented that “we have limited options with these patients, so it’s really exciting to see an initial trend toward efficacy, and their survival improvement was significant by several months.”
Dr. Shah was a moderator of the presidential symposium where the data were presented.
Comoderator Brooks D. Cash, MD, from the University of Texas Health Science Center at Houston, said that the advantage of EUS-RFA is that it’s only minimally invasive and appears to offer a significant survival advantage for patients with few effective treatment options.
He cautioned, however, that “it’s a small study and needs to be replicated in a larger venue and different sites as well, but I think it looks very promising.”
The investigators did not report a funding source for the study. Dr. Lopimpisuth, Dr. Shah, and Dr. Cash all reported having no relevant financial relationships to disclose.
CHARLOTTE, N.C. – In a small proof-of-concept study, patients with small unresectable pancreatic cancers treated with endoscopic ultrasound–guided radiofrequency ablation (EUS-RFA) had a more than twofold improvement in overall survival compared with historical controls with a similar disease history, investigators in Thailand found.
In a weighted analysis, median weighted overall survival – the primary outcome – was 14 months among 11 patients who underwent EUS-RFA, compared with 6.1 months for 35 matched controls, translating into a hazard ratio for death with EUS-RFA of 0.38 (P = .016), reported Chawin Lopimpisuth, MD, from King Chulalongkorn Memorial Hospital in Bangkok, Thailand.
Median weighted progression-free survival (PFS) was longer among cases than controls, but did not differ significantly, at 6.1 months and 3.9 months, respectively.
“In patients with unresectable pancreatic ductal adenocarcinomas that are less than 4 cm, EUS-RFA alone or combined with chemotherapy resulted in significantly improved overall survival and tended to improve progression-free survival with minimal adverse events,” Dr. Lopimpisuth reported at the annual meeting of the American College of Gastroenterology.
Small but unresectable tumors
Endoscopically guided radiofrequency ablation of pancreatic ductal tumors has been shown to be both feasible and safe in previous studies, he said, prompting his group to explore whether EUS-RFA could help to control the primary tumor and improve survival outcomes.
They enrolled 11 patients with primary pancreatic ductal adenocarcinoma tumors less than 4 cm in diameter that were unresectable due to blood vessel involvement or distant metastasis, and used propensity-score matching to pair them with a total of 35 controls. Controls were matched by tumor size, staging, age-adjusted Charlson Comorbidity Index, chemotherapy regimen received, and interactions between CCI, regimen, and staging.
The results were weighted to assure that covariate distribution among patients treated with chemotherapy only equaled that of patients who underwent EUS-RFA.
Patients underwent EUS-RFA with a 19-gauge needle, with 50 watts of energy delivered with an impedance of 100 ohms. Those patients deemed able to tolerate chemotherapy received that as well.
After a minimum of 1 year of follow-up, the median weighted survival, as noted before, was 14 months for patients who received EUS-RFA, compared with 6.1 months for controls.
Adjusted survival probabilities at 6 and 12 months were 73% and 64%, respectively, for patients in the EUS-RFA group, compared with 69% and 17% for controls. Adjusted PFS rates at 6 and 12 months were 55% and 36% in the EUS-RFA group, compared with 28% and 4% in the control group.
The only adverse event of significance was mild abdominal pain, reported by 8.3% of total EUS-RFA procedures.
Promising but preliminary
In an interview with this news organization, ACG President Samir A. Shah, MD, from Brown University and Miriam Hospital in Providence, R.I., who was not involved in the study, commented that “we have limited options with these patients, so it’s really exciting to see an initial trend toward efficacy, and their survival improvement was significant by several months.”
Dr. Shah was a moderator of the presidential symposium where the data were presented.
Comoderator Brooks D. Cash, MD, from the University of Texas Health Science Center at Houston, said that the advantage of EUS-RFA is that it’s only minimally invasive and appears to offer a significant survival advantage for patients with few effective treatment options.
He cautioned, however, that “it’s a small study and needs to be replicated in a larger venue and different sites as well, but I think it looks very promising.”
The investigators did not report a funding source for the study. Dr. Lopimpisuth, Dr. Shah, and Dr. Cash all reported having no relevant financial relationships to disclose.
CHARLOTTE, N.C. – In a small proof-of-concept study, patients with small unresectable pancreatic cancers treated with endoscopic ultrasound–guided radiofrequency ablation (EUS-RFA) had a more than twofold improvement in overall survival compared with historical controls with a similar disease history, investigators in Thailand found.
In a weighted analysis, median weighted overall survival – the primary outcome – was 14 months among 11 patients who underwent EUS-RFA, compared with 6.1 months for 35 matched controls, translating into a hazard ratio for death with EUS-RFA of 0.38 (P = .016), reported Chawin Lopimpisuth, MD, from King Chulalongkorn Memorial Hospital in Bangkok, Thailand.
Median weighted progression-free survival (PFS) was longer among cases than controls, but did not differ significantly, at 6.1 months and 3.9 months, respectively.
“In patients with unresectable pancreatic ductal adenocarcinomas that are less than 4 cm, EUS-RFA alone or combined with chemotherapy resulted in significantly improved overall survival and tended to improve progression-free survival with minimal adverse events,” Dr. Lopimpisuth reported at the annual meeting of the American College of Gastroenterology.
Small but unresectable tumors
Endoscopically guided radiofrequency ablation of pancreatic ductal tumors has been shown to be both feasible and safe in previous studies, he said, prompting his group to explore whether EUS-RFA could help to control the primary tumor and improve survival outcomes.
They enrolled 11 patients with primary pancreatic ductal adenocarcinoma tumors less than 4 cm in diameter that were unresectable due to blood vessel involvement or distant metastasis, and used propensity-score matching to pair them with a total of 35 controls. Controls were matched by tumor size, staging, age-adjusted Charlson Comorbidity Index, chemotherapy regimen received, and interactions between CCI, regimen, and staging.
The results were weighted to assure that covariate distribution among patients treated with chemotherapy only equaled that of patients who underwent EUS-RFA.
Patients underwent EUS-RFA with a 19-gauge needle, with 50 watts of energy delivered with an impedance of 100 ohms. Those patients deemed able to tolerate chemotherapy received that as well.
After a minimum of 1 year of follow-up, the median weighted survival, as noted before, was 14 months for patients who received EUS-RFA, compared with 6.1 months for controls.
Adjusted survival probabilities at 6 and 12 months were 73% and 64%, respectively, for patients in the EUS-RFA group, compared with 69% and 17% for controls. Adjusted PFS rates at 6 and 12 months were 55% and 36% in the EUS-RFA group, compared with 28% and 4% in the control group.
The only adverse event of significance was mild abdominal pain, reported by 8.3% of total EUS-RFA procedures.
Promising but preliminary
In an interview with this news organization, ACG President Samir A. Shah, MD, from Brown University and Miriam Hospital in Providence, R.I., who was not involved in the study, commented that “we have limited options with these patients, so it’s really exciting to see an initial trend toward efficacy, and their survival improvement was significant by several months.”
Dr. Shah was a moderator of the presidential symposium where the data were presented.
Comoderator Brooks D. Cash, MD, from the University of Texas Health Science Center at Houston, said that the advantage of EUS-RFA is that it’s only minimally invasive and appears to offer a significant survival advantage for patients with few effective treatment options.
He cautioned, however, that “it’s a small study and needs to be replicated in a larger venue and different sites as well, but I think it looks very promising.”
The investigators did not report a funding source for the study. Dr. Lopimpisuth, Dr. Shah, and Dr. Cash all reported having no relevant financial relationships to disclose.
AT ACG 2022
Maternal deaths show that ‘racism does exist among physicians’
Black mothers giving birth in hospitals are 53% more likely to die during childbirth than are Hispanic and White women, according to researchers who attributed the gap at least in part to bias among physicians and the health care system.
The United States is in the midst of a maternal healthcare crisis, said Robert White, MD, assistant professor of anesthesiology at Weill Cornell Medicine, New York, and lead author of the study. The maternal death rate among U.S. women in 2018, for instance, was 17.4 per 100,000 births, more than twice the figure in Canada (8.6 per 100,000 live births) and the United Kingdom (6.5 per 100,000 live births in 2016), according to the Commonwealth Fund.
“At baseline, our maternal mortality rates are higher than other comparable Western nations, and at the same time, there’s a huge spread in the maternal mortality ratio between White mothers and Black mothers, where Black mothers are experiencing maternal mortality about two or three times higher,” Dr. White told this news organization.
Previous research has shown racial disparities in rates of maternal mortality. But Dr. White said that his study controlled for income level, type of insurance, and other social factors that may have affected the health of the women.
“The research that I conducted is one of the largest of its kind, and the logistic regression model that we were able to run was able to control for a lot of these factors,” he said.
For the new study, presented at the 2022 annual meeting of the American Society of Anesthesiologists, Dr. White and his team analyzed data from 9.5 million deliveries across six states (California, Florida, Kentucky, Maryland, New York, and Washington) between 2007 and 2018. They found that 49,472 mothers (0.5%) either died in the hospital or experienced an injury during childbirth, which included damages to the brain, heart, eyes, or kidneys.
Overall, 0.8% of Black women experienced either a death or an injury, compared with 0.5% of Hispanic women and 0.4% of White women. The researchers concluded that Black women had a 53% increased chance of dying during childbirth in a hospital, even after adjusting for factors such as insurance type, hospital type, and income.
If income, insurance type, and other social factors aren’t driving this disparity in maternal mortality, what is? Dr. White said that the study didn’t uncover the underlying cause, but in his opinion, racial bias and systemic racism are likely contributing to the gap in deaths.
“I think the takeaway for physicians should be that we should humbly accept that prejudice, bias, and racism does exist among physicians,” Dr. White said.
Adi Davidov, MD, associate chair of obstetrics and gynecology at Staten Island (N.Y.) University Hospital, said that both anesthesiologists and ob.gyns. have been aware of these disparate health outcomes for years but have historically attributed the higher odds of injuries and death amongst Black women to health issues rather than racism.
“It is now quite evident that there is more to the story and that there is a degree of unconscious bias as well as systemic racism in health care that contributes to the disparities in outcomes,” said Dr. Davidov, who was not involved in the study.
Meanwhile, new data show that maternal mortality worsened during the COVID-19 pandemic, particularly for Black women. The rate of maternal death for Black women was 44 per 100,000 live births in 2019, 55.3 in 2020, and 68.9 in 2021, according to the U.S. Government Accountability Office. In contrast, White women had death rates of 17.9, 19.1, and 26.1, respectively.
“Bias or discrimination within the health care system can create communication challenges between providers and their patients, which may increase the risk of adverse outcomes,” the report stated.
What can be done
The most important thing physicians can do is to understand and acknowledge unconscious bias, Dr. Davidov told this news organization. “It is important to learn how to identify biases and make sure that it does not affect your medical decision making,” he said.
Dr. White suggested that physicians receive training in implicit bias and cultural competency and stay up to date on research regarding race and medicine as well as learning and using inclusive language.
He also urged physicians closely follow protocols for standard care for their discipline.
“Standardized care protocols have been shown to reduce variance between care of patients of different social structures and shown to decrease this disparity gap,” he said.
The study was supported by a Foundation for Anesthesia Education and Research Mentored Research Training Grant. Dr. White and Dr. Davidov report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Black mothers giving birth in hospitals are 53% more likely to die during childbirth than are Hispanic and White women, according to researchers who attributed the gap at least in part to bias among physicians and the health care system.
The United States is in the midst of a maternal healthcare crisis, said Robert White, MD, assistant professor of anesthesiology at Weill Cornell Medicine, New York, and lead author of the study. The maternal death rate among U.S. women in 2018, for instance, was 17.4 per 100,000 births, more than twice the figure in Canada (8.6 per 100,000 live births) and the United Kingdom (6.5 per 100,000 live births in 2016), according to the Commonwealth Fund.
“At baseline, our maternal mortality rates are higher than other comparable Western nations, and at the same time, there’s a huge spread in the maternal mortality ratio between White mothers and Black mothers, where Black mothers are experiencing maternal mortality about two or three times higher,” Dr. White told this news organization.
Previous research has shown racial disparities in rates of maternal mortality. But Dr. White said that his study controlled for income level, type of insurance, and other social factors that may have affected the health of the women.
“The research that I conducted is one of the largest of its kind, and the logistic regression model that we were able to run was able to control for a lot of these factors,” he said.
For the new study, presented at the 2022 annual meeting of the American Society of Anesthesiologists, Dr. White and his team analyzed data from 9.5 million deliveries across six states (California, Florida, Kentucky, Maryland, New York, and Washington) between 2007 and 2018. They found that 49,472 mothers (0.5%) either died in the hospital or experienced an injury during childbirth, which included damages to the brain, heart, eyes, or kidneys.
Overall, 0.8% of Black women experienced either a death or an injury, compared with 0.5% of Hispanic women and 0.4% of White women. The researchers concluded that Black women had a 53% increased chance of dying during childbirth in a hospital, even after adjusting for factors such as insurance type, hospital type, and income.
If income, insurance type, and other social factors aren’t driving this disparity in maternal mortality, what is? Dr. White said that the study didn’t uncover the underlying cause, but in his opinion, racial bias and systemic racism are likely contributing to the gap in deaths.
“I think the takeaway for physicians should be that we should humbly accept that prejudice, bias, and racism does exist among physicians,” Dr. White said.
Adi Davidov, MD, associate chair of obstetrics and gynecology at Staten Island (N.Y.) University Hospital, said that both anesthesiologists and ob.gyns. have been aware of these disparate health outcomes for years but have historically attributed the higher odds of injuries and death amongst Black women to health issues rather than racism.
“It is now quite evident that there is more to the story and that there is a degree of unconscious bias as well as systemic racism in health care that contributes to the disparities in outcomes,” said Dr. Davidov, who was not involved in the study.
Meanwhile, new data show that maternal mortality worsened during the COVID-19 pandemic, particularly for Black women. The rate of maternal death for Black women was 44 per 100,000 live births in 2019, 55.3 in 2020, and 68.9 in 2021, according to the U.S. Government Accountability Office. In contrast, White women had death rates of 17.9, 19.1, and 26.1, respectively.
“Bias or discrimination within the health care system can create communication challenges between providers and their patients, which may increase the risk of adverse outcomes,” the report stated.
What can be done
The most important thing physicians can do is to understand and acknowledge unconscious bias, Dr. Davidov told this news organization. “It is important to learn how to identify biases and make sure that it does not affect your medical decision making,” he said.
Dr. White suggested that physicians receive training in implicit bias and cultural competency and stay up to date on research regarding race and medicine as well as learning and using inclusive language.
He also urged physicians closely follow protocols for standard care for their discipline.
“Standardized care protocols have been shown to reduce variance between care of patients of different social structures and shown to decrease this disparity gap,” he said.
The study was supported by a Foundation for Anesthesia Education and Research Mentored Research Training Grant. Dr. White and Dr. Davidov report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Black mothers giving birth in hospitals are 53% more likely to die during childbirth than are Hispanic and White women, according to researchers who attributed the gap at least in part to bias among physicians and the health care system.
The United States is in the midst of a maternal healthcare crisis, said Robert White, MD, assistant professor of anesthesiology at Weill Cornell Medicine, New York, and lead author of the study. The maternal death rate among U.S. women in 2018, for instance, was 17.4 per 100,000 births, more than twice the figure in Canada (8.6 per 100,000 live births) and the United Kingdom (6.5 per 100,000 live births in 2016), according to the Commonwealth Fund.
“At baseline, our maternal mortality rates are higher than other comparable Western nations, and at the same time, there’s a huge spread in the maternal mortality ratio between White mothers and Black mothers, where Black mothers are experiencing maternal mortality about two or three times higher,” Dr. White told this news organization.
Previous research has shown racial disparities in rates of maternal mortality. But Dr. White said that his study controlled for income level, type of insurance, and other social factors that may have affected the health of the women.
“The research that I conducted is one of the largest of its kind, and the logistic regression model that we were able to run was able to control for a lot of these factors,” he said.
For the new study, presented at the 2022 annual meeting of the American Society of Anesthesiologists, Dr. White and his team analyzed data from 9.5 million deliveries across six states (California, Florida, Kentucky, Maryland, New York, and Washington) between 2007 and 2018. They found that 49,472 mothers (0.5%) either died in the hospital or experienced an injury during childbirth, which included damages to the brain, heart, eyes, or kidneys.
Overall, 0.8% of Black women experienced either a death or an injury, compared with 0.5% of Hispanic women and 0.4% of White women. The researchers concluded that Black women had a 53% increased chance of dying during childbirth in a hospital, even after adjusting for factors such as insurance type, hospital type, and income.
If income, insurance type, and other social factors aren’t driving this disparity in maternal mortality, what is? Dr. White said that the study didn’t uncover the underlying cause, but in his opinion, racial bias and systemic racism are likely contributing to the gap in deaths.
“I think the takeaway for physicians should be that we should humbly accept that prejudice, bias, and racism does exist among physicians,” Dr. White said.
Adi Davidov, MD, associate chair of obstetrics and gynecology at Staten Island (N.Y.) University Hospital, said that both anesthesiologists and ob.gyns. have been aware of these disparate health outcomes for years but have historically attributed the higher odds of injuries and death amongst Black women to health issues rather than racism.
“It is now quite evident that there is more to the story and that there is a degree of unconscious bias as well as systemic racism in health care that contributes to the disparities in outcomes,” said Dr. Davidov, who was not involved in the study.
Meanwhile, new data show that maternal mortality worsened during the COVID-19 pandemic, particularly for Black women. The rate of maternal death for Black women was 44 per 100,000 live births in 2019, 55.3 in 2020, and 68.9 in 2021, according to the U.S. Government Accountability Office. In contrast, White women had death rates of 17.9, 19.1, and 26.1, respectively.
“Bias or discrimination within the health care system can create communication challenges between providers and their patients, which may increase the risk of adverse outcomes,” the report stated.
What can be done
The most important thing physicians can do is to understand and acknowledge unconscious bias, Dr. Davidov told this news organization. “It is important to learn how to identify biases and make sure that it does not affect your medical decision making,” he said.
Dr. White suggested that physicians receive training in implicit bias and cultural competency and stay up to date on research regarding race and medicine as well as learning and using inclusive language.
He also urged physicians closely follow protocols for standard care for their discipline.
“Standardized care protocols have been shown to reduce variance between care of patients of different social structures and shown to decrease this disparity gap,” he said.
The study was supported by a Foundation for Anesthesia Education and Research Mentored Research Training Grant. Dr. White and Dr. Davidov report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Sexual health care for disabled youth: Tough and getting tougher
The developmentally disabled girl was just 10 years old when Margaret Thew, DNP, medical director of adolescent medicine at Children’s Wisconsin, Milwaukee, helped care for her. Providing that care was not emotionally easy. “Her brother’s friend sexually assaulted her and impregnated her,” Dr. Thew said.
The girl was able to obtain an abortion, a decision her parents supported. The alternative could have been deadly. “She was a tiny little person and would not have been able to carry a fetus,” Dr. Thew, a nurse practitioner, said.
Dr. Thew said she’s thankful that tragic case occurred before 2022. After the United States Supreme Court overturned Roe v. Wade in June, Wisconsin reverted to an 1849 law banning abortion. Although the law is currently being challenged, Dr. Thew wonders how the situation would have played out now. (Weeks after the Supreme Court’s decision, a similar case occurred in Ohio. In that case, a 10-year-old girl had to travel out of the state to obtain an abortion after having been raped.)
Talking to adolescents and young adults about reproductive health, whether regarding an unexpected pregnancy, the need for contraception, or to provide information about sexual activity, can be a challenge even for experienced health care providers.
The talks, decisions, and care are particularly complex when patients have developmental and intellectual disabilities. Among the many factors, Dr. Thew said, are dealing with menstruation, finding the right contraceptives, and counseling parents who might not want to acknowledge their children’s emerging sexuality.
Statistics: How many?
Because the definitions of disabilities vary and they represent a spectrum, estimates for how many youth have intellectual or developmental disabilities range widely.
In 2019, the National Survey of Children’s Health found that 1 in 4 children and adolescents aged 12-17 years have special health care needs because of disability. The American Community Survey estimates more than 1.3 million people aged 16-20 have a disability.
Intellectual disabilities can occur when a person’s IQ is below 70, significantly impeding the ability to perform activities of daily living, such as eating, dressing, and communicating. Developmental disabilities are impairments in physical, learning, language, and behavior, according to the United States Centers for Disease Control and Prevention. Among the conditions are attention-deficit/hyperactivity disorder, autism spectrum disorders, fragile X syndrome, learning and language problems, spina bifida, and other conditions.
Addressing common issues, concerns
April Kayser is a health educator for the Multnomah County Health Department, Portland, Ore. In 2016, Ms. Kayser and other experts conducted interviews with 11 youth with developmental and intellectual disabilities and 34 support people, either parents or professionals who provide services. The survey was part of the SHEIDD Project – short for Sexual Health Equity for Individuals with Intellectual/Developmental Disabilities – at Oregon Health and Science University (OHSU).
From their findings, the researchers compiled guidelines. They provided scenarios that health care providers need to be aware of and that they need to be ready to address:
- A boy, 14, who is unclear about what to do when he feels sexually excited and wants to masturbate but isn’t at home. He has been told that masturbation is appropriate in private.
- A 20-year-old woman who lives in a group home is pregnant. She confesses to her parents during a visit that another resident is her boyfriend and that he is the father of the child she is expecting.
- A 17-year-old boy wants to ask out another student, who is 15.
Some developmentally and intellectually disabled youth can’t turn to their parents for help. One person in the survey said his father told him, “You don’t need to worry about any of that stuff. You’re too young.” Another said the job of a health care provider was to offer reproductive and sex education “to make sure you don’t screw up in some bad way.”
One finding stood out: Health care providers were at the top of the list of those whom young people trusted for information about reproductive and sexual health, Ms. Kayser said. Yet in her experience, she said, health care professionals are hesitant to bring up the issues with all youth, “especially those with intellectual and developmental disabilities.”
Health care providers often talk both to the patient and to the parents. Those conversations can be critical when a child is developmentally or intellectually disabled.
Women with disabilities have been shown to have a higher risk for adverse outcomes of pregnancy, said Willi Horner-Johnson, PhD, associate professor at OHSU–Portland State University School of Public Health.
In a recent study, she and her colleagues analyzed data from the CDC’s National Survey of Family Growth that included self-reported disability status. They found that the number of women with disabilities who give birth is far higher than was previously thought.
The researchers found that 19.5% of respondents who gave birth reported at least one sensory, cognitive, or mobility-related disability, a rate that is much greater than the less than 1%-6.6% estimates that are based on hospital discharge data.
Her group reported other troubling findings: Women with disabilities are twice as likely to have smoked during their pregnancy (19% vs. 8.9%) and are more likely to have preterm and low-birthweight babies.
Clinicians play an important role
Dr. Horner-Johnson agreed with the finding from the Multnomah County survey that health care providers play an important role in providing those with intellectual and developmental disabilities reproductive health care that meets their needs. “Clinicians need to be asking people with disabilities about their reproductive plans,” she said.
In the Multnomah County report, the researchers advised health care providers to recognize that people with disabilities are social and sexual beings; to learn about their goals, including those regarding sex and reproductive health; and to help youth build skills for healthy relationships and sexual activity.
Dr. Horner-Johnson pointed out that the American College of Obstetricians and Gynecologists “recommends that clinicians discuss reproductive plans at every visit, for example, by asking one key question – ‘Would you like to become pregnant in the next year?’ – of every woman of reproductive age.”
Some women will not be able to answer that question, and health care providers at times must rely on a caregiver for input. But many women, even those with disabilities, could answer if given a chance. She estimated that only about 5% of disabled people are unable to communicate. “Clinicians defer to the caregiver more than they need to,” she said.
Clinicians are becoming better at providing care to those with disabilities, Dr. Horner-Johnson said, yet they have a way to go. Clinician biases may prevent some from asking all women, including those with disabilities, about their reproductive plans. “Women with disabilities have described clinicians treating them as nonsexual, assuming or implying that they would not or should not get pregnant,” she writes in her report.
Such biases, she said, could be reduced by increased education of providers. A 2018 study in Health Equity found that only 19.3% of ob.gyns. said they felt equipped to manage the pregnancy of a woman with disabilities.
Managing sexuality and sexual health for youth with disabilities can be highly complex, according to Margaret Thew, DNP, medical director of adolescent medicine at Children’s Wisconsin, Milwaukee. Challenges include the following:
- Parents often can’t deal with the reality that their teen or young adult is sexually active or may become so. Parents she helps often prefer to use the term “hormones,” not contraceptives, when talking about pregnancy prevention.
- Menstruation is a frequent concern, especially for youth with severe disabilities. Some react strongly to seeing a sanitary pad with blood, for example, by throwing it. Parents worry that caregivers will balk at changing pads regularly. As a result, some parents want complete menstrual suppression, Dr. Thew said. The American Academy of Pediatrics outlines how to approach menstrual suppression through methods such as the use of estrogen-progestin, progesterone, a ring, or a patch. In late August, the American College of Obstetricians and Gynecologists released its clinical consensus on medical management of menstrual suppression.
- Some parents want to know how to obtain a complete hysterectomy for the patient – an option Dr. Thew and the AAP discourage. “We will tell them that’s not the best and safest approach, as you want to have the estrogen for bone health,” she said.
- After a discussion of all the options, an intrauterine device proves best for many. “That gives 7-8 years of protection,” she said, which is the approved effective duration for such devices. “They are less apt to have heavy monthly menstrual bleeding.”
- Parents of boys with disabilities, especially those with Down syndrome, often ask for sex education and guidance when sexual desires develop.
- Many parents want effective birth control for their children because of fear that their teen or young adult will be assaulted, a fear that isn’t groundless. Such cases are common, and caregivers frequently are the perpetrators.
Ms. Kayser, Dr. Horner-Johnson, and Dr. Thew have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The developmentally disabled girl was just 10 years old when Margaret Thew, DNP, medical director of adolescent medicine at Children’s Wisconsin, Milwaukee, helped care for her. Providing that care was not emotionally easy. “Her brother’s friend sexually assaulted her and impregnated her,” Dr. Thew said.
The girl was able to obtain an abortion, a decision her parents supported. The alternative could have been deadly. “She was a tiny little person and would not have been able to carry a fetus,” Dr. Thew, a nurse practitioner, said.
Dr. Thew said she’s thankful that tragic case occurred before 2022. After the United States Supreme Court overturned Roe v. Wade in June, Wisconsin reverted to an 1849 law banning abortion. Although the law is currently being challenged, Dr. Thew wonders how the situation would have played out now. (Weeks after the Supreme Court’s decision, a similar case occurred in Ohio. In that case, a 10-year-old girl had to travel out of the state to obtain an abortion after having been raped.)
Talking to adolescents and young adults about reproductive health, whether regarding an unexpected pregnancy, the need for contraception, or to provide information about sexual activity, can be a challenge even for experienced health care providers.
The talks, decisions, and care are particularly complex when patients have developmental and intellectual disabilities. Among the many factors, Dr. Thew said, are dealing with menstruation, finding the right contraceptives, and counseling parents who might not want to acknowledge their children’s emerging sexuality.
Statistics: How many?
Because the definitions of disabilities vary and they represent a spectrum, estimates for how many youth have intellectual or developmental disabilities range widely.
In 2019, the National Survey of Children’s Health found that 1 in 4 children and adolescents aged 12-17 years have special health care needs because of disability. The American Community Survey estimates more than 1.3 million people aged 16-20 have a disability.
Intellectual disabilities can occur when a person’s IQ is below 70, significantly impeding the ability to perform activities of daily living, such as eating, dressing, and communicating. Developmental disabilities are impairments in physical, learning, language, and behavior, according to the United States Centers for Disease Control and Prevention. Among the conditions are attention-deficit/hyperactivity disorder, autism spectrum disorders, fragile X syndrome, learning and language problems, spina bifida, and other conditions.
Addressing common issues, concerns
April Kayser is a health educator for the Multnomah County Health Department, Portland, Ore. In 2016, Ms. Kayser and other experts conducted interviews with 11 youth with developmental and intellectual disabilities and 34 support people, either parents or professionals who provide services. The survey was part of the SHEIDD Project – short for Sexual Health Equity for Individuals with Intellectual/Developmental Disabilities – at Oregon Health and Science University (OHSU).
From their findings, the researchers compiled guidelines. They provided scenarios that health care providers need to be aware of and that they need to be ready to address:
- A boy, 14, who is unclear about what to do when he feels sexually excited and wants to masturbate but isn’t at home. He has been told that masturbation is appropriate in private.
- A 20-year-old woman who lives in a group home is pregnant. She confesses to her parents during a visit that another resident is her boyfriend and that he is the father of the child she is expecting.
- A 17-year-old boy wants to ask out another student, who is 15.
Some developmentally and intellectually disabled youth can’t turn to their parents for help. One person in the survey said his father told him, “You don’t need to worry about any of that stuff. You’re too young.” Another said the job of a health care provider was to offer reproductive and sex education “to make sure you don’t screw up in some bad way.”
One finding stood out: Health care providers were at the top of the list of those whom young people trusted for information about reproductive and sexual health, Ms. Kayser said. Yet in her experience, she said, health care professionals are hesitant to bring up the issues with all youth, “especially those with intellectual and developmental disabilities.”
Health care providers often talk both to the patient and to the parents. Those conversations can be critical when a child is developmentally or intellectually disabled.
Women with disabilities have been shown to have a higher risk for adverse outcomes of pregnancy, said Willi Horner-Johnson, PhD, associate professor at OHSU–Portland State University School of Public Health.
In a recent study, she and her colleagues analyzed data from the CDC’s National Survey of Family Growth that included self-reported disability status. They found that the number of women with disabilities who give birth is far higher than was previously thought.
The researchers found that 19.5% of respondents who gave birth reported at least one sensory, cognitive, or mobility-related disability, a rate that is much greater than the less than 1%-6.6% estimates that are based on hospital discharge data.
Her group reported other troubling findings: Women with disabilities are twice as likely to have smoked during their pregnancy (19% vs. 8.9%) and are more likely to have preterm and low-birthweight babies.
Clinicians play an important role
Dr. Horner-Johnson agreed with the finding from the Multnomah County survey that health care providers play an important role in providing those with intellectual and developmental disabilities reproductive health care that meets their needs. “Clinicians need to be asking people with disabilities about their reproductive plans,” she said.
In the Multnomah County report, the researchers advised health care providers to recognize that people with disabilities are social and sexual beings; to learn about their goals, including those regarding sex and reproductive health; and to help youth build skills for healthy relationships and sexual activity.
Dr. Horner-Johnson pointed out that the American College of Obstetricians and Gynecologists “recommends that clinicians discuss reproductive plans at every visit, for example, by asking one key question – ‘Would you like to become pregnant in the next year?’ – of every woman of reproductive age.”
Some women will not be able to answer that question, and health care providers at times must rely on a caregiver for input. But many women, even those with disabilities, could answer if given a chance. She estimated that only about 5% of disabled people are unable to communicate. “Clinicians defer to the caregiver more than they need to,” she said.
Clinicians are becoming better at providing care to those with disabilities, Dr. Horner-Johnson said, yet they have a way to go. Clinician biases may prevent some from asking all women, including those with disabilities, about their reproductive plans. “Women with disabilities have described clinicians treating them as nonsexual, assuming or implying that they would not or should not get pregnant,” she writes in her report.
Such biases, she said, could be reduced by increased education of providers. A 2018 study in Health Equity found that only 19.3% of ob.gyns. said they felt equipped to manage the pregnancy of a woman with disabilities.
Managing sexuality and sexual health for youth with disabilities can be highly complex, according to Margaret Thew, DNP, medical director of adolescent medicine at Children’s Wisconsin, Milwaukee. Challenges include the following:
- Parents often can’t deal with the reality that their teen or young adult is sexually active or may become so. Parents she helps often prefer to use the term “hormones,” not contraceptives, when talking about pregnancy prevention.
- Menstruation is a frequent concern, especially for youth with severe disabilities. Some react strongly to seeing a sanitary pad with blood, for example, by throwing it. Parents worry that caregivers will balk at changing pads regularly. As a result, some parents want complete menstrual suppression, Dr. Thew said. The American Academy of Pediatrics outlines how to approach menstrual suppression through methods such as the use of estrogen-progestin, progesterone, a ring, or a patch. In late August, the American College of Obstetricians and Gynecologists released its clinical consensus on medical management of menstrual suppression.
- Some parents want to know how to obtain a complete hysterectomy for the patient – an option Dr. Thew and the AAP discourage. “We will tell them that’s not the best and safest approach, as you want to have the estrogen for bone health,” she said.
- After a discussion of all the options, an intrauterine device proves best for many. “That gives 7-8 years of protection,” she said, which is the approved effective duration for such devices. “They are less apt to have heavy monthly menstrual bleeding.”
- Parents of boys with disabilities, especially those with Down syndrome, often ask for sex education and guidance when sexual desires develop.
- Many parents want effective birth control for their children because of fear that their teen or young adult will be assaulted, a fear that isn’t groundless. Such cases are common, and caregivers frequently are the perpetrators.
Ms. Kayser, Dr. Horner-Johnson, and Dr. Thew have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The developmentally disabled girl was just 10 years old when Margaret Thew, DNP, medical director of adolescent medicine at Children’s Wisconsin, Milwaukee, helped care for her. Providing that care was not emotionally easy. “Her brother’s friend sexually assaulted her and impregnated her,” Dr. Thew said.
The girl was able to obtain an abortion, a decision her parents supported. The alternative could have been deadly. “She was a tiny little person and would not have been able to carry a fetus,” Dr. Thew, a nurse practitioner, said.
Dr. Thew said she’s thankful that tragic case occurred before 2022. After the United States Supreme Court overturned Roe v. Wade in June, Wisconsin reverted to an 1849 law banning abortion. Although the law is currently being challenged, Dr. Thew wonders how the situation would have played out now. (Weeks after the Supreme Court’s decision, a similar case occurred in Ohio. In that case, a 10-year-old girl had to travel out of the state to obtain an abortion after having been raped.)
Talking to adolescents and young adults about reproductive health, whether regarding an unexpected pregnancy, the need for contraception, or to provide information about sexual activity, can be a challenge even for experienced health care providers.
The talks, decisions, and care are particularly complex when patients have developmental and intellectual disabilities. Among the many factors, Dr. Thew said, are dealing with menstruation, finding the right contraceptives, and counseling parents who might not want to acknowledge their children’s emerging sexuality.
Statistics: How many?
Because the definitions of disabilities vary and they represent a spectrum, estimates for how many youth have intellectual or developmental disabilities range widely.
In 2019, the National Survey of Children’s Health found that 1 in 4 children and adolescents aged 12-17 years have special health care needs because of disability. The American Community Survey estimates more than 1.3 million people aged 16-20 have a disability.
Intellectual disabilities can occur when a person’s IQ is below 70, significantly impeding the ability to perform activities of daily living, such as eating, dressing, and communicating. Developmental disabilities are impairments in physical, learning, language, and behavior, according to the United States Centers for Disease Control and Prevention. Among the conditions are attention-deficit/hyperactivity disorder, autism spectrum disorders, fragile X syndrome, learning and language problems, spina bifida, and other conditions.
Addressing common issues, concerns
April Kayser is a health educator for the Multnomah County Health Department, Portland, Ore. In 2016, Ms. Kayser and other experts conducted interviews with 11 youth with developmental and intellectual disabilities and 34 support people, either parents or professionals who provide services. The survey was part of the SHEIDD Project – short for Sexual Health Equity for Individuals with Intellectual/Developmental Disabilities – at Oregon Health and Science University (OHSU).
From their findings, the researchers compiled guidelines. They provided scenarios that health care providers need to be aware of and that they need to be ready to address:
- A boy, 14, who is unclear about what to do when he feels sexually excited and wants to masturbate but isn’t at home. He has been told that masturbation is appropriate in private.
- A 20-year-old woman who lives in a group home is pregnant. She confesses to her parents during a visit that another resident is her boyfriend and that he is the father of the child she is expecting.
- A 17-year-old boy wants to ask out another student, who is 15.
Some developmentally and intellectually disabled youth can’t turn to their parents for help. One person in the survey said his father told him, “You don’t need to worry about any of that stuff. You’re too young.” Another said the job of a health care provider was to offer reproductive and sex education “to make sure you don’t screw up in some bad way.”
One finding stood out: Health care providers were at the top of the list of those whom young people trusted for information about reproductive and sexual health, Ms. Kayser said. Yet in her experience, she said, health care professionals are hesitant to bring up the issues with all youth, “especially those with intellectual and developmental disabilities.”
Health care providers often talk both to the patient and to the parents. Those conversations can be critical when a child is developmentally or intellectually disabled.
Women with disabilities have been shown to have a higher risk for adverse outcomes of pregnancy, said Willi Horner-Johnson, PhD, associate professor at OHSU–Portland State University School of Public Health.
In a recent study, she and her colleagues analyzed data from the CDC’s National Survey of Family Growth that included self-reported disability status. They found that the number of women with disabilities who give birth is far higher than was previously thought.
The researchers found that 19.5% of respondents who gave birth reported at least one sensory, cognitive, or mobility-related disability, a rate that is much greater than the less than 1%-6.6% estimates that are based on hospital discharge data.
Her group reported other troubling findings: Women with disabilities are twice as likely to have smoked during their pregnancy (19% vs. 8.9%) and are more likely to have preterm and low-birthweight babies.
Clinicians play an important role
Dr. Horner-Johnson agreed with the finding from the Multnomah County survey that health care providers play an important role in providing those with intellectual and developmental disabilities reproductive health care that meets their needs. “Clinicians need to be asking people with disabilities about their reproductive plans,” she said.
In the Multnomah County report, the researchers advised health care providers to recognize that people with disabilities are social and sexual beings; to learn about their goals, including those regarding sex and reproductive health; and to help youth build skills for healthy relationships and sexual activity.
Dr. Horner-Johnson pointed out that the American College of Obstetricians and Gynecologists “recommends that clinicians discuss reproductive plans at every visit, for example, by asking one key question – ‘Would you like to become pregnant in the next year?’ – of every woman of reproductive age.”
Some women will not be able to answer that question, and health care providers at times must rely on a caregiver for input. But many women, even those with disabilities, could answer if given a chance. She estimated that only about 5% of disabled people are unable to communicate. “Clinicians defer to the caregiver more than they need to,” she said.
Clinicians are becoming better at providing care to those with disabilities, Dr. Horner-Johnson said, yet they have a way to go. Clinician biases may prevent some from asking all women, including those with disabilities, about their reproductive plans. “Women with disabilities have described clinicians treating them as nonsexual, assuming or implying that they would not or should not get pregnant,” she writes in her report.
Such biases, she said, could be reduced by increased education of providers. A 2018 study in Health Equity found that only 19.3% of ob.gyns. said they felt equipped to manage the pregnancy of a woman with disabilities.
Managing sexuality and sexual health for youth with disabilities can be highly complex, according to Margaret Thew, DNP, medical director of adolescent medicine at Children’s Wisconsin, Milwaukee. Challenges include the following:
- Parents often can’t deal with the reality that their teen or young adult is sexually active or may become so. Parents she helps often prefer to use the term “hormones,” not contraceptives, when talking about pregnancy prevention.
- Menstruation is a frequent concern, especially for youth with severe disabilities. Some react strongly to seeing a sanitary pad with blood, for example, by throwing it. Parents worry that caregivers will balk at changing pads regularly. As a result, some parents want complete menstrual suppression, Dr. Thew said. The American Academy of Pediatrics outlines how to approach menstrual suppression through methods such as the use of estrogen-progestin, progesterone, a ring, or a patch. In late August, the American College of Obstetricians and Gynecologists released its clinical consensus on medical management of menstrual suppression.
- Some parents want to know how to obtain a complete hysterectomy for the patient – an option Dr. Thew and the AAP discourage. “We will tell them that’s not the best and safest approach, as you want to have the estrogen for bone health,” she said.
- After a discussion of all the options, an intrauterine device proves best for many. “That gives 7-8 years of protection,” she said, which is the approved effective duration for such devices. “They are less apt to have heavy monthly menstrual bleeding.”
- Parents of boys with disabilities, especially those with Down syndrome, often ask for sex education and guidance when sexual desires develop.
- Many parents want effective birth control for their children because of fear that their teen or young adult will be assaulted, a fear that isn’t groundless. Such cases are common, and caregivers frequently are the perpetrators.
Ms. Kayser, Dr. Horner-Johnson, and Dr. Thew have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dupilumab-associated ocular surface disease in patients with AD: Unraveling the link
MONTREAL – , according to a study presented at the annual meeting of the International Society of Atopic Dermatitis.
In a prospective trial of 69 patients with AD starting dupilumab (Dupixent), baseline OSD was found in 91.3%, with about half of these patients reporting no symptoms, said investigator Roselie Achten, MD, from the National Expertise Center for Atopic Dermatitis at University Medical Center Utrecht, the Netherlands. Among these patients, ophthalmologic assessment revealed no OSD in 6 patients and mild OSD in 37 patients, but moderate and severe disease in 20 and 6 patients, respectively, she said, adding that 71% of the group also reported allergic conjunctivitis at baseline.
The patients enrolled in the study who started dupilumab were aged 36-38 years, with Eczema Area and Severity Index (EASI) scores of 14.7-16.5. Baseline ocular surface health was assessed with the Utrecht Ophthalmic Inflammatory and Allergic disease (UTOPIA) score. Tear fluid was collected to analyze biomarkers and dupilumab levels, and impression cytology was performed to collect conjunctival tissue cells for analysis of goblet cells. These measurements were repeated at 4 and 28 weeks after the start of therapy.
Over 28 weeks of treatment, 14.5% of patients experienced worsening of OSD, with worsening disease associated with a decline in the number of goblet cells. In addition, dupilumab treatment was associated with a significant decline in the production of Mucin5AC, suggesting a decline in function of the goblet cells. “Our hypothesis that the blocking effect of dupilumab on [interleukin-] IL-13 might lead to less goblet cells and less mucin production,” she explained.
In a subset of 48 patients, the researchers also detected significantly higher tear fluid dupilumab levels among those patients with more severe OSD, with comparable serum levels.
OSD has been reported in up to 34% of dupilumab-treated patients with AD and is the most frequently reported side-effect of this treatment, noted Dr. Achten. This side effect is not reported by other patients treated with dupilumab for other indications, she added, “suggesting that AD patients may have a predisposition to develop OSD during dupilumab treatment.”
Indeed, as recently noted by Vivian Shi, MD, from the department of dermatology, University of Arkansas for Medical Sciences, Little Rock, and colleagues, “for reasons not well understood, the incidence of conjunctivitis in dupilumab patients with asthma (0%-2.3%), chronic rhinosinusitis with nasal polyps (1.6%), or eosinophilic esophagitis (0%) is low to none; thus, patients with AD may be particularly susceptible.”
Dr. Achten said that dupilumab-treated patients with AD at her center are prescribed topical tacrolimus and ketotifen eye drops if they develop OSD.
Asked for comment, Melinda Gooderham, MD, who moderated the session, was impressed with the study. “I’d heard about the goblet cells, there were little bits of data here and there, but the tear analysis is something I hadn’t seen before. It was a nice series of experiments that pulled everything together,” she told this news organization. Dr. Gooderham, who is assistant professor at Queens University, in Kingston, Ontario, medical director at the SKiN Centre for Dermatology in Peterborough, Ontario, and consultant physician at Peterborough Regional Health Centre, said that she first began noticing dupilumab-related OSD as an early trial investigator for the drug. “When you put some patients on the drug it’s almost like tipping the balance – that little bit of mucin they’re dependent on is now reduced and it makes them more symptomatic,” she said.
Though she prescribes lubricating eye drops as prophylaxis for all her dupilumab-treated patients with AD, she recommends referring any patients who develop OSD to an ophthalmologist who is familiar with this specific side effect. “If they just see a random ophthalmologist who doesn’t know dupilumab, and doesn’t know the story around it, they could get any sort of diagnosis, or even be told to stop the medication altogether.”
The study was sponsored by Sanofi. Dr. Achten disclosed no other conflicts of interest. Dr. Gooderham is an investigator with Sanofi Genzyme for dupilumab.
A version of this article first appeared on Medscape.com.
MONTREAL – , according to a study presented at the annual meeting of the International Society of Atopic Dermatitis.
In a prospective trial of 69 patients with AD starting dupilumab (Dupixent), baseline OSD was found in 91.3%, with about half of these patients reporting no symptoms, said investigator Roselie Achten, MD, from the National Expertise Center for Atopic Dermatitis at University Medical Center Utrecht, the Netherlands. Among these patients, ophthalmologic assessment revealed no OSD in 6 patients and mild OSD in 37 patients, but moderate and severe disease in 20 and 6 patients, respectively, she said, adding that 71% of the group also reported allergic conjunctivitis at baseline.
The patients enrolled in the study who started dupilumab were aged 36-38 years, with Eczema Area and Severity Index (EASI) scores of 14.7-16.5. Baseline ocular surface health was assessed with the Utrecht Ophthalmic Inflammatory and Allergic disease (UTOPIA) score. Tear fluid was collected to analyze biomarkers and dupilumab levels, and impression cytology was performed to collect conjunctival tissue cells for analysis of goblet cells. These measurements were repeated at 4 and 28 weeks after the start of therapy.
Over 28 weeks of treatment, 14.5% of patients experienced worsening of OSD, with worsening disease associated with a decline in the number of goblet cells. In addition, dupilumab treatment was associated with a significant decline in the production of Mucin5AC, suggesting a decline in function of the goblet cells. “Our hypothesis that the blocking effect of dupilumab on [interleukin-] IL-13 might lead to less goblet cells and less mucin production,” she explained.
In a subset of 48 patients, the researchers also detected significantly higher tear fluid dupilumab levels among those patients with more severe OSD, with comparable serum levels.
OSD has been reported in up to 34% of dupilumab-treated patients with AD and is the most frequently reported side-effect of this treatment, noted Dr. Achten. This side effect is not reported by other patients treated with dupilumab for other indications, she added, “suggesting that AD patients may have a predisposition to develop OSD during dupilumab treatment.”
Indeed, as recently noted by Vivian Shi, MD, from the department of dermatology, University of Arkansas for Medical Sciences, Little Rock, and colleagues, “for reasons not well understood, the incidence of conjunctivitis in dupilumab patients with asthma (0%-2.3%), chronic rhinosinusitis with nasal polyps (1.6%), or eosinophilic esophagitis (0%) is low to none; thus, patients with AD may be particularly susceptible.”
Dr. Achten said that dupilumab-treated patients with AD at her center are prescribed topical tacrolimus and ketotifen eye drops if they develop OSD.
Asked for comment, Melinda Gooderham, MD, who moderated the session, was impressed with the study. “I’d heard about the goblet cells, there were little bits of data here and there, but the tear analysis is something I hadn’t seen before. It was a nice series of experiments that pulled everything together,” she told this news organization. Dr. Gooderham, who is assistant professor at Queens University, in Kingston, Ontario, medical director at the SKiN Centre for Dermatology in Peterborough, Ontario, and consultant physician at Peterborough Regional Health Centre, said that she first began noticing dupilumab-related OSD as an early trial investigator for the drug. “When you put some patients on the drug it’s almost like tipping the balance – that little bit of mucin they’re dependent on is now reduced and it makes them more symptomatic,” she said.
Though she prescribes lubricating eye drops as prophylaxis for all her dupilumab-treated patients with AD, she recommends referring any patients who develop OSD to an ophthalmologist who is familiar with this specific side effect. “If they just see a random ophthalmologist who doesn’t know dupilumab, and doesn’t know the story around it, they could get any sort of diagnosis, or even be told to stop the medication altogether.”
The study was sponsored by Sanofi. Dr. Achten disclosed no other conflicts of interest. Dr. Gooderham is an investigator with Sanofi Genzyme for dupilumab.
A version of this article first appeared on Medscape.com.
MONTREAL – , according to a study presented at the annual meeting of the International Society of Atopic Dermatitis.
In a prospective trial of 69 patients with AD starting dupilumab (Dupixent), baseline OSD was found in 91.3%, with about half of these patients reporting no symptoms, said investigator Roselie Achten, MD, from the National Expertise Center for Atopic Dermatitis at University Medical Center Utrecht, the Netherlands. Among these patients, ophthalmologic assessment revealed no OSD in 6 patients and mild OSD in 37 patients, but moderate and severe disease in 20 and 6 patients, respectively, she said, adding that 71% of the group also reported allergic conjunctivitis at baseline.
The patients enrolled in the study who started dupilumab were aged 36-38 years, with Eczema Area and Severity Index (EASI) scores of 14.7-16.5. Baseline ocular surface health was assessed with the Utrecht Ophthalmic Inflammatory and Allergic disease (UTOPIA) score. Tear fluid was collected to analyze biomarkers and dupilumab levels, and impression cytology was performed to collect conjunctival tissue cells for analysis of goblet cells. These measurements were repeated at 4 and 28 weeks after the start of therapy.
Over 28 weeks of treatment, 14.5% of patients experienced worsening of OSD, with worsening disease associated with a decline in the number of goblet cells. In addition, dupilumab treatment was associated with a significant decline in the production of Mucin5AC, suggesting a decline in function of the goblet cells. “Our hypothesis that the blocking effect of dupilumab on [interleukin-] IL-13 might lead to less goblet cells and less mucin production,” she explained.
In a subset of 48 patients, the researchers also detected significantly higher tear fluid dupilumab levels among those patients with more severe OSD, with comparable serum levels.
OSD has been reported in up to 34% of dupilumab-treated patients with AD and is the most frequently reported side-effect of this treatment, noted Dr. Achten. This side effect is not reported by other patients treated with dupilumab for other indications, she added, “suggesting that AD patients may have a predisposition to develop OSD during dupilumab treatment.”
Indeed, as recently noted by Vivian Shi, MD, from the department of dermatology, University of Arkansas for Medical Sciences, Little Rock, and colleagues, “for reasons not well understood, the incidence of conjunctivitis in dupilumab patients with asthma (0%-2.3%), chronic rhinosinusitis with nasal polyps (1.6%), or eosinophilic esophagitis (0%) is low to none; thus, patients with AD may be particularly susceptible.”
Dr. Achten said that dupilumab-treated patients with AD at her center are prescribed topical tacrolimus and ketotifen eye drops if they develop OSD.
Asked for comment, Melinda Gooderham, MD, who moderated the session, was impressed with the study. “I’d heard about the goblet cells, there were little bits of data here and there, but the tear analysis is something I hadn’t seen before. It was a nice series of experiments that pulled everything together,” she told this news organization. Dr. Gooderham, who is assistant professor at Queens University, in Kingston, Ontario, medical director at the SKiN Centre for Dermatology in Peterborough, Ontario, and consultant physician at Peterborough Regional Health Centre, said that she first began noticing dupilumab-related OSD as an early trial investigator for the drug. “When you put some patients on the drug it’s almost like tipping the balance – that little bit of mucin they’re dependent on is now reduced and it makes them more symptomatic,” she said.
Though she prescribes lubricating eye drops as prophylaxis for all her dupilumab-treated patients with AD, she recommends referring any patients who develop OSD to an ophthalmologist who is familiar with this specific side effect. “If they just see a random ophthalmologist who doesn’t know dupilumab, and doesn’t know the story around it, they could get any sort of diagnosis, or even be told to stop the medication altogether.”
The study was sponsored by Sanofi. Dr. Achten disclosed no other conflicts of interest. Dr. Gooderham is an investigator with Sanofi Genzyme for dupilumab.
A version of this article first appeared on Medscape.com.
FROM ISAD 2022
Time to ditch clarithromycin for H. pylori?
Rates of resistance to clarithromycin among Helicobacter pylori isolates in the United States and Europe are high enough to warrant discontinuation of empiric use of proton pump inhibitor (PPI)–based triple therapy that includes the antibiotic in these regions, a new study has found.
Overall, 22.2% of participants were resistant to clarithromycin – a rate that is above the currently recommended threshold of 15% or higher for avoidance of PPI-based triple therapy that includes clarithromycin.
, study investigator William Chey, MD, professor and chief, Division of Gastroenterology and Hepatology, Michigan Medicine, Ann Arbor, said in an interview.
Judith Kim, MD, a gastroenterologist at NYU Langone Health and clinical instructor of medicine at NYU Grossman School of Medicine, who wasn’t involved in the study, agrees.
“The use of PPI-based triple therapy is still common practice despite recent recommendations to avoid clarithromycin in areas with high resistance rates,” Dr. Kim told this news organization.
“This study shows that multiple parts of the United States and Europe have high resistance rates,” rendering clarithromycin-based regimens “more likely to ineffectively eradicate H pylori,” Dr. Kim said.
The study was published online in The American Journal of Gastroenterology.
Better options now available
Guidelines advise against the use of PPI-based triple regimens with clarithromycin for H. pylori infection in areas where resistance is 15% or higher or for patients who have previously received macrolides. However, up-to-date information on H. pylori antimicrobial resistance patterns is limited, especially in the United States.
Dr. Chey and colleagues assessed resistance rates to antibiotics commonly used to treat H. pylori in isolates from 907 adults with the infection in the United States and Europe. They included four U.S. subregions and five participating European countries.
In all U.S. subregions and European countries, clarithromycin resistance rates were above 15% except possibly in the United Kingdom, where the sample size was too small to provide a reliable estimate.
Three-quarters of the clarithromycin-resistant isolates were also resistant to metronidazole.
The study also found that, overall, 1.2% of patients had isolates that were resistant to amoxicillin, and 69.2% had isolates resistant to metronidazole. Resistance patterns were similar in the United States and Europe; metronidazole resistance was the most common (50%-79% of isolates), and amoxicillin was the least common (≤ 5%).
“Overall, these data provide robust evidence to support a shift away from the default empiric prescription of triple combinations containing a PPI and clarithromycin for H. pylori infection in the United States and Europe,” the study team writes.
The high prevalence of resistance, including dual resistance, highlights the need for antibiotic stewardship and resistance surveillance, as well as novel treatment strategies for H. pylori infection, they add.
Last spring, as previously reported, the United States Food and Drug Administration approved two vonoprazan-based treatments for H. pylori: Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin), both from Phathom Pharmaceuticals.
“Vonoprazan-based treatment may be superior to standard PPI triple therapy for clarithromycin-resistant infections based on prior studies and is a potential good option,” Dr. Kim said.
Still, she added, she “would most likely first recommend regimens that do not have clarithromycin, such as bismuth quadruple therapy.”
Study’s importance
Because the study drew upon the largest dataset to date on U.S. resistance rates, it should be used to more precisely guide first-line therapy decisions, said Richard Peek, Jr., MD, professor of medicine and director of gastroenterology at Vanderbilt University Medical Center, Nashville, Tenn.
“To date, there has been a dearth of information in the United States regarding H. pylori resistance rates, which has often led to the use of ineffective empiric therapies and inappropriate exposure to antibiotics,” Dr. Peek, who wasn’t involved in the study, told this news organization.
“These data are particularly exciting when viewed within the context of new genomic sequencing tests that can determine H. pylori resistance patterns using DNA isolated from the stomach or the stool,” he said.
Dr. Peek agreed that the recent approval of vonoprazan-based therapies “adds another regimen to the therapeutic armamentarium available for eradicating H. pylori, and its value seems to be particularly beneficial for eradication failures.”
The research was funded by Phathom Pharmaceuticals. Dr. Chey is a board member of the American College of Gastroenterology, GI on Demand, the International Foundation of Functional GI Disorders, and the Rome Foundation. He has received compensation as a consultant from AbbVie, Alfasigma, Allakos, Alnylam, Bayer, BioAmerica, Cosmo, Intrinsic Medicine, Ironwood Pharmaceuticals, QOL Medical, Nestle, Phathom Pharmaceuticals, RedHill Biopharma, Salix/Valeant, Takeda, Urovant, and Vibrant; grant/research support from BioAmerica, Commonwealth Diagnostics International, QOL Medical, Salix, and Vibrant; owns stock/stock options in GI on Demand and Modify Health; and owns patents relating to methods and kits for identifying food sensitivities and intolerances, digital manometry, and a rectal expulsion device. Dr. Peek and Dr. Kim report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Rates of resistance to clarithromycin among Helicobacter pylori isolates in the United States and Europe are high enough to warrant discontinuation of empiric use of proton pump inhibitor (PPI)–based triple therapy that includes the antibiotic in these regions, a new study has found.
Overall, 22.2% of participants were resistant to clarithromycin – a rate that is above the currently recommended threshold of 15% or higher for avoidance of PPI-based triple therapy that includes clarithromycin.
, study investigator William Chey, MD, professor and chief, Division of Gastroenterology and Hepatology, Michigan Medicine, Ann Arbor, said in an interview.
Judith Kim, MD, a gastroenterologist at NYU Langone Health and clinical instructor of medicine at NYU Grossman School of Medicine, who wasn’t involved in the study, agrees.
“The use of PPI-based triple therapy is still common practice despite recent recommendations to avoid clarithromycin in areas with high resistance rates,” Dr. Kim told this news organization.
“This study shows that multiple parts of the United States and Europe have high resistance rates,” rendering clarithromycin-based regimens “more likely to ineffectively eradicate H pylori,” Dr. Kim said.
The study was published online in The American Journal of Gastroenterology.
Better options now available
Guidelines advise against the use of PPI-based triple regimens with clarithromycin for H. pylori infection in areas where resistance is 15% or higher or for patients who have previously received macrolides. However, up-to-date information on H. pylori antimicrobial resistance patterns is limited, especially in the United States.
Dr. Chey and colleagues assessed resistance rates to antibiotics commonly used to treat H. pylori in isolates from 907 adults with the infection in the United States and Europe. They included four U.S. subregions and five participating European countries.
In all U.S. subregions and European countries, clarithromycin resistance rates were above 15% except possibly in the United Kingdom, where the sample size was too small to provide a reliable estimate.
Three-quarters of the clarithromycin-resistant isolates were also resistant to metronidazole.
The study also found that, overall, 1.2% of patients had isolates that were resistant to amoxicillin, and 69.2% had isolates resistant to metronidazole. Resistance patterns were similar in the United States and Europe; metronidazole resistance was the most common (50%-79% of isolates), and amoxicillin was the least common (≤ 5%).
“Overall, these data provide robust evidence to support a shift away from the default empiric prescription of triple combinations containing a PPI and clarithromycin for H. pylori infection in the United States and Europe,” the study team writes.
The high prevalence of resistance, including dual resistance, highlights the need for antibiotic stewardship and resistance surveillance, as well as novel treatment strategies for H. pylori infection, they add.
Last spring, as previously reported, the United States Food and Drug Administration approved two vonoprazan-based treatments for H. pylori: Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin), both from Phathom Pharmaceuticals.
“Vonoprazan-based treatment may be superior to standard PPI triple therapy for clarithromycin-resistant infections based on prior studies and is a potential good option,” Dr. Kim said.
Still, she added, she “would most likely first recommend regimens that do not have clarithromycin, such as bismuth quadruple therapy.”
Study’s importance
Because the study drew upon the largest dataset to date on U.S. resistance rates, it should be used to more precisely guide first-line therapy decisions, said Richard Peek, Jr., MD, professor of medicine and director of gastroenterology at Vanderbilt University Medical Center, Nashville, Tenn.
“To date, there has been a dearth of information in the United States regarding H. pylori resistance rates, which has often led to the use of ineffective empiric therapies and inappropriate exposure to antibiotics,” Dr. Peek, who wasn’t involved in the study, told this news organization.
“These data are particularly exciting when viewed within the context of new genomic sequencing tests that can determine H. pylori resistance patterns using DNA isolated from the stomach or the stool,” he said.
Dr. Peek agreed that the recent approval of vonoprazan-based therapies “adds another regimen to the therapeutic armamentarium available for eradicating H. pylori, and its value seems to be particularly beneficial for eradication failures.”
The research was funded by Phathom Pharmaceuticals. Dr. Chey is a board member of the American College of Gastroenterology, GI on Demand, the International Foundation of Functional GI Disorders, and the Rome Foundation. He has received compensation as a consultant from AbbVie, Alfasigma, Allakos, Alnylam, Bayer, BioAmerica, Cosmo, Intrinsic Medicine, Ironwood Pharmaceuticals, QOL Medical, Nestle, Phathom Pharmaceuticals, RedHill Biopharma, Salix/Valeant, Takeda, Urovant, and Vibrant; grant/research support from BioAmerica, Commonwealth Diagnostics International, QOL Medical, Salix, and Vibrant; owns stock/stock options in GI on Demand and Modify Health; and owns patents relating to methods and kits for identifying food sensitivities and intolerances, digital manometry, and a rectal expulsion device. Dr. Peek and Dr. Kim report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Rates of resistance to clarithromycin among Helicobacter pylori isolates in the United States and Europe are high enough to warrant discontinuation of empiric use of proton pump inhibitor (PPI)–based triple therapy that includes the antibiotic in these regions, a new study has found.
Overall, 22.2% of participants were resistant to clarithromycin – a rate that is above the currently recommended threshold of 15% or higher for avoidance of PPI-based triple therapy that includes clarithromycin.
, study investigator William Chey, MD, professor and chief, Division of Gastroenterology and Hepatology, Michigan Medicine, Ann Arbor, said in an interview.
Judith Kim, MD, a gastroenterologist at NYU Langone Health and clinical instructor of medicine at NYU Grossman School of Medicine, who wasn’t involved in the study, agrees.
“The use of PPI-based triple therapy is still common practice despite recent recommendations to avoid clarithromycin in areas with high resistance rates,” Dr. Kim told this news organization.
“This study shows that multiple parts of the United States and Europe have high resistance rates,” rendering clarithromycin-based regimens “more likely to ineffectively eradicate H pylori,” Dr. Kim said.
The study was published online in The American Journal of Gastroenterology.
Better options now available
Guidelines advise against the use of PPI-based triple regimens with clarithromycin for H. pylori infection in areas where resistance is 15% or higher or for patients who have previously received macrolides. However, up-to-date information on H. pylori antimicrobial resistance patterns is limited, especially in the United States.
Dr. Chey and colleagues assessed resistance rates to antibiotics commonly used to treat H. pylori in isolates from 907 adults with the infection in the United States and Europe. They included four U.S. subregions and five participating European countries.
In all U.S. subregions and European countries, clarithromycin resistance rates were above 15% except possibly in the United Kingdom, where the sample size was too small to provide a reliable estimate.
Three-quarters of the clarithromycin-resistant isolates were also resistant to metronidazole.
The study also found that, overall, 1.2% of patients had isolates that were resistant to amoxicillin, and 69.2% had isolates resistant to metronidazole. Resistance patterns were similar in the United States and Europe; metronidazole resistance was the most common (50%-79% of isolates), and amoxicillin was the least common (≤ 5%).
“Overall, these data provide robust evidence to support a shift away from the default empiric prescription of triple combinations containing a PPI and clarithromycin for H. pylori infection in the United States and Europe,” the study team writes.
The high prevalence of resistance, including dual resistance, highlights the need for antibiotic stewardship and resistance surveillance, as well as novel treatment strategies for H. pylori infection, they add.
Last spring, as previously reported, the United States Food and Drug Administration approved two vonoprazan-based treatments for H. pylori: Voquezna Triple Pak (vonoprazan, amoxicillin, clarithromycin) and Voquezna Dual Pak (vonoprazan, amoxicillin), both from Phathom Pharmaceuticals.
“Vonoprazan-based treatment may be superior to standard PPI triple therapy for clarithromycin-resistant infections based on prior studies and is a potential good option,” Dr. Kim said.
Still, she added, she “would most likely first recommend regimens that do not have clarithromycin, such as bismuth quadruple therapy.”
Study’s importance
Because the study drew upon the largest dataset to date on U.S. resistance rates, it should be used to more precisely guide first-line therapy decisions, said Richard Peek, Jr., MD, professor of medicine and director of gastroenterology at Vanderbilt University Medical Center, Nashville, Tenn.
“To date, there has been a dearth of information in the United States regarding H. pylori resistance rates, which has often led to the use of ineffective empiric therapies and inappropriate exposure to antibiotics,” Dr. Peek, who wasn’t involved in the study, told this news organization.
“These data are particularly exciting when viewed within the context of new genomic sequencing tests that can determine H. pylori resistance patterns using DNA isolated from the stomach or the stool,” he said.
Dr. Peek agreed that the recent approval of vonoprazan-based therapies “adds another regimen to the therapeutic armamentarium available for eradicating H. pylori, and its value seems to be particularly beneficial for eradication failures.”
The research was funded by Phathom Pharmaceuticals. Dr. Chey is a board member of the American College of Gastroenterology, GI on Demand, the International Foundation of Functional GI Disorders, and the Rome Foundation. He has received compensation as a consultant from AbbVie, Alfasigma, Allakos, Alnylam, Bayer, BioAmerica, Cosmo, Intrinsic Medicine, Ironwood Pharmaceuticals, QOL Medical, Nestle, Phathom Pharmaceuticals, RedHill Biopharma, Salix/Valeant, Takeda, Urovant, and Vibrant; grant/research support from BioAmerica, Commonwealth Diagnostics International, QOL Medical, Salix, and Vibrant; owns stock/stock options in GI on Demand and Modify Health; and owns patents relating to methods and kits for identifying food sensitivities and intolerances, digital manometry, and a rectal expulsion device. Dr. Peek and Dr. Kim report no relevant financial relationships.
A version of this article first appeared on Medscape.com.