User login
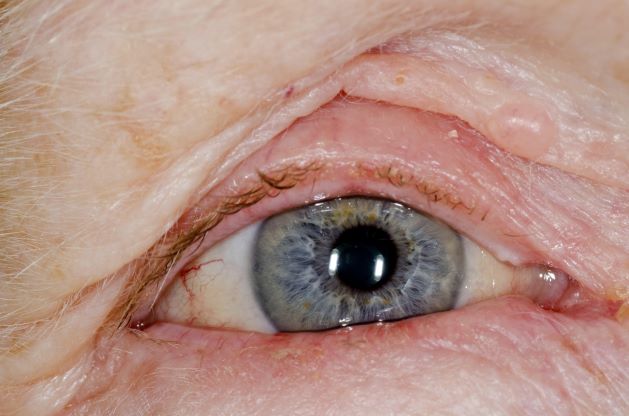
Red swollen eyelids
This patient's symptoms are consistent with a diagnosis of blepharitis.
Blepharitis is an inflammatory disorder of the eyelids that is frequently associated with bacterial colonization of the eyelid. Anatomically, it can be categorized as anterior blepharitis or posterior blepharitis. Anterior blepharitis refers to inflammation primarily positioned around the skin, eyelashes, and lash follicles and is usually further divided into staphylococcal and seborrheic variants. Posterior blepharitis involves the meibomian gland orifices, meibomian glands, tarsal plate, and blepharo-conjunctival junction.
Blepharitis can be acute or chronic. It is frequently associated with systemic diseases, such as rosacea, atopy, and seborrheic dermatitis, as well as ocular diseases, such as dry eye syndromes, chalazion, trichiasis, ectropion and entropion, infectious or other inflammatory conjunctivitis, and keratitis. Moreover, high rates of blepharitis have been reported in patients treated with dupilumab for atopic dermatitis.
Eye irritation, itching, erythema of the lids, flaking of the lid margins, and/or changes in the eyelashes are common presenting symptoms in patients with blepharitis. Other symptoms may include:
• Burning
• Watering
• Foreign-body sensation
• Crusting and mattering of the lashes and medial canthus
• Red lids
• Red eyes
• Photophobia
• Pain
• Decreased vision
• Visual fluctuations
• Heat, cold, alcohol, and spicy-food intolerance
The differential diagnosis for blepharitis includes bacterial keratitis, which is a serious ocular disorder that can lead to vision loss if not properly treated. Bacterial keratitis progresses rapidly and can result in corneal destruction within 24-48 hours with some particularly virulent bacteria. Patients with bacterial keratitis typically report rapid onset of pain, photophobia, and decreased vision.
Ocular rosacea should also be considered in the differential diagnosis of blepharitis, and the two conditions can co-occur. Patients with ocular rosacea may experience facial symptoms (eg, recurrent flushing episodes, persistent and/or recurrent midfacial erythema, papular and pustular lesions) in addition to ocular symptoms, which can range from minor irritation, foreign-body sensation, and blurry vision to severe ocular surface disruption and inflammatory keratitis.
Bacterial conjunctivitis involves inflammation of the bulbar and/or palpebral conjunctiva, whereas blepharitis involves inflammation of the eyelids only. Other conditions to consider in the diagnosis of blepharitis can be found here.
Given the unprecedented efficacy seen in clinical trials, dupilumab is emerging as a first-line therapeutic for moderate to severe atopic dermatitis. However, clinicians should be alert to ocular complications among their patients with atopic dermatitis who are being treated with dupilumab. In some patients, this may be because of preexisting meibomian gland disease and ocular surface disease. After a diagnosis of ocular complications, the continued use of dupilumab should be jointly evaluated by the ophthalmologist and dermatologist or allergist on the basis of the ocular risk vs systemic benefit. Treatment for blepharitis typically includes strict eyelid hygiene and topical antibiotic ointment; oral antibiotics can be beneficial for refractory disease.
William D. James, MD, Professor, Department of Dermatology, University of Pennsylvania, Philadelphia.
Disclosure: William D. James, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: Elsevier.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's symptoms are consistent with a diagnosis of blepharitis.
Blepharitis is an inflammatory disorder of the eyelids that is frequently associated with bacterial colonization of the eyelid. Anatomically, it can be categorized as anterior blepharitis or posterior blepharitis. Anterior blepharitis refers to inflammation primarily positioned around the skin, eyelashes, and lash follicles and is usually further divided into staphylococcal and seborrheic variants. Posterior blepharitis involves the meibomian gland orifices, meibomian glands, tarsal plate, and blepharo-conjunctival junction.
Blepharitis can be acute or chronic. It is frequently associated with systemic diseases, such as rosacea, atopy, and seborrheic dermatitis, as well as ocular diseases, such as dry eye syndromes, chalazion, trichiasis, ectropion and entropion, infectious or other inflammatory conjunctivitis, and keratitis. Moreover, high rates of blepharitis have been reported in patients treated with dupilumab for atopic dermatitis.
Eye irritation, itching, erythema of the lids, flaking of the lid margins, and/or changes in the eyelashes are common presenting symptoms in patients with blepharitis. Other symptoms may include:
• Burning
• Watering
• Foreign-body sensation
• Crusting and mattering of the lashes and medial canthus
• Red lids
• Red eyes
• Photophobia
• Pain
• Decreased vision
• Visual fluctuations
• Heat, cold, alcohol, and spicy-food intolerance
The differential diagnosis for blepharitis includes bacterial keratitis, which is a serious ocular disorder that can lead to vision loss if not properly treated. Bacterial keratitis progresses rapidly and can result in corneal destruction within 24-48 hours with some particularly virulent bacteria. Patients with bacterial keratitis typically report rapid onset of pain, photophobia, and decreased vision.
Ocular rosacea should also be considered in the differential diagnosis of blepharitis, and the two conditions can co-occur. Patients with ocular rosacea may experience facial symptoms (eg, recurrent flushing episodes, persistent and/or recurrent midfacial erythema, papular and pustular lesions) in addition to ocular symptoms, which can range from minor irritation, foreign-body sensation, and blurry vision to severe ocular surface disruption and inflammatory keratitis.
Bacterial conjunctivitis involves inflammation of the bulbar and/or palpebral conjunctiva, whereas blepharitis involves inflammation of the eyelids only. Other conditions to consider in the diagnosis of blepharitis can be found here.
Given the unprecedented efficacy seen in clinical trials, dupilumab is emerging as a first-line therapeutic for moderate to severe atopic dermatitis. However, clinicians should be alert to ocular complications among their patients with atopic dermatitis who are being treated with dupilumab. In some patients, this may be because of preexisting meibomian gland disease and ocular surface disease. After a diagnosis of ocular complications, the continued use of dupilumab should be jointly evaluated by the ophthalmologist and dermatologist or allergist on the basis of the ocular risk vs systemic benefit. Treatment for blepharitis typically includes strict eyelid hygiene and topical antibiotic ointment; oral antibiotics can be beneficial for refractory disease.
William D. James, MD, Professor, Department of Dermatology, University of Pennsylvania, Philadelphia.
Disclosure: William D. James, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: Elsevier.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's symptoms are consistent with a diagnosis of blepharitis.
Blepharitis is an inflammatory disorder of the eyelids that is frequently associated with bacterial colonization of the eyelid. Anatomically, it can be categorized as anterior blepharitis or posterior blepharitis. Anterior blepharitis refers to inflammation primarily positioned around the skin, eyelashes, and lash follicles and is usually further divided into staphylococcal and seborrheic variants. Posterior blepharitis involves the meibomian gland orifices, meibomian glands, tarsal plate, and blepharo-conjunctival junction.
Blepharitis can be acute or chronic. It is frequently associated with systemic diseases, such as rosacea, atopy, and seborrheic dermatitis, as well as ocular diseases, such as dry eye syndromes, chalazion, trichiasis, ectropion and entropion, infectious or other inflammatory conjunctivitis, and keratitis. Moreover, high rates of blepharitis have been reported in patients treated with dupilumab for atopic dermatitis.
Eye irritation, itching, erythema of the lids, flaking of the lid margins, and/or changes in the eyelashes are common presenting symptoms in patients with blepharitis. Other symptoms may include:
• Burning
• Watering
• Foreign-body sensation
• Crusting and mattering of the lashes and medial canthus
• Red lids
• Red eyes
• Photophobia
• Pain
• Decreased vision
• Visual fluctuations
• Heat, cold, alcohol, and spicy-food intolerance
The differential diagnosis for blepharitis includes bacterial keratitis, which is a serious ocular disorder that can lead to vision loss if not properly treated. Bacterial keratitis progresses rapidly and can result in corneal destruction within 24-48 hours with some particularly virulent bacteria. Patients with bacterial keratitis typically report rapid onset of pain, photophobia, and decreased vision.
Ocular rosacea should also be considered in the differential diagnosis of blepharitis, and the two conditions can co-occur. Patients with ocular rosacea may experience facial symptoms (eg, recurrent flushing episodes, persistent and/or recurrent midfacial erythema, papular and pustular lesions) in addition to ocular symptoms, which can range from minor irritation, foreign-body sensation, and blurry vision to severe ocular surface disruption and inflammatory keratitis.
Bacterial conjunctivitis involves inflammation of the bulbar and/or palpebral conjunctiva, whereas blepharitis involves inflammation of the eyelids only. Other conditions to consider in the diagnosis of blepharitis can be found here.
Given the unprecedented efficacy seen in clinical trials, dupilumab is emerging as a first-line therapeutic for moderate to severe atopic dermatitis. However, clinicians should be alert to ocular complications among their patients with atopic dermatitis who are being treated with dupilumab. In some patients, this may be because of preexisting meibomian gland disease and ocular surface disease. After a diagnosis of ocular complications, the continued use of dupilumab should be jointly evaluated by the ophthalmologist and dermatologist or allergist on the basis of the ocular risk vs systemic benefit. Treatment for blepharitis typically includes strict eyelid hygiene and topical antibiotic ointment; oral antibiotics can be beneficial for refractory disease.
William D. James, MD, Professor, Department of Dermatology, University of Pennsylvania, Philadelphia.
Disclosure: William D. James, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: Elsevier.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
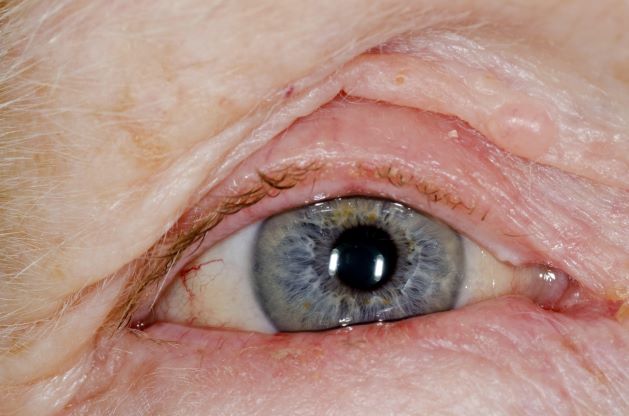
A 71-year-old woman was referred for an ophthalmologic examination by her dermatologist. The patient reports recent onset of red, swollen eyelids; ocular itching; and a burning sensation. Prior medical history includes severe atopic dermatitis, type 2 diabetes, and osteoarthritis. Current medications include metformin 1000 mg/d, celecoxib 200 mg/d, and clobetasol propionate 0.05% cream twice daily. The patient began receiving subcutaneous dupilumab 300 mg/once every 2 weeks about 6 weeks earlier.
New ACR vaccination guideline: Take your best shot
PHILADELPHIA – The new American College of Rheumatology Guideline for Vaccinations in Patients with Rheumatic and Musculoskeletal Diseases (RMDs) emphasizes that both adult and pediatric patients should receive recommended vaccinations whenever possible.
But the guideline, currently in press, also offers recommendations about whether and when to withhold vaccines from patients with RMDs, such as avoiding the use of live attenuated virus vaccines in patients who are on immunosuppressive drug regimens, such as conventional synthetic disease-modifying antirheumatic drugs (DMARDs), biologic DMARDs, or targeted synthetic DMARDs.

The new consensus guideline was formulated with the understanding that patients with RMDs are at increased risk for vaccine-preventable infections and more serious complications from infections, compared with the general population.
However, the guideline also acknowledges that the immunogenicity and safety of vaccines may differ among patients with RMDs, and that, depending on the patient age and disease state, individuals may benefit from modified vaccine indications, schedules, or modified medication schedules, said guideline panel member Anne Bass, MD, a rheumatologist at Hospital for Special Surgery and a professor of clinical medicine at Weill Cornell Medicine in New York, who presented the guideline with other panel members in a session outlining the recommendations at the annual meeting of the ACR.
“In addition, vaccination recommendations – since much of it relates to medications – really applies across diseases, and so the ACR felt that, rather than having vaccine recommendations tacked onto the end of treatment guidelines for each individual disease, that the topic should be discussed or tackled as a whole,” she said.
The guideline does not cover vaccinations in patients taking nonsteroidal anti-inflammatory drugs because this class of agents has minimal or no impact on antibody responses to vaccines. The guideline also does not address vaccinations against COVID-19 infections since the rapidly changing formulations would make the recommendations obsolete before they were even published, and because the U.S. Centers for Disease Control and Prevention provides up-to-date guidance on COVID-19 vaccinations in patients with compromised immunity, she said.
Guiding principles
The overarching principles of the guideline are to give indicated vaccines to patients with RMD whenever possible and that any decision to hold medications before or after vaccination consider the dosage used, RMD disease activity, and the patient’s risk for vaccine-preventable infection.

The guideline also states that “shared decision-making with patients is a key component of any vaccination strategy.”
Panel member Clifton O. Bingham III, MD, professor of medicine at Johns Hopkins University in Baltimore, outlined expanded indications for vaccinations against influenza, pneumococcal infections, varicella zoster virus (VZV) and human papillomavirus (HPV).
Influenza
The guideline conditionally recommends that patients with RMD aged 65 years and older and adults older than age 18 years who are on immunosuppressive medications should receive either high-dose or adjuvanted influenza vaccination rather than regular-dose vaccines.
“It’s recognized that the high-dose or adjuvanted vaccinations may be unavailable for patients when they’re seen in your practice,” Dr. Bingham said,” and we came out with two additional statements within the guidelines that said that any flu vaccine is recommended over no flu vaccinations, because we do know that responses are elicited, and a flu vaccination today is preferred over a flu vaccination delay.”
Pneumococcal vaccination
The panelists strongly recommended that patients with RMD younger than age 65 years who are on immunosuppressive medication receive pneumococcal vaccinations.
The ACR guideline is in sync with those issued by the CDC’s Advisory Committee on Immunization Practices, Dr. Bingham said. He urged audience members to visit a CDC-ACIP web page for more information on who should receive pneumococcal vaccination and when.
Recombinant varicella zoster
The recommendations strongly support that patients aged 18 years and over who are on immunosuppressive therapies should receive the recombinant VZV vaccine (Shingrix).
HPV
A less robust, conditional recommendation is for patients with RMDs who are between the ages of 26 and 45 years and on immunosuppressive medications to receive the HPV vaccine (if they have not already received the vaccine).
Non-live attenuated vaccines
Kevin Winthrop, MD, MPH, professor of infectious diseases and public health at Oregon Health & Science University, Portland, summarized the recommendations for managing immunosuppressive therapies in patients scheduled to receive vaccinations using killed or nonactive antigens.

“In influenza season, don’t pass up the opportunity to vaccinate,” he said, adding, “if you can wait on rituximab dosing, do it, and if you can’t, go ahead and vaccinate.”
The guidelines also recommend a 2-week methotrexate hold at the time of influenza vaccination; other DMARD dosing changes are likely not necessary at the time of vaccination, “but this is an area of fervent study, and I think in a year or two we’ll have more experimental hold data with regard to other DMARDs,” Dr. Winthrop said.
For other nonlive attenuated vaccinations, recommendations are similar to those for influenza, except with more flexible timing because these vaccinations are not seasonal. When and how to hold methotrexate is still up in the air, he said.
Additionally, it’s recommended that vaccinations be delayed in patients on high-dose prednisone until the drug is tapered to below 20 mg per day, and ideally to less than 10 mg per day, he said.
Live-attenuated vaccines
The guideline conditionally recommends deferring live-attenuated vaccines in patients on immunosuppressive drugs. It also recommends holding these medications “for an appropriate period before” vaccination and for 4 weeks afterward.
“Although the evidence around conventional synthetic DMARDs and TNF inhibitors is reassuring in terms of their safety at the time of live attenuated vaccines, as you can see the number of studies is quite small, and so the voting panel conditionally recommend against administering live-attenuated virus vaccines to patients who are on conventional synthetics, biologic, or targeted DMARDs,” Dr. Bass said.
In utero exposures
Most women with RMD who have recently given birth will consult their general pediatricians rather than rheumatologists for infant vaccinations, but pediatricians may not be aware of the affect that in utero exposures to biologic DMARDs can have on vaccine safety and immunogenicity in infants, Dr, Bass said.
“It’s important that you, as a provider, give your recommendations regarding infant rotavirus vaccination after in utero exposure to the pregnant rheumatic disease patient prior to delivery, and let that patient know that this is something that they should share with their pediatrician to be,” she advised audience members.
Getting the message out
In an interview, session moderator and guidelines panelist Lisa F. Imundo, MD, director of the center for adolescent rheumatology at Columbia University in New York, noted that rheumatologists don’t usually have the full schedule of pediatric vaccinations in stock and often leave the decisions about what to give – and when – to general practitioners.

“Pediatric rheumatologists sometimes will give patients flu vaccinations because they’re a high-risk population of patients, and we want to make sure that they’re getting it in a timely manner,” she said.
In addition, because pneumococcal polysaccharide vaccines are not indicated in the general pediatric population, children on biologic DMARDs who have completed their standard series of pneumococcal conjugate vaccines (PCV13 or PVC15) are recommended to get a 23-valent pneumococcal polysaccharide vaccine, Dr. Imundo said.
She also noted that communication between pediatric rheumatologists and general practitioners about vaccine recommendations can be challenging.
“It’s a huge issue, figuring out how we’re going to communicate all of this information to our pediatric colleagues,” she said. “With individual patients, we may sometimes remind doctors, especially with our younger patients who haven’t gotten their live vaccines, that they really shouldn’t get live vaccines until they’re off medication or until we arrange holding medication for some period of time.”
She said that ACR vaccine committee members are working with infectious disease specialists and guideline developers for the American Academy of Pediatrics to ensure guidelines include the most important vaccination recommendations for pediatric patients with RMDs.
The development process for the guidelines was supported by the ACR. Dr. Bass reported no relevant disclosures, Dr. Bingham disclosed consulting activities, grant/research support, and royalties from various corporate entities. Dr. Winthrop disclosed consulting activities for and research funding from various companies. Dr. Imundo reported no relevant financial relationships.
PHILADELPHIA – The new American College of Rheumatology Guideline for Vaccinations in Patients with Rheumatic and Musculoskeletal Diseases (RMDs) emphasizes that both adult and pediatric patients should receive recommended vaccinations whenever possible.
But the guideline, currently in press, also offers recommendations about whether and when to withhold vaccines from patients with RMDs, such as avoiding the use of live attenuated virus vaccines in patients who are on immunosuppressive drug regimens, such as conventional synthetic disease-modifying antirheumatic drugs (DMARDs), biologic DMARDs, or targeted synthetic DMARDs.
The new consensus guideline was formulated with the understanding that patients with RMDs are at increased risk for vaccine-preventable infections and more serious complications from infections, compared with the general population.
However, the guideline also acknowledges that the immunogenicity and safety of vaccines may differ among patients with RMDs, and that, depending on the patient age and disease state, individuals may benefit from modified vaccine indications, schedules, or modified medication schedules, said guideline panel member Anne Bass, MD, a rheumatologist at Hospital for Special Surgery and a professor of clinical medicine at Weill Cornell Medicine in New York, who presented the guideline with other panel members in a session outlining the recommendations at the annual meeting of the ACR.
“In addition, vaccination recommendations – since much of it relates to medications – really applies across diseases, and so the ACR felt that, rather than having vaccine recommendations tacked onto the end of treatment guidelines for each individual disease, that the topic should be discussed or tackled as a whole,” she said.
The guideline does not cover vaccinations in patients taking nonsteroidal anti-inflammatory drugs because this class of agents has minimal or no impact on antibody responses to vaccines. The guideline also does not address vaccinations against COVID-19 infections since the rapidly changing formulations would make the recommendations obsolete before they were even published, and because the U.S. Centers for Disease Control and Prevention provides up-to-date guidance on COVID-19 vaccinations in patients with compromised immunity, she said.
Guiding principles
The overarching principles of the guideline are to give indicated vaccines to patients with RMD whenever possible and that any decision to hold medications before or after vaccination consider the dosage used, RMD disease activity, and the patient’s risk for vaccine-preventable infection.
The guideline also states that “shared decision-making with patients is a key component of any vaccination strategy.”
Panel member Clifton O. Bingham III, MD, professor of medicine at Johns Hopkins University in Baltimore, outlined expanded indications for vaccinations against influenza, pneumococcal infections, varicella zoster virus (VZV) and human papillomavirus (HPV).
Influenza
The guideline conditionally recommends that patients with RMD aged 65 years and older and adults older than age 18 years who are on immunosuppressive medications should receive either high-dose or adjuvanted influenza vaccination rather than regular-dose vaccines.
“It’s recognized that the high-dose or adjuvanted vaccinations may be unavailable for patients when they’re seen in your practice,” Dr. Bingham said,” and we came out with two additional statements within the guidelines that said that any flu vaccine is recommended over no flu vaccinations, because we do know that responses are elicited, and a flu vaccination today is preferred over a flu vaccination delay.”
Pneumococcal vaccination
The panelists strongly recommended that patients with RMD younger than age 65 years who are on immunosuppressive medication receive pneumococcal vaccinations.
The ACR guideline is in sync with those issued by the CDC’s Advisory Committee on Immunization Practices, Dr. Bingham said. He urged audience members to visit a CDC-ACIP web page for more information on who should receive pneumococcal vaccination and when.
Recombinant varicella zoster
The recommendations strongly support that patients aged 18 years and over who are on immunosuppressive therapies should receive the recombinant VZV vaccine (Shingrix).
HPV
A less robust, conditional recommendation is for patients with RMDs who are between the ages of 26 and 45 years and on immunosuppressive medications to receive the HPV vaccine (if they have not already received the vaccine).
Non-live attenuated vaccines
Kevin Winthrop, MD, MPH, professor of infectious diseases and public health at Oregon Health & Science University, Portland, summarized the recommendations for managing immunosuppressive therapies in patients scheduled to receive vaccinations using killed or nonactive antigens.
“In influenza season, don’t pass up the opportunity to vaccinate,” he said, adding, “if you can wait on rituximab dosing, do it, and if you can’t, go ahead and vaccinate.”
The guidelines also recommend a 2-week methotrexate hold at the time of influenza vaccination; other DMARD dosing changes are likely not necessary at the time of vaccination, “but this is an area of fervent study, and I think in a year or two we’ll have more experimental hold data with regard to other DMARDs,” Dr. Winthrop said.
For other nonlive attenuated vaccinations, recommendations are similar to those for influenza, except with more flexible timing because these vaccinations are not seasonal. When and how to hold methotrexate is still up in the air, he said.
Additionally, it’s recommended that vaccinations be delayed in patients on high-dose prednisone until the drug is tapered to below 20 mg per day, and ideally to less than 10 mg per day, he said.
Live-attenuated vaccines
The guideline conditionally recommends deferring live-attenuated vaccines in patients on immunosuppressive drugs. It also recommends holding these medications “for an appropriate period before” vaccination and for 4 weeks afterward.
“Although the evidence around conventional synthetic DMARDs and TNF inhibitors is reassuring in terms of their safety at the time of live attenuated vaccines, as you can see the number of studies is quite small, and so the voting panel conditionally recommend against administering live-attenuated virus vaccines to patients who are on conventional synthetics, biologic, or targeted DMARDs,” Dr. Bass said.
In utero exposures
Most women with RMD who have recently given birth will consult their general pediatricians rather than rheumatologists for infant vaccinations, but pediatricians may not be aware of the affect that in utero exposures to biologic DMARDs can have on vaccine safety and immunogenicity in infants, Dr, Bass said.
“It’s important that you, as a provider, give your recommendations regarding infant rotavirus vaccination after in utero exposure to the pregnant rheumatic disease patient prior to delivery, and let that patient know that this is something that they should share with their pediatrician to be,” she advised audience members.
Getting the message out
In an interview, session moderator and guidelines panelist Lisa F. Imundo, MD, director of the center for adolescent rheumatology at Columbia University in New York, noted that rheumatologists don’t usually have the full schedule of pediatric vaccinations in stock and often leave the decisions about what to give – and when – to general practitioners.
“Pediatric rheumatologists sometimes will give patients flu vaccinations because they’re a high-risk population of patients, and we want to make sure that they’re getting it in a timely manner,” she said.
In addition, because pneumococcal polysaccharide vaccines are not indicated in the general pediatric population, children on biologic DMARDs who have completed their standard series of pneumococcal conjugate vaccines (PCV13 or PVC15) are recommended to get a 23-valent pneumococcal polysaccharide vaccine, Dr. Imundo said.
She also noted that communication between pediatric rheumatologists and general practitioners about vaccine recommendations can be challenging.
“It’s a huge issue, figuring out how we’re going to communicate all of this information to our pediatric colleagues,” she said. “With individual patients, we may sometimes remind doctors, especially with our younger patients who haven’t gotten their live vaccines, that they really shouldn’t get live vaccines until they’re off medication or until we arrange holding medication for some period of time.”
She said that ACR vaccine committee members are working with infectious disease specialists and guideline developers for the American Academy of Pediatrics to ensure guidelines include the most important vaccination recommendations for pediatric patients with RMDs.
The development process for the guidelines was supported by the ACR. Dr. Bass reported no relevant disclosures, Dr. Bingham disclosed consulting activities, grant/research support, and royalties from various corporate entities. Dr. Winthrop disclosed consulting activities for and research funding from various companies. Dr. Imundo reported no relevant financial relationships.
PHILADELPHIA – The new American College of Rheumatology Guideline for Vaccinations in Patients with Rheumatic and Musculoskeletal Diseases (RMDs) emphasizes that both adult and pediatric patients should receive recommended vaccinations whenever possible.
But the guideline, currently in press, also offers recommendations about whether and when to withhold vaccines from patients with RMDs, such as avoiding the use of live attenuated virus vaccines in patients who are on immunosuppressive drug regimens, such as conventional synthetic disease-modifying antirheumatic drugs (DMARDs), biologic DMARDs, or targeted synthetic DMARDs.
The new consensus guideline was formulated with the understanding that patients with RMDs are at increased risk for vaccine-preventable infections and more serious complications from infections, compared with the general population.
However, the guideline also acknowledges that the immunogenicity and safety of vaccines may differ among patients with RMDs, and that, depending on the patient age and disease state, individuals may benefit from modified vaccine indications, schedules, or modified medication schedules, said guideline panel member Anne Bass, MD, a rheumatologist at Hospital for Special Surgery and a professor of clinical medicine at Weill Cornell Medicine in New York, who presented the guideline with other panel members in a session outlining the recommendations at the annual meeting of the ACR.
“In addition, vaccination recommendations – since much of it relates to medications – really applies across diseases, and so the ACR felt that, rather than having vaccine recommendations tacked onto the end of treatment guidelines for each individual disease, that the topic should be discussed or tackled as a whole,” she said.
The guideline does not cover vaccinations in patients taking nonsteroidal anti-inflammatory drugs because this class of agents has minimal or no impact on antibody responses to vaccines. The guideline also does not address vaccinations against COVID-19 infections since the rapidly changing formulations would make the recommendations obsolete before they were even published, and because the U.S. Centers for Disease Control and Prevention provides up-to-date guidance on COVID-19 vaccinations in patients with compromised immunity, she said.
Guiding principles
The overarching principles of the guideline are to give indicated vaccines to patients with RMD whenever possible and that any decision to hold medications before or after vaccination consider the dosage used, RMD disease activity, and the patient’s risk for vaccine-preventable infection.
The guideline also states that “shared decision-making with patients is a key component of any vaccination strategy.”
Panel member Clifton O. Bingham III, MD, professor of medicine at Johns Hopkins University in Baltimore, outlined expanded indications for vaccinations against influenza, pneumococcal infections, varicella zoster virus (VZV) and human papillomavirus (HPV).
Influenza
The guideline conditionally recommends that patients with RMD aged 65 years and older and adults older than age 18 years who are on immunosuppressive medications should receive either high-dose or adjuvanted influenza vaccination rather than regular-dose vaccines.
“It’s recognized that the high-dose or adjuvanted vaccinations may be unavailable for patients when they’re seen in your practice,” Dr. Bingham said,” and we came out with two additional statements within the guidelines that said that any flu vaccine is recommended over no flu vaccinations, because we do know that responses are elicited, and a flu vaccination today is preferred over a flu vaccination delay.”
Pneumococcal vaccination
The panelists strongly recommended that patients with RMD younger than age 65 years who are on immunosuppressive medication receive pneumococcal vaccinations.
The ACR guideline is in sync with those issued by the CDC’s Advisory Committee on Immunization Practices, Dr. Bingham said. He urged audience members to visit a CDC-ACIP web page for more information on who should receive pneumococcal vaccination and when.
Recombinant varicella zoster
The recommendations strongly support that patients aged 18 years and over who are on immunosuppressive therapies should receive the recombinant VZV vaccine (Shingrix).
HPV
A less robust, conditional recommendation is for patients with RMDs who are between the ages of 26 and 45 years and on immunosuppressive medications to receive the HPV vaccine (if they have not already received the vaccine).
Non-live attenuated vaccines
Kevin Winthrop, MD, MPH, professor of infectious diseases and public health at Oregon Health & Science University, Portland, summarized the recommendations for managing immunosuppressive therapies in patients scheduled to receive vaccinations using killed or nonactive antigens.
“In influenza season, don’t pass up the opportunity to vaccinate,” he said, adding, “if you can wait on rituximab dosing, do it, and if you can’t, go ahead and vaccinate.”
The guidelines also recommend a 2-week methotrexate hold at the time of influenza vaccination; other DMARD dosing changes are likely not necessary at the time of vaccination, “but this is an area of fervent study, and I think in a year or two we’ll have more experimental hold data with regard to other DMARDs,” Dr. Winthrop said.
For other nonlive attenuated vaccinations, recommendations are similar to those for influenza, except with more flexible timing because these vaccinations are not seasonal. When and how to hold methotrexate is still up in the air, he said.
Additionally, it’s recommended that vaccinations be delayed in patients on high-dose prednisone until the drug is tapered to below 20 mg per day, and ideally to less than 10 mg per day, he said.
Live-attenuated vaccines
The guideline conditionally recommends deferring live-attenuated vaccines in patients on immunosuppressive drugs. It also recommends holding these medications “for an appropriate period before” vaccination and for 4 weeks afterward.
“Although the evidence around conventional synthetic DMARDs and TNF inhibitors is reassuring in terms of their safety at the time of live attenuated vaccines, as you can see the number of studies is quite small, and so the voting panel conditionally recommend against administering live-attenuated virus vaccines to patients who are on conventional synthetics, biologic, or targeted DMARDs,” Dr. Bass said.
In utero exposures
Most women with RMD who have recently given birth will consult their general pediatricians rather than rheumatologists for infant vaccinations, but pediatricians may not be aware of the affect that in utero exposures to biologic DMARDs can have on vaccine safety and immunogenicity in infants, Dr, Bass said.
“It’s important that you, as a provider, give your recommendations regarding infant rotavirus vaccination after in utero exposure to the pregnant rheumatic disease patient prior to delivery, and let that patient know that this is something that they should share with their pediatrician to be,” she advised audience members.
Getting the message out
In an interview, session moderator and guidelines panelist Lisa F. Imundo, MD, director of the center for adolescent rheumatology at Columbia University in New York, noted that rheumatologists don’t usually have the full schedule of pediatric vaccinations in stock and often leave the decisions about what to give – and when – to general practitioners.
“Pediatric rheumatologists sometimes will give patients flu vaccinations because they’re a high-risk population of patients, and we want to make sure that they’re getting it in a timely manner,” she said.
In addition, because pneumococcal polysaccharide vaccines are not indicated in the general pediatric population, children on biologic DMARDs who have completed their standard series of pneumococcal conjugate vaccines (PCV13 or PVC15) are recommended to get a 23-valent pneumococcal polysaccharide vaccine, Dr. Imundo said.
She also noted that communication between pediatric rheumatologists and general practitioners about vaccine recommendations can be challenging.
“It’s a huge issue, figuring out how we’re going to communicate all of this information to our pediatric colleagues,” she said. “With individual patients, we may sometimes remind doctors, especially with our younger patients who haven’t gotten their live vaccines, that they really shouldn’t get live vaccines until they’re off medication or until we arrange holding medication for some period of time.”
She said that ACR vaccine committee members are working with infectious disease specialists and guideline developers for the American Academy of Pediatrics to ensure guidelines include the most important vaccination recommendations for pediatric patients with RMDs.
The development process for the guidelines was supported by the ACR. Dr. Bass reported no relevant disclosures, Dr. Bingham disclosed consulting activities, grant/research support, and royalties from various corporate entities. Dr. Winthrop disclosed consulting activities for and research funding from various companies. Dr. Imundo reported no relevant financial relationships.
AT ACR 2022
Right ankle pain and swelling
This patient's findings are consistent with a diagnosis of psoriatic enthesitis.
Enthesitis is a hallmark manifestation of psoriatic arthritis (PsA). Approximately 30% of patients with psoriasis are estimated to be affected by PsA, which belongs to the spondyloarthritis (SpA) family of inflammatory rheumatic diseases.
An enthesis is an attachment site of ligaments, tendons, and joint capsules to bone and is a key inflammatory target in SpA. It is a complex structure that dissipates biomechanical stress to preserve homeostasis. Entheses are anatomically and functionally integrated with bursa, fibrocartilage, and synovium in a synovial entheseal complex; biomechanical stress in this area may trigger inflammation. Enthesitis is an early manifestation of PsA that has been associated with radiographic peripheral/axial joint damage and severe disease, as well as reduced quality of life.
Enthesitis can be difficult to diagnose in clinical practice. Symptoms include tenderness, soreness, and pain at entheses on palpation, often without overt clinical evidence of inflammation. In contrast, dactylitis, another hallmark manifestation of PsA, can be recognized by swelling of an entire digit that is different from adjacent digits. Fibromyalgia frequently coexists with enthesitis, and it can be difficult to distinguish the two given the anatomic overlap between the tender points of fibromyalgia and many entheseal sites. Long-lasting morning stiffness and a sustained response to a course of steroids is more suggestive of enthesitis, whereas a higher number of somatoform symptoms is more suggestive of fibromyalgia.
Enthesitis is included in the Classification Criteria for Psoriatic Arthritis (CASPAR) as a hallmark of PsA. While it can be diagnosed clinically, imaging studies may be required, particularly in patients in whom symptoms may be difficult to discern. Evidence of enthesitis by conventional radiography includes bone cortex irregularities, erosions, entheseal soft tissue calcifications, and new bone formation; however, entheseal bone changes detected with conventional radiography appear relatively late in the disease process. Ultrasound is highly sensitive for assessing inflammation and can detect various features of enthesitis, such as increased thickness of tendon insertion, hypoechogenicity, erosions, enthesophytes, and subclinical enthesitis in people with PsA. MRI has the advantage of identifying perientheseal inflammation with adjacent bone marrow edema. Fat-suppressed MRI with or without gadolinium enhancement is a highly sensitive method for visualizing active enthesitis and can identify perientheseal inflammation with adjacent bone marrow edema.
Delayed treatment of PsA can result in irreversible joint damage and reduced quality of life; thus, patients with psoriasis should be closely monitored for early signs of its development, such as enthesitis. A thorough evaluation of the key clinical features of PsA (psoriasis, arthritis, enthesitis, dactylitis, and spondylitis), including evaluation of severity of each feature and impact on physical function and quality of life, is encouraged at each clinical encounter. Because patients may not understand the link between psoriasis and joint pain, specific probing questions can be helpful. Screening questionnaires to detect early signs and symptoms of PsA are available, such as the Psoriasis Epidemiology Screening Tool (PEST), Psoriatic Arthritis Screening and Evaluation (PASE) questionnaire, and Toronto Psoriatic Arthritis Screening (ToPAS) questionnaire. These and many others may be used to help dermatologists detect early signs and symptoms of PsA. Although these questionnaires all have limitations in sensitivity and specificity for the diagnosis of PsA, their use can still improve early diagnosis.
The treatment of PsA focuses on achieving the least amount of disease activity and inflammation possible; optimizing functional status, quality of life, and well-being; and preventing structural damage. Treatment decisions are based on the specific domains affected. Nonsteroidal anti-inflammatory drugs and corticosteroid injections are first-line treatments for enthesitis. Early use of tumor necrosis factor inhibitors (TNF) (adalimumab, certolizumab pegol, etanercept, infliximab, and golimumab) is recommended. Alternative biologic disease-modifying agents are indicated when these TNF inhibitors provide an inadequate response. They include ustekinumab (dual interleukin [IL]-12 and IL-23 inhibitor), secukinumab (IL-17A inhibitor), and apremilast (phosphodiesterase-4 inhibitor) and may be considered for patients with predominantly entheseal manifestations of PsA or dactylitis. Biological disease-modifying agents approved for PsA that have shown efficacy for enthesitis include ixekizumab (which targets IL-17A), abatacept (a T-cell inhibitor), guselkumab (monoclonal antibody), and ustekinumab (monoclonal antibody). Tofacitinib and upadacitinib, both oral Janus kinase inhibitors, may also be considered.
Herbert S. Diamond, MD, Professor of Medicine (retired), Temple University School of Medicine, University of Pittsburgh; Chairman, Department of Medicine Emeritus, Western Pennsylvania Hospital, Pittsburgh, PA.
Herbert S. Diamond, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's findings are consistent with a diagnosis of psoriatic enthesitis.
Enthesitis is a hallmark manifestation of psoriatic arthritis (PsA). Approximately 30% of patients with psoriasis are estimated to be affected by PsA, which belongs to the spondyloarthritis (SpA) family of inflammatory rheumatic diseases.
An enthesis is an attachment site of ligaments, tendons, and joint capsules to bone and is a key inflammatory target in SpA. It is a complex structure that dissipates biomechanical stress to preserve homeostasis. Entheses are anatomically and functionally integrated with bursa, fibrocartilage, and synovium in a synovial entheseal complex; biomechanical stress in this area may trigger inflammation. Enthesitis is an early manifestation of PsA that has been associated with radiographic peripheral/axial joint damage and severe disease, as well as reduced quality of life.
Enthesitis can be difficult to diagnose in clinical practice. Symptoms include tenderness, soreness, and pain at entheses on palpation, often without overt clinical evidence of inflammation. In contrast, dactylitis, another hallmark manifestation of PsA, can be recognized by swelling of an entire digit that is different from adjacent digits. Fibromyalgia frequently coexists with enthesitis, and it can be difficult to distinguish the two given the anatomic overlap between the tender points of fibromyalgia and many entheseal sites. Long-lasting morning stiffness and a sustained response to a course of steroids is more suggestive of enthesitis, whereas a higher number of somatoform symptoms is more suggestive of fibromyalgia.
Enthesitis is included in the Classification Criteria for Psoriatic Arthritis (CASPAR) as a hallmark of PsA. While it can be diagnosed clinically, imaging studies may be required, particularly in patients in whom symptoms may be difficult to discern. Evidence of enthesitis by conventional radiography includes bone cortex irregularities, erosions, entheseal soft tissue calcifications, and new bone formation; however, entheseal bone changes detected with conventional radiography appear relatively late in the disease process. Ultrasound is highly sensitive for assessing inflammation and can detect various features of enthesitis, such as increased thickness of tendon insertion, hypoechogenicity, erosions, enthesophytes, and subclinical enthesitis in people with PsA. MRI has the advantage of identifying perientheseal inflammation with adjacent bone marrow edema. Fat-suppressed MRI with or without gadolinium enhancement is a highly sensitive method for visualizing active enthesitis and can identify perientheseal inflammation with adjacent bone marrow edema.
Delayed treatment of PsA can result in irreversible joint damage and reduced quality of life; thus, patients with psoriasis should be closely monitored for early signs of its development, such as enthesitis. A thorough evaluation of the key clinical features of PsA (psoriasis, arthritis, enthesitis, dactylitis, and spondylitis), including evaluation of severity of each feature and impact on physical function and quality of life, is encouraged at each clinical encounter. Because patients may not understand the link between psoriasis and joint pain, specific probing questions can be helpful. Screening questionnaires to detect early signs and symptoms of PsA are available, such as the Psoriasis Epidemiology Screening Tool (PEST), Psoriatic Arthritis Screening and Evaluation (PASE) questionnaire, and Toronto Psoriatic Arthritis Screening (ToPAS) questionnaire. These and many others may be used to help dermatologists detect early signs and symptoms of PsA. Although these questionnaires all have limitations in sensitivity and specificity for the diagnosis of PsA, their use can still improve early diagnosis.
The treatment of PsA focuses on achieving the least amount of disease activity and inflammation possible; optimizing functional status, quality of life, and well-being; and preventing structural damage. Treatment decisions are based on the specific domains affected. Nonsteroidal anti-inflammatory drugs and corticosteroid injections are first-line treatments for enthesitis. Early use of tumor necrosis factor inhibitors (TNF) (adalimumab, certolizumab pegol, etanercept, infliximab, and golimumab) is recommended. Alternative biologic disease-modifying agents are indicated when these TNF inhibitors provide an inadequate response. They include ustekinumab (dual interleukin [IL]-12 and IL-23 inhibitor), secukinumab (IL-17A inhibitor), and apremilast (phosphodiesterase-4 inhibitor) and may be considered for patients with predominantly entheseal manifestations of PsA or dactylitis. Biological disease-modifying agents approved for PsA that have shown efficacy for enthesitis include ixekizumab (which targets IL-17A), abatacept (a T-cell inhibitor), guselkumab (monoclonal antibody), and ustekinumab (monoclonal antibody). Tofacitinib and upadacitinib, both oral Janus kinase inhibitors, may also be considered.
Herbert S. Diamond, MD, Professor of Medicine (retired), Temple University School of Medicine, University of Pittsburgh; Chairman, Department of Medicine Emeritus, Western Pennsylvania Hospital, Pittsburgh, PA.
Herbert S. Diamond, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's findings are consistent with a diagnosis of psoriatic enthesitis.
Enthesitis is a hallmark manifestation of psoriatic arthritis (PsA). Approximately 30% of patients with psoriasis are estimated to be affected by PsA, which belongs to the spondyloarthritis (SpA) family of inflammatory rheumatic diseases.
An enthesis is an attachment site of ligaments, tendons, and joint capsules to bone and is a key inflammatory target in SpA. It is a complex structure that dissipates biomechanical stress to preserve homeostasis. Entheses are anatomically and functionally integrated with bursa, fibrocartilage, and synovium in a synovial entheseal complex; biomechanical stress in this area may trigger inflammation. Enthesitis is an early manifestation of PsA that has been associated with radiographic peripheral/axial joint damage and severe disease, as well as reduced quality of life.
Enthesitis can be difficult to diagnose in clinical practice. Symptoms include tenderness, soreness, and pain at entheses on palpation, often without overt clinical evidence of inflammation. In contrast, dactylitis, another hallmark manifestation of PsA, can be recognized by swelling of an entire digit that is different from adjacent digits. Fibromyalgia frequently coexists with enthesitis, and it can be difficult to distinguish the two given the anatomic overlap between the tender points of fibromyalgia and many entheseal sites. Long-lasting morning stiffness and a sustained response to a course of steroids is more suggestive of enthesitis, whereas a higher number of somatoform symptoms is more suggestive of fibromyalgia.
Enthesitis is included in the Classification Criteria for Psoriatic Arthritis (CASPAR) as a hallmark of PsA. While it can be diagnosed clinically, imaging studies may be required, particularly in patients in whom symptoms may be difficult to discern. Evidence of enthesitis by conventional radiography includes bone cortex irregularities, erosions, entheseal soft tissue calcifications, and new bone formation; however, entheseal bone changes detected with conventional radiography appear relatively late in the disease process. Ultrasound is highly sensitive for assessing inflammation and can detect various features of enthesitis, such as increased thickness of tendon insertion, hypoechogenicity, erosions, enthesophytes, and subclinical enthesitis in people with PsA. MRI has the advantage of identifying perientheseal inflammation with adjacent bone marrow edema. Fat-suppressed MRI with or without gadolinium enhancement is a highly sensitive method for visualizing active enthesitis and can identify perientheseal inflammation with adjacent bone marrow edema.
Delayed treatment of PsA can result in irreversible joint damage and reduced quality of life; thus, patients with psoriasis should be closely monitored for early signs of its development, such as enthesitis. A thorough evaluation of the key clinical features of PsA (psoriasis, arthritis, enthesitis, dactylitis, and spondylitis), including evaluation of severity of each feature and impact on physical function and quality of life, is encouraged at each clinical encounter. Because patients may not understand the link between psoriasis and joint pain, specific probing questions can be helpful. Screening questionnaires to detect early signs and symptoms of PsA are available, such as the Psoriasis Epidemiology Screening Tool (PEST), Psoriatic Arthritis Screening and Evaluation (PASE) questionnaire, and Toronto Psoriatic Arthritis Screening (ToPAS) questionnaire. These and many others may be used to help dermatologists detect early signs and symptoms of PsA. Although these questionnaires all have limitations in sensitivity and specificity for the diagnosis of PsA, their use can still improve early diagnosis.
The treatment of PsA focuses on achieving the least amount of disease activity and inflammation possible; optimizing functional status, quality of life, and well-being; and preventing structural damage. Treatment decisions are based on the specific domains affected. Nonsteroidal anti-inflammatory drugs and corticosteroid injections are first-line treatments for enthesitis. Early use of tumor necrosis factor inhibitors (TNF) (adalimumab, certolizumab pegol, etanercept, infliximab, and golimumab) is recommended. Alternative biologic disease-modifying agents are indicated when these TNF inhibitors provide an inadequate response. They include ustekinumab (dual interleukin [IL]-12 and IL-23 inhibitor), secukinumab (IL-17A inhibitor), and apremilast (phosphodiesterase-4 inhibitor) and may be considered for patients with predominantly entheseal manifestations of PsA or dactylitis. Biological disease-modifying agents approved for PsA that have shown efficacy for enthesitis include ixekizumab (which targets IL-17A), abatacept (a T-cell inhibitor), guselkumab (monoclonal antibody), and ustekinumab (monoclonal antibody). Tofacitinib and upadacitinib, both oral Janus kinase inhibitors, may also be considered.
Herbert S. Diamond, MD, Professor of Medicine (retired), Temple University School of Medicine, University of Pittsburgh; Chairman, Department of Medicine Emeritus, Western Pennsylvania Hospital, Pittsburgh, PA.
Herbert S. Diamond, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
A 42-year-old woman with a 20-year history of plaque psoriasis presents with complaints of a 3-month history of pain, tenderness, and swelling in her right ankle and foot, of unknown origin. Physical examination reveals active psoriasis, with a Psoriasis Area and Severity Index (PASI) score of 6.7 and psoriatic nail dystrophy, including onycholysis, pitting, and hyperkeratosis. Tenderness and swelling are noted at the back of the heel. The patient denies any other complaints. Laboratory tests are normal, including negative rheumatoid factor and antinuclear factor. MRI reveals soft tissue and bone marrow edema below the Achilles insertion.
Personalized breast screening a step closer to reality
say researchers.
“Several breast cancer risk prediction models have been created, but we believe this is one of the first models designed to guide breast screening strategies over a person’s lifetime using real data from a screening program,” said study author Javier Louro, PhD, Hospital del Mar Medical Research Institute, Barcelona, Spain.
“Our model might be considered a key for designing personalized screening aimed at reducing the harms and increasing the benefits of mammographic screening,” he said in a statement.
Someone with a low risk “might be offered screening with standard mammography every 3 or 4 years instead of 2 years,” Dr. Louro explained.
“Someone with medium risk might be offered screening with advanced 3D mammography every 3 years, while those at a high risk might be offered a new screening test with mammography or MRI every year.”
However, he cautioned that “all of these strategies are still theoretical and should be studied with regard to their effectiveness.”
Dr. Louro was talking about the new model at the 13th European Breast Cancer Conference.
Details of the new prediction model
To develop the new model, Louro and colleagues conducted a retrospective study of 57,411 women who underwent mammography in four counties in Norway between 2007 and 2019 as part of the BreastScreen Norway program, and followed them up to 2022.
The team gathered data on age, breast density, family history of breast cancer, body mass index, age at menarche, alcohol habit, exercise, pregnancy, hormone replacement therapy, and benign breast disease, and compared women with and those without a breast cancer diagnosis.
All of these 10 variables used were found to significantly explain part of the variability in the breast cancer risk.
Overall, the 4-year breast cancer risk predicted by the resulting model varied across the participants, from 0.22% to 7.43%, at a median of 1.10%.
Bootstrap resampling analysis revealed that the model overestimated the risk for breast cancer, at an expected-to-observed ratio of 1.10.
The largest effect on risk was from breast density on mammography. Women with dense breasts were at much higher risk: the adjusted hazard ratio was 1.71 for women with Volpara Density Grade 4 vs Grade 2 and was 1.37 when compared with Grade 3.
Exercise had a large impact on breast cancer risk, the researchers found. Women who exercised for 4 or more hours per week had an adjusted hazard ratio of 0.65 for breast cancer risk compared with women who never exercised. Although this effect of exercise reducing the risk for breast cancer is now widely known, it is not usually included in models that predict breast cancer risk, the team pointed out.
The team concluded that their prediction model could be used to personalize breast screening for women according to their risk assessment, although they acknowledge that more work is needed. This work is based on one screening program in one country, and similar studies in different settings are needed.
Reacting to the findings, Laura Biganzoli, MD, co-chair of the European Breast Cancer Conference and director of the Breast Centre at Santo Stefano Hospital, Prato, Italy, commented, “We know that breast screening programs are beneficial, but we also know that some people will experience potential harms caused by false-positives or overdiagnosis.”
“This research shows how we might be able to identify people with a high risk of breast cancer, but equally how we could identify those with a low risk. So it’s an important step toward personalized screening,” Dr. Biganzoli said.
This study was supported by a grant from Instituto de Salud Carlos III FEDER (grant PI/00047). No relevant financial relationships declared.
A version of this article first appeared on Medscape.com.
say researchers.
“Several breast cancer risk prediction models have been created, but we believe this is one of the first models designed to guide breast screening strategies over a person’s lifetime using real data from a screening program,” said study author Javier Louro, PhD, Hospital del Mar Medical Research Institute, Barcelona, Spain.
“Our model might be considered a key for designing personalized screening aimed at reducing the harms and increasing the benefits of mammographic screening,” he said in a statement.
Someone with a low risk “might be offered screening with standard mammography every 3 or 4 years instead of 2 years,” Dr. Louro explained.
“Someone with medium risk might be offered screening with advanced 3D mammography every 3 years, while those at a high risk might be offered a new screening test with mammography or MRI every year.”
However, he cautioned that “all of these strategies are still theoretical and should be studied with regard to their effectiveness.”
Dr. Louro was talking about the new model at the 13th European Breast Cancer Conference.
Details of the new prediction model
To develop the new model, Louro and colleagues conducted a retrospective study of 57,411 women who underwent mammography in four counties in Norway between 2007 and 2019 as part of the BreastScreen Norway program, and followed them up to 2022.
The team gathered data on age, breast density, family history of breast cancer, body mass index, age at menarche, alcohol habit, exercise, pregnancy, hormone replacement therapy, and benign breast disease, and compared women with and those without a breast cancer diagnosis.
All of these 10 variables used were found to significantly explain part of the variability in the breast cancer risk.
Overall, the 4-year breast cancer risk predicted by the resulting model varied across the participants, from 0.22% to 7.43%, at a median of 1.10%.
Bootstrap resampling analysis revealed that the model overestimated the risk for breast cancer, at an expected-to-observed ratio of 1.10.
The largest effect on risk was from breast density on mammography. Women with dense breasts were at much higher risk: the adjusted hazard ratio was 1.71 for women with Volpara Density Grade 4 vs Grade 2 and was 1.37 when compared with Grade 3.
Exercise had a large impact on breast cancer risk, the researchers found. Women who exercised for 4 or more hours per week had an adjusted hazard ratio of 0.65 for breast cancer risk compared with women who never exercised. Although this effect of exercise reducing the risk for breast cancer is now widely known, it is not usually included in models that predict breast cancer risk, the team pointed out.
The team concluded that their prediction model could be used to personalize breast screening for women according to their risk assessment, although they acknowledge that more work is needed. This work is based on one screening program in one country, and similar studies in different settings are needed.
Reacting to the findings, Laura Biganzoli, MD, co-chair of the European Breast Cancer Conference and director of the Breast Centre at Santo Stefano Hospital, Prato, Italy, commented, “We know that breast screening programs are beneficial, but we also know that some people will experience potential harms caused by false-positives or overdiagnosis.”
“This research shows how we might be able to identify people with a high risk of breast cancer, but equally how we could identify those with a low risk. So it’s an important step toward personalized screening,” Dr. Biganzoli said.
This study was supported by a grant from Instituto de Salud Carlos III FEDER (grant PI/00047). No relevant financial relationships declared.
A version of this article first appeared on Medscape.com.
say researchers.
“Several breast cancer risk prediction models have been created, but we believe this is one of the first models designed to guide breast screening strategies over a person’s lifetime using real data from a screening program,” said study author Javier Louro, PhD, Hospital del Mar Medical Research Institute, Barcelona, Spain.
“Our model might be considered a key for designing personalized screening aimed at reducing the harms and increasing the benefits of mammographic screening,” he said in a statement.
Someone with a low risk “might be offered screening with standard mammography every 3 or 4 years instead of 2 years,” Dr. Louro explained.
“Someone with medium risk might be offered screening with advanced 3D mammography every 3 years, while those at a high risk might be offered a new screening test with mammography or MRI every year.”
However, he cautioned that “all of these strategies are still theoretical and should be studied with regard to their effectiveness.”
Dr. Louro was talking about the new model at the 13th European Breast Cancer Conference.
Details of the new prediction model
To develop the new model, Louro and colleagues conducted a retrospective study of 57,411 women who underwent mammography in four counties in Norway between 2007 and 2019 as part of the BreastScreen Norway program, and followed them up to 2022.
The team gathered data on age, breast density, family history of breast cancer, body mass index, age at menarche, alcohol habit, exercise, pregnancy, hormone replacement therapy, and benign breast disease, and compared women with and those without a breast cancer diagnosis.
All of these 10 variables used were found to significantly explain part of the variability in the breast cancer risk.
Overall, the 4-year breast cancer risk predicted by the resulting model varied across the participants, from 0.22% to 7.43%, at a median of 1.10%.
Bootstrap resampling analysis revealed that the model overestimated the risk for breast cancer, at an expected-to-observed ratio of 1.10.
The largest effect on risk was from breast density on mammography. Women with dense breasts were at much higher risk: the adjusted hazard ratio was 1.71 for women with Volpara Density Grade 4 vs Grade 2 and was 1.37 when compared with Grade 3.
Exercise had a large impact on breast cancer risk, the researchers found. Women who exercised for 4 or more hours per week had an adjusted hazard ratio of 0.65 for breast cancer risk compared with women who never exercised. Although this effect of exercise reducing the risk for breast cancer is now widely known, it is not usually included in models that predict breast cancer risk, the team pointed out.
The team concluded that their prediction model could be used to personalize breast screening for women according to their risk assessment, although they acknowledge that more work is needed. This work is based on one screening program in one country, and similar studies in different settings are needed.
Reacting to the findings, Laura Biganzoli, MD, co-chair of the European Breast Cancer Conference and director of the Breast Centre at Santo Stefano Hospital, Prato, Italy, commented, “We know that breast screening programs are beneficial, but we also know that some people will experience potential harms caused by false-positives or overdiagnosis.”
“This research shows how we might be able to identify people with a high risk of breast cancer, but equally how we could identify those with a low risk. So it’s an important step toward personalized screening,” Dr. Biganzoli said.
This study was supported by a grant from Instituto de Salud Carlos III FEDER (grant PI/00047). No relevant financial relationships declared.
A version of this article first appeared on Medscape.com.
FROM EBCC-13
Decline in ambulatory function
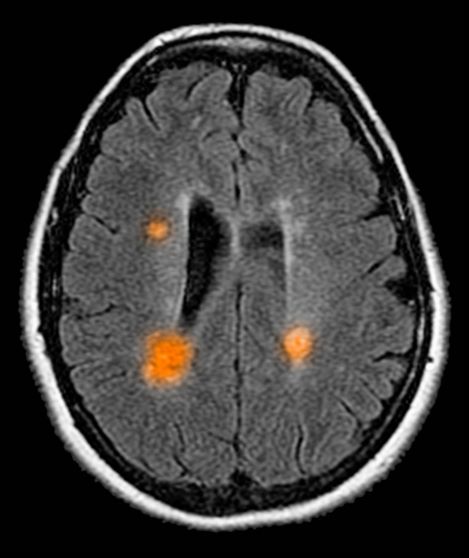
Based on this patient's history and presentation, the likely diagnosis is primary progressive multiple sclerosis (PPMS). PPMS represents around 10% of MS cases and tends to develop about a decade later than relapsing MS. Unlike other forms of MS, this phenotype progresses steadily instead of in an episodic fashion like relapsing forms of MS. Most patients with PPMS present with gait difficulty because lesions often develop on the spinal cord. While relapsing-remitting MS (RRMS) is much more common among women than men, men with MS are more likely to have the progressive form.
Although this patient's MRI ultimately points to multiple sclerosis, his functional deficits may initially suggest other conditions in the differential diagnosis. Brainstem gliomas typically manifest in unsteady gait, weakness, double vision, difficulty swallowing, dysarthria, headache, drowsiness, nausea, and vomiting. Transverse myelitis often presents with rapid-onset weakness, sensory deficits, and bowel/bladder dysfunction. Musculoskeletal and neurologic symptoms are common in Lyme disease. B12 deficiency can present with worsening weakness and a sensory ataxia that can present as balance difficulties, but it would not cause focal lesions on the MRI, nor would it present with bladder symptoms. In addition, the patient's steady decline in function rules out RRMS.
PPMS is diagnosed with confirmation of gradual change in functional ability (often ambulation) over time without remission or relapse. These criteria include 1 full year of worsening neurologic function without asymptomatic periods as well as two of these signs of disease: brain lesion, two or more spinal cord lesions, and oligoclonal bands or elevated Immunoglobulin G index. These timing-specific criteria can delay diagnosis, as seen here.
Ocrelizumab is the only FDA-approved disease-modifying therapy (DMT) proven to alter disease progression in ambulatory patients with PPMS. American Academy of Neurology guidelines recommend ocrelizumab for patients with PPMS who are likely to benefit from this therapy. While it is thought that DMTs are more effective at targeting inflammation in RRMS than nerve degeneration in PPMS, these agents may show benefit for patients with active PPMS (relapse and/or evidence of new MRI activity) rather than inactive disease. A recent PPMS study concluded that among patients with relapse or disease activity, DMTs were associated with a significant reduction of long-term disability risk. Together with immunomodulatory therapy, rehabilitation can help manage symptoms.
Krupa Pandey, MD, Director, Multiple Sclerosis Center, Department of Neurology & Neuroscience Institute, Hackensack University Medical Center; Neurologist, Department of Neurology, Hackensack Meridian Health, Hackensack, NJ.
Krupa Pandey, MD, has serve(d) as a speaker or a member of a speakers bureau for: Bristol-Myers Squibb; Biogen; Alexion; Genentech; Sanofi-Genzyme.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Based on this patient's history and presentation, the likely diagnosis is primary progressive multiple sclerosis (PPMS). PPMS represents around 10% of MS cases and tends to develop about a decade later than relapsing MS. Unlike other forms of MS, this phenotype progresses steadily instead of in an episodic fashion like relapsing forms of MS. Most patients with PPMS present with gait difficulty because lesions often develop on the spinal cord. While relapsing-remitting MS (RRMS) is much more common among women than men, men with MS are more likely to have the progressive form.
Although this patient's MRI ultimately points to multiple sclerosis, his functional deficits may initially suggest other conditions in the differential diagnosis. Brainstem gliomas typically manifest in unsteady gait, weakness, double vision, difficulty swallowing, dysarthria, headache, drowsiness, nausea, and vomiting. Transverse myelitis often presents with rapid-onset weakness, sensory deficits, and bowel/bladder dysfunction. Musculoskeletal and neurologic symptoms are common in Lyme disease. B12 deficiency can present with worsening weakness and a sensory ataxia that can present as balance difficulties, but it would not cause focal lesions on the MRI, nor would it present with bladder symptoms. In addition, the patient's steady decline in function rules out RRMS.
PPMS is diagnosed with confirmation of gradual change in functional ability (often ambulation) over time without remission or relapse. These criteria include 1 full year of worsening neurologic function without asymptomatic periods as well as two of these signs of disease: brain lesion, two or more spinal cord lesions, and oligoclonal bands or elevated Immunoglobulin G index. These timing-specific criteria can delay diagnosis, as seen here.
Ocrelizumab is the only FDA-approved disease-modifying therapy (DMT) proven to alter disease progression in ambulatory patients with PPMS. American Academy of Neurology guidelines recommend ocrelizumab for patients with PPMS who are likely to benefit from this therapy. While it is thought that DMTs are more effective at targeting inflammation in RRMS than nerve degeneration in PPMS, these agents may show benefit for patients with active PPMS (relapse and/or evidence of new MRI activity) rather than inactive disease. A recent PPMS study concluded that among patients with relapse or disease activity, DMTs were associated with a significant reduction of long-term disability risk. Together with immunomodulatory therapy, rehabilitation can help manage symptoms.
Krupa Pandey, MD, Director, Multiple Sclerosis Center, Department of Neurology & Neuroscience Institute, Hackensack University Medical Center; Neurologist, Department of Neurology, Hackensack Meridian Health, Hackensack, NJ.
Krupa Pandey, MD, has serve(d) as a speaker or a member of a speakers bureau for: Bristol-Myers Squibb; Biogen; Alexion; Genentech; Sanofi-Genzyme.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Based on this patient's history and presentation, the likely diagnosis is primary progressive multiple sclerosis (PPMS). PPMS represents around 10% of MS cases and tends to develop about a decade later than relapsing MS. Unlike other forms of MS, this phenotype progresses steadily instead of in an episodic fashion like relapsing forms of MS. Most patients with PPMS present with gait difficulty because lesions often develop on the spinal cord. While relapsing-remitting MS (RRMS) is much more common among women than men, men with MS are more likely to have the progressive form.
Although this patient's MRI ultimately points to multiple sclerosis, his functional deficits may initially suggest other conditions in the differential diagnosis. Brainstem gliomas typically manifest in unsteady gait, weakness, double vision, difficulty swallowing, dysarthria, headache, drowsiness, nausea, and vomiting. Transverse myelitis often presents with rapid-onset weakness, sensory deficits, and bowel/bladder dysfunction. Musculoskeletal and neurologic symptoms are common in Lyme disease. B12 deficiency can present with worsening weakness and a sensory ataxia that can present as balance difficulties, but it would not cause focal lesions on the MRI, nor would it present with bladder symptoms. In addition, the patient's steady decline in function rules out RRMS.
PPMS is diagnosed with confirmation of gradual change in functional ability (often ambulation) over time without remission or relapse. These criteria include 1 full year of worsening neurologic function without asymptomatic periods as well as two of these signs of disease: brain lesion, two or more spinal cord lesions, and oligoclonal bands or elevated Immunoglobulin G index. These timing-specific criteria can delay diagnosis, as seen here.
Ocrelizumab is the only FDA-approved disease-modifying therapy (DMT) proven to alter disease progression in ambulatory patients with PPMS. American Academy of Neurology guidelines recommend ocrelizumab for patients with PPMS who are likely to benefit from this therapy. While it is thought that DMTs are more effective at targeting inflammation in RRMS than nerve degeneration in PPMS, these agents may show benefit for patients with active PPMS (relapse and/or evidence of new MRI activity) rather than inactive disease. A recent PPMS study concluded that among patients with relapse or disease activity, DMTs were associated with a significant reduction of long-term disability risk. Together with immunomodulatory therapy, rehabilitation can help manage symptoms.
Krupa Pandey, MD, Director, Multiple Sclerosis Center, Department of Neurology & Neuroscience Institute, Hackensack University Medical Center; Neurologist, Department of Neurology, Hackensack Meridian Health, Hackensack, NJ.
Krupa Pandey, MD, has serve(d) as a speaker or a member of a speakers bureau for: Bristol-Myers Squibb; Biogen; Alexion; Genentech; Sanofi-Genzyme.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
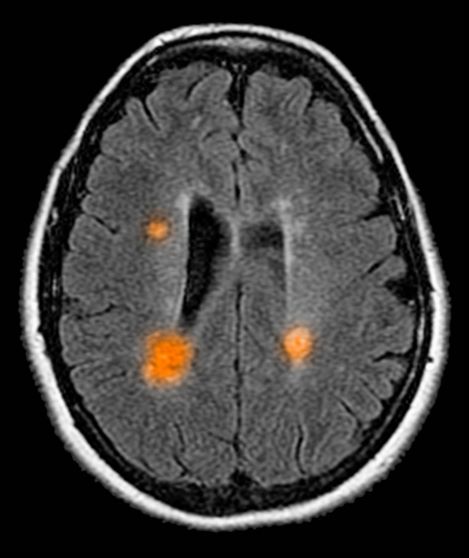
A 59-year-old man presents with worsening decline in ambulatory function and worsening bladder function. He reports "difficulty getting around" for the past year and a half, which he theorized might be because of arthritis, aging, or many years of biking. He presented to his primary care physician 2 months ago and was referred to rheumatology. His height is 5 ft 11 in and his weight is 166 lb (BMI 23.1). The patient subsequently reported a decreased attention span to the rheumatologist. He has no other significant medical or surgical history, though his brother has psoriatic arthritis. MRI shows multiple brain lesions without gadolinium enhancement and multiple spinal cord lesions.
Screen time may help concussion recovery
research shows.
Now a study suggests that getting back on TikTok and Snapchat may help, too.
After surveying 700 patients ages 8-16 following an injury, researchers for the Pediatric Emergency Research Canada A-CAP study team found that
A “moderate” amount was between 2 and 7 hours per day on various screens. “That includes their phones, computers, and televisions,” says lead author Molly Cairncross, PhD, of Simon Fraser University, Vancouver.
People in the study who reported either less or more screen time than that in the 7-10 days after injury also reported more symptoms, such as headaches and fatigue, during the first month. After that month, all the participants reported similar symptoms, regardless of their early screen use – suggesting that screen time makes little difference long term in pediatric concussion recovery.
The findings differ from a 2021 study by researchers at the University of Massachusetts, Boston, that found screen time slowed recovery. Why the clashing results? “I think what it comes down to are differences in study design,” says Dr. Cairncross. While the earlier study measured screen use in the first 48 hours, and recovery over 10 days, “we focused on screen time use over the first 7-10 days, and tracked recovery over 6 months,” she says.
“Taken together, the studies suggest a need to find balance – not too little and not too much time on screens for kids and teens following a concussion,” Dr. Cairncross says.
Ultimately, the findings support moderation rather than blanket restrictions on screen time as the best way to manage pediatric concussion, especially after the first 48 hours.
“It’s actually unsurprising,” says Sarah Brittain, MS, a speech-language pathologist and founder of Colorado Brain Recovery in Wheat Ridge, who was not involved in the study. “An early return to both cognitive and physical activity in a controlled fashion is really important. Sitting in a dark room and resting is not the answer and has been disproven in the literature.”
Old advice involved lying in a quiet, dark room for days, but recent evidence reveals that such “cocoon therapy” may actually prolong symptoms.
“With time, we have found this can negatively impact quality of life and depression scores, especially in teenagers,” says Katherine Labiner, MD, a child neurologist at Pediatrix Child Neurology Consultants of Austin, Tex., who was not involved in the study.
So, how might screens help? Dr. Labiner, Ms. Brittain, and Dr. Cairncross all point to the importance of connection – not the Internet kind, but the social kind. Children and teens use smartphones and computers to stay connected with peers, so banning screen time could have a negative impact on mental health by leading to loneliness, separation, and lack of social support.
“Depression can prolong the course of recovery,” says Ms. Brittain.
It’s worth noting that screen time could trigger visual symptoms in some patients, she says. “If someone feels worse within 2 minutes of being on a screen, that’s a good indicator that screens aren’t working for them,” Ms. Brittain says. “If being on a screen makes them dizzy or wiped out, or the words on the screen look like they’re moving when they’re not, that means it’s time to back off.”
She advises parents to watch for behavior changes like increased crankiness, impatience, and/or fatigue, which could mean that the child has returned to screen time – or any activity – too soon and should scale back until symptoms subside.
“The most important thing to stress with concussion is full recovery before complete return to activity,” Dr. Labiner says.
A version of this article first appeared on Medscape.com.
research shows.
Now a study suggests that getting back on TikTok and Snapchat may help, too.
After surveying 700 patients ages 8-16 following an injury, researchers for the Pediatric Emergency Research Canada A-CAP study team found that
A “moderate” amount was between 2 and 7 hours per day on various screens. “That includes their phones, computers, and televisions,” says lead author Molly Cairncross, PhD, of Simon Fraser University, Vancouver.
People in the study who reported either less or more screen time than that in the 7-10 days after injury also reported more symptoms, such as headaches and fatigue, during the first month. After that month, all the participants reported similar symptoms, regardless of their early screen use – suggesting that screen time makes little difference long term in pediatric concussion recovery.
The findings differ from a 2021 study by researchers at the University of Massachusetts, Boston, that found screen time slowed recovery. Why the clashing results? “I think what it comes down to are differences in study design,” says Dr. Cairncross. While the earlier study measured screen use in the first 48 hours, and recovery over 10 days, “we focused on screen time use over the first 7-10 days, and tracked recovery over 6 months,” she says.
“Taken together, the studies suggest a need to find balance – not too little and not too much time on screens for kids and teens following a concussion,” Dr. Cairncross says.
Ultimately, the findings support moderation rather than blanket restrictions on screen time as the best way to manage pediatric concussion, especially after the first 48 hours.
“It’s actually unsurprising,” says Sarah Brittain, MS, a speech-language pathologist and founder of Colorado Brain Recovery in Wheat Ridge, who was not involved in the study. “An early return to both cognitive and physical activity in a controlled fashion is really important. Sitting in a dark room and resting is not the answer and has been disproven in the literature.”
Old advice involved lying in a quiet, dark room for days, but recent evidence reveals that such “cocoon therapy” may actually prolong symptoms.
“With time, we have found this can negatively impact quality of life and depression scores, especially in teenagers,” says Katherine Labiner, MD, a child neurologist at Pediatrix Child Neurology Consultants of Austin, Tex., who was not involved in the study.
So, how might screens help? Dr. Labiner, Ms. Brittain, and Dr. Cairncross all point to the importance of connection – not the Internet kind, but the social kind. Children and teens use smartphones and computers to stay connected with peers, so banning screen time could have a negative impact on mental health by leading to loneliness, separation, and lack of social support.
“Depression can prolong the course of recovery,” says Ms. Brittain.
It’s worth noting that screen time could trigger visual symptoms in some patients, she says. “If someone feels worse within 2 minutes of being on a screen, that’s a good indicator that screens aren’t working for them,” Ms. Brittain says. “If being on a screen makes them dizzy or wiped out, or the words on the screen look like they’re moving when they’re not, that means it’s time to back off.”
She advises parents to watch for behavior changes like increased crankiness, impatience, and/or fatigue, which could mean that the child has returned to screen time – or any activity – too soon and should scale back until symptoms subside.
“The most important thing to stress with concussion is full recovery before complete return to activity,” Dr. Labiner says.
A version of this article first appeared on Medscape.com.
research shows.
Now a study suggests that getting back on TikTok and Snapchat may help, too.
After surveying 700 patients ages 8-16 following an injury, researchers for the Pediatric Emergency Research Canada A-CAP study team found that
A “moderate” amount was between 2 and 7 hours per day on various screens. “That includes their phones, computers, and televisions,” says lead author Molly Cairncross, PhD, of Simon Fraser University, Vancouver.
People in the study who reported either less or more screen time than that in the 7-10 days after injury also reported more symptoms, such as headaches and fatigue, during the first month. After that month, all the participants reported similar symptoms, regardless of their early screen use – suggesting that screen time makes little difference long term in pediatric concussion recovery.
The findings differ from a 2021 study by researchers at the University of Massachusetts, Boston, that found screen time slowed recovery. Why the clashing results? “I think what it comes down to are differences in study design,” says Dr. Cairncross. While the earlier study measured screen use in the first 48 hours, and recovery over 10 days, “we focused on screen time use over the first 7-10 days, and tracked recovery over 6 months,” she says.
“Taken together, the studies suggest a need to find balance – not too little and not too much time on screens for kids and teens following a concussion,” Dr. Cairncross says.
Ultimately, the findings support moderation rather than blanket restrictions on screen time as the best way to manage pediatric concussion, especially after the first 48 hours.
“It’s actually unsurprising,” says Sarah Brittain, MS, a speech-language pathologist and founder of Colorado Brain Recovery in Wheat Ridge, who was not involved in the study. “An early return to both cognitive and physical activity in a controlled fashion is really important. Sitting in a dark room and resting is not the answer and has been disproven in the literature.”
Old advice involved lying in a quiet, dark room for days, but recent evidence reveals that such “cocoon therapy” may actually prolong symptoms.
“With time, we have found this can negatively impact quality of life and depression scores, especially in teenagers,” says Katherine Labiner, MD, a child neurologist at Pediatrix Child Neurology Consultants of Austin, Tex., who was not involved in the study.
So, how might screens help? Dr. Labiner, Ms. Brittain, and Dr. Cairncross all point to the importance of connection – not the Internet kind, but the social kind. Children and teens use smartphones and computers to stay connected with peers, so banning screen time could have a negative impact on mental health by leading to loneliness, separation, and lack of social support.
“Depression can prolong the course of recovery,” says Ms. Brittain.
It’s worth noting that screen time could trigger visual symptoms in some patients, she says. “If someone feels worse within 2 minutes of being on a screen, that’s a good indicator that screens aren’t working for them,” Ms. Brittain says. “If being on a screen makes them dizzy or wiped out, or the words on the screen look like they’re moving when they’re not, that means it’s time to back off.”
She advises parents to watch for behavior changes like increased crankiness, impatience, and/or fatigue, which could mean that the child has returned to screen time – or any activity – too soon and should scale back until symptoms subside.
“The most important thing to stress with concussion is full recovery before complete return to activity,” Dr. Labiner says.
A version of this article first appeared on Medscape.com.
FROM PEDIATRICS
Novel vaccine approach halts disease after 23 years of breast cancer
A recent 6-month follow-up showed no evidence of new or recurrent disease, and scans showed regression of a distant bulky left adrenal metastasis, as well as at other sites.
A small site of residual hypermetabolism remains in the sternum, but this is thought to be related to scar tissue.
The patient, Stephanie Gangi, told Medscape Medical News that, before she entered into the trial for the novel cancer vaccine, she was “mentally and physically exhausted.” She had benefited from being diagnosed with hormone-positive breast cancer just as its treatment was evolving and progressing, which meant that, every time a treatment failed, “there was the next thing to try, which was great and kept me going.”
“But I will admit that, by age 66, and more than 20 years of cancer treatments, I was exhausted.”
Ms. Gangi, a New York City-based poet, essayist, and fiction writer, said she was “cautiously optimistic” about the cancer vaccine, but the “overriding thought was I wanted to avoid chemotherapy.”
“I was not really signing on for great outcomes, I was signing on for something that might keep chemo at bay. The biggest impact so far for me has been that, for the first time in more than a decade, I am not on any medication. That’s really amazing…and that means no side effects,” she said.
Ms. Gangi stopped the vaccine treatment this past July, and just over 3 months later, she is still “wrapping her head around” the fact that her cancer has regressed. “I’ve had breast cancer a long time,” she said, “and you can’t just snap your fingers and be fine.”
Although the two scans that she has had since the trial ended have been “astonishing,” she underlined that this is not about a ‘cure,’ but rather “clearing tumors for the first time in many years.”
“Cancer is sneaky and sinister, and it figures out how to circumvent all kinds of treatments,” she said, adding nevertheless that she is “happy and hopeful, and my family is thrilled, of course.”
Ms. Gangi was classed as having had a partial response to the cancer vaccine, one of a few in a small phase 1/2 trial at the Icahn School of Medicine at Mount Sinai in New York. One other patient also had a partial response, and one patient had a complete response.
However, six patients have progressive disease, and one has stable disease.
These results come from an interim analysis of 10 patients from the trial, and show a 30% response rate. They were presented at the recent annual meeting of the Society for Immunotherapy of Cancer.
The vaccine that was being tested combines local low-dose radiation, intramural Flt3L, which stimulates dendritic cells, and intravenous poly-ICLC, an immune stimulating factor, with the PD-1 inhibitor pembrolizumab (Keytruda).
The result is that, instead of making a vaccine in a laboratory and administering it, “we’re actually formulating it within the body,” lead author Thomas Marron, MD, PhD, professor of medicine (hematology and medical oncology) at Mount Sinai, said in an interview.
“What people don’t realize,” he said, is that bulky tumor sites contain “a lot of dead tumor, because they grow so fast and in a haphazard way.” This means that the immune system can be recruited to recognize the dead tumor and “gobble up the dead stuff that’s already there,” he added.
The hope is that the immune system will then kill not only “the tumor you are injecting into, but also tumors elsewhere in the body,” Dr. Marron said. “So you’re basically using your body’s own immune system and on and off switches to vaccinate the patient against their cancer.”
Another patient in the trial who had a complete response to the vaccine was William Morrison, with non-Hodgkin lymphoma (NHL).
Mr. Morrison was diagnosed in 2017, at which time he was enrolled onto a phase 1 trial of an earlier version of this novel vaccine treatment regimen. “Basically, they didn’t get the results they were hoping for, and I still had the lymphoma,” he said. In 2018, his indolent follicular lymphoma transformed into an aggressive diffuse large B-cell lymphoma, for which Mr. Morrison was given six cycles of chemotherapy. This put him into remission and cleared his lymphoma.
“But the remission lasted for maybe a little over a year,” he said.
The cancer came back, and at that point he was given the opportunity to enroll in the Mount Sinai trial. At the end of the treatment, “everything was clear.”
“I’ve been for PET scans every 6 months, and I just had a scan done the other week, and everything has been fine…I’ve been pretty excited. I was pretty lucky.”
“This recent one really has worked wonders,” he said, “When they gave me the good news the other day. I felt like a big weight had been lifted.”
Mr. Morrison also said that he did not experience any serious adverse events while being treated with the vaccine. “Other than a few minor things, I tolerated it pretty well,” he said.
In contrast, Ms. Gangi said she experienced “intense” flu-like symptoms that started in the first few days after the treatment and lasted for a couple of days.
Need to improve response rate
The current trial achieved responses in 30% of patients, which “is great, [but] we want to be at 100%,” said Dr. Marron.
“What we’re doing in the laboratory right now is using this as an opportunity to study what it is that’s special about those three people who responded and what’s not happening in the other seven people, and we have some initial data that we’re analyzing,” he said.
“We are seeing that the patients who responded have a much more robust response to the Ft3L in particular…and that could suggest that maybe we need a better Ft3L, or we could think about other ways to potentially manipulate this vaccine.
“Most of the patients who are referred to me are people who have run out of options…and that usually means they’ve had many different types of chemotherapy,” Dr. Marron commented. For example, Ms. Gangi had already been through 12 different chemotherapy regimens.
Chemotherapy suppresses the immune system, but it’s not only that — also having an effect are all the other treatments aimed at reducing nausea and allergic reactions to the anti-cancer therapy, Dr. Marron explained.
“By the time that I see a patient,” Dr. Marron said, “oftentimes their immune system is not optimal. So another way in which we would hope to see better responses is by moving this vaccine earlier in the treatment paradigm, and administering it to patients as their first or second treatment.”
Senior author Joshua Brody, MD, director of the Lymphoma Immunotherapy Program at Mount Sinai’s Tisch Cancer Institute, added that it “might be easy” to incorporate the vaccine into earlier lines of therapy.
He said in an interview that both immunotherapy and radiation therapy are “standard” treatments, and the key is “adding multiple ingredients together that don’t have cumulative toxicity.”
“You can’t just chemo one plus chemo two, because they have some of the same toxicities, but the delightful thing here is this therapy had been quite safe.
“So in theory it would be fairly easy to incorporate this into earlier lines of therapy, once we can get a bit more proof of principle,” Dr. Brody said.
Approached for comment, Ann W. Silk, MD, said that the results are “particularly impressive because we know anti-PD-1 plus radiation therapy does not work in hormone-positive breast cancer or lymphoma.”
Dr. Silk, an oncologist at the Dana-Farber Cancer Institute and assistant professor of medicine at Harvard Medical School in Boston, said in an interview that one advantage of this vaccine is that it “is not restricted to a certain number of antigens and does not rely on an algorithm.”
“I would love to see more data in hormone-positive metastatic breast cancer patients,” she added. “I would use this approach after the hormonal treatments stop working, but before chemotherapy.”
Dr. Silk also said that the safety profile “looks quite good, and I imagine this approach would result in a much better quality of life for patients as compared to chemotherapy.”
Details of the trial and results
The Mount Sinai researchers had previously developed a personalized genomic cancer vaccine, PGV-001, which showed promise in a phase 1 trial in 13 patients with solid tumors or multiple myeloma and a high risk of recurrence after surgery or autologous stem cell transplant.
Next, they worked to develop the concept further to turn the tumor into its own vaccine, which involved inducing anti-tumor responses in indolent NHL, which typically responds poorly to checkpoint blockade, by combining Ft3L, low-dose irradiation, and poly-ICLC.
The next phase 1 trial showed that this approach was feasible, but preclinical modeling suggested that the addition of PD-1 blockade could improve the cure rates. The researchers therefore conducted the current trial, recruiting 10 patients with indolent NHL, metastatic breast cancer, or head and neck squamous cell carcinoma (HNSCC).
Patients were given local radiation therapy on days 1 and 2, and intramural Ft3L to the same tumor on day 9, followed by eight intravenous injections of poly-ICLC over 6 weeks. On day 23, they received their first of eight doses of pembrolizumab.
Dr. Marron explained that the radiotherapy increases the amount of dead material for the immune system to work on by “killing some of the tumor cells,” adding: “We’re not trying to kill the whole tumor with the radiation…it just starts the process of releasing some more of that dead stuff.”
He explained that Ft3L is a human growth factor that simulates dendritic cells, “which I always say are the professor cells of the immune system,” as they tell the body “what’s good and what’s bad.”
The poly-ICLC is “basically like a fake virus,” Dr. Marron said, as it “turns on those immune cells that have taken up the tumor antigen in the neighborhood” of the tumor, so they “teach the immune system that there is something bad”.
Finally, the pembrolizumab is there to “take the foot off the brake of the immune system” and “grease the wheels a bit more,” he added, even though it does not work in all patients, or in all tumor types, including indolent NHL.
The trial was planned in two phases. In the first part, six patients were enrolled to assess the safety of the approach; the phase 2 stage of the trial followed a Simon’s Two-Stage design, with the aim of recruiting seven patients of each tumor type, followed by a further 12 patients if they showed a response.
The current interim analysis that was presented at the SITC meeting focused on the first 10 patients in the phase 2 part, who were enrolled between April 2019 and July 2022. This included six patients with metastatic breast cancer, three with indolent NHL, and one with HNSCC, all of whom completed their first disease response assessment.
All patients experienced treatment-related adverse events, largely comprising low-grade injection site reactions and flu-like symptoms linked to the poly-ICLC injections.
One patient experienced grade 3 pembrolizumab-related colitis, while another had self-resolving grade 3 fever following poly-ICLC injection.
The study was sponsored by Icahn School of Medicine at Mount Sinai and conducted in collaboration with Merck Sharp & Dohme LLC and Celldex Therapeutics. No relevant financial relationships were reported.
A version of this article first appeared on Medscape.com.
A recent 6-month follow-up showed no evidence of new or recurrent disease, and scans showed regression of a distant bulky left adrenal metastasis, as well as at other sites.
A small site of residual hypermetabolism remains in the sternum, but this is thought to be related to scar tissue.
The patient, Stephanie Gangi, told Medscape Medical News that, before she entered into the trial for the novel cancer vaccine, she was “mentally and physically exhausted.” She had benefited from being diagnosed with hormone-positive breast cancer just as its treatment was evolving and progressing, which meant that, every time a treatment failed, “there was the next thing to try, which was great and kept me going.”
“But I will admit that, by age 66, and more than 20 years of cancer treatments, I was exhausted.”
Ms. Gangi, a New York City-based poet, essayist, and fiction writer, said she was “cautiously optimistic” about the cancer vaccine, but the “overriding thought was I wanted to avoid chemotherapy.”
“I was not really signing on for great outcomes, I was signing on for something that might keep chemo at bay. The biggest impact so far for me has been that, for the first time in more than a decade, I am not on any medication. That’s really amazing…and that means no side effects,” she said.
Ms. Gangi stopped the vaccine treatment this past July, and just over 3 months later, she is still “wrapping her head around” the fact that her cancer has regressed. “I’ve had breast cancer a long time,” she said, “and you can’t just snap your fingers and be fine.”
Although the two scans that she has had since the trial ended have been “astonishing,” she underlined that this is not about a ‘cure,’ but rather “clearing tumors for the first time in many years.”
“Cancer is sneaky and sinister, and it figures out how to circumvent all kinds of treatments,” she said, adding nevertheless that she is “happy and hopeful, and my family is thrilled, of course.”
Ms. Gangi was classed as having had a partial response to the cancer vaccine, one of a few in a small phase 1/2 trial at the Icahn School of Medicine at Mount Sinai in New York. One other patient also had a partial response, and one patient had a complete response.
However, six patients have progressive disease, and one has stable disease.
These results come from an interim analysis of 10 patients from the trial, and show a 30% response rate. They were presented at the recent annual meeting of the Society for Immunotherapy of Cancer.
The vaccine that was being tested combines local low-dose radiation, intramural Flt3L, which stimulates dendritic cells, and intravenous poly-ICLC, an immune stimulating factor, with the PD-1 inhibitor pembrolizumab (Keytruda).
The result is that, instead of making a vaccine in a laboratory and administering it, “we’re actually formulating it within the body,” lead author Thomas Marron, MD, PhD, professor of medicine (hematology and medical oncology) at Mount Sinai, said in an interview.
“What people don’t realize,” he said, is that bulky tumor sites contain “a lot of dead tumor, because they grow so fast and in a haphazard way.” This means that the immune system can be recruited to recognize the dead tumor and “gobble up the dead stuff that’s already there,” he added.
The hope is that the immune system will then kill not only “the tumor you are injecting into, but also tumors elsewhere in the body,” Dr. Marron said. “So you’re basically using your body’s own immune system and on and off switches to vaccinate the patient against their cancer.”
Another patient in the trial who had a complete response to the vaccine was William Morrison, with non-Hodgkin lymphoma (NHL).
Mr. Morrison was diagnosed in 2017, at which time he was enrolled onto a phase 1 trial of an earlier version of this novel vaccine treatment regimen. “Basically, they didn’t get the results they were hoping for, and I still had the lymphoma,” he said. In 2018, his indolent follicular lymphoma transformed into an aggressive diffuse large B-cell lymphoma, for which Mr. Morrison was given six cycles of chemotherapy. This put him into remission and cleared his lymphoma.
“But the remission lasted for maybe a little over a year,” he said.
The cancer came back, and at that point he was given the opportunity to enroll in the Mount Sinai trial. At the end of the treatment, “everything was clear.”
“I’ve been for PET scans every 6 months, and I just had a scan done the other week, and everything has been fine…I’ve been pretty excited. I was pretty lucky.”
“This recent one really has worked wonders,” he said, “When they gave me the good news the other day. I felt like a big weight had been lifted.”
Mr. Morrison also said that he did not experience any serious adverse events while being treated with the vaccine. “Other than a few minor things, I tolerated it pretty well,” he said.
In contrast, Ms. Gangi said she experienced “intense” flu-like symptoms that started in the first few days after the treatment and lasted for a couple of days.
Need to improve response rate
The current trial achieved responses in 30% of patients, which “is great, [but] we want to be at 100%,” said Dr. Marron.
“What we’re doing in the laboratory right now is using this as an opportunity to study what it is that’s special about those three people who responded and what’s not happening in the other seven people, and we have some initial data that we’re analyzing,” he said.
“We are seeing that the patients who responded have a much more robust response to the Ft3L in particular…and that could suggest that maybe we need a better Ft3L, or we could think about other ways to potentially manipulate this vaccine.
“Most of the patients who are referred to me are people who have run out of options…and that usually means they’ve had many different types of chemotherapy,” Dr. Marron commented. For example, Ms. Gangi had already been through 12 different chemotherapy regimens.
Chemotherapy suppresses the immune system, but it’s not only that — also having an effect are all the other treatments aimed at reducing nausea and allergic reactions to the anti-cancer therapy, Dr. Marron explained.
“By the time that I see a patient,” Dr. Marron said, “oftentimes their immune system is not optimal. So another way in which we would hope to see better responses is by moving this vaccine earlier in the treatment paradigm, and administering it to patients as their first or second treatment.”
Senior author Joshua Brody, MD, director of the Lymphoma Immunotherapy Program at Mount Sinai’s Tisch Cancer Institute, added that it “might be easy” to incorporate the vaccine into earlier lines of therapy.
He said in an interview that both immunotherapy and radiation therapy are “standard” treatments, and the key is “adding multiple ingredients together that don’t have cumulative toxicity.”
“You can’t just chemo one plus chemo two, because they have some of the same toxicities, but the delightful thing here is this therapy had been quite safe.
“So in theory it would be fairly easy to incorporate this into earlier lines of therapy, once we can get a bit more proof of principle,” Dr. Brody said.
Approached for comment, Ann W. Silk, MD, said that the results are “particularly impressive because we know anti-PD-1 plus radiation therapy does not work in hormone-positive breast cancer or lymphoma.”
Dr. Silk, an oncologist at the Dana-Farber Cancer Institute and assistant professor of medicine at Harvard Medical School in Boston, said in an interview that one advantage of this vaccine is that it “is not restricted to a certain number of antigens and does not rely on an algorithm.”
“I would love to see more data in hormone-positive metastatic breast cancer patients,” she added. “I would use this approach after the hormonal treatments stop working, but before chemotherapy.”
Dr. Silk also said that the safety profile “looks quite good, and I imagine this approach would result in a much better quality of life for patients as compared to chemotherapy.”
Details of the trial and results
The Mount Sinai researchers had previously developed a personalized genomic cancer vaccine, PGV-001, which showed promise in a phase 1 trial in 13 patients with solid tumors or multiple myeloma and a high risk of recurrence after surgery or autologous stem cell transplant.
Next, they worked to develop the concept further to turn the tumor into its own vaccine, which involved inducing anti-tumor responses in indolent NHL, which typically responds poorly to checkpoint blockade, by combining Ft3L, low-dose irradiation, and poly-ICLC.
The next phase 1 trial showed that this approach was feasible, but preclinical modeling suggested that the addition of PD-1 blockade could improve the cure rates. The researchers therefore conducted the current trial, recruiting 10 patients with indolent NHL, metastatic breast cancer, or head and neck squamous cell carcinoma (HNSCC).
Patients were given local radiation therapy on days 1 and 2, and intramural Ft3L to the same tumor on day 9, followed by eight intravenous injections of poly-ICLC over 6 weeks. On day 23, they received their first of eight doses of pembrolizumab.
Dr. Marron explained that the radiotherapy increases the amount of dead material for the immune system to work on by “killing some of the tumor cells,” adding: “We’re not trying to kill the whole tumor with the radiation…it just starts the process of releasing some more of that dead stuff.”
He explained that Ft3L is a human growth factor that simulates dendritic cells, “which I always say are the professor cells of the immune system,” as they tell the body “what’s good and what’s bad.”
The poly-ICLC is “basically like a fake virus,” Dr. Marron said, as it “turns on those immune cells that have taken up the tumor antigen in the neighborhood” of the tumor, so they “teach the immune system that there is something bad”.
Finally, the pembrolizumab is there to “take the foot off the brake of the immune system” and “grease the wheels a bit more,” he added, even though it does not work in all patients, or in all tumor types, including indolent NHL.
The trial was planned in two phases. In the first part, six patients were enrolled to assess the safety of the approach; the phase 2 stage of the trial followed a Simon’s Two-Stage design, with the aim of recruiting seven patients of each tumor type, followed by a further 12 patients if they showed a response.
The current interim analysis that was presented at the SITC meeting focused on the first 10 patients in the phase 2 part, who were enrolled between April 2019 and July 2022. This included six patients with metastatic breast cancer, three with indolent NHL, and one with HNSCC, all of whom completed their first disease response assessment.
All patients experienced treatment-related adverse events, largely comprising low-grade injection site reactions and flu-like symptoms linked to the poly-ICLC injections.
One patient experienced grade 3 pembrolizumab-related colitis, while another had self-resolving grade 3 fever following poly-ICLC injection.
The study was sponsored by Icahn School of Medicine at Mount Sinai and conducted in collaboration with Merck Sharp & Dohme LLC and Celldex Therapeutics. No relevant financial relationships were reported.
A version of this article first appeared on Medscape.com.
A recent 6-month follow-up showed no evidence of new or recurrent disease, and scans showed regression of a distant bulky left adrenal metastasis, as well as at other sites.
A small site of residual hypermetabolism remains in the sternum, but this is thought to be related to scar tissue.
The patient, Stephanie Gangi, told Medscape Medical News that, before she entered into the trial for the novel cancer vaccine, she was “mentally and physically exhausted.” She had benefited from being diagnosed with hormone-positive breast cancer just as its treatment was evolving and progressing, which meant that, every time a treatment failed, “there was the next thing to try, which was great and kept me going.”
“But I will admit that, by age 66, and more than 20 years of cancer treatments, I was exhausted.”
Ms. Gangi, a New York City-based poet, essayist, and fiction writer, said she was “cautiously optimistic” about the cancer vaccine, but the “overriding thought was I wanted to avoid chemotherapy.”
“I was not really signing on for great outcomes, I was signing on for something that might keep chemo at bay. The biggest impact so far for me has been that, for the first time in more than a decade, I am not on any medication. That’s really amazing…and that means no side effects,” she said.
Ms. Gangi stopped the vaccine treatment this past July, and just over 3 months later, she is still “wrapping her head around” the fact that her cancer has regressed. “I’ve had breast cancer a long time,” she said, “and you can’t just snap your fingers and be fine.”
Although the two scans that she has had since the trial ended have been “astonishing,” she underlined that this is not about a ‘cure,’ but rather “clearing tumors for the first time in many years.”
“Cancer is sneaky and sinister, and it figures out how to circumvent all kinds of treatments,” she said, adding nevertheless that she is “happy and hopeful, and my family is thrilled, of course.”
Ms. Gangi was classed as having had a partial response to the cancer vaccine, one of a few in a small phase 1/2 trial at the Icahn School of Medicine at Mount Sinai in New York. One other patient also had a partial response, and one patient had a complete response.
However, six patients have progressive disease, and one has stable disease.
These results come from an interim analysis of 10 patients from the trial, and show a 30% response rate. They were presented at the recent annual meeting of the Society for Immunotherapy of Cancer.
The vaccine that was being tested combines local low-dose radiation, intramural Flt3L, which stimulates dendritic cells, and intravenous poly-ICLC, an immune stimulating factor, with the PD-1 inhibitor pembrolizumab (Keytruda).
The result is that, instead of making a vaccine in a laboratory and administering it, “we’re actually formulating it within the body,” lead author Thomas Marron, MD, PhD, professor of medicine (hematology and medical oncology) at Mount Sinai, said in an interview.
“What people don’t realize,” he said, is that bulky tumor sites contain “a lot of dead tumor, because they grow so fast and in a haphazard way.” This means that the immune system can be recruited to recognize the dead tumor and “gobble up the dead stuff that’s already there,” he added.
The hope is that the immune system will then kill not only “the tumor you are injecting into, but also tumors elsewhere in the body,” Dr. Marron said. “So you’re basically using your body’s own immune system and on and off switches to vaccinate the patient against their cancer.”
Another patient in the trial who had a complete response to the vaccine was William Morrison, with non-Hodgkin lymphoma (NHL).
Mr. Morrison was diagnosed in 2017, at which time he was enrolled onto a phase 1 trial of an earlier version of this novel vaccine treatment regimen. “Basically, they didn’t get the results they were hoping for, and I still had the lymphoma,” he said. In 2018, his indolent follicular lymphoma transformed into an aggressive diffuse large B-cell lymphoma, for which Mr. Morrison was given six cycles of chemotherapy. This put him into remission and cleared his lymphoma.
“But the remission lasted for maybe a little over a year,” he said.
The cancer came back, and at that point he was given the opportunity to enroll in the Mount Sinai trial. At the end of the treatment, “everything was clear.”
“I’ve been for PET scans every 6 months, and I just had a scan done the other week, and everything has been fine…I’ve been pretty excited. I was pretty lucky.”
“This recent one really has worked wonders,” he said, “When they gave me the good news the other day. I felt like a big weight had been lifted.”
Mr. Morrison also said that he did not experience any serious adverse events while being treated with the vaccine. “Other than a few minor things, I tolerated it pretty well,” he said.
In contrast, Ms. Gangi said she experienced “intense” flu-like symptoms that started in the first few days after the treatment and lasted for a couple of days.
Need to improve response rate
The current trial achieved responses in 30% of patients, which “is great, [but] we want to be at 100%,” said Dr. Marron.
“What we’re doing in the laboratory right now is using this as an opportunity to study what it is that’s special about those three people who responded and what’s not happening in the other seven people, and we have some initial data that we’re analyzing,” he said.
“We are seeing that the patients who responded have a much more robust response to the Ft3L in particular…and that could suggest that maybe we need a better Ft3L, or we could think about other ways to potentially manipulate this vaccine.
“Most of the patients who are referred to me are people who have run out of options…and that usually means they’ve had many different types of chemotherapy,” Dr. Marron commented. For example, Ms. Gangi had already been through 12 different chemotherapy regimens.
Chemotherapy suppresses the immune system, but it’s not only that — also having an effect are all the other treatments aimed at reducing nausea and allergic reactions to the anti-cancer therapy, Dr. Marron explained.
“By the time that I see a patient,” Dr. Marron said, “oftentimes their immune system is not optimal. So another way in which we would hope to see better responses is by moving this vaccine earlier in the treatment paradigm, and administering it to patients as their first or second treatment.”
Senior author Joshua Brody, MD, director of the Lymphoma Immunotherapy Program at Mount Sinai’s Tisch Cancer Institute, added that it “might be easy” to incorporate the vaccine into earlier lines of therapy.
He said in an interview that both immunotherapy and radiation therapy are “standard” treatments, and the key is “adding multiple ingredients together that don’t have cumulative toxicity.”
“You can’t just chemo one plus chemo two, because they have some of the same toxicities, but the delightful thing here is this therapy had been quite safe.
“So in theory it would be fairly easy to incorporate this into earlier lines of therapy, once we can get a bit more proof of principle,” Dr. Brody said.
Approached for comment, Ann W. Silk, MD, said that the results are “particularly impressive because we know anti-PD-1 plus radiation therapy does not work in hormone-positive breast cancer or lymphoma.”
Dr. Silk, an oncologist at the Dana-Farber Cancer Institute and assistant professor of medicine at Harvard Medical School in Boston, said in an interview that one advantage of this vaccine is that it “is not restricted to a certain number of antigens and does not rely on an algorithm.”
“I would love to see more data in hormone-positive metastatic breast cancer patients,” she added. “I would use this approach after the hormonal treatments stop working, but before chemotherapy.”
Dr. Silk also said that the safety profile “looks quite good, and I imagine this approach would result in a much better quality of life for patients as compared to chemotherapy.”
Details of the trial and results
The Mount Sinai researchers had previously developed a personalized genomic cancer vaccine, PGV-001, which showed promise in a phase 1 trial in 13 patients with solid tumors or multiple myeloma and a high risk of recurrence after surgery or autologous stem cell transplant.
Next, they worked to develop the concept further to turn the tumor into its own vaccine, which involved inducing anti-tumor responses in indolent NHL, which typically responds poorly to checkpoint blockade, by combining Ft3L, low-dose irradiation, and poly-ICLC.
The next phase 1 trial showed that this approach was feasible, but preclinical modeling suggested that the addition of PD-1 blockade could improve the cure rates. The researchers therefore conducted the current trial, recruiting 10 patients with indolent NHL, metastatic breast cancer, or head and neck squamous cell carcinoma (HNSCC).
Patients were given local radiation therapy on days 1 and 2, and intramural Ft3L to the same tumor on day 9, followed by eight intravenous injections of poly-ICLC over 6 weeks. On day 23, they received their first of eight doses of pembrolizumab.
Dr. Marron explained that the radiotherapy increases the amount of dead material for the immune system to work on by “killing some of the tumor cells,” adding: “We’re not trying to kill the whole tumor with the radiation…it just starts the process of releasing some more of that dead stuff.”
He explained that Ft3L is a human growth factor that simulates dendritic cells, “which I always say are the professor cells of the immune system,” as they tell the body “what’s good and what’s bad.”
The poly-ICLC is “basically like a fake virus,” Dr. Marron said, as it “turns on those immune cells that have taken up the tumor antigen in the neighborhood” of the tumor, so they “teach the immune system that there is something bad”.
Finally, the pembrolizumab is there to “take the foot off the brake of the immune system” and “grease the wheels a bit more,” he added, even though it does not work in all patients, or in all tumor types, including indolent NHL.
The trial was planned in two phases. In the first part, six patients were enrolled to assess the safety of the approach; the phase 2 stage of the trial followed a Simon’s Two-Stage design, with the aim of recruiting seven patients of each tumor type, followed by a further 12 patients if they showed a response.
The current interim analysis that was presented at the SITC meeting focused on the first 10 patients in the phase 2 part, who were enrolled between April 2019 and July 2022. This included six patients with metastatic breast cancer, three with indolent NHL, and one with HNSCC, all of whom completed their first disease response assessment.
All patients experienced treatment-related adverse events, largely comprising low-grade injection site reactions and flu-like symptoms linked to the poly-ICLC injections.
One patient experienced grade 3 pembrolizumab-related colitis, while another had self-resolving grade 3 fever following poly-ICLC injection.
The study was sponsored by Icahn School of Medicine at Mount Sinai and conducted in collaboration with Merck Sharp & Dohme LLC and Celldex Therapeutics. No relevant financial relationships were reported.
A version of this article first appeared on Medscape.com.
FROM SITC 2022
Midodrine may be comparable to albumin for PICD prevention in ACLF
WASHINGTON – , according to the results of a randomized controlled trial.
Albumin protected 80% of patients from PICD 6 days after paracentesis, whereas midodrine protected 84%, a difference that was not statistically significant. However, albumin was associated with a slightly higher incidence of adverse events and higher costs, said Mithun Sharma, MD, during his presentation at the annual meeting of the American Association for the Study of Liver Diseases.
Midodrine may be a safer and cost-effective option for these patients, said Dr. Sharma, of the department of hepatology and liver transplantation, AIG Hospitals, Hyderabad, India.
But he cautioned that given the small size of the open-label study, with only 25 patients in each arm, the results should be considered as proof of concept and need to be validated in larger studies.
PICD common in ACLF
PICD is caused by fluid shift during paracentesis, leading to a decrease in effective circulating blood volume.
The incidence of PICD after large-volume paracentesis in patients receiving albumin ranges from 12% to 20%, Dr. Sharma noted.
Albumin has been shown in several trials to be effective at reducing the incidence of PICD in patients undergoing paracentesis, but this agent requires IV infusion and is comparatively costly, he said.
In contrast, midodrine, a selective alpha-adrenergic agonist usually prescribed for orthostatic hypotension, may help to prevent PICD through its mechanism of action, maintaining mean arterial pressure (MAP).
In two small studies comparing albumin infusion in patients undergoing paracentesis with 8 liters of fluid removal, midodrine was either inferior to albumin or had no beneficial effect, Dr. Sharma said.
Patients with ACLF, however, have paracentesis with much lower fluid volumes, typically with less than 5 liters removed, and may be good candidates for midodrine.
Study details
Dr. Sharma and colleagues tested their hypothesis that in patients with ACLF undergoing modest-volume paracentesis, with fluid removal below 5 liters, midodrine could prevent PICD by increasing MAP, with an efficacy similar to that of intravenous 20% human albumin infusions.
They enrolled 50 patients with ACLF defined by Asian Pacific Association for the Study of the Liver criteria who were undergoing paracentesis with 3- to 4-liter fluid volumes.
They defined PICD as at least a 50% increase in plasma renin activity (PRA) over baseline on the 6th day following paracentesis.
The patients were randomly assigned to receive either intravenous 20% human albumin infusions toward the end of paracentesis or midodrine-hydrochloride 7.5 mg three times daily starting 2 hours before paracentesis. Because of the difference in drug delivery methods, the study could not be blinded to treatment type.
Patients’ mean arterial pressures were recorded daily, renal parameters and serum electrolytes were monitored on days 3 and 6, and blood samples were tested for PRA on day 1 and day 6.
The most common acute and chronic hepatic insults and baseline characteristics of the patients were similar between the groups, with alcohol-related liver disease the most common underlying etiology of cirrhosis.
The incidence of PICD at day 6, the primary endpoint, did not differ significantly between the groups, although mean PRA levels on day 6 were numerically higher in the midodrine group. There was a significant rise in the absolute PRA volume from baseline (P = .006), but this rise did not meet the PICD definition.
Researchers found no significant differences between the two groups in absolute change in PRA, and no significant changes in either group in MAP, creatinine, or sodium levels.
Complications and costs
PICD developed in four patients assigned to the albumin group and five patients assigned to the midodrine group; however, this difference was not significant. Fluid overload occurred in only one patient, in the albumin group.
No cases of hypertension or urinary retention arose in either group.
Grade I/II hepatic encephalopathy occurred 2-3 days after paracentesis in three patients on albumin and in two patients on midodrine.
Acute kidney injury was seen in three patients on albumin and in one patient on midodrine.
At 28 days after paracentesis, three patients in the albumin group had died, all from sepsis and multiorgan failure, while four patients in the midodrine group had died, three from sepsis and multiorgan failure and one from an upper gastrointestinal bleed.
Two patients in the albumin group and one patient in the midodrine group underwent liver transplant 1 month after paracentesis.
A cost-effectiveness analysis showed that the mean cost of albumin infusions was about sixfold higher than that of oral midodrine.
More data needed
Session moderator Shiv K. Sarin, MD, from the Institute of Liver and Biliary Sciences in New Delhi, India, who was not involved in the study, commented that while midodrine is a good drug and generally safe, he would wait to use it in patients who needed modest-volume paracentesis until more data are published.
Dr. Sarin also emphasized that albumin is “mandatory” for protecting patients who require large-volume paracentesis, and that it would be “unethical” not to use it in that clinical situation.
The study was internally supported. Dr. Sharma and Dr. Sarin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WASHINGTON – , according to the results of a randomized controlled trial.
Albumin protected 80% of patients from PICD 6 days after paracentesis, whereas midodrine protected 84%, a difference that was not statistically significant. However, albumin was associated with a slightly higher incidence of adverse events and higher costs, said Mithun Sharma, MD, during his presentation at the annual meeting of the American Association for the Study of Liver Diseases.
Midodrine may be a safer and cost-effective option for these patients, said Dr. Sharma, of the department of hepatology and liver transplantation, AIG Hospitals, Hyderabad, India.
But he cautioned that given the small size of the open-label study, with only 25 patients in each arm, the results should be considered as proof of concept and need to be validated in larger studies.
PICD common in ACLF
PICD is caused by fluid shift during paracentesis, leading to a decrease in effective circulating blood volume.
The incidence of PICD after large-volume paracentesis in patients receiving albumin ranges from 12% to 20%, Dr. Sharma noted.
Albumin has been shown in several trials to be effective at reducing the incidence of PICD in patients undergoing paracentesis, but this agent requires IV infusion and is comparatively costly, he said.
In contrast, midodrine, a selective alpha-adrenergic agonist usually prescribed for orthostatic hypotension, may help to prevent PICD through its mechanism of action, maintaining mean arterial pressure (MAP).
In two small studies comparing albumin infusion in patients undergoing paracentesis with 8 liters of fluid removal, midodrine was either inferior to albumin or had no beneficial effect, Dr. Sharma said.
Patients with ACLF, however, have paracentesis with much lower fluid volumes, typically with less than 5 liters removed, and may be good candidates for midodrine.
Study details
Dr. Sharma and colleagues tested their hypothesis that in patients with ACLF undergoing modest-volume paracentesis, with fluid removal below 5 liters, midodrine could prevent PICD by increasing MAP, with an efficacy similar to that of intravenous 20% human albumin infusions.
They enrolled 50 patients with ACLF defined by Asian Pacific Association for the Study of the Liver criteria who were undergoing paracentesis with 3- to 4-liter fluid volumes.
They defined PICD as at least a 50% increase in plasma renin activity (PRA) over baseline on the 6th day following paracentesis.
The patients were randomly assigned to receive either intravenous 20% human albumin infusions toward the end of paracentesis or midodrine-hydrochloride 7.5 mg three times daily starting 2 hours before paracentesis. Because of the difference in drug delivery methods, the study could not be blinded to treatment type.
Patients’ mean arterial pressures were recorded daily, renal parameters and serum electrolytes were monitored on days 3 and 6, and blood samples were tested for PRA on day 1 and day 6.
The most common acute and chronic hepatic insults and baseline characteristics of the patients were similar between the groups, with alcohol-related liver disease the most common underlying etiology of cirrhosis.
The incidence of PICD at day 6, the primary endpoint, did not differ significantly between the groups, although mean PRA levels on day 6 were numerically higher in the midodrine group. There was a significant rise in the absolute PRA volume from baseline (P = .006), but this rise did not meet the PICD definition.
Researchers found no significant differences between the two groups in absolute change in PRA, and no significant changes in either group in MAP, creatinine, or sodium levels.
Complications and costs
PICD developed in four patients assigned to the albumin group and five patients assigned to the midodrine group; however, this difference was not significant. Fluid overload occurred in only one patient, in the albumin group.
No cases of hypertension or urinary retention arose in either group.
Grade I/II hepatic encephalopathy occurred 2-3 days after paracentesis in three patients on albumin and in two patients on midodrine.
Acute kidney injury was seen in three patients on albumin and in one patient on midodrine.
At 28 days after paracentesis, three patients in the albumin group had died, all from sepsis and multiorgan failure, while four patients in the midodrine group had died, three from sepsis and multiorgan failure and one from an upper gastrointestinal bleed.
Two patients in the albumin group and one patient in the midodrine group underwent liver transplant 1 month after paracentesis.
A cost-effectiveness analysis showed that the mean cost of albumin infusions was about sixfold higher than that of oral midodrine.
More data needed
Session moderator Shiv K. Sarin, MD, from the Institute of Liver and Biliary Sciences in New Delhi, India, who was not involved in the study, commented that while midodrine is a good drug and generally safe, he would wait to use it in patients who needed modest-volume paracentesis until more data are published.
Dr. Sarin also emphasized that albumin is “mandatory” for protecting patients who require large-volume paracentesis, and that it would be “unethical” not to use it in that clinical situation.
The study was internally supported. Dr. Sharma and Dr. Sarin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
WASHINGTON – , according to the results of a randomized controlled trial.
Albumin protected 80% of patients from PICD 6 days after paracentesis, whereas midodrine protected 84%, a difference that was not statistically significant. However, albumin was associated with a slightly higher incidence of adverse events and higher costs, said Mithun Sharma, MD, during his presentation at the annual meeting of the American Association for the Study of Liver Diseases.
Midodrine may be a safer and cost-effective option for these patients, said Dr. Sharma, of the department of hepatology and liver transplantation, AIG Hospitals, Hyderabad, India.
But he cautioned that given the small size of the open-label study, with only 25 patients in each arm, the results should be considered as proof of concept and need to be validated in larger studies.
PICD common in ACLF
PICD is caused by fluid shift during paracentesis, leading to a decrease in effective circulating blood volume.
The incidence of PICD after large-volume paracentesis in patients receiving albumin ranges from 12% to 20%, Dr. Sharma noted.
Albumin has been shown in several trials to be effective at reducing the incidence of PICD in patients undergoing paracentesis, but this agent requires IV infusion and is comparatively costly, he said.
In contrast, midodrine, a selective alpha-adrenergic agonist usually prescribed for orthostatic hypotension, may help to prevent PICD through its mechanism of action, maintaining mean arterial pressure (MAP).
In two small studies comparing albumin infusion in patients undergoing paracentesis with 8 liters of fluid removal, midodrine was either inferior to albumin or had no beneficial effect, Dr. Sharma said.
Patients with ACLF, however, have paracentesis with much lower fluid volumes, typically with less than 5 liters removed, and may be good candidates for midodrine.
Study details
Dr. Sharma and colleagues tested their hypothesis that in patients with ACLF undergoing modest-volume paracentesis, with fluid removal below 5 liters, midodrine could prevent PICD by increasing MAP, with an efficacy similar to that of intravenous 20% human albumin infusions.
They enrolled 50 patients with ACLF defined by Asian Pacific Association for the Study of the Liver criteria who were undergoing paracentesis with 3- to 4-liter fluid volumes.
They defined PICD as at least a 50% increase in plasma renin activity (PRA) over baseline on the 6th day following paracentesis.
The patients were randomly assigned to receive either intravenous 20% human albumin infusions toward the end of paracentesis or midodrine-hydrochloride 7.5 mg three times daily starting 2 hours before paracentesis. Because of the difference in drug delivery methods, the study could not be blinded to treatment type.
Patients’ mean arterial pressures were recorded daily, renal parameters and serum electrolytes were monitored on days 3 and 6, and blood samples were tested for PRA on day 1 and day 6.
The most common acute and chronic hepatic insults and baseline characteristics of the patients were similar between the groups, with alcohol-related liver disease the most common underlying etiology of cirrhosis.
The incidence of PICD at day 6, the primary endpoint, did not differ significantly between the groups, although mean PRA levels on day 6 were numerically higher in the midodrine group. There was a significant rise in the absolute PRA volume from baseline (P = .006), but this rise did not meet the PICD definition.
Researchers found no significant differences between the two groups in absolute change in PRA, and no significant changes in either group in MAP, creatinine, or sodium levels.
Complications and costs
PICD developed in four patients assigned to the albumin group and five patients assigned to the midodrine group; however, this difference was not significant. Fluid overload occurred in only one patient, in the albumin group.
No cases of hypertension or urinary retention arose in either group.
Grade I/II hepatic encephalopathy occurred 2-3 days after paracentesis in three patients on albumin and in two patients on midodrine.
Acute kidney injury was seen in three patients on albumin and in one patient on midodrine.
At 28 days after paracentesis, three patients in the albumin group had died, all from sepsis and multiorgan failure, while four patients in the midodrine group had died, three from sepsis and multiorgan failure and one from an upper gastrointestinal bleed.
Two patients in the albumin group and one patient in the midodrine group underwent liver transplant 1 month after paracentesis.
A cost-effectiveness analysis showed that the mean cost of albumin infusions was about sixfold higher than that of oral midodrine.
More data needed
Session moderator Shiv K. Sarin, MD, from the Institute of Liver and Biliary Sciences in New Delhi, India, who was not involved in the study, commented that while midodrine is a good drug and generally safe, he would wait to use it in patients who needed modest-volume paracentesis until more data are published.
Dr. Sarin also emphasized that albumin is “mandatory” for protecting patients who require large-volume paracentesis, and that it would be “unethical” not to use it in that clinical situation.
The study was internally supported. Dr. Sharma and Dr. Sarin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE LIVER MEETING
Extreme temperature shifts tied to increase in hate speech
, according to researchers from the Potsdam Institute for Climate Impact Research.
What to know
- Analyzing over four billion tweets posted on the social media platform Twitter in the United States, researchers found that hate speech increased across climate zones, income groups, and belief systems when temperatures were too hot or too cold outside.
- The minimum number of hate tweets appears to occur when temperatures are between 15° and 18° C (59° to 65° F). The precise feel-good temperature window varies a little across climate zones, depending on what temperatures are common in those regions.
- When temperatures rose or fell from the feel-good temperature margin, online hate increased up to 12% for colder temperatures and up to 22% for hotter temperatures.
- The United Nations defines hate speech as cases of discriminatory language with reference to a person or a group on the basis of their religion, ethnicity, nationality, race, color, descent, gender, or other identity factor.
- The consequences of more aggressive online behavior can be severe, as hate speech has been found to have negative effects on the mental health of online hate victims, especially for young people and marginalized groups. It can also be predictive of hate crimes in the offline world.
A version of this article first appeared on Medscape.com.
This is a summary of the article, “Temperature Impacts on Hate Speech Online: Evidence From Four Billion Tweets,” published by The Lancet Planetary Health on September 1, 2022. The full article can be found on thelancet.com.
, according to researchers from the Potsdam Institute for Climate Impact Research.
What to know
- Analyzing over four billion tweets posted on the social media platform Twitter in the United States, researchers found that hate speech increased across climate zones, income groups, and belief systems when temperatures were too hot or too cold outside.
- The minimum number of hate tweets appears to occur when temperatures are between 15° and 18° C (59° to 65° F). The precise feel-good temperature window varies a little across climate zones, depending on what temperatures are common in those regions.
- When temperatures rose or fell from the feel-good temperature margin, online hate increased up to 12% for colder temperatures and up to 22% for hotter temperatures.
- The United Nations defines hate speech as cases of discriminatory language with reference to a person or a group on the basis of their religion, ethnicity, nationality, race, color, descent, gender, or other identity factor.
- The consequences of more aggressive online behavior can be severe, as hate speech has been found to have negative effects on the mental health of online hate victims, especially for young people and marginalized groups. It can also be predictive of hate crimes in the offline world.
A version of this article first appeared on Medscape.com.
This is a summary of the article, “Temperature Impacts on Hate Speech Online: Evidence From Four Billion Tweets,” published by The Lancet Planetary Health on September 1, 2022. The full article can be found on thelancet.com.
, according to researchers from the Potsdam Institute for Climate Impact Research.
What to know
- Analyzing over four billion tweets posted on the social media platform Twitter in the United States, researchers found that hate speech increased across climate zones, income groups, and belief systems when temperatures were too hot or too cold outside.
- The minimum number of hate tweets appears to occur when temperatures are between 15° and 18° C (59° to 65° F). The precise feel-good temperature window varies a little across climate zones, depending on what temperatures are common in those regions.
- When temperatures rose or fell from the feel-good temperature margin, online hate increased up to 12% for colder temperatures and up to 22% for hotter temperatures.
- The United Nations defines hate speech as cases of discriminatory language with reference to a person or a group on the basis of their religion, ethnicity, nationality, race, color, descent, gender, or other identity factor.
- The consequences of more aggressive online behavior can be severe, as hate speech has been found to have negative effects on the mental health of online hate victims, especially for young people and marginalized groups. It can also be predictive of hate crimes in the offline world.
A version of this article first appeared on Medscape.com.
This is a summary of the article, “Temperature Impacts on Hate Speech Online: Evidence From Four Billion Tweets,” published by The Lancet Planetary Health on September 1, 2022. The full article can be found on thelancet.com.
Chest tightness and wheezing
This patient's physical examination and imaging findings are consistent with a diagnosis of acute severe asthma. Agitation, breathlessness during rest, and a respiratory rate > 30 breaths/min are some manifestations of an acute severe episode. During severe episodes, accessory muscles of respiration are usually used, and suprasternal retractions are often present. The heart rate is > 120 beats/min and the respiratory rate is > 30 breaths/min. Loud biphasic (expiratory and inspiratory) wheezing can be heard, and pulsus paradoxus is often present (20-40 mm Hg). Oxyhemoglobin saturation with room air is < 91%. As the severity increases, the patient increasingly assumes a hunched-over sitting position with the hands supporting the torso, termed the tripod position.
Asthma is a chronic, heterogenous inflammatory airway disorder characterized by variable expiratory flow; airway wall thickening; respiratory symptoms; and exacerbations, which sometimes require hospitalization. According to the World Health Organization, asthma affected an estimated 262 million people in 2019. The presence of airway hyperresponsiveness or bronchial hyperreactivity in asthma is an exaggerated response to various exogenous and endogenous stimuli. Mechanisms implicated in the development of asthma include direct stimulation of airway smooth muscle and indirect stimulation by pharmacologically active substances from mediator-secreting cells, such as mast cells or nonmyelinated sensory neurons. The degree of airway hyperresponsiveness is associated with the clinical severity of asthma.
Acute severe asthma is a life-threatening emergency characterized by severe airflow limitation that is unresponsive to the typical appropriate bronchodilator therapy. As a result of pathophysiologic changes, airflow is severely restricted in severe asthma, leading to premature closure of the airway on expiration; impaired gas exchange; and dynamic hyperinflation, or air-trapping. In such cases, urgent action is essential to thwart serious outcomes, including mechanical ventilation and death.
Asthma severity is defined by the level of treatment required to control a patient's symptoms and exacerbations. According to the 2022 Global Initiative for Asthma (GINA) guidelines, a severe asthma exacerbation describes a patient who talks in words (rather than sentences); leans forward; is agitated; uses accessory respiratory muscles; and has a respiratory rate > 30 breaths/min, heart rate > 120 beats/min, oxygen saturation on air < 90%, and peak expiratory flow ≤ 50% of their best or of predicted value. Given the heterogeneity of asthma, patients with acute severe asthma may present with a variety of signs and symptoms, including dyspnea, chest tightness, cough and wheezing, agitation, drowsiness or signs of confusion, and significant breathlessness at rest.
Exposure to external agents, such as indoor and outdoor allergens, air pollutants, and respiratory tract infections (primarily viral), are the most common causes of asthma exacerbations, which vary in severity. Numerous other factors can trigger an asthma exacerbation, including exercise, weather changes, certain foods, additives, drugs, extreme emotional expressions, rhinitis, sinusitis, polyposis, gastroesophageal reflux, menstruation, and pregnancy. Importantly, a patient with known asthma of any level of severity can experience an asthma exacerbation, including patients with mild or well-controlled asthma.
Patients with a history of poorly controlled asthma or a recent exacerbation are at risk for an acute asthma exacerbation. Other risk factors include poor perception of airflow limitation, regular or overuse of short-acting beta agonists, incorrect inhaler technique, and suboptimal adherence to therapy. Comorbidities associated with risk for an acute asthma exacerbation include obesity, chronic rhinosinusitis, inducible laryngeal obstruction (vocal cord dysfunction), gastroesophageal reflux disease, chronic obstructive pulmonary disease, obstructive sleep apnea, bronchiectasis, cardiac disease, and kyphosis due to osteoporosis (followed by corticosteroid overuse). The lack of a written asthma action plan and socioeconomic factors are also associated with increased risk for a severe exacerbation.
In the emergency department setting, pharmacologic therapy of acute severe asthma should consist of a short-acting beta agonist, ipratropium bromide, systemic corticosteroids (oral or intravenous), and controlled oxygen therapy. Clinicians may also consider intravenous magnesium sulfate and high-dose inhaled corticosteroids. Once stable, patients should be treated with optimal asthma-controlling therapy, as outlined in GINA guidelines. Optimizing patients' inhaler technique and adherence to therapy are imperative, and comorbidities should be appropriately managed. Nonpharmacologic interventions, such as smoking cessation, pulmonary rehabilitation, exercise, weight loss, and influenza/COVID-19 vaccination, are also recommended as indicated.
Zab Mosenifar, MD, Medical Director, Women's Lung Institute; Executive Vice Chairman, Department of Medicine, Cedars Sinai Medical Center, Los Angeles, California.
Zab Mosenifar, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's physical examination and imaging findings are consistent with a diagnosis of acute severe asthma. Agitation, breathlessness during rest, and a respiratory rate > 30 breaths/min are some manifestations of an acute severe episode. During severe episodes, accessory muscles of respiration are usually used, and suprasternal retractions are often present. The heart rate is > 120 beats/min and the respiratory rate is > 30 breaths/min. Loud biphasic (expiratory and inspiratory) wheezing can be heard, and pulsus paradoxus is often present (20-40 mm Hg). Oxyhemoglobin saturation with room air is < 91%. As the severity increases, the patient increasingly assumes a hunched-over sitting position with the hands supporting the torso, termed the tripod position.
Asthma is a chronic, heterogenous inflammatory airway disorder characterized by variable expiratory flow; airway wall thickening; respiratory symptoms; and exacerbations, which sometimes require hospitalization. According to the World Health Organization, asthma affected an estimated 262 million people in 2019. The presence of airway hyperresponsiveness or bronchial hyperreactivity in asthma is an exaggerated response to various exogenous and endogenous stimuli. Mechanisms implicated in the development of asthma include direct stimulation of airway smooth muscle and indirect stimulation by pharmacologically active substances from mediator-secreting cells, such as mast cells or nonmyelinated sensory neurons. The degree of airway hyperresponsiveness is associated with the clinical severity of asthma.
Acute severe asthma is a life-threatening emergency characterized by severe airflow limitation that is unresponsive to the typical appropriate bronchodilator therapy. As a result of pathophysiologic changes, airflow is severely restricted in severe asthma, leading to premature closure of the airway on expiration; impaired gas exchange; and dynamic hyperinflation, or air-trapping. In such cases, urgent action is essential to thwart serious outcomes, including mechanical ventilation and death.
Asthma severity is defined by the level of treatment required to control a patient's symptoms and exacerbations. According to the 2022 Global Initiative for Asthma (GINA) guidelines, a severe asthma exacerbation describes a patient who talks in words (rather than sentences); leans forward; is agitated; uses accessory respiratory muscles; and has a respiratory rate > 30 breaths/min, heart rate > 120 beats/min, oxygen saturation on air < 90%, and peak expiratory flow ≤ 50% of their best or of predicted value. Given the heterogeneity of asthma, patients with acute severe asthma may present with a variety of signs and symptoms, including dyspnea, chest tightness, cough and wheezing, agitation, drowsiness or signs of confusion, and significant breathlessness at rest.
Exposure to external agents, such as indoor and outdoor allergens, air pollutants, and respiratory tract infections (primarily viral), are the most common causes of asthma exacerbations, which vary in severity. Numerous other factors can trigger an asthma exacerbation, including exercise, weather changes, certain foods, additives, drugs, extreme emotional expressions, rhinitis, sinusitis, polyposis, gastroesophageal reflux, menstruation, and pregnancy. Importantly, a patient with known asthma of any level of severity can experience an asthma exacerbation, including patients with mild or well-controlled asthma.
Patients with a history of poorly controlled asthma or a recent exacerbation are at risk for an acute asthma exacerbation. Other risk factors include poor perception of airflow limitation, regular or overuse of short-acting beta agonists, incorrect inhaler technique, and suboptimal adherence to therapy. Comorbidities associated with risk for an acute asthma exacerbation include obesity, chronic rhinosinusitis, inducible laryngeal obstruction (vocal cord dysfunction), gastroesophageal reflux disease, chronic obstructive pulmonary disease, obstructive sleep apnea, bronchiectasis, cardiac disease, and kyphosis due to osteoporosis (followed by corticosteroid overuse). The lack of a written asthma action plan and socioeconomic factors are also associated with increased risk for a severe exacerbation.
In the emergency department setting, pharmacologic therapy of acute severe asthma should consist of a short-acting beta agonist, ipratropium bromide, systemic corticosteroids (oral or intravenous), and controlled oxygen therapy. Clinicians may also consider intravenous magnesium sulfate and high-dose inhaled corticosteroids. Once stable, patients should be treated with optimal asthma-controlling therapy, as outlined in GINA guidelines. Optimizing patients' inhaler technique and adherence to therapy are imperative, and comorbidities should be appropriately managed. Nonpharmacologic interventions, such as smoking cessation, pulmonary rehabilitation, exercise, weight loss, and influenza/COVID-19 vaccination, are also recommended as indicated.
Zab Mosenifar, MD, Medical Director, Women's Lung Institute; Executive Vice Chairman, Department of Medicine, Cedars Sinai Medical Center, Los Angeles, California.
Zab Mosenifar, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's physical examination and imaging findings are consistent with a diagnosis of acute severe asthma. Agitation, breathlessness during rest, and a respiratory rate > 30 breaths/min are some manifestations of an acute severe episode. During severe episodes, accessory muscles of respiration are usually used, and suprasternal retractions are often present. The heart rate is > 120 beats/min and the respiratory rate is > 30 breaths/min. Loud biphasic (expiratory and inspiratory) wheezing can be heard, and pulsus paradoxus is often present (20-40 mm Hg). Oxyhemoglobin saturation with room air is < 91%. As the severity increases, the patient increasingly assumes a hunched-over sitting position with the hands supporting the torso, termed the tripod position.
Asthma is a chronic, heterogenous inflammatory airway disorder characterized by variable expiratory flow; airway wall thickening; respiratory symptoms; and exacerbations, which sometimes require hospitalization. According to the World Health Organization, asthma affected an estimated 262 million people in 2019. The presence of airway hyperresponsiveness or bronchial hyperreactivity in asthma is an exaggerated response to various exogenous and endogenous stimuli. Mechanisms implicated in the development of asthma include direct stimulation of airway smooth muscle and indirect stimulation by pharmacologically active substances from mediator-secreting cells, such as mast cells or nonmyelinated sensory neurons. The degree of airway hyperresponsiveness is associated with the clinical severity of asthma.
Acute severe asthma is a life-threatening emergency characterized by severe airflow limitation that is unresponsive to the typical appropriate bronchodilator therapy. As a result of pathophysiologic changes, airflow is severely restricted in severe asthma, leading to premature closure of the airway on expiration; impaired gas exchange; and dynamic hyperinflation, or air-trapping. In such cases, urgent action is essential to thwart serious outcomes, including mechanical ventilation and death.
Asthma severity is defined by the level of treatment required to control a patient's symptoms and exacerbations. According to the 2022 Global Initiative for Asthma (GINA) guidelines, a severe asthma exacerbation describes a patient who talks in words (rather than sentences); leans forward; is agitated; uses accessory respiratory muscles; and has a respiratory rate > 30 breaths/min, heart rate > 120 beats/min, oxygen saturation on air < 90%, and peak expiratory flow ≤ 50% of their best or of predicted value. Given the heterogeneity of asthma, patients with acute severe asthma may present with a variety of signs and symptoms, including dyspnea, chest tightness, cough and wheezing, agitation, drowsiness or signs of confusion, and significant breathlessness at rest.
Exposure to external agents, such as indoor and outdoor allergens, air pollutants, and respiratory tract infections (primarily viral), are the most common causes of asthma exacerbations, which vary in severity. Numerous other factors can trigger an asthma exacerbation, including exercise, weather changes, certain foods, additives, drugs, extreme emotional expressions, rhinitis, sinusitis, polyposis, gastroesophageal reflux, menstruation, and pregnancy. Importantly, a patient with known asthma of any level of severity can experience an asthma exacerbation, including patients with mild or well-controlled asthma.
Patients with a history of poorly controlled asthma or a recent exacerbation are at risk for an acute asthma exacerbation. Other risk factors include poor perception of airflow limitation, regular or overuse of short-acting beta agonists, incorrect inhaler technique, and suboptimal adherence to therapy. Comorbidities associated with risk for an acute asthma exacerbation include obesity, chronic rhinosinusitis, inducible laryngeal obstruction (vocal cord dysfunction), gastroesophageal reflux disease, chronic obstructive pulmonary disease, obstructive sleep apnea, bronchiectasis, cardiac disease, and kyphosis due to osteoporosis (followed by corticosteroid overuse). The lack of a written asthma action plan and socioeconomic factors are also associated with increased risk for a severe exacerbation.
In the emergency department setting, pharmacologic therapy of acute severe asthma should consist of a short-acting beta agonist, ipratropium bromide, systemic corticosteroids (oral or intravenous), and controlled oxygen therapy. Clinicians may also consider intravenous magnesium sulfate and high-dose inhaled corticosteroids. Once stable, patients should be treated with optimal asthma-controlling therapy, as outlined in GINA guidelines. Optimizing patients' inhaler technique and adherence to therapy are imperative, and comorbidities should be appropriately managed. Nonpharmacologic interventions, such as smoking cessation, pulmonary rehabilitation, exercise, weight loss, and influenza/COVID-19 vaccination, are also recommended as indicated.
Zab Mosenifar, MD, Medical Director, Women's Lung Institute; Executive Vice Chairman, Department of Medicine, Cedars Sinai Medical Center, Los Angeles, California.
Zab Mosenifar, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.

A 32-year-old Black man presents to the emergency department with severe dyspnea, chest tightness, and wheezing. The patient is sitting forward in the tripod position and appears agitated and confused. Use of accessory respiratory muscles and suprasternal retractions are noted. He reports an approximate 2-week history of rhinorrhea, cough, and mild fever, for which he has been taking an over-the-counter nonsteroidal anti-inflammatory agent and cough suppressant. His prior medical history is notable for obesity, type 2 diabetes, allergic rhinitis, mild asthma, and hypercholesterolemia. The patient is a current smoker (17 pack-years). Pertinent physical examination reveals a respiratory rate of 48 breaths/min, heart rate of 135 beats/min, 87% oxygen saturation, and peak expiratory flow of 300 L/min. Low biphasic wheezing can be heard. Rapid antigen and PCR tests for SARS-CoV-2 detected by nasopharyngeal swabs both come back negative. Chest radiography is ordered and shows pulmonary hyperinflation with bronchial wall thickening.
