User login
Topical POLG nanoemulsion improves dryness and itchiness in atopic dermatitis
Key clinical point: Daily continuous use of 10% phytosteryl/octyldodecyl lauroyl glutamate (POLG) nanoemulsion improved several dry skin symptoms and itchiness in patients with atopic dermatitis (AD).
Major finding: Significant improvement was observed with POLG nanoemulsion in itchiness as early as at 3 weeks (P < .05) and dryness at 6 weeks (P < .01). By 6 weeks, scaliness and smoothness of the skin were also significantly improved (P < .01).
Study details: Findings are from a clinical study including patients with AD who received 10% POLG nanoemulsion for 6 weeks.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Takada M et al. A nano-emulsion containing ceramide-like lipo-amino acid cholesteryl derivatives improves skin symptoms in patients with atopic dermatitis by ameliorating the water-holding function. Int J Mol Sci. 2022;23(21):13362 (Nov 1). Doi: 10.3390/ijms232113362
Key clinical point: Daily continuous use of 10% phytosteryl/octyldodecyl lauroyl glutamate (POLG) nanoemulsion improved several dry skin symptoms and itchiness in patients with atopic dermatitis (AD).
Major finding: Significant improvement was observed with POLG nanoemulsion in itchiness as early as at 3 weeks (P < .05) and dryness at 6 weeks (P < .01). By 6 weeks, scaliness and smoothness of the skin were also significantly improved (P < .01).
Study details: Findings are from a clinical study including patients with AD who received 10% POLG nanoemulsion for 6 weeks.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Takada M et al. A nano-emulsion containing ceramide-like lipo-amino acid cholesteryl derivatives improves skin symptoms in patients with atopic dermatitis by ameliorating the water-holding function. Int J Mol Sci. 2022;23(21):13362 (Nov 1). Doi: 10.3390/ijms232113362
Key clinical point: Daily continuous use of 10% phytosteryl/octyldodecyl lauroyl glutamate (POLG) nanoemulsion improved several dry skin symptoms and itchiness in patients with atopic dermatitis (AD).
Major finding: Significant improvement was observed with POLG nanoemulsion in itchiness as early as at 3 weeks (P < .05) and dryness at 6 weeks (P < .01). By 6 weeks, scaliness and smoothness of the skin were also significantly improved (P < .01).
Study details: Findings are from a clinical study including patients with AD who received 10% POLG nanoemulsion for 6 weeks.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Takada M et al. A nano-emulsion containing ceramide-like lipo-amino acid cholesteryl derivatives improves skin symptoms in patients with atopic dermatitis by ameliorating the water-holding function. Int J Mol Sci. 2022;23(21):13362 (Nov 1). Doi: 10.3390/ijms232113362
Emollient use in the first year of life does not protect against atopic dermatitis in the long term
Key clinical point: Daily application of emollients during the first year of life did not prevent the development of atopic dermatitis (AD) in the long term.
Major finding: A similar proportion of children in the emollient and standard skincare groups were clinically diagnosed with AD between 12 and 60 months (31% and 28%, respectively; adjusted relative risk 1.10; 95% CI 0.93-1.30).
Study details: Findings are from the multicenter, parallel, Barrier Enhancement for Eczema Prevention trial including 1394 infants at high risk of developing AD who were randomly assigned to receive emollient for the first year plus standard skincare or only standard skincare.
Disclosures: This study was funded by the UK National Institute for Health and Care Research Health Technology Assessment. Some authors declared receiving personal fees, grants, or research funding from or serving as an investigator or director for several sources.
Source: Bradshaw LE et al. Emollients for prevention of atopic dermatitis: 5-year findings from the BEEP randomized trial. Allergy. 2022 (Oct 19). Doi: 10.1111/all.15555
Key clinical point: Daily application of emollients during the first year of life did not prevent the development of atopic dermatitis (AD) in the long term.
Major finding: A similar proportion of children in the emollient and standard skincare groups were clinically diagnosed with AD between 12 and 60 months (31% and 28%, respectively; adjusted relative risk 1.10; 95% CI 0.93-1.30).
Study details: Findings are from the multicenter, parallel, Barrier Enhancement for Eczema Prevention trial including 1394 infants at high risk of developing AD who were randomly assigned to receive emollient for the first year plus standard skincare or only standard skincare.
Disclosures: This study was funded by the UK National Institute for Health and Care Research Health Technology Assessment. Some authors declared receiving personal fees, grants, or research funding from or serving as an investigator or director for several sources.
Source: Bradshaw LE et al. Emollients for prevention of atopic dermatitis: 5-year findings from the BEEP randomized trial. Allergy. 2022 (Oct 19). Doi: 10.1111/all.15555
Key clinical point: Daily application of emollients during the first year of life did not prevent the development of atopic dermatitis (AD) in the long term.
Major finding: A similar proportion of children in the emollient and standard skincare groups were clinically diagnosed with AD between 12 and 60 months (31% and 28%, respectively; adjusted relative risk 1.10; 95% CI 0.93-1.30).
Study details: Findings are from the multicenter, parallel, Barrier Enhancement for Eczema Prevention trial including 1394 infants at high risk of developing AD who were randomly assigned to receive emollient for the first year plus standard skincare or only standard skincare.
Disclosures: This study was funded by the UK National Institute for Health and Care Research Health Technology Assessment. Some authors declared receiving personal fees, grants, or research funding from or serving as an investigator or director for several sources.
Source: Bradshaw LE et al. Emollients for prevention of atopic dermatitis: 5-year findings from the BEEP randomized trial. Allergy. 2022 (Oct 19). Doi: 10.1111/all.15555
Topical prebiotics and postbiotics effective and well tolerated in mild-to-moderate atopic dermatitis
Key clinical point: A topical formulation containing a mixture of prebiotics and postbiotics was effective and well tolerated in patients with mild-to-moderate atopic dermatitis (AD).
Major finding: After 15 weeks, the SCORing AD index (−59.2%; P < .001) and the PRURISCORE (−64.1%; P < .001) reduced significantly, with 68.0% of patients reporting the tolerability of the drug as “very good” or “excellent.”
Study details: Findings are from a study including 396 patients with mild or moderate AD who received a topical formulation containing a mixture of prebiotics and postbiotics.
Disclosures: This work was supported by the Istituto Ganassini di Ricerche Biochimiche, Italy. The authors declared no conflicts of interest.
Source: Gelmetti C et al. Topical prebiotics/postbiotics and PRURISCORE validation in atopic dermatitis. International study of 396 patients. J Dermatolog Treat. 2022 (Oct 17). Doi: 10.1080/09546634.2022.2131703
Key clinical point: A topical formulation containing a mixture of prebiotics and postbiotics was effective and well tolerated in patients with mild-to-moderate atopic dermatitis (AD).
Major finding: After 15 weeks, the SCORing AD index (−59.2%; P < .001) and the PRURISCORE (−64.1%; P < .001) reduced significantly, with 68.0% of patients reporting the tolerability of the drug as “very good” or “excellent.”
Study details: Findings are from a study including 396 patients with mild or moderate AD who received a topical formulation containing a mixture of prebiotics and postbiotics.
Disclosures: This work was supported by the Istituto Ganassini di Ricerche Biochimiche, Italy. The authors declared no conflicts of interest.
Source: Gelmetti C et al. Topical prebiotics/postbiotics and PRURISCORE validation in atopic dermatitis. International study of 396 patients. J Dermatolog Treat. 2022 (Oct 17). Doi: 10.1080/09546634.2022.2131703
Key clinical point: A topical formulation containing a mixture of prebiotics and postbiotics was effective and well tolerated in patients with mild-to-moderate atopic dermatitis (AD).
Major finding: After 15 weeks, the SCORing AD index (−59.2%; P < .001) and the PRURISCORE (−64.1%; P < .001) reduced significantly, with 68.0% of patients reporting the tolerability of the drug as “very good” or “excellent.”
Study details: Findings are from a study including 396 patients with mild or moderate AD who received a topical formulation containing a mixture of prebiotics and postbiotics.
Disclosures: This work was supported by the Istituto Ganassini di Ricerche Biochimiche, Italy. The authors declared no conflicts of interest.
Source: Gelmetti C et al. Topical prebiotics/postbiotics and PRURISCORE validation in atopic dermatitis. International study of 396 patients. J Dermatolog Treat. 2022 (Oct 17). Doi: 10.1080/09546634.2022.2131703
Atopic dermatitis patients with good clinical response or conjunctivitis may opt for longer dupilumab dosing interval
Key clinical point: A longer dupilumab dosing interval might be a good treatment option for patients with atopic dermatitis (AD) who have achieved good clinical response (GCR) or report treatment-related conjunctivitis with a previous dupilumab treatment (600 mg followed by 300 mg every 2 weeks).
Major finding: In the GCR group, the mean Eczema Area and Severity Index (EASI) score was 28.22, which reduced significantly to 0.44 among patients receiving dupilumab once every 3 weeks (Q3W) and to 0.19 among patients receiving dupilumab once every 4 weeks (Q4W) after >60 weeks (both P < .0001). EASI improved after 18 weeks in the treatment-resistant conjunctivitis group (P < .0001).
Study details: Findings are retrospectively collected data of 59 adult patients with AD who implemented Q3W (84.75%) or Q4W (15.25%) dupilumab dosing interval due to GCR or conjunctivitis.
Disclosures: This study did not receive any funding. Some authors declared serving as speakers, investigators, consultants, or advisory board members, or receiving personal fees from several sources.
Source: Patruno C et al. Dupilumab dose spacing after initial successful treatment or adverse events in adult patients with atopic dermatitis: A retrospective analysis. Dermatol Ther. 2022 (Oct 13). Doi: 10.1111/dth.15933
Key clinical point: A longer dupilumab dosing interval might be a good treatment option for patients with atopic dermatitis (AD) who have achieved good clinical response (GCR) or report treatment-related conjunctivitis with a previous dupilumab treatment (600 mg followed by 300 mg every 2 weeks).
Major finding: In the GCR group, the mean Eczema Area and Severity Index (EASI) score was 28.22, which reduced significantly to 0.44 among patients receiving dupilumab once every 3 weeks (Q3W) and to 0.19 among patients receiving dupilumab once every 4 weeks (Q4W) after >60 weeks (both P < .0001). EASI improved after 18 weeks in the treatment-resistant conjunctivitis group (P < .0001).
Study details: Findings are retrospectively collected data of 59 adult patients with AD who implemented Q3W (84.75%) or Q4W (15.25%) dupilumab dosing interval due to GCR or conjunctivitis.
Disclosures: This study did not receive any funding. Some authors declared serving as speakers, investigators, consultants, or advisory board members, or receiving personal fees from several sources.
Source: Patruno C et al. Dupilumab dose spacing after initial successful treatment or adverse events in adult patients with atopic dermatitis: A retrospective analysis. Dermatol Ther. 2022 (Oct 13). Doi: 10.1111/dth.15933
Key clinical point: A longer dupilumab dosing interval might be a good treatment option for patients with atopic dermatitis (AD) who have achieved good clinical response (GCR) or report treatment-related conjunctivitis with a previous dupilumab treatment (600 mg followed by 300 mg every 2 weeks).
Major finding: In the GCR group, the mean Eczema Area and Severity Index (EASI) score was 28.22, which reduced significantly to 0.44 among patients receiving dupilumab once every 3 weeks (Q3W) and to 0.19 among patients receiving dupilumab once every 4 weeks (Q4W) after >60 weeks (both P < .0001). EASI improved after 18 weeks in the treatment-resistant conjunctivitis group (P < .0001).
Study details: Findings are retrospectively collected data of 59 adult patients with AD who implemented Q3W (84.75%) or Q4W (15.25%) dupilumab dosing interval due to GCR or conjunctivitis.
Disclosures: This study did not receive any funding. Some authors declared serving as speakers, investigators, consultants, or advisory board members, or receiving personal fees from several sources.
Source: Patruno C et al. Dupilumab dose spacing after initial successful treatment or adverse events in adult patients with atopic dermatitis: A retrospective analysis. Dermatol Ther. 2022 (Oct 13). Doi: 10.1111/dth.15933
Long-term efficacy of baricitinib in moderate-to-severe atopic dermatitis
Key clinical point: Baricitinib demonstrated long-term (52 weeks) efficacy in reducing disease severity in patients with moderate-to-severe atopic dermatitis (AD).
Major finding: At week 52, >45% of patients achieved ≥75% improvement in the Eczema Area and Severity Index (EASI), with a mean improvement of 56.8 points in the total EASI score.
Study details: Findings are from the phase 3, BREEZE-AD5 study including 146 patients with moderate-to-severe AD who were assigned to receive 2 mg baricitinib, of which 98 patients participated in the open-label extension, BREEZE-AD6 study.
Disclosures: This study was funded by Eli Lilly and Company, under license from Incyte Corporation. Five authors declared being employees and shareholders of Eli Lilly, and the other authors reported ties with several sources, including Eli Lily.
Source: Simpson E et al. Baricitinib 2 mg for the treatment of atopic dermatitis in North America: Long-term efficacy and patient-reported outcomes. Dermatol Ther. 2022 (Oct 21). Doi: 10.1111/dth.15954
Key clinical point: Baricitinib demonstrated long-term (52 weeks) efficacy in reducing disease severity in patients with moderate-to-severe atopic dermatitis (AD).
Major finding: At week 52, >45% of patients achieved ≥75% improvement in the Eczema Area and Severity Index (EASI), with a mean improvement of 56.8 points in the total EASI score.
Study details: Findings are from the phase 3, BREEZE-AD5 study including 146 patients with moderate-to-severe AD who were assigned to receive 2 mg baricitinib, of which 98 patients participated in the open-label extension, BREEZE-AD6 study.
Disclosures: This study was funded by Eli Lilly and Company, under license from Incyte Corporation. Five authors declared being employees and shareholders of Eli Lilly, and the other authors reported ties with several sources, including Eli Lily.
Source: Simpson E et al. Baricitinib 2 mg for the treatment of atopic dermatitis in North America: Long-term efficacy and patient-reported outcomes. Dermatol Ther. 2022 (Oct 21). Doi: 10.1111/dth.15954
Key clinical point: Baricitinib demonstrated long-term (52 weeks) efficacy in reducing disease severity in patients with moderate-to-severe atopic dermatitis (AD).
Major finding: At week 52, >45% of patients achieved ≥75% improvement in the Eczema Area and Severity Index (EASI), with a mean improvement of 56.8 points in the total EASI score.
Study details: Findings are from the phase 3, BREEZE-AD5 study including 146 patients with moderate-to-severe AD who were assigned to receive 2 mg baricitinib, of which 98 patients participated in the open-label extension, BREEZE-AD6 study.
Disclosures: This study was funded by Eli Lilly and Company, under license from Incyte Corporation. Five authors declared being employees and shareholders of Eli Lilly, and the other authors reported ties with several sources, including Eli Lily.
Source: Simpson E et al. Baricitinib 2 mg for the treatment of atopic dermatitis in North America: Long-term efficacy and patient-reported outcomes. Dermatol Ther. 2022 (Oct 21). Doi: 10.1111/dth.15954
Long-term efficacy of baricitinib in moderate-to-severe atopic dermatitis
Key clinical point: Baricitinib demonstrated long-term (52 weeks) efficacy in reducing disease severity in patients with moderate-to-severe atopic dermatitis (AD).
Major finding: At week 52, >45% of patients achieved ≥75% improvement in the Eczema Area and Severity Index (EASI), with a mean improvement of 56.8 points in the total EASI score.
Study details: Findings are from the phase 3, BREEZE-AD5 study including 146 patients with moderate-to-severe AD who were assigned to receive 2 mg baricitinib, of which 98 patients participated in the open-label extension, BREEZE-AD6 study.
Disclosures: This study was funded by Eli Lilly and Company, under license from Incyte Corporation. Five authors declared being employees and shareholders of Eli Lilly, and the other authors reported ties with several sources, including Eli Lily.
Source: Simpson E et al. Baricitinib 2 mg for the treatment of atopic dermatitis in North America: Long-term efficacy and patient-reported outcomes. Dermatol Ther. 2022 (Oct 21). Doi: 10.1111/dth.15954
Key clinical point: Baricitinib demonstrated long-term (52 weeks) efficacy in reducing disease severity in patients with moderate-to-severe atopic dermatitis (AD).
Major finding: At week 52, >45% of patients achieved ≥75% improvement in the Eczema Area and Severity Index (EASI), with a mean improvement of 56.8 points in the total EASI score.
Study details: Findings are from the phase 3, BREEZE-AD5 study including 146 patients with moderate-to-severe AD who were assigned to receive 2 mg baricitinib, of which 98 patients participated in the open-label extension, BREEZE-AD6 study.
Disclosures: This study was funded by Eli Lilly and Company, under license from Incyte Corporation. Five authors declared being employees and shareholders of Eli Lilly, and the other authors reported ties with several sources, including Eli Lily.
Source: Simpson E et al. Baricitinib 2 mg for the treatment of atopic dermatitis in North America: Long-term efficacy and patient-reported outcomes. Dermatol Ther. 2022 (Oct 21). Doi: 10.1111/dth.15954
Key clinical point: Baricitinib demonstrated long-term (52 weeks) efficacy in reducing disease severity in patients with moderate-to-severe atopic dermatitis (AD).
Major finding: At week 52, >45% of patients achieved ≥75% improvement in the Eczema Area and Severity Index (EASI), with a mean improvement of 56.8 points in the total EASI score.
Study details: Findings are from the phase 3, BREEZE-AD5 study including 146 patients with moderate-to-severe AD who were assigned to receive 2 mg baricitinib, of which 98 patients participated in the open-label extension, BREEZE-AD6 study.
Disclosures: This study was funded by Eli Lilly and Company, under license from Incyte Corporation. Five authors declared being employees and shareholders of Eli Lilly, and the other authors reported ties with several sources, including Eli Lily.
Source: Simpson E et al. Baricitinib 2 mg for the treatment of atopic dermatitis in North America: Long-term efficacy and patient-reported outcomes. Dermatol Ther. 2022 (Oct 21). Doi: 10.1111/dth.15954
Moderate-to-severe atopic dermatitis: No increased infection risk with long-term dupilumab use
Key clinical point: In patients with moderate-to-severe atopic dermatitis (AD), continuous long-term dupilumab treatment was not associated with an increased risk for overall systemic/cutaneous infections.
Major finding: At 4 years, the overall infection rate was 71.27 number of patients with ≥1 event per 100 patient-years (nP/100 PY), with most infections being mild to moderate in severity, and only a very small number of infections resulted in treatment discontinuation (0.34 nP/100 PY). The rate of total skin infections decreased from 28.10 to 11.48 nP/100 PY from week 16 to year 4.
Study details: Findings are from the analysis of the LIBERTY AD OLE study including 2677 patients with moderate-to-severe AD who received dupilumab, of which 13.1% completed treatment up to week 204.
Disclosures: This research was sponsored by Sanofi and Regeneron Pharmaceuticals, Inc. Four authors declared being employees and shareholders of Regeneron Pharmaceuticals. Three authors declared being employees or holding stock options in Sanofi. The other authors reported ties with several sources, including Regeneron and Sanofi.
Source: Blauvelt A et al. No increased risk of overall infection in adults with moderate-to-severe atopic dermatitis treated for up to 4 years with dupilumab. Adv Ther. 2022 (Nov 1). Doi: 10.1007/s12325-022-02322-y
Key clinical point: In patients with moderate-to-severe atopic dermatitis (AD), continuous long-term dupilumab treatment was not associated with an increased risk for overall systemic/cutaneous infections.
Major finding: At 4 years, the overall infection rate was 71.27 number of patients with ≥1 event per 100 patient-years (nP/100 PY), with most infections being mild to moderate in severity, and only a very small number of infections resulted in treatment discontinuation (0.34 nP/100 PY). The rate of total skin infections decreased from 28.10 to 11.48 nP/100 PY from week 16 to year 4.
Study details: Findings are from the analysis of the LIBERTY AD OLE study including 2677 patients with moderate-to-severe AD who received dupilumab, of which 13.1% completed treatment up to week 204.
Disclosures: This research was sponsored by Sanofi and Regeneron Pharmaceuticals, Inc. Four authors declared being employees and shareholders of Regeneron Pharmaceuticals. Three authors declared being employees or holding stock options in Sanofi. The other authors reported ties with several sources, including Regeneron and Sanofi.
Source: Blauvelt A et al. No increased risk of overall infection in adults with moderate-to-severe atopic dermatitis treated for up to 4 years with dupilumab. Adv Ther. 2022 (Nov 1). Doi: 10.1007/s12325-022-02322-y
Key clinical point: In patients with moderate-to-severe atopic dermatitis (AD), continuous long-term dupilumab treatment was not associated with an increased risk for overall systemic/cutaneous infections.
Major finding: At 4 years, the overall infection rate was 71.27 number of patients with ≥1 event per 100 patient-years (nP/100 PY), with most infections being mild to moderate in severity, and only a very small number of infections resulted in treatment discontinuation (0.34 nP/100 PY). The rate of total skin infections decreased from 28.10 to 11.48 nP/100 PY from week 16 to year 4.
Study details: Findings are from the analysis of the LIBERTY AD OLE study including 2677 patients with moderate-to-severe AD who received dupilumab, of which 13.1% completed treatment up to week 204.
Disclosures: This research was sponsored by Sanofi and Regeneron Pharmaceuticals, Inc. Four authors declared being employees and shareholders of Regeneron Pharmaceuticals. Three authors declared being employees or holding stock options in Sanofi. The other authors reported ties with several sources, including Regeneron and Sanofi.
Source: Blauvelt A et al. No increased risk of overall infection in adults with moderate-to-severe atopic dermatitis treated for up to 4 years with dupilumab. Adv Ther. 2022 (Nov 1). Doi: 10.1007/s12325-022-02322-y
Exposure to wildfire air pollution increases atopic dermatitis risk in older adults
Key clinical point: Air pollution due to a wildfire increased the rate of clinic visits for atopic dermatitis (AD), especially at a 0-week lag, in adults aged ≥65 years.
Major finding: In adults aged ≥65 years, the adjusted rate of clinic visits for AD during a week with a wildfire was 1.4 (95% CI 1.1-1.9) times the rate during weeks without wildfire and every 1-unit increase in the mean weekly smoke plume density score increased the rate of clinic visits for AD by 1.3 (95% CI 1.1-1.6) times.
Study details: This study analyzed the data of outpatient dermatology visits for AD (5529 visits) and itch (1319 visits).
Disclosures: This study did not report the source of funding. Dr. Grimes declared receiving grants from the University of California, San Francisco.
Source: Fadadu RP et al. Association of exposure to wildfire air pollution with exacerbations of atopic dermatitis and itch among older adults. JAMA Netw Open. 2022;5(10):e2238594 (Oct 26). Doi: 10.1001/jamanetworkopen.2022.38594
Key clinical point: Air pollution due to a wildfire increased the rate of clinic visits for atopic dermatitis (AD), especially at a 0-week lag, in adults aged ≥65 years.
Major finding: In adults aged ≥65 years, the adjusted rate of clinic visits for AD during a week with a wildfire was 1.4 (95% CI 1.1-1.9) times the rate during weeks without wildfire and every 1-unit increase in the mean weekly smoke plume density score increased the rate of clinic visits for AD by 1.3 (95% CI 1.1-1.6) times.
Study details: This study analyzed the data of outpatient dermatology visits for AD (5529 visits) and itch (1319 visits).
Disclosures: This study did not report the source of funding. Dr. Grimes declared receiving grants from the University of California, San Francisco.
Source: Fadadu RP et al. Association of exposure to wildfire air pollution with exacerbations of atopic dermatitis and itch among older adults. JAMA Netw Open. 2022;5(10):e2238594 (Oct 26). Doi: 10.1001/jamanetworkopen.2022.38594
Key clinical point: Air pollution due to a wildfire increased the rate of clinic visits for atopic dermatitis (AD), especially at a 0-week lag, in adults aged ≥65 years.
Major finding: In adults aged ≥65 years, the adjusted rate of clinic visits for AD during a week with a wildfire was 1.4 (95% CI 1.1-1.9) times the rate during weeks without wildfire and every 1-unit increase in the mean weekly smoke plume density score increased the rate of clinic visits for AD by 1.3 (95% CI 1.1-1.6) times.
Study details: This study analyzed the data of outpatient dermatology visits for AD (5529 visits) and itch (1319 visits).
Disclosures: This study did not report the source of funding. Dr. Grimes declared receiving grants from the University of California, San Francisco.
Source: Fadadu RP et al. Association of exposure to wildfire air pollution with exacerbations of atopic dermatitis and itch among older adults. JAMA Netw Open. 2022;5(10):e2238594 (Oct 26). Doi: 10.1001/jamanetworkopen.2022.38594
Atopic dermatitis: Dupilumab serum levels not associated with treatment response or adverse effects
Key clinical point: In patients with atopic dermatitis (AD), serum dupilumab levels at week 16 were not associated with treatment response or adverse effects due to dupilumab during the first year of treatment.
Major finding: Serum dupilumab levels at 16 weeks were not associated with the prediction of treatment response at 52 weeks (≥90% improvement in the Eczema Area and Severity Index; odds ratio [OR] 0.96; P = .34) or adverse events during the first year of treatment (OR 1.01; P = .83).
Study details: Findings are from a prospective clinical cohort study including 295 patients with AD who started dupilumab and had treatment week 16 serum samples available.
Disclosures: This study was funded by AbbVie, Eli Lilly, and other sources. The authors declared receiving consulting fees, speaking fees, investigator fees, or research funding from several sources.
Source: Spekhorst LS et al. Association of serum dupilumab levels at 16 weeks with treatment response and adverse effects in patients with atopic dermatitis: A prospective clinical cohort study from the BioDay registry. JAMA Dermatol. 2022 (Nov 2). Doi: 10.1001/jamadermatol.2022.4639
Key clinical point: In patients with atopic dermatitis (AD), serum dupilumab levels at week 16 were not associated with treatment response or adverse effects due to dupilumab during the first year of treatment.
Major finding: Serum dupilumab levels at 16 weeks were not associated with the prediction of treatment response at 52 weeks (≥90% improvement in the Eczema Area and Severity Index; odds ratio [OR] 0.96; P = .34) or adverse events during the first year of treatment (OR 1.01; P = .83).
Study details: Findings are from a prospective clinical cohort study including 295 patients with AD who started dupilumab and had treatment week 16 serum samples available.
Disclosures: This study was funded by AbbVie, Eli Lilly, and other sources. The authors declared receiving consulting fees, speaking fees, investigator fees, or research funding from several sources.
Source: Spekhorst LS et al. Association of serum dupilumab levels at 16 weeks with treatment response and adverse effects in patients with atopic dermatitis: A prospective clinical cohort study from the BioDay registry. JAMA Dermatol. 2022 (Nov 2). Doi: 10.1001/jamadermatol.2022.4639
Key clinical point: In patients with atopic dermatitis (AD), serum dupilumab levels at week 16 were not associated with treatment response or adverse effects due to dupilumab during the first year of treatment.
Major finding: Serum dupilumab levels at 16 weeks were not associated with the prediction of treatment response at 52 weeks (≥90% improvement in the Eczema Area and Severity Index; odds ratio [OR] 0.96; P = .34) or adverse events during the first year of treatment (OR 1.01; P = .83).
Study details: Findings are from a prospective clinical cohort study including 295 patients with AD who started dupilumab and had treatment week 16 serum samples available.
Disclosures: This study was funded by AbbVie, Eli Lilly, and other sources. The authors declared receiving consulting fees, speaking fees, investigator fees, or research funding from several sources.
Source: Spekhorst LS et al. Association of serum dupilumab levels at 16 weeks with treatment response and adverse effects in patients with atopic dermatitis: A prospective clinical cohort study from the BioDay registry. JAMA Dermatol. 2022 (Nov 2). Doi: 10.1001/jamadermatol.2022.4639
More weight loss with surgery than new obesity meds: meta-analysis
SAN DIEGO – but glycemic control was similar after either treatment.
However, researchers have yet to directly compare bariatric surgery with new dual and even triple agonists that are in development.
The review by Shohinee Sarma, MD, MPH, and Patricia Palcu, MD, from the University of Toronto, was published in Obesity. Dr. Sarma also presented the findings virtually at the Obesity journal symposium at ObesityWeek® 2022.
Eric Ravussin, PhD, outgoing editor-in-chief of Obesity, explained to in an interview that this is one of five articles the editors chose from about 20 papers submitted for consideration for the symposium, and it was selected because it is a first review and meta-analysis of this direct comparison.
It showed that in “a straight head-to-head comparison, weight loss is larger by about 20 kg (44 lb) with bariatric surgery versus a GLP-1 agonist, but the improvement in glycemia (carbohydrate metabolism) was similar,” said Dr. Ravussin, from Pennington Biomedical Research Center, Louisiana State University, Baton Rouge.
Study limitations, which the authors also acknowledge, include that this was a small review of small studies: There were only six studies and 322 patients.
Moreover, the data are from 2007 to 2017, and newer weight-loss drugs are more potent.
Most studies in the review compared bariatric surgery with liraglutide, Dr. Ravussin noted, whereas, “we have now better GLP-1 agonists like semaglutide,” as well as drugs that are combinations of a GLP-1 agonist with another agonist or agonists.
“Tirzepatide, for example, which is a combination of a GLP-1 agonist and a [glucose-dependent insulinotropic polypeptide (GIP) agonist], is showing results that are very close to weight loss with bariatric surgery,” he observed.
There are quite a few other drugs in development, too, he continued, which are going to approach the weight loss obtained with bariatric surgery.
Novo Nordisk is coming out with a combination of an amylin analog (cagrilintide) and a GLP-1 agonist (semaglutide), he noted. “There are others coming in with GLP-1 and glucagon [dual agonists], and there is even a ... combo called triple G, which is a glucagon, GLP-1, and GIP [agonist].”
We now need a head-to-head comparison between bariatric surgery versus a combination drug like tirzepatide in a large population, he said.
“This is an exciting period,” Dr. Ravussin summarized, “because, 10 years ago, nobody thought that [results with] pharmacotherapy can approach bariatric surgery. Now we have other drugs that are still in development that are going to approach really close bariatric surgery.”
In an email to this news organization, Dr. Sarma noted that “due to the potent weight loss and glycemic benefits of GLP-1 agonists, patients who wish to avoid the risks of bariatric surgery may wish to discuss the option of medical therapy with their health professionals.”
“For next steps,” she said, “we need long-term studies comparing the weight-lowering, glycemic, and cardiovascular benefits of GLP-1 agonists in comparison to bariatric surgery for better counseling in obesity treatment.”
Three RCTs, three observational studies
The researchers searched the literature for randomized controlled trials (RCTs) and observational studies up to April 21, 2021, which directly compared absolute weight loss with a GLP-1 agonist – liraglutide, dulaglutide, semaglutide, exenatide, lixisenatide, and albiglutide (which are approved by the U.S. Food and Drug Administration or Health Canada) – versus any type of bariatric surgery including Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy, gastric banding, and biliopancreatic diversion.
The studies included patients aged 18 and older with a body mass index (BMI) greater than 25 kg/m2.
Secondary outcomes included change in BMI, and for patients with type 2 diabetes, change in A1c.
The researchers identified three RCTs and three observational studies, with diverse drugs and diverse types of bariatric surgery, which enrolled 13 to 134 patients, with follow-up from 6 months to 10 years.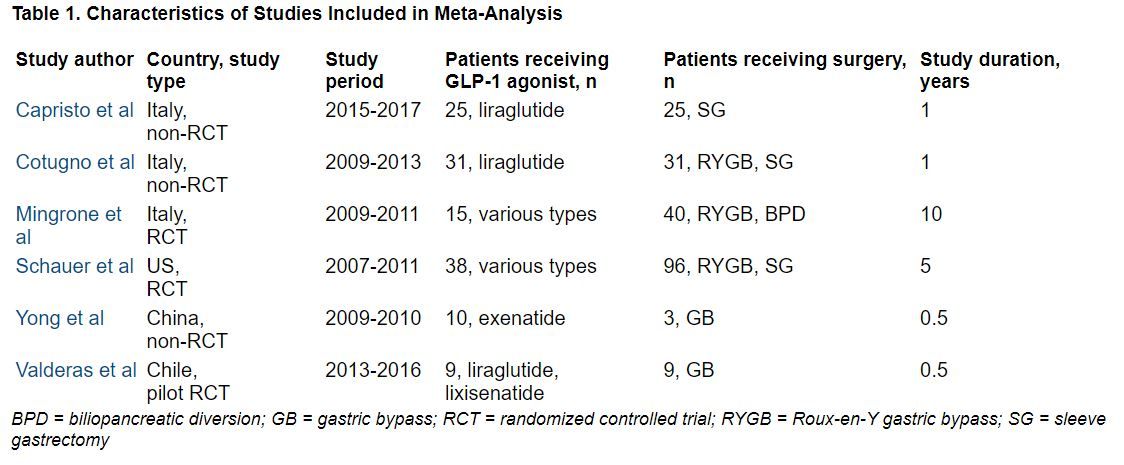
During follow-up, the overall mean weight loss was 22.7 kg greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 25.1 kg greater in the two non-RCTs with these data (Capristo et al. and Cotugno et al.).
The overall mean decrease in BMI was 8.2 kg/m2 greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 10.6 kg/m2 greater in the three non-RCTs with these data.
The overall mean decrease in A1c was 1.28% lower in the three RCTs with these data, and it was 0.9% lower in the one non-RCT with these data.
“In adults with obesity, bariatric surgery still confers the highest reductions in weight and BMI but confers similar effects in glycemic control when compared with GLP-1 agonists,” the researchers summarize.
Dr. Sarma received funding from the Clinical Investigator Program. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – but glycemic control was similar after either treatment.
However, researchers have yet to directly compare bariatric surgery with new dual and even triple agonists that are in development.
The review by Shohinee Sarma, MD, MPH, and Patricia Palcu, MD, from the University of Toronto, was published in Obesity. Dr. Sarma also presented the findings virtually at the Obesity journal symposium at ObesityWeek® 2022.
Eric Ravussin, PhD, outgoing editor-in-chief of Obesity, explained to in an interview that this is one of five articles the editors chose from about 20 papers submitted for consideration for the symposium, and it was selected because it is a first review and meta-analysis of this direct comparison.
It showed that in “a straight head-to-head comparison, weight loss is larger by about 20 kg (44 lb) with bariatric surgery versus a GLP-1 agonist, but the improvement in glycemia (carbohydrate metabolism) was similar,” said Dr. Ravussin, from Pennington Biomedical Research Center, Louisiana State University, Baton Rouge.
Study limitations, which the authors also acknowledge, include that this was a small review of small studies: There were only six studies and 322 patients.
Moreover, the data are from 2007 to 2017, and newer weight-loss drugs are more potent.
Most studies in the review compared bariatric surgery with liraglutide, Dr. Ravussin noted, whereas, “we have now better GLP-1 agonists like semaglutide,” as well as drugs that are combinations of a GLP-1 agonist with another agonist or agonists.
“Tirzepatide, for example, which is a combination of a GLP-1 agonist and a [glucose-dependent insulinotropic polypeptide (GIP) agonist], is showing results that are very close to weight loss with bariatric surgery,” he observed.
There are quite a few other drugs in development, too, he continued, which are going to approach the weight loss obtained with bariatric surgery.
Novo Nordisk is coming out with a combination of an amylin analog (cagrilintide) and a GLP-1 agonist (semaglutide), he noted. “There are others coming in with GLP-1 and glucagon [dual agonists], and there is even a ... combo called triple G, which is a glucagon, GLP-1, and GIP [agonist].”
We now need a head-to-head comparison between bariatric surgery versus a combination drug like tirzepatide in a large population, he said.
“This is an exciting period,” Dr. Ravussin summarized, “because, 10 years ago, nobody thought that [results with] pharmacotherapy can approach bariatric surgery. Now we have other drugs that are still in development that are going to approach really close bariatric surgery.”
In an email to this news organization, Dr. Sarma noted that “due to the potent weight loss and glycemic benefits of GLP-1 agonists, patients who wish to avoid the risks of bariatric surgery may wish to discuss the option of medical therapy with their health professionals.”
“For next steps,” she said, “we need long-term studies comparing the weight-lowering, glycemic, and cardiovascular benefits of GLP-1 agonists in comparison to bariatric surgery for better counseling in obesity treatment.”
Three RCTs, three observational studies
The researchers searched the literature for randomized controlled trials (RCTs) and observational studies up to April 21, 2021, which directly compared absolute weight loss with a GLP-1 agonist – liraglutide, dulaglutide, semaglutide, exenatide, lixisenatide, and albiglutide (which are approved by the U.S. Food and Drug Administration or Health Canada) – versus any type of bariatric surgery including Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy, gastric banding, and biliopancreatic diversion.
The studies included patients aged 18 and older with a body mass index (BMI) greater than 25 kg/m2.
Secondary outcomes included change in BMI, and for patients with type 2 diabetes, change in A1c.
The researchers identified three RCTs and three observational studies, with diverse drugs and diverse types of bariatric surgery, which enrolled 13 to 134 patients, with follow-up from 6 months to 10 years.
During follow-up, the overall mean weight loss was 22.7 kg greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 25.1 kg greater in the two non-RCTs with these data (Capristo et al. and Cotugno et al.).
The overall mean decrease in BMI was 8.2 kg/m2 greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 10.6 kg/m2 greater in the three non-RCTs with these data.
The overall mean decrease in A1c was 1.28% lower in the three RCTs with these data, and it was 0.9% lower in the one non-RCT with these data.
“In adults with obesity, bariatric surgery still confers the highest reductions in weight and BMI but confers similar effects in glycemic control when compared with GLP-1 agonists,” the researchers summarize.
Dr. Sarma received funding from the Clinical Investigator Program. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – but glycemic control was similar after either treatment.
However, researchers have yet to directly compare bariatric surgery with new dual and even triple agonists that are in development.
The review by Shohinee Sarma, MD, MPH, and Patricia Palcu, MD, from the University of Toronto, was published in Obesity. Dr. Sarma also presented the findings virtually at the Obesity journal symposium at ObesityWeek® 2022.
Eric Ravussin, PhD, outgoing editor-in-chief of Obesity, explained to in an interview that this is one of five articles the editors chose from about 20 papers submitted for consideration for the symposium, and it was selected because it is a first review and meta-analysis of this direct comparison.
It showed that in “a straight head-to-head comparison, weight loss is larger by about 20 kg (44 lb) with bariatric surgery versus a GLP-1 agonist, but the improvement in glycemia (carbohydrate metabolism) was similar,” said Dr. Ravussin, from Pennington Biomedical Research Center, Louisiana State University, Baton Rouge.
Study limitations, which the authors also acknowledge, include that this was a small review of small studies: There were only six studies and 322 patients.
Moreover, the data are from 2007 to 2017, and newer weight-loss drugs are more potent.
Most studies in the review compared bariatric surgery with liraglutide, Dr. Ravussin noted, whereas, “we have now better GLP-1 agonists like semaglutide,” as well as drugs that are combinations of a GLP-1 agonist with another agonist or agonists.
“Tirzepatide, for example, which is a combination of a GLP-1 agonist and a [glucose-dependent insulinotropic polypeptide (GIP) agonist], is showing results that are very close to weight loss with bariatric surgery,” he observed.
There are quite a few other drugs in development, too, he continued, which are going to approach the weight loss obtained with bariatric surgery.
Novo Nordisk is coming out with a combination of an amylin analog (cagrilintide) and a GLP-1 agonist (semaglutide), he noted. “There are others coming in with GLP-1 and glucagon [dual agonists], and there is even a ... combo called triple G, which is a glucagon, GLP-1, and GIP [agonist].”
We now need a head-to-head comparison between bariatric surgery versus a combination drug like tirzepatide in a large population, he said.
“This is an exciting period,” Dr. Ravussin summarized, “because, 10 years ago, nobody thought that [results with] pharmacotherapy can approach bariatric surgery. Now we have other drugs that are still in development that are going to approach really close bariatric surgery.”
In an email to this news organization, Dr. Sarma noted that “due to the potent weight loss and glycemic benefits of GLP-1 agonists, patients who wish to avoid the risks of bariatric surgery may wish to discuss the option of medical therapy with their health professionals.”
“For next steps,” she said, “we need long-term studies comparing the weight-lowering, glycemic, and cardiovascular benefits of GLP-1 agonists in comparison to bariatric surgery for better counseling in obesity treatment.”
Three RCTs, three observational studies
The researchers searched the literature for randomized controlled trials (RCTs) and observational studies up to April 21, 2021, which directly compared absolute weight loss with a GLP-1 agonist – liraglutide, dulaglutide, semaglutide, exenatide, lixisenatide, and albiglutide (which are approved by the U.S. Food and Drug Administration or Health Canada) – versus any type of bariatric surgery including Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy, gastric banding, and biliopancreatic diversion.
The studies included patients aged 18 and older with a body mass index (BMI) greater than 25 kg/m2.
Secondary outcomes included change in BMI, and for patients with type 2 diabetes, change in A1c.
The researchers identified three RCTs and three observational studies, with diverse drugs and diverse types of bariatric surgery, which enrolled 13 to 134 patients, with follow-up from 6 months to 10 years.
During follow-up, the overall mean weight loss was 22.7 kg greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 25.1 kg greater in the two non-RCTs with these data (Capristo et al. and Cotugno et al.).
The overall mean decrease in BMI was 8.2 kg/m2 greater in the bariatric surgery groups than in the GLP-1 agonist groups in the two RCTs with these data (Migrone et al. and Schauer et al.), and it was 10.6 kg/m2 greater in the three non-RCTs with these data.
The overall mean decrease in A1c was 1.28% lower in the three RCTs with these data, and it was 0.9% lower in the one non-RCT with these data.
“In adults with obesity, bariatric surgery still confers the highest reductions in weight and BMI but confers similar effects in glycemic control when compared with GLP-1 agonists,” the researchers summarize.
Dr. Sarma received funding from the Clinical Investigator Program. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT OBESITYWEEK®