User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
In America, cancer patients endure debt on top of disease
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Autoimmune disease patients’ waxing, waning response to COVID vaccination studied in-depth
A new study in The Lancet Rheumatology examines the strength and duration of SARS-CoV-2 vaccine–induced immunoglobulin-G antibody responses over time for patients with a variety of autoimmune diseases, compared with healthy controls.
The presence of humoral antibodies to SARS-CoV-2 has been shown to correlate with protection against COVID infection. But for patients with immune-mediated inflammatory diseases (IMIDs), host response to COVID infection or to vaccination is affected by the immune dysfunction imposed by the IMID and by the use of immune-modulating drugs to treat it.
This new study finds a weaker – as shown previously – and less sustained immune response to SARS-CoV-2 vaccines in patients with a variety of IMIDs, including rheumatoid arthritis, spondyloarthritis, psoriasis, inflammatory bowel diseases, and other systemic autoimmune diseases such as lupus. It also points toward the possibility of adjusting treatment and vaccination schedules and strategies for these patients based on their antibody levels, among other factors, to preserve best protection against severe COVID.
“It is important to assess immune response in these patients to see if they still have protection against severe COVID infection,” said lead author David Simon, MD, senior clinical scientist in clinical immunology and rheumatology at University Hospital Erlangen (Germany). “We know that antibody response is an immune correlate. Therefore, it is important to see how large and durable the immune response is to the coronavirus vaccine in these IMID patients, and whether specific drugs or therapies have negative effects on their immune response.”
What was studied?
For this large prospective cohort study, researchers registered 5076 coronavirus-vaccinated individuals. They analyzed serum samples obtained between December 15, 2020, and December 1, 2021, from 2,535 patients diagnosed with IMIDs and participating in a prospective coronavirus study program at the Deutsches Zentrum Immuntherapie in Erlangen. The IMID patients had a mean age of 55.0 years, and 58.9% were women.
A healthy control group of 1,198 individuals without IMID who had a mean age of 40.7 years, including 53.8% men, was also recruited for the analysis. All approved coronavirus vaccines were included, following standard vaccination schedules. Antibody response was measured over time by an enzyme-linked immunosorbent assay from 8 weeks after first vaccination to week 40.
Among the findings, the healthy controls had higher postvaccine antibody levels than did those with IMIDs. But the majority of vaccinated patients with IMID were able to build up a humoral immune response to SARS-CoV-2. Patients who were taking B-cell inhibitors like rituximab (Rituxan, Genentech; and biosimilars) and T-cell inhibitors like abatacept (Orencia, Bristol Myers Squibb) for IMIDs had significantly poorer antibody response.
Greater age and the use of combination therapies for IMIDs, compared with monotherapy, further reduced immune response to the vaccine. In terms of vaccination modality, messenger RNA–based vaccines induced higher antibody levels than did vector-based vaccines. The researchers noted that patients with IMID who were given a third vaccine dose could actually catch up well with the antibody responses observed in healthy controls.
“We looked at whether different IMIDs had a different humoral response, and we also assessed if there are effects from different therapeutic strategies,” Dr. Simon explained. “It doesn’t matter so much what kind of IMID patients have; much more important is the specific drug treatment and its impact on their antibody response.” Some participants were advised to briefly stop taking some immunosuppressive treatments before or after vaccination.
One of Dr. Simon’s coauthors, statistician and rheumatologist Koray Tascilar, MD, added, “This research is important because we looked not only at who responded less, which has been previously established, but who are at greater risk of losing their immune response, and how quickly.”
Need to take care
“Most treatments we as rheumatologists give to our patients don’t affect their SARS-CoV-2 humoral response,” Dr. Simon said. “However, there are specific drugs that are associated with lower antibody response. With respect to those drugs, we have to be more careful.”
It is important to be able to tell patients which drugs are safe and won’t have a negative impact on their immune response to vaccinations, Dr. Tascilar said. “But it would be too strong to say we’re ready to choose therapies based on their potential impact on protection against COVID. Yes, there is a risk from catching COVID, but we need to balance that risk with the risk of not giving patients the medications that are necessary to treat their rheumatologic condition.”
These diseases are serious, sometimes life-threatening. “We might think of strategies for how to mitigate the risk of underprotection from COVID that is brought about by these treatments,” he said. For example, offering boosters sooner or more frequently, or prophylactically treating with monoclonal antibodies.
“This study, along other recent studies, has found that antibody levels in patients with immune-mediated diseases wane more rapidly than in healthy controls, and this is especially true of those on medications that interfere with the B and T cells and anticytokine therapies,” Rebecca Haberman, MD, assistant professor, division of rheumatology, New York University Langone Health, noted in an email to this news organization.
“While there is no known antibody level that specifically correlates with clinical protection, and each patient needs to be thought of individually, these findings support the use of supplemental booster dosing in patients with immune-mediated inflammatory diseases,” Dr. Haberman said, adding that her own research in this area has shown similar results.
“As a rheumatologist, I would be more likely to encourage my patients – especially those on immunomodulatory medications – to get boosted.”
Dr. Tascilar said his study does not directly answer the question of whether an earlier booster shot would be an effective strategy for patients with IMID. “In our department, we have an early boosting strategy, based on level of immune response.” But the decision of revaccination or not, and when, is based on a number of factors, not only on the level of antibodies. “It’s just part of the instruments we are using.”
The study was supported by the Deutsche Forschungsgemeinschaft. Dr. Simon and Dr. Tascilar declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study in The Lancet Rheumatology examines the strength and duration of SARS-CoV-2 vaccine–induced immunoglobulin-G antibody responses over time for patients with a variety of autoimmune diseases, compared with healthy controls.
The presence of humoral antibodies to SARS-CoV-2 has been shown to correlate with protection against COVID infection. But for patients with immune-mediated inflammatory diseases (IMIDs), host response to COVID infection or to vaccination is affected by the immune dysfunction imposed by the IMID and by the use of immune-modulating drugs to treat it.
This new study finds a weaker – as shown previously – and less sustained immune response to SARS-CoV-2 vaccines in patients with a variety of IMIDs, including rheumatoid arthritis, spondyloarthritis, psoriasis, inflammatory bowel diseases, and other systemic autoimmune diseases such as lupus. It also points toward the possibility of adjusting treatment and vaccination schedules and strategies for these patients based on their antibody levels, among other factors, to preserve best protection against severe COVID.
“It is important to assess immune response in these patients to see if they still have protection against severe COVID infection,” said lead author David Simon, MD, senior clinical scientist in clinical immunology and rheumatology at University Hospital Erlangen (Germany). “We know that antibody response is an immune correlate. Therefore, it is important to see how large and durable the immune response is to the coronavirus vaccine in these IMID patients, and whether specific drugs or therapies have negative effects on their immune response.”
What was studied?
For this large prospective cohort study, researchers registered 5076 coronavirus-vaccinated individuals. They analyzed serum samples obtained between December 15, 2020, and December 1, 2021, from 2,535 patients diagnosed with IMIDs and participating in a prospective coronavirus study program at the Deutsches Zentrum Immuntherapie in Erlangen. The IMID patients had a mean age of 55.0 years, and 58.9% were women.
A healthy control group of 1,198 individuals without IMID who had a mean age of 40.7 years, including 53.8% men, was also recruited for the analysis. All approved coronavirus vaccines were included, following standard vaccination schedules. Antibody response was measured over time by an enzyme-linked immunosorbent assay from 8 weeks after first vaccination to week 40.
Among the findings, the healthy controls had higher postvaccine antibody levels than did those with IMIDs. But the majority of vaccinated patients with IMID were able to build up a humoral immune response to SARS-CoV-2. Patients who were taking B-cell inhibitors like rituximab (Rituxan, Genentech; and biosimilars) and T-cell inhibitors like abatacept (Orencia, Bristol Myers Squibb) for IMIDs had significantly poorer antibody response.
Greater age and the use of combination therapies for IMIDs, compared with monotherapy, further reduced immune response to the vaccine. In terms of vaccination modality, messenger RNA–based vaccines induced higher antibody levels than did vector-based vaccines. The researchers noted that patients with IMID who were given a third vaccine dose could actually catch up well with the antibody responses observed in healthy controls.
“We looked at whether different IMIDs had a different humoral response, and we also assessed if there are effects from different therapeutic strategies,” Dr. Simon explained. “It doesn’t matter so much what kind of IMID patients have; much more important is the specific drug treatment and its impact on their antibody response.” Some participants were advised to briefly stop taking some immunosuppressive treatments before or after vaccination.
One of Dr. Simon’s coauthors, statistician and rheumatologist Koray Tascilar, MD, added, “This research is important because we looked not only at who responded less, which has been previously established, but who are at greater risk of losing their immune response, and how quickly.”
Need to take care
“Most treatments we as rheumatologists give to our patients don’t affect their SARS-CoV-2 humoral response,” Dr. Simon said. “However, there are specific drugs that are associated with lower antibody response. With respect to those drugs, we have to be more careful.”
It is important to be able to tell patients which drugs are safe and won’t have a negative impact on their immune response to vaccinations, Dr. Tascilar said. “But it would be too strong to say we’re ready to choose therapies based on their potential impact on protection against COVID. Yes, there is a risk from catching COVID, but we need to balance that risk with the risk of not giving patients the medications that are necessary to treat their rheumatologic condition.”
These diseases are serious, sometimes life-threatening. “We might think of strategies for how to mitigate the risk of underprotection from COVID that is brought about by these treatments,” he said. For example, offering boosters sooner or more frequently, or prophylactically treating with monoclonal antibodies.
“This study, along other recent studies, has found that antibody levels in patients with immune-mediated diseases wane more rapidly than in healthy controls, and this is especially true of those on medications that interfere with the B and T cells and anticytokine therapies,” Rebecca Haberman, MD, assistant professor, division of rheumatology, New York University Langone Health, noted in an email to this news organization.
“While there is no known antibody level that specifically correlates with clinical protection, and each patient needs to be thought of individually, these findings support the use of supplemental booster dosing in patients with immune-mediated inflammatory diseases,” Dr. Haberman said, adding that her own research in this area has shown similar results.
“As a rheumatologist, I would be more likely to encourage my patients – especially those on immunomodulatory medications – to get boosted.”
Dr. Tascilar said his study does not directly answer the question of whether an earlier booster shot would be an effective strategy for patients with IMID. “In our department, we have an early boosting strategy, based on level of immune response.” But the decision of revaccination or not, and when, is based on a number of factors, not only on the level of antibodies. “It’s just part of the instruments we are using.”
The study was supported by the Deutsche Forschungsgemeinschaft. Dr. Simon and Dr. Tascilar declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study in The Lancet Rheumatology examines the strength and duration of SARS-CoV-2 vaccine–induced immunoglobulin-G antibody responses over time for patients with a variety of autoimmune diseases, compared with healthy controls.
The presence of humoral antibodies to SARS-CoV-2 has been shown to correlate with protection against COVID infection. But for patients with immune-mediated inflammatory diseases (IMIDs), host response to COVID infection or to vaccination is affected by the immune dysfunction imposed by the IMID and by the use of immune-modulating drugs to treat it.
This new study finds a weaker – as shown previously – and less sustained immune response to SARS-CoV-2 vaccines in patients with a variety of IMIDs, including rheumatoid arthritis, spondyloarthritis, psoriasis, inflammatory bowel diseases, and other systemic autoimmune diseases such as lupus. It also points toward the possibility of adjusting treatment and vaccination schedules and strategies for these patients based on their antibody levels, among other factors, to preserve best protection against severe COVID.
“It is important to assess immune response in these patients to see if they still have protection against severe COVID infection,” said lead author David Simon, MD, senior clinical scientist in clinical immunology and rheumatology at University Hospital Erlangen (Germany). “We know that antibody response is an immune correlate. Therefore, it is important to see how large and durable the immune response is to the coronavirus vaccine in these IMID patients, and whether specific drugs or therapies have negative effects on their immune response.”
What was studied?
For this large prospective cohort study, researchers registered 5076 coronavirus-vaccinated individuals. They analyzed serum samples obtained between December 15, 2020, and December 1, 2021, from 2,535 patients diagnosed with IMIDs and participating in a prospective coronavirus study program at the Deutsches Zentrum Immuntherapie in Erlangen. The IMID patients had a mean age of 55.0 years, and 58.9% were women.
A healthy control group of 1,198 individuals without IMID who had a mean age of 40.7 years, including 53.8% men, was also recruited for the analysis. All approved coronavirus vaccines were included, following standard vaccination schedules. Antibody response was measured over time by an enzyme-linked immunosorbent assay from 8 weeks after first vaccination to week 40.
Among the findings, the healthy controls had higher postvaccine antibody levels than did those with IMIDs. But the majority of vaccinated patients with IMID were able to build up a humoral immune response to SARS-CoV-2. Patients who were taking B-cell inhibitors like rituximab (Rituxan, Genentech; and biosimilars) and T-cell inhibitors like abatacept (Orencia, Bristol Myers Squibb) for IMIDs had significantly poorer antibody response.
Greater age and the use of combination therapies for IMIDs, compared with monotherapy, further reduced immune response to the vaccine. In terms of vaccination modality, messenger RNA–based vaccines induced higher antibody levels than did vector-based vaccines. The researchers noted that patients with IMID who were given a third vaccine dose could actually catch up well with the antibody responses observed in healthy controls.
“We looked at whether different IMIDs had a different humoral response, and we also assessed if there are effects from different therapeutic strategies,” Dr. Simon explained. “It doesn’t matter so much what kind of IMID patients have; much more important is the specific drug treatment and its impact on their antibody response.” Some participants were advised to briefly stop taking some immunosuppressive treatments before or after vaccination.
One of Dr. Simon’s coauthors, statistician and rheumatologist Koray Tascilar, MD, added, “This research is important because we looked not only at who responded less, which has been previously established, but who are at greater risk of losing their immune response, and how quickly.”
Need to take care
“Most treatments we as rheumatologists give to our patients don’t affect their SARS-CoV-2 humoral response,” Dr. Simon said. “However, there are specific drugs that are associated with lower antibody response. With respect to those drugs, we have to be more careful.”
It is important to be able to tell patients which drugs are safe and won’t have a negative impact on their immune response to vaccinations, Dr. Tascilar said. “But it would be too strong to say we’re ready to choose therapies based on their potential impact on protection against COVID. Yes, there is a risk from catching COVID, but we need to balance that risk with the risk of not giving patients the medications that are necessary to treat their rheumatologic condition.”
These diseases are serious, sometimes life-threatening. “We might think of strategies for how to mitigate the risk of underprotection from COVID that is brought about by these treatments,” he said. For example, offering boosters sooner or more frequently, or prophylactically treating with monoclonal antibodies.
“This study, along other recent studies, has found that antibody levels in patients with immune-mediated diseases wane more rapidly than in healthy controls, and this is especially true of those on medications that interfere with the B and T cells and anticytokine therapies,” Rebecca Haberman, MD, assistant professor, division of rheumatology, New York University Langone Health, noted in an email to this news organization.
“While there is no known antibody level that specifically correlates with clinical protection, and each patient needs to be thought of individually, these findings support the use of supplemental booster dosing in patients with immune-mediated inflammatory diseases,” Dr. Haberman said, adding that her own research in this area has shown similar results.
“As a rheumatologist, I would be more likely to encourage my patients – especially those on immunomodulatory medications – to get boosted.”
Dr. Tascilar said his study does not directly answer the question of whether an earlier booster shot would be an effective strategy for patients with IMID. “In our department, we have an early boosting strategy, based on level of immune response.” But the decision of revaccination or not, and when, is based on a number of factors, not only on the level of antibodies. “It’s just part of the instruments we are using.”
The study was supported by the Deutsche Forschungsgemeinschaft. Dr. Simon and Dr. Tascilar declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE LANCET RHEUMATOLOGY

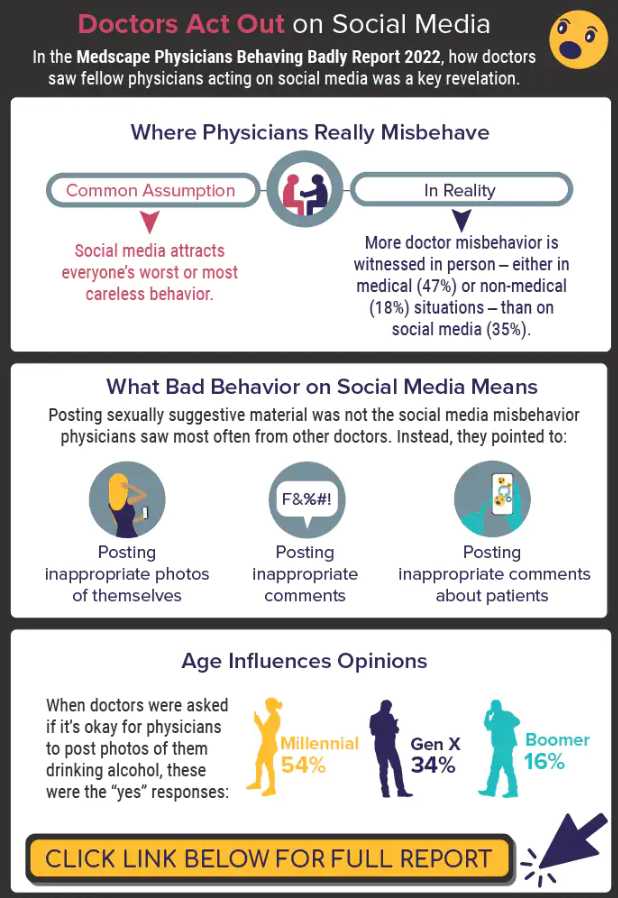
Infographic: Is physician behavior on social media really so bad?
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.
The medical profession is held to a high standard of personal conduct, so physicians keep a sharp eye out for how fellow doctors behave. That goes for social media as well as in-person conduct.
(and it’s not as egregious as you might think). If you’re interested in delving deeper into the data, check out the Medscape Physicians Behaving Badly Report 2022.
A version of this article first appeared on Medscape.com.
Paxlovid reduces risk of COVID death by 79% in older adults
The antiviral drug Paxlovid appears to reduce the risk of dying from COVID-19 by 79% and decrease hospitalizations by 73% in at-risk patients who are ages 65 and older, according to a new study published in The New England Journal of Medicine.
The pill, which is a combination of the drugs nirmatrelvir and ritonavir, received FDA emergency use authorization in December 2021 to treat mild to moderate disease in ages 12 and older who face high risks for having severe COVID-19, hospitalization, and death.
“The results of the study show unequivocally that treatment with Paxlovid significantly reduces the risk of hospitalization and death from COVID-19,” Doron Netzer, MD, the senior study author and a researcher with Clalit Health Services, Tel Aviv, told The Jerusalem Post.
“We are the country’s leader in the provision of giving Paxlovid to relevant patients,” he said. “It was given to patients all over the country, with medical teams monitoring the patients who took the pills.”
, the news outlet reported. The research team analyzed information from Clalit’s electronic medical records. The health care organization covers about 52% of the Israeli population and almost two-thirds of older adults. More than 30,000 COVID-19 patients in Israel have been treated with the drug so far.
Dr. Netzer and colleagues looked at hospitalization and death data for at-risk COVID-19 patients ages 40 and older between Jan. 9 and March 31, when the original Omicron variant was the dominant strain in Israel. During that time, more than 1.1 million Clalit patients were infected with COVID-19, 109,000 patients were considered at-risk, and 3,900 patients received the drug.
The average age of the patients was 60, and 39% of the patients were 65 and older. Overall, 78% of the patients had previous COVID-19 immunity due to vaccination, prior infection, or both.
Among ages 65 and older, the rate of COVID-19 hospitalization was 14.7 cases per 100,000 person-days among treated patients, compared with 58.9 cases per 100,000 person-days among untreated patients. This represented a 73% lower chance of being hospitalized.
Among ages 40-64, the rate of hospitalization due to COVID-19 was 15.2 cases per 100,000 person-days among treated patients, compared with 15.8 cases per 100,000 person-days among untreated patients. The risk of hospitalization wasn’t significantly lower for this age group.
Among ages 65 and older, there were two deaths from COVID-19 in 2,484 treated patients, compared with 158 in the 40,337 untreated patients. This represented a 79% lower chance of dying from COVID-19.
Among ages 40-64, there was one death from COVID-19 in 1,418 treated patients, compared with 16 in the 65,015 untreated patients. The risk of death wasn’t significantly lower for this age group.
For both age groups, a lack of previous COVID-19 immunity and a previous hospitalization were most strongly linked to high rates of hospitalization during the Omicron wave.
The researchers noted that they didn’t break down the data on ages 40-64 who had cancer and other severe conditions that weaken the immune system. These patients may be more likely to benefit from Paxlovid, they said, though future studies will need to analyze the data.
The study didn’t receive any financial or in-kind support, the authors said.
A version of this article first appeared on WebMD.com.
The antiviral drug Paxlovid appears to reduce the risk of dying from COVID-19 by 79% and decrease hospitalizations by 73% in at-risk patients who are ages 65 and older, according to a new study published in The New England Journal of Medicine.
The pill, which is a combination of the drugs nirmatrelvir and ritonavir, received FDA emergency use authorization in December 2021 to treat mild to moderate disease in ages 12 and older who face high risks for having severe COVID-19, hospitalization, and death.
“The results of the study show unequivocally that treatment with Paxlovid significantly reduces the risk of hospitalization and death from COVID-19,” Doron Netzer, MD, the senior study author and a researcher with Clalit Health Services, Tel Aviv, told The Jerusalem Post.
“We are the country’s leader in the provision of giving Paxlovid to relevant patients,” he said. “It was given to patients all over the country, with medical teams monitoring the patients who took the pills.”
, the news outlet reported. The research team analyzed information from Clalit’s electronic medical records. The health care organization covers about 52% of the Israeli population and almost two-thirds of older adults. More than 30,000 COVID-19 patients in Israel have been treated with the drug so far.
Dr. Netzer and colleagues looked at hospitalization and death data for at-risk COVID-19 patients ages 40 and older between Jan. 9 and March 31, when the original Omicron variant was the dominant strain in Israel. During that time, more than 1.1 million Clalit patients were infected with COVID-19, 109,000 patients were considered at-risk, and 3,900 patients received the drug.
The average age of the patients was 60, and 39% of the patients were 65 and older. Overall, 78% of the patients had previous COVID-19 immunity due to vaccination, prior infection, or both.
Among ages 65 and older, the rate of COVID-19 hospitalization was 14.7 cases per 100,000 person-days among treated patients, compared with 58.9 cases per 100,000 person-days among untreated patients. This represented a 73% lower chance of being hospitalized.
Among ages 40-64, the rate of hospitalization due to COVID-19 was 15.2 cases per 100,000 person-days among treated patients, compared with 15.8 cases per 100,000 person-days among untreated patients. The risk of hospitalization wasn’t significantly lower for this age group.
Among ages 65 and older, there were two deaths from COVID-19 in 2,484 treated patients, compared with 158 in the 40,337 untreated patients. This represented a 79% lower chance of dying from COVID-19.
Among ages 40-64, there was one death from COVID-19 in 1,418 treated patients, compared with 16 in the 65,015 untreated patients. The risk of death wasn’t significantly lower for this age group.
For both age groups, a lack of previous COVID-19 immunity and a previous hospitalization were most strongly linked to high rates of hospitalization during the Omicron wave.
The researchers noted that they didn’t break down the data on ages 40-64 who had cancer and other severe conditions that weaken the immune system. These patients may be more likely to benefit from Paxlovid, they said, though future studies will need to analyze the data.
The study didn’t receive any financial or in-kind support, the authors said.
A version of this article first appeared on WebMD.com.
The antiviral drug Paxlovid appears to reduce the risk of dying from COVID-19 by 79% and decrease hospitalizations by 73% in at-risk patients who are ages 65 and older, according to a new study published in The New England Journal of Medicine.
The pill, which is a combination of the drugs nirmatrelvir and ritonavir, received FDA emergency use authorization in December 2021 to treat mild to moderate disease in ages 12 and older who face high risks for having severe COVID-19, hospitalization, and death.
“The results of the study show unequivocally that treatment with Paxlovid significantly reduces the risk of hospitalization and death from COVID-19,” Doron Netzer, MD, the senior study author and a researcher with Clalit Health Services, Tel Aviv, told The Jerusalem Post.
“We are the country’s leader in the provision of giving Paxlovid to relevant patients,” he said. “It was given to patients all over the country, with medical teams monitoring the patients who took the pills.”
, the news outlet reported. The research team analyzed information from Clalit’s electronic medical records. The health care organization covers about 52% of the Israeli population and almost two-thirds of older adults. More than 30,000 COVID-19 patients in Israel have been treated with the drug so far.
Dr. Netzer and colleagues looked at hospitalization and death data for at-risk COVID-19 patients ages 40 and older between Jan. 9 and March 31, when the original Omicron variant was the dominant strain in Israel. During that time, more than 1.1 million Clalit patients were infected with COVID-19, 109,000 patients were considered at-risk, and 3,900 patients received the drug.
The average age of the patients was 60, and 39% of the patients were 65 and older. Overall, 78% of the patients had previous COVID-19 immunity due to vaccination, prior infection, or both.
Among ages 65 and older, the rate of COVID-19 hospitalization was 14.7 cases per 100,000 person-days among treated patients, compared with 58.9 cases per 100,000 person-days among untreated patients. This represented a 73% lower chance of being hospitalized.
Among ages 40-64, the rate of hospitalization due to COVID-19 was 15.2 cases per 100,000 person-days among treated patients, compared with 15.8 cases per 100,000 person-days among untreated patients. The risk of hospitalization wasn’t significantly lower for this age group.
Among ages 65 and older, there were two deaths from COVID-19 in 2,484 treated patients, compared with 158 in the 40,337 untreated patients. This represented a 79% lower chance of dying from COVID-19.
Among ages 40-64, there was one death from COVID-19 in 1,418 treated patients, compared with 16 in the 65,015 untreated patients. The risk of death wasn’t significantly lower for this age group.
For both age groups, a lack of previous COVID-19 immunity and a previous hospitalization were most strongly linked to high rates of hospitalization during the Omicron wave.
The researchers noted that they didn’t break down the data on ages 40-64 who had cancer and other severe conditions that weaken the immune system. These patients may be more likely to benefit from Paxlovid, they said, though future studies will need to analyze the data.
The study didn’t receive any financial or in-kind support, the authors said.
A version of this article first appeared on WebMD.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Vaccine hope now for leading cause of U.S. infant hospitalizations: RSV
Respiratory syncytial virus (RSV) is the leading cause of U.S. infant hospitalizations overall and across population subgroups, new data published in the Journal of Infectious Diseases confirm.
Acute bronchiolitis caused by RSV accounted for 9.6% (95% confidence interval, 9.4%-9.9%) and 9.3% (95% CI, 9.0%-9.6%) of total infant hospitalizations from January 2009 to September 2015 and October 2015 to December 2019, respectively.
Journal issue includes 14 RSV studies
The latest issue of the journal includes a special section with results from 14 studies related to the widespread, easy-to-catch virus, highlighting the urgency of finding a solution for all infants.
In one study, authors led by Mina Suh, MPH, with EpidStrategies, a division of ToxStrategies in Rockville, Md., reported that, in children under the age of 5 years in the United States, RSV caused 58,000 annual hospitalizations and from 100 to 500 annual deaths from 2009 to 2019 (the latest year data were available).
Globally, in 2015, among infants younger than 6 months, an estimated 1.4 million hospital admissions and 27,300 in-hospital deaths were attributed to RSV lower respiratory tract infection (LRTI).
The researchers used the largest publicly available, all-payer database in the United States – the National (Nationwide) Inpatient Sample – to describe the leading causes of infant hospitalizations.
The authors noted that, because clinicians don’t routinely perform lab tests for RSV, the true health care burden is likely higher and its public health impact greater than these numbers show.
Immunization candidates advance
There are no preventative options currently available to substantially cut RSV infections in all infants, though immunization candidates are advancing, showing safety and efficacy in clinical trials.
Palivizumab is currently the only available option in the United States to prevent RSV and is recommended only for a small group of infants with particular forms of heart or lung disease and those born prematurely at 29 weeks’ gestational age. Further, palivizumab has to be given monthly throughout the RSV season.
Another of the studies in the journal supplement concluded that a universal immunization strategy with one of the candidates, nirsevimab (Sanofi, AstraZeneca), an investigational long-acting monoclonal antibody, could substantially reduce the health burden and economic burden for U.S. infants in their first RSV season.
The researchers, led by Alexia Kieffer, MSc, MPH, with Sanofi, used static decision-analytic modeling for the estimates. Modeled RSV-related outcomes included primary care and ED visits, hospitalizations, including ICU admission and mechanical ventilations, and RSV-related deaths.
“The results of this model suggested that the use of nirsevimab in all infants could reduce health events by 55% and the overall costs to the payer by 49%,” the authors of the study wrote.
According to the study, universal immunization of all infants with nirsevimab is expected to reduce 290,174 RSV-related medically attended LRTI (MALRTI), 24,986 hospitalizations, and cut $612 million in costs to the health care system.
The authors wrote: “While this reduction would be driven by term infants, who account for most of the RSV-MALRTI burden; all infants, including palivizumab-eligible and preterm infants who suffer from significantly higher rates of disease, would benefit from this immunization strategy.”
Excitement for another option
Jörn-Hendrik Weitkamp, MD, professor of pediatrics and director for patient-oriented research at Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said in an interview there is much excitement in the field for nirsevimab as it has significant advantages over palivizumab.
RSV “is a huge burden to the children, the families, the hospitals, and the medical system,” he said.
Ideally there would be a vaccine to offer the best protection, he noted.
“People have spent their lives, their careers trying to develop a vaccine for RSV,” he said, but that has been elusive for more than 60 years. Therefore, passive immunization is the best of the current options, he says, and nirsevimab “seems to be very effective.”
What’s not clear, Dr. Weitkamp said, is how much nirsevimab will cost as it is not yet approved by the Food and Drug Administration. However, it has the great advantage of being given only once before the season starts instead of monthly (as required for palivizumab) through the season, “which is painful, inconvenient, and traumatizing. We limit that one to the children at highest risk.”
Rolling out an infant nirsevimab program would likely vary by geographic region, Ms. Kieffer and colleagues said, to help ensure infants are protected during the peak of their region’s RSV season.
The journal’s RSV supplement was supported by Sanofi and AstraZeneca. The studies by Ms. Suh and colleagues and Ms. Kieffer and colleagues were supported by AstraZeneca and Sanofi. Ms. Suh and several coauthors are employees of EpidStrategies. One coauthor is an employee of Sanofi and may hold shares and/or stock options in the company. Ms. Kieffer and several coauthors are employees of Sanofi and may hold shares and/or stock options in the company. Dr. Weitkamp reported no relevant financial relationships.
Respiratory syncytial virus (RSV) is the leading cause of U.S. infant hospitalizations overall and across population subgroups, new data published in the Journal of Infectious Diseases confirm.
Acute bronchiolitis caused by RSV accounted for 9.6% (95% confidence interval, 9.4%-9.9%) and 9.3% (95% CI, 9.0%-9.6%) of total infant hospitalizations from January 2009 to September 2015 and October 2015 to December 2019, respectively.
Journal issue includes 14 RSV studies
The latest issue of the journal includes a special section with results from 14 studies related to the widespread, easy-to-catch virus, highlighting the urgency of finding a solution for all infants.
In one study, authors led by Mina Suh, MPH, with EpidStrategies, a division of ToxStrategies in Rockville, Md., reported that, in children under the age of 5 years in the United States, RSV caused 58,000 annual hospitalizations and from 100 to 500 annual deaths from 2009 to 2019 (the latest year data were available).
Globally, in 2015, among infants younger than 6 months, an estimated 1.4 million hospital admissions and 27,300 in-hospital deaths were attributed to RSV lower respiratory tract infection (LRTI).
The researchers used the largest publicly available, all-payer database in the United States – the National (Nationwide) Inpatient Sample – to describe the leading causes of infant hospitalizations.
The authors noted that, because clinicians don’t routinely perform lab tests for RSV, the true health care burden is likely higher and its public health impact greater than these numbers show.
Immunization candidates advance
There are no preventative options currently available to substantially cut RSV infections in all infants, though immunization candidates are advancing, showing safety and efficacy in clinical trials.
Palivizumab is currently the only available option in the United States to prevent RSV and is recommended only for a small group of infants with particular forms of heart or lung disease and those born prematurely at 29 weeks’ gestational age. Further, palivizumab has to be given monthly throughout the RSV season.
Another of the studies in the journal supplement concluded that a universal immunization strategy with one of the candidates, nirsevimab (Sanofi, AstraZeneca), an investigational long-acting monoclonal antibody, could substantially reduce the health burden and economic burden for U.S. infants in their first RSV season.
The researchers, led by Alexia Kieffer, MSc, MPH, with Sanofi, used static decision-analytic modeling for the estimates. Modeled RSV-related outcomes included primary care and ED visits, hospitalizations, including ICU admission and mechanical ventilations, and RSV-related deaths.
“The results of this model suggested that the use of nirsevimab in all infants could reduce health events by 55% and the overall costs to the payer by 49%,” the authors of the study wrote.
According to the study, universal immunization of all infants with nirsevimab is expected to reduce 290,174 RSV-related medically attended LRTI (MALRTI), 24,986 hospitalizations, and cut $612 million in costs to the health care system.
The authors wrote: “While this reduction would be driven by term infants, who account for most of the RSV-MALRTI burden; all infants, including palivizumab-eligible and preterm infants who suffer from significantly higher rates of disease, would benefit from this immunization strategy.”
Excitement for another option
Jörn-Hendrik Weitkamp, MD, professor of pediatrics and director for patient-oriented research at Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said in an interview there is much excitement in the field for nirsevimab as it has significant advantages over palivizumab.
RSV “is a huge burden to the children, the families, the hospitals, and the medical system,” he said.
Ideally there would be a vaccine to offer the best protection, he noted.
“People have spent their lives, their careers trying to develop a vaccine for RSV,” he said, but that has been elusive for more than 60 years. Therefore, passive immunization is the best of the current options, he says, and nirsevimab “seems to be very effective.”
What’s not clear, Dr. Weitkamp said, is how much nirsevimab will cost as it is not yet approved by the Food and Drug Administration. However, it has the great advantage of being given only once before the season starts instead of monthly (as required for palivizumab) through the season, “which is painful, inconvenient, and traumatizing. We limit that one to the children at highest risk.”
Rolling out an infant nirsevimab program would likely vary by geographic region, Ms. Kieffer and colleagues said, to help ensure infants are protected during the peak of their region’s RSV season.
The journal’s RSV supplement was supported by Sanofi and AstraZeneca. The studies by Ms. Suh and colleagues and Ms. Kieffer and colleagues were supported by AstraZeneca and Sanofi. Ms. Suh and several coauthors are employees of EpidStrategies. One coauthor is an employee of Sanofi and may hold shares and/or stock options in the company. Ms. Kieffer and several coauthors are employees of Sanofi and may hold shares and/or stock options in the company. Dr. Weitkamp reported no relevant financial relationships.
Respiratory syncytial virus (RSV) is the leading cause of U.S. infant hospitalizations overall and across population subgroups, new data published in the Journal of Infectious Diseases confirm.
Acute bronchiolitis caused by RSV accounted for 9.6% (95% confidence interval, 9.4%-9.9%) and 9.3% (95% CI, 9.0%-9.6%) of total infant hospitalizations from January 2009 to September 2015 and October 2015 to December 2019, respectively.
Journal issue includes 14 RSV studies
The latest issue of the journal includes a special section with results from 14 studies related to the widespread, easy-to-catch virus, highlighting the urgency of finding a solution for all infants.
In one study, authors led by Mina Suh, MPH, with EpidStrategies, a division of ToxStrategies in Rockville, Md., reported that, in children under the age of 5 years in the United States, RSV caused 58,000 annual hospitalizations and from 100 to 500 annual deaths from 2009 to 2019 (the latest year data were available).
Globally, in 2015, among infants younger than 6 months, an estimated 1.4 million hospital admissions and 27,300 in-hospital deaths were attributed to RSV lower respiratory tract infection (LRTI).
The researchers used the largest publicly available, all-payer database in the United States – the National (Nationwide) Inpatient Sample – to describe the leading causes of infant hospitalizations.
The authors noted that, because clinicians don’t routinely perform lab tests for RSV, the true health care burden is likely higher and its public health impact greater than these numbers show.
Immunization candidates advance
There are no preventative options currently available to substantially cut RSV infections in all infants, though immunization candidates are advancing, showing safety and efficacy in clinical trials.
Palivizumab is currently the only available option in the United States to prevent RSV and is recommended only for a small group of infants with particular forms of heart or lung disease and those born prematurely at 29 weeks’ gestational age. Further, palivizumab has to be given monthly throughout the RSV season.
Another of the studies in the journal supplement concluded that a universal immunization strategy with one of the candidates, nirsevimab (Sanofi, AstraZeneca), an investigational long-acting monoclonal antibody, could substantially reduce the health burden and economic burden for U.S. infants in their first RSV season.
The researchers, led by Alexia Kieffer, MSc, MPH, with Sanofi, used static decision-analytic modeling for the estimates. Modeled RSV-related outcomes included primary care and ED visits, hospitalizations, including ICU admission and mechanical ventilations, and RSV-related deaths.
“The results of this model suggested that the use of nirsevimab in all infants could reduce health events by 55% and the overall costs to the payer by 49%,” the authors of the study wrote.
According to the study, universal immunization of all infants with nirsevimab is expected to reduce 290,174 RSV-related medically attended LRTI (MALRTI), 24,986 hospitalizations, and cut $612 million in costs to the health care system.
The authors wrote: “While this reduction would be driven by term infants, who account for most of the RSV-MALRTI burden; all infants, including palivizumab-eligible and preterm infants who suffer from significantly higher rates of disease, would benefit from this immunization strategy.”
Excitement for another option
Jörn-Hendrik Weitkamp, MD, professor of pediatrics and director for patient-oriented research at Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said in an interview there is much excitement in the field for nirsevimab as it has significant advantages over palivizumab.
RSV “is a huge burden to the children, the families, the hospitals, and the medical system,” he said.
Ideally there would be a vaccine to offer the best protection, he noted.
“People have spent their lives, their careers trying to develop a vaccine for RSV,” he said, but that has been elusive for more than 60 years. Therefore, passive immunization is the best of the current options, he says, and nirsevimab “seems to be very effective.”
What’s not clear, Dr. Weitkamp said, is how much nirsevimab will cost as it is not yet approved by the Food and Drug Administration. However, it has the great advantage of being given only once before the season starts instead of monthly (as required for palivizumab) through the season, “which is painful, inconvenient, and traumatizing. We limit that one to the children at highest risk.”
Rolling out an infant nirsevimab program would likely vary by geographic region, Ms. Kieffer and colleagues said, to help ensure infants are protected during the peak of their region’s RSV season.
The journal’s RSV supplement was supported by Sanofi and AstraZeneca. The studies by Ms. Suh and colleagues and Ms. Kieffer and colleagues were supported by AstraZeneca and Sanofi. Ms. Suh and several coauthors are employees of EpidStrategies. One coauthor is an employee of Sanofi and may hold shares and/or stock options in the company. Ms. Kieffer and several coauthors are employees of Sanofi and may hold shares and/or stock options in the company. Dr. Weitkamp reported no relevant financial relationships.
FROM THE JOURNAL OF INFECTIOUS DISEASES
ACC fills gaps on guidance for nonstatin therapies for LDL-C lowering
To address current gaps in expert guidance on newer nonstatin agents, the American College of Cardiology has issued an expert consensus decision pathway on the role of nonstatin therapies in LDL cholesterol lowering for risk reduction in atherosclerotic cardiovascular disease (ASCVD).
Since the publication of the most recent AHA/ACC cholesterol guidelines in 2018, a number of newer nonstatin medications have become available for management of lipid-associated risk, including bempedoic acid, inclisiran, evinacumab, and icosapent ethyl.
These medications were not addressed in the 2018 AHA/ACC Guideline on the Management of Blood Cholesterol.
The 53-page document – 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk – was published online in the Journal of the American College of Cardiology.
The new expert consensus document provides guidance for clinicians until the next formal guidelines are produced, Donald Lloyd-Jones, MD, chair of the writing committee, told this news organization.

The writing group focused on three key areas regarding the use of nonstatin therapies where recent scientific evidence is still under review and clinical trials are still underway:
- In what patient populations should newer nonstatin therapies be considered?
- In what situations should newer nonstatin therapies be considered?
- If newer nonstatin therapies are to be added, which therapies should be considered and in what order to maximize patient benefit and preference?
The document provides algorithms that endorse the four evidence-based patient groups identified in the 2018 guidelines and assumes that the patient is currently taking or has attempted to take a statin, given that that is the most effective initial therapy, the writing group says.
“The algorithms have been streamlined for ease of use by clinicians to help them identify who may need adjunctive nonstatin medications, to provide thresholds for consideration of those medications, and to provide a prioritization of those medications based on the strength of available evidence of efficacy,” said Dr. Lloyd-Jones, chair of the department of preventive medicine at Northwestern University’s Feinberg School of Medicine, Chicago.
“We hope that these pathways will assist the decision-making process for clinicians and patients,” he added.
He also noted that statins remain the “most important first-line therapy for reducing ASCVD risk, because of their efficacy, safety, and low cost. However, for some patients, there are now options if statins do not fully achieve the goals for reducing ASCVD risk or if statins are not tolerated at effective doses.”
“The new expert consensus document highlights that higher-risk patients should be considered more often for adjunctive therapy and provides user-friendly decision pathways to assist in considering the reasonable choices available under different clinical scenarios,” Dr. Lloyd-Jones said.
The document has been endorsed by the National Lipid Association.
This research had no commercial funding. Dr. Lloyd-Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
To address current gaps in expert guidance on newer nonstatin agents, the American College of Cardiology has issued an expert consensus decision pathway on the role of nonstatin therapies in LDL cholesterol lowering for risk reduction in atherosclerotic cardiovascular disease (ASCVD).
Since the publication of the most recent AHA/ACC cholesterol guidelines in 2018, a number of newer nonstatin medications have become available for management of lipid-associated risk, including bempedoic acid, inclisiran, evinacumab, and icosapent ethyl.
These medications were not addressed in the 2018 AHA/ACC Guideline on the Management of Blood Cholesterol.
The 53-page document – 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk – was published online in the Journal of the American College of Cardiology.
The new expert consensus document provides guidance for clinicians until the next formal guidelines are produced, Donald Lloyd-Jones, MD, chair of the writing committee, told this news organization.
The writing group focused on three key areas regarding the use of nonstatin therapies where recent scientific evidence is still under review and clinical trials are still underway:
- In what patient populations should newer nonstatin therapies be considered?
- In what situations should newer nonstatin therapies be considered?
- If newer nonstatin therapies are to be added, which therapies should be considered and in what order to maximize patient benefit and preference?
The document provides algorithms that endorse the four evidence-based patient groups identified in the 2018 guidelines and assumes that the patient is currently taking or has attempted to take a statin, given that that is the most effective initial therapy, the writing group says.
“The algorithms have been streamlined for ease of use by clinicians to help them identify who may need adjunctive nonstatin medications, to provide thresholds for consideration of those medications, and to provide a prioritization of those medications based on the strength of available evidence of efficacy,” said Dr. Lloyd-Jones, chair of the department of preventive medicine at Northwestern University’s Feinberg School of Medicine, Chicago.
“We hope that these pathways will assist the decision-making process for clinicians and patients,” he added.
He also noted that statins remain the “most important first-line therapy for reducing ASCVD risk, because of their efficacy, safety, and low cost. However, for some patients, there are now options if statins do not fully achieve the goals for reducing ASCVD risk or if statins are not tolerated at effective doses.”
“The new expert consensus document highlights that higher-risk patients should be considered more often for adjunctive therapy and provides user-friendly decision pathways to assist in considering the reasonable choices available under different clinical scenarios,” Dr. Lloyd-Jones said.
The document has been endorsed by the National Lipid Association.
This research had no commercial funding. Dr. Lloyd-Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
To address current gaps in expert guidance on newer nonstatin agents, the American College of Cardiology has issued an expert consensus decision pathway on the role of nonstatin therapies in LDL cholesterol lowering for risk reduction in atherosclerotic cardiovascular disease (ASCVD).
Since the publication of the most recent AHA/ACC cholesterol guidelines in 2018, a number of newer nonstatin medications have become available for management of lipid-associated risk, including bempedoic acid, inclisiran, evinacumab, and icosapent ethyl.
These medications were not addressed in the 2018 AHA/ACC Guideline on the Management of Blood Cholesterol.
The 53-page document – 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk – was published online in the Journal of the American College of Cardiology.
The new expert consensus document provides guidance for clinicians until the next formal guidelines are produced, Donald Lloyd-Jones, MD, chair of the writing committee, told this news organization.
The writing group focused on three key areas regarding the use of nonstatin therapies where recent scientific evidence is still under review and clinical trials are still underway:
- In what patient populations should newer nonstatin therapies be considered?
- In what situations should newer nonstatin therapies be considered?
- If newer nonstatin therapies are to be added, which therapies should be considered and in what order to maximize patient benefit and preference?
The document provides algorithms that endorse the four evidence-based patient groups identified in the 2018 guidelines and assumes that the patient is currently taking or has attempted to take a statin, given that that is the most effective initial therapy, the writing group says.
“The algorithms have been streamlined for ease of use by clinicians to help them identify who may need adjunctive nonstatin medications, to provide thresholds for consideration of those medications, and to provide a prioritization of those medications based on the strength of available evidence of efficacy,” said Dr. Lloyd-Jones, chair of the department of preventive medicine at Northwestern University’s Feinberg School of Medicine, Chicago.
“We hope that these pathways will assist the decision-making process for clinicians and patients,” he added.
He also noted that statins remain the “most important first-line therapy for reducing ASCVD risk, because of their efficacy, safety, and low cost. However, for some patients, there are now options if statins do not fully achieve the goals for reducing ASCVD risk or if statins are not tolerated at effective doses.”
“The new expert consensus document highlights that higher-risk patients should be considered more often for adjunctive therapy and provides user-friendly decision pathways to assist in considering the reasonable choices available under different clinical scenarios,” Dr. Lloyd-Jones said.
The document has been endorsed by the National Lipid Association.
This research had no commercial funding. Dr. Lloyd-Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
No benefit of routine stress test POST-PCI in high-risk patients
New randomized trial results show no benefit in clinical outcomes from active surveillance using functional testing over usual care among high-risk patients with previous percutaneous coronary intervention (PCI).
At 2 years, there was no difference in a composite outcome of death from any cause, MI, or hospitalization for unstable angina between patients who had routine functional testing at 1 year and patients receiving standard care in the POST-PCI trial.

“Our trial does not support active surveillance with routine functional testing for follow-up strategy in high-risk patients who undergo PCI,” first author Duk-Woo Park, MD, division of cardiology, Asan Medical Center, University of Ulsan, Seoul, South Korea, said in an interview.
The researchers said their results should be interpreted in the context of previous findings from the ISCHEMIA trial that showed no difference in death or ischemic events with an initial invasive versus an initial conservative approach in patients with stable coronary artery disease and moderate to severe ischemia on stress testing.
“Both the ISCHEMIA and POST-PCI trials show the benefits of a ‘less is more’ concept (i.e., if more invasive strategies or testing are performed less frequently, it will result in better patient outcomes),” the authors wrote. Although characteristics of the patients in these trials “were quite different, a more invasive therapeutic approach (in the ISCHEMIA trial) as well as a more aggressive follow-up approach (in the POST-PCI trial) did not provide an additional treatment effect beyond a conservative strategy on the basis of guideline-directed medical therapy.”
Results were presented at the annual congress of the European Society of Cardiology and published online simultaneously in the New England Journal of Medicine.
‘Compelling new evidence’
In an editorial accompanying the publication, Jacqueline E. Tamis-Holland, MD, Icahn School of Medicine at Mount Sinai, Mount Sinai Morningside Hospital, New York, also agreed that this new result “builds on the findings” from the ISCHEMIA trial. “Collectively, these trials highlight the lack of benefit of routine stress testing in asymptomatic patients.”
Dr. Tamis-Holland pointed out that many of the deaths in this trial occurred before the 1-year stress test, possibly related to stent thrombosis, and therefore would not have been prevented by routine testing at 1 year. And overall, event rates were “quite low, and most likely reflect adherence to guideline recommendations” in the trial. For example, 99% of patients were receiving statins, and 74% of the procedures used intravascular imaging for the PCI procedures, “a much greater proportion of use than most centers in the United States,” she noted.
“The POST-PCI trial provides compelling new evidence for a future class III recommendation for routine surveillance testing after PCI,” Dr. Tamis-Holland concluded “Until then, we must refrain from prescribing surveillance stress testing to our patients after PCI, in the absence of other clinical signs or symptoms suggestive of stent failure.”
Commenting on the results, B. Hadley Wilson, MD, executive vice chair of the Sanger Heart & Vascular Institute/Atrium Health, clinical professor of medicine at University of North Carolina at Chapel Hill, and vice president of the American College of Cardiology, said that for decades it’s been thought that patients who had high-risk PCI needed to be followed more closely for potential future events.
“And it actually turned out there was no difference in outcomes between the groups,” he said in an interview.
“So, I think it’s a good study – well conducted, good numbers – that answers the question that routine functional stress testing, even for high-risk PCI patients, is not effective or cost effective or beneficial on a yearly basis,” he said. “I think it will help frame care that patients will just be followed with best medical therapy and then if they have recurrence of symptoms they would be considered for further evaluation, either with stress testing or angiography.”
High-risk characteristics
Current guidelines do not advocate the use of routine stress testing after revascularization, the authors wrote in their paper. “However, surveillance with the use of imaging-based stress testing may be considered in high-risk patients at 6 months after a revascularization procedure (class IIb recommendation), and routine imaging-based stress testing may be considered at 1 year after PCI and more than 5 years after CABG [coronary artery bypass graft] (class IIb recommendation).”
But in real-world clinical practice, Dr. Park said, “follow-up strategy for patients who underwent PCI or CABG is still undetermined.” Particularly, “it could be more problematic in high-risk PCI patients with high-risk anatomical or clinical characteristics. Thus, we performed this POST-PCI trial comparing routine stress testing follow-up strategy versus standard-care follow-up strategy in high-risk PCI patients.”
The researchers randomly assigned 1,706 patients with high-risk anatomical or clinical characteristics who had undergone PCI to a follow-up strategy of routine functional testing, including nuclear stress testing, exercise electrocardiography, or stress echocardiography at 1 year, or to standard care alone.
High-risk anatomical features included left main or bifurcation disease; restenotic or long, diffuse lesions; or bypass graft disease. High-risk clinical characteristics included diabetes mellitus, chronic kidney disease, or enzyme-positive acute coronary syndrome.
Mean age of the patients was 64.7 years; 21.0% had left main disease, 43.5% had bifurcation disease, 69.8% had multivessel disease, 70.1% had diffuse long lesions, 38.7% had diabetes, and 96.4% had been treated with drug-eluting stents.
At 2 years, a primary-outcome event had occurred in 46 of 849 patients (Kaplan-Meier estimate, 5.5%) in the functional-testing group and in 51 of 857 (Kaplan-Meier estimate, 6.0%) in the standard-care group (hazard ratio, 0.90; 95% confidence interval, 0.61-1.35; P = .62). There were no between-group differences in the components of the primary outcome.
Secondary endpoints included invasive coronary angiography or repeat revascularization. At 2 years, 12.3% of the patients in the functional-testing group and 9.3% in the standard-care group had undergone invasive coronary angiography (difference, 2.99 percentage points; 95% CI, −0.01 to 5.99 percentage points), and 8.1% and 5.8% of patients, respectively, had a repeat revascularization procedure (difference, 2.23 percentage points; 95% CI, −0.22 to 4.68 percentage points).
Positive results on stress tests were more common with nuclear imaging than with exercise ECG or stress echocardiography, the authors noted. Subsequent coronary angiography and repeat revascularization were more common in patients with positive results on nuclear stress imaging and exercise ECG than in those with discordant results between nuclear imaging and exercise ECG.
POST-PCI was funded by the CardioVascular Research Foundation and Daewoong Pharmaceutical Company. Dr. Park reported grants from the Cardiovascular Research Foundation and Daewoong Pharmaceutical Company. Dr. Tamis-Holland reported “other” funding from Pfizer outside the submitted work. Dr. Wilson reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
New randomized trial results show no benefit in clinical outcomes from active surveillance using functional testing over usual care among high-risk patients with previous percutaneous coronary intervention (PCI).
At 2 years, there was no difference in a composite outcome of death from any cause, MI, or hospitalization for unstable angina between patients who had routine functional testing at 1 year and patients receiving standard care in the POST-PCI trial.
“Our trial does not support active surveillance with routine functional testing for follow-up strategy in high-risk patients who undergo PCI,” first author Duk-Woo Park, MD, division of cardiology, Asan Medical Center, University of Ulsan, Seoul, South Korea, said in an interview.
The researchers said their results should be interpreted in the context of previous findings from the ISCHEMIA trial that showed no difference in death or ischemic events with an initial invasive versus an initial conservative approach in patients with stable coronary artery disease and moderate to severe ischemia on stress testing.
“Both the ISCHEMIA and POST-PCI trials show the benefits of a ‘less is more’ concept (i.e., if more invasive strategies or testing are performed less frequently, it will result in better patient outcomes),” the authors wrote. Although characteristics of the patients in these trials “were quite different, a more invasive therapeutic approach (in the ISCHEMIA trial) as well as a more aggressive follow-up approach (in the POST-PCI trial) did not provide an additional treatment effect beyond a conservative strategy on the basis of guideline-directed medical therapy.”
Results were presented at the annual congress of the European Society of Cardiology and published online simultaneously in the New England Journal of Medicine.
‘Compelling new evidence’
In an editorial accompanying the publication, Jacqueline E. Tamis-Holland, MD, Icahn School of Medicine at Mount Sinai, Mount Sinai Morningside Hospital, New York, also agreed that this new result “builds on the findings” from the ISCHEMIA trial. “Collectively, these trials highlight the lack of benefit of routine stress testing in asymptomatic patients.”
Dr. Tamis-Holland pointed out that many of the deaths in this trial occurred before the 1-year stress test, possibly related to stent thrombosis, and therefore would not have been prevented by routine testing at 1 year. And overall, event rates were “quite low, and most likely reflect adherence to guideline recommendations” in the trial. For example, 99% of patients were receiving statins, and 74% of the procedures used intravascular imaging for the PCI procedures, “a much greater proportion of use than most centers in the United States,” she noted.
“The POST-PCI trial provides compelling new evidence for a future class III recommendation for routine surveillance testing after PCI,” Dr. Tamis-Holland concluded “Until then, we must refrain from prescribing surveillance stress testing to our patients after PCI, in the absence of other clinical signs or symptoms suggestive of stent failure.”
Commenting on the results, B. Hadley Wilson, MD, executive vice chair of the Sanger Heart & Vascular Institute/Atrium Health, clinical professor of medicine at University of North Carolina at Chapel Hill, and vice president of the American College of Cardiology, said that for decades it’s been thought that patients who had high-risk PCI needed to be followed more closely for potential future events.
“And it actually turned out there was no difference in outcomes between the groups,” he said in an interview.
“So, I think it’s a good study – well conducted, good numbers – that answers the question that routine functional stress testing, even for high-risk PCI patients, is not effective or cost effective or beneficial on a yearly basis,” he said. “I think it will help frame care that patients will just be followed with best medical therapy and then if they have recurrence of symptoms they would be considered for further evaluation, either with stress testing or angiography.”
High-risk characteristics
Current guidelines do not advocate the use of routine stress testing after revascularization, the authors wrote in their paper. “However, surveillance with the use of imaging-based stress testing may be considered in high-risk patients at 6 months after a revascularization procedure (class IIb recommendation), and routine imaging-based stress testing may be considered at 1 year after PCI and more than 5 years after CABG [coronary artery bypass graft] (class IIb recommendation).”
But in real-world clinical practice, Dr. Park said, “follow-up strategy for patients who underwent PCI or CABG is still undetermined.” Particularly, “it could be more problematic in high-risk PCI patients with high-risk anatomical or clinical characteristics. Thus, we performed this POST-PCI trial comparing routine stress testing follow-up strategy versus standard-care follow-up strategy in high-risk PCI patients.”
The researchers randomly assigned 1,706 patients with high-risk anatomical or clinical characteristics who had undergone PCI to a follow-up strategy of routine functional testing, including nuclear stress testing, exercise electrocardiography, or stress echocardiography at 1 year, or to standard care alone.
High-risk anatomical features included left main or bifurcation disease; restenotic or long, diffuse lesions; or bypass graft disease. High-risk clinical characteristics included diabetes mellitus, chronic kidney disease, or enzyme-positive acute coronary syndrome.
Mean age of the patients was 64.7 years; 21.0% had left main disease, 43.5% had bifurcation disease, 69.8% had multivessel disease, 70.1% had diffuse long lesions, 38.7% had diabetes, and 96.4% had been treated with drug-eluting stents.
At 2 years, a primary-outcome event had occurred in 46 of 849 patients (Kaplan-Meier estimate, 5.5%) in the functional-testing group and in 51 of 857 (Kaplan-Meier estimate, 6.0%) in the standard-care group (hazard ratio, 0.90; 95% confidence interval, 0.61-1.35; P = .62). There were no between-group differences in the components of the primary outcome.
Secondary endpoints included invasive coronary angiography or repeat revascularization. At 2 years, 12.3% of the patients in the functional-testing group and 9.3% in the standard-care group had undergone invasive coronary angiography (difference, 2.99 percentage points; 95% CI, −0.01 to 5.99 percentage points), and 8.1% and 5.8% of patients, respectively, had a repeat revascularization procedure (difference, 2.23 percentage points; 95% CI, −0.22 to 4.68 percentage points).
Positive results on stress tests were more common with nuclear imaging than with exercise ECG or stress echocardiography, the authors noted. Subsequent coronary angiography and repeat revascularization were more common in patients with positive results on nuclear stress imaging and exercise ECG than in those with discordant results between nuclear imaging and exercise ECG.
POST-PCI was funded by the CardioVascular Research Foundation and Daewoong Pharmaceutical Company. Dr. Park reported grants from the Cardiovascular Research Foundation and Daewoong Pharmaceutical Company. Dr. Tamis-Holland reported “other” funding from Pfizer outside the submitted work. Dr. Wilson reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
New randomized trial results show no benefit in clinical outcomes from active surveillance using functional testing over usual care among high-risk patients with previous percutaneous coronary intervention (PCI).
At 2 years, there was no difference in a composite outcome of death from any cause, MI, or hospitalization for unstable angina between patients who had routine functional testing at 1 year and patients receiving standard care in the POST-PCI trial.
“Our trial does not support active surveillance with routine functional testing for follow-up strategy in high-risk patients who undergo PCI,” first author Duk-Woo Park, MD, division of cardiology, Asan Medical Center, University of Ulsan, Seoul, South Korea, said in an interview.
The researchers said their results should be interpreted in the context of previous findings from the ISCHEMIA trial that showed no difference in death or ischemic events with an initial invasive versus an initial conservative approach in patients with stable coronary artery disease and moderate to severe ischemia on stress testing.
“Both the ISCHEMIA and POST-PCI trials show the benefits of a ‘less is more’ concept (i.e., if more invasive strategies or testing are performed less frequently, it will result in better patient outcomes),” the authors wrote. Although characteristics of the patients in these trials “were quite different, a more invasive therapeutic approach (in the ISCHEMIA trial) as well as a more aggressive follow-up approach (in the POST-PCI trial) did not provide an additional treatment effect beyond a conservative strategy on the basis of guideline-directed medical therapy.”
Results were presented at the annual congress of the European Society of Cardiology and published online simultaneously in the New England Journal of Medicine.
‘Compelling new evidence’
In an editorial accompanying the publication, Jacqueline E. Tamis-Holland, MD, Icahn School of Medicine at Mount Sinai, Mount Sinai Morningside Hospital, New York, also agreed that this new result “builds on the findings” from the ISCHEMIA trial. “Collectively, these trials highlight the lack of benefit of routine stress testing in asymptomatic patients.”
Dr. Tamis-Holland pointed out that many of the deaths in this trial occurred before the 1-year stress test, possibly related to stent thrombosis, and therefore would not have been prevented by routine testing at 1 year. And overall, event rates were “quite low, and most likely reflect adherence to guideline recommendations” in the trial. For example, 99% of patients were receiving statins, and 74% of the procedures used intravascular imaging for the PCI procedures, “a much greater proportion of use than most centers in the United States,” she noted.
“The POST-PCI trial provides compelling new evidence for a future class III recommendation for routine surveillance testing after PCI,” Dr. Tamis-Holland concluded “Until then, we must refrain from prescribing surveillance stress testing to our patients after PCI, in the absence of other clinical signs or symptoms suggestive of stent failure.”
Commenting on the results, B. Hadley Wilson, MD, executive vice chair of the Sanger Heart & Vascular Institute/Atrium Health, clinical professor of medicine at University of North Carolina at Chapel Hill, and vice president of the American College of Cardiology, said that for decades it’s been thought that patients who had high-risk PCI needed to be followed more closely for potential future events.
“And it actually turned out there was no difference in outcomes between the groups,” he said in an interview.
“So, I think it’s a good study – well conducted, good numbers – that answers the question that routine functional stress testing, even for high-risk PCI patients, is not effective or cost effective or beneficial on a yearly basis,” he said. “I think it will help frame care that patients will just be followed with best medical therapy and then if they have recurrence of symptoms they would be considered for further evaluation, either with stress testing or angiography.”
High-risk characteristics
Current guidelines do not advocate the use of routine stress testing after revascularization, the authors wrote in their paper. “However, surveillance with the use of imaging-based stress testing may be considered in high-risk patients at 6 months after a revascularization procedure (class IIb recommendation), and routine imaging-based stress testing may be considered at 1 year after PCI and more than 5 years after CABG [coronary artery bypass graft] (class IIb recommendation).”
But in real-world clinical practice, Dr. Park said, “follow-up strategy for patients who underwent PCI or CABG is still undetermined.” Particularly, “it could be more problematic in high-risk PCI patients with high-risk anatomical or clinical characteristics. Thus, we performed this POST-PCI trial comparing routine stress testing follow-up strategy versus standard-care follow-up strategy in high-risk PCI patients.”
The researchers randomly assigned 1,706 patients with high-risk anatomical or clinical characteristics who had undergone PCI to a follow-up strategy of routine functional testing, including nuclear stress testing, exercise electrocardiography, or stress echocardiography at 1 year, or to standard care alone.
High-risk anatomical features included left main or bifurcation disease; restenotic or long, diffuse lesions; or bypass graft disease. High-risk clinical characteristics included diabetes mellitus, chronic kidney disease, or enzyme-positive acute coronary syndrome.
Mean age of the patients was 64.7 years; 21.0% had left main disease, 43.5% had bifurcation disease, 69.8% had multivessel disease, 70.1% had diffuse long lesions, 38.7% had diabetes, and 96.4% had been treated with drug-eluting stents.
At 2 years, a primary-outcome event had occurred in 46 of 849 patients (Kaplan-Meier estimate, 5.5%) in the functional-testing group and in 51 of 857 (Kaplan-Meier estimate, 6.0%) in the standard-care group (hazard ratio, 0.90; 95% confidence interval, 0.61-1.35; P = .62). There were no between-group differences in the components of the primary outcome.
Secondary endpoints included invasive coronary angiography or repeat revascularization. At 2 years, 12.3% of the patients in the functional-testing group and 9.3% in the standard-care group had undergone invasive coronary angiography (difference, 2.99 percentage points; 95% CI, −0.01 to 5.99 percentage points), and 8.1% and 5.8% of patients, respectively, had a repeat revascularization procedure (difference, 2.23 percentage points; 95% CI, −0.22 to 4.68 percentage points).
Positive results on stress tests were more common with nuclear imaging than with exercise ECG or stress echocardiography, the authors noted. Subsequent coronary angiography and repeat revascularization were more common in patients with positive results on nuclear stress imaging and exercise ECG than in those with discordant results between nuclear imaging and exercise ECG.
POST-PCI was funded by the CardioVascular Research Foundation and Daewoong Pharmaceutical Company. Dr. Park reported grants from the Cardiovascular Research Foundation and Daewoong Pharmaceutical Company. Dr. Tamis-Holland reported “other” funding from Pfizer outside the submitted work. Dr. Wilson reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2022
Rivaroxaban outmatched by VKAs for AFib in rheumatic heart disease
Contrary to expectations, vitamin K antagonists (VKAs) reduced the risk for ischemic stroke and death, compared with the factor Xa inhibitor rivaroxaban, (Xarelto, Janssen) in patients with rheumatic heart disease and atrial fibrillation (AFib), in the INVICTUS trial.
Patients receiving a VKA, typically warfarin, had a 25% lower risk for the primary outcome – a composite of stroke, systemic embolism, myocardial infarction, or death from vascular or unknown causes outcome – than receiving rivaroxaban (hazard ratio, 1.25; 95% confidence interval, 1.10-1.41).
This difference was driven primarily by a significant reduction in the risk for death in the VKA group, and without a significant increase in major bleeding, reported Ganesan Karthikeyan, MD, from the All India Institute of Medical Sciences in New Delhi.
“VKA should remain the standard of care for patients with rheumatic heart disease and atrial fibrillation,” he concluded in a hotline session at the annual congress of the European Society of Cardiology.
The study, simultaneously published in the New England Journal of Medicine, is the first randomized controlled trial to assess anticoagulant therapy in patients with rheumatic heart disease and AFib.

“Who could have possibly guessed these results? Certainly not me,” said invited discussant Renato D. Lopes, MD, MHS, PhD, Duke Clinical Research Institute, Durham, N.C. “To me, this is one more classical example of why we need to do randomized trials, since they are the only reliable way to determine treatment effects and drive clinical practice.”
Evidence gap
Rheumatic heart disease affects over 40 million people, mainly living in low- and low- to middle-income countries. About 20% of symptomatic patients have AF and an elevated stroke risk, but previous AFib trials excluded these patients, Dr. Karthikeyan noted.
INVICTUS was led by the Population Health Research Institute in Hamilton, Ont., and enrolled 4,565 patients from 24 countries in Africa, Asia, and Latin America who had rheumatic heart disease, AFib or atrial flutter, and an increased stroke risk caused by any of the following: CHA2DS2VASc score of 2 or more, moderate to severe mitral stenosis (valve area ≤ 2.0 cm2), left atrial spontaneous echo contrast, or left atrial thrombus.
Participants were randomly assigned to receive rivaroxaban, 20 mg once daily (15 mg/d if creatinine clearance was 15-49 mL/min), or a VKA titrated to an international normalized ratio (INR) of 2.0-3.0.
Warfarin was used in 79%-85% of patients assigned to VKA, with the percentage varying between visits. The INR was in therapeutic range in 33.2% of patients at baseline, 65.1% at 3 years, and 64.1% at 4 years.
During an average follow-up of 3.1 years, the primary outcome occurred in 446 patients in the VKA group (6.49% per year) and 560 patients in the rivaroxaban group (8.21% per year). The restricted mean survival time for the primary outcome was 1,675 vs. 1,599 days, respectively (difference, –76 days; 95% CI, –121 to –31 days; P for superiority < .001).
The rate of stroke or systemic embolism was similar between the VKA and rivaroxaban groups (75 vs. 94 events), although ischemic strokes were significantly lower with VKA (48 vs. 74 events).
No easy explanation
Deaths were significantly lower with VKA than rivaroxaban, at 442 versus 552 (restricted mean survival time for death, 1,608 vs. 1,587 days; difference, −72 days; 95% CI, –117 to –28 days).
“This reduction is not easily explained,” Dr. Karthikeyan acknowledged. “We cannot explain this reduction by the reduction in stroke that we saw because the number of deaths that are prevented by VKA are far larger than the number of strokes that are prevented. Moreover, the number of deaths were mainly heart failure or sudden deaths.”
Numbers of patients with major bleeding were also similar in the VKA and rivaroxaban groups (56 vs. 40 patients; P = .18), although numbers with fatal bleeding were lower with rivaroxaban (15 vs. 4, respectively).
By design, there were more physician interactions for monthly monitoring of INR in the VKA group, “but we do not believe such a large reduction can be explained entirely by increased health care contact,” he said. Moreover, there was no significant between-group difference in heart failure medications or hospitalizations or the need for valve replacement.
Almost a quarter (23%) of patients in the rivaroxaban group permanently discontinued the study drug versus just 6% in the VKA group.
Importantly, the mortality benefit emerged much later than in other trials and coincided with the time when the INR became therapeutic at about 3 years, Dr. Karthikeyan said. But it is unknown whether this is because of the INR or an unrelated effect.
More physician contact
Following the presentation, session cochair C. Michael Gibson, MD, Baim Institute for Clinical Research, Harvard Medical School, Boston, questioned the 23% discontinuation rate for rivaroxaban. “Is this really a superiority of warfarin or is this superiority of having someone come in and see their physician for a lot of checks on their INR?”
In response, Dr. Karthikeyan said that permanent discontinuation rates were about 20%-25% in shorter-duration direct oral anticoagulant trials, such as RELY, ROCKET-AF, and ARISTOLE, and exceeded 30% in ENGAGE-AF with 2.8 years’ follow-up.
“So, this is not new,” he said, adding that 31.4% of rivaroxaban patients did so for valve replacement surgery and subsequently received nonstudy VKA.
Dr. Lopes said it is important to keep in mind that INVICTUS enrolled a “very different population” that was younger (mean age, 50.5 years), was much more often female (72.3%), and had fewer comorbidities than patients with AFib who did not have rheumatic heart disease in the pivotal trials.
“It will be interesting to see the treatment effect according to mitral stenosis severity, since we had about 30% with mild mitral stenosis and additionally 18% of patients without mitral stenosis,” he added.
Co–principal investigator Stuart J. Connolly, MD, from the Population Health Research Institute, said physician contacts may be a factor but that the mortality difference was clear, highly significant, and sufficiently powered.
“What’s amazing is that what we’re seeing here is something that hasn’t been previously described with VKA or warfarin, which is that it reduces mortality,” he said in an interview.
Rivaroxaban has never been shown to reduce mortality in any particular condition, and a meta-analysis of other novel oral anticoagulants shows only a small reduction in mortality, caused almost completely by less intracranial hemorrhage than warfarin, he added. “So, we don’t think this is a problem with rivaroxaban. In some ways, rivaroxaban is an innocent bystander to a trial of warfarin in patients with rheumatic heart disease and atrial fibrillation.”
Dr. Connolly said more work is needed to explain the findings and analyses are planned to see which patients are at highest risk for death as well as looking at the relationship between INR control and outcomes.
“We need to do more research on what it is about VKA that could explain this,” he said. “Is it affecting the myocardium in some way, is it preventing fibrosis, is there some off target effect, not on the anticoagulation system, that could explain this?”
Athena Poppas, MD, chief of cardiology at Brown University, Providence, R.I., and past president of the American College of Cardiology, said “INVICTUS is an incredibly important study that needed to be done.”
“The results – though disappointing and surprising in some ways – I don’t think we can explain them away and change what we are doing right now,” she said in an interview.
Although warfarin is a cheap drug, Dr. Poppas said, it would be tremendously helpful to have an alternative treatment for these patients. Mechanistic studies are needed to understand the observed mortality advantage and low bleeding rates but that trials of other novel anticoagulants are also needed.
“But I’m not sure that will happen,” she added. “It’s unlikely to be industry sponsored, so it would be a very expensive lift with a low likelihood of success.”
In an editorial accompanying the paper, Gregory Y.H. Lip, MD, University of Liverpool (England), pointed out that observational data show similar or even higher risks for major bleeding with rivaroxaban than with warfarin. “To improve outcomes in these patients, we therefore need to look beyond anticoagulation alone or beyond a type of anticoagulation drug per se. Indeed, a one-size-fits-all approach may not be appropriate.”
The study was funded by an unrestricted grant from Bayer. Dr. Karthikeyan and Dr. Poppas reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Contrary to expectations, vitamin K antagonists (VKAs) reduced the risk for ischemic stroke and death, compared with the factor Xa inhibitor rivaroxaban, (Xarelto, Janssen) in patients with rheumatic heart disease and atrial fibrillation (AFib), in the INVICTUS trial.
Patients receiving a VKA, typically warfarin, had a 25% lower risk for the primary outcome – a composite of stroke, systemic embolism, myocardial infarction, or death from vascular or unknown causes outcome – than receiving rivaroxaban (hazard ratio, 1.25; 95% confidence interval, 1.10-1.41).
This difference was driven primarily by a significant reduction in the risk for death in the VKA group, and without a significant increase in major bleeding, reported Ganesan Karthikeyan, MD, from the All India Institute of Medical Sciences in New Delhi.
“VKA should remain the standard of care for patients with rheumatic heart disease and atrial fibrillation,” he concluded in a hotline session at the annual congress of the European Society of Cardiology.
The study, simultaneously published in the New England Journal of Medicine, is the first randomized controlled trial to assess anticoagulant therapy in patients with rheumatic heart disease and AFib.
“Who could have possibly guessed these results? Certainly not me,” said invited discussant Renato D. Lopes, MD, MHS, PhD, Duke Clinical Research Institute, Durham, N.C. “To me, this is one more classical example of why we need to do randomized trials, since they are the only reliable way to determine treatment effects and drive clinical practice.”
Evidence gap
Rheumatic heart disease affects over 40 million people, mainly living in low- and low- to middle-income countries. About 20% of symptomatic patients have AF and an elevated stroke risk, but previous AFib trials excluded these patients, Dr. Karthikeyan noted.
INVICTUS was led by the Population Health Research Institute in Hamilton, Ont., and enrolled 4,565 patients from 24 countries in Africa, Asia, and Latin America who had rheumatic heart disease, AFib or atrial flutter, and an increased stroke risk caused by any of the following: CHA2DS2VASc score of 2 or more, moderate to severe mitral stenosis (valve area ≤ 2.0 cm2), left atrial spontaneous echo contrast, or left atrial thrombus.
Participants were randomly assigned to receive rivaroxaban, 20 mg once daily (15 mg/d if creatinine clearance was 15-49 mL/min), or a VKA titrated to an international normalized ratio (INR) of 2.0-3.0.
Warfarin was used in 79%-85% of patients assigned to VKA, with the percentage varying between visits. The INR was in therapeutic range in 33.2% of patients at baseline, 65.1% at 3 years, and 64.1% at 4 years.
During an average follow-up of 3.1 years, the primary outcome occurred in 446 patients in the VKA group (6.49% per year) and 560 patients in the rivaroxaban group (8.21% per year). The restricted mean survival time for the primary outcome was 1,675 vs. 1,599 days, respectively (difference, –76 days; 95% CI, –121 to –31 days; P for superiority < .001).
The rate of stroke or systemic embolism was similar between the VKA and rivaroxaban groups (75 vs. 94 events), although ischemic strokes were significantly lower with VKA (48 vs. 74 events).
No easy explanation
Deaths were significantly lower with VKA than rivaroxaban, at 442 versus 552 (restricted mean survival time for death, 1,608 vs. 1,587 days; difference, −72 days; 95% CI, –117 to –28 days).
“This reduction is not easily explained,” Dr. Karthikeyan acknowledged. “We cannot explain this reduction by the reduction in stroke that we saw because the number of deaths that are prevented by VKA are far larger than the number of strokes that are prevented. Moreover, the number of deaths were mainly heart failure or sudden deaths.”
Numbers of patients with major bleeding were also similar in the VKA and rivaroxaban groups (56 vs. 40 patients; P = .18), although numbers with fatal bleeding were lower with rivaroxaban (15 vs. 4, respectively).
By design, there were more physician interactions for monthly monitoring of INR in the VKA group, “but we do not believe such a large reduction can be explained entirely by increased health care contact,” he said. Moreover, there was no significant between-group difference in heart failure medications or hospitalizations or the need for valve replacement.
Almost a quarter (23%) of patients in the rivaroxaban group permanently discontinued the study drug versus just 6% in the VKA group.
Importantly, the mortality benefit emerged much later than in other trials and coincided with the time when the INR became therapeutic at about 3 years, Dr. Karthikeyan said. But it is unknown whether this is because of the INR or an unrelated effect.
More physician contact
Following the presentation, session cochair C. Michael Gibson, MD, Baim Institute for Clinical Research, Harvard Medical School, Boston, questioned the 23% discontinuation rate for rivaroxaban. “Is this really a superiority of warfarin or is this superiority of having someone come in and see their physician for a lot of checks on their INR?”
In response, Dr. Karthikeyan said that permanent discontinuation rates were about 20%-25% in shorter-duration direct oral anticoagulant trials, such as RELY, ROCKET-AF, and ARISTOLE, and exceeded 30% in ENGAGE-AF with 2.8 years’ follow-up.
“So, this is not new,” he said, adding that 31.4% of rivaroxaban patients did so for valve replacement surgery and subsequently received nonstudy VKA.
Dr. Lopes said it is important to keep in mind that INVICTUS enrolled a “very different population” that was younger (mean age, 50.5 years), was much more often female (72.3%), and had fewer comorbidities than patients with AFib who did not have rheumatic heart disease in the pivotal trials.
“It will be interesting to see the treatment effect according to mitral stenosis severity, since we had about 30% with mild mitral stenosis and additionally 18% of patients without mitral stenosis,” he added.
Co–principal investigator Stuart J. Connolly, MD, from the Population Health Research Institute, said physician contacts may be a factor but that the mortality difference was clear, highly significant, and sufficiently powered.
“What’s amazing is that what we’re seeing here is something that hasn’t been previously described with VKA or warfarin, which is that it reduces mortality,” he said in an interview.
Rivaroxaban has never been shown to reduce mortality in any particular condition, and a meta-analysis of other novel oral anticoagulants shows only a small reduction in mortality, caused almost completely by less intracranial hemorrhage than warfarin, he added. “So, we don’t think this is a problem with rivaroxaban. In some ways, rivaroxaban is an innocent bystander to a trial of warfarin in patients with rheumatic heart disease and atrial fibrillation.”
Dr. Connolly said more work is needed to explain the findings and analyses are planned to see which patients are at highest risk for death as well as looking at the relationship between INR control and outcomes.
“We need to do more research on what it is about VKA that could explain this,” he said. “Is it affecting the myocardium in some way, is it preventing fibrosis, is there some off target effect, not on the anticoagulation system, that could explain this?”
Athena Poppas, MD, chief of cardiology at Brown University, Providence, R.I., and past president of the American College of Cardiology, said “INVICTUS is an incredibly important study that needed to be done.”
“The results – though disappointing and surprising in some ways – I don’t think we can explain them away and change what we are doing right now,” she said in an interview.
Although warfarin is a cheap drug, Dr. Poppas said, it would be tremendously helpful to have an alternative treatment for these patients. Mechanistic studies are needed to understand the observed mortality advantage and low bleeding rates but that trials of other novel anticoagulants are also needed.
“But I’m not sure that will happen,” she added. “It’s unlikely to be industry sponsored, so it would be a very expensive lift with a low likelihood of success.”
In an editorial accompanying the paper, Gregory Y.H. Lip, MD, University of Liverpool (England), pointed out that observational data show similar or even higher risks for major bleeding with rivaroxaban than with warfarin. “To improve outcomes in these patients, we therefore need to look beyond anticoagulation alone or beyond a type of anticoagulation drug per se. Indeed, a one-size-fits-all approach may not be appropriate.”
The study was funded by an unrestricted grant from Bayer. Dr. Karthikeyan and Dr. Poppas reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Contrary to expectations, vitamin K antagonists (VKAs) reduced the risk for ischemic stroke and death, compared with the factor Xa inhibitor rivaroxaban, (Xarelto, Janssen) in patients with rheumatic heart disease and atrial fibrillation (AFib), in the INVICTUS trial.
Patients receiving a VKA, typically warfarin, had a 25% lower risk for the primary outcome – a composite of stroke, systemic embolism, myocardial infarction, or death from vascular or unknown causes outcome – than receiving rivaroxaban (hazard ratio, 1.25; 95% confidence interval, 1.10-1.41).
This difference was driven primarily by a significant reduction in the risk for death in the VKA group, and without a significant increase in major bleeding, reported Ganesan Karthikeyan, MD, from the All India Institute of Medical Sciences in New Delhi.
“VKA should remain the standard of care for patients with rheumatic heart disease and atrial fibrillation,” he concluded in a hotline session at the annual congress of the European Society of Cardiology.
The study, simultaneously published in the New England Journal of Medicine, is the first randomized controlled trial to assess anticoagulant therapy in patients with rheumatic heart disease and AFib.
“Who could have possibly guessed these results? Certainly not me,” said invited discussant Renato D. Lopes, MD, MHS, PhD, Duke Clinical Research Institute, Durham, N.C. “To me, this is one more classical example of why we need to do randomized trials, since they are the only reliable way to determine treatment effects and drive clinical practice.”
Evidence gap
Rheumatic heart disease affects over 40 million people, mainly living in low- and low- to middle-income countries. About 20% of symptomatic patients have AF and an elevated stroke risk, but previous AFib trials excluded these patients, Dr. Karthikeyan noted.
INVICTUS was led by the Population Health Research Institute in Hamilton, Ont., and enrolled 4,565 patients from 24 countries in Africa, Asia, and Latin America who had rheumatic heart disease, AFib or atrial flutter, and an increased stroke risk caused by any of the following: CHA2DS2VASc score of 2 or more, moderate to severe mitral stenosis (valve area ≤ 2.0 cm2), left atrial spontaneous echo contrast, or left atrial thrombus.
Participants were randomly assigned to receive rivaroxaban, 20 mg once daily (15 mg/d if creatinine clearance was 15-49 mL/min), or a VKA titrated to an international normalized ratio (INR) of 2.0-3.0.
Warfarin was used in 79%-85% of patients assigned to VKA, with the percentage varying between visits. The INR was in therapeutic range in 33.2% of patients at baseline, 65.1% at 3 years, and 64.1% at 4 years.
During an average follow-up of 3.1 years, the primary outcome occurred in 446 patients in the VKA group (6.49% per year) and 560 patients in the rivaroxaban group (8.21% per year). The restricted mean survival time for the primary outcome was 1,675 vs. 1,599 days, respectively (difference, –76 days; 95% CI, –121 to –31 days; P for superiority < .001).
The rate of stroke or systemic embolism was similar between the VKA and rivaroxaban groups (75 vs. 94 events), although ischemic strokes were significantly lower with VKA (48 vs. 74 events).
No easy explanation
Deaths were significantly lower with VKA than rivaroxaban, at 442 versus 552 (restricted mean survival time for death, 1,608 vs. 1,587 days; difference, −72 days; 95% CI, –117 to –28 days).
“This reduction is not easily explained,” Dr. Karthikeyan acknowledged. “We cannot explain this reduction by the reduction in stroke that we saw because the number of deaths that are prevented by VKA are far larger than the number of strokes that are prevented. Moreover, the number of deaths were mainly heart failure or sudden deaths.”
Numbers of patients with major bleeding were also similar in the VKA and rivaroxaban groups (56 vs. 40 patients; P = .18), although numbers with fatal bleeding were lower with rivaroxaban (15 vs. 4, respectively).
By design, there were more physician interactions for monthly monitoring of INR in the VKA group, “but we do not believe such a large reduction can be explained entirely by increased health care contact,” he said. Moreover, there was no significant between-group difference in heart failure medications or hospitalizations or the need for valve replacement.
Almost a quarter (23%) of patients in the rivaroxaban group permanently discontinued the study drug versus just 6% in the VKA group.
Importantly, the mortality benefit emerged much later than in other trials and coincided with the time when the INR became therapeutic at about 3 years, Dr. Karthikeyan said. But it is unknown whether this is because of the INR or an unrelated effect.
More physician contact
Following the presentation, session cochair C. Michael Gibson, MD, Baim Institute for Clinical Research, Harvard Medical School, Boston, questioned the 23% discontinuation rate for rivaroxaban. “Is this really a superiority of warfarin or is this superiority of having someone come in and see their physician for a lot of checks on their INR?”
In response, Dr. Karthikeyan said that permanent discontinuation rates were about 20%-25% in shorter-duration direct oral anticoagulant trials, such as RELY, ROCKET-AF, and ARISTOLE, and exceeded 30% in ENGAGE-AF with 2.8 years’ follow-up.
“So, this is not new,” he said, adding that 31.4% of rivaroxaban patients did so for valve replacement surgery and subsequently received nonstudy VKA.
Dr. Lopes said it is important to keep in mind that INVICTUS enrolled a “very different population” that was younger (mean age, 50.5 years), was much more often female (72.3%), and had fewer comorbidities than patients with AFib who did not have rheumatic heart disease in the pivotal trials.
“It will be interesting to see the treatment effect according to mitral stenosis severity, since we had about 30% with mild mitral stenosis and additionally 18% of patients without mitral stenosis,” he added.
Co–principal investigator Stuart J. Connolly, MD, from the Population Health Research Institute, said physician contacts may be a factor but that the mortality difference was clear, highly significant, and sufficiently powered.
“What’s amazing is that what we’re seeing here is something that hasn’t been previously described with VKA or warfarin, which is that it reduces mortality,” he said in an interview.
Rivaroxaban has never been shown to reduce mortality in any particular condition, and a meta-analysis of other novel oral anticoagulants shows only a small reduction in mortality, caused almost completely by less intracranial hemorrhage than warfarin, he added. “So, we don’t think this is a problem with rivaroxaban. In some ways, rivaroxaban is an innocent bystander to a trial of warfarin in patients with rheumatic heart disease and atrial fibrillation.”
Dr. Connolly said more work is needed to explain the findings and analyses are planned to see which patients are at highest risk for death as well as looking at the relationship between INR control and outcomes.
“We need to do more research on what it is about VKA that could explain this,” he said. “Is it affecting the myocardium in some way, is it preventing fibrosis, is there some off target effect, not on the anticoagulation system, that could explain this?”
Athena Poppas, MD, chief of cardiology at Brown University, Providence, R.I., and past president of the American College of Cardiology, said “INVICTUS is an incredibly important study that needed to be done.”
“The results – though disappointing and surprising in some ways – I don’t think we can explain them away and change what we are doing right now,” she said in an interview.
Although warfarin is a cheap drug, Dr. Poppas said, it would be tremendously helpful to have an alternative treatment for these patients. Mechanistic studies are needed to understand the observed mortality advantage and low bleeding rates but that trials of other novel anticoagulants are also needed.
“But I’m not sure that will happen,” she added. “It’s unlikely to be industry sponsored, so it would be a very expensive lift with a low likelihood of success.”
In an editorial accompanying the paper, Gregory Y.H. Lip, MD, University of Liverpool (England), pointed out that observational data show similar or even higher risks for major bleeding with rivaroxaban than with warfarin. “To improve outcomes in these patients, we therefore need to look beyond anticoagulation alone or beyond a type of anticoagulation drug per se. Indeed, a one-size-fits-all approach may not be appropriate.”
The study was funded by an unrestricted grant from Bayer. Dr. Karthikeyan and Dr. Poppas reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2022
COVID-19 vaccine safe in patients with heart failure
Patients with heart failure (HF) who received two doses of COVID mRNA vaccines were not more likely to have worsening disease, venous thromboembolism, or myocarditis within 90 days than similar unvaccinated patients, in a case-control study in Denmark.
Moreover, in the 90 days after receiving the second shot, vaccinated patients were less likely to die of any cause, compared with unvaccinated patients during a similar 90-day period.
Caroline Sindet-Pedersen, PhD, Herlev and Gentofte Hospital, Hellerup, Denmark, and colleagues presented these findings at the annual congress of the European Society of Cardiology.
Major risk is not receiving vaccine
These results “confirm that the major risk for patients with HF is not receiving vaccination for COVID-19,” Marco Metra, MD, who was not involved with this research, said in an interview.

Dr. Metra was coauthor of an ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic, published online ahead of print November 2021 in the European Heart Journal.
The guidance explains that patients with HF are at increased risk for hospitalization, need for mechanical ventilation, and death because of COVID-19, and that vaccination reduces the risk for serious illness from COVID-19, Dr. Sindet-Pedersen and colleagues explained in a press release from the ESC.
However, “concerns remain,” they added, “about the safety of the SARS-CoV-2 mRNA vaccines in heart failure patients, due to a perceived increased risk of cardiovascular side effects.”
The study findings suggest that “there should be no concern about cardiovascular side effects from mRNA vaccines in heart failure patients,” Dr. Sindet-Pedersen and colleagues summarized.
The results also “point to a beneficial effect of vaccination on mortality” and “indicate that patients with HF should be prioritized for COVID-19 vaccinations and boosters,” they added.
“There are ongoing concerns about the safety of COVID-19 vaccination in fragile patients and patients with heart failure,” said Dr. Metra, professor of cardiology and director of the Institute of Cardiology of the Civil Hospital and University of Brescia (Italy).
“These concerns are not based on evidence but just on reports of rare side effects (namely, myocarditis and pericarditis) in vaccinated people,” he added.
Dr. Metra also coauthored a position paper on COVID-19 vaccination in patients with HF from the Heart Failure Association of the ESC, which was published online October 2021 in the European Journal of Heart Failure.
“The current study,” he summarized, “shows a lower risk of mortality among patients vaccinated, compared with those not vaccinated.
“It has limitations,” he cautioned, “as it is not a prospective randomized study, but [rather] an observational one with comparison between vaccinated and not vaccinated patients with similar characteristics.
“However, it was done in a large population,” he noted, “and its results confirm that the major risk for patients with HF is not receiving vaccination for COVID-19.”
95% of patients with HF in Denmark double vaccinated
The group did not analyze the types of all-cause death in their study, Dr. Sindet-Pedersen clarified in an interview.
Other studies have shown that vaccines are associated with improved survival, she noted. For example, bacillus Calmette-Guérin vaccines and the measles vaccines have been linked with a decreased risk for nonspecific mortality in children, and influenza vaccines are associated with decreased all-cause mortality in patients with HF.
The rates of vaccination in this study were much higher than those for patients with HF in the United States.
In a study of 7,094 patients with HF seen at the Mount Sinai Health System between January 2021 and January 2022, 31% of patients were fully vaccinated with two doses and 14.8% had also received a booster, as per Centers for Disease Control and Prevention guidance. However, another 9.1% of patients were only partially vaccinated with one dose, and 45% remained unvaccinated by January 2022,
In the current study, “the uptake was very high,” Dr. Sindet-Pedersen noted, that is, “95% of the prevalent heart failure patients in 2021 received a vaccine.”
“It might be that the last 5% of the patients that did not receive a vaccine were too ill [terminal] to receive the vaccine,” she speculated, “or that was due to personal reasons.”
The researchers identified 50,893 patients with HF who were double vaccinated in 2021 and they matched them with 50,893 unvaccinated patients with HF in 2019 (prepandemic), with the same age, sex, HF duration, use of HF medications, ischemic heart disease, cancer, diabetes, atrial fibrillation, and admission with HF within 90 days.
Almost all patients in the vaccinated group received the Pfizer/BioNTech mRNA vaccine (92%) and the rest received the Moderna mRNA vaccine (8%), in 2021.
The patients had a mean age of 74, and 64% were men. They had HF for a median of 4.1 years.
During the 90-day follow-up, 1,311 patients in the unvaccinated cohort (2.56%) and 1,113 patients in the vaccinated cohort (2.23%) died; there was a significantly lower risk for all-cause death in the vaccinated cohort versus the unvaccinated cohort (–0.33 percentage points; 95% CI, –0.52 to –0.15 percentage points).
The risk for worsening heart failure was 1.1% in each group; myocarditis and venous thromboembolism were extremely rare, and risks for these conditions were not significantly different in the two groups.
The researchers and Dr. Metra declared they have no relevant financial disclosures. Dr. Metra is editor-in-chief of the European Journal of Heart Failure and senior consulting editor of the European Heart Journal.
A version of this article first appeared on Medscape.com.
Patients with heart failure (HF) who received two doses of COVID mRNA vaccines were not more likely to have worsening disease, venous thromboembolism, or myocarditis within 90 days than similar unvaccinated patients, in a case-control study in Denmark.
Moreover, in the 90 days after receiving the second shot, vaccinated patients were less likely to die of any cause, compared with unvaccinated patients during a similar 90-day period.
Caroline Sindet-Pedersen, PhD, Herlev and Gentofte Hospital, Hellerup, Denmark, and colleagues presented these findings at the annual congress of the European Society of Cardiology.
Major risk is not receiving vaccine
These results “confirm that the major risk for patients with HF is not receiving vaccination for COVID-19,” Marco Metra, MD, who was not involved with this research, said in an interview.
Dr. Metra was coauthor of an ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic, published online ahead of print November 2021 in the European Heart Journal.
The guidance explains that patients with HF are at increased risk for hospitalization, need for mechanical ventilation, and death because of COVID-19, and that vaccination reduces the risk for serious illness from COVID-19, Dr. Sindet-Pedersen and colleagues explained in a press release from the ESC.
However, “concerns remain,” they added, “about the safety of the SARS-CoV-2 mRNA vaccines in heart failure patients, due to a perceived increased risk of cardiovascular side effects.”
The study findings suggest that “there should be no concern about cardiovascular side effects from mRNA vaccines in heart failure patients,” Dr. Sindet-Pedersen and colleagues summarized.
The results also “point to a beneficial effect of vaccination on mortality” and “indicate that patients with HF should be prioritized for COVID-19 vaccinations and boosters,” they added.
“There are ongoing concerns about the safety of COVID-19 vaccination in fragile patients and patients with heart failure,” said Dr. Metra, professor of cardiology and director of the Institute of Cardiology of the Civil Hospital and University of Brescia (Italy).
“These concerns are not based on evidence but just on reports of rare side effects (namely, myocarditis and pericarditis) in vaccinated people,” he added.
Dr. Metra also coauthored a position paper on COVID-19 vaccination in patients with HF from the Heart Failure Association of the ESC, which was published online October 2021 in the European Journal of Heart Failure.
“The current study,” he summarized, “shows a lower risk of mortality among patients vaccinated, compared with those not vaccinated.
“It has limitations,” he cautioned, “as it is not a prospective randomized study, but [rather] an observational one with comparison between vaccinated and not vaccinated patients with similar characteristics.
“However, it was done in a large population,” he noted, “and its results confirm that the major risk for patients with HF is not receiving vaccination for COVID-19.”
95% of patients with HF in Denmark double vaccinated
The group did not analyze the types of all-cause death in their study, Dr. Sindet-Pedersen clarified in an interview.
Other studies have shown that vaccines are associated with improved survival, she noted. For example, bacillus Calmette-Guérin vaccines and the measles vaccines have been linked with a decreased risk for nonspecific mortality in children, and influenza vaccines are associated with decreased all-cause mortality in patients with HF.
The rates of vaccination in this study were much higher than those for patients with HF in the United States.
In a study of 7,094 patients with HF seen at the Mount Sinai Health System between January 2021 and January 2022, 31% of patients were fully vaccinated with two doses and 14.8% had also received a booster, as per Centers for Disease Control and Prevention guidance. However, another 9.1% of patients were only partially vaccinated with one dose, and 45% remained unvaccinated by January 2022,
In the current study, “the uptake was very high,” Dr. Sindet-Pedersen noted, that is, “95% of the prevalent heart failure patients in 2021 received a vaccine.”
“It might be that the last 5% of the patients that did not receive a vaccine were too ill [terminal] to receive the vaccine,” she speculated, “or that was due to personal reasons.”
The researchers identified 50,893 patients with HF who were double vaccinated in 2021 and they matched them with 50,893 unvaccinated patients with HF in 2019 (prepandemic), with the same age, sex, HF duration, use of HF medications, ischemic heart disease, cancer, diabetes, atrial fibrillation, and admission with HF within 90 days.
Almost all patients in the vaccinated group received the Pfizer/BioNTech mRNA vaccine (92%) and the rest received the Moderna mRNA vaccine (8%), in 2021.
The patients had a mean age of 74, and 64% were men. They had HF for a median of 4.1 years.
During the 90-day follow-up, 1,311 patients in the unvaccinated cohort (2.56%) and 1,113 patients in the vaccinated cohort (2.23%) died; there was a significantly lower risk for all-cause death in the vaccinated cohort versus the unvaccinated cohort (–0.33 percentage points; 95% CI, –0.52 to –0.15 percentage points).
The risk for worsening heart failure was 1.1% in each group; myocarditis and venous thromboembolism were extremely rare, and risks for these conditions were not significantly different in the two groups.
The researchers and Dr. Metra declared they have no relevant financial disclosures. Dr. Metra is editor-in-chief of the European Journal of Heart Failure and senior consulting editor of the European Heart Journal.
A version of this article first appeared on Medscape.com.
Patients with heart failure (HF) who received two doses of COVID mRNA vaccines were not more likely to have worsening disease, venous thromboembolism, or myocarditis within 90 days than similar unvaccinated patients, in a case-control study in Denmark.
Moreover, in the 90 days after receiving the second shot, vaccinated patients were less likely to die of any cause, compared with unvaccinated patients during a similar 90-day period.
Caroline Sindet-Pedersen, PhD, Herlev and Gentofte Hospital, Hellerup, Denmark, and colleagues presented these findings at the annual congress of the European Society of Cardiology.
Major risk is not receiving vaccine
These results “confirm that the major risk for patients with HF is not receiving vaccination for COVID-19,” Marco Metra, MD, who was not involved with this research, said in an interview.
Dr. Metra was coauthor of an ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic, published online ahead of print November 2021 in the European Heart Journal.
The guidance explains that patients with HF are at increased risk for hospitalization, need for mechanical ventilation, and death because of COVID-19, and that vaccination reduces the risk for serious illness from COVID-19, Dr. Sindet-Pedersen and colleagues explained in a press release from the ESC.
However, “concerns remain,” they added, “about the safety of the SARS-CoV-2 mRNA vaccines in heart failure patients, due to a perceived increased risk of cardiovascular side effects.”
The study findings suggest that “there should be no concern about cardiovascular side effects from mRNA vaccines in heart failure patients,” Dr. Sindet-Pedersen and colleagues summarized.
The results also “point to a beneficial effect of vaccination on mortality” and “indicate that patients with HF should be prioritized for COVID-19 vaccinations and boosters,” they added.
“There are ongoing concerns about the safety of COVID-19 vaccination in fragile patients and patients with heart failure,” said Dr. Metra, professor of cardiology and director of the Institute of Cardiology of the Civil Hospital and University of Brescia (Italy).
“These concerns are not based on evidence but just on reports of rare side effects (namely, myocarditis and pericarditis) in vaccinated people,” he added.
Dr. Metra also coauthored a position paper on COVID-19 vaccination in patients with HF from the Heart Failure Association of the ESC, which was published online October 2021 in the European Journal of Heart Failure.
“The current study,” he summarized, “shows a lower risk of mortality among patients vaccinated, compared with those not vaccinated.
“It has limitations,” he cautioned, “as it is not a prospective randomized study, but [rather] an observational one with comparison between vaccinated and not vaccinated patients with similar characteristics.
“However, it was done in a large population,” he noted, “and its results confirm that the major risk for patients with HF is not receiving vaccination for COVID-19.”
95% of patients with HF in Denmark double vaccinated
The group did not analyze the types of all-cause death in their study, Dr. Sindet-Pedersen clarified in an interview.
Other studies have shown that vaccines are associated with improved survival, she noted. For example, bacillus Calmette-Guérin vaccines and the measles vaccines have been linked with a decreased risk for nonspecific mortality in children, and influenza vaccines are associated with decreased all-cause mortality in patients with HF.
The rates of vaccination in this study were much higher than those for patients with HF in the United States.
In a study of 7,094 patients with HF seen at the Mount Sinai Health System between January 2021 and January 2022, 31% of patients were fully vaccinated with two doses and 14.8% had also received a booster, as per Centers for Disease Control and Prevention guidance. However, another 9.1% of patients were only partially vaccinated with one dose, and 45% remained unvaccinated by January 2022,
In the current study, “the uptake was very high,” Dr. Sindet-Pedersen noted, that is, “95% of the prevalent heart failure patients in 2021 received a vaccine.”
“It might be that the last 5% of the patients that did not receive a vaccine were too ill [terminal] to receive the vaccine,” she speculated, “or that was due to personal reasons.”
The researchers identified 50,893 patients with HF who were double vaccinated in 2021 and they matched them with 50,893 unvaccinated patients with HF in 2019 (prepandemic), with the same age, sex, HF duration, use of HF medications, ischemic heart disease, cancer, diabetes, atrial fibrillation, and admission with HF within 90 days.
Almost all patients in the vaccinated group received the Pfizer/BioNTech mRNA vaccine (92%) and the rest received the Moderna mRNA vaccine (8%), in 2021.
The patients had a mean age of 74, and 64% were men. They had HF for a median of 4.1 years.
During the 90-day follow-up, 1,311 patients in the unvaccinated cohort (2.56%) and 1,113 patients in the vaccinated cohort (2.23%) died; there was a significantly lower risk for all-cause death in the vaccinated cohort versus the unvaccinated cohort (–0.33 percentage points; 95% CI, –0.52 to –0.15 percentage points).
The risk for worsening heart failure was 1.1% in each group; myocarditis and venous thromboembolism were extremely rare, and risks for these conditions were not significantly different in the two groups.
The researchers and Dr. Metra declared they have no relevant financial disclosures. Dr. Metra is editor-in-chief of the European Journal of Heart Failure and senior consulting editor of the European Heart Journal.
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2022
Artificial intelligence poised to change paradigm of CV risk prevention
Causal-based algorithm personalizes strategies
Typically, artificial intelligence (AI) is applied to analyze a complex set of variables to make correlations not readily made by unassisted observation. But an AI offshoot, sometimes referred to as causal AI, incorporates causation not just association, and it appears capable of changing the paradigm for preventing cardiovascular (CV) events.
“Causal AI is a new generation of AI algorithms that empowers AI to move beyond prediction to help guide clinical decision-making for each individual,” reported Brian A. Ference, MD, director of research in translational therapeutics, University of Cambridge (England).

In a novel study testing this premise, called CAUSAL AI, this approach was explored with two major risk factors, elevated LDL cholesterol (LDL-C) and elevated systolic BP (SBP). Based on a deep learning algorithm that studied the impact of these risk factors on the biology of atherosclerosis, causal effects of these risk factors were assessed and then embedded in risk estimation.
Causal AI can predict treatment effect
The study showed that the accuracy of risk prediction can be improved markedly with causal AI, but, more importantly, it suggests that causal AI can predict the impact of specific actions to reduce this risk in the context of the patient’s trajectory toward CV events.
“Risk-estimating algorithms are used to select patients at high risk who may benefit from interventions to reduce risk, but they do not include the causal effects of changes in LDL-C and SBP,” Dr. Ference explained.
As a result, they “may not accurately estimate the baseline risk of cardiovascular events caused by a person’s LDL-C or SBP level or the benefit of treating these risk factors,” he added.
In the CAUSAL AI study, presented at the annual congress of the European Society of Cardiology, risk prediction embedded with causal AI demonstrated the ability to match predicted events with actual events in several large sets of patient data.
“Embedding causal effects into risk-estimating algorithms accurately estimates baseline cardiovascular risk caused by LDL and SBP and the benefit of lowering LDL, SBP, or both beginning at any age and extending for any duration,” Dr. Ference said.
Deep-learning AI evaluated more than 300 gene variants
The deep-learning AI was based on Mendelian randomization studies evaluating 140 gene variants associated with LDL-C and 202 variants associated with SBP.
In one test of the predictive impact of causal AI, risk prediction was first conducted in 445,771 participants in the UK Biobank with the Joint British Societies (JBS3) risk calculator. Relative to actual events in this population, the JBS3 alone “consistently underestimated the increased risk caused by elevated LDL, blood pressure, or both” over the lifetime of the patient, according to Dr. Ference.
It also systematically overestimated the risk of cardiovascular events among participants with lower LDL-C, blood pressure, or both.
However, after embedding the causal effect of LDL and blood pressure, “the same algorithm was able to precisely predict the risk of cardiovascular events,” Dr. Ference said. The improved accuracy resulted in “nearly superimposable observed and predicted event curves over time.”
Embedded causal effects precisely predicts outcomes
Causal AI, embedded into risk analyses, was also able to correct for inaccurate risk benefit derived from short-term clinical trials. These also “systematically underestimate the benefit of lowering LDL, blood pressure, or both,” according to Dr. Ference.
“By contrast, after embedding causal effects of LDL and blood pressure into the algorithm, the same algorithm precisely predicted the benefit of lowering LDL, blood pressure, or both at every age, once again producing superimposable observed and predicted event curves.
In another evaluation conducted by Dr. Ference and coinvestigators, the JBS3 algorithm was applied to several major trials, such as the Heart Protection Trial and HOPE-3. By itself, the JBS3 algorithm predicted less benefit than actually observed.
“After embedding causal effects of LDL and blood pressure, the same algorithm was able to precisely predict the benefit of lowering LDL, blood pressure, or both observed in the trials after 3-5 years,” Dr. Ference reported.
In a sensitivity analysis, the accuracy of the prediction remained largely similar across stratifications by risk factors, such as male sex, presence of diabetes, family history of cardiovascular disease, and other variables. It was also similar across participant age prior to a cardiovascular event and all durations of follow-up.
The data presented by Dr. Ference provides compelling evidence that JBS3, which is widely used in the United Kingdom for risk estimates, does not accurately estimate the risk of cardiovascular disease caused by elevated LDL or SBP. It also fails to estimate the benefit of treating these risk factors.
“Therefore, they cannot be used to determine the optimal timing, intensity, and duration of therapies to prevent cardiovascular events,” Dr. Ference said.
By embedding the causal effects of LDL-C and blood pressure through an AI-based algorithm, the benefit of treatment can be estimated accurately “beginning at any age and lasting for any duration, thus providing the essential information to inform individual treatment decisions about ultimate timing, intensity, and duration,” according to Dr. Ference.
Routine application awaits further steps
Despite the promise of this concept, there are many steps to be taken before it is introduced into the clinic, asserted designated discussant Folkert Asselbergs, MD, PhD. In addition to testing the accuracy in multiple populations, “we have to do the trials as well,” meaning prospective evaluations to validate the concept is meaningful for improving outcomes.
However, he does not doubt that the concept of causal AI is promising and likely to have a meaningful impact on cardiology after further validation.
“Causal AI is a crucial step that we need to take for more efficient health care,” he said. One reason he expressed caution is that several risk scores enhanced by AI, although not necessarily causal AI, have shown only “modest predictive value” in several studies that he cited.
“Hopefully the data presented from the CAUSAL AI study will really help us take a step up in the discussion to see how we can really benefit by including genetic information in an AI framework to include causality in predicting risk and predicting benefit of treatment,” said Dr. Asselbergs, professor of precision medicine, University of Utrecht (the Netherlands) Medical Center.
Dr. Ference reported financial relationships with more than 15 pharmaceutical companies. Dr. Asselbergs reported no potential conflicts of interest.
Causal-based algorithm personalizes strategies
Causal-based algorithm personalizes strategies
Typically, artificial intelligence (AI) is applied to analyze a complex set of variables to make correlations not readily made by unassisted observation. But an AI offshoot, sometimes referred to as causal AI, incorporates causation not just association, and it appears capable of changing the paradigm for preventing cardiovascular (CV) events.
“Causal AI is a new generation of AI algorithms that empowers AI to move beyond prediction to help guide clinical decision-making for each individual,” reported Brian A. Ference, MD, director of research in translational therapeutics, University of Cambridge (England).
In a novel study testing this premise, called CAUSAL AI, this approach was explored with two major risk factors, elevated LDL cholesterol (LDL-C) and elevated systolic BP (SBP). Based on a deep learning algorithm that studied the impact of these risk factors on the biology of atherosclerosis, causal effects of these risk factors were assessed and then embedded in risk estimation.
Causal AI can predict treatment effect
The study showed that the accuracy of risk prediction can be improved markedly with causal AI, but, more importantly, it suggests that causal AI can predict the impact of specific actions to reduce this risk in the context of the patient’s trajectory toward CV events.
“Risk-estimating algorithms are used to select patients at high risk who may benefit from interventions to reduce risk, but they do not include the causal effects of changes in LDL-C and SBP,” Dr. Ference explained.
As a result, they “may not accurately estimate the baseline risk of cardiovascular events caused by a person’s LDL-C or SBP level or the benefit of treating these risk factors,” he added.
In the CAUSAL AI study, presented at the annual congress of the European Society of Cardiology, risk prediction embedded with causal AI demonstrated the ability to match predicted events with actual events in several large sets of patient data.
“Embedding causal effects into risk-estimating algorithms accurately estimates baseline cardiovascular risk caused by LDL and SBP and the benefit of lowering LDL, SBP, or both beginning at any age and extending for any duration,” Dr. Ference said.
Deep-learning AI evaluated more than 300 gene variants
The deep-learning AI was based on Mendelian randomization studies evaluating 140 gene variants associated with LDL-C and 202 variants associated with SBP.
In one test of the predictive impact of causal AI, risk prediction was first conducted in 445,771 participants in the UK Biobank with the Joint British Societies (JBS3) risk calculator. Relative to actual events in this population, the JBS3 alone “consistently underestimated the increased risk caused by elevated LDL, blood pressure, or both” over the lifetime of the patient, according to Dr. Ference.
It also systematically overestimated the risk of cardiovascular events among participants with lower LDL-C, blood pressure, or both.
However, after embedding the causal effect of LDL and blood pressure, “the same algorithm was able to precisely predict the risk of cardiovascular events,” Dr. Ference said. The improved accuracy resulted in “nearly superimposable observed and predicted event curves over time.”
Embedded causal effects precisely predicts outcomes
Causal AI, embedded into risk analyses, was also able to correct for inaccurate risk benefit derived from short-term clinical trials. These also “systematically underestimate the benefit of lowering LDL, blood pressure, or both,” according to Dr. Ference.
“By contrast, after embedding causal effects of LDL and blood pressure into the algorithm, the same algorithm precisely predicted the benefit of lowering LDL, blood pressure, or both at every age, once again producing superimposable observed and predicted event curves.
In another evaluation conducted by Dr. Ference and coinvestigators, the JBS3 algorithm was applied to several major trials, such as the Heart Protection Trial and HOPE-3. By itself, the JBS3 algorithm predicted less benefit than actually observed.
“After embedding causal effects of LDL and blood pressure, the same algorithm was able to precisely predict the benefit of lowering LDL, blood pressure, or both observed in the trials after 3-5 years,” Dr. Ference reported.
In a sensitivity analysis, the accuracy of the prediction remained largely similar across stratifications by risk factors, such as male sex, presence of diabetes, family history of cardiovascular disease, and other variables. It was also similar across participant age prior to a cardiovascular event and all durations of follow-up.
The data presented by Dr. Ference provides compelling evidence that JBS3, which is widely used in the United Kingdom for risk estimates, does not accurately estimate the risk of cardiovascular disease caused by elevated LDL or SBP. It also fails to estimate the benefit of treating these risk factors.
“Therefore, they cannot be used to determine the optimal timing, intensity, and duration of therapies to prevent cardiovascular events,” Dr. Ference said.
By embedding the causal effects of LDL-C and blood pressure through an AI-based algorithm, the benefit of treatment can be estimated accurately “beginning at any age and lasting for any duration, thus providing the essential information to inform individual treatment decisions about ultimate timing, intensity, and duration,” according to Dr. Ference.
Routine application awaits further steps
Despite the promise of this concept, there are many steps to be taken before it is introduced into the clinic, asserted designated discussant Folkert Asselbergs, MD, PhD. In addition to testing the accuracy in multiple populations, “we have to do the trials as well,” meaning prospective evaluations to validate the concept is meaningful for improving outcomes.
However, he does not doubt that the concept of causal AI is promising and likely to have a meaningful impact on cardiology after further validation.
“Causal AI is a crucial step that we need to take for more efficient health care,” he said. One reason he expressed caution is that several risk scores enhanced by AI, although not necessarily causal AI, have shown only “modest predictive value” in several studies that he cited.
“Hopefully the data presented from the CAUSAL AI study will really help us take a step up in the discussion to see how we can really benefit by including genetic information in an AI framework to include causality in predicting risk and predicting benefit of treatment,” said Dr. Asselbergs, professor of precision medicine, University of Utrecht (the Netherlands) Medical Center.
Dr. Ference reported financial relationships with more than 15 pharmaceutical companies. Dr. Asselbergs reported no potential conflicts of interest.
Typically, artificial intelligence (AI) is applied to analyze a complex set of variables to make correlations not readily made by unassisted observation. But an AI offshoot, sometimes referred to as causal AI, incorporates causation not just association, and it appears capable of changing the paradigm for preventing cardiovascular (CV) events.
“Causal AI is a new generation of AI algorithms that empowers AI to move beyond prediction to help guide clinical decision-making for each individual,” reported Brian A. Ference, MD, director of research in translational therapeutics, University of Cambridge (England).
In a novel study testing this premise, called CAUSAL AI, this approach was explored with two major risk factors, elevated LDL cholesterol (LDL-C) and elevated systolic BP (SBP). Based on a deep learning algorithm that studied the impact of these risk factors on the biology of atherosclerosis, causal effects of these risk factors were assessed and then embedded in risk estimation.
Causal AI can predict treatment effect
The study showed that the accuracy of risk prediction can be improved markedly with causal AI, but, more importantly, it suggests that causal AI can predict the impact of specific actions to reduce this risk in the context of the patient’s trajectory toward CV events.
“Risk-estimating algorithms are used to select patients at high risk who may benefit from interventions to reduce risk, but they do not include the causal effects of changes in LDL-C and SBP,” Dr. Ference explained.
As a result, they “may not accurately estimate the baseline risk of cardiovascular events caused by a person’s LDL-C or SBP level or the benefit of treating these risk factors,” he added.
In the CAUSAL AI study, presented at the annual congress of the European Society of Cardiology, risk prediction embedded with causal AI demonstrated the ability to match predicted events with actual events in several large sets of patient data.
“Embedding causal effects into risk-estimating algorithms accurately estimates baseline cardiovascular risk caused by LDL and SBP and the benefit of lowering LDL, SBP, or both beginning at any age and extending for any duration,” Dr. Ference said.
Deep-learning AI evaluated more than 300 gene variants
The deep-learning AI was based on Mendelian randomization studies evaluating 140 gene variants associated with LDL-C and 202 variants associated with SBP.
In one test of the predictive impact of causal AI, risk prediction was first conducted in 445,771 participants in the UK Biobank with the Joint British Societies (JBS3) risk calculator. Relative to actual events in this population, the JBS3 alone “consistently underestimated the increased risk caused by elevated LDL, blood pressure, or both” over the lifetime of the patient, according to Dr. Ference.
It also systematically overestimated the risk of cardiovascular events among participants with lower LDL-C, blood pressure, or both.
However, after embedding the causal effect of LDL and blood pressure, “the same algorithm was able to precisely predict the risk of cardiovascular events,” Dr. Ference said. The improved accuracy resulted in “nearly superimposable observed and predicted event curves over time.”
Embedded causal effects precisely predicts outcomes
Causal AI, embedded into risk analyses, was also able to correct for inaccurate risk benefit derived from short-term clinical trials. These also “systematically underestimate the benefit of lowering LDL, blood pressure, or both,” according to Dr. Ference.
“By contrast, after embedding causal effects of LDL and blood pressure into the algorithm, the same algorithm precisely predicted the benefit of lowering LDL, blood pressure, or both at every age, once again producing superimposable observed and predicted event curves.
In another evaluation conducted by Dr. Ference and coinvestigators, the JBS3 algorithm was applied to several major trials, such as the Heart Protection Trial and HOPE-3. By itself, the JBS3 algorithm predicted less benefit than actually observed.
“After embedding causal effects of LDL and blood pressure, the same algorithm was able to precisely predict the benefit of lowering LDL, blood pressure, or both observed in the trials after 3-5 years,” Dr. Ference reported.
In a sensitivity analysis, the accuracy of the prediction remained largely similar across stratifications by risk factors, such as male sex, presence of diabetes, family history of cardiovascular disease, and other variables. It was also similar across participant age prior to a cardiovascular event and all durations of follow-up.
The data presented by Dr. Ference provides compelling evidence that JBS3, which is widely used in the United Kingdom for risk estimates, does not accurately estimate the risk of cardiovascular disease caused by elevated LDL or SBP. It also fails to estimate the benefit of treating these risk factors.
“Therefore, they cannot be used to determine the optimal timing, intensity, and duration of therapies to prevent cardiovascular events,” Dr. Ference said.
By embedding the causal effects of LDL-C and blood pressure through an AI-based algorithm, the benefit of treatment can be estimated accurately “beginning at any age and lasting for any duration, thus providing the essential information to inform individual treatment decisions about ultimate timing, intensity, and duration,” according to Dr. Ference.
Routine application awaits further steps
Despite the promise of this concept, there are many steps to be taken before it is introduced into the clinic, asserted designated discussant Folkert Asselbergs, MD, PhD. In addition to testing the accuracy in multiple populations, “we have to do the trials as well,” meaning prospective evaluations to validate the concept is meaningful for improving outcomes.
However, he does not doubt that the concept of causal AI is promising and likely to have a meaningful impact on cardiology after further validation.
“Causal AI is a crucial step that we need to take for more efficient health care,” he said. One reason he expressed caution is that several risk scores enhanced by AI, although not necessarily causal AI, have shown only “modest predictive value” in several studies that he cited.
“Hopefully the data presented from the CAUSAL AI study will really help us take a step up in the discussion to see how we can really benefit by including genetic information in an AI framework to include causality in predicting risk and predicting benefit of treatment,” said Dr. Asselbergs, professor of precision medicine, University of Utrecht (the Netherlands) Medical Center.
Dr. Ference reported financial relationships with more than 15 pharmaceutical companies. Dr. Asselbergs reported no potential conflicts of interest.
FROM ESC CONGRESS 2022