User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Majority of muscle symptoms with statins not caused by treatment
In the vast majority of people who experience muscle pain or weakness while taking a statin, those symptoms are not related to the statin, a new individual patient data meta-analysis of randomized controlled trials shows.
The Cholesterol Trialists Collaboration meta-analysis examined 19 large randomized double-blind trials that compared statin therapy with placebo and involved almost 124,000 patients.
“Our results show that, in people who experience muscle symptoms in the first year of taking a statin, those symptoms are actually due to the statin in only 1 of 15 of those people. For the other 14 of the 15 people who experience muscle symptoms in the first year of taking a statin, that muscle pain is not due to the statin,” lead investigator Colin Baigent, MD, said.
After the first year, there was no difference in muscle symptoms between patients taking a statin or those taking placebo.
Dr. Baigent, who is director of the Population Health Research Unit at the University of Oxford (England), presented the data on Aug. 29 at the European Society of Cardiology 2022 Congress.
It was also simultaneously published online in The Lancet.
Dr. Baigent explained that statins very rarely cause serious muscle adverse effects with biochemical evidence of cellular damage, such as myopathy (which occurs in less than 1 in 10,000 patients per year) and rhabdomyolysis (which occurs in about 0.2 per 10,000 patients per year).
The effect of statins on other less serious muscle symptoms without biochemical evidence of cellular damage is less clear, but misinformation about the risks have arisen from nonrandomized studies, with social media and press reports suggesting that the risk for muscle symptoms with statins is extremely common, Dr. Baigent said.
In response to this, the Cholesterol Trialists Collaboration put together a new program of data collection, validation, and analysis to provide reliable information from large double-blind randomized trials that are free from bias and confounding.
“Overall, when we look at all these data, we find there is about a 3% relative increase in the risks of experiencing muscle pain or weakness with a statin versus with placebo,” Dr. Baigent reported.
Muscle pain or weakness was reported by 16,835 of 62,028 patients taking a statin, (27.1%), compared with 16,446 of 61,912 patients taking placebo (26.6%), for a rate ratio of 1.03 (95% confidence interval, 1.01-1.06).
In absolute terms, the results show a rate of 166 reports of muscle symptoms per 1,000 patient-years in those taking a statin, compared with 155 per 1,000-patient-years in those taking placebo in the first year. This gives a rate ratio of 1.07 and an excess of 11 cases of muscle pain or weakness per 1,000 patients in the first year of statin therapy.
“The very small excess of muscle symptoms in the statin patients were generally mild, with most patients able to continue treatment,” Dr. Baigent added.
After the first year, the rate of muscle pain or weakness was exactly the same in the statin and placebo groups, at 50 per 1,000 patient-years.
“Therefore, for the vast majority of people who experience muscle pain or weakness on a statin, those symptoms are not due to the statin itself. It is due to something else, which could be ageing, thyroid disease, or exercise,” Dr. Baigent said. “After the first year of taking a statin, there is no excess risk of muscle pain or weakness at all.”
“To summarize, the excess risk of muscle pain or weakness with statin use is tiny, and almost nonexistent after the first year,” he added.
“Muscle pain is very common in the general population, and it was very common in both patients taking a statin and those given placebo in these randomized trials. We can only detect a difference by looking at all the data combined in this enormous study. And we now know for sure that over 90% of cases of muscle symptoms experienced by people taking a statin are not due to the statin.”
The researchers also looked at statin intensity and found that the more intense statins tend to cause slightly more muscle pain. “There was also some evidence, although this was not very clear, that the muscle pain with the more intensive statins may persist for longer than 1 year,” Dr. Baigent said.
But in terms of different moderate-intensity and high-intensity statins, there was no evidence of differences in muscle pain between the individual statin brands, he added.
Better patient information needed
Dr. Baigent called for better information in statin package inserts about the real risk for muscle symptoms with these drugs.
“We need to do a better job of communicating the real risk of muscle symptom to patients who are taking statins and to their doctors. At the moment, doctors often stop statins if patients complain of muscle pain, but our data show that in 14 out of 15 times, they would be wrong for doing that. Stopping the statin is nearly always a mistake,” he commented.
“At present, the package inserts include a whole load of rubbish from observational studies, which are completely unreliable,” he added. “This is of no value to patients. They go through this information and find several symptoms they are experiencing, which they attribute to the drugs. We really need to divide up the information into the evidence that we really know for sure and then the more speculative stuff.”
Dr. Baigent also highlighted the large benefits of statins, compared with the small risk for muscle symptoms.
“While statins may cause 11 patients per 1,000 to experience some mild muscle pain in the first year of taking these drugs, and this was reduced to none in subsequent years, statins, when used for the primary prevention of cardiovascular disease, prevent 25 cardiovascular events per 1,000 patients every year they are taken. And for secondary prevention this rises to 50 events prevented per 1,000 patients each year,” he noted.
The individual participant data meta-analysis involved 23 trials with information on almost 155,000 patients. All trials included at least 1,000 patients and at least 2 years of scheduled treatment. Adverse-event data were collected for all individual participants in 19 large randomized double-blind trials comparing statin therapy with placebo (123,940 patients) and in four randomized double-blind trials comparing more-intensive with less-intensive statin therapy (30,724 patients).
In the four trials of more-intensive versus less-intensive statin therapy, high-intensity regimens (atorvastatin 40-80 mg daily or rosuvastatin 20-40 mg daily) resulted in a larger relative increase in the rate of muscle pain or weakness than moderate-intensity regimens, with rate ratios of 1.08 (95% CI, 1.04-1.13) and 1.02 (95% CI, 1.00-1.05), respectively.
‘Reassuring information’
Discussant of the study at the ESC Hotline session, Erin Bohula, MD, Brigham and Women’s Hospital, Boston, said this new analysis had many strengths and used a rigorous approach to look at the issue of muscle symptoms with statins.
She pointed out some challenges, including the fact that the definition of adverse muscle events has changed over time and differed in the various trials, with heterogeneous data capture across trials. “So, this was a Herculean task to harmonize this very complicated dataset.”
Dr. Bohula concluded: “I think this is a very significant undertaking, resulting in a rich dataset that enhances our understanding of muscle symptoms related to statin use. The take-home for me is that muscle symptoms are a common complaint in the general population but are very rarely attributable to statins. This is very reassuring to me, and I hope it is reassuring to patients and can help us encourage them with adherence, given the clear cardiovascular benefits of statins.”
Chair of the ESC Hotline session at which the study was presented, Gabriel Steg, MD, Hôpital Bichat, Paris, asked whether some statin patients who experienced muscle symptoms with the drugs in active run-in periods in the trials may have been excluded from the main trials, so that this information might not have been captured, but Dr. Baigent replied that they also examined those data, which had been accounted for in the analysis.
“That’s really good news,” Dr. Steg commented. “This study is going to be one more tool in our response to statin skeptics and I think, as such, this work is a really a service to public health.”
The meta-analysis was funded by the British Heart Foundation, the U.K. Medical Research Council, and the Australian National Health and Medical Research Council.
A version of this article first appeared on Medscape.com.
In the vast majority of people who experience muscle pain or weakness while taking a statin, those symptoms are not related to the statin, a new individual patient data meta-analysis of randomized controlled trials shows.
The Cholesterol Trialists Collaboration meta-analysis examined 19 large randomized double-blind trials that compared statin therapy with placebo and involved almost 124,000 patients.
“Our results show that, in people who experience muscle symptoms in the first year of taking a statin, those symptoms are actually due to the statin in only 1 of 15 of those people. For the other 14 of the 15 people who experience muscle symptoms in the first year of taking a statin, that muscle pain is not due to the statin,” lead investigator Colin Baigent, MD, said.
After the first year, there was no difference in muscle symptoms between patients taking a statin or those taking placebo.
Dr. Baigent, who is director of the Population Health Research Unit at the University of Oxford (England), presented the data on Aug. 29 at the European Society of Cardiology 2022 Congress.
It was also simultaneously published online in The Lancet.
Dr. Baigent explained that statins very rarely cause serious muscle adverse effects with biochemical evidence of cellular damage, such as myopathy (which occurs in less than 1 in 10,000 patients per year) and rhabdomyolysis (which occurs in about 0.2 per 10,000 patients per year).
The effect of statins on other less serious muscle symptoms without biochemical evidence of cellular damage is less clear, but misinformation about the risks have arisen from nonrandomized studies, with social media and press reports suggesting that the risk for muscle symptoms with statins is extremely common, Dr. Baigent said.
In response to this, the Cholesterol Trialists Collaboration put together a new program of data collection, validation, and analysis to provide reliable information from large double-blind randomized trials that are free from bias and confounding.
“Overall, when we look at all these data, we find there is about a 3% relative increase in the risks of experiencing muscle pain or weakness with a statin versus with placebo,” Dr. Baigent reported.
Muscle pain or weakness was reported by 16,835 of 62,028 patients taking a statin, (27.1%), compared with 16,446 of 61,912 patients taking placebo (26.6%), for a rate ratio of 1.03 (95% confidence interval, 1.01-1.06).
In absolute terms, the results show a rate of 166 reports of muscle symptoms per 1,000 patient-years in those taking a statin, compared with 155 per 1,000-patient-years in those taking placebo in the first year. This gives a rate ratio of 1.07 and an excess of 11 cases of muscle pain or weakness per 1,000 patients in the first year of statin therapy.
“The very small excess of muscle symptoms in the statin patients were generally mild, with most patients able to continue treatment,” Dr. Baigent added.
After the first year, the rate of muscle pain or weakness was exactly the same in the statin and placebo groups, at 50 per 1,000 patient-years.
“Therefore, for the vast majority of people who experience muscle pain or weakness on a statin, those symptoms are not due to the statin itself. It is due to something else, which could be ageing, thyroid disease, or exercise,” Dr. Baigent said. “After the first year of taking a statin, there is no excess risk of muscle pain or weakness at all.”
“To summarize, the excess risk of muscle pain or weakness with statin use is tiny, and almost nonexistent after the first year,” he added.
“Muscle pain is very common in the general population, and it was very common in both patients taking a statin and those given placebo in these randomized trials. We can only detect a difference by looking at all the data combined in this enormous study. And we now know for sure that over 90% of cases of muscle symptoms experienced by people taking a statin are not due to the statin.”
The researchers also looked at statin intensity and found that the more intense statins tend to cause slightly more muscle pain. “There was also some evidence, although this was not very clear, that the muscle pain with the more intensive statins may persist for longer than 1 year,” Dr. Baigent said.
But in terms of different moderate-intensity and high-intensity statins, there was no evidence of differences in muscle pain between the individual statin brands, he added.
Better patient information needed
Dr. Baigent called for better information in statin package inserts about the real risk for muscle symptoms with these drugs.
“We need to do a better job of communicating the real risk of muscle symptom to patients who are taking statins and to their doctors. At the moment, doctors often stop statins if patients complain of muscle pain, but our data show that in 14 out of 15 times, they would be wrong for doing that. Stopping the statin is nearly always a mistake,” he commented.
“At present, the package inserts include a whole load of rubbish from observational studies, which are completely unreliable,” he added. “This is of no value to patients. They go through this information and find several symptoms they are experiencing, which they attribute to the drugs. We really need to divide up the information into the evidence that we really know for sure and then the more speculative stuff.”
Dr. Baigent also highlighted the large benefits of statins, compared with the small risk for muscle symptoms.
“While statins may cause 11 patients per 1,000 to experience some mild muscle pain in the first year of taking these drugs, and this was reduced to none in subsequent years, statins, when used for the primary prevention of cardiovascular disease, prevent 25 cardiovascular events per 1,000 patients every year they are taken. And for secondary prevention this rises to 50 events prevented per 1,000 patients each year,” he noted.
The individual participant data meta-analysis involved 23 trials with information on almost 155,000 patients. All trials included at least 1,000 patients and at least 2 years of scheduled treatment. Adverse-event data were collected for all individual participants in 19 large randomized double-blind trials comparing statin therapy with placebo (123,940 patients) and in four randomized double-blind trials comparing more-intensive with less-intensive statin therapy (30,724 patients).
In the four trials of more-intensive versus less-intensive statin therapy, high-intensity regimens (atorvastatin 40-80 mg daily or rosuvastatin 20-40 mg daily) resulted in a larger relative increase in the rate of muscle pain or weakness than moderate-intensity regimens, with rate ratios of 1.08 (95% CI, 1.04-1.13) and 1.02 (95% CI, 1.00-1.05), respectively.
‘Reassuring information’
Discussant of the study at the ESC Hotline session, Erin Bohula, MD, Brigham and Women’s Hospital, Boston, said this new analysis had many strengths and used a rigorous approach to look at the issue of muscle symptoms with statins.
She pointed out some challenges, including the fact that the definition of adverse muscle events has changed over time and differed in the various trials, with heterogeneous data capture across trials. “So, this was a Herculean task to harmonize this very complicated dataset.”
Dr. Bohula concluded: “I think this is a very significant undertaking, resulting in a rich dataset that enhances our understanding of muscle symptoms related to statin use. The take-home for me is that muscle symptoms are a common complaint in the general population but are very rarely attributable to statins. This is very reassuring to me, and I hope it is reassuring to patients and can help us encourage them with adherence, given the clear cardiovascular benefits of statins.”
Chair of the ESC Hotline session at which the study was presented, Gabriel Steg, MD, Hôpital Bichat, Paris, asked whether some statin patients who experienced muscle symptoms with the drugs in active run-in periods in the trials may have been excluded from the main trials, so that this information might not have been captured, but Dr. Baigent replied that they also examined those data, which had been accounted for in the analysis.
“That’s really good news,” Dr. Steg commented. “This study is going to be one more tool in our response to statin skeptics and I think, as such, this work is a really a service to public health.”
The meta-analysis was funded by the British Heart Foundation, the U.K. Medical Research Council, and the Australian National Health and Medical Research Council.
A version of this article first appeared on Medscape.com.
In the vast majority of people who experience muscle pain or weakness while taking a statin, those symptoms are not related to the statin, a new individual patient data meta-analysis of randomized controlled trials shows.
The Cholesterol Trialists Collaboration meta-analysis examined 19 large randomized double-blind trials that compared statin therapy with placebo and involved almost 124,000 patients.
“Our results show that, in people who experience muscle symptoms in the first year of taking a statin, those symptoms are actually due to the statin in only 1 of 15 of those people. For the other 14 of the 15 people who experience muscle symptoms in the first year of taking a statin, that muscle pain is not due to the statin,” lead investigator Colin Baigent, MD, said.
After the first year, there was no difference in muscle symptoms between patients taking a statin or those taking placebo.
Dr. Baigent, who is director of the Population Health Research Unit at the University of Oxford (England), presented the data on Aug. 29 at the European Society of Cardiology 2022 Congress.
It was also simultaneously published online in The Lancet.
Dr. Baigent explained that statins very rarely cause serious muscle adverse effects with biochemical evidence of cellular damage, such as myopathy (which occurs in less than 1 in 10,000 patients per year) and rhabdomyolysis (which occurs in about 0.2 per 10,000 patients per year).
The effect of statins on other less serious muscle symptoms without biochemical evidence of cellular damage is less clear, but misinformation about the risks have arisen from nonrandomized studies, with social media and press reports suggesting that the risk for muscle symptoms with statins is extremely common, Dr. Baigent said.
In response to this, the Cholesterol Trialists Collaboration put together a new program of data collection, validation, and analysis to provide reliable information from large double-blind randomized trials that are free from bias and confounding.
“Overall, when we look at all these data, we find there is about a 3% relative increase in the risks of experiencing muscle pain or weakness with a statin versus with placebo,” Dr. Baigent reported.
Muscle pain or weakness was reported by 16,835 of 62,028 patients taking a statin, (27.1%), compared with 16,446 of 61,912 patients taking placebo (26.6%), for a rate ratio of 1.03 (95% confidence interval, 1.01-1.06).
In absolute terms, the results show a rate of 166 reports of muscle symptoms per 1,000 patient-years in those taking a statin, compared with 155 per 1,000-patient-years in those taking placebo in the first year. This gives a rate ratio of 1.07 and an excess of 11 cases of muscle pain or weakness per 1,000 patients in the first year of statin therapy.
“The very small excess of muscle symptoms in the statin patients were generally mild, with most patients able to continue treatment,” Dr. Baigent added.
After the first year, the rate of muscle pain or weakness was exactly the same in the statin and placebo groups, at 50 per 1,000 patient-years.
“Therefore, for the vast majority of people who experience muscle pain or weakness on a statin, those symptoms are not due to the statin itself. It is due to something else, which could be ageing, thyroid disease, or exercise,” Dr. Baigent said. “After the first year of taking a statin, there is no excess risk of muscle pain or weakness at all.”
“To summarize, the excess risk of muscle pain or weakness with statin use is tiny, and almost nonexistent after the first year,” he added.
“Muscle pain is very common in the general population, and it was very common in both patients taking a statin and those given placebo in these randomized trials. We can only detect a difference by looking at all the data combined in this enormous study. And we now know for sure that over 90% of cases of muscle symptoms experienced by people taking a statin are not due to the statin.”
The researchers also looked at statin intensity and found that the more intense statins tend to cause slightly more muscle pain. “There was also some evidence, although this was not very clear, that the muscle pain with the more intensive statins may persist for longer than 1 year,” Dr. Baigent said.
But in terms of different moderate-intensity and high-intensity statins, there was no evidence of differences in muscle pain between the individual statin brands, he added.
Better patient information needed
Dr. Baigent called for better information in statin package inserts about the real risk for muscle symptoms with these drugs.
“We need to do a better job of communicating the real risk of muscle symptom to patients who are taking statins and to their doctors. At the moment, doctors often stop statins if patients complain of muscle pain, but our data show that in 14 out of 15 times, they would be wrong for doing that. Stopping the statin is nearly always a mistake,” he commented.
“At present, the package inserts include a whole load of rubbish from observational studies, which are completely unreliable,” he added. “This is of no value to patients. They go through this information and find several symptoms they are experiencing, which they attribute to the drugs. We really need to divide up the information into the evidence that we really know for sure and then the more speculative stuff.”
Dr. Baigent also highlighted the large benefits of statins, compared with the small risk for muscle symptoms.
“While statins may cause 11 patients per 1,000 to experience some mild muscle pain in the first year of taking these drugs, and this was reduced to none in subsequent years, statins, when used for the primary prevention of cardiovascular disease, prevent 25 cardiovascular events per 1,000 patients every year they are taken. And for secondary prevention this rises to 50 events prevented per 1,000 patients each year,” he noted.
The individual participant data meta-analysis involved 23 trials with information on almost 155,000 patients. All trials included at least 1,000 patients and at least 2 years of scheduled treatment. Adverse-event data were collected for all individual participants in 19 large randomized double-blind trials comparing statin therapy with placebo (123,940 patients) and in four randomized double-blind trials comparing more-intensive with less-intensive statin therapy (30,724 patients).
In the four trials of more-intensive versus less-intensive statin therapy, high-intensity regimens (atorvastatin 40-80 mg daily or rosuvastatin 20-40 mg daily) resulted in a larger relative increase in the rate of muscle pain or weakness than moderate-intensity regimens, with rate ratios of 1.08 (95% CI, 1.04-1.13) and 1.02 (95% CI, 1.00-1.05), respectively.
‘Reassuring information’
Discussant of the study at the ESC Hotline session, Erin Bohula, MD, Brigham and Women’s Hospital, Boston, said this new analysis had many strengths and used a rigorous approach to look at the issue of muscle symptoms with statins.
She pointed out some challenges, including the fact that the definition of adverse muscle events has changed over time and differed in the various trials, with heterogeneous data capture across trials. “So, this was a Herculean task to harmonize this very complicated dataset.”
Dr. Bohula concluded: “I think this is a very significant undertaking, resulting in a rich dataset that enhances our understanding of muscle symptoms related to statin use. The take-home for me is that muscle symptoms are a common complaint in the general population but are very rarely attributable to statins. This is very reassuring to me, and I hope it is reassuring to patients and can help us encourage them with adherence, given the clear cardiovascular benefits of statins.”
Chair of the ESC Hotline session at which the study was presented, Gabriel Steg, MD, Hôpital Bichat, Paris, asked whether some statin patients who experienced muscle symptoms with the drugs in active run-in periods in the trials may have been excluded from the main trials, so that this information might not have been captured, but Dr. Baigent replied that they also examined those data, which had been accounted for in the analysis.
“That’s really good news,” Dr. Steg commented. “This study is going to be one more tool in our response to statin skeptics and I think, as such, this work is a really a service to public health.”
The meta-analysis was funded by the British Heart Foundation, the U.K. Medical Research Council, and the Australian National Health and Medical Research Council.
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2022

Online tool IDs people with genetic mutations linked to cancer
(PGVs) in a diverse spectrum of cancer susceptibility genes.
The PREMMplus online tool was developed and validated by researchers at the Dana-Farber Cancer Institute, Boston using three cohorts involving more than 30,000 individuals who had undergone multigene hereditary cancer risk testing.
The study was published online in the Journal of Clinical Oncology.
“Our findings show that PREMMplus has the potential to change the model by which patients and family members are referred for genetic testing and counseling,” senior author Sapna Syngal, MD, MPH, with Dana-Farber/Brigham and Women’s Hospital, Boston, said in an institution news release.
Traditionally, when there is concern about a family cancer history, the individual is referred to a genetics clinic, where a counselor takes a complete family history.
“At a time when there’s a shortage of genetic counselors, PREMMplus can help streamline risk assessment and ensure that their time can be focused on where they’re most needed – helping people understand the results of genetic testing and the options available when a cancer-susceptibility gene is found,” Dr. Syngal says.
Online tool
The tool uses clinical data (age, sex, ethnicity, and personal/family history of 18 cancers) to determine an individual’s likelihood of harboring a PGV in 19 cancer susceptibility genes.
A PREMMplus score of 2.5% or greater had a 89%-94% sensitivity and > 97% negative predictive value (NPV) for identifying individuals with PGVs in 11 well-defined “category A” high-penetrance cancer risk genes: APC, BRCA1, BRCA2, CDH1, EPCAM, MLH1, MSH2, MSH6, biallelic MUTYH, PMS2, and TP53.
These PGVs “represent diverse types of inherited cancer risk for which there are established risk-reduction guidelines,” the study team says. Cancers associated with these PGVs include breast, ovarian, colorectal, pancreatic, and prostate cancer, as well as those that make up Lynch syndrome.
The ability of PREMMplus to identify individuals with PGVs in “moderate-penetrance” cancer risk genes (such as CHEK2 and ATM) was somewhat reduced but was still “quite strong” (84%-90% sensitivity and > 93% NPV), the study team reports.
In an interview, Dr. Syngal said her ultimate vision of this online tool is that it will be adapted into the electronic medical record (EMR).
“Through the EMR, it might somehow get pushed out to people before an oncology or primary care appointment or before a mammography or colonoscopy. Then by the time they come in, the doctor or nurse practitioner has the information and can refer them for genetic testing if appropriate,” Dr. Syngal explained.
The tool is not currently available for routine clinical use. The goal is to make it available online in a couple of months.
Dr. Syngal said two versions will be available. One will be a user-friendly version that can be filled out directly by patients and that will tell whether someone passes the threshold of needing genetic testing. The patient would then take that information to their primary care doctor.
With the second version, the doctor and patient would fill out the information together during an office visit.
PREMMplus would be free for the individual patient or provider.
“What we hope is that hospital systems will use it and that insurance companies will also use it as a way to say who needs testing and who to approve for testing,” Dr. Syngal told this news organization.
“For a hospital system or a genetic testing company, for example, that wants to integrate it into their direct-to-consumer platform, they would have to take out a license from Dana-Farber, and cost would be negotiated with each entity based on how they’re going to use it,” Dr. Syngal said.
Funding for the research was provided by the National Institutes of Health. A complete list of author disclosures is available with the original article.
A version of this article first appeared on Medscape.com.
(PGVs) in a diverse spectrum of cancer susceptibility genes.
The PREMMplus online tool was developed and validated by researchers at the Dana-Farber Cancer Institute, Boston using three cohorts involving more than 30,000 individuals who had undergone multigene hereditary cancer risk testing.
The study was published online in the Journal of Clinical Oncology.
“Our findings show that PREMMplus has the potential to change the model by which patients and family members are referred for genetic testing and counseling,” senior author Sapna Syngal, MD, MPH, with Dana-Farber/Brigham and Women’s Hospital, Boston, said in an institution news release.
Traditionally, when there is concern about a family cancer history, the individual is referred to a genetics clinic, where a counselor takes a complete family history.
“At a time when there’s a shortage of genetic counselors, PREMMplus can help streamline risk assessment and ensure that their time can be focused on where they’re most needed – helping people understand the results of genetic testing and the options available when a cancer-susceptibility gene is found,” Dr. Syngal says.
Online tool
The tool uses clinical data (age, sex, ethnicity, and personal/family history of 18 cancers) to determine an individual’s likelihood of harboring a PGV in 19 cancer susceptibility genes.
A PREMMplus score of 2.5% or greater had a 89%-94% sensitivity and > 97% negative predictive value (NPV) for identifying individuals with PGVs in 11 well-defined “category A” high-penetrance cancer risk genes: APC, BRCA1, BRCA2, CDH1, EPCAM, MLH1, MSH2, MSH6, biallelic MUTYH, PMS2, and TP53.
These PGVs “represent diverse types of inherited cancer risk for which there are established risk-reduction guidelines,” the study team says. Cancers associated with these PGVs include breast, ovarian, colorectal, pancreatic, and prostate cancer, as well as those that make up Lynch syndrome.
The ability of PREMMplus to identify individuals with PGVs in “moderate-penetrance” cancer risk genes (such as CHEK2 and ATM) was somewhat reduced but was still “quite strong” (84%-90% sensitivity and > 93% NPV), the study team reports.
In an interview, Dr. Syngal said her ultimate vision of this online tool is that it will be adapted into the electronic medical record (EMR).
“Through the EMR, it might somehow get pushed out to people before an oncology or primary care appointment or before a mammography or colonoscopy. Then by the time they come in, the doctor or nurse practitioner has the information and can refer them for genetic testing if appropriate,” Dr. Syngal explained.
The tool is not currently available for routine clinical use. The goal is to make it available online in a couple of months.
Dr. Syngal said two versions will be available. One will be a user-friendly version that can be filled out directly by patients and that will tell whether someone passes the threshold of needing genetic testing. The patient would then take that information to their primary care doctor.
With the second version, the doctor and patient would fill out the information together during an office visit.
PREMMplus would be free for the individual patient or provider.
“What we hope is that hospital systems will use it and that insurance companies will also use it as a way to say who needs testing and who to approve for testing,” Dr. Syngal told this news organization.
“For a hospital system or a genetic testing company, for example, that wants to integrate it into their direct-to-consumer platform, they would have to take out a license from Dana-Farber, and cost would be negotiated with each entity based on how they’re going to use it,” Dr. Syngal said.
Funding for the research was provided by the National Institutes of Health. A complete list of author disclosures is available with the original article.
A version of this article first appeared on Medscape.com.
(PGVs) in a diverse spectrum of cancer susceptibility genes.
The PREMMplus online tool was developed and validated by researchers at the Dana-Farber Cancer Institute, Boston using three cohorts involving more than 30,000 individuals who had undergone multigene hereditary cancer risk testing.
The study was published online in the Journal of Clinical Oncology.
“Our findings show that PREMMplus has the potential to change the model by which patients and family members are referred for genetic testing and counseling,” senior author Sapna Syngal, MD, MPH, with Dana-Farber/Brigham and Women’s Hospital, Boston, said in an institution news release.
Traditionally, when there is concern about a family cancer history, the individual is referred to a genetics clinic, where a counselor takes a complete family history.
“At a time when there’s a shortage of genetic counselors, PREMMplus can help streamline risk assessment and ensure that their time can be focused on where they’re most needed – helping people understand the results of genetic testing and the options available when a cancer-susceptibility gene is found,” Dr. Syngal says.
Online tool
The tool uses clinical data (age, sex, ethnicity, and personal/family history of 18 cancers) to determine an individual’s likelihood of harboring a PGV in 19 cancer susceptibility genes.
A PREMMplus score of 2.5% or greater had a 89%-94% sensitivity and > 97% negative predictive value (NPV) for identifying individuals with PGVs in 11 well-defined “category A” high-penetrance cancer risk genes: APC, BRCA1, BRCA2, CDH1, EPCAM, MLH1, MSH2, MSH6, biallelic MUTYH, PMS2, and TP53.
These PGVs “represent diverse types of inherited cancer risk for which there are established risk-reduction guidelines,” the study team says. Cancers associated with these PGVs include breast, ovarian, colorectal, pancreatic, and prostate cancer, as well as those that make up Lynch syndrome.
The ability of PREMMplus to identify individuals with PGVs in “moderate-penetrance” cancer risk genes (such as CHEK2 and ATM) was somewhat reduced but was still “quite strong” (84%-90% sensitivity and > 93% NPV), the study team reports.
In an interview, Dr. Syngal said her ultimate vision of this online tool is that it will be adapted into the electronic medical record (EMR).
“Through the EMR, it might somehow get pushed out to people before an oncology or primary care appointment or before a mammography or colonoscopy. Then by the time they come in, the doctor or nurse practitioner has the information and can refer them for genetic testing if appropriate,” Dr. Syngal explained.
The tool is not currently available for routine clinical use. The goal is to make it available online in a couple of months.
Dr. Syngal said two versions will be available. One will be a user-friendly version that can be filled out directly by patients and that will tell whether someone passes the threshold of needing genetic testing. The patient would then take that information to their primary care doctor.
With the second version, the doctor and patient would fill out the information together during an office visit.
PREMMplus would be free for the individual patient or provider.
“What we hope is that hospital systems will use it and that insurance companies will also use it as a way to say who needs testing and who to approve for testing,” Dr. Syngal told this news organization.
“For a hospital system or a genetic testing company, for example, that wants to integrate it into their direct-to-consumer platform, they would have to take out a license from Dana-Farber, and cost would be negotiated with each entity based on how they’re going to use it,” Dr. Syngal said.
Funding for the research was provided by the National Institutes of Health. A complete list of author disclosures is available with the original article.
A version of this article first appeared on Medscape.com.
FDA authorizes updated COVID boosters to target newest variants
The agency cited data to support the safety and efficacy of this next generation of mRNA vaccines targeted toward variants of concern.
The Pfizer EUA corresponds to the company’s combination booster shot that includes the original COVID-19 vaccine as well as a vaccine specifically designed to protect against the most recent Omicron variants, BA.4 and BA.5.
The Moderna combination vaccine will contain both the firm’s original COVID-19 vaccine and a vaccine to protect specifically against Omicron BA.4 and BA.5 subvariants.
As of Aug. 27, BA.4 and BA.4.6 account for about 11% of circulating variants and BA.5 accounts for almost all the remaining 89%, Centers for Disease Control and Prevention data show.
The next step will be review of the scientific data by the CDC’s Advisory Committee on Immunization Practices, which is set to meet Sept. 1 and 2. The final hurdle before distribution of the new vaccines will be sign-off on CDC recommendations for use by agency Director Rochelle Walensky, MD.
This is a developing story. A version of this article first appeared on WebMD.com.
The agency cited data to support the safety and efficacy of this next generation of mRNA vaccines targeted toward variants of concern.
The Pfizer EUA corresponds to the company’s combination booster shot that includes the original COVID-19 vaccine as well as a vaccine specifically designed to protect against the most recent Omicron variants, BA.4 and BA.5.
The Moderna combination vaccine will contain both the firm’s original COVID-19 vaccine and a vaccine to protect specifically against Omicron BA.4 and BA.5 subvariants.
As of Aug. 27, BA.4 and BA.4.6 account for about 11% of circulating variants and BA.5 accounts for almost all the remaining 89%, Centers for Disease Control and Prevention data show.
The next step will be review of the scientific data by the CDC’s Advisory Committee on Immunization Practices, which is set to meet Sept. 1 and 2. The final hurdle before distribution of the new vaccines will be sign-off on CDC recommendations for use by agency Director Rochelle Walensky, MD.
This is a developing story. A version of this article first appeared on WebMD.com.
The agency cited data to support the safety and efficacy of this next generation of mRNA vaccines targeted toward variants of concern.
The Pfizer EUA corresponds to the company’s combination booster shot that includes the original COVID-19 vaccine as well as a vaccine specifically designed to protect against the most recent Omicron variants, BA.4 and BA.5.
The Moderna combination vaccine will contain both the firm’s original COVID-19 vaccine and a vaccine to protect specifically against Omicron BA.4 and BA.5 subvariants.
As of Aug. 27, BA.4 and BA.4.6 account for about 11% of circulating variants and BA.5 accounts for almost all the remaining 89%, Centers for Disease Control and Prevention data show.
The next step will be review of the scientific data by the CDC’s Advisory Committee on Immunization Practices, which is set to meet Sept. 1 and 2. The final hurdle before distribution of the new vaccines will be sign-off on CDC recommendations for use by agency Director Rochelle Walensky, MD.
This is a developing story. A version of this article first appeared on WebMD.com.
Omega-3 fatty acids and depression: Are they protective?
New research is suggesting that there are “meaningful” associations between higher dietary intake of omega-3 fatty acids and lower risk for depressive episodes.
In addition, consumption of total fatty acids and alpha-linolenic acid was associated with a reduced risk for incident depressive episodes (9% and 29%, respectively).
“Our results showed an important protective effect from the consumption of omega-3,” Maria de Jesus Mendes da Fonseca, University of the State of Rio de Janeiro, and colleagues write.
The findings were published online in Nutrients.
Mixed bag of studies
Epidemiologic evidence suggests that deficient dietary omega-3 intake is a modifiable risk factor for depression and that individuals with low consumption of omega-3 food sources have more depressive symptoms.
However, the results are inconsistent, and few longitudinal studies have addressed this association, the investigators note.
The new analysis included 13,879 adults (aged 39-65 years or older) participating in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) from 2008 to 2014.
Data on depressive episodes were obtained with the Clinical Interview Schedule Revised (CIS-R), and food consumption was measured with the Food Frequency Questionnaire (FFQ).
The target dietary components were total polyunsaturated fatty acids (PUFA) and the omega-3 fatty acids: alpha-linolenic acid, eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and docosapentaenoic acid (DPA).
The majority of participants had adequate dietary intake of omega-3 fatty acids, and none was taking omega-3 supplements.
In the fully adjusted model, consumption of fatty acids from the omega-3 family had a protective effect against maintenance of depressive episodes, showing “important associations, although the significance levels are borderline, possibly due to the sample size,” the researchers report.
In regard to onset of depressive episodes, estimates from the fully adjusted model suggest that a higher consumption of omega-3 acids (total and subtypes) is associated with lower risk for depressive episodes – with significant associations for omega-3 and alpha-linolenic acid.
The investigators note that strengths of the study include “its originality, as it is the first to assess associations between maintenance and incidence of depressive episodes and consumption of omega-3, besides the use of data from the ELSA-Brasil Study, with rigorous data collection protocols and reliable and validated instruments, thus guaranteeing the quality of the sample and the data.”
A study limitation, however, was that the ELSA-Brasil sample consists only of public employees, with the potential for a selection bias such as healthy worker phenomenon, the researchers note. Another was the use of the FFQ, which may underestimate daily intake of foods and depends on individual participant recall – all of which could possibly lead to a differential classification bias.
Interpret cautiously
Commenting on the study, David Mischoulon, MD, PhD, professor of psychiatry, Harvard Medical School, and director of the depression clinical and research program at Massachusetts General Hospital, both in Boston, said that data on omega-3s in depression are “very mixed.”
“A lot of the studies don’t necessarily agree with each other. Certainly, in studies that try to seek an association between omega-3 use and depression, it’s always complicated because it can be difficult to control for all variables that could be contributing to the result that you get,” said Dr. Mischoulon, who is also a member of the Anxiety and Depression Association of America and was not involved in the research.
A caveat to the current study was that diet was assessed only at baseline, “so we don’t really know whether there were any substantial dietary changes over time, he noted.

He also cautioned that it is hard to draw any firm conclusions from this type of study.
“In general, in studies with a large sample, which this study has, it’s easier to find statistically significant differences. But you need to ask yourself: Does it really matter? Is it enough to have a clinical impact and make a difference?” Dr. Mischoulon said.
The ELSA-Brasil study was funded by the Brazilian Ministry of Science, Technology, and Innovation and by the Ministry of Health. The investigators have reported no relevant financial relationships. Dr. Mischoulon has received research support from Nordic Naturals and heckel medizintechnik GmbH and honoraria for speaking from the Massachusetts General Hospital Psychiatry Academy. He also works with the MGH Clinical Trials Network and Institute, which has received research funding from multiple pharmaceutical companies and the National Institute of Mental Health.
A version of this article first appeared on Medscape.com.
New research is suggesting that there are “meaningful” associations between higher dietary intake of omega-3 fatty acids and lower risk for depressive episodes.
In addition, consumption of total fatty acids and alpha-linolenic acid was associated with a reduced risk for incident depressive episodes (9% and 29%, respectively).
“Our results showed an important protective effect from the consumption of omega-3,” Maria de Jesus Mendes da Fonseca, University of the State of Rio de Janeiro, and colleagues write.
The findings were published online in Nutrients.
Mixed bag of studies
Epidemiologic evidence suggests that deficient dietary omega-3 intake is a modifiable risk factor for depression and that individuals with low consumption of omega-3 food sources have more depressive symptoms.
However, the results are inconsistent, and few longitudinal studies have addressed this association, the investigators note.
The new analysis included 13,879 adults (aged 39-65 years or older) participating in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) from 2008 to 2014.
Data on depressive episodes were obtained with the Clinical Interview Schedule Revised (CIS-R), and food consumption was measured with the Food Frequency Questionnaire (FFQ).
The target dietary components were total polyunsaturated fatty acids (PUFA) and the omega-3 fatty acids: alpha-linolenic acid, eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and docosapentaenoic acid (DPA).
The majority of participants had adequate dietary intake of omega-3 fatty acids, and none was taking omega-3 supplements.
In the fully adjusted model, consumption of fatty acids from the omega-3 family had a protective effect against maintenance of depressive episodes, showing “important associations, although the significance levels are borderline, possibly due to the sample size,” the researchers report.
In regard to onset of depressive episodes, estimates from the fully adjusted model suggest that a higher consumption of omega-3 acids (total and subtypes) is associated with lower risk for depressive episodes – with significant associations for omega-3 and alpha-linolenic acid.
The investigators note that strengths of the study include “its originality, as it is the first to assess associations between maintenance and incidence of depressive episodes and consumption of omega-3, besides the use of data from the ELSA-Brasil Study, with rigorous data collection protocols and reliable and validated instruments, thus guaranteeing the quality of the sample and the data.”
A study limitation, however, was that the ELSA-Brasil sample consists only of public employees, with the potential for a selection bias such as healthy worker phenomenon, the researchers note. Another was the use of the FFQ, which may underestimate daily intake of foods and depends on individual participant recall – all of which could possibly lead to a differential classification bias.
Interpret cautiously
Commenting on the study, David Mischoulon, MD, PhD, professor of psychiatry, Harvard Medical School, and director of the depression clinical and research program at Massachusetts General Hospital, both in Boston, said that data on omega-3s in depression are “very mixed.”
“A lot of the studies don’t necessarily agree with each other. Certainly, in studies that try to seek an association between omega-3 use and depression, it’s always complicated because it can be difficult to control for all variables that could be contributing to the result that you get,” said Dr. Mischoulon, who is also a member of the Anxiety and Depression Association of America and was not involved in the research.
A caveat to the current study was that diet was assessed only at baseline, “so we don’t really know whether there were any substantial dietary changes over time, he noted.
He also cautioned that it is hard to draw any firm conclusions from this type of study.
“In general, in studies with a large sample, which this study has, it’s easier to find statistically significant differences. But you need to ask yourself: Does it really matter? Is it enough to have a clinical impact and make a difference?” Dr. Mischoulon said.
The ELSA-Brasil study was funded by the Brazilian Ministry of Science, Technology, and Innovation and by the Ministry of Health. The investigators have reported no relevant financial relationships. Dr. Mischoulon has received research support from Nordic Naturals and heckel medizintechnik GmbH and honoraria for speaking from the Massachusetts General Hospital Psychiatry Academy. He also works with the MGH Clinical Trials Network and Institute, which has received research funding from multiple pharmaceutical companies and the National Institute of Mental Health.
A version of this article first appeared on Medscape.com.
New research is suggesting that there are “meaningful” associations between higher dietary intake of omega-3 fatty acids and lower risk for depressive episodes.
In addition, consumption of total fatty acids and alpha-linolenic acid was associated with a reduced risk for incident depressive episodes (9% and 29%, respectively).
“Our results showed an important protective effect from the consumption of omega-3,” Maria de Jesus Mendes da Fonseca, University of the State of Rio de Janeiro, and colleagues write.
The findings were published online in Nutrients.
Mixed bag of studies
Epidemiologic evidence suggests that deficient dietary omega-3 intake is a modifiable risk factor for depression and that individuals with low consumption of omega-3 food sources have more depressive symptoms.
However, the results are inconsistent, and few longitudinal studies have addressed this association, the investigators note.
The new analysis included 13,879 adults (aged 39-65 years or older) participating in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) from 2008 to 2014.
Data on depressive episodes were obtained with the Clinical Interview Schedule Revised (CIS-R), and food consumption was measured with the Food Frequency Questionnaire (FFQ).
The target dietary components were total polyunsaturated fatty acids (PUFA) and the omega-3 fatty acids: alpha-linolenic acid, eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and docosapentaenoic acid (DPA).
The majority of participants had adequate dietary intake of omega-3 fatty acids, and none was taking omega-3 supplements.
In the fully adjusted model, consumption of fatty acids from the omega-3 family had a protective effect against maintenance of depressive episodes, showing “important associations, although the significance levels are borderline, possibly due to the sample size,” the researchers report.
In regard to onset of depressive episodes, estimates from the fully adjusted model suggest that a higher consumption of omega-3 acids (total and subtypes) is associated with lower risk for depressive episodes – with significant associations for omega-3 and alpha-linolenic acid.
The investigators note that strengths of the study include “its originality, as it is the first to assess associations between maintenance and incidence of depressive episodes and consumption of omega-3, besides the use of data from the ELSA-Brasil Study, with rigorous data collection protocols and reliable and validated instruments, thus guaranteeing the quality of the sample and the data.”
A study limitation, however, was that the ELSA-Brasil sample consists only of public employees, with the potential for a selection bias such as healthy worker phenomenon, the researchers note. Another was the use of the FFQ, which may underestimate daily intake of foods and depends on individual participant recall – all of which could possibly lead to a differential classification bias.
Interpret cautiously
Commenting on the study, David Mischoulon, MD, PhD, professor of psychiatry, Harvard Medical School, and director of the depression clinical and research program at Massachusetts General Hospital, both in Boston, said that data on omega-3s in depression are “very mixed.”
“A lot of the studies don’t necessarily agree with each other. Certainly, in studies that try to seek an association between omega-3 use and depression, it’s always complicated because it can be difficult to control for all variables that could be contributing to the result that you get,” said Dr. Mischoulon, who is also a member of the Anxiety and Depression Association of America and was not involved in the research.
A caveat to the current study was that diet was assessed only at baseline, “so we don’t really know whether there were any substantial dietary changes over time, he noted.
He also cautioned that it is hard to draw any firm conclusions from this type of study.
“In general, in studies with a large sample, which this study has, it’s easier to find statistically significant differences. But you need to ask yourself: Does it really matter? Is it enough to have a clinical impact and make a difference?” Dr. Mischoulon said.
The ELSA-Brasil study was funded by the Brazilian Ministry of Science, Technology, and Innovation and by the Ministry of Health. The investigators have reported no relevant financial relationships. Dr. Mischoulon has received research support from Nordic Naturals and heckel medizintechnik GmbH and honoraria for speaking from the Massachusetts General Hospital Psychiatry Academy. He also works with the MGH Clinical Trials Network and Institute, which has received research funding from multiple pharmaceutical companies and the National Institute of Mental Health.
A version of this article first appeared on Medscape.com.
FROM NUTRIENTS
Children and COVID: New cases increase; hospital admissions could follow
New cases of COVID-19 in children were up again after 2 weeks of declines, and preliminary data suggest that hospitalizations may be on the rise as well.
, based on data collected by the American Academy of Pediatrics and the Children’s Hospital Association from state and territorial health departments.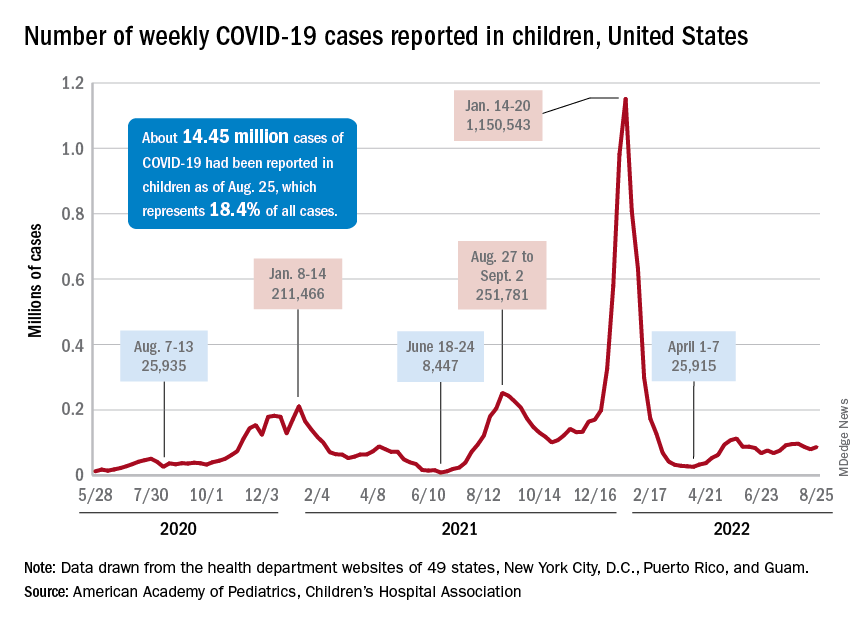
A similar increase seems to be reflected by hospital-level data. The latest 7-day (Aug. 21-27) average is 305 new admissions with diagnosed COVID per day among children aged 0-17 years, compared with 290 per day for the week of Aug. 14-20, the Centers for Disease Control and Prevention reported, while also noting the potential for reporting delays in the most recent 7-day period.
Daily hospital admissions for COVID had been headed downward through the first half of August, falling from 0.46 per 100,000 population at the end of July to 0.40 on Aug. 19, the CDC said on its COVID Data Tracker. Since then, however, admissions have gone the other way, with the preliminary nature of the latest data suggesting that the numbers will be even higher as more hospitals report over the next few days.
Vaccine initiations continue to fall
Initiations among school-age children have fallen for 3 consecutive weeks since Aug. 3, when numbers receiving their first vaccinations reached late-summer highs for those aged 5-11 and 12-17 years. Children under age 5, included in the CDC data for the first time on Aug. 11 as separate groups – under 2 years and 2-4 years – have had vaccine initiations drop by 8.0% and 19.8% over the 2 following weeks, the CDC said.

Through their first 8 weeks of vaccine eligibility (June 19 to Aug. 15), 4.8% of children under 5 years of age had received a first vaccination and 1.0% were fully vaccinated. For the two other age groups (5-11 and 12-15) who became eligible after the very first emergency authorization back in 2020, the respective proportions were 25.0% and 16.0% (5-11) and 33.8% and 26.1% (12-15) through the first 8 weeks, according to CDC data.
New cases of COVID-19 in children were up again after 2 weeks of declines, and preliminary data suggest that hospitalizations may be on the rise as well.
, based on data collected by the American Academy of Pediatrics and the Children’s Hospital Association from state and territorial health departments.
A similar increase seems to be reflected by hospital-level data. The latest 7-day (Aug. 21-27) average is 305 new admissions with diagnosed COVID per day among children aged 0-17 years, compared with 290 per day for the week of Aug. 14-20, the Centers for Disease Control and Prevention reported, while also noting the potential for reporting delays in the most recent 7-day period.
Daily hospital admissions for COVID had been headed downward through the first half of August, falling from 0.46 per 100,000 population at the end of July to 0.40 on Aug. 19, the CDC said on its COVID Data Tracker. Since then, however, admissions have gone the other way, with the preliminary nature of the latest data suggesting that the numbers will be even higher as more hospitals report over the next few days.
Vaccine initiations continue to fall
Initiations among school-age children have fallen for 3 consecutive weeks since Aug. 3, when numbers receiving their first vaccinations reached late-summer highs for those aged 5-11 and 12-17 years. Children under age 5, included in the CDC data for the first time on Aug. 11 as separate groups – under 2 years and 2-4 years – have had vaccine initiations drop by 8.0% and 19.8% over the 2 following weeks, the CDC said.
Through their first 8 weeks of vaccine eligibility (June 19 to Aug. 15), 4.8% of children under 5 years of age had received a first vaccination and 1.0% were fully vaccinated. For the two other age groups (5-11 and 12-15) who became eligible after the very first emergency authorization back in 2020, the respective proportions were 25.0% and 16.0% (5-11) and 33.8% and 26.1% (12-15) through the first 8 weeks, according to CDC data.
New cases of COVID-19 in children were up again after 2 weeks of declines, and preliminary data suggest that hospitalizations may be on the rise as well.
, based on data collected by the American Academy of Pediatrics and the Children’s Hospital Association from state and territorial health departments.
A similar increase seems to be reflected by hospital-level data. The latest 7-day (Aug. 21-27) average is 305 new admissions with diagnosed COVID per day among children aged 0-17 years, compared with 290 per day for the week of Aug. 14-20, the Centers for Disease Control and Prevention reported, while also noting the potential for reporting delays in the most recent 7-day period.
Daily hospital admissions for COVID had been headed downward through the first half of August, falling from 0.46 per 100,000 population at the end of July to 0.40 on Aug. 19, the CDC said on its COVID Data Tracker. Since then, however, admissions have gone the other way, with the preliminary nature of the latest data suggesting that the numbers will be even higher as more hospitals report over the next few days.
Vaccine initiations continue to fall
Initiations among school-age children have fallen for 3 consecutive weeks since Aug. 3, when numbers receiving their first vaccinations reached late-summer highs for those aged 5-11 and 12-17 years. Children under age 5, included in the CDC data for the first time on Aug. 11 as separate groups – under 2 years and 2-4 years – have had vaccine initiations drop by 8.0% and 19.8% over the 2 following weeks, the CDC said.
Through their first 8 weeks of vaccine eligibility (June 19 to Aug. 15), 4.8% of children under 5 years of age had received a first vaccination and 1.0% were fully vaccinated. For the two other age groups (5-11 and 12-15) who became eligible after the very first emergency authorization back in 2020, the respective proportions were 25.0% and 16.0% (5-11) and 33.8% and 26.1% (12-15) through the first 8 weeks, according to CDC data.
Distorted time perception during the pandemic tied to stress, poor mental health
ranging from difficulty keeping track of the days of the week to feeling that the hours either crawled by or sped up, new research suggests.
Results showed the sense of present focus, blurring weekdays and weekends together, and uncertainly about the future were reported by over 65% of the 5,661 survey respondents. And more than half reported the experience of feeling “time speeding up or slowing down,” report the investigators, led by E. Alison Holman, PhD, professor at the University of California, Irvine.
Significant predictors of these time distortions included being exposed to daily pandemic-related media and having a mental health diagnosis prior to the pandemic; secondary stress such as school closures and lockdown; financial stress; lifetime stress; and lifetime trauma exposure.
“Continuity between past experiences, present life, and future hopes is critical to one’s well-being, and disruption of that synergy presents mental health challenges,” Dr. Holman said in a news release.
“We were able to measure this in a nationally representative sample of Americans as they were experiencing a protracted collective trauma, which has never been done before, and this study is the first to document the prevalence and early predictors of these time distortions,” added Dr. Holman.
The findings were published online in Psychological Trauma: Theory, Research, Practice, and Policy.
Unique opportunity
During the pandemic, many people’s time perspective (TP), defined as “our view of time as it spans from our past into the future,” shifted as they “focused on the immediate, present danger of the COVID-19 pandemic and future plans became uncertain,” the investigators wrote.
Studies of convenience samples “suggested that many people experienced time slowing down, stopping, and/or speeding up as they coped with the challenges of the pandemic” – a phenomenon known as temporal disintegration (TD) in psychiatric literature.
Dr. Holman said in an interview that she researched TD after the Sept.11, 2001 World Trade Center attacks.
“We found that people who experienced that early sense of TD, the sense of ‘time falling apart,’ were more prone to getting stuck in the past and staying focused on the past event,” which led to feeling “more distress over time,” she said.
Research examining the prevalence of and psychosocial factors predicting TD are “quite rare” and studies examining TD “during an unfolding, protracted collective trauma are even rarer,” the researchers note. The COVID pandemic “presented a unique opportunity to conduct such a study,” the researchers wrote.
For their study, the investigators surveyed participants in the NORC AmeriSpeak online panel, a “probability-based panel” of 35,000 U.S. households selected at random from across the country.
The study was conducted in two waves: the first survey was administered March–April 2020, the second in September–October 2020.
Speeding up, slowing down
At wave 2, participants completed a 7-item index of TD symptoms experienced over the previous 6 months. To adjust for psychological processes that may have predisposed individuals to experience TD during the pandemic, the researchers included a Wave 1 measure of future uncertainty as a covariate.
Prepandemic health data had been collected prior to the current study.
Wave 1 participants completed a checklist reporting personal, work, and community-wide exposure to the COVID outbreak, including contracting the virus, sheltering in place, and experiencing secondary stressors. The extent and type of pandemic-related media exposure were also assessed.
At wave 2, they reported the extent of exposure to the coronavirus, financial exposures, and secondary stressors. They also completed a non–COVID-related stress/trauma exposure checklist and were asked to indicate whether the trauma, disaster, or bereavement took place prior to or during the pandemic.
The final sample consisted of 5,661 adults (52% female) who completed the wave 2 survey. Participants were divided into four age groups: 18-34, 35-49, 50-64, and 65 and older.
The most common experiences (reported by more than 65% of respondents) included being focused on the present moment, feeling that weekdays and weekends were the same, and feeling uncertain about the future.
Over half of respondents (50.4%) reported feeling as though time was speeding up, and 55.2% reported feeling as though time was slowing down. Some also reported feeling uncertain about the time of day (46.4%) and forgetting events they had just experienced (35.2%).
When the researchers controlled for feeling uncertain about the future, they found that women reported more TD than men (b = 0.11; 95% confidence interval, 0.07-0.14; P < .001).
At wave 1, associations were found between TD and COVID-related media exposure, prepandemic mental health diagnoses, and prepandemic non–COVID-related stress and trauma. At wave 2, associations were found between TD and COVID-related secondary and financial stressors (P < .001 for all).
In contrast, COVID-related work exposure at wave 1, being 45-59 years old, and living in the Midwest region were negatively associated with TD.
“The sense of the flow of the past into the present, and the present into the future is important for our mental health,” Dr. Holman said. “We need to remember who we have been, how that shaped who we are today, and where we want to go with our lives.”
Staying in the present moment is “good, when you’re doing it mindfully. But you still need to feel you can shape and work toward the future and have some sense of control,” she added.
Dr. Homan also recommended time-perspective therapy, which helps patients with PTSD to “build continuity across time – to understand and learn from the past, live in the present, and move toward the future.”
Widespread distortion
In an interview, Ruth Ogden, PhD, a lecturer at Liverpool (England) John Moores University, said the findings “confirm those reported in Europe, South America, and the Middle East, that widespread distortion to time was common during the pandemic and that distortions to time were greatest amongst those most negatively affected by the pandemic.”
The results also support her own recent research in the United Kingdom “suggesting that distortions to time during the pandemic extend to our memory for the length of the pandemic, with most people believing that lockdowns lasted far longer than they actually did,” said Dr. Ogden, who was not involved with Dr. Holman and colleagues’ current study.
“This type of subjective lengthening of the pandemic may reinforce trauma by making the traumatic period seem longer, further damaging health and well-being,” she noted. “As the negative fallouts of the pandemic continue, it is important to establish the long-term effects of time distortions during the pandemic on mental health and well-being.”
The study was funded by U.S. National Science Foundation and the National Institute on Minority Health and Health Disparities. The investigators reported no relevant financial relationships. Dr. Ogden receives funding from the Wellcome Trust.
A version of this article first appeared on Medscape.com.
ranging from difficulty keeping track of the days of the week to feeling that the hours either crawled by or sped up, new research suggests.
Results showed the sense of present focus, blurring weekdays and weekends together, and uncertainly about the future were reported by over 65% of the 5,661 survey respondents. And more than half reported the experience of feeling “time speeding up or slowing down,” report the investigators, led by E. Alison Holman, PhD, professor at the University of California, Irvine.
Significant predictors of these time distortions included being exposed to daily pandemic-related media and having a mental health diagnosis prior to the pandemic; secondary stress such as school closures and lockdown; financial stress; lifetime stress; and lifetime trauma exposure.
“Continuity between past experiences, present life, and future hopes is critical to one’s well-being, and disruption of that synergy presents mental health challenges,” Dr. Holman said in a news release.
“We were able to measure this in a nationally representative sample of Americans as they were experiencing a protracted collective trauma, which has never been done before, and this study is the first to document the prevalence and early predictors of these time distortions,” added Dr. Holman.
The findings were published online in Psychological Trauma: Theory, Research, Practice, and Policy.
Unique opportunity
During the pandemic, many people’s time perspective (TP), defined as “our view of time as it spans from our past into the future,” shifted as they “focused on the immediate, present danger of the COVID-19 pandemic and future plans became uncertain,” the investigators wrote.
Studies of convenience samples “suggested that many people experienced time slowing down, stopping, and/or speeding up as they coped with the challenges of the pandemic” – a phenomenon known as temporal disintegration (TD) in psychiatric literature.
Dr. Holman said in an interview that she researched TD after the Sept.11, 2001 World Trade Center attacks.
“We found that people who experienced that early sense of TD, the sense of ‘time falling apart,’ were more prone to getting stuck in the past and staying focused on the past event,” which led to feeling “more distress over time,” she said.
Research examining the prevalence of and psychosocial factors predicting TD are “quite rare” and studies examining TD “during an unfolding, protracted collective trauma are even rarer,” the researchers note. The COVID pandemic “presented a unique opportunity to conduct such a study,” the researchers wrote.
For their study, the investigators surveyed participants in the NORC AmeriSpeak online panel, a “probability-based panel” of 35,000 U.S. households selected at random from across the country.
The study was conducted in two waves: the first survey was administered March–April 2020, the second in September–October 2020.
Speeding up, slowing down
At wave 2, participants completed a 7-item index of TD symptoms experienced over the previous 6 months. To adjust for psychological processes that may have predisposed individuals to experience TD during the pandemic, the researchers included a Wave 1 measure of future uncertainty as a covariate.
Prepandemic health data had been collected prior to the current study.
Wave 1 participants completed a checklist reporting personal, work, and community-wide exposure to the COVID outbreak, including contracting the virus, sheltering in place, and experiencing secondary stressors. The extent and type of pandemic-related media exposure were also assessed.
At wave 2, they reported the extent of exposure to the coronavirus, financial exposures, and secondary stressors. They also completed a non–COVID-related stress/trauma exposure checklist and were asked to indicate whether the trauma, disaster, or bereavement took place prior to or during the pandemic.
The final sample consisted of 5,661 adults (52% female) who completed the wave 2 survey. Participants were divided into four age groups: 18-34, 35-49, 50-64, and 65 and older.
The most common experiences (reported by more than 65% of respondents) included being focused on the present moment, feeling that weekdays and weekends were the same, and feeling uncertain about the future.
Over half of respondents (50.4%) reported feeling as though time was speeding up, and 55.2% reported feeling as though time was slowing down. Some also reported feeling uncertain about the time of day (46.4%) and forgetting events they had just experienced (35.2%).
When the researchers controlled for feeling uncertain about the future, they found that women reported more TD than men (b = 0.11; 95% confidence interval, 0.07-0.14; P < .001).
At wave 1, associations were found between TD and COVID-related media exposure, prepandemic mental health diagnoses, and prepandemic non–COVID-related stress and trauma. At wave 2, associations were found between TD and COVID-related secondary and financial stressors (P < .001 for all).
In contrast, COVID-related work exposure at wave 1, being 45-59 years old, and living in the Midwest region were negatively associated with TD.
“The sense of the flow of the past into the present, and the present into the future is important for our mental health,” Dr. Holman said. “We need to remember who we have been, how that shaped who we are today, and where we want to go with our lives.”
Staying in the present moment is “good, when you’re doing it mindfully. But you still need to feel you can shape and work toward the future and have some sense of control,” she added.
Dr. Homan also recommended time-perspective therapy, which helps patients with PTSD to “build continuity across time – to understand and learn from the past, live in the present, and move toward the future.”
Widespread distortion
In an interview, Ruth Ogden, PhD, a lecturer at Liverpool (England) John Moores University, said the findings “confirm those reported in Europe, South America, and the Middle East, that widespread distortion to time was common during the pandemic and that distortions to time were greatest amongst those most negatively affected by the pandemic.”
The results also support her own recent research in the United Kingdom “suggesting that distortions to time during the pandemic extend to our memory for the length of the pandemic, with most people believing that lockdowns lasted far longer than they actually did,” said Dr. Ogden, who was not involved with Dr. Holman and colleagues’ current study.
“This type of subjective lengthening of the pandemic may reinforce trauma by making the traumatic period seem longer, further damaging health and well-being,” she noted. “As the negative fallouts of the pandemic continue, it is important to establish the long-term effects of time distortions during the pandemic on mental health and well-being.”
The study was funded by U.S. National Science Foundation and the National Institute on Minority Health and Health Disparities. The investigators reported no relevant financial relationships. Dr. Ogden receives funding from the Wellcome Trust.
A version of this article first appeared on Medscape.com.
ranging from difficulty keeping track of the days of the week to feeling that the hours either crawled by or sped up, new research suggests.
Results showed the sense of present focus, blurring weekdays and weekends together, and uncertainly about the future were reported by over 65% of the 5,661 survey respondents. And more than half reported the experience of feeling “time speeding up or slowing down,” report the investigators, led by E. Alison Holman, PhD, professor at the University of California, Irvine.
Significant predictors of these time distortions included being exposed to daily pandemic-related media and having a mental health diagnosis prior to the pandemic; secondary stress such as school closures and lockdown; financial stress; lifetime stress; and lifetime trauma exposure.
“Continuity between past experiences, present life, and future hopes is critical to one’s well-being, and disruption of that synergy presents mental health challenges,” Dr. Holman said in a news release.
“We were able to measure this in a nationally representative sample of Americans as they were experiencing a protracted collective trauma, which has never been done before, and this study is the first to document the prevalence and early predictors of these time distortions,” added Dr. Holman.
The findings were published online in Psychological Trauma: Theory, Research, Practice, and Policy.
Unique opportunity
During the pandemic, many people’s time perspective (TP), defined as “our view of time as it spans from our past into the future,” shifted as they “focused on the immediate, present danger of the COVID-19 pandemic and future plans became uncertain,” the investigators wrote.
Studies of convenience samples “suggested that many people experienced time slowing down, stopping, and/or speeding up as they coped with the challenges of the pandemic” – a phenomenon known as temporal disintegration (TD) in psychiatric literature.
Dr. Holman said in an interview that she researched TD after the Sept.11, 2001 World Trade Center attacks.
“We found that people who experienced that early sense of TD, the sense of ‘time falling apart,’ were more prone to getting stuck in the past and staying focused on the past event,” which led to feeling “more distress over time,” she said.
Research examining the prevalence of and psychosocial factors predicting TD are “quite rare” and studies examining TD “during an unfolding, protracted collective trauma are even rarer,” the researchers note. The COVID pandemic “presented a unique opportunity to conduct such a study,” the researchers wrote.
For their study, the investigators surveyed participants in the NORC AmeriSpeak online panel, a “probability-based panel” of 35,000 U.S. households selected at random from across the country.
The study was conducted in two waves: the first survey was administered March–April 2020, the second in September–October 2020.
Speeding up, slowing down
At wave 2, participants completed a 7-item index of TD symptoms experienced over the previous 6 months. To adjust for psychological processes that may have predisposed individuals to experience TD during the pandemic, the researchers included a Wave 1 measure of future uncertainty as a covariate.
Prepandemic health data had been collected prior to the current study.
Wave 1 participants completed a checklist reporting personal, work, and community-wide exposure to the COVID outbreak, including contracting the virus, sheltering in place, and experiencing secondary stressors. The extent and type of pandemic-related media exposure were also assessed.
At wave 2, they reported the extent of exposure to the coronavirus, financial exposures, and secondary stressors. They also completed a non–COVID-related stress/trauma exposure checklist and were asked to indicate whether the trauma, disaster, or bereavement took place prior to or during the pandemic.
The final sample consisted of 5,661 adults (52% female) who completed the wave 2 survey. Participants were divided into four age groups: 18-34, 35-49, 50-64, and 65 and older.
The most common experiences (reported by more than 65% of respondents) included being focused on the present moment, feeling that weekdays and weekends were the same, and feeling uncertain about the future.
Over half of respondents (50.4%) reported feeling as though time was speeding up, and 55.2% reported feeling as though time was slowing down. Some also reported feeling uncertain about the time of day (46.4%) and forgetting events they had just experienced (35.2%).
When the researchers controlled for feeling uncertain about the future, they found that women reported more TD than men (b = 0.11; 95% confidence interval, 0.07-0.14; P < .001).
At wave 1, associations were found between TD and COVID-related media exposure, prepandemic mental health diagnoses, and prepandemic non–COVID-related stress and trauma. At wave 2, associations were found between TD and COVID-related secondary and financial stressors (P < .001 for all).
In contrast, COVID-related work exposure at wave 1, being 45-59 years old, and living in the Midwest region were negatively associated with TD.
“The sense of the flow of the past into the present, and the present into the future is important for our mental health,” Dr. Holman said. “We need to remember who we have been, how that shaped who we are today, and where we want to go with our lives.”
Staying in the present moment is “good, when you’re doing it mindfully. But you still need to feel you can shape and work toward the future and have some sense of control,” she added.
Dr. Homan also recommended time-perspective therapy, which helps patients with PTSD to “build continuity across time – to understand and learn from the past, live in the present, and move toward the future.”
Widespread distortion
In an interview, Ruth Ogden, PhD, a lecturer at Liverpool (England) John Moores University, said the findings “confirm those reported in Europe, South America, and the Middle East, that widespread distortion to time was common during the pandemic and that distortions to time were greatest amongst those most negatively affected by the pandemic.”
The results also support her own recent research in the United Kingdom “suggesting that distortions to time during the pandemic extend to our memory for the length of the pandemic, with most people believing that lockdowns lasted far longer than they actually did,” said Dr. Ogden, who was not involved with Dr. Holman and colleagues’ current study.
“This type of subjective lengthening of the pandemic may reinforce trauma by making the traumatic period seem longer, further damaging health and well-being,” she noted. “As the negative fallouts of the pandemic continue, it is important to establish the long-term effects of time distortions during the pandemic on mental health and well-being.”
The study was funded by U.S. National Science Foundation and the National Institute on Minority Health and Health Disparities. The investigators reported no relevant financial relationships. Dr. Ogden receives funding from the Wellcome Trust.
A version of this article first appeared on Medscape.com.
FROM PSYCHOLOGICAL TRAUMA: THEORY, RESEARCH, PRACTICE, AND POLICY
Nearly 30% of U.S. cancer deaths linked to smoking
Nearly 123,000 cancer deaths – or
That corresponds to more than 2 million person-years of lost life and nearly $21 billion in annual lost earnings.
“During the past few decades, smoking has substantially declined in the U.S., followed by great declines in mortality from lung cancer and some other smoking-related cancers,” said lead author Farhad Islami, MD, senior scientific director of cancer disparity research at the American Cancer Society.
Despite this “remarkable progress, our results indicate that smoking is still associated with about 30% of all cancer deaths and substantial lost earnings in the U.S., and that more work should be done to further reduce smoking in the country,” he said.
The study was published online in the International Journal of Cancer.
Dr. Islami and colleagues had found that lost earnings from cancer deaths in 2015 came to nearly $95 billion. Other research showed that a substantial portion of lost earnings from cancer deaths could be traced to cigarette smoking, but estimates were more than a decade old.
To provide more recent estimates and help guide tobacco control policies, Dr. Islami and colleagues estimated person-years of life lost (PYLL) and lost earnings from cigarette smoking-related cancer deaths in 2019.
Of the 418,563 cancer deaths in adults ages 25-79 years, an estimated 122,951 could be linked to cigarette smoking. That corresponds to 29.4% of all cancer deaths and roughly 2.2 million PYLL. Translated to lost earnings, the authors estimated $20.9 billion total, with average lost earnings of $170,000 per cancer death linked to smoking.
By cancer type, lung cancer accounted for about 62%, or $12.9 billion, of the total lost earnings linked to smoking, followed by esophageal cancer (7%, or $1.5 billion), colorectal cancer (6%, or $1.2 billion), and liver cancer (5%, or $1.1 billion).
Smoking-related death rates were highest in the 13 “tobacco nation” states with weaker tobacco control policies and a higher rate of cigarette smoking. These states are Alabama, Arkansas, Indiana, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Ohio, Oklahoma, South Carolina, Tennessee, and West Virginia.
The lost earnings rate in all 13 tobacco nation states combined was about 44% higher, compared with other states and the District of Columbia combined, and the annual PYLL rate was 47% higher in tobacco nation states.
The researchers estimated that if PYLL and lost earnings rates in all states matched those in Utah, which has the lowest rates, more than half of the total PYLL and lost earnings nationally would have been avoided. In other words, that would mean 1.27 million PYLL and $10.5 billion saved in 2019.
Ending the ‘scourge of tobacco’
To kick the smoking habit, health providers should “screen patients for tobacco use, document tobacco use status, advise people who smoke to quit, and assist in attempts to quit,” Dr. Islami said.
Getting more people to screen for lung cancer in the United States is also important, given that only 6.6% of eligible people in 2019 received screening.
In a statement, Lisa Lacasse, president of the American Cancer Society Cancer Action Network, said this report “further demonstrates just how critical reducing tobacco use is to ending suffering and death from cancer.”
To end the “scourge of tobacco,” local, state, and federal lawmakers need to pass proven tobacco control policies, she said.
These include regular and significant tobacco tax increases, thorough statewide smoke-free laws, and enough funding for state programs to prevent and stop smoking. It also means ensuring all Medicaid enrollees have access to all services that can help smokers quit as well as access to all FDA-approved medications that help users stop smoking.
“We have the tools to get this done, we just need lawmakers to act,” Ms. Lacasse said.
A version of this article first appeared on WebMD.com.
Nearly 123,000 cancer deaths – or
That corresponds to more than 2 million person-years of lost life and nearly $21 billion in annual lost earnings.
“During the past few decades, smoking has substantially declined in the U.S., followed by great declines in mortality from lung cancer and some other smoking-related cancers,” said lead author Farhad Islami, MD, senior scientific director of cancer disparity research at the American Cancer Society.
Despite this “remarkable progress, our results indicate that smoking is still associated with about 30% of all cancer deaths and substantial lost earnings in the U.S., and that more work should be done to further reduce smoking in the country,” he said.
The study was published online in the International Journal of Cancer.
Dr. Islami and colleagues had found that lost earnings from cancer deaths in 2015 came to nearly $95 billion. Other research showed that a substantial portion of lost earnings from cancer deaths could be traced to cigarette smoking, but estimates were more than a decade old.
To provide more recent estimates and help guide tobacco control policies, Dr. Islami and colleagues estimated person-years of life lost (PYLL) and lost earnings from cigarette smoking-related cancer deaths in 2019.
Of the 418,563 cancer deaths in adults ages 25-79 years, an estimated 122,951 could be linked to cigarette smoking. That corresponds to 29.4% of all cancer deaths and roughly 2.2 million PYLL. Translated to lost earnings, the authors estimated $20.9 billion total, with average lost earnings of $170,000 per cancer death linked to smoking.
By cancer type, lung cancer accounted for about 62%, or $12.9 billion, of the total lost earnings linked to smoking, followed by esophageal cancer (7%, or $1.5 billion), colorectal cancer (6%, or $1.2 billion), and liver cancer (5%, or $1.1 billion).
Smoking-related death rates were highest in the 13 “tobacco nation” states with weaker tobacco control policies and a higher rate of cigarette smoking. These states are Alabama, Arkansas, Indiana, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Ohio, Oklahoma, South Carolina, Tennessee, and West Virginia.
The lost earnings rate in all 13 tobacco nation states combined was about 44% higher, compared with other states and the District of Columbia combined, and the annual PYLL rate was 47% higher in tobacco nation states.
The researchers estimated that if PYLL and lost earnings rates in all states matched those in Utah, which has the lowest rates, more than half of the total PYLL and lost earnings nationally would have been avoided. In other words, that would mean 1.27 million PYLL and $10.5 billion saved in 2019.
Ending the ‘scourge of tobacco’
To kick the smoking habit, health providers should “screen patients for tobacco use, document tobacco use status, advise people who smoke to quit, and assist in attempts to quit,” Dr. Islami said.
Getting more people to screen for lung cancer in the United States is also important, given that only 6.6% of eligible people in 2019 received screening.
In a statement, Lisa Lacasse, president of the American Cancer Society Cancer Action Network, said this report “further demonstrates just how critical reducing tobacco use is to ending suffering and death from cancer.”
To end the “scourge of tobacco,” local, state, and federal lawmakers need to pass proven tobacco control policies, she said.
These include regular and significant tobacco tax increases, thorough statewide smoke-free laws, and enough funding for state programs to prevent and stop smoking. It also means ensuring all Medicaid enrollees have access to all services that can help smokers quit as well as access to all FDA-approved medications that help users stop smoking.
“We have the tools to get this done, we just need lawmakers to act,” Ms. Lacasse said.
A version of this article first appeared on WebMD.com.
Nearly 123,000 cancer deaths – or
That corresponds to more than 2 million person-years of lost life and nearly $21 billion in annual lost earnings.
“During the past few decades, smoking has substantially declined in the U.S., followed by great declines in mortality from lung cancer and some other smoking-related cancers,” said lead author Farhad Islami, MD, senior scientific director of cancer disparity research at the American Cancer Society.
Despite this “remarkable progress, our results indicate that smoking is still associated with about 30% of all cancer deaths and substantial lost earnings in the U.S., and that more work should be done to further reduce smoking in the country,” he said.
The study was published online in the International Journal of Cancer.
Dr. Islami and colleagues had found that lost earnings from cancer deaths in 2015 came to nearly $95 billion. Other research showed that a substantial portion of lost earnings from cancer deaths could be traced to cigarette smoking, but estimates were more than a decade old.
To provide more recent estimates and help guide tobacco control policies, Dr. Islami and colleagues estimated person-years of life lost (PYLL) and lost earnings from cigarette smoking-related cancer deaths in 2019.
Of the 418,563 cancer deaths in adults ages 25-79 years, an estimated 122,951 could be linked to cigarette smoking. That corresponds to 29.4% of all cancer deaths and roughly 2.2 million PYLL. Translated to lost earnings, the authors estimated $20.9 billion total, with average lost earnings of $170,000 per cancer death linked to smoking.
By cancer type, lung cancer accounted for about 62%, or $12.9 billion, of the total lost earnings linked to smoking, followed by esophageal cancer (7%, or $1.5 billion), colorectal cancer (6%, or $1.2 billion), and liver cancer (5%, or $1.1 billion).
Smoking-related death rates were highest in the 13 “tobacco nation” states with weaker tobacco control policies and a higher rate of cigarette smoking. These states are Alabama, Arkansas, Indiana, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Ohio, Oklahoma, South Carolina, Tennessee, and West Virginia.
The lost earnings rate in all 13 tobacco nation states combined was about 44% higher, compared with other states and the District of Columbia combined, and the annual PYLL rate was 47% higher in tobacco nation states.
The researchers estimated that if PYLL and lost earnings rates in all states matched those in Utah, which has the lowest rates, more than half of the total PYLL and lost earnings nationally would have been avoided. In other words, that would mean 1.27 million PYLL and $10.5 billion saved in 2019.
Ending the ‘scourge of tobacco’
To kick the smoking habit, health providers should “screen patients for tobacco use, document tobacco use status, advise people who smoke to quit, and assist in attempts to quit,” Dr. Islami said.
Getting more people to screen for lung cancer in the United States is also important, given that only 6.6% of eligible people in 2019 received screening.
In a statement, Lisa Lacasse, president of the American Cancer Society Cancer Action Network, said this report “further demonstrates just how critical reducing tobacco use is to ending suffering and death from cancer.”
To end the “scourge of tobacco,” local, state, and federal lawmakers need to pass proven tobacco control policies, she said.
These include regular and significant tobacco tax increases, thorough statewide smoke-free laws, and enough funding for state programs to prevent and stop smoking. It also means ensuring all Medicaid enrollees have access to all services that can help smokers quit as well as access to all FDA-approved medications that help users stop smoking.
“We have the tools to get this done, we just need lawmakers to act,” Ms. Lacasse said.
A version of this article first appeared on WebMD.com.
FROM THE INTERNATIONAL JOURNAL OF CANCER
Drinking black tea linked to lower risk of dying from cardiovascular disease
Drinking tea has several reported health benefits, but most studies have been conducted in regions where green tea predominates.
The findings come from a prospective study of nearly 500,000 participants in the UK Biobank cohort, among whom drinking black tea was common. They suggest that drinking black tea may be associated with a moderately lower all-cause mortality risk, and the risk was lowest among those drinking two or more cups of tea per day.
The study was published online in Annals of Internal Medicine.
During a median follow-up of 11.2 years, those who drank at least two cups of tea each day had a lower all-cause mortality risk, reported Maki Inoue-Choi, PhD, and colleagues from the National Cancer Institute in Bethesda, Md.
After multivariate adjustment, the hazard ratios for death among tea drinkers, compared with no tea intake, were similar across intake levels: 0.95 for daily intake of up to 1 cup, 0.87 for 2-3 cups, 0.88 for 4-5 cups, 0.88 for 6-7 cups, 0.91 for 8-9 cups, and 0.89 for 10 or more cups.
Drinking tea also showed an inverse association with mortality from cardiovascular disease (adjusted HRs ranging from 0.98 to 0.76), ischemic heart disease (aHRs ranging from 1.03 to 0.74), and stroke (aHRs ranging from 0.92 to 0.48 ), However, the researchers added that “no clear trend was seen for cancer or respiratory disease mortality, with associations among higher intake categories tending toward the null.”
There is “no clear answer” as to why no association was observed between tea consumption and cancer mortality in the current study, Dr. Inoue-Choi said at a press briefing. Notably, the effects were apparent regardless of whether milk or sugar was added to tea, tea temperature, or genetic variations in caffeine metabolism among participants.
She and her colleagues controlled for these factors, as well as numerous others that could confound the results, including coffee consumption and baseline health and demographic characteristics..
The study subjects were 498,043 adults with a mean baseline age of 56.5 years. About 85% reported drinking tea, 90% reported drinking black tea, and most drank two to three cups (29%), four to five cups (26%), or six to seven cups (12%) per day.
A limitation of the study is the lack of information on certain aspects of tea intake, such as portion size and tea strength, the authors noted.
Tea is among the most frequently consumed beverages worldwide, and studies from places where green tea is popular, like China and Japan, have demonstrated health benefits. Data from places where black tea is more commonly consumed have been lacking and have provided conflicting results, Dr. Inoue-Choi said.
A presumed mechanism of action related to tea consumption is reduced oxidative stress and inflammation thanks to "polyphenols and flavonoids, namely catechins and their oxidated products," the authors explained. Oxidative stress and inflammation may promote carcinogenesis; therefore, reducing oxidative stress and inflammation may improve endothelial function, they added.
“While these findings may offer reassurance to tea drinkers, they do not indicate that people should start drinking tea or change their tea consumption for health benefits,” Dr. Inoue-Choi said, explaining that “the results need to be replicated in future studies and extended in other diverse populations.”
This study was funded by the National Cancer Institute Intramural Research Program and the NCI division of cancer epidemiology & genetics. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This article was updated 8/31/22.
Drinking tea has several reported health benefits, but most studies have been conducted in regions where green tea predominates.
The findings come from a prospective study of nearly 500,000 participants in the UK Biobank cohort, among whom drinking black tea was common. They suggest that drinking black tea may be associated with a moderately lower all-cause mortality risk, and the risk was lowest among those drinking two or more cups of tea per day.
The study was published online in Annals of Internal Medicine.
During a median follow-up of 11.2 years, those who drank at least two cups of tea each day had a lower all-cause mortality risk, reported Maki Inoue-Choi, PhD, and colleagues from the National Cancer Institute in Bethesda, Md.
After multivariate adjustment, the hazard ratios for death among tea drinkers, compared with no tea intake, were similar across intake levels: 0.95 for daily intake of up to 1 cup, 0.87 for 2-3 cups, 0.88 for 4-5 cups, 0.88 for 6-7 cups, 0.91 for 8-9 cups, and 0.89 for 10 or more cups.
Drinking tea also showed an inverse association with mortality from cardiovascular disease (adjusted HRs ranging from 0.98 to 0.76), ischemic heart disease (aHRs ranging from 1.03 to 0.74), and stroke (aHRs ranging from 0.92 to 0.48 ), However, the researchers added that “no clear trend was seen for cancer or respiratory disease mortality, with associations among higher intake categories tending toward the null.”
There is “no clear answer” as to why no association was observed between tea consumption and cancer mortality in the current study, Dr. Inoue-Choi said at a press briefing. Notably, the effects were apparent regardless of whether milk or sugar was added to tea, tea temperature, or genetic variations in caffeine metabolism among participants.
She and her colleagues controlled for these factors, as well as numerous others that could confound the results, including coffee consumption and baseline health and demographic characteristics..
The study subjects were 498,043 adults with a mean baseline age of 56.5 years. About 85% reported drinking tea, 90% reported drinking black tea, and most drank two to three cups (29%), four to five cups (26%), or six to seven cups (12%) per day.
A limitation of the study is the lack of information on certain aspects of tea intake, such as portion size and tea strength, the authors noted.
Tea is among the most frequently consumed beverages worldwide, and studies from places where green tea is popular, like China and Japan, have demonstrated health benefits. Data from places where black tea is more commonly consumed have been lacking and have provided conflicting results, Dr. Inoue-Choi said.
A presumed mechanism of action related to tea consumption is reduced oxidative stress and inflammation thanks to "polyphenols and flavonoids, namely catechins and their oxidated products," the authors explained. Oxidative stress and inflammation may promote carcinogenesis; therefore, reducing oxidative stress and inflammation may improve endothelial function, they added.
“While these findings may offer reassurance to tea drinkers, they do not indicate that people should start drinking tea or change their tea consumption for health benefits,” Dr. Inoue-Choi said, explaining that “the results need to be replicated in future studies and extended in other diverse populations.”
This study was funded by the National Cancer Institute Intramural Research Program and the NCI division of cancer epidemiology & genetics. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This article was updated 8/31/22.
Drinking tea has several reported health benefits, but most studies have been conducted in regions where green tea predominates.
The findings come from a prospective study of nearly 500,000 participants in the UK Biobank cohort, among whom drinking black tea was common. They suggest that drinking black tea may be associated with a moderately lower all-cause mortality risk, and the risk was lowest among those drinking two or more cups of tea per day.
The study was published online in Annals of Internal Medicine.
During a median follow-up of 11.2 years, those who drank at least two cups of tea each day had a lower all-cause mortality risk, reported Maki Inoue-Choi, PhD, and colleagues from the National Cancer Institute in Bethesda, Md.
After multivariate adjustment, the hazard ratios for death among tea drinkers, compared with no tea intake, were similar across intake levels: 0.95 for daily intake of up to 1 cup, 0.87 for 2-3 cups, 0.88 for 4-5 cups, 0.88 for 6-7 cups, 0.91 for 8-9 cups, and 0.89 for 10 or more cups.
Drinking tea also showed an inverse association with mortality from cardiovascular disease (adjusted HRs ranging from 0.98 to 0.76), ischemic heart disease (aHRs ranging from 1.03 to 0.74), and stroke (aHRs ranging from 0.92 to 0.48 ), However, the researchers added that “no clear trend was seen for cancer or respiratory disease mortality, with associations among higher intake categories tending toward the null.”
There is “no clear answer” as to why no association was observed between tea consumption and cancer mortality in the current study, Dr. Inoue-Choi said at a press briefing. Notably, the effects were apparent regardless of whether milk or sugar was added to tea, tea temperature, or genetic variations in caffeine metabolism among participants.
She and her colleagues controlled for these factors, as well as numerous others that could confound the results, including coffee consumption and baseline health and demographic characteristics..
The study subjects were 498,043 adults with a mean baseline age of 56.5 years. About 85% reported drinking tea, 90% reported drinking black tea, and most drank two to three cups (29%), four to five cups (26%), or six to seven cups (12%) per day.
A limitation of the study is the lack of information on certain aspects of tea intake, such as portion size and tea strength, the authors noted.
Tea is among the most frequently consumed beverages worldwide, and studies from places where green tea is popular, like China and Japan, have demonstrated health benefits. Data from places where black tea is more commonly consumed have been lacking and have provided conflicting results, Dr. Inoue-Choi said.
A presumed mechanism of action related to tea consumption is reduced oxidative stress and inflammation thanks to "polyphenols and flavonoids, namely catechins and their oxidated products," the authors explained. Oxidative stress and inflammation may promote carcinogenesis; therefore, reducing oxidative stress and inflammation may improve endothelial function, they added.
“While these findings may offer reassurance to tea drinkers, they do not indicate that people should start drinking tea or change their tea consumption for health benefits,” Dr. Inoue-Choi said, explaining that “the results need to be replicated in future studies and extended in other diverse populations.”
This study was funded by the National Cancer Institute Intramural Research Program and the NCI division of cancer epidemiology & genetics. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This article was updated 8/31/22.
FROM ANNALS OF INTERNAL MEDICINE
At-home test for oral/throat cancer launched in U.S.
Recently, a home test for oral and throat cancer was launched in the United States, and it is being marketed directly to the general public, aimed at former or current tobacco users and anyone 50 years or older.
Individuals can order the test – CancerDetect Test for Oral & Throat Cancer – directly from its maker, Viome Life Sciences, for $399.
The test is being marketed under the agency’s “laboratory developed test” rubric.
People who qualify and buy the test are mailed a saliva collection tube, which they fill and mail back. The company then analyzes the RNA for changes in human cells and the oropharyngeal microbiome that are associated with cancer. During a 15-minute telemedicine conference – included in the $399 cost – those who test positive are told to follow up with a secondary care center for a definitive diagnosis.
For people who test positive but have no visible lesion to biopsy, doctors will likely opt for surveillance, computer scientist Guruduth Banavar, PhD, Viome’s chief technology officer, told this news organization.
Dr. Banavar said people have been buying the test every day since it was launched in early August, but he declined to give specific sales figures.
CancerDetect’s tagline is “test at home for peace of mind.” The test “brings unprecedented accuracy to early cancer detection and prevention,” the company said in a press release announcing the launch.
The test showed an overall specificity of 94% and sensitivity of 84.2%-90% for cancer in Viome’s latest study, which is posted on medRxiv.org as a preprint. Banavar said it has been submitted to a top-tier medical journal.
Viome plans to market CancerDetect “in every possible way” to consumers, including social media, Dr. Banavar said. CancerDetect is not sold on Amazon at the moment, but the company sells another at-home test for gut microbiome plus cellular health on the website.
As for outreach to the medical community, “we will start doing that with dentists first” and then eventually oncologists and other doctors, but “our primary target is to get out to the consumers themselves,” Dr. Banavar said.
Viome’s main goal is to help consumers be proactive regarding their health, he said.
An expert opinion
The marketing push means that sooner or later, oncologists will likely have to deal with a patient who tests positive on CancerDetect, so this news organization turned to numerous experts for their thoughts. None had heard about the test, but one responded with comments.
“I am happy to see industry working on strategies for the early detection of oral and throat cancers,” and CancerDetect has “potential,” said surgical oncologist Saral Mehra, MD, MBA, chief of head and neck surgery at Yale University, New Haven, Conn.
However, after reviewing the study posted on medRxiv, Dr. Mehra advised caution. He said he was concerned about false negative results leading to missed cancers and false positives leading to unnecessary anxiety and testing.
According to the medRxiv preprint, the test was developed and validated using saliva samples from 1,175 people 50 years or older as well as adults with a history of tobacco use.
In the 230-sample validation cohort, CancerDetect correctly classified 18 out of 20 people with oral squamous cell carcinoma (OSCC) and 64/76 with oropharyngeal squamous cell carcinoma (OPSCC), yielding sensitivities of 90% and 84.2%, respectively.
The test also correctly identified 126/134 people as cancer free, for a specificity of 94%.
Results were similar between early and late-stage disease, but mixed in subgroups. Among people younger than age 50, for instance, 4/4 (100%) with OSCC and 2/3 (66.7%) with OPSCC were correctly classified as positive. Among older people, 15/17 (88.2%) with OSCC and 62/73 (84.9%) with OPSCC were correctly classified
Commenting on the results, Dr. Mehra noted that “the power of the study, especially for subgroup analysis, was low,” and investigators “used both advanced-stage and early-stage cancer patients in the model, while the target population for this test is early stage.
“The research needs to be tightened significantly on specific target populations, the models adjusted to really limit false negatives, and a plan [put in place] to act upon positive results,” he said.
Also, the ability of CancerDetect to pick up premalignant lesions – “the greatest value in a screening test” – is not clear, he added.
Viome’s Dr. Banavar said that CancerDetect is in its first iteration, and the test uses machine learning, so its diagnostic performance will improve with the ongoing addition of real-world data.
The company is organizing a pivotal trial to gain formal FDA approval, with results expected in a year and a half or so, he said.
Viome is pushing ahead with its RNA diagnosis technology for the entire range of alimentary canal cancers and disorders, including inflammatory bowel disease. The company has partnered with pharmaceutical companies, including GSK, for vaccines, Dr. Banavar said.
Dr. Mehra reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Recently, a home test for oral and throat cancer was launched in the United States, and it is being marketed directly to the general public, aimed at former or current tobacco users and anyone 50 years or older.
Individuals can order the test – CancerDetect Test for Oral & Throat Cancer – directly from its maker, Viome Life Sciences, for $399.
The test is being marketed under the agency’s “laboratory developed test” rubric.
People who qualify and buy the test are mailed a saliva collection tube, which they fill and mail back. The company then analyzes the RNA for changes in human cells and the oropharyngeal microbiome that are associated with cancer. During a 15-minute telemedicine conference – included in the $399 cost – those who test positive are told to follow up with a secondary care center for a definitive diagnosis.
For people who test positive but have no visible lesion to biopsy, doctors will likely opt for surveillance, computer scientist Guruduth Banavar, PhD, Viome’s chief technology officer, told this news organization.
Dr. Banavar said people have been buying the test every day since it was launched in early August, but he declined to give specific sales figures.
CancerDetect’s tagline is “test at home for peace of mind.” The test “brings unprecedented accuracy to early cancer detection and prevention,” the company said in a press release announcing the launch.
The test showed an overall specificity of 94% and sensitivity of 84.2%-90% for cancer in Viome’s latest study, which is posted on medRxiv.org as a preprint. Banavar said it has been submitted to a top-tier medical journal.
Viome plans to market CancerDetect “in every possible way” to consumers, including social media, Dr. Banavar said. CancerDetect is not sold on Amazon at the moment, but the company sells another at-home test for gut microbiome plus cellular health on the website.
As for outreach to the medical community, “we will start doing that with dentists first” and then eventually oncologists and other doctors, but “our primary target is to get out to the consumers themselves,” Dr. Banavar said.
Viome’s main goal is to help consumers be proactive regarding their health, he said.
An expert opinion
The marketing push means that sooner or later, oncologists will likely have to deal with a patient who tests positive on CancerDetect, so this news organization turned to numerous experts for their thoughts. None had heard about the test, but one responded with comments.
“I am happy to see industry working on strategies for the early detection of oral and throat cancers,” and CancerDetect has “potential,” said surgical oncologist Saral Mehra, MD, MBA, chief of head and neck surgery at Yale University, New Haven, Conn.
However, after reviewing the study posted on medRxiv, Dr. Mehra advised caution. He said he was concerned about false negative results leading to missed cancers and false positives leading to unnecessary anxiety and testing.
According to the medRxiv preprint, the test was developed and validated using saliva samples from 1,175 people 50 years or older as well as adults with a history of tobacco use.
In the 230-sample validation cohort, CancerDetect correctly classified 18 out of 20 people with oral squamous cell carcinoma (OSCC) and 64/76 with oropharyngeal squamous cell carcinoma (OPSCC), yielding sensitivities of 90% and 84.2%, respectively.
The test also correctly identified 126/134 people as cancer free, for a specificity of 94%.
Results were similar between early and late-stage disease, but mixed in subgroups. Among people younger than age 50, for instance, 4/4 (100%) with OSCC and 2/3 (66.7%) with OPSCC were correctly classified as positive. Among older people, 15/17 (88.2%) with OSCC and 62/73 (84.9%) with OPSCC were correctly classified
Commenting on the results, Dr. Mehra noted that “the power of the study, especially for subgroup analysis, was low,” and investigators “used both advanced-stage and early-stage cancer patients in the model, while the target population for this test is early stage.
“The research needs to be tightened significantly on specific target populations, the models adjusted to really limit false negatives, and a plan [put in place] to act upon positive results,” he said.
Also, the ability of CancerDetect to pick up premalignant lesions – “the greatest value in a screening test” – is not clear, he added.
Viome’s Dr. Banavar said that CancerDetect is in its first iteration, and the test uses machine learning, so its diagnostic performance will improve with the ongoing addition of real-world data.
The company is organizing a pivotal trial to gain formal FDA approval, with results expected in a year and a half or so, he said.
Viome is pushing ahead with its RNA diagnosis technology for the entire range of alimentary canal cancers and disorders, including inflammatory bowel disease. The company has partnered with pharmaceutical companies, including GSK, for vaccines, Dr. Banavar said.
Dr. Mehra reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Recently, a home test for oral and throat cancer was launched in the United States, and it is being marketed directly to the general public, aimed at former or current tobacco users and anyone 50 years or older.
Individuals can order the test – CancerDetect Test for Oral & Throat Cancer – directly from its maker, Viome Life Sciences, for $399.
The test is being marketed under the agency’s “laboratory developed test” rubric.
People who qualify and buy the test are mailed a saliva collection tube, which they fill and mail back. The company then analyzes the RNA for changes in human cells and the oropharyngeal microbiome that are associated with cancer. During a 15-minute telemedicine conference – included in the $399 cost – those who test positive are told to follow up with a secondary care center for a definitive diagnosis.
For people who test positive but have no visible lesion to biopsy, doctors will likely opt for surveillance, computer scientist Guruduth Banavar, PhD, Viome’s chief technology officer, told this news organization.
Dr. Banavar said people have been buying the test every day since it was launched in early August, but he declined to give specific sales figures.
CancerDetect’s tagline is “test at home for peace of mind.” The test “brings unprecedented accuracy to early cancer detection and prevention,” the company said in a press release announcing the launch.
The test showed an overall specificity of 94% and sensitivity of 84.2%-90% for cancer in Viome’s latest study, which is posted on medRxiv.org as a preprint. Banavar said it has been submitted to a top-tier medical journal.
Viome plans to market CancerDetect “in every possible way” to consumers, including social media, Dr. Banavar said. CancerDetect is not sold on Amazon at the moment, but the company sells another at-home test for gut microbiome plus cellular health on the website.
As for outreach to the medical community, “we will start doing that with dentists first” and then eventually oncologists and other doctors, but “our primary target is to get out to the consumers themselves,” Dr. Banavar said.
Viome’s main goal is to help consumers be proactive regarding their health, he said.
An expert opinion
The marketing push means that sooner or later, oncologists will likely have to deal with a patient who tests positive on CancerDetect, so this news organization turned to numerous experts for their thoughts. None had heard about the test, but one responded with comments.
“I am happy to see industry working on strategies for the early detection of oral and throat cancers,” and CancerDetect has “potential,” said surgical oncologist Saral Mehra, MD, MBA, chief of head and neck surgery at Yale University, New Haven, Conn.
However, after reviewing the study posted on medRxiv, Dr. Mehra advised caution. He said he was concerned about false negative results leading to missed cancers and false positives leading to unnecessary anxiety and testing.
According to the medRxiv preprint, the test was developed and validated using saliva samples from 1,175 people 50 years or older as well as adults with a history of tobacco use.
In the 230-sample validation cohort, CancerDetect correctly classified 18 out of 20 people with oral squamous cell carcinoma (OSCC) and 64/76 with oropharyngeal squamous cell carcinoma (OPSCC), yielding sensitivities of 90% and 84.2%, respectively.
The test also correctly identified 126/134 people as cancer free, for a specificity of 94%.
Results were similar between early and late-stage disease, but mixed in subgroups. Among people younger than age 50, for instance, 4/4 (100%) with OSCC and 2/3 (66.7%) with OPSCC were correctly classified as positive. Among older people, 15/17 (88.2%) with OSCC and 62/73 (84.9%) with OPSCC were correctly classified
Commenting on the results, Dr. Mehra noted that “the power of the study, especially for subgroup analysis, was low,” and investigators “used both advanced-stage and early-stage cancer patients in the model, while the target population for this test is early stage.
“The research needs to be tightened significantly on specific target populations, the models adjusted to really limit false negatives, and a plan [put in place] to act upon positive results,” he said.
Also, the ability of CancerDetect to pick up premalignant lesions – “the greatest value in a screening test” – is not clear, he added.
Viome’s Dr. Banavar said that CancerDetect is in its first iteration, and the test uses machine learning, so its diagnostic performance will improve with the ongoing addition of real-world data.
The company is organizing a pivotal trial to gain formal FDA approval, with results expected in a year and a half or so, he said.
Viome is pushing ahead with its RNA diagnosis technology for the entire range of alimentary canal cancers and disorders, including inflammatory bowel disease. The company has partnered with pharmaceutical companies, including GSK, for vaccines, Dr. Banavar said.
Dr. Mehra reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
How do you live with COVID? One doctor’s personal experience
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”

“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.
Early in 2020, Anne Peters, MD, caught COVID-19. The author of Medscape’s “Peters on Diabetes” column was sick in March 2020 before state-mandated lockdowns, and well before there were any vaccines.
She remembers sitting in a small exam room with two patients who had flown to her Los Angeles office from New York. The elderly couple had hearing difficulties, so Dr. Peters sat close to them, putting on a continuous glucose monitor. “At that time, we didn’t think of COVID-19 as being in L.A.,” Dr. Peters recalled, “so I think we were not terribly consistent at mask-wearing due to the need to educate.”
“Several days later, I got COVID, but I didn’t know I had COVID per se. I felt crappy, had a terrible sore throat, lost my sense of taste and smell [which was not yet described as a COVID symptom], was completely exhausted, but had no fever or cough, which were the only criteria for getting COVID tested at the time. I didn’t know I had been exposed until 2 weeks later, when the patient’s assistant returned the sensor warning us to ‘be careful’ with it because the patient and his wife were recovering from COVID.”
That early battle with COVID-19 was just the beginning of what would become a 2-year struggle, including familial loss amid her own health problems and concerns about the under-resourced patients she cares for. Here, she shares her journey through the pandemic with this news organization.
Question: Thanks for talking to us. Let’s discuss your journey over these past 2.5 years.
Answer: Everybody has their own COVID story because we all went through this together. Some of us have worse COVID stories, and some of us have better ones, but all have been impacted.
I’m not a sick person. I’m a very healthy person but COVID made me so unwell for 2 years. The brain fog and fatigue were nothing compared to the autonomic neuropathy that affected my heart. It was really limiting for me. And I still don’t know the long-term implications, looking 20-30 years from now.
Q: When you initially had COVID, what were your symptoms? What was the impact?
A: I had all the symptoms of COVID, except for a cough and fever. I lost my sense of taste and smell. I had a horrible headache, a sore throat, and I was exhausted. I couldn’t get tested because I didn’t have the right symptoms.
Despite being sick, I never stopped working but just switched to telemedicine. I also took my regular monthly trip to our cabin in Montana. I unknowingly flew on a plane with COVID. I wore a well-fitted N95 mask, so I don’t think I gave anybody COVID. I didn’t give COVID to my partner, Eric, which is hard to believe as – at 77 – he’s older than me. He has diabetes, heart disease, and every other high-risk characteristic. If he’d gotten COVID back then, it would have been terrible, as there were no treatments, but luckily he didn’t get it.
Q: When were you officially diagnosed?
A: Two or 3 months after I thought I might have had COVID, I checked my antibodies, which tested strongly positive for a prior COVID infection. That was when I knew all the symptoms I’d had were due to the disease.
Q: Not only were you dealing with your own illness, but also that of those close to you. Can you talk about that?
A: In April 2020, my mother who was in her 90s and otherwise healthy except for dementia, got COVID. She could have gotten it from me. I visited often but wore a mask. She had all the horrible pulmonary symptoms. In her advance directive, she didn’t want to be hospitalized so I kept her in her home. She died from COVID in her own bed. It was fairly brutal, but at least I kept her where she felt comforted.
My 91-year-old dad was living in a different residential facility. Throughout COVID he had become very depressed because his social patterns had changed. Prior to COVID, they all ate together, but during the pandemic they were unable to. He missed his social connections, disliked being isolated in his room, hated everyone in masks.
He was a bit demented, but not so much that he couldn’t communicate with me or remember where his grandson was going to law school. I wasn’t allowed inside the facility, which was hard on him. I hadn’t told him his wife died because the hospice social workers advised me that I shouldn’t give him news that he couldn’t process readily until I could spend time with him. Unfortunately, that time never came. In December 2020, he got COVID. One of the people in that facility had gone to the hospital, came back, and tested negative, but actually had COVID and gave it to my dad. The guy who gave it to my dad didn’t die but my dad was terribly ill. He died 2 weeks short of getting his vaccine. He was coherent enough to have a conversation. I asked him: ‘Do you want to go to the hospital?’ And he said: ‘No, because it would be too scary,’ since he couldn’t be with me. I put him on hospice and held his hand as he died from pulmonary COVID, which was awful. I couldn’t give him enough morphine or valium to ease his breathing. But his last words to me were “I love you,” and at the very end he seemed peaceful, which was a blessing.
I got an autopsy, because he wanted one. Nothing else was wrong with him other than COVID. It destroyed his lungs. The rest of him was fine – no heart disease, cancer, or anything else. He died of COVID-19, the same as my mother.
That same week, my aunt, my only surviving older relative, who was in Des Moines, Iowa, died of COVID-19. All three family members died before the vaccine came out.
It was hard to lose my parents. I’m the only surviving child because my sister died in her 20s. It’s not been an easy pandemic. But what pandemic is easy? I just happened to have lost more people than most. Ironically, my grandfather was one of the legionnaires at the Bellevue-Stratford Hotel in Philadelphia in 1976 and died of Legionnaire’s disease before we knew what was causing the outbreak.
Q: Were you still struggling with COVID?
A: COVID impacted my whole body. I lost a lot of weight. I didn’t want to eat, and my gastrointestinal system was not happy. It took a while for my sense of taste and smell to come back. Nothing tasted good. I’m not a foodie; I don’t really care about food. We could get takeout or whatever, but none of it appealed to me. I’m not so sure it was a taste thing, I just didn’t feel like eating.
I didn’t realize I had “brain fog” per se, because I felt stressed and overwhelmed by the pandemic and my patients’ concerns. But one day, about 3 months after I had developed COVID, I woke up without the fog. Which made me aware that I hadn’t been feeling right up until that point.
The worst symptoms, however, were cardiac. I noticed also immediately that my heart rate went up very quickly with minimal exertion. My pulse has always been in the 55-60 bpm range, and suddenly just walking across a room made it go up to over 140 bpm. If I did any aerobic activity, it went up over 160 and would be associated with dyspnea and chest pain. I believed these were all post-COVID symptoms and felt validated when reports of others having similar issues were published in the literature.
Q: Did you continue seeing patients?
A: Yes, of course. Patients never needed their doctors more. In East L.A., where patients don’t have easy access to telemedicine, I kept going into clinic throughout the pandemic. In the more affluent Westside of Los Angeles, we switched to telemedicine, which was quite effective for most. However, because diabetes was associated with an increased risk of hospitalization and death from COVID, my patients were understandably afraid. I’ve never been busier, but (like all health care providers), I became more of a COVID provider than a diabetologist.
Q: Do you feel your battle with COVID impacted your work?
A: It didn’t affect me at work. If I was sitting still, I was fine. Sitting at home at a desk, I didn’t notice any symptoms. But as a habitual stair-user, I would be gasping for breath in the stairwell because I couldn’t go up the stairs to my office as I once could.
I think you empathize more with people who had COVID (when you’ve had it yourself). There was such a huge patient burden. And I think that’s been the thing that’s affected health care providers the most – no matter what specialty we’re in – that nobody has answers.
Q: What happened after you had your vaccine?
A: The vaccine itself was fine. I didn’t have any reaction to the first two doses. But the first booster made my cardiac issues worse.
By this point, my cardiac problems stopped me from exercising. I even went to the ER with chest pain once because I was having palpitations and chest pressure caused by simply taking my morning shower. Fortunately, I wasn’t having an MI, but I certainly wasn’t “normal.”
My measure of my fitness is the cross-country skiing trail I use in Montana. I know exactly how far I can ski. Usually I can do the loop in 35 minutes. After COVID, I lasted 10 minutes. I would be tachycardic, short of breath with chest pain radiating down my left arm. I would rest and try to keep going. But with each rest period, I only got worse. I would be laying in the snow and strangers would ask if I needed help.
Q: What helped you?
A: I’ve read a lot about long COVID and have tried to learn from the experts. Of course, I never went to a doctor directly, although I did ask colleagues for advice. What I learned was to never push myself. I forced myself to create an exercise schedule where I only exercised three times a week with rest days in between. When exercising, the second my heart rate went above 140 bpm, I stopped until I could get it back down. I would push against this new limit, even though my limit was low.
Additionally, I worked on my breathing patterns and did meditative breathing for 10 minutes twice daily using a commercially available app.
Although progress was slow, I did improve, and by June 2022, I seemed back to normal. I was not as fit as I was prior to COVID and needed to improve, but the tachycardic response to exercise and cardiac symptoms were gone. I felt like my normal self. Normal enough to go on a spot packing trip in the Sierras in August. (Horses carried us and a mule carried the gear over the 12,000-foot pass into the mountains, and then left my friend and me high in the Sierras for a week.) We were camped above 10,000 feet and every day hiked up to another high mountain lake where we fly-fished for trout that we ate for dinner. The hikes were a challenge, but not abnormally so. Not as they would have been while I had long COVID.
Q: What is the current atmosphere in your clinic?
A: COVID is much milder now in my vaccinated patients, but I feel most health care providers are exhausted. Many of my staff left when COVID hit because they didn’t want to keep working. It made practicing medicine exhausting. There’s been a shortage of nurses, a shortage of everything. We’ve been required to do a whole lot more than we ever did before. It’s much harder to be a doctor. This pandemic is the first time I’ve ever thought of quitting. Granted, I lost my whole family, or at least the older generation, but it’s just been almost overwhelming.
On the plus side, almost every one of my patients has been vaccinated, because early on, people would ask: “Do you trust this vaccine?” I would reply: “I saw my parents die from COVID when they weren’t vaccinated, so you’re getting vaccinated. This is real and the vaccines help.” It made me very good at convincing people to get vaccines because I knew what it was like to see someone dying from COVID up close.
Q: What advice do you have for those struggling with the COVID pandemic?
A: People need to decide what their own risk is for getting sick and how many times they want to get COVID. At this point, I want people to go out, but safely. In the beginning, when my patients said, “can I go visit my granddaughter?” I said, “no,” but that was before we had the vaccine. Now I feel it is safe to go out using common sense. I still have my patients wear masks on planes. I still have patients try to eat outside as much as possible. And I tell people to take the precautions that make sense, but I tell them to go out and do things because life is short.
I had a patient in his 70s who has many risk factors like heart disease and diabetes. His granddaughter’s Bat Mitzvah in Florida was coming up. He asked: “Can I go?” I told him “Yes,” but to be safe – to wear an N95 mask on the plane and at the event, and stay in his own hotel room, rather than with the whole family. I said, “You need to do this.” Earlier in the pandemic, I saw people who literally died from loneliness and isolation.
He and his wife flew there. He sent me a picture of himself with his granddaughter. When he returned, he showed me a handwritten note from her that said, “I love you so much. Everyone else canceled, which made me cry. You’re the only one who came. You have no idea how much this meant to me.”
He’s back in L.A., and he didn’t get COVID. He said, “It was the best thing I’ve done in years.” That’s what I need to help people with, navigating this world with COVID and assessing risks and benefits. As with all of medicine, my advice is individualized. My advice changes based on the major circulating variant and the rates of the virus in the population, as well as the risk factors of the individual.
Q: What are you doing now?
A: I’m trying to avoid getting COVID again, or another booster. I could get pre-exposure monoclonal antibodies but am waiting to do anything further until I see what happens over the fall and winter. I still wear a mask inside but now do a mix of in-person and telemedicine visits. I still try to go to outdoor restaurants, which is easy in California. But I’m flying to see my son in New York and plan to go to Europe this fall for a meeting. I also go to my cabin in Montana every month to get my “dose” of the wilderness. Overall, I travel for conferences and speaking engagements much less because I have learned the joy of staying home.
Thinking back on my life as a doctor, my career began as an intern at Stanford rotating through Ward 5B, the AIDS unit at San Francisco General Hospital, and will likely end with COVID. In spite of all our medical advances, my generation of physicians, much as many generations before us, has a front-row seat to the vulnerability of humans to infectious diseases and how far we still need to go to protect our patients from communicable illness.
A version of this article first appeared on Medscape.com.
Anne L. Peters, MD, is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She has published more than 200 articles, reviews, and abstracts; three books on diabetes; and has been an investigator for more than 40 research studies. She has spoken internationally at over 400 programs and serves on many committees of several professional organizations.