User login
VIDEO: Checklists Improve Outcomes, Require Care-team Buy-in
50 Practical Medication Tips at End of Life
Patients with a life-limiting illness frequently experience pain and other symptoms. It is important to pay close attention when medication therapy is used to manage these symptoms. Occasionally, practitioners need to be creative in selecting, dosing, administering, and discontinuing medications at the end of life because of the patient’s changing health care needs.
In the video below, Dr. Kathryn Walker and Dr. Lynn McPherson of the University of Maryland discuss the role of the pharmacist in the hospital and hospice settings, as well as a few of their favorite medication tips and tricks in end-of-life care.
This article offers practical end-of-life medication tips including, but not limited to, medication administration; guidance on how to increase and decrease doses; medication selection for difficult to-treat patients; alternative dosage formulations; routes of medication administration; debridement medication regimens; and appropriate drug therapy selection. Dr. McPherson and Dr. Walker discuss how to deal with changing the goals of care for your dying patients and their families. They offer suggestions on how to integrate some helpful end-of-life medication tips into your practice.
*For a PDF of the full article, click on the link to the left of this introduction.
Patients with a life-limiting illness frequently experience pain and other symptoms. It is important to pay close attention when medication therapy is used to manage these symptoms. Occasionally, practitioners need to be creative in selecting, dosing, administering, and discontinuing medications at the end of life because of the patient’s changing health care needs.
In the video below, Dr. Kathryn Walker and Dr. Lynn McPherson of the University of Maryland discuss the role of the pharmacist in the hospital and hospice settings, as well as a few of their favorite medication tips and tricks in end-of-life care.
This article offers practical end-of-life medication tips including, but not limited to, medication administration; guidance on how to increase and decrease doses; medication selection for difficult to-treat patients; alternative dosage formulations; routes of medication administration; debridement medication regimens; and appropriate drug therapy selection. Dr. McPherson and Dr. Walker discuss how to deal with changing the goals of care for your dying patients and their families. They offer suggestions on how to integrate some helpful end-of-life medication tips into your practice.
*For a PDF of the full article, click on the link to the left of this introduction.
Patients with a life-limiting illness frequently experience pain and other symptoms. It is important to pay close attention when medication therapy is used to manage these symptoms. Occasionally, practitioners need to be creative in selecting, dosing, administering, and discontinuing medications at the end of life because of the patient’s changing health care needs.
In the video below, Dr. Kathryn Walker and Dr. Lynn McPherson of the University of Maryland discuss the role of the pharmacist in the hospital and hospice settings, as well as a few of their favorite medication tips and tricks in end-of-life care.
This article offers practical end-of-life medication tips including, but not limited to, medication administration; guidance on how to increase and decrease doses; medication selection for difficult to-treat patients; alternative dosage formulations; routes of medication administration; debridement medication regimens; and appropriate drug therapy selection. Dr. McPherson and Dr. Walker discuss how to deal with changing the goals of care for your dying patients and their families. They offer suggestions on how to integrate some helpful end-of-life medication tips into your practice.
*For a PDF of the full article, click on the link to the left of this introduction.
Kids' Outcomes Equal Across Pediatric, Adult Trauma Centers
CHICAGO – Outcomes for children seen at pediatric trauma centers were not significantly different than for children seen at adult trauma centers, according to a review of more than 45,000 pediatric injuries.
The finding "has significant policy implications because it means that emergency medical services do not have to triage patients according to specialty care centers," and it informs discussions about pediatric access to trauma care, said researcher Dr. Cassandra Villegas of the University of Arizona in Tucson.
Trauma accounts for approximately one-third of all pediatric mortality, but there are only 170 pediatric-specific trauma centers in the United States, which "means that the vast majority of pediatric patients that are injured are actually managed and evaluated at adult trauma centers," Dr. Villegas said at the annual clinical congress of the American College of Surgeons.
Nonetheless, data on pediatric outcomes for children treated at pediatric vs. adult trauma centers have not been conclusive, and most previous studies have focused on metropolitan or state pediatric centers, she said.
Dr. Villegas and her colleagues reviewed data from the National Trauma Database for 2007-2008 that included 27 pediatric trauma centers and 30 adult (mixed care) centers that had pediatric beds. Most (90%) of the 30 mixed care centers provided all acute pediatric services, while 10% shared these services with another medical center. All of the pediatric centers and 90% of the mixed care centers had pediatric intensive care units. The pediatric centers were significantly more likely to be university hospitals than were the mixed centers (85% vs. 53%).
The researchers analyzed outcomes for children aged 0-14 years, including 33,327 patients treated at pediatric centers and 12,605 patients treated at mixed centers.
After controlling for multiple variables including injury characteristics, Dr. Villegas and her associates found that in-hospital mortality – the primary outcome – was twice as high at mixed centers as at pediatric centers (2% vs. 1%), but this difference was not significant. The median length of stay was 2 days at all centers, although ICU admission rates were higher at mixed centers vs. pediatric centers (26% vs. 14%).
Approximately one-third of the patients seen at either type of center had an Injury Severity Score (ISS) in the 9-15 range, said Dr. Villegas. Falls were the most common type of injury, accounting for 49% of cases at pediatric centers and 37% of cases at mixed centers.
The patients at mixed centers were more likely than those at pediatric centers to be hypotensive (18% vs. 10%).
The study was limited by several factors, including the low incidence of pediatric mortality, the lack of uniform coding for death on arrival, and differences in ICU admission practices, said Dr. Villegas.
However, the findings suggest that there are no differences in outcomes for children treated at pediatric vs. mixed care centers, she said.
Dr. Villegas reported having no financial conflicts of interest.
CHICAGO – Outcomes for children seen at pediatric trauma centers were not significantly different than for children seen at adult trauma centers, according to a review of more than 45,000 pediatric injuries.
The finding "has significant policy implications because it means that emergency medical services do not have to triage patients according to specialty care centers," and it informs discussions about pediatric access to trauma care, said researcher Dr. Cassandra Villegas of the University of Arizona in Tucson.
Trauma accounts for approximately one-third of all pediatric mortality, but there are only 170 pediatric-specific trauma centers in the United States, which "means that the vast majority of pediatric patients that are injured are actually managed and evaluated at adult trauma centers," Dr. Villegas said at the annual clinical congress of the American College of Surgeons.
Nonetheless, data on pediatric outcomes for children treated at pediatric vs. adult trauma centers have not been conclusive, and most previous studies have focused on metropolitan or state pediatric centers, she said.
Dr. Villegas and her colleagues reviewed data from the National Trauma Database for 2007-2008 that included 27 pediatric trauma centers and 30 adult (mixed care) centers that had pediatric beds. Most (90%) of the 30 mixed care centers provided all acute pediatric services, while 10% shared these services with another medical center. All of the pediatric centers and 90% of the mixed care centers had pediatric intensive care units. The pediatric centers were significantly more likely to be university hospitals than were the mixed centers (85% vs. 53%).
The researchers analyzed outcomes for children aged 0-14 years, including 33,327 patients treated at pediatric centers and 12,605 patients treated at mixed centers.
After controlling for multiple variables including injury characteristics, Dr. Villegas and her associates found that in-hospital mortality – the primary outcome – was twice as high at mixed centers as at pediatric centers (2% vs. 1%), but this difference was not significant. The median length of stay was 2 days at all centers, although ICU admission rates were higher at mixed centers vs. pediatric centers (26% vs. 14%).
Approximately one-third of the patients seen at either type of center had an Injury Severity Score (ISS) in the 9-15 range, said Dr. Villegas. Falls were the most common type of injury, accounting for 49% of cases at pediatric centers and 37% of cases at mixed centers.
The patients at mixed centers were more likely than those at pediatric centers to be hypotensive (18% vs. 10%).
The study was limited by several factors, including the low incidence of pediatric mortality, the lack of uniform coding for death on arrival, and differences in ICU admission practices, said Dr. Villegas.
However, the findings suggest that there are no differences in outcomes for children treated at pediatric vs. mixed care centers, she said.
Dr. Villegas reported having no financial conflicts of interest.
CHICAGO – Outcomes for children seen at pediatric trauma centers were not significantly different than for children seen at adult trauma centers, according to a review of more than 45,000 pediatric injuries.
The finding "has significant policy implications because it means that emergency medical services do not have to triage patients according to specialty care centers," and it informs discussions about pediatric access to trauma care, said researcher Dr. Cassandra Villegas of the University of Arizona in Tucson.
Trauma accounts for approximately one-third of all pediatric mortality, but there are only 170 pediatric-specific trauma centers in the United States, which "means that the vast majority of pediatric patients that are injured are actually managed and evaluated at adult trauma centers," Dr. Villegas said at the annual clinical congress of the American College of Surgeons.
Nonetheless, data on pediatric outcomes for children treated at pediatric vs. adult trauma centers have not been conclusive, and most previous studies have focused on metropolitan or state pediatric centers, she said.
Dr. Villegas and her colleagues reviewed data from the National Trauma Database for 2007-2008 that included 27 pediatric trauma centers and 30 adult (mixed care) centers that had pediatric beds. Most (90%) of the 30 mixed care centers provided all acute pediatric services, while 10% shared these services with another medical center. All of the pediatric centers and 90% of the mixed care centers had pediatric intensive care units. The pediatric centers were significantly more likely to be university hospitals than were the mixed centers (85% vs. 53%).
The researchers analyzed outcomes for children aged 0-14 years, including 33,327 patients treated at pediatric centers and 12,605 patients treated at mixed centers.
After controlling for multiple variables including injury characteristics, Dr. Villegas and her associates found that in-hospital mortality – the primary outcome – was twice as high at mixed centers as at pediatric centers (2% vs. 1%), but this difference was not significant. The median length of stay was 2 days at all centers, although ICU admission rates were higher at mixed centers vs. pediatric centers (26% vs. 14%).
Approximately one-third of the patients seen at either type of center had an Injury Severity Score (ISS) in the 9-15 range, said Dr. Villegas. Falls were the most common type of injury, accounting for 49% of cases at pediatric centers and 37% of cases at mixed centers.
The patients at mixed centers were more likely than those at pediatric centers to be hypotensive (18% vs. 10%).
The study was limited by several factors, including the low incidence of pediatric mortality, the lack of uniform coding for death on arrival, and differences in ICU admission practices, said Dr. Villegas.
However, the findings suggest that there are no differences in outcomes for children treated at pediatric vs. mixed care centers, she said.
Dr. Villegas reported having no financial conflicts of interest.
FROM THE ANNUAL CLINICAL CONGRESS OF THE AMERICAN COLLEGE OF SURGEONS
Major Finding: In-hospital mortality for children aged 0-14 years was twice as high for those treated at mixed centers as for those treated at pediatric centers (2% vs. 1%), but this difference was not significant.
Data Source: The data come from the National Trauma Database for 2007-2008, and included 33,327 patients treated at pediatric centers and 12,605 patients treated at mixed centers.
Disclosures: Dr. Villegas reported having no financial conflicts of interest.
Is This Golfer's Pacemaker Malfunctioning?
ANSWER
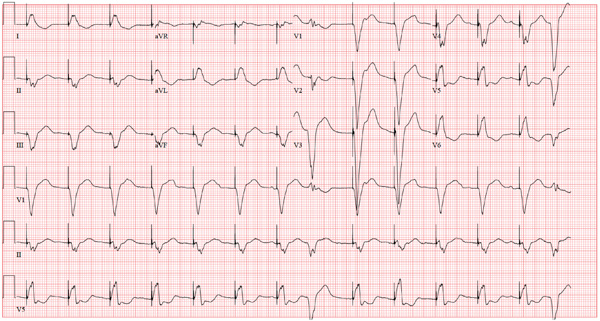
The ECG reveals an atrial-sensed and ventricular-paced rhythm of 83 beats/min. In this case, the pacemaker is functioning appropriately as programmed.
Pacemaker code consists of three letters: The first refers to the chamber(s) paced, the second to the chamber(s) sensed, and the third to the pacemaker’s response to a sensed beat. This patient has a pacing lead in the right atrium and one in the right ventricle and is programmed DDD. Each D in this case stands for dual: The first to indicate that both leads are programmed to pace, the second to indicate that both chambers may be sensed, and the third to indicate that the response to sensing can be either to inhibit or trigger a ventricular-paced beat in response to what happens in the atrium. Hence, there are four possible scenarios with a DDD pacemaker: AS-VS (atrial sensed-ventricle sensed; eg, intrinsic AV conduction requiring no pacing), AS-VP (atrial sensed-ventricle paced), AP-VS (atrial paced-ventricle sensed), and AP-VP (atrial paced-ventricle paced).
In this case, the atrial rate (83 beats/min) is faster than the pacemaker’s lower programmed rate. In order to see atrial pacing on the ECG, the intrinsic atrial rate would have to be less than the programmed rate of 60 beats/min. As soon as the pacemaker senses atrial conduction (either spontaneous or paced), it starts a timer (programmed at 130 ms in this case). If there is no spontaneous ventricular depolarization by the end of the timer, the pacemaker delivers an impulse to the ventricle, resulting in a paced ventricular beat. An often-made mistake (as this case illustrates) is the assumption that if one does not see pacing spikes, the pacemaker is not functioning properly.
ANSWER
The ECG reveals an atrial-sensed and ventricular-paced rhythm of 83 beats/min. In this case, the pacemaker is functioning appropriately as programmed.
Pacemaker code consists of three letters: The first refers to the chamber(s) paced, the second to the chamber(s) sensed, and the third to the pacemaker’s response to a sensed beat. This patient has a pacing lead in the right atrium and one in the right ventricle and is programmed DDD. Each D in this case stands for dual: The first to indicate that both leads are programmed to pace, the second to indicate that both chambers may be sensed, and the third to indicate that the response to sensing can be either to inhibit or trigger a ventricular-paced beat in response to what happens in the atrium. Hence, there are four possible scenarios with a DDD pacemaker: AS-VS (atrial sensed-ventricle sensed; eg, intrinsic AV conduction requiring no pacing), AS-VP (atrial sensed-ventricle paced), AP-VS (atrial paced-ventricle sensed), and AP-VP (atrial paced-ventricle paced).
In this case, the atrial rate (83 beats/min) is faster than the pacemaker’s lower programmed rate. In order to see atrial pacing on the ECG, the intrinsic atrial rate would have to be less than the programmed rate of 60 beats/min. As soon as the pacemaker senses atrial conduction (either spontaneous or paced), it starts a timer (programmed at 130 ms in this case). If there is no spontaneous ventricular depolarization by the end of the timer, the pacemaker delivers an impulse to the ventricle, resulting in a paced ventricular beat. An often-made mistake (as this case illustrates) is the assumption that if one does not see pacing spikes, the pacemaker is not functioning properly.
ANSWER
The ECG reveals an atrial-sensed and ventricular-paced rhythm of 83 beats/min. In this case, the pacemaker is functioning appropriately as programmed.
Pacemaker code consists of three letters: The first refers to the chamber(s) paced, the second to the chamber(s) sensed, and the third to the pacemaker’s response to a sensed beat. This patient has a pacing lead in the right atrium and one in the right ventricle and is programmed DDD. Each D in this case stands for dual: The first to indicate that both leads are programmed to pace, the second to indicate that both chambers may be sensed, and the third to indicate that the response to sensing can be either to inhibit or trigger a ventricular-paced beat in response to what happens in the atrium. Hence, there are four possible scenarios with a DDD pacemaker: AS-VS (atrial sensed-ventricle sensed; eg, intrinsic AV conduction requiring no pacing), AS-VP (atrial sensed-ventricle paced), AP-VS (atrial paced-ventricle sensed), and AP-VP (atrial paced-ventricle paced).
In this case, the atrial rate (83 beats/min) is faster than the pacemaker’s lower programmed rate. In order to see atrial pacing on the ECG, the intrinsic atrial rate would have to be less than the programmed rate of 60 beats/min. As soon as the pacemaker senses atrial conduction (either spontaneous or paced), it starts a timer (programmed at 130 ms in this case). If there is no spontaneous ventricular depolarization by the end of the timer, the pacemaker delivers an impulse to the ventricle, resulting in a paced ventricular beat. An often-made mistake (as this case illustrates) is the assumption that if one does not see pacing spikes, the pacemaker is not functioning properly.
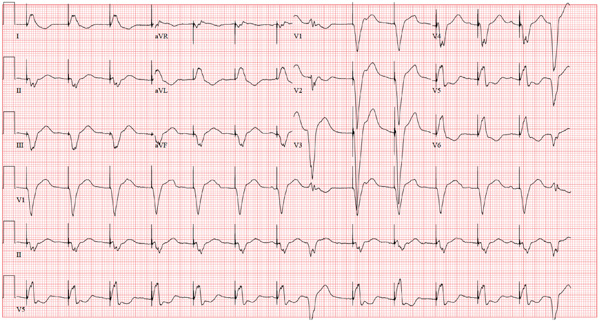
A 75-year-old man has a history of New York Heart Association Class II congestive heart failure (CHF), coronary artery disease (CAD) with coronary artery by-pass graft (CABG) surgery, and aortic stenosis with a bioprosthetic aortic valve replacement (AVR). He developed second-degree heart block (Mobitz II) following his four-vessel CABG and AVR four years ago, requiring placement of a dual-chamber pacemaker. He has been asymptomatic and plays golf two to three times per week. One week ago, he went to an urgent care center for treatment of a laceration on his leg and was told that part of his pacemaker wasn’t working. He presents to you now for follow-up on the pacemaker. Medical history is also remarkable for COPD, left inguinal hernia repair, hyperlipidemia, and bilateral cataracts. Family history is positive for CAD, diabetes, and stroke. He has a remote history of smoking and drinks one martini after each golf game. His medications include aspirin, lovastatin, and metoprolol. He has no drug allergies. The review of systems is negative except for a recent repair to a 3-cm laceration on the left leg. Physical examination reveals a well-developed, pleasant man in no distress. His height is 74” and weight, 179 lb. Blood pressure is 118/84 mm Hg; pulse, 80 beats/min and regular; respiratory rate, 14 breaths/min; temperature, 98.8°F; and O2 saturation, 97% on room air. Pertinent physical findings include a well-healed pacemaker site without signs of recent trauma. The lungs are clear in all fields, the cardiac exam is within normal limits, and there is no jugular venous distention. The abdomen is benign, and there is no peripheral edema. The laceration repair on his left leg is healing well (no erythema, induration, wound separation, or dehiscence). The pacemaker is programmed DDD at a lower rate of 60 beats/min and an upper rate of 120 beats/min, with paced and sensed atrioventricular (AV) delays programmed at 130 ms. An ECG reveals the following: a ventricular rate of 83 beats/min; PR interval, not measured; QRS duration, 162 ms; QT/QTc interval, 480/564 ms; P axis, unmeasurable; R axis, 254°; and T axis, 56°. What is your interpretation of this ECG? Is there any indication that the pacemaker is not functioning?
Is Leprosy the Cause of This Girl's Lesion?
ANSWER
The correct answer is postinflammatory hypopigmentation (choice “c”), in this case secondary to eczema in a classic antecubital location. Leprosy (choice “a”) is more common than one might imagine, but it does not appear overnight and does not involve overt inflammation. Vitiligo (choice “b”) does not appear suddenly and rarely involves the type of inflammation seen in this case. Lichen sclerosis et atrophicus (choice “d”) is an inflammatory condition that presents with hypopigmentation and epidermal atrophy; however, it is gradual in onset and would not exhibit papulosquamous inflammation.
DISCUSSION
The more color in the skin, the more the loss of that color stands out. Patients and families with darker skin are often understandably upset by the contrast. Providers need a differential for pigment loss, including the items mentioned—some of which have the potential to be dreadfully serious.
Two relevant facts stand out in this case: the rapidity of onset and the history of eczema, in which secondary pigment loss can occur. As mentioned, it is especially obvious in those with darker skin. Fortunately, once the eczema calms down, the hypopigmentation resolves and normal color returns.
Paradoxically, it’s not at all unusual to see postinflammatory hyperpigmentation, especially in those with skin of types IV and V (eg, African-Americans, some Hispanics, and those of Indian ancestry). Eczema is a common cause, but the inflammation can be from almost any source, including trauma, burns, or even acne.
Had this patient’s diagnosis not been obvious, a biopsy might have been indicated due to the serious nature of some of the items in the differential. Vitiligo, for example, can be very disfiguring, especially on a dark-skinned individual. It tends to become widespread and permanent, unless it’s caught and treated early on. Other conditions involving hypopigmentation include sarcoidosis, lupus, and morphea.
All of these conditions are unusual, if not rare, compared with atopic dermatitis (AD), which this patient has. AD is so common that almost 20% of newborns develop it. Eczema is one of the more typical manifestations, along with dry, sensitive skin, seasonal allergies, and reactive airway disease. Corroboration of the diagnosis is usually easily accomplished by taking a family history.
TREATMENT
Fortunately, this patient’s hypopigmentation will resolve quickly with treatment of her eczema, using a low-strength steroid cream (eg, hydrocortisone 2.5% cream or ointment). But a good portion of the “treatment” of AD is done by educating the family about the nature of the condition, as well as providing reassurance about the absence of the more serious items in the differential.
ANSWER
The correct answer is postinflammatory hypopigmentation (choice “c”), in this case secondary to eczema in a classic antecubital location. Leprosy (choice “a”) is more common than one might imagine, but it does not appear overnight and does not involve overt inflammation. Vitiligo (choice “b”) does not appear suddenly and rarely involves the type of inflammation seen in this case. Lichen sclerosis et atrophicus (choice “d”) is an inflammatory condition that presents with hypopigmentation and epidermal atrophy; however, it is gradual in onset and would not exhibit papulosquamous inflammation.
DISCUSSION
The more color in the skin, the more the loss of that color stands out. Patients and families with darker skin are often understandably upset by the contrast. Providers need a differential for pigment loss, including the items mentioned—some of which have the potential to be dreadfully serious.
Two relevant facts stand out in this case: the rapidity of onset and the history of eczema, in which secondary pigment loss can occur. As mentioned, it is especially obvious in those with darker skin. Fortunately, once the eczema calms down, the hypopigmentation resolves and normal color returns.
Paradoxically, it’s not at all unusual to see postinflammatory hyperpigmentation, especially in those with skin of types IV and V (eg, African-Americans, some Hispanics, and those of Indian ancestry). Eczema is a common cause, but the inflammation can be from almost any source, including trauma, burns, or even acne.
Had this patient’s diagnosis not been obvious, a biopsy might have been indicated due to the serious nature of some of the items in the differential. Vitiligo, for example, can be very disfiguring, especially on a dark-skinned individual. It tends to become widespread and permanent, unless it’s caught and treated early on. Other conditions involving hypopigmentation include sarcoidosis, lupus, and morphea.
All of these conditions are unusual, if not rare, compared with atopic dermatitis (AD), which this patient has. AD is so common that almost 20% of newborns develop it. Eczema is one of the more typical manifestations, along with dry, sensitive skin, seasonal allergies, and reactive airway disease. Corroboration of the diagnosis is usually easily accomplished by taking a family history.
TREATMENT
Fortunately, this patient’s hypopigmentation will resolve quickly with treatment of her eczema, using a low-strength steroid cream (eg, hydrocortisone 2.5% cream or ointment). But a good portion of the “treatment” of AD is done by educating the family about the nature of the condition, as well as providing reassurance about the absence of the more serious items in the differential.
ANSWER
The correct answer is postinflammatory hypopigmentation (choice “c”), in this case secondary to eczema in a classic antecubital location. Leprosy (choice “a”) is more common than one might imagine, but it does not appear overnight and does not involve overt inflammation. Vitiligo (choice “b”) does not appear suddenly and rarely involves the type of inflammation seen in this case. Lichen sclerosis et atrophicus (choice “d”) is an inflammatory condition that presents with hypopigmentation and epidermal atrophy; however, it is gradual in onset and would not exhibit papulosquamous inflammation.
DISCUSSION
The more color in the skin, the more the loss of that color stands out. Patients and families with darker skin are often understandably upset by the contrast. Providers need a differential for pigment loss, including the items mentioned—some of which have the potential to be dreadfully serious.
Two relevant facts stand out in this case: the rapidity of onset and the history of eczema, in which secondary pigment loss can occur. As mentioned, it is especially obvious in those with darker skin. Fortunately, once the eczema calms down, the hypopigmentation resolves and normal color returns.
Paradoxically, it’s not at all unusual to see postinflammatory hyperpigmentation, especially in those with skin of types IV and V (eg, African-Americans, some Hispanics, and those of Indian ancestry). Eczema is a common cause, but the inflammation can be from almost any source, including trauma, burns, or even acne.
Had this patient’s diagnosis not been obvious, a biopsy might have been indicated due to the serious nature of some of the items in the differential. Vitiligo, for example, can be very disfiguring, especially on a dark-skinned individual. It tends to become widespread and permanent, unless it’s caught and treated early on. Other conditions involving hypopigmentation include sarcoidosis, lupus, and morphea.
All of these conditions are unusual, if not rare, compared with atopic dermatitis (AD), which this patient has. AD is so common that almost 20% of newborns develop it. Eczema is one of the more typical manifestations, along with dry, sensitive skin, seasonal allergies, and reactive airway disease. Corroboration of the diagnosis is usually easily accomplished by taking a family history.
TREATMENT
Fortunately, this patient’s hypopigmentation will resolve quickly with treatment of her eczema, using a low-strength steroid cream (eg, hydrocortisone 2.5% cream or ointment). But a good portion of the “treatment” of AD is done by educating the family about the nature of the condition, as well as providing reassurance about the absence of the more serious items in the differential.

The parents of this 8-month-old infant are alarmed by skin changes that occurred practically overnight on the child’s arm—especially since the child’s grandparents suggested it might represent vitiligo or even leprosy. The child’s pediatrician thought “ringworm” was more likely, but the clotrimazole cream he recommended was no help. The child has an extensive history of atopy, including eczema affecting the trunk and face. The parents have used topical steroid cream on the affected areas with some good effect, but the loss of color in the antecubital site has made them reluctant to use the product on this new site. Examination shows a papulosquamous lesion, 3.5 cm in diameter, on the left lateral antecubital area, with marked central hypopigmentation. The child and her parents are Vietnamese, with type IV skin, making the pigment loss all the more obvious. The periphery of the lesion, in addition to being bumpy and scaly, is moderately inflamed. The rest of the child’s skin is dry but otherwise unremarkable.

Pregnancy Registries: Advantages and Disadvantages
Despite the fact that prescription medications are commonly used by pregnant women, for most products and for new drugs in particular, there is typically little to no human safety information available to aid clinicians and patients in managing risk. As randomized clinical trials are usually not considered ethical to perform in pregnancy, observational epidemiologic studies are often the next best option to address human pregnancy exposure. An increasingly common approach to gathering human safety data is postmarketing pregnancy registries.

These pregnancy registries are initiated many times by agreement between the manufacturer and a regulatory agency as a postmarketing commitment or requirement following shortly after drug approval. Furthermore, because use of a new drug in pregnant women might be relatively rare, a pregnancy registry may be the only feasible method for gathering preliminary safety information as quickly as possible so that potential signals might be detected and clinical decision making can be better informed.
Pregnancy registries vary in design, but all involve collection of data on exposure to the drug of interest in pregnant women, and collection of outcome data for those pregnancies. The primary outcome of interest is typically major congenital anomalies; some registries also collect outcome data on fetal/infant growth, preterm delivery, pregnancy loss, specific neonatal outcomes, and postnatal longer term growth and development. The rates of these outcomes can be compared with general population reference rates, or rates occurring in a specific comparison group that might be more similar to the exposed women, for example, in terms of the underlying maternal condition being treated by the drug.

In addition to early information on a new drug, some of the major advantages of many pregnancy registry designs are the ability to collect information on the exposure and other pregnancy details before the mother knows what the outcome of her pregnancy will be; direct collection of exposure information from the mother herself, so that important factors such as drug and alcohol use, dose, and exact timing of exposure to the drug of interest; information on important other factors such as tobacco, alcohol, and multivitamin use.
The most challenging aspect of pregnancy registries is recruitment, for which registries largely depend on obstetric providers and other specialty physicians. Although low numbers of recruited pregnancies may be caused by limited use of a new drug, clearly most pregnancy registries enroll a very small fraction of all exposed pregnancies that are in existence. A second, related issue is that there may be bias in the self-selection of women who do find out about the registry and agree to participate, thus raising questions about the generalizability of the findings. A third issue is that many registries experience high rates of "lost to follow-up," in which outcome information is unobtainable from the health care provider or the pregnant woman – in some cases as high as 40%. There is also a concern about bias involved with the timing in gestation when a pregnancy enters a registry, such as the later in gestation a pregnancy is enrolled, the more likely that prenatal diagnosis, pregnancy loss, or other adverse outcomes have already occurred – thus making the enrollment essentially retrospective.

Another concern is that few registries have a concurrently enrolled group of unexposed women for purposes of comparison. Thus, their findings are commonly compared to external reference statistics which may not be the most appropriate. Finally, in some registries, the absence of information on individual dose and specific timing in gestation of exposure may preclude evaluating the biological plausibility of any registry findings. All of these issues can lead to long delays in accumulation of sufficient information to draw meaningful inferences, and potential concerns about interpretation of results.
How can awareness of pregnancy registries and more representative enrollment of exposed women be improved? A variety of methods are used to inform physicians and their patients about existing pregnancy registries for the purpose of encouraging referrals, including the Food and Drug Administration website, information in product labeling and on product websites, direct to provider or direct to consumer advertising, and in commonly used resources for clinicians such as this column and Reprotox, an information system developed by the Reproductive Toxicology Center. However, with the rapidly increasing number of registries, it is challenging for physicians to remain current on which medications are being monitored through a registry, what the criteria for enrollment are, and how a physician or patient can find out more. Pregnancy registry designs that are disease based – such as encompassing all medications used to treat a specific disease in pregnancy – help simplify the referral process by broadening the criteria for enrollment. Particularly for specialty physicians, this can ease the burden of identifying eligible women for enrollment.

How can enrollment be accomplished as early as possible in pregnancy (after exposure, but before the outcome is known), and how can more complete ascertainment of exposure and outcome be improved? An approach that some registries have used to address this is by "direct to consumer" campaigns. Registries such as the Organization of Teratology Information Specialists (OTIS) Autoimmune Diseases in Pregnancy Registry require that the pregnant woman herself enroll in the study, and therefore, the study is marketed directly to those women, although physician referral is encouraged. At least in this case, this has led to low rates of lost to follow-up (less than 5%), recruitment timing that is typically before the seventh or eighth week of gestation, and collection of specific information on dose and timing in gestation of exposure.
Multiple drug, disease-based, multiple sponsor registries such as the Antiretroviral Drugs in Pregnancy Registry, the North American Antiepileptic Drugs in Pregnancy Registry (patients call 888-233-2334), and the National Pregnancy Registry for Atypical Antipsychotics (866-961-2388) offer distinct advantages but are not always feasible for a specific product. A national pregnancy registry for all new drugs has been suggested as another solution to many of the challenges facing single product registries and to streamline referral and follow-up. In addition, including pregnant women in selected preapproval studies has several advantages. Finally, creative new technologies for earlier and more complete ascertainment and referral, such as use of electronic medical records, should be fully explored. The need for safety information on new drugs is urgent.
Dr. Chambers is professor of pediatrics and family and preventive medicine at the University of California, San Diego. She is director of the California Teratogen Information Service and Clinical Research Program. Dr. Chambers is a past president of the Organization of Teratology Information Specialists and past president of the Teratology Society. Dr. Cohen directs the perinatal psychiatry program at Massachusetts General Hospital, which provides information about pregnancy and mental health. Dr. Koren is professor of pediatrics, pharmacology, pharmacy, and medical genetics at the University of Toronto. He heads the Research Leadership for Better Pharmacotherapy During Pregnancy and Lactation at the Hospital for Sick Children, Toronto, where he is director of the Motherisk program. Mr. Briggs is a pharmacist clinical specialist at the outpatient clinics of Memorial Care Center for Women at Miller Children’s Hospital in Long Beach, Calif.; a clinical professor of pharmacy at the University of California, San Francisco; and an adjunct professor of pharmacy at the University of Southern California, Los Angeles, and Washington State University, Spokane. He also is coauthor of "Drugs in Pregnancy and Lactation." Dr. Cohen is the principal investigator on the National Pregnancy Registry for Atypical Antipsychotics, which is sponsored by multiple atypical antipsychotic manufacturers.
Dr. Chambers, Dr. Koren, and Mr. Briggs said they had no relevant financial disclosures.
Despite the fact that prescription medications are commonly used by pregnant women, for most products and for new drugs in particular, there is typically little to no human safety information available to aid clinicians and patients in managing risk. As randomized clinical trials are usually not considered ethical to perform in pregnancy, observational epidemiologic studies are often the next best option to address human pregnancy exposure. An increasingly common approach to gathering human safety data is postmarketing pregnancy registries.
These pregnancy registries are initiated many times by agreement between the manufacturer and a regulatory agency as a postmarketing commitment or requirement following shortly after drug approval. Furthermore, because use of a new drug in pregnant women might be relatively rare, a pregnancy registry may be the only feasible method for gathering preliminary safety information as quickly as possible so that potential signals might be detected and clinical decision making can be better informed.
Pregnancy registries vary in design, but all involve collection of data on exposure to the drug of interest in pregnant women, and collection of outcome data for those pregnancies. The primary outcome of interest is typically major congenital anomalies; some registries also collect outcome data on fetal/infant growth, preterm delivery, pregnancy loss, specific neonatal outcomes, and postnatal longer term growth and development. The rates of these outcomes can be compared with general population reference rates, or rates occurring in a specific comparison group that might be more similar to the exposed women, for example, in terms of the underlying maternal condition being treated by the drug.
In addition to early information on a new drug, some of the major advantages of many pregnancy registry designs are the ability to collect information on the exposure and other pregnancy details before the mother knows what the outcome of her pregnancy will be; direct collection of exposure information from the mother herself, so that important factors such as drug and alcohol use, dose, and exact timing of exposure to the drug of interest; information on important other factors such as tobacco, alcohol, and multivitamin use.
The most challenging aspect of pregnancy registries is recruitment, for which registries largely depend on obstetric providers and other specialty physicians. Although low numbers of recruited pregnancies may be caused by limited use of a new drug, clearly most pregnancy registries enroll a very small fraction of all exposed pregnancies that are in existence. A second, related issue is that there may be bias in the self-selection of women who do find out about the registry and agree to participate, thus raising questions about the generalizability of the findings. A third issue is that many registries experience high rates of "lost to follow-up," in which outcome information is unobtainable from the health care provider or the pregnant woman – in some cases as high as 40%. There is also a concern about bias involved with the timing in gestation when a pregnancy enters a registry, such as the later in gestation a pregnancy is enrolled, the more likely that prenatal diagnosis, pregnancy loss, or other adverse outcomes have already occurred – thus making the enrollment essentially retrospective.
Another concern is that few registries have a concurrently enrolled group of unexposed women for purposes of comparison. Thus, their findings are commonly compared to external reference statistics which may not be the most appropriate. Finally, in some registries, the absence of information on individual dose and specific timing in gestation of exposure may preclude evaluating the biological plausibility of any registry findings. All of these issues can lead to long delays in accumulation of sufficient information to draw meaningful inferences, and potential concerns about interpretation of results.
How can awareness of pregnancy registries and more representative enrollment of exposed women be improved? A variety of methods are used to inform physicians and their patients about existing pregnancy registries for the purpose of encouraging referrals, including the Food and Drug Administration website, information in product labeling and on product websites, direct to provider or direct to consumer advertising, and in commonly used resources for clinicians such as this column and Reprotox, an information system developed by the Reproductive Toxicology Center. However, with the rapidly increasing number of registries, it is challenging for physicians to remain current on which medications are being monitored through a registry, what the criteria for enrollment are, and how a physician or patient can find out more. Pregnancy registry designs that are disease based – such as encompassing all medications used to treat a specific disease in pregnancy – help simplify the referral process by broadening the criteria for enrollment. Particularly for specialty physicians, this can ease the burden of identifying eligible women for enrollment.
How can enrollment be accomplished as early as possible in pregnancy (after exposure, but before the outcome is known), and how can more complete ascertainment of exposure and outcome be improved? An approach that some registries have used to address this is by "direct to consumer" campaigns. Registries such as the Organization of Teratology Information Specialists (OTIS) Autoimmune Diseases in Pregnancy Registry require that the pregnant woman herself enroll in the study, and therefore, the study is marketed directly to those women, although physician referral is encouraged. At least in this case, this has led to low rates of lost to follow-up (less than 5%), recruitment timing that is typically before the seventh or eighth week of gestation, and collection of specific information on dose and timing in gestation of exposure.
Multiple drug, disease-based, multiple sponsor registries such as the Antiretroviral Drugs in Pregnancy Registry, the North American Antiepileptic Drugs in Pregnancy Registry (patients call 888-233-2334), and the National Pregnancy Registry for Atypical Antipsychotics (866-961-2388) offer distinct advantages but are not always feasible for a specific product. A national pregnancy registry for all new drugs has been suggested as another solution to many of the challenges facing single product registries and to streamline referral and follow-up. In addition, including pregnant women in selected preapproval studies has several advantages. Finally, creative new technologies for earlier and more complete ascertainment and referral, such as use of electronic medical records, should be fully explored. The need for safety information on new drugs is urgent.
Dr. Chambers is professor of pediatrics and family and preventive medicine at the University of California, San Diego. She is director of the California Teratogen Information Service and Clinical Research Program. Dr. Chambers is a past president of the Organization of Teratology Information Specialists and past president of the Teratology Society. Dr. Cohen directs the perinatal psychiatry program at Massachusetts General Hospital, which provides information about pregnancy and mental health. Dr. Koren is professor of pediatrics, pharmacology, pharmacy, and medical genetics at the University of Toronto. He heads the Research Leadership for Better Pharmacotherapy During Pregnancy and Lactation at the Hospital for Sick Children, Toronto, where he is director of the Motherisk program. Mr. Briggs is a pharmacist clinical specialist at the outpatient clinics of Memorial Care Center for Women at Miller Children’s Hospital in Long Beach, Calif.; a clinical professor of pharmacy at the University of California, San Francisco; and an adjunct professor of pharmacy at the University of Southern California, Los Angeles, and Washington State University, Spokane. He also is coauthor of "Drugs in Pregnancy and Lactation." Dr. Cohen is the principal investigator on the National Pregnancy Registry for Atypical Antipsychotics, which is sponsored by multiple atypical antipsychotic manufacturers.
Dr. Chambers, Dr. Koren, and Mr. Briggs said they had no relevant financial disclosures.
Despite the fact that prescription medications are commonly used by pregnant women, for most products and for new drugs in particular, there is typically little to no human safety information available to aid clinicians and patients in managing risk. As randomized clinical trials are usually not considered ethical to perform in pregnancy, observational epidemiologic studies are often the next best option to address human pregnancy exposure. An increasingly common approach to gathering human safety data is postmarketing pregnancy registries.
These pregnancy registries are initiated many times by agreement between the manufacturer and a regulatory agency as a postmarketing commitment or requirement following shortly after drug approval. Furthermore, because use of a new drug in pregnant women might be relatively rare, a pregnancy registry may be the only feasible method for gathering preliminary safety information as quickly as possible so that potential signals might be detected and clinical decision making can be better informed.
Pregnancy registries vary in design, but all involve collection of data on exposure to the drug of interest in pregnant women, and collection of outcome data for those pregnancies. The primary outcome of interest is typically major congenital anomalies; some registries also collect outcome data on fetal/infant growth, preterm delivery, pregnancy loss, specific neonatal outcomes, and postnatal longer term growth and development. The rates of these outcomes can be compared with general population reference rates, or rates occurring in a specific comparison group that might be more similar to the exposed women, for example, in terms of the underlying maternal condition being treated by the drug.
In addition to early information on a new drug, some of the major advantages of many pregnancy registry designs are the ability to collect information on the exposure and other pregnancy details before the mother knows what the outcome of her pregnancy will be; direct collection of exposure information from the mother herself, so that important factors such as drug and alcohol use, dose, and exact timing of exposure to the drug of interest; information on important other factors such as tobacco, alcohol, and multivitamin use.
The most challenging aspect of pregnancy registries is recruitment, for which registries largely depend on obstetric providers and other specialty physicians. Although low numbers of recruited pregnancies may be caused by limited use of a new drug, clearly most pregnancy registries enroll a very small fraction of all exposed pregnancies that are in existence. A second, related issue is that there may be bias in the self-selection of women who do find out about the registry and agree to participate, thus raising questions about the generalizability of the findings. A third issue is that many registries experience high rates of "lost to follow-up," in which outcome information is unobtainable from the health care provider or the pregnant woman – in some cases as high as 40%. There is also a concern about bias involved with the timing in gestation when a pregnancy enters a registry, such as the later in gestation a pregnancy is enrolled, the more likely that prenatal diagnosis, pregnancy loss, or other adverse outcomes have already occurred – thus making the enrollment essentially retrospective.
Another concern is that few registries have a concurrently enrolled group of unexposed women for purposes of comparison. Thus, their findings are commonly compared to external reference statistics which may not be the most appropriate. Finally, in some registries, the absence of information on individual dose and specific timing in gestation of exposure may preclude evaluating the biological plausibility of any registry findings. All of these issues can lead to long delays in accumulation of sufficient information to draw meaningful inferences, and potential concerns about interpretation of results.
How can awareness of pregnancy registries and more representative enrollment of exposed women be improved? A variety of methods are used to inform physicians and their patients about existing pregnancy registries for the purpose of encouraging referrals, including the Food and Drug Administration website, information in product labeling and on product websites, direct to provider or direct to consumer advertising, and in commonly used resources for clinicians such as this column and Reprotox, an information system developed by the Reproductive Toxicology Center. However, with the rapidly increasing number of registries, it is challenging for physicians to remain current on which medications are being monitored through a registry, what the criteria for enrollment are, and how a physician or patient can find out more. Pregnancy registry designs that are disease based – such as encompassing all medications used to treat a specific disease in pregnancy – help simplify the referral process by broadening the criteria for enrollment. Particularly for specialty physicians, this can ease the burden of identifying eligible women for enrollment.
How can enrollment be accomplished as early as possible in pregnancy (after exposure, but before the outcome is known), and how can more complete ascertainment of exposure and outcome be improved? An approach that some registries have used to address this is by "direct to consumer" campaigns. Registries such as the Organization of Teratology Information Specialists (OTIS) Autoimmune Diseases in Pregnancy Registry require that the pregnant woman herself enroll in the study, and therefore, the study is marketed directly to those women, although physician referral is encouraged. At least in this case, this has led to low rates of lost to follow-up (less than 5%), recruitment timing that is typically before the seventh or eighth week of gestation, and collection of specific information on dose and timing in gestation of exposure.
Multiple drug, disease-based, multiple sponsor registries such as the Antiretroviral Drugs in Pregnancy Registry, the North American Antiepileptic Drugs in Pregnancy Registry (patients call 888-233-2334), and the National Pregnancy Registry for Atypical Antipsychotics (866-961-2388) offer distinct advantages but are not always feasible for a specific product. A national pregnancy registry for all new drugs has been suggested as another solution to many of the challenges facing single product registries and to streamline referral and follow-up. In addition, including pregnant women in selected preapproval studies has several advantages. Finally, creative new technologies for earlier and more complete ascertainment and referral, such as use of electronic medical records, should be fully explored. The need for safety information on new drugs is urgent.
Dr. Chambers is professor of pediatrics and family and preventive medicine at the University of California, San Diego. She is director of the California Teratogen Information Service and Clinical Research Program. Dr. Chambers is a past president of the Organization of Teratology Information Specialists and past president of the Teratology Society. Dr. Cohen directs the perinatal psychiatry program at Massachusetts General Hospital, which provides information about pregnancy and mental health. Dr. Koren is professor of pediatrics, pharmacology, pharmacy, and medical genetics at the University of Toronto. He heads the Research Leadership for Better Pharmacotherapy During Pregnancy and Lactation at the Hospital for Sick Children, Toronto, where he is director of the Motherisk program. Mr. Briggs is a pharmacist clinical specialist at the outpatient clinics of Memorial Care Center for Women at Miller Children’s Hospital in Long Beach, Calif.; a clinical professor of pharmacy at the University of California, San Francisco; and an adjunct professor of pharmacy at the University of Southern California, Los Angeles, and Washington State University, Spokane. He also is coauthor of "Drugs in Pregnancy and Lactation." Dr. Cohen is the principal investigator on the National Pregnancy Registry for Atypical Antipsychotics, which is sponsored by multiple atypical antipsychotic manufacturers.
Dr. Chambers, Dr. Koren, and Mr. Briggs said they had no relevant financial disclosures.

Radiation Therapy With or Without Temozolomide in Treating Patients With Low-Grade Glioma
Objectives: This phase III trial asks whether the addition of temozolomide (Temodar) to radiation therapy can improve progression-free survival and/or overall survival of patients with grade 2 glioma at the most recent pathological diagnosis.
Key entry or exclusion criteria: Patients with a previous pathological diagnosis of grade 3 or 4 are excluded, as are patients with prior radiotherapy, cytotoxic chemotherapy, radiosurgery, or investigational therapy for the brain tumor. Prior surgery is permitted.
Locations: 173 sites
Goal: 540 patients
Study sponsor: Eastern Cooperative Oncology Group in collaboration with the National Cancer Institute.
Link for more information: clinicaltrials.gov/ct2/show/study/NCT00978458
NIH clinical trials identifier: NCT00978458
Objectives: This phase III trial asks whether the addition of temozolomide (Temodar) to radiation therapy can improve progression-free survival and/or overall survival of patients with grade 2 glioma at the most recent pathological diagnosis.
Key entry or exclusion criteria: Patients with a previous pathological diagnosis of grade 3 or 4 are excluded, as are patients with prior radiotherapy, cytotoxic chemotherapy, radiosurgery, or investigational therapy for the brain tumor. Prior surgery is permitted.
Locations: 173 sites
Goal: 540 patients
Study sponsor: Eastern Cooperative Oncology Group in collaboration with the National Cancer Institute.
Link for more information: clinicaltrials.gov/ct2/show/study/NCT00978458
NIH clinical trials identifier: NCT00978458
Objectives: This phase III trial asks whether the addition of temozolomide (Temodar) to radiation therapy can improve progression-free survival and/or overall survival of patients with grade 2 glioma at the most recent pathological diagnosis.
Key entry or exclusion criteria: Patients with a previous pathological diagnosis of grade 3 or 4 are excluded, as are patients with prior radiotherapy, cytotoxic chemotherapy, radiosurgery, or investigational therapy for the brain tumor. Prior surgery is permitted.
Locations: 173 sites
Goal: 540 patients
Study sponsor: Eastern Cooperative Oncology Group in collaboration with the National Cancer Institute.
Link for more information: clinicaltrials.gov/ct2/show/study/NCT00978458
NIH clinical trials identifier: NCT00978458
Less Liver Cancer in HCV Patients Given Antiviral Therapy
Antiviral therapy may reduce the risk of hepatocellular carcinoma in patients with hepatitis C infections, Dr. Nina Kimer reported in the Oct. 22 issue of BMJ Open, published online.
Moreover, the effect seems to persist regardless of whether sustained virologic response is achieved.
Dr. Kimer, of Copenhagen University Hospital, Hvidovre, Denmark, and colleagues conducted a meta-analysis of trials looking at hepatitis C-related cirrhosis or fibrosis (BMJ Open 2012;2:e001313 [doi:10.1136/bmjopen-2012-001313]).
The primary analysis focused on randomized controlled trials, although prospective cohort studies with control groups were included in sensitivity analyses.
The authors searched the Cochrane Library, PubMed, EMBASE, and Web of Science databases, as well as reference lists from relevant papers, conference proceedings, and the World Health Organization Trial Search Portal.
Studies looking at HIV and chronic hepatitis B were excluded, for a total of eight randomized trials and five prospective cohort studies.
The duration of therapy (which included pegylated interferon in two trials, interferon plus ribavirin in one trial, and interferon monotherapy in the remaining trials) varied from 1 to 5 years. Follow-up ranged from 2 to 8.7 years.
Overall, the authors found that 81 of 1,156 patients who received antiviral therapy and 129 of 1,074 control patients who received no therapy developed hepatocellular carcinoma.
The relative risk for antiviral therapy, compared with no treatment, was 0.53 (95% confidence interval, 0.34-0.81).
"The corresponding number needed to treat to prevent one case of [hepatocellular carcinoma] was eight patients," added the researchers.
And while the effect of antivirals was more pronounced among patients with a virological response (RR 0.15; 95% CI, 0.05-0.45), there was nevertheless a clear reduction in risk for nonresponders to antivirals, with a relative risk of 0.57, compared with controls (95% CI 0.37-0.85).
"Although the intervention was more beneficial among sustained virological responders than nonresponders, there was a clear effect in both patient groups. ... Antiviral therapy may have beneficial effects on the risk of developing HCC that are unrelated to the virological response."
On the other hand, there was no reported effect of antiviral therapy on all-cause mortality, liver-related mortality, or liver-related morbidity in this population.
Dr. Kimer conceded several limitations to this analysis. "Only two of the included trials evaluated pegylated interferon, which is the current standard treatment for chronic hepatitis C."
Moreover, the duration of treatment in several included studies was "relatively long, which may increase the proportion of responders."
Finally, Dr. Kimer added that the researchers were unable to perform subgroup analysis to determine which treatment duration or dose is best.
"Based on the duration of follow-up and the lack of clear evidence concerning morbidity or mortality, we cannot exclude that interferon delays rather than prevents carcinogenesis," concluded the investigators.
Nevertheless, the "protection from HCC might be even better among patients in current antiviral therapy since the proportion of virological responders continues to increase with ongoing improvements in therapy," they wrote.
"Additional randomized trials with longer follow-up are still warranted to determine whether this is the case," they noted.
The authors disclosed having no outside funding and no competing interests related to this study.
sustained virologic response, hepatitis C-related cirrhosis, fibrosis,
Antiviral therapy may reduce the risk of hepatocellular carcinoma in patients with hepatitis C infections, Dr. Nina Kimer reported in the Oct. 22 issue of BMJ Open, published online.
Moreover, the effect seems to persist regardless of whether sustained virologic response is achieved.
Dr. Kimer, of Copenhagen University Hospital, Hvidovre, Denmark, and colleagues conducted a meta-analysis of trials looking at hepatitis C-related cirrhosis or fibrosis (BMJ Open 2012;2:e001313 [doi:10.1136/bmjopen-2012-001313]).
The primary analysis focused on randomized controlled trials, although prospective cohort studies with control groups were included in sensitivity analyses.
The authors searched the Cochrane Library, PubMed, EMBASE, and Web of Science databases, as well as reference lists from relevant papers, conference proceedings, and the World Health Organization Trial Search Portal.
Studies looking at HIV and chronic hepatitis B were excluded, for a total of eight randomized trials and five prospective cohort studies.
The duration of therapy (which included pegylated interferon in two trials, interferon plus ribavirin in one trial, and interferon monotherapy in the remaining trials) varied from 1 to 5 years. Follow-up ranged from 2 to 8.7 years.
Overall, the authors found that 81 of 1,156 patients who received antiviral therapy and 129 of 1,074 control patients who received no therapy developed hepatocellular carcinoma.
The relative risk for antiviral therapy, compared with no treatment, was 0.53 (95% confidence interval, 0.34-0.81).
"The corresponding number needed to treat to prevent one case of [hepatocellular carcinoma] was eight patients," added the researchers.
And while the effect of antivirals was more pronounced among patients with a virological response (RR 0.15; 95% CI, 0.05-0.45), there was nevertheless a clear reduction in risk for nonresponders to antivirals, with a relative risk of 0.57, compared with controls (95% CI 0.37-0.85).
"Although the intervention was more beneficial among sustained virological responders than nonresponders, there was a clear effect in both patient groups. ... Antiviral therapy may have beneficial effects on the risk of developing HCC that are unrelated to the virological response."
On the other hand, there was no reported effect of antiviral therapy on all-cause mortality, liver-related mortality, or liver-related morbidity in this population.
Dr. Kimer conceded several limitations to this analysis. "Only two of the included trials evaluated pegylated interferon, which is the current standard treatment for chronic hepatitis C."
Moreover, the duration of treatment in several included studies was "relatively long, which may increase the proportion of responders."
Finally, Dr. Kimer added that the researchers were unable to perform subgroup analysis to determine which treatment duration or dose is best.
"Based on the duration of follow-up and the lack of clear evidence concerning morbidity or mortality, we cannot exclude that interferon delays rather than prevents carcinogenesis," concluded the investigators.
Nevertheless, the "protection from HCC might be even better among patients in current antiviral therapy since the proportion of virological responders continues to increase with ongoing improvements in therapy," they wrote.
"Additional randomized trials with longer follow-up are still warranted to determine whether this is the case," they noted.
The authors disclosed having no outside funding and no competing interests related to this study.
Antiviral therapy may reduce the risk of hepatocellular carcinoma in patients with hepatitis C infections, Dr. Nina Kimer reported in the Oct. 22 issue of BMJ Open, published online.
Moreover, the effect seems to persist regardless of whether sustained virologic response is achieved.
Dr. Kimer, of Copenhagen University Hospital, Hvidovre, Denmark, and colleagues conducted a meta-analysis of trials looking at hepatitis C-related cirrhosis or fibrosis (BMJ Open 2012;2:e001313 [doi:10.1136/bmjopen-2012-001313]).
The primary analysis focused on randomized controlled trials, although prospective cohort studies with control groups were included in sensitivity analyses.
The authors searched the Cochrane Library, PubMed, EMBASE, and Web of Science databases, as well as reference lists from relevant papers, conference proceedings, and the World Health Organization Trial Search Portal.
Studies looking at HIV and chronic hepatitis B were excluded, for a total of eight randomized trials and five prospective cohort studies.
The duration of therapy (which included pegylated interferon in two trials, interferon plus ribavirin in one trial, and interferon monotherapy in the remaining trials) varied from 1 to 5 years. Follow-up ranged from 2 to 8.7 years.
Overall, the authors found that 81 of 1,156 patients who received antiviral therapy and 129 of 1,074 control patients who received no therapy developed hepatocellular carcinoma.
The relative risk for antiviral therapy, compared with no treatment, was 0.53 (95% confidence interval, 0.34-0.81).
"The corresponding number needed to treat to prevent one case of [hepatocellular carcinoma] was eight patients," added the researchers.
And while the effect of antivirals was more pronounced among patients with a virological response (RR 0.15; 95% CI, 0.05-0.45), there was nevertheless a clear reduction in risk for nonresponders to antivirals, with a relative risk of 0.57, compared with controls (95% CI 0.37-0.85).
"Although the intervention was more beneficial among sustained virological responders than nonresponders, there was a clear effect in both patient groups. ... Antiviral therapy may have beneficial effects on the risk of developing HCC that are unrelated to the virological response."
On the other hand, there was no reported effect of antiviral therapy on all-cause mortality, liver-related mortality, or liver-related morbidity in this population.
Dr. Kimer conceded several limitations to this analysis. "Only two of the included trials evaluated pegylated interferon, which is the current standard treatment for chronic hepatitis C."
Moreover, the duration of treatment in several included studies was "relatively long, which may increase the proportion of responders."
Finally, Dr. Kimer added that the researchers were unable to perform subgroup analysis to determine which treatment duration or dose is best.
"Based on the duration of follow-up and the lack of clear evidence concerning morbidity or mortality, we cannot exclude that interferon delays rather than prevents carcinogenesis," concluded the investigators.
Nevertheless, the "protection from HCC might be even better among patients in current antiviral therapy since the proportion of virological responders continues to increase with ongoing improvements in therapy," they wrote.
"Additional randomized trials with longer follow-up are still warranted to determine whether this is the case," they noted.
The authors disclosed having no outside funding and no competing interests related to this study.
sustained virologic response, hepatitis C-related cirrhosis, fibrosis,
sustained virologic response, hepatitis C-related cirrhosis, fibrosis,
FROM BMJ OPEN
Major Finding: Antiviral therapy for hepatitis C carried a relative risk of 0.53 for developing hepatocellular carcinoma, compared with no treatment (95% confidence interval, 0.34-0.81).
Data Source: A meta-analysis of randomized controlled trials.
Disclosures: The authors disclosed having no outside funding and no competing interests related to this study.
Hospitalists Can Be Prime Partners in QI, Patient Safety Efforts
NEW YORK—Hospitalists are poised to become key allies with hospital quality and safety officers nationwide, according to veteran hospitalist Jennifer Myers, MD, FHM, director of quality and safety education for Penn Medicine in Philadelphia.
Addressing hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium at Mount Sinai School of Medicine in New York, Dr. Myers said that while the challenges associated with quality improvement (QI) are many, HM leaders have the in-house relationships and respect to push the issue.
"There's really no other specialty more perfectly poised to lead this work," she told more than 180 symposium attendees Friday.
Dr. Myers, in an address titled "Enhancing Patient Safety," told The Hospitalist that HM leaders pursue three broad goals: to participate in QI programs already in place, to help create or foster a culture focused on addressing mistakes, and to teach those lessons to young physicians.
She urged physicians to actively report on mistakes and near misses, and earnestly address the processes that led to them. If a vehicle to discuss the mistakes doesn't exist at an institution, hospitalists can push to start one, she said. If a hospital doesn't have an electronic incident reporting system, a hospitalist can push to get one. "This is the goal," Dr. Myers added. "People coming to work and feeling they can be safe and report errors in the spirit of improvement."
She noted that many hospitalists already oversee quality and safety programs without any formal training. She recommended some of those physicians consider the Quality and Safety Educators Academy (QSEA), a three-day academy designed as a faculty development program and sponsored by SHM and the Alliance for Academic Internal Medicine (AAIM). The academy is March 7-9, 2013, in Tempe, Ariz.
NEW YORK—Hospitalists are poised to become key allies with hospital quality and safety officers nationwide, according to veteran hospitalist Jennifer Myers, MD, FHM, director of quality and safety education for Penn Medicine in Philadelphia.
Addressing hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium at Mount Sinai School of Medicine in New York, Dr. Myers said that while the challenges associated with quality improvement (QI) are many, HM leaders have the in-house relationships and respect to push the issue.
"There's really no other specialty more perfectly poised to lead this work," she told more than 180 symposium attendees Friday.
Dr. Myers, in an address titled "Enhancing Patient Safety," told The Hospitalist that HM leaders pursue three broad goals: to participate in QI programs already in place, to help create or foster a culture focused on addressing mistakes, and to teach those lessons to young physicians.
She urged physicians to actively report on mistakes and near misses, and earnestly address the processes that led to them. If a vehicle to discuss the mistakes doesn't exist at an institution, hospitalists can push to start one, she said. If a hospital doesn't have an electronic incident reporting system, a hospitalist can push to get one. "This is the goal," Dr. Myers added. "People coming to work and feeling they can be safe and report errors in the spirit of improvement."
She noted that many hospitalists already oversee quality and safety programs without any formal training. She recommended some of those physicians consider the Quality and Safety Educators Academy (QSEA), a three-day academy designed as a faculty development program and sponsored by SHM and the Alliance for Academic Internal Medicine (AAIM). The academy is March 7-9, 2013, in Tempe, Ariz.
NEW YORK—Hospitalists are poised to become key allies with hospital quality and safety officers nationwide, according to veteran hospitalist Jennifer Myers, MD, FHM, director of quality and safety education for Penn Medicine in Philadelphia.
Addressing hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium at Mount Sinai School of Medicine in New York, Dr. Myers said that while the challenges associated with quality improvement (QI) are many, HM leaders have the in-house relationships and respect to push the issue.
"There's really no other specialty more perfectly poised to lead this work," she told more than 180 symposium attendees Friday.
Dr. Myers, in an address titled "Enhancing Patient Safety," told The Hospitalist that HM leaders pursue three broad goals: to participate in QI programs already in place, to help create or foster a culture focused on addressing mistakes, and to teach those lessons to young physicians.
She urged physicians to actively report on mistakes and near misses, and earnestly address the processes that led to them. If a vehicle to discuss the mistakes doesn't exist at an institution, hospitalists can push to start one, she said. If a hospital doesn't have an electronic incident reporting system, a hospitalist can push to get one. "This is the goal," Dr. Myers added. "People coming to work and feeling they can be safe and report errors in the spirit of improvement."
She noted that many hospitalists already oversee quality and safety programs without any formal training. She recommended some of those physicians consider the Quality and Safety Educators Academy (QSEA), a three-day academy designed as a faculty development program and sponsored by SHM and the Alliance for Academic Internal Medicine (AAIM). The academy is March 7-9, 2013, in Tempe, Ariz.
Localized Hospitalist Teams Enhance Workflow Productivity
Using localized inpatient teams of hospitalists and physician assistants in single nursing units can boost physicians' productivity, hospital efficiency, and patient outcomes, according to a study in the Journal of Hospital Medicine.
The study, "Impact of Localizing General Medical Teams to a Single Nursing Unit," compared the effectiveness of using localized medical teams with nonlocalized teams in caring for patients in the nursing unit of an academic medical center from April to mid-July 2010. The localized team members received 51% fewer paged messages, logged more encounters with patients, and generated more relative value units (RVUs) during the workday compared with the nonlocalized teams, researchers reported.
These findings point to an overall significant increase in team productivity. The risk of 30-day readmissions and the patient charges incurred remained the same.
Lead author Siddhartha Singh, MD, MS, associate chief medical officer at Froedtert Hospital and the Medical College of Wisconsin in Milwaukee, says the study's most surprising finding was that patients averaged longer length of stay (LOS) under localized team care. However, Dr. Singh says, "if somebody wants to try out localization, the big message from our study is that it's a good thing as far as workflow is concerned."
Dr. Singh hopes the research will spark future studies about localized hospitalist teams and the optimal amount of localization needed to improve productivity and efficiency.
"When others try to localize patients, they need to be careful of 100% localization," he says. "My sense is, without having studied this any further, there's a sweet spot that optimizes the care provided to the patients [and maximizes] hospital efficiency and physician assistant productivity. I'm hoping that the next set of research on this topic tries to investigate that."
Using localized inpatient teams of hospitalists and physician assistants in single nursing units can boost physicians' productivity, hospital efficiency, and patient outcomes, according to a study in the Journal of Hospital Medicine.
The study, "Impact of Localizing General Medical Teams to a Single Nursing Unit," compared the effectiveness of using localized medical teams with nonlocalized teams in caring for patients in the nursing unit of an academic medical center from April to mid-July 2010. The localized team members received 51% fewer paged messages, logged more encounters with patients, and generated more relative value units (RVUs) during the workday compared with the nonlocalized teams, researchers reported.
These findings point to an overall significant increase in team productivity. The risk of 30-day readmissions and the patient charges incurred remained the same.
Lead author Siddhartha Singh, MD, MS, associate chief medical officer at Froedtert Hospital and the Medical College of Wisconsin in Milwaukee, says the study's most surprising finding was that patients averaged longer length of stay (LOS) under localized team care. However, Dr. Singh says, "if somebody wants to try out localization, the big message from our study is that it's a good thing as far as workflow is concerned."
Dr. Singh hopes the research will spark future studies about localized hospitalist teams and the optimal amount of localization needed to improve productivity and efficiency.
"When others try to localize patients, they need to be careful of 100% localization," he says. "My sense is, without having studied this any further, there's a sweet spot that optimizes the care provided to the patients [and maximizes] hospital efficiency and physician assistant productivity. I'm hoping that the next set of research on this topic tries to investigate that."
Using localized inpatient teams of hospitalists and physician assistants in single nursing units can boost physicians' productivity, hospital efficiency, and patient outcomes, according to a study in the Journal of Hospital Medicine.
The study, "Impact of Localizing General Medical Teams to a Single Nursing Unit," compared the effectiveness of using localized medical teams with nonlocalized teams in caring for patients in the nursing unit of an academic medical center from April to mid-July 2010. The localized team members received 51% fewer paged messages, logged more encounters with patients, and generated more relative value units (RVUs) during the workday compared with the nonlocalized teams, researchers reported.
These findings point to an overall significant increase in team productivity. The risk of 30-day readmissions and the patient charges incurred remained the same.
Lead author Siddhartha Singh, MD, MS, associate chief medical officer at Froedtert Hospital and the Medical College of Wisconsin in Milwaukee, says the study's most surprising finding was that patients averaged longer length of stay (LOS) under localized team care. However, Dr. Singh says, "if somebody wants to try out localization, the big message from our study is that it's a good thing as far as workflow is concerned."
Dr. Singh hopes the research will spark future studies about localized hospitalist teams and the optimal amount of localization needed to improve productivity and efficiency.
"When others try to localize patients, they need to be careful of 100% localization," he says. "My sense is, without having studied this any further, there's a sweet spot that optimizes the care provided to the patients [and maximizes] hospital efficiency and physician assistant productivity. I'm hoping that the next set of research on this topic tries to investigate that."