User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Alcohol consumption habits can predict gout tophi
The more years a person drinks alcohol, the kind of alcohol consumed, and the amount consumed can help to predict gout tophi, researchers say in a newly published paper in Arthritis Care and Research.
The study, led by Lin Han, PhD, of the gout laboratory, Shandong provincial clinical research center for immune diseases and gout, Affiliated Hospital of Qingdao (China) University, helps clarify the already-established relationship between alcohol consumption and gout tophi.
Additionally, the effects of drinking alcohol on ultrasound (US)–detected tophi and subcutaneous tophi (subtophi) were evaluated separately for the first time in this work, the authors say.
Tophi may be underdiagnosed because they are hard to find with only a physical exam. US can help with early detection, especially with small clusters of crystals or those found deep in the tissues, and offers good diagnostic accuracy with high specificity.
“Unlike subtophi, which represent long-term subcutaneous MSU [monosodium urate] deposition over many years, US-detected tophi represent the early stage of tophi in both intra- and extra-articular settings,” the authors write.
This cross-sectional study in China included 554 patients with gout who had joint ultrasound and physical exams through the Affiliated Hospital of Qingdao University. Physicians gathered medical histories using the Biobank Information Management System.
Physicians also tracked alcohol consumption patterns through the biobank information, which included answers to a detailed drinking questionnaire.
Patients were classified as either nondrinkers (no history of drinking; n = 141), former drinkers (n = 60), or current regular drinkers (n = 353). Current regular drinkers were asked further questions about their drinking patterns, including how long they have been drinking, type of alcohol they drink, and how much and how often they drink. In China, the average drink is considered to contain 10 g of alcohol, according to the World Health Organization.
Results from US and clinically detected tophi
Compared with nondrinkers, excessive drinkers (more than 70 g/week); long-term drinkers (at least 10 years), and spirits drinkers had a greater proportion, size, and number of US-detected tophi and subtophi (all P < .05).
After adjusting for confounders, the researchers found that excessive drinking was significantly associated with having US-detected tophi (odds ratio, 1.79) and subtophi (OR, 2.00). Similar associations were found for consumption of alcohol for at least 10 years (OR, 1.96 for US-detected tophi; OR, 2.17 for sub-tophi) and drinking spirits (OR, 1.81 for US-detected tophi; OR, 2.10 for subtophi). All comparisons were P < .05.
Among patients who already have US-detected tophi or subtophi, moderate drinking (70 g/week or less) was linked with larger or multiple tophi (all P < .05).

Angelo Gaffo, MD, section chief of rheumatology at the Birmingham VA Medical Center and associate professor of medicine in the division of rheumatology at the University of Alabama at Birmingham, said in an interview that the results are likely generalizable.
“I wouldn’t expect them to be specific to the Chinese population,” he said.
Most of the 554 patients were male (97.8%) and had no family history of gout (79.8%). The median duration of gout was 4 years, and the average age was 45.1 years.
Dr. Gaffo noted the population age was fairly young and the average duration of gout in these patients was fairly short. He also noted most had small tophi that were detected only by ultrasound and small numbers of tophi overall.
“I would like to see how these results will replicate in a population that has had gout for, say, 10 years on average,” he said.
Dr. Gaffo says he explores alcohol history with his patients with gout. If they are frequent drinkers, he encourages them to cut back.
“At the very least,” he said, “you have to restrict your intake to no more than 1-2 servings per week,” he said. “For some patients, even minimal amounts of alcohol intake can be associated with the development of flares.”
Still, research like this, he says, can help physicians point to evidence in their advice to patients about alcohol use.
He noted that the authors found the association between different types of alcohol and tophi was independent of serum urate level.
“That surprised me,” Dr. Gaffo said. “That’s a very unique finding.”
This work was supported by grants from the National Natural Science Foundation of China, the Natural Science Foundation of Shandong Province, Qingdao applied basic research project, National College Students’ Innovation and Entrepreneurship Training Program, and Shandong Provincial Science Foundation for Outstanding Youth Scholars.
The authors of the study and Dr. Gaffo report no relevant financial relationships.
The more years a person drinks alcohol, the kind of alcohol consumed, and the amount consumed can help to predict gout tophi, researchers say in a newly published paper in Arthritis Care and Research.
The study, led by Lin Han, PhD, of the gout laboratory, Shandong provincial clinical research center for immune diseases and gout, Affiliated Hospital of Qingdao (China) University, helps clarify the already-established relationship between alcohol consumption and gout tophi.
Additionally, the effects of drinking alcohol on ultrasound (US)–detected tophi and subcutaneous tophi (subtophi) were evaluated separately for the first time in this work, the authors say.
Tophi may be underdiagnosed because they are hard to find with only a physical exam. US can help with early detection, especially with small clusters of crystals or those found deep in the tissues, and offers good diagnostic accuracy with high specificity.
“Unlike subtophi, which represent long-term subcutaneous MSU [monosodium urate] deposition over many years, US-detected tophi represent the early stage of tophi in both intra- and extra-articular settings,” the authors write.
This cross-sectional study in China included 554 patients with gout who had joint ultrasound and physical exams through the Affiliated Hospital of Qingdao University. Physicians gathered medical histories using the Biobank Information Management System.
Physicians also tracked alcohol consumption patterns through the biobank information, which included answers to a detailed drinking questionnaire.
Patients were classified as either nondrinkers (no history of drinking; n = 141), former drinkers (n = 60), or current regular drinkers (n = 353). Current regular drinkers were asked further questions about their drinking patterns, including how long they have been drinking, type of alcohol they drink, and how much and how often they drink. In China, the average drink is considered to contain 10 g of alcohol, according to the World Health Organization.
Results from US and clinically detected tophi
Compared with nondrinkers, excessive drinkers (more than 70 g/week); long-term drinkers (at least 10 years), and spirits drinkers had a greater proportion, size, and number of US-detected tophi and subtophi (all P < .05).
After adjusting for confounders, the researchers found that excessive drinking was significantly associated with having US-detected tophi (odds ratio, 1.79) and subtophi (OR, 2.00). Similar associations were found for consumption of alcohol for at least 10 years (OR, 1.96 for US-detected tophi; OR, 2.17 for sub-tophi) and drinking spirits (OR, 1.81 for US-detected tophi; OR, 2.10 for subtophi). All comparisons were P < .05.
Among patients who already have US-detected tophi or subtophi, moderate drinking (70 g/week or less) was linked with larger or multiple tophi (all P < .05).
Angelo Gaffo, MD, section chief of rheumatology at the Birmingham VA Medical Center and associate professor of medicine in the division of rheumatology at the University of Alabama at Birmingham, said in an interview that the results are likely generalizable.
“I wouldn’t expect them to be specific to the Chinese population,” he said.
Most of the 554 patients were male (97.8%) and had no family history of gout (79.8%). The median duration of gout was 4 years, and the average age was 45.1 years.
Dr. Gaffo noted the population age was fairly young and the average duration of gout in these patients was fairly short. He also noted most had small tophi that were detected only by ultrasound and small numbers of tophi overall.
“I would like to see how these results will replicate in a population that has had gout for, say, 10 years on average,” he said.
Dr. Gaffo says he explores alcohol history with his patients with gout. If they are frequent drinkers, he encourages them to cut back.
“At the very least,” he said, “you have to restrict your intake to no more than 1-2 servings per week,” he said. “For some patients, even minimal amounts of alcohol intake can be associated with the development of flares.”
Still, research like this, he says, can help physicians point to evidence in their advice to patients about alcohol use.
He noted that the authors found the association between different types of alcohol and tophi was independent of serum urate level.
“That surprised me,” Dr. Gaffo said. “That’s a very unique finding.”
This work was supported by grants from the National Natural Science Foundation of China, the Natural Science Foundation of Shandong Province, Qingdao applied basic research project, National College Students’ Innovation and Entrepreneurship Training Program, and Shandong Provincial Science Foundation for Outstanding Youth Scholars.
The authors of the study and Dr. Gaffo report no relevant financial relationships.
The more years a person drinks alcohol, the kind of alcohol consumed, and the amount consumed can help to predict gout tophi, researchers say in a newly published paper in Arthritis Care and Research.
The study, led by Lin Han, PhD, of the gout laboratory, Shandong provincial clinical research center for immune diseases and gout, Affiliated Hospital of Qingdao (China) University, helps clarify the already-established relationship between alcohol consumption and gout tophi.
Additionally, the effects of drinking alcohol on ultrasound (US)–detected tophi and subcutaneous tophi (subtophi) were evaluated separately for the first time in this work, the authors say.
Tophi may be underdiagnosed because they are hard to find with only a physical exam. US can help with early detection, especially with small clusters of crystals or those found deep in the tissues, and offers good diagnostic accuracy with high specificity.
“Unlike subtophi, which represent long-term subcutaneous MSU [monosodium urate] deposition over many years, US-detected tophi represent the early stage of tophi in both intra- and extra-articular settings,” the authors write.
This cross-sectional study in China included 554 patients with gout who had joint ultrasound and physical exams through the Affiliated Hospital of Qingdao University. Physicians gathered medical histories using the Biobank Information Management System.
Physicians also tracked alcohol consumption patterns through the biobank information, which included answers to a detailed drinking questionnaire.
Patients were classified as either nondrinkers (no history of drinking; n = 141), former drinkers (n = 60), or current regular drinkers (n = 353). Current regular drinkers were asked further questions about their drinking patterns, including how long they have been drinking, type of alcohol they drink, and how much and how often they drink. In China, the average drink is considered to contain 10 g of alcohol, according to the World Health Organization.
Results from US and clinically detected tophi
Compared with nondrinkers, excessive drinkers (more than 70 g/week); long-term drinkers (at least 10 years), and spirits drinkers had a greater proportion, size, and number of US-detected tophi and subtophi (all P < .05).
After adjusting for confounders, the researchers found that excessive drinking was significantly associated with having US-detected tophi (odds ratio, 1.79) and subtophi (OR, 2.00). Similar associations were found for consumption of alcohol for at least 10 years (OR, 1.96 for US-detected tophi; OR, 2.17 for sub-tophi) and drinking spirits (OR, 1.81 for US-detected tophi; OR, 2.10 for subtophi). All comparisons were P < .05.
Among patients who already have US-detected tophi or subtophi, moderate drinking (70 g/week or less) was linked with larger or multiple tophi (all P < .05).
Angelo Gaffo, MD, section chief of rheumatology at the Birmingham VA Medical Center and associate professor of medicine in the division of rheumatology at the University of Alabama at Birmingham, said in an interview that the results are likely generalizable.
“I wouldn’t expect them to be specific to the Chinese population,” he said.
Most of the 554 patients were male (97.8%) and had no family history of gout (79.8%). The median duration of gout was 4 years, and the average age was 45.1 years.
Dr. Gaffo noted the population age was fairly young and the average duration of gout in these patients was fairly short. He also noted most had small tophi that were detected only by ultrasound and small numbers of tophi overall.
“I would like to see how these results will replicate in a population that has had gout for, say, 10 years on average,” he said.
Dr. Gaffo says he explores alcohol history with his patients with gout. If they are frequent drinkers, he encourages them to cut back.
“At the very least,” he said, “you have to restrict your intake to no more than 1-2 servings per week,” he said. “For some patients, even minimal amounts of alcohol intake can be associated with the development of flares.”
Still, research like this, he says, can help physicians point to evidence in their advice to patients about alcohol use.
He noted that the authors found the association between different types of alcohol and tophi was independent of serum urate level.
“That surprised me,” Dr. Gaffo said. “That’s a very unique finding.”
This work was supported by grants from the National Natural Science Foundation of China, the Natural Science Foundation of Shandong Province, Qingdao applied basic research project, National College Students’ Innovation and Entrepreneurship Training Program, and Shandong Provincial Science Foundation for Outstanding Youth Scholars.
The authors of the study and Dr. Gaffo report no relevant financial relationships.
FROM ARTHRITIS CARE AND RESEARCH
Type 1 diabetes control worse in racially segregated teens
Racial residential segregation was significantly associated with poor glycemic control in Black adolescents with type 1 diabetes, according to data from 144 individuals.
Racial residential segregation is considered a form of systemic racism that involves limited access to resources, including health care resources, Deborah A. Ellis, MD, of Wayne State University, Detroit, and colleagues wrote in a poster presented at the annual meeting of the American Diabetes Association.
In the study, the researchers recruited youth aged 10-15 years with type 1 diabetes from seven pediatric clinics in two large U.S. cities. The mean age of the participants was 13.3 years, and the mean hemoglobin A1c was 11.5%.
Diabetes management was based on self-reports using the Diabetes Management Scale (DMS). Racial residential segregation, which refers to the separation of groups within a geographic area, was determined using data from the U.S. Census using Location Quotient (LQ) at the block group level; this showed the ratio of the Black population to the total population, compared with the same ratio in the metropolitan area.
The mean family income was $34,163, and the mean LQ was 3.04, “indicating residence in highly segregated neighborhoods,” the researchers wrote.
Overall, racial residential segregation was significantly associated with A1c (P = .001) but not with DMS (P = .311). The researchers also conducted a stepwise multiple regression analysis including age, insulin delivery method, neighborhood adversity (a 9-item composite with variables including percentage of persons living in poverty, percentage of households with no vehicle), and family income. They found that only age, insulin delivery method, and racial residential segregation had significant impacts of A1c levels.
The study was limited by several factors, including the use of self-reports.
However, the results are consistent with previous studies showing the potential negative health effects of structural racism, the researchers wrote. The findings suggest that racial residential segregation has an independent effect on glycemic control in Black youth with type 1 diabetes, and consequently, “advocacy and policy making to address such inequities could improve diabetes population health.”
Location makes a difference
“Poor neighborhoods have been associated with high rates of obesity, hypertension, type 2 diabetes and high cholesterol,” Romesh K. Khardori, MD, professor of medicine at Eastern Virginia Medical School, Norfolk, said in an interview. However, “not much is known about impact of racial segregation on type 1 diabetes,” said Dr. Khardori, who was not involved in the study.
Dr. Khardori was not surprised by the current study findings. “In our practice, Black youth coming from racially segregated or low-income housing projects often tend have poor diabetes control, with repeated admissions to local hospitals for managing acute/chronic complications of type 1 diabetes,” he said.
The current findings reflect Dr. Khardori’s clinical experience and highlight the need for clinicians to recognize the increased risk for poor glycemic control and poor outcomes in this vulnerable population.
More research is needed to expand the observations of the current study, Dr. Khardori said. Future researchers also should “involve community leaders and politicians to educate and garner more support for mitigation efforts.”
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Ellis and Dr. Khardori had no financial conflicts to disclose.
Racial residential segregation was significantly associated with poor glycemic control in Black adolescents with type 1 diabetes, according to data from 144 individuals.
Racial residential segregation is considered a form of systemic racism that involves limited access to resources, including health care resources, Deborah A. Ellis, MD, of Wayne State University, Detroit, and colleagues wrote in a poster presented at the annual meeting of the American Diabetes Association.
In the study, the researchers recruited youth aged 10-15 years with type 1 diabetes from seven pediatric clinics in two large U.S. cities. The mean age of the participants was 13.3 years, and the mean hemoglobin A1c was 11.5%.
Diabetes management was based on self-reports using the Diabetes Management Scale (DMS). Racial residential segregation, which refers to the separation of groups within a geographic area, was determined using data from the U.S. Census using Location Quotient (LQ) at the block group level; this showed the ratio of the Black population to the total population, compared with the same ratio in the metropolitan area.
The mean family income was $34,163, and the mean LQ was 3.04, “indicating residence in highly segregated neighborhoods,” the researchers wrote.
Overall, racial residential segregation was significantly associated with A1c (P = .001) but not with DMS (P = .311). The researchers also conducted a stepwise multiple regression analysis including age, insulin delivery method, neighborhood adversity (a 9-item composite with variables including percentage of persons living in poverty, percentage of households with no vehicle), and family income. They found that only age, insulin delivery method, and racial residential segregation had significant impacts of A1c levels.
The study was limited by several factors, including the use of self-reports.
However, the results are consistent with previous studies showing the potential negative health effects of structural racism, the researchers wrote. The findings suggest that racial residential segregation has an independent effect on glycemic control in Black youth with type 1 diabetes, and consequently, “advocacy and policy making to address such inequities could improve diabetes population health.”
Location makes a difference
“Poor neighborhoods have been associated with high rates of obesity, hypertension, type 2 diabetes and high cholesterol,” Romesh K. Khardori, MD, professor of medicine at Eastern Virginia Medical School, Norfolk, said in an interview. However, “not much is known about impact of racial segregation on type 1 diabetes,” said Dr. Khardori, who was not involved in the study.
Dr. Khardori was not surprised by the current study findings. “In our practice, Black youth coming from racially segregated or low-income housing projects often tend have poor diabetes control, with repeated admissions to local hospitals for managing acute/chronic complications of type 1 diabetes,” he said.
The current findings reflect Dr. Khardori’s clinical experience and highlight the need for clinicians to recognize the increased risk for poor glycemic control and poor outcomes in this vulnerable population.
More research is needed to expand the observations of the current study, Dr. Khardori said. Future researchers also should “involve community leaders and politicians to educate and garner more support for mitigation efforts.”
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Ellis and Dr. Khardori had no financial conflicts to disclose.
Racial residential segregation was significantly associated with poor glycemic control in Black adolescents with type 1 diabetes, according to data from 144 individuals.
Racial residential segregation is considered a form of systemic racism that involves limited access to resources, including health care resources, Deborah A. Ellis, MD, of Wayne State University, Detroit, and colleagues wrote in a poster presented at the annual meeting of the American Diabetes Association.
In the study, the researchers recruited youth aged 10-15 years with type 1 diabetes from seven pediatric clinics in two large U.S. cities. The mean age of the participants was 13.3 years, and the mean hemoglobin A1c was 11.5%.
Diabetes management was based on self-reports using the Diabetes Management Scale (DMS). Racial residential segregation, which refers to the separation of groups within a geographic area, was determined using data from the U.S. Census using Location Quotient (LQ) at the block group level; this showed the ratio of the Black population to the total population, compared with the same ratio in the metropolitan area.
The mean family income was $34,163, and the mean LQ was 3.04, “indicating residence in highly segregated neighborhoods,” the researchers wrote.
Overall, racial residential segregation was significantly associated with A1c (P = .001) but not with DMS (P = .311). The researchers also conducted a stepwise multiple regression analysis including age, insulin delivery method, neighborhood adversity (a 9-item composite with variables including percentage of persons living in poverty, percentage of households with no vehicle), and family income. They found that only age, insulin delivery method, and racial residential segregation had significant impacts of A1c levels.
The study was limited by several factors, including the use of self-reports.
However, the results are consistent with previous studies showing the potential negative health effects of structural racism, the researchers wrote. The findings suggest that racial residential segregation has an independent effect on glycemic control in Black youth with type 1 diabetes, and consequently, “advocacy and policy making to address such inequities could improve diabetes population health.”
Location makes a difference
“Poor neighborhoods have been associated with high rates of obesity, hypertension, type 2 diabetes and high cholesterol,” Romesh K. Khardori, MD, professor of medicine at Eastern Virginia Medical School, Norfolk, said in an interview. However, “not much is known about impact of racial segregation on type 1 diabetes,” said Dr. Khardori, who was not involved in the study.
Dr. Khardori was not surprised by the current study findings. “In our practice, Black youth coming from racially segregated or low-income housing projects often tend have poor diabetes control, with repeated admissions to local hospitals for managing acute/chronic complications of type 1 diabetes,” he said.
The current findings reflect Dr. Khardori’s clinical experience and highlight the need for clinicians to recognize the increased risk for poor glycemic control and poor outcomes in this vulnerable population.
More research is needed to expand the observations of the current study, Dr. Khardori said. Future researchers also should “involve community leaders and politicians to educate and garner more support for mitigation efforts.”
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Ellis and Dr. Khardori had no financial conflicts to disclose.
FROM ADA 2022
Add AFib to noncardiac surgery risk evaluation: New support
Practice has gone back and forth on whether atrial fibrillation (AFib) should be considered in the preoperative cardiovascular risk (CV) evaluation of patients slated for noncardiac surgery, and the Revised Cardiac Risk Index (RCRI), currently widely used as an assessment tool, doesn’t include the arrhythmia.
But consideration of preexisting AFib along with the RCRI predicted 30-day mortality more sharply than the RCRI alone in an analysis of data covering several million patients slated for such procedures.

Indeed, AFib emerged as a significant, independent risk factor for a number of bad postoperative outcomes. Mortality within a month of the procedure climbed about 30% for patients with AFib before the noncardiac surgery. Their 30-day risks for stroke and for heart failure hospitalization went up similarly.
The addition of AFib to the RCRI significantly improved its ability to discriminate 30-day postoperative risk levels regardless of age, sex, and type of noncardiac surgery, Amgad Mentias, MD, Cleveland Clinic, told this news organization. And “it was able to correctly up-classify patients to high risk, if AFib was there, and it was able to down-classify some patients to lower risk if it wasn’t there.”
“I think [the findings] are convincing evidence that atrial fib should at least be part of the thought process for the surgical team and the medical team taking care of the patient,” said Dr. Mentias, who is senior author on the study published in the Journal of the American College of Cardiology, with lead author Sameer Prasada, MD, also of the Cleveland Clinic.
The results “call for incorporating AFib as a risk factor in perioperative risk scores for cardiovascular morbidity and mortality,” the published report states.
Supraventricular arrhythmias had been part of the Goldman Risk Index once widely used preoperatively to assess cardiac risk before practice adopted the RCRI in the past decade, observe Anne B. Curtis, MD, and Sai Krishna C. Korada, MD, University at Buffalo, New York, in an accompanying editorial.
The current findings “demonstrate improved prediction of adverse postsurgical outcomes” from supplementing the RCRI with AFib, they write. Given associations between preexisting AFib and serious cardiac events, “it is time to ‘re-revise’ the RCRI and acknowledge the importance of AFib in predicting adverse outcomes” after noncardiac surgery.
The new findings, however, aren’t all straightforward. In one result that remains a bit of a head-scratcher, postoperative risk of myocardial infarction (MI) in patients with preexisting AFib went in the opposite direction of risk for death and other CV outcomes, falling by almost 20%.
That is “hard to explain with the available data,” the report states, but “the use of anticoagulation, whether oral or parenteral (as a bridge therapy in the perioperative period), is a plausible explanation” given the frequent role of thrombosis in triggering MIs.
Consistent with such a mechanism, the group argues, the MI risk reduction was seen primarily among patients with AFib and a CHA2DS2-VASc score of 2 or higher – that is, those at highest risk for stroke and therefore most likely to be on oral anticoagulation. The MI risk reduction wasn’t seen in such patients with a CHA2DS2-VASc score of 0 or 1.
“I think that’s part of the explanation, that anticoagulation can reduce risk of MI. But it’s not the whole explanation,” Dr. Mentias said in an interview. If it were the sole mechanism, he said, then the same oral anticoagulation that protected against MI should have also cut the postoperative stroke risk. Yet that risk climbed 40% among patients with preexisting AFib.
The analysis started with 8.6 million Medicare patients with planned noncardiac surgery, seen from 2015 to 2019, of whom 16.4% had preexisting AFib. Propensity matching for demographics, urgency and type of surgery, CHA2DS2-VASc score, and RCRI index created two cohorts for comparison: 1.13 million patients with and 1.92 million without preexisting AFib.
Preexisting AFib was associated with a higher 30-day risk for death from any cause, the primary endpoint being 8.3% versus 5.8% for those without such AFib (P < .001), for an odds ratio of 1.31 (95% confidence interval, 1.30-1.32).
Corresponding 30-day ORs for other events, all significant at P < .001, were:
- 1.31 (95% CI, 1.30-1.33) for heart failure
- 1.40 (95% CI, 1.37-1.43) for stroke
- 1.59 (95% CI, 1.43-1.75) for systemic embolism
- 1.14 (95% CI, 1.13-1.16) for major bleeding
- 0.81 (95% CI, 0.79-0.82) for MI
Those with preexisting AFib also had longer hospitalizations at a median 5 days, compared with 4 days for those without such AFib (P < .001).
The study has the limitations of most any retrospective cohort analysis. Other limitations, the report notes, include lack of information on any antiarrhythmic meds given during hospitalization or type of AFib.
For example, AFib that is permanent – compared with paroxysmal or persistent – may be associated with more atrial fibrosis, greater atrial dilatation, “and probably higher pressures inside the heart,” Dr. Mentias observed.
“That’s not always the case, but that’s the notion. So presumably people with persistent or permanent atrial fib would have more advanced heart disease, and that could imply more risk. But we did not have that kind of data.”
Dr. Mentias and Dr. Prasada report no relevant financial relationships; disclosures for the other authors are in the report. Dr. Curtis discloses serving on advisory boards for Abbott, Janssen Pharmaceuticals, Sanofi, and Milestone Pharmaceuticals; receiving honoraria for speaking from Medtronic and Zoll; and serving on a data-monitoring board for Medtronic. Dr. Korada reports he has no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Practice has gone back and forth on whether atrial fibrillation (AFib) should be considered in the preoperative cardiovascular risk (CV) evaluation of patients slated for noncardiac surgery, and the Revised Cardiac Risk Index (RCRI), currently widely used as an assessment tool, doesn’t include the arrhythmia.
But consideration of preexisting AFib along with the RCRI predicted 30-day mortality more sharply than the RCRI alone in an analysis of data covering several million patients slated for such procedures.
Indeed, AFib emerged as a significant, independent risk factor for a number of bad postoperative outcomes. Mortality within a month of the procedure climbed about 30% for patients with AFib before the noncardiac surgery. Their 30-day risks for stroke and for heart failure hospitalization went up similarly.
The addition of AFib to the RCRI significantly improved its ability to discriminate 30-day postoperative risk levels regardless of age, sex, and type of noncardiac surgery, Amgad Mentias, MD, Cleveland Clinic, told this news organization. And “it was able to correctly up-classify patients to high risk, if AFib was there, and it was able to down-classify some patients to lower risk if it wasn’t there.”
“I think [the findings] are convincing evidence that atrial fib should at least be part of the thought process for the surgical team and the medical team taking care of the patient,” said Dr. Mentias, who is senior author on the study published in the Journal of the American College of Cardiology, with lead author Sameer Prasada, MD, also of the Cleveland Clinic.
The results “call for incorporating AFib as a risk factor in perioperative risk scores for cardiovascular morbidity and mortality,” the published report states.
Supraventricular arrhythmias had been part of the Goldman Risk Index once widely used preoperatively to assess cardiac risk before practice adopted the RCRI in the past decade, observe Anne B. Curtis, MD, and Sai Krishna C. Korada, MD, University at Buffalo, New York, in an accompanying editorial.
The current findings “demonstrate improved prediction of adverse postsurgical outcomes” from supplementing the RCRI with AFib, they write. Given associations between preexisting AFib and serious cardiac events, “it is time to ‘re-revise’ the RCRI and acknowledge the importance of AFib in predicting adverse outcomes” after noncardiac surgery.
The new findings, however, aren’t all straightforward. In one result that remains a bit of a head-scratcher, postoperative risk of myocardial infarction (MI) in patients with preexisting AFib went in the opposite direction of risk for death and other CV outcomes, falling by almost 20%.
That is “hard to explain with the available data,” the report states, but “the use of anticoagulation, whether oral or parenteral (as a bridge therapy in the perioperative period), is a plausible explanation” given the frequent role of thrombosis in triggering MIs.
Consistent with such a mechanism, the group argues, the MI risk reduction was seen primarily among patients with AFib and a CHA2DS2-VASc score of 2 or higher – that is, those at highest risk for stroke and therefore most likely to be on oral anticoagulation. The MI risk reduction wasn’t seen in such patients with a CHA2DS2-VASc score of 0 or 1.
“I think that’s part of the explanation, that anticoagulation can reduce risk of MI. But it’s not the whole explanation,” Dr. Mentias said in an interview. If it were the sole mechanism, he said, then the same oral anticoagulation that protected against MI should have also cut the postoperative stroke risk. Yet that risk climbed 40% among patients with preexisting AFib.
The analysis started with 8.6 million Medicare patients with planned noncardiac surgery, seen from 2015 to 2019, of whom 16.4% had preexisting AFib. Propensity matching for demographics, urgency and type of surgery, CHA2DS2-VASc score, and RCRI index created two cohorts for comparison: 1.13 million patients with and 1.92 million without preexisting AFib.
Preexisting AFib was associated with a higher 30-day risk for death from any cause, the primary endpoint being 8.3% versus 5.8% for those without such AFib (P < .001), for an odds ratio of 1.31 (95% confidence interval, 1.30-1.32).
Corresponding 30-day ORs for other events, all significant at P < .001, were:
- 1.31 (95% CI, 1.30-1.33) for heart failure
- 1.40 (95% CI, 1.37-1.43) for stroke
- 1.59 (95% CI, 1.43-1.75) for systemic embolism
- 1.14 (95% CI, 1.13-1.16) for major bleeding
- 0.81 (95% CI, 0.79-0.82) for MI
Those with preexisting AFib also had longer hospitalizations at a median 5 days, compared with 4 days for those without such AFib (P < .001).
The study has the limitations of most any retrospective cohort analysis. Other limitations, the report notes, include lack of information on any antiarrhythmic meds given during hospitalization or type of AFib.
For example, AFib that is permanent – compared with paroxysmal or persistent – may be associated with more atrial fibrosis, greater atrial dilatation, “and probably higher pressures inside the heart,” Dr. Mentias observed.
“That’s not always the case, but that’s the notion. So presumably people with persistent or permanent atrial fib would have more advanced heart disease, and that could imply more risk. But we did not have that kind of data.”
Dr. Mentias and Dr. Prasada report no relevant financial relationships; disclosures for the other authors are in the report. Dr. Curtis discloses serving on advisory boards for Abbott, Janssen Pharmaceuticals, Sanofi, and Milestone Pharmaceuticals; receiving honoraria for speaking from Medtronic and Zoll; and serving on a data-monitoring board for Medtronic. Dr. Korada reports he has no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Practice has gone back and forth on whether atrial fibrillation (AFib) should be considered in the preoperative cardiovascular risk (CV) evaluation of patients slated for noncardiac surgery, and the Revised Cardiac Risk Index (RCRI), currently widely used as an assessment tool, doesn’t include the arrhythmia.
But consideration of preexisting AFib along with the RCRI predicted 30-day mortality more sharply than the RCRI alone in an analysis of data covering several million patients slated for such procedures.
Indeed, AFib emerged as a significant, independent risk factor for a number of bad postoperative outcomes. Mortality within a month of the procedure climbed about 30% for patients with AFib before the noncardiac surgery. Their 30-day risks for stroke and for heart failure hospitalization went up similarly.
The addition of AFib to the RCRI significantly improved its ability to discriminate 30-day postoperative risk levels regardless of age, sex, and type of noncardiac surgery, Amgad Mentias, MD, Cleveland Clinic, told this news organization. And “it was able to correctly up-classify patients to high risk, if AFib was there, and it was able to down-classify some patients to lower risk if it wasn’t there.”
“I think [the findings] are convincing evidence that atrial fib should at least be part of the thought process for the surgical team and the medical team taking care of the patient,” said Dr. Mentias, who is senior author on the study published in the Journal of the American College of Cardiology, with lead author Sameer Prasada, MD, also of the Cleveland Clinic.
The results “call for incorporating AFib as a risk factor in perioperative risk scores for cardiovascular morbidity and mortality,” the published report states.
Supraventricular arrhythmias had been part of the Goldman Risk Index once widely used preoperatively to assess cardiac risk before practice adopted the RCRI in the past decade, observe Anne B. Curtis, MD, and Sai Krishna C. Korada, MD, University at Buffalo, New York, in an accompanying editorial.
The current findings “demonstrate improved prediction of adverse postsurgical outcomes” from supplementing the RCRI with AFib, they write. Given associations between preexisting AFib and serious cardiac events, “it is time to ‘re-revise’ the RCRI and acknowledge the importance of AFib in predicting adverse outcomes” after noncardiac surgery.
The new findings, however, aren’t all straightforward. In one result that remains a bit of a head-scratcher, postoperative risk of myocardial infarction (MI) in patients with preexisting AFib went in the opposite direction of risk for death and other CV outcomes, falling by almost 20%.
That is “hard to explain with the available data,” the report states, but “the use of anticoagulation, whether oral or parenteral (as a bridge therapy in the perioperative period), is a plausible explanation” given the frequent role of thrombosis in triggering MIs.
Consistent with such a mechanism, the group argues, the MI risk reduction was seen primarily among patients with AFib and a CHA2DS2-VASc score of 2 or higher – that is, those at highest risk for stroke and therefore most likely to be on oral anticoagulation. The MI risk reduction wasn’t seen in such patients with a CHA2DS2-VASc score of 0 or 1.
“I think that’s part of the explanation, that anticoagulation can reduce risk of MI. But it’s not the whole explanation,” Dr. Mentias said in an interview. If it were the sole mechanism, he said, then the same oral anticoagulation that protected against MI should have also cut the postoperative stroke risk. Yet that risk climbed 40% among patients with preexisting AFib.
The analysis started with 8.6 million Medicare patients with planned noncardiac surgery, seen from 2015 to 2019, of whom 16.4% had preexisting AFib. Propensity matching for demographics, urgency and type of surgery, CHA2DS2-VASc score, and RCRI index created two cohorts for comparison: 1.13 million patients with and 1.92 million without preexisting AFib.
Preexisting AFib was associated with a higher 30-day risk for death from any cause, the primary endpoint being 8.3% versus 5.8% for those without such AFib (P < .001), for an odds ratio of 1.31 (95% confidence interval, 1.30-1.32).
Corresponding 30-day ORs for other events, all significant at P < .001, were:
- 1.31 (95% CI, 1.30-1.33) for heart failure
- 1.40 (95% CI, 1.37-1.43) for stroke
- 1.59 (95% CI, 1.43-1.75) for systemic embolism
- 1.14 (95% CI, 1.13-1.16) for major bleeding
- 0.81 (95% CI, 0.79-0.82) for MI
Those with preexisting AFib also had longer hospitalizations at a median 5 days, compared with 4 days for those without such AFib (P < .001).
The study has the limitations of most any retrospective cohort analysis. Other limitations, the report notes, include lack of information on any antiarrhythmic meds given during hospitalization or type of AFib.
For example, AFib that is permanent – compared with paroxysmal or persistent – may be associated with more atrial fibrosis, greater atrial dilatation, “and probably higher pressures inside the heart,” Dr. Mentias observed.
“That’s not always the case, but that’s the notion. So presumably people with persistent or permanent atrial fib would have more advanced heart disease, and that could imply more risk. But we did not have that kind of data.”
Dr. Mentias and Dr. Prasada report no relevant financial relationships; disclosures for the other authors are in the report. Dr. Curtis discloses serving on advisory boards for Abbott, Janssen Pharmaceuticals, Sanofi, and Milestone Pharmaceuticals; receiving honoraria for speaking from Medtronic and Zoll; and serving on a data-monitoring board for Medtronic. Dr. Korada reports he has no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA Volara ventilator warning upgraded to full recall
The Food and Drug Administration has changed the warning about the Volara system to a Class I recall, the most severe level of recall, which is reserved for products that may cause injury or death. At the time of the warning, one injury had been associated with the product; as of June 23, there have been two deaths and one complaint, according to the FDA’s release.
Normally, the Volara system is used for breathing treatments that are administered at home. The medical device company that manufactures it, Baxter International, says the product is designed to help expand the airways and clear mucus for patients who use it. But because of recent product malfunctions, patients are at risk of choking on mucus, developing an infection in their lungs that cuts off their ability to take in oxygen, or in the worst cases, developing brain injury and death.
The risk is especially high because Volara is designed to be used in outpatient settings, not in the hospital under the supervision of a health care professional. It’s supposed to require less supervision than other ventilators. But if there is a problem with the device, or if it’s not connected properly, or if no one is available to assist, people are more likely to be harmed.
People who use the Volara ventilator system at home or people who assist in the use of it should be on alert for these problems. But the FDA advises that patients continue using the therapy if the device has been recommended by a doctor. The device should be used with extra precaution, and patients should be monitored for signs of distress, the release says. Problems while using the device should be reported to the FDA’s Medwatch database.
In addition to these reports, Baxter and its subsidiary company Hillrom say they will update the instructions for the device and will dispatch trainers to make home visits for users. The contact information for the company, as well as additional resources, are listed at the bottom of the release.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has changed the warning about the Volara system to a Class I recall, the most severe level of recall, which is reserved for products that may cause injury or death. At the time of the warning, one injury had been associated with the product; as of June 23, there have been two deaths and one complaint, according to the FDA’s release.
Normally, the Volara system is used for breathing treatments that are administered at home. The medical device company that manufactures it, Baxter International, says the product is designed to help expand the airways and clear mucus for patients who use it. But because of recent product malfunctions, patients are at risk of choking on mucus, developing an infection in their lungs that cuts off their ability to take in oxygen, or in the worst cases, developing brain injury and death.
The risk is especially high because Volara is designed to be used in outpatient settings, not in the hospital under the supervision of a health care professional. It’s supposed to require less supervision than other ventilators. But if there is a problem with the device, or if it’s not connected properly, or if no one is available to assist, people are more likely to be harmed.
People who use the Volara ventilator system at home or people who assist in the use of it should be on alert for these problems. But the FDA advises that patients continue using the therapy if the device has been recommended by a doctor. The device should be used with extra precaution, and patients should be monitored for signs of distress, the release says. Problems while using the device should be reported to the FDA’s Medwatch database.
In addition to these reports, Baxter and its subsidiary company Hillrom say they will update the instructions for the device and will dispatch trainers to make home visits for users. The contact information for the company, as well as additional resources, are listed at the bottom of the release.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has changed the warning about the Volara system to a Class I recall, the most severe level of recall, which is reserved for products that may cause injury or death. At the time of the warning, one injury had been associated with the product; as of June 23, there have been two deaths and one complaint, according to the FDA’s release.
Normally, the Volara system is used for breathing treatments that are administered at home. The medical device company that manufactures it, Baxter International, says the product is designed to help expand the airways and clear mucus for patients who use it. But because of recent product malfunctions, patients are at risk of choking on mucus, developing an infection in their lungs that cuts off their ability to take in oxygen, or in the worst cases, developing brain injury and death.
The risk is especially high because Volara is designed to be used in outpatient settings, not in the hospital under the supervision of a health care professional. It’s supposed to require less supervision than other ventilators. But if there is a problem with the device, or if it’s not connected properly, or if no one is available to assist, people are more likely to be harmed.
People who use the Volara ventilator system at home or people who assist in the use of it should be on alert for these problems. But the FDA advises that patients continue using the therapy if the device has been recommended by a doctor. The device should be used with extra precaution, and patients should be monitored for signs of distress, the release says. Problems while using the device should be reported to the FDA’s Medwatch database.
In addition to these reports, Baxter and its subsidiary company Hillrom say they will update the instructions for the device and will dispatch trainers to make home visits for users. The contact information for the company, as well as additional resources, are listed at the bottom of the release.
A version of this article first appeared on Medscape.com.
Aging HIV patients face comorbidities and hospitalizations
Thanks to effective treatment, people with HIV are living longer. But as they age, they face higher rates of age-related comorbidities and hospitalizations, according to a recent study of hospitalized patients.
Decision-makers will need to allocate resources, train providers, and plan ways to manage chronic diseases, such as diabetes and cancer, among geriatric HIV inpatients, according to the authors.
“There will be more [HIV] patients with age-related chronic conditions at an earlier age and who will utilize or will have a unique need for [health care for] these geriatric conditions,” first author Khairul A. Siddiqi, PhD, University of Florida, Gainesville, said in an interview. “Eventually, that may increase inpatient resource utilization and costs.”
The study was published online in HIV Medicine.
Aging with HIV
Analyzing the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project, the authors compared characteristics and comorbidities linked to hospital stays among people with HIV (HSWH) to those linked to hospital stays among people without HIV (HSWOH).
The NIS is a database of hospital records that captures 20% of discharges in the United States and covers all payers. Data in this analysis covered the years 2003-2015.
Among HSWH, patients aged 50 or older accounted for an increasing proportion over time, from fewer than 25% in 2003 to over 50% by 2015, the authors found. The subgroup aged 65-80 had risen from 2.39% to 8.63% by 2015.
The authors also studied rates of eight comorbidities, termed HIV-associated non-AIDS (HANA) conditions: cardiovascular, lung, liver, neurologic, and kidney diseases; diabetes; cancer; and bone loss.
The average number of these conditions among both HSWH and HSWOH rose over time. But this change was disproportionately high among HSWH aged 50-64 and those aged 65 and older.
Over the study period, among patients aged 65 or older, six of the eight age-related conditions the researchers studied rose disproportionately among HSWH in comparison with HSWOH; among those aged 50-64, five conditions did so.
The researchers are now building on the current study of HSWH by examining rates of resource utilization, such as MRIs and procedures, Dr. Siddiqi said.
Study limitations included a lack of data from long-term facilities, potential skewing by patients hospitalized multiple times, and the inherent limitations of administrative data.
A unique group of older people
Among people with HIV (PWH) in the United States, nearly half are aged 50 or older. By 2030, this group is expected to account for some 70% of PWH.
“We need to pay attention to what we know about aging generally. It is also important to study aging in this special population, because we don’t necessarily know a lot about that,” Amy Justice, MD, PhD, professor of medicine and of public health at Yale University, New Haven, Conn., said in an interview. Dr. Justice was not involved in the study.
The HIV epidemic has disproportionately affected people of color, men who have sex with men, and people with a history of injection drug use, Dr. Justice said.
“We don’t know about aging with [a] past history of injection drug use. We don’t even know much about aging with hepatitis C, necessarily,” she said. “So there are lots of reasons to pay some attention to this population to try to optimize their care.”
In addition, compared with their non–HIV-affected counterparts, these individuals are more susceptible to HANA comorbidities. They may experience these conditions at a younger age or more severely. Chronic inflammation and polypharmacy may be to blame, said Dr. Justice.
Given the burden of comorbidities and polypharmacy in this patient population, Dr. Siddiqi said, policy makers will need to focus on developing chronic disease management interventions for them.
However, Dr. Justice added, the risk for multimorbidity is higher among people with HIV throughout the age cycle: “It’s not like I turn 50 with HIV and all of a sudden all the wheels come off. There are ways to successfully age with HIV.”
Geriatric HIV expertise needed
Dr. Justice called the study’s analysis a useful addition to the literature and noted its implications for training.
“One of the biggest challenges with this large bolus of folks who are aging with HIV,” she said, “is to what extent should they be cared for by the people who have been caring for them – largely infectious disease docs – and to what extent should we really be transitioning their care to people with more experience with aging.”
Another key question, Dr. Justice said, relates to nursing homes and assisted-living facilities, whose staff may lack experience caring for HIV patients. Training them and hospital-based providers is crucial, in part to avoid key errors, such as missed antiretroviral doses, she said: “We need to really think about how to get non-HIV providers up to speed.”
That may begin by simply making it clear that this population is here.
“A decade ago, HIV patients used to have a lower life expectancy, so all HIV studies used to use 50 years as the cutoff point for [the] older population,” Dr. Siddiqi said. “Now we know they’re living longer.”
Added Dr. Justice: “Previously, people thought aging and HIV were not coincident findings.”
The study was funded by the Office of the Vice President for Research at the University of South Carolina. The authors and Dr. Justice disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Thanks to effective treatment, people with HIV are living longer. But as they age, they face higher rates of age-related comorbidities and hospitalizations, according to a recent study of hospitalized patients.
Decision-makers will need to allocate resources, train providers, and plan ways to manage chronic diseases, such as diabetes and cancer, among geriatric HIV inpatients, according to the authors.
“There will be more [HIV] patients with age-related chronic conditions at an earlier age and who will utilize or will have a unique need for [health care for] these geriatric conditions,” first author Khairul A. Siddiqi, PhD, University of Florida, Gainesville, said in an interview. “Eventually, that may increase inpatient resource utilization and costs.”
The study was published online in HIV Medicine.
Aging with HIV
Analyzing the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project, the authors compared characteristics and comorbidities linked to hospital stays among people with HIV (HSWH) to those linked to hospital stays among people without HIV (HSWOH).
The NIS is a database of hospital records that captures 20% of discharges in the United States and covers all payers. Data in this analysis covered the years 2003-2015.
Among HSWH, patients aged 50 or older accounted for an increasing proportion over time, from fewer than 25% in 2003 to over 50% by 2015, the authors found. The subgroup aged 65-80 had risen from 2.39% to 8.63% by 2015.
The authors also studied rates of eight comorbidities, termed HIV-associated non-AIDS (HANA) conditions: cardiovascular, lung, liver, neurologic, and kidney diseases; diabetes; cancer; and bone loss.
The average number of these conditions among both HSWH and HSWOH rose over time. But this change was disproportionately high among HSWH aged 50-64 and those aged 65 and older.
Over the study period, among patients aged 65 or older, six of the eight age-related conditions the researchers studied rose disproportionately among HSWH in comparison with HSWOH; among those aged 50-64, five conditions did so.
The researchers are now building on the current study of HSWH by examining rates of resource utilization, such as MRIs and procedures, Dr. Siddiqi said.
Study limitations included a lack of data from long-term facilities, potential skewing by patients hospitalized multiple times, and the inherent limitations of administrative data.
A unique group of older people
Among people with HIV (PWH) in the United States, nearly half are aged 50 or older. By 2030, this group is expected to account for some 70% of PWH.
“We need to pay attention to what we know about aging generally. It is also important to study aging in this special population, because we don’t necessarily know a lot about that,” Amy Justice, MD, PhD, professor of medicine and of public health at Yale University, New Haven, Conn., said in an interview. Dr. Justice was not involved in the study.
The HIV epidemic has disproportionately affected people of color, men who have sex with men, and people with a history of injection drug use, Dr. Justice said.
“We don’t know about aging with [a] past history of injection drug use. We don’t even know much about aging with hepatitis C, necessarily,” she said. “So there are lots of reasons to pay some attention to this population to try to optimize their care.”
In addition, compared with their non–HIV-affected counterparts, these individuals are more susceptible to HANA comorbidities. They may experience these conditions at a younger age or more severely. Chronic inflammation and polypharmacy may be to blame, said Dr. Justice.
Given the burden of comorbidities and polypharmacy in this patient population, Dr. Siddiqi said, policy makers will need to focus on developing chronic disease management interventions for them.
However, Dr. Justice added, the risk for multimorbidity is higher among people with HIV throughout the age cycle: “It’s not like I turn 50 with HIV and all of a sudden all the wheels come off. There are ways to successfully age with HIV.”
Geriatric HIV expertise needed
Dr. Justice called the study’s analysis a useful addition to the literature and noted its implications for training.
“One of the biggest challenges with this large bolus of folks who are aging with HIV,” she said, “is to what extent should they be cared for by the people who have been caring for them – largely infectious disease docs – and to what extent should we really be transitioning their care to people with more experience with aging.”
Another key question, Dr. Justice said, relates to nursing homes and assisted-living facilities, whose staff may lack experience caring for HIV patients. Training them and hospital-based providers is crucial, in part to avoid key errors, such as missed antiretroviral doses, she said: “We need to really think about how to get non-HIV providers up to speed.”
That may begin by simply making it clear that this population is here.
“A decade ago, HIV patients used to have a lower life expectancy, so all HIV studies used to use 50 years as the cutoff point for [the] older population,” Dr. Siddiqi said. “Now we know they’re living longer.”
Added Dr. Justice: “Previously, people thought aging and HIV were not coincident findings.”
The study was funded by the Office of the Vice President for Research at the University of South Carolina. The authors and Dr. Justice disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Thanks to effective treatment, people with HIV are living longer. But as they age, they face higher rates of age-related comorbidities and hospitalizations, according to a recent study of hospitalized patients.
Decision-makers will need to allocate resources, train providers, and plan ways to manage chronic diseases, such as diabetes and cancer, among geriatric HIV inpatients, according to the authors.
“There will be more [HIV] patients with age-related chronic conditions at an earlier age and who will utilize or will have a unique need for [health care for] these geriatric conditions,” first author Khairul A. Siddiqi, PhD, University of Florida, Gainesville, said in an interview. “Eventually, that may increase inpatient resource utilization and costs.”
The study was published online in HIV Medicine.
Aging with HIV
Analyzing the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project, the authors compared characteristics and comorbidities linked to hospital stays among people with HIV (HSWH) to those linked to hospital stays among people without HIV (HSWOH).
The NIS is a database of hospital records that captures 20% of discharges in the United States and covers all payers. Data in this analysis covered the years 2003-2015.
Among HSWH, patients aged 50 or older accounted for an increasing proportion over time, from fewer than 25% in 2003 to over 50% by 2015, the authors found. The subgroup aged 65-80 had risen from 2.39% to 8.63% by 2015.
The authors also studied rates of eight comorbidities, termed HIV-associated non-AIDS (HANA) conditions: cardiovascular, lung, liver, neurologic, and kidney diseases; diabetes; cancer; and bone loss.
The average number of these conditions among both HSWH and HSWOH rose over time. But this change was disproportionately high among HSWH aged 50-64 and those aged 65 and older.
Over the study period, among patients aged 65 or older, six of the eight age-related conditions the researchers studied rose disproportionately among HSWH in comparison with HSWOH; among those aged 50-64, five conditions did so.
The researchers are now building on the current study of HSWH by examining rates of resource utilization, such as MRIs and procedures, Dr. Siddiqi said.
Study limitations included a lack of data from long-term facilities, potential skewing by patients hospitalized multiple times, and the inherent limitations of administrative data.
A unique group of older people
Among people with HIV (PWH) in the United States, nearly half are aged 50 or older. By 2030, this group is expected to account for some 70% of PWH.
“We need to pay attention to what we know about aging generally. It is also important to study aging in this special population, because we don’t necessarily know a lot about that,” Amy Justice, MD, PhD, professor of medicine and of public health at Yale University, New Haven, Conn., said in an interview. Dr. Justice was not involved in the study.
The HIV epidemic has disproportionately affected people of color, men who have sex with men, and people with a history of injection drug use, Dr. Justice said.
“We don’t know about aging with [a] past history of injection drug use. We don’t even know much about aging with hepatitis C, necessarily,” she said. “So there are lots of reasons to pay some attention to this population to try to optimize their care.”
In addition, compared with their non–HIV-affected counterparts, these individuals are more susceptible to HANA comorbidities. They may experience these conditions at a younger age or more severely. Chronic inflammation and polypharmacy may be to blame, said Dr. Justice.
Given the burden of comorbidities and polypharmacy in this patient population, Dr. Siddiqi said, policy makers will need to focus on developing chronic disease management interventions for them.
However, Dr. Justice added, the risk for multimorbidity is higher among people with HIV throughout the age cycle: “It’s not like I turn 50 with HIV and all of a sudden all the wheels come off. There are ways to successfully age with HIV.”
Geriatric HIV expertise needed
Dr. Justice called the study’s analysis a useful addition to the literature and noted its implications for training.
“One of the biggest challenges with this large bolus of folks who are aging with HIV,” she said, “is to what extent should they be cared for by the people who have been caring for them – largely infectious disease docs – and to what extent should we really be transitioning their care to people with more experience with aging.”
Another key question, Dr. Justice said, relates to nursing homes and assisted-living facilities, whose staff may lack experience caring for HIV patients. Training them and hospital-based providers is crucial, in part to avoid key errors, such as missed antiretroviral doses, she said: “We need to really think about how to get non-HIV providers up to speed.”
That may begin by simply making it clear that this population is here.
“A decade ago, HIV patients used to have a lower life expectancy, so all HIV studies used to use 50 years as the cutoff point for [the] older population,” Dr. Siddiqi said. “Now we know they’re living longer.”
Added Dr. Justice: “Previously, people thought aging and HIV were not coincident findings.”
The study was funded by the Office of the Vice President for Research at the University of South Carolina. The authors and Dr. Justice disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HIV MEDICINE
Autoimmune disorder drugs top list of meds linked to headache
DENVER – in a federal side effect database that anyone can contribute to, according to a new study presented at the annual meeting of the American Headache Society.
“Surprising findings included the significant number of immunosuppressants and immunomodulators present in the data,” study lead author Brett Musialowicz, a medical student at Robert Wood Johnson Medical School, New Brunswich, N.J., said in an interview. “Additionally, our data provides evidence that suggests that several medications belonging to these drug classes were less likely to be associated with medication-induced headaches,” raising questions about the mechanism.

Drugs most frequently linked to headaches
The researchers launched their study to better understand headache as a side effect of medication use, Mr. Musialowicz said. They analyzed entries from the Food and Drug Administration’s Adverse Event Reporting System for the period from July 2018 to March 2020 and listed the top 30 most commonly reported medications linked to headaches and their reported odds ratio. According to a website devoted to pharmacovigilance training, ROR refers to “the odds of a certain event occurring with your medicinal product, compared with the odds of the same event occurring with all other medicinal products in the database.”
After generic and brand name data was consolidated, the drug most frequently linked to headaches was apremilast with 8,672 reports, followed by adalimumab (5,357), tofacitinib (4,276), fingolimod (4,123), and etanercept (4,111). These drugs treat autoimmune disorders such as psoriasis, multiple sclerosis, and Crohn’s disease.
The other drugs in the top 15 ranked by frequency are treatments for hepatitis C (4 drugs), pulmonary arterial hypertension (4 drugs), arthritis (1 drug), and asthma (1 drug).
Of the top 30 drugs most frequently linked to headaches, the pulmonary hypertension drug epoprostenol – ranked 23rd – had the highest ROR at 12.8. The next highest were the hepatitis C drugs glecaprevir and pibrentasvir, tied at 10th in the frequency analysis and both with an ROR of 9.4.
“Pulmonary arterial dilators and vasodilators are believed to cause headaches by sensitizing extracranial arteries. Clinical evidence suggests there a vascular component to some types of headache,” Mr. Musialowicz said. “Monoclonal antibodies are suggested to cause headache by means of an immune response. Several monoclonal antibodies are in trials targeting [the calcitonin gene-related peptide] receptor, which is believed to be involved in migraine headache. These trials will help further elucidate the mechanisms of headache and potential drugs to treat these conditions.”
Is the data useful?
Stewart Tepper, MD, a neurologist at Geisel School of Medicine at Dartmouth, Hanover, N.H., who’s familiar with the study findings, discounted the new research in an interview. He noted that any member of the public can contribute to the federal database of adverse effects (drug manufacturers are required to contribute to it), and the data says nothing about denominators.
“It’s not a reasonable way to evaluate adverse effects, to just have everyone and their uncle saying ‘This particular drug did this to me.’ It’s not in any way useful,” he said. However, he added that the database sometimes “gives you a bit of a signal so you can go back and try to get scientifically collected data.”
When asked to respond, study coauthor and neurologist Pengfei (Phil) Zhang, MD, of Robert Wood Johnson Medical School, noted that the FDA created the database “for a reason.” He also noted that the researchers used a statistical analysis technique – ROR – that was invented to adjust for weaknesses in databases.
No study funding is reported. Mr. Musialowicz reported no disclosures. Dr. Zhang has received honorarium from Alder Biopharmaceuticals, Board Vitals, and Fieve Clinical Research. He collaborates with Headache Science Incorporated without receiving financial support, and he has ownership interest in Cymbeline. Another author reports research grant support from the American Epilepsy Society and the New Jersey Health Foundation. Dr. Tepper reported multiple disclosures.
DENVER – in a federal side effect database that anyone can contribute to, according to a new study presented at the annual meeting of the American Headache Society.
“Surprising findings included the significant number of immunosuppressants and immunomodulators present in the data,” study lead author Brett Musialowicz, a medical student at Robert Wood Johnson Medical School, New Brunswich, N.J., said in an interview. “Additionally, our data provides evidence that suggests that several medications belonging to these drug classes were less likely to be associated with medication-induced headaches,” raising questions about the mechanism.
Drugs most frequently linked to headaches
The researchers launched their study to better understand headache as a side effect of medication use, Mr. Musialowicz said. They analyzed entries from the Food and Drug Administration’s Adverse Event Reporting System for the period from July 2018 to March 2020 and listed the top 30 most commonly reported medications linked to headaches and their reported odds ratio. According to a website devoted to pharmacovigilance training, ROR refers to “the odds of a certain event occurring with your medicinal product, compared with the odds of the same event occurring with all other medicinal products in the database.”
After generic and brand name data was consolidated, the drug most frequently linked to headaches was apremilast with 8,672 reports, followed by adalimumab (5,357), tofacitinib (4,276), fingolimod (4,123), and etanercept (4,111). These drugs treat autoimmune disorders such as psoriasis, multiple sclerosis, and Crohn’s disease.
The other drugs in the top 15 ranked by frequency are treatments for hepatitis C (4 drugs), pulmonary arterial hypertension (4 drugs), arthritis (1 drug), and asthma (1 drug).
Of the top 30 drugs most frequently linked to headaches, the pulmonary hypertension drug epoprostenol – ranked 23rd – had the highest ROR at 12.8. The next highest were the hepatitis C drugs glecaprevir and pibrentasvir, tied at 10th in the frequency analysis and both with an ROR of 9.4.
“Pulmonary arterial dilators and vasodilators are believed to cause headaches by sensitizing extracranial arteries. Clinical evidence suggests there a vascular component to some types of headache,” Mr. Musialowicz said. “Monoclonal antibodies are suggested to cause headache by means of an immune response. Several monoclonal antibodies are in trials targeting [the calcitonin gene-related peptide] receptor, which is believed to be involved in migraine headache. These trials will help further elucidate the mechanisms of headache and potential drugs to treat these conditions.”
Is the data useful?
Stewart Tepper, MD, a neurologist at Geisel School of Medicine at Dartmouth, Hanover, N.H., who’s familiar with the study findings, discounted the new research in an interview. He noted that any member of the public can contribute to the federal database of adverse effects (drug manufacturers are required to contribute to it), and the data says nothing about denominators.
“It’s not a reasonable way to evaluate adverse effects, to just have everyone and their uncle saying ‘This particular drug did this to me.’ It’s not in any way useful,” he said. However, he added that the database sometimes “gives you a bit of a signal so you can go back and try to get scientifically collected data.”
When asked to respond, study coauthor and neurologist Pengfei (Phil) Zhang, MD, of Robert Wood Johnson Medical School, noted that the FDA created the database “for a reason.” He also noted that the researchers used a statistical analysis technique – ROR – that was invented to adjust for weaknesses in databases.
No study funding is reported. Mr. Musialowicz reported no disclosures. Dr. Zhang has received honorarium from Alder Biopharmaceuticals, Board Vitals, and Fieve Clinical Research. He collaborates with Headache Science Incorporated without receiving financial support, and he has ownership interest in Cymbeline. Another author reports research grant support from the American Epilepsy Society and the New Jersey Health Foundation. Dr. Tepper reported multiple disclosures.
DENVER – in a federal side effect database that anyone can contribute to, according to a new study presented at the annual meeting of the American Headache Society.
“Surprising findings included the significant number of immunosuppressants and immunomodulators present in the data,” study lead author Brett Musialowicz, a medical student at Robert Wood Johnson Medical School, New Brunswich, N.J., said in an interview. “Additionally, our data provides evidence that suggests that several medications belonging to these drug classes were less likely to be associated with medication-induced headaches,” raising questions about the mechanism.
Drugs most frequently linked to headaches
The researchers launched their study to better understand headache as a side effect of medication use, Mr. Musialowicz said. They analyzed entries from the Food and Drug Administration’s Adverse Event Reporting System for the period from July 2018 to March 2020 and listed the top 30 most commonly reported medications linked to headaches and their reported odds ratio. According to a website devoted to pharmacovigilance training, ROR refers to “the odds of a certain event occurring with your medicinal product, compared with the odds of the same event occurring with all other medicinal products in the database.”
After generic and brand name data was consolidated, the drug most frequently linked to headaches was apremilast with 8,672 reports, followed by adalimumab (5,357), tofacitinib (4,276), fingolimod (4,123), and etanercept (4,111). These drugs treat autoimmune disorders such as psoriasis, multiple sclerosis, and Crohn’s disease.
The other drugs in the top 15 ranked by frequency are treatments for hepatitis C (4 drugs), pulmonary arterial hypertension (4 drugs), arthritis (1 drug), and asthma (1 drug).
Of the top 30 drugs most frequently linked to headaches, the pulmonary hypertension drug epoprostenol – ranked 23rd – had the highest ROR at 12.8. The next highest were the hepatitis C drugs glecaprevir and pibrentasvir, tied at 10th in the frequency analysis and both with an ROR of 9.4.
“Pulmonary arterial dilators and vasodilators are believed to cause headaches by sensitizing extracranial arteries. Clinical evidence suggests there a vascular component to some types of headache,” Mr. Musialowicz said. “Monoclonal antibodies are suggested to cause headache by means of an immune response. Several monoclonal antibodies are in trials targeting [the calcitonin gene-related peptide] receptor, which is believed to be involved in migraine headache. These trials will help further elucidate the mechanisms of headache and potential drugs to treat these conditions.”
Is the data useful?
Stewart Tepper, MD, a neurologist at Geisel School of Medicine at Dartmouth, Hanover, N.H., who’s familiar with the study findings, discounted the new research in an interview. He noted that any member of the public can contribute to the federal database of adverse effects (drug manufacturers are required to contribute to it), and the data says nothing about denominators.
“It’s not a reasonable way to evaluate adverse effects, to just have everyone and their uncle saying ‘This particular drug did this to me.’ It’s not in any way useful,” he said. However, he added that the database sometimes “gives you a bit of a signal so you can go back and try to get scientifically collected data.”
When asked to respond, study coauthor and neurologist Pengfei (Phil) Zhang, MD, of Robert Wood Johnson Medical School, noted that the FDA created the database “for a reason.” He also noted that the researchers used a statistical analysis technique – ROR – that was invented to adjust for weaknesses in databases.
No study funding is reported. Mr. Musialowicz reported no disclosures. Dr. Zhang has received honorarium from Alder Biopharmaceuticals, Board Vitals, and Fieve Clinical Research. He collaborates with Headache Science Incorporated without receiving financial support, and he has ownership interest in Cymbeline. Another author reports research grant support from the American Epilepsy Society and the New Jersey Health Foundation. Dr. Tepper reported multiple disclosures.
AT AHS 2022
Recommended headache treatments get mixed reception in EDs
DENVER – a new study finds. But the use of diphenhydramine (Benadryl) more than doubled even though guidelines caution against it, while recommended drugs such triptans and corticosteroids were rarely prescribed.
From 2007-2010 to 2015-2018, researchers reported at the annual meeting of the American Headache Society, a database reveals that opioid use in headache cases at EDs fell from 54% to 28%. Diphenhydramine use grew from 17% to 36% (both (P < .001). The percentage of cases in which EDs sought neuroimaging stayed stable at about 36%, a number that the study authors described as too high.

“Future studies are warranted to identify strategies to promote evidence-based treatments for headaches and appropriate outpatient referrals for follow-up and to reduce unnecessary neuroimaging orders in EDs,” lead author Seonkyeong Yang, MS, of the University of Florida, Gainesville, said in an interview.
Ms. Yang said researchers launched the study to update previous data in light of changes in opioid prescribing and the 2016 release of American Headache Society guidelines for the treatment of acute migraines in the ED setting. The research was published in the Journal of Clinical Medicine.
Headache treatment in the ED
For the study, researchers analyzed data from the U.S. National Hospital Ambulatory Medical Care survey and focused on adults who had a primary discharge diagnosis of headache.
For the 2015-2018 period, per weighted numbers, the survey encompassed 10.2 million headaches mostly among people younger than 50 (71%), female (73%), and White (73%). Migraines made up 33% of the total, with nonspecified headache accounting for almost all of the remainder (63%).
In 68% of cases, two or more medications were administered in the ED. This number rose to 83% among patients with migraine. But most of the time (54%), no medications were prescribed at discharge.
Among recommended medications, antiemetics – the most commonly used class of drugs in these patients – were prescribed 59% of the time in both 2007-2010 and 2015-2018 (P = .88). Usage of acetaminophens and NSAIDs grew from 37% to 52% over that time period.
Despite recommendations, the use of ergot alkaloids/triptans and corticosteroids remained low (less than 6% of the time).
“Several factors may contribute to the underuse of triptans in EDs, including their cardiovascular contraindications, ED physicians’ unfamiliarity with injectable triptans, higher costs, and treatment failures with triptans before ED visits,” Ms. Yang said. “We observed an upward trend in dexamethasone use over time. However, it was still underutilized. [The corticosteroid was only used 3.5% of the time from 2015-2018.] The 2016 AHS guideline strongly recommends dexamethasone use to prevent migraine recurrence after ED discharge. Identifying patients at high risk of headache recurrence for dexamethasone use may further improve patient outcomes of acute headache management in ED settings.”
Ms. Yang also reported that the use of diphenhydramine grew even though it’s not recommended. “Diphenhydramine is more likely to be used to prevent akathisia, a side effect of some antiemetics [that is, dopamine receptor antagonists] in headache-related ED visits,” she said. “However, the 2016 AHS guideline recommends against diphenhydramine use due to its limited efficacy in relieving headache pain. In addition, there is also conflicting evidence on diphenhydramine’s efficacy in preventing akathisia when coadministered with antiemetics. Diphenhydramine use requires caution due to its sedative effect and abuse potential.”
As for medication combinations, Ms. Yang said “the most broadly used therapy among headache-related ED visits in 2007-2010 was an opioid with an antiemetic (21.0%), which decreased to 6.6% in 2015-2018. Meanwhile, the combined use of acetaminophen/NSAIDs with antiemetic and diphenhydramine increased substantially from 3.9% to 15.7% and became the most prevalent therapy in 2015-2018. Opioid monotherapy use gradually decreased during the study period [from 8.8% to 1.9%].”
Evidence-based treatments underutilized
Commenting on the findings, New York University Langone neurologist and headache researcher Mia Tova Minen, MD, MPH, noted in an interview that AHS guidelines do not indicate acetaminophen/NSAIDs, diphenhydramine, and corticosteroids for the acute treatment of migraine. “The recommended treatments are sumatriptan subcutaneous, IV metoclopramide, and IV prochlorperazine. Steroids can be helpful in the prevention of migraine recurrence but not for the acute treatment of the migraine itself,” she said. “We need to ensure that patients with migraine get the top evidence-based treatments for migraine.”
As for diphenhydramine, she said it “is not a treatment for headache disorders. It does not have proven efficacy. It is sometimes given to reduce side effects of more acute treatments of headache, but it can make patients fatigued and keep them in the ED longer.”
Overuse of neuroimaging
Ms. Yang also highlighted study data about the frequency of neuroimaging. “Understandably, ED physicians do not want to miss any life-threatening secondary headaches like stroke,” she said. “However, other factors also contribute to the overuse of neuroimaging in headache-related ED visits: patient demands, financial incentives, a busy ED practice where clinical evaluation is replaced by tests, and ED physicians’ unfamiliarity with ICHD-3 diagnostic criteria for primary headache disorders. There is still much room for improvement in neuroimaging use for headaches in ED settings.”
For her part, Dr. Minen said scans are often performed reflexively and can be overused. “A CT scan is really only good in the case of acute trauma to rule out a fracture or a bleed or if there are signs of an emergent neurologic emergency like herniation or if a MRI is contraindicated. An MRI of the brain is typically the best test to examine brain tissue, though sometimes vessel imaging is also warranted. In the case of no red flags and a normal neurologic exam, the use of neuroimaging is low yield.”
The research has no funding. Ms. Yang and two other authors disclosed research funding from Merck. Dr. Minen reports no disclosures.
DENVER – a new study finds. But the use of diphenhydramine (Benadryl) more than doubled even though guidelines caution against it, while recommended drugs such triptans and corticosteroids were rarely prescribed.
From 2007-2010 to 2015-2018, researchers reported at the annual meeting of the American Headache Society, a database reveals that opioid use in headache cases at EDs fell from 54% to 28%. Diphenhydramine use grew from 17% to 36% (both (P < .001). The percentage of cases in which EDs sought neuroimaging stayed stable at about 36%, a number that the study authors described as too high.
“Future studies are warranted to identify strategies to promote evidence-based treatments for headaches and appropriate outpatient referrals for follow-up and to reduce unnecessary neuroimaging orders in EDs,” lead author Seonkyeong Yang, MS, of the University of Florida, Gainesville, said in an interview.
Ms. Yang said researchers launched the study to update previous data in light of changes in opioid prescribing and the 2016 release of American Headache Society guidelines for the treatment of acute migraines in the ED setting. The research was published in the Journal of Clinical Medicine.
Headache treatment in the ED
For the study, researchers analyzed data from the U.S. National Hospital Ambulatory Medical Care survey and focused on adults who had a primary discharge diagnosis of headache.
For the 2015-2018 period, per weighted numbers, the survey encompassed 10.2 million headaches mostly among people younger than 50 (71%), female (73%), and White (73%). Migraines made up 33% of the total, with nonspecified headache accounting for almost all of the remainder (63%).
In 68% of cases, two or more medications were administered in the ED. This number rose to 83% among patients with migraine. But most of the time (54%), no medications were prescribed at discharge.
Among recommended medications, antiemetics – the most commonly used class of drugs in these patients – were prescribed 59% of the time in both 2007-2010 and 2015-2018 (P = .88). Usage of acetaminophens and NSAIDs grew from 37% to 52% over that time period.
Despite recommendations, the use of ergot alkaloids/triptans and corticosteroids remained low (less than 6% of the time).
“Several factors may contribute to the underuse of triptans in EDs, including their cardiovascular contraindications, ED physicians’ unfamiliarity with injectable triptans, higher costs, and treatment failures with triptans before ED visits,” Ms. Yang said. “We observed an upward trend in dexamethasone use over time. However, it was still underutilized. [The corticosteroid was only used 3.5% of the time from 2015-2018.] The 2016 AHS guideline strongly recommends dexamethasone use to prevent migraine recurrence after ED discharge. Identifying patients at high risk of headache recurrence for dexamethasone use may further improve patient outcomes of acute headache management in ED settings.”
Ms. Yang also reported that the use of diphenhydramine grew even though it’s not recommended. “Diphenhydramine is more likely to be used to prevent akathisia, a side effect of some antiemetics [that is, dopamine receptor antagonists] in headache-related ED visits,” she said. “However, the 2016 AHS guideline recommends against diphenhydramine use due to its limited efficacy in relieving headache pain. In addition, there is also conflicting evidence on diphenhydramine’s efficacy in preventing akathisia when coadministered with antiemetics. Diphenhydramine use requires caution due to its sedative effect and abuse potential.”
As for medication combinations, Ms. Yang said “the most broadly used therapy among headache-related ED visits in 2007-2010 was an opioid with an antiemetic (21.0%), which decreased to 6.6% in 2015-2018. Meanwhile, the combined use of acetaminophen/NSAIDs with antiemetic and diphenhydramine increased substantially from 3.9% to 15.7% and became the most prevalent therapy in 2015-2018. Opioid monotherapy use gradually decreased during the study period [from 8.8% to 1.9%].”
Evidence-based treatments underutilized
Commenting on the findings, New York University Langone neurologist and headache researcher Mia Tova Minen, MD, MPH, noted in an interview that AHS guidelines do not indicate acetaminophen/NSAIDs, diphenhydramine, and corticosteroids for the acute treatment of migraine. “The recommended treatments are sumatriptan subcutaneous, IV metoclopramide, and IV prochlorperazine. Steroids can be helpful in the prevention of migraine recurrence but not for the acute treatment of the migraine itself,” she said. “We need to ensure that patients with migraine get the top evidence-based treatments for migraine.”
As for diphenhydramine, she said it “is not a treatment for headache disorders. It does not have proven efficacy. It is sometimes given to reduce side effects of more acute treatments of headache, but it can make patients fatigued and keep them in the ED longer.”
Overuse of neuroimaging
Ms. Yang also highlighted study data about the frequency of neuroimaging. “Understandably, ED physicians do not want to miss any life-threatening secondary headaches like stroke,” she said. “However, other factors also contribute to the overuse of neuroimaging in headache-related ED visits: patient demands, financial incentives, a busy ED practice where clinical evaluation is replaced by tests, and ED physicians’ unfamiliarity with ICHD-3 diagnostic criteria for primary headache disorders. There is still much room for improvement in neuroimaging use for headaches in ED settings.”
For her part, Dr. Minen said scans are often performed reflexively and can be overused. “A CT scan is really only good in the case of acute trauma to rule out a fracture or a bleed or if there are signs of an emergent neurologic emergency like herniation or if a MRI is contraindicated. An MRI of the brain is typically the best test to examine brain tissue, though sometimes vessel imaging is also warranted. In the case of no red flags and a normal neurologic exam, the use of neuroimaging is low yield.”
The research has no funding. Ms. Yang and two other authors disclosed research funding from Merck. Dr. Minen reports no disclosures.
DENVER – a new study finds. But the use of diphenhydramine (Benadryl) more than doubled even though guidelines caution against it, while recommended drugs such triptans and corticosteroids were rarely prescribed.
From 2007-2010 to 2015-2018, researchers reported at the annual meeting of the American Headache Society, a database reveals that opioid use in headache cases at EDs fell from 54% to 28%. Diphenhydramine use grew from 17% to 36% (both (P < .001). The percentage of cases in which EDs sought neuroimaging stayed stable at about 36%, a number that the study authors described as too high.
“Future studies are warranted to identify strategies to promote evidence-based treatments for headaches and appropriate outpatient referrals for follow-up and to reduce unnecessary neuroimaging orders in EDs,” lead author Seonkyeong Yang, MS, of the University of Florida, Gainesville, said in an interview.
Ms. Yang said researchers launched the study to update previous data in light of changes in opioid prescribing and the 2016 release of American Headache Society guidelines for the treatment of acute migraines in the ED setting. The research was published in the Journal of Clinical Medicine.
Headache treatment in the ED
For the study, researchers analyzed data from the U.S. National Hospital Ambulatory Medical Care survey and focused on adults who had a primary discharge diagnosis of headache.
For the 2015-2018 period, per weighted numbers, the survey encompassed 10.2 million headaches mostly among people younger than 50 (71%), female (73%), and White (73%). Migraines made up 33% of the total, with nonspecified headache accounting for almost all of the remainder (63%).
In 68% of cases, two or more medications were administered in the ED. This number rose to 83% among patients with migraine. But most of the time (54%), no medications were prescribed at discharge.
Among recommended medications, antiemetics – the most commonly used class of drugs in these patients – were prescribed 59% of the time in both 2007-2010 and 2015-2018 (P = .88). Usage of acetaminophens and NSAIDs grew from 37% to 52% over that time period.
Despite recommendations, the use of ergot alkaloids/triptans and corticosteroids remained low (less than 6% of the time).
“Several factors may contribute to the underuse of triptans in EDs, including their cardiovascular contraindications, ED physicians’ unfamiliarity with injectable triptans, higher costs, and treatment failures with triptans before ED visits,” Ms. Yang said. “We observed an upward trend in dexamethasone use over time. However, it was still underutilized. [The corticosteroid was only used 3.5% of the time from 2015-2018.] The 2016 AHS guideline strongly recommends dexamethasone use to prevent migraine recurrence after ED discharge. Identifying patients at high risk of headache recurrence for dexamethasone use may further improve patient outcomes of acute headache management in ED settings.”
Ms. Yang also reported that the use of diphenhydramine grew even though it’s not recommended. “Diphenhydramine is more likely to be used to prevent akathisia, a side effect of some antiemetics [that is, dopamine receptor antagonists] in headache-related ED visits,” she said. “However, the 2016 AHS guideline recommends against diphenhydramine use due to its limited efficacy in relieving headache pain. In addition, there is also conflicting evidence on diphenhydramine’s efficacy in preventing akathisia when coadministered with antiemetics. Diphenhydramine use requires caution due to its sedative effect and abuse potential.”
As for medication combinations, Ms. Yang said “the most broadly used therapy among headache-related ED visits in 2007-2010 was an opioid with an antiemetic (21.0%), which decreased to 6.6% in 2015-2018. Meanwhile, the combined use of acetaminophen/NSAIDs with antiemetic and diphenhydramine increased substantially from 3.9% to 15.7% and became the most prevalent therapy in 2015-2018. Opioid monotherapy use gradually decreased during the study period [from 8.8% to 1.9%].”
Evidence-based treatments underutilized
Commenting on the findings, New York University Langone neurologist and headache researcher Mia Tova Minen, MD, MPH, noted in an interview that AHS guidelines do not indicate acetaminophen/NSAIDs, diphenhydramine, and corticosteroids for the acute treatment of migraine. “The recommended treatments are sumatriptan subcutaneous, IV metoclopramide, and IV prochlorperazine. Steroids can be helpful in the prevention of migraine recurrence but not for the acute treatment of the migraine itself,” she said. “We need to ensure that patients with migraine get the top evidence-based treatments for migraine.”
As for diphenhydramine, she said it “is not a treatment for headache disorders. It does not have proven efficacy. It is sometimes given to reduce side effects of more acute treatments of headache, but it can make patients fatigued and keep them in the ED longer.”
Overuse of neuroimaging
Ms. Yang also highlighted study data about the frequency of neuroimaging. “Understandably, ED physicians do not want to miss any life-threatening secondary headaches like stroke,” she said. “However, other factors also contribute to the overuse of neuroimaging in headache-related ED visits: patient demands, financial incentives, a busy ED practice where clinical evaluation is replaced by tests, and ED physicians’ unfamiliarity with ICHD-3 diagnostic criteria for primary headache disorders. There is still much room for improvement in neuroimaging use for headaches in ED settings.”
For her part, Dr. Minen said scans are often performed reflexively and can be overused. “A CT scan is really only good in the case of acute trauma to rule out a fracture or a bleed or if there are signs of an emergent neurologic emergency like herniation or if a MRI is contraindicated. An MRI of the brain is typically the best test to examine brain tissue, though sometimes vessel imaging is also warranted. In the case of no red flags and a normal neurologic exam, the use of neuroimaging is low yield.”
The research has no funding. Ms. Yang and two other authors disclosed research funding from Merck. Dr. Minen reports no disclosures.
AT AHS 2022
Artificial intelligence: The Netflix of cancer treatment
Chemotherapy, now streaming at just $15.99 a month!
It’s a lazy Sunday and you flip on Netflix, looking for something new to watch. There’s an almost-overwhelming number of shows out there, but right at the top of the recommended list is something that strikes your fancy right away. The algorithm behind the scenes is doing its job well, winnowing the universe of content right down to the few things you’ll find relevant, based on what you’ve watched and liked in the past.

Now, the almighty content algorithm is coming for something a little more useful than binge watching obscure 80s sitcoms: cancer treatment.
By plugging the fully sequenced genomes of nearly 10,000 patients with 33 different types of cancer into an algorithm powered by the same sort of artificial intelligence used by Netflix, researchers from London and San Diego found 21 common faults in the chromosomes of tumors, which they called copy number signatures. While cancer is a complex disease, when faults occur in those copy number signatures, the results were similar across the board. If X genetic defect occurs within a tumor, Y result will happen, even across cancer types. For example, tumors whose chromosomes had shattered and reformed had by far the worst disease outcomes.
The eventual hope is that, just as Netflix can predict what you’ll want to watch based on what you’ve already seen, oncologists will be able to predict the course of a cancer, based on the tumor’s early genetic traits, and get ahead of future genetic degradation to prevent the worst outcomes. A sort of “Oh, your tumor has enjoyed The Office. Might we suggest a treatment of 30 Rock” situation. Further research will be required to determine whether or not the cancer algorithm can get us part 2 of “Stranger Things 4” a week early.
Pay criminals, cut crime?
What is the best method for punishing those who commit wrongdoing? Fines? Jail time? Actually, no. A recent study says that financial compensation works best.
In other words, pay them for their actions. Really.
Psychologist Tage S. Rai, PhD, of the University of California, San Diego, Rady School of Management, found that people who hurt others or commit crimes are actually doing it because they think it’s the right thing to do. The results of this study say play at the angle of their morality. When that’s compromised, the offender is less likely to do it again.
Four different experiments were conducted using an online economics game with nearly 1,500 participants. Dr. Rai found that providing a monetary bonus for inflicting a punishment on a third party within the game cut the participants’ willingness to do it again by 50%.
“People punish others to signal their own goodness and receiving compensation might make it seem as though they’re driven by greed rather than justice,” he said.
The big deterrent, though, was negative judgment from peers. People in the study were even more hesitant to inflict harm and gain a profit if they thought they were going to be judged for it.
So maybe the answer to cutting crime isn’t as simple as slapping on a fine. It’s slapping on shame and paying them for it.
A conspiracy of chronobiologic proportions
The Golden State Warriors just won the NBA championship – that much is true – but we’ve got some news that you didn’t get from ESPN. The kind of news that their “partners” from the NBA didn’t want them to report. Unlike most conspiracy theories, however, this one has some science behind it.

In this case, science in the form of a study published in Frontiers in Physiology says that jet lag had a greater effect on the Boston Celtics than it did on the Warriors.
“Eastward travel – where the destination time is later than the origin time – requires the athlete to shorten their day (known as a phase advance). During phase advance, athletes often struggle to fall asleep at an earlier bedtime, leading to sleep loss and, consequently, potential impaired physiological performance and motivation the next day,” senior author Elise Facer-Childs, PhD, of Monash University, Melbourne, said in written statement.
Dr. Facer-Childs and associates took a very close look at 10 seasons’ worth of NBA games – 11,481 games, to be exact – and found “that eastward (but not westward) jet lag was associated with impaired performance for home (but not away) teams.” The existence of a pro-Western bias against teams that traveled eastward for their home games was clear:
- The chance of winning for eastern teams was reduced by 6.0%.
- They grabbed 1.3 fewer rebounds per game.
- Their field goal percentage was 1.2% lower.
And here’s the final nail in the conspiracy coffin: The NBA knew about the jet lag effect and changed the schedule of the finals in 2014 in a way that makes it worse. Before that, the higher-seeded team got two home games, then the lower-seeded team had three at home, followed by two more at the home of the higher seed. Now it’s a 2-2-1-1-1 arrangement that leads to more travel and, of course, more jet lag.
The study was published during the championship series, so the investigators suggested that the Celtics “might benefit from chronobiology-informed strategies designed to mitigate eastward jet lag symptomatology.”
So there you have it, sports fans/conspiracy theorists: You can’t chase Steph Curry around the court for 48 minutes without the right chronobiology-informed strategy. Everyone knows that.
Being hungry can alter your ‘type’
Fasting and being hungry can be a dangerous mix for becoming “hangry” and irritable, but did you know being hungry can also affect your attraction to other people?

Evidence has shown that being hungry can affect important things such as decision-making, memory, cognition, and function. It might affect decision-making in the sense that those six tacos at Taco Bell might win out over grilled chicken breast and veggies at home, but can hunger make you think that the person you just swiped right on isn’t really your type after all?
We’ll leave that up to Valentina Cazzato of Liverpool (England) John Moores University and associates, whose study involved 44 people, of whom 21 were women in their early 20s. The participants were shown computer-generated images of men and women of different sizes. The same background was used for each picture and all the expressions of the models were neutral. Participants were asked to rate each image on how much they liked it. One study was done on participants who had been fasting for 12 hours, and the second was done on those who had just eaten something.
The subjects generally preferred slim models over more rounded ones, but not after fasting. When they were hungry, they found the round human bodies and faces more attractive. So, yes, it’s definitely possible that hunger can alter your attraction to others.
“Future work might seek to elucidate the relationship between physiological states of hunger and shifts in appreciation of the human bodies and whether this relationship might be mediated by individual traits associated with to beholder’s body adiposity,” said researchers.
Chemotherapy, now streaming at just $15.99 a month!
It’s a lazy Sunday and you flip on Netflix, looking for something new to watch. There’s an almost-overwhelming number of shows out there, but right at the top of the recommended list is something that strikes your fancy right away. The algorithm behind the scenes is doing its job well, winnowing the universe of content right down to the few things you’ll find relevant, based on what you’ve watched and liked in the past.
Now, the almighty content algorithm is coming for something a little more useful than binge watching obscure 80s sitcoms: cancer treatment.
By plugging the fully sequenced genomes of nearly 10,000 patients with 33 different types of cancer into an algorithm powered by the same sort of artificial intelligence used by Netflix, researchers from London and San Diego found 21 common faults in the chromosomes of tumors, which they called copy number signatures. While cancer is a complex disease, when faults occur in those copy number signatures, the results were similar across the board. If X genetic defect occurs within a tumor, Y result will happen, even across cancer types. For example, tumors whose chromosomes had shattered and reformed had by far the worst disease outcomes.
The eventual hope is that, just as Netflix can predict what you’ll want to watch based on what you’ve already seen, oncologists will be able to predict the course of a cancer, based on the tumor’s early genetic traits, and get ahead of future genetic degradation to prevent the worst outcomes. A sort of “Oh, your tumor has enjoyed The Office. Might we suggest a treatment of 30 Rock” situation. Further research will be required to determine whether or not the cancer algorithm can get us part 2 of “Stranger Things 4” a week early.
Pay criminals, cut crime?
What is the best method for punishing those who commit wrongdoing? Fines? Jail time? Actually, no. A recent study says that financial compensation works best.
In other words, pay them for their actions. Really.
Psychologist Tage S. Rai, PhD, of the University of California, San Diego, Rady School of Management, found that people who hurt others or commit crimes are actually doing it because they think it’s the right thing to do. The results of this study say play at the angle of their morality. When that’s compromised, the offender is less likely to do it again.
Four different experiments were conducted using an online economics game with nearly 1,500 participants. Dr. Rai found that providing a monetary bonus for inflicting a punishment on a third party within the game cut the participants’ willingness to do it again by 50%.
“People punish others to signal their own goodness and receiving compensation might make it seem as though they’re driven by greed rather than justice,” he said.
The big deterrent, though, was negative judgment from peers. People in the study were even more hesitant to inflict harm and gain a profit if they thought they were going to be judged for it.
So maybe the answer to cutting crime isn’t as simple as slapping on a fine. It’s slapping on shame and paying them for it.
A conspiracy of chronobiologic proportions
The Golden State Warriors just won the NBA championship – that much is true – but we’ve got some news that you didn’t get from ESPN. The kind of news that their “partners” from the NBA didn’t want them to report. Unlike most conspiracy theories, however, this one has some science behind it.
In this case, science in the form of a study published in Frontiers in Physiology says that jet lag had a greater effect on the Boston Celtics than it did on the Warriors.
“Eastward travel – where the destination time is later than the origin time – requires the athlete to shorten their day (known as a phase advance). During phase advance, athletes often struggle to fall asleep at an earlier bedtime, leading to sleep loss and, consequently, potential impaired physiological performance and motivation the next day,” senior author Elise Facer-Childs, PhD, of Monash University, Melbourne, said in written statement.
Dr. Facer-Childs and associates took a very close look at 10 seasons’ worth of NBA games – 11,481 games, to be exact – and found “that eastward (but not westward) jet lag was associated with impaired performance for home (but not away) teams.” The existence of a pro-Western bias against teams that traveled eastward for their home games was clear:
- The chance of winning for eastern teams was reduced by 6.0%.
- They grabbed 1.3 fewer rebounds per game.
- Their field goal percentage was 1.2% lower.
And here’s the final nail in the conspiracy coffin: The NBA knew about the jet lag effect and changed the schedule of the finals in 2014 in a way that makes it worse. Before that, the higher-seeded team got two home games, then the lower-seeded team had three at home, followed by two more at the home of the higher seed. Now it’s a 2-2-1-1-1 arrangement that leads to more travel and, of course, more jet lag.
The study was published during the championship series, so the investigators suggested that the Celtics “might benefit from chronobiology-informed strategies designed to mitigate eastward jet lag symptomatology.”
So there you have it, sports fans/conspiracy theorists: You can’t chase Steph Curry around the court for 48 minutes without the right chronobiology-informed strategy. Everyone knows that.
Being hungry can alter your ‘type’
Fasting and being hungry can be a dangerous mix for becoming “hangry” and irritable, but did you know being hungry can also affect your attraction to other people?
Evidence has shown that being hungry can affect important things such as decision-making, memory, cognition, and function. It might affect decision-making in the sense that those six tacos at Taco Bell might win out over grilled chicken breast and veggies at home, but can hunger make you think that the person you just swiped right on isn’t really your type after all?
We’ll leave that up to Valentina Cazzato of Liverpool (England) John Moores University and associates, whose study involved 44 people, of whom 21 were women in their early 20s. The participants were shown computer-generated images of men and women of different sizes. The same background was used for each picture and all the expressions of the models were neutral. Participants were asked to rate each image on how much they liked it. One study was done on participants who had been fasting for 12 hours, and the second was done on those who had just eaten something.
The subjects generally preferred slim models over more rounded ones, but not after fasting. When they were hungry, they found the round human bodies and faces more attractive. So, yes, it’s definitely possible that hunger can alter your attraction to others.
“Future work might seek to elucidate the relationship between physiological states of hunger and shifts in appreciation of the human bodies and whether this relationship might be mediated by individual traits associated with to beholder’s body adiposity,” said researchers.
Chemotherapy, now streaming at just $15.99 a month!
It’s a lazy Sunday and you flip on Netflix, looking for something new to watch. There’s an almost-overwhelming number of shows out there, but right at the top of the recommended list is something that strikes your fancy right away. The algorithm behind the scenes is doing its job well, winnowing the universe of content right down to the few things you’ll find relevant, based on what you’ve watched and liked in the past.
Now, the almighty content algorithm is coming for something a little more useful than binge watching obscure 80s sitcoms: cancer treatment.
By plugging the fully sequenced genomes of nearly 10,000 patients with 33 different types of cancer into an algorithm powered by the same sort of artificial intelligence used by Netflix, researchers from London and San Diego found 21 common faults in the chromosomes of tumors, which they called copy number signatures. While cancer is a complex disease, when faults occur in those copy number signatures, the results were similar across the board. If X genetic defect occurs within a tumor, Y result will happen, even across cancer types. For example, tumors whose chromosomes had shattered and reformed had by far the worst disease outcomes.
The eventual hope is that, just as Netflix can predict what you’ll want to watch based on what you’ve already seen, oncologists will be able to predict the course of a cancer, based on the tumor’s early genetic traits, and get ahead of future genetic degradation to prevent the worst outcomes. A sort of “Oh, your tumor has enjoyed The Office. Might we suggest a treatment of 30 Rock” situation. Further research will be required to determine whether or not the cancer algorithm can get us part 2 of “Stranger Things 4” a week early.
Pay criminals, cut crime?
What is the best method for punishing those who commit wrongdoing? Fines? Jail time? Actually, no. A recent study says that financial compensation works best.
In other words, pay them for their actions. Really.
Psychologist Tage S. Rai, PhD, of the University of California, San Diego, Rady School of Management, found that people who hurt others or commit crimes are actually doing it because they think it’s the right thing to do. The results of this study say play at the angle of their morality. When that’s compromised, the offender is less likely to do it again.
Four different experiments were conducted using an online economics game with nearly 1,500 participants. Dr. Rai found that providing a monetary bonus for inflicting a punishment on a third party within the game cut the participants’ willingness to do it again by 50%.
“People punish others to signal their own goodness and receiving compensation might make it seem as though they’re driven by greed rather than justice,” he said.
The big deterrent, though, was negative judgment from peers. People in the study were even more hesitant to inflict harm and gain a profit if they thought they were going to be judged for it.
So maybe the answer to cutting crime isn’t as simple as slapping on a fine. It’s slapping on shame and paying them for it.
A conspiracy of chronobiologic proportions
The Golden State Warriors just won the NBA championship – that much is true – but we’ve got some news that you didn’t get from ESPN. The kind of news that their “partners” from the NBA didn’t want them to report. Unlike most conspiracy theories, however, this one has some science behind it.
In this case, science in the form of a study published in Frontiers in Physiology says that jet lag had a greater effect on the Boston Celtics than it did on the Warriors.
“Eastward travel – where the destination time is later than the origin time – requires the athlete to shorten their day (known as a phase advance). During phase advance, athletes often struggle to fall asleep at an earlier bedtime, leading to sleep loss and, consequently, potential impaired physiological performance and motivation the next day,” senior author Elise Facer-Childs, PhD, of Monash University, Melbourne, said in written statement.
Dr. Facer-Childs and associates took a very close look at 10 seasons’ worth of NBA games – 11,481 games, to be exact – and found “that eastward (but not westward) jet lag was associated with impaired performance for home (but not away) teams.” The existence of a pro-Western bias against teams that traveled eastward for their home games was clear:
- The chance of winning for eastern teams was reduced by 6.0%.
- They grabbed 1.3 fewer rebounds per game.
- Their field goal percentage was 1.2% lower.
And here’s the final nail in the conspiracy coffin: The NBA knew about the jet lag effect and changed the schedule of the finals in 2014 in a way that makes it worse. Before that, the higher-seeded team got two home games, then the lower-seeded team had three at home, followed by two more at the home of the higher seed. Now it’s a 2-2-1-1-1 arrangement that leads to more travel and, of course, more jet lag.
The study was published during the championship series, so the investigators suggested that the Celtics “might benefit from chronobiology-informed strategies designed to mitigate eastward jet lag symptomatology.”
So there you have it, sports fans/conspiracy theorists: You can’t chase Steph Curry around the court for 48 minutes without the right chronobiology-informed strategy. Everyone knows that.
Being hungry can alter your ‘type’
Fasting and being hungry can be a dangerous mix for becoming “hangry” and irritable, but did you know being hungry can also affect your attraction to other people?
Evidence has shown that being hungry can affect important things such as decision-making, memory, cognition, and function. It might affect decision-making in the sense that those six tacos at Taco Bell might win out over grilled chicken breast and veggies at home, but can hunger make you think that the person you just swiped right on isn’t really your type after all?
We’ll leave that up to Valentina Cazzato of Liverpool (England) John Moores University and associates, whose study involved 44 people, of whom 21 were women in their early 20s. The participants were shown computer-generated images of men and women of different sizes. The same background was used for each picture and all the expressions of the models were neutral. Participants were asked to rate each image on how much they liked it. One study was done on participants who had been fasting for 12 hours, and the second was done on those who had just eaten something.
The subjects generally preferred slim models over more rounded ones, but not after fasting. When they were hungry, they found the round human bodies and faces more attractive. So, yes, it’s definitely possible that hunger can alter your attraction to others.
“Future work might seek to elucidate the relationship between physiological states of hunger and shifts in appreciation of the human bodies and whether this relationship might be mediated by individual traits associated with to beholder’s body adiposity,” said researchers.
Children and COVID: Vaccines now available to all ages
The COVID-19 prevention effort in children enters its next phase as June draws to a close, while new pediatric cases continued on a downward trend and hospitalizations continued to rise.
The COVID-19 vaccines from Pfizer-BioNTech and Moderna were approved for use in children as young as 6 months, the Centers for Disease Control and Prevention announced on June 18.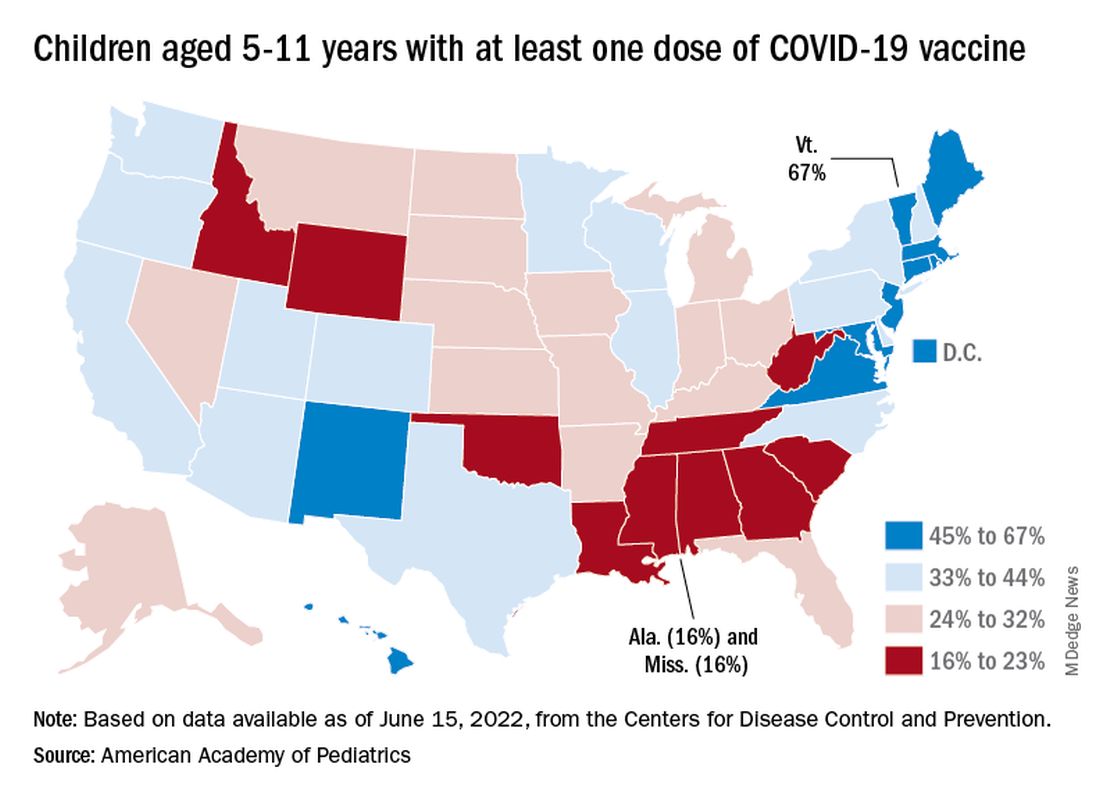
“We know millions of parents and caregivers are eager to get their young children vaccinated. ... I encourage parents and caregivers with questions to talk to their doctor, nurse, or local pharmacist to learn more about the benefits of vaccinations,” CDC Director Rochelle P. Walensky, MD, MPH, said in a written statement.
There are, however, indications that many parents are not that eager. Another 11% said “they will only do so if they are required,” Kaiser noted.
The vaccination experience with children aged 5-11 years seems to agree with those numbers. As of June 16, more than 7 months after the vaccine became available, just over 36% had received at least one dose and about 30% were fully vaccinated, CDC data show.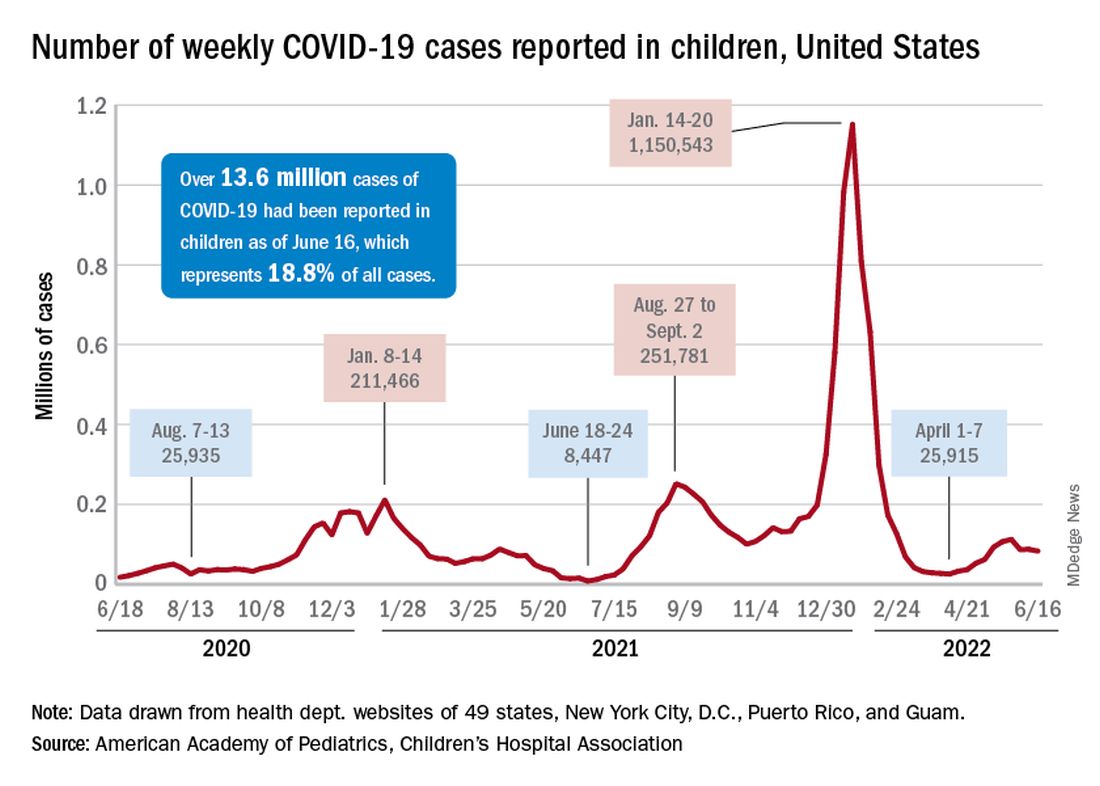
There are, according to the American Academy of Pediatrics, still five states where less than 20% of eligible 5- to 11-year-olds have received an initial vaccination. Among children aged 12-17, uptake has been much higher: 70% have received at least one dose and 60% are fully vaccinated, the CDC said.
Trends for new cases, hospitalizations diverging
COVID incidence in children, meanwhile, dropped for the second time in 3 weeks. There were 83,000 new cases reported during June 10-16, a decline of 4.8% from the previous week, according to the AAP and the Children’s Hospital Association.
New cases had risen by a very slight 0.31% during the week of June 3-9 after dropping 22% the week before (May 27 to June 2). Total cases in children have surpassed 13.6 million, which represents 18.8% of cases in all ages since the start of the pandemic, the AAP and CHA said in their weekly COVID report.
New admissions of children with confirmed COVID-19, however, have continued to climb since early to mid April. On June 16, the rate for children aged 0-17 years was up to 0.31 per 100,000, compared with the 0.13 per 100,000 recorded as late as April 11, the CDC said on its COVID Data Tracker.
The COVID-19 prevention effort in children enters its next phase as June draws to a close, while new pediatric cases continued on a downward trend and hospitalizations continued to rise.
The COVID-19 vaccines from Pfizer-BioNTech and Moderna were approved for use in children as young as 6 months, the Centers for Disease Control and Prevention announced on June 18.
“We know millions of parents and caregivers are eager to get their young children vaccinated. ... I encourage parents and caregivers with questions to talk to their doctor, nurse, or local pharmacist to learn more about the benefits of vaccinations,” CDC Director Rochelle P. Walensky, MD, MPH, said in a written statement.
There are, however, indications that many parents are not that eager. Another 11% said “they will only do so if they are required,” Kaiser noted.
The vaccination experience with children aged 5-11 years seems to agree with those numbers. As of June 16, more than 7 months after the vaccine became available, just over 36% had received at least one dose and about 30% were fully vaccinated, CDC data show.
There are, according to the American Academy of Pediatrics, still five states where less than 20% of eligible 5- to 11-year-olds have received an initial vaccination. Among children aged 12-17, uptake has been much higher: 70% have received at least one dose and 60% are fully vaccinated, the CDC said.
Trends for new cases, hospitalizations diverging
COVID incidence in children, meanwhile, dropped for the second time in 3 weeks. There were 83,000 new cases reported during June 10-16, a decline of 4.8% from the previous week, according to the AAP and the Children’s Hospital Association.
New cases had risen by a very slight 0.31% during the week of June 3-9 after dropping 22% the week before (May 27 to June 2). Total cases in children have surpassed 13.6 million, which represents 18.8% of cases in all ages since the start of the pandemic, the AAP and CHA said in their weekly COVID report.
New admissions of children with confirmed COVID-19, however, have continued to climb since early to mid April. On June 16, the rate for children aged 0-17 years was up to 0.31 per 100,000, compared with the 0.13 per 100,000 recorded as late as April 11, the CDC said on its COVID Data Tracker.
The COVID-19 prevention effort in children enters its next phase as June draws to a close, while new pediatric cases continued on a downward trend and hospitalizations continued to rise.
The COVID-19 vaccines from Pfizer-BioNTech and Moderna were approved for use in children as young as 6 months, the Centers for Disease Control and Prevention announced on June 18.
“We know millions of parents and caregivers are eager to get their young children vaccinated. ... I encourage parents and caregivers with questions to talk to their doctor, nurse, or local pharmacist to learn more about the benefits of vaccinations,” CDC Director Rochelle P. Walensky, MD, MPH, said in a written statement.
There are, however, indications that many parents are not that eager. Another 11% said “they will only do so if they are required,” Kaiser noted.
The vaccination experience with children aged 5-11 years seems to agree with those numbers. As of June 16, more than 7 months after the vaccine became available, just over 36% had received at least one dose and about 30% were fully vaccinated, CDC data show.
There are, according to the American Academy of Pediatrics, still five states where less than 20% of eligible 5- to 11-year-olds have received an initial vaccination. Among children aged 12-17, uptake has been much higher: 70% have received at least one dose and 60% are fully vaccinated, the CDC said.
Trends for new cases, hospitalizations diverging
COVID incidence in children, meanwhile, dropped for the second time in 3 weeks. There were 83,000 new cases reported during June 10-16, a decline of 4.8% from the previous week, according to the AAP and the Children’s Hospital Association.
New cases had risen by a very slight 0.31% during the week of June 3-9 after dropping 22% the week before (May 27 to June 2). Total cases in children have surpassed 13.6 million, which represents 18.8% of cases in all ages since the start of the pandemic, the AAP and CHA said in their weekly COVID report.
New admissions of children with confirmed COVID-19, however, have continued to climb since early to mid April. On June 16, the rate for children aged 0-17 years was up to 0.31 per 100,000, compared with the 0.13 per 100,000 recorded as late as April 11, the CDC said on its COVID Data Tracker.
Baclofen shows limited role in GERD
A randomized clinical trial indicated that add-on baclofen may be of benefit to patients on adequate doses of proton pump inhibitors (PPI) with refractory gastroesophageal reflux disease (GERD). However, the benefit was limited to a subset of patients with positive symptom association probability (SAP), which was calculated using 24-hour combined multichannel intraluminal impedance and pH monitoring (24h pH-MII).

“Empirical add-on therapy with baclofen in GERD patients with persisting typical symptoms in spite of double-dose PPI therapy does not seem justified. The use of baclofen should be limited to patients who display a positive SAP for typical reflux symptoms (heartburn and/or regurgitation) during PPI therapy,” researchers led by Ans Pauwels, PhD, MPharmSc, of the Catholic University of Leuven (Belgium) concluded in Alimentary Pharmacology & Therapeutics.
Asked to comment, Philip Katz, MD, professor of medicine and director of GI Function Laboratories at Weill Cornell Medicine and a co-author of some recent GERD guidelines said, “What it tells me is that baclofen may be useful to a patient population that has an accurate diagnosis of reflux hypersensitivity. The difficulty with this study is that the patients you would expect to be helped by baclofen, which were patients who satisfied the criteria for true GERD, didn’t have any improvement.”
PPIs are effective at reducing acid reflux and promoting esophageal healing in GERD patients, but they have little effect on non-acid reflux. Heartburn is most often tied to acid reflux, but regurgitation occurs with similar frequency during both acid and non-acid episodes.
Up to 50% of patients still have reflux despite PPI treatment, and many of these patients will respond to higher PPI doses. However, those who don’t respond are left with few treatment choices.
Reflux events generally occur during transient lower esophageal sphincter relaxations (TLOSRs), and this mechanism is predominant in mild and moderate GERD. A gamma-aminobutyric acid type B receptor agonist, baclofen reduces TLOSRs and associated reflux episodes following meals. Few studies have examined the clinical potential of baclofen in refractory GERD, and it generally is only used after determining that ongoing weakly acidic reflux is responsible for symptoms, using 24h pH-MII.
The study included about 60 patients who underwent 24-hour monitoring while taking a PPI twice daily. Over a 2-week run-in period, participants filled out daily diaries and were randomized to placebo or baclofen 3 times daily over 4 weeks. The baclofen dose was 5 mg for the first week, then 10 mg for the next 3 weeks.
At the end of treatment, 24h pH-MII was repeated. The researchers found no significant decreases in non-acid reflux events after placebo treatment (corrected P = .74) and a trend towards a reduction following baclofen treatment (corrected P = .12).
Although the results won’t change his practice significantly, Dr. Katz congratulated the authors on the thoroughness of the study. However, he noted that wellbeing is a difficult endpoint to study: “The importance of this study to me is that it confirms that baclofen shouldn’t be used empirically, since there was no improvement in patients who were functional, and it was hard to find improvement in any group. This reinforces the need for a thorough work-up of the patient with GERD.”
The drug also had some tolerability issues: 16% of patients on baclofen discontinued its use because of adverse events such as drowsiness, dizziness, headache, and nausea.
An important limitation of the study is that the researchers recruited patients with persistent GERD symptoms despite use of PPIs. “Calling it refractory GERD is tricky because they didn’t prove they had GERD before they were enrolled in the study. That being said, the researchers did a very rigorous, very careful study to try and find potentially some place that baclofen might benefit patients,” said Dr. Katz.
The authors of the study and Dr. Katz have no relevant financial disclosures.
A randomized clinical trial indicated that add-on baclofen may be of benefit to patients on adequate doses of proton pump inhibitors (PPI) with refractory gastroesophageal reflux disease (GERD). However, the benefit was limited to a subset of patients with positive symptom association probability (SAP), which was calculated using 24-hour combined multichannel intraluminal impedance and pH monitoring (24h pH-MII).
“Empirical add-on therapy with baclofen in GERD patients with persisting typical symptoms in spite of double-dose PPI therapy does not seem justified. The use of baclofen should be limited to patients who display a positive SAP for typical reflux symptoms (heartburn and/or regurgitation) during PPI therapy,” researchers led by Ans Pauwels, PhD, MPharmSc, of the Catholic University of Leuven (Belgium) concluded in Alimentary Pharmacology & Therapeutics.
Asked to comment, Philip Katz, MD, professor of medicine and director of GI Function Laboratories at Weill Cornell Medicine and a co-author of some recent GERD guidelines said, “What it tells me is that baclofen may be useful to a patient population that has an accurate diagnosis of reflux hypersensitivity. The difficulty with this study is that the patients you would expect to be helped by baclofen, which were patients who satisfied the criteria for true GERD, didn’t have any improvement.”
PPIs are effective at reducing acid reflux and promoting esophageal healing in GERD patients, but they have little effect on non-acid reflux. Heartburn is most often tied to acid reflux, but regurgitation occurs with similar frequency during both acid and non-acid episodes.
Up to 50% of patients still have reflux despite PPI treatment, and many of these patients will respond to higher PPI doses. However, those who don’t respond are left with few treatment choices.
Reflux events generally occur during transient lower esophageal sphincter relaxations (TLOSRs), and this mechanism is predominant in mild and moderate GERD. A gamma-aminobutyric acid type B receptor agonist, baclofen reduces TLOSRs and associated reflux episodes following meals. Few studies have examined the clinical potential of baclofen in refractory GERD, and it generally is only used after determining that ongoing weakly acidic reflux is responsible for symptoms, using 24h pH-MII.
The study included about 60 patients who underwent 24-hour monitoring while taking a PPI twice daily. Over a 2-week run-in period, participants filled out daily diaries and were randomized to placebo or baclofen 3 times daily over 4 weeks. The baclofen dose was 5 mg for the first week, then 10 mg for the next 3 weeks.
At the end of treatment, 24h pH-MII was repeated. The researchers found no significant decreases in non-acid reflux events after placebo treatment (corrected P = .74) and a trend towards a reduction following baclofen treatment (corrected P = .12).
Although the results won’t change his practice significantly, Dr. Katz congratulated the authors on the thoroughness of the study. However, he noted that wellbeing is a difficult endpoint to study: “The importance of this study to me is that it confirms that baclofen shouldn’t be used empirically, since there was no improvement in patients who were functional, and it was hard to find improvement in any group. This reinforces the need for a thorough work-up of the patient with GERD.”
The drug also had some tolerability issues: 16% of patients on baclofen discontinued its use because of adverse events such as drowsiness, dizziness, headache, and nausea.
An important limitation of the study is that the researchers recruited patients with persistent GERD symptoms despite use of PPIs. “Calling it refractory GERD is tricky because they didn’t prove they had GERD before they were enrolled in the study. That being said, the researchers did a very rigorous, very careful study to try and find potentially some place that baclofen might benefit patients,” said Dr. Katz.
The authors of the study and Dr. Katz have no relevant financial disclosures.
A randomized clinical trial indicated that add-on baclofen may be of benefit to patients on adequate doses of proton pump inhibitors (PPI) with refractory gastroesophageal reflux disease (GERD). However, the benefit was limited to a subset of patients with positive symptom association probability (SAP), which was calculated using 24-hour combined multichannel intraluminal impedance and pH monitoring (24h pH-MII).
“Empirical add-on therapy with baclofen in GERD patients with persisting typical symptoms in spite of double-dose PPI therapy does not seem justified. The use of baclofen should be limited to patients who display a positive SAP for typical reflux symptoms (heartburn and/or regurgitation) during PPI therapy,” researchers led by Ans Pauwels, PhD, MPharmSc, of the Catholic University of Leuven (Belgium) concluded in Alimentary Pharmacology & Therapeutics.
Asked to comment, Philip Katz, MD, professor of medicine and director of GI Function Laboratories at Weill Cornell Medicine and a co-author of some recent GERD guidelines said, “What it tells me is that baclofen may be useful to a patient population that has an accurate diagnosis of reflux hypersensitivity. The difficulty with this study is that the patients you would expect to be helped by baclofen, which were patients who satisfied the criteria for true GERD, didn’t have any improvement.”
PPIs are effective at reducing acid reflux and promoting esophageal healing in GERD patients, but they have little effect on non-acid reflux. Heartburn is most often tied to acid reflux, but regurgitation occurs with similar frequency during both acid and non-acid episodes.
Up to 50% of patients still have reflux despite PPI treatment, and many of these patients will respond to higher PPI doses. However, those who don’t respond are left with few treatment choices.
Reflux events generally occur during transient lower esophageal sphincter relaxations (TLOSRs), and this mechanism is predominant in mild and moderate GERD. A gamma-aminobutyric acid type B receptor agonist, baclofen reduces TLOSRs and associated reflux episodes following meals. Few studies have examined the clinical potential of baclofen in refractory GERD, and it generally is only used after determining that ongoing weakly acidic reflux is responsible for symptoms, using 24h pH-MII.
The study included about 60 patients who underwent 24-hour monitoring while taking a PPI twice daily. Over a 2-week run-in period, participants filled out daily diaries and were randomized to placebo or baclofen 3 times daily over 4 weeks. The baclofen dose was 5 mg for the first week, then 10 mg for the next 3 weeks.
At the end of treatment, 24h pH-MII was repeated. The researchers found no significant decreases in non-acid reflux events after placebo treatment (corrected P = .74) and a trend towards a reduction following baclofen treatment (corrected P = .12).
Although the results won’t change his practice significantly, Dr. Katz congratulated the authors on the thoroughness of the study. However, he noted that wellbeing is a difficult endpoint to study: “The importance of this study to me is that it confirms that baclofen shouldn’t be used empirically, since there was no improvement in patients who were functional, and it was hard to find improvement in any group. This reinforces the need for a thorough work-up of the patient with GERD.”
The drug also had some tolerability issues: 16% of patients on baclofen discontinued its use because of adverse events such as drowsiness, dizziness, headache, and nausea.
An important limitation of the study is that the researchers recruited patients with persistent GERD symptoms despite use of PPIs. “Calling it refractory GERD is tricky because they didn’t prove they had GERD before they were enrolled in the study. That being said, the researchers did a very rigorous, very careful study to try and find potentially some place that baclofen might benefit patients,” said Dr. Katz.
The authors of the study and Dr. Katz have no relevant financial disclosures.
FROM ALIMENTARY PHARMACOLOGY & THERAPEUTICS